IN PORTUGAL, SPAIN, FRANCE, AND
THE NETHERLANDS,
FROM THE BATTLE OF ROLIÇA, IN 1808, TO THAT OF
WATERLOO, IN 1815;
WITH ADDITIONS RELATING TO THOSE IN THE CRIMEA IN
1854-1855.
SHOWING
THE IMPROVEMENTS MADE DURING AND SINCE THAT PERIOD IN THE
GREAT ART AND SCIENCE OF SURGERY ON ALL THE
SUBJECTS TO WHICH THEY RELATE.
REVISED TO OCTOBER, 1855.
BY G. J. GUTHRIE, F.R.S.
SIXTH EDITION.
PHILADELPHIA:
J. B. LIPPINCOTT & CO.
1862.
TO
The Right Honorable
The Lord Panmure,
SECRETARY OF STATE FOR THE WAR DEPARTMENT,
ETC. ETC. ETC.,
THESE COMMENTARIES
ARE, BY PERMISSION,
INSCRIBED,
BY HIS LORDSHIP’S VERY OBEDIENT
AND FAITHFUL SERVANT,
G. J. GUTHRIE.
Twenty months have elapsed since the Introductory Lecture was published in The Lancet; fifteen others succeeded at intervals, and fifteen have been printed separately to complete the number of which the present work is composed. Divested of the historical and argumentative, as well as of much of the illustrative part, contained in the records whence it is derived, it nevertheless occupies 585 pages—the essential points therein being numbered from 1 to 423.
Sir De Lacy Evans, in some observations lately made in the House of Commons on the subject of a Professorship of Military Surgery in London, alluded to these Lectures in the most gratifying manner; he could not, however, state their origin, scope, or object, being unacquainted with them.
On the termination of the war in 1814, I expressed in print my regret that we had not had another battle in the south of France, to enable me to decide two or three points in surgery which were doubtful. I was called an enthusiast, and laughed at accordingly. The battle of Waterloo afforded the desired opportunity. Sir James M’Grigor, then first appointed Director-General, offered to [6] place me on full pay for six months. This would have been destructive to my prospects in London; I therefore offered to serve for three, which he was afraid would be called a job, although the difference between half-pay and full was under sixty pounds; and our amicable discussion ended by my going to Brussels and Antwerp for five weeks as an amateur. The officers in both places received me in a manner to which I cannot do justice. They placed themselves and their patients at my entire disposal, and carried into effect every suggestion. The doubts on the points alluded to were dissipated, and the principles wanting were established. Three of the most important cases, which had never before been seen in London nor in Paris, were sent to the York Military Hospital, then at Chelsea. The rank I held as a Deputy Inspector-General precluded my being employed. It was again a matter of money. I offered to do the duty of a staff-surgeon without pay, provided two wards were assigned to me in which the worst cases from Brussels and Antwerp might be collected. The offer was accepted; and for two years I did this duty, until the hospital was broken up, and the men transferred to Chatham. In the first year a Course of Lectures on Military Surgery was given. The inefficiency of such a Course alone was soon seen, for Surgery admits of no such distinctions. Injuries of the head, for instance, in warfare, usually take place on the sides and vertex; in civil life, more frequently at the base. They implicate each other so inseparably, although all the symptoms are not alike or always present, that they cannot be disconnected with propriety. This equally obtains in other [7] parts; and my second and extended Course was recognized by the Council of the Royal College of Surgeons as one of General Surgery.
When the Court of Examiners of the Royal College of Surgeons of England—of which body I have been for more than twenty years a humble member—confer their diploma after examination on a student, they do not consider him to have done more than laid the foundation for that knowledge which is to be afterward acquired by long and patient observation. When a student in law is called to the bar, he is not supposed to be therefore qualified to be a Queen’s counsel, much less a judge or a chancellor. The young theologian, admitted into deacon’s orders, is not supposed to be fitted for a bishopric. When the young surgeon is sent, in the execution of his duties, to distant climes, where he has few and sometimes no opportunities of adding to the knowledge he had previously acquired, it is apt to be impaired; and he may return to England, after an absence of several years, less qualified, perhaps, than when he left it. To such persons a course of instruction is invaluable. It should be open to them as public servants gratuitously, and should be conveyed by a person appointed and paid by the Crown. He should be styled, in my opinion, the Military Professor of Surgery, and be capable, from his previous experience and his civil opportunities, of teaching all things in the principles and practice of surgery connected with his office, although he may and should annually select his subjects. Leave of absence for three months might be advantageously granted to officers in turn for the purpose of at[8]tending these lectures, and the Professor should certify as to their time having been well employed. For thirty years I endeavored to render this service to the Army, the Navy, and the East India Company, from the knowledge I had acquired of its importance. To the Officers of these services my two hospitals, together with Lectures and Demonstrations, were always open gratuitously, as a mark of the estimation in which I held them. By the end of that period the enthusiasm of the enthusiast who wished for another battle in 1814 had oozed out, like the courage of Bob Acres in “The Rivals,” at the ends of his fingers. The course of instruction was discontinued, but not until such parts were printed, under the title of “Records of the Surgery of the War,” as were not before the public, in order that teachers of civil or systematic surgery should be acquainted with them.
4 Berkeley Street, Berkeley Square,
June 21, 1853.
The rapid sale of the fifth, and the demand for a sixth edition of this work, enable me to say that the precepts inculcated in it have been fully borne out and confirmed by the practice of the Surgeons of the Army now in the Crimea in almost every particular. To several of these gentlemen I desire to offer my warmest thanks for the assistance they have afforded. Their names are given with the cases and observations they have been so good as to send me, and a fuller “Addenda” shall be made from time to time, as I receive further information from them, and others who will, I hope, follow the example they have thus set. More, however, has been done; they have performed operations of the gravest importance at my suggestion, that had not been done before, with a judgment and ability beyond all praise; and they have modified others to the great advantage of those who may hereafter suffer from similar injuries. They have thus proved that if the Administrative duties of the Medical Department of the Army have not been free from public animadversion, that its practical and scientific duties have merited public approbation; which I am satisfied, from what they have already done, they will continue to deserve.
[10] The precepts laid down are the result of the experience acquired in the war in the Peninsula, from the first battle of Roliça in 1808, to the last in Belgium, of Waterloo in 1815, which altered, nay overturned, nearly all those which existed previously to that period, on all points to which they relate. Points as essential in the Surgery of domestic as in military life. They have been the means of saving the lives, and of relieving, if not even of preventing, the miseries of thousands of our fellow-creatures throughout the civilized world.
I would willingly imitate the example lately indulged in, by many of the best Parisian surgeons, of detailing circumstantially the improvements they have made in practical and scientific surgery; the manner in which they were at first contested, and the universal adoption of them which has succeeded, were it not that I might run the risk of being accused of gratifying some personal vanity, while only desirous of drawing the attention of the public to the merits of the men who so ably served them in the last war, nearly all of whom are no more; and who have passed away, as I trust their successors will not, with scarcely a single acknowledgment of their services, except the humble tribute now offered by their companion and friend.
4 Berkeley Street, Berkeley Square,
October 7, 1855.
ON GUNSHOT WOUNDS, ETC.
1. A wound made by a musket-ball is essentially contused, and attended by more or less pain, according to the sensibility of the sufferer, and the manner in which he may be engaged at the moment of injury. A musket-ball will often pass through a fleshy part, causing only the sensation of a sudden and severe, although sometimes of a trifling blow. If it merely strike the same part without rupturing the skin, the pain is often great. Major King, of the Fusiliers, was killed at New Orleans by a musket-ball, which struck him on the pit of the stomach, leaving only the mark of a contusion.
2. Wounds from musket-balls, particularly of the face, sometimes bleed considerably at the moment of injury, and for some little time afterward, although no large vessel shall be injured to render the bleeding inconvenient or dangerous. The application of a tourniquet is then seldom if ever necessary, unless a vessel of some magnitude should be partially torn or divided.
3. When a limb is carried away by a cannon-shot, any destructive bleeding usually ceases with the faintness and failure of strength subsequent on the shock, and a hemorrhage thus spontaneously suppressed does not generally return; it is the effort of nature to save life. The application of a tourniquet is rarely necessary, unless as a precau[26]tionary measure, when it should be applied loosely, and the patient, or some one else, shown how to tighten it if necessary. A musket-ball will often pass so close to a large artery, without injuring it, as to lead to the belief that the vessel must have receded from the ball by its elasticity. A ball passed between the femoral artery and vein of a soldier at Toulouse without doing more injury than a contusion, but it gave rise to inflammation and closure of the vessels, followed by gangrene of the extremity. General Sir Lowry Cole was shot through the body at Salamanca, immediately below the left clavicle; a part of the first rib came away, and the artery at the wrist became, and remained, much diminished in size. General Sir Edward Packenham was shot through the neck on two different occasions, the track of each wound being apparently through the great vessels. The first wound gave him a curve in his neck, the second made it straight. His last unfortunate wound, at New Orleans, was directly through the common iliac artery, and killed him on the spot. Colonel Duckworth, of the 48th Regiment, received a ball through the edge of his leather stock, at Albuhera, which divided the carotid artery, and killed him almost instantaneously.
4. Secondary hemorrhage of any importance from small vessels does not often occur. On the separation of the contused parts, or sloughs, a little blood may be occasionally lost; but it is then generally caused by the impatience of the surgeon, or the irregularity of the patient, and seldom requires attention.
5. A large artery does sometimes give way by ulceration between the eighth and the twentieth days; but the proportion is not more than four cases in a thousand, requiring the application of a ligature; exclusive of those formidable injuries caused by broken bones, or the inordinate sloughing caused by hospital gangrene, when not properly treated.
6. A certain constitutional alarm or shock follows every serious wound, the continuance of which excites a suspicion of its dangerous nature, which nothing but its subsidence, and the absence of symptoms peculiar to the internal part presumed to be injured, should remove. The opinion given under such circumstances should be very guarded; for if this symptom of alarm should continue, great fears may be entertained of hidden mischief. Colonel Sir W. Myers was shot, at Albuhera, at the head of the Fusilier Brigade, at [27] the moment of victory, by a musket-ball, which broke his thigh, and lodged. The continuance of the alarm and anxiety satisfied me it had done other mischief. He died next morning, of mortification of the intestines. General Sir Robert Crawford was wounded at the foot of the smaller breach at the storming of Ciudad Rodrigo, by a musket-ball, which entered the outer and back part of the shoulder, and came out at the axilla. There was a third wound, a small slit in the side, apparently too small to admit a ball. The continuance of the anxiety and alarm pointed out some hidden mischief, which I declared had taken place; and when he died his surgeon found the ball loose in his chest. It had been rolling about on his diaphragm. Surgery was not sufficiently advanced in those days to point out the situation, or to authorize an attempt for the removal of the ball. It must in future be done.
This constitutional alarm and derangement are not always present to so marked an extent. A soldier at Talavera was struck on the head by a twelve-pound shot, which drove some bone into, and some brain out of his head: he was walking about, complaining but little, immediately after the accident, although he died subsequently.
7. It is not always possible, from their appearance, to decide which opening is the entrance, which the exit of an ordinary sized round ball; or when two holes are distant from each other, to ascertain whether they have been caused by one, or by two distinct balls. When a ball is not impinging with much impetus, it may become a penetrating, without being much of a contused wound, which will close in and heal with little suppuration. If the ball do not press upon, or interfere with some important part, the slight degree of irritation which follows may give rise to the formation of a sac, which adheres to it and possibly keeps it quiet for years, if not for life.
8. The wound made by the entrance of an ordinary musket-ball is usually circular, depressed, of a livid color, and capable of admitting the little finger, the exit being more ragged, and not depressed. It is sometimes little more than a small slit or rent, although at others, as in the face or in the back of the hand, it may be much torn, giving to an otherwise simple wound a more frightful appearance, such as is not usually seen in the thigh, or other equally firm fleshy part.
[28] 9. Wounds from flattened or irregular-shaped musket-balls, pieces of shells, or other sharp-edged destructive instruments, are often very much lacerated, and their entrance is less marked. The part thus torn can generally be preserved, and the wound healed with comparatively little loss of substance.
10. When it is desirable to ascertain the exact course of a ball, and, if possible, the internal part injured by it, the sufferer should be placed in the position he was in when he received the injury, with especial reference to the probable situation of the enemy, when that will often become very intelligible which was before indistinct. My attention was directed, after the battle of Toulouse, to a soldier, whose foot was gangrenous without an apparent cause, he having received merely a flesh wound in the thigh, not in the exact course of the main artery, which, nevertheless, I said was injured. On placing the man in the same position with regard to us, that he supposed himself to have been in toward the enemy when wounded, the possibility of such an injury was seen; and dissection after death proved the correctness of the opinion.
11. When one opening only can be seen, it is presumed the ball has lodged; but this does not follow, although the finger of the surgeon may pass into the wound for some distance. At the battle of Vimiera, I pulled a piece of shirt, with a ball at the bottom of it, out of the thigh of an officer of the 40th Regiment, into which it had gone for at least three inches. After the battle of Toulouse, a ball, which penetrated the surface of the chest, and passed under the pectoral muscle for two inches, was ejected by the elasticity of the rib against which it struck. Scarcely any inconvenience followed, and the officer rapidly recovered. After the battle of Waterloo, I was requested to decide whether a young officer should be allowed to die in a few days, or to have a chance for his life by losing his leg above the knee. The joint was open, the suppuration profuse. A large or grape-shot was supposed to be lodged in the head of the tibia. The limb was amputated, and he is now alive, forty years afterward, but no shot was found in his limb. It had dropped out after doing the injury.
12. The treatment of simple gunshot or flesh wounds should be, under ordinary circumstances, as simple as themselves. Nothing should be applied but a piece of linen or [29] lint, wetted with cold water; this may be retained by a strip of sticking-plaster, or any other thing applicable for the purpose of keeping the injured part covered. A compress of linen, or other similar substance, moistened with cold or iced water when procurable, will be useful; and a few inches of a linen bandage may be sewed on, to prevent the compress from changing its position during sleep. When the wound becomes tender, a little oil, lard, or simple ointment may be placed over it. A roller, as a surgical application, is useless, if not injurious. At the first and second battles in Portugal, every wound had a roller applied over it; it soon became stiff, bloody, and dirty. They did no good, were for the most part cut off with scissors, and thus rendered useless. When really wanted, at a later period, they were not forthcoming. An advancing army cannot, and ought not to carry casks full of rollers into the field; and the apothecary-general had better have instead, two casks or boxes full of good wax candles; for, although every regimental surgeon ought to have four in his panniers, kept as carefully for emergencies as his capital instruments, they will require from time to time to be replaced. No roller should be more than two inches and a quarter wide, and made of good, strong, coarse linen, very much, in fact, the reverse of the rollers which have until lately been supplied to the army.
13. Cold or iced water may be used as long as cold is grateful to the sufferer. When it ceases to be so, it should be exchanged for warm, applied in any convenient way which modern improvements have suggested, whether by piline, gutta-percha, oiled silk, etc. An evaporating poultice may be used in private life, but no poultices should be permitted in a military hospital, until the principal surgeon is satisfied they are necessary. They are generally cloaks for negligence, and sure precursors of amputation in all serious injuries of bones and joints. They are properly used to alleviate pain, stiffness, swelling, the uneasiness arising from cold, and to encourage the commencing or impeded action of the vessels toward the formation of matter. As soon as the effect intended has been obtained, the poultice should be abandoned, and recourse again had to water, hot or cold, with compress and bandage. I was in the habit of calling a poultice when misapplied a cover-slut.
14. Many simple flesh wounds are cured in four weeks; the greater part in six. Fresh air and cold water are essen[30]tial. Purgatives may be occasionally given, and abstinence is an excellent remedy. Emetics, bleeding, and something approaching to starvation as to solids, are of great importance if the sufferers should be irregular in their habits, or the inflammatory symptoms run high. In weakly persons, a generous diet with tonic remedies will be necessary.
15. In wounds of muscular parts inflammation usually occurs from twelve to twenty-four hours after the injury, and the vicinity of the wound becomes more sensible to the touch, with a little swelling and increase of discoloration. A reddish serous fluid is discharged, and the limb becomes stiff and nearly incapable of motion, from its causing an increase of pain. These symptoms are gradually augmented on or about the third day; the inflammation surrounding the wound is more marked; the discharge is altered, being thicker; the action of the absorbents on the edges of the wound may be observed; and, on the fourth or fifth, the line of separation between the dead and living parts will be very evident. The wound will now discharge purulent matter mixed with other fluids, which gradually diminish as the naturally healthy actions take place. The inside of the wound, as the process of separation proceeds, changes from a blackish-red color to a brownish yellow, moistened by a little good pus. On the fifth and sixth days, the outer edge of the separating slough is distinctly marked, and begins to be displaced; the surrounding inflammation extends to some distance, the parts are more painful and sensible to the touch; the discharge is more purulent, but not great in quantity. On the eighth or ninth day, the slough is, in most cases, separated from the edges of the track of the ball, and hanging in the mouth of the wound, although it cannot yet be disengaged; the discharge increases, and the wound becomes less painful to the patient, although frequently more sensible when touched.
If there be two openings, the exit of the ball, or the counter-opening, is in general much the cleaner, being often in a fair granulating state before the entrance of the ball is free from slough. If the inflammation have been smart, the limb is at this time a little swollen and discolored for some distance around; fibrin and serum are thrown out into the cellular membrane, or areolar tissue, as it is now termed; the redness diminishes; the sloughs are discharged, together with any little extraneous substances which may be in the [31] wound; and there is frequently a slight bleeding, if the irritable granulations are roughly treated. The limb on the twelfth, and even fifteenth day, retains the appearance of yellowness and discoloration which ensues from a bruise, and which continues a few days longer. The sloughs do not, sometimes, separate until this period, and, in persons slow to action, not even until a later one. The wound now contracts; the middle portion of the track first closes, and is no longer pervious; the lower opening soon heals, while the upper, or that usually made by the entrance of the ball, continues to discharge for some time, and toward the end of six weeks, or sometimes two months, finally heals with a depression and cicatrix, marking distinctly the nature of the injury that has been received.
16. The state of constitution, the difficulties and distresses of military warfare, exposure to the inclemency of the weather, the season of the year, or the imprudence of individuals, will sometimes bring on a train of serious symptoms, in wounds apparently of the same nature as others in which no such evils occur. After the first two or three days, the symptoms gradually increase, the swelling is much augmented, the redness extends, and the pain is more severe and constant. The wound becomes dry, stiff, with glistening edges, the general sensibility is increased, the system sympathizes, the skin becomes hot and dry, the tongue loaded, the head aches, the patient is restless and uneasy, the pulse full and quick; there is fever of the inflammatory kind. The swelling of the part increases from deposition in the areolar tissue to a considerable extent above and below the wound, and the inflammation, instead of being entirely superficial or confined to the immediate track of the ball, spreads widely. The wound itself the sufferer can hardly bear to be touched; it discharges but little, and the sloughs separate slowly. Pus soon begins to be secreted more copiously, not only in the track of the wound, but in the surrounding parts; sinuses may form in the course of the muscles, or under the fascia, and considerable surgical treatment be necessary, while the cure is protracted from three to four, and even to six months; and is often attended for a longer period with lameness, from contraction of the muscles or adhesions of the areolar tissue. The parts, from having been so long in a state of inflammation, are much weaker, and if the injury have been in the lower extremity, the leg [32] and foot swell on any exertion, which cannot be performed without pain and inconvenience for a considerable time. The treatment should be active; the patient, if robust, ought to be bled if no endemic disease prevail, vomited, purged, kept in the recumbent position, and cold applied so long as it shall be found agreeable to his feelings; when that ceases to be the case, warm fomentations ought to be resorted to, but they are to be abandoned the instant the inflammation is subdued and suppuration well established. The feelings of the patient will determine the period, and it is better to begin a day too soon than one too late. If the inflammation be superficial, leeches will not be of the same utility as when it is deep seated; but then they must be applied in much greater numbers than are usually recommended. The roller and graduated compresses, or pressure made by slips of adhesive plaster under them, are the best means of cure in the subsequent stages, with change of air, and friction to the whole extremity, which alone, when early and well applied, will often save months of tedious treatment. If the limb become contracted and the cellular membrane thickened, it is principally by friction (shampooing) that it can be restored to its natural motion.
17. If the ball should have penetrated without making an exit, or have carried in with it any extraneous substances, the surgeon must, if possible, ascertain its exact situation, and remove it and any foreign bodies which may be lodged; indeed, if there be time, every wound should be examined so strictly as to enable the surgeon to satisfy himself that nothing has lodged. This is less necessary where there are two corresponding openings evidently belonging to one shot; but it is imperiously demanded of the surgeon, where there is one opening only, even if that be so much lacerated as to lead to the suspicion of its being a rent from a piece of shell; for it is by no means uncommon for such missiles, or a grape-shot, to lodge wholly unknown to the patient, and to be discovered by the surgeon at a subsequent period, when much time has been lost and misery endured. A soldier during the siege of Badajoz had the misfortune to be near a shell at the moment of its bursting, and was so much mangled as to render it necessary to remove one leg, an arm, and a testicle, (a part of the penis and scrotum being lost.) In one of the flesh wounds in the back part of the thigh and buttock a large [33] piece of shell was lodged, and kept op considerable irritation until it was removed. The man recovered.
18. In examining a wound, a finger should be gently introduced, if possible, in the course of the ball, to its utmost extent; in parts connected with life, or liable to be seriously injured, it is the only sound usually admissible. While this examination is taking place, the hand of the surgeon should be carefully pressed upon the part opposite where the ball may be expected to lie, by which means it may perhaps be brought within reach of the finger, and for want of which precaution, it may be missed by a very trifling distance. While the finger is in the wound the limb may be thrown as nearly as possible into that action which was about to be performed on the receipt of the injury, when the contraction of the muscles and the relative change of the parts will more readily allow the course of the ball to be followed. If this should fail, attention should be paid to the various actions of the limb, the attendant symptoms arising from parts affected, and what may be called the general anatomy of the whole circle of injury. A muscle, in the act of contraction, may oppose an obstacle to the passage of an instrument in the direction the ball has taken, especially if it should have passed between tendons or surfaces loosely connected by cellular membrane; as by the side of, or between the great blood-vessels, which by their elasticity may make way for the ball, and yet impede the progress of a sound. When the ball is ascertained to have passed beyond the reach of the finger, a blunt silver sound or elastic bougie may be used, and the opposite side of the limb should be carefully examined, and pressure made on the wounded side, when it will probably be found more or less deeply seated. If the ball should not be discoverable by these means, the surgeon should consider every symptom, and every part of anatomy connected with the wound, before he decides on leaving the ball to the operations of nature.
19. It is unnecessary to dilate a wound without a precise object in view, which might render an additional opening requisite. This dilatation or opening, when made, should always be carried through the fascia of the limb. A wound ought not to be dilated because such operation may at a more distant period become necessary. The necessity should first be seen, when the operation follows of course.
Suppose a man be brought for assistance with a wound [34] through the thigh, in the immediate vicinity of the femoral artery, which he says bled considerably at the moment of injury, but the hemorrhage had ceased. Is the surgeon warranted in cutting down upon the artery, and putting ligatures upon it on suspicion? Every man in his senses ought to answer, No. The surgeon should take the precaution of applying a tourniquet loosely on the limb, and of placing the man in a situation where he can receive constant attention in case of need; but he is not authorized to proceed to any operation, unless another bleeding should demonstrate the injury and the necessity for suppressing it. By the same reasoning, incisions are not to be made into the thigh on the speculation that they may be hereafter required. If the confusion which has enveloped this subject be removed, and bleeding arteries, broken bones, and the lodgment of extraneous substances be admitted to be the only legitimate causes for dilating wounds in the first instance, the arguments in favor of primary dilatation in other cases must fall to the ground.
When the inflammation, pain, and fever run high, the tension of the part being great, an incision should be made by introducing the knife into the wound, and cutting for the space of two or three inches, according to circumstances, in the course of the muscles, carefully avoiding any other parts of importance. The same should be done at the inferior or opposite opening, if mischief be seriously impending, not so much on the principle of loosening the fascia as on that of taking away blood from the part immediately affected, and of making a free opening for the evacuation of the fluids about to be effused.
It is no less an advantageous practice in the subsequent stages of gunshot wounds, where sinuses form and are tardy in healing. A free incision is also very often serviceable when parts are unhealthy, although there may not be any considerable sinus. Upon the necessity of it where bones are splintered, there is no occasion in this place to insist.
20. In making incisions for the removal of balls in the vicinity of large vessels, particularly in the neck, the hand should always be unsupported, in order to prevent an accident from any sudden movement of the patient. This caution is the more necessary on the field of battle, where many things may give rise to sudden alarm. At the affair [35] of Saca Parte, near Alfaiates, in Portugal, I stationed myself behind a small watch-tower, and the wounded were first brought to this spot for assistance. A howitzer had also been placed upon it, being rising ground, and at the moment I was extracting a ball situated immediately over the carotid artery, the gun was fired, to the inexpressible alarm of surgeon, patient, and orderly, who bolted in all directions. From my hand being unsupported, no mischief ensued, and the operation was completed as soon as all had recovered their usual serenity. When a ball is discovered on the opposite side of a limb, through which it has nearly penetrated, but has not had sufficient power to overcome the resistance and elasticity of the skin, it should be removed by incision. An opening is thus obtained for the evacuation of any matter which may be formed in the long track of such a wound, and any other extraneous bodies are more readily extracted. When a ball has penetrated half through the thick part of the thigh, in such a direction that it cannot readily be removed by the opening at which it entered; or, from the vicinity of the great vessels, it may be considered unadvisable to cut for it in that direction; or if the ball cannot be distinctly felt by the finger through the soft parts, it ought not to be sought for at the moment, for an incision of considerable extent will be required to enable the surgeon to extract it. Much pain will be caused, and higher inflammation may follow than would ensue if the wound were left to the efforts of nature alone, by which, in time, the ball would in all probability be brought much nearer to the surface, and might be more safely extracted. It frequently happens, that after a few days or weeks, a ball will be distinctly felt in a spot where the surgeon had before searched for it in vain. A wound will frequently close without further trouble, the ball remaining without inconvenience in its new situation; and the patient not being annoyed by it, does not feel disposed to submit to pain or inconvenience for its removal. A very strong reason for the extraction of balls during the first period of treatment, if it can be safely accomplished, is, that they do not always remain harmless, but frequently give rise to distressing or harassing pains in or about the part, which often oblige the sufferer to submit to their extraction at a later period, when their removal is infinitely more difficult; and may be more distressing than at the moment of injury.
[36] Nothing appears more simple than to cut out a ball which can be felt at the distance of an inch, or even half an inch below the skin, but the young surgeon often finds it more difficult than he expected, because he makes his incision too small; and cannot at all times oppose sufficient resistance to prevent the ball from retreating before the effort he makes for its expulsion with the forceps or other instrument. The ball also requires to be cleared from the surrounding cellular substance, to a greater extent than might at first be imagined; for all that seems to be required is, that a simple incision be made down to the surface of it, when it will slip out, which is not usually the case. When a ball has been lodged for years, a membranous kind of sac is formed around it, which shuts it in as it were from all communication with the surrounding parts. If it should become necessary to extract a ball which has been lodged in this manner, the membranous sac will often be found to adhere so strongly to the ball that it cannot be got out without great difficulty, and sometimes not without cutting out a portion of the adhering sac.
It often occurs that a ball lodges and cannot be found, especially where it has struck against a bone, and slanted off in a different direction. If the ball should lodge in the cellular tissue between two muscles, it often descends by its gravity to a considerable distance, and excites a low degree of irritation, which slowly brings it to the surface, or terminates in abscess. Colonel Ross, of the Rifle Brigade, was wounded at the battle of Waterloo by a musket-ball, which entered at the upper part of the arm and injured the bone. More than one surgeon had pointed out the way by which it had passed under the scapula and lodged itself in some of the muscles of the back. About a year afterward I extracted it close to the elbow, the ball lying at the bottom of an abscess, which was only brought near the surface by time, by the use of flannel, and by desisting from all emollient applications.[1]
[1] Various instruments have been invented for the removal of balls which have been deeply lodged in soft parts; but little assistance has been derived from them hitherto, although many of them are very ingenious.
21. A ball will frequently strike a bone, and lodge, without causing a fracture, although it will a fissure. It will even go through the lower part of the thigh-bone, between [37] or a little above the condyles, merely splitting without separating it, and some balls have lodged in bones for years, with little inconvenience. It should nevertheless be a general rule not to allow a ball to remain in a bone, if it can be removed by any reasonable operation. The rule is not entirely devoid of exception. Lieutenant-Colonel Dumaresq, aid-de-camp to the present Lord Strafford, was wounded at Waterloo by a ball which penetrated the right scapula, and lodged in a rib in the axilla. The thoracic inflammation nearly cost him his life, but he ultimately quite recovered, and died many years afterward of apoplexy, the ball remaining enveloped in bone.
22. When a bayonet is thrust into the body it is a punctured wound made by direct pressure; when of little depth, much inconvenience rarely ensues, and the part heals slowly, but surely, under the precaution of daily pressure. A punctured wound, extending to considerable depth, labors under disadvantages in proportion to the smallness of the instrument, and the differences of texture through which it passes. When the instrument is large, the opening made is in proportion, and does not afford so great an obstacle to the discharge of the fluids poured out or secreted as when the opening is small. Lance wounds are therefore less dangerous than those inflicted by the bayonet. When a small instrument passes deep through a fascia, it makes an opening in it which is not increased by the natural retraction of parts, inasmuch as it is not sufficiently large to admit of it; and which opening, small as it is, may be filled or closed up by the soft cellular tissue below, which rises into it, and forms a barrier to the discharge of any matter which may be secreted beneath. If the instrument should have passed into a muscle, it is evident that if that muscle were in a state of contraction at the moment of injury, the punctured part must be removed to a certain distance from the direct line of the wound when in a state of relaxation, and vice versa. The matter, secreted, and more or less in almost every instance will be secreted, cannot in either case make its escape, and all the symptoms occur of a spontaneous abscess deeply seated below a fascia. That inflammation should spread in a continuous texture is not uncommon; that matter, when confined, should give rise to great constitutional disturbance is, if possible, less so; but that this disturbance takes place without the occurrence of inflamma[38]tion, or the formation of matter, may be doubted; and it may be concluded that there is no peculiarity in punctured wounds that may not be accounted for in a satisfactory manner. Serious effects have been attributed to injuries of nerves, but without sufficient reason; nevertheless, those who have seen locked-jaw follow a very simple scratch of the leg from a musket-ball, more frequently than from a greater injury, are not surprised at any symptoms of nervous agitation that may occur after punctured wounds. As many bayonet wounds through muscular parts heal with little trouble, it is time enough to dilate them when assistance seems to be required. Cold water should be used at first; care should be taken not to apply a roller or compress of any kind over the wound; matter, when formed, should be frequently pressed out, and, if necessary, a free exit should be made for it.
23. A great delusion is cherished in Great Britain on the subject of the bayonet—a sort of monomania very gratifying to the national vanity, but not quite in accordance with matter of fact. Opposing regiments, when formed in line, and charging with fixed bayonets, never meet and struggle hand to hand and foot to foot, and this for the very best possible reason, that one side turns round and runs away as soon as the other comes close enough to do mischief; doubtless considering that discretion is the better part of valor. Small parties of men may have personal conflicts after an affair has been decided, or in the subsequent scuffle if they cannot get out of the way fast enough. The battle of Maida is usually referred to as a remarkable instance of a bayonet fight; nevertheless, the sufferers, whether killed or wounded, French or English, suffered from bullets, not bayonets. The late Sir James Kempt commanded the brigade supposed to have done this feat, but he has assured me that no charge with the bayonet took place, the French being killed in line by the fire of musketry; a fact which has of late received a remarkable confirmation in the published correspondence of King Joseph Bonaparte, in which General Regnier, writing to him on the subject, says: “The 1st and 42d Regiments charged with the bayonet until they came within fifteen paces of the enemy, when they turned, et prirent la fuite. The second line, composed of Polish troops, had already done the same.” Wounds from bayonets were not less rare in the Peninsular war. It may be that all those who were [39] bayoneted were killed, yet their bodies were seldom found. A certain fighting regiment had the misfortune one very misty morning to have a large number of men carried off by a charge of Polish lancers, many being also killed. The commanding officer concluded they must be all killed, for his men possessed exactly the same spirit as a part of the French Imperial guard at Waterloo. “They might be killed, but they could not by any possibility be taken prisoners.” He returned them all dead accordingly. A few days afterward they reappeared, to the astonishment of everybody, having been swept off by the cavalry, and had made their escape in the retreat of the French army through the woods. The regiment from that day obtained the ludicrous name of the “Resurrection men.”
The siege of Sebastopol has furnished many opportunities for partial hand to hand bayonet contests, in which many have been killed and wounded on all sides, but I do not learn that in any engagements which have taken place regiments advanced against each other in line and really crossed bayonets as a body; although the individual bravery of smaller parties was frequently manifested there, as well as in the war in the Peninsula.
ON INFLAMMATION, MORTIFICATION, ETC.
24. In some very rare cases, an intense, deep-seated inflammation supervenes after some days, almost suddenly and without any obvious cause. The skin is scarcely affected, although the limb—and this complaint has hitherto been observed only in the thigh—is swollen, and exceedingly painful. If relief be not given, these persons die soon, and the parts beneath the fascia lata appear after death softened, stuffed, and gorged with blood, indicating the occurrence of an intense degree of inflammation, only to be overcome by general blood-letting; and especially by incisions made through the fascia from the wound, deep into the parts, so as to relieve them by a considerable loss of blood, and by the removal of any pressure which the fascia might cause on the swollen parts beneath.
[40] 25. Erysipelatous inflammation is marked by a rose or yellowish redness, tending in bad constitutions to brown or even to purple, but in all cases terminating by a defined edge on the white surrounding skin. It frequently spreads with great rapidity, so that the limb, and even the whole skin of the body, may be in time affected by it, the redness subsiding and even disappearing in one part, while it extends in another direction. When this inflammation attacks young and otherwise healthful persons of apparently good constitution, it should be treated by emetics, purgatives, and diaphoretics, in the first instance, with, perhaps, in some cases, bleeding. When the habit of body is not supposed to be healthy, bleeding is inadmissible, and stimulating diaphoretics, combined with camphor and ammonia, will be found more beneficial after emetics and purgatives; these remedies may in turn be followed by quinine and the mineral acids, with the infusion and tincture of bark. Little reliance can be placed on large doses of cinchona in powder; they nauseate and therefore distress.
When the inflammation extends deeper than the skin, into the areolar or cellular tissue, it partakes more of the nature of the healthy suppurative inflammation, commonly called phlegmonous, is accompanied by the formation of matter, and tends to the sloughing or death of this tissue at an early period. The redness in this case is of a brighter color, although equally diffuse, and with a determined edge; the limb is more swollen and tense, and soon becomes quagmiry to the touch. The skin is then undermined, and soon loses its life, becomes ash colored and gangrenous in spots, and separates, giving exit to the slough and matter which now pervade the whole extremity affected. If the patient survive, it will probably be with the loss of the whole of the skin and the cellular substance of the limb.
As soon as the inflamed part communicates the springy, fluctuating sensation approaching, but not yet arrived at the quagmiry feel alluded to, an incision should be made into it, when the areolæ or cells of the cellular tissue will be seen of a bright leaden color, and of a gelatinous appearance, arising from the fluid secreted into them, being now nearly in the act of being converted into pus. The septa, dividing the tissue into cells, have not at this period lost their life, and the fluid hardly exudes, as it will be found to do a few hours later, when the matter deposited has become purulent. [41] When this change has taken place, the patient is in danger, and if relief be not given, he will often sink under the most marked symptoms of irritative fever of a typhoid type. Nature herself sometimes gives the required relief by the destruction of the superincumbent skin; but this part is tough, offers considerable resistance, and does not readily yield until the deep-seated fascia is implicated, and the muscular parts are about to be laid bare.
An incision made into the inflamed part through the cellular tissue, down to the deep-seated fascia, which should not be divided in the first instance, gives relief. One of four inches in length usually admits of a separation of its edges to the amount of two inches, by which the tension of the skin, which principally causes the mischief which follows the inflammation, is removed. As many incisions are required as will relieve this tension, according to the extent of the inflammation, which is also relieved by the flow of blood, but that requires attention, as it is often considerable, particularly if the deep fascia be divided on which the larger vessels are found to lie. If the necessary incisions be delayed until the quagmiry feeling is fully established, the skin above it is generally undermined and dies. The following case is given as the first known in London, in which long incisions were made for the cure of this disease, and their effect in relieving the constitutional irritation is so strongly marked as to need no further explanation:—
Thomas Key, aged forty, a hard drinker, was admitted into the Westminster Hospital, under my care, on the 21st of October, 1823, having fallen and injured his left arm against a stool, four days previously. On the 30th, the skin being very tense, the part springy, and yielding the boggy feel described, pulse 120, mind wandering, I proposed, in consultation with my colleagues, to make incisions into the part, but which were considered to be unusual and improper. On the 31st, the pulse being 140, and everything indicating a fatal termination, I refrained from any further consultation, although directed by the rules of the hospital; and, after my old Peninsular fashion, made an incision eight inches long into the back of the arm, and another of five on the under edge, in the line of the ulna, down to the fascia, which was in part divided; one vessel bled freely. The next day, November 1, the pulse was 90; the man had slept, and said he had had a good night. The [42] incision on the back of the arm was augmented to eleven inches; and from that time he gradually recovered, being snatched as it were from the jaws of death.
This case, published at the time, has been the exemplar on which this most successful practice has been followed throughout the civilized world—a practice entirely due to the war in the Peninsula.
When this kind of inflammation attacks the scrotum, which it sometimes, although rarely, does, as a sporadic disease, independent of any urinary affection, incisions into it should be made with great caution, not extending beyond the discolored spots, in consequence of the loss of blood which would ensue from the great vascularity of the part. They should be confined to, and not extend beyond, the parts obviously falling into a state of slough or of mortification.
26. Mortification is the last and most fatal result of inflammation, although it may occur as a precursor of it in the neighboring parts, and not as a consequence. The essential distinction is, between that which is idiopathic or constitutional and that which is local; and has not existed long enough to implicate the system at large, or to become constitutional. Idiopathic or constitutional mortification, sphacelus or gangrene, may be humid or dry. Humid, when the death of the part has been preceded by inflammation and a great deposition of fluid in it, followed by putrefaction and decomposition, as after an attack of erysipelas following an injury. It may then be said to be acute. Dry, when preceded by little or no deposition of fluid in it, and followed by a drying, shriveling, and hardening of the part, nearly in its natural form and shape, unless exposed to external causes usually leading to putrefaction. The most remarkable instances have occurred in persons suffering from typhus fever, and exposed to cold, without sufficient covering or care. When it occurs in old persons, or in those who have lived on diseased rye or other food, it may be called chronic. The gangrene which follows wounds has been termed traumatic, which explains nothing but the fact of its following an injury.
Local mortification may be the effect of great injury applied direct to the part, or of an injury to the great vessels of the limb. It may occur from intense cold freezing the part, or from intense heat burning or destroying it.
[43] 27. It sometimes happens that a cannon-ball strikes a limb, and without apparently doing much injury to the skin, so completely destroys the internal textures that gangrene takes place almost without an effort on the part of nature to prevent it. This kind of injury was formerly attributed to the wind of a ball; but no one who has seen noses, ears, etc. injured or carried away, and all parts of the body grazed, without such mischief following, can believe that either the wind, or the electricity collected by it, can produce such effect.
The patient is aware of having received a severe blow on the part affected, which does not show much external sign of injury, the skin being often apparently unhurt or only grazed; the power of moving the part is lost, and it is insensible. The bone or bones may or may not be broken, but in either case the sufferer, if the injury be in the leg, is incapable of putting it to the ground. After a short time the limb changes color in the same manner as when severely bruised, and the necessary changes rapidly go on to gangrene. The limb swells, but not to any extent, and more from extravasation between the muscles and the bones than from inflammation, which, although it is attempted to be set up, never attains to any height. The mortification which ensues tends to a state between the humid and the dry, and rather more to the latter than the former. These cases are not of frequent occurrence, and are not commonly observed until after the blackness of the skin, and the want of sensibility and motion attract attention; for the patient is generally stupefied at first by the blow, and the part or parts about the injury feel benumbed. I made these cases an object of particular research after the battle of Waterloo, but could find only one among the British wounded. The man stated that he had received a blow on the back part of the leg, he believed from a cannon-shot, which brought him to the ground, and stunned him considerably. On endeavoring to move, he found himself incapable of stirring, and the sensibility and power of motion in the limb were lost. The leg gradually changed to a black color, in which state he was carried to Brussels. When I saw it, the limb was black, apparently mortified, and cold to the touch; the skin was not abraded; the leg was not so much swollen as in cases of humid gangrene; the mortification had extended nearly as high as the knee; there was no appearance of a line of separation; and [44] the signs of inflammation were so slight that amputation was performed immediately above the knee. On dissecting the limb, I found that a considerable extravasation of bloody fluid had taken place below the calf of the leg, and in the cavity thus formed some ineffectual attempts at suppuration had commenced. The periosteum was separated from the tibia and fibula; the popliteal artery was, on examination, found closed in the lower part of the ham by coagulated lymph, proceeding from a rupture of the internal coat of the vessel. Two inches below this the posterior tibial and fibular arteries were completely torn across, and gave rise, in all probability, to the extravasation. The operation was successful. The proper surgical practice in such cases is to amputate as soon as the extent of the injury can be ascertained, in order that a joint may not be lost, as the knee was in this instance. It is hardly necessary to give a caution not to mistake a simple bruise or ecchymosis for mortification. To prevent such an error leading to amputation, Baron Larrey has directed an incision to be previously made into the part, and to this there can be no objection.
When a large shot or other solid substance has injured a limb to such an extent only as admits of the hope of its being possible to save it, this hope is sometimes found to be futile, at the end of three or four days, from a failure of power, in the part below the injury, to maintain its life for a longer time: mortification is obviously impending. In military warfare, uncontrollable events often render amputation unavoidable in such a case. Under more favorable circumstances, the surgeon should be guided by the principle laid down of constitutional and local mortification; and, although the line cannot perhaps be distinctly drawn between them at the end of three, four, or more days, it will be better to err on the side of amputation than of delay. If the limb should be swollen or inflamed to any distance, with some constitutional symptoms, in a doubtful habit of body, the termination will in general be unfavorable, whichever course be adopted, more particularly if the amputation must be done above the knee. The consideration of the circumstances in which the patient is placed, his age, and habit of body, should have great weight in forming a decision in the first instance, as to the propriety of attempting to save the limb, which ought only to be done in persons of good constitution and apparent strength.
[45] 28. Whenever the main artery of a limb is injured by a musket-ball, mortification of the extremity will frequently be the result, particularly if it be the femoral artery; it will be of certain occurrence if both artery and vein are injured, although they may not be either torn or divided. There may not then be such a sudden loss of blood, in considerable quantity, as to lead to the suspicion of the vessel being injured. The fact is known from the patient’s soon complaining of coldness in the toes and foot, accompanied by pain, felt especially in the back part or calf of the leg, or in the heel, or across the instep, together with an alteration of the appearance of the skin of the toes and instep, which, when once seen, can never be mistaken. It assumes the color of a tallow candle, and soon the appearance of mottled soap. Although there may be little loss of temperature under ordinary circumstances of comfort, there is a feeling of numbness, but it is only at a later period that the foot becomes insensible. This change marks the extent of present mischief. The temperature of the limb above is somewhat higher than natural, and some slight indications of inflammatory action may be observed as high as the ham, and the upper part of the tibia in front; it is at these parts that the mortification usually stops when it is arrested. The general state of the patient, during the first three or four days, is but little affected, and there is not that appearance of countenance which usually accompanies mortification from constitutional causes. In a day or two more, the gangrene will frequently extend, when the limb swells, becomes painful, and more streaked or mottled in color; the swelling passes the knee, the thigh becomes œdematous, the patient more feverish and anxious, then delirious, and dies.
An extreme case will best exemplify the practice to be pursued. A soldier is wounded by a musket-ball at the upper part of the middle third of the thigh, and on the third day the great toe has become of a tallowy color and has lost its life. What is to be done? Wait with the hope that the mortification will not extend. Suppose that the approaching mortification has not been observed until it has invaded the instep. What is to be done? Wait, provided there are no constitutional symptoms; but if they should present themselves, or the discoloration of the skin should appear to spread, amputation should be performed forthwith, for such cases rarely escape with life if it be not [46] done. Where in such a case should the amputation be performed? I formerly recommended that it should be done at the part injured in the thigh. I do not now advise it to be done there at an early period, when the foot only is implicated; but immediately below the knee, at that part where, if mortification ever stops and the patient survives, it is usually arrested; for the knee is by this means saved, and the great danger attendant on an amputation at the upper third of the thigh is avoided. The upper part of the femoral artery, if divided, rarely offers a secondary hemorrhage. The lower part, thus deprived by the amputation of its reflex blood, can scarcely do so; and if it should, the bleeding may be suppressed by a compress. The blood will be dark colored. If the upper end should bleed, the blood will be arterial, and by jets, and the vessel must be secured by ligature.
29. When from some cause or other amputation has not been performed, and the mortification has stopped below the knee, it is recommended to amputate above the knee after a line of separation has formed between the dead and the living parts. This should not be done. The amputation should be performed in the dead parts, just below the line of separation, in the most cautious and gentle manner possible, the mortified parts which remain being allowed to separate by the efforts of nature. A joint will be saved, and the patient have a much better chance for life.
30. A wound of the axillary artery rarely leads to mortification of the fingers or hand. If it should do so, the principle of treatment should be similar, although the saving of the elbow is not so important as that of the knee: neither is the amputation in the axilla, below the tuberosities of the humerus, as dangerous as that above the knee.
31. Mortification after the sudden application of intense cold or heat is to be treated on similar principles.
32. When a nerve or plexus of nerves conveying sensation and motion, and going to a part, or an extremity of the body, is divided, the part or limb is deprived of three great qualities: motion, sensation, and the power of resisting with effect the application of a degree of heat or of cold, which is innocuous when applied in a similar manner to the opposite or sound extremity. In other words, it will be scalded by hot water and frost-bitten by iced or even cold water, [47] which are harmless when applied to another and a healthy part.
An officer received, at the battle of Salamanca, two balls, one under the left clavicle, which was supposed to have divided the brachial plexus of nerves, as the arm dropped motionless and without sensation to the side. The other ball passed through the knee-joint, which suppurated. The left side of the chest became affected; he suffered from severe cough, followed by hectic fever, and was evidently about to sink. As a last chance, I amputated his leg above the knee, after which he slowly recovered. Fourteen years afterward he showed me his arm in the same state, and told me he had been indicted for a rape, but that the magistrates, seeing the wooden leg and the useless arm, while admitting the attempt, would not assent to the committal of the offence.
33. When one nerve only of several going to an extremity such as the arm and hand, is divided, the loss sustained is confined to the extreme part more immediately supplied by the injured nerve. Thus, if the ulnar nerve only be divided, the little finger and the adjacent side of the ring finger suffer, perhaps in some degree the inner side of the thumb and the adjoining fingers; if the median nerve, the thumb and other fingers; if the radial, the back of the hand next the thumb. In some instances there seems to be a kind of collateral communication by which a degree of sensibility is after a time recovered.
34. If any foreign substance should lodge in and continue to irritate the nerve, the wounded part often becomes so extremely painful as not to be borne; the nerve at that part forms a tumor of a most painful character, requiring removal, or in extreme cases even the amputation of the extremity.
35. After an ordinary amputation, the extremity of a nerve enlarges so as to resemble a leek, and if this should adhere to the cicatrix of the wound, painful symptoms, referred to the toes and other parts of the removed leg, are experienced often to an almost unbearable degree; the end of the nerve should be removed. The pain apparently felt in and referred to the toes is merely the effect of irritation of the extremity of the nerve.
36. Wounds or injuries of nerves, which do not entirely divide the trunk, or a principal branch given off from a [48] plexus of nerves, may give rise to general as well as to local symptoms; that is, by sympathy, connection, or continuity of disease, other nerves and organs of the body are affected. This applies also to the spinal marrow, when the injury does not destroy at once. General Sir James Kempt was wounded at the storming of the castle of Badajoz, on the inside of the left great toe, by a musket-ball which, from the appearance of a slit-like opening, was supposed to have rebounded from the bone, but was discovered a fortnight afterward flattened and lying between it and the next toe. Inflammation had ensued, followed by great irritability and numerous spasmodic attacks, appearing to render locked-jaw probable. The spasms soon became general, extending from the foot to the head, but tetanus did not take place. On his return to England, they gradually subsided, but he did not sleep at night for a year. After the battle of Waterloo the spasms became more frequent and troublesome, attacking the muscles at the back of the neck and throat, causing considerable anxiety. The attack was often traced to exposing the foot to cold or to undue pressure, and frequently to derangement of stomach, although he was most regular in diet. After the lapse of six or seven years these severe symptoms subsided; but during the last forty years of his life he suffered occasionally from them.
Admiral Sir Philip Broke received a cut with a sword on boarding the Chesapeake, on the left side of the back of the head, which went through his skull, rendering the brain visible; the wound healed in six months, although splinters of bone came away for a year. A second cut on the right side did not penetrate the bone. After a temporary paralysis of the right side, he recovered, with a loss of power and a disordered sensation in the second, third, and little fingers of the right hand, aggravated by cold weather and by mental anxiety.
Seven years afterward, he fell from his horse, and suffered from concussion of the brain, which added to his former sensations by rendering the left half of his whole person incapable of resisting cold, or of evolving heat. In a still atmosphere abroad, at 68° Fahr., he said, “the left side requires four coatings of stout flannel, which are augmented as the thermometer descends every two degrees and a half, to prevent a painful sense of cold; so that when it stands at the freezing point the quantity of clothing of the affected [49] side becomes extremely burdensome. When exposed to a breeze, or even in moving against the air, one or even two oilskin coverings are necessary in addition, to prevent a sensation of piercing cold driving through the whole frame. Moderate horse exercise and generous diet improved the general health; the warm bath caused a distressing effect; the shower bath, cold or tepid, increased the paralytic affection. Frictions, with remedies of all kinds, increased it also, and so did sponging with vinegar and water, as well as any violent, stimulating, quick excitement, or earnest attention to any particular subject. The Admiral died unrelieved, twenty-six years after the receipt of the injury, of disease of the bladder.”
37. Brigade-Major Bissett was wounded on horseback, in the Kaffir war, by a musket-ball, which entered on the outside of the lower part of the left thigh, passed upward across the perineum, wounding the rectum within the anus—from which part he lost a quantity of blood—and came out through the pelvis on the opposite side. The course of this ball was accounted for by the fact that he saw the Kaffir who shot him standing some yards below him when he fired. The ball, in its passage upward and across the thigh, injured the great sciatic nerve, and the consequence is continued pain in the toes, instep, and foot, with contraction of the muscles, and lameness, together with the usual incapability of bearing heat or cold, particularly the latter, against which he is peculiarly obliged to guard. The skin shows no sign of discoloration or derangement. Position gives the explanation why the ball took such a peculiar course; the symptoms show the nature of the injury. From other effects he has perfectly recovered, but his leg is comparatively useless, while it is a constant source of suffering.
38. The cases related in the Lectures on wounds of arteries, of mortification taking place in the foot and leg, after the division of the principal artery in the thigh, show that the maintenance of the life of a part depends on the blood. The cases now related show that neither an injury nor the division of the principal nerve, nor, perhaps, of all the nerves going to a part, will destroy that life. The complete failure of the circulation, in a part such as the foot, impairs, but does not totally destroy, the sensibility imparted by the nerves, until after the loss of life has taken [50] place, or until decomposition is about to occur. An injury then to the nerve causes great pain, not usually at the part injured, but in the extreme parts supplied by it; some loss of the power of motion; some deprivation of its ordinary sensibility, as shown by a feeling of numbness, and an incapability, to a certain extent, of resisting heat or cold. When all the nerves have been divided, the power of moving the limb is lost, as well as its sensibility in a general sense. The temperature remains at a natural standard under ordinary circumstances, but no extra evolution of heat can take place by which cold is resisted, nor any absorption of it, which perhaps renders the application of a high temperature, particularly when combined with moisture, dangerous. The circulation is capable of maintaining the ordinary heat of a part, although it is deprived of the influence of the special nerves of sensation and of motion; but a greater evolution of heat appears to depend on something communicated by the nerves in a state of integrity. In the case of Sir P. Broke, this something appeared to be derived from the brain, on which part the wound was inflicted, and the transmission of which was interrupted by the injury. The evolution of animal heat has of late been supposed to be dependent on electricity, from the resemblance which exists between it and the nervous power, although the attempts to identify them have not been successful. That the evolution of heat is the result of nervous power, appears to be indisputable; in what that power consists, physiologists have yet to ascertain.
39. The best means of mitigating the pain, independently of the application of warmth—and cold rarely does good, as the sufferer soon finds out—is by the application of stimulants to the whole of the extremity affected, followed by narcotics. The tinctures of iodine and lytta, the oleum terebinthinæ, the oleum tiglii or cajeputi, the liquor ammoniæ or veratria, may be used in the form of an embrocation, of such strength as to cause some irritation on the skin, short, however, of producing any serious eruption. After the parts have been well rubbed, opium, belladonna, or henbane may be applied in the form of ointment; or the tincture of opium, henbane, or aconite may in turn be applied on linen. Great advantage has been derived in many neuralgic pains from the application of an ointment of aconitine, carefully prepared, in the proportion of one grain to a [51] drachm of lard, at which strength it will sometimes irritate almost to vesication, as well as allay pain.
When the pains return from exposure to cold, particularly in the lower extremity, great advantage has been derived from cupping on the loins, from purgatives, opiates, and the warm bath. Benefit has been obtained occasionally from quinine, and from belladonna, aconite, and stramonium, administered internally in small doses frequently repeated, but not suffered to accumulate without purgation; as the accumulated effects are sometimes dangerous.
AMPUTATIONS, ETC.
40. When the wound of an extremity is of so serious a nature as to preclude all hope of saving the limb by scientific treatment, it should be amputated as soon as possible.
41. An amputation of the upper extremity may almost always be done from the shoulder-joint downward, without much risk to life. When necessary, the sooner it is done the better.
42. An amputation of any part of the lower extremity below the knee may be done forthwith, with nearly an equal chance of freedom from any immediate danger, as of the upper extremity at or near the shoulder-joint.
43. It is otherwise with amputations above the middle of the thigh, and up to the hip-joint. They are always attended with considerable danger.
44. There can be no doubt that if the knife of the surgeon could in all cases follow the ball of the enemy or the wheel of a railway carriage, and make a clean good stump, instead of leaving a contused and ragged wound, it would be greatly to the advantage of the sufferer; but as this cannot be, and an approach to it even can rarely take place, the question naturally recurs,—At what distance of time, after the receipt of the injury or accident, can the operation be performed most advantageously for the patient?
45. In order to answer this question distinctly, it should be considered with reference to distinct places of injury:—
1st. When injuries require amputation of the arm below [52] the shoulder-joint, or of the leg below the knee, these operations may be done at any time from the moment of infliction until after the expiration of twelve or twenty-four hours, without any detriment being sustained by the sufferer with regard to his recovery; although every one, under such circumstances, must be desirous to have the operation over. The surgeon having several equally serious cases of injury of the head or trunk brought to him at the same time as two requiring amputation of the upper extremity, may defer the latter more safely perhaps than the assistance he is also called upon to give to the other cases, the postponement of which may be attended with greater danger.
2d. This state embraces those great injuries in which the shoulder is carried away with some injury to the trunk; or the thigh is torn off at or above its middle, rendering an amputation of the upper third, or at the hip-joint, necessary. It is this or nearly this state which alone implies a doubt as to the propriety of immediate amputation, and demands further investigation. It is the state to which attention is earnestly drawn for future observation.
46. It has been implied, if not actually maintained, that a man could have his thigh carried away by a cannon-shot without being fully aware of it, or, if aware of it, that it did not cause much alarm—in fact, that it did not materially signify as to his apprehension, whether the ball took off his limb or the tail of his coat, or only grazed his breeches. An instance of this kind has not fallen under my observation.
47. A surgeon on the field of battle can rarely have a patient brought to him, requiring amputation, under less time than from a quarter to half an hour; a surgeon in a ship may see his patient in less than five minutes after the receipt of the injury; and to the surgeons of the navy we must hereafter defer for their testimony as to the absence or presence of the constitutional alarm and shock to which I have alluded, and to what degree they follow, immediately after the receipt of such injury. The question must not be encumbered and mystified by a reference to all sorts of amputations after all sorts of injuries, but to the one especial injury, viz., that of the upper third of the thigh.
48. My experience, which may be erroneous, like everything human, has taught me, that when a thigh is torn, or nearly torn off, by a cannon-shot, there is always more or less loss of blood, suddenly discharged, which soon ceases in [53] death, or in a state approaching to syncope. When the great artery has been torn, this fainting saves life, for an artery of the magnitude of the common femoral does not close its canal by retracting and contracting in the same manner as a smaller vessel; it can only diminish it; and the formation of an external coagulum is necessary to preserve life, which the shock, alarm, and fainting, by taking off the force of the circulation, aid in forming; and without which the patient would bleed to death. An amputation, in this state of extreme depression, might destroy life, although aided by the exhibition of chloroform.
49. If the cannon-shot, or other instrument capable of crushing the upper part of a thigh, should not divide the principal artery, and the sufferer should not bleed, it is possible he may be somewhat in the state alluded to in which the patient, for he may not be called sufferer, is said to be just as composed as if he had only lost a portion of his breeches. Nevertheless few have seen a man lose even a piece of his skin and of his breeches by a cannon-shot, without perceiving that he was indisputably frightened. Dr. Beith, surgeon of the Belleisle, hospital ship, in the Baltic, informs me that Mr. Wrottesley, of the Engineers, was struck by a cannon-shot, at Bomarsund, on the upper part of his right thigh, which shattered it and his hand, which was resting upon it. His leg was also broken by a splinter from the gun which the ball had previously struck. The femoral artery was not injured, and it was said he lost but little blood. He, however, never rallied from the blow, but sank in twenty minutes after he was brought to Dr. Beith. The constitutional shock and alarm were great; countenance sunk and pallid, pulse scarcely perceptible.
“An East Indian, twenty-two years of age, of healthy aspect, in the month of October, 1854, when proceeding on a shooting excursion, at Moulmein, in Burmah, was most severely wounded by the accidental explosion of his gun, the entire charge of large shot lodging in the center of the left thigh, and causing a bad compound fracture, with fearful laceration of the soft parts. I was asked to see the patient by Dr. Reynolds, the staff-surgeon of the station, at half-past seven A.M., an hour after the injury had been inflicted, and found him laboring under most urgent collapse and great nervous depression. It was of course impossible to save the limb, but I suggested delay for some hours, and the moderate [54] use of stimulants, till the system had in some degree recovered its equilibrium. Such was the case at five P.M., and the flap operation was done while the man was under the full influence of chloroform, (three drachms being required for that purpose.) When placed in bed, he became conscious, but never rallied, and died in half an hour.
“Very little blood was lost during the operation, and the impression on my mind was, that it would have been wiser to have steadily but carefully continued the use of stimulants during the operation, and thus have counteracted the shock of the latter following on that of the injury, from which the system had only partially recovered.”—Case by Dr. Dane, Surgeon to the Forces.
Deputy Inspector-General Taylor informs me that “a young muscular man, of the siege-train, had his left thigh nearly carried off at its middle by a cannon-shot at Sebastopol. The soft parts on the inside, including the artery, escaped laceration; the remaining soft parts and large pieces of bone were entirely carried away, the injury extending above the middle of the bone. The muscles on the fore part of the other thigh were extensively laid bare and injured. The prostration was great; pulse feeble; the man’s spirits were good, and he desired amputation under chloroform. The left thigh was amputated at the upper third. The chloroform, administered on a pocket-handkerchief, lightly folded, and held over the nose and mouth, speedily took effect. I am under the impression that the chloroform not only caused insensibility to pain, but supported the system during the operation, although the man died an hour after its completion. Nevertheless, I think the chloroform enabled the man to bear the operation better than he would have done without it.”
This case does not quite meet my proposition as to the effect of chloroform when the thigh has been carried off nearer the hip-joint, with rupture of the principal artery; cases which have hitherto been usually lost, whether amputation is performed or not.
50. While some persons, under the loss of a thigh high up, are reduced to a state of syncope, or nearly approaching to it, which renders them almost or even entirely speechless, others are said to suffer extreme pain, and earnestly entreat assistance, under which circumstances amputation should be performed forthwith. In the former, the admin[55]istration of stimulants may render the operation less immediately dangerous. In the latter, they will be beneficial, and may save life.
51. Chloroform, or other similar medicaments, may produce an effect in such cases as yet unknown. Its careful administration may not destroy the ebbing powers of life, and may render an amputation practicable, which could not otherwise be performed without the greatest danger. It may be otherwise; the point, however, is to be ascertained, although in all cases of great suffering its use should be unhesitatingly adopted.
Much difference of opinion having taken place on the subject of chloroform, I requested Dr. Snow, who has superintended its use in many of our hospitals, and in almost all the cases of serious operation in private life, to draw up his observations and opinions in the most compendious form possible, which he has been so good as to do, in the following terms:—
“Chloroform may be given with safety and advantage to every patient who requires, and is in a condition to undergo, a surgical operation. A state of great depression, from injury or disease, does not contra-indicate the use of chloroform. This agent acts as a stimulant in the first instance, increasing the strength of the pulse, and enabling the patient, in a state of exhaustion, to go through an operation much better than if he were conscious.
“Persons who have died from the effects of chloroform had disease of the heart, or of some other vital organ, but the majority had a sound state of constitution; and it seems probable that the average health of persons who have been the subject of accident has been at least as good as that of those who have taken chloroform without ill effects. From these and other considerations I am of opinion that accidents from chloroform are to be prevented by care in its administration, and not by the selection or rejection of cases for its employment.
“When animals are made to breathe air containing not more than four or five per cent. of the vapor of chloroform till death ensues, the breathing ceases very gradually, being first rendered laborious and then feeble, and the heart continues to beat for a minute or two after respiration has ceased. During this interval, while the heart is still beating, the animal can be easily restored by artificial respira[56]tion. This mode of death from chloroform might undoubtedly take place in the human subject, if a person were to go on giving it regardless of the symptoms; but a careful examination of all the recorded cases of death from this agent shows that it has not occurred in this manner. On the contrary, the symptoms of danger have in every instance come on suddenly, and the action of the heart has been arrested at the same moment as the breathing, or even before it. This is precisely the way in which the lower animals die when they are compelled to breathe air containing eight or ten per cent. of the vapor of chloroform. It is therefore evident that the cause of death is the inhalation of the vapor of chloroform not sufficiently diluted with common air.
“It requires more chloroform to suspend the functions of the ganglionic nerves, which preside over the contractions of the heart, than to suspend the functions of the medulla oblongata and the nerves of respiration; but the action of the heart may be arrested by the direct effect of this agent. Chloroform, when inhaled, is absorbed by the blood in the lungs, passes at once to the left cavities of the heart, and is immediately sent through the coronary arteries to every part of that organ, in less time, probably, than it can reach the brain; or, supposing the respiration to be suddenly arrested by the action of the chloroform on the brain, the vapor, not being sufficiently diluted, is present in large quantities in the lungs at the moment when the breathing ceases; and becoming absorbed, in addition to that which was already in the blood, has the effect of paralyzing the heart.
“Twenty-five minims of chloroform produce only twenty-six cubic inches of vapor, and as one hundred cubic inches of air, at 60° Fahr., will take up fourteen cubic inches of vapor, and at 70° will take up twenty-four cubic inches, if fully saturated, it is quite possible that the air during inhalation may contain ten per cent. of the vapor, if means be not taken to prevent it. Under these circumstances, each hundred cubic inches of air would contain nearly ten minims of chloroform, and this might be taken into the lungs at once by a rather deep inspiration. The average quantity of chloroform present in the blood of an adult, when sufficiently insensible for a surgical operation, is eighteen minims, while twenty-four minims are as much as can be present in the system at one time with safety. The absorption of [57] a little more than thirty minims would have the effect of causing death, even if it were equally diffused throughout the circulation. It must be evident, therefore, that to take ten minims of chloroform into the lungs at one inspiration, when insensibility is almost complete, must be attended with danger.
“Robust persons, accustomed to hard work or violent exercise, are very apt to become affected with rigidity of the muscles and struggling, when nearly insensible from chloroform; and they often hold the breath for a time, and then draw a deep inspiration. It is under these circumstances that several of the accidents from chloroform have taken place, and extreme care is required to give the chloroform more than usually diluted with air, when this state of unconscious struggling and rigidity occurs.
“The most important point to attend to, in the exhibition of chloroform, is to insure that the vapor shall be sufficiently diluted with air during the whole process of inhalation. This may be effected with a suitable apparatus and proper attention, or if an inhaler be not at hand, the chloroform should be diluted with one or two parts by measure of rectified alcohol. One or two drachms of this may be placed on a hollow sponge, and repeated when required. The spirit has the effect of limiting the quantity of chloroform which rises in vapor, while very little of the diluent is inhaled, since, from its lower volatility, the greater part of it remains on the sponge or handkerchief employed to exhibit the chloroform.
“When the chloroform vapor is so diluted that it does not constitute more than four or five per cent. of the respired air, its effects become developed very gradually and regularly. The suspension of the sensibility of the conjunctiva at the border of the eyelids is the best sign that the patient will bear the operation without flinching, and the inhalation should immediately be left off if the breathing become stertorous. The pulse is not a very important guide in the exhibition of chloroform, for the two following reasons: 1st, if the vapor be sufficiently diluted with air, the pulse cannot be seriously affected by it; and 2d, if it be not so diluted, the pulse may cease suddenly, without previous warning of danger.
“If the vapor of chloroform be sufficiently diluted with air, it is practically impossible that any accident, really due [58] to this agent, should occur. In case of accident, however, artificial respiration, very promptly and efficiently performed, is the only means which affords a prospect of restoring the patient—at all events, this is the only means found to restore animals when it was obvious they would not recover spontaneously. The prospect of success from artificial respiration will depend on the greater or less extent to which the heart is affected by the direct action of the chloroform.”
Mr. Syme, in his “Clinical Observations,” delivered in the Royal Infirmary in Edinburgh, recommends, in cases of approaching death from the use of chloroform, that the tongue should be drawn forward by means of a pair of artery forceps, by which it is presumed the epiglottis is raised, and a greater facility afforded for the admission of atmospheric air, the inconvenience resulting from two small holes in the tip of the tongue being amply compensated by the preservation of life.
Nevertheless, I am of opinion that attention should be paid to the pulse, and whenever it begins to fail or flutter, the inhalation of chloroform should be arrested; for respiration and the pulse often cease almost simultaneously, and in some instances have done so irrecoverably.
I formerly said that chloroform might be used with advantage in all cases of injury requiring amputation, save one, and in that one experience was wanting to decide the point. It is when a thigh has been carried off by a cannon-ball, or destroyed at its upper part by any other means, such as the wheels of a railway carriage or other weighty machine. When the thigh is carried off by a cannon-shot, the artery being torn across, there is so great a shock and so great a loss of blood at the moment, followed by fainting, or such faintness as leads to the belief that the sufferer is dying, and some do actually die without an effort at recovery. In such a case, or in one somewhat similar, Dr. Snow and others think chloroform would act as a stimulus, and that it would enable the patient to bear the operation of amputation with success, which he otherwise might not have done. It may be so; but, as I believe nothing in surgery until fairly tried and found to answer, I refrain, for the present, from expressing a positive opinion, save that the trials should be made with great caution, inasmuch as the observations which have been made in the Crimea have not been sufficiently numerous or so decisive as to settle the point in [59] favor of the chloroform, although they confirm all the others to which allusion has been made. In these cases a tourniquet cannot be applied, and the sudden loss of blood saves the life of the sufferer for the time, by suppressing the bleeding; which suppression, I have long since pointed out, is effected in the artery at the groin, by the formation of a coagulum, and not by the contraction and retraction of the vessel into the shape of the neck of a claret bottle, which would take place at the lower third of the same artery in the thigh under a similar injury; in which case, also, the bleeding would cease by the unassisted efforts of nature. If the artery, there or elsewhere, should, on the contrary, be only partially divided, the person would bleed to death, unless surgery of some kind should come to his aid.
52. When the sufferer is brought to the surgeon at the end of half an hour, having lost a limb below the thigh or shoulder by a cannon-shot, he will often be found in a state of such great depression as to be likely to be destroyed by the infliction of a serious and painful operation like amputation, unless chloroform should relieve it. This has occurred to me so often as to induce me formerly to recommend delay for four, six, or even eight hours, if the unfortunate person did not suffer much, and appeared likely to be revived by the proper use of stimulants. If he should be in great pain, the limb should be removed under chloroform.
53. This recommendation originated from the fact that, as one seriously wounded man has as much claim as another to the attention of the surgeon, all could not be attended to at the same time; and the success following the deferred cases of amputation was as great, if not greater, than in those on which the operation was more immediately performed.
54. The advantageous results of primary amputations, or those done within the first twenty-four, or at most forty-eight hours, over secondary amputations, or those done at the end of several days, or of three or four weeks, have been so firmly and fully established as no longer to admit of dispute.
55. When an amputation is deferred to the secondary period, a joint is often lost. A leg which might have been cut off below the knee in the first instance is frequently obliged to be removed above the knee when done in the second.
[60] 56. In the secondary period after great injuries, the areolar and muscular textures near the part injured are often unhealthy, the bones are in many instances inflamed internally, and their periosteal membranes deposit on the surrounding parts so much new ossific matter as frequently to envelop in a few days the ligatures on the vessels, and render them immovable, necrosis of the extremity of the bone following as a necessary consequence, thus protracting the cure for months.
57. Sloughing of the stump, accompanied by inflammation of the vein or veins leading to the cava, frequently takes place. This state of stump is often followed by purulent deposits in and upon the different viscera, and principally in the cavities of the chest. Where febrile diseases are endemic, they often prevail; the constitutional irritation is great; the stumps do not unite, or, if apparently united, open out and slough, and frequently after a few days implicate the veins.
58. In the first edition of my work on Gunshot Wounds, and on the great operations of Amputation, published in 1815, I said, alluding to secondary operations: “In the most favorable state of the stump, the diseased parts do not extend very deep; yet inflammation is frequently communicated along the vein, which is found to contain pus, even as far as the vena cava.” “When I have met with this appearance, I have always considered the vessels as participating in (not originating) the disease, which had existed some days, and thereby more quickly destroying the patient.” I further said that after secondary amputations, the febrile irritation, allayed by the operation, sometimes returns, and more or less rapidly cuts off the patient by an affection of some particular internal part or viscus, especially of the lungs. “If it be the lungs, and they are most usually affected, the breathing becomes uneasy; there is little pain when the disease is compared with pneumonia or pleuritis; the cough is dry and not very troublesome; the pulse having been frequent, there is but little alteration; the attention of the surgeon is not sufficiently drawn by the symptoms to the state of the organ, and in a very short time all the symptoms are deteriorated: blisters are employed, perhaps blood-letting, but generally in vain; and the patient dies in a few hours, as in the last stage of inflammation of the lungs, in which effusion or suppuration has taken place.” “My atten[61]tion was drawn to it after losing several cases in this way, as a circumstance of more than common accident, from its having happened to a young officer to whom I was paying considerable attention, (at Salamanca.) Since that I had one well-marked case at Santander, of a sudden and fatal affection of the lungs after amputation of the thigh, which was under the immediate care of Dr. Irwin,” and of myself as the principal medical officer. The late Mr. Rose, of the Guards, communicated a case, after amputation of the arm, to Sir James M’Grigor, who forwarded it to me; and my old friend, the late Mr. Boutflower, who served frequently under me during the latter part of that war, and aided me in all my labors and views, forwarded to me, at the same time, two cases from Fuenterabia, which terminated fatally after amputation of the arm, from the deposition of a considerable quantity of pus in the cavity of the thorax. “So insidious,” he said, “was the approach of the disease, that, except a difficulty of breathing which supervened a few hours before death, there were no symptoms indicating the existence of such a morbid affection.” No further notice was taken of this disease by any one in any of the hospitals on entering France in 1813, neither at St. Jean de Luz, nor Bayonne, nor Pau, St. Sever, Tarbès, or Orthez, until after the battle of Toulouse, where the following cases occurred, which I published previously to any one else in 1815.
A soldier suffered amputation of the thigh five weeks after the injury, in consequence of a gunshot fracture at Toulouse, he being in a very reduced state, the discharge profuse, the pain great, hectic fever severe. The third day after the operation, from which he scarcely rallied, he complained of difficulty in swallowing, and pain in the situation of the thyroid gland, which was found next morning to be inflamed. In spite of the means employed, he died on the fourth day of this attack, or the seventh after the amputation, in a state of great emaciation. On dissection, the whole substance of the thyroid gland was destroyed, a deposit of good pus occupying its place, which descended by the sides of the trachea and œsophagus to the sternum, and had all but found its way into the larynx, between the cricoid and thyroid cartilages on the right side.
Daniel Lynch, wounded through the knee-joint at the battle of Toulouse, on the 12th of April, 1814, had his thigh amputated by the late Mr. Boutflower, on the 8th of May. [62] The night succeeding the operation he passed comfortably. Next day, the 9th, the febrile symptoms were augmented. On the 10th he was worse; pulse 150. On the 11th he was better. On the 16th he was considered to be in a state of convalescence, and went on improving until the 22d, when fever recurred. On the 28th his stomach became very irritable; the stump appeared to be nearly healed, the discharge being small, and of good quality; one ligature remained. 30th: Pulse 110; tongue of a brownish hue. During the 31st and 1st of June he got worse, and died. The stump appeared to have united externally, except where the ligatures came out; but, on cutting through the line of adhesion, the muscular parts within were evidently unhealthy; the bone was surrounded for some distance by a case of osseous matter, including the remaining ligature, which could not be removed by any force short of breaking it. The femur was bare, and showed marked signs of absorption having commenced; three inches of it must have come away if the man had lived. The extremity of the vein was in a sloughing state.
Having dissected the other extremity for a clinical lecture I was occasionally in the habit of giving on particular cases, a semi-transparent membranous bag, containing good pus, was found accidentally on the tibialis posticus muscle. The blood in the perineal vein outside of it was coagulated; there were little or no marks of inflammation, and the matter appeared to have been deposited without any. The inner side of the soleus muscle seemed simply to be discolored.
The first edition, containing these facts, which were before unknown, and which furnish another laurel to the surgery of the Peninsular war, having been published before the battle of Waterloo, the opinions and facts stated therein became matters for public discussion, and the reports made by my friends from Brussels, Antwerp, Yarmouth, and Colchester, confirmed all the facts, and, I may add, all the opinions of the slightest importance. They were published in the second edition in 1820, and again more pointedly in the third, published June 18, 1827.
59. Forty years have passed away since I stated my opinion, that inflammation of the veins is of two kinds—the adhesive or healthy, from which the sufferers usually recover, as in the cases of women laboring under the disease called [63] phlegmasia dolens, and the irritating or unhealthy, occurring after operations; the disease being communicated by continuity to the vein, rather perhaps than originating in it. I then said I did not believe that pus is carried from the inside of the vein to the general circulation, the office of the vein as a carrier of blood ceasing on the inflammation taking place in its internal tissue, although I admit that the blood in a vitiated state, from the commencing disease in the stump, or in the system, may have for some time passed along it into the general circulation. The inflammation thus commencing may extend upward and downward, and across to the opposite side of the body, as I first demonstrated in 1825, in the case of Jane Strangemore, p. 47. I never saw it actually in the heart, the sufferers dying by the time it had reached as high as the diaphragm, and in general before it had got so far.
60. When a person, after undergoing amputation, is about to suffer from unhealthy inflammation of the veins, the pulse quickens, and continues above 90, usually rising from 100 to 130. The stomach becomes irritable; there are frequent attacks of vomiting, generally of a bilious character, accompanied by the usual symptoms of fever. A few days after the commencement of the complaint, there is usually a well-marked rigor, followed perhaps by others, but exacerbations and remissions of fever are common. The skin gradually assumes a yellowish tinge, the perspiration is excessive, the bowels irregular, the pulse becomes weaker and more irritable, the emaciation is considerable, and the patient gradually sinks; or the febrile symptoms may subside, with the exception of the frequency of the pulse, the patient rallies a little, but while he says he is better, and the appetite even returns, the deterioration in appearance becomes more marked, more deathlike, even while eating, and an accession of fever rapidly closes the scene. The stump is often not more painful than under ordinary circumstances, neither is there any remarkable pain or tenderness in the course of the vessels.
61. The practical points are, to draw blood with caution, on the accession of fever, provided a remittent or typhoid form does not prevail; to open out the stump as soon as possible, even by a division of the external adhesions, the inner parts being usually unsound; to envelop it in a large warm poultice; to apply cold above, even ice if procurable, [64] in the course of the great vessels, and to soothe the system by calomel, opium, and saline diaphoretic remedies, followed by stimulants, cordials, quinine, and acids.
Private A. Clarke, 79th Regiment, had his thigh broken by a musket-ball a little above the knee-joint, at Waterloo, and was admitted into the clinical ward of the York Hospital, in London, in November, 1816. The bone being in a state of necrosis, Mr. Guthrie amputated the thigh high up, on the 20th of January, 1817. Pulse before and after the operation 104. On the 25th, pulse 120; skin cool; tongue moist; appeared weak and irritable. During the 26th and 27th, symptoms of low fever came on. 28th, suffered severely from vomiting, general fever, greater prostration of strength; stump had not united, but discharged good pus. 30th, skin assumed a yellow tinge.
On the 1st of February, had a rigor resembling a fit of ague, and Mr. Guthrie declared his suspicion of the formation of matter, probably in the liver, and of inflammation of the veins of the stump. The symptoms gradually assumed the character of typhus gravior, and on the 8th he died. On dissection the liver was found enlarged, and weighing six pounds; the other viscera were sound. On examining the stump an abscess containing four ounces of good pus was found in the under part, near the bone. The femoral vein and those going to that part of the stump were inflamed, and contained coagulated blood, lymph, and purulent matter, the disease extending from the femoral to the vena cava. The rigors on the 1st February marked the formation of matter, the typhoid symptoms its continuance, and the inflammation of the veins. Union was discouraged from the first dressing.
The following case is so highly instructive on all points, that it is transcribed from the London Medical and Physical Journal for 1826:—
Jane Strangemore, aged twenty-eight, was admitted into the Westminster Hospital, September 24, 1823, with an elastic swelling of the whole of the knee-joint, measuring twenty-seven inches and a half in circumference. The thigh was amputated by Mr. Guthrie on Saturday, the 27th, the bone being sawn through just below the trochanter. She suffered a good deal from pain after the operation. An opiate was administered and repeated, and she passed a good night.
[65] 28th.—The pulse, which previous to the operation was 80, has increased to 100; there is, however, little heat of skin, and she appears easy. Some aperient medicine, and saline draughts to be given every four hours. Toward the evening, she vomited a quantity of bilious matter; pulse 120. Three grains of calomel and one of opium, followed by the common aperient mixture, were ordered, and an enema. Equal parts of ether and laudanum to be applied to the region of the stomach, to which part pain was referred.
October 1st.—Better in all respects, but looking irritable and ill; no pain anywhere; no sickness; appetite good; pulse still quick.
8th.—Two ligatures have come away; the wound looks well; the edges have nearly healed; eats meat, and with a good appetite.
9th.—Not so well; pulse 120; skin hot; feels ill; complains of pain in the other leg and thigh, which disturbed her rest. Was well purged, and the leg fomented; the pain was principally felt in the calf and in the heel.
10th.—Pulse 130; tongue furred; vomiting again of bile; the pain in the thigh, extending upward to the groin and downward to the heel, is intolerable, particularly in the latter part; the thigh and leg much swelled, and tender to the touch, although without redness; the swelling elastic, yet yielding to the pressure of the finger, but not in any manner like an œdematous limb. Mr. Guthrie pronounced the disease this morning to be inflammation of the veins, extending from the opposite side; but after a careful examination, and on pressure, no pain was felt in the course of the iliac vessels of that side, and the stump looked well, save at one small point corresponding to the termination of the femoral vein.
17th.—The symptoms continued nearly the same during the week, the sickness of stomach and purging of bilious matter abating at intervals.
20th.—Less pain in the limb, which is swollen and tender to the touch, the superficial veins being all very much enlarged. The groin more swollen and tender; sickness gone, and her appetite returning; she is allowed good nourishing simple diet. The stump has been poulticed since the 9th, to promote suppuration.
25th.—During these five days it was interesting to see the patient eat, and desire solid food, and, in her extremely [66] emaciated state, seem to enjoy it. The bowels occasionally deranged. Pulse always from 125 to 136. Is slightly jaundiced in color, but declares that she is better, and will get well.
27th.—Gradually sank in the evening, and died; the limb having everywhere diminished in size, except at the groin, where the swelling was more circumscribed, resembling the appearance of a chronic abscess approaching the surface. On examination after death, the termination of the vein on the face of the stump was open, and in a sloughy state; above that, for the distance of four inches, and as high as Poupart’s ligament, the inside of the vein bore marks of having been inflamed, but the inflammation seemed to have been of an adhesive character; above that point, the inflammation appeared to have been of an irritative or erysipelatous kind, had gone on to suppuration, and the vein was filled with purulent matter, lymph, and blood, partly coagulated and partly broken down. These appearances extended up the cava as high as the diaphragm, and traces of inflammation could be distinctly observed almost in the auricle. The disease had passed along the right external iliac and its branches; it had descended along the left iliac vein and its branches in the pelvis to the uterus, and along the limb to the sole of the foot. At the left groin the iliac vein, becoming femoral, was greatly distended with pus, apparently of good quality, and, if the patient had lived a day or two longer, it would have been discharged by a natural effort, as in chronic abscess; the viscera were healthy.
During the last days of this woman’s life, no blood was returned from the lower half of the body, unless by the superficial veins; yet she was comparatively easy, although of a yellow hue, emaciated to the utmost, so as to represent a living skeleton; in this state, with a pulse at 130, craving for and eating a whole mutton-chop and more at a time, with the most deathlike countenance it is possible to conceive.
These two cases mark the course, the symptoms, and the termination of inflammation of the veins after amputation, in as clear (if not a more clear) and distinct manner as any which have since been published, and which they preceded; nevertheless, most authors of more modern date overlook the first, and some appear to avoid as much as possible noticing the second.
[67] 62. After the battle of Waterloo, the wounded of the same regiment were sent indiscriminately, some to Brussels, others to Antwerp. Those who remained at Brussels suffered principally from inflammatory fever after amputation; those at Antwerp, from the epidemic fever prevailing at the time, beginning us an intermittent and ending often in typhus; facts of great importance to recollect, as showing the influence of malaria. The following are instances of endemic fever after secondary amputation, ending in subacute inflammation of the lungs and effusion into the chest:—
Charles Brown, 92d Regiment, forty years of age, at that time a healthy man, was wounded on the 18th June by two musket-balls in the right hand and wrist; he was admitted into the hospital at Antwerp on the 25th June. On the 5th July, the arm was swollen above the elbow; discharge profuse and fetid; countenance sallow and dejected; fever. 8th: Arm amputated above the elbow. 9th, 10th, 11th: A little increase of fever. 12th: A paroxysm of intermittent, to which he had been subject occasionally since he had been at Walcheren. On removing the dressing, the edges of the stump were retorted; discharge copious and fetid; respiration hurried; thirst; skin hot and yellowish; pulse 90. 14th: Intermittent returned; head affected in consequence of long continuance in the hot bath. 15th: Complains to-day of fullness and pain in the left side; pulse 100; skin of a deeper tinge of yellow; a sense of suffocation when in the horizontal position. A blister was applied to the whole of the side of the chest. 16th: Was delirious during the night; vomited frequently; became insensible at the hour when the paroxysm of intermittent fever was expected to return; and died in the evening. On opening the chest, the lungs were found adhering to the pleuræ costales in several places, and were hepatized; a quantity of serum and lymph was contained in the left pleura, so as to compress the lung, in which there was a small abscess. The liver was twice the natural size.
J. Lomax, of the Guards, was wounded at Waterloo, suffered amputation of the right arm on the 23d August, and arrived at the General Hospital, Colchester, on the 27th, in a state of high fever, and unable to give any distinct account of himself. He had had the ague, he said, for many days, which left him for a short time, but returned when on board ship; on the 25th he was attacked by pain in the side, [68] which was very severe on the 26th, on which day a blister was applied, which greatly relieved him. The stump had an unhealthy appearance, the edges of the wound evincing a disposition to separate. On the 28th he was free from pain; fever unabated, with a tendency to delirium. He sank rapidly on the 30th, and died on the 31st, notwithstanding the use of the most powerful stimuli. A quantity of serum was found on dissection in the left side of the chest, and the pleura pulmonalis on each side was covered with a thick layer of coagulable lymph. The pericardium was distended with fluid. The liver was enormously enlarged, pushing up the diaphragm, and displacing the lung, having in its substance a large abscess containing at least a quart of pus. The stump did not exhibit any peculiar appearance.
O. Sweeney, 90th Regiment, aged nineteen, was wounded in the hand on the 18th of June, 1815, and taken to Brussels. On the 5th of July he left for England, and arrived at Colchester on the 14th. The wound shortly after assumed an unhealthy appearance; hemorrhage took place, and the arm was amputated on the 30th. The day after, he had severe rigors for fifteen minutes, followed by fever. The next day he was better, and appeared to be doing well until the 6th of August, when fever recurred. Stump quite healthy in appearance. On the 7th, he was attacked by vomiting and purging, which lasted several hours, and reduced him much, returning at intervals until the evening of the 8th. Small quantities of wine and opium agreed best, and a blister was applied to the scrobiculus cordis. On the 9th, he complained of pain and tenderness in the abdomen, which were relieved by fomentations and an enema. The stump looked well, and discharged healthy pus in small quantity; the ligature on the brachial artery came away. On the 10th, his strength failed, and the tongue and teeth were covered with a dark sordes. The adhesions of the stump appeared disposed to separate. At night he was restless, with low delirium; and on the 11th died, with the complete facies Hippocratica. On raising the sternum, the pleura of the left lung was found adhering to that of the ribs, and covered by a thick layer of coagulable lymph. The lung was highly inflamed; and on cutting into its substance, a number of small tubercles was observed. The pericardium and left cavity of the thorax contained more than the usual [69] quantity of fluid. During the progress of this case, eleven days from the amputation no one symptom existed which could induce a suspicion of inflammation going on in the thorax. The stump was in a sloughing state, but the disease did not extend along the brachial veins.
Thomas Haynes, 23d Light Dragoons, aged nineteen, was wounded by a spear on the back of the left forearm, at Waterloo; the wound appeared to do well until he left Brussels for England, when it assumed an unfavorable appearance, and on his arrival at Colchester, on the 14th of July, it was in a sloughing state. The pain was excessive, and the tenderness around the whole circumference of the sore was so great that he could not suffer the slightest pressure with the finger. He was largely bled, and a solution of sulphuric acid, one drachm to twelve ounces of water, was applied twice a day to the whole surface, and the whole kept wet with cold water; this treatment was continued until the 21st, during which period he was bled five times, to about twenty ounces each time. The acid solution was increased in strength from one drachm to an ounce, and care was taken that the sloughing portions only were touched with it. His health was considerably amended, and on the whole a favorable result was expected. At two on the 22d, however, a sudden hemorrhage took place, to the amount of three pints; a second ensuing on the 23d, the arm was amputated. The pulse continued quick; in other respects he was doing well, until the 25th, when some accession of fever took place, and increased. He was bled to ten ounces, and purged. On the 26th, the line of incision in the stump appeared to be healed; and with the exception of the pulse at 140, he had no unpleasant symptom on the 27th, and was free from pain of every kind. On removing the center strap, which had been allowed to remain, a large collection of matter of good quality issued. On the 28th, he was much the same. On the 29th, the countenance had assumed a deathlike paleness; pulse 120, intermitting every fifth pulsation; breathing short and laborious, with some pain in the chest, and every symptom of effusion having taken place. He died at two P.M., six days after the amputation.
The only morbid appearance found on dissection was a large quantity of serous fluid in the pericardium, which was distended by it, and on both sides of the chest. The heart and lungs, with their membranes, were quite sound. On [70] examining the stump, the sanative process was found to have been entirely confined to the integuments. No appearance of granulation could be perceived on the muscular surface.
This last case is worthy of especial observation, on account of the manner in which sulphuric acid was used for the sloughing state, from one drachm to one ounce of the acid to twelve ounces of water, not as something new, but as an ordinary application; and I am doubtful whether there is any case on record of such use, anterior to it. Is the external use of strong acids in sloughing cases also due to the war in the Peninsula? Delpech says Yes,—a testimony I shall confirm in its proper place.
I have departed, in some degree, in the foregoing observations, from the aphorismal form I had prescribed for myself in the commencement of these Commentaries. I have done so as an act of justice to those officers who served at Toulouse, Brussels, Antwerp, and Colchester, in 1814 and 1815, who are all now no more, and who labored hard in the then early investigation of these different states of disease, and have not received the reward they merited of public acknowledgment. I have endeavored, as the late Chancellor of the Exchequer says in his life of Lord George Bentinck, to preserve for them the chastity of their honor.
63. Mr. Hunter, in 1793, described the appearances and the fatal results of inflammation of the veins, as a consequence of injuries inflicted on the surrounding parts, but I apprehend I was the first person to point out the prevalence of this complaint after secondary amputation, and its intimate connection with certain low inflammatory attacks, attended by destructive purulent depositions, particularly in the chest, and their more chronic deposit in other parts. Mr. Rose, of the Guards, published some observations in the fourteenth volume of the Medical and Chirurgical Transactions, in 1828, confirming the remarks made by me in print thirteen years before, but without referring to them. Mr. Arnott has an able paper on that subject in the fifteenth volume. M. Sedillot thinks he has detected globules of pus in different parts of the circulating system in persons who had died of this disease. Mr. Henry Lee, 1850, one of the last English writers on the subject, professedly doubts the accuracy of the observation; this point remains among others for further investigation. He admits, however, that [71] in cases where, from long-continued disease, there have been repeated introductions of vitiated fluids into the circulation, the blood loses much of its coagulating power, which prevents the admission of purulent matter by the veins, by forming coagula with it in them, thus constituting he thinks the essential disease. When the coagulating power of the blood is thus lost, he thinks it possible that pus-globules may then be found circulating in it. Other late writers, and lastly Dr. Hughes Bennett, think these diseases are dependent on the introduction of a peculiar animal poison. Attention should be paid by the medical officers of the public service, whenever there is a war, to the state of the blood, and to the inner lining of the diseased veins under the microscope;[2] and all those gentlemen, when in London, should study its use, under Mr. Quekett, at the College of Surgeons, to whose lectures they have the right of admission, and to whose kindness they will all soon feel greatly indebted. I am not aware that the writers referred to have added anything to the practical facts I had related so long before, which is much to be regretted. It is of little use, although it is a step in the right direction, to describe a disease, or even to show why and wherefore it destroys, unless a means of prevention or of cure can also be indicated.
[2] The India Company have supplied the principal hospital of each presidency with one good microscope at least; one of these, with a person who understands its use, should be attached (but is not) to the principal hospitals during the present war in the East.
64. In the irritable and sloughing state of stump alluded to, hemorrhages frequently take place from the small branches, or from the main trunks of the arteries, in consequence of ulceration; and it is not always easy to discover the bleeding vessel, or, when discovered, to secure it on the face of the stump; for as the ulcerative process has not ceased, and the end of the artery which is to be secured is not sound, no healthy action can take place; the ligature very soon cuts its way through, and the hemorrhage returns as violently as before, or some other branch gives way; and under this succession of ligatures and hemorrhages the patient dies.
Some surgeons have, in such cases, preferred cutting down upon the principal artery of the limb, in preference to performing another amputation, even when it is practicable; [72] and they have sometimes succeeded in restraining the hemorrhage for a sufficient length of time to allow the stump to resume a more healthy action. This operation, although successful in some cases, will generally fail, and particularly if absolute rest cannot be obtained, when amputation will become necessary. The same objection of want of success may be made to amputation; on a due comparison of the whole of the attending circumstances, the operation of tying the artery in most cases is to be preferred in the first instance, and if that prove unsuccessful, then recourse is to be had to amputation; but this practice is by no means to be followed indiscriminately. The artery ought to be secured with reference to the mode of operating, as in aneurism, but the doctrines of this disease are not to be applied to it, because it is still a wounded vessel with an external opening.
To obviate all doubts, the part from which the bleeding comes should be well studied, and the shortest distance from the stump at which compression on the artery commands the bleeding carefully noted; at this spot the ligature should be applied, provided it be not within the sphere of the inflammation of the stump. In case the hemorrhage should only be restrained by pressure above the origin of the profunda, and repeated attempts to secure the vessel on the surface of the stump have failed, amputation is preferable to tying the artery in the groin, when the strength of the patient will bear it.
When hemorrhage takes place after amputation at or below the shoulder-joint, it is a dangerous occurrence. An incision should then be made through the integuments and across the great pectoral muscle, when the artery may be readily exposed, and a ligature placed upon it without difficulty anywhere below the clavicle.
If the state of the stump in any of these cases should appear to depend upon the bad air of the hospital, the patient had better be exposed to the inclemency of the weather than be allowed to remain in it.
In crowded hospitals, hemorrhages from the face of an irritable stump are not unfrequent, and often cause a great deal of trouble and distress. It is not a direct bleeding from a vessel of sufficient size to be discovered and secured by ligature, but an oozing from some part of the exposed granulations, which are soft, pale, and flaccid. On making pressure on them the hemorrhage ceases, but shortly after [73] reappears, and even becomes dangerous. This hemorrhage is usually preceded by pain, heat, and throbbing in the surface from which it proceeds. There is irritation of the habit generally, and a tendency to direct debility. The proper treatment consists in the removal of the patient to the open air, with an antiphlogistic regimen in the first instance, followed by the use of quinine and acids; cold to the stump, in the shape of pounded ice or iced water. Escharotic and stimulating applications should be used with caution. If any of the styptics which are sometimes announced as infallible could be relied upon, their application in these cases would be most advantageous. The solution of the perchloride of iron is the best.
APHORISMS FOR AMPUTATIONS, ETC.
65. Amputation of a limb is the last resource and the opprobrium of surgery, as death is of the practice of physic; it being, notwithstanding, impossible to do impossibilities, and save a limb or a life which can no longer be preserved. Art and science at that point cease to be useful.
66. At the commencement of the war in the Peninsula, all surgeons believed it to be impossible to compress in an effective manner the artery of the thigh against the bone, as it passes over the edge of the pubes, and that the loss of blood on its division must be so formidable as to be murderous. This was merely a surgical delusion, which maintained its ground in London until the end of 1815, when the French soldier, whose thigh I had successfully taken off at the hip-joint, after the battle of Waterloo, without first tying the femoral artery, was shown to all disbelievers. It was the great point in advance in English and European surgery, and one great result of the practice of that war.
67. This great, indeed most important fact, having been established, the surgery of amputation was deprived of nearly all its terrors. Confidence, and with it coolness, were obtained; and many young surgeons diligently sought for an operation on the hip-joint as the ne plus ultra of [74] operative boldness and dexterity, much after the fashion of the young lady pianistes, who do not consider themselves in any way advanced on the road to perfection until they can play at least the overture to Guillaume Tell, if not the Galop Chromatique of Listz, nearly as well as the composer himself.
68. As a tourniquet cannot be applied in this amputation, nor even at that of the shoulder-joint, without doing harm, its inutility in the greatest operations is proved; and recourse should not be had to it in the smaller or less dangerous ones, provided sufficient assistance can be obtained. When the surgeon has only one assistant, he should apply a tourniquet, or even if he should have several bad ones on whom he cannot depend.
69. There is always more blood lost, and particularly in secondary amputations, when a tourniquet is used than when the principal artery is compressed by one assistant, and two others are ready to press on the outside of the flaps, or upon the divided vessels, with the ends of their fingers; the force necessary to prevent the passage of blood through the common femoral, or the axillary artery, being merely that of the finger and thumb, applied in a very gentle manner, or even of the end of the forefinger of a competent person. I have rarely applied a tourniquet since 1812, and few persons have done more formidable operations under more difficult circumstances. The ancient illusion with regard to the necessity for tourniquets in amputation must be given up, except by incompetent persons, or by those who are fearful and superstitious, and do not like to depart from the ways of their forefathers.
70. A tourniquet is useful when loosely applied after an operation, and the attendant should be taught how to turn it, so as to suppress any serious bleeding which may take place until the surgeon can be procured. It may be, although it rarely is, necessary on the field of battle. The surgeon need not, therefore, load himself or his assistant, as formerly, with a sackful, for a thoroughly useful tourniquet can be made in a moment with a pebble and a pocket-handkerchief, or a roller. The great point is to know where and how to apply it. When gentlemen called surgeons by warrant are sent to an army, as many were to that in Spain and France, with only the knowledge of a druggist, having been refused a commission on account of their ignorance, it is [75] necessary this instruction should be especially given to them; and this horrible fact is recorded with the hope it may be useful in preventing any such atrocious proceedings in future. Peace or humane societies, if they cannot prevent a war, may interfere with advantage on this point, to divest it of some of its horrors. At the battle of Inkerman, a young officer, the son of a friend of mine, was wounded in the leg by a musket-ball, which caused much loss of blood. A tourniquet was applied, instead of the required operation being performed, and he was sent on board a transport from Balaklava. The leg mortified, as a matter of course, and was amputated. He died, an eternal disgrace to British surgery, or rather to the nation which will not pay sufficiently able men, and therefore employs ignorant ones—the best they can get for the money.
71. When circular operations were performed in the olden time, particularly on the thigh, the skin, when divided, was dissected, and turned up like the cuff of a coat—a painful proceeding, as unnecessary as it was barbarous. Forty years have elapsed since I demonstrated its absurdity, and showed that the first incision in the thigh should include the fascia lata, any deep attachments it might have should follow, when the parts thus divided ought to be retracted as a whole, to form a proper covering for the stump.
It was at the same time shown that, in whatever way, and however clumsily and tediously, the muscles might be divided, it did not prevent the successful result of the operation, provided the bone was cut short, so as to form a cone, with an elongated or depressed point.
72. The nicking of the periosteum, and pushing it upward and downward, so as to leave a space for the saw, was at the same time forbidden, as leading to necrosis of the part of the bone thus denuded, if unremoved by the saw. The saw was also directed to be held perpendicularly to, and not across, the bone, nor even diagonally to it—an apparently trivial, but yet great improvement. The last part divided is an outer and thin layer of hard bone, which does not so readily splinter on the side as on the under part, by the weight of the leg.
73. The limb to be amputated is not to be held by the assistant in the manner described and usually shown in books: one hand ought not to be above the knee, but below and by the side of it, the other grasping the calf, so that [76] the limb may be duly supported, and drawn inward or outward, in the opposite direction to the saw, as it divides the last layers of the bone.
74. The common integuments of the stump should be drawn together, in primary amputations, by sutures formed of flexible leaden wires; by threads of silk, if leaden wires be not attainable. The vessels which bleed should be carefully secured by single yet fine threads of dentists’ or other strong silk, one end to be cut off in primary amputations. In secondary amputations, when the parts are not always sound, both ends of the ligature should be cut off, and in such cases the edges of the wound should be brought in contact only, with a layer of fine linen between them, without the expectation of, or the desire for, union taking place.
75. The removal of a limb should not occupy two minutes, but the securing the blood-vessels should be done without reference to time; when carefully effected, there is little fear of secondary bleeding, and the stump should be closed at once. It has been lately recommended not to close the stump for four, six, or eight hours after the operation; but this is not advisable, unless the depressed state of the patient, or other causes, should have rendered it impossible to secure, in a proper manner, all the vessels which are likely to bleed. It will be less painful and dangerous to delay, in such cases, than to have to reopen the stump.
76. When the edges of the incision have been brought together by the hands of the assistants, and by the sutures indicated, strips of some kind of agglutinative plaster without resin should be applied between them, and a little wet lint over the incision, retained by two cross-pieces of rollers, the ends of which are maintained in their situation by another roller applied round the body and over the upper part of the thigh, including the extremities of the two cross-pieces; but this roller is not to be applied over the end of the stump. When the war came well in, stump-caps, as they were called, went out, being worse than useless. The stump should be supported on a soft pillow, so as to be as comfortable as possible, and protected by a cradle from accidental injury.
If inflammation, accompanied by pain, should take place, cold or iced water should be applied, particularly in primary amputations. In secondary ones, warm fomentations or light warm poultices will be more advantageous, all constriction [77] by sutures or plasters being removed, the parts being simply approximated to each other. Attention should be paid to the directions in aphorism 61.
77. This amputation essentially owes its existence to the wars of the French Revolution. M. Bourgery says Blandin performed it three times in 1794; once successfully. Baron Larrey did it seven times during his different campaigns, and he says one or two persons who had survived were seen during their cure by an officer in Russian Poland, but they never reached France. Nevertheless, I always assume that one at least did recover, whether he was really seen or not, being a compliment and a reward justly due to the zeal and ability of my old friend the Baron, to whom the surgery of France is so much indebted. This operation was first done in Spain by the late Mr. Brownrigg, at Elvas, in 1811, and by myself after the siege of Ciudad Rodrigo, but none of our patients ultimately recovered. I operated on a French soldier at Brussels soon after the receipt of the injury at Waterloo; he survived; and he was the first and the only man seen for a long time afterward in either London or Paris. The biographer of Baron Larrey says he was present at, and advised the operation to be done; but that is an error, as the Baron did not visit Brussels until after I had left it for Antwerp; neither had I any knowledge of the Baron’s writings in 1811 or 1812, when my first operation was done in Portugal. Eighteen or twenty ways have been suggested for doing this operation, and twenty persons are believed to have survived its performance, several of whom may be living at the present time.
A very extensive destruction of the soft parts, the femur remaining entire, does not authorize the removal of the limb in the first instance, unless the main artery be also injured. Captain Flack, of the 88th Regiment, was struck by a large cannon-shot at Ciudad Rodrigo, on the outside and anterior part of the left thigh, which tore up and carried away nearly all the soft parts from the groin, or bend of the thigh, below Poupart’s ligament, to within a hand’s-breadth of the knee. It was an awful affair. He was supposed to be dying, was returned dead, and his commission was given to another. Left to die in the field hospital after the town was stormed, [78] and finding himself thus deserted by his own friends, he claimed my aid as a stranger. I took him five leagues to my hospital at Aldea del Obispo. The femoral artery lay bare for the space of nearly four inches, in a channel at the bottom of the wound; the whole, however, gradually closed in, and he recovered.
If the injury is on the back part, a flap should be made in amputation from the fore part. If the wound should be on the outside, the flap is to be made from the inside, and vice versa, the object being to make the stump as long as possible. A wound of the artery, accompanied by a fracture of the femur, requires amputation, for although many would survive either injury alone, none would, it may be apprehended, surmount both united.
If after a fracture in course of treatment, the principal artery should be wounded by some accidental motion of the bone, amputation should in general be resorted to. A ligature on the artery higher up would fail, and the operation of seeking for both ends of the injured vessel would cause so much mischief in an unsound part that the consequences would in all probability be fatal.
78. When the femur is suffering from a malignant disease, commencing in the periosteum, or in its cancellated internal structure, I am reluctantly obliged to say, from experience, that the removal of the whole bone at the hip-joint offers the best, perhaps the only chance of success. In such cases, the operator has in general the power of selecting his mode of proceeding.
It may be laid down as a principle in all cases of accident, whether from shot, shell, or railway carriages, that no man should suffer amputation at the hip-joint when the thigh-bone is entire. It should never be done in cases of injury when the bone can be sawn through immediately below the trochanter major, and sufficient flaps can be preserved to close the wound thus made. An injury warranting this operation should extend to the neck, or head of the bone, and it may be possible, as I have proposed, even then to avoid it by removing the broken parts.
79. The principle being established, as a general rule in all cases of recent injury, that the femur must be broken at least as high as the trochanter to constitute an imperative case for this operation, the next point of importance relates to the manner of forming the first incisions. The instruc[79]tions and recommendations to be found in books for the performance of this operation are frequently inapplicable, and are not to be depended upon; the errors occurring from the operation having been considered and performed on the dead body and not on the living; on the normal and not on the injured state of parts. Thus, for instance, it is recommended that an assistant should rotate the knee outward or inward, to show the head of the femur; to which recommendation there is the insuperable objection, that no person should suffer this operation who has a knee, or half a thigh, or even a third of one, to move by the rotary process. Pure theorists in surgery have decided upon having a large flap made on the fore part of the thigh, and a smaller one behind, regardless of the fact that this cannot be done in many cases requiring a primary operation from the nature of the injury; although it may be done in many secondary cases, in which this severe operation would not have been required if the limb had been amputated in the first instance. It is the mode recommended by Mr. Brownrigg, who in his operations, which were secondary ones, had a choice of integument, and it is, perhaps, under these circumstances, the best.
Baron Larrey tied the femoral artery in the first instance, and then made two lateral flaps; but this operation, dependent on the fear of hemorrhage, was never performed in the British army.
80. My first successful operation, performed in 1815, was done from without inward, the flaps being anterior and posterior, the artery being compressed against the pubis.
The patient is to be laid on a low table, or other convenient thing, in a horizontal position; an assistant, standing behind and leaning over, compresses the external iliac artery becoming femoral, as it passes over the edge of the pubis. The surgeon, standing on the inside, commences his first incision some three or four inches directly below the anterior spinous process of the ilium, carries it across the thigh through the integuments, inward and backward, in an oblique direction, at an equal distance from the tuberosity of the ischium to nearly opposite the spot where the incision commenced; the end of this incision is then to be carried upward with a gentle curve behind the trochanter, until it meets with the commencement of the first; the second incision being rather less than one-third the length of the first. The integuments, including the fascia, being retracted, the [80] three gluteal muscles are to be cut through to the bone. The knife being then placed close to the retracted integuments, should be made to cut through everything on the anterior part and inside of the thigh. The femoral or other large artery should then be drawn out by a tenaculum or spring forceps, and tied. The capsular ligament being well opened, and the ligamentum teres divided, the knife should be passed behind the head of the bone thus dislocated, and made to cut its way out, care being taken not to have too large a quantity of muscle on the under part, or the integuments will not cover the wound, under which circumstance a sufficient portion of muscular fiber must be cut away. The obturatrix, gluteal, and ischiatic arteries are not to be feared, being each readily compressed by a finger until they can be duly secured. The capsular ligament, and as much of the ligamentous edge of the acetabulum as can be readily cut off, should be removed. The nerves, if long, are to be cut short. The wound is then to be carefully cleansed, and brought together by three or more soft leaden sutures in a line from the spine of the ilium toward the tuberosity of the ischium. The ligatures are to be brought out between the sutures, and some adhesive strips of plaster applied to support them. A little wet lint is to be placed over the wound, and some well-adapted compress under the lower flap; the whole to be retained by a soft bandage. In my successful case there was a shot-hole in the under flap, which did good service; and from having seen its use, I have no objection to a small perpendicular slit being made in the lower flap, and a strip of linen introduced to prevent adhesion. The immediate union of the flaps cannot be expected, nor is it often to be desired.
This mode of proceeding is more certain of making good flaps where integuments are scarce. Where the integuments will admit of the anterior flap being made by the sharp-pointed puncturing knife dividing the parts after it has been passed across from without inward, there is no objection to this proceeding, and some prefer it. I have had two such knives added to each of the cases of instruments supplied to the army for the purpose.
Professor Langenbeck, when lately in London, informed me he had performed amputation at the hip-joint several times in the Holstein war, and he believed more than once successfully; making the anterior flap by the pointed knife, [81] cutting from within outward, but the posterior one by cutting through the integuments from without inward, as I have recommended in high amputation below the joint, in order to make the flap of a more equal and proper thickness. One point to be attended to is to leave as little as possible of the internal tendinous structure of the great gluteus muscle, as it does not readily unite with other parts; a second, not to leave too much muscle on the under part; and a third, to remove as much as possible of the ligamentous structure about the joint. The after-treatment will be the same as in other formidable cases. The shock, however, of the injury, and of the amputation, will render blood-letting unnecessary. Cordials, in small quantities, with opiates and a good but light nourishing diet, should be given. The wound should be wetted with cold water, and the patient constantly watched, so that hemorrhage may be arrested if it should take place. In an otherwise successful operation performed by Mr. C. G. Guthrie, at the Westminster Hospital, the patient was lost on the third day from this cause.
Mr. Brownrigg’s operation is to be done in the following manner: The patient is to be placed on a low table and properly secured, with the nates projecting over its edge, the artery being compressed. The surgeon enters the pointed knife between the spine of the ilium and the trochanter major, and carries it across the thigh, as near as may be to the head and neck of the femur, until the point appears on the inside, near the scrotum, which should have been previously drawn away. The knife is to cut slowly downward, to make a flap, under which, and behind the knife, an assistant inserts his four fingers, in order to be able to grasp the flap and aid in compressing the principal artery, as the operator completes the flap, which it is intended should be a large one, as shown in the diagram, fig. 1.
Fig. 1.
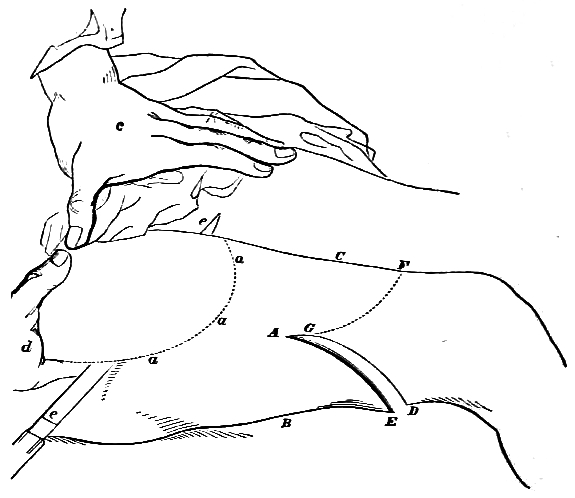
Amputation of the Hip-joint as performed by Mr. Brownrigg.
(Upper figure.)
a a a, anterior flap in dotted lines;
c, thumb compressing the artery on the pubis;
d, fingers introduced under the flap;
e, the straight knife, entrance and exit of.
(Lower figure.)
Flap Amputation as performed by Mr. Luke, on the lower half of the thigh.
A, middle of the outside of the thigh and point of entrance of knife;
B, under part;
C, upper part;
A to E, the under flap;
G to F, dotted line of upper flap, beginning short of commencement of under flap.
The assistant holding up the flap, the surgeon cuts the attachment of the gluteus medius muscle, from the upper edge of the trochanter, if it has not been already done, opens the capsular ligament of the joint, and divides the ligamentum teres. The head of the bone can then be readily withdrawn from the acetabulum. The knife being placed behind the head of the bone and the trochanter, should be carried obliquely downward and backward, so as to form a shorter flap behind than was made before. The amputations of the hip-joint, performed in the Crimea, have not, I understand, been as successful as the ability with which they were performed might have led the operators to expect.
Fig. 2.
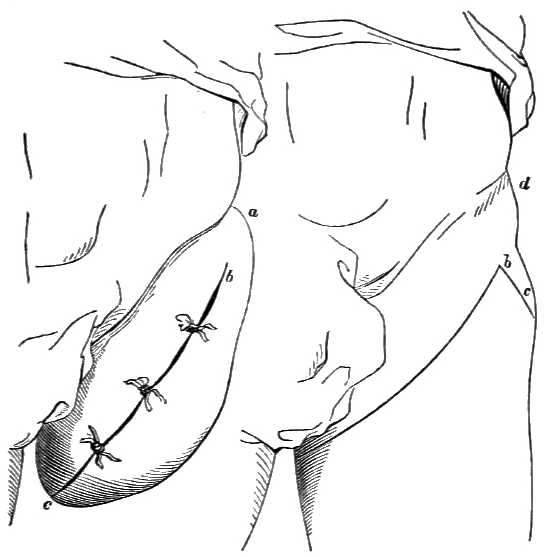
Mr. Guthrie’s operation.
Left side—
a, anterior superior spine of ilium;
b, commencement of anterior incision, continued by the black line;
c, the posterior incision joining the anterior one.
(Second figure.)
b c, line of incision marked by three sutures.
81. Amputation by the circular incision is to be done in the following manner: When a tourniquet is used, which it should not be, if the surgeon can depend on his assistants, the pad should be firm and narrow, and carefully held directly over the artery, while the ends of the bandage in which it is contained are pinned together. The strap of the tourniquet is then to be put round the limb, the instrument itself being directly over the pad, with the screw entirely free; the strap is then to be drawn tight and buckled on the outside, so as to prevent its slipping, and yet not to interfere with the screw. Should the screw require to be turned more than half its number of turns, the strap is not sufficiently tight, [84] or the pad has not been well applied. The patient being placed on a table at a convenient height, the assistants are carefully to retract the integuments upward, and put them on the stretch downward, by which means their division is more easily and regularly accomplished. The surgeon, standing on the outside, passes his hand under the thigh and round above quite to the outside, and there he begins his incision with the heel of the knife, and with a quick, steady movement, carries it round the thigh until the circular division of the skin, cellular membrane, and fascia has been completed. The skin cannot be sufficiently retracted unless the fascia be divided, and as the division of the skin is certainly the most painful part of the operation, it ought never to be done by two incisions, when the largest thigh can most readily and speedily be encircled by one. If the fascia should not be completely divided by the first circular incision, it is to be cut with the point of the knife, together with any attachment to the bone or muscles beneath. The amputating knife is then to be applied close to the retracted fascia and integuments, and the outermost muscles are to be divided by a circular incision, with any portion of the fascia that may not have equally retracted. This incision completed, the knife is immediately to be placed close to the edge of the muscular fibers which have retracted, and the remainder of the soft parts divided to the bone in the same manner. In making these two incisions, care should be taken to cut at least half an inch on each side of the great artery by one incision, which should be either the first or second, as may be most convenient. The muscles attached to the bone are then to be separated with a scalpel for about three inches in large thighs, by which means the bone will be fairly imbedded when sawed off. The common linen retractor is next to be placed on the limb, and the muscles steadily kept back while the bone is sawed through. The periosteum may or may not be divided by one circular cut of the scalpel after the retractor has been put on. The heel of the saw is then to be applied and drawn toward the surgeon, so as to mark the bone, in which furrow he will continue to cut with long and steady strokes, the point of the saw slanting downward in a perpendicular direction until the bone be nearly divided, when the saw is to be more lightly pressed upon, to avoid splintering it, which this manner of sawing will also tend to prevent. During this operation [85] the thigh should be held steadily above, and in such a manner below that the part to be cut off does not weigh or drag on the bone above; at the same time it must not be pressed inward or upward, or it will prevent the motion of the saw or splinter the bone. The retractor is then to be removed, the great artery to be pulled out by a tenaculum passed through its sides, separated a little from its attachments, and firmly tied with a two-threaded, strong ligature, provided dentists’ silk be not used, and the tenaculum is not to be withdrawn until this has been accomplished; any other vessels that show themselves may be secured, and compression should for an instant be taken off the main artery, when others will start. If used, the tourniquet should now be removed, and the small remaining vessels will be discovered. If the great vein continue to bleed after some pressure has been made upon it, a single-threaded ligature should be put over it; but this should not be done if it can be avoided, and only when the loss of a little blood might be dangerous. If the cancellated part of the bone bleed freely, the thumb of the left hand pressed steadily upon it, while the vessels are tying, will in a short time suppress the hemorrhage. Any inequality of bone should be removed by forceps. The ligatures should now be shortened, one end of each thread being cut off; the stump is to be sponged with cold water and dried, the bandage rolled steadily down the thigh; the muscles and integuments brought forward and placed in apposition, horizontally across the face of the stump, and retained by leaden sutures and adhesive plasters carefully applied, from below upward, and from above downward; the ligatures being brought out nearly as straight as possible, in two or three places between the slips of plaster, unless both ends have been cut short. A compress of lint is to be placed over and under the wound, supported by two slips of bandage, in the form of a Maltese cross, vertically and horizontally, and the whole secured by a few more turns of the bandage. No stump-cap is to be applied; the stump is to be raised a little on a proper pillow from the bed, in which the patient lies on his back; and if the bone appear to press too much against the upper flap, the body may be a little raised, which will relieve it.
In secondary amputation of the thigh, the integuments may not be sound, and will not retract, in which case they must be dissected back to an equal distance all round. If [86] the muscles are much diminished in size, or flabby, they should be left even longer than may appear necessary for the formation of a good stump; and this is to be done more especially on the under part, for the bone will frequently protrude under these circumstances, when enough has been supposed to have been preserved. In all these cases the bone should be shorter than usual, and the skin should, if possible, retain its attachments to the parts beneath. No inconvenience can ever arise from too much muscle and skin in a circular stump; but it does sometimes from too much skin alone.
In primary operations there will be from three to seven vessels to be tied; in secondary ones, from ten to sixteen, and even then there may be an oozing from the stump. In this case a little delay in searching for the vessels is necessary; the tourniquet and all tight bandages should be removed, and the stump well sponged with cold water before it is dressed. A certain degree of oozing is to be expected from all stumps, although it does not always occur: but when there is really any hemorrhage, so that blood distills freely through the dressings, the stump should be opened, when the bleeding vessel will generally be discovered readily, though not visible before. A stump under these circumstances should not be closed in the first instance; the parts should be merely approximated until all bleeding has ceased.
When the operation is performed near the knee, the gradual thickening of the thigh prevents the retraction of the integuments, and has an effect upon the vessels of the stump; both of which evils are avoided after the circular incision has been completed, by making a cut, an inch and a half in length, in the integuments through the fascia on each side, in the horizontal direction in which they are recommended to be placed, after the operation is finished; but this will very rarely be necessary.
82. Amputation of the thigh, by the flap operation, is best accomplished by the method adopted by Mr. Luke, of the London Hospital, which is as follows: The patient being placed so that the thigh projects beyond the table, the surgeon stands with his left hand toward the body, or on the outside when amputating the right, and on the inside when amputating the left thigh. The knife to be used ought to be narrow, pointed, and longer by two or three inches than the diameter of the thigh at the place of ampu[87]tation. The point of the knife should be entered mid-distance between the anterior and posterior surfaces of the thigh, which may be effected with accuracy, if the eye is brought to a level with the thigh, when the middle point is easily determined. The posterior flap is to be formed first, by carrying the knife transversely through the thigh, so that its point shall come out on the opposite side, exactly midway between the anterior and posterior surfaces. In traversing the thigh, the knife should pass behind the bone, and will be more or less remote from it in different individuals, according to the greater or less development of the posterior muscles, when, by cutting obliquely downward, to the extent of from four to six inches, according to the thickness of the thigh, a posterior flap is formed. The anterior flap is effected, not by making a flap, but by commencing an incision through the integuments and muscles on the side of the thigh opposite to the surgeon, at a little distance anterior to the extremity of the posterior flap. This incision is made from without inward, through the integuments, so as to form an even curve, and without angular irregularity, over the thigh, to near the base of the posterior flap on the side on which the surgeon stands. The length of this flap is determined by that of the posterior. It will therefore vary from four to six inches, as before stated; and for its completion will require a second, or perhaps a third, application of the knife. In the two flaps thus made, the division of almost all the soft structures is included, a few only immediately surrounding the bone remaining uncut. These are to be divided by a circular sweep of the knife, at the part where it is intended to saw the bone; in this way it is sufficiently denuded for the application of the saw. The flaps being held back by an assistant, the bone is to be sawn through in the usual way. In amputations of the lower part of the thigh it usually happens that the ischiatic nerve lies upon the surface of the posterior flap, and should be removed. It occasionally occurs, although not frequently, that the popliteal artery is cut obliquely at its commencement; but in amputations above the passage of the arterial trunk through the tendon of the triceps, this does not take place, the division of the artery being usually included in the circular sweep made after the formation of the flaps. The divided arteries having been carefully secured, the flaps are to be brought together and retained by three sutures [88] passed through the integuments at equal distances from each other, and from the extremity or base of the flaps. It appears to be a matter of considerable importance not only that their edges should be kept in apposition, but that their whole surfaces should be kept in accurate contact. For this purpose, the following method of dressing is adopted: The edges, in the intervals between the sutures, are to be held together by strips of adhesive plaster about one inch in breadth. A compress of lint is then to be fitted over each flap, that upon the posterior being the larger. The compresses are to cover the flaps only, and not to extend over the extremity of the bone, where their pressure would probably be ill endured. The posterior compress is made large, that it may serve as a cushion on which the thigh rests when the patient is placed in bed. The compresses are to be retained in position by one or two strips of plaster, and supported by a bandage applied carefully round the stump. If this be properly accomplished, the whole surfaces of the flaps will be kept accurately in contact with each other, and complete union may be reasonably expected. By securing the perfect apposition and support of the entire surfaces in accurate contact, the disposition to the issue of blood from small vessels is also obviated to a great extent, and it is even probable that vessels of a larger diameter than the smallest, which would bleed if not restrained, are, by the pressure of the opposing surface, prevented from doing so, and the probability of secondary hemorrhage is diminished. Experience has demonstrated the fact that primary union of the flaps is most effectually procured in the great majority of amputations thus treated. Indeed, non-union of the flaps is the exception; union, the rule. In the subsequent treatment of the stump, care must be taken to prevent an accumulation of discharge in the tracks of the ligatures; and the dressings must be renewed according to circumstances having reference to the quantity of discharge, and the uneasiness of the patient. The line of division of the integuments of the two flaps is situated, at first, in the center of the face of the stump; but when the flaps have united, a gradual change takes place in the position of the cicatrix: it recedes, by degrees, to the posterior aspect of the thigh, and the bone abuts upon the anterior flap, by which alone it is eventually covered, and the cicatrix is thus removed from its pressure.
[89] 83. A protrusion of bone is a disagreeable occurrence after amputation; it will sometimes happen after sloughing of the stump, without any fault of the operator. If, on completing the operation, it is evident the bone cannot be well covered, a sufficient portion should be at once sawn off, and the error remedied.
When the bone protrudes at a subsequent period to the extent of an inch or more, it should be removed by operation, an incision being made on, and down to, the bone, and the saw applied where it is sound. The chain saw, when at hand, answers well, and some should be supplied for the use of the principal hospitals with every army. The protruded end of bone should be held steadily by pincers, or it may be introduced into a hollow tube, which fixes it firmly.
When the bone has been badly sawn through, or split in the act of dividing the last layer, or the periosteum is unduly separated, the end will often exfoliate with the split, which may extend up for several inches, giving rise to the formation of abscesses, causing much suffering, and occupying a great length of time before the ring of bone and the split portion exfoliate, and the stump becomes quite sound. A splinter of this kind may even require to be removed at a late or at a distant period, from the nervous irritation and suffering it may occasion. This irritation has been often attributed to the extremity of the principal nerve, which always enlarges, assumes a bulbous form, and is painful on pressure, when made for the purpose, although not so under ordinary circumstances. This enlargement never requires removal, unless it should adhere to the cicatrix, or be the subject of disease incidentally occasioned in it. The great sciatic nerve became early thus enlarged in the thigh of the late Marquess of Anglesea, and was mistaken for disease, for which he was advised to have it removed, it being painful on pressure, and therefore the supposed cause of the tic douloureux under which he labored. Consulted on the propriety of this operation, his leg-maker, Mr. Pott, being present, who had also lost a leg above the knee, I requested his lordship to squeeze Mr. Pott’s bulbous nerve, in the same manner as the doctor had squeezed his lordship. He did so, and Mr. Pott roared and sprang from the floor in a manner which quite satisfied Lord Anglesea.
REMOVAL OF THE HEAD OF THE FEMUR, ETC.
84. The removal of the head of the thigh-bone from its place in the hip-joint, after it has been separated in a measure from its attachments by disease of a scrofulous nature, is an operation which has been several times successfully performed, and life has been thereby preserved without much suffering or risk to the patient. In this case, the head of the bone is found lying outside the cavity, from which it has been drawn by the action of the muscles. A step further must be taken, and this operation must some day be done in cases of fracture of the head or neck of this bone caused by an external wound—cases which have hitherto been invariably fatal, or in which life has been preserved by amputation at the hip-joint.
The great advance which operative surgery has made within the last forty years, and the success which has followed the removal of the head of the humerus, the whole of the elbow, the ankle, and even the knee-joint, render it imperative on surgeons of ability to endeavor to save life without the performance of so formidable an operation as that of the removal of the whole limb, more particularly when the health is good and the parts sound, with the exception of those immediately injured.
The cases which seem more particularly favorable for this operation are those in which the head or neck of the bone is broken by a musket-ball. Picture to yourselves a man lying with a small hole either before or behind in the thigh, no bleeding, no pain, nothing but an inability to move the limb, to stand upon it, and think that he must inevitably die in a few weeks, worn out by the continued pain and suffering attendant on the repeated formation of matter burrowing in every direction, unless his thigh be amputated at the hip-joint, or he be relieved by the operation which, I insist upon it, ought first to be performed.
85. In order to do this operation with precision, the surgeon should make himself well acquainted with the anatomy of the parts; and as the war in the Russian Empire may [91] offer opportunities for its performance, a recapitulation of the essential points to be noticed may be useful. Two limbs should be injected so as to show the great arteries distinctly, and one should be dissected so that every part may be brought into view at once. That being done, attention should be directed to two points, the great trochanter and the round head of the thigh-bone in its socket, which is directly below and a little internal to the anterior superior spinous process of the ilium.
When the thigh is bent in the dissected limb, the head of the bone will be seen rolling in the socket very distinctly, and, in order to lay it bare for removal, the muscles, etc. around it must be divided. The first, on the anterior and outer part, is the tensor vaginæ femoris; this should be divided; outside this the gluteus medius must be cut, going to be inserted into the upper and outer part of the top of the great trochanter; deeper, and between these two last, lies the gluteus minimus, winding forward to be inserted into the anterior portion of the same part. Now, let the great gluteus muscle be cut through backward in a curve, and the insertions of four muscles at one part—viz., the pit or fossa immediately behind the great trochanter—will be brought into view: these are the pyriformis, the gemelli, reckoned as one muscle, and the obturatores externus and internus. They should all be cut through within half an inch from their insertion. The square muscle lying or placed immediately below them, and running from the ischium to the inter-trochanteric line, is the quadratus femoris; it must be cut across. The head of the femur will now be seen to roll in the socket on the least motion being given to the knee. The surgeon should then open into the exposed joint with great care, when by a gentle rotation of the knee inward the head of the thigh-bone will be readily dislocated outward. The ligamentum teres, or the round ligament, as it is termed, although it is triangular at its origin, should now be divided, with as much of the capsular ligament as may be necessary, when everything will be ready for the application of the saw.
Pause a moment, and view the parts before the saw is applied. Two strong muscles are inserted into the small trochanter by a common tendon, the iliacus internus and psoas magnus. This insertion should remain untouched if the fracture should not extend below the little trochanter. [92] It is not always necessary to injure them, and they will be of great use afterward, if the operation should prove successful. If the neck of the bone be broken through, rotating the thigh as directed may not assist much in dislocating its head. But then, the separation of the fractured parts may be readily completed, and the piece detached, when the remaining part of the head of the bone will be more easily removed. The sawing may be accomplished with the greatest ease by a small common saw, or by the improved chain saw, which will do good service. The arteries to be divided are all of small size. Filled with red injection, they are so small as scarcely to be seen; and they could not give any trouble; for the wound is so large as to give easy access to every part, and readily admit of any bleeding vessel being tied without difficulty. The round ligament should be cut off close to its origin in the acetabulum, and any portion of the capsular ligament and cartilaginous edge of the acetabulum which can be quickly removed with it, but no time should be unnecessarily lost in trying to remove the cartilaginous lining of the cavity itself, which will be gradually absorbed. The sawn end of the femur should now be brought up into the cavity, and kept there if possible by a supporting splint and bandage, with the hope that it may become rounded and adhere by a newly-formed ligamentous structure, in the same manner as the end of the humerus does to the glenoid cavity of the scapula, when similarly treated. The edges of the wound are then to be brought in apposition, and retained so by two or three sutures. The gluteus magnus slides over the trochanter major, having a bursa between them, and this part will not readily throw out granulations. The surgeon may therefore be less solicitous about the accuracy of the apposition of the edges at the under part, through which the discharge will more easily pass. The outside must, however, be supported by sticking-plaster and bandage compress, to prevent any bagging, and to keep all parts in contact. The saving the periosteum of as much of the femur to be taken away, as strongly recommended by MM. Flourens and Baudens in the excision of the head of the humerus, should be attempted, although not easy of execution. (Aph. 118.)
86. The surgeon should now do the operation on the undissected limb. The first cut through the skin, integuments, and fascia lata should be a curved one, beginning just over [93] the inner edge of the tensor vaginæ femoris muscle, as shown on the other leg, curving downward and outward, so as to pass across the bone an inch at least below the trochanter major, when it should turn upward to the extent of three inches or more, as the size of the limb may require. This incision or flap should, when complete, divide, in addition to the integuments, the fascia lata, the tensor vaginæ femoris, and part of the gluteus maximus. The flap thus formed must be raised or turned up by an assistant, to enable the operator to get at and divide the parts below, in the order before named. It is not necessary to stop to tie any bleeding vessel until the operation is finished, for little or no blood will be lost.
Pause again. The surgeon has just done nearly the outer half of the operation as to cutting, for removing the whole limb at the joint; and if he should now find that the bone is so much shattered in the shaft that he cannot hope to save the limb, there is no difficulty in removing it. To do this, place your long knife inside the bone, with the middle of its edge resting against the outer edge of the iliacus and psoas muscles, and at one firm cut of a strong hand let it cut its way inward, forming an inner flap, your assistant steadily compressing the femoral artery against the bone above. This artery and the great profunda will both be divided; seize them with the finger and thumb of the left hand, and place a ligature, or assist in placing one, on each branch with the right; or, if the trunk of the profunda should have been cut very short, tie the main trunk of the femoral. Let the ligature be a single thread of strong dentists’ silk, with which I have successfully tied the common iliac, and no fear need be entertained of its not holding fast if you tie it reasonably tight. The idea usually entertained that a great artery cannot be closed by the ordinary process of nature under a ligature, if a branch be given off near it, is erroneous. I never placed reliance on this opinion unless in the accidental circumstance of the outside of the orifice of the branch being in contact with the ligature, the irritation caused by which outside may not be sufficient to close the orifice within, and the common iliac artery of one of the two cases in which I tied it successfully (the patient dying a year afterward) may be seen in the Museum of the College of Surgeons. It is tied about an inch from the aorta, and was pervious on each side of the ligature, which has closed [94] the vessel to no greater extent than its own width, proving all the facts I have mentioned so frequently on this subject. As to the smaller vessels, they will give no trouble, being easily commanded, each by the point of a finger. I have not done this operation of removing the head and neck of the femur on a healthy living man after an accident, but it must be done, and I am satisfied it will in the end succeed. It was done in the 3d Division of the army in the Crimea after the engagement of the 18th of June. The continuity of the head with the shaft was not altogether destroyed, the fracture being principally confined to the great trochanter and the trochanteric ridge. It was at first thought the operation might be dispensed with, but as great irritation ensued, with every prospect of considerable mischief, the head, neck, and both trochanters were excised. On the 6th of July the man was doing well, but unfortunately he was attacked by cholera three days afterward, and died. This operation has since been done by Mr. Blenkin, of the Grenadier Guards; the result will be stated hereafter.
Amputation at the hip-joint should not be performed, unless the head and neck of the thigh-bone be injured; and it ought not to be done if they be, unless the shaft of the thigh-bone be extensively broken also. The operation I have recommended should be its substitute, and I hope yet to see a man walking with ease and comfort on whom it has been performed. The recommendation thus given is the result of the experience of former times, of the whole of the war in the Peninsula and at Waterloo, matured by that of the last forty years in London hospitals, and by a due consideration of the state of surgery throughout all civilized Europe and America. Surgery is never stationary, and surgeons of the present day must continue to show that it is as much a science as an art.
87. Wounds of the knee-joint from musket-balls, with fracture of the bones composing it, require immediate amputation; for although a limb may be sometimes saved, it cannot be called a recovery, or a successful result, where the limb is useless, and is a constant source of irritation and distress after several mouths of acute suffering have been endured, to obtain even this partial relief from impending death. For one limb thus saved, ten lives will be lost; and the sufferer is often glad, after months and years have elapsed, to lose the limb thus saved, more particularly when [95] the ball has lodged in the articulating surface of either of the bones. Amputation at a secondary period, in these cases, does not afford half the chance of success, for many will not survive the inflammation and the fever which will ensue. The amputation should therefore be immediate, unless excision can be substituted for it, and it is a point to be hereafter decided whether excision may not almost always be so substituted when the wound is made by a musket-ball, and the popliteal artery and nerve are not injured.
88. Compound fractures of the patella, without injury to the other bones, admit of delay, provided the bone be not much splintered. If the ball should have pierced the center of the patella, and passed out nearly in an opposite direction behind, the limb will not be saved. If the ball have struck the patella on its edge, and gone through it transversely, opening into the joint, it will very rarely be saved; but if it be merely fractured, there is hope under the most rigorous antiphlogistic treatment, and delay is proper. A ball will occasionally penetrate the capsular ligament, and lodge in the knee-joint, with little injury to the bones. If it cannot be extracted without opening extensively into the cavity of the joint, and the extraction of the ball is absolutely necessary, amputation or excision had better be performed at first, for it will be ultimately necessary. The condyles of the femur and the lower part of the bone being spongy, a ball may pass through them or between them, and fall into the knee-joint, or it may make a prominence on the side of the patella, without passing out, or immediately interrupting the motion of the leg, for the soldier may walk some distance afterward. The popliteal artery may also be divided in addition, and either of these cases will render amputation necessary, for the ball must be taken out on the fore part, and the general inflammation of the joint will either destroy the patient in a short time, or, after much distress and hazard, leave him no alternative but amputation. If a ball lodge in the condyles of the femur within the capsular ligament, and cannot be easily extracted, excision or amputation is advisable; for the limb, if preserved, will not be a useful one. If the ball, on the other hand, lodge without the capsular ligament, and cannot readily be extracted, the wound should be healed as soon as possible; and, although it may cause some little inconvenience to the knee-joint, the limb and life of the patient may be [96] saved, as I have seen in many instances, when a continuance of persevering efforts to extract the ball would have exposed both to great danger. Many cases of wounds in the knee-joint, in which the capsular ligament has been wounded, and the articulation opened into without injury to the bones, do well, such as simple incised wounds made with a clean cutting instrument. The success attending all wounds of the knee-joint depends entirely upon absolute rest, upon the antiphlogistic mode of treatment being rigidly enforced, on the healthy state of the atmosphere, and on the locality being free from endemic disease. The limb is to be placed in the straight position, a splint to be put beneath it, in order to prevent any motion, and cold or iced water to be applied, especially in summer, to diminish the increasing heat. General bleeding may be had recourse to in sufficient quantity to keep all general inflammatory action in due bounds; but it is on local blood-letting that the surgeon must principally rely for the prevention of inflammation. Cupping can sometimes be performed with marked effect; but leeches are more serviceable when they can be procured in sufficient numbers; from twenty to forty, or more, may be applied at a time; whenever the sensation of heat is felt, and is accompanied by pain, they should be repeated until these symptoms subside. The necessity for the local abstraction of blood is so great that it should never be lost sight of for a moment; for if suppuration take place throughout the cavity of the joint, it is followed, in most instances, by ulceration of the cartilages and caries of the bones. By local and general bleeding, the application of cold, rigid abstinence, and the straight position, a recovery may sometimes be effected; but wounds of the knee-joint, however simple, should always be considered as of a very dangerous nature, infinitely more so than those of the shoulder, the elbow, or the ankle. When a poultice is applied to a gunshot wound of this kind, I consider it the precursor of amputation. Col. Donnellan, of the 48th Regiment, was wounded, at the battle of Talavera, in the knee-joint, by a musket-ball, which gave him so little uneasiness that he could scarcely be persuaded to proceed to the rear. At a little distance from the fire of the enemy, we talked over the affairs of the moment, when, tossing his leg about on his saddle, he declared he felt no inconvenience from the wound, and would go back, as he saw his corps was very much exposed. After he had stayed [97] with me a couple of hours, I persuaded him to go into the town. This injury, although at first to all appearance so trifling, proceeded so rapidly as to prevent any relief at last being obtained from amputation, and caused his death in a few days.
89. Excision of the knee-joint is an operation formerly attended with so little success that it has been but rarely performed until lately. The result will, in all probability, be more favorable in cases of injury from musket-balls, in which the femur and tibia have both been much injured, without so much mischief being inflicted on the soft parts as would have rendered amputation necessary. In such cases, provided every accommodation, and particularly absolute rest and good air, can be obtained for the sufferer, excision should be attempted, in preference to the amputation recommended in 84 and 85. Some cases of success have lately been published by Mr. Jones, of the island of Jersey; some by Mr. Syme, Mr. Mackenzie, Dr. Gurdon Buck, Mr. Fergusson, and others. Mr. Jones’s method of operating is here transcribed, as sent to me by himself:—
“In my first case, the incisions were in this form H, two lateral, one along each side of the joint, and a transverse one immediately over the middle of the patella. The flaps were then dissected upward and downward, the patella removed—and I do not see that any advantage can be gained by keeping it, even if not diseased—the crucial and lateral ligaments were then divided, and the joint completely opened. The leg was afterward bent backward on the thigh, and the diseased portion of the femur was cleared, and removed with an ordinary amputating saw. The same method was followed with the tibia: the bones were then placed in juxtaposition, the flaps brought together by means of a few stitches, and the limb placed in a species of fracture-box. Water-dressing was applied. In the second case, I followed very nearly the same plan, with the exception of my first incisions, which were made something in a horseshoe shape. In the third case, I removed a considerable portion of integument, and, I conceive, with marked advantage. In the two former cases, I think the cure was protracted by preserving all the diseased external parts.”
Dr. Gurdon Buck, of the United States of America, in a case of anchylosis, with deformity, after a gunshot wound, removed the knee-joint by a transverse incision from one [98] condyle to the other across the lower margin of the patella. A longitudinal incision intersected this, extending four inches above and below it. The flaps being dissected up, the joint was opened into by an incision across the ligamentum patellæ at the inferior edge of the bone, and also across the lateral ligaments. The adhesions of the articular surfaces were broken up by forced flexion very gradually applied. A slice was then removed with the common amputating saw from the surface of the condyles of the femur, including the pulley-like surface, care being taken to make this section on a plane parallel with the surfaces of support upon which the condyles rest, when the body is erect. The articular surface of the tibia was next removed on a level with the upper extremity of the fibula, after the insertions of the capsular ligament had been dissected up from the posterior half of the circumference of the head of the bone. The broad, fresh-cut bony surfaces, which were very vascular and healthy, admitted of accurate coaptation without stretching the tendons and other parts in the ham. To secure them in close contact, and prevent displacement, a flexible iron wire was passed through both bones on either side, and the two ends twisted and left out between the flaps of skin. The patella, being disorganized and softened, was removed, except the superior margin, which affords insertion to the quadriceps muscle. The flaps of integument having been trimmed, were brought together by sutures and adhesive plaster, and the limb placed in a fracture-box. The constitutional fever was moderate, and disappeared in a fortnight. Suppuration never exceeded half an ounce daily. At the end of five weeks and a half the wires became loose, and were removed. No exfoliation followed. At the end of nine weeks the wound had entirely healed, and the limb could be raised bodily from the bed. There is no mobility between the bones; the difference in the length of the limb, as compared with the other, is one inch and a half, which permits the foot to clear the surface of the ground, which cannot be done when the limb is of the same length as the other.
Mr. Jones, since the publication of his original cases, has in a subsequent one not only preserved the patella, but even the ligamentum patellæ, which he considers to be a great improvement when it can be effected; he operated in the following manner: A longitudinal incision down to the bone, four inches in extent, was made on each side of the[99] knee-joint, midway between the vasti and the flexors of the leg. These two cuts were then connected by a transverse one just over the prominence of the tubercle of the tibia, care being taken not to cut the ligamentum patellæ. The flap was turned upward; the patella and its ligament were freed, drawn over the internal condyle, and kept there by means of a broad, flat, and turned-up spatula. The joint was thus exposed, the synovial capsule was divided as far as could be seen, when the leg was forcibly bent, the crucial ligaments, almost breaking in the act, only required a slight touch of the knife to divide them completely. The articular surfaces of the bones were now completely brought into view, when the diseased portions were removed by suitable saws, the soft parts being kept aside by assistants; the external condyle had been hollowed out by a large abscess, so that it was necessary to saw off (obliquely) another portion of the carious bone, and to gouge out the remainder, until the healthy cancellous structure was reached. The articular surface of the patella had also to be gouged until sound bone was attained. The bones were brought into apposition, and the patella and its ligament replaced, as nearly as possible; at the end of seven weeks the patient, twelve years old, was able to turn the limb from side to side, and ultimately recovered.
This little boy I saw walking firmly on his leg, an admirable instance of conservative surgery. It is, nevertheless, an operation which ought not to be done on the field of battle, unless perfect quiescence and every desired accommodation can be obtained, and no endemic disease prevail.
90. Amputation of the leg is performed in two ways—by the circular incision and by two flaps, the circular incision being only applicable to the calf. In either way the stump should, if possible, be seven inches long, for the more convenient application of an artificial leg, which is now made with a socket to fit the stump, instead of resting against the bent knee, unless the stump be too short for its proper adaptation otherwise.
The operation by the circular incision is performed by necessity in the thick part of the leg, and the bone is usually sawn through about four inches from the patella, so that, when the stump has healed, there may be sufficient length of bone left to support with steadiness the weight of the body on the knee, and that greater facility may be given to[100] the motion of the leg, from the preservation of the insertion of the flexor tendons. The most eligible place for the application of the tourniquet, when used, is about one-third of the length of the thigh from the knee, on the inside, where the artery perforates the tendon of the triceps muscle, and where it can be most conveniently compressed against the bone by a small firm pad, the instrument being on the outside, or opposite the pad; or the compress may be placed between the hamstring tendons, a little distance from the hollow behind the joint, the instrument itself being on the fore part of the thigh. In this method the pad must be thicker, and the compression is more painful, and not more secure. The surgeon should stand on the inside of the leg to be operated upon, that he may more readily saw the fibula at the same time as the tibia, by which the chance of splintering the fibula is diminished; for this bone is held much more steadily under the saw when the tibia is undivided, whatever pains may otherwise be taken by the assistants to secure it. The limb should be a little bent, and the circular incision made with the smaller amputating knife through the skin and integuments to the bone on the fore part, and to the muscles on the outside and back part; and as the attachment of the skin to the bone will not readily allow its retraction, it must be dissected back all round, and separated from the fascia, the division of which in the first incision would avail nothing, from its strong attachments to the parts beneath. The muscles are then to be cut through, nearly on a level with the first incision, down to the bones. The interosseous ligament between the tibia and fibula is to be divided with the catlin; and as several of the muscles cannot retract in consequence of their attachment to the bones, they are to be separated with the knife; in the same manner the inter-muscular septa, or expansions running between them, are to be divided, as they would else prevent their retraction. The retractor with three slips is now to be put on, the center slip running between the bones, by which the soft parts may be pulled back to a sufficient distance, any adhering part being divided by the point of the knife. The bones are to be sawn through with the usual precautions, and the retractor removed, when the three principal arteries should be secured: the anterior tibial, on the fore part of the interosseous ligament, between the tibia and fibula; the peroneal artery behind the fibula; and the[101] posterior tibial near it, more inward and behind the tibia; this artery will frequently, however, contract very much, and will only show itself on the compression being taken off the artery above. It in general causes more trouble to secure it than the others, and I have two or three times seen, even in London hospitals, the needle dipped round it in despair, when merely pulling out the artery with the tenaculum, and dissecting a little round it, would have shown the small retracted bleeding vessels arising from it, and have prevented, in all probability, a secondary hemorrhage. The tourniquet, if used, being removed, the smaller vessels tied, and the stump sponged with cold water and dried, the integuments and muscles should be brought forward as much as possible, and the strips of adhesive plaster applied from side to side—that is, the wound is to be closed vertically or nearly so, that the strips of plaster may not in any way press upon the fore part of the tibia, by which its protrusion will be avoided, an occurrence which almost invariably follows when the line of approximation is horizontal and the strips of plaster press upon the bone. If the spine of the tibia be sharp, it should be removed by the saw, whether the operation be done by the circular incision or by the use of flaps.
91. The flap operation, as performed by Mr. Luke, differs from that of the thigh in some particulars. There is a greater variety in the proportion which the soft parts in the posterior flap bear to those in the anterior, and the distance from the bones at which the limb is transfixed in the first step of the operation is subject to such variety that, when the calf is large, the mid-point for the introduction of the knife lies at some distance from the posterior aspect of the bones; in a small calf, it is close to it. The course of the knife through the limb is oblique instead of transverse, for the purpose of accommodating the line of incision to the plane of the two bones. The anterior flap is formed in the same way as in the thigh amputation, but it has proportionately more integuments and is thinner; yet its base and length are rendered equal to the base and length of the posterior flap, and may be adjusted evenly with it when the stump is dressed. In the circular division of the remaining soft parts, after the formation of the flaps, there is a necessary variation in the proceedings, from the circumstance of there being two bones united by interosseous membrane. It may, however, be accomplished by sweeping the knife[102] around the more distant bone of the two, its point being afterward carried between the bones through the interosseous membrane. While the knife is between the bones, its edge may be so turned that the membrane may be divided longitudinally to any convenient extent for the easy introduction of a retractor, and the soft parts around the bone nearest to the operator may subsequently be divided by a sweep of the knife in a manner similar to that adopted for the division of parts around the more distant bone. The sawing of the bones and dressing of the stump are accomplished as in the thigh amputation; but more care is required to avoid pressure on the acute margin of the tibia, (which, when very sharp, should be removed,) and to prevent the pendulous state of the flaps.
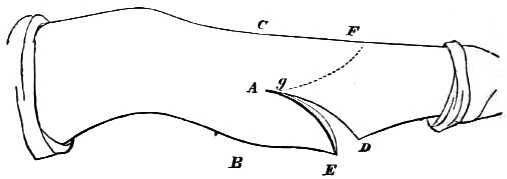
A. The mid-point between B and C, at which the knife is introduced for carrying it across the limb.
A to D. The course of the incision to form the posterior flap, E.
F to g. The course of the incision to form the anterior flap.
When the nature of the injury renders amputation necessary at or immediately below the tuberosity of the tibia, the operation may be done with safety. Baron Larrey recommended the removal of the head of the fibula in such cases; I have done it with impunity, and thereby made a better stump than if it had not been done; but as the articulating surface of the head of the fibula does sometimes enter into the composition of the knee-joint, and as this cannot be known beforehand, the removal of this portion of the fibula is not advisable, neither must the tibia be sawn through above the tuberosity lest the capsular ligament be implicated. As an operation by which the knee-joint is saved, it is important; for although the stump is very short, it forms a solid support for the body, enables the patient to walk without the aid of a stick, and admits of the adaptation of an artificial leg. The skin, in these cases, must be saved in every direction by flaps, to form a covering. When in [103] sufficient quantity, the operation may be done by the circular incision, as much muscle as possible being saved to aid in forming a covering on the under and outer sides. The posterior tibial artery will be found to have retracted behind the head of the bone, whence it, or others which may bleed, must be drawn out. The nerves should be cut as short as possible.
92. This operation should be performed in the following manner: Begin the incision behind the external malleolus, an inch and a half above its lower extremity, and carry it downward and then forward across the front of the ankle-joint, then under the internal malleolus and upward, close behind this process, to the extent of an inch and a half; this incision should merely divide the skin, and should not, on any account, wound the subjacent parts. Raise the flap thus made, and, placing the leg on its inside, detach and turn aside the peronei tendons from the groove behind the external malleolus. Cut through the external lateral ligaments of the ankle-joint, keeping the knife close to the end of the fibula; then, with the large bone-scissors or nippers, cut through the fibula from one-half to three-quarters of an inch above its junction with the tibia, and, after dividing the ligamentous fibers connecting the two bones, remove the malleolus externus. Turn the leg on to its outer side, and cut through the internal lateral ligament close to the tibia, to avoid wounding the posterior tibial artery; this will allow the foot to be dislocated outward, and the lower end of the tibia to be brought well out through the wound. An assistant keeping the foot and tendons out of the way, the lower end of the tibia is to be removed by a fine saw to the same extent as the fibula, or as high as the injury or [104] disease requires. The articulating surface, or injured part of the astragalus, is then to be removed, after which the foot is to be returned to its proper position, and the cut surfaces of the tibia and astragalus brought into close approximation, and so kept by suture, strapping, and bandage. The limb is to be placed on an outside leg-splint, having a foot-piece to it; and in order to prevent any matter oozing, an opening should be maintained on the outside of the joint, with a corresponding hole in the dressing and splint for this purpose, until the recovery is completed. The shot-hole will sometimes answer the purpose, when the injury is inflicted by a musket-ball. There are no vessels to tie, unless wounded accidentally.
93. If this bone should be much shattered, and the injury nearly confined to it alone, it may be removed in the following manner: Make a semilunar incision down to the bone from the posterior angle of the inner malleolus, across the sole of the foot to the external malleolus, the convexity of the flap being forward. This flap being turned back, the tendo Achillis is brought into view, and is to be separated from its attachment or cut across above it. The point of junction between the calcis and astragalus having been ascertained, the ligamentous fibers are to be cut through and the joint between them opened, when the knife is to be carried from behind forward, in order to divide the interosseous ligament between them. Some ligamentous fibers passing between the calcis and cuboid bones are then to be cut through, when the os calcis may be dissected out without difficulty. The posterior tibial artery and nerve will be divided.
This bone was first removed for disease of its substance by Mr. Hancock, and the operation has been done several times since by Mr. Greenhow and others with success.
94. When the bones of the leg are not injured, although those of the tarsus are so far destroyed as to render amputation necessary, the operation introduced by Mr. Syme for removing the foot at the ankle-joint will be well adapted for this injury, provided the soft parts have not been so much destroyed as to prevent the formation of the covering flap or flaps. His directions are:—
[105] “Pressure should be made on the tibial arteries by the finger of an assistant or a tourniquet applied above the ankle. The only instruments required are a knife, the blade of which should not exceed four inches in length, and a saw. The foot being held at a right angle to the leg, the point of the knife is introduced immediately below the malleolar projection of the fibula, rather nearer its posterior than anterior edge, and then carried straight across the bone to the inner side of the ankle, where it terminates at the point exactly opposite its commencement. The extremities of the incision thus formed are then joined by another passing in front of the joint.

“The operator next proceeds to detach the flap from the foot bone, and for this purpose, having placed the fingers of his left hand over the prominence of the os calcis, and inserted the point of his thumb between the edges of the plantar incision, guides the knife between the bone and nail of the thumb, taking great care to cut parallel with the bone and to avoid scoring or laceration of the integuments. He then opens the joint in front, carries his knife outward and downward on each side of the astragalus so as to divide the lateral ligaments, and thus completes the disarticulation. Lastly, the knife is carried round the extremities of the tibia and fibula so as to afford room for applying the saw, by means of which the articular projections are removed, together [106] with the thin connecting slice of bone covered by cartilage. The vessels being then tied, and the edges of the wound stitched together, a piece of wet lint is applied lightly over the stump, without any bandage, so as to avoid the risk of undue pressure in the event of the cavity becoming distended with blood, which would be apt to occasion sloughing of the flap. When recovery is completed, the stump has a bulbous form, from the thick cushion of dense textures that cover the heel, and readily admits of being fitted with a boot.
“The advantages which I originally anticipated from this operation were—first, the formation of a more useful support for the body than could be obtained from any form of amputation of the leg; and, secondly, the diminution of risk to the patient’s life, from the smaller amount of mutilation, the cutting of arterial branches instead of trunks, the leaving entire the medullary hollow and membrane, and the exposure of cancellated bone, which is not liable to exfoliate like the dense osseous substance of the shaft. From my own experience, amounting to upwards of fifty cases, and that of many other practitioners who have adopted amputation at the ankle, I now feel warranted to state that these favorable expectations have been fully realized, and that, in addition to its other advantages, this operation may be regarded as almost entirely free from danger to life.”
This operation has not answered, in some of the hospitals in London, the expectations entertained of it from its success in Edinburgh, the flap formed from the under part, or heel, having frequently sloughed. This, Mr. Syme declares, is the fault of the operators, and not of the operation, sufficient attention not having been paid to make the flap of a proper length, and no more, and to preserve the posterior tibial artery intact, until it has divided into its plantar branches. He insists, with reason, that the operation should be done exactly as he has described it in the following explanation:—
“A transverse incision should be carried across the sole of the foot, from the tip of the external malleolus, or a little posterior to it, (rather nearer the posterior than the anterior margin of the bone,) to the opposite point on the inner side, which will be rather below the tip of the internal malleolus, but can be readily determined by placing the thumb and finger at opposite sides of the heel. If the incision be car[107]ried farther forward, a considerable inconvenience is experienced from the greater length of the flap; and I believe a great deal of the difficulty that has been attributed to the operation has arisen from this source—the operator getting into the hollow of the os calcis, cuts and haggles, in striving to clear the prominence of the bone, with the desperate energy of an unfortunate mariner embayed on a lee shore in a gale of wind. Another incision is then to be carried across the instep, joining the ends of the former. The next point to be attended to is, that in separating the flap of skin from the os calcis you must cut parallel to the bone. This is of the greatest importance, since when the flap is detached from the bone, its only supply of nourishment must be the branches which run through it parallel to the surface; and if, instead of keeping parallel to the surface, you cut on the flap as a butcher does when he skins a sheep—you will, by scoring it in this way, necessarily cut across these branches. I have reason to believe—nay, to know—that the sloughing which has occurred in some cases has been due to these defects in the performance of the operation; the flap having been cut too long, difficulty has been experienced in separating it from the calcaneum, and this has led to the scoring of the flap, which has been inevitably followed by death of a portion or the whole of it.”
Domestic surgery, or that of civil life, has in these operations of excision of the ankle-joint, and of amputation at that part, repaid her Amazonian sister of military warfare for the improvements she has introduced into the great art and science of surgery; and a degree of generous emulation will be excited and maintained between them, which, it may be hoped, will, during the present war in the East, add much to its scientific and preservative character.
95. A musket-ball will seldom pass through the foot without injuring a joint of some kind, or wounding a tendon or nerve; and the injury to the fascia, which is very strong on the sole of the foot, and frequently covered by much thickened integument, is always attended with inconvenience. The extraction of balls, of splinters of bone, of pieces of cloth, and the discharge of matter become more difficult, and often cause so much disease as ultimately to render amputation of the foot necessary. Tetanus is a frequent consequence of these injuries, and is a disease, in its acute form, certainly irremediable by any operation or medicine at pres[108]ent known. Amputation has always failed in my hands, although it was strongly recommended by Baron Larrey. The operative surgery of the foot should be done as soon after the injury as it can be conveniently accomplished; for a large, clean, incised wound is a safe one, compared with a torn surface of much less extent, and a splintered bone with extraneous substances; as a ball lodged in the foot is always very dangerous, great attention should be paid in the examination of even slight wounds. A cannon-shot can seldom strike the foot without destroying it altogether; it may, however, strike the heel and destroy a considerable part of the os calcis, without rendering amputation necessary, if the ankle-joint be untouched; for by due attention in removing the spicula of bone at first, and by making free openings for the discharge of matter in every direction in which it may appear inclined to insinuate itself, the limb may be preserved in a useful state.
The following case, from the surgeon of the 44th Regiment, in the Crimea, is an instance of the removal of the foot after the manner recommended by the late M. Roux, every effort having previously been made to save it: “Chloroform having been administered, an incision was commenced immediately in front of and below the internal malleolus; this was carried downward and forward until it reached the center of the sole of the foot. From the extremity of this a second incision was made nearly at right angles, extending backward along the sole and upward over the attachment of the tendo Achillis to the os calcis. A third incision was carried from this round and below the external malleolus to meet the first at its commencement. Disarticulation of the ankle-joint was made from the outside, the soft parts put well on the stretch by forcibly depressing the foot, when, by successive sweeps of the scalpel, care being taken to keep the edge close to the bone, the os calcis was separated from its connection with the soft parts. The plantar arteries were divided at the very extremity of the flap. The operation was completed by sawing off the two malleoli and the thin scale of the articulating surface of the tibia. The anterior tibial and the two plantar arteries each required a ligature. Sutures were inserted, and the flap supported by strips of wet lint. The operation was performed on the 4th of July. The stump was dressed the second day after the operation. There had been no hemorrhage; the flap was partially ad[109]herent; on the outer side the skin was red, tense, and shining; the sutures were very tight; they were removed from this part; no appearance of sloughing.
“July 26th.—The ligatures came away upon the sixth day; no sloughing of the flap occurred; a small abscess formed both on the outside and inside of the leg, just where the malleoli were sawn off. These were opened; the redness of the skin rapidly disappeared after this. The line of incision is now entirely healed at the outer part; the inner is not so far advanced, but is doing well. The flap is becoming a firm, round cushion; and the pressure, when he walks, will fall upon the skin taken from the sole of the foot. The advantages which this operation appears to possess are, that the flap is not so large and baggy as in the early stage after Syme’s amputation; it is performed with greater facility and rapidity, and there is less chance of wounding the posterior tibial artery.”
The accompanying sketch is of the astragalus and calcis of the right foot, with a ball lodged on the inside, where it joins the smaller apophysis of the os calcis. The round spot (No. 3) represents the ball, and the tendons of the anterior tibial and of the common flexor muscles of the toes must have been divided by it; the proper flexor of the great toe is at some little distance below, and unhurt; the posterior tibial nerve and the artery, about to divide into the two plantars, are still farther distant. In this case the ball might and ought to have been removed by the gouge, the small chisel, the screw, or other instrument supplied for this purpose, as soon as possible after the injury. Nothing was done, however; inflammation and ulceration extended into the ankle-joint, and the amputation of the foot by the flap operation at the joint was performed and failed. The leg became affected; and the case ended in amputation of the thigh, from which the man recovered, and was sent to England. I know not his name, nor the regiment he belonged to, nor the surgeon who attended him, nor any more of the case, as the bone only has been sent to me from Scutari as a personal attention.
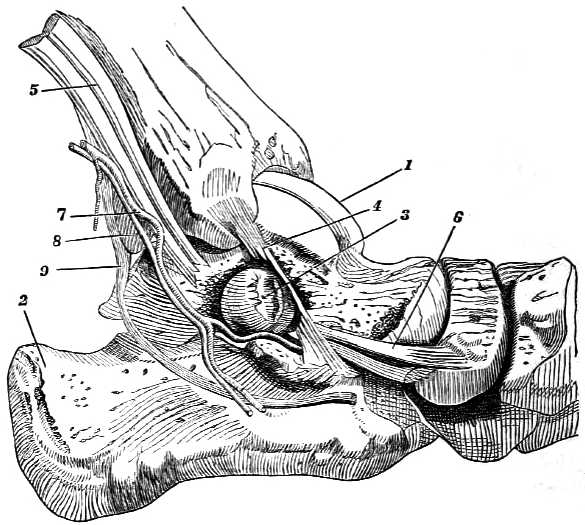
1. Astragalus.
2. Os calcis.
3. The ball.
4. Ligament descending from the tibia, torn by the ball.
5. Tendons of tibialis anticus and flexor communis cut across by the ball.
6. The other end of the same tendons.
7. The posterior tibial artery dividing into two branches.
8. The posterior tibial nerve.
9. The tendon of the flexor proprius pollicis.
If the ball had entered to a greater depth, the proper operation would have been to remove the bone altogether, which is a difficult and disagreeable operation, even when done in cases in which this bone has been dislocated, and is projecting under the skin. It is much more so when in its [110] proper place; less so when the ends of the tibia and fibula are also removed for disease of these parts, in which case, the bone being softened, it yields readily to the scissors, by which it should be divided, and to which it opposes, when sound, a great resistance from its solidity. The removal of the astragalus alone has been successfully performed for disease in children, in two instances, by Mr. Statham, of University College Hospital, and has been strongly recommended by Dr. Buchanan, of Glasgow, and others. The operation, according to Mr. Statham’s method, is to be done as follows: An incision, four and a half inches long, is to be commenced within the anterior edge of the fibula, and carried down in a straight line beyond the anterior end of the metatarsal bone of the little toe; a second incision, about an inch in length, should then be made from the center of the wound downward [111] toward the sole of the foot, for the purpose of giving room. The integuments are then to be raised from the bone, from the upper edge of the first incision, carrying with them the extensor tendons toward the inside of the foot, to give more room for ulterior proceedings, without injuring them. The under joint of a pair of short, strong scissors, such as are supplied in the capital cases of instruments, ought then to be pushed under the neck of the astragalus, at the hollow, where it is attached by a strong interosseous ligament to the os calcis. The upper blade being then closed upon the bone, it may be divided, but not without considerable force. The articulating end of the astragalus with the os naviculare can then be easily removed by a strong pair of forceps, its ligamentous attachments being first divided by the knife. In order to extract the remaining portion of bone, the under blade of the strong scissors must be again pushed under it from before backward, and made to cut it in two. The outer part being now separated from the internal end of the fibula, care being taken not to injure the perpendicular ligament going from that bone to the os calcis, this piece should be forcibly removed by strong forceps—an operation which could not be easily borne unless chloroform were used. The remaining piece or pieces must follow, when an examination should be made by the finger to ascertain that none remain. The parts should be brought together, a little lint and cold water applied, the limb placed on a splint, and interfered with afterward as little as possible. The wood-cut represents the forceps for extracting a ball imbedded in the astragalus.
Many years have elapsed since I stated that muscles might be cut across without, or with very little, inconvenience resulting from their division. Mr. Stanley has lately shown that tendons even may be cut across with little disability [112] following, in a boy who had suffered an injury to the wrist; inflammation followed, with disease of the bones; and Mr. Stanley, instead of amputating the hand, made a flap on the back of it through the tendons. He removed seven of the small bones—all, indeed, except the trapezium supporting the thumb. The tendons reunited, and the boy has a remarkably good motion of the hand and fingers—proving the propriety of an operation which does so much credit to Mr. Stanley.
The astragalus may be also removed by a similar flap operation dividing the extensor tendons of the toes, commencing on the outside of the fibula, and being carried round in front, but not so far as to injure the tibialis anticus tendon, nor the anterior tibial artery and nerve; or, when the incision reaches the edge of the outer extensor, the whole of them are to be separated from the parts beneath, and drawn inward, when the operation of removing the bone is to be completed, as in the former instance. But many surgeons believe that when tendons are forcibly drawn aside, after being separated from their attachments, they are apt to slough, and that their division would, in most cases, be less injurious. In neither operation need tendon, artery, vein, or nerve of any importance be divided.
It may perhaps be stated that less regard is paid generally to gunshot wounds of the foot in which balls lodge than is desirable; and that other methods of operating may be devised for removing the astragalus less difficult in their performance, and more advantageous for the sufferers. The other bones of the instep and foot should be treated in a similar manner when balls lodge in them. Their removal may be more readily effected.
96. Wounds from cannon-shot injuring the fore part of the foot are better remedied by amputation at the joints of the tarsus with the metatarsus, than by sawing these bones across; but when the injury affects only one or two toes, they may be removed separately, recollecting that it is of greater importance to preserve the great toe than any other, and that this toe is worth preserving alone, when any one of the others would be rather troublesome than useful. Musket-balls seldom commit so much injury as to require amputation as a primary operation, although they may frequently render it necessary as a secondary one. The splinters of bone are to be removed, the ball and extraneous [113] substances are, if possible, to be taken out; and if the bones, tendons, and blood-vessels are so much injured as to render the attempt to preserve them useless, amputation is to be performed. If the preservation of the limb be thought practicable—and it generally will be so in wounds from musket-balls—the attempt must be made under the most rigid antiphlogistic treatment, the local application of leeches and cold water from the first, with free openings for the subsequent discharge. Musket-balls seldom injure the metatarsal bones so as to require their removal with their toes, and under the treatment above mentioned these wounds will in general be healed without further operation. Wounds from grape-shot occasionally render the removal of the metatarsal bone of the great toe at the tarsus necessary, although much should be done to save it. The little and adjacent toes are also sometimes removed at the tarsus, the middle ones but seldom, as it is not an easy operation to perform, in consequence of the naturally close attachment of these bones, and the additional compactness they have acquired from the pressure of the shoe. Hemorrhage from the arteries of the foot authorizes amputation in a very slight degree, even when superadded to other causes; for the incisions necessary to secure the bleeding vessels will not, in general, add much to the original injury, unless they be very extensive; while, on the contrary, they render the wound less complicated and more manageable.
97. Amputation at the tarsus, when it is proposed to save the flap from the under part of the foot, is performed in the following manner: The joints of the metatarsus with the tarsus having been well ascertained, an incision is to be made across the foot, in the direction of the joints, but from half to three-quarters of an inch nearer the toes, and the integuments drawn back over the tarsus. From the extremities of this incision, two others are to be made along the sides of the great and little toes, for about two inches and a half, according to the thickness of the foot; the ends of these two incisions are to be united by a transverse one down to the bone, on the sole of the foot, the corners being rounded off. The flap thus formed on the under part is to be dissected back from the metatarsal bones, including as much of the muscular parts as possible, as far as the under part of the joints of the tarsus. The metatarsal bones are now to be removed by cutting into and dislocating each joint from [114] the side, commencing on the outside, by placing the edge of the knife immediately above, but close to the projection made by the posterior part of the metatarsal bone supporting the little toe, which prominence is always readily perceived. The arteries are to be secured, any long tendons and loose capsular ligament to be removed with the knife or scissors, and the under flap, formed from the sole of the foot, is to be raised up so as to make a neat stump when brought in contact with the upper portion of integuments that was first turned back; the whole to be retained in this position by sutures, adhesive plaster, and bandage. When the skin of the under part of the foot is much torn, which is not uncommon in a wound made by a fragment of a shell, the flap cannot be formed from it; in this case it must in a great measure be saved from the upper part; but the integuments being here so much thinner, the flap is not so good a defense against external violence, and will be more readily affected by cold. The metatarsal bones may be sawn across in a straight line, in preference to removing them at the joint; and although the whole may be sawn across at once with more ease than any one of them individually, except the outer ones, yet the stump is never so much protected from external violence as when the operation is performed at the joints of the tarsus.
98. Amputation of the foot, leaving the astragalus and calcis, may, in certain cases of injury anterior to these bones, be performed with advantage, care being taken to make the under flap so large that the line of cicatrization may be on the upper and anterior edge of the stump, rather than transversely across the face of it, in order to render it firmer, and better able to resist and sustain any pressure which may be applied to it.
The limb being placed on the table, and held by an assistant, the surgeon ascertains the situation of the joint formed by the junction of the astragalus with the scaphoides, which will be indicated by the prominence on the inside of the tarsus, discoverable by passing the finger forward from the malleolus internus toward the side of the great toe. The joint of the os cuboides with the os calcis on the outside is always to be found about half an inch behind the projection formed by the posterior part of the metatarsal bone of the little toe. The under part of the foot being firmly held in the palm of the surgeon’s hand, he places the point of the [115] thumb on the external joint, and that of the forefinger over the internal one; these indicate a transverse oblique line for the first incision, which should commence near the thumb, and be continued with a semilunar sweep, the convexity toward the toes, until it terminates at the side of the foot where the forefinger was placed. The joint between the astragalus and scaphoides is now to be opened, by directing the knife from within obliquely outward toward the projection of the metatarsal bone of the little toe. These bones are then to be dislocated by pressure, and the ligaments retaining them divided. The joint between the os cuboides and the os calcis is next to be opened from without inward, and the bones dislocated. The strong inter-articular ligament being cut, and the joint largely opened, the knife is to be passed between the under surfaces of the scaphoides and cuboides, and the soft parts adhering to them, and a flap cut from behind forward sufficiently large to cover the wound, which is then to be dressed in the usual manner.
99. Mr. Wakley, jun., has lately performed a successful operation for the removal of the astragalus and calcis, deserving of imitation in peculiar cases. It is done as follows:—
“The patient being under chloroform, the diseased foot (the left) having been drawn forward, so as to be free from the table, an incision was made from malleolus to malleolus, directly across the heel. A second incision was next carried along the edge of the sole, from the middle of the first to a point opposite the astragalo-scaphoid articulation, and another on the opposite side of the foot, from the vertical incision to the situation of the calcaneo-cuboid joint. These latter incisions enabled the operator to make a flap about two inches in length from the integument of the sole. In the next place a circular flap of integument was formed between the two malleoli posteriorly, the lower border of the flap reaching to the insertion of the tendo Achillis. This flap being turned upward, the tendon was cut through, and the os calcis, having been disarticulated from the astragalus and cuboid bones, was removed, together with the integument of the heel included between the two incisions. The lateral ligaments connecting the astragalus with the tibia and fibula were next divided, and the knife was carried into the joint on each side, extreme care being observed to avoid wounding the anterior tibial artery, which was in view. The [116] astragalus was then detached from the soft parts in front of the joint and from its articulation with the scaphoid bone, and the malleoli were removed with the bone-nippers. The only artery requiring ligature was the posterior tibial. Dur[117]ing the few minutes the operation lasted, the patient did not manifest the slightest symptoms of pain or uneasiness. On bringing the edges of the flaps together, they were found to fit with accuracy, and were secured by twelve interrupted sutures. The wounds were covered by several folds of lint, and supported by a light bandage. The patient, who had lost but very little blood, was then removed to his bed.

The incisions above described are here marked out on a healthy foot.
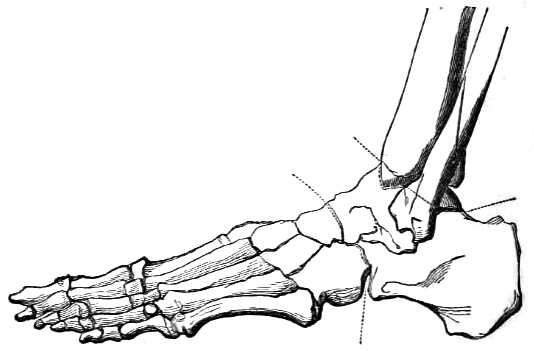
The skeleton of the foot will at the same time show the amount of bone removed.
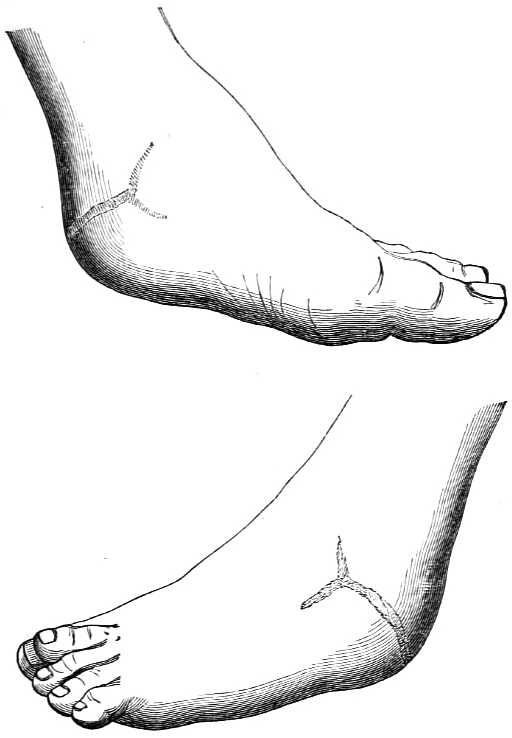
These drawings exhibit the present condition of both sides of the foot—the amount of deformity is less than might have been expected.
“On the 21st of February he was discharged the hospital, exactly two months after the operation, to go into the country, the foot being well, with the exception of a small open[118]ing. He came again up to town on the 15th of April, and has become stout. The sinus on the left side of the foot had closed, but a slight collection of matter had formed a little above the instep; this was discharged by means of a puncture with the lancet, and he was directed to return to the country, and dash cold water over the foot two or three times daily. On the 10th of June he returned to town to his employment. There was then not the vestige of a wound, the last opening having completely closed. He was ordered to wear a high-heeled boot. He is now a healthy-looking man, and walks very well.”
As the posterior tibial must be divided, the preservation of the anterior artery is essentially necessary; the success of the operation depends upon it. This artery, accompanied by its vein and nerve, lies close upon the astragalus; the artery may be said to be even attached to it, a point requiring the greatest attention in dissecting out the bone without injuring this vessel, which is seen under the scalpel.
100. Amputation of a single metatarsal bone, on the outside or inside of the foot, is to be done by an incision round the root of the toe, terminating in a line on the outside of the foot, which is continued down to the joint of the tarsus. The integuments are turned back above and below from the metatarsal bone, which is to be dissected out, with the toe attached to it, and the flaps brought together so as to leave but one line of incision. In military surgery, there is always a wound; and when the removal of the bone is necessary, it is in general an extensive one, with loss of substance, so that a covering cannot be saved in this way, especially on the upper part of the foot, when struck by a ball or piece of shell. The surgeon, therefore, must be prepared to look for his covering on the under part, where he will occasionally not be able to procure it in sufficient quantity, and it must not be forgotten that the neighboring parts will often be injured. The object must then be to save the integuments from such parts as are uninjured, so as to cover in the wound as nearly as possible when the bone has been removed. In doing this, the first incision should commence at the upper part and inside of the toe, and be carried round so as to separate the toe from its attachment to its fellow. If the injury be entirely on the upper part, the continuation of this incision must be so regulated as to form the whole of the flap from below, and its commencement above must be con[119]tinued round the injured part so as to meet the lower end near the articulation of the bone with the tarsus, and vice versa. If the ball have gone directly through, destroying the integuments above and below, the incisions must surround the injured part in such a manner, on the upper and under side of the foot, as to allow the flaps to be formed in every other part, except where the injury was inflicted, from which granulations must arise. By saving skin everywhere else, the wound will be much diminished in size, will heal sooner, will be less liable to suffer from external violence and less obnoxious to the subsequent pain which generally at intervals attends wounds of this kind.
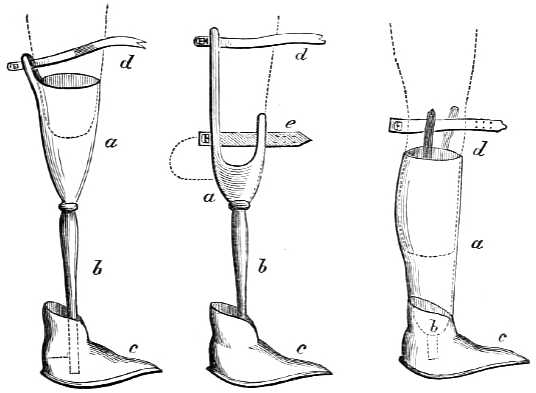
Amputation above Knee.
a, wooden bucket for stump;
b, pin to attach foot;
c, the rolling foot;
d, straps of attachment to body.
Amputation below Knee, No. 1.
a, wooden shape to receive knee;
b, pin;
c, rolling foot;
d, e, straps of attachment.
Amputation below Knee, No. 2.
a, wooden bucket to receive the whole of stump;
b, fixture to foot;
c, rolling foot;
d, straps for knee.
101. M. de Beaufoy has invented a foot for the wooden pin used by the soldiers in the Invalides, at Paris, who had suffered amputation above or below the knee; this, Mr. Bigg, of Leicester Square, has tried on some old soldiers at Chelsea Hospital; one of them reports that he has not only found[120] his step to be steadier, but that he could walk twice the distance in the same time that he could with his ordinary pin-leg.
The advantage of the invention is, that whereas a common wooden pin only gives one point of support, and consequently the body is obliged to raise itself so as to describe an arc, of which the end of the wooden pin is the center, the curved foot acts like a series of levers, each successive point of it being a fulcrum. The precaution should be taken to have the aperture at a, fig. 2, for the insertion of the pin, made square, to prevent its turning when in use.
PRIMARY AMPUTATION, ETC.
102. An upper extremity should not be amputated for almost any accident which can happen to it from musket-shot; and there is scarcely an injury of the soft parts likely to occur which would authorize amputation as a primary operation.
103. If the head or articulating extremity of the bone entering into the composition of the shoulder-joint be merely or slightly injured by musket-shot, the arm ought to be saved with some defect of motion in the joint. The wound should be enlarged in the first instance, to allow of a sufficient examination with the point of the finger, and any loose pieces of bone should be removed. Inflammation is to be restrained within due bounds until suppuration has been established, when, if a clear depending opening should not exist for the discharge of the matter poured out, it should be made, and any loose portions of bone removed. The principal points to attend to are, the prevention of sinuses around the joint, by the formation of dependent openings, position, perfect quietude, due support, the methodical application of bandages, and occasional mild stimulating injections into the wound. A simple incised wound penetrating the joint, and even injuring the bone, does not call for any immediate operation. An attempt should be made to effect a cure by the first intention, which can only be managed by means of proper position and support.
[121] 104. If the head of the bone be much splintered, or if a ball have gone through it, that portion should be sawn off; for a part thus injured has often been a source of great inconvenience and suffering for many years afterward—during, in fact, the remainder of the life of the sufferer; which misery would have been avoided by the excision of the head of the bone in the first instance—an operation which ought in fact to be done even at a later period, if it had not been performed at the time when the injury was received. Secondary operations of this kind are never so successful as primary ones, and great discrimination should be exercised in attempting to save the head of the bone, or, in other words, to avoid the operation for its removal.
105. When the splinters extend far into the shaft of the humerus, it may be proper to amputate the whole extremity, especially if the great artery be also wounded; but the shaft is seldom broken in such accidents to any great extent, and amputation should be confined almost to injuries from cannon-shot or shells, or heavy machinery, destructive of the soft parts as well as of the bone.
106. When the injury done to the upper arm is so extensive that it cannot be saved, although the head of the humerus be not injured, the amputation should take place immediately below the tuberosities, and not at the joint, which latter operation always renders the shoulder flatter, and the appearance of the person more unseemly, than when the head of the bone is left in its place.
107. It will frequently happen that the arm may be irrecoverably shattered, and the thorax partake in a less degree of the injury, there being apparent only some slight contusion or grazing of the skin; if low down, the elasticity of the false ribs may have prevented the integuments being much injured in appearance, although the blow has been violent; yet the force of the large shot may have ruptured the liver or spleen. If higher up, it may perhaps fracture the ribs, in addition to a more severe contusion of the integuments. When these accidents occur, the symptoms arising from the wound or contusion of the trunk of the body are to be first considered. If they do not indicate a speedy dissolution of the patient, or the prospect of such an event in two or three days, the operation ought to be performed, and a chance of recovery given to the sufferer, which he would not have, the arm being retained, and the injury of the chest[122] remaining the same. The danger to be apprehended in the more favorable cases is from inflammation, and this will be rather diminished than increased by the operation; the danger of deferring which is manifest and certain, while the injury committed in the thorax or abdomen is not ascertained, and its effects may be obviated. If the termination should be unfavorable, it can only be a matter of regret for the sake of the individual, and not for the non-performance of a duty. If the cavity of the chest be laid open, or several ribs beaten in, or a stuffing of the lungs take place from a large ruptured blood-vessel—all of which circumstances are obvious, and cannot be mistaken—the operation would, in all probability, be useless. A hemorrhage of short duration, or the expectoration of blood in moderate quantities, although a dangerous symptom, is not to be considered as depriving the patient of a reasonable chance for life, for it frequently follows blows from more common causes, from which many people recover. If the operation be delayed to ascertain what injury may have been done to the chest, from the symptoms that will follow, the danger resulting from both will be increased; and even when it has been ascertained that there is but little mischief existing in the thorax, the operation can no longer be performed with the same propriety, in consequence of the inflammation which has supervened; and the patient will probably die, when he would have recovered under a more decided mode of treatment.
108. A round shot or flat piece of shell may strike the arm, after rebounding from the ground, or when nearly exhausted in force, without breaking the skin, or only slightly doing it, yet all the parts within may be so much injured as not to be able to recover themselves: the bone may be considerably broken or splintered, the muscles and nerves greatly contused. The injury may not, perhaps, be quite so extensive. The bone may be merely fractured, and yet the soft parts will often be so much destroyed as not to be able to carry on their usual actions. A ruptured blood-vessel may, with an apparently slight external wound of this nature, pour out its blood between the muscles, and inject the arm to nearly double its size, all of which are causes rendering an operation necessary, and requiring decision, for inflammation will, and mortification may, ensue in a short time, when the most favorable moment for operation will have been lost.
109. Amputation at the shoulder-joint is an operation of[123] little surgical importance. The fear formerly entertained of loss of blood has passed away, and every surgeon now knows that if he should happen to cut the axillary artery unintentionally, it can be held between the forefinger and thumb, without difficulty or danger, until a ligature can be placed upon it. No accomplished surgeon of the present day should give himself the least concern about compressing the subclavian artery. It is, on the contrary, better, when the arm is raised from the side preparatory to entering or using the knife, that the surgeon should then feel the pulsation of the artery in the axilla, that he may the more easily avoid, and subsequently command it. The axillary artery does not throw out much blood at each pulsation, and a little pressure with the end of the forefinger will always prevent bleeding, until the surgeon is prepared to take hold of the vessel with the tenaculum or forceps. The operator should, in fact, divest himself of all fear of hemorrhage. When gentlemen are afraid, however, and cannot help it, (for Henry IV. of France, ce roy si vaillant, always felt an inconvenient intestinal motion when a fight began,) compression may be made upon the subclavian artery by the thumb of an assistant, the round handle of a key, or the padded end of the handle of a tourniquet; the latter forms the best pad, and is usually at hand.
110. The great point to be attended to in performing the operation is to save skin to cover the stump. The directions, therefore, which are usually given for doing it after any particular method can only be occasionally useful; for the surgeon may not always be able to select the parts to be divided or retained. In cases of malignant disease of the bone and periosteum of the middle of the arm, my experience directs the removal of the whole of the bone at the joint, and not the amputation below the head; although the appearance of the integuments, and of the bone itself, would seem to encourage the attempt to preserve the roundness of the shoulder. In such cases, the removal of the extremity at the joint may be done by any one of the many ways which have been recommended for its performance. In none should the acromion or coracoid process be exposed, unless previously injured. Neither is it necessary to lose time, or to give pain, by depriving the glenoid cavity of its cartilage; but it should always be borne in mind that if the nerves be not shortened after the removal of the arm, [124] they may be included in or adhere to the cicatrix, and cause, during a long life, much distressing pain to the sufferer.
111. Amputation at the shoulder-joint, performed immediately after the receipt of an injury, is now a very simple operation, for which simplicity English surgery is also indebted to the Peninsular war. As a secondary operation, or done at a later period, when the parts are all impacted together, it is less so. In both stages it is absolutely necessary to remember—1st. That, except in cases of disease, and not of injury, the shaft of the bone must be broken; and that all the directions usually given for rotation of the arm inward and outward during the operation are unnecessary cruelties not to be attempted, and rarely to be effected if attempted, with a broken bone. 2d. That the arm should always be raised from the side and supported by the hand of an assistant, who can feel, if he please, at any time of the operation, the pulsation of the axillary artery; and all operative methods are hereby condemned in which this precautionary measure is not the first step.
112. Operation by two flaps, external and internal.—The outer—beginning nearly an inch below the acromion process, the hair in the axilla having been previously removed—is to be carried down with a gentle curve so deeply as to divide the deltoid muscle, and to show the long head of the triceps at its under and outer edge. The second incision is to be carried in a similar direction on the inside, through the deltoid muscle, but need not divide the insertion of the pectoralis major, which should be exposed. These flaps being held back, the joint will be seen and readily opened into at its upper part, by cutting upon the head of the bone, in doing which the long tendon of the biceps will be divided, allowing the head of the humerus to drop from the glenoid cavity sufficiently to admit the forefinger of the left hand, on which the supra-spinatus, infra-spinatus, and teres minor may be cut through externally, as they go to be inserted into the great tuberosity, and the thick tendon of the sub-scapularis muscle internally, where it is attached to the smaller tuberosity. The head of the bone is then readily drawn out from the glenoid cavity, when the inner flap, including the axillary artery, vein, and nerves, may be taken hold of between the two forefingers and thumb of an assistant, while the surgeon, with one sweep of the knife, divides all the remaining parts below. The axillary [125] and the posterior circumflex arteries will have to be secured; the anterior circumflex, when arising from the posterior, is frequently cut off with it; the nerves are to be shortened; the flaps brought together by sutures; and an especial pad placed upon the pectoralis major, to prevent unnecessary retraction, if possible.
113. The operation by one, or nearly one upper flap, is to be performed when the under soft parts of the arm have been destroyed, and the bone broken. It may be done by thrusting a small, two-edged knife through the integuments and under the deltoid muscle, from side to side, to form a flap; or it may be made by commencing an incision an inch above the posterior fold of the armpit, and carrying it over the arm in a curved form, the convexity being downward, to the same height on the anterior fold; the lowest part of the incision being five fingers’ breadth from the point of the acromion, the posterior end or point of it being somewhat higher than the anterior one. The flap being turned up, and the tendon of the pectoralis major divided, the head of the bone is to be exposed and separated as before stated, as much as possible of the integuments being preserved on the under part of the arm. This will often be best done by dissecting out the head and broken pieces of bone, and then preserving in succession every piece of sound integument, before the artery, vein, and nerves are divided.
114. Lisfranc and many French and continental surgeons recommend the operation to be done with a pointed, double-edged knife, in the following manner: The arm being approximated to the trunk, in a state of half pronation, the point of the knife is to be entered at a small triangular space, which may be perceived on the inside of the fullness of the shoulder, bounded above by the scapular extremity of the clavicle and a small part of the acromion; on the inside, by the coracoid process; and on the outside, by the head of the humerus. The knife thus entered obliquely is to be passed across to the outside, opening in its passage into the joint, when, by sliding the knife forward over the head of the bone, while the deltoid is raised up by the operator or an assistant, a flap is to be formed, during which proceeding the arm is to be raised from the side, to facilitate its performance. If this flap be well made, the upper part of the capsular ligament, the tendons of the long head of the biceps, and the supra-spinatus are divided, and the tendons of the [126] infra-spinatus, teres minor, and sub-scapularis are also cut through in part, if not entirely. The upper and posterior flap is thus completed.
In the second step of the operation, the surgeon passes the knife behind the head of the humerus, and makes the under and anterior or inner flap, by cutting downward and inward, including in it a very small portion of the deltoid, the pectoralis major, latissimus dorsi, teres major, the triceps, coraco-brachialis, the short head of the biceps, and the vessels and nerves, when the limb is separated from the body. The flaps are nearly of the same size, and are to be brought together by sutures.
In the secondary operation, or that done several weeks after the receipt of the injury, in consequence of the attempt to save the arm having failed, it should be borne in mind that the soft parts will often be found so altered and impacted together that they will not yield or separate; and nothing is gained but by each cut of the knife, causing thereby some little delay, inconvenience, and loss of time.
115. Amputation of the arm immediately below the tuberosities of the humerus ought to be done in the following manner: The arm being raised from the side, and an assistant having compressed, or being ready to compress, the subclavian artery, the surgeon commences his incision one or two fingers’ breadth beneath the acromion process, and carries it to the inside of the arm, below the edge of the pectoral muscle, then under the arm to the outside, where it is to be met by another incision, begun at the same spot as the first, below the acromion process. The integuments, thus divided, are to be retracted, and the muscular parts cut through, until the bone is cleared as high as the tuberosities. The artery will be seen at the under part, and should be pulled out by a tenaculum or spring forceps, and secured as soon as divided. The bone is best sawn, the surgeon standing on the outside; the nerves should be cut short, and the flaps brought together by two or three silk or leaden sutures. There are few or no other vessels to tie, and the cure is completed in the usual time, while the rotundity of the shoulder is preserved. This operation is similar to that already recommended for the amputation at the joint, which in many cases it is intended to supersede.
116. Excision of the head of the humerus.—The point governing the modus operandi of this operation is, and [127] ought to be, the fact that, under the most favorable state of recovery which can take place, the shoulder-joint usually becomes so stiff that its ordinary motions may be considered to be lost. Operative processes which have for their principal object the sparing of the deltoid muscle are unnecessary, for, if spared, it is as useless as if it had been cut; and it seems to have been forgotten that, when cut, it reunites, and becomes nearly as strong as before it was injured. It is the joint that cannot be moved, not the muscle which has lost its power. I prefer, therefore, in doing this operation, in cases of some standing, to make a short crescentic flap by an incision across the anterior part of the shoulder, as in the operation of amputation, which, on being turned up, leaves the joint exposed. The edge of the knife being applied to the head of the bone in a line below, but immediately under the acromion process, divides the capsular ligament, and with it the long tendon of the biceps, on which the arm drops from the socket, or glenoid cavity, and allows the finger to be introduced, when the three muscles inserted into the great tuberosity may be cut through, and the sub-scapularis inserted into the small tuberosity will also be divided. The head of the bone is then readily brought out, and may be easily detached from any surrounding connections, and sawn off with little or almost no loss of blood. The elbow is to be supported, so as to bring the end of the sawn bone in apposition with the glenoid cavity. The flap may be allowed to unite with the parts below as soon as it will, the shot-holes, if any, being in general sufficient to allow of such discharge as may be necessary.
In cases of recent injury, considerable aid will be obtained in keeping the sawn end of the humerus in apposition with the glenoid cavity, by not dividing the long tendon of the biceps. This must be done by dissecting it out of its groove in the humerus, between the tuberosities, and by cutting through the capsular ligament vertically, so as to follow it up to its attachment to the upper edge of the glenoid cavity, when it may be easily drawn aside with a blunt hook, until the operation has been completed—a proceeding difficult of accomplishment in old cases of disease or injury, and in them not necessary nor advisable.
The accompanying sketch shows the head of the humerus of the right arm or side, with a ball lodged in it, a relic from Inkerman, sent to me as an especial mark of attention by [128] one of the medical officers at Scutari, but without the name of the man, the regiment he belonged to, or the surgeon who performed the operation for its removal. The following account was wrapped round the bone. It commences a day or two after the operation was done at Scutari, and shows that the man died from an affection of the lungs, not uncommon, as was first shown during the late war, after operations following extensive suppurations:—
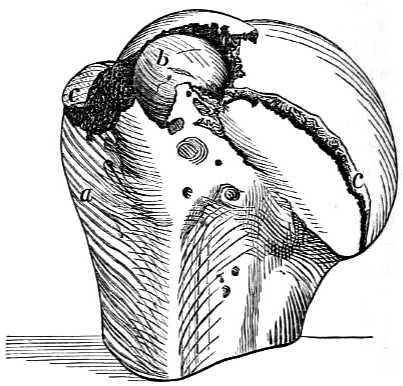
a. The head of the humerus sawn off below the tuberosities.
b. The ball.
c c. Fractures of the head of the bone.
“Pulse soft, 120. He passed a rather restless night, although he had another opiate at one A.M., and partially removed the dressings. In the morning he was better; he took some tea and a little wine with arrow-root, but was very much depressed in spirits. The wound looked well, there being less discharge, and of a more healthy character; no increased inflammation around the wound, but no tendency to union by the first intention on removal of the stitches. He was put upon farinaceous diet, with four ounces of wine and beef-tea. He continued to do well till the evening of the 16th, when he complained of tightness of the chest and slight cough. Harshness of respiratory murmur and increased vocal resonance, but no crepitation, could be detected on the right side on auscultation; he complained also of pain[129] in the hypogastrium and slight diarrhœa. At bedtime he had a sedative antimonial draught, after which he rested well, but perspired profusely. On being particularly questioned, he admitted that he had had diarrhœa several times since landing at Varna, and had had bloody stools after the battle of Alma, for which, however, he had never been off duty; he had also frequently been troubled with cough, and two of his family, he understood, died of consumption. For two days he continued to improve in spirits, to take his food better, and the wound assumed a healthy granulating appearance, but a very small portion of the end of the humerus appeared white, as if going to necrose. On the evening of the 18th his breathing was more oppressed, and his countenance flushed and anxious. On examination of the chest, the lower two-thirds of the right lung were dull on percussion; bronchial breathing in the lower half, with crepitation above; in the left lung loud sub-crepitus; diarrhœa had also supervened during the day, but was checked for the time by an opiate enema. From this date his strength gradually sank; the diarrhœa returned again and again, in spite of repeated opiate enemata and small doses of Dover’s powder with hyd. c. cretâ. The surface of the wound assumed a less healthy appearance; the respiration became more labored, and he gradually sank till Saturday, November the 25th, when he died at half-past ten A.M.
“On examination of the head of the bone, after its removal, there was found an irregular, rugged cavity in the cancellated tissue, about an inch long, by half an inch broad, extending nearly transversely from the smaller to the greater tuberosity, and above the latter a musket-ball was found deeply imbedded, its external convex surface being on a level with the articular cartilage. From this several small fissures radiated over the globular head, and from each end of the cavity a much deeper one extended round the anatomical neck, separating the articular portion of the bone, in two-thirds of its circumference, from the shaft.
“At the post-mortem examination, the surface of the wound looked black and sloughy near the seat of injury, but more healthy in the direction of the incisions. A small portion of the end of the humerus was of a pearly white, in progress of necrosing; but around the shaft, immediately below this, and in the glenoid cavity, the process of repair had commenced. Both lungs were found engorged with[130] frothy serum; the lower two-thirds of the right lung hepatized; traces of old tubercle in apices of both lungs, with miliary tubercle scattered throughout the whole substance of the left and upper part of the right. The whole tract of the colon, from the cæcum to the rectum, presented traces of ulceration, the ulcers being seldom larger than a split pea, with hardened, elevated edges; the bases in some instances were formed by the peritoneum only; generally they were scattered irregularly, but occasionally they were found in rows corresponding to the long diameter of the gut. In the rectum the ulceration was more extensive, in some parts the size of a farthing, the edges very irregular, and the direction more transverse.” These appearances precisely resemble those observed during the autopsy in cases of death from consumption, and are not therefore peculiar to the dysentery under which he had suffered.”
117. Professor B. Langenbeck, in order to save the deltoid muscle, proposed and practiced the operation in the following manner, during the Danish war in Sleswick-Holstein, with success in several instances: Begin the incision through the integuments and deltoid muscle immediately below the anterior border of the acromion, and continue it directly downward, over the minor tuberosity of the humerus, to the extent of four inches. Separate the parts, open the sheath of the long tendon of the biceps muscle, and draw out and hold it on one side with a blunt hook. Rotate the arm outward, (if it will rotate,) to facilitate the division of the tendon of the sub-scapularis; then rotate the arm inward, to aid in the division of the tendons of the supra-spinatus, infra-spinatus, and teres minor muscles, inserted into the great tuberosity. Complete the division of the capsular ligament, push the bone through from below, using the arm as a lever if you can, and saw it off. No arteries of consequence are wounded.
This operation would not be so easy of execution as is supposed, in cases in which the head and neck of the humerus are broken from the shaft; it would be very difficult of execution in old cases in which the soft parts are so hardened and impacted as to admit of little or no motion.
The extent to which the shaft of the humerus may be removed with the head cannot be distinctly defined. The greater the distance, the less will be the chance of the bone uniting to the glenoid cavity, in such a manner as to render[131] it a useful limb, whether by the formation of a ginglymoid joint, or by anchylosis. In the present state of our knowledge the bone should not be sawn lower than the insertion of the deltoid muscle. If the arm were preserved by an operation below that part, it is probable that the bone, however supported, would not become attached to the glenoid cavity. It might however become useful, by some artificial help, as has occurred in cases of false joint in the middle arm, after ununited fractures.
118. Excision of the head of the humerus is not to be done in every instance of compound fracture of that bone, as the following cases will show:—
Lieutenant Madden, 52d Regiment, was wounded at the assault of Badajos in 1812, by a musket-ball, which fractured the head of the humerus, and lodged in it. The broken pieces were from time to time removed by incisions, together with the ball, and he ultimately preserved a very serviceable arm. He is now a very zealous member of the Church of England.
Robert Masters, 40th Regiment, was wounded at the battle of Toulouse, on the 12th of April, 1814, by a musket-ball in the right shoulder, which lodged in the head of the bone. Shown to me a few days afterward as a case for amputation at the shoulder-joint, I directed the excision of the head of the bone as soon as the parts became more quiescent. Under venesection, purgatives, leeches, the constant application of cold, and low diet, the high inflammatory symptoms which had supervened subsided, and, six weeks after the accident, the ball, and part of the head of the humerus, were removed, after an incision had been made through the external parts for the purpose. Three mouths after the receipt of the injury, the man was sent to England, with no other inconvenience than that resulting from the loss of motion in the shoulder, which was stiff. The use of the forearm was preserved, and a limited one of the upper arm, by moving the shoulder-bone on the trunk.
Private Oxley, 23d Regiment, was wounded at the battle of Toulouse, in April, 1814, by a musket-ball, which entered at the anterior edge of the deltoid muscle, passed across the head of the humerus, injuring it in its course, and went out near the posterior edge of the muscle, through which, at its middle part, the deficiency in the rotundity of the head of the humerus could be distinctly felt. Shown to me a few[132] days afterward as a slight but peculiar wound, it was marked as a case for excision, if circumstances should render it necessary. No bad symptoms, however, supervened; the man only complained of the restraint put upon him, and the lowness of his diet. Some pieces of bone came away, or were removed, and in July he was sent to England, the wound being healed and free from pain; the shoulder stiff. The lower arm he used as before the accident.
General Lord Seaton suffered from a nearly similar wound, at the taking of Ciudad Rodrigo, and recovered with a good use of his arm.
These cases were fortunate in their results, but such do not always follow. Major C. was wounded in one of the battles in the Pyrenees, in 1813, by a musket-ball, which injured the head of the left humerus from side to side. Thirty years afterward the wounds still discharged, and gave him great uneasiness. A probe discovered much diseased bone. I advised the excision of the head of the bone, to which he would not assent. His courage had been broken by continued suffering.
Ensign Moore, of the Bengal army, was wounded at Sobraon, on the 10th February, 1846, by a musket-ball, which passed through the anterior and inner part of the deltoid muscle, one inch and a half below the inner part of the acromion process, struck and went through the head of the bone, which it splintered, and made its exit behind, in front of, but near the inferior angle of the scapula. He remained in camp three days, and was sent to hospital at Ferozapore, where he suffered much from inflammation, pain, etc., and after a month was sent to Subaltro in the Hills, where some pieces of bone came away, during which time he suffered severely, and was much weakened by it and the discharge. On the 20th October, 1846, he was removed to Bunda, in Bundeleund; here more bone came away, accompanied by much discharge. Thence he proceeded in April, 1847, to Juanpore, where he suffered three attacks of inflammation, two of them very severe; the constitutional disturbance was great. The posterior wound was reopened, and a large quantity of offensive matter discharged. On the 7th of August, 1847, the suppuration is stated to have been still great, and the strength very much reduced, on which account he was recommended to proceed to Europe. On the 9th June, 1848, the wounds were healed, the last piece of[133] bone having come away about ten days before. The pieces of bone are from the head and from the part adjoining. The head of the bone is greatly diminished in size, so much so as to appear to have been almost entirely removed; the joint is stiff, if not anchylosed, the shoulder flat, the under use of the arm perfect, that of the upper part dependent on the motion of the shoulder-blade. The removal of the head of the bone, immediately after the receipt of the injury, would have been the best course to have pursued, for the arm when the cure took place was not in a better state than it would have been in if the operation had been performed at first, and the patient would have been spared two years of great suffering, not unattended with considerable danger.
M. Baudens, in a very able paper, an extract of which, made by himself, is published in the “Comptes Rendus” of the French Academy of Sciences, for February, 1855, on the Resection of the Head of the Humerus, seems to have overlooked, or not to have seen, the foregoing observations, as he assumes, as a consequence of his own observations on fourteen primary cases of which one only died, that the resection of the head of the humerus ought to be the rule in surgery when a ball has broken this part, and that amputation of the limb should be the exception—a point long since settled in my surgical works.
He considers that surgical writers in general have supposed that the bone remains suspended in the middle of the muscles, which does not accord with his practice, nor with the remarks made by me on this subject.
He recommends the following mode of operating: The arm being slightly turned outward and backward, the point of a small, straight amputating knife is to be entered on the outside of the coracoid process, immediately over the head of the humerus; lower the hand and carry the point of the knife in a straight line for ten or twelve centimeters downward, always applied to the bone, which serves as a guide.
If the incision thus made should not be large enough to expose the head of the humerus, a transverse subcutaneous one should be made through the muscular fibers toward the superior angle. If it be sufficiently large and open, this is not necessary. The long tendon of the biceps will be seen at the bottom of the incision, and is to be cut across.
Bring opposite the incision, by rotating the arm, first the great tuberosity, then the smaller one, in order to divide the[134] four muscles attached to them. The division of these parts will largely open the joint, when the elbow being carried backward and upward, the head of the bone will protrude. Detach gently the periosteum, slip the chain saw behind and below the head of the bone, so as to leave the periosteum as much uninjured as possible, doing in fact a sub-periosteal extirpation.
Tie the vessels, cover the upper end of the humerus with the periosteum thus saved like a hood, and keep it in contact with the glenoid cavity.
He maintains that when a ball has broken the head of the humerus, if the removal of the head be not effected, one of three things follows: the operation is performed subsequently, or the patient dies of purulent deposits, or recovers with a stiff joint, accompanied by fistulous openings of a disagreeable nature.
He contends that a ginglymoid joint is always formed by his method, which enables the sufferer to make much greater use of it than if the operation were performed in any other way; but it will be very difficult of performance if the bone should be so much injured as to prevent the tuberosity following the motion to be given to the elbow, and is not therefore recommended.
119. If, from some complication of injury, the axillary or other artery should give way during the treatment, the extremity is not to be amputated. The artery is to be secured by one ligature applied above the opening in it and by another below it, the surgeon always bearing in mind the fact that the proper way to get at the axillary artery is by cutting across the fibers of the pectoral muscle, and not in their direction, and that it will be better to amputate the arm than to tie the subclavian artery above the clavicle.
120. Amputation of the arm by the common circular incision should only be practiced in the space between the lower edge of the insertion of the pectoralis major and the elbow-joint; and rarely in cases of injury from musket-balls. No common flesh-wound, made either by cannon or musket-shot, even including a division of the artery, absolutely demands this operation, the bone being uninjured. If, in addition to a destructive flesh-wound, the bone be broken, or if it be mashed with the muscles by an oblique stroke of a round shot, or the forearm be carried away or destroyed, it is admissible. It is to be done in the following manner: [135] An assistant draws up the integuments with both hands; another does the same downward, if the parts admit of it; the forearm is to be moderately bent. The integuments are to be divided by a circular incision, and retracted. The muscles and vessels are then to be cut through by one sweep of the knife, if it can be done. The muscles adhering to the bone are next to be separated from it to the extent of two inches. The retractor is to be applied, and the periosteum divided by one circle of the knife around the bone, and in the circle thus cut the saw is to work until the bone is divided; attention being paid to the directions already given to saw in a perpendicular, not slanting direction. The artery or arteries are to be tied, the surface of the stump cleansed with warm and then with cold water, and dried. Leaden sutures are useful.
121. Mr. Luke performs the operation by two flaps on the same principle as in the thigh. There is a close resemblance in the manner of amputating the arm by the double-flap operation to that adopted for the amputation of the thigh. The first flap is made posteriorly to the bone, by transfixing the limb, for which purpose the knife is entered at the mid-point between the anterior and posterior surfaces, carried transversely across the limb, and made to cut toward the posterior surface, in an oblique direction, until all the soft structures are divided. It is necessary, in entering the knife, to bear in mind that the bone lies opposite to the mid-point, and that, in carrying the knife across the limb, it would strike against the surface of the bone, unless means were adopted for its prevention. This is easily done by grasping the structures which are to form the posterior flap between the fingers and thumb of the left hand, and by drawing them backward during the time the knife is entering at the mid-point and being carried across the limb. Having formed the posterior flap, the anterior one is formed as in amputation of the thigh, by cutting inward from the surface toward the bone with a sweep, which will make this flap equal in length to the posterior. The operation is completed by dividing the remaining soft parts by means of a cut carried circularly around the bone, and by sawing the bone in the line of division. The after-treatment is the same as in the thigh.
122. Excision of the elbow-joint.—An incised wound of moderate extent into the elbow-joint, cutting off with it[136] a part of the condyle of the humerus, or the head of the radius, or a part of the ulna, demands the removal of the injured piece of bone only. The forearm should be bent, and the antiphlogistic treatment fully carried out. A ball fracturing the olecranon, or other portion of a single bone, although opening into the joint, does not immediately require any operation.
If a ball should lodge in the lower part of the humerus, or in either of its condyles, it should be removed as quickly as possible by the trephine, or other appropriate instrument.
When the articulating ends of the humerus, radius, and ulna are wholly or in part injured by a musket-ball, it was formerly the custom to amputate the arm in such instances of great mischief—an operation which should be superseded by that of excision of the joint, by which the forearm will be saved, and considerable use of it retained.
To perform this operation, a straight, strong-pointed knife is to be pushed into the joint behind, immediately above but close to the olecranon process, and exactly at its inner edge, to avoid the ulnar nerve, which lies between it and the inner condyle, to which it may be considered to be affixed. The incision thus begun is to be carried outwardly to the external part of the humerus, dividing the insertion of the triceps. At each end of this transverse cut an incision is to be made upward and downward for about two inches each way, the three resembling the letter H. The flaps thus made being turned up and down, the olecranon should be sawn across, together with the great sigmoid cavity and the coronoid process of the ulna, the insertion of the brachialis internus having been previously separated from the coronoid process. Before this is done, the ulnar nerve should be separated with its attachments from the inner condyle, and turned aside to avoid injury. The joint being now fully exposed, the head of the radius may be sawn off or cut through with the strong spring scissors if possible, above the tubercle into which the biceps tendon is inserted. The extremity of the humerus should next be pushed through the wound, and the broken end sawn off, a spatula or other thin solid substance being placed underneath it, to prevent the brachial artery or median nerve being injured. Any hemorrhage which there may be having ceased, the forearm is to be bent, the bones are to be placed in apposition, and the incisions approximated by sutures and sticking-plaster, duly supported by[137] compress and bandage, so that union may take place if possible, particularly of the transverse wound first made. The arm should be supported by a sling, and dressed early, as the shot-hole or holes must remain open and discharging. Some motion of the new joint to be formed may be expected under gentle passive movements; but as a stiff joint cannot always be avoided, the arm should be kept bent.
123. Amputation of the elbow-joint has been recommended, but not frequently performed. It may be done in any way by which good covering can be obtained, and it has been supposed that the long stump thus made is more useful if the olecranon process be sawn across, and left with the triceps attached to it, than if it be removed. When the parts are sound, a flap may be made in front by introducing a straight, double-edged knife over the outer condyle, and carrying it across and through the soft parts over the opposite or inner condyle, when by cutting downward and outward a flap is to be formed of from three to four fingers’ breadth in length. A shorter flap is to be made behind, when both are to be raised, and the bleeding vessels previously secured, the external lateral ligament being divided. The radius is to be separated from the humerus, when the olecranon may be sawn across, or, if the arm be bent, separated from the humerus without difficulty. The flaps are to be brought together and retained in the usual manner.
124. Amputation of the forearm is seldom required after wounds from musket-balls. The bones can be readily got at, and large pieces removed with ease. The arteries can be cut down upon and secured without difficulty, except at the upper part, and even there with some little sacrifice of muscular parts, which are not to be spared. The fascia may be divided freely in every direction, and as mortification from defect of nourishment rarely takes place in the fingers, as it does in the toes, when the great arteries of the limb have been injured, every effort should be made to save a forearm, however badly it may at first appear to be injured.
The flap operation is to be preferred to the circular, particularly when done a little above the wrist; to which operation Baron Larrey and the surgeons of France particularly objected during the late war. Having done it most successfully since 1806, however, it is recommended as preferable to any other, even when the injury admits of its being done neat the carpus. When the nature of the injury does not[138] admit of two equal flaps being formed, it must be done by two unequal ones, or even by one, it being important for the fixing of an artificial hand or other help to have a long stump.
The arm being placed and held firmly in the intermediate position between pronation and supination, with the thumb uppermost, so that the radius and ulna are in one line, a sharp-pointed straight knife is to be entered close to the inner edge of the radius, and brought out below at the inner edge of the ulna. It is then to be carried forward for half an inch, and made to cut its way out with a gentle inclination, so as to form a semicircular flap. Re-entered at the same point as before, a similar flap is to be made on the outside, the position of the bones being a little altered to admit of its easy execution. The two flaps are to be turned back; the tendon of the supinator radii longus, and all other tendinous, muscular, or interosseous fibers, not cut through, are then to be divided, and the linen retractor run between the bones, which are to be sawn across at the same time. All pressure being taken off, the tendons and the vessels, if long, are to be cut short, and the arteries to be tied, after which the flaps are to be brought together by sutures, and retained by sticking-plaster, compress, and bandage.
125. When the operation is to be performed above the middle of the arm, it may be done by the circular incision.
The arm being placed with the thumb uppermost, an assistant should retract the integuments as much as possible, while the operator makes a circular incision through them. They are then to be drawn up for nearly an inch. The muscles on the inside of the arm should be divided by one slanting cut to the bones; then those on the outside. The bones are to be cleared by cutting through any muscular fibers attached to them, when the interosseal ligament should be divided, and the linen retractor passed between the bones, which may be sawn through at the same time without difficulty. The stump is to be dressed in the usual manner. The operation may be done by cutting through the integuments and muscles at once in an oblique manner, until the flaps thus formed shall be sufficiently large to make a thick cushion over the ends of the bones.
126. Amputation at the wrist, or the joint of the radius and ulna with the first row of the bones of the carpus, has[139] been recommended by some surgeons as preferable to amputation above the ends of the radius and ulna. The hand being placed midway between pronation and supination, the soft parts are to be divided by a circular incision beginning from half an inch to an inch below the ends of the radius and ulna. The integuments being turned up without the tendons, they are to be divided, and the joint is to be opened into before the spinous process of the radius; and, while the hand is pressed down, the knife should divide all the soft parts, and separate the carpus from the radius and ulna. The wound is to be closed by sutures in the usual manner. When a circular incision cannot be made, in consequence of the nature of the injury, and this operation is still preferred, a covering for the bones must be obtained wherever it can be procured, by one or more flaps.
127. In all injuries of the hand, the value of a thumb and a finger, or of two fingers, or even of one, should be borne in mind, and no part should be removed that can be saved, and appears likely to be of use. When cannon-shot, large splinters of shells, or grape-shot have struck the hand, amputation will often be necessary; but the foregoing precept should never be forgotten.
A musket-ball fairly passing through the hand generally fractures two metacarpal bones, although a small ball may pass between them without breaking either. The wounds should be enlarged, and the broken ends of the bone sawn off, or the splinters removed, and the points of bone smoothed off, the tendons to be carefully preserved, and vigorous antiphlogistic measures adopted. The tendency to tetanus or trismus will be best obviated by such measures, the incisions, when necessary, being made in the direction of the bones and tendons. Any hemorrhage which can ensue will be readily commanded by ligature, by torsion of the vessel, or by a small graduated compress and bandage, when those are inapplicable. Injuries by musket-balls to the metacarpal bones rarely take place without implicating one or more flexor or extensor tendons, and the consequence is that the fingers to which they belong are often bent inward toward the palm, constituting a defect less inconvenient, however, than if the finger remained straight and immovable.
128. When one or more fingers are destroyed, and the metacarpal bones injured, they are to be sawn or cut off, but not removed at the carpus, although an opening into the[140] joint of the carpus will generally do well, if skin can be saved to cover it. In all cases of amputation of one or more fingers, the metacarpal bones, if injured, should be left as long as possible, and particularly that of the index finger, when the thumb remains. In all cases it is better, if possible, to leave the heads of the metacarpal bones in their places, rather than open into the joint of the carpus, if it can be avoided. If the articulating heads must come out, a strong, thin scalpel is to be pushed in between the bones, the ligaments cut through above, below, and at the sides, and care should be taken, in removing one or two of these bones, not to dislocate the others, and the joint should be covered by a flap or flaps made for the purpose, the sides of the remaining fingers being covered in a similar manner. This succeeds admirably, when the two outer bones and fingers only are taken away.
129. The phalanges of the fingers may be removed by making a flap from the upper or under part, or from both, or from the sides. The square flap from the upper part of the finger is preferable, when the joint with the metacarpal bone is to be operated upon, the commencing points of the flap being united by a transverse incision on the under part of the joint. It should be recollected, that in all these excisions the larger end of bone belongs to that which is not removed, as may be shown by bending the finger; and that the ligamentous attachment between the metacarpal bones, connecting a middle one to its fellows on each side, should be cut through, when the joint will be easily dislocated. Attention should be paid to the division of the lateral ligaments, in the removal of any of the bones of the fingers.
Professor B. Langenbeck has operated in some instances, and he says successfully, without the loss of the finger, by sawing off, in his first case, the articulating ends of the first phalanx and of the metacarpal bone of the forefinger, in consequence of an injury from a rotating piece of machinery; in another, the ends of the first and second phalanges of the middle finger after a severe laceration; and in a third case, by sawing off the end of the second phalanx, and removing the whole of the bone of the third of the forefinger from the soft parts, leaving the nail; the man recovering with a shortened but useful finger. In all these cases the flexor and extensor tendons were from the first uninjured.
M. Langenbeck has also removed the metacarpal bone of[141] the thumb in the following manner: “An incision is to be made along the whole length of the bone toward the palmar aspect, thus avoiding the tendons. Then free both articulating extremities, separate the soft parts from the body of the bone, which is to be drawn outward by a strong pair of forceps, with two bent points or teeth at each extremity. To prevent the shortening or drawing inward of the thumb, it is to be kept straight and duly extended by a splint and other apparatus.” He recommends, with Flourens, the preservation of as much as possible of the periosteum, and uses for its detachment a small curved knife with a square end. Separating the periosteum from the bone is more easily directed than done. Professor Quekett, at my request, made some trials on the humerus to ascertain the point, and found that the periosteum could not be separated from the cartilaginous covering of the head of the bone, in the manner proposed, although it could be done by scraping half an inch below the insertion of the capsular ligament, and a sufficient portion saved to cover the sawn end of the bone, in the manner recommended by M. Baudens.
SECONDARY AMPUTATIONS, ETC.
130. Secondary amputations, or those performed after the lapse of six or more weeks from the receipt of an injury, when suppuration has been fully established, are not as successful in military as in civil hospitals, in which these operations are more commonly performed for incurable diseases than for injuries. When, however, they are done in them for injuries, they are not equally successful.
131. In military warfare these amputations are frequently done from necessity, not choice, after the first forty-eight hours; and especially after four or five days to the end of six weeks, in parts which have been lately, or are still affected by some of the accompaniments of inflammation, or are in a state of irritation. In these cases the cellular or areolar tissue has become firmer and more compact than usual; the muscles are not perfectly healthy; the blood-vessels are[142] larger and more numerous, and ready to assume actions unusual to them in a state of health. Where the bones have been diseased, much bony matter may be deposited between the muscles, and in some cases the vessels even are surrounded by it. After a few hours’ remission, the constitutional symptoms often return, the wound sloughs, and secondary hemorrhage is not an infrequent consequence. The ligatures are a source of irritation, and prevent union, which, in fact, should not in such cases be attempted, and, if attempted, will as rarely succeed.
132. In these states of constitutional derangement, inflammation of the veins and sloughing of the stump are not uncommon, augmented by, if not dependent in some degree on, the state of the atmosphere, which in autumn, the season for many military movements, gives rise to endemic fevers, and even to dysenteries and cholera, which the soldier is often so unfortunate as to acquire in crowded hospitals. If the man should escape with life, a joint will frequently be lost which might have been saved, if the operation had been performed in the first instance below it. When the injury is in the thigh, this is a most important point for consideration.
133. If the sufferer should escape these dangers, there remain the sudden and usually disastrous affections from depositions of matter in the viscera, alluded to in aphorisms 58, 59, 60, 61, and 62, which are by no means so common when the patient is in better health; the connection of these with inflammation of the veins deserves a more close investigation than has as yet been bestowed upon it by civil or by military surgeons since attention was first drawn to it by me in 1815.
134. In secondary amputations in parts which have partaken of the extensive irritation which accompanies the original injury, more of the soft parts must be preserved, although they cannot be said to be unsound. In other words, the bone must be cut shorter, or the stump will be conical and bad, particularly if sinuses containing pus are found to run up between the muscles, or between them and the bone itself—a state very likely to give rise subsequently to caries.
In sawing the bone, it may be again stated, the point of the saw should incline downward, and when two-thirds of the bone have been divided, it should be made to cut per[143]pendicularly, whereby the side next the operator is the last part divided; the hazard of splintering the bone at that moment will then be avoided, particularly if the limb to be removed be held with great steadiness.
135. In secondary amputations, twice, nay, three times the number of arteries will often bleed as in primary ones. In the thigh, the femoral artery should be drawn out with a tenaculum or spring forceps, and tied firmly with a single thread of dentists’ silk, one of the two ends being cut off close to the knot. The smaller the vessel, the smaller the thread required. Torsion or twisting the smaller vessels, so as to rupture their inner coats, answers very well in cases in which many small ones bleed. When a nerve is known to accompany an artery, it should be carefully separated from it.
136. If the bleeding should continue from above the ligature on the extremity of an artery, it is generally caused by some small branch given off from it, which has been cut so close to the trunk of the vessel as not to have been observed. In that case, the artery itself should be drawn out by the tenaculum or spring forceps until the bleeding point can be seen, and a ligature placed above it, when the piece below should be cut off with the first ligature applied. This inconvenience will be in general avoided by taking care to divide the principal artery at one stroke of the knife, and with it half an inch at least of the surrounding tissues, if the operation be done by the circular incision; if by flaps, the extent of the exposed arteries should be carefully examined, and the ligatures applied at the highest point of exposure, when all below should be removed.
137. When a tourniquet is used, and applied too close to the incised parts, it often prevents, even when loosened, the principal vessel from being found, from its having pressed on the ends of the muscles. If one be used, it should be removed as soon as possible after the principal artery has been secured. The repeated tightening and loosening of the tourniquet will cause more vessels to bleed in the end, and more blood to be lost, than if it had not been used; it ought not, therefore, to be resorted to when good assistance is procurable. In cases of this kind, in which the stump may not cease to ooze, the circulation being good, and sponging with cold water not effectual, the wound should not be finally closed for two, four, or more hours, until the oozing has[144] ceased, and the parts can be freed from the coagulated blood, and brought together.
138. In cases in which union is not expected to take place, both ends of the ligature should be cut off; for union of the external parts is not to be desired in many instances of secondary amputation, particularly after serious injuries; the inflammation consequent on which has in some degree implicated the structures divided in the operation, rendering them less liable to take on the healthy action of adhesion. The soft parts should be simply approximated by two or more sutures, the edges of the wound having a piece of lint or fine linen between them. This precaution should be particularly attended to after a great battle, when it is perceived that from the air, the crowded state of the hospital, or the season of the year, the stumps, although they may appear to unite in the first instance externally, do not in reality do so internally.
139. It has been proposed to use ligatures made of cat-gut or other animal substances, which may be cut short, and left in the wound to be absorbed. This has taken place in some instances, while in others little abscesses have followed, allowing their discharge, and not expediting the cure, so that the practice has not prevailed; it is said that greater success has attended in America ligatures used in this way made of very fine shreds of the strong tendons of the large deer of that country. Ligatures should not be applied on large veins when they continue to bleed, if it can be avoided, although it has frequently been done without subsequent inconvenience. A little delay and moderate pressure will generally suffice to arrest the bleeding.
140. If the surgeon find, after completing the operation, that the bone cannot be sufficiently covered to make a good stump, a piece should be sawn off at once, and the error remedied, with little comparative inconvenience to what would occur afterward, if the bone be too long. No false shame should prevent its being done. If, however, the error have occurred, and the end of bone should become uncovered during the process of healing, it may be allowed to separate of itself, as it cannot be sawn off at this period without difficulty and much suffering; for an exposed surface will then remain, from which an exfoliation will take place before the stump can heal. In cases of great protrusion, an incision should be made down to the bone, which should be firmly[145] held by strong forceps, or by a tube in which it will fit, when it is to be sawn off by the chain saw at a sound part, above that which has been exposed. The wound, in all cases, should be well supported by compress and bandage, to secure a good stump; whence the necessity for the bone being shorter than in those secondary amputations which are done at the period of election, and which will, on the contrary, often unite without difficulty. In primary operations, cold water is most applicable in the first instance; in secondary amputations, warmth by fomentations, rather than by even the lightest of poultices.
141. A fracture of a bone, however simple it may be in its nature, is said to be compound when accompanied by an external opening in, or a wound of, the soft parts, communicating with the broken bone—a complication which usually gives rise to ulcerative inflammation and suppuration throughout the whole extent of the injury, preventing thereby those milder processes being effected which, under the more favorable circumstances of the skin being unbroken, lead to a speedy union of the broken parts; whence the desire manifested by the surgeon, in ordinary cases of compound fracture, to close the external wound, if possible, but which, from the nature of a gunshot wound, it is useless to attempt. A fracture is said to be comminuted when the bone is crushed, as by a heavy wheel passing over it. It may still, however, be a simple fracture, that is, without an external wound; and in that state it is much less dangerous than a similar injury accompanied by an external opening, however small, the edges of which cannot be immediately and permanently reunited.
142. An arm or a leg, as a general rule, is not to be amputated in the first instance for a compound fracture caused by a musket-ball, unless the ball be of large size, and the bone much shattered. An effort should always be made to save it; and, under reasonable circumstances with regard to the extent of injury, the comfort, climate, and ordinary good health of the sufferer, the object will frequently be obtained under good surgical treatment.
143. It is not so with the thigh. After the battle of Toulouse, forty-three of the best of the fractures of the[146] thigh were attempted to be saved under my direction, and even selection. Of this number thirteen died; twelve were amputated at the secondary period, of whom seven died; and eighteen retained their limbs. Of these eighteen, the state three months after the battle was: five only could be considered well, or as using their limbs; two more thought their limbs more valuable, although not very serviceable, than a wooden leg; and the remaining eleven wished they had suffered amputation at first. Of the officers with fracture of the femur, one (having been taken prisoner during the action) died under the care of the French surgeons, by whom he was skillfully treated; the other has preserved a limb, which he rather wishes had been exchanged for a wooden leg.
In the five successful cases, the injury was in all at or below the middle of the thigh. In the thirteen others who retained their limbs, the injury was not above the middle third; and of those who died unamputated, several were near or in the upper third, and either died before the proper period for secondary amputation, or were not ultimately in a state to undergo that operation. Of the seven amputations which died, two were at the little trochanter, by the flap operation; and the others were for the most part unfavorable cases. In one case only was the head or neck of the bone fractured. The man lived for two months, and, from the dreadful sufferings he endured, it was much regretted that he had not lost his limb at the hip-joint at first. The operation ought, however, to have been the removal of the head and neck of the bone; but he was not seen in time by those who could or would have done this operation, which was then, however, only contemplated for the first time.
Nearly all the wounded, after this battle, had every possible assistance and comfort, from the second day after the action. The hospitals were well supplied with bedsteads—no inconsiderable point in the treatment of fractures—and several of the surgeons had been in almost every battle from the commencement of the war. The medicines and materials for their treatment were in profusion. The sick and wounded (1359 in number, including 117 officers) were in charge of two deputy inspectors-general, ten staff-surgeons, six apothecaries, and fifty-one assistant-surgeons; and the whole worked from morning until evening with the greatest assiduity. The surgery of the British army was then at the highest point of perfection it attained during the war; and[147] this enumeration is given to show the number of medical men required under the most favorable circumstances for 1500 wounded men, if they are to have all the aid surgery can give them. Doctors are not the most ornamental part of an army perhaps, but there are days in a campaign when many poor fellows find them to be the most useful.
Every broken thigh or leg was in the straight position, and the success was greater than on any previous occasion. Nevertheless, with all these advantages, there can be little doubt that if amputation had been performed in the first instance, on the thirty-six out of the forty-three who died or only partially recovered, some twenty would have survived, able, for the most part, to support themselves with a moderate pension, instead of there being perhaps five, or at most ten, nearly unable to do anything for themselves. Baron Larrey, with the élite of the military surgeons of France, as well as of those of Germany, have maintained this opinion; and the result of the practice as yet observed in the Crimea essentially confirms it, partly from the greater extent of mischief done to the bone by the large needle two-ounce rifle bullets of the Russians, and partly perhaps from the want of the accommodation and appliances which the circumstances of the siege of Sebastopol did not admit of. In the present state of our knowledge, it is perhaps the safest practice, particularly under doubtful circumstances, in which it cannot be ascertained whether rest, the best surgical care, and comfort may not be wanting; without all which a favorable result cannot be expected.
144. War is an agreeable occupation, trade, or professional employment for the few only, not for the many; and particularly not for the poor, when they have the misfortune to have their limbs broken by musket-shot. There are very few men in England who know what are the first principles of a medico-military movement with an army in the field; and it will not materially signify whether there should be even one so instructed, until the nation at large shall be impressed with the idea that no expense, no trouble, ought to be spared to obtain for their soldiers so unhappily injured the utmost comfort and accommodation that can be procured for them, as well as the best surgical assistance. The first was little attended to in England during three-fourths of the Peninsular war; and the latter was supposed to be obtained, when the demand was urgent, by giving a warrant to kill or cure to persons as dressers who were unable to undergo an[148] examination with any prospect of success, and prove themselves worthy a commission. Many a gallant soldier lost his life from the want of that proper attendance and care alluded to; many a desolate and unhappy mother mourned the loss of a son she need not have mourned for under happier circumstances, and who might have been the support, the happiness, of her declining years. Yet England calls herself the most humane, as well as the greatest, nation upon earth; she claims to be the most civilized, and she may be so; but certainly, in the case of those who have hitherto fallen in her defense, she could not on many occasions have been more careless or less compassionate. I have endeavored to impress on the directors of the East India Company in particular the injustice, the carelessness, of their treatment of the wounded soldiers of the royal army of Great Britain. My remonstrances have hitherto been in great part useless. It is to be hoped, however, that the present War Minister will cause an official public inquiry to be made into this matter, for that alone can cause this grievance to be redressed. Old habits are not to be overcome but by public opinion.
145. The peculiar difficulty in treating a gunshot fracture takes place when the bone is splintered for some distance, as well as broken. In these cases, inflammation occurs internally in the membranous covering of the cancellated structure of the bone, ending in the death of the parts affected; while the periosteum takes on that peculiar action externally which ends in the deposition of ossific matter around the splinters which have lost their life, and are enveloped by it. The bony matter, at first small in quantity, is gradually augmented, and deposited for some distance in the surrounding parts, so that it has been known to include the neighboring vessels and nerves in less than twenty days; at the end of a few weeks the quantity of ossific deposit is often very remarkable. Each splinter of bone becomes the sequestrum of a necrosis, in a similar manner as it is known to occur in the bones of young persons spontaneously affected by that disease, with this essential difference, that in the idiopathic disease there is only one, as if worm eaten, sequestrum, perhaps the length of the shaft of the bone, easily removable by one operation, while there may be in the traumatic disease several dead centers of ossific deposit, each of which requires to be removed by an operation to effect a cure. This new bony deposit will often be half an inch and[149] more in thickness, and at a late period is as hard as the old bone. The repetition of operations required in such cases is very distressing, particularly in the thigh, in which the disease often continues for months, and even for years.
The following case, related by Colonel Wilton, is instructive: “Lieutenant Timbrell, late of my old regiment, the 31st, had both his thighs broken at the battle of Sobraon; he would not allow amputation, so the doctor put him in a boarded ‘dooley,’ and his legs in a kind of trough. As I was also wounded, I used to see him almost daily, and I never heard him complain except the days when the doctor tried to extend his legs. Some time after our return to England (perhaps seven or eight months) I went to visit him, and found him quite recovered, and able to enjoy a day’s shooting as well as most people. He showed me many pieces of bone which had come away from his wounds, and appeared to have lost about three inches of his height; his limbs were rather bowed. He is now paymaster of the 6th Foot; and when I saw him, a few days before he embarked for the Cape, he was as active as ever, although I do not think he could either run or jump.”
146. A musket-ball will often lodge in the less dense parts of bones, such as the great trochanter or the condyles of the femur, without fracturing the bone; it will sometimes even pass through the femur above and between the condyles, merely splitting, but without separating the bone in parts or pieces. Balls sometimes lodge in the shaft of the femur without breaking it, and frequently do so in the tibia, the humerus, the bones of the cranium, and even in others of less size. Balls thus lodged will sometimes remain for years—nay, during a long life—without causing much inconvenience. It is, however, generally the reverse, and they are often the cause of so much irritation and distress that the sufferers are willing to have them, and even their limbs, removed at last at any risk. Whenever, then, a ball can be felt sticking in a bone, although it cannot be brought into view, it should, if possible, be dislodged and removed by the trephine, by small chisels, by small, strong-pointed curved elevators, or by any of the screws invented for the purpose, which have sometimes been found efficient. An apparently useful instrument of this kind is attached to the forceps for extracting balls; it is more frequently used in France than in England. When the ball can be seen as well as felt, the[150] surgeon must be guided by his own experience and judgment with respect to the most fitting instruments. It is to be removed if possible, whatever may be the means used for its abduction, after the wound has been properly enlarged for the purpose.
147. When a ball merely grazes a bone without breaking it, and passes through the limb, and no splinters can be felt by the finger, dilatation is unnecessary in the first instance; although some small splinters may be cast off subsequently, or a layer of bone may exfoliate, requiring assistance for their removal.
The bone may be fractured in a case of this kind transversely, and will require only the simplest treatment in an almost similar manner.
148. If the ball should enter and be flattened against the bone without breaking it, and lodge against it or in the soft parts, it should be sought for and removed. When the ball is flattened and the bone broken, it may lie between the broken extremities, and even lodge in one of them, rendering the case more complicated, and the necessity for close investigation more urgent. A leaden ball when striking on the sharp edge of a long bone, such as the spine of the tibia, has been known to be divided on it, without the bone being broken. This has happened in the arm.
149. When a ball strikes the shaft of a bone, such as the femur, directly and with force, it shatters it often in large, long, and pointed pieces, retaining their attachment to the muscles inserted into them. A fracture of this nature in the middle of the thigh will often extend downward into the condyles, and as high as, although rarely into, the trochanters. These are cases for immediate amputation.
150. Gunshot fractures of the head and neck of the femur have hitherto been fatal injuries, unless the whole extremity has been removed. It is hoped death may be prevented without this most formidable operation, by the removal of the head and neck of the bone, according to aphorism 85. If the upper third of the femur below the trochanter be badly fractured, and an attempt be made to save the limb, death generally occurs after several weeks of intense suffering, more particularly when the bone is broken by the large two-ounce balls now used by the Russians in the Crimea.
The least dangerous and the most likely to be saved are fractures of the lower third, or at most of the lower half, of the thigh-bone. When they do not communicate with the[151] knee-joint, an attempt ought always to be made to save the limb.
151. The preservation of a femur fractured by a musket-ball, when splintered to any extent, ought only to be attempted if the principal splinters can be removed. When the splinters of the femur are long and large, it has been supposed that if they retain their attachment to the soft parts, they may be placed in apposition and preserved. This may be doubted. It ought, however, only to be attempted under the most favorable circumstances, and will not often succeed even then. In the humerus it is different. An examination by the finger in the first instance is necessary to ascertain the extent of the injury to the bone, and to enable the surgeon to remove the broken portions, as well as the ball or any extraneous substances which may be in the wound. The incisions necessarily required for this purpose in the thigh are sometimes neglected, or the surgeon refrains from making them from the great thickness of the muscular parts, and from the wound having taken place on the inside, near the great vessels, so as to render incisions of sufficient size or extent in some degree dangerous. The thickness of the muscular parts is not a sufficient reason for avoiding an incision, neither is the vicinity of the great vessels and nerves, although they may not be divided; if the situation of the bone on the outside of the thigh be attended to, the broken portions may sometimes be got at at that part, if not on the inside. If this cannot be done, amputation had better be had recourse to. The object of the examination of such a wound being to ascertain the state of the fracture, and to remove the splinters and any extraneous substances, the extent and number of the incisions must depend on them; the true principle of what has been called dilatation of wounds. If the ball should have merely struck and grazed the bone, and passed out, causing a transverse fracture only, there is no necessity for making incisions at the moment, although one or more may be subsequently required to aid in the discharge of an exfoliated piece of bone, or of a splinter which may have been overlooked. If the ball lodge deeply in the soft parts, after breaking the bone, it should be removed, if practicable, by a second or counter-opening, and a free vent should always be made for the discharge. It may, however, be laid down as a general rule, that whatever is likely to be required during the first few days had better be done on the first than on the second or third; for after inflammation has[152] commenced, any handling or examination of the limb, however gently made, gives great pain.
152. After the first incisions have been made, and the larger splinters, which can be felt, have been removed, a secondary danger occurs from those which are smaller, and may have been overlooked, or not been discovered. This arises from the enveloping of these splinters in the new ossific matter described as being formed by the inflamed periosteum. This evil must be prevented by a careful examination of the wound when suppuration has been fully established, and the sensibility of the parts is in some degree diminished; when, if loose splinters of bone can be felt, they ought to be removed by incisions carefully and gently made to the extent which may be required. If this be not done early, the ossific deposit will take place around, and shut them in, even if the wound should close, which it usually will not. Their retention is accompanied by a firm thickening of the part, and in due course of time a spot of inflammation implies the formation of an abscess, and an ulcerated opening through the new bony deposit. When this abscess breaks externally, the probe will pass through the hole in the new bone, and rest on the rough, dead, and now perhaps movable splinter, the extraction of which can alone afford permanent relief. The earlier this is done the softer the ossific matter will be; at an early period, it will cut like Parmesan cheese intermixed with lime. If deferred until the bony matter is quite hard, it must be cut through with the chisel, or bone scissors or forceps, the application of which sometimes requires great force.
153. The successful treatment of a gunshot fracture of the thigh cannot be effected while the patient is lying on a little straw or a mat on the ground, and proper bedsteads should always form a part of the hospital stores of an army in the field. There is one in use at the Westminster Hospital, and another at the Royal Westminster Ophthalmic Hospital, which may be taken as models. Each, when complete, with mattress, etc., costs ten pounds, and, with a second inclined plane and mattress, might answer for two fractures; six may be easily carried in any common or spring cart wherever they are wanted. They would alleviate the sufferings, the horrible torments, many suffer unnecessarily. There is a very good and even cheaper one in use in the London Hospital, well worthy attention. An instrument or iron machine, movable from bed to bed, has been invented by Dr. Thom[153]son, of Stratford-on-Avon, which lifts a man readily from his bed, and, after he has been dressed, lays him down again with ease in a similar manner to the bedstead alluded to. It has, however, the advantage of being movable, while the apparatus in the bedstead is fixed. Lord Strafford has sent one to his regiment, the Coldstream Guards, and Dr. Thomson has sent another. Young backs and young knees only can bend for consecutive hours over men lying on the ground. Doctors of fifty years of age cannot do it; they are physically unequal to the labor. A staff-surgeon half a century old on a field of battle is almost an absurdity in the art, if not in the science of surgery: he ought to be promoted to the rank of inspector. The custom of the present day is to promote men more on account of the length of their services than because of their value: whereas, to make good physicians and surgeons, it should be from their value, combined with a due regard to a moderate yet sufficient length of service, which certainly should never exceed, even if it amounted to, twenty years; ten or twelve, in time of war, would be better,—a matter of expense against life and human misery.
154. The position of the patient in a gunshot fracture of the thigh or leg is of the utmost importance. He should lie on his back, and the limb should be straight. It is almost impossible to keep a man’s thigh in the bent position, or on its side, without his turning on his back, and the union of the bone, if it take place at all, must then be at an angle. The bent position forward, or on an inclined plane, is defective, inasmuch as the matter, which must necessarily be secreted in great quantity, will gravitate backward in spite of every care to prevent it. When a proper bedstead is used, a slightly inclined plane will sometimes be advantageous at a later period, when the body may also be raised, even to the erect position, the principal object being to take off the action of the two muscles inserted into the smaller trochanter, which, with the rotators behind, raise and evert the upper end of the broken bone. This direction outward should be met by a similar direction of the lower part of the bone, and by the application, from time to time, of a proper splint, compress, and bandage on the elevated bone, if they can be borne with perfect ease.
155. Splints are of various kinds, and made of different substances. The discovery of gutta-percha has enabled some to be made of that substance, which, when moulded into sheets, of from one to two or three eighths of an inch[154] in thickness, can be rendered soft and pliable by the application of hot water, regaining its firmness as it dries. Splints can thus be made of any size or length, and of any form, with apertures, if necessary, for the passage of the discharge from the wounds. Leather tanned without oil, and called splint-leather, is equally useful; if, when dried, the splints thus made become too hard, and press unequally, they can be softened by hot water, and removed and replaced with little comparative inconvenience.
One wooden splint of more than the length of the limb, somewhat similar to that called Desault’s, is absolutely necessary for the thigh, if it can be borne, which it rarely can, as a means of extension, or rather of preserving length. A shorter one on the inside, and one behind, will sometimes be required to complete the set A short one may be wanting for occasional use in front.
156. The bones of the leg being more exposed, admit of greater liberties being taken with them, and of larger portions, or even parts, being taken away successfully, than ought to be attempted in the thigh. A leg should, therefore, be seldom amputated for a fracture from a musket-ball. The splinters should be removed to almost any extent and number, and irregular portions sawn off from both ends, if they should be thus implicated. If one bone of the leg remain uninjured, the case becomes comparatively simple. The position should be straight on the heel, as a general rule, admitting of few exceptions.
157. The best apparatus for a compound fracture of the leg in either civil or military surgery, particularly in the latter, is that contrived by Mr. Luke, which may be seen in use at the London Hospital, and is supplied by Mr. M’Lellan, 3 Turner Street, Whitechapel Road. It is a simple iron cradle of small size, such as is used to guard a limb from the weight of the bedclothes, composed of three bars or large segments of a circle, united at their middles and ends or sides, as all cradles are, by a bar of iron of equal thickness. This is placed on a board a little wider than itself, with a ledge or bar at each side to prevent the cradle from moving, aided by two buttons or little pieces of wood on each side, which, being movable, turn over the iron bars, and thus render the board and cradle one firm piece. In this the leg is to be slung, to the center bar above, by ordinary tapes. A splint made of copper, to prevent rust or injury, hollowed to receive the leg, extending beyond the[155] foot with a footboard, and beyond the condyles of the femur above, enables the tapes to be passed under the limb for slinging it; while from the extension of the splint beyond the condyles, it causes the leg and thigh to move together, in a manner which will often prevent the pain which follows a sudden motion of the patient. Solid wooden side splints are still wanting, and these should have holes cut in them to allow a vent for the discharge and for the application of dressings; or if a portion of the splint, say the middle, should require removal altogether for this purpose, the upper and lower parts may be united by a semicircular bar of iron, at the pleasure of the surgeon; within this the dressings may be applied, and by it the splint will be rendered firm.[3] When the leg is thus slung, the knee will be somewhat bent, the thigh raised, the muscles of the leg behind relaxed, and the patient can be moved with much greater facility than with any other apparatus; one great advantage of this apparatus is, that it can be used with effect even if the patient be obliged to lie on the ground. It admits of being slung as a whole in a spring-cart, by additional but strong, elastic straps fastened to or applied on the under part of the board, and thus a double slinging motion may be obtained when the sufferer is obliged to be moved.
[3] This apparatus has, I think, been improved upon at the Bristol Hospital by the addition of a bar on each side of the center one.
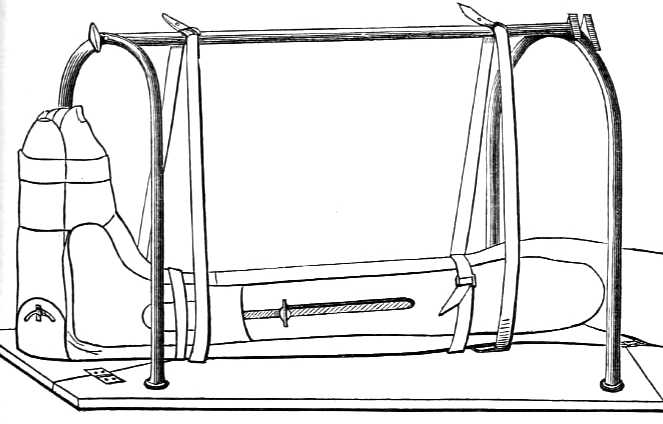
These splints are so portable that they may be carried into the field or upon the deck of a ship, to bring the patient to the surgeon.
In using the apparatus, the back of the leg and lower end of the thigh are to be evenly supported on a pad placed on the leg-rest; a splint is to be placed on each side of the leg, and the whole secured by straps carried around near the knee and ankle. The leg is then to be suspended by two straps from the bar of the cradle placed over the leg as represented, so as to swing without touching the folding board on which the cradle is placed. The foot should be secured to the foot-piece by a bandage.
Solid splints, and a firmly-fixed cradle, under which the leg may hang, may be said to be the sine qua non of the treatment of a gunshot fracture of the leg. The French in the Crimea have an apparatus called a GOUTTIÈRE, to be hereafter noticed.
158. Half-a-dozen pairs of long poles made light and of tough wood, which might always be replaced without difficulty, and a good thick ticking for each pair, having a case or pipe on each side in which the poles might run, ought to be a part of the surgical stores of every regiment on service in time of war. Two short irons, having at each end a ring through which the poles may run, will keep the ticking or sacking extended, and the patient flat and immovable unless shaken by accident. The sacking will roll up into little compass, if the poles should not be forthcoming or are not wanted, and, when the ground is damp, will make an excellent bedstead as well as a covering for the doctor. If four legs be added to each bearer, a great facility will be obtained on halting when the carriers are tired, the sufferer being raised from the ground, which in muddy or boggy places is very desirable.
159. The arm, when fractured by musket-shot, admits even of more strenuous efforts being made to save it; from its smaller size, and the more ready exposure of the bone or bones when badly broken, the danger is less. If an artery should yield by ulceration, it should be laid bare by operation, and a ligature placed on each bleeding end. An additional or second wound in the forearm only complicates the case, and the loss of a finger or two does not augment the danger. In fact, amputation should rarely take place in the first instance, and only in the second when mortification has commenced, or the strength and health of the patient will[157] no longer bear the drain upon them. The head of the bone should be removed, with as much of the shaft as may be injured; the elbow-joint should be excised, if the condyles are destroyed and the joint injured; if the middle of the bone should be destroyed, the upper and lower ends of it should be approximated. A great advantage is derived from the facility with which the upper extremity can be supported as compared with the lower, and the aid to the general health which may be obtained from the locomotion sufferers with broken arms are capable of undergoing.
160. In making incisions for the removal of splinters of bone, both at an early and at a late period, particularly in the latter, when the soft parts are all impacted together, and nothing is gained beyond what is cut, the course of the trunks of nerves, as well as of the great arteries, should be carefully attended to, and those parts avoided; for a successful cure of the fracture will be much deteriorated in value, if accompanied by a loss of motion or of sensation in the hand or fingers.
161. Splints for the arm should be made of solid materials, although light; some a little hollowed, and at a right angle, to correspond with the bend of the arm, and to admit of a little motion of the radius and of the forearm and hand, which relieves the position, is more comfortable for the sufferer, and tends to prevent stiffness of the elbow. The pads of lining for the splints should be made of cleaned or carded wool, rather than of tow or old linen, protected by some one or other of the modern modifications of caoutchouc or gutta-percha.
162. The medical treatment of compound fractures should be directed to allay pain and to prevent as far as possible any excess of general irritation and fever; to sustain, at a subsequent period, the strength of the sufferer by appropriate medicines, good and sufficient diet, and a free circulation of air, without all which little can be expected, to say nothing of absolute rest and those ordinary attentions and comforts so necessary for the restoration of health.
163. The following returns are illustrative of the principles recommended with reference to primary and secondary amputations. The first two show the seats of injury in 1359 persons wounded and admitted into hospital after the battle of Toulouse. The fifth return should be considered rather as an approximation to the truth than as the exact truth, as [158] it does not include those who died on the field of Waterloo, but those only who reached Brussels, and does not include those who were sent to Antwerp.
No. 1.—Return of Surgical Cases treated and Capital Operations performed in the General Hospital at Toulouse, from April 10th to June 28th, 1814.
| DISEASES AND STATE OF WOUNDS. |
Total treated. |
Died. | Dis- charged to duty. |
Transferred to Bourdeaux. |
Proportion of death to the number treated. |
| Head | 95 | 17 | 25 | 53 | 1 in 5-10/17 |
| Chest | 96 | 35 | 14 | 47 | 1 in 2-35/96 |
| Abdomen | 104 | 24 | 21 | 59 | 1 in 4-1/3 |
| Super’r extrem’s | 304 | 3 | 96 | 205 | 1 in 101 |
| Inferior ditto | 498 | 21 | 150 | 327 | 1 in 23-5/7 |
| Comp’d fractures | 78 | 29 | ... | 49 | 1 in 2-20/29 |
| Wounds of spine | 3 | 3 | ... | ... | 1 in 1 |
| Wounds of joints | 16 | 4 | ... | 12 | 1 in 4 |
| Amputations— | |||||
| Arm 7} Leg and thigh 41} |
48 | 10 | ... | 38 | 1 in 5-1/3 |
| Total | 1242 | 146 | 306 | 790 | 1 in 8-128/145 |
Wounded officers 117, not included, making a total of 1359, among whom thirteen cases of tetanus occurred, all of which proved fatal.
No. 2.—Officers.
| NATURE Of WOUNDS. |
Admitted. | Dis- charged. |
Sent to Bordeaux. |
Died. | Remaining. |
| Head | 6 | 4 | 1 | ... | 1 |
| Chest | 10 | 2 | 2 | ... | 6 |
| Abdomen | 1 | ... | ... | ... | 1 |
| Sup’r extremities | 33 | 9 | 15 | ... | 9 |
| Inferior ditto | 49 | 12 | 21 | 1 | 15 |
| Comp’d fractures | 7 | ... | 1 | 2 | 4 |
| Slight wounds | 11 | 7 | 2 | ... | 2 |
| Total | 117 | 34 | 42 | 3 | 38 |
[159] One secondary amputation of the arm occurred, and recovered; four of the inferior extremities, of which one died from tetanus. The thirty-eight remaining eventually went to Bordeaux, and thence to England.
No. 3.—Return of Capital Operations performed at the Hospital Stations of the Army in Spain, between the 21st of June and 24th of December, 1813, including the battles of Vittoria, the Pyrenees, and San Sebastian, to the entrance into France.
| STATIONS. | OPERATIONS. | No. operated upon. |
Died. | Dis- charged cured. |
Under treat- ment. |
REMARKS. |
| Vittoria | Shoulder- joint |
13 | 10 | 2 | 1 | |
| Upper extremities |
108 | 58 | 40 | 10 | ||
| Lower ditto |
148 | 95 | 38 | 15 | ||
| Trepan | 3 | 3 | ||||
| Santander | Upper extremities |
22 | 5 | 8 | 9 | |
| Lower ditto |
23 | 9 | 6 | 8 | ||
| Bilbao | Shoulder- joint |
5 | 5 | {The great {number {of amputations at {this station {was in part {occasioned by {hospital {gangrene. |
||
| Upper extremities |
146 | 48 | 46 | 52 | ||
| Lower ditto |
68 | 36 | 16 | 16 | ||
| Aneurism | 1 | 1 | ||||
| Passages | Shoulder- joint |
1 | ... | ... | 1 | |
| Upper extremities |
11 | 1 | 3 | 7 | ||
| Lower ditto | 14 | 6 | 3 | 5 | ||
| Trepan | 3 | 2 | 1 | |||
| Aneurism | 1 | 1 | ||||
| Vera | Upper extremities |
12 | 4 | 8 | ||
| Lower ditto | 5 | 3 | 2 | |||
| Total | 584 | 287 | 173 | 124 | ||
| Recapitulation:— | ||||||
| Shoulder- joint |
19 | 15 | 2 | 2 | ||
| Upper extremities |
299 | 116 | 105 | 78 | ||
| Lower ditto |
258 | 149 | 65 | 44 | ||
| Trepan | 6 | 5 | 1 | |||
| Aneurism | 2 | 2 | ||||
If one-sixth of the number remaining under treatment be considered to have died, which is a low calculation, the deaths will stand to the recoveries as 300 dead to 276 recovered, or a loss of more than one-half of the secondary operations.
[160] No. 4.—Capital Operations performed in the Field with Divisions of the Army during the same period.
| DIVISIONS. | OPERATIONS. | Number operated upon. |
Died. | Dis- charged cured. |
Under treatment. |
Tetanus occurred. |
REMARKS. | |
| Cavalry | Upper extremities | 3 | 1 | 2 | ||||
| Lower ditto | 3 | 2 | 1 | |||||
| First division |
Shoulder-joint | 3 | ... | 2 | ... | ... | 1 | Sent to General Hospital. |
| Upper extremities | 14 | 1 | 3 | 5 | ... | 5 | ||
| Lower ditto | 10 | 2 | ... | 1 | 1 | 6 | ||
| Trepan | 2 | 2 | ||||||
| Second | Shoulder-joint | 1 | ... | 1 | ||||
| Upper extremities | 16 | ... | 5 | 6 | ... | 5 | Sent to General Hospital. |
|
| Lower ditto | 21 | 3 | 6 | 7 | ... | 5 | ||
| Aneurism | 1 | ... | ... | 1 | ||||
| Third | Shoulder-joint | 1 | ... | ... | 1 | |||
| Upper extremities | 17 | 2 | ... | 15 | ||||
| Lower ditto | 10 | ... | 2 | 8 | ||||
| Fourth | Upper extremities | 10 | ... | 10 | ||||
| Lower ditto | 20 | ... | 20 | |||||
| Fifth | Shoulder-joint | 12 | ... | 8 | 2 | ... | 2 | Sent to General Hospital. |
| Upper extremities | 57 | 1 | 36 | 2 | ... | 18 | ||
| Lower ditto | 41 | 10 | 13 | 2 | ... | 16 | ||
| Sixth | Shoulder-joint | 1 | 1 | |||||
| Upper extremities | 7 | ... | 5 | ... | ... | 2 | Sent to General Hospital. |
|
| Lower ditto | 6 | 1 | 1 | 3 | ... | 1 | ||
| Seventh | Upper extremities | 18 | ·· | 3 | 1 | ... | 14 | Sent to General Hospital. |
| Lower ditto | 9 | 1 | ... | 1 | ... | 7 | ||
| Light division |
Shoulder-joint | 1 | ... | ... | ... | ... | The whole of these cases sent to the General Hospital; results not known at the division. |
|
| Upper extremities | 21 | ... | ... | ... | ... | |||
| Lower ditto | 8 | ... | ... | ... | ... | |||
| Trepan | 4 | ... | ... | ... | ... | |||
| Total | 317 | 27 | 118 | 55 | 1 | |||
| Recapitulation:— | ||||||||
| Shoulder-joint | 19 | 1 | 11 | 3 | ... | 4 | Sent to General Hospital. |
|
| Upper extremities | 163 | 5 | 64 | 29 | ... | 65 | ||
| Lower ditto | 128 | 19 | 43 | 22 | ... | 44 | ||
| Trepan | 6 | 2 | ... | ... | ... | 4 | ||
| Aneurism | 1 | ... | ... | 1 | ... | |||
[161] Of 310 amputations 25 died, 172 recovered in the field, and 113 were sent to the rear, of whom one-sixth may be considered to have died, making a total of 45 deaths in 310 cases—the proportion of upper extremities to lower in the 310 being as 182 to 128, thus greatly influencing the result, which is consequently much more favorable than if the numbers had been reversed. The proportion of upper to lower extremities in the secondary amputations, as by return No. 3, is equally in favor of the upper, and can only be accounted for, when compared with Return No. 4, by the army being constantly in motion and the hospitals at a distance. The difference of results at the several stations is also remarkable; it is so with the divisions in the field. The 3d and 4th divisions, under Staff-Surgeons Lindsey and Boutflower, kept their amputations with them in bivouac, and their success is remarkable; that of the 4th division has no parallel. The light division, on outpost duty, could not keep their amputations. These two returns include 886 amputations.
The labors of the surgeons of the army may be judged of by the fact that, during the last three months of the year to which these returns refer—viz., from September 25th to December 24th, 1813—the number of sick and wounded amounted to 37,144, a number nearly equal to that of the whole army.
[162] No. 5.—Return of Capital Operations, Primary and Secondary, performed in the British General Hospitals, Brussels, or brought in from the Field between 16th June and 31st July, 1815.
| OPERATIONS. | |||||||||||||
| General total. | |||||||||||||
| Primary operations. | |||||||||||||
| Died. | |||||||||||||
| Remaining. | |||||||||||||
| Proportion of deaths to operations. |
|||||||||||||
| Secondary operations. | |||||||||||||
| Died. | |||||||||||||
| Remaining. | |||||||||||||
| Proportion of deaths to operations. |
|||||||||||||
| Total remaining. | |||||||||||||
| Of these doubtful. |
|||||||||||||
| Transferred to Antwerp. |
|||||||||||||
| REMARKS. | |||||||||||||
| Shoulder- joint |
8 | 6 | 1 | 5 | 1 to 6 | 12 | 6 | 6 | 1 to 2 | 11 | |||
| Hip-joint | 1 | ... | ... | ... | ... ... | 1 | ... | 1 | ... ... | 1 | ... | ... | A French soldier, who recovered. |
| Thigh | 148 | 54 | 19 | 35 | 1 to 3 | 94 | 43 | 51 | 1 to 2 | 86 | 9 | 4 | |
| Leg | 93 | 43 | 7 | 26 | 1 to 6 | 50 | 16 | 34 | 1 to 3 | 60 | ... | 4 | |
| Arm | 72 | 21 | 4 | 17 | 1 to 5 | 51 | 13 | 38 | 1 to 4 | 55 | ... | 6 | |
| Forearm | 39 | 22 | 1 | 21 | 1 to 22 | 17 | 5 | 12 | 1 to 3 | 33 | ... | 3 | |
| Carotid artery tied |
1 | ... | ... | ... | ... ... | 1 | ... | 1 | ... ... | 1 | ... | ... | |
| Trephine | 2 | ... | ... | ... | ... ... | 2 | 1 | 1 | 1 to 2 | 1 | ... | 1 | |
| Total | 374 | 146 | 32 | 104 | ... ... | 228 | 84 | 144 | ... ... | 248 | 9 | 18 | |
CHARACTERS OF HOSPITAL GANGRENE.
164. This most destructive disease owes its names of hospital gangrene, phagedena, gangrenosa, pourriture d’hôpital, sloughing ulcer, etc. etc. to the different appearances the affected parts assume on different occasions, according to the intensity of the morbid poison applied, and possibly also to the state of constitution of the individual attacked. The peculiar nature of this poison has not yet been ascertained. Professor Brugmans says that in 1797, in Holland, charpie composed of linen threads cut of different lengths, which, on inquiry, it was found had been already used in the great hospitals in France, and had been subsequently washed and bleached, caused every ulcer to which it was applied to be affected by hospital gangrene; and the fact that this disease was readily communicated by the application of instruments, lint, or bandages which had been in contact with infected parts, was too firmly established by the experience of every one in Portugal and Spain to be a matter of doubt. Its character as a thoroughly contagious disease is indisputable. Its capability of being conveyed through the medium of the atmosphere to an ulcerated surface is also admitted, although some have thought that the infection was not always applied to the sore, but affected it secondarily, through the medium of the constitution. Brugmans says that hospital gangrene prevailed in one of the low wards at Leyden in 1798, while the ward or garret above it was free. The surgeon made an opening in the ceiling between the two, in order to ventilate the lower or affected ward, and in thirty hours three patients who lay next the opening were attacked by the disease, which soon spread through the whole ward. Our experience in Portugal and Spain confirmed this fact, and left no doubt on the mind of any one who had frequent opportunities of seeing the disease, that one case of hospital gangrene was capable of infecting not only every ulcer in the ward, but in every ward near it, and ultimately throughout the hospital, however large. The disease, as long as it remains unaltered by[164] destructive applications, may be considered to be infectious as well as contagious.
This infection can penetrate the dressings so as to affect the ulcer through them, although requiring a difference of time in different parts of the body. Ulcers on the lower extremity experienced the influence of the morbid poison in general at an earlier period than those on the upper extremity; and a wound might be seen in a healthy state on the arm, while one on the leg had been evidently suffering from this disease for some days, if the complaint had become mild, or somewhat chronic. If the morbid poison were in its active state, then the deterioration of the ulcers on the arm was almost if not quite contemporaneous with that on the leg.
165. Mr. Blackadder has given the following account of the disease from inoculation in his own person, which is, therefore, more to be relied upon than any other:—
“While engaged in examining the stump of a patient who had died from this disease, I accidentally wounded one of my fingers with the point of a double-edged scalpel, but so slightly that not a drop of blood made its appearance, and on this account I did not consider any particular precautionary means necessary. In the course of about sixty hours, however, the wound had become inflamed, and I was attracted to it by an occasional smart, stinging sensation, which ultimately extended a considerable way up the arm. On the fourth day the inflammation had increased, and the stinging sensation was almost constant. Headache, nausea, and general indisposition followed, with frequent chills, which increased very much toward evening; but which, with the other symptoms, were considerably relieved by the use of neutral salts, the pediluvium, and warm diluents. A vesicle, having a depression in its center, and containing a watery fluid of a livid color, was now forming upon a hard and elevated base; the surrounding integuments became tumefied, of an anserine appearance, and extremely sensitive to the touch; at about the distance of the fourth of an inch from the base of the tumor, a very distinct areola, of a bluish-red color, made its appearance, and remained visible for several days. At this period, circumstances rendered it necessary for me to be exposed to wet, to undergo considerable fatigue, and immediately afterward to travel to a considerable distance. The inflammation, however, gradually subsided, but[165] the stinging, accompanied by a burning sensation, still continued, and the sore had no disposition to heal; yet it did not enlarge externally, but was disposed to burrow under the integuments. This phagedenic disposition was ultimately got the better of by laying open the sore, and by repeated applications of caustic; but it was two months before a complete cicatrix had formed. The new cuticle remained for a length of time extremely sensitive to the touch; and it was upwards of six months before it had acquired the color of the surrounding integuments.”
166. M. Delpech was disposed to consider that the misfortunes and sufferings of the French army had a great depressing influence on the soldiers, from which at other times they would have been exempted, and that this aided the propagation of the malady; but many soldiers of the British army, free from these particular depressing causes, suffered in a similar manner. Dr. Tice, at Coimbra, says:—
“An uncommon depressing affection of the mind often exists among persons suffering from this disease, painful to witness—a morbid dejection, or apathy, which could scarcely be removed, and on which, in very bad cases, no impression could be made. In others, the humane solicitations of the medical officers have failed against the influence of oppressive gloom, amounting to despair. Expectation and hope seemed to be exiled from their minds by the dominion of painful despondency, which, prevailing in melancholy disorder, seemed uncontrolled or checked by the intrusive importunities of the present, or the consciousness of a future existence.”
A wound attacked by hospital gangrene in its most concentrated and active form presents a horrible aspect after the first forty-eight hours. The whole surface has become of a dark-red color, of a ragged appearance, with blood, partly coagulated, and apparently half putrid, adhering at every point. The edges are everted, the cuticle separating from half to three-quarters of an inch around, with a concentric circle of inflammation extending an inch or two beyond it; the limb is usually swollen for some distance, of a shining white color, and not peculiarly sensible, except in spots, the whole of it being perhaps edematous or pasty. The pain is burning, and unbearable in the part itself, while the extension of the disease, generally in a circular direction, may be marked from hour to hour; so that in from[166] another twenty-four to forty-eight hours, nearly the whole of the calf of a leg, or the muscles of a buttock, or even of the wall of the abdomen, may disappear, leaving a deep, great hollow, or hiatus, of the most destructive character, exhaling a peculiar stench, which can never be mistaken, and spreading with a rapidity quite awful to contemplate. The great nerves and arteries appear to resist its influence longer than the muscular structures, but these at last yield; the largest nerves are destroyed, and the arteries give way, frequently closing the scene, after repeated hemorrhages, by one which proves the last solace of the unfortunate sufferer. I have seen all the largest arteries of the extremities give way in succession, and until the progress of the disease was arrested by proper means, the application of a ligature was useless. The joints offer little resistance; the capsular and synovial membranes are soon invaded, and the ends of the bones laid bare. The extension of this disease is, in the first instance, through the medium of the cellular structure of the body. The skin is undermined, and falls in; or a painful red, and soon black patch, or spot, is perceived at some distance from the original mischief, preparatory to the whole becoming one mass of putridity, while the sufferings of the patient are extreme. A complaint of this kind cannot be local, even if a local origin be admitted; the accompanying fever is usually dependent on the previous state and general constitution of the patient, modified by the season of the year, or the prevailing type of febrile disease.
This gangrenous disease does not always prevail in this, its most concentrated form; the destroying process assumes more of a sloughing than of a gangrenous character, whence Delpech has denominated it pulpous, rather than gangrenous. It is in its nature almost equally destructive, although not quite so formidable in appearance. It may attack the whole surface of an ulcer at once, or in distinct points, all, however, rapidly extending toward each other, until they constitute one whole. The red of the granulations becomes of a more violet color, and the change is accompanied by burning, a pain not usually felt in the part, while a layer of ash-colored matter is soon seen covering them, which adheres so firmly as not to be readily removed; or, if separated, shows that it is a substance formed upon the surface, and constituting a part of the granulations themselves, which are ultimately confounded with it.
[167] About the end of the first week, and sometimes much later, this kind of ulcer becomes more painful, the edges or the circumference of the wound assume a browner hue, and the parts become somewhat pasty, the whitish color of the part particularly affected being opaque, gray, and soft. It may be said that the false membrane, having become very thick, has lost the little vitality it possessed, and become putrid; the discharge, which had been partly suppressed, now reappears, not as pus, but as a fetid ichor, exhaling the peculiarly offensive stench of this disease. This pulpy, yellowish, putrid substance becomes thicker, and extends deeply; it invades the whole substance of a muscle, under which a probe may be passed, and the instrument brought out through it, with the loss, perhaps, of some striæ of blood, from parts which are not yet actually destroyed; the mass is, however, adherent, although its extent diminishes by the putrefaction and wasting away of its surface.
There are two characters always peculiar to this disease, in which it differs from all other gangrenous ulcers from ordinary causes; these are, the circular form it assumes after a very few days, even in its slighter varieties, and its peculiar odor or stench.
167. If this disease were entirely a local complaint, caused by the application of a morbid poison, giving rise to the destructive changes described on the surface of an ulcer, it should be followed by febrile or constitutional symptoms at the end of several days only; and Delpech is disposed to think that in such cases these constitutional symptoms take place from and after the sixth day. If it were entirely a constitutional disease, giving rise to the destructive changes described as taking place on the surface of an ulcer, the febrile symptoms should precede the changes in the ulcerated surface. That the febrile symptoms do seem to follow the appearance of the local alteration, is in many cases indisputable; that they precede or accompany the local symptoms in many other cases, is indubitable; and that the disease in a mild state, although yet capable of committing much mischief, is neither preceded nor followed by febrile or constitutional symptoms, cannot be doubted. The febrile symptoms themselves differ essentially from each other when they do occur, generally partaking the character of the endemic fever prevailing in the country at the season at which they appear. The fever is sometimes inflammatory, sometimes typhoid,[168] and occasionally resembles the bilious remittent of the summer and autumn in hot climates, and ends in typhus. It is probable that a want of attention to these circumstances decided the opinions entertained by different individuals as to the general character of the febrile symptoms, and of the treatment to be pursued for their removal. That this disease was generally considered a constitutional complaint, until nearly the end of 1813, must be admitted; and it was the very indifferent success which attended its treatment by constitutional means and simple detergent applications, which caused the surgeons of the British army to view it more as a local disease, capable of giving rise to severe constitutional symptoms—a change of opinion which was materially influenced by the knowledge that the French surgeons more generally considered, with Pouteau, that it was local in the first instance, and treated it by the actual cautery. In my hands, constitutional treatment, and every kind of simple mild detergent applications, always failed, unless accompanied by absolute separation, the utmost possible extent of ventilation, and the greatest possible attention to cleanliness; and not even then without great loss of parts in many instances. This induced me, at Santander, in November and December, 1813, to try the mineral acids, not as then generally used as stimulants or detersives, but as caustics. This proceeding was always, however, accompanied by a constitutional treatment, regulated by the nature of the symptoms, which at that station were never benefited by bleeding, although it had proved so effectual, without the local remedies, at the neighboring sea-port of Bilbao.
168. Dr. Boggie, the great advocate for constitutional treatment, says that under him, at Bilbao, in 1813, where caustic applications were not used, or only as detersives, the disease was arrested by blood-letting to the amount of one or two pounds, and, in some cases, to the extent of three or four. He admits, however, that bleeding must be resorted to with the greatest caution in persons of less robust constitutions, who may have lingered long in hospital, or suffered much from ill health; and that in some cases it is altogether inadmissible—an acknowledgment which is decisive, in my mind, that constitutional treatment is only auxiliary. He says he never saw the puncture made by the lancet affected by this disease; a convincing proof to me, who have seen it, that the virulence of the complaint, as an infectious disease, was[169] subsiding at Bilbao when the treatment he introduced proved so effectual.
In one case at Santander, in which hospital gangrene in the hand and arm and tetanus existed together, they were both cured by venesection, which failed as signally in doing the least good in a case in the next bed, under nearly similar circumstances.
Dr. Boggie admits that “in that form of gangrene named phagedena, a very great destruction of parts may sometimes take place without the constitution being much affected by it. Now, if blood-letting be used in such a case, or even in the advanced stage of the true inflammatory gangrene, when disorganization has taken place, and the system is sinking under the consequent debility, the vital powers being nearly exhausted, the result must be obvious; but when it is used with caution, and in cases where it is really applicable, it will be found to be a most valuable remedy.” In all cases, Dr. Boggie, like every one else, had recourse to emetics, purgatives, and such other general treatment as the febrile symptoms appeared to indicate. As local applications, he recommends cold water, alone or mixed with a small portion of acetic acid, constantly applied and frequently renewed. Poultices and warm applications he objects to; and after the sloughs separate, he approves of dry lint and weak solutions of sulphate of zinc. Should the sloughs adhere after the inflammation has abated, warm, stimulating ointments, and sometimes weak solutions of the nitrate of silver or of the mineral and vegetable acids, may be had recourse to.
169. To Mr. Blackadder must be attributed the introduction of the use of Fowler’s solution of arsenic as an escharotic, in November, 1813, while he was at Passages; it answered remarkably well in arresting the progress of the disease, and was afterward found to be equally efficient in the hospitals at Antwerp. The only objection to its use that I am aware of is, that it caused in some few cases slight symptoms of its poisonous effect having taken place on the bowels, apparently from absorption,—an inconvenience which might become a serious evil, and which caused a preference to be given to the mineral acids, which act equally well without incurring a similar risk of evil. Mr. Blackadder, stationed on the same coast, within about forty miles of Dr. Boggie at Bilbao, took a diametrically opposite view of[170] this complaint to the doctor; and believing the disease to be purely local in the first instance, considered venesection as almost always unnecessary, although he admitted that cases may occur in which the abstraction “of a small quantity of blood would be likely to be attended with more good than harm; but certainly,” he adds, “blood-letting is an operation which ought to be avoided as much as possible in gangrenous phagedena, particularly when the previous injury has been extensive, such as that of a penetrating gunshot wound.”
Dr. Walker, who served at Bilbao at the same time, concludes an able report in the following terms:—
“Lately, however, the disease put on a milder form, and the sloughing did not proceed with that rapidity that it did at first, nor was the fever so violent. And more lately still, since the setting in of the cold weather, the type of the fever seems to have changed entirely, and to have put on the inflammatory type, so as to require strong evacuants, and even bleeding, which has been used with the greatest success by Staff-Surgeon Boggie, who has for a considerable time had the more immediate care of the patients of this description at the Cordeleria Hospital.”
170. “When this disease does not proceed rapidly, and is confined to the ulcerative form,” Delpech says, “it may be removed by stimulant applications, such as vinegar, the vegetable and mineral acids, the Egyptian ointment, etc.” Of these he prefers vinegar applied on lint, after having rubbed or scraped off any false or pulpy membrane which appears to conceal the surface of the ulcer. “Some good effect,” he adds, “has been observed from the careful application of powdered charcoal to the whole surface of the sore, which,” he says, “ought not to be in the gangrenous, or pulpy, or putrid state, but merely ulcerative or phagedenic; and not even then, when this peculiar ulceration assumes a deeply hollowed-out form, rapidly filled with an abundant and tenacious discharge.” Of constitutional treatment he evidently thinks little; and, while he admits the propriety and necessity of treating every accompanying state of fever, whether it be inflammatory, catarrhal, bilious, remittent, etc., by its appropriate means, he does not seem to think they have much influence on the local disease, although he firmly believes that the suppression of the local disease materially assists in arresting, in a great measure, such constitutional[171] symptoms as may be dependent on it, unless influenced by some peculiarity of constitution. His principal local remedy was the hot iron or actual cautery applied to every part.
He says (page 86) some surgeons of the Anglo-Portuguese army of Lord Wellington had assured him that the mineral acids, the hydrochloric, nitric, and sulphuric, had been frequently employed in the British hospitals in Spain with success; and he particularly mentions M. Guthrie, Inspecteur au Service de Santé, as the person from whom he especially received his information; thus establishing the fact that the use of the mineral acids in a dilute and concentrated state was known to, and had been essentially introduced into practice by, the surgeons of the British army during the war in Spain—a fact which admits of no dispute as to the origin of its use.
171. In India, Mr. Taylor, late surgeon 29th Regiment, now a deputy inspector-general in the medical department in the Crimea, reports:—
“Hospital gangrene appeared among the wounded of the 29th Regiment a little later than in the hospitals of other corps. The disease declared itself, on the 18th of January, in a stump case; and between that date and the 26th of the same month fifteen cases had come under treatment. At first I could tell, by the peculiar dark, florid countenance of the patient, that his wound had taken on the gangrenous affection; yet I cannot say that there was, in these cases, any marked inflammatory fever. Subsequently, in the prevalence of the disease, this dark-red color of the face was neither well marked nor by any means so constant. In many cases the disease seemed purely local; but in the great majority there was certainly much feverish constitutional disturbance accompanying the local affection, and often preceding it. My experience of the disease, as it occurred among the wounded at Ferozepore, does not enable me to determine, satisfactorily to myself, whether it be essentially a local or a constitutional affection. I am inclined to place it in the former category; and there is no doubt whatever in my mind that the essential means of treatment are local.
“In the treatment of this disease, I proceeded regularly on one plan, and found that so efficacious that I was not inclined to try any other. The plan adopted was, the application of the strong nitric acid, so as completely to cut off the diseased from the sound part, or part so far sound as[172] only to be affected with inflammation. The acid, however, required to be rubbed in with the blunt end of the probe, so that it not only destroyed the cuticle, but killed the cutis vera, and probably the cellular membrane underneath. The narrow yellow ring of dead skin thus formed separated like a piece of leather, generally carrying with it the whole slough, and leaving a clean, healthy surface, as well as edges to the wound. I never attempted to apply the acid to the surface underneath the slough, neither is such an application necessary; the vital seat of the disease is in its circumference, however large the area. I must admit that the disease sometimes crossed the acid boundary, and a second, and even a third application of the remedy was required; but this was rare. Neither was constitutional treatment neglected, but this varied according to the state of the patient; emetics, purgatives, saline medicines, and low diet being sometimes required; while in other instances ether, ammonia, laudanum, and generous diet were administered.
“When speaking of the symptoms of this disease, I should have mentioned that a burning, gnawing sensation was sometimes loudly complained of. The application of the acid soon removed that pain, and the acid itself did not often seem to produce much suffering. In one instance, deemed a favorable one, I tried venesection, and I fear did mischief. Calomel and antimonials were useful. I did not try the arsenical solution. The change of air, which the march of the wounded, on their return to Kussowlee, occasioned, certainly had a very beneficial effect on all the gangrenous and sloughing sores.
“At the same time that hospital gangrene was prevalent at Ferozepore, some wounds took on a malignant fungous affection, which spread over the healthy surface like the hospital gangrene. The dirty, fibrous-looking, fungous growth rose considerably above the edges of the wound, partially overlapping them; these edges were inflamed, but not livid and vesicated as in the cases of gangrene; but here also the disease took the circular or oval form. The affection here noticed I observed only in wounds of the forearm and hand; Colonel Barr’s wound, which was of the forearm near the wrist, took on this disease. The application of nitric acid in the same way as for hospital gangrene eventually checked its progress.
“In no case that came under my observation did the gan[173]grene directly prove fatal, though in many cases it contributed largely in bringing about an unfavorable termination.”
172. Conclusions. First.—Hospital gangrene never occurs in isolated cases of wounds.
Second.—It originates only in badly-ventilated hospitals, crowded with wounded men, among and around whom cleanliness has not been too well observed.
Third.—It is a morbid poison, remarkably contagious, and is infectious through the medium of the atmosphere applied to the wound or ulcer.
Fourth.—It is possibly infectious, acting constitutionally, and producing great derangement of the system at large, although it has not been satisfactorily proved that the constitutional affection is capable of giving rise to local disease, such as an ulcer; but if an ulcer should occur from accidental or constitutional causes, it is always influenced by it when in its concentrated form.
Fifth.—The application of the contagious matter gives rise to a similar local disease, resembling and capable of propagating itself, and is generally followed by constitutional symptoms.
Sixth.—In crowded hospitals the constitutional symptoms have been sometimes observed to precede, and frequently to accompany, the appearance of the local disease.
Seventh.—The local disease attacks the cellular membrane principally, and is readily propagated along it, laying bare the muscular, arterial, nervous, and other structures, which soon yield to its destructive properties.
Eighth.—The sloughing of the arteries is rarely attended by healthy inflammation, filling up their canals by fibrin, or by that gangrenous inflammation which attends on mortification from ordinary causes, and alike obliterates their cavities. The separation of the dead parts is, therefore, accompanied by hemorrhage, which, when from large arteries, is usually fatal.
Ninth.—The operation of placing a ligature on the artery at a distance, or near the seat of mischief, does not succeed, because the incision is soon attacked with the disease, unless it has been arrested in the individual part first affected, and the patient has been separated from all others suffering from it.
Tenth.—The local disease is to be arrested by the appli[174]cation of the actual or potential cautery: an iron heated red hot, or the mineral acids pure, or a solution of arsenic, or of the chloride of zinc, or of some other caustic which shall penetrate the sloughing parts, and destroy a thin layer of the unaffected part beneath them. If a sinus or sinuses have formed under the skin or between the muscles, from the extension of disease in the cellular or areolar structure, they must be laid open, and the cautery applied; for if any part affected be left untouched or undestroyed by the acid, the disease will recommence and spread from that point. The parts touched by the acids or cautery may be defended by cloths or other material, wetted with hot or cold water according to the feelings of the sufferers, and poultices of various kinds may be had recourse to, if unavoidable.
Eleventh.—After the diseased parts have been destroyed by the actual or potential cautery, they cease in a great measure to be contagious, and there is less chance of the disease being propagated to persons having open wounds or ulcerated surfaces. A number of wounded thus treated are less likely to disseminate the disease than one person on whom constitutional treatment alone has been tried.
Twelfth.—The pain and constitutional symptoms occasioned by the disease, considered as distinct from the symptoms which may be dependent on disease endemic in the country, are all relieved, and sometimes entirely removed, by the destruction of the diseased surface, which must, however, be carefully and accurately followed, to whatever distance and into whatever parts it may extend, if the salutary effect of the remedies is to be obtained.
Thirteenth.—On the separation of the sloughs, the ulcerated surfaces are to be treated according to the ordinary principles of surgery. They cease to eliminate the contagious principle, and do not require a specific treatment.
Fourteenth.—The constitutional or febrile symptoms, whenever or at whatever time they occur, are to be treated according to the nature of the fever they are supposed to represent, and especially by emetics, purgatives, and the early abstraction of blood if the fever be purely inflammatory, and by less vigorous means if the fever prevailing in the country be of a different character. Pain should be alleviated by opium, which should be freely administered.
Fifteenth.—The essential preventive measures are separation, cleanliness, and exposure to the open air,—the first [175] steps toward that cure which cauterization will afterward in general accomplish.
Sixteenth.—If the sufferer be very young, or of a weakly habit, his strength will frequently require to be supported in the most efficient manner by a due administration of cinchona bark, wine, and a generous diet,—means often found essentially necessary after all severe attacks of debilitating diseases.
The formidable nature of this terrible disease, before the local application of caustic remedies was fully adopted, will be best understood by the following document.
Return of the Number of Cases of Hospital Gangrene which have appeared at the Hospital Stations in the Peninsula between 21st June and 24th December, 1813.
| STATIONS. | No. of cases occurred. |
Discharged cured. |
Died. | Under treatment. |
No. operated upon. |
REMARKS. |
| Santander | 160 | 72 | 85 | 53 | 25 | {Most of these {cases were sent {from Vittoria. |
| Bilbao | 972 | 557 | 387 | 28 | 183 | |
| Vittoria | 441 | 349 | 88 | 4 | 74 | |
| Passages | 41 | 2 | 2 | {Thirty-seven {transferred {to Santander. |
||
| Vera | ... | ... | ... | ... | ... | {Vera, being almost {on the field {of battle, {had no case. |
| 1614 | 980 | 512 | 85 | 282 |
ON WOUNDS OF ARTERIES, ETC.
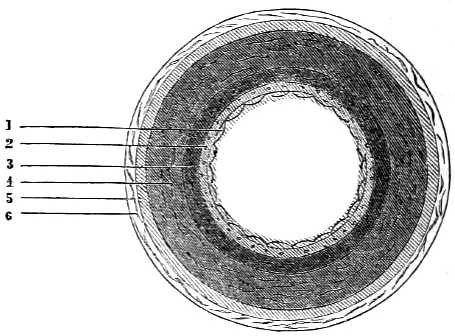
173. The efforts resorted to by nature for the suppression of serious hemorrhages depend on the capabilities of the arteries as resulting from their structure, into which it becomes an object of importance minutely to inquire. With this view, the old division of an artery into three coats may be continued, the difference between ancient and modern anatomy being in their subdivision into different textures or layers. The annexed diagram shows the edge of a large artery, which has been divided circularly, and magnified so as to exhibit six layers in a distinct manner; each of the three ancient coats is divided into two. The inner or old serous coat is shown to be separable into two: the epithelial, marked 1, and the fenestrated, marked 2. The middle coat is also separated into two: the inner, or muscular, marked 3, and the outer, or elastic, marked 4. The outer coat is divisible also into two layers, the inner, marked 5, and the outer, marked 6; number 5 being composed more of elastic fibers: number 6 more of areolar fibers, by which tissue, in a less condensed state, the arteries of the extremities are attached to their sheaths. Such may be considered to be [177] the general composition of a large artery, each particular structure remaining to be examined.
No. 1.
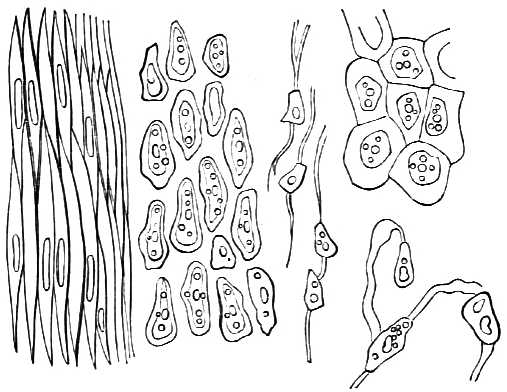
OLD. MIDDLE. YOUNG.
174. If a small portion of the inner coat of an artery be gently scraped with a knife, or if the inside of the cheek be treated in a similar manner, a little white soft substance is brought away on it, called epithelium, a name given to it by Ruysch, from the delicate layer of epidermis investing the female nipple, έπι, upon, θηλή, a nipple. The epithelium of the human body is divided into three kinds by microscopists—the tesselated, pavement, or scaly; the cylindrical, or conical; and the spheroidal, or glandular. The tesselated, as it exists in arteries, is represented in diagram No. 1, in three different stages—in the young person, in middle age, and in the very old person; one stage gradually degenerating or changing into the other, at each different period of life. It is composed of a single layer of nucleated cells, of a flat, oval, round, hexagonal, or polygonal form, and about 1/1400 of an inch in diameter, the nucleus in each cell containing within itself one or more nucleoli, and even several paler granules. The epithelium has a thickness proportioned to the friction or pressure to which it is exposed, particularly when covering the skin. In the arteries of the young, and in the mammalia generally, the epithelium is [178] strongly marked; in older persons, all traces both of cells and nuclei have disappeared. It lines not only the internal surface of the arteries and veins, but the mouth with its mucous glands; the conjunctiva of the eye; the pharynx and œsophagus; the vagina and cervix uteri; the entrance of the female urethra, and the serous membranes.
The conical or cylindrical is composed of cells closely set together, of a conical, cylindrical, or pyramidal form, about 1/1200 of an inch long, each cell inclosing a flat nucleus, with nucleoli. It lines the urethra in the female, from the entrance where the tesselated ends, and extends inward to the urinary tubules of the kidneys; the greater part of the male organs in a similar manner; the digestive canal and gland-ducts, from the cardia to the anus.
The spheroidal or glandular epithelium consists of cells, more or less circular or spherical in figure, each having a large nucleus in its center. The epithelium is met with in all glandular organs, such as the liver, kidney, lachrymal, and salivary glands, and in these cells the proper secretion of the gland is developed. The tesselated and cylindrical kinds are, on the contrary, more or less protective.
The two first kinds are sometimes ciliated, by the addition, at their free extremities, of several fine, pellucid, blunt, and pliant hairlike processes or cilia, about 1/5000 of an inch long, which are, during life, in constant motion. This kind of epithelium, known as the ciliary, lines the whole respiratory track of mucous membrane; the palpebral conjunctiva, as opposed to the tesselated on the eyeball; the ventricles of the brain; the posterior half of the uterus, and the Fallopian tubes.
The epithelium is placed upon the second layer of the internal coat, which, from certain appearances of apertures or windows, has been called the perforated or fenestrated layer. (See diagram No. 2.) It can be peeled off in small pieces only, and shows under a power of 250 diameters a series of well-marked fibers running in almost parallel lines upon a comparatively structureless membrane, resembling the inner layer of the cornea, as in the left-hand figure of the diagram, the fibers being arranged in the length of the vessel. They frequently bifurcate, and almost immediately join again, so that an oval space, resembling a hole, is perceived. This is not always a hole or perforation, as it is generally described to be, as may be seen and proved by the [179] fact that the supposed opening is sometimes filled up by small bodies, like nuclei, as if the oval space were occupied by a cell. This fenestrated layer varies in thickness in different vessels, and is more strongly developed in the lower animals than in man; by some authorities it is not regarded as a distinct layer, but as the innermost layer of longitudinal fibers belonging to the middle coat. When this layer is very thick, the fibers which are yellow do not all run in the direction of the length of the vessel, for others crossing at right angles may sometimes be observed, as delineated in the right-hand figure of diagram No. 2. These two layers compose the ancient inner coat of an artery, and are frequently the seat of disease.
No. 2.
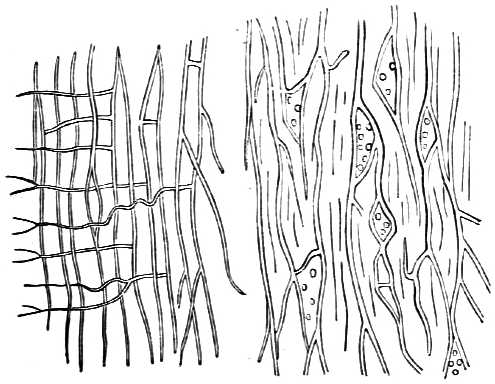
The middle coat, as it was termed, forms by much the greatest part of the thickness of an artery, and, generally speaking, is of a more or less yellow color. It appears fibrous to the naked eye, and can be peeled off not unfrequently in a series of circular layers; when examined microscopically, it is seen to be composed of two sets of fibers arranged in a circular direction. The inner layer is composed principally of muscular fibers, of the organic or involuntary kind. (See line marked 3 on the circular diagram.) The outer layer, marked line 4 on the same diagram, is made up chiefly of elastic fibers, with a much smaller [180] amount of the muscular or contractile element. These conjoined layers form the muscular coat of Mr. Hunter, the fibrous or contractile coat of later anatomists, who denied its muscularity from the supposed absence of fibrin—an error fallen into from chemical science being unequal at that time to its discovery, or rather of its more elementary part, called protein, the principal constituent both of albumen and fibrin, which two are now found to differ from each other in the addition only of three per cent, of sulphur. Mülder says, in his “Animal and Vegetable Chemistry,” (Part II. p. 307:) “The combinations of sulpho-phospho protein (fibrin and albumen) and of sulpho-protein casein with acids, alkalies, and salts are especially remarkable. Protein is soluble in weak alkalies. Since, therefore, the serum of the blood is always slightly alkaline, being a proteate of soda, with sulphur and phosphorus, it keeps the sulpho-phospho protein in solution. This property is the cause of the blood remaining in a liquid state—a chief requisite for animal life.
“If a weak alkaline solution of protein be neutralized by an acid, the solubility of sulpho-phospho protein is greatly diminished. The sulphuric and phosphoric acids, by not dissolving protein, stanch bleeding. Acetic acid, by which protein is dissolved, does not, neither does the hydrochloric.
“Protein, according to Mülder—although it is doubted by Liebig—is a complex substance, consisting of several heterogeneous organic compounds united into one whole, easily acted upon by strong reagents.
“If a protein compound be brought into contact with an alkali, ammonia is immediately disengaged, and the alkaline solution can hardly be made weak enough to prevent the disengagement of ammonia. If either fibrin or coagulated albumen be dissolved in a weak potash lye, ammonia is always perceptible. Protein, therefore, is always in a state of decomposition, as serum is alkaline.”
In diagram No. 3, fig. 3, the organic or involuntary muscular fibers of the intestine are shown, consisting of more or less flattened bands, the fibers of which are soft, and marked with minute granules, sometimes exhibiting traces of nuclei. These purely muscular fibers are most abundant next to the inner coat of the artery, and diminish in number as they approach the outer layer, their place being occupied [181] by firmer and more elastic fibers of a yellow color, seen collectively in the circular diagram, as line 4, and separately in diagram 3, fig. 4, and in diagram 4.
No. 3.
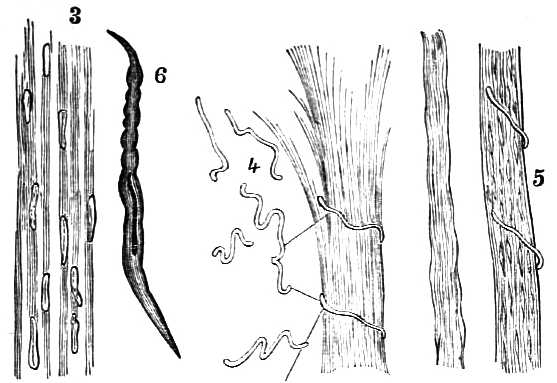
No. 4.
The involuntary muscular fibers of an artery do not always form a continuous layer; they are often smaller than those found in the intestines, bladder, and uterus, and occur as fusiform cells, detached from each other, and having a large, club-shaped nucleus, as shown at fig. 6 in diagram 3.
The voluntary muscular fibers differ from the involuntary, in having cylindrical fibers of much larger size, with transverse and longitudinal[182] markings, unlike the flattened fibers of less size of the involuntary muscles, which have also a faintly granular appearance, instead of the more determined transverse and longitudinal lines of the voluntary muscles.
The outer or elastic layer of the ancient middle coat, represented by line 4 in the circular diagram, contains muscular fibers, but it is formed principally of strong, elastic fibers difficult of separation, and, when torn across, have curled extremities, as shown in the diagram marked 4, differing only in size from those found in the ligaments of the spine, and in the ligamentum nuchæ of quadrupeds, as shown in the separate diagram marked 4.
The external coat of an artery, divided also into two layers, is shown on the circular diagram by lines 5 and 6. These two layers are composed of the yellow elastic fibers last noticed, and another set of fibers, white in color and inelastic in structure, arranged in various directions; the inner layer predominating in yellow elastic, the outer layer in white inelastic fibers, constituting a firm investment to all the other layers of which the artery is composed. The white [183] inelastic fibers are shown in diagram No. 3, fig. 5, with a yellow elastic fiber curling round them. The constant crossing and recrossing of these two sets of fibers form certain spaces, which, when not in a compact form, become real spaces, meshes, or areolæ, constituting what is now called areolar tissue, rather than the cellular of the older anatomists, from the circumstance that the areolæ communicate, and that perfect cells in any tissue do not. These elements of areolar tissue can be readily distinguished by the action of acetic acid, under which reagent the white fibers will almost disappear, leaving only a slight trace of fibers containing oval nuclei, as seen and marked in diagram 3, fig. 5. It is seen when unraveled in b, diagram 5.
No. 5.
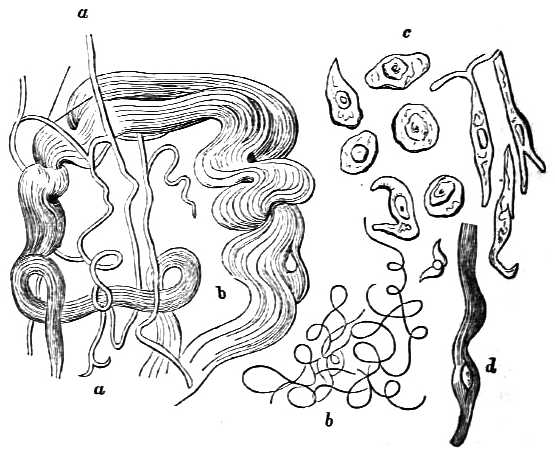
a. Yellow elastic fibers.
b. White inelastic fibers.
c. Nuclei.
d. Fiber, with nucleus.
The inner layer of the middle coat, or muscular coat, as it may be justly termed, forms, it will be seen, the greatest part of the thickness of the wall of certain arteries, and in some instances, as in the anterior tibial artery, constitutes nearly the entire thickness of the vessel. The internal coat in all is frequently seen puckered in a longitudinal direction.
175. The arteries are supplied with blood by vessels of small size, which do not come off immediately from the part of the artery they are destined to supply, but principally from neighboring vessels. They are called vasa vasorum. They are arranged precisely in the same manner as those of the areolar tissue. A few of these vessels penetrate as far as the middle or muscular coat, but do not reach the inner, which has no vessels, proximity to the circulating fluid being apparently sufficient for its nutrition.
Arteries are supplied with nervous influence by branches from the sympathetic system running in their walls, and through their connection by ganglions with the organs they supply with blood.
176. The cells, nuclei, and nucleoli alluded to are supposed to be thus produced. In a shapeless, consistent, sometimes almost gelatinous mass, to which the name of cyto-blastema or formative substance has been given, containing the materials requisite for the production of cells, small, round grains or nucleoli are perceived in the act of formation. Around these grains a layer of granular matter is deposited, which continually increases in thickness, and constitutes the kernel or nucleus. This is oval shaped or round, almost always opaque, has a granular surface, and is considered to be a vesicle, a little cell itself. From the sur[184]face of this kernel a small, very thin transparent vesicle is raised, appearing as a segment of a sphere, which soon expands, and becomes so large, when full grown, that the kernel lies as a minute corpuscle upon its interior wall; the material for its formation being supplied by the cyto-blastema, it is converted into a vesicle by the kernel which is first formed, its embryo existing in the formative substance.
The first trace of organization is the production of a small, perceptible body, or nucleolus, which deposits on the surface a granular substance from the cyto-blastema, to give rise to a little producing organ, the kernel or nucleus. This further transforms the surrounding cyto-blastema into a granular surface, from which the vesicle is formed, raised, expanded, and filled with a liquid, in which vesicle thus enlarged the kernel remains inclosed and adhering to a certain spot of its wall.
If two nucleoli lie close to one another, they coalesce and become one solid mass, capable of producing one cell only, containing one kernel and two nucleoli. This view is that of Schleiden and Schwann, supported by Mülder, but not entirely approved by Henle; inasmuch as no kernel can be perceived in the cells of many cellular systems while in the act of formation. In the elementary parts of animals which have long since lost their cellular form, the remnants of kernels are frequently found, as has been demonstrated in the preceding diagrams. The manner, however, in which the elementary first-seen granules are formed in the cyto-blastema, science has not yet been able to discover. The chemists have proved that all elementary organic substances consist of carbon, hydrogen, oxygen, and nitrogen, susceptible of endless modifications of their respective forces, under which an organic molecule or ovum is produced, and after that, under certain circumstances, an animal such as man.
177. When the current of blood through the main trunk of the arteries of an extremity is cut off, the circulation is carried on by the collateral branches. This collateral circulation is more perfect, more active in young persons during the increase or growth of the body, than it is either at maturity or in the decline of life. The important point is not, however, alone referable to the time of life at which the continuity and permeability of the main trunk cease to exist, but to the nature of the disease or injury which has given rise to it.
When an aneurismal limb has been injected, on which an [185] operation has not been performed, the collateral vessels have all been found larger and more fully shown than on the opposite side, although not to the same extent as in cases of a similar nature in which the operation has been done.
It is necessary that this enlargement of the collateral branches should lake place at an early period, because in many cases of aneurism the artery beyond or below the tumor is obliterated long before any operation is performed. The main supply of blood has been already cut off from the extremity, and the operation adds very little to the derangement of the circulation which has for some time taken place below the tumor.
When an operation has been successfully performed for aneurism, and the patient has died some time afterward, dissection has shown various arteries enlarged, both above and below the part where the trunk was obliterated by the ligature; and not only an enlargement of arteries, which, from their regularity have received names, but others have been developed not usually known to exist, or not of a size to be conveniently traced. These through their frequent anastomoses bring the blood at last into several large trunks, by which it is again conveyed to the original vessel below all and every obstruction which may have taken place; thus compensating by a circuitous route for the loss of the direct supply. The principal object of inquiry is, do these vessels always exist, or at what period of time do they begin to enlarge, so as to enable them to carry on the circulation, in the manner in which it is presumed to be done?—for few will assert that the enlargement of these particular collateral vessels was an accidental play of nature, and existed previously to the commencement of the disease or injury for which the operation was performed. On this point, the theory of the operation for aneurism and its applicability to wounded arteries appears to hinge; and, what is of more importance, on which the practice resulting from it depends.
Two distinct kinds of collateral circulation are at present acknowledged: one by direct large communicating arteries; the other through the direct medium of the capillary vessels inosculating with each other. Where direct communicating arteries exist, little subsequent change beyond enlargement takes place in them. It is otherwise with the indirect capillary vessels. When the radial or ulnar artery has been divided in the hand, the blood will not only flow readily [186] from each end of the divided vessel, but equally red and arterial from both, the communication being through direct arterial branches from one vessel to the other. It will also be red and arterial if the division take place at the wrist, and may be so in the brachial; but if the femoral in the lower part of the thigh be wounded, the color of the blood issuing from the lower end of the artery, if any issue at all, will be dark or venous. It is so, because it has been obtained from the capillary arteries, which in this case being empty received blood by regurgitation from the veins, the valves of which when present do not prevent its reflux course. If a limb be injected and carefully dissected four or five days after a ligature has been placed during life high up on the principal trunk, the capillary vessels will be seen to be well injected; but few or none will be found large enough to admit of their inosculation being traced throughout. If another limb be injected and dissected, some sixty days after the ligature has been applied, a difference will be distinctly observed between the two preparations. In the latter, the capillaries will not appear to be so fully injected, but several larger and more tortuous vessels will be found in situations where they were not expected to exist; and the anastomoses of these one with another, generally by arches, may be traced to their communication with the principal trunk, both above and below the obliterated part. If an incision were made in the nearest pervious portion of the lower part of an artery in the thigh of a person who had undergone this operation, arterial blood would issue from it. The communication would have become direct by communicating branches, and the capillaries would have returned to their accustomed duties.
178. During the first twenty-four hours after the division of an artery such as the femoral, or the application of a ligature, the temperature of the limb is commonly diminished; after that period, and as the action of increase takes place, the temperature is usually from three to five degrees higher than in the opposite healthy limb. At the end of from eighteen to twenty-eight days, in a successful case, it is found to be equal in both.
It is asserted by some sanguine supporters of the all-powerful influence of the collateral circulation, that it is sufficient at all times, and under all natural circumstances, to maintain the life of the extremity. The practice of the Peninsular war proved the fallacy of this opinion in too [187] many instances to admit of any doubt of its inadequacy to do so in the lower extremity after the division of the femoral artery, under ordinary circumstances. The fact of enlargement or of a new development of vessels having taken place after the commencement of disease or the reception of an injury, has been demonstrated by dissection, and it is through them the life of the limb is to be preserved; but time is required for their development. When a limb is lost through mortification, as the consequence of a division or obstruction of the principal artery, it usually takes place after the infliction of a sudden injury, in consequence of these collateral branches not having had time to enlarge.
179. The collateral circulation is therefore not the same, and is not in the same stage of preparation, in a limb suffering from a divided or wounded artery, as in one in which an aneurism has for some time existed; this is the reason why mortification is more common after wounded arteries than after operations for aneurism.
PROPER TREATMENT OF WOUNDED ARTERIES, ETC.
180. The due appreciation of the means adopted by nature and by art for the suppression of hemorrhage, as well as the proper treatment of wounded arteries, is owing to the surgery of the war in the Peninsula. They were suspected after the battles of Roliça, Vimiera, Oporto, and Talavera, but did not receive their complete development until after the battle of Albuhera. It was not until after that of Toulouse they were partially admitted; and it is only of late that they have been almost everywhere acknowledged, taught, and practiced.
Previously to the time of Mr. Hunter, the diseased or dilated state of the coats of an artery which constitutes an aneurism was, when it occurred in the ham, very often fatal. The operation of Anel, first performed in 1710, of cutting down to the artery, and placing a ligature upon it immediately above the dilated part, was not approved, and Mr. Pott, the great contemporary of Mr. Hunter, recommended in bad cases that amputation should be resorted to in the [188] first instance; although Desault had succeeded, in 1783, in a case of popliteal aneurism, in which, after the manner of Anel, he had placed the ligature on the artery a little above the aneurismal swelling in the ham. Mr. Hunter’s contemplative mind, aided by his knowledge of anatomy and of disease, led him to believe that the ligature thus applied on the artery in the ham failed, because the vessel was unsound at that part, and was therefore incapable of taking on those healthy actions necessary for the obliteration of its canal above the ligature, which are known to take place when the artery is in a normal state. He concluded that this was sufficient to account for the failures, without especially taking into consideration the difficulty of applying the ligature in the ham immediately above the aneurismal sac, and of the probability of the sac suppurating when thus molested; an occurrence aiding materially in the necessity for the loss of the limb by amputation, performed then under circumstances of constitutional irritation, which would render it less likely to be attended with success.
From the consideration of these and other circumstances, Mr. Hunter was induced to propose, in 1785, that the ligature should not be placed on the artery near the tumor in the ham, but at a greater distance on the fore part or middle of the thigh, and Scarpa subsequently recommended it to be placed even higher—a recommendation which has been generally followed, and the spot now selected for this operation is at the lower part of the upper third of the thigh. This operation was therefore performed not only for aneurism, but improperly for a wound of the artery, not only in the ham, but even in the leg; it consequently failed in almost every instance of traumatic injury, thus rendering amputation necessary, which was generally followed by death.
181. The Hunterian theory implies:—
1. That the artery is in general sound at the part in the front of the thigh selected for operation, while it is usually unsound in the popliteal space behind, or in the ham, where Desault operated, and Anel recommended it to be done; that operation is now abandoned on the continents of Europe and America, as well as in England.
2. That a ligature can readily be placed upon it at a distance from the disease in the fore part of the thigh, and will usually be followed by success as far as concerns the obliteration of the artery immediately below the part on which it is applied.
[189] 3. That the artery being aneurismal, the collateral branches had begun to enlarge, so as to be better able to carry on the circulation, after the supply of blood to the lower part of the limb by the main trunk had been cut off.
4. That no branches of importance are usually given off between the ligature on the artery on the fore part of the thigh and the sac of the aneurism in the ham.
5. That if such branches were ever given off, and brought the blood from their collateral communications back into the main artery below the ligature, and thence into the sac, so as to renew its pulsatory movements, they would ultimately disappear, from the impelling force not being sufficient to prevent a gradual coagulation taking place, which would soon fill up the cavity of the sac, and thus prevent its further enlargement; at which stationary point a process of removal by absorption would begin and continue, until the diseased sac with its contents had diminished, if not entirely disappeared, leaving only a trace behind of its former existence, the process thus described being frequently assisted by a commencing obliteration of the artery immediately below the aneurism. The essential point in this theory, which has immortalized the name of Hunter in surgery, depends on the integrity of the aneurismal sac, which ultimately retains, as a general rule, subject to rare exceptions, any blood which may be brought into it, either by the collateral branches from above, or from below by what may be called regurgitation, until it has become coagulated, when the sac is so filled up that no more blood can pass into it to cause its further distention, or any ulterior evil.
This theory of Mr. Hunter, then so new, so beautiful in itself, was eagerly embraced by nearly all the civilized world; and surgeons were not content with applying it to cases of diseased or aneurismal arteries, to which it is especially applicable, but they extended it indiscriminately to cases of wounded arteries, to which the practice of the war in Spain proved it was inapplicable, and in which I have, since 1811, maintained it could only succeed as a matter of accident, not of principle.
182. The essential features of the theory opposed to Mr. Hunter, with respect to wounded arteries, and called mine, are:—
1st. That the artery at the wounded part is free from previous disease, and may be expected to take on those healthy actions which, after the application of a ligature, lead to the [190] obliteration of its canal, and the consequent suppression of hemorrhage.
2d. That the circulation of the blood by the collateral branches is less free in a sound limb than in one which has suffered during several weeks from the formation of an aneurism.
3d. That this freedom of circulation is less in the lower than in the upper extremity, under all circumstances.
4th. That mortification of the foot and leg, and often of the whole limb, followed by the death of the person, is a common occurrence after a ligature has been placed high up on the artery in the thigh, in consequence of a wound; while it is not so common an occurrence when such operation is performed in the same place for an aneurism of several weeks’ duration. If the vein be also wounded, mortification is almost inevitable.
5th. That mortification of the hand and arm rarely follows the application of a ligature to the artery of the upper extremity in any part of its course, however near the heart.
6th. That when the collateral vessels are capable of carrying on the circulation through the lower extremity, the lower end of the divided artery bleeds dark or venous-colored blood, while its upper end bleeds scarlet or arterial-colored blood. In the upper extremity, the color of the blood from the lower end of the divided artery is little altered—a consequence of the greater freedom of anastomosis, or of the freer collateral circulation in the upper extremity. Facts of the greatest importance in surgery.
7th. That whenever the collateral vessels are not capable of carrying on the circulation of a limb, mortification or death of the part ensues; and that whenever this collateral circulation is sufficient to maintain the life of the limb, blood must pass into the artery below the wound, and must, as a general rule, pass up and out through the lower end of the divided artery, unless prevented by the application of a ligature, or by some accidental circumstance, forming an exception to the rule, but not the rule itself.
8th. That the collateral branches are capable of bringing blood into the artery above the aneurismal sac and between it and the ligature, is admitted in the Hunterian theory, which blood the aneurismal sac receives, and usually retains. [191] When the artery is a wounded artery, and the ligature is applied at a distance above the wound, blood is often brought into it below the ligature in a similar manner; but as there is no aneurismal sac to receive and retain it, the patient bleeds perhaps to death, unless surgery come to his assistance.
9th. The presence of an aneurismal sac in one case, and its absence in the other, is the essential difference destructive of the Hunterian theory for the treatment of aneurism being applicable to that of wounded arteries.
10th. The processes for the natural suppression of hemorrhage are somewhat different in the upper and lower ends of an artery, and are less capable of resistance in the lower. This end frequently yields to the pressure of the blood regurgitating from below, and renews a bleeding which may have been suppressed for weeks, unless its closure has been rendered more permanent by the application of a ligature.
11th. The absence of the aneurismal sac renders the application of two ligatures absolutely necessary, one on each end of a divided artery, or one above and one below the wound, if the artery should not be divided; constituting the most essential feature of my theory, and the principal point to be attended to in the treatment of wounded arteries.
12th. This bleeding from the lower end of the vessel, which is more or less of a venous color, and issues in a continuous stream, may be restrained by compression properly made on the course of the lower part of the wounded artery; but in no instance should recourse be had to a ligature on a distant part of the artery above the seat of injury, until every other possible effort to arrest the hemorrhage from the lower end of the vessel has failed.
13th. The great principles of surgery to be observed in cases of wounded arteries, and which ought never to be absent from the mind of the surgeon, are two in number:—
1. That no operation ought to be performed on a wounded artery unless it bleed.
2. That no operation is to be done for a wounded artery in the first instance but at the spot injured, unless such operation not only appears to be, but is impracticable.
183. The means adopted by nature for the suppression of hemorrhage have been investigated by Celsus, Rufus, Galen, Œtius, etc., down to Dr. Jones, the most important English writer on this subject; but the methods of inquiry they all [192] adopted appear to have been insufficient and unequal to the object in view. They bled an animal until he died, and then reasoned on the manner or means by which the bleeding was suppressed, when it was in fact arrested by death. It is obvious, then, that it is only when nature has not been interfered with, and the patient has not died from bleeding continued to the last moment, but has, on the contrary, lived some time after the hemorrhage has ceased, that the processes by which its suppression has been accomplished can be fairly investigated. These processes essentially depend on the size and variations of structure in an artery, which have been shown to be dissimilar in large and small arteries, and not even quite alike in the upper and lower ends of the same artery—facts which were elicited from observations made on men on the field of battle during the Peninsular war, and consequently not liable to error. It was then proved that arteries of moderate dimensions, such as the middle part of the femoral or the axillary, tibial or brachial, and particularly all below these in size, are capable, by their own intrinsic powers, when completely divided, of arresting the passage of the blood through them without any assistance from art, or from the surrounding parts in which they are situated. The establishment of this fact overthrew at once the theory which relates to the importance of, and necessity for, the sheath of the vessel, and the offices it performs in suppressing hemorrhage in vessels of this size, and in a great measure that supposed to be derived from the formation of an external coagulum, the bouchon of the French.
184. When the femoral artery has been fairly divided in the lower part of the thigh, the patient has, in almost all the cases which have come under observation, either died without assistance, or the hemorrhage has ceased spontaneously. Having been thus arrested for twelve hours, the efforts of nature are usually sufficient to prevent its return from the upper, although not from the lower end of the vessel; but then it is of venous and not of arterial color—a fact I first demonstrated, and which is now acknowledged to be of the greatest importance. The great evil to be dreaded in such cases is not from hemorrhage from the upper end of the divided artery, but from the lower, and from mortification of the foot.
The upper end of an artery retracts on being divided, and this retraction is accompanied by a contraction of the cut [193] extremity of the vessel, which assumes the shape of the neck of a French wine-bottle or Florence oil-flask. The contraction is confined in the first instance to its very extremity, so that the barrier opposing the flow of blood is formed by this part alone. The contraction, however, goes on increasing for the space of an inch; it is usually filled up with an internal coagulum of a round, pyramidal shape, adhering firmly to the contracted end of the artery, loose at its apex, and extending frequently as far as the first collateral branch, but rarely under any circumstances beyond two inches; the very orifice of the artery on the outside being in a few days covered by a layer of a yellowish green-colored substance or fibrin, which indicates its situation in a remarkable manner. Some of these processes are continued even after the external wound has healed; the artery generally goes on diminishing and contracting as far as it is useless, so that of three or four inches, from one to two may be impervious, the remainder being contracted, although still permeable by a probe. An accompanying nerve, where there is one, would do the reverse, the cut extremity would become enlarged or bulbous, gradually diminishing as it is traced upward, until it regains its proper size.
The processes adopted by nature for closing the lower end of a divided artery of the size of the femoral at the inferior part of the thigh are somewhat different from those employed at the upper or opposite extremity. The retraction or contraction of the lower end of a divided artery is neither so perfect nor so permanent as at its upper end, and the small internal coagulum is in many instances altogether wanting, or very defective in its formation. The closure of the lower orifice being less perfectly accomplished than of the upper, it is the more likely to suffer from secondary hemorrhage, which may be distinguished from that from the upper end of the artery at an early period after the accident, by the venous color of the blood, and from its flowing or welling out in a continuous stream, as water rises from a spring, and not with an arterial impulse.
The retracting and contracting powers in the lower end of a divided artery are nevertheless considerable, and are sufficient in some cases to nearly close the lower end of the femoral artery when divided by amputation above the knee. When the femoral artery is cut across, the lower portion of the vessel is emptied by its last efforts, combined with the [194] action of the capillaries. When the collateral circulation is powerful, blood soon regurgitates into the artery, but the force of the regurgitation can be in no proportion to that of the propulsion at the other or upper divided end of the vessel, which will generally be able to resist this impulse, while the lower one often opens and bleeds after the lapse of a few days. In all the cases I have had an opportunity of examining, in which hemorrhage had taken place from the lower end of the artery, the following appearances were observable after the interval of from four to five days.
The same kind of yellowish-green matter marks and conceals the situation of the lower extremity of the artery in the wound as it does the upper. It is, however, thinner where it immediately covers the end of the artery, which in none of these cases was contracted in the conical manner described as taking place in the upper extremity. On the introduction of a probe with the greatest gentleness into the artery from below, it usually makes its appearance at a point on the yellow space, raising a thin portion as it protrudes. On laying open the artery, the orifice would seem to have been once closed by this layer of fibrin, but with a less degree of contraction than the upper end of the same artery; the layer still, however, forming an obstacle sufficient to cover and close three-fourths of the orifice, the blood having flowed through the remaining fourth, which had probably given way by accident; which accident is usually some sudden or continued motion being given to the extremity or part injured, and which motion it is imperatively necessary to avoid, when the lower end of a wounded artery has not been secured by ligature.
A soldier, who had his arm carried away by the bursting of a shell at the siege of Ciudad Rodrigo, was brought to me shortly afterward. The axillary artery, becoming brachial, was torn across, and hung down lower than the other divided parts, pulsating to its very extremity. Pressed and squeezed in every way between my fingers in order to make it bleed, it still resisted every attempt, although apparently by the narrowest possible barrier, which appeared to be at the end of the artery, and formed by its contraction. The orifice of the canal was marked by a small red point, to which a very slight and thin layer of coagulum adhered, the removal of which had no influence on the resistance offered by the very extremity of the artery [195] to the passage of blood through it. In this, and in another instance of a similar nature, the end of the artery being cut off at less than an eighth of an inch from the extremity, it bled with its usual vigor. In both, the vessel for near that distance was contracted so as to leave little or no canal at its orifice, which in these cases was filled by a coagulum of the size and shape of a very small pin.
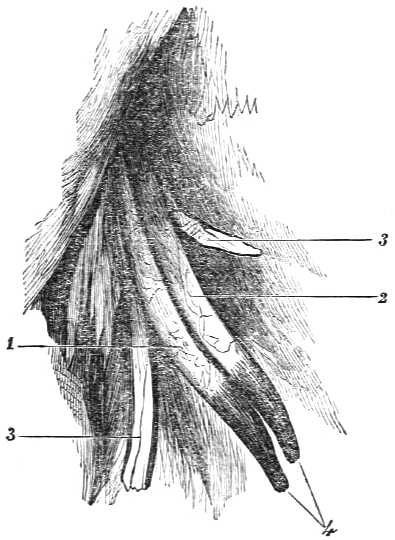
1. Axillary artery.
2. Axillary vein.
3, 3. Branches of axillary plexus of nerves.
4. Curved, pointed and plugged ends of the artery and vein.
The vessels are here represented as they lay exposed in the lacerated parts. The pointed and plugged ends of the vessels were of a dark coagulum color, while above both artery and vein had a reddish, vascular appearance, and were held in close relation by their sheath. The artery bent distinctly to the very base of the coagulum.
Mr. Deputy Inspector-General Taylor informs me that a soldier of the 44th Regiment was struck by a cannon-shot on the 21st of June, 1855, in front of Sebastopol; it carried his left arm away from the shoulder, leaving the artery, vein, and nerves exposed as in the accompanying sketch. The thought, he says, crossed my mind, as I held the artery between my finger and thumb, that it might be for the benefit [196] of the patient to place a ligature on the artery at the highest point, exposed, cutting off the part below, having had a precisely similar case at Ferozeshah, in India, in which the soldier recovered without the artery being tied, or any hemorrhage recurring. The shot, in carrying away his arm, struck him very severely on the chest, and I fear has injured the lungs, but there is so much ecchymosis that the presence or absence of sounds cannot be distinguished by the stethoscope. Of this injury of the chest the man died some days after its receipt. The body was buried without examination, but no hemorrhage had taken place from the wound.
Private J. Barnes, 29th Regiment, on the 16th of May, 1811, at the battle of Albuhera, received a musket-ball in the right thigh, behind and above the knee, inclining downward and inward, close to the condyles of the femur, and in the direction of the femoral artery becoming popliteal; it bled violently at the moment, and so continued for a few minutes, during which time he conceives he lost two quarts of blood. It then ceased, and he was dressed in the usual slight manner, and remained two days upon the field of battle, until removed to Valverde, nine miles, on a bad road, on men’s shoulders, in a blanket converted into a bearer. He was considered as one of the slighter cases, until the gentleman in immediate charge of him requested me to see him, on account of his toes being in a state of mortification.
On the evening of the 3d of June, eighteen days after the accident, the man was placed on a bullock car, to be removed with the rest of the wounded to Elvas, the mortification of the foot having ceased to increase, and a line of separation having been formed. Shortly after the cars moved, I was informed that he was bleeding from the wound: it evidently appeared to flow from the popliteal artery; and as it issued slowly, I supposed from the lower divided end. The foot being partly lost, I determined on amputation above the knee, which was performed at Olivença. The amputated limb was sent after me to Elvas, that it might be examined at leisure. I carefully traced the course of the wound, and found in it a little coagulated blood, but could not see the mouth of the vessel. A probe passed into the upper end of the artery was obstructed before it reached the ulcerated surface by nearly an inch; and on passing it up the lower one, it was stopped exactly in the middle of the track of the [197] ball, by a veil or substance drawn across the mouth of the vessel, which, on careful examination, showed the point of the probe at one part of the circle, although too small to let it through; from this part I conceive the hemorrhage came. The divided ends were one inch apart. The upper, or femoral portion, for nearly an inch, contained a firm coagulum, filling up that part of the artery, which had contracted like the neck of a claret bottle. The lower or popliteal portion of the artery had a very peculiar appearance; the substance drawn across appeared to have closed it completely at one time, and to have given way from the rough motion of the car at the point now open, which was very small even when the sides of the artery were approximated. A very little soft coagulum was behind it; and if the man had not been removed, the vessel might have remained secure. This case shows very distinctly the means adopted by nature for the suppression of hemorrhage from both ends of a divided artery.
Corporal Carter, of the pioneers of the 29th Regiment, was wounded at the battle of Roliça, in August, 1809, by a musket-ball, which passed through the anterior and upper part of the forearm, fracturing the ulna. Shortly afterward a profuse hemorrhage took place, and the staff-surgeon in charge tied the brachial artery. In the night the hemorrhage recurred, and the man nearly bled to death. The arm was then amputated, when the ulnar artery was found in an open and sloughing state.
Remarks.—A simple incision to expose the wounded artery, and placing two ligatures upon it, would have saved this man his arm and his life.
At the battle of Vimiera, which followed a few days afterward, a soldier received a somewhat similar wound, save that the brachial artery bled forthwith, the hemorrhage being stopped by the tourniquet. Warned by the preceding case, I cut down on the artery, carefully avoiding the nerve, which had been tied in the former instance, and found the artery more than half divided. It was secured by a ligature above and below the wound: the bleeding did not afterward return, and the man recovered.
185. Thomas Carryan, of the 3d Regiment, was wounded at Albuhera, on the 16th of May, 1811, on the inside of the calf of the right leg, the ball passing out on the fore and outside of the tibia: it bled considerably for some minutes, when [198] it ceased, and the hemorrhage did not return until the 15th of June, on which day a little blood followed the dressings, and increased on the patient making any exertion; so that on the 4th, the gentleman under whose care he was tied the femoral artery on the outside of the sartorius muscle, which suppressed the hemorrhage for that day, the limb continuing with little or no interruption of the same temperature to the hand as the other. On the 5th, the original wound had a bad appearance, and some coagulated blood was readily pressed out of it; on the 6th, a greater quantity came away; and on the 7th, the exertion of using the bed-pan was followed by a stream of arterial blood, which ceased on tightening the precautionary tourniquet.
The limb was amputated above the ligature on the artery. Its dissection showed the anterior tibial artery to have been destroyed for some distance, and the muscles on the back part of the leg nearly in a gangrenous state. The patient died a few days afterward.
Remarks.—If an incision had been made in the leg so as to expose the artery, and ligatures had been placed on it above and below the wound, the man, in all probability, would not have died.
Sergeant William Lillie, of the 62d Regiment, aged thirty-two, was wounded in the right thigh, on the 10th of April, at the battle of Toulouse, by a musket-ball, which passed through, in an oblique direction downward and inward, close to the bone, describing a track of seven inches. The ball was extracted behind on the field. He said he had bled a good deal on the receipt of the injury, which he had stopped by binding his sash round the limb. The discharge from the wound was considerable; it appeared, however, to be going on well until the 20th of the month, when, on making a sudden turn in bed, dark-colored blood flowed from both orifices of the wound in considerable quantity. I had given an order, as the Deputy Inspector-General in charge of all the wounded, that no operation should be performed on a wounded artery without a report being sent to me, and an hour at least granted for a reply, unless the case were of too urgent a nature to admit of it. It appeared to be so in this instance, and before I arrived Mr. Dease had performed the operation for aneurism at the lower part of the upper third of the thigh. I could only express my regret that it had been done, and point out the probability of the recurrence of the [199] hemorrhage from the lower end of the artery, which took place on the 7th of May, when the limb was amputated, and the man subsequently died. On examination the artery was found to have been divided exactly where it passes between the tendon of the triceps and the bone. The upper portion of the artery thus cut across was closed. A probe introduced into it from above would not come out at the face of the wound, although the impulse given to this part on moving it was observable in the middle of a large, yellowish-green spot, which I had previously declared to be the situation of the extremity of the artery which had contracted behind this, in the shape of a claret bottle, for about an inch, having within it a small coagulum. The lower end of the artery from which the hemorrhage had taken place was marked by a spot of a similar character; but on passing a probe upward from the popliteal space, it came out at a very small hole in the extremity of the artery, in the center of the yellow spot, the canal of the artery not being contracted and diminished, but only apparently closed by a layer of the yellowish-green matter laid over it, and adhering to its circumference.
Sergeant Baptiste Pontheit, of the French 64th Regiment, was wounded by a musket-ball at the battle of Albuhera, on the upper and fore part of the thigh; it passed out behind, in the direction of the femoral artery. He lost a great quantity of blood before the hemorrhage ceased, but the wound went on well until the 26th, ten days after the battle, when he felt something give way in his thigh, and found himself bleeding from the wound, which, however, soon ceased on pressing his hand upon it. In the afternoon, on again moving, he lost about half a pint of florid blood, which induced the surgeon on duty to place a tourniquet on the limb. When at leisure (in the course of two hours) I removed the tourniquet, and as no hemorrhage occurred, and there was no swelling in the vicinity of the wound, I replaced the dressing with a precautionary screw tourniquet, explaining to him its use, and the probable nature of his wound, together with the operation requisite to be performed in case of further bleeding.
On turning in bed at night he lost a little more blood, which ceased on his tightening the tourniquet, which was shortly after loosened. In the morning, everything being removed, there appeared some swelling about the wound, the [200] opening of which was filled up by a coagulum: gentle pressure being made, it readily turned out, and was followed by a stream of arterial blood, leaving little doubt of the femoral artery being wounded. Compression being effected in the groin, I made an incision three inches and a half in length, taking the wound as a central point, and exposed the femoral artery and vein: both were wounded, the former being half destroyed in its circumference, surrounded with coagulated blood, and appearing as if it had sloughed from being touched by the ball, the course of which was directly past it, and would have carried it away if it had not been for the elasticity of the artery. A ligature placed above, and another below the wound, secured both artery and vein; the incised wound was brought together by adhesive plaster, and the limb placed in a relaxed position. The operation was of short duration; he lost little or no blood, but, the circulation was very languid, and the man exceedingly low. The warmth of the leg and foot was soon below the standard of the other; warm flannels were applied, and some brandy was given to him. In the evening the heat was more natural, and the man returned thanks for the humanity and kindness shown to him, congratulating himself and me upon the success of an operation which he had supposed would be infinitely more severe. The next morning he ate a tolerable breakfast, but felt a pricking sensation in the calf of the leg, which was as warm to the hand as the other, but the foot was cold. The second day the swelling of the limb, its appearance, and discoloration on the under part, indicated approaching mortification, which on the third was evident, and on the fourth, at mid-day, he died, the limb up to the wound being nearly all in a gangrenous state. No adhesion had taken place in the wound, or in the artery, which showed the inner coat cut, the ligatures being firm, and no coagulum behind them.
Captain St. Pol, of the 7th or Royal Fusiliers, was wounded in the ham from behind, while in the ditch at the foot of the great breach at Badajos. He fell instantly, and lost, as he thinks, a considerable quantity of blood. On recovering he was raised from the ground, and walked a few paces prior to his being carried to his tent, where I saw him in the afternoon of the next day, the 7th. The leg had ceased to bleed before his arrival in camp. A substance could be felt on the inner side of the patella, which, by the sensation communi[201]cated to the finger on moving, appeared to be the ball, which was extracted. Some dark-colored blood issued from the cavity; the ball was lying loose and unconnected; the finger, on being passed into the joint, which was swollen, discovered no splinters of bone, and the entrance of the ball behind would not admit the finger. His having walked some distance on the leg, and the absence of any splinters between the articulating extremities of the bones, induced Dr. Armstrong, the surgeon of his regiment, and myself to think that the ball had entered with little injury to the bone; and after stating to the patient the little hope we had of ultimately saving the limb, independently of the great danger to which he was exposed, compared to the certainty of the operation of amputation at the moment, we recommended its being done, but he would not consent. The next day he was removed to Badajos on a litter, the heat of the tent being unsupportable.
On the morning of the 9th I saw him early, when the want of circulation in the foot was evident from its having lost its natural color and warmth; the knee was swollen, but not painful, and I had no doubt that the artery had been divided by the ball. The marbled appearance and tallow-white color soon indicated the loss of the leg above the calf; and vesications had formed on the foot, already of a green color.
On the 12th, the extent of the gangrene was defined on the back of the knee up to the original wound at its lower edge, gradually receding as it advanced to the fore part of the leg, which for three inches below the knee was apparently sound; the uneasiness of the knee being moderate, and the incised wound looking perfectly healthy, although the latter had not united.
On the 16th, the separation of the dead from the living parts having taken place behind, and being well marked and commencing on the fore part, the limb was amputated as low down as possible. Sixteen vessels were tied; the parts were gently brought together, without any hope of union. According to subsequent experience, this operation should not have been performed. The dead parts only should have been removed, and the stump left to nature until the health was perfectly restored.
On the 24th he died.
On examining the amputated limb, the popliteal nerve was found untouched, the ball having passed on the inside; [202] the popliteal vein was also entire, having a small tumor adhering to its under part between it and the artery, the divided end of which was closed by a yellowish-green firm substance readily distinguishing it from the surrounding parts. On clearing the whole from the bone, and making a small circular opening into the tumor, which was elastic and covered with brown fibrous layers, it proved to be an aneurismal sac, smooth on the inside, containing florid arterial blood and some little coagula. The artery, on being carefully opened to the closed end, appeared to have been injured above the part divided by the ball, and communicated with the sac by a small fissure or rupture. The end of the artery was then slit up, so as to show the very little thickness of the closing substance and the great original contraction of the diameter of the vessel. There was no internal coagulum, neither was there any laid over the external part of the artery; between it and the bone there was a coagulum about the size of a small phial cork. The other end of the artery could not be found, from the gangrenous state of the parts.
Private P. Turnbull, of the grenadiers of the 74th Regiment, of good stature, was wounded on the 10th of April, 1814, at Toulouse, by a musket-ball passing from the inside to the outside of the middle of the thigh; he says it bled considerably at first, but the bleeding soon ceased; the wound was not painful, and he thinks he observed the leg and foot to be colder than the rest of his body for the first two or three days, but did not much attend to it, further than conceiving the numbness, coldness, and impeded power of motion as natural to the wound.
On the 18th of April, the gentleman in charge of this patient pointed him out to me as an extraordinary case of gangrene coming on without, as he supposed, any sufficient cause. The wound on the outside of the thigh, or the exit of the ball, was nearly healed, and that on the inside was without inflammation or tumefaction, and with merely a little hardness to be felt on pressure. The pulsation of the artery could be distinctly felt to the edge of the wound, but not below it; the leg was warm, the gangrene confined to the toes. The artery of the other thigh could be distinctly traced down to the tendon of the triceps. As he was at a small hospital, about two miles from town, on the field of battle, I did not see him again until the 20th, and afterward on the 23d, when, although the gangrenous portion included [203] all the toes, it had the appearance of having ceased. Satisfied that it would again extend, I left directions with the assistant-surgeon that the limb should be amputated below the knee.
The surgeon, whom I had not seen, and who did not understand the subject, disobeyed the order, conceiving that there must be some mistake. On visiting the hospital, a little after daylight on the 25th, I was greatly annoyed at finding that the operation had not been done, and that the mortification had begun to spread the evening before. It was then too late. On the 26th it was above the ankle, with considerable swelling up to the knee. At night the man died; and the next morning, at six o’clock, I removed the femoral artery from Poupart’s ligament to its passage through the triceps, which part was affected by the mortification.
The ball had passed between the artery and vein in the spot where the vein is nearly situated behind it and adherent only by cellular membrane, through which the ball made its passage, the coats of the vein being little injured, and those of the artery not destroyed in substance, although bruised; it was at this spot much contracted in size, and filled above and below by coagula, which prevented the transmission of blood, and the vein above and below the wound was filled by a coagulum and was also impassable. This preparation is unique; it is perhaps the only one in existence proving the elasticity which vessels possess, and their capability of avoiding to a certain extent an injury about to be inflicted upon them. It is in the museum at Chatham.
186. When a round and small ligature is properly applied to an artery of a large size, such as the femoral, the sides of the vessel are brought together in a folded, plaited, or wrinkled manner; the ancient inner and middle coats of the artery, including the modern four, are divided, while the outer one remains entire and apparently unhurt. If the ligature be removed, an impression or indentation made by it on the outer coat will remain as a mark; and if the artery be slit open in a careful manner, the division of the inner coats will be obvious. These changes were known to Desault, and are mentioned by Deschamps in his work on the Ligature of Arteries. They were more satisfactorily proved to occur by Dr. Jones, and have been clearly stated by Mr. Hodgson and others. The remaining part of the process differs from the account they have given, and, according to observations [204] I have had opportunities of making on the living and on the dead, is as follows: the inner and middle coats, formed by four distinct layers or structures, are not only divided, but the inner ones particularly appear to be curled inward on themselves, so that the cut edge of one half or side is not applied to its fellow in the usual way of two surfaces, but by curling inward meets its opponent on every point of a circle, and in this way forms a barrier inside that of the external coat, which is tied around it by the ligature; so that, in fact, when a small ligature is firmly tied, its direct pressure is not applied to the inner coats, which have been divided and have curled away from it, but to the two layers of the outer coat, which are in consequence of that pressure made to ulcerate or slough—processes which could scarcely fail to take place also in the other coats if they were subjected to pressure in a similar manner. The cut edges of the four inner layers being from this provision of nature perfectly free, are capable of taking on the process of inflammation, which stops at the adhesive stage. This they do by the effusion of lymph or fibrin both within and without, to a greater or less extent as the case may require. The outer coat of the artery must either yield by ulceration or sloughing, or the ligature must remain until it is decomposed and destroyed. It usually yields by sloughing, in consequence of its being deprived of life by the pressure of the ligature, which is left at liberty by the ulceration which takes place in the sound part of the artery immediately above and below the part strangulated, which part is frequently brought away in the noose. The artery does not always yield by sloughing, particularly if it be a large one and the ligature thick and soft. In this case, a part of the outer coat, and particularly the white, inelastic substance, from its folding or plaiting under the ligature, seems to escape that degree of pressure necessary to destroy it; and when the remaining part yields, it continues entire, and is only removed by a subsequent process of ulceration occasioned by its irritation as an extraneous body.
In such cases, the layers of the external coat could not close around the inner ones, which are thus shown to be capable of forming an effectual barrier without it, although it materially assists in giving greater strength to the cicatrix, by the effusion of fibrin which takes place within, without, and around.
[205] While this process is going on without, and at the very extremity of the artery, the vessel is gradually contracted above it, and its coats become more or less inflamed, soft, and vascular. The inner layers are seen to be wrinkled transversely, and a small coagulum of blood is formed within them. This sometimes completely fills the artery, but it is more common for a small, tapering coagulum to be formed, adhering by its base to the extremity of the vessel; the white color of which renders it distinctly observable, when contrasted either with the coagulum or the inner coat of the artery, which latter is usually of a red or scarlet color while the inflammatory action is going on. A coagulum, contrary to the usually received opinion, is not absolutely necessary to the permanent closure of the artery, although it certainly assists in maintaining it. An artery is also supposed to contract gradually up to its first collateral branch; but this is not always the case, and depends entirely on the use for which the branch is required. After amputation at the middle of the arm, the artery will go on diminishing in size up to the subscapular branch, the circumflex arteries diminishing in proportion, in consequence of their being so much less necessary than before the operation. In several instances the principal artery has remained pervious below the collateral branch, the next immediately above the part where the ligature has been applied. Neither will the presence of a collateral branch immediately above where the ligature has been placed upon the artery always, although it sometimes may, interfere with the consolidation of the wound, and the closure of the canal of the vessel. It may impede the process, and render it for a time less safe, and in some instances it may prevent it altogether, but I have so often seen large arteries, heal after division close to the giving off of a considerable branch, that I consider them to be always capable of doing so, provided they are naturally sound. If they are not sound, it is very doubtful what process may take place; but it will be less likely to be a healthy one, if interfered with by the immediate proximity of a collateral branch. The power which suppresses hemorrhage in a bleeding artery resides, it must be borne in mind, in the very extremity of the vessel itself. It is, however, advisable to take care that a ligature shall be applied above [206] rather than immediately below a branch given off from a trunk, more particularly when it may be doubted whether the trunk is free from disease.
In 1834 I placed a ligature of strong dentists’ silk on the right common iliac artery of a lady of middle age for a swelling in the hip, supposed to be a gluteal aneurism, which, after commencing the operation, was found to occupy a considerable part of the iliac region. The lady died a year afterward, and it was then found that the ligature had been applied at the distance of five-eighths of an inch from the bifurcation of the aorta, and three-eighths of an inch above the origin of the internal iliac, independently of the line of separation between the parts of the iliac divided by the ligature, which did not seem to be wider than the ligature itself. The separated ends were united at the point of separation by new matter, the orifice or end of each being closed by a very narrow barrier, the inner coat of the artery being redder than natural, somewhat irregular and contracted, and containing hardly any coagulum. The fact was thus proved in the largest artery in the body save one, that a coagulum is not necessary for the safety of the union, while the immediate vicinity of so large a vessel as the internal iliac, to say nothing of the aorta itself, also proves that the danger hitherto expected from the neighborhood of a collateral branch is more imaginary than real—two great facts the practice of the Peninsular war led me to declare, and which ought no longer to be doubted.
The preparation exemplifying these points is in the museum of the Royal College of Surgeons, together with the ligature still carrying in its noose the portion of the artery it strangulated and brought away with it.
187. A ligature should always be round and small, provided it be sufficiently strong. The strength of a ligature is variously estimated; some surgeons trying it by the strength of their own fingers, others by what they conceive to be the resisting power of the coats of the artery, in which perhaps they may err. The only way in which a surgeon can hope to acquire correct information on this point is by trying on the dead body what force of fingers is required to cut the inner coats of arteries of various sizes; and then taking the least force required for this purpose, to ascertain whether he can easily pull the ligature over or off the divided end of the artery. If a surgeon will take the trouble [207] to do this, he will find that he has estimated the necessary force much too highly, and that he is in more danger of breaking his ligature than of failing to secure the artery. Hemorrhage has, however, been known to occur from the ligature having slipped off the end of an artery, which had been divided in the operation for aneurism, although I have never seen it happen after amputation, where the vessels were tied with a small, firm ligature. It constitutes a valid objection to the division of the artery between the ligatures, when two are applied.
A ligature composed of one strong thread of dentists’ silk, well waxed, is sufficiently firm for the largest artery. It does not, however, much signify what may be the shape, size, form, or substance of ligatures, when they are applied to arteries in a sound state, provided they are not too large, are fairly and separately tied, and with a sufficient degree of force to retain the ligature in its situation until separated by the usual processes of nature, which generally take from fourteen to thirty days for their completion.
188. When arteries are unhealthy, the selection and proper application of a ligature are points of great importance. A larger although yet a small, round ligature should be fairly, evenly, and firmly, although not so forcibly applied as on a sound artery; without the intervention of any substance whatever between it and the cellular covering of the vessel. The secondary hemorrhages which are recorded by different writers as prone to occur, and which did take place, happened, I am disposed to believe, more from the application of improper ligatures than from any other cause; for the inner coat of an artery is so prone to take on the adhesive state of inflammation that if a strong, small ligature be applied in the manner directed, it is more than probable that the closure of the artery will be effected. Ulceration will, however, sometimes take place on the inner coat of the vessel, and slowly extend outward, undoing in its progress any steps which may have been begun for the consolidation of the extremity of the artery. When a secondary hemorrhage does occur from this or from any other cause, it is usually from the beginning of the second to the fourth week; but there is no security for the patient until after the ligature has come away, unless it is retained an inordinate length of time, from having included some substances which do not readily yield under irritation, such [208] as the extremity of a nerve, or a slip of ligament which is not sufficiently compressed in the noose of the ligature.
Secondary hemorrhage may also take place from the extension of ulceration or sloughing to the artery from the surrounding parts, and perhaps as frequently as from any other cause; but when mortification occurs, there is no secondary hemorrhage, unless in that species which is called hospital gangrene. The advantages to be derived from the application of a strong, small ligature, from the least possible disturbance of the surrounding parts, and from absolute quietude, while the healing processes are going on, must be so obvious as to require no further observation. An undue interference with the ligature, by pulling at it, cannot be too earnestly deprecated at an early period; although, at a subsequent time, some force is occasionally required for its removal after amputation.
THE FEMORAL ARTERY, ETC.
189. When the femoral artery is cut across in the upper part of the thigh, whether it be done by a cannon-shot, a musket-ball, or a knife, the patient does not always bleed to death at once, although he frequently dies after a time in consequence of the shock and the loss of blood.
At the battle of Toulouse a large shot struck an officer and two men immediately behind him, and nearly tore off the right thigh of each. The artery was divided about, or less than three inches below Poupart’s ligament. I saw the officer shortly afterward, in consequence of his surgeon saying it was a case for amputation at the hip-joint. The bleeding had ceased, the pulse was feeble; the countenance ghastly, bedewed with a cold sweat, and with every indication of approaching dissolution. The house being at an advanced point, and close to one of the French redoubts, the fire of round shot and musketry was so severe upon and around it as to induce me to remain, until the battery should be taken by the troops then advancing upon our flank. In [209] order to occupy my time usefully, I returned to the officer, and found he had just expired. Desirous of seeing by what means the hemorrhage had been arrested, I cut down upon the artery, took it carefully out, and found that its divided end was irregularly torn; a slight contraction had taken place just above, but not sufficient to have been of the slightest utility in suppressing the bleeding, which was in fact prevented by an external coagulum, which filled up the ragged extremity of the vessel, and which in a few days, if he had lived, would have been removed with the purulent discharge, an internal one forming in the mean time, the extremity of the artery also contracting and retracting, so that a secondary hemorrhage might not have taken place, indeed would not in the generality of instances.
At Salamanca I had the opportunity of examining the thigh of a French soldier, whose femoral artery had been divided perhaps even higher up by a cannon-shot. He lived until the next morning, when I saw him, no operation whatever having been attempted, nor a tourniquet applied. He died exhausted, but not from any immediate bleeding, which, when once stopped, had not returned. The artery was in a similar state to the preceding one, with this slight difference, that the orifice was a little more contracted; the external coagulum filled up the ragged end of the artery, and was slightly compressed within by the contraction, which kept it in its place. The rest of the coagulum filled the hollow in the surrounding parts, which the retraction of the artery had occasioned. In this case, so unlike those I have hitherto noticed, the first natural cause giving rise to the suppression of the bleeding was the diminution of the power of the heart; the second, the formation of a coagulum in the hollow of the sheath left by the retraction of the artery. Contraction had begun, but had done nothing essential. (See Aph. 413.)
In other instances in which I have examined the extremities of such large arteries when divided, the appearances have been more or less of a similar nature; unless where the persons had died immediately, when the torn extremities were found quite open, with little surrounding coagulum. I have, however, seen persons wounded in this manner live for several days, when I have found, after death, the extremity of the artery open, and no appearance of blood having passed [210] into it below Poupart’s ligament. The consent necessary between the inner coat of the artery and the blood for the free passage of blood had been destroyed by the injury.
190. A small puncture in an artery, made with a needle, will sometimes heal, as it generally does in dogs. I have, however, seen several instances in which the femoral artery was wounded by a tenaculum, during amputation, and a secondary hemorrhage followed, requiring the application of a ligature. A larger puncture, or a longitudinal slit of from one to two lines in extent, does not commonly unite, except under pressure, although the edges of the wound may not always separate so as to allow blood to issue in any quantity. It sometimes only oozes out, and occasionally does not do even that, unless some obstacle to the circulation takes place below, when blood is propelled with a jet; and the edges of the cut having thus been separated, blood continues to be thrown forth in considerable quantity. In an artery of the size of the temporal, a small longitudinal slit may sometimes heal without the canal of the artery being obliterated, although this very rarely takes place in one of a large calibre.
In all cases of punctured wounds, when pressure can be effectually made, and especially against a bone, it should be tried in a graduated manner over the part injured, in the course of the artery above and below the wound, and if in an extremity, over the whole limb generally, the motions of which should be effectually prevented, and absolute rest enjoined, if the artery is of any importance. This should be continued for two, three, or more weeks, according to the nature of the injury.
A medical student, being desirous of bleeding his friend, also a student, in the arm, opened the ulnar artery, which in this case was very superficial. On discovering the error he had committed, he closed the wound, and applied a firm compress and bandage, under which it healed. On applying the ear to the part, it sounded like an aneurism, although there was scarcely any tumor, the thrilling sound being apparently occasioned by friction against the cut edges of the artery. This thrilling noise diminished, and the vessel immediately below the wound gradually recovered its pulsation, except at the exact situation of the injury, where none could be distinguished. It was obliterated at that part for the length of the eighth of an inch.
[211] The master tailor of the 40th Regiment, tempted by the approaching prospect of plunder, was induced, on the night of the assault on Badajos, to give up the shears, and arm himself with the halbert, and was properly rewarded for his temerity by a wound from a pike in the right arm, from which, he says, he bled like a pig, and became very faint. On his arrival at the spot indicated for surgical assistance, he fainted; but this was attributed to the unwarlike propensities of the man, rather than to any sufficient cause. The wound was not more than one-third of an inch long, a little below the edge of the pectoralis major, and immediately over the artery. The arm and hand were numb and cold; the pulse was not distinguishable at the wrist, and it appeared to cease at the place of injury, which was harder and a little more swollen than natural. He said that his pulse had always been felt by the doctors in the usual place. The wound healed without any trouble. On the 1st of May the pulsation of the artery could be felt a little below the wound. On any exertion he had a good deal of unpleasant numbness in the thumb and forefinger. A small cicatrix formed at the place of the wound, which was otherwise quite natural to the touch. This case proves that when a large artery is wounded in man by a sharp cutting instrument, to a certain but moderate extent the process of cure takes place through inflammation and by the obliteration of that part of the canal of the vessel. Continental surgeons have since sacrificed whole hecatombs of animals to prove this fact, which had been so many years before recorded in England as having occurred in man.
It has not been satisfactorily proved in man that a large artery, such as the femoral or even the brachial, has been opened to the extent of one-third or a fourth of its circumference, and that the wound has healed without the canal becoming impervious. A smaller wound of a large artery may close without obstructing the canal of the vessel, but the part is not so firm or so solid as before, and may yield, and give rise to an aneurism, having apparently the characters of a small true, as opposed to the spurious diffused, or even circumscribed swelling, which more usually follows a similar accident.
Colonel Fane was wounded by an arrow in the right side of the neck, opposite the bifurcation of the carotid, which caused a considerable loss of blood at the moment. The [212] wound healed, leaving only a mark where the point of the arrow had entered. Some time afterward he observed a small swelling at the part, which, from its pulsation, was declared to be an aneurism. Uneasy about it, he asked my opinion at Badajos, after the siege. It had not increased, but it caused him some anxiety, and I promised to place a ligature on the common carotid if the aneurism should increase in size. He was unfortunately killed in action a year afterward, by a shot through the head.
191. When a large artery, such as the brachial, is cut transversely to a fourth of its circumference in man, it forms a circular opening as in animals; and if the artery be large, the bleeding usually continues until the person faints, or it is arrested by pressure. In dogs the bleeding commonly ceases without any assistance from art, and without the animal being exhausted; in horses and sheep the bleeding usually continues till the animals die; while in man, even with the best aid from compression, hemorrhage will in all probability recur, unless the circulation be altogether arrested. If the external opening only should be closed, a spurious, circumscribed aneurism will be the consequence in so small an artery as the temporal, and a ligature will sometimes be required above and below a little aneurism of this description. In a larger artery the spurious aneurism may or may not be diffused.
When an artery of this size is completely divided, it is less likely to continue to bleed than if it had been only wounded. When it is merely cut or torn half through, but not completely divided in the first instance, it is in the same state with regard to hemorrhage as if it had partially given way by ulceration. It can neither retract nor contract, and will continue to bleed until it destroys the patient, unless pressure be accurately applied and maintained until further assistance can be procured. The practice to be pursued is to divide the vessel, if it be a small one, such as the temporal artery, when it will be enabled to retract and contract; and the bleeding will in general permanently cease under pressure, especially when it can be applied against the bone. If the artery is of a larger class, and continues to bleed, it should be sufficiently exposed by enlarging the wound; a ligature should be applied above and below the opening in the vessel, which may or may not be divided between them at the pleasure of the surgeon.
[213] In June, 1829, I happened to be at Windsor, on a visit to my old friend, the late Dr. Ferguson, and was called to a young gentleman, the upper part of whose right femoral artery had been accidentally cut by the point of a scythe. On dilating the wound, a tourniquet being on the limb, black blood flowed freely from it; on unscrewing the tourniquet by degrees, arterial blood showed itself, and the upper end of the artery was secured by ligature when the tourniquet was removed. Venous-looking or black blood then again flowed in greater abundance than before, evidently from a large vessel. This I restrained by pressure made below the wound with the thumb of the left hand, while I laid bare the lower part of the artery, from a slit in which, near an inch in length, the black blood was seen to flow. A ligature passed around the vessel below the wound suppressed the bleeding. The artery was not divided, and the young gentleman perfectly recovered, and has continued well until this day. The absolute necessity for two ligatures was here well shown, as well as the flow of dark-colored blood from the lower end of the artery. This gentleman is now an officer in the army, and suffers no inconvenience from his accident.
192. When a large artery is wounded at some depth from the surface, and the external opening is small, blood not only issues through the opening, but is often forced into the cellular structure of the limb to a considerable distance; the pulsation of the tumor is observable, and the thrill or sound which accompanies a ruptured artery is distinct. If a large quantity of blood, partly in a fluid, partly in a coagulated state, be collected immediately over and around the wound in the artery, the tumor may not pulsate or give forth any sound, if the coagulated blood be in considerable quantity, although some elevation of the tumor may be observed corresponding to the pulse.
This rising or pulsation of the swelling often depends on the impulse given to the whole, as a mass, by the artery against which it is lying, and not upon blood circulating through it. An impulse of this kind is distinguishable in a bronchocele which lies immediately over and in contact with the carotid artery. It is the same when blood is extravasated by the rupture of several small vessels, in consequence of the passage of a wheel over the limb, especially in the thigh, where a swelling containing fluid blood will sometimes pulsate in a well-marked manner, until it gradu[214]ally diminishes as the blood coagulates, when the motion becomes a mere elevation at each stroke of the heart. The whizzing sound or thrill attendant on a ruptured artery is in these cases wanting, being a very diagnostic mark of this accident; although where there is true aneurism, and it has burst, forming a diffused and spurious one, the thrill may be wanting; but the history of these cases enables a surgeon to distinguish between them. If several ounces of blood are thrown out, and remain fluid, they ought to be evacuated, or suppuration will ensue. If they become coagulated, the mass will be gradually absorbed. Fluid blood should be evacuated by a small opening, and the part afterward treated by compress and bandage. If the fluid or partly coagulated blood should increase in quantity, and the swelling continue to enlarge and pulsate, the extension of the mischief should be arrested by opening the swelling and securing the artery by ligature. When the external opening is enlarged, and the clots which filled it up are at all disturbed, arterial blood begins to flow, and the finger will readily follow the track through which it passes down to the artery, if it should not be too far distant. If the incision be made sufficiently large to enable the operator to remove these clots of blood with rapidity, the finger will more readily pass down to the wound in the artery, which, if a large one, may be thus easily discovered, if within reach and sight, provided the tourniquet be thoroughly unscrewed, and the surgeon is not afraid. A ligature should then be placed above and below the opening in the artery.
When an artery is wounded, and the external opening in the integument heals so as to prevent the blood from issuing through it, a traumatic, spurious, circumscribed, or diffused aneurism is said to form, according to the facility which is offered by the structure of the parts for the confinement or diffusion of the extravasated blood. A traumatic aneurismal tumor of this nature differs essentially from aneurism which has taken place as a consequence of disease, and not of direct injury. If a spurious aneurism form from disease, the artery is in general unsound for some distance above and below the tumor. In the aneurismal tumor from a wound, the artery is perfectly sound, except as far as concerns the seat of injury. There is, then, not only a great and essential difference between these two kinds of aneurism as regards their nature, but also with respect to the collateral circulation,[215] and the operation to be performed for their cure; and the surgeon may not overlook these facts.
A school-boy, about fourteen years of age, let a pen-knife drop from his hand while sitting down, and drew his knees suddenly toward each other to catch the falling knife; the point was thus forced into the inner and middle part of the thigh, and wounded the femoral artery. The medical man on the spot put a plaster on the little incision in the integuments, and the wound quickly healed. The boy complained of uneasiness, but was supposed to be making more of it than necessary, and was made to go into school as usual. The limb, however, began to swell, and the boy was brought to London, supposed to be suffering from abscess, and placed under the care of Mr. Keate, who, suspecting the evil, carefully introduced the point of a lancet, and, after a clot of blood had been forced out, a jet of arterial blood flew across the room. The hemorrhage was arrested by pressure below Poupart’s ligament, while Mr. Keate enlarged the opening in the integuments, and removed two washhand-basinsful of coagulated blood. He then put his finger on a large opening in the artery, under which two ligatures were passed by means of an eye-probe, and the artery was divided between them. The muscles had been cleanly dissected, and the cavity extended from the fork internally, and trochanter externally, to the knee. There was much less suppuration than could have been expected. The ligatures were detached about the usual time, and the patient entirely recovered.
This admirable case should be imprinted on the mind of every surgeon. With the hope that it will be so, I refrain from commenting on three or four cases which have occurred within the last two years, in which, from neglect of the precept inculcated by it, very distressing if not fatal consequences ensued.
193. There is no precept more important than that which directs that no operation should be done on a wounded artery unless it bleed, inasmuch as hemorrhage once arrested may not be renewed, in which case any operation must be unnecessary. The following case shows how firmly the principles on which wounded arteries ought to be treated were fixed in my mind in the year 1812; and there is no case during that eventful period to which I look back with more satisfaction than the following:—
John Wilson, of the 23d Regiment, was wounded at the[216] battle of Salamanca by a musket-ball, which entered immediately behind the trochanter major, passed downward, forward, and inward, and came out on the inside of the anterior part of the thigh. The ball could not have injured the femoral artery, although it might readily have divided some branch of the profunda. Several days after the receipt of the injury, I saw this man sitting at night on his bed, which was on the floor, with his leg bent and out of it, another man holding a candle, and a third catching the blood which flowed from the wound, and which had half filled a large pewter basin. A tourniquet with a thick pad was placed as high as possible on the upper part of the thigh, and the officer on duty was requested to loosen it in the course of an hour; that was done, and the bleeding did not recommence. The next day, the patient being laid on the operating table, I removed the coagula from both openings, and tried to bring on the bleeding by pressure and by moving the limb; it would not, however, bleed. As there could be no other guide to the wounded artery, which was evidently a deep-seated one, I did not like to cut down into the thigh without it, and the man was replaced in bed, and a loose precautionary tourniquet applied. At night the wound bled smartly again, and the blood was evidently arterial. It was soon arrested by pressure. The next day I placed him on the operating table again, but the artery would not bleed. This occurred a third time with the same result. The bleedings were, however, now almost immediately suppressed, whenever they took place, by the orderly who attended upon him; care having been taken to have a long, thick pad always lying over the femoral artery, from and below Poupart’s ligament, upon which he made pressure with his hand for a short time. Absolute rest was enjoined. The hemorrhage at last ceased without further interference, and the man recovered.
This case was one of considerable interest at the time, and is the model one on which the treatment of all such injuries should be founded. If the wound had bled, I should have introduced my finger, and enlarged it transversely, continuing the incision until the opening was sufficiently large to see to the bottom of the wound or the bleeding part. It is necessary in such cases to be attentive to the course of the great vessels and nerves, but not to the safety of muscular fibers, the division of which leads to[217] no permanent injury. As pressure on the main trunk led to the ultimate suppression of the hemorrhage, it may be said that a ligature placed high up on the femoral artery would not only have done the same, but would have relieved the man from the anxiety necessarily dependent on the momentary fear of a recurrence of the hemorrhage. There are two objections to this method of proceeding: the likelihood of mortification taking place, which in similar cases has been known to occur; and the possibility of the hemorrhage being renewed through the anastomosing branches. The temporary suspension of the circulation by pressure does little or no harm, more particularly where the pad used is so thick and narrow as to cause it to fall principally on the artery, and only in a slight degree on the surrounding parts, which by a little attention may be readily accomplished. It is not then good practice to cut down upon an artery on the first occurrence of hemorrhage, unless it be so severe or so well marked as to leave no doubt of its being from the main trunk of the vessel itself; nor is it then advisable to do so, except the artery continue to bleed; for many a hemorrhage, supposed to have taken place from the main trunk of an artery, has been permanently stopped by a moderately continued pressure exercised in the course of the vessel, and sometimes on the bleeding part itself; particularly if the blood be of a dark color, indicating that it comes from the lower end of the vessel.
A painter could not have had a better subject for a picture illustrative of the miseries which follow a great battle, than some of the hospitals at Salamanca at one time presented. Conceive this poor man, late at night, in the midst of others, some more seriously injured than himself, calmly watching his blood—his life flowing away without hope of relief, one man holding a lighted candle in his hand, to look at it, and another a pewter washhand-basin to prevent its running over the floor, until life should be extinct. The unfortunate wretch next him with a broken thigh, the ends lying nearly at right angles for want of a proper splint to keep them straight, is praying for amputation or for death. The miserable being on the other side has lost his thigh; it has been amputated. The stump is shaking with spasms; it has shifted itself off the wisp of straw which supported it. He is holding it with both hands, in an agony of despair. These Commentaries are written to prevent as far as possible such horrors; and [218] they may be prevented by efficient and well-appointed medical officers; but there must also be greater attention to these points than has hitherto been given by the government of the country.
Don Bernardino Garcia Alvarez, captain of the regiment of Laredo, thirty years of age, was wounded at the battle of Toulouse by a musket-ball, which passed through the thigh, a little above its middle. The wound was not considered a dangerous one until the 30th, twenty days after the injury, when a considerable bleeding took place; and as the vessel from which it came seemed to be very deeply seated, the Spanish surgeon in charge tied the common femoral artery. I saw the gentleman in consequence of this having been done. The hemorrhage was suppressed by the operation, and the limb soon recovered its natural temperature, but gangrene made its appearance on the great toe on the third day afterward. It did not seem to increase, but the limb swelled as if nature were endeavoring to set up sufficient action to maintain its life; and this continued until the tenth day after the operation, when he died, completely exhausted. On the dissection of the limb, the femoral artery was found to be perfectly sound in every part below where the ligature had been applied. The vessel which bled could not be discovered; but it was certainly a branch from the profunda, and not the femoral itself. In this case the ligature of the femoral artery destroyed the patient, and the practice pursued must be condemned. The gunshot wound should have been largely dilated, at both orifices if necessary, until the wounded vessel was discovered, which possibly had not been completely divided by the ulcerative or sloughing process which had taken place, and its division would in all probability have suppressed the bleeding.
A young gentleman, aged twelve, accompanying his brothers shooting, in December, 1844, was struck in the upper part of the left thigh by a duck-shot, which entered about three inches below Poupart’s ligament, a little to the inner side of the femoral artery. He bled until he fainted, and was taken home. There was no return of the bleeding for three days, during which time the limb was exceedingly painful, and soon began to enlarge. After this occasional and considerable bleedings took place, the limb still continuing to increase in size. Fomentations and poultices were applied; irritative fever set in, and the pain was in[219]tense. At the end of a fortnight the small hole made by the shot appeared to be healed over by a thin skin of a blue color, which tint extended for some distance. The limb was enormously swollen, with a feeling of distention, which induced the surgeon to puncture the most prominent part with a lancet. After some clots of blood had been removed, an alarming arterial hemorrhage took place. The femoral artery was now tied high up, below Poupart’s ligament. The bleeding was in some measure restrained, but not suppressed, and after a short time it returned at intervals with augmented violence, until death ensued, three weeks after the accident.
Remarks.—If an incision had been made into the thigh in the course of the wound when the bleeding returned on the third day, and both ends of the wounded artery had been tied, the boy would in all probability have recovered. The ligature placed on the femoral artery above the wound in it did restrain for a short time the flow of blood, but could not prevent its flowing from perhaps both ends of the vessel, until it destroyed the patient. A ligature on the external iliac would only have caused it to be deferred for a day or two, until the collateral branches had enlarged, or else he would have died of mortification.
This really formidable case shows most distinctly the necessity for always observing the rule of tying the wounded artery at the part injured, in order that the mistake may not be made of placing a ligature on the wrong artery—the constriction of which may cost the patient his life, while it may not prevent a return of the bleeding. It also shows that no loss of blood from a diffused aneurism can equal the danger which must be encountered, and the mistakes which may be made, by not laying it open, and seeing the hole in the artery, or its divided extremities.
Captain Seton, a short man, fat of his age, was wounded in a duel, in 1845, in the upper part of the right thigh, a little above and in front of the great trochanter, the wound being continued across the thigh, its internal opening being about the middle of the fold of the left or opposite groin. He lost a great deal of blood at the time, the issue of which ceased on his fainting. Ten days after the duel his countenance was blanched, his pulse rather quick and feeble. On examining the wounds, that on the right hip (the opening of entrance) was circular, filled with a dry, depressed slough,[220] and there was a narrow, faint blush of redness round its margin. In the left groin the opening of exit was marked by a jagged slit, already partly closed by a thin cicatrix. There was extensive mottled purple discoloration (ecchymosis) of the skin in both groins, and over the pubes, scrotum, and upper part of the right thigh. In the right groin was found a large, oval, visibly pulsating tumor, its long diameter extending transversely from about an inch and a half on the inner side of the anterior superior spinous process of the ilium to about opposite the linea alba, and its lower margin projecting slightly over Poupart’s ligament into the upper and inner part of the thigh. On handling this tumor, it appeared elastic but firm, very slightly tender, and not capable of any perceptible diminution in bulk by gradual and continued pressure. The pulsation was distinct in all parts of the swelling, and was equally evident whether the fingers were pressed directly backward, or whether they were placed at its upper and lower margins, and pressed toward the base of the tumor, in a direction transversely to its long axis, the parts being for the time relaxed. The femoral artery was slightly covered by the swelling, and the pulsations of that vessel were with some difficulty distinguished in the upper third of the thigh, below the margin of the tumor. This appeared to depend partly on the natural obesity of the patient, and partly on a considerable degree of general swelling of the thigh. Pressure on the femoral artery or over the abdominal aorta did not arrest the pulsation in the tumor, and in the former situation was attended with severe pain. Under these circumstances it was deemed advisable to apply a ligature on the external iliac artery, and give the patient a chance of the occurrence of coagulation in the tumor, and closure of the wounded vessel, before the free re-establishment of the circulation through the femoral artery. In the present case it was supposed that mortification of the limb was all the less likely to occur from the circumstance that the greater part of the effusion appeared in front of the abdominal parietes, and therefore exercised less pressure on the femoral vein than if further extension into the thigh had taken place. The danger of peritonitis was by this proposal made a new element in the calculation; but it was estimated that the chances of this and of mortification of the limb, taken together, were less unfavorable than the chances of immediate and secondary hemorrhage attaching to the operation of tying the[221] artery at the spot injured. The operation being completed, the right foot, leg, and thigh were enveloped in lamb’s-wool and flannel, and the limb elevated on an inclined plane of pillows, so as to favor the return of blood as much as possible, and prevent venous congestion. The day on which the operation was performed was passed in considerable pain, the patient being restless, and complaining of a sense of burning in the limb. An anodyne, however, secured him a tolerably good night’s rest. The day after the limb was found altogether diminished in bulk, and its temperature equal to that of the healthy limb; no return of pulsation had taken place in the tumor. The same evening some tenderness and tension of the abdomen came on, though the bowels had been kept in a regular state by occasional small doses of castor-oil. In the morning of the second day, pain in the belly, with increased tension, hurried breathing, short, dry cough, and tenderness over the lower part of the abdomen, were observed. Pulse quicker and small. Leeches were applied, and three-grain doses of calomel, with a little Dover’s powder, ordered every three hours. The symptoms, however, became rapidly worse; the patient complained of severe pain in the right leg, and a sensation of great heat over the whole body, although the actual temperature was rapidly falling below the natural standard. The right leg also became cold sooner than the left. At seven P.M. he became more easy, and expressed an opinion that he should “do well;” but in little more than half an hour he expired.
Examination after death.—Swelling and ecchymosis of the right thigh, particularly at the upper part, and in the right iliac region; also swelling and ecchymosis of the scrotum, chiefly in the right side, with general tumefaction of the abdominal parietes below the umbilicus. A wound into which the little finger could be passed was on the upper and outer aspect of the right thigh, about three inches below the crest of the ilium and about an inch nearer the mesial line than the great trochanter, and on the left side another smaller wound, situated about the external aperture of the left spermatic canal. The first-mentioned wound was open; the lips of the latter were partially adherent. The course of the wound was traced from the outside through a dense layer of fat about two inches in thickness, (on an average.) It had divided one of the superficial branches of the femoral artery, about half an inch below Poupart’s ligament, and[222] about an inch from the main body of the femoral artery; this had caused a false aneurism. The sac contained about three ounces of blood. Blood was also effused into the cellular structure of the scrotum, and downward beneath the sartorius muscle. The wound passed through the cellular tissue, across the pubes, and emerged about the situation of the left external spermatic ring, without having divided the cord on either side, and was quite superficial to the bladder. No other artery appeared to have been wounded. When the parietes of the abdomen were reflected, a considerable quantity of sero-purulent fluid was found in the abdominal cavity; and on different parts of the large and small intestines patches of acute inflammation were observed, particularly on the ascending arch of the colon. The peritoneum adjoining the wound of the operation was inflamed, and approaching to gangrene: it had not been injured by the knife during the operation. The intestines were unusually large, and distended with flatus. The other abdominal viscera were healthy, but loaded to an extraordinary degree with fat. The ligature had been properly applied to the iliac artery; the vein was not injured; the surface of the wound and the cellular tissue in the neighborhood of the artery were sloughy. There was some enlargement of the right limb, but apparently no mortification. The femoral artery was pervious; the course of the wound was through a bed of fat, fourteen inches in length, and three inches in depth, over the pubes, and no muscular substance was injured; the blood found in the aneurismal sac was firmly coagulated, and there was no mark of recent oozing from the injured artery.
Remarks.—If this gentleman had been wounded at the foot of the breach in the wall of Ciudad Rodrigo, in January, he might, to his great dissatisfaction, have been one of eleven officers whom I saw lying dead, and as naked as they were born, on the face of the breach of Badajos, in April. He would have been saved by one doctor, or an old woman, and a little cold water, in 1812, and did die of seven in 1845, after an operation most brilliantly performed, but done in the wrong place, even if any operation had been necessary, which it was not. The case is an experimentum crucis of principles.
The first error committed in this case was in calling and believing a wounded artery to be a circumscribed, false, or diffused traumatic aneurism. Nothing can be called an[223] aneurism, by which word a dilated vessel or a diseased shut or closed sac is understood, which has one or more holes in it, made by a ball, or by anything else, the wound or track of which remains open. It is simply a case of wound in which an artery has been divided or injured, and while this track of the ball remains open, no ingenuity of argument can make it otherwise. When the external openings made by the ball have closed, the case may then be called, if there be a collection of blood, whether fluid or coagulated, one of circumscribed, false, diffused traumatic aneurism, or anything else that philologists may please to designate it. The dissection report proved this case to be simply a small collection of blood, three ounces and a half, or seven small tablespoonfuls—communicating with two open wounds. Calling this an aneurism, or a shut sac of any kind, was then the first and fundamental error, as fatal as erroneous.
The second error consisted in the belief, contrary to all experience, that any sac or bag, or collection of blood by whatever name it may be called, having two openings leading to, or into it, and communicating with the atmosphere, could be augmented to any dangerous extent by the further pouring out of blood from an artery of any size, or from any artery at all, without some of such extravasated blood being discharged or forced out through one or both of the open external wounds in sufficient quantity to show that the opening in the vessel was not closed.
The first two errors, or defects of principles, gave rise to the third, viz.: the belief that an operation was necessary where none was required, the dissection having proved that the whole idea of the nature of the injury was a mistake: there was no large artery wounded; the small one, which had been wounded, had ceased to bleed; the quantity of blood extravasated did not exceed seven small tablespoonfuls. The third mistake could not have taken place if the first two errors had not been committed.
The fourth error occurred from its being taken for granted that the femoral artery was wounded; and that ascertaining the fact by opening the small swelling which contained only three and a half ounces of blood, would be followed by a fatal hemorrhage; which supposition arose from this swelling receiving a pulsatory motion from its vicinity to the femoral artery—a mistake which should not have occurred; for it had long before been said, (page 16 of my published[224] lectures:) “The motion or pulsation of the swelling often depends on the impulse given to the whole as a mass, by the great artery against which it is lying, and not upon blood circulating through it. When blood is extravasated by the rupture of small vessels in consequence of the passage of a wheel over the limb—especially in the thigh, where I have seen a swelling containing fluid blood pulsate in an almost alarming manner, until it gradually diminished as the blood coagulated, when the motion became a mere elevation at each stroke of the heart—the whizzing sound or thrill attendant on a ruptured artery (of a size to require a ligature being understood) is in these cases wanting, constituting a very distinguishing mark of this accident.”
Surgeons fifty years ago were afraid of hemorrhage from the femoral artery, but the practice of the Peninsular war dissipated such fears. The reason given for not laying open the wound, and looking at the bleeding artery, in this case, is ingenious, but not tenable. The patient is said to have lost a large quantity of blood; and if this were even a fact, which may, however, be doubted, is there a case on record of a serious wound of the femoral artery, such as this was supposed to have been, in which that vessel has been successfully secured by ligature, without the patient having equally lost so large a quantity of blood as to be supposed to be about to die? It has always been so; the reason, however specious, is not valid, and cannot be admitted.
The fifth error arose from imagining that the considerable loss of blood supposed to have taken place would have rendered the patient incapable of bearing more; for it is a recorded fact that those operations high up on the femoral artery, from which patients have recovered, have never been done without great losses of blood having been previously sustained; and if the patient was so weakened that his heart and arteries could not bear the abstraction from their contents of a few ounces more blood—supposing such loss to be inevitable—how could they have power to drive or force the blood through the limb by the collateral channels, in a manner sufficient to support its life, when the main trunk was cut off within the pelvis? They could not do it—they have rarely done it under such circumstance; they could not have done it in this case; and if the patient had not died within the first forty hours of inflammation of the peritoneum, to which accident he ought not to have been ex[225]posed, he would have died of mortification within forty hours more, which had already commenced, as shown by the swelling of the limb and pain in the calf of the leg, which almost invariably attend such mortification.
The sixth error consisted in the belief that if the femoral artery had been wounded, a ligature on the external iliac would have permanently arrested the bleeding. It would, in all probability, have done no such thing, beyond a day or two—perhaps even only for the moment. It is a delusion, persisted in notwithstanding the most clear and positive proofs to the contrary. The patient will die of mortification from the want of blood in the limb, if the circulation be not re-established; and if this should take place, blood must find its way into the lower end of the wounded artery, and perhaps even into the upper, and renew the hemorrhage.
If the femoral artery had been wounded, as was supposed in this case, but not completely divided, it must and would have continued to bleed through the external wound, until the patient died, or a ligature had been placed upon it. It has been said that, in the case as it actually occurred, the little artery, which was divided and which had not bled for some days, could not have been safely tied, if it had bled again, because it was only an inch long; but this is said in defiance of every sort of proof which has been given to the contrary.
As far back as 1815 I said: “There was no foundation for the theory which declared that a ligature when placed on an artery such as the femoral would fail, if in the immediate vicinity of a collateral branch, in consequence of the flow of blood through this vessel preventing the obstruction and consolidation of the main branch for a distance sufficient to enable it to resist the impulse of the blood behind.” This was said from pure practical facts, free from all kinds of theory; and the preparation before alluded to, in the museum of the College of Surgeons, in which I tied the common iliac artery, will show the mark of a simple thread around it, and a single line of adhesion resisting the whole power of the heart, the canal above the spot not being obliterated.
The seventh error committed in this case was in contravening the great surgical precept, formed on no inconsiderable experience during the early part of the war in the[226] Peninsula, “not to perform an operation on an artery until it bleed.”
194. When a wound occurs in the thigh, implicating the femoral artery or its branches, and the bleeding cannot be restrained by a moderate but regulated compression on the trunk of the vessel, and perhaps on the injured part, recourse should be had to an operation, by which both ends of the wounded artery may be secured by ligature; and the impracticability of doing this should be ascertained only by the failure of the attempt. If the lower end of the artery cannot be found at the time, the upper only having bled, a gentle compression maintained upon the track of the lower may prevent mischief; but if dark-colored blood should flow from the wound, which may be expected to come from the lower end of the artery, and compression does not suffice to suppress the hemorrhage, the bleeding end of the vessel must be exposed, and secured near to its extremity.
The instruments which have been invented for the cure of aneurism, by compressing the main trunk of the artery, will be found eminently useful, if applied with care, in many cases of hemorrhage in which it may be doubtful what vessel is actually injured, as in the case of Wilson, page 215, and in cases also of wounds of the hand or foot in which bleeding occurs through the medium of collateral branches. These instruments, although they cannot conveniently be placed in the capital cases of instruments, should be in store, whether with divisional or general hospitals.
MORTIFICATION, ETC.
195. The gangrene, mortification, or sphacelus, consequent on a wound of the main artery of the lower extremity, is, in the first instance, local and dry, unless putrefaction be induced by heat. (See Aphorism 28.) The following case is a good example of this and of all the other points laid down as principles or facts:—
A gentleman received an injury in the upper part of the[227] left thigh, parallel to but a little below Poupart’s ligament, from the shaft of a van. The late Messrs. Heaviside, Howship, and Chevalier were sent for immediately, and my attendance was desired next day. I called the attention of these gentlemen to the tallowy-white and mottled appearance of the foot and lower part of the leg, and assured them that the femoral artery was injured, and the femoral vein in all probability also, from the rapid appearance of the first signs of dry gangrene. In this they would not believe, until the shrinking and drying of the foot and leg became obvious, the course of the tendons on the instep and toes being marked by so many dark-red lines under the drying skin above them. The amputation I recommended below the knee they would not hear of, although they reluctantly admitted the fact of the mortification. On the eighteenth day after the accident, blood flowed from the wound in quantity, of a dark-venous color. This bleeding I pronounced to be from the lower end of the artery. My three friends, in whose hands the case was, could not understand this, and placed a ligature on the external iliac artery, which did not arrest the bleeding. They now, although too late, saw their error, and desired me to do what I pleased, and a ligature secured the lower end of the artery from which the blood flowed. The man died exhausted a few days afterward.
This is a remarkable case, deserving the most serious attention. According to the principle laid down at first as a general rule, the thigh should have been amputated at the seat of injury the morning after the accident, when the signs of mortification of the foot were obvious. But it must be borne in mind that amputations at the trochanter major or hip-joint are most formidable and not generally successful operations; in consequence of which I have recommended another course, deserving, in such cases, of the most deliberate consideration and trial. (See Aphorism 29.) The leg should have been amputated immediately below the knee, as I had ordered it to be done in the case of Turnbull, (page 202,) because that is the part in all such cases at which nature seems capable of arresting the progress of the mortification, if the constitution and powers of the sufferer are good, and equal to the calls upon them. The impairing, the destructive influence a mortified leg exerts on the whole system is removed, and an amputation substituted for it of comparatively little moment. When the hemorrhage took[228] place, the lower end of the artery should have been tied. The upper end never bled, and the ligature on the iliac artery was useless. In this case, it is probable, as the vein was also injured, that the life of the part at and above the knee might not have been preserved, and the patient would have died.
In a case of the kind in which the artery was wounded at the lower part of the thigh instead of the upper, amputation at or just below the wound may be the proper course; this amputation, although dangerous, being much less so than one at the upper part of the thigh or hip-joint. Nevertheless, amputation should not be had recourse to unless the extension of the mortification is beyond a doubt.
196. In Aphorism 29, it is strongly recommended not to amputate a thigh when mortification has stopped just below the knee, and a line of separation has been formed between the dead and the living parts—an opinion formed on a principle laid down in opposition to those usually received by the profession at large, and which have been entertained from the fact that amputations done under these circumstances are commonly fatal.
Richard Cook, aged fifty, a mason, while sitting on a square block of stone, on the 23d of February, was struck by another, which drove the popliteal space or ham against the edge of the block on which he sat, causing him great pain, and otherwise greatly bruising the leg, although no bones were fractured, nor was the skin torn. The limb, on his admission into the Westminster Hospital half an hour afterward, was much larger than the other, and of a dark reddish-blue color, evidently from the bruise or extravasation of blood, which appeared to be still issuing from the vessel or vessels, as the limb continued to increase in size, until it became at last greatly swollen. The pulsation of neither the anterior nor the posterior tibial artery could be distinguished through the swelling the next morning. The bowels were opened, and a cold spirit lotion was applied to the calf and around the leg, and the swelling somewhat subsided, the limb becoming quite a blue-black, which, with the tenseness of the parts, distinctly indicated the effusion of a large quantity of blood. It was soon obvious that greater mischief had occurred than had been expected; and on the 2d of March, as vesications, filled with a bloody fluid, were formed on the outside of the leg, over the fibula, and the [229] whole limb was manifestly about to pass into a state of gangrene, if it had not already done so, I prepared everything for tying the popliteal or other arteries, if found necessary, and made a long and deep incision on the outer and back part of the leg, through the integuments and muscles posterior to the fibula, and removed a considerable quantity of coagulated blood from between the muscles and from a large cavity which extended upward into the ham, without causing further hemorrhage; in no part of that cavity could an artery be felt. The patient’s countenance and body had assumed a jaundiced hue; the pulse was very quick; the tongue foul; the countenance sunken; the skin hot; the head wandering. Poultices of linseed-meal and stale beer were applied, with gentle, stimulating applications. Brandy and wine were ordered in proper quantities every hour or two, with sufficient doses of the muriate of morphia at night to allay irritation and induce sleep. The incision, together with these remedies, gave great relief, and on the 7th the man seemed to have been saved from a state of the most imminent danger. On the 8th the pulse was 112, the tongue clean, the skin of a whiter color, the bowels opened by injections; eight ounces of brandy were given in the twenty-four hours; wine, with sago, arrow-root, jelly, oranges, and anything he chose to ask for. The greatest cleanliness was observed, and the chloride of lime was used in profusion all around him. The mortification of the limb was complete; a line of separation formed about four inches below the knee in front, and extended behind toward the ham. On the 26th, the dead parts having almost entirely separated from the bones all round, those which remained were cut through where dead, the bones were sawn about five inches below the knee, and the lower part of the limb removed, leaving an irregular, and, in part, a granulating stump, with an inch of bone projecting from it. On the 24th of May this portion was found to be loose; diluted nitric acid had been applied to its surface, and on the 20th of June it separated. On the 16th of August Cook left the hospital in good health, with a very good stump, having cost the hospital £57 in extra diet. In this case, there can be little doubt of the popliteal artery having been torn; and if the incision made on the 2d had been had recourse to during the first two or three days, and the artery sought for, and secured if found bleeding, it is possible the mortification might have been pre[230]vented; although it is probable, from the pressure arising from the great extravasation and coagulation of blood, that the collateral circulation was so much impeded as not to have been able to maintain the life of the limb below even during that time. The incision made on the 2d saved the life of the patient, by taking off the tension of the part, and relieving thereby in a remarkable manner the constitutional irritation which hourly appeared likely to destroy him; indeed, no one expected anything but his dissolution. When the line of separation had formed, he was evidently unequal to undergo the operation of amputation, in order to make a good stump, without great risk, and the dead parts were therefore merely separated for the sake of cleanliness and comfort. Experience has demonstrated in too many cases of the kind that the formal operation of amputation at this time, as recommended by most modern surgeons, would in all probability have cost him his life.
The application of powdered charcoal, particularly that made from bog earth, or of areca wood, or Macdougall’s disinfecting powder, or of the disinfecting liquids now in use, such as the chlorides of lime, sodium, and zinc, removes in a great degree the intolerable odor which renders the room of the sufferer unbearable, and essentially interferes with his amendment. Incisions should be made into the dead parts to allow the evacuation of the fluids contained within them, while the parts themselves may be removed from time to time; so that when the period arrives at which an amputation is considered advisable, the bones, if of the leg, may be sawn through at or below the line of separation, and nearly the whole of the mortified soft parts removed, so as to leave little of those which are dead and offensive. This operation is done without the patient feeling it; it gives rise to no irritation, inconvenience, or danger; Nature is not interfered with in her operations; and in due time the parts which remain are separated and fall off, leaving a stump more or less good, but which will always bear the application of a wooden leg; and thus the knee-joint is saved—a saving of no small importance to the patient, and a new precept in surgery.
197. The following cases may be considered conclusive:—
A private of the 5th division of infantry received a wound at the battle of Salamanca from a musket-ball, which passed across the back part of the right leg, from above downward [231] and inward. It entered about two inches below and behind the head of the fibula, and passed out near the inner edge of the tibia. There was little blood lost at the time, and it was considered to be a simple wound; eight days after the injury, some blood flowed with the discharge; this increased during the night, and, on examining the limb on the morning of the ninth day, it was evidently injected with blood, which flowed of a scarlet color from both orifices. It being doubtful which vessel was wounded—whether it was the trunk of the popliteal artery, or the posterior tibial or peroneal after its division into these branches—it was thought advisable to place a ligature on the femoral artery about the middle of the thigh, which suppressed the hemorrhage. The case was now shown to me, as one in proof of the incorrectness of the opinion I had a few days before stated, of the impropriety of such an operation being done. The seeming success did not long continue; hemorrhage again took place from the original wound, and the limb was then amputated. The posterior tibial artery had been injured, and had sloughed. The man died.
Remarks.—A straight incision, directly through the back of the calf of the leg, of six inches in length, and two ligatures on the wounded artery, would have saved this man’s leg and life.
Henry Vigarelie, a private in the German legion, was wounded on the 18th of June, at the battle of Waterloo, by a musket-ball, which entered the right leg immediately behind and below the inner head of the tibia, inclining downward, and under or before a part of the soleus and gastrocnemius muscles, and coming out through them, four inches and three-quarters below the head of the fibula, nearly in the middle, but toward the side of the calf of the leg. In this course it was evident that the ball must have passed close to the posterior tibial and peroneal arteries; but, as little inflammation followed, and no immediate hemorrhage, it was considered to be one of the slighter cases. On the latter days of June he occasionally lost a little blood from the wound, and on the 1st of July a considerable hemorrhage took place, which was suppressed by the tourniquet, and did not immediately recur on its removal. It bled, however, at intervals, during the night; and on the morning of the 2d it became necessary to reapply the tourniquet, and to adopt some means for his permanent relief.
[232] The man had lost a large quantity of blood from the whole of the bleedings; his pulse was 110, the skin hot, tongue furred, with great anxiety of countenance: the limb was swollen from the application of the tourniquet from time to time, a quantity of coagulated blood had forced itself under the soleus in the course of the muscles, increasing the size of the leg, and florid blood issued from both openings on taking the compression off the femoral artery. On passing the finger into the outer opening, and pressing it against the fibula, a sort of aneurismal tumor could be felt under it, and the hemorrhage ceased, indicating that the peroneal artery was in all probability the vessel wounded.
In this case there was, in addition to the wound of the artery, a quantity of blood between the muscles, which in gunshot wounds, accompanied by inflammation, is always a dangerous occurrence, as it terminates in profuse suppuration of the containing parts, and frequently in gangrene. Its evacuation therefore became an important consideration, even if the hemorrhage had ceased spontaneously.
The leg having been condemned for amputation above the knee, the officers in charge were pleased to place the man at my disposal: and being laid on his face, with the calf of the leg uppermost, I made an incision about seven inches in length in the axis of the limb, taking the shot-hole nearly as a central point, and carried it by successive strokes through the gastrocnemius and soleus muscles down to the deep fascia, when I endeavored to discover the bleeding artery; but this was more difficult than might be supposed, after such an opening had been made. The parts were not easily separated, from the inflammation that had taken place; and those in the immediate track of the ball were in the different stages from sphacelus to a state of health, as the ball in its course had produced its effect upon them, or their powers of life were equal or unequal to the injury sustained.
The sloughing matter mixed with coagulated blood readily yielded to the back of the knife, but was not easily dissected out. The spot which the arterial blood came from was distinguished through it, but the artery could not be perceived, the swelling and the depth of the wound rendering any operation on it difficult. To obviate this inconvenience, I made a transverse incision outward, from the shot-hole to the edge of the fibula, which enabled me to turn back two[233] little flaps, and gave greater facility in the use of the instruments employed. I could now pass a tenaculum under the spot whence the blood came, which I raised a little with it, but could not distinctly see the wounded artery in the altered state of parts, so as to secure it separately. I therefore passed a small needle, bearing two threads, a sufficient distance above the tenaculum to induce me to believe it was in sound parts, but including very little in the ligature, when the hemorrhage ceased; another was passed in the same manner below, and the tenaculum withdrawn. The coagula under the muscles were removed, the cavity washed out by a stream of warm water injected through the external opening, the wound gently drawn together by two or three straps of adhesive plaster, and the limb enveloped in cloths constantly wetted with cold water. The patient was placed on milk diet.
On the 4th, two days after the operation, the wound was dressed, and looked very well; the weather being very hot, two straps of plaster only were applied to prevent the parts separating. On the 5th a poultice was laid over the dressings, in lieu of the cold water, the stiffness becoming disagreeable. On the 6th, as the wound, although open in all its extent, did not appear likely to separate more, the plasters were omitted, and a poultice alone applied. On the 8th and 9th it suppurated kindly; and on the 10th, or eight days from the operation, the ligatures came away, the limb being free from tension, and the patient in an amended state of health, his medical treatment having been steadily attended to.
The man was brought to England, to the York Hospital at Chelsea, and walked about without appearing lame, although he could not do so for any great distance. He suffered no pain, except an occasional cramp in the ball of the foot, and some contraction of the toes, which took place generally when he rose in a morning, and continued for a minute or two, until he put them straight with his hand; this I did not attribute to the operation, but to some additional injury done to the nerves by the ball in its course through the leg.
This case, which has been followed by many others equally successful, even after the femoral artery had been ineffectually tied, established the practice now followed in England by all educated surgeons; and is another of those great[234] additions to surgery for which science is indebted to the Peninsular war.
198. It may be permitted to repeat, that if an artery such as the axillary be laid bare previously to an operation for amputation at the shoulder, and the surgeon take it between his finger and thumb, he will find that the slightest possible pressure will be sufficient to stop the current of blood through it. Retaining the same degree of pressure on the vessel, he may cut it across below his finger and thumb, and not one drop of blood will flow. If the artery be fairly divided by the last incision which separates the arm from the body, without any pressure being made upon it, it will propel its blood with a force which is more apparent than real. All that is required to suppress this usually alarming gush of blood is to place the end of the forefinger directly against the orifice of the artery, and with the least possible degree of pressure consistent with keeping it steadily in one position the hemorrhage will be suppressed. It is more important to know that if the orifice of the artery, from a natural curve in the vessel, or from other accidental causes, happen at the same time to retract and to turn a little to one side, so as to be in close contact with the side or end of a muscle, the very support of contact will sometimes be sufficiently auxiliary to prevent its bleeding.
In amputation at the hip-joint, the femoral and profunda arteries are frequently divided at or just below the origin of the latter, and bleed furiously if disregarded; but the slightest compression between the finger and thumb stops both at once. They never have given me the smallest concern in these operations, or others of a similar nature; and surgeons should learn to hold all arteries that can be taken between the finger and thumb in great contempt. It is quite impossible for a man to be a good surgeon—to do his patient justice in great and difficult operations attended by hemorrhage, unless he has this feeling—unless his mind is fully satisfied of the truth of these observations. While his attention ought to be directed to other important circumstances, it is perhaps absorbed by the dread of bleeding, by the idle fear that he will not be able to compress the artery and restrain the bleeding from it—that he may have half a dozen vessels bleeding at once—that his patient will die on the table before him. Once fairly in dismay, and the patient is really in danger; but, endowed with that confidence[235] which is only to be acquired through precept supported by experience, he surveys the scene with perfect calmness: taking the great artery between the finger and thumb of one hand, he places the points of all the other fingers, of both hands if necessary, on the next largest vessels; or he presses the flaps or sides of the wound together until his other hand can be set at liberty by an assistant, or in consequence of a ligature having been passed around the principal artery. This is a scene sufficient to try the presence of mind of any man; but he is not a good surgeon who is not equal to it—who does not delight in the recollection of it when his patient is in safety, and his recovery assured. It was in consequence of what was then considered the too great boldness of the practice that my old friend, Sir Charles Bell, whose loss to science cannot be too much regretted, represented me seated on a pack saddle on the back of a bourro, (Anglice, a jack-ass,) on the top of the Pyrenees, expatiating on their merits (which he did not believe) to the descendants of the Bearnois of Henri Quatre on one side, and to the children of the lieges of Ferdinand and Isabella on the other; but no one now disputes their accuracy. The surgery of the Peninsular war was many years in advance of the surgery of civil life.
199. The principles laid down for the treatment of wounded arteries in the lower extremity are equally to be observed with respect to those of the upper. There is, however, little or no fear of mortification taking place in the upper extremity, the collateral circulation being more direct and free; while there is greater danger from this cause of hemorrhage from the lower end of the artery, if a ligature should not have been placed upon it, or if it should not be retained a sufficient length of time.
200. The error of placing a ligature on the subclavian artery above the clavicle, for a wound of the axillary below it, should never be committed. One person dies for one who lives after this operation, when performed under favorable circumstances, independently of the loss which may be sustained by a recurrence of bleeding from the original wound, which is always to be expected and ought to take place; when it does not happen, it is the effect of accident, which accident in all probability occurs from the state of absolute rest having been carefully observed.
201. The necessity for an aneurismal sac below the[236] clavicle, and for its remaining and continuing to remain intact, until the cure is completed, when the subclavian artery has been tied above, is rendered unmistakable by the following case:—
Ambrose C. was admitted into the Charing Cross Hospital, in August, 1848, in consequence of a bruise from a sack of beans; there was axillary aneurism, extending under the pectoral muscle up to the clavicle. A ligature was applied in the usual situation on the outside of the scalenus muscle, and came away on the twenty-second day. The aneurismal sac suppurated, and burst three days afterward, when a quantity of pus and blood, partly fluid, partly coagulated, but very offensive, was discharged. The opening was enlarged, and everything appeared to be going on well, at which time I saw him. On the nineteenth day after the ligature came away, I visited him again with Mr. Hancock, and merely observed that he must keep himself very quiet, and I thought he would do well. In the evening he died from hemorrhage, while eating some gruel. On examination after death, the artery was found to be sound, except where it communicated with the sac by an opening three-quarters of an inch in length. The ligature had been applied midway between the thyroid axis and the first of the thoracic branches. There was a small coagulum, of half an inch in length, both internal and external to the ligature, but not extending to the branch above or below it. The artery was of its natural size as far as the remains of the sac, but beyond it the axillary artery was diminished; the remains of the sac were void of coagulum, except where it communicated with the artery, to which opening a small coagulum had adhered, but had given way at its lower part, and thus caused his death. Between the opening and the ligature, five large branches entered into or were given off by the artery, and through some of these blood was brought round by the collateral branches in an almost direct manner, so that the man’s life depended on the resistance offered by the small coagulum after the sac had given way; proving in an exemplary manner the value of the sac remaining entire.
If this case will not convince the incredulous, it would be useless to bring even the sufferers in such cases from their graves, to affirm the fact of the inapplicability of the theory of aneurism to the treatment of a wounded artery—of the [237] impropriety of placing a ligature on the subclavian artery above the clavicle, for a wound of the artery below it.
Corporal W. Robinson, 48th Regiment, was wounded at the battle of Toulouse, by a piece of shell, which rendered amputation of the right leg immediately necessary, and so injured the right arm as to cause its loss close to the shoulder-joint eighteen days afterward. At the end of a month the ligatures had separated, and the wound was nearly healed, although a small abscess had formed on the inside, near where the upper part of the tendon of the pectoralis major had been separated from the bone. Sent to Plymouth, this little abscess formed again, and was opened on the 2d of August, three months after the amputation. The next day blood flowed so impetuously from it as to induce the surgeon to make an incision, and seek for the bleeding vessel, which could not be found. The late Staff-Surgeon Dease, warned by the case of Sergeant Lillie, (page 198,) strongly objected to the subclavian artery being tied above the clavicle, and, true to the principle inculcated at Toulouse, advised the application of a ligature below the clavicle on a sound part of the artery, but as near as possible to that which was diseased. The operation was done by the senior officer, Mr. Dowling, who carried an incision from the clavicle downward through the integuments and great pectoral muscle, until the pectoralis minor was exposed. This was then divided, and a ligature placed beneath it on the artery where it was sound, at a short distance from the face of the stump, where it was diseased. The man recovered without further inconvenience.
202. In all those cases in which it has been supposed necessary to place a ligature on the artery above the clavicle, after a failure in the attempt to find the artery below it, the failure has occurred from the error committed in not dividing the integuments and great pectoral muscle directly across from the lower edge of the clavicle downward. It is quite useless dividing these parts in the course of the fibers of the muscle, and the case of Robinson is the model on which all such operations should be done. If this operation had not succeeded, the ligature of the artery above the clavicle was a further resource; but as the artery was sound below, with the exception of the end engaged in the face of the stump, the operation was successful; no doubt should be entertained in such cases of the propriety of an operation [238] which is attended with little risk, compared with that which destroys one man for every one it saves.
203. Punctured wounds of the arteries of the arm and forearm ought to be treated by pressure applied especially to the part injured, and to the limb generally; but when the bleeding cannot be restrained in this manner, in consequence of the extent of the external wound, the bleeding artery is to be exposed, and a ligature applied above, and another below the part injured, whether the artery be radial, ulnar, or interosseal.
204. When the external wound closes under pressure, and blood is extravasated in such quantity under the fascia and between the muscular structures as is not likely to be removed by absorption under general pressure, the wounded artery should be laid bare by incision and secured in a similar manner, even at the expense of any muscular fiber which may intervene.
205. When an aneurismal tumor forms some time after such an accident, in the upper part of the forearm in particular, the application of a ligature on the brachial artery is admissible, on the Hunterian principle.
206. When the ulnar artery is wounded in the hand, which is comparatively a superficial vessel, two ligatures should be placed upon it in the manner hereafter to be directed. When the opening is small, pressure may be tried.
207. When the radial artery is wounded in the hand, in which situation it is deep seated, the case requires greater consideration. When there is a large open wound, and the bleeding end or ends of the artery can be seen, a ligature should be placed on each; but this cannot always be done without more extensive incisions than the tendinous and nervous parts will justify.
208. When search has been made by incisions through the fascia, (as extensively as the situation of the tendons and nerves in the hand will permit,) which are best effected by introducing a bent director under it, the current of blood, through either the ulnar or the radial artery at the wrist, or even through both, should be arrested in turn by pressure, which in most cases of this kind will succeed, if properly applied, and thus show the vessel injured. The bleeding point should be fully exposed, and all coagula removed, when a piece of lint, rolled tight and hard, but of a size only sufficient to cover the bleeding point, should be laid upon it. A [239] second and larger hard piece should then be placed over it, and so on, until the compresses rise so much above the level of the wound as to allow the pressure to be continued and retained on the proper spot, without including the neighboring parts. A piece of linen, kept constantly wet and cold, should be applied over the sides of the wound, which should not be closed so as to allow of any blood being freely evacuated; and if the back of the hand be then laid on a padded splint, broader than the hand, a narrow roller may be so applied as to retain the compresses in their proper situation, without making compression on or impeding the swelling of the adjacent parts, the fingers being bent, in order to relax the palmar aponeurosis—a proceeding which should never be neglected in any operation in the palm of the hand. It has been lately proposed by M. Thierry, a French surgeon, to raise and bend the arm, as a means of impeding the circulation where the artery passes over the elbow-joint, and the proposal deserves adoption, but not to the extent he recommends, which cannot be long submitted to. Pressure made at the same time on the radial or ulnar artery, or on both, by a piece of hard wood two inches long, shaped like a flattened pencil, is much more effectual, and more to be depended upon. When from the bones being broken, or the hand so swollen, or from other circumstances, pressure, however lightly and carefully applied, cannot be borne in the manner directed, and the attempts to secure the artery at the bleeding spot have failed, and pressure on the radial or ulnar artery has been equally unsuccessful, in consequence of the swelling or other circumstances, both may be tied at the wrist in preference to placing a ligature on the brachial artery, although that even must be done as a last resource, if the bleeding should still continue. If it be asked why not do this in the first, rather than in the last instance, the answer is, that it has so often failed to prevent a renewal of the bleeding from both ends of a wounded artery in the hand, that complete dependence cannot be placed upon it, particularly if there should be a division high in the arm of the brachial into the radial and ulnar arteries. When, however, the arteries leading to the wound have been secured, either by pressure or ligature, NEAR to the part, and the bleeding returns by the collateral circulation, which in the hand is so free, the arresting the supply of blood through the main trunk may and often has suppressed the hemorrhage, at all [240] events for a sufficient time to enable the injured parts to recover themselves, provided the forearm is bent and raised, and the person kept at rest in the most restricted manner, without which this operation will in all probability fail. It is in these cases that the instrument alluded to, page 226, will be useful, rendering the ligature on the trunk of the vessel unnecessary, more particularly if the bleeding should appear to depend on some peculiarity in the structure of the coats of the artery.
209. When the obstacle to the application of pressure arises from the injured state of the metacarpal bone or bones, one or more should be removed, with the fingers if necessary, so as to expose a clear and new surface, on which the bleeding vessels may be seen and secured. In some cases, particularly if there should be a hemorrhagic tendency in the arterial system generally, as known from previous accidents, the first compress may be wetted with the perchloride of iron, the ol. terebinth., the dilute sulphuric acid, or the tincture of matico; these remedies may be also administered internally. Some new styptics have lately been much lauded in Malta and other places, but sufficient proofs have not been given of their efficiency.
210. When the radial artery is wounded as it turns from the back to the inside of the hand, to form the deep-seated palmar arch, it meets a branch of the ulnar nerve about to terminate in the muscles of the thumb. If the treatment by pressure above recommended should not succeed, the muscles forming what is called the web, between the thumb and metacarpal bone of the forefinger, should be cut through, and the bleeding vessel exposed. They are the adductor pollicis on the inside, and the abductor indicis on back of the hand.
WOUNDS OF THE ARTERIES, ETC.
211. The precept so strongly insisted upon, that no operation should be done on a wounded artery unless it bleed, and at the place from which it bleeds, has been particularly opposed with reference to the neck, the opponents believing that placing a ligature on the primitive carotid is an operation not attended with much risk, and that it may therefore be done as a precautionary measure when the wounded part does not bleed; this statement is an error. Of thirty-eight cases collected by Dr. Norris in 1847, in which this vessel was tied for aneurism, twenty-six died, and twelve suffered from affection of the brain, the frequency of which occurrence has been singularly overlooked by practical surgeons; although proving, in a very marked manner, that the operation of tying the primitive carotid is not a trifling affair, and that the success, when compared with the failures, is only as one and one. A much more important objection is the difficulty of deciding, in many cases of wounds of the neck, what artery is wounded, and what trunk should be tied; whether it be the external carotid or its branches, or the internal, or the vertebral artery. Errors have been committed on all these points by men of the greatest anatomical and surgical knowledge; the trunk of a sound artery having been tied instead of that of a wounded one, inflicting thereby on the patient a second and useless wound, more dangerous, perhaps, than the original one it was intended to relieve.
When Professor of Anatomy and Surgery to the College of Surgeons in 1830, I stated that in wounds of the neck which rendered it advisable to place a ligature on some part of the carotid, on account of the supposed impracticability of laying bare the bleeding orifice, it was generally the external carotid which should be secured, rather than the primitive trunk; there not being sufficient reason for cutting off the supply of blood to the head by the internal carotid, unless the operation on the external carotid should fail. This direction should be implicitly followed.
[242] 212. A man was wounded by a ball in the side of the neck, and suffered severely from secondary hemorrhage. Some days after being brought into the hospital, M. Breschet, unable to arrest the bleeding, was about to apply a ligature to the common carotid, when the man died in time to prevent it. On examination after death, the vertebral was found to be the artery wounded, between the second and third vertebræ. The ligature of the carotid, had he lived a little longer, would have been a useless addition to his misery.
Professor Chiari, of Naples, tied the trunk of the left common carotid on the 18th of July, 1829, on account of a false aneurism below the mastoid process, consecutive to a wound made by a sharp-pointed instrument under the angle of the jaw. The man died on the ninth day, and the wounded artery was found to be the vertebral, between the transverse processes of the first and second vertebræ. M. Ramaglia says, a man, thirty-nine years of age, was wounded by a sharp-cutting, penetrating instrument, below the left ear, from which an aneurismal swelling resulted. The common carotid was tied, but as this did not arrest the pulsations of the aneurism, the ligature was removed, and the patient, after suffering from various accidents, died, when the vertebral was found to be the artery wounded.
M. Maisonneuve, of Paris, lately laid the following most instructive case before the Academy of Medicine: A lady was shot by her husband, who stood close to her, with a pistol loaded with ball. The wound was inflicted on the anterior part of the neck, on a level with the left side of the cricoid cartilage. The hemorrhage had been considerable when the surgeons, Messrs. Maisonneuve and Favrot, arrived, though the wound looked at first as if the ball had not penetrated deeply. There were pain and numbness of the left arm; respiration, voice, and deglutition were, however, normal. On examining with the probe, it was found that the cricoid cartilage had been bared, and that the ball had then run from above downward, leaving the trachea and œsophagus internally, and the common carotid artery, the internal jugular vein, and the pneumogastric nerve externally, and was impacted in the body of the sixth cervical vertebra, where it could easily be felt. Some attempts at extraction were made, but they caused so much pain that they were given up. The patient was bled six times in four[243] days, and had large doses of opium; she improved considerably under this treatment, and the inflammation was very moderate.
On the eighth day hemorrhage occurred at the wound, and again on the ninth, but it ceased of itself on each occasion. When, however, it broke out a third time, the surgeons proceeded at once to search for the bleeding vessel. An incision about three inches long was made on the anterior edge of the sterno-mastoid muscle, a little external to the wound inflicted by the ball; the carotid sheath was then brought into view, and the vessels were found intact. The cricoid cartilage and the first rings of the trachea were afterward seen to have been grazed by the ball, which was found implanted in the body of the sixth cervical vertebra, whence it was easily extracted. Severe hemorrhage ensued immediately upon the removal of the ball, the blood seeming to proceed from the vertebral artery, which appeared to have been wounded within the canal formed by the foramina of the transverse processes. By placing the finger on the hole left by the ball, the orifice whence the blood issued was distinctly seen; forceps were applied to it, and held firmly for a little while to arrest the hemorrhage. An aneurismal needle, with a very small curve, was then made to carry a double thread behind the vessel. One of these was used to tie the artery above, and the other below the aperture whence the blood issued.
The operators at first thought they were mistaken in supposing that they had tied the vertebral artery, as the vessel seemed quite free, while it is known to be protected by the transverse processes in that locality, and believed they had secured the inferior thyroid. The hemorrhage ceased at once, and some smaller vessels were then tied, among which was the inferior thyroid artery. Everything went on favorably at first; the threads fell on the ninth day after the deligation of the vessel, and the patient remained in a satisfactory state for the next five days, when severe febrile symptoms, unpreceded by shivering, set in; and on the eighteenth day after the operation, the twenty-seventh after the infliction of the wound, the patient was suddenly seized with a violent pain in the cervical region, cried out loudly, and fell into deep coma, which lasted for about seven hours, when she expired, notwithstanding the most strenuous means were used to rouse her.
[244] On the post-mortem examination, the course of the ball was found as stated above, viz., it had run from the integuments to the body of the sixth cervical vertebra, leaving the trachea and œsophagus internally, and the carotid sheath and its contents externally, untouched. The inferior thyroid artery was wounded just before it reaches the thyroid gland, and had a firm clot, about half an inch in length, filling its cylinder. The transverse process of the sixth cervical vertebra was fractured, and had left the wounded vertebral artery unprotected. The vessel above and below the wound in its coats was filled with a firm clot for about an inch in each direction. The body of the sixth cervical vertebra had been perforated by the ball, which had dug for itself a canal communicating with the cavity of the spine by a small aperture, evidently of very recent formation. This aperture resulted clearly from the necrosis of the thin shell of bone which formed the bottom of the canal. The cancelous texture of the body of the vertebra was infiltrated with pus, and a sero-purulent fluid was found in the spinal canal, both in the cellular tissue external to the dura mater and in the sub-serous texture of the meninges. No other lesion existed in any other part of the frame.
213. M. S., a female, aged fifty-three, was admitted into the Westminster Hospital, with a large, movable tumor in the neck, under the sterno-mastoid muscle of the right side. An operation having been commenced for its removal, the tumor was found to be of a more than doubtful character, and to dip down between and behind the great vessels of the neck. In the course of the operation, the external carotid was opened a little above its bifurcation, and a ligature was applied on the common carotid. The bleeding was not in the least arrested; a ligature was then placed on the external carotid above the hole in the artery, which still continued to pour out blood; a third ligature was now put upon the internal carotid, with no better success. A fourth ligature was then applied on the external carotid, below the hole in it, including the superior thyroid, which was given off at that part; after which the bleeding ceased, and never returned. Three ligatures came away in three weeks; the fourth remained during five weeks. The patient recovered from the operation, but the tumor grew again, and the woman died exhausted at the end of six months. On examination after death, the arteries referred to were found to[245] be obliterated for some distance above and below the parts injured.
The utter inefficiency of everything but the two ligatures, the one immediately above, the other immediately below the part opened, could not be more distinctly proved, if a case were even invented for the purpose; and the fact could not be more satisfactorily shown that in every case of wounded—not aneurismal—artery in the neck, one ligature should be applied above, and another below the opening in the injured vessel, and not one alone on the common trunk, even if that should be the part injured.
It is argued that when a man has his internal carotid cut on the inside of his throat, by a foreign body of any kind thrust through his mouth, the artery cannot be tied by two ligatures at the wounded part through the mouth, not even if it were enlarged from ear to ear. What, then, is to be done? The artery should be secured by ligature by an incision made on the outside of the neck. This being admitted, the question then is, shall the wounded artery be laid bare at the part injured, or two inches or so lower down, where the main trunk can be most easily got at by men of even very moderate anatomical knowledge?—an operation which has frequently failed, although it has frequently succeeded, and is therefore most approved. I am willing, for the present, to consider it nearly impracticable to tie the internal carotid safely from the outside of the neck, at the part wounded, without great anatomical knowledge, and to accept, for the moment, as the proper operation, the ligature of the common trunk of the carotid, at the distance of two or more inches, being the operation of Anel; but I venture to ask, with what fairness can this operation, thus done on one side of the neck, at the distance of two inches, the other side remaining sound, be considered similar to that of Mr. Hunter, done on the thigh for a wound in the calf of the leg, at the distance of perhaps twenty inches, with all the intervening collateral branches perfectly sound? It cannot be considered an analogous operation, with propriety or fairness, nor ought the one to be compared with the other, although it is done; and thus the subject is mystified to all those who do not understand it thoroughly. It is because English surgeons miscall this the operation of Hunter, that French surgeons claim the operation of Hunter as that of Anel, and deny the priority of Hunter, although[246] the two operations are essentially distinct. The operation of Anel for aneurism of the popliteal artery would be destructive; the operation of Hunter for a wound of the popliteal artery would be equally so.
This point must, however, be pressed further. Let us suppose that the internal carotid has been opened by a wound inflicted through the mouth, and death is about to follow, unless the hole in the artery can be tied up. How is it to be done? The Hunterian theorists say it is impracticable to tie the artery at the wounded part, and the primitive trunk must therefore be secured.
Let us now suppose that a ligature has been placed on the common carotid, and the bleeding continues; what is to be done? By the Hunterian and Anellian theorists there is nothing more to be done—the patient must die. By my theory there is another operation to be done, and the patient need not necessarily die. As there is already a wound in the neck made by the surgeon, there would be little difficulty, by extending it, in ascertaining that the blood came from the brain, and that nothing but a ligature on the internal carotid artery above the part wounded through the mouth could save the patient; and why not do this operation at first, and place a ligature above and another below the wound in the artery?
214. It is with great satisfaction I quote the opinion of M. Velpean on this subject, as showing the greater advance Parisian surgeons have made than even many of high attainments in London: “In hemorrhage from the neck, the mouth, the throat, the ear, or the skull, everything should be done to reach the branch of the carotid which has been wounded, rather than tie the carotid itself.” Alluding to a wound of the inferior pharyngeal artery, he says: “The search for this artery will cause but little or no inconvenience, for the same incision will suffice for the ligature of the external or internal carotid, the lingual, the facial, or the superior thyroid artery, if it become necessary, each artery being capable of being taken hold of and compressed, until the one which is really wounded is ascertained.” He further adds: “Surgeons found it formerly more convenient and sure to tie the primitive trunk of the carotid, for all arterial diseases of the head, than to tie the external or internal carotid or their branches; but this is not admissible in the present day.” Operating for a tumor on the left temple, which he consid[247]ered aneurismal, he first tied the common trunk of the carotid, and then the internal. The tumor diminished in size, but hemorrhage took place from the wound, and was frequently repeated until the sixteenth day, when the patient died hemiplegic. The hemorrhage came from the external carotid, and the blood escaped through the upper opening of the common carotid. He says himself he ought to have tied the external carotid also; or, after the first bleeding, have applied a ligature on the upper end of the common trunk.
215. Dr. Twitchell, of Keene, N. H., United States, says a soldier, in a sham fight, in 1807, received a wound, from the wadding of a pistol, on the right side of the head, face, and neck, which was much burned. A large wound was made in the mouth and pharynx; nearly the whole of the parotid gland, with the temporal, masseter, and pharyngeal muscles, was destroyed. The neighboring bones were shattered, and the tongue injured. The hemorrhage was not copious, although the external carotid and its branches were divided. Ten days after the accident, the sloughs had all separated, and left a large circular aperture, of from two to three inches in diameter, at the bottom of which might be seen distinctly the internal carotid artery, denuded from near the bifurcation of the common trunk to where it forms a turn to enter the canal in the temporal bone. Directly on this part there was a dark speck, of a line or two in diameter, which suddenly gave way while Dr. Twitchell was in the house. With the thumb of his left hand he compressed the artery against the base of the skull, and effectually controlled the hemorrhage. The patient fainted. As soon as he recovered, the doctor says: “I proceeded to clear the wound from blood, and having done this I made an incision with a scalpel downward, along the course of the artery, to more than an inch below the point where the external branch was given off, which, as stated above, had been destroyed at the time of the injury. Having but one hand at liberty, I depended upon the mother of the patient to separate the sides of the wound, which she did, partly with a hook, and occasionally with her fingers. At length, partly by careful dissection, and partly by using my fingers and the handle of the scalpel, I succeeded in separating the artery from its attachments; and, passing my finger under it, I raised it up sufficiently for my assistant to pass a ligature round it. She tied it with a sur[248]geon’s knot, as I directed, about half an inch below the bifurcation.” Dr. Twitchell removed his thumb, and sponged away the blood, not doubting that the hemorrhage was effectually controlled; but, to his surprise and disappointment, the blood immediately began to ooze from the rupture in the artery, and in less than ten minutes it flowed with a pulsating jet. He compressed it again with his thumb, and began to despair of saving his patient, but resolved to make another attempt. Raising his thumb, he placed a small piece of dry sponge directly over the orifice in the artery, and renewed the compression till a rather larger piece of sponge could be prepared. He placed that upon the first, and so went on, pressing the gradually enlarged pieces obliquely upward and backward against the base of the skull, till he had filled the wound with a firm cone of sponge, the base of which projected two or three inches externally. He then applied a linen roller in such a manner as to press firmly upon the sponge, passing it in repeated turns over the head, face, and neck. On the 30th of December the patient was discharged cured, several fragments of bone and two teeth from the upper jaw having been cast off. Some deformity remained, in consequence of the depression on the side of the face.
The inutility of tying the primitive trunk for a wound of the internal carotid is distinctly shown in this case, which is no less valuable from the fact demonstrated, that if the internal carotid can be exposed and injured within the angle of the jaw by an accident, it can be exposed and secured by ligature at the same part by an operation.
216. When, then, the internal carotid is wounded through the mouth, what operation is to be performed? That of placing a ligature above, and another below the opening made into it; and after much consideration, and many trials, the following operative process is recommended to the attention of those who are best acquainted with the subject:—
An incision is to be begun opposite to and on the outside of the extremity of the lobe of the ear, and carried downward in a straight line, until it reaches a little below the angle of the jaw, at the distance of nearly half an inch, more or less, as may be found most convenient from the form of the neck. This incision exposes the parotid gland without injuring it. A second is then to be made from the extremity of the first, extending at a right angle forward, under or along the base[249] of the lower jaw, until the end of it is opposite the first molar tooth. This incision should divide the skin, superficial fascia, platysma myoides muscle, and the facial artery and vein. The second molar tooth should then be removed, and the jaw sawn through at that part. Then cut through the deep fascia, the mylo-hyoideus muscle, and the mucous membrane of the floor of the mouth, exposing the insertion of the internal pterygoid muscle, which is to be divided. The surgeon will next be able to raise and partially evert the angle of the jaw, and thus obtain room for the performance of the remaining part of the operation, which should be effected by the pointed but blunt end of a scalpel, or other instrument chosen for the purpose of separating, but not of cutting. The styloid process of the temporal bone may then be readily felt, and exposed by the separation of a little cellular membrane, and with it the stylo-hyoid muscle, which is to be carefully raised and divided. The external carotid artery will thus be brought into view, together with the stylo-pharyngeus muscle and the glosso-pharyngeal nerve attached to it. These are to be drawn inward by a blunt hook, when, if care be taken to avoid the pneumogastric nerve, the internal carotid may be felt, seen, and secured by ligature with comparative facility outside the tonsil, there being between them the superior constrictor of the pharynx, which, in a case of wound through the mouth, must have been divided. The pneumogastric nerve should be drawn outward, and the external carotid artery also, if in the way. The division of the jaw will not lead to further inconvenience, as the bone always reunites, when divided, with little difficulty. That this operation requires a thorough knowledge of the anatomy of the parts, is true; and this can only be acquired by repeated dissections.
217. The nearest successful case to the operation thus recommended was performed by Dr. Keith, of Aberdeen.
E. Kennedy, aged twenty-five, accidentally swallowed a pin, the head of which could be felt below and behind the left tonsil, covered by the lining membrane of the pharynx; it could not be extracted by any attempt made for its removal. The membrane was snipped by a pair of probe-pointed scissors, to expose the head of the pin. This was followed by the discharge of mouthfuls of arterial blood, and it was evident that the internal carotid artery had been injured. Pressure on the common carotid stopped the[250] bleeding, and the operation of placing a ligature on the internal carotid was effected in the following manner: The patient’s head being supported by a pillow, her face was turned toward the right shoulder, when an incision was made from below the ear along the ramus of the lower jaw to below its angle. No hemorrhage occurred, and the vessel was speedily exposed and secured by a double ligature passed under it, with less difficulty than the depth of the vessel would lead one to expect. One ligature arrested the flow of blood, and the other was therefore withdrawn. The woman recovered, without any return of the bleeding. Dr. Keith, aware of the necessity for tying the other end of the artery, if it should bleed, watched the case day and night until the period of danger had passed away. The pin gave no trouble, until felt by the patient as about to go down the œsophagus, which it did to her great satisfaction and relief from further anxiety.
LIGATURE OF THE COMMON ILIAC ARTERY, ETC.
218. The operation for placing a ligature on the aorta should not be done by making an opening through the front of the abdomen, as has hitherto been proposed. It should in future be attempted and executed nearly in the same manner as the operation for placing a ligature on the common iliac, which has succeeded. The aorta bifurcates usually on the body of the fourth, or on the inter-vertebral substance between it and the fifth vertebra, although it may be higher or lower—a fact which cannot be ascertained previously to the operation; the most usual place is nearly opposite to the margin of the umbilicus on the left side. It is about half an inch above this that the ligature should be placed on the aorta, if this operation is ever done again, rather lower than higher, on account of the origin of the inferior mesenteric artery. As the aorta is to be reached by carrying the finger along the common iliac, the comparative situation of that vessel is next to be estimated.
The length of the two common iliac arteries varies according to the stature of the patient, and the place at which the[251] aorta bifurcates. The common iliacs again divide into the external and internal iliacs, which division is usually opposite to the sacro-iliac symphysis. The length of the common iliac artery is therefore tolerably well defined, as scarcely ever exceeding two inches and three-quarters, and seldom being less than two inches. The external iliac is a little longer than the common iliac, and the place of subdivision of the common iliac into external and internal can always be ascertained, during an operation, by tracing the external iliac upward to its junction with the internal to form the common trunk, which proceeds upward and inward to the aorta. The left margin of the umbilicus being taken as a point opposite to that which may be presumed to be the part at which the aorta divides, and the situation of the external iliac becoming femoral being clearly ascertained, a line drawn between the two will nearly indicate the course of these two vessels; sufficiently so, at all events, to enable the operator to mark with his eye, or with ink, the place where he expects to tie the artery; and to regulate the length of the incision, so that this ideal spot may correspond to its center. It is necessary to recollect, also, that the whole of one hand and part of the other must be introduced into the wound, to enable the operator to pass a ligature round the artery, and to tie the knots: so that an external excision of less extent than five inches will not suffice, and six will afford a facility in operating, which will save pain to the patient and inconvenience to the operator. In calculating the length of the incision, allowance must be made for the size, obesity, and muscularity of the patient. If a rule be placed on the crest of each ilium, about one inch and a half behind the anterior superior spinous process, it will pass in a well-formed man across the junction of the fifth lumbar vertebra with the upper part of the sacrum, and a little way behind where the common iliac divides into external and internal. The center of an incision, six inches in length, beginning about half an inch above Poupart’s ligament, and about the same distance to the outside of the inner ring, and carried upward, will fall nearly on a line with this point. The incision should be nearly parallel to the course of the epigastric artery, but a little more to the outside, in order to avoid it and the spermatic cord, and having a gradual inclination inward toward the external edge of the rectus muscle; the patient being on his back, with the head and shoulders[252] raised, and the legs bent on the trunk. The aponeurosis of the external oblique muscle having been opened inferiorly, is to be slit up for the whole length of the external incision; and the director having been first passed under the internal oblique muscle, through a small opening carefully made into it, it is to be divided in a similar manner. The transversalis is then to be cut through at the under part, and its tendinous expansion divided at the upper part, the greatest precaution being taken by the finger to prevent the peritoneum being injured. The fascia transversalis is then to be torn through at the lower and outer part, so that the fingers may be passed inward from the ilium, and the peritoneum detached from the iliac fossa, and turned with its contents inward, by a gradual and sidelong movement of the fore and second fingers inward and upward, until, passing over the psoas muscle, the external iliac artery is discovered by its pulsation. It is then to be traced upward and inward toward the spine, when its origin and that of the internal iliac from the common trunk will be felt. The point of the forefinger will then be nearly in the center of a line drawn from the umbilicus to the anterior superior spine of the ilium; hence the necessity for an incision six inches in length, if the artery is to be tied high up, which is to be accomplished by tracing it in a similar manner to its origin from the aorta.
The common trunk of the iliac arteries and the aorta itself may be tied by the same method of proceeding; the only difference which can be practiced with advantage will be to make the incision a little longer at its upper part, no inconvenience arising from the addition to the length of the external wound, while the subsequent steps of the operation will be much facilitated by it. The following method of proceeding, adopted in two cases in which I placed a ligature on the common iliac artery with a successful result, will bring the operation so graphically before the reader that it cannot be misunderstood, and may be readily followed in operating: I began the operation, the patient lying on the back, by an incision on the fore part of the abdomen, commencing an inch and a half below the inside of the anterior spine of the ilium, and the same distance within it, carrying it upward, and diagonally inward toward the edge of the rectus muscle above the umbilicus, so that the incision was between six and seven inches long. If the incision be made more outwardly, toward the side in a straight or vertical line from the ilium[253] toward the ribs, great difficulty will be experienced in turning over the peritoneum with its contents, so as to place the finger on the last lumbar vertebra—an inconvenience which will be avoided by making the incision diagonally, and of the length directed.
After dividing the common integuments, the three layers of muscles were cut through in the most careful manner; the division of the transversalis muscle was attended with some difficulty, inasmuch as there was but little fascia transversalis, and the peritoneum was remarkably thin—as thin as white silver paper. On attempting to reach the under part on the inside of the ilium, so as to turn the peritoneum over, which in sound parts is always done without the least difficulty, I found that it could not be done on account of the tumor which projected inward adhering to it; some bleeding took place from the large veins which surrounded it, giving rise to the caution not to proceed further in that direction. At this moment, in spite of the greatest possible care that could be taken by Mr. Keate, who raised and protected the peritoneum, a very small nick was made in it, sufficient to show the intestine through it. Perceiving that I could not tie the internal iliac as I had at first intended, and that I must place the ligature on the common iliac, I tried to gain a greater extent of space upward; but where the tendon of the transversalis muscle passes directly across from the lower ribs to aid in forming the sheath of the rectus, the peritoneum is usually so thin and so closely attached to it that it can only be separated with great difficulty. I knew this from the operation I had before performed, when, in spite of all the precaution I could then take, the peritoneum was at this spot slightly opened. It occurred in the present instance, and the right lobe of the liver was thus exposed.
The opening thus made on the fore part of the abdomen was not large enough to admit two hands. The peritoneum being, however, separated a little from the posterior wall of the abdomen from the outside, by the fingers, for a cutting instrument was inadmissible, four of the fingers of one hand were introduced beneath it, and it was turned a little over toward the opposite side. In doing this it must be remembered that the peritoneum must be raised, the hand being pushed toward the back as little as possible, in order to avoid getting behind the fat commonly found in that part of[254] the body, which would lead to the under edge of the psoas muscle instead of the upper surface, and thus render the operation embarrassing.
The peritoneum being carefully drawn over with its contents, I found I could only get one hand, or a little more, underneath it in search of the artery, the tumor below preventing any further detachment of the peritoneum in that direction. I therefore passed my finger across the psoas muscle, and it rested on the fifth lumbar vertebra. The common iliac artery was not to be felt, however, even as high up as the fourth lumbar vertebra, nor was the aorta; they had both risen with the peritoneum, and my finger resting on the spine was beneath them. Mr. Keate endeavored to raise or draw over the peritoneum, to give me an opportunity of seeing the vessels, but it could not be done. However, he felt the pulsation of the iliac artery, which had been raised with the peritoneum, to which I found it adhering. Carefully separating it with the end of the forefinger of the right hand, I passed a single thread of strong dentists’ silk, as it is termed, in a common solid aneurismal needle, by the aid of the thumb and forefinger of the left hand, round the artery without seeing it. I could then bring the artery a little forward by means of the aneurismal needle, when it appeared to be perfectly clear, and from the distance of the bifurcation of the aorta above, which could be distinctly felt, I calculated that the common iliac was tied exactly at its middle part. All pulsation below immediately ceased.
The two ends of the ligature were twisted, and the peritoneum replaced in its proper situation, care being taken that the two small openings into it should be well covered under the skin, so that they might not be in the line of the incision, and that they should be covered by newly divided healthy parts, so that they might thus adhere to each other. Three strong sutures and three or four smaller ones were put in through the skin, in order to prevent the parts bursting asunder from the movements of the patient. This operation was only formidable, as a whole, from the circumstance that space could not be obtained for the introduction of both hands; for, strange as it may appear, the safety of and ease in doing the operation depend on the first incision in the fore part of the abdomen being so large that the peritoneum containing the bowels may be freely drawn over by the ex[255]panded hands of the assistant, so that the operator can see what he is doing beneath. In my first case the whole of the parts under the peritoneum could be distinctly seen, and several gentlemen (not in the profession) who were present saw the common iliac artery in its natural situation.
The patient suffered little or nothing from the operation, which was performed on the Saturday; there was no augmentation of the pulse until Sunday evening, when it rose to 120; she then experienced some pain, which was materially diminished, although not altogether removed, by the abstraction of fourteen ounces of blood. At four in the morning, Mr. Hancock, now senior surgeon to the Charing Cross Hospital, took away fourteen ounces more, after which she had not a bad symptom. The bowels were not moved for the first four days. The temperature of the limb diminished, but not much, which may be attributed to its having been constantly rubbed night and day by two persons; and a hot brick, or bottles of hot water, covered with flannel, having been applied to the feet, of the temperature of from 120° to 140°. One nurse rubbed the lower part of the limb, and another the upper, for three days and three nights; if an interval of a few minutes occurred, a hot flannel was put on the limb. The friction was very slight, so as not to injure the cuticle. The patient occasionally dozed a little; still the same gentle friction was kept up. The ligature came away on the twenty-sixth day after the operation. The external incision healed very readily, but was followed, as is usual in all extensive wounds of the muscular wall of the abdomen, by a slight herniary projection, requiring the support of an abdominal bandage.
The situation of the ureter and rectum on the left side in this operation, and of the ureter and cæcum with its appendix on the right side, should be well understood, and it should be known that the ureter rises with the peritoneum. The relative situation of the common iliac artery and vein should be particularly attended to, when passing the ligature around the vessel. On the left side, the artery lies external and anterior to its commencement; on the right, the artery passes over the commencement of the vena cava and the left iliac vein, which do not follow the peritoneum when drawn toward the opposite side. The bowels should be thoroughly well evacuated before the operation is performed, but purgatives should not be given for some days after it has been done.[256] The food should be liquid, and inflammation should be subdued by leeches, general bleeding, fomentations, and opium.
219. The aorta may be as readily tied by this mode of proceeding as the common iliac; and I am satisfied it is in this way such an operation ought to be performed, provided it become necessary to attempt it, which I suspect it will not be; for when an aneurism has formed so high up that it prevents the application of a ligature on the side on which the disease is situated, the common iliac will be more readily tied above it, instead of the aorta, by performing the operation on the opposite or sound side of the body; for as a ligature can be applied with great ease on the sound side on the middle of the common iliac artery, it requires very little more knowledge and dexterity to pass over to the opposite or diseased side, and tie the artery above the aneurismal tumor, the size of which would have prevented the operation being done on its own or the affected side. The placing a ligature on the aorta for an aneurism in the pelvis will thus be rendered unnecessary—a most important result, deduced from the operation described.
220. If the internal iliac is to be tied, the operator traces it downward from its origin, in preference to passing his finger from the external iliac artery inward in search of it. Having placed the point of his forefinger on the vessel at the part where he intends to pass his ligature, he scratches with the nail upon and on each side of it, so as to separate it from its cellular attachments, and from the vein which accompanies, but lies behind it. Thus far the operator proceeds by feeling; but it is now necessary that the sides of the wound should be separated, and kept apart by blunt spatulæ curved at the ends, so as to take up as little space as possible, and not to injure the peritoneum. The surgeon should, if possible, see the artery, and the ligature carried on the eye of a bent probe, or a convenient aneurismal needle, should be passed under it from within outward, when it should be taken hold of with the forceps; the probe or needle should then be withdrawn, and the ligature firmly tied twice, or with a double knot. Great care must be taken to avoid everything but the artery. The peritoneum which covers it and the ureter which crosses it must be particularly kept in mind. The situation of the external iliac artery and vein, which have been crossed to reach it, must always be recollected,[257] and, if there be sufficient space, they should be kept out of the way, and guarded by the finger of an assistant.
221. The external iliac artery has been so often and so successfully tied that a description of the two methods of proceeding commonly adopted will suffice, with a few additional remarks. The first, recommended by Mr. Abernethy, is in accordance with the operations on the common, and on the internal iliac. The patient being laid on his back, with the shoulders slightly raised, and the legs bent on the trunk, an incision is to be made about three inches and a half in length in the direction of the artery, terminating over or a little above Poupart’s ligament. The aponeurosis of the external oblique muscle will be exposed, and an opening being made into it, a director is to be introduced, and it is to be slit up to the extent of the external incision. The internal oblique and transversalis muscles are then to be “nicked,” so as to allow a director or the point of the finger to be introduced below them, when they also are to be divided, the finger separating them from the fascia transversalis and the peritoneum. The fascia transversalis running from Poupart’s ligament to the peritoneum is now to be torn through with the nail, immediately over the pulsating artery, and the peritoneum is to be separated by the finger, and pushed upward until sufficient room has been obtained; which in this, as well as in all other operations on the iliac arteries, is sometimes difficult on account of the protrusion of the intestines covered by the peritoneum, when the patient is not sufficiently tranquil. The artery is yet at some depth; it is covered by a dense cellular membrane, connecting it to the vein on its inside, which must be torn through with the nail. The anterior crural nerve is separated from the artery by the psoas muscle, at the outer edge of which it lies. The aneurismal needle should be passed between the vein and the artery, and the point made to appear on the outside of the latter.
In this operation the ligature is placed on the external iliac, above where it gives off the epigastric and the circumflexa ilii arteries; as the operation is very much the same as that already described, with the exception of the incision being shorter and nearer to Poupart’s ligament, it is obvious, if it were found necessary from disease to tie the artery higher up, or even to tie the common iliac, that it might be done by merely enlarging the wound. It is therefore the[258] best mode of proceeding when the aneurismal swelling in the groin has encroached on Poupart’s ligament.
Another method has been recommended by Sir Astley Cooper, which is perhaps more followed where there is little doubt of the artery being sound.
“The patient being placed in the recumbent posture, on a table of convenient height, the incision is to be begun within an inch of the anterior superior spinous process of the ilium, and is to be extended downward in a semicircular direction to the upper edge of Poupart’s ligament. This incision exposes the tendon of the external oblique muscle; in the same direction the above tendon is to be cut through, and the lower edges of the internal oblique and transversalis abdominis muscles exposed; the center of these muscles is then to be raised from Poupart’s ligament; the opening by which the spermatic cord quits the abdomen is thus exposed, and the finger passed through this space is directly applied upon the iliac artery, above the origin of the epigastric and circumflexa ilii arteries. The iliac artery is placed upon the outer side of the vein; the next step in the operation consists in gently separating the vein from the artery by the extremity of a director, or by the end of the finger. The solid curved aneurismal needle is then passed under the artery, and between it and the vein from without inward, carrying a ligature, which, being brought out at the wound, the needle is withdrawn, and the ligature is then tied around the artery, as in the operation for popliteal aneurism. One end of the ligature being cut away, the other is suspended from the wound, the edges of which are brought together by adhesive plaster, and the wound is treated as any other containing a ligature.”
This method of operating will suffice when the artery is to be tied for an aneurism which does not extend as high as Poupart’s ligament. When it does, the operator will be so much inconvenienced by it, while the sound part of the artery above the tumor will be so much in a hollow behind it in the pelvis, that a ligature cannot readily be passed around it; the disturbance to the peritoneum will be much greater, and much more likely to give rise to peritonitis, than if the incision were made an inch longer on the face of the abdomen. The surgeon, instead of searching for the artery, as Sir Astley Cooper has directed, through the passage by which the spermatic cord quits the abdomen, and thus passing the[259] fingers directly under the peritoneum, will find it very much for his own ease, and for the advantage of his patient, to pass his fingers under the peritoneum from the inside of the wall of the ilium, from which it readily separates, and thus approach the artery from the outside instead of from below. He will obtain more room, reach the artery easily above the origin of the circumflexa ilii, and avoid that disturbance of the peritoneum, in applying the ligature, which often leads to inflammation. The ligature should be passed under the artery from within outward, so as to avoid the vein, which I have seen injured by passing the needle from without inward.
If the surgeon have unluckily divided the epigastric artery, either in this or in any other operation, all that he has to do is to enlarge the incision, and tie both ends of the divided vessel; I have no hesitation in saying it will not be of any consequence, either in this operation or in one for hernia.
222. In all cases of aneurism of the gluteal and sciatic arteries, the internal iliac artery should be tied, instead of an operation on the part itself. In all cases of wounds of those arteries, which are the only ones rendering an operation for placing a ligature on these vessels necessary, the wound should in a great measure regulate the course of the incision. The operation is an act of simple division, first through the common integuments for the space of five inches, then through and between the fibers of the gluteus muscle to the same extent; a dense aponeurosis covering the vessels is to be next divided, when the bleeding will lead to the injured vessel. Place the body on the face, turn the toes inward; commence the incision one inch below the posterior spinous process, and one inch from the sacrum; carry it on toward the great trochanter in an oblique direction to the extent of five inches. Divide the gluteus muscle and the aponeurosis beneath it, and seek for the artery as it escapes through the upper and anterior part of the sciatic notch, lying close to the bone. If the vessels of the gluteus muscle bleed, so as to be troublesome, and cannot be stopped by compression, they must be secured.
If the sciatic artery be the vessel injured, the incision should be made in the same direction, but about an inch and a half lower down. If the course of the wound render it doubtful which artery has been injured, the incision should be as nearly as possible between the two lines directed, the[260] wound being always the best guide; care should be taken in every instance to include nothing in the ligature but the artery.
Dr. Tripler, of the United States Army, was called to a person who had fallen backward with great force on a glass bottle, which had thus been driven into the right buttock, within an inch of the ischiatic notch. The fingers passed into the wound could be felt on the inside of the thigh. The man was deluged with blood, and in a state of syncope. The wound was plugged and bandages applied. Several hemorrhages took place, and on the thirteenth, five days after the receipt of the injury, the wound was enlarged, and the gluteal artery tied as it emerged from the pelvis. The bleeding ceased for three hours, when it returned with as much force as ever. After various ineffectual attempts to suppress the bleeding by pressing on the external iliac and femoral arteries, it was determined to tie the internal iliac, which was done in a very satisfactory manner, and the bleeding did not return. The man died three days after the operation, and an examination after death took place; but, strange to say, no notice is taken, no mention whatever is made of the wounded vessel. It is simply remarked that the last ligature was found embracing the internal iliac artery an inch below the bifurcation, and a firm coagulum already deposited above the point of ligation.
According to the principles laid down in this work, two errors were committed in this case. The first, in tying the gluteal artery as it emerged from the pelvis. The second, in tying the internal iliac, which was unnecessary. The bleeding which caused this operation to be resorted to is described as a welling up of the vital fluid, as returning slowly and sluggishly; the color is not alluded to. It is probable that the gluteal artery was not divided, but only wounded; and if the injured part had been sought for, and one ligature applied above, and another below the wound in it, the hemorrhage would not have returned, and life perhaps might not have been lost.
The operations were highly honorable to the gentlemen concerned, as proving their anatomical knowledge. The principle on which they acted I presume to condemn.
223. Compression should never be made on the femoral artery when a ligature is about to be placed upon it for aneurism, because the pulsation is thereby suppressed, and[261] the most important guide to the vessel is at the same time taken away. When the artery has been wounded near the groin, and is bleeding, compression must be had recourse to in the first instance to arrest the hemorrhage; the first incisions must therefore be made without the information which the pulsation gives as to the precise situation of the artery, although a finger may be allowed to rest, or a mark be made on the part, beneath which the artery could be felt before the pressure was applied. The external incision should always be made longer or shorter in proportion to the depth at which the artery is situated. It should be at least one-third longer in the middle than at the upper part of the thigh; for, while a long incision always facilitates the subsequent steps of the operation, it never does harm, unless it is out of all reasonable proportion. The center of the incision should be, if possible, directly over that part of the artery on which it is intended to apply the ligature; but no inconvenience will arise from its being applied nearer its upper extremity. The patient being laid on his back, and properly supported, the knee is to be bent and turned outward, by which the head of the femur will be rolled in the acetabulum, and the femoral artery will be more distinctly felt at the upper part of the thigh, below Poupart’s ligament. It lies on the psoas muscle, having the vein on its inside, and the anterior crural nerve about half an inch on its outside, having passed between the psoas and iliacus muscles, although some branches soon approach the artery, and run down on the external part of the sheath. The relative position of the parts having been duly considered, an incision is to be made directly in a line over the pulsating artery, and carried through the skin, cellular tissue, and superficial fascia, down to the deep-seated or fascia lata of the thigh. If an absorbent gland should be in the way, it must be turned aside or removed. The arteria profunda femoris is given off about two inches below Poupart’s ligament, on the back part of and outside the femoral, while three or four small vessels spring from half an inch to an inch below it on the fore part, and one or other of these may be divided. They are the superficial epigastric, the superficial pudic, the superficial circumflex of the ilium, and probably an artery supplying the absorbent glands. If they bleed so as to be troublesome, they must be secured, more particularly if the femoral artery is to be tied below them.[262] The fascia lata is now to be divided, with that part of the fascia transversalis which, descending beneath Poupart’s ligament, forms the sheath of the artery, when the vessel will be exposed. In dividing this fascia and sheath, the point of the knife is always to be directed to the center of the artery, so that if it be cut by accident it may be seen, when the only result will be the necessity for the application of a ligature above and one below it. The artery being fully exposed, as ascertained by the pulsation being felt by the finger, it is to be separated from its cellular attachment to the sheath on each side by a blunt or silver knife; and the aneurismal needle or probe, armed with a strong single thread of dentists’ silk, is to be passed under it from the inner or pubic side outward, by which all injury to the vein from the round point of the needle or probe will be avoided. Two common knots are to be made in the usual manner, when one thread may be cut off, or the two twisted together and brought carefully out of the wound; the edges of which are then to be duly approximated and retained in that situation by sticking-plaster and a moderate compress, secured in a similar manner. The knee is to be bent forward to relax the parts, and laid on the outside with a pillow beneath it.
The needle will pass more easily under the artery if the thigh be bent on the trunk; before the knots are tied, the surgeon should ascertain that pressure on the part or artery, which he has nearly surrounded by the ligature, suppresses the pulsation in the tumor below.
224. The point of a sword entering the anterior part of the thigh two inches below Poupart’s ligament, and wounding the superficial femoral artery, will necessitate the application of two ligatures, one above and the other below the wound in the vessel; but as the profunda under ordinary circumstances is given off posteriorly at this spot, it is possible the upper ligature may be placed on the main artery a little above the bifurcation. The result might, and would probably be, on some sudden movement of the patient, a recurrence of the hemorrhage by regurgitation from the profunda into the main trunk below the ligature; and thus through the wound in the artery, the lower ligature assisting by the obstacle it offers to the passage of blood through it. In such a case, the wound should be reopened, and the profunda sought for and tied. It has been argued that the ligatures, being applied close to the origin of collateral[263] branches, must fail. This error has been demonstrated, (Aph. 186,) and need not be further insisted upon. That it should still be maintained by some surgeons and teachers, who prefer old jog-trot theories to demonstrated facts, and cannot perceive that an exception is not a fundamental rule, is much to be regretted.
225. The operation for popliteal aneurism lower down in the thigh is to be done in the following manner:—
The surgeon, having turned the knee outward and bent the leg inward into the tailor’s sitting position, to show the course of the sartorius muscle, should trace the artery from the groin downward, until it appears to pass under that muscle. The external incision, four inches in length, made in the course of the artery, should pass over this point one inch, so that when the fascia lata is divided, the sartorius muscle may be seen crossing over to the inside at the lower extremity of the wound. The fascia lata is to be divided upward for the space of two inches of the incision. The forefinger is then to be introduced into the wound, and pressure made with it rather outwardly, when it will readily distinguish the pulsation of the artery, still included in its sheath. This is to be opened by slight and repeated touches of the knife directly over the center of the line of the vessel, or it may be divided on the director, when the artery will be exposed. The point of the forefinger will easily recognize it from the roundness and firmness of the feeling communicated by it, as well as by its pulsation; and the end of the nail, or handle of the scalpel or blunt knife, will separate it with facility from its attachments, to such an extent as to admit the blunt point of the solid, unyielding aneurism needle to be passed beneath it from the pubic side. If the point of the needle do not readily come through the cellular attachments of the artery on the outside, this part must be touched lightly with the scalpel, or rubbed with the nail until the ligature is exposed, which should then be taken hold of with the forceps and one end drawn out, while the instrument with the other end is withdrawn. The operator, taking both ends of the ligature, which has been in this manner passed under the artery, between the fingers of one hand, presses upon the artery with the forefinger of the other, so as to arrest the course of the blood in it, when, if there be an aneurism blow, the pulsation in it will cease. The ligature is then to be pressed upward as far as the[264] artery has been detached, and is to be tied with a double knot. The wound is to be dressed as in the previous case with adhesive plaster and compress, but without a bandage; and the patient is to be placed in bed, with his knee bent forward, or resting on the outside, if more agreeable to him.
The operation is done in this manner on that part of the femoral artery which is not covered by muscle, and all interference with the sartorious is avoided. It is the improvement on the Hunterian operation recommended by Scarpa, and ought always to be adopted. This method obviates all discussion as to placing the ligature on the outside of the sartorious muscle, or as to the fear of injuring the absorbents; as to the saphena vein, it can always be seen, and its course traced up the thigh and avoided. After the first incision has been made and completed down to the fascia lata, that part is to be divided to the extent of two inches, but this must be dependent on circumstances; the object being to obtain a view of the sheath containing the artery, the opening into which, after the first touch of the knife, may be completed with the assistance of the director under it. The artery will be less disturbed in its lateral attachments by an opening into the sheath, of three-quarters of an inch in length, than by one of half the extent, as it will admit of the aneurism needle being passed under it with more facility, and consequently with less disturbance to the surrounding parts. There is no reason to believe that a free opening into the fascia of the thigh has ever done mischief, or even one made in the sheath, provided the artery has not been unnecessarily disturbed.
The warmth of the limb operated upon should be maintained by gentle friction from the toes upward to the knee; when left at rest it should be enveloped in flannel. The wound should not be dressed until the fourth day, the limb being kept quite quiet; the patient should move as little as possible in bed, and the part of the heel on which the limb rests should be examined from time to time, as it may under pressure become gangrenous.
Suppression of the secretion of urine is not uncommon during the first twenty-four hours after all these operations; it may be gradually removed by the patient’s taking mild diluent drinks. The constitutional irritation is frequently great, the pulse rising in forty-eight hours from 85 to 120;[265] if this continue until the third day, when the fear of mortification will have passed away, it should be moderated by the abstraction of a small quantity of blood. In some cases of this kind I have had occasion to bleed twice, and with the happiest effect, the pulse having fallen in consequence to its natural standard. The medicines given at the same time were saline draughts every six hours, with from four to six or more drops of Battley’s solution of opium. The ligatures come away on and about the fifteenth day. In many cases they remain a much longer time without inconvenience.
226. The popliteal artery is never to be secured by ligature, unless wounded and bleeding. Under ordinary circumstances, an incision should be made at least three inches long in the course of the wound, the patient being laid on his face and the limb extended. If the injury to the artery has been committed where it lies in the ham between the heads of the gastrocnemius muscle, the bleeding and the pulsation will point out its situation. The integuments and fascia having been divided, the posterior saphena vein and nerve, if seen, are to be avoided and drawn aside, when, by carefully separating some dense cellular or areolar membrane and drawing the heads of the gastrocnemius from each other, the bleeding artery will be seen as well as the vein and nerve. The nerve should be drawn inward with a blunt hook and the vein carefully drawn outward.
“On the 2d of February, 1855, a young gentleman, aged nineteen, had a heavy mortising chisel thrown at him, which entered the upper part of the calf of the leg. There was arterial bleeding, which a man near him stopped by keeping his finger on the wound. I saw him two hours after the accident; there was bleeding ‘per saltum;’ presumed that the posterior tibial was cut. Consulting with two other surgeons, he was turned over on the table; the limb was distended, and a firm clot filled up the cavity; I pressed moderately upon either side of the wound, but there was no return of hemorrhage. The patient was therefore put to bed, a bandage applied, and an assistant left in charge. The day following there was less tension in the calf; no hemorrhage. Having recently read a case by Butcher, in the ‘Dublin Quarterly,’ upon the treatment of wounded arteries by compression, I followed out his rules. The case did well up to February 13th, when he had a sudden and severe pain in the calf of the leg, which was much distended, and the clot[266] pulsating strongly. In a few minutes a large stream burst out, so large that I was satisfied it could not be from the posterior tibial. I put my finger in the sinus and found that its direction was first backward, then backward and upward. I again proposed to dilate the wound and search for the vessel, when an objection was started by one of my friends, that if the artery were wounded immediately on its division, there would not be sufficient space for the clot to form. As this objection was made, and I failed to combat it, I summoned the consulting surgeon of the district. After carefully considering the case, he strongly advised a fair trial should still be given to compression. Hemorrhage returned upon the 16th. A consultation advised ligature of the femoral artery, which operation I did. Bleeding returned on the 25th, and on the 26th I cut down and found a small slit in the popliteal, and put a ligature above and below it, which saved the life of the patient.”
227. The posterior tibial, or the peroneal artery, or both, if wounded at the same time, are to be tied according to the principles laid down in Aphorism 197, page 231. An incision, from six to seven inches long, should be made nearer to the inner edge of the leg than to the center, and should be carried through the gastrocnemius muscle, the plantaris tendon, and soleus muscle, down to the deep fascia, under which the arteries lie with their accompanying veins, having the posterior tibial nerve on the fibular side of the artery. If the incision has been made in the upper part of the calf of the leg, the peroneal artery will be exposed by it; but if it be certain that the peroneal artery is the vessel injured, the incision should be made toward the fibular side of the leg. When the surgeon has divided the fascia, he will find this artery covered by the fleshy fibers of the flexor longus pollicis muscle, at any distance below three inches and a half from the head of the fibula; these fibers being divided, the artery will be found close to the inside of the bone. Above that part the artery is under the fascia, and upon the tibialis posticus muscle. It has not an accompanying nerve. Both arteries will be readily found by either of the incisions, if the surgeon be acquainted with their situation.
The posterior tibial artery may require to be tied between the ankle and the heel. In this situation its pulsation may be felt, and that will be the best guide to the artery. It has the tendons of the tibialis anticus, and of the flexor digitorum[267] communis, nearer to the malleolus than itself, and distant about a quarter of an inch; there is a vein on each side of the artery. Posterior to this is the posterior tibial nerve, and nearer the heel the tendon of the flexor longus pollicis. To tie the artery near the heel, its pulsation should be felt, and an incision more than two inches long made upon it, through the common integuments and superficial fascia; a strong aponeurosis will be found beneath, covering the sheath of the vessels and adhering to the tendons. This aponeurosis must be carefully opened on a director passed beneath it, and then the sheath of the vessels: the artery should be tied with a single ligature, unless wounded. The nerve is nearer the heel.
The posterior tibial artery may be tied a couple of inches higher up in the small part of the leg, by making the incision on the tibial edge of the soleus muscle, under which it lies.
228. The posterior tibial artery, an inch and a quarter or from that to an inch and a half below the inner ankle, gives off the internal plantar artery, and assumes the name of external plantar. The internal and smaller artery passes forward on the inside of the foot, under the origin of the abductor pollicis, to the outer or metatarsal side of the great toe.
The external plantar artery, from the point of division, takes a course curved toward the heel to the metatarsal bone of the little toe, which is prominent, being a distance of about three inches; during this course it is covered by the integuments, lateral ligament of the joint, a quantity of granular fat, the thick plantaris fascia, the origin of the abductor of the great toe, and the flexor brevis of the other toes. The artery may then be felt and seen near the os calcis, having the nerve and vein to the inner side; and lying on the accessorius muscle and its fascia, at the depth, in ordinary cases, of about an inch and a half. The plantar fascia extends in considerable strength from the os calcis forward to the toes, and divides into two portions opposite the first phalanx of each, which are inserted laterally into the sheaths of the flexor tendons, and the sides of the ligaments connecting the phalanges to the metatarsal bones. This fascia should, when necessary, be slit up at the part injured, or a bent probe forcibly passed under it to the required extent, when any intervening muscular fibers should be divided until[268] the bleeding point is perceived, when a ligature above and another below the wound should be placed upon the artery.
The external plantar artery, on reaching the metatarsal bone of the little toe, runs forward, in nearly a straight line, between the middle and outer divisions of the plantar fascia, the section of which will expose it as far forward as the end of the metatarsal bone.
229. The anterior tibial artery is to be tied at that part of its course at which it may be wounded. When the operation is done for aneurism, it should be performed a short distance above the tumor, and sometimes a second operation below it will become necessary. If the aneurism should be situated so high up and so close to the origin of the vessel as not to admit of a ligature being applied anterior to the interosseous ligament, it may be placed on the femoral artery of the thigh, and the result awaited. If it appeared likely to succeed at first, and yet the pulsation returned, the artery should be tied below the tumor, because the return of pulsation would probably depend on the blood regurgitating into the vessel.
In order to tie the anterior tibial artery after it has passed from the back to the fore part of the leg through the interosseous space, and over the interosseous ligament, and for one-third of its descent toward the instep, draw a line from the head of the fibula to the base of the great toe, which will nearly describe its course. An incision four inches in length is to be made in this line down to the fascia covering the muscles; if the foot be bent upward, and again extended, the bellies of the tibialis anticus and extensor digitorum communis muscles will be more distinctly seen. The fascia is to be divided for the whole length of the incision between them; they are then to be separated for the same distance by the scalpel and the finger; the artery will be found close on the interosseous ligament, between its two venæ comites.
A case has been supposed, in which a knife, a sword, or other narrow instrument, having penetrated the upper part of the leg, has wounded the anterior tibial artery just after it has been given off from the posterior tibial, behind the interosseous space or ligament. The bleeding is free, and from the wound in the front of the leg, although the artery cannot be secured, from the narrowness of the space between the tibia and fibula, behind which space it is situated. This very peculiar injury, which may, however, occur at any time, can[269]not be known until an incision has been made on the fore part of the leg, and the bleeding point seen so deep between the bones as not to admit of two ligatures being placed on the artery above and below it. In such a case, an incision is to be made through the calf of the leg, when the artery can be secured without difficulty. No great inconvenience, it is apprehended, would result from the two operations. If the sword wound should have been a small one, although deep, compression on its surface would in all probability have been had recourse to in the first instance; which, while it prevented the flow of blood externally, would scarcely impede its effusion above the fascia and under the soleus muscle, the distention of which and of the calf of the leg would, to a careful observer, point out the evil, and lead to the operation being done in the first instance through the calf of the leg.
In the middle third of the leg the origin of the extensor proprius pollicis intervenes between the tibialis anticus and the extensor communis digitorum muscles. The anterior tibial nerve, a branch of the peroneal, attaches itself to the artery a little above this middle part, and is usually found in front of it, although it is not constantly in that situation: care should always be taken to avoid it.
In the lower part of the leg the artery lies on the tibia, having the tendons of the extensor digitorum communis on the outside, and that of the extensor proprius pollicis on the inside, by which it is overlapped, being also covered by the fascia and the integuments.
On the instep this artery runs over the astragalus, the naviculare, and the os cuneiforme internum, to the base of the metacarpal bone supporting the great toe. It here divides into two branches: one dips down between the first and second metatarsal bones, to join the terminating branch of the external plantar artery, rendering the collateral circulation free; the other passes on to the inside of the great, and the opposite sides of the first and second toes. The artery is always to be found on the fibular side of the tendon of the extensor proprius pollicis.
THE COMMON CAROTID ARTERY, ETC.
230. The carotid artery may be tied, in almost any part of its course, in the following manner: The patient being seated, with the shoulders supported, so that the light may fall on the neck, the head is to be bent a little forward, to relax the muscles on the fore part. An incision is then to be made on the line of the inner edge of the sterno-cleido-mastoideus muscle, by which the integuments, the platysma myoides, and the superficial cervical fascia are to be divided. The extent of this incision, in persons with long necks, may be from a line beginning parallel with the cricoid cartilage to within about half an inch of the sternal end of the clavicle: when the neck is very short, it must be begun as high up as the lower edge of the thyroid cartilage, so as to be as nearly as possible three inches in length. The sterno-cleido-mastoideus muscle is then to be drawn outward, with any vein which may be seen attached to its under edge. The pulsation of the artery under the finger will point out its situation, and the sterno-hyoideus and sterno-thyroideus muscles being drawn and kept inward, the omo-hyoideus will be seen crossing in the upper part of the hollow thus formed by the separation of these parts. The central tendinous portion of this muscle is attached and fixed by the deep cervical fascia, and lies immediately over the sheath of the vessels, particularly over the jugular vein. This fascia, which is strong although thin, is to be carefully divided below the muscle, immediately over the center of the artery, the position of which is to be accurately ascertained by the finger. At or beneath the same spot, the sheath of the artery is to be opened; and the long, thin nerve, the descendens noni, which runs upon the sheath, will at this part be seen inclining to the tracheal side of the artery. It is to be separated and drawn inward with the muscles. If the sheath of the artery be carefully opened immediately over its center, the jugular vein will scarcely interfere with it. But as it has been known to enlarge suddenly under the exertions or excitement of the[271] patient so as to overlap the artery, it has been recommended to make gentle pressure on the vessel at the upper part of the incision, and below if necessary, in order to prevent that occurrence. The aneurismal needle is then to be introduced and passed under the artery from without inward, by which the jugular vein and the par vagum nerve will be avoided, more particularly if the sheath of the vessels has been undisturbed, save where it has been opened immediately over the artery. The point of the aneurismal needle is to be brought out close to the inside of the artery within its sheath, by which means all danger will be avoided of injuring either the recurrent or the sympathetic nerves which lie behind or to the inside of it. As to the œsophagus, thoracic duct, or thyroid artery, they are not likely to be injured by any common operator; but he should be aware that on the left side, if he be obliged to operate low down, he may meet with greater inconvenience from the jugular vein, which is more anterior to the artery, and rather overlaps it, while on the right side it inclines outward from it.
The carotid artery may be tied higher up in the following manner: The incision in this instance should be begun a little below where the former one was commenced, and should be continued upward for the same length of three inches, in a line extending toward the angle of the jaw. The head should be laid back to enable this to be done, and ought to be kept in that position by an assistant. The artery at this part of the neck is covered by the integuments, the platysma myoides muscle, and the fascia. After the muscle has been divided, the strong fascia must be carefully raised with the forceps and opened, and the operator will do wisely if he divide it upward and downward on a director. With the end of the scalpel or a blunt knife he should separate the cellular tissue from the veins, which appear in this situation, and are often the source of much embarrassment. The sheath of the artery is to be opened over the center of the vessel, and the ligature is to be passed around it as before. The descendens noni nerve runs in general on the outside of the artery in this part of the neck, and afterward crosses over to the tracheal side. The par vagum, which lies in the angle formed posteriorly by the apposition of the carotid artery and jugular vein, to which latter it is more particularly attached, is to be avoided on introducing the aneurismal needle; and on bringing it out on the inside,[272] the same attention must be paid to prevent injury to the great sympathetic or any of its branches. The surgeon in both these operations should draw the ligature first a little outward and then inward, so as to enable him to ascertain that he has included in it nothing but the artery, which is to be tied with two knots; one end may be cut off, or both may be twisted together, and brought out of the wound opposite where the vessel has been tied. The integuments should be accurately closed by adhesive plaster, and the patient put to bed with the head bent forward, and properly supported. He should eat as little solid food as possible until after the ligatures have come away, and observe even greater precautions as to quietude than in other instances.
231. The external carotid artery may be tied by an operation conducted in a similar manner. After the first incisions have been made, and the strong cervical fascia divided, the operator must feel for the pulsating vessel, which will be found on a line parallel with the cornu of the os hyoides, below which part the common trunk usually divides into the external and internal carotids, the external being the more superficial and internal of the two at their origin. The external carotid turns with its convexity inward; nearly opposite to but rather above the os hyoides it is crossed by the ninth or lingual nerve, the digastric and stylo-hyoid muscles; it should be tied below this part.
When any of the branches of the external carotid has been wounded, it ought to be tied by a similar operation at both ends, at the part wounded. If the surgeon cannot do this, and the hemorrhage demand it, the trunk of the external carotid is the vessel on which the ligature should be placed, not that of the common carotid.
232. The internal carotid artery, when wounded near the bifurcation of the common carotid, is to be secured by two ligatures, and the steps in the operation are the same as those for exposing the external carotid, the surgeon recollecting that the internal carotid is more deeply seated and to the outside of the external. A ligature may be placed on the internal or external carotid, close to the bifurcation, with safety; but if the wound of either vessel should encroach on the bifurcation, one ligature should be applied on the common trunk and another above the part wounded; but as neither of these would control the collateral circulation through the uninjured vessel, whichever of the two it[273] might be, a third ligature should be placed on it above the bifurcation.
When the internal carotid is wounded through the mouth, at the upper part of the neck, it should be secured by the operation described on page 248, Aph. 216.
233. The arteria innominata arises from the upper part of the arch of the aorta, generally on a line nearly parallel with the upper edge of the cartilage of the second rib, ascends obliquely toward the right side, and usually divides opposite the sterno-clavicular articulation into the right subclavian and the right carotid arteries; the last of which appears to be its continuation, although the smaller in size. The arteria innominata is about two inches in length, rarely exceeding two inches and a half, although it is very variable both in length and situation, so much so as sometimes to render the operation of placing a ligature upon it during life impracticable. It is covered by the right vena innominata, which receives the left at a right angle, near the origin of the artery. Exterior to the vena innominata are the sterno-thyroideus and sterno-hyoideus muscles, some strong fascia covering the vein at its upper part, and the first bone of the sternum. The arteria innominata may ascend higher in the neck before it divides, in which case its pulsation will be perceptible in front of the trachea, and the subclavian artery will cross higher in the neck, which is one reason for not continuing the external incision down to the sterno-clavicular articulation in the operation on the right carotid. The subclavian artery, given off behind or a little above the articulation, proceeds outwardly for the space of one inch before it reaches the inner edge of the scalenus anticus muscle, which is about half an inch in width; so that the subclavian artery, when it clears the outer edge of the scalenus anticus muscle in a tall man, is not more than one inch and a half or three-quarters from its origin, even to the spot at which a ligature is usually placed upon it. The first branch given off is the vertebral on the upper and back part of the artery, distant half an inch from the carotid at the bifurcation. The thyroid axis is given off at the anterior and upper part of the artery, a quarter of an inch more outwardly, and the internal mammary often arises directly opposite from the anterior and inferior part of the artery, descending into the chest behind the junction of the first and second ribs with their cartilages. The inner edge[274] of the scalenus anticus muscle is close to these two last vessels. The phrenic nerve, crossing this muscle obliquely, lies on the outside of the thyroid axis, and on the inside of the internal mammary artery; having crossed the subclavian artery at this part, it descends between it and the junction of the internal jugular and subclavian veins to the chest. Internal to this, some small branches of the great sympathetic nerve, which lies behind, pass over the artery; and still more internal, but distant about a quarter of an inch from the carotid artery, the par vagum crosses likewise. The only point at which the subclavian artery can be tied internal to the edge of the scalenus anticus muscle is at this point, on the inside of the par vagum, in a space scarcely more than one-quarter of an inch in width, to which the carotid will be the best guide. It would appear that a ligature may be as readily applied around the innominata, immediately below the bifurcation, as around the subclavian, although little or no reliance can be placed on success attending either operation.
From this view of the parts it will be evident that the operation may be done in the following manner: Raise the shoulders of the patient, and allow the head to fall backward, by which the artery will be drawn a little from within the chest. Let an incision be made over and down to the sterno-cleido-mastoideus muscle, the sternal origin of which, and nearly the whole of the clavicular origin, should be divided on a director, carefully introduced below it, avoiding some small veins which run below and parallel with its origin. An incision is now or previously to be made, two inches in length, through the integuments, along the inner edge of the muscle, which will admit of its being raised and turned upward and outward. Some cellular texture being torn through, the sterno-hyoideus muscle is brought into view, and should be divided on a director. The sterno-thyroideus is then to be cut through in a similar manner. A strong fascia and some cellular texture here cover the artery, having the nerves above mentioned running beneath it, the carotid being to the inside, the internal jugular vein to the outside. By following the carotid downward, the finger will rest on the innominata and on the origin of the subclavian, and a ligature may be placed on either. If on the innominata, the aneurismal needle (and several kinds should be at hand) should be passed from without inward,[275] immediately below the bifurcation, close to the vessel. If on the subclavian, the surgeon must recollect that there is only about a quarter of an inch of this artery on which the ligature can be applied; this small space being bounded internally by the carotid artery, and externally by the par vagum above, and the vertebral artery below. The ligature should be applied close to the vertebral artery, the needle being passed from below upward, the greatest care being taken to avoid the recurrent nerve, which separates from the par vagum at this part, and winds under the subclavian and carotid arteries, to be continued upward to the larynx. If the ligature be placed on the arteria innominata, the same care must be taken to draw the par vagum outward, and to avoid the recurrent nerve. The edges of the wound should be brought together and dressed in the usual manner, the head being bent forward on the trunk, and maintained in that position, in order to relax the parts, and admit of their being kept in apposition.
This operation ought only to be performed in cases of aneurism of the subclavian artery, in which it is presumed that the disease extends as far as the external edge of the scalenus anticus muscle, but not more inwardly. The arteria innominata has certainly been tied five, if not six times in vain, and in two or three other instances the attempt failed, the operator not succeeding in his object. In Dr. Mott’s case the ligature came away on the fourteenth day, but the patient died from hemorrhage, in consequence of ulceration of the artery, on the twenty-sixth day after the operation. Dr. Graëfe’s patient also died from hemorrhage on the sixty-seventh day. It is evident, from these cases, that a man may live so long after the operation as to show that he does not die from its immediate effects, or from any that must necessarily take place. It is therefore possible that if the operation be often repeated it may eventually be successful.
234. The left subclavian artery rises perpendicularly out of the chest like the innominata, but on a plane much posterior to it, so that at the part where the vertebral artery is given off, which is about an inch and a half from the origin of the artery, it lies nearly an inch deeper from the surface than the vessel on the opposite side. It is covered by, or is more directly connected with, the important parts which are also in the vicinity of the right subclavian. The pleura adheres to it, and can scarcely avoid being torn in putting a[276] ligature around it. The par vagum is parallel with and anterior to it. The internal jugular vein and the left vena innominata lie over it. The thoracic duct and œsophagus are connected with it; and the carotid artery is in front. So that with the most careful dissection it is not a very easy matter to place a ligature upon the ascending portion of the left subclavian artery, without doing more mischief than is compatible with the life of the patient.
Aneurisms of the arch of the aorta have been sometimes known to appear so far beyond the outer edge of the scalenus anticus muscle as to impress the surgeon with the idea that they arose from the subclavian artery, and that an operation on that vessel might be attended with success. This error is not likely, however, to occur in the present day, for the stethoscope will always point out the existence of such an aneurism within the chest, and will therefore demonstrate the impropriety of the operation. Aneurisms of this nature are usually attended by some circumstances indicating their more internal origin, independently of the information derived from the stethoscope. An operation should only be attempted when the case is free from doubt.
Whenever an aneurismal tumor in the neck is accompanied by any alteration of the sterno-clavicular articulation, the case is clearly one totally unfitted for any operation. The same may be said of any case of aneurismal swelling, either internal or external to it, in which the stethoscope applied on the sternum in the course of the arteria innominata, or of the arch of the aorta, indicates disease. A swelling at the root of the carotid is more likely to be an aneurism of the arch of the aorta, or of the arteria innominata, than of the carotid itself. The stethoscope will remove all doubt.
235. The subclavian artery has been frequently tied above the clavicle, external to the scalenus anticus muscle. It should be done in the following manner: The patient being placed horizontally on the table, in such a situation that the light may be directed into the hollow in the bottom of which the artery is to be tied, the shoulder is to be depressed, and an incision made along the edge of the clavicle, commencing one inch nearer the sternum than the clavicular edge of the sterno-cleido-mastoideus muscle, and carried outward to the extent of three inches and a half or four inches. The platysma myoides and the superficial fascia are to be divided,[277] taking care not to injure the external jugular vein, which should be drawn to the outer side of the wound. By this incision the edges of the trapezius and sterno-cleido-mastoideus muscles will be exposed.
The object of the operation is in the first instance to reach the outer edge of the anterior scalenus muscle: this lies immediately below the outer edge of the clavicular portion of the sterno-cleido-mastoideus, and the division of a portion of this part of the muscle will greatly facilitate the subsequent steps of the operation, although it may be done without it. The artery will be found crossing over the first rib at the very edge of the attachment of the scalenus anticus to it; but a quantity of cellular substance and fascia intervenes, which must be torn through before it can be exposed. This should be done with a blunt, round-pointed knife, in a line parallel with the first incision, but more immediately over the outer edge of the scalenus muscle. The omo-hyoideus muscle passing obliquely across the root of the neck will be in this manner exposed, which should be clearly done, because it narrows the space in which the operation is to be performed to a small triangle; the outside and apex of which is formed by this muscle, the inside by the scalenus anticus, the base by the rib, above it the subclavian vein, and above it again, but under the clavicle, the supra-scapular artery and vein. The blunt knife, working in the triangular space, will first expose one or more of the nerves of the axillary plexus, which again diminishes the space; more inwardly the scalenus anticus will be felt, and should be seen by tearing through the thin fascia which lies behind the omo-hyoideus, and is connected with it. The point of the finger, assisted if necessary by the blunt knife, should be passed along the edge of the muscle until it rests on the first rib, and at the angle formed between the muscle and the rib the artery will be found and known by its pulsation. The operator should detach the artery in a slight degree from its connections, with the nail of the forefinger, and the aneurismal needle should be passed in preference from below upward, by which the pleura will be avoided. After the ligature has been passed under the artery, the vessel should be pressed upon with the finger, while the ligature is firmly held in the other hand, by which the circulation through the artery will be stopped. The pulsation in the tumor and at the wrist should cease, when the ligature may be tied with a[278] double knot; for doing this, one or two steel probes, having a ring at the end, placed at a right angle with the shaft, will afford great assistance.
In some instances, particularly in short-necked persons, the omo-hyoideus lies close to the clavicle, and requires to be drawn upward and outward from it. In others, the lowest nerve of the axillary plexus lies over the artery, and may be mistaken for it. When the veins coming from the neck are large and numerous, great care should be taken to avoid injuring them, as they frequently cause not only much hemorrhage, but great delay. Great care must also be taken in all these operations to prevent the ingress of air into any of the veins which may by accident be opened, as its admission in quantity has occasioned sudden death, although the entrance of a few bubbles may not be so dangerous as has been supposed.
236. When the axillary artery is to be tied for a wound caused by a sharp-pointed or other instrument which has been forced through the pectoral muscle or under it from the axilla, the patient is to be firmly supported or placed in the horizontal position, the arm to be slightly separated from the body, and an incision made in the course of the axillary artery, through the integuments, superficial fascia, and the great pectoral muscle—in fact, through the anterior fold of the armpit. The length of the incision will depend on the part at which the artery is to be secured. The parts divided being separated, the pectoralis minor will be seen crossing to the coracoid process at the upper part of the wound, and the artery may be felt below it, inclosed in its cellular sheath, with the nerves of the arm and its venæ comites. All other modes of attempting this operation are unworthy consideration, and ought to be discarded as dangerous and insufficient.
At the lower edge of the pectoralis minor, the artery is crossed by the outer of the venæ comites, which passes between the external cutaneous and the external origin of the median nerve, at the spot where they separate from the plexus. The artery may be tied below this separation, or the nerves and vein may be drawn to the outside, and the artery tied above the union of the external with the internal root of the median nerve as high as the origin of the arteria thoracica acromialis, the pectoralis minor being either raised and pushed upward, or divided if necessary. The internal[279] root of the median nerve is in connection with the internal cutaneous and ulnar nerves; the larger of the venæ comites is to the inside and behind, but as it ascends it receives its fellow, and with the cephalic vein forms in front of the artery the subclavian vein.
237. The brachial artery can be traced by its pulsation from the lower edge of the teres major muscle to below the bend of the arm, where it is covered by the pronator radii teres muscle. At first it is on the ulnar side of the humerus, resting on the triceps, and slightly overlapped by the coraco-brachialis and biceps muscles. In the middle of the arm it rests on the tendon of the coraco-brachialis, is close to the bone, and lies under the lower edge of the biceps; in which situation it may always be compressed by bending the forearm, so as to cause the belly of the biceps to enlarge, when pressure made immediately below it will arrest the circulation in the brachial artery. It then crosses toward the anterior part of the arm, and rests on the brachialis anticus muscle until it passes the bend of the elbow. It is accompanied by two veins, which are connected with it by a loose cellular membrane forming a sheath. The external cutaneous and median nerves lie a little to the outside of the artery in the upper third of the arm. In the middle third the median nerve lies generally in front of, but sometimes between the artery and the bone, and is on the inside at the inferior part. The internal cutaneous nerve runs parallel with but superficial to the artery, the ulnar nerve nearer but posterior to it. When a ligature is to be placed on the brachial artery in the upper part of its course, the incision should be made about three inches in length, directly on the line of the pulsating vessel, by which all mistakes will be avoided. The integuments should be divided carefully, that the internal cutaneous nerve may not be injured; the fascia is then to be cut through and the forearm bent, when the vessels and nerves will be relaxed. The artery is to be separated from its veins, one on each side; and it must be recollected that the external cutaneous and median nerves are to the radial side of the artery, the internal cutaneous and the ulnar nerves to the ulnar side of it. In the middle of the arm the median nerve lies immediately over the artery, except in those cases where it passes behind it; when it lies in front it may be mistaken for the artery, from the pulsation being communicated to it. The incision should be to the same extent of three inches,[280] directly in the course of the artery, and the ligature should be passed from the ulnar to the radial side of the vessel, in order to avoid the possibility of including either the internal cutaneous or the ulnar nerve, and for the purpose of excluding both the veins.
238. The brachial artery, a little below the bend of the arm, divides into the radial and ulnar arteries—the radial being the continuation of the brachial in direction, the ulnar in size. The brachial artery, at the bend of the arm, is cushioned on the brachialis internus muscle, having the tendon of the biceps on the outside, the median nerve on its inside, which is at first continued on the same side of the artery, which now takes the name of ulnar. This vessel inclines toward the ulna for about an inch, and then passes between the two origins of the pronator radii teres muscle; the median nerve crosses it at this part to get into the middle of the arm, and is then separated from it by the ulnar origin of the muscle. The artery continues its course, inclining outwardly, under the pronator radii teres, the flexor carpi radialis, the palmaris longus, and the flexor sublimis muscles, lying on the flexor profundus. On clearing the ulnar edge of the flexor sublimis, it is covered by the flexor carpi ulnaris, the course of the artery having been obliquely under these muscles to the extent of two inches. To tie it in any part of this course, they must be more or less divided, and the only difficulty or danger arises from the median nerve, which lies deeper under the radial origin of the pronator teres. But the whole of the muscular fibers may be divided, without injuring the nerve, by successive and careful incisions through them until the artery and nerve are exposed, and a ligature may then be applied above and below the wound in the vessel. It may be supposed, by way of elucidation, that a man has received a wound from a sword through the flexor muscles, which injures also the ulnar artery, as may be presumed from its situation and the continued and impetuous flow of blood. It may be further supposed that this wound is in a slanting direction from the ulna toward the radius. The surgeon, if he thinks he can calculate the point at which the artery is injured, should cut down upon it in the direction of the fibers of the intervening muscles, and even through them until he reaches the artery; but if he has erred in his calculation, he should introduce a probe into the wound, and, after having ascertained the line[281] it has taken, he should cut, if necessary, across the muscular fibers in that direction until he exposes the bleeding artery; if he be careful not to divide the median nerve, no inconvenience will arise from the operation. (Aph. 184, page 192.)
239. If the ulnar artery be wounded near its origin, through the radial side of the pronator teres muscle, an incision should be made through the integuments and the aponeurosis of the biceps muscle; the pronator muscle being then exposed, it is to be drawn inward and downward, or toward the ulna, and the dissection continued until the median nerve is brought into view. The probe introduced through the original wound will lead to the artery, the pulsation of which will be felt and the bleeding seen. Where the nerve crosses the artery, the vessel will be found above or to the radial side of it, and to the ulnar side below. It may be tied above without dividing a muscular fiber; but at the part where the nerve crosses, and below it, some fibers of the pronator teres must be divided, and in some cases the whole of them, before the artery can be properly secured by two ligatures; but this division is of little or no consequence, as the muscular fibers reunite without difficulty.
240. To tie the ulnar artery in the middle third of the arm, the surgeon should bend the wrist, and trace upward the tendon of the flexor carpi ulnaris as far as it can be felt. At the point where it becomes indistinct, an incision should be commenced and carried upward for the space of four inches; the fascia is then to be divided to the same extent, when the flexor carpi ulnaris may readily be traced upward by its tendon, which is on the radial side of it; this muscle may then be easily separated from the flexor sublimis, beneath the edge of which the artery will be found covered by the deep-seated fascia, having a vein on each side, and the ulnar nerve to the ulnar side of it. By this method of proceeding the artery will be readily exposed, which is not always the case by any other manner of operating, and it may be tied as high up as where it passes from under the flexors of the arm.
The ulnar artery may be easily tied near the wrist, where it is most superficial. Bend the wrist, and make the flexor carpi ulnaris act, when the tendon will be felt internal to the styloid process of the ulna; make an incision two inches and a half in extent along the radial edge of this tendon, dividing the fascia of the arm which covers it. The artery[282] will be felt below the deep-seated fascia, and, on dividing it, will be seen with its venæ comites, the ulnar nerve being behind it; that nerve must be avoided, in the application of a ligature.
241. The radial artery may be secured by ligature with great ease in any part of its course to the wrist. At the upper third of the arm, the radial artery is covered by the approximation of the supinator radii longus and pronator radii teres muscles. To expose it at this part, a line may be drawn from the middle of the bend of the arm to the thumb, which will indicate its course; or the supinator radii longus being put into action, an incision is to be made from the bend of the arm obliquely outward along its ulnar edge to the extent of three inches, avoiding the median vein, but dividing the integuments and the fascia. The supinator muscle is then to be gently separated from the pronator radii teres by the handle of the knife, and the artery will be felt covered by the deep-seated fascia; on the division of which, it will be seen with its venæ comites lying on some adipose membrane, and on some branches of the musculo-spiral nerve, which separate it from the tendon of the biceps, and are to be carefully avoided. The musculo-spiral nerve itself lies nearer the radius, rendering it advisable to pass the aneurismal needle from that side.
In the middle third of the forearm, the inner edge of the supinator radii longus marks the line of the incision, which should be to the extent of three inches. The fascia being divided, the supinator longus is to be separated from the flexor carpi radialis, and, on the division of the deep fascia, the artery will be found passing with its venæ comites over the insertion of the pronator radii teres and the radial origin of the flexor digitorum sublimis. The musculo-spiral nerve lies close to the radial side of the artery.
Near the wrist, the radial artery may be tied with great facility. Make an incision two inches and a half long on the radial side of the tendon of the flexor carpi radialis, which becomes prominent on bending the wrist; the superficial and deep fasciæ are to be divided, when the artery and its veins will be exposed; the nerve has not accompanied the artery to this point, where it lies on the pronator quadratus, whence it turns below the styloid process of the radius to the back of the hand.
The radial artery, on giving off the superficialis volæ to[283] the palm of the hand, near the end of the radius, inclines outward, and, when between its styloid process and the trapezium, lies beneath the two first extensors of the thumb. Passing onward to reach the angle formed by the metacarpal bones of the thumb and forefinger, it lies first in a triangular space between these two extensor muscles and the third, in which situation a ligature may readily be placed upon it by a simple incision. Proceeding onward, the artery passes under the third extensor and lies to the outside of it, where it may also be secured by ligature without difficulty, just before it dips into the palm and gives off the principal artery to the thumb. After the radial artery has reached the inside of the hand, to form the deep-seated palmar arch, it crosses the metacarpal bones nearly at a right angle, covered by all the muscles, tendons, and nerves of the palm. A branch of the ulnar nerve is here seen going to the muscles of the thumb. If the graduated compression recommended in Aphorism 208, page 238, together with due pressure on the radial and ulnar arteries at the wrist, should fail to arrest the bleeding from a wound at this part, the two muscles, forming what may be and is called the web, between the thumb and forefinger should be divided until the wounded artery can be seen. These muscles are the adductor pollicis on the inside, and the adductor indicis on the back of the hand; and their division would lead to little or no inconvenience. If a man, in opening an oyster, were to divide these muscles by an accidental thrust of his knife, it would not be considered a serious accident, although some surgeons might be dismayed if desired to divide them surgically, to expose the artery at the spot where it has been wounded.
INJURIES OF THE BRAIN.
242. Injuries of the head affecting the brain are difficult of distinction, doubtful in their character, treacherous in their course, and for the most part fatal in their results. The symptoms which appear especially to indicate one kind of accident are frequently met with in another. It may even[284] be said that there is no one symptom which is presumed to demonstrate a particular lesion of the brain, which has not been shown to have taken place in another of a different kind. Examination after death has often proved the presence of a most serious injury the existence of which had not even been suspected; and death has often ensued immediately, or shortly after the most marked and alarming symptoms, without any adequate cause for the event being discovered on dissection. One man shall lose a considerable portion of his brain without its being productive at the moment of the slightest apparent functional inconvenience; while another shall fall, and shortly die without an effort at recovery, in spite of any treatment which may be bestowed upon him, after a very much slighter injury inflicted apparently on the same part. During the war with the United States, in 1814, a soldier in Canada was struck by a ball which lodged in the posterior part of the side of the head; the wound healed, and the man returned to his duty. Twelve months afterward, having got drunk, he fell in the streets of Montreal, and died. The ball was found lying on the corpus callosum, where it had made a small hole or sac for itself. After the battle of Waterloo, I recommended, in the case of a soldier similarly wounded, that nothing should be done unless symptoms arose demanding the use of the trephine; as none occurred, and the wound healed, the man was sent home to Colchester, where he got drunk, and fell dead in the marketplace. The ball was lodged deeply in a cyst in the posterior lobe of the brain. Persons rarely live with a foreign body lodged in the anterior lobe of the brain, although many recover with the loss of a portion of the brain at that part. An injury of apparently equal extent is more dangerous on the forehead than on the side or middle of the head, and much less so on the back part than on the side. A fracture of the vertex is of infinitely less importance than one at the base of the cranium, which, although not necessarily fatal, is always attended with the utmost danger. The treatment of these several injuries (although they may be at first sight apparently similar) cannot, and must not be alike in all—a fact which should always be borne in mind in their management. In civil life, both in hospitals and among private persons, injuries of the base of the cranium are most frequently met with, because they are generally the consequence of falls; while in military life injuries of the base of[285] the skull are rare, and those of other parts are common. The practice of the military surgeon, with respect to injuries of the cranium and its contents, is therefore more successful, all things considered, than that of the surgeon in civil life, and particularly in a great metropolis; this may perhaps account for some of the discrepancies in opinion which have existed between them.
243. Many physiologists have thought they could indicate the part of the brain injured from the symptoms which followed, and there are some which do not admit of dispute as to their cause; but there are very many which at present do not admit of being distinctly traced to their source. Birds, small quadrupeds, fishes, and reptiles will live for some weeks after nearly all the contents of the skull have been removed. Sensation, volition, memory, judgment, sight, hearing, and all other sensations are lost by the removal of the cerebral hemispheres. The mobility of the iris is destroyed, not by the removal of the hemispheres, but of the corpora quadrigemina. If the cerebellum be cut away, a bird can no longer jump, walk, or retain its natural position, but it can move and live. When the medulla oblongata, or medulla spinalis, or the nerves of these parts, have been divided, muscular contraction ceases, and all power of movement is lost. Life is destroyed because respiration ceases when the medulla oblongata is divided at or immediately below the origin of the eighth pair of nerves. The removal of any one of these nervous parts in the lower animals only weakens the powers of those which remain. In man it destroys them, and life is extinguished.
244. Respiration consists of four movements—1, the opening of the mouth and dilatation of the nostrils; 2, the opening of the glottis; 3, the elevation of the ribs; 4, the contraction of the diaphragm. The division of the dorsal spinal marrow, below the origin of the phrenic nerve, paralyzes the movement of the ribs; above the phrenic nerves it paralyzes the diaphragm, and respiration ceases; the yawning or opening of the mouth and glottis alone remain. On dividing the point of origin of the par vagum, the movements of the glottis cease. On slicing the upper part of the medulla oblongata instead of the lower, from before backward, the opening or yawning of the mouth ceases; another slice, and the dilatations of the nose are arrested, and the inspiratory movements of the trunk alone remain.[286]
While the power of motion in each part seems thus to be dependent on isolated points of the medulla oblongata and the medulla spinalis, an indirect or connecting influence is admitted to take place between them and the remaining parts of the brain; and whatever may be its nature or extent in animals, there can be no doubt of its being so infinitely greater in man as to be essentially different; for none of these experiments can be made either artificially or accidentally on any one of these parts in him, without being productive of the ultimate if not almost immediate death of the whole.
Dr. Marshall Hall, in the comprehensive and luminous view he has taken of the nervous system, supposes that each sentient and motor nerve of the spinal marrow is further endowed with an excito-motor power for reflex action. He calls these generally excito-motor nerves, and considers them to be connected with a part of the medulla spinalis, distinct from that portion which is strictly an appendage to the brain. Incident nerves arise from the skin and certain mucous membranes, and convey impressions from them to the spinal marrow. Reflex nerves convey back the nervous influence excited through the medium of the incident nerves, to the voluntary muscles in which they terminate; and Dr. Marshall Hall further considers that these nerves, and the part he calls the true spinal cord, constitute the true spinal system which presides over ingestion and exclusion, retention and egestion; and consequently that its influence is exerted upon the muscles which belong to the entrances and outlets of the animal frame; or, in other words, upon the sphincters, and the muscles of deglutition and of respiration; and that the true spinal system maintains the tone of the whole muscular system. Stimulating an incident or excitor nerve of the extremities, by tickling or pricking the sole of the foot or the palm of the hand after sensation is apparently destroyed, causes a special muscular contraction or motion in the limb, if the excito-motor system be uninjured. Irritating the eyelashes induces contraction of the eyelids; and the irritation of one will sometimes cause contraction of both. Tickling the verge of the anus induces contraction of the sphincter muscle. Irritating the fauces and the root of the tongue, by pressing it down with the handle of a spoon, induces an action of deglutition. Respiration is excited by irritating or exciting the trifacial or fifth pair of nerves, by throwing cold water[287] on the face, and stimulating the nostrils; by influencing the spinal nerves by a similar use of cold water to the body and chest, and by tickling or stimulating the sides, soles of the feet, and verge of the anus.
The great object or value of these and other facts and physiological experiments is to enable us to conclude, as far as possible, what part, what great division of the brain or spinal marrow is most seriously injured, more particularly with respect to the prognosis than to the treatment. Great severity and persistence of the symptoms lead to the belief that the part of the brain or spinal marrow on which they depend is directly injured rather than indirectly affected, and that the result is more likely to be fatal. Permanent insensibility and loss of motion may depend on cerebral mischief only. The loss of the mobility of the iris implies an affection of the tubercula quadrigemina. Convulsions, vomiting, a drawing up of the limb not affected by paralysis, stertor, a difficulty in swallowing, strabismus, and relaxed sphincters, show derangement of the spinal functions; which is well marked when tickling the eyelashes does not cause closing of the lid, of the verge of the anus no contraction of the sphincter, of the sole of the foot no motion of the toes.
245. In order to simplify the investigation of Injuries of the Head, they have been divided into two great classes: one denominated Injuries from Concussion; the other, Injuries from Compression or Irritation of the Brain. By the term Concussion of the Brain, a certain indefinable something, or cause of evil which cannot be demonstrated, is understood to have taken place; the effect of which is often clearly proved by the almost instantaneous death of the individual, or by a succession of symptoms which quickly lead to his destruction. The term concussion is very aptly and forcibly illustrated by the homely but striking expression in use in the sister country, when a man has been suddenly killed by a fall on the head, “that the life has been shook out of him.” On a dissection of the brain in a pure case of this kind, no trace of injury or even of derangement of any part of it can be perceived. Life is extinct, but the brain is intact. The immaterial has been separated from the material part, by an injury apparently inflicted on the very seat of life, with as little apparent derangement of its structure as if death had occurred in a secondary manner from the abstraction of blood by a rupture of the heart.
[288] Modern surgery has in fact added nothing to our information on the subject, perhaps from the peculiar difficulties of the case, which may not admit of removal in the present state of our knowledge; although all writers seem to coincide in opinion that a sudden stoppage of the circulation of the blood is the more immediate cause of death. That the positive shock communicated to the brain from one side to the other, and the repercussion which follows from its resiliency, are capable of giving rise to a direct and visible injury, is indisputable. It usually forms on what may be termed the edges of the hemispheres, which appear to be discolored, bruised, and sometimes torn, so as to have caused the term laceration to be given to this kind of injury. This mischief, however, is most commonly found in the examination of those persons who have survived the accident for some days, and is therefore only a predisposing cause of death.
246. When an injury is not immediately fatal, and life, although for a time in imminent danger, is not destroyed, yet fluctuates on the verge of destruction, gradually to be restored, again to fail, and at the end of several days to be eventually extinguished, the changes which take place in the functions of the brain during this period are accompanied by alterations which are observable in its appearance. The assemblage of phenomena which have taken place constitute inflammation; and it is only by that vigorous treatment which subdues inflammatory action that a person in whom they have occurred can be preserved. The immaterial part of man is so intimately connected with his material part that they cannot be suddenly separated without the material part receiving an irrecoverable though often an imperceptible detriment; the bonds which unite them cannot be temporarily loosened without a derangement taking place, which appears to require for its recovery the aid of some of those processes of nature which are known to occur in the restoration to health of other parts of the body. A moderate shock is often immediately followed by sickness, faintness, weakness, and in a few hours by a slight headache, from which the person quickly recovers without further inconvenience; or the headache may remain for several days the sole symptom or sign of an injury having been sustained; the slightest possible approach to that action which we call inflammation having sufficed to effect a cure. One step[289] further, the headache continues, the stomach sympathizes, there is little or no desire for food, the whole person feels more or less deranged, and the pulse quickens. A smart purgative will perhaps relieve all these manifestations of approaching evil, but the loss of a little blood will be more certainly efficacious.
A child ten years of age fell over the banisters into the passage, and struck its forehead. It was taken up apparently lifeless, but it soon appeared that it was only stunned; it breathed deeply, looked about vacantly, and could not speak; it then vomited, and gradually recovered its speech and senses. A brisk purgative was all that was required to remove the slight headache which followed on the subsequent day.
In more dangerous cases which ultimately prove fatal, the laceration of the brain alluded to complicates the mischief as well as the symptoms, and is perhaps the actual cause of death. It has, however, been demonstrated that a slighter injury of the kind, giving rise to long-continued symptoms, need not necessarily be fatal; in which case it is supposed that the cure is effected by adhesion, and not by granulation accompanied by the secretion of purulent matter.
247. When a concussion of the brain has rendered the sufferer insensible and motionless, the countenance is deadly pale, (the reverse of what takes place in sanguineous apoplexy;) the pulse is not discoverable: the man does not appear to breathe. It is useless to open his veins, for they cannot bleed until he begins to recover; and then the loss of blood would probably kill him. It is as improper to put strong drinks into his mouth, for he cannot swallow; and if he should be so far recovered as to make the attempt, they might possibly enter the larynx and destroy him. If he should appear to breathe, and be made to inhale very strong stimulating salts, it will probably give rise to inflammation of the inside of his nose and throat, to his subsequent great distress. Mild stimulants and disagreeably smelling substances held to the nose, together with partial as well as general friction with the warm hands, are the best means to be adopted, and should be continued until it be ascertained that life is extinct. If the patient should recover, some signs of breathing will be discoverable, followed by a distinct inspiration, repeated at so distant an interval as to[290] render its recurrence uncertain. At last respiration is satisfactorily established, and the pulse, which was doubtful at the commencement of the restoration to existence, becomes perceptible, although often irregular, and sometimes continues so until reaction has taken place. With this partial recovery of the natural functions of the body, vomiting is apt to supervene, and is one of the earliest and most satisfactory symptoms of returning sensibility. It was formerly supposed to be peculiar to cases of concussion, but it is often present in cases evidently of compression or irritation from external violence. The breathing becomes in general quite free; and although it is occasionally labored, it is rarely stertorous, a symptom which may be considered, when permanent, as a more distinct sign of continued irritation, or of compression and of extravasation, than of concussion. The sensibility of the surface, however, is not fully re-established, the patient is not cognizant of any injury committed upon him, and if he should recover, has no recollection of what has passed. This first stage does not last long, and with the partial re-establishment of the functions of the lungs and of the heart, and of the circulation of the blood through the brain, although irregularly or insufficiently performed, the second stage may be supposed to begin. The patient is still in a state of stupefaction, although now perhaps sensible to personal maltreatment; and in this condition he may remain for many days; he draws away or moves the part aggrieved; he may be able to answer in a monosyllable correctly or otherwise to questions loudly put, as if to rouse him from slumber; but if the answer should be longer, it will generally be incoherent. The pupils are for the most part in a medium or in a contracted state, but rarely dilated. Stimulants were formerly given at and up to this point, with a view of reviving and restoring the patient to greater activity, and to prevent a relapse into his former state. Dissection has, however, proved that it is a state in which congestion is about to be followed by inflammation of the brain or of its membranes; that the stage succeeding to this is one of active inflammation, even if the patient should eventually recover; and if he relapse into that state of stupefactive insensibility which precedes death, sufficient evidence to account for his decease may be found in the laceration of the substance of the brain, in small extravasations in various parts, or in other mischief which may not perhaps be expected. Pre[291]viously to this stage of fatal termination, the muscles are not relaxed, and do not lose their tone, as in a similarly fatal case of compression of the brain; the urine does not flow involuntarily until after the spinal marrow has been some time seriously implicated, and death is at hand. This renders it necessary, in all cases of injury of the head, to attend to the state of the bladder, which may become distended, and render the use of the catheter necessary. The urine will be acid as long as the catheter is required, and will become alkaline as soon as it dribbles away involuntarily. The bowels will at an early period be confined, and more powerful doses of aperient medicines will be required than are needed under more ordinary circumstances, although the sphincter ani may be relaxed, and the power of retention be lost from the first, provided the injury has been very severe. When the feces pass involuntarily, it is presumed that the cerebro-spinal axis is seriously affected, and that the excito-motory system is greatly impaired, if not wholly destroyed. When a person is insensible, it is not always easy or convenient to ascertain whether the feces pass involuntarily from loss of power of the sphincter ani, or are discharged from the ordinary action of the bowels, of which the patient cannot give notice. It may be inferred when the urine flows in a stream, although apparently in an involuntary manner, that the power of the detrusor muscle of the bladder is only impaired. In general, certain efforts are made to evacuate the bowels, although the person may be upon the whole unconscious of the act, showing that the defect is not essentially in the sphincter ani, but in the want of consciousness in the brain.
Vomiting should not be solicited, as it may do harm when in excess, but when slight, it has appeared to be beneficial. The more simple the treatment during this the period of commencing reaction, the more likely is it to be ultimately successful. The period at which insensibility ceases, and the re-establishment of the natural functions of respiration and of the circulation begins, must always be uncertain.
248. The termination of the first and the commencement of the second or really inflammatory stage, or that tending to recovery, is marked on dissection by the vessels of the brain and of its membranes being full of blood, and showing those appearances which are indicative of inflammation. If the patient is to recover, the stupefaction, or assoupissement,[292] continues, although a greater degree of sensibility prevails; the pulse becomes regular, if it were not so before; the skin is hotter than natural; the patient can often be induced to show his tongue, which is white, and to answer shortly, and tell where he feels pain, although he often answers incorrectly; he can sometimes put out his hand and help himself, and occasionally even get out of bed. He usually turns to avoid the light, and the pupils are for the most part contracted; but no reliance can be placed on the state of the pupils at this period of the complaint; both are sometimes dilated, or one is dilated and the other contracted—sometimes dilating on the admission of light, sometimes contracting; or they may not be in the least changed until shortly before death. An alteration from the ordinary state of the pupils does not prove the absence or presence of any serious general injury, but only that a particular part of the brain has been more or less affected. The breathing at this period is free, and not in the least noisy or stertorous, unless the concussion be complicated with irritation occurring from lesion of the brain or its membranes, or of the medulla oblongata. The patient may remain in this state without any sensible alteration for several days, or he may, as is more commonly the case when restoration to health is to follow, recover his speech as well as his general sensibility; nevertheless he frequently speaks more or less incoherently, mutters to himself as if thinking of something, and wanders at night, becoming even delirious, and requiring restraint to keep him in bed. Inflammation of the brain is now fully established and must be subdued. It is at or about this period that other symptoms occur, which are frequently enumerated as those indicative of concussion—it should be added, of concussion in its latter stage. The pulse becomes quicker, perhaps full or hard, varying from 84 to 90, and even to 100. In such cases, an augmented pulsation of the carotids may often be observed, and is considered by some to be confirmative of the fact of concussion, although it is by no means a sign to be entirely depended upon. Such a person will not be comatose, but watchful, sleeps little or none, talks incoherently, or is often really delirious, refuses food if offered, drinks with avidity, has a hot skin, and a white tongue. If other symptoms occur, such as spasms or convulsions, the absolute loss of any sense, or paralysis of any or the whole of a part, the case is complicated by laceration[293] of the brain, compression, or other causes of mischief, from the effects of which, if he cannot be relieved by blood-letting, he gradually sinks into a state of coma, and dies.
The deviations which take place from the usual and ordinary modes of breathing are supposed to offer distinctive signs of the nature of the injury which has taken place, but they are uncertain; they mark the degree of injury, and perhaps the part injured, rather than anything else. Stertorous breathing has always been considered a sign of extravasation causing compression of the brain. Many cases, however, have occurred of slight extravasation with partial loss of power of one-half the body, accompanied by great numbness, without any stertor in breathing; but a well-marked case of large extravasation has rarely or never been observed without it, or another peculiarity of breathing which is less thought of, although an equally characteristic and dangerous sign of such mischief having taken place when it is permanent; this is a peculiar whiff or puff from the corner of the mouth, as if the patient were smoking. This, when observed among other urgent symptoms, is usually followed by death. Stertorous breathing and the whiff or puff at the corner of the mouth are presumed to indicate an injury to the cerebro-spinal axis as well as to the cerebrum; but whether the injury be direct or indirect is uncertain, although it is frequently accompanied by extravasation or laceration. When the breathing is only oppressed or labored or heavy, neither extravasation nor lesion to any extent can in general be discovered after death. The surgeon will then practically be right in considering the stertor or whiff in breathing to be accompanied by, if not directly dependent on, extravasation or lesion; and the heavy or labored breathing to be dependent generally on a derangement of function, which is not perceptible on examination. If there be truth in experimental anatomy, stertorous breathing ought to be dependent on a direct affection of the medulla oblongata; nevertheless there can be no doubt that a temporary stertor or a puff at the corner of the mouth may exist without it, as a consequence of too great an abstraction of blood.
An officer, exercising his regiment under a hot sun in Portugal, suddenly fell back on his horse, and was carried home insensible and breathing stertorously; from this state he soon recovered, feeling weak in his lower limbs and incapable of influencing the sphincter ani, which was soon fol[294]lowed by incontinence of urine. His intellectual faculties were never affected after the first insensibility; and on the third day he rode on a mule, with care, twenty miles to Lisbon. Many months elapsed before he recovered the necessary command over the sphincter ani. Years have elapsed, and he cannot now always retain his urine. In this case the spinal marrow would seem to have been principally affected.
It is important to recollect that the stupefaction or insensibility of concussion is coeval with the injury, and that as few cases of compression of the brain occur without some degree of concussion, the insensibility may in many instances depend on it. The stupefaction peculiar to compression, demanding relief by blood-letting or by operation, is that which comes on some two or more hours after the accident, and is caused by congestion or by extravasation; it must also be distinguished from that which appears after several days, and is the consequence of inflammatory action and effusion. The pulse has been supposed to offer a diagnostic sign of the nature of the mischief which has taken place in the brain; pressure or extravasation, it is said, being attended by a slow and labored action of the heart. This may be admitted as a general, but by no means as a certain rule, for many of the largest extravasations, and many of the most diffused, have been accompanied throughout by a very quick pulse. When the physiological doctrines of the circulation are duly considered, as well as the experiments on which they are founded, it will be evident that the action of the heart may be influenced by other causes than those occurring from the part of the brain apparently injured. Pressure made purposely on the brain or dura mater in man during life is always followed, when carried to too great an extent, by a diminution in the frequency of the pulse, and even by syncope.
When the stage of depression is slowly passing into that of excitement, and inflammation is about to be set up, bleeding may be had recourse to; but what quantity of blood, if any, should be taken away, is often doubtful. The loss of six, eight, or even of ten ounces can do no harm, if it do no good, and it may enable the surgeon to form a more accurate judgment of the state or degree of the complaint than he could otherwise have done.
A laboring man, thirty years of age, fell from a height[295] of fifteen feet, on the back of his head, a small puffy tumor being perceivable near the junction of the right parietal with the occipital bone. He was insensible and motionless; countenance deadly pale; circulation weak in the arms, but more marked in the carotids; respiration heavy and slow; pupils much dilated and fixed; no relaxation of the sphincters. Hot-water bottles were applied to the feet, and friction to the body generally. In the afternoon he became warmer; some reaction seemed to be taking place, accompanied by slight twitchings of the face, and shiverings. At four o’clock he was bled to sixteen ounces, in consequence of the pulse having become fuller, although soft and 96 in the minute. The surface was warm and moist, and he was so far sensible as to complain, on being pressed for an answer, of pain at the part of the head injured. The bleeding was discontinued, in consequence of its bringing on convulsive movements ending in syncope; the pupils contracted, the countenance became deadly white, and he breathed on the right side of his mouth for a few minutes, with the whiff or puff so peculiar in cases of compression of the brain. On recovering from his swoon, the pulse became regular and 85 in number, the skin warm and moist, and the pupils more sensible to their proper stimulus. The bladder, which had been a little distended, acted voluntarily. The next day he was perfectly collected, and complained only of a little pain in the head. Pulse 84; was quiet and slept during a part of the night. The bowels acted under the influence of the calomel and colocynth given the evening before, and of a senna draught in the morning. He quickly recovered, without any further bad symptoms.
The effects of a large abstraction of blood at too early a period are well shown in this case, especially by the convulsions and by the peculiar kind of breathing.
249. When the period of excitement or of inflammation has begun, and the patient, although disposed to coma, is still irrational and impatient when roused, he is not to be left to await the effects of a blistering plaster or of a dose of physic, as has been recommended in such cases, but ought to be bled sitting up in bed to whatever extent may be necessary to relieve the symptoms, or at least to cause a near approach to fainting, for nothing less can relieve such a person effectually, and give him a fair chance for life. The bleeding must be steadily repeated as the symptoms recur until relief[296] has been obtained, or until it becomes evident that the powers of the patient cannot resist the inroads of the disease and of the efforts made for its cure. The quantity of blood that may be lost in two or three days by powerful, healthy men is sometimes enormous, amounting to 100, 150, and even 200 ounces, with the happiest effect. The following case, which was one of inflammation tending to effusion, will show the extent to which it ought to be carried in an elderly person of a different habit of body:—
A gentleman, sixty-seven years of age, had suffered for three weeks from occasional attacks of gout in his right foot, which he had himself treated by simple means, taking the pulvis ipecacuanhæ compositus at night to relieve pain. Once or twice his family had observed that his head was, for a short time, not so clear as usual; but no suspicion of further evil was entertained until he awoke one morning, evidently talking incoherently. As the gout had nearly disappeared from his feet, sinapisms were applied to both; purgatives and diaphoretics were freely administered, and he appeared to be relieved. On the third morning he became more loquacious and forgetful, was occasionally incoherent, and complained of a certain loss of power, and of numbness in the right side. Pulse 84, full and regular; tongue white; some confusion of ideas was evident, with slight headache. He was cupped at ten in the morning to ten ounces, without advantage; as all the symptoms appeared to be increasing, at four in the afternoon sixteen ounces of blood were taken from the arm, which produced a marked effect for some time. At ten at night, the symptoms having returned, and the blood drawn being very much cupped and buffed, twelve ounces more were taken from the arm, when the pulse quickened and began to intermit; he appeared to be about to faint, and the object seemed to be attained. Calomel and opium were then given every four hours, until the mouth became affected; but the essential symptoms were already subdued, and the patient recovered, with a slight sensation of numbness and loss of power of the right side of the body and head.
The necessary effect was in this case produced by the loss of forty ounces of blood. In a younger and more vigorous man it might have required three or four times as much to have been taken away by repeated bleedings, before the ob[297]ject could have been attained; of this the following case is a good instance:—
Mr. B., having jumped out of a carriage, the horses of which were running away at full gallop, fell on his face, and was found insensible and motionless. Some cold water having been poured upon him, he gradually recovered, and afterward ate a hearty dinner, drank a bottle of port wine, and walked home, a distance of three miles. He thought himself quite well the next morning, and went to bathe; but on returning about noon he felt uneasy, lay down on a sofa, began to talk incoherently, and was soon quite delirious. At one o’clock he was bled, but the symptoms of inflammation were not completely subdued until he had lost eighty-four ounces of blood, the last quantity being taken away at eleven at night. The vigorous treatment adopted in this case during the first ten hours in all probability saved the life of the patient.
250. It sometimes happens that congestion precedes inflammation to such an extent as to give rise to stupefaction and symptoms of compression.
A Portuguese soldier of General Harvey’s brigade of the fourth division of infantry was struck by a musket-ball at the first siege of Badajos, on the top and toward the back part of the head; it divided the soft parts, and grazed the bone without fracturing it. He walked from the trenches to the rear, and said he was not much hurt. About five or six hours afterward, he was found apparently asleep, and could not be awakened, on which I was asked to see him. Finding the pulse at 60, regular and full, although compressible, I directed him to be raised and blooded until he fainted. When he had lost some twenty ounces of blood, he opened his eyes, recovered his senses, and knew those about him. The next day he went to the rear, free from all symptoms, and rejoined some time afterward, in apparent good health, although he complained more than was usual to him of the heat of the sun.
In some less important cases of injury, one bleeding will answer the purpose; cupping and leeches may also be resorted to with advantage; but in all very severe ones general blood-letting is the only trustworthy source of relief. It should always be done with effect, the finger examining the opposite pulse, and regulating the amount to be taken away. At an early period of concussion, the quantity drawn should not be[298] large; it should increase with the urgency for its abstraction, and diminish with the frequency of the repetition, being always, however, carefully regulated by the effect. The inability of blood-letting to overcome the disease will be shown by the increase in frequency of the pulse, its diminution in power under slight compression, its greater softness, together with the persistence of the other symptoms.
It is in these cases that repeated small bleedings, to the amount of six or eight ounces, ought to be resorted to, when it is doubtful whether the loss of blood can or cannot be borne; they may then be considered not as curative, but as explorative measures, although they sometimes prove very effective; and when not properly regulated, the reverse.
In all these, and in other more desperate cases, the effect of mercury, provided it has been early and rapidly administered, may yet be decisive. Calomel, combined with another and not less important remedy, opium, ought to be given every two or three hours until the effects of both are fairly induced.
Blisters should never be applied to the head until after the leading symptoms of inflammation have been overcome; they will do more good at a later period, applied between the shoulders or on the nape of the neck. They should be dressed with mercurial and savine, or other stimulating ointment.
The hair should be cut close in ordinary cases, or shaved off in the more serious ones. The head should be raised in bed, and kept wet with a cold evaporating lotion, or one composed of two ounces of the nitrate of potash, one of the muriate of ammonia, one pint of vinegar, and five of water, made in small quantities at a time, as may be required; or with a small quantity of pounded ice and water in a large bladder. Perfect quietude, cold drinks, at pleasure, and nearly absolute starvation should be enforced.
The different points of practice which have been noticed are well illustrated by the following case, in which the symptoms of concussion were complicated by those which are commonly observed in compression of the brain:—
An old man, when cleaning windows, fell from some steps on his forehead, which he slightly cut and bruised, the left temporal artery being divided by another small cut: it bled profusely until the hemorrhage was arrested by a surgeon. He remained in a state of insensibility for nearly two hours,[299] when he rallied, and answered questions, although imperfectly. Pulse quicker than natural, and intermittent. He shortly afterward relapsed into a state of insensibility, with convulsions, stertorous breathing, puffing at the corner of the mouth, and complete loss of voluntary motion: the pulse could scarcely be felt. This convulsive fit lasted about ten minutes, when his respiration became natural, and his pulse was restored. The insensibility continued for an hour, when it was attempted to bleed him, but the pulse fell immediately, and it was not persisted in. He soon, however, became quite sensible, sat up in bed, and vomited some blood. In the afternoon he had another and slighter fit, from which he quickly recovered. On the third day he was free from all bad symptoms, and said, when asked, that he had only a very slight headache. The pulse occasionally intermitted. On the fourth he declared he was starved, became snappish and irritable, complained of pain in the head, and had a quick and irregular pulse. On the fifth he got up and dressed himself, had another slight convulsive fit, and fell into a state of stupefaction, for which bleeding gave little relief; and in the evening he died. From the first period of his improving until his death, sensation and motion remained. On examination, a starred fracture without depression was found corresponding to the wound on the forehead, continuing to the base of the frontal bone, across the ethmoid, over the body of the sphenoid bone, breaking off the posterior clinoid processes, and extending to the basilar process of the occipital bone, but not quite to the foramen magnum. The anterior lobe of the right hemisphere of the cerebrum was lacerated to the extent of an inch; that part was surrounded by the usual appearances of inflammation. Some blood was extravasated on the tentorium, beneath the posterior lobe of the brain, and lymph was effused over the whole of its surface, between the arachnoid membrane and the pia mater. The trephine, if resorted to, would have only added to the mischief.
Inebriation from spirituous liquors may complicate a case at its earliest period, from the stupefaction it occasions; but the odor of the spirits is usually demonstrative of the fact, and the stomach-pump in such cases is an admirable remedy.
251. Mania sometimes supervenes on concussion, as the[300] inflammatory symptoms subside. It is best treated by the different preparations of opium.
George Grey, aged forty-five, a stout man, fell from an omnibus, Nov. 1, 1839, and received a blow on the right parietal bone, a little behind the coronal suture. He lies on his back in a state of stupefaction, although sensible when pinched, but is restless, and suffers from convulsive motions of the mouth and limbs; pupils fixed, the right being more dilated than the left; pulse 120; heat of skin natural; respiration deep and rapid, without stertor; the sphincters not relaxed. A turpentine enema was given, and a calomel pill was swallowed with great difficulty. The head was shaved, and a cold lotion applied; he soon afterward became violent, and required the restraint of a tight jacket. The pulse fell in the afternoon to 84.
Nov. 2d.—Passed a restless night without sleep, and has a wild appearance: pulse 96, and regular. At twelve o’clock became sensible, and gave a confused account of the accident. Was freely purged, and a quarter of a grain of the acetate of morphia was given every four hours: the first at seven, the second at eleven, and the third at three in the morning.
3d.—Has passed a quiet night, but with little sleep; the morphia has had a soothing effect; talks rationally, although a little confusedly, and recognized his mother, who says he received a violent blow on the head three years ago, which has rendered him mad ever since whenever he drinks too much. Pulse 72; bowels open, and is free from restraint. At seven in the evening, he suddenly started up in bed, saying some one was going to murder him. Half a grain of the acetate of morphia quieted him; it was repeated at half-past twelve and at half-past four, and kept him quiet, although he did not sleep.
4th.—He was collected, quiet, and free from restraint; pulse 96, rather full; secretions natural. The morphia was continued in adequate doses for a few days, and he gradually recovered.
252. Concussion induces affections of the brain and of its membranes of an equally serious nature, at a more distant period of time, when the stage of stupefaction and insensibility is wanting; it is to guard against such an occurrence that persons who suffer from falls or severe blows on the head usually lose blood. A gentleman was thrown from his[301] gig near Hounslow, and received a very severe shock and several bruises, without feeling much hurt, or being aware that his head had actually touched the ground. He came up to town, went to bed, and got up next morning suffering only from a slight headache, and stiff from his bruises, of which, however, he thought nothing. On the second day I saw him in consequence of headache, throbbing in the temples, sickness, and general malaise or discomfort. Being a stout young man, thirty ounces of blood were taken from the arm in a sitting posture, until he nearly fainted, after which he was relieved. In the evening, the symptoms having all returned, pulse 88, and full, he was bled in the erect position until he fainted, forty ounces being taken away. The blood of the morning was buffed and cupped, and the bowels had acted freely. On the morning of the third day the pulse, which had become fuller, yielded to the loss of twenty-four ounces of blood, and in the afternoon, on its rising again, to sixteen more; after which the symptoms gradually subsided, and he appeared to be restored to health, with one interruption from irregularity in diet, requiring the further loss of blood by cupping behind the ears, and some sharp purgation. His cure was not, however, permanent; for having dined out a month afterward, he became delirious during the night, and required to lose sixteen ounces of blood in the morning, which relieved, but did not cure him. Some pain remained in his head, the pulse continued at 90, the tongue was white, with thirst, loss of appetite, and watchfulness. Calomel and opium were now administered until the mouth became affected, when he quickly got well; although a slight relapse or two afterward convinced him that he could not drink nor lead an irregular life with impunity.
There are no cases of convalescence after disease or injury which require more care than those which follow injuries of the head. Relapses, from apparently trifling causes, are extremely frequent, and gradually but certainly undermine the health; they are, in fact, connected with chronic derangement of the brain, or of its membranes; and unless successfully met, generally end, after the lapse of a few weeks or months, in irritative fever and death. In many instances, particularly among poor people subject to privations and of irregular habits, in whom an injury of the head has not originally been of any apparent importance, such a state of irritation, if it occur, combined with debility, is very difficult to[302] manage; it requires a combination of local as well as of general means for its cure. A few leeches and blisters may be applied alternately over the part affected, with great advantage; and a mild, nourishing diet, with gentle alteratives and tonics, will expedite the cure, especially when aided by perfect repose and a fresher atmosphere. An issue in the arm, which establishes a gentle but permanent drain, will often be found an efficacious remedy.
WOUNDS OF THE HEAD.
253. Compression of the brain means a diminution of the size of certain parts of it, resulting from the pressure of an extraneous body, whether it be fluid or solid, in consequence of which particular symptoms are generally known to ensue. When they occur, it is said that the sufferer is laboring under symptoms of compression of the brain, and apoplexy from the rupture of a blood-vessel may be considered as the best form or illustration of the complaint. These symptoms sometimes take place from the presence of a foreign substance, such as a point or piece of bone, which from the smallness of its size can hardly compress, although it may displace; and it is then said that the symptoms arise from irritation of the brain. Many of them have also been found to occur from loss of blood, or the absence of pressure, or from insufficient pressure arising from changes in the circulation; and several different opinions have been entertained on all the points connected with these subjects. It has been argued that as the brain is incompressible, no compression can take place. There is no proof, however, of the fact of its being incompressible as a whole, although it has been stoutly maintained by Monro secundus, Sir C. Bell, and others.
The brain is surrounded by membranes capable of secreting a halitus or a fluid whenever it may be necessary to fill up space; it is intersected by partitions apparently for the prevention of jar and pressure, and is permeated in every[303] part by vessels of various sizes, both venous and arterial. It has been presumed that it contains at all times the same quantity, or nearly the same quantity, of blood, in consequence of its freedom from atmospheric pressure, through the intervention of the bones of the skull. If this conjecture be correct, the quantity cannot be materially increased, unless something be displaced to make room for the addition; nor can it be essentially diminished without something being added to supply its place. The question turns, however, very much on the words “materially increased or diminished;” for a very small additional quantity may be the cause of serious mischief, and the subtraction of even less may give rise to great cerebral disturbance; but there can be little doubt that the actual quantity contained in the head is less at one time than at another, the deficiency being usually on the side of the arteries; when congestion takes place, it is for the most part venous. When a person is about to faint on the first passage of a catheter through the urethra, the blood deserts his face, he feels sick, his pulse nearly ceases, and he would faint if he were allowed to remain in the erect position. Let his head now be bent down between his knees for a minute; his face fills with blood, his brain does the same, and he recovers almost immediately. Young ladies, when about to faint, are prevented from doing so by these means being adopted, which they declare, nevertheless, to be very unladylike, although they may be doctorial and effective.
254. The motions of the brain covered by the dura mater are but little observable under ordinary circumstances when a circular portion of bone has been removed by the trephine; the surface of the dura mater remains in general perfectly LEVEL; it is of a reddish-silvery color, and is firmly attached to the cut edge of the bone. The surface is raised, however, on a full expiration, and it falls on a deep inspiration. Fluid secreted or placed upon it is seen to move synchronously with the pulse; but the dura mater never rises up into the hole made by the removal of the bone, unless some fluid be retained beneath it. If the quantity of fluid extravasated or collected under it be large, it rises immediately on the removal of the bone; but the protrusion of this membrane does not always take place for some hours afterward if the fluid be more diffused. The motions of the brain, when the dura mater is thus protruded into the opening, become very[304] indistinct, even if they can be perceived. These two points, viz., the protrusion into the opening and the absence of pulsation, are important facts, little noticed by surgical writers, to be borne in mind in connection with the practice to be pursued.
If we sometimes see the natural and ordinary size of the brain diminished under pressure, and that certain symptoms, such as insensibility, syncope, convulsions, and paralysis, are consequent on this state, and are relieved by the removal of the pressure and the restoration of the compressed brain to its ordinary state, we may safely conclude that some derangement takes place in its integral parts, which may be best understood by the word compression. If we further consider that compression can rarely exist without irritation, and that sometimes of a formidable nature, there does not appear to be so much difficulty in the subject as is frequently represented, although the physiological explanation may not be so simple. In the present state of our knowledge, we apprehend that in many cases approaching to apoplexy, in which the symptoms are similar to those arising from compression, all, or nearly all, the vessels, as far as we can ascertain, are actually full of blood, instead of being partially empty and containing less than the natural quantity. When we see a patient, lying in a state of insensibility with a fracture of the cranium, immediately recover his senses after the application of the trephine and the removal of a large coagulum of blood, we are apt to suppose that the coagulum of blood and the insensibility stand in the relation to each other of cause and effect. It is not unreasonable to conclude that the pressure of the extravasated blood confined by the bone had occasioned the insensibility, and that this did not depend alone upon some few vessels containing less blood than usual; for the brain must be considered as a whole in all these investigations, and reference should not be made to its vascular structures only in explanation of the cause of its derangements.
255. When compression of the brain is caused by an extravasation of blood, the patient is insensible, breathes slowly, loudly, and in a heavy, labored manner, or with stertor, and cannot be awakened, although the noisy breathing may be for a time suspended. The breath is sometimes emitted from the corner of the mouth, like a whiff or puff of smoke, and with something of a similar noise: this, when[305] permanent, is a more dangerous symptom than the common snoring or stertorous breathing. He sometimes froths at the mouth, and occasionally appears convulsed, but neither hears nor sees, nor takes the least notice of those about him. The countenance is generally flushed if the shock or blow has been slight, pale or livid if it should have been great. The pulse is usually slower than natural, sometimes irregular or intermitting, occasionally quick, even from the receipt of the injury. The pupils of the eyes may be contracted or dilated, being dependent for their condition more perhaps on the part of the brain affected than on the degree of injury. They are generally more contracted in the first instance than dilated; they may afterward pass into a medium or doubtful state; one may be even dilated, and the other not. In general, as the mischief is continued and augmented, they become dilated and immovable. The eyes may be turned upward, or may be fixed in the center, or be drawn irregularly outward or inward, causing strabismus, which is, however, a more rare occurrence. If the eyelids should be partially open, tickling the cilia or the conjunctiva of the ball with a straw or a feather will cause them to close, if the spinal cord be sound. The mouth and lips are more or less compressed, and fluids run out at the corners, unless placed on the very back of the tongue by a long, narrow spoon, when they are swallowed with difficulty. Paralysis of one side of the face and hemiplegia are common; paraplegia is more rare. In both kinds of palsy one part in one limb may be more completely affected than another, in which convulsive twitchings are sometimes present, as well as a frequent drawing up of the limb of the unaffected side. Tickling the soles of the feet or the palms of the hands will sometimes cause retraction of the toes or fingers when the limbs are apparently motionless; pricking them gently with a pin will often give rise to convulsive startings and tremblings of all the muscles of the extremity when tickling fails, showing that the capability to move the part remains, although the will to do so is wanting. The leg or arm is sometimes drawn toward the body when separated from it; it more often falls from the hand as if it belonged to the body of a dead person; the muscles are occasionally more stiff and rigid, and some power of motion remains, although but little of sensation; sometimes sensation is perfect when motion is lost, and sensation may be lost on one side and motion on[306] the other. The urine at first retained may ultimately pass involuntarily, as well as the feces; nevertheless, irritating the verge of the anus will excite motion and contraction in the sphincter ani, if the functions of the spinal cord be not destroyed. The action of the involuntary muscles is little impaired in general, and the secretions are but slightly affected; when it is otherwise, the injury must have extended to the ganglionic system, and the whole of the nervous centers must be materially implicated.
The loss of motion, or of the power of moving parts of the body, is either perfect or imperfect according to the degree of injury which has been inflicted, varying from a sense of feebleness to an almost utter incapability of moving the part. It is accompanied in general by defective sensation, or numbness, or by the complete loss of sensation and of the power of resisting heat and cold; the whole side, or one extremity, or a part only of an extremity may be affected, and not the whole. The mischief which gives rise to the loss of motion usually occurs on the side of the brain opposite to that part of the body which is paralytic. This was known and stated by Hippocrates, and the subject has been pursued to the most complete demonstration by modern anatomists.
The pathological proofs are not less complete. Desault and Bichat were by no means satisfied that the paralysis which followed an injury always took place on the opposite side; and some pathologists since their time, while admitting the fact, have shown that there may be exceptions. It is acknowledged, although it is not clearly and satisfactorily accounted for as to the face, that an extravasation of blood into one hemisphere of the cerebrum, or even of the cerebellum, can cause paralysis of the complete half of the body on the opposite side. It has been demonstrated that the right side of the body and the left side of the face may be paralytic at the same time and from the same injury apparently of the left side of the head, the mischief which caused the paralysis of the right side being found, in by far the greater number of instances, on the left side of the brain, and that which gave rise to the paralysis of the left side of the face to have been caused by an injury in the course of the portio dura of the seventh pair of nerves when about to leave, or after it had left, the brain.
Burdach found, in 268 cases of lesion of one side of the brain, that 10 presented paralysis on both sides of the body,[307] and 250 of one side; in 15 of these the paralysis was on the same side as the injury. Convulsions took place in 25 cases on the same side as the disease; in 3, on the opposite side. In cases of lesion of one corpus striatum, there were, in 36 instances, paralysis of the opposite side, and 6 with convulsions of the same side, and in no instance convulsions of the opposite side. In 28 cases of cerebral lesion of one side, the muscles of the opposite side of the face were paralyzed; in 10, those of the same side. Paralysis of the eyelid was in 6 cases on the same side, in 5 on the opposite side. Paralysis of the muscles of the eyeball occurred in 8 cases on the same side, in 4 on the opposite; paralysis of the iris, in 5 cases on the same side and in 5 on the opposite, the tongue being generally drawn toward the paralyzed side of the face.
A man fell down stairs and received an injury on the head from the fall which rendered him nearly insensible at the moment. There were no signs or appearances on the outside of the head indicative of any serious mischief, nor were any found on examination after death. The pulse was quick, and rose to 140; the left side was paralytic; the breathing not stertorous, but accompanied by a little puff on the right side of the mouth; the pupils somewhat dilated; he could not speak, convulsions supervened, and he died the day afterward. On dissection, the peculiar flatness of the convolutions of the brain on the right side was so remarkable, when compared with that of the left, as to leave little doubt of its having been occasioned by something which had pressed them forcibly upward against the inside of the cranium; and, on slicing off a portion of the brain, a larger coagulum of blood was found below than is usually observed to exist without the almost immediate death of the patient. The same thing has been so distinctly marked in other instances that no doubt can be entertained of those convolutions of the brain which were situated between the coagulum and the cranium having undergone a considerable degree of compression. It is worthy of remark that the pulse of this person was always regular and remarkably quick from the first examination after the receipt of the injury until the period of his death, showing, perhaps, that the action of the heart is not affected directly by pressure acting only on the upper surface of the brain.
256. Convulsive actions of the muscles, or positive con[308]vulsive fits, are always important symptoms; yet they seem in some persons to be dependent on idiosyncrasy, particularly when they appear early, and after the loss of blood, in which case they are less dangerous. They occur at different periods after the receipt of the injury, and have been supposed to depend in general upon laceration of the substance of the brain, although experiments on animals would seem to show that they may be caused directly by irritation of the cerebro-spinal axis within the skull, in which case the patients are more likely to recover. They have been observed particularly on the side opposite to that which is paralytic, so as to give rise to the idea that the paralysis is dependent on injury of one side of the cerebrum, and convulsions on injury of the other. When the effect of the mischief is so great as to cause complete paralysis, convulsive twitches do not take place, although they frequently precede, and may in many cases be considered as premonitory signs, while the evil which gives rise to the paralysis is gradually accumulating. When the paralysis is not complete, the side so affected suffers sometimes from slight convulsive twitches, while well-marked spasms prevail in the other, leading to the belief that, while paralysis is an affection of only half the brain of the opposite side, or of half the spinal marrow of the same side, convulsions are the effect of a more general irritation, capable, however, of being confined to a part; for partial convulsive motions do very frequently occur without any paralysis accompanying them on the opposite side. Several cases have occurred in which the convulsions have ceased, and the patients recovered after the removal of a portion of bone which was irritating the brain; but convulsions have generally been the forerunners of death when the seat of injury was unknown and effective relief could not be given. When they occur in cases apparently of pure concussion, accompanied by inflammation of the brain or of its membranes, and the patient recovers after many days of the strictest antiphlogistic treatment, it is possible that the brain may have been lacerated, and the cure have been effected by adhesion. Convulsions, it must be remarked, are among the most common symptoms of inflammation of the membranes of the brain, without any such lesion of its substance, although they are frequently wanting. They may be expected to take place about and after the fifth day in injuries of the head, when inflammation of the brain or of its[309] membranes is about to extend to or to become continuous with the neighboring parts, and may be more or less severe, varying from a state of partial trembling of a limb to that of general agitation and restlessness of the body generally—from a slight, irregular movement of the eyelids, or of the muscles of the face, to the more marked spasmodic startings of the whole of one side, grinding of the teeth, and contraction of the limbs. It is far different with those convulsive movements which, at a late period, become nearly permanent, or with rigid spasms, resembling tetanus, in which the body is drawn in different directions, forward, backward, or to one side. These are for the most part forerunners of death. Examination after death, in such cases, has frequently shown nothing discoverable beyond inflammation of the pia mater, and an effusion of fluid, generally purulent, on the surface of the brain, or in its ventricles, or between the pia mater and the tunica arachnoides.
The three following cases are intended to show the different forms of paralysis that ensue after injuries accompanied by compression or irritation of the brain:—
Charles Murray, private in the 2d battalion of 1st Foot Guards, aged thirty-three, was wounded on the 18th of June, at Waterloo, by a piece of shell which struck him on the superior part of the left parietal bone. He remained insensible about half an hour, and on recovering from that state, was affected with nausea and some bleeding from the left ear, and found himself unable to move his right arm and right leg, which hung as if they were dead, and had lost their feeling. Admitted into the Minimes General Hospital at Antwerp on the 29th; he suffered much from pain in the head, which was relieved by his being twice bled. The paralytic affection having remained without change from the moment he was wounded, a piece of the parietal bone, about three-fourths of an inch long, and several smaller fragments, were extracted four days after admission into the hospital, two perforations with the trephine having been necessary. Immediately after the removal of the bone he recovered the use of his right arm and leg, so far as to be able to move them, and to be sensible of their being touched. He gradually recovered by the 14th of August, so as to be sent to the General Hospital at Yarmouth, never having had a bad symptom, the only defect remaining on the right side being an inability to grasp any[310]thing in his hand with force. The pulsation of the brain was still visible at the bottom of the wound for about the space of half the circumference of the crown of the trephine. September 16th, 1815: the wound has filled up with healthy granulations, and has nearly cicatrized. A small sinus remains at the superior part, through which the edge of the bone can be felt. His health has been invariably good, although he has suffered a good deal of pain twice previously to the coming away of little pieces of bone, and toward evening he has been generally subject to slight vertigo. Discharged cured.
William Mitchel, of the Royals, aged forty, was wounded by a musket-ball on the 18th of June, at Waterloo; it struck the side of the head near the vertex, and, passing across through the sagittal suture, fractured and depressed both parietal bones. When he had recovered his senses he suffered great pain in the part, and found that he had lost the use of BOTH his legs, and was benumbed even from the loins and lower part of the chest; he was often sick, and felt low and ill. On the 28th, ten days after the battle, the trephine was applied in two places, and the whole of the detached and depressed portions of bone were removed. The sickness, lowness of spirits, and general illness immediately subsided, and the loss of power in the lower extremities gradually began to diminish, but he was not able to walk without assistance until the first week in August. On the 10th he arrived at Yarmouth, not having had a bad symptom after the depressed bone had been removed; and by the end of September he was discharged, able to walk well with the assistance of a stick.
Mr. Keate has mentioned to me a case, in which the injury and the paralysis were apparently on the same, or the right side. The paralysis, although positive, was not so complete as to render the patient quite incapable of moving the arm and leg, which were frequently convulsed, but the convulsions, which were observable in both, were more marked on the opposite or left side. On examination after death, the most serious injury was found to be a fracture of the right parietal and temporal bones, extending to the petrous portion of the latter, and beyond it; this, with a rather large extravasation of blood under and in the course of the fracture, appeared to be sufficient not only to destroy life, but to have caused paralysis of the left side, which, however, it[311] did not do. Another extravasation, rather less in quantity, had, however, taken place under the upper and anterior portion of the left parietal bone, which enabled Mr. Keate fully to account for the paralysis which took place on the right side. According to the surgery of the French Academicians of the beginning of the eighteenth century, this man would have been trephined or trepanned on the left side of the head in search of an extravasation by contre-coup; but accident or chance alone could have led to the right spot, as it was by no means opposed to that on the other side.
257. A simple fissure or fracture of the skull is of no more importance than a fracture of any other bone in the body, unless it implicate the brain; it should be managed according to the ordinary principles of surgery. These principles, however, involve a treatment diametrically opposite to that practiced by many surgeons, almost unto the present day.
If the integuments or scalp be divided, and the bone fissured, these principles should be carried out, by endeavoring to procure the union of the divided parts, as was generally done during the war in all such injuries from sabre-cuts as did not quite penetrate the skull—a practice that was found to be eminently successful, even when union did not take place. The general treatment should be similar to that insisted on in concussion, of which the following may perhaps be considered a sufficient example:—
A soldier in Lisbon, partly in liquor, received a blow from a spade which cut the upper part of the head across the sagittal suture, and rendered him senseless. He soon got better, and a slight fissure or fracture without depression was discovered. His head was shaved, kept raised, wet and cold, and the divided parts brought together by sticking-plaster; he was bled to twenty-four ounces, purged, starved, and kept quiet in a dark room. Slept well, but said that his head felt painful, as if something tight was tied around it. Pulse 96, small and hard; bowels not open. Blood was taken from the arm to the amount of forty ounces, when he appeared about to faint. Calomel and jalap, followed by infus. sennæ cum magnes. sulphate, were given, and acted well, and he was greatly relieved. The calomel was continued every six hours. In the evening, however, the pain and tightness of the head returned, with a pulse of 110,[312] hard and full; these symptoms were removed by the loss of twenty-four ounces of blood. He remained easy until the evening of the next or the third day, when the pulse quickened to 120, became small and hard, and he complained of severe pain in the head. It was evident that inflammation of the brain or of its membranes had commenced, and that it must be subdued; he was therefore bled until he fainted, forty ounces having been taken away. This entirely relieved him, and calomel and jalap, senna and salts were again administered with great effect. On the fourth day he was easy, the pulse 94, soft and full, the mouth being tender from the mercury. The wound did not heal by adhesion, but by granulation; and under the continuance of the starving and purging system he gradually got well without any more bad symptoms, having been saved by the loss of one hundred and twenty-eight ounces of blood in three days.
The vigorous and decided abstraction of blood saved the man, and, with the mercury, in all probability prevented the occurrence of those evils which our predecessors sought to obviate by removing a portion of bone. They believed the bone could not be fractured without an extravasation taking place beneath; and some took credit to themselves for placing wedges between the broken edges, in order to allow the escape of the blood or of the matter which might be formed below it. That blood may be effused, and matter may be formed, is indisputable, even under the most active treatment; but that an operation by the trephine will anticipate and prevent these evils, cannot be conceded in the present state of our knowledge; and the rule of practice is at present decided, that no such operation should be done until symptoms supervene distinctly announcing that compression or irritation of the brain has taken place. It is argued that when these symptoms do occur, it will be too late to have recourse to the operation with success. This may be true, as such cases must always be very dangerous; but it does not follow, and it never has been, nor indeed can it be shown, that the same mischief would not have taken place, if the operation had been performed early.
258. When a simple fracture, which in its slightest form is called a capillary fissure, takes place, the dura mater must be separated from it at that part to a certain extent, and some small vessels must be torn through. It does not follow, however, that blood must necessarily be poured out in[313] such a quantity that it will not be absorbed. Dissection, on the contrary, has established the fact that it will be absorbed even in cases of fracture of greater extent, where it has been seen that a larger quantity had been extravasated. As the effusion of a larger, or of so large a quantity of blood as to prove eventually mischievous, does not usually take place, except under other circumstances than those of a simple fracture, the ordinary practice ought not to be to seek for that which is not likely to be found. The dura mater is rarely separated beyond the limits of the fracture, and it is more likely to recover without any further exposure or interference than with it. The dura mater, however, may be separated to a considerable extent from the bone in more severe injuries, and a quantity of blood is often extravasated upon it. When this does occur, the commotion or shock which occasioned the fracture, the separation of the dura mater, and the extravasation will generally have caused other more important although less perceptible derangements. These show themselves after the lapse of a few days, by giving rise to inflammation of the brain or of its membranes, of which such patients more usually die, than of the separation of the dura mater, or of the extravasation of a small quantity of blood. The case is no longer one of simple fissure or fracture of the cranium, and the nature and severity of the symptoms which have supervened must regulate the practice to be pursued.
259. After the receipt of a severe blow, or of a gunshot fracture of the head, which has not even stunned the person at the moment, he may walk to the surgeon, the wound be dressed, and he may converse with his fellows as if nothing had happened; yet in a short time he may become heavy, stupid, drowsy, and unwilling to move, with a slow pulse and a pallid countenance. Inflammation has not yet had time to set in, and extravasation has not always taken place. If the loss of a moderate quantity of blood should relieve such a person, it shows that congestion had occurred, perhaps on the surface of the brain under the injured spot, on recovering from which, by the unassisted efforts of nature, he would still be liable to inflammation. I have repeatedly seen a sharp bleeding from an incision made to allow a complete examination of the part in such a case, cause the restoration of the patient to his natural state. A return of untoward symptoms during the progress of the case does not always[314] indicate essential mischief; they will be removed, if of a temporary nature, by a further moderate bleeding, by purgatives, and by greater restriction in diet, through irregularities in which these secondary attacks most usually occur. If the loss of blood should not relieve the symptoms, the case is probably complicated by a separation of the dura mater, or by an extravasation having taken place between the dura mater and the bone, or even in or on the surface of the brain.
260. When a fracture takes place at the anterior inferior angle of the parietal bone, or in any part of the course of the middle meningeal artery, it often gives rise to a more serious injury, which nothing but an operation can remove. The artery is always in a groove, and is often even imbedded in the bone at its lower part, and may be torn at the moment of fracture, giving rise to a gradual extravasation of blood on the surface of the brain, which can be borne to a considerable extent without causing any particular symptoms, although a sudden and considerable effusion causes immediate insensibility. When the extravasation is gradual, the patient walks away after the accident, and converses freely, becoming oppressed slowly, and in the end insensible, as the last drops of blood which are effused render the compression effective. When these symptoms occur after a wound in this particular part, the bone should be immediately examined; if there be no obvious fracture, and relief cannot be obtained by the abstraction of blood, the trephine should be resorted to as a last resource; for if there be truth in the statements so confidently made of fracture of the inner table of the bone from concussion of the outer without fracture, it is here especially that we may be permitted to look for it. The hemorrhage in the greater number of these cases takes place slowly, and the effused blood depresses the brain by separating the dura mater from the neighboring bone—a process, however, which can hardly occur unless the injury has been so violent as to rupture its attachments to the bone; for the brain generally yields rather than the attachments of the dura mater, and is depressed, the hollow or cavity thus formed being filled up by the coagulum, which becomes thicker and thicker until insensibility is induced. Blood effused between the dura mater and the bone readily fills up in the first instance all the space formed by the disruption of the membrane; for the force with which the blood is poured out from the artery[315] overcomes the resistance offered by the brain, which gradually yields and sinks unto that point at which its natural functions can no longer be carried on. If the attachments of the dura mater be strong, and the separation which has taken place between it and the bone be small, the blood effused is compressed by the bone on one side, on which it can exert no influence, and is resisted by the dura mater, which will recede no further on the other. The wounded artery in such a case is soon compressed by its own coagulum, and the effusion is comparatively trifling, giving rise, according to its nature, either to the primary symptoms of compression from extravasation, or to the secondary ones dependent in all probability on inflammation and suppuration of the part, and of irritation and compression of the brain beneath. If, on the contrary, the separation of the dura mater from the bone be extensive, the quantity of extravasated blood may be considerable and the brain will be greatly depressed. Experience has demonstrated that persons have recovered after large coagula have been removed; but in all these cases the brain had not lost its resiliency, and was seen to regain its natural level on the removal of the depressing cause, the person often opening his eyes and recognizing and speaking to those about him; but this does not take place when the brain remains depressed after the blood has been removed.
A French artillery driver was knocked off his horse by a musket-ball, which struck him on the anterior and inferior portion of the right parietal bone, during a charge made by General Brennier, at the battle of Vimiera, on the British infantry under the command of the late Sir Ronald Fergusson. I took him under my care, thinking from his freedom from bad symptoms and the slightness of the fracture that he would probably do well. The next morning I found him apparently dying. A portion of bone being removed, a thick coagulum of blood appeared beneath, apparently extending in every direction. Three more pieces of bone were taken away and the coagulum, which appeared to be an inch in thickness, was removed with difficulty with the help of a feather. The brain did not, however, regain its level, and the man shortly after died. The middle meningeal artery was torn across on the outside of the dura mater; the wound did not pass through to the inside, and there was[316] no blood beneath the dura mater. The convolutions of the brain were depressed and flattened by the pressure.
A soldier of the 29th Regiment was struck on the right parietal bone in a similar manner, shortly after daylight, at the battle of Talavera, during the first attack on the hill, the key of the British position. He walked to me soon afterward to the place where the wounded of the evening before had been collected in the rear. Being otherwise employed, I heard his story but could not attend to him at the moment, and found him some time afterward insensible, with a slow, intermitting pulse, breathing loudly, and supposed to be dying. The fractured parts were sufficiently broken to admit of the introduction of two elevators, by means of which they were gradually removed, together with a large coagulum of blood which had depressed the brain. When this had been done the brain regained its level, the man opened his eyes, looked around, knew and thanked me. The pulse and breathing became regular; he said he suffered only a little pain in the part, and should soon get well. He died, however, on the third day.
During the battle of Salamanca a soldier of the 27th Regiment was brought to me, who had walked to the rear, and had fallen down insensible within a few yards of the hospital station. I found a considerable fracture, with depression at the inferior part of the parietal bone before and above the ear. The end of the elevator having been introduced, a small piece of bone was first raised, then another, and a third, when a thick coagulum was exposed and removed. The dura mater was not separated from the bone around to any extent, and the coagulum, although thick, was not large. The brain, which had been depressed, regained its level immediately; the man recovered his senses, and was cured of his wound, but remained unfit for service. The artery did not bleed after it had been exposed.
The rule in surgery, to remove the bone in such cases, is absolute.
261. Fractures of the skull are stated, from almost the earliest records of surgery, to occur on one side of the head in consequence of blows received on the other. The facts which ancient authors have collected and related on this point are so numerous and so well attested that it appears almost more than skeptical to doubt their accuracy, however seldom they may be now observed.
[317] A counter-fracture or fissure of one parietal or temporal bone, caused by a blow on the opposite one, is of such rare occurrence that it is in general unnoticed by later writers on injuries of the head. It is not so, however, with respect to a fracture at the base of the cranium from a blow on the vertex, or on the back part of the head—a kind of accident which occurs more frequently perhaps than any other in civil life—because persons who suffer from fractures of the skull do so more generally by falling from a height, or from being pitched on their heads, than by direct blows or other injuries. This accident principally depends on the superincumbent weight of the body pressing on the unsupported flat and thin base of the skull, and is but little connected with the unyielding nature of the spine; for it occurs to as great an extent in consequence of falls from a short distance without any impetus, as from falls from a great height. Some of the worst cases take place by the sufferer having been thrown from the back of a horse by the sudden starting of the animal, without any running away. Although in these cases a fissure may often be traced to the foramen magnum, the great fracture is essentially distinct, extending from the petrous portion of the temporal bone on each side, across, and between the sphenoid bone and the os frontis, and even separating the edges of the coronal suture nearly to the opposite side.
A noted gambler was thrown from his horse, and pitched on the top of his head at the door of the Westminster Hospital, late at night; he was taken up insensible, and died shortly afterward. The skull was fractured quite round from the vertex to the base, and from side to side, so that the fore and back parts might have been easily separated into halves, if the soft parts had been removed. Fractures of the base of the cranium are generally fatal, but not always so; for some persons live a considerable time afterward, and appear to die from other causes; so that partial, if not perfect recovery is possible.
H. Cochrane, forty-five years of age, fell a distance of twenty feet upon his head, and was taken up apparently lifeless, bleeding largely from the ears, nose, and mouth, but more particularly from the ears. He was seen within half an hour of the accident. He was then quite insensible; the surface of the body cold; pulse about 68, and very feeble; in three hours after the accident he was bled to six[318]teen ounces, when his pulse rose to 76, and the breathing, which before was rather oppressed, became more free. He was ordered six grains of calomel, followed by moderate doses of senna, till the bowels should be relieved.
He continued progressively mending, but in a state of stupidity, accompanied by extreme listlessness; answered questions sullenly, and frequently rested upon one arm without appearing conscious of pain; the mouth was drawn to the left side, to which there had been a slight tendency for some days; the tongue not at all affected.
He continued under treatment for three weeks longer, soon after which he was permitted to resume his employment, the mouth being still drawn in some degree to the left side. His habits became silent and solitary, but he performed his task with the greatest exactness. He was occasionally subject to vertigo, particularly in hot weather, after any violent exertion or taking a small quantity of beer; a pint of ale would render him stupid or insensible. Six months afterward he was found dead, lying in a ditch.
Sectio cadaveris.—The nasal bones were fractured by a blow which had made a transverse incision in the upper part of the face. The femur was found fractured upon the right side, and the scalp puffy and ecchymosed on the left. On removing the skull-cap, the dura mater appeared perfectly healthy, without any sign of extravasated blood upon the surface. Beneath the pia mater on the left side the sulci of the brain were filled with black blood, apparently very recently effused. The brain was removed without the least violence, when a lesion was found upon its inferior surface, corresponding to the petrous portion of the right temporal bone. The dura mater in this situation was externally of its natural structure, and adhered with its usual degree of firmness to the bone beneath. The arachnoid and pia mater were here deficient; the lesion consisted of a cavity about fifteen lines in length, nine in breadth, and three in depth, coated with a light-yellow lining, which also adhered to the corresponding portion of the inner surface of the dura mater, which completed the walls of the cavity inferiorly; it contained a turbid serum, in which were seen floating numerous but exceedingly minute white globules. The portion of the brain in this situation did not appear to have been disturbed by the recent violence, except that from the upper part of the cavity a probe was admitted without any resistance into the [319] descending horn of the right lateral ventricle, which, with the one on the opposite side, was filled with a large quantity of bloody serum, none of which, however, had escaped into the cavity beneath. The brain generally appeared perfectly healthy, and not more vascular than usual. Even within a line of the yellow deposit above mentioned there appeared not the slightest change of structure. On removing the dura mater from the base of the skull, indications of a former fracture were discovered, leading vertically down through the squamous portion of the temporal bone, whence it appeared to have been continued along the anterior part of the petrous portion into the Vidian canal; the edges of this fracture, both internally and externally, had been rounded by absorption; it was met at right angles by another which ran across the base of the petrous portion of the temporal bone. The direction of the last fracture was marked by numerous small, rough particles of bone, which adhered so slightly to the rest that they separated on maceration. The transverse ligament of the second vertebra was ruptured, and the atlas forced forward. The connection between the articular processes of the second and third cervical vertebræ on the right side had also been separated by the fall which had caused death.
William Clayton, forty-four years of age, was admitted on the 31st of July, 1841, into the Westminster Hospital, having received a blow on the RIGHT side of his head from the handle of a windlass, by which his skull was fractured. The fracture extended downward from the parietal bone across the temporal, and in all probability through its petrous portion, as blood flowed freely from the ear for the first six hours; he was stunned for a few minutes at first, but became sensible by the time he was brought to the hospital. The bleeding from the ear was followed by the discharge of a fluid resembling water—which is a very dangerous symptom, as it usually flows from the sac of the arachnoid membrane—and afterward at intervals by a discharge of blood and matter, particularly, he said, on coughing; he was also quite deaf, with a little pain on the right side of the head. The bowels were well opened, and he lost sixteen ounces of blood. On the evening of the third of August, the fourth day after the accident, paralysis of the muscles of the RIGHT side of the face supplied by the portio dura came on, or was first observed. Pulse 80. He was well purged, but lost no blood, as he was apparently weak and the pulse soft; it fell[320] next day to 72. Mercury was now administered twice a day until the mouth became sore. On the eighteenth of September he was discharged, cured of the paralysis, the wound on the head being open, and a piece of bone bare and likely to exfoliate. October 8. Readmitted in consequence of great headache after drunkenness, with numbness of the toes and fingers; he was well purged, and felt relieved. He remained in the hospital for a month, his mouth being again slightly affected, occasionally drinking in spite of all remonstrance; he then returned to his work on the piers of Westminster bridge. On the eighth of June several small pieces of bone came away; and the wound nearly healed. The course of the fracture can be traced, in consequence of the scalp having adhered to the bone, causing a slight depression and hardness, which can be felt by the finger, extending down to the ear.
An hostler was thrown on his head from a horse, and was carried to the Westminster Hospital late at night in a state of stupefaction; no other injury could be discovered. The next morning he could answer questions, although not always correctly; complained of pain in his head, had bled from the ears all night, and had vomited some blood two or three times. Pupils dilated, but they contracted on bringing a lighted candle near them; the left eyelid more open than the right; pulse 52; very restless, and constantly turning in bed. V. S. ad ℥xxiv. Calomel and colocynth: salts and senna. Cold to the head. The pulse rose to 60 after the loss of blood. 2d day. Is delirious; bleeding from the ears but trifling; complains of pain in the head; bowels open; passes urine freely; pulse 54, a little irregular. Y. S. ad ℥xvj gave relief. Continue calomel, and salts and senna. 3d day. Restless all night; headache and thirst; bowels open. V. S. ad ℥xiv relieved the pain in the head. Pulse 56. 4th day. Restless and delirious at night; pulse 60, regular; bowels open; headache. V. S. ad ℥xiv. No discharge from the ears. 6th day. Slightly paralytic on the left side of the face, tongue drawn to that side; headache, restless, delirious; feces and urine passed unconsciously; pulse 80. V. S. ad ℥xx. Pulse rose to 100, and was weaker. Calomel, gr. iii every six hours. 7th day. Pulse 88, compressible; restless at all times, delirious at night; bowels open, but he is more conscious of everything. 8th day. Pulse 80, small, intermitting; occasionally slept a little, and[321] is generally better; bowels well purged; paralysis of the face continues. Has taken a little farinaceous food. Continue calomel and inf. sennæ. 10th day. Improved; slept tolerably well. 12th day. Continues to improve. Omit the calomel, but continue the infus. sennæ. 16th day. Is better. Paralysis lessened. Recollects he was thrown from a horse, but nothing else. Is free from pain, but very weak. Mouth a little sore.
After this time he gradually recovered, but was for a long time unable to work, or to undergo any exposure. A very little more mischief, and he would have gradually sunk, and died after the seventh day, instead of slowly recovering.
INJURIES OF THE HEAD.
262. A fracture of the inner or vitreous table of the skull, as it has been termed from its peculiar brittleness, as opposed to the greater toughness of the outer, is a rare occurrence without some signs of depression or fracture of the outer table, or detachment of the pericranium.
Mr. S. Cooper says: “One case of this kind, attended with urgent symptoms of compression, I trephined at Brussels. A large splinter of the inner table was driven more than an inch into the brain, and on its extraction the patient’s senses and power of voluntary motion instantly returned. The part of the skull to which the trephine was applied did not indicate externally any depression, although the external table came away in the hollow of the trephine, leaving the inner table behind.”
The records of eighteen centuries have produced but little information on this most interesting subject: and if the cases were collected which have been overlooked by authors, as well as those which have been altogether omitted, little would be gained; it may be concluded, therefore, that although such things have happened, they are of rare occurrence. I have never, in the great number of broken heads I have had under my care on many different and[322] grand occasions, actually known the inner table to be separated from the outer, without positive marks of an injury having been inflicted on the bone or pericranium. Although it is not possible to doubt the fact of fracture of the inner table having occurred, without apparent injury to the outer, it is very desirable in a practical point of view not to bear it too strongly in mind; for if a surgeon should be prepossessed with the idea that the inner table may be so readily fractured and separated from the diploe placed between it and the outer table, and thus cause irritation or pressure on the brain, few persons who had received a knock on the head, followed by any serious symptoms, without fracture or depression, would escape the trephine, and the worst practice would be again established. An operation should never be performed under the expectation that such an accident may have happened, unless it be apparently required by the urgency of the symptoms indicating compression or irritation of the brain, which cannot be relieved by other means, and are about to prove fatal.
It is by no means intended to imply by these remarks that a blow on the head will not frequently detach the dura mater from the inner table by rupturing its vessels, and thus give rise to compression or irritation of the brain from the effusion of blood or the formation of matter; or that the inner table may not from the same cause become diseased, and thus lead to ulterior mischief; but these are altogether different states of injury, and require a different consideration.
Mr. Deane, of Chatteris, in Cambridgeshire, had occasion to examine the head of a young man after death from a blow on the left side, just below the parietal protuberance, there being only a slight detachment of the pericranium, but no fracture. On removing the skull-cap, a very distinct fracture of the inner table, about three-quarters of an inch long, was seen corresponding to the external part injured, extending outwardly as far as the diploe, but no farther. The dura mater adhered firmly everywhere, except at this part, and for some distance around, a quantity of fluid blood being interposed between it and the bone. If this man had outlived the first symptoms, he would not, in all probability, have recovered without an operation for the removal of the extravasated blood.
263. Severe effects do not always take place in such cases[323] in the course of the first treatment, but occur afterward; or the unfavorable symptoms, never having been entirely removed, increase so much at a later period as to render the aid of operative surgery necessary for the removal of the bone, in order to save life.
M. A. Farnham, aged twenty-three, a stout, healthy-looking girl, received a blow, two years before, from a stone falling from a door-way under which she was passing; it struck her upon the left side of the head at a spot an inch anterior to the parietal prominence, the weight of the stone and the space through which it fell making the estimated force with which it struck the head equal to sixteen pounds. The immediate effect of the blow was insensibility, followed by acute fixed pain in the head, which has ever since continued to mark the seat of injury. A week after the receipt of the blow she began to lose the power of moving the right arm, there being, however, no loss of sensation or any disturbance of the cerebral functions.
During the following twelve mouths the symptoms remained unchanged; this period was spent in several London hospitals; not having derived any relief while in any of these institutions, she became an out-patient of the Westminster Hospital.
The arm and leg of the right side were quite paralytic, the former, which had previously been flaccid, having now become remarkably rigid, its temperature being below that of the opposite side; vision, particularly of the left eye, imperfect, the pupils, however, acting naturally; hearing on that side also affected; memory bad; respiration frequently slow and almost stertorous; the countenance had assumed a dull, heavy expression, and she manifested an unusual tendency to sleep.
April 1st, 1841.—Mr. Guthrie this day removed a disk of bone from the exact point in the parietal region to which she referred the pain. The portion of bone presented no evidence of disease; its thickness varied from two and a half to four lines, the latter measurement corresponding to the part most distant from the sagittal suture; the vessels of the diploe bled freely, the dura mater was quite healthy, and without any very evident motion.
On visiting her an hour after the operation, she raised the previously paralytic arm several inches from the bed, and was able to bend and extend the fingers. The pain in[324] the head was considerably less, and her countenance, before dull and heavy, was now remarkably animated. Sensation had returned in the arm, and partially in the leg. Her pulse was calm, and the skin cool.
Ten hours after the operation she was attacked with rigors, followed by pyrexia and all the symptoms of commencing inflammation of the brain. By the immediate abstraction of blood, which was three times repeated during the succeeding twelve hours, whenever the pain in the head or the force of the circulation increased, every bad symptom was removed. In the course of three days the paralysis had completely disappeared, sight and hearing again became perfect, and after passing through a speedy convalescence, she quitted the hospital completely recovered.
She has since had some relapses of pain and uneasiness in the head, but is altogether a different person, although of a very hysterical temperament. The cicatrix on the head is firm, and she considers herself to have been cured by the operation.
264. The inner table is sometimes broken in a peculiar manner, and to this attention was first drawn in my lectures, since trepanning has ceased to be the rule of practice in all cases of fractures. It occurs from the blow of a sword, hatchet, or other clean-cutting instrument, which strikes the head perpendicularly, and makes one clean cut through the scalp and skull into the brain. This kind of cut is usually considered as a mere solution of continuity, and not as a fracture, the bone being apparently only divided, with scarcely any crack or fissure extending beyond the part actually penetrated by the instrument. When the outer table alone has been divided, the wound in the scalp should be treated as a simple incised one, and united as quickly as possible, a practice of which I have seen several successful instances. When the instrument even penetrates to the diploe, the same course should be pursued; for although the external wound may not unite by the adhesive process, and some small exfoliations may occur, it is not common for serious consequences to ensue under that strictly antiphlogistic plan of treatment to which all persons with such injuries should be subjected.
265. When the sword or ax has penetrated the inner table, the case is of a much more serious nature; for this part will be broken almost always to a greater extent than[325] the outer table. It may be separated from it, and driven into the membranes, if not into the substance of the brain itself, the surface of the bone showing merely a separation of the edges of the cut made into it. These cases should all be examined carefully. The length of the wound on the top, or side, or any part of the head which is curved and not flat, will readily show to what depth the sword or ax has penetrated. A blunt or flat-ended probe should in such cases be carefully passed into the wound, and being gently pressed against one of the cut edges of the bone, its thickness may be measured, and the presence or absence of the inner table may thus be ascertained. If it should be separated from the diploe, the continued but careful insertion of the probe will detect it deeper in the wound. A further careful investigation will show the extent in length of this separation, although not in width; and will in all probability satisfy the surgeon that those portions of bone which have thus been broken and driven in are sticking in or irritating the brain. In many such cases there has not been more than a momentary stunning felt by the patient; he says he is free from symptoms, that he is not much hurt, and is satisfied he shall be well in a few days.
An officer was struck on the head, in Halifax, Nova Scotia, by a drunken workman with a tomahawk, or small Indian hatchet, which made a perpendicular cut into his left parietal bone, and knocked him down. As he soon recovered from the blow, and suffered nothing but the ordinary symptoms of a common wound of the head with fracture, it was considered to be a favorable case, and was treated simply, although with sufficient precaution. He sat up, and shaved himself until the fourteenth day, when he observed that the corner of his mouth on the opposite side to that on which he had been wounded was fixed, and the other drawn aside; and that he had not the free use of the right arm so as to enable him to shave. He was bled largely, but the symptoms increased until he lost the use of the right side, became comatose, and died. On examination, the inner table was found broken, separated from the diploe, and driven through the membranes into the brain, which was at that part soft, yellow, and in a state of suppuration.
Mr. B., of the 29th Regiment, when in Halifax, Nova Scotia, was struck, in a drunken frolic, on the anterior part of the left parietal bone, with his own sword, which was a straight,[326] heavy one, and a wound about two inches long was made in the side of his head through the bone. His little finger was cut at the same time, and it was not until the finger had been dressed that I was asked to look at the head, which he declared had nothing the matter with it. He was vomited, and purged, and the next morning bled, and as symptoms of inflammation of the membranes of the brain came on or increased, the bleedings were repeated, the quantity taken at each time being gradually diminished. He lost 250 ounces of blood in five days, after which he gradually although slowly recovered, some small spiculæ of bone coming away during the cure. Returning to England, the vessel was taken off the Scilly Islands, and he was sent to Verdun, where he remained several years, until liberated by the peace of 1814, when he rejoined his regiment, which had served in the Peninsula, and had returned to North America. It was soon found that he became outrageous on drinking a very little wine, and was odd in his manner, and had a great propensity to set out walking for hours without apparently knowing what he was about, or where he was going. When his regiment came immediately in front of the enemy, he was found going over to their lines, without being aware of what he was doing; and he was at last obliged to be sent to England, having evidently become deranged. This gentleman has ever since been confined in a private mad-house. His brother offered to allow the bone to be removed; but after thirty years of derangement a recovery could not be expected, and it was declined. If the examination I have since learned to be proper in such cases, had been made at the time, the inner table of the bone would have been found broken and depressed; and he might now have been in health both of mind and body.
I removed, in Lisbon, in the hospital appropriated to the wounded French prisoners in 1812, a portion of bone by the trephine, which had been fractured by a sword some months before: the wound had not healed, and some pieces of bone were depressed. One piece, in particular, of the inner table, was sticking in and irritating the dura mater, and was in all probability the immediate cause of the fits from which the patient had been suffering. He recovered.
A British soldier received a wound at the affair of El Boden, in front of Ciudad Rodrigo, from a sword, on the top of the head; he accompanied me to Alfaiates, on the retreat[327] of the army. The bone was apparently only cut through, yet the inner table was depressed, and felt rugged when examined with the probe. The symptoms of inflammation increasing on the fourth day, and not being relieved by copious bleeding, I removed a central portion of the cut bone by one large crown of the trephine, and took away several small pieces which were sticking into the dura mater, after which all the symptoms gradually subsided.
266. The whole of the French wounded, who remained on the ground or were taken prisoners after the battle of Salamanca, were under my care, and among them there were several severely wounded by sword-cuts received in the charges of heavy cavalry made by Generals Le Merchant and Bock. The cerebellum was laid bare in two cases without any immediate bad effect. In one particular case, which recovered, (after the battle of Waterloo,) the brain was seen pulsating for several weeks; and the statements made to me by the different officers at Brussels and Antwerp, and afterward at Yarmouth and Colchester, entirely confirmed the observations I had made, and the recommendations I have inculcated on this particular point as resulting from the practice of the Peninsular war.
267. It would appear that too much stress is laid upon a difference which is supposed to exist in the danger of trephining a man on the first or on the seventh day after an accident; and that an error may be committed in believing that the trephine is a more dangerous instrument on the first day than on the seventh. The question is not whether the man is to be trephined or not, but which will be the best and safest day or time to do the operation. I do not hesitate to say the first, believing the violence to be greater when done on parts already in a state of inflammation, than when they are sound. When the inner table has pierced the membranes and gone into the brain itself, the individual will in most cases ultimately die miserably of the accident if not relieved by art. It is less safe to let him designedly run the certain risk of cerebral irritation, which when once excited is often indomitable, than to remove the cause, and endeavor to prevent the evil. If the cerebral irritation only manifested its effects on the surface of the dura mater by causing suppuration there, delay might be admitted; but as it usually gives rise under these circumstances to the formation of matter on the surface, and even in the substance of the brain, where it[328] is deadly, “la chirurgie expectante” cannot be allowed. Lastly, there is not more danger of a hernia cerebri, as has been supposed, when the operation is done early, than when it is done at a later period; on the contrary, the patient has a much better chance of escape from hernia cerebri, and from all other evil, when the local and the general treatment are decided and efficient.
If, on attempting to remove a fragment buried in the brain, serious convulsive movements should be excited, it would be proper to desist from all further attempts to extract the splinters until the brain has become more quiescent.
It is necessary to recollect that the brain appears to be insensible, or nearly so, when first exposed; and it has rarely occurred that a serious convulsion or anything beyond vomiting has taken place on the removal of a piece of bone from the brain; nor will any difficulty be found in removing such small fragments as can be seen with a pair of forceps duly adapted for the purpose. It is impossible to say at what period of time the brain may become irritable, and no longer admit of its being touched without convulsive movements ensuing; but when this state of irritation has commenced, and its existence is proclaimed by the excitement which takes place on touching the fragment of bone, the surgeon should at once desist from all attempts to remove the foreign body. The brain under ordinary circumstances is much more likely to recover from an injury, all foreign or irritating matters having been removed, than when suffering from their presence.
268. The establishment of the principles which ought to regulate the practice of surgery in cases of fracture with depression of the inner table of the skull, is of the greatest importance. The principle being laid down that it is right and proper to examine all such wounds with a blunt, flat probe, in order to ascertain if possible whether the inner table be depressed and broken, the question necessarily arises, what is to be done when such depression and breaking down of the inner table have been ascertained to have taken place? There can be no hesitation in answering, that in all such cases the trephine should be applied, although no symptoms should exist, with the view of anticipating them. The old doctrine, it may be said, in regard to fractures generally, is revived in these cases, but on a principle with which our predecessors were not sufficiently acquainted. A patient[329] very often survives a mere depression of the skull; he may, and occasionally does survive, a greater depression of the inner than of the outer table; but it has not been shown that he ever does survive and remain in tolerable health, after a depression with fracture of the inner table, when portions of it have been driven into the dura mater. If cases could be advanced of complete recovery after such injuries, they would not supersede the practice recommended, unless they were so numerous as to establish the fact that injuries of the dura mater and brain by pieces of bone sticking in them are curable without an operation, and without leaving any serious defects. There are great objections to the trephine being applied in ordinary cases of fracture, not attended by symptoms of further mischief; but the nature of the cases particularly referred to having been ascertained, the practice should be prompt and decisive in every instance in which the surgeon is satisfied that there is not merely a slight depression or separation of the inner table, but that several points of it have been driven into the dura mater. If one trephine will suffice, the central point being applied close to the edge of the middle of the wound in the bone, it should be applied there; but if the cut be longer, and the spiculæ of bone extend upward and downward in its length, a small trephine should be applied as near each end as may be judged advisable, and one edge of the cut bone should be removed by the straight saw, of which Paré and Scultetus made such use in ancient times, and which Mr. Hey of Leeds revived in modern surgery; or the small straight saw may be used alone, if the object of removing a portion of bone can be attained without the trephine. By these means sufficient room will be obtained to remove the broken pieces of bone which are irritating the dura mater and brain. The danger resulting from the application of the trephine, in such cases, bears no proportion to the risk incurred by leaving the broken portions of bone as a constant cause of irritation.
269. There is an essential difference between a depression of the skull in a CHILD and in an ADULT. In the child the inner table is not brittle—it bends equally and does not break; it very often does little mischief when depressed, and gradually recovers its level. The brain in young persons is softer and less consistent, and can accommodate itself[330] more readily to pressure for a limited time, without ultimate mischief, than the brain of an adult; so that a continuance of the most urgent symptoms can alone authorize the application of the trephine in children, and in young persons under fifteen or sixteen years of age. A similar bending of the long bones in young children is often observed at an early period in life.
270. The propriety of dividing the scalp in an adult, in order to examine the state of the bone beneath, when evidently depressed, thus rendering a simple although comminuted fracture a compound one, is a matter of very great importance, the decision of which rests upon the still more essential point—viz., whether a depressed portion of bone ought or ought not to be removed? This again must depend upon the nature and extent of the depression, for many persons who have suffered from such a misfortune have recovered without the depressed portion being raised. It is a question of degree or extent, upon which every surgeon must form a judgment from his own observation and experience.
The difference between a simple and a compound fracture of the leg is often considerable; it is more often dependent on degree. When the fracture is nearly transverse, and the skin is cleanly divided, the difference between it and a simple fracture of the same part is little more than one of time. This may be the case with an injury of the head; the difference between the two states in fractures of the skull has, however, been much exaggerated; so much so, that no reliance can be placed on the supposition that there is more real danger in a case of fracture with depression in which the scalp has been divided, than when it has been only bruised, and not divided. I admit that theoretically it ought to be otherwise, but theory and practice do not always correspond. In all cases in which a fracture with marked depression is known to have occurred in an ADULT, it is good practice to ascertain the nature and extent of the depression. It is imperatively necessary if accompanied by symptoms of compression.
If the result of a great number of comparative trials should be in favor of never, under any circumstances, raising a depressed portion of bone in an adult, but of leaving it to the efforts of nature, an incision in order to ascertain the state of parts below ought not to be made; but as such[331] a result is not likely to be obtained, the practice recommended appears to be the best.
The scalp should be divided, in such cases as may require the operation, by a straight, crucial, or such other shaped incision as may be found most convenient to the surgeon; but no part should be removed which can be preserved with the hope of maintaining its life.
271. The cranium, together with the fracture and depression, being exposed, the question whether the trephine should be applied or not is next to be determined. If the operation by the trephine, or that of sawing a piece of bone out of the head, were not in itself dangerous, there could be no hesitation about its use; but it is a dangerous operation, especially in crowded hospitals, and ought not to be resorted to when it can be avoided. If any ten healthy persons were trephined in a hospital, one would in all probability die from the effects of the operation, and three or four more might have a narrow escape from the inflammation of the brain and its membranes, or the other consequences which would probably ensue. It is not the admission of air, which has been even lately supposed to do mischief, that is to be dreaded in these cases, but the same kind of irritation which often follows the abstraction of a piece of bone under other and more ordinary circumstances at a later period of time.
The following cases are illustrative of many important points:—
William Rogers, aged nineteen, of the 32d Regiment, was wounded on the 16th of June by a musket-ball, which entered at the inferior angle of the left parietal bone, knocked him down, and for a few minutes rendered him insensible. On recovering his mental powers, he found that he was unable to speak, not so much (as he said afterward) from the want of power to form words, as from the incapacity of giving them sound. He was conscious of everything passing around him, and reasoned correctly. He retired out of the reach of shot, and then lay down for the night. On the following morning, he went to Brussels, where he was examined and dressed. On the morning of the 18th he reached Antwerp on horseback, very giddy, and overwhelmed with fatigue, fasting, and watching; he was admitted into the Minimes General Hospital and put to bed, when he soon fell into a sound sleep, which with some tea refreshed him much.
June 19th. The ball was found to have passed obliquely[332] upward and backward at least two inches, and could be distinctly felt with a probe. It gave more the idea of having raised the outer table than that of having depressed the inner. The defect in speech was in some measure diminished, and this with giddiness were the only symptoms of compression. A poultice was placed over the wound, a brisk purgative given, and spoon diet ordered.
20th. The pain and giddiness having increased, with annoyance from noise and exposure to light, twenty-six ounces of blood were taken from the arm. The following day the purgative was repeated, and the patient was much relieved. Everything went on well, the wound was nearly healed, and he was considered almost fit to be discharged, when, on the 16th of July, the wound began to open; on the 18th it was dilated and a portion of the cranium removed by the forceps; this was soon followed by symptoms of inflammation of the brain; twenty ounces of blood were taken immediately from the arm, purgatives and diaphoretics were ordered, and the strictest abstinence enjoined. 23d. Venesection was repeated, as well as the other means usually adopted to reduce high action. 24th. Completely relieved. 26th. Another portion of the cranium removed, the dura mater being fully exposed; the general health in the best state.
August 3d. Doing remarkably well; the wound healthy; the pulsation of the brain evident; the power of speech perfectly restored. The ball yet remains in, according to the opinion of the patient, (who is a fine, intelligent lad,) and he thinks it has gradually descended toward the petrous portion of the left temporal bone. Sent to England at the end of the month, the wound being healed.
When I saw this man at Antwerp I gave my opinion, without hesitation, that the bone and the ball ought to have been removed in the first instance, when he would have had a better chance for perfect recovery. The operation, when afterward performed for the removal of the loose pieces of bone, placed his life in great jeopardy. He was discharged the service with the ball lodged, and it is more than probable that he did not long survive, which he might have done if the ball had been removed when it was first felt within the skull.
In the following case the ball could not perhaps have been removed in the first instance with propriety; it might,[333] however, have been lying on the dura mater, or near it, within reach, and the actual state of things ought to have been ascertained, the surgeon afterward deciding whether any further operation were necessary.
Thomas O’Brien, 28th Regiment, aged twenty-three, was wounded by a musket-ball on the 16th of June at Quatre Bras; the bullet penetrated the occipital bone below and to the right of the junction of the lambdoidal and sagittal sutures. On his arrival at Colchester, the wound was healthy in appearance and healing rapidly. It appeared from his own account that for some hours after the injury he was totally deprived of sight; since that time he has been constantly more or less affected with headaches, for which he has been prescribed occasional cathartics and low diet. He has also been affected with pain and weakness in both eyes, but more particularly in the right. While at Brussels, and during his progress to Ostend, he lived very irregularly, and was frequently intoxicated. The external wound was entirely healed on the 20th of July, and no suspicion existed that the ball was lodged in the brain. On the 25th matter was perceived under the scalp, and was evacuated yesterday. To-day, the 27th, he complains of increase of headache; pulse small and quick. V. S. ad ℥vj. Haust. cathart. statim. 28th. In the course of this day his symptoms have become very urgent; he is restless, with a very quick pulse; an extensive crucial incision was made in the site of the original wound, and now for the first time it was discovered that the ball had penetrated the brain; several loose pieces of bone were extracted; a considerable quantity of arterial blood was suffered to flow from the small vessels divided in the incision. His bowels had been well opened by the cathartic. The most vigorous treatment was continued, but the symptoms notwithstanding increased, and he died on the morning of the 29th of July.
The ball was found lodged nearly two inches deep in the substance of the right posterior lobe of the brain; a considerable quantity of pus surrounded it; some inflammation of the brain and its membranes was observed, but much less than might have been expected.
A. Clutterbuck, 61st Regiment, aged twenty-five, was wounded in the back of the head by a musket-ball at the battle of Toulouse, on the 10th of April, 1814. He felt little inconvenience from the wound during the first two[334] days. On the 14th he complained of severe pain in the head, giddiness, and dimness of sight; the face was flushed, pulse hard and frequent. Twenty ounces of blood were taken from the arm, and the wound enlarged so as to expose the cranium. The upper part of the os occipitis was found fractured by the ball, and a circular portion of it, about the size of a shilling, was depressed and fractured. 15th. Pain in the head much abated; no giddiness, dimness of sight, or any unfavorable symptom; pulse still hard. V. S. ad ℥xx. To be well purged. 19th. He was bled again this day to the extent of twelve ounces, as a matter of precaution. 23d. Continues free from any bad symptom. May 8th. The wound is now much contracted, and he feels no inconvenience. A small portion of the bone still feels bare to the probe, but the greater portion of the depressed piece is covered with healthy granulations. No exfoliation has taken place. May 24th. The wound is nearly healed; he is in good health and spirits, and without inconvenience.
This case may be properly contrasted with that of O’Brien, as showing by the result the difference between an uninjured and an injured brain. If the fractured and depressed bone had not been at the back part of the head, it is probable the depressed portion would have been removed in the first instance, as it certainly would have been after the 15th, if the unfavorable symptoms had not yielded to the general treatment; but the bone would then have been removed under much more unfavorable circumstances than at first.
The following case is related to show the extent to which blood-letting may frequently be carried to preserve life. There having been no reason to believe that the symptoms depended on fractured and depressed bone, the scalp was not divided; and as the symptoms were coeval with and not consecutive to the injury, they were therefore supposed to depend on concussion rather than on compression of the brain. If the trephine had been applied on the fourth day because the insensibility continued, the additional injury would in all probability have proved fatal. If the depletion of all kinds had been less effective, the inflammation of the brain or of its membranes would certainly have terminated in the effusion of lymph or the formation of matter, which the use of the trephine would not have prevented nor removed.
George Mills, an artillery driver, aged twenty-eight, was[335] admitted into the Dépôt de Mendicité Hospital, Toulouse, May 29, 1814, in consequence of having been thrown from his horse on his head against the ground. He had fallen on the right side of the os frontis, immediately above the eye, where the surface of the skin appeared to be scratched and bruised, but the bone was not depressed: he was bled freely, but remained insensible. The next morning he was again bled to twenty ounces, which operation was repeated in the evening. On the 29th, the temporal artery was opened, and a vein in his arm at the same time, the breathing being strong and sonorous, the eyes closely shut, and he lying quite insensible; the pulse before the bleeding was quick and small; after he had lost about eight ounces of arterial and eight ounces of venous blood, it became fuller, and the breathing was somewhat relieved; the slightest touch gave him pain, and he shrunk from pressure made directly above the eye. The temporal artery was again opened in the evening, and ten ounces of blood were taken away. A purgative and a stimulating enema were ordered, and cold was constantly applied to the head.
30th. He has been freely purged and appears more collected; the pulse is still quick and small; breathing very free; the irritability continues and he complains of pain on pressing the head. The purgative and the enema were repeated, and ten ounces of blood were drawn from the temporal artery, after which he attempted to speak. 31st. Passed a good night; the pulse is quick and small; pain in the head still great; was again bled to twelve ounces, and the purgative was repeated. June 1st. Pulse quick; there is not so much pain in the injured part, and he appears more sensible; was bled to twenty-four ounces, and the purgative was repeated. 3d. Was again bled to ten ounces. From this time until the 20th, he gradually improved, and was then discharged cured.
The treatment in these cases was the same, although in one there was no fracture, and in the other two there was fracture with depression. The broken portions of bone did not, in Clutterbuck, appear to press unequally on the dura mater, and it was presumed that the moderate degree of pressure which ensued from the depression might be borne with impunity, as it did not seem likely to be accompanied by the projection inward of any pointed pieces which might irritate the brain. The result confirmed the supposition and[336] justified the treatment. If the examination of the depressed part had led to the apprehension that such points of bone did exist, and were sticking into and irritating the dura mater or brain, they would have been removed, in the belief that although they might not at the moment have given rise to any other symptoms than those which depended on the blow, the time would come when they would scarcely fail to cause those which usually accompany the formation of matter within the skull. If this danger should also be avoided, the subsequent evils which have been noticed as occurring at a later period, and which ultimately require the same operation for the relief of the patient after months of acute suffering, might be encountered; for although a person may temporarily recover from an injury in which a portion of bone has been allowed to remain a source of irritation to the brain, it does not follow that such recovery should be permanent. If there be a doubt on the mind of the surgeon, whether there be or be not any pieces of bone depressed and irritating the brain or its membranes, he should wait; this is the real difference between the surgery of the latter part of the Peninsular war and that of the olden time.
272. When a fracture is accompanied by depression, and the broken portion or portions of bone would seem to be driven into the dura mater or the brain, or to press so unequally upon them that as much mischief is likely to ensue from leaving as from removing them, especially in an adult or a middle-aged man, less harm will in general follow from ascertaining the fact by dividing the scalp and removing the broken pieces than by doing nothing, more particularly when the presence of a foreign body has been ascertained. If there be no symptoms indicative of mischief below the fractured part, the surgeon must then decide, after the best estimate he is able to make, of the probable evil which will occur from allowing the broken or depressed portions of bone to remain.
A French grenadier was brought to the field hospital the second day after the battle of Salamanca; he had received a blow on the left side of the head, probably from a piece of shell, which had caused a contusion and swelling on the left parietal bone, with a graze of the scalp, but without any opening communicating with the bone. This swelling, on examination, was so soft, and the feeling of depressed bone beneath so distinct, combined with the fact of the continued[337] lethargic state of the patient, that an incision was made into it, when the bone beneath was found broken into several small pieces. On clearing away the blood, two pieces which were loose were readily raised and removed by the elevator and forceps, and egress given to an ounce or two of blood, which were extravasated beneath, apparently from the rupture of the vessels passing between the dura mater and the bone. The patient regained his senses in the course of the night and morning of the third day, and under a strictly antiphlogistic regimen gradually recovered, some other small pieces of bone coming away, one or two others apparently reuniting to the uninjured parts, showing that it is not always necessary to remove every portion of bone which may be broken, provided any bond of union remains, and principally that which exists between it and the dura mater.
These different cases stand out in bold relief as eminently successful and opposed to those said to have been equally so under la chirurgie expectante. They tend to show that however good a general rule may be, it may admit of many and important exceptions; and they prove that experience, aided by sound and correct observation, is essentially necessary for the formation of a scientific surgeon.
273. In young persons the brain will bear a greater degree of pressure and of irritation with impunity than it will in persons of mature age. By far the greater number of cases in which recovery has taken place after fracture and depression of the skull with injury of the brain, and even loss of its substance, have occurred in children or in persons under the adult age; greater reliance may therefore be placed on the powers of nature in them; and recourse may be had less frequently to the aid of operative surgery in order to prevent mischief than in older persons, even when the bone is fractured as well as depressed. It will be found, and the remark is important, that the cases of fracture and depression reported to have been successfully treated without operation, have occurred principally in young persons.
The result of my experience has rendered it imperative to remove at once all portions of bone or foreign substances which have materially injured the dura mater in adults, although no symptoms of compression should be observed. If the wound in the dura mater should not be sufficiently large to allow the offending body to be extracted through it,[338] the opening must be enlarged to enable it to be withdrawn without further laceration.
274. Depressed portions of bone, accompanied by fracture at the back part of the head, need not necessarily be removed in the first instance. When the fractured and depressed bone is accompanied by symptoms of compression in an adult, which continue after the usual antiphlogistic means and remedies have been employed in vain, and appear to increase rather than to diminish, the broken and depressed portion should be raised; for although the brain will bear and accommodate itself to pressure in many persons in a manner which could not be either foreseen or expected, it will not do so in all; and the removal of the bone offers the best chance for relief, whether the mischief has arisen from the pressure made by it or occurs from the extravasation of blood beneath. When the principal symptom of compression is a severe fixed pain in the part, although the state of the fracture and depression would not alone have rendered the removal of the bone positively necessary, it is advisable to do so when this symptom is present.
The greatest discrimination is required in cases where the extent of the injury is not so manifest and in which there is more room for doubt. In most cases in which a slight or moderate degree of fracture and depression of the skull has taken place, the symptoms of concussion are present as well as those of compression. The symptoms of concussion are, however, coeval with the injury, and although those of compression may take place almost instantaneously, they more usually occur at a later period of time. The symptoms of concussion may nevertheless continue for days, more particularly the insensibility, or that state which is approaching to it, complicating the case and embarrassing the practitioner. In a child or young person the symptoms of compression or irritation, when they appear even at a secondary period, may pass away under further moderate depletion; but in an adult any undue delay in giving the necessary relief, by the removal of the depressed portion of bone, will in general be destructive to the patient. It is the irritation caused by the depressed bone on the dura mater, and communicated to the brain, which gives rise to the unfavorable symptoms and to the formation of matter which follows them.
A gentleman received a blow on the side of the head, which knocked him down and deprived him of his senses,[339] from which state he partially recovered, and vomited; some stupefaction, however, remained, although he could be made to answer by a little importunity. Pulse 62, irregular, breathing slow, the pupils contracting under the influence of light; the integuments where the blow was received were soft and swollen, in all probability from an extravasation of blood beneath. The next day the pulse was full and regular, the pupils were dilated, vomiting had taken place several times, and the patient answered correctly on being sharply questioned. He was bled largely, purgatives were administered, and cold was steadily applied to the head. He was bled the next day; on the third the left arm became paralytic, the pupils continued dilated, and on the fifth day paralysis implicated the left leg as well as the arm. There could now be no doubt that the brain was suffering from compression; but as the nerves of the excito-motory system were unaffected, and the functions of ingestion and egestion were satisfactorily accomplished, it was thought advisable to trust to the efforts of nature. The swelling of the scalp was painful.
A week afterward the general symptoms were the same, or only slightly augmented by fever; but, as the swelling of the scalp was more painful, it was opened, and a quantity of matter was evacuated, the bone beneath being fractured and depressed. As this operation gave some relief, it was thought advisable to wait, with the hope that the benefit thus obtained might prove permanent. The patient did not improve, however; and as the symptoms of fever increased, and were accompanied at last by rigors and great pain in the head, the depressed portions of bone were removed, and about half an ounce of purulent matter escaped from between the dura mater and the bone. The relief given this time was effective, and the patient perfectly recovered. “La chirurgie expectante” placed this man’s life in the greatest jeopardy. It was only saved at the last moment by the aid of that surgery which ought not to have been withheld when the paralysis, by affecting the leg as well as the arm, demonstrated the extension of the mischief within the head. In this instance the operation was successful, but it is not in general so serviceable when delayed to so late a period. It is in cases of this serious nature often a means of prevention rather than of cure.
275. When a severe blow, accompanied by a shock, as from a fall, has been received on the head, and the skull is[340] so thick and strong as to be able to resist the violence thus offered without being broken, or is only slightly fractured, the vibration or trémoussement is directly communicated to the brain, giving rise to laceration or bruising of its structure in various situations, to the rupture and separation of the vessels of the dura mater from the bone to which they are attached, and to derangement of other parts, which will in all probability be followed by inflammation, and may even terminate in the formation of matter under the dura mater as well as above it, and even in the brain itself. It is said to take place by “contre-coup” when the mischief occurs in any other part of the head than that which is struck, numerous instances of which are given by the older French authors. They were probably cases of laceration, the consequence of concussion of the brain, and not relievable by the art of surgery; but the injury which the older surgeons particularly distinguished as by “contre-coup” was where the blow was on one side, and a fracture took place or matter was formed in a circumscribed spot on the other; these cases did sometimes, they say, although rarely, admit of relief by operative surgery. These cases, unaccompanied by fracture, do not appear to take place under the improved method of treatment by larger depletion, by antimony, and by the early use of mercury. In the event, however, of their occurring, there is no surgeon of the present day who would attempt an operation of exploration on the opposite side of the head to the injury, without some sign of mischief existing at that part; although such operation, if done, might accidentally be followed by success.
TUMORS OF THE SCALP, ETC.
276. When the periosteum covering the bone is bruised, or the bone is merely deprived of this membrane, it does not follow that it should die or exfoliate. In many instances the wound will gradually close up and heal, as if no such accident had happened. A blow or bruise on the head often[341] gives rise to a swelling or tumor, from the rupture of the small vessels passing into the cellular membrane between the scalp and the pericranium; the tumor in these cases appears immediately after the receipt of the injury as a soft swelling, and is usually found to contain blood, which in most instances is removed by absorption in the course of from two to three weeks. In some cases inflammation supervenes, and one part becomes tender and appears to point; into this a small incision should be made to allow the blood and matter to escape, when gentle compression should be resorted to in order to induce the parts to unite. Swellings of this kind in new-born infants, occurring from pressure during delivery, may be readily mistaken for deficiencies of the occipital and parietal bones, if it were not for the absence of all motion, which under such circumstances would be communicated to them from the brain. The blood effused in the cellular membrane raises the border of the swelling, which becomes harder than the neighboring parts, while the center remains soft and yielding, giving a sensation to the finger as if the bone beneath were wanting, or, after a blow, the idea that the bone beneath is depressed. If such a swelling be unnecessarily opened, considerable inflammation and suppuration will often follow, to the great inconvenience of the patient; this will in general be avoided by the use of a moderately stimulating cold lotion.
277. In other cases of tumors, which are called secondary in contradistinction to the preceding, the patients go on well for eight, nine, or more days, at the end of which time they complain of headache, giddiness, nausea, restlessness, thirst, and generally of fever. A few days more, frequently from the thirteenth to the fifteenth day, rigors, sometimes severe, are superadded, and a swelling, if not observed before, is now perceived on the spot where the injury had been received, if the integuments have not been divided; or, if there be a wound, it loses its healthy red appearance, and assumes a yellowish, unhealthy color, which is accompanied by a thinner and more acrid discharge. From this time the symptoms gradually increase, the patients become delirious, convulsed, comatose, and die; and matter is found between the skull and the dura mater, or in or on the substance of the brain. If this secondary swelling be divided, and the fluid evacuated, which is not good pus, the pericranium will be found detached and the bone bare.
[342] It has been stated that a bone so circumstanced would not be found to bleed on being scraped, and that, by attending to the want of hemorrhage from the outside of the cranium, the extent of the evil might be ascertained, and that so long as a denuded, discolored bone will bleed on being scraped, it may be considered that the dura mater is attached below, and that no operation should be performed.
The essential difference between the primary and the secondary swellings is to be found in the fact that, although the bone be exposed, and even in some degree may have changed its color in the primary swelling when matter has formed, the febrile symptoms will subside after its evacuation, healthy granulations will spring up, and little or no exfoliation will take place. In the secondary swelling none of these favorable symptoms or appearances will take place, for the bone is incapable of maintaining its life, and must die. If the outer table only be implicated, it may exfoliate; but if there be reason to believe that matter has collected beneath, on the dura mater, the bone should be removed by the trephine.
Inflammation of the dura mater proceeding to suppuration, or the formation of matter between it and the bone, appears to have been a much more common consequence of injuries of the head in former times than at present. It is not now of frequent occurrence in London hospitals.
As blows on the head and the structure and functions of the brain are the same at present as formerly, the difference in regard to such cases can only depend on the difference of treatment. It is, in fact, infinitely more depletory now, and therefore less operative. Blood is taken away in larger quantities, although to this there are exceptions, depending on the constitution of the patient, which will not always admit of it, while the potassio-tartrate of antimony and mercury are by most surgeons administered at an early period.
Suppuration, or the formation of pus on the surface of the dura mater, not being, under the strictly antiphlogistic and mercurial system, so common as formerly, sufficient attention has not perhaps been paid to another evil which frequently accompanied it in former times, viz., suppuration on the surface and in the substance of the brain itself; for the greater number of those who died with fracture and depression of the skull, and whose cases are recorded, suffered also[343] from alteration of the structure or substance of the brain, and the formation of matter within it or upon its surface. This termination might not have taken place in a large proportion of the cases in which it occurred if the depressed bone had been raised to its level, and the irritation arising from undue or unequal pressure had been avoided. It must be admitted, however, that an internal part of the brain may receive such a shock at the moment of injury, as well as an external part, that no treatment can arrest the progress of the mischief, although it may be delayed; and when the patient dies, after four, five, or more weeks of alternate hope and suffering, matter may be found in some part of the brain where an injury was not suspected.
Purulent matter may be formed beneath the dura mater in a confined spot, or it may be diffused generally over the surface of the brain, in which case the sufferer has no chance of relief.
278. The operation of incising the dura mater, to admit of the discharge of blood or matter from beneath, and even of puncturing the brain, has not been much resorted to in England; this may be an error. The records of surgery supply many cases where it might have been done with advantage, and some in which it was done with the greatest benefit to the patient. It is not an operation which ought to be performed without signs sufficiently demonstrative of the necessity for doing it.
I have seen, on the removal of a portion of bone by the trephine, the dura mater rise up rapidly into the opening so as to attain the level of the surface of the skull, totally devoid, however, of that pulsatory motion which usually marks its healthy state. An opening into it, under these circumstances, has allowed a quantity of blood or of purulent matter to escape, proving that the unnatural elevation of the dura mater was caused by the resiliency of the brain when the opposing pressure of the cranium was removed. This tense elevation, its abnormal color, and the absence of pulsation are positive signs of there being a fluid beneath, requiring an incision into the dura mater for its evacuation. It is a point scarcely noticed in English surgery—one which was not in the slightest degree understood at the commencement of the war in the Peninsula.
A. Monro, of the 42d Regiment, was wounded on the 10th of April, at Toulouse, by a musket-ball, which fractured the[344] left parietal bone slightly, without depressing any part of it. No symptoms followed requiring more than ordinary attention until the 23d, up to which time he had been kept on low diet, for the most part in bed, and had been bled and purged. On the evening of that day he became feverish, and hasty and odd in manner, and the pulse quickened; he declared himself, however, to be quite well, and submitted to be bled and physicked with great reluctance, calomel combined with opium being given him at short intervals. On the 24th he complained of pain in the head, which he said was very slight, and that upon the whole he was quite well, and would not be bled nor have anything done. He was bled largely by force, which lowered the strength of the pulse, but did not relieve any of the symptoms of irritation of the brain. On the 25th he was evidently worse, although he declared himself to be quite well; he talked a little incoherently; the pupils were dilated; the pulse quick but regular; the countenance was changed; he was sensible, apparently, upon all points except that of being much worse, which he resolutely denied, saying he was better and would soon be well. Satisfied that matter was forming, or had formed, in or on his brain, I desired that the trephine might be applied on the fractured part and the bone removed. This, however, he would not permit the officers in charge to do, and they awaited my return in the afternoon, when, finding him much worse, I directed it to be done by force, three of his own regiment with others attending to assist the surgeons. He called upon these men by name not to allow him to be murdered in cold blood, declared he was getting well, and would get well if let alone, and prayed them to avenge his death on the doctors if they meddled with him. The surgeons were dismayed, and requested that the operation, which they said required great care, should be performed by me, their chief. I therefore removed the bone; and the moment it was taken away the dura mater rose up in the opening to the level of the surrounding bone, and remained without any pulsatory motion. I had no doubt of matter being beneath, and that, from his general state, the man would die. I did not therefore think it prudent, under all the circumstances, to do more than warn his comrades that, when dead, they would see the whole brain beneath in a state of suppuration. He died that night; and the next day they saw the whole of the left hemisphere soft, yellow, and cov[345]ered with matter, to their great surprise and satisfaction at the accuracy of the diagnosis.
Absalom Lorimer, of the 42d Regiment, was wounded by a musket-ball on the 10th of April, 1814, at the battle of Toulouse, which carried away a small portion of the scalp just above the right temple, fracturing the bone slightly, but without any depression. No symptoms occurred demanding more than ordinary attention for the first fortnight, during which period he had been bled once, purged, and kept on low diet. On the 25th, he complained of pain in his head around the wound, shooting to the back part; pulse 60; pupils dilated. An incision having been made to the bone, the pericranium was found detached, and the bone fractured, but without any obvious depression. V. S. ad ℥xx, calomel and colocynth: as the pain continued, the bleeding was repeated in the evening. 26th. Pain in the head greatly relieved; pulse 60; bowels torpid. Ten ounces of blood were taken from the temporal artery, and the calomel and colocynth, salts and senna were repeated. On the morning of the 29th, the symptoms of compression having increased, the trephine was had recourse to, and the fractured portion of bone was removed: a layer of coagulated blood was found on the dura mater, which puffed up into the opening. In the evening he became convulsed, the pulse intermitted, and he died. On examination, a large abscess was found in the right hemisphere of the brain, having the ventricle for its base, with some matter on the surface of the brain, and between the dura mater and the bone at the base of the cranium.
On the morning of the day that I performed this operation, I had done another of the same kind at the Hôpital des Minimes; the dura mater rose up in a similar manner without pulsation into the opening made by the removal of the circular piece of bone by the trephine; on puncturing it a considerable quantity of pus oozed out. The opening was enlarged; and the flow of matter was daily encouraged, until it gradually diminished, and ceased with the formation of granulations, and the drawing in and cicatrization of the part.
279. It has been supposed theoretically that a wound through the dura mater was particularly dangerous, in consequence of the tunica arachnoides which lines it being a serous membrane; and that, if the inflammation which en[346]sued did not cease at the adhesive stage, by the consolidation of the surface which covered the pia mater with that which lined the dura mater, a diffuse inflammation would necessarily follow, which might spread over its whole extent. This has not been found practically to be the case; and if a simple wound of the dura mater be a danger that ought to be avoided, the risk run cannot be put in comparison with that which accompanies the continuous irritation depending on the presence of a spicula of bone, which has passed through the dura mater, and is irritating the brain beneath. It has also been supposed theoretically that the danger would be diminished if the pia mater were wounded also, as the brain would project and fill the wound; but the accuracy of this opinion may be doubted. If the dura mater were injured through error or design, I should not think the evil lessened by adding to it a wound of the pia mater, and perhaps also of the brain.
By those who have been accustomed to the terrible injuries which occur in military warfare, in which large portions of the brain are sometimes exposed, and even lost, without much inconvenience following, the exposure of or the opening into the dura mater is not considered of so much importance as it is by those who have had fewer opportunities of seeing such awful cases; while the formation and retention of matter below the bones of the cranium is, on the other hand, more dreaded by those who have often seen their ill effects than by those who have not had many occasions for observing them; by whom, however, they are often considered, when they do take place, to be irremediable by art.
280. Gunshot wounds of the skull are attended by certain peculiarities. In ordinary circumstances there is usually an external wound and a fracture more or less comminuted, with depression; this wound will almost always require to be enlarged by a simple incision, so as to show the extent of the depression or the size of the broken and depressed portions of bone. When the bone is scarcely injured, and the periosteum is only bruised, or when the bone is even deprived of this covering, it does not follow that it should die or even exfoliate. In many instances the wound will gradually close in and heal, as if no such evil had occurred; and in those which do not terminate so favorably, the cure may only be delayed by the exfoliation of a layer or scale of[347] bone from its outer surface, unless the mischief should have implicated the parts beneath.
A musket-ball striking directly against a bone sometimes makes a hole not larger than itself, with or without any radiating fracture; and one large trephine, if properly applied, will often embrace the whole of the mischief, and admit of the removal of the broken pieces. As a center-pin cannot be used, the trephine may be made to turn very well in most cases in a flat but thick bar of iron, having a hole in the middle, of such a size only as will allow the polished outside of the trephine to turn in it. Sufficient support for the instrument will be obtained by this means until it has made a groove in the bone for itself, when the operation may be continued as it would be in an ordinary case after the removal of the center-pin.
When a musket-ball ranges along the side or top of the head, it may break the outer, and depress and fracture the inner table to a considerable extent, for the space even of three or more inches. The broken portions of bone may in general be removed by means of good forceps and a straight saw; and no good reason can be given for delaying the operation unless the nature of the injury be doubtful, when it may be as well to wait for symptoms. It sometimes happens, although rarely, that a ball sticks so firmly in the bone that it cannot be extracted by working round it in any ordinary way with a pointed instrument. The difficulty usually arises from the ball having half buried itself in the diploe, so little of it being exposed as not to admit of a firm hold being taken of it. The large trephine, used in the way pointed out, has several times overcome this difficulty. The removal of the outer table has been sufficient where the inner one has not been driven into the dura mater; when any doubt is entertained on this point both should be removed.
281. A ball or other foreign substance may penetrate the brain directly or obliquely. When the ball penetrates the brain directly, it is not often that it can be removed, and the sufferer very rarely survives beyond a few days, even if the ball has been extracted; more particularly if the injury have occurred in the anterior part of the substance of the brain; several persons, however, have recovered, in whom the injury occurred toward the back part of the head, the ball being allowed to remain. It will be better in all such cases to allow the ball to remain, which it will often do for[348] many days, until circumstances render it necessary to endeavor to find it. When it can be felt immediately under the surface of the brain, it ought to be removed like any other foreign substance.
Dr. Rogers relates the history of an excellent case, in which a young man aged nineteen received a wound on the frontal bone, just above the center of the left superciliary ridge, from the bursting of a gun on the 10th of July. It was not until the 4th of August that he discovered a piece of iron lodged within the head, in the bottom of the wound, (from which a considerable quantity of brain had come away,) which he extracted the next day. It proved to be the breech-pin of the gun, three inches in length, and three ounces in weight. By the tenth of December his patient was perfectly cured.
When a ball strikes the head obliquely, it may enter and pass out or lodge. Nearly all these cases die, but one occasionally escapes, and none should be allowed to die without assistance. When the entrance and exit of the ball are obvious, and not far distant from each other, the splinters of bone should be removed; and if the little bridge between the openings should be injured, the whole should be taken away by the straight saw; an operation which cannot, however, be necessary in the first instance, if the portion of bone be apparently sound.
At the battle of Talavera, a soldier of the 48th Regiment was brought to me in a state of insensibility; he had received a musket-ball on the upper part of the right side of the frontal bone, where it had entered, and had evidently passed backward; it could be followed by the probe rubbing against the bone for nearly four inches. The scalp over this point was soft, as if blood were effused below; and on dividing it, a fracture was seen bulging rather outward. The trephine was applied forthwith, and the bone removed, together with the ball, which only wanted a little more impetus to have come through. The brain was injured, and the man died two days afterward.
A French grenadier was wounded at the battle of Salamanca by a musket-ball, which struck him on the right side of the head, penetrated the temporal muscle, and lodged in the bone beneath, giving rise to symptoms of compression. On dividing the parts, I found that the ball had fractured and driven in a part of the temporal bone, one portion of[349] the ball being above, and the other below the broken bone. The upper half of the ball was readily removed, but several small portions of bone were raised by the elevator and forceps before the remaining portion of the ball could be drawn from under the bone, which was not depressed, the ball having been cut in two by its edge. The dura mater was bruised, but not torn through. The wound suppurated freely; several pieces of bone exfoliated, and the patient was ultimately discharged in progress toward a cure.
A small ball sometimes becomes so flattened by striking against the skull as to remain undiscovered when care is not taken in the examination. A soldier was wounded at the storming of San Sebastian by a ball on the side of the head, which was supposed not to have lodged. The wound did not heal, a small opening remaining, although no exfoliation took place, and the bone did not seem to be bare. On dividing the scalp to ascertain the cause of the delay in healing, a small ball, quite flat, was found; it had sunk down a little below the hole left for the discharge to which by its irritation it had given rise.
When a larger ball or a piece of a shell strikes the head, the fracture is usually extensive, and portions of bone, or a piece of the shell itself, are often lodged in the substance of the brain. There is nothing peculiar in the management of these cases, which are for the most part unfortunate.
282. A suture may be separated by a musket-ball, which impinges with a moderate degree of force directly upon it, but not without great danger. It can, however, only happen in young persons in whom the sutures are not obliterated as they are in elderly ones; in general it takes place when the ball happens to lodge as it were between the bones concerned in the formation of the suture. The first case of the kind which came under my observation occurred at the taking of Oporto. I met with a second at Albuhera, a third at Salamanca, and a fourth in a slighter degree at Orthez.
A heavy dragoon was wounded at the battle of Salamanca by a musket-ball in the body, which caused him to fall from his horse, injuring the top of his head. Little attention was paid to him until mischief was suspected from the lethargic state into which he fell, which could only be attributed to the blow on the head, where a tumor was observable. This, on being divided, showed a separation of the[350] edges of the sagittal suture, from which some blood flowed. Two crowns of the trephine were applied on the twelfth day, in order to admit of the free discharge of some blood which had been extravasated from a wound in the longitudinal sinus, after which the symptoms subsided, and the patient gradually recovered.
A ball may pass apparently through the fore part of the head from side to side without doing much mischief beyond depriving the sufferer of sight. It does not in these cases injure the brain, but passes immediately below it and through the back part of both orbits. In four such cases the recovery was rapid, but the blindness was irremediable.
283. The danger of injury to the frontal sinuses has been greatly exaggerated, and vanishes in a great degree when attention is paid to their structure. The uncertainty of the depth of the cavity between the tables of the bone, and the irregularity of the exposed surface of the inner table, which may through carelessness be mistaken for depression, should be remembered.
A soldier of the 29th Regiment was wounded at the battle of Talavera by a ball, which struck him on the lower part of the right side of the forehead, fracturing the external wall of the frontal sinus. On examination, the ball could be felt lodged in the sinus, whence it was readily removed by enlarging the opening, and the man recovered without any bad symptoms.
At the storming of Badajos, a soldier of one of the regiments engaged at the little breach was struck by a small ball about the size of a swan-shot; it penetrated the frontal sinus of the right side, and stuck in the inner table, the outer being considerably injured and splintered by the blow. The splinters having been removed, the small ball could be seen sticking in the inner table of the bone, whence it was easily extracted, leaving the dura mater bare beneath. He was sent to Elvas, and recovered with a good and firm cicatrix.
After a wound of the frontal sinus has healed, the air has been known to raise up the integuments of the forehead into an elastic crepitating swelling whenever the patient blew his nose, so that a compress and bandage on the part were required for its relief; but these cases are very rare.
284. Wounds of the bony parts within the orbit are often attended by the most serious consequences. A boy, nine years of age, was struck by his playfellow with the end of a[351] thick iron wire on the right eye, which blackened it. There was no external wound; but as there was some bloody chemosis at the upper part and the inside, there was a probability of the wire having penetrated deeply, although the opening could not be discovered by the probe. The accident had happened two days before, but he did not think himself ill. He was well purged, and cold water was applied externally. Two days after, he complained of sickness, headache, and some pain over the brow. He was bled freely from the temple of that side by leeches, and well purged by calomel and jalap. On the sixth day his mother reported him as having been delirious and restless all night. He was found stupefied, answering with difficulty and incoherently; pulse very quick, skin hot and dry, with some convulsive twitches of the face and arms; pupils slightly obeying the influence of a strong light, but not dilated. He was again bled freely from the temple, but his breathing became more difficult, he fell into a comatose state, and died in the night. On examining the head, the stiff iron wire was found to have passed under the upper eyelid, between it and the eye, through the posterior part of the orbitar plate of the frontal bone and into the anterior lobe of the brain, which was softened at that part, and bedewed with matter.
A woman, who had been struck by her husband on the left eye with a tobacco-pipe, while preparing her frying-pan for cooking, knocked him down with the pan, and ruptured his right eye, which was lost. She then pulled out a piece of the pipe which was sticking in the orbit, between the lid and upper and inside of her own eye, which was uninjured. She complained of little but the bruise, and rather brought her husband than herself for advice. Bled and purged, she did not complain of anything for several days, when she said she had been very ill all night, with nausea, headache, and shivering; with hot and dry skin, pulse very quick, the upper eyelid paralytic; she looked very ill, became delirious at night, and died two days after the first complaint of serious illness. On examination, half an inch of the red waxed end of the tobacco-pipe was found to have gone through the sphenoid bone, by the side of the sella turcica, and to have lodged in the brain, whence it was removed bedewed with pus, the brain being yellow and softened around it.
A wound of the longitudinal or lateral sinuses, allowing a[352] free discharge of the blood poured out, is of comparatively little consequence. It is, on the contrary, a very fatal injury when the blood is permitted to accumulate.
285. A protrusion of the brain, often improperly called a fungus cerebri, is of two kinds, and occurs at different periods of time. The first kind is principally composed of coagulated blood, usually appears immediately after, or within two days after, the injury, and is generally fatal. The second takes place at a later period, although it has occurred on the third or fourth day, and is formed for the most part of brain. These protrusions rarely take place when a considerable portion of the skull has been lost or removed, the brain then being able to expand to such an extent as the inflammatory impulse from within may render necessary. When the opening is small, and the dura mater has not been injured, it has seldom been observed. It is then principally when the opening in the skull has been of greater extent than the size of one piece of bone removed by the trephine, the dura mater having yielded either in consequence of the injury or by ulceration, that this evil takes place; it is not, under proper treatment, a fatal, although it is always an extremely dangerous occurrence.
In the first kind of protrusion, the dura mater must necessarily be torn to some extent, and the tumor which comes through it is of a dark-brown color, glazed and covered in general by the pia mater. These protrusions were accompanied, in every case I have seen, by delirium and other symptoms of inflammation of the brain and of its membranes, and not by coma, until near the fatal termination of the disease. I have seen them torn off by the patients themselves during life, or before death; and satisfied myself that they all arose from hemorrhage into the substance of the brain, probably immediately below its surface, which became more elevated as the inflammation proceeded, and was gradually protruded at the part where there was the least opposition. When the tumor was torn off, little hemorrhage ensued, but a dark-brown blood cavity was seen in the substance of the brain; and when cut off and examined, the protruded part seemed to be covered by the pia mater, with or without a layer of cerebral matter, and was made up generally of coagulated blood. No case of this kind recovered.
In the second kind of protrusion, or that which usually although not necessarily takes place when the first or active[353] inflammatory symptoms are on the decline, the tumor is formed of the substance of the brain. It has been supposed that in whatever manner a case of hernia cerebri may arrive at a favorable termination, there must inevitably be a loss of brain proportionate to the extent of the protrusion—a conclusion which the experience of the Peninsular war did not confirm, while it may lead to the establishment of an erroneous practice for the too early removal of the protrusion. The loss of a portion of one of the hemispheres of the brain is now known to occasion little or no inconvenience in many instances, either to the intellectual or corporeal faculties; nevertheless, as the precise quantity of brain which a person may lose with impunity has not been ascertained, it may be as well not to deprive a patient of any, provided its removal can be dispensed with; and that it may be so dispensed with, the practice of that war gave positive proof in several instances, by the protruded part being gradually withdrawn within the skull, the wound having afterward healed by the ordinary processes of nature.
There were three cases of recovery from a protrusion of the brain after the battle of Toulouse.
Bernard Duffy, 40th Regiment, aged twenty-four, was wounded on the 10th of April, and admitted into the Caserne de Calvete Hospital, on the 13th, with fracture and depression of the upper part of the os frontis. Some portions of detached bone were removed; he was largely bled and purged.
On the 14th, he complained of severe pain in the head, giddiness, dimness of sight, and drowsiness. The pupils were much dilated; pulse 60, and full. An incision was made down to the bone, and the divided arteries were allowed to bleed freely. One perforation was made by the trephine, and the whole of the detached and depressed pieces of bone, which were of considerable size, were removed, one of them having penetrated the dura mater.—15th. Has less pain in the head; pulse full and slow; pupils dilated, with a tendency to coma, but he is sensible when spoken to. V. S. ad ℥xxiv. Continue the purgatives.—18th. Is less drowsy; pupils more contracted. The surface of the dura mater is sloughy, and a small, dark-colored excrescence is rising up through the opening in the cranium.—22d. The fungus cerebri has considerably increased in size during the last few days; in other respects he is doing well.—24th.[354] The wound looks clean; the discharge is healthy. The fungus increases in size, and is rather above the edges of the wound; some sloughs have separated from it, and it has now a red and tolerably clean appearance.—26th. The wound granulates regularly; the excrescence seems to enlarge rather at the base than at the upper part; it was touched slightly with lunar caustic without any pain or unpleasant symptom being produced.—30th. Continues doing well. The pupils are still somewhat dilated, but contract readily on the admission of light; appetite good; bowels regular; and the patient says he has no complaint. Discharge from the wound healthy; the fungus is prevented from increasing by a slight application of the argenti nitras every second day. He has not required any medicine for some time past.—May 6th. The wound has closed around the fungus, which is a little above its edges; it is touched slightly every day with lunar caustic or the sulphate of copper. The pulsation of the brain elevating and depressing the fungus is perfectly distinct; no constitutional derangement. Was discharged cured to Bordeaux.
William Donaldson was admitted, on the 13th of April, 1814, into the Dépôt de Mendicité Hospital, having received a gunshot wound in the head on the 10th of April, which fractured the right parietal bone to a considerable extent. The brain protrudes; pulse quick and small; bowels open. V. S. ad ℥xvi.—14th. The pulsation of the brain is evident, and the protrusion increases; he complains of no particular pain; the discharge is profuse, and of a thin, black, watery quality; pulse 90; bowels freely open. V. S. ad ℥xvi. Continue the purgatives.—15th. The pulse and bowels natural, the protrusion has scarcely increased; discharge profuse, and still gleety; a small compress was laid over the dressings, and a bandage was lightly applied.—16th. Pulse and secretions natural; the wound looks more healthy; the discharge something better in appearance; the fungus does not increase.—19th. Is doing well, and does not complain of pain; functions natural; the protrusion somewhat less; discharge good. A small quantity of cloth has come away.—21st. Discharge improved. Continue the purgatives.—26th. The protrusion evidently diminishes, and begins to heal at the edges.—30th. The hernia cerebri has considerably diminished; secretions natural; a small quantity of bone has come away; discharge diminished.—May 4th. The wound is[355] healing rapidly; the patient is now permitted to get out of bed, and has half diet. Another very small piece of bone has come away.—10th. The wound is now nearly healed.—Between the 15th and the 25th several small pieces of bone came away.—On the 26th, on introducing the probe, a small piece of bone followed it; and on further examination a large piece was felt quite loose, and was removed by incision. Discharged cured to Bordeaux.
Gentle pressure was made on the protrusions, according to the feelings of the individuals, in both these cases; when made too firmly, it gave rise to swimmings and pain in the head, retardation of the pulse, a sense of sickness and fainting, and on one occasion to syncope. Pressure could only be borne when very lightly applied while the protrusion was increasing, but could be gradually augmented when it became stationary, and during its diminution and secession. The pressure was continued until after the wound had healed.
I had occasion, at Santander, to remove a portion of bone, including the upper part of the lambdoidal suture of the right side, from the head of a soldier of the Light Division, in consequence of symptoms of irritation having come on after an irregularity in drinking. He had been wounded by a musket-ball on the heights of Vera, which had fractured and depressed the skull at that part some weeks before. A piece of bone was depressed, and had irritated the dura mater at the part; the membrane had some matter upon its surface, and was evidently abraded. The operation gave relief, but a tumor soon sprang up, evidently composed of brain. The patient was again bled, purged, and starved; calomel and opium were given in moderate doses, and the protrusion ceased to increase; about the same time it changed color, became yellow, fetid, softer, and soon wasted away, pieces of dead matter separating at each dressing, until it sunk within the level of the skull; after which healthy granulations sprung up, and the wound healed.
In the fatal cases, paralysis, accompanied by stupor and other symptoms of compression of the brain, invariably supervened before death.
The preceding cases prove that persons may recover after having had a protrusion of the brain, without as well as with the loss of a portion of its substance, the difference in all probability between the cases being dependent on the de[356]gree of mischief which gave rise to them. In the fatal cases I have seen, the protrusion was manifestly a part of the substance of the brain, and firmer than the hemisphere beneath, which was soft, pulpy, and of a yellow and sometimes of a reddish color, the lateral ventricle being filled with a sero-purulent matter, pus being also spread over the surface and intermingled with the pulpy structure, into which the brain had been changed. The protrusion was the consequence of low inflammation of the brain; and greater caution had been necessary during the progress of the mischief than had been enforced. It was the observation of this, and of other circumstances not less important, which led me to enjoin that rigid system of management insisted upon in all cases of injury of the head. There can be no doubt that the formation of many of these protrusions was aided by the opening made in the dura mater, which would have restrained their growth if it had been sound. The dura mater therefore should never be opened if it can be avoided.
It has been proposed to destroy protrusions of the brain with escharotics, and by ligature; and more faith has sometimes been placed in the knife for their early removal than in the more deferred operations of nature. Greater reliance may, however, be placed on the efforts of nature, assisted by a methodical treatment of the low inflammatory state of the brain, and by such pressure at a later period as can be borne with comfort, and persisted in with propriety.
286. It has been supposed that abscess of the liver followed injuries of the head in a more peculiar manner than injuries of other parts of the body, an opinion upon which too much reliance should not be placed; for experience has induced me to think that unless the liver be really injured by a fall or blow, it only becomes affected in a secondary manner, in a similar way to the lungs or other viscera, or to the joints or other parts. The new disease in these cases is always insidious in its nature and progress, and for the most part fatal in its result, as has been explained at length, (Aph. 59, p. 62, et seq.)
287. When a person has received a serious blow on the head, which has given rise to an exfoliation of the bone, or to a very slight depression of the skull, he is rarely restored to his previous healthy and natural state. The scalp adheres firmly to the bone beneath, instead of sliding loosely over it, and a deep hollow is formed, which would imply[357] that greater mischief had been done and a greater loss of bone had been sustained than had actually occurred. This is the more remarkable when pieces of bone have been removed. Major D., of the Indian army, was wounded on the left side of the forehead, at its upper part, by a musket-ball, at the assault of Maheidpoor. Several pieces of bone were removed, and the pulsation of the brain was evident under the discharge. The point of a little finger passes into the hole left by the cicatrization of the wound, to a greater extent than might be expected. This officer suffers from headaches, augmented or brought on by any exertion of body or mind. He cannot bear exposure to the heat of the sun. He can scarcely drink three glasses of wine without feeling their effect. Persons so afflicted can bear no great exertion of any kind. They fall down under exposure to heat. They are easily inebriated, rendered furious by a small quantity of liquor, and often become stupefied, comatose, or even die suddenly. In addition to these evils, which may be avoided by care, many are subjected to fits, which are apparently epileptic; and others suffer from such intolerable pain in the part injured, as well as in the head generally, as to be desirous of seeking relief by an operation, even at the risk of life.
These injuries are often accompanied during their progress by mental defects which time does not always remove. The memory is very often much impaired; it is frequently defective as to things as well as to persons. The sight of one or of both eyes may be impaired, or even lost. Ptosis, or a falling of the upper lid, is not an uncommon although a more curable defect. Speech is not only difficult, but the power of uttering certain words is often lost; a language is occasionally for a time forgotten, and a sort of conventional one has even been adopted, under my own observation. The more serious evils which befall these unfortunate sufferers are aberrations of mind, rendering some degree of restraint necessary, or a state of fatuity, which is not less distressing. These intellectual defects are often accompanied by various states of lameness or debility, from which there is but little hope of recovery. Pathologists have supposed that concussion of the brain is frequently accompanied by, and may indeed be essentially dependent on, small extravasations of blood in various parts of or throughout the brain, not larger than the point or head of a small pin, constituting, in[358] fact, a derangement which, when general, is destructive of life, and, when partial, may sometimes be the cause of the various defects which follow injuries of the head.
288. It is an interesting fact that a person who has been shot in the head, or has fallen from the top of a house, so as to become insensible, has no knowledge of the circumstance; and when, after several days or weeks, he regains his senses, he has no recollection of the injury, or of having received the wound; or if he should have fallen from a height, he only remembers that he was aware he was about to fall, but of the actual descent, or of the injury, he knows nothing.
289. The trephine, which is worked by turning the hand, and makes therefore only a half turn, necessarily saws unequally; but the operator has the advantage of being able to press with it on any particular part as the sawing of the bone draws to a close, and can thus cut any portion of the bone which is thicker than the rest without wounding the dura mater. The division and yielding of the last layer of bone is very sensibly felt by the hand, and when sawing, the surgeon can use the trephine as a slight lever with great effect, by pressing on a particular part, or from side to side, and the inner layer of the vitreous table may be in this manner as much broken as sawn through. The piece to be removed should never be brought away in the crown of the trephine, but should be raised by the forceps and lever; whenever a rough edge of the inner table remains, it should be carefully rounded off with the lenticular or blunt-ended instrument commonly used for that purpose.
290. Whenever there has been a loss of the integuments or scalp, so that this part cannot be brought over the opening made by the removal of the bone, some fine soft cotton should be laid on the dura mater, so that a slight degree of support may be given to that membrane, more particularly when it is thought that it may not be necessary to examine it for two or three days. When circumstances appear to render a daily inspection necessary, the cut portions of the scalp should be brought over the opening, and retained by a slight compress and bandage kept constantly wet and cold. The dura mater usually changes color and becomes more red; a layer of lymph is seen adhering to it, from which granulations arise and spring up until they touch the scalp, to which they unite, or cicatrization takes place. When the[359] patient dies early from other causes, and the calvarium has been raised, the discolored spot on the dura mater marks the place from over which the bone was removed. I have seen this in a state of slough, and the only apparent discoverable mark of disease.
One of the improvements in modern surgery is to be found in the restriction which has gradually been placed on the repeated use of the trephine on the same person, and on the removal of large portions of the skull. Cases are not, however, wanting in the older authors which would appear to justify the proceeding, although it may perhaps be said that they only show how great an extent of injury may sometimes be committed with impunity.
Saviard trepanned one person twenty times. Russ Martel and Le Gendre, surgeons to the King of Navarre, say that in the year 1686 they took away nearly both parietal bones, and the patient recovered and lived for thirty years afterward, half his body, however, being paralyzed. Marechal applied the trephine twelve times successfully, Gooch thirteen times, Desportes twelve times. Saviard says that he had under his care a woman whose parietal bones, together with a great part of the occipital and frontal, separated at the end of two years after a blow; the bones thus separated resembled a calvarium sawn off a dead person. No fungus or hernia took place, and she lived for several years afterward.
Dr. Drummond, deputy inspector-general of hospitals, has published the case of a seaman belonging to H.M.S. “Mutine,” who in 1845 fell down some stone steps at Sierra Leone, receiving a contused wound on the scalp, for which he was admitted into the Royal Naval Hospital at Plymouth in October of the same year. The bone, which was not supposed to have been injured, was then found to be denuded of its pericranium to some extent, (left side of occipital.) After an attack of erysipelas, followed by numerous purulent deposits under the scalp, necrosis went on rapidly; there was oozing of pus from beneath the diseased bones, and gaping of the coronal and sagittal sutures, the brain pulsating very distinctly in the spaces. In July, 1846, he was removed to Melville Naval Hospital at Chatham. During the six years he has been under observation, there have been repeated attacks of erysipelas, followed by profuse suppuration. Both tables of the bones have suffered in[360] some places; in others only the external. About five square inches have been lost from the right side of the frontal, right parietal, and squamous part of the right temporal. The whole of the occipital to within a short space of the foramen magnum is deficient, with the exception of about two inches in the center of the bone, which are now undergoing the process of separation. On the left side, Dr. Drummond adds, there has been less destruction of the bones, but extensive caries was going on there, and fetid pus was being discharged from several openings at the date when the case was reported, (April, 1851.) At no point was there any tendency to reproduction of bone, or arrest of the disease.
291. The removal of a large portion of the skull may be necessary where the broken portions are deprived of their natural support and connections, but as little should be taken away as possible. When the loss of sense and motion is accompanied by fracture, and continues to increase rather than to diminish, after the necessary and usual means have been adopted for its relief, a piece of bone should be removed. If blood should be found in any quantity on the dura mater, it may be necessary to take away more bone to admit of its free discharge; for although the gradual pressure of the brain from within will tend to expel it, this object may not be attained in sufficient time, and the patient may be lost. The older surgeons in these cases were anxious to ascertain how far or to what extent the dura mater was separated from the skull, and they often removed large portions of bone accordingly; although their practice should not be implicitly followed, repeated observation has shown that modern surgeons have often fallen too much into the opposite extreme of doing nothing. When blood has been evacuated in this manner, the parts must pass from a state of inflammation into that of suppuration before the dura mater can again adhere to the superincumbent bone, and care must be taken that the matter shall have a free discharge. If symptoms of fever, followed by those of commencing compression, should supervene from the granulations arising from the dura mater filling up the opening and preventing its exit, they should be excised; or if the matter should have gravitated in a direction which does not admit of its being discharged, the opening in the skull should be increased so as to remove the impediment, and thereby lessen the danger.
[361] A layer of blood is often extravasated very thinly over the whole surface of the brain and cannot be removed, although it may be absorbed. It is, on the other hand, often collected in larger quantity on the basis of the cranium, whence it will not be absorbed and cannot be removed. It may be extravasated without reference to the part on which the blow has been received, giving rise in the end to symptoms of epilepsy or apoplexy, for the relief of which no surgical operation can avail; but when a blow has been undoubtedly received on a part of the skull, and any sign of mischief can be perceived on or in that part, the removal of the bone is permissible.
292. The wind of a cannon-ball has been supposed to exert some influence on the brain when passing close to the head; there is, however, no valid foundation for the opinion. An officer of the fifth division was struck by a cannon-shot, during the assault of Badajos, on the right side of the head and face. It carried away the right eye and the whole face, the left eye hanging in the orbit, the floor of which was destroyed. A part of the lower jaw remained on the left side, but a great part of the tongue was gone. He had lost a large quantity of blood, but was quite sensible. In the middle of the next day he suffered much from the want of water to moisten his throat, which could not be procured. After a distressing delay of three or four hours under a hot sun, a small quantity was obtained, the arrival of which he observed; and while I was giving directions relative to its distribution, I felt a gentle tap on my shoulder, and on turning round saw this unfortunate man standing behind me, a terrific object, holding out a small cup for water, not one drop of which he could swallow. Alone among strangers, he felt that every kindness in our power to offer was bestowed upon him, and he contrived to write his thanks with a pencil, which he gave me when he pressed my hand at parting at eleven at night. I was glad at sunrise to find he had just expired.
293. When a portion of bone is as it were sliced off with the scalp and adheres to it firmly, the scalp and bone should be reapplied; and the cure will often be effected without difficulty. When the portion of bone cut off and hanging to the scalp, which is turned down, has but little adherence, it should be removed.
A German dragoon was brought to me in front of Ma[362]drid, who had received a slicing cut of this kind on the top and side of the head, which caused a portion of the scalp and parietal bone to be turned down over the ear, uncovering the dura mater. Replaced and retained in its situation, the flap and bone appeared to adhere, and the man recovered. In the case of a Portuguese soldier cut down by the French cavalry in a sortie during the second investment of Badajos, a portion of bone cut off with a flap was quite loose, and was removed. The patient did equally well.
In the museum of the Royal College of Surgeons there are ten skulls which have suffered from very severe slicing cuts. They appear to have been collected from the burial-place of some establishment for invalid soldiers in Germany. The portions of bone thus sliced, and they are large pieces, were once detached, and afterward reunited a little out of their proper places, so that the points of separation and of union can be distinctly seen. These fissures are all in a certain state of progress toward being filled up by bone, and the patients must have lived some months, if not years, after the receipt of their respective injuries; for bone is deposited apparently with difficulty and most carefully in all such cases, so as not to irritate the membranes of the brain. The opening in the first instance is filled up by granulations, over which a thin skin is formed; this afterward becomes firmer and harder, being in some cases, where the trephine had been used, a thin but strong membranous expansion extending from one edge of bone to the other. In others it is thicker and more solid, and in a few instances osseous matter is deposited in its circumference, so as in part to fill up the opening, the edges of the bony circle made by the trephine becoming gradually thinner as they appear to grow inward. It is common for an exfoliation to take place in such cases from the edges of the cut bone, and from the circle made by the trephine. It has been occasionally observed, after death, that the circular cut edge of the bone does not become thin in the manner described, but that a sort of ridge forms around and within it.
When the scalp is torn down without being much bruised, and a large flap extending from the occiput to the forehead falls down on the shoulder, covered with blood or dirt, the flap should be cleansed and restored to its place. When it is large, two or three sutures may be necessary to keep it in its proper situation. The flap may not entirely adhere under[363] any management, but it will do so in parts; and care should be taken to evacuate at an early period any matter which may form by small but sufficient incisions made where required; this will in general be above and about the ear. When the flap is much bruised, the attempt at adhesion by close apposition will be useless until after suppuration has taken place, when a well-regulated pressure will do much toward expediting the cure.
294. Erysipelas occurs in two forms: when the skin has the ordinary redness characteristic of the complaint, and when the color of the skin is not altered or is whiter than natural, but puffed, tense, and shining, the inflammation being seated beneath the tendinous expansion of the occipito-frontalis muscle.
The general treatment should be regulated by the powers of the patient and the state of the constitution, (Aph. 24, page 39.) The local treatment of the first form essentially depends on puncturing the red and inflamed skin all over with the point of a lancet, assisting the flow of blood by warm fomentations. The punctures should be repeated, if necessary. The second form is to be treated by incisions, perhaps the greatest improvement of the surgery of the Peninsular war.
The scalp in such cases is in a state of general puffiness, causing the head to look considerably larger than usual, but without redness; it retains the impression of the finger. Incisions are to be made in the scalp from two to four or six inches in length, united by others, if necessary. The scalp will often be upward of an inch in thickness, and filled with a fluid partly serous, partly purulent. The small arteries bleed freely, and should be allowed to do so as long as may be desirable, when the hemorrhage should be arrested by pressure. The head should be fomented. The essential points are, to take off tension, and to allow the free discharge of any fluid which may be secreted. The moment the parts around a wound have become puffy, the surface of the wound changing from a red to a yellowish color, with a thin discharge instead of good pus, an incision should be made through them, and repeated, if necessary. It relieves the tension and the irritative fever, and prevents the delirium which would follow; which neither bleeding, purging, nor the other constitutional remedies which the state of fever may indicate will remove. If it should be neglected, sup[364]puration and sloughing will extend under the tendon of the occipito-frontalis, or the fascia of the temporal muscle, and the greatest danger will be incurred from this additional cause.
WOUNDS OF THE CHEST.
295. Wounds penetrating the wall of the chest, and implicating any part or portion of its cavity or contents, are among the most dangerous of injuries. They require in their treatment a more careful attention and a greater extent of knowledge than most others which befall mankind. The means which the improved methods of auscultation have afforded cause the progress of the symptoms which follow to be less obscure, and lead to a less doubtful practice than formerly; while they render a knowledge of this branch of medical science an essential part of the education of a surgeon.
296. Incised or punctured wounds, from swords, lances, bayonets, or knives, require a treatment essentially distinct on many points from that of gunshot wounds, especially in the commencement. On this early treatment so much depends, that details of the more serious or more important cases are rarely found among the records of injuries sustained on the field of battle, where so much is often to be done, and so few are to be found to do it.
The simplest of the more serious results from injuries not penetrating the chest is the occurrence of inflammation, either of its lining membrane, giving rise to what is called pleuritis, or of the substance of the lung, termed pneumonia, or of both, constituting what has been named pleuro-pneumonia; but many severe blows on the chest are not followed by such serious consequences.
On the 17th August, 1808, in the act of leaving the village of Colombeira to ascend the heights of Roliça, a soldier was shot in the leg: he jumped up three or four feet, and made a considerable outcry. A second was struck at the same time by a ball on the shoulder, which did not penetrate, but gave him great pain. A third received a ball on[365] his buff-leather belt, on the right breast. The noise made by these two blows was unmistakable. I saw this man fall, and supposed he was killed: the ball, however, had only gone through his belt, and made a mark on his chest, over the cartilage of the fourth rib, the hardness and elasticity of which had prevented further mischief. He recovered in a short time, spat a little blood in the night, and after a large bleeding was enabled to accompany me on the 20th to Vimiera, ready for the fight next morning.
A soldier was struck on the hill of Talavera,[4] on the breast-plate by a ball, which, as he believed, had gone through his body. He was as white as a sheet, and desperately frightened. On opening his coat, I found the ball had indented the breast-plate, and made a round, red mark on the skin, without going deeper. I did not see him again for several days, until after crossing the bridge of Arzobispo, on the retreat to Truxillo. He was then engaged in disemboweling a fine fat wild hog, among a herd of which we had, unluckily for them, just fallen. He recognized me at once; said that, as I told him, he had been more frightened than hurt; that he had been bled largely and well physicked, and after two or three days had thought no more of it. I am bound to add that, in gratitude, he offered me a leg of the pig, which, having nothing to eat, I could not but accept. It supplied a dinner for three others who are now no more.
[4] The Duke of Wellington received a blow from a spent ball at the same time, near the left clavicle.
A soldier of the 40th Regiment slipped from the ladder on which he was attempting to scale the wall near the great breach of Badajos, and fell on his cartridge-box, which hurt his left side so much as to render him unable to move for some time. On the 8th of April he was much worse. The part injured was painful to the touch; the difficulty of breathing considerable; cough hard, with little expectoration; pulse 90, skin hot, appetite gone, tongue white. V. S. ad ℥xvj, and aperients. 9th. Better; pain less; expectoration more in quantity, and viscid. V. S. ad ℥xii; antimonials. 10th. Pain still felt on coughing; expectoration reddish; difficulty of breathing greater. Pil. cal. et antim. c. opio; V. S. ad ℥xvj. He gradually recovered (his mouth having become slightly sore) from what was manifestly an attack of pneumonia.[366] A gentleman, in 1835, fell from his shooting-pony on his powder-horn, which bruised his right side from the seventh to the last rib, and, as he said, knocked the breath out of his body, and hurt him so much as to render him incapable of walking from one room to another from pain in the side, back, and thigh. No bones were broken. The pain, on the second day, was augmented on breathing and on attempting to cough. The third day he was purged, and blooded to sixteen ounces, which gave some relief; but as the symptoms increased on the fourth day, he was more carefully examined. His right side could not bear pressure. The respiratory murmur was distinct, but accompanied by a crepitating rhonchus under the part injured. Cough troublesome; expectoration mucous, viscid, and of a reddish tinge. Antim. p. tart. and sulphas magnesiæ, every four hours. V. S. ad ℥xiv. On the fifth day, the symptoms being little altered, he was cupped on the part affected to fourteen ounces. On the sixth, the pain was only felt on coughing, or on drawing a very full breath; expectoration redder and thicker; pulse quicker. The rhonchus was quite as distinct. V. S. ad ℥xij, and the medicines to be continued. After this he quickly recovered and the natural respiration became distinct.
Lieutenant Cooke Tylden Patterson, of the Light Division, was struck on the left breast by a musket-ball, on the morning of the 15th of July, 1813, in front of the village of Vera, in the Pyrenees. He fell on his back breathless, as if he were killed. While waiting the order to advance, he had been reading Gil Blas in Spanish, and on receiving it, had hastily put the book in the breast pocket of his coat. The ball had struck this, but, unable to penetrate it, had fallen on the ground at his feet, completely flattened on one side, and marked with the impression of the braid of his coat. A piece of the cover of the book, about the size of a half-crown, was driven in, and the leaves throughout were indented by the ball. It was some days before the effects of the blow entirely subsided.
A soldier of the 97th Regiment was struck at the unsuccessful assault of Fort Christoval, opposite Badajos, by a musket-ball, which went through his brass breast-plate and coat, drove his shirt through the skin, and against the sternum, which it was not able to penetrate. He fell, and was supposed to be killed, but he soon recovered and ran to[367] the rear. The ball was found flattened between his shirt and coat. The part of the chest was very black next day, the spot struck by the ball being much bruised. It was necessary to bleed him largely. When the integuments are painful, although merely bruised, the diluted tincture of arnica is a useful application, and Scheele’s hydrocyanic acid, six drops to an ounce of water, is said to be efficacious.
Major Lightfoot was struck by a musket-ball on the left breast; it went through his clothes, the integuments and the outer part of the great pectoral muscle, and slanted inward for three inches toward the sternum, to which distance its track could be followed. It was evident that the ball had neither lodged nor penetrated, for no serious symptoms ensued. In all probability it had been ejected the way it went in by the elasticity of the cartilages of the ribs near the sternum.
297. In order to understand, or to become in any way acquainted with the changes from the natural structure which are going on under derangement in the chest, even from simple injuries, it is always necessary to have recourse to auscultation, and sometimes, although more rarely, to percussion, if the external parts are not too tender. Under all circumstances both sides of the chest should be examined by the stethoscope. As the ordinary breathing of an individual is rarely sufficiently strong to enable the auscultator to hear it with distinctness, the patient should be desired to inspire fully and more quickly than usual, without much effort, and without noise from the mouth or nose, or retaining his breath. The inspiration and the expiration are both to be carefully observed.
When the ear is firmly and equably applied to the chest of a healthy young person, a very distinct and long-continued sound is heard at the moment of inspiration, and another at that of expiration. This is called the vesicular or respiratory murmur, and is dependent on the air fully permeating and distending the air-vesicles of the lungs. It has been poetically compared to the sound of a gentle gale rustling in a thick summer foliage—to the whisper of a retiring wave on a sandy beach in a calm day. It is soft, scarcely sonorous, equable, and during inspiration continuous. In childhood it is louder than in adult persons, arising probably from the greater activity of the lungs in young than in elderly people. This is called, and especially when perceptible in[368] adults, puerile respiration, as opposed to their ordinary, or what in old persons may be called senile. It is more marked during inspiration.
When the stethoscope is applied in the situation of the great bronchial passages, as over the first bone of the sternum, under the clavicle, in the center of or between the shoulder-blades, a different sound is usually but not always distinguishable, when the patient breathes fully, arising from the passage of the air through these bronchial tubes. It is compared to the noise made on blowing through a reed or quill, and is called bronchial or tubular respiration. When heard in other parts of the chest, it is a morbid sound. If the stethoscope be applied over the trachea, the sound is louder, rougher, and more intense, and is called tracheal respiration. On listening over the trachea during speaking, the voice sounds as if it were passing into the ear, and the words are distinct—tracheophony. This, if heard in any other part of the chest, is a sign of disease, for in the natural state the voice is heard only to resound through the chest, but the words are not heard if the other ear be stopped. When heard, the sound has been called pectoriloquy, and is supposed to imply the existence of a cavity at that part; but the word is unnecessary, or, if used, it means that the cavern or hollow communicating directly with the trachea gives forth a similar or nearly similar sound, a natural sound in an unnatural position. The essential difference between bronchophony and tracheophony in the investigation of disease is, that in the latter the voice apparently speaks through the stethoscope into the ear of the auscultator, while in the former it is heard with scarcely less distinctness, but at the distal end of the instrument. Over the larynx it is louder, hoarser, and rougher.
The length of the sound in inspiration, as compared with that of expiration, has been said to be as five to two. One is louder and longer than the other, a difference requiring attention from the circumstance that morbid sounds of great import are heard in inspiration, which do not prevail during expiration. When any other difference is perceptible between them, so that they more nearly resemble each other in duration or in intensity, or when expiration is prolonged, some structural alteration may be suspected in old persons, some disease in young ones. When little or no respiratory murmur can be heard after symptoms of inflammation have existed for some time, the case is very serious, implying that[369] effusion into the cavity, or condensation of the lung, has taken place to a considerable extent.
298. The number of inspirations in a minute in the adult and elderly persons varies from eighteen to twenty-two in a state of health: from twenty-two to twenty-six in children. The stroke of the pulse is generally as four to one. If the inspirations are eighteen, the pulse will in general be seventy-two. Both may be slower, although they are often quicker under disease. When the breathing is slower, it commonly indicates some affection of the nervous system; when very rapid, some important lesion within the chest.
The theory of percussion is founded upon three elementary sounds, which are produced when a solid, a liquid, or a gaseous body is struck; all others are varieties of these. The sensation of resistance which is experienced at the same time bears an exact relation to the density of these bodies—hence the resistance when a solid substance is struck is greater than when a gaseous one is under percussion. The liver, the thorax in a case of pleuritic effusion, and the distended stomach after a long fast, afford good examples of these elementary sounds. To employ percussion successfully, it is necessary that the strokes be uniform in force and quickness, and that the finger or pleximeter be so applied to the surface that no space exists between them, otherwise such a sound will be elicited as may give rise to an incorrect diagnosis.
It having been stated that a sound lung never fills the bag of the pleura, particularly toward the diaphragm, at least during ordinary respiration, I requested Mr. Quekett, the Resident Conservator of the College of Surgeons, to ascertain this by experiments on some sheep at the moment of their being killed; and it appeared from them that the base of the lung is always in contact with the surface of the diaphragm.
299. In ordinary expiration the chest diminishes in size. The ribs which have been raised recede, by the elasticity of their cartilages, and by the return of the ligaments, to their state of rest; the elevated muscles become relaxed, while others belonging to the lower part of the trunk and abdomen contract. The diaphragm is relaxed, and pushed upward by the viscera of the abdomen, pressed upon by the muscles of its wall, if it should not be drawn upward by the attraction of the lung, which when distended endeavors by its elas[370]ticity to return upon itself, and to occupy less space than the capacity of the chest will afford. The lung, invested by an elastic, special, and transparent membrane, and covered by the pleura pulmonalis, is composed of an immense number of air vesicles, the largest being equal in size to the fourth part of a millet-seed. These air vesicles, crowded together, each communicating with a fine bronchial tubule, are separated from each other into groups by a condensed cellular tissue, thicker where it surrounds these lobules, which alternately form, when aggregated together, a lobe, whence it is called interlobular tissue. An artery and vein form a very minute net-work around each vesicle. These vesicles may become filled with water; when dilated by air, they constitute what is called emphysema of the lung. The lung in man is constantly applied to the internal surface of the chest, the pleura or serous membrane covering the lung being closely applied to the pleura lining the wall, and one surface glides upon the other, moistened by a secretion in just sufficient quantity to effect this object. If the lower intercostal muscles of a young animal be removed to a sufficient extent, the lung and the diaphragm may be seen applied to the inside of the pleura lining the rib, and ascending and descending in concert, the lungs moving vertically, not horizontally. The diaphragm ascending, covered by its pleura, is in a similar manner applied to the lower part of the wall of the chest, which had been filled by the lung during inspiration. After death the lung remains closely applied to the pleura, recedes on an opening being made into that membrane, and may collapse, provided no adhesions exist to prevent it.
300. When inflammation of the pleura takes place, the gliding motion is not effected silently, but with a peculiar noise, called by the French frottement. When the lung is inflamed, the respiratory murmur is changed in that part, or is overcome by a peculiar sound, which can be distinctly investigated by the ear—rhonchus crepitans. Hence the great value of auscultation.
In the following observations it is not intended to give a history of, or even the whole of the symptoms and consequences of inflammation of the pleura and the lungs; but only to draw attention to such of the principal facts as it may be necessary to consider when these inflammations and their consequences are caused by external injuries.
Acute idiopathic inflammation of the pleura usually com[371]mences by rigors, preceded perhaps by some signs of general uneasiness, which soon become those of great febrile excitement. Pain is early felt in the side in the course of the sixth, seventh, and eighth ribs, or at the point corresponding generally to the seat of the inflammation. It is usually sharp and darting, is called a stitch, occupies rather a small space, (the point de côté of the French,) and is always increased by drawing a full breath or by coughing. The breathing is short, from the disinclination to fill the chest, by which the pain would be increased; it is hurried, and sometimes takes place as if by jerks, from the necessity for its repetition, in consequence of the smallness of the quantity of air admitted at each attempt. When the attack is very severe the patient tries to breathe with the healthy side only, the lower ribs of the affected side being moved but slightly, and with evident caution. If the inflammation have been caused by extreme violence, pain will also be felt, particularly at the part injured.
When inflammation has affected the pleura covering the diaphragm, especially when caused by external violence, the pain will be felt lower down, so as to lead to the suspicion that it is also abdominal. When jaundice supervenes, it occurs from the extension of disease through the substance of the diaphragm, as is occasionally seen in wounds implicating the chest, the diaphragm, and the liver.
A cough is not a constant accompaniment of the first stage of disease; when present, it is usually dry, slight, infrequent, and does not attract attention, unless accompanied by a thin, frothy mucous expectoration, indicating the presence of bronchitis; of pneumonia, if reddish. The patient usually lies on his back while the pain is severe, and has a great indisposition to turn fully on to the affected side. At a later period, when effusion has taken place, the pain usually subsides, and he turns on the side affected to relieve the difficulty of breathing, caused by the pressure of the fluid on the sound lung through the bulging of the mediastinum; but the manner of lying, or decubitus, is of little importance, and should be subservient to the feelings of the patient, who is sometimes comfortable only when raised to nearly an erect position.
When the complaint is not subdued at an early period, an effusion of serous fluid, more or less in quantity, takes place. The whole cavity of the side affected has been known to be filled in from twenty-four to forty-eight hours, giving rise to[372] symptoms dependent on the degree to which the effusion has taken place; this is the evil which in injuries penetrating the cavity of the chest is most to be feared. When the external wound has been closed, or is so partially closed as not to allow the escape of the effused fluid, it is commonly the immediate cause of the death of the patient. Its secretion and early evacuation are therefore the most important points to be attended to in wounds of the chest.
The respiratory murmur becomes less distinct as soon as the pain prevents the ordinary distention of the affected side of the chest, and diminishes the quantity of air which usually penetrates the lung in any given time. As soon as a thin layer of fluid commences to be thrown out between the pleuræ, this murmur becomes fainter, and when it is complete, it ceases. If the patient can bear percussion, the side affected yields a dull, dead sound instead of the ordinary clear, sonorous one of health. The position of the patient when erect, by causing the fluid to descend, may allow of the respiratory murmur being heard at the upper part of the chest; and it may be perceived in front, but not behind, when he lies on his back, until the cavity is filled, when the sound altogether ceases. At the spot in the back corresponding to the root of the lung, or at any other point at which a previously formed adhesion may retain the lung against the wall of the chest, some respiratory murmur may yet be distinguished, until this part of the lung shall also have yielded to the general compression, so as to be temporarily impervious, or have become solidified under the continuance and extension of disease. While this is taking place in the affected side, the other lung is called upon to make up the work of aerification of the blood; it labors harder, its functions become more energetic, and that side of the chest is more distended; the respirations become quicker, fuller, and louder, and the vesicular murmur is said to resemble that of a child—in fact, to be puerile.
When the lung begins to be compressed by the circumambient fluid and the respiratory murmur ceases, a peculiar modification of the respiration through the large bronchial tubes may be heard, constituting bronchial respiration. It occurs in pneumonia, in pulmonary apoplexy, and in tubercular disease when the lung is solidified. When the voice is heard through the stethoscope in these complaints, the peculiar sound emitted is called bronchophony.
[373] In pleuritic effusion, the voice, when carefully examined, sometimes obtains a character not previously noticed, but of comparatively little importance, called œgophony, a sound which may be easily confounded with bronchophony, of the latter of which it is a modification more often alluded to than observed. Laennec says: “Simple œgophony consists in a peculiar resonance of the voice, which accompanies or follows the articulation of words. It appears to be sharper than natural, more acute and somewhat silvery, vibrating, as it were, on the surface of the lung more as an echo of the voice than as the voice itself. It rarely enters the tube of the stethoscope, less frequently traverses it completely. It has besides another peculiar character, which is constant, and from which I have taken its name. It is a trembling, bleating, or shaking sound, like that of a goat, the tone of which animal it greatly resembles. When it occurs near a large bronchial tube, as in the root of the lungs, a more or less marked bronchophony is often superadded.” This sound may pervade the whole side; it is usually, however, most distinct near the inferior angle of the scapula, the patient being erect. It only exists where the effused fluid is small in quantity, and is never a dangerous symptom; its return, after it has been present and has disappeared, is a sign that a part of the effused fluid has been removed. It is a sign principally of value in distinguishing between pleuritis and pleuro-pneumonia and pure pneumonia, in which latter disease it is not heard, as in that complaint fluid is not thrown out into the cavity of the pleura.
301. In pneumonia or inflammation of the substance of the lung, as distinct from any implication of the pleura, which, however, most frequently obtains after blows on, and in cases of penetrating wounds of, the chest, the symptoms differ. The ordinary febrile symptoms are similar to those of pleurisy, only more intense; they usually precede for a day or two the local symptoms of difficult respiration, pain, and cough. The dyspnœa varies in different people. In some it is only a slight embarrassment of breathing, admitting of partial removal by accelerating the number of the respirations, which are augmented from twenty to thirty, forty, and upwards, and in children to sixty and seventy, marking a great degree of distress and of extent of inflammation, from which, when they are so frequent, persons rarely recover. The patient can scarcely speak or lie down,[374] and is obliged to be supported in that which he finds to be the least uneasy position. Pain is not always present; it is even said to be more frequently absent when the substance of the lung is affected, and not the pleura. That pain is not a necessary concomitant of pneumonia, is admitted, but that it is usually present, and with great intensity in many cases, cannot be doubted. When present, it is usually an early symptom, deep seated below the sternum, under the breast, extending to the scapula. When in the sides it is more acute and fixed, and is probably conjoined with the pain of pleurisy.
The pulse is quick and sharp, occasionally full and hard, at the commencement of this complaint in young and healthy persons, although it is sometimes small and weak from the beginning, where there is little general power; but this rarely occurs in cases of injury, and is not to be relied upon in opposition to other symptoms.
The cough is usually dry in the commencement of idiopathic pneumonia, rarely recurring by paroxysms, and is without any particular indication; it is soon, however, accompanied with a slight mucous expectoration, which, after some twenty-four or forty-eight hours, begins to assume certain and peculiar characters of the utmost importance as indicating the existence and the different stages of the disease. On the second or third day the expectoration becomes bloody. Each sputum, spit, or crachat of the French is composed of mucus intimately combined with blood—that is, not simple streaks or striæ of blood, as in catarrh; nor is it pure blood, as in hemoptysis. Each sputum is either of a yellow, or rusty, or even red color, according to the quantity of blood intimately mixed with the mucus. These sputa are at the same time tenacious and viscous, adhering so intimately together as to form a homogeneous transparent whole, readily gliding, however, from the basin in which they are held on sufficient inclination being given to it. At this period or stage of the disease, the sputa adhere strongly to each other, but the mass is not sufficiently viscid to stick to the sides of the vessel. When no further change takes place in the sputa the inflammation rarely passes beyond the first stage of obstruction or engorgement, or swelling. When they attain to a more viscous state, and adhere to the inside of the vessel in which they have been received, the progress of the inflammation to the second stage, or that of hepatiza[375]tion, may be feared. In almost every case where the viscidity of the expectorated matter increases, respiration becomes dull or bronchial, percussion of the chest yields a duller sound than before, and the inflammation has attained its highest degree. The expectoration, after being some time stationary, changes its character. If the complaint is to terminate by resolution, or by death, or to pass into a chronic state, the redness and viscidity gradually diminish, and at last disappear. If the rust color and the viscidity should return, there has been a relapse, which the reappearance of the other symptoms will show. When the inflammation is of the most serious nature, and about to terminate fatally, the expectoration diminishes, and at last ceases. In some cases it only diminishes because it cannot be discharged; it accumulates in the trachea, in the larynx, and in the bronchi, until the patient is destroyed. In some rare cases the matter secreted is spit up nearly to the last, and in others, still more rare, the approach of death in the last stage is characterized by a brown expectoration which cannot be mistaken for either of the others which preceded it. If the pneumonia pass into the chronic state, the expectoration becomes yellowish, or somewhat greenish, and at last is purely catarrhal.
Delirium is not an uncommon symptom when the inflammation of the lung is intense in persons of powerful constitutions, particularly during the exacerbation of fever in the night. It yields with the other symptoms when relief is obtained. When, however, it comes on at a later period of the complaint, or when the accompanying fever is not purely inflammatory, or in persons weakened by exhaustion and privation, it is usually a fatal symptom if continued. When mild, it often occurs after repeated and efficient bleedings, which have subdued, but not entirely removed the disease; and yields to opiates and gentle stimulants, by which the pain is removed, although it sometimes remains in a milder degree than before.
The ear discovers, soon after the commencement of the disease, that the natural murmur cannot be distinctly heard, it having been at first partly obscured, and after a time entirely superseded by a peculiar noise, called a crepitating or crepitous rattle or rhonchus. In its purest state it has been likened to the sound of a lock of hair rubbed close to the ear, or to that made by rumpling a fine piece of parch[376]ment; or again, to that which is produced by what under ordinary circumstances is called the crepitation of salt, when scattered in small quantities on red-hot coals. This crepitating rhonchus is heard at first in a small part of the lung, generally at the lower rather than at the upper part; it marks the first stage of the disease. It is not of long continuance; the vesicular murmur is either restored, or the crepitating rhonchus ceases to be heard, in consequence of the second stage to this, or that of hepatization, having commenced; the small air-vesicles are no longer pervious; the sound of the breathing, which is now heard, is that of the air more forcibly driven into the larger bronchial tubes causing bronchial respiration, which is no longer a vesicular or crepitating, but a whiffing sound, like that caused by blowing forcibly through a quill, or as if little gusts of air were blown in or blown out. The voice betrays to the ear of the auscultator another sign; it descends into the pervious bronchi, and being conveyed to the ear through the solid lung, gives rise to that peculiarity of voice called bronchophony, a correct knowledge of which can only be acquired by repeated observation.
When the inflammation of the lung is confined to a small and deeply-seated spot, auscultation may not at first reveal the evil; or it may possibly be overlooked, through the sound part of the lung becoming more active, and giving forth in consequence a stronger and more puerile breathing, which may mislead the listener.
When the vesicular murmur cannot be heard, when the rhonchus or crepitating râle or sound is not present, and bronchial respiration and bronchophony only can be distinguished, the case is one of great anxiety and danger. The second stage of hepatization is passing into the third, or purulent infiltration, of which auscultation shows no further signs, although the matter secreted may be expectorated, in proof of what has taken place. Pus is thus formed, which it is steadily maintained by some pathologists is not deposited in the form of abscess, but is infiltrated throughout the parenchymatous substance of the lung, finding its way into larger bronchial tubes, or being poured out from some parts of their secreting surface; the accuracy of this statement, however, as a rule, may be doubted, from some dissections having proved the reverse.
302. The effects of inflammation of the pleura are well[377] marked; the first is to diminish, if not to annul, the secretion of the exhalation, or halitus, by which it is lubricated; so that its surfaces can no longer glide without noise upon each other. The patient is often made aware of the difference by some uneasy internal sensation; the auscultator, by a rubbing or creaking sound emitted as the inflamed pleuræ, no longer smooth and polished, rub against each other, and become covered by a thick, effused matter, although not actually separated by a liquid. It is a sound which cannot exist after separation has taken place by the intervention of a fluid, or after adhesions have formed; it is, therefore, an early and transitory sign, is frequently interrupted, and returns, as if by jerks, three or four times repeated in succession. The pleura when inspected, after being attacked by inflammation, shows at first but little sign of derangement on its serous surface. It quickly, however, exhibits numberless small vessels, carrying red blood, which are principally seated in the sub-serous cellular tissue, reddening the membrane more deeply in one part than another. These soon begin to take on a new action, leading to the deposition of coagulable lymph or fibrin, which adheres to the inflamed surfaces. These deposits soon assume the determinate form of very thin layers, constituting what are called false membranes; while a serous or sero-purulent effusion takes place, even to filling the cavity of the chest, and which may or may not be ultimately absorbed. When coagulable lymph is first deposited, and about to form a false membrane, it is soft, of a grayish-white color, and does not possess any appearances of organization. Red points are, after a time, perceived in it, which soon become red lines or streaks, on the surface. This organization of the lymph does not depend on the period which has elapsed from the commencement of the complaint. It is seen in the first day of the disease in some cases; it is altogether absent in others, and depends much on the state and habit of the patient. The lymph is sometimes deposited in small drops or spots; in others, in patches of a greater or less size, varying according to the extent of the inflammation which has produced them. When a false membrane is once fully formed, it becomes itself a secreting surface, and may go on augmenting its thickness to so great a degree as materially to diminish the cavity of the chest. I have seen the pleura with a solid deposit of this kind much more than an inch in thickness. In general,[378] it is found in distinct layers, superimposed one upon the other. Whatever may be their thickness, they commonly admit of being separated from each other. The false membranes thus formed, resembling areolar tissue in their properties, may ultimately become cartilaginous, and even bony. When simple adhesions form between the pleuræ, they become lengthened with time; and, although they impede the motion of the lung at first, and may give rise to some uneasy sensations, they gradually become elongated, and give no further inconvenience. The fluid thrown out is serous; is often mingled with flocculi or lymph, which are seen floating in it; it is therefore more or less turbid, resembling whey. It is often nearly colorless and transparent; when the consequence of injury, it is often tinged with blood, forced out from the capillary vessels of the pleura, or of the false membrane, if not caused by the deposition of the fluid coagulated in the first instance after the receipt of the injury.
The quantity of fluid thus thrown out varies from an ounce to several pints; it gravitates according to the position of the patient, unless, when from old adhesions between the pleuræ, it is confined to particular parts. When the cavity of the pleuræ is free, and the fluid is in quantity, it compresses the lung, and diminishes its size by pressing or squeezing the air out of it; it is thus pressed toward the vertebral column, and so greatly diminished in size and augmented in density as to be useless for the purposes of respiration. While the lung is undergoing this compression to its utmost, the mediastinum also yields, and bulges into the opposite side of the chest, carrying the heart more or less with it; so that when the left side of the thorax is thus affected, the heart is seen and heard to beat on the right. The diaphragm now yields in turn, more on the left than on the right side, from the obstacle to its descent afforded by the liver. The intercostal muscles and ribs resist the internal pressure for a considerable length of time, even for weeks; they at last, however, yield; the ribs may even turn a little outward, while the interspaces in thin persons are said to fill out, so as to render that side of the chest nearly smooth, the size of that side, when measured, being larger than the other, in some instances even by two inches, but this rarely occurs unless the fluid within is purulent, and the disease of long standing.
303. After a time, and particularly in wounds of the[379] chest, the effused fluid becomes purulent, the lung, compressed to a small, flattened surface, adheres to the spine by what was its root, if no adventitious attachments have retained it in a different position; and the pleura has become a thick, yellowish-white, irregular, honey-combed sort of covering for it, as well as completely lining the chest. The serous as well as the purulent effusion are both free from any unpleasant odor; unless a kind of gangrene has taken place, when the latter becomes very offensive, and of a greenish-black color, as well as the substance of the false membranes extending to and sometimes beneath the pleura covering the condensed lung, into which openings have even thus been made.
In some cases the surface of the pleura is covered with small tubercles, some as large as a filbert; in others it appears to have a reticular or honey-combed appearance; and in particular cases, large irregularities or excavations may be observed in it when much thickened, being evidently spots of ulceration, which, if they had proceeded, would have ended by allowing passage to the matter outward, until it formed an external abscess, implicating in all probability one or more of the ribs; thus giving rise to an exfoliation which, by being separated internally, might in time be the cause of further mischief, if not previously covered by a thin layer of false membrane. When chronic pleurisy succeeds to a more acute attack, or they alternate with each other, particularly after penetrating wounds of the chest, several layers seem to be laid down one upon the other. This deposit is never so thick upon the pleura pulmonalis; nevertheless it is thick enough in most instances to prevent the lung from again dilating, the substance of it being generally quite permeable to, although so compressed as to be deprived of, air. It is then flattened, drawn upward toward its root against the mediastinum and spinal column, unless by some previous adhesion such a course has been prevented, and it adheres, as it has been often known to do, to the side of the chest. As that adhesion may occur in more than one spot, so may the effusions or deposits take place between them, constituting circumscribed sacs, and rendering the case more complicated.
304. The changes which take place in the structure of the lung in pneumonia are three in number: 1. Engorge[380]ment. 2. Hepatization. 3. Purulent infiltration. The formation of an abscess or vomica, and the occurrence of gangrene, may be omitted, as well as of chronic disorders, in the views about to be taken of the disease from injury.
In the first stage of inflammatory obstruction, or that of engorgement, the lung has assumed externally a livid-red or violet color. It is heavier and firmer than in its healthy state, and the natural feeling of crepitation, although greatly diminished, is not extinct. The lung retains the impression of the finger, and pits on pressure as if it contained a liquid, although air-bubbles can yet be distinguished in it, and its cellular or spongy texture is still to be observed. On cutting into it, a quantity of sanguineous or turbid fluid flows from it, mingled with numerous minute air-bubbles. In some places the color of the incised surface is darker and more compact, showing that some progress has been made toward the stage of hepatization. It nevertheless tears with greater facility than in a healthy state.
In the second stage, or that of the red softening of Andral, the hepatization of Laennec—the latter term being in most common use, from the lung assuming somewhat the appearance of liver in solidity and weight—the lung does not crepitate, no air-bubbles pass out of it, but a thick, bloody fluid exudes on pressure, and it sinks for the most part in water. The color is somewhat less red or violet than in the first stage, and lighter and more varied in color when cut into. The openings of the larger vessels and of the bronchi, when cut across, are observed as white specs; the interlobular tissue is thicker and more marked in lines running in different directions; while many little granular points can be discovered, especially with a glass, apparently of a more solid material than the surrounding parts.
The word solidity, or solidification, is sufficiently explanatory in contradistinction to the naturally pervious and crepitating state of the lung. Andral believed that hepatization arises from an excessive congestion of blood, and not from any deposition of lymph. It is not easy, however, to understand, in the present state of our knowledge, how acute inflammation can go on for three or more days without secretion and deposition being added to congestion. That hepatization, or impermeability to air, may take place in the typhoid pneumonia in twenty-four hours, and that it as suddenly seems to be removed, is hardly conclusive, as it[381] shows merely that a thoroughly well-loaded lung ceases to be permeable to air until a part of the load shall have been displaced.
When the lung, inflamed to the second stage, or that of hepatization, is about to be restored to a state of health, a slight crepitation or crackling begins again to be heard at the end of each inspiration; and as this increases, (the rhonchus crepitans redux of Laennec,) the bronchial respiration and voice gradually, or after a time, diminish, until they entirely disappear; while a mucous râle or rattle commences, the index of that free expectoration by which pneumonia usually terminates.
In the third stage of morbid change, or that of purulent infiltration, the lung is of a lighter color, from the intermixture of a new matter in its substance, although in the first degree it preserves its firmness and granular structure. The new secretion is of an opaque, straw or yellow color, and puriform in its nature. This is discoverable more particularly in spots; but as the disease proceeds, it pervades the whole substance of the lung, which becomes softer and more moist, and is easily broken down by the fingers, the granular structure having disappeared. It is more or less a purulent sort of sponge, in which all of the lung that can be perceived under a strong light may be resolved into small blood-vessels, bronchial tubes, and interlobular septa.
These three degrees or stages of inflammation may be met with in the same lung, for the most part gradually intermingling one with the other. The lower part of the lung being ordinarily first affected, is usually the seat of the purulent infiltration of the third stage; while in the tubercular affection, which ends in phthisis, the disease commonly begins in the upper part.
Resolution or recovery from even this, the last of the morbid changes which have been observed, may take place, although it is less likely to do so after idiopathic than traumatic inflammation, in which the lung was previously healthy, and the constitution unimpaired.[382]
GENERAL BLOOD-LETTING, ETC.
305. The first and most essential remedy in the treatment of pleuritis and pneumonia from injury is bleeding, which should be resorted to in every case, whenever the febrile excitement is really inflammatory. All old people, under such circumstances, unless in a cachectic state, bear at least one bleeding well; they often bear more; and no fact is more important, in opposition to the opinions commonly entertained on this subject. In young people, who have not been reduced in health and strength by privations and hard service, the bleeding should be repeated until the desired object has been effected; the quantity required to be drawn in inflammation, particularly after injuries, is often very great. It may almost become a question, in some cases, whether a patient shall be allowed to die of the disease, or from loss of blood; for convalescence is rapid in proportion as the inflammation is of small extent, and has been early subdued. As the first stage of pneumonia only lasts from twelve hours to three days before it passes into the second, and the second from one day to three before matter begins to be deposited, no time should be lost to prevent these evils taking place, if the patient is to be saved, without incurring a risk, from which few escape with health, even if life be ultimately preserved. Bleeding in inflammation of the pleura, in young and healthy persons, should therefore be effected with an unsparing hand, until an impression has been made on the system—until the pain and the difficulty of breathing have been removed—until the patient can draw a full breath, or faints; and the operation should be repeated, from time to time, every three or four hours, according to the intensity of the recurrence, or the persistence of the essential symptoms. The pulse does not often indicate the extent or severity of the inflammation, although it often expresses the amount of the constitutional irritability of the person. It is sometimes exceedingly illusory as a guide, and is never to be depended upon in the earlier stages of[383] disease, when accompanied by pain and great oppression of breathing. Whenever the pulsations of the heart are proportionally much stronger than those of the arteries, we may bleed without fear, and with the certainty of finding the pulse rise; but if the heart and pulse are both weak, the abstraction of blood will almost always occasion complete prostration of strength, and may be fatal.
306. When many years ago in charge of a regiment of infantry, on the top of the Berry Head, the outermost point of Torbay, the men thus greatly exposed were attacked by pneumonia. According to the practice taught in London, I bled my patients three and four times in the first forty-eight hours. I first drew sixteen ounces, then fourteen, then twelve, then abstracted, as the complaint continued, eight ounces; gave tartar emetic, so as to keep up nausea; then calomel, antimony, and opium, and lost my patients. I examined the bodies of all, and found that they had lived to what is now called the third stage of pneumonia, combined in almost all with pleuritis, with effusion, and the formation of false membranes. The disease was essentially a pleuro-pneumonia, varying in different degrees, as the pleura or the lungs were principally affected; and I saw with regret that the disease had not in any way been arrested; that the means employed had been insufficient. What was to be done? My sixteen ounces of blood were increased to thirty, but it would not do. It was evident that, to succeed, no limit should be placed to the abstraction of blood in the first instance, but the decided incapability of bearing its further loss. Every man was therefore bled, when he came into the hospital, until he fainted, and the bleeding was repeated every four hours, or even oftener, as long as pain or difficulty of breathing remained; under this improved practice all recovered.
The lesson learned at Berry Head was not forgotten during the five subsequent years passed in British North America. The men were as healthy, the winds were sharper and colder, the vicissitudes of all kinds greater. Rum was cheaper, newer, and stronger than the gin of Torbay. The local inflammations were often as severe, whether of the pleura or of the lungs, and by no means less so of the bowels. A grenadier, some six feet three inches high, broad, and well framed in proportion, had drank a gallon of rum during the afternoon, and very narrowly escaped, even with the loss of[384] nearly as much of his blood, abstracted in a few hours. His first bleeding was into the washhand-basin, until he fainted, lying on his back, and the bleedings were repeated as soon as he began to feel pain, and whenever he felt a return of the pain he used to put his arm out of bed to have the vein reopened, for Jack Martin was a very gallant fellow. This is given as an extreme case, to be borne in mind under circumstances somewhat similar, particularly after injuries. In common cases of well-marked pleuritis from injury in strong and healthy persons, it is now not unusual to abstract blood by those who rely on its efficiency, until the pain and difficulty of breathing are relieved, or fainting is about to take place. The patient should be raised in bed, the opening in the vein should be large, the flow of blood free. The quantity will vary from sixteen ounces to three times that amount in different people; but the important point is to repeat it as soon as the pain or difficulty in breathing returns. It rarely happens that one bleeding, to whatever extent it may be carried, will suffice to remove the symptoms; and recurrence should be had to this remedy as often as the pain and oppression require, and THE FORCE OF THE HEART will bear it, especially during the first two or three days. It will often be necessary to have recourse to it in smaller quantities for the next four or six days, and again in less quantity on any return of the inflammatory symptoms. Where the patient is likely to faint, he should be bled in the recumbent position; and as it is advisable to take away a sufficient quantity of blood, great care should be taken, by arresting its flow for a time, by giving stimulants, by admitting fresh air, and by sprinkling with cold water, to prevent syncope, which is sometimes dangerous in elderly persons, who may be subject to and who are not readily recovered from it. In the second stage of the complaint, profuse and repeated bleedings do not answer as well; they do not remove the evil which has occurred, although they may prevent its increase. Blood should then be drawn in such quantity only as will relieve the action of the heart, restless under its efforts to propel the blood through a hepatized lung. The quickness of pulse, the cough, the difficulty of breathing, must now be aided and relieved by other means; for although the pulse is not a certain indication, on which dependence can be placed in the early stage of this complaint, the breathing generally is; and as long as the respiration is oppressed,[385] blood should be carefully abstracted, until it becomes manifest that the effect has been to quicken the pulse, while it materially diminishes its power, when it is forbidden.
307. A cupped and buffy state of the blood, together with a firm coagulum, is a satisfactory proof of the propriety of bleeding in the first stage of the disease; but after the effect of mercury on the system has been produced, it cannot be depended upon with the same degree of certainty. When the propriety of further venesection is doubtful, the greatest advantage may be obtained from the use of leeches and from cupping, particularly in cases of injury to the chest. Leeches may be applied by tens and twenties at a time; and when they have ceased to bleed into a warm bread and water or evaporating poultice, they may be replaced by as many more, until the pain and the oppression are removed. Cupping is always to be had recourse to when leeches cannot be obtained, and, when well done, it is frequently to be preferred; cupping to sixteen ounces will usually be found equivalent to forty or more leeches. Both these means often relieve to a greater extent, with less general depression, than a smaller quantity of blood taken from the arm, and are, therefore, at such times more advisable. When blood cannot be obtained from the veins, the arteries must furnish it; and both temporal arteries have been opened with the best effect in injuries of the chest, when blood could not be obtained from the arm, or from the external jugular vein.
308. The effects of bleeding were of old found to be different under different circumstances and in different climates. Asclepiades remarks that while phlebotomy was fatal at Rome and at Athens, it was beneficial in the Hellespont. Nevertheless, at a much later period, Baglivi says: “In Romano, phlebotomia est princeps remedium in plenritide.”
In the Crimea blood-letting has not been so favorably viewed, nor found so serviceable nor so necessary; although the abstraction of smaller quantities than those indicated above, and less frequently repeated, has been found eminently beneficial, the difference being dependent on climate and the impaired vigor of the sufferers.
The remedy first to be administered, and most to be depended upon in the first stage, is tartar emetic, which usually gives rise to vomiting, purging, and possibly to sweating; it should not be omitted because such effects are produced in the first instance. After a few, perhaps three or four doses,[386] the vomiting usually ceases, the stomach tolerates its introduction, and its gradual increase from six to nine, twelve, twenty, or more grains in the twenty-four hours, is often borne not only with impunity, but with great advantage. Vomiting and purging are not desirable, as the effects of tartar emetic are more rapid and beneficial when they give rise to no particular evacuation beyond that of general perspiration. The most valuable remark of Laennec on its use is, “that by bleeding we almost always obtain a diminution of the fever, of the oppression, and of the bloody expectoration, so as to lead the patients and the attendants to believe that recovery is about to take place; after a few hours, however, the unfavorable symptoms return with fresh vigor; and the same scene is renewed often five or six times after as many venesections. On the other hand, I can state that I have never witnessed these renewed attacks under the use of tartar emetic.” He further says that the same favorable results do not occur from its use in pleurisy or in inflammation of serous membranes, as in pneumonia.
309. Mercury is a remedy of the greatest importance in serous inflammations, such as pleuritis, although of less value than tartar emetic in the first stage of pneumonia, than which it would appear to be more efficient in the later period of the stages of hepatization and infiltration, though some physicians place entire confidence on its efficacy in all. It is of most value when combined with opium. Some suppose that the opium merely prevents the irregular action of the mercury; others, in some papers printed in the journals for 1801, state that opium has a distinct curative effect, being capable, when given in large doses, of subduing inflammation, and more particularly of allaying pain, relieving the cough and irritation, and of procuring sleep; in which opinion I fully concur. Opium is highly advantageous in irritable and nervous persons, and will frequently relieve the nervous pain, the pleurodynia which remains after pleuritis, when nothing else succeeds. Calomel in large doses is usually preferred to all other forms, but a difference of opinion has occurred as to what is a large dose; whether two, three, four, six, ten, or twelve grains are large doses, and whether they shall be given every one, two, three, four, or six hours. It has been attempted to solve this question by supposing that in highly inflammatory cases in healthy persons, from three to six, and even to twelve grains, may be given twice[387] or three times a day, with better effect than smaller ones more frequently repeated; but this has not been made manifest.
In cases less inflammatory or complicated with gastric derangement, the disease assuming more of a general than of a local character, the excretions being vitiated, the skin dry and hot, and the tongue loaded, from gr. iss to gr. iij of calomel, combined with three grains of Dover’s powder, may be advantageously given every second or third hour, the great object being to affect the gums as quickly as possible. This is not effected in some cases by any of the quantities given until after a considerable lapse of time, while in others it is accomplished by less than half a dozen grains of the remedy. It has not been ascertained that twenty-four or forty grains given in two or four doses in twenty-four hours will affect the mouth more rapidly than three grains every two hours for the same time, neither is it less liable to cause irritation; while the third or half a grain of opium given every two hours seems to keep up the effect of that remedy with great advantage. It does not materially signify which method is adopted in strong and healthy persons, although the smaller doses are most satisfactory to all parties when the patient is weak and irritable, while the large and less frequent doses often excite great apprehension. It is argued that calomel in large doses never causes the dysentery nor the severe ptyalism produced by smaller doses; that it acts more quickly, and that after giving twenty grains, and repeating it in six hours, any other medicines may be given without interfering with it, although the strictest attention must be paid to diet, generally confining it to very small sups of warm whey. Very serious derangements do, however, follow the exhibition of the large as well as of the small doses, inasmuch as it is impossible to know beforehand what quantity will cause a severe salivation or diarrhœa, which it may be difficult to arrest.
310. It may be concluded that, of the two heroic internal remedies, tartar emetic and calomel, recommended for the cure of inflammation of the chest, tartar emetic is the more appropriate for inflammation of the lungs or pneumonia, provided it be not accompanied by symptoms of gastric inflammation; in which case its use should be superseded by leeches to the epigastrium, and saline aperients, lest the irritation, vomiting, and purging should increase the evil. But[388] care must be taken that one inflammation shall not be allowed to increase, while attention is principally paid to the other, and symptoms of irritation, the gastro-enterite of the French physicians, are not to be mistaken for gastritis. Mercury, in the form of calomel, is more to be depended upon in inflammation of the pleura, over which, as well as over inflammation of serous membranes in other parts of the body, it exercises a remarkable influence.
311. Blisters are never useful during the continuance of acute inflammation of the chest, although their use is indicated when the patient is much exhausted, the pulse weak, and the breathing continues difficult; or in cases in which the disease proceeds slowly, or is becoming chronic, when they often do much good. The same may be said of dry cupping, mustard poultices, and other cutaneous rubefacients, such as the ol. terebinth. used hot, which often do much good in the commencement and termination of slight attacks, or of their supervention on chronic disease, or after injuries.
In the acute stages simple drinks only should be allowed. As soon as the inflammatory action has subsided, the lightest farinaceous nourishment, gradually augmented by the addition of broths, jellies, eggs, fish, and lastly of animal food, should be substituted. The temperature of the room ought to be moderate and equal.
Inflammation of the lungs frequently terminates by the deposition of a white or lateritious sediment in the urine, which is considered a critical evacuation, not however to be relied upon, unless accompanied by a remission of the important symptoms. A moderate diarrhœa and a profuse perspiration are also signs of a favorable crisis.
312. Inflammation of the chest has been hitherto considered as accompanied by inflammatory fever as an essential character, but this is by no means always the case. In large cities, and among troops after hard service, in which they have been subjected to much privation, and in certain epidemics, the accompanying fever often partakes of a low or typhoid character, and becomes infinitely more dangerous. This modification of disease I have known from my earliest years, in different climates, in all of which it proved most fatal. It is a disease formed of a local inflammation accompanied by general symptoms of a low asthenic type of fever, combined with those of marked derangement of the stomach,[389] intestines, or liver, as shown by a dry black, or red black, or brown tongue, offensive breath, diarrhœa, vomiting of a dark-colored or greenish fluid, watery or sanious expectoration, great thirst, headache, a feeble and quick pulse, low delirium, and great prostration of strength. It was marked, on the banks of the Guadiana, by the discharge of lumbrici by the mouth and by the anus. This disease has always appeared to arise from peculiar circumstances, and to disappear when they ceased to exist; such as great privations and exposure to cold and fatigue, the use of ardent spirits without sufficient food, bad air, or other depressing causes. It is sometimes epidemic. The fever is typhoid, the local inflammation latent, and the symptoms of it masked. It may be complicated with inflammation of the stomach and intestines; it may occur in cases of erysipelas, or after wounds or injuries attended with large secretions of purulent matter, or with other complaints. While the symptoms of low fever are general and well marked, those of the latent affection of the lung are not so prominent or even observable. The patient complains but little, and sometimes not at all, of his chest, until attention is drawn to it by a slight cough, and difficulty of respiration, attended by a character of countenance which usually indicates embarrassment in the functions of the lung. It may be brought on by a common non-penetrating injury of the chest.
In typhoid pneumonia, general bleeding, if admissible, is to be had recourse to with extreme caution, even in young and robust persons. Local depletion is oftentimes useful, and perhaps ought to be alone relied upon. The great dependence is on calomel and opium, and after such local depletion as may be thought advisable, counter-irritation by blistering, and the administration of stimulants, such as camphor, ammonia, and wine, in small and repeated quantities. Mild aperients only should be employed, and anodyne injections are frequently useful. While auscultation has thrown a clear and steady light on the nature of the mischief which is going on, it has added little or nothing dissimilar to the practice pursued some forty years ago. The nature of the hepatization or solidification which takes place in the lung in typhoid pneumonia has given rise to some difference of opinion among morbid anatomists, who incline to believe, from the rapidity with which it takes[390] place, and with which it is sometimes removed, that it depends more on passive congestion, and on a typhoid alteration of the state of the blood, than on an altered action in the vessels of the part. This opinion does not seem to be fully supported by dissection, unless it be generally admitted that gray hepatization, and the third stage of disease of the lungs in pneumonia, mean simple congestion.
When the patient survives the imminence of danger in which he is placed by the attack of the disease, and the expectoration becomes copious, with great emaciation, quick pulse, and hectic fever, a slight infusion of senega or of cinchona with ammonia, with a mild and well-regulated diet, and change of air and climate, answer best in aiding recovery.
A typhoid pleuritis is presumed to exist, as a distinct disease from typhoid pneumonia, although the analogy between them is admitted to be close; like it the disease is latent and more frequently pointed out by the sinking of the powers of life than by any new suffering. The signs of effusion may be discovered on auscultation, and the treatment is essentially similar; blistering and counter-irritants being perhaps more useful, if time be granted for their application.
313. Empyema, from εν, in, and πυον, pus,—a name given to all collections of fluids in, and to the operation for evacuating them from, the cavity of the chest. Empyema is not a special disease, but the result of another; commonly of acute or chronic pleurisy, or of injuries of the chest, which give rise to inflammation, ending in suppuration. When it occurs from the effusion of a serous fluid, constituting a local dropsy, it is usually the result of disease of the heart, or of the great vessels, and is accompanied or preceded by symptoms indicating the existence of those complaints, in which case it is not likely to be benefited by any operation. The disease is then denominated hydrothorax. The serous fluid is generally transparent, although more or less tinged with blood, when thrown out in persons who die within a few days after receiving a wound of the chest. It may, and does occasionally, contain in these cases a large quantity of blood; but an early effusion of blood is not uncommon in very acute cases of pleuritis. It is usually more or less turbid when the result of ordinary inflammation, although the presence of albuminous or purulent matter is not constant. Whether colorless, transparent, turbid, or purulent, it remains free from fetor, unless gangrene has occurred inter[391]nally, or some communication with the atmosphere has taken place by an external opening.
While the fluid remains transparent, the appearance of the pleura is little changed, but when it has become turbid in any great degree, or flocculent, or purulent, the pleura has lost its natural appearance. In its simplest character, when the fluid is puriform, particularly if the inflammation have not been very active, it is covered with a layer of whitish inorganic sediment, which can be scraped off by the scalpel. This is sometimes quite red, as if loaded with blood which had been deposited upon it. Whenever pleuritic symptoms continue beyond the ordinary period of about three weeks, or, after a temporary abatement, are followed by those of effusion, which are not in turn removed, the occurrence of empyema may be suspected.
Empyema may form from a pulmonic abscess bursting, or a gangrenous spot being detached and falling into the cavity of the pleura. An abscess in the liver or other parts may also communicate with the pleura, and abscesses formed from injury or otherwise in the wall of the chest may also give rise to it. It is usually, however, caused by acute inflammation, by penetrating injuries, or by the introduction of foreign substances. It should, however, be borne in mind that when it occurs from wounds, the external opening must have healed, or the complaint would be simply a wound in the chest, with a discharge from the cavity of the side affected. A true surgical case of empyema, following an injury of the chest, in which the wound has healed, is not to be ascertained but by the same means as in a case arising entirely from internal causes, unless the protrusion of the cicatrix should indicate the presence of matter behind it.
314. The symptoms by which the termination of inflammation in effusion may be known: are dyspnœa, or difficulty of breathing, which is greater when the effusion has taken place rapidly, less when it has been gradual; subsidence of pain; inability to lie on the unaffected or sound side, which subsides, or is entirely removed, after the operation has been performed and the fluid evacuated, although it should be replaced by air in consequence of the lung being unable to resume its natural position. When the effused fluid has filled one side of the chest, that side is evidently enlarged, and this can be distinctly seen when the dilatation does not exceed half an inch, measuring by a tape from the spinous[392] process of a vertebra behind to the center of the sternum. The ribs are nearly, if not quite, immovable, and partially raised, offering a strong contrast to the active motion of the ribs on the other side. The intercostal spaces in these persons may be more or less filled up, rendering the whole surface smooth and soft. In some very severe cases the external parts become edematous, so that the ribs cannot be felt, and this sign, although not always present, is certainly pathognomonic when it takes place at a late period of the disease. When the effusion is into the left side of the chest, the heart is frequently pushed over with the mediastinum to the right side, and its pulsation can be seen and felt to the right side of the sternum; or it may descend with the diaphragm into the epigastrium—changes which are not so extensive or remarkable when the effusion is into the right side, as the liver materially impedes the descent of the diaphragm, and the heart is already in the left side, in which it is sometimes raised rather than depressed. It is said that if the hand be placed over the affected side, while the patient speaks with a tolerably loud voice, and a strong vibration is felt in the part, the case is not one of empyema; but this is as uncertain a sign and as little to be depended upon as the dullness on percussion which sometimes takes place under the sternum in empyema. The cough and expectoration offer nothing peculiar, unless a communication exist between the lung and the cavity of the chest, when the expectoration in general becomes very fetid and disagreeable. The febrile symptoms depend on the activity of the previous disease, and the rapidity with which the effusion has taken place.
Night-sweats, it has been supposed, never accompany the hectic fever of empyema, unless there be tubercles in the lungs or pleura—a remark which cannot be depended upon.
315. Two symptoms have been insisted upon by older authors as distinctive of effusion in the chest, which more modern ones are disposed to doubt, particularly in the early stages of the disease. One is an edematous swelling of the back, the other a protrusion of the intercostal spaces. A third may be added when the effused fluid is blood, which is that the edematous swelling becomes ecchymosed, or red, or bruised looking, from the effusion of blood into the cellular membrane beneath the skin, over the whole space occupied by the blood within. That the first two symptoms do[393] assuredly indicate the presence of pus, cannot be doubted; and that the third is a sign that the effused fluid is blood, has not been disproved; but it must be borne in mind that they are late, not early symptoms, and the operation should not be delayed until they are present, if other signs should appear to demand its performance. Valentin was the first to notice the ecchymosis of the side and back when the chest was full of blood, a sign which Larrey particularly insists upon, but which certainly does not appear so early as to be distinctive, when other symptoms exist which almost render it certain. The swelling does not arise from transudation of matter through the pleura, but from irritation transmitted through it, as in any other deep-seated abscess. Dilatation of the chest is usually an early symptom, although a considerable effusion may exist without it, or with but a slight elevation of the intercostal spaces. When the complaint is distinct, these spaces are elevated to a level with the ribs, so that the surface becomes perfectly smooth and equal; a farther protrusion is a very rare occurrence. Effusion indeed of serous fluid to a considerable extent, so as to displace the heart, may take place without the intercostal spaces being elevated, which is only believed to occur when the intercostal muscles have become paralyzed. When the matter has been evacuated, the muscles recover their tone, and the intercostal spaces reappear.
In all cases of empyema in which the lung is so bound down by adhesions that it cannot be expanded by the continued process of respiration, a cure can only be accomplished by an alteration of the form of the affected side of the chest, by which its cavity is diminished, and often nearly obliterated. This is an effort of nature. The pleura changes its character, becomes so thick as materially to diminish the cavity, the diaphragm ascends, the heart leans to that side in many instances, the spine curves, the ribs thicken and become flatter, and close in upon each other, abolishing the intercostal spaces.
Treatment.—As long as the febrile symptoms consequent on the inflammation continue to any extent, medicines will be of but little avail, and counter-irritants should be avoided. When they have subsided, purgatives and diaphoretics may be tried, in combination with tonics and a light but good nourishing diet. Blisters applied frequently upon a large[394] surface often do good. When these means fail, the operation must be resorted to.
316. It has not been satisfactorily decided whether the operation for empyema was first performed on Phalereus, Jason, or Prometheus; it is therefore said of all three that, being expected to die of an abscess in the lungs declared to be incurable, they went into battle for the purpose of getting killed; but being only run through the body, they all recovered, in consequence of the escape of the purulent matter through the holes thus made. The operation was performed by Hippocrates and his successors, by the knife, by caustic, and by the hot iron. Ambrose Paré was the first who recommended a trocar and canula, and many instances of success in all ways are recorded. The modern methods are by the trocar and canula, and by incision. Whenever auscultation, percussion, or succussion give reason to believe that a fluid is collected, which medicine has not been nor is able to remove, the simple operation by the trocar and canula should be performed. If fluid should pass through the small canula generally used by way of exploration, a larger one may be introduced in its place if thought advisable. In ordinary cases, the little wound should be closed immediately after the evacuation of the fluid; it usually heals without difficulty, and the operation may be repeated if necessary. Care should be taken that the point of the instrument is perfectly sharp, or it may separate the thickened false membrane from the inside wall of the chest, and, by pushing it before it, prevent the fluid from passing through the canula when the trocar is withdrawn.
317. The place of election, in England, for a puncture, in ordinary cases, is usually between the fifth and sixth ribs, counting from above, and between the sixth and seventh from below, and at one-third the distance from the spinous processes of the vertebræ, or two-thirds from the middle of the sternum. If there should be any protrusion of the intercostal spaces, it may be a rib or two lower down. The point of the instrument should be introduced a little nearer the lower than the upper rib, and pressed on until all resistance has been overcome. It is entered nearer the lower rib to avoid the intercostal artery, and yet not touching the rib lest it should induce a too forcible contraction of the inter[395]costal muscles, by which the operator might be inconvenienced.
If the person should be very fat, or the puffing of the integuments considerable, it may not be easy to feel the ribs, in which case even recourse should not be had to incision. When the arm is placed by the side, and bent forward at a right angle so that the hand rests on the ensiform cartilage, the inferior angle of the scapula will correspond in general, but not always, with the interval between the seventh and eighth ribs at the back part. The attachment, however, of the last of the true ribs, the seventh, to the xyphoid cartilage, can always be ascertained in front, and an error of importance cannot well take place, as the object in making a puncture by measurement is to avoid the diaphragm. Freteau, of Nantes, says that he performed the operation on the left side between the tenth and eleventh ribs, and on the right side between the ninth and tenth in more than thirty dead bodies, and always opened into the cavity of the chest, commencing the incision close to the edge of the latissimus dorsi muscle, or about three inches and a half from the spine—an operation which in this place should be done by incision, and not by the trocar. When there is reason to believe that there is an extraneous body to be extracted, such as a ball, the place of election is of importance, as it is desirable it should be a little above the diaphragm in order to facilitate its extraction; for although, by carefully shifting the position of the patient, a ball or a piece of bone may be brought to rest against the opening, it will not be easily taken hold of unless it lie upon the diaphragm, a point which will be hereafter further elucidated. When an external swelling indicates the presence of matter, and there is reason to believe it communicates with the inside of the chest, the opening should be made into the tumor, and is then called the “operation by necessity,” which is not an uncommon occurrence after gunshot wounds. It is not, however, always done in the most convenient place, and should then be repeated lower down, which will also be sometimes necessary in consequence of the matter collected in this way being cut off by adhesions from the general cavity.
When the operation by incision alone was performed, the success was certainly not great. In modern practice (after the operation by puncture) it has been much greater, which may be attributed to the operation having been had recourse[396] to at an earlier period, or about the end of the third week. After wounds penetrating the chest which do not admit the effused fluid to flow out, it should be done much earlier.
It is possible that both sides of the chest may be affected; but both sides may not be punctured in succession, for an error in puncturing both, or even the sonorous or sound side instead of the dull or affected side, has been almost immediately destructive of life.
318. The admission of atmospheric air into the cavity of the chest during this operation has been much deprecated, and many inventions have been recommended for its prevention, but it is scarcely possible to prevent some air getting in. It is often seen to do so; it has been proved by auscultation to have done so, and is usually absorbed in a few hours. In one case which I saw it gave rise to distressing symptoms from pressure on the lung, but was removed by a common syringe, to the great relief of the patient. In all these cases two things must be considered: Can the compressed lung expand so as to fill the chest when the fluid is withdrawn? The answer must be, in many cases it is so bound down by adhesions that it can dilate but slowly, if at all. If it be asked whether a vacuum is formed in the chest, the answer will be, no; and it will then be admitted, on consideration, that air always finds its way into the chest, and never does harm to persons in health. When mischief does ensue after an operation or an injury, it usually occurs from the irritation caused in a particular state of constitution, and not from the admission of air. A change in the appearance of the discharge has been frequently found to follow, and to depend upon, an accidental derangement of stomach, and to return to its more normal state on the derangement being removed. If the wound into a cavity can be closed and healed, the air will remain with impunity until absorbed. If the wound cannot be healed, unhealthy inflammation may be propagated from it to the whole cavity with which it communicates, but this is not the effect of the admitted air.
Dr. H. M. Hughes has published several cases of pneumothorax in the first part of the of the volume of “Guy’s Hospital Reports” for 1852. In the sixth case, which he calls a genuine example of pneumothorax from rupture of one or more of the vesicles of an emphysematous lung, the patient died speedily; and, on examination, he says: “It is also an interesting fact that no evidence of inflammatory[397] action existed in the pleura, as it indicates that air in a healthy serous membrane does not excite inflammation;”—a Peninsular dogma I have been forty years inculcating, and which I trust is at last admitted as an established fact. How long it may be before it is generally taught, is another matter; for surgeons, like other men, often adhere with tenacity to preconceived opinions, however erroneous, particularly as they advance in life and have ceased to desire to learn more than they already know.
319. In all cases of serous effusion, there can be little doubt that the fluid should be wholly evacuated and the wound closed. When the fluid is purulent, a permanent drain should be early established. It is not, however, common for the operation to be repeated several times without the serous discharge becoming purulent; and, in such cases, it usually becomes necessary at last to allow the wound to remain open until the discharge shall cease of itself. Whenever more than one opening is necessary, and the first is made between the fifth and sixth ribs, the succeeding ones should be made lower down; so that when it is thought right to leave the last puncture to become fistulous, it may be made as near the diaphragm as may be thought consistent with the safety of that part.
When a doubt exists as to the probability of more than one puncture being sufficient, and it seems likely that a third, or even more, will be required, the surgeon may anticipate this necessity by introducing a piece of soft gum-elastic catheter through the canula into the chest to the extent of about three inches, enough being left outside to admit of its being secured by tapes and adhesive plaster; through this a certain quantity of the fluid may be drawn off daily until it ceases to be discharged. The elastic tube bends with the heat, and applies itself to the inside of the ribs. If the lung should rub against it, which can be ascertained by a blunt probe, the elastic tube should be removed, and the external wound kept open by a softer plug. In all these operations, care should be taken to prevent the occurrence of inflammation. The accession of pain in the part, of difficulty of breathing, of fever, should be met by the abstraction of a few ounces of blood by cupping, by dry-cupping, by mercury in small doses, by rest, by diet, etc., and, if a tube have been introduced, by its removal.
The propriety of injecting stimulating or even simple fluids[398] into the cavity of the chest has been often advocated, and as frequently repudiated. Warm water or milk and water is certainly admissible, and has been found very useful, particularly when there is an adventitious cause keeping up the irritation, which may possibly be brought to the opening by the sudden abstraction of the injection. Pieces of cloth and bits of exfoliated bone have been floated out by throwing in an injection of tepid milk and water. The opening, in a case of this kind, should be made between the eleventh and twelfth ribs behind.
Dr. Wendelstadt, of Hersfield, in the year 1810, in the twenty-third year of his age, suffered an attack of pleurisy, which became chronic, and ended in effusion. After severe suffering for six months, he was able to attend to his professional duties. The ribs of the right side protruded, but the intercostal spaces did not; the whole side was motionless on respiration taking place. The circumference of the chest continued to increase, and fluctuation within became evident on succussion. In June, 1819, having undergone another attack of pleurisy, he submitted to the operation for empyema, as offering some hope of preserving life. When a pint of fluid had been discharged, the wound was closed, and he experienced great relief. The next day a third of a quart was taken away twice in the day, and on the third day as much more; but he thought this was too much, as he became greatly exhausted, and feared that suffocation was impending. He was recovered by stimulants. On the fourth day the fluid was thicker in consistence, and fetid, and continued more or less so for a fortnight. It was then allowed to flow as it would at each dressing. Astringent injections were used for six weeks, but were then abandoned, and he gradually recovered his strength. Thirteen years afterward, in 1830, the wound was still open, discharging twice a day, sometimes only half a drachm, sometimes three or four ounces daily. The right side had altogether shrunk, and did not move on inspiration; he had no cough, and was otherwise in good health; a piece of a rib became loose, and was removed at the end of thirteen years, when the report of the case terminated, the patient being in health.
It may be remarked on this case, that the admission of air did no harm; that the lung remained compressed; that the whole side thickened and flattened, as a consequence, so as to obliterate the cavity; but the cure would not have been[399] effected even then, if the piece of carious rib had not been discovered and removed.
Mr. Winter, secretary to Admiral Sir C. Napier, was wounded by two musket-balls, one in the arm, while the other entered between the inferior edge of the left scapula and the thorax, which it penetrated, fracturing a rib in its progress, and lodged. He fell, and spat up some blood, and as symptoms of inflammation supervened in twenty-four hours, he was bled largely; this was repeated frequently until these symptoms were subdued. He was after a time sent to the Marine Hospital, Lisbon, in a miserable plight, suffering from hectic fever, with a flushed face, hot skin, glassy eye, great prostration of strength, cough, restlessness, dyspnœa, and copious night-sweats. The wound discharged a watery, sanious, fetid matter in quantity, and he was unable to do anything but eat, and for food he had a great craving. From this state, under good treatment, he gradually recovered his strength, and on the 18th of June, 1834, a piece of the rib was removed. The wound remained open with a great purulent discharge, which kept him in a reduced state; a little more than one year after the injury, he reached London, and was taken into the Westminster Hospital. The left side of the chest was flattened and contracted, and the lung was doing very little in the respiratory way; the wound discharging a quantity of matter, which he could readily evacuate by making the opening the dependent point, but not otherwise. On enlarging the external wound, so as to make the opening into the chest direct, I found a round-pointed gum-elastic bougie could pass into it for four inches, and, on bending it down, for six inches more, it having to pass over a thickened pleura, and false membrane of an almost cartilaginous nature, for the extent of an inch, before it could be felt to be in a large cavity. As it did not appear that he had any chance of recovery, unless another opening were made lower than the sixth rib, in a more dependent position, I proposed the operation, but he would not submit; and after a time he left the hospital and went into the country, where he died.
A non-commissioned officer, of the 2d Division of cavalry, was wounded at the battle of Albuhera, on the 10th of July, 1811, in several places, by the lances of the Polish cavalry; one of these penetrated the left side of the chest behind, immediately below and in front of the inferior angle of the scapula. He spat and coughed up blood, and lost so much[400] from the wound that he became insensible, the bleeding having been stopped by a part of his shirt being bound upon it tightly by means of his woolen sash. Brought to the village of Valverde, my attention was drawn to him some days afterward, in consequence of the difficulty of breathing having increased so that he was obliged to be raised nearly to an upright position, as well as from his inability to rest on the part wounded, round which a dark-blue inflammatory swelling had taken place, the wound having closed. An incision being made into it, a quantity of bloody purulent matter and clots of blood flowed from it. The incision was then enlarged, so as to allow of a direct opening into the cavity of the chest, which was kept open. The relief was immediate. He was removed to Elvas, apparently doing well, some three weeks afterward.
This case offered the nearest approach I have seen to the ecchymosed edema described by Valentin as accompanying effusions of blood into the cavity of the chest; and, as well as the following, is an instance of operations, not by election, but by necessity.
A French soldier had been wounded at Almaraz by a musket-ball, which went through the right side of the chest, in a line nearly horizontal from a little below and to the outside of the nipple, backward. The first symptoms having subsided, he gradually descended the Tagus to Lisbon, where, after some months of continual discharge, the wounds closed, first the back, and then the front. He did not recover his strength, always looking sickly, and suffering from pain, difficulty of breathing, and other inconveniences, which did not prevent his walking about in the confined space to which he was doomed as a prisoner of war. My attention was drawn to him in consequence of an obvious fullness of the intercostal spaces, of the great difficulty of breathing, and of a puffy inflammatory swelling which was forming around and at the seat of the wound in front. Through this I made an incision into the cavity of the chest, the walls of which, on introducing the finger through the opening, appeared to be very much thicker than usual. A large quantity of pus was discharged, and the man was relieved, but this amelioration was not of long continuance, and he gradually sank and died. On opening the body, the inside of the wall of the chest was found to be half an inch in thickness, in consequence of a firm deposition on the pleura, of a yellowish-ash color, honey[401]-combed or ulcerated, as it were, in plates, particularly where the opening had been made. The lung was shrunk up from the anterior and lower part of the chest, but adhered to the wounded part behind, and was covered by a layer of false membrane of considerable thickness. The wound through the lung could not be distinctly traced, from its being diseased throughout.
At Santander, in October of the same year, 1813, I received some eight hundred wounded in the affairs of Le Saca, Vera, etc. One of the Light Division had been shot through the left side of the chest: the posterior wound had closed, but a sufficiently large quantity of matter was discharged through a small anterior one to show that there must be some depot from which it proceeded. The wound was laid open into the cavity of the chest, and free vent given to a quantity of matter. Some small pieces of rib were discharged, and a bit of something like the cloth of his coat also came away. He could lie on either side, and hopes were entertained of his recovery, until after I left Santander in December, to join the army in France, when he suffered a relapse of inflammation, and died.
A soldier of the German Legion was wounded at Waterloo by a lance between the sixth and seventh ribs of the left side. He spat up much blood for several days, and was carried to Antwerp, where he remained for several months, suffering from great difficulty of breathing and other distress in his chest, which recurred from time to time, although the wound had healed. He was admitted into the York Hospital, Chelsea, in the spring of 1816, in consequence of an attack of inflammation, of which he died. On examining the body, the lung of the right side was found to be greatly inflamed, and full of purulent fluid, which caused his death. The left or wounded side was found to contain a small quantity of pus, the cavity being very much diminished by the great thickening of the pleura and the falling in of the ribs, which were thicker, greatly flattened, and changed in form; the lung, shrunk or collapsed, was covered by a thick adventitious membrane, and bound down against the spine, leaving a long, small space between the pleuræ, which once had doubtlessly been full of matter. The mediastinum and heart appeared to lean toward the left side, aiding in this manner in the obliteration of the cavity, which must take place if a permanent cure be effected in empyema. I have seen two[402] cases in which this obliteration appeared to be complete: one in a soldier, who had been wounded in the chest; the other in a gentleman, the subject of empyema, in private life. In both the spine was also distorted, the side wasted, the nipple lower than the other. The breathing of the opposite side was more marked and developed. It might have been called puerile.
320. Pneumothorax means an effusion of air and of the matter of a tubercular abscess from disease into the cavity of the chest, or from an injury or a wound in the lung. When pneumothorax is the consequence of disease of long standing, the patient may be sensible of a sudden pain, which does not abate, and which is accompanied by an equally sudden increase of the difficulty of breathing, for which he cannot account. He feels relief by lying on his back or on the affected side, rarely on the other, although the difficulty of breathing may increase, so as to render the further continuance of life doubtful, while the prostration of strength is considerable. The muscles of respiration are all in rapid and powerful action; the heart is displaced to the right side when the complaint attacks the left, and it will be displaced somewhat to the left when the right is affected; in some cases it even descends into the epigastrium, or is otherwise removed from its natural situation, even toward the axilla, although the left side is supposed to be more obnoxious to this complaint than the right. The pulse becomes exceedingly quick and small, countenance pale, nights sleepless. The affected side is oftentimes evidently dilated, and the intercostal spaces may be less marked, or partly filled up, when the respiratory motion given to the parts under ordinary circumstances is seen to be deficient. But these differences, as well as that which can be obtained by comparing both sides by measurement, are not so marked as when the cavity is filled with fluid, of which in pneumothorax there is always a small quantity effused.
Percussion, beginning from above, in the erect position, will give, in cases in which it is ascertained that respiration is null, a clear tympanitic sound, as low as the level of the fluid, when it changes abruptly to a dull sound, or that indicating the presence thereof. If the patient be then placed in the recumbent position, the clear sound can be heard above, the dull one below, demonstrating the change in the situation of the air and fluid. Auscultation, in addition to[403] the absence of respiration, when the chest is fully expanded, discovers no respiratory murmur; but a peculiar sound called tintement métallique, or metallic tinkling, is heard at intervals, particularly on the patient’s coughing, speaking, or breathing. It may be imitated by dropping a pin into a large wine-glass, but it more nearly resembles the sound of a jew’s-harp in the hands of a child: once heard it cannot be mistaken. It is a sound distinctive of pneumothorax.
“Mr. Cornish, a medical practitioner, having suffered an attack of pleuritis, nearly expired from suffocation on Monday, the 29th December, 1828. He was lying on his right side, breathing most laboriously; countenance sunk; pulse between 130 and 140; had had no sleep for many nights. The action of all the respiratory muscles was painful to behold; no perceptible difference in the size or shape of the two sides. The right emitted an extremely dull sound; the left sounded hollow throughout. The apex of the heart was beating rather to the right of the right nipple. The respiration was loud and rattling in the right side; metallic tinkling distinct in the left; expectoration muco-purulent, with specks of blood, and many black particles. Mr. Guthrie, who saw him for the first time, made a short incision between the sixth and seventh ribs, and cautiously opened the pleura, when a rush of air issued forth with a hissing noise, strong enough to have extinguished several candles. The patient turned on his back, breathed with comparative freedom, and expressed his gratitude for the operation. No fluid issued from the wound when made a dependent opening. On the 31st, the difficulty of breathing and the metallic tinkling had returned, the wound having closed. The wound was reopened and enlarged; the pulse fell to 120; the metallic tinkling ceased to be heard; the patient took some nourishment and an opiate at night.
“Jan. 1st, 1829.—Has slept several hours; breathing easy; pulse reduced in frequency; appetite good. A canula was placed in the wound, when large quantities of air came through it on each expiration; the heart beat two inches nearer the central line of the thorax than before. During the night he became greatly oppressed, and died next day. On raising the sternum, the heart was found rather to the right of the median line of the chest. The left lung was collapsed to one-fifth of its natural dimensions. The vacant space was filled with air, and about fourteen ounces of turbid[404] serous fluid. The pleuræ costalis and pulmonalis presented marks of inflammation of a few weeks’ standing—viz., some thin false membranes, which were easily separated by scraping with the scalpel. There were no marks of more recent pleurisy. A tube was inserted into the trachea, and air blown into the lungs. The left lung expanded to a certain extent, and air was heard to bubble out, when an aperture was immediately recognized at the division between the two lobes, through which the air rushed forth and extinguished a taper that was held near it. The aperture was circular, fistulous, and capable of admitting a crow-quill, and was found to communicate with a very small excavation, formed by the softening down of some tuberculous matter; into this small excavation a bronchial tube was seen to enter. Thus, the communication between the trachea and the cavity of the chest was distinctly traced. The left lung presented some trifling tuberculation, but was not materially diseased.”
William Griffin, aged eighteen, was admitted into the Westminster Hospital on September 14th. Ten days before his admission into the hospital he discharged a pistol against the left side of his chest, causing a wound corresponding to the middle of the eighth rib, from which a very small quantity of blood escaped. The medical practitioner who was called to him at the time passed a probe to the extent of four inches into the wound. The wound had nearly cicatrized, but he became the subject of acute pain, diffused over the whole of the left side of the chest, accompanied by fever and frequent cough, dyspnœa, and inability of lying on the right side. After the lapse of a week he was transferred by his surgeon to the medical wards under Dr. Roe, at which time he had begun to expectorate purulent matter of an extremely fetid character, occasionally mixed with blood. His respiration was hurried, the right side of the chest expanding much more freely than the left; the lower three-fourths of the affected side were dull on percussion; tubular respiration could be detected at the upper part, but at the lower no air appeared to enter; well-marked modifications of voice existed over the whole of that side of the chest. By measurement no difference in the relative size of the chest was observed, but the intercostal spaces of the left side remained motionless daring expiration. The heart could be felt feebly pulsating at the epigastrium.
October 15th.—He suffered from a violent paroxysm of[405] coughing, during which great dyspnœa suddenly came on. He sat propped up in bed; respiration was almost ineffectual, his face livid and covered by a cold, clammy sweat, pulse scarcely perceptible at the wrist, and his extremities were becoming cold. On examining the chest, the left side, before quite dull, now afforded tympanitic resonance on percussion, which, together with the total loss of respiration and the presence of metallic tinkling, proved the existence of pneumothorax. A trocar was introduced between the sixth and seventh ribs, and was followed by an escape of gas with about five drachms of pus, both of a very fetid character; the canula becoming obstructed, a larger one was then passed through the opening, but not more than half an ounce of pus escaped; it was then withdrawn, and found to be blocked up by what appeared to be disintegrated lung. Being greatly relieved, no further attempts at evacuating the fluid were then made.
At night, during a paroxysm of coughing, six ounces of fetid pus escaped by the opening, after which he felt relieved. A second gush of sanious fluid, to the amount of five ounces, containing small masses of sloughing membrane, subsequently took place. Cavernous respiration at the upper half of the lung, mixed with gurgling and metallic tinkling. Expectoration muco-purulent and offensive.
21st.—Has somewhat improved, but suffers from accessions of fever toward evening, and perspires very profusely during the night; the cough is less frequent, and he expectorates freely, the sputa being of a purulent, fetid character. Scarcely any discharge from the side.
Nov. 5th.—Has remained in nearly the same condition until yesterday, when he ceased to expectorate, and has since become much worse; his skin is now intensely hot; face flushed; tongue brown and coated; pulse jerking, but feeble and frequent; the opening in the chest has quite healed.
A second opening was now made about an inch external to the former one, and a canula introduced, but not more than one ounce of pus escaped, the instrument becoming blocked up by portions of sloughing tissue; during a paroxysm of coughing, which occurred a few hours afterward, several ounces of fetid sanguineous pus were forced through the wound.
16th.—Since the last report he has been slowly sinking— [406] is emaciated to an extreme degree. The wound originally produced by the pistol-ball, as well as those made by the trocar, have become fistulous, so that during respiration the air passes into the chest, and is expelled with as much freedom as that passing by the trocar. Expectoration has continued very copious, about a pint and a half having been passed in every twelve hours; large sloughs have formed upon the nates and hips, his intellect wanders, and he has frequent syncope. Died on the 5th of December.
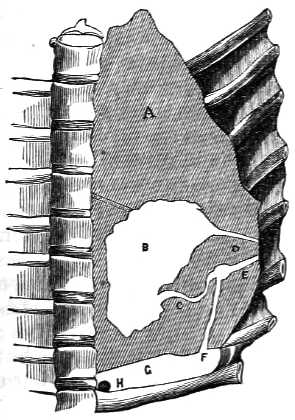
A. Section of the lung, made vertically.
B. Section of the abscess communicating by the sinus,
C, with the circumscribed cavity,
D, in which the bullet had been
lodged after its entrance by the sinus, E.
F. The sinus by which the ball had
passed into the pleural cavity, G.
Opposite the 7th and 8th ribs the lung is
quite adherent.
H. The ball.
Sectio cadaveris.—The pleural cavity of the left side contained about ten ounces of purulent matter mixed with blood, and floating in it were numerous masses of white, curd-like matter, at the bottom of which, in the angle formed by the diaphragm with the spine, was found a pistol-ball partly covered by albuminous matter and discolored. Fluid injected into the left bronchus was found to issue freely from an opening at the most depending part of the lung, communicating with a small cavity, the interior of which was lined by the same thick membrane met with in cases of chronic phthisical disease; from the upper part of this cavity two other sinuses were formed, the one passing externally and terminating by an adhesion of the lung with the ribs at the point where the ball had entered; the other was longer and more tortuous, passing deeply in the substance of the lung, and ending in a large abscess capable of containing five or six ounces of pus. The lung was at its lower part firmly attached to the ribs by intervening false membrane, while the upper part was free, and had become compressed toward the spinal column. The substance of that part of the lung not involved in the abscess was infiltrated with pus, and[407] the greater number of the bronchial tubes were filled up by masses of curdy matter similar to those found floating in the effused fluid. The natural division of the lung into lobes was quite destroyed by the pleuritic adhesions of one to the other, while the pleura lining the parietes was covered by rugged layers of false membrane of irregular thickness, but readily detached. No trace of tubercular deposit could be found, and the lung of the opposite side was quite healthy. Since the first publication of these cases the operation has been so frequently and, in many instances, so successfully performed, as to leave no doubt of the advantages to be derived from it.
321. Lord Beaumont was wounded by a pistol-ball on the 13th of February, 1832, when standing sideways. It entered the right side of the chest a little below the nipple, appeared to pass under the lower end of the sternum, just above or about the xyphoid cartilage, and to have lodged in the cartilage of the last of the true ribs of the left side near its junction with the bone, in consequence of a round projection at that part resembling a pistol-ball, but which, on being exposed, showed only a knob of cartilage which might have been a natural formation; no further steps were therefore taken. The injury had been received about four o’clock—it was now five; he could lay flat on his back; had little or no pain or oppression.—Seven o’clock: Breathing became oppressed, and accompanied by pain; vesicular murmur distinct in both lungs; pulse 96; bleeding to thirty-two ounces.—Nine o’clock: Difficulty of breathing; the pain greater; was again bled until the pulse failed, although he did not faint; the relief great.—Half-past ten: Oppressive breathing again returned; pulse very low and quick; thirty-six leeches applied; relief obtained.—Half-past twelve: Thirty-six more leeches.—Half-past two: Thirty leeches were again applied. In all, four pints of blood were taken from the arm, and one hundred and two leeches were applied to the chest, the bleeding being encouraged afterward; during the first ten hours live grains of calomel and four of the compound extract of colocynth had been given, and now forty minims of Battley’s solution of opium were administered.
14th.—Eight o’clock: Slept after four o’clock; on waking took an aperient draught, and is much easier; pulse 120, soft, small, and weak.—Three P.M.: On the dyspnœa return[408]ing twenty-one leeches were applied, and the oppression was relieved; an enema given, which acted freely.—Half-past twelve: A returning oppression relieved by eleven leeches; calomel repeated, and thirty minims of solution of opium.
15th.—Eight A.M.: Slept at intervals; little or no expectoration, no blood; thinks he would faint if he sat up in bed; pulse 130, soft, small, and weak; little pain; lies tolerably flat; respiratory murmur distinct on both sides.—Nine P.M.: Oppression returned; twenty-four leeches; repeat calomel and colocynth; an enema, after which the bowels became free.—Evening: Six grains of calomel, and opium draught.
16th.—Eight A.M.: Had forty-eight leeches applied at intervals twice during the night; slept at intervals, and is easier; no pain in the chest; pulse 108.—Evening: An enema; six grains of calomel, and one grain of opium.
17th.—Eight A.M.: Slept during the night, and is better; pulse 108, soft; breathes freely; no pain.—Evening: Has had leeches applied twice during the day, making in all 245, and each time with relief; an enema,—calomel and opium as before.—Twelve at night: More oppression, and, as the pulse was fuller and quicker, a vein in the arm was opened, but only four ounces of blood could be obtained.
18th.—Eight A.M.: Slept at intervals, although very restless; pulse 120, fuller; oppression in breathing returning; bleeding to twenty ounces, which caused him to faint; senna draught.—Evening: Has been much relieved by the bleeding; blood cupped and buffy; twenty leeches; enema; calomel and opium. In the night, at two o’clock, the dyspnœa returning, twenty-two leeches were applied, and thirty minims of solution of opium given.
19th.—Eight A.M.: Easier, quieter, better; pulse 110, soft; can lie quite flat on his back. The wound discharged so little that the external parts were dilated inward toward the sternum, until the pulsation of an artery could be seen, perhaps the internal mammary, which it was not thought advisable to disturb; respiratory murmur not distinct at night; enema; calomel, opium, and twenty leeches.
20th.—At three in the morning, being greatly oppressed, thirty leeches were applied, and at eight o’clock twenty more, which quite relieved him, but left him in a state of great exhaustion, sick, and faint. A little arrow-root relieved the faintness; discharge from the wound free, and accompanied[409] by air; bowels open.—Ten at night: Calomel, and forty minims of the solution of opium.
21st.—Eight A.M.: Has now, for the first time, a hope of life: pulse 112, soft; no pain; can turn on his side, but fears to hurt himself; wound discharges freely; has had a small piece of bread for the first time.—Four P.M.: Restless, but better; senna and sulphate of magnesia mixture.—Eight P.M.: Oppressed; pulse 120; twelve leeches; calomel, and thirty minims of the solution of opium, at night.
23d.—Oppression at night relieved by six leeches; slept afterward; breath slightly affected by the mercury, which was omitted in consequence; ten grains of the compound extract of colocynth given at night, with thirty minims of the solution of opium.
25th.—Free from pain; breathes easily and without difficulty; can turn in bed with ease; slept well; the discharge from the wound is free; takes farinaceous food, oranges, tea, etc. He gradually improved until the 13th of March.—On the previous Friday, the 9th, he removed from Bond Street to Mount Street; and on the 13th, amused himself by washing all over in a small back room without a fire; caught cold, and acquired a troublesome cough, which was quieted on the 14th, at night, by opium.—On the 15th, A.M., it was evident that some mischief had been done; pulse 120; breathing difficult; was bedewed with a cold sweat; respiratory murmur indistinct on both sides; on the left, not heard below the fourth rib; although the whole side sounded sonorously, it evidently contained air, the tintement métallique being very remarkable. The wound having closed very much, and the distance to the left cavity of the pleura under the sternum being considerable, a piece of sponge tied around the eye of a small gum-elastic catheter was introduced, so as to enlarge the track of the ball, and give passage to the air from the left side of the chest. This was done at five o’clock P.M., and at ten, on its being withdrawn, air rushed out in a very manifest manner, to his great relief. The metallic tinkling, which was distinct before the instrument was withdrawn, instantly ceased, but could be reproduced by closing the opening. The small gum catheter was therefore reintroduced with the eye projecting beyond the sponge, and retained, air passing through it; cough very troublesome.
March 17th.—Better; pulse 100; bowels open; cough[410] easier; expectorates freely a rouillée, or reddish muco-purulent matter.
18th.—Easier and better; breathing on the left side not heard below the fourth rib; discharge free; the permanent gum catheter taken out, but passed in daily. After this he slowly recovered, and continued to enjoy good health until the summer of 1854, when he died of what was supposed to be ulceration of the stomach, being an admirable instance of the treatment to be followed in such cases. When there is not an opening to enlarge, one should be made with the trocar.
It has been stated by the latest writers on pneumothorax, that tympanitic resonance on percussion, and the absence of respiration, are not pathognomonic signs of pneumothorax, as these physical signs may exist without it, and pneumothorax may exist without them. The metallic tinkling, in addition to the absence of all appearance of disease in the abdomen, will be conclusive of the presence of this disease.
322. Emphysema, from εν and φυσαω, to inflate; the diffusion of air into a part of or throughout the cellular tissue of the body. It has been said to take place after a wound of the chest, but without an injury of the lung, from the air passing through the wound into the cavity during inspiration; and by accumulation and subsequent compression under the act of expiration, giving rise to all the symptoms of the disease; a complaint more theoretical than real.
Emphysema, as a medical disease, is opposed to the surgical disease, in not being an extravasation of air into the cavity of the chest, but a dilatation of the air-cells formed for its reception. It is of two kinds, Vesicular and Interlobular—vesicular when dependent on the enlargement of one or more air-cells; interlobular when, from the sudden rupture of an air-cell, the air has found its way into the interlobular structure of the lung. A third and very rare kind has been added, in which air, being extravasated under the pleura, has raised it in the form of a pouch. The morbid appearances these diseases afford, and the symptoms they give rise to, do not fall within the range of surgical skill; and are not frequently within the controlling power of medical science and ability.
Emphysema is free from redness, and is distinguished from edema, or the swelling containing a serous fluid which is also colorless, by its not pitting on pressure, or retaining the[411] mark of the finger. It is, on the contrary, elastic; and the displacement of the air, on pressing on the part, gives rise to a peculiar noise, resembling the crackling of a dry bladder partly filled with air on its being compressed, usually called crepitation. This swelling extends as the air introduced increases in quantity until the whole of the areolar tissue of the body may be fully distended.
Emphysema most commonly occurs from fractured ribs, a point from one or more of which abrades the surface of the lung. Through the opening thus made, the air escapes into the sac of the pleura, and thence by the side of the broken part of the ribs into the cellular membrane. The distress in breathing arises from the air being diffused over the surface of the lung, which it gradually causes to collapse under the pressure exercised by the act of expiration; while, at the same time, the mediastinum yielding, the opposite lung suffers in a similar way, although to a less extent, until the aerification of the blood is so greatly obstructed as at last to interfere with life, unless relief be obtained by the equalization of the pressure made on the lung by the compressed air in the cavity of the pleura, with that exercised on the inside of the lung through the glottis.
In ordinary but not severe cases of fractured ribs, a slight degree of emphysema is frequently observed over the injured part, implying that the lung has been wounded; such a case requires the application of a compress, wetted with a little spirit and cold water, retained by a bandage. The great art in the treatment of broken ribs by compress and bandage consists in their proper application, which can only be ascertained by the feelings of the patient. The application of a broad flannel bandage, so as to restrain the motions of the chest, and to cause the sufferer to breathe by the diaphragm, has been recommended from the earliest periods of surgery; but many persons with injured or broken ribs cannot bear the pressure of a bandage, while others derive much ease from its use. A tight bandage generally disagrees when the injury has been sustained at the lower part of the chest, and is more frequently useful when the fracture is above the fifth or sixth rib.
When the emphysematous swelling extends so as to invade a considerable portion of the body, the further diffusion of air should be prevented by punctures made through the skin in such places as may be thought necessary, and in ex[412]treme cases even by incisions; but these are things more often spoken of and written about than practiced, or than are even necessary.
323. Mr. J. Bell had so alarmed all military surgeons by stating, in his able discourses on the Nature and Cure of Wounds, that emphysema was “peculiarly frequent in gunshot wounds of the chest, both at the orifice of entrance and of exit of the ball,” that they thought of little else. They could not withstand the brilliant manner in which this remarkable error—for error it is—was expressed. To such of us as had served in the first part of the war in Portugal it was no longer a bugbear; we slept in peace after the battles of Roliça and Vimiera, of Corunna, of Oporto, and Talavera—laughing, perhaps, a little at the credulity of the surgical portion of mankind; for the opening made by a musket-ball rarely admits of emphysema. A slanting wound made by a pistol-ball may sometimes give rise to it. After long and tortuous wounds made by swords or lances it is seen more frequently, but then it takes place shortly after the receipt of the injury.
A soldier, at the battle of Albuhera, was wounded in the right side of the chest by a sword, which had passed slantingly under the shoulder-blade, from which injury he did not suffer much, until the whole side as well as the body and neck began to swell and impede his breathing, which was effected with some difficulty and with any ease only when sitting up. The external wound was enlarged until I could distinctly hear the air rush out and see the part where the weapon had penetrated between the ribs; upon which he declared himself relieved, when the wound was closed by compress and bandage. It did not unite, however; active inflammation of the cavity of the chest ensued, requiring frequent and considerable losses of blood for its suppression. At the end of three weeks the man was sent to Elvas, in a favorable state for recovery.
324. When an opening is made into the cavity of the chest in the dead body, the lung recedes from the pleura lining its wall, for some distance; it is said to collapse; but this does not take place in anything like the same extent in the living body; and if the continued admission of air through the wound be prevented, it scarcely takes place at all; or, should it have done so, the air is usually absorbed and the lung quickly recovers its natural dimensions and[413] functions. Neither does a wound in the chest, when kept open, usually cause this collapse to the extent which it is generally supposed to do in the living body. The lung can be seen in motion and performing its office, although imperfectly, as it does not fill the cavity of the pleura. When the lung has been wounded by a ball actually going through its substance, it does not necessarily collapse; and abrasions or deeper injuries of its surface lead to no such result. To cause the complete collapse of a living lung, its surface must be compressed by a fluid, as in empyema, or by confined air, as in emphysema or in pneumothorax.
In extreme cases, when the patient can no longer lie down, but sits up, supported, in the greatest agony of respiration, approaching to suffocation, the face and lips swollen and blue, the pulse almost imperceptible and countless, an opening should be made into the chest by a small trocar and canula, for the purpose of evacuating the highly compressed and compressing air, and to allow the expansion of the lung after its evacuation. When this compressed air has been drawn off, as in the case of Lord Beaumont, the compressing power being removed, the lung expands in part, if not entirely, in spite of the breach in it, and the mediastinum and heart return to their natural situation, the distress in breathing is removed, the failing circulation is restored, and the opposite lung resumes its functions.
The course then to pursue in such extreme cases is merely to puncture the chest, evacuate the air, withdraw the canula, and close the opening. The life of the patient having been thus saved, time is given for the wound in the lung to heal under the usual inflammatory processes, provided it will do so without a recurrence of the mischief. This, if it should take place, must be met by another puncture, or the opening in the chest should be made permanent in order to equalize the pressure of the air in the cavity.
The incisions (the “taillades” of the French) into the cavity of the chest formerly recommended, should only be resorted to when the means indicated have failed, which they will rarely do when combined in the first instance with an antiphlogistic treatment, aided by sedatives, and if necessary by cordials.
The advantages to be derived from auscultation in these cases are evident. Its value has been sufficiently shown, and[414] the ear or the stethoscope should be resorted to at least three times in every twenty-four hours, in every case, however trifling it may appear to be, until the absence of danger has been ascertained.
SIMPLE INJURIES OF THE CHEST, ETC.
325. The most simple injury, perforating the wall of the chest, is a stab by a triangular sword, a small knife, or other weapon, which may or may not abrade the surface of the lung, and which is usually attended by little pain, although it often gives rise to considerable alarm. It might be supposed that a very slight wound of the lung would be followed by some expectoration of blood, but this does not always take place; and although its presence may be considered demonstrative of the injury, its absence is no proof of the contrary; for a considerable injury from a stab or from a musket-ball may be inflicted, with scarcely any sign of blood in the matter expectorated. If the pleuræ are in their natural state, a small quantity of air may enter the chest, but the opening will require to be direct and tolerably large before the lung will separate or shrink from the wall on that account; if adhesions should have been previously formed between the pleuræ preventing it, they will be for the advantage of the sufferer.
In a simple incised wound, injuring the lung perhaps extensively, as supposed from the bleeding from the mouth, no examination by probes or other instruments need or ought to be made as a general rule; but the wound should be immediately closed by sutures after the external parts have been sufficiently examined to satisfy the surgeon that no portion of the offending instrument has been broken off, or other extraneous matters are sticking in the part.
The advantages derived from the closure of punctured wounds of the chest in former times led to the practice of sucking them by the mouths of irregular practitioners, generally the drum-major of the regiment, when the patient was a soldier; and the consequences, although in some[415] instances apparently miraculous, were in others quite as unfortunate.
That bleeding may take place from the lung into the cavity of the chest is indisputable, but little or no blood will escape through a small wound; and its continuing to flow from such a wound will be a presumptive if not a conclusive proof that some artery external to the pleura has been wounded. Sucking, under ordinary circumstances, of a small wound, unattended by bleeding, does good by attracting the natural fluids to the parts, and thus causing them to swell so as to be placed in apposition in the most advantageous manner for their reunion. Punctured wounds of small size, therefore, may be sucked chirurgically if any one be willing to do it, after which a bit of gold-beater’s skin, or dry lint, should be placed upon the wound, supported by a compress covered by adhesive plaster; these dressings should not be removed for several days.
326. The patient should lie on the wounded part, as a general rule, if he can conveniently bear it, not for the purpose of allowing any effused blood or fluid to flow out, unless some particular reason require the precaution of keeping the wound open, but to allow the pleura covering the lung to be as closely applied as may be to the pleura lining the wall of the chest, with the hope that the adhesive process may take place between these parts, and by this means cut off the wound from the general cavity of the pleura, a proceeding due to the practice of the Peninsular war, yet so little attended to at the present time by some teachers of surgery, who seem to confound the practice thus recommended in incised wounds penetrating the cavity of the chest with that which should be adopted in gunshot wounds, that few students obtain even a reasonable degree of knowledge on this subject. Teachers are entitled to prefer any mode of treatment they please, but they should be careful not to neglect the opinions of others, whose authority, derived from experience, they are bound at least to notice, even if it should be to disapprove.
327. Incised wounds of even greater extent ought not to be examined by the probe or finger; no disturbance of any kind should be permitted unless the cartilage or bone be injured. The external parts should be brought together as closely as possible, so as to facilitate in every way their union, and the processes which it is desirable should go on[416] within. The external parts or skin and cellular membrane cannot be kept in perfect and continued apposition without sutures, and the proper method of proceeding is to sew up the wound in the skin with a needle and fine silken thread in a continuous manner, including absolutely nothing but so much of the cut edges as will retain the thread; a small piece of gold-beater’s skin or lint should then be laid over the stitches and retained by a compress and adhesive plaster.
In a simple case of this kind little or nothing is effused into the cavity or secreted from the membranes of the chest, which will interfere with the processes which may have happily begun, and which it is desirable should be aided by the absolute quiescence of the patient, to whom no medicine should be given which may render any movement of the body necessary. It was formerly supposed that the greatest object to be attained was the prevention of inflammation, and a man was no sooner stabbed by his opponent than he was blooded and purged by his surgeon, regardless of the necessity which existed for perfect rest and the presence of a certain amount of inflammation, in order to enable nature to carry on those processes which are essential for the restoration of the injured parts. This inflammation should be allowed to commence without interference and to continue in a moderate degree until the object shall have been effected. It should only be interrupted or subdued when it is supposed to be about to exceed that degree which experience has pointed out as likely to be useful.
328. When the most courageous persons are wounded in parts essential to life, there is more or less alarm or shock created by the injury; although it has been gravely argued that a man does not always know when he is actually shot or run through the body. A continued state of anxiety and depression after an accident of this kind is a disagreeable accompaniment of the injury, during which little should be done beyond the giving a little cordial, and quieting the apprehensions of the patient, leaving him to rest, if possible, after the necessary applications have been made. If a gradual improvement take place, if the pulse rise, if the patient resume more of his natural appearance, and that state of commencing excitement which is denominated reaction follow, hope may then be entertained. The general symptoms, as long as they continue within ordinary bounds, are of little importance; the local ones, significative of action[417] commencing in the injured part, are, however, to be carefully watched. They are those of inflammation of the pleura, and it may be of the lung. This inflammation begins slowly, and a day may elapse before it is well marked; for, when persons have died within the first few hours after such injuries, the pleura has often shown but little sign of inflammatory action. Auscultation should always be resorted to from the moment of injury, and constantly used throughout the treatment. Whenever it is concluded that adhesion between the two pleuræ has failed to take place, the direction to lie on the wounded side ceases to be of importance. Until this period no food whatever should be allowed, and thirst should be allayed by small quantities of water.
329. A punctured, incised, or gunshot wound, going fairly through both cavities of the chest, is usually believed to be quickly if not immediately mortal—an opinion generally correct with respect to wounds made by musket-balls, although it is certainly not the case with regard to punctured wounds, and does not always occur in those made by pistol or musket-balls.
Sergeant-Major Richards, of the 29th Regiment, received thirteen sword or bayonet wounds, and other injuries, on the heights of Roliça, on the 17th August, 1808—one particularly through each side of the chest, between the ribs, as if the small-sword had made a wound of larger size than usual. He had distinguished himself greatly in covering the body of his commanding officer, and was beaten down before the British column, which had been repulsed, could rally and recover its ground. He was an object of particular attention to me, for the few minutes he lived after I saw him; he had coughed up a little blood, and died gasping, as if suffocated, the chest laboring on each side to do its work in vain. His commanding officer, Colonel the Hon. George Lake, lay dead by his side, killed instantaneously by a musket-ball, which passed from the upper part of the left through the right side of the chest.
A French gentleman, fencing with his pupil in July, 1834, received a blow under the right axilla in a very violent lunge, whereby the button of the foil was broken off, and the foil itself passed into and through the back part of the thorax, the point coming out between the sixth and seventh ribs on the left side near the angles. There was but little bleeding. The chief symptoms were those of great inflammation of the[418] contents of the cavity, which gave way to full and repeated bleeding from the arm, with perfect rest and almost starvation. He recovered very favorably, and was quite well in about eight weeks. He remains well, and is following his profession as a teacher of fencing.
330. When an incised wound into the chest is large and direct, injuring the lung, two very important points usually demand immediate attention. The first is to relieve the oppressed state of the breathing; the second, to suppress the bleeding.
In large penetrating wounds of the chest, with injury of the lung, it has been observed that the patient has breathed most easily when the external wound has been covered; and has been hardly able to breathe when it was opened, which is attributed to the air getting into that side of the thorax in inspiration, instead of entering the lung by the trachea. If the wound admit of being well closed, the difficulty of breathing diminishes; adhesion may take place, and the inflammatory action within the chest may terminate; but if the inflammatory symptoms continue, adhesion does not take place, and the secretion and effusion of a quantity of serous fluid are the consequence. This secretion of fluid is the natural consequence of inflammation which has passed the stage of adhesion, whether the injury of the chest have occurred from a stab or from a gunshot. It is the leading fact in the treatment of these injuries, hitherto disregarded by writers on this subject, but on the proper management of which, in both instances, a successful result principally depends. If the closure of the wound lead, in the course of a few days, to the re-establishment of the breathing, and the antiphlogistic means employed to the cessation of all urgent inflammatory symptoms, adhesion has most likely taken place, or is about to take place, in the neighborhood of the wound, and the patient will in all probability recover without much further suffering. If this should not occur, and effusion take place, the wound should be reopened, or the fluid otherwise evacuated.
A soldier of the 9th Regiment was wounded at Roliça, in 1808, by the point of a sword in the left side; it penetrated the chest, making a wound somewhat more than an inch long, through which air passed readily, accompanied by a very little frothy blood, which was also spit up on any effort being made to cough, leaving no doubt of the lung[419] having been injured, that viscus appearing to be retained against the wall of the chest. As the edges of the wound could not be accurately kept in apposition by adhesive plaster, two sutures were applied through the skin, and the man was desired to lie on the injured side, with the hope that adhesion might take place, as there appeared to be no effusion of blood into the cavity. He was freely bled on each of the two days following the receipt of the wound, and gradually recovered.
A French soldier was brought into the village after the battle of Vimiera, wounded by a sword in the right side of the chest. He said he had lost a good deal of blood; was very pale; pulse small; extremities cold; breathing hurried and oppressed; had spit up some blood. On removing the handkerchief, a gaping wound presented itself, an inch and a half long, through which the cavity of the chest could be seen, the lung having receded. The wound did not bleed. As adhesive plasters would not keep the edges of the skin in perfect contact if he attempted to move, they were sewn together, and after the application of a compress he was much relieved. The next day all the symptoms were alleviated, and after the supervention of some serious inflammatory symptoms, he was forwarded to Lisbon, for embarkation for France, in a fair state of recovery.
It was the successful results of these cases which led to the closure of all such wounds in the first instance, with the hope of preventing thereby the extension of the inflammation to the whole sac of the pleura, which in many instances it succeeds in doing; and thus that which was done in the first instance from apparent necessity, rather than scientifically adopted, became a rule of practice, which may be laid down as a principle to be followed in similar cases. When persons thus wounded are neglected, the wound remains open, and the cavity of the pleura passes into a state of suppuration, after all the symptoms of acute pleuritis or of pleuro-pneumonia have taken place.
331. If the union of a large incised or other wound by the adhesive process does not take place, a bloody, serous fluid oozes out from under the dressings, if the oppression of breathing should not have led to their removal; the patient is relieved by the discharge, which, after a time, as the case proceeds toward recovery, will become less in quantity and more purulent in quality.
[420] If the union of the divided parts should take place externally, and the general as well as local symptoms become more urgent, there can be little doubt of a collection of some kind having taken place, and then auscultation and percussion, if the latter can be borne, become of the greatest importance. From the moment the wound is closed the ear becomes the most important guide; the only one in fact to be depended upon as to what is going on within the chest. The case is one of pleuritis, perhaps of pleuro-pneumonia, and hence the reason that the symptoms and treatment of these complaints have been more fully noticed than might be considered to appertain to the province of surgery. The effusion of a bloody, serous fluid comes on, after a penetrating injury, from the third until the seventh or ninth day, by which time the cavity of the pleura may be filled; puncturing the chest between the sixth and seventh ribs at the point of election, or reopening the wound, should be early resorted to for its evacuation.
A picket of Portuguese infantry being surprised by a sudden rush of French cavalry from the town, during the first unsuccessful siege of Badajos, were nearly all sabred. The survivors were brought to me. Two had been run through one side of the chest, and one through both sides; the last died a few minutes after I saw him. The other two seemed to be nearly in a similar situation from loss of blood by the mouth and from the wounds. These were immediately closed by stitches, compresses, and adhesive plasters. A little hot brandy and water was given to each, and they were laid aside without hope of recovery. They did not die, however; the breathing became more easy, the distress less, and the pulse more distinct; reaction after a time took place. The next morning, the siege being abandoned, they were removed to Elvas, where I afterward heard they were doing well.
A soldier of the Third Division of Infantry, under the command of Sir James Kempt, was wounded at Waterloo, by a straight sword or sabre, which penetrated the left side of the chest. He fell, and lost a considerable quantity of blood from the mouth as well as from the wound, and was supposed to be dying. On showing some signs of life, the wound was covered by a part of his shirt; and on his arrival at the Elizabeth Hospital in Brussels, four days afterward, it was closed. On the ninth day, when my attention was[421] drawn to him, he was sitting up in great distress, from difficulty of breathing, his hand pressed upon the wounded part, the cicatrix of which was red, swollen, and projecting. I recommended the assistant-surgeon in charge to open this with an abscess lancet, which he did, giving vent to a very large quantity of bloody and purulent matter, to the great relief of the patient for several days, although he did not ultimately recover.
The advantage derived from the closure of the wounds in these cases was manifest. It relieved the breathing, and caused the hemorrhage to cease, aided, in all probability, by the exhausted state of the patients. The relief to the breathing was at the moment the most essential point, the wounds of entrance being nearly two inches long, and the free admission of air quite unopposed; the lung had receded from the opening.
332. The important question of hemorrhage, in cases of incised wounds admitting of being accurately closed, remains for consideration. In many instances, the quantity of blood effused is trifling, and in others, although greater, it is absorbed without being productive of evil. In a third class, the quantity extravasated is larger than can be absorbed, although it does not flow in an inconvenient or dangerous manner through the wound, and may ultimately become coagulated and adherent to the diaphragm and spine in the angle between them, when the patient lies long on his back. In the worst or most alarming cases, the loss of blood is and has been so great that its suppression offers the only chance for the continuance of life. It is between these two last cases only that a difference of opinion exists as to the treatment to be pursued: one party desiring that the effused blood, if moderate in quantity, should be allowed to discharge itself, the wound being kept open; the other, that under all circumstances, whether the quantity of blood poured out be small or great, the wound should be closed, and the result awaited. The right course is, I apprehend, to remove all the blood which can be evacuated by position, provided it can be done without danger to the patient, rather than to allow it to fill the chest; but as the bleeding vessel in the lung cannot readily be got at, if seen, nor be secured by ligature with advantage, it is advisable, if the bleeding continue, to close the wound, and allow the cavity of the pleura to be filled, until the lung shall be sufficiently com[422]pressed to cause the hemorrhage to cease, if the person survive so long. The first object is to save life; after that, if time be given, the next will be to relieve the loaded cavity. After the wound has been closed, and the patient has so far recovered that reaction has begun to take place, it may be concluded that the bleeding has ceased. The chest should then be most carefully auscultated from day to day, so that its respiratory state may be known, particularly with regard to the increase of effusion, which will then be serous. This will not take place until after the third, and not perhaps before the fifth or sixth day, in any considerable quantity; when, if it should have occurred, the wound should be reopened, or another opening made at the most convenient place for the evacuation of the effused blood and serum. It is probable that the wound of the vessel in the lung which furnished the blood will be closed in five or six days: while it is of great importance that the lung should be early relieved from pressure, that it should be allowed to expand, and not be bound down by false membranes; which will be the case if the compressing fluid be not removed, and the inflammatory symptoms subdued. There is no object to be gained but the suppression of the hemorrhage by retaining the blood and serum within the chest; while the probability of a return of the bleeding is not great after an opening has been made, and the blood and serum have been evacuated, although much mischief will inevitably follow the effused fluids remaining too long.
Repeated observation has shown that in sabre-wounds penetrating the chest and lung, which have not united, and from which no excessive hemorrhage has occurred, a great discharge of serous fluid usually takes place from the cavity, which, gradually diminishing, becomes purulent, and at last ceases, without the function of the lung being destroyed; while, if the wound had been early closed, and the fluid collected too long retained, the functions of the lung would be impaired, and a counter-opening, for the relief of the resulting empyema, may be unavailing. Whenever, therefore, the adhesive process between the pleuræ has failed, and great effusion has taken place, the sooner it is discharged the better.
In addition to the closure of the wound, it is desirable to arrest the hemorrhage by other means, if possible, such as the abstraction of blood from the arm to such an extent as[423] it may be considered the patient can bear, the administration of the acetate of lead with opium, turpentine, matico, or the mineral acids; and the external and internal use of cold or iced water, if it can be borne. If there be reason to believe that a rib or ribs have been injured—that any extraneous body is inclosed in the wound—or, from its appearance, that it will certainly reopen, an incision should be made in the part injured, for the purpose of giving the necessary assistance. The cure, however, will not only be assisted, but mainly effected, by procuring a depending opening by means of the small trocar and canula introduced as low down as auscultation will authorize; the introduction of this instrument will give the desired information on the one hand, and do little or no harm on the other.
A soldier of the 3d Regiment of Infantry was wounded by a lance at the battle of Albuhera, in the left side, between the fifth and sixth ribs; and was thrown down, bleeding from the mouth and from the wound, which was afterward closed by his comrades, by confining upon it a piece of his shirt folded up for the purpose. Brought to the hospital, at the village of Valverde, he appeared ten days afterward to be dying from difficulty of breathing. On enlarging the opening in the integuments, a quantity of blood, partly fluid, partly coagulated, issued from the cavity of the chest. The wound was kept open to allow the discharge of this, and of a reddish, watery fluid, which, after a few days, became purulent. At the end of three weeks I sent him to Elvas, doing well, and with but little discharge from the wound.
A heavy dragoon, of the German Legion, was wounded at the battle of Salamanca by a sword, which penetrated the cavity of the right side of the chest, between the sixth and seventh ribs. He fell from his horse, and lost a considerable quantity of blood from the mouth and from the wound. On examining the wound next day, a black coagulum was seen filling up the orifice, the cellular membrane around being considerably ecchymosed, and little doubt existed that the oppression in breathing under which he labored was caused by blood effused into the cavity. On separating the edges of the wound with a director, several ounces of blood, half fluid, half coagulated, were evacuated by making the external opening, which was enlarged, quite dependent. The lung was then seen in contact with the external opening of the wound, having expanded as the pressure of the blood was[424] removed from it. The wound was closed simply by lint, compress, and adhesive plaster, without bandage; the man was largely bled, and placed upon his wounded side on the ground, being the most comfortable position, in some degree relieved from the oppression in breathing. Two days after, the wound discharged freely a reddish-colored watery fluid, evidently from the cavity of the chest, the exit of which was aided by keeping the wound generally dependent. This continued for several days, the fluid gradually becoming less in quantity, and purulent; under careful management he was able to go to the rear, nearly well, by the end of October.
333. On the subject of the ecchymosis, which Valentin considers to be a pathognomonic sign of effusion of blood within the chest, he says: “It is very dissimilar to that which occurs after a blow or wound, and which takes place shortly after the accident, beginning around the wound, if there be one, and extending from it. The patient also complains of pain when the bruised part is pressed by the fingers. These characters are not observed in the ecchymosis, the sign of effusion, which always takes place near the angles of the lower or false ribs descending toward the loins. Its color is identical with that which appears on the abdomen of persons some time after death, a bright violet, (violet très éclairci.) It appears about ten days after the receipt of the injury, sometimes later.” The same sort of thing, he thinks, takes place when the cavity of the chest is filled with pus, but that edematous swelling is without discoloration.
334. In order to be explicit on points so important as those of which I have treated, I have thought it right to lay down certain general conclusions, subject to occasional deviations:—
a. All incised or punctured wounds of the chest should be closed as quickly as possible by a continuous suture through the skin only and a compress supported by adhesive plasters, the patient being afterward placed on the wounded side—a precept which is absolute only with respect to incised wounds capable of being united by suture in the manner directed.
b. As soon as the presence of even a serous fluid in the chest is ascertained to be in sufficient quantity to compress the lung, a counter-opening should be made in the place of election for its evacuation by the trocar and canula, which may be afterward enlarged; unless the reopening of the[425] wound should be thought preferable, which will not be the case unless it should be low in the chest.
c. If blood flow freely from a small opening, the wound should be enlarged so as to show whether it does or does not flow from within the cavity. If it evidently proceed from a vessel external to the cavity, that vessel must be secured by torsion or by a ligature applied on it, all the other methods recommended being simply surgical absurdities.
d. If blood flow from within the chest in a manner likely to endanger life, the wound should be instantly closed; but as the loss of a reasonable quantity of blood in such cases, say from two to three pounds, will be beneficial rather than otherwise, this closure may be delayed until syncope takes place or until a further loss of blood appears unadvisable.
e. If the wound in the chest have ceased to bleed, although a quantity of blood is manifestly effused into the cavity of the pleura, the wound may be left open, although lightly covered, for a few hours, if the effused or extravasated blood should seem likely to be evacuated from it when aided by position; but as soon as this evacuation appears to have been effected, or cannot be accomplished, the wound should be closed. It must be borne in mind that the extravasation which does take place is usually less than is generally supposed—a point which auscultation will in all probability disclose.
f. If the cavity of the pleura be full of blood, and the oppression of breathing and the distress so great as to place the life of the patient in immediate danger from suffocation, the wound should be reopened, if it have been closed, or freely enlarged, if small, to such an extent as will allow a clear evacuation of the effused blood. It has been supposed that in such a case the lung does not sufficiently collapse, and the bleeding is therefore continued because the vessel cannot contract; but the lung will usually collapse under pressure of the air, unless prevented by previously-formed adhesions, when the hemorrhage may possibly cease—instances of which are said to have taken place, and the practice should therefore be borne in mind.
WOUNDS OF THE CHEST, ETC.
335. Gunshot wounds of the chest, penetrating the cavity, are always exceedingly dangerous. After the battle of Toulouse, on the 10th of April, 1814, one hundred and six cases of wounds in the chest in officers and soldiers, in all of whom the cavities were not penetrated, were received into hospital. Between the 12th of April and the 28th of June thirty-five died, fourteen were discharged to duty, and fifty-seven were transferred to Bordeaux to proceed to England, some to die, some to be pensioned, but few in all probability to return to the service—being an ultimate loss of nearly one-half, if the fifty-seven cases sent to England could be traced. M. Menière, in giving an account of the wounded carried to the Hôtel-Dieu of Paris, in the three remarkable days of July, 1830, where every case was immediately taken care of, says forty cases were received into the hospital; of these twenty died; he states the case of ten more, seriously wounded, who recovered; and he gives the names of seven more, in six of whom the cavity of the chest was not perforated, and alludes to three wounded by small-swords, who recovered—the loss being thus one-half, even if the rest happily and perfectly recovered, which may be doubted, thus showing that with the ablest assistance the Hôtel-Dieu of Paris could afford the loss was one-half. After the battle of Waterloo the loss was much greater; with the army on the Sutlej the loss was deplorable, in consequence of the want of a sufficient number of medical officers and of means—a state of destitution to which I have drawn the attention of the directors of the East India Company in the strongest possible terms, but which they will not rectify, but which will some day, I hope, become the subject of Parliamentary discussion, and, I doubt not, of public reprobation. That the wounds of the chest with the army in the Crimea will afford a more satisfactory result, cannot, I fear, be expected, and for similar reasons.
336. When a musket-ball fairly passes through the cavity[427] of the chest, the orifice of entrance is round, depressed, dark colored, and more or less bloody in the first instance; the orifice of exit is generally more of a rugged slit or tear than a hole. The alarm is great, and the powers of life are much depressed. The wounds may or may not bleed; the sufferer may spit up more or less blood; respiration may be difficult, countenance pale, extremities cold, pulse variable—symptoms dependent on particular constitutions and circumstances connected with the extent of the injury.
It has been said that balls are apt to run round the body, coming out at a point opposite to that at which they entered, without penetrating the cavity of the chest; this, whenever it does take place, is a rare exception to a general rule, dependent on the ball being reflected from something solid which it cannot penetrate, such as a button, a piece of money, a rib, etc. If the ball run under the integuments exterior to the fascia covering the intercostal muscles, it is usually marked by a tenderness in its course on touching the part and a discoloration of the skin. A ball may, however, run between two ribs for some distance, injuring the muscular structures between them without penetrating the cavity, in which case, after the first moments of alarm have passed away, the symptoms indicative of a penetrating wound either cease or do not occur, although those of inflammation of the pleura or lung may and often do follow to a considerable extent.
When the ball cannot be traced, the absence of symptoms, after the first period of alarm has subsided, will enable the surgeon to form the surest prognosis; their absence, however, cannot too certainly be relied on.
A ball will occasionally rebound from the sternum, leaving merely a black mark; from the spongy nature of that bone in which they frequently lodge, they require the application of the trephine. If a ball should be felt through a wound in the sternum, the broken portions of bone should be removed by the small saw or by the trephine, and the ball extracted.
337. An enlargement of the wound, the “debridement” of the French, does no harm beyond the pain it occasions, unless there be something to be removed, when an incision becomes necessary, in many instances, for the removal of extraneous bodies or for the evacuation of blood, etc. When a wound from a musket-ball appears likely to have penetrated the cavity of the chest, and is too small to admit the[428] end of the finger, the opening ought to be enlarged so as to allow its introduction as far as the ribs, in order to ascertain whether those bones have sustained any injury, or whether anything is lodged exterior to or within them. It is not necessary that a man should be cut simply because he has been shot; and an enlargement of the wound should be of no greater extent than is absolutely necessary for the purpose intended. When pieces of shell, or of a sword or lance, are broken off and partly lodged in the cavity of the thorax, which is more likely to happen when they enter through the large muscles of the back, they will require larger incisions to give room for their removal. Great praise was given of old to Gerard, surgeon-in-chief of La Charité in Paris, who, having perceived that a small sword, after going through a rib, was broken off close to it, thought it advisable to make an incision through the intercostal muscles into the chest, and then to introduce his forefinger, armed at the end with a thimble, with which he pressed back the point of the broken blade. In a case of this kind, the surface and outer edge of the bone should be removed, until the piece of steel can be firmly seized and withdrawn by a fine pair of pincers or pliers.
When a ball sticks firmly between two ribs, it requires some care to remove it, as the rib both above and below may be more or less interested, although not actually fractured. The attempt should be made during inspiration, when the lower rib should be depressed, and some thin but not sharp-pointed instrument like an elevator should be gently pressed around and under the looser edge of the ball, in order to extricate it.
When a musket-ball fractures a rib, there ought to be no hesitation about the propriety of enlarging the wound, to allow the splintered portions of bone to be removed. It is possible that in doing this some pieces of cloth or other matters may be extracted, which might else glide into the cavity of the thorax, or stick in the lung itself.
A soldier of one of the regiments on the left of the position of Talavera was brought to me, wounded by a ball in the left side of the breast; it had struck the sixth rib, and passed out about four inches nearer the back. As the point of the finger indicated the presence of broken bone, I enlarged the anterior wound, and then found that the ball had driven some spiculæ of bone into the surface of the[429] lung, which appeared to have been previously attached to the pleura costalis at that part. These having been removed, together with a piece of coat which had been carried in with the ball, a small, clean wound was left, which gradually healed up, the man accompanying me on the retreat over the bridge of Arzobispo.
338. When a ball impinges with force on the center of one of the ribs, and passes into or through the chest, the bone is usually broken into several splinters of different lengths, some of which frequently accompany the ball in the commencement of its course, or are even carried into the substance of the lung, together with a part of the wadding of the gun, or of the clothes of the patient. These should if possible be extracted if they can be seen, and the sharp ends of the rib rounded off. When the ball fractures a rib on passing out of the chest, the splinters are driven outwardly, and should be removed by incision.
339. When a ball strikes a cartilage of one of the ribs, it does not punch out a piece as it were, but merely divides and passes through it, bending it inward, rarely tearing away a portion. The parts of the cartilage thus bent and turned inward are to be drawn outward, and replaced by the end of the finger, a bent probe, or other curved instrument.
A ball, when striking obliquely but with force on the chest, will frequently penetrate, and then run round, between the lung and the pleura lining the wall of the chest, for a considerable distance, before it makes its exit. In this case the lung may be only slightly bruised, without the pleura pulmonalis or costalis being more than ruffled. In others the lung shows a distinct track or hollow made by the ball. A shade deeper, and the ball penetrates, and forms not a hollow, but a canal. The patient in all these cases spits blood, and the first symptoms are severe; they frequently, however, subside, and are not always followed, under proper treatment, by effusion, although it may always be expected.
340. When a ball fairly passes through the lung, it leaves a track more or less bruised, which continues for a time to bleed according to the size of the vessels which are injured, thus making a wound more dangerous as it approaches the root of the lung where the vessels are largest. More or less blood is spit up, or, if effused, it[430] gravitates in the chest, until it rests on the diaphragm or other most depending part, according to the position of the patient. If it should be in quantity, the filling up of the chest may be ascertained by auscultation, if the wound be closed. As the quantity of effused blood increases, the lung becomes more and more compressed, until at last the hemorrhage ceases under pressure, if the wound be covered; and the patient is saved for the moment, unless he should die of asphyxia, from the lung on the other side being also compressed through the bulging of the mediastinum on it; to prevent which, if possible, the wound should be reopened or enlarged, so as to take off the pressure of the effused and perhaps coagulated blood. If the person wounded shall have suffered formerly from inflammation, and the lung has adhered in consequence to the wall of the thorax, at the parts where the ball enters and goes out, the cavity of the chest will not be opened, and the track only of the ball will communicate with the external parts, unless the ball shall have perforated some of the large vessels, when he will continue to bleed by the mouth. The pressure of the blood effused into the track of the ball, which may become coagulated, will sometimes suffice, under even these circumstances, to effect the suppression of the hemorrhage which the loss of blood, the faintness of the patient, and the weakness of the circulation, under proper treatment, will materially assist in rendering permanent.
General Sir G. Lowry Cole, G.C.B., was struck at the battle of Salamanca, on the 22d of July, 1812, by a musket-ball, which entered immediately below the clavicle, fractured the first rib, and, inclining inward, came out through the scapula behind; as he spat blood for three days, the upper part of the lung was shown to have been injured. The ball appeared to have passed so close to the under part of the subclavian artery that the greatest fears were entertained for his safety; more particularly as a marked difference in the size of the pulse was perceived in the left arm, which did not exist before. He remained three days on the field of battle, in a Portuguese officer’s tent I always carried with me. Under repeated bleedings, and the strictest antiphlogistic treatment, several splinters having come away, and a large piece of the rib and of the scapula having exfoliated, he gradually recovered, so as to be able to resume the command of the Fourth Division in October at Madrid.[431] The subclavian artery never resumed its power, and the radial always beat less forcibly on the left side. He perfectly recovered his health, the respiratory murmur of the lung being natural. He died suddenly in 1844, from rupture, I believe, of an aneurism of the abdominal aorta.
A dragoon of the King’s German Legion, shot in a nearly similar manner on the same occasion, suffered more severely: the clavicle and first rib were splintered to a greater extent, and he lost a large quantity of blood by the mouth. The splinters having been removed, after enlarging both wounds for that purpose, and the inflammatory symptoms subdued, he appeared to be going on favorably for three weeks; when, having eaten some meat obtained irregularly, he suffered what seemed to be a bilious attack of vomiting and purging, attended by fever and oppression in the chest; an ipecacuanha emetic having been given with full effect, relieved him much. During the efforts to vomit, the wounds discharged a quantity of sero-purulent fluid, a piece of the cloth of his coat, and another of bone, which had gone in with the ball, and in all likelihood had been lying with the matter at the bottom of the chest. After this he slowly recovered. This case is peculiarly instructive.
General Sir Andrew Barnard, G.C.B., was wounded when in command of the Rifle Brigade, at the passage of the Nivelle, on the 10th November, 1813, by a musket-ball, which entered between the second and third ribs, in front of the right side of the chest, passed directly through the cavity and through the shoulder-blade, from under the integuments covering which it was removed. He not only felt but heard the sound of the ball as it struck him, and he fell from his horse. Blood gushed from his mouth, and continued to do so until after he was completely exhausted by bleeding from the arm to the amount of two quarts. He was again bled at night, and the subsequent morning, which relieved all the material symptoms. During six weeks he suffered from difficulty of breathing and cough, and from night-sweats. Some pieces of bone and cloth came away from the wounds, with a free discharge in the first instance, which gradually diminished until the wound closed. In eight weeks he was able to resume his command.
[432] More than forty years afterward I found the lung pervious; the vesicular murmur could be freely heard even up to the situation of the wounds, to the internal parts of which it may be concluded the lung adhered, from the sound conveyed to the ear on auscultation. He suffered little or no subsequent inconvenience from the injury, and died in January, 1855, aged 82.
Case of Major-General Broke, by himself.—Toward the close of the battle of Orthez, on the 27th of February, 1814, a musket-shot struck me between the second and third ribs on the right side, near the breast-bone. I was then on horseback, being aid-de-camp to Lieutenant-General Sir Henry Clinton, commanding the Sixth Division. The sensation was precisely as if I had been struck a violent blow with the point of a cane, but it did not unhorse me. I was attended in a very short time by the surgeon of the 61st Regiment, when, on removing my clothes, the air and blood bubbled out from the wound as I drew my breath. The surgeon, turning me on my face, discovered the ball to be lodged under the thin part of the blade-bone. This he cut through and extracted the ball, and with it pieces of my coat, waistcoat, and shirt, which were lodged between the ribs and the blade-bone. This occurred about four P.M. I was then removed to the town of Orthez, a distance of about three miles, and in the course of the afternoon the veins of both arms were opened in at least seven different places, but scarcely any blood came away; breathing became exceedingly painful in a day or two, and I felt nearly suffocated, when, in the evening, my brother, Sir Charles Broke Vere, arrived with my friend, Mr. Guthrie, who examined me carefully. The agony of drawing breath was such that I could scarcely endure it. He opened one of the temporal arteries, and desired that it might be allowed to bleed without interruption. He afterward left me to visit some other wounded men, and returned in about three hours, when I told him that I felt relieved, and had much less of the suffocating pain in breathing. He then opened the other temporal artery, directing as before that its bleeding should not be checked. I shortly after that dropped asleep, and on waking could breathe freely; my recovery was progressive from that time, the wound in front, where the ball entered, being the first closed; but both were healed at the end of about eight weeks, and in about ten I was able to rejoin the army at Bordeaux.
H. G. Broke, Major-General. [433]
He is now, in 1855, in perfect health, the respiratory murmur being free all over the chest.
The Duke of Richmond, then Earl of March, was wounded by a musket-ball at the battle of Orthez, while at the head of his company in the 52d Light Infantry. He was standing at the moment with his right face toward the enemy. The ball entered that side of the chest, between the fourth and fifth ribs, nearly in a line with the lower edge of the scapula. He fell to the ground with great violence, and was speechless for some time. He stated to me at a subsequent period that the sensation he felt at the moment was as if he had been “cut in two.”
On immediate examination there was no other opening to be found but the one where the ball had entered; nor were the medical officers able to feel the ball anywhere under the skin or under the muscles.
The wound having been dressed he was laid on a door and removed to Orthez, about three miles from the scene of action, during which he complained of excruciating pain, extending from the wound to the top of the os ilii on the same side, the pain being much aggravated by frequent and severe cough, with copious expectoration of frothy mucus, and much florid blood; respiration hurried; countenance pale.
The moving him to Orthez occupied nearly three hours; a great part of the ground being very rough and broken, the men could not well step together, and the consequent unavoidable shaking and jolting caused him much pain. On his arrival at Orthez, he was extremely languid, with a tendency to syncope. Pulse feeble; extremities rather cold.
Seven in the evening: After having been faint for an hour, he became hot and restless; pulse 108, and full; skin more hot, and the respiration short and more hurried. After he was placed in bed hemorrhage from the wound took place to a very considerable extent. Eight ounces of blood were taken from the arm. (Could bear no more.)
15th inst., nine A.M.: After the bleeding he became more quiet, and had less pain; but he has since become very restless, and the pain returned, with a full, hard, and frequent pulse. The wound has again discharged a very considerable quantity of blood. Bleeding repeated as before.
Nine P.M.: Deputy-Inspector Thomson and Staff-Surgeon Maling examined the wound. Mr. Maling introduced his[434] finger (the whole length) between the ribs into the wound without any interruption to its progress, and without being able to reach the termination of the passage of the ball; and Dr. Thomson then passed a probe (its whole length) straight into the chest, with a similar result; thus leaving no doubt on the minds of all present that the ball had passed directly into the posterior part of the chest.
Midnight: The blood last taken is very buffy; and there has again been an immense discharge of blood, etc. from the wound; the sheets, mattresses, etc. are saturated with it; and on the floor, under the bed, there is a large pool of blood which had soaked through the bedding. Pulse 114, low and frequent; cough and expectoration as before; pain violent, and great restlessness. Repeat the bleeding.
Mem.—Perhaps enough has now been stated to show the nature of the wound; and any further detailed statement of his lordship’s sufferings, or the treatment of his case, would be unnecessary. On the latter point, however, it may be mentioned that, exclusive of the general treatment, he was bled seven times between the evening of the 27th of February and the morning of the 2d of March, the cough, expectoration, breathing, pain, etc. being much relieved by each bleeding.
A. Hair, M.D.
Mr. Guthrie saw the Earl of March on the same day as Colonel Broke, and suggested that no further efforts should be made to find the ball, while the treatment adopted should be steadily pursued; and in 1846, he pointed it out lying under the edge of the base of the scapula. His grace is now, 1855, in good health, and the chest, well formed, sounds clearly and healthily in every part, even at the point injured.
341. The ball in passing through the lung, in these cases, destroyed the life of that part only which it touched; and although air would pass out at the time, this would not be of long continuance. The wounds being kept covered, the lung did not and does not usually, in similar instances, collapse or recede from the wall of the chest, but quickly recovers its state of expansion, however impaired it may be at the moment by the injury. The track made by the ball gradually suppurates and heals, leaving merely a depression or cicatrix on the surface attached around or in part to the wall of the chest by adhesion. The track through the lung[435] may be readily seen in such cases after death; although during life it interferes so little with the respiratory murmur as not to be observable, unless by its greater distinctness, from the thinness of the intervening parts.
Mrs. M. was wounded by a small pistol-ball, which entered on the right side from behind, between the seventh and eighth ribs, just under the arm when hanging down, and passed out in front over the cartilage of the sixth rib, more than an inch from the pit of the stomach. She had not spit blood, and the ear declared the lung to be pervious to air at the wounded part, which raised a hope that the ball might not have penetrated the cavity, although it might have injured the pleura. As she suffered great pain twenty-four hours after the injury, the breathing being oppressed, Mr. Adams bled her into a hand-basin, until about to faint. She lost nearly thirty ounces of blood, but her symptoms were quite relieved, so as to render any other bleeding during her treatment unnecessary. At the end of the third day she spat a very little blood after removal in a carriage to another lodging, and then gradually recovered. After four different stethoscopic investigations, I came to the conclusion that the ball had not struck the lung in the first instance, although the lung adhered to the pleura costalis, and suffered from some abrasion or ulceration at that point, which gave rise to the expectorated blood.
These cases are instances of wounds of the upper part of the lung, which are in general more dangerous than those of the lower, from the vessels being larger, and from the greater difficulty with which any extravasated blood or fluids can escape. They also prove that when blood is poured out in small quantity, it may be absorbed, but what that quantity may amount to is doubtful.
342. In cases in which the external opening or wound does not communicate freely with the cavity of the chest, the principal danger arises from the inflammation of the pleura ending in effusion, which, if not evacuated, leads to the loss of the individual. It is the great fact to be attended to in the treatment of pistol wounds of the chest, or those made by small balls which do not pass out. All the persons I have seen die from small balls have died with the affected cavity more or less full of fluid. The post-mortem reports of all persons killed in England in duels by wounds through the chest, unwittingly attest this fact, as well as the [436] insufficiency of the surgical treatment they received; and the necessity, for the future, for its amendment. It is in these cases that the stethoscope is most valuable—its frequent use indispensable. When the respiratory murmur ceases to be heard except at what is the upper part of the chest, whatever the position of the patient may be, it is full time to enlarge the original opening, or to draw off the fluid by the trocar and canula.
Laennec thought that when a considerable effusion took place in pleuro-pneumonia, filling the posterior part of the chest when the patient lay on his back, it nevertheless diffused itself over the whole surface of the lung; but dissection has shown, in cases of wounds, that the fore part of the lung may be applied to the anterior part and sides of the ribs, while a serous effusion fills the hollow behind, the respiratory murmur being distinctly heard above it. It is the most important fact to ascertain, particularly in pistol or small penetrating wounds of the chest, in which the opening is not sufficiently large to allow any fluid effused to run out.
Sir C. B. was wounded by a pistol-ball in the back, which passed into the chest through the lower part of the lung of the right side, and lodged on the inside of the wall of the chest in front of the same side, sticking in and against a rib, but giving rise to no external marks or signs of mischief at that part, so as to admit of an operation for its removal. The inflammatory symptoms having been restrained, it was nevertheless obvious that the cavity of the chest was full of fluid, and that the oppression in breathing arose from it, and not from the injury done to the lung. The stethoscope was then unknown, the ear was not in use; my older colleagues were obstinate; they would not hear of an operation for enlarging the wound into the chest; and as our patient was, unfortunately for him, shot in London, instead of at the pass of Roncesvalles, or on the bridge over the Bidassoa at Irun, we let him die on the eighth or ninth day, without all the aid which surgery might have given him. It is possible he would not have recovered under any circumstances, from the ball having lodged, and from his advanced age.
A soldier of the Fifth Division of Infantry was wounded at Toulouse by a musket-ball, which entered between the fourth and fifth ribs of the right side, near the sternum, and [437] came out behind nearly opposite, fracturing the ribs, the splinters of which were removed. The first symptoms of inflammation, having been in some degree subdued by the sixth day, were followed by those more immediately indicating effusion; such, particularly, as great oppression, difficulty of breathing, and inability to lie in the recumbent position, which induced me to introduce, after a little pressure, a gum-elastic catheter into the posterior wound, through which a quantity of red, serous fluid was withdrawn, exceeding, perhaps, three pints by measure. On the removal of the catheter the discharge of fluid ceased, and, under a strict antiphlogistic treatment, the man gradually recovered, so as to be sent to England in the following June. If the symptoms of oppression had returned, I should have repeated the operation perhaps lower down. Auscultation, if it had been then known, would have smoothed away many doubts and difficulties.
A soldier of the 40th Regiment was wounded at Toulouse on the 10th of April by a musket-ball, which entered about two inches below the nipple of the right breast, passed through the cavity and the lung, and came out behind at a nearly opposite point, injuring the ribs above and below, without entirely destroying their continuity. He was bled largely on the morning of the 11th, and again at night. On the 12th the bleeding was repeated; some small pieces of ribs were extracted from both orifices, and some part of his dress from the anterior one. He spat blood when he coughed, and respiration was difficult. Calomel, opium, and antimony were given in pills every six hours, and the bleedings were repeated daily, and sometimes oftener, for the first eight days, during which time a free discharge, at first serous, afterward purulent, took place from the wound, after which the inflammatory symptoms subsided; the cough became easier, the expectoration less, and free from blood; breathing easy. The calomel was omitted; a mild farinaceous diet was allowed instead of a little gruel, and a very little bread and milk. In a fortnight the wounds began to heal. On the 1st of May, some small pieces of rib were removed from the anterior wound, after which both gradually closed, and he was forwarded to Bordeaux on his way to England in the beginning of June, cured.
Corporal Dunleary, of the 69th Regiment, was wounded on the 16th of June, 1815, at Quatre Bras, by a musket-ball, [438] which entered the thorax, fracturing the seventh rib on the fore part of the right side, and lodged. He said he had lost a large quantity of blood from the mouth, and some from the wound, between that and the 19th, when he was brought to the hospital in Brussels. The pulse was then quick and hard, respiration difficult and anxious, and a bloody discharge issued from the wound on every respiration; bowels confined since the accident; was bled to forty-four ounces; saline purgatives, with calomel, antimony, and opium, were given until the 29th of June, when the wound discharged good pus. From this time, at different periods for six weeks, he lost ninety-two ounces more blood, being strictly placed on milk diet. Several pieces of rib exfoliated. He was sent home on the 31st of August, declaring himself quite as well as ever he had been in his life; the ball remaining undiscovered.
A soldier of the Fusilier Brigade was struck by a musket-ball on the right side of the front of the chest, at the battle of Albuhera; it entered between the fifth and sixth ribs, passed through the lungs, and lodged. Three days afterward, when the first symptoms were in part subdued, he complained of pain in a particular spot, nearly opposite to where the ball had entered, at which part something could be felt deeply seated. An incision being made, the ball was found lodged in the intercostal muscles between the ribs, whence it was easily removed. A considerable discharge of reddish-colored serum followed, with great mitigation of the symptoms, after which, under strict treatment, the man recovered, and was sent to Elvas with every prospect of a cure.
Lieutenant-Colonel Harcourt and Major Gillies, of the 40th Regiment, were both shot through the chest, at the head of the regiment, at the successful assault of Badajos; the wounds were as nearly similar as possible, from before directly backward. They were taken to the same tent, and treated alike with the same care by the late Mr. Boutflower, the surgeon of the regiment, with whom I saw them daily. The inflammatory symptoms ran high in both. In Major Gillies, a tough old Scotchman, they could not be subdued, and he died, at the end of a few days, of pleuro-pneumonia. Colonel Harcourt slowly recovered, and died Marquis d’Harcourt, near Windsor, more than twenty-five years after[439]ward, suffering little or no inconvenience from his chest, when I last saw him.
Captain Cane, 23d Fusiliers, was wounded at the affair of Saca Parte, in front of Alfaiates, in 1812, by a musket-ball, which struck him below and a little to the outside of the left nipple, fractured the rib, and entered the chest, giving rise to the sensation as if the ball had passed diagonally downward and backward to the loins of the same side. He spat blood, and was very faint. The next day he could scarcely breathe, was in great pain, continued flushed and anxious; pulse 100. He was bled into a washhand-basin until he fainted, and every day afterward, some days twice, to a less extent, for ten days, and once again until syncope was induced, on an accession of symptoms after an imprudence in taking a little wine, which nearly smothered him, he said. Some pieces of flannel shirt, of braces, coat, etc. were removed from the wound, and several portions of bone gradually followed, together with a quantity of matter, which continued to flow from May until the end of the following September, when the wound healed.
On the 23d Jan., 1821, I had an opportunity of examining this gentleman. My report says, he is never free from a little pain in the loins, where the ball is supposed to be, and cannot take a full inspiration without pain in the chest; expectorates more or less constantly, and occasionally a little blood about once in three or four months in half congealed lumps. Cannot ride or take any exercise because it brings on the pain. The cicatrix shows a large, deep hole, and the deficiency of the rib is well marked. The side of the chest is altogether contracted and flatter; the heart has been moved behind the sternum; the beat of the apex being on the other side of the xiphoid cartilage, and that of the heart, as a whole, is more indistinct than usual. In other ways in good health. It is possible that the ball may be lodged in or be retained by layers of coagulable lymph in the angle formed between the diaphragm, the ribs, and the spine.
William Downes, of the 11th Regiment of infantry, aged thirty-three, was wounded by a musket-ball, on the 31st of August, 1813, in the Pyrenees; it fractured the fourth rib of the left side, passed through the chest, and came out behind through the scapula. He spat a good deal of blood, although little flowed from the wound. The next day he was bled largely twice, to relieve the bleeding from the lung, [440] and was sent to Passages, where he was bled daily; and thence, a ship being ready, to Santander, where he arrived on the 14th of September. A free, bloody, purulent discharge took place from the anterior wound, but little from the posterior, and he expectorated a bloody, purulent matter, and occasionally a little blood. Toward the end of September the sanguineous expectoration ceased; but the soft parts of the chest had sloughed and separated under an attack of hospital gangrene, from which he had a narrow escape during the month of October. The wound in the chest gradually closed during the month of November; and on the 14th of December he was discharged convalescent, his health tolerably good, but his breathing by no means free; no expectoration. The left arm was impaired in power, in consequence of the mischief done to the muscles of the fore part of the chest and shoulder by the hospital gangrene. The chest was altogether somewhat flattened and shrunk, but there did not seem to be any diseased action going on within.
Case of Lieutenant-Colonel Dumaresq, aid-de-camp to Lord Strafford, by himself.—While turning round, after a successful charge of infantry, at Hougomont, on the 18th of June, 1815, I was wounded by a musket-ball, which passed through the right scapula, penetrated the chest, and lodged in the middle of the rib in the axilla, which was supposed to be broken. When desired to cough by the medical officer who first saw me, almost immediately after receiving the wound, some blood was intermixed with the saliva. I became extremely faint, and remained so about an hour and a half, after which I rode four or five miles to the village of Waterloo, where I was bled, which relieved me from the great difficulty I had in breathing; this difficulty was accompanied by a severe pain down my neck, chest, and right side. I was much easier until the evening of the 19th; but in the course of the night, the difficulty of breathing becoming much greater, and the spasmodic affection having very much increased, I was bled seven times, until the middle of the next day.—20th. I continued better, but was then seized with the most violent spasms imaginable in my neck, chest, and stomach. I could scarcely breathe at all, and was in the greatest possible pain; I was again bled twice very largely, and my stomach and chest fomented for a length of time with warm water and flannels. I passed a very tolerable night, and continued pretty well until two o’clock the following day, [441] when I was again very largely bled, by which I was very much relieved. I continued pretty well, and free from much pain; but my pulse having very much increased, and having a good deal of fever, on the 23d I was bled again; after this I continued free from much pain or difficulty of respiration, and on the 26th was removed into Bruxelles, when I came under your care. I forgot to mention that when I was so violently attacked I had two lavements most vigorously applied; salts, etc. proving of no avail, took digitalis, commencing with ten drops every four hours, increasing to fifteen from the second day.
N.B.—Up to this period, the 2d of July, the devil a bit have I eaten.
The ball in this case was lodged in the rib, which ultimately became thickened around it. He recovered with good health, but with occasional spasms in the chest; and died of apoplexy, in Australia, twenty-five years afterward. His doggerel lines show the buoyant and unconquerable spirit of a soldier, who knew that his chance of recovery was small. It was a most gallant, a most friendly spirit. Peace to his manes.
If the ball had caused a greater degree of irritation, I was prepared to cut down upon the rib, and remove a part of it, if necessary; for I have seen balls so situated slip from their lodgment, roll on the diaphragm, and cause general inflammation, suppuration of the cavity, and death, which must almost always ensue in such cases, unless the ball can be removed, and the matter evacuated by an operation to be hereafter described.
General Macdonald, of the Royal Artillery, was present at Buenos Ayres, when a bombarder of that corps received a wound from a two-pound shot, which went completely through the right side, so that when led up to the general, who was lying on the ground, he saw the light quite through him, and supposed he was of course lost. This, however, did not follow, and some months afterward the man walked into General (then Captain) Macdonald’s room, so far re[442]covered from the injury as to be able to undertake several parts of his duty before he was invalided; thus proving the advantage of a shot, however large, going through rather than remaining in the chest.
Appearances After Death, Etc.
343. The appearances after death differ materially even in apparently similar wounds.
A French soldier, shot through the right side of the chest at the siege of Badajos, died in December, 1812, in Lisbon, apparently of consecutive phthisis. The ball had gone through the chest from before directly backward; the posterior wound was closed; the anterior one was fistulous, and discharged a small quantity of matter, of which he spat up daily a large quantity until he died. The lung was diseased throughout, and contained several vomicæ or small abscesses, from which the matter expectorated was secreted. The track of the ball was nearly filled up, although the part immediately around was harder than usual. The lung adhered in many places to the wall of the chest, which was much flattened.
In other cases, portions of wadding, of leather belts, of splinters of different lengths, pieces of buttons, and even balls, have been found loose in the chest, showing the necessity for an especial and decided treatment.
A French soldier was wounded by a musket-ball at the battle of Waterloo; it penetrated the chest, fracturing the second rib, then passed through the lung, and went out behind in nearly a straight line, close to the spine. Left on the field of battle for five days before he was brought to Brussels, he was nearly dead with difficulty of breathing and other symptoms of inflammation, from which he recovered in the course of the next ten days, under repeated bleedings and the strictest antiphlogistic regimen. At the end of this time, when apparently doing well, an accession of inflammation and of all his bad symptoms took place, destroying him at the end of four weeks from the receipt of the injury. On[443] dissection, the lung was found adherent to the chest by false membranes of some thickness, with a quantity of purulent fluid in the cavity. The track of the ball was in a suppurating state, and two pieces of rib were found in the center of its course. The whole of the lung appeared to be filled with a sero-purulent fluid, which could be readily squeezed out.
John Roth, of the 5th battalion of the 60th Regiment, aged twenty-nine, had been wounded by two balls, one on the 10th of April, 1814, at the battle of Toulouse, which grazed the left temporal bone; the other had gone through the upper part of the right chest, in the Pyrenees, the autumn before. Both wounds had healed. He was seized on the 8th of May, after a little intemperance, with pains in his body and joints, pain in the chest, and cough, with bloody expectoration; skin hot, tongue foul, and bowels confined. On the 9th he was bled, and purged by calomel, antimony, and salts. On the 10th symptoms augmented, pulse 120, small, and wandering, but no pain in the head. Repeat the medicines. Head shaved and cold applied; bleeding to ten ounces. 11th. Every symptom increased; great pain on touching the chest; pulse 126; skin hot. On the 12th passed his urine and feces involuntarily; and on the 13th he died, his body being covered by petechiæ.
The head, on examination, showed pus under the dura mater, at and behind the situation of the wound he had received. The right lung adhered to the walls of the chest where the ball had entered and passed out, the track made by it being very visible, indurated, and inflamed, from the last attack: the parts otherwise sound; no fluid in the cavity.
Mr. Drummond was wounded by a pistol-ball in the back, low down, about two inches from the spine, and three inches from the inferior angle of the scapula; it was afterward found to have entered between the eleventh and twelfth ribs, and to have passed between the base of the lung and the diaphragm, abrading the former, and passing through the latter into the abdomen, ultimately lodging in the fat under the skin, over the cartilage of the eighth rib of the left side, nearly at an opposite point in front. From the absence of all symptoms of shock and alarm, it was hoped by some that the ball might have run round, but on the removal of the little ball its course could not be traced. This occurred on[444] Friday. On Saturday morning at five o’clock he suffered great uneasiness and difficulty of breathing, accompanied by a particular catch or jerk in respiration, indicating a wound of the diaphragm. The stethoscope and the ear attested the clearness of the respiratory murmur in every part of the chest, which sounded well, and I was satisfied the lung was not materially injured; twelve ounces of blood were drawn with difficulty from both arms. At ten o’clock, the jerk and difficulty of breathing being greater, the left temporal artery was opened, as no blood could be drawn from the veins; five ounces only could be obtained; a dose of calomel and a senna draught had been followed by the discharge of a teaspoonful or two of blood, leaving no doubt on my mind that the ball had penetrated the cavity of the abdomen, as well as of the chest, and that a bowel had been injured. With a constitution apparently unequal to bear an inflammation of the most dangerous character, or the remedies necessary to subdue it, the prospect was but melancholy. Thirty-six leeches were applied around the wound in front, but they drew little blood. Pulse from 108 to 112. Dr. Hume, Mr. B. Cooper, and Mr. Jackson were added in consultation on Monday at twelve, when the jerk became worse, the oppression in breathing greater. Muriate of morphia, half a grain; at two, bled to twelve ounces; blood very buffy; calomel, two grains, opium, half a grain, every two hours. In the evening, bleeding, repeated to fourteen ounces; no more would flow. Tuesday morning, at five, bled again to twelve ounces. The ear now indicated effusion for the first time. It was not, however, in sufficient quantity to render the evacuation of the fluid necessary. After this he gradually sank, and died on Wednesday morning. He lost on the whole fifty-six ounces of blood. On examination after death, it was found that the ball, after entering the cavity of the chest, had slightly abraded the left lung at its lower and inferior edge, which was covered by recent lymph, the lung being internally sound. The left side of the chest contained nearly a pint of red-colored serum. The ball had perforated the diaphragm, grazed the fat of the left kidney, passed through the great omentum below the stomach, to the part where it was extracted, injuring apparently no important organ in the abdomen in its transit, but giving rise to an effusion of blood from some small vessel which had sloughed, the blood being partly coagulated and partly diffused to the[445] amount of many ounces; its loss appeared to have been the immediate cause of death.
A gamekeeper’s gun burst at the Red House, Battersea, and a small part of the lock entered the middle of the left arm, and passed upward into the axilla, where it could not be traced by Mr. Keate, who saw him within an hour after the accident. The symptoms which followed were those of inflammation of the chest, and were subdued by active treatment; the wound healed, and he returned to his occupation in Wiltshire. Having exposed himself to the night air some weeks afterward, the inflammation of the chest returned, and he died. On opening the thorax, one edge of the bit of iron was found impacted in the surface of the lung, the other edge was rubbing against the inside of the sixth rib, which was nearly worn through by the constant friction it underwent during respiration; there was also a mark on the pericardium as of a cicatrix, and of a graze on the surface of the heart.
Among the French prisoners in Lisbon, in the spring of 1813, I saw a man in whose chest a ball had entered midway between the fifth and sixth ribs, and lodged; from this a constant and considerable discharge of purulent matter took place. The ball was found after death lying between the diaphragm and the spine, surrounded by coagulable lymph, and adhering by its envelope to the spine and diaphragm at the angle formed between them; there was a very thickened pleura costalis; the lung was shrunk and attached by membrane almost equally thickened across the chest, the lower part of which was filled in the upright position by the discharge, which was only evacuated in quantity when the opening of the wound was made dependent.
A case was met with after the battle of Waterloo, among the French wounded, which was somewhat similar. A portion of rib had been driven in, and the assistant-surgeon was aware that the ball could occasionally be felt. The man died at the end of a fortnight, the cavity containing a quantity of sero-purulent bloody matter. The lung had been injured by the ball, which had fallen loose into the cavity of the chest.
344. The removal of splinters of bone, or of other foreign bodies from the lung, has occupied the attention of surgeons from the earliest periods, and some of them proposed to draw a piece of cambric or other things through the chest, for the[446] purpose of removing them. These extreme measures have been abandoned; but there can be no doubt of the propriety of removing as many of these causes of irritation as can be either seen or felt. If the ball have broken a rib, the orifice of entrance especially should be enlarged as early and as carefully as possible, so as to give an opportunity for the removal of the splinters and of all angular points of bone which may be turned inward. A little addition to the original opening can do no harm, and if the lung should not collapse, or should it be adherent, it will enable the surgeon to see whether any splinters are impacted in it, and to remove them. It is possible that the end of the finger even may be introduced, and the lung felt, if it should not have receded too far; as it is insensible to such an operation, no evil will ensue; but all probings with small, sharp-pointed instruments should be avoided. That wadding, buttons, pieces of cloth, and of bone have been frequently coughed up, I have had experience; but although it is said that even balls have been thus brought up, I have not had an opportunity of seeing them.
An officer was wounded by a musket-ball on the 9th of July, 1745; it passed through the chest, entering in front, fracturing the seventh rib near its junction with the cartilage attaching it to the sternum, and passing out behind near the angle of the same rib, which it again broke, together with the one immediately below it. M. Guerin enlarged the openings of entrance and of exit to the extent of nearly two inches, by dividing the pleura, the intercostal muscles, and the integuments from within outward. Several splinters of the rib injuring the lung were removed, the smallest of which might be half an inch or six lines long, by two wide. A tent was then passed through the wound. The patient suffered much, and spat a great deal of blood; pulse feeble, extremities cold. He was bled three times the first night, and twenty-six times during the first fifteen days, the seton being retained in the chest the whole time. On the twenty-second day, a piece of cloth was felt by the finger, after removing the seton, and was extracted; a splinter was also felt, but so deeply that it could not be removed without enlarging the incision. As the inflammatory symptoms were re-excited, he was bled for the twenty-ninth time. On the thirtieth day these symptoms had so much increased that the seton was withdrawn, under the impression that it was doing[447] more harm than good, and the thirty-first bleeding was effected. The next morning the patient complained of something pricking him within, and the parts left between the two original wounds, after the incisions which had already been made, were divided. The chest was now open from the articulation of the head of the rib with the sixth and seventh vertebræ behind, nearly to the cartilage in front; and the whole course of the ball was seen; it had made a groove in the surface of the lung, in the substance of which a splinter was sticking. This was extracted, and the wound dressed simply, after which the patient gradually improved, and was quite cured in four months.
The two first incisions for the removal of the splinters were necessary. The tent or seton drawn through the chest was an error; and although the fortunate result of the case depended probably on the removal of the splinters of bone sticking in the lung, few would survive the formidable operation performed for their removal. The case is suggestive and instructive.
345. When the lung can be seen through the opening made by the ball, or after some moderate enlargement for the purpose of removing any splintered pieces of rib or any spiculæ which can be felt or seen, the object is attained. I have not had experience of the utility of large incisions for the purpose of making the lung more visible, although the importance of extracting foreign substances in the first instance is inculcated, provided their situation can be ascertained.
A Spanish soldier, wounded at the battle of Toulouse, was brought to me the same evening, shot through the right side of the chest, between the fifth and sixth ribs, one of which was fractured, the ball passing out nearly opposite behind. On removing the splinters by the aid of an incision, I found that the lung was adherent to the inside of the chest, and was enabled to withdraw from within the lung some splinters of bone and a part of his coat. He left Toulouse apparently doing well; but natives of warm climates rarely suffer from such severe attacks of inflammation as those of northern habits and constitutions.
A soldier of the German Legion was wounded at the battle of Waterloo, the 13th of June, 1815, by a musket-ball, which entered between the seventh and eighth ribs in front, about two inches from the sternum on the right side,[448] passing out behind. He died in York Hospital, Chelsea, in the month of January following, where he was taken after some drunken fits, which induced an attack of pneumonia. A fistulous opening existed, and had discharged a little matter, which was gradually diminishing; the sinus was from six to seven inches long, extending into and nearly through the base of the lung, and was lined by a mucous membrane, the lung around being thickened to the extent of from a quarter to half an inch. There was but little fluid in the cavity, although the lung on both sides showed signs of recent inflammation, without which he would in all probability have recovered. The orifices of entrance and of exit through the lung adhered to the walls of the chest, thus separating the track of the ball from the general cavity of the pleura, which would in all probability have led to his ultimate recovery, if it had not been for his intemperance.
346. When a ball, or portion of bone, leather, cloth, wadding, or other foreign substance is driven into the cavity of the pleura, it usually gives rise to fatal results, constituting, therefore, cases of the greatest importance, to which attention has not been sufficiently given, but on which too much cannot be bestowed, if life is to be preserved by the art of surgery. The neglect of these cases has probably arisen from the insufficiency of the means of ascertaining their nature—an insufficiency which auscultation has in some measure removed, and which the science of surgery may still further diminish. The presence of a ball, a piece of bone, or of any other substance, lying upon or rolling about on the pleura covering the diaphragm, must give rise to more or less irritation and inflammation, and consequently to suppuration, or the formation of matter upon the surface of that membrane in its thickened state, until, in all probability, the foreign substance has been removed or the person has wasted away and perished.
A dragoon of the King’s German Legion was wounded between the eighth and ninth ribs at the battle of Salamanca. The ball had entered and lodged; the symptoms were severe; the breathing laborious. As the discharge from the wound was not free, I enlarged the opening, removed some scales of bone, a bit of cloth which stuck between the ribs, the lower of which was broken, and evacuated a great quantity of bloody-colored fluid, not purulent. After a few days the discharge became purulent, and, as he felt something, as he[449] thought, roll within him, which he supposed might be the ball, I contemplated again enlarging the wound, so as to be able to see whether anything were loose in the cavity; but a sudden relapse of inflammation, from drinking some brandy, carried him off. On examination, the ball was found lying loose on the diaphragm in the chest, and might, with some enlargement of the wound, have been extracted.
A French prisoner of war, who had been wounded near Almaraz by a musket-ball, which had lodged in the left side of the chest, was sent to Lisbon in 1812, with a considerable discharge through the wound, and died there. The ball was found in the angle formed between the diaphragm and the spine, enveloped in coagulable lymph, by which it was attached to the spine; there were some splinters of bone inclosed with it.
A soldier of the 29th Regiment was wounded at Talavera by a musket-ball, which penetrated the right side of the chest, between the fourth and fifth ribs, and lodged. He died the day after, and on opening the body, I found that the ball had passed through the lung, and was lying loose on the ribs behind, near the union of the diaphragm with the spine.
Major-General Sir Robert Crawford was wounded at the foot of the smaller breach at the storming of Ciudad Rodrigo, by a musket-ball, which passed through the posterior fold of the armpit and entered the side of the chest in the axilla by a small opening or slit, apparently too small to allow a ball to pass through. I saw him a few minutes afterward with Dr. Robb, under whose care he remained, when, from the general anxiety manifested, I was satisfied as to the severity of the injury. The symptoms were not at first urgent, but their continuance and augmentation, in spite of the most rigorous antiphlogistic treatment, led, in a few days, to his death. On examination of the body, the ball was found lying on the diaphragm; the cavity of the chest contained a large quantity of very turbid serum; false membranes had formed on the lung, which was compressed toward the spine, and at the upper part retained the mark of an injury as from a ball which had not had force enough to penetrate and lodge.
Baron Larrey has had the good fortune to meet with some remarkable cases of this kind. In the first he did not see the man for some weeks after the wound had been in[450]flicted, the ball entering at the upper edge of the fourth rib, about an inch from its junction with the cartilage. By means of a bent and flexible sound introduced through the wound, he distinguished a hard, metallic substance at the bottom of the cavity of the chest, which he supposed to be the ball, nearly in the situation of the place where the operation for empyema is usually performed. This operation having been done, about twelve ounces of pus escaped, and the ball was discovered rather flattened. It was easily removed with the aid of a pair of polypus forceps. After this there was every prospect of recovery, until the patient, having unfortunately one day drank too much brandy, was attacked by enteritis, and died.
William Barrett, of the Life Guards, a middle aged, muscular man, of full habit, was wounded by a musket-ball at the battle of Waterloo; it fractured the third and fourth ribs behind on the left side, and broke the left arm. He was brought to Brussels, where the inflammatory symptoms were subdued by repeated general and local bleedings, and the other ordinary but strictly antiphlogistic means, during the first six weeks, by which time the external wound had nearly closed, and no trace of the ball could be perceived. At the end of this time, Staff-Surgeon Collier, now Inspector-General of Hospitals, under whose care he was, and who furnished me with these particulars of the case, which I saw in Brussels, finding that his symptoms became worse, that he had rigors and evening exacerbations, and that the difficulty of breathing had increased almost to suffocation, decided on opening into the cavity of the chest and following the course of the ball. This he did by a deep incision, which enabled him to remove some pieces of the ribs, which were denuded but not detached. A bag-like protrusion was then felt between the ribs near their angles, which was opened, and nearly two pints of thick, fetid pus escaped, the relief which followed being as complete as sudden. The wound was dressed from the bottom, and every means adopted, except introducing a tent, to prevent its closing, but in vain; the opening closed, and matter again collected, requiring a second incision for its removal. Between these two operations small bleedings were resorted to most beneficially. A short gum-elastic catheter was introduced into the cavity of the chest after the second incision; very little matter, however,[451] was secreted. From this time he gradually recovered, and was sent to England, cured, in November.
347. The presence of a ball, rolling about on the diaphragm, can now be ascertained by means of the stethoscope at an early period, so as to admit of an operation being undertaken with confidence for its removal; while the knowledge acquired by auscultation or percussion, of the filling of the chest by fluid, whether serous, bloody, or purulent, is at the same time incontestibly demonstrated. The presence of a ball, or of any other foreign body, decides the question as to the place where the opening into the chest should be made. On this point the information derived from the practice of the French surgeons in Algeria is valuable.
M. Baudens, whose labors I again refer to with great pleasure, says that he has also seen splinters of bone and even a ball, surrounded by a cyst formed by the pseudo-membranes of inflammation, cut off from the general cavity, and confined in the angular space formed behind between the rib, the diaphragm, and the spine. In one case, M. Baudens introduced a sonde à dard, such as is used in the high operation for the stone, between the second and third ribs, and made it project behind between the eleventh and twelfth. He then cut down upon it, and extracted a ball and some splinters of the rib. The wound thus made was then closed, the upper one being sucked dry daily by a pump. The patient recovered in forty days.
A., 54th Regiment, was brought to the hospital at Algiers, on the 22d of October, 1833, wounded eleven days before by a ball, which, having broken the right clavicles was lost in the chest, without any sign of effusion having taken place; he appeared to be going on well, until suddenly he complained of pain about the middle of the sixth rib, which could not be removed by the means employed, and was accompanied by a great discharge from the wound. On the 10th of November he died. The clavicle and the first rib had been fractured, and an abscess had formed behind them, the size of a hen’s egg, containing several splinters of bone, which had stuck in and afterward separated from the lung. The ball had passed from above downward and outward, forming a sinus, which terminated at the middle of the sixth rib, to which this part of the lung was attached; the posterior three-fourths of this canal were[452] closed; the anterior fourth contained two splinters of bone, one of which was about to fall into the abscess in front. The sixth rib was broken, although it had not been perceived during life; and a small digital cavity was formed at this part in it by the ball, surrounded by portions of lymph, floating loosely from its edges; from this the ball had been detached, and had given rise to the inflammation which destroyed him. The ball had fallen on the diaphragm, where it was lying loose, surrounded by a quantity of purulent matter.
M. Baudens says himself, and rightly, that the operation of opening into the chest should have been performed in the eleventh intercostal space, and that the wound in front should have been enlarged.
M. Baudens relates another case, in which the posterior wound, situated near the angle of the tenth rib, had healed, the anterior one, half an inch below the clavicle, giving issue to an abundant and weakening suppuration. The lung above this was permeable to air, but the respiratory murmur could not be heard below it. To draw off this offensive fluid, he adapted an empty caoutchouc bag to a gum-elastic canula, which he affixed against the orifice of the wound, and thus sucked out six pints in five days. Some days later the wound behind reopened, and a piece of bone was discharged from it, which saved the man’s life. Two years afterward he was seen in good health.
The desire to have as dependent an opening in the chest as possible in these injuries has been manifested by all surgeons of experience; and the interspaces between the ninth and tenth, and between the tenth and eleventh ribs, have been often selected for this purpose; but as the operation was formerly done with the trocar, the abdomen was as often opened as the thorax, and death was frequently thus caused, even if it would not have been occasioned by the disease. To prevent, or to avoid this evil, M. Baudens advises its being performed at three fingers’ distance from the spine, by incision, and he says he has frequently done it with success, although he does not give any circumstantial directions as to the operative method to be pursued. I therefore caused several experiments and dissections to be made in the workroom of the College of Surgeons by Mr. Quekett, with the following results:—
348.—1. That a trocar and canula pushed in between the[453] eleventh and twelfth ribs, in a diagonal direction upward, on a line with the angle of the ribs generally, will in the dead body invariably enter the cavity of the chest without injuring the diaphragm.
2. That the same operation performed on the living body would, in all probability, if done at the moment of expiration, first enter the thorax, then pierce the diaphragm, and thus open into the cavity of the abdomen,—a difference in result to be explained by reference to the anatomy and physiology of the parts concerned; showing that this operation, when required on man, should always be done cautiously by incision, and not by puncture with the trocar and canula.
On examining the lower part of the chest from within, after removing the pleura, the diaphragm is seen forming the boundary between the thorax and the abdomen, commencing from the transverse process of the first lumbar vertebra, and forming an arch under which the upper part of the psoas muscle passes, (the ligamentum arcuatum proprium.) From this part extends another aponeurotic arch along the lower border, to the end of the last rib, called the false ligamentum arcuatum, (ligament cintré du diaphragme of Cruveilhier,) which is nothing more than the upper edge of the anterior layer of the aponeurosis of the transversalis muscle, folded upon itself in all its extent. The diaphragm is afterward attached to the lower border of the twelfth, and in succession to the eleventh, tenth, ninth, eighth, seventh, and sometimes to the sixth, ribs, counting from below upward. The external intercostal muscles are distinctly seen between the ribs, extending from the spine until they meet and are concealed by the fibers of the internal intercostal muscles, near the angles of the ribs. The vessels and nerves, after passing on the external intercostal muscles, subsequently run between them and the internal ones.
The lower intercostal arteries arise from the aorta on each side, and before they enter the space between the ribs give off a branch passing backward to the vertebral canal and the posterior muscles of the spine. The eleventh and twelfth intercostal arteries, covered at first by the pillar of the diaphragm, ascend on leaving the vertebræ to reach the under edges of the ribs, and are accompanied by a vein and nerve. The tenth intercostal artery, and those immediately above it, run almost horizontally, and nearly in the mid[454]-spaces of the ribs, as far as their angles, at which part a small artery is commonly given off, which descends from the main trunk at an acute angle to the rib below, and may be injured in opening into the chest, and be perhaps mistaken, in operating, for the intercostal artery itself. From the angles each artery runs in a groove in the under edge of the rib as far as the anterior third, when they all become very much diminished in size, and, leaving the grooves, run in the middle of the intercostal spaces, until lost in their different anastomoses with the branches of the epigastric, phrenic, lumbar, and circumflexa ilii arteries.
In making an opening into the chest between the tenth and eleventh, or between the eleventh and twelfth ribs, the artery will not be injured, provided the opening be made below the middle of the intercostal space, which is wider between the eleventh and twelve ribs than between those above it. The vein is situated above the artery, and proceeds to the vena azygos major on the right, and to the smaller azygos vein on the left side.
The intercostal nerves are the anterior branches of the dorsal nerves, and lie below the arteries under the pleura upon the external intercostal muscles, until they approach the angles of the ribs, where they enter between the layers of the intercostal muscles.
It is worthy of observation that the pleura is necessarily continued over the inside of the twelfth rib to line the different attachments of the diaphragm, and that an incision may always be made into the chest above this point, if done carefully.
On removing the integuments of the back, covering the muscles and the lower ribs, the broad expanse of the latissimus dorsi muscle is brought into view, extending from the ilium and spine upward and outward, and covering all the parts of importance beneath in the operation to be described. On the removal of the lower part of this muscle the serratus posticus inferior is seen, of a somewhat quadrilateral form, arising by a thin aponeurosis common to it and to the latissimus dorsi, from the spinous processes of the three superior lumbar vertebræ and the two inferior dorsal, and proceeding upward and outward to be inserted by four flat, tendinous digitations into the four lower ribs.
If this muscle be separated from its origins and turned outward, or divided in the middle, and its two portions reflected, the posterior spinal or long muscles running in and[455] filling up the groove or hollow of the side of the spine will now be distinctly seen, composed chiefly of the sacro-lumbalis and the longissimus dorsi muscles, sometimes called as a whole the erector spinæ or the sacro-spinal muscle. This, which forms a thick mass over the beginning of the tenth, eleventh, and twelfth ribs, is not to be divided or interfered with beyond a very few at most of its external fibers; the opening into the chest about to be made should begin at its external edge and go through the external intercostal muscle, which is now exposed on a plane below it.
The eleventh and twelfth ribs, unlike all those which precede them, except the first, have only one surface of articulation with the corresponding vertebræ, to which they are attached, instead of two facettes articulating—one with the body of the vertebra above, the other with that below. They form, particularly the twelfth, a more acute angle with the spine than the other, which gives to them their greater degree of obliquity, while the freedom of their cartilaginous extremities enables the twelfth, particularly, to be depressed or separated by a moderate force from the rib above to a greater extent than at any other part, by which means a foreign body of larger size may be removed from between them more readily than elsewhere.
349. Operation.—The eleventh and twelfth ribs having been distinctly traced, and the obliquity of their descent from the spine having been clearly made out, the patient ought, if possible, to be placed on a stool, with the upper part of the chest supported by a pillow on a table before him. An incision should then be made over the intercostal space between these ribs, three inches long and slightly curved, through the integuments down to the latissimus dorsi muscle, and as the mass of long spinal muscles is usually three inches in width, and can in general be seen, the incision should commence two inches from but between the spinous processes of the eleventh and twelfth vertebræ, and be continued obliquely or diagonally downward in the course of the interspace between these ribs. The latissimus dorsi and the serratus posticus inferior muscles having been divided at the upper part where they cover the longissimus dorsi or the long spinal muscular mass alluded to, its edge becomes apparent; from this point the latissimus and the serratus are to be further divided downward. The external intercostal muscle being thus exposed, its fibers should be[456] scratched through or separated in the middle of the interspace between the ribs, which can now be seen as well as felt. A director should be introduced below the muscle, on which it may be carefully cut through, as well as any fibers of the internal intercostal muscle which may extend as far as the wound thus made. The pleura will then be exposed, and if the cavity of the chest contain fluid in any quantity, it can scarcely fail to project in such a manner as to convey to the finger the assurance of its being beneath. An opening may then be carefully made into it at the upper part of the incision close to the external vertical fibers of the spinal mass of muscles, at the moment of inspiration, and on the existence of fluid being ascertained by its discharge, the opening should be enlarged by a director previously introduced under the pleura, the patient being desired to draw a full breath at the time, in order that the diaphragm may descend as low as possible. If there should not be any fluid in the chest, the diaphragm, in ascending during expiration, may be applied to the inside of the pleura lining the chest as high even as the fifth rib, counting from above, and might easily be divided with the pleura, if great care were not taken to make the opening during the process of inspiration.
In all cases of wounds of the chest, in which auscultation points out the presence of a ball rolling loose on the diaphragm, this operation should be performed for its removal, and may save the life of the sufferer. It would, perhaps, have done so in the case of Sir Robert Crawford. At a later period the presence of a foreign body, perhaps, can only be known by the sounds or defect of sounds which may be observed at the back part of the chest, in which the ball or other foreign bodies lodge or become enveloped by matters confining them in that situation.
HERNIA OF THE LUNG, ETC.
350. Hernia of the lung, as a consequence of a wound in the chest which has healed, is a complaint of rare occurrence. It appears to take place when the intercostal mus[457]cles have been much injured and are deficient, the opening through them being merely covered by the common integuments which have yielded to the pressure exerted from within. It has been supposed that it might be mistaken for the thinning of parts from the formation of matter within, or empyema. The early occurrence of the abscess after the receipt of the injury forbids the supposition, while the ear, applied to the protruded part which is most prominent during EXPIRATION or coughing, perceives not only a crepitation, felt equally by the touch, but the natural respiratory murmur stronger, softer, but less vailed and more like the sound given out by a pulmonary lobule inflated close to the ear, but without enlargement of the part.
A portion of lung will sometimes protrude during the efforts made by the sufferer to breathe, particularly in expiration, when the wound is left open and the lung is sufficiently free to admit of it. When protruded, it sometimes happens that the efforts of nature are not sufficient for its retraction, and it remains filling up the opening into the thorax. A large portion of lung is rarely protruded, except through an opening which readily admits of its return; but when the wound is small, the return of a portion of protruded lung, when it is not positively strangulated, should not be interfered with. The surface of the lung is but little sensible; touching it causes no apparent pain, and its adhesion to the edges of the cut pleura is more advantageous than its separation from it. It should, therefore, be allowed to remain or be only so far returned, if it can be so managed, as to rest within the edges of the divided pleura and fill up the gap made by the incision, over which the integuments should be accurately drawn and retained. The adhesion of the lung to the pleura costalis arrests the inflammation, and may prevent its progress to other parts of the cavity. That the inflammation may extend farther into the substance of the lung, is possible, but when the sufferers are otherwise healthy, the chance of evil from pneumonia is less than from inflammation of the general cavity. Whenever the protruded lung has been completely returned, more inflammation has followed than where it has been allowed to remain under the precautions recommended. Three cases were brought under my notice at Brussels, after the battle of Waterloo, which were not interfered with, greatly to the advantage of[458] the patients. It is rare, however, to see a protrusion of the lung after a gunshot wound.
The protruded lung, when left uncovered and unprotected, soon loses its natural brilliancy, dies quickly, shrinks, and becomes livid, without being gangrenous. In such cases the protruded part may be removed, but it should never be separated at its base from its attachment to the pleura costalis by which it is surrounded.
351. Wounds of the diaphragm were known to the older surgeons from the time of Paré; they were aware that these wounds were not immediately, although generally, mortal. They knew that the viscera of the abdomen did sometimes pass through such wounds into the cavity of the chest, but they did not know that a wound of the diaphragm never closes, except under rare and particular circumstances; that it remains an opening during the rest of the life of the sufferer, ready at all times to give rise to a hernia which may become strangulated and destroy the patient, unless relieved by an operation as yet unperformed, but to which attention is especially directed—a fact first pointed out by me early in the war in the Peninsula.
A soldier of the 29th Regiment was wounded at the battle of Talavera, and died in four days after the receipt of the ball, which went through the chest into the liver. I found, on examining the body, an opening in the central part of the diaphragm of an oval shape, the edges smoothing off as if they were inclined to become round; this opening was nearly two inches long, evidently ready to allow either the stomach or the intestines to pass through it on any exertion.
Captain Prevost, aid-de-camp to Sir E. Packenham, was wounded by a musket-ball, on the 27th September, 1811, on the heights of Saca Parte. It penetrated the chest from behind, splintering the ninth and tenth ribs of the left side, and made its exit a little below and to the right of the xiphoid cartilage. A good deal of blood was lost from the posterior wound, but he did not spit up any. He was carried to Alfaiates, and there he threw up a small quantity of bloody matter by vomiting. The posterior wound was enlarged and continued to discharge some blood, the intercostal artery being in all probability wounded. Sixteen ounces of blood were taken from the arm, giving great relief, and the bowels were opened by the sulphate of magnesia.
[459] Sept. 29th.—Bleeding to eighteen ounces; on the 30th he was bled again to thirty-two ounces, from which great relief was obtained; he fainted, however, on making a trifling exertion to relieve his bowels.
Oct. 1st.—Accession of symptoms as yesterday, relieved by bleeding in a similar manner; bowels open.
3d.—The inflammatory symptoms recurred this morning, and were again removed by the abstraction of sixteen ounces of blood. Beef-tea.
5th.—Passed a sleepless night, and was evidently suffering from considerable internal mischief; wandered occasionally; pulse quick, 120, and small; felt very weak and desponding. A little light, red wine given, with beef-tea and bread; opium night and morning.
6th and 7th.—Much the same; pulse always quick, with much general irritability.
15th.—The wounds discharged considerably, particularly the posterior one; has a little cough; pulse continues very quick; spasms of the diaphragm troubled him for the first time, and caused great pain and uneasiness; they were relieved by opium in large and repeated doses.
On the 18th the spasmodic affection of the diaphragm and the pain returned with great violence, so as to threaten his dissolution, which took place on the 20th.
On examination, I found that the ball had passed through the under part of the inferior lobe of the left lung, and through the pericardium under the heart, through the tendinous part of the diaphragm, and into the liver, before it made its exit. The wound in the lung was suppurating; the matter and fluid from the cavity of the chest had a free discharge by the shot-hole; the edges of the wound in the diaphragm were smooth as if cicatrized, leaving between them an elliptical opening an inch long. The injury to the liver was through the substance of the anterior part of its right lobe; the matter having a free discharge, and generally slightly yellow, as if tinged with bile in small quantity. The skin did not show a yellowish tinge, neither were the conjunctivæ discolored.
A soldier of the 23d Regiment was wounded at the same affair, by a musket-ball, on the right side; it fractured the sixth rib, from three to four inches from the sternum, and passed out behind, between the ninth and tenth ribs, near the spine. The rib being fractured, the splinters were re[460]moved after an enlargement of the wound by incision, when the opening into the cavity of the chest was manifest, air being discharged freely from it. The shock in the first instance was great; but after a time reaction took place, and he lost a considerable quantity of blood in six bleedings during the first sixty hours. The discharge, at first serous and bloody, gradually became purulent, and the occurrence of jaundice showed that the diaphragm and liver had in all probability been injured. Under the administration of calomel, antimony, and opium, this symptom was gradually disappearing, when I left him to rejoin the army. He was sent to the rear at the end of ten weeks nearly well.
On the day preceding the battle of Fuentes d’Onor, in 1811, Sergeant Barry was wounded in the chest. The ball entered close to the nipple of the left breast, and passed out at the back, between the eighth and ninth ribs. The anterior opening of the wound soon healed, but the posterior one did not do so for a considerable period, when he became affected by such severe cough, with expectoration, that his medical attendant deemed it proper to reopen it. The symptoms were relieved, and portions of his shirt and jacket were discharged. After this his health improved so rapidly as to enable him soon to rejoin his corps. The wound in the back repeatedly opened and healed—generally at intervals of twelve or fourteen months; but for five or six years it ceased to do so. His appetite was small and delicate; flatulence was much complained of; and if the stomach at any time happened to be overloaded, vomiting occurred. He died of mortification of the left leg, January 4th, 1833.
On examination, the whole of the stomach and the greater part of the transverse arch of the colon were found in the left cavity of the chest, having passed through an opening in the diaphragm extending about three inches in a transverse direction, near the center of the dorsal attachments of that muscle. The peritoneum lining the diaphragm was firmly attached to the parts passing through it.
The wound in this instance was through muscular, not tendinous parts. The preparation is in the museum at Chatham, No. 63, Class 6.
A French soldier was admitted into the Gensd’armerie Hospital at Brussels, in consequence of a wound from a musket-ball, at the battle of Waterloo, which entered behind between the eighth and ninth ribs, near the spine, and lodged[461] internally. After many severe symptoms and much suffering, he died on the 1st of December, worn out by the discharge, which often amounted to a pint daily, for the free exit of which the external wound had been early enlarged. On examination, the lung was slightly ulcerated on its surface, opposite to where the ball had entered, and a little matter contained in a sac had formed between it and the wall of the chest. That the ball had gone on was proved by the fact of there being an opening in the tendinous part of the diaphragm, through which a portion of the stomach had passed into the chest, from which it was easily withdrawn. The ball could not be found in the abdomen; in all probability, it had passed into the intestine and had been discharged per anum, as has happened in other instances.
James Wilkie, 12th Light Dragoons, aged thirty-four, was suddenly attacked, at four P.M. of the 6th September, 1815, with violent pain in the umbilical and epigastric regions, accompanied with nausea and great irritability of stomach; pulse small, rapid, and regular. Assistant-Surgeon Egan visited him half an hour after the attack, bled him freely, and caused the abdomen to be fomented with hot water; a large blister was applied to the seat of pain, an ounce of castor-oil was given, and emollient and laxative clysters were occasionally administered. At night the symptoms abated, and he slept about three hours. The next morning his countenance exhibited that appearance of haggardness and anxiety which have always been alarming indications; pulse feeble and rapid; the pain severe; at noon he vomited from two to three ounces of black, fetid blood in a fluid state; the pulse became very feeble. At four P.M. the pain increased, he ejected from his stomach from four to six ounces of dark, fluid blood that had less fetor; and at six the same evening he expired in pain.
This man, on the 18th of June, at Waterloo, received a punctured wound from a sword, which entered about an inch below the inferior angle of the scapula on the left side, penetrated the thorax, appeared to have passed through the diaphragm, the point of the weapon coming out on the opposite side of the chest between the first and second false ribs. The wounds were quite healed, and he apparently enjoyed good health, when he arrived from Brussels in August.
Appearances on dissection.—On opening the abdomen,[462] the whole of the intestines, with the exception of the duodenum, were in a high state of inflammation. On tracing the duodenum upward a very small portion of the stomach was found in its natural situation; while, on opening the thorax, a large spherical tumor was seen in its left cavity, containing two quarts or upwards of black, fluid, fetid blood. This sac was soon seen to be the stomach, which had protruded through the aperture in the diaphragm, by which it was so firmly embraced as to render the communication between the portion of the stomach in the thorax and that in the abdomen impervious to each other. The hernial sac and its contents were supported by the diaphragm. The left lung exhibited a shriveled, contracted appearance, as if its function had been impeded by the pressure of the sac and its contained fluid. The cicatrix and the course of the sword were well marked. The cardiac and pyloric orifices of the stomach were in the natural cavity.
S. Fletcher, 31st Regiment, wounded at Sobraon on the 10th of February, 1846; died at Chatham, February, 1847. On opening the thorax, the greater part of the stomach, and a foot and a half of the transverse arch of the colon, with the omentum attached, were found in the left pleural cavity. There was an opening in the diaphragm with a rounded margin two inches and a half in diameter, two inches to the left of the œsophagus. The stomach, colon, and omentum adhered firmly, at one part, to the pleura covering the diaphragm and lining the ribs to the extent of a few inches, although otherwise loose and free in the cavity. The parts in the aperture of the diaphragm were free from adhesions, and the finger passed easily through the opening from below upward. Two cicatrixes were to be seen on the left side of the chest—one between the eleventh and twelfth ribs, close to the transverse processes of the vertebræ; the other between the eighth and ninth ribs, three inches and a half from the cartilages. The preparation is in the museum at Chatham.
352. These cases confirm the fact that wounds of the diaphragm, whether in the muscular or the tendinous part, never unite, but remain with their edges separated, ready for the transmission between them of any of the loose viscera of the abdomen which may receive an impulse in that direction. That parts of these viscera do pass upward and back again, cannot be doubted; and it is probable that in[463]carceration may take place for a length of time before strangulation occurs from some sudden and distending impulse giving rise to it.
When the solid viscera of the abdomen are injured, as well as the diaphragm against which they are applied in their natural situation, the wound may sometimes be considered a fortunate one; for the liver or spleen may adhere to the opening in the diaphragm and fill up the space between its edges.
A wound of the diaphragm may be suspected from the course of the ball, particularly when it passes across the chest below the true ribs. It is necessarily accompanied by an opening into the cavity of the abdomen, and is by so much the more dangerous. The symptoms will partake of an injury to both, although they are principally referable to that of the chest, and are those of intense inflammation, accompanied by a difficulty of breathing, which in the case of Mr. Drummond was a peculiar sort of jerk; in that of Captain Prevost it was more spasmodic. The risus sardonicus, hiccough, pain on the top of the shoulder, and loss of power of the arm, which were all more or less present, in all probability depended on some larger fibrils of the phrenic nerve being wounded. The treatment should be antiphlogistic, with a free external opening for the discharge of matter. The accession of jaundice shows an injury to the liver; vomiting of blood or its passage per anum indicates a wound of the stomach or intestines.
353. When the patient recovers, the probability of a hernia taking place into the chest through the diaphragm should be explained to him. If any reason should exist for the belief that it had occurred, he should be doubly cautious as to eating and drinking in small quantities only, and remaining in the erect position for some time after each meal; he should carefully avoid a stooping posture and all muscular exertion or straining. If symptoms of strangulation should come on, an opening made into the abdomen would appear to offer the only chance for life. The hernia may perhaps be drawn back into its place in the abdomen; but if firm adhesions have formed between the protruded parts and the edges of the opening in the diaphragm, the case must be treated as one of adherent strangulated rupture in any other part, by a simple division of the stricture in the most convenient situation. The opening should be a straight[464] incision through the wall of the abdomen, large enough to admit the hand, immediately over the part where the diaphragm is supposed to be injured. It should be closed by a continuous suture through the skin. This operation, now for the first time recommended, although apparently formidable, cannot be compared as to danger with the incisions of twelve and fourteen inches long through the wall of the abdomen, which have been in some instances successfully made for the removal of diseased ovaria.
354. Wounds of the heart are for the most part immediately fatal. Many persons have, however, been known to live for hours, nay days, and even weeks, with wounds which could scarcely be otherwise than destructive; and several cases are recorded in which the cicatrixes discovered after death, in persons known to have been wounded in the vicinity of the heart, have shown that even severe wounds of that most important organ are not necessarily fatal. As our knowledge of the nature of the injury inflicted can never be distinct, it follows that every wound should be considered as curable until it is unfortunately proved to be the contrary.
355. Auscultation and percussion, and principally auscultation of the whole precordial region, have afforded means of judging of injuries of the heart which were not formerly known. A vertical line, coinciding with the left margin of the sternum, has about one-third of the heart, consisting of the upper portion of the right ventricle, and the whole of the left, on the left. The apex of the heart beats between the cartilages of the fifth and sixth left ribs, at a point about two inches below the nipple and an inch on its external side; or, if one leg of a compass be fixed at a point midway between the junction of the cartilage of the fifth rib on the left side with the rib and sternum, and a circle of two inches in diameter be drawn around, it will define as nearly as possible the space of the precordial region occupied by the heart while uncovered, except by the pericardium and some loose cellular texture. In the rest of the precordial region it is covered, and separated from the walls of the chest by the intervening lung.
If the chest of the dead subject be transfixed with long needles, it will be found that the center of the first bone of the sternum corresponds with the lower edge of the left subclavian vein and to the arch of the aorta crossing the trachea, the center of the second bone to the upper edge of the[465] appendix of the right ventricle, and the center of the third bone to the right side of the right auricle, the right ventricle being lower down. A needle penetrating the chest at the costal extremity of the fifth rib, close to the upper edge of its cartilage, will touch the septum of the ventricle. The apex of the heart is an inch and a half below this, and inclined to the left side.
The semilunar valves of the pulmonary artery correspond to a spot a little below the center of the third bone of the sternum. The aortic valves are a few lines below and behind the pulmonary. The mitral valves are a little lower, and still more deeply seated. The pulmonary artery, after touching the sternum, inclines to the left, and is found close to the sternum between the second and third ribs. The aorta ascends to the first bone, and crosses it to form the arch.
One-third of the heart, consisting of the upper part of the right ventricle and of the whole of the right auricle, is beneath the sternum; the remainder of the right, with the left ventricle and auricle, are to the left side of that bone.
356. On applying the ear to the precordial region, the patient being in the erect position, two sounds are distinguishable in a healthy heart—one duller and more prolonged, the other clearer and shorter; between these there is scarcely an appreciable interval. The period of repose is sufficiently marked before the first or duller sound returns. Of the time thus occupied, one-half is filled up by the first or dull sound, one-quarter by the second or sharp sound, one-quarter by the pause or period of repose.
Twenty-nine theories have been proposed, each accounting for the sounds of the heart. The theory of Dr. Billing appears to prevail at present, which supposes that the sounds thus heard “are caused by the valves, which, being membranous, each time they resist the reflux of the blood are thrown into a state of sudden tension, which produces sound.”
The impulse of the heart, as far as it can be felt by the touch, depends much on the position in which the body is placed. In the erect position, it is heard between the fifth and sixth ribs. In the recumbent posture, the impulse is almost imperceptible. It is perhaps more observable when the body is turned on the right side, but decidedly more so when it is turned on the left. A clearer sound proceeds from a thin, and a duller sound from a thick heart; a sound of greater extent from a large heart, and a sound of less[466] extent from a small one. A more forcible impulse is given by a thick heart, and one more feeble by a thin one; the impulse is conveyed to a longer distance from a small heart.
From a clearer sound we believe in the probability of an attenuated heart, but we argue its certainty from a clearer sound joined with a weaker impulse. A stronger impulse denotes the probability of a hypertrophied heart, but we argue its certainty from a stronger impulse with a diminished sound.
The terms endocardial and exocardial are used to designate the alterations which take place in the sounds of the heart under disease—endocardial when they occur within the heart, and exocardial when they take place upon its surface. The endocardial murmur of disease, or bellows-sound, takes the place of and is substituted in certain cases for the first or second, or even for both the healthy or normal sounds. The exocardial murmur of disease is heard with the normal sounds, but confusing and overpowering, sometimes overwhelming, them by its rubbing or crumpling noise. The natural sounds exist, although rendered imperceptible by the greater distinctness and nearer approach of the unnatural or unhealthy ones.
The heart apart from the pericardium never moves without a sound; the pericardium apart from the heart never gives out one. Under disease the heart gives out the natural sound, diminished, exaggerated, or modified, or it may be totally altered. The sounds given out by a diseased pericardium must always be new, (there being no old ones,) and are described as rubbing, or to-and-fro sounds. The pleura, when diseased, being a serous structure, like the inner membrane of the pericardium, gives out less marked but somewhat similar sounds (the “frottement” of the French) in particular stages of disease.
The alterations in the ordinary sounds constituting the endocardial murmurs of the heart under disease depend principally on the altered state of the endocardium, or membrane lining its cavities; the sounds given off, and called exocardial, on an altered state of the serous membrane of the pericardium, reflected over the outer surface of the heart. The endocardial or bellows-sound, when it accompanies the normal sounds of the heart, may result from any kind of derangement affecting the internal membrane of that organ, particularly rheumatic inflammation, or from any force which[467] may compress its cavities; or it may depend on the altered quality of the blood, from anemia. It should be present after excessive hemorrhages have greatly reduced the powers of the sufferer. When this murmur or sound occurs after injury in the vicinity of the heart, and is accompanied by fever, it indicates inflammation of the lining membrane, although no local pain, no palpitations, no irregular movements of the heart be present.
When a murmur or sound is heard of a different kind, possessing the character of friction, of surfaces moving backward and forward on each other, or to and fro, it is the sign of inflammation of the membrane covering the heart, as well as of that lining the fibrous external tissue of the pericardium. The signs of both external and internal inflammation may be present at the same time, and they frequently are in cases of acute rheumatism.
357. When the heart is supposed to be wounded, even without much loss of blood, there is fainting; palpitation; irregular movement or total cessation of its action; coldness of the extremities; ghastliness of countenance, succeeded by great anxiety; a sense of anguish; an intermission or cessation of pulse, followed, if the patient should survive, by reaction, which renders it very frequent and sometimes increases its impulse; while the anxiety is increased by pain, sometimes intolerable, referred to the part. These symptoms imply a serious injury, although they may not all be present, and many of them differ in intensity. If the patient should survive, the ordinary sounds of the heart will return, with more or less irregularity, accompanied after a few hours by the endocardial murmur, although something like it may perhaps be observed from the first period of injury. The friction or attrition sound, indicating the presence of inflammation of the pericardium, may be absent; it will not be discernible, if a layer of blood be effused into the cavity of that membrane; while the natural sounds of the heart are rendered more indistinct as the heart is separated from the walls of the chest by the effusion which distends the pericardium, and impedes the regular action of the heart, but cannot compress it, as an empyema does the lung. If inflammation take place without an effusion of blood, the friction sound will be heard, and will usually continue even after some effusion of serum and of lymph has occurred, as the quantity of serum secreted is rarely sufficient to prevent the[468] effused and attached portions of lymph from rolling against each other.
The presence of a larger quantity of fluid may be more distinctly known by percussion, if it can be borne in cases of injury, the degree and extent of the dullness being the measure of its existence and accumulation. It may extend over a part or over the whole of the precordial region, reaching as high as the second, or even the first rib, beneath the sternum, and even under the cartilages of the ribs of the right side.
358. That the heart when wounded is capable of recovery by the permanent closure of the wound, in a few rare instances, is indisputable; and it would seem, from a consideration of the different cases which have been recorded, that such recovery takes place in consequence of there being but little blood discharged through the wound, or into the cavity of the pericardium, or into that of the pleura. The absence or the cessation of the hemorrhage by the contraction of the wound, or the formation of a coagulum, is the first step toward a cure, and it was to one or other of these circumstances that most of those who survived the injury for several days or weeks owed their existence for the time, although they usually died from the effects of inflammation, more of the inner lining and outer covering than of the substance of the heart itself.
If the wound be inflicted by a musket or pistol-ball, it cannot be closed, although pressure may be made upon it for a time, so as to suppress the external flow of blood. If this should succeed, it is more than probable that the hemorrhage will continue internally, and that the patient may die after much suffering, principally from oppression, caused by the escape of blood into the cavity of the chest.
If the wound be a stab, the external opening may be accurately closed, and the escape of blood prevented; but as the pressure of the blood in the pericardium is unequal to restrain the action of the heart, blood forced out through the opening fills the cavity of the pleura, and causes suffocation, unless from some accidental circumstance the opening in the heart becomes obstructed, and the bleeding ceases.
If all the circumstances be considered, there can be no doubt of the propriety of closing the wound in the first instance, if the flow of blood be excessive and appear likely to endanger life. It seems to be as little doubtful that the[469] wound should be reopened after a time, if the danger from suffocation be imminent. The relief obtained by the escape of a little blood may be efficacious, while it does not necessarily follow, although it is more than probable it will be so, that its place will be occupied by a further extravasation of blood, which will prove fatal. It is a choice of difficulties, and death from hemorrhage is easier than death from suffocation.
In the case of the Duc de Berri, whose right ventricle was wounded, and who died from loss of blood, Steifensand reprehends Dupuytren for having opened the external wound every two hours, to prevent suffocation; but if death were actually impending from the filling of the cavity of the chest being about to cause suffocation, there was nothing to be done but to give relief at all hazards.
359. When the sufferer has recovered from the imminent danger attendant on the infliction of the injury, and the pericardium is believed to be so full of blood or of serum as to prevent in a great measure the movements of the heart, it has been proposed by Baron Larrey to open the pericardium by the following operation—equally, as he thinks, applicable in an ordinary case of hydrops pericardii:—
“An oblique incision is to be made from over the edge of the ensiform cartilage, to the united extremities of the cartilages of the seventh and eighth ribs. The cellular tissue being divided with some fibers of the rectus and external oblique muscles, there remains only a portion of the peritoneum called its false layer, above the pericardium, which can be seen after the division of all the intervening cellular tissue, projecting between the first and second digitations of the diaphragm. Into this the bistoury is to be entered, with the precaution of doing it with the edge turned upward, and directed a little from right to left, to avoid the peritoneum. The smallest portion possible of the anterior border of the diaphragm is next to be divided, where it is attached to the inner part of the cartilage of the seventh rib. The internal mammary artery is to the outside. The patient should be placed perpendicularly, and supported on his bed, which inclines the anterior part and base of the pericardium to the fore part of the chest.”
Skielderup recommends this operation to be done by first trepanning the sternum a little below the spot where the cartilage of the fifth rib is united to that bone, at which part[470] the periosteum lining it offers considerable resistance, and should not be divided by the trephine. Below this there is a triangular space formed by the separation of the layers of the mediastinum, free from cellular tissue, and tending a little more to the left than to the right. The apex of this triangle is opposite the fifth rib; its base touches the diaphragm. The bone having been removed, the patient is made to lean forward, when the projection of the pericardium will enable the operator to feel that a quantity of fluid is within, and to open it with safety.
360. J. Dierking, a stout, muscular man of the 3d Regiment of German Hussars, was wounded at the battle of Waterloo by a lance, which penetrated the chest between the fifth and sixth ribs, and was then withdrawn. He fell from his horse, lost a good deal of blood by the mouth, and some by the wound, and was carried to Brussels without any particular attention being drawn to the injury. His strength not being restored, while he suffered from palpitations of the heart, and other uneasy sensations in the chest, he was sent to England to be invalided; and in November, 1815, was admitted into the York Hospital, Chelsea, in consequence of an attack of pneumonia, of which he died in two days, without attention being particularly drawn to the cicatrix of the wound.
On examining the body, I found that the lance, having injured the edge of the cartilage of the rib, passed through the inferior lobe of the left lung, the track being marked by a depressed, narrow cicatrix. It then perforated the pericardium under the heart, and sliced a piece of the outer edge of the right ventricle, which, being attached below, turned over and hung down from the heart to the extent of two inches, when in the fresh state, the part of the ventricle from which it had been sliced being puckered and covered by a serous membrane like the heart itself. The lance then penetrated the central tendon of the diaphragm, making an oval opening, easily admitting the finger, the edges being smooth and well defined. It then entered the liver, on the surface of which there was a small, irregular mark or cicatrix. The heart in front was attached to the pericardium by some strong bands, the result of adhesive inflammation, but the general appearance of the serous membrane showed that this had not been either great or extensive. The pericardium was not thickened.[471]
If this man had lived long enough, he might have furnished an instance of hernia of the stomach or of intestine into the pericardium. The preparation is in the military museum at Chatham, Class 1, Div. 1, Sect. 7, No. 156.
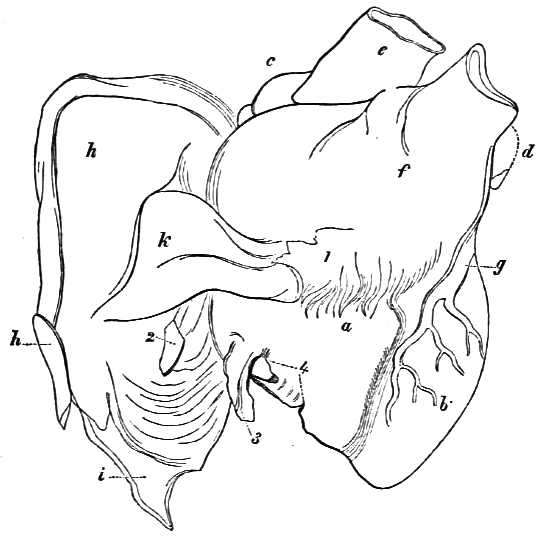
a, right ventricle;
b, left ditto;
c, right auricle;
d, left ditto;
e, aorta;
f, pulmonary artery;
g, coronary ditto;
h, a portion of the cartilages of the ribs seen on the inside;
i, a portion of the diaphragm;
k, the pericardium.
1, a portion of the pericardium reflected to show abnormal adhesions to the surface of the heart;
2, aperture of wound through the diaphragm and the pericardium;
3, pendulous slice off the substance of the right ventricle;
4, puckered cicatrix of the wound of the ventricle.
That the heart, when exposed, is insensible, or nearly so, to the touch, was known to Galen and to Harvey. Galen is said to have removed a part of the sternum and pericardium, and to have laid his finger on the heart. Harvey did the same to the son of Lord Montgomery, who was wounded in the chest. Professor J. K. Jung not only introduced needles into the hearts of animals, but also galvanized them without disadvantage, although Admiral Villeneuve is supposed to have died suddenly from running a long pin into his heart, which scarcely left the mark of its entrance.
That persons may die from the shock of a blow on the[472] heart, need not be doubted, and that they do die when little blood is lost, is admitted. History preserves the fact that Latour d’Auvergne, Captain of the 46th demi-brigade, who had obtained the honorable title of “Premier Grenadier de France,” fell and died immediately after receiving a wound from a lance at Neustadt, in the month of July of the sixth year of the Republic; it struck the left ventricle of the heart near its apex, but did not penetrate its cavity. He was, however, sixty-eight years of age.
361. In wounds of the heart, all extraneous matters should be removed, if possible, and all inflammatory symptoms should be subdued by general bleeding, by leeches, by calomel, antimony, opium, etc. The chest should be examined daily by auscultation. If the cavity of the pleura should fill with blood, it ought to be evacuated to give a chance for life, and if the pericardium should become permanently distended by fluid, it should be evacuated.
Lacerations and ruptures of the heart have frequently taken place from blows or other serious contusions.
Ollivier, who devoted much time to reading and collecting the observations made by different writers on the injuries of the heart, says: “That of forty-nine cases of spontaneous rupture of the heart, thirty-four were of the left ventricle, eight only of the right, two of the left auricle, three of the right, and that in two cases both ventricles were torn in several places; and that these results were in an inverse proportion to those which occurred after blows or contusions; the right ventricle being ruptured in eight out of eleven cases, the left ventricle three times; the auricles being also torn in six of these eleven cases; the ruptures not being confined to one spot, but taking place occasionally in several different parts, or even in the same ventricle.” In eight of these cases he had noticed, the heart was ruptured in several places. That a spontaneous rupture may be cured as well as a wound, seems likely, from a case reported by Rostan, of a woman who died after fourteen years’ suffering with pain about the heart, and was found to have the ventricle ruptured. A cicatrix was observed to the left side of the recent rupture, half an inch in extent in every direction, in which the new matter was evidently different from the natural structure of the heart.[473]
WOUNDS OF THE INTERNAL MAMMARY ARTERY, ETC.
362. Wounds of the internal mammary and intercostal arteries have so much occupied the attention of theoretical surgeons, and so many inventions have been broached for the suppression of hemorrhage, particularly from the latter, that it becomes consolatory to know that bleeding from these vessels rarely takes place; that the inventions are more numerous than the case requiring them, and that no notice need be taken of them, they being as unnecessary as they are useless. I have never had occasion to see a distinct case of hemorrhage from an internal mammary artery, but if bleeding should take place from a wound in its neighborhood, of a nature to lead to the belief that it came from this vessel, the wound should be enlarged until the part whence the blood flows can be ascertained, when, if it be from that artery, the vessel should be twisted or secured by ligatures, and if these methods should be impracticable, the wound should be closed and the result awaited.
The following method of operating for the application of a ligature on this vessel has been proposed by M. Goyraud. It may be done with ease in the three first intercostal spaces, it offers some difficulties in the fourth, is very difficult in the fifth, and is scarcely to be done lower down. An incision two inches in length is to be made near the side of the sternum from without inward, at an angle of forty-five degrees with the axis of the body. The middle of this incision should be three or four lines distant (a quarter of an inch) from the bone, and in the center of the intercostal space, within which the vessel is to be found. The skin, cellular substance, and the great pectoral muscle having been divided, the aponeurosis of the external intercostal muscle with the muscular fibers of the inner intercostal muscle are to be separated and torn through with a director, until the artery and its two venæ comites are laid bare at the distance of three lines from the edge of the sternum, lying before the fibers of the triangularis sterni muscle, which separates these vessels from the pleura. A bent probe, or other proper instrument,[474] can then be readily passed under the artery. The vessel can only be secured in this way when injured at the upper part of the chest; below this it must bleed into the cavity, unless there be an open wound.
363. The intercostal artery, although often injured, rarely gives rise to hemorrhage so as to require a special operation for its suppression; but whenever it does so happen, the wound should be enlarged so as to show the bleeding orifice, which should be secured by one ligature if distinctly open, and by two if the vessel should only be partially divided. The vessel is sometimes so small as to be easily twisted, or its end sufficiently bruised as well as twisted, to arrest the hemorrhage. It lies between the two layers of intercostal muscles, and in the middle of the ribs it runs in a groove in the under part of each.
I have had occasion to twist and bruise the end of an artery bleeding in an intercostal space, and I have tied the vessel under the edge of the rib; but I have not met with any of the great difficulties usually said to be experienced in suppressing a hemorrhage from this artery, when the wound was recent, and the parts were sound; no reliance should be placed on the hypotheses often entertained on this subject.
When the parts are unsound, and the hemorrhage is secondary, greater difficulty is sometimes experienced in arresting it, because the ligature easily cuts its way through the softened parts, and styptics are liable to fall into the cavity of the chest.
The late General Sir G. Walker, G.C.B., after scaling the wall of Badajos, with the fifth division, was wounded by a musket-ball, which struck the cartilages of the lower ribs of the right side, broke the bones, penetrated the chest, and then passed outward. He remained in Badajos under my care during the first three weeks, with many of the other principal officers who were wounded; and overcame the first inflammatory symptoms in a satisfactory manner. After I left him the wound sloughed, some part of the cartilages separated, and one of the intercostal arteries bled, although the bleeding was arrested once by ligature, and afterward, on its return, by different contrivances; each time it reappeared his life was placed in considerable jeopardy from it and the discharge from the cavity of the chest, which was profuse. The bleeding was ultimately arrested by the oil of[475] turpentine, applied on a dossil of lint, and pressed on the bleeding spot by the fingers of assistants until the hemorrhage ceased. He recovered after a very tedious treatment, with a considerable flattening of the chest, and a deep hollow at the lower part of the side, whence portions of the rib, and of the cartilages had been removed.
A young man, aged fifteen, was wounded by small shot in the chest, between the first and second ribs, and near the sternum, at the distance of about forty-eight paces. He ran about six hundred paces, fell, and died thirty-eight hours afterward. On opening the injured cavity of the thorax, it was found to contain twenty-eight ounces of blood, the lung having collapsed to one-fourth its natural size. An opening on its upper part corresponded to the external one in the paries; but the track of the shot could not be traced into its substance for more than two inches and three-quarters; a lacerated spot was, however, perceived at the lower edge of the sixth rib, about two inches from its head, at which part the intercostal artery was found to be torn through; the shot could not be found, and there was no opening in the skin behind.
The discussions which took place on this case led to the statement of an anatomical fact—that when a man is standing erect, a line drawn horizontally from the upper border of the second rib in front would touch the upper edge of the fifth rib behind, and that very little inclination, viz., an inch and a half, was necessary to make the shot wound the intercostal artery of the sixth. Auscultation would have made known the extravasation, and relief might have been given by an incision over the spot where uneasiness was felt; for the loss of blood was not sufficient of itself to destroy life, unless some other injury had been sustained, which was not perceived.
364. Wounds of the neck which are made with swords, or by knives or razors, by persons attempting to destroy themselves, are to be treated on two great principles. The first is, not to place the parts in contact until all hemorrhage has ceased, lest the patient be suffocated. In the mean time, while any oozing continues, a soft sponge should be placed between the edges of the cut. When the larynx or trachea is obstructed by a quantity of blood, it may be sucked out, or drawn up by an exhausting pump, and it may be advisable in some cases to introduce a tube. If the[476] trachea be cut across, a stitch will be necessary to keep the ends in contact. The second is, to keep the divided parts in contact afterward, by position and bandage, but not by suture. If the œsophagus be wounded, nourishment should be administered by a gum-elastic tube introduced through the nares into the stomach. It is almost unnecessary to add that the artery, if wounded, should be secured by ligature. A hole in the internal jugular vein may be closed by a thread passed around it when raised by a tenaculum.
Captain Hall, of the 43d Regiment, was wounded by a ball which passed between the upper part of the back of the larynx and the termination of the pharynx, without causing much further inconvenience than the loss of voice. In this instance it must have been the superior laryngeal nerve that was injured, and not the recurrent, yet the voice could only be heard in a whisper, and was not completely recovered for years. If a ball should lodge in the trachea, it must be removed by the operation of laryngotomy or tracheotomy, if the original wound cannot be enlarged; although Birch, says Christopher Wren, hung up a man wounded in this way by the heels, when the ball dropped out through the glottis and mouth. General Sir E. Packenham, who was killed at New Orleans by a ball which went through the common iliac artery, had been twice shot through the neck in earlier life. The first shot, which went through high up from right to left, turned his head a little to the right. The second shot, from left to right, brought it straight. My kind and excellent friend had ever afterward a great respect and regard for the doctors and a strong feeling for the wounded. The recollection of that regard, and the advantages derived from it, have made me sometimes think it might be advantageous for the unfortunate as well as for the doctors if every general could be at least shot once through the neck or the body, before he was raised to the command of an army in the field; for there is nothing like actual experience of suffering to make men feel for their fellow-creatures in distress. A Minister at War would not perhaps be the worse for a little personal experience in this matter.
365. Wounds of the face made by swords or sharp-cutting instruments should be always retained in contact by sutures. When the cut is of small extent, and not deep, the skin only should be included by the thread, and that in[477] the slightest possible manner, and the part supported by adhesive plaster and bandage. When the cheek is divided into the mouth, one, two, or more sutures may require to be inserted more deeply, but the deformity of a broad cicatrix will in general be avoided, by carefully sewing up the whole line, taking the very edge of skin only; and a cut in the bone or bones of the cheek should not prevent the attempt being made to unite the external wound over it.
Incised or even lacerated wounds of the eyelids and brows should be united by suture, as far as can possibly be done in the first instance, by which a subsequent painful operation may be avoided; great care should be taken in doing this; the suture must be inserted through the eyelid, and a leaden thread is often the best, the first being introduced at the very edge of the lid, and two, or as many more afterward as may be necessary. They may remain for three or more days, as circumstances seem to require. If the eye be wounded, any part protruding beyond the sclerotic coat should be cut off with scissors; but the eye, however injured, should not be removed unless the ball be detached in every direction, or destroyed. The treatment should be strictly antiphlogistic, in order to prevent suppuration of the eyeball, which may in general be effected, if too much injury have not been done to it, and if the treatment be sufficiently decided and well continued. These observations apply to the nose and ears, and all parts not actually separated—or, if separated, for a short time only—should be replaced in the manner directed, and every attempt made to procure reunion. If this should fail, surgery may yet be able to yield assistance by replacing the loss by a piece of integument dislodged from the neighboring parts—a proceeding requiring a separate consideration. Injuries from musket-balls are often attended by considerable laceration, particularly when near the eyelids. Whenever this occurs, the parts likely to adhere should be brought together by suture, after any splinters of bone which may present themselves, or can be seen or felt, have been removed from the holes made by the ball. If the bones should be broken, and not splintered, they will frequently reunite under proper management.
366. Wounds of the eye from small shot are remediable when these small bodies lodge in the cornea or sclerotica, whence they may be removed by any sharp-pointed instru[478]ment. When a shot or piece of a copper cap is driven through the cornea, into the iris, or lies in the anterior chamber, it should be removed by an incision to the extent of about one-fourth or one-fifth of the cornea, near its junction with the sclerotica, but in these cases a cataract, if not amaurosis, frequently results. When the shot passes through all the coats of the eye, it can neither be seen nor removed with safety; vision will be lost, much pain may be endured, and the eye will frequently be destroyed by suppuration, or by a gradual softening, and ultimate diminution in size. A contused wound from a large shot which only injures the coats of the eye, but does not perforate them, will oftentimes be cured by a proper antiphlogistic treatment, which in all cases should be most strictly enforced, although loss of sight is a frequent consequence after such injuries.
When a ball lodges behind the eye, it usually causes protrusion, inflammation, and suppuration of that organ. If it be not discovered by the usual means, its lodgment may be suspected from the gradual protrusion and inflammation of the eye itself. If it be discovered, it should be removed together with the eye, if such proceeding be necessary for its exposure. If suppuration have commenced in the eye, a deep incision into the organ will arrest, if not prevent, the horrible sufferings about to take place, and allow of the removal of the offending cause. If the eye remain in a state of chronic disease and suffering, a similar incision will give the desired relief. If the chronic state of irritation affect the other eye, the incision and sinking of the ball of the one first affected or injured is urgently demanded, and should not be delayed. If the back part of the eye be left with the muscles attached to it, a stump remains, against which an artificial eye may be fitted, so as sometimes to render the loss of the natural one almost unobservable.
367. I have several times seen both eyes destroyed and sunk by one ball, with little other inconvenience to the patient; one eye sunk, the other amaurotic, and both even amaurotic, almost without a sign of injury, by balls which had passed from side to side through both orbits, but behind the eyes. When the eye becomes amaurotic from a lesion of the first branch of the fifth pair of nerves, the pupil does not become dilated; the iris retains its usual action, although the retina may be insensible and vision destroyed. This was well shown in the case of the late Major-General Sir A.[479] Leith, who was wounded by a sword in the forehead, this nerve being divided. It has so often occurred as to leave no doubt of the fact, and of the error formerly existing on this point.
368. Penetrating wounds implicating the bones of the face are always distressing. When the bones of the nose are carried away, there must always be some deformity remaining, although there is oftentimes but little suffering. When these bones are merely splintered and depressed, great pains should be taken to keep them properly elevated. If the duct of the parotid gland be implicated by an incised wound, care should be taken to divide the cheek into the mouth, if it should not have been already done, and to keep the incised wound open until the external one is closed. If a salivary fistula have formed externally, from inattention or otherwise, it must be treated according to the ordinary methods adopted in such cases. When a wound of the gland itself becomes fistulous, and weeps, which is a rare occurrence, it will be best treated by actual or potential cauterization, if moderate pressure should fail. When these wounds are of some extent, they are often followed by partial paralysis, in consequence of the seventh pair of nerves being injured, when the mouth is drawn somewhat to the other side. When the lachrymal bones or sac are injured by balls or swords, the tears usually continue through life to run over, and give inconvenience, although much good may be done by early attention to the injuries of this part. Wounds injuring the upper jaw are oftentimes followed by much suffering, and by permanent inconvenience.
General Sir Colin Halkett, G.C.B., was wounded on the 18th of June, at Waterloo, when in front of his brigade, which was formed in squares for the reception of the French cavalry, by a pistol-ball, fired by the officer commanding them, which struck him in the neck, and gave him great pain, but without doing much mischief. A second shot shortly afterward wounded him in the thigh, and he was obliged to leave the field toward the close of the day, by a third musket-ball, which struck him on the face, when standing sideways toward the enemy. It entered a little below the outer part of the cheek-bone on the left side, and, taking an oblique direction downward and forward, shattered and destroyed in its course several of the double teeth in the upper jaw, fracturing the palate from its posterior part, for[480]ward to the front teeth. The ball then took a direction obliquely upward, destroying the teeth of the opposite side of the upper jaw, which bone it also broke, and lodged under the fleshy part of the cheek. These wounds gave great pain, and until the ball was removed, the left ear was totally insensible to sound and all external impressions, although the general suffered much from distressing noises in his ear. These subsided on the removal of the ball some days afterward.
The treatment of this wound, however, was most painful; the extraction of several pieces of bone was necessary at different times, during the three following years, before the wounds were finally closed. Considerable derangement of health followed, the deafness remains; and the general has ever since been subjected to attacks in the head of an increasing and most distressing nature.
369. Wounds of the lower jaw are perhaps more common, and are certainly more troublesome than those of the upper; they are more difficult of management, and, for the most part, end in greater deformity, unless particular care be taken to prevent it, and then only in very severe cases, by operations which were formerly not in use, but which the intrepidity of the surgeons of the present day have deprived of all their terrors. I mean the methodical division of the soft parts, the sawing off and removal of the broken pieces of bone, and the rounding off of those parts of the jaw which may remain irregular and pointed. M. Baudens has given two good examples of the success of this proceeding during his campaigns in Algeria. In the first case, the ball entered at the middle of the left cheek, and came out by the side of the spinous process of the seventh cervical vertebra. The ascending ramus of the lower jaw was broken into numerous splinters. M. Baudens divided the soft parts down to the bone, entering the straight bistoury four lines, or the third of an inch, below the articulation of the jaw with the temporal bone. He then carried it downward, and a little obliquely forward, so as to terminate it in the fibers of the masseter muscle, about half an inch below the base of the bone. This incision was begun below the seventh pair of nerves, and exposed the parotid gland divided vertically at its middle part. The splinters were removed, a part of the pterygoideus internus muscle was divided, and a projecting point of bone attached to it sawn off. He then separated[481] the attachments of the buccinator, temporal, and pterygoideus externus muscles, divided the ligaments, and removed the coronoid and articulating processes, taking care to avoid the fifth and seventh pairs of nerves. The bleeding from two arteries was suppressed by twisting their ends; and the parts were afterward brought together by sutures, which remained for eight days. A month after the operation the patient ate solid food, and in six weeks was cured. In the second case, the ball entered near the left commissure of the lip, and came out behind on the side of the middle of the neck; three inches of the jaw were splintered, the ends of the bone being sharp and angular. In order to remove the splinters, and to prevent the evils anticipated, M. Baudens divided the lip from the angle downward and outward, below the base of the bone, as far back as the edge of the masseter muscle. He then separated the flaps, and sawed the jaw across, first near the symphysis, and then behind, outside the attachment of the masseter. The facial artery was twisted, four sutures were inserted, and the jaw duly supported. The patient was bled twice, and in six weeks was cured; at the end of that time he could eat solid food. After the healing of such wounds, mechanical means are often necessary to enable the sufferer to eat and to live without causing disgust to his neighbors and his friends.
It is said there are fifteen men in the Hôtel des Invalides, in Paris, wearing silver masks on the lower part of their faces, in consequence of injuries of this kind.
Colonel Carleton was an instance of a ball fracturing the jaw directly through its body, near where the masseter muscle is attached on both sides; the jaw was broken into three pieces, besides splinters; several teeth were knocked out, and the tongue very much hurt. By sawing off the splinters both from within and without, and by cleansing and supporting the parts with great care, he recovered after a length of time, the deformity after such a wound being much less than might be expected.
370. Incised wounds of the tongue do sometimes give rise to hemorrhage somewhat difficult to restrain, particularly if it occur a few days after the receipt of the injury, when the tongue is swollen and painful. It does not so frequently occur after gunshot wounds. As the vessels of one side do not communicate with those of the other, any bleeding which continues after the artery of one side has been properly[482] secured, can only take place from a wound of the artery of the other, which must then also be tied. This should be done by drawing the tongue as far as possible out of the mouth by a flat pair of forceps, which may be easily effected at an early period, when it is not tender and painful. At a later date, and under difficult circumstances, various styptics, such as the mineral acids, nitrate of silver, etc., will be useful. The actual cautery has been recommended, but I have never seen it used in such cases.
371. One of the most curious instances of the lodgment of a foreign body in the face occurred in the person of Captain Fritz, at Ceylon; his gun burst in his hand, and drove the iron breech into the forehead, whence it descended into the nares, and, at the end of a year, part of it made its appearance in the mouth, through the palate. He died eight years afterward, having suffered much inconvenience from the offensive discharge it occasioned. When the iron was removed, it had obviously injured no part of any material importance to life. I have seen balls descend in this way into the throat and soft palate, and have removed them from both places with success, and from the hard palate with equal surprise and advantage to the patient. I have known a ball lodge in the superior maxillary sinus for months, and even for years, before it was removed, or the death of the patient proved the fact.
STRUCTURE OF AN INTESTINE, ETC.
372. If an intestine be divided circularly in any part, its walls will be found to be composed of three principal coats or tunics, which are—commencing from the inside—the mucous, the muscular, and the serous or peritoneal, each being separated from the other by a layer of areolar tissue. A diagram thus made would show a transverse division of the intestine, and eight distinct if not all different parts. Beginning from without, viz., serous or peritoneal, areolar or sub-serous; longitudinal muscular, areolar; transverse muscular, areolar or sub-mucous, and epithelial. The mucous[483] coat in man has a peculiarity not observable in animals, of ledges or shelves projecting into its cavity.
When the mucous coat of the duodenum is examined with the naked eye, the first part of its course presents a tolerably smooth appearance, gradually, however, becoming irregular in transverse folds, which are so numerous, marked, and regular in the jejunum and ileum as to have obtained from the earliest times the name of valvulæ conniventes. They are most strongly marked in the jejunum, and gradually disappear toward the lower part of the ileum, the inner surface of the large intestines being still smoother than any part of the small, although large pouches or cells are formed in the colon by a peculiar arrangement of the muscular coat. These valves never extend completely round the inside of the intestine, and rarely more than half or two-thirds, although they sometimes bifurcate. They have a velvety appearance, which has obtained for this coat the name of villous as well as that of mucous.
Valvulæ conniventes are peculiar to man; none exist in the ourang-outang or chimpanzee. In the frog there are valvular folds, appearing, at first sight, like the valvulæ conniventes of the human subject; but, on a careful examination, they are found to be mere elevations, without villi. In the tortoise there are similar folds, running however in a longitudinal or opposite direction. In the rhinoceros the mucous membrane is raised up into villiform processes, somewhat like the valvulæ conniventes, or large villi; but they are not villi, as each process is covered with other projections which really are villi. A valvula connivens consists of two layers of mucous membrane and sub-mucous tissue, but the muscular coat is not continued into it.
373. When examined microscopically, the velvety appearance is found to consist of innumerable small processes which have been called villi, each villus being composed principally of a very thin, transparent basement or germinal membrane, forming a sheath or case, inclosing within it an artery, a vein, a capillary plexus, and an absorbent vessel termed lacteal. A nerve has not been discovered, although it is presumed to exist. These villi are longest in the duodenum, and gradually diminish in number and in size from 1/25 to 1/50 of an inch. Between these villi or projections, holes or openings are observable, termed the follicles of Lieberkühn, who first described them; they resemble inverted villi, being[484] in some instances as deep as the villi are long. Unlike the villi, they are found throughout the intestines. The villi in every part in common with all mucous membranes are covered, and the follicles are lined by epithelium, which in this instance is the columnar, situated on the basement membrane, each column being attached by its pointed extremity. A layer of this epithelium extends between the villi, down to the lower part of each follicle, each column being, generally speaking, shorter and rounder than when covering the villi.
The office of the epithelium of the villi has been stated to be protective, that of the follicles to be secretive. A villus, when duly magnified, is seen to have a bulbous extremity without an opening, and to be covered by epithelium when the intestine is in a state of quiescence, uncalled upon for any purpose of digestion. When digestion commences, the epithelium, according to the researches of Mr. Goodsir, is separated and thrown off. As the chyme begins to pass along the small intestine, an increased quantity of blood circulates in the capillaries of the gut. In consequence of this increased flow of blood, or from some other cause, the internal surface of the gut throws off the epithelium of both villi and follicles, which is intermixed with the chyme in the cavity of the gut. The cast-off epithelium, forming 19/20ths of the covering of the villus, is of two kinds, that which covers the villi, and which from the duty it performs may be termed protective, and that which lines the follicles and may be termed secretive, each column having a nucleus situated at some part of it, and bulging out that part.
The villi being now turgid with blood, erected and naked, and covered by the chyme mingled with the cast-off epithelia, commence their functions. The summit of the villus becomes at first somewhat flattened and crowded under the basement membrane with a number of newly-formed and perfectly spherical vesicles, varying from 1000 to less than 2000 of an inch in size. Toward the body of the villus or the inner edge of the vesicular mass, minute granular or oily particles are situated in great numbers, and gradually pass into the granular texture of the substance of the villus. As the process advances lacteal vessels are shown passing up from the root of the villus, subdividing and looping as they approach the spherical mass, which in this stage has become more distinctly vesicular, although no distinct communication can be detected between them. The blood-vessels[485] and capillaries shown in injected preparations are now seen colored red with their own blood, and running up to the basement membrane, looping with each other immediately beneath it, and ending in one or more venous trunks. The vesicles, quite distended and grouped in masses, push forward the membrane, and give to it by these inequalities an appearance resembling that of a mulberry.
The minute vesicles above noticed fulfill the important office of absorption, by drawing into their cavities through their walls, by a process called endosmosis, that portion of the chyme necessary to form chyle; when filled with it they burst or dissolve, their contents being thus discharged into the texture or substance of the villus, fit to be taken up by the granular vesicles interspersed among the terminal loops of the lacteals, and communicating with their trunks, running up from the root of the villus in their center. Absorption is thus shown to be effected by closed vesicles, and not by vessels opening on the surface of the villus.
The débris and the contents of the dissolved chyle cells, etc. pass into the looped net-work of lacteals, as in other lymphatics. When the gut contains no more chyme, the flow of blood to the mucous membrane diminishes, the development of new vesicles ceases, the lacteals empty themselves, the villi become flaccid, and the cast-off epithelium is reproduced, apparently from the nuclei in the basement membrane, in the intervals of digestion, showing that this function should only be induced at regular periods, the presumed special use of the epithelium being to prevent, in a measure, the absorption of any effete or other matters which might exert a deleterious influence oh the system, the epithelium of the follicles now secreting a mucus which may be considered protective.
In the large intestines there are no villi, but the whole surface is covered with follicles which must be capable of absorbing as well as of secreting, as it is ascertained that persons can be nourished and kept alive for many weeks by nutritious enemata which do not pass into the small intestines.
374. On examining the mucous membrane of the stomach, its follicular structure is immediately seen, the follicles resembling much in appearance those of the intestine; but in the stomach minute tubes are found opening into the bottom[486] of each follicle, fulfilling in all probability a different office, the follicles being lined by columnar epithelium, the tubes by spheroidal or glandular epithelium; it is therefore presumed that the gastric juice is secreted by the tubes, the mucus by the follicles. The tubes differ in the middle and lower parts of the stomach, by being longer or more deeply seated, and more numerous as they approach the pylorus, showing in all probability a difference of function between the upper and middle, and the pyloric or lower extremity of the organ.
The intestines are supplied with glands, not apparently for the purposes of absorption, but of secretion; these require attention. They are the duodenal of Brunner, the agminated of our countryman, Nehemiah Grew, and of Peyer, and the solitary, which are found in the lower part of the small and in the whole course of the large intestines.
The glands of Brunner are situated at the commencement of the duodenum, within an inch of the pylorus, and are not visible until the serous and muscular coats have been removed from without. They appear to the naked eye like the little white eggs of an insect. Under the microscope each little gland is found to be lobulated, very much resembling a small portion of a salivary gland or pancreas, each lobule having an excretory duct, which unites with those from other lobules to form one larger one opening on the mucous surface of the bowel. The lobules themselves are made up of vesicles, within which the secretory cells are discernible.
The agminated glands of Grew and Peyer, by the latter of whom they were more minutely described, occur in oval patches at irregular distances throughout the jejunum and ileum, and are situated on the side immediately opposite the part where the mesentery is united to the bowel. Each gland resembles somewhat a Florence oil-flask in shape, the small end or mouth, which is more or less pointed, projecting through among the villi or the follicles. They are composed of cells, supplied by capillary vessels, which Mr. Quekett says have the peculiarity of being unsupported by areolar tissue, and are termed by him, in consequence, naked. These are the glands which are found more or less diseased after phthisis and fevers which have terminated fatally. The oval form of the patches is retained, although considerably raised above the general surface of the mucous membrane,[487] and when injected the parts around are more vascular, the ulcerated portion being less so than usual.
The solitary glands are best seen in the cœcum and appendix vermiformis. They are well developed in the fœtus, projecting slightly above the mucous membrane. Each gland may be considered as one of the agminated form much enlarged, and when the free surface is very flat, an opening may be easily seen in the center. These glands also are frequently the seat of ulceration in fever and dysentery, and particularly in phthisis. The follicles partake of this disease, and the whole mucous coat may be destroyed. In some cases there is an attempt at healing, and the edges of the ulcers become more vascular and even villous.
The sub-mucous areolar tissue—the tunica nervosa of Haller, the fibrous lamella of Cruveilhier—separating yet connecting the mucous with the muscular coat of the intestine, is composed of the yellow elastic and of the white or non-elastic fibers, the latter of which predominate. It is more firmly connected with the mucous than with the muscular coat, and in it the blood-vessels and nerves are supported prior to their distribution in the mucous membrane. This sub-mucous tissue or structure prevails also in the stomach, and is often much altered by disease, becoming thicker, and assuming a more dense and sometimes an almost gristly hardness. It is an important part in the surgical treatment of wounds of the intestines, being firmer, stronger, and more elastic in reptiles, and more distinct in carnivorous than in herbivorous animals or in man.
375. The muscular coat of the intestines is in two layers, the internal being composed of fibers running transversely, the outer fibers running longitudinally; they are thickest in the duodenum and rectum. They are of the involuntary or unstriped kind, as opposed to the voluntary or striped, which are of large size, and characterized by striæ running transversely and longitudinally.
The involuntary fibers, on the contrary, are much smaller in size, are always more or less flattened, and present no trace of striæ or stripes, although the interior appears granular, with an occasional nucleus. The heart is a remarkable exception to this rule, being an involuntary organ, with striped fibers differing in size, resembling in this respect those of a voluntary muscle.
The peritoneal coat is formed of the white fibers, under a[488] structureless or basement membrane, covered by tesselated epithelium, constituting a serous and secreting membrane.
376. Wounds and injuries of the abdomen are essentially of three kinds—1. Affecting the paries or wall. 2. Opening or extending into its cavity. 3. Wounding or injuring its contents.
The wall of the belly is, when severely hurt, liable to a permanent defect, as the ordinary result of a severe bruise. It is the formation of a ventral rupture. A division of the wall to any extent by a sharp-cutting instrument is usually followed by a similar consequence; and it never fails to occur in the openings made by a musket-ball penetrating into or passing through the cavity.
Captain Tarleton, of the 7th or Royal Fusiliers, was struck on the left iliac region by a large, flat piece of shell, at the battle of Albuhera, in 1811. The surface was not abraded, although the iron caused a very severe and painful bruise; the whole of that side of the belly became quite black, and the remaining part much discolored. Some months afterward he drew my attention to the part, and I then found that the whole of the muscular portion of the wall had been removed by absorption to the extent of the immediate injury from the piece of shell, the tendinous parts alone remaining under the integuments. These protruded on any effort, constituting a circular-shaped ventral rupture, with a large base, which required the application of a pad and bandage for its repression.
Mr. Smith, a deputy-purveyor, received a blow on the side of the fore part of the belly from the end of a spanker-boom, which knocked him down, and gave rise for some time to much inconvenience. He showed the part to me in Lisbon, in 1813, in consequence of the formation of a ventral hernia to the extent of the spot originally injured. In neither of these cases was such a result expected; no rupture of the fibers of the muscles was distinguished at the time, and it was supposed that the sufferers would recover without any permanent defect. The absorption of the muscular fibers was therefore a subsequent process; whether this result may or may not be prevented in similar cases by a more active or a longer-continued treatment, with the early application of a retaining bandage, is yet to be ascertained. It may be that some muscular fibers were actually ruptured and others bruised in these cases; but the extent of the absorption[489] was greater than the apparent injury would seem to have warranted.
Abscesses form from neglected injuries of this kind, and give rise to the most serious apprehensions of their bursting into the cavity of the abdomen, which, however, they very rarely do. The safety of the peritoneum and its capability of affording sufficient resistance to the progress of the matter through it seem to depend upon the strength of the fibrous structure on its outer or muscular side; the inner or really serous surface being very delicate, and offering but little resistance to the application of any moderate degree of force.
An officer, whose name I forget, was wounded at the assault of Ciudad Rodrigo, in 1812, by a musket-ball, on the left side and fore part of the abdomen, near the crest of the ilium: it made a wound about four inches in length, cutting away the muscles of the abdominal wall so deeply as to lead to the exposure, and, as I feared, to the ulceration of the peritoneum, when the sloughs should separate. Under these circumstances, although not belonging to my division, I took him with me from the field to the divisional hospital at Aldea Gallega, some ten miles from the battlefield. Granulations sprang up, however, from the bottom and sides of the wound, which gradually closed in and healed without further difficulty.
377. It has been supposed theoretically, to be a matter of importance to discriminate between the orifice of entrance of a ball passing through the abdomen or its wall, and that of its exit. Practically speaking, it is a matter of indifference; the part on which the ball impinges is usually distinguished by a more circular and depressed appearance, while the opening of exit more frequently resembles a tear or slit, the edges of which are rather disposed to protrude.
A ball striking obliquely against the wall of the abdomen has been said to run sometimes nearly round under the skin, or between the muscles and the peritoneum, a proceeding upon the recurrence of which little expectation need be placed. It may, however, do something of the kind for a considerable distance, passing even over or between the spinous processes of the vertebra behind. In such cases, when they actually occur, the course of the ball will usually be marked by a line on the skin, more or less of a reddish-blue color; and the constitutional alarm, if it should occur[490] at all, will subside early. A ball may, however, pass under and between the muscular layers of the wall of the belly, (or run nearer to the peritoneum for several inches,) giving rise to great anxiety, until the sloughs have separated from the openings of entrance and of exit, at which parts they prevail to a greater extent than in the middle of the track of the projectile. In some few instances an opening will require to be made in the middle of this track or course of the ball, for the evacuation of pus or of other extraneous matters which may be detained in it.
When a ball lodges in the wall of the abdomen and is deeply situated, it sometimes escapes notice, and when found is often better left alone unless it prove troublesome. When it approaches the surface, it may be removed if it cause inconvenience. When removed after the lapse of twenty or more years, I have found some dense cellular membrane forming a sac around and adhering to the ball, which is usually more or less flattened and irregular.
378. Injuries of the wall of the abdomen from cuts or stabs affecting the muscular and tendinous parts are said to be frequently troublesome, and even dangerous, from their giving rise to pain, vomiting, and severe general derangement. This only occurs when suppuration takes place, and, from some accidental circumstance, the matter does not find a ready exit, but collects between the muscles, or within or under their aponeurotic sheaths. This is indicated by the pain and swelling of the part, proceeding sometimes to the formation of an abscess, which ought to be prevented, if possible, by an early enlargement of the wound, so as to remove the cause of irritation, and the obstacle to the free discharge of the secreted matter. If the swelling should become prominent in a more convenient situation than the spot of injury, it should be opened at that part.
In these and in all other serious injuries of the abdomen, the recumbent position, with a relaxed state of the muscles, should be observed for several days at least. The antiphlogistic plan of treatment should be fully enforced, especially by leeching, bleeding, and spare diet, and in due time the part should be supported by a proper bandage.
The late General Sir John Elley was wounded in the last charge of heavy cavalry at Waterloo, by the point of a sabre, which entered nearer the extremity of the ensiform cartilage than the umbilicus, causing a wound about two inches in[491] length, penetrating the stomach. From this he recovered in due time without any severe symptoms, but with a small hernia of that organ, which remained until his death, giving rise occasionally to some gastric inconvenience when he did not keep a gentle pressure on it by a retaining bandage.
379. Severe blows, or contusions from falls or from the concussion of foreign bodies, may give rise not only to injury of the internal parts of the abdomen, followed by inflammation, but to rupture of the hollow as well as of the more solid and fixed viscera, and death.
William Fletcher, of the 18th Hussars, a healthy man, thirty-seven years of age, received a kick from a horse, immediately above the os pubis, on the 15th of April, 1810, (about a league from Cartaxo, on the Tagus;) great tension of the belly soon followed, with excessive pain and vomiting. The pulse rose rapidly. He was bled to syncope twice during the day, to the extent of sixteen ounces each time. In the evening he was removed to Cartaxo, and taken into hospital; the pain continued, accompanied by retching, without much vomiting; the abdomen was constantly fomented with hot water, and injection was thrown up, and two ounces of infusion of senna with salts were given every two hours. In spite, however, of the most active treatment, he died on the 17th. On dissection, the peritoneum was found to contain a large collection of fluid, partaking of a fecal character; the bowels appeared to have suffered to the greatest extent, and a laceration was discovered in the ileum.
A child, just able to walk, was placed under my care in the Westminster Hospital, in consequence of its having received some injury on the side of the belly, from having been tossed up into the air by its father with his right hand, and caught in its descent in the crutch formed by the thumb and fingers of the left, on the thumb of which it unfortunately at last fell; this caused the child great pain, which was soon followed by considerable swelling and inflammation of the belly, of which it died. On examination after death, the small intestine was discovered to have been ruptured by the end of the thumb, from which extravasation of its contents into the abdomen had ensued.
The first effect of a rupture of the intestine must be the extravasation of such gas as may be contained in or secreted from it, giving rise to the sudden swelling, as well as to the[492] sudden effusion, of part of its contents, but which, from the support of continuity, and of the general pressure of the abdominal parietes, is perhaps more gradually poured out. The rapid swelling and tension of the belly is perhaps then a distinguishing symptom of a rupture of the intestines.
A Spanish soldier was brought to me, near the conclusion of the battle of Toulouse, in consequence of having been struck obliquely by a cannon-shot on the right side of the abdomen and back, which appeared to be badly braised, although no abrasion of the skin had taken place. The shock was great, however; he was unable to move his limbs, and appeared likely to die, which he did in fact, in the course of the night, having passed bloody urine, but without any reaction having taken place. On making an incision through the skin, which was then quite a blue black, although not torn, all the soft parts were found reduced to a state approaching to the appearance of jelly; the spine was injured, the right kidney ruptured, and the cavity of the abdomen full of blood.
A soldier of the 40th Regiment was struck by a ricochet cannon-shot, on the last day of the siege of Ciudad Rodrigo. He saw the ball, which destroyed his left forearm so as to render amputation necessary, strike the ground a little distance from him, before he was himself injured. He thought, from the sort of shock he received, that it had also struck his belly; but this I should not have credited, if it had not been for a bruise across the umbilical region without actual abrasion of the integuments, on which account my attention was drawn to him on the fourth day after the injury, at the hospital of Aldea Gallega. He had been bled in consequence of complaining of pain, and because of the quickness of pulse and the fever which had ensued, and which were attributed to irritation after amputation. The belly was swollen and tender under pressure. Calomel, antimony, and opium were given: he was bled again, and blisters were applied. The stump took on unhealthy action, and he died a fortnight after the receipt of the injury. The abdomen, when opened, was found to contain a quantity of opaque serous fluid, mixed with shreds of coagulable lymph. The omentum and intestines were of a dark color, and loaded with blood, distinctly indicating the chronic state of inflammation which had taken place.
If the injury should not destroy the patient, but prove[493] sufficient to give rise, after several weeks, to effusion into the cavity, the fluid should be evacuated by the trocar.
When the fixed viscera are ruptured by severe blows, such as those received by falls or from cannon-shot, the sufferers usually die from hemorrhage and not from inflammation. The arm has been carried away, and the liver ruptured without almost a sign of injury to the skin of the abdomen, death ensuing from hemorrhage.
380. When an incised wound is made through the wall of the abdomen to any extent, except perhaps in the linea alba, the muscular parts are rarely found to unite in a more perfect manner than when they are ruptured and bruised. In those cases in which I have tied the common iliac artery by an incision on the face of the lateral part of the abdomen, the patients recovering afterward, the incision through the muscular wall did not remain united, although union appeared to have taken place in the first instance, and a herniary protrusion formed in the course of the greater part of the line of the wound.
The constant occurrence of this non-union, except by skin and cellular membrane, led me to repudiate the introduction of ligatures through other parts for the purpose of keeping them in apposition, as it does not lead to the permanent cohesion of the parts, while it exposes the sufferers to all the dangers which the irritation of sutures commonly occasions, thus offering another instance of the improvement surgery owes to the war in the Peninsula.
Chelius recommends “several flat ligatures to be introduced through the skin and muscles, the needle being placed close to the muscular surface of the peritoneum.” Graëfe (section 514) is declared to be of the same opinion, he recommending, however, that a soft tape should be substituted for a ligature. Reference is made to Weber in support of this practice, to which Mr. South, the translator, does not raise any objection.
381. In all simple wounds of the wall of the belly of moderate extent, the edges of the wound should be brought together by means of a small needle and a fine silk thread passed through the skin and the loose cellular membrane only which is in contact with it, by a continuous suture without puckering, in the manner a tailor would fine-draw a hole in a coat. This gives a certain degree of support to the parts beneath; and if proper attention be paid to maintain[494] a well-regulated, relaxed position of the muscles, no great separation takes place in wounds of a reasonable extent, and little or none in a wound of smaller dimensions. An effective support should be also given by strips of adhesive plaster extending to some distance around the body; a bandage rarely does good, and will assuredly do mischief, unless it be very carefully applied and watched, so as only to give support and not to make undue pressure. The position of the patient is of the greatest importance; its essential object is to bring the edges of the incision, and especially of that in the peritoneum, as nearly as possible in apposition, so that the space between them may be more easily filled up by the opposing peritoneum forming the anterior layer of the omentum, or by the outer covering of the intestine if the omentum should not intervene. This is to be effected by the gentlest inclination of the body toward the wound which may be supposed capable of keeping these parts in apposition; for although the omentum and intestines are often capable of undergoing a considerable degree of motion from side to side, independently of that peculiar wormlike movement on themselves which in the intestines is called peristaltic, they very frequently do not wander from place to place in the manner which has been sometimes attributed to them, but remain, under proper care, so far stationary as to admit of the cut edges of the wounded peritoneum adhering to the healthy peritoneum opposed to them, when they will be retained in contact with it. The serous surfaces of the peritoneum which are in contact with each other soon offer on one part, and accept on the other, the process of adhesion through the medium of lymph or fibrin deposited between them. If this adhesion take place, it extends for some little distance from the wounded part, which it thus closes up and cuts off from all communication with the general cavity of the belly; the previous admission of air—the bugbear of surgeons of the olden times—being of no sort of consequence. The adhesive process is the effect of inflammation extending to a certain point, and ending in the deposition of fibrin. When it exceeds this, the secretion of a quantity of serous fluid, together with threads of flocculent matter, marks the excess of inflammation; it is diffused over more or less of the peritoneum lining the wall of the belly, covers its contained viscera, and prevents that adhesion from taking place which is the safeguard of the patient.
[495] 382. Absolute quietude is no less to be observed. It must, however, be steadfastly continued; the slightest alteration of position should be forbidden. Motion should not on any account, nor for any reason whatever, be allowed, if it can by any possibility be avoided. In the position in which the patient is placed he should be rigorously maintained until adhesion has been effected or all hope of it has passed away. The practice of the older surgeons was to purge such persons vigorously, in order to remove from their bowels any peccant matters that might be in them; in the same manner they recommended persons should be purged who had undergone the operation for strangulated hernia—both which proceedings the experience of the war enabled me to condemn, as being not only contrary to the right medical treatment of such cases, but to the physiological and surgical principles on which it ought to be founded, a condemnation the accuracy of which is now universally admitted, although the source from which it is derived is not so universally acknowledged. No purgative medicine whatever should be given to a person with a penetrating wound of the abdomen. No food should enter his mouth; and no more water even should be allowed than may be found requisite to moisten the lips and allay any intolerable thirst which may ensue. This precaution need not be carried out so strictly if it could be readily ascertained that an intestine was not wounded; but as this knowledge, however satisfactory it would be, cannot always be obtained, and ought not in the generality of instances to be sought for, the restriction should be fully observed if possible. In all cases of injury of the belly there is more or less shock, alarm, and anxiety. It is sometimes remarkably great, even when the mischief has not been considerable. When little or no injury has been inflicted on the intestines, the natural and usual action of expelling the contents is generally delayed beyond the time at which in health it would in all probability have occurred. When nature shall point out by the sensations of the patient an inclination to perform this function, it may be assisted by an injection of warm water or of any mild laxative which may facilitate the process and prevent any unnecessary action of the abdominal muscles, against which the patient should be cautioned. The attendants should be forewarned that the position of the patient is not to be interfered with under any circumstances, the necessary[496] arrangements being made by bedsteads of a proper construction, or by other simple means which are sufficiently well known.
383. The custom of directing a man to be bled forthwith, as well as purged, because he has been stabbed, was another error much in esteem by the older surgeons, but which experience did not sanction, and it could not therefore be approved. The abstraction of blood before reaction has taken place delays its occurrence as well as the commencement of that inflammatory stage which is to be so salutary in its result in favorable cases. It tends to prevent the agglutinative process from taking place, and thus aids the diffusion of inflammation over the whole surface of the peritoneum. The general abstraction of blood is to be ordered, and regulated as to quantity by the symptoms of inflammation which may accompany or follow reaction. The quantity of blood required to be taken away in these cases is usually large, particularly at an early period. With the army in the Crimea, the abstraction of large quantities could not in general be borne and has not been found serviceable, nor has it been found so necessary to repeat the bleedings as in persons more favorably situated. It is, however, often a nice point to determine when blood enough has been abstracted with advantage, as too much may be taken away as well as too little—the former being marked, after death, by the general diffusion of a slight degree of inflammation, without the concomitant sign of effusion of serum. Leeches applied in considerable number will often be found more beneficial, particularly at a late period, when the sufferer may not be able to bear a general abstraction of blood. The patient, after leeches have been once applied and their good effect has been ascertained, will often ask for them himself on the recurrence of pain or on its increase; and from twenty to sixty, or even eighty, may be applied in some instances of great danger with advantage.
The pulse is by no means a guide in the management of these cases; a small, low, and sometimes not even a hard pulse being more strongly indicative of an overpowering state of inflammation than is a quick and full pulse; much more depends on the pain, the anxiety, and the general oppression than on the apparent state of the circulation. Before general and local bleeding cease to be employed with[497] advantage, calomel, antimony, and opium will render essential, nay, most important, service.
The extensive incisions made of late years into the abdomen for the removal of ovarian tumors, with fair success, confirm what I have constantly repeated in my lectures for the last thirty-five years, that penetrating wounds of the abdomen, without injury to the viscera, when properly treated, are not so dangerous as they were generally supposed to be.
384. In penetrating wounds of the belly, the offending instrument frequently passes in for a considerable distance, sometimes separating or pushing the viscera aside without injuring them, at others inflicting upon them wounds more or less severe. In fatal cases of stabs from knives and sharp instruments, the intestines have been usually injured by the point, although when the lapse of three or four days before death takes place, the small wound is not readily perceived.
W. Carpenter, private, 1st battalion, 43d Regiment, was accidentally wounded, March 19th, 1812, by a comrade, the small end of a ramrod entering about two inches below the navel, passing in a direction upward, penetrating the second lumbar vertebra, and protruding an inch and a half on the opposite side.
On examining the wound, the ramrod was found firmly fixed in the bone. It was endeavored at first to extract it by a gentle turn, making extension at the same time, but this failed. Force was then applied on the opposite side, by fixing the broad end of a ramrod on the point of the protruding one, which was laid bare by an incision, when by a smart stroke with a stone it was driven back and removed. Bleeding to twenty ounces.
March 20th.—Has slept several hours during the night; passed urine two or three times; suffers slight pain occasionally on turning himself in bed; has the perfect use of his lower extremities; pulse rather full; skin cool; repeat bleeding to twenty ounces.
22d.—No evacuation since the 20th; pulse rather full; bleeding to twenty-two ounces; sulphate of magnesia, one ounce. Seven o’clock A.M.: Medicine operated three or four times; feels no pain in passing water.
23d.—Has passed a good night; wounds dressed; is allowed a small proportion of bread with his tea.
[498] 28th.—So far recovered as to be able to be removed to Elvas.[5]
That a blunt instrument, like the small end of a ramrod, should be forced between the loose viscera of the abdomen without wounding any of them, may be easily conceived, but that balls or sharp-pointed swords should do so, is not to be understood so easily. Ambrose Paré, our own Wiseman, Ravaton, Lamotte, Muys, and others, however, have related instances of this kind, in which the patients recovered in an inconceivably short space of time; but these and other recoveries of a similar nature must be considered as exceptions to general rule.
[5] He marched with his regiment, in the summer, to Valladolid, and was drowned in the Douro.—G. J. G.
385. Wounds penetrating the wall of the belly, when made by cutting or lacerating instruments, or by musket-balls, are usually followed, if to any extent, by a protrusion of some portion of the contents of the cavity, generally of the omentum or intestine, if not of both. This may take place at the rounded orifice of entrance of a ball, as well as at the more slit-like opening of exit, which, if the patient should recover, becomes closed by a thin tendinous-like expansion, under the cicatrix formed by the common integuments. These soon yield to the general pressure on the abdominal cavity, and admit of the formation at the part of a ventral rupture, requiring the application of a restraining bandage.
386. When a piece of omentum only protrudes, the direction given by the latest writers on surgery is, that it shall be returned into the cavity of the abdomen whence it came, the finger following to ascertain that it is quite free; after which the wound is to be carefully closed by sutures applied close to the peritoneum, so that the omentum may not again protrude through it. Having objected already to the manner of employing the suture, I now object to the treatment of the omentum, and do not approve of its being so dextrously returned by the finger within the peritoneum to its natural loose situation. I desire, on the contrary, that it may be retained between the cut edges of the peritoneum, but without the slightest pressure or possible strangulation, in order that by its retention it may more readily adhere to these edges, and thus form a more certain barrier against the ex[499]tension of inflammation than is likely to take place when moving at liberty in the cavity of the abdomen, however closely it may be supposed to be applied to the inner surface of its paries.
It sometimes happens that a portion of omentum is altogether without the cavity of the abdomen, and the opening through which it has protruded seems too small to allow its restoration to the cavity. The latest authors on this subject recommend a blunt director to be introduced between the upper edge of the wound and the protruded part, be it omentum or intestine, or both, upon which a blunt-ended bistoury is to be passed into the cavity as far as the enlargement of the wound seems to require, after which the director and the bistoury are to be withdrawn together. I altogether dissent from this. It is scarcely ever necessary to enlarge the opening in the peritoneum, the obstacle to reduction being situated in the tendinous expansion or aponeurosis of the wall of the belly, a slight division of which will give sufficient space for the restoration of the protruded part in almost every instance. I have unavoidably opened into the cavity of the peritoneum, and have seen it done in other instances, but no inconvenience follows small openings not exceeding a quarter of an inch in length, when they are properly covered over by the healthy parts. It is therefore important in all cases to have as small an opening as possible in the peritoneum, and certainly no addition should be made to the size of a small opening if it can by any possibility be avoided, however indifferent half an inch, more or less, may be in the length of a large one. All protruded parts, whether omentum or intestine, should be gently cleansed with warm water, and the fingers of the surgeon should be wetted in a similar manner, the mesentery being returned first if protruded, then the intestine, and lastly the omentum; the two former under all circumstances; the latter not so, if it be adherent or inflamed, torn or jagged, or in a state of suppuration or gangrene. It should in these cases be left to itself, and treated in the most simple manner; a ligature should never be applied to it, neither should it be spread out and cut off, as was formerly recommended, as it will gradually retract and be withdrawn into the cavity of the abdomen. If suppuration should take place in its substance, and the swelling of the part lead to its constriction, or the formation of matter under the integuments or between the[500] layers of muscular or tendinous fibers, these may be carefully divided.
Evan Thomas, aged seventeen, was admitted into the Westminster Hospital, Sept. 1st, 1828, having been stabbed with a dinner-knife immediately above the umbilicus; the wound was three-quarters of an inch long; the omentum protruded and could not be returned until the skin, cellular membrane, and fascia had been divided; the opening in the peritoneum was then distinctly seen, against the inside of which the omentum was left, the wound in the skin being sewed up by the continuous suture. In the evening he was bled to sixteen ounces, and, as he had thrown up his dinner, an enema only was administered. On the 2d, the belly being tense and slightly painful, although he was not in constant pain, the blood drawn before being buffy, twenty-two ounces more were taken away, a purgative enema administered, and, as the bowel was not believed to be injured, four grains of calomel and six of the compound extract of colocynth were given, with a draught of senna and salts every four hours. 3d. The bowels open; no pain and scarcely any uneasiness on pressure; abdomen soft. No food; barley-water and gruel; pulse 84. On the 6th the sutures were removed, the wound having reunited. He was then made an out-patient, having a comfortable home.
A soldier of the Second Division of Infantry received several stabs from a lance in different parts of the body, at the battle of Albuhera, as the lancers rode past him, while lying on the ground, one only being of any importance: it was on the right side and lower part of the belly, and through it a portion of omentum protruded. On this being reduced, the epigastric artery, which had been divided, bled freely; a ligature was readily applied, and the wound closed by the continuous suture. The patient, after undergoing a very rigorous treatment, recovered.
A Spanish soldier was wounded in a scuffle in Madrid, in 1812, at the gate of the British Hospital, near the Prado, into which he was brought, with a wound on the right side of the abdomen, near and below the umbilicus, through which a portion of omentum protruded about the size of a small orange. As this could not readily be returned, I carefully enlarged the wound at its under part, some three or four hours afterward, by dividing the skin, and then found that it was the aponeurotic or tendinous expansion of[501] the muscles going to form the sheath of the rectus, which prevented the return of the omentum into the belly; on the division of this part it slipped back without difficulty, but as it did not recede further than the peritoneum I left it there, and closed the wound, which was about an inch long, by sewing it up in the manner described. He was bled and starved, and was delivered up to the proper authorities out of danger, with his wound nearly healed, when the army evacuated the place.
A Spanish soldier was wounded at the battle of Toulouse by a musket-ball, which passed in on one side and came out at the other, carrying with it a portion of omentum which gradually became as large as an orange, in which state I saw it four days after the accident. Little had been done; he had not suffered much pain, although the abdomen was tender; he had vomited; passed blood with his motions; was feverish and ill. I visited this man every three or four days; he suffered from privations of every kind, yet each time I found him better. The protruded omentum gradually diminished in size, and was at last drawn into the wound in the abdomen and covered by granulations. He left Toulouse before me, nearly well.
If the omentum be greatly bruised or injured it may be cut off, and the vessels tied if bleeding; but it should not be returned further than the edges of the peritoneum, over which the external wound is to be closed.
Ravaton wrote a hundred years ago: “The views of a surgeon must be very confined who advises the application of a ligature to the omentum when protruding from the cavity of the belly in a healthy state. It is a cruel and deadly maneuver, contrary to reason and experience. To restore it to its place is so simple, just, and reasonable, that I am surprised it does not occur to every one. The reduction is easily effected. It is sometimes difficult to retain the reduced part except by sutures. I admit that when the omentum is strangulated, gorged with blood, black, and about to become gangrenous, the result of its restoration to the cavity may be doubted: yet experience has demonstrated that it is the safest mode of proceeding, taking care not to close the wound entirely, but to leave an opening at the lower part to give vent to any effusion or suppuration that may take place.”
387. When a portion of intestine is protruded without[502] being wounded, it is to be returned, whatever may be its state, unless it be soft and unresisting between the fingers, of a dull blue or black color, and to every surgical eye deprived of life or mortified. At any state previous to this (to Englishmen) almost certainly fatal condition, it should be restored into the cavity of the abdomen. When a portion of intestine is thus returned, three directions are given by most modern surgeons, and especially by Chelius, section 517, on which his English editor makes no comment; and which may therefore be considered to be those which are commonly taught in London, but of which I entirely disapprove. The first is, that the peritoneum is to be divided in cases where an obstacle is interposed to the return of the intestine; this I aver to be less necessary for the intestine than for the omentum. The second is that, “after the reduction, the forefinger must be introduced into the cavity of the belly in order to ascertain that the intestines have not passed into the interspaces of the muscles”—a precaution which is unnecessary, and may do much mischief. The third is, that the patient is then to be placed “in such a posture as that the intestines should least press against the wound,” to which direction I object. The surgeon should certainly take care that the intestine does not pass between the layers of muscle, nor anywhere else than into the cavity of the belly. So far, however, from the intestines being pushed away from the cut peritoneum, the most favorable position for it would be to be applied against the edges of the cut membrane, and even rising up for the least possible distance, without or above it, the great object to be desired being to facilitate adhesion by as perfect an apposition of these parts as possible, while the external wound is accurately closed by the continuous suture, and duly supported by adhesive plaster, compress, and a bandage, provided it be methodically applied. The next best thing which can happen is that, every part being relaxed, and the patient perfectly quiescent, the intestine should press so steadily and yet so gently against the wounded peritoneum that it will be kept in constant apposition with it without protruding through it.
A soldier of the Artillery was stabbed in two places, in 1812, with a long knife, by a townsman, late in the evening, and was carried into the hospital for the sick and wounded French prisoners in Lisbon. The wound in the belly was situated somewhat more than an inch to the right side of[503] the umbilicus, and was about an inch in length from above downward; through it a considerable protrusion of small intestine, without any omentum, had taken place. This was distended by flatus, and of a dark-brown color when I first saw it, some time after the receipt of the injury. The bowel being constricted by the tendinous expansion of the muscular fibers, the latter was carefully divided by a blunt-pointed curved bistoury passed under its upper edge, and resting on the back of the nail of the forefinger, by which the intestine was guarded; the flatus having been pressed out of the intestine, which was gently washed with warm water, it was restored to the cavity of the abdomen. Of the part which had apparently first protruded, the peritoneal coat and a few fibers of the longitudinal layer of muscle were divided to the extent of half an inch, the remaining portion of the gut being unhurt. The skin was then sewed up by a fine continuous suture, and adhesive plaster and a compress duly applied. A good deal of alarm was evinced, the pulse was very small, and the man faint. The other wound was in the back, about half an inch in extent, and near the inferior angle of the right scapula. It appeared to be a penetrating wound, but not giving rise to any peculiar symptoms, he was placed in bed on his back, with his legs raised, and the body slightly bent. Early the next morning, the officer on duty found it necessary to bleed him largely, to forty ounces, according to my directions, on account of pain which had come on in his bowels and in his back, accompanied by difficulty of breathing, the skin being hot and the pulse quick and hard. The cellular membrane around the wound in the back was emphysematous; there was a slight cough, accompanied by an expectoration slightly tinged with blood. The bleeding removed the essential symptoms, but the pain and difficulty of breathing returning next day, it was repeated to eighteen ounces, with an equally good effect. It was necessary to repeat it on the third, fourth, and fifth days, when the pain ceased to return, and the pulse, instead of being small and hard, became softer and fuller. The bowels were open naturally on the third day, and the emphysema had gradually disappeared, no food being allowed, and very little drink for some days, and then only in small quantities of the simplest kind. The threads were removed with scissors on the sixth day, and the man was free from complaint, although very weak, at the end of five weeks.
Madame Doucet was applied to a hundred years ago, by a[504] soldier, who having been struck by a halbert, had a wound made across his abdomen from above the ilium, through which a quantity of intestine protruded, which he carried in his hat, enveloped in his shirt. Having had to walk between three and four miles, in the heat of July, to the old lady, his bowels were as dry as parchment by the time he arrived. She therefore bathed them in warm milk and water until they became soft and natural in appearance, returned them into the cavity of the belly, and sewed up the wound with a well-waxed silken thread—thus setting an example which ought to be followed in 1855. The man recovered.
388. When the protruded intestine is wounded, the case is complicated, and much depends on the size of the wound. A mere puncture, or a very small cut, is often of no consequence, and does not require any treatment; the bowel should merely be returned to the cavity of the belly, and the symptoms of inflammation closely watched, and, if possible, steadily subdued.
It is advisable, in investigating this subject further, to consider the abdomen as devoid of cavity during life and health, the contained parts being so gently pressed upon by the containing and retaining muscular parietes around as to enable them all to carry on their ordinary functions, unless suffering from some derangement, exclusive of that which might arise from a deficiency of the pressure usually exercised upon them; but that this pressure can, or generally will, prevent the effusion of the contents of a bowel when ruptured, if the wound be half an inch in length, or that it will prevent the extravasation of blood from an artery or vein of moderate dimensions, if torn, is contrary to facts now considered indisputable, as I have frequently had occasion to verify. That a mere puncture of the intestine does not allow the effusion of air, much less of the contents of the bowel, is not doubted. When the contents of the bowel have been poured out, without an external opening in the paries through which they might escape, inflammation and death have ensued at no long distance of time. When blood is poured out from the great vessels, as in rupture of the liver or spleen—of which instances will be adduced—the general cavity may be filled; but when the injury is less extensive, or the lesion less important, the blood usually gravitates toward the back or sinks into the pelvis. It is possible that blood may be effused in small quantity, and be then confined, under the general[505] pressure of the wall of the abdomen and the resistance offered by its contents, to a particular spot, whence it may be absorbed after coagulation; or, by commencing decomposition, give rise to irritation, and be discharged through the external wound, if one exist, or through the bowel with which it may happily be in contact.
A soldier, belonging to the Second Division of Infantry, was wounded by the Polish Lancers at the battle of Albuhera, in several places slightly, and in the abdomen severely, a penetrating wound having been made an inch long, between the umbilicus and the crest of the ilium on the left side. Brought to me the day after at Valverde, the edges of the wound were stitched together and dressed simply. He said it had bled freely at first, and was then painful. Treated antiphlogistically and sharply, the inflammatory symptoms gradually subsided. The bowels were relieved by gentle aperients, there being no reason to suppose they had been wounded. A small, oval swelling was soon perceived under the wound, which was tender to the touch, indicating mischief of some kind. The edges of the wound, which did not unite fully, although they were retained in contact, at last separated, and allowed about a wineglassful of bloody matter to pass out, which reduced the swelling and removed the uneasiness and pain of which he complained. After this he gradually recovered, and was discharged to Elvas, and thence to Lisbon.
389. Whenever large effusions of blood have occurred, the sufferers have usually been lost, from the occurrence of peritoneal inflammation. That small ones may be absorbed, cannot be doubted. I have seen instances of their having been discharged by the bowel, although I have never been so fortunate as to see a general formation of matter from effusion, and to have opened the abdomen for the evacuation of its contents with success; nevertheless, I do contemplate that such cases may occur, and surgery may come to their relief with good effect.
The important conclusions to be deduced from the observations of those who have made experiments on the intestines of living animals are—First, that wounds not exceeding four lines in length, (or the third part of an inch,) no matter what their direction may be, are not so apt, as might be supposed, if left to themselves, to be succeeded by extravasation of the contents of the intestinal tube; and that, in the[506] majority of cases, nature, properly aided by art, is fully competent to effect reparation. Secondly, that wounds of the bowels to the extent of six lines, whether transverse, oblique, or longitudinal, are almost always, if not invariably, followed by the escape of the contents of the bowel, and the consequent development of fatal peritonitis. It may, therefore, be concluded, from experiments made on animals, as far as they can be relied upon with reference to man, that every wound in the bowel, of such an extent as shall not admit of its being temporarily filled up by the protrusion and eversion of its internal or mucous coat, which always takes place as an effort of nature to close the wound, ought, if possible, to receive assistance from art, and that can only be given with advantage in the first instance.
Mr. Travers tied a thin ligature firmly round the duodenum of a living dog; the ends were cut off, the parts returned, and the external wound properly closed. On the fifteenth day, the cure being completed, the dog was killed. A portion of omentum, connected with the duodenum, was lying within the wound, and the folds contiguous to the tied part of the intestine adhered to it in several points. A slight depression was observed around the duodenum, the internal or mucous surface of which was more vascular than usual; a transverse fissure marked the seat of the ligature. “The lymph,” Dr. Gross observes, “which is effused upon the external surface of a bowel, consequent upon such an operation, gives the part at first a rough, uneven appearance; but, if the animal survive several months, it is generally no easy matter to determine the seat of the injury from the external appearance of the part. Internally, the cicatrization is almost as complete, the continuity of the mucous membrane being everywhere established, leaving scarcely even a seam at the original seat of constriction. The rapid manner in which the ligature cuts its way from without inward obviates the evils which might arise from the occlusion of the passage. In an experiment, in which the dog was killed upon the eleventh day after the application of the ligature, the canal of the bowel was completely restored, and the bond of connection between the divided parts was firm and organized.”
Similar effects are produced when a small ligature is applied around the edges of a wound from two to three lines in diameter, provided it be drawn with sufficient firmness not to slip off. The process of reparation is not, however, so[507] speedily completed, owing to the breach being much wider than when a ligature is simply placed around the tube. The mucous membrane requires a longer period for its reproduction, and the quantity of lymph deposited around and inclosing the ligature is proportionally greater.
390. The idea of sewing together, and thereby restoring the continuity of a wounded bowel, is attributed to four master surgeons, as they were called, of Paris, in the thirteenth century, who, having united their efforts for the relief of the sick poor in that city, procured, it is said, a portion of the trachea of an animal, one end of which they introduced into the upper part of the divided bowel, and the remaining piece into the lower, and then brought the divided ends into contact, and retained them by as many sutures as appeared to be necessary. Their writings, in which this operation is described, are lost. Peter de Argelata, who lived about the middle of the fifteenth century, says that Jemerius, Roger, and Theodoric supported the intestine by a canula of elder-wood, while Gilbert de Salicetti condemns both the use of the trachea and the elder-wood tube, and recommends, if anything be used, that it should be the dry and hardened bowel of some animal. These ancient surgeons believed that a transverse division of the intestine was necessarily a fatal injury, and only resorted to the methods they recommended when the division was less complete. Duverger de Maubeuge, in the beginning of the eighteenth century, apparently unaware of what had been done before his time, brought forward this method of the four masters as an invention of his own. He cut off a portion of mortified intestine in a case of strangulated hernia, introduced a piece of the trachea of a calf, brought the divided intestine over it, and fastened it by a suture. The trachea was passed on the twenty-first day, and the external wound was closed by the forty-fifth, the patient recovering.
Ramdohr, a German surgeon, who lived in the early part of the last century, seems to have been the first to join the ends of a divided bowel by introducing the upper end within the lower. He removed two feet of mortified intestine in a case of strangulated hernia—performed this operation on the ends of the bowel, retained the parts by stitches, and his patient perfectly recovered. Heister says the mortified parts were in his possession. (Haller, Disputat. Anatom., vol. vi., Observ. Med. Miscel., 18.) Since his time, many of the most[508] eminent surgeons of France, Italy, America, and Great Britain have turned their attention to this subject; but the conclusion at which I have arrived is that the continuous suture is, in all cases of serious injury, the most simple and the best.
391. In making a continuous suture, a fine needle and a waxed silken thread should be introduced through the gut, beginning on the inside close to one end of the cut part, and bringing it out on the peritoneal surface a little more than a line distant from where it entered. The needle is then to be carried to the opposite side through the bowel from without inward, and the sewing thus continued until completed, each stitch being about the sixth part of an inch asunder, and about that distance from the edge of the cut. The threads or stitches should not be drawn close until the whole are inserted, when, on being drawn moderately tight one after another, the cut edge of the intestine should be turned inward by a blunt probe, so that the peritoneal surfaces shall be in contact under the stitches and in the best situation for union, the mucous coat forming a ridge within, the outside being perfectly smooth, the stitches not being too tight, while the end may be secured by a knot made by a turn of the thread over the needle. This done, the intestine should be returned into the cavity of the abdomen, and events awaited. Recoveries more frequently follow wounds of the colon than of the jejunum or ilium; but the result must always be doubtful, being dependent on many causes which the surgeon can neither foresee nor control.
TREATMENT OF INCISED WOUNDS, ETC.
392. When an incised wound in the intestine is not supposed to exceed a third of an inch in length, no interference should take place; for the nature and extent of the injury cannot always be ascertained without the committal of a greater mischief than the injury itself. When the wound in the external parts has been made by an instrument not larger than one-third or from that to half an inch in width, no attempt to probe or to meddle with the wound, for the pur[509]pose of examining the intestine, should be permitted. When the external wound has been made by a somewhat broader and longer instrument, it does not necessarily follow that the intestine should be wounded to an equal extent; and unless it protrude, or the contents of the bowel be discharged through the wound, the surgeon will not be warranted in enlarging the wound in the first instance to see what mischief has been done. It may be argued that a wound four inches long has been proved to be oftentimes as little dangerous as a wound one inch in length; yet most people would prefer having the smaller wound, unless it could be believed that the intestine was injured to a considerable extent. Few surgeons, even then, would like to enlarge the wound to ascertain the fact, unless some considerable bleeding or a discharge of fecal matter pointed out the necessity for such an operation. When the wounded bowel protrudes, or the external opening is sufficiently large to enable the surgeon to see or feel the injury by the introduction of his finger, there should be no difficulty as to the mode of proceeding.
393. A puncture or cut which is filled up by the mucous coat so as to be apparently impervious to air does not demand a ligature. An opening which does not appear to be so well filled up as to prevent air and fluids from passing through it cannot usually be less than two lines in length, and should be treated by suture. When the opening is small, a tenaculum may be pushed through both the cut edges, and a small silk ligature passed around, below the tenaculum, so as to include the opening in a circle, a mode of proceeding I have adopted with success in wounds of the internal jugular vein without impairing its continuity; or the opening, if larger, may be closed by two or more continuous stitches made with a very fine needle and silk thread, cut off in both methods close to the bowel, the removal of which from the immediate vicinity of the external wound is little to be apprehended under favorable circumstances. The threads or sutures will be carried into the cavity of the bowel, as has been already stated, if the person survive, and the external part of the wounded bowel will either adhere to the abdominal peritoneum or to one or other of the neighboring parts.
When the intestine is more largely injured in a longitudinal or transverse direction, or is completely divided as far[510] as or beyond the mesentery, the continuous suture is absolutely necessary.
394. When the abdomen has been penetrated, and considerable bleeding takes place, but not from the intestine, it is necessary to look for the wounded vessel. When it comes from one of the mesenteric arteries or from the epigastric, the wound is to be enlarged until the bleeding artery be exposed, when ligatures are to be placed on its divided ends if they both bleed, the external wound being accurately closed. I have seen the epigastric artery tied several times with success.
A Portuguese caçador on picket was wounded at the second siege of Badajos in a sally made by some French cavalry. He had three or four trifling cuts on the head and shoulders, and one across the lower part of the belly on the right side. He bled profusely, and, when brought to me, had lost a considerable quantity of blood which came through a small wound made by the point of a sabre. This wound I enlarged until the wounded but undivided artery became visible; upon this two ligatures were placed, and the external wound was sewed up. The peritoneum was open to a small extent, but the bowel did not protrude; and the patient (not being an Englishman, and therefore not so liable to inflammation) recovered after being sent to Elvas.
A soldier of the same regiment, cut down at the same time, died as soon as he was brought into camp, having been severely wounded in the chest and abdomen. He was said to have died from hemorrhage, from a wound in the belly, two inches in length, made by one of the long-pointed swords of the French dragoons. I had the curiosity to enlarge the wound, and found one of the small intestines had been cut half across, another part injured, and that the blood came from an artery which had been opened by the point of the sword in going through the mesentery, which wound had caused his death.
395. When this operation cannot be done successfully or with advantage to the patient, whose life is in jeopardy from the continued drain, the wound should be closed by suture, and a compress laid over it and retained by a bandage methodically applied for the purpose of aiding the muscular parietes in keeping up that pressure on the viscera which may be useful in arresting the flow of blood from the wounded part. If the bleeding continue, or, having been arrested,[511] should recur, and the belly become in consequence distended, the sutures being evidently so tense as to be likely to cut their way out, or if the blood should ooze out between the stitches, they may be in part removed in order to give immediate relief. When the belly becomes very painful, tense, and manifestly full after a punctured wound, and not tympanitic from the extrication of air or the distention of the bowel by it, the wound should be enlarged to allow the evacuation of the extravasated blood, which cannot be absorbed when in such quantity. The orifice of a small gunshot wound, which is not sufficiently direct to communicate with the cavity and to allow the issue of blood extravasated in the quantity alluded to, should be enlarged to such an extent as to effect that object.
396. Blood effused in moderate quantity, and circumscribed by the pressure exercised upon the contents of the abdomen by its parietes, may readily be evacuated by the wound, provided it be sufficiently open; and the patient may recover, if the inflammation which must necessarily ensue should not be communicated along the peritoneum throughout the cavity, or if it should be subdued in time. If the blood be in small quantity, it coagulates, and may be absorbed; but if in such a quantity as cannot be absorbed, or from any other cause which may prevent its removal by this means, it becomes after a time a source of irritation, and nature sometimes commences early to cut it off from the general cavity by surrounding it with fibrin—a result which, however desirable, can rarely be expected.
When extravasated blood is thus cut off from the general cavity, and cannot be absorbed or be by accident carried off through an opening in the bowel, a change takes place by which it ceases to be bland and harmless, and causes it to excite inflammation and its ordinary consequence, suppuration, if the patient survive so long. This occurs, for the most part, after the first inflammatory symptoms have subsided, from the tenth to the twelfth, or even to a later, day, when the renewal of irritation is accompanied by an increase of the general symptoms, by a more local pain, and by a circumscribed swelling of some part near the wound, in which fluctuation may perhaps be distinguished even during the existence of the general tenderness of the whole abdomen. Under such circumstances, when it is proposed to make an incision into this part, if it should be thought advisable to[512] do such an operation, it may safely be preceded by an exploring needle or a very fine trocar and canula, which will demonstrate the fact of the purulent and sanious depot, without doing in such a case perhaps any mischief, if the expectations of the surgeon should not be realized. If the exploring needle should show that a bloody, purulent, or other fluid is really distending the abdomen, no doubt ought to be entertained about enlarging the original wound and making a depending opening.
Ravaton, in his twenty-fifth observation, relates the case of a soldier who was wounded five days before by the point of a sabre, to the right of the umbilicus. When the man was brought to him, the belly was swollen, hard, and very painful, with vomiting, hiccough, etc., announcing the approach of death. Believing that the abdomen contained a fluid, either effused or secreted, he made an opening into the cavity immediately above Poupart’s ligament or the outside of the internal opening of the ring of the right side, when, finding that nothing came from the cavity, he passed his finger upward along the iliac vessels, and, after tearing up some membranous adhesions, evacuated a pint of coagulated blood and fetid, serous fluid. He then introduced a dossil of lint into the wound to keep it open, fomented and oiled the belly, round which he applied a bandage, and placed the patient on his face. The bad symptoms diminished during the night, and the patient declared himself better in the morning. From the fifth to the tenth day of the wound he was in extreme danger. On the eleventh, the bed was inundated with a purulent matter of an almost insupportable smell. The cavity of the abdomen was injected and cleansed, the ordinary dressings applied, and the greatest cleanliness observed. He was subsequently dressed three times a day in a similar manner; portions of omentum were occasionally drawn away with the forceps. His strength was well supported by every kind of nourishment. The night-sweats continued until the thirty-third day, and on the seventy-second he was discharged from the hospital, cured. The discharge at first was serous, and only became purulent on the sixth day after the operation.
Thomas M’Mahon, 76th Regiment, aged twenty-two, was admitted into the Garrison Hospital, Portsmouth, upon the 13th of June, 1845, with all the symptoms of strangulated inguinal hernia of the left side, of two days’ standing, for[513] which the usual operation was performed. Everything went on favorably till the morning of the fourth day after the operation, when he made a sudden effort to go to the close-stool, which was immediately followed by the descent of a considerable portion of intestine and omentum, accompanied with profuse hemorrhage from a small artery on the surface of the intestine, which was taken up and tied, and the parts returned into the abdominal cavity. The greatest excitement followed, with all the symptoms of acute inflammation. These were treated by general bleeding to the extent of fifty ounces, and sixty leeches to the abdomen, with other antiphlogistic remedies. On the morning of the seventeenth day from the performance of the operation, a piece of intestine came away with the fecal contents of the bowels, after which the patient experienced relief in all his symptoms, and appeared to gain health and strength, and after a time the wound seemed disposed to close, three weeks after the sloughing of the intestine. On the sixth day afterward the evacuations ceased, attended with acute tenderness of the abdomen, which began to swell fast. The means adopted had not the slightest effect, and the patient was considered past relief, unless it could be obtained by an external opening. I accordingly made an incision over the site of the former wound, and carefully opened the intestine, to the extent only to allow the tube of the stomach-pump to be inserted, when there was an immediate discharge of flatus and some feculent matter, and the patient expressed himself relieved. By the further use of the stomach-pump apparatus, I was enabled to extract a quantity of feculent matter by the artificial opening, and after some hours the patient was completely relieved from the dangerous symptoms he was suffering from. The artificial opening was left patent for two months, when the bowels again gave evidence of acting naturally. The artificial wound was not, however, closed till the 22d of August, 1845; a week after the bowels appeared to act freely and naturally.
The patient from this time got well and strong, and was discharged to his duty on the 10th of October, 1845, since which period he continued to perform all the duties of a soldier most efficiently, without experiencing any inconvenience to his general health or constitution, until the 6th of October, 1846, when he died of inflammation of the brain, at Fort George, in Scotland. On dissection, the abdominal[514] viscera, including the intestinal canal, appeared perfectly healthy; but on a minute examination of the portion of small intestine (found to be the ileum) situated in the inguinal region of the side operated upon, directly opposite to the cicatrix of the external wound, it was discovered to be firmly attached to the abdominal parietes, by an adventitious membrane, to the extent of two lines, which then diverged, and formed itself into a canal of a funnel shape for about five inches and a quarter in length, of a homogeneous structure, which united itself with the continuous intestinal tube. By this wonderful provision of nature the healthy functions were uninterruptedly carried on, and permanently continued, without any pain or detriment to the patient’s general health. On appearance, Jan. 23d, 1847.
A. Maclean, M.D., late Surgeon, 76th Regiment.
Cases of extravasation or of effusion, terminating by the formation of a sac, pouch, reservoir, or foyer surrounding it, while the rest of the cavity remains free from inflammation, are so rare in natives of our northern climates that I am indisposed to infer that they do take place, except as very accidental circumstances. The fact that such things do take place should be borne in mind, and surgery should not be wanting in giving its aid, under all well-considered and reasonable circumstances. It is easier to do nothing than to think and to act.
The general treatment to be pursued in the acute period of all these cases of inflammation has been sufficiently marked—antiphlogistic to the utmost extent consistent with propriety, by bleeding, leeching, and cupping; the repeated administration of enemata; the early exhibition of mercury and opium, and subsequently of gentle aperients.
397. Continental surgeons, and by pre-eminence Baron Larrey, who is followed on this point by most French surgeons, inculcate the necessity of enlarging the wounds made by a musket-ball in the wall of the belly, although the Baron is particular in confining it to the muscular parts; M. Baudens, one of the latest writers on the subject, points out the additional tendency this gives to the formation of hernia, and furnishes therefore the soundest reason for not doing it without an especial cause. When a slip of the muscular or tendinous structures interferes with the quiescence of the wound; when it is desirable to introduce a finger to make[515] an examination; when it is necessary to divide a portion to allow the restoration of protruded parts, no one will doubt the propriety of the direction. But when neither these nor any other good or sufficient reason can be given for such an operation as that of enlarging the wound (débridant la plaie) simply because it has been usual so to do, at the risk of making a large hernial protrusion instead of a smaller one, it is unnecessary. It gives rise to some bleeding, but that is really nothing; it makes a cut instead of a hole, by which nothing essential is gained; and as this enlargement of the wound can always be accomplished when it may become necessary from a sufficient cause, such interference, especially on the fore part or the sides of the abdomen, may be safely omitted.
398. When a musket-ball, passing across the abdomen, comes out behind through the thick muscles of the back, with perhaps a slit-like opening in the skin, through which some urine, and perhaps fecal fluid or matter may also pass, such wounds should be enlarged both superficially and deeply. There is here an object to be gained, and the operation is necessary. There is no objection to its being done when it is even supposed that these fluids or matters are likely to be soon or ultimately discharged through it, as it is desirable that any secretions or effusions which cannot be evacuated by the natural passages should have every reasonable opportunity offered of making their escape.
399. When it is obvious, from internal hemorrhage, or from the discharge of fecal matter, or from the introduction of the finger, by which it can be felt, that a large hole or rent has been made in an intestine, the wound should then be enlarged so as to allow its being brought into sight, when the edges should, if required, be smoothed, and the continuous suture applied in the manner directed, Aph. 391.
400. When a musket-ball penetrates the cavity of the belly, it may pass across in any direction without injuring the intestines or solid viscera. It usually does injure one or the other, and it has been known to lodge without doing much mischief. The symptoms are generally indicated by the parts injured, although in all the general depression and anxiety are remarkable; their continuance marks the extent if not the nature of the mischief.
The following cases of the survivors of hundreds who[516] died under similar wounds, during the war beginning with the battle of Roliça in Portugal, in August, 1808, and ending with that of Waterloo, in June, 1815, may be read with a melancholy interest, as showing what sometimes will happen in a few rare instances, and even then as more dependent on the wantonness of nature than on the united efforts of science and of art.
A soldier of the brigade of heavy cavalry, under General Le Marchant, advancing in line to charge the French infantry at Salamanca, on which occasion the general was killed, was struck by a musket-ball, which entered in front, between the umbilicus and the ilium of the left side and came out behind on the opposite side above the right haunch-bone, thus traversing the body. The bowel protruded in front, but was uninjured, and was easily restored to its place. He remained at the field hospital with me for the first three days and was rigorously treated, as well as afterward in the San Domingo Hospital, where he gradually recovered, and was ultimately sent to the rear.
Captain Slayter Smith, of the 13th Dragoons, being engaged at Campo Mayor, on the 25th of March, 1811, was shot by a pistol-ball, which entered at the left hip, three inches and a half from the junction of the ilium with the sacrum, an inch and a half below its crest, and came out about three inches below the navel, and one inch to its right side. He felt a terrible shock, but did not faint or fall from his horse.
“There was a protrusion of bowel from the wound in front of about three inches; but little blood issued from it. The hemorrhage from the wound in my back was very copious. A French officer, with three or four of his men, were so near me that he called out ‘Rendez vous, mon officier,’ to which I replied, ‘Pas encore, monsieur,’ and rode away with my bowel in my hand.
“I reached the field hospital shortly afterward, when the protrusion was returned without enlarging the orifice, and no stitch was put into the wound then or afterward. It was dressed merely with lint and adhesive plaster. I begged earnestly for a glass of Madeira, which, after a little hesitation on the part of the surgeon, was given to me; but they afterward thought it necessary to bleed me; but little blood followed the insertion of the lancet. This was the only time I was bled. In the morning I found the bed saturated with[517] blood, which had trickled through to the floor, and had escaped from the wound behind.
“Before a month had elapsed I and all the wounded were removed to Elvas on bullock-cars, and a desperate journey it was.
“On my arrival, inflammation began in the wound in front, accompanied with great swelling and pain. The swelling was laid open and a quantity of matter was evacuated, followed by an angry-looking protrusion, which was carefully washed with warm water, and poulticed; when the inflammation had subsided, the wound was dressed as before, with lint confined by adhesive plaster. When the protrusion was touched by the hand I experienced a nauseous and disgusting sensation, to which in comparison the application of the knife or lancet was a flea-bite.
“I arrived in England in June, and in September went to Brighton. Soon afterward I felt terrible pains in the right side of my back, in a line with the wound, through the ilium, or rather above it, where a kind of tumor formed. For several days I suffered agony from it; and one night, completely worn out, I fell into a long and deep sleep, and awaking late in the morning I found all pain and excrescence gone, and nothing remaining but a tenderness of the part on pressure with the finger. I underwent much from violent spasms in the stomach, which I never had before I was wounded. I recovered, however, sufficiently to rejoin my regiment the following spring in the Peninsula, and was soon afterward again wounded in a skirmish by a spent shot in the left shoulder, which, however, was of no moment, though I was compelled to return to England on sick leave, in October, 1812, as the spasms increased with greater severity, incapacitating me from doing my duty, and at times rendering me totally helpless.
“I now gradually recovered my health, and in the spring of 1815, accompanied the 10th Hussars to Belgium, and served at Waterloo.
“My health gave way again in 1821, and I certainly was in a precarious state for three or four years, but I gradually recovered, and by dint of great care and attention to diet I am now (1853) in robust health, and can take the strongest exercise with impunity.”
John Richardson, of the 1st Royal Dragoons, was wounded[518] at the battle of Waterloo by a musket-ball, which entered two and a half inches above the umbilicus, and passed out on the left side, close to the lumbar vertebræ. He threw up a considerable quantity of blood, and the stomach was so irritable that nothing would remain on it. He complained of pain, which cut him right across, as he termed it; his eyes were suffused and face flushed; had headache; pulse 130. Thirty ounces of blood were taken from the arm, emollient injections thrown up the rectum, and poultices applied to the wounds.
June 20th.—Some blood came away with the injections during the night; great pain in the right side and shoulder; saline draughts are returned tinged with bile and blood; pulse 130. Bled to sixteen ounces; injections and poultices continued.
21st.—A draught was ejected mixed with blood, and a quantity of bilious fluid; diarrhœa during the night; the feces were mixed with blood; pulse 120; skin hot. Bleeding to twelve ounces; blood sizy.
22d.—Slept a little during the night; had several alvine evacuations of a bilious fluid mixed with blood. The tension of the belly is not so great. He still complains of pain. Tea remains on his stomach. Bleeding to twelve ounces; fomentations and poultices to the belly; chicken and beef broths; injections frequently.
24th.—Feels considerable relief from the tension of the abdomen having subsided; threw up his tea and a quantity of clotted blood this morning.
26th.—Had a bad night; pulse 125, and full. Complains of great pain in the hepatic region, and backward toward the spine. Bleeding to sixteen ounces. ℞.—Hydrarg. chlorid. gr. iv; conf. rosæ. gr. ix; to be made into two pills, one to be taken twice a day.
30th.—Vomiting in the night, mixed with blood; tea, etc. remain on the stomach this morning; pulse 108.
July 5th.—The adnatæ have a yellow tinge; in other respects he is doing well. ℞.—Chlorid. hydrarg. gr. x; extr. colocynth. comp. ʒj: to be made into ten pills, one to be taken three times a day.
20th.—The wound perfectly healed; is cleaning his accoutrements, boots, etc. Was discharged on the 28th of July, perfectly recovered.
Owen M’Caffrey, aged thirty-three, first battalion 95th[519] Regiment, was wounded on the 18th of June at the battle of Waterloo, by a musket-ball, which penetrated the cavity of the abdomen on the right side, about midway between the superior anterior spinous process of the ilium and the linea alba. When admitted into the Minimes General Hospital three days after, he was in the most deplorable state; the whole abdomen was tense and exquisitely tender; the pulse small and wiry; vomiting incessant, with hiccough and ghastly visage. From this period to the 24th, he was thrice largely blooded, and the strictest antiphlogistic plan was laid down and rigidly adhered to. Laxative injections were administered, the whole of the abdomen was frequently fomented, and opiates were administered to allay the irritability of the stomach, and to procure ease and rest. On the 25th the wounded intestine sloughed, and the feces escaped by the external orifice, the adherence of the two surfaces of the peritoneum preventing any, even the smallest portion, getting into the cavity of the abdomen.
26th.—The high inflammatory action having been reduced, milk, rice, and sugar, and the farinaceous part of the potato were allowed.
July 1st.—No very alarming symptom remains. Half a fowl ordered for his dinner, and the greatest attention to personal cleanliness directed to be paid.
7th.—Strength slowly but gradually returning. The action of the large intestines is daily kept up by stimulating injections.
14th.—Progress to recovery satisfactory. The injections are daily repeated, and the discharge by the natural passage increases. The wound contracts and looks healthy. Is enabled to sit up, and has recovered his cheerfulness.
28th.—Still improving; ultimately recovered.
The situation of the ball was never ascertained.
A soldier of la Jeune Garde Imperiale was struck by a ball, which entered to the right and a little below the umbilicus and passed out on the left or opposite side, about two inches above the crest of the ilium. It was supposed to have passed along the canal of the great arch of the colon. Fecal matter, much tinged with bile, passed by both openings. The symptoms of inflammation were severe for the first few days, but gradually yielded to the means employed, when the bowels began to act regularly by the aid of mild injections, and the discharge from the wounds gradually[520] lessened; the man was much reduced, but otherwise in good health, and was sent to France from Brussels, nearly well.
A soldier of the Third Division of Infantry was wounded during the assault of Ciudad Rodrigo, by a ball which entered and lodged in the left side of the back, about midway between the spine and a line drawn to the upper part of the crest of the ilium, from which opening the contents of the bowel were discharged. Left among the dead and those who were supposed to be dying at the field hospital, in the rear of the trenches, I sent him, with all those of different corps who were wounded, to my own hospital at Aldea Gallega, some ten miles off. Here, under a sufficiently vigorous treatment, of which bleeding, starvation, and quietude were the prominent features, he gradually recovered. On the fifth day the ball passed per anum, and on two or three different occasions afterward portions of his coat, flannel shirt, and breeches. Fecal matter passed readily through the wound, while the bowels were gently solicited by common injections for some time; but the wound gradually closed in, and the man regained his health, and was sent to the rear with a slight colored discharge from the wound, not quite free from odor.
Ensign Wright, 61st Regiment, was wounded by a musket-ball, on the morning of the 10th of April, at Toulouse. The ball passed through the abdominal parietes on the right of the linea alba, nearly half way betwixt the umbilicus and the pubes, and lodged. Sense of debility, tremor, nausea, small, feeble pulse, and pain in the lower part of the abdomen were the immediate symptoms.
Peritonitic and enteritic symptoms of considerable violence having begun to manifest themselves on the 11th, copious and repeated evacuations of blood were made by order of Mr. Guthrie, the Deputy Inspector-General in charge of all the wounded. Fomentations were applied to the belly; abstinence in food and drink was strictly enjoined, and the most rigid antiphlogistic regimen followed. The same practice was pursued during the 12th, 13th, and 14th, venesection being performed either two or three times every day, as the augmented state of the local and general inflammatory symptoms seemed to require. The bowels during the above period had continued perfectly free, and the dejections were tolerably natural in color, but rather dark, and extremely fetid. He had been frequently troubled with nausea and[521] vomiting of bilious matter. Two small doses of castor-oil had been exhibited.
Toast and water, tea, boiled milk-and-water, with a little soft bread soaked in it, and mutton and chicken-broth in small quantities at a time, were all that was allowed him for food and drink.
April 15th.—Pulse above 100, weak and small; temperature natural; the tongue clean. Continued affected with a degree of nausea and vomiting, after drinks especially; and some diarrhœa was present.
17th.—Was bled last night to twelve ounces, in consequence of increased pain of abdomen and augmented pyrexia; to-day quiet and easy, and has had several stools.
18th.—Diarrhœa and tenesmus troublesome during the night; ball voided with the feces at six A.M.; it is somewhat flattened, as if from impinging on a stone; has felt easy since. Continue antiphlogistic regimen.
19th.—Diarrhœa abated; but the abdomen is tense and painful on pressure. He is distressed with nausea and vomiting; pulse 100, and sharp; great thirst; tongue dry. Bleeding to sixteen ounces; abdomen fomented.
20th.—Bleeding was repeated last night from persistence of the symptoms of peritonitis. Blood drawn very buffy; has had several loose stools during the night. He is to-day easy; abdomen now scarcely painful. Fomentations continued.
29th.—This morning the abdomen was tense and painful on pressure; he was affected with nausea, and had had vomiting repeatedly during the night; thirst and pyrexia. Fomentations were applied from time to time, and yielded relief. Suspect that he has not observed the prescribed regimen.
May 1st.—Pain of abdomen and bilious vomitings during the night; has had three loose stools. Pulse 110, hard and small; thirst urgent. Blood let to fainting; fomentations continued.
2d.—Last night he was again bled to two ounces, when fainting supervened. He passed a quiet night; had two liquid stools; abdomen not painful, nor is he sick at stomach, nor thirsty. To keep himself warm, particularly the belly.
11th.—Suspect he has been rather irregular in diet.[522] Passed a bad night, partly in delirium; has vomited much; has obviously pain on pressure of the abdomen, but appears studious to conceal it; pulse 112, small and not soft; temperature increased; tongue red; thirsty; three liquid stools. The stomach to be kept warm; ten drops of tincture of digitalis in half an ounce of mist. acaciæ, to be taken three times a day; diet of milk and farinaceous food; for drink, infusion of tea in small quantities. Eight o’clock.—Pulse 120, soft; feels easier, and has not vomited. Ordered a foot-bath.
13th.—Molested by pains, nausea, and vomiting during the night; pulse 110, not soft; skin cool, but is thirsty, and his tongue is of a vermilion color, and arid; confesses that he has hitherto disguised his feelings, as well as other circumstances connected with his case, particularly his manner of living. Digitalis continued; blister to be applied to the epigastric region, and the foot-bath repeated in the evening.
14th.—Bad night; pulse 112; skin hot; pain of abdomen not urgent; no vomiting, but is affected with nausea. Digitalis continued. Four o’clock.—Pulse 100; feels nauseated; no pain of abdomen. Digitalis occasionally.
16th. Eight A.M.—The tendency to vomit continues. One grain and a half of chloride of mercury with a grain and a half of opium, made into a pill, to be taken in the morning; to be bled. Seven P.M.—Vomits whatever he swallows in any quantity; skin hot; thirst great; tongue red; two motions; says abdomen is not painful; pulse 112. A blister to be again applied to the epigastrium; foot-bath in the evening; repeat the mucilaginous mixture for cough.
17th.—Rested ill; blister has not risen; cough has been severe and continues so; two motions; pulse 120, and not soft; cough augmented by deep inspiration, and pain produced. Take blood from the arm to eight ounces; foot-bath in the evening; continue pill.
18th.—Bad night; cough gone; respiration easy; pulse 100; skin cool and moist; no thirst; one motion of a natural kind. Repeat mucilage and the calomel and opium pill.
24th.—Has this morning experienced a severe attack of dyspnœa, attended by cough and pain of chest, both increased by full inspiration. Pulse 120; face flushed; says he caught cold from exposure to the night air. Bled im[523]mediately, and as much blood taken as his strength would permit; foot-bath repeated in the evening.
25th.—Six ounces of blood drawn; surface buffy; bad night; cough, pain, and pyrexia abated this morning; in the evening severe dyspnœa; cough and pain of chest have recurred; pulse 120. Six ounces of blood to be drawn, should strength permit; mucilaginous mixture to be continued; another blister to be applied to the chest.
28th.—In a fair way of recovery; was discharged for England in June, with little or no complaint.
John Murray, Surgeon to the Forces.
Sergeant Matthews, of the 28th Regiment, was wounded at Waterloo by a musket-ball, about an inch below the umbilicus, a little to the right side, which lodged. He walked to a village in the rear, where he remained for three days, having been bled each day to fainting, before he was removed to Brussels, where my attention was particularly attracted to him, in consequence of his having passed the ball (a small rifle one) per anum, three days after his arrival, or the sixth from the receipt of the wound. The wound was healed by the end of August; and he felt so well that he marched to Paris with other convalescents, to joint his regiment. After some weeks he got drunk, and suffered from an attack of pain in the bowels, in the situation of the wound, requiring active treatment. On attempting one day to have a motion, he found, after many efforts, that something blocked up the anus, and on taking hold of and drawing it out, he found it was a portion of the waistband of his breeches, including a part of the button-hole—a fact verified by Staff-Surgeon Dease, who wrote to me an account of this peculiar case. After this the man recovered without further difficulty, although, as in all such cases, there was a herniary projection. He was afterward subject to costiveness, to pain in the part after a copious meal, probably from the stretching of the adhesions formed between the intestine and the abdominal peritoneum, which inclined him to bend his body forward to obtain relief.
In all such cases, the extraneous substance having lodged, and mainly injured in all probability the vitality of the part which assists in the lodgment, the ball becomes covered with a layer of coagulable lymph or fiber, capable of retaining it in its new situation, whence it is gradually removed by[524] ulceration, or by the sloughing of the injured parts into the cavity of the bowel; much in the same manner as an abscess in the liver is evacuated into the duodenum or neighboring intestine, to which it may become attached. It is always fortunate when the canal from the external wound is cut off by the deposition of lymph, as it expedites the cure, and renders the injury less formidable; but if this should not take place, the contents of the bowel are discharged through it for a greater or shorter length of time, until the canal between the parts gradually closes, and cicatrization takes place, in default of which an artificial anus may remain in addition to the natural one, the functions of the bowels generally being performed with more or less difficulty.
The two following very interesting cases of abdominal injury having been received while these pages were passing through the press, are here inserted:—
A man in the 19th Regiment was wounded through the abdomen, and survived nineteen hours, the ball entering near to the umbilicus, and passing out close to the sacrum. On the post-mortem examination, the small intestines were found to have been wounded no less than sixteen times by the ball in its passage. When wounded, he was stooping in the act of defecation.
T. Alexander, Deputy Inspector-General.
5th August, 1855.
On the evening after the battle of Alma, as my regiment was halting on the brow of a hill, previous to bivouacking, a wounded Russian officer, apparently in great pain, was perceived on the other side of the ravine. Passing over to where he lay, I found that he had been wounded by a musket-ball, that had entered the lumbar region directly over the spine. As he was enabled in his agony to crawl on his hands and knees, it was evident there was no paralysis, and on passing a probe I found the ball had avoided the spine, but as I could not pass in the instrument more than an inch, I was left in uncertainty as to its further course.
He was removed to my hospital tent, when I tried, but with little success, to remove the excessive pain from which he was suffering. In about two hours after he took my finger and placed it on a hard substance imbedded in the walls of the abdomen, and on cutting down on this I perceived a musket-ball. Previous to extracting it, however, I[525] observed a white, glistening substance oozing from the wound, which, on carefully removing with the probe, proved to be a portion of tape-worm, about a yard and a half in length. I then extracted the ball, and again another portion of the worm presented, which measured about two yards and a half in length. It was now complete, though cut in two evidently by the ball, and the two portions, one containing the head and the other the tail, were soon writhing on the table.
The patient experienced immediate relief; the pain had ceased; he slept well, and on the following morning he was free from thirst, with a tolerably quiet pulse. Unfortunately the order arrived for all prisoners and wounded to be sent to the rear, and I lost sight of the case.
What was the cause of this agony of pain? Evidently the writhing of the worm, or why should it so suddenly cease on the worm’s liberation? The abdomen must have been entered by the ball, or how could the worm’s exit have been effected? Nevertheless, but for its presence, the patient was so free from constitutional symptoms on the following morning that a surmise might really have arisen that the ball had passed round the abdomen without injury to the peritoneum.
Rt. De Lisle, Surgeon,
4th K. O. Regiment.
Camp before Sebastopol, August 8th, 1855.
ABNORMAL OR ARTIFICIAL ANUS, ETC.
401. In some cases of wounds of the intestine the continuity of the bowel is not sufficiently re-established; the external wound remains open, and becomes indurated and fistulous, giving passage to the fecal matters, and rendering the sufferers very miserable. These cases are of rare occurrence among the hardy natives of Great Britain and Ireland, and comparatively little has been done or even recommended in this country for the relief of this misfortune.
When an intestine has lost a more or less considerable[526] part of its substance at a particular spot, and an artificial anus is about to be formed, it adheres to the peritoneum around the inside of the external wound, although the adhesion is of little extent or width, and forms but a narrow barrier for the protection of the cavity of the abdomen. The upper end of the bowel is more open than the lower, the caliber of which is contracted in size, and is sometimes even difficult to find; while its opening is partially closed by a sort of septum extending across, or from where the two portions of a divided gut have come irregularly in contact with each other by their sides, without uniting in the first instance in their length; or from the falling in especially of the posterior part of the lower end, to which the upper has become united. The projection thus formed in the tube is called by the French eperon or promontoire, valve or spur, ridge or septum; it directs the fecal matter through the external wound, while it obstructs its passage into the lower part of the bowel. There is generally great difficulty in ascertaining the fact of the existence and exact situation of this valve during life; in distinguishing the upper from the lower end of the intestine, as well as the nature and extent of the adhesions by which the injured intestine is retained in its situation. If the absence of such a valve can be satisfactorily made out—and it is sometimes wanting—the external opening may be successfully closed by compression, or by operation. If the valve should exist, its removal by a preliminary operation is necessary; it has been attempted in France with various but somewhat doubtful success.
402. When a portion of small intestine has been lost by mortification or otherwise, and the patient has recovered with an unnaturally situated or artificial anus, the intestine, although at first in contact with the wall of the abdomen, is gradually, in many cases though not in all, retracted into the cavity—it has been supposed by the dragging of the mesentery upon it at the point of union of the divided extremities outside where the eperon or valve is formed; and it is said that this dragging has even led to the gradual disappearance of the valve, admitting thereby of the contents passing more readily from the upper part of the intestine into the lower, and consequently laying the foundation for a cure. This dragging of the intestine, or its movements under the different motions of the body, in some cases cause an elongation of the membrane formed under the adhesive process,[527] by which the intestine is attached to the inside of the wall of the abdomen in the same manner as adhesions are elongated between the pleuræ, and a sac or pouch is thus formed between the cut ends of the intestine and the fistulous external opening which Scarpa was the first fully to demonstrate and explain, and which he called an entonnoir, infundibulum, or funnel. If, then, in an old case, a small portion of the wall of the abdomen be removed in the form of a V, the internal opening at the apex of the V, if small, would be made into a sort of funnel, while the outer incision would remove all the hardened fistulous parts—an operation which is sometimes required to be done when the external opening is not free, and fecal matters have insinuated themselves between the aponeurotic parts, giving rise to abscesses and other small fistulous openings in different directions. It is necessary to bear the formation of this pouch in mind as well as that of the valve, in order to understand the operations proposed for the relief or cure of this complaint.
If simple compression fail in the first instance to prevent the passage of the feces, which never can be thoroughly controlled from the want of a sphincter and the uncertainty of pressure, the method of Desault may be adopted. This consists in gradually dilating the external wound so as to enable the operator to discover the open ends of the bowel, when a tent is to be introduced into the lower end, and afterward into the upper, being fastened by a thread passed around its middle. A pyramidal-shaped pad is then to be placed over the opening, and compression made by bandage upon it so as to press the whole inward. The size of the tent is to be gradually enlarged until the contents of the gut begin to pass downward with ease, when a well adjusted pressure is to be made on the fistulous opening only, to prevent all oozing from it until the internal parts have had time to close.
403. Dupuytren invented a pair of forceps, consisting of a male and female branch, to be applied separately, one on each side of the valve or eperon, to the extent of an inch or an inch and a half at most, when they were to be closed by a screw until they had compressed the part between them sufficiently to destroy its life. The separation of the valve included within the forceps would take place by the usual processes of ulceration in its immediate proximity, and by adhesion of the parts external to the bowels to those sur[528]rounding them. The inflammation, however, did not always stop at the adhesive stage, and death has been the result as well as a successful cure.
404. Mr. Trant has invented an instrument he calls a propeller, for pressing back the eperon, an account of which is given in the Dublin Medical Press, May 14th, 1845. He used this in one case with complete success. The instrument by its formation admits of being passed through the artificial anus, and of being placed on the eperon at the bottom of the wound, where it can be retained for a considerable time without producing the slightest inconvenience. It does not, while in the intestines, offer any obstruction to the passage of the fecal matters flowing along the cavity of the tube. It acts as a forceps in retaining the anterior wall of the intestine in close contact with the posterior surface of the abdominal parietes, while the propeller is pressing back the eperon toward the spine; consequently the danger of separating the delicate adhesions in this situation is prevented, otherwise a fatal extravasation into the cavity of the abdomen might ensue. The instrument was made by Mr. Reed, of Dublin, and merits further trial, being apparently less dangerous than the other methods recommended in similar cases. Whatever may be the method employed for the cure of an artificial anus by operation, it cannot be doubted that the patient must be exposed to all the dangers which may result from inflammation, for which he must be prepared beforehand, and the symptoms of which must be met and subdued as they arise; or, if this cannot be accomplished, the mechanical means, if any be used that can be taken away, must be removed, and quiet, if possible, restored by their abstraction and by the treatment adopted. In successful cases, a small aperture will frequently remain, constituting a fecal fistula instead of an artificial anus. This will sometimes become irritable, inflame, ulcerate, or burst, discharging the solid contents of the bowel, although, on the subsidence of the irritation, the part under pressure usually returns to its former state.
405. Wounds and injuries of the liver, whether incised or penetrating, occurring from blows or from musket-balls, are very serious, although not necessarily fatal. Some few persons recover altogether, some few with more or less of permanent disability. The remainder die during the first or inflammatory stage, or in the secondary one, which follows[529] from the twelfth or fourteenth day after the primary symptoms have in some measure subsided.
The symptoms which ensue after a wound of the liver are those common to inflammation of the cavity of the abdomen, with the addition of those peculiar to the organ—pulse often smaller and less perceptible than in peritonitis; discoloration of the skin, eyes, and urine, amounting even to jaundice, although this is not an immediate symptom, neither is it always present. The pain is not confined to the part, but extends to the umbilicus, while the pain symptomatic of inflammation of the liver—viz., pain in the top of the right shoulder—is felt early, and is often accompanied by cramps of the muscles of the arms and numbness of the fingers. The usual symptoms of anxiety and depression are present, and the stomach shows by its irritability that it has partaken of the shock given to the system. The bowels are usually confined, but I have known blood passed from them when it was not supposed that the stomach or intestines had been wounded; the discharge from the wound is either of blood or bile, or both, mixed with a serous effusion which afterward becomes purulent. Wounds of the gall-bladder are, as far as is known, fatal—the effusion of bile which immediately takes place giving rise to inflammation which, with other causes, destroys the sufferer at the end of a few days. If the gall-bladder be adherent to the peritoneum from any previous inflammation, a wound in it need not prove mortal, as the effusion would be avoided, and there is no reason to believe that an injury to this part would be otherwise more vital than that of any other of the viscera of the abdomen.
The late Lieut.-General Sir S. Barns, when Lieut.-Colonel of the Royals, was wounded at the battle of Salamanca by a musket-ball, which injured the cartilages of the false ribs, a portion of the rib being removed and passed out through the liver. A bilious discharge continued several weeks from the wound, and his life was saved with great difficulty. He returned to his duties, although suffering from a dragging pain and weight in the side, which any exertion increased. In the autumn of 1819 he was attacked by acute inflammation; the pain in the right side, extending over the stomach and umbilicus, was constant and acute, and increased on pressure; the pulse small, indeed scarcely perceptible; the extremities cold; the countenance depressed and anxious; bowels confined; stomach rather irritable. A number of[530] leeches were applied, and other remedies administered. The constant pain, which was increased by pressure, could only be relieved by loss of blood, although every other symptom seemed to forbid depletion. Twenty ounces of blood were taken from the arm, which caused a diminution of the pain, and gave relief for an hour; the pain then returned, and twelve ounces more blood were taken away, with the most beneficial effect; a blister was applied over the part, and a dose of calomel and opium was repeated. Shortly afterward he became tranquil; the extremities lost their coldness; and, although the pain continued in a slight degree for several hours, and much soreness remained for many days, he quickly recovered. Two months afterward he had another and equally severe attack, in consequence of walking about two miles rather hastily; from that he was relieved in a similar manner. Whenever he bent his body, a portion of the rib appeared to press in upon the liver, and often gave him acute, darting pain; and one day, on pulling on his boot in haste with some bodily exertion, a third attack ensued. In order to prevent the bending of the body forward, and to confine the motion of the liver, which seemed liable to injury from the irregular points of bone which could be readily distinguished above it, stays, made with iron plates instead of whalebone, were adapted to his body, and from these he derived great comfort.
Corporal Macdonald, first battalion, 79th Regiment, was wounded on the 16th of June at Quatre Bras, by a musket-ball, which entered the abdomen, splintered the eighth rib on the right side, passed through the liver, and was supposed to have lodged on the opposite side, as he says he felt the ball strike the left side, on which he was not able to lie for a long time. Lost but little blood at the time; was dressed superficially, and arrived in Brussels on the 19th, laboring under considerable fever. Bleeding to thirty-six ounces. For seven successive days the bleeding was repeated, to from twelve to sixteen ounces each day, when a large, bilious, and purulent discharge took place from the wound, on which the inflammatory symptoms appeared to subside, until the 30th of June, when bleeding took place from the wound during the night to the extent of twenty ounces, and then ceased spontaneously. On the 15th of July the hemorrhage recurred with so much fever as to warrant twenty ounces of blood being taken from the arm, and this[531] was repeated the next day. The bilious discharge ceased in the middle of August, and on the 2d of September he was discharged convalescent.
Lieutenant Edward Hooper, first battalion, 38th Regiment, was wounded by a musket-ball on the 9th of December, 1812. It passed through the anterior edge of the liver, and, glancing round the ribs, was cut out about two inches from the spine.
On his being wounded, he could scarcely believe his shoulder was not the part affected. His pulse was intermitting; the breathing hurried and laborious, and in a short time the tunicæ conjunctivæ became yellow. He was very largely bled, and warm fomentations were applied to the abdomen, from which, and the bleeding, he received some temporary relief; but, in consequence of his removal that night to the rear, the symptoms were much aggravated on the morning of the 10th. He complained of acute pain over the whole abdomen, increased on pressure; vomiting; quick, hard, and wiry pulse, (no pain referred to the wound.) The bleeding was repeated ad deliquium, warm fomentations and an enema also repeated, and a saline mixture, with a very few drops of tincture of opium, to allay the irritability of the stomach. On the following evening the vomiting had ceased; his pulse was less frequent and hard; pain less. On the 11th, after passing a very restless night, the pulse again rose; the abdomen became tense but not very painful, and he made ineffectual efforts to stool. He was again bled, a large blister was applied over the abdomen, and an ounce of castor-oil was given immediately. The blister acted well, and the purgative gave him three copious stools of dark and fetid feces. On the 12th he complained of twitching pains, referred to the right shoulder, and was ordered one grain of calomel, with two of antimonial powder, three times a day.
Jan. 13th.—Was free from pain; pulse fuller and less frequent; urine clear; tension of abdomen subsided. The calomel and antimony were continued, and some light nourishment was allowed. From this day a gradual amendment took place. The calomel was continued until his mouth became slightly affected; and, as his bowels were in general torpid, from the deficient secretion of bile, a mild purgative was given every two or three days, as occasion required, and an ounce of the infusion of calumba, with quassia, three or four times daily.
[532] A soldier of the 48th Regiment was struck by a musket-ball at Albuhera, on the upper part of the right hypochondrium, over the liver; it came out behind, at a point immediately corresponding to that in front. Blood and bile were discharged from the wounds in considerable quantity, and his case was considered to be hopeless. Brought to me at Valverde, the next day, he was bled largely several times; the wounds were dressed simply, and he was kept perfectly quiet, and his bowels gently open. The skin became of a yellow color, his strength failed under the treatment, and he became thin, and looked ill. At the end of three weeks he was sent to Elvas, where he gradually improved, and was forwarded thence to Lisbon and to England, with his wounds healed.
An officer was wounded in one of the battles in the Pyrenees, by a musket-ball, which penetrated the outer part of the right hypochondrium, at the edge of the false ribs, and lodged. Blood and bile flowed in considerable quantity; the skin became yellow, the pain and swelling of the abdomen were considerable, and he was given over as lost. Under a vigorous and careful treatment he gradually recovered, so as to be sent to England, with a fistulous opening at the orifice of entrance. I examined the wound in 1817, three years afterward, and found that a large blunt probe passed inward toward the stomach and liver for the distance of five inches, where it ended apparently in a sort of sac. Purulent and bilious matters were constantly discharged from the wound; his countenance was sallow; his digestion bad; he suffered from constant uneasiness, if not pain, and was altogether out of health. I saw him once annually for several years, and found that I could sometimes strike the ball with the probe; that he frequently, after an attack of pain and derangement, passed matter by stool, after which the pain and uneasiness about the wound ceased. I had hopes the ball would some day pass through the opening thus made, and had thoughts of enlarging the external wound, and of endeavoring to extract the ball with a long pair of forceps. He ceased at last to pay his annual visit, and I suspect he died in one of the attacks I have alluded to. This ball must have passed very close to, if it did not penetrate, the gall-bladder.
I have never had an opportunity of extracting a ball from the liver during life, although I have seen persons live many weeks into whose livers balls had penetrated; and I have been acquainted with three persons who had been[533] wounded through the liver, to whom little subsequent inconvenience was occasioned.
406. Portions of the liver have been removed in some instances; in one case, related by Blanchard, a small piece of liver was removed with the forceps. The patient dying of fever three years afterward, a small piece of the liver near the external wound was found wanting. Dieffenbach gives a case in which a small protruded portion was cut off with scissors, without any bad consequence. Dr. Macpherson, in the ‘London Medical Gazette’ for January, 1846, has related the case of a Hindoo, a large piece of whose liver protruded through a wound an inch in length, made by a spear in the right hypochondriac region. A ligature was applied tightly around its base, and the piece cut off, rather than make such an enlargement of the wound as might allow the restoration of the protruded liver. The arteries bled from the cut surface, and required to be tied, and a double ligature was put through the stump of liver and tied on each side. The part was not pushed back into the abdomen, but allowed to remain in the wound. The symptoms were mild, the ligatures came away on the ninth day, and the man returned to his home in three weeks.
These cases may be considered exceptions to the general rule, which directs the return of all protruded parts. The retention of the part from which the piece was cut off within the divided parts of the wound was agreeable to the principles I have inculcated with respect to wounds of all the cavities.
407. Wounds of the stomach are usually fatal, although some persons escape when these injuries are confined to its anterior and upper surface, and do not penetrate both sides, in which case effusion into the cavity of the abdomen, and consequent inflammation, can scarcely fail to ensue. It is fortunate for the patient, when they occur, that the stomach should be empty. If it should not be so, the contents may possibly be ejected shortly after the receipt of the wound, but it is not advisable to excite vomiting by remedies, or by means adapted for that purpose. In a perfectly quiescent state, the general compression of the contents of the abdomen by its walls may prevent effusion under ordinary circumstances, and this state should be maintained as rigidly as possible. The apparent course of the wound indicates the probable mis[534]chief, which is especially confirmed by vomiting of blood, great anxiety, depression of countenance, a cold, clammy skin, pain in the part, hiccough, and by the discharge of the contents of the stomach, if the wound be sufficiently open to allow it; pulse low and sometimes intermittent. If effusion of the contents of the stomach should not occur, the external wound, if an incised one, should be closed by suture, and the patient kept in the utmost state of quietude, in a somewhat elevated position, the abdominal muscles being relaxed. Neither food nor drink should enter the stomach, although thirst should be allayed by wetting the tongue and mouth. The bowels should be relieved by enemata, and the belly fomented. Bleeding and leeching, as frequently repeated as the symptoms appear to require, must be carried to the greatest extent that can be permitted with safety.
When the external wound is so large as to enable the wounded stomach to be seen, the cut edges of the wound in it should be brought together by the continuous suture, as in the intestines; and the external wound should be closed in a similar manner, the end of the ligature on the wound of the stomach being cut off close to the viscus, that organ being left perfectly free, with the hope that the thread will be carried into its cavity, while the outside adheres to the peritoneum opposed to it.
When the stomach pours its contents through an external opening, too small to allow its being examined, it is desirable that the wound should be enlarged, if a doubt be entertained of the passage being free. It is a sufficient reason for such an operation to allow the opening in the stomach to be seen. It is very probable that effusion will take place into the cavity of the abdomen if it be not done, and the death of the patient will follow. It is very probable he will die if it be done, and therefore in such cases little has hitherto been attempted. I am of opinion, however, that in the case I have last alluded to, a blunt hook may be sometimes introduced through the wound into the stomach, so as to keep it stationary while the external opening is carefully enlarged, and that it ought to be done in such cases, and the wound in the stomach closed in the manner recommended. I have never had a case under my care in which I could have done this; but I have seen some die in whom it might have been done; and it deserves to be considered when surgeons shall be in sufficient numbers on the field of battle to[535] attend to such recommendations, and to the after-treatment these cases require.
When the stomach is injured by a musket-ball, and its contents are discharged externally, the edges of the wound, not being in a condition to unite, must remain open for several days. The person should be placed in the mean time in the most easy and comfortable position which may enable the contents of the stomach to be readily passed out externally, if they show any disposition to be thus evacuated. The external wound should be dilated as far as the peritoneum, if it should be required, so as to admit of the passage being direct, and symptoms must be awaited and treated as they arise. If the patient should survive the first or inflammatory stage, he should be supported by clysters composed of strong beef-tea or veal broth, given five or six times during the twenty-four hours. When it may be expected that the wound in the stomach has closed, or that the injured portion has adhered to the neighboring parts, warm jellies and light broths may be frequently given in small quantities, but solid food should be forbidden until complete recovery has taken place. I have seen inattention to this precaution in more than one instance prove fatal.
408. Fistulous openings have been known to follow wounds of the stomach, and to continue for years. The case related by Dr. Beaumont of the American army, of St. Martin, who, in 1822, received an extensive wound in the stomach, which became fistulous, admitting of a variety of most interesting inquiries being made into the process of digestion, is remarkable.
Hevin has related some of the most interesting cases of those who had swallowed knives, etc., by design or by accident, and whose stomachs were opened for their removal. The most ridiculous story of the whole is an instructive one, however. Some young students, desirous of punishing a young woman who had offended them, cut short the hair of the tail of a large pig, and when frozen hard, forcibly pushed it up her anus, leaving a couple of inches only hanging out of the small end or tip. The hairs having been cut short caught in the gut when attempts were made to draw out the tail, and gave her inexpressible pain. The most serious symptoms followed during six days, and every attempt having failed, Marchetti was applied to. He prepared a hollow tube two feet long, large enough to receive the thickest part[536] of the pig’s tail, to the end of which he fastened a strong waxed cord, which he drew through the tube. This he carefully introduced into the anus, pushing it over the pig’s tail, until he drew the whole of it into the tube, which he then brought away, including the tail, to the great relief of the sufferer.
409. The necessity for an operation so grave as that of opening the stomach must be shown by the presumed impossibility of the foreign substances being dissolved, or of their passing out of it by any other means, while the continued distress they occasion more than equals the risk which is likely to be incurred. The offending substance ought to be felt through the wall of the abdomen, and the incision for its removal should be made between the recti muscles in the linea alba, unless the foreign body have actually pierced the stomach, and can be felt to the outside of the rectus muscle, at which part the incision ought to be made obliquely in the direction of the fibers of the external oblique muscle, all bleeding vessels being secured before the peritoneum is opened. This having been accomplished, the protruding body should be extracted by such an enlargement of the opening in the stomach as may be actually necessary. When the substance does not protrude, although it can be felt through the wall of the stomach, it will be advisable, if possible, to draw it toward the upper or smaller curvature of the stomach rather than to the lower, avoiding the coronary vessels, and taking a medium distance for the opening from the cardiac orifice, and thereby such advantage as may be derived from gravitation. The wound in the stomach should be united by the continuous suture, and the external wound should be closed in a similar manner. The patient ought to be kept in bed in an easy erect position.
410. Injuries of the spleen have been usually fatal, from hemorrhage filling the general cavity of the abdomen, especially when they have arisen from rupture of that organ, which I have several times seen occur in consequence of falls, or from blows from cannon-shot, which have not opened into the cavity or exposed the viscus. Wounds from musket-balls have for the most part destroyed the sufferers, either from hemorrhage or from inflammation. I have not seen nor heard, during the Peninsular war, of a wound in the abdomen through which the spleen protruded, the patient recovering. Instances have occurred in which[537] this part has been removed in man after its exposure by injury. A case is said to have taken place after the battle of Dettingen, in which the spleen, covered with dirt, was cut off, and the patient recovered. In another case the spleen, found without the wound at the end of twenty-four hours, was cold, black, and mortified. The surgeon placed a ligature above this part, and cut off three inches and a half of the spleen; a large artery was tied, and the remaining portion of the viscus was returned into the cavity of the belly, the ligature hanging to it, and the patient got well.
Wounds from stabs with a bayonet, or a sabre, or long-pointed sword are frequently fatal, either from hemorrhage or from inflammation; but I have seen accidentally, after death, cicatrixes in the spleen corresponding to external marks, indicative of a former wound. The treatment, in all such cases, should be to encourage the discharge of blood from the part, in the first instance; then to close the external wound if an incised one, to place the patient on the injured side, and to subdue all unnecessary inflammation by bleeding, leeching, absolute rest, and starvation. The application of warm fomentations where an oozing of blood may be expected to take place cannot be recommended, and cold should be substituted if agreeable to the feelings of the patient. When the blow or wound does not cause the death of the individual by hemorrhage or acute inflammation, a chronic state of disease may supervene, which, if not duly combated, will ultimately destroy him. The early administration of calomel and opium, and the repeated application of blisters, will, in these cases, as well as in those of wounds of the liver, be of the greatest service. Effusion or suppuration may take place as well as in those cases which have been noticed, when other viscera have been injured; although instances of such terminations are not recorded, it does not follow that they have not taken place.
411. Wounds affecting the kidney have been less fatal than those of the spleen, although they are scarcely less dangerous, from the complications by which they are attended; the successful cases on record are not numerous, and the practice to be pursued can only be general. The results, when not fatal, have been for the most part unknown, from the patients either lingering on or recovering after they have been discharged from the service. I saw two cases of[538] this nature after the battle of Waterloo. In one, the ball had passed through the abdomen, entering a little below and to the left of the umbilicus, and coming out behind nearly opposite and close to the spine. No fecal matter was discharged from the front wound, but some came through the posterior one, accompanied by a small quantity of urine, indicating a lesion of the kidney or of the ureter at its upper part. The symptoms, at first severe, had subsided under proper treatment, and there was every probability that the sufferer would eventually recover, although I was unable to trace the case after the man left Brussels. In the other, pain was principally felt in the testis and the spermatic cord of the side injured.
An officer was wounded on the right side, on the 9th December, 1813, the ball being cut out behind; his case was considered hopeless. An hour afterward, on being moved to the fire, he desired to make water, and then passed what appeared to him to be a quantity of blood. Carried to the rear on a wagon for three leagues, he suffered beyond description, passed bloody water again, and on his arrival in quarters was bled and had an enema administered. He then became delirious, was bled several times, had blisters applied to the abdomen, suffered from pain at the top of the right shoulder, and took no other nourishment but tea for fourteen days. He gradually recovered, and at the end of seven weeks was sent to England. After remaining some time in London, he joined the depot of his regiment. In consequence of this exertion, he suffered an attack of fever and peritoneal inflammation; and a tumor formed in the site of the posterior wound, which was opened, and discharged several ounces of matter of a urinous odor. Another abscess formed, and was opened. During this time he suffered great pain and became greatly emaciated; the urine diminished in quantity with the frequent calls to pass it. He lingered in this state until the end of July. The flow of matter from the wound was great, and had a urinous smell. The desire to make water was incessant; but it passed only by drops, and brought him to a state of frenzy; the discharge from the wounds, which had been lessening for two days before, suddenly stopped; the pain and pressure of urine became intolerable; he remained at last in a state of the greatest torture for about three minutes, when, during an effort, a burst of urine took place, colored with blood,[539] forcing out with it a hard lump, shaped like a short, thick shrimp, three-quarters of an inch long, which proved, when examined next day, to be the cloth which had been driven in by the ball. It must have passed from the pelvis of the kidney or the ureter into the bladder. It was hard, was covered by a black crust, and was thought to be a stone when passed. It could not, however, have been long in the bladder, or it would have been covered by the triple phosphates, and have formed the nucleus of a calculus requiring to be removed by operation.
Le Capitaine Negre, of the French Infantry of the Line, was struck on the left side above the hip, at the battle of Albuhera, by a musket-ball, which went through the upper part of the sigmoid flexure of the colon, and came out behind, injuring apparently the fourth and fifth lumbar vertebræ. As urine came through this opening, the ureter or lower part of the kidney must have been wounded; and, as he had lost the use of one leg and much of that of the other, the spinal marrow must also have been injured. He was left on the field of battle, supposed to be about to die, and was brought to me to the village of Valverde, three days afterward, in a most distressing state. The inflammatory symptoms had been and were severe; the pain he suffered on any attempt to move him was excessive; the discharge of feces from the anterior wound, and of urine from the posterior one and by the usual ways, rendered him miserable, and he at last implored me to allow the box of opium pills, of which one was given at night to each man who stood most in need of them, to be left within his reach, if I would not kindly do the act of a friend and give them to him myself. He died at the end of ten days, after great suffering, constantly regretting that our feelings as Christians caused their prolongation.
412. Wounds of the spermatic cord are of infrequent occurrence, and rarely lead to fatal, although often to inconvenient consequences.
I have removed the bruised and shattered remains of a testis and epididymis to expedite the cure, and I have been obliged to do so at a later period in consequence of the wounded portion becoming enlarged and diseased. These occurrences are rare; the wound in the testis usually heals kindly; but the portion which remains, however, is probably of little use, although the patient does not like to lose it.[540] A gentleman in perfect health was struck accidentally in the right testis by two shot, while out shooting partridges. The shot lodged, and gave rise to uneasiness, and after a time to an enlargement, which could not be distinguished from medullary sarcoma. I removed the testis, and the wound healed kindly. The lumbar glands had, however, taken on the disease, and he died of their great enlargement and the general mischief which ensued within the year. The preparation is in the museum of the College of Surgeons.
I have not had occasion to tie an artery, even when the penis has been as good as amputated. If bleeding should take place in the progress of the cure, a large catheter should be introduced into the urethra, as a point on which pressure may be made laterally; for I am not aware of any other use it can be, unless the urethra be also torn, when a moderate-sized catheter should be kept in it permanently, if it can be borne, to aid in the healing of the surrounding parts with as little contraction as possible of the canal. When the corpus spongiosum has been carried away or sloughs with the urethra, there is usually some injury done at the same time to the corpora cavernosa, and the part becomes contracted and curved when distended. I have not seen any of these cases since the introduction into practice of the methods which have been recommended by Dieffenbach and others for the formation of a new urethra by borrowing from the neighboring parts; but several might certainly have been benefited by such treatment.
A married soldier, of the 29th Regiment, was wounded on the heights of Roliça, in August, 1808, by a small musket-ball, which went through both corpora cavernosa from side to side. The man suffered very little inconvenience, and the wounds healed very well. He seemed to consider the injury as of no importance to himself, but had some idea there might be a difference of opinion in another party. There is usually a deficiency of substance at the part after such wounds, and sometimes on inconvenient curve or twist, such as often takes place when the corpora cavernosa and the corpus spongiosum are injured or ruptured from other causes.
WOUNDS OF THE PELVIS, ETC.
413. Wounds of the pelvis from musket-balls injuring its contents are of common occurrence, and, although frequently fatal, often permit a considerable length of treatment before they destroy the sufferers or admit of their recovery. In many instances fistulous openings remain for years. The orifices of entrance and of exit of the ball lead to little information. It is only from the absence of paralysis or of hemorrhage, or of those signs which indicate the lesion of any of the organs contained within the pelvis, that the surgeon can form an estimate of the evil which has been committed; even when parts of the greatest importance are injured, such as the bladder or the rectum, the general symptoms are occasionally of little moment.
When paralysis occurs, which it rarely does unless the spinal marrow be injured, the functions of the bladder and of the rectum are implicated, and there is but little pain. When the nerves only are injured, the paralysis is not complete; it usually affects one side more than the other, is a numbness rather than a paralysis, and is accompanied by severe pain, sometimes at the seat of injury, but more usually extending to the thigh and to the extremities of the nerves in the foot. I was consulted in a case of wound from a pistol-shot, in the last dorsal or upper lumbar vertebra, of several years’ standing, in which the paralysis of both limbs was complete. The patient had a great desire to have the cicatrix opened, and the ball followed and extracted, and would willingly have submitted to such an operation, but he could not find any one in London or Paris willing to attempt it.
When a ball appears to cross or pass even from side to side of the pelvis, it is not always easy to say whether it has penetrated the cavity or not, until symptoms indicative of such injury appear; the less done to such wounds the better. When a ball enters, strikes a bone, and lodges, it is very desirable to ascertain its situation, in order that it may be at[542] once removed, if it can possibly be done with but little comparative danger; for balls which lodge in these flat bones may often be removed, and the comfort of the patient assured by a timely operation, instead of proving the source of much torment and misery for many years by their being allowed to remain.
The late Colonel Wade, one of the most distinguished officers of his rank in Spain, was wounded at the battle of Albuhera, in 1811, by a musket-ball on the left side; it passed through the ilium, and was supposed to have narrowly avoided opening into the cavity of the abdomen. It could not be followed beyond the bone. The inflammatory symptoms were subdued in the usual time, and he gradually recovered his health, some pieces of bone coming away from time to time. A small fungous protrusion and discharge continued from the wound for several years, with a certain degree of pain, and of occasional lameness in the leg and thigh. The wound closed sometimes for a few months, and reopened after an attack of pain, with great lameness and swelling of the hip, and a discharge of matter from the original site. An abscess at last formed under the gluteus maximus, and was opened at its anterior and lower edge. This gave great relief and prevented the irritation of the upper and anterior original wound, the matter finding a more ready passage. I often assured him I could distinguish the ball very deeply seated; and in the summer of 1846, thirty-five years after the receipt of the injury, it had descended so far that I passed a probe under it at the distance of two inches and a half from the lower opening. He was to have come to London as early as his duties would possibly permit, in the spring of 1847, to have had it removed, when he was suddenly cut off by apoplexy, to the great regret of all who knew him.
The late General Sir Hercules Packenham, G.C.B., was wounded at the assault of Badajos by a musket-ball, April 6th, 1812, which deprived him of the use of the thumb and little finger, and partially of the hand; and by another which struck him on the right iliac region, passing in just below Poupart’s ligament and outwardly through the ilium. Eight pieces of bone came away at Elvas, and eleven more, in 1813, in London. He went to Baréges in 1814-15-16-17, with the hope that the ball might be loosened and removed, but in vain; it never could be found. A small quantity of[543] inoffensive glutinous matter, sometimes streaked with blood, was discharged occasionally from the seat of the injury. At times the wound became painful and very troublesome for a week or ten days together, after which little inconvenience was felt in the limb.
Colonel Sir J. M. Wilson, now of Chelsea Hospital, was wounded in seven different places by three musket-balls on the left hip, at the Chippewa, near the Falls of Niagara, on the 5th of July, 1814. One, which struck him a little before the trochanter, passed upward through the ilium, (from which several pieces of bone came away on four or five different occasions,) and lodged against or in the spinal column, rendering the left leg quite powerless, and impairing the power of the right. He fell. Shortly after an Indian warrior came up, placed his foot on his neck, drew out his scalping-knife, seized his hair, and was in the act of beginning to scalp him, when a shot passed through his chest and laid him prostrate by the side of his intended victim, who thus happily escaped. The numbness and inability to put the limb to the ground continued from eighteen months to two years, during which time he was on crutches. After this he gradually recovered, always suffering more or less. The pain in the back is often most excruciating, coming on without any apparent cause, except perhaps from change of weather. He limps after walking a couple of miles, and if exercise be continued, pain ensues. He married in 1824, has several children, and is obliged to lead a very regular, quiet life, without which he breaks down. The great suffering he experiences, at the end of near forty years, is, however, from the pain in the back, sense of coldness in the left leg, and numbness accompanied by pain in the course of the nerves. He is equally sensible to heat in a close atmosphere, which he is obliged to avoid. The alvine and urinary secretions, etc. have always been impaired or deranged since the wound was received. He is troubled with painful affections and a train of nervous feelings of the whole system, attributable to the injury. The ball can of late be felt at the bottom of a soft swelling in the loins; but the colonel, since the affair of the Indian, has no predilection for cold steel, and protests as loudly against the scalpel of the surgeon as the scalping-knife of the Indian.
A soldier, of the Fourth Division of Infantry, was wounded at the battle of Salamanca by a musket-ball, which entered[544] immediately above the right ilium, passed across, and made its exit nearly opposite on the left side, going nearer to the back than to the wall of the abdomen. He was supposed to be killed, but had recovered a little life when brought to me at the field hospital some hours afterward. The belly was swollen, generally tympanitic, and some hemorrhage had taken place from the wound of entrance, and he was unable to move the leg of that side. On reaction taking place, he was bled repeatedly, and treated antiphlogistically with the aid of calomel, opium, and antimony. He was removed to the San Domingo Hospital, and on the sixth day the bowels were relieved naturally. A small quantity of fecal matter was passed for several days with the discharge from the wound, but this gradually ceased, and the man ultimately recovered without any particular defect, except weakness and occasional pain and derangement of bowels, on any irregularity.
John Bryan, 1st Light Battalion of the King’s German Legion, was wounded on the 17th of June near Quatre Bras by a musket-ball, which entered at the groin, and made its exit behind. He was transported to Brussels, with his foot and leg in a state of mortification. Wine and other stimulants were freely given, and he rallied a little on the 23d and 24th. On the 25th, the stomach rejected everything except brandy and opium. On the 26th, a line of separation seemed to be about to form between the dead and the living parts, although he was evidently failing. He died on the 28th, eleven days after the receipt of the injury. On examination after death the ball was found to have completely divided the external iliac artery; about a pint of coagulated blood, mixed with some excessively fetid pus, was collected in the pelvis; the ends of the wounded artery had receded considerably from each other, and a coagulum had formed in each, which was easily squeezed out, the orifice of the upper end only being a little contracted. There were signs of some peritoneal inflammation having taken place; the intestines had not been wounded, and the ball, in passing out, had splintered the upper edge of the back part of the ilium.
General Sir Edward Packenham was killed instantaneously at New Orleans, by hemorrhage from a nearly similar wound, in which the common iliac artery was divided.
414. I have removed balls on different occasions which[545] have lodged in the bones of the pelvis, and always with the greatest advantage, when done early. I have seen much evil result from their being allowed to remain, as they caused not only frequent distress, but at last gave rise to disease in the bone, derangement of the general health, and death. When the ball can be felt impacted in the bone, incisions through muscular parts of little consequence should not be spared to expose it. If an error exists at this moment, it is that too little is done, rather than too much. Too great reliance is placed on the efforts of nature, and not enough on the resources of art. The constant meddling with a wound is not recommended; nevertheless, much may be done by careful investigation from time to time, of which La Motte gives a good example in his fifty-first observation.
A grenadier was wounded at the battle of Dettingen, in 1743, by a musket-ball, which entered above Poupart’s ligament, near the opening of the external oblique muscle on the left side, and lodged. Thirteen days after his reception into the hospital at Landau, La Motte felt with the probe what he thought was the ball lying on the outside of the psoas muscle against the bone. He made the patient lie on his face, and touched the foreign body every day in order to loosen it. On the thirty-fifth day he was satisfied it was the ball, and on the forty-fifth, after many attempts, it was at last extracted. His fifty-second observation relates to a case as nearly similar as possible to those of Sir H. Packenham and Colonel Wade. He made several deep and long incisions in search of the ball, which he could not find; the wound became fistulous, and at the end of a year closed, in all probability to reopen from time to time.
The difference in practice between 1743 and 1855 ought to be, that in 1855 the ball should be found first, and the deep and long incisions made afterward for its extraction; which do not preclude any previous external openings that may be necessary to facilitate the first examination.
Captain Campbell was wounded by a pistol-ball, on the 5th of September, 1805; it penetrated the abdomen on the middle of the right side, and was extracted from nearly the same situation on the left; from its irregular denticulated shape, it would appear to have impinged against a vertebra. He complained of violent pain in the loins and belly, with numbness and pain of the left leg and thigh, and suffered[546] also from the greatest oppression, anxiety, and sickness. An enema was administered, and twenty-four ounces of blood were taken from the arm; lower extremities nearly paralyzed; anxiety and oppression great at night. Blood-letting to ten ounces. Cannot pass his urine; hot fomentations; and at twelve at night sixteen more ounces of blood were drawn. At three P.M., had three motions, the two last containing apparently a pint of pure blood. Pain and other symptoms being urgent, eight ounces more blood were taken away. At six P.M., passed urine for the first time, highly tinged with blood; has had two motions, also mixed with blood. Pain continuing, ten ounces of blood were abstracted, although occasionally almost fainting on any movement; belly fomented. At eight at night, sixty drops of laudanum. At ten, being very restless, twenty drops more, which procured some sleep, although he vomited frequently; belly relieved by the fomentation; three stools mixed with blood.
Sept. 6th.—All the symptoms relieved; passes blood with his urine; sickness and vomiting troublesome; pulse 90, rather firm than feeble. One o’clock.—Complains of violent pain in the left leg and thigh, belly, and loins; pulse 116, full and strong. Blood-letting to sixteen ounces. Barley-water with niter for common drink. Six P.M.—Pulse 96; bowels open, with discharge of blood; symptoms generally relieved. Tincture of opium, twelve drops at night.
8th.—Slept better; less pain; paralysis continues. In the evening symptoms aggravated; lost twelve ounces of blood; enema, etc. repeated; pulse 120.
9th, 10th, 11th, 12th.—Pulse 96; bowels open; urine bloody; is generally better.
15th.—Wound of exit healed; urine bloody; bowels open. Chicken-broth for the first time.
20th.—The opening of entrance having nearly closed was enlarged, and a free exit allowed for the matter.
Oct. 20th.—Wounds quite closed; is free from pain, is able to move about the house on crutches; warm, stimulating applications to the limbs seem to have given most relief.
Nov. 20th.—Paralytic affection gone; he can now mount his horse, and has only a feeling of numbness and torpor in the left leg and thigh.
415. The general opinion which formerly prevailed, that wounds of the bladder, by musket-balls, were for the most[547] part mortal, is now known to be erroneous. When the bladder is wounded below, where it is not covered by the peritoneum, persons do sometimes recover by what may be considered the almost unaided efforts of nature. A large number of cases came under my observation at Brussels and at Antwerp, and many had already died. Persons rarely recover in whom urine has found its way into the general cavity of the abdomen. They generally die of inflammation in from three to six days.
When the bladder is wounded where it is covered by the peritoneum, and the opening or openings do not by some accident permit the urine to flow into the cavity of the abdomen, the patient may be free from immediate danger for a short time, although very anxious and greatly depressed in countenance and manner, and even sick to vomiting. The pain is not commonly severe at first, and if he can make water, which in all such cases it is desirable to prevent by having recourse to the catheter, it is more or less colored or mixed with blood. If the urine should not escape into the cavity of the abdomen, the ordinary inflammation which must necessarily ensue takes place and affects the internal surface of the bladder. The desire to pass urine becomes greater, and is frequently insupportable, while it can in some cases be only passed by drops. In others these symptoms are less urgent. Nevertheless, the natural action of the bladder, or, in those severe cases, the additional efforts which are made for its expulsion by the abdominal muscles, may cause the urine to be forced through the wound into the cavity of the abdomen, whence the advantage to be obtained from the early use of the elastic catheter. When the orifices of entrance and of exit are free, and low down in the pelvis, the urine may run out without much immediate mischief ensuing. But as this cannot always be known, an elastic gum catheter should be introduced from the first and fixed in the bladder, in every case where the nature of the injury is doubtful, until the urine ceases to flow through the wounds. It must, however, be recollected that in some cases in which it has caused great irritation, by being introduced too early, while the bladder was very sensitive, the patients have been much relieved by its removal. The principle is nevertheless incontrovertible in all doubtful cases; the urine should be allowed to drop out of the catheter nearly as fast as it passes into the bladder, when this organ[548] is very irritable; great pains should also be taken that the end of the instrument should be within, but not too far within the bladder, so as to excite irritation by rubbing against its sides, or to allow its end rising above the urine which might in this way collect below it, and at last escape through the wounds.
416. The inflammatory actions are to be subdued by general bleeding, the application of leeches, the administration of diluent drinks in moderate quantity, the exhibition of gentle aperients, such as castor-oil, and by enemata. Opium in all these cases is an important remedy, principally in the shape of morphia. Opium in substance, when introduced into the rectum in the shape of a suppository, or dissolved in half an ounce or an ounce of water as an enema, should be repeated in such quantities, beginning with two grains, as will procure ease.
417. The urine, in most cases of injury below the peritoneum, flows readily through the wound of entrance, if not of exit, in the first instance, and care should be taken, by enlarging the posterior wound, that no obstacle within reach shall prevent it; but after inflammation has been established, the parts swell, and as the sloughs begin to separate, its passage is often obstructed; the elastic catheter, if not used before, will then render important service by allowing the sloughs to be separated without the healthy parts being irritated by the urine being retained. After a time the urine may be only drawn off in small quantities through the catheter, as frequently as circumstances may render advisable. The permanent use of the catheter in these cases will often prevent the urine from forming any devious paths as it proceeds outward, ending in abscesses and fistulous openings, causing much discomfort and even misery. It is not common for blood to be poured into the bladder in such a quantity as to cause much inconvenience; it coagulates with equal proportions of urine, and a silver catheter should be used, by which it may be broken up and rendered more easy of solution by injections of warm water. When the neck of the bladder or the prostatic part of the urethra has been divided so that a catheter cannot be efficiently used, surgery must come with more immediate aid to the assistance of the sufferer, by making a clear and free opening from the perineum for the evacuation of the urine and of the discharge from the wound. If a ball lodge in or near the bladder, or[549] in the prostate, it must be removed by an operation in the perineum.
A soldier of the Light Division was wounded on the heights of Vera, in the Pyrenees. A musket-ball had entered behind near the sacrum and lodged. He was bled twice, in consequence of suffering pain in the part, but was not otherwise much disturbed. There was at first a difficulty in passing urine, but this gradually subsided, although he always suffered pain in micturition, which was frequent and distressing. He remained in this state until December, when he passed, with considerable effort and after much difficulty, a hard piece of his jacket about half an inch in length, larger than the orifice of the urethra, through which it was forced. As it was not incased by calcareous matter, it could not have been long in the bladder, but must have been lodged near it before it ulcerated its way in, giving rise to the constant desire and irritation which he had so long experienced. His symptoms then subsided, although they had not entirely disappeared when he left for England.
A French soldier was wounded by a musket-ball on the back part of the right hip, at Almaraz, on the Tagus, was taken prisoner, and sent to Lisbon in the autumn of 1813. The ball had lodged, but gave him little inconvenience at the time beyond some pain in the course of the sciatic nerve, subsequently followed by defect of motion on the right side. Four months after the injury pain came on about the region of the bladder, with great desire to pass urine, which he could not do when standing, but which dribbled away when lying down. When quiet he suffered little, but great pain followed any attempt at continued motion. A catheter could be introduced, but with great difficulty when it reached the prostate gland, which was exceedingly tender to the touch. After a time the instrument could not be passed, and the man was in great agony until something appeared to give way, and a discharge of matter took place, when the urine followed, and he was relieved. An abscess had formed, in all probability from the proximity of the ball, which still could not be felt. The man recovered, retaining, however, his former state of lameness and defect of power, although relieved from the vexatious irritation of the bladder.
A soldier of the Fourth Division of Infantry was wounded at the battle of Toulouse, while entering a redoubt, by a musket-ball, which entered at the left groin, and, crossing[550] the pelvis, came out on the upper part of the opposite hip behind. The urine flowed from both wounds and from the rectum, indicating that the ball had passed between these parts, and a little feces came from the posterior wound for three weeks. The pain and suffering were not great, and principally arose from retention of urine, requiring the use of the catheter, which was left in, and changed from time to time, until the urine flowed by the side of it, instead of through the wounds, which it did occasionally for some weeks in drops, but not in any quantity; after which the wounds gradually closed, and the man was sent to England cured.
A soldier of the Cavalry of the King’s German Legion was struck, at the battle of Salamanca, by a musket-ball, which entered just above the pubes a little to the right side, and came out below on the opposite nates. The urine flowed readily through both wounds for the first three days, and he suffered afterward from great pain and distress about the region of the bladder, from which he could not expel any urine, neither would it pass by either wound. I immediately introduced a catheter, drew off a moderate quantity of urine, and then fixed it in the bladder, desiring him to draw off his urine every hour when awake. This he did, often leaving the stopper out at night. The urine flowed after a few days through the posterior wound, and then ceased. The catheter was washed from time to time, and was at last withdrawn, as the urine began to flow by the side of it, and the wound had finally closed when he left the San Domingo Hospital.
Captain Martin received a wound from a musket-ball at the siege of Ciudad Rodrigo; it entered just above the pubes, passed through the bladder and rectum, and came out behind, splintering the sacrum, the contents of both viscera being freely discharged through this opening. As he suffered but little inconvenience from the urine, very little of which passed by the urethra, that passage was not interfered with in the first instance. Inflammatory symptoms were kept within due bounds, the rectum was carefully washed out by emollient enemata, and his food rendered as light as possible. Under this treatment he gradually improved; the anterior wound first healed, and subsequently the posterior one, leaving him comparatively well when he left me for Lisbon on his way to England.
[551] 418. These cases give, however, a brighter view of the nature of these wounds than they frequently justify; extravasation of urine, inflammation, and death are not of infrequent occurrence in cases to which strict attention is not paid; and great misery is often caused from the irritation of the bladder and the discharge which follows, until the constitution is undermined and death ensues.
Captain Sleigh, of the 100th Regiment, was wounded at the battle of Chippewa, on the 5th of July, 1814, by a musket-ball, which entered the left groin immediately over Poupart’s ligament, by the side of the spermatic vessels, injuring in its course the anterior brim of the pelvis. It thence passed through the bladder obliquely across the pelvis, and terminated its course beneath the integuments in the right buttock, whence it was immediately extracted. Blood and urine flowed incessantly from the groin; the quantity of blood lost was considerable. He complained much of pain in the hypogastric region; the abdomen was tense and painful to the touch, and he had an almost continued inclination to micturate; but his attempts, after the most painful efforts, were entirely frustrated. The anxiety was great, the respiration hurried, and the pulse quick and fluttering. He was bled to the extent of thirty ounces; an enema was given; fomentations applied to the belly; and the catheter introduced—all which afforded him some relief. The next day he was removed to the rear, a distance of seventeen miles, in an open wagon, partly during the inclemency of the night, and was quite worn out by so long a journey. He was carried thence on board ship, and landed at York on the morning of the 9th of July, the fourth day after he received his wound.
July 9th.—Abdomen tense and painful to the touch; severe pain in the perineum; great inclination to void urine, but fruitlessly; wound in the groin sloughy, discharges urine and blood mixed with a small quantity of pus; posterior wound healthy, no discharge of urine from it; catheter attempted to be passed without success. Ordered an ounce and a half of castor-oil immediately.
10th.—Passed a restless night; had two copious stools; voided a few drops of urine by the urethra; still great inclination to pass urine. Ordered two grains of extract of opium made into a pill.
11th.—All the painful sensations much relieved; abdomen[552] less tense; a small piece of bone extracted from the urethra about an inch in length, of the thickness of a crow-quill; a little urine followed more freely.
15th.—Complains of severe pain in the spermatic cord; discharge from groin more offensive; wound filled with large maggots; bowels open.
19th.—Wound of groin looks clean; a small piece of bone discharged by the urethra, and a piece of cloth extracted from the groin.
24th.—A small piece of bone extracted from the groin.
August 5th.—Passes a good deal of pus and urine by the urethra.
29th.—Posterior wound much inflamed and very painful upon pressure. A poultice to be frequently applied.
Sept. 1st.—An abscess has burst; a piece of cloth has been extracted; urine and pus are discharged by both wounds.
12th.—Doing well; wounds closing.
16th.—Bladder resuming its power; discharge of matter from groin very trivial.
Oct. 4th.—Posterior wound closed.
30th.—Wound of groin closed; urine, passed by the natural passage, mixed with pus.
At first it was supposed that only the fundus of the bladder was wounded; but when the collection of matter took place in the right buttock, and a piece of cloth was extracted from it, the urine following, it was evident that both sides of the bladder had been transfixed by the ball; and that, probably, the urine from the commencement had been prevented flowing posteriorly by the intervention of this foreign body. An elastic gum catheter could not be passed into the bladder on account of the piece of bone which had forced its way into the urethra, and from its being obstructed afterward by smaller pieces of bone.
When I saw this gentleman some time afterward, it appeared to me that the purulent discharge from the urethra was not from the inner membrane of the bladder, but was probably caused by some dead bone of the pelvis having a communication with the bladder by a fistulous opening.
A soldier, of the King’s German Legion, was struck, at Waterloo, by a musket-ball, which entered a little way above the pubes, and lodged. The symptoms which immediately followed were by no means severe, although he passed a[553] little bloody urine at first; the external wound closed without difficulty. He complained of pain at the neck of the bladder, and had a great desire to pass urine, with other signs of stone in the bladder, which induced me to pass a sound, when I found that the ball was lying loose in that viscus. On his arrival at the York Hospital, at Chelsea, from Brussels, he became, with the French soldier, whose thigh had been amputated at the hip-joint, an object of great attention. I performed the operation for the removal of the ball in the presence of a large concourse of military and medical persons. It was done in less than two minutes; but the calculus, composed of the triple phosphates, which had formed around the ball, yielded, and broke under the forceps. The pieces were removed separately. The ball, being heavy, fell below the neck of the bladder, which, being healthy, yielded to the pressure, and allowed it to sink on the rectum, where it could not be caught by the forceps, until it had been raised by a finger in the bowel. The bladder was then well washed out, so as to remove all the pieces that might remain, and the man was placed in bed. He was bled once in consequence of some apprehension of pain; but he had not a bad symptom, and rapidly recovered.
The symptoms of irritation did not, however, entirely pass away, as could have been wished, and I began to fear that some small pieces of calculus had been overlooked; when, one morning, after considerable effort, he passed a ring of sandy calcareous matter, which had formed around the orifice of the bladder, and which, being dislodged, had fortunately entered the urethra, along which it was forced by the urine. It was evidently formed of the phosphates in minute portions, which had become agglutinated together, around the meatus of the bladder. This he took with him to Hanover, where it, himself, and the cicatrixes of his wound, and of his operation, attracted great notice. The ball, which was flattened on one side, I kept in a small box, together with the pieces of calculus which were extracted, and showed them annually at my lecture on this subject for many years. One evening, however, I unfortunately left my little box on the table after lecture; and when I recollected, and returned for it, I found that some gentleman had borrowed it, and has not yet returned it. At the battle of Chillianwallah a similar wound took place; the ball formed the nucleus of a calculus, and was removed successfully by a gentleman in the[554] service of the East India Company, whose name I have not been able to learn.
The following case, from Baron Percy, is in point: A young man was wounded by a pistol-shot, which entered just above the os pubis, through the linea alba, wounded the bladder, and lodged. The belly swelled; a tumor formed in the perineum; no urine passed; the bowels were confined, and fever ran high, with a tendency to delirium. Believing that the tumor in the perineum, and the fluctuation he thought he perceived, might be caused by extravasated urine, he punctured it with a trocar, and evacuated a large quantity of bloody urine. This induced him to enlarge the opening, and carry it on to the bladder, through which he brought out the ball, some shirt, and several clots of blood. The man was bled nine times in all; the urine after a time passed in the ordinary way, and the patient slowly recovered.
An officer was wounded near Bayonne, by a musket-ball, on the left side; it passed through the ilium across the pubes, and made its exit through the gluteus maximus of the opposite side, but lower down. Urine flowed through both wounds at first very readily, but none of any moment came by the urethra, from which some blood occasionally oozed. The attempt to pass a catheter failed, although the desire to make water was urgent and painful. After a few days the passage of urine by the external wounds became obstructed, apparently by the sloughs; great pain and misery were experienced; fever ran high; rigors and delirium followed extravasation of urine, and death closed the scene. The mischief here arose from the catheter not having been passed into the bladder, which could not be effected, from the prostatic part of the urethra or the neck of the bladder having been injured.
419. Surgery in such, or in nearly similar cases, requires a catheter or staff to be passed down the urethra as far as it will go; an incision should then be made upon it, from the center or across the perineum, and the urethra divided on the staff until the finger rests upon the wounded parts, when, in all probability, a straight catheter, with the aid of the forefinger in the rectum, can be carried through them into the bladder. The urine will then have a direct passage outward, instead of coming indirectly from the bladder by the wounds. If the straight catheter cannot be passed, which can scarcely occur, the central incision is to be continued[555] from the point of obstruction into the bladder, guided by the finger in the rectum. A free opening from the bladder offers the only hope of safety.
420. The rectum may be wounded without any other organ being injured within the pelvis; of this I have seen several instances. Captain Gordon, of the navy, was struck by a rifle-ball toward the lower part of one side of the sacrum, after being knocked down by one he had received on the head, and by another in the neck and back. The ball, which passed into the rectum, made its exit on the opposite side of the sacrum, and stercoraceous matters were evacuated by both wounds. The pain was severe; the limbs were deprived of much of their power of motion, and the next day the bladder was incapable of expelling its contents. This was relieved by the catheter, and the rectum was kept clear by warm, mild enemata, while the inflammatory symptoms were subdued by bleeding, opium, starvation, and rest. At the end of three months he was able to walk, but with some difficulty, on account of defective power in one leg. Some small pieces of bone came away and the wounds closed, although he was subject to an occasional slight opening of the orifice of entrance, from which a little matter was discharged, when it again closed. He remained more or less lame until his death, which took place with the loss of the ship he commanded, in a hurricane, on the coast of North America.
A French soldier was wounded at the battle of Salamanca by a ball, which entered by the side of the sacrum, and lodged. Having been rode over and bruised, he was taken prisoner, and brought to me on the field of battle. From this wound he suffered comparatively little, except from a difficulty of passing urine. On the third day after his arrival at the San Carlos Hospital, or the sixth from the receipt of the injury, he passed the ball per anum. The wound quickly closed, and he aided his comrades as an orderly in the hospital afterward.
421.—1. Severe blows on the abdomen give rise to the absorption of the muscular structures, and the formation of ventral hernia, in many instances; this may, in some measure, be prevented during the treatment, by quietude, by the local[556] abstraction of blood, and by the early use of retaining bandages.
2. Abscesses in the muscular wall of the abdomen, from whatever cause they arise, should be opened early; for although the peritoneum is essentially strong by its outer surface, it is but a thin membrane, and should be aided surgically as much as possible.
3. Severe blows, attended by general concussion, frequently give rise to rupture of the solid viscera, such as the liver and the spleen, causing death by hemorrhage. When the hollow viscera are ruptured, such as the intestines or the bladder, death ensues from inflammation.
4. Incised wounds of the wall of the abdomen to any extent rarely unite so perfectly (except, perhaps, in the linea alba) as not to give rise to ventral protrusions of a greater or less extent.
5. As the muscular parts rarely unite in the first instance after being divided, sutures should never be introduced into these structures.
6. Muscular parts are to be brought into apposition, and so retained principally by position, aided by a continuous suture through the integuments only, together with long strips of adhesive plaster, moderate compression, and sometimes a retaining bandage.
7. Sutures should never be inserted through the whole wall of the abdomen, and their use in muscular parts under any circumstances is forbidden; unless the wound, from its very great extent, cannot be otherwise sufficiently approximated to restrain the protrusion of the contents of the cavity. The occurrence of such a case is very rare.
8. Purgatives should be eschewed in the early part of the treatment of penetrating wounds of the abdomen. Enemata are to be preferred.
9. The omentum, when protruded, is to be returned by enlarging the wound through its aponeurotic parts if necessary, but not through the peritoneum, in preference to allowing it to remain protruded, or to be cut off.
10. A punctured intestine requires no immediate treatment. An intestine, when incised to an extent exceeding the third part of an inch, should be sewn up by the continuous suture in the manner recommended, Aph. 391.
11. The position of the patient should be inclined toward the wounded side, to allow the omentum or intestine being[557] closely applied to the cut edges of the peritoneum. Absolute rest, without the slightest motion, should be observed. Food and drink should be restricted, when not entirely forbidden.
12. If the belly swell, and the propriety of allowing extravasated or effused matters to be evacuated seem to be manifest, the continuous suture or stitches should be cut across to a certain extent, for the purpose of giving this relief.
13. If the punctured or incised wound be small, and the extravasation or effusion within the cavity seem to be great, the wound should be carefully enlarged, and the offending matter evacuated.
14. A wound should not be closed until it has ceased to bleed, or until the bleeding vessel has been secured, if it be possible to do so. When it is not possible so to do, the wound should be closed, and the result awaited.
15. A gunshot wound penetrating the cavity can never unite, and must suppurate. If a wounded intestine can be seen or felt, its torn edges may be cut off, and the clean surfaces united by suture. If the wound can neither be seen nor felt, it will be sufficient for the moment to provide for the free discharge of any extravasated or effused matters which may require removal.
16. A dilatation or enlargement of a wound in the abdomen should never take place, unless in connection with something within the cavity rendering it necessary.
17. If the epigastric, circumflexa ilii, or other artery in the wall of the abdomen, be injured and bleed, the wound should be enlarged, and the bleeding vessel secured by ligature. If the main trunk or the external iliac artery be sought for and tied, the patient will in all probability die.
18. When balls lodge in the bones of the pelvis, they should be carefully sought for and removed, if it can be done with propriety and safety.
19. In a wound of the bladder, an elastic gum catheter should be kept in the urethra, frequently without a stopper, until the wound is presumed to be healed—unless its presence should prove injurious, from excess of irritation, not removed by allowing the urine to pass through it by drops as it is brought into the bladder.
20. In all cases in which a catheter cannot be introduced, in consequence of the back part of the urethra or the neck[558] of the bladder being injured, an opening for the discharge of the urine should be made from the perineum into the bladder. It is essential to the preservation of life.
21. The treatment of all these injuries must be eminently antiphlogistic, principally depending on general and local blood-letting, absolute rest, abstinence from food, and in some cases almost even from drink, the frequent administration of enemata, and the early exhibition of mercury, and especially of opium, in the different ways usually recommended, with reference to the part injured.
422. As the operation for opening into the colon may be necessary, after an injury of that part, as well as from disease below it, the following method, recommended by Mr. Hilton, is briefly transcribed from the Reports of Guy’s Hospital. A line drawn parallel to the spinous processes directly downward from the angle of the seventh, eighth, or ninth rib across the costo-iliac space to the crest of the ilium, will correspond with the outer edge of the erector spinæ muscle and the apices of the transverse processes. A measured inch outwardly corresponds with the outer edge of the quadratus lumborum muscle. A vertical incision, two inches long, made at the extremity of the measured inch, should divide the skin, cellular tissue, and the tendon of the internal oblique muscle, and expose the outer edge of the quadratus lumborum muscle. Any bleeding vessels to be secured. The last dorsal nerve, if seen lying across the upper part of the incision, should be divided, to prevent the occurrence of pain from its being engaged in the cicatrix. The transversalis abdominis muscle is then to be divided vertically to nearly the same extent of two inches, parallel to the edge of the quadratus, when a quantity of loose lobulated fat will be seen, which should be partly removed and partly displaced by the blunt end of a director, in the vertical direction of the original incision, when the intestine will be brought into view. Any bleeding vessels should be secured, and pressure made on the abdomen, which will cause the intestine to become more prominent at the bottom of the incision. A silk ligature is now to be passed into the bowel and through the integuments at the upper part, so as to fix the intestine above, when a second ligature is to be applied in a similar manner below. The intestine is then to be opened between them, care being taken to apply another[559] ligature above and below it, if the intestine should not appear to be firmly held in its place. If a vessel in its wall should bleed, it must be tied. Inflammation, pain, and restlessness should be obviated as far as possible by fomentations, opiates, and diaphoretics, and strict attention paid to cleanliness and the comfort of the patient, until the first symptoms have passed away, and he is able to assume the erect position.
423. These commentaries are restricted to those points which constitute, in a great degree, what the French call la haute chirurgie. They are published that every soldier should have the opportunity of knowing how he ought to be treated, when suffering for a country not too grateful for the services rendered by her bravest sons; and I have labored with the hope that some few of them, when they find that their limbs, perhaps their lives, have been saved under the precepts I have laid down, may acknowledge, when I am beyond that bourn whence no traveler returns, that they owe them, under the will of God, to those efforts I, more than any one else, have made, and continue to make, for the adoption of that practice which led to their preservation.
Several reports and cases having reached me from various medical officers in the Crimea, too late for publication in their proper places, I have thought it best to notice some generally as to results, others particularly. Chloroform has been freely administered in all the Divisions of the army save the Second, and has been generally approved; one death only, as far as is known, having occurred directly from its administration, of which Staff-Surgeon Gordon, P.M.O. of the Second Division, has favored me with the following report:—
Martin Kennedy, 62d Regiment, aged 32 years, a healthy soldier, having accidentally wounded one of his fingers by his musket going off, and the medical officer in charge considering it necessary to remove it, was brought under the influence of chloroform, but, according to his (the surgeon’s) statement, only about ʒij could have been inhaled. He had commenced the operation, when the patient suddenly expired. On the post-mortem examination, beyond a little fatty deposit on the external surface of the left ventricle, together with a degree of hypertrophy of the same, no morbid appearance existed. The usual restoratives were resorted to, but ineffectually.
The following case, furnished by Assistant-Surgeon Hannan, 49th Regiment, is given as an illustration of the success of amputation without chloroform in the Second Division:—
Patrick Kenny, 49th Regiment, aged 22. This soldier, while on duty in the trenches on the 21st of July, received a compound comminuted fracture of the right humerus, extending from its middle third to the head of the bone. The integuments of the outer and upper part of the shoulder were carried away. There was also a contused and lacer[562]ated wound of the left knee, opening into the joint, with comminuted fracture of the patella, these injuries being caused by pieces of shell. He was seen a quarter of an hour after admission by Dr. Gordon, P.M.O., who removed the arm at the shoulder-joint, making a sufficient flap from the integuments of the axilla. The thigh was then amputated in its lower third. These operations were performed in immediate succession without the administration of chloroform. The thigh healed nearly by the first intention—all the ligatures having come away by the fourteenth day. The shoulder healed by granulation—the ligature of the axillary artery coming away on the twenty-first day. During the progress of treatment he had not any constitutional disturbance further than three slight attacks of diarrhœa. He is now up and about, and goes to England by the next opportunity.
In the worst cases of amputation at the hip-joint, or at the upper third of the thigh, chloroform has appeared to cause insensibility to pain without diminishing the powers of the sufferer, when given with due caution or not carried so far as to affect the pulse or respiration. (See Aphor. 51.) The evidence on this point is sufficient to authorize surgeons to administer it in all such cases, with the expectation that it will always prove advantageous, an accidental death, such as has been observed from its use, being independent of the nature of the injury. The amputations performed at the hip-joint, at least six in number, have not been successful as to the result, although the sufferers bore them well in the first instance, offering every prospect of recovery for days and even for weeks.
Deputy Inspector-General Taylor informs me, and his opinion is corroborated by all the medical officers, that the labors the troops had to perform, the privations they suffered, the frequent insufficiency of their food, the want of proper clothing, with other depressing causes, had so deprived them of that power British soldiers generally possess, that all the operations of importance performed on the lower extremities were more or less unsuccessful, while those on the upper were as remarkable for their success. This deprivation of power, it is said, was even more observable in the French army; and he informs me that most of their surgeons had declined performing any of the great operations usually done on the upper third of the thigh, in conse[563]quence of their almost certain failure, preferring to let the injuries take their course, even unto the death of the sufferers, rather than hasten their dissolution by any operation usually considered and often found to be conservative; a lamentable state of things from which governments may draw an inference of the utmost importance, viz., that to guard against the effects of disease as well as of injuries, the utmost pains should be taken to preserve the health and maintain the vigor of their soldiers. A matter of expense as well as of arrangement.
This statement is corroborated by Deputy Inspector-General Alexander, who informed me, on the 3d of August, 1855, that “during the whole of this campaign, where we have had ample opportunities of testing the use of chloroform, both after the battles of the Alma and Inkerman, as well as throughout the whole siege operations before Sebastopol, up to the present period, no operations whatever of any consequence (save with one or two exceptions, and then at the patients’ own request,) have been performed in the Light Division, without first placing the patient under the influence of chloroform, and in no single instance have either the medical officers of the Division, or myself, seen any bad results follow, or had to reject its use, but quite the contrary. Of course, in such a campaign, many operations of the most serious character, both on the upper and lower extremities, have been performed in the Division by the different medical officers as well as by myself. At the Alma, I operated upon three patients at the hip-joint, two being our own men and the third a Russian. All the three patients were first placed under chloroform, with the results above stated. In the case of a soldier of the 90th Regiment, whose right arm I removed at the shoulder-joint on the 10th of July, for great destruction of the soft parts and extensive injury to the humerus, the patient was so low when placed on the table that brandy and water was given to him, and he was then immediately afterward placed under chloroform. When I had finished, it was found that his pulse was stronger than before commencing the operation. In Sir T. Trowbridge’s case, in which I had to remove both feet, one at the ankle-joint and the other above it, he was placed under chloroform for both operations, a few minutes having been allowed to elapse before giving it to him again for the second operation, and with the best results. Both feet were much injured [564] by round shot, the bones of both being completely smashed with great destruction of the soft parts, so much so, that in the case at the ankle-joint I had to form the flap from the cushion of the heel. I, however, did not remove the articular surface of the lower end of the tibia, as recommended by Mr. Syme, and the wound healed well. Of the three cases mentioned at the hip-joint, two were performed on the 21st, and the Russian on the 22d of September. At one of the former I was assisted by the late Dr. Mackenzie, from Edinburgh. All three were carried down on the 22d, to be placed on board ships for conveyance to Scutari. It has been reported to me that one of the two operated on, on the 21st, Peter Sullivan, 33d Regiment, died at Scutari General Hospital on the 11th of October, three weeks from the date of the operation, ‘from excessive debility.’ Nothing could be ascertained about Peter Cleary, 23d Fusiliers; it is therefore most likely that he died on the passage.
“The Russian died on the 22d of October, ‘from great debility and extensive sloughing.’
“A shoulder-joint case in the 90th Regiment never had a bad symptom, and the wound is all but healed. The flap in this case was made from the axillary portion of the arm, the deltoid having been all but destroyed.
“The flap operation has been invariably performed in the Light Division, with but two exceptions, viz., one of the arm and the other of the thigh.”
Excision of the head, neck, and trochanter of the femur, with portions of the shaft, has been performed at least six times before Sebastopol. The result has been unfavorable in five, although in all there were well-grounded expectations of success for weeks. In one case by Mr. Blenkins, of the Grenadier Guards, he informs me, it was for the first three or four weeks very favorable. The man, however, sank at the end of the fifth week from deposition of matter in the knee-joint. (See p. 42 et seq.) Of the second case, which occurred in the general hospital in the camp and ended fatally, I have no further notice. The third, in the 68th Regiment, in charge of Mr. O’Leary, the operation performed on the 19th of August, was going on most favorably on the 5th of October.
Private Thomas M’Kenena, aged twenty-five, was struck by a fragment of shell, on the 19th of August, over the great trochanter of the left femur. The wound, nearly an inch in [565] length, extended down to the bone, which was distinctly fractured. Some loose scales could be felt at the bottom of the wound. On examination, the injury appeared to be a transverse fracture of the neck of the thigh-bone, apparently involving the joint.
After a consultation with superior medical officers, it was decided that excision should be performed, which was done without difficulty. No vessels required ligature, although the man lost a considerable quantity of blood.
The excised parts, which are herewith forwarded, show that the nature of the injury was different from what it was supposed to be, and that the head of the bone was intact.
After the wound, about five inches long, had been sewn up, the limb was placed in a sling made of strong canvas, and was swung from a beam over the man’s cot, the bed being raised.
This method of treatment was adopted with a view to encourage approximation of the upper end of the bone to the pelvis, and by pressure on the sides of the limb to prevent the accumulation of matter among the tissues. The man progresses favorably.
Diet was very generous.
J. C. O’LEARY,
Surgeon, 68th Light Infantry.
Camp, 4th Division, Crimea, Sept. 14, 1855.
The bones removed are in the museum of the Royal College of Surgeons.
The fourth case is given at length by Staff-Surgeon Crerar, as follows:—
Private William Smith, First Battalion First Royals, was brought to hospital from the Greenhill trenches, in front of Sebastopol, about twelve P.M., on the 6th of August. On questioning him, I ascertained that an hour or so before he was struck by a fragment of an exploded grenade, which first broke into small pieces a water canteen which was suspended over the left hip, and then made an opening or wound about the size of a shilling nearly a quarter of an inch posterior to the great trochanter. Crepitus was quite distinct on moving the limb; and I easily ascertained, on exploring the wound with my finger, that a fracture through the trochanter had taken place, but was quite unable to ascertain to what extent upward and downward the fracture extended. [566] I accordingly solicited a consultation with Deputy Inspector-General Taylor and Staff-Surgeon Paynter. After a careful examination, (the patient being under the influence of chloroform,) the femur was discovered to be comminuted. Excision at the hip-joint being recommended by these officers, in which opinion I concurred, I proceeded to perform the operation by commencing an incision, nine inches in length, in a line with and two inches posterior to the anterior superior spinous process of the ilium, and carrying it down in a straight line directly over the trochanter major; a second incision about two and a half inches in length was made, commencing immediately below the trochanter backward through the gluteus maximus; by a little easy dissection the seat of fracture was exposed, the trochanter was found broken into several portions, detached and imbedded in the contused muscles around, from which they were at once removed. The fracture was found to extend obliquely inward about an inch and a half along the shaft of the bone. The femur was now protruded through the wound, and I sawed off the whole of the fractured bone, leaving a smooth, clean surface; I then proceeded to disarticulate the head of the femur, which was effected without difficulty. Scarcely three ounces of blood were lost, and little or no shock was induced; only one small bleeding point was secured near the tail of the wound, and the divided parts were brought together by two sutures and bands of adhesive plaster.
At twelve A.M., two hours after the operation on the 7th instant, his pulse being rather feeble, he was ordered some wine and water.
7th, vespere.—Countenance cheerful, voice strong; says he intends keeping up his pluck, and is sure he will get well; has no inclination to take the beef-tea ordered for him, but has had some arrow-root and wine. To have a morphia draught at bedtime.
8th.—Passed a good night; limb in a good position; retracted about two inches; wound looks healthy; pulse 100, soft; has made urine freely; skin moist; bowels were opened freely in the night.
9th.—Slept well at night; says that he feels very comfortable; skin moist; pulse 120; sutures were removed, and the wound allowed to gape; it has a remarkably healthy appearance. To go on with the simple water dressing, chicken-broth, arrow-root, and wine.
[567] Vespere.—Has been very cheerful all day; limb has retracted about another half inch; pulse 112.
10th.—Passed a more restless night, in consequence of not having the morphia draught as early as the previous night; has had several hours’ sleep this morning, and is more refreshed; pulse, on waking, from 114 to 120, skin comfortable; no sign of distress in his aspect; wound suppurating healthily; bowels were opened again once last night.
10th, vespere.—Has been very easy all day; skin cool; tongue normal; pulse 120, soft and regular; has had to-day two eggs, one ounce of arrow-root, two gills of wine, and two pints of chicken-broth, all of which he relished much. To have a grain of acetate of morphia in solution at bedtime.
11th.—Slept soundly all night; when I visited him, at six A.M., he had just awoke; pulse 115, soft; appears contented and comfortable.
Vespere.—Doing well; wound continues to look healthy; position of limb good; has consumed a fair quantity of chicken-broth, beef-tea, arrow-root, and three gills of sherry to-day; pulse 113 at eight P.M.
12th.—Bowels were opened in the night; the introduction of the bed-pan gave him a good deal of annoyance; the air of the hut was rather stagnant last night, and he did not sleep as well as usual; pulse 120, soft; tongue continues clean and moist; there is more discharge from the wound to-day.
Vespere.—The progress of the case is most satisfactory; had a fresh egg, tea, and toast for breakfast, his own selection, which he appeared to relish greatly; at twelve he had two mutton-chops and a glass of wine, and at five P.M., a pint of chicken-broth, with bread, and a second glass of wine. The morphia draught as usual.
13th.—Continues to look happy and contented. Healthy-looking granulations are evident over two-thirds of the wound; swelling of limb subsiding; discharge from wound healthy; pulse 114, regular and soft; all the symptoms are so very favorable that I have every reason to expect a successful issue.
14th.—A small slough at the lower part of the wound, remainder healthy and clean; tongue a little too dry this morning, and he has more thirst than usual; pulse 118. To have [568] effervescing draughts of bicarbonate of potassa and citric acid three times a day; to continue simple water dressing.
Vespere.—Thirst not so urgent; tongue cleaner and moister; has a feeling of fullness in the abdomen. To have his usual morphia draught and an ounce of castor-oil at bedtime.
15th.—Passed three large stools in the night, with great relief; aspect resigned, and his spirits continue good; slough has come away; pulse 118, soft and regular; skin tolerably cool.
Vespere.—Felt a good deal exhausted to-day from the heat, which was very great—ninety-two degrees.
16th.—Looks heavy and out of spirits this morning; discharge has increased, but is of a better quality since the slough separated; tongue dry, inclined to brown; pulse the same, skin rather hot; continue effervescing draughts every third hour.
Vespere.—Tongue more moist, less thirst. When asked how he felt, he replied, with a great deal of life in his countenance, “I am very well, and I feel very comfortable;” asked for a mutton-chop early in the day, which he got, and appeared to like; he had at different times in the day arrow-root, chicken-broth, and wine.
17th.—Wound looks very healthy, and the general symptoms very favorable to-day; tongue clean and moist; less thirst; skin cooler; had him removed to a fresh bed without a great deal of pain or trouble; limb retracted less than three inches; position now good since he was shifted.
18th.—Very much worse this morning; had a rigor about ten A.M. yesterday; features now sharpened and pinched; tongue dry and brown; pulse thready, about 125.
Vespere.—Continues in a very low state; wound has a very healthy appearance; discharge healthy, but not as abundant as it was; has had besides wine, a pint and a half of porter, mutton-broth, and a chop to-day; zinc lotion to the wound.
19th.—When I visited him at six A.M. to-day, I was much pleased to find him looking quite cheerful; pulse soft, 112; skin cool and moist, paler than usual; wound doing well. Continue zinc lotion to the sore, and to have his choice to-day of mutton-broth, beef-tea, or chicken-broth; arrow-root to be given twice, four gills of sherry or port as usual.
Vespere.—No change to report.
[569] 20th.—Looking rather pale, and features pinched; pulse better, about 100, soft; skin cool; tongue more coated than usual, inclined to be dry. I fear this case is a bad one, not likely to terminate as we so much desire.
Vespere.—Has been very uneasy all day; skin hot; tongue dry.
21st, six A.M.—Has just awoke, having been asleep since nine last night; says that he feels stronger; aspect certainly improved since the last visit; coating on the tongue thicker, brown; the pulse has more strength than it had yesterday; no feeling of uneasiness; wound looking remarkably well, and discharging laudable pus; asks for cold drinks; to have his choice of iced soda, tamarind, toast or rice water; diet the same as yesterday.—Eleven A.M.: has fallen off very much since the morning, features pinched and blue; pulse irregular, small, and wiry.—Twelve nocte: continues to sink; died at half-past twelve P.M.
Examination of the limb six hours after death.—Cut surfaces of femur perfectly smooth; bone easily denuded of its periosteum; acetabulum smooth; muscles infiltrated with pus; nature had not made the slightest attempt to repair the loss.
What would the result have been if amputation at the hip-joint had been performed? The same. The vis medicatrix naturæ is not sufficient to carry our sick through such formidable operations; it is no fault of the surgeons. A better and a more liberal allowance of animal and vegetable food during health is required, if England expects her soldiers to survive severe operations, disease and wounds. An attempt to save the limb, for the very same reason, would, most undoubtedly, have been a failure. Our Minié rifle-ball fractures of the femur all sink under conservative surgery. Our amputations above the middle of the thigh have a like issue; it is truly disheartening.
J. CRERAR, Surgeon, 68th Regiment.
Camp before Sebastopol, 24th August.
Dr. Crerar was greatly distressed by the loss of this man, and the manner in which he expresses his grief is declaratory of his feelings. The excised bones are in the museum of the Royal College of Surgeons.
The fifth, by Dr. Hyde, ended fatally on the sixth day.
[570] Corporal Benjamin Shehan, 41st Regiment, advanced with his corps, about twelve o’clock, on the 8th of September, to storm the Redan. Having succeeded in getting into the work, the regiment was afterward obliged to retire; in the retreat to our trenches he was wounded, and lay on the field till the following day, when he was brought to the hospital of the Royal Sappers and Miners. On examining the wound, it was found that a grape-shot had entered at the great trochanter, and, passing inward and a little forward, had passed out at the groin of the same side, about an inch below Poupart’s ligament, externally to, and a little in front of, the femoral vessels. The lower fragment of the fracture protruded through the external wound, and the introduction of the finger discovered a comminuted state of the neck of the bone.
Excision of the joint having been decided on, the operation was performed in the presence of Deputy Inspector-General Taylor, Staff-Surgeon Dr. Paynter, and Surgeon Elliot, Ordnance Department.
Operation performed about one P.M. 9th of September.—An incision, about four inches in length, commencing a little above the trochanter, was carried downward along the outer side of the femur. The lower fragment, for about an inch of its extent, was cleared of its attachments. An assistant holding the thigh below, and pushing the bone upward and outward, so as to bring the fragment through the incision, about an inch of the bone was then sawed off. The head of the bone was next dissected from the socket; this part of the operation was considerably facilitated by an assistant catching a firm hold of the neck by means of a pair of tooth forceps, then rotating the head, and using slight force to dislodge it from the cavity, the operator dividing the capsular and round ligaments, the latter of which is more easily and safely divided at the lower and outer side of the articulation. The upper part of the trochanter was next dissected out, and several small spiculæ of bone removed. The edges of the incision were then brought together by sutures, and a bandage applied. It was not found necessary to tie any vessel, and there was very little hemorrhage. The man bore the operation well, and was returned to his bed in good spirits, and with a good pulse.
10th.—Passed a good night; slept pretty well; pulse 106, soft; skin cool; in good spirits.
[571] 11th.—Slept some hours; pulse 106, soft; bowels open; tongue furred, but moist. Wound dressed and looking well; some healthy discharge.
13th.—Going on apparently very well; pulse still 106; countenance good. Vespere: Complains of an increase of pain in the hip, but otherwise says he feels much as usual; pulse small and rapid. Ordered wine and arrow-root.
14th.—Died at six this morning.
The autopsy showed a considerable cavity filled with sanies in the situation of the operation, but no other fractured bone was discovered. The articulating surface of the acetabulum was coated by a fetid, pasty substance.
GEO. HYDE, M.D., Staff-Surgeon.
The sixth, by Staff-Surgeon Coombe, also ended fatally.
Private James Nadauld, aged twenty-one, First Battalion Rifle Brigade, was admitted into the Castle Hospital, Balaklava, upon the 16th of July, 1855, five days after the receipt of a gunshot injury of the right shoulder. Upon the 19th of July the head of the humerus was excised, and the ball was found impacted in it. The healing process went on most favorably, and the man was discharged upon the 26th of August, quite well, for the purpose of proceeding to England. The excised bone is in the museum of the Royal College of Surgeons.
W. H. McANDREW, M.D.,
Surgeon, 57th Regiment.
Camp, Sebastopol, Sept. 14th, 1855.
Private John Purcell, 57th Regiment, aged twenty-one, was wounded upon the 18th of June, in the unsuccessful assault upon the Redan, by a Minié rifle-ball, which passed directly through the head of the humerus, but did not touch the glenoid cavity. Upon the 22d of June, the head of the bone was excised; and upon the 26th of August, the man was discharged from hospital, quite well, for the purpose of proceeding to England. The excised bone is in the museum of the Royal College of Surgeons.
W. H. McANDREW, M. D.,
Surgeon, 57th Regiment.
Camp, Sebastopol, Sept. 14th, 1855.
The following case of wound of the larynx is instructive:—
Lieutenant Charles H. Evans, 55th Regiment, aged nine[572]teen years, was wounded on the evening of the 5th of August, 1855, about eleven o’clock P.M., while on duty in the trenches. The ball entered the right side of the neck, close to the angle of the jaw, and passed apparently between the hyoid bone and the arytenoid cartilages, and then downward, having its exit below the cricoid cartilage on the left side. The pharynx and larynx were wounded, and the trachea was contused and displaced. Respiration somewhat hurried; a quantity of mucus collects in the trachea, and is expectorated in fits.
About seven o’clock P.M. of the 6th, the respiration becoming more difficult, with a degree of lividity of the lips, indicative of the non-oxygenation of the blood, it was deemed advisable to have recourse to tracheotomy, which, in consequence of the displacement of the parts and the swelling, was effected with considerable difficulty. The usual tubes were found too short for the purpose, and a large silver catheter was inserted, through which the air passed freely. Whenever he attempted to drink, the liquid passed into the trachea through the openings caused by the ball. From the operation no benefit arose, and he continued very restless until within an hour of his decease, which took place about twenty-six hours after the receipt of the wound. The voice was never heard above a whisper.
Post-mortem examination, twelve hours after death. The ball would appear to have passed through the hyo-thyroid membrane, fracturing and shattering the thyroid cartilage. The membrane lining the glottis was torn and destroyed. The vessels escaped without injury, the ball having passed anteriorly.
ARCHD. GORDON. M.D.,
Staff-Surgeon, 1st Class, in Med. Charge, 2d Division.
Camp before Sebastopol, September 3, 1855.
Deputy Inspector-General Taylor, who was present during the operation, adds: “The want of a longer tracheal tube than is commonly supplied for such operations was obvious, and is a good practical hint. For the first time in my life I found my two forefingers transfixing a man’s neck from side to side. The fingers did not cause any cough or irritation, but those symptoms were occasioned by the least attempt to swallow water. The thyroid cartilage was separated into two pieces.”
[573] The following cases, one of wound of the profunda femoris, the other of the popliteal, deserve attention:—
Late in the afternoon of the 14th of August, Private George Irvine, aged twenty-five, was brought from the trenches, having been struck by a Minié-ball of the largest size, which had penetrated the left thigh, about two inches below Poupart’s ligament, just in the course of the femoral artery. The ball passed slightly outward, fracturing the femur, and was cut out at the back of the limb, completely flattened. As there was considerable hemorrhage, both venous and arterial, no examination with the finger was permitted. Dr. Taylor, superintending the Division, having been informed of the case, a consultation was held.
Amputation at the hip-joint was forbidden by the prostration of the man, who had lost much blood before he was brought to camp. Excision of the head of the femur was also inadmissible, from the evident wound of a large artery, with probably that of a large vein. Search for the wounded artery, for the purpose of applying a ligature, was then determined upon, but before the operation had well proceeded, the hemorrhage was so great that it was found impossible to continue it, and pressure by means of graduated compresses was resorted to, with complete success.
On the following morning an operation was still out of the question. Prostration continued, with great irritability of stomach, and a small, quick pulse. No return of hemorrhage, though the pressure of the tourniquet was but very slight.
On the 16th, the pulse was more quick and irritable, with the same irritability of stomach, and urgent thirst. He had passed a better night, however. At the consultation this morning, the circulation through the posterior tibial artery was so evident that the question of the femoral artery being wounded was set at rest. It was decided, as no return of hemorrhage had occurred, that the case should be left to nature.
On the 17th, he suffered from starting pains in the thigh. There was less irritability of stomach, but the pulse was very small and weak. During the night there was slight hemorrhage, owing to his restlessness, but it was easily arrested by a turn or two of the tourniquet.
On the evening of the 20th, this restlessness increased; delirium set in, and early in the morning of the 22d he died.
[574] The limb was examined after death, when the following appearances presented:—
Femoral artery intact. Femoral vein wounded, with more than half its caliber shot away. At about two inches from its origin there was a wound of the profunda artery, on which an aneurism, nearly the size of a pigeon’s egg, had formed, and passed upward through the wound made by the ball. The profunda vein was intact. The injured vessels having been removed for preservation, the bone was then cut down upon, when a fracture, nearly transverse, and not at all comminuted, was observed below the trochanters. No splitting of bone upward; downward its outer plate was slightly cracked, but nothing more. The preparation is in the museum of the Royal College of Surgeons.
Private James Ross, a lad of eighteen, was brought up from the trenches, on the morning of the 3d inst., having had his right leg blown off below the knee by a round shot. He had lost a very large quantity of blood before the tourniquet was applied, and was consequently so much collapsed that an operation was out of the question. He was therefore dressed and the tourniquets (two had been put on) removed. He never rallied, and died on the 12th, nine days after the receipt of the injury. No hemorrhage ever occurred, though all pressure had been removed from the artery.
R. V. DE LISLE,
Surgeon, 4th King’s Own Regiment.
Camp before Sebastopol, Sept. 14, 1855.
The following is worthy of publication, as showing the successful effects of strychnia, when carried to the extreme verge of propriety, in injuries of the spinal cord.
Sergeant William Aldridge, 46th Regiment, aged 39 years, during a sortie from Sebastopol, was knocked down in the trenches, and his back formed a bridge over which Russians and English passed. The result was serious injury to the spine, causing paralysis of the lower extremities and bladder. The pain was excruciating, and the patient could not be moved in bed for several weeks.
On the 4th of March, 1855, he was placed under my charge in the military hospital at Portsmouth, when he complained of great pain and tenderness along the spine, and incontinence of urine, together with wandering day dreams and insomnolency at night. Solution of the muriate[575] of morphia ʒj was prescribed without any effect. (ʒj contains 1 gr.) The dose was gradually increased to ʒij of the solution.
15th March.—Fell out of bed during the night, trying to hide himself. Is wandering, and fancies that he has deserted from the Crimea, and will be shot. The narcotic has been omitted for several days. Strychnia was now ordered, one-sixth of a grain three times a day.
20th.—Continues much the same, with slight twitchings of the face.
25th.—Has been unconscious for three days. Now complains of intense pain in the back and violent cold perspiration.
28th.—Returning consciousness; feels easier, having slept uninterruptedly for forty-eight hours. Expressed a desire to make his will, and send to Dublin for his wife; both wishes were complied with.
30th.—Sensation and motion are gone from the lower extremities, and the urine is still passed involuntarily. One-eighth of a grain of strychnia was ordered twice a day.
31st.—Is powerfully under the influence of the remedy, with convulsive movements of the upper and lower extremities; wild stare and fixed jaws. The lower extremities had not moved for several months previously. This paroxysm lasted for one hour under my own observation, after which the muscles became relaxed, the face bedewed with a gentle perspiration, and resumed its ordinary tranquil appearance.
April 2d.—Feels greatly relieved from pain, and is comparatively comfortable; sleeps calmly. His appearance is entirely changed; looks natural; features calm; is cheerful, and reads the papers. Strychnia was omitted for some days after the last paroxysm, and replaced by the tincture of the sesquichloride of iron with quassia, and a generous diet.
6th.—Continues to improve. Has now and then slight twitchings in the legs and arms. The strychnia was resumed and omitted, as the symptoms indicated, to the end of the month.
May 1.—Is greatly improved; goes about the balcony in a chair. Returning sensation in the right leg. Bladder still not under the control of the will.
20th.—Sensation much improved in both legs, and motion increasing in the right leg.
25th.—Convulsive movements all over the body, resulting[576] from the use of the strychnine. Lower extremities decidedly improved both in motion and sensation.
June 1st.—Maintains his improved condition. Recommenced the strychnine to-day, without any marked effect at the moment.
10th.—Violent tetanic spasms followed the employment of the remedy, producing considerable increase of motion in both extremities. The paroxysms usually continue about fifteen minutes, when the muscular system resumes its ordinary appearance.
20th.—Continues the same. Strychnia not resumed since last entry, as occasional twitchings occur about the head and face, and he is now affected by the smallest dose.
July 1st.—General health excellent.
10th.—Continues to improve daily in regaining the use of his limbs. Is now able to walk on the ramparts with crutches, but is exceedingly sensitive to every change of weather—damp always causing pain in the spine. Continued to improve to the end of the month.
August 1st.—No change worthy of note.
14th.—Discharged to Chatham.
T. H. BURGESS, M.D.,
Military Hospital, Portsmouth.
The following case of injury of the abdomen, sent to me by Dr. Rooke, civil surgeon with the army in the field, is very remarkable:—
Robert Cousins, aged 20, 77th Regiment, was admitted into the general hospital, camp, June 8th, with severe injuries caused by a round shot, which struck him when he was on duty in the advanced trenches. When the shot struck him he was standing up, half-face toward the enemy, his right arm extended in front of the right hip; he was in the act of reaching his water-can, which rested against the parapet of the trench.
On admission he was in a state of semi-collapse, the integuments of the right hand and forearm greatly lacerated, the wrist-joint laid open, the bones of the carpus comminuted; the radius and ulna were also fractured at the middle third. There was a lacerated wound in the right iliac region, the size of the palm of the hand; over this space the skin and muscles of the abdominal wall were torn away, the peritoneum lining it was also lacerated, and at the bottom [577] of the wound was seen a coil of intestine in situ; there was no tendency to protrusion, nor were its coats at all injured. The crest and body of the ilium were much comminuted, the fracture extending downward between the anterior superior and anterior inferior spinous processes. The anterior superior spinous process was broken off. There was another wound just below the great trochanter; this apophysis was also shattered. The right limb was two inches shorter than its fellow, the foot everted, but, from the great comminution of the pelvis and the extreme pain produced by examination, it was not satisfactorily made out that the neck of the femur was fractured, but the shortening of the limb and eversion of the foot were in favor of that diagnosis. The injuries which the patient had received were considered mortal; it was thought unnecessary cruelty to amputate the forearm. Such pieces of the ilium as were loose were removed; wet lint applied to the wounds; and brandy and water with opiates were ordered. One of his comrades volunteered to watch over him, and he was left, as all thought, to die. The next day (June 9th) he had partially rallied from the state of collapse; had taken liquid nourishment—beef-tea, arrow-root, etc. There was no pain or tenderness of the abdomen; had passed his water without difficulty. The surface of the abdominal wound was sloughy; intestine still visible; complains of pain in the arm. It was not yet considered advisable to perform any operation. He was ordered opium gr. j every four hours; also a dose of morphia at night, arrow-root, beef-tea, and port wine, which he prefers to brandy.
10th.—Has rallied completely; no pain or tenderness of the abdomen; complains greatly of his arm, and is anxious that something should be done. He slept well after taking the morphia; his face is tranquil, breathing natural, pulse weak; no irritability. Deputy Inspector-General Taylor saw the case in consultation with Dr. Mouat, P. M. O. of the hospital. It was decided to amputate the forearm. This was done at the upper third; chloroform was administered, and produced no ill effects. He was ordered any fluid nourishment he might fancy, with port wine, and an opiate at night.
11th.—No symptoms of peritonitis; suffers no pain; tongue clean and moist; pulse quiet; passes his water regularly; the bowels have not acted. The abdomen is quite [578] soft and fallen, not the slightest tenderness on pressure. To continue on the same plan. He could now give some account of the way in which he was wounded. He stated that he thought it must have been a round shot that struck him. It first struck his arm, then entered the right iliac region, emerging at the lower wound. The surface of the wound in the iliac region is in a sloughy state from the severe bruising of the parts. The coil of intestine is still visible at the bottom of the wound.
12th.—No symptoms of peritonitis; bowels have not acted; tenderness down the outside of the thigh, with redness of the skin, and pitting upon pressure. Stump dressed to-day and looking well.
13th.—No unfavorable constitutional symptoms. The outer part of the thigh is tender and the skin red; free incisions were made; the fascia was sloughy. He takes nourishment; has eight ounces of port wine daily, eggs, arrow-root, and essence of beef. Bowels not acted.
21st.—He had no symptoms worthy of remark since the 13th. The bowels have not been moved; he complained to-day of not being able to pass his motions. Two injections of warm water were administered in the course of the day. He passed a large quantity of hardened feces, which relieved him greatly. The sloughs are separating from the incisions in the thigh; the crest and ala of the ilium are exposed; healthy granulations are springing up from the bottom of the wound. Stump healing favorably.
July 26.—The case has progressed without a bad symptom. At first it was thought that the greater part of the ala of the ilium would exfoliate, but some red points appeared on the surface, and the concavity of the bone became covered with granulations. The exfoliation was limited to the anterior part of the crest of the ilium, which separated on the 17th instant. At various times pieces of bone have been removed as they became detached; there are others still left to come away. The granulations on the upper wound are on a level with the skin of the abdomen. The crest of the ilium is covered with granulations; the wound is contracting, but there is a deficiency of skin to cover the projecting portion of the ilium. The lower wound is also open, and has been enlarged to remove pieces of bone; the incisions in the thigh have healed. The bowels have acted regularly without medicines until to-day, when he required a castor-oil [579] injection. The right thigh is more than two inches shorter than the left; union appears to have taken place; he has no pain on motion. The dead bone that still remains alone prevents the wounds from closing, their surfaces being covered with healthy granulations. His general health is good. He has taken at intervals some oleum jecoris aselli, and, for a mild attack of bronchitis under which he suffered at the end of June, expectorants and diaphoretics. There has not been a single symptom of any abdominal complication. He has an opiate at night. The stump has been healed nearly three weeks.
September 14th.—Since the last report no unfavorable symptoms have occurred. The stump of the forearm has been healed some weeks; his health is good; indeed, from first to last, he has not had a single symptom denoting constitutional disturbance. All the dead bone from the crest of the ilium has separated; the wound of the abdomen is skinned over, with the exception of a small spot about the size of a sixpence. This is healthy, and is gradually healing. The bowels act regularly. There are still two sinuses on the outer side of the thigh—one above, the other below, the great trochanter. On probing these, dead bone is felt, which has not yet separated. The right limb is about three inches shorter than the left, is freely movable in any direction without pain. He can raise the knee from the pillow, but cannot lift the heel from the bed; he can, however, turn himself over on to the left side without assistance. The prominence of the crest of the ilium is greatly diminished from loss of bone. The trochanter major is unusually projecting; the natural appearance of the hip-joint is entirely gone. The injuries to the bones have been so severe, it is difficult to say what changes have occurred. The ilium and pubis have been greatly comminuted, the fracture most probably extending through the acetabulum. Immediately below Poupart’s ligament, to the outside of the femoral artery, a hard substance is felt beneath the skin. This, when he was admitted, was at first supposed to have been a piece of a shell, but it is now thought to be a portion of the pubis driven downward upon the thigh.
He may now be said to be convalescent.
John Shehan, aged nineteen, 57th Regiment, was wounded in the left thigh before the Redan, on the 18th of June. He [580] was brought to the general hospital, and placed under the charge of a gentleman of considerable skill and experience. The wound presented two openings, an anterior and a posterior; the latter offered greater facilities for examination than the former; the finger, passed from behind, detected several fragments, which were removed, and as a tolerably uniform surface of bone (vide specimen) was then felt, it was determined, after consultation, to make an attempt to save the limb. The injured extremity was accordingly bound up with a long splint in the most careful manner, and matters promised favorably for a time. He, however, complained of a good deal of suffering in the limb from time to time, gradually wasted, suffered from diarrhœa, and finally sank on the 6th of August. On examination post-mortem, I found the chief organs in a normal condition. There was some congestion of the ilium, and the colon presented a few points of ulceration. The condition of the parts in the left lower extremity was very remarkable. Beneath the integuments, all the muscular and other textures, from the seat of injury to the groin, were converted into a soft, broken-down, black, rotten mass; and I may here observe that this low but intense disorganizing process, extending through the greater part of the limb, has presented itself in several of my examinations of somewhat similar injuries, and appears to me to be connected with a peculiar pathological state in which all the vital organs remain sound, but the vis vitæ is remarkably reduced below par. The fractured bone it is unnecessary to describe. The vertical and cross infraction of the fragments and its almost “arborescent” appearance are most remarkable. I look upon it as a specimen of no ordinary value, conveying more than one most useful lesson. The bones are in the museum of the Royal College of Surgeons.
R. D. LYONS,
Pathologist to the Army in the East.
Camp before Sebastopol, August 30, 1855.
Private William Leah, 30th Regiment, aged twenty-one, was brought to me on the 27th of June, while I was on duty in the trenches, with fracture of the external condyle of the humerus of left arm, by a musket-ball, which had entered the joint between it and head of radius, and had made its exit over olecranon process of ulna. Artery uninjured. On [581] being sent to camp, the joint was excised by Mr. Dowse, surgeon of the regiment. The patient progressed favorably, and the wound has been healed for nearly a month. He can use all the muscles of the forearm, except the flexor of the little finger, and is regaining the motion possessed by the elbow-joint.
DAVID MILROY, M.D.,
Assistant-Surgeon, 30th Regiment.
Camp, Second Division, Heights of Sebastopol, Sept. 5, 1855.
J. Maguire, 31st Regiment, aged twenty, wounded in the advanced trenches.
July 12, five A.M.—Carried into hospital, wounded by a splinter of shell in left elbow and on left hip. The splinter struck him in an oblique direction, from behind, fracturing olecranon process and internal condyle of humerus, lacerating and otherwise injuring the joint, the ulnar nerve being also injured. The splinter continuing its onward course, inflicted a lacerated wound on the hip, with comminuted fracture of about the anterior fifth of the crest of the ilium, several small pieces of bone being driven in on the peritoneum, causing pain on the slightest motion. All the loose portions of bone were removed, and several others separated from the muscles. Abdomen painful, and swollen at that side. Abdomen continued painful during the day; bowels acted; he also passed water freely.
13th.—Pain in abdomen much less; little, if any, constitutional disturbance; elbow extremely painful; the pain accompanied with partial paralysis of the little and ring fingers. Staff-Surgeon Dr. Gordon having seen him, and not apprehending any danger from the wound in the side, the operation for excision of the elbow-joint was determined on, and performed under chloroform, by a single straight incision passing through the original wound, including the upper and lower fourths of the forearm and arm. There was very little hemorrhage. The arm was then put up in an angular splint. It continued to progress favorably, the greater part healing by the first intention. There was some suppuration, but a free exit being given to the matter, it did not retard recovery.
August 19th.—This patient was discharged from the regimental hospital, to general hospital, Balaklava. The [582] wound nearly healed; sensation partially restored to the fingers; slight motion at the bend of the elbow; but he has not power to raise the hand.
THOMAS J. ATKINSON,
Assistant-Surgeon, 31st Reg. in Med. Charge.
Camp before Sebastopol, Sept. 1, 1855.
Private Anthony Murray, aged twenty-eight, 41st Regiment, a healthy man, was struck, while on duty in the trenches before Sebastopol, on the night of the 23d of July, 1855, by a portion of a shell, which penetrated the left elbow-joint; the head of the radius and the outer half of the articulating surface of the humerus were comminuted, fragments being impacted in the cancelous structure of the humerus, and driven in between that bone and the ulna. Excision of the joint having been determined on, it was performed in the following manner: a straight incision was made along the posterior surface of the joint, the olecranon cut through, and the extremities of the several bones removed in succession; the parts were then brought together by suture, and the limb placed in a flexed position; about a third of the wound healed by the first intention; no inflammation supervened. On the 3d of August the wound was granulating in a healthy manner; on the 22d, it had almost healed, and the limb was put up permanently, the forearm at right angles to the arm; on the 31st, some union had taken place between the bones; the man can move the thumb and three fingers; he is free from pain; his health is very good, and he appears to be progressing favorably in every respect.
J. E. SCOTT, M.D., Surgeon, 41st Regiment.
August 31st, 1855.
Private Jesse Lockhurst, 31st Regiment, aged twenty-six, was wounded in the advanced trenches, 17th of August, 1855.
August 17th.—Six o’clock A.M., carried into regimental hospital, having received an extensive lacerated wound of right cheek: very little apparent hemorrhage, but the power of deglutition was completely lost, and respiration impeded. On making an examination of the wound, it was ascertained that the right superior maxillary bone was fractured, and a portion of the hard palate with the molar teeth driven in on the tongue; there was a large piece of shell or shot lodged [583] at the bottom of the wound, lying on left palate, and, as far as could be ascertained, on the back of pharynx. Staff-Surgeon Dr. Gordon being present, the ball, after much labor, was extracted, and found to be a grape-shot of seventeen and a half ounces weight. During the operation it was found necessary to dilate the wound by dividing the lip near its external angle—the portions of bone that were removed were the alveolar process, with all the molar teeth, including part of the palate and a portion of the orbital plate and nasal process of the superior maxillary bone, and all the malar bone. There was no serious hemorrhage during the operation, nor immediately after the extraction of the shot. The cheek was then plugged with lint and the wound brought into apposition by sutures. The man experienced immediate relief after the operation, sat up in bed, washed out his mouth, and drank some water; he seemed extremely thankful, and blessed the doctors. During the night and part of the next day there was some oozing from the mouth. No bad symptom occurred until the 20th, when an active hemorrhage came on from the back of the palate. The exact source could not be ascertained. He became very weak and almost pulseless; but the hemorrhage was eventually restrained by means of ice and plugging the wound with lint moistened in tincture of matico. Iced drinks occasionally.
31st.—The man is now doing extremely well, can talk, and takes a pint of jelly daily; the external wound is not yet quite healed, in consequence of the saliva flowing through it. The right eye is uninjured, and sight unaffected.
September 1st.—He has just been discharged to general hospital, Balaklava, from the regimental hospital.
THOS. J. ATKINSON, Assistant-Surgeon,
31st Regiment, in Med. Charge.
Camp before Sebastopol, September 1, 1855.
On the morning of July 24th, Private Francis O’Brien, a lad of eighteen, was brought from the trenches, with a wound from a musket-ball in the right temple. It entered about two inches above the orbit, passed downward, and drove out a large portion of the supra-orbital ridge, which appeared to be imbedded in the upper eyelid, and was cut down upon by the medical officer in the trenches, in mistake for the ball, which it certainly very much resembled. As no [584] ball could be found, it was supposed to have passed out at the opening of entrance.
The finger when passed into the wound could feel the pulsation of the brain, yet from that day to the present no symptom of cerebral disturbance has appeared, unless it be that since his convalescence the muscles of the face work convulsively when he feels faint and weak from remaining too long in the erect posture. About a month after admission, the detached portion of the bone above the orbit was removed from the eyelid, though with considerable difficulty, and on the following morning the ball fell from the wound, much to the poor lad’s horror, who thought his eye had dropped out.
Both wounds have now healed, but he is unable to raise the right eyelid; the eye is perfect, but apparently without power of vision, though sensible to the stimulus of light, for on turning the wounded side to the light, the left pupil contracts. His general health is good.
R. V. DE LISLE,
Surgeon, 14th King’s Own Regiment.
Camp, Sept. 10.
Private Joseph Bourke, 17th Regiment, admitted on 9th of September, 1855, with fracture of anterior superior angle of right parietal bone, with depression of about one-third of an inch, for the size of a florin. No attempt was made to elevate the depressed portion. Has not had a bad symptom. Wound of scalp nearly healed.
W. P. WARD,
Surgeon, 17th Regiment.
Private Michael Caffrey, 88th Regiment, wounded at the attack upon the Redan on the 8th of September, was brought to the hospital of the 38th Regiment on the morning of the 9th. A round rifle-ball struck him at the anterior part of the left parietal bone, and passed through the brain in a line which brought it out at the vertex, fracturing the parietal bone of the opposite side; the ball at its entrance split, and one-half pushing before it a small piece of bone, both lodged at the entrance; the other half of the ball was found lodged in the brain at the upper and back part, having detached a circular portion of the skull.
A director was passed along the track of the wound, and [585] the scalp laid open; the brain was found to protrude through the fracture. In this condition the patient lived for eleven days, utterly unconscious of everything passing around him, the urine and feces coming away involuntarily. There was paralysis of the opposite side.
A post-mortem examination showed the brain to have been reduced to a pultaceous mass only in the direction of the passage of the missile; the remaining portion of the wounded hemisphere and that of the opposite side were healthy.
The absence of the usual train of head symptoms, and the length of time which so extensive an injury permitted life to remain, render this case worthy of some remark.
FREDERIC WALL,
Surgeon, 38th Regiment.
Camp before Sebastopol, Sept. 20, 1855.
Private William Doyle, 19th Regiment, aged nineteen years, was wounded in the head by a rifle-ball, in the advanced trench of the right attack, on August the 30th. The scalp and pericranium were cut about two inches, and a portion of the cranium, a little in advance of the posterior and superior angle of the right parietal bone, close to the sagittal suture, about an inch in length and half an inch in breadth, was depressed. According to statement the man was rendered perfectly senseless and motionless, from the instant of being struck by the bullet. On reaching camp he presented all the usual symptoms indicating compression; pupils dilated and fixed, warm surface, total unconsciousness, complete paralysis, etc. On examination of the depressed portion of bone, no opening whatever could be felt; the edges of the sunk bone and the bone adjoining were in contact, and it was presumed to be an ordinary case of fracture with depression simply. Some very minute portions of cerebral substance were observed to be mixed with the clot of blood about the wound, such as might be squeezed through a fissure. Trephining being determined on, it was performed at once, and the depressed bone raised without difficulty. No relief of symptoms followed. The dura mater bulged slightly upward into the opening. On passing the finger over its surface, a little beyond the space exposed by the trephine, a defined cut edge was felt about an inch in ad[586]vance of the depressed piece of bone, being the boundary of an opening into the cerebral substance.
Three hours after arrival in camp the patient died. On examination post-mortem, a wedge-like section of the ball was found to have entered and penetrated the cerebral substance; it was discovered in the anterior lobe on the right side, just above the orbitar plate. It had not completely penetrated, but was lying just above the membrane covering the lobe. The ball—a conical rifle-ball with three cannelures—was cut smoothly from apex to base, as if by a sharp knife. This must have been done by the edge of broken bone above the opening made in the parietal bone, one-half of the ball flying off, the other entering the skull. On close examination, several very small points of lead were found to be imbedded along the margin of the bone alluded to. The depressed portion of bone, directly after the piece of ball entered, must have sprung up again by its own resiliency, or been forced up by sudden pressure from within, so that no evidence of an aperture, but merely a fissure and depression remained. The inner table was separated, and nearly detached, for a space rather more extensive than that of the depressed part of the outer table. The superior longitudinal sinus was wounded by the sharp edge of the broken inner table, and a very considerable quantity of blood extravasated upon the surface of the brain.
The portion of bone implicated in this injury has been preserved.
THOMAS LONGMORE,
Surgeon, 19th Regiment.
Camp before Sebastopol.
Six amputations at the hip-joint (if not more) have been performed in the Crimea, and all the sufferers have died, a loss which has not been experienced in civil life under any circumstances, many persons having survived the operation for years. It has been fairly attributed to the depressing causes from which the army suffered, and for which the government has been blamed; although the great functionaries appear to me to have less to account for than their subordinates, as far as regards deficiencies in the treatment of the sick and wounded.
[587] The operation for removing the head of the femur from its connection with the hip, leaving the limb for future use, was first recommended by me as a substitute for amputation at the hip-joint, and has been done in at least six instances, one only surviving. I limited the operation to injuries of the head and neck of the bone, or with little extension beyond these two parts, being cases which hitherto invariably died unless amputation at the hip-joint were performed, and which it was and is hoped the operation of excision might render unnecessary; but it must be done under happier circumstances, and perhaps with greater restriction. The success which has followed the removal of the head of the humerus from the shoulder-joint even with as much as one-third of the shaft, as low as the insertion of the deltoid muscle, has led to the belief that as much may be done in the thigh; and in the hope that it might be so, a considerable portion of the shaft of the femur has been removed with the head and neck in the cases alluded to, so that an approximation of the remainder of the shaft to the cavity of the joint has not been possible. If the operation performed by Surgeon O’Leary, 68th Regiment, (page 564,) which at the end of seven weeks is reported as doing well, although the pulse remained between 80 and 100, should succeed, it is doubtful whether the limb will be of any use or better than an artificial leg, from the extent of the bone removed, which will prevent the formation of a firm joint or union. The sling used in this case has been considered very advantageous by all who have seen the man, and proves how much may be done in all cases of compound fractures by similar appliances, but which has not yet been done. A correct judgment cannot, however, be formed as to the value of this operation until it has been performed on one of those cases in which a ball shall simply lodge in the head or neck of the femur without injuring the shaft of the bone—an accident which has been so frequently observed in the head of the humerus, and of which I have sent two preparations to the museum of the College of Surgeons. (See page 127.)
It has been already stated that the loss of life after amputations performed for gunshot fractures of the upper part of the thigh has been so great, both in the French and English armies, that such operations have been nearly abandoned.
The Russians, at the commencement of the siege of Sebas[588]topol, made use of a conical rifle bullet, flat at the base, weighing nearly one ounce and three-quarters. Latterly they have used a larger conical one, with three grooves around the circumference of the base of the cone, which is hollowed out to receive a cup, and shows a projection on the inside of the hollow. This ball is near two inches long, and weighs somewhat more than one ounce and three-quarters.
The balls formerly used by the French army were twenty to the pound, and by the English, sixteen. The balls alluded to are nine to the pound. When this Russian ball strikes soft parts only, such as the thigh, it merely makes a larger hole than the common bullet, into which the finger passes easily, and the wound heals as readily. Whenever it strikes a bone, it would appear to break it more extensively, and to require more certainly the amputation of the limb; although the smaller French ball used in former days, when it struck a bone, disabled the sufferer as effectually for all future service, yet it might not as certainly lead to his death.
Dr. Lyons not only transmitted to me the case, related page 579, of John Shehan, but has since sent me the broken bones, which confirm everything I have said on this subject, page 321. The sound bone above the fracture has become more solid; the splinters not having been removed are lying across, and prevent the approximation or union of the ends of the old bone, while the effort made by nature to effect this object by the deposition of new ossific matter, adds to the evil by fixing these splinters in so solid a manner that they cannot escape or be removed by any other means than that of forcible abstraction, after painful and perhaps dangerous operations, each splinter possibly requiring a separate one. Shehan’s case was one for amputation from the first, if he had been in a state to undergo it with a prospect of success.
The treatment of gunshot fractures of the leg ought to have been more successful than it has been, even when both bones were broken; the want of success may be in part attributed to the remissness which has taken place in supplying the necessary, nay, the essential appliances, by means of which much suffering might have been alleviated, perhaps prevented, even if cures could not have been effected.
In performing the operation for the excision of portions of the extremities of bones, a chain saw is a most desirable [589] aid on many occasions. There was not one with the British army in the Crimea, and when wanted, they were borrowed from the French ambulances. It was only on the 30th of September last some were ordered to be sent out, and they cannot yet have arrived. In a lecture I delivered on the 14th of April last in the Theater of the College of Surgeons, as its President, by permission of the Council, the proceeding being unusual, I drew attention, for the express purpose, to the necessity which existed for the Crimean army being supplied with a machine capable of being moved from bed to bed, by means of which the unfortunate soldier could be raised in the extended state, and after being washed, his wounds dressed, and his bedclothes changed, he might be again laid down with comparatively little uneasiness. Fifty of them would not cost £300, but there are none in the Crimea, except two, one sent to the Coldstream Guards, by Lord Strafford at his own expense, and one which the makers placed at my disposal. I hear that three have been ordered lately, like the chain saw, when too late, for many are now no more who stood in the greatest need of them, and without which machine they had little chance of being saved.
On the 14th of April, 1855, I published a lecture, in which I gave a sketch of an apparatus for slinging a broken leg, which instrument I declared to be a sine qua non in the successful treatment of a gunshot fracture of the leg. By permission of the Duke of Newcastle, I sent out forty-six sets complete for every part of the body, the year preceding. They were, I am told, left at Varna; and four medical officers, of character and knowledge, who have lately returned from the East, assure me within the last week that no such, or any similarly useful, apparatus was ever seen in the hospitals in front of Sebastopol. Other instances of remissness of equal importance might be adduced, if it were not useless to advert to them; for we delight, I believe, in being admitted by foreigners to be a wonderful people in the mismanagement of our affairs in the first instance, however important or trivial. It is, I believe, an admitted maxim, that the right men should be in the right place—the square ones in the square holes, the round ones in the round holes; but there is another one of equal importance, viz., that the right thing should be in the right place at the right time, without which teaching or practicing surgery becomes of little value.
[590] Amputation at the knee-joint has been done, I hear, in six cases since the taking of Sebastopol; four are dead; one is doing well under Mr. Blenkins, of the Guards, and the other yet survives. Excision of the knee-joint has been performed since the taking of Sebastopol in one case by Staff-Surgeon Lakin, and is doing well.
The excisions performed on the head of the humerus, and on the bones composing the elbow-joint, have been very successful. There is, however, a circumstance to which I am desirous of drawing attention, viz., that the head of the humerus should never be removed in amputations, when it is uninjured, however close the destruction below may have approached it. The round head of bone left in the socket preserves the squareness of the shoulder, and renders the loss of the arm less unseemly. It tends to prevent the inclination the body generally has to the opposite side, and its being left adds nothing to the difficulties of the operation. The excisions of the ankle-joint have been numerous and more successful than might have been expected under the depressing causes alluded to.
For the preparations of the head of the humerus and of the astragalus, referred to at pages 110 and 128, I have since learned I am indebted to Deputy Inspector-General Macgregor; and I am particularly so to Assistant-Surgeon Gregg, of the 17th Regiment, for the great care he has bestowed on several of the specimens of injury sent to me.
Wounds penetrating the cavities of the chest and abdomen have been no less fatal than those of the lower extremities. The same want of power has been exhibited in them; the same inability to bear the means of cure which, under happier circumstances, have proved successful.
I hope to receive reports on wounds of arteries, on secondary hemorrhage, and on injuries of the head, so as to enable me to remove any doubts which may exist on these points; and I beg to assure those officers who will favor me with their opinions and facts, that they shall be duly reported in another “Addenda.”
I cannot conclude these remarks without expressing my sense of the great practical ability displayed by very many of the medical officers in the Crimea, of their devotion, of their self-denial—qualities which ought to obtain for them the special approbation of the nation.
October 18, 1855.
THE END
PUBLISHED BY
J. B. LIPPINCOTT & Co.,
PHILADELPHIA.
Will be sent by mail, post paid, on receipt of the price by the Publishers.
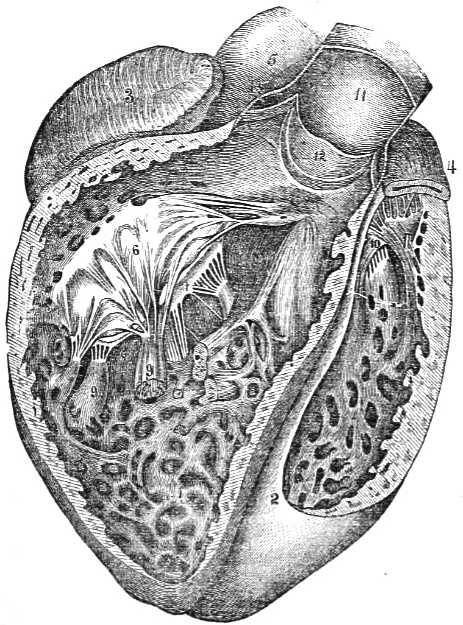
View of the Heart, with the anterior portions of the ventricles removed.
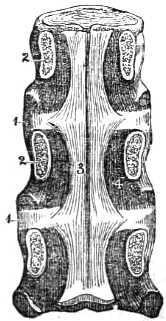
Dorsal Vertebra.
Human Anatomy: An Elementary Text-book for Students. By Joseph Leidy, M.D., Professor of Anatomy in the University of Pennsylvania. Elegantly illustrated from numerous original drawings. One vol. 8vo. $5.00
Notes on the Surgery of the War in the Crimea, with Remarks on the Treatment of Gunshot Wounds. By George H. B. Macleod, M.D., F.R.C.S., Surgeon to the General Hospital in Camp before Sebastopol, Lecturer on Military Surgery in Anderson’s University, Glasgow, etc. etc. One vol. 12mo. $1.50.
SUMMARY OF CONTENTS.
Chap. I.—The History and Physical Characters of the Crimea. The Changes of the Seasons during the occupation by the Allies. The Natives, and their Diseases.
Chap. II.—Drainage of the Camp. Water Supply. Latrines. Food. Cooking. Fuel. Clothing. Housing. Duty. Effect of all these combined on the health and diseases of the soldiers. Hospitals. Distribution of the Sick. Nursing, male and female. Transport.
Chap. III.—The Campaign in Bulgaria, and its effects on the subsequent health of the troops. The Diseases which appeared there, and during the Flank March, as well as afterward in the Camp before Sebastopol.
Chap. IV.—Distinction between Surgery as practiced in the Army and Civil Life. Soldiers as patients, and the character of the Injuries to which they are liable. Some peculiarities in the Wounds and Injuries seen during the war.
Chap. V.—The “Peculiarities” of Gunshot Wounds, and their General Treatment.
Chap. VI.—The Use of Chloroform in the Crimea. Primary and Secondary Hemorrhage from Gunshot Wounds. Tetanus. Gangrene. Erysipelas. Frost-bite.
Chap. VII.—Injuries of the Head.
Chap. VIII.—Wounds of the Face and Chest.
Chap. IX.—Gunshot Wounds of the Abdomen and Bladder.
Chap. X.—Compound Fracture of the Extremities.
Chap. XI.—Gunshot Wounds of Joints. Excision of Joints, etc. etc.
Chap. XII.—Amputation.
IN PRESS.
By Henry H. Smith, M.D., Surgeon-General of the State of Pennsylvania.
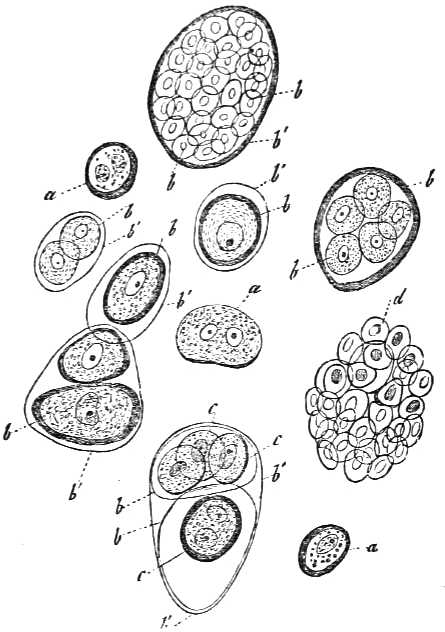
Cartilage cells from a fibrous, velvety, articular cartilage of the condyle of the femur of man, magnified 350 diameters.
Manual of Human Microscopical Anatomy. By A. Kolliker, Professor of Anatomy and Physiology in Wurzburg. Translated by Geo. Bush, F.R.S., and Thomas Huxley, F.R.S. Edited, with notes and additions, by J. Da Costa, M.D. Illustrated by 313 engravings on wood. One vol. 8vo. $3.75.
It would be useless for us to attempt a review of this work, for the text is so fully illustrated by engravings, and is so intimately associated with them, that we cannot extract any part as a sample of the style, without weakening its force, for the want of its accompanying illustration. The book must be read and studied before an adequate idea can be formed of its value and excellence. The book comes from such high authority, and is indorsed by such competent judges, as to make it at once indispensable to the student of microscopic anatomy. We hope it will have an extensive circulation.—Western Lancet.
The reputation of Professor Kolliker, acquired by his former and larger work on microscopical anatomy, will be enhanced by this text book on Histology, for such it is destined to be pre eminently. The text is fully illustrated by engravings, greatly adding to the value of the work, and accompanied by explicit explanations of the figures. We commend it to the profession, and to students especially, as worthy of their patronage.—N. Y. Medical Gazette.
A Systematic Treatise, Historical, Etiological, and Practical, on the principal diseases of the interior valley of North America, as they appear in the Caucasian, African, Indian, and Esquimaux varieties of its population. By Daniel Drake, M.D. Edited by S. Hanbury Smith, M.D., formerly Professor of the Theory and Practice of Medicine in Starling Medical College, Ohio; and Francis G. Smith, M.D., Professor of the Institute of Medicine in the medical department of Pennsylvania College, Philadelphia. One vol. 8vo. Sheep, $5.00.
Dr. Drake’s great reputation, and his extensive practice in the western country, gives great value and decisive authority to this treatise on the diseases prevalent in the valley of the Mississippi. While the work is of great interest to the general practitioner in other parts of the country, to the Western and Southwestern members of the medical profession it will hereafter be considered an indispensable book of reference and instruction.
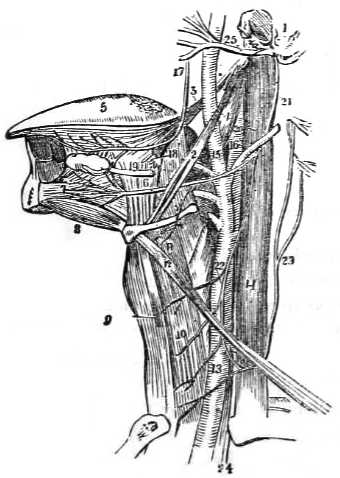
Nerves of the neck and tongue.
The United States Dissector; or, Lessons in Practical Anatomy. By William E. Horner, M.D., late Professor of Anatomy in the University of Pennsylvania. Fifth edition, carefully revised, and entirely remodeled. By Henry H. Smith, M.D., fellow of the College of Physicians of Philadelphia, etc. With one hundred and seventy-seven new illustrations. One vol. demi 8vo. $2.00.
This is a new and revised edition of one of the most popular works on dissection which has ever been published in this country. The editor has carefully revised the text, modified its order, added an entire set of new illustrations, and introduced such recent subjects as the progress of science rendered necessary.
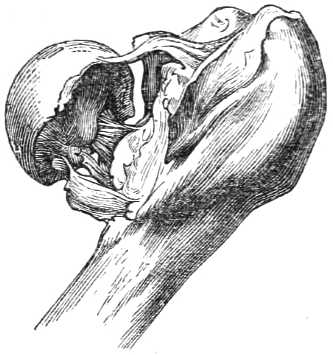
Old Inter-Capsular Fracture, with considerable shortening.
A Treatise on Fractures. By Professor J. F. Malgaigne, of Paris. With over one hundred Illustrations. Translated from the French, with notes and additions, by John H. Packard, M.D. One vol. 8vo. $4.00.
Malgaigne’s Treatise has enjoyed so wide a circulation and such well-deserved renown, that we must own to a feeling of surprise at learning that before the appearance of the present work no attempt has been made to present so popular an author in an English dress. The present book, a contribution to our literature from America, is the work of a gentleman whose name is not otherwise known to us, and is one which we can conscientiously pronounce very valuable.... A very useful book indeed, and one which we hope will have an extensive circulation.—British and Foreign Med. Chir. Review.
Must be regarded as a monument, conspicuous and to be admired, even among the noble monuments of the medical literature of his [the author’s] country. As a solid, complete, substantial, highly-finished work, we know of none that is its superior; it can, with justice, be regarded as a model in scientific literature.—North American Med. Chir. Rev.
It affords us sincere pleasure to be able to welcome the appearance, in an English dress, of this valuable treatise. The annotations which Dr. Packard has appended to it are numerous, and appear to us to be of much practical value, adapting, as they do, the treatment of fractures to the generally received and most approved American methods.—Journal of the Medical Sciences.
Notes of M. Bernard’s Lectures on the Blood, with an Appendix, giving an account of the latest studies of M. Robin, the celebrated microscopist. By Walter Franklin Atlee M.D. One vol. 12mo. Cloth, 75 cents.
A Treatise on the Practice of Medicine. By Geo. B. Wood, M.D., Professor of the Theory and Practice of Medicine in the University of Pennsylvania. Fourth edition, improved. Two vols. 8vo. $7.00.
This is far the best work on the practice of medicine in the English language, and we recommend it strongly to the attention of our readers. It is much fuller than Dr. Watson’s admirable lectures, while it is less lengthy than the Library or Cyclopædia of Medicine; and it has this further advantage over the two last-named works—that while they are far behind, it is a fair reflex of the actual state of knowledge.—London Medical Times and Gazette.
The Dispensatory of the United States: Consisting of—
1. A treatise on Materia Medica, or the natural, commercial, chemical, and medical history of the substances employed in medicine, and recognized by the Pharmacopœias of the United States and Great Britain;
2. A treatise on Pharmacy: Comprising an account of the preparations directed by the American and British Pharmacopœias, and designed especially to illustrate the Pharmacopœia of the United States; and
3. A copious Appendix, embracing an account of all substances not contained in the official catalogues, which are used in medicine, or have any interest for the physician or apothecary. By Geo. B. Wood, M.D., Professor of the Theory and Practice of Medicine in the University of Pennsylvania, etc. etc., and Franklin Bache, M.D., Professor of Chemistry in the Jefferson Medical College of Philadelphia, etc. etc. Eleventh edition, much enlarged. One vol. 8vo. $6.00.
This work has been thoroughly revised, with many alterations and additions, so as to bring it fully up to the level of the present state of materia medica and pharmacy. It embraces the substance of the recently revised United States and British Pharmacopœias, with a commentary on all that is new in those publications. Nothing, indeed, has been omitted in the revision which could render it worthy of the confidence it has enjoyed.
A Treatise on Therapeutics and Pharmacology, or Materia Medica. By Geo. B. Wood, M.D., Professor of the Theory and Practice of Medicine in the University of Pennsylvania, Senior Physician of the Pennsylvania Hospital, one of the authors of the United States Dispensatory, author of a Treatise on the Practice of Medicine, etc. etc. Two vols. 8vo. $7.00.
In his preface Dr. Wood gives the following account of his opportunities for acquiring knowledge and forming just views on the subjects embraced in this treatise:—
“Almost from the commencement of his professional life the author has given peculiar attention to this branch of medical knowledge. For a period of about thirty years, before 1850, when he was transferred to the professorship which he now occupies, he was engaged in teaching materia medica, first as a private lecturer, and afterwards successively in the Philadelphia College of Pharmacy and the University of Pennsylvania. His position, therefore, rendered constant investigations into the properties, effects, and uses of remedies necessary in order at once to do justice to his pupils and avoid discredit to himself. Most of those whom he now addresses are probably aware that he is one of the authors of the United States Dispensatory. To provide the original materials for his portion of that work, and to gather from time to time the knowledge requisite for its maintenance upon a level with the progressive condition of medical science, unremitting diligence was essential in prosecuting inquiry and investigation in the whole field of pharmacology. In addition to the ordinary professional opportunities, he has for about twenty years held the office of one of the physicians of the Pennsylvania Hospital, which has given him facilities for testing the value of remedies greater than any amount of private practice could afford. Few persons have had greater advantages or stronger inducements than himself for acquiring the knowledge requisite for the production of a work of this kind.”
Introductory Lectures and Addresses on Medical Subjects. Delivered chiefly before the medical classes of the University of Pennsylvania. By Geo. B. Wood, M.D., LL.D., President of the American Philosophical Society, Professor of the Theory and Practice of Medicine, and of Clinical Medicine, in the University of Pennsylvania, etc. etc. One vol. 8vo. $1.75.
A Treatise on the Diseases and Physical Education of Children. By John Eberle, M.D., late Professor of the Theory and Practice of Medicine in Transylvania University, etc. etc. Fourth edition, with notes and large additions by Thomas D. Mitchell, A.M., M.D., Professor of the Theory and Practice of Medicine in the Philadelphia College of Medicine, late Professor of Materia Medica and Therapeutics in Transylvania University, Lecturer on Obstetrics and the Diseases of Women and Children, etc. etc. One vol. 8vo. $2.50.
Dr. Eberle’s “Treatise” has long been regarded by the medical profession as the best and most comprehensive work on the diseases and physical education of children. Dr. Mitchell has made considerable additions to it, introducing many topics not treated of by Dr. Eberle, every one of which he considers entitled to a place in a work on the diseases of the infant race. The large addition of matter thus made to the work has proved to be both acceptable and useful.
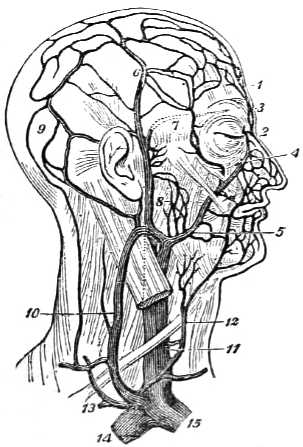
Veins of the head and neck.
Elements of Human Anatomy: General, Descriptive, and Practical. With over 400 illustrations. By T. G. Richardson, M.D., Demonstrator of Anatomy in the Medical Department of the University of Louisville, and one of the attending Surgeons to the Louisville Marine Hospital. One vol. 8vo. $3.00.
It is an amply sufficient text-book, and the preceptor may confidently place it in the hands of his pupils as such. The wood-cuts are numerous and elegant, and serve admirably to illustrate the text.—New Jersey Medical Reporter.
Our author claims for his work the improvement of having general, de[623]scriptive, and practical anatomy in the same volume; the arrangement of the section devoted to practical anatomy so as to secure the greatest possible economy of material; and lastly, in the substitution of English for Latin terms, wherever it appeared to be practicable and judicious.—N. Y. Medical Times.
A Practical Treatise on Venereal Diseases; or, Critical and Experimental Researches on Inoculation applied to the study of these affections: With a therapeutical summary and special formulary. By Ph. Ricord, M.D., Surgeon of the Venereal Hospital of Paris, Clinical Professor of Special Pathology. Translated from the French by A. Sidney Doane, A.M., M.D. Thirteenth edition. One vol. 8vo. $1.50.
M. Ricord’s reputation as a lecturer and practitioner in Paris is of the highest order. He is distinguished for his sound and philosophical views upon a disease which carries terror wherever it appears, and whose consequences are often felt by the innocent as well as the guilty. The first part of the book partakes of the philosophical spirit of its author, while in the pages devoted to the treatment of syphilis, M. Ricord has spread out the results of thousands of cases coming under his observation.
A Dictionary of Domestic Medicine and Household Surgery. By Spencer Thomson, M.D., L.B.C.S. Edinb. First American, from the last London edition. Revised, with additions, by Henry H. Smith, M.D., Professor of Surgery in the Pennsylvania University. One vol. 12mo. $1.50.
This work has received the highest encomiums from the critical journals of the day. “Many a useful life,” remarks a British periodical, “might have been spared, and many an insidious disease checked in the bud, had such works as that of Dr. Thomson been earlier in existence. To the traveler by sea or by land, to the settler and the emigrant, far from medical aid, it must prove invaluable.”
The work has been carefully adapted to the American climate and habits by Dr. Henry H. Smith, of Philadelphia, whose contributions to the volume have greatly added to its value. It is the standard book of domestic medicine. The arrangement of the subjects in alphabetical order renders it extremely convenient for prompt reference and consultation.
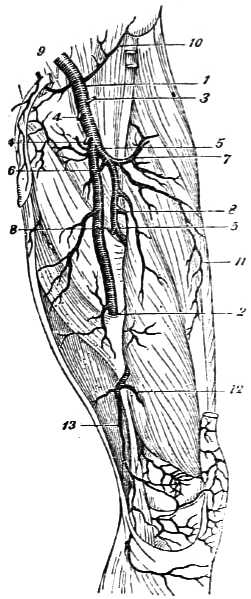
A new arrangement of the London Dissector, with numerous modifications and additions; containing a concise description of the Muscles, Nerves, Blood-vessels, Viscera, and Ligaments of the Human Body as they appear on Dissection. With Illustrations. By D. Hayes Agnew, M.D., Lecturer on Anatomy, and Surgeon to the Philadelphia Hospital, (Blockley.) One vol. 12mo. $1.00.
This work has been adapted to the use of the American student by altering the arrangement and changing the nomenclature in many cases; by adding the ligamentous system; by illustrations; by erasing what was unnecessary, and presenting the whole as nearly as possible in the topographical order. The work, as now published in this American edition, has been prepared with a single eye to the faithful economy of the student’s time.
A Practical Treatise on Diseases of the Urinary and Generative Organs in both Sexes. Part I.—Non-specific Disease. Part II.—Syphilis. By William Acton, late Surgeon to the Islington Dispensary, and formerly Externe at the Female Venereal Hospital, Paris. From the second London edition. With additional Illustrations and Colored Plates. One vol. 8vo. $4.00.
This work is intended to be used by the student as a complete Text-book on the subjects of which it treats; and, at the same time, to supply data for the surgeon desirous of learning the most modern treatment of the protean forms of Syphilis, as well as materially to assist the practitioner who, in the witness-box, is liable to be cross-examined on many of the most intricate questions of generation, absorption, or contagion.
Transcriber’s Notes:
A number of typographical errors have been corrected silently.
Archaic spellings have been retained.
Cover image is in the public domain.
Alt Text for images are in the public domain.
“Remarks” heading added to Table of Contents.
Index, Index of Cases, and Medical Works added to the Table of Contents.
Amputation of arm index to page 156 is deduced, only “ 56” was printed.
Index references page 649 which does not exist.