*** START OF THE PROJECT GUTENBERG EBOOK 60822 ***
Transcriber’s Note:
The cover image was created by the transcriber and is placed in the public domain.
PUBLICATIONS FROM
THE UNIVERSITY OF PITTSBURGH
SCHOOL OF MEDICINE
Studies on Epidemic Influenza
COMPRISING
Clinical and Laboratory Investigations
BY
Members of the Faculty
of the
School of Medicine
UNIVERSITY OF PITTSBURGH
1919
TABLE OF CONTENTS
|
|
Page |
| |
| History and Epidemiology of Epidemic Influenza |
9–33 |
| |
| |
James I. Johnston, M.D., F.A.C.P.,
Assistant Professor of Medicine. |
|
| |
| A Clinical Description of Influenza as It Appeared in the Epidemic of 1918–19 |
35–63 |
| |
| |
J. A. Lichty, Ph.M., M.D.,
Associate Professor of Medicine. |
|
| |
| The Urine and Blood in Epidemic Influenza |
65–79 |
| |
| |
P. I. Zeedick, M.D.,
Demonstrator in Medicine. |
|
| |
| The Treatment of Influenza |
81–95 |
| |
| |
W. W. G. Maclachlan, M.D., C.M.,
Assistant Professor of Medicine. |
|
| |
| The Prevention of Epidemic Influenza with Special Reference to Vaccine Prophylaxis |
97–153 |
| |
| |
S. R. Haythorn, M.D.,
Director of the Singer Memorial Research Laboratories. |
|
| |
| Physiological and Physiological Chemical Observations in Epidemic Influenza |
155–160 |
| |
| |
C. C. Guthrie, Ph.D., M.D.,
Professor of Physiology. |
|
| |
| The Bacteriology of Epidemic Influenza with a Discussion of B. Influenzæ as the Cause of This and Other Infective Processes |
161–205 |
| |
| |
W. L. Holman, B.A., M.D.,
Professor of Bacteriology. |
|
| |
| The Pathology of Epidemic Influenza |
207–293 |
| |
| |
Oskar Klotz, M.D., C.M.,
Professor of Pathology. |
|
5
PREFACE
This report is based upon a series of investigations carried on
during the epidemic of influenza at Pittsburgh. This epidemic
reached Pittsburgh about the last week of September, 1918,
rapidly spreading through the community during the first days
of October. Pittsburgh had been warned of its coming through
the experience of Boston, where the epidemic made its appearance
during the late days of August. To a certain extent the
warning from the East permitted the making of preparations to
control its ravages. But even with the attempt for the protection
of public health the epidemic advanced with all its virulence,
rapidly picking out the susceptible individuals and leading to a
high death rate.
At the time of the coming of the epidemic there were stationed
at Pittsburgh two military camps, comprising about 7,000 men.
It was with the presence of the disease among these men that
our investigations were chiefly concerned. The men at their
respective camps (on the campus of the University of Pittsburgh
and at the Carnegie School of Technology) were housed in barracks
which had been erected only a short time previously. These
barracks contained large dormitories, in which the individuals
freely mingled with each other. In them there was no opportunity
of complete isolation, and by this means of housing good
opportunity was available for the propagation of any communicable
infectious disease. The ordinary sanitary arrangements
for these groups were well provided. The first cases of recognized
influenza made their appearance on October 2. On this
day two men were found with the disease and were isolated. On
the following day there were four, and on the third day eight.
It was soon recognized that the increasing number of the infected
cases was growing so rapidly that definite arrangements for their
segregation and care had to be undertaken. This was provided
for on October 4, when the Elizabeth Steel Magee Hospital was
in part taken over by the military authorities and wards were
rapidly adapted for the coming epidemic. For the foresight in
making the adequate arrangements for its control and management
we shall always remain indebted to Major E. W. Day. His
6indefatigable work in the early days of the epidemic will always
be remembered, and the fact that the epidemic was kept within
reasonable bounds of control was the result of his stringent
quarantine regulations along with the organization of his medical
forces. Working under his direction, Capt. H. H. Hendershott
undertook the management of the hospital and rendered
most efficient service. The capacity of the hospital was soon
overburdened, so that from a normal 150–bed institution it was
on the sixth day of its conversion into an emergency hospital
carrying more than 300 cases of influenza. This hospital in itself
was unable to accommodate all of the cases falling ill, and provision
for these had to be made in some of the municipal institutions.
On October 5, 1918, the Medical School of the University
of Pittsburgh undertook to provide the laboratory facilities for
the emergency Military Hospital. It was at first intended to equip
only those laboratory departments which were deemed essential
for the clinical care of the patients in the wards. Inasmuch,
however, as the epidemic of influenza was spreading with alarming
rapidity throughout the city, it was deemed advisable to close
the Medical School and to place at the disposal of the Military
Hospital all the laboratory facilities which could in any way be
of use in the care and study of the influenza patients. This
permitted the establishment of departments in pathology, bacteriology,
physiology, physiological-chemistry and clinical microscopy.
The following workers partook in the investigations
which were here carried out: Dr. Oskar Klotz, director of laboratories;
physiology, Dr. C. C. Guthrie (chief), Dr. A. Rhode, Dr.
M. Menten, Mrs. C. C. Macklin, Miss S. Waddell and Miss M. Lee;
bacteriology, Dr. W. L. Holman (chief), Miss A. Thorton, Miss
C. Prudent and Miss R. Jackson; pathology, Dr. Oskar Klotz
(chief), Mr. A. D. Frost, Mr. J. L. Scott and Miss A. Totten;
clinical microscopy, Miss R. Thompson, Mr. M. Marshall and Mr.
H. Mock; records, Miss H. Turpin. Intensive work was undertaken
by each over a period of about five weeks, when the epidemic
was again on the road to disappearance and few new cases were
being admitted. These laboratories discontinued their work at
the Military Hospital on November 9.
The clinical observations which are contained in this report
were made at the Mercy Hospital. This institution set aside
upward of 100 beds for the care of the overflow which could not
7be accommodated at the Military Hospital. It is unfortunate
that the clinical observations and the laboratory findings contained
in this report were not made upon the same cases. With
the number of cases suddenly thrust upon the medical staff of
the army, it was not possible for them to devote detailed attention
to clinical investigation. Furthermore, during the progress of
the epidemic these medical officers were transferred to new posts,
so that it was impossible to obtain a summary of the clinical
findings at the Military Hospital by any of the officers who had
but recently been detailed to the work. We were fortunate,
however, that the clinical investigations were carried out on a
similar group of cases to those studied by the laboratory, and it
might be said that their clinical findings on the patients housed
at the Mercy Hospital are parallel with those observed in other
institutions. Necessarily the researches carried out during such
an epidemic were intensive, and all the workers in the various
branches feel that if they had to live through another such
plague they would be much better prepared to approach their
problem. During the heat of such investigations valuable time
is often lost in perfecting methods of technique, and one sorrowfully
finds oneself without available material when the technical
work has been accomplished but the epidemic has passed by. In
the studies in bacteriology we were fortunate in having some of
the technical difficulties for the isolation of the B. influenzæ
previously solved. It may be that this in part explains the
broad success which Dr. Holman has had in isolating the B. influenzæ
from so many cases. In other fields the road was less
broken, and it was not until late in the course of the epidemic
that results were obtained in the investigation which seemed to
point to valuable leads.
Dr. S. R. Haythorn, director of the Singer Memorial Laboratory,
early in the epidemic became interested in the protection
of individuals against the infection. In certain quarters much was
claimed for the immunity which could be conferred by vaccination,
either by the inoculation of pure B. influenzæ vaccines or
by mixed vaccines. Hoping for some results by the use of
such vaccines, Dr. Haythorn undertook the preparation of these
materials. The value of this procedure could only be estimated
after the lapse of some time and at a period when the epidemic
was again waning.
8The clinical work at Mercy Hospital was carried on under the
direction of Dr. J. A. Lichty, and assisted by Dr. W. W. G. Maclachlan,
Dr. P. I. Zeedick, Dr. F. Klein and Dr. W. J. Fetter. By
the close co-operation of the members of this group it was possible
to put the clinical findings of one or other member to severe
test, so that the recorded observations and deductions are of the
greater value and less flavored by the personal element. This is
of the more value, since, with the great amount of work which
had to be done at the time of the height of the epidemic, it was
often not possible for the same individual to bestow the amount
of time upon each and all cases as he desired.
We are much indebted to Dr. Ogden M. Edwards, dean of the
School of Medicine, for making available the facilities for carrying
out the work, and for encouraging the publication of the
reports.
9
HISTORY AND EPIDEMIOLOGY OF INFLUENZA
By James I. Johnston, M. D.
The history of epidemic influenza extends back with definite
authenticity to the Middle Ages, with a fair amount of assurance
to the beginning of the Christian Era and with presumptive reliability
even before that period. Beyond this statement, nothing
definite can be said until the first epidemic reported by Short and
found in the English Annals in the year 1510. This, the first
reliable record, presented some features not unlike those occurring
in the present epidemic. Two or three striking things stand
out in this record—namely, the presence of nose bleed, pneumonia
and the very great danger to gravid women. Here, for the
first time, the meteorological conditions were elaborately studied
and persistently dwelt upon. One other impressive thing, also
reported by Short, was that in 1580 the disease showed a tendency
to return after a period of quiescence. Attention is called to this
because the epidemic, while it was exceedingly prevalent in the
months of August and September, became pandemic in October
and November. Another feature was that during the years intervening
between 1580 and 1658 sporadic cases of this disease were
frequently reported. During the latter year another epidemic
appeared in the month of April. In 1657 and 1658 at London the
summer was very warm, the winter came on early, there was
much snow and the spring was very moist.
The prevailing opinion at this time, and the first stated by
Willis, was that the widespread disease was due to the weather
influences on the circulation, poisoning the blood of the patients,
and “not blasts of malignant air.” The disease prevailed in the
large cities, recurring again in the autumn in an extensive form
through the villages and country. Sydenham, in his communication
on the epidemic in 1675, wrote emphatically on the influence
of the infection on pregnant women, and here used the term
“tussis epidemicus” as a name for the disease. The summer of
1675 was wet with an inconstant autumn. La Grippe prevailed in
10France and Germany, according to Atmuller. In England in 1676,
the autumn was pleasant, but suddenly became cold and moist.
La Grippe then started in Germany during September after a
summer and a beginning autumn which was very rainy. Molyneux
in his description of the epidemic of 1693 in Dublin called attention
to a feature, very striking to the recent pandemic, that the
aged to a great extent escaped the infection. This would seem a
somewhat unique feature until that epidemic is compared with
the present one. In 1729 Morgagni and others stated that over
all Europe the winter of 1728 was very rigorous, the spring was
cold and the summer and autumn very variable, while January
and February of that year were very moist. Huxham in his
record of 1729, the fifth extensive one on record in the English
Annals, which extended into 1733, stated from his study at
Plymouth that the epidemic was exceedingly mild in the year
1733, and, with the exception of infants and consumptive old
people, the mortality was very low. Like many of his predecessors,
he emphasized greatly the conditions of the weather at
the time and presented an elaborate study of it. The epidemic of
1732 was one of the longest and most persistent, extending up to
1737. All authors do not hesitate to attribute as a cause the very
frequent variations of temperature which characterized this
period. Of this epidemic Arbuthnot also emphasized the importance
of the air, assigning the prevalence and widespread features
of the disease to the thick and frequent fogs. From November,
1732, until March, 1733, this disease spread from Germany to
Italy and thence to England. He called attention to a very
striking feature—namely, that people in prisons and in hospitals
escaped the disease. This, as we know, where such institutions
are placed under preventive quarantine, is not such a unique
feature during this present scourge. He, more than former
writers, devoted pages to the elaborate and accurate description
of instruments for meteorological observation and their findings,
which meteorological records were published in detail, covering
the whole period of a year—June, 1732, to June, 1733—with
almost daily regularity. Huxham in 1737 in his record first used
the term “epidemic catarrhal fever”—a name often used subsequently
to describe this disease. Here attention was first called
to the prostration which characterized the convalescents, and his
belief that consumption frequently followed the disease. The
11next epidemic, which occurred in 1742 and 1743, was also reported
by Huxham, who stated that the weather was very rigorous. This
disease, according to his description, extended over all Europe,
and the term “influenza” seems to have been first used by him
during this time. The cases were mild in England, but more
severe in Southern Europe. Whytt in his record of the epidemic
of 1758 was the first who did not consider that the air condition
or the seasons had the significance attributed to them by former
writers, since the weather conditions during the prevalence of the
disease were generally mild and dry. In Edinburgh at this time
not even one out of seven escaped. Nevertheless, he did not hesitate
to express his opinion that the disease did not spread by contagion
from one person to another. One other observation of his
is worthy of note, which is: that frequent relapses occurred when
patients were re-exposed too soon after the first infection and
such relapses were much more severe than the original disease.
The epidemic of 1762 called forth the opinion of Baker, emphasizing
an opinion already expressed by Whytt, that the origin of
epidemic disease is not due to changeable winds nor to their
nature or character as recorded by the barometer. This epidemic
also prevailed over all Europe and appears to have begun following
sharp alterations of cold and moisture. In 1766 in Spain,
France and other parts of Europe the epidemic appears to have
begun after a warm summer, followed by an autumn moist and
cold. In 1767 Heberden placed on record his observations during
this period, but nothing new was reported. In 1775 the disease
began in Germany in the summer after a dry and warm spring
and spread over all Europe. During the prevalence of the disease
in 1775 a questionnaire was sent to the leading English physicians,
and letters from Fothergill, Sir John Pringle, Heberden, Reynolds
and others seemed to express a consensus of opinion that weather
conditions had nothing to do with the prevalence or spread of the
disease, and that the cause and reason for its spread were unknown.
Following sharp alterations in temperature in 1780, the
disease appeared in France and then throughout the world. The
epidemic of 1782 began in Russia, starting January 2 at St.
Petersburg. The thermometer underwent a variation of 40
degrees and the same day 4,000 were afflicted with La Grippe.
It reached Koenigsburg in March, Copenhagen in April, London
in May, France in June and July, Italy in July and August, Spain
12and Portugal in August and September, and then reached America.
Edward Gray, writing of the epidemic of 1782 for the first time,
expressed emphatically his opinion on the contagiousness of the
disease and stated what we now know—that close contact is
necessary. To him also is attributed the opinion first mentioned
by him, that there is a possibility of carriers in this disease.
During this time Dr. Hamilton, in a published letter, protested
against venesection in influenza, a practice long prevalent, and
Hogarth called attention to the fact that the disease began in
cities and villages first and that it was brought to these places by
visitors from without.
The first American writer on this subject was Noah Webster
in 1647 and 1655. Following him was Warren, writing of the
epidemic of 1789 and 1790, just 100 years before the last and
greatest epidemic which preceded the present one. Rush and
Drake also reported this epidemic. During that epidemic which
prevailed in America from September to December, 1789, and
appeared again in the spring of 1790, President Washington
suffered a very severe attack. The year before, in 1788, when
the epidemic prevailed abroad, the summer temperature in Paris
was very variable, variations of 8, 10 and 12 degrees occurring
on various days. La Grippe predominated all the time. The same
variations were true in Vienna. At the end of the year 1799 the
epidemic struck Russia, following very cloudy, misty weather,
was prevalent in Lithuania in January of the year 1800 and in
Poland during February.
The next great epidemic occurred in 1802 and 1803, was very
general, beginning in France and coinciding with a cold and moist
autumn following a very dry summer. It was of six months’
duration in England. Many schools, jails, asylums and workhouses,
although located in the area swept by this plague, at first
escaped. As mentioned before, this striking feature has not been
so unique in subsequent epidemics. One feature noticed here
and commented upon freely was that elsewhere throughout the
country there seemed to arise endemic foci. During this time
there was also the prevailing belief that the disease was followed
by phthisis. One other observation made here, which was accurate,
lasting and is accepted today, was that no family was
affected en masse, but always one individual case occurred first,
to be followed by general infection of the others. At this time
13early bleeding was still adhered to. The French spoke of seven
varieties of the disease, but one can only see in the classification
emphasis laid on certain individual symptoms in this disease of
complex symptomatology. During this epidemic pneumonia is
said to have been very infrequent. The disease was particularly
fatal to pregnant women, and the patients suffering from pulmonary
tuberculosis were hurried off by the influenza.
Burns, writing of the epidemic of 1831, mentioned that in 1810
the disease was very widespread in China and Manila, and also
emphasized the fact mentioned in many works that certain epidemics
prevailed among animals at the same time, stating that
in 1831 these diseases were of choleric nature. This epidemic
began in 1830 in the East, reached Paris in the summer of 1831,
reappeared in Europe in 1833, following the same route that
cholera had taken in 1832. In the epidemic of 1833, Hingeston
also laid great stress on the fact that horses were often affected.
These features, as mentioned by Burns and Hingeston, are frequently
quoted by authors, and such observations seem to have
been widely accepted.
One of the greatest epidemics of influenza began in 1836 and
extended until 1837, and was called at this time epidemic catarrh.
It began in England in January, spread to France, and during all
the time that it was in Paris there were continual penetrating
rains with cold and humidity. At Montpelier on February 20,
1837, the thermometer passed from 12 to 15 degrees above to
2 and 3 degrees below zero, and it was then that La Grippe
appeared suddenly. In reply to the circular letter sent out by
the Council of the Provincial Medical Association of England,
comprising 18 questions, the following opinions prevailed. The
disease was greatest from September to February; the great
prevalence of the epidemic in all parts of the kingdom was recognized—attacks
were irrespective of age, sex or temperament; it
was milder in children, and the aged suffered most from it.
Further, the disease was extensive in all neighborhoods; the mortality
was 1 in 50, old age predisposed to fatal termination, and
the duration of the disease occupied two periods, one terminating
in 4 or 5 days and one in 5 to 14 days. Also relapses were
frequent; those exposed to employment in the open air were not
more liable to the disease than others; there was no proof of the
disease being communicated from one person to another, and influenza
14aggravated an existent pneumonia or pulmonary phthisis.
And finally previous attacks of influenza offered no protection;
the symptoms were uniform; the most common of unusual symptoms
were those of meningitis, inflammation of the lungs and
syncope, and aside from ordinary care and treatment, general
venesection was not endorsed. Evidence of fine weather and good
telluric conditions were at this time also appended. The same
symptoms and complications, particularly those of the lungs,
occurred irrespective of seasons, civilization or place. It was believed
and stated that the plague described in Homer was probably
influenza. For the first time there is noticed here a point
well worth consideration—the association of other epidemics with
influenza, either anticipating, following or superseding. That
some such association may follow the present pandemic is not to
be entirely ignored. For example, cholera is already reported as
prevailing abroad, following an earlier influenza outbreak. During
the period, as if anticipating bacteriology, one writer
explained the epidemic in an article called “The Dust of Regular
Winds,” and Groves (1850) wrote on “Epidemics Examined, or
Living Germs as a Source of Disease.”
In 1846 and 1847 a slight epidemic occurred in London, Paris,
Nancy and Geneva. In France during the last week of 1857, and
extending into January and February, 1858, there was a mild
epidemic. During this period there alternated frequent frosts
with soft weather, misty and humid. Among the numerous small
epidemics between 1837 and 1889, one occurred on the continent
of Europe in 1860, but little of value or interest was noted. In
Paris in March, after great and sharp variations in temperature,
a series of epidemics extended from 1870 to 1875. These were
unimportant. Atmospheric modifications occupied first rank in
the minds of some as a cause for the outbreaks. Rapid changes
from hot to cold or from cold to hot were given weight. Other
undetermined modifications of conditions were probably important.
In a recent article published by Loy McAfee (J. A. M. A., 1917,
72, 445) he discussed the confusion which existed between the
diagnosis of cerebro-spinal meningitis and epidemic influenza in
1863. These were believed the same by some—that is, the same
disease of varying degree. There was a great diversity of opinion
among clinicians at this time, and the American Medical Association
15appointed a committee to make an investigation. McAfee
quotes from the Medical and Surgical History of the War of the
Rebellion that in 1861 and 1862 an epidemic existed among the
troops called epidemic catarrh, which was afterward changed to
read acute bronchitis. In September, 1861, there existed an
epidemic of influenza in one of the regiments which lasted more
than two weeks, and in another camp there was a similar epidemic
at the same time. It is stated that there were in all 168,715
cases among the white troops, with a mortality of 650, and 22,648
among the negro troops, with a mortality of 255, making about
4 per thousand, and over 11 per thousand, respectively.
The next great epidemic, and the last until the present,
occurred in the years 1889 and 1892, and was pandemic in its
nature. The death rate during this time was lower in the cities
than in the country. This was probably due to the fact that
the greatest mortality was among children and old people, and
as old people were generally left in the country, this explains the
observation. The highest number of deaths was among males,
believed to be due to the exposure and fatigue of work. Forty
per cent. of the world’s population was said to have been attacked
during this period. The yearly or seasonal repetition, as shown
in this pandemic, had occurred in other epidemics. In the great
pandemic of 1889 and 1890, five decades after the last important
epidemic, it was stated that the medical profession found itself
confronted by a new disease of which it had knowledge through
medical history, so also in our time few physicians recognized at
first the reappearance of influenza. This 1889 epidemic is extensively
reported in the literature, and has been elaborately worked
out by many observers. One important feature has been emphasized
by Leichtenstern, which, although recognized by the profession
after the last epidemic had been fully reported and
recorded, is not appreciated by the profession during the present
epidemic—namely, that while shortly after the last epidemic
there were smaller relightings of the infection throughout various
parts of the country, those diseases which we erroneously
call grippe or influenza, occurring commonly in the spring and
fall, are in no way connected with the disease with which we are
dealing, and which occurs at rather long intervals. Any speculation
in regard to these periods, which history has shown to
be fairly wide apart, has very little basis. This pandemic, like
16many of former days, is believed to have originated in Asia,
and from there to have spread over Europe and hence over
the world. The disease spread rapidly over countries, affected
probably about 40 per cent. of the world’s population, disappeared
rapidly after several weeks, was thought to have had
nothing to do with weather conditions, had a great morbidity
but small mortality, and affected all ages and occupations. There
is no doubt, as stated by some, that the development of traffic
and travel was a large factor in the rapid and extensive spread
of influenza during this pandemic. The course which the disease
followed, springing from its supposed beginning in Asia, has been
fully and amply described by writers after that period, but the
great rapidity of its dissemination over all countries is the most
remarkable feature in the epidemiology of any disease. This,
during 1889, made many prominent physicians disregard the
opinion that influenza spread by contagion and accept again the
opinion expressed by observers of epidemics in former ages, that
miasma as a pathogenic agent was responsible for its distribution;
but anyone who reads closely the history of this epidemic,
and in the light of modern medical science, must feel that the
rapidity of distribution was nowhere greater than the most
speedy means of transportation. This very necessary close connection
was demonstrated also in regard to the mode of spread
of the disease; the large cities and the commercial centers were
affected earlier, smaller and country districts followed later,
railroad towns were more frequently attacked than isolated villages,
and even from jails, prisons and workhouses, where quarantine
was immediately attempted, as well as from remote villages
where the disease had been brought, there could be traced
a zone of infection spreading into the country. One interesting
point was raised at this time—namely, that in some places it
seemed to spread by leaps and bounds, and at other places
radiating as stated above.
The old controversy of whether influenza is distributed in a
radiating manner or in so-called leaps and bounds is believed to
be settled by consensus of opinion that it occurs in both ways.
An opinion expressed by the study at this time as to whether
influenza spreads more rapidly than any other infectious disease
is found in the statement that the contagion is markedly virulent,
the micro-organisms are easily conveyed from their original seat
17in the mucous membrane by coughing, sneezing and expectoration,
the great number of persons who, though slightly affected,
carried on their ordinary way of life without hindrance, the
probable longevity of the organisms in convalescents, the brief
period of incubation of two or three days, the susceptibility of all
people of every age and vocation, and the possibility of carrying
the contagion by merchandise and even through short distances
in the air, are all suggestive reasons for this. No one at present
accepts the so-called miasmatic nature of the contagion. Proofs
are ample to show that one case must be present in a locality
or even family, although it may be frequently overlooked, from
which the epidemic spreads. During this period of 1889 and
1890 the duration of the actual epidemic period in different localities
in Europe was from four to six weeks. This was subsequently
shown to be consistent with the recorded reports from
the various cities in the United States. Following this pandemic
in the first part of the year in 1891 there were numerous epidemic
outbreaks in various parts of America, including New Orleans,
Chicago, Boston, and simultaneously in England. Strange to
say, at this time neither Germany nor France had such epidemics,
although both were exposed by travelers, particularly
from England and America. The question was raised at that
time whether the Germans, French or other continental nations
were more immune than Americans and English. In the fall of
1891 and the entire winter of 1892 the disease was extensively
prevalent both in Europe and Northern America. In these later
epidemics there was no definite direction of spread. They probably
would come more clearly under the so-called radiation from
numerous rural districts. In almost every case at the point of
its origin in these countries the epidemic developed and spread
slowly, lasting months and with very varying morbidity and
mortality. They had none of the explosive characteristics of
the pandemic. The general diminished morbidity of the later
epidemic, the diminished geographic distribution of the disease
and the scarcely recognizable character of its contagion, its slow
development and extension over several months, the continuous
diminution in frequency and in intensity since its onset in 1889,
have been explained by presumptive successive lessening of susceptibility
of the population, possibly due to acquired immunization.
Observers at that time, as well as ourselves, could question
this last statement.
18There was observed one noteworthy thing about seasons.
While the great pandemic of 1889 and 1890 had no definite connection
with seasons, the epidemic types which followed in 1891
and 1892 seemed to show a lighting up in either spring or fall,
remaining dormant in the summer months. It has also been
shown by the history of former epidemics that almost all the
pandemics started from Russia in the fall, winter and spring
months. Such was the case in 10 of the great pandemics of
1729 to 1889. This, no doubt, was the reason so many of the
former historical writers were impressed by seasons and meteorological
conditions. The statement made by observers during
the epidemic that influenza presented two phases, one pandemic
and the other endemic, and that each follows different epidemiological
rules, seems possible. The question raised during the last
epidemic of the spread of the disease in families, the disease
occurring at high altitudes and even at sea, we know does not
interfere with the recognition of its spread by direct contagion.
Definite examples of families or villages being infected by a
returned member of such family or citizen from abroad are
reported frequently, and even the appearance of the disease in
isolated places has often been traced and verified from a definite
source, to say nothing of the question of carriers and those supposed
to be suffering from other diseases.
Striking examples are shown also in this epidemic that many
institutions, frequently those isolated from the world, were
markedly exempt until, through servants or outside visitors, the
disease gained access to them. This gave a most favorable field
for the study of invasion, spread and decline of the disease.
Observations made at this time in regard to hospitals seemed to
suggest that certain institutions were more or less exempt,
although not closed institutions, while others suffered from the
first. These two types of hospital invasion are hard to reconcile.
Great stress was laid in this epidemic upon the very great
morbidity and the low mortality. Simple, uncomplicated influenza
at this time was looked upon as a disease that was rarely dangerous
to life. Studies have shown that after this period there
seemed to have been lessened morbidity. As previously stated,
nearly all the numerous pandemics at various times have had
their origin in Russia and arose in the late autumn or winter
months. This pandemic of 1889 and the succeeding severe epidemics
19in Europe and North America in the years of 1891 and
1892 occurred almost exclusively in the cold weather, the summer
remaining free. It is generally believed now, and was at the end
of that pandemic, that atmospheric or telluric conditions had
nothing to do with the spread. The origin of epidemics following
the pandemics seemed to be influenced in their recurrence by the
season of the year. It was conceded by observers in that pandemic
also that contagion might be carried by merchandise and
even flies and healthy individuals.
1918 Epidemic in Large Cities
In the city of Boston during the week ending August 28, at the
Naval Station at the Commonwealth Pier, 50 cases of influenza
occurred and within the next two weeks more than 2,000 were
reported in the naval forces of the First Naval District. Of these
5 per cent. developed broncho-pneumonia with a mortality of more
than 60 per cent. From here it probably spread to Camp Devens
and thence ran rapidly over the country. There can hardly be a
question that it spread along the lines of traffic. Up to November
9 there were reported 3,339 cases among the civilian population
of Boston. There were 3,430 deaths from influenza, the presumption
being that these were due to bronchial pneumonia,
although not reported as such. The deaths from all forms of
pneumonia were reported as 942, making in all 4,372 deaths from
September 7 to November 9. This discrepancy—that is more
deaths than reported cases of influenza—is due to the fact that
influenza was not made a reportable disease until the date of
October 4, fully a month from the time the epidemic appeared.
The weather conditions were generally fair and no noted abnormality
is recorded as compared with other years. The statement
of the Health Department of this city was that, after a practical
disappearance of influenza in October, there was a slight recurrence
in November and a more pronounced recurrence about the
first of December, since which time the cases have slowly but
steadily decreased, until at present—December 21—the fatalities
attributable to influenza are about 20 daily.
In the city of New York the epidemic first appeared September
18. Up to and including December 27 there were reported to
the Department of Health 136,061 cases of influenza and 21,388
20cases of pneumonia. The number of deaths since September 18
was 11,725 attributed to influenza in the death certificates filed
in the Health Department and 11,601 attributed to pneumonia.
The epidemic reached its peak during the week of October 19,
slowly subsided and was practically at an end on November 9.
While the epidemic is reported as ending on this date, the mortality
rate from influenza and pneumonia is still very much above
normal. No particular features concerning the meteorological
conditions were noted, except that in this city the weather was
clear and delightful during the months of September and October
when the epidemic was rampant.
In the city of Philadelphia on July 22 the Health Department
issued its first health bulletin on so-called Spanish influenza,
announcing the possible spread of this disease into the United
States. On September 18 a warning was issued against an epidemic,
the department starting a public campaign against coughing,
sneezing and spitting. On September 21 the Bureau of
Health made influenza a reportable disease. At this time the
authorities stated an epidemic of influenza was recognized as
existing among the civil population of similar type to that found
in the naval stations and cantonments; that a large percentage
of cases was accompanied by pneumonia; that patients should be
isolated and attendants wear masks; that isolation be practiced
for a period of ten days after recovery to prevent carriers; that
patients be guarded against relapse and that the public be cautioned
against large assemblages and crowded places, as well as
to avoid coughing, sneezing and spitting. On October 3 the
churches, saloons and theatres were closed, funerals were made
private and food handlers were required to protect their wares.
The number of cases reported from September 23 to November 8
was 48,131, but the Bureau states, from a rough estimate, the
number of cases was probably 150,000. The total number of
deaths reported was 7,915 from influenza and 4,772 from pneumonia
in all its forms, the presumption being that the deaths
during this period were due to influenzal pneumonia. The
weather condition during this time is recorded as mild and fair.
The influenza cases began to be reported in Cleveland on
October 5, and up to December 20, 22,703 cases had been recorded.
Certificates recording deaths due to influenza alone numbered
2,497, while pneumonia amounted to 833. The epidemic was at
21its height in the latter half of October and the weather was
spoken of as pleasant fall weather. During the week of October
26 the epidemic reached its greatest height, abated in the week
ending November 23, increased later, but showed a drop for the
week ending December 21.
The epidemic first reached Chicago on September 21, and
from that date on it rapidly increased throughout the city for a
period of 26 days until October 17, when it reached its maximum
both in the number of deaths from influenza and from pneumonia.
On that day the total number of deaths from influenza and from
pneumonia reported was 2,395. From September 21 until November
16 there were reported 37,921 cases of influenza and
13,109 cases of pneumonia. On September 8 at the Great Lakes
Naval Training Station, which is 32 miles north of the city, an
extensive outbreak of influenza occurred. This was 13 days
before the outbreak in the city of Chicago itself. Camp Grant,
located at Rockford, 92 miles northwest of the city, suffered an
outbreak on September 21. A suggestion of the likelihood that
influenza was prevalent in this country in a mild and unrecognized
form in the spring of this year is shown by the fact that
numerous local outbreaks of acute respiratory diseases were
brought to the attention of the Health Department of Chicago.
These occurred especially in large office buildings and in industrial
departments. The total number of deaths from influenza
and pneumonia during 14 weeks was 51,915. This would indicate
that a very great number of cases were not reported to the
Bureau of Health until they died or else there must have been a
large number of deaths due to lobar pneumonia. One naturally
obtains from these figures the impression that the disease was
not recognized for a long time, that the pneumonia must have
been called lobar pneumonia, and that the actual figures gathered
by this city, as well as others, must have been greatly confused
at the onset of the epidemic. It is not unlikely that records from
many of the army cantonments and naval stations may be considered
from the same viewpoint. Weather conditions were considered
normal at the height of the epidemic, the weather being
dry. There has been a flare-up of influenza recently, but not in
sufficient numbers to justify calling it epidemic.
In the city of Louisville, Ky., the epidemic started September
26, and the total number of cases up to December 21 is reported
22as being 9,445. Out of this number 772 deaths occurred from
pneumonia. No distinction is made here between broncho-pneumonia
and lobar pneumonia, but the presumption from the records
of other cities at this time is that these were cases of broncho-pneumonia
following influenza. The weather was described as
being delightful fall weather. The statement is made by the
authorities that while the epidemic is still prevalent, it is confined
largely to children and is rapidly abating.
The first case in the city of St. Louis was reported about October
7, and up to December 23 there had been 31,531 cases reported
to the Bureau of Health. They recorded 1,920 deaths with
influenza given as a contributing cause. Preceding the time when
the epidemic was at its height the weather was fair and warm,
and the statement is made that, “without going into the matter
exactly, we have been of the opinion that damp, rainy weather
has been a help in controlling the disease.” The opinion was
expressed by the Commissioner of Health that the disease had
now abated.
No information could be obtained as to when the epidemic first
reached the city of New Orleans, but during the months of October
and November 43,954 cases of influenza were recorded. Of
this number 2,188 died from a combination of influenza and pneumonia.
They stated in their health report that during the period
from January 1 to December 31 there were 239 deaths attributable
to broncho-pneumonia. The weather was mild and on
December 24 the epidemic was stated to have abated.
The city of Minneapolis recorded its first case on October 7,
but the authorities expressed their belief that a few cases had
appeared before that date. Up to December 21, 15,000 cases had
been reported to the Bureau of Health and of these there had been
735 deaths from broncho-pneumonia. They had in their city a
late, rainy fall and up to that period they had had no cold weather.
The record obtained from the city of San Francisco stated that
the epidemic first appeared September 23 and that it was very
widespread in that city early in October. There were two invasions
and 53,260 cases reported. At the height of the epidemic
more than 2,000 cases were reported in one week; 188 deaths
occurred from influenzal pneumonia. The following week, after
the institution of mask wearing, in which between 80 and 90 per
cent. of the population concurred, it was stated that the number
23of cases decreased to about 200. It was stated that the weather
was generally very fair during the epidemic.
From the city of Portland, Oregon, the following information
was obtained: The epidemic first appeared October 11, with a
second one toward the end of the year. There were 8,079 cases
reported, with 658 deaths from influenza and 250 from pneumonia.
Weather conditions were stated to be varied, but the
health officer believed that during the worst wave the weather
was clear and dry, with easterly wind. He believed that a decrease
in influenza was noticed immediately after a Chinook wind and
warm rain. Similar observations were made by Coutant in
Manila.
A weather comparison of 12 large cities, well distributed over
the United States, studied during this pandemic of influenza and
checked with normal weather during that of many years, shows:
Boston, fair with no abnormality; New York, clear and delightful,
no abnormality; Philadelphia, mild and fair; Pittsburgh, mild
and cloudy; Cleveland, pleasant fall weather; Chicago, normal
and dry; Louisville, delightful fall weather; St. Louis, fair and
warm-damp, rainy weather later seemed to control the epidemic;
New Orleans, mild; Minneapolis, a rainy fall and no cold weather,
which is unusual there; San Francisco, generally fair, and Portland,
Oregon, clear and dry.
The Epidemic in Universities and Colleges
At Bryn Mawr College, in Pennsylvania, an institution devoted
to the higher education of women, located within 10 miles of the
city of Philadelphia, the epidemic occurred at the beginning of
the college year—October 1. This college at the time had an
enrollment of 465 students. There were 85 cases of influenza,
with an additional 25 who suffered from influenza in their homes.
There were no deaths from pneumonia. The weather conditions
were clear and warm, and since November 29 there have been no
new cases occurring in the college and only three or four of the
students have been ill at their homes since that time.
24
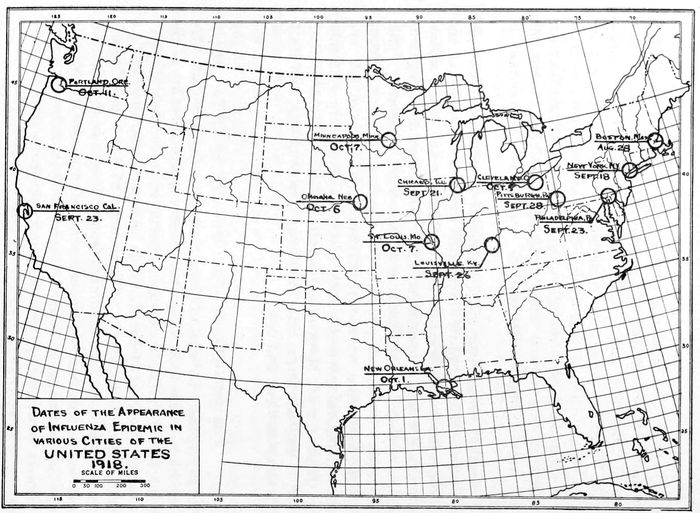
Dates of the Appearance of Influenza Endemic in various Cities of the UNITED STATES
1918.
25The enrollment at Smith College, Northampton, Mass., was
2,103, and the first case of influenza appeared with the arrival
of the students on September 18 and reached its height on September
30. All group gatherings indoors were stopped from
October 3 to October 18, and the epidemic was over by October
20. A recurrence began November 15 and continued until December
17. There were 182 cases in the first epidemic and 100 cases
in the second. There were only two deaths from influenza
pneumonia. During the rise of the epidemic the weather was
rainy, followed by good, clear weather. The change in weather
conditions seemed to make no difference. The second epidemic
was still prevalent when the students left for their holidays.
In Wellesley College, where there were enrolled 1,593 students,
the epidemic first appeared on September 18. Up to the middle of
December they had had 280 cases. During six weeks of the
epidemic 265 cases were reported and only one death occurred
from broncho-pneumonia. For the most part, bright and sunny
days were present, with only a few cloudy and rainy days. This
college has not been without cases since September, but the
epidemic lasted only about six weeks.
In a communication from Columbia University it is stated that
the epidemic appeared during the week beginning September 22.
No records were available for the student body at the time of
inquiry, but in the Student Army Training Corps of 2,200 men
between 8 and 9 per cent. had the disease during the period from
October 1 to December 14. In this army group during this period
two deaths from influenza and pneumonia occurred. The weather
conditions in the city during this time were considered normal
for fall weather—that is, mostly clear, with high winds. The
opinion expressed was that the epidemic was still prevalent and
increasing, and that a return wave seemed to be more virulent
and affected the children of the city more than had the first one
in the early fall.
There were enrolled at Harvard on October 1, 3,193 students.
The first case of influenza occurred on September 20. There were
227 cases of influenza reported; of these there were 46 cases of
broncho-pneumonia, with five deaths. There were two waves to
the epidemic; the first wave height was in October and the second
the last of November. The weather conditions were not severe
nor particularly unfavorable at either time. The epidemic abated
at the university largely because of the demobilization of the
Student Army Training Corps. At that time it was still prevalent
in Cambridge and Greater Boston.
26At Yale University the disease first appeared in the New
Haven Hospital on September 21. There were registered in all
departments of the university 2,265 students. Up to the date of
December 24, 1,013 cases have been treated. The number of
deaths from broncho-pneumonia has been 249. At the height of
the epidemic, which occurred in the third week of October, typical
fall weather prevailed. An unusually clear, dry October with
very little rain, much sunshine and rather low humidity was the
weather report.
During the period of the epidemic at Princeton that university
had 1,050 students, and the first cases appeared shortly after the
opening of the college term on September 24. As a precautionary
measure, every case, when even only suspicious, was sent to the
infirmary. In all, there were about 70 cases in the university
and about 45 cases from the United States School of Military
Aeronautics. Only one member in the latter school died of pneumonia.
There were no deaths among the students at the university.
In this part of the country the weather was most
delightful all autumn, being warm and dry, very little rain
having occurred since the end of July. At the date of the inquiry
the epidemic had disappeared—that is, about December 21—there
being only two very mild cases under suspicion. In the town of
Princeton, outside of the university, the conditions were much
more serious than in the university itself. Influenza appeared
in the homes of many of the poor people of the immigrant class,
so that it was not uncommon for four or five members of one
family to be infected at once. In one family of seven, five serious
cases of pneumonia developed. An emergency hospital was opened
by the authorities and 40 cases of pneumonia were treated. Of
these approximately one-half died. At the time this report was
furnished the epidemic seemed to have disappeared.
The number of students enrolled at the University of Virginia
was 957. The first cases occurred as early as September 24.
There were 290 of these in number, and three died of broncho-pneumonia.
The epidemic was reported as having abated on
December 15, but a few cases appeared after that date.
1918 Epidemic at Pittsburgh
At the Army General Hospital No. 24, located at Hoboken, a
few miles outside of the city of Pittsburgh, on September 28
27two soldiers were taken ill and, with the disease unrecognized,
they were removed to the cantonment hospital at Point Breeze,
within the city proper. The men were found a few days later
to be suffering from influenza, and from this presumable source an
epidemic spread rapidly among the troops and student soldiers
located here.
From September 28 until November 20, 1,392 cases of influenza
occurred among the enlisted men. How the infection reached the
first two cases at Hoboken is not known. The command here
consisted of the Student Army Training Corps of the University
of Pittsburgh, and Carnegie Institute of Technology, Motor
Mechanics of the University of Pittsburgh and the Ordnance and
Quartermasters’ Department on detached service. The strength
of this command was approximately 7,000. The first case
appeared on September 30 and the diagnosis was made on the
following day. Beginning October 13, all soldiers of this group
were inoculated with two 1 cc. doses of vaccine, obtained from the
New York State Board of Health. At the height of the epidemic
there were about 840 soldier patients in the several hospitals
of the city at one time. Cubicles were used in the hospitals,
and in the barracks a floor space of 50 square feet was
allowed to each man. The men slept alternately head to foot,
with paper screens intervening, which were changed daily. In
company formation they were instructed to gargle their throats
and clean their teeth morning and night under the supervision
of their officers. Strict military quarantine was maintained
throughout the entire camp, no congregating was allowed, classes
were suspended and only open-air drills were permitted. For the
entire command there were 220 cases of pneumonia, with 99
deaths, an average mortality of 44 per cent. The dishes were
boiled in the hospitals, and sanitary dishwashers were used in all
mess halls. The kitchen help and personnel were inoculated with
influenza vaccine, with apparently good results. The Magee
Hospital, with 375 beds, was under strict military control. When
this was full, all others were treated in the civilian hospitals.
In the city of Pittsburgh the disease was not made reportable
until October 5. However, one case was reported on October 1,
and it was known that there were a few isolated cases in Pittsburgh
previous to that date. During the months of October,
November and up to December 21 there were 23,268 cases of
influenza reported, and the deaths were 1,374 from lobar pneumonia
28and 678 from broncho-pneumonia. We cannot but feel
that most of the deaths reported during the period of the epidemic
as lobar pneumonia were broncho-pneumonia associated
with influenza. It was well known among civilians that true
lobar pneumonia was exceedingly rare and has remained so up
to the present time. This is especially noticeable, as this is the
time of the year when lobar pneumonia is usually widespread in
Western Pennsylvania. This district was particularly favored
with a mild fall and winter. On October 1 the first case was
reported, on October 15 the epidemic reached its peak—on that
day 957 persons being reported ill with the disease. From October
16 until October 28 it maintained an average of 600 cases
daily; from October 29 until October 31 there was a sharp decline
from 600 cases daily down to 200 cases daily. From November
1 until December 21 the decline has been uniform, and on this
latter date 58 cases of influenza and 7 of pneumonia were reported.
The height of the epidemic was reached between October
15 and October 29. During the period of the epidemic in Pittsburgh,
from October 1 until December 15, 62 days were recorded
as cloudy, or partially cloudy, and only 14 days as clear, although
the cloudy days seemed distributed and not in decided groups.
The mean temperature for October was 58 degrees, with normal
54.9; for November, 44 degrees, normal 42.9; for December, 41
degrees, normal 34.7. The precipitation in October was 3.08, as
against a normal of 2.36; in November, 1.79, with normal 2.55;
and in December, 3.50, normal 2.73. From a study of these
weather reports we see that the epidemic occurred during a
period of abnormally warm, cloudy and slightly more moist
autumnal season than usual, but these variations were relatively
slight and far from decided. The confusion of diagnosis between
lobar pneumonia and broncho-pneumonia, associated with or following
influenza, occurred in the Pittsburgh health reports as
well as in other cities. The presumption that almost all, if not
all, of the cases reported as pneumonia of different types were
really cases of influenzal pneumonia, seems justified.
Epidemic Incidents in Institutions and Towns of Western Pennsylvania
During the time the epidemic was at its height in Pittsburgh
the Western Pennsylvania Institution for the Blind was in session.
29This school is located in the heart of the educational center
and was surrounded by the barracks of the Student Army Training
Corps of the University of Pittsburgh and the Carnegie Institute
of Technology. When the influenza was recognized as epidemic
in this neighborhood, the attending physician at this
institution advised a quarantine against the public. The children
were refused visitors in the buildings, and the usual week-end
trips home were forbidden. This school was continuously in
session from September 24 until November 30. During this time
there was not a single case of influenza in the school and the
children were free from any infectious disease. On December 1
the pupils returned to school after the Thanksgiving holiday,
and one week later, on December 8, the first case of influenza
appeared. In a period of five days following 15 cases developed.
It was considered wise to close the school, and all well children
were sent to their homes. The institution was kept closed until
January 1, since which time no cases have developed. Very few
of these children had influenza at home, and only one death
occurred.
A reliable report, subsequently confirmed by the health officer,
stated that in Masontown, Pa., the start and course of the epidemic
were very striking. A dance was held in the town and the
musicians were brought from nearby cities. One of the musicians
employed was not very well upon his arrival, and became so ill
that after the dance he was put to bed in the hotel. He was
found to be suffering from influenza when examined the following
day, and from him as the primary case the town was swept
by the epidemic.
In Mercer, Pa., the physician to the Board of Health reported
that during September they had a general epidemic of coryza
and sneezing, with slight fever, which lasted for three or four
days. This was looked upon by the people as hay fever. In the
midst of this, or about September 16, a man, 74 years of age,
who had been away from home, developed true influenza, followed
by pneumonia, from which he recovered about October 10.
Another man, employed in Greenville, a nearby town, where
influenza was already prevalent, returned to his family here
suffering from the disease. The whole family and all who were
exposed to this family were infected. From this family as a
focus the disease spread rapidly in every direction. There were
30about 350 cases in the town of 2,000 inhabitants, and there were
9 deaths. Sporadic cases have occurred since, ranging in number
from one to a dozen at a time. These numbers do not include
scores of cases called colds by the people, but it seems that all
these cases had an influenza element.
In the town of New Castle it was not possible to trace the onset
of the influenza epidemic to a definite case. As the health officer
stated, several cases were reported at once.
The first case of influenza in Indiana, Pa., of which there was
any definite knowledge occurred on September 15. A clothing
merchant who had just arrived from New York, where he had
been buying stock for his store, was the first case identified. The
next case occurred several weeks later, the disease being contracted
at the mining town of Coal Run, in Indiana County.
A man resident in Sharpsburg who had suffered from influenza
visited friends in Fraser Township, Allegheny County, to convalesce.
Previous to his coming that section had been free from
the disease. He was still coughing at the time, and, moreover,
he is said to have been a great talker and visited largely among
the neighbors of his host. Threshings in that part of the township
were going on and these he also attended. The date of his
coming was October 13. By October 15 his hostess was taken ill.
By October 16 some of the threshers were affected, and by October
17 enough were sick to break up the work of threshing.
Eventually all the men engaged became ill, and 11 families were
infected from this source.
Summary
Reviewing the history of former epidemics and pandemics, I
have gained the impression, as have many others, that we are
not dealing with any new disease. Further, our knowledge of
this pandemic with its high incidence of broncho-pneumonia
shows that it is in no way markedly different from that of former
manifestations of influenza. One is impressed by the fact that
in different outbreaks of this disease of complex symptomatology
certain symptoms or complications have been prominent, overshadowing
others, and making such complications the striking
feature at the time. The failure to recognize that these varying
features are merely different manifestations of one disease has
31resulted in much confusion. The observation made in the last
epidemic—and one which can be endorsed during the present
plague—is that influenza has been and is the most widespread,
rapid and extensive of all diseases. One thing also that
attracts attention at the present time is the long period existing
between the several pandemics. Whether, as one observer during
the present pandemic has stated, it requires a long period for
the infection to become active and easily carried, or whether
any possible reason can be suggested for these phenomena, admits
of no satisfactory explanation. The outstanding feature during
this epidemic is the complication of broncho-pneumonia, and yet,
from very early times, this complication has been repeatedly
spoken of as a striking characteristic. Reviewing the health
reports from the large cities of deaths from pneumonia, the presumptive
opinion seems justified that almost all, if not all, pneumonias
reported as associated with influenza were of the broncho-pneumonia
type. The infrequent presence, indeed the rare finding,
of lobar pneumonia during this period in Pittsburgh seems
to verify the aforesaid opinion. The great frequency and the
high mortality of broncho-pneumonia were particularly noted
during the present epidemic. During the present epidemic the
great mortality among pregnant women was another striking
feature, and yet this is by no means new, having been recorded
by some of the earliest writers. Such also may be said of the
recurrence of the disease in the same patient. One important
observation brought out in the study of the pandemic of 1889 to
1892 was that the ordinary infections occurring in the spring
and fall known as grippe or La Grippe are in no way connected
with the pandemics which have occurred. There seems to be a
consensus of opinions among the records of the more recent epidemics,
as well as during the present pandemic, that weather
conditions in no way influence the spread of the disease. Furthermore,
a study of weather conditions throughout the United
States, and particularly those of our own city, seem to bear out
the truth of this observation. While clinicians during other
epidemics expressed their belief in the incident of a primary case
producing infection, it has only been during the present one that
such an opinion has not been assailed. The large number of
military training camps and cantonments have undoubtedly
offered splendid opportunity for the spread of influenza. The
32futility of attempting to control it even under normal conditions
is still questionable. Consistent with former reported invasions
of the disease, the present epidemic lasted a definite period. This
period was about six weeks in most of our large cities, colleges
and institutions, extending approximately from October 1 to
November 15.
It is imperative to note the accurate clinical observations recorded
from the numerous epidemics of the past by men with
far less data to go upon than is available at the present day. The
high morbidity among the personnel of many of our hospitals and
institutions where the infection occurred and the relatively low
mortality deserve attention. This may be partly explained
by the methods of treatment of those infected, but not entirely.
The great likelihood of carriers of influenza, who either are not
ill or who are suffering from very mild infection, is an observation
also noted by former writers which cannot be ignored. The
value of the masks has not been established, although they have
been extensively used in many parts of the country. Frequent
throat lavage was generally accepted as a rational preventive
measure. Relightings of the disease have been noted in most of
our cities after the subsidence of the epidemic. Vaccination
against influenza is fully discussed in Dr. Haythorn’s paper in
this series.
The presence of influenza in San Quentin prison, California,
in April, 1918 (Public Health Reports, May 9, 1919); an epidemic
of respiratory disease in Chicago in the spring of 1918; the report
of Soper of influenza in our army camps in March and April,
1918; the occurrence of influenza in Porto Rico in June; influenza
on a United States Army transport from San Francisco, as
reported by Coutant, seem to point to the possibility that influenza
had a footing in America long before the disease became pandemic.
The view held by some that the beginning of influenza
was in America, subsequently being transferred to Europe and
then reimported here, is worthy of consideration. Coutant believed
the disease originated in Manila, others that it traveled from “a
permanent endemic focus in Turkestan,” and there are many
other theories which attempt to discover the original source of
the disease. The question is today an unsettled one. The pandemic
of influenza in its severest form swept so suddenly over
the world that before the profession realized it or had become
33stabilized it had changed its character and the great plague was
gone. The consequence has been that we have really learned
little that is new and have done scarcely more than establish on
a firm basis many of the opinions formed after the great outbreak
of some 30 years ago. Because transportation is today more
rapid than it was at that time, so the spread of the disease has
been correspondingly swift. Our modern life, the congregating
crowds in theatres, moving-picture houses and in lecture halls, as
well as of the men in our training camps, the development of
street cars and the more frequent traveling by train—these and
many more changes in our mode of living have served to aggravate
the conditions favoring the widespread distribution of the
infecting agent. A higher proportion of the population was,
therefore, attacked than in any previous pandemic, and the period
during which the disease was widely prevalent has for the same
reason been relatively much shorter.
The characters differed somewhat in different regions, but the
evidence shows clearly that we are not dealing with any new
disease. It will be years before we are able to fully analyze the
data that have been collected from such wide sources and by so
large a body of trained men, so that important epidemiological
facts may still be forthcoming from the material already at hand.
We are too close to the events to get the most helpful perspective,
and the object of this report has been to add, in however small a
degree, to the general knowledge of this great pandemic as it has
appeared to us in Pittsburgh and its surroundings.
35
A CLINICAL DESCRIPTION OF INFLUENZA AS IT APPEARED IN THE EPIDEMIC OF 1918–1919
The epidemics of influenza which have been recorded from
time to time during the past few centuries have always contributed
an interesting chapter to the history of medicine. The
protean character of the disease with its many complications is
always an excuse for another attempt at the description of the
clinical manifestations of a recent epidemic. This is not, however,
the only incentive at the present time for describing the
clinical aspect of the disease as it appeared in the epidemic
through which we have just passed. The study of the disease
from other aspects, such as the pathological, the bacteriological
and the physiological, by well-organized groups of workers has
made it necessary to co-ordinate, if possible, the clinical findings
in every detail with these apparently basic principles. It would
be interesting to review here the peculiarly fortunate circumstances
which have led to the investigations. On account of
the great war many temporary laboratory organizations which
otherwise would not have existed were in operation, and these
organizations, moreover, were keen to undertake any laboratory
problem which might arise. The present epidemic presented the
opportunity, and that the work was taken up with great enthusiasm
is evidenced by the reports coming from the various army
hospitals, base hospitals and civilian hospitals throughout the
world. The permanent laboratories connected with medical
schools and with institutions for medical research took up the
problems with equal endeavor. This brief reference is made only
to call attention to the fact that from such organizations a great
mass of information has come which must be critically reviewed
and coordinated before it can add to the permanent fund of our
knowledge of the disease under consideration.
36The material upon which the following clinical observations
have been made is peculiarly adapted to review because it consists
of two distinct groups of patients which were admitted to
the Mercy Hospital. One group of 153 men was composed of
soldiers between the ages of 18 and 23, which had been recently
inducted into the Student Army Training Corps, and were living
in barracks in the immediate vicinity of the hospital. Another
group consisted of civilians (394), ranging from youth to old age,
which came from various parts of the city and surrounding towns
and country. The first group came to the hospital early, or as
soon as the disease was recognized; the second group came
usually after several days of illness had elapsed, or when a complication
had already arisen. Many of this group had been ambulatory
cases for the first part of the disease. The entire number
of patients admitted to the Mercy Hospital from the first admission,
September 21 to December 1, the end of the quarantine,
was 547. After December 1 very few simple influenza cases were
admitted. These 547 cases form the basis of the observations
which will be referred to in this paper.
From the last great epidemic or pandemic of influenza, that
of 1889 and 1890, have come clinical descriptions which should
be reviewed before speaking of the clinical manifestations which
have characterized the present epidemic as shown in the two
groups studied.
One of the best descriptions of that epidemic was given by
Dr. O. Leichtenstern in Nothnagel’s Encyclopedia of Practical
Medicine. This contribution, among many others, describing the
epidemic of 1889 and 1890 is one of the first to refer to the
Pfeiffer bacillus as being etiologically associated with the disease.
It differs, therefore, greatly from descriptions of previous epidemics.
Leichtenstern says: “The typical influenza consists of
a sudden pyrexia of from one to several days duration, commencing
with a rigor, and accompanied by severe headache, generally
frontal, with the pains in the back and limbs, by prostration
quite out of proportion to other symptoms and marked loss
of appetite.” He continues by saying that to these characteristic
symptoms may be added the catarrhal phenomena arising from
the affection of the respiratory tract, particularly the upper
(coryza) and “occasionally” the lower, the trachea and bronchi.
This description is so in accord with the symptoms of uncomplicated
37influenza as found in the present epidemic that very little
need be added. Any difference which may occur in the description
of the disease is likely to be accounted for by the peculiarity
of onset, whether in the upper or lower respiratory tract, and by
the different ways of interpreting complications which may have
arisen. It is evident from this description that the upper
respiratory tract was affected more generally than the lower in
the epidemic of 1889 and 1890. In the present epidemic it can
safely be said that the reverse was the usual state of affairs. It
was a rather unusual occurrence when the affection was limited
only to the nose, pharynx, larynx, trachea and larger bronchi. A
very large number, no doubt, had a peculiar œdema, a so-called
“wet lung,” which we shall discuss later; others went on to a
capillary bronchitis or a bronchiolitis, and a large number had
broncho-pneumonia. This sequence we shall attempt to show in
the statistics at hand. In some cases the lesion in the lower
respiratory tract seemed to be primary, there having been no
initial coryza. At least none was observed and no history was
obtained.
Prodromal Stage and Communicability
The length of the prodromal stage—the stage from the time
of contact to the earliest onset of symptoms—has always led to
interesting observations and discussion. In this epidemic we
have rather definite information bearing upon this subject.
A young married farmer living in a rural community where
no influenza had occurred up to the time of the present experience
went to a city about 40 miles distant. On the train he sat
in the same seat with a man who was apparently ill, and who
was sneezing and coughing. He was in the city only a few hours,
and was not in any place of congregation except the railway
train. Forty-eight hours after his return to his home he noticed
the first symptoms and began a mild course of influenza. About
50 hours later his wife was taken with the same symptoms, and
in two days more their only child was afflicted. Other members
of the household were also afflicted, and one of them died of
pneumonia.
It might be interesting to quote a similar observation made by
Macdonald and Lyth, of York, England, published in a recent
issue of the British Medical Journal (November 2, 1918, p. 488),
which corroborates this experience. They say: “We traveled
38from London together on Thursday, October 3, by train, leaving
King’s Cross at 5.30 P. M., arriving in York at 9.30, and as we
were leaving the carriage a young flying officer, who had come
the whole way with us and was coughing and sneezing at intervals,
informed us that he was ill and had had influenza for several
days. On Saturday, October 5, we both became ill and had developed
typical attacks of influenza. With both of us the illness
developed suddenly with laryngitis; in both the first signs were a
severe attack of coughing; and in both the time was noted fairly
accurately as being between 2 and 2.30 P. M. One case was quite
mild, the temperature never over 101. The other was more
severe; the temperature arose to 104½ and the catarrh extended
to the bronchi. His wife and two children also developed influenza,
and in their case the symptoms showed suddenly, about
2 P. M., on Monday, October 7. Now we are convinced that we
became infected from our traveling companion during the train
journey—more likely toward the end of the journey; and if we
take the time of infection as 9.30, this fixes the incubation period
for both of us at a minimum of 41 hours, with a maximum
margin of error of 4 hours. The three cases developing in the
family of one of us point to a similar incubation period, as their
illness started almost exactly 48 hours after his, and as it is
likely that the infection would not take place until a few hours
after the first symptom, the incubation period in these three
cases must have been nearly the same as our own two.
“It can be readily understood that we were in no position to
conduct extensive bacteriological examinations, but a culture
taken from the posterior nares of one of us on October 10 with a
guarded swab showed colonies of Pfeiffer’s bacillus and of micrococcus
catarrhalis.”
This observation is so convincing, I have quoted it at length
and in full.
The communicability of influenza has been observed by all, and
the ease with which it passes from one individual to another
noted. One observation made by us was of considerable interest.
In a house where a patient lay sick with a severe attack of
influenza for nearly three weeks several members of the household
passed the door of the sick room a number of times daily,
and yet they did not contract the disease. This is in marked
contrast with the immediate contact between the two physicians
39and the young flying officer, who sat in the same railway carriage
compartment for four hours. The same observation was made in
the hospital among nurses in direct contact with patients. A
large number of these contracted the disease, while those not
immediately associated with influenza patients almost invariably
escaped. This speaks strongly against the idea that the epidemic
was a so-called “plague,” or that it passed without intermediate
means through the air and pervaded all places.
From information thus far at hand it seems, therefore, that
the prodromal stage, or stage of incubation, is one which covers
about 48 hours, and that it is usually without symptoms unless
it be a peculiar prostration which had been described by some
patients. It would also appear from the experiences just narrated
that it was necessary to be in rather close contact with a
patient, so that there could be an exchange of respired air before
infection could take place.
Duration of the Disease
In all descriptions of the disease the duration is spoken of as
“several days, more or less,” “a three-day fever,” or “a seven-day
fever.” Because of the careful supervision under which the
soldiers were kept while in the barracks an excellent opportunity
was afforded to note the duration of uncomplicated cases. The
shortest time observed was 1 day, and the longest 10 days. The
average duration of temperature among 87 soldiers without
inflammation of the lungs or other certain complications was
6⅓ days. Among the civilians the shortest time of pyrexia was
a few hours only, while the longest in 73 male patients was 14
days, and in 84 female patients was 16 days. The average length
of pyrexia in the males was 4⅝ days, and in the females was
5¼ days.
While the very definite clinical description of the former epidemics
of a so-called uncomplicated influenza seems to have
served satisfactorily to the present time, the laboratory studies
and the possibly more thorough clinical observations which have
been carried out recently in this epidemic make it necessary to
present anew the whole disease picture of influenza, with the hope
of suggesting a classification more in accord with our present
knowledge of the disease.
40
Forms and Varieties of Influenza
A few words as to “forms” or varieties of influenza might be
helpful before suggesting a classification of symptoms. In former
epidemics of influenza considerable importance was attached to
the early manifestations or first symptoms as characterizing the
“form” of influenza which was in evidence in the individual
patient. These were reported as a “respiratory form,” a “nervous
form,” a “gastro-intestinal form,” and other forms—circulatory,
renal, psychic, etc. In the epidemic of 1889 and 1890 particularly
these types were noted, and they have been described in the subsequent
small epidemics, practically characterizing them as being
of one or the other, and frequently as being without any respiratory
symptoms. In the study of our group of cases in the present
epidemic every effort was made to recognize the non-respiratory
cases, but we were unable to find a single case which did not have
definite respiratory symptoms, either early or late, in addition
to any other symptoms present. Only occasionally were nausea,
vomiting and diarrhea or tachycardia, or certain neuroses or
psychoses, the leading symptoms. The respiratory symptoms in
some cases seemed to be at the onset primarily of the lower
respiratory system—that is, without the preliminary coryza.
These usually ran a rapidly fatal course, characterized by marked
cyanosis and confusingly irregular chest signs. We would say,
therefore, in so far as our experience goes in this epidemic, we
are not justified in speaking of any particular forms except the
respiratory form, and whenever pronounced manifestations occurred
justifying a characterization of any other form they could
more easily be interpreted as a complication, or the manifestation
of a coincident disease, or of a severe toxæmia.
The classification of the symptoms, therefore, takes into consideration
largely those symptoms arising from the respiratory
system. We are of the impression that the pathology demonstrated
by Dr. Klotz and described by others justifies the following
classification. Clinically we would recognize two distinct
groups of epidemic cases.
The first includes those without lung involvement having
symptoms arising from the upper respiratory tract, including the
trachea and the larger bronchi. These were practically without
any chest signs except for the rather indefinite signs of an acute
41bronchitis, and the only symptoms referable to the respiratory
tract were a coryza, soreness of the throat, hoarseness and a
cough of varying degree and character. If to these symptoms
are added those of Leichtenstern just mentioned, one will have a
good description of a so-called simple, uncomplicated influenza.
The second includes those with lung involvement and associated
with physical chest signs, in some indefinite and confusing,
while in others definitely conforming with the existing pathology.
These symptoms and chest signs were those associated at one
time with what appeared to be an acute œdema of the lungs. At
another time the physical signs were those of a bronchiolitis
(capillary bronchitis), or most frequently of a broncho-pneumonia,
of an isolated type or of a massive type. Finally there
were some forms of lobar pneumonia which at times we were
unable to differentiate from a true lobar (croupous) pneumococcic
pneumonia.
Influenza Without Lung Involvement
Of the group without lung involvement nothing further would
seem necessary to be said in addition to what one finds in standard
text-books describing the disease picture of former epidemics.
The incidence of influenza of this type among our group was as
follows: Of 153 soldiers 93, or about 60 per cent., had a so-called
simple, uncomplicated influenza, and of the 394 civilians 185, or
about 52 per cent., had no lung involvement. There are a few
points in which the symptoms of the present epidemic seem to be
so peculiar that they merit special consideration.
The Temperature
This can be described as showing a sudden rise to 102–104, at
which point it is maintained for a few days, and subsides by
lysis in a few days more. A typical chart is as follows:
42
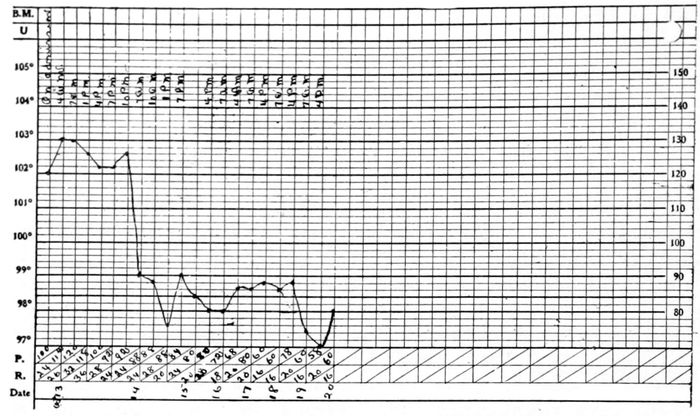
Or the temperature might fall one or two degrees for a day
or so after the first rise, and then go up again for one or two
more days, and subside by lysis as is shown in Chart II.
This would occur without our being able to find any lung lesion
unless we accept the acute œdema or wet lung as a complication,
43and this we were rarely able to recognize by any definite physical
signs in the chest. Cyanosis frequently accompanied this second
rise of temperature, and was later interpreted as being associated
with the so-called wet lung. When the temperature remained up
longer than five days it could safely be concluded that lung involvement
must be present.
The Pulse and Respirations
The pulse was invariably slow, or rather out of proportion to
the temperature. Even when the patient seemed very ill the
pulse remained from 84 to 96, and of surprisingly good quality.
This was noted also when some of the more severe pulmonary
involvements or some complications arose. The pulse frequently
did not become rapid until shortly before death. The respirations
in an uncomplicated case also remained about normal. The
rate was not accelerated until lung complications arose, and then
a gradually increasing rate was often the first herald of oncoming
danger and a sign of grave prognostic import. The relation of
the pulse phenomena toward the end of a fatal case was most
remarkable. The respiratory rate was accelerated, as has been
noted above, but the pulse rate frequently remained unchanged,
being characteristically slow. In a patient seen in consultation
with Dr. Lester H. Botkin, of Duquesne, Pa., death took place
while we were in the sick room. It was a case of apparently
uncomplicated influenza of seven days’ duration. The respirations
were rapid and the pulse was only 96. In the last five
minutes of life the heart beats as observed with the stethoscope
never varied, until they suddenly ceased; during the same time
the respiratory efforts were only three agonal ones, the last being
a minute or so before the last heart beat. There were no physical
signs of consolidation at any time recognized in this case, but
we feel that the lung, had we seen it at autopsy, would in all
likelihood have shown the peculiar hemorrhagic and œdematous
character so often observed in the fatal cases.
There were, of course, marked exceptions to the description
of slow pulse and later rapid respirations observed. In some the
pulse rate and respirations increased, together with or without
definite signs of a grave complication.
44
Cyanosis
This was recognized early in the epidemic. It was sometimes
preceded by a peculiar flushing of the face, such as accompanies
belladonna poisoning. It might be noticed in the very first days
of the attack. The cyanosis was looked upon as being a very
early symptom of lung involvement. With our later knowledge
from autopsies, and especially as shown by Dr. Klotz, we feel it
was surely an accompaniment of, or may even have preceded, the
changes in the lung which have been designated as œdematous,
“wet” or cyanotic. At the earliest appearance of the cyanosis we
were frequently unable to find any change in the physical signs
of the chest. Of course, the indefinite signs of an acute bronchitis
were present, and in some cases an additional “impaired
resonance” was noted over one or both lower lobes, but when this
was definitely present other more definite signs soon followed,
and our case was shifted suddenly from Group I, i. e., without
apparent lung involvement, to Group II, i. e., with definite lung
involvement. This cyanosis was noticed first in the face, and
frequently was marked on the dorsal surface of the hands. It
was not unlike the cyanosis which may sometimes be seen when
large doses of certain coal tar derivatives are taken. In fact, the
question arose whether in the epidemic of 1889 and 1890, when
the coal tar derivatives were prescribed with such freedom and
with accompanying cyanosis and apparently such deleterious
effects, the cyanosis may not after all have been due more largely
to the infection than to the medication. After that epidemic it
was said: “Influenza has slain its thousands, but the coal tar
products have slain their tens of thousands.” There was no gross
hæmaturia or hæmoglobinuria present in these cases, although
a few red blood cells were seen microscopically. There was, however,
epistaxis, sometimes early in the disease or later associated
with the cyanosis. In a few cases there was hæmoptysis, which
we regard as always arising in cases where the wet or hemorrhagic
lung was present. Cyanosis in disease of the lungs, and
especially in the terminal stage of lobar pneumonia, is a familiar
and common occurrence, but the cyanosis observed in this epidemic
seemed quite different from the ordinary. The points of
difference were these: (a) it came early in the disease; (b) it
seemed to be more generally present when very little lung involvement
could be demonstrated physically, and was just as likely to
45disappear when more definite chest signs were demonstrable;
(c) it was not associated with embarrassment of respiration;
(d) it had no relation with a demonstrable circulatory disturbance.
The pulse did not become rapid; the quality of the pulse
did not change; the right heart was not dilated, as is so frequently
the case in the terminal stage of a lobar pneumonia when
cyanosis appears; (e) and finally there was no associated œdema
of the lungs, or at least that œdema of the lungs which occurs
in the later stage of lobar pneumonia, when the pulse becomes
rapid, when there is rapid and labored respiration, when the right
heart dilates, when there is cold perspiration, and when the signs
of impending death are plainly evident. The cyanosis of influenzal
pneumonia seemed to be due to an entirely different
cause or combination of conditions from those present in lobar or
pneumococcic pneumonia. The cyanosis of influenzal pneumonia
was, therefore, most confusing, and became all the more so when
it was recognized that it did not yield to the respiratory and
circulatory stimulants usually employed when cyanosis is present.
The inhalation of oxygen was resorted to rather routinely early
in the epidemic. It seemed to temporarily influence the cyanosis,
but the results were not permanent, and the outcome of the cases
did not seem to be different from those in which oxygen inhalations
were not used.
The blood pressure in those cases in which cyanosis was
observed was invariably low. This seemed to be due to the infection,
for in several private patients not belonging to this group
of patients with previously known high blood pressures the blood
pressure was observed as much lower throughout the course of
the infection.
Leucopenia
The peculiar behavior of the white blood corpuscles will be discussed
more fully in another paper of this series. Our remarks
will deal more particularly with the clinical observations and
interpretations. The leucocytes fell below the normal from the
very onset of the disease; they varied very little regardless of
great changes in temperature; they did not always increase, or if
they did increase at all it was comparatively little, even in an
extensive invasion of the lungs or in severe complications. Concerning
the leucopenia we have no explanation to suggest, save
46that it is a clinical characteristic of the disease. Our first thought
was that the infection came on so suddenly and profoundly there
was no time for a leucocyte reaction. But when we recall other
diseases associated with a leucopenia, notably typhoid fever,
which does not come on with such suddenness, our explanation
for the leucopenia of influenza does not seem to hold. The leucopenia
must be simply a peculiar toxic blood reaction characteristic
of the Pfeiffer bacillus invasion. Such an explanation has long
been accepted in the Eberth bacillus infection.
Asthenia
A condition which was frequently noted by the patient was an
indescribable weakness and prostration which appeared early,
sometimes before any other symptoms were noted or before any
elevation of temperature. The young soldier was in apparent
perfect condition when he arose in the early morning. During
the “setting up” exercises he did not feel so fit, and a few hours
later appeared extremely weak. When his condition was called
to the attention of the medical officers he was found to have a
slight elevation of temperature and was sent to his bed.
In former epidemics, as also in this one, marked prostration
was recognized as coming at the height of the disease and remaining
persistently during convalescence. But it does not seem
to be recorded as among the first symptoms.
Influenza with Lung Involvement
Of the group with lung involvement much may be written from
a clinical standpoint, and much confusion may be brought about.
Especially is this so if one has no definite idea of the pathology
present, or if one enters into a discussion of the character of the
infection—a point upon which there is as yet no unanimity of
opinion. From the many reports which have been put forth
from the base hospitals of the various cantonments, and also
from the reports coming from civilian practice, it is evident that
scarcely any two groups of laboratory men or any two individuals
of those separate groups have the same idea as to the bacteriology
and the pathology peculiar to this epidemic.
As long as there is this confusion and element of doubt in the
minds of those to whom we are accustomed to look, the clinician
47must necessarily speak with considerable hesitancy, especially
when he attempts to interpret the physical signs observed. In
our own group the observations of Klotz, Guthrie, Holman and
others have given us an interpretation of our clinical findings
which, at present at least, is more or less satisfactory. We shall
definitely keep in mind their observations and conclusions as we
go on with the description of the physical signs of the chest in
cases having lung involvement.
In the description of this group it will readily be seen that the
lower respiratory tract stood the brunt of the infection. Of the
153 soldiers under our care, 60, or about 40 per cent., were recognized
as having pneumonia. Of these, 34 had undoubted demonstrable
signs, while 26 were questionable, and yet from the temperature
and other symptoms we concluded there was a pneumonia.
Of the 394 civilians, 189, or about 50 per cent., had
pneumonia. Of this group there were again some 28 or 30 in
which the diagnosis was doubtful, according to the ordinary way
of making a diagnosis, but we felt sure from the temperature
course that more than a simple influenza was present. In the
description of the physical findings of the chest in these influenzas
with lung involvement it will be readily seen why the
diagnosis must sometimes be in doubt.
Before referring to the physical signs it might be well to
describe the condition and general appearance of the patient
when the lungs became involved. The patient who had been
progressing with an apparently simple influenza, with no chest
signs except those of bronchitis or tracheitis, occasionally slightly
cyanotic, became more cyanotic, the elevation of temperature
continued longer than three to seven days, or if it came to the
normal began to rise again, his respirations gradually increased
and the pain in the chest became well localized. One could safely
assume that the patient had developed a lesion in the chest. This
could not always be localized during the first few hours or on the
first day. The evidence of increased bronchial disturbance was
frequently recognized, and later impairment of resonance and
diminished breath sounds associated with “a few crackles” were
noted. This, so far as we can tell, may have been the only evidence
of the stage of œdema or “wet lung.” After this, as the
disease advanced, definitely increased vocal fremitus and rather
definite tubular breathing with greater impairment of resonance
48were noticed. These signs were usually observed first at the apex
of the left lower lobe, and from here they extended forward along
the inter-lobar sulcus, or downward along the spinal column. If
the lesion was noticed first on the left side, in a day or two it was
found more or less definitely in the right lower lobe also. It
seemed to occur more frequently first in the body of the right
lobe, instead of in the apex of the lobe as on the left side. In both
lobes it might spread to contiguous areas and form a massive
consolidation, or it might be found in small separate areas, some
of which would clear up in a day, while others would persist.
The expectoration was frothy, containing either blood or
masses of yellowish, greenish purulent material floating in a
watery sanguiolent or clear fluid, or enmeshed in frothy mucus.
The amount of expectoration in some cases was enormous, but
as a rule it was scanty. It was thick and ropy at times and distinctly
annoying to the patient.
At this stage the physical signs were very much in accord with
those of broncho-pneumonia. In a few hours sometimes, or in a
day, the small areas of consolidation became confluent and massive
consolidation was formed. It appeared as though the whole
lobe would in time become solid, as in a true lobar pneumonia. Or
the original areas may apparently have cleared and other areas
involved, became the centers of massive consolidations. In many
cases both lower lobes were thus similarly affected, and one had
the physical signs of a double lobar pneumonia. However, nearly
always a small angle of the lobe remained clear, thus differing
from the entire lobe involvement characteristic of a true croupous
pneumonia. Other signs, such as the absence of vesicular breathing
and presence of the crepitant râle, moist râles of all sizes to
very coarse râles, could be noted. As in certain stages of a complete
consolidation, the lung might be dry; no râles present, but
definite tubular breathing present. This in a day or two, or after
a longer time, might give the signs of resolution. The stage of
resolution, however, was almost invariably prolonged, sometimes
extending over weeks. With these variable lung signs were often
mingled the signs of a fibrinous or serofibrinous pleurisy, which
occasionally but remarkably infrequently went on to effusion or
empyæma.
[Click on any image for larger version]
49As stated above, the demonstrable pathology was in the lower
lobe, and more frequently in the left than in the right, only occasionally
in the middle lobe, and never, we might say, in the upper
lobes. The very earliest definite signs were found at the apex of
the left lower lobe.
This observation seems to be entirely contradictory to that of
the pathologist, who found in 65 per cent. of all cases coming to
autopsy a lesion in all the lobes of the lungs (Klotz). The only
explanation we can give which seems at all satisfactory to us is
that the pathology in the upper and middle lobes must not have
been sufficient, or must have been of such a nature that it did not
yield the physical signs, i. e., definite impaired percussion resonance,
increased vocal fremitus and tubular breathing, with varying
shades of moist râles—signs upon which we insisted before
we were willing to state definitely that there is a demonstrable
pneumonia present.
In this description it has been attempted to follow the order of
invasion in a lung which seemed to go through the entire course
of the disease. There were, necessarily, all degrees of the
process, some cases showing few signs and yet being remarkably
ill, and others all of the signs with very little other evidence of
serious illness.
We were continually impressed with the notion that the
pathology in the lung, at least the pathology demonstrable
physically, did not tell the whole story of the case, and that the
outcome depended as much or possibly more upon a general
infection or toxæmia of which the recognized condition in the
respiratory system was only a small part. We were particularly
impressed with this in the success or failure following the application
of any therapeutic measures. It was quite a common
remark, therefore, in the wards of the hospital among those associated
in the work that “the patient died too quickly to permit
of the succession of the various stages of pneumonia”; or, in the
autopsy room, that if the patient had lived long enough he would
have had demonstrable, well-recognized pathology of the lung,
instead of the cyanotic, wet, spongy lung which was found.
The temperature course in the pulmonary cases was characterized
by its irregularities, and by its being entirely out of harmony
with the extent and severity of the lung invasion in so far as it
could be interpreted by the physical signs. The temperature as
described in a simple influenza might not come to the normal in
the time of three to seven days, and might even go higher, with
50no demonstrable chest signs, but with every other evidence of
lung involvement. Later the temperature might come down by
lysis, which was the usual way, and the chest signs gradually
or suddenly become evident. The temperature might remain
normal throughout the rest of the course, and a lobe or even
both lower lobes of the lungs be as solid as in a true lobar
pneumonia. Occasionally the temperature fell by crisis, but there
was no associated change in the physical signs of the chest. In
short, the temperature seemed to run a course entirely independent
of the physical signs in the chest. In two remarkable
cases seen in consultation on two consecutive days the physicians
in charge declared that no signs of consolidation could be found,
though all other evidences of pneumonia were present. In the
12 hours which had elapsed from the time the last examination
was made the temperature fell by crisis. At the consultation,
to the surprise of the family physicians, we found both lower
lobes consolidated, it having occurred apparently with the crisis.
Both patients were healthy-looking, robust, young men, and both
recovered with delayed resolution. In the convalescence of such
cases, if the patient got up too soon or if any other indiscretion
took place, a relighting of the lung occurred. From the above
description it can be readily seen that a diagnosis of the conditions
in the chest in influenzal pneumonia was frequently impossible,
because one had to abandon all his previous ideas of pneumonia,
in so far as onset, crisis, blood picture, sputum, temperature,
respiratory and circulatory phenomena, physical signs and
prognosis were concerned.
Assistance from the laboratory was meager, especially in the
early days of the epidemic. This was due largely to the inability
to get laboratory workers in sufficient numbers to follow the
work through, but more largely to the fact that we were unable
to interpret the unusual laboratory results which were available.
When we were once fully aware of the difficulties in diagnosis
which confronted us, we utilized every practical means at our
disposal. Among these was an examination of the chest with
the X-ray. On account of lack of facilities and of help, it was
impossible to make routine X-ray examinations of the chest in
all cases. Besides, it was difficult to interpret the X-ray findings,
on account of the unusual character of the lesions. Also, many
of the patients were so desperately ill one hesitated to disturb
51them. We hear that other clinics had similar experiences, and
that very little substantial help came from the X-ray, except in
cases with complications. Several attempts were made to determine
the kind of shadow, if any, the “cyanotic, œdematous,
wet” lung would make, but no satisfactory observations have
been forthcoming. From our own observations and from the discussions
of other observers, it would seem to us that the stereoscopic
examination of these chests is the only possible way of
getting satisfactory plate readings in these cases where the
pathology seems so lawless in its extent and peculiar in its distribution.
This method of examination, however, demands facilities
convenient at the bedside and perfect co-operation of the
patient—difficult conditions to meet under the circumstances. In
the acute cases, when the desire to make a diagnosis not only of
the presence but of the extent of the disease was keen, X-ray
examination was largely impractical. In cases of delayed resolution,
or in cases with complications with prolonged convalescence,
X-ray examinations were extremely helpful.
Diagnosis of Influenzal Pneumonia
In the consideration of any disease the well-trodden path of a
painstaking history, a thorough physical examination, and reliable
laboratory investigation, together with an intelligent interpretation,
will usually lead to a definite diagnosis. In certain
diseases, as is well known, the stress must be placed about equally
on all of these factors, while in others one or other factor predominates.
In influenzal pneumonia, until more is known of the
etiology (bacteriology) and of the pathological changes and of
the physiological disturbances, the controlling factor in the
diagnosis (we feel embarrassed to admit) must be the history.
This is true not only of the diagnosis of influenza with or without
pulmonary involvement, but is also true of the diagnosis of the
various complications, and will be found to be particularly true
in the recognition of the bizarre sequelæ, which no doubt in the
succeeding months or years will be attributed to or will follow in
the train of influenza.
With the knowledge that there is a prevailing epidemic of
influenza and that the manifestations are largely in the respiratory
tract, any pulmonary disturbance will necessarily make one
52suspicious of the presence or the oncoming of an influenzal pneumonia
in the patient under consideration. The history of the
onset, as of simple influenza, is the greatest factor. This with a
continued temperature, cough, cyanosis, slow pulse, continued
asthenia, or even an unusual leucopenia, may have a greater
weight in determining the diagnosis of lung involvement than
will the apparently definite or, as it may happen, the confusing
chest signs. To differentiate from ordinary bronchitis, broncho-pneumonia
and catarrhal pneumonia, one need only refer additionally
to the severity and persistency of the disease when it is
of the influenzal type, as compared with the mildness of the
ordinary type. To differentiate it from croupous pneumonia, one
need only compare the confusing symptom picture of the influenzal
pneumonia with the definite, clear picture of ordinary
pneumonia; or the confusing kaleidoscopic chest signs of the one
with the definite, clear-cut signs of the other. The laboratory
thus far has been the smallest factor in making the diagnosis,
in that sputum examinations, blood examinations, blood cultures
and urine examinations are mostly negative in their results, or
at least the findings are not specific. We do not, however, mean
to indicate that these tests are not of the greatest value. The
leucopenia is the one outstanding feature which seems to have
separated this infection from other acute lung infections, excepting
miliary tuberculosis. The differentiation of influenzal pneumonia
from an acute tuberculous process in the lung may be
difficult, especially if there is no reliable history available. However,
the fact that pulmonary tuberculosis usually begins at the
apices of the lungs and influenzal pneumonia at the bases or at the
apices of the lower lobes is quite helpful. Of course, the examination
of the sputum for tubercle bacilli will be a deciding factor.
The differentiation between influenzal pneumonia and diseases
of the pleura is one which practically rarely needs to be made,
for there seem to be very few cases of influenzal infection of the
lungs in which the pleura is not also involved to a greater or
lesser extent.
Complications
In considering the complications of influenza one again comes
up squarely against the question: What is influenza and what is
the specific micro-organism responsible for it? If the Pfeiffer
53bacillus is the specific cause, what pathology can be attributed
to it? It has been an almost universal observation that the lesions
in the lungs and pleura which characterized the group of cases
with lung involvement rarely yielded a pure culture of the Pfeiffer
bacillus, and that secondly in a large percentage of cases the
Pfeiffer bacillus apparently was absent, and that other micro-organisms,
such as the pneumococcus, streptococcus, micro-organisms
commonly found in the pneumonic processes, were
present and predominated. The question arises, therefore, may
not all the influenzas with lung involvement be complications of
influenza? It is our feeling that Pfeiffer bacillus is present
throughout the respiratory tract in all cases, and while it may
of itself produce a lesion like a broncho-pneumonia or a lobar
pneumonia, it chiefly prepares the soil for other germs which may
happen to be present, and which are more commonly found in the
pneumonias. We, therefore, look upon the lesion commonly found
in the lung as being a part of rather than a complication of influenza,
and look upon lesions elsewhere, due to the influenzal or
other micro-organisms, as a definite complication.
There is no doubt that the most frequent complication of
influenza, especially in the present epidemic, is in connection
with the pleural membranes. When one recalls that pneumonia
rarely occurs without there being also a pleuritis, and also when
one recognizes that in an influenzal infection of the lungs the
specific micro-organism, together with any other micro-organism
which may happen to be present, seems to run riot, apparently
abandoning its usual mode of invasion, it can be readily understood
why this complication is so frequent and so varied. The
pleurisy was usually of the fibrinous type, and rarely was accompanied
with demonstrable fluid. Of the 153 soldiers in only 3
was fluid detected in the chest, and of the 394 civilians only 10
showed fluid. In many more cases fluid was suspected, but X-ray
examinations and free needling of the chest showed that we had
misinterpreted the physical signs.
After our experience in the epidemic of pneumonia in the spring
of 1918, when the disease was also so prevalent in the cantonments,
we of course expected to see many cases of empyæma
and lung abscess in the present epidemic. In this we were agreeably
disappointed. Only one case of empyæma and only one case
with abscess of the lung were found up to the time of collecting
54our data and the compiling of our statistics. Both of these were
among the civilians. From our experience since the compiling of
our statistics, we are inclined to believe that this low incidence
of empyæma may not altogether represent the real state of
affairs, as we have since received in the hospital several cases
of empyæma, as well as of abscess of the lung, which seemed to
have followed an influenzal infection which had occurred three or
four months previously. One of these cases was a particularly
remarkable one, in that the patient had already been admitted to
the hospital twice since his initial attack of influenza in October
for suspected pleurisy with effusion. We were unable to find any
fluid with the needle, though we felt certain of having demonstrated
it a number of times physically and with the X-ray. About
eight weeks after the second admission, however, pus was found
after several needlings in the left chest, axillary space, apparently
along the inter-lobar sulcus. This case was a good example
of many we have seen in which a pneumonia, or possibly, as we
see it now, a pleurisy, or even a localized empyæma, seemed to
confine itself about the sulcus or fissure between the upper and
lower lobes of the lung. Frequently the process began posteriorly,
apparently at the apex of the lower lobe, and traveled
forward and downward across the axillary space until it appeared
in the anterior part of the chest. In most cases we interpreted
our signs as those of a consolidated lung, and scarcely knew
whether the consolidation was in the upper part of the lower lobe
or in the lower part of the upper, or in both. In some cases we
suspected a localized empyæma or an abscess in the sulcus, but in
none did we find pus after exploring with the needle until this
recent case occurred. The passage of the needle in this case,
which was done several times before pus was found, always gave
the impression that it was going through dense fibrous tissue
for some distance before the abscess was finally found. From
this experience, and from the extensive and irregular invasion of
the pleura which we have seen demonstrated at autopsies, there
can be no doubt that the clinical history of the complications of
influenza in this epidemic is not a closed chapter.
In six patients there was a purulent inflammation of the
pharynx, larynx and trachea. It was extensive and produced
profound general symptoms, dyspnœa and profuse purulent expectoration.
The lungs were clear, but the patient seemed for
55a time in danger of death. The condition was considered a grave
complication. There was only one case of acute sinusitis, one case
of antrum disease, and only four cases of middle ear infection were
recognized. This is in marked contrast to other epidemics which
have occurred to our knowledge in the past fifteen years or more,
and which have been spoken of as influenza or “grippe.” Disease
of the tonsils, middle ear disease, mastoid disease and sinus disease
occurred with great frequency in those sporadic epidemics.
This again seems to show that the deep respiratory tract was
more generally and more severely affected in this epidemic than
the upper respiratory tract.
With the exception of the pleura, the serous membranes were
remarkably free from infection. Only one case of acute endocarditis,
three cases of meningitis (all pneumococcic), none of
pericarditis, peritonitis or arthritis were recognized among the
547 cases of influenza.
The kidneys did not seem to be involved in the infection. Albumen
was present in the urine, as might be expected in febrile
conditions, but no evidence of acute clinical nephritis, such as
suppression of urine, general œdema or uræmia, was recognized.
The condition of the urine in this epidemic will be described more
in detail in another paper of this series.
A peculiar pathological process in the muscles was brought to
our attention by Dr. Klotz, who demonstrated a myositis or
hyaline degeneration of the lower end of the recti abdominalis.
This lesion is carefully described in the pathological section.
After our attention had been called to this lesion we recognized
several cases clinically having the same condition. One was in
the right sterno-cleido-mastoid muscle and another was in the
left ilio-psoas muscle. This last patient while he was convalescing
developed a severe pain in the left hip, extending upward
into the lumbar region and downward into the thigh. His decubitus
was like that of one suffering with psoas abscess. Every
test available was made to confirm this diagnosis, but all the
findings were negative. The patient rested in the hospital, in bed,
for some time, gradually improved, and eventually made a complete
recovery.
In several cases we also detected an osteitis, especially of the
bodies of the vertebræ. One was of the cervical vertebræ and
the other of the dorsal. The first died after intense suffering.
56An autopsy was not obtained. The other had a plaster cast
applied as in Pott’s disease, and improved sufficiently to leave the
hospital in comfort. One hesitates under the circumstances to
attribute these bone lesions definitely to the same infecting
micro-organism which was responsible for the epidemic of influenza,
as it might easily have happened that a coincident quiescent
tuberculous lesion was present and relighted during the
epidemic. However, in one case from the service of Dr. J. O.
Wallace the possibility of the bone lesions being due to the
Pfeiffer bacillus was demonstrated. This was a child of 16
months with an epiphysitis of the upper end of the tibia. The
inflamed area was incised and pus was found. A smear at the
time showed the B. influenzæ, which was grown in pure culture.
A most interesting complication noted in a few of our cases
was a transient glycosuria. The first case brought to our attention
was a middle-aged female, who complained of failure of
vision. Upon making an ophthalmoscopic examination a papillitis
of a mild type was noticed. This led to a careful study of
the urine, and sugar was found in a small amount for a short
period of three days, although the glycosuria readily disappeared
by cutting down the carbohydrate intake, the vision came back
to normal more slowly. In fact, it was almost one month before
the symptoms and signs of the retinal change had entirely disappeared.
It is interesting in this connection to recall similar
cases referred to in Allbutt’s System of Medicine, vol. vi, on
influenza, following the epidemic of 1890 in England. Other
transient glycosurias showed no visual changes. We do not consider
these to be true cases of diabetes mellitus. In all a transient
hyperglycæmia was also noted.
Pregnancy
A condition which can scarcely be considered as a complication
of influenza, but which, however, was a large factor in increasing
the mortality among women, was pregnancy. Among the cases
included in this study were five pregnant women, who came to
the hospital and were referred to the medical service. As soon
as a complication relative to the existing pregnancy arose they
were referred to the Obstetrical Department. On account of the
57great amount of work in caring for the influenzal patients, and
on account of the scarcity of physicians and nurses, we were
unable to follow these cases closely enough to give any such
definite data as we wish. Three miscarried or went into premature
labor. Happily only one of them died. The two which did
not miscarry recovered and left the hospital well.
We very soon recognized in consultation with the obstetricians
that the pregnant woman was in a really dangerous condition
if she contracted influenza. She was likely to have a termination
of her pregnancy in the height of the infection, no matter
how recent or how remote pregnancy had taken place. If pregnancy
did not terminate, the chances of recovery were less than
those of the non-pregnant woman; if it did terminate, the
chances for recovery were still less. To the pregnant woman
with pneumonia very little hope of recovery could be offered. I
am indebted to Dr. Paul Titus, of the Obstetrical Department of
the School of Medicine, University of Pittsburgh, for a report
which includes the cases seen by himself and his assistant, Dr.
J. M. Jamison, during this epidemic. Dr. Titus was kind enough
to include in his report certain conclusions which merit consideration.
The report is as follows: “A series of 50 cases, at
all stages of gestation. Interruption of pregnancy occurred in
21, or 42 per cent., of the cases; 29, or 58 per cent., in which
pregnancy was uninterrupted. Mortality of pregnant women
developing epidemic influenza is higher than that of ordinary
individuals, even though their pregnancy is undisturbed, since
14 of the 29 in whom pregnancy was not interrupted died, an
incidence of 482
10 per cent. If a pregnant woman miscarries or
falls into labor, the mortality increases to 809
10 per cent. (17 of
the 21 in whom pregnancy was interrupted died). The period
of gestation has less influence on the outcome than the interruption
itself. Of 10 at term, 3 lived and 7 died after delivery.
“Two main features of this condition as a complication of pregnancy
are: First, pregnant women developing epidemic influenza
are liable to an interruption of their pregnancy (42 per cent.
aborted, miscarried or fell into labor); second, the prognosis,
which is already grave on account of the existence of pregnancy,
becomes more grave if interruption of pregnancy occurs.
58“The cause of the frequency of interruption of pregnancy is
probably a combination of factors: (1) The theory of Brown-Sequard
that a lowering of the carbon-dioxid content of the blood
causes strong uterine contractions sufficient to induce labor.
(2) The toxæmia causes the death of the fœtus, particularly if
not mature, when it acts as a foreign body and is extruded (10
premature fœtuses were born dead, while 1 was born alive,
although 9 out of 10 at full term were born alive and survived).
“The cause of the frequency of death following interruption of
pregnancy is also due in all probability to a combination of
factors: (1) Shock incident to labor. (2) Increase from muscular
labor of carbon-dioxid in blood already overloaded by the deficiency
of the diseased respiratory organs. (3) Sudden lowering
of intra-abdominal pressure by the delivery. (4) Lowering of
blood pressure by the hemorrhage of the delivery. (5) Strain of
labor on an already impaired myocardium.”
If one had been told a year ago that an epidemic could occur
which would result in the death of 60 per cent. of all pregnant
women affected, it would have been thought too unlikely to warrant
any consideration. Though the effect upon pregnancy of
the acute infectious diseases forms an important chapter in the
pathology of pregnancy, it seems that the profession, and in this
the obstetrician is no exception, has never realized how pernicious
and tragic the results of an influenzal epidemic can be in a community.
From the experience in previous epidemics we cannot
but feel that the infection in the present epidemic was unusually
fatal. Whitridge Williams (“Text-book of Obstetrics”) speaks
of the interruption of pregnancy as having occurred in 6 out of
7 cases with one observer, and in 16 out of 21 in another, while
a third has found it only twice in 41 cases. However, none of
these writers speaks of having had a death.
Sequelæ
In referring to some of the associated conditions of influenza
one scarcely knows whether to consider them as complications
or sequelæ. The pathological process certainly had its origin
from the influenzal attack, but at times apparently assumed an
inactive stage. The patient is usually free from any specific
influenzal symptoms, but retains for a long time other symptoms
59referable to various organs, or he may have been normal for a
shorter or a longer period and then suddenly develop symptoms
apparently independent of the previous infection. It may be well
to consider all such conditions which followed the febrile attack,
whether immediately or more remotely, as sequelæ, and I shall
therefore speak of them as such.
The first and probably the most interesting and confusing are
the conditions found in the lungs following influenza. A chronic
bronchitis, an old bronchiectasis, or a previous tuberculous lesion
in whatsoever stage, may present acute symptoms and signs
which are difficult to interpret. The question always arises in
the individual case—is this a process due to the recent influenzal
attack, or was it there before the attack? Is it of streptococcic,
pneumococcic, or tuberculous origin? The history of previous
diseases of the lungs may help to arrive at a diagnosis. The history
of the severity of the influenzal attack is of very little help,
because the apparently mildest attack may be followed by the
most profound changes in the lungs, and the gravest attack with
a history of definite lung infection may leave the lungs without
a trace of the previous pathology. The physical examination is
helpful, of course, in determining whether the lesion is at the
apices or at the bases, and from this a reasonably safe inference
may be drawn as to whether it is from a previous tuberculous
lesion or a recent influenzal infection. The Roentgenologist depends
almost entirely upon this localization. If the linear striæ
are only at the apex, it is probably tuberculous; but if they are
only at the base, or also at the base, it is likely to be an influenzal
lung. In fact, the Roentgenologist with his present information
is ready to admit that it is most difficult to speak definitely of
the lungs in these cases. The possibility of confusing the post-influenzal
lung with a tuberculous lesion is not peculiar to this
epidemic. After the epidemic of 1889 and 1890 the same condition
was observed by clinicians. Dr. Roland G. Curtin, of Philadelphia,
in 1892 and 1893 conducted a series of clinics at the
Philadelphia Hospital, in which he spoke of the “non-bacillary
form of phthisis,” and showed case after case which he said
might be diagnosed as pulmonary tuberculosis, but because of
the recent epidemic and the absence of the tubercle bacillus he
diagnosed them as post-influenzal lung.
60In the present stage of our knowledge, many of these post-influenzal
lungs will not be diagnosed properly until sufficient
time is given for either the lung to clear up or the tubercle bacillus
to appear in the sputum. We would emphasize the importance
at the present time of finding the tubercle bacillus in all
suspicious lung lesions before giving a positive opinion as to the
tuberculous nature, even though the physical signs are very
definite.
Another group of sequelæ is that due to thyroid disturbance,
or disturbance of the endocrin system in general. Since the epidemic
a number of patients have been seen who noticed an
enlargement of a previously normal thyroid gland or greater
enlargement of a previously hypertrophied gland. In the same
way the symptoms of hyperthyroidism appeared, new in some
or a recrudescence in others.
In some of these there was a disturbance of carbohydrate
metabolism, as shown by an occasional glycosuria and an increase
in the blood sugar, or by a possible disturbance of the suprarenals,
as brought out by the administration of adrenalin hypodermatically
(Goetsch test). In the application of this test in
post-influenzal patients it appeared that the whole endocrin system
was in a state of imbalance.
It appears to us not at all improbable that the so-called psychoneuroses
of which fatigue, nervousness, irritability and tachycardia
play such an important part might also be explained in the
same way. These constitute a group of sequelæ which were frequently
recognized after previous epidemics, and which are again
coming to the foreground.
We are of the opinion, on account of the apparent absence of
any specific pathology of the gastro-intestinal tract and its
appendages during the attack of influenza, that the sequelæ
referred to the digestive system are largely due to exacerbations
of previous physiological disturbances or pathological processes.
The patient with a previous peptic ulcer has a recurrence of his
ulcer. The patient with an infection of the biliary tract has an
acute exacerbation, or may have an attack of biliary colic. In
fact, there seem to have been many more cases of this kind since
the epidemic than before, and most of the patients date the time
of the onset from a period soon after recovering from influenza.
61Very few, if any, patients in our experience have exhibited
sequelæ due to disease of the cardio-vascular or genito-urinary
systems. It may be that these will appear later when the more
remote effects of an acute infection are recorded.
A very commonplace sequel, but of more or less interest, is the
tendency to furunculosis. Our attention was particularly called
to the associated hyperglycæmia. The blood sugar readings varied
from 0.2 to 0.41. There was no glycosuria, acetone or diacetic
acid. We have no explanation to offer for this, although one
might dilate readily on many attractive theories. The hyperglycæmia,
one may add, was readily reduced by a lowered carbohydrate
intake, which also had a curative action on the furunculosis.
Finally we would mention the peculiar epidemic which has
been observed apparently over the world, encephalitis lethargica.
We do not for a moment put ourselves on record as regarding this
disease as a post-influenzal affair, but no one will deny that it has
a peculiar time relation to the epidemic; and further, that its distribution
is apparently identical. Its bacteriology seems to be
unknown. Its local pathology in the mid-brain is not peculiar or
at variance with encephalitis produced by known organisms. We
have seen five cases; three of whom had had undoubted influenza,
while the other two were entirely free from even the slightest
suggestion of any type of illness previous to the attack. All of
these cases recovered. It has been stated that following the 1890
epidemic a clinical condition was observed in Europe which bears
a close resemblance to what has been termed at the present time
encephalitis lethargica.
Prognosis and Mortality of Influenza
In giving a prognosis of influenza one has to take into consideration
the peculiar manifestations of the disease, especially
the possible and sudden changes which are liable to take place
in the lungs. The points which lead one to feel that the outlook
is grave occur in about the following order, which is also about
the order of the severity of the symptoms. First, cyanosis.
This usually appeared quite early and was considered a forerunner
of definite lung infection. It may have been a symptom
only of the “wet lung,” to which reference has been made, but
it was usually followed with definitely recognized pathology in
62the chest, and it immediately made the outlook unfavorable.
Second, continuation of elevated temperature. If the temperature
fell to normal in three or four days, the outlook was, of
course, good; but if it went up again, or if the temperature did
not fall in that time, the chances were that there was a lung
involvement, even though the chest signs were negative or only
those of an acute bronchitis. Strange to say, however, when
definite chest signs were once recognized, the height of the temperature
or the continuation of fever was not so important a
prognostic factor. Third, increase in pulse rate. The pulse, as
was noted before, was unusually slow, even though the patient
seemed desperately ill; when, however, it began to increase in
rate the condition was usually very grave. Fourth, the extent
of lung involvement. This was of very little prognostic value.
Both lower lobes might be solid, and yet if there was no cyanosis
and the pulse and respirations were satisfactory, the outlook
was rather good. On the other hand, there might be the slightest
involvement of the lung, and if the pulse were rapid and cyanosis
present the outlook was grave. Fifth, depression and stupor, or
loss of so-called “morale.” If the patient remained clear in his
mind, bright and hopeful, no difference how extensive the involvement
or how grave the symptoms, the prospect of recovery was
better. This is, of course, not peculiar to influenza, but it seemed
particularly striking during the epidemic. Sixth, a gradually
rising rate in respiration, which often was not more than two per
minute per day, if progressive, even in the absence of other
untoward signs, conveyed a serious prognosis.
Our mortality among the civilians in comparison with the soldiers
was exceedingly high. The first cases seen by us were
among the soldier patients sent to the hospital. These were as
fine a lot of healthy young men as one can well imagine. They
came to the hospital comparatively early in the infection. After
the first week it appeared as though our experience would be
entirely different from those in other localities, for we had very
few deaths. In another week our mortality began to rise, but
never as high as among the civilians, as will be seen by the
following figures.
Of the 153 soldiers 87 were without lung involvement, and of
these none died; 66 had lung involvement, and of these 16 died.
Mortality among the 153 was 10 per cent. Of the 394 civilians
63157 were without lung involvement, and of these 1 died; 237 had
lung involvement, or some other complication, and of these 93
died. Mortality among the 394 was 23.6 per cent.
It will be seen that the mortality in the civilians was more than
twice as high as in the soldiers. It has already been mentioned
that the soldiers were ordered to the hospital promptly. The
civilian patients, on the other hand, were later in coming to the
hospital, some of them appearing when they had already developed
serious complications. Another factor in determining the
mortality were the ages of the patients. The soldiers ranged from
18 to 34 years, with an average of 20 years. The civilians
ranged from 6 months to 73 years, with an average of 30 years.
Generally speaking, the greater the age the higher was the mortality.
A third factor which should be considered in determining the
actual mortality is the result of later complications and sequelæ.
The figures as given are those of 547 patients, 110 of whom had
died in the Mercy Hospital and 437 of whom had been discharged
therefrom between September 22 and November 30, 1918, the
length of the quarantine. Those who were discharged had been
up and about for a week or 10 days before leaving the hospital.
From our experience with post-influenzal patients admitted to the
Mercy Hospital since November 30, we are of the opinion that
some of the patients discharged before November 30 as recovered
may have later developed sequelæ which might have proved fatal.
No follow-up system has been pursued as yet which enables us
to speak definitely and statistically of the present condition of
those discharged.
This compilation does not readily lend itself to drawing any
more specific conclusions, but we cannot desist from expressing
our opinion that in the clinical study of this recent epidemic we
find very little that may not have been observed by clinicians in
previous epidemics.
65
THE URINE AND BLOOD IN EPIDEMIC INFLUENZA
By Peter I. Zeedick, M. D.
Epidemic influenza, unlike other acute infectious processes as
diphtheria and scarlet fever, seemingly attacks the kidney in a
rather mild manner. This statement refers only to the uncomplicated
cases, as other bacterial or toxic agents do play a part
in the nephritides occurring so often with the pneumonias or
other complications following influenza. It is, however, true that
in many simple epidemic cases there is evidence of a transient
mild nephritis, or possibly, more correctly stated, a nephrosis.
Some writers observed albuminuria in 80 per cent. of the cases,
while the incidence in other reports varies from 4 to 66 per cent.
It is not always stated with reference to these figures that the
patients clinically were free from the common complication—pneumonia.
The findings of various observers differ greatly,
but they all agree that acute nephritis as a serious sequel is
somewhat rare.
In the literature of the past epidemics general acknowledgment
has been accorded to the presence of albumin in the urine
during the acute stage of the disease. Many times this has
received no further notice or comment than “febrile albuminuria.”
The association of occasional hyaline and granular casts has also
been mentioned. One is impressed with the fact that the older
observers laid but little emphasis on the urinary findings. It
also seems to be true that nephritis as a clinical entity is not
prone to follow the epidemics. In general, our conclusions from
the last epidemic are about the same.
The data for this paper was obtained from examination of 994
specimens of urine from 750 patients; of this number 517 specimens
were examined at the Magee Hospital, where members of
the S. A. T. C., all young men, were treated, and 447 specimens
from the Mercy Hospital, where, in addition to the S. A. T. C.,
we had men, women and children. On account of the large
66amount of material and work on hand, as a rule only one specimen
of urine was examined from each patient, but where complications
were suspected repeated daily examinations were made.
We have grouped our results in tables, so that the various points
may be more readily followed.
Table I shows the urinary findings of uncomplicated influenza
cases admitted to the wards of the Mercy Hospital. None of
these cases developed pneumonia and, after running the usual
course, recovered. We would call attention to the fact that 25
per cent. showed albuminuria. The amount of albumin was
never excessive, and very often was little more than a faint trace.
On the other hand, we have had a few patients where a previous
kidney lesion was known to be present, and naturally in these
cases a heavy cloud of albumin was met with. The albuminuria
was almost always a transient affair, lasting only during the
acute part of the illness, and would rightly come under the class
of febrile albuminuria. We regard it as being more the evidence
of nephrosis than a nephritis. As a rule, the time for the
appearance of albumin was after the fever had been present for
at least two or three days. One rarely met with it in the short
attacks of influenza where the temperature came to normal in
less than 72 hours. A certain time factor appeared to be necessary
in order for the nephrosis to develop. Another point of
interest is the presence of red and white blood cells seen relatively
frequently during the early days of the illness. One
wonders if this finding is analogous to the bleeding from the
nose and lung so often met with at the onset of the disease. The
red blood cells were seen microscopically, and only very rarely
did we encounter a smoky urine.
67TABLE I
URINE ANALYSIS IN CASES OF UNCOMPLICATED INFLUENZA AT THE MERCY HOSPITAL
| Day of Disease |
Total No. of Specimens |
Specific Gravity |
Alb. |
R.B.C. |
Casts |
| 1001–10 |
1011–20 |
1021–30 |
1031–40 |
| 2 |
118 |
8 |
31 |
61 |
18 |
29 |
17 |
8 |
| 3 |
97 |
8 |
15 |
62 |
12 |
23 |
10 |
11 |
| 4 |
51 |
9 |
22 |
17 |
3 |
11 |
7 |
|
| 5 |
24 |
4 |
2 |
14 |
4 |
5 |
3 |
4 |
| 6 |
11 |
|
|
8 |
3 |
4 |
|
|
| 7 |
25 |
|
10 |
14 |
1 |
8 |
|
|
| 8 |
12 |
|
2 |
8 |
2 |
6 |
|
3 |
| 9 |
4 |
|
2 |
1 |
1 |
2 |
|
|
| 18 |
2 |
|
1 |
1 |
|
|
|
|
| Totals |
344 |
29 |
95 |
186 |
44 |
88 |
37 |
26 |
TABLE II
URINE ANALYSIS IN CASES OF UNCOMPLICATED INFLUENZA AT THE MAGEE HOSPITAL
| Day of Disease |
Total No. of Specimens |
Specific Gravity |
Alb. |
R.B.C. |
Casts |
| 1001–10 |
1011–20 |
1021–30 |
1031–40 |
| 1 |
101 |
6 |
22 |
49 |
24 |
5 |
|
3 |
| 2 |
127 |
1 |
17 |
75 |
34 |
13 |
|
3 |
| 3 |
82 |
3 |
13 |
55 |
11 |
13 |
1 |
4 |
| 4 |
36 |
1 |
14 |
18 |
3 |
4 |
|
2 |
| 5 |
40 |
2 |
9 |
24 |
5 |
6 |
1 |
2 |
| 6 |
23 |
1 |
5 |
15 |
2 |
7 |
1 |
3 |
| 7 |
5 |
|
1 |
4 |
|
3 |
|
2 |
| 8 |
5 |
1 |
|
4 |
|
|
|
|
| 9 |
2 |
1 |
|
1 |
|
|
|
|
| 10 |
10 |
1 |
3 |
5 |
1 |
2 |
|
1 |
| 11 |
3 |
|
|
3 |
|
2 |
|
1 |
| 12 |
3 |
|
1 |
2 |
|
2 |
1 |
|
| 13 |
1 |
|
1 |
3 |
|
|
|
|
| 14 |
1 |
|
|
1 |
|
|
|
|
| 15 |
5 |
|
1 |
4 |
|
|
|
|
| Totals |
447 |
17 |
87 |
263 |
80 |
57 |
4 |
21 |
The results shown in Table II illustrate the urinary findings
at the Magee Hospital, and, as in the previous table, include cases
of influenza which did not develop pneumonia. The specimens
examined were obtained from young, healthy men, between the
68ages of 20 and 32, and showed albumin in 13 per cent. of the
cases. This age factor probably accounts for the lower incidence
of albuminuria for this group.
TABLE III
URINE ANALYSIS IN CASES OF PNEUMONIA (INFLUENZAL) AT THE MERCY HOSPITAL
| Day of Disease |
Total No. of Specimens |
Specific Gravity |
Alb. |
R.B.C. |
Casts |
| 1001–10 |
1011–20 |
1021–30 |
1031–40 |
| 1 |
47 |
4 |
14 |
25 |
2 |
36 |
7 |
6 |
| 2 |
22 |
1 |
8 |
9 |
4 |
19 |
1 |
4 |
| 3 |
9 |
2 |
3 |
3 |
1 |
7 |
1 |
|
| 4 |
6 |
1 |
3 |
2 |
|
4 |
1 |
|
| 5 |
6 |
1 |
|
5 |
|
5 |
|
1 |
| 6 |
16 |
2 |
7 |
7 |
|
13 |
2 |
7 |
| 7 |
9 |
|
5 |
3 |
1 |
8 |
|
|
| 8 |
3 |
|
1 |
2 |
|
3 |
|
|
| 9 |
3 |
|
2 |
|
|
2 |
|
|
| 10 |
1 |
|
|
|
|
1 |
|
|
| 11 |
|
|
|
|
|
|
|
|
| 12 |
3 |
|
2 |
1 |
|
2 |
|
|
| 13 |
4 |
|
1 |
3 |
|
3 |
|
1 |
| 14 |
2 |
|
|
2 |
|
2 |
|
|
| 15 |
|
|
|
|
|
|
|
|
| 16 |
|
|
|
|
|
|
|
|
| 17 |
|
|
|
|
|
|
|
|
| 18 |
1 |
|
|
1 |
|
1 |
|
|
| 19 |
|
|
|
|
|
|
|
|
| 20 |
1 |
|
1 |
|
|
|
|
|
| Totals |
133 |
11 |
47 |
63 |
8 |
106 |
13 |
19 |
Table III includes the urinary findings of patients diagnosed
as influenzal pneumonia. In this table the term “Day of Disease”
indicates the day on which the physical signs of pneumonia could
be demonstrated, and not the day on which the patient was taken
ill with influenza. The incidence of albuminuria—79 per cent.—is
very high, while the presence of casts and red blood cells is
low. These results are really what one would expect. As we
have noticed in the late stages of uncomplicated influenza a
greater tendency for urinary changes to become apparent, one
would, therefore, most likely find considerable urinary disturbance
in the pneumonia immediately following the epidemic disease.
Pneumococcic pneumonia is prone to be accompanied by
69an albuminuria. So when we have both influenzal and pneumococcic
etiological factors involved, it is but natural to have
most of the patients showing signs of kidney disturbance. The
amount of albumin present, although generally greater than in
uncomplicated influenza, was not excessive. At times there was
little more than a trace. We noted the relative scarcity of casts—a
condition which differs greatly from our past experience in the
ordinary lobar pneumococcic pneumonia. On the transient nature
of this kidney involvement we have considerable positive evidence,
but there is no question that the time required for the
urine to return to normal is longer after pneumonia than uncomplicated
influenza. We have observed but one or two cases which
afterward returned to us presenting clinical signs of acute
nephritis. In fact, in going over our hospital records of the
winter and spring we noted that an unusually small number of
acute nephritics have been admitted. This would seem to be
evidence that, as has been noted in the past, the kidney is not a
vulnerable organ in this epidemic disease.
TABLE IV
URINE ANALYSIS IN CASES OF PNEUMONIA (INFLUENZAL) AT THE MAGEE HOSPITAL
| Day of Disease |
Total No. of Specimens |
Specific Gravity |
Alb. |
R.B.C. |
Casts |
| 1001–10 |
1011–20 |
1021–30 |
1031–40 |
| 1 |
3 |
|
|
2 |
1 |
1 |
|
1 |
| 2 |
12 |
|
1 |
10 |
1 |
8 |
|
6 |
| 3 |
4 |
|
|
4 |
|
1 |
1 |
1 |
| 4 |
9 |
1 |
2 |
4 |
2 |
6 |
|
6 |
| 5 |
8 |
|
4 |
4 |
|
6 |
|
5 |
| 6 |
8 |
|
5 |
3 |
|
7 |
2 |
6 |
| 7 |
4 |
|
2 |
2 |
|
3 |
|
2 |
| 8 |
10 |
|
2 |
8 |
|
5 |
2 |
5 |
| 9 |
4 |
|
2 |
2 |
|
4 |
3 |
4 |
| 10 |
6 |
|
1 |
5 |
|
6 |
3 |
5 |
| 11 |
1 |
|
1 |
|
|
1 |
|
1 |
| 12 |
1 |
|
1 |
|
|
1 |
|
|
| 13 |
|
|
|
|
|
|
|
|
| 14 |
|
|
|
|
|
|
|
|
| 15 |
2 |
|
2 |
|
|
1 |
|
1 |
| Totals |
70 |
1 |
20 |
45 |
4 |
49 |
11 |
40 |
70Table IV includes specimens obtained at the Magee Hospital
from patients diagnosed as pneumonia. The results among
these young students were very similar to those of the previous
chart, where all ages were included. However, casts and red
blood cells were more regularly noted.
From the four tables, we are able to note one or two common
facts. In acute uncomplicated influenza albuminuria occurred 57
times in 447 specimens, or 13 per cent., at the Magee Hospital.
Here we dealt entirely with the young adult. At the Mercy Hospital
88 positive results of albumin in 344 specimens, or 26 per
cent., from patients of all types were recorded. The common
total would be 781 specimens examined, and 141, or 17 per cent.,
showing albumin.
With the advent of pneumonia the incidence of albuminuria
was increased. At the Magee Hospital it was seen 49 times in
70 examinations, or 70 per cent.; while at the Mercy Hospital 106
positive results were found in 133 specimens examined, a percentage
of 79. The combined figures, therefore, would show 155
out of 203, or 76 per cent.
The incidence of albuminuria for the epidemic in all its phases
would be, from our figures, 400 in 994 specimens, or 40 per cent.
Red blood cells were present in 5 per cent. of the influenza
cases, and in 11 per cent. of the pneumonias. This was always
a microscopic observation, save in the case of a slightly smoky
urine. Even microscopically the red cells were not numerous.
We noted them at times quite early in the disease in some of the
severe cases which presented epistaxis and hematemesis. Possibly
one might consider the early presence of red blood cells in
the urine as a condition analogous to those just mentioned,
although we never saw anything suggesting free hemorrhage
from the kidney. It is probably better to regard the red cells
as a manifestation of an acute nephrosis of toxic origin.
Casts were found in 35 per cent. of the cases showing albuminuria.
We are inclined to feel that this observation is somewhat
low, but at the same time we have noted that in uncomplicated
influenza one frequently sees albumin without casts.
We were also impressed with the fact that casts were not as
prominent a feature in the influenzal pneumonias as they are in
frank lobar pneumonia of essentially pneumococcic origin.
71During the course of routine examinations several transient
glycosurias were seen. Their transient character was the outstanding
feature. The quantity of sugar was very moderate—our
figures were never above 1 per cent.—and the daily amount
of urine was always within normal limits. Acetone and diacetic
acid were absent. A few observations on the blood sugar showed
a rise (.2 to .25), which readily came to normal with treatment.
Clinically these cases were not classed as diabetes mellitus, but
rather as a nervous complication of influenza, involving in some
way the carbohydrate metabolism, probably through the central
nervous system. One case of special interest, which is mentioned
elsewhere, was the association of glycosuria with almost total
blindness from a very intense optic œdema. Sugar (1 per cent.)
was present on the day of admission, while only a trace was noted
on the two following days, and from then on the urine was free
from sugar. How many days the sugar had been present before
admission to the hospital we cannot say, but we could trace the
failure of vision back to almost the day of its onset, which was
three weeks previous to our first examination. The eye symptoms
were the only complaints. The patient had had a moderately
sharp attack of influenza a little over two weeks before
the first sign of failure of vision had appeared. We may add
that the vision returned slowly to normal several weeks after
admission. The urine and blood sugar were normal, on a general
diet, over a period of one month while in the hospital. Unfortunately,
we have had no further record of this patient regarding
the urine, but her vision still remains normal. Cases of this type
were observed in England after the 1890 epidemic, and are referred
to in Allbutt’s “System of Medicine,” vol. i, on influenza.
Our other glycosuria cases did not present changes in the fundus
of the eye. The glycosuria and glycæmia were transient, and we
feel that they do not represent diabetes mellitus. Most of the
patients of this class had long since recovered from an attack of
influenza, and came to the hospital usually for treatment of
various nervous conditions, which at times simulated neuritis, or
otherwise one saw manifestations of general nervousness, not
unlike hyperthyroidism. In all probability, we were dealing with
a hyperglycæmia associated with a hyperactive thyroid gland.
So, after all, the glycosuria, even though rare, is not bewildering.
Symptoms and signs of toxic goitre in direct relation to the
72epidemic we claim to have seen, and one is justified, temporarily
at least, in having the thyroid gland father our transient
glycosuria.
In relation to the positive sugar findings, we have had numerous
negative examples of almost equal interest. Furunculosis is
a very common sequel of the epidemic. It is well known that
in furunculosis there is a hyperglycæmia, but no glycosuria and
no acetone or diacetic acid in the urine. All our blood sugar
readings were above the normal, and at times unusually high.
They varied from .2 to .41. This last unusually high amount was
in a young physician with recurrent furunculosis following
influenza. There was no glycosuria at any time. Elimination
of carbohydrates not only brought the blood sugar to normal
limits in the course of a week, but also assisted in the cure of the
furunculosis, but in a longer time. In all of this group we saw no
incidence of polyuria or glycosuria.
Hematology
There is very little evidence, as shown in the literature, that
special study on the blood during past influenzal epidemics has
been made. A few references to alterations in the count of cells
have been reported for the last epidemic (1890), but they are,
as a rule, very brief statements. Cabot notes a normal leucocyte
count in two-thirds of the cases, and a moderate increase in the
rest. Several observers call attention to the leucopenia during
the height of the disease, with a subsequent rise after the temperature
has fallen to normal. According to Rieder and Herman
(American Journal of Medical Science, 1893, cv. 696), the leucocytes
were not increased in simple influenza, and only very
slightly in the pneumonia following this disease. Herman also
noticed a decline in the leucocytes in pneumonia as a fatal ending
ensued. This finding was one of the few recorded for the 1890
epidemic. Emerson (Emerson Clinic Diagnosis, 1911, 558) found
in influenza almost one-half of the cases showing more than
10,000 leucocytes, some even reaching 25,000. He further notes
that early in the disease the count may be low, 3,000 to 5,000, but
it usually rose sharply, to fall again when the temperature comes
to normal. He lays stress on obtaining a leucocyte curve for each
case in order to get a true picture of what changes occur. The
past epidemic has brought out many observations on this subject.
73They vary somewhat, as is to be expected, but a common
factor seems to be more or less basic—namely, a leucopenia or
a normal count is the most significant single blood picture we
have of uncomplicated influenza. Further, a leucocytosis is fairly
generally, and we believe correctly, interpreted as evidence of a
secondary bacterial invasion in this particular epidemic, and
usually of the respiratory system. The leucopenia is as much a
part of the clinical picture of influenza as it is of typhoid
fever. Leucocytosis always means secondary invasion by other
organisms.
During the recent epidemic the clinical laboratory department
of the School of Medicine, University of Pittsburgh, has made
747 blood counts on influenza cases. In most of the cases blood
counts were made as a routine, while repeated counts were done
only on selected patients.
The following table indicates the leucocyte count for our series,
comprising the epidemic in all of its phases. There are a few
general points which appear striking that we may refer to at this
time, and leave until later the discussion of the minor details.
One-third of the counts, including, as they do, many cases of
pneumonia, showed a leucopenia, while 70 per cent. of the total
number fell under 10,000. This last group contains more pneumonias
and other complications than simple influenza. But 5 per
cent. of the cases counted showed more than 20,000. All of these
undoubtedly had pneumonia or some other complication. Comparing
this finding with our experience in the past before the
epidemic with the pneumococcic lobar pneumonia, one sees at
once that, as far as this type of clinical observation is concerned,
the two pneumonias are totally different. The writer remembers
but one case of lobar pneumonia which showed a persistent white
count falling below 10,000. Certainly in this community lobar
pneumonia and low leucocyte counts were unusual combinations
until the present epidemic. Further, the evident depression of
leucocytosis even where there was an actual increase is indicated
by 95 per cent. of our counts being below 20,000. This leads us
to state that the pneumococcus, although present in practically
all of our pneumonias, produced in only a small percentage of the
bloods we examined its characteristic increase. The toxic factor
of this influenzal epidemic certainly causes a marked change in
the white cells of the blood.
| MERCY HOSPITAL |
MAGEE HOSPITAL |
| Leucocyte Count. |
Influ. |
Influ. Pn. |
Influ. Compl. |
Total |
% |
Influ.
Influ. Pn.
Influ. Compl. |
% |
Total |
% |
| 2000 or less |
|
2 |
|
2 |
38 |
1 |
28 |
3 |
32 |
| 2000–3000 |
3 |
3 |
1 |
7 |
13 |
20 |
| 3000–4000 |
7 |
12 |
4 |
23 |
34 |
57 |
| 4000–5000 |
14 |
13 |
9 |
36 |
41 |
77 |
| 5000–6000 |
17 |
16 |
6 |
39 |
42 |
81 |
| |
|
|
|
|
|
|
|
|
|
| 6000–7000 |
15 |
13 |
6 |
34 |
40 |
59 |
37 |
93 |
38 |
| 7000–8000 |
7 |
8 |
5 |
20 |
36 |
56 |
| 8000–9000 |
8 |
14 |
8 |
30 |
37 |
67 |
| 9000–10000 |
15 |
9 |
8 |
32 |
39 |
71 |
| |
|
|
|
|
|
|
|
|
|
| 10000–12000 |
4 |
12 |
9 |
25 |
20 |
44 |
27 |
69 |
25 |
| 12000–14000 |
1 |
1 |
8 |
10 |
28 |
38 |
| 14000–16000 |
5 |
3 |
2 |
10 |
22 |
33 |
| 16000–18000 |
3 |
2 |
2 |
7 |
16 |
23 |
| 18000–20000 |
2 |
2 |
2 |
6 |
15 |
21 |
| |
|
|
|
|
|
|
|
|
|
| 20000–22000 |
|
1 |
1 |
2 |
2 |
4 |
5 |
6 |
3 |
| 22000–24000 |
|
|
1 |
1 |
8 |
9 |
| 24000–26000 |
|
|
1 |
1 |
4 |
5 |
| 26000–28000 |
|
|
|
|
2 |
2 |
| 28000–30000 |
|
|
1 |
1 |
3 |
4 |
| |
|
|
|
|
|
|
|
|
|
| 30000–32000 |
|
|
|
|
|
3 |
3 |
3 |
2 |
| 32000–34000 |
|
|
|
|
|
3 |
3 |
| 34000–36000 |
|
|
|
|
|
3 |
3 |
| 36000–38000 |
|
|
|
|
|
|
|
| 38000–40000 |
|
|
|
|
|
1 |
1 |
| 40000–42000 |
|
|
|
|
|
2 |
2 |
| |
|
|
|
|
|
|
|
|
|
| |
|
|
|
287 |
|
460 |
|
747 |
|
The blood picture in uncomplicated influenza is a normal one
for the red cells and the hæmoglobin, but the white cells are
characteristically altered. We have made many observations on
the red blood cells, and from all aspects the picture appears to be
normal. Similarly, there is nothing significant about the hæmoglobin
estimations. Where we have slight alteration in the red
count and in the hæmoglobin it is probably safer not to attribute
the change to the epidemic. We have no records showing a
secondary anæmia due to the initial epistaxis.
75A leucopenia or a normal count is what one should see in most
of the uncomplicated influenzal cases. We are almost ready to
say that any estimation above normal limits means secondary
bacterial invasion. The count may remain low throughout the
illness, rising to the normal rapidly as the temperature falls. We
do not regard a leucocytosis at the end of an epidemic case as
part of the blood picture. Our experience is that with convalescence
the normal count returns and remains within normal
bounds. Very often hidden sinus infection is responsible for
some of the post-influenzal leucocytoses. The leucopenia may
vary from a slightly subnormal count to a point well below
2,000. Most of the simple epidemic cases showed some degree
of leucopenia. As far as we have been able to estimate, we are
led to believe that one should not lay any special stress on the
grade of leucopenia as being of prognostic significance in uncomplicated
influenza. Many of the mildest clinical types showed
very low counts, and vice versa. There is, however, a prognostic
relation to be noted with reference to a falling white count in the
pneumonia, but this we shall mention again later. The onset of
the leucopenia corresponds to the onset of the disease. It was
present with the earliest cases we examined, and remained fairly
stationary, although we have records of its fluctuating slightly
one way or the other. But one must remember in this regard
the personal error in blood counting, and also particularly the
error of the apparatus. For careful work only those counting
chambers and pipettes should be used that have a Bureau of
Standards certificate. The duration of the leucopenia was fairly
close to the duration of the disease.
How many cases of influenza of several days’ illness having
about 12,000 leucocytes, a few sticky râles in the chest, but no
signs of definite consolidation, have been observed by the clinicians?
These cases recover without further change, and the
diagnosis is handed in as influenza without a complication being
mentioned. In collecting the blood reports from this group the
12,000 cells accordingly must be considered as having occurred
in a simple influenza. We hold that this is not a case of uncomplicated
epidemic disease. There is undoubted evidence, as is
acknowledged by the clinician, of a bronchiolitis; and how many
lungs showing a bronchiolitis at autopsy fail to have a broncho-pneumonia?
True it may not be demonstrable by our physical
76examination. This is often the origin of many high counts in
what apparently is considered uncomplicated influenza.
The blood picture of the pneumonia following the epidemic
was more or less constant, although at the same time the features
of the count may be quite different. One could roughly
divide the results into three groups: (1) leucocytosis, (2) leucopenia,
(3) intermediate or normal. Some pneumonias could be
followed during their course through all of these classes. Before
discussing the white count we can briefly dismiss the other
phases of the blood examination by stating that the red blood
cells and hæmoglobin presented nothing by the usual examinations
which was of special significance, or in any way characteristic.
As an example of the group showing a leucocytosis let us
follow a patient through an acute influenzal attack, followed by
a pneumonia with a subsequent recovery. An initial leucopenia,
gradually or suddenly changing into a very moderate leucocytosis
(10,000–15,000), was noted at the onset of the pneumonia. During
the course of the complication the number of cells in the
majority of cases increased, but rarely advanced beyond 20,000.
With lysis or crisis the count dropped toward normal, and by the
time the lung signs had disappeared the white cells were at the
usual number, or very slightly increased. The point which
seemed to us to be of importance was that, even although we had
a leucocytosis, it was nothing like the count that one would expect
for a lobar pneumonia. Of course, there were a few high counts,
but looking at the group as a whole they were relatively low.
There are a number of variations to this form of blood picture
which we might briefly consider. We have observed secondary
rises in the leucocyte count concurrent with a new lung involvement.
This type was the one so prone to develop into a condition
of non-resolution, fibrosis and ultimate death, with a continuous
moderately high leucocytosis to the end. Another variation
which we learned to fear was the fall of leucocytes to normal or
subnormal after a primary rise, when the clinical course of the
case in no way indicated a crisis or lysis pending. Seemingly,
the longer the primary leucocytosis had been present the more
serious was the subsequent leucopenia. We regard this form of
secondary leucopenia, if one may use such a term, as a prognostic
sign of some value. As in lobar pneumonia, a high leucocyte
count has been, as a rule, a favorable feature.
77The second group, or those showing a leucopenia throughout
their course, was by no means an unusual thing. This is a cardinal
point—in fact, one of the most striking clinical features of
the epidemic. The leucopenia here does not have the prognostic
value that it seems to have in the group just referred to previously.
We have observed cases go through a pneumonia with
4,000–5,000 white cells in a relatively easy manner. When, however,
the leucocytes fall to 3,000 or under, one may be reasonably
sure that the outcome is doubtful, even with the general condition
of the patient at the time favorable. In the pneumonias of this
group which died the leucocytes have always fallen to about 2,000
cells. We have a number of observations taken from one-half
to four hours before death showing counts in the immediate
neighborhood of 2,000, but never below this number. Where
recovery has taken place the cells go forward to the normal,
more or less keeping pace with the general clinical picture.
Of group three there is not much to say, except that on one
hand it tends toward a leucocytosis, and on the other to a leucopenia.
This group comprises a considerable number of the pneumonias.
We are not in a position to say anything regarding the
relative mortality of this group. The development of a leucopenia
from these cases after a period of some stability in the
leucocytic curve is of bad prognostic import. Not infrequently
we have noticed rather wild abrupt rises to 20,000 in the leucocytes
toward the late half of the disease. This curve was nearly
always sustained until the end, which, as a rule, was recovery.
We do not need to consider at any length the effect on the
leucocyte count of complications not of lung origin. Acute sinuses
in head, otitis media and meningitis always produced a variable
moderate leucocytosis. The change was not so marked in meningitis,
as our cases were all preceded by a pneumonia which had
independently invoked a slight leucocytic response. As a complication
of the pneumonia we have noted an abrupt rise following
an acute pleuritis with effusion, and similarly after the onset
of an empyema. These complications seemed to be able to induce
a leucocytosis with more certainty and ease than the more
serious pneumonic condition. Possibly, as they occurred toward
the end of the infection, the toxic factor of the epidemic influenza
was more or less spent, and the secondary invader had a freer
hand to act in its normal way.
78Differential counts were made in 194 cases, including influenza,
influenzal pneumonia and influenzal complications. We have
taken the average percentage of each type of cell for the groups,
which are purely numerical divisions based on the leucocytic
count. No differentiation is made for the various clinical divisions
of the epidemic in the following table:
| Leucocytes 2,000–8,000. |
| |
P. |
E. |
L.M. |
S.M. |
Trans. |
| Total counts 86 |
66% |
1% |
13% |
17% |
3% |
| |
| Leucocytes 8,000–10,000. |
| |
P. |
E. |
L.M. |
S.M. |
Trans. |
| Total counts 33 |
69% |
1% |
11% |
16% |
3% |
| |
| Leucocytes 10,000–20,000. |
| |
P. |
E. |
L.M. |
S.M. |
Trans. |
| Total counts 45 |
76% |
2% |
10% |
19% |
3% |
| |
| Leucocytes 20,000–30,000. |
| |
P. |
E. |
L.M. |
S.M. |
Trans. |
| Total counts 17 |
79% |
2% |
8% |
7% |
4% |
| |
| Leucocytes 30,000–40,000. |
| |
P. |
E. |
L.M. |
S.M. |
Trans. |
| Total counts 13 |
85% |
1% |
5% |
6% |
3% |
The differential count in general indicates an increase in the
polymorphonuclear leucocytes as the total leucocytic number
increases. This is really what one would expect. There also
seems to be an increase of the large mononuclear cells, with a
slight diminution in the small mononuclear elements, particularly
in the count below 10,000. Abnormal cells were encountered
very seldom. One can hardly say that the epidemic has a
characteristic differential blood picture, except, perhaps, that an
increase of the large mononuclears is present in the low counts.
This, however, may hold true for any leucopenia.
Conclusions
1. Epidemic influenza is often accompanied by a transient
slight albuminuria with a few red blood cells and casts. Acute
nephritis as a clinical entity does not appear to be other than a
rare sequel.
792. Epidemic influenza tends to produce a leucopenia.
3. A leucocytosis in influenza, as a rule, indicates a secondary
infection.
4. The pneumonia following influenza shows, as a rule, but a
very moderate leucocytosis, while, on the other hand, the presence
of a leucopenia is by no means infrequent.
We are greatly indebted to Miss R. Thompson, Messrs. Mock,
Frost, Marshall and Scott for their assistance in this work at
the Magee Hospital.
81
THE TREATMENT OF INFLUENZA
By W. W. G. Maclachlan, M. D.
One may frankly say there is no specific treatment for influenza.
Possibly we are in error in introducing the discussion,
particularly on treatment with such a definite and unsatisfactory
conclusion. The same statement has been made after all the
previous pandemics, and one wonders whether a like remark is
going to apply to the next similar scourge. The past two or three
months should bring to the medical profession a certain humility
which should stimulate a keener sense of research, especially as
we now have at our disposal highly organized laboratories where
unsolved problems can be viewed from almost any angle. Yet
we are really, save here and there, putting our forces together
in the study of the disease. It is obvious that a fleeting epidemic
makes a most difficult subject for study, especially during a time
when there is a paucity of physicians. May we not hope, however,
that some researches on the disease may be forthcoming,
so that we may safely feel that at least preventive or protective
measures will be possible?
There is no one who is able to say that this or that drug has
not been thoroughly tried. The alkalies, salicylates, antipyretics,
quinine and the sedatives have all been freely used in the last as
well as the present epidemic. Each group of drugs has its following,
although it appears to be a general rule in this epidemic
to use the antipyretics (coal tar products) as little as possible.
From the distant past we have numerous records of treatment.
Willis (1658) emphasized the value of sweating and the use of
diaphoretics, but at the same time he states that in mild cases
the cure is left to nature; Sydenham (1675) claimed considerable
value in fresh air. He also paid more attention to restricting the
diet, and was not favorable to the use of anodynes. One certainly
obtains the impression from the records of past epidemics
that many of the general principles in treatment were similar to
what are now in vogue. Medicinal remedies, of course, varied
greatly, but to enumerate them would be merely giving a résumé
82of the progress of therapeutics. Sufficient is it to say that influenza
has certainly, since the earliest days, given therapeutists an
ample opportunity to test their wares.
The outstanding respiratory complication, pneumonia, has
added a very undesirable phase to the disease. In fact, the
greater part of the mortality was due to this serious sequela.
Some interesting points have been brought out in serum and
blood therapy for this type of pneumonia. The use of whole
blood or serum from convalescent patients in cases of pneumonia
opens up a new and not unlikely fruitful means of treatment.
The method of treatment possibly may be applicable as an emergency
measure in other diseases, as has been shown in the case
of scarlet fever and poliomyelitis. We also have the anti-pneumococcic
sera available for therapeutic use. The drugs and the
general treatment of the pneumonia are virtually the same for
the last two epidemics.
The protean manifestations of the 1890 epidemic, with its
unusual nervous sequelæ, have not been seen to any extent, as
far as we yet know. In fact, the present epidemic appears to be
relatively free from complications other than those occurring in
the lung during the acute course of the disease. Hence, in all
likelihood, there will be less of the nervous after effects to be
treated. It is, however, too early to hope that the nervous system
is going to escape.
In another part of this volume the vaccine therapy is discussed
in detail, so that we shall not repeat what has been brought out
in that article. We would, however, emphasize the value of
honest and accurate clinical reports of the use of vaccines, in
order to establish their present status in epidemic influenza.
Overestimation and commercialism are very likely to ruin a
method of treatment, even when it may be of value in a certain
phase of the disease. If we do not carefully weigh the pros and
cons of the vaccine treatment in this epidemic from a purely
scientific and coldly neutral attitude, we are simply doing the
public and ourselves an injustice.
The treatment of influenza as the disease presented itself
to us in this community will be considered under three divisions—acute
influenza, pneumonia, and other complications.
83
Acute Influenza
There is one important thing to be done in the treatment of
influenza, whether the infection be mild or severe. Have the
patient go to bed as soon as possible. In most of the acute
attacks the individual went to bed of his own accord; but there
were, unfortunately, too many instances where the patient refused
to surrender, trying, as we say, to fight the attack. Some
appeared to be able to accomplish this feat. But how many of
our cases of fatal pneumonia can be clearly linked up with this
group of the mild or subacute preliminary course? No matter
how light the attack may appear to be, the patient should be told
of the necessity of remaining in bed until the pulse, respiration
and temperature have returned to the normal and remained normal
for at least five days. At the onset a hot bath, with care to
avoid chilling, followed by a drink of hot lemonade and a Dover’s
powder, gave considerable relief to the patient.
The value of good nursing cannot be overestimated. The nurse
must see that the patient is always well covered and kept warm,
not even permitting him to rise in bed to reach for a drink; also
the regulation of the temperature of the room should be carefully
watched. The main point is to have plenty of fresh air. We
have noticed that the patient appeared more comfortable if the
air was slightly warmed. Water should be given at regular intervals.
Under no consideration should an acute influenza case be
allowed to get up to go to the toilet.
At the onset, and while the febrile attack is still present, there
is little desire for food—but one does not need to worry about the
question of nourishment in such an acute illness. Milk, cream,
cocoa, gruels and fruit juices may be given at first, and as the
fever subsides the diet increased. We have found that the appetite
returned to normal very readily. In view of the urinary
findings indicating a slight transient nephritis, meat broths are to
be avoided until the convalescent stage is reached. We have been
very guarded in recommending cold sponging in acute influenza.
As a rule, it was not necessary. The icebag to the head is often
of great value in the intense headache, which is so frequent. It
is our opinion that in the treatment of uncomplicated influenza
what has just been mentioned constitutes the important part.
Most physicians would agree with this. However, when we
84advance to drug therapy, we come into the personal realm of
likes and dislikes of drugs and methods of usage.
We do not intend in any way to give our views in a dogmatic
manner, nor to touch upon all of the remedies that have been
advanced. At the onset of the disease a moderate calomel purge,
followed by a saline, was given in all cases. We were practically
free from the so-called intestinal type of influenza which was
seen in some other communities, consequently we did not hesitate
to use calomel. Castor oil or magnesium sulphate was given
afterward, as was found necessary. Abdominal distention was
rarely seen, and when it occurred a plain soapsuds enema with
turpentine was administered.
Quinine sulphate (gr. iii-v, three times a day) combined with
phenyl-salicylate (gr. v) was a routine measure. We often noticed
deafness after a very few doses of quinine. It was then discontinued.
Acetyl-salicylic acid (gr. v, three to six times a day)
seemed to have a palliative effect on the severe headaches,
although during the height of the disease the general muscular
aching did not appear to be relieved by its use. It was not used
routinely. These drugs possibly made the patients more comfortable,
but we were very skeptical as to their influence on the
general infection. The raising of the leucocyte count by quinine
in influenza appears very unlikely. The use of alkaline salts has
been a general procedure, particularly as we are now on the
alkaline wave of therapeutics. Sodium bicarbonate was added
to the drinking water of all patients (two drams to the quart).
We gave this salt for its diuretic effect. In a few cases more active
diuresis by the alkalines was readily and easily produced by the
use of “imperial drink” three or four times a day. We felt that
good kidney elimination was of considerable importance.
The use of tartrates and citrates, as in “imperial drink” in
a condition where we know some kidney impairment is present,
is possibly flying in the face of danger—especially in view of the
fact that these salts are so available in the production of experimental
nephritis. But we have only to see their application in
the human in mercury bichloride poisoning, where an intense
nephrosis usually develops, to fully realize that these salts may
be given without danger to the kidney. We do not suggest that
the kidney lesions of influenza and mercury bichloride poisoning
85are the same. We are merely bringing out this point of analogy
in support of their use in certain desirable cases.
The respiratory symptoms gave us more concern than any
other phase of the uncomplicated case. The irritating, distressing,
non-productive cough suggested both a sedative and
expectorant. Ammonium chloride (gr. iii-v, t. i. d.) was the usual
expectorant. It seemed to increase in value with the more chronic
type of case. It is our impression with those acute hacking
coughs that the sedatives produced more gratifying results.
Elixir terpin hydrate with heroin, codeine and occasionally morphine
were preferred. When good results were noted sedatives
were given liberally. Steam inhalations combined with tr. benzoin
co., followed by spraying the throat with medicated liquid
petroleum, gave some relief. The tendency to œdema, however,
as we saw it in the cases complicated by pneumonia made us
hesitate to use inhalations. Possibly the fear was groundless.
Morphine (grs. ⅙) was given for sleeplessness, and it was
repeated if necessary.
Cardiac stimulants were rarely needed. The tincture of digitalis
was the choice, but in the uncomplicated cases was very
seldom used.
At the beginning of the epidemic we prescribed whisky in
almost every case. Our idea was that it would have a sedative
action. At the present time we are very doubtful of its value.
Toward the end of the epidemic we used it very moderately. The
results obtained possibly depended for the most part upon the
type of patient. Some of the soldiers asked to have it discontinued,
not from any moral point of view, while others wished
more frequent doses. The elderly patients seemed to appreciate
this remedial agent to a fuller extent.
Pneumonia
The pneumonia following the original infection was, from the
standpoint of physical diagnosis, often difficult of diagnosis in its
early stages. The infection commencing as an influenza would
at times pass imperceptibly into pneumonia, and obviously the
points brought out in the previous paragraphs on treatment were
applied until the diagnosis of pneumonia had been established.
86Some new factors were peculiar to the pneumonia and demanded
further changes in the handling of the cases.
We would again emphasize the value of careful nursing to
conserve the patients’ strength. They should be kept warm, well
covered, with plenty of fresh air. Water should be given regularly
and abundantly. The diet should be light, one depending
a good deal upon the severity of the case. We believe it is safer
to limit the diet to fluids while the infection is still pronounced,
but as soon as the crisis has passed one may increase the diet
freely and fairly rapidly.
Regular elimination from the bowel should be helped by the
use of castor oil every other day, the dosage made to comply with
the patient. We noticed much less abdominal distention in this
form of pneumonia than one is accustomed to see in the ordinary
lobar pneumonia. If distention were present, plain soap enemas
with turpentine gave very satisfactory results. Turpentine
stupes also are of considerable value. Rest at night is needed.
When a hypnotic was necessary we gave morphine (gr. ⅙), and
repeated if the desired results were not obtained.
The day is coming when we are going to isolate our pneumonia
cases. This was almost an impossibility during the stress of the
past epidemic, but we know that temporary and fairly satisfactory
methods can be applied. Many hospitals provided for a type
of isolation. In a pneumonia ward sheets stretched between the
beds keep the fine spray which a heavy cough always produces
from spreading over the next two or three beds. This method is
simple and can be easily carried out. We feel almost certain of
having seen convalescent influenza cases develop pneumonia from
the adjacent pneumonia patients. As much as is physically possible,
the uncomplicated influenza and the pneumonia cases should
be separated. Further, it is to be kept in mind that reinfection
by another group of pneumococcus is quite possible, even in a
ward containing only pneumonia patients.
We did not observe any special effect of quinine, salol, salicylates
after the pneumonia had developed and, therefore, these
drugs were discontinued. Digitalis in the form of the tincture
was at first made a routine measure, but toward the middle of
the epidemic we stopped this routine usage and gave it only as it
appeared to be indicated. Our impression was that the heart
87was not involved as it is in ordinary pneumonia. A slow, full
pulse, as was so often the rule, did not seem to require digitalis.
For more rapid action of the drug one of the hypodermic digitalis
preparations or strophanthin was given.
Caffein sodium benzoate or salicylate seemed to be of considerable
value given hypodermically every two or three hours, the
last dose at 4 P. M. Its action as a respiratory stimulant and also
as a diuretic was what we desired to obtain. The drug was used
fairly early in the pneumonia, and although it was never prescribed
routinely we gave it frequently.
Atropine was indicated whenever signs of œdema were evident.
Its action was not always successful, but in certain severe cases
we believe that large repeated doses of atropine saved a few lives.
One-fiftieth (1
50 gr.) grain hypodermically, repeated every hour
for several doses, was usually well borne. We noticed twice in
each of two cases after using small doses (1
100 every four hours)
a peculiar rapid cyanosis not associated with dyspnœa develop.
This reaction remained, however, for only a short time, about 15
to 20 minutes, but it was rather alarming while it lasted.
The drug therapy is not very satisfactory in lobar pneumonia,
and it is less so in the form of pneumonia which follows influenza.
There is practically nothing essentially new in the drug
and general treatment of this serious complication over what was
shown in 1890, or even in the earlier epidemics, save that our
nursing and hygienic measures are undoubtedly better.
The addition of an immune serum (anti-pneumococcus serum
No. 1) to the treatment of pneumonia is a milestone in the history
of the handling of this disease, but we must keep in mind
that the pneumonia of the past epidemic was not the usual pneumococcic
lobar pneumonia. That the pneumococcus was present
in a great many cases is shown in another article of this series,
but we also know that the B. influenzæ was present in many, and
that it played an active part in the disease is evidenced by the
constant low blood count or actual leucopenia. A leucopenia in
true lobar pneumonia is most unusual in the United States. The
rarity of Type I pneumococcus was noteworthy. We were practically
unable to get any anti-pneumococcic serum which was
known to be of value at the time of the epidemic, so naturally
could not apply this method of treatment as was desired. About
88half a dozen 50 cc. bottles were in possession of the army medical
officers here, but they unfortunately could get no further supply
after this was used. We would have liked very much to have
combined the anti-pneumococcic serum in Type I cases with the
citrated convalescent blood, as was used by us during the epidemic.
The anti-pneumococcic chicken serum of Kyes should also
be considered. This serum has had but a very localized trial,
but from competent observers who have given it to a considerable
extent in some of the army camps we are led to believe that it
has a very definite value. Major Lawrence Litchfield informed
the writer that he had observed excellent results with Kyes
chicken serum during the past epidemic in the treatment of pneumonia.
This serum was not available for our use. It is to be
hoped that further experience with Kyes serum will be favorable,
because from the practical standpoint in the treatment of pneumonia
it has many commendable features. Again, we desire to
point out that the use of anti-pneumococcus sera in influenzal
pneumonia may not be a fair test of their true value.
Very early in the epidemic we realized that the pneumonia was
of unusual severity and most difficult to treat satisfactorily. We
were at once impressed by our helplessness, particularly in those
patients showing cyanosis. Nothing we did seemed to vary the
course of the pneumonia after this sign was evident.
Our work in the epidemic began about October 10 on receiving
a large batch of soldiers, about 100, from the Student Army
Training Corps of the University of Pittsburgh. At the end of
the first week several points were impressed on our mind.
Firstly, in the severe cases of pneumonia; and in the early part
of the epidemic most of the pneumonia was severe, the mortality
was excessive, much higher than we have been accustomed to
experience in Pittsburgh, where, as a rule, our hospital ward
pneumonia is a very severe infection. Secondly, the wide variation
in the severity of the epidemic as presented in the student
soldiers coming from identical surroundings and conditions, the
mildness on the one hand and the malignant character of the
influenza on the other, was a very striking feature. This led to
our adopting a form of treatment which was quite successful.
We worked purely on the hypothesis that those individuals
recovering from a mild or moderate influenza infection developed
89a higher grade of immunity than those in whom the disease was
more severe or fatal, and this immunity could be transferred to
another. This, of course, was merely inference. If the mild
cases did present a higher immunity, one would naturally think
that immune bodies would be present in the blood, and that in
transfusion from cases which had recovered one might have a
measure of therapeutic value for this epidemic. Recently
Spooner, Scott and Heath and others have demonstrated specific
agglutins in the serum of patients convalescing from the epidemic.
On October 17 we gave whole citrated blood from a convalescent
case of uncomplicated influenza to an influenzal pneumonia
patient. The result in this case was strikingly good, and
for the following five or six weeks this method was frequently
used. We decided to give the whole blood instead of the serum,
as we were able to treat the cases more readily and rapidly in this
way. Our method of transfusion was, fortunately, very simple.
We had treated but a few cases when the report of McGuire
and Redden appeared. These observers working in the Naval
Hospital at Chelsea, Mass., presented very excellent results in
the use of immune serum from convalescent influenza cases in
the treatment of pneumonia. They reported 30 recoveries out of
37 cases, with 1 death, and 6 cases still under treatment at the
time of their report. This form of treatment began at Chelsea
on September 28, 1919. In Texas, on October 15, Brown and
Sweet gave two cases of influenzal pneumonia citrated blood from
convalescent influenza patients. Their two cases recovered. Our
published results, although not showing such excellent figures
as from the Chelsea observers, agree very well with their work.
Since that time a number of confirmatory reports have been
brought forward. Ross and Hund have shown that this method
has been of value in their hands, and recently a further statement
from McGuire and Redden tends to confirm their first views
as to the value of immune serum from convalescent patients.
Their last report giving a mortality of 6 in 151 cases of pneumonia
cannot be other than positive proof of the value of this
method of treatment.
As the technical side of the work has been given in several
articles, we hardly think it necessary to again review it in detail.
A few phases should, however, be recalled. It would seem that
90either serum or the whole citrated blood may be used. Solis-Cohen
and his group of workers believe that whole blood has
stronger bactericidal properties than defibrinated blood or the
plasma. But yet one cannot complain, even on a theoretical basis,
against the results obtained with serum by McGuire and Redden.
The use of whole blood increases the detail of the procedure, in
that the agglutination reactions must be estimated. Unfavorable
results in this regard also naturally cut down the supply of
available donors. In a military hospital a dearth of donors does
not arise, but in civilian practice the problem is very different.
In our work we never gave more than 100 cc. of whole blood;
usually the amount varied between 50 cc. and 75 cc. On account
of the small amount we felt that isoagglutination would not be
a serious factor, and in more than 200 injections we failed to see
any evidence of ill results from this source. Giving up to 500 cc.,
as was done by Ross and Hund, is probably a different affair, and
accurate agglutination tests are essential. We feel that if the
case is treated sufficiently early in the disease as much good can
be shown to occur after 50 cc. as after 100 cc. of blood. We do
believe, however, that the pooling of sera, where one is able to
carry out this method, as it means a liberal supply of donors, is
really the method of choice. Syphilis must be ruled out, both
clinically and serologically.
As we emphasized previously, the problem presented in the
army hospital and in civilian practice is a little different. We
have had some experience with both sides. Fortunately, the
greater part of our work was with the Student Army Training
Corps, where army conditions were more or less carried out.
There was never any difficulty in getting donors. In fact, the
idea of giving blood appealed to these young fellows. In civilian
life it is, in our experience, a more difficult problem. The usual
personnel of the public ward has always its fair percentage of
positive Wassermann reactors, and the type of individual is quite
different from the young soldier. For a relative or friend we
could easily get a donor, but this group would cover only a small
percentage of the cases one wished to treat. The technique of
giving blood can be reduced to a very simple procedure, and
by no means should be regarded as a difficult surgical undertaking.
Combining the receiving apparatus of Ross and Hund
91(J. A. M. A., 72, 1919, p. 642) with the syringe method for giving
the blood which we suggested in our previous article makes an
ideal arrangement.
The results depend upon the time of treatment. The earlier
the pneumonia is recognized the better are the chances of recovery.
It is our belief that the majority of influenza cases
which kept a fairly high temperature for more than four days
had a lung lesion, even if we could not make out definite consolidation.
As the convalescent influenza serum may have value only
for the influenza infection, it would, therefore, appear but logical
that a late pneumonia which almost always has other organisms
present would not react as favorably. We have seen very few of
the deeply cyanotic type recover even with serum. The essential
rule is to treat them before this stage develops.
We have observed little or no change in the leucocyte count,
even after successful treatment, and taking our group as a whole
we are rather surprised at this result. Other observers have
noticed a marked increase in the leucocytes as the case reacted
favorably to the injections. We agree with McGuire and Redden
that the patients with counts below 10,000, as a rule, show the
best results. This possibly indicates that the influenza infection
is predominating, and that the usual secondary invaders (pneumococcus
and streptococcus) are at this time playing but a little
part. Hence the value of early treatment is apparent.
From the published results of different workers and our own
experience, we feel that influenza immune serum or whole citrated
blood given early in the pneumonia is of undoubted value—in fact,
almost specific. If the epidemic reappears next year, unless some
other better method is forthcoming, we would advise its more
general use, and would suggest the collection of pooled serum as
early as possible in the epidemic.
At the end of this article there is appended a series of our ward
record charts of patients who developed pneumonia following the
influenza. These charts are shown to indicate the results of
giving immune convalescent citrated blood in pneumonia. The
ones presented are from some of the group which recovered. We
have, of course, the charts from the fatal cases, but as they do
not bring out any special point, save that there was little or no
change after treatment, we are omitting them. It is not our
92idea, however, to give the impression that we have had nothing
but success with this method of treatment. It might be well to
emphasize some of the salient points which are brought out.
(1) The regularity of the drop in temperature after the injection
is almost generally demonstrated.
(2) The occasional chill following the injection seemed to have
no untoward results.
(3) The leucocytes show, as a rule, little or no variation after
transfusion. Our work agrees with McGuire and Redden’s statement
that the cases with a leucocyte count under 10,000 give
the best results with immune serum.
(4) The time of injection in many of the cases was by no
means ideal, in that the disease was advanced; and again in many
the injection should have been repeated sooner. This, however, is
no fault of ours.
(5) One injection of 50 cc. of citrated blood from a good donor,
if given early enough, may be all that is necessary. Several
charts bear out this statement.
(6) The day of disease is dated from the onset of the influenza.
The demonstrable signs of pneumonia correspond roughly to the
initial rise in temperature following the influenza. The day of
disease of the pneumonia is not indicated on the chart, as this
information we have obtained from the daily notes.
Complications
The epidemic was well spent before we observed many complications,
save those referable to the lung. Later various forms
of sequelæ have been appearing. One must guard, however,
against the danger of attributing all of our ills to the past epidemic.
We are not going to give in detail the treatment of these
various conditions, nor even mention all of the many complications.
The main points, however, we desire to emphasize.
We have previously considered pneumonia, which is the principal
complication with simple influenza, and the two are closely
allied. As an end result of the pneumonia, non-resolution and
fibrosis of the lung are of first importance. We cannot say very
much on the treatment of this condition. The duration varied
from a few to several weeks, and recovery was infrequent. Our
treatment aimed at supplying as much nourishment as was possible
93to give, with, in addition, good nursing. The treatment
otherwise was purely of a general hygienic type. Tepid sponging
appeared to give considerable relief from the profuse sweating
these patients so often had. Drugs were of value only for some
local effect. We wonder if carefully handled vaccine therapy at
the onset of such a complication might not prove of some value.
The autogenous would be the one of choice.
Empyema was not found to be as prevalent as one would
imagine. With so much non-resolution of lung following the
pneumonia we were surprised to see so little empyema. All
delayed resolutions we explored with the needle, so we feel that
the condition, if present, would have been recognized. The treatment
of empyema need not be given any special emphasis. It is,
as of old, a surgical affair. One or two new points in the technique
have been brought out in the way of drainage, but possibly
they have not been sufficiently tried to lay any stress upon them
at present. Dakin’s solution in certain chronic cases appeared
of value. Our empyema cases did well.
Pleurisy with effusion was observed a number of times, although
it has been our experience to find a very few large
effusions. Pleural puncture often gave negative results, even
when the signs did appear to indicate the condition. We aspirated
the fluid when present. The end results were always good. In
only one case did we have to repeat the aspiration for reaccumulation
of fluid.
Chronic bronchitis, accompanied at times with considerable
dyspnœa, has been seen on several occasions. There is very
likely associated with this condition some fibrosis of lung, and
probably some organization of small bronchioles themselves.
Expectoration has been variable, profuse or scanty, mucoid or
purulent. We consider rest in bed, with as full a diet as possible
to build up the general condition of the patient, the best form of
treatment. These cases had little or no temperature, and consequently
at first absolute rest was not considered necessary, but
we now regard it as the essential part of the treatment. Atropine
and heroin are of value at certain times. We confess to have
seen very little benefit from the expectorants. We are rather
surprised that this sequela is not of more frequent occurrence.
94Phlebitis, in our series usually of the formal vein, occurred
about as often as it does in typhoid fever. The end result, however,
is much better than in typhoid. We have seen only one
case where “the milk leg” has resulted. Rest and elevation of
the limb were all that we required. In the acute stage, if pain was
present, a light, carefully applied icebag was added. It is important
to rest the limb for at least two or three weeks, and to
caution the patient against remaining on the feet too long for
some weeks after recovery.
We saw a great deal of acute sinus infection, often occurring
even while the attack of influenza was present, but, as a rule,
this complication followed the attack. At times several weeks
intervened. The ethmoidal sinuses are most susceptible, but a
considerable number of acute frontal sinus infections were noted,
the latter often immediately following or occurring during the
acute period of the influenza attack. The majority of these
infections appeared transient, and disappeared with a little local
treatment. In fact, in frontal sinusitis cold applications seemed
to be all that was necessary. With some of the more chronic
infections nose and throat surgery has been followed by relief of
symptoms. Acute suppurative otitis media, considering the number
of influenza patients, was not common. Ear drum puncture
was done if necessary. We saw one case of acute mastoiditis
develop. The mastoid process was opened and drained.
Acute suppurative meningitis, following or associated with
pneumonia, appeared on three occasions. The pneumococcus was
cultured from the spinal fluid in all cases. Anti-pneumococcus sera
intraspinally (Type I or the Kyes serum) should be given. The
Type I serum is of value in a similar group infection. We have
had no experience with this method, but some recoveries from
pneumococcus meningitis have been reported after the early use
of serum given into the spinal canal.
Following the 1890 epidemic cases complaining of blindness
or partial loss of vision, with optic œdema or neuritis and a
glycosuria, were occasionally observed. We have seen one of this
type, and several transient glycosurias without eye signs or
symptoms. The glycosuria may be of nervous origin. Our
method of treatment was one of elimination and rest. The gastro-intestinal
tract was emptied with calomel, and afterward a
morning saline was given for a few days. Hot packs were
95administered, one a day for about two weeks. The patient was
instructed to drink as much water as possible, and we eliminated
sugar, bread and the 20 per cent. vegetables from the diet. The
glycosuria lasted for three days, while the vision, although beginning
to improve at once after treatment, took five weeks to
return to normal. The patient was kept in bed for three weeks.
How long the glycosuria had been present before admission to
the hospital we do not know. The transient glycosuria group
without the eye manifestations required very little treatment.
They also showed a transient hyperglycemia. A carbohydrate
free diet very rapidly cleared up these cases. After a time we
decided to watch the course of this group on a non-restricted
diet, even with sugar, and we found that they all returned to
normal (blood and urine), in a few days clearly indicating their
transient nature. We do not regard this process as a diabetes
mellitus. We do not give the hot packs, although free elimination
by bowel was attained in all. These cases were recognized
only through routine urine examination.
Furunculosis with a high blood sugar, in one case 0.41, without
glycosuria was a very interesting complication. We saw a great
deal of furunculosis, always with the increased blood sugar from
0.2 to 0.3, but never with glycosuria. Reducing the carbohydrates,
or even a fast day with good intestinal elimination, had
excellent results.
Neuritis and general debility have often been associated with
nasal or tonsilar infection, which when surgically corrected led
to the disappearance of symptoms and improvement of health.
Finally, we wish to refer to an isolated case of acute osteomyelitis
which was incised, and from the purulent fluid present in the
bone B. influenzæ was grown in pure culture. This is a very
unusual complication, and is of particular interest on account
of the positive bacteriological finding. The patient made an
uneventful recovery.
| McGuire and Redden |
Jour. A. M. A., 1918; lxxi, p. 1311. |
| McGuire and Redden |
Jour. A. M. A., 1919; lxxii, p. 709. |
| Brown and Sweet |
Jour. A. M. A., 1918; lxxi, p. 1565. |
| Ross and Hund |
Jour. A. M. A., 1919; lxxii, p. 640. |
| Spooner, Scott and Heath |
Jour. A. M. A., 1919; lxxii, p. 155. |
| Maclachlan and Fetter |
Jour. A. M. A., 1918; lxxi, p. 2053. |
| Heist and Cohen |
Jour. Immunol., 1918; iii, p. 261. |
| Kyes |
Jour. Med. Res., 1918; xxxviii, p. 495. |
96[Click on image for larger version]
97
THE PREVENTION OF EPIDEMIC INFLUENZA WITH SPECIAL REFERENCE TO VACCINE PROPHYLAXIS
By Samuel R. Haythorn, M. D.
INTRODUCTION
In developing practical measures for the prevention or control
of influenza epidemics, preventive medicine faces one of the most
difficult problems of modern times. By means of quarantine,
protective vaccination and instructions in personal hygiene many
of the diseases which formerly ravaged the world have been
brought under control. At first glance it would seem to be a
simple matter to apply the principles which we have found successful
against these diseases to influenza and let it go at that,
but in the recent epidemic many of the formerly successful
measures were tried and found to be either inefficient, inapplicable,
or at least of doubtful value.
During the pandemic there was little time to think collectedly,
and no time to analyze procedures, and even now it is far from
easy to determine what things were done wisely and what things
were of no practical value. There exists the greatest difference
of opinion as to what measures should again be used when the
need arises, and what ones should be discarded. For instance,
there are confirmed exponents of prophylactic vaccines, and
equally able men who are convinced of their uselessness; enthusiastic
advocates of the face mask, and almost as many objectors;
those who would close schools, churches, theatres, etc., and those
who claim that such measures serve only to prolong the epidemic.
One naval officer is said to have stated that he had accumulated
figures either to prove or to disprove the usefulness of any preventive
measure yet recommended. There is, in short, a chaos
of opinions with followers who vary from the one extreme of
believing there is “virtue in all things” to those of the other
extreme who state that every susceptible person develops the
98disease in the degree of his susceptibility, regardless of any and
all preventive measures used. While there remain so many
points on which definite, concrete knowledge is lacking, and so
much controversy over the relative value of various measures,
this paper can do little more than state the facts and discuss
their bearing on prevention as impartially as possible.
Great progress has been made in controlling contagious diseases
in recent years—a fact which can be easily verified by
anyone who will compare the sick reports of the Great World War
with those of any war previous to the beginning of the present
century. The diseases which have been most easily controlled
have been those against which prophylactic vaccines or prophylactic
sera have been developed. Smallpox, dysentery and
typhoid fever have lent themselves readily to control by protective
vaccination, while reliable temporary immunity can be
afforded by the administration of sera for protection against
diphtheria and tetanus. These are by no means all, but are
probably the most striking illustrations; and with such examples
before us, the greatest hope for the prevention of influenza
apparently lies in the development of a prophylactic vaccine
against it.
History of Prophylactic Vaccination in General
The name vaccine came from “vacca,” or cow, and was originally
applied by Jenner (1796) to the virus taken from cowpox
pustules for prophylactic inoculation against smallpox. It
has come to be loosely applied to all forms of preventive inoculations
except sera. We have, therefore, a variety of vaccines
which differ in their nature and method of preparation. Some
are produced by growing the virus in insusceptible animals, some
are composed of attenuated viruses, and most common of all are
the bacterial vaccines, sometimes called “bacterins,” which are
prepared from killed cultures of bacteria. Sera are used in
prophylaxis, as well as treatment, and are made by bleeding and
separating off the serum from animals which have been immunized
against the cause of the disease in question. Sera and
vaccines are wholly different products, and the distinction should
be made in discussing them, although there is a common tendency,
particularly among lay writers, to use the words interchangeably.
99Smallpox is the classical example of a disease which
can be completely controlled by universal vaccination. The parasite
causing smallpox has never been certainly demonstrated, but
over a century ago Jenner showed that cowpox, a localized, non-fatal
disease, protected against smallpox. Modern methods have
proven that a cow inoculated with smallpox virus develops cowpox,
and that thereafter the virus loses its power to produce
smallpox when it is returned to man. Instead, it causes a local
pustule, and confers immunity to smallpox over a considerable
length of time. Rabies is another example in which the exact
cause of the disease is still in doubt, and in which a protective
vaccine has proven of great value. Rabies vaccine was developed
by Pasteur, and is prepared by drying the spinal cords of rabbits
that have been killed by a highly virulent rabies virus. Typhoid,
dysentery, pneumonia and several other diseases of known etiology
have been more or less controlled by the use of vaccines
made from their respective bacterial causes. These vaccines are
of the “killed bacteria” type of vaccines, and credit for their
application to human disease belongs to Sir Almroth Wright
(1896). The preparation of bacterial vaccines is very simple.
Bacteria which are known to cause a certain disease are isolated
in pure culture, grown on artificial media, killed either by chemicals
or heat, standardized either by counting, or drying and
weighing, and suspended in salt solution for subcutaneous injection.
Salt suspension vaccines are usually given in three or four
increasing doses, about one week apart. Le Moignic and Pinoy
(58) first elaborated a lipovaccine for triple typhoid vaccination,
which was used extensively in France during the war.
Whitmore, Fennel and Peterson have recently also advised the
drying of killed bacteria and the suspension of them in oil. This
method makes it possible to give a single massive dose of bacteria
which is sufficiently large to completely immunize the
individual against the disease, and which prolongs the immunizing
period by allowing slow absorption over a period of several
weeks. These vaccines are called lipovaccines, have been adopted
in the United States Army as the standard typhoid vaccine, and
promise in time to supersede the salt suspensions entirely from a
commercial standpoint. Many other modifications in the preparation
of bacterial vaccines have been advised, notably the class
known as sensitized vaccines. These are prepared by incubating
100bacterial vaccines for a time with the serum taken from animals
already immunized against them. The serum apparently absorbs
many of the toxic substances, and permits the injection of more
efficient doses. Besredka advised the use of living cultures which
had been incubated with immune sera, on the basis that vaccines
so prepared were very active and non-toxic. The sensitizing
treatment, however, does not stop the growing powers of the
bacteria, and vaccines of the Besredka type are generally considered
dangerous and so are little used. Sensitized killed bacterial
vaccines, on the other hand, are quite popular.
When a sufficiently large dose of vaccine is given to an individual
there is usually a transient rise in temperature for from
12 to 48 hours; the local focus of injection becomes sore and
inflamed, and a white count often shows an actual increase in the
number of polymorphonuclear leucocytes in the general circulation.
A series of doses are usually given. If after a few days
blood is withdrawn from the patient and immuniological tests
made, it will generally be found that the patient’s leucocytes take
up bacteria, and particularly the type of bacteria of which the
vaccine was composed, more readily and in greater numbers than
the leucocytes of the ordinary individual. Wright and Douglas
(52) and Neufeld and Rimpau (53) have shown that this effect
of increased phagocytosis is brought about by the vaccine through
the production of substances which act specifically on the bacteria
and render them more susceptible to inclusion within the
white cells. These substances belong to the group of antibodies,
and are known as “opsonins” or “bacteriotropins,” and are
specific for any given bacteria. Moreover, the serum of the
patient will, as a rule, be found to have developed the faculty
of agglutinating and bacteriolysing suspensions of the specific
organism injected and of fixing complement in the presence of
an antigen prepared from that organism. In animal work it has
been possible to go still farther, for it can be shown that the
resistance of the animal can be raised until it is no longer possible
to kill it with the same dose which is found to be fatal for
the unimmunized animals. Not only has animal work made it
possible to determine the protective powers of vaccines, but it
has also served to show the specific nature of the protective
power and the relative extent to which “group” or “crossed”
protection can be conferred by vaccinating with closely allied
101organisms—as, for instance, paratyphoid bacilli in typhoid fever.
The non-toxic nature of vaccines is also determined by animal
experiment before such preparations are injected into humans.
The most successful prophylactic bacterial vaccine which has
been developed so far is that for typhoid fever. A comparison
of the occurrence of typhoid fever in the United States Army
before and since the use of anti-typhoid vaccine is all that need
be cited to convince one of its value. At the time of the Spanish
War there was no vaccination against typhoid fever, and there
were 20,738 cases, with 1,580 deaths, among 107,973 men who
remained in the camps in the United States during the war (54).
During the summer of 1911, the maneuver division of the
United States Army, having 12,801 men, all of whom had been
vaccinated against typhoid fever, were stationed at San Antonio,
Texas. Two cases of typhoid fever developed among them, and
neither case died. Among the civilian population of the city,
living under usual conditions during the same time, there were
49 cases of typhoid fever, with 19 deaths. Since 1912, typhoid
vaccination has been compulsory in the United States Army, and
the largest epidemic of typhoid fever which I have found reported
so far during the late war was that at Camp Greene (55), Charlotte,
N. C., where 18 cases developed. Only 12 of these men
had received the complete series of immunizing doses. For a
complete discussion of the value of typhoid vaccine the interested
reader is referred to Gay’s Monograph (56) on typhoid fever.
Prophylactic Vaccination Against Influenza
The hope of finding an early solution to the vaccine problem
in influenza appeared to be in the development of a prophylactic
“bacterial vaccine” similar to that which proved so efficient for
typhoid. In his discussion of the vaccine problem in pneumonia,
Fennel pointed out that, theoretically, any disease of microbic
origin in which spontaneous recovery is at all possible should
yield to specific prophylactic measures. The difficulty, however,
of preparing a bacterial vaccine for influenza comparable to that
for typhoid fever is that the unquestioned cause of influenza has
yet to be determined. The probable cause of influenza is the
Pfeiffer bacillus, but its relationship has not been proven beyond
question. On the other hand, the innocence has likewise not been
proven, as Dr. Holman in his article of this series has ably shown.
102It is not my intention to go deeply into the question of etiology,
but simply to bring out a few points which a priori seemed to
indicate that the reasonable solution of vaccine prophylaxis was
in the preparation of a pure Pfeiffer bacillus suspension.
The experiments in man lead to very surprising results. Rosenau,
Keegan, Goldberger and Lake, at Gallops Island, Boston,
Mass., (1) inoculated volunteers with pure culture of B. Pfeiffer,
with secretions of the upper air passages and with blood from
typical cases of influenza. Sixteen men, of whom 13 were supposedly
non-immune, had Pfeiffer bacilli installed into their nasal
passages, and none of them developed the disease. Secretions
filtered and unfiltered also gave negative results. Contact with
well-developed early cases also failed. McCoy and Richey (1a)
conducted similar experiments in San Francisco, with negative
results. The men of the latter group had been vaccinated with a
mixed streptococcic vaccine, which may have played some part.
Had the experiments with the Pfeiffer bacillus been negative
and the other experiments positive, they would have shown that
the bacillus of Pfeiffer was not the cause of influenza; but since
all attempts were negative, it merely brought out the fact that
there had been a change, due probably to some immune factor,
which seemed to have acted alike on the Pfeiffer bacillus and all
other types of virus present, and to have made them all innocuous.
These experiments still leave the cause of influenza in question.
Those who are opposed to the Pfeiffer bacillus being the cause
of influenza in its epidemic form base their position on the
points that the common finding of the bacillus might be accounted
for on the grounds of its being a secondary rather than a primary
invader; that while it is not so common at ordinary times, it
does occur with other organisms in whooping cough and sometimes
in chronic diseases of the air passages, and that the rules
of Koch have not been complied with in that the organism
has not been found in every case of the disease; that where it
has been grown in pure culture and inoculated into man and animals,
it has either produced no disease, or the lesions which followed
have not been typical of epidemic influenza. On the side
of those who believe that the Pfeiffer bacillus is the chief cause,
or, at any rate, that it is partly responsible for epidemic influenza,
are the facts of its fairly constant presence in the purulent
bronchial secretion of patients suffering from epidemic influenza;
103its relatively uncommon occurrence at other times; its known
pathogenicity in occasional cases of meningitis, and in the inflammation
of the bony sinuses of the head and face; the relative
immunity of nearly all common laboratory animals and the fact
that the attempts to transfer epidemic influenza from man to
man failed not only when Pfeiffer bacilli were used, but also when
direct contact and direct coughing by the patient into the face
of the volunteer were tried. The argument that many cantonment
laboratories failed to find the organisms loses weight when
we find that the percentage of positives increased where the
material examined was removed directly from the lungs at
autopsy, where special cultural methods were in use and where
the laboratory personnel was large enough to devote a sufficient
amount of time to each individual culture. All of these points
indicate that the organism was overlooked in a great many
instances. In our laboratory we found the examination of sputa
very unsatisfactory because of the great amount of contamination,
and because the bacillus seemed to lose its ability to grow
after a relatively short time in the sputum in vitro. Moreover,
I am convinced that the bacillus changes its morphology to such
an extent under varying conditions as to make it impossible of
identification when present among other organisms in sputum
smears. The failure of animal inoculations is also not conclusive
evidence against the Pfeiffer organism, because guinea pigs,
rats and mice have a natural immunity for them. Rabbits are
only slightly susceptible, and then only to intravenous injections.
The mixture of the Pfeiffer bacillus with any one of several other
pathogenic organisms will increase the pathogenicity of both.
Monkeys inoculated intracranially develop a typical Pfeiffer bacillus
meningitis.
Whatever the ultimate outcome of the investigations as to
the parasitic cause of epidemic influenza, the Pfeiffer bacillus
was the generally accepted cause at the beginning of the 1918
epidemic, though it was at once realized that most of the deaths
were due to complicating pneumonias and to secondary infections
with other organisms. Under the circumstances, one of two
courses was open: (a) the acceptance of the Pfeiffer bacillus as
the presumptive cause of influenza and the preparation of a
specific prophylactic vaccine against infections with that organism;
or (b) the use of a mixed bacterial vaccine containing the
104common and most deadly secondary infecting organisms, designed
to increase the patient’s general resistance by decreasing his
susceptibility to the allied, collateral and secondary infecting
agents. Attempts were made along both lines, with more or less
unsatisfactory results.
The Attempt to Develop a Specific Prophylactic Vaccine by the Use of Pure Pfeiffer Strains
By a specific prophylactic vaccine for any given disease, we
mean a material which when inoculated into an individual will
actively protect that individual against the given disease. In
infectious diseases, the immunizing material is usually of microparasitic
origin (in contrast to desensitizing substances used in
pollen diseases and those due to unusual sensitiveness to foreign
proteins), and is specific only for the disease caused by the microparasite
from which the material was prepared. With the knowledge
in hand during the epidemic, the logical plan seemed to be
to prepare a pure Pfeiffer bacillus vaccine, the object of which
was to eliminate primary infection with that organism and thus
prevent the secondary invaders from obtaining a fertile soil.
While specific Pfeiffer bacillus vaccines had been tried in treatment,
the field was a comparatively new one so far as prevention
was concerned. Many of the biological products companies had
so-called influenza vaccines on the market for treatment purposes,
and many of these contained Pfeiffer bacilli. A few preparations
of pure strains of the bacilli were also available, but I
was unable to find any records of their use for prophylaxis.
Lacy (2) reported two cases of sinusitis treated with autogenous
vaccines made from pure Pfeiffer strains—one patient improved
rapidly and the other showed no change. Investigation of several
of the other references on influenza vaccines showed that mixed
vaccines had been used in each instance. The work of Flexner
and Wolstein (3, 4 and 5) indicated that active immunizing substances
could be prepared from the Pfeiffer bacillus, although
they worked with serum instead of vaccines. They prepared an
anti-influenza-meningitis serum by immunizing goats and horses.
These sera cured monkeys of experimentally produced influenzal
meningitis. The sera showed agglutinins and bacteriotropins
for Pfeiffer bacilli, as well as positive fixation tests in dilutions
of 1 in 100, but they contained no lysins. The serum was offered
105for intradural use in treating influenzal meningitis, but was
found to have no value when used in human cases.
The first references which we have found on the use of pure
Pfeiffer bacillus vaccines for the prevention of epidemic influenza
were those of Leary (6), (7), and of Rosenau (8). Shortly after
the appearance of the first influenza cases in Boston, Leary used
a vaccine prepared from several strains of Pfeiffer bacilli both
for the treatment of influenza and for its prevention. The vaccine
for the latter purpose was given to medical students and
nurses, and the first results were apparently very encouraging.
Continued use has not been convincing. Barnes (9) reported an
attempt to protect the employees and patients of an institution
near Woonsocket. On October 9 a case of influenza developed in
the female ward, and was followed five days later by another.
On October 22 the disease appeared in the male ward, and the
same day 172 employees and patients were given their first inoculation
with Leary’s vaccine. Doses of 400, 800 and 1,200 million
bacilli were given at 24–hour intervals. All persons who had
developed influenza before the three doses had been completed
were excluded from the computation of the disease incidence,
which was found to be 20 per cent. both among vaccinated and unvaccinated
individuals. The mortality rate was 16 per cent. for
the 25 cases among the vaccinated, and 15.8 per cent. among 57
unvaccinated patients. The result failed to show any protective
qualities for the vaccine.
The best controlled vaccine experiment in which Leary’s vaccine
was used was that reported by Hinton and Kane (10), and
was carried out at the Monson State Hospital for epileptics. The
hospital had a population of 979 inmates, ranging from 4 years
of age to senility; of these 461 were vaccinated and 518 were not.
Vaccination was begun on October 6, and three doses of 400, 800
and 1,200 million were given at 24–hour intervals. The first case
of influenza developed a few hours after vaccination was completed,
but there were no more cases before October 12, when five
cases developed. The table shows the result of the work, and
that the vaccine failed to protect.
|
Population. |
No. of Cases. |
% of Cases. |
No. of Deaths. |
% of Deaths. |
| Vaccinated |
461 |
163 |
35.4% |
28 |
17.1% |
| Unvaccinated |
518 |
178 |
32.4% |
24 |
13.4% |
106Attempts to protect by the use of Leary’s influenza vaccine
were made in 11 other Massachusetts institutions, but the results
cannot be used to compare the incidence and mortality rates
between the vaccinated and unvaccinated, because the epidemic
was either on the wane, or at least well advanced when the vaccinations
were begun. The reports are of great interest in
showing the large number of vaccinations which failed to protect.
In the Taunton State Hospital about 800 were vaccinated, and
among them there were 81 cases of influenza and 17 deaths from
pneumonia, even though the epidemic was on the wane when
vaccinations were begun.
In the Gardner State Colony 834 were vaccinated after the
peak of the epidemic had passed. This number included all but
15 of the inmates who had not contracted influenza up to that
time. Out of this group, 62 vaccinated individuals developed the
disease.
At the Massachusetts School for Feeble-Minded 457 inmates
were selected for vaccination and controls. Of the 234 vaccinated,
56 developed influenza. Of the 223 unvaccinated, 185
developed influenza, with 16 pneumonias and 12 deaths. The vaccinated
group, however, were a more vigorous group of individuals
to begin with, and represented a higher mental grade
than the unvaccinated group, so that the evidence was considered
of questionable value.
At the Wrentham State School the influenza epidemic was
well under way before vaccinations were begun, and hence the
susceptible individuals were in a large part either affected or
infected with the disease. Of 1,198 unvaccinated persons, 758
developed influenza, giving a morbidity rate of 63 per cent. Of
128 vaccinated, 13 developed influenza and 1 died. Physicians in
this institution believe that the vaccinated were not as ill as the
unvaccinated patients.
In the Medfield State Hospital, having a total population of
1,940,421 cases of influenza, with 63 deaths, had occurred before
vaccinations were begun. Of the remaining unattacked inmates
902 were vaccinated. After the completion of vaccination one
new case appeared among the unvaccinated, and there were none
among the vaccinated.
107At the North Hampton State Hospital there were 9 cases of
influenza, 4 of whom died, among 444 unvaccinated individuals,
and 9 cases, with 1 death, among 563 vaccinated patients.
Among 506 patients vaccinated at the Westborough State Hospital
there developed 15 cases of influenza, 2 of which terminated
fatally. Of the 415 unvaccinated controls, 25 developed influenza
and there were no deaths. At the time vaccinations were completed
only 13 had developed influenza.
In the Worcester State Hospital vaccination was carried out
after the epidemic had entirely subsided.
At the Bridgewater State Hospital no vaccines were used, but
the morbidity rate was 29.9 per cent., as contrasted with 32.9
per cent. among the unvaccinated at Monson.
At the Danvers State Hospital the population of 853 adults
was divided into three sections. One section was vaccinated with
the Leary vaccine, one section with an unheated influenza vaccine
prepared by Dr. Rosenau at the Chelsea Naval Hospital, and one
section held as controls. The epidemic had, however, reached its
height before vaccination was begun, and no information as to
the relative value of the vaccines could be determined.
In Hinton’s (11) report the analysis covered the studies on
about 6,000 vaccinated individuals, which represented slightly
less than half of the population of 12 Massachusetts State institutions.
Hinton’s conclusions were as follows: “The heated suspension
of influenza bacilli used as a prophylactic vaccine did not
prevent influenza, lessen its severity nor its complications, and, as
far as could be ascertained, resulted in no harm.”
About the same time that Leary was working on his vaccine,
Rosenau prepared an unheated suspension of Pfeiffer bacilli,
isolated from cases of influenza of the existing epidemic, which
he used at the Chelsea Naval Hospital and in an experiment at
the Pelham Bay Naval Training Station. The writer is indebted
to Surgeon-General of the Navy W. C. Braisted for the data
from which this report was compiled—the report of the Sanitary
Officer of the station not having been completed at the time the
information was furnished. The vaccine experiment was made
in the isolation regiment, which had remained practically free of
influenza. Inoculations were begun on September 30, when 638
men were given the first dose of vaccine, 833 men being held as
controls. On October 4 the second dose was given to 589 men,
108and vaccination was completed on October 8, when 565 men were
inoculated. This group comprised the total number who received
three inoculations. On October 14 practically all of these men
were transferred, so that it was very difficult to get a complete
record. Those cases which developed influenza prior to October
10 have been omitted by the writer, both from the control and
vaccinated groups, because it is unfair to consider the incidence
of influenza among controls which developed prior to the time
the inoculations were completed in the vaccinated group. Between
October 10 and October 24 there were 27 cases of influenza
which developed among the vaccinated, and 30 among the controls,
giving a morbidity rate of 3.6 per cent. among the 833
controls, as compared to 4.7 per cent. among the 565 vaccinated
men. Emphasis is laid on the fact that these morbidity rates
were calculated for both groups on the number of cases that
appeared after vaccination had been completed. The result failed
to show protective qualities in the vaccine.
Influenza vaccines for prophylaxis were also prepared in great
quantities by the New York City Board of Health, and were made
under the direction of W. H. Parke. No reports on the value of
their vaccines have as yet appeared, and the writer has been
unsuccessful in obtaining any data on the matter. The Parke
vaccine was made in the following way: A large number of
strains of Pfeiffer bacilli were isolated from cases of influenza
during the epidemic. These were grown on a veal infusion agar
containing 1 per cent. peptone, 0.5 per cent. of sodium chloride,
5 per cent. chemically pure glycerin, and the reaction of which
was made neutral to phenolthalein in the cold. The agar was
melted, and from 3 per cent. to 5 per cent. of citrated horse blood
was added to it at a temperature above 95° C. The media was
then slanted and cooled in 6 × 1 inch test tubes. Most of the
vaccines contained about 17 different strains of Pfeiffer bacilli.
The strains were inoculated separately on a series of slants, and
at the end of 24 hours the cultures were washed off with sterile
water and the washings from each series were placed in a separate
bottle. Smears were then made to determine whether or
not gram positive organisms were present, and as soon as each
bottle was found to be free from contamination the contents
were pipetted off into a 1,000 c.c. flask, and the dilution with
sterile salt solution containing 0.25 per cent. phenol made. All
109of the strains were mixed together in the large flask. A sample
was then removed for standardization by Wright’s method, and
the flask was submerged for one hour in water at 53° C. Transplants
for sterility were made and watched for 48 hours. The
vaccine was then diluted so that each cubic centimeter contained
1,000,000,000 Pfeiffer bacilli. Prophylactic vaccination was carried
out by giving ½ c.c., 1 c.c. and 1½ c.c. doses at seven-day
intervals.
Author’s Vaccine
At the request of the Department of Public Health of the city
of Pittsburgh, the writer undertook to prepare Parke’s vaccine
in large quantities. The vaccine was to be prepared under the
direction of a committee consisting of Drs. Oskar Klotz, W. L.
Holman, E. W. Willetts, George L. Hoffman and the writer, and
the vaccine was to be turned over to the City Health authorities
for distribution in the community. The work was carried out
at the Singer Memorial Laboratory, and was begun the same day
that the committee was appointed. Thirteen strains of Pfeiffer
bacilli were used. Holman contributed six strains, isolated at
autopsies done by Klotz at the Magee Hospital. Other fresh
cultures were furnished by Willetts; Wiese, of the City Laboratory,
and by the Singer Laboratory. The media used was that
recommended by the New York Board of Health, save that
sheep’s blood was used instead of horse blood because of convenience.
The same technique was employed, with the exception
that a modification of the Hopkins method of standardization
was used instead of the Wright method. This was done
because Pfeiffer bacilli are extremely small, tend to form unbreakable
clumps and tangles, and so increase the difficulties of
making satisfactory counts, either by means of the Wright
method or with the Helber-Glynn counting chamber, that the
methods are independable. Opalescent standards permit of such
enormous variations that it was decided to use the Hopkins
method, or a slight modification which we found so satisfactory
that we will give our method here in detail.
Method of Standardization
When the sample was removed for standardization it contained
not only a thick suspension of Pfeiffer bacilli, but also bits of
110agar and blood-stained debris. It was necessary to rid the suspension
of the gross contamination, and this was done at first by
filtering it through sterile glass wool filters, and later by centrifuging
it at slow speed for about 10 minutes. The suspension
then contained little but the Pfeiffer bacilli, and was placed
in the Hopkins tube and centrifuged for ½ hour on the sixth
contact of the rheostat. This gave the per cent. of Pfeiffer
bacilli in the suspension, and the necessary dilutions to make
1,000,000,000 per cubic centimeter were readily determined. The
Hopkins tube consists of a centrifuge tube, with a capillary tube
sealed on at the smaller end. The centrifuge tube is graduated
in 10 c.c., 5 c.c. and 1 c.c. amounts, and the capillary portion is
graduated in 0.01, 0.02, 0.03, 0.04 and 0.05 c.c. amounts. To
standardize the vaccine, 10 c.c. of the sample was centrifuged in
the tube and the amount of sediment read on the capillary scale.
If the amount of bacilli fell between the graduations, an additional
amount of sample was added, so that the sediment reached
one of the graduated lines, the exact amount of sample added
being noted. The percentage of the suspension could thus be
determined by dividing the number of c.c. of sample used into
the amount of the sediment obtained, and the number of bacteria
calculated according to Hopkins table. The table available to
us did not list the Pfeiffer bacillus, but according to it a 1 per
cent. suspension of staphylococcus contains 10 billion organisms
to the cubic centimeter, and we estimated that Pfeiffer bacilli
were about half the size of staphylococci. This assumption was
borne out by a number of Wright’s method counts on standardized
suspension of bacilli. We, therefore, calculated that a 1
per cent. suspension of Pfeiffer bacilli should contain about 20
million organisms. Then, if 10 c.c. contain 0.02 c.c. of bacterial
sediment, the per cent. was calculated by taking 0.02
10 = 0.2 per
cent., the strength of the suspension. If 1 per cent. contains
20 billion, then 0.2 per cent. contains 4 billion per c.c. In order
to get a 100 million per c.c. suspension, it would be necessary to
dilute the original suspension 40 times.
Every method of standardization is more or less inaccurate,
but the above described method gave a fairly uniform product.
Drying and weighing is claimed by many to be more accurate,
but even with this procedure a fair amount of non-bacterial sediment
is present in the material to be weighed.
111After the vaccine was completed, cultures were made from
the final dilutions and were watched for 48 hours. Mice and
guinea pigs were injected with the first samples to make certain
that the material was non-toxic. Two laboratory employees also
volunteered and received full doses before the first batch of vaccine
was released. The first five litres were turned over to the
Red Cross on October 31, one week from the day the work was
begun. In three more days the laboratory reached a capacity
of 10 litres a day, and on the fifth day the order was received to
discontinue preparation of the vaccine.
Relatively little of our vaccine was given out, and in the rush
it was not possible to determine which physicians had been given
our vaccine and which had received commercial mixed products,
so there is no data on its protective powers.
As soon as we found that there was no call for prophylactic
vaccines, we planned some animal experiments; but inasmuch as
we were unable to get our cultures of Pfeiffer bacilli virulent
enough to kill mice or guinea pigs, the minimum lethal dose could
not be determined, and without it it was impossible to determine
the protective value of the vaccine. Mr. Purwin, in our laboratory,
injected a 25–gram mouse intravenously with 2 c.c. of a
milk thick suspension of Pfeiffer bacilli without killing the animal.
He was successful in getting a small needle into the tail
vein and in slowly injecting the whole amount. The mouse was
sick for about 36 hours, but entirely recovered. Guinea pigs
were insusceptible to very large doses. Had we succeeded by
means of a vaccine in completely immunizing a man against
Pfeiffer bacilli, we still would have been uncertain that he was
immune to influenza in its “epidemic” form.
The absence of virulence in our laboratory strains may not
mean that the cultures were non-virulent when first isolated, but
it suggests the uselessness of attempting to make active vaccines
from strains kept on artificial media for months or years, such
as those commonly offered for sale by commercial houses.
The loss of virulence in strains that have been isolated for
some time is interesting in the light of Parker’s (12) work upon
toxine production by Pfeiffer bacilli. She found that toxic filtrates
appeared in infusion broth cultures in from 6 to 8 hours,
and that 2 c.c. of a 20–hour filtrate would kill a medium-sized
rabbit in from 1 to 3 hours. It was also found that the poison
112deteriorated so rapidly that, in order to determine its toxicity,
the tests had to be made on the same day that the filtrate was
obtained. Parker succeeded in making an anti-serum against the
poison, which appeared to be antitoxic for it both in vitro and
in vivo. This work is interesting, and may be a step toward the
development of a practical prophylactic serum.
Conclusion
From the above data, it is apparent that there is very little to
indicate that an immunity to epidemic influenza is conferred by
the use of a prophylactic vaccine composed of inert Pfeiffer
bacilli alone. If a desirable vaccine is to be obtained through
the use of these organisms, there must be radical changes in the
mode of preparation of the vaccine or in the size of the doses
given.
The Attempt to Protect Against Epidemic Influenza by the Use of Mixed Vaccines
For some years commercial houses have been carrying mixed
vaccines for the treatment of colds, which they called influenza
vaccines. These preparations were made up usually of six or
more different varieties of bacteria, and all of them were of
similar composition. There was more or less variation in the
doses, both as far as the total number of bacteria and the relative
number of the different types were concerned. A typical example
of a so-called “mixed influenza vaccine” may be given about as
follows:
| B. Influenza (Pfeiffer) |
25 |
to |
400 |
million per c.c. |
| M. Catarrhalis |
25 |
to |
400 |
million per c.c. |
| B. Friedlander |
25 |
to |
400 |
million per c.c. |
| Pneumococci |
25 |
to |
400 |
million per c.c. |
| Streptococci |
25 |
to |
400 |
million per c.c. |
| Staph. Albus-Aureus |
50 |
to |
800 |
million per c.c. |
| |
|
|
|
|
| Totals |
175 |
to |
2800 |
million per c.c. |
These vaccines were recommended in the various catalogues
for use either alone or together with other vaccines in the prophylaxis
and treatment of common colds, and in acute and chronic
diseases of the respiratory tract. As a matter of fact, they had
113been used very little in prophylaxis, and had failed to show very
much value in treatment. In discussing these vaccines from the
standpoint of treatment, R. M. Pearce (13) had the following to
say: “A mixed vaccine for common ‘colds’ containing several
organisms (staphylococcus, streptococcus, pneumococcus, micrococcus
catarrhalis group, bacillus of Friedlander group, diphtheroid
group, bacillus influenza) is one of the most recent
bacterial ‘shotgun’ mixtures, which takes the chance of one lucky
bull’s-eye in seven shots.” “No one can claim a scientific or even
a common-sense basis for the treatment of a cold by such a
mixture.” Catarrhal mixed vaccines of a similar kind were
refused acceptance by the committee on “New and Non-efficial
Remedies” of the American Medical Association, in June, 1918
(14), on the grounds that insufficient evidence of their therapeutic
value had been furnished by their manufacturers.
While the above illustrates the status of “mixed vaccine” for
therapeutic purposes, it is a well-recognized fact that it is possible
to produce an immunity for most of the bacteria composing
such vaccines, if killed cultures of the various strains are injected
in sufficiently large doses. Again referring to Pearce’s article,
we find the statement: “Prophylactic vaccination rests on a sound,
scientific basis of experimental studies and clinical observation.”
The attempt to protect against epidemic influenza by the use
of mixed vaccines was based largely on the following points. The
medical profession was confronted by a rapidly approaching
deadly epidemic, against which ordinary measures of control had
failed. The epidemic was supposed to be due to a primary infection
with Pfeiffer’s bacillus, but all of the fatal cases were found
to have profound secondary or symbiotic infections, with one or
more of the strains contained in the “mixed vaccines.” It was
known that mixed bacterial proteins, even though they were not
actually specific, possessed certain qualities of producing reactions
unfavorable to infections in general, which were characterized
by a temporary rise in temperature, by an increase in the
number of leucocytes, and by a more or less demonstrable amount
of active immunity against each one of the contained bacterial
toxins. The artificial production of a leucocytosis was especially
desirable, because a characteristic of epidemic influenza was the
failure of leucocytosis on the part of the infected individual. In
other words, mixed vaccines were used because they were the
114only available substances which offered the hope of creating a
reaction against the secondary invaders which were so commonly
the cause of death in influenza.
Since Pittsburgh’s experience with prophylactic vaccination
had chiefly to do with the use of commercially prepared mixed
vaccines, a brief history of the local experience with them may
be of interest.
About the time that the first cases of influenza were being
reported from the Pittsburgh district, articles on preventive
vaccines as used in Boston and at some of the camps began to
appear in the daily papers, shortly after which came the
announcement that the Carnegie Steel Company was offering
free vaccination to their employees and to the families of their
employees. Dr. W. O. Sherman, chief surgeon for the company,
advocated the use of the vaccine because he hoped to increase
the immunity to secondary infection and to produce an active
leucocytosis in the vaccinated individuals, and at the same time
to allay panic among the employees at a time when an interruption
of manufacturing and mining pursuits might be disastrous
to the entire country; and he did it with the assurance that if
the vaccine did no good, it would at least do no harm. He took
steps to arrange for the collection of data by which he hoped
to determine whether or not the vaccine as used by their company
did any good. His report has not yet appeared. Other
large corporations at once instituted prophylactic vaccinations
with commercial “mixed vaccines.”
In contrast to the altogether laudable efforts of these companies
to protect their employees, a complete history of the
vaccine episode in this community necessitates the recounting of
a very different phase in the matter. When it became known
that corporations were vaccinating their employees, people in
general naturally began to investigate. Physicians’ offices were
besieged by persons who either demanded vaccination at once or
wanted to know whether or not there was “anything in it.”
Conscientious physicians in their turn called up the offices of the
medical societies, the various laboratories, and telegraphed everywhere
trying to get some definite data before recommending the
vaccine to their patients. It was impossible to answer the question
definitely, because it was a new procedure and purely in the
experimental stage. On the whole, the medical profession
115handled the situation in a competent and dignified manner, for
the great majority gave vaccines only after a full explanation
to the effect that its value was in doubt, or else refused to give
it altogether. There were some, however, who were not conscientious,
and the unscrupulous practitioner seldom had a better
chance to impose upon the public. The demand for vaccine soon
exceeded the supply, and it is claimed that there were doctors
who gave any type of vaccine they could obtain without regard
to its bacterial make-up or intended purpose. Anti-diphtheritic
serum was given in many instances, and it is said that even
normal salt was used. Statements to the effect that exorbitant
sums were being charged and that guarantees of prevention
were being made resulted in the Red Cross Society undertaking
the distribution of the vaccine. To protect itself, the Medical
Society issued the following notice in the weekly bulletin for
October 26, 1918:
The Society wishes it understood that at present there is no
vaccine, serum or inoculation which will secure anyone against
influenza. It is desirable that everyone should avoid hysteria and
consider only the reports which are officially given out by the
Health Department, since of late various methods of prophylaxis
and treatment have found their way into the daily newspapers,
and these may prove harmful rather than do good.
Almost simultaneously the daily papers published the report of
Surgeon-General Blue, of the United States Bureau of Public
Health, which expressed practically the same opinion. It was not
the intention of either of these articles to criticise the practice
of vaccination, but merely to warn the public against profiteering
and fraudulent guarantees. They had the unexpected effect,
however, of causing people to completely lose faith in prophylactic
vaccines, and in many instances to become actually antagonistic
to them. It was during this period that the preparation
of vaccines from pure influenza strains was undertaken, under
supervision of the County Society and for distribution through
the Department of Public Health. Two days after the first supply
of this vaccine was ready the Red Cross authorities telephoned
that there was no further call for vaccine. The man in
charge of the distribution stated concretely that “the bottom
had dropped out of the vaccine business.” A few days later the
116Department of Health issued an order to stop the preparation of
the vaccine.
Many pharmacies, having small supplies of vaccines, realized
the great call for it and the difficulty of obtaining a new supply,
and were also guilty of commercialism. Certain of the large
biological product companies were no exception. One house
issued a hand-bill, printed in red on a yellow background, which
stated: “Epidemic influenza is due to the influenza bacillus. The
present epidemic of influenza has a tendency to develop pneumonia.
The use of our influenza bacillus vaccine No. ——
will abort the influenza and avoid pneumonia and other sequelæ.
When pneumonia has developed, it can be reduced to less than
one-third the mortality and duration usual with other methods of
treatment,” etc. Practically all of the above statements are still
unproven, and probably will never be shown to be true. Such a
bulletin undoubtedly lays this firm of vaccine manufacturers
open to prosecution under the law protecting against false and
fraudulent advertising. Several fairly well-authenticated incidents
occurred in which the representatives of vaccine houses
offered factory managers and others share and share alike in the
profits, if the brand of vaccine made by them was used. It is
on such happenings as the above that the writer advocates legal
measures, allowing Boards of Health to control the advertising
of remedies and distribution of biological products during epidemics.
How much Pittsburgh will learn from the experience with
vaccines will depend on the numerous analyses of data which
were acquired during the epidemic.
Data on the Prophylactic Value of Mixed Vaccines
Proof of the prophylactic value of mixed vaccines for epidemic
influenza depends entirely upon the results of its practical
application to human subjects in times when the disease is
prevalent. Animal determinations are out of the question, because
it has not been possible to produce the epidemic form of
influenza experimentally. If all people were equally susceptible
and were equally exposed, it would be a simple matter to compare
the number of vaccinated persons who developed the disease
with the number of unvaccinated persons who contracted it; but
since many thousands were vaccinated and some of them contracted
117the disease in spite of it, and a greater number of persons
who were not vaccinated entirely escaped, the analysis is
extremely difficult.
The time element is a big factor. In instances where vaccination
was completed in a community before the epidemic appeared
there, the figures are worth more than those in which vaccination
was undertaken after the epidemic had become established.
This is true, because the most susceptible persons in a community
developed the disease as soon as they were exposed, the less susceptible
ones were not attacked until later, and the insusceptible
ones escaped altogether. Whenever vaccination is begun during an
epidemic, the persons vaccinated for prophylactic purposes are
necessarily chosen from those who have not yet developed an
attack. The later in the epidemic that vaccination is begun, the
greater will be the number of persons selected for vaccination
from among those more or less naturally immune. Then, if the
total number of cases among the vaccinated is compared with
the total number of cases among the unvaccinated, the apparent
value of the vaccine is increased; but the estimation is not a fair
one, because the vaccinated group is unavoidably selected from
among relatively immune persons, while the controls include all
of the very susceptible people who were suffering from the disease
at the time vaccination was begun. Where vaccination is
begun after the epidemic is advanced, the only figures worth
while are those obtained by a day-by-day or a week-by-week comparison
between the number of cases developing among controls
and the number of cases appearing among those vaccinated, and
by beginning that comparison at a time subsequent to the day on
which the prophylactic inoculations were completed.
Aside from the interpretation of the results there is possibly
a more serious reason for objecting to the beginning of vaccination
during an epidemic. This lies in the danger of producing
a temporary negative phase in the patient, which makes him
somewhat more susceptible to natural infection for a few hours
immediately following each administration.
McCoy (15) outlined the requirements necessary for an ideal
vaccine experiment as follows: 1. The community should be as
large as possible, and should number at least 10,000 persons.
2. The conditions under which they live should be as nearly equal
as possible. 3. The turnover, or rather the change in population,
118should be as small as possible. 4. The social service should be
efficient and reliable, so that it can be definitely ascertained when
anyone becomes sick and what the disease is from which he
is suffering. 5. Fifty per cent. should be vaccinated before the
epidemic arrives, and the other 50 per cent. should be held as
controls.
No examples were found which came up to the above requirements,
but there were some instances in which vaccination was
completed before the epidemic appeared, and some in which we
were able to get a week-by-week comparison between vaccinated
and unvaccinated groups. Most of the data which has been
reported shows that vaccination was begun about the last of the
second or the first of the third week of the epidemic, and in some
instances not until after the peak was passed. Add to this the
fact that the vaccine was given in from three to four doses, at
from three to seven day intervals—a course which required in
the neighborhood of two weeks for completion—and it is obvious
that the full protective powers of the vaccine were not acquired
by the individual until the worst of the epidemic was over and
the number of cases were rapidly subsiding.
In order to get the best understanding from these experiments,
the data will be presented in three series: I. Those instances in
which vaccination was completed before the epidemic appeared.
II. Those instances in which it is possible to compare the relative
occurrence of influenza in both the vaccinated and unvaccinated
groups after vaccination was completed. III. Those instances in
which vaccination was begun after the epidemic appeared and
in which comparisons of total figures only are available.
Series I. Those Instances in Which Vaccination Was Completed Before the Epidemic Appeared
1. The only instance in the Pittsburgh community in which
vaccination was completed before the epidemic appeared is that
reported from the Dixmont Hospital, Dixmont, Pa., and furnished
me through the courtesy of Dr. Hutchinson (16). The institution
had a population of about 1,000 patients and 300 employees.
Prophylactic vaccination was begun on October 20, and was completed
about November 6. Each c.c. of the vaccine used contained
200,000,000 each of B. Pfeiffer, Micrococcus Catarrhalis, B. Friedlander,
119Pneumococci, Streptococci and Staphylococci, both Aureus
and Albus. Four doses were given of 4 minims, 8 minims, 12
minims and 16 minims, respectively. Inoculations were carried
out at four-day intervals. Owing to the isolation of the institution
from the general community, the first case did not appear
until two weeks later—namely, on November 20. The results are
shown by the table.
|
Population. |
No. of Cases. |
% of Cases. |
No. of Deaths. |
% of Deaths. |
| Vaccinated |
600 |
44 |
7.3% |
0 |
0% |
| Unvaccinated |
700 |
69 |
9.8% |
9 |
1.2% |
None of the vaccinated patients developed pneumonia, though
there were 15 cases among the unvaccinated.
This experiment shows a slight percentage in favor of vaccination,
and indicates that there was some decrease in the severity
of the secondary infections.
2. The experiment reported by McCoy, Murray and Teeter (17)
showed quite opposite results from the above, and was an excellent
example of a small though completely controlled test. In
an asylum for the insane in San Francisco all of the patients
under 41 years of age were divided into two groups—one group
was kept as controls and the other was given a vaccine furnished
by F. O. Tonney, of the Chicago Health Department. The vaccine
contained 500,000,000 each of B. Influenza, Pneumococcus
I, II and III, 1,500,000,000 Pneumococcus IV, 1,000,000,000 Streptococcus
Hæmolyticus and 500,000,000 Staphylococci. Doses of
0.5 c.c., 1 c.c. and 1½ c.c., which were given at 48–hour intervals.
Inoculation was completed on November 15, and the first case of
influenza appeared on November 26. The table shows the result.
|
Vaccinated. |
Not Vaccinated. |
| Persons in group |
390 |
390 |
| Cases of influenza |
119 |
103 |
| Cases of pneumonia |
23 |
17 |
| Number of deaths |
10 |
7 |
3. The report of Minaker and Irvine (18) included several
groups of men, the first two of which apparently belonged in our
first series. They used a vaccine, each c.c. of which contained
5,000,000,000 B. Pfeiffer, 3,000,000,000 each of Pneumococcus I
120and II, 1,000,000,000 Pneumococcus III, 100,000,000 Streptococcus
Hæmolyticus. In all, they vaccinated 11,179 persons.
(a) Their first group numbered 4,950 persons in quarantine at
the Naval Training Station. The quarantine was maintained for
24 days, and no influenza appeared during that time. Three
thousand five hundred and fourteen of them were released at a
time when there were still 200 to 300 cases of influenza being
reported daily in San Francisco. Out of the 3,514 men, 15 had
influenza, and there were no deaths.
(b) At the Mare Island Navy Yards 1,950 marines were released
immediately after completion of the inoculation. They
were turned into Valejo and San Francisco, where influenza was
at its height. Only 35 cases, with 1 death, occurred, and these
developed shortly after the men were released in San Francisco.
This group was controlled with an unvaccinated group of 8,232
persons who remained at Mare Island, and 1,296 cases of influenza,
with 65 deaths, occurred among the controls.
(c) At San Pedro 3,100 were vaccinated, and of these 53 had
influenza, and there were no deaths. The occurrence among these
was compared with the prevalence of the disease in Los Angeles,
but this part of the report leaves much to be desired in the way
of the relative dates, etc.
(d) The fourth group, consisting of 1,080 civilians, developed
14 cases, with no deaths. However, vaccination of this group
was not completed until 21 days after the pandemic had appeared
in the community. Minaker’s and Irvine’s analyses show a favorable
percentage for vaccination in the first two groups, but their
groups three and four were not sufficiently well controlled to be
of much help.
4. In a report which appeared during October, 1918, Eyer and
Lowe (29) published the results of prophylactic inoculation of
1,000 New Zealand troops with a mixed catarrhal vaccine. They
controlled their experiments with 19,000 New Zealand troops
who were not inoculated. A comparison of the incidence of acute
respiratory disease and influenza during the primary wave of
the epidemic as it appeared during June and July, gave two cases
among the vaccinated troops and an average of 43.2 cases per
thousand among the controls.
Later they reported (58) the results of much larger experiments
as carried out at 17 different camps and hospitals. The
vaccine which they used was a typical “mixed” vaccine, save that
121the authors emphasized the advantage of using strains not more
than three generations removed from the body. At some of the
camps their reports were unfavorable, but upon the whole their
results, as summarized below, were most encouraging. In most
instances inoculations were completed just prior to the arrival
of the autumn epidemic.
Out of a total average strength of 21,759, approximately
16,104 men received full prophylactic vaccination, and approximately
5,700 were uninoculated, or had received only 1 dose;
3,366 cases of influenza developed—15 per cent.; 1.3 per cent.
occurred among the vaccinated, while 4.1 per cent. developed in
the uninoculated; 8 per cent. of the severe cases among the protected
died, as compared to 23 per cent. among the uninoculated.
The death rate for all infected cases was 0.26 per cent. among the
inoculated and 2.2 per cent. among the uninoculated.
Notanda.—All of the above reports, comprising the “Series I”
experiments, indicate that mixed vaccines reduced the number of
severe illnesses and lowered the death rate to some extent.
Series II. Those Instances in Which It Is Possible to Compare the Relative Occurrence in Both Vaccinated and Unvaccinated Groups After Vaccination Was Completed
1. The report on prophylactic vaccination at the Hospital for
the Insane at Retreat, Pa., was very kindly furnished by Dr.
Charles B. Maberry (20). When the epidemic approached, the
institution was placed in quarantine and remained free from
influenza until October 28, when two cases appeared in nurses
who had broken quarantine. Influenza spread in the male ward,
but the female wards were kept free during the whole of the
epidemic. There were 370 male patients, but 60 were in the
infirmary and were not included in the calculation. Out of 310
patients, 210 received vaccines. Ordinary commercial mixed
vaccine was used, and vaccination was begun two days after
influenza appeared. During the first week there were 40 cases
of influenza, 6 of which occurred among those who had received
a single dose of the vaccine. After the first week there were
38 cases of influenza, with 10 pneumonias and 5 deaths, among
the unvaccinated, giving a morbidity rate of 38 per cent. and a
122mortality rate of 5 per cent. In the vaccinated group there were
no cases after vaccination was completed. Maberry states
further that in ward III the only cases which appeared subsequent
to vaccination were in six patients who refused preventive
inoculations. This appears to be the most favorable of any of the
reports.
2. Nurses on duty in hospitals everywhere suffered greatly
from influenza, and those of Pittsburgh were no exception. Some
of the hospitals vaccinated the nurses during the epidemic and
some did not, and it was hoped that by getting a week-by-week
comparison of the number of cases among vaccinated and non-vaccinated
nurses some reliable data would be obtained. A circular
letter sent to all of the hospitals in the community contained
a blank asking for the number of nurses, date of appearance
of the epidemic, use of vaccine, dates of inoculations, and
for a week-by-week occurrence of influenza in each group. Only
7 hospitals complied with the request, and of them only 5 sent
complete data. Complete reports were received from the Allegheny
General, Columbia, Presbyterian, South Side and St. Francis
Hospitals. Of a total of 336 nurses in these 5 institutions,
38 developed influenza in the first week, 48 in the second, 39 in
the third, 43 in the fourth, and 45 subsequent to the fourth week,
making a total of 213—a morbidity of 63 per cent. The Mercy
and St. Margaret’s Hospitals reported the total number of nurses
and the occurrence of influenza among them, and adding in their
reports there were 521 nurses on duty in 7 hospitals, with 257
cases of influenza, giving a morbidity rate of 50 per cent.; 28
cases of pneumonia and 11 deaths, giving a 2 per cent. mortality
rate. The total figures from hospitals where vaccines were used
are against vaccination, due partly to the fact that vaccination
was started late. In these hospitals the morbidity was 66 per
cent. and the death rate 3 per cent. In the hospitals where
vaccines were not used the morbidity rate was 20 per cent. and the
death rate 1.2 per cent. No dependable data was obtained, but
the report from the South Side Hospital was interesting. Of 60
nurses on duty, 36 had influenza and 2 died. Of this number
19 were stricken the first week. Three days after the first cases
were admitted to the hospital vaccination was begun, and was
given to most of the nurses still on duty. Of those taking vaccines
20 developed influenza and 1 died during the period of
123immunization, but after the inoculations were completed there
were no more cases in either group.
During the epidemic it was said that benefit was derived from
the use of vaccines on nurses at the West Penn Hospital, but
the writer was unable to obtain a report from this institution.
The collected data on nurses was useless, though it is interesting,
in that it shows the possibility of making figures prove almost
anything you want them to prove.
Series III. Those Instances in Which Vaccination Was Begun After the Epidemic Appeared, and in Which Comparisons of Total Figures Only Are Available
Undoubtedly the largest attempt at prophylaxis against epidemic
influenza through the use of “mixed vaccines” was that
made under the direction of Dr. W. O. Sherman for the Carnegie
Steel and H. C. Frick Coke Companies. The results which Dr.
Sherman hoped to attain when he planned using the vaccine and
collecting the data have already been given. Commercial mixed
vaccines similar to those described under the “Series I” experiment
were used, and four doses, three days apart, were given.
Inoculations were begun on October 20, 1918, and were completed
during the first week of November. Vaccine was administered
to the employees and their families without charge. Later cards
were given to all employees, and they were made to fill them out
and return them. On the cards were blanks calling for the
name, age, sex, color, number of inoculations, whether or not
the employee himself or any member of his family had had
influenza, and how many days the sick individuals had been in
bed. Each mill and mine was then supplied with a set of blank
forms providing for a complete statistical record of the number
of inoculations and the total incidence of influenza, pneumonia
and death. From the reports of the respective mills and mines
the total figures given in the charts were compiled.
Difficulties were encountered in every part of the work. The
vaccine demand was so great that the products of three different
firms were used. So many doctors were in service that most of
the vaccine had to be given by carefully coached nurses. The
bulletins of the United States Bureau of Public Health and of
the Allegheny County Medical Society, with their warnings about
influenza vaccines being only in the experimental stage, appeared
124just at the time the work was begun and caused a great many
to refuse to complete vaccination after one or two doses had been
given. So few medical men were left that it was impossible to
have them see all cases and so determine the nature of many of
the illnesses which were occurring. It was assumed, therefore,
that any employee who had fever and was sick for a period of
three days had influenza, and that any who were confined to bed
for seven days or more had pneumonia. The figures of the central
offices were made up from the reports of 14 steel mills, 1
cement factory, 4 warehouses and 57 mining districts. The accuracy
of data depended on the careful work of a great many local
statistical workers, which made individual variations hard to
control. The greatest difficulty of all, however, lay in finding a
common basis for comparisons of the incidence of influenza,
pneumonia and death in the vaccinated and non-vaccinated
groups, since the data on the former group included the occurrence
only after the peak of the epidemic had been passed, and
that of the latter group included the occurrence for the entire
epidemic.
The total figures are given in the three charts.
| CHART I. |
|---|
| |
| Carnegie Steel Company. |
| |
| All Works Except Homestead, City Mills, Columbus, Lucy and Isabella. |
| |
| Statistical Report on Inoculation Against Influenza. |
| |
| 1. Number of employees who had influenza |
5,728 |
18% |
| |
| 2. Number of employees who did not have influenza |
24,956 |
|
| |
|
|
|
| Total number of employees |
|
30,684 |
|
| |
| 3. Total number of persons inoculated |
One inoculation |
2,983 |
|
| |
Two inoculations |
3,675 |
|
| |
Three inoculations |
4,626 |
|
| |
Four inoculations |
10,053 |
|
| |
|
|
|
| |
Total |
21,337 |
|
| |
| 4. Cases influenza developed after |
No inoculations |
2,133 |
23% |
| |
One inoculation |
745 |
25% |
| |
Two inoculations |
776 |
21% |
| |
Three inoculations |
794 |
17% |
| |
Four inoculations |
1,280 |
12% |
| |
|
|
|
| |
Total |
5,728 |
|
| |
| 1255. Cases influenza pneumonia developed after |
No inoculations |
804 |
37% |
| |
One inoculation |
356 |
48% |
| |
Two inoculations |
403 |
52% |
| |
Three inoculations |
321 |
40% |
| |
Four inoculations |
459 |
36% |
| |
|
|
|
| |
Total |
2,343 |
|
| |
| 6. Deaths from influenza and “flu Pneumonia” after |
No inoculations |
104 |
4.7% |
| |
One inoculation |
32 |
4.3% |
| |
Two inoculations |
33 |
4.2% |
| |
Three inoculations |
21 |
2.6% |
| |
Four inoculations |
33 |
2.5% |
| |
|
|
|
| |
Total |
223 |
3.9% |
| |
| |
| CHART II. |
|---|
| |
| H. C. Frick Coke Company. |
| |
| Statistical Report on Inoculation Against Influenza. |
| |
| 1. Number of employees who had influenza |
5,248 |
31.4% |
| |
| 2. Number of employees who did not have influenza |
11,464 |
|
| |
|
|
|
| Total number of employees |
|
16,712 |
|
| |
|
|
|
| 3. Total number of persons inoculated |
No inoculations |
3,122 |
|
| |
One inoculation |
2,483 |
|
| |
Two inoculations |
2,548 |
|
| |
Three inoculations |
3,550 |
|
| |
Four inoculations |
5,009 |
|
| |
|
|
|
| |
Total |
13,590 |
|
| |
| 4. Cases influenza developed after |
No inoculations |
1,495 |
47.9%
of (3 |
| |
One inoculation |
634 |
25.5% |
| |
Two inoculations |
770 |
30.2% |
| |
Three inoculations |
1,078 |
30.4% |
| |
Four inoculations |
1,271 |
25.0% |
| |
|
|
|
| |
Total |
5,248 |
|
| |
| 1265. Cases influenza pneumonia developed after |
No inoculations |
94 |
6.3%
of (4 |
| |
One inoculation |
33 |
5.2% |
| |
Two inoculations |
42 |
5.4% |
| |
Three inoculations |
69 |
6.4% |
| |
Four inoculations |
85 |
6.7% |
| |
|
|
|
| |
Total |
323 |
6.1%
of (4 total |
| |
|
|
|
| 6. Deaths from influenza and “flu |
No inoculations |
30 |
2.0%
of (4 |
| |
One inoculation |
13 |
2.0% |
| |
Two inoculations |
21 |
2.9% |
| |
Three inoculations |
16 |
1.5% |
| |
Four inoculations |
37 |
2.9% |
| |
|
|
|
| |
Total |
117 |
2.2%
of (4 |
| |
| |
| CHART III. |
|---|
| |
| Bessemer & Lake Erie Railroad. |
| |
| Statistical Report on Inoculation Against Influenza. |
| |
| 1. Number of employees who had influenza |
1,275 |
24% |
| |
| 2. Number of employees who did not have influenza |
3,986 |
|
| |
|
|
|
| Total number of employees |
|
5,261 |
|
| |
| 3. Total number of persons inoculated |
No inoculations |
3,091 |
|
| |
One inoculation |
232 |
|
| |
Two inoculations |
249 |
|
| |
Three inoculations |
479 |
|
| |
Four inoculations |
1,210 |
|
| |
|
|
|
| |
Total |
2,170 |
|
| |
| 4. Cases influenza developed after |
No inoculations |
705 |
55% |
| |
One inoculation |
111 |
48% |
| |
Two inoculations |
91 |
36% |
| |
Three inoculations |
129 |
27% |
| |
Four inoculations |
239 |
19% |
| |
|
|
|
| |
Total |
1,275 |
|
| |
| 1275. Cases influenza pneumonia developed after |
No inoculations |
283 |
40%
of (4 |
| |
One inoculation |
75 |
67% |
| |
Two inoculations |
59 |
64% |
| |
Three inoculations |
51 |
42% |
| |
Four inoculations |
69 |
28% |
| |
|
|
|
| |
Total |
537 |
|
| |
| 6. Deaths from influenza and “flu Pneumonia” after |
No inoculations |
40 |
5.6%
of (4 |
| |
One inoculation |
5 |
4.5% |
| |
Two inoculations |
0 |
|
| |
Three inoculations |
0 |
|
| |
Four inoculations |
3 |
4.3% |
| |
|
|
|
| |
Total |
48 |
|
Charts I and III show a decrease in the incidence of influenza
in direct proportion to the number of inoculations given. This
finding would have been very important had vaccination been
completed before the epidemic appeared. There is, however, no
convincing evidence in either of these charts that the vaccine cut
down the relative number of pneumonias, or decreased the death
rate to any appreciable extent. Chart I also shows the interesting
fact that influenza occurred slightly more often among those
who had one inoculation than among those who were not vaccinated
at all.
Chart II would indicate that influenza occurred much less frequently
in the vaccinated than in the control group, but a closer
analysis brings out the contradictory finding that influenza
occurred at the same rate in the group of 634 persons who had
only 1 dose that it did in the group of 1,271 who completed the
course.
The reports from the separate communities were so conflicting
that to attempt to analyze them leads only to confusion.
No reports of harmful effects from the use of the vaccine were
received, and several physicians who attended sick employees
say that, even though the figures do not show it, they feel certain
that the vaccinated persons in general were not as sick as
those who were not vaccinated.
On account of the conditions under which the vaccinations
were done and the reports compiled, Dr. Sherman has not felt
128justified in making a report, fearing that erroneous conclusions
might be drawn from the data. We are greatly indebted to him
for the use of his reports, without which our account of the
influenza epidemic in Pittsburgh would have been very incomplete.
2. Another large steel corporation who used vaccine but
asked that their names be withheld furnished the following
report. During the epidemic the company offered free vaccination
to its 27,000 employees and their families. Commercial
mixed vaccines were used, three injections given, and vaccination
begun on October 19, which was about the time of the peak of the
epidemic in Pittsburgh. The results include a record of all
employees who lost over six days between October 1 and November
30.
| EMPLOYEES |
Morbidity |
Pneumonia |
Mortality |
| No. |
% |
No. |
% |
No. |
% |
| Received only one dose |
3,895 |
511 |
13.13 |
31 |
0.8 |
28 |
0.72 |
| Received only two doses |
3,329 |
414 |
12.44 |
40 |
1.2 |
19 |
0.57 |
| Received all three doses |
9,897 |
468 |
4.75 |
46 |
0.46 |
32 |
0.32 |
| Total of above |
17,119 |
1393 |
8.14 |
117 |
0.68 |
79 |
0.46 |
| Received no doses |
10,036 |
1522 |
15.17 |
154 |
1.53 |
106 |
1.06 |
| Total for both groups |
27,155 |
2915 |
11.66 |
271 |
1.10 |
185 |
0.76 |
Before satisfactory conclusions can be drawn from these
figures it is necessary to know how many of the 10,036 persons
became sick before vaccination, and whether or not the rate of
decrease in this group was not similar to that shown by the
number of patients who developed influenza during the intervals
between their doses of vaccine. The relatively high percentage
of cases following the first and second doses are capable of
explanation on one, or perhaps on all, of the three following
grounds: (a) the general subsidence of the epidemic, which
showed a rapid decrease by the time the third dose was given;
(b) the increased protection afforded by the three doses of vaccine,
and (c) the broken resistance of the patient following sudden
sensitization by the vaccine.
3. Rosenow (21) prepared a mixed vaccine by growing the
various bacteria in glucose broth, for from 18 hours to 36 hours,
129centrifuging and suspending the sediment in salt solution and
making up the vaccine on a percentage basis.
| Pneumococci, Types I (10 per cent.), II (14 per cent.) and III (6 per cent.) |
30 per cent. |
| Pneumococci Group IV and the allied green-producingdiplostreptococci described |
30 per cent. |
| Hemolytic Streptococci |
20 per cent. |
| Staphylococcus Aureus |
10 per cent. |
| Influenza bacillus |
10 per cent. |
Most of the vaccine was distributed within a radius of 200
miles of Rochester, Minn., but samples were furnished to physicians
all over the country, who agreed to return statistics on its
use. No evidence was found that this vaccine caused a temporary
break in the resistance of the user. Out of a total of 20,972
persons vaccinated, 14.6 cases of influenza, 1.8 cases of pneumonia,
with 1.8 mortality, occurred per thousand in the six weeks
following vaccination. As controls, he took “such persons in
institutions, colleges, factories and communities where vaccine
was used, and included only those reports which contained accurate
data as to the incidence and mortality among them.” Among
61,753 such controls he found 229 cases of influenza, 15.7 cases of
pneumonia and 3.4 deaths per thousand. He concluded from his
results that “it appears possible to afford a definite degree of
immunity by prophylactic inoculations to persons against the
more serious respiratory infections during the present epidemic.”
It is quite difficult to agree with Rosenow in his interpretation
of the figures as presented by him, inasmuch as he made no
allowance for the stage of the epidemic at which vaccination was
carried out, either among the vaccinated or the non-vaccinated.
Such a comparison would be well nigh impossible where the vaccine
was sent in varying quantities to such a large number of
places.
4. League Island Report (22). Vaccines were used as a preventive
in 50 persons, most of whom were hospital apprentices
and in the wards 12 to 15 hours a day. Other precautions were
used, such as masks, but not a single case developed in the group.
The vaccine was used as a curative agent in 50 uncomplicated
cases; none of the patients injected early developed pneumonia.
1305. Puget Sound Navy Yards Report (23). The vaccine used
at this station was made from hæmolytic streptococci, no other
organisms being used; 4,212 men were vaccinated, and not one
died from influenza. Among 111 Philippinos isolated and vaccinated
there occurred only 2 cases. Among 361 marines vaccinated
early there occurred 2 cases. Among 62 marines at the
ammunition depot who were vaccinated early there occurred
3 cases, only 1 of which occurred after completion of vaccination.
Among 662 bluejackets at Seattle Training Camp only 10 men
developed the disease. Among 83 at the aviation corps there were
32 cases—31 of them developed the disease within a few hours
after the first injection. There were no deaths in any of the
above groups. The period of observation was closed on October
21, and so few cases of influenza appeared subsequent to that
date that it seemed that the epidemic was practically over at the
time the data was obtained.
6. Kitano (24) used a vaccine for prophylaxis containing
0.2 m.g. of Pfeiffer bacilli per c.c. on 10,300 persons with encouraging
results. He used vaccine for treatment on 87 patients,
without any deaths. In the same group were 270 cases treated in
the usual way, with 23 per cent. mortality. The vaccine lessened
the severity, shortened the period of illness, and lowered the
mortality.
7. Wynn (25) used mixed vaccines in the treatment of influenza,
and believed they aborted the disease if given early.
8. Norman White (26) states that vaccination in India would
be impractical, because the disease is so brief and severe that
it would be over before innumerable doctors could complete
inoculations.
9. Whitingham and Sims (27) reported the use of a mixed
vaccine in an institution where 156 were inoculated and 149
were not. The case incidence was 5 per cent. among the vaccinated
and 12 per cent. among the controls. No statement of
the stage of the epidemic at which vaccination was done is mentioned
in the report.
10. Cadham (28) reported on inoculations in a military hospital
and in the civilian population near Winnipeg. Of 282 vaccinated
soldiers admitted to the hospital, 17 had pneumonia and
5 died. Of 238 not vaccinated, 41 had pneumonia and 17 died.
Among 24,184 civilians given two doses, 9.7 per cent. had influenza
131and 0.5 per cent. had pneumonia and 0.09 per cent. died.
Among 85,941 controls, 24.8 per cent. had influenza, 2.2 per cent.
pneumonia and 0.66 per cent. died. Cadham states that most of
the inoculations were made early in the epidemic, but no accurate
statistics were kept on the point.
11. A conference was held at the British War Office on October
14, 1918 (30), to discuss prophylactic vaccination and vaccines
for treatment of influenza. Elaborate plans regarding dosage
and gathering of statistics were made.
Notanda.—For reasons already given, the reports in Series III
fail to give very reliable data on which to base a knowledge of the
value of preventive vaccination against epidemic influenza.
The Attempt to Prevent Pneumonia as a Complication of Influenza Through the Use of Lipovaccine
Whitmore, Fennel and Peterson (31) developed a method of
preparing an oily suspension of killed bacteria which they called
“lipovaccine.” The method was used at first in making typhoid
and dysentery vaccines. The advantages of lipovaccines (32)
over salt suspensions are: the prevention of autolysis of the
bacteria, thus increasing the length of time during which the
vaccine remains active; the slow absorption of the dose, allowing
the patient to continue to absorb immunity-producing substances
over a period of days or weeks; the administration of a single
massive dose, which does away with the three doses necessary
when salt suspensions are used; and perhaps, also, the direct
reduction in the toxicity of the dose by the lipoid material.
Based upon the classification of pneumococci by Dochez and
Gillespie (33) in this country, and by Lister (34), (35), (36) in
South Africa, and upon the latter’s successful use of anti-pneumonia
vaccine on the Rand, an anti-pneumonia lipovaccine was
prepared at the Army Medical School which contained approximately
10,000,000,000 each of types I, II and III pneumococci.
The vaccine was made by growing the pneumococci in dextrose
broth, centrifuging them out of the broth with a sharpless milk
centrifuge, drying the sediment at 55° C., weighing it out so
that each cubic centimeter of the finished vaccine contains
0.83 m.g. of each type, and making a suspension of them in olive
oil. More recently cotton-seed oil has been used.
132The result of the use of a salt suspension pneumococcus vaccine
at Camp Upton was published by Cecil and Austin (37). A study
of the agglutination and protective power of the serum of 42 persons
vaccinated against pneumococcus types I, II and III demonstrated
that a definite immune response could be secured to types
I and II but not to type III. Twelve thousand five hundred and
nineteen men were vaccinated at the camp, and most of the men
received three or four inoculations at intervals of from five to
seven days. The men were under observation for ten weeks, and
during that time no cases of pneumonia of the three fixed types
occurred among those who had received two or more injections.
In a control of approximately 20,000 men there were 26 cases of
pneumonia of types I, II and III. The incidence of pneumococcus
type IV pneumonia was less among the vaccinated than among
the unvaccinated groups. There were, however, 17 cases of pneumonia
among the vaccinated men, compared to 173 cases of pneumonia
among the controls. The annual pneumonia death rate for
vaccinated groups in the army was 0.83 per one thousand, and for
unvaccinated groups was 12.8.
Fennell reported the use of pneumo-lipovaccine in Washington
during the influenza epidemic, but the number of cases cited by
him were too small to permit of definite conclusions. His results
appeared favorable.
Cecil and Vaughan (37a) reported on the results of vaccination
with pneumo-lipovaccine at Camp Wheeler; 13,460 men, comprising
80 per cent. of the camp, were inoculated. Most of these
men were under observation for 2 or 3 months after vaccination,
and there occurred among them 32 cases of pneumococcus types
I, II and III pneumonia. In one-fifth of the camp which was not
vaccinated there occurred 43 cases of pneumonia. They observed
that influenza caused a marked reduction in the resistance to
pneumonia among vaccinated as well as non-vaccinated men. Of
155 cases of pneumonia of all types, which developed one week
or more after vaccination, 133 were secondary to influenza. The
death rate among vaccinated men one week or more after vaccination
was 12.2 per cent., whereas the death rate for 327 cases
of all types of pneumonia which occurred among unvaccinated
groups was 22.3 per cent. The death rate for primary pneumonia
among vaccinated groups was 11.9 per cent., and among unvaccinated
31.8 per cent. It was found that protective bodies do not
133begin to appear in the serum after lipovaccines are given until
the eighth day after the injection. Twenty-four cases of pneumonia
occurred in the first week after vaccination. In their conclusions
Cecil and Vaughan state that there was no evidence
whatever that pneumococcus vaccine predisposed the individual,
even temporarily, toward either pneumococcus or streptococcus
pneumonia. Most of the reactions after vaccination were mild,
but one disagreeable feature was that in a certain percentage
there persisted a small fluctuating mass at the site of the injection.
Lacy saw a number of these cysts aspirated, and the
contents were found to be a sterile, oily fluid, with many leucocytes
present. In one instance the primary reaction disappeared
within a few days after vaccination, but recurred after four
months and persisted for several weeks.
Notanda.—The army lipovaccine apparently offers a certain
definite amount of protection against pneumonia, which was the
most dangerous complication of influenza. The protective substances
do not appear in the serum until eight days have elapsed
after the vaccination, and while no definite evidence has appeared
to show that there is a temporary increase in susceptibility
immediately after vaccination, the best results would undoubtedly
be obtained where the dose is given something more than eight
days before the appearance of the epidemic. The indications are
that the vaccine will not protect against influenza, but that the
complication of pneumonia is less likely to occur in the vaccinated
than in the unvaccinated individual.
Summary
Records of attempts to confer immunity to influenza by the
use of vaccines have been separated into related groups and
studied. Those where pure Pfeiffer strains were used have been
considered in one group. Those where mixed vaccines were used
have been analyzed in three sub-groups or series, depending on
the relation between the times of vaccination and of the advent
of the epidemic, upon whether or not a week-by-week comparison
of the occurrence of influenza among vaccinated and unvaccinated
groups was made, and upon whether or not statistics for total
comparison alone were available. The third group included the
reports of the use of army pneumo-lipovaccines for the prevention
of the secondary pneumonia complications of influenza.
134
Conclusions
From our statistics we conclude that:
1. There is as yet no evidence that vaccines composed purely
of strains of Pfeiffer bacilli will confer immunity to epidemic
influenza.
2. The only data which can be used as a basis for estimating
the value of mixed vaccines as a preventive for epidemic influenza
must be obtained from experiments in which vaccination was
either completed before the epidemic appeared, or in which week-by-week
comparisons between the number of cases occurring in
the vaccinated and unvaccinated groups can be made.
3. Data obtained from experiments conducted under the above
qualifications is inconclusive, but presents little evidence of the
value of mixed vaccines in protecting against influenza. There
is, however, an indication that mixed vaccines used prior to the
arrival of the epidemic will lessen the number and the severity
of secondary pneumonias, and will probably lower the death rate
to a small degree.
4. The army pneumo-lipovaccine apparently offers some protection
against primary infections with types I, II and III pneumococci,
and a somewhat lesser amount of protection against
secondary pneumococcic infections with these strains following
influenza.
5. While it is impossible to say that the large number of
influenza cases developing almost immediately after vaccination
would not have occurred anyway, it is at least suggestive that a
temporary break occurs in the resistance after the inoculation,
and that unusual care should be taken by persons who have been
recently vaccinated, particularly when they are in the midst of
an epidemic disease.
Part II. General Prophylactic Measures
One of the most remarkable things about the 1918 pandemic
was the great rapidity with which it spread to all parts of the
world. From the report of the first cases which landed in Boston
until the epidemic arrived in San Francisco the time consumed
was less than two months, and the peaks of the two epidemics
were just about one month apart. Apparently no part of the
world escaped. Asia, Europe, Africa, North and South America,
135and some of the remote islands of the Pacific, all reported large
epidemics, with high mortality and great suffering. The deplorable
failure of precautionary measures in controlling the spread,
or at least in limiting the disease, may be offset in a measure
by the unusual conditions under which almost everybody had
been living. Vast numbers from all over the world were gathered
together because of the war. Thousands of men were housed
together in army camps or in training cantonments. Other
thousands were doing relief work or engaged in the manufacture
of munitions. Most of those at home were doing double duty,
and were on a severe nervous strain. Everyone everywhere was
working to the limit and was consequently fatigued. The necessities
of war had cut down the amounts of food generally, and
sugar and fat rations particularly. Traffic, both between nations
and at home, had never been so great nor accommodations so
insufficient. So that it is likely that all of these and many more
changes in the daily routine of individuals led to a condition of
lowered resistance, and at the same time increased their chances
of exposure. One point, at least, stands out prominently, and
that is that “influenza as it occurred clinically during the first
great wave was different from those cases which appeared later.”
This was seen in the acuteness of the onset, in the severity of
symptoms, and in the high mortality rate. Therefore, any
measure which afforded protection, if only for the time being, is
worthy of retrial.
In view of the fact that recurrences have followed closely in
the wake of all former influenza epidemics, and with the hope of
stimulating concerted investigation of preventive measures, the
American Public Health Association (57), at its meeting in
Chicago in December, 1918, appointed a committee to outline
“a provisional working formula, based on the facts and opinions
brought out at the meeting.” A summary of the opinions as
taken from the report of the committee is given here. They
reported that the disease was probably due to some micro-organism
or virus as not yet identified; that while it was known
as “influenza,” it was not known to be identical with the disease
generally known under that name; that there was no known
laboratory method of differentiating it from ordinary colds,
bronchitis, etc.; that there was no known laboratory method of
determining when a patient ceased to be infective; and that the
136deaths from influenza were due to secondary pneumonia resulting
from an invasion by one or more forms of streptococci, or by
one or more forms of pneumococci, or by the so-called influenza
bacillus or bacillus of Pfeiffer. Because of the clear and concise
manner in which this report brings out the opinions held, at the
time, by a majority of the medical profession a portion of the
report is given here verbatim.
“Evidence seems conclusive that the infective micro-organisms
or virus of influenza is given off from the noses and mouths of
infected persons. It seems equally conclusive that it is taken
in through the mouth or nose of the person who contracts the
disease, and in no other way except as a bare possibility through
the eyes by way of the conjunctivæ or tear ducts.
“If it be admitted that influenza is spread solely through discharges
from the nose and throats of infected persons, finding
their way into the noses and throats of other persons susceptible
to the disease, then, no matter what the causative organism or
virus may ultimately be determined to be, preventive action
logically follows the principles named below, and, therefore, it
is not necessary to wait for the discovery of the specific micro-organism
or virus before taking such action.
“1. Break the channels of communication by which the infective
agent passes from one person to another.
“2. Render persons exposed to infection immune, or at least
more resistant, by the use of vaccines.
“3. Increase the natural resistance of persons exposed to the
disease by augmented healthfulness.”
The ways and means of carrying out these principles are many
and varied, and it is merely the intention of this paper to put
together a sort of digest of some of the more important arguments
for and against some of the seemingly more important
measures proposed.
Methods Proposed for Breaking the Channels of Communication
(a) Rigid quarantine for all persons suffering from the disease
and all contacts. During the epidemic quarantine was advocated
by many people. It was pointed out that the disease spread most
rapidly in camps, in ships, and in quarters generally where large
numbers of persons were closely associated; that it was quite as
137contagious and more rapidly fatal than most diseases which are
regularly quarantined; that while it was admitted that there is
no laboratory method to make certain the diagnosis, and no
method of telling how long convalescents are capable of transmitting
the disease, as there is, for instance, in diphtheria, still
there is no question of the value of the arbitrary quarantine used
in measles, scarlet fever and smallpox, all of which are diseases
in which the parasitic causes are not known. Further, the
opinion was expressed that complete isolation and quarantine
would not only protect the community from influenza, but that
it would also in a measure protect the patient from contact with
numerous outside strains of pneumococci and streptococci, and
so lessen secondary infection and reduce the general mortality.
There are many reasons why quarantine is not applicable
in epidemic influenza. Most important of all is probably the
inability to make certain the diagnosis, especially during the
early stages in light cases. This would work detrimentally in
several ways. Really ill patients would delay calling a physician
until late, for fear of unnecessary quarantine. Many needless
and unjust quarantines would result when the diagnosis was
uncertain and the physician anxious to carry out quarantine
measures efficiently. Many patients would have contacts running
about and infecting their neighborhoods while a delayed diagnosis
was being made. Influenza was so contagious during the
epidemic that it would have necessitated general quarantine
not only of all infected persons but also of all contacts to have
obtained any favorable results, and since nearly everyone was
either a patient or a contact, all lines of business would literally
have been paralyzed by the procedure. If it is true that the
infected person is most dangerous to others before he has developed
symptoms himself, he is a carrier impossible of detection
and control. Points in favor of the hypothesis that infected
persons spread the disease before they develop symptoms are
found in the following facts. As the disease passed from community
to community officials became alert for the appearance
of the first case. In army barracks and in large institutions it
was often possible to determine the first case at its development.
The case was, in many instances, removed at once and isolated,
but I have seen no instance in which such a measure was successful
in curbing the disease. As subsequent cases appeared they
138were likewise immediately removed, but the cases continued to
spread just the same. Bloomfield (38) cited the incident of a
student who spent a few hours visiting his sister in a part of the
country where there had been no influenza. He appeared well at
the time, but six hours after his return to school he developed
influenza. Two days after the contact the sister came down with
the disease. On the other hand, he told of a student who did not
contract the disease, though he slept for two nights in the same
bed with his roommate, who had returned to school with a well-developed
case of influenza. The unsuccessful attempts to transmit
influenza in the experiments of Rosenau (37), McCoy (37a)
and others already cited would indicate that the cases from whom
the material was taken were no longer infectious, although some
of them had been showing symptoms for only about 12 hours.
Bloomfield observed that the general use of face masks in the
wards did not alter the course of the epidemic, and stated that if
face masks are protective, infection from early unisolated cases
must be assumed.
Provided influenza is generally transmitted during the period
of incubation, a theory which seems consistent with the facts,
rigid quarantine for epidemic influenza is impracticable and probably
useless.
Partial Isolation by Means of the Cubicle System
The so-called cubicle system consists in the dividing of rooms,
or more particularly of wards, into small compartments by means
of suspending sheets from wires so that each bed is separated
from its neighbor. Capps (39) reported favorably on the method
as used at Camp Grant, where sheets or halves of tents were
suspended from wires or from the mosquito netting frames
which were a part of the standard beds. Doctors, nurses and
attendants were forced to wear masks in the wards, and patients
were not allowed out of the cubicles without them. In discussing
this paper Thayer emphasized the value of screening, masking
and the wearing of gowns, and also recommended thorough washing
of the hands between the examination of each two patients;
and Emerson called attention to the fact that the first demonstration
of the cubicle system as an adequate means of preventing
acute respiratory diseases was made at the Pasteur Institute of
139Paris, where it had been in operation for 10 years. The latter
stated that the system had been used in various hospitals in
America and was essential for the care of diphtheria, measles and
scarlet fever. He further indicated that if the technique of personal
cleanliness of nurses, doctors and attendants could be perfected,
it was probable that the height of the cubicle partition
could be reduced to that of a “red string.” The method certainly
seems worthy of consideration and trial, particularly in large
general hospitals and public institutions.
The Use of the Face Mask
The question of the value of wearing a gauze mask over the
mouth and nostrils during an influenza epidemic is still an open
one. Masks, however, have been found useful in protecting
against some other diseases of respiratory origin. In December,
1917, Weaver (40) reported favorably on the use of gauze masks
in the Durand Hospital of Infectious Diseases. The masks were
used by nurses in attendance upon patients with contagious diseases,
and also by patients who were convalescing from diphtheria,
meningitis or pneumonia and who were in the same wards
with those having other respiratory diseases. In a later article
Weaver (41) stated that by the use of masks they had been able
to reduce the percentage of diphtheria carriers among their
nurses in the diphtheria wards to 5.2 per cent., as compared
to the average of 23.25 per cent. during the 20 months immediately
preceding their adoption of their use. He recommended
the general use of masks for physicians when in contact with all
types of respiratory diseases. In March, 1918, Capps (39a)
reported encouraging results in the control of infections through
the masking of all patients at Camp Grant. During the epidemic
the wearing of masks became quite general, and was very popular
in many sections.
Several sets of laboratory experiments have been carried out
recently to determine whether the masks are of practical value
or not. The experiments have generally consisted in spraying
cultures of living bacteria over sterile bacterial plates which were
protected by one or more layers of gauze. A number of variations
were made in the manner in which this was done: (a) the
distance between the nozzle of the spray and the mask was
140varied, and the distance between the plate and the mask kept constant;
(b) the distance between the plate and the mask varied,
and the distance between the nozzle and the mask kept constant;
(c) the use of masks both over the nozzle of the spray and over
the plate being kept constant, and the distance between the two
masks varied. In a somewhat different set of experiments the
mask was placed over the mouth of a person, who was told to
talk or cough over an agar plate, and the bacterial plate being
held at various measured distances from the face. By counting
the number of colonies which developed upon the plates it was
possible to get fairly reliable data as to the efficiency with which
the bacteria were intercepted by the gauze. Weaver (42) found
that if enough gauze was used, it would filter out all of the bacteria
passing from the spray in the direction of the plate. The
efficiency of the mask being in direct proportion to the fineness
of the mesh and the number of layers employed. Doust and Lyon
(43) made a series of experiments to determine the distance
through which droplets are carried when expelled under different
circumstances. They found that in ordinary speech infected
material is projected for about four feet, and that during coughing
the material is carried about ten feet. They demonstrated
that masks of medium meshed gauze, two to ten layers thick,
worn by the person coughing did not prevent the passage of
infectious material into the air, but that a three-layer buttercloth
mask was much more efficient. Haller and Colwell (44)
used three distinct sets of experiments—one with the mask over
the mouth of the patient, one with the mask over the plate, and
the third with masks over both—and concluded that a five-layer
mask made up of 24 × 20 mesh protected the plate in the second
series of experiments. They suggested marking one side of the
mask, so that it would always be worn with the same side out.
Leete (45), in England, by a similar series of experiments concluded
that a dry mask of six to eight layers of butter muslin
worn by a contact would protect him against droplet-carried
infections. Dannenberg (46) suggested making the gauze mask
over a copper screen wire frame to give it shape and keep it away
from the mouth, thus keeping it relatively dry. All observers
agree that masks while dry are more efficient than they are after
they have become moist.
141The efficiency of the mask has also been widely discussed from
the clinical standpoint. Mink (47) in discussing their use at the
Great Lakes Training Station said that he had no objection to the
mask as it is “intended to be worn,” but that as it “was worn” by
the medical corps men at the station 8 per cent. of those who
used the mask developed influenza, as compared to 7.75 per cent.
of those who did not; 30 per cent. of the dental officers at the
station developed the disease in spite of the fact that they were
all accustomed to wear masks during their work. In discussing
the mask Vaughan (48) said: “With reference to the mask, I
am strongly of the opinion that we have overestimated its
value. * * * When I went to Camp Devens they were not
using the mask. I called the doctors together and told them its
use was not compulsory, but I said: ‘Every doctor who took care
of cases of pneumonic plague and did not wear a mask died from
it, and every man who cared for pneumonic plague cases and
didn’t wear a mask did contract it.’” They were then allowed
to choose for themselves. It has been pointed out that the epidemic
dropped off at once in San Francisco with the universal
compulsory use of the mask on the street, but it is also said that
the epidemic in Los Angeles, which ran a course parallel to that
in San Francisco and in which masks were only indiscriminately
used, began to drop off simultaneously. While it is difficult to
get at the facts, it seems that, provided epidemic influenza is
carried through the air or by means of droplets, the universal
use of masks should decrease the number of exposures. The
claim has been made that masks merely tend to prolong the epidemic,
and that susceptible persons develop the disease after
the epidemic proper has passed. If the mask will protect the
susceptible individual until the virulence of the disease has
decreased, it will better that individual’s chances for recovery,
and so is worth the trouble.
General Closing Orders
In most large cities orders were issued closing churches and
theatres and prohibiting public gatherings of all kinds. In New
York these places of public gathering were not closed, and it has
been pointed out, as an argument against closing orders in the
future, that the death rate there was less than in Boston, Philadelphia,
142Pittsburgh, etc. Copeland (49), of the New York Board
of Health, stated that the unventilated picture shows were closed,
but that the theatres were used as places of public instruction.
New York’s relatively low death rate was difficult of explanation,
but it is very certain that it had nothing to do with the fact that
closing orders were not in vogue. If it were possible to obtain
the figures, it would be interesting, indeed, to compare the death
rate from influenza among New York’s theatre-attending public
during the epidemic with the death rate of the community in
general.
Generally speaking, any unnecessary public gatherings are
inadvisable during any epidemic. While our exact knowledge of
the mode of transmission of influenza is incomplete, it is unquestionably
a contact disease. People who have been exposed and who
have not yet contracted the disease are known to have transmitted
it to a third person. A certain number of people from
infected homes will attend public gatherings as long as they are
able, for it is impossible to get together any large group of persons
all of whom are going to play fair. It is true that these
meeting places may be used in a measure to allay panic and to
instruct the public in health measures, but there are many efficient
and far less dangerous methods of accomplishing the same
results. Vaughan in discussing assemblies in large halls mentioned
that in a hall at Camp Forest, which held 9,000 people,
the individuals had a space of about 16 inches laterally between
their noses. He pointed out that if many of them were talking,
coughing or sneezing, the air contamination would soon become so
great that it could make little difference whether there was a
roof over the building or not. He emphasized the fact that it is
just as possible to crowd men in the open as it is indoors. Ventilation
is undoubtedly an important factor, but it cannot correct
overcrowding. As far as the educational value of the public
gatherings was concerned, it may be observed that regular
attendants of theatres and moving-picture houses during the
year of 1918 had become quite accustomed to appeals regarding
all sorts of public movements from speakers who appeared
between the acts, or pictures, but that the closing of these places
threw a wholesome scare into them which made them pay far
closer attention to prophylactic measures than almost anything
143that could have happened. “Object-lessons are always superior
to didactic teaching.” In Chicago a new argument for the closing
of theatres was advanced. It was said that with no place to go
many people retired earlier and obtained more than their accustomed
amount of rest. It was believed that this aided in increasing
their natural resistance. The argument that the closing of
these places served only to delay the epidemic is an argument
in favor of the measure, because the virulence of the disease
decreased rapidly as the epidemic progressed.
The Closing of Schools
Boards of Health generally were opposed to the closing of the
public schools. This position gave rise to innumerable clashes
with anxious parents. The health authorities took the position
that children were relatively insusceptible to influenza; that while
they were quiet in a well-ventilated schoolroom they were little
exposed; that those who coughed or sneezed could be examined
at once, and that daily school inspection would lead to early discoveries
of all cases, so that doctors and nurses could take
immediate steps to treat the patients and to protect the families
from which they came. Copeland advocated the continuance of
the schools in New York, and based his position on the fact that
out of 1,000,000 children in New York City 700,000 came from
tenement homes. He believed these children were far better off
in school, where they received daily medical attention, than upon
the streets or in unhygienic homes.
In Pittsburgh the school children were quizzed as to the number
of sick at home, and this gave valuable information on the
stage of the epidemic. They were sent home with printed warnings
against sneezing, coughing and spitting, and were thus used
as a means of instructing their parents. The Pittsburgh schools
were kept open until the sickness of a number of teachers and
the withdrawal of many scholars made it advisable to close.
Three very potent arguments have been brought forward in
favor of closing the schools: (1) As long as the schools are open
children from infected homes are forced into contact with children
from uninfected homes, and we are at present unaware of
the extent to which the disease may be carried by a third person.
(2) Children in as yet uninfected homes which are comfortable
144and hygienic are far better off than they are in school, and can
hardly be considered in the same class with children from unclean
tenements. (3) If the period of greatest contagion is before
symptoms develop, inspection, while valuable for the institution
of treatment, cannot hope to aid in curbing the epidemic. It is
evident that different measures must be employed in applying
closing orders to crowded cities, moderately large towns and
rural districts. The difficulty lies in determining the best means
for serving each community.
The Closing of Public Dance Halls
Public dances should undoubtedly be prohibited during epidemics.
They not only present all the bad features of other
public gatherings, but during the dancing people are brought in
very close contact and often breathe directly into each other’s
faces. In addition, air currents are stirred up and a certain
amount of dust is raised. During the exercise the dancers
breathe more rapidly and deeply, thus inhaling unusually large
amounts of dust, droplets and contaminated air. Another feature
is found in the “resistance-breaking” element of alternate overheating
and rapid cooling of the body.
Regulation of Public Eating and Drinking Places
Public eating places are a necessity and cannot be closed.
People should be cautioned against using them as places of
amusement and of congregation during epidemics. Boards of
Health should feel it just as much their duty to see to the
sterilization of dishes and eating utensils as they do to the
enforcing of any other public health functions, and they should
also insist on the daily inspection of the employees of such
establishments. The beer saloon question may be passed over
for the present, but the soda-water fountain as conducted during
the 1918 epidemic was undoubtedly a great menace. Ice cream,
syrupy mixtures, etc., of various kinds are readily contaminated
by pathogenic organisms which may serve as secondary infectors,
if in no other capacity. The syrups, moreover, adhere to the
spoons and glasses, which are rarely thoroughly washed and are
practically never sterilized between customers. The use of paper
145dishes and glasses is probably a step in the right direction, but
the spoons should be thoroughly washed and sterilized. The fact
that soda-water employees are not always selected for high-grade
intelligence, and are generally left largely to their own
hygienic procedures, makes the chances of transferring infections
at these places enormous. If soda fountains are allowed
to continue business at all during the epidemics, it should be only
under the very strictest supervision by Boards of Health. The
scalding of all utensils should be enforced by law.
People generally should be cautioned to use exceptional cleanliness
in the preparation of all foods in the home. In discussing
the recent epidemic Lynch and Cummings (50) stated that “the
mess-kit wash water proved the major route of transmission
from sick to well in the army.” Vaughan said: “I am pretty
certain, not convinced, that hand-to-mouth infection is of more
importance than droplet infection.”
Regulation of Traffic
Business must be conducted in epidemic as well as in normal
time, and employees must go to and from their places of occupation.
In cities where the distance from the residence to the
business districts is great, street cars and other public conveyances
must be used. Their use undoubtedly increases the number
of contacts and leads to a wider distribution of the disease,
but, like eating in public restaurants, it is a chance which many
have to take. Few places offer better opportunities for exposure
than street cars—where people of all grades of intelligence, representing
all states of health and degrees of cleanliness and
uncleanliness, are crowded closely together, breathe into each
other’s faces, and handle the same straps and supports.
In Pittsburgh the cars have a seating capacity for from 30
to 50 persons, but during the morning and evening hours they
are crowded to capacity, and are commonly seen to carry more
than 100 passengers at a time. Here, too, the unkempt, indifferent
foreign element is conspicuous, and these people are known
to disregard all hygienic teachings. A few days after the
appearance of the epidemic the street cars were placarded with
warnings against coughing, spitting and sneezing. The cards
instructed people who became ill to go home, to go to bed and
146to remain there until they were well. Later a second order
appeared which gave notice that all windows in street cars were
to be kept raised six inches and that no heat was to be allowed
in the car. The order was intended to improve ventilation, and,
for a wonder, it was enforced. During the first few days the
weather was fine, warm and clear, and the draught caused by
the open windows brought no discomfort; but later the weather
became cold and several days of drizzling rain set in. The cars
with open windows became very uncomfortable, but the streetcar
employees insisted upon obeying the order to the letter. No
judgment was exercised by them, and the windows were kept
open night and day, cold or warm, crowded or empty, in fair
and rainy weather alike, and no heat was allowed to be turned
on. Many people preferred standing to exposing their backs and
necks to the cold draughts, and it is more than likely that such
use of open windows did far more harm than good. As above
quoted, Vaughan pointed out that crowding is just as dangerous
out of doors as indoors, and it is certain that crowding in cold,
draughty cars is dangerous, both from the close contact and
because of the added danger of lowering bodily resistance.
In an attempt to decrease the crowding on public conveyances
the so-called “stagger-hour” system was adopted in New York.
Under this arrangement manufacturers and business houses
changed their working hours in such a way that the morning and
evening travel was spread out and the average number of people
carried per hour was proportionately decreased.
Looking backward over the methods used to decrease the spread
through the use of public conveyances, it seems that the following
procedures have the best claims for retrial: (1) Placarding the
cars. This appeared to reduce the amount of coughing and
sneezing, even in face of the fact that the cars were unusually
draughty and chilly. (2) The adoption of the “stagger-hour”
system where the practice is feasible. (3) The instruction of the
people to use the street cars as little as possible.
Enforcement of Anti-Spitting Ordinances
All street cars and trains carry anti-spitting notices either
to the effect that spitting will be prohibited on penalty and fine
and imprisonment, or giving stated amounts of the fine. Yet
147spitting is constantly indulged in in these places and one
rarely sees or hears of the enforcement of the law. If the ordinance
was worth making a law, it is certainly worth enforcing,
and yet there is probably no law so flagrantly broken. Ordinary
police officers pay no attention to the enforcement of the spitting
ordinance and have been known to refuse to even reprimand
spitters. The incident of a sanitary officer wearing a uniform and
a cap, indicating to the public his official position, who was seen
sitting in the smoking car in a local suburban train and spitting
profusely on the floor has been recounted on very reliable authority.
Another incident is known in which a street car conductor
was asked by one passenger to stop another who was expectorating
abundant mucoid sputum upon the floor. The conductor
replied that he had orders not to notice such things. It is no
wonder that people are indifferent to such impotent measures.
Whether it is possible to convey epidemic influenza or not by
means of sputum, it is certain that tuberculosis is spread in this
way, and that influenza predisposes to tuberculosis and causes old
healed tuberculous foci to become active. People should be made
to understand that they may have tuberculosis without knowing
it themselves, and that by spitting it may be transmitted to other
persons. Spitting by persons aware that they have tuberculosis
is criminal negligence and such persons should undoubtedly be
prosecuted. If a person knows that he has tuberculosis and
deliberately spreads about the infection so that other persons
contract the disease and die from it, he is directly responsible for
the deaths. It would be hard to imagine trying to control manslaughter
committed in any other way by merely putting up signs
in conspicuous places forbidding the act. The average boy
acquires the spitting habit between the ages of 8 and 12 years,
and in many instances carries it to the grave. The one possible
way of stopping spitting seems to lie in teaching the dangers of
it to children, beginning in the kindergarten and emphasizing it
throughout the child’s education. It is possible that in this way
spitting may become obsolete in two or more generations.
Increasing Natural Resistance by Augmented Healthfulness
If there is any way of increasing the natural resistance against
epidemic influenza, it is a most desirable goal toward which to
work, but it must first be determined along what lines the effort
148is to be directed. It was not the aged, the unconditioned nor the
physically unfit who suffered most from influenza, but was rather
the best trained, most healthful and most robust young persons
we had. Those in the army had been selected because of their
physical fitness and they had further received excellent physical
training in the various camps and cantonments. It would not be
possible to bring any large percentage of the general public up to
such a stage of “augmented healthfulness” as healthfulness is
generally understood. It has been said that men in the military
camps were more commonly infected because they were more
active, went about more and were, therefore, more frequently
exposed. In one particular this statement is true, for men marching
rapidly and exercising violently breathe more deeply and at
a faster rate than they do under ordinary conditions, so that they
naturally draw greater quantities of air into their lungs. It was
an obvious fact that those persons given to sedentary lives were
less often affected than the active and vigorous. Practically
speaking, it would seem that during influenza epidemics people
should be instructed to take more than the usual amount of sleep
and rest, to indulge only in mild exercises, to eat good, wholesome
food, to wear warm clothing, to seek mental and physical relaxation
at home, and, above all, to avoid crowds and public gatherings.
In some instances the constant use of oils in the nose and throat
was advised, the theory being that the oil served the double purpose
of preserving the healthy condition of the mucous membranes
by lessening crusting, crevicing and drying, and of mechanically
protecting from infection by the presence of the layer of oil.
Many of the different liquid paraffins, both medicated and in the
natural state, were used. It is probably advisable to apply such
oils either with a swab or from a medicine dropper, rather than to
attempt to spray them, since in the latter method there is some
danger of blowing infectious material down into the trachea and
larynx.
It is hardly necessary to point out the importance of augmented
cleanliness of the mouth, teeth and throat by means of mild antiseptic
washes and tooth-cleansing materials during an epidemic.
General Measures
Public Health Administration
Unless one had had a wide experience in the administrative
149side of public health matters, it would be useless for him to try
to discuss the details of handling any sort of an epidemic, and
even then local conditions vary so much in different cities and
States that each administrator’s experience must differ greatly.
The difficulty with reports of epidemics by public health officials
is usually found in the fact that the reports are impersonal compilations
and convey no idea to the reader, or rather to the
student (for no mere reader is attracted to them), of what situations
were faced, of what difficulties were in the way, of how the
conditions were met, or what the administrator after due reflection
would advise doing next time under similar circumstances.
In the face of inexperience the writer ventures the following suggestions
for improvement, though no originality is claimed for
the ideas.
The administrative powers should be centralized in one individual,
or in an executive officer acting for a competent board of
advisers, who should be endowed with the powers to carry out the
measures which seem best suited to meet the situation at hand,
and who should be beyond the pale of political interference and
in position to prevent political fiascos, built more or less directly
on health regulations.
The United States Public Health Service should work toward
standardizing health laws and penalties for all States.
Thorough enforcement of ordinances requiring the reporting
of all cases and all deaths as now demanded by public health
rulings should be insisted upon. These reports are so important
to a knowledge of the progress of the epidemic that the section on
preventive medicine of the American Medical Association (51)
has just advised the consideration of eliminating from membership
in the Association any physician who willfully fails or refuses
to comply with the regulations requiring the reporting of communicable
diseases. Additional information can be obtained by
daily canvasses of the schools, when open, of the large industries,
and of the daily admissions to hospitals. Data on the daily
facilities for the handling of additional cases in hospitals should
be on file in the office of the administrator of health.
Printed instructions giving in detail the proper procedures for
isolation of the patient and the protection of the family should be
supplied to physicians for distribution at the first visit to suspected
cases.
150
Desirable Laws
Some specific laws governing the following points would be of
great advantage during the progress of an epidemic: (a) A law
providing for the commandeering by boards of health of vaccines,
sera or other substances for which a sudden unusual demand
may occur, and for the distribution of such substances by the
authorities to the public at the prices ordinarily asked. (b) A
law permitting the exclusion from the daily papers by boards of
health of advertisements containing obviously false and fraudulent
statements relative to the epidemic. (c) A law permitting
the health authorities to go into public eating places and demand
proper sterilization of dishes and eating utensils with the alternative
of closing the establishment. (d) A set of laws making
the penalties sufficient to prevent violations of the regulations.
Education of the Public
From the beginning to the end of an epidemic the health
authorities, aided by the medical profession, should take the
public wholly into their confidence. At the first news of the
approach of the disease a general bulletin should be issued giving
all of the main facts that are available. This was done in a way
by the American Public Health Service, but the bulletin reached
only a small fraction of the people, and although parts of it
appeared later in the daily papers, it was pretty generally
missed. The papers should be used freely and the space paid for
when necessary, so that the news of the epidemic is featured
emphatically. The establishment of a question and answer
department or a bureau of information would take care of a
great deal in the way of denying misinformation. The public
should be encouraged to report helpful facts of all kinds, but
with the understanding that no rumors would be published without
investigation and confirmation. In this way it would be
possible to prevent articles advising harmful and useless remedies
from reaching the press, and aid in suppressing some of the
“Sure Cures,” so many of which appeared to abuse the confidence
of the unwary during the 1918 epidemic. Several such
cures have been most interestingly discussed in a recent bulletin
of the United States Public Health Service. The bulletin divides
the “Sure Cures” into three different classes, as follows: “First
151comes the individual who has a specific remedy, the formula of
which he will sell for a price * * *; next comes the person
with a pseudo-scientific treatment, e. g., isotonic sea water,
‘orzono therapy,’ ‘harmonic vibrations.’ * * * Still another
type, who gives freely of his advice that humanity may be
spared from pestilence.” Among the latter are found advice for
placing sulphur in the shoes, wearing of amulets, inhaling of
alcohol, chloroform, etc., as well as numerous religious and mental
science treatments, etc. A frank statement of facts and a discussion
of the ridiculous side of many of these claims would
undoubtedly benefit the entire public. The placarding of the cars
and the warnings posted in conspicuous places no doubt helped
greatly, and this method undoubtedly should be continued. As
long as theatres are allowed to remain open, speakers may be
used to advantage to emphasize important points. The County
Medical Societies should be asked to appoint committees for
supplying information or for seeing that the information given
to the public is authoritative. In large cities committees may
be organized among hospital superintendents, so that the heartiest
co-operation between health authorities and hospitals will
be available. The ever-ready aid of the Red Cross and of every
other auxiliary body should be employed to the fullest extent to
allay apprehension and relieve suffering.
Summary
The exact knowledge of the mode of transmission of epidemic
influenza is still wanting, but it is known to be spread by contact.
Attention should be directed toward every practical means of
decreasing the number and intimacy of contacts. Publicity campaigns
and other educational measures should be pushed strongly.
Health Departments should adopt a policy of preparedness during
inter-epidemic times, should make every effort to centralize and
standardize their work, and should take steps to obtain sufficient
legal backing, so that upon the appearance of the epidemic they
can take the lead, speak with authority and enforce their ordinances
and measures. The physician’s duty is to inform himself
on the value of the various measures, and if he is at odds with
the public health methods, he should settle them between epidemics,
so that when he is called upon to carry out public health
152orders he can do it to the letter and without criticism. Laymen
should learn that quiet living without violent exercise, the keeping
of good hours, the avoidance of public gatherings and of
unnecessary exposure is the best policy to pursue during influenza
epidemics. They should strictly obey the orders of those who
have specialized in the control of epidemics, and all business men
must stand ready to help in every possible way and to make their
business interests subservient to the public good.
BIBLIOGRAPHY
| 1. |
Rosenau, Keegan, Goldberger and Lake |
Public Health Report, 1919; xxxiv, No. 2, p. 33. |
| 1a. |
McCoy and Richey |
Public Health Report, 1919; xxxiv, No. 2, p. 34. |
| 2. |
Lacy |
Jour. Lab. and Clin. Med., 1918; iv, p. 55. |
| 3. |
Wollstein |
Jour. Exper. Med., 1911; xiv, p. 73. |
| 4. |
Flexner |
Jour. Amer. Med. Assoc., 1913; lxi, p. 1872. |
| 5. |
Park and Williams |
Bacteriology, 1914 Edition; p. 437. |
| 6. |
Leary |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 2098. |
| 7. |
Leary |
Amer. Jour. Public Health, 1918; viii, p. 755. |
| 8. |
Rosenau |
Preliminary report furnished through Surgeon-General of the Navy W. C. Braisted. |
| 9. |
Barnes |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 1849. |
| 10. |
Hinton and Kane |
The Commonwealth Mass. State Dept. Health, 1918; vi, Nos. 1 and 2, p. 28. |
| 11. |
Hinton and Kane |
Hinton’s Report. |
| 12. |
Parker |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 476. |
| 13. |
Pearce |
Jour. Amer. Med. Assoc., 1913; lxi, p. 2115. |
| 14. |
Committee on New and Non-Official Remedies |
Jour. Amer. Med. Assoc., 1918; lxx, p. 1967. |
| 15. |
McCoy |
Personal Communication. |
| 16. |
Hutchinson |
Dixmont Hospital Report. |
| 17. |
McCoy, Murray and Teeter |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 1997. |
| 18. |
Minaker and Irvine |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 847. |
| 19. |
Sherman |
Report. |
| 20. |
Maberry |
Report from Hospital for Insane, Retreat, Pa. |
| 21. |
Rosenow |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 31. |
| 22. |
Beaver, Boles and Case |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 265. |
| 23. |
Ely, Lloyd, Hitchcock and Nickson |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 24 |
| 24. |
Kitano |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 1575. |
| 25. |
Wynn |
Pract. London, 1919; cii, p. 77. |
| 26. |
Norman White |
Lancet., 1919; i, p. 707. |
| 27. |
Whitingham and Sims |
Lancet., 1918; ii, p. 865. |
| 15328. |
Cadham |
Lancet., 1919; ii, p. 885. |
| 29. |
Eyre and Lowe |
Lancet., 1918; ii, p. 485. |
| 30. |
Conference British War Office |
|
| 31. |
Whitmore, Fennel and Peterson |
Jour. Amer. Med. Assoc., 1918; lxx, p. 427; also p. 902. |
| 32. |
Fennel |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 2115. |
| 33. |
Dochez and Gillespie |
Jour. Amer. Med. Assoc., 1913; lxi, p. 727. |
| 34. |
Lister |
Publications of the South African Institute for Medical Research, No. 2, 1913. |
| 35. |
Lister |
Publications of the South African Institute for Medical Research, No. 8, 1916. |
| 36. |
Lister |
Publications of the South African Institute for Medical Research, No. 10, 1917. |
| 37. |
Cecil and Austin |
Jour. Exper. Med., 1918; xxviii, p. 19. |
| 37a. |
Cecil and Vaughan |
Jour. Exper. Med., 1919; xxix, p. 457. |
| 38. |
Bloomfield |
Johns Hopkins Bull., 1919; xxx, p. 1. |
| 39. |
Capps |
War Med., Vol. ii, p. 371. |
| 39a. |
Capps |
Jour. Amer. Med. Assoc., 1918; lxx, p. 910. |
| 40. |
Weaver |
Jour. Amer. Med. Assoc., 1918; lxx, p. 76. |
| 41. |
Weaver |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 1405. |
| 42. |
Weaver |
Jour. Infect. Dis., 1919; xxiv, p. 218. |
| 43. |
Doust and Lyon |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 1216. |
| 44. |
Haller and Colwell |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 1213. |
| 45. |
Leete |
Lancet., 1919; i, p. 392. |
| 46. |
Dannenberg |
Jour. Amer. Med. Assoc., 1918; lxx, p. 99. |
| 47. |
Mink |
Jour. Amer. Med. Assoc. 1918; lxxi, p. 2175. |
| 48. |
Vaughan |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 2100. |
| 49. |
Copeland |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 2173. |
| 50. |
Lynch and Cummings |
Jour. Amer. Med. Assoc., 1918; lxxi, p. 2174. |
| 51. |
Amer. Med. Association |
Public Health Report, 1919; xxxiv, p. 1413. |
| 52. |
Le Moignie and Pinoy |
Compt. rendu. Soc. Biol., 1916; lxxix, pp. 201 and 352. |
| 52a. |
Wright and Douglas |
Proc. Royal Soc. Med., 1904; lxxiii, p. 128, and lxxiv, p. 147. |
| 53. |
Neufeld and Rimpau |
Zeitschr. f. Hyg., 1905; li, p. 283. |
| 54. |
Rosenau |
Prevent. Med. and Hyg., 1918. |
| 55. |
Brown, Palfrey and Hart |
Jour. Amer. Med. Assoc., 1919; lxxii, p. 463. |
| 56. |
Gay |
Typhoid fever. (Published by Macmillan Co., 1918.) |
| 57. |
Eyre and Low |
Lancet. I, April 5, 1919; p. 557. |
155
PHYSIOLOGICAL AND PHYSIOLOGICAL CHEMICAL OBSERVATIONS IN EPIDEMIC INFLUENZA
By C. C. Guthrie, Ph. D., M. D.
The material consisted of cases in the acute stage of epidemic
influenza with and without clinical pulmonary involvement
(alveolar); of convalescents, and of normal individuals without
influenzal history.
It was hoped that it would be possible to follow selected cases
over considerable time periods, observation to compromise coordinated
clinical as well as laboratory data, but the exigencies of
the situation rendered this impossible. Unfortunately, this limits
the value of the studies. But since similar observations were
made on cases ranging from normal to the gravest severity—in
fact, preceding death but a few hours in some instances—and
from the nature of the findings, certain conclusions are clearly
warranted.
It is regrettable that the data on certain points is not more
extensive, and particularly that other methods of observation
were not employed. As an example of the latter, measurements
and analyses of expired air may be given, as this was planned
from the beginning and unsuccessful efforts made to provide the
required apparatus. In view, however, of the circumstances of
the investigation, it is felt that the studies made are, on the
whole, reasonably comprehensive and complete. And it is only
fair here to acknowledge that this was rendered possible by the
cordial and practical support of the Medical School, the military
authorities, the director of the laboratories, clinical colleagues,
particularly Dr. W. W. G. Maclachlan, and last, but not of less
importance, of the members of the department who made the
studies.
In presenting the results, it is deemed most expedient and
practical to omit extensive tabulations and to summarize the data
under each subject.
From the report it will be obvious that certain studies were in
preliminary stages at the termination of the investigation. This
156was due in certain instances to the lateness of their undertaking,
or time consumed in providing essential equipment and methods;
or to disappearance of suitable cases due to waning of the
epidemic.
Results
Circulation
For the most part, cases showing marked clinical symptoms
were studied. The pulse in severe cases frequently was weak
and rapid but regular. In some cases it was less rapid than the
clinical state would seem to indicate.
Arterial Blood Pressure was low; systolic pressure in severe
cases ranging downward from 95, and diastolic down to 40 or
under. In patients in early stages of convalescence the pressure
showed a marked advance toward normal levels. Arterial blood
pressure seemed a reliable general index of the condition of the
patient.
Venous Blood Pressure.—The observations included patients
who a few hours later expired. The Von Recklinghausen method
was used. No marked abnormality was observed, so other
methods of observation were deemed superfluous.
Respiration
In severe cases, frequently it was rapid and of shallow character;
but, like the pulse, often it was less rapid than the clinical
state would seem to indicate.
Cyanosis of dark hue and marked degree was prevalent in the
earlier severe cases, and in some cases appeared entirely out of
proportion to the state of circulation and respiration and to the
post-mortem findings as reported by Dr. Klotz.
Blood
Hemorrhage being not uncommon, the blood was tested for
coagulability, but in this respect no marked departure from the
normal range was noted.
Coagulation.—Coagulation time was observed by stirring blood
in a test tube with a wire and noting the time of the appearance
of fibrin and by means of a Biffi-Brooks coagulimeter. The
extreme ranges observed were from 2½ to 5½ minutes. The
157average by defibrination was 3 minutes and 36 seconds, and by
the Biffi-Brooks method 4 minutes and 38 seconds.
Red Corpuscles.—Osmotic resistance. A number of bloods
were examined by observing their resistance to osmotic laking
by exposure to a series of hypotonic sodium chloride solutions.
Though some differences were observed, from the evidence
obtained, it is not permissible to conclude that such variations
were constant or of a significant magnitude.
Color on exposure to air. It was early observed that venous
blood from cyanotic patients was very slow to take on arterial
hue on exposure to air.
Plasma Bicarbonate.—The plasma bicarbonate was determined
in seven cases by Miss Waddell by the method of Van Slyke and
Cullen. In all except one of these the results were within the
normal range as given by Van Slyke. Three were in the lower
normal range, being 54.1, 55.1 and 60.5 respectively, expressed
in terms of cubic centimeters of CO2 reduced to 0°, 760 mm. Hg.
pressure, bound as bicarbonate by 100 c.cm. of plasma. Three
were in the median range, being 64, 65.5 and 71 c.cm. In one case
the bicarbonate CO2 was reduced to 46.6 c.cm.
There seemed to be no constant relation between the apparent
severity of the clinical condition of the patient and the bicarbonate
reading. In the one case in which this was found to be
reduced below Van Slyke’s lower normal limit the blood was taken
only a few hours before death.
Hemoglobin Per Cent.—As determined by the Sahli hemoglobinometer
(by Miss Lee) and as estimated by the total oxygen
capacity (Van Slyke method) (by Dr. Rohde and Mrs. Macklin),
the hemoglobin content ranged within normal levels.
Relative Volume of Corpuscles.—A limited number of hematokrit
tests on severe cases gave results in normal levels.
Spectroscopic Studies.—Sera obtained from 20 post-mortem
bloods were examined spectroscopically. In eight an absorption
band in the red was observed. In some instances such a band
was observed in blood obtained shortly after death and before
coagulation had occurred, while other similar bloods, as well as
bloods obtained at longer intervals after death, exhibited no
such band. A similar band was observed in one case from blood
obtained from a patient about 12 hours before death from pneumonia
following influenza. Medication was not a causative
158factor. To ammonium sulphide the band in the red reacted as
methemoglobin and the position (as estimated by Dr. Menten)
corresponded with methemoglobin. Oxyhemoglobin bands in
such bloods occupied normal positions as determined by Dr.
Menten. On diluting such bloods with water no abnormality in
character or position bands was observed, save in one instance
(No. 778 below). This does not, however, disprove the possibility
of such abnormality in the hemoglobin within the cells, for
moderate dilution only of serum rendered the band in the red
invisible, presumably by dilution.
Detailed examination of the absorption bands was made with a direct reading wave-length
Hilger Spectroscope (which was calibrated by line spectra derived from salts added to an
alcohol flame) by Dr. Menten. This spectroscope had an accuracy of about two Angstroms.
In all, seven post-mortem bloods were examined, viz. autopsy numbers 756, 761, 763, 773,
778, 784, and 787. In five of these, sufficient serum was obtained to make readings. All
gave the two characteristic oxyhemoglobin bands in the blue-green with centers of the bands at
λ 758μμ λ and 542μμ. The second oxyhemoglobin band varied slightly in width in the different
samples. In addition to the two oxyhemoglobin bands in each of four of the above sera, viz:
Nos. 756, 763, 767 and 787, an absorption band in the red was found with the center of the
band as follows: Number 756 at λ 627μμ, number 761 at λ 634μμ, number 763 at λ 625μμ, and
number 787 at λ 634μμ. These bands varied considerably in intensity and could only be
identified when the two oxyhemoglobin bands were merged and appeared as one broad band.
As controls for the position of the oxyhemoglobin bands two normal bands were examined,
which showed two bands with centers also at λ 758μμ and λ 543μμ. For comparison of the
methemoglobin bands of the above post-mortem bloods, a sample of this hemoglobin compound
was made by adding potassium ferricyanide to normal blood until the solution became brownish
in color. The center of this methemoglobin band was found at λ 634μμ. In blood from
autopsies number 773 and number 778 sufficient serum could not be obtained to make a reading.
To each of these bloods distilled water was added. The laked blood of 778 gave a
methemoglobin band with the center at λ 632μμ on examination 24 hours after autopsy.
Similar treatment of corpuscles five days subsequently gave no indication of the presence of
any methemoglobin spectroscopically.
From the serum and from the laked corpuscles of number 784 no trace of methemoglobin
was found when the blood was examined a few hours after removal at autopsy.
Oxygen Capacity.—The total oxygen capacity was determined
by the Van Slyke method (by Dr. Rohde and Mrs. Macklin). At
this stage the more pronounced type of influenza had subsided,
but in early convalescence the capacity was within normal ranges.
Other studies using different technique gave concordant results,
but there were indications that oxygen was more slowly
absorbed than normally.
Oxygen Content of Venous Blood measured by the Van Slyke
method (by Dr. Rohde and Mrs. Macklin) on the same bloods
examined for total oxygen capacity seemed to indicate a mild
deficiency as compared to normal bloods.
159Gases, Kinds, Quantity and Rate Yielded to Vacuum.—In general
it may be said that quantitative differences observed are not
considered fundamental, but that the studies indicate abnormal
slowness in oxygen absorption.
Gases, Quantity and Rate of Absorption on Exposure to Air
After Extraction by Pump.—The results emphasize slowness of
oxygen absorption as compared to normal blood.
The material to be examined was exhausted for three minutes in the receiver of the Van
Slyke apparatus. One c.cm. was then transferred, with as little exposure to air as possible,
to a small empty bottle, which was then closed and placed in communication with a calibrated,
horizontal tube, containing a segment of alcohol, which served the dual purpose of a seal
and an air volume change indicator. (See Fig. 1.) The apparatus was made in duplicate and
mounted on a common base, so that simultaneous readings on different samples could be
made. After establishing the zero position of the alcohol segment, the base on which the
bottles were mounted was vigorously shaken in a uniform manner. Ten seconds after the
period of shaking, the volume readings were taken. Successive periods of shaking and
reading were conducted at 30-second intervals, until the test was completed. Actual volume
changes were then calculated, tabulated and plotted.
The greater confidence is placed on the results obtained by observing the color of the blood,
as described below; but since then the method has been checked up and the results indicate
that the findings were of sufficient accuracy to warrant their inclusion in this report.[1]
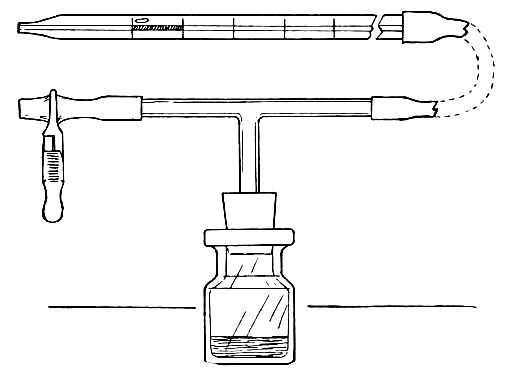
Effect of Addition of Serum on Behavior on Exposure to Air.—The
persistence of venous hue of blood exposed to air was noted
above. It was observed that the addition of serum from the
same blood conspicuously shortened the time required for such
blood to acquire an arterial hue. The addition of normal serum
was more effective in this respect than pathological serum.
Measurements of the rate of absorption of such blood after the
addition of serum indicated acceleration of oxygen absorption.
160From this it would seem that the oxygen transmitting capacity
of the serum was diminished.
Effect of Addition of Dry Sodium Bicarbonate on Behavior on
Exposure to Air.—The addition of a small quantity of dry sodium
bicarbonate to a blood refractory to arterialization on exposure
to air enormously accelerated the process, as judged by the color.
To what extent the change in color may have been due to causes
other than oxygen absorption was not determined.
Comment
The most significant positive findings were evidence of deficiency
of serum oxygen transmitting capacity or rate, and the
detection in serum of an absorption band in the red corresponding
to methemoglobin. The presence of the abnormal substance
giving rise to the absorption band is considered of special interest
as indicating abnormal chemical conditions in the blood, rather
than material change in hemoglobin oxygen capacity.
161
THE BACTERIOLOGY OF EPIDEMIC INFLUENZA WITH A DISCUSSION OF B. INFLUENZÆ AS THE CAUSE OF THIS AND OTHER INFECTIVE PROCESSES
By W. L. Holman, B. A., M. D.
Introduction
In a study of the bacteriology of a respiratory disease such as
influenza, the technical difficulties encountered are very great
and must be overcome before we can draw useful conclusions
from the results obtained or attempt to determine the etiological
factors. The important methods of attacking such a problem
include: (1) the study of stained smears and cultures from the
various available materials, along with the demonstration of the
bacteria in the lesions found in the disease by a study of sections;
(2) tests with the various materials to determine the presence
of the causative agent, which includes experiments on man and
animals and is more inclusive than the mere study of the bacteria
isolated; (3) immunological studies of man suffering from
the disease, or of man and animals treated with the materials
from the disease; (4) pathological, clinical and epidemiological
studies linked with the above.
Many of the difficulties and sources of error in these methods
are manifest to all, but certain points may be indicated as more
important in the phases of the work on which I am to report.
General Methods of Investigation
Stained smears from the material available. The choice of the
material is of first importance. Sputum to be of any real value
must be obtained from the deeper portions of the respiratory
tract, should be as free as possible from the secretions of the
buccal cavity, and should be washed in saline before it is used.
These are considered among the first requirements in the study
of lung infections by the pneumococci and are equally important
in influenza. Swabs from the nasopharynx should be obtained
with the same precautions as are demanded in meningococcal
162work. The other available material—such as blood, lung puncture
fluid, pleural fluid and spinal fluid—must be collected with
the greatest care.
The staining methods should, naturally, include those which
will bring out the various types of bacteria, and must include
the Gram method, using dilute alcoholic fuchsin (1-20) as the
counterstain. The varying morphology of the B. influenzæ and
its frequent minute size make it difficult to detect. It is not the
only Gram negative small bacillus seen in smears from the
throat, but when it occurs in the typical schools, or where there
are numerous bacilli to be seen, its characteristics are quite
definite. I have recently isolated an anærobic Gram negative
bacillus from a series of swabs from the buccal cavity which
suggests in many ways the morphology of the B. influenzæ, which
will indicate one of the many difficulties to be met with in the
study of stained smears. They are, nevertheless, of great use as
a control on cultures, and most helpful in the study of the
material from sources other than the respiratory tract.
Cultures of the bacteria from the various materials. Here we
have the greatest difficulty of all. The medium chosen determines
the bacteria which will appear to predominate, and there is
no single medium that will answer all purposes. Streptococci
will appear to be in excess when serum broth is used, as I have
previously shown; pneumococci with Avery’s pneumococcus
medium; and staphylococci, the Gram negative cocci, and the diphtheria
group with Loeffler’s serum. Ordinary blood agar is perhaps
the best general medium for direct and secondary plating.
There have been many special media devised for growing the
B. influenzæ, but the one I have used most and found particularly
helpful is heated blood agar made after the general method of
Voges.
The extremely tiny colony of B. influenzæ on ordinary blood
agar makes it particularly difficult to detect, and one is apt to
get the wrong impression of its numbers from the macroscopic
appearance of the plate. In attempts at isolation there must be a
liberal use of media in picking colonies, as many suspicious ones
will turn out to be immature growths of B. xerosis, M. pharyngis
(or M. catarrhalis), streptococci, or more rarely pneumococci and
other organisms. Replating from such picks is frequently necessary,
163and further plates, from the original culture on heated blood
agar, must often be made before the B. influenzæ can be isolated.
The care required in all stages of the isolation of this organism,
the unstinted use of media for plating and for picks, the number
of stained smears to be studied, and the further transfers necessary
to verify results, all these limit the amount of material
which can be studied with any degree of accuracy. If further
the streptococci, the pneumococci, the Gram negative cocci, the
capsulated Gram negative bacilli and many others are to receive
any attention, it can readily be appreciated that a few cases
carefully studied are of far more value than a large number
hurriedly examined in an uncertain routine.
The pathological study of the same cases on which I have done
the bacteriology will be found in Dr. Klotz’s paper in these communications,
and I will merely refer to some of the bacterial findings
in the sections of the lungs and bronchi. The more inclusive
methods which have been used in attempts to determine the
etiological factor in influenza we have been unable to attempt,
but I will refer later in this paper to the findings of the investigations
of others. Immunological studies have been limited to
a few investigations on the presence of agglutinins, complement
binding substance, skin reactions and the amount of complement
present in the sera of certain patients. The epidemiological and
clinical studies are reported by Drs. Johnston and Lichty in this
series of reports.
Material Studied
The material used in the study I am reporting included swabs
from the large bronchi and fluid from the lungs and pleural
cavities of 32 autopsies, as well as blood cultures from 22
patients and swabs from the nasopharynx of 31 individuals.
Fifteen sera were tested for fixation of complement with an
antigen made from several strains of B. influenzæ. Fourteen
other sera were tested for agglutinins. Complement content
was determined in the sera of 25 patients. Skin tests after the
Von Pirquet method were done on 14 convalescents, and carefully
stained nasopharyngeal smears without cultures were
studied from 48 patients.
164The chief attention was given to the study of the autopsy
material and we concentrated on the isolation of B. influenzæ.
At the same time we did not neglect the other bacteria making
up the flora of the bronchi, lungs and pleural cavity in these
cases. The various types were isolated and most of them fully
identified.
Technique
Direct smears were made on sterile slides of all material
studied and stained by Gram’s method. The counterstain was
always alcoholic fuchsin diluted 1-20 in distilled water. Direct
cultures were made on a human blood agar plate containing 5
per cent. blood, which was further smeared just before use with
defibrinated blood. This latter procedure was later discarded,
as it did not appear to assist to any marked extent the growth of
B. influenzæ. Blood broth containing a few drops of defibrinated
blood and blood agar slants smeared with blood were also used.
Heated blood agar (2-3 c.cm. of defibrinated human blood added
to 100 c.cm. of ordinary agar at a temperature of from 90 to
100° C., or as the agar comes from the sterilizer) was used in the
last nine cases to replace the blood agar slant in the direct cultures
and as the medium of choice for transfers of the B. influenzæ.
I prefer the ordinary blood agar plate to the heated blood plate
because the former gives readings which are very helpful in
distinguishing colonies of various types. B. influenzæ appears as
clear, tiny, pinpoint, inert colonies. B. xerosis or the pseudodiphtheria
group gives more opaque but often rather similar
colonies. Gram negative cocci as M. pharyngis siccus have dry,
raised, soon becoming wrinkled, inert colonies, varying greatly
in size; M. catarrhalis, more moist, inert colonies. The cocci of
the streptococcus viridans group appear as very small colonies
with greening, or are not infrequently inert, while thin, flattened
colonies with central thickening may sometimes be noted. Those
of the streptococcus hemolyticus group occur as small, frequently
nipple-like colonies with clear, wide zones of hemolysis; pneumococci
as moderately small, moist, dewdrop-like colonies with
center collapsing early and with greening; streptococcus or
pneumococcus mucosus as larger, watery, sticky colonies with
greening and frequently an early clearing near the colonies.
TABLE I.
BACTERIOLOGY OF THIRTY-TWO AUTOPSIES FROM INFLUENZA CASES.
| Autopsy Number. |
Date. |
Day of Disease. |
Hours P.M. |
DIRECT SMEAR—GRAM’S METHOD. |
B. Influenzæ |
Pneumcocci. |
Strept. Mococci. |
Hemolytic Strept. |
S.P.A. |
Other Cocci. |
Other G—B. |
Other Bacteria. |
NOTES. |
| Bronch. |
Lung. |
Pleural Fluid. |
|
| 741 |
1918 Oct. 9 |
3 |
16 |
G +staph. Few pneumo-like. Few chains of elong. cocci. |
0 |
+ |
0 |
|
|
|
+ |
G+ diploc. |
|
|
Nine plates used to isolate B.I. Sp.a. overgrew all cultures. B.I. seen in blood smear agar in 24 hours. |
| 743 |
11 |
5 |
8 |
Br. G—bac. from coccoid to short threads. Mostly scattered. Some phagocyted. Fewer G +cooci in short chains. |
+ |
0 |
– |
|
Pleural fluid and seen as diplos in direct smear. |
|
|
Br. G + diploc. not like pneumo. |
Br. lux. white almost coccoid. |
|
Pericard, fluid and liver juice, no growth. |
| 744 |
11 |
7 |
11 |
Br. G—bac. moderately stout about in small groups and scattered. G+diploc (pneumo) also G— threads. Phago. of both in a few cells. |
+ |
– |
0 |
Lung + |
|
|
|
M. tetrag. in Br. M. pharyng. in Br. |
|
|
Pneumococcus from lung. No attempt after first plate to isolate B.I. |
| 745 |
12 |
10 |
6 |
Br. G +–large bac., strept. short, G—B, few, very short, no threads. |
+ |
0 |
– |
|
|
Pleural fluid, also seen in smear. |
Pl. fluid, also seen in smears. |
|
|
|
Swab from ruptured rectus. Sterile. No material from lung. |
| 746 |
12 |
5 |
½ |
Br. G—B very short, no threads. Irregularly scattered. More seen in left bronchus. A few cells phagocyted. |
+ |
– |
0 |
|
|
|
|
Strept. viridans from bronchus. |
B. coli from bronchi and lung. |
B. xerosis from bronchus. |
The overgrowth of B. coli in lung material prevented further attempts to isolate B.I. |
| 747 |
13 |
6 |
3 |
Br. G+diploc, fairly numerous. G—B tiny, as diplos and in long threads scattered or in small groups. Pleural fluid and lung no bacteria seen. |
+ |
– |
– |
|
|
|
Bronchus and pleural fluid. |
Strept. viridans from bronchi and lung. |
|
B. subtilis group from pleural fluid. |
Five picks from blood agar plate failed to recover B.I. from lung. |
| 748 |
13 |
4 |
4 |
Br. nothing like B. I. seen. G+ small elong. diplo. Numerous G + diploc. in lung. Comparatively few Q-B, very short. |
– |
+ |
0 |
Lung+, not isolated from bronchus. |
|
|
|
Strept. viridans from bronchus. |
|
|
B.I. not seen nor isolated from the bronchi. |
| 749 |
14 |
4 |
15 |
Br. G+large pneumo like, many G+large bacilli, single and in pairs. Few G—B very tiny and widely scattered; lung, heavy mixture as in bronchi. |
– |
– |
0 |
Bronchus Lung? |
|
|
Bronchus and lung. |
|
B. coli from bronchus and lung. |
|
The overgrowth of B. coli prevented any further attempts to isolate B.I. |
| 750 |
14 |
9 |
6 |
Br. G+B large like B. welchii, G—rather stout coccoid forms, G+C in pairs and short chains. Tiny G—coccoid forms like B. I. Lung G+ pneumo-like and caps, chains; no B. I. |
– |
– |
0 |
Bronchus? Lung? |
|
|
|
|
B. coli from bronchi and lungs. |
|
B. coli again present as in No. 749. Direct smear suggests heavy contamination. |
| 751 |
14 |
7 |
6 |
Br. G +cocci large elong.? caps, also G +C in flat pairs. G—coccoid forms. Lung, numerous bacteria. G+strept. with flattened cocci. Some G-short forms? |
– |
– |
+ |
|
Pleura. Lung. Bronchus. |
|
|
M. tetragenous from bronchus. |
|
Spore-bearer with tiny cols, pleur. B. xerosis from bron. |
|
| 752 |
15 |
13 |
15 |
Br. G+pneumo-like. G+B smaller than B. welchii, occasionally tiny G -diplobacillus. Lung, G+chains of cocci Gram weak. Few G—tiny bacilli scattered or in groups. |
– |
+ |
0 |
Bronchus and lung. |
|
|
|
Strep. viridans from bronchus and lungs. |
|
|
B.I. like seen in original culture on blood agar but not isolated from bronchus. |
| 756 |
16 |
8 |
18 |
Br. numerous G+B. B welchii like. G—B large and few tiny. G+round diploc. Pl. fluid almost pure pneumo-like, few G-forms probably the same. |
– |
0 |
– |
|
|
|
Pleural fluid. |
Strep. viridans from bronchus. |
B. coli from bronchus and pleural fluid. |
B. xerosis from bronchus. |
Compare No. 749 and 750. Fluid from lung not obtained for culture. |
| 757 |
16 |
6 |
14 |
Br. G—B tiny, to medium. G—like M. catarrhalis. G+cocci, pairs and chains. Few B. W. like. Lung, many G—B like B. I. Some cells filled, also G—cocci. M. catarrhalis like and rare B. welchii like. |
+ |
+ |
0 |
Bronchus and lung. |
|
|
Bronchus and lung. |
M. tetragenous? from lung. |
|
B. xerosis from bronchus. |
This case 14 hours P. M. gave B.I. from all the material. |
| 758 |
16 |
14 |
16 |
Br. pneumo-like in excess. G—B from tiny to forms stouter than B. I. Few strept. rare M. catarrhalis. Lung, pneumo-like. Phago. |
+ |
? |
0 |
Bronchus and lung. |
|
|
|
M. catarrhalia-like from lung. Strep. viridans from lung and bronchus. |
B. coli from bronchus. |
|
The B. coli did not prevent the isolation of B.I. like seen in original blood agar cultures of lung. |
| 761 |
17 |
7 |
19 |
Br. pneumo-like. B. I. like common, M. catarrhalis like. Both B.I. and M. catarrhalis phagocyted. B.I. single or in threads. Some typical groups. Lung, pneumo, caps, rare, M. catarrhalis like. |
+ |
– |
0 |
Bronchus and lung. |
|
|
Bronchus and lung. |
|
B. coli from bronchus. |
|
Even after 19 hours P. M. the B.I. was isolated. |
| 762 |
17 |
10 |
12 |
Br. numerous B.l. like typical, also many pneumo. and M. catarrh. Lung same. M. catarrh. phagocyted. B.I. smear, many phagocyted, many pneumo. |
+ |
+ |
+ |
Pleural fluid and bronchus. |
|
|
|
M. catarrh. like from lung and bronchus. |
|
B. xerosis from lung. B. subtilis from bronchus. |
|
| 763 |
17 |
11 |
13 |
Lung, pneumo-like, slight phagocytosis. Pl. fl., pneumo and few strept., slight phagocytosis. |
0 |
– |
– |
Pleural fluid. |
|
|
|
|
|
|
No growth from lung on plate. B.I. like seen in original culture from pleural fluid. No material from bronchus. |
| 764 |
17 |
9 |
6 |
Br. B.I. smear. Cells crowded. Pneumo-like fewer, occasional G—stouter thread. |
+ |
0 |
0 |
Bronchus. |
|
|
|
Staph, albus from bronchus. |
|
|
Material only from bronchi. |
| 765 |
17 |
9 |
16 |
Br. pneumo. B.I. few scattered. G+flattened diploc. Phago. of B.I. and pneumo. Lung, pneumo-like, rare strept. very questionable G—B free and in cells. |
+ |
+ |
0 |
|
|
Lung. |
|
M. catarrh. from bronchus and lung. |
B. coli from bronchus and lung. |
|
|
| 767 |
18 |
10 |
14 |
Br. rather round pneumo-like with caps. B.I. few. Scattered, also in cells. Lung, few bacteria. G+strep. often phagocyted. |
– |
– |
0 |
Bronchus. |
Lung. |
|
Bronchus. |
|
|
|
Blood culture 15
10 gave pure growth of pneumo. mucosus. |
| 770 |
19 |
11 |
9 |
Br. crowded with B.I. like. Few G+cocci and fewer M. catarrh. like. Pl. fluid G+flattened pairs, pus cells, phagocyted. |
+ |
+ |
– |
Bronchus. |
|
|
Bronchus, lung, pleural fluid. |
|
|
|
|
| 773 |
21 |
20 Recurrence. |
3 |
Br. few bacteria G+and G—pneumo-like. Rare G+–thread. Lung, pneumo and rare strept. Pl. fluid, pneumo-oat shapes, etc. |
– |
– |
– |
|
|
|
Bronchus. |
Strept. viridans bronchus. Sarcina albus lung. |
|
B. xerosis from bronchus. G + B lux. white pleura. fluid. |
No growth from lung except sarcina. Only 2 colonies from pleural fluid on blood agar plates. |
| 778 |
24 |
23 |
17 |
Br. B.I. smear. Fewer large pneumo. Lung, G + small diploc. Few B.I. like. Pl. fluid, few cells, no bacteria. |
+ |
+ |
– |
Bronchus and lung. |
|
|
Lung. |
|
Non-motile, non-fermenting, lux, white from bron. |
|
Ten plates and 30 picks were done for the isolation of B.I. |
| 781 |
26 |
5 |
4 |
Br. crowded with staph. like. Fewer G—B, larger than B.I., few M. catarrhalis like. Lung G+ small staph. like, caps, cocci in pairs and chains. Few tiny G—B. Pl. fluid pneumo-like and elong. cocci in chains capsulated. |
– |
+ |
– |
|
Lung and pleural fluid. |
|
Bronchus and lung abscess. |
Staph. albus and sarcina from pleural fluid. |
|
|
B.I. like seen from 24 hour Ht. blood agar from bronchi and lung but only isolated from lung on replating. Bl. culture 25
10 sterile. |
| 782 |
26 |
8 |
3 |
Br. numerous B.I. like scattered, some phagocyted. Fewer G+ flat pairs with capsule. |
+ |
– |
0 |
|
Bronchus and lung. |
|
|
|
|
|
No B.I. like on 24-hour Ht. blood agar from lung. |
| 783 |
26 |
8 |
1 |
Br. G+small caps, pneumo-like. Lung poor smear, occasional pneumo-like. |
+ |
– |
0 |
Lung. |
|
|
Bronchus. |
M. catarrh. like bronchus. |
|
|
No B.I. like on 24-hour Ht. blood agar from lung. |
| 784 |
28 |
8 |
6 |
Br. capsulated pneumo-like, few strep. Lung, chiefly pneumo-like. few G—B like B.I., also G—pneumo-like. |
+ |
+ |
0 |
Bronchus and lung. |
Bronchus and lung? |
|
|
M. catarrh. like bronchus. |
|
|
Numerous B.I. like on 24-hour Ht. blood agar of bronchi and fewer from lung. Isolated by replating. |
| 786 |
29 |
4 |
2 |
Br. G+cocci in round pairs and rather flat chains, suggested caps. Tiny G—B very rare. Lung streptococci flattened, often phagocyted. |
+ |
– |
0 |
Bronchus. |
|
Bronchus and lung. |
|
Staph, albus from bronchus. |
|
|
Pleural fluid not collected sterilly, Haemol. strept. isolated. |
| 787 |
29 |
8 |
2 |
Br. numerous pneumo-like, bacillary forms. A rare suspicious B.I. like, some of these in cells. Lung, caps, elongated diplos, and chains of elong. cocci. |
+ |
+ |
0 |
|
|
|
Bronchus and lung. |
|
B.M.C. from bronchi. |
|
All the bacteria isolated were seen in 24-hour Ht. blood agar cultures from bronchi and lung. |
| 791 |
Nov. 1 |
6 |
6 |
Br. few bacteria. G+pneumo-like round, G—B and threads, size varies, like B.I. Lung, G + caps, pneumo. G+Large B. few suspicious G—coccoid forms. Pl. fl. caps, pneumo and caps, elong. chains. |
+ |
+ |
– |
Bronchus and pleural cavity. |
|
|
Bronchus and lung. |
|
|
|
Replated from Ht. blood agar to isolate B.I. from lung. |
| 792 |
2 |
6 |
3 |
Br. caps, pneumo-like bac. forms and chains. G-caps, pneumo-like. Few G—B. questionable. Lung. caps, pairs and chains of elong. cocci, in cells. Pl. fluid, numerous caps, chains of diploc. |
+ |
+ |
– |
Bronchus, lung and pleural fluid. |
|
|
|
Staph. albus, lung, strept. viridans lung, M. catarrh. like lung and bronchi. |
|
|
B.I. like seen on 24-hour Ht. blood agar from bronchi and lung but not pleural fluid. |
| 793 |
4 |
10 |
3
2 |
Br. M. catarrh. and G+cocci, few bacteria, few G—B. Ear, G+cocci. |
– |
– |
– |
?Throat. |
|
Bronchus, lung, arm vein, spleen ear. |
Throat, ear and bronchus. |
Strept. viridans from throat. |
B. coli from throat. |
|
B.I. like never seen except from throat which may have been B. coli. |
| |
|
|
|
Total |
20 |
13 |
2 |
20 |
6 |
4 |
16 |
|
|
|
|
| |
|
|
|
B. influenzæ found—Percentage |
66½ |
46 |
14 |
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| |
|
|
|
Total percentage for B. influenzæ |
|
78 |
% |
|
|
|
|
|
|
|
|
- EXPLANATORY NOTE.
-
- B.I.—B. influenzæ.
- S.P.A.—Staphylococcus pyogenes aureus.
- M. pharyog—Micrococcus pharyngis siccus.
- Br.—Bronchus.
- Phago.—phagocytosis.
- Ht.-Heated blood agar.
- B. W.—B. welchii.
165Staphylococci develop opaque, paint-like colonies of varying size,
with or without hemolysis, and so do other less frequently found
bacteria give more or less distinctive colonies. The heated blood
agar does not show these differences.
The colonies most liable to be confused with those of B. influenzæ
are, therefore, those of B. xerosis, immature colonies of
the Gram negative cocci and certain colonies of the streptococcus
viridans group. Transfers should always be made to heated
blood agar of all colonies suggestive of B. influenzæ, or when
the growth of the B. influenzæ has only occurred in the more
crowded portions of the plate, and it is difficult to pick pure
cultures, attempted pickings should be made to this medium for
further platings. It is frequently necessary to make further
blood agar plates from the original blood agar, blood broth or
heated blood agar cultures after longer incubation periods,
depending on the findings in smears from these media. The
heated blood agar is the best of these to encourage the growth
of B. influenzæ. It must, however, be used at once, or within a
very few days of its preparation, and cannot be kept on hand as
a stock medium. I have not found it as useful for plating
because of the difficulty of differentiating colonies. The phenomenon
of the star-like and more luxuriant growth of the colonies
of B. influenzæ about colonies of other bacteria has often been
noted, and will be referred to in a later portion of this report.
Here it may be said that this is at times a marked feature of
certain mixtures and must be recognized in studying the plates.
The finding of B. influenzæ in picks from apparently isolated
colonies of other forms is not uncommon, and is the same type
of difficulty which I have discussed in papers on streptococci. It
is important to recall, in connection with cultures taken from
the lungs at autopsy, the experimental work of Norris and Pappenheimer,
who showed that B. prodigiosus put in the mouth
immediately after death could be recovered from the lungs in
over 50 per cent. of the cases studied.
Results of the Author
In Table I are shown my results from the 32 cases which came
to autopsy. The B. influenzæ was isolated from one or more
sources in 25, making a total of 78 per cent. Most of the negative
166cases probably also had this organism, but I did not grow
it from the material which I used for culturing. The work of
others would indicate that it may have been present in other
regions, such as the sinuses of the head or other portions of the
lung and respiratory tract. The positive results show B. influenzæ
present in 20 out of 30 cases from the bronchi; in 13 of 28
from the lungs; in 2 of 14 from the pleural cavity; in 9 of 26
from both bronchi and lung where both were cultured; in 8 of
26 from the bronchi with the lung negative; in 3 of 26 from the
lung with the bronchi negative; once of 10 from the pleural
cavity with both the bronchi and the lung negative, and once
from all three sources.
The negative results occurred in seven cases. In three of
these (749, 750, 756) B. coli overgrew the cultures from the
bronchus, in two also from the lung, and in one, without lung
culture, from bronchus and pleural cavity. The mere presence
of B. coli, however, did not preclude the isolation of B. influenzæ,
as is seen in cases 746, 758, 761 and 765. The finding of B. coli
would suggest a post-mortem invasion. The hours after death
before the autopsy was done were in these seven cases, ½,
15, 6, 18, 16, 19, 16, respectively. That delay in performing the
autopsy, as emphasized by Spooner, Scott and Heath, adds
to the difficulty is self-evident, but successful isolations of
B. influenzæ have been obtained after even longer periods than
in the negative cases (761). In the fourth negative case (763)
the bronchus was not cultured. A pneumococcus was grown
from the pleural cavity and no growth was obtained from the
lung. In the original culture from the pleural cavity influenza-like
forms were seen but could not be isolated. In the fifth case
(767) a blood culture three days before death gave a growth of
pneumococcus mucosus which was also grown from the lung at
autopsy. Direct smear from the bronchus showed very few
influenza-like forms. Our sixth negative finding was in a case
of 20 days’ illness, the patient having had a recurrence (773).
Staphylococcus pyogenes aureus, streptococcus viridans and
B. xerosis were grown from the bronchus. Only a sarcina form
grew from the lung, and a further probable air contamination
occurred on the media from the cultures of the pleural cavity.
The B. xerosis colonies were confusing, picked as possible B. influenzæ,
167and, before this was discovered, the overgrowth prevented
further attempts to isolate the influenza bacilli. The last unsuccessful
case was one with a general infection of a hemolytic
streptococcus from an acute otitis media. The streptococcus was
isolated from the bronchus, lung, spleen, arm vein and the middle
ear at autopsy.
It will be seen that in these seven negative cases technical
difficulties prevented the isolation of the B. influenzæ, even if it
had been present. I would not, therefore, conclude that the
organisms were necessarily absent, but rather that we have
failed either to secure material from the focus of infection or on
account of the other reasons mentioned.
It is very evident that a variety of secondary organisms very
frequently overgrow the field and become numerically predominant.
In our first case staphylococcus pyogenes aureus overgrew
all the other organisms present in cultures from the lung
material. B. influenzæ was, however, seen in the original 24-hour
blood agar culture. It required 9 blood agar plates before the
organism could be isolated. In another case 10 plates were used
for the isolation.
The findings of the bacteria in the lung sections are particularly
interesting and instructive. The entire series of cases have
not been completely studied, so I am unable to tabulate the findings.
In cases 761 and 762 sections of the lung showed influenza-like
bacilli to be almost pure in the earlier stages of the process,
while in areas with purulent foci pneumococcus-like and other
Gram positive cocci were also numerous. In some cases B. influenzæ-like
organisms were to be seen in overwhelming numbers.
In others they were scarce, while in some nothing resembling
B. influenzæ could be found in the sections. Positive cultures
were often independent of whether the influenza-like forms were
to be seen in smears or sections or not, although they were found
in the great majority of the cases. The findings in the direct
smears and the bacteriological results make useful material for
comparison.
Swabs from the nasopharynx were cultured from 31 individuals;
nearly all of these were cases suspected of diphtheria
or as carrying the diphtheria bacillus, and no particular effort
was made to isolate the B. influenzæ. They were seen in the
168mixed culture occasionally. In the last eight cases the heated
blood agar, ordinary blood agar and Loeffler’s serum were seeded
from the throat swabs. B. influenzæ practically overgrew all
the other bacteria from seven of these cases on the heated blood
agar medium and was isolated without difficulty; all eight showed
M. catarrhalis. The two other media gave little or no evidence
of the presence of B. influenzæ. As I have said above, our attention
was concentrated on the autopsy material. These cultures
from the throat were simply made to demonstrate the usefulness
of the heated blood agar.
TABLE II
BACTERIA SEEN IN DIRECT SMEARS FROM NASOPHARYNX
| Type of Disease. |
Number of Patients. |
B. Influenzæ-Like. |
Pneumococcus-Like. |
M. Catarrhalis-Like. |
| Early |
24 |
14 |
17 |
6 |
| Serious |
13 |
13 |
13 |
9 |
| Convalescent |
11 |
8 |
11 |
6 |
| Total |
48 |
35 |
41 |
21 |
| Percentage of positives |
|
73 |
86 |
43 |
Direct Smears from Nasopharyngeal Swabs
It is recognized by most of the modern investigators that little
reliance can be put on the finding of B. influenzæ-like bacilli in
direct smears. The organism is markedly pleomorphic, occurring
as extremely small coccoid forms up to threads of various lengths.
Notwithstanding these morphological variations the organisms
are usually seen as tiny bacilli, and these are considered as the
typical form. We carried out a series of microscopical examinations
of carefully made smears from the throats of patients with
influenza. Particular attention was given to the occurrence of
organisms resembling in morphology and staining B. influenzæ,
pneumococci and M. catarrhalis. We have divided the cases
roughly into three types—early, serious, and convalescent. Table
II shows our results. The term B. influenzæ-like was used for
the typical morphological picture so often described. Dr. Frost
and Mr. Scott carried out this portion of our work and their
results are interesting.
169Blood cultures were done on 22 cases. Pneumococcus mucosus
was grown from one patient who three days later came to
autopsy (Case 767). In another case pneumococcus-like organisms
were seen in smears from the dextrose broth flask after
24 hours’ incubation. These, for some unknown reason, did not
grow on blood agar plates. After 48 hours smears made on
blood agar from the original flask gave a growth of B. influenzæ
and a M. catarrhalis-like organism. I consider this result a very
unsatisfactory one, being quite unable to explain the failure to
grow the pneumococci-like forms on transfer. Possibly the
acidity developed might account for it.
TABLE III
AGGLUTINATION TESTS WITH SERA OF CONVALESCENT INFLUENZA PATIENTS
| Dilution of Serum |
+ |
+– |
– |
| Convalescents |
1-1 |
3 |
0 |
2 |
| 1-10 |
5 |
2 |
7 |
| 1-40 |
2 |
3 |
9 |
| 1-80 |
0 |
1 |
13 |
| 1-160 |
0 |
0 |
14 |
| Normal Controls |
1-10 |
1 |
2 |
0 |
| 1-40 |
0 |
1 |
2 |
The complete agglutination as would be indicated by +++ or ++ was
not seen.
Agglutination tests were carried out with the sera of 14 convalescents
and 3 normal individuals. A polyvalent emulsion of
strains of the influenza bacillus isolated from our cases was used.
The results are shown in Table III. Tubes were incubated at
37.5° C. The results did not indicate anything in the nature of a
specific reaction. Dr. Frost carried out this work during the
height of the epidemic, but we were unable to continue it further.
A short review of the work of others will be found near the end
of this paper. Miss Thompson and Mr. Mock studied complement
fixation, using the sera of 15 convalescents against an antigen
of B. influenzæ. Their results were negative. The antigen
appeared to be slightly more anti-complementary than were
170emulsions of staphylococcus or B. coli. Huntoon also noted this
anti-complementary character of emulsions of B. influenzæ.
Attempts were made to estimate the amount of complement
present in the fresh blood serum of influenza patients. The
technique was to use a 1-4 dilution of the patient’s serum, adding
measured amounts of this to a 1 per cent. blood emulsion, with
1 unit of amboceptor and determine the smallest amount necessary
to bring about complete hemolysis. This test was carried
out on eight patients ill for only a few days. The average
amount of the dilute serum was 0.181 c.cm. Fifteen patients, convalescent
after a moderate illness, gave an average of 0.276 c.cm.
Two patients seriously ill with temperatures of 104.3° F. and
105° F. required 0.4 c.cm. to bring about complete hemolysis. We
would not like to draw any very definite conclusions where we
are dealing with such small fractional differences. This lessening
of complement has been noted in other infectious diseases and
may be important in the questions of immunity in influenza.
Dr. Frost carried out a number of cutaneous tests after the
method of Von Pirquet, using a polyvalent, weakly alkaline
emulsion of influenza bacilli in 25 per cent. glycerin. Eleven
convalescents were tested and none of them showed any local or
general reaction. The suggestion that these results may indicate
an increase in resistance is discussed in another place. A number
of strains of pneumococci which we had isolated from our
autopsy cases were differentiated by the agglutination method.
Type I was found 3 times; type II, 10 times; type IV, 9 times.
Four showed agglutination with both type I and type II sera.
Type IV pneumococcus was isolated in one case from the right
and left bronchus as well as the lung. In another case the same
type pneumococcus was recovered from the lung and pleural
fluid. These results are similar to those found by numerous
workers.
The Hemophilic Bacteria
The discovery by Pfeiffer of the hemophilic character of the
bacillus found by him in cases of influenza opened up a new group
of micro-organisms known as the hemophilic bacteria. Davis
(1915) has laid particular stress on the group character of these
bacilli, and the more they are studied the more clear does it
become that there are several distinct members. The B. influenzæ
171is by far the most important as well as the most frequently
found of the group and is considered as the type organism.
All these bacteria require for their growth the presence of
some form of hemoglobin. The actual amount necessary may
be very small, and Davis suggested that it may have a catalytic
action. A great deal of work has been done in attempts to discover
just what portions of the hemoglobin are necessary to
bring about this phenomenon. In our discussion on media for
the influenza bacillus we will briefly describe some of the various
hemoglobin preparations that have been used successfully. It
must at this point be emphasized that blood is very useful in
many media to stimulate the growth of a great variety of bacteria,
and the transfers made from such luxuriantly growing
cultures may grow very poorly or not at all on ordinary media,
and this might easily lead to erroneous conclusions on the hemophilic
character of the organisms studied. There are certain
bacteria which grow so much better on media containing blood
that such media are sometimes necessary for their isolation,
although after a few transfers they will grow on ordinary media.
This is true for bacillus pertussis, and throughout the literature
a good deal of confusion has arisen in not recognizing this temporary
hemophilic character of certain bacteria. The true hemophilic
bacteria do not grow except in the presence of hemoglobin
in some form or other. The problem becomes almost academic
when we consider the small amounts of hemoglobin that are
necessary. Davis has shown that a dilution of 1 in 180,000 is
sufficient, and in the interesting discussion between Cantani and
Ghon and Preyss it was demonstrated that hematin or other
hemoglobin product was necessary in the agar before B. influenzæ
would grow in the presence of other bacteria, and that this
hematin could be derived from the blood in the meat which was
used in making the basic infusion.
Symbiosis.—The fact that other bacteria can bring to growth
the influenza bacillus on media otherwise unsuited to its needs
brings up the interesting problem of symbiosis, which is one of the
most important characters of the influenza bacillus. Not only do
other bacteria make possible the growth of B. influenzæ on media
on which the influenza bacillus will not grow, but they stimulate
a better growth on blood agar and other more or less favorable
media. Grassberger first noted this stimulating character of
172other bacteria and described and illustrated the very large
colonies of B. influenzæ which develop in the neighborhood of
colonies of staphylococcus and other bacteria. Staphylococci
killed by heat were found to have a similar effect. Meunier
nicely described this phenomenon by using the term satellites
for the circles of B. influenzæ colonies which develop about the
colonies of other bacteria. A great number of workers have
since noted this characteristic relationship between B. influenzæ
and other bacteria, and occasionally have laid stress on its importance
in the problems of the infections by the influenza bacillus.
Allen particularly emphasized the probable importance of this in
discussing the problem of carriers of B. influenzæ as sources of
danger. There seems no doubt that this symbiotic relationship
depends on so altering the hemoglobin products as to render
them more readily available for the influenza bacillus. This is
indicated by the fact that on various media containing hemoglobin,
altered so that it encourages the growth of B. influenzæ,
no such symbiotic stimulation can be demonstrated. This phenomenon
is quite peculiar to this bacillus, distinguishes it from
most of the other members of the group, and should be always
determined before an organism is classed as B. influenzæ.
Other Hemophilic Bacteria.—The question of a pseudo-influenza
bacillus was first raised by Pfeiffer and has been studied by many
workers after him. Grassberger, who carefully investigated this
problem, worked more particularly with two strains showing the
extreme of variation between the small characteristic morphology
of the B. influenzæ and the thread forms supposed to be characteristic
of the so-called pseudo-influenza bacillus. The great
majority of workers have agreed with him in concluding that this
morphological variation is not sufficient nor constant enough to
justify separating two such groups. Nevertheless many reports
indicate peculiar tendencies of certain strains toward thread
formation. There seems to be suggestive evidence that the
organism described by Cohen in 1909 under the name B. meningitidis
cerebrospinales septicemicus is different from true
B. influenzæ. Although the cultural characters were apparently
identical, this organism was definitely pathogenic for guinea pigs
and rabbits. The involvement of joints in the cases reported
by Longo and others would suggest a greater pathogenic power
for these strains. Prasek and Zatelli reported a similar bacillus
173from meningitis, and Davis found that his meningitis strains
were more pathogenic for rabbits than were others. Wollstein
has studied this question very carefully and found a marked
difference between the strains from the meninges and those from
the respiratory tract in their pathogenicity for rabbits. The
strains with a tendency to thread formation were usually also
those grown from the meninges, but she concluded from the
results of serological tests that all strains of B. influenzæ are of
one race, irrespective of their origin or virulence. The question
is still an open one, as Batten and others described strains from
the meninges which are non-pathogenic, and Ritchie found his
strains from meningitis pathogenic for guinea pigs but not for
rabbits. The irregularity and wide divergence in the results of
blood cultures may have a definite relationship to these differences
in the pathogenicity of strains.
Other hemophilic bacteria include the bacillus described by
Friedberger under the name of B. hemoglobinophilus canis.
This organism is to be found in the preputial secretion of dogs.
It does not show the phenomenon of symbiosis, and I have found
that it grows rather more freely and is more resistant to drying
than is the influenza bacillus. Krage has confirmed Friedberger’s
findings growing this bacillus from 60 per cent. of his dogs,
and believed it a pyogenic organism just as B. influenzæ may be.
The hemophilic and hemolytic organisms described by Davis,
which he isolated from pathological urine, were non-symbiotic
and non-pathogenic. Koch has described a similar organism
from puerperal infection. Whether the hemophilic organism
described by Thalhimer from the uterus in a case of puerperal
infection, those found by Cohen in urethral discharge in one
case and the pelvic exudate of another, and the findings of Kretz
in pyelitis, Wright in pyelonephrosis and Klieneberger in cystitis
cases, possibly refer to this same bacillus is, of course, uncertain.
Pritchett and Stillman found a somewhat similar bacillus, which
they called Bacillus X, from the mouths of 24 persons. It was
hemophilic and hemolytic, stouter than B. influenzæ and showed
long tangled threads in blood broth. It was non-pathogenic and
is probably the same as Davis’ organism.
Davis described another hemophilic bacillus from a patient
with purulent foci which was non-hemolytic and non-symbiotic.
It was grown from an abscess of the shoulder joint, the blood
174and the bronchial secretion of an infant. Cyanosis was a marked
feature of this case. Paranhos described a hemophilic bacillus
from meningitis, which, however, was Gram positive, and Moon
reported an anærobic hemophilic bacillus from an infection of
the ethmoid sinus. The work of Jordan would suggest that there
may be two groups of B. influenzæ based on the indol production.
Morphology.—The morphology of B. influenzæ has received
more than usual attention. In what we consider its characteristic
form, it is an extremely small bacillus, usually single but sometimes
in pairs, and not infrequently exhibiting polar staining. In
direct smears, where there are many bacteria present, they are
frequently arranged in the schools so frequently described. The
development of thread forms is today considered quite characteristic
for B. influenzæ. The organisms vary from moderately long
bacillary forms to very long twisted or curled threads suggesting
leptothrix. In such cultures chains of tiny bacilli are also quite
often noted. At the other extreme we have exceedingly tiny
coccoid forms, resembling in size the B. bronchisepticus, which,
as Ferry has shown, are small enough to pass through many
grades of filters.
It is the thread forms, as discussed above, that have received
most attention in relation to the so-called pseudo-influenza bacillus.
The observations of Wollstein, Lacy and many others
showed these forms to be common in meningeal infections and
that, as a rule, they are more pathogenic for animals than other
strains. Another interesting and important observation is that
emphasized by Dick and Murray of the possible confusion of
these forms with Gram negative leptothrix. That this confusion
is liable to occur is illustrated by reports such as Macdonald
finding leptothrix in a meningeal infection, now looked upon as
an example of influenzal meningitis, and the probable B. influenzæ
reported by Dick, and, as quoted by Dick and Murray, the
finding of a Gram negative leptothrix as the cause of broncho-pneumonia
by Kato. The 2 per cent. leptothrix reported by
Nuzum and his co-workers from the recent epidemic may be still
another example. Equally important is the recognition of the
great frequency of this thread development in the majority of
B. influenzæ cultures on ordinary blood agar media, or even in
the water of condensation of fresh blood agar tubes. The delayed
growth of this bacillus on ordinary blood agar would lead to its
175being frequently overlooked unless smears are made, and the
irregular thread forms are recognized as being the B. influenzæ.
This development of thread forms was particularly noted in my
work before pickings were made to the Voges heated blood agar,
but because I had been forewarned by discussing these morphological
variations with Lacy, I was able to recognize them as
forms of B. influenzæ. Most of my early isolations showed these
predominating, and they were also noticed in cultures sent from
the Public Health Laboratory at Washington. These cultures on
further transfer, however, showed in 24 hours the typical small
form on ordinary blood agar as well as on the Voges medium.
On the latter the development of thread forms was greatly
delayed and frequently did not appear at all, although after long
periods other abnormal, swollen and irregular shapes sometimes
developed.
Media in Growth of B. Influenzæ
The discovery of the hemophilic character of B. influenzæ has
been confirmed by a long list of investigators. The agar smeared
with pigeon blood as used by Pfeiffer has not, however, been
found fully satisfactory and many modifications have been made.
The fact that hemoglobin in some form is necessary for the
growth of these bacteria has led to a great deal of study in
attempts to discover the chemical part, or parts, essential for
this purpose. Hemoglobin in very small amount, as shown by
Davis and others, is sufficient to make media suitable for growing
B. influenzæ. This fact has led to much confusion, owing
to the difficulty of eliminating all possible sources from which
some form of hemoglobin might enter the media. Kitasato used
a glycerin agar and succeeded in growing the influenza bacillus
for 10 transfers. Pielicke, however, did not consider that Kitasato
was actually dealing with the influenza bacillus, but that
he as well as Babes, Bruschettini and Markel had most probably
streptococci in their cultures. Besson held the same view of
Kitasato’s organism. It would further appear from the illustrations
of Klein that he also grew streptococci and not the B. influenzæ.
The first culture of the influenza bacillus was probably
obtained by Bujiwid in February, 1890. He grew on agar
smeared with the spleen pulp of an influenzal patient a tiny
bacillus which he was unable to grow on blood free medium, but
176he did not appreciate its importance until Pfeiffer’s article
appeared. Teissier in his book on “L’ Influenza en Russie” mentioned
this culture.
The hemophilic character of these bacteria indicates that they
are rather strict parasites, and despite the researches of Nastjukoff
with various egg media, and Cantani with a number of
supposedly non-hemoglobin additions to the agar, as well as the
studies on symbiosis, with other bacteria, by Cantani, Neisser,
Luerssen and many others, it still remains true that some form
of hemoglobin is necessary for their growth. Fresh blood either
incorporated in the medium or smeared on the surface is not the
best medium for these bacteria. Altered hemoglobin is much
more favorable, and a variety of methods have been devised to
bring about those alterations which stimulate the growth of
B. influenzæ. One of the earliest, as well as one of the very best,
of these is the method of Voges, who added blood to melted
agar at a temperature of about 100° C. I have found this
medium exceptionally suited to growing B. influenzæ, and I consider
it excellent for the primary culture from the original
material, for pickings from plates and to obtain a heavy growth
of B. influenzæ for any purpose. The medium was used by Delius
and Kolle (1897), Grassberger (1898), who spoke very highly
of it, and Paltauf (1899), who said that the use of this medium
made the demonstration of B. influenzæ possible when only a
very few were present. A great many other workers have used
it with success, and during the recent epidemic it has gradually
found its place. Levinthal’s medium (1918) is practically the
same, although he boiled and filtered the agar after the addition
of the blood. The growth of B. influenzæ on the Voges agar can
properly be described as luxuriant, and to anyone only accustomed
to the use of ordinary blood agar it is an agreeable
surprise to see this supposedly delicate bacillus growing so
remarkably well.
Various other methods have been used to bring about this
beneficial change in hemoglobin. Gioelli (1896) used a medium
made up of 1.1 per cent. hemoglobin and 21.5 per cent. malt
extract. This is reddish brown in color, becomes clear when
neutralized with potassium hydrate and remains so on heating.
This added to agar is reported as very favorable in growing this
bacillus. Ghon and Preyss described a medium made up of meat,
177peptone, salt and agar prepared in the ordinary way, but not
filtered for at least a week, and then only roughly. This medium
is favorable for symbiotic growths. He further used beef blood
heated in a soda solution and blood heated in water as hemoglobin
preparations to be added to agar. Thalhimer found an
amorphous hemoglobin medium to be more favorable than when
a purer hemoglobin was used. W. F. Robertson found a hemoglobin
agar, prepared by allowing sheep’s blood to clot, decanting
off most of the serum, freezing and then thawing what remains
and adding 1 c.c. of this to an agar tube at about 60° C., to be
very favorable for the growth of B. influenzæ. Cantani used a
blood treated with pepsin and hydrochloric acid, digested some
days in the incubator, filtered and made weakly alkaline. This
mixture was heated for a few minutes, refiltered and added to
the medium. He speaks of it as extraordinarily good for B. influenzæ.
Blood treated with trypsin has been used by Matthews,
Averill, Young and Griffiths, Harris, A. Fleming and others.
Fleming further found that this alteration in hemoglobin can be
brought about in a number of other ways. Blood boiled in agar
(suggesting the Voges agar) and the tubes slanted while hot,
blood boiled in water, the clotted blood precipitated and the
clear fluid added to agar, or more rapidly by adding equal quantities
of sulphuric acid to the blood and a similar amount of
potassium hydrate he obtained altered blood suitable for media.
He reported that by any of these methods he could obtain a
medium very stimulating to the growth of B. influenzæ. By the
addition of brilliant green (1 in 500,000) he inhibited the growth
of staphylococcus, streptococcus and pneumococcus. For storing
cultures of B. influenzæ Fleming found a minced meat medium
with the addition of blood to be the best. I have found this
medium without the blood to be an excellent one for keeping
a great variety of cultures. Bernstein and Loewe have reported
the use of gentian violet (1 in 5,000) for the same purpose as the
brilliant green used by Fleming. Avery’s oleate blood agar
medium he reported to be largely selective. It checked the
growth of pneumococci and streptococci, but gave luxuriant
growths of B. influenzæ. Pritchett and Stillman have used it
with excellent results recovering B. influenzæ from a very high
percentage of the cases studied.
178The use of symbiotic bacteria has been extensively studied in
investigations of the biology of B. influenzæ, and it has been
shown, as noted elsewhere, that such accessory bacteria will
bring to growth B. influenzæ on media otherwise quite unsuited
to its needs. It has been further found that on various preparations
of hematin agar, on which B. influenzæ refused to grow,
such media could be rendered favorable for their growth by the
addition of living or freshly killed cultures of staphylococcus and
many other bacteria. And although the method is well known,
it has not been extensively used for the purposes of isolation.
Many of the workers, however, have pointed out the importance
of looking for growth of the influenza bacillus in the neighborhood
of the more easily grown bacteria which almost always
develop in cultures from the respiratory tract. Grassberger has
particularly studied this problem and has made practical application
of the method. Accidental contamination of plates with air
bacteria have made possible, in some instances, the isolation of
B. influenzæ—as, for example, in the finding of Heyrovsky from
a case of empyema of the gall bladder—while other workers have
pointed out the difficulty of demonstrating growth where B. influenzæ
is pure in the material cultured, and the comparative ease
and relative luxuriance of growth where other bacteria are
present. To just what this stimulating effect is due has been
much discussed, and it is generally agreed that the hemoglobin
is markedly changed and rendered more available by the action
of these germs. It is to be noted that on a medium containing
blood altered by heating or by the various methods as described
by Fleming the foreign bacteria no longer show any symbiotic
action on B. influenzæ. Grassberger considered the effect of the
bacteria on the blood to be the same as that of heating. Allen
laid particular stress on this symbiotic character. He used a
staphylococcus, either living or killed, in making his cultures
and noted the difficulty of growing B. influenzæ from material
in which it occurred pure. W. F. Robertson made use of these
facts of symbiosis for both isolation and stimulation of growth.
He employed alternate drills of M. catarrhalis or pneumococcus
with the B. influenzæ, and Brown and Orcutt used strains of
hemolytic streptococci for the same purpose. The latter authors
considered that the beneficial effect of the streptococci was
merely due to the setting free of the hemoglobin. The fact that
179similar results are to be obtained by the use of non-hemolytic
bacteria as well as forms giving green color changes to the blood
makes this explanation untenable. In my own studies I have
confirmed the results of several previous workers. I have found
that B. influenzæ is stimulated in its growth by the presence
near it of colonies of staphylococcus pyogenes aureus and albus,
pneumococci, streptococcus viridans and hemolyticus and other
bacteria. The largest colonies of the bacillus I have obtained
were those growing near the periphery of a colony of an air
nocardia. I have also noted that emulsions of a staphylococcus
killed by boiling for five minutes, when added to ordinary blood
agar, had a marked stimulating effect, although no evidence of
hemolysis was present. This effect was practically absent if the
emulsion was boiled for 15 minutes, or after being killed was
left at room temperature for several days. There was no evidence
of these stimulating effects by any of these methods when
heated blood agar was used, the colonies on this medium growing
equally large by themselves. Comparative studies of the effect
of different bacteria can be simply carried out as follows: Smear
evenly the surface of an ordinary blood agar plate with an emulsion
of B. influenzæ. Seed this plate at various points with
minimal amounts of the various bacteria. After various periods
of incubation the size of the B. influenzæ colonies about the
other bacterial growths can be estimated, and impression preparations
on cover glasses will give very interesting pictures.
The growth of B. influenzæ in primary cultures from sputa
and similar sources is to be explained by the probable presence
of traces of blood or altered hemoglobin as well as the symbiotic
relationship with other bacteria. Fichtner used fresh heated
sputum (60 to 65° C.) in place of blood, and Richter a medium
made with sterilized pus. Parker, in her study of a filterable
poison produced by the B. influenzæ, found veal infusion broth
with 10 per cent. defibrinated blood heated to 75° C. until the
blood coagulated and settled on standing to be the best for the
purpose. Jordan in his study of indol production by these bacteria
used a meat infusion broth with 5 per cent. sheep’s blood
added at 90° C. or over and filtered through cotton or paper.
Wittingham and Sims noted that in using blood from influenza
cases the bacteria frequently did not grow, more especially
B. influenzæ; and Rivers found human blood poorer than cat or
180rabbit blood for growing this organism, as did Minaker and
Irvine. It would seem clear from this review of some of the
suggestive work on the methods of growing B. influenzæ that
little attention should be given to the results of many workers,
where ordinary media were used, particularly when the difficulties
of isolation were not appreciated.
B. Influenzæ as a Pathogenic Bacterium
If B. influenzæ is the causative agent in clinical influenza,
there is certainly ample evidence that it is pathogenic to man.
The symptoms of toxemia, which are so manifest in the pandemic
disease as well as in the sporadic cases, would indicate that the
etiological agent is markedly toxicogenic. Animal experiments
by Pfeiffer, and a long list of investigators following him, would
seem to show that the majority of cultures of B. influenzæ do
not have any power of establishing themselves in the animal
tissue. Killed cultures showed equally as high toxic effects as
the living, and so it was generally concluded that many of the
general effects in influenzal infections were of a toxic nature.
There are many exceptions to the above-mentioned failures to
produce infections in animals. Cantani obtained very constant
positive results by subdural injections. He first clearly showed
that killed cultures were markedly toxic and that virulence could
be raised very definitely by animal passage. By injecting brain
emulsion with a culture he obtained a subcutaneous abscess in
a rabbit which after eight days still contained the living
organism. Nastjukoff found that animals with a lowered resistance,
or definitely ill from, for example, an artificial tuberculosis,
became infected while others did not. Jacobson showed that
B. influenzæ injected with streptococci caused a definite mixed
infection, and that after six passages the influenza bacillus alone
could produce a fatal infection. Saathoff (1907) confirmed
Jacobson’s findings and found pneumococci equally effective.
Davis (1915) also confirmed the principle established by Jacobson
of the symbiotic relation of other bacteria to infection with
B. influenzæ. He used a culture of a non-virulent staphylococcus
pyogenes aureus, and was able to produce death invariably in
guinea pigs after intraperitoneal injection. From the heart’s
blood, as a rule, only the hemophilic bacillus was recovered. He
also found animal passage increased the virulence, and further
181that M. catarrhalis and an avirulent streptococcus had the same
effect as the staphylococcus. Slatineanu (1901) found that he
could infect animals with B. influenzæ if the cultures were
injected along with weak solutions of lactic acid, and that after
animal passage by this method the bacillus became more virulent
and would eventually kill by itself. It must not be forgotten
in this connection that strains of B. influenzæ from meningitis
cases are frequently definitely pathogenic for animals. The
importance of considering these various factors in a discussion
of infection by this organism is, of course, very evident. Ecker
found his strains pathogenic for mice after subcutaneous injection,
and the bacilli were readily obtained from the heart’s blood.
Spooner and his co-workers from their results of more than a
hundred intraperitoneal injections concluded that the organism
is not pathogenic for mice.
In all animal experiments it is of the greatest importance that
the bacteria be known which may interfere in the experiments
through spontaneous infection (often liable to be induced by the
injection) from the animal’s own flora, as well as the greater
susceptibility of previously diseased animals (Nastjukoff). It
would appear from the results of Bruschettini and Cornil and
Chantemesse in the early days of the influenza bacillus, and
those of Lamb and Brannin in their recent study, that these
authors did not seriously consider the spontaneous infection of
guinea pigs and rabbits with B. bronchisepticus or the bacillus
of rabbit septicæmia, both morphologically, very similar to
B. influenzæ. Rosenow in his experiments with streptococci from
cases of influenza has also apparently failed to realize the importance
of the lung lesions produced by the B. bronchisepticus in
guinea pigs as reported by Theobald Smith, myself and many
others.
Parker has found a filterable poison from the influenza bacillus
which developed rapidly (6 to 8 hours) in a special heated blood
broth medium, deteriorated rapidly even in the cold, and killed
rabbits in quantities of 2 c.c. in from 1 to 3 hours. Rabbits
could further be immunized against this poison, and their sera
protected other rabbits against fatal doses. This is the first time
that a true powerful toxine has been obtained. Couret and
Herbert obtained toxine from B. influenzæ in Avery’s oleate
broth. Huntoon and Ross also clearly demonstrated toxine production
182by this organism so that it would appear, with this confirmation,
that the B. influenzæ can be definitely classed among
the toxine producers. Toxemia being the most striking clinical
characteristic of influenza, we have in these findings very strong
evidence of the etiological importance of this hemophilic bacillus
to the disease. A very interesting observation was made by
Latapie that the serum of a goat immunized against influenza
bacillus is toxic if it is used shortly after the injection of the
microbes, but that this toxicity is absent three weeks after the
last injection. It would appear to me that the evidence of a
filterable virus from the secretions of the respiratory tract does
not eliminate the very probable toxine from such materials. The
production of toxine by this organism probably depends, as is
the case with very many of our toxine formers, on the most
favorable combinations of conditions. That it is not readily
formed in artificial cultures, or that it is very unstable if formed,
is evidenced by the frequent failures of a great many workers.
It has been suggested that different symbiotic conditions in the
respiratory tract determine the amount of toxine produced.
Huntoon found a high toxine production in mixed cultures with
streptococci. This, however, does not appear to be necessary,
as there is ample evidence of severe toxemia from pure infections
with B. influenzæ in various parts, such as the accessory sinuses
of the head, the meninges, the lungs and other parts of the
respiratory tract.
It is not fundamentally necessary that a toxine producing
organism be present in overwhelming numbers before it can be
accepted as the cause of the toxemia. Nor, on the other hand,
must we have toxemia every time the organism is found. The
prevalent idea among bacteriologists would appear to be the
reverse of what I have just stated. It would, indeed, be extremely
difficult to make bacteriological diagnoses of a great many of our
diseases, where the etiological factor is well established, if these
conditions were required. We do not do so, for example, in
diphtheria, examinations of stools for typhoid, nor in infections
with the tetanus bacillus. We recognize carrier cases of meningococcus,
B. typhosus, hemolytic streptococci and many others,
without detracting seriously from their importance in definite
types of infection. Formerly the specificity of the different
bacteria for definite disease processes was very rigid, but today
183we interpret more broadly the finding of gonococcus in endocarditis,
the meningococcus in bacteremia, B. typhosus in osteomyelitis,
streptococci and pneumococci in all manner of infections
and many other bacteriological results. True it is that the
various bacteria show predilections for attacking certain tissues,
but the varying susceptibilities bring about the greatest variations
in the manifestations of these infections.
The B. influenzæ is not confined to the causation of severe
pandemic or epidemic influenza, but includes in its field purulent
bronchitis, meningitis, sinusitis, conjunctivitis and many other
pathological processes. It further should be recognized as a
relatively frequent cause of complications in measles and other
diseases.
Infections of the Respiratory Tract
The disease influenza is primarily an infection of the respiratory
tract. It varies from one of the most acute and fatal
diseases we know of through all grades of severity—from
chronic infections lasting over years to the familiar three or five
day fever. This graduation is to be found more or less marked
in all our bacterial infections, but would seem to be not generally
recognized or appreciated as occurring in infections with the
influenza bacillus. That Pfeiffer was dealing with one phase of
the disease when the influenza bacillus was discovered does not
invalidate the results of numerous workers which have been
added since then.
Probably the greatest confusion in attempts to get a clear
picture of this protean disease has been and is a non-recognition
of influenza as a frequent complication of other diseases, such as
measles (Jochmann, Susswein, Tedesko and very many others).
The second cause for this confusion has been the misinterpretation
of the facts demonstrating the rather frequent occurrence
of carriers. During an epidemic the vast majority of patients
show the disease as an upper respiratory infection of varying
degrees of intensity, but which usually subsides after periods
of from three to five days of fever. Along with this we have
other graded manifestations of further involvement of the tract
with laryngitis, bronchitis, bronchiolitis and all degrees of broncho-pneumonia.
To prevent the severe lung involvement prompt
treatment must be carried out, under which rest in bed is by
184long odds the most important. This will be discussed in another
paper of this series, and was particularly well demonstrated in
the results at the Naval Hospital as verbally reported to me by
D. G. Richey. The interesting point is that the infection can
be controlled, but this does not indicate the etiological factor as
different from that acting in the more severe cases.
The epidemiological evidence would seem to show very clearly
that the incubation period is approximately two days, and that a
period of six weeks is the usual limit for the severe wave of the
epidemic in different localities. In my opinion, during this period
every exposed individual in a community has received the influenza
bacillus in the respiratory tract, and that all the susceptible
individuals are attacked and show more or less evidence of the
infection. As a consequence of this general distribution we have
great numbers of individuals carrying the organism, and the
aftermath is to be noted in other and later manifestations of
the same infection.
Sporadic cases of influenza appear during inter-epidemic
periods and more or less healthy carriers are frequent. Scheller’s
study in Königsberg showed, if we can rely on his figures, that
the carriers were very numerous during an epidemic year (winter
1906-1907), being 24 to 33 per cent.; that as the epidemic
became less widespread (winter 1907-1908) it fell to 10 to 13
per cent.; as it was disappearing (summer 1908) he found only
1.5 to 3.3 per cent.; while when the epidemic was completely
over (winter 1908-1909) there were no carriers of B. influenzæ
found. These results are taken from studies of sputa and throat
smears of 138, 218, 155 and 185 cases, respectively, for the
periods mentioned. The monumental work of Tedesko, who reported
the results of 1,479 cultures, covering 11 years (1896-1906),
would indicate that B. influenzæ is continually present
in the population. However, in carefully analyzing his results,
it is very clear that in the great majority of his cases it was of
definite etiological significance. Lobular pneumonia, acute, purulent
and chronic bronchitis, and most frequently clinical influenza,
are the prominent diagnoses in all his tables. He was able to
grow B. influenzæ repeatedly from individual patients for many
months.
Lord in similar studies (1902, 1905, 1908) brought out somewhat
similar facts. He laid particular stress on the cases of
185chronic bronchitis with numerous B. influenzæ in the sputum
and a probable confusion of these with pulmonary tuberculosis.
He was able to follow a number of his patients for several years.
B. influenzæ was grown in culture from the sputum of one of
these in 1902; in November, 1903; in February, 1904, and in
February, 1905. In other cases the organism was shown to be
present by culture practically continuously for months and even
years. Lord, with Scott and Nye, in a recently published article
(1919) reviewed his former results and showed a relatively high
incidence of B. influenzæ in the respiratory tract of apparently
healthy people. Davis studied 534 cases, further indicating the
prevalence of this organism in the community.
The B. influenzæ has been recovered from the respiratory tract
during the clinically pure influenza, from the sputum and lung
in influenzal pneumonia, and from the purulent sputum in all
grades of bronchitis. These should all be looked upon as true
infections by the influenza bacillus, the varying manifestations
merely differing with the resistance of the individual. In the
epidemic in the fall of 1918 pneumonia was the outstanding
feature. Preceding this in the English publications we have
reports of outbreaks of purulent bronchitis. Macdonald and his
co-workers, finding the B. influenzæ frequently present, considered
the condition as one indication of a virulent infection by
this organism. Hammond, Rolland and Shore reported similar
cases, and Abrahams and his co-workers looked upon the cases
of purulent bronchitis as occupying a position, without any
definite line of demarcation, between those with definite broncho-pneumonia
on the one side and those with simple bronchial
catarrh on the other. H. E. Robertson emphasized the serious
nature of influenzal purulent bronchitis and the almost epidemic
character and rather high mortality of the outbreak in the winter
and spring of 1917-1918. There were also numerous mild outbreaks
of influenza before the overwhelming culmination of the
last three months of 1918, as reported by Orticoni and many
others and noted by Johnston in this series of papers. Greenwood
in an epidemiological study emphasized the point, previously
made evident by Parsons for the pandemic of 1889-1892,
that the mass attack is preceded by numbers of individual cases.
In this country it was noted during the winter of 1917-1918 and
the following spring that the B. influenzæ was rather frequently
186found in the respiratory infection in our army camps (Soper,
Cole and MacCallum and others).
It is well recognized that when the actual epidemic struck
there were comparatively few bacteriologists familiar with the
B. influenzæ. The real difficulties of isolation, the more favorable
media, the facts of symbiosis, the importance of carriers,
the varying manifestations of the infection and many of the
other vitally important points, although more or less fully reported
in the literature, were nevertheless practically unknown.
It was my own experience, and that of many others. This must
be seriously considered in analyzing many of the reports on bacteriological
findings throughout the period of the severe wave and
even after.
Results of Others During the Recent Pandemic
It will be impossible to review the numerous reports on the
recent epidemic that have appeared. Many of these can be discounted,
as far as the finding of B. influenzæ is concerned, for
the reasons mentioned above. The often quoted report of Little,
Garofalo and Williams, who did not even use a hemoglobin
medium, will serve as an example. Little attention should be
given to others where the large numbers of cases precluded the
requisite time and media necessary for such a difficult problem.
Friedlander and his co-workers in their report from Camp Sherman
made no mention of the number of sputa, throat swabs or
autopsies which they examined bacteriologically. The incidence
of influenza showed a total of 10,979 cases, 2,001 of pulmonary
œdema or pneumonia and 842 deaths. They recorded one culture
from the sputum with pneumococcus predominating which gave
two colonies of B. influenzæ, and this bacillus was grown from
the lung exudate at one autopsy. Their conclusions that “B. influenzæ
(Pfeiffer) has not been demonstrated as the causative
organism” is certainly true from their results, but that “the
frequency of its detection has not exceeded the frequency of its
existence under normal conditions” can hardly be considered as
established, if we accept the many results mentioned above as
indicating its presence during inter-epidemic times, unless they
mean by normal conditions practically complete freedom from
this organism.
187The prevalence of B. influenzæ in various sections of this
country may be indicated by the following reports chosen from
many available ones. Keegan, from the First Naval District
Hospital, found B. influenzæ 19 times from 23 in cultures grown
from the lungs. In 6 cases these cultures were pure. Medalia
reported from Camp McArthur the following. Out of 2,279 sputa
of influenza suspects, 76.8 per cent. showed “B. influenzæ” in
smears, and 445 sputa from cases of broncho-pneumonia showed
it in 54 per cent. It was found in culture in only 10.6 per cent.
of these last cases. He considered sputum smears of practical
diagnostic help. He further grew B. influenzæ twice from the
blood during life, once with a pneumococcus and once alone.
Necropsy cultures gave B. influenzæ in 2 of 3 cultures from the
brain, 19 of 34 from the heart, 19 of 36 from the spleen, 54 of
65 from both lungs, 50 of 62 from the right pleura and 47 of 62
from the left pleura. The percentage of positive results ranged
from 53 in the spleen to 83 in the lungs. Nuzum and his associates
only found B. influenzæ in 4 of 100 cases from the bronchial
secretions, but it is interesting to note that he grew it in
practically pure culture from both lungs of one case at autopsy.
Synnott and Clark in Camp Dix found streptococci and pneumococci
predominating, and, although making no particular
effort to study the B. influenzæ or determine its frequency, they
found it in the majority of cases when it was looked for. Blanton
and Irons reported as follows from Camp Custer. From cultures
of the nose and throat of 357 examined before the epidemic
struck, B. influenzæ was found in 5.1 per cent.; in 366 throat
cultures of influenza cases without physical signs of pneumonia
the same organism was grown in 44, or 8 per cent.; sputa typed
for pneumococci 740 times from influenza cases with pneumonia
gave isolations of B. influenzæ 38 times, or 5 per cent.—8 times
alone, but here it should be remarked that these latter isolations
were only attempted after the organism was suspected from the
morphological picture of the smears; from 280 autopsies B. influenzæ
was recovered 8 times from the lung and 3 times from the
heart’s blood. This report covered the period from the outbreak
of the epidemic, October 5 (or as given by Soper, September 30)
to October 22, at the outside a period of 22 days. During this
time 366 throat cultures, 510 blood cultures, 740 sputa typed for
pneumococci, 280 autopsies with cultures from both lung and
188heart’s blood, made a total of primary cultures of well over 2,000.
The technical difficulties would make it almost impossible to
handle such a mass of material and get reliable results for the
incidence of B. influenzæ.
Brem, Bolling and Casper in Camp Fremont found B. influenzæ
in 259 from 537 selected cases in swabs from the nasopharynx.
It was also noted in a fair number of other examinations. Opie
and his co-workers found B. influenzæ to be very frequent at
Camp Pike. Spooner, Scott and Heath isolated B. influenzæ at
Camp Devens from the sputa of 104 cases, from nasopharyngeal
swabs in 11 out of 18 attempts and from the pleural fluid 8 times
out of 45, twice pure. From 37 autopsies they found B. influenzæ
in 23 and in pure culture in at least 1 lobe of the lung in 16. From
82 blood cultures at autopsy B. influenzæ was recovered twice.
Nichols and Stimmel studied lung punctures during life and grew
the B. influenzæ from 7 out of 10 attempts, 5 times in pure culture.
Stone and Swift at Fort Riley found B. influenzæ in 18.7
per cent. of 928 sputa and in 5.2 per cent. of 77 sputa from fatal
cases. He recovered it from autopsy material; 21 times from 51
lungs, once alone; twice from 26 pleural fluids; twice from 30
heart bloods; 19 times from the sinuses of 40, and 9 times from
the ear and mastoid of 17 cases.
Lamb and Brannin at Camp Cody examined 80 typical cases
early in the epidemic. They found B. influenzæ predominated in
46 per cent. being present with pneumococci on 41 per cent. of the
plates. They also grew the influenza bacillus from a fair number
of other cases.
Wollstein and Goldbloom in the Babies Hospital of the City of
New York found the B. influenzæ in 13 of 17 sputa during life
and in both lungs of all 18 autopsies as well as in the heart’s blood
of one. Kotz found it in half of his 30 cases. Pritchett and Stillman
grew the influenza bacillus from 41 of 49 cases of influenza,
from 40 of 43 cases of influenza with broncho-pneumonia, from all
of six other broncho-pneumonia cases and from 11 of 20 cases of
lobar pneumonia, making a total of 98 positive findings from 118
or 82 per cent. They further found 25 positives from 54 convalescent
and 74 from 177 normal sputa. Wolbach found this
organism in pure culture in one or more lobes of the lungs of 9
from 23 cultured cases. It was demonstrated in 23 of 28 either
by culture or in section.
189Similar results are to be found in reports from Great Britain.
Martin noted a great increase in the numbers present as the
sputum became more purulent. Hicks and Gray found B. influenzæ
by culture in 75 per cent. of their cases. They were seen
in direct smears in only 70 per cent. Gotch and Wittingham considered
M. catarrhalis to be the etiological factor as it was found
in all of their 50 cases. B. influenzæ was grown in 8 per cent.,
although B. influenzæ-like bacilli, were seen in 62 per cent. of their
smears. Averill, Young and Griffiths studied the sputum from 41
cases and found B. influenzæ in 32. It is interesting that Macdonald
and Lyth determined the incubation period to be 41 hours
as a minimum in their own experience and that from the posterior
nares of one of them B. influenzæ was obtained.
Schofield and Cynn found the B. influenzæ in Korea. Kraus in
Brazil found it in the sputum in 62 per cent. of his cases of influenza.
It was also found in the organs of 27 who had died, being
in pure culture in five. It has further been found in France, Italy
and practically all parts of the world where investigations have
been made. The German literature is at present only available
in the report of the British Medical Research Committee which
is written in a more or less popular manner with a rather strong
tendency against the importance of B. influenzæ. Dietrich,
Simmonds, Bergmann and others, however, found B. influenzæ
rather frequently. Such quotations as “Uhlenhuth, a diehard of
bacteriologic orthodoxy, has clearly shown signs of uneasiness”
and “one empyema and one throat swab yielded the looked for
growth” will indicate why this review is of little use. It is certainly
necessary to “look for” the B. influenzæ to get results of
any worth.
Secondary, ancillary or symbiotic bacteria are of cardinal importance
in these infections. It has been considered by some
writers as characteristic for the influenza bacillus to be followed
so frequently with such a variety of secondary invaders. Sahli
looked upon the complex of B. influenzæ, pneumococcus and streptococcus
as the true etiological cause of influenza. Abrahams and
his associates discussed the symbiotic effect of the B. influenzæ
in raising the virulence of pneumococci previously present in the
patient and many other investigators lay stress on these symbiotic
relationships.
190Pneumococci appear to be the commonest of these secondary
micro-organisms judging from the various published reports, but
the fact must not be overlooked that, particularly in America, the
typing of pneumococci has drawn a disproportionate attention to
this group. Hemolytic streptococci have received much attention
(Ely and his co-workers and several others). M. catarrhalis
(Gotch and Wittingham and several of the British writers), members
of the B. mucosus capsulatus group (Nichols and Stimmel,
Rucker and Wenner), staphylococcus aureus (Patrick), various
ill-defined streptococci (Rosenow and several British writers),
capsulated cocci apparently different from pneumococci, B. pestislike
forms and many others have been given more or less attention,
often as clearly recognized secondary infections, but not
infrequently as of primary significance.
B. influenzæ, however, is the organism most regularly found in
this pandemic where carefully looked for, and the evidence of its
lowering the general resistance to bacterial invasion is very
strong. The experiments of Ghedini and Fedeli showing the
effect of the toxine on muscular tone and those of Ghedini and
Breccia who found a similar effect on blood vessels are worthy of
note.
The fact that the flora differs so widely in various regions is
what one might expect and many investigators have emphasized
the significance of this. Bacteria in the mouth and throat are
readily transmitted from individual to individual and under the
conditions in the training camps and our modern life, the development
of local flora is not surprising. That it is of very great
importance is recognized by all and it is often a determining
factor in the severity of the infection. Nevertheless, influenza in
this pandemic has been almost equally severe whatever the secondary
organism may have been.
I have discussed in another place the suggestion of the stimulating
effect of various bacteria on the growth and toxine production
of B. influenzæ. Huntoon showed the effect of hemolytic
streptococci in cultures to be helpful in toxine production. An
important point, however, is that no one bacterium has been
shown to be exclusive in thus affecting the growth on media of
the influenza bacillus, and in the animal experiments in raising
the invasive and pathogenic power of this organism the same
appears to be true. The infection in influenza, in the vast
191majority of cases, rapidly becomes a mixed one. The secondary
organisms at times completely dominating the field, at least as far
as numbers go, most frequently invade the blood stream and it
would appear often play the important role in many of the secondary
conditions.
Chronic Infections
B. influenzæ is a frequent finding in the sputum of patients with
chronic bronchitis, pulmonary tuberculosis and other chronic conditions
in the respiratory tract. Boggs recovered this bacillus
from two cases of bronchiectasis, Richards and Gurd had a similar
case and Tedesko reported several. The literature is filled
with references to the finding of B. influenzæ in cases of chronic
bronchitis. Those reported by Lord, Madison and Tedesko quoted
above will serve as examples. The frequent positive cultures in
cases of pulmonary tuberculosis so often referred to in reviews
of the literature and the significance of these findings, as pointed
out by Scheller, are important as bearing on the much debated
subject of the effect of influenza on this disease. These types of
chronic infection by the influenza bacillus should be more generally
recognized as they undoubtedly will become more numerous
following this last epidemic if we can judge from the experience
of the past.
Infections of the Pleura
The recovery of B. influenzæ from the pleural cavity is not
uncommon as is shown in the above review. The findings of
MacCallum, Cole and others during the spring of 1918 are particularly
interesting. Beall in 1906 reported a case of empyema
with large quantities of green pus in which B. influenzæ was
found in pure culture.
Sinuses of the Head
Infection of the accessory sinuses of the head has long been
recognized as occurring in influenza. Frankel found B. influenzæ
in 4 from 40 infected antra. Lindenthal, who was particularly
interested in the question of sporadic influenza, found the bacillus
in one or more of the head sinuses in six of eight carefully studied
cases. He considered that the B. influenzæ remained in these
192areas during inter-epidemic times and from hence caused the
sporadic outbreaks of influenza. Howard and Ingersoll reviewed
the literature up to 1898 and grew B. influenzæ from one of three
acute antral diseases. They did not find it, however, in 12 chronic
cases. Clemens believed the influenza bacillus to be present in
the sinuses rather frequently in cases where it was overgrown or
difficult to culture from the lower respiratory secretions. Moszkowski
grew it in one case from the pus of the antrum. Tedesko
recorded several positive results and many others are reported in
the literature.
The two cases reported by Lacy (1918), the findings during the
present epidemic by Stone and Swift of B. influenzæ in 13 of 28
sphenoidal and 6 of 12 ethmoidal sinuses cultured at necropsy,
those by Spooner, Scott and Heath, of B. influenzæ in four frontal
sinuses and in eight sphenoidal, and the recovery by Wolbach of
B. influenzæ in cultures from the sinuses in certain cases where
the lung cultures were negative, emphasize the importance and
frequency of the infection by this organism in these cavities.
Keegan, who laid particular stress on lung punctures and autopsy
examinations, pointed out that in throat cultures the probability
that the influenza focus is often not in the pharynx but in some
recess of the nasal cavity.
H. E. Robertson in the spring of 1918 reported the infection of
the sinuses in seven cases of tracheo-bronchitis with patches of
broncho-pneumonia and the growth of B. influenzæ from sphenoid,
ethmoid or frontal sinuses of all these cases. He also found this
organism in the sphenoid of six cases dying with various diseases
as well as in two accident cases with death under 24 hours. The
importance of these results was laid stress on by the author, not
only on account of the probable toxic absorption and the general
menace of spread, but, more particularly, because such individuals,
acting as carriers, could furnish foci for the spread of epidemics.
Eye and Ear
Infections of the eye by the influenza bacillus are quite common.
This subject is fully discussed by Axenfeld (text-book,
“The Bacteriology of the Eye”). Giani and Picchi found it in the
eye in 66 per cent. of influenza cases, in 90 per cent. of epidemic
conjunctivitis, and in the normal eye of 5.8 per cent. Wynekoop,
193in 1903, reported having found this organism in cases of conjunctivitis
in 1899. Guiral, in the recent epidemic, found influenza
bacillus constantly present in the secretions in cases of
what seemed to be Week’s conjunctivitis. Ulceration of the
cornea was rather common. One such case is mentioned in which
there was no pain in the eyes, but general symptoms of influenza.
The middle ear is also sometimes infected. Between the report
of Kossel in 1893 and that of Stone and Swift in 1918, who found
the middle ear and mastoid to contain B. influenzæ in 8 of 17
cases, there have been many references in the literature to this
complication by the influenza bacillus. The evidence indicates,
however, that in the middle ear, as in the pleural cavity, the
secondary bacteria are far more often the important ones.
Meninges
Influenzal meningitis seems to stand by itself as a manifestation
of the pathogenic effects of B. influenzæ. The literature is
too voluminous to review in this place, but the evidence would
seem to point to a more invasive and pathogenic type of this
organism, if not to a separate member of the group.
Invasion of the Blood Stream
The evidence in clinical influenza would suggest at times a
bacteremia in addition to the severe toxemia, which is such a
constant feature of the disease. Simultaneously with the discovery
of B. influenzæ, Canon reported finding bacilli of similar
morphology in blood smears, but was unable to grow them, and it
would appear at least doubtful that he was dealing with the
influenza bacillus. Meunier is probably the first who grew this
organism from the blood. He recovered it from 8 blood cultures
out of 10 in cases of broncho-pneumonia following measles, and
in one other case of broncho-pneumonia. A very full discussion
of this question is to be found in Canon’s book on “The Bacteriology
of the Blood in Infectious Diseases.” Of particular
interest are the results of Ghedini, who made a careful study of
28 influenza patients. B. influenzæ was grown from the blood in
18 of these at the height of the fever, while in the 10 negative
cases the disease was milder or the blood was taken only after
194the temperature had fallen. The amount of blood used was
20-30 c.c., and it was cultured in lecithin broth. In practically
all of his cases several cultures were taken, and in a number of
the positive cases negative results were obtained both before and
after the acme of the fever. He also grew the bacillus from 8 of
14 spleen punctures of these patients. Madison (1910) reported
the recovery of this bacillus from the blood of a patient with a
primary broncho-pneumonia who recovered. This author also
used about 30 c.c. of blood. Thursfield, in 1910, also reported
two cases of B. influenzæ bacteremia in which the organisms were
recovered at the height of the temperature. One had influenza,
the other phlebitis, and both recovered. Tedesko and several
others have found it in the heart’s blood in many cases, more
especially in broncho-pneumonia after measles.
During the present epidemic the positive cultures of this
bacillus from the blood have been rather infrequent. J. S. Fleming
had 2; 2 are quoted in the report of the Influenza Committee of
the Advisory Board to the D. G. M. S. (Peters and Cookson);
Medalia had 2 during life and 19 of 34 at autopsy; Orticoni, Barbie
and Leclerc in 5 of 10 blood cultures in one series, and 7 of 19
in another; Stone and Swift 2 at autopsy; McKeekin, in Australia,
influenza-like bacilli in 4; Blanton and Irons three times in the
heart’s blood, one of these pure; Spooner, Scott and Heath twice
in the heart’s blood at autopsy, and Wollstein and Goldbloom
from the heart’s blood in one child. In the majority of these
findings the bacillus was not found in pure culture. Abrahams
and his associates found the B. influenzæ along with a pneumococcus
and M. catarrhalis from the heart’s blood in one case.
In our positive blood culture there was evidence of the same
mixture being present.
Before drawing sweeping conclusions against the invasion of
the blood by B. influenzæ it must be remembered that the quantity
of blood used has been generally only about 10 c.c., and often
much less, the difficulty of observing growth if the culture is
pure has been largely overlooked, the use of more favorable media
than blood agar and the possible inhibitory action of influenzal
blood, as suggested by Wittingham and Sims, Rivers and others,
has not been considered, and further that sufficient care has
not been exercised to obtain blood at the most favorable period in
the disease. It may be recalled that the problem is quite similar
195to that of demonstrating the organisms in the blood in patients
with streptococcus viridans bacteremia.
All the available evidence, however, points to the invasion of
the blood in influenzal infections as being a very fleeting one.
Unless this is true, it would be surprising in the many hundreds
of blood cultures which have been taken in the concentrated
study of patients during the recent pandemic, if more successful
cultures had not been obtained. General infections with localization
of B. influenzæ in different parts of the body are here of
interest—such as that reported by Slawyk and others. Whether
the strains causing meningitis, and which apparently more frequently
invade the blood, are really different members of the
hemophilic group or only forms with a higher invasive power is
still, I believe, an open question.
Endocarditis
In endocarditis the B. influenzæ is probably, after streptococci,
the organism most frequently isolated from the blood. Rosenthal
from heart’s blood at autopsy, Schlangenhaufer, Jehle two cases,
Horder (1907) six cases, and who believed he was the first to
isolate B. influenzæ from the blood, Tedesko in a number at
autopsy, Spat, F. J. Smith, Saathoff, Libman four cases, Sacquepee,
McPhedran, Mann, Rainaford and Warren three cultures
from two patients, and a number of others all bear witness to its
frequency.
Other organs of the body are sometimes found to contain
B. influenzæ. Adrian, Schultes, Basile and Tedesko have all
recovered this organism from the diseased appendix. Several
years ago a bacillus, considered, to be B. influenzæ, was grown
from the pus of an appendix abscess in our laboratories. Wright
found it in pyelonephrosis. Klieneberger found influenza-like
bacilli in cases of cystitis. Menko reported the bacillus from
orchitis, and Cohn found numerous influenza-like bacilli in the
discharge from urethritis. Meunier found it in pure culture in
a case of osteoperiostitis. Huyghe, Besancon and Griffon recovered
it from infected joints, as did Pacchioni in a general infection.
Weil found it in the pus about the hip joint one month
after an attack of influenza. This short review serves to illustrate
that the influenza bacillus, although generally limited to
196infections in the respiratory tract, is, nevertheless, capable of
infecting other parts.
Immunity—Phagocytosis
Phagocytosis of the B. influenzæ has been very frequently
noted in the study of sputum smears. It has been observed,
moreover, that this phenomenon occurs most frequently when
the patient is on the road to recovery (Pfeiffer, Martin, and
others), and it may indicate an important reaction on the part
of the body to this organism. Tunnicliff in a recent report, however,
did not find the opsonic index to be raised above the normal
in her patients, and Tunnicliff and Davis had difficulty with a
spontaneous phagocytosis of this bacillus. This difficulty was to
a large extent absent in her later study.
Agglutination
Agglutination tests have been used by many investigators in
attempts to determine a specific reaction in the sera of persons
suffering from influenza. Such reactions develop, as we know,
against secondary infecting bacteria, so that unqualified conclusions
cannot be drawn that agglutinins in the sera of patients
against B. influenzæ indicate the etiological importance of this
organism. Vagedes using a dilution of 1-50 found 8 positives
among 27 patients tested. Lord found the test most inconstant.
Ghedini obtained useful results by using serum in dilutions 1-20
to 1-30, and had 17 positives from 28 influenza cases. He found
agglutinins present three to four days after the height of the
infection, and noted that the sera became practically normal after
three to four weeks. Fichtner, although he obtained agglutination
with sera of influenza patients in high dilutions (1-100 and
1-750), found his controls were often agglutinated, and consequently
drew no conclusions. Wollstein (1906) did a series of
agglutination tests, using various strains of B. influenzæ. The
sera of patients she found very unsatisfactory, but by immunizing
rabbits with this organism she obtained sera with titres up to 1 in
400. She could find no differences among the various strains
studied. Somewhat similar results were obtained by her in 1915
working with strains from the meninges and the respiratory
tract. Odaira carried out a rather extensive series of tests, using
197immunized rabbit sera and a special method of making his bacterial
emulsions. He was able to distinguish B. influenzæ from
both B. pertussis and the so-called Cohen’s bacillus of meningitis.
Friedberger’s dog bacillus, however, could not be differentiated
from B. influenzæ by this means. A. Fleming during the
recent epidemic had good results with the sera of 21 patients.
He incubated at 50° C. for two hours. He also used sera of
immunized rabbits and got marked agglutination against the
homologous strain, but varying results with other strains. He
noted some strains agglutinated readily, while others did not.
Eyre and Lowe noted an increase in agglutinins in the sera of
people vaccinated against the influenza bacillus. Couret and
Herbert could distinguish two types and a possible third among
their strains. Park and his co-workers found numerous types
by means of agglutination. Absorption of agglutinins was found
helpful by these last two workers. There are so many factors
capable of altering the sensitiveness of bacteria to agglutination,
as in the well-known experiments of Neufeld, that we must
recognize that much work is still to be done before we can properly
interpret the results of these agglutination tests.
Binding of Complement
Complement fixation tests were carried out by Odaira but his
results were much less satisfactory than those he obtained by
means of agglutination. Rapaport made an extensive study of
this test, using the sera of patients in various stages of convalescence.
Three hundred and fifteen convalescents showed 54.5
per cent. positive while 300 controls only gave 9.5 per cent.
positive results. Most of the positive cases were in patients
three to five days after their illness, but the reaction was found
in convalescents after from 1 to 45 days. Sera from acutely
ill patients at times showed negative or slightly positive reactions
but these same sera after keeping for some days and retesting
often gave strongly positive results. This would appear to be
a promising field for investigation.
Anaphylaxis
Hypersensitiveness was noted by W. F. Robertson in chronic
infections with B. influenzæ. Wollacott in a letter to the British
198Medical Journal suggested that the severity of the recent outbreak
of influenza may possibly be due to the development of a
state of anaphylaxis. There would seem to be at least some
evidence in favor of such a view in the fact that the severe outbreak
was preceded by epidemics of a milder form of influenza
and that the influenza bacillus was probably widely spread during
this time. Greenwood, as quoted above, noted that primary cases
always precede the mass attack. Of course, the term anaphylaxis
has been used to explain almost everything. Nevertheless,
the theory is interesting. The skin tests which we did for hypersensitiveness
were, as I have noted above, negative but there is
a possibility that the failure of the reaction may indicate a higher
resistance or even an antitoxin, now that the bacillus can be
classed as a toxicogenic one. Anti-influenza sera have been produced
by a few investigators (Latapie, Wollstein) but have not
found any practical application during this pandemic. Vaccination
is discussed elsewhere in these studies.
Experiments on the Human
There has never been in the history of medicine so many experiments
on human beings as have been carried out in the
attempts to discover the etiological factor in the recent pandemic
of influenza. Davis has called attention to a successful human
inoculation with pure cultures of B. influenzæ which he performed
in 1906. During the present investigation at least 200 men have
volunteered as experimental subjects, and the results of many
different methods of attempting to transmit the disease, have
been disappointing and inconclusive. I will not attempt to
review the reports at present available, as a great deal of the
work done has not yet appeared in print. The important point
is that the results do not affect the various views held as to
the causative agent in pandemic influenza nor the massive evidence
for transmission of the disease under natural epidemic
conditions.
It is my opinion, as expressed above, that practically all of
the population are rapidly infected during such a pandemic as
we have had. The resistant have escaped, and it would appear
to be very difficult to break down this resistance. The human
experiment carried out by Pettenkofer on himself and his assistant
199with vibrion choleræ is an example, but we have numerous
others demonstrating the same kind of phenomena in most of
our diseases of established bacterial origin. In diphtheria we
have an explanation in the varying antitoxic content of the sera,
but we really know very little of what are the actual factors in
preventing or determining infection among exposed individuals
in the natural history of most diseases. The reports of Leonard
Hill and Gregor are well worth reading in this connection, as
well as the editorial in the same number of the British Medical
Journal. We are not in a position to be very dogmatic on the
causes of epidemics. The mere presence of the bacteria or any
other living virus is not in itself sufficient to explain the phenomenon,
and one of the chief objects of this paper is to indicate
from the collected facts, that in the words of Flexner, “the case
against the influenza bacillus is not proved.”
Conclusions
1. B. influenzæ is one of a group of hemophilic bacteria and
there are probably strains of this organism which may be differentiated
which will lead to further subdivisions of the group.
2. B. influenzæ as we understand it today, is distinguished
by its morphological and staining characters; its requiring hemoglobin
in some form for its development; its showing symbiotic
reactions with other bacteria which stimulate its growth; the
production of a toxine and its usual low pathogenicity for
animals.
3. The media found most favorable for its growth are those
containing blood with the hemoglobin content altered in certain
ways, (1) by heating, (2) the addition of various chemicals,
(3) by the action of other bacteria or their products. The heated
blood agar I have found to be a most efficient and readily prepared
medium.
4. Since B. influenzæ is so difficult to isolate, it is necessary
to be very cautious in interpreting results unless the greatest
effort has been made to demonstrate the presence of this
organism.
5. B. influenzæ should be considered, from the evidence at
hand, as the bacterial causative agent in epidemic influenza, and
it should be recognized that secondary infections following the
200primary attack by this organism are both frequent and important.
This view I believe the logical one, unless much more
convincing evidence than we have today may demonstrate
another more probable living virus as the cause.
6. B. influenzæ is a frequent etiological factor in purulent
and chronic bronchitis, broncho-pneumonia and other acute and
chronic respiratory infections, in meningitis, endocarditis, sinusitis,
conjunctivitis and other conditions, as well as in complications
of many other diseases.
7. There are many carriers of the bacillus among our population,
both in apparently normal individuals and in those suffering
from chronic infections of bronchi, sinuses or other parts.
8. The problem of what constitutes resistance or susceptibility
to this infection are as far from solution as they are in
most other respiratory diseases, and the attempts to explain the
reasons for epidemics have been as futile as they are for meningitis
and many other respiratory epidemics.
9. It would not appear that the immunological reaction
against this infection has been discovered, but the possibility
of its being of an antitoxic nature opens an interesting field for
investigation.
BIBLIOGRAPHY
| Abrahams, Hallows and French |
Lancet., 1919; i, p. 1. |
| Abrahams, Hallows, Eyre and French |
Lancet., 1917; ii, p. 377. |
| Abstract of Foreign Literature on Influenza |
Jour. A. M. A., 1918; lxxi, p. 1573. |
| Adrian |
Quoted by Tedesko, q. v. |
| Allen |
Lancet., 1910; i, p. 1263. |
| Averill, Young and Griffiths |
British Med. Jour., 1918; ii, p. 111. |
| Avery |
Jour. A. M. A., 1918; lxxi, p. 2050. |
| Babes |
Deutsch. Med. Wochen., 1892; xviii, p. 113. |
| Batten |
Lancet., 1910; i, p. 16. |
| Basile |
Baumgarten Jahresb., 1907; xxiii., p. 284. |
| Beall |
Jour. A. M. A., 1906; xlvi, p. 1442. |
| Bernstein and Loewe |
Jour. Infect. Dis., 1919; xxiv, p. 78. |
| Besancon and Griffon |
Quoted by Scheller, q. v. |
| Besson |
Text-book, translated by Hutchens, 1913. |
| Blanton and Irons |
Jour. A. M. A., 1918; lxxi, p. 1988. |
| Boggs |
Amer. Jour. Med. Sci., 1905; cxxx, p. 902. |
| Brem, Bolling and Casper |
Jour. A. M. A., 1918; lxxi, p. 2138. |
| 201Brentz and Frye |
Woman’s Med. Jour., 1908; xviii, p. 73. |
| Brown and Orcutt |
Jour. Exper. Med., 1918; xxviii, p. 659. |
| Bruschettini |
Cent. f. Bakt. Abt. i., 1892; xi, p. 412. |
| Bruschettini |
Cent. f. Bakt. Abt. i., 1892; xii, p. 34. |
| Bruschettini |
Cent. f. Bakt. Abt. i., 1893; xiv, p. 253. |
| Bujivid |
Cent. f. Bakt. Abt. i., 1893; xiii, p. 554. |
| Canon |
Die Bakteriologie des Blutes bei Infektionskrankheiten Jena, 1905. |
| Canon |
Deutsch. Med. Wochen., 1892; xviii, p. 28. |
| Cantani |
Zeit. f. Hyg., 1896; xxiii, p. 265. |
| Cantani |
Cent. f. Bakt. Abt. i., 1897; xxii, p. 601. |
| Cantani |
Cent. f. Bakt. Abt. i., 1900; xxviii, p. 743. |
| Cantani |
Zeit. f. Hyg., 1901; xxxvi, p. 29. |
| Cantani |
Cent. f. Bakt. Abt. i., Orig., 1902; xxxii, p. 692. |
| Cantani |
Zeit. f. Hyg., 1903; xlii, p. 505. |
| Capaldi |
Cent. f. Bakt. Abt. i., 1896; xx, p. 800. |
| Clemens |
Munchen. Med. Wochen., 1900; p. 925. |
| Cohen |
Annales de l’Instit. Pasteur., 1909; xxiii, p. 273. |
| Cohen and Fitzgerald |
Cent. f. Bakt. Abt. i., Orig., 1910; lvi, p. 464. |
| Cohn |
Arch. f. Gyn., 1907; lxxxii, p. 695. |
| Cohn |
Cent. f. Bakt. Abt. i., ref., 1906; xxxviii, p. 23. |
| Cole and MacCallum |
Jour. A. M. A., 1918; lxx, p. 1146. |
| Cornil and Chantemesse |
Cent. f. Bakt. Abt., i., 1893; xiii, p. 489. |
| Couret and Herbert |
Report at meeting of Amer. Assoc. Path. and Bact., 1919. |
| Coutant |
Jour. A. M. A., 1918; lxxi, p. 1566. |
| Davis, D. J. |
Jour. Infect. Dis., 1907; iv, p. 73. |
| Davis, D. J. |
Arch. Int. Med., 1908; ii, p. 124. |
| Davis, D. J. |
Jour. Infect. Dis., 1910; vii, p. 599. |
| Davis, D. J. |
Amer. Jour. Dis. Child., 1911; i, p. 249. |
| Davis, D. J. |
Jour. A. M. A., 1915; lxiv, 1814. |
| Davis, D. J. |
Jour. Infect. Dis., 1917; xxi, p. 392. |
| Delius and Kolle |
Zeit. f. Hyg., 1897; xxiv, p. 327. |
| Dever, Boles and Case |
Jour. A. M. A., 1919; lxxii, p. 265. |
| Dick, G. F. |
Jour. A. M. A., 1918; lxx, p. 1529. |
| Dick, G. H. and Murray |
Jour. A. M. A., 1918; lxxi, p. 1568. |
| Dujarric de la Riviere |
Jour. Med. Res., 1918; xxxix, p. 39, review. |
| Dunn |
Jour. A. M. A., 1919; lxxi, p. 2128. |
| Ecker |
Jour. A. M. A., 1918; lxxi, p. 1482. |
| Ely, Lloyd, Hitchcock and Nickson |
Jour. A. M. A., 1919; lxxii, p. 24. |
| Eyre |
Jour. Path. and Bact., 1909; xiv, p. 160. |
| Eyre and Lowe |
Lancet., 1918; ii, p. 484. |
| Ferry |
Jour. Path. and Bact., 1915; xix, p. 488. |
| Fichtner |
Cent. f. Bakt. Abt., i, Orig., 1904; xxxv, p. 374. |
| Fichtner |
Baumgarten’s Jahresb., 1906; xxii, p. 207. |
| Finkler |
Cent. f. Bakt. Abt., i, 1896; xx, p. 807. |
| Fleming, A. |
Lancet., 1919; i, p. 138. |
| 202Fleming, J. S. |
Jour. A. M. A., 1918; lxxi, p. 2137. |
| Fraenkel |
Quoted by Howard, q. v. |
| Friedberger |
Cent. f. Bakt. Abt., i, Orig., 1903; xxxiii, p. 401. |
| Friedlander, McCord, Sladen and Wheeler |
Jour. A. M. A., 1918; lxxi, p. 1652. |
| Ghedini and Breccia |
Cent. f. Bakt. Abt., i, Ref., 1911; lvii, p. 567. |
| Ghedini and Fedeli |
Cent. f. Bakt. Abt., i, Ref., 1910; xlvii, p. 358. |
| Ghedini |
Baumgarten’s Jahresb., 1906; xxii, p. 207. |
| Ghedini |
Cent. f. Bakt. Abt., i, Orig., 1907; xliii, p. 407. |
| Ghon and Preyss |
Cent. f. Bakt. Abt., i, Orig., 1902; xxxii, p. 90. |
| Ghon and Preyss |
Cent. f. Bakt. Abt., i, Orig., 1904; xxxv, p. 531. |
| Giani and Picchi |
Cent. f. Bakt. Abt., i, Ref., 1906; xxxvii, p. 239. |
| Gioelli |
Cent. f. Bakt. Abt., i, 1898; xxii, p. 853. |
| Goodpasture |
Jour. A. M. A., 1919; lxxii, p. 724. |
| Gotch and Wittingham |
British Med. Jour., 1918; ii, p. 82. |
| Grassberger |
Zeit. f. Hyg., 1897; xxv, p. 453. |
| Grassberger |
Cent. f. Bakt. Abt., i, 1898; xxiii, p. 353. |
| Greenwood |
British Med. Jour., 1918; ii, p. 563. |
| Gregor |
British Med. Jour., 1919; i, p. 242. |
| Guiral |
Reviewed Jour. A. M. A., 1919; lxxii, p. 80. |
| Guizzetti |
Reviewed Jour. A. M. A., 1919; lxxii, p. 1111. |
| Hammond, Rowland and Shore |
Lancet., 1917; ii, p. 41. |
| Harris |
Lancet., 1918; ii, p. 877. |
| Heyrovsky |
Wien, Klin. Woch., 1904; xvii, p. 644. |
| Hicks and Gray |
Lancet., 1919; i, p. 419. |
| Hill, Leonard |
British Med. Jour., 1919; i, p. 238. |
| Holman |
Jour. Infect. Dis., 1914; xv, p. 293. |
| Holman |
Jour. Med. Res., 1916; xxxv, p. 151. |
| Horder |
Lancet., 1918; ii, p. 871. |
| Horder |
36th An. Rep. Loc. Govt. Bd., 1906; p. 279. |
| Howard and Ingersoll |
Amer. Jour. Med. Sci., 1898; cxv, p. 520. |
| Huntoon |
Report at meeting of Amer. Assoc. Path. and Bact., 1919. |
| Hurley |
Letter. Boston Med. Surg. Jour., 1918; clxxix, p. 691. |
| Huyghe |
Quoted by Scheller, q. v. |
| Influenza Committee Advis. Bd. to the D. G. M. S. |
British Med. Jour., 1918; ii, p. 509. |
| Jacobsohn |
C. r. Soc. Biol., 1901; xix, p. 553. |
| Jehle |
Quoted by Madison, q. v. |
| Jochmann |
Cent. f. Bakt. Abt. i, Ref., 1906; xxxviii, p. 661, and quoted by Scheller, q. v. |
| Jordan |
Jour. A. M. A., 1919; lxxii, p. 1542. |
| Keegan |
Jour. A. M. A., 1918; lxxi, p. 1051. |
| Keeton and Cushman |
Jour. A. M. A., 1918; lxxi, p. 1962. |
| Kinsella |
Jour. A. M. A., 1919; lxxii, p. 717. |
| Kitasato |
Deutsch. Med. Wochen., 1892; xviii, p. 28. |
| 203Klein |
British Med. Jour., 1892; p. 170. |
| Klieneberger |
Quoted by Scheller, q. v. |
| Koch |
Quoted by Davis, 1915; q. v. |
| Kossel |
Quoted by Ritchie, q. v. |
| Kotz |
Jour. Lab. Clin. Med., 1919; iv, p. 424. |
| Krage |
Baumgarten’s Jahresb., 1910; xxvi, p. 1063. |
| Kraus |
Jour. A. M. A., 1919; lxxii, p. 292. Medical News. |
| Kretz |
Cent. f. Bakt. Abt., i, 1898; xxiii, p. 24. |
| Krumbhaar |
Lancet., 1918; ii, p. 123. |
| Lacy |
Jour. Lab. and Clin. Med., 1918; iv, p. 55. |
| Lamb and Brannin |
Jour. A. M. A., 1919; lxxii, p. 1056. |
| Latapie |
C. r. Soc. Biol., 1904; lv, p. 1272. |
| Latapie |
Jour. Med. Res., 1918; xxxix, review. |
| Levinthal |
Zeit. f. Hyg., 1918; lxxxvi, p. 1. |
| Libman |
Trans. Assoc. Amer. Phys., 1912; xxvii, p. 157. |
| Lindenthal |
Wien. Klin. Wochen., 1897; x, p. 353. |
| Little, Garofalo and Williams |
Lancet., 1912; ii, p. 34. |
| Longo |
Baumgarten’s Jahresb., 1908; xxiv, p. 660. |
| Lord |
Boston Med. and Surg. Jour., 1902; cxlvii, p. 662. |
| Lord |
Boston Med. and Surg. Jour., 1905; clii, pp. 537 and 574. |
| Lord |
Jour. Med. Res., 1908; xix, p. 295. |
| Lord, Scott and Nye |
Jour. A. M. A., 1919; lxxii, p. 188. |
| Luerssen |
Cent. f. Bakt. Abt., i, Orig., 1904; xxv, p. 434. |
| MacCallum |
Monog. of Rockefeller Instit. for Med. Res., 1919; No. 10. |
| Macdonald and Lyth |
British Med. Jour., 1918; ii, p. 488. |
| Macdonald, Ritchie, Fox and White |
British Med. Jour., 1918; ii, p. 481. |
| Madison |
Amer. Jour. Med. Sci., 1910; cxxxix, p. 527. |
| Madison |
Jour. A. M. A., 1910; lv, p. 477. |
| Mann, Rainaford and Warren |
Med. Surg. Rep. of Roosevelt Hosp., 1915. |
| Martin, C. J. . |
British Med. Jour., 1918; ii, p. 281. |
| Matthews |
Lancet., 1918; ii, p. 104. |
| Medalia |
Boston Med. Surg. Jour., 1919; clxxx, p. 323. |
| Menko |
Quoted by Scheller. |
| Menschikow |
Cent. f. Bakt. Abt., i, Ref., 1906; xxxvii, p. 490. |
| Meunier |
Cent. f. Bakt. Abt., i, 1897; xxi, p. 689. |
| Meunier |
La Sam. Med., 1898. Quoted by Lord and Scheller, q. v. |
| Minaker and Irvine |
Jour. A. M. A., 1919; lxxii, p. 847. |
| Mix |
New York Med. Jour., 1918; cviii, p. 709. |
| Moon |
Quoted by Davis, 1915; q. v. |
| Moszkowski |
Cent. f. Bakt. Abt., i, Ref., 1902; xxxii, p. 272. |
| Munro |
British Med. Jour., 1919; i, p. 338. |
| Muir and Wilson |
British Med. Jour., 1919; i, p. 3. |
| McMeekin |
Reviewed Jour. A. M. A., 1919; lxxii. |
| 204McPhedran |
Canadian Med. Assoc. Jour., 1913; iii, p. 548 |
| Nastjukoff |
Cent. f. Bakt. Abt., i, 1895; xvii, p. 492. |
| Nichols and Stimmel |
Jour. A. M. A., 1919; lxxii, p. 174. |
| Norris and Pappenheimer |
Jour. Exper. Med., 1905; vii, p. 450. |
| Nuzum, Pilot, Stangl and Bonar |
Jour. A. M. A., 1918; lxxi, p. 1562. |
| Odaira |
Cent. f. Bakt. Abt., i, Orig., 1911; lxi, p. 289. |
| Oertel |
Canadian Med. Surg. Jour., 1919; ix, p. 339. |
| Opie, Freeman, Blake, Small and Rivers |
Jour. A. M. A., 1919; lxxii, pp. 108 and 556. |
| Orticoni and Barbie |
Reviewed Jour. A. M. A., 1919; lxxii, p. 228. |
| Orticoni, Barbie and Leclerc |
New York Med. Jour., 1918; cviii, p. 730. |
| Paltauf |
Wien. Klin. Wochen., 1899; xii, p. 576. |
| Paranhos |
Cent. f. Bakt. Abt., i, Orig., 1909; l, p. 607. |
| Park |
Reported at Meeting of Amer. Assoc. Path. and Bact., 1919. |
| Parker |
Jour. A. M. A., 1919; lxxii, p. 476. |
| Patrick |
Lancet., 1919; i, p. 137. |
| Pfeiffer |
Deutsch. Med. Wochen., 1892; xviii, p. 28. |
| Pfeiffer |
Zeit. f. Hyg., 1893; xiii, p. 357. |
| Pfeiffer and Beck |
Deutsch. Med. Wochen., 1893; xviii, p. 465. |
| Pieliche |
Berl. Klin. Wochen., 1894; xxxi, p. 534. |
| Poliak |
Wien. Klin. Wochen., 1908; xxi, p. 973. |
| Pritchett and Stillman |
Jour. Exper. Med., 1919; xxix, p. 259. |
| Rapaport |
Jour. A. M. A., 1919; lxxii, p. 633. |
| Richards and Gurd |
Montreal Med. Jour., 1907; xxxv, p. 541. |
| Richter |
Cent. f. Bakt. Abt., i, 1894; xxxi, p. 832. |
| Ritchie |
Jour. Path. and Bact., 1911; xiv, p. 615. |
| Rivers |
Bull. Johns Hopkins Hosp., 1919; xxx, p. 129. |
| Robertson, H. E. |
Jour. A. M. A., 1918; lxx, p. 1533. |
| Robertson, W. F. |
British Med. Jour., 1918; ii, p. 680. |
| Rosenow |
Jour. A. M. A., 1919; lxxii, p. 1604. |
| Rosenthal |
These. Paris., 1900. |
| Rucker and Wenner |
New York Med. Jour., 1918; cviii, p. 1066. |
| Saathoff |
Munch. Med. Wochen., 1907; p. 2220. |
| Sacquepee |
Paris Med., 1913; xxxv, p. 208. |
| Sahli |
Reviewed Jour. A. M. A., 1919; lxxii, pp. 686 and 111. |
| Scheller |
Cent. f. Bakt. Abt., i, Orig., 1909; l, p. 503. |
| Scheller |
Kolle and Wassermann, 1912; v, p. 1257. |
| Schlagenhaufer |
Quoted by Scheller, q. v. |
| Schofield and Cynn |
Jour. A. M. A., 1919; lxxii, p. 981. |
| Schultes |
Quoted by Scheller, q. v. |
| Slatineanu |
C. r. Soc. Biol., 1901; xxix, p. 850. |
| Slatineanu |
Cent. f. Bakt. Abt., i, Orig., 1906; xli, p. 185. |
| Slawyk |
Zeit. f. Hyg., 1899; xxxii, p. 443. |
| Smith, F. J. |
Lancet., 1908; i, p. 1201. |
| Smith, W. H. |
Jour. Boston Soc. Med. Sci., 1899; iii, p. 274. |
| 205Smith, Theobald |
Jour. Med. Res., 1913; xxix, p. 291. |
| Soper |
Jour. A. M. A., 1918; lxxi, p. 1899. |
| Soper |
Jour. Lab. Clin. Med., 1918; iii, pp. 560-567. |
| Spat |
Berl. Klin. Wochen., 1907; xliv, p. 1173. |
| Spooner, Scott and Heath |
Jour. A. M. A., 1919; lxxii, p. 155. |
| Stone and Swif |
Jour. A. M. A., 1919; lxxii, p. 487. |
| Strause and Bloch |
Jour. A. M. A., 1918; lxxi, p. 1568. |
| Susswein |
Wien. Klin. Wochen., 1901; xiv, p. 1149. |
| Synnott and Clark |
Jour. A. M. A., 1918; lxxi, p. 1816. |
| Tedesko |
Cent. f. Bakt. Abt., i, Orig., 1907; xliii, pp. 322, 432, 548. |
| Thalhimer |
Bull. Johns Hopkins Hosp., 1911; xxii, p. 293. |
| Thalhimer |
Cent. f. Bakt. Abt., i, Orig., 1914; lxxiv, p. 189. |
| Thursfield |
Quart. Jour. Med., 1910; iv, p. 7. |
| Tunnicliff |
Jour. A. M. A., 1918; lxxi, p. 1733. |
| Tunnicliff and Davis |
Jour. Infect. Dis., 1907; iv, p. 66. |
| Vagede |
Baumgarten’s Jahresb., 1903; xix, p. 244. |
| Voges |
Berl. Klin. Wochen., 1894; xxxi, p. 868. |
| Weil |
Cent. f. Bakt. Abt., i, Ref., 1910; xlvii, p. 359. |
| Wittingham and Sims |
Lancet., 1918; ii, p. 865. |
| Wolbach |
Bull. Johns Hopkins Hosp., 1919; xxx, p. 104. |
| Wollstein |
Jour. Exper. Med., 1906; viii, p. 681. |
| Wollstein |
Jour. Exper. Med., 1911; xiv, p. 73. |
| Wollstein |
Jour. Exper. Med., 1915; xxii, p. 445. |
| Wollstein and Goldbloom |
Amer. Jour. Dis. Child., 1919; xvii, p. 165. |
| Woollacott |
British Med. Jour., 1918; ii, p. 530. |
| Wright, J. H. |
Boston Med. Surg. Jour., 1905; clii, p. 496. |
| Wynekoop |
Jour. A. M. A., 1903; xl, p. 574. |
207
THE PATHOLOGY OF EPIDEMIC INFLUENZA
By Oskar Klotz, M. D., C. M.
The discussion to be entered into in this report will be limited
to an experience dealing with epidemic influenza as it was met
with in the emergency Military Hospital in Pittsburgh. We
shall largely confine our attention to the observations which
came directly under our supervision, and in as much as this
investigation was continued during the epidemic as it swept
over this district, the intensive study was limited to a time period
of about five weeks. During this period much material was
collected, which since then, has taken us a considerable time to
analyze. We have thought it more valuable to restrict our discussion
to this material in that it illustrates the pathological
lesions as they occurred during the acute stage of the disease.
We have not entered upon a discussion of the sequelæ or the
chronic lesions which are not uncommonly found following in the
wake of an acute epidemic nor do we deal with the lesions arising
in cases of sporadic influenza, such as are always with us. As
is so well illustrated in the literature, there is probably no disease
which has so many late complications and sequelæ as influenza.
The investigations upon the protean lesions have been fully reported
in numerous papers during the intervals between epidemics.
A comprehensive bibliography upon influenza will be
found at the end of the extensive report by Leichtenstern (1905).
There is very much less accurate information available upon the
actual lesions present during the acute disease when present in
epidemic or pandemic form, than upon the many clinical complications
in various systems and organs. In fact, our knowledge
of the pathology of influenza lies more largely in the field of
associated lesions such as the late events in the bronchi, the
sinuses of the head, abscesses, meningitis and other conditions,
rather to be viewed as complications than as portions of the
disease. There are relatively few thorough pathological analyses
of the influenza lesions as they are found in the acute epidemic
disease.
208A fair literature has already appeared upon epidemic influenza
from the many countries and regions over which the present
pandemic (1918) has swept. These reports by various authors
are offered from different viewpoints, some investigators being
impressed with certain features which they bring into marked
prominence in their reports. It thus happens that up to the
present there is a decided lack of uniformity in the opinions
expressed upon different phases of the subject. The nature of
the pathology of the past epidemic has given rise to many expressions
of opinion as well as dogmatic statements, which are found
to differ from those of others. It seems to us that this apparent
confusion arises partly through the somewhat different characteristics
of the disease as it has made its appearance in different
centers. We hear it repeatedly stated that the types found
in different military camps and urban communities were quite
unlike those of other regions. It is evident that such differences
in the clinical course actually did exist and that the epidemic
though having a common foundation upon which the disease process
was built differed in what might be looked upon as symbiotic
complications during the early and acute stages. Differences in
the nature of the findings in various communities also probably
lay in the fact that the bacterial flora associated with the causative
agent of influenza was quite different in different regions.
We mention this here so that a full appreciation will be obtained
for the differences in the pathological characters of the disease
as they are found in one region or another. We appreciate, of
course, that if the concomitant bacterial flora associated with the
underlying cause of influenza, differs in different regions, so, too,
will the bodily reactions differ within certain degrees. We are
becoming more familiar with different types of bacteria, and the
resulting inflammatory reaction which is often unique or at least
particular, and that not uncommonly the nature of the inflammatory
process suggests the type of bacterium involved. This
argument, of course, must not be driven too far, for we well
know that the same micro-organisms under different conditions
can cause types of inflammatory reactions wholly divergent.
In as much as our observations are confined to a particular
group of cases and the study of these was undertaken during
the five weeks of the acute epidemic, these results are not to be
compared with the collected statistics on influenza as they shall
209be made over a period beginning with the onset of the epidemic
and ending with the last vestiges remaining after months or it
may be years of time. Our observations are to be considered
only in the light of the events taking place during the height of
an epidemic wave. In as much as influenza presents itself
during an epidemic in different forms, we shall again mainly
limit the report upon our investigations of those cases having
respiratory lesions. Our acute observations were made upon
the tissues of those who had died of this disease. It is impossible,
or nearly so, to fully study the tissues of those with lesser
lesions and who recover. Hence, if we divide the influenza cases
into those (1) without pulmonary lesions and (2) those with
pulmonary lesions, we must state that all of our cases coming
to autopsy fall in the second group. It is true that one of these
having pulmonary lesions was not brought to his fatal termination
by them but by a septicæmia arising in the middle ear. He
had distinct lesions in his lungs. In other words, our autopsy
material represents epidemic influenza in which the lung was
definitely involved in an inflammatory state. In all but one of
these the pulmonary lesion was the cause of death.
No doubt, if opportunity had presented itself to follow a large
epidemic through months of its progress, during which late complications
in various portions of the body would make their
appearance, our analysis would give a different picture and the
pulmonary factor for the fatal termination would not be in such
prominence.
Of the first group, those cases of epidemic influenza not showing
pulmonary lesions, we will have very little to say, in as much
as the pathological investigations of them is impossible, or nearly
so, during the height of the disease.
Such cases apparently do not die at this period. I am willing
to admit that individuals without pulmonary involvement may
succumb, but I question whether their death has been due to
the result of the influenzal lesions, be it in nose, pharynx, larynx
or trachea, or be it in the intestine, but rather that the fatal
termination occurred later in the course of this complex disease,
when distant vital organs became involved or incapacitated in a
toxemia or secondary bacterial invasion. We must clearly distinguish
these cases from the clear-cut ones of epidemic influenza,
looking upon the new circumstances as complications aside from
210the original disease. Such, for example, is the case we have
mentioned where a fatal streptococcus bacteriæmia followed in
the wake of an otitis media. In our experience we have not had
a fatal case of the acute epidemic disease in which the lung was
not involved.
In types of epidemic disease such as we have just had, where
the epidemic wave has passed over in a period of four or five
weeks, there is always much to be regretted which has been left
undone. We tried as far as possible to gain all the information
available at the time of collecting our materials and of laying
aside such of the work which could be accomplished at a subsequent
date. The materials were collected from divergent sources
in the cadaver, and the more perishable substances were analyzed
immediately. During the period of the epidemic 32 autopsies
were performed and as much use as possible was made of each
for a thorough comprehension of the lesions.
Materials
During the period of our work 639 patients were admitted to
the hospital suffering from clinical influenza. The cases varied
in type from the very mild to the extremely ill. The majority
of the cases were of the type of “three-day fever.” Clinically
81 cases developed pneumonia, and of these, 35 died. It would,
of course, be impossible to say how many other individuals had
a pulmonary involvement which could not be recognized clinically.
In fact, some of the cases which did come to autopsy were only
recognized as having a pulmonary involvement when the lungs
were examined outside of the body. The physicians freely admitted
that the physical signs were quite unusual and unlike those
of the ordinary forms of pneumonia. In fact, except for the
fact that we were living in the midst of an epidemic of respiratory
infections, there was nothing to make the clinician suspect
that many of these cases had a pulmonary involvement.
Obviously, when the recognized signs of different types of pneumonia
made their appearance, the clinician did not fail to make
proper interpretation of the lung involvement. This, as we shall
discuss later, is an event superadded to a lung condition which
pathologically must be recognized as pneumonia (inflammation)
and which differs so decidedly from what we know of as croupous
or lobar pneumonia, as well as ordinary broncho-pneumonia that
211it would be incorrect to include them under this heading, although
the distribution of the lesion may have lobar, bronchial or lobular
characters.
| Date 1918 |
Patients Admitted |
Patients Discharged |
Cases in Hospital |
Deaths |
| October |
5 |
65 |
0 |
65 |
0 |
| 〃 |
6 |
23 |
0 |
88 |
0 |
| 〃 |
7 |
61 |
0 |
149 |
0 |
| 〃 |
8 |
77 |
0 |
225 |
1 |
| 〃 |
9 |
42 |
1 |
266 |
0 |
| 〃 |
10 |
35 |
1 |
300 |
0 |
| 〃 |
11 |
9 |
0 |
307 |
2 |
| 〃 |
12 |
2 |
16 |
290 |
3 |
| 〃 |
13 |
10 |
0 |
298 |
2 |
| 〃 |
14 |
1 |
18 |
278 |
3 |
| 〃 |
15 |
4 |
13 |
266 |
3 |
| 〃 |
16 |
9 |
23 |
248 |
4 |
| 〃 |
17 |
10 |
19 |
235 |
4 |
| 〃 |
18 |
16 |
34 |
217 |
0 |
| 〃 |
19 |
38 |
29 |
225 |
1 |
| 〃 |
20 |
27 |
0 |
252 |
0 |
| 〃 |
21 |
37 |
43 |
245 |
1 |
| 〃 |
22 |
33 |
7 |
270 |
0 |
| 〃 |
23 |
14 |
20 |
263 |
2 |
| 〃 |
24 |
20 |
17 |
266 |
0 |
| 〃 |
25 |
27 |
21 |
272 |
0 |
| 〃 |
26 |
10 |
29 |
250 |
0 |
| 〃 |
27 |
18 |
3 |
265 |
1 |
| 〃 |
28 |
10 |
31 |
243 |
3 |
| 〃 |
29 |
6 |
16 |
231 |
0 |
| 〃 |
30 |
11 |
27 |
215 |
1 |
| 〃 |
31 |
2 |
15 |
202 |
2 |
| November |
1 |
2 |
18 |
185 |
0 |
| 〃 |
2 |
4 |
18 |
170 |
1 |
| 〃 |
3 |
5 |
1 |
174 |
0 |
| 〃 |
4 |
2 |
19 |
156 |
1 |
| 〃 |
5 |
5 |
0 |
161 |
0 |
| 〃 |
6 |
4 |
16 |
149 |
0 |
| |
|
|
|
|
|
| Admissions. |
639 |
|
|
35 |
The individuals admitted to this hospital were obtained from
the two military camps at the University of Pittsburgh and the
Carnegie School of Technology. All of them were enrolled in
212the army service and ranged from the ages of 18 to 30. They
were vigorous individuals, who had passed their physical examinations
for the army. The epidemic made its appearance in
these camps on October 2, rapidly ascending from a report of
two ill on October 2, four on October 3, eight on October 4, to
65 on October 5. On October 11 there were 307 cases in the
hospital.
Of these cases 35 died, the day of death being indicated in the
following table.
| Day of Disease on Which Death Occurred |
Number of Cases |
| Third |
1 |
| Fourth |
3 |
| Fifth |
4 |
| Sixth |
4 |
| Seventh |
4 |
| Eighth |
5 |
| Ninth |
3 |
| Tenth |
4 |
| Eleventh |
3 |
| Thirteenth |
1 |
| Fourteenth |
1 |
| Twentieth |
1 |
| Twenty-third |
1 |
The time as indicated in the above table has no relation to the
length of time that the patients were ill of pneumonia, but refer
to the period of illness from the beginning of the influenza. The
duration of the pneumonia is indicated in another table.
Of the 35 fatal cases 32 came to autopsy. Facilities were available
to do the work very satisfactorily, in that the hospital was
well provided with a modern post-mortem room and its accessories.
The notes on the autopsies were taken immediately and
fully, and the materials for subsequent study were collected in
different types of preserving fluid. Portions of tissue were collected
from all of the organs for microscopical study, while fluids
from the chest, lungs, bronchi and heart were obtained for bacteriological
investigations and for some chemical analyses.
Added to the above material we also had the opportunity of
reviewing and studying the lesions of 18 autopsies performed by
213Dr. J. W. McMeans. These cases were very similar to our own
series, in that they were cases of epidemic influenza amongst
soldiers who were being cared for at the St. Francis Hospital.
The disease processes were quite alike in the two series, and the
analyses made by Dr. McMeans are comparable in our own and
serve as a means of checking our results obtained in another
institution. The similarity of the lesions in the lungs and other
organs serve to indicate that what is reported in this paper is an
index of the nature of the lesions of epidemic influenza as it
occurred in the Pittsburgh district. In a few instances the
autopsies performed by Dr. McMeans revealed more advanced
pulmonary lesions with abscess and gangrene than were noted in
the cases autopsied at the Military Hospital. The process, however,
in the two series of autopsies was identical.
General External Features
There were no external characteristics of the bodies which
were autopsied by us which were constant. Some features were
more commonly present than others. Of these the cyanosis of
the face, head, neck and shoulders, and in a few instances of the
upper extremities, attracted our attention more than any other.
This cyanosis was present in over one-half of the number of
cases, and it was confined almost always to the upper part of
the body. The face, ears and neck were always more affected
than other parts. This cyanosis bore no relation to the length of
time after death when the body was viewed, as we found that
when it was present during life it maintained its prominent
appearance for a long time after death.
The cyanosis differed from the bright hue or flush as it is at
times observed in ordinary pneumonia, the color in these instances
being of a dark purple, or better a purplish blue. The
lips and ears showed the most intense color. The cyanosis was
not associated with any evidence of œdema. The capillaries of
the tissues were filled with blood which was of a very dark character.
Cyanosis could also be seen in the finger tips about the
nails. This was more marked in the upper extremities than in
the lower. The skin of the body rarely showed any cyanosis,
these tissues being quite pale, or at times showing a slightly
yellowish tinge. In one instance the cyanosis of the head and
214neck was accompanied by a slight purplish rash upon the upper
portion of the chest. This rash was of a petechial kind, there
being slight hemorrhage into the tissues. The lesion, however,
was not of the blotchy purpuric type which has been observed
by others during this and past epidemics (Cole). This single case
is the only one where we had evidence of superficial hemorrhages
into the skin.
| |
Cyanosis |
|
No Cyanosis |
| No. |
Degree |
Distribution |
|
| 741 |
+ |
Chest and upper extremities |
747 |
| 743 |
+ + |
Face, neck and ears |
748 |
| 744 |
+ + + |
Head and neck (upper portion of chest and thighs mottled and purple) |
749 |
| 745 |
+ + |
Head and neck and upper extremities |
751 |
| 746 |
+ + |
Ears, neck and shoulders |
752 |
| 750 |
+ + |
Face, ears and neck |
764 |
| 756 |
+ + |
Neck, jaw, shoulders and upper extremities |
765 |
| 757 |
+ |
Face, neck, shoulders, arms and chest |
778 |
| 758 |
+ + + |
Face, ears, neck and upper chest |
782 |
| 761 |
+ |
Face, ears, neck and upper chest |
784 |
| 762 |
+ |
Ears, neck and chest |
786 |
| 763 |
+ |
Head and neck |
793 |
| 767 |
+ |
Face, ears and neck |
|
| 773 |
+ + |
Neck, ears and cheeks, extending moderately to upper chest. Hemorrhage into conjunctiva |
|
| 781 |
+ + |
Eyes, lips, ears and neck |
|
| 783 |
+ + |
Face, lips, neck and fingers |
|
| 787 |
+ + + |
Ears, neck and shoulders |
|
| 791 |
+ + |
Ears, neck and upper chest |
|
| 792 |
+ + |
Ears and back of neck |
|
| 19 |
|
+ Blotchy or slight 6 |
12 or |
| or |
|
++ Moderate 10 |
38.6% |
| 61.4% |
|
+++ Well marked 3 |
|
| 770 |
|
Fine petechial rash over upper chest. |
|
Occasionally we met with small hemorrhages lying in the
upper layers of the subcutaneous tissue. These lesions were
small and could not be seen from the external surface. Nevertheless,
215some of them seemed to have occurred in direct contact
with the deep cutis and surrounded portions of the deep skin
appendages. From an examination of our cases there was no
reason at the time of autopsy to lay any particular stress upon
the occurrence of these hemorrhages. Subsequently, it has come
to mind, and since learning of the unusual frequency of boils and
deep pustules making their appearance as post-influenzal sequelæ,
that these minute lesions may have a bearing upon the localization
of infection in the skin tissues. We must appreciate, of
course, that other factors of a constitutional nature probably
render the individual more susceptible to the invasion of the
staphylococcus, and that such factors are all-important in allowing
this organism to gain a foothold. Whether the decreased
sugar-tolerance with hyperglycemia, which has been observed
in the late stages of influenza, bears a relation to the increased
susceptibility, as appears to be the case in diabetes mellitus, is an
interesting point for further investigation. Other constitutional
states are also undoubtedly involved in the increased susceptibility
to the infection which the patient suffers. Elsewhere
(Dr. Holman) it is shown that the natural complement content
is considerably depressed during the height of the influenza.
With such factors present and with the available infecting micro-organisms,
it is possible that the minute deep skin hemorrhages
bear a relation to the immediate localization of the infection.
In two instances slight hemorrhages were observed into the
conjunctival tissues. In each case they were unilateral and occupied
the tissues contiguous to the inner canthus. In one case
there was well-marked icterus with yellow coloration of the
scleræ and skin. In this case the icterus was associated with
degenerative changes in the liver, there being no recognizable
obstruction to the bile passages. The icterus had come on quite
acutely and without any special clinical manifestations. In the
epidemic of 1890 jaundice was present in a considerable number
of cases (Medical Record, 1890, xxxvii, 473). Cole made similar
observations in the epidemic of influenza amongst the Canadian
soldiers. Œdema of the skin was not met with in any of our
cases. This point is worthy of comment, inasmuch as some
authors have been impressed with the serious damage taking
place in the kidney and the resulting incapacity of these organs.
216Although, as we shall point out later, the kidney tissues in these
cases showed a decided toxic degeneration, there was no evidence
that a glomerular damage of serious degree ever occurred. The
urinary excretion, as is pointed out in a report by Dr. Zeedick,
varies considerably with the intensity of the disease. It is unusual
to find derangement of kidney function to a degree to reflect seriously
upon the general bodily state. At least this has been our
experience in the present epidemic. Even where subsequently
we were able to demonstrate a considerable tubular degeneration
in the cortex of the kidney the change in the kidney function
was not of sufficient magnitude to lead to a water-retention to
be recognized in an anasarca. I wish to distinguish clearly at
this point the difference in finding an œdema in certain involved
tissue structures in various parts of the body and arising through
an inflammatory reaction due to the presence of peculiar focal
irritation, as compared with the accumulation of fluid in many
and irregular situations as it occurs through retention and faulty
excretion by the kidneys. Various organs as we have found—as,
for instance, the lung, heart and liver—showed a condition of
œdema which was not to be reconciled with an inadequate circulation
because of a cardiac or renal incompetency. These œdemas,
which we will discuss later, are local and are the result of damaging
influences inducted in and upon the tissues where they are
found.
Muscle
In all of our cases we have been struck with the excellent
physique of the individuals succumbing to this epidemic. All
were youths in the best of health, of good muscular build and
strong bony frame-work. Post-mortem rigidity set in fairly
rapidly after death. Where this rigidity had “set” for six or
more hours it required much force to change the position of the
muscles. The voluntary muscles of the thorax and abdomen were
always carefully observed, and in a number of instances the
muscles of the thigh were also examined. It was not possible
routinely to dissect the muscles of the extremities, so that we
are unable to give an accurate account of the occurrence of
degenerations in these structures. We have, however, observed
the reactions taking place in the pectorals, psoas and muscles of
217the abdominal parietes. Changes were observed with greatest
frequency in the recti of the abdomen. Degeneration occurred in
these muscles in 14 instances, while the same tissues suffered
rupture, in part or completely with hemorrhage, in six instances.
It was not uncommon to find marked degeneration in the lower
segment of the rectus muscle on one side, while degeneration
and hemorrhage had occurred in its fellow on the opposite side.
In four cases rupture of the entire belly of the muscle had taken
place, so that a considerable space had occurred between the
broken ends and a large clot of blood filled the intervening space.
This degeneration, which was seen only in the voluntary muscles,
was quite interesting and in its milder degrees was rather difficult
to detect. All gradations of loss of muscle color were seen. In
some instances the muscle simply seemed to have lost its meaty
lustre, while again in the more severe instances the muscle color
had changed from the bright red to an insipid yellow or clay
color. The most marked degeneration occurred in the midportions,
while the ends of the muscle masses at the points of
attachment were less involved. Complete rupture of the rectus
always occurred in the lowermost segment, a short distance above
the insertion into the pubic bone. At times the distribution of
the degeneration within the muscle was quite patchy, and irregular
islands of yellow about 2 cm. in diameter were splashed
through the muscle masses, which in themselves were paler than
normal. Where the muscle degeneration was advanced the tissue
was soft and at times even buttery. It resembled the character
of the degeneration observed in typhoid fever, although I have
no recollection amongst many enteric cases of having seen the
degeneration of the muscle occur so acutely. Recklinghausen
claimed that these hemorrhages were most unusual in influenza.
This is contrary to our findings.
Degenerations of a similar kind as those of the abdominal recti
were found in both pectorals. In the chest region, however, the
degeneration was less frequent and less severe. We observed it
only twice, and in neither instance had the degeneration led to
a rupture and hemorrhage of the muscle bundles. Kuskow
observed a single case of degeneration and hemorrhage of the
pectoral muscles. In the psoas muscle we observed degeneration
on two occasions, in one of which the lesion was associated with
a partial separation of the muscle fibers and hemorrhages into
218its substance. In one case clinically, but not coming to autopsy,
a lesion, which from its character we presume to have been a
degeneration, occurred in the sterno-mastoid, being accompanied
by hemorrhage and the development of a firm clot the size of a
hazel nut. In the subsequent history of this case the lesion
passed through an aseptic process of organization with contracture
so that the patient has recently been developing a “wryneck.”
Kohts in 1890 reported the finding of muscle degeneration
and abscesses in the arm. The condition arose as a late complication
of influenza.
From our experience at the autopsy table in observing the
relative frequency with which muscle degeneration occurs in the
severe cases of epidemic influenza, we feel convinced that numerous
cases which recover pass undiagnosed of this condition.
Furthermore we have evidence, as illustrated in a case observed
by Dr. McMeans, wherein a lesion which occurred in the gluteal
muscles was followed by a localizing infection at this site that
these muscle degenerations and hemorrhages may have serious
consequences. There are a number of instances in which post-influenzal
complications of the nature of deep-seated abscesses of
the extremities, thorax, and abdomen may have their explanation
for the localization in a primary muscle damage accompanied by
hemorrhage and followed by an infection of variable type. Cole
also comments upon the development of abscess in the deep
muscles where degeneration had taken place. In illustrating
some of our findings to Dr. J. Anderson he immediately recognized
such a condition in the pectoral muscles of a patient in
which he was unable to arrive at a conclusion of the pathological
events which had taken place. It is one of the noteworthy features
in this disease that the voluntary muscles of certain
regions are apt to suffer severe damage, while the heart and the
various unstriped muscular tissues are little if at all affected by
a similar process. It would be interesting to know whether the
lack of response and the delayed functional recovery on the part
of the muscles of the extremities in so many patients who have
suffered influenza is the result of the damaging influence of a
peculiar intoxication present in this disease. One of the features
in influenza is the prostration of the patient, and with it there is
definite muscular weakness. We have been prone to lay the responsibility
of this state entirely at the door of the nervous
219tissues. Here, however, we are able to offer evidence that quite
aside from the lesions arising in the nervous tissue, there is definite
muscle damage which, as we shall again discuss when
describing the microscopic features, incapacitates even to the
point of complete destruction the muscle elements in various
fields of the body. Before, however, being able to state that the
muscular weakness of the extremities is the result of such damage
by toxins it is necessary to obtain more definite information
regarding the frequency with which these degenerations occur
in the limbs. In our own material we are unable to discuss the
matter with adequate figures. We are, however, impressed with
the changes observed in the muscles which were available to us.
Naturally, too, a certain number of muscle degenerations have
escaped our detection because of our unfamiliarity with the
mildest grades. In fact, we have already discovered in our
microscopic studies that certain cases, which in the macroscopic
had escaped us, showed well-marked lesions under the microscope.
TABLE IV
MUSCLE DEGENERATION
| Abdominal Recti |
Pectoral |
Psoas |
| Toxic Degeneration |
Hemorrhage Into Rectus |
Toxic Degeneration |
Toxic Degeneration |
| 745 on 10th day |
745 both on 10th day |
756 on 8th day |
756 on 8th day |
| 749 on 4th |
752 both on 13th |
770 on 11th |
792 on 6th |
| 752 on 13th |
756 both on 8th |
|
|
| 756 on 8th |
764 both on 9th |
|
|
| 757 on 6th |
765 both on 9th |
|
|
| 762 on 10th |
778 both on 23d |
|
|
| 763 on 11th |
|
|
|
| 764 on 9th |
Rupture of |
|
|
| 765 on 9th |
Rectus |
|
|
| 767 on 10th |
|
|
|
| 770 on 11th |
745 right on 10th day |
|
|
| 778 on 23d |
756 both on 8th day |
|
|
| 783 on 8th |
778 right on 23d day |
|
|
| 791 on 6th |
|
|
|
We have convinced ourselves that the marked hemorrhage
taking place in the muscle tissue follows upon a primary degeneration
of this tissue and its spontaneous rupture. The amount
220of hemorrhage is in proportion to the degeneration and fracture
of the muscle elements. The hemorrhage does not precede the
muscular change, nor does it have any antecedent relation to the
actual tearing of the muscle fibers.
A much better appreciation of the muscle degeneration was
obtained in the microscopic studies of these tissues. The various
gradations of tissue change could be followed, which was not
possible in the naked-eye examinations. Some points respecting
this degeneration were quite noteworthy. Firstly, the process of
degeneration in its early stages and advancing through the acute
destructive periods was not accompanied by any inflammatory
reaction. Evidence of inflammatory exudate was obtained only
when the degeneration had proceeded to a degree permitting of
rupture with hemorrhage, or in the late stages when the areas of
marked muscle dissolution were undergoing repair. We have no
evidence to indicate that bacteria were present during the beginning
of the degenerative process. Bacteria could not be demonstrated
in section. The appearance of the tissue suggested a
purely toxic process which was selective in its action, picking
out voluntary striped muscle tissue and attacking certain muscle
groups in preference to others. It was also interesting to observe
in the early stages of the degeneration that individual fibers lying
amidst healthy and unchanged muscle elements would show
degeneration in many of its stages. This appearance was often
unique, particularly when in the early stages of the process the
involved fiber would still retain its normal position and shape
though markedly altered in its staining and chemical qualities.
The degeneration as observed in these cases showed many of
the characters like that of waxy degeneration seen in typhoid
fever. Similar appearances to these have also been described in
connection with the toxic degenerations which occur in the
vicinity of infections by the gas bacillus. In fact, all the stages
observed in the one can be seen in the other. They differ,
however, only in the degree to which final destruction takes
place and in the speed with which the degeneration is accomplished.
The character of the degeneration is well studied
in sections stained with hematoxylin and eosin, eosin-methylene
blue, and best of all in the phosphotungstic acid hematoxylin.
By the latter method one is able to follow clearly the grade
of degeneration as it effects the muscle striations. On the
221other hand, the peculiar waxy appearance of the early degenerating
fibers is best seen in sections stained with eosin or
fuchsin, where the striated muscle fibers are found to be
changed to a more intensely staining red body of homogeneous
character and devoid of all evidence of their original internal
architecture. These bland waxy fibers were often of the size and
shape like the normal. On the other hand, the fibers are also
not uncommonly swollen, stretching the sarcolemma to almost the
bursting point. Following this primary bland degeneration the
fiber takes on irregular shapes, becoming constricted and collapsed
at irregular intervals, so that islands of the waxy contents lie
within the sarcolemma, being separated from each other by constricted
areas in which the original myoplasm has undergone decomposition
and sometimes complete absorption. This irregular
destruction of the muscle contents often has a granular stage in
which the original muscle substance has become disintegrated.
The sarcolemma follows the condition within it, stretching when
the fiber is swollen and shrinking, or even becoming collapsed when
the inner substance is becoming liquified and absorbed. The
sarcolemma does not suffer the degenerative changes of the inner
fiber, nor can one observe nuclear changes in this sheath which
are significant.
When first studying this process of degeneration it appeared
to us that the earliest change was a loss of the transverse striations
and the subsequent disappearance of the longitudinal
fibrillæ. We have subsequently found that this is incorrect and
that the changes observed in the markings of the fibers were not
constant. At times the muscle substance would progress through
stages of degeneration up to the point of disintegration and dissolution
while the transverse striæ were still discernible in the
altered fiber. The one constant change that we have observed in
the degenerating fibers was the early loss of staining qualities
as obtained by the phosphotungstic acid hematoxylin. In such
preparations the earliest effect of the intoxication upon the
muscle fiber was a change in reaction to this stain. Sometimes
within a given fiber small irregular and poorly staining blotches
could be observed, while the remaining portion of the fiber was
normal in its appearance. Later these poorly staining areas
became larger, occupying the entire width of the fiber and being
distributed at irregular intervals in its length. Finally the characteristic
222staining quality was entirely lost, although in the
poorly colored cell transverse striations were still discernible and
a true waxy stage had not yet taken place.
At times the waxy degeneration advanced into the stage of
disintegration by an irregular destruction within the fiber. When
this occurred the fragments of waxy substance took on curious
coiled and grotesque shapes, while a granular destruction was
taking place in their periphery. Neither inflammation, œdema
nor a vascular reaction could be determined in these tissues of
mild or severe change. The reaction as is indicated in the table
occurred quite acutely and was not accompanied by fatty products
commonly seen in the slower forms of degeneration.
Gradually the debris of the degenerated fibers is absorbed and
the sarcolemma shrinks and collapses upon itself. During this
stage a reaction occurs in the sarcolemma with nuclear proliferation.
At times the last vestiges of the muscle fiber are seen to
be surrounded by a crown of nuclei and cells reminding one of
the appearance of the degenerating nerve cells in the Gasserian
ganglion in hydrophobia. The involved area becomes active in
appearance, showing proliferation of fibroblasts and the appearance
of occasional lymphocytes and plasma cells. Scar tissue
continues to develop in proportion to the amount of damage done.
In areas where hemorrhage had taken place the amount of scar
tissue is exaggerated, owing to a process of organization which is
taking place quite apart from the muscle degeneration. Thus
not a few scars scattered through the voluntary striped muscles
are the final outcome of this toxic degeneration occurring in
epidemic influenza. Some of these lesions may account for the
indefinite pains and symptoms of which the patient complains
for so many months after his acute illness. I refer particularly
to lesions occurring in the psoas and muscles of the back as possible
explanations for the partial invaliding of some individuals.
In a certain number of cases of acute influenza the patients
complain of severe abdominal pain, in the absence of any localizing
symptoms or evidence of intestinal derangement. Such was
the case with a number of the above cases coming to autopsy,
and the sole evidence we could offer was muscle degeneration with
or without massive hemorrhage. The abdominal pains complained
of were more of the nature of dull aches with occasional exacerbations
and shooting or lancinating “stitches.” Rarely was the
223patient able to define the position of the pain, not being able to
state whether it was within the abdomen or in the parietes.
Most frequently they claimed it was internal. We have on no
occasion demonstrated an intra-abdominal lesion which could
account for such pains. None of our cases was of the type of
“intestinal influenza.” We are, therefore, led to the conclusion
that the muscle degenerations of the various degrees, from the
slight with few muscle elements involved to the severe with
rupture and hemorrhage, account for a proportion of the clinical
symptoms of (muscle) pains and aches as well as weakness.
We cannot claim that coughing was a necessary factor in inducing
rupture of the abdominal recti. In some of the cases with rupture
severe coughing had not been observed during the illness.
Upper Respiratory Tract
The pathological changes found in the nose, pharynx and
larynx were of relatively slight importance and most variable in
their severity and incidence. The majority of individuals had
few clinical manifestations of disease in these parts. Some, however,
complained of dryness of the pharynx with slight feeling
of fullness. An examination of these parts revealed some congestion,
varying from a red injected mucosa to a bluish cyanosis.
In the nose the reaction was rarely as acute as is seen in infectious
coryza, but even where relatively little change was to be
seen in the tissues hemorrhage from the erectile tissue was not
uncommon during the acute stages. No particular lesion was to
be found associated with nose bleed. There was an unusual
absence of excessive secretion from nose and pharynx in the
majority of cases. One was also struck with the infrequency
with which the larynx was involved. A certain number of individuals
complained of hoarseness, and in them injection of the
vocal cords with some swelling was found. In many others, however,
even where an intense infectious process was present in
the lower respiratory tract the larynx was almost without change.
It was from the level below the larynx that the acute reaction
in the respiratory system was found.
In all of our cases the trachea showed definite inflammatory
reaction. Of the 32 cases there were 26 having an acute tracheitis,
5 with an acute mucopurulent inflammation and 1 with a
224reaction in the subacute stage. In the majority of the cases with
acute tracheitis there was a thin layer of exudate lying upon the
mucosal surface. At times the trachea was filled with a frothy
serous fluid, the greater part of which had its origin in the lung.
Nevertheless, as we shall point out later, we did obtain microscopical
evidence indicating that during the early acute stage
of the tracheitis a considerable serous exudate escapes from its
mucosa. This serous inflammatory reaction is an important one
for all of the mucosal structures upon which the virus of influenza
obtains a footing. This we have found true for the trachea,
bronchi and alveoli of the lungs. In some cases the exudate
was grey and lay in close contact with the injected tissues. At
first sight this grey exudate suggested necrosis, but it was readily
wiped from the underlying structure. Some leucocytes and cell
debris with many bacteria made up the content of this grey
exudate.
The macroscopic appearance of the trachea was that of an
intensely injected structure which had largely lost its normal
lustre. The naked eye could distinguish that anatomical change
had occurred in the surface tissue of the trachea and that there
was unusual evidence of intensely injected vessels lying in the
submucosa. In only one instance was there an appearance of a
true necrotic membrane lying upon the surface of this intensely
inflamed layer. This apparent membrane was found to consist
of a wide patch of desquamated epithelial cells which was lying
as a delicate necrotic plate upon the surface. This thin layer
was devoid of a meshwork of fibrin threads as usually accompanies
a true false membrane of other sources.
The early intense inflammatory reaction of the surface membrane
of the trachea was characteristic, and in our experience
was never exceeded in intensity by other infections. A desquamation
of the lining membrane was also a common finding.
Naturally this intense reaction so commonly found in the trachea
extended without interruption into the main bronchi and their
divisions. The finding of this continuous surface inflammation
is good evidence of the mode of spread of the infectious process
along these membranes, beginning in the upper portions and by
direct continuity involving more and more of the respiratory
tubes toward the lung.
225The varying grades in the intensity of the inflammatory reaction
upon the inner surface of the trachea was well illustrated in
the microscopic sections. Even with the different degrees of the
reaction there was a fairly constant character to the inflammation.
In this way the response was found to differ from that
commonly observed in ordinary infections of the respiratory
tract. The first striking feature is the marked response of the
vascular channels, both blood and lymphatic. The vessels lying
in the submucosa were found intensely engorged so that their
walls were stretched to the point of bursting. In fact, not a few
vessels were seen whose walls, probably under the stress of
intoxication and dilatation, had given way leading to a flooding
of the neighboring tissue with their contents. Where such vessels
lay close underneath the surface the hemorrhage escaped
into the lumen of the trachea. Accompanying this early vascular
response there was found a marked serous exudate leading to a
stretching of the submucosal tissues by distention of the interstitial
spaces. This reaction resembled an acute inflammatory
œdema and occupied the area between the mucosa and the inner
border of the cartilage rings. Beyond this region no response
was found. Thus in the earliest stages, and where the mucosa
was still intact, the main reaction was of the nature of an intense
serous inflammation with congestion of the blood vessels and
frequent interstitial hemorrhages.
Shortly following the development of the serous exudate in the
submucosal tissues, the epithelial lining is found to suffer from
the reaction. The serous exudate does not remain confined to the
interstitial tissues, but is poured out through the mucosa into
the trachea. It would appear that the amount of this clear
exudate may become greater than can be dealt with by the
mucosa, with the result that an accumulation of this serous fluid
takes place between this epithelial layer and its basement membrane.
We have repeatedly seen considerable stretches of the
mucosa lifted from the basement membrane and shed in large
plaques into the lumen. These mucosal cells at the time of their
desquamation retain fairly well their morphological characters,
and do not show evidence of necrosis prior to their removal.
Disintegration of these cells naturally occurs while lying in the
secretion of the trachea, and a variable cellular mass in stages of
disintegration may often be found both in smears and sections.
226When the epithelial cells are lifted in wide plates, a type of bleb
develops which is easily broken and then disintegrates.
The desquamation of the lining membrane is a fairly constant
occurrence in the cases coming to autopsy. In the majority of
those which we have examined the greater portion of the trachea
was completely denuded, save for small islands lying in the
recesses near the mouths of the mucous ducts. In one case this
lesion was accompanied by a process of ulceration, due in all
probability to the invasion by other micro-organisms. The denuded
tracheal surface usually shows a further inflammatory
reaction in which a cellular exudate then makes its appearance.
This reaction is mainly one in which lymphocytes and plasma
cells infiltrate the spaces previously occupied by the serous fluid.
The reaction is limited to the submucosa and does not extend into
the tissues beyond the cartilages. We have found only occasional
polymorphonuclear leucocytes lying close below the surface. During
this period, however, varying grades of degeneration may
occupy the upper layers. The basement membrane particularly
seems to suffer by losing its characteristic outline and staining
qualities. This membrane becomes swollen, softened and indefinite.
At times a homogeneous precipitate occurs along its free
surface giving rise to an appearance resembling a false membrane.
This deposit is, however, distinctively different from the
diphtheritic membrane of other infections. It is interesting,
however, that where such deposits and degeneration occur in
the basement membrane more or less degeneration and necrosis
also occur in the connective tissues immediately neighboring to it.
These tissues show a peculiar granular destruction and alter
their staining qualities. Moreover, and what is more important,
under these conditions the dilated blood vessels are found to
suffer from the injuries taking place in their neighborhood.
We have repeatedly found partially or completely thrombosed
capillaries, arterioles and venules in these surface layers. These
thromboses took place while the vessel was in its distended state
and thus produced a mold of the dilated vessel. This observation
is of importance in indicating the severity of the effect of the
virus and toxin upon the tissues of the trachea, and it is also of
importance to appreciate that this damaging influence is very
different from that which we encounter in pneumococcus infections,
and we shall point out in our discussion on lung a reaction
227very similar to that which takes place very superficially in the
trachea may also occur in the alveolar walls of the lung.
Having referred to the intensity of the responses of the blood
vascular system, we must also indicate the part played by the
lymphatics. Simultaneously with the reactions taking place
about the blood vessels of the trachea we observed similar
responses in the lymphatic channels. At first these dilated structures
contained only fluid. Later the migration of the lymphocytes
took place along these routes, and rarely micro-organisms
could be demonstrated either free or within an occasional leucocyte.
The sharp response of the lymphatics during the serous
inflammation is noteworthy, inasmuch as we have found that the
lymph glands lying about the respiratory tubes and lungs were
early in their response to the irritating virus.
Bacteria were demonstrated in the secretions lying upon the
surface of the trachea. In those specimens in which the mucous
membrane was still intact we attempted to demonstrate the
clustering of the micro-organisms about the ciliated cells as was
described by Mallory in whooping cough. Although the organisms,
and particularly small Gram negative bacilli, could be
demonstrated lying about these cells no characteristic arrangement
was found. Furthermore where the mucosa was still
attached to its basement membrane we were never able to demonstrate
organisms below the surface of the epithelial layer. In
several cases where the mucosa was lifted in bleb-like structures
a number of organisms were detected below the epithelial layer
and in contact with the basement membrane of the submucosa.
We have rarely demonstrated bacteria in the interstitial spaces
of the submucosa, even where large numbers of organisms were
lying upon the inner denuded surface.
The distinction which was made by the gross examination of
the trachea between the acute tracheitis with serous exudate,
subacute tracheitis and mucopurulent tracheitis was not so
readily distinguished in the microscopic sections. In the gross
the character of the exudate lying upon the surface was the main
guide suggesting the nature and intensity of the inflammatory
reaction. In the microscopic sections this exudate was largely
wanting, or was not sufficiently characteristic to confirm the
gross findings. On the other hand, differences in the nature of
the injury were to be found mainly in the reaction of the submucosa.
228As we have indicated above, the early inflammatory
reaction of the trachea is mainly evident in an intense congestion
accompanied by an inflammatory œdema of the submucosal
tissues, hemorrhage sometimes accompanying this response. In
the later stages of the reaction a cellular deposit takes the place
of the inflammatory œdema and usually consists of lymphocytes
and plasma cells. It is only in those cases where the intensity of
the irritant continues to act over a longer period of time that
a superficial necrosis with leucocytic infiltration makes its appearance.
The epithelial layer of the trachea is desquamated early
in the acute reaction, and hence a denudation of the surface is to
be found in all stages of the acute lesion. The mucous glands
have not been found to show any particular involvement in the
inflammatory process, and in the majority of instances they were
found to have escaped entirely the damaging effect of the virus.
Their response in an over-secretion of mucus may be the outcome
of a stimulation by toxins or soluble irritants; but on the
other hand, may also probably be a reflex response to the injury
of the mucosal surface, which being bared of its covering is
highly sensitive. The increased discharge of mucus from the
deep glands may well be a protective response to such injury.
Bronchi
The lesions in the bronchi were in every way comparable to
those in the trachea. The main bronchial tubes differ in no
material way from the structure of the trachea, and the extension
of the inflammatory process from above downwards leads
to a reaction in their walls similar to what has been above
described. As we follow the subdivisions of the bronchi we
gradually lose some of the characteristics contained in the larger
tubes. The mucous glands gradually become fewer and eventually
disappear. The cartilage rings become smaller and no longer
completely encircle the bronchus, and with the further diminution
in the size of these structures disappear entirely. A relatively
greater amount of muscle tissues takes the place of the
cartilage rings. This change in the anatomy of these structures
has a certain influence in modifying the character and distribution
of the inflammation.
229TABLE V
BRONCHITIS AND TRACHEITIS
| Acute bronchitis and tracheitis |
26 |
| Subacute bronchitis and tracheitis |
1 |
| Acute mucopurulent tracheitis |
5 |
| Acute purulent bronchitis |
2 |
| Acute mucopurulent bronchitis |
7 |
| Ulcers of trachea |
1 |
| Acute bronchiectasis |
1 |
Thus whereas we have indicated that the inflammation of the
trachea and of the large bronchi is of a peculiar kind and remains
confined to the tissue lying inwardly from the cartilage rings, we
found that where these structures give place to a loose muscle
tissue with a more extensive lymphatic drainage the zone of
inflammation is not so limited, but proceeds outwardly into the
neighboring tissues. We often use the terms bronchus and
bronchioles very freely without clearly distinguishing any real
difference. In a study of the inflammatory reactions of the
respiratory tubes in epidemic influenza (as well as in other infections)
it is best to accept the anatomical definition that the
bronchioles not only represent the minute tubules passing to the
alveoli, but also those small air passages which devoid of cartilage,
mucous glands and heavy connective tissue stroma are in
close relation to the parenchymatous tissues of the lung. These
soft muscular tubes possess blood and lymphatic vessels which
freely communicate with the blood vessels of the lung alveoli.
It is in association with these distant tubes that concomitant
inflammatory reactions are found in the alveoli and in the bronchial
tubes.
Desquamation of the epithelial lining is to be found in every
size of bronchial tube where the infection has caused an acute
inflammatory reaction. Throughout the pulmonary tissues where
the lung is found in some stage of influenzal pneumonia the
bronchial tubes, both large and small, are either entirely denuded
of the mucosa or show only remnants attached to irregular
areas. In the smaller passages dense clusters of desquamated
cells are sometimes found within the lumen and indicate the
accumulation of a desquamated epithelium obtained from portions
230of the tubular system in deeper portions of the lung. In
the early stages, this desquamation is accompanied by a serous
exudate and a certain amount of hemorrhage. Later we find
masses of leucocytes which fill up the tube, and though appearing
to arise from these structures have in fact largely come from
the lung alveoli. Like the larger bronchial tubes the distant
ramifications show relatively little cellular reaction in their walls
in the early period. It is only when the neighboring lung tissues
are extensively implicated in a purulent inflammation that we
find a similar exudate occupying the tissues of the bronchioles.
Polymorphonuclear leucocytes are equally distributed through
the region of the basement membrane, submucosa, muscular coat
and outer connective tissue layer. Some grades of degeneration
may occupy the inner surface wherein the basement membrane
first shows a homogeneous swelling and later a granular degeneration.
In a few instances where the small bronchioles have
communicated with regions with abscess formation an ulcerating
surface occupied the inner boundary.
The evidence in the smaller bronchial tubes, both those with
cartilage and those without, that an inflammatory reaction of
some degree may occupy the muscular coat is of importance.
We have found reactions of inflammation in the muscular coat
varying from a mild œdema and cellular exudate to an intense
polymorphonuclear leucocyte involvement. In the latter the
muscle fibers showed evidence of degenerative change and suggested
an acute weakening of this layer. We lay particular
importance upon this finding as indicating a causative factor in
the development of acute bronchiectasis as was met with in one
of our cases. In this particular instance the bronchi passing to
the lower lobes of each lung were unusually dilated and could be
followed, in the gross, to their distant extremities. The dilatation
was more or less uniform and no large pouches or cavities had
developed. A mucopurulent exudate was found occupying these
dilated tubes. Others have likewise observed the development
of acute bronchiectasis under these conditions. Goodpasture and
Burnett found that as early as the second to the fourth day one
of the striking appearances was the gaping dilated condition of
the infundibula, and the tendency to dilatation of the air passages
was manifested in a bronchiectasis in 4 out of 30 cases.
Boggs as well as Lord have reported upon chronic bronchiectasis
231associated with the B. influenzæ and there appeared to be evidence
that a certain percentage of cases recovering from influenza
permanently develop irregular dilatations of the bronchial tubes.
The recognition of inflamed bronchi or bronchioles was never
difficult. In the gross the presence of the abnormal exudate and
the intense injection of the mucosal surfaces always attracted
attention to the inflammatory state. Furthermore where the
mucosa had been desquamated the surface of these tubes was
found to be quite granular if closely observed. With moderate
magnification by means of a hand lens the granular appearance
was shown to be due to the engorged vessels. Much easier, of
course, was the recognition of the inflammatory reaction by the
microscope. The importance, however, of the bronchitis and
bronchiolitis lay in the amount of involvement which had
occurred in the neighboring tissues. As we, however, indicated
elsewhere, we do not doubt that many of the cases of three-day
fever have a state of tracheitis and bronchitis equal to that which
we have observed in many of our cases. Whether the inflammatory
reaction progressed beyond the firmer bronchial tubes to the
softer and more vascular structures would be difficult to say
where our evidence rests upon the clinical findings alone. It
is, however, probable that a certain number of the severe and
sharp attacks of influenza not only cause a tracheitis and bronchitis
of the larger tubes, but also extend more deeply into the
smaller ramifications tending to simulate the reactions which we
have above described. When we ask ourselves, however, how
distantly must the infection invade the smaller bronchial tubes
before involving the parenchymatous tissues of the lung we are
at a loss to enunciate a general rule. It is more than probable
that there are modifying influences which determine whether the
bronchitis with a certain amount of its bronchiolitis will progress
to a true pneumonia or will remain localized to these tubular
systems. I can well appreciate that in the event that a bronchitis
has an inflammatory reaction accompanied by much serous
exudate there is great danger of flooding the neighboring alveoli
with this inflammatory fluid and of carrying the large numbers
of the micro-organisms within the tubes to the air sacs of the
lung. Under these conditions the virus has an unusual ability to
develop the disease from one localized in the air passages to that
of a true pneumonia. It is probable that the peculiar early acute
reaction which is present in the air passages in epidemic influenza
is responsible for the extensive involvement of the lung in the
severe and dangerous form of inflammation.
232TABLE VI.
EXTENT AND DISTRIBUTION OF PNEUMONIA.
| Autopsy Number. |
Age. |
RIGHT LUNG. |
Type of Lesion. |
LEFT LUNG. |
Type of Lesion. |
Pleura. |
Abscess of Lung. |
Day of Disease. |
| Weight of Lung. |
Involvement of Lobes. |
Weight of Lung. |
Involvement of Lobes. |
| Upper. |
Middle. |
Lower. |
Upper. |
Lower. |
Right. |
Left. |
| 741 |
18 |
720 G. |
+ |
+ |
++ |
Lobar S. & H. |
850 G. |
+ |
++ |
Lobar S. & H. |
S.F. |
S.F. |
|
3d. |
| 743 |
20 |
825 G. |
+ |
+ |
+ |
Lobular S. & H. |
1375 G. |
+++ |
+++ |
Lobar S. & H. Early P. |
F. |
S.F. |
|
5th |
| 744 |
30 |
900 G. |
+ |
– |
++ |
Lobar and Lobular S. & H. |
900 G. |
++ |
++ |
Lobar S. & H. |
S.F. |
S.F. |
|
7th |
| 745 |
18 |
575 G. |
+ |
– |
++ |
Lobular S. & H. |
480 G. |
– |
++ |
B.P. with Necrosis. |
S.F. |
– |
+ |
10th |
| 746 |
21 |
900 G. |
+ |
++ |
+++ |
Lobar S. & H. |
650 G. |
+ |
+++ |
Lobar S. & H. |
– |
– |
|
5th |
| 747 |
27 |
1510 G. |
+++ |
++ |
+++ |
Lobar S. & H. |
1000 G. |
+++ |
+++ |
Lobar S. & H. |
S.F. |
– |
|
6th |
| 748 |
22 |
900 G. |
+ |
+ |
+++ |
Lobar and Lobular S. & H. |
1250 G. |
+ |
+++ |
Lobar S. & H. and B.P. |
– |
– |
|
4th |
| 749 |
23 |
1480 G. |
++ |
++ |
+++ |
Lobar S. & H. Slight Purulent. |
1250 G. |
++ |
+++ |
Lobar S. & H. Slight P. |
F. |
– |
|
4th |
| 750 |
24 |
1200 G. |
+++ |
+ |
+++ |
Lobar and Lobular. Early Purulent. |
825 G. |
+ |
+++ |
Lobar and Lobular. Early P. |
F. |
F. |
|
9th |
| 751 |
22 |
1250 G. |
– |
– |
+++ |
Lobar Purulent. |
610 G. |
± |
± |
B.P. slight. |
S.F. |
– |
|
7th |
| 752 |
27 |
1125 G. |
+++ |
+ |
+++ |
Lobar S. & H. |
775 G. |
± |
+++ |
B.P. and Lobar P. |
F. |
S.F. |
|
13th |
| 756 |
22 |
1000 G. |
++ |
++ |
++ |
Lobar S. & H. Slight Purulent. |
820 G. |
+++ |
++ |
Lobar and Lobular S. & H. |
F. |
S.F. |
|
8th |
| 757 |
21 |
815 G. |
++ |
– |
++ |
Lobular S. & H. |
1075 G. |
+++ |
+++ |
Lobar S. & H. and Purulent. |
F. |
F. |
|
6th |
| 758 |
22 |
1150 G. |
+++ |
+ |
+ |
Lobar Purulent |
1400 G. |
+++ |
+++ |
Lobar Purulent. |
F. |
F. |
|
14th |
| 761 |
21 |
1250 G. |
+++ |
++ |
+++ |
Lobar S. & H. and Lobular Purulent. |
550 G. |
+ |
+ |
Lobular S. & H. |
– |
– |
|
7th |
| 762 |
21 |
680 G. |
+ |
+ |
+ |
Lobular S. & H. |
750 G. |
+ |
+++ |
Lobar S. & H. and Lobular P. |
S.F. |
S.F. |
|
10th |
| 763 |
22 |
920 G. |
+ |
– |
+ |
B. P. and Lobar S. & H. |
540 G. |
– |
+ |
B.P. |
F.P. |
– |
|
11th |
| 764 |
23 |
725 G. |
– |
+ |
+ |
Lobular S. & H. |
550 G. |
+ |
+ |
B.P. |
– |
– |
|
9th |
| 765 |
25 |
1100 G. |
++ |
– |
++ |
Lobar S. & H. |
1400 G. |
– |
+++ |
Lobar S. & H. and Early P. |
– |
– |
|
9th |
| 767 |
25 |
1075 G. |
+ |
+++ |
+++ |
Lobar and Lobular S. & H. and Lobular Purulent. |
850 G. |
– |
++ |
Lobar S. & H. Lobular P. |
– |
F. |
|
10th |
| 770 |
21 |
900 G. |
++ |
++ |
++ |
Lobar S. & H. and Lobular Purulent. |
750 G. |
++ |
++ |
Lobar S. & H. Lobular P. |
S.F. |
F. |
+ |
11th |
| 773 |
22 |
2050 G. |
+++ |
++ |
+++ |
Lobar S. & H. and Purulent. |
780 G. |
– |
+++ |
Lobar S. & H. Lobular P. |
F. |
F. |
|
20th recurrence |
| 778 |
22 |
1100 G. |
++ |
+ |
++ |
Interstitial Pneumonia. |
975 G. |
++ |
++ |
Interstitial Pneumonia. |
S.F. |
S.F. |
|
23d |
| 781 |
21 |
1000 G. |
+++ |
++ |
+++ |
Lobar S. & H. |
540 G. |
+ |
+++ |
Lobar S. & H. Purulent. |
S.F. |
S.F. |
+ |
5th |
| 782 |
18 |
650 G. |
+ |
– |
++ |
Lobular S. & H. Slight Purulent. |
875 G. |
++ |
+++ |
Lobar S. & H. and Early P. |
F. |
F. |
|
8th |
| 783 |
21 |
1250 G. |
+++ |
+++ |
+++ |
Lobar S. & H. |
580 G. |
+ |
++ |
Lobar S. & H. |
S.F. |
S.F. |
|
8th |
| 784 |
21 |
1590 G. |
+++ |
+++ |
+++ |
Lobar Purulent. |
1400 G. |
+++ |
+++ |
Lobar S. & H. and Purulent. |
S.F. |
S.F. |
|
8th |
| 786 |
20 |
1100 G. |
++ |
+++ |
+++ |
Lobar S. & H. Slight Lobular Purulent. |
700 G. |
– |
++ |
Lobar S. & H. and Early P. |
S.F. |
– |
|
4th |
| 787 |
21 |
750 G. |
++ |
– |
++ |
Lobular S. & H. |
1125 G. |
+++ |
+++ |
Lobar S. & H. |
S.F. |
S.F. |
|
8th |
| 791 |
21 |
775 G. |
+ |
++ |
++ |
Lobular S. & H. and Purulent. |
1050 G. |
++ |
+++ |
Lobar S. & H. and Slight P. |
F. |
S.F. |
|
6th |
| 792 |
21 |
1050 G. |
+ |
+ |
+++ |
Lobar and Lobular S. & H. |
950 G. |
+ |
++ |
Lobar and Lobular S. & H. |
S.F. |
S.F. |
|
6th |
| 793 |
18 |
500 G. |
– |
– |
+ |
Slight Lobular S. & H. |
435 G. |
– |
+ |
Slight Lobular Purulent. |
– |
F. |
Strep. Bacteriemia. |
10th |
S—Serous. H—Hemorrhagic. P—Purulent. B.P.—Broncho-pneumonia. S.F.—Serofibrinous. F.—Fibrinous.
F.P.—Fibrinopurulent.
234It was very evident that the smaller bronchi and bronchioles
were much more readily involved in a severe inflammatory reaction
than the larger tubes. A purulent inflammation was not
uncommonly found in the bronchioles of the lung when a pneumonic
state with leucocytic infiltration was present. Even where
such purulent infiltration of the walls of the bronchioles was
readily demonstrable the trachea and main bronchi were devoid
of this intense reaction. These purulent inflammations were not
uniformly distributed in the bronchioles of the lung, but only
occurred in those regions where the parenchymatous tissues were
in themselves involved in a purulent reaction. It was difficult to
find the evidence whether the purulent bronchitis preceded or
followed the presence of a purulent pneumonia. The intimacy
of the lung tissues with those of the small bronchioles makes it
impossible for one or other of these structures to escape when
one of them is implicated in a purulent reaction. It is equally
important to appreciate that to a considerable extent the lung
tissue surrounding the small bronchioles becomes involved by a
direct radial extension through the walls of the thin respiratory
tubes. Such extension laterally is assisted by the free lymphatic
communication lying about the bronchioles and stretching into
the lung parenchyma. Purulent processes of the small air tubes
always showed a similar reaction in the interstitial tissues of the
neighboring air sacs.
Our material did not permit of following the bronchial reactions
to their conclusion. In some instances we have found that
where abscesses developed within the lung the contiguous bronchi
and bronchioles either became eroded or suffered intense suppurative
inflammatory lesions on their inner surface. The manner
in which repair of the more common inflammatory processes
of the bronchi is accomplished could not be demonstrated in the
cases dying during the acute stage. In one case an organizing
bronchitis was associated with an organizing lobular pneumonia.
In this instance the connective tissues were proliferating freely
from the inner wall of the bronchi, there being no evidence of a
basement membrane at the point where the connective tissue was
growing. The development of the connective tissue appeared to
235be spontaneous and was not taking place within an unresolved
fibrinous exudate. In as much as the fibrosing process was
largely scattered through all of the lobes, the numerical involvement
of the respiratory tubes was quite great. In this instance
the amount of obstruction which was imposed upon the respiratory
tissues by the fibrosing pneumonia and bronchitis was sufficient
to cause considerable distress and dyspnœa during the last
few days of the patient’s life. The amount of dyspnœa was out
of proportion to the clinical manifestations of pulmonary involvement,
and from a clinical point of view it was difficult to arrive
at a conclusion of the nature of the lung lesion.
Undoubtedly during the subsidence of the inflammatory process
within the bronchi the gradual restitution of the tissues
with little or no fibrosis is accompanied by a reproduction of
the lining membrane arising from the epithelial remnants in the
small mucous crypts. In a few cases lately coming to autopsy
where the patients had suffered an influenza five or six weeks
previously, the mucosa of the trachea and bronchi had assumed
its normal appearance and was fully clothed by a normal epithelial
covering.
Lung—Early Stage
We have just discussed the importance of the inflammation of
the trachea and bronchi in the cases of influenza. It is our belief
that every case of influenza has some tracheitis, and a great
many have both tracheitis and bronchitis. This is true in the
absence of localizing signs and symptoms, as was evident even
in these cases in which the simple influenza passed into its more
severe type with its pulmonary lesions. In many of these
instances clinical evidences of an inflammatory reaction in the
respiratory tubes were wanting, while the reactions observed at
autopsy were often astounding.
Just as we feel that simple influenza and inflammation of the
respiratory tubes go hand in hand, or better that these respiratory
localizations are the all-important ones in every case of
simple influenza, so, too, we are of the belief that the pulmonary
lesions bear the same relation to all cases of severe and fatal
epidemic influenza. We hold that no case comes to his death
through acute epidemic influenza without having a lesion in the
lung. The pulmonary condition, therefore, is of first importance
236and its analysis is imperative for a proper understanding of this
disease. There has been divided opinion as to the part played
by the pulmonary lesion in epidemic influenza, some holding that
it is to be looked upon as a part of the disease and others that
it must be viewed as a complicating lesion. Complications of
various kinds are very common, and there are a number of conditions
arising in the lung (abscess, gangrene, necrosis) which
must be viewed as complications. There is, however, a type of
pneumonia, and here I use the term in its broad sense, which is
not in truth a complication but merely a wider extent of involvement
of the respiratory tract by the same virus which is always
present to cause lesions in the respiratory tubes. The reaction
within the lungs is distinctive and differs from the pneumonias
which are met with under other conditions and with various
bacterial agencies. Nor are our findings in this matter unique
for this epidemic. They have been described and discussed in
the past. True it is that, like in the epidemic which has just
passed us, the incidence of clinical and pathological pneumonia
varied quite widely in different communities, so, too, the reports
of past epidemics do not give a uniform description of a pulmonary
lesion. Where, however, the analysis has been made
during the four weeks’ period of the acute epidemic and where
the descriptions have been recorded by painstaking observers, the
similarity with our present findings is very striking. I would
refer in particular to one report made in 1893 in Petrograd by
Kuskow. His report deals with 40 carefully studied cases in
which records both macroscopic and microscopic were accurately
made.
One of the great difficulties in placing an accurate interpretation
upon the pulmonary findings lies in the fact that true pneumonia
as seen in epidemic influenza in man has not been reproduced
in animals. Furthermore, as the majority of the fatal
human cases of epidemic influenza with their associated pneumonias
present a mixed infection of the lung tissues, it is difficult,
if not impossible, to indicate the lesions which have resulted
through the activity of one of these as against those induced by
the other bacteria present. In our own carefully studied cases
wherein bacteriological cultures were taken from every lung
there was not a single instance in which the influenza bacillus
was present in pure culture. This is more fully commented upon
237in the studies by Dr. Holman, but the point we wish to make
here is the difficulty in arriving at a conclusion in our material
as to the actual effects induced by any one type of organism.
As it is fully discussed by Dr. Holman we are convinced of the
importance of the influenza bacillus in this epidemic. We also
appreciate that pneumonia lesions in animals have been induced
by a variety of materials gained from influenza patients, but yet
in view of the abnormal manner of producing such lesions these
are hardly comparable to those in man. We may well expect
severe œdema, inflammation and hemorrhage, if in guinea pigs,
rabbits and monkeys we introduce by intra-tracheal insufflation
large quantities of fluid suspensions of bacteria. And thus we
find positive results obtained by the use of a filtrable virus,
streptococci, influenza bacilli and other organisms. The lung is
a sensitive tissue which quite readily responds to a variety of
irritants. In many respects some of these lesions simulate those
in influenza, but still we are far from the conclusion that the
disease, influenza, with all its manifestations has been actually
reproduced.
The pathology of the pulmonary lesions in acute epidemic
influenza is so distinctive that except for the late purulent stage
which may resemble types of reinfected and unresolved pneumonia
the condition cannot be confused with the stages of frank
lobar pneumonia. We appreciate that this is a very positive
statement, and that opposition will be taken by those who resting
their opinion upon individual factors may claim that a clear
distinction from other forms of pneumonia is not available. We,
however, base our opinion not upon a single feature, but upon
the combined pathological complex observed in many individual
cases. These features are mainly those seen in the type of the
lesion, the character of the distribution, extent of involvement
and the multiple stages so commonly present at one time in
different portions of the lung. The type lesion that has become
so well known in pneumococcus lobar pneumonia has its distinctive
stages which for teaching purposes are divided into the
stage of (1) congestion, (2) red hepatization, (3) gray hepatization
and (4) resolution. In dealing with lobar pneumonia from
the standpoint of illustrating these stages the majority of teachers
annually confess their inability to present for the student’s
study the stage of congestion. The student is impressed that
238the congestive stage of lobar pneumonia is very transient and
rapidly passes into the stage of red hepatization. Patients do
not die with pneumococcus pneumonia in the stage of congestion.
And this is also largely true of the stage of red hepatization,
which is but rarely seen at the autopsy table. This community
(Pittsburgh) gives its large quota to the mortality statistics of
pneumococcus pneumonia, but it is most unusual to meet with a
specimen of red hepatization except for the borders of the
advancing gray area. And, furthermore, red hepatization even
when found in the unusual cases shows remarkably little of this
character when seen under the microscope. True it is that a
certain number of red blood cells will be found in the alveoli and
a certain degree of congestion will occupy the alveolar walls, but
its extent is far less than what we may have hoped to demonstrate
to others. So that broadly speaking the intensely congested
lung with or without red hepatization is unusual in our
frank lobar pneumonia. This was quite the reverse in our cases
of acute epidemic influenza-pneumonia. Furthermore lobar pneumonia
in the great majority of instances illustrates a distribution
distinctive for the name. Massive lobar, or pneumococcus pneumonia
is found to occupy one or more lobes or parts of lobes.
The involved lobe is fairly uniform in the stage of the inflammatory
process. If it is in the early gray stage, this will be seen
with equal intensity in the different areas of the lobe. Patches
of pneumonia in different stages within the same lobe are not
to be found, while this finding is not uncommon in the pneumonias
of acute epidemic influenza. And lastly, the frequency
with which an inflammatory œdema occupied the lungs in the
cases of influenza was in quite striking contrast with the dry
fibrinous lesion of common pneumonia. This wet state of the
lung was but a stage in the inflammatory process varying in its
extent in the different periods, but nevertheless inducing a character
in the early pulmonary lesions which was quite foreign to
our usual finding. This wet state also assisted in modifying the
subsequent picture so that when the lung assumed its gray
appearance it was rather of a slimy character than of the firm
dry nature. In this late gray stage the slimy lung somewhat
resembled the appearance of unresolved pneumonia where this
condition had been brought about by a new infection upon the
original cause of the pneumonia.
239It is incorrect in influenza pneumonia to speak of the lesions
as lobar pneumonia or broncho-pneumonia if by these terms
we have in mind the pathological characters observed in the
pneumococcic pneumonia with its lobar or bronchial distribution.
Influenza-pneumonia appeared with both lobar and
lobular characteristics. Nearly every case had both types of
lesions present, but the nature of the inflammatory process is
so decidedly different from that of the ordinary endemic pneumonia
that a confusion in the interpretation is likely to arise
and in fact has already raised a considerable polemic. Influenza-pneumonia
is commonly lobar, lobular or bronchial in distribution.
It is, however, not of the characters that are associated
with the lesions designated under these terms. When, therefore,
we here use the word “lobar” we mean lobar in distribution but
not lobar in type. As will be seen from our table, it was usual
to have multiple lobes involved. But the lesions, not only in the
different lobes varied in their character and distribution, but
even within the same lobe a variety of types was present.
| Day of Pneumonia on Which Death Occurred |
No. of Cases |
| Second |
2 |
| Third |
4 |
| Fourth |
7 |
| Fifth |
6 |
| Sixth |
7 |
| Seventh |
3 |
| Eighth |
1 |
| Tenth |
1 |
| Twentieth |
1 |
To a certain degree we were able to analyze the types of the
lesions as they occurred in the different stages and progress of
the pulmonary inflammation. Briefly, these were as follows: the
earliest stage of congestion following rapidly upon the infection
from the bronchi was followed by (1) inflammatory œdema, (2)
hemorrhage, (3) cellular exudate (a. mononuclear cells, b. leucocytes,
c. interstitial infiltration) and (4) resolution or organization,
abscess, infarct and gangrene. The majority of our cases
240died during the stages of congestion, hemorrhage or early purulent
infiltration. In the early stages the amount of fibrin was
small or entirely absent, later, with the appearance of leucocytes,
some fibrin was present.
For the estimation of the time elapsing between the onset of
the pneumonia and death we are dependent upon the clinician.
This is often quite difficult to do, in as much as with a primary
respiratory disease, such as epidemic influenza represents, it is
very difficult to determine the time when there is a transition
from the inflammatory process of the upper respiratory tubes
to that of the pulmonary tissue. In many of the cases where from
the onset there was intense prostration and every evidence of
marked intoxication the clinical manifestations of localized processes
taking place in the respiratory system were very much
in the background and often of insidious progress. In four of
our cases it appeared as if the pulmonary manifestations had
made their appearance with the first sudden and severe onset of
the influenza. On the other hand, also, the clinical signs and
symptoms of lung involvement were different from those of frank
lobar pneumonia. We would, from our experience at the autopsy
table, say that where in the cases of epidemic pneumonia there
are present the signs of pulmonary consolidation like those of
true lobar pneumonia, that there has been an antecedent period
of a pulmonary lesion which passed unrecognized by the clinician.
To more clearly state the case, whereas in lobar pneumonia the
stage of congestion preceding the stage of red hepatization gives
rise to no signs whereby the clinician can indicate the time of
its onset or determine the time when it has passed into the succeeding
stage, and moreover, the stage of congestion is of short
duration to be measured in a period of a few hours, this stage
in epidemic influenza though equally indefinite in its clinical
manifestations is much prolonged, lasting not only a period of
hours but even a period of several days. It is this pulmonary
state which is difficult or even impossible to recognize in the
living. All gradations of it occur and the clinician can only
broadly suggest from all the evidence at hand, the period when
inflammation with definite exudate began in the lung. In as
much as the total length of illness of a number of cases was only
three, four and five days, whereas there was nothing at the onset
to suggest pulmonary involvement, we can estimate approximately,
241at least, the duration of the lung condition. This makes
it possible to give a relative estimate of the character of the
lesions present at different periods of time. The outstanding
finding, as we will discuss again, was that a distinct and peculiar
pulmonary reaction was primarily imposed upon the lung, which
made its appearance at periods different from those of frank
lobar pneumonia.
We were repeatedly surprised at finding death to have occurred
during the stage of acute congestion with some hemorrhage and
inflammatory œdema of lung and in the absence of any sign of
grey hepatization or purulent infiltration. In many of these
cases the involved areas of lung though heavy and œdematous,
were still partly air-containing and the amount of lung involvement
was insufficient, on the basis of mechanical interference,
in accounting for the severity of the clinical symptoms and the
fatal outcome. This must have impressed everyone dealing with
the autopsies during the acute epidemic. It immediately suggests
that in some cases at least the pulmonary lesion, in as far
as incapacitating the external respiratory system, was not the
sole or even the important cause of death, but that a condition
of intoxication, borne out by the evidence of damage in muscles,
blood and kidney is a large factor of danger in this disease.
We shall briefly describe the important pulmonary findings
as we have met with them in the successive stages of influenza-pneumonia.
This, we hope, will make clear the interpretation
of the pathology of the lung lesion of the epidemic as it came
under our observation.
The earliest pulmonary lesion which we encountered was one
of congestion, inflammatory œdema and hemorrhage. These
three conditions were usually present at the same time and were
found in the height of intensity in all of the cases dying within
the first four days of illness. During this early period these
manifestations of inflammation were not accompanied by definite
red or grey hepatization as might ordinarily be expected.
The lesions varied greatly in their intensity, the œdema always
being very prominent, while the hemorrhage varied from a
diffuse infiltration of the involved lobe or added to this, was
localized in massive collections four or five cm. in diameter and
commonly occupying the central portions of the lobes. We have
seen several hemorrhages lying in close proximity to each other
242with their borders coalescing and leading to a larger central
involvement. In the regions where the hemorrhage and inflammatory
œdema were diffuse, air was still present within the lung
tissue, sometimes to an extent permitting the lung tissue to float
on water but more often in quantity sufficient only to suspend
the tissue at various depths. On pressure the fine air bubbles
were recognized amidst the blood-stained fluid. Acute compensatory
emphysema often occupied the anterior borders of
the lobes or formed interstitial blebs beneath the pleura. The
quantity of fluid, inflammatory œdema and hemorrhage, contained
within these bulky lobes was often very surprising. A
lobe when compressed would leak fluid with the ease that it could
be obtained from a sponge. Out of the lower lobe on one occasion
we pressed 700 c.c. of limpid blood-stained exudate. The
acute emphysema which may make its appearance suddenly, is
TABLE VIII
Distribution of Pneumonic Lesions and Grades of Severity
| Degree of Involvement |
+ |
++ |
+++ |
Total |
| Left upper lobe |
10 |
6 |
7 |
23 |
| Left lower lobe |
4 |
10 |
17 |
31 |
| Right upper lobe |
12 |
8 |
9 |
29 |
| Right middle lobe |
10 |
9 |
4 |
23 |
| Right lower lobe |
5 |
9 |
18 |
3 |
| |
| All lobes were simultaneously involved in some grade of pneumonia in 18 cases—56 per cent. |
at times quite remarkable. It may appear very early in disease.
We have not met with a single case where the emphysema of
the lung led to a rupture of the air sacs and an interstitial infiltration
of air through lung, mediastinum, neck and subcutaneous
tissues. Some very remarkable cases are reported by different
authors where this emphysema was of astounding grade leading
to a crepitating infiltration throughout the mediastinum, neck
and the subcutaneous tissues over the thorax and abdomen as
low as the pubis. The milder grade of emphysema consisted
mainly of an abnormal expansion of the air sacs which were not
infiltrated by exudate and which probably had some effect in preventing
the diffusion of the inflammatory fluid from entering
243certain regions. These emphysematous areas could be readily
recognized by the naked eye along the anterior borders of the
lung as well as between the involved pneumonic patches within
the lung.
These lungs, involved in this early serous and hemorrhagic
exudate varied considerably in their appearance according to the
regional and quantitative involvement. As is seen from Table
viii, the lower lobes were more commonly occupied by massive
exudate than the upper, and the involvement of multiple lobes
was the usual. Still more remarkable is the fact that all lobes
were simultaneously involved in some grade of reaction (pneumonia)
in 56 per cent. of cases. In complicated influenza-pneumonia
Goodpasture and Burnett found the inflammatory reaction
in both lungs and involving to a greater or less degree the lobes
on each side. Most commonly this involvement consisted of a
lobar distribution in one or two lobes with a lobular or patchy
disposition of exudate in one or more of the remaining lobes.
Where the distribution was lobar the involved lobe was distended
to its fullest and the pleura tightly stretched over the
lung tissue which, heavy with fluid, was not solid but flabby.
The lung could be moulded under the finger and could be compressed
into various shapes. At first sight this flabby, heavy
lung tissue suggested the appearance of the waterlogged lung
which one encounters in renal disease or failing circulation. A
closer analysis, and particularly when the lung was sliced, showed
an entirely different character.
Where the inflammatory œdema was accompanied by much
focal hemorrhage the distribution was nodular and suggested
the appearance of the hemorrhagic lung of plague pneumonia.
It was this appearance which led to the suggestion that the
pandemic was not one of influenza but possibly of an infection
related to the eastern plague. The nodular masses of hemorrhage
at times occupied areas varying from the size of a walnut to
that of a golf ball and were localized amidst a relatively mildly
involved lung tissue making a sharp contrast between the involved
and relatively normal tissue. With the removal of the
lung from the body and the partial collapse of the aerated tissues
these nodules became still more prominent. The greater
the amount of hemorrhage within these areas the more solid
became the occupied tissue. Such sporadic distribution of hemorrhagic
244lesions occurred in the two most intense and rapidly
fatal cases. Both of these individuals died within 48 hours of
the time of onset of the lung conditions. In these two cases we
do not believe that the pulmonary lesions had been prolonged
over a time even as long as 36 hours but with the difficulty of
estimating the onset of the lung involvement we are giving a
liberal estimate of this time.
Besides meeting with the stages of congestion, œdema and
hemorrhage during the earliest days of the pulmonary lesions
we have found that they are to be encountered virtually through
all the stages of the fatal cases either as remnants of the original
reactions which had not been entirely obliterated by the succeeding
purulent process or as was so commonly found, new reactions
occurred in other regions of the lung so that, in the same individual,
inflammatory reactions of different stages of development
could be defined. I do not recollect a single autopsy of a
case dying during the acute period which did not show evidence
of some areas in the stages of this early acute reaction. Naturally
where resolution is well advanced within the lung all trace of
inflammatory exudate of various kinds is removed and where
such individuals with their resolved pneumonia are brought to
death through succeeding complications the above finding will
not be borne out. We limit, however, our statement to the findings
in the acute deaths.
We have previously intimated that the œdema present in the
early stages of the reaction is to be looked upon as an inflammatory
œdema or better as a true serous exudate, and must not
be confused with the transudation of fluids in non-inflammatory
conditions. We have on several occasions collected the fluid
expressed from the soggy lungs and have made some determinations
of their chemical qualities. The difficulty immediately
arises in separating the materials arising from cellular degeneration
from the natural constituents of the serous exudate. We
were unable to obtain specimens in which laked blood was not
present, so that even though the cellular constituents and fibrin
were removed, decomposition products could not be separated.
The analyses, however, gave a differentiation from the transudate
seen in renal and cardiac conditions.
During the period of the accumulation of this inflammatory
fluid the clinician could often recognize a profuse watery exudate
245within the lung or even observed an abundant serous discharge
arising in bronchi and trachea. At times the quantity of expectoration
was great. Frothy serous fluid accumulated in the air
passages and would periodically be expectorated. At other times
the hemorrhage was of quite serious extent and the patient
would suddenly bring up several mouthfuls or more of bright
blood. This pulmonary hemorrhage was without manifestations
different from the acute illness with cyanosis of other individuals.
The two most acute cases, which we have referred to
above, were of this kind, both of them having marked hæmoptysis
with the loss of upwards of a pint of blood at a time.
The early pulmonary lesion which we have described, we have
called acute serous pneumonia and acute hemorrhagic pneumonia
(or we might speak of it as an acute sero-hemorrhagic pneumonia)
and is one which is distinctive for epidemic influenza.
The cut surface of a lobe involved in this reaction is wet, glassy,
meaty and oozes much blood-stained fluid. It contains no visible
fibrin and presents no characters of a “cellular consolidation.”
As a serous inflammation of the lung it is unique. The further
remarkable character to the pulmonary lesion is that in advancing
through the other stages, it never passes through a stage
of “red hepatization.” Here again we have a distinctive difference
from the pneumococcus-pneumonia. From what we have
previously said about the nature of this early acute inflammation
of the lung in this disease it is apparent that red hepatization
has no place in its process. The stage of red hepatization
is attained only when the inflammatory reaction is accompanied
by certain constituents in the exudate, which upon coagulation
(separation out of the fibrin) renders the lobe dry and solid,
while there is a sufficient abundance of red blood cells and congestion
to maintain a dark red color. The hepatized lung on section
is dry, more or less granular, containing fibrin, red cells and
leucocytes within the alveoli. Extensive œdema is unusual except
in the cases of hypostatic pneumonia, which in well marked
cases bears some resemblance to the gross appearance of the
early influenza pneumonia. We have not encountered a single
case of the red meaty lung of influenza which showed evidence
of true red hepatization in the gross.
The microscopical examination of the lung tissue confirmed
the observations which were made in the gross. In the early
246stages of congestion the reaction was much more extensive than
what could be spoken of as a broncho-pneumonia. The capillary
dilatation in the alveolar walls occupied diffuse areas varying
from multiple lobules and areas several cm. in size to the
common diffuse congestion of an entire lobe. Capillaries were
distended to their full capacity and often this engorgement was
associated with the leakage of blood or a serous fluid. Not uncommonly
a clear serous fluid was exuded into the interstitial
tissues of the alveolar wall and collected within the air sacs.
The high albuminous content of this fluid was seen in the homogeneous
coagulation which occurred when the tissues were placed
in fixatives. The microscopical sections of such parts demonstrated
the coagulum occupying the alveoli as a clear homogeneous
substance containing relatively few cells and looking not unlike
the colloid deposit of the thyroid. The alveolar walls, themselves,
were infiltrated with fluid so that the distended tissues and vessels
made these structures thick and bulky. In our own observations
we were impressed by the differences of the early inflammatory
reaction from those ordinarily seen in pneumonia. Amongst
these differences was the quantity of fluid extruded into the lung
with a relative absence of fibrin. In some instances fibrin was
completely wanting, although small quantities could be demonstrated
in isolated areas. This observation upon the quantity of
fibrin can be made only during the early stage of the disease in
as much as after secondary infection of various kinds has become
implanted the presence of fibrin has become a variable
quantity often exceeding that seen in the early stages. This is
one of the points upon which the older authors have laid stress
in differentiating influenza pneumonia from others. In this we
fully concur. Whether this lack of fibrin in the inflammatory
exudate is a characteristic to be associated with the infection
by the B. influenzæ alone is hard to say, but in as much as it was
such a prominent finding we are led to lay some stress upon it.
It is, of course, to be realized, as with all other micro-organisms
that under certain conditions fibrin will form an important part
of the exudate even when the B. influenzæ is present. This
is true in the inflammatory reactions of the meninges present in
infections due to this bacillus. Under the conditions of epidemic
influenza where the lung lesion is the prominent and unique
247reaction this micro-organism fails by itself to bring out this
quality in the exudate.
Not uncommonly this stage of inflammatory œdema was accompanied
by various grades of hemorrhage, varying from the
presence of small aggregations of red cells to a complete flooding
of the lung tissue making it look not unlike a red infarct of lung,
save that the alveolar walls still showed an active circulation and
living cells. It was remarkable that even though there was such
an intense reaction taking place in the lung tissue there was
little or no evidence of a cellular exudate during this stage of
the process. Where much blood was extruded into the alveoli
occasional fibrin threads were found in the coagulum. In these
early cases the bronchicles and small bronchi were found to contain
an exudate similar to that in the alveoli. Not uncommonly
the vessels from which the red blood was escaping, could be
demonstrated in sections. The appearance of the vascular wall
suggested that a definite opening had occurred in the side of the
capillary from which the blood escaped. We were not able to
demonstrate a fatty or other type of degeneration in the cells of
the capillary walls. It is probable that the process of injury was
much too acute to permit of the demonstration of the products
of degeneration within the surviving cells.
The hemorrhagic lesions which had existed for a longer period
of time gradually showed a varying infiltration by wandering
cells. The earliest cells not belonging to those of the hemorrhage
or œdema appearing within the alveoli were mononuclear elements
partly arising from the alveolar walls and partly coming
from the circulation. Numerous mononuclear cells of epithelial
type desquamating from the inner surface of the alveoli accumulated
in the œdematous fluid and the hemorrhage within a short
time after their occurrence. These cells either appeared in
clusters or as single elements. Accompanying this were also large
mononuclear cells loaded with different quantities of pigment
which had apparently escaped from the lymphatic channels within
the alveolar walls. These latter cells belong to the wandering
endothelial type which are active in phagocytosis for foreign
material and which assist so largely in inducing the deposit of
carbon in the lungs and lymph glands. A third mononuclear cell
appearing early in the reaction was the lymphocyte. The numbers
and extent of distribution of this cell were not constant. We
248have seen it in some of the reactions where very few leucocytes
were to be seen, and where it constituted the main infiltrating cell
of the alveolar wall or the air sacs. We have previously mentioned
its presence in the inflammatory reactions of the bronchi.
Here we find it in the early response within the lung tissue and
appearing amidst a reaction which is intensely acute. It is not
long after the finding of these various cell elements that the
polymorphonuclear leucocyte wanders in large droves to numerically
overshadow the mononuclear cells. Nevertheless, the three
types above mentioned can be recognized in the exudate through
the succeeding stages of reactions in the lung. The large macrophage
shows its phagocytic properties in taking up numerous red
blood cells, lymphocytes and occasional leucocytes.
It is not difficult to demonstrate that the inflammatory reaction
within the bronchi and bronchioles precedes the responses within
the alveoli. Quite often one may find an acute bronchiolitis with
desquamation of the lining epithelium and the early serous exudate
lying amidst the lung parenchyma unaffected by any irritant
and reaction. There is every evidence that the bacteria reach the
lung tissue by extending along the walls of the respiratory tubes
and eventually reaching the air sacs either in the distant extremities
of the bronchioles or when they have arrived at the thin-walled
structures extend through them into the neighboring air
sacs.
It is during this early period that we are able to observe the
characteristics of the initial inflammatory exudate as we have
described it above. The serous exudate and the infiltration by
mononuclear cells appear early while the absence of fibrin also
attracts attention. In place of fibrin there appeared in a certain
number of cases a peculiar material of a hyaline nature which
becomes plastered against the borders of the air sacs forming
a fairly thick laminated structure and within which thread-formation
is not to be seen. Occasionally a few cells lie within
this hyaline substance. Some have referred to this as a type
of fibrin. We have found, however, that it does not give the
staining reactions for fibrin and does not appear to be of the
same composition. These masses are tightly welded to the alveolar
walls and the borders are often indistinguishable. In part
this material appeared to be made up of necrotic cells of the
septum which previously had suffered œdema and circulatory
249interference. We have found in a number of cases hyaline
thromboses of the fine capillaries with more or less necrosis of the
alveolar septum. At times the septum was entirely destroyed so
that a thick hyaline mass alone separated neighboring air sacs.
This hyaline necrosis resembles in part the superficial necrosis
which was observed along the borders of the denuded bronchi.
There is, however, more than necrosis of cells constituting this
deposit for the bulk of material eventually deposited is much
greater than could arise from tissue cells alone. These hyaline
masses have never been found to lie upon the alveolar wall with an
intact lining, but it is always accompanied by a loss of the lining
cells and more or less destruction of the wall itself. As to the
nature of the hyaline deposit which is laid down in lamellae we do
not know. Fibrin threads occasionally appear to arise from these
hyaline deposits and extend amidst the exudate in the air sac.
One cannot assume, however, that the fibrin and the hyaline
material have any relation to each other as their chemical characteristics
(and mode of deposition) appear to be quite different.
It has been suggested by some that this hyaline material represents
an imperfectly formed fibrin which has formed a jelly-like
clot, not having the property of developing the usual threads.
It is of importance to appreciate that the deposition of these
hyaline structures indicates a severe injury of the alveolar walls
not commonly observed in ordinary pneumonias.
In different areas of the same lung these constituents of the
early exudate may be observed in all proportions of admixture.
Each one of the elements of the exudate may largely overshadow
the others and prominently modify the appearance of the lesions.
Broadly speaking, however, the inflammatory œdema and hemorrhage
occupying the greatest part of the exudate in the lungs and
the absence of marked leucocytic response as well as the absence
of the characteristic fibrinous meshwork in the alveoli give to the
early influenza-pneumonia a character different from those which
we ordinarily see.
It is during this early phase of the reaction that the influenza
bacilli can be shown within the lung structures. The distribution
of bacteria is not uniform. Clusters of these minute bacilli
are found in the alveoli at irregular intervals, many of the air sacs
containing much exudate being quite free from organisms. When
present the bacteria appeared in tightly aggregated schools lying
250free amongst cells of the exudate, but also certain numbers being
incorporated within the large mononuclear cells. In some regions
organisms of the type of the influenza bacilli were alone seen,
while elsewhere again, and particularly where the exudate was
assuming purulent characters other bacteria of the nature of
streptococci, staphylococci and micrococcus catarrhalis, were also
found.
Lung—Secondary Stage
Following upon the primary reaction in the lung as above
described, a secondary reaction makes its appearance at variable
periods. This reaction is one in which the inflammatory exudate
resembles more closely but is not identical with the responses
which are observed in ordinary lobar, lobular and pneumococcus-pneumonia.
Whereas in the earlier period, the reaction is largely
one of a serous and hemorrhagic exudate accompanied by peculiar
hyaline deposits along the inner borders of the alveoli, later there
is seen a change in the quality of the exudate with the accumulation
of more cellular elements and some fibrin. The naked eye
appearance of the involved tissue changes considerably. The lung
tissue loses in weight but becomes more solid. The lung contains
less fluid and the cut surfaces are drier and the color of the reaction
changes from the dark congested appearance to one showing
all varieties of red and gray. This change from the flabby and
soggy pneumonia to the more definite type of consolidation occurs
in the regions which have been previously involved and is not to
be found in the lung areas which have escaped the early reaction.
The gray consolidation appears to be either a stage of the influenza-pneumonia
or is a new reaction superadded to those pulmonary
lesions induced by the primary infection.
It is sometimes difficult to recognize the beginning of this pneumonic
stage inasmuch as the gray color does not make its appearance
even with the presence of fairly large quantities of cellular
exudate. The amount of hemorrhage that originally lay in the
affected areas for a long time overshadows the presence of the
color of the cellular exudate. This is also true of the characters
that may be impressed by the presence of fibrin. Small quantities
of fibrin scattered through the congested and œdematous lung are
not readily recognized and the beginning of this secondary reaction
is also easily overlooked if one relies upon evidence of consolidation.
251More or less solid exudate may occupy a flabby lung
without permitting one to appreciate its presence in the gross
specimen. When, however, the deposit is of sufficient quantity to
change the color of the involved lobe and to alter its consistency,
one has little difficulty in recognizing the changes now taking
place. The earliest development of this change in the inflammatory
reaction was on the fourth day. In the majority of instances
the gray color and the consolidation made its appearance about
the sixth day. We have, however, on several occasions observed
hemorrhagic lesions as late as the seventh and eighth day, at
which time it was impossible to recognize a gray hue to the
exudate or the character of granular consolidation to the involved
lung.
The reaction naturally suggests the stage of gray hepatization
as we so well appreciate it in ordinary pneumococcus-pneumonia
and from the standpoint of its color and the greater solidification
of the lung tissue we might speak of it as such. Here, however,
it must be clearly distinguished from the gray hepatization of
ordinary pneumonia. This secondary lesion of influenza-pneumonia
has but little in common other than its color and the
development of a consolidation with true lobar pneumonia. It is
never as clear cut as we see it in the latter and the degree of the
“gray hepatization” is not uniformly distributed through the involved
lobe. One portion of the lobe will show a diffuse gray hue
while in other parts more decided lobular or patchy areas are
picked out in the advanced reaction. There is not the uniformity
of lobar involvement nor is the distribution as regular as one
obtains it in broncho-pneumonia. Furthermore, the character of
the consolidation differs very decidedly in showing such a variety
of hues in reds and grays and the cut surface is not the picture
of the dry granular consolidation of our endemic disease. The
gray areas are in all states of wetness and ooze a slimy fluid on
the cut surface. In the later stages this exudate is most profuse
resembling a sticky pus. In its appearance we were reminded of
the character seen in unresolved pneumonia as well as in the
pneumonias produced by the pneumococcus mucosus, and the B.
mucosus capsulatus. We would, therefore, avoid the use of the
term gray hepatization and in place of it, as the evidence with the
microscope confirms, use the term purulent pneumonia.
252There are three other characters which differentiate this gray
stage from those of ordinary pneumonias—(1) the irregular distribution,
(2) the friability of the involved tissue and (3) the
interstitial reaction. We have never observed such an irregularity
in the distribution of a gray stage of pneumonia as we have
seen it develop in acute influenza-pneumonia. All types of involvement
of the lobes are found in different cases and even sometimes
in the same case. The least frequent type has been the
broncho-pneumonia in its true form. Broncho-pneumonia as we
see it in children and the cases following measles is usually fairly
uniformly seeded through several lobes and the size of the individual
patches is about that of a split pea. The small bronchus
can be recognized about the center of the involvement. In those
instances one has studded through the lung tissue numerous small
swollen areas which are granular, dry and gray. Differing from
this the patchy distribution of the gray stage of influenza-pneumonia
had no regularity either in the size of the areas nor the distribution.
A lobe may show one or more patches. The patches
may be distributed toward one portion of the lobe more than
another. Furthermore the areas do not always encircle the small
bronchi but involve the terminal portion so that an entire lobule
is more commonly affected. The lobular type rather than the
peribronchial type is most commonly seen and it is often remarkable
how sharply the gray lobule is demarcated from the surrounding
congested lung tissue. On several occasions we observed
a single lobule in the gray stage while the remaining portion of
the lobe was in the serous and hemorrhagic condition. However,
multiple lobules are commonly seen closely associated in the
advancing inflammatory process. Such lobules show peculiar
geographical patches or leaflet-like configuration. Varying with
the number of lobules involved the extent of the gray change in
the lobes assumed more or less a lobar distribution. There was
no uniform position to this pneumonic state sometimes appearing
in the peripheral tissues of the lung, at other times lying centrally
with less involved or less advanced inflammatory reactions surrounding
it. Nevertheless, the gray stage made its appearance
more rapidly in the lower lobe than the upper and it was not
uncommon to find this condition appearing quite early in the
upper posterior portion of the lower lobes. This latter position
is the one which is recognized during life by the clinician as one
253of the earliest localizations of the demonstrable pneumonia. It is
reported by many that the first physical signs of consolidation are
to be obtained close to the lower angles of the scapulae.
There is no doubt that the character of the pneumonic process
in the epidemic influenza was not the same in all localities. There
have been not a few who have reported a large proportion of their
pulmonary lesions as a definite broncho-pneumonia with an interstitial
purulent involvement. The prominent reaction was a small
circumscribed yellow focus about the bronchioles from which a
bead of pus could be expressed. These pea-sized foci were scattered
through several or all lobes. It is this type of reaction
which appears to develop by a direct extension through the
bronchial walls and to remain quite localized in the alveoli
about these tubes. This reaction seems to be purulent from
its very beginning and does not pass through the stages as
we have described them above. There is more or less fibrin
present in the exudate, but usually not in the quantity observed
in lobar pneumonia. These lesions closely resemble those observed
in the post-measles pneumonia, and it is claimed are the result of
the same agent; the hemolytic streptococcus. In only one case did
we observe a lesion of this kind. The small areas of broncho-pneumonia
were confined to the left lower lobe and in the lower
portion of the upper lobe. Each area was about the size of a split
pea, was quite yellow and in fairly sharp contrast to the background
of an acute sero-hemorrhagic pneumonia. The subsequent
history of these interstitial purulent broncho-pneumonias
is like that in measles, where the tendency toward an organizing
pneumonia has been shown. The importance of the hemolytic
streptococcus in inducing purulent interstitial lesions of the lung
(and also of other organs) cannot be over-impressed. It is not
so much the type of the reaction during its acute stage which
attracts our attention, but the manner of the healing process. It
is more than probable that the organizing pneumonias of influenza,
not only of this distinct bronchial type, but also the lobular,
confluent and lobar variety have had an associated streptococcus
infection. The more intimate discussion of this type of pneumonia
has been given by MacCallum.
Our autopsy experience has led us to believe that the definite
clinical signs of pneumonia are associated with the development
of this gray consolidation of the lung. The lung tissue develops
254characters which permit the physical signs to be recognized. The
tissue is more solid and more readily transmits the bronchial
sounds. This is not true of the earlier stages where the inflammatory
process is contained within a lung tissue which still is
partially crepitant and when the so-called consolidation is due to
an inflammatory œdema and not to the more solid fibrinous and
cellular exudate. With the protean distribution of the gray lesion
one does not wonder at the clinical difficulties in mapping out or
even finding the consolidated tissues.
As soon as the lobes show this gray character and with the
progressive development of an acute interstitial purulent pneumonia,
the lung tissue becomes friable. All gradations of flabbiness
may still be obtained and in the early stages while the
cellular exudate is accumulating to change the color of the lung,
little variation from the tough character of the pulmonary tissues
can be recognized. When, however, a true gray character is
assumed by a portion of the lobe, the tissue becomes so soft that
it is handled with difficulty without rupture. The thumb can be
pressed into the gray mass and pus will well up around the invading
phalanx. The consistency in the late stages reminds one
of the pulpy tissues in acute splenitis. In cutting such lobes it is
almost impossible to obtain slices of the tissues, their own weight
often breaking such a segment. When allowed to rest on the
table for a few moments, the cut surface becomes coated with a
dirty yellow slime representing pus and products of disintegration
arising from the lung. The stroma and alveolar tissues are themselves
involved in the inflammatory process and many of them
have suffered complete or partial destruction so that they offer
but little resistance to pressure and serve as a poor supporting
stroma to the pulmonary tissues. The reaction which has taken
place within the lung producing both the gray color and the
destruction of the tissues is, indeed, an active suppurative one.
One would not be surprised to obtain not only a purulent lesion
wherein the cellular exudate occupies the air sacs and their walls
but also a further stage leading to a destruction of the tissues to
the extent that abscess cavities are produced. These we have met
with in several instances, some of them being small while others
were several centimeters in diameter. An abscess of larger extent
and having a destructive process which involved the surrounding
tissues so that one would speak of it as a process of gangrene, was
255observed by Dr. McMeans in one of his cases. A lobar distribution
of the purulent lesion takes place where multiple involved
lobules have fused in their periphery or where a suppurative flooding
of the tissues in this violent late reaction has taken place.
The question at once comes to mind whether this gray stage is
but the late event of what we have previously spoken of as influenza-pneumonia
or whether this condition is superadded to what
may begin as an influenza-pneumonia but end in a pulmonary
inflammation with a mixed infection. Dr. Holman was not able
to demonstrate a sufficient difference in the bacteriology of the
lobes in the gray stages from those in the early acute stage to be
able to say that the flora changes at a certain time during the
progress of the disease in the individuals. It is possible, and
there is some evidence in support of this, that the earlier stages
of the pneumonic process represent the reaction to the influenza
bacillus and that during this period the response is fairly uniform
and similar owing to the fact that this infection has but a short
incubation period and a high pathogenicity. In such an event the
particular micro-organism may bring about a peculiar response
of its own before the other organisms with which it is associated
have the opportunity of producing damage. Subsequently, however,
these secondary organisms impose their peculiar reactions
upon an altered lung, thus inducing an inflammatory lesion which
differs from the preceding reaction and also differs from the reaction
usually induced by those organisms upon relatively healthy
tissues. It is difficult to account for the very irregular distribution
of the gray lesions by an explanation concerning the influenza
bacillus alone, or by the characters peculiar to the secondary
infection. There is an entire want of character to these gray
lesions which makes them differ from other types of pneumonia
known to us.
It is well to lay particular stress upon this peculiarity in the
distribution and extent of the lesions within the lobes; and it is
also important to appreciate the difference in the appearance of
these gray areas from those of true lobar or broncho-pneumonia.
Finally there is another point in which this stage of the pneumonic
process differs from that of pneumococcus lobar pneumonia.
In frank lobar pneumonia the reactions taking place in
the involved portion of the lung are fairly uniform in all its parts.
The stage of red hepatization occupies about that amount of lung
256which subsequently shows itself in the state of gray hepatization.
In other words, all of those areas which appear gray are preceded
by this peculiar red consolidation, and all of the area occupied by
the red hepatization will pass through the phases of gray hepatization
before entering upon the final stage of resolution.
In influenza-pneumonia, on the other hand, the events taking
place in a given lobe are not uniform and various stages and
grades of the inflammatory reaction may be recognized at the
same time, some appearing red, some congested, some flooded
with blood in hemorrhage and others showing the purulent infiltration
by the appearance of gray patches upon the background
of red. Not only do the various reactions within the same lobe
fail to show similar grades of intensity and similar stages or time
of involvement, but we find that all of the red and hemorrhagic
areas are not destined to pass through the gray stages. At times
it is true an entire lung will enter into the purulent phase and if
this becomes extreme abscess and gangrene are almost certain to
develop. But often the purulent infiltration occupies only a few
or scattered lobules and resolution may take place in a lung where
the greater part of the lobes is occupied by the inflammatory
œdema and hemorrhage and has never become truly consolidated
by cellular and fibrinous exudate. This feature that the involved
lung tissues need not pass through the sequence of events which
is usually observed in frank lobar pneumonia is so distinctive
that it differentiates the character of the inflammatory reaction
very clearly. It may be that this is an indication of the unequal
distribution of the micro-organism and that the first infection
presumably by the bacillus influenzæ has been much more diffuse
and of wider extent than the secondary invading bacteria which
being distributed through the bronchial tree are more or less
localized to those lobules most severely involved. It is impossible
to claim for influenza-pneumonia as clear and sharp-cut stages as
we obtain them in the pneumococcus lobar pneumonia.
During the period of the intense purulent reaction in certain
portions of the lung, the intrinsic structures within the area also
partake in the damage and response. The suppurative infiltration
not only occupies the alveolar walls but also extends through the
tissues of the bronchioles, the arteries and the veins. The polymorphonuclear
leucocytes seem to migrate into all of the parenchyma
indicating some damage by bacterial invasion. On more
257than one occasion have we observed partial or incomplete thrombosis
of arterioles and capillaries whose walls showed an acute
suppurative reaction. Some of these thromboses are of importance,
being associated with the interference with a blood supply
not compensated by adequate anastomosis. Necrosis and small
areas of gangrene and abscess are to be found in the region of
the circulatory disturbances. It is also during this period of the
disease when the bronchi and their ramifications contain pus or
muco-pus, that the exudate from the alveoli readily finds its way
into the air passages and becoming mixed with the mucus from
these tracts forms a tenacious discharge.
The presence of large amounts of exudate within the bronchi
brought these structures into unusual prominence. This was particularly
true in the purulent stage of the reaction when beads of
sticky pus would well up from the cut bronchioles. We were
tempted on a number of occasions to speak of this in terms of
bronchiectasis but with the intense inflammatory reaction occupying
the bronchial wall and modifying its contour on this account
we avoided this diagnosis. In one instance, however, the lesion
was unmistakable. This was a case of purulent pneumonia (764)
dying on the ninth day of the disease. The distribution of his
pulmonary lesions was distinctly lobular, apparently following the
course of the bronchial distribution. The bronchi were followed
longitudinally and irregular pouchings of the lumen were very
apparent. The bronchi had suffered marked inflammatory reaction
which had also infiltrated the muscular tissues of the tubes.
Goodpasture and Burnett report finding two cases of acute bronchiectasis
associated with abscess and ulceration of the bronchi.
In our case the bronchiectasis was found bilateral but was more
marked in the lower lobes than the upper.
The lymphatic channels within the lung tissue are found active
in establishing an internal drainage to the neighboring thoracic
glands. The lymph vessels were often found filled with leucocytes
and variable amounts of serum. During this late stage only a few
of the endothelial leucocytes were observed wandering to or from
the lung with a load of pigment or cell debris. These wandering
endothelial cells, however, appeared to become loosened from their
normal situations and in the vicinity of lymphatic nodes or communicating
channels where these cells are prone to localize with
their carbon pigment, again assumed their spherical form and
258took on migratory properties entering into the nearby tissues and
scattering themselves in the looser structures. It is an interesting
point to note that these pigment carrying cells, ordinarily
assuming a latent existence when their cytoplasm has been
crowded with foreign particles will assume all the activities of
migrating cells when the œdema of the tissues alters the physical
properties not conducive to a stationary existence. These cells
will then be found to enter the lung alveoli, often appearing as
cells which have only recently picked up their carbon load.
When, however, the conditions of the experiment, that is, the
production of an inflammatory œdema in the lung, are produced
in the tissues of an individual with much anthracosis, he will,
during the period of his pneumonia and for some time during
convalescence, bring up a greater number of these cells in his
sputum than are ever obtained during the times when the lung is
not involved. We are convinced that inflammatory conditions of
the lung tend to reduce the total number of latent pigment bearing
cells present in the involved tissues, and in this way somewhat
reduce the grade of anthracosis.
A considerable discussion has arisen concerning the proper
nomenclature for the pneumonia or pneumonias found in epidemic
influenza. From some quarters have come the reports of a true
lobar pneumonia, from others a lobular or broncho-pneumonia
and others again claim that the reaction is an interstitial pneumonia
of varying distribution. It appeared to us that the gross
distribution of the lesions is not alone the criterion for a proper
appreciation of the inflammatory states which may arise within
the lung. I believe it has been amply demonstrated that the pneumonic
reactions appearing in different regions of the United
States as well as in different countries are not of a constant kind
when viewed alone in the light of the gross picture nor are they
constant from the standpoint of their bacteriology. We are of the
opinion that the earlier phases of the pulmonary reaction are
fairly constant in different places and that this constancy is
dependent upon the common virus which initiates the respiratory
lesion and which then permits a variety of micro-organisms invading
as secondary agents. The secondary agents vary with the
community and depending upon their nature the character of the
reaction differs from that in other places. It has been well
demonstrated that in some regions the hemolytic streptococcus
259is the important organism following the primary injury by the
initial virus. In other places the pneumococcus or the staphylococcus
or the M. catarrhalis is found to be of primary importance.
Up to the present it has not been shown that the influenza
bacillus is not the important organism causing the initial reaction
and being responsible for the opportunity of secondary invaders
leading to such diverse reactions in the lung. In our series we
have met with lobar, lobular, interstitial and broncho-pneumonic
types. We have not observed a case of the miliary bronchial reaction
as described and illustrated by Goodpasture and Burnett and
fully investigated by MacCallum. Moreover we have not met
with the type of purulent bronchitis as a characteristic lesion
preceding pulmonary involvement. The occurrence of pus within
the bronchi occurred not early in the pulmonary lesion but later
after the bronchi and bronchioles had passed through their stages
of acute, serous and hemorrhagic pneumonia and were entering
upon their secondary stage with pus production. The pulmonary
lesion had long preceded the appearance of pus in the bronchi.
We do not hold, however, that such relations between the pulmonary
lesion and the purulent bronchitis do not exist for there
is evidence that in particular regions this sequence of events was
closely observed.
We cannot, however, correlate our findings with the classification
of pneumonias as given by MacCallum. His claim for specific
types of pneumonia as a sequel to influenza is based upon his
statement that “no satisfactory evidence has been brought forward
to show that the epidemic influenza is a bacterial infection.
It is evidently a general or systematic infection not especially
affecting the respiratory tract and analogous in many respects,
as Bloomfield has pointed out, to the acute exanthematic diseases.”
Thus we are confronted by two schools concerning the nature of
influenza. The one claiming that epidemic influenza is essentially
a disease of the respiratory system and the other completely denying
this.
I am unable to understand the claims which are put forward
to substantiate the second view.
The classification of the pneumonias as suggested by MacCallum
would be valuable if it could be applied in a practical
manner. We find, however, that his description for the pneumococcus-pneumonia
hardly coincides with common observations on
260endemic pneumonia and if the description is to apply only to the
pneumonias associated with influenza wherein pneumococcus
alone is isolated we find that our own observations do not coincide
with this. The picture offered by MacCallum under this heading
was reproduced when the bacteriological findings illustrated the
presence of organisms other than the pneumococcus or combinations
of these. The most characteristic of his description is the
one for the streptococcus-pneumonia which when present alone
gives quite a unique picture. The picture, however, is to a certain
degree modified by the reactions which precede the streptococcus
in the lung. Furthermore to offer as a characteristic picture for
the influenza infection of the bronchi the presence of a thick
yellow pus is hardly complete inasmuch as this exudate appeared
only as a stage in the inflammatory process. The intense serous
and hemorrhagic response observed early in this type of infection
is more unique than the presence of pus which appears somewhat
later and which may occur with infections other than the B.
influenzæ. It has long been the hope in pathology to be able to
establish by the character of the tissue reaction, the nature of the
infecting agent. Up to the present this has been possible only
with a very few types of bacteria.
Lung—Stage of Resolution
The removal of the infection and the inflammatory exudate
from the lung tissue is accomplished slowly. Clinically the pulmonary
process clears up by lysis, and it is quite unusual to have
a crisis with the rapid disappearance of the serious manifestations.
It is difficult to obtain a clear conception of what takes
place in any individual case recovering from an influenza-pneumonia,
but if we have an understanding of what may occur in
the inflamed lung tissue in any one of the stages or varieties of
kind, we may visualize the changing character of the lung condition
tending toward the final restoration.
We have previously pointed out that the early stage of influenza-pneumonia
is one of congestion, œdema, hemorrhage and
more or less leucocytic infiltration, and that this reaction differs
materially from that observed in pneumococcus lobar pneumonia.
There being no stage of true red hepatization, it has also become
apparent that this peculiar primary reaction need not pass into
the stage of gray consolidation. Scattered areas in the lung pass
261from the condition of acute serous and hemorrhagic pneumonia
to a type of purulent pneumonia while much of the remaining
tissue continues in the state as seen in the early reaction. A certain
amount of cellular exudate makes its appearance but not
sufficient to lead to a true consolidation. This variety of reaction
is present from the fifth day of the pneumonia onwards and may
continue with all of its varieties through until the tenth or twelfth
day or even longer when recovery from the infection is beginning.
Thus the stage of resolution makes its appearance before the
inflammatory reaction in the involved lobes has assumed a common
character and where we are able to recognize different grades
of severity and different stages of inflammation within the same
lobe. Resolution taking place in such a lobe has responses occurring
in the different parts determined by the nature of the antecedent
reaction. We have found that those portions which have
not advanced beyond the stage of œdema and hemorrhage may
clear up with the disappearance of this early exudate and its
infection. In a neighboring portion the purulent inflammation
passes through phases differing somewhat from the preceding
but also tending toward the restoration of the parenchyma and
the disappearance of the inflammation. It would be incorrect to
consider the resolution of the early type of inflammatory reaction
as an abortive process inasmuch as it is not yet clear whether
this serous and hemorrhagic process is not the characteristic
inflammation of a peculiar micro-organism or organisms and that
when acting alone these bacteria do not in themselves stimulate
a further inflammatory response. Hence if it is true that there
is a peculiar inflammatory reaction of a non-suppurative and non-fibrinous
kind the manner of resolution will differ somewhat from
that where these other constituents of the exudate are present.
It becomes clear, therefore, that in influenza-pneumonia all of the
lung involved in the early peculiar inflammatory reaction need not
pass through those stages and reactions as we recognize them in
pneumococcus lobar pneumonia.
The resolution taking place in the areas of serous and hemorrhagic
pneumonia is accomplished largely by a reabsorption of
the fluid, autolytic disintegration of the red blood cells and a
certain amount of phagocytosis of red blood cells and their
debris. This resolution is quite rapidly accomplished, and the
clearing up of such an area may take place in a remarkably short
262period of time. The leucocytes and endothelial cells which are
present with every such reaction become active in phagocytosis
of bacteria, and we have repeatedly observed them crowded with
small Gram negative bacilli, whose morphology is similar to that
of the B. influenzæ. These areas contain but few bacteria of
other kinds. The exudate in the alveolar walls is also simple in
character and is readily removed. Slight suffusion of blood,
serous fluid, and migrating cells may occupy portions of the
alveolar walls during the acute reaction, but these, too, are easily
removed and the tissue rapidly resumes its normal character.
The vascular and lymphatic congestion again disappear and the
tissues which once were soggy return to a normal state without
leaving behind evidence of the pulmonary incapacity. The lining
epithelium of trachea, bronchi and alveoli is restored by proliferation
from the neighboring less injured parts.
If this early stage in influenza-pneumonia is to be compared
with the early reactions of endemic pneumonia, it is interesting
to note with what ease the resolution may be accomplished in
the former, whereas in the latter a further sequence of stages
must apparently be passed through before the lung is cleared
of its inflammatory products. As we have intimated before, the
early exudate in these two types of pneumonia differs very essentially,
the one being accompanied by much fibrin and leucocytes
which are present only in small quantities in the pulmonary
lesion of influenza.
Resolution of the other portions of the involved lobes in influenza
is not so easily accomplished. Where a progressive lesion
with its development of pus occupying both the air sacs and the
tissue of the lung, the outcome of attempts at repair are uncertain.
Complete resolution with complete disappearance of the
purulent exudate may take place as we see it in many other
regions occupied by a similar reaction; and where the purulent
response is not accompanied by material damage to the tissue the
restoration of the lung is so complete that upon its recovery no
evidence is left behind of the former injury, but in as much as
the presence of a purulent reaction in the lung is often of more
severe grade than this, a certain amount of tissue destruction
having been accomplished, the repair does not completely restore
the tissue to its former normal state. The purulent lesion, however,
is not uncommonly accompanied by minute capillary thromboses,
263tissue derangement, organic destruction, with even tissue
alteration amounting to abscess or gangrene, and it is too much
to hope that the lung may be completely restored. Minute
abscesses varying from microscopic size to large cavities, several
centimeters in diameter, were not unusual in the tissues severely
involved in the purulent reaction. Thus in these areas, resolution
can be accomplished only by a process of slow organization of
the damaged parts with the final production of fibrosis. These
fibroses are of variable extent depending upon the initial damage.
We have been very much struck with the speed with which this
process of organization may take place and the extent of the
lung tissue which may become involved in this late lesion. In
one of our cases we have evidence of marked fibrosis present on
the twenty-third day of his illness. Patches of organization varying
from one to four centimeters in diameter occupied the different
lobes of the lung. The new fibrous tissue was well developed
and the purulent reaction had largely disappeared. The fibrosis
obliterated the normal architecture of alveoli and bronchioles,
leaving only irregular islands of epithelium which assumed
grotesque glandular shapes and looked not unlike a new growth.
One of the interesting features of these late fibroses which
come to occupy various extents of the lung and bronchial tissues
is that the individual after recovering from his acute influenzal
lesions again passes, in about his third week, into a stage of
dyspnœa with manifestations out of proportion to the physical
signs or constitutional derangements which can be determined.
The dyspnœa is often the outstanding sign and the patient may
die in a state of asphyxia.
We have observed evidence of organization in its earlier reactions
taking place in the patches of gray consolidation. This
organization of the lung tissue takes place as an interstitial
fibrosis and as an alveolar organization. Masses of granulation
tissue grow out into and come to occupy the lumen of the air
sacs, while in other instances the new growth of tissue takes
place mainly in the alveolar walls converting them from thin
partitions to thickened and tough structures. In the cases in
which a purulent pneumonia was present for some time, and
where some of these tended towards repair, this type of restoration
with the new development of connective tissue was found.
The amount of fibrosis varied very much, and in many instances
264there was no evidence that obstruction to the bronchioles
occurred to a material degree. Hence, although we believe that
more or less organization occurs in all of those cases which have
passed through a purulent pneumonia, and that a permanent
mark is left upon the lung tissue, it is not probable that the
amount of involvement and final damage by fibrosis is sufficient
to seriously influence the pulmonary respiration. There is, however,
a certain percentage of cases in which this organization
and fibrosis does involve sufficient of the lung parenchyma and
bronchioles to interfere with the pulmonary ventilation.
Where the purulent pneumonia has markedly involved the
parenchyma, and particularly where vascular channels both large
and small have suffered, some of them by thrombosis, others by
a sclerotic thickening, the circulatory disturbance may be sufficiently
interfered with to infarct the area. The infarction usually
occupies the purulent area itself, and with the complete occlusion
of the circulation the resulting necrosis gives rise to an appearance
different from that usually seen in pulmonary infarcts. The
area may lie in the peripheral portion of the lobe or may occupy
deeper parts. The infarct is of a cream-white color, quite homogeneous,
and resembles the appearance of a local area of caseous
pneumonia. This appearance is brought about through the local
purulent consolidation undergoing necrosis. Some of these areas
rapidly develop a cavity through liquefaction of the exudate.
The localization of the inflammatory products not only upon
the surface of the air sacs but also in the stroma of the alveoli;
the interlobular trabeculæ, and about the vascular channels indicates
the intense effect of the virus of this disease. The exudate
is largely an indication of the point of action of the irritant upon
the tissues, and in influenza with its variety of bacteria in the
lung this is not limited to the surface membrane of the air sacs.
During this second stage of the reaction the purulent exudate
was found occupying all structures of the involved area. Damage
upon the component tissues was to be seen in the endothelium
of the capillaries, the muscle tissue of the bronchioles and arterioles,
the connective tissues and the epithelium. It was seldom
that bacteria were demonstrated in the interstitial parts, and it
would appear that the damage was the result of their toxins.
Hence, broadly speaking, the end result of the pneumonic
process in influenza is far more complex and indefinite than that
265in lobar pneumonia. Resolution may take place early with the
clearing up of the first products of the exudate; or it may be
delayed in association with the secondary purulent process which
not uncommonly occupies multiple lobes. Where the resolution
begins in purulent regions the final outcome is most variable,
depending upon the amount of damage which has been imposed
upon the lung tissue during the suppurative inflammation, ending
either in complete restoration or slight fibrosis of the lung, or
passing on to focal scarring of various degrees, sufficient to alter
the pulmonary capacity. In other instances the resolution is
delayed by the development of abscess, infarct and gangrene.
Here the final outcome is determined by the amount of tissue
involved in the destructive process, and the persistency with
which the infecting micro-organisms attack the local tissues and
the constitutional resistance of the individual. Those individuals
in whom resolution begins before there is much purulent pneumonia
stand the best chance of having the lung return to its
normal characteristics.
Pleura
Inflammation of the pleura was a complication which varied
in its extent and appearance. It appeared to us that a definite
interval lapsed between the development of the lesions in the
lung and the appearance of an inflammatory reaction upon the
pleural surfaces. Although we have recorded evidence of a
pleural reaction in 27 cases, this does not indicate that we have
met with that number of pleurisies of clinical severity. In this
group we include all gradations of pleural reaction from the
merest evidence of irritation and slight dulling of the surface to
the cases in which definite and marked inflammatory exudate
accumulated within the cavity. In many cases we observed a
slight increase in the amount of the fluid present in one or other
pleural cavity, while there was little or no macroscopic evidence
of a cellular or fibrinous exudate. An examination of the fluid
showed the presence of lymphocytes and endothelial cells in small
numbers, and sections of the pleural surface at points where a
slight dulling of the serous membrane was seen at autopsy
showed the presence of a very thin layer of a hyaline fibrin. By
taking these reactions as indicative of pleurisy we have recorded
2666 cases of acute fibrinous pleurisy, 20 of acute serofibrinous
pleurisy, and 1 of acute fibrino-purulent pleurisy.
An increase in the quantity of fluid in the pleural sacs was the
most common indication of pleural irritation. The quantity
varied from 50 to 500 c.c. of a clear or slightly turbid fluid. Not
uncommonly this fluid was blood stained and evidence of superficial
extravasation of blood could be recognized directly beneath
the pleural membrane. These serous reactions accompanied the
early acute stage, while hemorrhage was the accompaniment of
the early period of the influenzal pneumonia when similar hemorrhages
were found in the lung substance. The pleural reactions
were almost entirely confined to the visceral pleura, and only
in the very severe responses did we obtain a marked inflammatory
reaction with hemorrhage upon the chest wall. Goodpasture
and Burnett state that “there is commonly a moderate serous
effusion in one or both pleural cavities amounting to 50 or 250
cubic centimeters. The fluid is clear and has the color of blood-stained
serum. The pleural surfaces are smooth, shiny and wet,
though occasionally a thin, granular fibrinous exudate may be
seen by reflected light over limited areas. Often numerous small,
red, discrete, or confluent pleural hemorrhages are present over
consolidated portions, especially posteriorly on the surface of the
lower lobes.” Where organisms other than the influenza bacillus
had invaded the pleural sac and had been present for a sufficient
time to obtain a reaction, the serous type of exudate observed
in the early lesions changed to the turbid type of fluid accompanied
by more or less fibrin deposit. There was one case where
the intense reaction with fibrin and leucocytes gave rise to a new
character to the pleural exudate, a fibrino-purulent pleurisy or
empyema.
As we have subsequently learned the pleurisies developing late
in the course of the influenza and those which persist after the
pulmonary inflammation has passed are prone to be of a purulent
kind. There have been a fair number of cases of empyema
brought to our attention by the surgical department in the bacteriological
laboratory of the hospital, subsequent to the wave
of epidemic influenza. If one were to base his finding alone upon
observations obtained in the operating room, he would be impressed
by the fact that the pleurisy accompanying the epidemic
of influenza is of a purulent type. On the other hand, if one were
267alone to consider the findings at the autopsy table during the
five weeks of the epidemic, one would be of the opinion that the
pleurisy is of very minor consequence and of a serous type. It
is this changing picture which is particularly to be kept in mind.
And our experience indicates that during the height of the influenzal
lesions of the lung when the pulmonary lesions develop so
rapidly that we obtain a pleural reaction closely resembling the
inflammatory conditions in the lung and also containing bacteria
not unlike the pulmonary flora. Dr. Holman has obtained the
influenza bacillus and other varieties from the pleura during
these early periods of the pulmonary inflammation. It is more
than probable that just as in the infection of the lung tissue
where there is a change in the type of the bacteria present, so,
too, the flora of the pleura alters in the succeeding stages of the
pulmonary reaction. In the late event of empyema we have not
observed the influenza bacillus. The majority of the empyemas
possess hemolytic streptococci and occasionally pneumococci.
Heart
During the acute epidemic and while the disease was at its
height it was remarkable how few cases showed involvement of
the heart. It was the common observation that even during
intense illness the heart action remained fairly stable and did not
indicate an effect by intoxication as might be expected from the
severity of the illness. In as much as the majority of deaths
occurred within relatively few days of the onset of the severe
infection, the type of lesion that would be looked for in the heart
would be either bacterial inflammatory products within the pericardium,
myocardium or endocardium or toxic lesions of musculature
alone.
In our series we have encountered no cases of pericarditis.
This lesion in the experience of others has also been unusual,
and it would appear that bacterial invasion of this sac is accomplished
mainly in the presence of secondary infections localizing
in the neighboring pleura. It was not uncommon to find a slight
increase in the serous fluid in the sac, but this on no occasion
amounted to a hydropericardium. The fluid was always clear
and with no evidence of fibrin or cellular exudate. Petechial
hemorrhages scattered over the epicardium were noted in seven
268cases. In the majority of instances these minute hemorrhages
were scattered in small numbers over the ventricular walls. In
one instance these petechial hemorrhages were also present
through the myocardium, suggesting the influence of an intoxication
not upon the tissues of the heart as much as upon the
finer structures of the vascular channels. This is furthermore
borne out in the presence of petechial hemorrhages confined not
to one organ, but to various tissues and structures in the body.
More or less cloudy swelling or granular degeneration of the
muscle elements of the heart was not uncommon. It was sufficiently
pronounced in 12 cases to be readily detected by the
naked eye. A lesser amount was also observed in other cases
on microscopical examination. In only one instances was the
myocardial degeneration of such extent to lead to a definite and
recognizable weakening of the musculature. In this instance the
autopsy showed a flabby myocardium which was relatively soft
and easily broken and in which all the chambers of the heart
were decidedly dilated. This was the only case in which we were
convinced of a sufficient influence of the toxic effects upon the
musculature to permit a stretching of the walls, with failure of
function.
In a number of other instances, however, in which there was
more or less granular degeneration and cloudy swelling we found
that the right ventricle ceased in diastole without, however, the
capacity of the chamber being enlarged. We would make this
differentiation in speaking of dilatation of the heart. We have
met with 11 cases in which the right heart died in diastole, but
in which there was no evidence that the right ventricle had been
unduly expanded. In four cases there was evidence of an old
compensatory hypertrophy of the left ventricle in which the
cavity of this chamber was also slightly larger than normal. The
lesions in these four cases, however, bore no direct relation to
the results from the influenza infection. The appearance of the
musculature with moderate grade of cloudy swelling suggested
some œdema of the tissues. In the myocardium, œdema is difficult
to recognize, and we would not place great stress upon its
presence in mild degree.
The microscopic examination of the myocardium showing
cloudy swelling gave the usual picture as is seen with a variety
of infections. The muscle fibers showed a fine granular deposit
269in their cytoplasm and the staining quality of the tissue was
somewhat altered. The transverse striæ were less distinct than
normal, while not uncommonly the longitudinal fibrils became
more evident. Fatty degeneration was not encountered.
In the single case showing a definite and acute dilatation of the
ventricles the cause of the myocardial lesion could not be placed
at the door of the influenzal infection. This was the case suffering
from a secondary streptococcal bacteriæmia arising in the
middle ear. It is more than probable that the streptococcus was
the immediate cause of the acute muscle change and weakening.
In a number of cases we have studied the tissues of the bundle of
His, but we were unable to note any definite change.
It is interesting that the intoxication associated with acute
influenza is selective in localizing in certain muscle tissues. We
have previously indicated the intensity of muscle degenerations
occurring in the abdominal recti. Even in these cases where
these striped voluntary muscles were markedly affected the myocardium
showed nothing more than a mild or moderate grade of
cloudy swelling. We can only account for this in a difference
in the constitution of these muscular structures, some being of
such composition permitting of the localizing and damage by
the unknown intoxicant. It does not appear that the reason for
localization in certain tissues is in any way related to the character
of the blood supply, nor is it related to the activity of the
part.
In three cases we have found an inflammatory lesion of the
endocardial tissues. In all of them this consisted of a slight
acute verrucose mitral endocarditis. The lesions were very small,
consisting only of a fine granular deposit looking like grains
of sand localized along the border of the mitral leaflets. In no
instance was the leaflet injured or incapacitated. Unfortunately
the lesion not being suspected was encountered after the heart
had been removed and opened and when it was too late to make
bacteriological analyses. This point is greatly to be regretted,
in as much as it is of great importance to know whether some
distant lesions are induced through the influenza bacillus or its
symbiotic flora.
The majority of authors report but little upon the heart lesions
in influenza. Many deny that a heart involvement is to be found,
a few report an occasional endocarditis. Wallis and Kuskow
270found more or less myocardial change similar to what is usually
described as cloudy swelling. This reaction they point out differs
in no way from the degenerations arising from other types of
intoxications. Keegan in a series of about 23 autopsies found
only a single case with acute dilatation.
Abrahams, Hallows and French had an opportunity of observing
over 400 autopsies upon the influenza patients, and they comment
upon the infrequency of cardiac dilatation. A slight dilatation
of the right ventricle was seen in a few cases, and in no
instance did they find pericarditis or endocarditis. They comment
upon the heart condition as follows: “The most remarkable
feature about the heart is the general absence of dilatation. In
quite a large proportion of cases there has been no trace of dilatation;
in a fair number of others there has been some dilatation
of the right side, but this has seldom been extreme, perhaps
enough to cause the apex of the heart to be formed about equally
by right and left ventricles. Most often the heart has appeared
of normal dimensions and the apex has been formed entirely by
the left ventricle. This absence of dilatation accounts for the
clinical absence of orthopnœa.” In direct contradiction to the
above findings, the Advisory Board to the D. G. M. S., France,
report the findings in 30 autopsies of clinical influenza. Twenty-nine
of these 30 cases showed dilatation of the heart, chiefly of
the right side, but very commonly of the left side as well.
Twenty-one showed myocarditis and two endocarditis. In this
report it is stated that these patients showed evidence of obsolete
tuberculosis. It is possible that the condition of the patients
and the presence of an unusual complicating infection led to the
high incidence of cardiac involvement. The figures in this last
series are much too high when compared with the frequency of
heart involvement as found by the majority of other investigators.
A number of heart lesions not resulting from influenza were
observed. For none of them was there an antecedent history,
but in some cases the condition may have had an influence in
causing accessory cardiac embarrassment. One case had a
chronic interstitial myocarditis of the rheumatic type, three had
mild grades of chronic sclerotic mitral endocarditis, one a bicuspid
pulmonary valve and three showed old pericardial adhesions, one
271of them having a complete obliteration of the sac. The foramen
ovale was patent in six of the hearts.
Arteries
The arteries in these young adults were remarkably healthy,
and in none of them did we observe the characters of arteriosclerosis
or leutic lesions. On the other hand, evidence of superficial
fatty streaks lying in the intima of the aorta and some of
its large branches were not uncommon and are believed to have
had a relation to the acute infection of which they died. In only
four cases in the series of 32 autopsies was evidence of these
fatty streaks wanting. In about one-half of the remaining number
these fatty streaks were only slight or moderate in extent,
while in the rest of them these lesions were particularly prominent
and striking. They formed linear markings on the posterior
wall of the aorta, aggregating with particular prominence about
the intercostal arteries. The anterior wall was quite free from
them. The greater extent of these lesions lay in the descending
thoracic and was less marked in the arch and the abdominal
aorta. At times these fatty streaks were found to extend into
the large vessels of the neck and into the intercostal arteries, and
they were also found in the coronaries of the heart. It was
uncommon to observe their presence in the arteries of the
abdominal viscera.
This type of lesion has been discussed from the standpoint of
its etiology and its possible bearing upon true arteriosclerosis.
Some believe that the frequency of its finding in autopsy
material suggests the non-importance of its presence. This we
can hardly agree with. It is true that the presence of these
lesions does not materially incapacitate the aorta in acting as
the main channel for the distribution of blood. The lesions are
quite superficial in the intima and cause but little elevation on
the surface. The amount of roughening which the intima presents
to the blood is not great. Nevertheless, the presence of
these fatty streaks is an index of the disturbed metabolism of
the cholesterin products of the body. Under certain conditions
they make their appearance when there is a true hypercholesterinemia
such as is readily produced in the animal experiments
by feeding cholesterin. Under these circumstances the various
272tissues of the body, including the adrenal, the corpus luteum, the
spleen, liver and arteries, all participate in localizing cholesterin
in the form of cholesterin-ester in peculiar cells which have been
termed cholesterin-ester phagocytes. It has been shown that
cholesterin metabolism is quite readily altered in the human and
that the blood content will vary from the normal. In chronic
kidney disease, pregnancy, diabetes, chronic heart disease and
arteriosclerosis the blood cholesterin rises, while in many of the
acute infectious diseases the cholesterin in the blood is materially
diminished. It is particularly in these latter cases where fatty
streaks of the intima are prone to occur. Hence in human
pathology we more often meet with the development of fatty
streaks of the intima associated with a hypocholesterinemia than
with a hypercholesterinemia.
The fatty streaks of the intima of the aorta to which we are
referring are lesions quite aside from true endarteritis as well as
atheroma. In naked eye appearance the lesion is of a fatty
nature and suggests atheroma, but it differs from this well-known
lesion in the fact that the fatty materials, cholesterin-esters,
are contained within cells which are of uniform type and
have no reaction in their immediate vicinity. True atheroma
may occur in definite levels of the intima, most commonly in the
deepest portion, and is characterized by the fact that we are
dealing with a variety of fatty materials, neutral fat, fatty acids,
soap, cholesterin-ester and free cholesterin which lie between the
tissue cells forming a detritus following a process of true degeneration.
It is possible that some of the superficial fatty streaks
do give rise to a small atheromatous area by death of the cells
which primarily contain the fatty substances. Most commonly,
however, the fatty streaks do not progress directly to atheroma
but may entirely disappear, as we have seen it occur in our
experimental animals. At other times these fatty streaks are
followed by a slight thickening of the surface of the intima so
that the resemblance to early endarteritis is obtained. We do
not believe that these fatty streaks in themselves lead to the
chronic nodular thickening of the aorta, but that other factors
giving rise to a low grade inflammatory reaction must be present.
There appears to be a relation between the development of
these fatty streaks and the altered cholesterin metabolism,
brought about by pathological change in the blood, adrenal cortex
273and it may be in the liver. It is under these conditions where
these tissues are altered particularly by bacterial toxins in a
process of marked cloudy swelling that these intimal fatty
streaks arise. Analyses in other diseases have shown that such
organic changes lead to a diminution in the cholesterin content
of the blood, while at the same time there is neither an increased
intake nor an excessive output. It would appear that certain
types of tissues and cells are stimulated into activity to become
depots for the cholesterin which is not being properly handled
by the adrenal and other organs. These cells in the intima which
become active in taking up cholesterin-esters are types of endothelial
cells whose origin is not entirely clear. In these lesions
it is observed that the most superficial cells of the intima do not
show an overloading with the fatty compound, but that the cells
active in absorption lie at a level slightly beneath the endothelial
lining and form colonies as if arising through active division of
cells which are present in these parts. Active migration on the
part of these cells is not to be observed. They do not appear
to wander far from the location where they are found during the
acute process. The plaque may enlarge by proliferation and thus
enlarge the extent of the involved area. We have failed to find,
however, that these cells migrate into the lowermost portion of
the intima or into the media. The possibility that these cells
do arise from the endothelium lining the blood vessels has, up
to the present, not been excluded. If such is the case, the cells
appear to adopt a function which is not commonly observed in
normal arteries nor present in the endothelial cells lying immediately
above the fatty plaque.
We have searched various arterial systems in the cases of acute
epidemic influenza for inflammatory lesions lying in the adventitia
and media. These, up to the present, we have not discovered.
Some years ago a number of French authors reported the
development of acute non-suppurative influenza lesions in the
outer coats of arteries which at times had aneurysm as the outcome.
These cases, however, occurred during non-epidemic
periods, when the type of influenza of which the patient suffered
was quite different from that seen in pandemics. As far as we
know none of the reported cases of arteritis and aneurysm occurring
under these conditions has shown the presence of the influenza
bacilli in the arterial lesion. It is possible that sporadic
274influenza has complicating secondary infections which are of
importance in localizing in the arterial wall.
Occasional reports have been made upon the occurrence of
thrombosis immediately following an attack of influenza. These
thromboses have occurred in diverse regions, the brachial,
femoral, the mesenteric, and other arteries. It is possible that
the development of the deep hemorrhagic lesions of muscles in
the extremities are associated with thrombosis. It is impossible,
however, to demonstrate within such blood masses the presence
of thrombosed vessels which had preceded the hemorrhagic state.
It was, however, possible to demonstrate capillary thromboses
through the lung and in the submucosa of bronchi and trachea.
In these instances the damage to the vascular walls was brought
about by the action of the infection immediately surrounding
them, and was not associated with a process beginning within
the lumen of the channel. The type of thrombosis within the
lung to which we have referred in a previous discussion is interesting
in that it does not show the usual type of fibrin clotting,
but in place of fibrin threads a gummy homogeneous material is
deposited upon the vessel walls within which the red blood cells
soon undergo dissolution. It would appear that these thromboses
within the lung are dependent upon a toxic action on the
vessel wall and its plasma content.
Thromboses within venous channels are met with more often
than in arteries. The veins of the lower extremities are most
frequently affected, and yet amidst the many cases of influenza
it is an unusual occurrence. The various thromboses of larger
vessels usually occur as post-influenzal complications rather than
as accompaniments of the acute disease. It is possible that factors
other than those present during the acute stage play an
important part, and that the virus of influenza is not directly
the cause of the thrombosis.
Lymphatics of Lung and Mediastinum
One of the prominent reactions which was almost constantly
present as the inflammatory reaction involving the lymphatic
system of the chest. The lymph glands within the chest responded
to a marked degree in hyperplasia and commonly showed
enlargement quite out of proportion to what is usually observed in
275lobar pneumonia. These reactions were in direct relation to the
inflammatory processes of the lung and appeared to be involved
in proportion to the inflammation occupying the tissues drained
by them. Elsewhere in the body the lymph glands responded but
slightly, and often no change was observed in the lymphatics
of the abdomen, axilla and lower extremities. The systemic
intoxication thus had no effect upon distant lymph glands, and
even the presence of micro-organisms in the circulation did not
appear to cause responses in these tissues other than in the
neighborhood of the chest. Within the chest the lymphatic system
became involved through the presence of the various bacteria
migrating along the lymphatic channels as well as through its
activity in removing products of inflammation.
The response of the thoracic lymphatics, including those within
the lung and mediastinum, is observed in all stages of pneumonia.
But in epidemic influenza the reaction was much more prompt,
appearing in the early stages and rapidly developing tissue
changes along the channels and in the lymph nodes. The lymph
channels during the period of the early serous pneumonia became
dilated and filled with fluid with relatively few cells. The stroma
immediately surrounding became œdematous, so that in the gross
specimen the connective tissue between the lobules of lung were
sometimes easily seen as gray strands. At this time this tissue
was not increased in quantity and did not project above the level
of the cut lung. The fibrous tissue remained soft and pliable, but
formed quite wide strands. When the pulmonary reaction became
hemorrhagic, red blood cells, leucocytes and large mononuclears
were found mixed with the fluid in the lymphatics. We
had no way of determining the direction of the lymph flow from
the pulmonary tissues, but it was assumed that as there was no
excessive loss of serous fluid from the lung and the lymphatics
beneath pleura into the chest cavities that the fluid was draining
through the channels lying about the bronchi and vessels.
The further evidence of the direction of flow was seen in the
rapid and comparable responses which occurred in the lymph
glands along these routes. The glands about the bronchi and
at the hilus became enlarged, red and succulent. The glands were
often two and one-half centimeters in diameter. Their capsule
was thin and stretched and the gland was quite soft. Many of
them when cut open were almost diffluent.
276This acute lymph hyperplasia occurred in 30 of our cases. It
is impossible to indicate any particular type of infection as being
responsible for these lymphatic lesions. The nature of the bacteria
present in these 30 cases differed quite considerably: 25
showed influenza bacilli, 15 pneumococci, 18 streptococci, 8
M. catarrhalis and 17 staphylococci. In as much as the pulmonary
reaction was fairly constant in certain characteristics in
all of our cases, and as we believe that the influenza bacilli were the
very important factor in these reactions, it would appear that the
lymphatic responses are only a part of the general inflammation
of the respiratory organs. Comparison can also be made of the
character of the lymphatic changes with that occurring within
the pulmonary tissues. The lymphatics were filled with fluid
which dilated all the available sinuses; the lymph nodes were
œdematous and within them the reaction often had numerous
small hemorrhages.
The lesion within the lymph nodes following the early serous
inflammation was of a non-suppurative kind. The lymph follicles
lost their outline, and the lymphocytes were diffused through the
stroma so that no recognition of the germinal centers could be
found. The dilated sinuses within the lymph nodes were filled
with large mononuclear cells, of the type of endothelial cells,
along with some lymphocytes and leucocytes. Subsequently the
leucocytes increased very materially so that the lymphatic fluid
became purulent. Smears obtained from larger lymphatics
showed leucocytes and varieties of bacteria. This was particularly
true in those cases where the pulmonary lesion had itself
become purulent either localized in a patchy pneumonia or with
lobar involvement. Under these circumstances focal areas of
purulent infiltration were found within the tissues of the gland
occupying the regions of the former follicles and leading to
necrosis or abscess. Where such purulent reaction and abscess
formation were found within the lymph nodes there was remarkably
little reaction in the tissues of the immediate vicinity. No
attempt at the development of a pyogenic membrane or granulation
tissue was observed, though this probably does take place in
the cases recovering.
In only one instance did we observe the development of the
peculiar fibrosis along the lymphatic channels where the freshly
cut section of lung reveals prominent and raised demarcation
277between the lobules. This response has been described by MacCallum
as unique for the streptococcus inflammation of the lung.
The character of the exudate within the lymphatics with many
mononuclear cells and blood is not to be considered singular for
the influenza pneumonia. It has been found that in ordinary
lobar pneumonia, as well as in the pneumonia following measles,
the early pulmonary reaction is accompanied by the dilatation
of the lymphatic channels along the bronchi, containing serous
fluid, mononuclear cells, blood and leucocytes, while occasionally
thrombosis entangling bacteria is also encountered. It would
seem, however, that the lymphatics in epidemic influenza can
more readily recover their normal character when a streptococcus
infection is wanting.
In the late purulent lesions of the lung we have encountered
dilated lymphatic channels whose yellow contents could be recognized
by the naked eye. At times this could be followed for short
distances along the bronchi as narrow yellow cords, or when cut
transversely appeared as small dots close to the bronchi or vessels.
On pressure small droplets of pus may be evacuated, or
again where fibrin has led to a coagulation of the exudate a
yellow plug can be withdrawn from the channel. These small
plugs resembled the thick exudate seen within the bronchi and
often were misleading when first viewed. The distribution of the
purulent lymphatic masses was most irregular occupying only
local or patchy fields in the lung, particularly associated with
the purulent confluent pneumonia. In one instance such a lymphatic
appeared to be associated with the development of a small
abscess lying close to the bronchus.
Too much stress cannot be placed upon the importance of the
lymphatics in all forms of pneumonia. They play an important
role in the drainage of the lung during inflammation. In the
normal lung we hardly appreciate the lymphatic distribution
except in our observations upon anthracosis. But even under
these conditions when much carbon is deposited in conjunction
with the lymphatic system we do not gain a true appreciation of
the activity of the lymph channels and nodes during an acute process.
Bacteria may be demonstrated in acute infections of the
lung within the fluid and cells of the lymph channels. Less
easily may we demonstrate bacteria in the lymph nodes under
similar conditions, although when abscess has occurred their
278presence is readily recognized. The transport of bacteria is
accomplished not only by a passive migration of micro-organisms
in the fluid as it drains from the lung, but organisms are also
found within the leucocytes as they travel with the current.
Only occasionally have we demonstrated bacteria within the
wandering large mononuclear cells, although we have observed
them in a few instances within the cells lining the sinuses of
the nodes.
Whether the inflammation of the pleura is directly related to
the involvement of the pleural lymphatics we have not been able
to determine. In our series of cases pleurisy has not been a
prominent feature of the disease, and in many instances the
grade of involvement was so slight that it was not easily recognized
by the naked eye and showed only a slight reaction microscopically.
That the presence of bacteria within the intricate
plexus of lymphatics beneath the pleura may be responsible for
the development of an inflammation of this membrane may well
be the case, and in this way simulate the mode of transmission
of the infection as seen in lobar pneumococcus pneumonia and in
the streptococcus type of infection.
Abdominal Viscera
The lesions occurring in the abdominal viscera were of less
importance than those within the thorax. In none of the cases
of the epidemic was the intestinal type of the disease, described
in previous years, encountered. The changes found in the various
viscera were concomitant with evidences of intoxication as
observed clinically or at autopsy in other regions of the body.
We found no evidence that the bacteria of the disease localized in
the tissues of the abdominal viscera, and we were led to believe
that the alterations in morphology and function were the result
of diffusible toxins. The action of these toxins was either upon
the parenchymatous cells of the organs, as in the liver and kidney,
resulting in granular degeneration, or upon the capillaries
with the development of petechial or diffuse hemorrhage as was
encountered in the stomach, intestines and bladder. The absence
of definite localized inflammatory processes in these distant
tissues, including the abdominal lymphatics, speaks against the
probability of a bacteriæmia playing an important role in the
279disease. That transient bacteriæmias by the influenza bacillus
do occur has been repeatedly demonstrated, and that the organisms
associated with this bacillus may also enter the blood stream
has likewise been found. But these states are accessory to the
disease, and must be viewed as complications rather than the
rule. Hence the occasional observations by some, of bacterial
inflammatory reactions in liver and kidney must not be considered
a part of epidemic influenza, for in many cases it is wanting.
The majority of lesions of the abdominal viscera probably arise
through the action of the unknown toxin in the blood.
In the stomach and intestines the lesions were of two kinds,
(1) hemorrhage and (2) erosions. Petechial hemorrhages were
present in the stomach 15 times, in the intestines 4 times. These
small dots of blood extravasation, lying in the mucosa and submucosa,
differ in no way from those observed in other acute
infections and intoxications, save that the tendency for the leakage
of blood into the lumen of the viscera was more pronounced.
Often we could observe the presence of free and more or less
altered blood in the stomach and intestines, and in 12 cases the
amount was considerable, sufficient to be spoken of as melena.
It is probable that the oozing of blood takes place not only from
the areas visible to the eye as petechial hemorrhages, but also
from the more normal-looking mucosa of stomach and bowel.
The tendency to hemorrhage was not necessarily accompanied by
visible alterations in the epithelial layer of the mucosa, though
at times erosions were found. When hemorrhage could be
observed, the extravasation of blood occupied the superficial
layers of stroma, causing a separation of the tissues beneath the
epithelial layer. At times the submucosa was also infiltrated,
and in one instance the musculature. The lesions were isolated
and sporadic, but always about small capillary loops. It appeared
to us that the damage was primarily upon the vascular tissues
and particularly upon the endothelial walls of the fine channels.
Inflammation was not present, and the hemorrhage was more or
less passive—that is, a slow oozing rather than acute hemorrhage
by rhexis.
The second type of lesion of the gastro-intestinal canal was
erosion. This was of the nature of a defect in the mucosa,
usually multiple, small and well circumscribed. The tissue loss
was superficial. In their appearance these lesions were similar
280to those encountered in these parts in other infections, and also
as described by McMeans in experimental infections of animals.
The erosions appear to arise in a process of bland necrosis, limited
in the periphery by healthy tissue and not tending to enlarge. It
is probable that these erosions are associated in their development
with the petechial hemorrhages, being a sequel to the vascular
disturbance of the mucosa and subsequent digestion of the
injured tissue. Multiple lesions of the stomach were found 10
times and twice in the intestine. The largest was 1.25 cm. in
diameter. They are more common on the posterior than anterior
wall, and usually toward the lesser curvature. It is probable that
these defects are limited in their progress and heal readily.
The changes occurring in the liver were not of striking account.
Cloudy swelling was observed 13 times, usually of moderate
grade. The usual appearances with enlargement of the organ,
bulging of the parenchyma on section and a dull gray cut surface
were all that could be found. The one case with icterus was the
only one in which the natural discharge of bile from the liver
was interfered with through the swelling. Even in this case the
obstruction to the outflow of bile in the small channels was not
demonstrable in the microscopic sections, nor was there evidence
of unusual bile staining of the liver-points suggesting the possible
origin of the icterus in an unusual hemolysis. On no occasion
did we meet with recent inflammatory reactions in the gall
bladder or bile ducts, and we have no evidence that the organisms
of the infection are discharged from the body by these routes.
The cloudy swelling of the liver was accompanied by slight
œdema of these tissues in seven cases; and in six instances focal
necroses were observed. These focal necroses were similar in
appearance to those seen in typhoid fever, but were much less
frequent in the tissue. Only careful search revealed isolated pinhead
gray dots with depressed centers. They were most commonly
in the mid-zone of the lobule, and in the early stage were
without inflammatory reaction. Subsequently, leucocytes infiltrated
the area, but not in an amount to form pus. Bacteria
were never demonstrated in the areas of focal necrosis. Four
cases showed old adhesions about the gall bladder and in one a
gall stone was present.
281Lesions of the pancreas were not encountered. In a few cases
the lymph glands about the head of the pancreas were slightly
enlarged.
The spleen showed relatively little reaction and in only two
cases was it enlarged. Fourteen times a diagnosis of acute
splenitis was made on examination of the gross specimen. This
diagnosis rested upon the finding of a swollen spleen with tense
capsule and with a dark bulging pulp. The Malpighian bodies
were usually in part or completely obliterated, though in a few
instances these grayish nodules seemed even larger than normal.
These spleens contained an excess of blood within the pulp. In
one case several isolated areas appeared hemorrhagic as if a local
rupture of the tissues had occurred. The microscopic examination
of these specimens showed mainly a marked congestion of
the sinusoids, a diminution in the size of the lymphoid corpuscles
and some increase in the number of leucocytes within the blood
spaces and reticulum. Only occasionally did we observe a proliferative
reaction of the large mononuclear cells lying in the
reticulum. This proliferation was not sufficiently marked nor
uniformly present to be considered as characteristic. We did not
find abnormal deposition of blood pigment indicating an unusual
destruction of red blood cells within the spleen. It is interesting
to note that 5 of the 32 cases showed obsolete miliary tubercles
in the spleen.
Our analysis of the changes occurring in the kidney bore out
the clinical findings observed in the wards. Like in so many
acute infectious diseases urinary changes were commonly present.
These are in part dependent upon systemic changes in the metabolism
of tissues and not entirely the result of renal lesions. In
acute epidemic influenza there was no common characteristic in
the urinary output. The amount excreted in 24 hours was usually
diminished to a small extent, the color was darker, the specific
gravity slightly increased, as well as the total solids. There was
no marked change in the total quantity of output of any one of the
constituents as far as they were analyzed by us. Albumin was
present in the urine in variable amounts and in the more severe
cases casts were also present. There was only one case in which
the quantitative output was much diminished and where some fear
was entertained of development of acute uremic manifestations.
This individual, however, died before these made their appearance
282and before there was any evidence that the retention of
waste products was causing definite clinical symptoms.
In 30 cases coming to autopsy more or less cloudy swelling
was to be observed in the kidney. This reaction varied from a
very mild swelling and granular degeneration of the tubules of
the cortex to a decided parenchymatous degeneration with loss
of nuclear structure and erosion of some of the cells lining the
tubules. The convoluted tubules were always most markedly
involved. Occasionally this tubular degeneration was accompanied
by a desquamation of the lining cells of the glomerular
capsules. We were, however, unable to recognize an acute inflammatory
reaction in the interstitial tissue or in the glomeruli in
any of the cases, except the one which had developed a streptococcus
bacteriæmia as a sequel to an otitis media. The kidney
lesion reminded one very much of the toxic lesion which is
observed in the kidney in typhoid fever. Differing, however,
from the latter there was a variable congestion of the fine vessels
associated with the cyanosis which was present in a certain percentage
of these cases. At times the kidneys were quite wet
with blood from the venous engorgement.
The lesions in the kidney were of a toxic type and did not
resemble reactions following the presence of the bacteria in the
stroma of the organ. In the majority of instances in other diseases
where bacteria themselves locate in tissues we are able to
recognize focal lesions of acute necrosis or inflammation. In
epidemic influenza where a variety of micro-organisms within
the lung are able to reach distant structures in a bacteriæmia,
we would, because of their type, expect to find inflammatory
reactions of a definite kind. The absence of such reactions is
very suggestive that the bacteria do not commonly localize in the
kidney, but that their toxins alone affect it during its elimination.
We have also entirely missed the finding of any vascular
lesions in the renal system. Neither degeneration nor inflammatory
reactions of any of the coats of the blood vessels could be
distinguished.
The partial incapacity on the part of the kidneys must, therefore,
be viewed as a complication resulting from the effect of a
diffusible toxin reaching them by the blood stream. The damage
performed in this manner may be quite extensive upon the
secreting tissues of the tubules leading to an increased or decreased
283output of the urinary constituents. Because of the nature
of the lesion, it is probable that the kidney damage incurred
during the acute epidemic influenza is only temporary and not
permanent. Tubular degeneration is readily repaired, and in the
absence of an inflammatory reaction in the interstitial tissue
or the glomeruli avoids the development of a permanent mark or
derangement in the system. This is as we find it in typhoid
fever.
In two cases we observed very interesting lesions in the bladder.
These two individuals during life had been excreting
markedly blood-stained urine for some days preceding death.
In the one case the hemorrhage was so marked that on standing,
about one-tenth of the urine was composed of sedimented red
blood cells. It was assumed that the hemorrhage was of kidney
origin until the autopsy revealed a simple cloudy swelling of the
kidney associated with a hemorrhagic state of the submucosa
of the bladder. In both cases the posterior wall of the bladder
was heavily infiltrated with blood so that the mucosa was raised
from the surface and the prominent folds showed a superficial
erosion with small points of greenish necrosis. This bladder
hemorrhage was concomitant with hemorrhagic foci elsewhere
in the body, pericardium, pleura, stomach and intestine. Alone
in the bladder however, the hemorrhage formed a distinct mass
and allowed a considerable escape from the lesions on the surface.
These areas of hemorrhage were not infected and showed no
local inflammatory reaction. They also appeared to be toxic in
origin and resembled the hemorrhages occurring in the muscles
of the abdomen.
Changes in the adrenal gland were noted in 14 instances. In
all of these there was the picture of what is commonly known
as cloudy swelling of the cortex and, in addition to this, in three
cases small petechial hemorrhages were observed. The so-called
cloudy swelling of the adrenal consists largely in a loss of the
bright golden appearance of the cortical tissues accompanied by
soft œdematous swelling. The tissues change color to a brown or
clay color, and it is not uncommon to observe that the inner
zone of pigmentation is more diffuse. There is no sharp demarcation
between the layers of the cortex. With this alteration in
the outer structure of the adrenal, the medulla not uncommonly
284appears smaller. This change is more apparent than real, and
we have not been able to observe any definite lesion in the nervous
portion. At times we believed that the inner tissue appeared
more cellular, but it was not possible to determine any specific
alteration in the cells.
The changes in the adrenal cortex are comparable to those
observed in typhoid fever. The analyses of these tissues showed
that the cells were almost devoid of cholesterin bodies and few
doubly refractile globules could be demonstrated. This change
in the adrenal is by no means specific for any acute disease, it
being found in many of the severe infections. We regret that
systematic analysis of the blood serum in these cases was not
made to determine the cholesterin content. If the comparison
bears out with typhoid fever, we would expect to find that the
quantitative cholesterin of the blood is diminished. Some importance
attaches itself to the study of the cholesterin metabolism,
particularly in regard to the development of the peculiar fatty
streaks which develop in the aorta and other arteries during
these acute infections. It has been claimed that in the human
these streaks bear an analogy to those produced in the experimental
animals and that the arterial lesions are associated with
an altered activity on the part of the adrenal cortex in handling
the cholesterin compounds. In influenza there is evidence that
the adrenal does not function in a normal fashion and that the
storage of cholesterin-esters does not take place. From this,
however, we cannot conclude that the blood content is increased,
and, in fact, it is more than probable in comparing the other
reactions of the disease that it follows the changes as seen in
typhoid fever where the blood content of cholesterin is lowered.
In this way comparison with the experimentally produced arterial
lesions in animals is not clear, in as much as in the experimental
work a true hypercholesterinemia was induced. Nevertheless it
is possible that with the abnormal function on the part of the
adrenal the cholesterin materials are made more available for
absorption by other tissues and that a true hypercholesterinemia
is not necessarily a constant factor, even with the abnormal
accumulation of these substances in the intima. It may well be
that the normal activity of the adrenal is related to the presence
285of toxins in the circulation and an attempt by mobilizing cholesterin
to diminish the activity of these harmful substances.
OBSERVATIONS UPON THE PATHOLOGY OF EIGHTEEN CASES OF INFLUENZA
The recent epidemic of influenza has afforded a series of interesting
autopsies in view of the very extensive and peculiar
involvement that occurred in the lungs of the cases examined.
Ordinary lobar pneumonia, as we know it, was not observed,
although it must be said that the lungs many times exhibited a
consolidation of a lobar distribution. The usual dry granular
lung of the more common pneumonia was absent, and in its stead
a most unusual series of pictures was observed in the several
cases. A common feature of all cases was the œdema of the
lung tissue, which in the majority of instances contained such
an amount of fluid that it ran freely from the cut surface in
almost unlimited quantity. This fluid varied in its color and
consistence depending upon the age of the process. In the very
early cases the lungs were boggy, very congested, and a thin
serosanguinous fluid poured forth from the cut surface. It
actually appeared as though the fluid within the tissue was under
considerable pressure. At times blotchy deep red hemorrhages
occurred in the lung substance, and hemorrhages of a bright red
color were not infrequent in the pleura. That the circulation of
the lungs was much embarrassed was often prettily demonstrated
by the dilatation of the fine capillaries and lymphatics beneath
the pleura. These small vessels stood out prominently as a
meshwork more or less outlining the areas supplied by them.
Not only was the peculiar consolidation in lobar arrangement,
but also in many cases was there evidence of a lobular distribution.
Even in some cases where the entire lobe was consolidated
the cut surface presented a peculiar lobulation with patches of
lung tissue projecting above the general surface. The wet
trabeculated structure of the lung in this stage did not give the
impression of true red hepatization, but rather a structure
resembling spleen and at times a meaty, compact, glassy picture
not unlike thyroid.
286As the process advanced the appearance of the lung changed
from deep red to yellowish red and finally to a quite yellowish
gray color, still retaining, however, the very moist characters.
The fluid found in the lung changed its consistency from the
thin red type to a sticky, glairy variety which could be pulled
out in long strings. It was noted that the change in the character
of the fluid was accompanied by similar changes in the lung
structure, advancing in two cases to abscess formation of a
grape-bunch type. Here there was a rather extensive necrosis
and cavitation of lung substance in communication with the
bronchioles. However, there was also marked softening and
necrosis of lung in a number of cases where abscesses did not
develop, but the lesion was so advanced that the lung substance
was almost diffluent. An accompaniment of these advanced cases
were irregular yellow islands which appeared beneath the pleura.
At times they reached the size of a circle 2 cm. in diameter and
were slightly raised above the surrounding pleural surface. When
these were opened they were found to be areas of softened lung
substance. This reaction was so extensive in some lungs that
it resembled to a degree the appearance of a caseous pneumonia.
However, the former process appeared to be brought about by the
interference with the lymphatic drainage, as it was not uncommon
to see engorged yellow channels beneath the pleura as well
as enlarged lymph nodes at some distance from the hilus.
Another feature of the advanced cases were the plugs of ropy
yellow material which were contained within the bronchioles,
while in the early cases the bronchi and bronchioles showed
intense congestion of the mucosa with blood-stained fluid in their
lumina.
Of the more unusual reactions observed in the lungs an infarct
was found occupying a considerable part of the lower left lobe
in one case. There was a marked softening of the lung tissue
with reddish, mucky-looking lung substance arranged about small
irregular cavities. This reaction extended into the lung for a
distance of 4.5 cm. Bordering close on these softened areas
there was a dry mottled yellowish gray and deep red lung tissue.
Surrounding this area again were noted a number of small blood
vessels in which there were found yellowish granular plugs. One
plug in a vessel was found at a distance of 3 cm. from the base
287of the lobe, and another was found at a distance of 8 cm. from
the apex of the lobe. On further examination it was observed
that the base of this softened area was situated on the pleural
surface and that the apex was directed inward about a distance
of 6 cm. from the pleura. Bathing the cut surface there was a
glairy and very sticky material of a reddish yellow color. Near
the apex of this softened area in the lung there was found a
vessel about the size of a goose-quill in which there was a grayish
yellow granular plug. This plug was adherent to the vessel.
Within the small bronchioles there were plugs of a soft yellowish
brown material. The striking feature in addition to the softening
of the lung in a number of places was the glairy material of a
sticky nature which bathed the cut surface. A white infarct was
present in the spleen. The lung described above as well as
another showed gangrenous change. In the second of these two
abscesses had formed, and there was a communication between
the lung and pleural cavity in which there was a large amount of
sanguino-purulent fluid and a pyopneumothorax.
In a description of these reactions it must be added that the
early and late changes were not always observed independently,
but in most cases occurred together, giving the lung a peculiar
mottled red and yellow glassy appearance. More frequently the
congested œdematous reaction was observed singly, while the
purulent alteration usually was in combination with the former
type. The acute serous pneumonia was noted 13 times, 6 times
in combination with the purulent reaction and 7 times alone,
while the acute purulent pneumonia was found in 9 cases, 3 times
alone and 6 times with an acute serous process. In all but
3 of 18 cases there was evidence of a bronchial distribution. Two
of these three cases showed a massive œdematous lung with in
one case an extensive hemorrhage, while the third presented an
advanced purulent reaction with marked necrosis and softening.
An acute bronchitis which varied in character from a hemorrhagic
to a purulent one was present in all the cases. The reaction
observed within the bronchi in the individual cases corresponded
closely to the picture found in the lungs.
In all cases except one there was an exudate in one or both
pleural cavities. A serofibrinous pleurisy was noted in 11 cases
with, in 2 of this number, a fibrino-purulent reaction present
288in the opposite pleural cavity, while fibrino-purulent pleurisy
occurred alone in 6. In 6 cases pleurisy occurred on one side
only with the incidence equally divided in each cavity. Both
pleurae were involved in 9 cases. Seventeen of the 18 cases
showed both lungs involved. One case was an individual who had
had clinical influenza and during convalescence developed gangrenous
colitis and acute ascending myelitis which terminated
fatally. B. influenzæ was isolated from the bronchioles in the
lung of this individual.
The reaction of the body generally was evidenced by a widespread
distribution of petechial hemorrhages over serosal and
mucosal surfaces. However, certain other important lesions
were noted such as one acute vegetative mitral endocarditis,
two acute serofibrinous pericarditis, three cases in which focal
necroses were prominent in the liver and two examples of infarct
of spleen. Further, there were four cases of slight dilatation of
the right heart. The liver was usually swollen and œdematous
and the spleen presented evidence of an acute reaction, softening
and reddening of its pulp with at times slight enlargement.
As evidence of the virulent character of the infection from
which these patients suffered, there was not only present in the
lung a peculiar hemorrhage and purulent process, but also a
more or less widespread distribution of hemorrhages in other
parts of the body. The gastro-intestinal tract was most affected
with the stomach showing petechial hemorrhages in 17 of 18
cases and the small intestine in 15 of the same number. In the
gastric mucosa of three cases there were definite erosions, while
in two instances the duodenum presented an intense œdematous
and hemorrhagic appearance of its mucosa. Further hemorrhages
were observed on one occasion each in the mesentery and
in the mesenteric and retroperitoneal lymph nodes. In the latter
the mesenteric glands were so distended with hemorrhages that
a soft pulp spurted out when the glands were sectioned. Next
in order of frequency, hemorrhages were noted 9 times in the
pleura, 8 in the pelvis of the kidney, 6 in heart muscle and 3
each in pericardium and bladder. In one case of widespread distribution
of petechial hemorrhages there was a massive loose
hemorrhage into the lower recti abdominis. Further another
289case showed a large amount of a blood-stained fluid in the peritoneal
cavity.
Summary
In the analysis of the cases of acute epidemic influenza two
important features of the disease present themselves, (1) a
marked systemic intoxication with localized manifestations in
certain organs, and (2) inflammatory lesions of the respiratory
tract. These manifestations present themselves both to the
clinician and to the pathologist, and to each they have demonstrated
their importance in the disease. The pathologist not in
touch with the clinical manifestations of the toxæmia has more
closely linked the occurrence of these two factors with the actual
findings in the cadaver. But there are those who look upon
these factors as separate and distinct, viewing the toxæmia as
an individual process and as illustrating the uninvolved influenza,
while the inflammatory reaction of the respiratory tract is taken
to be a complication arising through the activity of secondary
invading organisms. This is the view held by MacCallum, who
compares influenza with the acute exanthemata wherein the
respiratory lesions are but secondary to the production of a
lowered resistance and an invasion by a variety of bacteria. Such
confusion presupposes an undetermined virus for influenza. In
confirmation to such views we have the reports upon a filterable
virus. Up to the present, however, the latter has been on insecure
grounds.
It would appear to us that, as has been discussed by Dr. Holman,
the case against the B. influenzæ not being the important
causative agent has not been proved. The demonstration by
others of a potent toxin from the B. influenzæ cannot be overlooked,
and although the actual disease has not been reproduced
in animals, there is evidence that this toxin will induce acute
degenerations in various tissues. Furthermore, the in vitro
symbiotic relation demonstrated for the B. influenzæ with other
organisms, as the pneumococcus, streptococcus, staphylococcus
pyogenes aureus and M. catarrhalis, gives ample support to the
claim for a similar symbiosis in the human tissues. The evidence
for the important primary relation of the B. influenzæ to epidemic
influenza is such that we cannot disregard it—at least,
290not before we can produce some definite positive evidence that
another demonstrable virus precedes it and produces those constitutional
effects which initiate the remaining sequelæ.
We must agree with Christian in the statement that all cases
dying during the acute stage of epidemic influenza have inflammatory
lesions in the respiratory tract and largely in the lung
(pneumonia). It is difficult to conceive of a disease comparable
to the acute exanthemata, which beginning as a separate and distinct
process ends fatally within 48 hours with a pneumonia
which is claimed to be secondary.
Epidemic influenza is an acute infectious process of the respiratory
tract, usually localizing in the upper respiratory system, but
often and in a fairly constant percentage of cases extending into
the lower portion of the same system and causing a type of broncho-pneumonia.
Accompanying the initial invasion there is a
marked systemic intoxication with lesions of degeneration arising
in a variety of tissues. These lesions of degeneration are to be
seen both locally in the respiratory system as well as in distant
parts, as in the muscles, kidney and liver. The primary damage
arising in the respiratory organs, and which we believe to be the
result of infection by the B. influenzæ, facilitates attacks by such
other bacteria as are available and pathogenic to man. The
secondary invaders are not constant in type, but we find variations
according to the localities where the epidemic takes place.
Just as there is a difference in the bacterial flora which constitutes
the secondary invasion, so, too, there is a variation in the
picture of the inflammatory process which appears in the lungs.
The occurrence of the miliary streptococcal broncho-pneumonia
has been met with in certain localities much more frequently than
in others; lobular and confluent pneumonia has been the prevailing
type in certain regions, while a lobar purulent pneumonia with
abscess and gangrene was most frequent with others. There
does not appear to be an individual and constant character in the
mode of distribution of the pneumonia in the lungs. That the
pneumonias were not the usual type otherwise seen, is fairly
agreed upon by all. The most astonishing feature presenting
itself to us was the frequency of death occurring in the early
stages of the inflammatory process and before the gray stage
had definitely developed. The gray stage of influenza pneumonia
291is a purulent pneumonia which often also constitutes an acute
interstitial pneumonia.
The extensive hemorrhage and inflammatory œdema of the
lung are striking during the early stages of the lung involvement.
The mononuclear infiltration which appears early and remains
for a variable time, until the purulent process is well under way,
is also unique. The hyaline deposit in the lung alveoli; the capillary
thrombosis and necrosis of the alveolar walls and bronchi
are important; while the tendency to abscess, infarct, gangrene
and incomplete resolution with fibrosis differentiates this type of
pneumonia from the common lobar variety.
As an organic evidence of the acute intoxication, none stands
out more prominently than the degeneration of the voluntary
muscles. These resemble the waxy degeneration of other bacterial
intoxications, and particularly that of typhoid fever. The
finding of these acute degenerations does not assist us in arriving
at a conclusion as to the nature of the poisonous body, whether
a true exotoxin. The presence, however, of such widespread
degenerative lesions in cases showing no naked eye change suggests,
at least, that the peculiar muscle weakness associated with
pain has its origin in this definite process and not in primary
nerve lesions.
Very interesting it is that the different muscular structures
are not equally affected by the intoxication. This is particularly
noteworthy in the heart and intestine. In neither of these structures
have we met with lesions comparable to those in the voluntary
muscles. Wherein this immunity resides we cannot state.
In our own series, as well as in the majority of others, there was
an unusual absence of evidence of myocardial weakness. In most
of those dying during the acute illness, the heart muscle was
found firm and the cavities not dilated. This finding was in
striking contrast to that found in acute lobar pneumonia where
dilatation of the right ventricle and auricle, along with muscle
degeneration, is almost the rule. In but one case of the present
series did we find myocardial degeneration leading to dilatation
of the cavities and causing death. And in this particular case
the intoxication was due to a streptococcus septicæmia arising
as a late sequel from the middle ear. The heart in influenza
withstands remarkably well the effects of an intoxication from
292the disease and carries the extra load imposed upon it by the
involved lung with little evidence of fatigue.
It is also worthy of attention to note that the kidney suffers
so little in this severe disease. Bacterial localization with inflammatory
concomitants does not occur, and there is no lasting
damage upon its structure. As in so many conditions of bacterial
poisoning, tubular degeneration, varying from a cloudy swelling
to a more acute damage, is to be found in a percentage of cases,
but complete restoration is rapidly obtained in convalescence.
It is unusual to find such severe renal damage to incapacitate
function to a degree to endanger life.
Finally we can add our evidence, gained from a study of the
pathology of epidemic influenza, that the primary disease induced
by the invasion of the B. influenzæ opens the way for secondary
infections of a variety of kinds, whose subsequent effect may be
more serious than initial lesions. The many late complications
which arise in this manner we have not investigated.
BIBLIOGRAPHY
| Abrahams, Hallows and French |
Lancet., 1919; i, p. 1. |
| Advisory Board to the D. G. M. S |
Brit. Med. Jour., 1918; ii, p. 505. |
| Blanton and Irons |
Jour. A. M. A., 1918; lxxi, p. 1988. |
| Boggs |
Johns Hop. Bull., 1905; xvi, p. 288. |
| Brooks and Cecil |
Brit. Med. Jour., 1918; ii, p. 496. |
| Chickering and Park |
Jour. A. M. A., 1919; lxxii, p. 617. |
| Christian |
Jour. A. M. A., 1918; lxxi, p. 1565. |
| Cole |
Brit. Med. Jour., 1918; ii, p. 566. |
| Cole |
Canadian Med. Assoc. Jour., 1919; ix, p. 41. |
| Dever, Boles and Case |
Jour. A. M. A., 1919; lxxii, p. 265. |
| Fildes, Baker and Thompson |
Lancet., 1918; ii, p. 697. |
| Fletcher |
Lancet., 1919; i, p. 104. |
| Friedlander, McCord, Sladen and Wheeler |
Jour. A. M. A., 1918; lxxi, p. 1652. |
| Goodpasture and Burnett |
U. S. Naval Med. Bull., 1919; xiii, No. 1. |
| Hall, Stone and Simpson |
Jour. A. M. A., 1918; lxxi, p. 1986. |
| Hunt |
Lancet., 1918; ii, p. 419. |
| Keegan |
Jour. A. M. A., 1918; lxxi, p. 1051. |
| Kuskow |
Virchows Archiv., 1895; cxxxix, p. 406. |
| Le Count |
Jour. A. M. A., 1919; lxxii, p. 650. |
| Lord |
Boston Med. and Surg. Jour., 1905; cl, p. 537. |
| Lyon |
Jour. A. M. A., 1919; lxxii, p. 924. |
| 293MacCallum |
Jour. A. M. A., 1919; lxxii, p. 720. |
| MacCallum |
Monog. Rock. Inst. for Med. Res., 1919; No. 10. |
| Muir and Wilson |
Brit. Med. Jour., 1919; i, p. 3. |
| McMeans |
Archives of Int. Med., 1917; xix, p. 709. |
| Nuzum, Pilot, Stangl and Bonar |
Jour. A. M. A., 1918; lxxi, p. 1562. |
| Oertel |
Canadian Med. Assoc. Jour., 1919; ix, p. 339. |
| Opie, Freeman, Blake, Small and Rivers |
Jour. A. M. A., 1919; lxxii, p. 556. |
| Speares |
Boston Med. and Surg. Jour., 1919; clxxx, p. 212. |
| Stone and Swift |
Jour. A. M. A., 1919; lxxii, p. 487. |
| Symmers |
Jour. A. M. A., 1918; lxxi, p. 1482. |
| Synnott and Clark |
Jour. A. M. A., 1918; lxxi, p. 1816. |
| Torrey and Grosh |
Amer. Jour. Med. Sci., 1919; clvii, p. 170. |
| Weber |
British Med. Jour., 1919; i, p. 8. |
| Wittingham and Sims |
Lancet., 1918; ii, p. 865. |
294
EXPLANATION OF PLATES
| Fig. i. |
Cyanosis of head and neck. |
| |
| Fig. ii. |
Acute tracheitis with desquamation of epithelium and superficial necrosis. |
| |
| Fig. iii. |
Acute serous and hemorrhagic pneumonia. |
| |
| Fig. iv. |
Acute serous pneumonia with massive hemorrhage. |
| |
| Fig. v. |
Acute hemorrhagic and purulent lobular pneumonia. The purulent process is seen to be advancing from the focal type to the more diffuse lobar by fusion of the neighboring lobules. |
| |
| Fig. vi. |
Acute purulent pneumonia. |
| |
| Fig. vii. |
Lobular fibrosing pneumonia. In this specimen the patches of new scar tissue formed irregular islands. The final stage of contraction of the scar had not taken place. |
| |
| Fig. viii. |
Acute serous pneumonia with some infiltration by mononuclear cells. |
| |
| Fig. ix. |
Acute hemorrhagic pneumonia. |
| |
| Fig. x. |
Hyaline deposits upon alveolar walls. In some areas the wall itself has suffered necrosis. |
| |
| Fig. xi. |
Acute purulent pneumonia. In other areas of the same lung the interstitial infiltration by leucocytes was more intense. |
| |
| Fig. xii. |
Acute lymph adenitis, showing the unusual numbers of endothelial cells while leucocytes are relatively infrequent. |
| |
| Fig. xiii. |
Rupture of abdominal rectus muscle with hemorrhage. The degeneration antecedent to the rupture is shown in the belly of the muscle. |

TRANSCRIBER’S NOTES
- Silently corrected typographical errors and variations in spelling.
- Anachronistic, non-standard, and uncertain spellings retained as printed.
- Footnotes have been re-indexed using numbers.
*** END OF THE PROJECT GUTENBERG EBOOK 60822 ***