Figs. 1 and 2
MILITARY MEDICAL MANUALS
General Editor:
SIR ALFRED KEOGH, G.C.B., M.D., F.R.C.P.
ARTIFICIAL LIMBS
BY
| A. BROCA | AND | DUCROQUET |
| Professor of Topographical Anatomy | Orthopædic Surgeon to the | |
| to the Faculty of Paris | Rothschild Hospital |
TRANSLATED AND EDITED BY
R. C. ELMSLIE, M.S., F.R.C.S.
Major R.A.M.C.(T.F.)
Orthopædic Surgeon to St. Bartholomew's Hospital, Surgeon to
Queen Mary's Hospital, Roehampton
WITH 208 ILLUSTRATIONS
UNIVERSITY OF LONDON PRESS, Ltd.
18 WARWICK SQUARE, LONDON, E.C. 4.
PARIS: MASSON ET CIE
120 BOULEVARD SAINT-GERMAIN
1918
The infinite variety of injuries which any war presents to the surgeon gives to military surgery a special interest and importance. The special interest and importance, in a surgical sense, of the great European War lies not so much in the fact that examples of every form of gross lesion of organs and limbs have been seen, for if we read the older writers we find little in the moderns that is new in this respect, but is to be found in the enormous mass of clinical material which has been presented to us and in the production of evidence sufficient to eliminate sources of error in determining important conclusions. For the first time also in any campaign the labours of the surgeon and the physician have had the aid of the bacteriologist, the pathologist, the physiologist and indeed of every form of scientific assistance in the solution of their respective problems. The clinician entered upon the great war armed with all the resources which the advances of fifty years had made available. If the surgical problems of modern war can be said not to differ sensibly from the campaigns of the past, the form in which they have been presented is certainly as different as are the methods of their solution. The achievements in the field of discovery of the chemist, the physicist and the biologist have given the military surgeon an advantage in diagnosis and treatment which was denied to his predecessors, and we are able to measure the effects of these advantages when we come to appraise the results which have been attained.
But although we may admit the general truth of these statements it would be wrong to assume that modern scientific knowledge was, on the outbreak of the war, immediately useful to those to whom the[vi] wounded were to be confided. Fixed principles existed in all the sciences auxiliary to the work of the surgeon, but our scientific resources were not immediately available at the outset of the great campaign; scientific work bearing on wound problems had not been arranged in a manner adapted to the requirements, indeed the requirements were not fully foreseen; the workers in the various fields were isolated, or isolated themselves pursuing new researches rather than concentrating their powerful forces upon the one great quest.
However brilliant the triumphs of surgery may be, and that they have been of surpassing splendour no one will be found to deny, experiences of the war have already produced a mass of facts sufficient to suggest the complete remodelling of our methods of education and research.
The series of manuals, which it is my pleasant duty to introduce to English readers, consists of translations of the principal volumes of the "Horizon" Collection which has been appropriately named after the uniform of the French soldier.
The authors, who are well-known specialists in the subjects which they represent, have given a concise but eminently readable account of the recent acquisitions to the medicine and surgery of war which had hitherto been disseminated in periodical literature.
No higher praise can be given to the Editors than to say that the clearness of exposition characteristic of the French original has not been lost in the rendering into English.
The medical volumes which have been translated for this series may be divided into two main groups, the first dealing with certain epidemic diseases including syphilis, which are most liable to attack soldiers, and the second with various aspects of the neurology of war. The last word on Typhoid Fever, hitherto "the greatest scourge of armies in time of war," as[vii] it has been truly called, will be found in the monograph by MM. Vincent and Muratet which contains a full account of recent progress in bacteriology and epidemiology as well as the clinical features of typhoid and paratyphoid fevers. The writers combat a belief in the comparatively harmless nature of paratyphoid and state that in the present war hæmorrhage and perforation have been as frequent in paratyphoid as in typhoid fever. In their chapter on diagnosis they show that the serum test is of no value in the case of those who have undergone anti-typhoid or anti-paratyphoid vaccination and that precise information can be gained by blood cultures only. The relative advantages of a restricted and liberal diet are discussed in the chapter on treatment, which also contains a description of serum-therapy and vaccine-therapy and the general management of the patient.
Considerable space is devoted to the important question of the carrier of infection. A special chapter is devoted to the prophylaxis of typhoid fever in the army. The work concludes with a chapter on preventive inoculation in which its value is conclusively proved by the statistics of all countries in which it has been employed.
MM. Vincent and Muratet have also contributed to the series a work on Dysentery, Cholera and Typhus which will be of special interest to those whose duties take them to the Eastern Mediterranean or Mesopotamia. The carrier problem in relation to dysentery and cholera is fully discussed, and special stress is laid on the epidemiological importance of mild or abortive cases of these two diseases.
In their monograph on The Abnormal Forms of Tetanus, MM. Courtois-Suffit and Giroux treat of those varieties of the disease in which the spasm is confined to a limited group of muscles, e. g. those of the head, or one or more limbs, or of the abdomino-thoracic muscles. The constitutional symptoms are less severe than in the generalised form of the disease, and the prognosis is more favourable.
The volume by Dr. G. Thilbierge on Syphilis in the Army is intended as a vade-mecum for medical officers in the army.
Turning now to works of neurological interest we have two volumes dealing with lesions of the peripheral nerves by Mme. Atanassio Benisty, who has been for several years assistant to Professor Pierre Marie at La Salpêtrière. The first volume contains an account of the anatomy and physiology of the peripheral nerves, together with the symptomatology of their lesions. The second volume is devoted to the prognosis and treatment of nerve lesions.
The monograph of MM. Babinski and Froment on Hysteria or Pithiatism and Nervous Disorders of a Reflex Character next claims attention. In the first part the old conception of hysteria, especially as it was built up by Charcot, is set forth, and is followed by a description of the modern conception of hysteria due to Babinski, who has suggested the substitution of the term "Pithiatism," i. e. a state curable by persuasion, for the old name hysteria. The second part deals with nervous disorders of a reflex character, consisting of contractures or paralysis following traumatism, which are frequently found in the neurology of war, and a variety of minor symptoms, such as muscular atrophy, exaggeration of the tendon reflexes, vasomotor, thermal and secretory changes, etc. An important section discusses the future of such men, especially as regards their disposal by medical boards.
An instructive companion volume to the above is to be found in the monograph of MM. Roussy and Lhermitte, which embodies a description of the psychoneuroses met with in war, starting with elementary motor disorders and concluding with the most complex represented by pure psychoses.
When the present war began, surgeons, under the influence of the immortal work of Lister, had for more than a quarter of a century concerned themselves[ix] almost exclusively with elaborations of technique designed to shorten the time occupied in or to improve the results obtained by the many complex operations that the genius of Lister had rendered possible. The good behaviour of the wound was taken for granted whenever it was made, as it nearly always was, through unbroken skin, and hence the study of the treatment of wounds had become largely restricted to the study of the aseptic variety. Septic wounds were rarely seen, and antiseptic surgery had been almost forgotten. Very few of those who were called upon to treat the wounded in the early autumn of 1914 were familiar with the treatment of grossly septic compound fractures and wounded joints, and none had any wide experience. To these men the conditions of the wounds came as a sinister and disheartening revelation. They were suddenly confronted with a state of affairs, as far as the physical conditions in the wounds were concerned, for which it was necessary to go back a hundred years or more to find a parallel.
Hence the early period of the war was one of earnest search after the correct principles that should be applied to the removal of the unusual difficulties with which surgeons and physicians were faced. It was necessary to discover where and why the treatment that sufficed for affections among the civil population failed when it was applied to military casualties, and then to originate adequate measures for the relief of the latter. For many reasons this was a slow and laborious process, in spite of the multitude of workers and the wealth of scientific resources at their disposal. The ruthlessness of war must necessarily hamper the work of the medical scientist in almost every direction except in that of providing him with an abundance of material upon which to work. It limits the opportunity for deliberate critical observation and comparison that is so essential to the formation of an accurate estimation of values; it often compels work to be done under such high pressure and such unfavourable conditions that it becomes of little value for[x] educative purposes. In all the armies, and on all the fronts, the pressure caused by the unprecedented number of casualties has necessitated rapid evacuation from the front along lines of communication, often of enormous length, and this means the transfer of cases through many hands, with its consequent division of responsibility, loss of continuity of treatment, and absence of prolonged observation by any one individual.
In addition to all this, it must be remembered that in this war the early conditions at the front were so uncertain that it was impossible to establish there the completely equipped scientific institutions for the treatment of the wounded that are now available under more assured circumstances, and that progress was thereby much hampered until definitive treatment could be undertaken at the early stage that is now possible.
But order has been steadily evolved out of chaos and many things are now being done at the front that would have been deemed impossible not many months ago. As general principles of treatment are established it is found practicable to give effect to them to their full logical extent, and though there are still many obscure points to be elucidated and many methods in use that still call for improvements, it is now safe to say that the position of the art of military medicine and surgery stands upon a sound foundation, and that its future may be regarded with confidence and sanguine expectation.
The views of great authorities who derive their knowledge from extensive first-hand practical experience gained in the field, cannot fail to serve as a most valuable asset to the less experienced, and must do much to enable them to derive the utmost value from the experience which will, in time, be theirs. The series covers the whole field of war surgery and medicine, and its predominating note is the exhaustive, practical and up-to-date manner in which it is handled. It is marked throughout not only by a[xi] wealth of detail, but by clearness of view and logical sequence of thought. Its study will convince the reader that, great as have been the advances in all departments in the services during this war, the progress made in the medical branch may fairly challenge comparison with that in any other, and that not the least among the services rendered by our great Ally, France, to the common cause is this brilliant contribution to our professional knowledge.
A glance at the list of surgical works in the series will show how completely the ground has been covered. Appropriately enough, the series opens with the volume on The Treatment of Infected Wounds, by A. Carrel and G. Dehelly. This is a direct product of the war which, in the opinion of many, bids fair to become epoch-making in the treatment of septic wounds. It is peculiar to the war and derived directly from it, and the work upon which it is based is as fine an example of correlated work on the part of the chemist, the bacteriologist and the clinician as could well be wished for. This volume will show many for the first time what a precise and scientific method the "Carrel treatment" really is.
The two volumes by Prof. Leriche on Fractures contain the practical application of the views of the great Lyons school of surgeons with regard to the treatment of injuries of bones and joints. Supported as they are by an appeal to an abundant clinical experience, they cannot fail to interest English surgeons, and to prove of the greatest value. It is only necessary to say the Wounds of the Abdomen are dealt with by Dr. Abadie, Wounds of the Vessels by Prof. Sencert, Wounds of the Skull and Brain by MM. Chatelin and De Martel, and Localisation and Extraction of Projectiles by Prof. Ombredanné and R. Ledoux-Lebard, to prove that the subjects have been allotted to very able and experienced exponents.
Alfred Keogh.
No attempt is made in this little book to describe all the artificial limbs and appliances that have been invented. Before the war these were very numerous, since then their number has become countless, and not a day passes without the appearance of some new model of greater or less ingenuity.
But all these special inventions, the utility of which we should not think of denying, are only of real practical value if the makers have followed out certain general principles in their manufacture. In the following pages we have attempted to indicate what these principles are.
Our experience has been gained in connection with the Fédération des Mutilés, where hundreds of disabled men have been examined and fitted, and where we have always tried to give to each that appliance which is best suited to his work.
For this indeed is the vital principle, and great disappointments will result if, for æsthetic reasons, every patient is given the same appliance, whether it be the leg known as the American leg or an elaborate artificial arm. More often than might be believed accurate imitation of the external form of the natural limb is incompatible with good functional use. This is particularly so in the upper limb.
Perhaps the readers of these pages will gain a clear understanding of these principles; and we shall have attained our object if by enabling them to understand certain typical appliances we make it possible for them to devise others which are at the same time strong, shapely and practical.
Throughout the volume it will be found that we[xiv] express a preference for the construction of artificial limbs for the lower limb out of wood, the method adopted by the Americans. This procedure, because strength and durability are so necessary, seems to us to constitute a very real advance; these considerations are, however, of much less importance in the case of the upper limb. It is a matter for regret that the French official instructions have not compelled our manufacturers to adopt this technique, too often the latter are inclined to keep to their old routine, but they can be induced to alter it, as we have proved by our success at the Fédération des Mutilés.
There is nothing revolutionary in such a suggestion. It has been adopted by the Belgian Government in the fitting centres which they have established; this is also the case with the English authorities, who, we understand, have even attracted from America special fitters for this work. We should have thought that we, in France, might have developed our national supply of artificial limbs in the same direction.
The details of the manufacture of artificial limbs naturally differ greatly in different countries. So much so that at first sight it might appear useless to introduce into England and America the account given in this work of the methods adopted in France. But, as the authors state in their preface, the principles remain the same whatever the details of the methods used. In the lower limb the essentials to be studied are the points upon which weight can be taken, the "Bearing Points," the proper method of fitting the stump, the principles of securing stability and the mechanism of the knee and ankle joints. These remain unalterable whatever be the material used and whatever be the details of manufacture.
In England it has for a long time been understood that every sailor or soldier who has lost a limb has the right to expect that he will be supplied with a good artificial substitute. And, further, it has been taken for granted that this will, in the case of the lower limb, be a full artificial leg and not a peg leg. Therefore the standard pattern has in England been a full limb, and the peg has only been supplied as a temporary appliance, and as an alternative appliance to be used when the other limb requires alteration or repair. For this reason the possibilities of the peg leg, except in its simplest form, have perhaps been neglected in this country, and a study of the French methods of making these peg legs, particularly the convertible peg leg, is well worth while.
The introduction of American artificial legs into[xvi] this country has not been so revolutionary in its results as it is apparently in France, for we have been accustomed for many years to make the bucket out of a single piece of willow. The alterations in our methods introduced recently from America are essentially the following—
1. The use of a sling which passing over the shoulders is attached to the leg below the knee in such a way as to act as a mechanism for extending the knee.
2. The manufacture of the leg portion out of a single piece of wood.
3. The abolition of the old tendon action for the ankle joint (which resembled the mechanism described on page 57) and its replacement by the ankle with movement limited by indiarubber buffers.
4. Covering the wooden part of the limb with a layer of raw hide or parchment, which certainly adds to the strength.
The sole remaining problem in the design of artificial legs appears to be the invention of a knee mechanism which will lock in any degree of flexion when a strain is put upon it, so that the wearer does not necessarily fall when his weight comes upon the limb with the knee flexed. A recent invention, still on its trial, seems to indicate that this problem is not incapable of solution.
In artificial arms the differences between the French and English patterns are greater than in artificial legs. But here again the principles remain the same. In England, also, we have worker's arms and show arms, but the latter tend to be more elaborate than the French patterns, mechanical movements being more developed. For this reason this pattern is usually called, in England, the mechanical arm. Instead of the single cord, looped round the opposite shoulder, and used to open the spring thumb (see p. 101), at least three such cords are used, actuated (1) by rounding the back; (2) by expanding the upper part of the chest, and (3) by raising or lowering the shoulder[xvii] on the side of the amputation. These may be used for various purposes, of which the chief are (1) flexing the artificial elbow; (2) working the elbow lock, and (3) actuating the thumb, fingers or appliances used instead of the hand. The chief other differences in the methods adopted in England are—
1. A smaller enclosure of the shoulder region for purposes of suspension, the limb being held on by a harness of straps. We, in fact, value mobility of the shoulder, and gain it at the expense of stability.
2. The use of various alternative patterns of elbow locks.
3. The appliances used instead of the hand are very different in pattern, although the principles for their construction remain as described here by the authors.
Much ingenuity has been expended on the design of mechanical artificial hands, with results which are satisfactory so far as they go, but which require much further development before the hand can possibly replace even a few of the appliances which can be substituted for it. For this reason it should be made an invariable rule that the artificial hand, however ingenious and however apparently perfect it may be, should be detachable, so that it may be replaced by other appliances.
R. C. E.
| PAGE | |
|---|---|
| GENERAL INTRODUCTION | v |
| PREFACE | xiii |
| INTRODUCTION TO THE ENGLISH EDITION | xv |
| CHAPTER I | |
| GENERAL CONSTRUCTION OF AN ARTIFICIAL LIMB | 1 |
| CHAPTER II | |
| GENERAL PRINCIPLES OF FITTING FOR THE LOWER LIMB | 6 |
| CHAPTER III | |
| ARTIFICIAL LIMBS FOR AMPUTATIONS THROUGH THE THIGH | 12 |
| I. Apparatus with bearing upon the ischium | 12 |
| 1. The shape of the top of the bucket | 13 |
| 2. Mode of suspension | 21 |
| 3. Walking on a peg leg and similar appliances | 28 |
| 4. Walking with free flexion of the knee | 33 |
| II. Limbs without bearing upon the ischium | 60 |
| CHAPTER IV | |
| ARTIFICIAL LIMB FOR DISARTICULATION AT THE HIP JOINT | 64 |
| CHAPTER V | |
| ARTIFICIAL LIMBS WITH FREE KNEE JOINT FOR AMPUTATION THROUGH THE LEG | 66 |
| I. Appliances with bearing upon the tuberosities of the tibia | 67 |
| II. Appliances with end bearing only | 77 |
| CHAPTER VI[xx] | |
| PARTIAL AMPUTATIONS OF THE FOOT | 81 |
| CHAPTER VII | |
| ARTIFICIAL LIMBS FOR AMPUTATION THROUGH THE FOREARM | 84 |
| I. Points of attachment | 85 |
| II. Elbow joint | 90 |
| III. The artificial hand and appliances | 96 |
| A. The artificial hand | 97 |
| B. Appliances for use in place of the hand | 108 |
| CHAPTER VIII | |
| ARTIFICIAL LIMBS FOR AMPUTATION THROUGH THE ARM | 129 |
| I. Artificial arm | 132 |
| II. Worker's arm | 138 |
| CHAPTER IX | |
| ARTIFICIAL LIMBS FOR DISARTICULATION THROUGH THE SHOULDER JOINT AND AMPUTATION THROUGH THE DELTOID MUSCLE | 143 |
| CHAPTER X | |
| SOME GENERAL PRINCIPLES IN THE RE-EDUCATION OF THE DISABLED | 145 |
| INDEX | 159 |
A prosthetic apparatus for any amputation is composed of two parts:
1. The artificial limb.
2. The attachment of this limb to the trunk.
The artificial limb itself is divided into two parts:
1. A conical socket.
2. A part which replaces the missing limb and is in fact a terminal functional appliance.
Two conditions must be considered, whether or not there remains attached to the trunk a segment of the limb capable of being fitted into the base of the artificial limb, to which it gives support, and to which, in addition, it can communicate movement. Accordingly the artificial limb differs essentially for:
1. Disarticulation of the shoulder and of the hip.
2. Amputation of the arm and of the thigh.
In the first case we attach to the trunk an instrument which is entirely passive.
In the second we attempt to turn to account the active movements of the stump.
These various parts do not lend themselves to[2] a general description applicable at once to the upper and lower limbs. Not only are the modes of attachment and the functional artificial limb quite different, but the bucket does not serve the same purposes.
The position of the scar.—The stump, which fits the bucket exactly, transmits to it two kinds of force:
1. The force of vertical pressure.
2. Lateral force corresponding to the angular movements of the joint above.
The lateral force is transmitted by the whole of one surface of the stump to the corresponding lateral surface of the bucket: by the anterior and posterior surfaces only in the case of hinge joints such as the elbow and the knee: by all surfaces in the case of joints with movements of circumduction such as the shoulder and the hip.
Vertical pressure exercised upwards or downwards may cause the limb to press upon the bucket at two points: (1) on the summit of the cone, i.e. on the extremity of the stump; (2) on the base of the cone, i.e. on the bony prominences around the last remaining joint. The adjustment is never sufficiently accurate for the relief due to the fitting of the stump in the bucket to be of much importance.
We should take it as a general rule that a scar cannot stand pressure or friction; and that in consequence, when we amputate under favourable conditions, we should arrange to place the scar in such a position that from our knowledge of the suitable prosthetic apparatus these two evils will be avoided. It should be added, however, that after perfect primary union, the narrow and mobile scar is very tolerant, but it must also be remembered—[3]especially as will be seen in the lower limb—that this condition is rarely realised in war surgery.
The length of the stump is often estimated by reference to that of the other limb; amputation at the upper, middle, or lower third of the thigh, of the leg, of the arm, or of the forearm. This is convenient, starting from a certain minimum length, but there is an absolute minimum length below which the stump has insufficient leverage and tends moreover to escape from the bucket.
Temporary and permanent apparatus.—For the irregular amputations of war surgery which have suppurated, more often than for those of civil practice, it is generally advisable, particularly in the lower limb, to use a temporary apparatus, of fairly good fit, for several weeks or even months before the permanent apparatus of more precise fit. The stump has to soften and shrink gradually; only when this has occurred can we make an accurately fitting bucket, by means of a cast if necessary.
Materials for making the bucket.—The first method of construction is that of leather reinforced with metal; a sheath strengthened with metal supports, is laced around the stump; the supports further give attachment, if there is room, to the artificial joints. This is an excellent principle, either for stumps which are still likely to diminish in size, or for the upper limb where exact fit is of secondary importance.
For buckets accurately fitted on a cast we employ:
Blocked leather, which loses shape and ought to be abandoned for artificial limbs for the lower extremity.[1]
[1] This we have attained at the Fédération des Mutilés, having forced the makers to abandon their routine. It seems to us therefore that the same result might be attained for the appliances furnished by the State, which are still made of leather.
Celluloid is the material of choice, but it has the defect of requiring the hand of an artist; commercial attempts on a large scale have so far yielded mediocre results.
Metal (zinc, sheet steel, aluminium), the defect of which is that the apparatus, particularly for the lower limb, is noisy. This is also an inconvenience in the metal joints of lateral steels of leather appliances and of the spiral springs in certain wooden apparatus, for this reason indiarubber is more often relied on for springs and accumulators.
Wood, for many years used for the commoner types of limbs for the lower extremity, is now, as the result of American influence, utilised for the making of apparatus hitherto termed "de luxe," but to-day serviceable, thanks to this technique.[2]
[2] Working in wood, to hollow out of a log of wood a bucket which fits the stump accurately, is no novelty. Some sixty years ago two Frenchman, Bailly, then Xavier, succeeded in such construction. But these appliances, like the common, cheap unshaped peg leg, split easily and were only made strong when the Americans conceived the idea of covering the outer surface with a layer of raw hide: strong, and therefore practical, for though we may resign ourselves to the frequent renewal of a peg leg at 25 francs, it is another matter with an appliance costing 300 to 400 francs. (Prices in peace time.)
(In England the standard patterns of artificial legs have for many years been made out of wood.—Ed.)
The adjustment to the stump is very exact; the contact with the surface where there is friction is soft and comfortable without padding; the appliance is light, strong and silent. The best woods appear to be English willow and lime. The bucket should not present any flaw or knot, this can be seen on the inner uncovered surface.
But we must emphasise the general fact that standardisation is impossible when the bucket is made of wood.[5] For the other parts it is possible but not for the bucket, which must be made specially for each patient, hollows being made for each bony point, which must be marked out and felt for with the fingers. A plaster cast would appear more exact: but by this means we do not mark out the bony points. Good results cannot be obtained, if, as certain people have tried, linear measurements are sent to a workshop whence an apparatus is forthwith despatched to a patient whom the maker has never seen.
Whether we are dealing with an amputation of the leg or an amputation of the thigh, the principle function of the artificial limb is to support the weight of the body. The bucket must therefore give support to this weight. Three bearing points are thus possible: at the base, upon the surface and upon the end of the stump.
1. Bearing upon the base.—The principal bearing is that which is taken by fitting the upper edge of the bucket under the bony prominences situated around the last joint preserved, i.e. the tuberosity of the ischium for the thigh, the head of the tibia for the leg.
2. Bearing upon the surface of the stump.—Certain makers attribute to this an importance which we believe to be imaginary, but which leads them to erroneous conclusions.
It is evident that if a conical stump which is jointless and which transmits the weight is fitted exactly, point downwards, into a conical bucket, supported below by a vertical pillar, the weight is transmitted by the friction of the part enclosed against the bucket, without any pressure upon the free end.[7] Whence it may be concluded that, as the end of the stump should not serve as a bearing point, we should prefer a terminal scar to lateral scars which might be rendered painful or even ulcerated by friction against the bucket.
But experience shows us that if the pressure of the bucket at this point is harmful to the lateral scars, it is not less so for most terminal scars.
The stump in its bucket is in fact a bone, furnished with soft parts upon which we cannot exert vertical pressure, without squeezing them back towards the base of the stump, thus exerting an upward tension of the terminal soft parts over the end of the bone. This is bound to occur unless there is a considerable length of soft parts beyond the end of the bone, that is unless more bone has been sacrificed than was necessary. In this way we get all the disadvantages of an end bearing without its advantages.
3. Direct end bearing.—This is only the principal bearing in certain special stumps which we shall indicate in due course; in some of these it is the sole bearing. In the case of apparatus for the usual amputations, above the epiphyseal enlargements, it is never more than a complementary or accessory bearing, although a very useful one.
To take pressure upon the end of the stump it is only necessary to stretch across the bucket at the right height a piece of material covered with felt. If the apparatus is made of leather, the support is taken upon a circular band of metal fixed to the lateral steels.
In order that direct pressure upon the stump may be possible, two conditions are indispensable: that there is no terminal scar; and that the extremity of the bone is well covered with a thick and non[8]adherent flap. Actually walking directly on the stump does not involve simply support by pressure, but also inevitable friction, of greater or less importance, caused by the backward and forward movement. This is only realised under the most perfect conditions if the skin is adapted by its structure to this movement. This is the case with the sole of the foot: where the epidermis and dermis are thick and the subcutaneous areolar tissue and deep fascia, continuous with it, enclose little cavities filled with globules of fat; these form a cushion, like little globules of liquid gliding over each other. The skin of the point and of the posterior surface of the heel is less suitable anatomically than that of the sole: it is, however, good, and it is for this reason that after amputation above the malleoli, it is possible to walk directly upon the cut surface of the tibia.
Nevertheless skin which is not prepared in this way by its normal structure can adapt itself to pressure and friction, provided that it is padded by a thick muscular layer, sheathed whenever possible with fibrous tissue. A skin which is not so lined, especially in fair and stout people, with thin and delicate skin, ulcerates easily as the result of friction or even of simple pressure, and bursæ and callosities form. See what happens to the skin on the dorsum and outer side of the foot in the case of talipes equino varus. The muscles of the flap will not remain over the bone in the condition of muscular tissue, they become fibrous—but they are useful because:
1. They interpose a fibrous layer of greater or less thickness between the bone and the skin, so that the latter remains movable over the end of the bone and is not directly compressed;
2. They adhere to the cut section of the bone forming a tendinous insertion, which renders their action on the bony lever more powerful.
A flap bears weight badly when the muscles have retracted around the bone, over which there is then nothing but skin. It is the same when the flap is stretched tightly across the end of the bone, the soft parts must remain soft and free.
Among the hundreds of cases of amputation of the leg or thigh that have passed before us in being fitted at the Fédération des Mutilés, there were many in which the presence of a terminal scar rendered the fitting of an apparatus difficult; we have never found this the case with a lateral scar; we have never seen the latter ulcerate rapidly as the result of pressure or friction in a properly made wooden bucket. So that it cannot be admitted that the proper covering of a stump is ever a matter of secondary importance.
Consequently we should consider, as a matter of principle, the circular method of amputating only as a last resort, and we ought to arrange the section of the soft parts so as to cover the end of bone as adequately as possible, and to bring the scars to one side.
We realise that in practice war surgery often necessitates deviations from the ideal. We often find ourselves in a dilemma—either the stump must be good but too short; or, being long, must be poor or even bad.
In the special case of the thigh, circular amputation in the lower third when it is carried out through healthy tissue and has not suppurated can be trimmed and sutured in such a way as to give an excellent scar, which is transverse and slightly posterior. In[10] this situation after these routine amputations, a linear scar which is supple and has healed by first intention, separated from the bone by a good cushion of muscular and fibrous tissue, causes little embarrassment, whatever its position; at the end of a few months it stands pressure and friction without harm. But we are considering war surgery and consequently we are often called upon to fit stumps in which the cicatrix is large, hard, and more or less irregular, in which the bone has suppurated and in which the neighbouring soft parts are indurated and scarred. These stumps are not, however, the results of the work of the worst surgeon.
Amputating through infected parts, resigning himself to healing by granulation and subsequent trimming by operation, he must take time and trouble to attain in the end a result which is good functionally, although at first sight unsightly. But it is this surgeon who is on the right road, rather than he who sends us good stumps which have not suppurated, because he has amputated through the thigh for a wound of the middle of the leg, or through the leg for a wound of the foot or even of the front of the foot.
It is clear, that for the stump effectually to play its part of a lever in its bucket, a certain definite length is necessary; and we ought to do everything possible to secure a length of at least 15 to 20 centimetres in a thigh stump, or 10 to 12 centimetres in a leg stump. But when this length is secured, there is no great functional difference between, for example, an amputation of the leg in the lower third or in the lower quarter, particularly if the fitter understands how to utilise direct end bearing. The[11] knowledge of this is of capital importance to the surgeon called upon to carry out secondary operations upon imperfect stumps, in determining whether it is possible to put an immediate stop to suppuration by drastic shortening, or whether he must preserve length and lose time by curretting the foci of inflammation in the bone.
There are two entirely different modes of fitting:
I. For amputations above the condyles, in which weight must always be borne upon the tuberosity of the ischium through the top of the bucket.
II. For amputations through the condyles (or for disarticulation of the knee) in which a direct end bearing may suffice.
(Amputation above the condyles.)
In the construction of an artificial limb for amputation through the thigh two entirely different principles may be used, according as it is desired to make the patient walk upon a rigid shaft, that is to say upon a peg, or upon an artificial leg proper, in which the knee bends in walking (known as the American leg).
But whichever principle is adopted, whatever material is chosen, wood or leather, and however exact the fit in the bucket may be, certain common rules govern:—
1. The shape of the top of the bucket by which[13] it is fitted to the top of the thigh and its bearing upon the ischium.
2. The attachment of the limb to the trunk.
To begin with we shall consider these two questions, and then temporary and permanent apparatus, the peg leg and the full artificial limb, will be described.
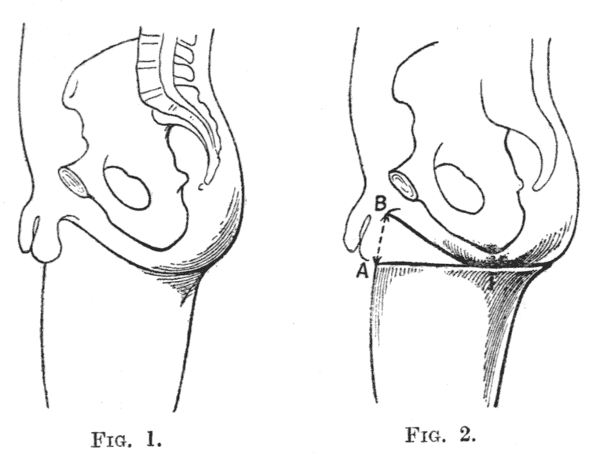
The tuberosity of the ischium is the sole bony point which can prevent the ascent of the limb when weight is applied. This tuberosity is situated in the posterior part of the perineum (Fig. 1), the anterior part of which is unable to stand pressure. It is necessary, therefore, to clear this part by cutting down the inner border in its anterior part, forming a perineal concavity, which rises posteriorly against the ischium (Fig. 3).
It is essential that the ischium should not be able to slip inside the bucket, otherwise the inner border will come in contact with the perineum: therefore the diameter of the bucket must be less than that of the limb, so that the ischium may rest upon its upper edge.
If the bucket is too large, the patient abducts the stump, so as to lower the inner border and prevent pressure on the perineum; he carries the leg away from the side as he walks, and this is both unsightly and fatiguing.
When an apparatus is completed, it is very easy to ascertain the site of the pressure on the ischium. The limb being put on, the ischium is fixed between the thumb and first finger, and it can then be ascertained whether it rests on the edge of the bucket or[14] lies within it. This can be determined more exactly, if whilst the fingers which mark the position of the ischium are kept within the bucket, the patient is told to raise his stump.
If the bucket is sufficiently narrow, it may be circular without the excavation for the perineum (Fig. 2). But this shape is unsatisfactory for another reason, because it results in a tendency for the limb to rotate inwards.
At the moment when the artificial limb is coming in contact with the ground as it takes a step, the pelvis is oblique (the iliac spine of the sound side lying posterior to that of the amputated side). The sound limb as it executes its step is carried forwards, and the pelvis which was oblique in one direction now becomes oblique in the opposite direction. This movement is transmitted to the femur in the stump, so that the artificial limb turns inwards relatively to the stump. With each step this rotation becomes little by little more perceptible, and after a time the patient is obliged to correct it by turning the artificial limb with his hand.
If, on the other hand, the front of the upper border of the bucket slopes downwards and inwards at an angle of about 45 degrees, when as a result of its weight the bucket turns inwards as the limb is swung, the base of the stump will come against a higher part of bucket; but when the pressure of the weight of the body returns, the stump, being forced into the bucket, will descend again along this slope, that is to say a passive external rotation of the artificial limb will be brought about, correcting at every step the tendency to internal rotation.
Figs. 1 and 2
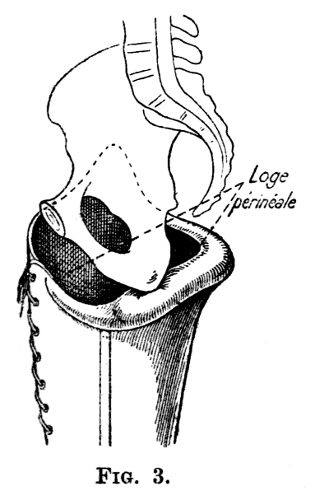
Fig. 3
In the upright position the rami of the pubis and ischium, between which stretches the perineum, slope downwards and backwards at an angle of about 45° with the horizontal. The tuberosity of the ischium bounds the perineum posteriorly, and is its lowest point. The rami of the pubis and ischium, corresponding to the genito-crural fold, mark the boundary between the thigh and the perineum. These bones are unable to stand the pressure of an artificial limb.
If the top of the bucket is narrower than the circumference of the top of the limb, measured below the ischium, it may be circular and still give support to the ischium, which will not slip into it. If the ischium does slip into the bucket, the result will be that it no longer serves as the support, the pressure coming instead upon the rami of the pubis and ischium and upon the perineum.
The constriction thus exerted upon the top of the stump may easily become insupportable. The correct solution of the problem is to cut down the upper border of the bucket opposite the perineum, letting it rise again posteriorly beneath the tuberosity of the ischium, and gain a good support there.
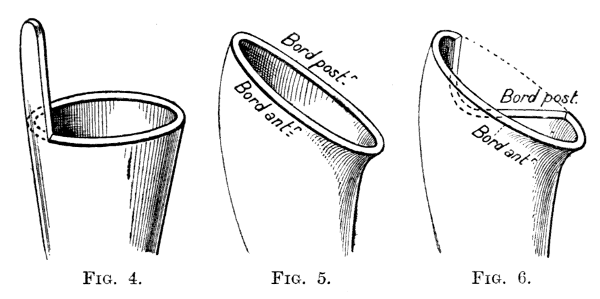
The same slope may be given to both edges of the[16] bucket (Fig. 5). This obliquity in the posterior part serves no useful purpose: it is better on the contrary to lower the posterior border combining this semioblique fitting with a rise beneath the ischium and a depression under the perineum (Fig. 6).
These conditions are easily carried out in a wellmade wooden bucket, represented in figures 8 and 9, in which it may further be seen that from the front it is convex outwards; from the side, convex forwards (Fig. 9). This form, which is that of some good American appliances, ought to be generally used.
The curve outwards, by drawing away the soft parts from it, frees the region of the ischium and allows the tuberosity of the ischium to press upon the bucket (Fig. 8).
If the thigh piece is curved forwards, and particularly if the limb is built with a very slight flexion of the knee, the stump remains slightly flexed at the hip and the patient feels as if he is sitting in the apparatus.
When the thigh piece is straight, an uncomfortable pressure is produced by the edge of the bucket against the ischium. It may be added that extension of the hip is very often impaired, particularly in patients with a short stump: The extensor muscles being divided, the flexors cause contraction into a flexed position, the more so the shorter the stump is. If the thigh piece is straight, the short stump cannot follow the movement of extension necessary in walking; it slips out of the bucket if the anterior lip of the latter is too low.
The principles are the same for the leather bucket, known as the French pattern.
Figs. 4,5 and 6
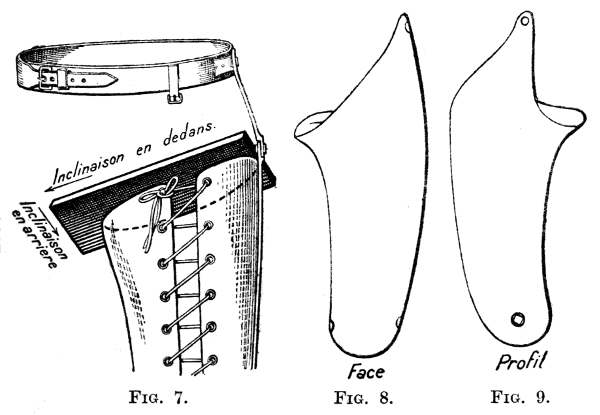
Figs. 7,8 and 9
Figure 4 shows the circular bucket (almost always too large) of the poor man's peg leg, attached to the body by a belt which is fastened to a projection upwards from the outer side of the bucket. Figure 5 shows the oblique bucket, with symmetrical anterior and posterior borders. Figure 6 one with the anterior border oblique, the posterior border being cut away. Figure 7 shows the double obliquity, downwards and backwards, of the bucket. The convexities of the bucket and thigh piece, in the type which we consider to be the best, are shown in figure 8 (convexity outwards), and figure 9 (convexity forwards).
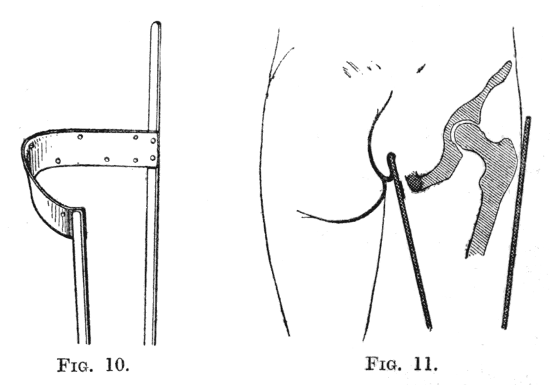
In this the thigh piece is strengthened by two lateral steels (to the lower end of which is fixed the[18] leg piece) joined posteriorly by a semicircular cross piece on which the ischium should rest (Fig. 13).
Figs. 10 and 11
The usual form hitherto has been that shown in figure 10. The cross piece was horizontal and formed simply a posterior semicircle; the lateral steels were straight. Consequently in this pattern these steels form a cone, in which the soft parts are not compressed on the inner side, nor drawn outwards, as in the apparatus previously described. Further, as long as the stump is not shrunken, the ischium covered on its inner side by soft parts sinks into the bucket, and it is the perineum which becomes the point of pressure (Fig. 11). Made of leather, the perineal concavity soon loses its shape and really no longer exists. Finally the bucket is circular, with the faults inseparable from that shape (Fig. 12).
In cases where it is felt necessary to employ leather, all these faults are easily corrected, by giving the cross piece the shape which we have described for the wooden bucket, and by prolonging it forwards[19] through two-thirds of the corresponding circumference, in the shape of an oblique bucket. (Dotted line in Fig. 12.)
If it is not strengthened, an oblique border of leather gives way, and after a few months' use allows rotation. The leather which extends from the termination of the metal ascends very steeply towards the trochanter, whilst the posterior border of the bucket, which is horizontal, curves downwards on the inner side to form the perineal concavity.
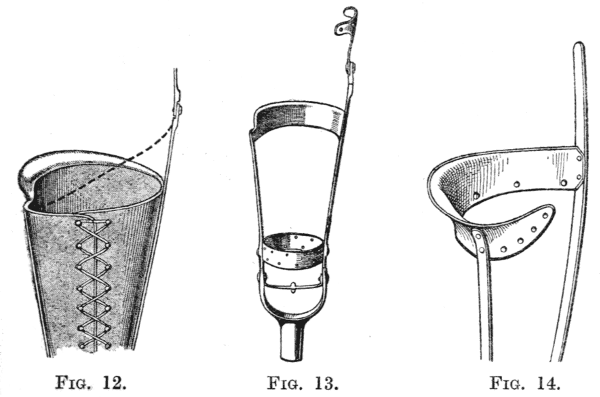
Figs. 12,13 and 14
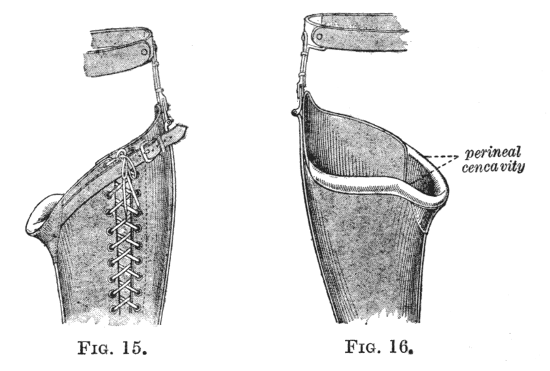
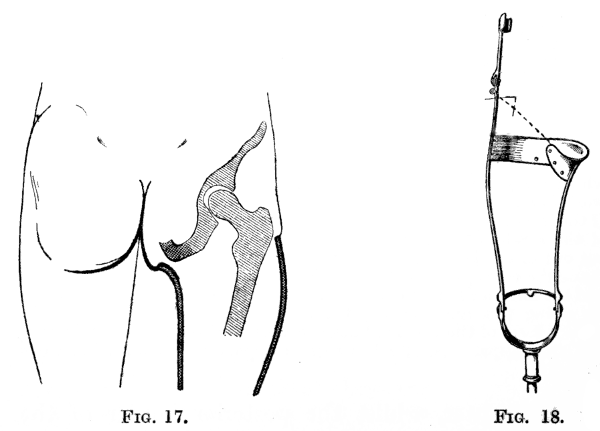
The ordinary leather bucket is mounted upon two lateral steels, which are joined by a posterior cross piece (Fig. 13). This framework is shown in figure 10, and covered with leather in figure 12. If the lateral steels are straight and divergent, this has all the defects of the straight circular bucket. The concavity for the perineum, cut out of the leather, soon loses its shape. It is, however, easy to shape the cross piece as shown in figure 14, with a perineal concavity and the anterior border oblique, following the dotted line in figure 12. By doing this and curving the steel uprights appropriately, the correct form of the wooden bucket can be copied exactly in a leather and steel apparatus. Such a correct apparatus is shown in figures 15 to 18.
In figure 14 is seen the metal framework; in figures[20] 15 and 16 that of the apparatus covered with leather; in figure 17 the support upon the ischium; and the possibility of making this appliance identical with the wooden bucket will be observed (Fig. 18).
Figs. 15 and 16
Figs. 17 and 18
Suspension of the thigh piece is essential, and is all the more important when the stump is short and consequently more liable to slip out of the bucket. For this purpose support may be taken either from the waist, upon the prominence of the iliac crests, or from the shoulders by means of braces. In the case of a long stump (amputation below the middle of the thigh) only one of these methods is necessary, we shall describe the usual methods:
The waist belt (French system) for leather appliances.
Braces (American system) for appliances of wood.
If the stump is short a combination of the two methods is best.
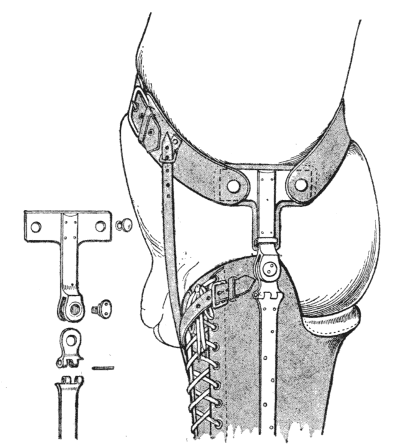
Figs. 19 and 20.—Simple pelvic suspension, with details of the joint at the hip.
A. Suspension by means of a waist belt.—For the peg leg made of leather the best method consists in placing a pelvic plate, which is attached to the hip steel, below the iliac crest (Figs. 20 to 24). A belt attached to the extremities of this plate surrounds the pelvis and passes above the iliac crest on the other side. The thigh piece is attached to this support, on the outer side, by articulation of the outer femoral steel with the hip steel; on the inner side, by a perineal strap. Braces complete the method of suspension of the apparatus (Fig. 21).
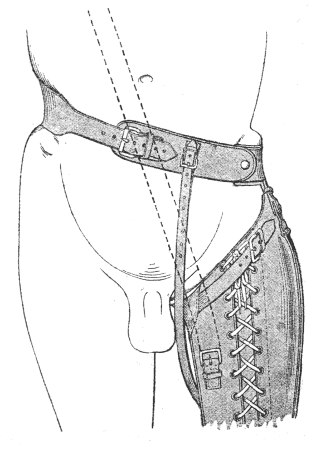
Fig. 21.
The axis of the metal joint between the outer femoral steel and the lower end of the T piece should be directly above the great trochanter (Fig. 20).
The femoral steel often breaks in the neighbourhood of this joint (Fig. 23); we have got over this difficulty by adding immediately beneath it a joint which allows of abduction (Fig. 19). A perineal strap limits this movement.
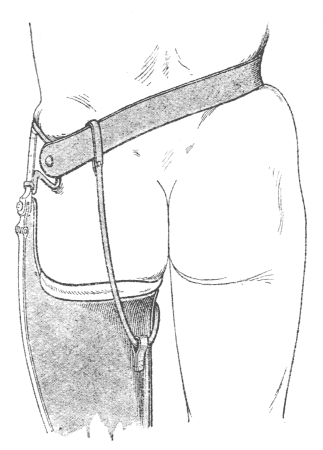
Fig. 22.
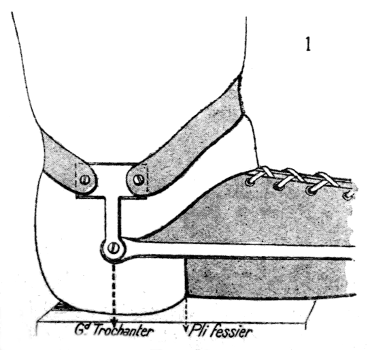
Fig. 23.
Suspension from the pelvis.
A metal hip piece is fixed below the iliac crest and held in place by a belt which passes above the iliac crest of the opposite side (Figs. 20 to 24). This piece is attached to the thigh bucket by a joint shown in figure 19 (see also Fig. 22), which allows both flexion and abduction of the hip, and which forms the suspension of the outer side of the limb. The inner border is suspended by means of a perineal strap, shown in figures 21 and 22. In figure 21 is shown how a suspending brace may be easily added. Figure 23 shows the action of a single hinge joint, allowing only flexion and extension at the hip joint. On page 27 will be seen similar joints which, however, move on the pelvic attachment as well as on the thigh piece. The object of this is to prevent the pinching of the abdominal wall by the top of the thigh bucket when the patient sits. It is indispensable in short stumps. On page 21 will be seen a joint which allows abduction of the hip, and thus relieves the strain upon the hinge joint; without it the latter is easily broken.
B. Suspension by means of braces (American method).—The American method of suspension has the advantage of leaving the pelvis free; the patient does not feel the pull of the hip piece. Besides, when the belt is used, if the patient sits down, the buttock on the side of the stump is raised, to an extent corresponding to the thickness of the bucket, an obliquity of the pelvis, which is both uncomfortable and unsightly, being produced. The braces being relaxed in the sitting posture, the patient can avoid this inconvenience; for the stump may be slipped partly out of its bucket, the upper extremity of which is then beyond the level of the edge of the chair. This[25] position is very comfortable, because it is normal, but the patient must replace his stump in the bucket whenever he stands up.
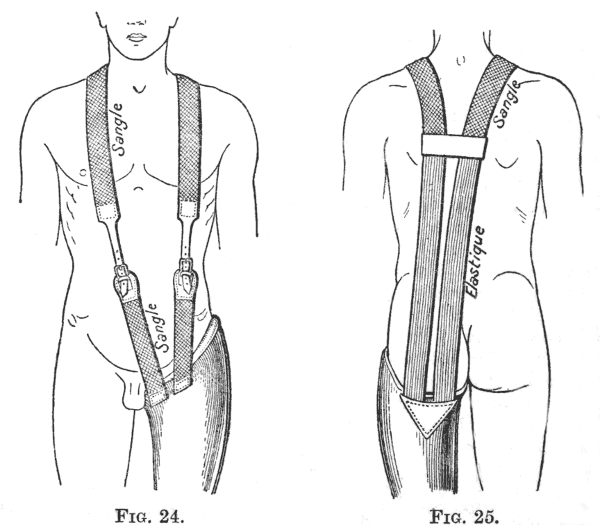
Figs. 24 and 25
Braces composed of straps passing over the shoulders and down the front, attached to the bucket by buckles. Posteriorly they are joined together by a cross strap between the scapulæ, and beyond this are continued in the form of elastic straps.
This form of suspension is essential for those artificial limbs with a free knee-joint, in which, as we shall see, the braces serve to extend the joint.
We illustrate here two methods of attaching the braces to the thigh piece, that which we use in the limb supplied by the Fédération (Figs. 24 and 25)[26] and that which is used in the American limb of Marks (Figs. 26 and 27).
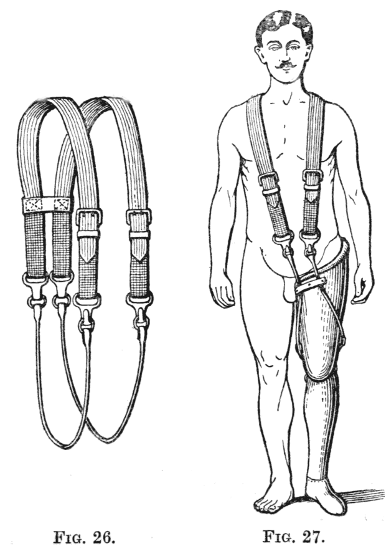
Fig. 26.—Braces which end below in looped thongs of leather.
Fig. 27.—These loops, held in to the thigh piece by passing beneath a loop of leather, pass over two pulleys about the middle of the inner and outer sides of the thigh piece respectively. The outer brace tends to abduct the limb if it is tightened.
C. Combined method of suspension.—If the stump is short the artificial limb must be attached both by a belt and by braces; the latter should be 5 to 6 centimetres wide.
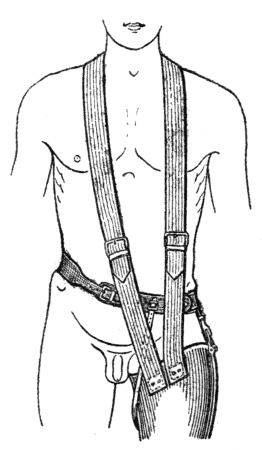
Fig. 28.
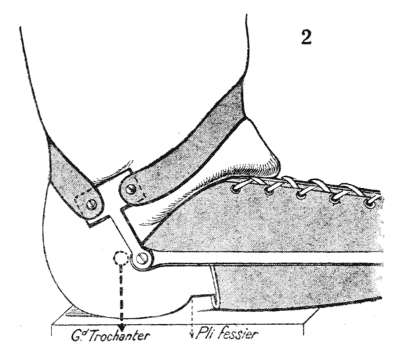
Fig. 29.
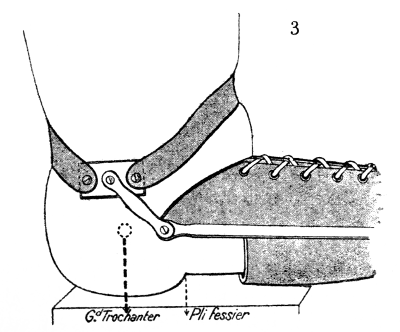
Fig. 30.
Combined suspension for short stumps.
Fig. 28.—Complete appliance.
Fig. 29 and 30 show the value of a flexion pivot between the hip piece and the pelvic plate. If there is no such pivot, the T piece undoubtedly rotates upon the belt, but not to a sufficient extent to prevent the thigh piece in rising and pinching the abdominal wall (Fig. 29). If there is a double joint the hip piece becomes oblique, thrusting the thigh piece forward and allowing the patient to sit erect (Fig. 30).
In these cases also, to prevent the stump escaping from the bucket when the hip is flexed, the front of the thigh piece is carried as high as possible; but if the appliance is furnished with a metal T piece, such as has been described (Fig. 29, see also Fig. 23), then this raised border prevents flexion of the hip by coming in contact with the abdominal wall when the patient sits down. This difficulty can be got over by making the top of the T piece movable; when the patient sits down the vertical piece of the T becomes oblique, the thigh piece comes forward, allows the stump to escape a little way and no longer presses against the abdominal wall (Fig. 30).
The belt may also be replaced by a leather corselet,[27] having fixed to it the hip piece that we have just described.
The braces by themselves are a poor method of attachment for a short stump.
In the sitting position the stump easily escapes from the bucket.
When the patient is standing the stump remains abducted, whilst the apparatus, as the result of its own weight hangs vertically, in this swaying position the lower extremity of the stump presses against the outer side of the bucket, whilst the inner edge of the bucket cuts into the flesh at the top of the thigh.
The rigid peg and the jointed peg.—The peg leg is a rigid rod, ending in a slight enlargement, which transmits the weight of the body, resting by means of the ischium upon the top of the bucket, directly to the ground.
The erect position is thus very secure, and stability in walking is also very good throughout the time when the artificial limb bears the weight.
To raise the limb from the ground and carry it forwards, the patient uses at the same time both flexion of the stump at the hip and movements of the pelvis (elevation, then rotation inwards) varying to some extent with his proficiency and with the length of the stump.
The old-fashioned peg leg, called the "poor man's peg," consists of a bucket continued into a rigid peg. If the support beneath the ischium is well made according to the principles described above, it is an excellent temporary limb.[3] This bucket of common wood, which is not specially shaped to the stump, is very economical; its imperfect fit is an advantage[29] in that the stump, which is still enlarged, cannot bear friction; as the stump assumes its true shape and diminishes in size, the bucket is packed. We would add that every patient, who is not rich enough to possess two complete artificial limbs should have in reserve an emergency peg leg, for occasions when the artificial limb requires repair.
[3] A number of temporary limbs have been designed, with buckets of lattice work or of plaster. The old-fashioned wooden peg, which is easily obtained, avoids all this additional work without any disadvantage.
As a permanent apparatus, with accurately fitted bucket, the rigid peg leg has two defects: it has not the appearance of a leg and foot, and when the patient is sitting the rigid peg is unsightly and inconvenient to him and to his neighbours. We have therefore designed and completed a jointed peg leg, the principle of which is as follows:
Below the thigh piece the peg is attached by a transverse joint, this joint being locked in the extended position when the patient is upright. The patient sets it free by manipulating the lock through the trousers, when he sits down; when he gets up again the locking in the extended position is automatic.
The fitting of this transverse joint may be carried out in two ways.
1. The upper end of the peg ends in a stirrup-shaped fork and the bolt passes through the two ends of this fork and through the lower end of the thigh piece (Figs. 31 to 33).
2. The lower extremity of the thigh piece has cut in it a central mortise into which fits a vertical plate, prolonged upwards from the middle of the leg piece. The bolt passes through this artificial tibial spine and through the two sides of the mortise in the thigh piece. If the hole in the tibial spine through which this bolt passes is square the hinge works securely (Figs. 34 to 36).
In this form the axle turns with the leg, in the first form this is also possible. But most often when the forked attachment is used it is fixed to a leather thigh piece, and each end of the fork is jointed independently to the corresponding end of the lateral steels of the thigh piece, without any complete transverse bolt. It is then the fork that revolves around these two joints.
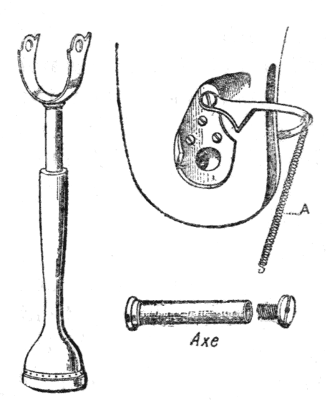
Figs. 31 to 33.—Fixation of the stirrup of the leg (Fig. 31) by a transverse bolt (Fig. 33), the aperture for which in the thigh piece is seen in Fig. 32. Double lock (Fig. 32).
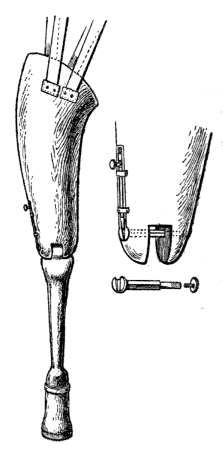
Figs. 34 to 36.—Attachment by mortise and tenon, with a bolt, square in section, passing through the knee. Single lock on the outer side.
If there is a complete transverse bolt, the joint can be securely locked by a single lock at one of its extremities (at the outer extremity) (Figs. 36 to 39).
If there are two lateral joints the single lock is insufficient, both joints must be fixed at once; unless this is done, that which is not fixed has a certain amount of play and is strained.
It is, however, simple, by means of a posterior semicircle, to joint the two locks and to work them together by a single movement (Fig 32).
For æsthetic reasons the wooden leg piece may be made in the shape of a leg and foot. But if the principle of the peg leg has been adopted, for an agricultural labourer for example, on account of its stability, it is better to use an appliance in which a "show leg" is fitted around the simple peg on days when appearance is more important than work (Figs. 37 to 45). The limb is thus rendered lighter, for the false calf consists of a simple layer of felt and it is very easy to replace the enlarged lower end of the peg by a foot.
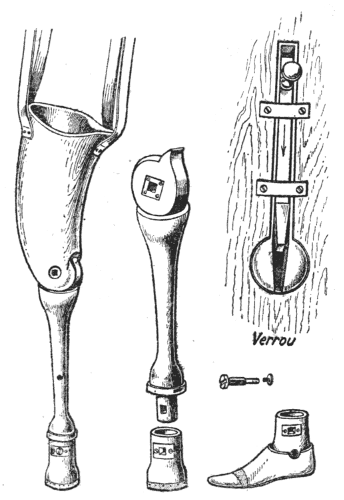
Figs. 37 to 40.—Attachment by a mortise, and show foot.
We show later two models of this sort, one with an American thigh piece of wood and a single lock upon a transverse axle, the other with a leather thigh piece and a double lock. The first (Figs. 37 to 40) is shown with an attachment by braces, and the second (Figs. 41 to 47) with an attachment by means of a waist belt; we have already explained when these two must be combined.
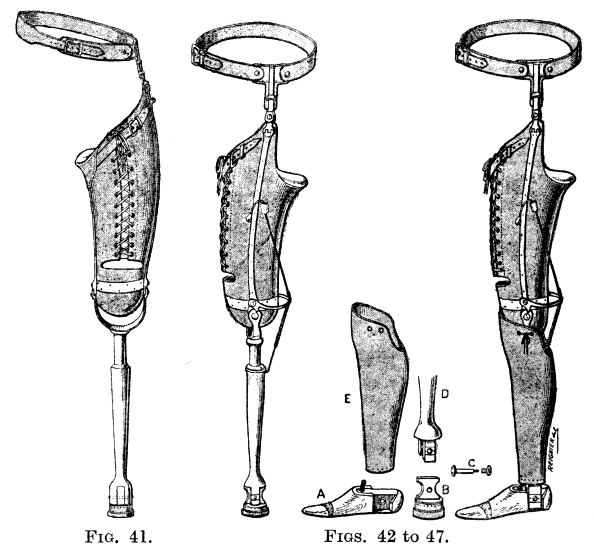
Figs. 41 to 47
Leather and steel peg leg, with show foot.
Figures 41 to 47 (leather appliance) should be compared with figures 37 to 40 (wooden appliance) which complete them in certain points. It is unnecessary to refer further to the method of fitting the bucket to the suspension, or to the method of attaching and locking the knee.
The peg—attached above by a stirrup or by a mortise, it does not matter which—ends below in a rectangular tenon which fits into a corresponding excavation in the upper surface of the terminal piece, whether peg or foot (Figs. 38 and 44). A transverse bolt, square in section, with a head at one end and a thread at the other, fixes these two parts together. By taking out this bolt the peg can be replaced by the foot or vice versâ.
If the attachment of the foot is made in the heel, a fixed foot is used (Figs. 43 and 45), but it is easy, by making the attachment higher, to use a foot with movable ankle joint (Fig. 40).
The attachment of the show calf piece around the peg is shown in figures 43 and 45.
Most often the wooden thigh piece is to be preferred;[33] the limb is lighter and may last four or five years instead of about two years.
We may add that leather loses its shape and the bucket becomes enlarged, producing inconveniences already described on page 18.
But leather—indespensable for certain stumps which cannot stand a wooden bucket—has the advantage that it can be employed as a temporary fitting. During the first weeks, sometimes even for the first months, the shrinking of the stump can be accommodated by lacing up the bucket, and, when shrinkage is complete, the leg part of this first apparatus can be attached to a wooden bucket which the improved condition of the stump now renders possible.
This form is a little more expensive (80 frs.) than "the poor man's leg," but I believe a great deal more comfortable. It may be added, that it is easy when the foot is fitted at the end of the apparatus to render flexion of the knee free and to attain the "American walk," of which we shall speak later. All that is necessary is to attach in front an artificial muscle of indiarubber, reaching from the thigh to the leg and an extending sling like that in the American limbs (see page 47).
This appliance which we call the "Fédération Leg," because we designed it at the Fédération des Mutilés, has already been imitated without its origin being acknowledged.
A. Design.—The oldest type, which will suffice for studying the general conditions of stability, is that[34] of Marks, with a fixed foot shaped out of the same piece of wood as the leg: the ankle joint—several types of which we shall describe later—does not affect the question of stability.
The appliance is made entirely of wood; it is strong and light.
Nothing need be added to the description already given of the fitting and method of attachment of the thigh piece, which ends below in a curved "condyle,"[4] which fits into the top of the leg piece. It is transfixed by a metal bolt, from each end of which a metal plate descends and is riveted into a corresponding groove in the leg.[5] This forms the axle which rotates in the thigh piece when the knee flexes or extends. Flexion of the knee is free. Extension is stopped just short of the straight line (see p. 16).
[4] The bucket and the condylar portion are made of two separate pieces of wood.
[5] The hole through which the bolt passes being cut in soft wood (willow or lime), must be strengthened by a cylinder of metal, of leather, or of harder wood (beech or service tree) in which the axle revolves.
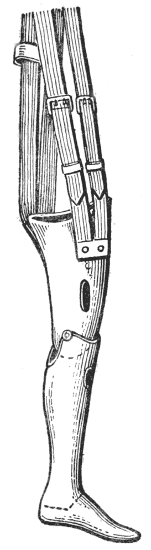
Fig. 48.—Marks leg with fixed foot.

Fig. 49.—Construction of the foot.
The foot is in equinus at an angle of 25° to 30° so that the heel is 2 or 3 centimetres from the ground (the usual height of the heel of a boot). The piece of wood which forms the instep and which is continuous with the[35] leg stops at a point corresponding to the middle of the metatarsus, and is only half the thickness of the foot. The rest of the foot is shaped of indiarubber stuck on to the instep piece; the wood and rubber being enclosed in a sheath of leather.
The foot should also point slightly outwards, as in the normal standing position.
To ascertain whether the limb is built so as to ensure equilibrium, a thread is stretched against its side so as to pass through the axes of the knee and ankle joints, if this cuts the ischial bearing point at its centre the equilibrium of the patient is assured. Equilibrium will be better still if the cord lies entirely behind the ischial bearing point, leaving in front of it the greater part of the thigh piece. The best method of ascertaining if the foot is properly mounted is to hold the limb in front of one by the thigh piece, with the knee bent at a right angle; it can then be seen whether the foot turns outwards at the correct angle.
It is not necessary to say anything more about the shape of the thigh piece (page 17).
The metal bolt which transfixes the knee must not allow any play; the hole through which it passes must be lined with hard wood or leather.
The indiarubber sole should be reinforced with several layers of canvas incorporated in the rubber, as the latter if not so reinforced perishes and cracks.
The appliance must further be examined after it is applied. The level of the iliac spines must be compared: the spine on the side of the amputation should be 2 cm. below that of the sound side.
Examine the position of the point of the foot. Make the patient sit down, see if the knees are on the same horizontal plane; if the sound knee is the higher[36] the leg piece is too short. The foot being fixed in the equinus position the patient must wear boots while the examination is being carried out.
B. Mechanism of walking.—In walking, a step being taken with the artificial leg, the toe of the foot is the last to leave the ground, the heel being raised and the knee straight. The limb is swung forward and raised by flexion of the hip: active flexion of the knee is impossible, but passive flexion occurs, owing to the weight of the leg piece, as the thigh is raised.
At this moment the leg piece is vertical, forming an angle with the thigh, from this position it must pass into one in which it is oblique forwards and downwards, in a straight line with the thigh, so that the knee may be fully extended when weight is again borne by the limb as the foot meets the ground. If at this moment the knee is flexed the limb will double up under the weight of the body.
The first contact of the limb with the ground should be at the heel with, as we have already said, the knee extended. Afterwards as the limb, which at first points obliquely forward and downwards, passes into the vertical position in which it must be at the period when it bears the whole of the weight, this complete extension becomes locked and transforms the limb into a rigid column.
This is brought about as explained on page 48 by mounting the foot in equinus, and we must here describe the methods by which the commencement of the movement of extension may be communicated to the leg so that the heel may be the first part of the foot to touch the ground.
These methods may be termed knee extending mechanisms. [37]They assist the passive action of the weight of the leg.
In fact the recurrence of extension is brought about by a pendulum movement of the leg, which, at first oblique downwards and backwards, swings into a downward and forward obliquity. But this movement is slow (the pendulum which marks one second is one metre long) and incomplete. The patient can make it complete with a little instruction, by extending the thigh slightly as soon as the foot touches the ground.
This may be sufficient if the stump is long; the leverage is good, and while the hip is being flexed a swing can be given to the thigh piece which accentuates the pendulum movement of the leg.
But with a short stump some special mechanism is essential to make sure that extension will be complete, otherwise the patient will be obliged to walk with short and calculated steps, to wait whilst the pendulum action produces extension of his knee and allows him to put weight upon his foot.
C. Mechanism for starting extension of the knee during the time the leg is swinging.—There are two methods which are generally combined:
1. Elastic traction by an artificial muscle.
2. The extending sling.
1. Artificial muscle.—The action of an artificial muscle made of elastic (noiseless) or of a coiled steel spring, is easily understood.
(a) The simplest method (that which is commonly used for infantile paralysis affecting the quadriceps) consists in fixing an elastic band divided into two slips, one on either side of the patella) between the front of the thigh and of the leg, about the middle of[38] each. (This is represented in figure 98 in our convertable leg.)
(b) When the apparatus includes the regular artificial knee the makers generally place this mechanism in the interior of the thigh and leg pieces, using methods which are often very ingenious. Of these we illustrate some on pages 40 onwards, with an explanatory description.
In describing these mechanisms, which may be called intra-condylar, it is necessary to speak at the same time of the stop to limit extension because, as will be seen, it is combined with the extending spring.
We have already said that rigidity in extension when the limb is vertical is essential, but whilst it is necessary for extension to be complete at this moment it is also necessary to prevent the knee being forced into the hyperextended position, as this would quickly strain the joint and render the limb useless.
This limitation of extension can be effected quite easily by the tension of a popliteal cord (see page 41. The knee in Marks leg), or by carrying the anterior border of the leg piece upwards in front of the thigh piece so that it impinges against the latter.
This method is not very good because it is noisy.
Moreover, the repeated impact against the leg piece may split the wood, so that if this method is adopted the stop must be reinforced by a binding of several layers of parchment.
We will first describe a mechanism the association of which with the extending sling will be seen on page 48.
α. To limit extension of the knee all that is necessary is to prolong the antero-posterior diameter of the knee bolt (which turns with the leg) by a horizontal wing,[39] which engages with a corresponding notch in the femoral condyle. We show here Figs. 50 and 51) a rather more complicated but still simple mechanism which is interesting because it can be combined with the action of the extending sling (see page 48).
It consists of a piece of metal curved on the flat, ending above in a cylinder through which the knee bolt passes, continued below into a cylindrical tail piece, which fits into a ring which is fixed inside the top of the calf. During flexion this plate moves in a median posterior window in the femoral condyle, becoming oblique at the same time as the tail piece sinks into the ring; during extension the tail piece rises in the ring and the interior flat surface engages against a corresponding groove in the femoral condyle (covered with leather to secure silence).
Figs. 50 and 51.—Internal mechanism to limit extension of the knee.
β. In the Marks knee an internal system of cords and springs serves at the same time both to limit[40] extension and to produce an elastic extending force. It is a system which is fairly simple and much used.
1. Limitation of extension is secured by a U-shaped cord, the extremities of which are fixed to a wooden cross piece (T), fixed in the thigh piece three centimetres above the axis of the joint. The cords leave the thigh through two lateral openings in the back of the thigh piece, and the loop passes through a ring halfway down the calf.
2. The extending force consists in a coiled steel spring the mechanism of which is combined with that of this cord. The lower half of the spring is enclosed in a copper tube lined with chamois leather to secure silence; its upper half or rather more is coiled around a wooden pin, which terminates above in a head which is cup shaped: it will be seen (Fig. 57)that if pressure is made on this head the spring is shortened and under compression.
This spring is fixed below (by means of a tenon which allows antero-posterior movement) upon a bracket in the calf which is continuous with the ring through which passes the check cord. The cup-shaped upper end is in contact with a ball which projects from the upper surface of the thigh piece between the two openings for the check cord (Fig. 53). It will be seen that when the knee is flexed the spring, the head of which lies below the axis of the joint, will be compressed at the same time as the check cord is relaxed) so that there is an elastic recoil tending to reproduce extension. The ball which rests on the top of the spring is fixed in such a manner as to be in the same horizontal plane as the axis of the knee: that is to say, it is in the same vertical plane as this axis when the knee is flexed to a right[41] angle (Fig. 52). Therefore in this position the spring has no tendency to produce either extension or flexion, that is to say the mechanism is now at dead point, and when the patient is sitting flexion to the right angle is maintained without any effort.
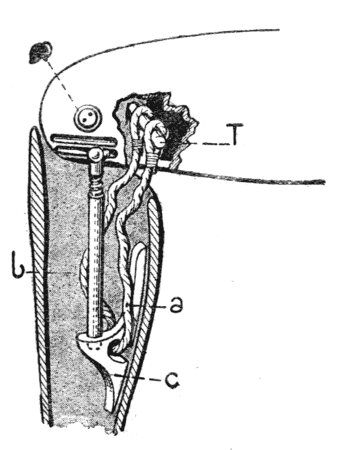
Fig. 52.
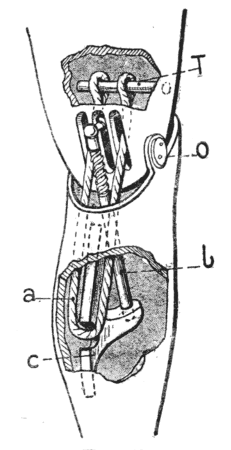
Fig. 53.
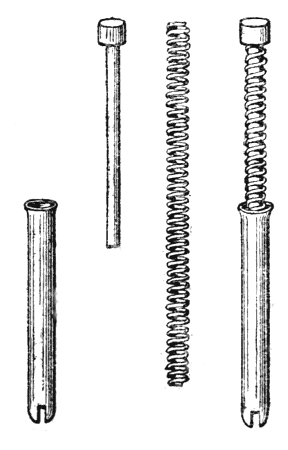
Figs. 54 to 57.
The Marks knee.
Figs. 52 and 53.—O, knee bolt. T, cross piece of wood, situated in the extended position above the knee bolt, in the flexed position behind it. C, bracket fixed halfway up the interior of the calf.
A U-shaped cord a passes through a hole in the bracket C and is attached at each end to the cross piece T; it limits extension. The two ends of the word enter the thigh piece by two apertures in the posterior surface, between which is fixed a metal ball which projects 2 cms. The extending spring is the rod b which is fixed to this ball and to a socket in the upper surface of the bracket. Figs. 54 to 57 show the parts of this spring: a tube, a spiral spring, and a rod with cup-shaped head. When the spring is in the tube and the rod in the spring (Fig. 57), it will be seen that pressure upon the head of the rod increases the tension of the spring.
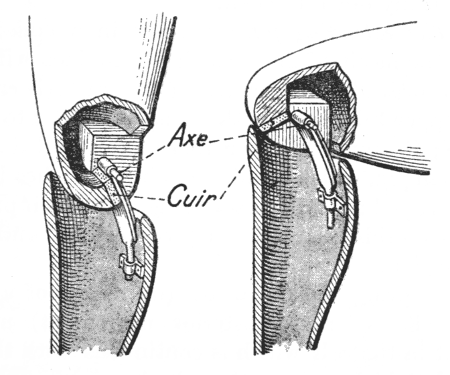
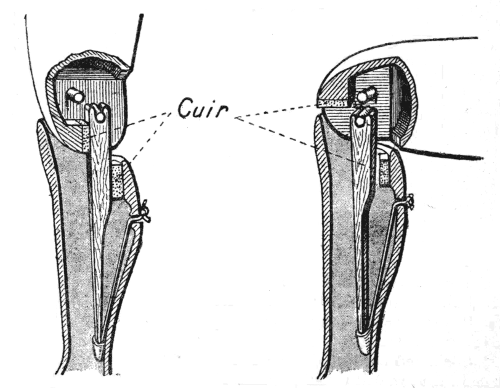
In the knee shown in figures 58 and 59 the extending mechanism is as follows. Directly behind the axis of the joint is a metal crossbar, upon which fits the grooved upper extremity of a piece of wood, the other end of which rests (like a lance) in a pocket which is suspended in the leg piece by an elastic band (the latter being kept stretched to a greater or less extent by a lace which emerges from the calf).
Figs. 58 and 59.—Elastic spring for extending the knee.
The elastic being slightly stretched when the knee is extended, it will be seen that the crossbar turning round the axis of the knee becomes lowered as the knee flexes, so that the elastic is stretched and[43] consequently opposes flexion; but when the knee is bent to a right angle the axis of the joint, the crossbar and the wooden rod are in the same vertical line; the mechanism is at a dead point just as we have already seen in the Marks knee, and the tension on the elastic presses the leg directly downwards without tending either to flex or to extend it.
Leather pads deaden the noise of the impact.
Extension is limited, as will be seen by comparing figures 58 and 59, by the vertical wooden rod meeting flat surfaces in the thigh and leg pieces simultaneously.
3. Extending slings.[6]—To the sling which passes over the shoulder on the side of the artificial limb, is attached a strap which passes down in front of the thigh piece and is attached to the upper third of the leg.
[6] This is an old French method used in Fouilloy's appliance, which has, however, only become generally used in the suspending braces of the American appliance.
When the patient raises the leg from the ground, the weight of the appliance makes it slip down the stump, tension is thus produced upon this strap and as a result the knee is extended. By an adroit movement of the shoulder this extension can be carried out actively.
When the limb rests upon the ground the weight of the body presses the stump down into the bucket, the tension on the strap is released and consequently the knee is free to flex.
On pages 44 to 48 will be found figures showing the principal points in this extending brace.
The braces, whether they have or have not an extending strap, may be constructed in three ways:
a. To ease the constant pressure exerted on the[44] shoulders by the strap which is stretched by the weight of the artificial limb, the brace may be made of elastic like the ordinary trousers brace. But the limb they carry is heavy, so they rapidly become overstretched and it is difficult to keep them properly adjusted.
b. The stretching is naturally diminished if the upper part of the brace is not elastic but an elastic section is inserted in its lower third, in front and behind.
c. But the patients almost always say that better command of the limb is obtained with inelastic braces. If the strap is wide on the shoulder, the pressure is well borne, and the lower attachment may be made narrower, consisting of a leather thong (Fig. 64).
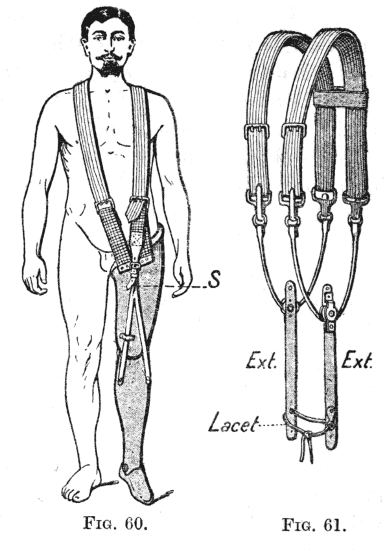
Figs. 60 and 61.
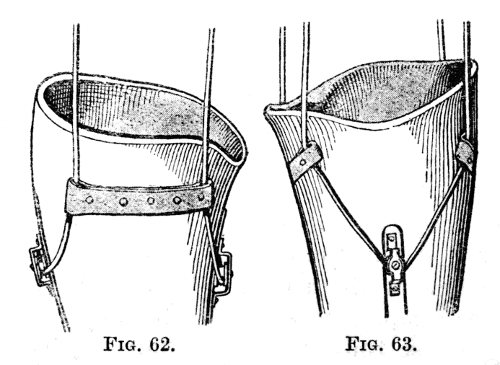
Figs. 62 and 63.
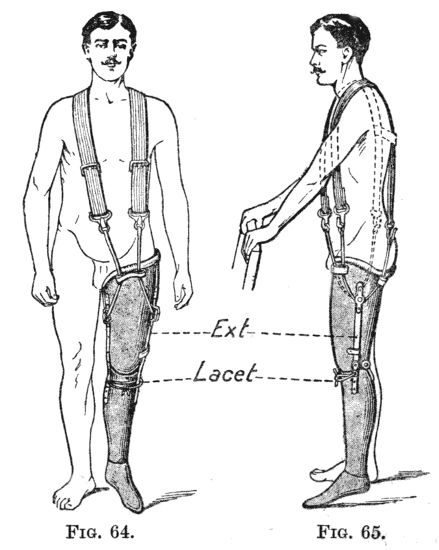
Figs. 64 and 65.
Fig. 60.—Fouilloy's Braces. Figs. 61 to 65.—Marks' braces. Fig. 61.—General construction of the braces. Figures 62 and 63.—Attachment at the sides of the thigh piece. Figures 64 and 65.—General view of the apparatus as worn.
To attach extension braces to the front of the leg piece the old and simple method adopted by Fouilloy may be used. It consists in attaching an elastic strap to the brace which passes over the shoulder on the side of the amputation (and which is fixed to the top of the thigh piece alongside of the other brace). The elastic strap ends in a bifurcated leather thong each branch of which (held in place by a loop of leather) descends obliquely alongside of the patella surface to be attached to the corresponding side of the leg in its upper third (Fig. 60.
In Marks' method the braces end below in loops made of a leather thong (Fig. 61). These are held against the thigh piece by passing under leather bands; they reach as far down as the upper third on the inner and outer sides of the thigh (Figs. 62 to 65).
To each of the loops, gliding on them by means of a pulley, is attached a leather strap which descends vertically to the upper third of the corresponding surface of the leg, being held in place by passing under[46] a leather band. These two straps are attached to each other in front by a lace, which draws them towards the middle line, and in this way brings their line of action forwards. The tighter the lace is drawn the more powerful will be the extending force.
Instead of attaching the extension brace to the leg piece it may be made to pass under a pulley in the interior of the knee. What actually happens is that the thigh piece drops, owing to its weight, when the limb is swung free; this throws a strain on the brace which is transmitted to the leg piece by the following mechanism. The metal stop described on page 39 which limits extension of the knee during the period of weight bearing, is prolonged upwards[47] and forwards beyond the hole through which the axis of the knee passes, this prolongation being furnished with two wooden pulleys (Fig. 69). The loops attached to the braces enter the front of the thigh piece, each by a separate opening, turn under the corresponding pulley and emerge again posteriorly (Figs. 66 to 68).
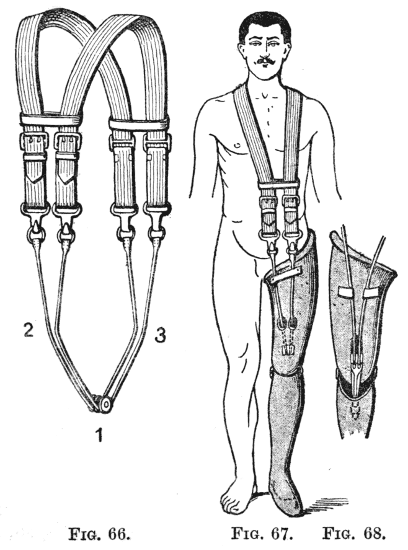
Figs. 66 to 68.
This mode of attachment has the advantage that when the limb is swung the movement does not take place upon the shoulders—which easily become chafed by the ordinary suspenders—but upon the pulleys upon which the leather thongs work.
The mechanism shown in figures 69 to 71 is interesting. When the metal lever moves around the axis of the knee joint, its lower end and the pulleys at the upper end travel in opposite directions: in flexion the pulleys move downwards and forwards, the lower end upwards and backwards; in extension they move in the opposite direction. Therefore when the limb is swung and the knee bends (Fig. 71), the thigh piece drops of its own weight, the braces tighten, raise the pulley and consequently make the lower end of the lever move downwards and forwards, thus extending the knee joint.
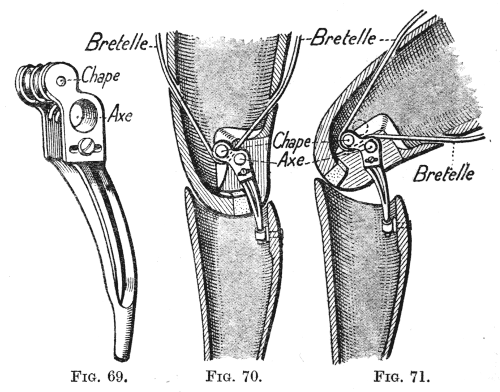
Figs. 69 to 71.
D. Mechanism to secure rigidity of the knee during weight hearing.—During the time that the healthy limb is raised from the ground and carried forwards there must be complete rigidity of the artificial limb in the extended position. This is[49] secured by mounting the foot in the equinus position. When it has been swung forwards, in taking a step, the limb comes in contact with the ground heel first; then, as the leg becomes vertical the entire sole lies flat on the ground; if the foot is in equinus this position is only possible with the knee hyperextended, or with full extension it may be possible for a very short period. So that it is the weight of the body that locks the limb in the extended position, the sole of the foot sloping obliquely downwards and forwards; and the weight being taken on the toe. There is[50] always a tendency to hyperextension, and to avoid straining the limb in this direction (as occurs in a living knee which is forced into the position of genu recurvatum by a talipes equinus) it is as well, as we have already said, to oppose it by some passive resistance, either in the form of a simple popliteal check cord or by a stop fixed to the front of the leg.
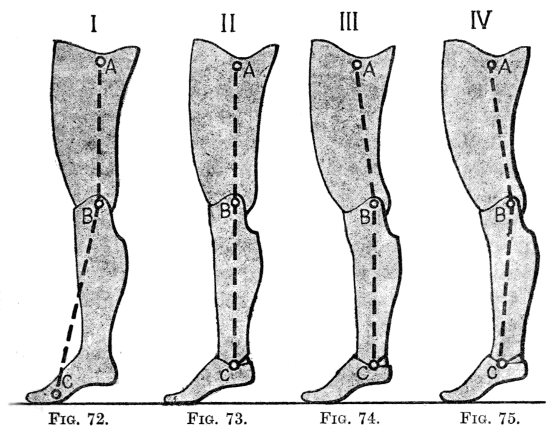
Figs. 72 to 75.
In Figure 72 the foot is fixed, the weight comes upon the point of the foot, and pressure upon the axis AB tends to close the angle ABC, i.e. to produce a genu recurvatum, and so to lock the knee in extension. If the foot is articulated, equilibrium is secured in the same way. Figures 73 to 75 are intended to show that in order that the axis ABC may not be vertical (Fig. 73) the axis B of the knee must be behind the perineal concavity in the bucket, and it is better if at the same time the axis of the ankle joint C is carried forward.
This extension is unlocked automatically at the moment when the weight is thrown forward on the healthy limb, the artificial limb rising on its toe and the knee commencing to bend because the braces are relaxed.
E. Movable ankle.—We have taken as our type a limb with a fixed foot. There are, however, a number of methods of attaching a foot with a movable ankle joint. The general principles and the mechanism for securing stability are those which we have already studied, but the gait is more supple, at the price it is true of somewhat delicate articulations and therefore of simplicity.
The foot is made of a single piece of wood; it is divided transversely at the level of the middle of the metatarsal bones, and the anterior part (shaped like toes) is attached by two pieces of leather, dorsal and plantar, between which are two indiarubber cylinders which keep the toe piece extended 15° to 20° when at rest, and which allow, when the foot is pressed on the ground, an extension to 45°.
This foot is mounted on the leg at an angle of 45° beyond the right angle, with an interposed rubber cylinder, which allows of the diminution of the angle to 25° or 30° but no further. It is important that flexion to a right angle should not be possible. In fact, a slight degree of equinus is essential in order to secure[51] the locking of the knee in extension, exactly as with the fixed foot (compare figures 73, 74 and 75 with figure 72), and as on the shoe there is always a heel which makes us walk normally in slight equinus, the two feet will be similar in appearance, the slight movement of the artificial foot being sufficient to allow a rolling movement of the sole upon the ground (Figs. 77 to 86).
Figs. 76 to 76A.
The figures 76 and 76A show the simplest and best known mechanism. On the upper surface of the foot two cavities are hollowed, one in front and one behind the bolt of the ankle joint, in each of these is placed a cylinder of rubber; the posterior cylinder is about twice as thick as the anterior. Above them the leg piece is fixed, it ends in front in a short instep which lies within the cavity hollowed out in the foot.
The foot is attached to the leg piece by a bolt made as follows: a steel tube fitting into two corresponding grooves in the leg and foot, is attached to the leg by being prolonged upward into a vertical rod, which is secured by a nut inside the leg piece.
Upon the steel tube moves a brass rod shaped like an inverted U, the two ends of which pass through the foot and fasten beneath it by two nuts (Fig. 82).
Raising the point of the foot further compresses[52] the anterior piece of rubber, lowering it relieves the pressure upon this piece and compresses the posterior piece. But the tension and the size of the pieces of rubber are such that they are under slight compression in the position of rest, the foot being in 30° of equinus. So that this foot is never loose. When pressure is made on the point of the foot it may come to within 15° or 20° of a right angle, but it returns to its angle of 30° as soon as the pressure ceases.
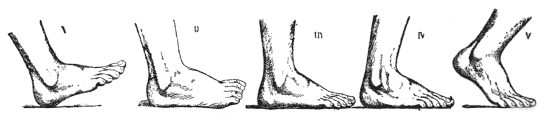
Figs. 77 to 81.
Contact of the sole with the ground in normal walking. Heel first then toe, with progressive dorsiflexion of the ankle joint. Compare with the contact of the artificial foot in figures 82 to 86.
With boots on, with heels of 2·5 centimetres the two feet are in the same position when the soles are flat on the ground.
The forepart of the foot (representing the toes and the anterior part of the metatarsals) is kept in this position (Fig. 76) in slight extension by a piece of rubber, compression of which allows an increase of extension of 15° to 20°.
When a step is taken, the heel of the foot first meets the ground, the leg pointing downwards and forwards. Then the whole sole comes to lie flat on the ground, the degree of equinus being increased, the posterior rubber compressed and the anterior relaxed (Figs. 82 and 83), but when the limb is vertical the sole still being flat on the ground, compression of the posterior diminishes and that on the anterior increases[53] (Fig. 84). This remains unchanged up to the moment when the foot leaves the ground, whilst the heel rises and the weight is borne on the toe piece of the foot, which is forced into extension (Figs. 85 and 86).
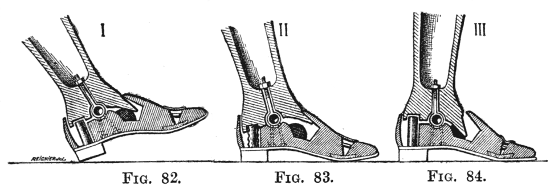
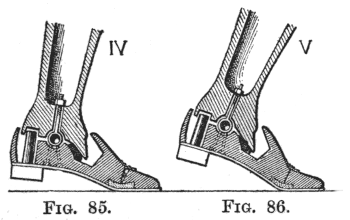
Figs. 82 to 86.
This method of using rubber cylinders is the simplest. Another method, good but more delicate, is shown in figures 87 and 88. In the leg below the calf are two cross pieces of wood; the lower placed transversely supports the upper which is antero-posterior and so increases its resistance to the cords which are attached to it.
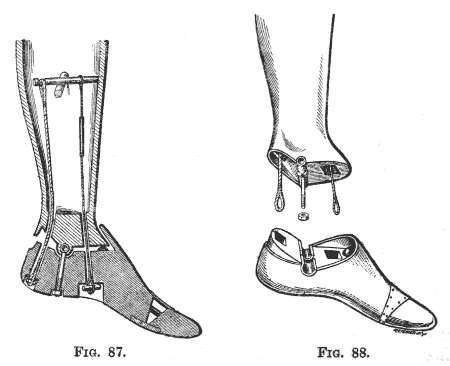
Figs. 87 and 88.
The shape of these pieces of wood can be seen in the figures and require no further explanation. The bolt of the ankle joint is the same as in the foot last described. To the antero-posterior cross piece are attached two cords, which pass through the foot and are attached beneath it, one under the heel, and the[54] other about the level of the midtarsal joint. The posterior cord is inelastic and stops dorsiflexion of the foot. The anterior has a section of elastic in it; it prevents the dropping of the foot whilst the limb is being swung. A small pad of rubber placed in front beneath the anterior part of the leg piece allows, by its compression, the partial correction of the equinus when the sole is pressed flat on the ground.
Some appliances allow the foot a little lateral mobility, by rotation around an antero-posterior axis, so that it may adapt itself to irregularities of the ground. We here illustrate the "Duplex foot," which is very ingenious but which has the defect that after a time the mechanism grates. The ankle attachment is carried out in the same way as in the limbs last described (in this particular limb it is[55] attached by cords), but the foot piece is divided as in a sub-astragaloid amputation; the lower surface of the astragaloid piece bears a median antero-posterior projection, tapering posteriorly and enlarged into a knob anteriorly, this lies in a corresponding groove in the heel piece; alongside this are two rubber cushions which are alternately compressed and relaxed as the foot inclines to one or other side.
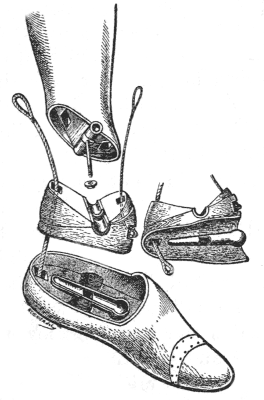
Fig. 89.—Duplex Foot.
This very ingenious combination, which, however, necessitates a rather complex mechanism, was devised by Palmer in 1850. It is carried out in the limb made by Frees, the mechanism of which will be seen to resemble that of the articulated foot shown on page 54 in figures 87 and 88.
Above the axis of the knee joint and at right angles to it is a wooden cross piece, to which are attached three cords, two behind the joint, one in front; these cords emerge from the thigh piece through an opening in its lower end (Figs. 90 to 92).
The posterior of these cords, made of hemp, ends inside the upper third of the leg. It limits the extension of the knee, exactly as described in the Marks leg.
The other two cords extend down to the foot, which is attached in a manner very similar to that shown on page 54, but with a single rubber cylinder behind, and with the instep cut obliquely so that when the joint is in the resting position of equinus there is an opening in front amounting to an angle of 15° to 20°. The posterior cord, of hemp, is attached in the heel; the anterior, made of catgut with an indiarubber section, enters the foot obliquely and is fixed a little in front of the middle of the sole.
When the knee flexes, the wooden cross piece tilts, its posterior end becoming lower, its anterior higher (Figs. 91 and 92), the elastic of the anterior cord is tightened, thus raising the front of the foot, whilst at the same time the heel cord is relaxed. Thus the mechanism which produces extension of the knee acts at the same time upon the foot; when the knee is straight the foot is plantar flexed to 20°, when the knee flexes the foot comes to a right angle. Thus the foot becomes dorsiflexed at the same time as the knee flexes, as in ordinary walking.
If the action in walking is watched, it will be seen that as the limb is swung forward, the toe is raised so as to clear the ground.[7]
[7] The mechanism of this artificial leg resembles that of the "tendon leg," which was in such common use in England before the present war that it is often called the English pattern.—(Ed.)
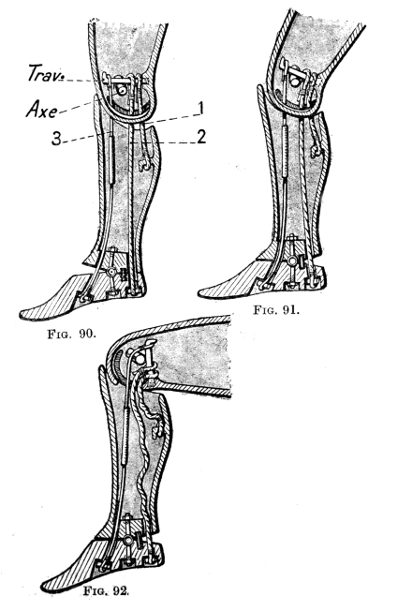
Fig. 92.—(Figs. 90 to 92. Foot and Knee of Frees.)
In the sitting position the anterior cord is not relaxed, there is no dead point, so that the knee always tends to extend. This is somewhat inconvenient.
Conversion of the articulated peg leg into the leg with free knee movement and vice versâ.
Whatever advantage it may be thought to possess, in our opinion the artificial leg with free knee joint is only suitable for sedentary occupations; it is not suitable for manual labourers and particularly for agricultural labourers who are obliged to get about on rough ground. Hence it is not uncommon for a patient who has been provided with an American leg to come and ask for a peg leg. In figures 93 to 95 it will be seen that it is a simple matter to transform the limb into an articulated peg. It is only necessary[59] to attach the stirrup-shaped fork of the peg to the thigh piece by the knee bolt, and to add the double lock. To this peg may be added, if desired, the show calf and foot described on page 32. The full artificial leg can be rebuilt whenever it is wished.
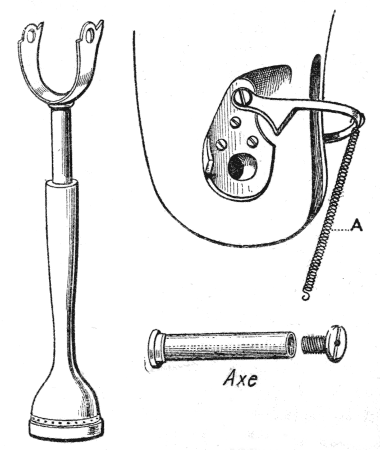
Figs. 93 to 95.
On the other hand, an articulated wooden peg leg, such as we have described under the name of the Federation leg, can be easily adapted for walking with a free knee. It is only necessary to unlock the knee joint and to add the artificial muscle or accumulator of elastic shown in figure 98. This supplies the extending force, the value of which we have shown on page 36. We consider that this appliance is excellent and we know patients who almost always[60] walk upon the peg, but who sometimes use a free knee for short walks. The conversion is simple and requires no special care. Under these conditions the fixed foot is almost always used; there is nothing to prevent the fitting of an articulated foot, but we have already seen that there is no great difference in walking between the old-fashioned fixed foot of the Marks leg and the more or less complicated articulated feet of more recent design.
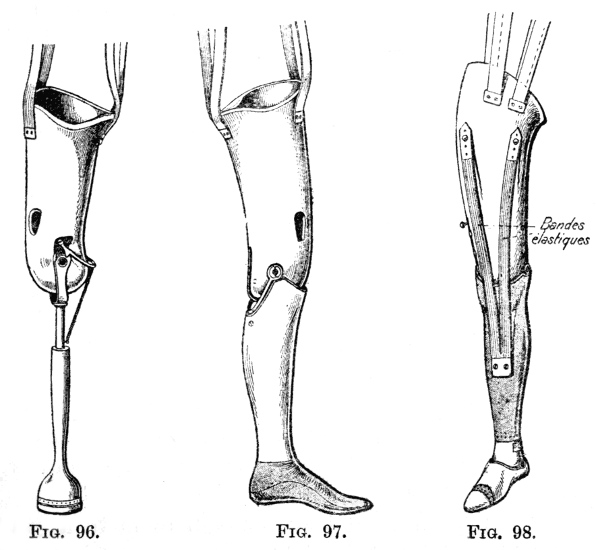
Figs. 96 to 98.
For amputations through the condyles of the femur, and similar amputations (disarticulation of the knee and very short stumps below the knee).
Certain orthopædists do not know how to fit an artificial limb to an amputation through the condyles of the femur; they come therefore to the conclusion that this is a bad operation, and ought to be replaced by an amputation above the condyles.
The two objections raised to this amputation are:—
1. That it is impossible to fit a wooden bucket because the bone at the lower end of the stump is larger than it is at a higher level.
2. That it does not leave enough room to fit an artificial knee joint at the right level.
These two objections are not valid, and, on the other hand, this amputation allows us to fit an artificial limb with complete end bearing, and this is a great advantage.
1. Fitting of the bucket.—The first difficulty is easily got over. All that is necessary is to cut away the front of the lower half of the bucket, and to cover in this opening with a lacing piece of leather. The[61] stump passes into the top of the bucket, comes out of this opening and then falls back into the enlarged lower end where it takes a direct bearing (Fig. 99).
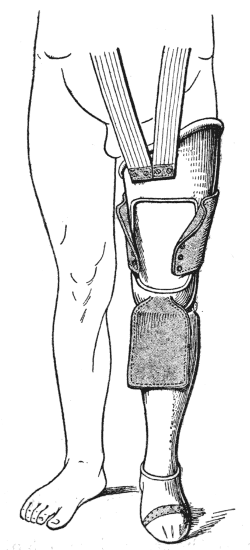
Fig. 99.—Limb with end bearing for amputation in the region of the condyles of the femur. Anterior part of the thigh bucket cut away to allow the insertion of the enlarged lower end of the stump.
2. Level of the knee joint.—It is clear that if the stump is too long it is impossible to fit a knee joint with a bolt right through at the same level as the opposite knee. The thigh piece would have to be prolonged downwards in order to allow of the insertion of this bolt.
This arrangement would not affect walking, but would be unsightly in sitting because of the inequality in the length of the thighs.
It is easy to overcome the difficulty by attaching the leg by two independent lateral hinge joints, without a bolt right through, using the stirrup-shaped fork and the double lock, if a peg is used. This method, as we have already stated, is not so strong, but this is to a large extent compensated for by the possibility of getting a direct end bearing.
3. Direct end bearing and suspension.—If the stump is well covered with a good anterior flap and if the lower end of the bucket is accurately moulded upon it with an interposed layer of felt, the patient can walk directly upon the end of the stump, without it being necessary to carry the bucket up against the ischium, simple braces being used as the means of suspension.
4. There is nothing special about the braces or about the extending strap if the knee is free, nor about the method of attaching the foot.
These limbs for long stumps do not require any spring to extend the knee, if one is wanted an artificial muscle is quite easily fitted.
We have taken as our type an amputation through the femoral condyles.
The covering of the stump is excellent, and pressure is taken upon tissues which are naturally adapted to it (the thick skin and fibrous tissue over the patella), specially if it has been possible to keep the patella in the flap and fix it across the cut surface of the femur (Gritti's operation).
The mechanical points in the fitting of an artificial limb for an amputation through the knee joint are the same. But this amputation seems to us to be inferior[63] to that through the condyles. The sacrifice of three centimetres in length is of no importance in an appliance with direct end bearing; and, on the other hand, disarticulation has several disadvantages:—
1. The enlargement of the femoral condyles, without any compensating advantage.
2. The bearing upon the two condyles, separated by a groove.
3. The insufficient covering of the condyles by the thin skin of the front of the leg.
The principles of fitting a limb are the same in amputations of the leg in which we are obliged to make the patient walk upon the bent knee (too short a stump, the position of the scars, persistent osteitis, the impossibility of straightening the knee when it is ankylosed or stiff in a flexed position), as in the old-fashioned kneeling pin leg.
A posterior transverse band, passing over the bent stump helps to hold the limb on.
Attempts have been made to attach to the pelvis, by means of a waist belt or braces, a wooden artificial limb whose upper end is fitted directly on to the tuberosity of the ischium. So far these have met with little success. In our opinion, the only really practical method is to enclose the whole stump and pelvis in a regular corset, and to attach the artificial limb to this corset.[8]
[8] Amongst English limb makers this moulded corset with the steel hip attachments is usually known as the "tilting table."—(Ed.)
The moulding of this corset upon the stump must be accurate.
The tuberosity of the ischium is the only bony point in the stump upon which pressure can be taken. The corset may be made of leather, but, until a new order is issued, the material of choice is celluloid, moulded upon a plaster of Paris cast, in spite of the disadvantage mentioned on page 4.
The limb is an articulated peg leg, with convertible knee joint and double lock, exactly the same as in the limb for amputation through the thigh.
It is attached to the pelvis (i.e. to the tilting table), as shown in figures 100 and 101, by a joint with a double anterior lock, which allows the patient to sit down by flexing the hip.
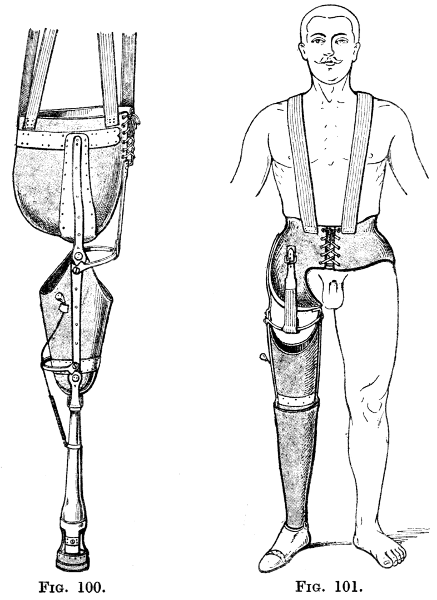
Figs. 100 and 101.
This general description and an examination of figures 100 and 101 will suffice to explain this appliance. It is comparatively rarely required, and its construction is difficult; we consider that the forms shown in the illustrations are the best. It is only possible to fit such an appliance when the conditions are good, when the scar is above and in front of the ischium, and when the latter is well covered.
If the leg stump is ten centimetres long, if the knee joint is freely mobile and capable of complete, or almost complete, active extension, and if there are no adherent scars around the tuberosities of the tibia, the American apparatus with free knee joint should be adopted.
Walking on the bent knee (as stated on page 63) with the "poor man's peg" may be allowed as a temporary measure, but the patient must be advised to give his knee a rest frequently in order to lessen the risk of stiffness in a flexed position.
There are two methods of fitting, corresponding with those we have described for the thigh.
1. For the ordinary amputations with bearing upon the top of the leg.
2. For amputation very low down with end bearing upon the extremity of the stump.
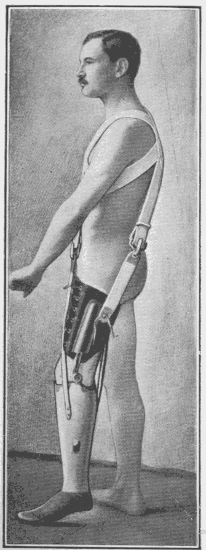
Fig. 102.—Limb fitted upon the patient. Note that he stands upon the toe, and that the knee is flexed.
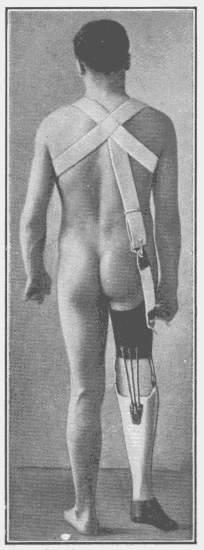
Fig. 103.—Posterior view of the same limb.
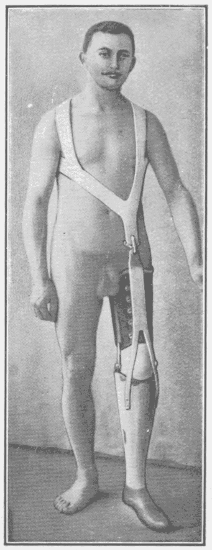
Fig. 104.—Anterior view of the same limb.
An artificial limb for amputation through the leg with a free knee joint is composed of two parts: a leg piece (with foot) which is fitted to the bony prominences around the top of the stump and supports them; and a suspensory apparatus which consists of a lacing thigh corset.
A. Leg Bucket.—The points on which the top of the bucket must be fitted are the internal tuberosity and the anterior tubercle of the tibia, and the head of the fibula, so that hollows corresponding to these must be carved out.
Pressure upon the head of the fibula is often painful, and a deep concavity is therefore carved out for it. The pressure then comes upon the external tuberosity of the tibia which, however, ordinarily bears little weight.
Whenever possible direct end bearing upon the termination of the stump should be used as an accessory to relieve the weight upon the tuberosities of the tibia; this is obtained as described on page 7. It is only possible if the scar is lateral and if there is a good thick posterior or external flap (in the upper third of the leg). An anterior flap is the least satisfactory.
It is also advisable—
That the inner surface and the anterior border of the tibia be divided obliquely, and that the fibula be divided at a higher level than the tibia.
The fibula must not take weight, it is too slender. In high amputations it has a tendency to tilt outwards, causing the double inconvenience of widening the stump and of projecting through the skin. If only 4 or 5 cms. of the fibula remain it is perhaps best to disarticulate and remove it.
With a fitting arranged in this way, we consider that the convenience of walking with a free knee can be assured to patients whose stumps measure only 10 cms. from the lower border of the patella.
These principles can be applied to a limb constructed either of wood or of leather.
The leather appliance (French method) is formed of a leather cylinder, strengthened by two laternal steels which articulate at the level of the knee joint with two similar steels in the thigh corset. Its upper edge may be strengthened anteriorly by a metal plate, but in practice the latter cannot be made to fit with precision the bony prominences enumerated above. It is actually the edge of the leather, adjusted by lacing, which supports tibial tuberosities, and therefore the precision of the fit is soon lost.
For this reason, for amputation below the knee, the American method of construction with a wooden bucket is demonstrably superior.
These limbs are infinitely more durable than the French. They may last three years, whereas the French limb used by a young and active patient is worn out at the end of the first year, and it was for this reason that a limb with a free knee joint used to be considered a luxury.[9]
[9] That is the reason that amputation at four fingers' breadth below the knee used to be called for the working class, amputation at "the seat of election," a name which is no longer applicable and which is liable to mislead the operator.
This wooden bucket is shaped very accurately to the bony prominences, and by passing the fingers over its inner surface the three hollows corresponding to the points of pressure enumerated above can be distinctly felt.
It is important to describe the shape of the upper edge of the bucket in order to guard against two points which may interfere with flexion—
I. Pinching of the tissues behind the knee.
II. The tendency of the stump, when it is short, to tilt forward in the bucket (Fig. 108).
Pinching of the flesh behind the knee in flexion takes place between the edge of the leg piece and that of the thigh corset.
If the top of the bucket is horizontal, it must inevitably occur, even if the edge of the thigh corset is well cut away (Fig. 106).
It can be avoided by cutting away these two edges into concavities opposite each other.
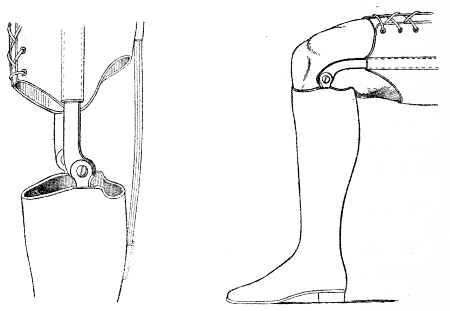
Figs. 105 and 106.—Limb in which the upper edge of the leg bucket is almost horizontal; in the sitting position (Fig. 106) the flesh at the back of the thigh is pinched even if the lower end of the thigh corset is well cut away.
In the French limbs made of leather it is usual to make the leg piece very high in front, i.e. as high as the middle of the patella. This is quite useless. The posterior border is cut down to a depth of two fingers' breadth below the axis of the joint. Pinching is thus avoided, but the posterior support is insufficient, the stump tilts forward as described above and the bucket gapes in front (Fig. 108). If the top of the bucket is horizontal—as in certain American limbs—there is, as we have already said, pinching of the popliteal tissues and compression of the popliteal vessels and nerves (Fig. 106). A concavity is therefore necessary, but one reaching to one finger's breadth below the axis of the joint is sufficient. In front the[71] edge of the bucket reaches up to the joint line, this is quite sufficient to enclose the bony prominences (Fig. 109).
The posterior concavity of the leg piece is combined with a concavity in the thigh piece varied in accordance with the thickness of the popliteal soft parts.
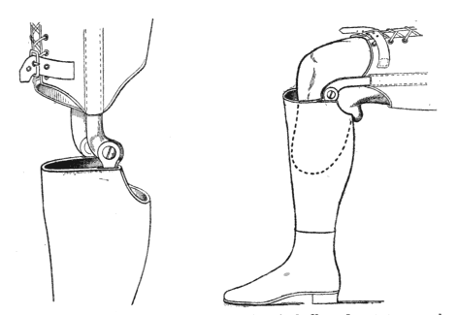
Figs. 107 and 108.—If the leg bucket is hollowed out too much at the back, the stump is tilted obliquely forward (Fig. 108), the knee loses contact with the bucket, and the flesh at the back of the thigh is pinched.
To diminish further the tendency of the stump to tilt forward the posterior edge of the bucket is flattened so that the shape of the top of the bucket is triangular with curved sides and angles much rounded (the anterior angle over the tuberosity of the tibia being obtuse). This is the natural shape of a section of the top of the calf. In this way the posterior muscles are flattened and no[72] longer tend to escape from the bucket when the knee is flexed. In figures 110 and 111 are shown two ways in which this flattened posterior margin may be shaped.
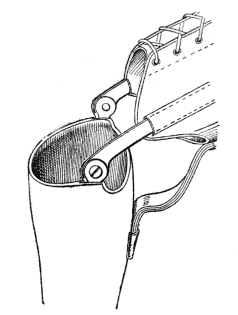
Fig. 109.
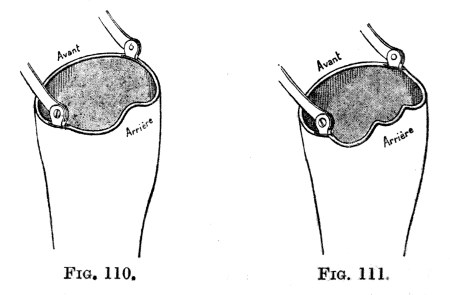
Figs. 110 to 111.
B. Suspension Apparatus.—The leg is attached (a) by a thigh corset taking its hold on the femoral condyles, and (b) by braces over the shoulders.
(a) The thigh corset is made of leather laced in front. Two lateral steels curving in sharply against the upper part of the condyles (Fig. 112) form the most effective part of the support. At their lower ends they are articulated with two steels passing up from the top of the leg to which they are attached. The joint (Fig. 113) is composed of a nut, A, into which fits a screw. Around the nut is a copper ring made to move with the femoral steel by means of a stop-notch. When the knee flexes and extends the wear comes upon this copper ring. The steels remain intact. If the joint works loose it is sufficient to renew the ring.
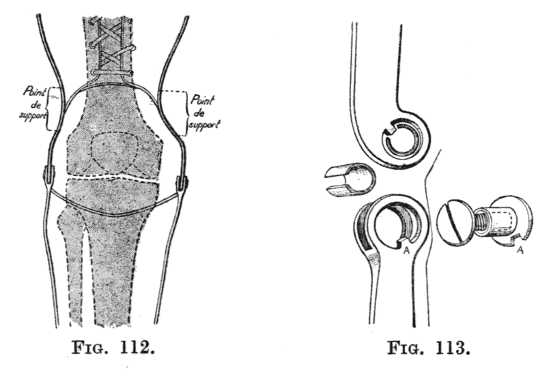
Fig. 112.—The thigh steels, curved in above the condyles, hold the limb on very securely.[10]
Fig. 113.—Details of the joint at the knee.
[10] In this illustration the joints are placed too low. They should be opposite the centre of rotation of the knee joint, i.e. a transverse line passing through the femoral condyles. (Ed.)
(b) The braces are a very useful addition which French orthopædists should employ systematically.[74] They increase the stability of the limb and allow the thigh piece to be laced less tightly, so that contraction of the thigh muscles is facilitated.
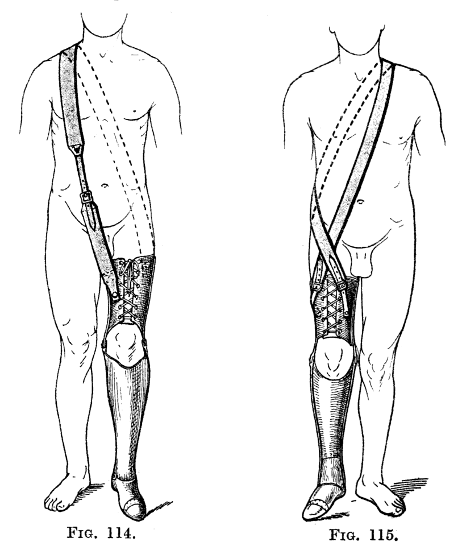
Figs. 114 and 115.
Support may be given by a strap from a waist belt as shown in figure 117, but proper braces are better. These braces pass over the shoulder of the sound side and are attached either to the thigh corset or to the leg piece of the artificial limb. Attachment to the thigh corset is made by a single strap either in front and behind (Fig. 114) or on either side of the front lacing, the ends of the strap crossing in[75] front of the groin (Fig. 115). It is a simple matter to add to the brace an extending strap, such as we have described for the artificial limb for amputation through the thigh (page 44). It is only necessary to terminate the brace in a strap from which two branches pass down in an inverted V and are fixed to the sides of the front of the leg piece (Figs. 116 and 117). This is unnecessary if the stump is long, for its leverage will then be good. It is, however, very useful for short stumps which give little power to[76] the action of the quadriceps. In the case of patients with a long stump an attempt has been made to abolish the thigh piece and suspend the limb exclusively by braces. This method, we believe, is inadequate even if it is completed by a transverse band above the knee (Figs. 118 and 119).
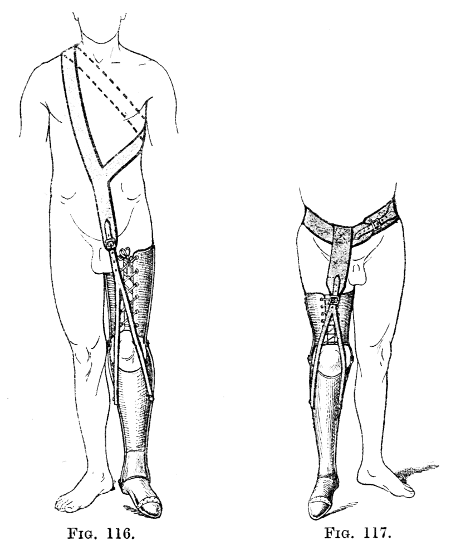
Figs. 116 and 117.
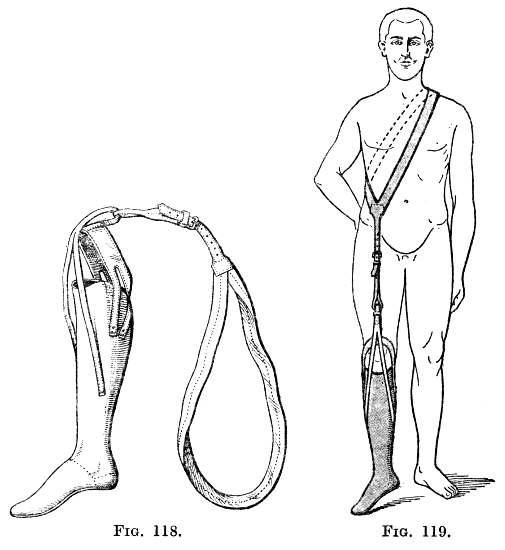
Figs. 118 and 119.
C. The Foot.—The foot, usually articulated, is fixed in exactly the same way as in a limb for an amputation through the thigh, i.e. it is mounted in the equinus position. But in this case, however, precautions must be taken against stretching of the posterior ligaments of the knee joint, because the equinus mechanically produces hyperextension of the knee, and a genu recurvatum may result. For this reason a strap must be fixed posteriorly between the thigh corset and the leg[77] piece to prevent full extension of the knee (popliteal check cord). This means that we make the patient stand and walk with slight flexion of the knee and with a corresponding elevation of the heel of the shoe (2-3 centimetres).
These appliances are suitable for certain amputations very low down in the leg which we must first define.
The orthopædist should consider the following operations as very low amputations of the leg, allowing of walking with end bearing only, and suitable for the same type of appliance:—
Supra-malleolar amputation.[11]
Disarticulation at the ankle joint.
Sub-astragaloid amputation.
Osteoplastic amputations through the os calcis[78] (or amputation in which the os calcis is retained entire after removal of the astragalus).
[11] In England, of course, this is always called Syme's amputation. It constitutes the type par excellence of the end-bearing stump. Upon a good Syme stump a patient may be able to walk ten miles without an artificial foot, wearing simply an "elephant boot." Amputations above the Syme level are not end bearing, however long the stump may be. The other amputations in this region seen in English war surgery are the various types of osteoplastic amputations in which a part of the os calcis is retained (Pirogoff's amputation, etc.). These have the following defects:—
(1) There is often sepsis between the tibia and the os calcis, necessitating re-amputation. Osteoplastic amputations are unsuitable for septic surgery.
(2) Ankylosis between the os calcis and the tibia is often imperfect so that the bulbous end of the stump is unstable.
(3) The stump is too long to allow of the fixation of a good artificial ankle joint beneath it. A Syme's amputation leaves two to two and a half inches clearance between it and the ground.
I have not yet seen a sub-astragaloid amputation in war surgery, and only once a disarticulation through the ankle joint, the latter could not bear pressure and it was necessary to convert it into a Syme's amputation. In fact, in this region there is Syme's amputation and a number of other far inferior amputations which should never be considered when a Syme's amputation is possible. (Ed.)
Certain limb makers consider these operations are bad for the same two reasons that we have already refuted in connection with amputation through the condyles of the femur, viz.—
(1) The stump being enlarged at its lower end will not fit into a wooden bucket.
(2) The stump is too long to allow an artificial foot to be fixed below it.
From this it simply follows: 1. That complete enclosure of the stump in a wooden bucket is impossible; 2. That pressure must be placed directly and exclusively upon the end of the stump.
The latter condition is only possible if the state of the soft parts allows the cutting of a thick plantar flap to cover the cut surface of the bone and if care be taken to resect the posterior tibial nerve in the flap.
We therefore draw special attention to the excellent elliptical supra-malleolar amputation with posterior flap (Guyon's method) in which it is sufficient to retain a bare finger's breadth of skin from the plantar surface in front of the point of the heel. It bears direct pressure well, perfectly if a layer of the os calcis is cut with the scissors from the area adjacent to the tendo-Achillis and applied under the cut end of the tibia.
For all these amputations the anterior flap is bad. The thin dorsal skin of the foot is incapable of withstanding the direct pressure which is indispensable for this method of fitting.
Even if it were true that under these long stumps it is impossible to insert an artificial foot for lack of space, the operations which we have enumerated[79] above should be recommended if the flap can be cut in the way we have indicated.
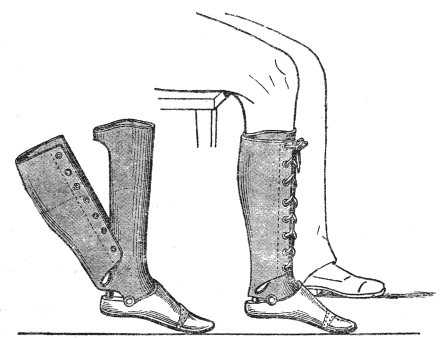
Figs. 120 and 121.
Their great advantage—and the reason for retaining as much length of bone as possible—is that they allow walking directly on the stump without an apparatus. It is sufficient to have a circular shoe made by any shoemaker consisting of a heel more or less thickened surmounted by a lacing gaiter reaching halfway up the leg. Guyon's amputation constitutes the limit up to which this "elephant boot" is possible.
It is an unsightly apparatus, but its simplicity and cheapness should be taken into consideration, for it is quite possible that a manual labourer, especially a countryman, to whom an artificial foot and an "elephant boot" are given, will reserve the former for Sunday and use the other for his daily work.
Appliances with Artificial Foot.—The wooden piece which partly encloses the stump consists of a block carved to the shape of the stump and padded with felt, it is prolonged in front by an instep reaching to the level of the middle of the metatarsus, and above by a grooved piece which reaches halfway up the leg and encloses the anterior half of the latter. A leather gaiter is fixed at the sides and back and extends up the leg, being laced in front over the wooden piece as a field boot is laced over the leather tongue. The foot may be mounted at right angles to the leg, but it is better mounted slightly in equinus.
The sole and toes are of rubber as described on page 35.
In studying figures 120 and 121 the following should be noted:—
1. The shape of the leg bucket in which an aperture behind permits the introduction of the stump which is enlarged at its lower end.
2. The mechanism by which the posterior gaiter laced in front fixes this leg bucket.
3. The articulation of the foot on a transverse axis.
This name should be applied to amputations in which the mobility of the ankle joint is retained, i.e. Chopart's amputation (midtarsal disarticulation), Lisfranc's amputation (tarso metatarsal disarticulation), amputation of several toes with their metatarsal bones, or amputation of all five toes.
1. The amputations of Chopart and Lisfranc.—Chopart's amputation has a grave defect: the anterior muscles have not sufficient leverage to oppose this gastrocnemius and soleus, and the posterior tarsal bones tilt forward so that the patient walks, not on the lower surface of the os calcis and the plantar skin, but on the head of the astragalus and of the os calcis and on a painful cicatrix. If certain precautions are taken (careful preservation of the fibrous plantar flap and suture to it of the anterior tendons) this defect is not invariably present, and it is an exaggeration to say that Chopart's amputation "has never given anything but disappointment." It should, however, only be practised if the technique is well understood, and even then it is rarely indicated, because it demands almost as much plantar skin as Lisfranc's amputation.
Nevertheless I have seen some good Chopart[82] stumps the result of operations by myself or by other surgeons; they should be fitted like the stumps resulting from Lisfranc's operation.
With regard to the latter, they can be easily and comfortably fitted, provided that the scar is dorsal and is not stretched over prominent bones.
If the first cuneiform is not well covered it can simply be removed, no functional disability results. It is mainly upon the plantar surface of the stump that pressure is borne, but pressure comes also upon the anterior surface when the foot is tilted downwards.

Fig. 122.
The fore part of the foot which constitutes the prosthetic apparatus consists of a block of wood, which reaches forward as far as the middle of the metatarsus and ends in a vertical plate in front of the stump. This block of wood is carved to the shape of the stump and lined with felt. It is attached to the leg by a leather gaiter which laces in front.
Anteriorly it is prolonged into an artificial toe piece similar to that already described for the artificial limb for amputation through the thigh.
This appliance is not indispensable. It is sufficient to use a piece of cork shaped to the anterior surface of the stump and filling up the anterior part of the boot, its advantage, however, is that once the patient is fitted with this appliance he can wear an ordinary boot.
2. Partial Amputation of the Fore Part of the Foot.—These are—
Transverse amputation through the metatarsal bones.
Disarticulation of one or more toes with their metatarsal bones.
Disarticulation of one or more toes.
For any of these amputations all that is required is an ordinary boot, fitted with a cork, which is shaped to fit the stump and which fills up the space left by the amputation.
In order that the patient may walk well the scar should be dorsal and should not be tense.
We consider that the difficulty of maintaining equilibrium after removal of the head of the first metatarsal, or even of the whole of this metatarsal bone, has been much exaggerated.
Removal of a marginal metatarsal bone (either alone or with its neighbour), tends to make the foot tilt into varus or valgus; so that the boot needs to be stiffened and the sole thickened to avoid this.
The constituent parts of an artificial arm are the same in principle as for those of an artificial leg, they are—
1. A means of attachment preventing the appliance from dropping as the result of its weight.
2. A socket, fitted to the stump and articulated with the last named at the elbow.
3. The terminal appliance, intended to replace as far as possible the amputated hand and, if possible, resembling it in appearance. In the case of the upper limb the advantages that wood possesses in giving strength and accuracy of fit do not apply, and the arm and the forearm pieces are made of leather, with lateral steels articulated at the elbow: this joint is active in the case of amputations of the forearm but purely passive in amputations of the arm.
We will commence by describing the appliance for amputation through the forearm, taking as our type amputation in the lower half. This will furnish an example which illustrates all the principles that should guide us, the ends we should have in view, and the means by which we can attain them.
When once we have studied the apparatus by[85] means of which the functions of the hand can as far as possible be replaced, a short description will suffice to explain what can be done when the loss of movement of the elbow and then a shorter and shorter stump in the upper arm oblige us to diminish the utility of the appliance.
We must study in turn: (1) The attachment of the upper arm socket; (2) the joint between this and the forearm socket; and (3) the appliances attached to the extremity of the forearm whether these take the shape of a hand or not.
1. Suspension.—In the exceptional amputation very low down, in which the roots of the thenar and hyperthenar eminences remain, the enlargement thus formed at the extremity of the forearm may be used for the attachment of a wristlet which may suffice to support the artificial appliance, provided that the latter is not intended for heavy work. In the latter case an attachment from the elbow at least must be added.
This method would evidently be out of the question in the usual class of case, viz. ordinary amputations through the forearm.
In these the attachment may be made in two ways:—
(1) To the humerus above the condylar enlargements, the epicondyle and the epitrochlea, the latter being much the more prominent.
(2) To the top of the shoulder, i.e. to the surface over the acromion and clavicle.
A. Attachment to the Elbow.—The simplest method[86] of attachment is that in which pressure is exerted upon the condyles of the humerus (Fig. 124). A leather armlet laced in front is furnished with two lateral steels, curved in above the condyles and articulated at the level of the centre of rotation of the elbow joint with two similar steels in the forearm piece (the socket).
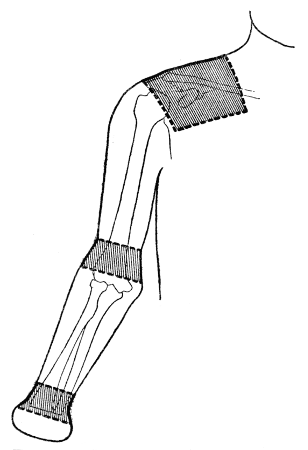
Fig. 123.—The three regions used as points of support, the shoulder, the elbow and the wrist.
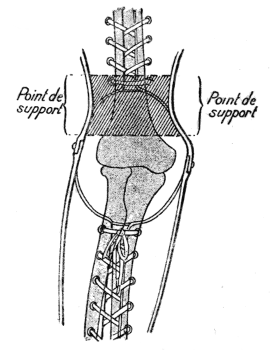
Fig. 124.—Suspension from the elbow. The side steels of the arm piece are curved in to fit upon the supra-condylar ridges of the humerus. A good method of suspension for long stumps, when the appliance is not to be used for heavy work. It should be supplemented in other cases by direct suspension from the shoulder.
This direct method of attachment is sufficient for a low amputation, in cases where the patient does not do hard work. But if the stump is short and if the patient has to carry fairly heavy weights the appliance is only prevented from slipping by a consider[87]able constriction of the arm, which results in a serious interference with muscular action.
B. Attachment to the Shoulder.—For this reason it is usually advisable to supplement this by an indirect attachment to the acromion and clavicle by means of a shoulder cap.
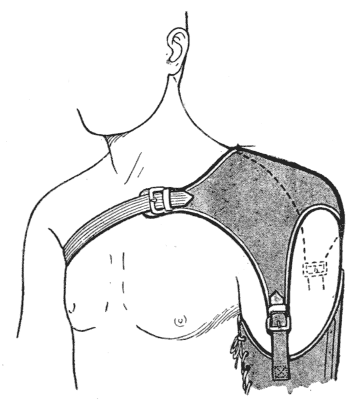
Fig. 125.
The firmest and strongest pattern consists of a piece of blocked leather, moulded to the shoulder, including the pectoral, supra-clavicular and scapular regions. This is kept in place by a strap which passes under the opposite axilla. It is cut away on the outer side of the acromion, the anterior and posterior borders being continued downwards on either side of the deltoid as two tapering straps to which the armlet is attached. In this way full liberty of movement is allowed to the shoulder (Fig. 125).
This pattern is strong, but cumbersome and heavy. It can be lightened by reducing it to an antero-posterior strap, 6 or 7 centimetres wide, over the clavicle and spine of the scapula, ending in front and behind at the level of the axillary folds in triangular enlargements. In the upper and inner angles of these are attached the ends of the axillary strap, to the lower and outer angles, prolongations from the armlet (Figs. 126 and 127).
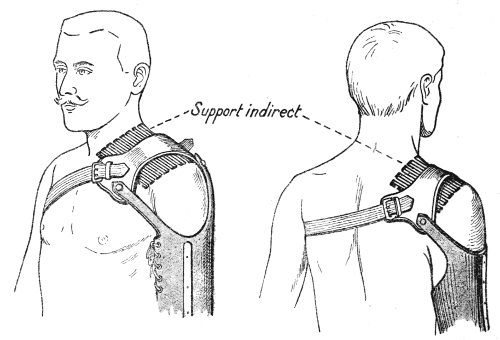
Figs. 126 and 127.
The lightest method, but obviously also the least secure, consists in suspending the armlet by two straps, anterior and posterior, which cross above the clavicle and then pass in the form of a loop under the opposite axilla (Fig. 128).
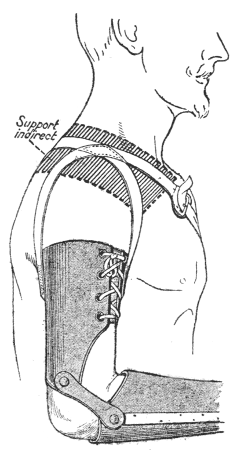
Fig. 128.
The choice between these three methods of attachment depends upon the profession of the patient and the strength required by it.
2. Resistance to Upward Pressure.—The artificial limb should be capable of resisting upward pressure, when a thrusting force is exerted by the hand. This is secured in the following three ways, the hand being presumed to hang vertically with the elbow straight:—
(1) By pressure of the end of the stump in the socket (in amputations low down with a palmar flap—for example, in disarticulation at the wrist joint).
(2) By pressure of the top of the forearm socket on the enlargement of the forearm below the elbow.
(3) By pressure of the inner side of the upper edge of the armlet against the axilla.
But, in actual work, thrusting movements are nearly always made with the elbow bent to a right angle or almost so, then the pressure transmitted through the forearm piece is borne almost entirely by the steels of the armlet.
3. Resistance to Rotation.—A well-adjusted artificial arm cannot rotate on the limb because—
(1) The forearm is elliptical in section and not circular, this is specially so in the lower third.
(2) Flexion of the elbow is only possible if the artificial joint is in the same plane as the axis of the elbow joint—that is, the sagittal plane.
(3) The axillary strap of the shoulder attachment prevents rotation.
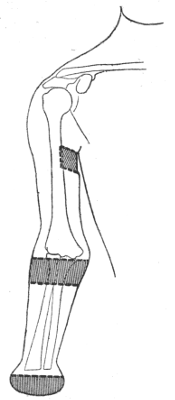
Fig. 129.—The three regions used as points of resistance to upward pressure.
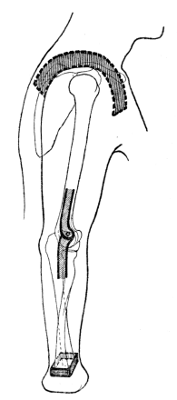
Fig. 130.—The three regions at which rotation of the apparatus may be prevented.
1. The Concavity of the Armlet.—At the elbow joint the pinching of the anterior soft parts on flexion is liable to take place in just the same way as occurs at the back of the knee in amputations through the leg. To avoid this it is necessary—
(1) That the axis of the joint should lie in a[91] prolongation of a line passing through the epicondyle and the epitrochlea.
(2) That the armlet and the forearm socket should be cut away in front in crescent-shaped concavities.
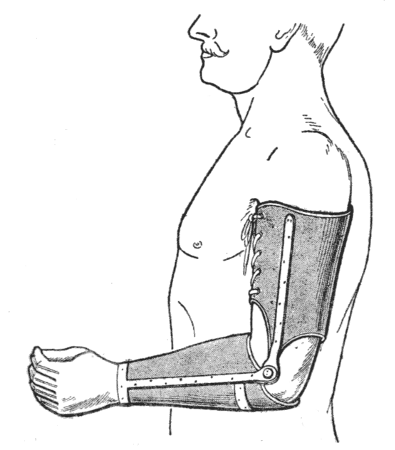
Fig. 131.—Limb for amputation in the middle third of the forearm.
The depth of these concavities is estimated when the limb is fitted. Both the arm and the forearm may be cut away freely without any resulting inconvenience, provided that the stump is long; but if the stump is short and includes only the upper third of the forearm, it is impossible to cut away the forearm socket sufficiently without depriving the stump of a proper hold in the socket, so that movements are not transmitted to the forearm lever with their proper force. Consequently the socket for the forearm must be cut away very little, and must be carried up to the level of the fold of the elbow when the joint is flexed. The flesh in front of the elbow will not be pinched if, the[92] forearm being fitted very accurately, the muscles of the upper arm are allowed free play, by cutting away the front of the armlet to half its height, but in this case an indirect attachment to the shoulder is essential.[12]
[12] Another difficulty in fitting a short forearm stump arises from the fact that the antero-posterior diameter of the forearm immediately below the elbow increases considerably when the joint is flexed, because of the contraction of the muscles arising from the condyles. If the forearm socket is made to fit closely when the elbow is extended it will be too small when the joint is flexed and will prevent full flexion. If it was made to fit with the elbow flexed, there is risk of the stump slipping out of the socket when the joint is extended. (Ed.)
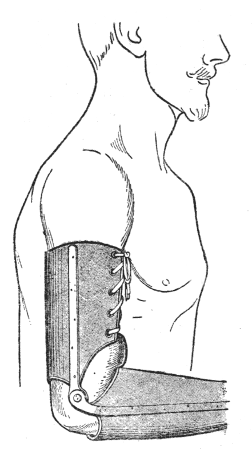
Fig. 132.—Bad apparatus for amputation in the upper third of the forearm. The front of the arm piece is insufficiently cut away.
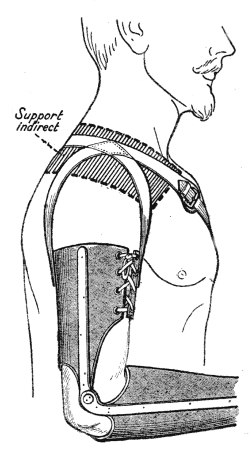
Fig. 133.—Good apparatus. The arm piece is well cut away, consequently the flesh does not bulge out.
2. Construction of the Joint.—In most cases this is a simple articulation between the steels of the arm and the forearm pieces by two hinge joints.
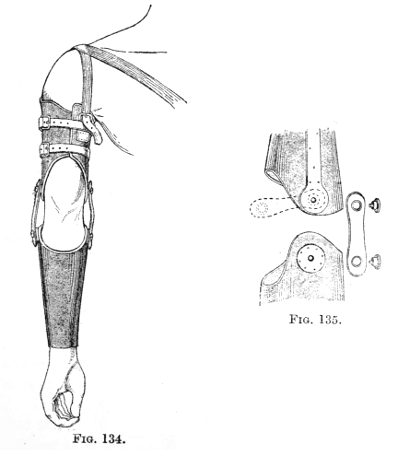
Fig. 134.—Limb for amputation through the lower third of the forearm, with elbow joint of strong leather.
Fig. 135.—Details of the joint.
The objection to this is that the movements of pronation and supination, if these are present in the stump, are abolished.
(a) Long Stump.—When the stump is long (amputation in the lower quarter) the following may be[94] used: The steels of the forearm socket are attached to the armlet, which is not furnished with steels, by two straight strips of hard leather jointed at each end with rivets to the corresponding piece of the limb. This allows a certain amount of torsion so that pronation and supination are to some extent possible. It is necessary to add an indirect attachment to the shoulder. Not only must the armlet, not being closely moulded over the condyles, be even when new laced so tightly as to be unbearable, but in addition the inevitable loss of shape of the unsupported leather will in every case soon interfere with proper support direct from the armlet (Figs. 134 and 135).
This method is, moreover, scarcely applicable to patients who will have to carry out heavy work.
(b) Short Stump.—The stump of an amputation in the upper third of the forearm is too short to be securely held in the forearm bucket. There is consequently a loss of power in the movements communicated, particularly in flexion, the arm of the lever being too short; in addition, the elbow joint in these cases is often a little stiff, so that flexion beyond a right angle is impossible (Figs. 136 to 138).
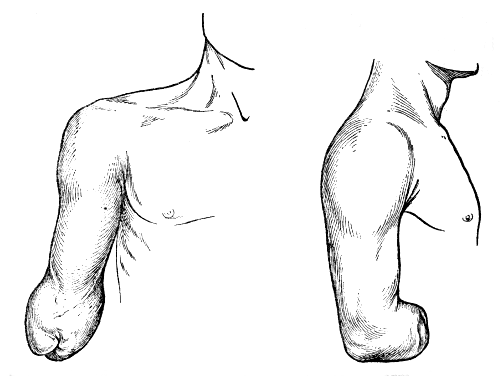
Figs. 136 and 137.—Amputation through the forearm above the upper third. The elbow joint does not flex beyond the right angle.
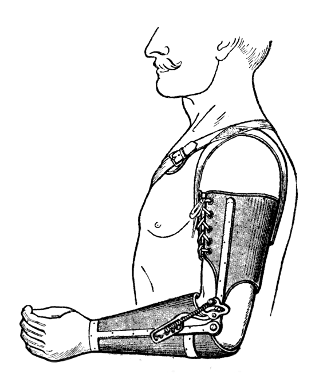
Fig. 138.—Limb for amputation through the upper third of the forearm. (For a description of the ratchet see page 135.)
The chief functional difficulty depends upon the fact that, with the elbow at a right angle, the anterior surface of the forearm stump is too short to support a weight; for example, a basket held by the handle. The stump escapes partly from the bucket when the forearm extends. It is therefore well in such cases to fix the elbow at a right angle by means of a ratchet identical with that used in the artificial arm for amputation above the elbow (Fig. 138).
At the extremity of their forearm almost all patients wish in the first place to wear something that is shaped like a hand. Many people—and even many medical men—consider that this "artificial hand" is really useful. In actual fact, by means of fairly simple contrivances, it can be used to enable the patient to eat, to write, to put on and take off his hat, but it is out of the question for it to do real work. For that an appliance, a tool in fact, adapted for use and not for appearance is necessary.
The limb, therefore, will, as a rule, end in a hand, but for workmen this hand will be capable of being unscrewed and replaced easily by one or more appliances.
Attempts have been made to construct so called universal hands and forceps which will serve for any sort of work, but up to the present none of these inventions have given satisfaction. And the practical solution of the problem in the present state of affairs consists in devising a special appliance for a particular trade, studying carefully the movements necessary in this trade.
A workman who in the course of his occupation carries out a number of different movements may thus have several appliances, which he selects as he requires them. For example, a locksmith must be able to hammer, to file, and to drill holes in succession.
We will describe first the hand properly so called, then the appliances. The former is suitable for clerks, and it is for them that the various improved patterns that we shall describe are made. The latter are suitable for manual workers to whom should be given[97] a hand in which the mechanism is reduced to a spring thumb grip and one or more special appliances.
These appliances will almost always be constructed to carry out the movements made by the left hand in the course of the work, because the first step in the re-education of a patient who has lost the right hand should always consist in training the remaining left hand to carry out the work hitherto entrusted to the missing right hand.
The hand, which is screwed into the end of the forearm socket in such a way that it is in semipronation when the arm hangs vertical, is nearly always made of wood, but occasionally of aluminium.[13]
[13] Hands are nearly always made of lime wood, which has the advantage of lightness, but the fingers are fragile and easily break. Instead of using hornbeam, which is hard but heavy, as the fragility only affects the fingers, some makers have overcome this difficulty by reinforcing the fingers by what they call a "philippeau."
The finger is divided throughout its whole length by a mortise 1·5 millimetres in width, in which are glued two layers of veneering wood (mahogany, rosewood, etc., extremely hard woods, or else a layer of hornbeam).
It may be a simple show hand without any joint. This pattern is no longer used. It may be jointed in one or in several fingers. We shall first consider certain principles of construction which we can explain by describing the chief mechanisms used.
Simple Spring Grip Thumb.—The simplest and most useful articulation is that of the thumb, which when at rest is kept by means of a spring in the flexed position, with the grip against the index finger which is partly flexed (as are also the other fingers).
In many cases the patient is content with this simple mechanism. He opens the spring with the[98] other hand and allows it to close on the object he wishes to grip (Figs. 139-145).
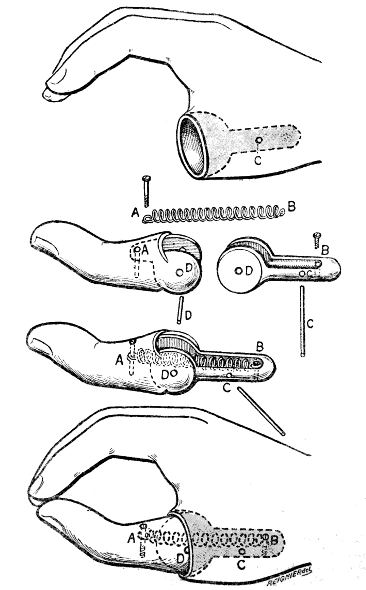
Figs. 139 to 142.—Mechanism of the passive spring thumb.
The thumb turns on the axle D upon a piece which fits by a tapered extremity C into a hollow cut out in the thenar eminence. The base of the thumb is rounded. The spring AB flexes the thumb.
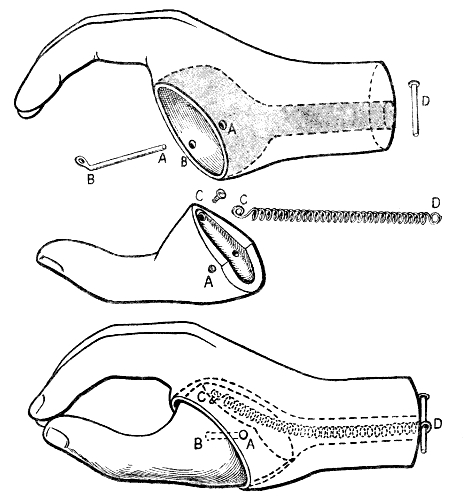
Figs. 143 to 145.—The Beaufort Thumb.
The model shown on page 98 is more mobile than this, in which the thumb turns on the axis AB, and is fitted directly into the thenar eminence. But in this type it will be seen that the spring CD which keeps the thumb flexed, reaches right up to the wrist, and is therefore longer and more powerful. The thumb is much stronger, and this is the mechanism usually adopted. It has the inconvenience that it requires a deep excavation of the thenar eminence, encroaching upon the root of the index finger, so that it is impossible to mount the thumb in this way when it is desired to fit a movable metacarpo-phalangeal joint to the index finger, either with a spring (Fig. 155) or without (Fig. 148).
The Automatic Thumb.—Active opening movement can be produced by the mechanism shown in figure[99] 146. A cord fixed behind the scapula of the opposite side by a ring which passes over the clavicle and under the axilla, extends down the posterior surface of the arm and forearm pieces, running in pulleys which keep[100] it in place. If the patient bends the elbow and at the same time brings the arm and both shoulders forward, rounding his back, the cord is tightened and pulls the thumb into the position of abduction and extension.
This narrow grip, between the tips of the thumb and index finger only, is not always convenient. A commercial traveller or a foreman could not easily hold with it the order book, in which he has to write. But if the thumb, held by a powerful spring, is parallel to the palm of the hand and grips against the other fingers, which are stretched out and not semiflexed, the grip will be strong and convenient, especially if a mechanism is introduced between the forearm and the hand, allowing the latter to be rotated at will into any position (Fig. 148).
As in the preceding case the thumb may have either a simple grip or an automatic grip opened voluntarily by a cord from the shoulder.
The following is a very interesting method which allows a fork or pen to be held, the automatic thumb being used. The fingers are half flexed, the index being separated from the middle finger, so that the handle of a pen can be inserted between them. The grip of the thumb is not against the tip of the index finger but against the outer side of the last phalanx of the middle finger, against which in consequence the handle of the object held will be pressed (Fig. 147).
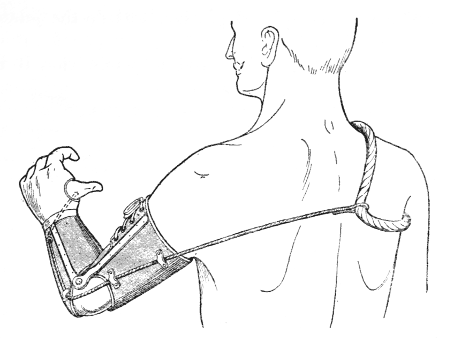
Fig. 146—Appliance with automatic thumb. The cord is fixed to a loop which passes round the sound shoulder. Abduction and forward movement of the shoulder and flexion of the elbow open the thumb.
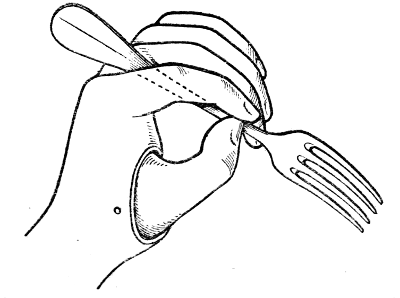
Fig. 147.—Hand with space between the index and middle fingers, wide enough to take the handle of a fork, which is held by pressure of the thumb against the side of the middle finger.
The extended fingers are better placed for gripping than the partially flexed fingers, although the latter are convenient to the patient in certain ways. Ball and socket joints are inserted at the interphalangeal joints. (Details are shown in figures 152 to 154.) These are so stiff that they maintain the position[101] in which they are placed passively, as do the joints of an artist's lay figure.
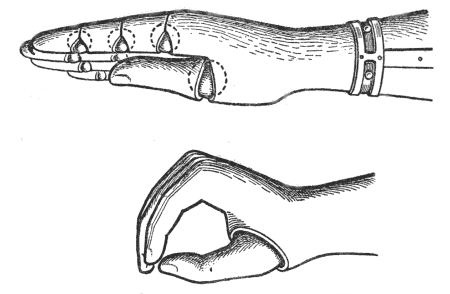
Fig. 148.—Articulated hand for commercial travellers. The thumb, lying parallel to the palm of the hand, takes a secure hold of such an article as a memorandum book.
Fig. 149.—The usual pattern of hand. The grip is too small.
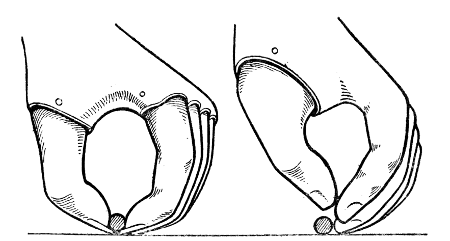
Fig. 150.—The index finger is the same length as the middle finger. The thumb and index fingers are furnished with nails. A small ball can be picked up.
Fig. 151.—The middle finger being longer than the index, the latter does not reach the surface of the table and the ball cannot be picked up.
If the fingers are rigid and in semiflexion it is[103] possible to articulate all the metacarpo-phalangeal joints, fitting them with a spring, which keeps them flexed, and arranging for active extension as already described for the thumb. All that is necessary is to terminate the cord by five separate strings instead of one. In certain special cases this arrangement may be useful (Figs. 155 to 157). It seems to us useless to render the interphalangeal joints automatic.
As to the attempt which Beaufort appears to have made to give movement to the wrist also, we do not believe that any practical result has as yet been attained.
For the relative length of the fingers and the utility of a nail on the thumb and on the index finger see figures 150 and 151.
In the usual pattern (Figs. 149 and 151) the fingers are semiflexed and the thumb grips against the index finger, which is shorter than the middle finger as in the natural hand. If it is desired to pick up a ball, for example (Fig. 151), it will be seen that the middle finger projects and gets in the way. For this reason it is advisable that the index finger be longer than the middle, and in addition it is useful to furnish the thumb and index finger with a little projection representing the nail (Fig. 150).
In figure 148 will be seen an arrangement which allows the thumb to grip not by the tip, but by the whole length of its palmar surface (to hold, for example, a notebook). The fingers of this hand have ball and socket joints constructed in the way shown in figures 152 to 154. The joints keep passively the[104] position in which they are placed. The attachment of the ball of the joint on an intermediate tenon is similar to that of the thumb shown on page 98. The articulation of the index finger prevents the sufficient excavation of the thenar eminence for the insertion of the Beaufort thumb with its powerful spring. The wrist rotates upon a bayonet joint.
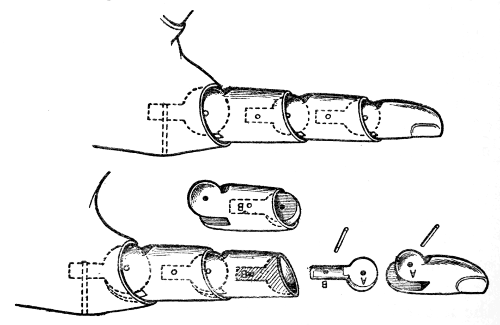
Figs. 152 to 154.
The fingers shown in figures 155 to 157 are joined together into a single piece, which articulates with the metacarpal part of the hand upon a transverse axis.
They are held in a position of flexion at the metacarpo-phalangeal joints by four palmar springs and they are opened away from the thumb by the action of a cord which bifurcates from the thumb cord on the back of the hand. The pull of this cord is exerted upon the upper angle of a triangle from the lower border of which four cords pass on to the back of the phalanges. Figure 156 shows detail of a finger. We know that attempts have been made to isolate[105] by surgical means the masses of the extensor and flexor muscles in the end of the stump, making from them little prominences, perforated with a tunnel which is lined with skin. The cords pass through the tunnels, and in this way are worked voluntarily. We are not sure that this is practicable.
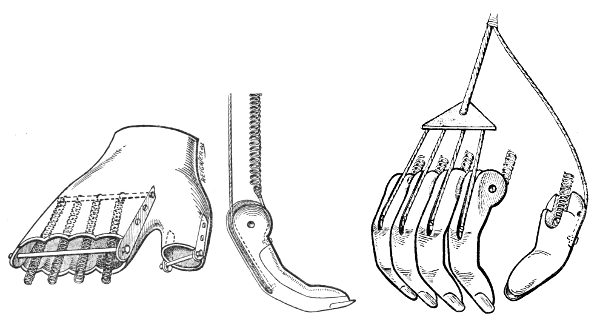
Figs. 155 to 157.—Automatic fingers.
In figure 155 are seen the cavity in which the finger portion works and the axis upon which movement takes place, also the four palmar springs. In figure 157 the arrangement of the cords. In figure 158 the attachment of the spring to the finger. This pattern, which we have designed and which is not patented, seems to us to be simpler than those in which the interphalangeal joints are also articulated and are automatic. It gives a more accurate grip between the tips of the thumb and index finger.
The Brunet Grip.—The Brunet grip is described here because of its resemblance to the automatic thumb, both being worked on the same principles.
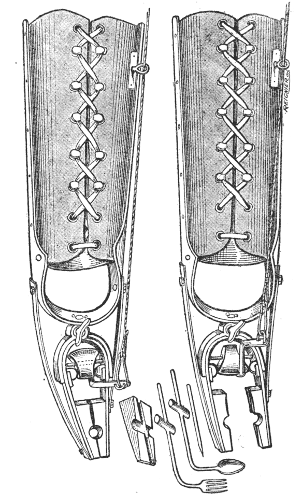
Figs. 158 and 159.
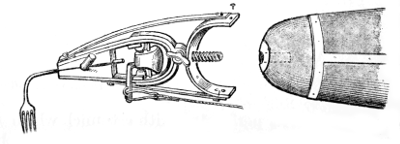
Fig. 160.
Brunet's Grip.[107]
Below the leather forearm piece, which laces up, the lateral steels are continuous with each other in the form of an arch, to which the grip is riveted.
The latter consists of a strong semicircular piece of metal facing downwards, ending in a pair of wide and thick jaws, like those of a locksmith's pliers. When the apparatus is at rest, these are kept in contact by the pressure of two powerful fixed springs, attached to the semicircle on the forearm above and to the jaws below. The external and dorsal spring is attached to the tip of its jaw, the internal and palmar (the side on which the manipulating cord is attached) to the base of it.
The pliers are opened in the following way:—
Inside the semicircle to which the jaws are attached, lies a cylinder with its ends cut obliquely; this rotates about a transverse axis, and when at rest lies with its longer side upward. To the palmar edge of the shorter side is attached a transverse eccentric, to which is hooked a cord actuated as described in figure 146. When this is drawn upward the cylinder rotates so that the wider side comes between the jaws of the pliers and opens them; when the cord is relaxed the springs turn the cylinder back again find the jaws close. Figures 158 and 159 show the appliance at rest and with the jaws open.
This appliance is patented and is made in one piece. We demonstrate in figure 160 that it would be very easy to make the pliers detachable from the forearm, with a screw connection, just as is done in the various other appliances which will be described.
The grip of the automatic thumb always lacks power, for two reasons. There is no room in the thenar eminence to fit a powerful spring and the grip has always a very narrow hold.
The Brunet grip is an actual pair of pliers, shaped like these and furnished with a powerful spring. It is opened by a cord like that of the automatic thumb. Figures 158 to 160 explain the mechanism. It is an excellent appliance with which the wearer can carry out the majority of the actions of everyday life. It has, however, the disadvantage that it is not shaped like a hand—a point to which patients attach much importance—and, moreover, it is a part of a patented appliance, for which an interchangeable hand is not manufactured. So that in order to have in addition an artificial hand, which is capable of being removed and replaced by one or more of the appliances which will be described later, it would be necessary for the patient to possess two complete artificial limbs, and changing from one to the other would evidently be inconvenient.
We generally prescribe this appliance for patients who have lost both arms, for one side and as a supplementary appliance.
There are other similar models into details of which it is unnecessary to enter. Those in which the grip is opened by movements of pronation and supination are obviously only suitable for certain rare cases (very long stumps, with free movement).
The general principle is to fit to the end of the forearm piece an attachment which can be screwed on or unscrewed at will and which carries an appliance which is adapted to the various more or less specialised movements of the patient's trade.
Naturally the results thus attained must always be imperfect; but however little perseverance and ingenuity he may possess, the patient finds that he is able to educate the remaining arm, even when it is the left, to replace the amputated one in a way that is often remarkable. It is to this education that attention must be specially directed in the workshops for the re-education of the maimed.
1. Knife and Fork.—The first necessity is to be able to eat, and by certain very simple devices a fork, spoon or knife may be fixed to a wooden hand, whether the thumb be mobile or not.
As a general rule if the patient has one arm intact, he uses the sound hand only for this purpose, but when both forearms have been lost an appliance is indispensable.
We have already described how in the hand with an automatic thumb, room can be left between the index and middle fingers for the handle of a spoon or fork. A direct grip can also be obtained with the hand shown in figure 147.
The hand with five automatic digits (p. 105) is usually arranged in such a way that it is possible to[110] hold a tumbler for drinking; but a patient with an amputation of one hand drinks with the other, and one who has lost both hands can drink with a straw.
These appliances have replaced that in which the knife or fork is attached to a block of wood which can be fitted into the palm of the hand when required. It is inconvenient to be obliged to carry these special implements about.
Raynal's fork-rest has the advantage over the last[111] mentioned that it fits any fork. Figure 161 shows very clearly its construction and the way in which it is used. The small special attachment, which is screwed in place, is not cumbersome and can quite well be carried in the pocket; it is, however, even more convenient to have an appliance which is capable of gripping the fork directly like those described previously.
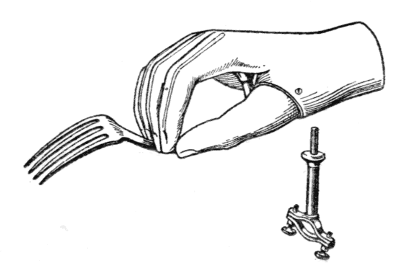
Fig. 161.—Raynal's fork rest.
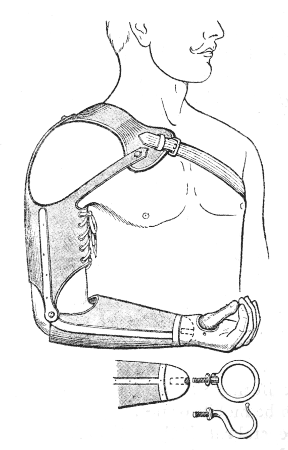
Fig. 162.—The termination of the forearm is a hemispherical piece of metal, furnished with a screw into which screw at will the hand, the hook or the ring.
2. Appliances for Workmen.—All the appliances that are attached to the arms in place of the artificial hand for performing various kinds of work are elaborated from two simple forms: the hook and the ring (for catching hold and carrying a parcel, for holding a handle, etc.). A glance at figure 162 will show the nature of these and the way in which they are used. But it will also be understood that if the simple ring and hook are useful for equally simple purposes they are altogether insufficient for skilled labourers[112] whose work entails a certain special adroitness, e.g. joiners, locksmiths, agricultural labourers, etc.
Many makers have realised this and have devised very ingenious implements, some of which we reproduce, though we are obliged to limit ourselves to certain types, for they can be varied in countless ways according to the needs of particular cases. The same workman, as we have already said, may have several appliances which he uses in turn as he needs them in the course of his work.
These appliances are constructed in two ways; some are fixed to the end of the forearm and are immobile, some are attached by means of a joint or joints and are capable of rotation in various directions.
(a) Fixed Appliances.—We illustrate here an appliance derived from the simple hook, the vine-dresser's claw, devised some time ago by Gripouilleau; branches of varying size can be held while the other hand saws them or cuts them with the pruning shears (Figs. 163 and 164).
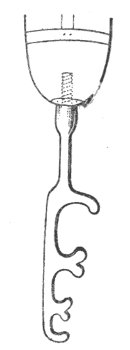
Fig. 163.—Vine dresser's hook. (Gripouilleau).
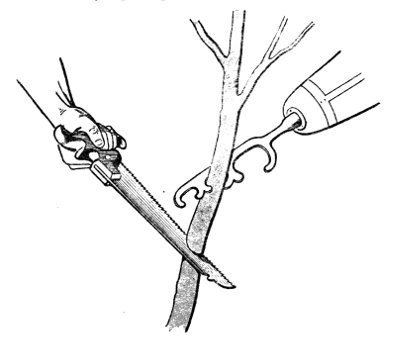
Fig. 164.—The branch is held in the grip by a leverage exerted by torsion.
This appliance of Gripouilleau, with a series of hooks, forms the basis of almost all the "pincer hands" constructed by M. Boureau and characterised by—
(1) The closure of the upper hook which is thus transformed into a ring, the two appliances being combined in one;
(2) The spring fixed to the straight side of the hook providing the grip necessary for holding articles. If the free end of the spring is turned up like the pointed toe of a mediæval shoe a sufficiently large opening is left between it and the straight edge of the hook to enable an object which is fixed mechanically or held by the other hand to be pushed into and gripped by the spring.
The simplest type of this mechanism is the postman's hand (Figs. 165 and 166).
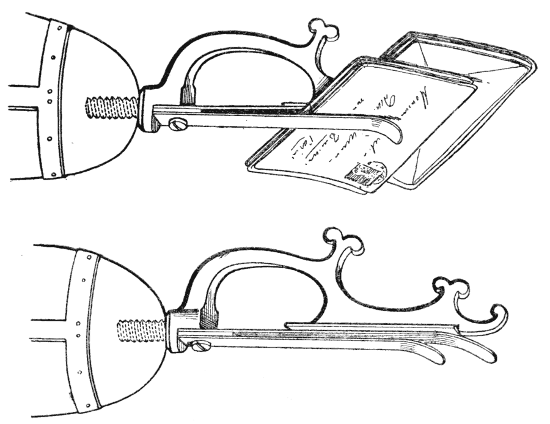
Figs. 165 and 166. Postman's hand.
The left hand of the postman who sorts letters has for its work to keep in the proper order the envelopes which are arranged in little packets; the right hand has only to push the letter into place between a flat spring, fixed to the wrist, and the back of the hook. If two or three springs are supplied the postman can arrange two or three packets of letters at the same time. He can also bind the packet with string.
The vine-dresser's hand is provided with this spring to hold small flat objects, but the second spring is wavy in outline, so that semilunar spaces are left between it and the first. Into these branches slip when the spring is pressed against them, and they are thus held more firmly, whilst being sawn or pruned,[114] than by the twisting action of the old pattern hook of Gripouilleau (Figs. 167 and 168).
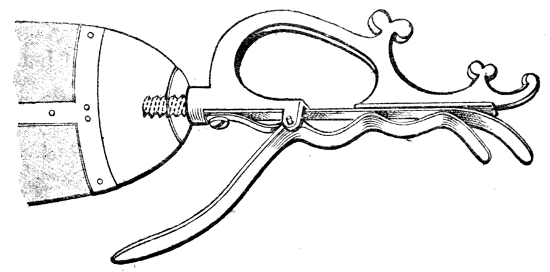
Fig. 167.—Horticulturist's hand.
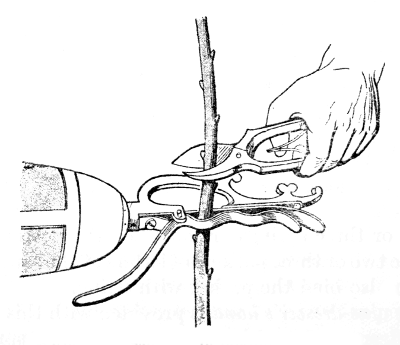
Fig. 168.—Method of holding a branch.
This thrust to seize the branch is somewhat rough, and is only possible in holding hard wood which there is no fear of bruising. For more delicate shoots (grafting vines indoors, preparation of cuttings), a grip is necessary which can be opened before seizing[115] hold of the object. This is accomplished by prolonging the spring towards the forearm as a handle, pressure upon which against the chest (when standing), or against the knee (when sitting), opens the grip, in which the graft, for example, is then placed in the opening of the correct size.
The packer's hand is very ingenious (Fig. 169). It has the hook pierced by an eye enabling a thread to be passed through a basket as with a curved needle. The jaws of the pincers are smooth at the tips, but further back they have a series of graduated notches in which tacks of different sizes can be held whilst they are driven in with the hammer. But of course a workman can only work quickly if he can hold a number of tacks of the same size in the palm of his hand, placing one under the hammer, relaxing his hold of it after the first gentle blow has fixed it, and getting the next ready while he drives it home.
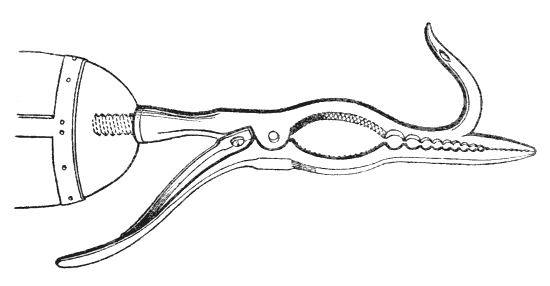
Fig. 169.—Packer's hand.
The plumber's hand (Fig. 170) is made in the shape of a pair of gas pliers, and ends in cutting edges with which wires can be cut. With them a bolt can be held whilst the other hand screws on the nut.
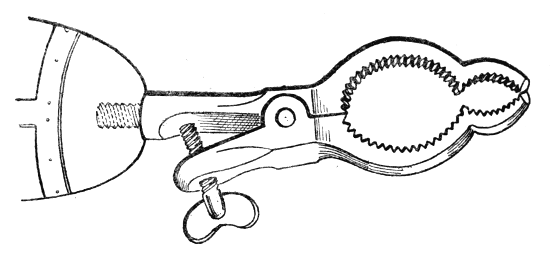
Fig. 170.—Plumber's hand.
The leather-cutter's hand (Figs. 171 and 172) should be able to hold the skin which the other hand cuts: it consists of a plate with a rough surface fixed to a ball and socket joint which allows it to turn in any direction, so that the other hand can follow the line to be cut which is often sinuous. This appliance may also be used to hold a drawing paper, a rule for cutting cardboard, or sheets of paper for binding.
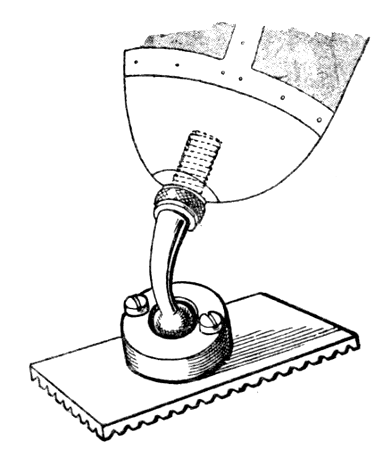
Fig. 171.—Leather-cutter's hand.
The examples that we have chosen amongst[117] Boureau's appliances for craftsmen will, we believe, be sufficient to explain the principles of their construction. These consist in studying the movements which are normally carried out by the passive hand (usually the left hand, but the right in left-handed people) and to devise an appliance accordingly, the sound hand always becoming the active hand.
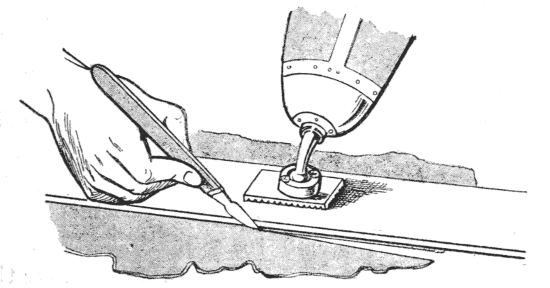
Fig. 172.—Leather-cutter's hand.
We could have described many more examples, but we shall only say a few words about the mechanic's hand, which is simply an adjustable spanner which can be automatically closed, terminating in toothed pliers to hold circular objects without the necessity for being screwed up. As a matter of fact, in all the work of a mechanic (sawing, filing, drilling, tightening screws, hammering, forging, and grinding) the left hand is only used for picking up and steadying the article to be manipulated. M. Boureau rightly considers that it is better to entrust this rôle to the artificial hand rather than to contrive to make the latter capable of sawing or of filing by means of the devices which we shall describe further on (p. 121 and following), ingenious and interesting though these may be.
From these appliances, adapted to certain particular grips, others have been devised for chair caning, soldering, and for enabling factory hands to work starting levers and brakes.
Thus each case must be studied separately and the workman furnished with one or several appliances according to his needs, making the necessary modifications from the existing patterns.
Several of these appliances are attached by a ball-and-socket joint like that described for the leather cutter: this is an intermediate form between the fixed appliance and the jointed appliances which will be described later.
Boureau recommends that the length of the forearm should be such that the artificial appliance reaches only as far as the level of the sound wrist. The work will then gain in precision. We believe that this principle holds good even for the true artificial hand, which should be made 3 to 4 centimetres shorter than the sound hand. But it must be realised that we shall be met with a difficulty, which we have already experienced. Comments are made upon the appearance of the arm and the wearer may sometimes be made to believe that this is due to faulty construction.
For certain special crafts the subject may be studied from another standpoint and an actual tool constructed which carries out the necessary actions like a machine worked by the forearm, so that in these special cases the artificial hand is the active hand.
At the Valentin Hauy Institute for the blind, where there has long been a brushmaking workshop, we have seen in use a very ingenious tool of this description[119] with a combined action for carrying out the entire manipulation of the thread which fixed the little bundles of bristles into the holes perforating the back of the brush. Results are so good that a blind and[120] maimed worker using this apparatus works more quickly than his comrades who have the use of both hands. It consists of a two-pronged claw surmounted by a small thimble-shaped projection and with a small hook, like a crochet hook projecting in front (Fig. 173). The hook first passes through one of the holes in the back of the brush, catches up the thread and draws it through the hole (Figs. 174 and[121] 175). The thread is then looped around the thimble, whilst the sound hand binds the little bundle of bristles into a twist of the loop (Fig. 176), and finally the bundle is fixed into the hole, the claw being used to draw the brush towards the worker (Fig. 177).
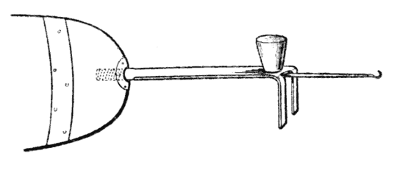
Fig. 173.—Brushmaker's hook.
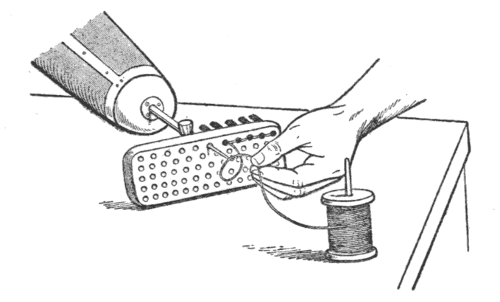
Fig. 174.—First movement. The string is picked up by the hook.
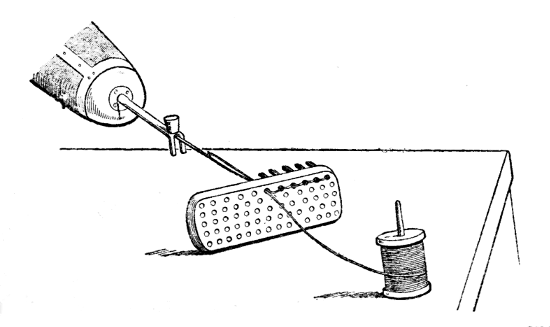
Fig. 175.—Second movement. The string is pulled through one of the holes perforated in the back of the brush.
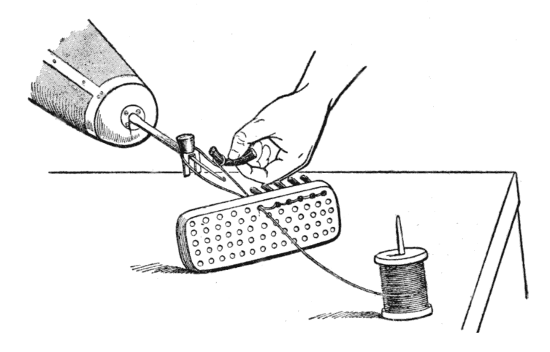
Fig. 176.—Third Movement. Catching the bundle of bristles.
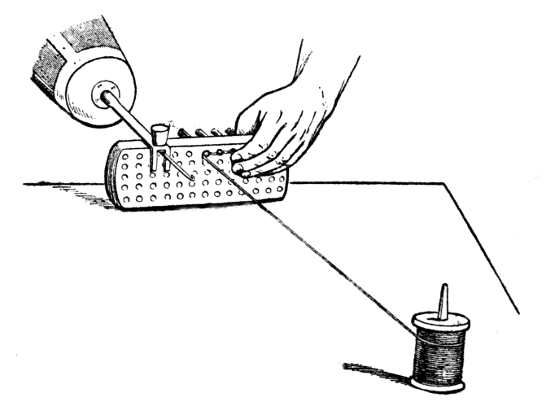
Fig. 177.—Fourth Movement. The bundle is fixed in the hole in the back of the brush.
(3) In place of an actual tool the detachable part may consist of a clamp on the principle of a ring into which the tool is inserted by the handle. The two principal methods are the screw and the American chuck. A glance at figures 178 and 179 will explain how the large handle of a tool intended for heavy work is controlled by means of a screw and rings.
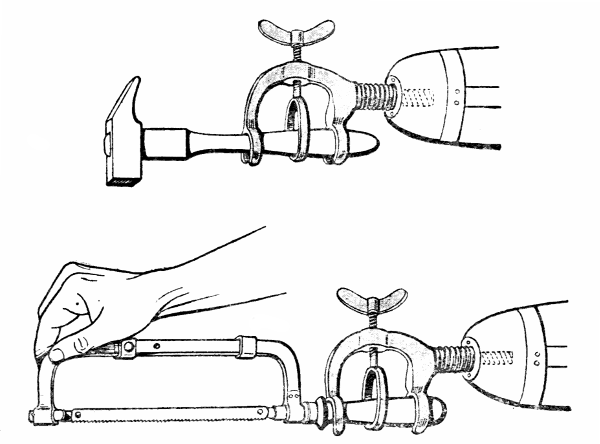
Figs. 178 and 179.—Nyrop's grip for hammer and saw.
At Rouen we have seen the disabled Belgians who had been re-educated wearing an ingenious T-shaped clamp by means of which the handle of a tool may be held either in the line of the axis of the forearm[122] or at right angles to this. This method is specially useful for manipulating a file which is worked with one hand while the other, in this case the sound hand, presses upon the free end. Usually the filing is done backwards and forwards, working from base to tip of the file, but sometimes, specially for final polishing, the file is held with both hands and worked from side to side.
The American chuck consists of a pair of metal jaws fixed at their base into a cylinder and appearing somewhat like the petals of a long corolla. Another cylinder is screwed over the first to control the opening[123] and shutting of the jaws. When this cylinder is unscrewed the jaws open and the handle of the tool can be inserted, when it is screwed up it closes the jaws and makes them grip the handle.
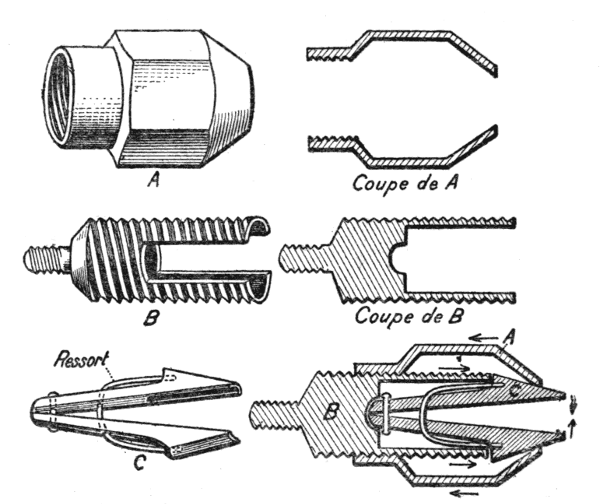
Figs. 180 to 185.—The American Chuck.
The pincers are composed of two jaws with vertical cylindrical grooves (to fit upon a handle), joined above by a ring (Fig. 185) and coupled by a spring C which keeps them apart. The pincers fit into a piece B (Fig. 182) cut on the outer side with a screw thread (Figs. 182 and 183) upon which the piece A is screwed up or down (Figs. 180 and 181). When screwed towards the point of the pincers it presses on the two jaws and closes them. When screwed in the opposite direction the pincers open automatically.
If the jaws open widely, the wooden handle of a tool can be held, but if the opening is small the unmounted tool must be fitted into them (Figs. 186 and 187). This method is specially useful for files, as it frequently happens that several files are required for the same piece of work and they can be changed rapidly.
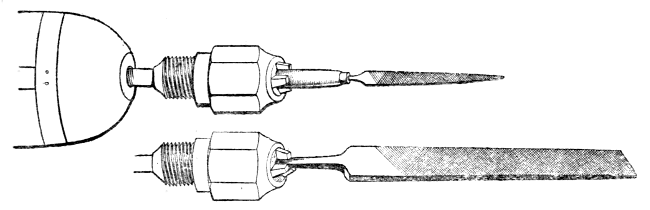
Figs. 186 and 187.—File fitted into the American chuck.
It must, however, be insisted upon that the principle of giving a passive rôle to the artificial hand is to be preferred.
(b) Appliances with Mobile Joints.—In the course of work the direction of the wrist is changing at every instant, flexion, extension, pronation, and supination occurring, sometimes in order to move around the object, sometimes in order to maintain a suitable position when the movements of the shoulder and elbow vary the direction of the forearm.
The consequence of this is that the worker learns to turn the piece of work around with his sound hand. To get over this difficulty passive joints are inserted[124] at the wrist, which allow the appliance to move when it is pressed against the piece of work and to take up the direction which suits the inclination of the forearm.
One of the simplest mechanisms—and one of the oldest, because it was designed by Gripouilleau—is that of the agricultural labourer's ring, intended to grip and manipulate the handle of a wheelbarrow or a plough. The ring is mounted on a transverse axis and moves in a horseshoe which in its turn revolves on a shank which is screwed into the forearm. The ring is provided with a screw, which may be tightened upon the handle if desired, but which is, however, rarely used (Figs. 188 to 190).
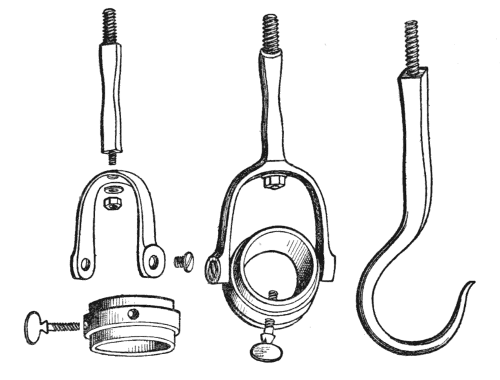
Figs. 188 to 190.—Agricultural hook and ring. (Gripouilleau.)
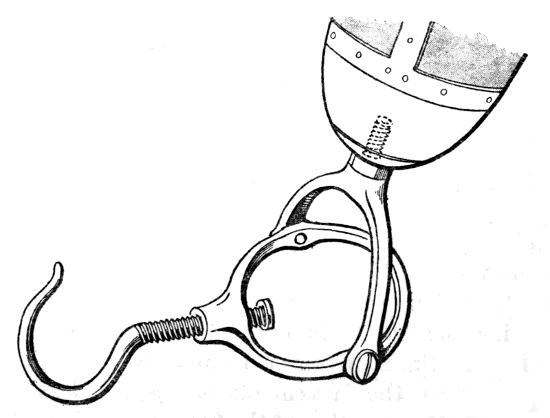
Fig. 191.—Combined hook and ring. (Boureau.)
The tram-driver's bell, represented in figure 192, is devised on the same principle. It moves on a transverse axis, and in figures 193 and 194 its utility in managing levers in driving a tram or a motor car will be easily seen. The rotation of the horseshoe on the axis of the forearm is not required.
Figs. 192 to 194. 1. Tram driver's and chauffeur's bell. 2. Method of use by a tram driver. 3. Management of a motor car lever. Pressure at the extremity and traction.
The "cardan" joint also allows movement in every direction: it consists of two semicircles of metal, placed at right angles, each working around a transverse axis, these axes being united in the form of a cross. The construction and working will[127] probably be understood without further explanation by a study of figures 195 to 198. The first two represent a system with a ball in the centre, which is well known commercially. The last two represent the simple universal joint generally used in orthopædic surgery. It is somewhat more cumbersome than the previous model.
Figs. 195 and 196.—Universal joint with ball.
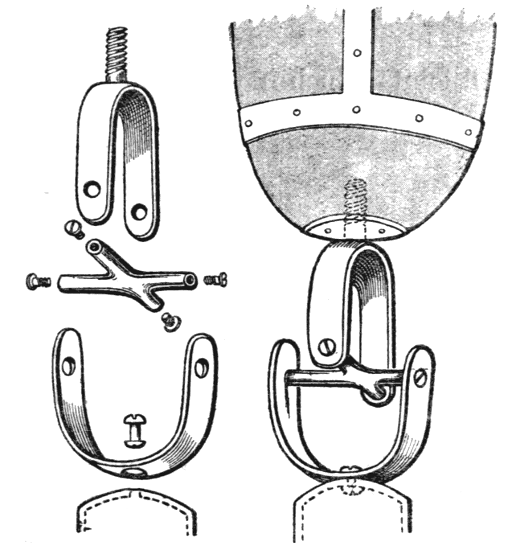
Figs. 197 and 198.—Simple universal joint.
The spade holder used at the agricultural centre at Limonest is mounted on a cardan (Fig. 199).
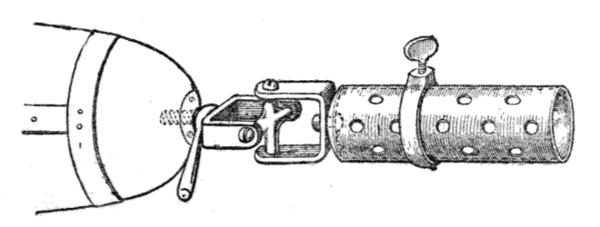
Fig. 199.—Gardener's cylindrical spade holder. A universal joint permits movements in every direction.
The joint can be fixed by a compression screw which is easily and quickly adjusted.
Where several tools are necessary each should be complete with its own universal joint.
Other methods of terminal passive articulations are—
(1) Ball joints which have already been described in connection with the fingers and which may be applied to the wrist.
(2) Bayonet joints which are only applicable to certain artificial hands which are not subjected to any great strain.
Figure 200 explains this mechanism as it is applied to the artificial hand represented in figure 148.
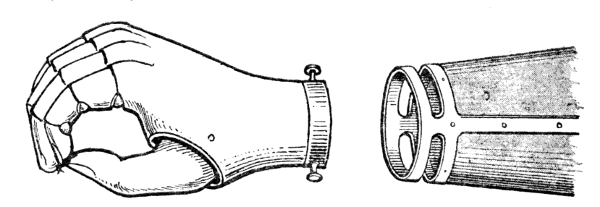
Fig. 200.
In this chapter we shall deal only with amputation of the arm below the upper third, i.e. with cases in which the stump is long enough to transmit movements to the artificial limb. Amputation through the deltoid muscle must be considered in association with disarticulation of the shoulder.
Below the arm socket is attached an artificial limb which represents the elbow joint, forearm, and hand.
There are two types to be described:—
1. The artificial arm proper, which has the external shape of the natural limb.
2. The worker's arm, a terminal appliance in which outward appearance is not considered.
The considerations as to the arm socket and its attachment by a shoulder cap are the same for the two types of appliance.
Attachment and Arm Socket.—The surface over the acromion and clavicle is the only point from which support can be given to an appliance for an amputation through the arm; the attachment is made by means of a shoulder cap.
The general shape of this shoulder cap and its[130] attachment by means of a strap passed under the opposite axilla are similar to those described for appliances for amputation through the forearm.
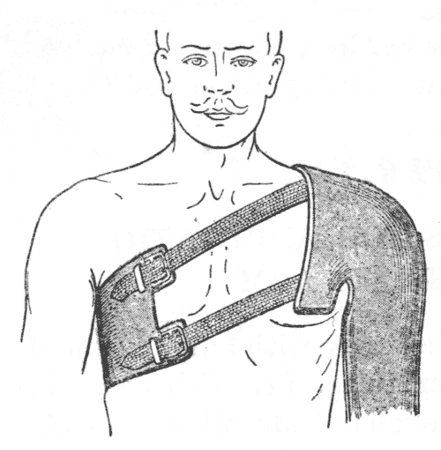
Fig. 201.
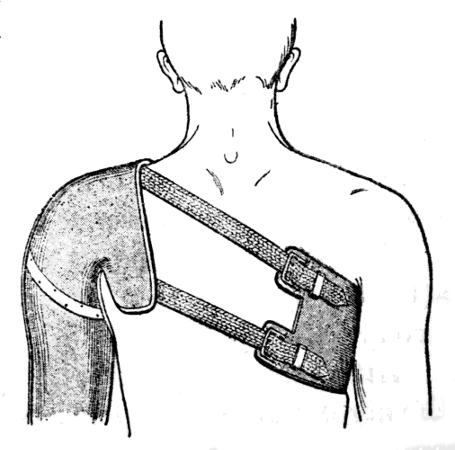
Fig. 202.
The larger the shoulder cap the more it extends forwards over the anterior wall of the axilla, upwards over the supra clavicular fossa, and backwards over the scapula, the more secure will be the support. The appliance is heavy and has no support other than the axillary strap. The latter has a tendency to ride upwards against the axilla where it exerts a pressure which may be uncomfortable. This may be relieved by attaching a vertical strap which is buttoned to the trouser belt.
But although this extensive enclosure of the thoracic region may not hinder the movements of the stump forwards and backwards, it must obviously interfere with the movement of abduction. No doubt this movement is the less important of the two, but we ought to try to preserve it as far as possible.
In short stumps we must abandon it. But if the stump is long and consequently has no tendency to escape from the socket, even if this slips down a little, movement may be retained by two methods.
The first consists in separating the arm socket from a large shoulder cap, and inserting a joint between (see page 87); but the appliance is then heavy and cumbersome. Moreover, although abduction can thus be easily attained, thrusting and pulling movements require a light appliance, and finally it is impossible to secure rotation.
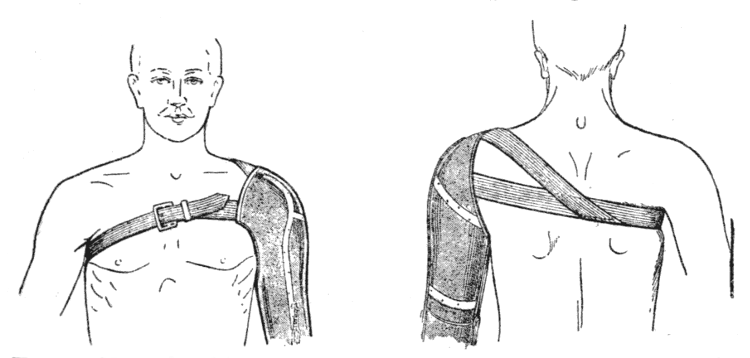
Figs. 203 and 204.—Shoulder fitting of small extent allowing abduction.
It is possible, on the other hand, by means of the other method, which consists in ending the shoulder cap at a line continued vertically upwards from the thoracic margin of the axilla. If the straps are strong and carefully adjusted the result is better than with the fitting over the scapula, so that this appliance is preferable. We here illustrate a method of fitting the straps which we consider a good one. From the posterior part of the ordinary axillary strap, a Y-shaped branch passes to the upper border of the shoulder cap above and in front of the clavicle, this[132] makes up for the small extent of the enclosure of the shoulder.
For the worker's arm a considerable enclosure without any joint is essential, in order to secure stability.
The arm bucket, usually continuous with the shoulder cap, is made of leather strengthened with steels.
The artificial arm is often abducted from the trunk, which constitutes an inconvenience. This is sometimes due to a fault in the alignment, the arm piece not being at right angles to the shoulder cap. It is, however, more often due to the cylindrical shape given to the arm bucket which forces it away from the trunk. The inner side of the bucket should be flattened so that it may hang vertically close to the thorax.
The details of construction are different for the true artificial arm and the worker's arm.
The arm and forearm pieces are both made of leather. There is no object in making them to lace, the stump is enclosed in a socket in which it need not fit very tightly, because, as we shall explain, this appliance is unsuitable for heavy work.
These two parts are strengthened with steels, which are articulated by hinge joints at the level of the elbow. We have to study—
1. The position of the steels and the direction of the axis of the joint.
2. The lock to fix the elbow joint in a flexed position.
1. Position of the Steels.—The stump can transmit to the arm socket the various movements grouped under the name of circumduction, but its hold does not enable it to transmit rotation.
It is therefore undesirable—although usual—to attach the steels on the arm and forearm to the inner and outer sides of the limb. If this is done, as rotation is impossible, flexion of the forearm at the elbow can only be carried out in the sagittal plane. But this movement is only exceptionally required; the elbow being flexed to the right angle and fixed in this position by a ratchet the limb forms a hook upon which an object may be hung, provided that the forearm lies transversely in contact with the abdomen and not antero-posteriorly. Flexion should therefore be in a plane which is almost the frontal plane (20° or 30° in front of this), and not in the sagittal plane. As there is no active rotation of the arm therefore the steels must be almost in the sagittal plane (the anterior a little external, the posterior a little internal).
In certain carefully constructed appliances the arm bucket is cut transversely above the elbow and between the two parts a bayonet joint is fixed where the arm can be rotated by the sound hand, so that the direction of the elbow movement can be altered.
2. Ratchet to fix the Elbow Joint in the Flexed Position.—When at rest the forearm should hang vertically. But the hand can only be used when the elbow is flexed to an obtuse angle or a right angle, the latter position being more often used. Therefore when the patient has bent the joint to the required angle with his sound hand, he must be able to fix it in this position.
This fixation is effected by means of a ratchet[134] attached to the outer side of the elbow, which can be locked or unlocked at will.
This ratchet consists of a flat metal plate with a prolongation upwards shaped like the handle of a fork. The end of this prolongation is attached to the arm steel by a pin joint about 3 centimetres above the axis of the elbow joint. The plate is pierced by a rectangular opening, one border of which is notched; it lies against the forearm steel, a catch projecting from which fits into the opening, this catch, situated 6 centimetres below the axis of the elbow, is of the same diameter as the notches with which it engages. The higher the notch with which engagement takes place the more nearly flexion approaches the right angle.
The width of the opening in the plate is twice the size of the catch, so that the joint works freely when the catch glides on the smooth edge and becomes fixed as soon as the catch engages in the notched border.
It is only necessary to arrange a lock, manipulated through the sleeve, to bring the smooth or the notched border in contact with the catch.
Suppose that the handle of the ratchet is prolonged behind the point at which it is hinged to the arm steel as a little lever furnished with a button, and that an elastic cord or spring is stretched from this button to a point on the postero-external border of the forearm, then if the lever points upwards and the notches are on the upper edge of the ratchet (as is the case in figure 205), the elastic, pulling the lever forwards, will press the ratchet down and make the notches engage with the catch on the forearm, if, on the other hand, the lever points downwards the elastic traction[135] will release the notches. The reverse occurs if the notches are on the lower edge.
It is then only necessary to arrange a mechanism by means of which this little lever can turn, with a stop which arrests it above at the vertical position, below at a point 45° beyond the horizontal.
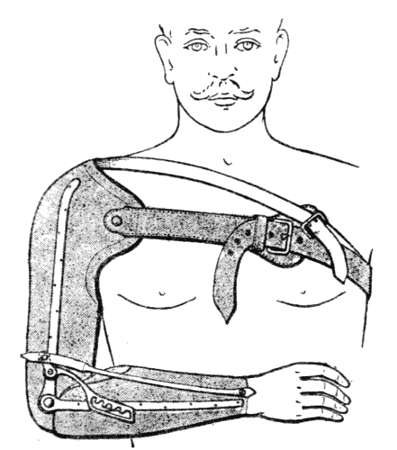
Fig. 205.—Elbow ratchet.
A simple mechanism of this sort is shown in figures 206 and 207. The joint surfaces of the ratchet and of the little lever each bear a shoulder, the former in front, the latter behind, extending over such a proportion of their circumference as will make them act as stops in the desired positions above and below.
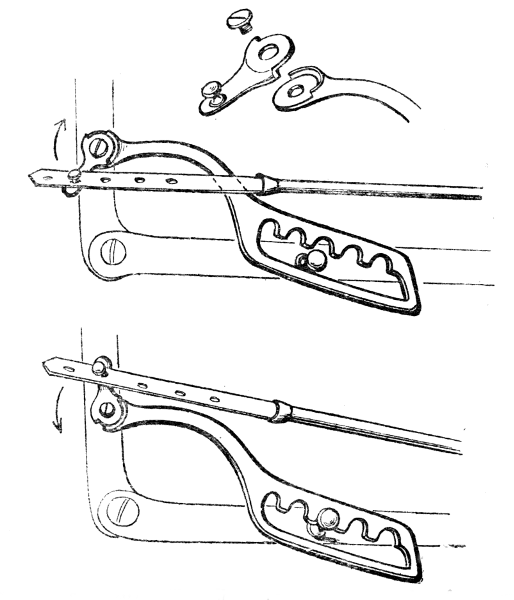
Figs. 206 and 207.—The elbow ratchet and mode of action of its lock.
A lock is thus provided which can be manipulated with the other hand.
In the particular pattern illustrated, traction is made by an elastic cord fixed to the centre of the back of the wrist and ending above in a leather strap pierced with holes which fix on the button of the lever. This arrangement allows of the adjustment necessitated by the gradual stretching of an elastic which is subjected to continuous tension.
A steel spring of this length (the whole length of the forearm) would be too heavy if it were sufficiently powerful. If it is desired to use this method the two ends of a powerful spring should be fixed, one to the button on the lever, the other to the catch on the forearm with which the ratchet engages.
The spring should always be in tension. As the distance between the joint on the arm and any point on the forearm increases as the elbow extends, it is better for the ratchet, with notches on its upper[137] edge, to be engaged when the button points upwards and free when it points downwards. In the opposite arrangement, which is often used, the tension is considerable without being useful when the forearm is vertical, and the mechanism soon wears out.
3. Hand and Other Appliances.—The hand attached to the end of the forearm has a spring thumb which may be passive or automatic. In the latter case, if the stump is long enough to allow considerable movements of the arm, the cord works in the way described on page 87, for amputation of the forearm. If the stump is short, traction must be exerted by movement of the shoulders, rounding the back.
The hand with a mobile wrist is never used with these amputations except in certain expensive appliances, in which in addition the four fingers may be articulated, as described on page 101. For the ordinary limb these delicate mechanisms are devoid of practical utility.
It is easy to replace the hand with interchangeable appliances, but when the patient has to do hard work this is not a satisfactory method.
The arm with the ratchet at the elbow is in fact suitable for use by a clerk. But it is not either strong enough or simple enough for manual labour. In our opinion the functional and practical value of an artificial arm, particularly for amputation above the elbow, is often exaggerated, however it does exist, especially in many branches of agricultural work. For the latter the slightness of the lateral steels—and especially of the joints at the elbow—makes the appliance insufficiently strong. The necessary delicacy of the ratchet and its manipulation through the sleeve by the sound hand are additional disadvantages.
If our object is to fit to an arm stump an appliance which will be at the same time strong and flexible, capable of carrying out rough and even vigorous work, we must abandon the attempt to imitate the natural shape of the arm.
The movements and strength of the stump must be transmitted to the object held by means of a rigid rod at the extremity of which the appliance for gripping is fixed. It is possible to fix around this rod a show arm with a hand and a passive spring thumb for wearing on special occasions, in exactly the same way as we fit the show leg round the peg. Figures 208 and 210 will show at a glance how this is done.
But, as far as our present experience goes, this is only an accessory added for æsthetic reasons. The true worker's arm consists of a strong metal rod fixed to the arm socket in a way that we must now study.
1. The Arm Socket.—We have already said that this must be continued into a shoulder cap of considerable extent, which may be perforated in the region of the point of the shoulder in order to render the appliance lighter. Abduction at the shoulder is thus sacrificed.
The arm socket is made of leather, open down the front and laced. By being laced it fits the stump more securely. It is strengthened by two steels which may be fixed in the frontal plane because, as we shall see, a passive rotation at the elbow joint is possible.
These steels are directly continuous below with a hemispherical steel cap, which is pierced in the axis of the limb by a hole into which is bolted the[139] connecting piece to which the rod which represents the forearm is attached.
2. Articulation at the Elbow.—The forearm consists of simple metal tube, attached beneath the arm socket by methods which depend upon the following principles.
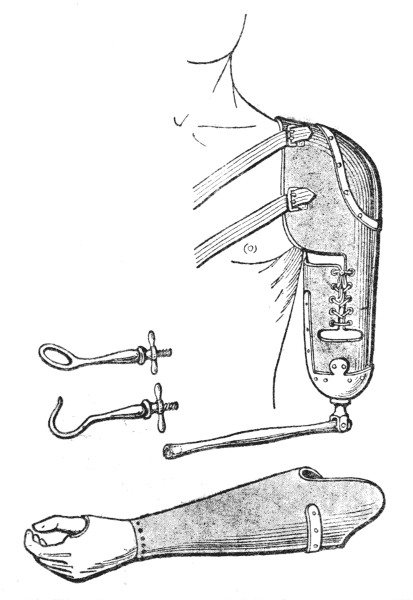
Figs. 208 and 209.—Worker's arm and show arm.
The worker's arm consists of a metal rod which swings backwards and forwards at the elbow and also rotates upon the arm socket. To the end of this rod an appliance can be screwed (a ring and hook are here shown). Around the worker's arm a show arm with a hand (Fig. 209) can be fixed. They are shown in place in Figure 210.
The only movements that the stump can transmit[140] to the arm socket are forward and backward movements hinging about the shoulder, and abduction. The first of these movements is the only really useful one for the workman. The downward pressure exerted by active extension of the elbow no longer exists; in order to press upon an object the sound hand must be used, for it is not practicable to make use of the weight of the body thrown forward for this purpose.
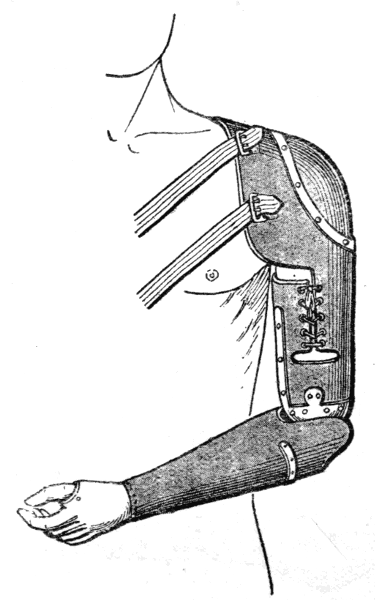
Fig. 210.—Show arm in position.
In backward and forward movements—considering, for example, the use of the file—the angle at the elbow opens when the arm is thrust forward and closes when it is pulled backwards. These passive[141] movements of the joint must not be impeded in any way, that is to say, the forearm must swing freely below the arm upon a transverse axis and it must also be able to rotate freely around a vertical axis.
These movements are secured in the ploughman's hand which was designed sixty years ago by Gripouilleau and in which the joint which we have shown as a method of attaching the mobile ring to the wrist is utilised. The forearm rod attached by a strong transverse pin swings freely in a little stirrup-shaped cap, which itself rotates around a bolt by which it is firmly fixed into the metal or wooden hemisphere which terminates the arm socket.[14]
[14] Wood, which was used by Gripouilleau, has been given up.
It is clear that this complete liberty of action has its disadvantages; the elbow joint can never be made to assume a fixed position against any passive resistance; moreover, in actual practice the useful range of either of these movements is small. For this reason attempts have been made to devise methods by which they can be limited in the various worker's arms which have been designed since the beginning of the war. In all these arms the mechanism of the elbow joint is derived from that of the ploughman's arm of Gripouilleau. Unfortunately none of these mechanisms in which a pressure screw is used for fixation possess any strength. At first sight, in a new appliance they appear attractive and work well, but it is well known to all mechanics that the thread of a screw which is in constant use quickly wears and then it is impossible to tighten it.
At the extremity of an artificial arm, whether it be an arm of natural shape or a worker's arm simplified to the form of a jointed rod, any of the appliances[142] already described for forearm amputations can be screwed on as required.
It is by the use of these appliances that Gripouilleau's old ploughman's arm, which ended in an interchangeable hook and ring, has been improved.
Apart from their actual economic value, results have been obtained by use of these terminal appliances, in many different skilled trades, which are of the greatest possible interest.
For reasons that we have indicated in describing the attachment of the elbow, the various attempts that have been made to give to the wrist a mobility that is under control have not so far led to the invention of an appliance that is both strong and durable. For this reason we consider that until something new is designed it is better to make the terminal appliance a fixed one.
So far as function is concerned these operations are identical; a short arm stump is incapable of transmitting movements to the socket of the artificial limb.
That is to say, our appliance will be a purely passive one, and at the present time it is useless to attempt to make any sort of worker's arm. We must aim simply at supplying a limb which imitates the external shape of the arm, with an elbow joint which can be locked with a ratchet. At most it is possible by a movement of the opposite shoulder to work an automatic thumb by means of a cord, as a rule, however, a simple spring thumb is preferred.
Nothing need be added to what has been said in the previous chapter about the elbow joint or the hand.
In the fitting of an attachment over the shoulder the amputation through the deltoid presents an actual advantage. For in this case the shape of the point of the shoulder is preserved, and the attachment[144] carried out as described on pages 87 and 130 fixes the appliance very securely.
If the entire humerus has been removed a very extensive enclosure of the front and back of the chest is essential and in order that the axilla may be in close contact with the top of the limb it is a good thing to stretch across this space a layer of some firm material.
These appliances can be used to steady a piece of paper upon which the patient is writing, to carry a parcel which is not too heavy with the elbow flexed, to grip an article with the thumb. A workman who is being re-educated for some occupation which is possible for a one-armed man, will usually—unless he is going out for pleasure—leave his artificial arm at home in the cupboard.
When a disabled man has been fitted with an artificial limb he has to learn a trade which will enable him to supplement his pension and provide for himself and his family. In our opinion, which we believe we have expressed more than once in this book, it is nearly always advisable to determine what profession will ultimately be possible before ordering the artificial limb. This principle is perhaps not always thoroughly understood, although there are fitting centres where it is fully recognised (a proof of this may be found in a recent article by Nové-Josserand and Bouget).
It is unnecessary to repeat that whilst every effort must be made to associate form with function, the latter is bound to take precedence of the former. It is, however, not always easy to impress upon patients, and more especially upon their protectors, that form is for Sundays and holidays, and function is for workdays.
The grave problem of re-education of amputation cases, and in a more general sense of all the maimed, now confronts us. We believe it to be worth while to indicate the general principles so far as they are at present understood.
At the outbreak of war the idea of the disabled in general, and particularly of those who had had a limb amputated, was often to give up any really active trade and to seek a "situation" generally as an official with no actual manual labour. It must be confessed that many people, especially the nurses, encouraged them in this, and possibly the latter would not deny having done so.
It has rapidly become evident that there are too many maimed to be supplied with situations as caretakers of public gardens or doorkeepers, and that they will not be able to gain a living by making tricoloured decanter-mats of string or raffia or artificial flowers, when bazaars organised for their benefit by tender-hearted souls have gone out of fashion.
One of us was present a short while ago at the following little scene:—
In a hospital where there were two amputation cases, one through the lower fourth of the thigh, the other through the middle of the leg, both agricultural labourers, a distinguished man of letters, actuated by the best intentions, asked them what they counted on being able to do after they had been fitted with artificial limbs. The first replied that he hoped to return to agricultural work, the second that he would never be able to do that but would look out for a "situation." Our friend was much surprised to hear us say that he would be ill employed in using his influence to obtain his desire for the second patient, because a man with only one leg could work on the land with almost no diminution of his ordinary capacity, even with the old-fashioned kneeling peg leg.
As Jean Camus has well said in a recent article in the Paris Médical, "We are beginning to pass beyond the phase when re-education of the maimed was left to chance. It is felt now that the frivolous efforts of benefactresses who, acting with the best intentions but without reflections, are delighted to be able to transform into a shorthand typist an honest farm labourer who had a strong attachment to the soil and could quite well return to it, must be avoided. Such feats are both culpable and absurd."
These fantastic ideas must be got rid of, and all our efforts must be co-ordinated, the complexity of the conditions to be dealt with being duly weighed.
Given a maimed man the first care should be to educate to the maximum all the uninjured and remaining parts. It is too often forgotten that among the parts remaining the brain plays a leading rôle, even the chief rôle, not only because it is the organ of "good will" without which all attempts at re-education are fruitless, but also because good will being given the intelligent man will succeed better and will be able to adapt himself to more delicate work. "Physiotherapy cannot be prescribed," says J. Camus, "as quinine is prescribed. The malarial patient who takes the latter medicine benefits whether he wishes to or not. The wounded man who submits each morning to his mechanotherapeutic treatment does not recover unless he wishes."
It is very difficult to make the layman understand this. He invariably takes for granted the good will of the patient, with all of whose complaints he sympathises, without for a moment realising that they sometimes degenerate into jeremiads, often with an ulterior motive. An examination by a doctor—[148]and an experienced doctor—is therefore necessary in order to determine under what physical and mental conditions an amputation case can be re-educated; so that he may understand that it is entirely to his interest to work as quickly and as well as possible, that begging is degrading, and above all that private charity is temporary and exhaustible; and that in consequence he must as quickly as possible put himself into a condition to supplement by a salary justly earned the pension or gratuity which is certain to be insufficient for his maintenance.
It can never be sufficiently insisted upon in dealing with the maimed that by resuming work, and on account of the functional improvement resulting from doing so, they need have no anxiety that their pension will be reduced, because the amount of this is based on the extent of the injury itself and on the man's rank, and not on his profession before he became a soldier. In the same rank the pension is the same for a surgeon or a lawyer, if both have lost a hand.
It is a deep-seated notion, instilled into the minds of injured workmen by the often suspicious folk who advise them, that if they begin work before their case has been settled their pension will be less.
It must be acknowledged on the other hand that the civil expert is often faced with a difficulty. As our law stands—and it is unfair—work cannot be resumed partially with provisional half-pay followed later by whole-time work with permanent salary. This difference is important to our wounded soldiers, who have everything to gain by a rapid and complete re-education and whose duty it is to do whole or part-time work while their legal position is being arranged and before the wound, in legal phraseology,[149] has become "consolidated," that is to say, before the completion of treatment.
It is only fair to add that the patients are not alone to blame and that the administration has for long been guilty of an error against which reaction is growing, viz. delaying re-education until the time when the local condition has become permanent and the patient has been discharged and has received his prosthetic apparatus.
This delay is deplorable, on both medical and social grounds. On medical grounds because in very many cases before treatment is quite complete the addition of carefully graduated and supervised work is an important part of the treatment. On social grounds because it is necessary to fight in every possible way against the common tendency of the patient to fall into habits of laziness and intemperance.
This is now understood, and almost everywhere to-day the wounded soldier can resume work in workshops attached to the centres of physiotherapy, and thus begin his re-education while continuing his treatment.
At a certain stage resumption of work becomes the best therapeutic agent of all.
It is obvious that this resumption of work cannot supply the place of certain special treatments such as electrical treatment during the regeneration of a nerve, balneotherapy, or graduated gymnastic exercises; but is it not true that work with its continual active movement is infinitely superior to passive mobilisation by means of apparatus however ingeniously the latter may be contrived? Morover it is surely a more efficacious course of mechanotherapy when the patient works for half[150] or all the day than is provided by the special course occupying only an hour or two.
The tendency to-day is in this direction, as, for example, at the Grand Palais, thanks to the efforts of J. Camus, and also in the agricultural centre of the XIIIth district under the direction of Belot and Privat. At a given moment all treatment may be suspended and the patient may devote himself exclusively to work with results the excellence of which Nepper and Vallée have demonstrated.
The workmen are then eligible for work in a town in private workshops, but so far this freedom has more inconveniences than advantages. A man whose working capacity is much reduced, and more especially a man who requires re-education, has no place in an ordinary workshop where neither the proprietor nor the foreman nor his fellow-workmen are in truth much inclined to concern themselves about him. Where actual education is necessary this is best supplied in special workshops where the patient will be among comrades handicapped like himself, whose progress he will be able to watch and whose efforts he will imitate, rather than among able-bodied workmen, by comparing himself with whom he is bound to be discouraged.
The problem has been solved by the Belgians in a remarkable establishment opened at Port-Villerz, and by the Austrians at Vienna under the direction of Spitzy, as Nové-Josserand and Bouget inform us, by delaying a maimed soldier's discharge from the army until his re-education is as complete as possible. This method has proved to be to the interest both of the individual and of the State, but we do not seem to have considered this solution, and it is still to be[151] feared that it would accord ill with the independence of our national character. The actual fact, though it has not been brought into prominence, is that our usual system of "watertight compartments" has been applied by adding to the centres of physiotherapy centres of agricultural or industrial re-education, the results obtained in which are dependent upon the efficiency of the director of physiotherapy.
This matter seems to have received very little special attention in connection with amputation cases. It is, however, of great utility to develop the strength and agility of the remaining limbs by suitable gymnastic exercises, to teach a man with only one leg, for example, to jump without an artificial limb and to climb a slippery rope or a ladder; or to train the left hand of a man who has lost his right; to develop the greatest possible strength in the stump by training it in movement combined with the exertion of force. In addition to this, early and provisional equipment with artificial limbs must become general. These temporary limbs are undoubtedly rudimentary contrivances, but they are functionally good and are useful on account of their mere weight.
In this connection the temporary arms used by Nové-Josserand and Bouget in their agricultural re-education centre are very interesting models. The great advantage of using a temporary limb is that the time required for the construction of the permanent apparatus, often a considerable period, is not lost in idleness, the mother of all the vices.
It was said at the beginning of the last chapter that whenever possible a disabled man should be[152] given a real trade and not one of those frivolous and trifling occupations which were at one time the fashion.
In the choice of a trade the ruling principle is that of aiming to restore as nearly as possible the man's former occupation. This principle should not, however, be carried to an extreme.
As Camus has justly said, by his previous work a man has stored up a mass of ideas, a fact which is too little realised, especially by himself. These include the manner of choosing, holding, and attacking the materials upon which he works, and of appreciating their qualities and faults; knowledge of their market value, of the value of the labour, etc. This should be utilised in his future work even though it be realised, as M. Bourillon has remarked, that the resumption of his trade in its entirety may be impossible.
With the tools that have been described a man who has lost his forearm may be able, for example, to undertake a locksmith's work and to execute correctly all the movements required in plying the trade. Granted; but how long will he take to make one piece, let us say, as well as his neighbour? If he produces little he will not find an employer to give him daily work, while if he does piecework, apart from the fact that it is not in good repute among those who are the actual leaders of the working classes, it will not be remunerative, and to earn 3 frs. a day when a comrade earns 10 or 12 frs. is practically an impossible solution.
The case may be cited of a woman suffering from congenital deficiency of the hand with a very short rudiment of the wrist which is only slightly mobile.[153] By means of contrivances which we need not describe, and with no prosthetic apparatus, she threads her needle and sews as quickly and as well as anybody. This is not an argument, for: (1) it is a congenital lesion and the educability of a child is well known; (2) the woman is extremely intelligent, and unhappily this favourable factor cannot always be counted upon. It would be wrong to conclude from this that a case of amputation at the wrist should be put to sewing.
It must never be forgotten that intelligence and will are factors of the first importance, so that however little intellectual capacity the disabled man may have, he is bound to profit by his passage through the school of re-education in learning to read and write if he is illiterate—this is more frequent than is usually believed—or to improve his knowledge if he has already had some instruction. It is, in fact, by brain work that many learn to replace their physical defect. Let us take, for example, a disabled bricklayer. If he is intelligent and is given a helping hand in the shape of the necessary instruction, he may become a builder on his own account in a small way when he knows how to make plans, work out estimates and keep accounts.
This is not a Utopian fancy. In the small towns and villages there are many owners of businesses such as masons, decorators, joiners, etc., workmen who cannot spell, but who are intelligent, have business minds and a gift for overseeing, who have given up the trowel and will build you a house as well as, or often better than, many "architects." It is with similar aims to these in view that a bricklayer should be re-educated when it is judged that his intellectual capacity is sufficiently great.
Where there is no intelligence education can do little. There are in civil life innumerable "casual labourers" with limbs intact who have never been able to learn a regular trade and who earn a miserable livelihood by doing what "turns up." Their situation becomes serious when they lose some of their physical capacity. They can, however, be rescued, particularly by encouraging them to become agricultural labourers. It is indeed especially agricultural labourers who should be urged to return to the land, and those mechanics who will be unable to work in a factory for the future should also be encouraged to take up this work. One reason for this is that the workman's arm—especially if it has not been too much elaborated—is useful for the execution of a considerable variety of work on the land. It is unnecessary to speak of cases of amputation below the knee, since their usefulness on the land may be taken for granted.
In the country as a matter of fact a man never dies of hunger; and this cannot be said of the town. Apart from actual cultivation of the land, which is in part impossible for the maimed, there are numerous and important occupations of which a town dweller would not think. It is when he goes to the centre of re-education in agricultural work, first of all to view it and then to work, that the disabled man takes note of what he can or cannot do, and of the work in connection with agriculture which is open to him, such as poultry rearing or bee keeping.
This applies to other employments than agriculture.
Apart from his actual trade which the workman can no longer ply with a sufficient return for his labour, he may be able to work at one or two of the accessory employments which would not of themselves[155] bring him in a living but which would yield a satisfactory supplementary income.
In certain re-education centres there seems to be a marked predilection for crafts in which the apprenticeship is short and the installation costs little, though these are in fact the characteristics of those trades which give the labourer a poor return, that is to say, time-work in a large or small workshop.
At the beginning of the war an attempt was made to show that there would never be enough tinkers, sabot makers, shoemakers, or saddlers in the country. It is quite a false idea that a disabled man can gain a living at one of these crafts in a village. It is true that he can do so if, working as an agricultural labourer, he can act as a barber in his spare time, and is capable of executing small jobs, especially repairs, which the villagers would readily give to him rather than have to go several miles to get them done. When the disabled man has this additional work in his hands he will gradually be able to ascertain whether the needs of the countryside and his own personal capacity are compatible with its development. In that case, however, he will be, in fact, a small proprietor buying his own tools and materials and fixing a retail price. But the great majority of workmen have no notion of such calculations and such organisation as are indispensable when a man runs a business even if he is alone. It follows, therefore, that the education of his mental, and especially his commercial, faculties must be considered, and it must be ascertained whether the man is likely to profit by such education. It is useless to install in a hamlet a shoemaker who is incapable of working except as an assistant, and in the town at the actual factories the prospects are poor.
Moreover, conditions of life in the disabled man's native place must be considered as a matter of importance. A man from the Mediterranean country has no idea beyond the cultivation of meadows, and one from Picardy none beyond the making of cane baskets for packing flowers.
Judgment is difficult, and in order that the choice may be exercised as reasonably as possible, the careful collaboration of the patient, the doctor and the managers of the workshops is essential. We repeat that this is one of the principal objects for which the centres of re-education are useful. There are some efficient men, we know, who without asking anything of anybody find quickly and unerringly the exact work that suits them. There is no need of anxiety in such cases.
A certain metal worker from the invaded area suffering from pseudarthrosis of the shoulder, whose wound we were treating, sent for his wife, and they began to rear geese. We know two cases of amputation of the right arm, an operative at an aeroplane works and a worker in stucco, who during their stay at hospital and before they had been supplied with artificial limbs, had taught themselves, the one technical design the other ornamental design. Both of them, as soon as they were discharged, have been taken on by their former masters, who no doubt were fully conscious that they were thus combining a good deed with good business. To come to a decision of any value, however, cases of this sort must not be taken as a criterion, for they are in fact exceptional. The majority of the men are in need of guidance.
The procedure employed at the Belgian centre of re-education at Port-Villerz consists in allowing[157] the patient to frequent the workshops at will for a few days, during which time he sees what is going on and is not slow to make his choice, which it appears rarely needs to be amended.
We have dealt chiefly with the conditions which are suitable for the re-education of a man who has lost an upper limb, or, speaking more generally, is disabled in one arm, for whom resumption of work in a workshop will often be out of the question. The question is easier of solution for the lower limb. Cases of amputation of the leg can work standing, if supplied with an artificial limb, at practically any trade. Cases of amputation of the thigh have numerous manual occupations open to them in which they sit for at least part of the time. It must be understood, however, that these professions which require skill can, as a rule, only be learnt in well-equipped workshops at the price of a fairly long apprenticeship. Two or three years are necessary to make a good mechanic, a good watchmaker, glass cutter, etc. This should not deter us in the case of fairly young men. The difficulty is to organise special workshops, often with a complicated equipment, where the maimed man can at least pick up the rudiments of the work, for it is not to be thought of that he can remain there during the whole time occupied in a complete training.
In conclusion, we should like to draw attention to the law of 1831, which regulates the distribution of pensions by means of groups classified according as the loss is of two limbs or of one. No distinction is made with regard to the seat of the amputation. But a man who has lost both legs and has been suitably equipped with artificial limbs can earn a fair wage,[158] whereas a man who has lost both arms is completely disabled so that he cannot even wash or dress himself. Among the amputation cases the difference is also considerable in the lower limb, between amputation through the leg and through the thigh, and even more in the upper limb, between an amputation retaining the movements of the elbow and one in which they are lost. There is, moreover, a great difference in the quality of stumps and the consequent utility of the artificial limb. It is of course impossible to allow with mathematical precision for all degrees of disablement, but the several general distinctions which we have enumerated could be taken into consideration without difficulty.
Printed in Great Britain for the University of London Press, Ltd., by Richard Clay & Sons, Ltd., London and Bungay.
THE UNIVERSITY OF LONDON PRESS, Ltd.
have pleasure in announcing the publication of the following series which covers the whole field of War Medicine and Surgery
Military Medical Manuals.
A Series of handy and profusely illustrated manuals translated from the French under the general Editorship of
SIR ALFRED KEOGH,
G.C.B., LL.D., M.D., F.R.C.P., Hon. F.R.C.S.
Late Director-General Army Medical Service
AND
Lt.-Gen. T. H. J. G. GOODWIN
C.B., C.M.G., D.S.O.
Director-General Army Medical Service
Each translation has been made by a practised hand and is edited by a specialist in the branch of surgery or medicine covered by the volume. It was felt to be a matter of urgent necessity to place in the hands of the medical profession a record of the new work and new discoveries which the war has produced, and to provide for everyday use a series of brief and handy monographs of a practical nature. The present series is the result of this aim. Each monograph covers one of the many questions at present of surpassing interest to the medical world, is written by a specialist who has himself been in close touch with the progress which he records in the medicine and surgery of the war. Each volume of the series is complete in itself, while the whole will form a comprehensive picture of the medicine and surgery of the Great War.
From the BRITISH MEDICAL JOURNAL: "The books are short and practical, and are founded upon the most recent clinical and laboratory experience."
THE TREATMENT OF INFECTED WOUNDS. By A. Carrel and G. Dehelly. Translated by Herbert Child, Capt. R.A.M.C., with Introduction by Sir Anthony A. Bowlby, K.C.M.G., K.C.V.O., F.R.C.S., Surgeon-General Army Medical Service. With 97 illustrations in the text and six plates. Second Edition, with additions.
Price 6/- net
Is as fine an example of correlated work on the part of the chemist, the bacteriologist, and the clinician as could well be wished for, and bids fair to become epoch-making in the treatment of septic wounds.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
THE SPECTATOR: "It would be hard to imagine a better set of books; they are well written, well translated, well illustrated, moderate in length, and moderate in price."
THE PSYCHONEUROSES OF WAR. By Dr. G. Roussy, Assistant Professor in the Faculty of Medicine, Paris, and J. Lhermitte, sometime Laboratory Director in the Faculty of Medicine, Paris. Edited by Colonel William Aldren Turner, C.B., M.D., and Consulting Neurologist to the Forces in England. Translated by Wilfred B. Christopherson. With 13 full-page plates.
Price 6/- net
"The Psychoneuroses of War" being a book which is addressed to the clinician, the authors have endeavoured, before all else, to present an exact semeiology, and to give their work a didactic character. After describing the general idea of the psychoneuroses and the methods by which they are produced, the authors survey the various clinical disorders which have been observed during the war.
THE CLINICAL FORMS OF NERVE LESIONS (Vol. I). By Mme. Athanassio Benisty, House Physician of the Hospitals of Paris (Salpêtrière), with a Preface by Professor Pierre Marie. Edited with a Preface by E. Farquhar Buzzard, M.D., F.R.C.P., Captain R.A.M.C.(T.), etc. With 81 illustrations in the text, and seven full-page plates.
Price 6/- net
In this volume will be found described some of the most recent acquisitions to our knowledge of the neurology of war. But its principal aim is to initiate the medical man who is not a specialist into the examination of nerve injuries. He will quickly learn how to recognise the nervous territory affected, and the development of the various clinical features; he will be in a position to pronounce a precise diagnosis, and to foresee the consequences of this or that lesion.
THE TREATMENT AND REPAIR OF NERVE LESIONS (Vol. II). By Mme. Athanassio Benisty. Edited by E. Farquhar Buzzard, M.D., F.R.C.P., Capt. R.A.M.C.(T.), etc. With 62 illustrations in the text and four full-page plates.
Price 6/- net
This volume is the necessary complement of the first. It explains the nature of the lesions, their mode of repair, their prognosis, and above all their treatment. It provides a series of particularly useful data as to the evolution of nerve-wounds—the opportunities of intervention—and the prognosis of immediate complications or late sequelae.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
"The importance of this comprehensive series can hardly be exaggerated. The French genius in its application to scientific medicine will be discovered here at its best and it will be found to be a distinct gain to have had this method of collaboration applied to so important an enterprise."
THE TREATMENT OF FRACTURES. By R. Leriche, Assistant Professor in the Faculty of Medicine, Lyons. Edited by F. F. Burghard, C.B., M.S., F.R.C.S., formerly Consulting Surgeon to the Forces in France. Vol. I.—"Fractures Involving Joints." With 97 illustrations from original and specially prepared drawings.
Price 6/- net
The author's primary object has been to produce a handbook of surgical therapeutics. But surgical therapeutics does not mean merely the technique of operation. Technique is, and should be, only a part of surgery, especially at the present time. The purely operative surgeon is a very incomplete surgeon in time of peace; "in time of war he becomes a public disaster; for operation is only the first act of the first dressing."
Vol. II.—"Fractures of the Shaft." With 156 illustrations from original and specially prepared drawings.
Price 6/- net
Vol. I. of this work was devoted to Fractures Involving Joints; Vol. II. (which completes the work) treats of Fractures of the Shaft, and is conceived in the same spirit—that is, with a view to the production of a work on conservative surgical therapeutics.
The author strives on every page to develop the idea that anatomical conservation must not be confounded with functional conservation. The two things are not so closely allied as is supposed. There is no conservative surgery save where the function is conserved. The essential point of the treatment of diaphysial fractures consists in the early operative disinfection, primary or secondary, by an extensive sub-periosteal removal of fragments, based on exact physiological knowledge, and in conformity with the general method of treating wounds by excision. When this operation has been carefully performed with the aid of the rugine, with the object of separating and retaining the periosteum of all that the surgeon considers should be removed, the fracture must be correctly reduced and the limb immobilised.
FRACTURE OF THE LOWER JAW. By L. Imbert, National Correspondent of the Société de Chirurgie, and Pierre Réal, Dentist to the Hospitals of Paris. With a Preface by Medical Inspector-General Février. Edited by J. F. Colyer, F.R.C.S., L.R.C.P., L.D.S. With 97 illustrations in the text and five full-page plates.
Price 6/- net
Previous to the present war no stomatologist or surgeon possessed any very extensive experience of this subject. Claude Martin, of Lyons, who perhaps gave more attention to it than anyone else, aimed particularly at the restoration of the occlusion of teeth, even at the risk of obtaining only fibrous union of the jaw. The authors of the present volume take the contrary view, maintaining the consolidation of the fracture is above all the result to be attained. The authors give a clear account of the various displacements met with in gunshot injuries of the jaw and of the methods of treatment adopted, the latter being very fully illustrated.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
THE SPECTATOR: "For our physicians and surgeons on active service abroad or in military hospitals at home these are the very books for them to dip into, if not to read through."
FRACTURES OF THE ORBIT AND INJURIES OF THE EYE IN WAR. By Felix Lagrange, Professor in the Faculty of Medicine, Bordeaux. Translated by Herbert Child, Captain R.A.M.C. Edited by J. Herbert Parsons, D.Sc., F.R.C.S., Temp. Captain R.A.M.C. With 77 illustrations in the text and six full-page plates.
Price 6/- net
Grounding his remarks on a considerable number of observations, Professor Lagrange arrives at certain conclusions which at many points contradict or complete what we have hitherto believed concerning the fractures of the orbit: for instance, that traumatisms of the skull caused by fire-arms produce, on the vault of the orbit, neither fractures by irradiation nor independent fractures; that serious lesions of the eye may often occur when the projectile has passed at some distance from it. There are, moreover, between the seat of these lesions (due to concussion or contact) on the one hand, and the course of the projectile on the other hand, constant relations which are veritable clinical laws, the exposition of which is a highly original feature in this volume.
HYSTERIA OR PITHIATISM, AND REFLEX NERVOUS DISORDERS. By J. Babinski, Member of the French Academy of Medicine, and J. Froment, Assistant Professor and Physician to the Hospitals of Lyons. Edited with a Preface by E. Farquhar Buzzard, M.D., F.R.C.P., Captain R.A.M.C.(T.), etc. With 37 illustrations in the text and eight full-page plates.
Price 6/- net
The number of soldiers affected by hysterical disorders is great, and many of them have been immobilized for months in hospital, in the absence of a correct diagnosis and the application of a treatment appropriate to their case. A precise, thoroughly documented work on hysteria, based on the numerous cases observed during two years of war, was therefore a necessity under present conditions. Moreover, it was desirable, after the discussions and the polemics of which this question has been the subject, to inquire whether we ought to return to the old conception, or whether, on the other hand, we might not finally adopt the modern conception which refers hysteria to pithiatism.
WOUNDS OF THE SKULL AND THE BRAIN. Clinical forms and medico-surgical treatment. By C. Chatelin and T. De Martel. With a Preface by the Professor Pierre Marie. Edited by F. F. Burghard, C.B., M.S., F.R.C.S., formerly Consulting Surgeon to the Forces in France. With 97 illustrations in the text and two full-page plates.
Price 7/6 net
Of all the medical works which have appeared during the war, this is certainly one of the most original, both in form and in matter. It is, at all events, one of the most individual. The authors have preferred to give only the results of their own experience, and if their conclusions are not always in conformity with those generally accepted, this, as Professor Pierre Marie states in his preface, is because important advances have been made during the last two years; and of this the publication of this volume is the best evidence.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
From THE TIMES: "A series of really first-rate manuals of medicine and surgery ... the translations are admirably made. They give us in English that clearness of thought and that purity of style which are so delightful in French medical literature and are as good in form as in substance."
LOCALISATION AND EXTRACTION OF PROJECTILES. By Assistant Professor Ombrédanne, of the Faculty of Medicine, Paris, and M. Ledoux-Lebard, Director of the Laboratory of Radiology of the Hospitals of Paris. Edited by A. D. Reid, C.M.G., M.R.C.S., L.R.C.P., Major (Temp.) R.A.M.C. With a Preface on Extraction of the Globe of the Eye, by Colonel W. T. Lister, C.M.G.. With 225 illustrations in the text and 30 full-page photographs.
Price 10/6 net
This volume appeals to surgeons no less than to radiologists. It is a summary and statement of all the progress effected by surgery during the last two and a half years. MM. Ombrédanne and Ledoux-Lebard have not, however, attempted to describe all the methods in use, whether old or new. They have rightly preferred to make a critical selection, and—after an exposition of all the indispensable principles of radiological physics—they examine, in detail, all those methods which are typical, convenient, exact, rapid, or interesting by reason of their originality: the technique of localisation, the compass, and various adjustments and forms of apparatus.
WOUNDS OF THE ABDOMEN. By G. Abadie (of Oran), National Correspondent of the Société de Chirurgie. With a Preface by Dr. J. L. Faure. Edited by Sir Arbuthnot Lane, Bart., C.B., M.S., Colonel (Temp.), Consulting Surgeon to the Forces in England. With 67 illustrations in the text and four full-page plates.
Price 7/6 net
Dr. Abadie has been enabled, at all the stations of the army service departments, to weigh the value of methods and results, and considers the following problems in this volume: (1) How to decide what is the best treatment in the case of penetrating wounds of the abdomen; (2) How to install the material organisation which permits of the application of this treatment, and how to recognise those conditions which prevent its application; (3) How to decide exactly what to do in each special case—whether one should perform a radical operation, or a palliative operation, or whether one should resort to medical treatment.
WOUNDS OF THE BLOOD-VESSELS. By L. Sencert, Assistant Professor in the Faculty of Medicine, Nancy. Edited by F. F. Burghard, C.B., M.S., F.R.C.S., formerly Consulting Surgeon to the Forces in France. With 68 illustrations in the text and two full-page plates.
Price 6/- net
Hospital practice had long familiarised us with the vascular wounds of civil practice, and the experiments of the Val-de-Grâce School of Medicine had shown us what the wounds of the blood-vessels caused by modern projectiles would be in the next war. But in 1914 these data lacked the ratification of extensive practice. Two years have elapsed, and we have henceforth solid foundations on which to establish our treatment. In a first part, Professor Sencert examines the wounds of the great vessels in general; in a second part he rapidly surveys the wounds of vascular trunks in particular, insisting on the problems of operation to which they give rise.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
GLASGOW HERALD: "The whole series is heartily commended to the attention and study of all who are interested in and responsible for the treatment of the injuries and diseases of a modern war."
THE AFTER-EFFECTS OF WOUNDS OF THE BONES AND JOINTS. By Aug. Broca, Professor of Topographical Anatomy in the Faculty of Medicine, Paris. Translated by J. Renfrew White, M.B., F.R.C.S., Temp. Captain R.A.M.C., and edited by R. C. Elmslie, M.S., F.R.C.S.; Orthopædic Surgeon to St. Bartholomew's Hospital, and Surgeon to Queen Mary's Auxiliary Hospital, Roehampton; Major R.A.M.C.(T.) With 112 illustrations in the text.
Price 6/- net
This new work, like all books by the same author, is a vital and personal work, conceived with a didactic intention. At a time when all physicians are dealing, or will shortly have to deal, with the after-effects of wounds received in war, the question of sequelae presents itself, and will present itself more and more. What has become—and what will become—of all those who, in the hospitals at the front or in the rear, have hastily received initial treatment, and what is to be done to complete a treatment often inaugurated under difficult circumstances?
ARTIFICIAL LIMBS. By A. Broca, Professor in the Faculty of Medicine, Paris, and Dr. Ducroquet, Surgeon at the Rothschild Hospital. Edited and translated by R. C. Elmslie, M.S., F.R.C.S., etc.; Orthopædic Surgeon to St. Bartholomew's Hospital, and Surgeon to Queen Mary's Auxiliary Hospital, Roehampton; Major R.A.M.C.(T.). With 210 illustrations.
Price 6/- net
The authors of this book have sought not to describe this or that piece of apparatus—more or less "newfangled"—but to explain the anatomical, physiological, practical and technical conditions which an artificial arm or leg should fulfil. It is, if we may so call it, a manual of applied mechanics written by physicians, who have constantly kept in mind the anatomical conditions and the professional requirements of the artificial limb.
TYPHOID FEVERS AND PARATYPHOID FEVERS (Symptomatology, Etiology, Prophylaxis). By H. Vincent, Medical Inspector of the Army, Member of the Academy of Medicine, and L. Muratet, Superintendent of the Laboratories at the Faculty of Medicine of Bordeaux. Second Edition. Translated and Edited by J. D. Rolleston, M.D. With tables and temperature charts.
Price 6/-net
This volume is divided into two parts, the first dealing with the clinical features and the second with the epidemiology and prophylaxis of typhoid fever and paratyphoid fevers A and B. A full account is to be found of recent progress in the bacteriology and epidemiology of these diseases, considerable space being given to the important question of the carrier in the dissemination of infection.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
From THE LANCET: "The names of the editors are sufficient guarantee that the subject matter is treated with fairness and discrimination."
DYSENTERIES, CHOLERA, AND EXANTHEMATIC TYPHUS. By H. Vincent, Medical Inspector of the Army, Member of the Academy of Medicine, and L. Muratet, Superintendent of the Laboratories at the Faculty of Medicine of Bordeaux. With an Introduction by Andrew Balfour, C.B., C.M.G., M.D., Lieut.-Col. R.A.M.C. Edited by George C. Low, M.A., M.D., Temp. Capt. I.M.S.
Price 6/- net
This, the second of the volumes which Professor Vincent and Dr. Muratet have written for this series, was planned, like the first, in the laboratory of Val-de-Grâce, and has profited both by the personal experience of the authors and by a mass of recorded data which the latter years of warfare have very greatly enriched. It will be all the more welcome, as hitherto there has existed no comprehensive handbook treating these great epidemic diseases from a didactic point of view.
ABNORMAL FORMS OF TETANUS. By MM. Courtois-Suffit, Physician of the Hospitals of Paris, and R. Giroux, Resident Professor. With a Preface by Professor F. Widal. Edited by Surgeon-General Sir David Bruce, K.C.B., F.R.S., LL.D., F.R.C.P., etc., and Frederick Golla, M.B.
Price 6/- net
Of all the infections which threaten our wounded men, tetanus is that which, thanks to serotherapy, we are best able to prevent. But serotherapy, when it is late and insufficient, may, on the other hand, tend to create a special type of attenuated and localised tetanus; in this form the contractions are as a general rule confined to a single limb. This type, however, does not always remain strictly monoplegic; and if examples of such cases are rare this is doubtless because physicians are not as yet very well aware of their existence. We owe to MM. Courtois-Suffit and R. Giroux one of the first and most important observations of this new type; so that no one was better qualified to define its characteristics. This they have done in a remarkable manner, supporting their remarks by all the documents hitherto published, first expounding the characteristics which individualise the other atypical and partial types of tetanus, which have long been recognised.
WAR OTITIS AND WAR DEAFNESS. Diagnosis, Treatment, Medical Reports. By Dr. H. Bourgeois, Oto-rhino-laryngologist to the Paris Hospitals, and Dr. Sourdille, former interne of the Paris Hospitals. Edited by J. Dundas Grant, M.D., F.R.C.S.(Eng.); Major R.A.M.C., President, Special Aural Board (under Ministry of Pensions). With many illustrations in the text and full-page plates.
Price 6/- net
This work presents the special aspects of inflammatory affections of the ear and deafness, as they occur in active military service. The instructions as to diagnosis and treatment are intended primarily for the regimental medical officer. The sections dealing with medical reports (expertises) on the valuation of degrees of disablement and claims to discharge, gratuity or pension, will be found of the greatest value to the officers of invaliding boards.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
MILITARY MEDICAL MANUALS
GUY'S HOSPITAL GAZETTE: "The series is a most valuable addition to the medical literature of the war.... We deem it to be almost indispensable to a medical officer, and have no hesitation in unreservedly recommending it."
SYPHILIS AND THE ARMY. By G. Thibierge, Physician of the Hôpital Saint-Louis. Edited by C. F. Marshall, F.R.C.S.
Price 6/- net
It seemed, with reason, to the editors of this series that room should be found in it for a work dealing with syphilis considered with reference to the army and the present war. The frequency of this infection in the army, among the workers in munition factories, and in the midst of the civil population where this is in contact with soldiers and mobilised workers, makes it, at the present time, a true epidemic disease, and one of the most widespread of epidemic diseases. Dr. Thibierge, whose previous labours guarantee his peculiar competence in these difficult and important questions, has, in writing this manual, very notably assisted in this work. But the treatment of syphilis has, during the last six years, undergone considerable modifications; the new methods are not yet very familiar to all physicians; and certain details may no longer be present to their minds. It was therefore opportune to survey the different methods of treatment, to specify their indications, and their occasionally difficult technique, which is always important if complications are to be avoided. It was necessary before all to state precisely and to retrace, for all those who have been unable to follow the recent progress of the therapeutics of venereal diseases, the characters and the diagnostic elements of the manifestations of syphilis.
MALARIA IN MACEDONIA: Clinical and Hæmatological Features. Principles of Treatment. By P. Armand-Delille, P. Abrami, G. Paisseau and Henri Lemaire. Preface by Professor Lavern, Membre de l'Institut. Edited by Sir Ronald Ross, K.C.B., F.R.S., LL.D., D.Sc., Lieut.-Col. R.A.M.C. With illustrations and a coloured plate.
Price 6/- net
This work is based on the writers' observations on malaria in Macedonia during the present war in the French Army of the East. A special interest attaches to these observations, in that a considerable portion of their patients had never had any previous attack. The disease proved to be one of exceptional gravity, owing to the exceptionally large numbers of the Anopheles mosquitoes and the malignant nature of the parasite (Plasmodium falciparum). Fortunately an ample supply of quinine enabled the prophylactic and curative treatment to be better organised than in previous colonial campaigns, with the result that, though the incidence of malaria among the troops was high, the mortality was exceptionally low. Professor Laveran, who vouches for this book, states that it will be found to contain excellent clinical descriptions and judicious advice as to treatment. Chapters on parasitology and the laboratory diagnosis of malaria are included.
An early announcement will be made in regard to further volumes under consideration.
The cost of postage per volume is: Inland 5d.; Abroad 8d.
LONDON: UNIVERSITY OF LONDON PRESS, LTD.,
18, Warwick Square, E.C.4
Transcriber's Note: All obvious spelling and punctuation errors have been corrected.