
Transcriber's Note:
The cover image was created by the transcriber and is placed in the public domain.
| CHAPTER I. INTRODUCTORY | 4 | |
| Introductions to Birth Control by Margaret H. Sanger, | ||
| Havelock Ellis, August Forel and G. F. Lydston. | ||
| CHAPTER II. THE ORIGIN AND PRACTICE OF BIRTH CONTROL IN VARIOUS COUNTRIES | 23 | |
| Genesis of Movement, | ||
| England, | ||
| Holland, | ||
| France, | ||
| United States, | ||
| Other Countries. | ||
| CHAPTER III. POPULATION AND BIRTH RATE | 43 | |
| Birth Control, by Havelock Ellis, | ||
| Population Facts in United States, | ||
| Birth Rate of British Empire, | ||
| Birth Rate of Other Countries (With Tables). | ||
| CHAPTER IV. INFANT MORTALITY | 93 | |
| General Statistics, | ||
| Results of Children’s Bureau Survey at Johnstown, Pa., by Emma Duke, | ||
| Manchester Report. | ||
| CHAPTER V. MATERNAL MORTALITY AND DISEASES AFFECTED BY PREGNANCY | 155 | |
| Children’s Bureau Report, by Grace L. Meigs, | ||
| Death Rates from Child Birth in Foreign Countries, | ||
| A Municipal Birth Control Clinic, | ||
| Tuberculosis, | ||
| Kidney Diseases, | ||
| Eclampsia, | ||
| Diabetes, | ||
| Pelvic Deformities, | ||
| Heart Disease, | ||
| Too Frequent Pregnancies, | ||
| Pernicious Vomiting. | ||
| CHAPTER VI. HARMFUL METHODS PRACTICED TO AVOID LARGE FAMILIES | 185 | |
| Coitus Interruptus, | ||
| Continence, | ||
| The Objects of Marriage, by Havelock Ellis, | ||
| Abortion. | ||
| CHAPTER VII. PROSTITUTION, FEEBLE-MINDEDNESS AND VENEREAL DISEASES | 197 | |
| The Social Evil, | ||
| Feeble-mindedness, | ||
| Syphilis, | ||
| Gonorrhea. | ||
| CHAPTER VIII. OTHER TRANSMISSIBLE DISEASES AND PAUPERISM | 223 | |
| Insanity, | ||
| Epilepsy, | ||
| Alcoholism, | ||
| Pauperism, | ||
| Child Labor. | ||
| CHAPTER IX. CONCLUSION: EMINENT OPINIONS | 245 | |
| The Progress of Holland, | ||
| Eminent Opinions | ||
| GLOSSARY | 250 | |
The purpose of the Appellant in presenting the various statistics and medical and social facts incorporated in the supplementary brief, entitled THE CASE FOR BIRTH CONTROL, is to give the Court a clear conception of the meaning of birth control. The historical stages through which this question has gone have been reviewed, its status in foreign countries outlined. Finally, the effects upon the commonwealth of the prohibition contained in the Section known as 1142 of the Penal Law have been made clear. Said Section comprises in its prohibition the very points of knowledge most necessary to human liberty, and has resulted in extreme harm to the individual, to the family and to society at large.
The idea of the social and racial value of knowledge to prevent conception is new in the United States, and therefore it has been difficult to get first-hand facts and comprehensive statistics with a local bearing. Consequently, the Appellant has been obliged to lay emphasis upon data from foreign countries where the subject has been exhaustively studied, both theoretically and practically. However, the American case for birth control, as presented in this compilation, is the most complete possible in view of the records available.
The material in this general introduction to the question of the prevention of conception comprises an article by Margaret H. Sanger and extracts from the works of Havelock Ellis, August Forel and G. F. Lydston, M.D. The last three are eminent authorities, whose opinions are selected as being the clearest exposition of the social philosophy—Birth Control.
NOTE: All the notations of pages and tables refer to original documents and not to the present volume.
(The following is the case for birth control, as I found it during my fourteen years’ experience as a trained nurse in New York City and vicinity. It appeared as a special article in “Physical Culture,” April, 1917, and has been delivered by me as a lecture throughout the United States. It is a brief summary of facts and conditions, as they exist in this country.)
For centuries woman has gone forth with man to till the fields, to feed and clothe the nations. She has sacrificed her life to populate the earth. She has overdone her labors. She now steps forth and demands that women shall cease producing in ignorance. To do this she must have knowledge to control birth. This is the first immediate step she must take toward the goal of her freedom.
Those who are opposed to this are simply those who do not know. Any one who like myself has worked among the people and found on one hand an ever-increasing population with its ever-increasing misery, poverty and ignorance, and on the other hand a stationary or decreasing population with its increasing wealth and higher standards of living, greater freedom, joy and happiness, cannot doubt that birth control is the livest issue of the day and one on which depends the future welfare of the race.
Before I attempt to refute the arguments against birth control, I should like to tell you something of the conditions I met with as a trained nurse and of the experience that convinced me of its necessity and led me to jeopardize my liberty in order to place this information in the hands of the women who need it.
My first clear impression of life was that large families and poverty went hand in hand. I was born and brought up in a glass factory town in the western part of New York State. I was one of eleven children—so I had some personal experience of the struggles and hardships a large family endures.
When I was seventeen years old my mother died from overwork and the strain of too frequent child bearing. I was left to care for the younger children and share the burdens of all. When I was old enough I entered a hospital to take up the profession of nursing.
In the hospital I found that seventy-five per cent. of the diseases of men and women are the result of ignorance of their sex functions. I found that 6every department of life was open to investigation and discussion except that shaded valley of sex. The explorer, scientist, inventor, may go forth in their various fields for investigation and return to lay the fruits of their discoveries at the feet of society. But woe to him who dares explore that forbidden realm of sex. No matter how pure the motive, no matter what miseries he sought to remove, slanders, persecutions and jail await him who dares bear the light of knowledge into that cave of darkness.
So great was the ignorance of the women and girls I met concerning their own bodies that I decided to specialize in woman’s diseases and took up gynecological and obstetrical nursing.
A few years of this work brought me to a shocking discovery—that knowledge of the methods of controlling birth was accessible to the women of wealth while the working women were deliberately kept in ignorance of this knowledge!
I found that the women of the working class were as anxious to obtain this knowledge as their sisters of wealth, but that they were told that there are laws on the statute books against imparting it to them. And the medical profession was most religious in obeying these laws when the patient was a poor woman.
I found that the women of the working class had emphatic views on the crime of bringing children into the world to die of hunger. They would rather risk their lives through abortion than give birth to little ones they could not feed and care for.
For the laws against imparting this knowledge force these women into the hands of the filthiest midwives and the quack abortionists—unless they bear unwanted children—with the consequence that the deaths from abortions are almost wholly among the working-class women.
No other country in the world has so large a number of abortions nor so large a number of deaths of women resulting therefrom as the United States of America. Our law makers close their virtuous eyes. A most conservative estimate is that there are 250,000 abortions performed in this country every year.
How often have I stood at the bedside of a woman in childbirth and seen the tears flow in gladness and heard the sigh of “Thank God!” when told that her child was born dead! What can man know of the fear and dread of unwanted pregnancy? What can man know of the agony of carrying beneath one’s heart a little life which tells the mother every instant that it cannot survive? Even were it born alive the chances are that it would perish within a year.
Do you know that three hundred thousand babies under one year of age die in the United States every year from poverty and neglect, while six hundred thousand parents remain in ignorance of how to prevent three hundred thousand 7more babies from coming into the world the next year to die of poverty and neglect?
I found from records concerning women of the underworld that eighty-five per cent. of them come from parents averaging nine living children. And that fifty per cent. of these are mentally defective.
We know, too, that among mentally defective parents the birth rate is four times as great as that of the normal parent. Is this not cause for alarm? Is it not time for our physicians, social workers and scientists to face this array of facts and stop quibbling about woman’s morality? I say this because it is these same people who raise objection to birth control on the ground that it may cause women to be immoral.
Solicitude for woman’s morals has ever been the cloak Authority has worn in its age-long conspiracy to keep woman in bondage.
When I was in Spain a year ago, I found that the Spanish woman was far behind her European sisters in readiness or even desire for modern freedom. Upon investigation as to the cause of this I found that there are over five thousand villages and towns in Spain with no means of travel, transportation and communication save donkeys over bridle paths. I was told that all attempts to build roads and railroads in Spain had been met with the strongest opposition of the Clergy and the Government on the ground that roads and railroads would make communication easier and bring the women of the country into the cities where they would meet their downfall.
Do we who have roads and railroads think our women are less moral than the Spanish women? Certainly not. But we in this country are, after all, just emerging from the fight for a higher education of women which met with the same objection only a few years ago.
We know now that education has not done all the dreadful things to women that its opponents predicted were certain to result. And so shall we find that knowledge to control birth, which has been in the hands of the women of wealth for the past twenty-five years, will not tend to lower woman’s standard of morality.
Statistics show us that the birth-rate of any given quarter is in ratio with and to its wealth. And further figures prove that in large cities the rich districts yield a birth-rate of a third of that of the poor districts. In Paris for every 1,000 women between the ages of 15 and 50 the poor districts yield 116 births and the rich districts 34 births. In Berlin conditions are approximately the same. For every 1,000 women between the ages of 15 and 50 the poor districts yield 157 births while the rich yield 47. This applies also to all large cities the world over.
It can be inferred from these figures that the women of wealth use means to control birth which is condemned when taught to the poor. But the menace to our civilization, the problem of the day, is not the stationary birth-rate 8among the upper classes so much as the tremendous increase among the poor and diseased population of this country....
Is woman’s health not to be considered? Is she to remain a producing machine? Is she to have time to think, to study, to care for herself? Man cannot travel to his goal alone. And until woman has knowledge to control birth she cannot get the time to think and develop. Until she has the time to think, neither the suffrage question nor the social question nor the labor question will interest her, and she will remain the drudge that she is and her husband the slave that he is just as long as they continue to supply the market with cheap labor.
Let me ask you: Has the State any more right to ravish a woman against her will by keeping her in ignorance than a man has through brute force? Has the State a better right to decide when she shall bear offspring?
Picture a woman with five or six little ones living on the average working man’s wage of ten dollars a week. The mother is broken in health and spirit, a worn out shadow of the woman she once was. Where is the man or woman who would reproach me for trying to put into this woman’s hands knowledge that will save her from giving birth to any more babies doomed to certain poverty and misery and perhaps to disease and death.
Am I to be classed as immoral because I advocate small families for the working class while Mr. Roosevelt can go up and down the length of the land shouting and urging these women to have large families and is neither arrested nor molested but considered by all society as highly moral?
But I ask you which is the more moral—to urge this class of women to have only those children she desires and can care for, or to delude her into breeding thoughtlessly. Which is America’s definition of morality?
You will agree with me that a woman should be free.
Yet no adult woman who is ignorant of the means to prevent conception can call herself free.
No woman can call herself free who cannot choose the time to be a mother or not as she sees fit. This should be woman’s first demand.
Our present laws force woman into one of two ways: Celibacy, with its nervous results, or abortion. All modern physicians testify that both these conditions are harmful; that celibacy is the cause of many nervous complaints, while abortion is a disgrace to a civilized community. Physicians claim that early marriage with knowledge to control birth would do away with both. For this would enable two young people to live and work together until such time as they could care for a family. I found that young people desire early marriage, and would marry early were it not for the dread of a large family to support. Why will not society countenance and advance this idea? Because it is still afraid of the untried and the unknown.
9I saw that fortunes were being spent in establishing baby nurseries, where new babies are brought and cared for while the mothers toil in sweatshops during the day. I saw that society with its well-intentioned palliatives was in this respect like the quack, who cures a cancer by burning off the top while the deadly disease continues to spread underneath. I never felt this more strongly than I did three years ago, after the death of the patient in my last nursing case.
This patient was the wife of a struggling working man—the mother of three children—who was suffering from the results of a self-attempted abortion. I found her in a very serious condition, and for three weeks both the attending physician and myself labored night and day to bring her out of the Valley of the Shadow of Death. We finally succeeded in restoring her to her family.
I remember well the day I was leaving. The physician, too, was making his last call. As the doctor put out his hand to say “Good-bye,” I saw the patient had something to say to him, but was shy and timid about saying it. I started to leave the room, but she called me back and said:
“Please don’t go. How can both of you leave me without telling me what I can do to avoid another illness such as I have just passed through?”
I was interested to hear what the answer of the physician would be, and I went back and sat down beside her in expectation of hearing a sympathetic reply. To my amazement, he answered her with a joking sneer. We came away.
Three months later, I was aroused from my sleep one midnight. A telephone call from the husband of the same woman requested me to come immediately as she was dangerously ill. I arrived to find her beyond relief. Another conception had forced her into the hands of a cheap abortionist, and she died at four o’clock the same morning, leaving behind her three small children and a frantic husband.
I returned home as the sun was coming over the roofs of the Human Bee-Hive, and I realized how futile my efforts and my work had been. I, too, like the philanthropists and social workers, had been dealing with the symptoms rather than the disease. I threw my nursing bag into the corner and announced to my family that I would never take another case until I had made it possible for working women in America to have knowledge of birth control.
I found, to my utter surprise, that there was very little scientific information on the question available in America. Although nearly every country in Europe had this knowledge, we were the only civilized people in the world whose postal laws forbade it.
The tyranny of the censorship of the post office is the greatest menace to liberty in the United States to-day. The post office was never intended to be a moral or ethical institution. It was intended to be mechanically efficient; 10certainly not to pass upon the opinions in the matter it conveys. If we concede this power to this institution, which is only a public service, we might just as well give to the street car companies and railroads the right to refuse to carry passengers whose ideas they do not like.
I will not take up the story of the publication of “The Woman Rebel.” You know how I began to publish it, how it was confiscated and suppressed by the post office authorities, how I was indicted and arrested for bringing it out, and how the case was postponed time and time again and finally dismissed by Judge Clayton in the Federal Court.
These, and many more obstacles and difficulties were put in the path of this philosophy and this work to suppress it if possible and discredit it in any case.
My work has been to arouse interest in the subject of birth control in America, and in this, I feel that I have been successful. The work now before us is to crystallize and to organize this interest into action, not only for the repeal of the laws but for the establishment of free clinics in every large center of population in the country where scientific, individual information may be given every adult person who comes to ask it.
In Holland there are fifty-two clinics with nurses in charge, and the medical profession has practically handed the work over to nurses. In these clinics, which are mainly in the industrial and agricultural districts, any woman who is married or old enough to be married, can come for information and be instructed in the care and hygiene of her body.
These clinics have been established for thirty years in Holland, and the result has been that the general death-rate of Holland has fallen to the lowest of any country in Europe. Also, the infant mortality of Amsterdam and The Hague is found to be the lowest of any city in the world. Holland proves that the practice of birth control leads to race improvement; her increase of population has accelerated as the death-rate has fallen.
In England, France, Scandinavia, and Germany, information regarding birth control is also freely disseminated, but the establishment of clinics in these countries is not so well organized as it is in Holland, with the consequence that the upper and middle classes, as in this country, have ready access to this knowledge, while the poor continue to multiply because of their lack of it. This leads, especially in France, to a high infant mortality, which, rather than a low birth-rate, is the real cause of her decreasing population.
We in America should learn a lesson from this, and I would urge immediate group action to form clinics at once. We have in this country a splendid foundation in our hospital system and settlement work. The American trained nurse is the best equipped and most capable in the world, which enables us, if we begin work at once, to accomplish as much in ten years’ time as the European countries have done in thirty years.
11The clinic I established in the Brownsville district of Brooklyn accomplished at least this: it showed the need and usefulness of such an agency.
The free clinic is the solution for our problem. It will enable women to help themselves, and will have much to do with disposing of this soul-crushing charity which is at best a mere temporary relief.
Woman must be protected from incessant childbearing before she can actively participate in the social life. She must triumph over Nature’s and Man’s laws which have kept her in bondage. Just as man has triumphed over Nature by the use of electricity, shipbuilding, bridges, etc., so must woman triumph over the laws which have made her a childbearing machine.
RACE REGENERATION. HAVELOCK ELLIS. New Tracts for the Times. Cassell & Co., Ltd., London, New York, Toronto and Melbourne. 1911.
Henry Havelock Ellis: L.S.A. Hon. Member Medico-legal Society of New York. Hon. Fellow of the Chicago Academy of Medicine; Foreign Associate of the Societe Medico-Historique of Paris, etc.; General Editor of the Contemporary Science Series (1889); born Croydon, Surrey, 2nd Feb., 1859; belonging on both sides to families connected with the sea; spent much of childhood on sea, (Pacific, etc.); educated, private schools; St. Thomas’s Hospital; engaged in teaching in various parts of New South Wales, 1875–79. Returned to England and qualified as medical man, but only practiced for a short time, having become absorbed in scientific and literary work. Edited the Mermaid Series of Old Dramatists, 1887–89. Publications: The New Spirit, 1890; The Criminal, 1890 (4th edition revised and enlarged 1910); Man and Woman, a Study of Human Secondary Sexual Characters, 1894 (5th edition revised and enlarged 1914); Sexual Inversion, being Vol. II of Studies in the Psychology of Sex, 1897 (3rd edition revised and enlarged 1915); Affirmations, 1897; The Evolution of Modesty, etc., being vol. I of the studies in Psychology of Sex, 1899 (3rd edition revised and enlarged, 1910); The 19th Century; A Dialogue in Utopia, 1900; A Study of British Genius, 1904; Analysis of the Sexual Impulse, 1903, (2nd edition revised and enlarged 1913); Sexual Selection in Man, 1905; Erotic Symbolism, 1906; Sex in Relation to Society, being vols. 3, 4, 5 and 6 of studies in psychology of sex; The Soul of Spain, 1908; The World of Dreams, 1911; The Task of Social Hygiene, 1912; Impressions and Comments, 1914; Essays In War Time, 1916.
When we survey the movement of social reform which has been carried on during the past one hundred years, we thus see that it is proceeding in four stages. 1—The effort to clear away the gross filth of our cities, to improve the dwellings, to introduce sanitation, and to combat disease. 2—The 12attempt to attack the problem more thoroughly by regulating conditions of work, and introducing the elaborate system of factory legislation. 3—The still more fundamental step of taking in hand the children who have not yet reached the age of work, nationalizing education, and ultimately pushing back the care and over-sight of infants to the moment of birth. 4—Finally, most fundamental step of all, the effort, which is still only beginning to provide the conditions of healthy life even before birth. It must be remembered that this movement in all its four stages is still in active progress among us. It is not mere ancient history. On the contrary, it is a movement that is constantly spreading and at every point becoming more thorough, more harmoniously organized. Before long it will involve a national medical service, which will impose on doctors as their primary duty, not the care of disease, but the preservation of health. We have to realize at the same time that this movement has been exclusively concerned, not with the improvement of the quality of human life, but exclusively with the betterment of the conditions under which life is lived. It tacitly assumed that we have no control over human life and no responsibility for its production. It accepted human life—however numerous it might be in quantity, however defective in quality—as a God given fact, which it would be impious to question. It heroically set itself to the endless task of cleansing the channels down which this muddy torrent swept. It never went to the source. Only take care of the soil, these workers at social reform said in effect, and the seed is no matter. That, as we can now see, was a silly enough position to take up. P. 26.
Here we have been spending enormous enthusiasm, labor and money in improving the conditions of life, with the notion in our heads that we should thereby be improving life itself, and after 70 years we find no convincing proof that the quality of our people is one whit better than it was when for a large part they lived in filth, were ravaged by disease, bred at random, soaked themselves in alcohol, and took no thought for the morrow. Our boasted social reform has been a matter of bricks and mortar—a piling up of hospitals, asylums, prisons and workhouses—while our comparatively sober habits may be merely a sign of the quietly valetudinarian way of life imposed on a race no longer possessing the stamina to withstand excess.
One of the most obvious tests of our degree of success in social reform directed to the betterment of social conditions is to be found in the amount of our pauperism, and the condition of our paupers. If the amelioration of the conditions of life can effect even a fraction of what has been expected of it, the results ought to be seen in the diminution of our pauperism, and the improvement of the condition of our paupers. Yet so far as numbers are concerned, the vast army of our paupers has remained fairly constant during the whole period of social reform, if indeed it has not increased. As to the ineffectiveness of our methods the Royal Commissioners, especially perhaps in their Minority Report, have shed much light. It was to be expected that these muddled methods should be most marked in all that concerns the beginnings of life, for that is precisely where our whole treatment of social 13reform has been most at fault. Children under 16 form nearly one-third of the paupers relieved. In the United Kingdom the Poor Law authorities have on their books as outdoor paupers, 50,000 infants under four years of age. As regards the annual number of births in the Poor Law institutions of the United Kingdom, there are not even definite statistics available, but it is estimated in the Minority Report that the number is probably over 15,000, 30% of these being legitimate children, and 70% illegitimate. There is no system in the treatment of mothers; and often not the most elementary care in the treatment of the infants. It is scarcely surprising that though the general infant mortality is excessively high, the infant mortality of the workhouse babies is two or three times as high as that among the general population. And the Royal Commissioners pathetically ask, “To what is this retrogression due? It cannot be due to lack of expenditure, or to lack of costly and elaborate machinery.” No, it certainly is not. It is in large part due, as we are now just beginning to recognize, to the concentration of our activities on the mere conditions of life, to our neglect of the betterment of life itself. We have failed to realize that the whitening of our sepulchres will not limit the number of corpses placed in those sepulchres. It is the renewal of the spirit within that is needed, not alone the improvement of material conditions, but the regeneration of life. If we wish to realize more in detail the slight extent to which our efforts to better the conditions of life have raised the quality of life itself, we have but to turn to the problem of the feebleminded, which during recent years has attracted so much attention. It is necessary to remember that this feeblemindedness is largely handed on by heredity. Exact investigation has now shown that feeblemindedness is inherited to an enormous extent. Some years ago, Dr. Ashby, speaking from a large experience, estimated that at least 75% of feebleminded children are born with an inherited tendency to mental defect. More precise investigation has shown since that this estimate was under the mark. Dr. Tredgold, who in England has most carefully studied the heredity of the feebleminded, found that in over 82% there is a bad nervous inheritance. Heredity is the chief cause of feeblemindedness, and Tredgold has never seen a normal child born of two feebleminded parents. The very thorough investigation of the heredity of the feebleminded which is now being carried on at the institution for their care at Vineland, N. J., shows even more decisive results. By making careful pedigrees of the families to which the inmates at Vineland belong it is seen that in a large proportion of cases feeblemindedness is handed on from generation to generation, and is transmissible through three generations, though it sometimes skips a generation. Not only is feeblemindedness inherited, and in a much greater degree than has been hitherto suspected, but the feebleminded tend to have a much larger number of children than normal people. The average number of children of feebleminded people seems to be usually about one-third more than in normal families, and is sometimes very much greater. Page 26–36.
And it is not only in themselves that the feebleminded are a burden on 14the present generation and a menace to future generations. They are seen to be often a more serious danger when we realize that in large measure they form the reservoir from which the predatory classes are recruited. This is for instance the case as regards the fallen. Feebleminded girls of fairly high grade may often be said to be predestined to immorality if left to themselves, not because they are vicious, but because they are weak and have little power of resistance. They cannot properly weigh their actions against the results of their actions, and even if they are intelligent enough to do that, they are still too weak to regulate their actions accordingly. Moreover, even when, as so often happens among the high grade feebleminded, they are quite able and willing to work, after they have lost their respectability by having a child, the opportunities of work become more restricted and they drift into prostitution. Criminality again is associated with feeblemindedness in the most intimate way. Not only do criminals tend to belong to large families, but the families that produce feebleminded offspring also produce criminals. P. 40.
Closely related to the great feebleminded class, and from time to time falling into crime are the inmates of workhouses, tramps and the unemployable. The so-called able-bodied inmates of our workhouses are frequently found on medical examination to be more than 50% cases of mental defectives, equally so whether they are men or women. P. 42.
We have found that this movement for social reform, while it has been inevitable and necessary, and is even yet by no means at an end, is not fulfilling, and cannot fulfil the expectations of those who set it in motion. It has even had the altogether undesigned and unexpected result of increasing the burden it was intended to remove. Whatever the exact action of natural selection may be, as soon as we begin to interfere with it, and improve the conditions of life by caring for the unfit, enabling them to survive and to propagate their like, as they will not fail to do, insofar as they belong to the unfit stocks, then we are certainly, without intending it, doing our best to lower the level of life. We increase, or at best retain the unfit, while at the same time we burden the fit with the task of providing for the unfit. In this way we deteriorate the general quality of life in the next generation, except insofar as our improvement of the environment may enable some to remain fit, who under less favorable conditions would join the unfit. It is now possible for us to realize how the way lies open to the next great forward step in social reform. On the one hand the progressive movement of improvement in the conditions of life, by proceeding steadily back, as we have seen, to the conditions before birth, renders the inevitable next step a deliberate controlled life itself. On the other hand, the new social feeling which has been generated by the task of improving the conditions of life, and of caring for those who are unable to care for themselves, has made possible a new explanation of responsibility to the race. We have realized practically and literally that we are “our brother’s keepers.” We are beginning to realize that we are the keepers of our children of the race that is to come after us. Our sense of social responsibility is becoming 15a sense of racial responsibility. It is that enlarged sense of responsibility which renders possible what we call the regeneration of the race. We cannot lay too much stress on this sense of responsibility for it is its growth which alone renders possible any regeneration of the race. So far as practical results are concerned, it is not enough for men of science to investigate the facts and the principles of heredity and to attempt to lay down the laws of eugenics, as the science which deals with the improvement of the race is now called. It is not alone enough for moralists to preach. The hope of the future lies in the slow development of those habits, those social instincts arising inevitably out of the actual facts of life, and deeper than science, deeper than morals. The new sense of responsibility, not only for the human lives that now are, but the new human lives that are to come, is a social instinct of this fundamental nature. Therein lies its vitality and its promise. It is only of recent years that it has been rendered possible. Until lately, the methods of propagating the race continued to be the same as those of savages thousands of years ago. Children “came” and their parents disclaimed all responsibility for their coming; the children were sent by God, and if they all turned out to be idiots, the responsibility was God’s. That is all changed now. It is we who are more immediately the creators of men. We generate the race; we alone can regenerate the race. We have learned that in this, as in other matters, the Divine Force works through us and that we are not entitled to cast the burden of our evil actions on to any higher Power. The voluntary control of the number of offspring which is now becoming the rule in all civilized countries in every part of the world has been a matter of concern to some people, who have realized that however desirable under the conditions, it may be abused. But there are two points about it which they should do well always to bear in mind. In the first place, it is the inevitable result of the advance in civilization. Reckless abandonment to the impulse of the moment, and careless indifference to the morrow, the selfish gratification of individual desire at the expense of probable suffering to lives that will come after, this may seem beautiful to some people, but it is not civilization. All civilization involves an ever-increasing forethought for others, even for others who are yet unborn. In the second place, it is not only inevitable, but it furnishes us with the one available lever for raising the level of our race. In classic days, as in the East, it was possible to consider infanticide as a permissible method for attaining this end. That is no longer possible to us. We must go further back. We must control the beginnings of life. And that is a better method, even a more civilized method, for it involves greater forethought, and a finer sense of the value of life. To-day, all classes in the community, save the lowest and most unfit, exercise some degree of forethought and control in regulating the size of their families. That it should be precisely the unfit who procreate in the most reckless manner is a lamentable fact, but it is not a hopeless fact, and there is no need for the desperate remedy of urging the fit to reduce themselves in this matter to the level of the unfit. That would merely be a backward movement of civilization. It is education, sobriety, and some degree of well-being which lead to the control 16of the size of families, and as it is social amelioration which brings this result about, it is a result that we may view with equanimity. It used to be feared that a falling birth rate was a national danger. We now know that this is not the case, for not only does a falling birth rate lead to a falling death rate, but in this matter no nation moves by itself. Civilization is international, though one nation may be a little before or behind another. Hitherto France has been ahead, but all other nations have followed. In Germany, for instance, sometimes regarded as a rival of England, the birth rate has fallen just as in England. Russia indeed is an exception, but Russia is not only behind England, but behind Germany in the march of civilization; its birth rate is high, its death rate is high; a large proportion of its population live on the verge of famine. We are not likely to take Russia as our guide in this matter; we have gone through that stage long ago. But at the stage we have now reached it is no longer a question of gaining control over the production of the new generation, but of using that control, and of using it in such a way that we may help to leave the world better than we found it. “What has posterity done for me that I should do anything for posterity,” someone is said to have asked? The answer is that to the human race that went before him he owes everything, and that he can only repay the debt to those who come after him. There is more than one way in which we can repay our debt to the race, but there is no better way than by leaving behind us those who are fit to carry on the tasks of life to higher ends than we have ourselves perhaps been able to attain. Children have been without value in the world because there have been too many of them; they have been produced by a blind and helpless instinct, and have been allowed to die by the hundred thousand. For more than half a century after the era of social reform set in there was no decline at all in the enormous infant mortality. It has only now begun, as the inevitable accompaniment of the decline in the birth rate. Not the least service done by the fall in the birth rate has been to teach us the worth of our children. We possess the power, if we will, deliberately and consciously to create a new race, to mold the world of the future. As we realize our responsibility we see that our new power of control is not merely for the end of limiting the quantity of human life, perhaps for a selfish object, but for the high end of improving its quality. It is in our power not only to generate life, but, if we will, to regenerate life. If we realize that possibility, and if we understand how the course of civilization has now brought it within our grasp, we have reached the heart of our problem. Our greatest foe, apart from indifference, is ignorance. Even science in this field is only beginning to feel its way, while the mass have still to unlearn many prejudices of the past. P. 48–54.
Galton, during the last years of his life, believed that we are approaching a time when eugenic considerations will become a factor of religion, and when our existing religious conceptions will be reinterpreted in the light of a sense of social needs, so enlarged as to include the needs of the race which is to come. Certainly for those who have been taught to believe that man was in 17the first place created by God, it should not be difficult to realize the divine nature of the task of human creation which has since been placed in the hands of man, to recognize it as a practical part of religion, and to cherish a sense of its responsibility. P. 63.
THE SEXUAL QUESTION. August Forel. A Scientific, Psychological, Hygienic and Sociological Study. Translated by C. F. Marshall, M.D., F.R.C.S. Late Assistant Surgeon to the Hospital for Diseases of the Skin. London.
August Forel: Doctor of Philosophy honoris causa; Doctor of Laws honoris causa. Born September 1848 at Morges, Switzerland. Educated at University of Zurich and Vienna. In 1873 assistant physician at the district insane asylum at Munich; 1877, Privat-dozent at the University; 1879, Privat-dozent and then Professor at Zurich, and until 1898 Director of the State Insane Asylum at Burgholzli near Zurich. Works: Experience et remarques crit. sur les sensations des insectes (in 4 vol. of Recueil Zoolog. suisse Genf. 1886–7) Giftapparat u. d. Analdrusen der Ameisen, 1878; Les Fourmis de la Suisse, 1874; Errichtg. v. Trinkerasylen, 1891; D. Hypnotismus; Gehirn und Seele; Hygiene der Nerven und des Geistes; Die Sexuelle Frage; Verbrecher und Konstit. Seelenabnormitat; Ges. Hirnanah. Abhandl; Sinnesleben d. Insekten; Kulturstrebungen der Gegenwart.
He discovered in 1885 the seat of the auditory nerves in the brain; researches into the psychology of ants.
We must not forget that among our brutal, yet human ancestors, the struggle for life demanded the cruel and wanton exposure or slaughter of all weak and decrepit individuals, and that epidemic diseases, plagues, and pests ravaged the peoples without mercy. Of course our present civilization has put up a barrier against all this. Yet for that very reason, the blind and thoughtless propagation of degenerate, tainted and enfeebled individuals is another atrocious danger to society. But then the sexual appetite cannot be legislated out of existence, or killed by repressive measures. We can but consider all legislation and all police measures which are intended to regulate the sexual intercourse in the human family as absolute failures, as inhuman, in fact as downright detrimental to the race. Exacting laws have never improved the morals of any race or nation, hypocrisy and secret evasion are the only results obtained. It would be better by far if steps were taken to enlighten the masses on the questions of sexual heredity and degeneration. Wisdom of this kind does not corrupt.
The law of heredity winds like a red thread through the family history of every criminal, of every epileptic, eccentric and insane person. And we 18should sit still and watch our civilization go into decay and fall to pieces without raising the cry of warning and applying the remedy?
The sexual appetite is very pronounced in tuberculous persons. They marry and beget children in the most wanton fashion. The law cannot and does not prevent them, and the carnal instinct is not to be killed. What is to be done when law and religion forbid the application of preventive measures and even prosecute the person that recommends them? Local diseases and pathological conditions in the woman (at times in man also) within wedlock, may render parturition and immediate danger to the life of the mother or of the child, or of both together. Surely in such cases it is the bounden duty of the physician to intervene and counsel against, nay absolutely forbid impregnation. Well, how is it to be done? Must husband and wife who love each other be separated? It would be unnatural, in fact it is quite impossible. Or should they abandon sexual intercourse altogether and live like brother and sister? Well, a few exceptionally cold natures may have will power enough to carry into effect such a pact. But in 99 out of 100 cases the interdict of the sexual act sends the husband to satisfy his cravings elsewhere and contract disease, or he falls in love with another woman and wrecks home and family. Similar conditions may be brought about by other causes as well. Take for instance, the poor working man, or mechanic, who has already six or seven children, and whose wife is unusually fertile, giving birth to children year after year. The wages of the father do not suffice to properly support them all. The food that can be purchased with the slender means is not at all adequate. Rent and other bills fall behind and they get in debt. They are both young yet. What is to be done? If they follow the natural law there will be an increase in the family every year. Moreover, these ever-recurring labors weaken the constitution of the mother and sap away her strength. Starvation? Sexual continence in wedlock? It is curious indeed to hear rich men, well fed clergymen, pious zealots and reformers, leaning back in comfortable chairs discussing this burning question and bewailing the immorality of the common people. Statistics prove that these very people who extol to the poor all the blessings of a poor family never live up to their teachings, either in theory or in practice. The majority of these apostles of morality have no children at all or at the utmost two or three. Why should that be so? What interesting reading it would make if the sexual history of these persons were followed up and printed.
Many hygienic reasons and the most elemental laws of humanity demand that the wife who is fertile above the average should have a rest of at least 18 months between each succeeding pregnancy. But this cannot be achieved in the natural course of events except in very rare cases without wrecking the marriage. If we crystallize this sexual social question we arrive at the following conclusions: There are a great many cases, especially of a pathological character, but none the less, also, in normal and sound individuals, in which procreation within wedlock or without either definitely or temporarily either 19for the mother or the child, or for both, and for that reason should be interdicted. Very few men and a very small proportion of women—no matter how firmly they may be resolved—are capable of suppressing their sexual needs. Even if they succeed the consequences are generally of a disastrous nature, loss of marital love, secret illicit relations with others, and subsequent infidelity, nervous disorders, impotence, etc. In all these cases we are confronted with the following dilemma: 1—In the unmarried person: onanism or prostitution, or both. Is that morality? Such people must either forever forego love, marriage, and normal lawful sexual intercourse, or face sterility in wedded life. 2—Within marriage: onanism, prostitution and infidelity, or the adoption of rational preventive measures. I leave it to the reader, and to the law maker to pick out the correct alternative and to arrive at the one possible decent and ethical solution of these conflicting questions.
It seems almost incredible that in some countries medical men who are not ashamed to throw young men into the arms of prostitution, blush when mention is made of anti-conceptional measures. P. 427b.
A year, at least, should elapse between parturition and the next conception; this gives approximately two years between the confinements. In this way the wife keeps in good health and can bear healthy children at pleasure. It is certainly better to procreate seven children, than to procreate 14, of which seven die, to say nothing of the mother, who rapidly becomes exhausted by uninterrupted confinements. P. 430.
It is quite certain that the sexual life of man can never raise above its present state without being freed from the bonds of mysticism and religious dogma, and based on a loyal and unequivocal human morality which will recognize the normal wants of humanity, always having as its principle object the welfare of posterity. P. 459.
The true task of a political economy which has the true happiness of man at heart should be to encourage the procreation of happy, useful, healthy and hard-working individuals. To build an ever increasing number of hospitals, asylums for lunatics, idiots and incurables, reformatories, etc., to provide them with every comfort and manage them scientifically, is undoubtedly a very fine thing, and speaks well of the progress and development of human sympathy. But what is forgotten is that by concerning ourselves almost exclusively with human ruins, the results of our social abuses, we gradually weaken the force of the healthy portion of the population. By attacking the roots of the evil and limiting the procreation of the unfit we shall be performing a work which is much more humanitarian, if less striking in effect. Formerly, our economists and politicians hardly have considered this question, and even now very few are interested in it because it brings no honors, nor money, as we do not ourselves see the fruits of such efforts. In short, we amuse ourselves with repairing the ruins, but are afraid to attack what makes these ruins. P. 465–6.
20The anti-conceptional measures recommended have been often condemned, sometimes as immoral, sometimes as contrary to aesthetics. To interfere in this way with the action of nature is said to injure the poetry of love and the moral feeling, and at the same time to disturb natural selection. There are several replies to these objections. In the first place, it is wrong to maintain that man cannot encroach on the life of nature. If this were the case, the earth would now be a virgin forest, and a great many plants and animals would not have been adapted to the use of man. We have proved without deference, often with a brutal hand, to the misfortune of art and poetry, that we are capable of successfully meddling with the machinery of nature, even in what concerns our own persons.
The aesthetic argument appears, at first sight, more valid. It is unnecessary, however, to discuss matters of taste. From all points of view, the details of coitus leave much to be desired from the aesthetic point of view, and such a slight addition as a protective does not appear to make any serious difference. P. 497–8.
She, (woman) ought to develop herself strongly and healthily by working along with man in body and mind by procreating numerous children when she is strong, robust and intelligent. But this does not nullify the advantage that may accrue from limiting the number of conceptions when the bodily and mental qualities are wanting in the procreators. P. 332.
One of the most difficult and important future tasks of social science toward humanity is to set free sexual relations from the tyranny of religious dogmas by placing them in harmony with the true and purely human laws of natural science. P. 357.
In no animal do we find the abuses which man is permitted to practice toward his wife and children. P. 368.
The law should abandon its useless and even harmful chicanery concerning the questions of sexual relations and love, and regulate more carefully the duties of parents toward their children, and thus protect future generations against the abuses of the present generation. P. 377.
It is important to bear in mind that modern legislation on marriage often favors the reproduction of criminals, lunatics and invalids, while it hinders the production of healthy children by men who are intelligent, honest and robust. When an abnormal, unhealthy man is married his wife is obliged to submit to the conception of tainted children. What we require is more personal liberty for healthy, adaptable individuals and more restrictions for the abnormal, unhealthy and dangerous. The civil law of the future will have to take these facts into consideration if it wishes to keep level with scientific progress. P. 393.
21THE DISEASES OF SOCIETY AND DEGENERACY. THE VICE AND CRIME PROBLEM. G. F. Lydston, M.D., Professor of Genito-Urinary Surgery, State University of Illinois. Prof. of Criminal Anthropology, Chicago, Kent College of Law; Member of the American Medical Association, etc., etc. The Riverton Press, Chicago, 1912.
The responsibility of rearing a large number of useful and upright citizens is a little too great for the poor family drudge who manipulates the wash board with one hand, holding a squealing baby with the other, and simultaneously attempts to keep in control a dozen other demonstrative and lusty children. She has a difficult task before her, even where her environment is favorable to the rearing of children, but where the children are brought into contact with evil associates as they are very likely to be when parental control is so lax as it necessarily is under such circumstances, they are not likely to become either ornamental or useful factors in our social system. If more attention were paid to quality of both parentage and children, and less fretting done as to the possible disasters to the nation incidental to small numbers of children, it would be better for the race. At the present day, when practically no attention is paid to stirpiculture in the human species, it seems absurd to worry about diminution in size of the American family. Is the function of the wife altogether that of a breeding machine? Has she no personal rights? Should she be sacrificed to posterity? Is it always her duty to rear a large family? Unhesitatingly I answer no to each question. The perpetuation of the race depends upon matrimony, it is true. It is not however woman’s function merely to increase numbers at the expense of her own life and comfort. This is a fallacy and an injustice to womanhood, and should be contradicted from the house-tops. The woman who is merely a beast of burden, a breeder of children, is a failure in modern life. Quality of progeny is not conserved along such lines, and quality, not quantity, makes for the elevation of the human race. Woman should not be sacrificed to posterity. Something is due her as a social integer. She is entitled to life, liberty and the pursuit of happiness. She, as well as man, comes within the provisions of the constitution. Better a single child properly reared by a happy contented mother than a dozen ill-fed, unkempt, dirty, vicious and half-baked hoodlums. “Multiply and replenish the earth” was once sound doctrine, but it does not uniformly fit modern conditions. The scriptural injunction should be qualified. The multiplication should not extend beyond the parents capacity to comfortably rear and educate their children, nor beyond the number consistent with the preservation of the mother’s health and happiness.
In the countries covered by this chapter Birth Control has been recognised as a legitimate science; leagues advocating the prevention of conception have been formed; and the leading authorities have approved the practice as being the foundation of a better social structure.
THE CONTROL OF BIRTHS. MARY ALDEN HOPKINS. Harper’s Weekly, April 10th, 1915.
The European laws on this subject are in striking contrast to ours. They treat contraception and abortion as two separate matters. The laws against abortion are strict. The laws concerning contraception are directed against distasteful advertising but not against private advice or public propaganda. In England the applicant must state in writing over his or her signature that he or she is married or about to be married. In Holland formulas and methods may be supplied privately, but must not be publicly advertised. In Germany there is no law on the matter, but sentiment is strongly opposed to advertising. In Switzerland it is forbidden to advertise or circularize. In Norway and Sweden advertising is not expected. Italy and France have no law on the subject. In Russia advertising in the newspapers is common. Everywhere in Europe contraceptives are for sale at pharmacies.
The Birth Control Movement is antagonistic to the general practice of abortion. The Hungarian senate, a few years ago, declared that the limitation of families by prevention of conception was absolutely necessary in order to check the wide-spread evil of attempted abortion.
Our present laws confuse the issue by classing—in a shockingly ignorant fashion,—contraception, abortion, and pornography, in the same category. The group is treated in the New York State Penal Code under the astonishing title of “Indecent Articles.” The eye of the law distinguishes no difference between the books of August Forel, a scientist revered in laboratories all over the world, and the obscene penny postcard sold by some slinking vendor.
24THE MALTHUSIAN LEAGUE OF ENGLAND. The Origin and History of Birth Control in Great Britain. Reprinted from The Malthusian, April, 1880.
Little improvement can be expected in morality until the production of large families is regarded in the same light as drunkenness, or any other physical excess.—John Stuart Mill, 1872.
In obedience to the request of the Nestor of political economists of Europe, the distinguished editor of the Journal des Economistes of Paris, M. Joseph Garnier, we give a short account of the reasons which led to the foundation of the Malthusian League, the latest product of the nineteenth century’s ideas in the direction of social progress. It gives us unfeigned pleasure to be the means of making the most thorough of all French writers on the doctrines of our English latter-day economists acquainted with the position which the great population question has recently assumed in this country. It is not, we believe, too much to allege that the most advanced thinkers of this country are at this moment well aware of the existence of the new-Malthusian remedy for the evils of society. How this has come to pass we proceed at once to show.
It was not long after the publication of Mr. Malthus’ work that some thoughtful men began to notice that in modern France the late marriage customs of most European states were replaced to a certain extent by prudence after marriage. Mr. Francis Place was one of the first to write a work on population, in which he recommended the physical checks so commonly made use of by the French parents for adoption in England. He is said to have remonstrated with Mr. Malthus about an expression in the first edition of his essay, in which he spoke of such checks under the head of Vice, and the tradition is that Malthus left out the expression in his subsequent edition: and, as he himself had two children, Mr. Porter (of Nottingham) believes that Mr. Malthus was, like Mr. Mill (the father of John Stuart Mill), himself a believer in the conjugal prudence practised by the better class of peasantry and townspeople. Mr. Place is also said to have converted Mr. Robert Owen, the socialist to his opinion, and it is believed that Mr. Owen owed the success of his colony of New Lanark to a knowledge of this point, which he communicated to his workmen. Mr. Robert Dale Owen, a son of Robert Owen, emigrated in his youth to the United States of America, and became before his death, in 1877, one of the foremost citizens of the western republic. That gentleman, having doubtless heard the question discussed by his father, Mr. Francis Place, and other friends in London, was induced in 1830 to publish a now well-known treatise on the population question, entitled Moral Physiology, a work written with the most philanthropic design and couched in the most careful language consistent with clearness and the attainment of its end, in which he gave a description of the above-mentioned physical checks. This work was, however, written subsequently to the publication of Mr. 25Richard Carlile’s tract, entitled Every Woman’s Book, which was a most outspoken work, written by one of those fearless thinkers who have done so much to complete the reformation in England and secure freedom of speech and of the press for this country. Had it not been for him and his co-workers, England might at this day have been in as backward a condition as modern Spain. Dr. Charles Knowlton, an able physician of Boston, Massachusetts, U.S.A., was the next person who wrote upon this question in his now famous little pamphlet, the Fruits of Philosophy, wherein there was contained a good deal of popular information on physiology, and a careful account of the checks spoken of by Mr. Dale Owen and Mr. Carlile. This work was followed after a long interval by a small pamphlet by Mr. Austin Holyoake, entitled Large and Small Families, which, in company with the tracts by Carlile, Owen, and two other works were sold for many years by booksellers of the ultra-liberal party, latterly styled the Secularists.
In 1876 the Fruits of Philosophy, after circulating without notice for forty years, was suddenly attacked as an obscene publication under an Act of Parliament called “Lord Campbell’s Act,” and a bookseller in Bristol, of the name of Cook, was sentenced to two years’ imprisonment for selling it. The London publisher of the work, Mr. C. Watts, was also prosecuted for selling it, but, on submission, was let off with merely the payment of costs, or about two hundred pounds fine. The work would have been suppressed had not Mr. C. Bradlaugh, the head of the Secularist party and editor of the National Reformer, the most advanced liberal journal in England, in company with a young but already most distinguished lady, Mrs. Annie Besant, come forward and sold it openly. In order to try the case, Mr. Bradlaugh and Mrs. Besant entered into partnership in a publishing establishment in Stonecutter Street, Farringdon Street, London, and sold the Fruits of Philosophy quite openly, sending copies of it to the city authorities. Mr. Bradlaugh had for many years been an avowed Malthusian, and the lady also was quite convinced of the importance of the question. Both were determined that no bigoted society should put the work under the ban of the law without a fight for it. The case was first tried at Guildhall, and was sent on to the Court of Queen’s Bench, before the Lord Chief Justice Cockburn. The trial began on the 18th of June, 1877, and lasted three days. The jury contained, among other persons of wealth and position, the name of Arthur Walter, Esq., the son of the proprietor of the Times journal. After a most powerful defence, in which Mrs. Besant and Mr. Bradlaugh delivered speeches which told most powerfully upon the judge and all present in the Court, the jury delivered the following verdict: “We are unanimously of the opinion that the book in question (the Fruits of Philosophy) is calculated to deprave public morals; but at the same time we entirely exonerate the defendants from any corrupt motives in publishing it.” The judge—who had charged quite in favor of the defendants—would have let them off with a nominal fine, but, influenced by the information that they intended carrying on the sale of the work, strangely sentenced them to a heavy imprisonment and fine. Fortunately, the higher Court of Appeal 26decided that there had been an error in the indictment, and thus the defendants were set free. The prosecution has not been repeated since that date.
The excitement caused by the trial led to the formation of a society called The Malthusian League, which was set on foot as a means of opposing both active and passive resistance to the attempts made to stifle discussion on the population question. Mr. Bradlaugh had commenced such a league many years previously, but the time was not ripe for it. The first meeting of the League was held in the Minor Hall of the Hall of Science, Old Street, on July 17th, 1877, for the election of officers. That meeting elected Dr. C. R. Drysdale president, and Mrs. Annie Besant honorary secretary, in company with Mr. Hember and Mr. R. Shearer. The Council of the League consisted of Messrs. Bell, Brown, Dray, Page, Mr. and Mrs. Parris, Mr. and Mrs. Rennick, Messrs. Rivers, Seyler, G. Standing, Truelove, and Young. Mr. Swaagman was elected treasurer to the League.
Very soon after the formation of the League, another prosecution of Mr. Edward Truelove, bookseller, of High Holborn, took place in the Queen’s Bench on February 1st, 1878. The works he was prosecuted for were quite of the same character as Knowlton’s Fruits of Philosophy, and were entitled: More Physiology, a most philanthropic pamphlet by Mr. Robert Dale Owen, Senator of the United States, and another pamphlet entitled Individual, Family and National Poverty. Mr. Truelove was most effectually defended by Mr. William Hunter, and the case fell through, as one of the jury considered the book quite moral and philanthropic in its tendencies. The secretary for the “Society for the Suppression of Vice,” Mr. Collette by name, followed up the prosecution, and Mr. Truelove was tried in the Central Criminal Court on May 9th, 1878, and condemned to a fine of fifty pounds and an imprisonment of four months duration, which he underwent. An immense meeting was held in St. James Hall, on the evening of June 6, 1878, to protest against this disgraceful treatment of an honest man like Mr. Truelove, at which the president of the League took the chair, and enthusiastic addresses were delivered by Mrs. Besant and Mr. Bradlaugh.
The trial of Mrs. Besant and Mr. Bradlaugh lasted several days, and aroused a greater interest in the subject than had been known since the days of Malthus. The English Press was full of the subject; scientific congresses gave it their attention; many noted political economists wrote about it; over a hundred petitions were presented to Parliament requesting the freedom of open discussion; meetings of thousands of persons were held in all the large cities; and as result, a strong Neo-Malthusian League was formed in London.
From the small beginning described in the above article the English work has spread over all the rest of the world. The following is a list of the leagues having membership in the Federation Universelle de la Regeneration Humaine, in which the English organization has always played a leading part:
England (1877).—The Malthusian League. Periodical, The Malthusian.
Holland (1885).—De Nieuw-Malthusiaansche Bond. Secretary, Dr. J. Rutgers, 9 Verhulststraat, Den Haag. Periodical, Het Gellukkig Huisgezin.
Germany (1889).—Sozial Harmonische Verein. Secretary, Herr M. Hausmeister, Stuttgart. Periodical, Die Sozial Harmonie.
France (1895).—Génération Consciente. 27 Rue de la Duée, Paris XX.
Spain (1904).—Liga Española de Regeneración Humana. Secretary, Señor Luis Bulffi, Calle Provenza 177, Pral, la, Barcelona. Periodical, Salud y Fuerza.
Belgium (1906).—Ligue Néo-Malthusienne. Secretary, Dr. Fernand Mascaux, Echevin, Courcelles. Periodical: Génération Consciente, 27 Rue de la Duée, Paris XX.
Switzerland (1908).—Group Malthusien. Secretary, Valentin Grandjean, 106 Rue des Eaux Vives, Geneva. Periodical, La Vie Intime.
Bohemia-Austria (1901).—Zadruhy. Secretary, Michael Kacha, 1164 Zizhov, Prague.
28Portugal.—Paz e Liberdade, Revista Anti-Militarista e Neo-Malthusiana. E. Silva, junior, L. da Memória, 46 r/e, Lisbon.
Brazil (1905).—Sección brasileña de propaganda. Secretaries: Manuel Moscosa, Rua de’Bento Pires 29, San Pablo; Antonio Dominiguez, Rua Vizcande de Moranguapez 25, Rio de Janeiro.
Cuba (1907).—Sección de propaganda. Secretary, José Guardiola, Empedrado 14, Havana.
Sweden (1911).—Sallskapet for Humanitar Barnalstring. President: Mr. Hinke Bergegren, Vanadisvagen 15, Stockholm, Va.
Flemish Belgium (1912).—National Verbond ter Regeling van het Kindertal. President, M. L. van Brussel, Rue de Canal, 70, Louvain.
Italy (1913).—Lega Neomalthusiana Italiana. Secretary, Dr. Luigi Berta, Via Lamarmora 22, Turin. Periodical, L’Educazione Sessuale.
Africa.—Ligue Néo-Malthusienne, Maison du Peuple, 10 Rampe Magenta, Alger.
The English organization, with headquarters in London, has for its officers some of the most distinguished men and women in England:
The following are some extracts from the League’s rules:
That the objects of this Society be:—
1. To spread among the people, by all practicable means, a knowledge of the law of population, of its consequences, and of its bearing upon human conduct and morals.
2. To urge upon the medical profession in general, and upon hospitals and public medical authorities in particular, the duty of giving instruction in hygienic contraceptive methods to all married people who desire to limit their families, or who are in any way unfit for parenthood; and to take any other steps which may be considered desirable for the provision of such instruction.
1. “That population (unless consciously and sufficiently controlled) has a constant tendency to increase beyond the means of subsistence.”
2. That the checks which counteract this tendency are resolvable into positive or life-destroying, and prudential or birth-restricting.
3. That the positive or life-destroying checks comprehend the premature death of children and adults by disease, starvation, war, and infanticide.
4. That the prudential or birth-restricting check consists in the limitation of offspring (1) by abstention from or postponement of marriage, or (2) by prudence after marriage.
5. That prolonged postponement of marriage—as advocated by Malthus—is not only productive of much unhappiness, but is also a potent cause of sexual vice and disease. Early marriage, on the contrary, tends to ensure sexual purity, domestic comfort, social happiness and individual health; but 30it is a grave social offence for men and women to bring into the world more children than they can adequately house, feed, clothe, and educate.
6. That over-population is the most fruitful source of pauperism, ignorance, crime, and disease.
7. That it is of great importance that those afflicted with hereditary disease, or who are otherwise plainly incapable of producing or rearing physically, intellectually and morally satisfactory children, should not become parents.
8. That the full and open discussion of the Population Question in all its necessary aspects is a matter of vital moment to Society.
It has been the object of this organization during these years to carry on the theoretical propaganda of Birth Control mainly among the educators, consisting of clergymen, physicians, scientists, sociologists, economists and others who in turn would form a strong, reliable public opinion who would force the dissemination of practical information among that element of society who are propagating the diseased and unfit.
It is only within the last few years that this League has begun to distribute information to prevent conception. Thousands of copies of this leaflet have been distributed in nearly every country throughout the civilized world except The United States of America where laws prevent its circulation.
Notice.—The Council of the Malthusian League, while continuing to regard this as a matter which is strictly within the province of the medical profession, and which ought to be taken over by them, has compiled a leaflet entitled “Hygienic Methods of Family Limitation,” for the benefit of those desirous of limiting their families, but who are ignorant of the means of doing so, and unable to get medical advice on the subject. This leaflet can only be issued, however, to persons over twenty-one years of age who are either married or about to be married, and who declare their conscientious belief that family limitation is justifiable on personal and national grounds. Anyone wishing to obtain a copy of this leaflet must write his or her name and address clearly upon both of the forms of declaration below, and send them to the Hon. Secretary. The sealed leaflet will then be sent them. In order to encourage family limitation among the poorest classes, no charge will be made either for the leaflet or postage, but it is hoped that those who can afford it will enclose stamps for postage or a small donation to help the League in its work.
Under no circumstances whatever can the practical leaflet be supplied without a properly filled up declaration, nor can more than one copy be supplied 31to the same person. Those wishing to help others, may have additional copies of the declaration form to hand on.
The Malthusian League regrets that it is unable to comply with applications for this leaflet from the United States.
Interest in the subject did not confine itself to England, for in 1878 at an International Medical Congress in Amsterdam the subject was discussed with great enthusiasm. A paper prepared and read by Mr. S. Van Houten (later Prime Minister) caused a wider interest in the matter and a year later the Neo-Malthusian (or Birth Control) League of Holland was organized. Charles R. Drysdale, then President of the English League, attended the conference.
As is usual in such causes, many of the better educated and intelligent classes adopted the practice at once, as did the better educated workers; but the movement had as yet no interest among the poorest and most ignorant. The League set to work at once to double its efforts in these quarters. Dr. Aletta Jacobs, the first woman physician in Holland, became a member of the League, and established a clinic where she gave information on the means of prevention of conception free to all poor women who applied for it.
All classes, especially the poor, welcomed the knowledge with open arms, and requests came thick and fast for the League’s assistance to obtain the necessary appliances free of charge. The consequence has been that for the past twelve years the League has labored chiefly among the people of the poorest districts. Dr. J. Rutgers and Madame Hoitsema Rutgers, two ardent advocates of these principles, have devoted their lives to this work. Dr. Rutgers says that where this knowledge is taught there is a reciprocal action to be observed: “In families where children are carefully procreated, they are reared carefully; and where they are reared carefully, they are carefully procreated.”
The Neo-Malthusian (or Birth Control) League of Holland has over 7,000 men and women in its membership, and more than fifty nurses whom it indorses.
These nurses are trained and instructed by Dr. Rutgers in the proper means and hygienic principles of the methods of Birth Control. They are established in practice in the various towns and cities throughout Holland. They advise women as to the best method to employ to prevent conception. They work mainly in the agricultural and industrial districts, or are located near them; and their teachings include not only the method of prevention of conception, but instruction in general and sexual hygiene, cleanliness, the uselessness 32of drugs, and the non-necessity of abortions. (The Council of the Neo-Malthusian or Birth Control League calls attention to the fact that it has for its sole object the Prevention of Conception, and not the causing of abortion.)
The clinic organized by Dr. Jacobs,—the first clinic in the world for the organized dissemination of information on Birth Control,—proved so efficient and beneficial to the standards of the community that others were opened and established until there are now more than fifty in operation.
There is no doubt that the establishment of these clinics is one of the most important parts of the work of a Birth Control League. The written word and written directions are very good, but the fact remains that even the best educated women have very limited knowledge of the construction of their generative organs or their physiology. What, then, can be expected of the less educated women, who have had less advantages and opportunities? It is consequently most desirable that there be practical teaching of the methods to be recommended, and women taught the physiology of their sex organs by those equipped with the knowledge and capable of teaching it.
It stands to the credit of Holland that it is perhaps the only country where the advocates of Birth Control have not been prosecuted or jailed; because the laws regarding the liberty of the individual and the freedom of the press uphold it, and protect its practise.
Despite the outbreak of war, the progress of the League has been most satisfactory. The membership increased from 5,057 at the beginning of 1914 to 5,521 at the end; and branches now exist in twenty-eight towns in Holland. The list of officers and correspondents alone now occupies four pages of the Report, and comprises nearly two hundred names. As these are of persons in every part in the country, it will be realised how great are the facilities for everyone to obtain practical information. Besides the great amount of advice given by the trained workers, 7,200 copies of the League’s booklet giving practical advice on methods of family limitation (birth control) were supplied. It is instructive to see, in the reports from the various branches open statements that Mrs. X (full name given) helped 149 women and supplied seven gross of preventives, the kinds being clearly specified. The branch reports give particulars of nearly 1,300 women personally instructed in preventive methods by trained workers, but the war prevented the returns from being anything like complete. And this in a country of only six million inhabitants.—The Malthusian, London, July 15, 1915.
There is no doubt that the Neo-Malthusian (Birth Control) League of Holland stands as the foremost in the world in organization, and also as a practical example of the results to be obtained from the teaching of the prevention of conception. Aside from the spreading influence of these ideas in Belgium, Italy, and Germany, Holland presents to the world a statistical record which proves unmistakably what the advocates of Birth Control have claimed for it.
The infantile mortality of Amsterdam and The Hague is the lowest of any cities in the world, while the general death rate and infantile mortality of Holland has fallen to be the lowest of any country in Europe. These statistics also refute the wild sayings of those who shout against Birth Control and claim it means race suicide. On the contrary, Holland proves that the practice of anti-conceptional methods leads to race improvement, for the increase of population has accelerated as the death rate has fallen. There has also been a rapid improvement in the general physique and health of the Dutch people, while that of the high birth rate countries, Russia and Germany, is said to be rapidly deteriorating.
The following figures will suffice to show some of the improvements which have been going on in Holland since 1881, the time the League became actively engaged in the work:—
Taken from Annual Summary of Marriages, Births, and Deaths in England and Wales, etc., for 1912.[1]
| Amsterdam (Malthusian (Birth Control) League started 1881; Dr. Aletta Jacobs gave advice to poor women, 1885.) | ||||
|---|---|---|---|---|
| 1881–85 | 1906–10 | 1912 | ||
| Birth Rate | 37.1 | 24.7 | 23.3 | per 1,000 of population |
| Death Rate | 25.1 | 13.1 | 11.2 | per 1,000 of population |
| Infantile Mortality: (Deaths in first year) |
203 | 90 | 64 | per thousand living births |
| The Hague (now headquarters of the Neo-Malthusian (Birth Control) League) | ||||
| 1881–85 | 1906–10 | 1912 | ||
| Birth Rate | 38.7 | 27.5 | 23.6 | per 1,000 of population |
| Death Rate | 23.3 | 13.2 | 10.9 | per 1,000 of population |
| Infantile Mortality: (Deaths in first year) |
214 | 99 | 66 | per thousand living births |
| Rotterdam.[2] | ||||
| 1881–85 | 1906–10 | 1912 | ||
| Birth Rate | 37.4 | 32.0 | 29.0 | per 1,000 of population |
| Death Rate | 24.2 | 13.4 | 11.3 | per 1,000 of population |
| Infantile Mortality (Deaths in first year) |
209 | 105 | 79 | per thousand living births |
| Fertility and Illegitimacy Rates. | ||||
| 1880–2 | 1890–2 | 1900–2 | ||
| Legitimate Fertility | 306.4 | 296.5 | 252.7 | Legitimate birth per 1,000 Married Women aged 15 to 45. |
| Illegitimate Fertility | 16.1 | 16.3 | 11.3 | Illegitimate births per 1,000 Unmarried Women, aged 15 to 45. |
| The Hague. | ||||
| 1880–2 | 1890–2 | 1900–2 | ||
| Legitimate Fertility | 346.5 | 303.9 | 255.0 | |
| Illegitimate Fertility | 13.4 | 13.6 | 7.7 | |
| Rotterdam. | ||||
| 1880–2 | 1890–2 | 1900–2 | ||
| Legitimate Fertility | 331.4 | 312.0 | 299.0 | |
| Illegitimate Fertility | 17.4 | 16.5 | 13.1 | |
1. These figures are the lowest in the whole list of death rates and infantile mortalities in the summary of births and deaths in cities in this Report.
2. Lowest figure for the Continent.
34There has been a marked improvement in the labor conditions in Holland during these last ten years especially, wages having increased and hours of labor decreased, with the cost of living taking a comparatively very small rise.
There is no country in Europe where the educational advantages are so great as in Holland.
That the Birth Control propaganda has been a success in Holland any one travelling through that delightful, clean and cheerful country can testify.
In that enlightened country, Holland, the teaching by the medical profession of the most hygienic methods of birth limitation has enabled the poor to have small families which they could raise to be physically and morally better equipped than formerly, and what is most interesting to observe is that, whether as a result of this or for some other reason, the families among the well-to-do are not nearly as small as in other countries.—Dr. S. Adolphus Knopf, in The Survey for November, 1916.
Germany was the next to follow, in 1889, when Herr Max Hausmeister and Herr Karl Lotter founded the Sozial Harmonische Verein, with its paper Die Sozial Harmonie. Like the English League, this society has confined its teachings to the theoretical and economic aspects of the subject, in which it has especially distinguished itself. In Germany all such doctrines are of course anathema, but the enormous decline in the birth-rate in several towns testifies to the refusal of the German people to be hectored into misery. All the signs point at present to an extraordinary ferment of new ideas in Germany, and a large number of other movements are more or less openly Neo-Malthusian.—From The Malthusian (London), January, 1909.
The German Sozial Harmonische Verein, founded in 1889, by Herr Max Hausmeister, has continued its quiet, but effective, work, and its periodical, Die Sozial Harmonie, has contained many articles of great economic value. A remarkable feature in Germany, however, has been the rapid rise of the Mutterschutz Society, under the able presidency of Dr. Helene Stocker, a society which aims at obtaining greater security and freedom for married and unmarried mothers, and at securing better conditions for the rearing of their offspring. Neo-Malthusianism (Birth Control) is becoming an important feature of this work, and is also dealt with in the Zeitschrift fur Sexual-wissenschaft, a scientific journal devoted to sex matters. The birth-rate of Prussia has seen one of the most rapid declines, from 36.2 in 1901 to 33.7 in 1906, and 33.0 in 1907; while the death-rates for the same years have been 20.5, 17.9, and 17.8, and the infantile mortalities 200, 177, and 168 respectively. The birth-rate of Berlin in 1907 was 24.3, or below that of London, 26.8.—From The Malthusian (London) for July 15th, 1909.
France differs from all other countries in having realized the individual advantages of the practice of birth control long before any other country in Europe. It is said that the sale of the lands (forfeited by the Emigrés or confiscated by the Commune after the Revolution) to the people, together with the law of equal inheritance in accordance with the principles of Liberty, Equality and Fraternity adopted for their guidance formed the chief incentive to restriction of the numbers of the family.
The birth-rate declined in an irregular manner from 1870 to the present time, especially among the wealthy classes, while the poor and ignorant continued to be burdened with large families. This led M. Paul Robin in 1896 to form the French Ligue de la Regeneration Humaine, and to employ his enormous energy and enthusiasm towards the formation of leagues in other 36countries. Bohemia, Spain, Brazil, Belgium, Cuba, Africa and Switzerland formed leagues in succession, most of them circulating periodicals dealing with Neo-Malthusian (Birth Control) theory and practice. At the same time M. Robin formed a Federation Universelle de la Regeneration Humaine, in which the various leagues have been associated and which has held two international meetings—the first at Paris in 1900 and the second at Liege in 1905.—From The Malthusian (London) January, 1909.
Fifteen years after the founding of M. Robin’s work, the propaganda in France is very complete and intense. Theoretical or practical, it appears under many forms. It acts through books, pamphlets, leaflets, journals, lectures, pictures, and even songs. Tens of thousands of theoretical volumes and pamphlets are disseminated, hundreds of thousands of leaflets are distributed. The practical pamphlets find their success in rapidly disappearing editions. In every part of the land—in town, and even country—lectures are given, and numerous militant workers diffuse the good tidings in multitudes of papers. The centers of our propaganda are too numerous to be fully quoted. In the first rank are the societies exclusively Neo-Malthusian (Birth Control), which, in fact, each carry on in their own manner the work undertaken by Regeneration. The most active, the most enterprising, and the most combative of these organizations, Génération Consciente, multiplies its efforts, extends its action, and prospers unceasingly. Again there exists a different class of propagandists—the individual—who, without periodical, place or society, works by disseminating not only the pamphlets, leaflets, and books, but also the means of prevention.—From The Malthusian (London) of September 15, 1910.
France has her population practically under control, and can increase or diminish at will according to the prospects of good or bad times. (See Page 37 for French Birth and Death Rate).—From The Malthusian (London) of April 15th, 1909.
France has set the example of real civilization and other nations are following her more or less rapidly according to their advancement in culture.
There has been a tendency to ascribe the low birth-rate in France to infertility or degeneracy, although this is patently absurd to all those who are acquainted with the French people. For the low birth-rate of France is practically entirely due to prudential control of families among married people who make no pretense to the avoidance of preventive intercourse.
Dealing with the conditions of the people in France there is little that does not compare favorably with all other old countries. The average duration of life is about fifty years, which is nearly the highest in Europe. The 37infantile mortality is the worst feature,[3] but it has been declining for some years.
3. Note: This is a problem of hygiene and infant welfare. If the same care were given the babies of France as is being given the infants of other advanced countries there is little doubt that the mortality rate would decline proportionately.—M. H. S.
There is no “too old at thirty-five” difficulty in France, elderly men being employed where boys are (in other countries); there is no unemployment worth speaking of; there is no land problem, and house rents, instead of being forced up by excess of demand, are actually lowered by excess of supply, so that the “unearned increment” is frequently negative.—From The Malthusian (London) for April 15th, 1909.
Writing of France in 1879, a few years after the close of the disastrous Franco-Prussian War, Johannes Swaagman said:
“France, notwithstanding the heavy war indemnity of five milliards, and perhaps an equal expenditure of her own war material, is now the only country that has a surplus on its estimated budget, and can even dream of reducing taxation. Besides this, large sums are being spent on improvements, with a view of accelerating commerce and industry.
“France has still many things to learn, notably as regards hygiene, but we have no hesitation in asserting that as regards the solution of the most distressing problems which humanity has to face and as regards general happiness and culture she is far ahead of all other countries and she has simply led the way in the direction in which all other nations are bound to follow, and in which they are already hastening.”—From The Malthusian (London) of April 15th, 1909.
Strong and vigorous movements exist in Switzerland, Belgium, Hungary, Spain, Norway, Sweden, Denmark and Italy, while there are somewhat less active ones in Russia, Japan, India, and even China. I will not take the space to furnish the details of the movement in these countries because they are mainly inspired in their activities from those well organized Leagues already mentioned.
The actual facts as regards the French birth-rate are constantly misrepresented. Taking the actual population, this appears to have been 24.8 millions in 1783, 28.9 millions in 1806, and to have gone on more or less steadily increasing to 39.26 millions in 1907. Exceptions to this increase have taken place six times since 1881, there being a deficit or excess of deaths over births of 38,446 in 1890, of 10,505 in 1891, of 20,041 in 1892, of 17,813 in 1895, of 3825,988 in 1900, and of 19,920 in 1907. Despite these deficits the natural increase, or excess of births over deaths, was 1,232,744 in the twenty-five years from 1881 to 1905, while the total increase, including immigration, etc., was 1,690,000 during the same period. It is worthy of note also in view of the suggestions that the deficit is about to become chronic, and that France is therefore a “dying nation,” that in 1893 and 1894, after three years of deficits, there were excesses of 7,000 and 39,000; in 1897 and 1898 of 93,700 and 108,000; and in 1901 of 72,000. There has been no report since 1907, but Le Jour Officiel of Paris has given the figures for the first six months of 1908, which show an increase of 12,066, partly due to a rise of 8,657 in the births and partly a decline of 8,416 in the deaths.—From The Malthusian (London) of April 15th, 1909.
| BIRTH RATE IN FRANCE | ||
|---|---|---|
| Compiled from The Malthusian (London), for April 15th, 1909 | ||
| Year | Increase | Decrease |
| 1890 | 38,446 | |
| 1891 | 10,505 | |
| 1892 | 20,041 | |
| 1893 | 7,000 | |
| 1894 | 39,000 | |
| 1895 | 17,813 | |
| 1896 | No record available | |
| 1897 | 93,700 | |
| 1898 | 108,000 | |
| Total for 8 years | 247,700 | 86,800 |
| 86,800 | ||
| ——————— | ||
| Total increase | 160,900 | |
| ——————— | ||
| Rate of increase per year (approximately) | 20,100 | |
| Increase in total population from 1783 to 1907 | 15,000,000 | |
It is interesting to know that the present agitation for the dissemination of knowledge to prevent conception, as expressed in the various leagues throughout the world to-day had its greatest impetus and inspiration from two books written by Americans in the United States.
39The first of these was a pamphlet entitled “Moral Physiology,” written by United States Senator Robert Dale Owen, son of Robert Owen, which was published in New York City in 1830 and gave a description of the physical checks made use of in France, where it was the custom to limit the number of children to the means at the command of the family. This book was much read and commented favorably upon in America.
So favorably did this publication appeal to the thinking minds of the time, that Dr. Charles Knowlton, an able Boston physician, on reading Owen’s pamphlet, was so struck by its importance as a contribution to the science of hygiene that he brought out a similar work in 1833, entitled “The Fruits of Philosophy.” His book was addressed to young married people and gave a popular description of the anatomy of the organs of reproduction, especially in the female, and a somewhat more detailed account of the physical checks to prevent conception than had been given in Owen’s pamphlet.
“The Fruits of Philosophy” circulated unchallenged for more than forty years, and finally, in 1876, was attacked as an obscene publication under the new act of Parliament called “Lord Campbell’s Act,” and a bookseller of Bristol, England, was sentenced to two years’ imprisonment for selling it.
This work would have been suppressed altogether had not Charles Bradlaugh and Mrs. Annie Besant, two ardent defenders of British liberty, come forward and volunteered to sell it in order to test the case in the English courts. The trial, as has been described herein under the title of “Birth Control League of England,” attracted great attention to this philosophy throughout the world. It is a sad commentary upon the legislative bodies of this country that up to the present every attempt by advocates of this principle to discuss this subject and awaken our people to its needs has been met with prosecution and jail sentences.
During these last forty years the movement has made rapid progress in all civilized countries except the United States. In this progressive matter we find ourselves classed with Russia, Japan, India and China, where national interest is concerned with quantity of human beings rather than with quality.
But during the last five years the subject has come forcibly to the front, mainly through prosecutions. Again a message has gained a hearing from the dock which it could never have won from the platform.
The people of this country are now awakened to the need of knowledge to prevent conception. Social workers, nurses, and members of the medical profession find their work hampered and their activities nullified by oppressive laws denying the individual the right of health, life and the pursuit of happiness.
The most advanced thinkers in America are with us in this movement, the sentiment being largely in favor of the establishment of clinics, similar 40to those in Holland, where the poor and overburdened mothers may come for advice to be given by doctors, nurses or others competent to instruct.
Following are some of the names of men and women in the United States who stand for the dissemination of such knowledge, have allied themselves to this great humanitarian cause, and have come out in the press for birth control as a national necessity:
Dr. Abram Jacobi, ex-president, American Medical Association, New York City.
Dr. Hermann M. Biggs, State Commissioner of Health, New York.
Dr. John N. Hurty, secretary, State Board of Health, Indiana.
Dr. Godfrey R. Pisek, professor of diseases of children, New York Post-Graduate Medical School and Hospital, New York City.
Dr. J. W. Trask, United States Public Health Service, Washington, D. C.
Dr. Ira S. Wile, editor, American Medicine, member Board of Education, New York City.
Dr. John A. Wyeth, professor of surgery and president of the New York Polyclinic Medical School and Hospital, ex-president of the American Medical Assn., and New York Academy of Medicine, New York City.
41Dr. S. Adolphus Knopf, professor of medicine, department of Phthisio-therapy, at New York Post-Graduate Medical School and Hospital, New York City.
Dr. Lydia Allen de Vilbiss, formerly of New York State Department of Health, now in charge of the division of Child Hygiene of the State Board of Health of Kansas.
Rev. Dr. Frank Crane, formerly pastor of the Union Congregational Church, Worcester, Mass., now notable writer of editorial articles for New York Globe, etc.
Rev. Dr. Percy Stickney Grant, rector, Protestant Episcopal Church of the Ascension, New York City.
Rev. Dr. Frank Oliver Hall, minister, Church of the Divine Paternity, New York City.
Rev. Dr. John Haynes Holmes, minister, Unitarian Church of the Messiah, New York City.
Rev. Dr. Harvey Dee Brown, minister, Unitarian Church of the Messiah, New York City.
Rev. Dr. Stephen S. Wise, rabbi of the Free Synagogue, New York City.
Rev. Dr. Sidney E. Goldstein, rabbi of the Free Synagogue, New York City.
Rev. Dr. Waldo Adams Amos, rector, Protestant Episcopal Church of St Paul, Hoboken, N. J.
Physicians, scientists, economists, social workers and others interested in the forward march of this country are simply marking time in progress until it is decided whether or not the medical profession and its assistants have the legal right to impart information to prevent conception to those who need it. A favorable decision would permit men and women to stem the incoming tide of feebleminded, unfit, degenerate individuals who undermine our present social structure and place a burden on generations yet unborn.
In this chapter it is demonstrated that a high birth rate invariably means a high death rate, particularly a high infant mortality. Where a knowledge of methods to prevent conception results in a lowering of the birth rate, proportionately more of those children born survive, and a healthier, sturdier population is the result.
It may be said that Nature has been seriously troubled with the problem of reproduction even from the first creation of life. Our own doubts and difficulties in that sphere are but a continuation of those experienced on the earth long before Man’s ancestors descended from the forest trees. Nature’s first insistent impulse was for reproduction, and so the lowlier organisms increase at an enormous rate, though by far the greater number of the creatures thus produced are doomed to early destruction by other creatures which prey upon them. Then sex arose and developed. And the object of sex may be said to act as a check on reproduction, and not, as we have sometimes too hastily assumed, to ensure reproduction, for that was already more than fully ensured by other methods already in existence. The device of sex rendered reproduction more difficult, but in decreasing the quantity of offspring it at the same time improved their quality. As the sexual process increased in complexity the individuals produced equally grew more complex and better equipped to resist the dangers they were subjected to. Fishes are spawned by the thousand, but only a few come to maturity. The higher mammals produce but few offspring and surround them with parental care until they are able to lead their own lives with a fair chance of surviving. Thus the sexual process in its finally developed form may be regarded as a mechanism for subordinating quantity to quality, and so promoting the evolution of life to ever higher stages.
This process, which is plain to see on the largest scale throughout living nature, may be more minutely studied, as it acts within a narrower range, in the human species. Here we statistically formulate it in the terms of birth-rate 44and death-rate; by the mutual relationship of the two courses of the birth-rate and the death-rate we are able to estimate the evolutionary rank of a nation, and the degree in which it has succeeded in subordinating the primitive standard of quantity to the higher and later standard of quality.
It is especially in Europe that we can investigate this relationship by the help of statistics which in some cases extend for nearly a century back. We can trace the various phases through which each nation passes, the effects of prosperity, the influence of education and sanitary improvement, the general complex development of civilisation, in each case moving forward, though not regularly and steadily, to higher stages by means of a falling birth-rate, which is to some extent compensated for by a falling death-rate, the two rates nearly always running parallel, so that a temporary rise in the birth-rate is usually accompanied by a rise in the death-rate,—by a return, that is to say, to the conditions which we find at the beginning of animal life,—and a steady fall in the birth-rate is always accompanied by a fall in the death-rate.
The modern phase of this movement, soon after which our precise knowledge begins, may be said to date from the industrial expansion, due to the introduction of machinery, which Professor Marshall places in England about the year 1760. That represents the beginning of an era in which all civilised and semi-civilised countries are still living. For the earlier centuries we lack precise data, but we are able to form certain probable conclusions. The population of a country in those ages seems to have grown very slowly and sometimes even to have retrograded. At the end of the sixteenth century the population of England and Wales is estimated at five millions and at the end of seventeenth at six millions,—only 20% increase during the century—although during the nineteenth century the population nearly quadrupled. This very gradual increase of the population seems to have been by no means due to a very low birth-rate, but to a very high death-rate. Throughout the Middle Ages a succession of virulent plagues and pestilences devastated Europe. Smallpox, which may be considered the latest of these, used to sweep off large masses of the youthful population in the eighteenth century. The result was a certain stability and a certain well-being in the population as a whole, these conditions being, however, maintained in a manner that was terribly wasteful and distressing.
The industrial revolution introduced a new era which began to show its features clearly in the early nineteenth century. On the one hand, a new motive had arisen to favor a more rapid increase of population. Small children could tend machinery and thereby earn wages to increase the family takings. This led to an immediate result in increased population and increased prosperity. But on the other hand, the rapid increase of population always tended to outrun the rapid increase of prosperity, and the more so since the rise of sanitary science began to drive back the invasions of the grosser and more destructive infectious diseases which had hitherto kept the population down. The result was that new forms of disease, distress, and 45destitution arose; the old stability was lost, and the new prosperity produced unrest in place of well-being. The social consciousness was still too immature to deal collectively with the difficulties and frictions which the industrial era introduced, and the individualism which under former conditions had operated wholesomely now acted perniciously to crush the souls and bodies of the workers, whether men, women or children.
As we know, the increase of knowledge and the growth of the social consciousness have slowly acted wholesomely during the past century to remedy the first evil results of the industrial revolution. The artificial and abnormal increase of the population has been checked because it is no longer permissible in most countries to stunt the minds and bodies of small children by placing them in factories. An elaborate system of factory legislation was devised, and is still ever drawing fresh groups of workers within its protective meshes. Sanitary science began to develop and to exert an enormous influence on the health of nations. At the same time the supreme importance of popular education was realised. The total result was that the nature of “prosperity” began to be transformed, instead of being, as it had been at the beginning of the industrial era, a direct appeal to the gratification of gross appetites and reckless lusts, it became an indirect stimulus to higher gratifications and more remote aspirations. Foresight became a dominating motive even in the general population, and a man’s anxiety for the welfare of his family was no longer forgotten in the pleasure of the moment. The social state again became more stable, and more “prosperity” was transformed into civilisation. This is the state of things now in progress in all industrial countries, though it has reached varying levels of development among different peoples.
It is thus clear that the birth-rate combined with the death-rate constitutes a delicate instrument for the measurement of civilisation, and that the record of these combined curves registers the upward or downward course of every nation. The curves, as we know, tend to be parallel, and when they are not parallel we are in the presence of a rare and abnormal state of things which is usually temporary or transitional.
It is instructive from this point of view to study the various nations of Europe, for here we find a large number of small nations, each with its own statistical system, confined within a small space and living under fairly uniform conditions. Let us take the very latest official figures (which are usually for 1913) and attempt to measure the civilisation of European countries on this basis. Beginning with the lowest birth-rate, and therefore in gradually descending rank of superiority, we find that the European countries stand in the following order: France, Belgium, Ireland, Sweden, the United Kingdom, Switzerland, Norway, Scotland, Denmark, Holland, the German Empire, Prussia, Finland, Spain, Austria, Italy, Hungary, Serbia, Bulgaria, Roumania, Russia. If we take the death-rate similarly, beginning with the lowest rate and gradually descending to the highest, we find the following 46order: Holland, Denmark, Norway, Sweden, Switzerland, the United Kingdom, Belgium, Scotland, Prussia, the German Empire, Finland, Ireland, France, Italy, Austria, Serbia, Spain, Bulgaria, Hungary, Roumania, Russia.
Now we cannot accept the birth-rates and death-rates of the various countries exactly at their face value. Temporary conditions, as well as the special composition of a population, not to mention peculiarities of registration, exert a disturbing effect. Roughly and on the whole, however, the figures are acceptable. It is instructive to find how closely the two rates agree. The agreement is, indeed, greater at the bottom than at the top; the eight countries which constitute the lowest group as regards birth-rate are the identical eight countries which furnish the heaviest death-rates. That was to be expected; a very high birth-rate seems fatally to involve a very high death-rate. But a very low birth-rate (as we see especially in the case of France) is not invariably associated with a very low death-rate though it is never associated with a high death-rate. This seems to indicate that those qualities in a highly civilised nation which restrain the production of offspring do not always or at once produce the eugenic racial qualities possessed by hardier peoples living under simpler conditions. But with these reservations it is not difficult to combine the two lists in a fairly concordant order of descending rank. Most readers will agree, that taking the European populations in bulk, without regard to the production of genius (for men of genius are always a very minute fraction of a nation), the European populations which they are accustomed to regard as standing at the head in the general diffusion of character, intelligence, education, and well-being, are all included in the first twelve or thirteen nations, which are the same in both lists though they do not follow the same order. These peoples, as peoples—that is, without regard to their size, their political importance, or their production of genius—represent the highest level of democratic civilisation in Europe.
It is scarcely necessary to add that various countries outside Europe equal or excel them; the death-rate of the United States, so far as statistics show, is the same as that of Sweden, that of Ontario, still better, is the same as Denmark, while the death-rate of the Australian Commonwealth with a medium birth-rate, is lower than that of any European country, and New Zealand holds the world’s championship in this field with the lowest death-rate of all. On the other hand, some extra-European countries compare less favorably with Europe: Japan, with a rather high birth-rate, has the same high death-rate as Spain, and Chili, with a still higher birth-rate, has a higher death-rate than Russia. So it is that among human peoples we find the same laws prevailing as among animals, and the higher nations of the world differ from those which are less highly evolved precisely as the elephant differs from the herring, though within a narrower range, that is to say, by producing fewer offspring and taking better care of them.
The whole of this evolutionary process, we have to remember, is a natural process. It has been going on from the beginning of the living world. But 47at a certain stage in the higher development of man without ceasing to be natural, it becomes conscious and deliberate. It is then that we have what may properly be termed Birth Control. That is to say that a process which had before been working slowly through the ages, attaining every new forward step with waste and pain, is henceforth carried out voluntarily, in the light of the high human qualities of reason and foresight and self-restraint. The rise of birth control may be said to correspond with the rise of social and sanitary science in the first half of the nineteenth century, and to be indeed an essential part of that movement. It is firmly established in all the most progressive and enlightened countries of Europe, notably in France and in England; in Germany, where formerly the birth-rate was very high, birth control has developed with extraordinary rapidity during the present century. In Holland its principle and practice are freely taught by physicians and nurses to the mothers of the people, with the result that there is in Holland no longer any necessity for unwanted babies, and this small country possesses the proud privilege of the lowest death-rate in Europe. In the free and enlightened democratic communities on the other side of the globe, in Australia and New Zealand, the same principles and practice are generally accepted, with the same beneficent results. On the other hand, in the more backward and ignorant countries of Europe, birth control is still little known, and death and disease flourish. This is the case in those eight countries which come at the bottom of both our lists.
Even in the more progressive countries, however, birth control has not been established without a struggle which has frequently ended in a hypocritical compromise, its principles being publicly ignored or denied and its practice privately accepted. For at the great and vitally important point in human progress which birth control represents, we really see the conflict of two moralities. The morality of the ancient world is here confronted by the morality of the new world. The old morality, knowing nothing of science and the process of Nature as worked out in the evolution of life, based itself on the early chapters of Genesis, in which the children of Noah are represented as entering an empty earth which it is their business to populate diligently. So it came about that for this morality, still innocent of eugenics, recklessness was almost a virtue. Children were given by God, if they died or were afflicted by congenital disease, it was the dispensation of God, and, whatever imprudence the parents might commit, the pathetic faith still ruled that “God will provide.” But in the new morality it is realised that in these matters Divine action can only be made manifest in human action, that is to say through the operation of our own enlightened reason and resolved will. Prudence, foresight, self-restraint—virtues which the old morality looked down on with benevolent contempt—assume a position of the first importance. In the eyes of the new morality the ideal woman is no longer the meek drudge condemned to endless and often ineffectual child-bearing, but the free and instructed woman, able to look before and after, trained in 48a sense of responsibility alike to herself and to the race, and determined to have no children but the best.
Such were the two moralities which came into conflict during the nineteenth century. They were irreconcilable and each firmly rooted, one in ancient religion and tradition, the other in progressive science and reason. Nothing was possible in such a clash of opposing ideas but a feeble and confused compromise such as we still find prevailing in various countries of old Europe. It was not a satisfactory solution, however inevitable, and especially unsatisfactory by the consequent obscurantism which placed difficulties in the way of spreading a knowledge of the methods of birth control among the masses of the population. For the result has been that while the more enlightened and educated have exercised a control over the size of their families, the poorer and more ignorant—who should have been offered every facility and encouragement to follow in the same path—have been left, through a conspiracy of secrecy, to carry on helplessly the bad customs of their forefathers. This social neglect has had the result that the superior family stocks have been hampered by the recklessness of the inferior stocks.
Such is the situation to-day when we find America entering this field. Up till now America had meekly accepted at Old Europe’s hands the traditional prescription of our Mediterranean book of Genesis, with its fascinating old-world fragrance of Mount Ararat. On the surface, the ancient morality had been complacently, almost unquestionably accepted in America, even to the extent of permitting a vast extension of abortion—a criminal practice which ever flourishes where birth-control is neglected. But to-day we suddenly see a new movement in the United States. In a flash, America awoke to the true significance of the issue. With that direct vision of hers, that swift practicality of action, and above all, that sense of the democratic nature of all social progress, we see her resolutely beginning to face this great problem. In her own vigorous native tongue we hear her demanding: “What in the thunder is all the secrecy about anyhow?” And we cannot doubt that America’s own answer to that demand will be of immense significance to the whole world.
BIRTH CONTROL. MARY ALDEN HOPKINS, in Harper’s Weekly, 1915.
No one knows what the birth rate of the United States is, or what it ever has been. Every European country knows its birth rate and its death rate, because every birth and every death is registered. Where the number of births, the number of deaths and the number of the population are all known, it is an easy matter to calculate the rates per thousand. But in the international tables of vital statistics our country’s figures are omitted.
Our 1910 census announced that 23 states had “fairly complete” death 49registration. They recorded about 90% of their deaths. But the birth registration situation was shocking. The New England States, Pennsylvania and Michigan were the only acceptable states. The figures for the cities of Washington, D.C., and New York City passed muster also. The 1910 census birth rate is not yet published, but the 1900 census made shift to figure it out by means of the number of the population’s increase and the death rate. This would be surer if the death rate were not itself approximate. However, the calculated rates were, birth rate, 35.1 per 1000 population; death rate, 17.4 per 1000; excess of births over deaths 17.7 per 1000. Comparing these rates with the rates of the European countries for the same decade, we find ourselves near the head of the list for high birth rate, near the foot of the list for low death rate, and increasing faster than any other nation. These figures leave nothing to be desired from an emotional viewpoint. But they leave much to be desired in the way of accuracy. In addition to our lack of statistics we are confused by the effect of immigration.
The birth rate of every civilized country is falling. The following comparison of national birth rates is based on the ten largest countries of Europe. The less important ones show the same general characteristics. Asiatic countries must be excluded as they have no reliable vital statistics. The United States must be considered separately because both our mortality records and our birth registration are so defective that only approximate calculations can be made. The maximum birth rate preceding the present decline occurred in France 1811–20; in Norway, Sweden, Finland, Austria and Prussia 1821–30; Belgium 1831–40; Denmark 1851–60; Scotland and Spain 1861–70; England, Wales, Ireland, Hungary, Switzerland, Germany, Bavaria, Saxony, and the Netherlands 1871–80; Portugal, Italy, Serbia and Roumania, 1881–90.
The figures of the following table are taken from the Report of the Registrar General of Great Britain for 1910. Five year periods are used in place of single years to eliminate variations of exceptional years.
Seventy-third Annual Report of the Registrar-General of Births, Deaths and Marriages in England and Wales, 1910, London. Pub. by His Majesty’s Stationery Office. Printed by Darling and Sons, Ltd., Bacon St., E. London. 1912.
| Yearly Number of Births per 1000 Inhabitants. | ||
|---|---|---|
| 1881–5 | 1906–10 | |
| Russia (European) | 49.1 | 47.7[4] |
| Hungary | 44.6 | 36.7 |
| German Empire | 37.0 | 34.3[4] |
| Spain | 36.4 | 33.6 |
| Austria | 38.2 | 33.6 |
| Italy | 38.0 | 32.6 |
| 50The Netherlands | 34.8 | 29.6 |
| Belgium | 30.7 | 27.7[4] |
| England and Wales | 33.5 | 26.6 |
| France | 24.7 | 19.7 |
4. Figures for previous five years.
The countries are arranged in order of their 1906–10 rates.
By subtracting the figures in the second column from the first we obtain the fall in the rates between 1881–5 and 1906–10. Russia, in 1910, had the highest birth rate, and had suffered the slightest diminution, only 1.4 per thousand. Curiously Hungary, standing second in line, showed the greatest fall, 7.9. England and Wales, far down the scale, had a drop of 6.9 per thousand. Italy, The Netherlands, France, and Austria kept a fairly even pace with a fall of around 5. Belgium, Spain, and the German Empire lost only about 3 per thousand.
Much discussion has arisen concerning the cause of this decline. Two distinct stages occur in the fecundity of animal life. In the species below the human race it is checked by biological causes. In the human race it is checked by social and economic causes. As the scale of life rises, the number of offspring become fewer. The higher the animal, the fewer the offspring.
When we reach the human animal, we find in addition to pestilence, war, and “acts of God,” various forms of voluntary check. Semi-civilized countries manage the affair rather crudely; in India the Ganges is hardly yet free from infant corpses, and in China girl babies show an assisted mortality. More civilized countries limit the birth rate more felicitously, reducing the number of marriages and advancing the age of marriage, by imposing social, ethical, and financial obligations. This decreases the number of possible children. These indirect checks held back the increase of population so slightly, evenly and over so long a period as to be hardly perceptible. In the seventies appeared a phenomenon of spectacular novelty—the small family. Harmless methods of contraception had been perfected, the knowledge disseminated, and the means supplied. The birth rate, which had slowly declined through aeons, from eggs by the millions to yearly babies, dropped with dizzying rapidity.
As the birth rates of the nations fall, so fall the death rates. Here are the death rates for the same ten nations for the same years as the previous birth rate table.
| 51 | ||
| Yearly Number of Deaths per 1,000 Inhabitants | ||
|---|---|---|
| 1881–5 | 1906–10 | |
| Russia (European) | 35.4 | 30.9[5] |
| Hungary | 33.1 | 25.0 |
| Spain | 32.6 | 24.3 |
| Austria | 30.1 | 22.3 |
| Italy | 27.3 | 21.0 |
| German Empire | 25.3 | 19.9[5] |
| France | 22.2 | 19.2 |
| Belgium | 20.6 | 17.0[5] |
| England and Wales | 19.4 | 14.7 |
| The Netherlands | 21.4 | 14.3 |
5. Figures for previous five years.
A comparison of the two tables shows immediately that the countries having the highest birth rate have also the highest death rate. Russia, which heads the list in births, heads the list in deaths. Hungary comes second in both lists. Next come, in a slightly altered order, the four countries, German Empire, Spain, Austria and Italy. An exception occurs in France which has the unusual combination of a low birth rate and a medium death rate. Belgium, and England and Wales occupy the same position in both lists with low birth rates and low death rates. The Netherlands is the notable country with its medium birth rate and its low death rate. The Neo-Malthusians love to mention at this point that this country has governmental encouragement in teaching contraception.
The increase of a country is the difference between its birth rate and its death rate. The population of a country depends, not upon its birth rate, but upon its birth rate, minus its death rate. If the two are identical, the population is stationary. This happened in France in the 1891–5 period. The number of births per thousand inhabitants was exactly the number of deaths per thousand inhabitants. The rest of the world tolled the knell for France. But France instead of declining into the have-been nations showed that a controlled birth rate can be raised as well as lowered. Slowly and apparently intentionally she raised her rate during the succeeding years.
Decline and rise of French Birth rate: 1881–5, 2.5; 1886–90, 1.1; 1891–5, 0.0; 1896–1900, 1.2; 1901–5, 1.6; 1906–10, .7. Nor has France since those early nineties allowed her birth rate to fall below her death rate.
The populations of European nations are increasing, because the death rates are falling faster than the birth rates.
If we subtract the deaths per thousand inhabitants, given in the second table, from the births per thousand inhabitants given in the first table, we shall have the natural rate of increase. In every single case the number of 52births is greater than the number of deaths—so every country is increasing in population.
| Natural Increase in Population per 1,000 Inhabitants | ||
|---|---|---|
| 1881–5 | 1906–10 | |
| Russia (European) | 13.7 | 16.8[6] |
| The Netherlands | 13.4 | 15.3 |
| German Empire | 11.7 | 14.4[6] |
| Hungary | 11.5 | 11.7 |
| England and Wales | 14.1 | 11.5 |
| Italy | 10.7 | 11.4 |
| Austria | 8.1 | 11.3 |
| Belgium | 10.1 | 10.7[6] |
| Spain | 3.8 | 9.3 |
| France | 2.5 | .7 |
6. Figures for previous five years.
From the second column we find that Russia is increasing most rapidly. The Netherlands comes second in rate of increase—an honorable position to which the regulationists point triumphantly when they assert that control of the birth rate does not mean the ruin of the nation. The German Empire comes next, with Hungary following. England stands fifth in the rating of increase, and England takes the position with woeful lamentations. Italy, Austria, Belgium, and Spain are near the foot of the list, and France brings up the rear a long, long way behind. France is the only one that is anywhere in sight of a stationary population.
Excepting France and England, every one of these countries is increasing at a faster rate than formerly, because though the birth rate has fallen fast, the death rate has fallen faster. By comparing the second column showing the increase in the 1906–10 period with the first column showing the increase in the 1881–5 period, in the preceding table, we see how much each country is gaining in her rate of increase. This increase may or may not be considered desirable according to whether one wishes to conserve the food supply or increase the army. To every one it presents an interesting condition. It is unexpected to find with a falling birth rate an increasingly increasing population,—always excepting France and England.
When we are considering the growth of population it is not the births but the survivals that count; and it is a remarkable fact, of which illustrations will appear anon, that comparatively few of those who have made strong remarks on the birth-rate question seem to have realised this. The child that 53perishes before entering on a productive existence is not an asset to the numbers or efficiency of the community, but a drain upon it for which there is no compensating gain.
We shall now study the principal parts of our Empire seriatim, and it will suffice if we consider Great Britain and Ireland, Australasia, Canada, South Africa, and India.
England and Wales.—Special attention should be given to this diagram (Fig. 2), as, apart from England’s intrinsic Imperial importance, it exhibits changes typical of those taking place in the majority of civilised countries at the present time. Our Registrar-General’s Reports give us figures starting from the year 1853, and it will be seen that there was a fairly definite rise in the birth-rate till the year 1876, after which there set in that rapid and steady decline which we hear so much about to-day.
As to the cause of this remarkable decline, it is now pretty generally known that the chief factor is the voluntary reduction of the fertility rate (the average number of children to a marriage). Further, the decline has been largely a class one, affecting first the richer and more cultured classes, rapidly extending through the various grades of the middle classes until it has now reached the skilled artizans, but not the poorest and most unskilled laborers.
The evidence for these contentions is briefly (a) that just before the year 1876 an actuarial enquiry made by Mr. Ansell on behalf of the National Life Assurance Society revealed the fact that the average number of children to a family in the upper and professional classes at that time was somewhat over five, while the average for the whole population was 4.63 according to the Registrar-General’s Report; (b) that the birth-rate reckoned on the number of married women has since fallen from 304.1 per thousand in 1876 to 196.2 in 1911; (c) that families are now notoriously very small among the professional classes; and (d) that the birth-rate in some of the poorest districts of our large towns is still about as high as it was in 1876. We have not yet got the detailed returns of families for the census of 1911 in England and Wales; but for Scotland, where the variations in the birth-rate have been very similar, Dr. J. C. Dunlop, in a paper read before the Royal Statistical Society the other day, gave these details. The average number of children to a family among the poorest unskilled laborers is still about seven, while it is only 3.91 for medical practitioners, 4.33 for the clergy, and 3.76 for army officers.
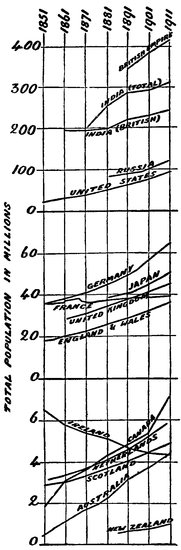
Fig. 1.—POPULATION OF VARIOUS COUNTRIES.
VARIATIONS IN BIRTH RATE &c., IN ENGLAND & WALES
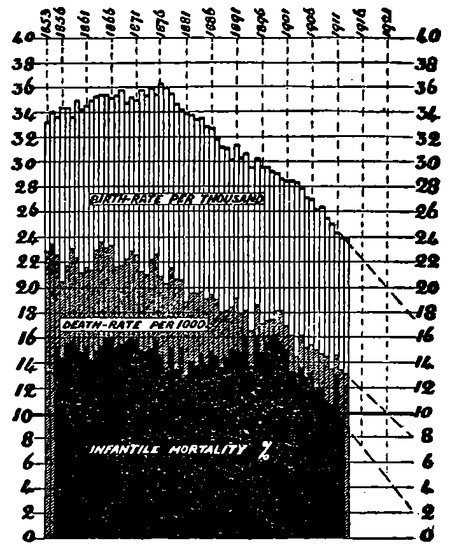
Fig. 2.—ENGLAND AND WALES.
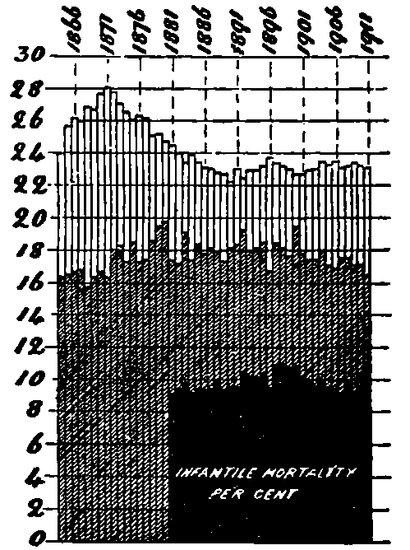
Fig. 3.—IRELAND.
Turning at once, however, to the accompaniments of these changes in the birth-rate, we find that the death-rate has also shown very decided changes, although the temporary fluctuations prevent our locating them with the same precision. For between fifteen and twenty years after 1853 the general deathrate 54was approximately stationary, or perhaps slightly rising; but since then there has been a rapid and steady fall from about 22 per thousand to a little over 13. The infantile mortality, after various minor fluctuations, has fallen very rapidly since 1900. The net result of these changes is that the rate of 55natural increase of population (excess of birth-rate over death-rate) during the last five years has averaged 11 per thousand, which is nearly the same as in the first five years 1853–57, when it was 11.7 per thousand, although it temporarily increased to 14.3 per thousand in the quinquennium 1874–78. The cry of “depopulation” or of “race suicide” has little more justification to-day when our birth-rate is only 24 and the average family probably between three and four children than it had in 1855 with a birth-rate of 34 and an average of 5 births per marriage. In an article in the Daily Telegraph of January 17 last, a writer pointed out that mortality was very high among the large families of the seventeenth and eighteenth centuries, and asked: “If to lose half, or more than half, their children was common among well-to-do people, how did poor folks fare?”
The actual rise of the population, after allowing for migration, is, of course, given by the census returns. Fig. 1 shows the variation of the total population of the United Kingdom and of England and Wales, from 1850 onwards.
Many of you will have heard alarmist statements from various quarters to the effect that our population is rapidly becoming stationary owing to the combined results of a declining birth-rate and an accelerated emigration. In the Fortnightly Review for February last an article on “The Danger of Unrestricted Emigration,” by Mr. Archibald Hurd, contained a characteristic statement of this kind:—“The population of Ireland and Scotland is rapidly declining, and that of England and Wales is now practically stagnant, the natural increase only slightly exceeding the outflow due to emigration.”
We will deal with Ireland in a moment; but as regards both England and Wales and Scotland the statement appears entirely unwarranted. The actual increase of population in England and Wales between the censuses of 1901 and 1911 was 10.9 per cent., which is only a little below the “natural” increase (in Wales it reached the unprecedentedly high increase of 18.1 per cent.); while in Scotland the actual increase of population was 6.4 per cent. over the decade. Probably these alarms were due to consideration of emigration apart from immigration or from return of our own emigrants.[7] The actual increase of population for the whole of the United Kingdom was 9.1 per cent.; and this has only been exceeded twice in the past six decades.
7. Further investigation appears to indicate that the official statistics concerning emigration and immigration are very unreliable. The Statistical Abstract for the United Kingdom for 1912 gives the total emigration in the ten years 1901–10 as 4,724,233, and the total immigration 2,409,490, leaving an outward balance of 2,314,723. In the same period there were 11,628,493 births and 6,780,266 deaths, giving a natural increase of 4,848,227; and since the actual increase by the census returns was 3,757,944, the net loss by emigration could only have been 1,091,283 or less than half of the officially recorded number. Thus it appears that little over one-fifth of our natural increase is lost by emigration. (Since writing this, I find the Registrar-General admits the returns prior to 1908 were defective.)
56We need not consider Scotland further, as its variations resemble those of England and Wales.
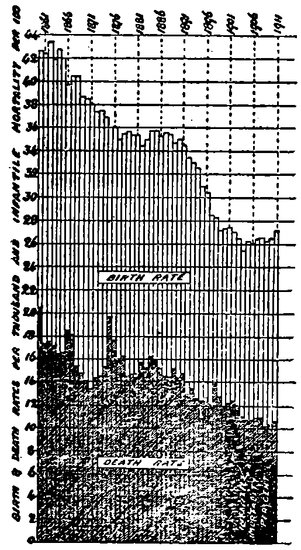
Fig. 4.—AUSTRALIA.
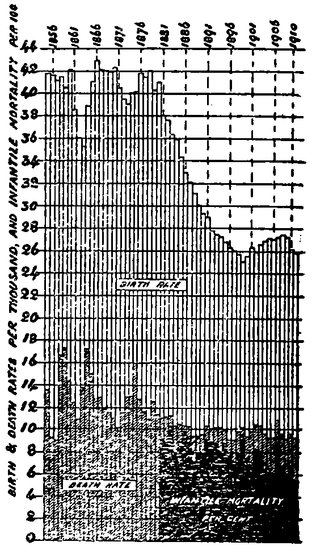
Fig. 5.—NEW ZEALAND.
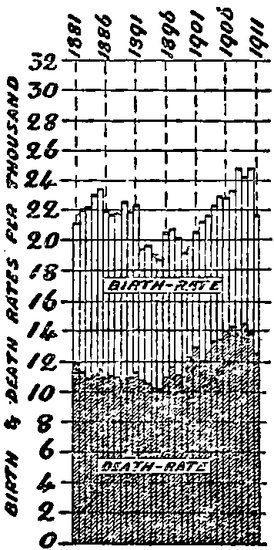
Fig. 6.—ONTARIO, CANADA.
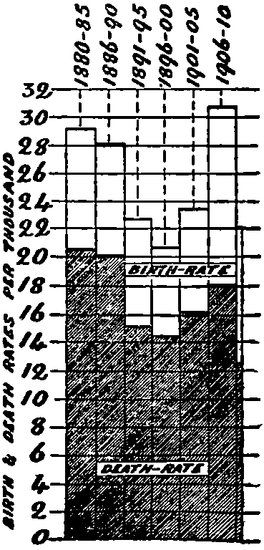
Fig. 7.—TORONTO.
Ireland.—Ireland’s statistics differ so much from those of most other countries that they merit special consideration. In Fig. 3 are shown the variations of its birth and death-rates. From these it appears that, for many years past, Ireland has had very low but practically steady birth-and death-rates. 57On further studying the matter, however, we find that Ireland’s low birth-rate is not due to small families, but to a low marriage rate (probably due to immigration of young people). The fertility rate of its women has remained high and steady, 283 per thousand in 1881, and 289 in 1901. The excess of births over deaths has averaged 6 per thousand recently, although it was much higher forty-five years ago. But the terrible poverty succeeding the famine produced the great tide of emigration which has reduced the population from eight to little over four millions. It should be observed, however, that it is late in the day to deplore the depopulation of Ireland, as it has now practically ceased. The fall of population was 11.8 per cent. between the censuses of 1851 and 1861, but only 1.7 per cent. between those of 1901 and 1911; while in the closing years of the decade, the Registrar-General’s returns gave the population as almost exactly stationary. It is highly probable that the next census will show an increase in the population of Ireland for the first time since 1846.
We may now turn to the various parts of our Empire overseas, and it will be sufficient if we consider the four principal divisions: Australasia, Canada, Union of South Africa, and India. The order is chosen as dealing with the populations of British origin first.
Australasia.—Australia and New Zealand both call for particular attention in this connection, as family limitation appears to be very general in them, and many authorities have spoken about it in strong terms. Mr. Roosevelt, for example, wrote as follows in 1911: “The rate of natural increase in New Zealand is actually lower than in Great Britain, and has tended steadily to decrease; while Australia increases so slowly that, even if the present rate were maintained, the population would not double itself in the next century.”
Again, the Bishop of London, last year appears to have told the North-West Australian Diocesan Association “that the birth-rate in Australia is going down even more rapidly than at home (United Kingdom), and that he did not know how we are going to keep Australia even British.”
In addition to these grave warnings, fears have been continually expressed concerning the danger of Australia from the Japanese or Chinese. We are told also that from the industrial point of view Australia is calling out for population; and a law giving a bonus of £5 for each child was passed a twelve-month ago. It would appear, therefore, that the birth-rate question is a very serious one in Australasia, especially when we are aware that determined attempts at checking the resources of family limitation have signally failed.
Let us now examine the actual figures for the variation of the birth-rate, etc., and compare them with the above statements. These are given in Figs. 4 and 5.
In both countries the birth-rate fifty years ago was remarkably high (well 58over 40 per thousand), and it has since fallen very rapidly to 26 or 27 per thousand. But in both of them the death-rate has fallen somewhat, and they now have the lowest death-rates in the world, that of New Zealand having been about 9.5 per thousand for many years past. So, instead of increasing slowly, their rate of natural increase by excess of births over deaths is actually the highest in the world (with the possible exception of Bulgaria). The natural increase of New Zealand during the last five years has been more than 50 per cent. greater than in Great Britain, instead of being less, as stated by Mr. Roosevelt; and instead of the birth-rate going on falling, it has, on the contrary, risen lately. The natural increase of Australia is 16 per thousand, which would cause the population to double in forty-four years, or to become five times as large in a century. The Australian birth-rate has been well maintained during the past seven years, and the death-rate has slightly declined; so the natural increase has slightly accelerated.
The foregoing statements are, of course, quite independent of immigration, and the following are the actual census figures for the increase of population.
| 1860 | 1870 | 1880 | 1890 | 1900 | 1910 | |
|---|---|---|---|---|---|---|
| Australia, population | 1,145,585 | 1,647,766 | 2,231,531 | 3,151,355 | 3,765,339 | 4,425,083 |
| Per cent. increase in decade | 43.8 | 35.5 | 41.2 | 19.5 | 17.5 | |
| New Zealand, population | 625,508 | 768,278 | 1,002,679 | |||
| Per cent. increase in decade | 22.6 | 30.5 |
It is worthy of note that in Australia, which is supposed to be needing population so much, the actual increase in the last two decades has been only slightly in excess of the natural increase. This means that the net immigration must have been very small, or that nearly as many people must have left Australia as entered it—a curious commentary on the alleged need for them.[8] New Zealand, on the other hand, shows a phenomenally large increase by the combination of natural increase and immigration.
8. In the five years 1901–05 there was an actual net loss of over 16,000 persons by excess of emigration.
It will be well at this point to examine the justification for the yellow peril theory as regards Australia. Japan has certainly moved in the opposite direction to Australia in having increased its birth-rate from 26 to 33 per thousand between 1891 and 1910. But its general and infantile mortality have also increased. Thus its natural increase to-day is only 12.5 per thousand as against the 16 or 17 per thousand of Australia and New Zealand, while its actual rate of increase is far short of theirs. Although the population of Japan is about ten times that of the whole of Australasia, every year makes the proportionate disparity of numbers less instead of greater; while as regards health, physique and financial resources, the advantage, of course, lies heavily with our people. That Australasia will be well advised to look 59to her defences may be granted; but there seems no reason whatever to be dissatisfied with the increase of her population.
Canada.—Little can be said about this part of our Empire, owing to paucity of statistical information; but that little is most interesting and significant. As regards the total population, the census returns show a very rapid increase, that of 34 per cent. (from 5,371,315 in 1901 to 7,204,838 in 1911) being without parallel in modern times. When we come to consider the birth-rate, however, a remarkable phenomenon appears. The only part of the Dominion for which vital statistics appear to be available is the Province of Ontario. Fig. 6 shows that the birth-rate of Ontario was only 22 or 23 per thousand in the eighties, and actually dropped to 19 in 1895, since then it has recovered (owing to an increased marriage-rate) to about 25 per thousand. Its lowest birth-rate was equal to that of France to-day. But the death-rate had also fallen—namely, to 10 per thousand, so that the natural increase was 9 per thousand, or not much behind that of most civilised countries. This fact may be commended to the consideration of those who think that the slow rate of increase of the French population is due to its low birth-rate.
The remarkable phenomenon now appears. The increase of the birth-rate in Ontario to 25 per thousand has been accompanied, not by a corresponding rise in the natural increase, but by an increase of the death-rate to 14 per thousand! So the additional births appear to have populated the graveyards rather than the country. It has been suggested to me by Dr. Stevenson that the increase in the birth and death rates of Ontario may be exaggerated, in that due allowance has not been made by the Canadian authorities for the effect of immigration. But even making the fullest allowance for this, there can be no doubt that both the birth and death rates have risen, and by nearly the same amount. The city of Toronto (Fig. 7) is a most striking example of the same phenomenon.
There need be no great difficulty in understanding this result. We have continually heard in the papers recently of poverty and unemployment in most of the large towns of Canada. Although the resources of the country are no doubt enormous, they can only be brought relatively slowly into operation, owing to the shortness of the summer and the difficulties of transport. The frequently quoted statement that her food exports show signs of lessening indicates that the inability of food to keep pace with an unrestricted population will prove true here as elsewhere.
Canada offers excellent opportunities for sturdy efficient workers, and will be able to support an immense population some day. But any attempt to crowd it rapidly with children or inefficient town-bred immigrants will only raise the death-rate, unemployment and labor unrest. The lives of women settlers are generally exceedingly strenuous and trying; and this, in combination 60with the long distances from medical or other help, makes the bringing up of large families very precarious.
South Africa.—Beyond the fact that the population of the Union of South Africa increased from 5,175,824 in 1904 to 5,973,394 in 1911 (i.e., an increase of 15.4 per cent. in seven years) little information appears to be available. The white population seems to have increased from 1,116,806 to 1,276,242 (i.e., by 14.28 per cent.) in the interval, while the native population increased from 3,491,056 to 4,019,006 (i.e., by 15.12 per cent.). But since no figures as to birth-rates are available nothing can be said beyond the fact that the actual increase works out at about 20 per thousand per annum, which is fairly high.
India.—We now turn from colonies mainly occupied by our own race and exhibiting our modern characteristics to a most marked degree, and come to our great Eastern possession which has preserved the ancient traditions of rapid reproduction. Writer after writer has launched into panegyrics on “the glorious fertility of the East,” and the Bishop of Ripon a few years ago issued this impressive warning: “Learn from the East. If we could but bring ourselves to do so, perhaps at no very distant period the Yellow Peril might turn out to be the White Salvation.”
That India is a country of high birth-rate is of course notorious. The custom of almost universal child marriage, and the anxiety which prevails among some (apparently not all) of the religious sects for a large posterity would alone render this inherently probable. According to the Statesman’s Year Book for 1913 the average birth-rate for India in the three years 1908–10 was 37.7 per thousand. This, however, was “officially but imperfectly recorded,” and the census report for 1901 gave the probable birth-rate for India as 48.8 per thousand. This figure is not at all an unlikely one, for the same rate has prevailed in Russia and parts of Egypt; but such figures as have appeared in the 1911 census report seem to confirm the lower estimate. Here are the figures for three of the important provinces:—
| Total for decade 1901–11 | Percentage of Population 1901 | Excess Births, – Deaths | Actual Increase | |||
|---|---|---|---|---|---|---|
| Births | Deaths | Births | Deaths | |||
| Bengal, Behar and Orissa | 29,351,442 | 25,373,322 | 39.10 | 33.80 | 3,978,120 | 4,552,293 |
| Punjab | 8,286,261 | 8,843,708 | 40.8 | 43.5 | –557,447 | 355,383 |
| Assam | 1,883,545 | 1,564,022 | 35.70 | 29.65 | 319,523 | 489,892 |
It is possible that these figures are correct, even without any restraint upon births, as the census report of 1901 mentioned that premature and repeated maternity combined with chronic under-nutrition appeared to lead to exhaustion and loss of fertility. In any case, however, the birth-rate counts among the highest at the present day.
But when we turn to the death-rate and the natural and actual increase of population there seems little reason for congratulation. The death-rate, 61given by the Statesman’s Year Book, for the three years above quoted was no less than 34.3, leaving a natural increase of only 3.4 per thousand—the lowest in our Empire, and nearly as low as that of France. The figures for Bengal, etc., above only show a natural increase of 4.7 per thousand, half that of Ontario at its lowest birth-rate of 19 per thousand; those for the Punjab reveal, despite the high birth-rate, an actual diminution of population by excess of deaths over births.
The emigration from India appears to be so infinitesimal in comparison with its population that the actual increase represents the natural increase almost exactly. In Fig. 1 is shown the variation of population in the whole of India and in the British Provinces according to the census returns.
| 1872 | 1881 | 1891 | 1901 | 1911 | |
|---|---|---|---|---|---|
| Total population | 206,162,360 | 263,896,330 | 287,314,671 | 294.361.056 | 315.001.099 |
| Per cent. increase in decade | 23.1 | 13.1 | 2.4 | 7.0 | |
| British Provinces | 195,840,000 | 199,200,000 | 221,380,000 | 231,600,999 | 244,279,888 |
| Per cent. increase in decade | .08 | 1.6 | 11.0 | 4.5 | 5.5 |
Thus the rate of increase of population has been exceedingly slow except as regards the totals for 1881 and 1891, and for the British Provinces in 1891. But the Census Commissioners themselves state that the first few enumerations rapidly increased in completeness, which probably accounted for a good deal of the two former increases; while as regards the British Provinces, there was an increase in area of no less than 25 per cent. between 1881 and 1901, which heavily discounts the increase of 11 per cent. in population in 1891. The average increase in the British Provinces comes out at only 4.3 per cent. per decade over the whole period from 1861 to 1911; so when the increase of area is taken into account it may be doubted whether there has been any great excess of births over deaths at all.
A more absolute contradiction to the theory that a “glorious fertility” produces numbers and vigor it would be difficult to conceive. India is a land of famine. We all know of the terrible holocausts of 1876–8 when over five million perished, and that of 1899–1901, which was held responsible for over a million deaths, besides numerous smaller ones. But as Mr. W. S. Lilly has written in India and its Problems, “We may truly say that in India, except in the irrigated tracts, famine is chronic—endemic. It always has been.” Sir Frederick Treves in his charming work, The Other Side of the Lantern, has expressed the same opinion, and he says:—“These are some of the great hordes who provide in their lean bodies victims for the yearly sacrifice to cholera, famine, and plague.” The average death-rate of 34.3 per thousand, which is probably underestimated, means, with a population of 315 millions, over ten million deaths annually. Were the Indian death-rate 10 per thousand as in Australasia, there would be only three million deaths. Hence, unless medical authorities can give good reason for postulating an inherent racial predisposition to premature death among the inhabitants of India, this means 62that at least seven millions of lives are wasted annually by starvation or the diseases to which it renders them an easy prey.
There can be no doubt in the mind of anyone who studies the figures, that India is a chronically, seriously over-populated country, despite the oft-quoted dictum of Sir William Hunter. That India might produce food enough to feed her present population need not be contested. But that any action on the part of the authorities will succeed in providing for an increase of ten millions annually is inconceivable. The whole Empire owes a tribute of gratitude and admiration to Sir A. Cotton whose magnificent irrigation schemes have so greatly increased the possibilities of agriculture. They have no doubt been the real cause of the 7 per cent. increase of population in the last decade. This, however, only means providing for two out of the seven millions to be saved; and irrigation like everything else has its limits.[9] Nothing will remove starvation, pestilence, misery and unrest from India, except the adoption by her people of the parental prudence of western nations.
9. In the article on India in the “Encyclopaedia Britannica” it is stated that the Irrigation Commission of 1901–03 emphatically asserted that irrigation alone could not cure famine.
The idea has been constantly put forward that the religious prejudices of the Indian population make such a contingency impossible. Is it certain, however, that this is so? The Census Report of 1901 suggested that in Assam some restraints upon births had been in vogue. In 1911, again, the Vice-President of the Calcutta Municipality, Babu Nilambara Mukerji, M.A., called attention to the extreme poverty caused by over-population, and strongly advocated such restraints. His address seems to have been received with considerable favor, and I have been asked to write articles for prominent native papers on the subject.
The project of encouraging emigration from India has, of course, been put forward. But the recent experiences in South Africa and elsewhere hardly favor this proposition, and Mr. Archer in an interesting article on “India and Emigration,” in the Daily News of December 26, pointed out that the real difficulty of over-population could not be appreciably lessened in this way.
Ceylon.—In view of the foregoing, reference may be made to Ceylon which has published its birth and death rates continuously since 1881, though I do not know what reliance can be placed on them. Fig. 8 shows that the birth-rate has rapidly risen from 27 to 41 per thousand, but that the death-rate and infantile mortality have also greatly increased.
The Empire.—The top line in Fig. 1 shows the increase of the population of the whole of our Empire according to the Statistical Abstract just issued. The figures are as follows:—
| Census | 1891 | 1901 | 1911 |
|---|---|---|---|
| Population | 345,356,000 | 385,572,000 | 417,268,000 |
| Per cent. increase in decade | 11.6 | 8.3 |
63Of course the increase from 1891 to 1901 was swelled by the addition of the Union of South Africa, etc., but the addition in the second period probably fairly represents the natural increase. The countries which go to swell this increase are those in which small families are the rule, and have rates of increase varying from 11 to 17 per thousand. It is India with the highest birth-rate which pulls down the average.
The population of the world is now probably about 1,800,000,000, and increasing at the rate of 5 per cent. or 6 per cent. in a decade. So our Empire includes about a quarter of the world’s population and is increasing more rapidly than the remainder.
No consideration of this subject would be complete if comparison were not made with the more important nations outside our own Empire. If Imperialist security depends upon numbers, it is relative, not absolute, numbers which count, and our attitude towards the falling birth-rate must depend upon what is happening among our rivals.
France.—The case of France appears to be the chief cause of the fears concerning the declining birth-rate, and she is variously spoken of as “dying,” “becoming depopulated,” “decadent,” etc. In Fig. 9, I have collected the vital statistics for France over the whole period of her declining birth-rate, i.e. from before the Revolution. They show the following characteristics:—
1. France is not becoming depopulated. Her population has been slowly but steadily rising ever since the Franco-German war, both actually and by excess of births over deaths, although in some years the deaths have exceeded the births.
2. The excess of births over deaths in the last decade 1901–10, though small, is double that of the previous decade, notwithstanding that the birth-rate fell from 22.2 to 20.6. It averaged about 48,000 per annum.
3. In 1781–84, before the decline of the birth-rate set in, the birth-rate had the high value of 38.9 per thousand. But instead of this giving a high natural increase of population, the death-rate was no less than 37 per thousand, giving an excess of births over deaths of only 1.9 per thousand—little more than that (1.2) of the last decade.
4. The enormous fall of the birth-rate from 38.9 to 20.6 per thousand, has been accompanied by a fall in the death-rate from 37 to 19.4 per thousand. Thus a fall of 18.3 in the birth-rate has been accompanied by a fall of 17.6 in the death-rate, and only a drop of .7 per thousand in the rate of increase.
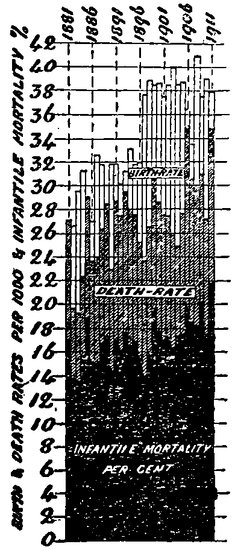
Fig. 8.—CEYLON.
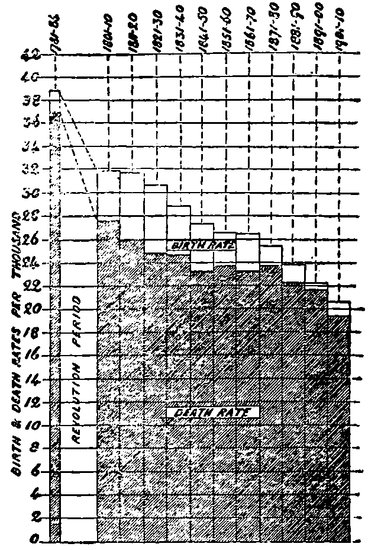
Fig. 9.—FRANCE.
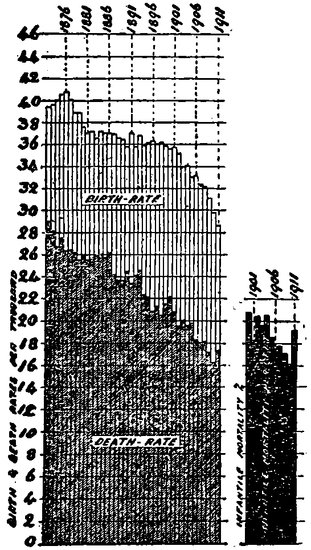
Fig. 10.—GERMANY.
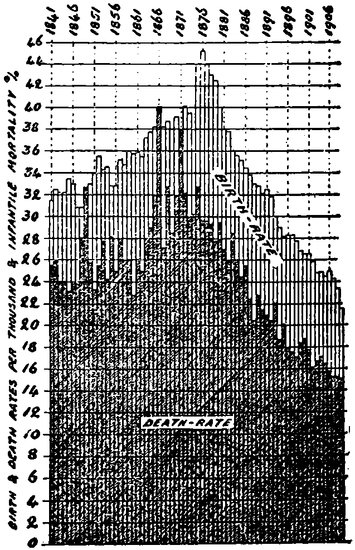
Fig. 11.—BERLIN.
5. The present low rate of natural increase in France is not necessarily due to its low birth-rate, as Ontario in Canada, with a similar birth-rate, had a death-rate of 10 per thousand, or a natural increase of 9 per thousand—nearly as great as our own. The low increase of France is therefore due to 65its high death-rate, not to its low birth-rate, and an explanation or remedy should be found for the former before objection is made to the latter.
6. Possibly as a result of the present agitation in France in favor of large families, the births in the first half of last year increased by 8,000 over those of the corresponding period of 1912. Instead of producing a greater increase of population, the deaths increased by 12,000, so that the survivals actually diminished.
It appears from the foregoing that while it is true that France is increasing in population much more slowly than other countries, there is no justification for believing that an increased birth-rate would populate it more rapidly. Much more likely is it that the result would be the same as that shown in Ontario and other countries—a higher death-rate without any advantage as regards numbers.
Germany.—As France is held up as the awful example of a low birth-rate, so is Germany regarded as the good example of a high one. It is certainly fear of Germany that is responsible for so much of the anxiety concerning our birth-rate.
That the population of Germany is increasing very rapidly is quite true, and it certainly has also a relatively high birth-rate. (Fig. 10). But the birth-rate has fallen rapidly since 1876, and despite this the natural increase of population has actually accelerated, because the death-rate has fallen still more rapidly. As the German death-rate is still considerably above the 9 or 10 per thousand line, there is plenty of room for this process to continue. The curve of actual increase of population in Fig. 1, shows that it has become exceedingly high of late years, despite the great fall in the birth-rate.
Those, however, who still think that Germany’s high birth-rate is a source of advantage to her may be consoled to know it will not continue long. The fall in the last few years has been phenomenal; and the statement made in a German paper a few days ago that at the present rate the German birth-rate will be down to that of France in ten years’ time appears to be justified. The birth-rates of her large towns are already close to this point (Berlin 20.4, Hamburg 21.8, Dresden 20.2, Munich 21.9, while that of London is still about 24) and the country districts are sure to follow. But the example of Berlin is a most striking one as to the fallacy of regarding high birth-rates as conducive to rapid increase. Fig. 11 shows that the birth-rate of Berlin rose with great rapidity from 32 per thousand in 1841 to over 45 in 1876, since when it has fallen even more rapidly. But, neglecting sudden variations due to war and epidemics, the death-rate has risen and fallen in such close correspondence as to produce comparatively little change in the rate of natural increase. The variation of the infantile mortality is very similar. On all grounds, therefore, it seems difficult to see what advantage Germany has derived 66from her high birth-rate, and the disadvantages were so obvious that it is little wonder that the German people have decided in favor of a low one.
Austria shows very similar variations to Germany.
Russia.—Russia has the largest population of any European nation, 120,588,000 in 1911. Its birth-rate for many years was the highest in the world, very nearly 50 per thousand. But its death-rate and infantile mortality have been the highest in Europe, so that its rate of increase of population, though rapid, has been less than that of New Zealand or Australia. Over two millions of unnecessary deaths have taken place annually, and one infant in every four (or over a million annually) dies in its first year. The war with Japan, a country of half its population and a much lower birth-rate, strikingly illustrated the inefficacy of mere numbers. In the Standard of March 6, it was stated that although the general recruiting standard in Russia is lower than in Austria, France, Germany, or Great Britain, the rejections in many localities reach the enormous figure of 70 per cent.
The Netherlands.—The foreign countries already dealt with are quite sufficient to give us a fair idea of our position among the great powers as regards the birth-rate question. No thoughtful person, however, can fail to see that this has another aspect which has generally been quite overlooked. It will therefore be of special interest to study the record of a nation in which this has been kept in view for many years. Holland is an intensely patriotic country, and its need for military efficiency is beyond dispute. It is inconceivable that her statesmen could contemplate a policy in any way detrimental to this. Yet it appears that in 1881 an organisation having as its direct object the reduction of the birth-rate, especially among the poor, was formed in Amsterdam, and that it received the warm support of Dr. van Houten, Minister of the Interior, and of Mynheer N. G. Pierson, the Finance Minister. It was thus enabled to conduct an energetic propaganda in favor of small families among the poorest classes, whose means or health did not permit them to do justice to large families. In 1895 its work had become so appreciated that it was approved by Royal Decree as one of the Societies of Public Utility. To-day it is a large and flourishing association with medical and other helpers in all the great centers. Thus in Holland the diminution of the birth-rate has been favored and directed on humanitarian and eugenic lines; and there has been a tendency for the State to become more individualistic in character, rather than to adopt that policy of State assistance which has been forced on most other nations by the gravity of their social problems, and which, by pressing on the educated classes, has led them seriously to restrict their numbers.
The results of their policy as regards the numbers and health of the population can be seen from Fig. 12. The birth-rate has fallen steadily and rapidly, especially in the last decade. The death-rate, however, has fallen so much more rapidly, that it has now reached 12.3 per thousand in 1912—the 67lowest figure in Europe; and the natural increase has reached 15.7 per thousand, the highest figure in Western Europe. The infantile mortality has also fallen more rapidly than in any other country. Indeed, Amsterdam and The Hague, the principal centres of the propaganda, had the lowest general and infantile mortality of all the great cities of the world, according to our Registrar-General’s Annual Summary for 1912.
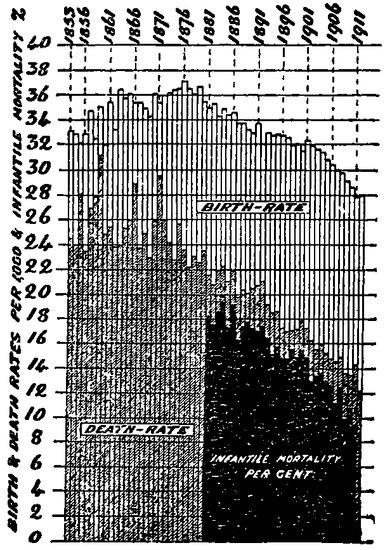
Fig. 12.—THE NETHERLANDS.
When we turn from the question of numbers to the physical and social condition of the people, the results are even more gratifying. Those who have traveled in Holland will, I think, admit that the country looks prosperous, and the men, women and children robust and contented. Slums such as we have in our great cities seem practically non-existent; nor is there any sign of the stunting and anaemia so noticeable in our large towns, and even in our countryside. Dr. Soren Hansen in the Eugenics Congress of 1912 stated that the average stature of the Dutch people had increased by four inches in the last fifty years. The army records given in the official Year Book of the Netherlands are also most striking. The number of young men drawn annually for conscription by lot has increased from 27,559 in 1865 to 48,509 in 1911 (out of a population of 6,000,000); and of these the proportion over 5 ft. 7 in. in height has increased from 24.5 per cent. to 47.5 per cent., while that of those under 5 ft. 2½ in. has fallen from 25 per cent. to under 8 per cent. This is doubtless due to the fact that in Holland the poorest and least fit have been encouraged to be prudent, while in our country they have been having the largest families—the fitter classes having smaller families in 68consequence. Real wages which have fallen here and in Germany have apparently gone up in Holland, and her agriculture has rapidly improved. In every way that I have been able to test, her prosperity and progress has been most satisfactory. Moreover, Holland stands next to ourselves as a successful coloniser. Her possessions in the East and West Indies occupy an area of 783,000 square miles with a population of 38,000,000 (seven times her own population), 81,000 being Europeans. Germany, with a home population ten times greater, has colonies aggregating 1,029,000 square miles with a population of only 14,000,000 inhabitants, of whom but 25,000 are whites.
In view of all these records I cannot think that any unbiassed person will be able to avoid the conclusion that large numbers and national efficiency are not to be secured by a high birth-rate, especially in the lower strata of society. High birth-rates to-day invariably mean high general and infantile death-rates, and, when accompanied by humanitarian legislation, a serious process of reversed selection.
The explanation of this apparent paradox lies in the fact, which never seems to be properly understood, that the population of the world and of nearly all countries is constantly being kept in check by insufficiency of food. A French statistician, M. Hardy, has calculated (and his figures, though challenged by great authorities, have now been accepted) that if the total food production of the world were fairly distributed among its inhabitants, the ration of proteids available for each would only be two-thirds of that recognised as necessary for efficiency. Mr. Seebohm Rowntree has shown that large numbers of families in our own country—the richest in the world—have deficiencies of protein in their diet by amounts up to 40 per cent., and over 2,500,000 adult male workers have wages of 25s. a week or less, upon which with the present cost of living and rent in towns it is impossible to bring up more than three children properly. As a result, whenever families are large a considerable proportion of the children die, and of those who survive many grow up stunted and incapable of assimilating a good training. The over-crowding caused by large families with an ever decreasing margin for rent is also a potent cause of disease and of immorality—the latter evil being further greatly intensified by the economic difficulties in the way of marriage that are the chief bar to the prevention of those terrible diseases for which the Royal Commission, presided over by our Chairman, is investigating a remedy.
That the rate of increase of population of a country depends in almost every case upon its power of feeding its people by its own or imported food, and not upon its birth-rate, is a matter which statesmen will have to recognise; and those who are anxious for the increase of the population of our 69country and Empire, should turn their attention to the acceleration of food production instead of deploring the declining birth-rate. No intelligent person will claim that the food producing possibilities of the world are exhausted, but it does appear difficult to increase them at more than a very slow rate (probably at present not more than 6 per cent. or 7 per cent. in a decade); and the world’s population cannot increase faster than the food does. Irrigation in India has been followed by an increase in population far greater than before, and encouragement of agriculture or of the industries which bring food to this country is the only means by which our increase of population can be accelerated. No shuffling of the incidence of taxation, and no humanitarian schemes, will affect it—except prejudicially by favoring the increase of the inefficient rather than the efficient. Nor will emigration, the panacea of the orthodox Imperialist, solve the problem. We do not want effective producers to leave us, and these are the only people our colonies really desire. Our town-bred weaklings are frequently less fitted to succeed in the Colonies than at home, as the experience of Canada appears to testify. It has been said that “no Empire can survive which is rotten at the core”; and if we persist in the policy of encouraging the excessive reproduction of the poor, of taxing the capable for their support, of keeping about a third of our men and women unmarried, and of seeing many of our best emigrate for want of decent prospects at home, we need not be surprised if our Imperial efficiency diminishes.
On the other hand, if we consider the example of Holland we may be assured that a further fall in the birth-rate among the poorer classes will be accompanied by an immediate and progressive improvement in their conditions, by a checking of the output of physical and mental defectives, and by a gain in the national efficiency, and probably also in the rate of increase of our population. As the Bishop of Ripon said at the Church Congress of 1910: “If the diminution of the birth-rate could be shown to prevail among the unfit, we might view the phenomenon without apprehension, and we might even welcome the fact as evidence of the existence of noble and self-denying ideals.” There is no reason why the death-rate in any part of our Empire should be higher than the 9 per thousand of New Zealand, where poverty as we know it scarcely exists. The birth-rate of Great Britain can therefore fall to 20 per thousand before our normal natural increase of 11 per thousand is reduced. As this paper is being concluded, the Registrar-General’s figures for 1913 have come to hand, and show that the fall of the birth-rate in the last three years has been accompanied by a recovery in the natural increase to 10.8 per thousand.
In the accompanying diagrams white strips imply birth-rates, shaded strips death-rates, and black strips infantile mortality, or deaths of children under one year. The amount of the white strip visible above the shaded strip is, of course, the excess of birth over death-rate, or the rate of natural increase of population.
Fig. 1.—Shows the relation between birth and death-rates and infantile mortality in various countries in 1901–05.
Fig. 2.—Relation between birth-rate and corrected death-rates in various countries. (This shows that France is healthier than appears in Fig. 1.)
Fig. 3.—Shows relation between birth and death-rates from various causes in five districts of London.
Fig. 4.—Relation between the birth-rate and death-rate for various arrondissements of Paris in 1906. (Note that the increase in the Elysée quarter is as high as the average in the quarters of high birth-rate.)
Figs. 5 and 6.—Variations of the total population of birth- and death-rates in the United Kingdom and the German Empire. (Note that the fall in the death-rate corresponds fairly closely to that in the birth-rate.)
Fig. 7.—The same for France. (Note that the population is still increasing, although slowly.)
Fig. 8.—Birth and death-rates for France since 1781. (Note that the rate of increase of population in 1781 was no higher with a birth-rate of 39 per 1,000 than in 1901–6 with a birth-rate of only 21 per 1,000. A fall of 17.8 per 1,000 in the birth-rate has resulted in a fall of 17.5 per 1,000 in the death-rate.)
Fig. 9.—Birth and death-rates and infantile mortality for England and Wales. Also marriage rate, fertility of married women, illegitimacy, and variation of diseases. (Note that the illegitimate birth-rate has fallen to half since the fall of the birth-rate set in.)
Fig. 10.—Birth and death-rates and infantile mortality in the Netherlands. (Notice the rapid increase of population as the death-rate falls, and the great fall of infantile mortality, probably due to the practical work of the Dutch Neo-Malthusian Birth Control League among the poor.)
Figs. 11–13.—Protestant Countries. (Notice the correspondence between the birth and the death-rates and infantile mortality in all.)
Figs. 14–16.—Roman Catholic Countries. (Note that the fall of the 71birth-rate has taken place almost equally with that in the Protestant countries, and with the same result.)
Figs. 17–20.—The only four countries in which the birth-rate is approximately stationary. (Notice that the death-rate has not fallen—except perhaps in Russia—and that the infantile mortality has not fallen. Also that the highest birth-rate produces the highest death rate and infantile mortality, and the lowest birth-rate the lowest mortality.)
Figs. 21–24.—The only four countries with rising birth-rates. The death rate and infantile mortality have increased in every one.
Fig. 25.—Australia. The death-rate has fallen with the birth rate, and is now only about 10 per 1,000.
Fig. 26.—New Zealand. The only country in which the fall in the birth-rate has not produced a fall in the death-rate, and which is not therefore over populated. The infantile mortality is the lowest in the world, and the death-rate less than 10 per 1,000, which gives us an ideal which we can reach in all countries by lowering the birth-rate sufficiently.
Fig. 27.—The City of Toronto. The birth-rate has fallen and afterwards risen. The death-rate has fallen with the birth-rate, and afterwards risen, indicating that the improvements in sanitation have not been the cause of the falling death rate in other countries.
Fig. 28.—Berlin. The birth-rate rose rapidly from 1841 to 1876, and afterwards fell even more rapidly. The death-rate, except for epidemics and wars, rose and fell in almost precise correspondence with the birth-rate.
Fig. 29.—Berlin. The dotted area shows the fertility rate or births per 1,000 married women, and indicates the remarkably rapid fall since 1876. The correspondence of the infantile mortality with the birth-rate shown in Fig. 28 is very close.
Figs. 30 and 31.—Europe and Western Europe. These show that the total population of Europe is increasing faster the more the birth-rate falls, while in Western Europe the birth and death-rates correspond almost exactly. Calculations made from this show that about 25,000,000 fewer births and deaths have occurred in Europe since 1876, due to the fall in the birth-rate caused by the Knowlton Trial and the Neo-Malthusian movement. It should be noted that in the great majority of cases the decline of the birth-rate commenced in 1877, the year of the Knowlton Trial.
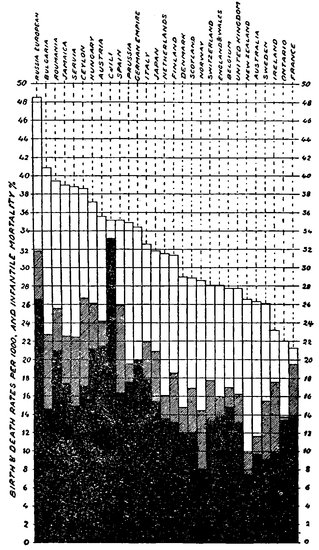
Fig. 1.
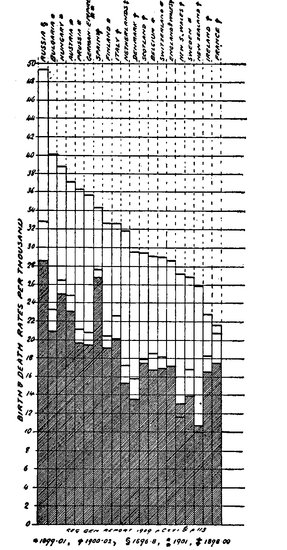
Fig. 2.
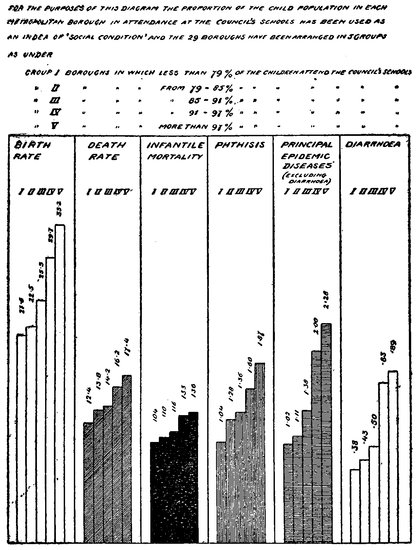
Fig. 3.
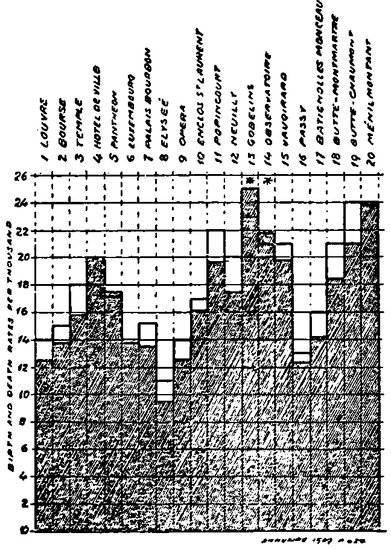
Fig. 4.
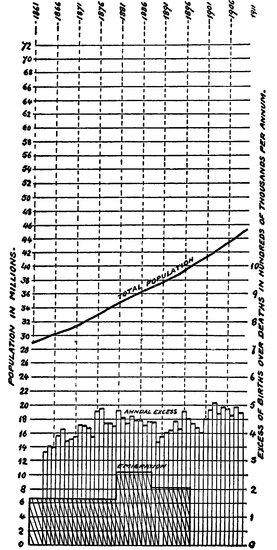
Fig. 5.
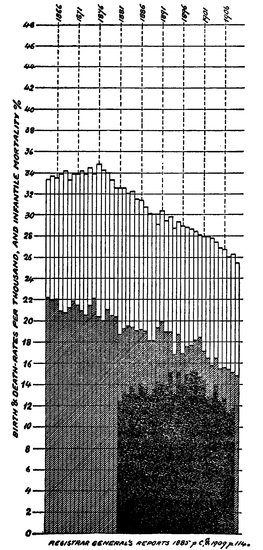
Fig. 5a
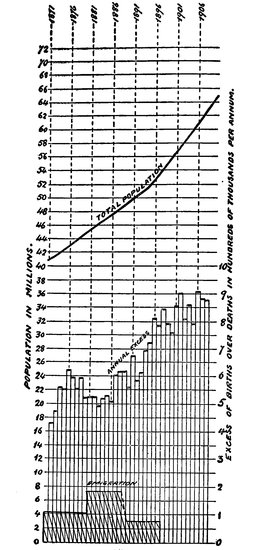
Fig. 6
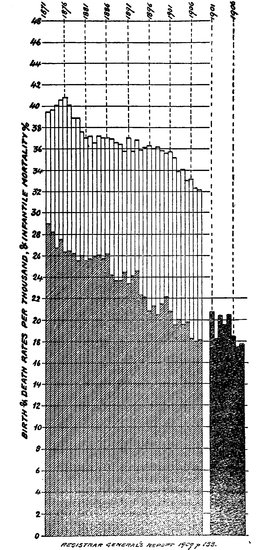
Fig. 6a.
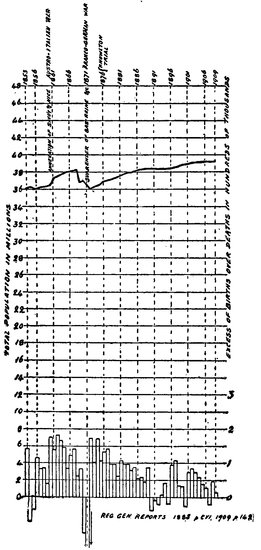
Fig. 7
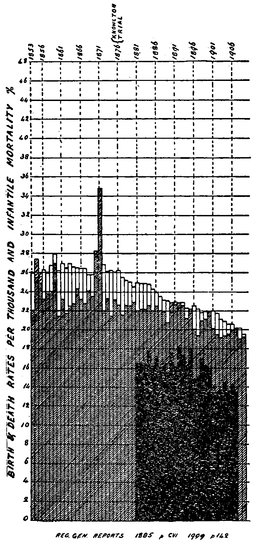
Fig. 7a.
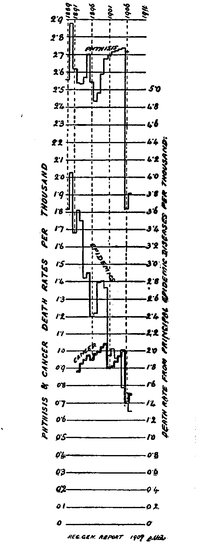
Fig. 7b.
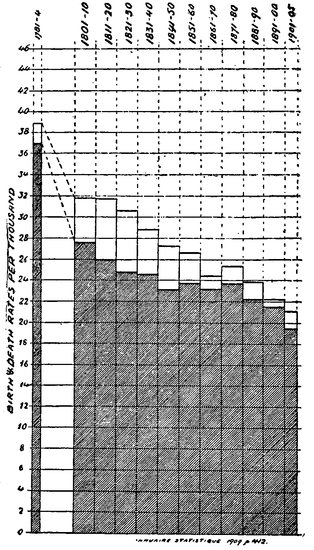
Fig. 8.
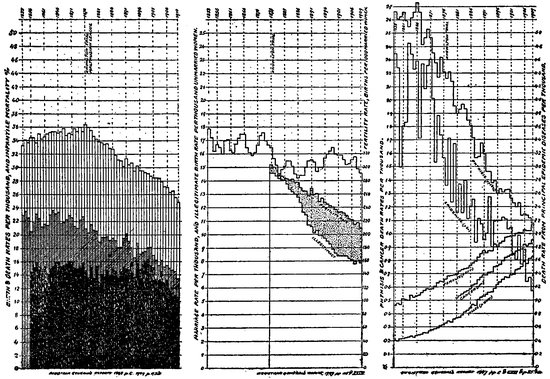
Fig. 9
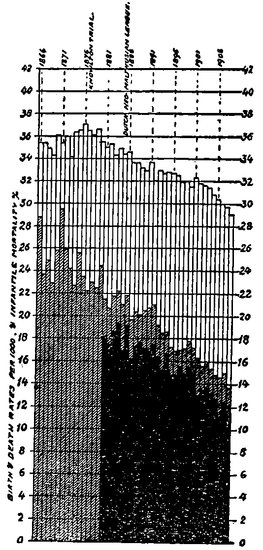
Fig. 10.
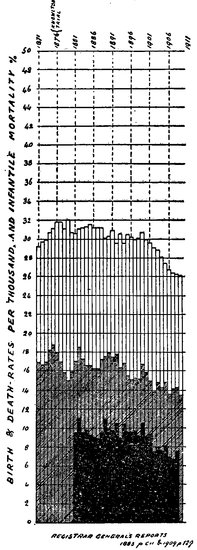
Fig. 11.
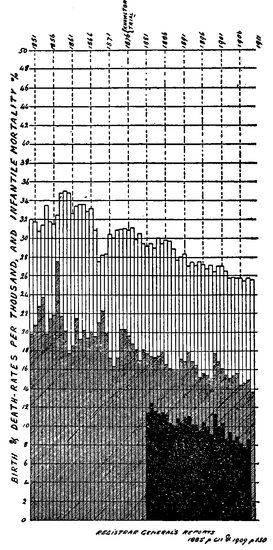
Fig. 12.
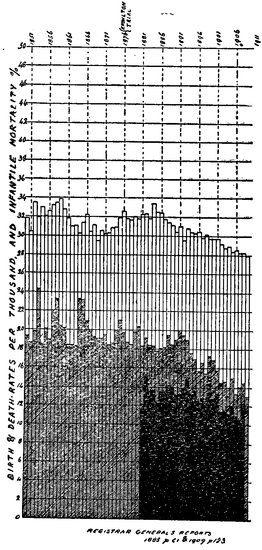
Fig. 13.
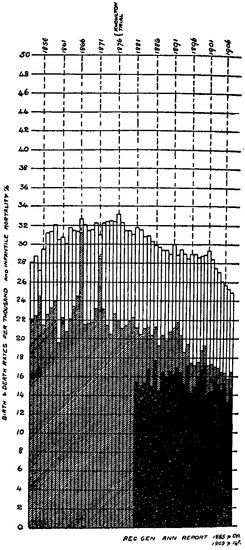
Fig. 14.
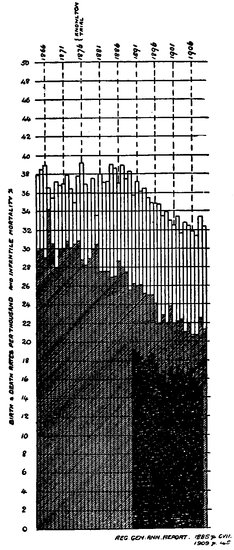
Fig. 15.
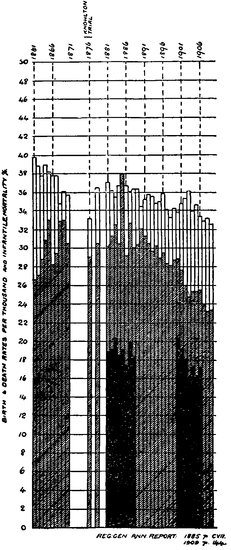
Fig. 16.
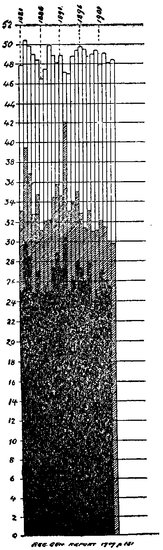
Fig. 17
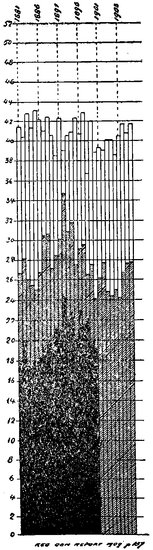
Fig. 18
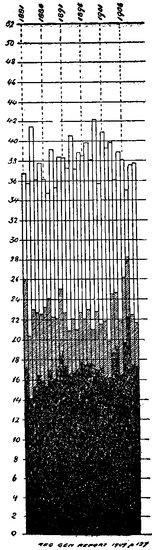
Fig. 19
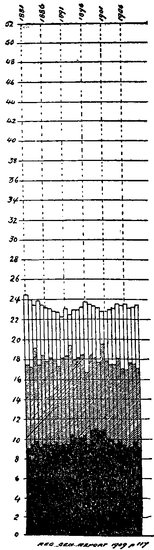
Fig. 20
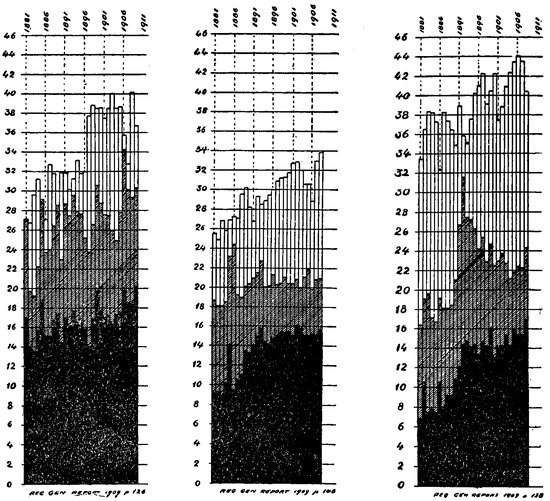
Figs. 21-23
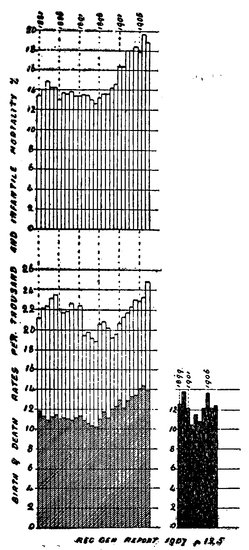
Fig. 24
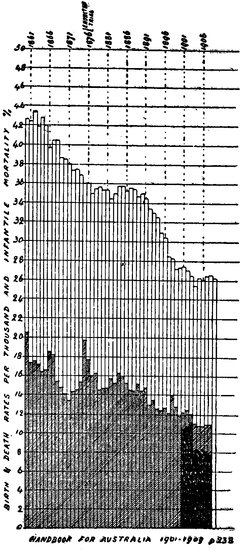
Fig. 25
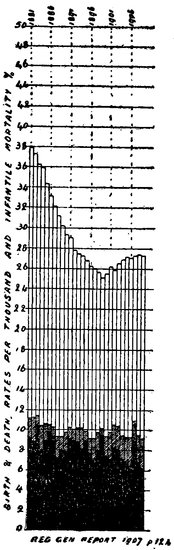
Fig. 26
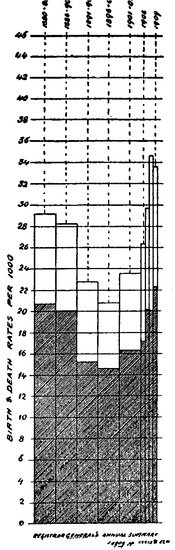
Fig. 27
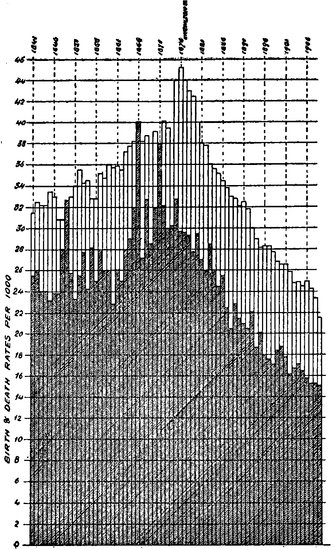
Fig. 28
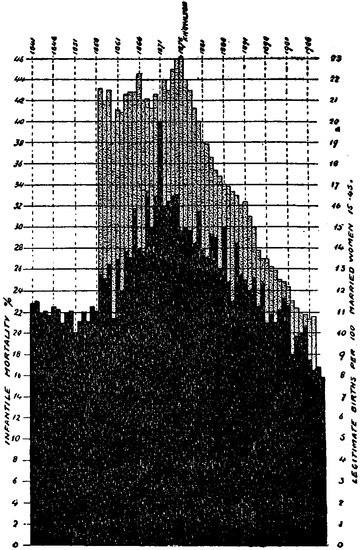
Fig. 29
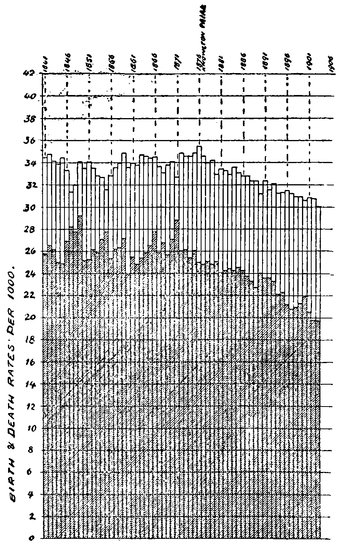
Fig. 30
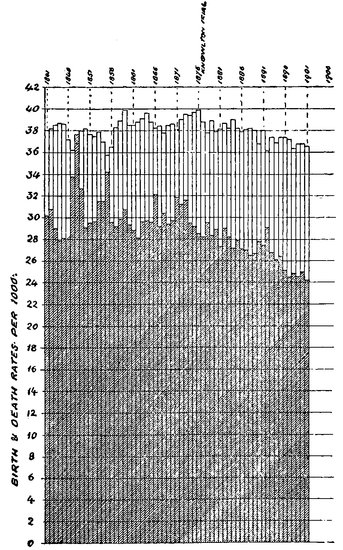
Fig. 31
In the preceding pages it was stated that a high birth-rate is always accompanied by a high infant mortality. The material presented in this chapter demonstrates the fact that ignorance of methods to prevent conception forces the wives of ill-paid wage-workers to bear an excess of unwanted children. Figures are adduced to show an appalling death rate of infants under five years of age and the economic distress of the survivors in families unwanted and too large.
MEDICAL GYNECOLOGY. Howard A. Kelly, A.B., M.D., LLD., Professor of Gynecological Surgery in Johns Hopkins University, and Gynecologist to the Johns Hopkins Hospital, etc. D. Appleton Co. New York and London, 1912.
As long as a community can rest content in the belief that a large infant mortality is the natural method of reducing the race of the unfit, the doctrine of laissez-faire can be accepted with complaisance. If, however, it seems probable that the influence of environment must be reckoned as a greater cause of infant mortality and of physical unfitness than the influence of heredity, it may be wiser for society, as it certainly will be easier, to preserve the lives and health of the children born, than to stimulate an increase in a birth rate now diminishing. As it is an open question whether the race as a whole suffers mental and physical deterioration from a diminished rate of production among the superior stocks, it is unquestionably a matter of public policy, as well as of common humanity, that conditions of living in communities should be made favorable to the preservation of the life and health of all infants and children. P. 41.
EUGENICS AND RACIAL POISONS. Prince A. Morrow, M.D. Pamphlet published by the Society of Sanitary and Moral Prophylaxis, N. Y., 1912.
Observation shows that the class known as degenerates is increasing much more rapidly than the general population and that their average duration of life has been lengthened. Diseases may be cured, but degeneracy, which is usually due to some inherited defect in the physical, mental or moral nature 94of the individual, is rarely amenable to curative treatment. It is only through applied eugenics that the vast volume of disease and degeneracy which flows through the channels of heredity can be prevented. Obviously this can be accomplished only through education and legislative restriction upon the procreation of the unfit.
In the making of the child, the mother not only contributes one half of the ancestral qualities which enter into its constitution, but furnishes all the nutrition and energy which serve to support its life. From this point of view the mother is the supreme parent of the child, she is the source of its life and from her blood is drawn the material which contributes to its growth and development. The welfare of the mother is the welfare of the child. We have thus come to recognize the dominant influence of the mother’s relation to the health, as well as the life of the race. A high standard of physical motherhood is the most favorable asset of a nation. Havelock Ellis, in his recent work, on the Psychology of Sex, says, “Nations have begun to recognize the desirability of education, but they have scarcely yet come to recognize that the nationalization of health is even more important than the nationalization of education. If it were necessary to choose between the task of getting children educated and the task of getting them well born and healthy, it would be better to abandon education. There have been many great people who never dreamed of national systems of education; there has been no great people without the art of producing healthy and vigorous children.”
Newman, the distinguished author of the work on “Infant Mortality” declares that the problem of infant mortality is not one of sanitation alone, or housing, or indeed of poverty as such, it is mainly a question of motherhood.
It is not probable that the scientific methods which have been successfully applied to plants and the selective breeding of animals will ever replace the haphazard methods of human reproduction.
There is no fact better established than that a man can transmit only that which he is. If his system is weakened by excess or tainted with disease he can beget only physical weakness, or beings tainted with disease. The syphilitic, the consumptive, the epileptic, the alcoholic, should not produce his kind.
NEO-MALTHUSIANISM AND RACE HYGIENE IN “PROBLEMS IN EUGENICS.” Vol. 2. London, 1913. Dr. Alfred Ploetz, President of the Int. Soc. for Race Hygiene.
Arthur Geissler concluded from a study of about 26,000 births of unselected marriages among miners that the mortality of children was least in 95the four first-born, and then increased to a very high rate. Following are Geissler’s figures, (marriages with only one or two children are omitted).
| Deaths during first year | |
|---|---|
| 1st born children | 23% |
| 2nd born children | 20% |
| 3rd born children | 21% |
| 4th born children | 23% |
| 5th born children | 26% |
| 6th born children | 29% |
| 7th born children | 31% |
| 8th born children | 33% |
| 9th born children | 36% |
| 10th born children | 41% |
| 11th born children | 51% |
| 12th born children | 60% |
INFANT MORTALITY. Results of a Field Study in Johnstown, Pa., based on Births in one calendar year. By Emma Duke, Infant Mortality Series, No. 3. Bureau Publication No. 9. U. S. Department of Labor, Children’s Bureau.
The pamphlet embodies the result of a field study in Johnstown, Pa., based on one calendar year. The inspection was made in 1913, of the 1911 babies, so that even the last born baby included had reached its first birthday—or rather had had a chance to reach its first birthday; many of them were dead long before that day. Every mother of a 1911 baby was visited. She was questioned about the health of that child and all her other children. The report takes up the familiar factors—neighborhood environment, sanitary conditions, sewage, housing, nativity, attendance at birth, feeding, age of mother, and like matters. Full information is given on these points. Then the report considers infant mortality from a novel viewpoint—the relation of the death rate to the size of the family. The Johnstown statistics include families varying in number from one child to ten and over, and varying in health from none living to all living. The result of the study of infant mortality in relation to the size of the family is thus stated: “The statistics, based on the results of all her reportable pregnancies, show a generally higher infant mortality rate where the mother has had many pregnancies, but there is not always an increase from one pregnancy to the next.” The following table shows this tendency. It is based on the reproductive histories of 1,491 married mothers who had 5,617 births. Miscarriages are not included.
| 96 | |
| Infant Mortality Rate for all Children borne by Married Mothers: Table 36 | |
|---|---|
| Number of Pregnancies. | Infant Mortality Rate. |
| 1 and 2 | 108.5 per 1,000 |
| 3 and 4 | 126.0 per 1,000 |
| 5 and 6 | 152.8 per 1,000 |
| 7 and 8 | 176.4 per 1,000 |
| 9 or more | 191.9 per 1,000 |
| Average | 149.9 per 1,000 |
In contemplating these figures we think immediately of wage-earning mothers away from home, ignorant feeding, and lack of care. These are powerful factors in raising the death rate.
Of all the 1911 babies who died before they were a year old, 37% died in the first month of life. So much pain and misery and then no baby after all. All the skill in the world could not have saved those babies who lived only long enough to die.
The infant mortality rate for the babies whose fathers earn under $521 is almost twice as great as for those born into families in the most prosperous group. These figures strengthen the conclusion reached in the study of the babies born in 1911, namely that the economic factor is of far-reaching importance in determining the baby’s chance of life.
One of the tables showing the influence of the economic factor, is calculated on the basis of 1,434 live-born babies with fathers. 187 of these babies succumbed during the first year, giving a general mortality rate of 130.7 per 1,000. In these families a very few of the mothers worked outside the homes.
| Father’s earnings | Live-births | Deaths 1st year | Infant mortality rate |
|---|---|---|---|
| Under $625 | 384 | 82 | 213.5 |
| $625 to $899 | 385 | 47 | 122.1 |
| $900 or more | 186 | 18 | 96.8 |
| Ample | 476 | 40 | 84.0 |
Expressed in words, this table asserts that when the family income is under $625 a year, the children born alive die before the first birthday at the rate of 213.5 to the 1,000. In striking contrast when the income is $900 or more, they die only 96.8 to the 1,000. “Ample” was the expression used when the investigator could not obtain exact information as to the amount, but saw no evidence of actual poverty. The same ratio held good when it was calculated for the native-born mothers alone and when it was calculated for the foreign-born mothers alone. Even where mothers are American-born women, staying at home to look after their children, the amount of money to be spent on the child strongly influences its chance of life and death.
97According to this table the superiority which children in indigent households show over children in well-to-do households is preeminent skill in dying. When father earns $12 a week the children die at the rate of 213 per 1,000; but when father earns $18 a week, only 96 children per 1,000 pass away the first year of their lives. The lower the father’s wages, the higher the babies’ death rate. Many a death certificate should read, “Died of poverty.”
The following table is compiled from the 5,617 children borne by 1,491 married mothers, in Johnstown, Pa.
| Order of Birth | Deaths per 1,000 |
|---|---|
| 1st and 2nd born children | 138.3 |
| 3rd and 4th born children | 143.2 |
| 5th and 6th born children | 177.0 |
| 7th and 8th born children | 181.5 |
| 9th and later born children | 201.1 |
Apparently the size of the family has much to do with the child’s chance of living, and apparently the earlier in the succession the child is born, the better chance of life it possesses. Death warrants await the coming of the youngest born.
| Table 42.—Infant mortality rate for all children of married mothers included in this investigation, distributed according to the father’s earnings. | |
|---|---|
| Father’s annual earnings | Infant mortality rate |
| Under $521 | 197.3 |
| $521 to $624 | 193.1 |
| $625 to $779 | 163.1 |
| $780 to $899 | 168.4 |
| $900 to $1,199 | 142.3 |
| $1,200 to $1,200 and over | 102.2 |
The term infant mortality, used technically, applies to deaths of babies under 1 year of age. An infant mortality rate is a statement of the number of deaths of such infants in a given year per 1,000 births in the same year. Some countries include stillbirths in making the computations, but this method is not generally followed in this country nor has it been followed in this report.
Ordinary procedure is to compare the live births in a single calendar year with the deaths of babies under 12 months of age occurring in that same year, even though those who died may not have been born within the calendar year of their death. The infant mortality rates in this report, however, have not been computed on the usual basis, but for the purpose of securing greater accuracy in measuring the incidence of death this bureau has considered, in making the computation, only so many of the babies born in the year 1911 as could be located by its agents, and has compared with this number the number of deaths within this group of babies who died within one year of birth, even though some of these deaths may have occurred during the calendar year 1912.
Infant mortality can be accurately measured in no other way than by means of a system of completely registering all births as well as all deaths. In 1911 the United States Bureau of Census regarded the registration of deaths as being “fairly complete (at least 90 per cent. of the total)” in 23 States, but the same degree of completeness in the registration of births was found only in the New England States, Pennsylvania, and Michigan, and in New York City and Washington, D.C. An exact infant mortality rate for the United States as a whole cannot be computed owing to this generally incomplete registration. In the 1911 census report on mortality statistics, however, the infant mortality rate is estimated at 124 per 1,000 live births. How this estimated rate compared with the computed rates for other countries is shown in the following summary:
| 102 | ||||
| Deaths of Children under 1 Year of Age per 1,000 Live Births, by Quinquennial Periods from 1901 to 1910, and also for the Single Calendar Years 1909 to 1910.[10] | ||||
|---|---|---|---|---|
| COUNTRY. | 1901 to 1905 | 1906 to 1910 | 1909 | 1910 |
| Chile | 306 | 315 | 315 | 313 |
| Russia (European) | ([11]) | |||
| Austria | 215 | |||
| Hungary | 212 | 204 | 212 | 194 |
| Prussia | 190 | 168 | 164 | 157 |
| Jamaica | 174 | 191 | 174 | 188 |
| Spain | 173 | |||
| Ceylon | 171 | 189 | 202 | 176 |
| Italy | 168 | 155 | ||
| Japan | 154 | 166 | ||
| Servia | 149 | |||
| Belgium | 148 | 137 | ||
| Bulgaria | 148 | |||
| France | 139 | 120 | ||
| England and Wales | 138 | 117 | 109 | 105 |
| The Netherlands | 136 | 114 | 99 | 108 |
| Switzerland | 134 | 115 | ||
| Finland | 131 | 117 | 111 | 118 |
| Scotland | 120 | 108 | ||
| Denmark | 119 | 98 | ||
| Province of Ontario | 114 | 127 | 131 | 123 |
| Ireland | 98 | 94 | 92 | 96 |
| Australian Commonwealth | 97 | 78 | 72 | 75 |
| Sweden | 91 | 72 | ||
| Norway | 81 | 72 | ||
| New Zealand | 75 | 70 | 62 | 68 |
10. From the Seventy-third Annual Report of the Registrar General of Births, Deaths, and Marriages in England and Wales (1910). London, 1912.
11. Available only for the period from 1896 to 1900, when it was 261.
When it had been decided by the Children’s Bureau to make infant mortality the subject of its first field study and to include all babies born in a given calendar year, regardless of whether they lived or died during their first year, advice and cooperation were enlisted of mothers, physicians, nurses, and others experienced in the care of children, and also of trained investigators and statisticians, in the preparation of a schedule which was submitted to them for criticism.
With its limited force and funds it was not possible for the Children’s Bureau to extend its inquiries throughout the entire United States. It was therefore decided to make intensive studies of babies born in a single calendar year in each of a number of typical areas throughout the country that offered contrasts in climate and in economic and social conditions, the results to be eventually combined and correlated. It was necessary to restrict the choice of the first area to a place of such size as could be covered thoroughly within a reasonable time by the few agents available for the work.
Johnstown, Pa., was the first place selected. It is in a State where birth registration prevails, and hence a record of practically all babies could be secured; it is of such size that the work could be done by a small force within a reasonable period, and it seemed to present conditions that could with interest be contrasted with conditions typical of other communities. Moreover, the State commissioner of health and the State registrar of vital statistics 103were both working zealously to enforce birth-registration laws; both were actively interested in reducing infant mortality, and they welcomed a study of the subject in their State. In Johnstown the mayor, the president of the board of health, the health officer, and other local officials all showed the same spirit of hearty cooperation and interest.
Inasmuch as the study was confined to babies born in a single calendar year and work was begun in January, 1913, the latest year in which the babies could have been born and still have attained at least one full year of life was 1911.
Work was begun on January 15, 1913, with the transcription from the original records at Harrisburg of the names and other essential facts entered on the birth certificates of babies born in 1911, and, if the baby had died during its first year of life, items on the death certificate were also copied.
In the meantime the people of Johnstown through the press, and through the clergy in the foreign sections, had been informed of the purpose and plan of the investigation. Without the friendly spirit thus aroused and the interest manifested by the Civic Club and other organizations the work could not have been brought to a successful issue. The investigation was absolutely democratic; every mother of a baby born in 1911, rich or poor, native or foreign, was sought, and it is interesting to note refusals were met with in but two cases.
The original plan was to limit the investigation to those babies born in the calendar year selected whose births had been registered, the purpose being to secure facts concerning a definite group and not to measure the completeness of birth registration. Shortly after beginning the work, however, agents of this bureau were told that the Serbian women in Johnstown seldom had either a midwife or a physician at childbirth; that they called in a neighbor or depended upon their husbands for help at such times, or that they managed alone for themselves, and that therefore their babies usually escaped registration. The omission of these babies meant the exclusion of a number of mothers in a group that was too important racially to be omitted from an investigation embracing all races and classes. Accordingly a list of babies christened in the Serbian Church and born in the year 1911 was secured and an attempt made to locate them. In addition an agent called at each house in the principal Serbian quarter to inquire concerning births in 1911. A number of unregistered babies of Serbian mothers were thus found and included in the investigation.
The agents were sometimes approached by mothers of babies born in 1911 who resented being omitted from the investigation simply for the reason that their babies’ births had not been registered. The agents were therefore instructed to interview mothers thus accidentally encountered and to include their babies in the investigation. But no additional baptismal records were copied nor was a house-to-house canvass made of the city; in fact, no further 104means were resorted to to locate unregistered babies for the purpose of including them in the investigation.
There were 1,763 certificates copied at Harrisburg, and 1,383 of the babies named in them were reached by the agents. In addition, 168 babies for whom there were no birth certificates, but who were located in the ways just noted, were included, making a total of 1,551 completed schedules secured.
Of the 380 not included in the investigation there were 149 who could not be located at all; 220 others had moved out of reach—that is, into another city or State; 6 of the mothers had died; 3 could not be found at home after several calls, and 2 refused to be interviewed.
From the following summary of data recorded on the certificates of the 380 unlocated babies just referred to it appears that the infant mortality rate (134.3) among them is almost the same as that (134) shown in Table 1 for babies included in the investigation. In reality, however, it is perhaps a little higher, as some of these babies no doubt died outside of Johnstown and their deaths were recorded elsewhere.
| NATIONALITY OF MOTHER. | Total births. | Live births. | Still-births. | SEX OF BABY. | ATTENDANT AT BIRTH. | Certificate showing deaths during first year. | |||
|---|---|---|---|---|---|---|---|---|---|
| Male. | Female. | Physician. | Midwife. | Unknown. | |||||
| Total | 380 | 350 | 30 | 227 | 153 | 158 | 180 | 33 | 47 |
| Native | 134 | 118 | 16 | 76 | 58 | 122 | 5 | 7 | 12 |
| Foreign | 246 | 232 | 14 | 151 | 95 | 36 | 184 | 26 | 35 |
| Slovak, Polish, etc | 43 | 41 | 2 | 27 | 16 | 4 | 37 | 2 | 3 |
| Croatian and Servian | 13 | 11 | 2 | 10 | 3 | 7 | 6 | 5 | |
| Magyar | 1 | 1 | 1 | 1 | |||||
| German | 8 | 8 | 6 | 2 | 2 | 5 | 1 | 2 | |
| Italian | 41 | 39 | 2 | 26 | 15 | 3 | 36 | 2 | 4 |
| Syrian and Greek | 7 | 6 | 1 | 3 | 4 | 3 | 4 | 1 | |
| British | 7 | 7 | 3 | 4 | 5 | 2 | |||
| Austrian (not otherwise specified) | 123 | 116 | 7 | 73 | 50 | 19 | 89 | 15 | 20 |
| Not reported | 3 | 3 | 2 | 1 | 3 | ||||
The rate of infant mortality is regarded as a most reliable test of the sanitary condition of a district. (Sir Arthur Newsholme, Elements of Vital Statistics, p. 120. London, 1899.)
Johnstown is a hilly, somewhat Y-shaped area of about 5 square miles which spreads itself out into long, narrow, irregularly shaped strips, detached by rivers and runs and steep hills. In some places it is not over a quarter of a mile wide, but its extreme length is about 4 miles. The city is composed of 10521 wards and is an aggregation of what were formerly separate unrelated boroughs or towns. The names of these different sections, together with the numerical designations of the wards included in or comprising them, are shown in the following table. This table gives for each section not only the total population according to the Federal census of 1910, but also the number of live-born babies included in the investigation and the number and proportion of deaths among such babies during their first year.
| Table 1.—Distribution of Population, Live Births and Deaths During First Year, and Infant Mortality Rate According to Section of Johnstown, for all Children Included in this Investigation. | ||||
|---|---|---|---|---|
| SECTION OF CITY AND WARD. | Population, 1910.[12] | Total live-born babies. | Deaths during first year of babies born in 1911 | Infant mortality rate. |
| The whole city | 55,482 | 1,463 | 196 | 134.6 |
| Down-town section (wards 1, 2, 3, 4) | 5,944 | 80 | 4 | 52.0 |
| Kernville (wards 5, 6) | 6,070 | 104 | 6 | 57.7 |
| Homerstown (ward 7) | 4,476 | 109 | 17 | 156.0 |
| Roxbury (ward 8) | 2,862 | 85 | 19 | 117.6 |
| Conemaugh Borough (wards 9, 10) | 5,282 | 136 | 16 | 117.6 |
| Woodvale (ward 11) | 3,945 | 107 | 20 | 271.0 |
| Prospect (ward 12) | 1,893 | 55 | 11 | 200.9 |
| Peelorville (ward 13) | 1,443 | 13 | 4 | ([13]) |
| Minersville (ward 14) | 2,403 | 72 | 9 | 125.0 |
| Cambria City (wards 15, 16) | 8,706 | 310 | 55 | 177.4 |
| Moxham (ward 17) | 5,735 | 157 | 14 | 39.2 |
| Morrellville (wards 18, 19, 20) | 5,757 | 194 | 15 | 32.5 |
| Coopersdale (ward 21) | 968 | 36 | 8 | ([13]) |
12. Federal census of 1910.
13. Total live births less than 50; base therefore considered too small to use in computing an infant mortality rate.
To learn where the babies die is perhaps the first step in solving the infant mortality problem. The modern health officer recognizes this and generally has in his office a wall map upon which are indicated sections, wards, city blocks, and sometimes even houses. As infant deaths are reported, pins are stuck in the map in the proper places, a density of pins on any part of the map indicating, of course, where deaths are most numerous, although the percentage of infant deaths may not be the highest.
The highest infant mortality rate, 271, is found in the eleventh ward, known as Woodvale, although this is neither the most populous ward nor the one having the largest number of births. The infant mortality rate here, however, is double the rate for the city as a whole and more than five times as great as it is for the most favorable ward.
This is where the poorest, most lowly persons of the community live—families of men employed to do the unskilled work in the steel mills and the mines. They are for the most part foreigners, 78 per cent. of the mothers interviewed in this ward being foreign born.
106Through Woodvale runs the main line of the Pennsylvania Railroad. To the north of the tracks rises a steep hill, toward the top of which is Woodvale Avenue, the principal street north of the railroad. (See plate A.) Sewer connection is possible for the houses along this avenue, as a sewer main has recently been installed, but the people have not in all cases gone to the expense of having the connection made, and in other cases where they have done so sometimes only the sinks are connected with the sewer and the yard privy is retained.
On the streets above Woodvale Avenue dwellings are more scattered and the appearance is more rural. A few of the families still have to depend upon more or less distant springs for their water, although city water is quite generally available throughout Woodvale.
The streets near the bottom of the hill, as Plum Street, for example, are so much below the level of the sewer mains that they can not be properly drained into the sewer. Private drain pipes from houses are buried a few feet below the surface and protrude from the sides of the hills, dripping with house drainage which flows slowly into ditches and forms slimy pools. (See Plates B and C.)
None of the streets on the north side of the railroad track are paved; sidewalks and gutters are lacking. In cold weather the streets are icy and slippery and even dangerous on account of the grade. In warm weather they are frequently slippery and slimy with mud.
Maple Avenue is the principal street of that part of Woodvale lying to the south of the railroad tracks, and it is the only properly paved and graded street in Woodvale. The streets on this side of the tracks, however, are not in as bad a condition as those to the north, nor are the drainage and general sewerage conditions as offensive as north of the tracks, but many of the streets are nevertheless muddy and filthy. (See Plate D.)
Prospect ranks next to Woodvale in infant mortality, having a rate of 200. This section, lying along a steep hill and above one of the big plants of the steel company, has not a single properly graded, drained, and paved street. The sewers are of the open-ditch type, and the natural slope of the land toward the river is depended upon for carrying off the surface water that does not seep into the soil. The closets are generally in the yard and are either dry privies or they are situated over cesspools. Some of the people who live on the lower part of the slope have wells sunk directly in the course of the drainage from above. (See Plate E.)
Cambria City, which is composed of the two most populous wards of Johnstown, has the third highest infant mortality rate, 177.4. It has a large foreign element, as is evidenced by the fact that 90.6 per cent. of the mothers interviewed were foreign born. It is situated along the river, between the hills of Minersville and Morrellville, and somewhat to the north of Prospect. 107The sewage from other residential sections and from the steel mills above them empties into the river at this point. In warm, dry seasons the river is low, flows slowly, and forms foul-smelling pools.
Sewer connection is possible for most of the houses in Cambria City, although all are not connected. Some, on the streets bordering the river, have private drain pipes that empty out into the stream. Others have their kitchen sinks connected with the sewer but still retain yard privies, which, of course, are not sewer connected.
There is considerable crowding of houses on lots, rear houses being commonly built on lots intended for but one house. Density of population and house congestion are greater here than elsewhere in the city.
The streets of Cambria City are somewhat better graded and more generally paved than those of Woodvale, but muddy streets and unpaved sidewalks nevertheless exist here. Broad Street, however, which is the business thoroughfare and runs through the center of the section, is the widest and best constructed street in Johnstown. Bradley Alley, on the other hand, running the length of Cambria City and parallel to Broad Street, is the most conspicuous example in the city of a narrow lane or alley used as a residence street. A number of small dwellings, generally housing more than one family, have their frontage on this alley, which is 19 feet 10 inches in width and without sidewalks. It is unpaved and in bad condition, generally being either muddy or dusty and littered with bottles, cans, and other trash. (See Plates F. and G.)
Homerstown has an infant mortality rate of 156, ranking fourth among the several sections of Johnstown in this respect. It has a fairly prosperous and somewhat suburban appearance, but its comparatively high infant mortality rate can perhaps be partly accounted for by the bad street conditions and the fact that refuse of all sorts is dumped into the shallow river at this point.
Minersville is a district where a high rate would be expected from prevailing conditions. The rate is 125, or less than the average for the city but more than double that for the most favorable sections. This ward is built on a hill and so located that the rising clouds of grit-laden smoke from the steel mills envelop it much of the time. Only one street in this section is well paved, and this is seldom clean. Houses on some of the streets near the top of the hill are not sewer connected, and streams of waste water trickle down the hill and give rise to unpleasant odors. (See Plates H and I.)
Conemaugh Borough, with an infant mortality rate of 117.6, ranks sixth in this respect among the sections into which Johnstown has been divided. It comprises wards 9 and 10 and begins at the edge of the down-town section and spreads upward over the hills to the southwest. Some of the houses on streets near the top of the hill are not sewer connected, and streams of water 108constantly trickle down the numerous alleys and streets that descend the hill. (See Plate J.) This section makes a very unfavorable first impression because of the open drainage and of the many dirty, badly paved streets. (See Plate K.) Unlike some of the other wards, it has a rather evenly distributed population and is without the vast uninhabited areas and acutely congested spots found in some other sections. On the whole there is little crowding on the lots and there are many good-sized yards. One-third of the population is foreign born. Of these the Italians are the most numerous. Despite certain ugly spots this section has not the unwholesome atmosphere that characterizes Woodvale and to a lesser extent Prospect, Cambria City, and Minersville.
The infant mortality rate of 117.6 per thousand in Roxbury is the same as that of Conemaugh Borough. For reasons not plainly apparent the rate here is higher than in Moxham, Morrellville, Kernville, or the down-town section, although it appears to be as favorably conditioned as these sections are from a social, economic, and sanitary standpoint. Here, as in all these sections, however, are many conditions not conducive to health. For example, parts of Franklin Street are in bad repair. The roadway is full of ruts and holes; the street, which is seldom sprinkled, is dusty in dry weather and muddy in wet weather, and in front of good houses along one section of this street runs an open ditch that receives house drainage.
Moxham has the eighth highest infant mortality rate, it being 89.2. Conditions here are generally rather favorable, although there is some complaint that at “high water” the sewage received by one of the runs in this section backs into some of the houses and then the sinks and water-closets overflow. Some of the homes here, near the city limits, are not supplied with city water but are still dependent upon wells and springs.
One of the three wards constituting Morrellville (ward 18) has a rural appearance; there is little house crowding on lots, big yards are common, and the streets are not paved. It is, however, marred by an offensive open-ditch sewer. Ward 19 of Morrellville has a more finished, less rural appearance. One of its objectionable features is that house drainage and the bloody waste of slaughterhouses are emptied into a shallow stream that flows through it. Ward 20 adjoins ward 19, and although it spreads out into a suburb it appears for the most part to be a comfortable and busy little village. Strayer’s Run winds about here and receives sewage. The fact that it is without a guardrail in some places and that the railing is inadequate in others makes it a source of danger, and according to common report such accidents as children falling into the stream have occurred. The infant mortality rate for Morrellville is 82.5.
Kernville, a section with a considerable proportion of prosperous people, has a very favorable infant mortality rate, it being 57.7. Parts of this section, 109however, are on a hill stretching upward from Stony Creek, which is both unsightly and offensive in warm weather and when the water is low.
The down-town section, i.e., wards 1, 2, 3, and 4, where are to be found many of the best conditioned houses, the homes of many of the well-to-do people, has the lowest infant mortality rate in the city, it being but 50.
No infant mortality rate is presented in the tables for Coopersdale or for Peelorville. In the first-named section only 36 live-born infants were considered, and 8 of them died in their first year. But this high rate need not be considered as especially significant, as the base number is small for such a computation. Coopersdale, however, is a suburban-appearing community in which one would expect the infant mortality rate to be low.
Peelorville is that part of the thirteenth ward which adjoins Prospect. A number of company houses are located here in which sanitary conditions are fairly good. The ward seems to have good drainage and no sewage nuisances. It is a community of wage earners and not of prosperous homes. Only 18 babies are included in the report for this district, one of whom died. With such a small base the infant mortality rate is not significant. (See Plate L.)
The general inadequacy of the sewerage system which has been indicated for the city as a whole is due in part to the fact that the city is largely an aggregation of sections, formerly independent of Johnstown itself, which have been annexed at different periods. Some of these boroughs had sewer systems more or less developed when they were taken into Johnstown; others had none. Not only the sewerage of Johnstown but that of outlying boroughs pollutes the two shallow rivers, the Conemaugh and the Stony Creek, that flow through Johnstown. These are burdened with more waste than they can properly carry away, and the deposits which are left on the rocks in various sections of both rivers create nuisances that are the subject of much complaint, especially during the warm summer months. (See Plates M, N, O, and P.) At various times agitation has been started to improve the rivers which, as they flow through Johnstown, are, at the low-water stage, little better than swamps of reeking slime from the waste matter emptied into them from the hundreds of sewers along their banks. The pipes through which waste matter is emptied into the streams go only to the river edge, leaving their mouths uncovered and making the river beds at times pools of slowly flowing filth. These unsightly, malodorous conditions could be remedied if pipes were extended out into the middle of the streams, where the water is deeper.
110With the exception of sprinkling a few wagon loads of lime along the banks of the streams each year, the city has done nothing to abate the nuisances arising from the use of these rivers as sewers or to restrain the coal and steel companies from allowing the drainage from mines and mills to enter the streams.
The engineer’s records show that Johnstown had in 1911 a total of 41.1 miles of sewers and 36 sewer outlets, and 82 miles of streets, 52.7 miles being paved. The alleys in Johnstown are generally inhabited. They are narrow and without sidewalks. Their length is 52.88 miles and 47.35 miles are unpaved. The combined length of streets and alleys is 134.88 miles. A comparison of this combined length of streets and alleys with the 41.1 miles of sewers having 36 outlets shows the inadequacy of the sewer system.
Not only is there an absence of paving, but the roadways are in very bad condition. A protest by “A Citizen” in the Democrat of June 26, 1913, says that there are nine months in the year when it would be impossible for the proposed fire-department automobile engines to attend a fire in the seventh, eighth, eleventh, seventeenth, eighteenth, nineteenth, twentieth, and twenty-first wards owing to the condition of the streets.
The scavenger system is also very defective. Citizens are required to pay for the removal of their ashes, trash, and garbage. Garbage collections are not made by the municipality, but by private contractors, and any sort of receptacle, covered or uncovered, can or box, is pressed into service by householders. It is by no means uncommon to find streets and alleys littered with ashes, garbage, bottles, tin cans, beer cases, and small kegs. Dirty streets are by no means exceptional in Johnstown, even though the State of Pennsylvania has a law (act of Apr. 20, 1905) which provides for the punishment of any person who litters paved streets. It reads, in part, as follows (sec. 7 of Pamphlet Laws, 227):
“From and after the passage of this act, it shall be unlawful, and is hereby forbidden, for any person or persons to throw waste paper, sweepings, ashes, household waste, nails, or rubbish of any kind into any street in any city, borough, or township in this Commonwealth, or to interfere with, scatter, or disturb the contents of any receptacle or receptacles containing ashes, garbage, household waste, or rubbish which shall be placed upon any of said paved streets or sidewalks for the collection of the contents thereof.
“Any person or persons who shall violate any of the provisions of this act shall, upon conviction thereof before any magistrate, be sentenced to pay the cost of prosecution and to forfeit and pay a fine not exceeding $10 for each offense, and in default of the payment thereof shall be committed and imprisoned in the county jail of the proper county for a period not exceeding ten days.”
In a report on infant mortality to the registrar general of Ontario, 1910, 111Dr. Helen MacMurchy says: “Improve the water supply, the sewerage system, and the system of disposing of refuse; introduce better pavements, such as asphalt, and at once there is a decline in infantile mortality.” All these are sanitary features in need of great improvement in Johnstown, and unquestionably a lowered infant mortality rate would reward any efforts for their betterment.
In Johnstown the so-called “double” house predominates, usually frame. The double house is in reality two semidetached houses built upon a single lot. Rows of three or more houses of two, three, or four rooms each are common, and they are known locally as three-family, or six-family houses, as the case may be. Sometimes these are “rear houses,” that is, they are built behind other houses that face the street, on the same lots and in fact are approached by way of a narrow alley running alongside the house that has its frontage directly on the street. For this type of house water-closets or privies are often in rows in the yard or court that is used in common by all families. (See Plates Q and R.) In some places they are too few in number to permit each family to have the exclusive use of one.
Johnstown has three or four comparatively high-grade apartment houses, and in several office buildings rooms are rented to families for housekeeping. These are generally taken by native families.
In one of these office buildings the two lower floors are used for business purposes and the two upper floors are given over entirely to tenement purposes. From 40 to 50 families live here, many of whom have but one room. To serve the 20 or 25 families on each floor there is one bath and toilet room for men and another for women. Adjoining the toilet rooms is a small room containing garbage cans and trash receptacles for the use of the tenants.
The sanitary conditions in some of the best tenements or apartments, however, are not up to the standards of other cities, and in those occupied by the poorer people conditions are much worse than are usually permitted to exist in cities having large tenement houses in great numbers, where a tenement-house problem is recognized as such and active efforts are made by the municipality to improve conditions.
An absolute measure of the importance of each single housing defect in a high mortality rate can not be secured from this study. But it is not without interest to note that in homes where water is piped into the house the infant mortality rate was 117.6 per thousand, as compared with a rate of 197.9 in homes where the water had to be carried in from outdoors. Or that in the homes of 496 live-born babies where bathtubs were found the infant mortality rate was 72.6, while it was more than double, or 164.8, where there 112were no bathtubs. Desirable as a bathtub and bodily cleanliness may be, this does not prove that the lives of the babies were saved by the presence of the tub or the assumed cleanliness of the persons having them. In a city of Johnstown’s low housing standards, the tub is an index of a good home, a suitable house from a sanitary standpoint, a fairly comfortable income, and all the favorable conditions that go with such an income.
The same trend of a high infant mortality rate in connection with other housing defects is noted in the next table.
| Table 3.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality Rate, According to Housing Conditions. | |||
|---|---|---|---|
| Deaths during First Year | |||
| HOUSING CONDITIONS | Live births | Number | Infant mortality rate |
| Total | 1,463 | 196 | 134.0 |
| Dry homes | 808 | 99 | 122.5 |
| Moderately dry homes | 336 | 47 | 139.9 |
| Damp homes | 319 | 50 | 156.7 |
| Bath | 496 | 36 | 72.6 |
| No bath | 965 | 159 | 164.8 |
| Not reported | 2 | 1 | ([14]) |
| Water supply in house | 1,173 | 138 | 117.6 |
| Water supply outside | 288 | 57 | 197.9 |
| Not reported | 2 | 1 | ([14]) |
| City water available | 1,333 | 176 | 132.0 |
| City water not available | 128 | 19 | 148.4 |
| Not reported | 2 | 1 | ([14]) |
| Yard clean | 801 | 80 | 99.9 |
| Yard not clean | 632 | 107 | 169.3 |
| No yard | 28 | 8 | ([14]) |
| Not reported | 2 | 1 | ([14]) |
| Water-closet | 739 | 80 | 108.3 |
| Yard privy | 722 | 115 | 159.3 |
| Not reported | 2 | 1 | ([14]) |
14. Total live births less than 50; base therefore considered too small to use in computing an infant mortality rate.
The following summary may be of interest in indicating some relation between infant mortality and cleanliness or uncleanliness combined with dryness or dampness of homes:
| Table 4.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality, According to Cleanliness and Dryness of Home. | |||
|---|---|---|---|
| Deaths during First Year | |||
| TYPE OF HOME | Live births | Number | Infant mortality rate |
| All types | 1,463 | 196 | 134.0 |
| Clean | 943 | 107 | 113.5 |
| Moderately clean | 354 | 58 | 163.8 |
| Dirty | 166 | 31 | 186.7 |
| Dry | 807 | 99 | 122.7 |
| Damp | 656 | 97 | 147.9 |
| Clean: | |||
| Dry | 581 | 61 | 105.0 |
| Damp | 362 | 46 | 127.1 |
| Moderately clean: | |||
| Dry | 158 | 27 | 170.9 |
| Damp | 196 | 31 | 158.2 |
| Dirty: | |||
| Dry | 68 | 11 | 161.8 |
| Damp | 98 | 20 | 204.1 |
113Dirt is doubtless unhealthful, but the amount of ill health or the number of infant deaths caused by a home being dirty can hardly be measured, when, as is usually the case, the dirt is accompanied by so many other bad conditions arising from poverty. For example, a home in close proximity to railroad tracks or mills whose stacks send forth clouds of soot, smoke, and ashes is generally the poorly built home of those who have neither time nor means to secure and retain cleanliness under such difficulties.
Overcrowding in homes is another factor the relative importance of which can not be exactly determined, because of its close connection with other ills. But the degree of overcrowding is greatest in the small cheaper houses, those of one, two, three, or four rooms. The average number of persons per room in the homes of all live-born babies for whom the data were secured was found to be 1.38. Homes of four rooms were more numerous than those of any other size and they housed an average of 1.58 persons per room. The number of babies in homes of various sizes with the number of persons per room for homes of each size was as follows:
| Table 5.—Number of Babies Living in Homes of Each Specified Size, and Average Number of Persons Per Room in Homes of Each Size. | ||
|---|---|---|
| Size of home | Live-born babies | Persons per room |
| All homes | 1,463 | |
| 1 room | 33 | 4.42 |
| 2 rooms | 165 | 2.27 |
| 3 rooms | 147 | 1.83 |
| 4 rooms | 526 | 1.58 |
| 5 rooms | 222 | 1.22 |
| 6 rooms | 233 | 1.07 |
| 7 rooms | 38 | .96 |
| 8 rooms | 43 | 0.83 |
| 9 rooms | 22 | .93 |
| 10 rooms | 4 | .88 |
| 11 rooms | 4 | .64 |
| 12 rooms | 1 | .75 |
| 13 rooms | 1 | .69 |
| 14 rooms | 2 | .43 |
| Not reported | 22 | |
In homes of one, two, three, or four rooms or where the number of occupants ranged from 4.42 to 1.58 persons per room the infant mortality rate was 155, as compared with a rate of but 101.8 in larger homes, where the number ranged from 1.22 to 0.43 persons per room.
The 1910 census returns show that the greatest overcrowding was in ward 15, where the average number of persons per dwelling was 9.9. Wards 16, 11, and 14 came next with rates of 8.3, 7.7, and 7.2 respectively. The infant mortality rate for these four wards is 190.2, which is over one-third more than the rate for the whole city.
The mortality rate among infants who slept in a room with no other person than their parents was much lower than among those who slept in a room with more than two persons. The babies that slept in separate beds also had a much lower infant mortality rate than those who did not sleep alone, as shown in the next table. (Table omitted.)
In presenting statistics on sleeping and ventilation, only the babies who lived at least one month have been considered, for the reason that so many deaths during the first month of life were due to prenatal causes.
114The incidence shown in the foregoing table is significant, even though it can by no means be deduced therefrom that the health of a large proportion of babies was so impaired by sleeping with older and more or less unhealthy persons that death resulted. But irregular night feeding and overfeeding are undoubtedly harmful, and the mother is tempted to subject the baby to this when it sleeps with her and disturbs her rest.
Of the 1,389 babies who lived at least one month, 600, or 43.2 per cent., lived in homes where the baby slept in a room with not more than two other persons. The fact that the baby slept in a room with no more persons than its parents generally argues that the family’s means permitted them to have one or more additional rooms for other members of the family, but in other cases, of course, merely that there were no other persons in the family.
Almost every home visited had means for good ventilation of the baby’s room at night, yet but 604, or 43.5 per cent., of the 1,389 babies who lived at least a month slept at night in well-ventilated rooms—that is, in rooms where, according to the mother’s statement, a window was open all night. Some mothers opened windows when the weather was neither cold nor damp; or opened them in a hall or room adjoining that where the baby slept; others emphatically stated that at night the windows were “always shut tight.” The babies subjected to differences of ventilation show corresponding variations in infant mortality rates.
A high death rate in badly ventilated homes can not be charged wholly to bad air. The mother who did not, or could not, provide proper ventilation was generally the mother without the means or the knowledge necessary to enable her to care for her baby properly in other respects, and yet the marked differences suggest that ventilation is itself a very important ally of the baby in its first year of struggle for existence.
In many rooms that were poorly ventilated, windows were not opened for the reason that the room was not properly heated and the houses themselves were flimsy and drafty. The problem in such houses is to keep warm. If the windows were frequently or constantly opened, the houses would be too cold to live in. In some localities the outside air is so laden with soot, ashes, dirt, and smoke that every effort is made to keep it out of the house.
The foreigners, who generally have the most miserable homes, are not dirty people who select bad living conditions through innate poor judgment, low standards, and lack of taste. The squalid homes which housed the natives and later the Germans and the Irish until the present type of immigrants came to do the more poorly paid work were the only homes available within the purchasing power of their low wages. The new immigrants demanded practically nothing and the owners did practically nothing in the matter of improving these homes, which naturally became more and more squalid as time went on. An excessive infant mortality rate and insanitary homes in unhealthful sections were found to be coexistent.
The investigation embraced 860 babies of native mothers (of whom 6 were negroes) and 691 babies of foreign mothers, making a total of 1,551. The infant mortality rate for the entire group was 134 per 1,000 live births; for the babies of native mothers 104.3, and for those of foreign mothers 171.3. The stillbirth rate for native mothers having children in 1911 was less than that for foreign mothers, being 52.3, as compared with 62.2 per 1,000 total births.
The line between the natives and foreigners is very sharply drawn in Johnstown. The native population as a rule knows scarcely anything about the foreigners, except what appears in the newspapers about misdemeanors committed in foreign sections. The report of the Immigration Commission[15] comments “on the attitude of the police department toward foreigners ... with regard to Sunday desecration,” and states that “the Croatians are accustomed to spend Sunday in singing, drinking, and noisy demonstrations. The police have been instructed to show no leniency on account of ignorance of the municipal regulations, and, without any attempt at explaining the laws, they arrest the offenders in large numbers.” Again, it states: “They are arrested more often for crimes that make them a nuisance to the native population than for mere infractions of the law.... Few arrests are made for immorality among foreigners.” “Sabbath desecration” is the crime foreigners are most frequently charged with.
15. United States Immigration Commission Reports, Volume VIII., “Immigrants in Industries: Part 2, Iron and Steel Manufacturing in the East,” p. 387. Reference is to Johnstown and is a very true picture of various immigrant institutions and of the comparative progress and assimilation of different races there. Although the immigration report was made five years before our investigation, conditions remain practically the same.
Foreigners are employed largely in the less skilled occupations of the steel mills, which operate 24 hours a day, seven days a week. At the time the investigation was made some of the men in the steel mills worked for a period of two weeks on a night shift of 14 hours, then two weeks on a day shift of 10 hours, and back again to the night shift of 14 hours for another two weeks, and so on. When shifts were changed, one group of men was required to work throughout a period of 24 hours instead of for the usual 10 or 14 hour period and another group had 24 hours off duty. Some departments of the steel mills, however, shut down on Sundays, and in some departments for certain occupations an eight-hour day prevails, but these more favorable conditions do not prevail among the majority of the unskilled foreign workers whose homes were visited.
The foreigners who work on a 24-hour shift in a mill on one Sunday frequently “desecrate” their alternate free Sabbath by “singing, drinking, and noisy demonstrations,” in spite of the known danger of arrest for “crimes 116that make them a nuisance to the native population” or for “Sabbath desecration,” laws concerning which are strictly enforced in Johnstown; for example, children are not permitted to play in public playgrounds on Sunday and mercantile establishments are required to be closed on that day. Also, it is “unlawful for any person or persons to deliver ice cream, or to sell or deliver milk from wagon or by person carrying same, within the city on the Sabbath day, commonly called Sunday, after 12 o’clock m.” The ordinance from which the foregoing sentence was quoted became a law on January 25, 1914.
The foreign group having the highest infant mortality rate is the Serbo-Croatian[16] where infant deaths numbered 263.9 per 1,000 live births.
16. A distinct and homogenous race, from a linguistic point of view, among Slavic peoples. They are divided into the groups “Croatian” and “Servian,” on political and religious grounds, the former being Roman Catholics and the latter Greek Orthodox. Their spoken language is the same but they can not read each other’s publications, for the Croatians use the Roman alphabet, or sometimes the strange old Slavic letters, while the Servians use the Russian characters fostered by the Greek Church.
Three Krainers have also, for convenience, been included in this group. Krainers are Slovenians from the Austro-Hungarian Province of Carniola and are designated “close cousins of the Croatians but with a different though nearly related language” by Emily Greene Balch in her book entitled “Our Slavic Fellow Citizens.”
The men of the Serbo-Croatian group are fine looking and powerful and are employed in the heavy unskilled work of the steel mills and the mines. They greatly outnumber the women of their race in Johnstown, and a man with a wife frequently becomes a “boarding boss”; that is, he fills his rooms with beds and rents out sleeping space to his fellow countrymen at from $2.50 to $3 a month each. The same bed and bedding is sometimes in service both night and day to accommodate men on the night and the day shifts of the steel mills.
The wife, without extra charge, makes up the beds, does the washing and ironing, and buys and prepares the food for all the lodgers. Usually she gets everything on credit and the lodgers pay their respective shares biweekly. These conditions exist to some extent among other foreigners, but are not as prevalent among other nationalities in Johnstown as among the Serbo-Croatians.
In a workingman’s family, it is sometimes said, the woman’s work-day is two hours longer than the man’s. But if this statement is correct in general, the augmentation stated is insufficient in these abnormal homes where the women are required to have many meals and dinner buckets ready at irregular hours to accommodate men working on different shifts.
The Serbo-Croatian women who, more than any of the others, do all this work are big, handsome, and graceful, proud and reckless of their strength. During the progress of the investigation, in the winter months, they were frequently seen walking about the yards and courts, in bare feet, 117on the snow and ice-covered ground, hanging up clothes or carrying water into the house from a yard hydrant.
Whether it harmed them to expend their force and vigor as they did could not be determined in individual cases, but their babies are the ones who died off with the greatest rapidity, their infant mortality rate being 263.9, as compared with the rates of 171.3 for all the foreign; 104.3 for the natives; and 134 for the entire group as shown in Table 18. Excluding babies of Serbo-Croatian mothers, the infant mortality rate for babies of foreign mothers is but 159.7.
The Italian mothers visited in Johnstown bore 75 children in 1911, 4 being stillborn. The infant mortality rate among the live born was 183.1, the highest of any racial group excepting the Serbo-Croatian, where it was 263.9.
The Italians have been in Johnstown somewhat longer than the Serbo-Croatians and they seem to have a little firmer grip on the community life there. Their homes are a shade better, a trifle cleaner, and somewhat less crowded than those of the Serbo-Croatians, although their hygienic standards seem little if any higher and they rank no better in literacy. The women do not perform the arduous duties that are the lot of so many of the Serbo-Croatian women; they have not the robust physique of the latter and the men are not found in those branches of the steel industry which require the extraordinary strength possessed by the Serbo-Croatians. The occupations of the Italian fathers were found to be more diversified than those of the Serbo-Croatians, some being fruit, grocery, or cheese merchants; steamship agents; bricklayers, carpenters, or workers at other skilled and semiskilled trades.
The infant mortality rate in the group designated “Slovak, Polish, etc.” is 177.1. In this group are included all the Slavic races represented in the investigation excepting the Serbo-Croatian. The babies of Slovak[17] mothers were found to be most numerous, there being 276 of them. There were 108 babies of Polish,[18] 2 of Bohemian,[19] and 7 of Ruthenian[20] mothers. In addition, 118one baby of a Scandinavian (Danish) mother was included, not because Scandinavians bear the least racial resemblance to the Slavic races, but because the few Scandinavians in Johnstown happened to be on about the same economic footing as the “Slovak, Polish, etc.”
17. Slovaks occupy practically all except the Ruthenian territory of northern Hungary; also found in great numbers in southeast Moravia. They are the Moravians conquered by Hungary. In physical type no dividing line can be drawn between Slovaks and Moravians. It is often claimed that Slovak is a Bohemian dialect.
18. The west Slavic race native to the former Kingdom of Poland. For the most part they adhere to the Roman rather than the Greek Orthodox Catholic Church.
19. The westernmost division or dialect of the Czech and the principal people or language of Bohemia. Czech is the westernmost race or linguistic division of the Slavic (except Wendish, in Germany), the race or people residing mainly in Bohemia and Moravia.
20. Also known as Little Russians; live principally in southern Russia; also share Galicia with the Poles but greatly surpassed by Poles in number. In language and physical type resemble Slovaks. Generally Greek Orthodox, but a few are Greek Catholics of the Roman Catholic Church, whose priests marry, and are separated from other Roman Catholics by marked religious differences.
The rate for this group is lower than that for either the Serbo-Croatians or the Italians, but it is nevertheless very high and one exceeded by only a few European countries, as shown by the table on page 12.
Some of the “Slovaks, Poles, etc.,” live in the same squalid sections as the Serbo-Croatians, and in the same type of inferior houses, but on the whole they have been in Johnstown longer, are more prosperous, and are therefore beginning to move from Cambria City and Woodvale, where formerly practically all lived, into more desirable sections. Those who have been in this country longest and intend to stay here are buying homes with large yards in the less crowded sections and are raising vegetables and flowers. Others, however, still remain in poor neighborhoods and sometimes buy houses there for from $300 to $600 each, built close together on rented ground.
Lodgers are by no means uncommon among the people in this group, but usually their homes are cleaner, less crowded, and possessed of more comforts than those of the Serbo-Croatians and Italians.
The British[21] infant mortality rate in Johnstown is 129 and the German 127.7. The British and Germans in Johnstown are more prosperous than the Slavic, Magyar, Jewish, Italian, Syrian, and Greek peoples, and regard the others as “foreigners.” It was strange to hear a man, one who could speak English, say, “We are not foreigners; we are Germans.” The British and Germans occupy the same relative position economically that they occupy in the infant mortality scale with relation to other races.
21. English, Irish, Scotch, and Welsh included in the term British.
In the Magyar group, of 38 babies born alive 4 died in their first year, making an infant mortality rate of 105.3, which is almost as low as that for babies of native mothers. The Magyars are little if any better off than the other “foreigners” among whom they live, but they possess somewhat higher standards of living. They live in poor neighborhoods and have inferior houses, but their homes are cleaner and they themselves somewhat more alert, personally cleaner, and less illiterate than the other foreigners.
There were but 10 babies of Hebrew mothers and 12 of Syrian and Greek mothers; among these there were no deaths. These groups are too small numerically to be significant in a comparative race study of infant mortality.
In all there were but 88 stillbirths included in the investigation. They were more numerous proportionately among the Germans than among the mothers of any of the other nationalities. No single nationality group, however, has a very large representation, and hence a comparison of the rate for one with that for another nationality is not as significant as the difference in rate between native and foreign mothers. Although a special study of the causes of stillbirths was not made in connection with a study of deaths of infants during their first year of life, nevertheless the incidence of these births among the different nationality groups is believed to be of some interest, and therefore shown in the next table. (Omitted.)
The native mother usually had a physician at childbirth; the foreign-born, a midwife. The more prosperous of the foreign mothers, however, departed from their traditions or customs and had physicians, while the American-born mothers, when very poor, resorted to midwives. The midwives usually charged $5, and sometimes only $3; they waited for payment or accepted it in installments, and they performed many little household services that no physician would think of rendering.
Two-thirds of those having no attendant were Serbo-Croatians. It was a Polish woman, however, who gave the following account of the birth of her last child:
At 5 o’clock Monday evening went to sister’s to return washboard, having just finished day’s washing. Baby born while there; sister too young to assist in any way; woman not accustomed to midwife anyway, so she cut cord herself; washed baby at sister’s house; walked home, cooked supper for boarders, and was in bed by 8 o’clock. Got up and ironed next day and day following; it tired her, so she then stayed in bed two days. She milked cows and sold milk day after baby’s birth, but being tired hired some one to do it later in week.
This woman keeps cows, chickens, and lodgers; also earns money doing laundry and char work. Husband deserts her at times; he makes $1.70 a day. A 15-year-old son makes $1.10 a day in coal mine. Mother thin and wiry; looks tired and worn. Frequent fights in home.
The infant mortality rate was lower for babies delivered by physicians than for those delivered by midwives or for those at whose birth no properly qualified attendant was present. This is not necessarily an indication of the 120quality of the care at birth, although in some cases the inefficiency of the midwife may have directly or indirectly caused deaths, just as in some instances a physician’s inefficiency may have caused them. The midwife, however, is resorted to by the poor, and in their homes are found other conditions that create a high infant mortality rate.
Frequently the Serbo-Croatian women dispense altogether with any assistance at childbirth; sometimes not even the husband or a neighbor assists. Over 30 per cent. of the births among the women of that race took place without a qualified attendant. More than one-half of those delivered by midwives, less than one-fifteenth of those delivered by physicians, and about one-fifth of those delivered without a qualified attendant had babies who died in their first year of life.
Fifteen of the 19 Serbo-Croatian women whose babies died under 1 year of age kept lodgers.
In Johnstown the midwife is resorted to principally by the poor. Recent laws that the State is now trying to enforce require that the standard for the practice of midwifery be raised. If this can be done midwives might become definitely helpful persons in the community. One or two of the intelligent graduate midwives in Johnstown have been an educational force among the foreign mothers for some years past. On the other hand there were others who were so dirty and so ignorant that they were a menace to the public health.
There are differences in the infant mortality rate between the babies of literate and the babies of illiterate mothers; between those with mothers who can speak English and those with mothers who can not; and between babies of the mothers who have been in this country for a considerable period and those of the newer arrivals. Comparisons of this nature are confined to the foreign mothers, as only three cases of illiteracy were found among native mothers, and the other comparisons would not, of course, be applicable in any case to native mothers.
22. By literacy is meant ability to read and write in any language and not simply in English.
The next table shows that the infant mortality rate among the children of illiterate foreign mothers was 214, or 66 per thousand greater than the rate among literate foreign mothers.
| 121 | ||||||
| Table 13.—Distribution of Births and of Deaths During First Year, Infant Mortality Rate, and Number and Per Cent of Stillbirths, According to Literacy of Foreign Mothers. | ||||||
|---|---|---|---|---|---|---|
| LITERACY OF FOREIGN MOTHERS. | Total births. | Live births. | STILLBIRTHS. | DEATHS DURING FIRST YEAR. | ||
| Number. | Per cent. | Number. | Infant mortality rate. | |||
| Foreign mothers | 691 | 648 | 43 | 6.2 | 111 | 171.3 |
| Literate | 445 | 419 | 26 | 5.8 | 62 | 148.0 |
| Illiterate | 246 | 229 | 17 | 6.9 | 49 | 214.0 |
The next table shows that babies whose mothers can not speak English were characterized by a more unfavorable infant mortality rate than other babies.
| Table 14.—Distribution of Births and of Deaths During First Year, Infant Mortality Rate, and Number and Per Cent of Stillbirths, According to Ability of Foreign Mother to Speak English. | ||||||
|---|---|---|---|---|---|---|
| ABILITY TO SPEAK ENGLISH. | Total births. | Live births. | STILLBIRTHS. | DEATHS DURING FIRST YEAR. | ||
| Number. | Per cent. | Number. | Infant mortality rate. | |||
| Foreign mothers | 691 | 648 | 43 | 6.2 | 111 | 171.3 |
| Speak English | 263 | 247 | 16 | 6.1 | 36 | 145.7 |
| Can not speak English | 428 | 401 | 27 | 6.3 | 75 | 187.0 |
In addition to a consideration of the babies according to their mothers’ ability to speak English, it is of interest to note the infant mortality rates among babies whose mothers have been in this country for different periods of time.
The high infant mortality rate for the children of newer immigrants, illiterates, and those who can not speak English is perhaps affected by the fact that they are at the same time generally of the poorest families and are housed in the most insanitary and unhealthful part of the city.
The age of the mother is frequently believed to be a factor in the health of the child. The highest infant mortality rate was found to be that for the group of babies with mothers over 40 years of age, and the lowest for babies of mothers from 20 to 24 years of age.
| Table 16.—Distribution of Births and of Deaths During First Year, Infant Mortality Rate, and Number and Per Cent of Stillbirths, According to Age of Mother. | ||||||
|---|---|---|---|---|---|---|
| AGE OF MOTHER. | Total births. | Live births. | STILLBIRTHS. | DEATHS DURING FIRST YEAR. | ||
| Number. | Per cent. | Number. | Infant mortality rate. | |||
| All mothers | 1,551 | 1,463 | 88 | 5.7 | 196 | 134.0 |
| Under 20 | 105 | 95 | 10 | 9.5 | 13 | 136.8 |
| 20 to 24 | 476 | 454 | 22 | 4.6 | 55 | 121.1 |
| 25 to 29 | 410 | 391 | 19 | 4.6 | 56 | 143.2 |
| 30 to 39 | 480 | 449 | 31 | 6.5 | 61 | 135.9 |
| 40 and over | 80 | 74 | 6 | 7.5 | 11 | 148.6 |
The youngest mothers have a higher stillbirth rate than other mothers, and the oldest group of mothers has the next highest rate. In this connection not only the foregoing table is of interest, but also Table XII, based upon the entire reproduction histories of the mothers included in this study. As all the children borne by these mothers are included, the base numbers in the latter table are larger and the figures therefore somewhat more significant.
A baby who comes into the world has less chance to live one week than an old man of 90, and less chance to live a year than one of 80.—Bergeron.
The most dangerous time of life is early infancy; even old age seldom has greater risk. Death strikes most often in infancy. The Johnstown babies died during their first year of life at the rate of 134 per 1,000 born alive, and they paid their heaviest toll in their very earliest days. If the total of 196 deaths had been distributed evenly throughout the 12 months, 8.3 per cent. of the babies would have died each month and 25 per cent. during each quarter. But instead of that 37.8 per cent. died in the first month; 9.2 per cent. in the second, and 8.2 per cent. in the third, or over 55 per cent. in the first quarter.
| 123 | ||
| Table 17.—Number and Per Cent Distribution of Deaths of Babies, by Age at Death. | ||
|---|---|---|
| AGE AT DEATH. | DEATHS OF BABIES OF ALL MOTHERS. | |
| Number. | Per cent. distribution. | |
| Total deaths in first year | 196 | 100.0 |
| First quarter | 108 | 55.1 |
| First month | 74 | 37.8 |
| First week | 45 | 23.0 |
| Less than 1 day and 1 day | 30 | 15.3 |
| 2 days | 4 | 2.0 |
| 3 to 6 days | 11 | 5.6 |
| Second week | 14 | 7.1 |
| Third week | 7 | 3.6 |
| Fourth week | 8 | 4.1 |
| Second month | 18 | 9.2 |
| Third month | 16 | 8.2 |
| Second quarter | 42 | 21.4 |
| Third quarter | 31 | 15.8 |
| Fourth quarter | 15 | 7.7 |
The large number of deaths in the first few hours or days of life indicates that many babies are born with some handicap and that in many instances the mother has been subjected to some condition which resulted in the birth of a child incapable of withstanding the ordinary strain of life. Of the 45 babies who died in Johnstown less than a week after birth, 38 died of prematurity, congenital debility or malformations, or injuries received at birth. In one other case the cause of death was given as “bowel trouble” and in six other cases it was not clearly defined. In addition to the 45 babies just referred to as having died in their first week, 12 died later either from prematurity or from congenital defects.
Of the deaths from causes arising after birth, 52 were attributed by the attending physicians to diarrhoea and enteritis, 50 to respiratory diseases; and 44 to some other or to some ill-defined cause.
| Table 18.—Distribution of Deaths During First Year and Infant Mortality Rate, According to Cause of Death and Nativity of Mother. | ||||||
|---|---|---|---|---|---|---|
| CAUSE OF DEATH. | DEATHS DURING FIRST YEAR OF BABIES OF— | |||||
| All mothers. | Native mothers. | Foreign mothers. | ||||
| Number. | Infant mortality rate. | Number. | Infant mortality rate. | Number. | Infant mortality rate. | |
| All causes | 196 | 134.0 | 85 | 104.3 | 111 | 171.3 |
| Diarrhea and enteritis | 52 | 35.5 | 17 | 20.9 | 35 | 54.0 |
| Respiratory diseases | 50 | 34.2 | 19 | 23.3 | 31 | 47.8 |
| Premature births | 24 | 16.4 | 11 | 13.5 | 13 | 20.1 |
| Congenital debility or malformation | 19 | 12.9 | 5 | 6.1 | 14 | 21.6 |
| Injuries at birth | 7 | 4.8 | 6 | 7.4 | 1 | 1.5 |
| Other causes or not reported | 44 | 30.1 | 27 | 33.1 | 17 | 26.2 |
124The latest census report on mortality statistics characterizes diarrhoea and enteritis as the “most important preventable cause of infant mortality” in the United States, and numerically at least it proves to be the most important cause of infant death in Johnstown.
Holt[23] says that one of the most striking facts about diarrheal diseases in infants is their prevalence during the summer season. In Johnstown the infant diarrheal deaths were least prevalent in the first quarter of the year, next in the second, next prevalent in the fourth, and most prevalent in the third or summer quarter.
23. The Diseases of Infancy and Childhood, by L. Emmett Holt. p. 345. New York, 1912.
| Table 19.—Distribution of Deaths, According to Cause of Death and Quarter of Calendar Year in which Death Occurred. | |||||
|---|---|---|---|---|---|
| CAUSE OF DEATH. | All deaths. | QUARTER OF CALENDAR YEAR IN WHICH DEATH OCCURRED. | |||
| First. | Second. | Third. | Fourth. | ||
| All causes | 196 | 54 | 29 | 74 | 39 |
| Diarrhea and enteritis | 52 | 3 | 5 | 32 | 12 |
| Respiratory diseases | 50 | 24 | 8 | 7 | 11 |
| Premature births | 24 | 7 | 5 | 9 | 3 |
| Congenital debility or malformation | 19 | 5 | 2 | 8 | 4 |
| Injuries at birth | 7 | 5 | 1 | 1 | |
| Other causes or not reported | 44 | 10 | 8 | 18 | 8 |
Our figures are too small to admit of broad generalizations or a very full discussion of infant deaths according to the period of the year.
This excess of infant deaths from diarrhea in the summer months has been established by statistics in many countries, and the cause of such an excess has been the subject of much discussion, but as yet there is no general agreement. Liefmann and Lindemann[24] conclude, however, that in this field of controversy there are certain facts which are at present well established, these being the dependence of the high summer mortality on methods of feeding, on hot weather, and on the living and social condition of the parents. The last factor mentioned by these authors, including as it does housing conditions, economic status, and degree of intelligence, is becoming more and more the subject of study and investigation. It has been shown that the distinctly harmful effect of hot weather on the infant is increased when the housing conditions are bad; in overcrowded homes with bad ventilation the indoor temperature may be many degrees higher than the outdoor temperature. The ignorance and carelessness of mothers has also been shown to increase the bad effect of hot weather. With hygienic care, including cool baths, much fresh air, and careful feeding, many infants are able to pass through extremely hot weather without diarrheal disturbances.
24. Liefmann, H., and Lindemann, H., Die Lokalization der Sauglingsterblichkeit und ihre Beziehungen zur Wohnungsfrage. Med. Klinik 1912, pp. 8, 1074.
Respiratory diseases were reported as a cause of death with almost as great frequency as diarrheal diseases. As shown by Table 19, these deaths occurred principally in the colder months of the first and fourth quarters of the calendar year.
Food is recognized as of such importance in relation to infant mortality that studies of this subject frequently resolve themselves into studies of feeding only. Invariably these demonstrate the truth of the statement of Dr. G. F. McCleary[25] that “in human milk we have a unique and wonderful food for which the ingenuity of man may toil in vain to find a satisfactory substitute.” Many mothers, however, still fail to appreciate the risk their young babies face in being given any except the natural infant food, and consequently babies are in large numbers wholly or partly weaned from the breast in the earliest months of their lives.
25. Infantile Mortality and Infants’ Milk Depots. London.
Breast feeding is far more general, comparatively, among the poorer mothers than among the well to do, as shown by the following summary which gives the number and per cent. of babies of mothers with husbands earning varying incomes, who had been completely weaned from the breast when they were 3, 6, or 9 months of age, respectively. For each of the periods indicated the percentage completely weaned from the breast is much greater in the groups where earnings are highest.
| Table 20.—Distribution of Babies Alive at 3, 6, and 9 Months of Age by Type of Feeding at Each of Said Ages, According to Annual Earnings of Father and Nativity of Mother. | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| ANNUAL EARNINGS OF FATHER AND NATIVITY OF MOTHER. | BABIES LIVING AT AGE OF— | ||||||||
| 3 months. | 6 months. | 9 months. | |||||||
| Total. | Completely weaned from breast. | Total. | Completely weaned from breast. | Total. | Completely weaned from breast. | ||||
| Number. | Per cent. | Number. | Per cent. | Number. | Per cent. | ||||
| Total | 1,355 | 193 | 14.2 | 1,313 | 250 | 19.0 | 1,282 | 358 | 27.5 |
| Under $624 | 341 | 22 | 6.5 | 322 | 32 | 9.9 | 309 | 57 | 18.4 |
| $625 to $899 | 358 | 48 | 13.4 | 351 | 63 | 17.9 | 342 | 85 | 24.9 |
| $900 and over[26] | 629 | 114 | 18.1 | 616 | 146 | 23.7 | 608 | 201 | 33.1 |
| Not reported[27] | 27 | 9 | 33.3 | 24 | 9 | 37.5 | 23 | 10 | 43.3 |
| Mother native | 765 | 155 | 20.3 | 747 | 195 | 26.1 | 735 | 251 | 34.1 |
| Under $624 | 69 | 10 | 14.5 | 66 | 13 | 19.7 | 65 | 18 | 27.7 |
| $625 to $899 | 180 | 36 | 20.0 | 177 | 46 | 26.0 | 173 | 55 | 31.8 |
| $900 and over[26] | 491 | 100 | 20.4 | 482 | 127 | 26.3 | 476 | 168 | 35.3 |
| Not reported[27] | 25 | 9 | 36.0 | 22 | 9 | 40.9 | 21 | 10 | 47.6 |
| Mother foreign | 590 | 38 | 6.4 | 566 | 55 | 9.7 | 547 | 102 | 18.6 |
| Under $624 | 272 | 12 | 4.4 | 256 | 19 | 7.4 | 244 | 39 | 16.0 |
| $625 to $899 | 178 | 12 | 6.7 | 174 | 17 | 9.8 | 169 | 30 | 17.8 |
| $900 and over[26] | 138 | 14 | 10.1 | 134 | 19 | 14.2 | 132 | 33 | 25.0 |
| Not reported[27] | 2 | 2 | 2 | ||||||
26. Includes those reported as earning “ample.” “Ample,” as used in this report has a somewhat technical meaning; when information concerning the father’s earnings was not available and the family showed no evidences of poverty, the word “ample” was used. When, however, the family was clearly in a state of abject poverty, it was included in the group “Under $521.”
27. Unmarried mothers’ babies also included.
126Breast feeding, wholly or in part, is continued for a longer period by foreign than by native mothers, as indicated in the preceding table, showing that 20.3, 26.1, and 34.1 per cent. of the native mothers’ babies as compared with 6.4, 9.7, and 18.6 per cent. of the foreign mothers’ babies had been weaned from the breast at the age of 3, 6, and 9 months, respectively.
| Table 25.—Distribution of All Births, Live Births, and Stillbirths and of Deaths During First Year, and Infant Mortality Rate, According to Sex of Baby and Nativity of Mother. | ||||||
|---|---|---|---|---|---|---|
| SEX OF BABY AND NATIVITY OF MOTHER. | All births. | Live births. | STILLBIRTHS. | DEATHS DURING FIRST YEAR. | ||
| Total. | Rate per 1,000 births. | Total. | Infant mortality rate. | |||
| BABIES OF NATIVE MOTHERS. | ||||||
| Total number | 860 | 815 | 45 | 52.3 | 85 | 104.3 |
| Male: | ||||||
| Number | 433 | 406 | 27 | 62.4 | 46 | 113.3 |
| Per cent. | 50.3 | 49.8 | 60.0 | 54.1 | ||
| Female: | ||||||
| Number | 427 | 409 | 18 | 42.2 | 39 | 95.4 |
| Per cent. | 49.7 | 50.2 | 40.0 | 45.9 | ||
| BABIES OF FOREIGN MOTHERS. | ||||||
| Total number | 691 | 648 | 43 | 62.2 | 111 | 171.3 |
| Male: | ||||||
| Number | 380 | 355 | 25 | 65.8 | 59 | 166.2 |
| Per cent. | 55.0 | 54.8 | 58.1 | 53.2 | ||
| Female: | ||||||
| Number | 311 | 293 | 18 | 57.9 | 52 | 177.5 |
| Per cent. | 45.0 | 45.2 | 41.9 | 46.8 | ||
The extent to which the native and foreign mothers in Johnstown relinquished a part of their household duties as the time for their confinement approached is shown below:
| Table 26.—Distribution of Births According to Time of the Mother’s Relinquishment of Part of Household Duties Before Confinement, by Nativity of Mother. | |||
|---|---|---|---|
| TIME OF RELINQUISHMENT OF PART OF HOUSEHOLD DUTIES BEFORE CONFINEMENT. | All births. | To native mothers. | To foreign mothers. |
| All mothers | 1,551 | 860 | 691 |
| No household duties relinquished to day of confinement | 1,350 | 695 | 655 |
| Part of duties relinquished: | |||
| Less than 7 days before confinement | 3 | 1 | 2 |
| 7 to 13 days before confinement | 7 | 5 | 2 |
| 2 weeks to 1 month before confinement | 16 | 12 | 4 |
| 1 month or more before confinement | 174 | 146 | 28 |
| Had no household duties | 1 | 1 | |
Among the 174 babies of mothers who relinquished part of their household duties a month before confinement, the infant mortality rate was 112.5, as compared with 136.7 for those of other mothers.
| 127 | ||||
| Table 27.—Distribution of Births and of Deaths During First Year, and Infant Mortality Rate, According to Time of Relinquishment of Part of Household Duties of Mother Before Confinement. | ||||
|---|---|---|---|---|
| TIME OF RELINQUISHMENT OF PART OF HOUSEHOLD DUTIES BEFORE CONFINEMENT. | All births. | Live births. | Deaths during first year. | Infant mortality rate. |
| All mothers | 1,551 | 1,463 | 196 | 134.0 |
| No cessation or less than 1 month | 1,376 | 1,302 | 178 | 136.7 |
| 1 month or more | 171 | 160 | 18 | 112.5 |
| No housework | 1 | 1 | ||
To what extent the relinquishment of household duties at a given time directly affected the health of the child can not be definitely shown. A relation may exist, but on the other hand the difference in the mortality rate may be due to the fact that the mothers could afford to give consideration to their condition and escape some of their heaviest tasks as their pregnancy approached its end, and were members of families who were thoughtful of them and relieved them of these tasks or employed extra household assistance at such times.
Another indication of intelligence and of comfortable surroundings is the care given a mother in the early days of her baby’s life, particularly if she is a nursing mother. The duration of her rest period before the resumption of part of her household duties is one measure of this. The foreign mothers, with less education, more numerous and arduous tasks, less opportunity for leisure, and smaller incomes, begin to resume their housework sooner than the native mothers with young babies.
| Table 28.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality Rate, According to Time of Mother Resuming Part of Household Duties After Confinement, by Nativity of Mother. | |||||
|---|---|---|---|---|---|
| TIME OF RESUMING PART OF HOUSEHOLD DUTIES AFTER CONFINEMENT. | LIVE BIRTHS TO— | DEATHS DURING FIRST YEAR. | |||
| All mothers. | Native mothers. | Foreign mothers. | Total. | Infant mortality rate. | |
| Total | 1,463 | 815 | 648 | 196 | 134.0 |
| 8 days or less | 467 | 44 | 423 | 79 | 169.2 |
| 9 to 13 days | 560 | 446 | 114 | 70 | 125.0 |
| 14 days or more | 427 | 318 | 109 | 41 | 96.0 |
| Mother died or not reported | 9 | 7 | 2 | 6 | ([28]) |
28. Total number of live births less than 50; base therefore considered too small to use in computing an infant mortality rate.
The fact that a mother takes up her housework in the early days of her baby’s life does not necessarily increase the danger of its death. In some cases, however, mothers stated that the quantity of their breast milk was noticeably impaired when they got up and resumed their work too soon. Naturally this would affect the baby’s nutrition. In other cases a mother’s 128cares and duties may be so absorbing that she can not give the baby full attention. Whatever the exact explanation, attention should be called to the greater frequency of infant deaths when the mother resumed household duties very soon after childbirth.
A statement of the time of the mother’s resumption of household duties in full, like that giving the time of resumption in part, shows that the native mothers have the longer period of rest.
| Table 29.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality Rate, According to Time of Mother Resuming all Household Duties After Confinement, by Nativity of Mother. | |||||
|---|---|---|---|---|---|
| TIME OF RESUMING ALL HOUSEHOLD DUTIES AFTER CONFINEMENT. | LIVE BIRTHS TO— | DEATHS DURING FIRST YEAR. | |||
| All mothers. | Native mothers. | Foreign mothers. | Total. | Infant mortality rate. | |
| Total | 1,463 | 815 | 648 | 196 | 134.0 |
| 8 days or less | 219 | 13 | 206 | 37 | 168.9 |
| 9 to 13 days | 182 | 132 | 50 | 30 | 164.8 |
| 14 days or more | 1,053 | 663 | 390 | 123 | 116.8 |
| Mother died or not reported | 9 | 7 | 2 | 6 | ([29]) |
29. Total live births less than 50; base therefore considered too small to use in computing an infant mortality rate.
The infant mortality rates for all mothers in the group just referred to, according to the time of resuming housework in full after childbirth, show fewer infant deaths proportionately when the mother has had a longer rest; that is, a rest of two weeks or more.
A grouping of babies according to the income of the father shows the greatest incidence of infant deaths where wages are lowest, and the smallest incidence where they are highest, indicating clearly the relation between low wages and ill health and infant deaths.
For all live babies born in wedlock the infant mortality rate is 130.7. It rises to 255.7 when the father earns less than $521 a year or less than $10 a week, and falls to 84 when he earns $1,200 or more or if his earnings are “ample.”[30] The variation in the infant mortality rate from one earnings group to another is not perfectly regular and consistent, but if any two or more 129consecutive groups are combined an invariable lowering of the infant mortality rate from one such combined group to that next higher results.
30. “Ample” as used in this report has a somewhat arbitrary meaning. When information concerning the father’s earnings was not available and the family showed no evidences of actual poverty, the word “ample” was used. If no information concerning earnings was available when, on the other hand, the family was clearly in a state of abject poverty, then the income was tabulated as “Under $521.”
| Table 30.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality Rate, According to Annual Earnings of Father and Nativity of Mother, for Legitimate Live-Born Babies. | |||
|---|---|---|---|
| ANNUAL EARNINGS OF FATHER ACCORDING TO NATIVITY OF WIFE. | Total live births. | Deaths during first year. | Infant mortality rate. |
| Total | 1,431 | 187 | 130.7 |
| Under $625 | 384 | 82 | 213.5 |
| Under $521 | 219 | 56 | 255.7 |
| $521 to $624 | 165 | 26 | 157.6 |
| $625 to $899 | 385 | 47 | 122.1 |
| $625 to $779 | 224 | 24 | 107.1 |
| $780 to $899 | 161 | 23 | 142.9 |
| $900 or more | 186 | 18 | 96.8 |
| $900 to $1,199 | 138 | 14 | 101.4 |
| $1,200 or more | 48 | 4 | 83.3 |
| Ample[1] | 476 | 40 | 84.0 |
| Husbands with native wives | 785 | 76 | 96.8 |
| Under $625 | 80 | 16 | 200.0 |
| Under $521 | 32 | 9 | ([31]) |
| $521 to $624 | 48 | 7 | 145.8 |
| $625 to $899 | 193 | 20 | 103.6 |
| $625 to $779 | 86 | 6 | 69.8 |
| $780 to $899 | 107 | 14 | 130.8 |
| $900 or more | 129 | 10 | 77.5 |
| $900 to $1,199 | 92 | 7 | 76.1 |
| $1,200 of more | 37 | 3 | ([31]) |
| Ample[1] | 383 | 30 | 78.3 |
| Husbands with foreign wives | 646 | 111 | 171.8 |
| Under $625 | 304 | 66 | 217.1 |
| Under $521 | 187 | 47 | 251.3 |
| $521 to $624 | 117 | 19 | 162.4 |
| $625 to $899 | 192 | 27 | 140.6 |
| $625 to $779 | 138 | 18 | 130.4 |
| $780 to $899 | 54 | 9 | 166.7 |
| $900 or more | 57 | 8 | 140.6 |
| $900 to $1,199 | 46 | 7 | 152.2 |
| $1,200 or more | 11 | 1 | ([31]) |
| Ample[32] | 93 | 10 | 107.5 |
31. Total live births less than 50; base therefore considered too small to use in computing an infant mortality rate.
In considering the babies of native and of foreign mothers separately in the foregoing table, similar variations in mortality rates according to earnings of father are found, although the foreign infant death rate is higher in each group. The foreign are less numerous both actually and relatively in the higher wage groups.
130The foreigners of a given wage group almost always live in a poorer neighborhood than the natives earning the same amount. The foreigners go where they find their own countrymen, most of whom are poor, and hence even those who earn a fair wage find themselves, until they become Americanized, surrounded by poor conditions and an ignorant class of people.
It is of interest to note what per cent. of the native and what per cent. of the foreign are in the several earnings groups. The next table shows this for all married mothers and not simply for those of live-born babies as in the foregoing table.
| Table 31.—Number and Per Cent of Mothers by Nativity, According to the Annual Earnings of Husband. | ||||||
|---|---|---|---|---|---|---|
| ANNUAL EARNING OF HUSBAND. | ALL MOTHERS. | NATIVE MOTHERS. | FOREIGN MOTHERS. | |||
| Number. | Per cent. | Number. | Per cent. | Number. | Per cent. | |
| Total | 1,491 | 100.0 | 816 | 100.0 | 675 | 100.0 |
| Under $521 | 233 | 15.6 | 36 | 4.4 | 197 | 29.2 |
| $521 to $624 | 174 | 11.7 | 50 | 6.1 | 124 | 18.4 |
| $625 to $779 | 229 | 15.4 | 86 | 10.5 | 143 | 21.2 |
| $780 to $899 | 166 | 11.1 | 108 | 13.2 | 58 | 8.6 |
| $900 to $1,199 | 146 | 9.8 | 98 | 12.0 | 48 | 7.1 |
| $1,200 and over | 50 | 3.4 | 39 | 4.8 | 11 | 1.6 |
| Ample[33] | 493 | 33.1 | 399 | 48.9 | 94 | 13.9 |
The 1,491 married mothers included in the foregoing table bore 1,517 babies in 1911, the excess being due to plural births. The 33 unmarried mothers and their 34 babies (one mother had twins), although included in some of the general tables, are not included in those relative to the earnings of the husband.
In localities where large numbers of women are engaged in industrial work, comparisons are frequently made of the death rates among their babies with those of the babies of mothers not so engaged. In Johnstown, however, industrial occupations are not open to women, and but 3.1 per cent. of the mothers visited went outside their homes to earn money. All mothers who gained money by keeping lodgers or in any other way are, for convenience, designated “wage-earning” mothers, even though their earnings were not in the form of a definite wage at stated periods.
Although not industrially engaged, nearly one-fifth of the mothers did resort to some means of supplementing the earnings of their husbands. Usually they kept lodgers. This was done by the foreign mothers principally, exactly one-third of whom had lodgers, as compared with less than 1 per cent. 131of the native women. Usually work done outside the home consisted either of char work or of assisting husbands in their stores. Generally these stores were in the same building with the home.
When a mother of a young baby does not give her full time to her duties within the home but resorts to means of earning money, it generally indicates poverty. This is true to a greater degree in Johnstown than in places which have many inducements for women to work. In Johnstown, with its excess of males, especially in the foreign population, the woman’s services are particularly needed to make the home.
In the group where the husband earns $10 a week or less—that is, under $521 a year—many of the women are wage earners. In each group showing better earnings for the husband the number and percentage of wage-earning wives decline. Such a tabulation as the following almost automatically fixes the minimum wage on which a man, wife, and a child or two can live with any degree of comfort in Johnstown at about $780 a year. When the husband’s wage is less than $780 a year, it is shown that the wives, in considerable number, must be wage earners. As shown in the next table, in nearly half of the families where the husband earns $10 a week or less (less than $521 a year), the wife resorted to some means of earning money; when he earned as much as $900 a year, only 8.9 per cent. of the wives worked, and in the small group where the man earns as much as $1,200 a year, only 1 in 50.
| Table 32.—Number and Per Cent of Husbands with Wage-Earning Wives, by Nativity of Wife and Annual Earnings of Husband. | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| ANNUAL EARNINGS OF HUSBAND. | TOTAL HUSBANDS. | HUSBANDS HAVING NATIVE WIVES. | HUSBANDS HAVING FOREIGN WIVES. | ||||||
| Number. | Husbands with wage-earning wives. | Number. | Husbands with wage-earning wives. | Number. | Husbands with wage-earning wives. | ||||
| Number. | Per cent. | Number. | Per cent. | Number. | Per cent. | ||||
| Total | 1,491 | 278 | 18.6 | 816 | 26 | 3.2 | 675 | 252 | 37.3 |
| Under $521 | 233 | 111 | 47.6 | 36 | 9 | 25.0 | 197 | 102 | 51.8 |
| $521 to $624 | 174 | 57 | 32.8 | 50 | 3 | 6.0 | 124 | 54 | 43.5 |
| $625 to $779 | 229 | 51 | 22.3 | 86 | 4 | 4.7 | 143 | 47 | 32.9 |
| $780 to $899 | 166 | 25 | 15.1 | 108 | 6 | 5.6 | 58 | 19 | 32.8 |
| $900 to $1,199 | 146 | 13 | 8.9 | 98 | 1 | 1.0 | 48 | 12 | 25.0 |
| $1,200 and over | 50 | 1 | 2.0 | 39 | 11 | 1 | 9.1 | ||
| “Ample”[34] | 493 | 20 | 4.1 | 399 | 3 | .8 | 94 | 17 | 18.1 |
It is impossible to judge from statistics alone whether or not the work done by an individual woman, either her own housework or work for money, is so excessive as to affect her during pregnancy or while nursing to the extent of reacting on the health of the baby; but the fact is that the infant mortality rate is higher among the babies of wage-earning mothers than 132among others, being 188 as compared with a rate of 117.6 among the babies of nonwage-earning mothers. Wage-earning mothers and low-wage fathers are in practically the same groups, and it is difficult to secure an exact measurement of the comparative weight of the two factors in the production of a high infant mortality rate.
| Table 33.—Distribution of Live Births and of Deaths During First Year, and Infant Mortality Rate for Babies of Wage-earning and Nonwage-earning Mothers, According to Annual Earnings of Father. | ||||||
|---|---|---|---|---|---|---|
| ANNUAL EARNINGS OF FATHER. | MOTHER A WAGE EARNER. | MOTHER NOT A WAGE EARNER. | INFANT MORTALITY RATE. | |||
| Live births. | Number of deaths in first year. | Live births. | Number of deaths in first year. | Mother a wage earner. | Mother not a wage earner. | |
| Total | 266 | 50 | 1,165 | 137 | 188.0 | 117.6 |
| Under $521 | 105 | 26 | 114 | 30 | 247.6 | 263.2 |
| $521 to $624 | 53 | 8 | 112 | 18 | 150.9 | 160.7 |
| $625 to $779 | 48 | 6 | 176 | 18 | 127.1 | 102.3 |
| $780 or over, or “ample”[35] | 60 | 10 | 763 | 71 | 166.7 | 93.1 |
Of the 1,551 birth included in this investigation 34, or 2.2 per cent., occurred out of wedlock. Nine of the 32 illegitimate babies who were born alive died during their first year. It is recognized that these figures are a very small base from which to draw conclusions concerning the effect of illegitimacy on the infant mortality rate. It is of interest, nevertheless, to note that the findings for this small group are similar to those of countries which compute an infant mortality rate for legitimate and illegitimate children separately, that is, a rate for illegitimates more than twice as high as for children born in wedlock.
| Table 34.—Distribution of Births and of Deaths During First Year, and Infant Mortality Rate, According to Legitimacy. | ||||
|---|---|---|---|---|
| LEGITIMACY. | Total births. | Live births. | DEATHS DURING FIRST YEAR. | |
| Number. | Infant mortality rates. | |||
| Illegitimate | 34 | 32 | 9 | 281.3 |
| Legitimate | 1,517 | 1,431 | 187 | 130.7 |
Thirty-two, or 3.7 per cent., of the 860 native mothers, as compared with 2, or 0.3 per cent., of the 691 foreign mothers visited, had illegitimate children in 1911.
In addition to the data relating exclusively to babies born in 1911, a statement was secured from each mother as to the number and duration of each of her pregnancies and the result thereof; that is, the number of children she had borne, alive or dead, the number of miscarriages she had had, and the age at death of each live-born child who had died. Although this information was secured for all mothers, tabulations are presented of the data furnished by married mothers only. Comparatively few single mothers reported more than one child, and information from them on this point is not believed to be as reliable as that from married mothers.
The 1,491 married mothers of babies born in 1911 had had an aggregate of 5,554 pregnancies, resulting in 5,617 births, the excess of 63 births over pregnancies being due to plural births. Eight hundred and four of these children died under 1 year of age, making an infant mortality rate of 149.9 for all their babies, as compared with the rate of 134 for those born in 1911. The stillbirths of these women numbered 194, or 4.5 per cent. of the total number of births; miscarriages reported numbered 191, but these were not added to the total reportable[36] pregnancies.
36. “Reportable” pregnancies are those terminating either in the birth of a live child or of a dead child when the period of gestation exceeds 28 weeks; that is, when its registration or report is required by law.
Details as to the infant mortality rates for all babies born to native and foreign mothers included in this study, not only in the year 1911 but at any other time, are presented in the next table, which classifies the babies according to the total number of reportable pregnancies that their mothers had had, to and including the pregnancy resulting in the 1911 birth.
| Table 35.—Distribution of Mothers, of Live Births, and of Deaths During First Year, and Infant Mortality Rate for Babies of Native and Foreign Married Mothers, According to the Number of Reportable Pregnancies. | ||||||
|---|---|---|---|---|---|---|
| REPORTABLE PREGNANCIES FOR MARRIED MOTHERS. | Number of married mothers. | NUMBER OF BABIES. | INFANT MORTALITY RATE AMONG BABIES OF— | |||
| Born alive. | Died in first year. | All mothers. | Native mothers. | Foreign mothers. | ||
| Total | 1,491 | 5,363 | 804 | 149.9 | 113.1 | 184.6 |
| 1 | 339 | 322 | 35 | 108.7 | 75.9 | 183.7 |
| 2 | 283 | 544 | 59 | 108.5 | 76.5 | 156.7 |
| 3 | 214 | 626 | 92 | 147.0 | 118.0 | 177.6 |
| 4 | 186 | 723 | 78 | 107.9 | 99.4 | 116.3 |
| 5 | 147 | 704 | 103 | 146.3 | 86.1 | 191.5 |
| 6 | 94 | 546 | 88 | 161.2 | 157.4 | 163.6 |
| 7 | 83 | 555 | 78 | 140.5 | 100.0 | 173.8 |
| 8 | 54 | 426 | 95 | 223.0 | 157.6 | 272.7 |
| 9 | 33 | 283 | 41 | 144.9 | 128.4 | 155.2 |
| 10 or more | 58 | 634 | 135 | 212.9 | 164.5 | 257.6 |
The statistics, based upon the results of all her reportable pregnancies, show a generally higher infant mortality rate where the mother has had many 134pregnancies, but there is not always an increase from one pregnancy to the next. This is more clearly shown when the pregnancies are grouped as in the next table.
| Table 36.—Infant Mortality Rate for all Children Borne by Married Mothers, According to Specified Number of Reportable Pregnancies. | |
|---|---|
| REPORTABLE PREGNANCIES FOR MARRIED MOTHERS. | Infant mortality rate. |
| Total | 149.9 |
| 1 and 2 | 108.5 |
| 3 and 4 | 126.0 |
| 5 and 6 | 152.8 |
| 7 and 8 | 176.4 |
| 9 or more | 191.9 |
This tendency is shown in still another form of summary: Combinations of four or less pregnancies are, for convenience, considered as group 1, while the combinations of over four are designated group 2. The differences in rates in the two groups are notable. The infant mortality rate is much lower for the first than for the second group.
| Table 37.—Infant Mortality Rate for All Children Borne by Married Mothers, According to Specified Number of Reportable Pregnancies, by Groups | |
| REPORTABLE PREGNANCIES FOR MARRIED MOTHERS. | Infant mortality rate. |
|---|---|
| GROUP 1. | |
| 2 or less | 108.5 |
| 3 or less | 124.7 |
| 4 or less | 119.2 |
| GROUP 2. | |
| Over 4 | 171.5 |
| Over 5 | 178.8 |
| Over 6 | 183.9 |
This influence of the size of the family upon the infant mortality rate is shown in the computations giving the relative infant mortality rate for the different children borne by married mothers. The rate is most favorable for the second-born child, being 131.2. Among first born it is 143.6; for tenth or later born children 252.3.
| Table 38.—Infant Mortality Rate for All Children Borne by Married Mothers, According to the Order in which the Child was Born | |
|---|---|
| ORDER OF BIRTH. | Infant mortality rate. |
| First-born child | 143.6 |
| Second-born child | 131.2 |
| First and second born children | 138.3 |
| Third-born child | 144.2 |
| Fourth-born child | 142.0 |
| Third and fourth born children | 143.2 |
| Fifth-born child | 178.1 |
| Sixth-born child | 175.5 |
| Fifth and sixth born children | 177.0 |
| Seventh-born child | 192.1 |
| Eighth-born child | 165.4 |
| Seventh and eighth born children. | 181.5 |
| Ninth-born child | 128.2 |
| Tenth or later born child | 252.3 |
| Ninth and later born children | 201.1 |
135The next table gives a further elaboration of the same data; that is, it shows the infant mortality rate where such rates are lowest and highest, respectively, according to the age of the mother at the child’s birth and the order in which the child was born. Attention is again directed to the fact that the statistics presented in this section on “Reproductive histories” are based upon the total number of reportable pregnancies; that is, in addition to the pregnancies resulting in births in 1911, all prior pregnancies of the women considered in the investigation have been included.
| Table 39.—Lowest and Highest Infant Mortality Rates, According to Age of Mother at Birth of Child and the Order in which Child was Born. | ||||
|---|---|---|---|---|
| ORDER OF BIRTH. | INFANT MORTALITY RATES, ACCORDING TO MOTHER’S AGE. | |||
| Lowest mortality. | Highest mortality. | |||
| Mother’s age. | Mortality rate. | Mother’s age. | Mortality rate. | |
| All children | 20–24 | 140.0 | Under 17 | 367.3 |
| First child | 25–29 | 92.1 | 17–19 | 190.4 |
| Second child | 25–29 | 100.3 | 17–19 | 178.6 |
| Third child | 30–39 | 106.4 | 25–29 | 160.8 |
| Fourth child | 30–39 | 122.4 | 20–24 | 155.0 |
| Fifth child | 30–39 | 105.8 | 25–29 | 236.6 |
| Sixth child | 30–39 | 164.8 | 25–29 | 171.4 |
The difference in size of family for native and foreign mothers of different ages are indicated in the next table. The total and average number of live-born children, not reportable pregnancies, are given.
| Table 40.—Total and Average Number of Live-Born Children Borne by Married Mothers Having Either a Live Birth or a Stillbirth in 1911, Classified by Nativity and Age of Mother. | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| AGE OF MOTHER AT BIRTH OF CHILD IN 1911. | ALL MARRIED MOTHERS. | NATIVE MARRIED MOTHERS. | FOREIGN MARRIED MOTHERS. | ||||||
| Total. | Live-born children. | Total. | Live-born children. | Total. | Live-born children. | ||||
| Number. | Average. | Number. | Average. | Number. | Average. | ||||
| All ages | 1,465 | 5,363 | 3.7 | 801 | 2,600 | 3.2 | 664 | 2,763 | 4.2 |
| Under 20 years | 81 | 96 | 1.2 | 62 | 70 | 1.1 | 19 | 26 | 1.4 |
| 20 to 24 years | 456 | 908 | 2.0 | 258 | 483 | 1.9 | 198 | 425 | 2.1 |
| 25 to 29 years | 389 | 1,261 | 3.2 | 196 | 536 | 2.7 | 193 | 725 | 3.8 |
| 30 to 39 years | 459 | 2,480 | 5.4 | 240 | 1,188 | 5.0 | 219 | 1,292 | 5.9 |
| 40 years and over. | 80 | 618 | 7.7 | 45 | 323 | 7.2 | 35 | 295 | 8.4 |
The next table shows all losses of pregnancy sustained by 628 mothers and the rate of loss per 1,000 births for mothers having different numbers of births or reportable pregnancies. For all mothers it was 188.4. “Loss,” 136as here used, means the sum of infant deaths (or deaths in first year) and stillbirths.
| Table 41.—Aggregate Number of Births, Losses, and Rate of Loss Per 1,000 Births, According to Number of Births per Mother. | |||
|---|---|---|---|
| NUMBER OF BIRTHS PER MOTHER. | Aggregate number of births. | Aggregate number of losses. | Rate of loss per 1,000 births. |
| Total | 5,617 | 1,058 | 188.4 |
| 1 | 335 | 53 | 158.6 |
| 2 | 554 | 87 | 157.0 |
| 3 | 648 | 113 | 174.4 |
| 4 | 748 | 109 | 145.7 |
| 5 | 740 | 133 | 179.7 |
| 6 | 576 | 119 | 206.6 |
| 7 | 574 | 104 | 181.2 |
| 8 | 432 | 102 | 236.1 |
| 9 | 324 | 65 | 200.6 |
| 10 or more | 686 | 173 | 252.2 |
The influence of the economic factor on infant mortality among the babies born prior to 1911 can not be determined with exactness, as no inquiry was made concerning earnings of the father when the other children were born. But it is believed that his earnings during the year following the birth of the 1911 baby can be regarded as an index of the economic standing of the family for some time past. In individual cases, of course, revolutionary changes in the family’s income may have occurred, but for the great mass of people in the group considered it is not likely that within such a short space of time as that covered by the child-bearing period of the women considered—most of whom had not had numerous pregnancies—marked changes had taken place. If these known earnings are accepted as an index, the following variations are found to occur in the infant mortality rate for all the babies of whom a record was secured:
| Table 42.—Infant Mortality Rate for all Children of Married Mothers Included in this Investigation, Distributed According to the Father’s Earnings. | |
|---|---|
| FATHER’S ANNUAL EARNINGS. | Infant mortality rate. |
| Under $521 | 197.3 |
| $521 to $624 | 193.1 |
| $625 to $779 | 163.1 |
| $780 to $899 | 168.4 |
| $900 to $1,199 | 142.2 |
| $1,200 and over | 102.2 |
The infant mortality rate for the babies whose fathers earn under $521 is almost twice as great as for those born into families in the most prosperous group. These figures strengthen the conclusion reached in the study of the 137babies born in 1911, namely that the economic factor is of far-reaching importance in determining the baby’s chance of life.
| Table V.—Distribution of Live Births and of Deaths During First Year, According to Number of Persons and Number of Rooms per Family. | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PERSONS PER FAMILY (NOT INCLUDING BABY). | All live born babies. | NUMBER OF BABIES WHO WERE BORN ALIVE AND NUMBER OF SUCH BABIES WHO DIED DURING FIRST YEAR IN HOMES HAVING— | |||||||||||
| 1 room | 2 rooms | 3 rooms | 4 rooms | 5 rooms | 6 rooms | 7 rooms | 8 rooms | 9 rooms | 10 rooms and over. | Unknown number of rooms. | |||
| {Births | 1,463 | 33 | 165 | 147 | 526 | 222 | 233 | 38 | 43 | 22 | 12 | 22 | |
| Total | {Deaths | 196 | 3 | 29 | 24 | 79 | 20 | 20 | 6 | 6 | 4 | 2 | 3 |
| {Births | 24 | 3 | 7 | 4 | 6 | 2 | 2 | ||||||
| 2 | {Deaths | 19 | 1 | 5 | 4 | 6 | 1 | 2 | |||||
| {Births | 275 | 14 | 46 | 35 | 96 | 29 | 37 | 4 | 6 | 1 | 7 | ||
| 3 | {Deaths | 31 | 5 | 4 | 12 | 2 | 3 | 3 | 2 | ||||
| {Births | 234 | 7 | 44 | 20 | 83 | 40 | 23 | 4 | 5 | 2 | 2 | 4 | |
| 4 | {Deaths | 30 | 1 | 12 | 5 | 9 | 2 | 1 | |||||
| {Births | 229 | 27 | 24 | 88 | 31 | 43 | 4 | 5 | 1 | 1 | 5 | ||
| 5 | {Deaths | 22 | 1 | 6 | 9 | 1 | 4 | 1 | |||||
| {Births | 182 | 2 | 21 | 17 | 56 | 37 | 34 | 5 | 7 | 2 | 1 | ||
| 6 | {Deaths | 18 | 4 | 8 | 2 | 3 | 1 | ||||||
| {Births | 164 | 2 | 10 | 20 | 50 | 32 | 30 | 9 | 6 | 3 | 1 | 1 | |
| 7 | {Deaths | 15 | 1 | 2 | 6 | 1 | 3 | 1 | 1 | ||||
| {Births | 107 | 2 | 5 | 14 | 37 | 16 | 18 | 4 | 6 | 2 | 3 | ||
| 8 | {Deaths | 17 | 2 | 6 | 3 | 1 | 2 | 1 | 1 | 1 | |||
| {Births | 79 | 2 | 2 | 6 | 27 | 13 | 13 | 6 | 2 | 4 | 4 | ||
| 9 | {Deaths | 8 | 1 | 2 | 2 | 1 | 2 | ||||||
| {Births | 58 | 1 | 1 | 2 | 26 | 7 | 15 | 1 | 1 | 3 | 1 | ||
| 10 | {Deaths | 15 | 1 | 11 | 2 | 1 | |||||||
| {Births | 36 | 1 | 1 | 16 | 3 | 10 | 3 | 2 | |||||
| 11 | {Deaths | 4 | 1 | 1 | 1 | 1 | |||||||
| {Births | 21 | 1 | 1 | 10 | 2 | 6 | 1 | ||||||
| 12 | {Deaths | 5 | 2 | 1 | 1 | 1 | |||||||
| {Births | 20 | 1 | 13 | 4 | 1 | 1 | |||||||
| 13 | {Deaths | 4 | 3 | 1 | |||||||||
| {Births | 8 | 1 | 5 | 2 | |||||||||
| 14 | {Deaths | 2 | 1 | 1 | |||||||||
| {Births | 6 | 3 | 2 | 1 | |||||||||
| 15 | {Deaths | 1 | 1 | ||||||||||
| {Births | 4 | 4 | |||||||||||
| 16 | {Deaths | 2 | 2 | ||||||||||
| {Births | 3 | 1 | 1 | 1 | |||||||||
| 17 | {Deaths | ||||||||||||
| {Births | 5 | 1 | 1 | 1 | 1 | 1 | |||||||
| 18 | {Deaths | 1 | 1 | ||||||||||
| {Births | 2 | 2 | |||||||||||
| 19 | {Deaths | ||||||||||||
| {Births | 3 | 1 | 1 | 1 | |||||||||
| 20 | {Deaths | 1 | 1 | ||||||||||
| {Births | 1 | 1 | |||||||||||
| 22 | {Deaths | 1 | 1 | ||||||||||
| {Births | 1 | 1 | |||||||||||
| 23 | {Deaths | ||||||||||||
| Not | {Births | 1 | 1 | ||||||||||
| reported. | {Deaths | ||||||||||||
| 138 | |||||||||||||||
| Table VIII.—Distribution of Deaths of Infants at Specified Age, According to Cause of Death of Infant and Nativity of Mother. | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CAUSE OF DEATH OF INFANT AND NATIVITY OF MOTHER. | Total deaths under 1 year of age. | AGE AT DEATH. | |||||||||||||
| Less than 1 week. | 1 week but less than 1 month. | 1 month but less than 1 year. | |||||||||||||
| Total. | 1 day or less. | 2 days. | 3 to 6 days. | Total. | 1 week but less than 2. | 2 weeks but less than 3. | 3 weeks but less than 1 month. | Total. | 1 month but less than 2. | 2 months but less than 3. | 3 months but less than 6. | 6 months but less than 9. | 9 months and over. | ||
| All causes | 196 | 45 | 30 | 4 | 11 | 29 | 14 | 7 | 8 | 122 | 18 | 16 | 42 | 31 | 15 |
| Native mothers | 85 | 25 | 18 | 3 | 4 | 9 | 2 | 1 | 6 | 51 | 9 | 7 | 18 | 12 | 5 |
| Foreign mothers | 111 | 20 | 12 | 1 | 7 | 20 | 12 | 6 | 2 | 71 | 9 | 9 | 24 | 19 | 10 |
| Diarrhea and enteritis | 52 | 1 | 1 | 5 | 3 | 2 | 46 | 5 | 4 | 17 | 15 | 5 | |||
| Native mothers | 17 | 1 | 1 | 16 | 3 | 1 | 5 | 5 | 2 | ||||||
| Foreign mothers | 35 | 5 | 3 | 2 | 30 | 2 | 3 | 12 | 10 | 3 | |||||
| Respiratory diseases | 50 | 3 | 3 | 47 | 7 | 4 | 15 | 13 | 8 | ||||||
| Native mothers | 19 | 19 | 2 | 2 | 8 | 5 | 2 | ||||||||
| Foreign mothers | 31 | 3 | 3 | 28 | 5 | 2 | 7 | 8 | 6 | ||||||
| Premature births | 24 | 21 | 19 | 2 | 3 | 3 | |||||||||
| Native mothers | 11 | 11 | 11 | ||||||||||||
| Foreign mothers | 13 | 10 | 8 | 2 | 3 | 3 | |||||||||
| Congenital debility or malformation | 19 | 10 | 7 | 1 | 2 | 6 | 2 | 3 | 1 | 3 | 1 | 2 | |||
| Native mothers | 5 | 4 | 3 | 1 | 1 | 1 | |||||||||
| Foreign mothers | 14 | 6 | 4 | 1 | 1 | 5 | 2 | 3 | 3 | 1 | 2 | ||||
| Injuries at birth | 7 | 7 | 3 | 2 | 2 | ||||||||||
| Native mothers | 6 | 6 | 3 | 2 | 1 | ||||||||||
| Foreign mothers | 1 | 1 | 1 | ||||||||||||
| Other or not reported | 44 | 6 | 1 | 1 | 4 | 12 | 6 | 1 | 5 | 26 | 5 | 6 | 10 | 3 | 2 |
| Native mothers | 27 | 3 | 1 | 1 | 1 | 8 | 2 | 1 | 5 | 16 | 4 | 4 | 5 | 2 | 1 |
| Foreign mothers | 17 | 3 | 3 | 4 | 4 | 10 | 1 | 2 | 5 | 1 | 1 | ||||
| 139 | ||||||||
| Table X.—Distribution of Births to Married Wage-earning Mothers, According to Husband’s Annual Earnings and Nativity and Earnings of Mother. | ||||||||
|---|---|---|---|---|---|---|---|---|
| NATIVITY AND ANNUAL EARNINGS OF MARRIED MOTHER. | Total births. | BIRTHS TO MARRIED WAGE-EARNING MOTHER WITH HUSBAND EARNING ANNUALLY— | ||||||
| Under $521. | $521 to $624. | $625 to $779. | $780 to $899. | $900 to $1,199. | $1,200 and over. | Ample.[37] | ||
| All wage-earning mothers | 281 | 112 | 57 | 51 | 25 | 14 | 1 | 21 |
| Under $53 | 20 | 6 | 5 | 1 | 4 | 1 | — | 3 |
| $53 to $103 | 57 | 23 | 12 | 11 | 7 | 3 | — | 1 |
| $104 to $207 | 89 | 46 | 16 | 19 | 3 | 3 | — | 2 |
| $208 to $311 | 60 | 23 | 16 | 12 | 4 | 3 | 1 | 1 |
| $312 and over | 46 | 14 | 8 | 8 | 7 | 2 | — | 7 |
| Not reported | 9 | — | — | — | — | — | 2 | 7 |
| Native wage-earning mothers | 26 | 9 | 3 | 4 | 6 | 1 | — | 3 |
| Under $53 | 6 | 2 | 1 | — | 2 | 1 | — | — |
| $53 to $103 | 5 | 2 | 1 | 2 | — | — | — | — |
| $104 to $207 | 5 | 1 | 1 | 2 | 1 | — | — | — |
| $208 to $311 | 4 | 3 | — | — | 1 | — | — | — |
| $312 and over | 3 | 1 | — | — | 2 | — | — | — |
| Not reported | 3 | — | — | — | — | — | — | 3 |
| Foreign wage-earning mothers | 255 | 103 | 54 | 47 | 19 | 13 | 1 | 18 |
| Under $53 | 14 | 4 | 4 | 1 | 2 | — | — | 3 |
| $53 to $103 | 52 | 21 | 11 | 9 | 7 | 3 | — | 1 |
| $104 to $207 | 84 | 45 | 15 | 17 | 2 | 3 | — | 2 |
| $208 to $311 | 56 | 20 | 16 | 12 | 3 | 3 | 1 | 1 |
| $312 and over | 43 | 13 | 8 | 8 | 5 | 2 | — | 7 |
| Not reported | 6 | — | — | — | — | 2 | — | 4 |
| 140 | |||||||||||||||
| Table XI.—Distribution of Results of Reportable Pregnancies (Live Births and Stillbirths) and Miscarriages, According to Number per Mother and Nativity of Mother. | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NUMBER OF REPORTABLE PREGNANCIES PER MOTHER AND NATIVITY OF MOTHER. | REPORTABLE PREGNANCIES AND RESULTS THEREOF. | MISCARRIAGES IN ADDITION TO REPORTABLE PREGNANCIES. | |||||||||||||
| Total pregnancies. | Total births. | Excess due to plural births. | Number of mothers. | Live births. | Stillbirths. | Number of miscarriages reported. | Number of mothers reporting miscarriages. | ||||||||
| Number. | Number of mothers having live births. | Deaths in first year. | Number of still-births. | Number of mothers having still-births. | Per cent. of all births. | Total mothers. | Per cent. of all mothers. | ||||||||
| Number. | Number of mothers having babies die. | Infant mortality rate. | |||||||||||||
| All married mothers | 5,554 | 5,617 | 63 | 1,491 | 5,363 | 1,465 | 804 | 509 | 149.9 | 254 | 194 | 4.5 | 191 | 130 | 8.7 |
| 1 | 339 | 343 | 4 | 339 | 322 | 318 | 35 | 34 | 108.7 | 21 | 21 | 6.1 | 8 | 8 | 2.4 |
| 2 | 566 | 576 | 10 | 283 | 544 | 279 | 59 | 54 | 108.5 | 32 | 28 | 5.6 | 23 | 16 | 5.7 |
| 3 | 642 | 650 | 8 | 214 | 626 | 214 | 92 | 75 | 147.0 | 24 | 23 | 3.7 | 26 | 18 | 8.4 |
| 4 | 744 | 752 | 8 | 186 | 723 | 180 | 78 | 64 | 107.9 | 29 | 21 | 3.9 | 22 | 18 | 9.7 |
| 5 | 735 | 740 | 5 | 147 | 704 | 147 | 103 | 67 | 146.3 | 36 | 31 | 4.9 | 20 | 14 | 9.5 |
| 6 | 564 | 568 | 4 | 94 | 546 | 93 | 88 | 60 | 161.2 | 22 | 13 | 3.9 | 23 | 14 | 14.9 |
| 7 | 581 | 586 | 5 | 83 | 555 | 83 | 78 | 48 | 140.5 | 31 | 22 | 5.3 | 27 | 15 | 18.1 |
| 8 | 432 | 437 | 5 | 54 | 426 | 54 | 95 | 42 | 223.0 | 11 | 7 | 2.5 | 15 | 9 | 16.7 |
| 9 | 297 | 299 | 2 | 33 | 283 | 33 | 41 | 20 | 144.9 | 16 | 11 | 5.4 | 13 | 8 | ([38]) |
| 10 or more | 654 | 666 | 12 | 58 | 634 | 58 | 135 | 45 | 212.9 | 32 | 17 | 4.8 | 14 | 10 | 17.2 |
| Native | 2,717 | 2,744 | 27 | 816 | 2,600 | 801 | 294 | 206 | 113.1 | 144 | 115 | 5.2 | 136 | 92 | 11.3 |
| 1 | 234 | 236 | 2 | 234 | 224 | 222 | 17 | 17 | 75.9 | 12 | 12 | 5.1 | 7 | 7 | 3.0 |
| 2 | 346 | 351 | 5 | 173 | 327 | 170 | 25 | 23 | 76.5 | 24 | 21 | 6.8 | 18 | 13 | 7.5 |
| 3 | 333 | 338 | 5 | 111 | 322 | 111 | 38 | 31 | 118.0 | 16 | 16 | 4.7 | 21 | 15 | 13.5 |
| 4 | 376 | 377 | 1 | 94 | 362 | 94 | 36 | 31 | 99.4 | 15 | 13 | 4.0 | 13 | 10 | 10.6 |
| 5 | 325 | 326 | 1 | 65 | 302 | 65 | 26 | 21 | 86.1 | 24 | 19 | 7.4 | 13 | 10 | 15.4 |
| 6 | 222 | 222 | 37 | 216 | 37 | 34 | 22 | 157.4 | 6 | 5 | 2.7 | 17 | 9 | ([38]) | |
| 7 | 266 | 267 | 1 | 38 | 250 | 38 | 25 | 18 | 100.0 | 17 | 11 | 6.4 | 25 | 13 | ([38]) |
| 8 | 184 | 187 | 3 | 23 | 184 | 23 | 29 | 17 | 157.6 | 3 | 2 | 1.6 | 8 | 5 | ([38]) |
| 9 | 117 | 118 | 1 | 13 | 109 | 13 | 14 | 7 | 128.4 | 9 | 6 | 7.6 | 4 | 3 | ([38]) |
| 10 or more | 314 | 322 | 8 | 28 | 304 | 28 | 50 | 19 | 164.5 | 18 | 10 | 5.6 | 10 | 7 | ([38]) |
| 141 | |||||||||||||||
| Foreign | 2,837 | 2,873 | 36 | 675 | 2,763 | 664 | 510 | 303 | 184.6 | 110 | 79 | 3.8 | 55 | 38 | 5.6 |
| 1 | 105 | 107 | 2 | 105 | 98 | 96 | 18 | 17 | 183.7 | 9 | 9 | 8.4 | 1 | 1 | 1.0 |
| 2 | 220 | 225 | 5 | 110 | 217 | 109 | 34 | 31 | 156.7 | 8 | 7 | 3.6 | 5 | 3 | 2.7 |
| 3 | 309 | 312 | 3 | 103 | 304 | 103 | 54 | 44 | 177.6 | 8 | 7 | 2.6 | 5 | 3 | 2.9 |
| 4 | 368 | 375 | 7 | 92 | 361 | 92 | 42 | 33 | 116.3 | 14 | 8 | 3.7 | 9 | 8 | 8.7 |
| 5 | 410 | 414 | 4 | 82 | 402 | 82 | 77 | 46 | 191.5 | 12 | 12 | 2.9 | 7 | 4 | 4.9 |
| 6 | 342 | 346 | 4 | 57 | 330 | 56 | 54 | 38 | 163.6 | 16 | 8 | 4.6 | 6 | 5 | 8.3 |
| 7 | 315 | 319 | 4 | 45 | 305 | 45 | 53 | 30 | 173.8 | 14 | 11 | 4.4 | 2 | 2 | ([38]) |
| 8 | 248 | 250 | 2 | 31 | 242 | 31 | 66 | 25 | 272.7 | 8 | 5 | 3.2 | 7 | 4 | ([38]) |
| 9 | 180 | 181 | 1 | 20 | 174 | 20 | 27 | 13 | 155.2 | 7 | 5 | 3.9 | 9 | 5 | ([38]) |
| 10 or more | 340 | 344 | 4 | 30 | 330 | 30 | 85 | 26 | 257.6 | 14 | 7 | 4.1 | 4 | 3 | ([38]) |
38. Not shown when base is less than 50.
| 142 | |||||||||||||||
| Table XII.—Distribution of Results of Reportable Pregnancies (Live Births and Stillbirths) and Miscarriages, According to Number per Mother and Age of Mother at Each Pregnancy. | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NUMBER OF REPORTABLE PREGNANCIES AND AGE OF MOTHER AT BIRTH OF BABY BORN IN 1911. | REPORTABLE PREGNANCIES. | LIVE BIRTHS. | BABIES DYING IN FIRST YEAR. | STILLBIRTHS. | MISCARRIAGES. | ||||||||||
| Total. | Resulting births. | Number of mothers. | Number. | Number of mothers. | Number. | Number of mothers. | Infant mortality rate. | Number. | Number of mothers. | Per cent. of all births | Number reported. | Mothers reporting. | |||
| Number. | Excess over pregnancies.[39] | Number. | Per cent. of all mothers. | ||||||||||||
| All married mothers | 5,554 | 5,617 | 63 | 1,491 | 5,363 | 1,465 | 804 | 509 | 149.9 | 254 | 194 | 4.5 | 191 | 130 | 8.7 |
| Under 20 years | 107 | 108 | 1 | 89 | 96 | 81 | 12 | 11 | 125.0 | 12 | 12 | 11.1 | |||
| 20 to 24 years | 933 | 946 | 13 | 461 | 908 | 456 | 140 | 115 | 154.2 | 38 | 29 | 4.0 | 19 | 18 | 3.9 |
| 25 to 29 years | 1,316 | 1,329 | 13 | 395 | 1,261 | 389 | 185 | 132 | 146.7 | 68 | 55 | 5.1 | 46 | 27 | 6.8 |
| 30 to 39 years | 2,570 | 2,595 | 25 | 466 | 2,480 | 459 | 382 | 207 | 154.0 | 115 | 84 | 4.4 | 95 | 66 | 14.2 |
| 40 years and over | 628 | 639 | 11 | 80 | 618 | 80 | 85 | 44 | 137.5 | 21 | 14 | 3.3 | 31 | 19 | 23.8 |
| Average age: 28 years. | |||||||||||||||
| 1 reportable pregnancy | 339 | 343 | 4 | 339 | 322 | 318 | 35 | 34 | 108.7 | 21 | 21 | 6.1 | 8 | 8 | 2.4 |
| Under 20 years | 74 | 75 | 1 | 74 | 67 | 66 | 8 | 7 | 119.4 | 8 | 8 | 10.7 | |||
| 20 to 24 years | 178 | 179 | 1 | 178 | 176 | 175 | 18 | 18 | 102.3 | 3 | 3 | 1.7 | 3 | 3 | 1.7 |
| 25 to 29 years | 57 | 58 | 1 | 57 | 54 | 53 | 4 | 4 | 74.1 | 4 | 4 | 6.9 | 3 | 3 | 5.3 |
| 30 to 39 years | 30 | 31 | 1 | 30 | 25 | 24 | 5 | 5 | ([40]) | 6 | 6 | ([40]) | 2 | 2 | ([40]) |
| Average age: 23 years. | |||||||||||||||
| 2 reportable pregnancies | 566 | 576 | 10 | 283 | 544 | 279 | 59 | 54 | 108.5 | 3 | 28 | 5.6 | 23 | 16 | 5.7 |
| Under 20 years | 24 | 24 | 12 | 21 | 12 | 3 | 3 | ([40]) | 3 | 3 | ([40]) | ||||
| 20 to 24 years | 312 | 317 | 5 | 156 | 302 | 154 | 42 | 37 | 139.1 | 15 | 13 | 4.7 | 6 | 6 | 3.8 |
| 25 to 29 years | 148 | 151 | 3 | 74 | 141 | 73 | 9 | 9 | 63.8 | 10 | 9 | 6.6 | 5 | 3 | 4.1 |
| 30 to 39 years | 78 | 80 | 2 | 39 | 76 | 38 | 5 | 5 | 65.8 | 4 | 3 | 5.0 | 12 | 7 | ([40]) |
| 40 years and over | 4 | 4 | 2 | 4 | 2 | ||||||||||
| Average age: 25 years. | |||||||||||||||
| 3 reportable pregnancies | 642 | 650 | 8 | 214 | 626 | 214 | 92 | 75 | 147.0 | 24 | 23 | 3.7 | 26 | 18 | 8.4 |
| Under 20 years | 9 | 9 | 3 | 8 | 3 | 1 | 1 | ([40]) | 1 | 1 | ([40]) | ||||
| 20 to 24 years | 231 | 234 | 3 | 77 | 227 | 77 | 40 | 31 | 176.2 | 7 | 6 | 3.0 | 7 | 6 | 7.8 |
| 25 to 29 years | 285 | 288 | 3 | 95 | 277 | 95 | 41 | 33 | 148.0 | 11 | 11 | 3.8 | 14 | 7 | 7.4 |
| 30 to 39 years | 108 | 110 | 2 | 36 | 105 | 36 | 8 | 8 | 76.2 | 5 | 5 | 4.5 | 4 | 4 | ([40]) |
| 40 years and over | 9 | 9 | 3 | 9 | 3 | 2 | 2 | ([40]) | 1 | 1 | ([40]) | ||||
| Average age: 26 years. | |||||||||||||||
| 4 reportable pregnancies | 744 | 752 | 8 | 186 | 723 | 186 | 78 | 64 | 107.9 | 29 | 21 | 3.9 | 22 | 18 | 9.7 |
| 20 to 24 years | 156 | 160 | 4 | 39 | 148 | 39 | 28 | 21 | 189.2 | 12 | 6 | 7.5 | 3 | 3 | ([40]) |
| 25 to 29 years | 300 | 301 | 1 | 75 | 290 | 75 | 26 | 23 | 89.7 | 11 | 10 | 3.7 | 10 | 6 | 8.0 |
| 30 to 39 years | 252 | 255 | 3 | 63 | 249 | 63 | 21 | 17 | 84.3 | 6 | 5 | 2.4 | 6 | 6 | 9.5 |
| 40 years and over | 36 | 36 | 9 | 36 | 9 | 3 | 3 | ([40]) | 3 | 3 | ([40]) | ||||
| Average age: 29 years. | |||||||||||||||
| 5 reportable pregnancies | 735 | 740 | 5 | 147 | 704 | 147 | 103 | 67 | 146.3 | 36 | 31 | 4.9 | 20 | 14 | 9.5 |
| 20 to 24 years | 50 | 50 | 10 | 49 | 10 | 9 | 7 | 183.7 | 1 | 1 | 2.0 | ||||
| 25 to 29 years | 280 | 283 | 3 | 56 | 266 | 56 | 51 | 31 | 191.7 | 17 | 15 | 6.0 | 6 | 4 | 7.1 |
| 30 to 39 years | 375 | 377 | 2 | 75 | 361 | 75 | 40 | 27 | 110.8 | 16 | 14 | 4.2 | 12 | 8 | 10.7 |
| 40 years and over | 30 | 30 | 6 | 28 | 6 | 3 | 2 | ([40]) | 2 | 1 | ([40]) | 2 | 2 | ([40]) | |
| Average age: 30 years. | |||||||||||||||
| 6 reportable pregnancies | 564 | 568 | 4 | 94 | 546 | 93 | 88 | 60 | 161.2 | 22 | 13 | 3.9 | 23 | 14 | 14.9 |
| 20 to 24 years | 6 | 6 | 1 | 6 | 1 | 3 | 1 | ([40]) | |||||||
| 25 to 29 years | 132 | 133 | 1 | 22 | 127 | 21 | 23 | 17 | 181.1 | 6 | 1 | 4.5 | 6 | 3 | ([40]) |
| 30 to 39 years | 360 | 362 | 2 | 60 | 347 | 60 | 54 | 36 | 155.6 | 15 | 11 | 4.1 | 13 | 9 | 15.0 |
| 40 years and over | 66 | 67 | 1 | 11 | 66 | 11 | 8 | 6 | 121.2 | 1 | 1 | 1.5 | 4 | 2 | ([40]) |
| Average age: 33 years. | |||||||||||||||
| 7 reportable pregnancies | 581 | 586 | 5 | 83 | 555 | 83 | 78 | 48 | 140.5 | 31 | 22 | 5.3 | 27 | 15 | 18.1 |
| 25 to 29 years | 98 | 99 | 1 | 14 | 90 | 14 | 23 | 13 | 255.6 | 9 | 5 | 10.0 | 2 | 1 | ([40]) |
| 30 to 39 years | 392 | 395 | 3 | 56 | 377 | 56 | 45 | 28 | 119.4 | 18 | 15 | 4.6 | 19 | 11 | 19.6 |
| 40 years and over | 91 | 92 | 1 | 13 | 88 | 13 | 10 | 7 | 113.6 | 4 | 2 | 4.3 | 6 | 3 | ([40]) |
| Average age: 34 years. | |||||||||||||||
| 8 reportable pregnancies | 432 | 437 | 5 | 54 | 426 | 54 | 95 | 42 | 223.0 | 11 | 7 | 2.5 | 15 | 9 | 16.7 |
| 25 to 29 years | 16 | 16 | 2 | 16 | 2 | 8 | 2 | ([40]) | |||||||
| 30 to 39 years | 408 | 413 | 5 | 51 | 403 | 51 | 87 | 40 | 215.9 | 10 | 6 | 2.4 | 15 | 9 | 17.6 |
| 40 years and over | 8 | 8 | 1 | 7 | 1 | 1 | 1 | ([40]) | |||||||
| Average age: 35 years. | |||||||||||||||
| 9 reportable pregnancies | 297 | 299 | 2 | 33 | 283 | 33 | 41 | 20 | 144.9 | 16 | 11 | 5.4 | 13 | 8 | 24.2 |
| 30 to 39 years | 207 | 208 | 1 | 23 | 195 | 23 | 32 | 15 | 164.1 | 13 | 8 | 6.3 | 5 | 4 | ([40]) |
| 40 years and over | 90 | 91 | 1 | 10 | 88 | 10 | 9 | 5 | 102.3 | 3 | 3 | 3.3 | 8 | 4 | ([40]) |
| Average age: 37 years. | |||||||||||||||
| 10 or more reportable pregnancies | 654 | 666 | 12 | ([41])58 | 634 | 58 | 135 | 45 | 212.9 | 32 | 17 | 4.8 | 14 | 10 | 17.2 |
| 30 to 39 years | 360 | 364 | 4 | 33 | 342 | 33 | 85 | 26 | 248.5 | 22 | 11 | 6.0 | 7 | 6 | ([40]) |
| 40 years and over | 294 | 302 | 8 | 25 | 292 | 25 | 50 | 19 | 171.2 | 10 | 6 | 3.3 | 7 | 4 | ([40]) |
| Average age: 39 years. | |||||||||||||||
39. 143Excess of births over pregnancies due to plural births.
40. Rate not computed because of small base.
41. Includes 21 having 10 pregnancies; 16 having 11; 11 having 12; 6 having 13; 3 having 14; 1 having 16.
| 144 | |||||||||||||||
| Table XIII.—Distribution of Results of Reportable Pregnancies (Live Births and Stillbirths) and Miscarriages, According to Number per Mother and Husband’s Earnings. | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SPECIFIED NUMBER OF PREGNANCIES FOR ALL MARRIED MOTHERS AND ANNUAL EARNINGS OF HUSBAND. | REPORTABLE PREGNANCIES. | LIVE BIRTHS. | BABIES DYING IN FIRST YEAR. | STILLBIRTHS. | MISCARRIAGES. | ||||||||||
| Total. | Resulting births. | Number of mothers. | Number. | Number of mothers. | Number. | Number of mothers. | Infant mortality rate. | Number. | Number of mothers. | Per cent. of all births | Number reported. | Mothers reporting. | |||
| Number. | Excess over pregnancies.[42] | Number. | Per cent. of all mothers. | ||||||||||||
| All reportable pregnancies | 5,554 | 5,617 | 63 | 1,491 | 5,363 | 1,465 | 804 | 149.9 | 509 | 254 | 194 | 4.5 | 191 | 130 | 8.7 |
| Husband earns: | |||||||||||||||
| Under $521 | 938 | 946 | 8 | 233 | 902 | 227 | 178 | 197.3 | 110 | 44 | 31 | 4.7 | 27 | 17 | 7.31 |
| $521 to $624 | 691 | 700 | 9 | 174 | 668 | 173 | 129 | 193.1 | 75 | 32 | 25 | 4.6 | 22 | 14 | 8.0 |
| $625 to $779 | 816 | 826 | 10 | 229 | 797 | 227 | 130 | 163.1 | 88 | 29 | 21 | 3.5 | 21 | 15 | 6.6 |
| $780 to $899 | 611 | 616 | 5 | 166 | 588 | 163 | 99 | 168.4 | 61 | 28 | 23 | 4.5 | 30 | 19 | 11.4 |
| $900 to $1,199 | 574 | 581 | 7 | 146 | 548 | 143 | 78 | 142.3 | 48 | 33 | 24 | 5.7 | 25 | 18 | 12.3 |
| $1,200 and over | 196 | 199 | 3 | 50 | 186 | 49 | 30 | 161.3 | 18 | 13 | 9 | 6.5 | 8 | 6 | 12.0 |
| Ample[43] | 1,728 | 1,749 | 21 | 493 | 1,674 | 483 | 160 | 95.6 | 109 | 75 | 61 | 4.3 | 58 | 41 | 8.3 |
| 1 reportable pregnancy | 339 | 343 | 4 | 339 | 322 | 318 | 35 | 108.7 | 34 | 21 | 21 | 6.1 | 8 | 8 | 2.4 |
| Husband earns: | |||||||||||||||
| Under $521 | 48 | 48 | 48 | 43 | 43 | 11 | 11 | 5 | 5 | ||||||
| $521 to $624 | 23 | 23 | 23 | 22 | 22 | 2 | 2 | 1 | 1 | 1 | 1 | ||||
| $625 to $779 | 46 | 48 | 2 | 46 | 46 | 44 | 6 | 5 | 2 | 2 | 2 | 2 | |||
| $780 to $899 | 35 | 35 | 35 | 32 | 32 | 3 | 3 | 3 | 3 | ||||||
| $900 to $1,199 | 38 | 39 | 1 | 38 | 36 | 35 | 4 | 4 | 3 | 3 | |||||
| $1,200 and over | 13 | 13 | 13 | 13 | 13 | 1 | 1 | ||||||||
| Ample[43] | 136 | 137 | 1 | 136 | 130 | 129 | 8 | 61.5 | 8 | 7 | 7 | 5.1 | 5 | 5 | |
| 2 reportable pregnancies | 566 | 576 | 10 | 283 | 544 | 279 | 59 | 108.5 | 54 | 32 | 28 | 5.6 | 23 | 16 | 5.7 |
| Husband earns: | |||||||||||||||
| Under $521 | 62 | 64 | 2 | 31 | 62 | 31 | 11 | 176.4 | 11 | 2 | 2 | 3.1 | |||
| $521 to $624 | 72 | 74 | 2 | 36 | 68 | 36 | 8 | 177.6 | 6 | 6 | 6 | 8.1 | 3 | 1 | |
| $625 to $779 | 110 | 111 | 1 | 55 | 108 | 55 | 17 | 157.4 | 16 | 3 | 3 | 2.7 | 2 | 2 | 4.4 |
| $780 to $899 | 56 | 56 | 28 | 53 | 28 | 9 | 169.8 | 7 | 3 | 3 | 5.4 | 4 | 2 | ||
| $900 to $1,199 | 46 | 46 | 23 | 41 | 23 | 2 | 2 | 5 | 5 | 4 | 4 | ||||
| $1,200 and over | 16 | 16 | 8 | 14 | 7 | 1 | 1 | 2 | 1 | 1 | 1 | ||||
| Ample[43] | 204 | 209 | 5 | 102 | 198 | 99 | 11 | 55.6 | 11 | 11 | 8 | 5.3 | 9 | 6 | 5.9 |
| 145 | |||||||||||||||
| 3 reportable pregnancies | 642 | 650 | 8 | 214 | 626 | 214 | 92 | 147.0 | 75 | 24 | 23 | 3.7 | 26 | 18 | 8.4 |
| Husband earns: | |||||||||||||||
| Under $521 | 114 | 115 | 1 | 38 | 110 | 38 | 27 | 245.5 | 23 | 5 | 4 | 4.3 | 5 | 3 | |
| $521 to $624 | 102 | 104 | 2 | 34 | 101 | 34 | 16 | 158.4 | 13 | 3 | 3 | 1.9 | 1 | 1 | |
| $625 to $779 | 84 | 84 | 28 | 82 | 28 | 13 | 158.5 | 11 | 2 | 2 | 2.4 | 3 | 2 | ||
| $780 to $899 | 87 | 87 | 29 | 83 | 29 | 6 | 72.3 | 6 | 4 | 4 | 4.6 | 5 | 4 | ||
| $900 to $1,199 | 57 | 58 | 1 | 19 | 55 | 19 | 11 | 200.0 | 8 | 3 | 3 | 5.2 | 7 | 3 | |
| $1,200 and over | 6 | 7 | 1 | 2 | 7 | 2 | 1 | 1 | |||||||
| Ample[43] | 192 | 195 | 3 | 64 | 188 | 64 | 18 | 95.7 | 13 | 7 | 7 | 3.6 | 5 | 5 | 7.8 |
| 4 reportable pregnancies | 744 | 752 | 8 | 186 | 723 | 186 | 78 | 107.9 | 64 | 29 | 21 | 3.9 | 22 | 18 | 9.7 |
| Husband earns: | |||||||||||||||
| Under $521 | 104 | 104 | 26 | 101 | 26 | 13 | 128.7 | 9 | 3 | 2 | 1.9 | 4 | 2 | ||
| $521 to $624 | 88 | 89 | 1 | 22 | 86 | 22 | 10 | 116.3 | 9 | 3 | 1 | 3.4 | 2 | 2 | |
| $625 to $779 | 136 | 137 | 1 | 34 | 129 | 34 | 19 | 147.3 | 15 | 8 | 6 | 5.8 | 3 | 2 | |
| $780 to $899 | 96 | 97 | 1 | 24 | 95 | 24 | 13 | 136.8 | 12 | 2 | 1 | 2.1 | 3 | 3 | |
| $900 to $1,199 | 56 | 58 | 2 | 14 | 55 | 14 | 4 | 72.7 | 2 | 3 | 1 | 5.2 | 2 | 2 | |
| $1,200 and over | 40 | 41 | 1 | 10 | 39 | 10 | 5 | 4 | 2 | 2 | 2 | 2 | |||
| Ample[43] | 224 | 226 | 2 | 56 | 218 | 56 | 14 | 64.2 | 13 | 8 | 8 | 3.5 | 6 | 5 | 8.9 |
| 5 reportable pregnancies | 735 | 740 | 5 | 147 | 704 | 147 | 103 | 146.3 | 67 | 36 | 31 | 4.9 | 20 | 14 | 9.5 |
| Husband earns: | |||||||||||||||
| Under $521 | 130 | 131 | 1 | 26 | 125 | 26 | 21 | 168.0 | 12 | 6 | 6 | 4.6 | 3 | 3 | |
| $521 to $624 | 90 | 91 | 1 | 18 | 85 | 18 | 20 | 235.3 | 12 | 6 | 5 | 6.6 | 3 | 1 | |
| $625 to $779 | 100 | 100 | 20 | 99 | 20 | 18 | 181.8 | 13 | 1 | 1 | 1.0 | 3 | 2 | ||
| $780 to $899 | 110 | 110 | 22 | 106 | 22 | 13 | 122.6 | 8 | 4 | 4 | 3.6 | 3 | 2 | ||
| $900 to $1,199 | 65 | 66 | 1 | 13 | 60 | 13 | 6 | 100.0 | 5 | 6 | 4 | 10.0 | |||
| $1,200 and over | 30 | 30 | 6 | 26 | 6 | 10 | 6 | 4 | 3 | 2 | 1 | ||||
| Ample[43] | 210 | 212 | 2 | 42 | 203 | 42 | 15 | 73.9 | 11 | 9 | 8 | 4.2 | 6 | 5 | |
| 6 reportable pregnancies | 564 | 568 | 4 | 94 | 546 | 93 | 88 | 161.2 | 60 | 22 | 13 | 3.9 | 23 | 14 | 14.9 |
| Husband earns: | |||||||||||||||
| Under $521 | 132 | 132 | 22 | 124 | 21 | 26 | 209.7 | 14 | 8 | 3 | 6.1 | 2 | 2 | ||
| $521 to $624 | 60 | 60 | 10 | 59 | 10 | 9 | 152.5 | 8 | 1 | 1 | 1.7 | 6 | 2 | ||
| $625 to $779 | 114 | 115 | 1 | 19 | 110 | 19 | 14 | 127.3 | 11 | 5 | 2 | 4.3 | 3 | 2 | |
| $780 to $899 | 48 | 48 | 8 | 48 | 8 | 7 | 6 | 4 | 2 | ||||||
| $900 to $1,199 | 72 | 74 | 2 | 12 | 70 | 12 | 12 | 171.4 | 9 | 4 | 3 | 5.4 | 4 | 3 | |
| $1,200 and over | 12 | 12 | 2 | 11 | 2 | 3 | 1 | 1 | 1 | ||||||
| Ample[43] | 126 | 127 | 1 | 21 | 124 | 21 | 17 | 137.1 | 11 | 3 | 3 | 2.4 | 4 | 3 | |
| 146 | |||||||||||||||
| 7 reportable pregnancies | 581 | 586 | 5 | 83 | 555 | 83 | 78 | 140.5 | 48 | 31 | 22 | 5.3 | 27 | 15 | 78.1 |
| Husband earns: | |||||||||||||||
| Under $521 | 91 | 92 | 1 | 13 | 88 | 13 | 13 | 147.7 | 8 | 4 | 4 | 4.3 | 4 | 2 | |
| $521 to $624 | 56 | 56 | 8 | 51 | 8 | 15 | 294.1 | 6 | 5 | 4 | 8.9 | 1 | 1 | ||
| $625 to $779 | 98 | 101 | 3 | 14 | 97 | 14 | 16 | 164.9 | 9 | 4 | 3 | 4.0 | |||
| $780 to $899 | 35 | 35 | 5 | 32 | 5 | 6 | 5 | 3 | 2 | 3 | 1 | ||||
| $900 to $1,199 | 84 | 84 | 12 | 79 | 12 | 7 | 88.6 | 5 | 5 | 2 | 6.0 | 5 | 3 | ||
| $1,200 and over | 21 | 22 | 1 | 3 | 22 | 3 | 1 | 1 | 2 | 1 | |||||
| Ample[43] | 196 | 196 | 8 | 186 | 28 | 20 | 107.5 | 14 | 10 | 7 | 5.1 | 12 | 7 | ||
| 8 reportable pregnancies | 432 | 437 | 5 | 54 | 426 | 54 | 95 | 223.0 | 42 | 11 | 7 | 2.5 | 15 | 9 | 16.7 |
| Husband earns: | |||||||||||||||
| Under $521 | 120 | 120 | 15 | 117 | 15 | 31 | 265.0 | 12 | 3 | 2 | 2.5 | 5 | 2 | ||
| $521 to $624 | 96 | 98 | 2 | 12 | 94 | 12 | 22 | 234.0 | 10 | 4 | 2 | 4.1 | 1 | 1 | |
| $625 to $779 | 40 | 41 | 1 | 5 | 41 | 5 | 11 | 4 | 2 | 1 | |||||
| $780 to $899 | 48 | 49 | 1 | 6 | 46 | 6 | 11 | 5 | 3 | 2 | 5 | 3 | |||
| $900 to $1,199 | 24 | 24 | 3 | 24 | 3 | 6 | 3 | 1 | 1 | ||||||
| $1,200 and over | 16 | 16 | 2 | 16 | 2 | 3 | 2 | 1 | 1 | ||||||
| Ample[43] | 88 | 89 | 1 | 11 | 88 | 11 | 11 | 125.0 | 6 | 1 | 1 | 1.1 | |||
| 9 reportable pregnancies | 297 | 299 | 2 | 33 | 283 | 33 | 41 | 144.9 | 20 | 16 | 11 | 5.4 | 13 | 8 | |
| Husband earns: | |||||||||||||||
| Under $521 | 81 | 82 | 1 | 9 | 80 | 9 | 15 | 187.5 | 6 | 2 | 2 | 2.4 | 3 | 2 | |
| $521 to $624 | 72 | 72 | 8 | 70 | 8 | 10 | 142.9 | 6 | 2 | 1 | 2.8 | 3 | 3 | ||
| $625 to $779 | 18 | 18 | 2 | 15 | 2 | 3 | 1 | 1 | 1 | ||||||
| $780 to $899 | 18 | 19 | 1 | 2 | 17 | 2 | 5 | 2 | 2 | 2 | |||||
| $900 to $1,199 | 18 | 18 | 2 | 18 | 2 | 2 | 2 | ||||||||
| $1,200 and over | 18 | 18 | 2 | 16 | 2 | 2 | 1 | ||||||||
| Ample[43] | 72 | 72 | 8 | 67 | 8 | 9 | 134.3 | 4 | 5 | 4 | 6.9 | 6 | 2 | ||
| 147 | |||||||||||||||
| 10 or more reportable pregnancies | 654 | 666 | 12 | 58 | 634 | 58 | 135 | 212.9 | 45 | 32 | 17 | 4.8 | 14 | 10 | 17.2 |
| Husband earns: | |||||||||||||||
| Under $521 | 56 | 58 | 2 | 5 | 52 | 5 | 10 | 192.3 | 4 | 6 | 1 | 10.3 | 1 | 1 | |
| $521 to $624 | 32 | 33 | 1 | 3 | 32 | 3 | 17 | 3 | 1 | 1 | 1 | 1 | |||
| $625 to $779 | 70 | 71 | 1 | 6 | 70 | 6 | 16 | 228.6 | 4 | 1 | 1 | 1.4 | 2 | 1 | |
| $780 to $899 | 78 | 80 | 2 | 7 | 76 | 7 | 26 | 342.1 | 7 | 4 | 2 | 5.0 | 3 | 2 | |
| $900 to $1,199 | 114 | 114 | 10 | 110 | 10 | 24 | 218.2 | 8 | 4 | 3 | 3.5 | 2 | 2 | ||
| $1,200 and over | 24 | 24 | 2 | 22 | 2 | 5 | 1 | 2 | 1 | 8.3 | |||||
| Ample[43] | 280 | 286 | 6 | 25 | 272 | 25 | 37 | 136.0 | 18 | 14 | 8 | 4.9 | 5 | 3 | |
42. Excess of births over pregnancies due to plural births.
| 148 | ||||||
| Table XIV.—Distribution According to Number of Pregnancies and Age Groups of Married Mothers Classified by Nativity. | ||||||
|---|---|---|---|---|---|---|
| MOTHER’S AGE AND NUMBER OF REPORTABLE PREGNANCIES. | ALL MOTHERS. | NATIVE MOTHERS. | FOREIGN MOTHERS. | |||
| Number. | Per cent. | Number. | Per cent. | Number. | Per cent. | |
| Total pregnancies | 1,491 | 100.0 | 816 | 100.0 | 675 | 100.0 |
| 1 | 339 | 22.7 | 234 | 28.7 | 105 | 15.6 |
| 2 | 283 | 19.0 | 173 | 21.2 | 110 | 16.3 |
| 3 | 214 | 14.4 | 111 | 13.6 | 103 | 15.3 |
| 4 | 186 | 12.5 | 94 | 11.5 | 92 | 13.6 |
| 5 | 147 | 9.8 | 65 | 8.0 | 82 | 12.1 |
| 6 | 94 | 6.3 | 37 | 4.5 | 57 | 8.4 |
| 7 | 83 | 5.6 | 38 | 4.7 | 45 | 6.7 |
| 8 | 54 | 3.6 | 23 | 2.8 | 31 | 4.6 |
| 9 | 33 | 2.2 | 13 | 1.6 | 20 | 3.0 |
| 10 and over | 58 | 3.9 | 28 | 3.4 | 30 | 4.4 |
| Under 20 years, total pregnancies | 89 | 100.0 | 66 | 100.0 | 23 | 100.0 |
| 1 | 74 | 83.1 | 55 | 83.3 | 19 | 82.6 |
| 2 | 12 | 13.5 | 10 | 15.2 | 2 | 8.7 |
| 3 | 3 | 3.4 | 1 | 1.5 | 2 | 8.7 |
| 20 to 24 years, total pregnancies | 461 | 100.0 | 261 | 100.0 | 200 | 100.0 |
| 1 | 178 | 38.6 | 114 | 43.7 | 64 | 32.0 |
| 2 | 156 | 33.8 | 86 | 33.0 | 70 | 35.0 |
| 3 | 77 | 16.7 | 42 | 16.1 | 35 | 17.5 |
| 4 | 39 | 8.5 | 14 | 5.4 | 25 | 12.5 |
| 5 | 10 | 2.2 | 4 | 1.5 | 6 | 3.0 |
| 6 | 1 | .2 | 1 | 0.4 | ||
| 25 to 29 years, total pregnancies | 395 | 100.0 | 199 | 100.0 | 196 | 100.0 |
| 1 | 57 | 14.5 | 45 | 22.6 | 12 | 6.1 |
| 2 | 74 | 18.7 | 46 | 23.1 | 28 | 14.3 |
| 3 | 95 | 24.1 | 40 | 20.1 | 55 | 28.1 |
| 4 | 75 | 19.0 | 40 | 20.1 | 35 | 17.9 |
| 5 | 56 | 14.2 | 17 | 8.5 | 39 | 19.9 |
| 6 | 22 | 5.6 | 7 | 3.6 | 15 | 7.7 |
| 7 | 14 | 3.5 | 4 | 2.0 | 10 | 5.1 |
| 8 | 2 | .4 | 2 | 1.0 | ||
| 30 to 39 years, total pregnancies | 466 | 100.0 | 245 | 100.0 | 221 | 100.0 |
| 1 | 30 | 6.4 | 20 | 8.2 | 10 | 4.5 |
| 2 | 39 | 8.4 | 29 | 11.8 | 10 | 4.5 |
| 3 | 36 | 7.7 | 25 | 10.2 | 11 | 5.0 |
| 4 | 63 | 13.5 | 33 | 13.5 | 30 | 13.6 |
| 5 | 75 | 16.1 | 40 | 16.3 | 35 | 15.8 |
| 6 | 60 | 12.9 | 24 | 9.8 | 36 | 16.3 |
| 7 | 56 | 12.0 | 28 | 11.4 | 28 | 12.7 |
| 8 | 51 | 10.9 | 23 | 9.4 | 28 | 12.7 |
| 9 | 23 | 4.9 | 8 | 3.3 | 15 | 6.8 |
| 10 and over | 33 | 7.1 | 15 | 6.1 | 18 | 8.1 |
| 40 years and over, total pregnancies | 80 | 100.0 | 45 | 100.0 | 35 | 100.0 |
| 2 | 2 | 2.5 | 2 | 4.4 | ||
| 3 | 3 | 3.8 | 3 | 6.7 | ||
| 4 | 9 | 11.3 | 7 | 15.6 | 2 | 5.7 |
| 5 | 6 | 7.5 | 4 | 8.9 | 2 | 5.7 |
| 6 | 11 | 13.8 | 5 | 11.1 | 6 | 17.1 |
| 7 | 13 | 16.3 | 6 | 13.3 | 7 | 20.0 |
| 8 | 1 | 1.3 | 1 | 2.9 | ||
| 9 | 10 | 12.5 | 5 | 11.1 | 5 | 14.3 |
| 10 and over | 25 | 31.3 | 13 | 28.9 | 12 | 34.3 |
| 149 | |||||||||
| Table XV.—Distribution of Married Mothers by Losses Sustained, According to Nativity of Mother and Number of Possible Losses. | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| NUMBER OF BIRTHS OR POSSIBLE LOSSES AND NATIVITY OF MOTHER. | DISTRIBUTION OF MOTHERS ACCORDING TO NUMBER OF LOSSES. | ||||||||
| Number of mothers. | 1 loss. | 2 losses. | 3 losses. | 4 losses. | 5 losses. | 6 losses. | 8 losses. | 10 or more losses. | |
| All mothers | 1,491 | 399 | 121 | 60 | 24 | 13 | 8 | 1 | 2 |
| 1 birth | 335 | 53 | |||||||
| 2 births | 277 | 67 | 10 | ||||||
| 3 births | 216 | 73 | 14 | 4 | |||||
| 4 births | 187 | 55 | 13 | 8 | 1 | ||||
| 5 births | 148 | 48 | 19 | 11 | 1 | 2 | |||
| 6 births | 96 | 44 | 13 | 8 | 2 | 1 | 2 | ||
| 7 births | 82 | 22 | 19 | 10 | 2 | 1 | |||
| 8 births | 54 | 18 | 8 | 10 | 4 | 2 | 2 | ||
| 9 births | 36 | 9 | 10 | 5 | 1 | 1 | 2 | ||
| 10 or more births | 60 | 10 | 15 | 4 | 13 | 7 | 1 | 1 | 2 |
| Native mothers | 816 | 199 | 59 | 19 | 5 | 6 | 1 | 1 | |
| 1 birth | 232 | 29 | |||||||
| 2 births | 170 | 36 | 5 | ||||||
| 3 births | 111 | 35 | 7 | 1 | |||||
| 4 births | 98 | 33 | 6 | 3 | |||||
| 5 births | 65 | 19 | 10 | 4 | |||||
| 6 births | 38 | 19 | 7 | 1 | 1 | ||||
| 7 births | 37 | 10 | 8 | 3 | 1 | ||||
| 8 births | 21 | 8 | 5 | 3 | |||||
| 9 births | 15 | 4 | 4 | 3 | 1 | ||||
| 10 or more births | 29 | 6 | 7 | 1 | 4 | 5 | 1 | ||
| Foreign mothers | 675 | 200 | 62 | 41 | 19 | 7 | 7 | 2 | |
| 1 birth | 103 | 24 | |||||||
| 2 births | 107 | 31 | 5 | ||||||
| 3 births | 105 | 38 | 7 | 3 | |||||
| 4 births | 89 | 22 | 7 | 5 | 1 | ||||
| 5 births | 83 | 29 | 9 | 7 | 1 | 2 | |||
| 6 births | 58 | 25 | 6 | 7 | 2 | 2 | |||
| 7 births | 45 | 12 | 11 | 7 | 2 | ||||
| 8 births | 33 | 10 | 3 | 7 | 4 | 2 | 2 | ||
| 9 births | 21 | 5 | 6 | 2 | 1 | 2 | |||
| 10 or more births | 31 | 4 | 8 | 3 | 9 | 2 | 1 | 2 | |
| 150 | ||||
| Population, Registered Births, Deaths of Infants under 1 Year of Age, and Infant Mortality Rates for Registration States and Registration Cities having a Population of at Least 50,000 in 1910. | ||||
|---|---|---|---|---|
| AREA. | DEATHS[44] OF INFANTS UNDER 1 YEAR OF AGE. | |||
| Population in 1910. | Births.[45] | Number. | Per 1000 births.[46] | |
| REGISTRATION STATES. | ||||
| Connecticut | 1,114,756 | 27,291 | 3,476 | 127 |
| Maine | 742,371 | 15,578 | 2,108 | 135 |
| Massachusetts | 3,366,416 | 86,765 | 11,377 | 131 |
| Michigan | 2,810,173 | 63,566 | 7,912 | 124 |
| New Hampshire | 430,572 | 9,385 | 1,373 | 146 |
| Pennsylvania | 7,665,111 | 202,631 | 28,377 | 140 |
| Rhode Island | 542,610 | ([47])6,595 | ([47])1,111 | ([47])168 |
| Vermont | 355,956 | 7,343 | 791 | 168 |
| REGISTRATION CITIES OF 50,000 POPULATION OR OVER IN 1910. | ||||
| Connecticut: | ||||
| Bridgeport | 102,054 | 2,976 | 367 | 123 |
| Hartford | 98,915 | 2,411 | 286 | 119 |
| New Haven | 133,605 | 3,772 | 406 | 108 |
| Waterbury | 73,141 | 2,150 | 320 | 149 |
| Washington, D. C. | 331,069 | 7,016 | 1,068 | 152 |
| Portland, Me. | 58,571 | 1,163 | 167 | 144 |
| Massachusetts: | ||||
| Boston | 670,585 | 17,760 | 2,246 | 126 |
| Brockton | 56,878 | 1,359 | 134 | 99 |
| Cambridge | 104,839 | 2,462 | 293 | 119 |
| Fall River | 119,295 | 4,591 | 854 | 186 |
| Holyoke | 57,730 | 1,702 | 362 | 213 |
| Lawrence | 85,892 | 3,165 | 529 | 167 |
| Lowell | 106,294 | 2,630 | 607 | 231 |
| Lynn | 89,336 | 2,218 | 216 | 97 |
| New Bedford | 96,652 | 3,873 | 685 | 177 |
| Somerville | 77,236 | 1,728 | 174 | 101 |
| Springfield | 88,926 | 2,438 | 302 | 124 |
| Worcester | 145,986 | 3,918 | 536 | 137 |
| Michigan: | ||||
| Detroit | 465,766 | 11,960 | 2,138 | 179 |
| Grand Rapids | 112,571 | 2,693 | 329 | 122 |
| Saginaw | 50,510 | 897 | 130 | 145 |
| Manchester, N. H. | 70,063 | 1,939 | 375 | 193 |
| New York, N. Y. | 4,766,883 | 129,316 | 6,159 | 125 |
| Bronx Borough | 430,980 | 10,926 | 11,047 | 96 |
| Brooklyn Borough | 1,634,351 | 43,128 | 5,063 | 117 |
| Manhattan Borough | 2,331,542 | 66,112 | 8,900 | 135 |
| Queens Borough | 284,041 | 7,095 | 865 | 122 |
| Richmond Borough | 85,969 | 2,055 | 284 | 138 |
| Pennsylvania: | ||||
| Allentown | 51,913 | 1,406 | 202 | 144 |
| Altoona | 52,127 | 1,392 | 166 | 119 |
| Erie | 66,525 | 1,713 | 197 | 116 |
| Harrisburg | 64,186 | 1,308 | 169 | 129 |
| Johnstown | 55,482 | 1,628 | 268 | 165 |
| Philadelphia | 1,549,008 | 38,666 | 5,334 | 138 |
| Pittsburgh | 533,905 | 15,059 | 2,259 | 150 |
| Reading | 96,071 | 2,370 | 336 | 142 |
| Scranton | 129,867 | 3,512 | 520 | 148 |
| Wilkes-Barre | 67,105 | 1,840 | 269 | 146 |
| Rhode Island: | ||||
| Pawtucket | 51,622 | ([48]) | 191 | ([48]) |
| Providence | 224,326 | ([48]) | 827 | ([48]) |
44. Exclusive of stillbirths.
45. Provisional figures; exclusive of stillbirths.
46. Based on provisional figures for births.
47. The figures for Rhode Island are exclusive of Providence and Pawtucket.
48. Returns of births not received from State board in time for inclusion.
151It will be seen by this table that Johnstown is among the 10 cities of more than 50,000 population which had an infant mortality rate of 1910 in excess of 150 per 1,000 births. These 10 cities and their respective rates are as follows: Lowell, Mass., 231; Holyoke, Mass., 213; Manchester, N. H., 193; Fall River, Mass., 186; Detroit, Mich., 179; New Bedford, Mass., 177; Lawrence, Mass., 167; Johnstown, Pa., 165; Washington, D. C., 152; and Pittsburgh, Pa., 150.
It should be borne in mind that the absolute infant mortality rate of 134, computed for the group of babies included in this investigation, that is, for those born in Johnstown in 1911, can not be compared with any of the approximate rates in the foregoing table, since the basis of computation is entirely different. But the method used in this report seemed to be the only practicable one for our purpose, namely, to measure the infant mortality rate in different districts of the city where the babies are subjected to varying conditions.
152Conditions similar to those existing in Johnstown were found in Chicago by Dr. Alice Hamilton, Bacteriologist in the Memorial Institute for Infectious Diseases, Hull House. The results of a study made of 1,600 families in the neighborhood was published in 1910. The investigation was undertaken to find out the truth or falsity of a general feeling among the district nurses that a high birth rate was accompanied by a high death rate. It was found that a high birth rate was not so much accompanied as outrun by a high death rate. The number of children live-born was compared with the number of children who reached the age of three, so it is a study of child mortality, rather than of infant mortality. The child mortality rate rises and falls very much as does the infant mortality rate in Johnstown. A table calculated from the data of all the families shows an ascending mortality rate:
| No. in Family | Child Mortality Rate |
|---|---|
| 4 children and less | 118 |
| 6 children and more | 267 |
| 7 children and more | 280 |
| 8 children and more | 291 |
| 9 children and more | 303 |
Expressed in words this table says that child mortality increases as the number of children per family increases, until we have a death rate in families of eight and more, which is two and a half times as great as that in families of four children and under.
The findings of the bureau’s earlier study in Johnstown, Pa., are confirmed in many respects by the findings in Manchester—the coincidence of a high infant mortality rate with low earnings, poor housing, mother’s work, and large families.
The mortality rate among the 1,564 live-born babies studied in Manchester was 165 per 1,000 births, which is considerably higher than the estimated rate for the whole country.
Manchester is primarily a textile town, and the textile mills employed 36.3 per cent. of all the fathers of babies born in Manchester during the 12 153months covered by the study. Of the fathers, 13.7 per cent. were earning less than $450 per year; 48.5 per cent. less than $650; 22.9 per cent. $850 or more; 6.4 per cent. $1,250 or more.
Of the babies with fathers earning less than $450, about 1 in 4 died before it was 12 months old. The great majority of the babies had fathers in the wage group from $450 to $849, and of these about 1 in 6 died. Of the babies whose fathers earned $850 but less than $1,050, 1 in 8 failed to survive. Where the fathers earned $1,050 or more, 1 baby in 16 died in the first year.
Where families lived two or more persons per room, the infant death rate was twice as high as where they lived less than one person per room. The babies living in houses occupied by a single family died at the rate of 86.1 per 1,000, but those in tenements occupied by more than six families died at the rate of 236.6 per 1,000.
When the mother was a wage earner the baby’s chances of living were less than when she was not. Babies of mothers who had worked at some time during the year before the baby’s birth died at the rate of 199.2 per 1,000, while babies of nonworking mothers died at the rate of 133.9. Babies of mothers employed away from home some time during the year after childbirth while the baby was still alive and under four months old had a rate of 277.3, while babies of mothers not employed during that time had a rate of 122.
Babies of foreign-born mothers did not fare so well as babies of native mothers. The differences of rates, however, are only partly accounted for by their lower earnings. The largest foreign element in Manchester is Canadian French, and among them the infant mortality rate, 224 per 1,000 live births, is greater than that among any other group of the population, although their earnings are in general higher than those of other foreigners.
Sheer size of family appears to be one factor in this high Canadian-French rate, one-third of their babies being sixth or later in order of birth, while over one-sixth of these mothers had had from 9 to 18 children. These Canadian-French babies in families of 6 or more children died at the rate of 246.2 per 1,000 and the rate rises to 277.2 per 1,000 when only babies ninth or later in order of birth are considered.
This chapter shows that the female death-rate is much greater during the child-hearing age than at other periods and notably greater than the male death-rate at any period. The outstanding fact is that this abnormal female death-rate, between the ages of 15 and 45, must be ascribed to too frequent pregnancies and to those diseases of the lungs, heart and kidneys which are hastened by pregnancy. Ninety-five per cent. of such deaths could be averted by the dissemination of knowledge to prevent conception.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL BIOLOGICAL AND HYGIENIC ASPECTS. E. HEINRICH KISCH, M.D., Professor of the German Medical Faculty of the University of Prague, Physician to the Hospital and Spa of Marienbad, Member of the Board of Health, etc. Translated by M. Eden Paul, M.D. Rebman Co., New York.
It is astonishing to observe the number of full term deliveries and miscarriages that a woman will experience within a comparatively short period of time, as is seen too frequently among the laboring classes, and more especially, among the factory workers. If we assume the original mortality of childbirth to be 6 per mille, a woman who in the course of 15 years undergoes labor (at full term or prematurely) 16 times, runs a risk of death to be expressed by the ratio of 6 × 16 = 96 per mille; that is to say, on the average of 1,000 women who became pregnant as often as this, nearly one in ten will die in childbed. P. 278.
In certain serious general disorders, in diseases of the heart, or of the lungs, in pelvic deformity, and in pathological changes of the female reproductive organs, it may be right to employ means for the prevention of pregnancy—not merely sexual abstinence, but actual measures to prevent fertilization. P. 395.
Based upon the observations of Schauta and Fellner, the latter author advances the rule that in the case of a woman suffering from disease, marriage should be forbidden only when the mortality from the disease in question is not less than 10%. In this category we must include severe cases only 156of pulmonary tuberculosis, whilst cases of laryngeal tuberculosis will, according to this rule, be absolutely unfit for marriage. Among heart affections contra-indicating marriage, he includes mitral stenosis, other valvular affections in which there is serious disturbance of compensation, and myocarditis; he considers marriage inadmissible also in cases of chronic nephritis, and among surgical affections, in case of malignant tumor. No case in which during a previous pregnancy the patient has been affected by one of the following diseases; viz. severe chorea, mental disorders, severe epilepsy, pulmonary tuberculosis which progressed much during pregnancy, morbus cordis, with considerable disturbance of compensation, severe heart trouble due to Graves disease—in all such cases a repetition of pregnancy should be avoided. P. 261.
A study of maternal mortality, by Dr. Grace L. Meigs, head of the hygiene division of this bureau, has been undertaken as a direct corollary to the infant mortality inquiry. The sickness or death of the mother inevitably lessens the chances of the baby for life and health. A large proportion of the deaths of babies occur in the first days and weeks of life, and these early deaths can be prevented only through proper care of the mother before and at the birth of her baby.
In the introduction to the report on “Maternal mortality in connection with childbearing,” issued as a supplement to his report as medical officer of the local government board of Great Britain for 1914–15, Sir Arthur Newsholme says:
The present report is intended to draw attention to this unnecessary mortality from childbearing, to stimulate further local inquiry on the subject, and to encourage measures which will make the occurrence of illness and disability due to childbearing a much rarer event than at present.
The attainment of these ends is important as much in the interest of the child as of its mother. That the welfare of the child is wrapped up in that of the mother was fully recognized in the board’s circular letter of 31st July, 1914, and the schedule appended to that letter; and each year it is becoming more fully realized that, in order to insure healthy infancy and childhood, it is necessary that, both during pregnancy and at and after the birth of the 157infant, increased maternal care and guidance and medical assistance should be provided.
The Children’s Bureau studies of infant mortality in town and country reveal clearly the connection between maternal and infant welfare and make plain that infancy can not be protected without the protection of maternity.
In her report Dr. Meigs undertakes to do no more than to assemble and interpret figures already published by the United States Bureau of the Census and in the mortality reports of various foreign countries and to state accepted scientific views as to the proper care of maternity. She shows that maternal mortality, although in great measure preventable, is not decreasing in the United States. Her report reveals an unconscious public neglect due to age-long ignorance and fatalism. As soon as the public realizes the facts to which Dr. Meigs calls attention it doubtless will awake to action, and suitable provision for maternal and infant welfare will become an integral part of all plans for local protection of public health.
The report is summarized as follows:
“In 1913 in this country at least 15,000 women, it is estimated, died from conditions caused by childbirth; about 7,000 of these died from childbed fever, a disease proved to be almost entirely preventable, and the remaining 8,000 from diseases now known to be to a great extent preventable or curable. Physicians and statisticians agree that these figures are a great underestimate.
“In 1913 the death rate per 100,000 population from all conditions caused by childbirth was but little lower than that from typhoid fever; this rate would be almost quadrupled if only the group of the population which can be affected, women of childbearing age, were considered.
“In 1913 childbirth caused more deaths among women 15 to 44 years old than any disease except tuberculosis.
“The death rate due to this cause is almost twice as high in the colored as in the white population.
“Only 2 of a group of 15 important foreign countries show higher rates from this cause than the rate in the registration area of the United States. The rates of three countries, Sweden, Norway, and Italy, which are notably low, show that low rates for these conditions are attainable.
“The death rates from childbirth and from childbed fever for the registration area of this country are not falling; during the 13 years from 1900 to 1913 they have shown no demonstrable decrease. These years have been marked by a revolution in the control of certain other preventable diseases, such as typhoid, diphtheria, and tuberculosis. During that time the typhoid rate has been cut in half, the rate of tuberculosis markedly reduced, and the rate for diphtheria reduced to less than one-half. During this period the death rate from childbirth has decreased in England and Wales, Ireland, Australia, 158and Japan. The other foreign countries studied show stationary or slightly increasing rates. The death rate from childbed fever has decreased only in England and Wales, Ireland, and Scotland.
“These facts point to the need in this country and in foreign countries of higher standards of care for women at the time of childbirth.
“The low standards at present existing in this country result chiefly from two causes: (1) General ignorance of the dangers connected with childbirth and of the need for proper hygiene and skilled care in order to prevent them; (2) difficulty in the provision of adequate care due to special problems characteristic of this country. Such problems vary greatly in city and in country. In the country inaccessibility of any skilled care, due to pioneer conditions, is a chief factor.
“Improvement will come about only through a general realization of the necessity for better care at childbirth. If women demand better care, physicians will provide it, medical colleges will furnish better training in obstetrics, and communities will realize the vital importance of community measures to insure good care for all classes of women.”
While the figures given by Dr. Meigs are a startling indication of the great number of maternal fatalities occurring in various parts of the country, no estimates can be made of the number of mothers who survive only to suffer from a degree of preventable ill health which limits or defeats the well-being and happiness of their households.
MATERNAL MORTALITY FROM ALL CONDITIONS CONNECTED WITH CHILD BIRTH IN THE UNITED STATES AND CERTAIN OTHER COUNTRIES. By Grace L. Meigs, M.D. U. S. Department of Labor, Children’s Bureau, 1917.
For the last two decades civilized countries have been absorbed in the problem of preventing the enormous and needless waste of human life represented by their infant death rates. The importance of this problem has been felt more keenly in the last two years in the countries now at war; in these countries the efforts toward saving the lives of babies have redoubled since the war began. Side by side with this problem, another, which is only of late finding its true place, is that of the protection of the lives and health of mothers during their pregnancy and confinement. This is a question so closely bound up with that of the prevention of infant mortality that the two can not be separated.
159It is now realized that a large proportion of the deaths of babies occur in the first days and weeks of life, and that these deaths can be prevented only through proper care of the mother before and at the birth of her baby. It is also realized that breast feeding through the greater part of the first year of the baby’s life is the chief protection from all diseases; and that mothers are much more likely to be able to nurse their babies successfully if they receive proper care before, at, and after childbirth. Moreover, in the progress of work for the prevention of infant mortality it has become ever clearer that all such work is useful only in so far as it helps the mother to care better for her baby. It must be plain, then, to what a degree the sickness or death of the mother lessens the chances of the baby for life and health.
This question has also another side. Each death at childbirth is a serious loss to the country. The women who die from this cause are lost at the time of their greatest usefulness to the State and to their families; and they give their lives in carrying out a function which must be regarded as the most important in the world.
Questions then of the most vital interest to the whole Nation are these: How are the lives of the mothers in this country and other countries being protected? To what degree are the diseases caused by pregnancy and childbirth preventable? If preventable, how far are they being prevented in this country? Has there been the same great decrease in the last few years in sickness and death from these causes as that which has marked the great campaigns against other preventable diseases such as typhoid, tuberculosis, or diphtheria? How do the conditions in the United States compare with those in other countries?
Puerperal septicemia (childbed fever).—The fact is now well known that puerperal septicemia, or childbed fever, is in reality a wound infection, similar to such an infection after an accident or an operation, and that it can be prevented by the same measures of cleanliness and asepsis which are used so universally in modern surgery to prevent infection. The proof of the nature of this disease is one of the tremendous results of the scientific discoveries which were made in the latter part of the nineteenth century.
During the early part of that century childbed fever was one of the greatest hospital scourges known. It occurred also in private practice; but in hospitals where there was great opportunity for the spreading of infection the death rate from this disease was appalling. The average death rate in hospitals in all countries was 3 to 4 per cent. of all women confined; sometimes it reached 10 to 20 per cent. and even over 50 per cent. during short periods of epidemics. In the face of this terrific mortality many obstetrical hospitals were closed. Commissions were appointed to investigate the cause of these epidemics, and medical congresses devoted sessions to the discussion of the problem. In 1843 Oliver Wendell Holmes, and in 1847 Semmelweiss, 160published articles stating the theory that this fever was similar to a wound infection and was due chiefly to the carrying of infectious material on the hands of attendants from one case to another.
In 1913 in the “death-registration area” of the United States 10,010 deaths were reported as due to conditions caused by pregnancy and childbirth. Of these deaths, 4,542 were reported as caused by puerperal septicemia or childbed fever.
Using the death-registration area as a basis, we are justified in estimating that in 1913 in the whole United States 15,376 deaths were due to childbirth, and 6,977 of these were due to childbed fever. As will be shown later, these figures are without doubt a gross underestimate. As it is, they are striking enough—almost 7,000 deaths in one year in this country due to childbed fever, a disease to a large degree easily preventable; and over 8,000 due to the other diseases caused by pregnancy and confinement, most of which are preventable or curable by means well known to science.
The death rate from all diseases caused by pregnancy and confinement in 1913 in the registration area was 15.8 per 100,000 population (which includes all ages and both sexes). The death rate from puerperal septicemia was 7.2.
These figures, however, mean little to us unless we compare them with the death rates from other preventable diseases. In the same year and area the typhoid rate was 17.9 per 100,000 population; the rate from diphtheria and croup 18.8. The highest death rate from any one disease was that from tuberculosis, 147.6 per 100,000 population. Any such comparison with the rates from diseases to which both sexes and all ages are liable is of course very misleading; but in spite of that fact it is interesting to note that typhoid fever, the disease against which so great an amount of effort is now directed, has a rate at present but 2 per 100,000 population higher than that from the diseases caused by pregnancy and confinement.
Death rates per 100,000 women.—The death rates from childbirth are approximately doubled when worked on the basis of 100,000 women. This will be seen when Tables IV and III (p. 50) are compared. The former gives for the period 1900 to 1910, the annual death rates per 100,000 women in the group of 11 States which were in the death-registration area in 1900, the latter the death rates per 100,000 population in the same group of States for 161the same period. It is evident that the rates in Table IV for each year are slightly more than twice those in Table III for the same year.
Death rates per 100,000 women of childbearing age.... Again, a much higher but a more accurate death rate from these diseases is found when the basis taken is the group which alone is affected by these diseases—women of childbearing age. When the rate is based not upon 100,000 population of both sexes and all ages but upon 100,000 women 15 to 44 years of age, the rate as ordinarily given is multiplied several times.
In 1900, the only year for which the rates can be computed, the death rate in the registration area per 100,000 women 15 to 44 years of age from all diseases of pregnancy and confinement was 50.3; from puerperal infection, 21.6. The corresponding rates for the same year per 100,000 population were 13.1 and 5.6. In this year, therefore, the rates are almost quadrupled when based on that group of the population which alone can be affected by these diseases.
Moreover, the death rates as ordinarily given per 100,000 population conceal the fact that the diseases of pregnancy and childbirth are indeed among the most important causes of death of women between 15 and 44 years of age; the actual number of deaths shows this to be the case. In 1913 in the registration area these diseases caused more deaths than any other one cause of death except tuberculosis. In that year there were, among women 15 to 44 years of age, 26,265 deaths from tuberculosis; 9,876 deaths from the diseases of pregnancy and confinement; 6,386 from heart disease; 5,741 from acute nephritis and Bright’s disease; 5,065 from cancer; and 4,167 from pneumonia. Other diseases, such as typhoid, appendicitis, and the infectious diseases show far fewer deaths.
Death rates per 1,000 live births.—This rate, as will be shown repeatedly throughout the report gives a far clearer picture of the actual risk of childbirth than do any of the rates so far considered. This rate can be given only for one year, 1910, and only for the provisional birth-registration area for that year. The rate from all diseases caused by pregnancy and confinement is 6.5, from puerperal septicemia, 2.9, and from all other diseases of pregnancy and confinement, 3.6 per 1,000 live births. That is, in this area for every 154 babies born alive one mother lost her life.
Are the death rates from these diseases in the death-registration area of the United States higher or lower than those in other civilized countries? Have these rates in other countries been falling or rising in the last 13 years, while the rates of this country have been apparently stationary? These questions, 162like all those of comparative international statistics, are of immense interest, but they involve many difficulties and sources of error. They should be considered in reading the following summary.
In order to make possible a comparison of the death rates from these causes for 15 foreign countries with those for the United States, an average rate has been computed for the years 1900 to 1910 for each of the countries, using the same method as that in use in the United States. When the 16 countries studied are arranged in order, with the one having the lowest rate first, the death-registration area of the United States stands fourteenth on the list. (See Table XII, p. 56.) Only two countries, Switzerland and Spain, have higher rates; many of the countries, however, show rates differing but little from that of the United States. Markedly low rates are those of Sweden (6), Norway (7.8), and Italy (8.9); a strikingly high rate is that of Spain (19.6).
The death rate from childbirth per 1,000 live births is not available for the death-registration area of the United States, but can be given only for the small number of States and cities included in the provisional birth-registration area and for one year, 1910. (See p. 31.) This rate, 6.5, is considerably higher than that for 1910 of any of the countries studied. When the average rates for a number of years of the 15 countries are reckoned per 1,000 live births and arranged in order, it will be seen that the same group of countries—Sweden, Italy, and Norway—shows the lowest rates. (See Table XIII, p. 56.) Spain in this table shows the rate which is next to the highest, while Belgium now has the highest rate. For a comparative study of the rates of these countries the rates per 1,000 live births give undoubtedly the clearest picture of the actual conditions.
These rates show a wide variation. While in Sweden but one mother is lost for every 430 babies born alive, in Belgium one mother dies for every 172 babies, and in Spain one for every 175 babies born alive. The rates in Belgium and Spain are two and a half times as high as the rate in Sweden.
Far more significant than a comparison of actual death rates of various countries is a comparison of the changes which have occurred in these death rates in each country in recent years. England and Wales, Ireland, Japan, New Zealand, and Switzerland have shown a decrease in the death rate per 1,000 live births from all diseases caused by pregnancy and confinement; but, in this group, only in England and Wales and in Ireland has the death rate from puerperal septicemia decreased; in the other three countries this rate has remained practically the same, though the total rate has decreased.
In Australia, Belgium, Hungary, Italy, Norway, Prussia, Spain, and Sweden both the rate from childbirth and that from puerperal septicemia remained almost stationary during the periods studied.
163The total rate for Scotland shows a definite increase, though the rate from puerperal septicemia has decreased. (See Table XVI, p. 66.)
Communities are still to a great extent indifferent to or ignorant of the number of lives of women lost yearly from childbirth; many communities which are proud of their low typhoid or diphtheria rates ignore their high rates from childbed fever. Communities are only beginning to realize that among their chief concerns is the protection of the babies born within their limits, and necessarily also of the mothers of those babies before and at confinement.
The statistics of causes of death are available only for a certain portion of the United States, included in the so-called “death-registration area.” Unlike other civilized countries, the United States has no uniform laws for the registration of births and deaths. Moreover, the efficiency of enforcement of existing laws varies greatly in the different States. The Bureau of the Census in 1880 therefore established a “death-registration area,” which comprises “States and cities in which the registration of deaths is returned as fairly complete (at least 90 per cent. of the total), and from which transcripts of the deaths recorded under the State laws or municipal ordinances are obtained by the Bureau of the Census.” In 1880 this area included but 17 per cent. of the total population of the United States. As States and cities have passed better laws and obtained better enforcement they have been added to the registration area; the latter has increased greatly in size, but even in 1913 included only 65.1 per cent. of the population of the United States. For the remaining 34.9 per cent. of the population of the country we have no reliable statistics. This 34.9 per cent. includes the population of the greater number of the Southern States and of many Middle Western and Western States outside of certain registration cities in these States which are included in the area. No statements can be made, therefore, of the number of deaths from any cause in the United States as a whole; only an estimate can be made on the assumption that for any cause of death the same rate prevails in the remainder of the United States as in the death-registration area.
The registration of births is still more incomplete in this country than is the registration of deaths. For 1910 the United States Bureau of the Census established a “provisional birth-registration area,” including the New England States, Pennsylvania, Michigan, New York City and Washington, D. C.
Death rates per 1,000 births.—As shown above, the method of computation of death rates which gives the clearest picture of the hazards of childbirth is that which takes into account only the women giving birth to children in that year. This is the method in use in a large number of foreign countries. The advantages of the method are self-evident. A demonstration of 164the superiority of this method of computation is obtained by a study of the tables giving the death rates from these diseases for foreign countries. In certain countries, as for instance Belgium and Hungary, there has been in recent years an apparent fall in the average death rates as computed per 100,000 population, while the average rates computed per 1,000 live births have remained stationary or risen. This phenomenon is due, evidently, to a decline in the birth rate in these countries during these years, and shows how misleading the rates as given per 100,000 population undoubtedly are in countries with declining birth rates. Whether a fall in the birth rate has occurred in the United States is not known. If it has occurred in the registration area, it would mean that the slight rise in rates per 100,000 population between 1900 and 1913 means a greater rise in rates computed according to the number of births. Such an error might compensate for the opposite error due to the more complete registration of deaths from childbirth in the later years of this period.
Miscarriages are not reportable in any country, although a number of miscarriages (as the term is usually defined) probably are reported as stillbirths in certain countries. The fact that women having miscarriages are not considered in the base would lead to a somewhat higher death rate than that which would express absolutely the number of deaths per 1,000 women at risk.
Far more valuable than a comparison of average rates of foreign countries is a study of the rates of each country for a series of years in order to discover whether they are decreasing or increasing and to compare such changes in the various countries. While it may be dangerous on account of different countries, no such source of error is attached to the comparison of rates in the same country for a number of years. The period 1900 to 1913 (or the latest year for which figures are available) is a very short one for a study of a change in death rates. It would have been far more interesting to study the death rates for a long series of years in each country, choosing a period beginning before the introduction of methods of asepsis. But such a study for the complete list of countries considered was not thought advisable, because of the difficulties caused by variations in classification of causes of death in the earlier years.
In order to study the rates for any increase or decrease occurring during the last 13 years, the rates per 1,000 live births will be used rather than those per 100,000 population. In several countries—Belgium, Hungary, Italy, Norway, Prussia, and Spain—the rate from childbirth per 100,000 population apparently has fallen during the period, while the rate per 1,000 live births has 165remained almost the same, or has risen. The cause of this inconsistency is the fact that in these countries the birth rate or the proportionate number of births to the number of inhabitants has decreased.
Number of deaths of women from 15 to 44 years of age in the death-registration area from each cause and class of causes included in the abridged International List of Causes of Death (revision of 1909),[49] 1913.
49. Except No. 25, diarrhea and enteritis (under 2 years), and No. 34, senility.
(Computed from figures in Mortality Statistics, 1913, pp. 338 to 349, in which causes of death are given according to the detailed International List of Causes of Death.)
| Abridged International List No. | Cause of death. | Number of deaths. |
|---|---|---|
| 13, 14, 15 | Tuberculosis of the lungs, tuberculous meningitis, other forms of tuberculosis | 26,265 |
| 31, 32 | Puerperal septicemia (puerperal fever, peritonitis) and other puerperal accidents of pregnancy and labor | 9,876 |
| 19 | Organic diseases of the heart | 6,386 |
| 29 | Acute nephritis and Bright’s disease | 5,741 |
| 16 | Cancer and other malignant tumors | 5,065 |
| 22 | Pneumonia | 4,167 |
| 35 | Violent deaths (suicide excepted) | 3,262 |
| 1 | Typhoid fever | 2,706 |
| 30 | Noncancerous tumors and other diseases of the female genital organs | 2,669 |
| 26 | Appendicitis and typhlitis | 1,620 |
| 36 | Suicide | 1,562 |
| 23 | Other diseases of the respiratory system (tuberculosis excepted) | 1,458 |
| 18 | Cerebral hemorrhage and softening | 1,398 |
| 24 | Diseases of the stomach (cancer excepted) | 940 |
| 27 | Hernia, intestinal obstruction | 854 |
| 28 | Cirrhosis of the liver | 598 |
| 9 | Influenza | 489 |
| 17 | Simple meningitis | 484 |
| 8 | Diphtheria and croup | 330 |
| 12 | Other epidemic diseases | 312 |
| 6 | Scarlet fever | 307 |
| 5 | Measles | 304 |
| 3 | Malaria | 250 |
| 21 | Chronic bronchitis | 184 |
| 20 | Acute bronchitis | 90 |
| 33 | Congenital debility and malformations | 24 |
| 11 | Cholera nostras | 18 |
| 4 | Smallpox | 16 |
| 7 | Whooping cough | 9 |
| 2 | Typhus fever | 2 |
| 10 | Asiatic cholera | |
| 37 | Other diseases | 11,688 |
| 38 | Unknown or ill-defined diseases | 458 |
166A MUNICIPAL BIRTH CONTROL CLINIC. MORRIS H. KAHN, M. D., in New York Medical Journal for April 28, 1917.
Showing that large families among the poor are the result of ignorance of methods to prevent conception among the mothers.
The following studies were undertaken with a view to determining whether there was an actual need and demand for birth control education and whether such a demand, if it existed, could be supplied with any effect by a scientifically conducted clinic in the dispensaries of the Department of Health of the City of New York; we felt that it might be of scientific and sociological interest to publish a report and an analysis of the observations made, probably the first of their kind in this country. Section 1142 of our Penal Code was ignored in conducting this birth control study.
The social and economic status of the patients was fairly uniform, about the same as that of patients attending the other dispensary institutions in this city. A tabulation of the results was made under the following headings: Name and nationality; age; number of years married; number of living children and their ages; number of deceased children; number of miscarriages or abortions; contraceptive methods known or practised. More or less complete data were secured in 464 cases.
The average number of procreative years of married life was 16.1, the age of fifty years being considered in this study as the end of the procreative period for the seventy-two women who were older than that. The average number of living children was 3.27 and of deceased children 1.2, making a total average of 4.47 children born to each family. Of the 464 women, 176, or three eighths, had had abortions or miscarriages, the total number of such interruptions of pregnancy being 324, or an average of 1.8 each for the women involved.
Of the 464 women, 192 knew of no contraceptive methods and therefore had used none. The remaining 272 women knew of one or more methods, more or less effectual, for the prevention of conception. Of the 192 women who were ignorant of the use of contraceptives, practically one half, or 104, had a history of abortions, with a total of 202 abortions, or an average of two apiece. In contrast with this, of the 272 women who knew of one or more contraceptives, only one fourth, or seventy-two, had undergone abortions, with a total of 122 abortions, or an average of only 1.6 apiece.
A further analysis of our tables shows an interesting and striking relationship between ignorance of methods for the prevention of conception and the number of children. Sixty-eight women had had three children each. Of these, twenty-six, or thirty-eight per cent., were ignorant of contraceptives. Twenty-eight women had had four children each. Of these fourteen, or fifty per cent., were ignorant of contraceptives. Fifty-five women had had five children each. Of these thirty were ignorant of contraceptives, or fifty-four 167per cent. Thirty-two women had had six children each. Of these twenty were ignorant of contraceptives, or sixty-two per cent. Forty women had had seven children each. Of these thirty-eight were ignorant of contraceptives, or ninety-five per cent. Twenty-one women had had eight children each. Of these twenty were ignorant of contraceptives, or ninety-five per cent. Forty-four women had had nine or more children each, and of these all were ignorant of contraceptive measures. Arranged in tabular form, these data would appear as follows:
| Number of Women | Number of Children | Number Ignorant of Contraceptives | Percentage |
|---|---|---|---|
| 68 | 3 | 26 | 38 |
| 28 | 4 | 14 | 50 |
| 55 | 5 | 30 | 54 |
| 32 | 6 | 20 | 62 |
| 40 | 7 | 38 | 95 |
| 21 | 8 | 20 | 95 |
| 44 | 9 to 17 | all | 100 |
It is sometimes stated by opponents of birth control that contraceptive methods are known by every married person and that the fault and immorality of having a large family of unprovided for dependents lies not in ignorance of contraceptives but rather in a lack of determination on the part of one or both parents to use preventive measures; in other words, that the failure to use contraceptives results from the inconvenience attending some methods and also from the influence of religious sentiment.
The above data, however, tend to show that ignorance of contraceptives not only is a great factor in the production of large families, but is also a great factor in increasing the number of abortions. From the fact that two thirds of these women knew absolutely no contraceptive method, while the methods used by many of the others were ineffectual or positively harmful, it is apparent that there is a definite opportunity for educating these women in methods of regulating conception. That there is need and demand for such education is voiced in unmistakable language by the multitude of poor who seek advice from all practising physicians.
Prof. Theodate L. Smith, director of the Library Department, Child Study Institute, Clark University, investigated the records of the families of early graduates of Yale University (1701 to 1745) and of Harvard University (1658 to 1690); and found that of the wives of Harvard men, 37.3 per cent. died under the age of 45 years, while of the wives of Yale men, 40 per cent. died under 50 years. Prof. Smith also showed that there is a tendency for families very large in the first generation to die out in the third or fourth generation. One family of twenty children, by two wives, has living descendent 168by one son only, one daughter being untraceable. A family of ten brothers and sisters, only two of whom lived until 50, produced three surviving children, who in turn have produced one, and that a sickly specimen. Another family had fourteen in the first generation, eight in the second, six in the third and only two in the fourth.—Mary Alden Hopkins in Harper’s Weekly, June, 1915.
OBSTETRICS. A Text Book for the Use of Students and Practitioners. J. Whitridge Williams, Professor of Obstetrics, John Hopkins University, Obstetrician-in-Chief to the John Hopkins Hospital, Gynaecologist to the Union Protestant Infirmary, Baltimore, Md. D. Appleton & Co. 1912.
As a rule, all diseases which subject the organism to a considerable strain are much more serious when occurring in the pregnant woman. In general it may be said that pregnancy exerts a deleterious influence upon all chronic organic maladies, while its effect is usually less marked in acute infectious processes. The latter, however, frequently lead to premature delivery and the additional physical strain attending the latter matter render the course of the disease much less favorable. Page 489.
“Owing to the well known fact that pulmonary tuberculosis usually progresses much more rapidly after child bearing, it is advisable that tubercular women take every precaution to avoid the possibility of conception.” Page 383.
It would appear therefore that in the vast majority of cases the disease (tuberculosis) is not transmitted directly from the mother to the fetus, and that the latter is born with a tendency to tuberculosis, rather than with the disease itself. Hence it follows that the children of tubercular mothers should be brought under the best hygienic surroundings, and should not be suckled by their mothers. In view of the fact that the tubercular process usually becomes exacerbated either during pregnancy or after child birth, most authorities recommend that abortion be induced as a matter of routine in all tubercular women, and many that they be rendered sterile by artificial means. This appears to be a somewhat too extreme point of view, but I consider that abortion should be induced in the first pregnancy occurring after the onset of the disease, and whenever it makes its appearance during the early months of pregnancy. Page 494.
169THE PRACTICE OF OBSTETRICS. In original contributions by American Authors. Edited by Reuben Peterson, A.B., M.D., Professor of Obstetrics and Gynaecology in the University of Michigan, Ann Arbor, Mich. Obstetrician-in-Chief to the University of Michigan Hospital. Lea Bros. & Co. Philadelphia and New York. 1907. Chapter IX.
Exact observations on a large number of cases have demonstrated beyond doubt that with very rare exceptions a pregnancy exerts a harmful effect upon the course of the disease (tuberculosis). Page 344.
So seriously is the tubercular process affected by a concomitant pregnancy that it seems the duty of the physician to warn every tubercular girl against marriage. Especially deleterious to the patient are pregnancies which follow each other at short intervals. In such instances the patient must be strongly advised against a new impregnation. It hardly can be denied that in some of these cases artificial sterilization may be justified. An additional argument in favor of this procedure is the comparative frequency with which, if not the infection itself, at least a marked disposition to it is transmitted to the fetus in utero. P. 344.
A TEXT BOOK OF OBSTETRICS. Barton Cooke Hirst, M.D., Professor of Obstetrics in the University of Pennsylvania; Gynaecologist to the Howard and Orthopaedic and the Philadelphia Hospitals, etc. W. B. Saunders Co. 1909.
The influence of pregnancy upon tuberculosis is most unfavorable and in women predisposed to tuberculosis, gestation may be the determining factor in lighting up an attack. It is the duty of a physician to advise strongly against marriage and maternity in the case of a woman already infected, or predisposed to tuberculosis. If the patient is pregnant an induction of labor should be considered. P. 427.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D., Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
Women with tuberculosis should not marry, first, because this aggravates their own disease. Second, they may infect the husband, and third, they propagate tuberculous children. Knowing the tendency for a latent tuberculosis 170to break out in pregnancy, marriage is to be forbidden. If the woman marries, she should avoid conception. P. 481.
If tuberculosis of the lungs is manifested in early pregnancy, if there is fever, wasting, hemoptysis and advancing consolidation, that is, the process seems to be florid, abortion should be induced without delay. Trembley, of Saranac Lake induces abortion in the early months in all cases. Urgent symptoms of cardiac nature, persistent hemoptysis and dyspnea may require emptying of the uterus. Complicating nephritis, heart disease, and contracted pelvis, which is said to be more frequent in the tuberculous, will give early indications for interference. P. 481.
TUBERCULOSIS. Jos. B. De Lee.
The woman should be instructed how to avoid pregnancy in the future. Something must be done until the woman is cured of her tuberculosis, so that she may safely go through a confinement, because every accoucheur recoils with horror from the task of repeatedly doing abortions on these tuberculous women. P. 482.
THE PRACTICE OF OBSTETRICS. Designed for the use of Students and Practitioners of Medicine. J. Clifton Edgar, Prof. of Obstetrics and Clinical Midwifery in the Cornell University Medical College; Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity and Dispensary; Consulting Obstetrician to the New York Maternity and Jewish Maternity Hospitals. 5th Edition. Revised. P. Blakiston’s Co., Phil.
The subject of the relationship between tuberculosis and pregnancy has recently attained an increased degree of importance through the agitation in favor of the justification of abortion in the tuberculous pregnant woman. P. 314.
Statistics appear to show, according to Lancereaux, that a considerable number of cases of tuberculosis develop solely as a result of pregnancy. If pregnancy can thus affect health, how much more likely would it be for the disease to assert itself in a woman who is a fit subject for it, or in one who is actually consumptive. In the former class are so called candidates for tuberculosis who have a family history of the disease of much significance under these circumstances. One should strongly dissuade girls with tubercular history and antecedents from early marriage, fearing that repeated childbearing will infallibly light up the dreaded malady. What has been said of the candidate for tuberculosis applies with the same, or greater force in the case of so-called latent tuberculosis and of apparent recovery from the disease. Present 171sentiment is beginning to dissuade such women from marriage, not less for their own benefit than for the sake of posterity, and all organized movements which are seeking to eradicate tuberculosis from the world lay much stress on discouraging marriage in tuberculosis suspects. Until this view prevails there will necessarily be some justification for interrupting a pregnancy already under way. P. 314.
Sanatoria for consumptives do not care to admit pregnant women, and this prohibition is equivalent to ranking them as incurable. The fact that a candidate for tuberculosis runs a very great risk of becoming consumptive through childbirth is a most stubborn one, and when in addition to becoming a consumptive herself she also brings into the world an individual who is likely to become tubercular, it readily becomes apparent that the question of the propriety of therapeutic abortion is bound to become an issue in the future in the practice of obstetrics. P. 315.
A tubercular woman may go through gestation with no undue acceleration of her malady, only to succumb after delivery to acute general tuberculosis, or acute tubercular pneumonia. P. 315.
Tubercular pregnant women also show no little tendency to abort. P. 316.
TUBERCULOSIS A PREVENTABLE AND CURABLE DISEASE. S. Adolphus Knopf, M.D.; Professor of Phthisio-therapy at the New York Post-Graduate Medical School and Hospital; Associate Director of the Clinic for Pulmonary Disease of the Health Department; Attending Physician to the Riverside Sanitorium for Consumptives of the City of New York, etc. Moffat Yard & Co., 1909. New York.
We have emphasized the fact that tuberculosis is very rarely directly hereditary, but that what is often transmitted by tuberculous parents is a weakened system, or physiological poverty. Nevertheless it is evident that tuberculous individuals ought not to marry, and when tuberculosis develops in a married couple it is best that they should have no children. P. 354.
PULMONARY TUBERCULOSIS. Its Modern Prophylaxis and the Treatment in Special Institutions and at Home. S. Adolphus Knopf, M.D. P. Blakiston’s Sons & Co., Phil., 1899.
If conception has taken place in a tuberculous woman institute treatment, preferably in a sanatorium near the home of the patient. But as Treaudeau says, it is essential that the treatment be continued for a long time afterwards, and I should like to add that a repetition of pregnancy must be prevented. P. 283.
172THE TUBERCULOSIS PROBLEM AND SECTION 1142 OF THE PENAL CODE OF THE STATE OF NEW YORK. S. Adolphus Knopf, M.D. Reprinted from the New York Medical Journal for June 12th, 1915.
There seems to be no difference of opinion in the minds of men and women who have studied rational eugenics and sociology concerning the necessity of beginning to work with the preceding generation, and of teaching parents that quality is better than quantity, and that a large number of children, underfed or of mental, moral and physical inferiority, means race suicide, while the reverse means race preservation.
I cannot defend my attitude better than by telling you the conclusions I have arrived at in my study of the tuberculosis situation in the United States. In the families of the poor where there are usually numerous children, it really matters little whether it is the father or the mother who is acutely tuberculous. Since almost invariably they live in close and congested quarters, are underfed and insufficiently clad, it is of relatively rare occurrence when most of the children do not become infected with tuberculosis. In some of our tuberculosis clinics where we insist on an examination of all the children of the tuberculous parents visiting these special dispensaries, we find as many as fifty per cent. of the children to be afflicted with tuberculosis as the result of postnatal infection. In taking the history of a patient in my private consultation work, it is my invariable custom to ask whether he comes from a large family, and if so whether he was among the first or latter born children. As a rule, especially among the poor, it proves to be one of the latter born, (the fifth, sixth, seventh, eighth, ninth, etc.) who contracts tuberculosis, and I believe this to be because when he came to the world there were already many mouths to feed and food was scant, for the father’s income rarely increases with the increase of the family; and the mother, worn out with repeated pregnancies, cannot bestow upon the latter born children the same care which was bestowed upon the first. We know tuberculosis to be a preventable and curable disease, but we also know that it is the disease of poverty, privation, malnutrition, and bad sanitation. P. 4.
I do not know the penalty to be visited upon a physician who offends the majesty of the law as set forth in section 1142 of the penal code, but I for one am willing to take the responsibility before the law and before my God for every time I have counselled, and every time I shall counsel in the future, the prevention of a tuberculous conception, with a view to preserving the life of the mother, increasing her chances of recovery, and, last, but not least, preventing the procreation of a tuberculous race. P. 5.
173THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch, M.D., Professor of the German Medical Faculty of the University of Prague; Physician to the Hospital and Spa of Marienbad; Member of the Board of Health, etc. Translated by M. Eden Paul, M.D. Rebman Co., New York.
As regards the marriage of any woman suffering from tuberculosis we must take into consideration a fact that medical experience has conclusively established, namely, that the processes of generation have an unfavorable influence upon pulmonary tuberculosis. P. 259.
During pregnancy tuberculosis advances with such rapid strides that pregnancy and lying-in accelerate the fatal event. In some cases of consumption it is the first pregnancy that is the most perilous, but in other cases a later pregnancy proves more perilous. P. 260.
Dr. S. Adolphus Knopf, M.D., Professor of Medicine, Department of Phthisio-therapy of the New York Post Graduate Medical School and Hospital; Senior Visiting Physician to Riverside Hospital-Sanatorium for the Consumptive Poor of the City of New York, etc.
Of the 150,000 who it is estimated die annually from tuberculosis in the United States, I venture to say 50,000 have been bread winners. Estimating the value of such a single life to the community at only about $5,000, this makes a loss of $250,000,000 each year. Another third, I venture to say, represents children at school age. They have died without having been able to give any return to their parents or to the community. Making the average duration of their young life only 7.5 years, and estimating the cost to parents and the community at only $200 per annum, the community loses another $75,000,000. The value of lives of little babes, children below and above school age, adolescents not yet bread winners, and men and women no longer able to earn their living can not be estimated in exact figures, but is reasonable to suppose the total annual financial loss from tuberculosis in the United States to be at least half a billion dollars. This does not include the expenditures for hospitals, sanatoria, clinics, dispensaries, colonies, preventoria and other agencies, devoted to the solution of the tuberculosis problem.
In the face of these figures and the suffering, misery and disappointment of parents who lose their children after having tenderly loved and cared for them for some years, I wonder if there can be any doubt in the minds of sane men that it would have been better if these children had never been born. Surely all this is race suicide instead of race preservation.
Not so very long ago I was asked by a young colleague to aid in the diagnosis of tuberculosis in a day laborer. The man earned $12 a week, was 174thirty-six years of age on the day the examination and diagnosis was made, had been married fourteen years, and his eleventh child had been born on his last birthday; four or five had already died, two of them of tuberculous meningitis. A glance at the rest of the family showed that nearly all of them were predisposed to tuberculosis, if not already infected, and that a few years of continued underfeeding and bad housing would finish their earthly career. With two or three children to provide for the family might have lived in relative comfort; with better food and better home environments the father might never have become tuberculous and none of the children might have contracted the disease. The commonwealth would have been the gainer by two or three mentally and physically vigorous future citizens.
Only a few days ago, while an article for the Journal of Sociologic Medicine was in preparation, an Italian woman presented herself to me for examination. She gave her age as fifty-six, and had married quite young. She had borne her husband seventeen children, of which, however, only four were living. Some had died in infancy, some at school age, and some during adolescence. What useless suffering! What useless economic loss to the individual family and society at large. Upon examination, I found the woman’s mental condition even worse than her physical status. The repeated pregnancies, the frequent diseases in the family, thirteen deaths among her children, had made a mental and physical wreck of her. Yet the woman belonged to the better and well-to-do class of our population of Italian birth. What would her condition have been if she had also had to share in the struggle for the existence of the family, and had had to work in sweatshops or factories, as so many of the poor Italians have to do?
When pregnancy means danger to the life of the mother, or exacerbation of an existant mental or physical ailment, as, for example, tuberculosis, which is always aggravated by child-bearing, every conscientious physician should do his utmost to prevent childbirth in such an invalid.
Where there is tuberculosis or any other serious transmissible disease in one or both of the parents, or there is danger that it may be transmitted to the offspring, it should not only be the right but the sacred duty of the physician to prevent the conception of any physically and mentally handicapped offspring destined to become a burden to the community.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American Authors. Edited by Reuben Peterson, A.B., M.D., Professor of Obstetrics and Gynecology in the University of Michigan, Ann Arbor, Mich. Obstetrician and Gynecologist in Chief to the University of Michigan Hospital. Lea Bros. & Co., Phil. and New York. 1907. Chapter XIX.
Pephritis. From statistics we find that even excluding the cases of 175eclampsia, the maternal mortality from nephritis during pregnancy is 33%, and the fetal mortality between 50% and 60%. P. 352.
Women suffering from a chronic nephritis should be advised strongly against marriage, especially in the presence of a cardiac or pulmonary lesion. Married women should be warned against impregnation. P. 354.
Pyelitis. “On account of the increased dangers of pyelitic and especially of a pyelonephritic process during pregnancy, women suffering from these diseases should be warned against marriage. Married women should be warned against a new impregnation, on account of the marked tendency of pyelitis to recur with every pregnancy.” P. 355.
PRACTICAL OBSTETRICS. Thos. Watts Eden. Obstetrician, Physician and Lecturer on Midwifery and Gynecology, Charing Cross Hospital; Consulting Physician to Queen Charlotte’s Lying-in-Hospital; Surgeon to In-Patient Chelsea Hospital for Women. 4th Edition. C. V. Mosby Co. 1915.
Certain of the conditions enumerated form absolute indications for the induction to abortion. These are nephritis, (a form of kidney disease), uncompensated valvular lesions of the heart, advanced tuberculosis, insanity, irremediable malignant tumors, hydatidiform mole, uncontrollable uterine haemorrhage, and acute hydramnios. P. 652.
PRINCIPLES AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D., Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital and Dispensary, and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
All forms of nephritis have a very bad influence on the pregnancy, abortion and premature labor being common. (66% Hofmeier) Seitz found that only from 20% to 30% of the children survived. One of the causes of habitual death of the fetus, abortion, and premature labor is chronic nephritis. P. 497.
“The children of nephritics are usually puny and pale.” P. 497.
Both mother and child are seriously jeopardized by chronic nephritis, the mortalities being about 30% respectively. P. 497.
Women with chronic nephritis should not marry, and if married, should not conceive. P. 498.
Diabetes. Sterility is common. Abortion and premature labor occur in 33% of the pregnancies. The children, if the pregnancy goes to term, often die shortly after birth, the total mortality being 66%. P. 502.
176True diabetes has a very bad diagnosis. Offergold found over 50% mortality. Of the children 51% were still born, 10% died within a few days after birth, and 5% more before six months. P. 503.
If a woman comes under treatment with a history of diabetes it is best to terminate the pregnancy at once. P. 503.
THE PRACTICE OF OBSTETRICS. Designed for the use of Students and Practitioners of Medicine. J. Clifton Edgar. Professor of Obstetrical and Clinical Midwifery in the Cornell University Medical College; Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity Dispensary; Consulting Obstetrician to the New York Maternity and Jewish Hospitals. 5th Edition, Revised. P. Blakiston’s & Co., Philadelphia.
Statistics appear to show that labors in these women, (diabetes) are quite apt to end unfavorably, in one or another way. When diabetic women become pregnant their disease usually takes a turn for the worse. According to Lecorche, true diabetes who become pregnant, usually succumb to the disease within a short time after delivery. P. 305.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. By Joseph B. De Lee, M.D.
Over 20% of women with eclampsia die and statistics show that 10% of such cases developed in the maternities. For the child the chances are not good, nearly one half of the children dying as a result, that is, due to: prematurity, toxemia, asphyxiation by repeated convulsions of the mother, drugs administered to the mother, and injuries sustained during birth, especially forced delivery. Eclampsia is more easily developed in a pregnant woman because the kidneys are carrying an increased burden, and too often diseased through the pregnancy changes. The cause of eclampsia are unknown but in 20% of cases the convulsions begin during pregnancy, in 60% during labor, and in 20% after delivery. Page 365.
The treatment is to stop the gestation at a point before either mother or child, or both, are in danger either to life or to health. Page 1041.
MATERNAL MORTALITY. Grace L. Meigs, M.D., U. S. Department of Labor. 1917.
Puerperal albuminuria and convulsions, called also eclampsia, or toxemia of pregnancy, is a disease which occurs most frequently during pregnancy 177but may occur at or following confinement. It is a relatively frequent complication among women bearing their first children. When fully established its chief symptoms are convulsions and unconsciousness. In the early stages of the disease the symptoms are slight puffiness of the face, hands, and feet; headache; albumen in the urine; and usually a rise in blood pressure. Very often proper treatment and diet at the beginning of such early symptoms may prevent the development of the disease; but in many cases where the disease is well established before the physician is consulted, the woman and baby can not be saved by any treatment. In the prevention of deaths from this cause it is essential, therefore, that each woman, especially each woman bearing her first child, should know what she can do, by proper hygiene and diet, to prevent the disease; that she should know the meaning of these early symptoms if they arise, so that she may seek at once the advice of her doctor; and that she should have regular supervision during pregnancy, with examination of the urine at intervals.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. Joseph B. De Lee, M.D. Page 514.
Without doubt pregnancy has a bad effect on the course of this disease. It may develop a latent diabetes, there being cases where severe symptoms appeared only during successive pregnancies, and others where the disease grew progressively worse each time. Coma occurs in 30% of the cases and is almost always fatal. It may be brought on by a slight shock in pregnancy, but more often during and just after labor. Delivery seems to have a worse effect than most surgical operations, causing collapse, coma, or sudden death. Bronchitis has been noted in the puerperium, and this has been found to eventuate in tuberculosis. True diabetes has a very bad prognosis, authorities finding over 50% mortality, of which 30% died in coma, within two and one half years, and too often the child dies in utero.
MATERNAL MORTALITY. Grace L. Meigs, M.D., U. S. Department of Labor, 1917.
Some obstruction to labor in the small size or abnormal shape of the pelvic canal causes many deaths of mothers included in the class “other accidents of labor” and also many stillbirths. If such difficulty is discovered before labor, proper treatment will in almost all cases insure the life of mother and child; if it is not discovered until labor has begun, or perhaps until it has continued for many hours, the danger to both is greatly increased. Every 178woman, therefore, should have during pregnancy—and above all during her first pregnancy—an examination in which measurements are made to enable the physician to judge whether or not there will be any obstruction to labor. A case in which a complication of this kind is found requires the greatest skill and experience in treatment, but with such treatment the life and health of the mother are almost always safe.
PRINCIPLES AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D., Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital and Dispensary, and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
No subject in medicine presents greater difficulties in all its aspects than this one, (treatment of contracted pelves) and none demands such art or practical skill. Science aids little here. P. 709.
Outside factors must also be considered: 1—The environment, whether the parturient is in a squalid tenement, in the country, in a home where every appliance is attainable, or in a well equipped maternity. 2—Whether in the hands of a general practitioner or a trained specialist. 3—If the patient is a Catholic, all medically indicated procedures not being permitted. 4—The age of the parturient, and the probability of her having more children. Even with these enumerations, the possible factors which might influence a labor, or our decision regarding the course to pursue have not all been mentioned. P. 709.
THE PRACTICE OF OBSTETRICS. Designed for the use of Practitioners and Students of Medicine. J. Clifton Edgar, Professor of Obstetrics and Clinical Midwifery in the Cornell University Medical College. Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity Dispensary; Consulting obstetrician to the New York Maternity and Jewish Maternity Hospitals. 5th Edition, Revised. P. Blakiston’s & Co., Phila.
A knowledge of the female bony pelvis is the very alphabet of obstetrical science, and the foundation of obstetrical art. This structure is most important since it is from the disproportion between its size and that of the fetus, or from its abnormal shape that many of the difficulties of labor arise.
179PRACTICAL OBSTETRICS. Thos. Watts Eden. Obstetrician; Physician and Lecturer on Midwifery and Gynecology, Charing Cross Hospital; Consulting Physician to Queen Charlotte’s Lying-in-Hospital; Surgeon to In-Patient Chelsea Hospital for Women. 4th Edition. C. V. Mosby Co. 1915.
The general course of labor is modified by pelvic contractions in various ways. 1—Abnormal presentations are three or four times commoner in contracted than in normal pelves. 2—Prolapse of the cord is much commoner than in normal pelves. 3—When natural delivery occurs labor is prolonged and the mechanism is modified. 4—Unless the true conjugate is at least 3¼ inches, even with artificial aid the survival of the child is seriously jeopardized. 5—The maternal risks are increased by the greater length and difficulty of the labor and by the frequent necessity of employing artificial methods of delivery. 6—The fetal risks are increased in natural delivery by severe compression of the head during its passage through the narrow pelvis, and other circumstances by the operations required to effect delivery, some of which involve the destruction of the fetus. P. 409.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American authors. Edited by Reuben Peterson, A.B., M.D. Lea Bros. & Co., Phil. and New York. 1907.
Labor complicated by anomalies of the Bony Pelvis. John F. Moran, M.D.
The frequency with which pelvic contraction occurs can only be determined with relative accuracy. There is in existence a comparatively large amount of statistical data on this subject, but the reports of different investigators vary within wide limits, and these variations are naturally not to be explained entirely on the assumption of racial conditions, or geographic distribution. Between these wide limits are arrayed the figures of about 20 modern observers in different parts of the civilized world who have reported statistics of cases. The combined figures of 19 observers include a total of over 150,000 cases examined for pelvic contraction. In these cases the average of contraction is found to be about 10%. Williams concludes that contracted pelves occur in from 7% to 8% of the white women of this country. P. 658–659.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch, M.D. Professor of the German Medical faculty of the University of Prague; Physician to the Hospital and Spa of Marienbad; Member of the Board of Health, etc. Translated by M. Eden Paul, M.D. Rebman Co., New York.
These are cases (severe heart disease) in which, in my opinion, it is the 180physician’s duty to concern himself with the subject of the use of preventive measures, and having regard for the preservation of a woman’s life, and uninfluenced by any false delicacy, but with simple earnestness to inform his patient with respect to the needful prophylactic measures. The artificial termination of pregnancy, which unquestionably is often justified in women suffering from heart disease, but which unfortunately is apt to have very unfavorable results, will rarely need to be discussed if by the proper employment of preventive measures care is taken that pregnancy does not recur too frequently. P. 255.
OBSTETRICS. A Text Book for the use of Students and Practitioners. Whitridge Williams, Professor of Obstetrics, Johns Hopkins University; Obstetrician in Chief to the Johns Hopkins Hospital; Gynecologist to the Union Protestant Infirmary, Baltimore, Md. D. Appleton & Co., 1912.
Some authorities recommend that women suffering from heart lesions should be dissuaded from marriage, or if married, from becoming pregnant. This, however, appears to be an extreme view, though of course when the lesion is serious and the compensation faulty the dangers of child-bearing should be carefully explained. P. 498.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American authors. Edited by Reuben Peterson, A.B., M.D., Professor of Obstetrics and Gynecology in the University of Michigan, Ann Arbor, Mich.; Obstetrician and Gynecologist-in-Chief to the University of Michigan Hospital. Lea Bros. & Co., Phil. and New York. 1907. Chapter XIX.
“Leyden claims that about 40% of all women with serious heart lesions meet their death in connection with childbirth. Still greater than the demands upon the heart during pregnancy are those made by labor. The strain, mental excitement, and especially the sudden changes in the blood pressure, conditions which are well recognized as extremely harmful to every patient with a chronic heart lesion, and which cannot be avoided in the course of labor, make the situation extremely dangerous.” (Hugo Ehrenfest, M.D.) P. 357.
“The prognosis for the fetus is unfavorable. Fellner, whose figures undoubtedly are low, places the frequency of premature, spontaneous interruption of pregnancy as 20%, other writers at from 40% to 60%.” P. 358.
“No marriage for the unmarried, no pregnancy for the married, no nursing for the confined,” is a statement which has been made by a French author, and has been accepted by many writers. It is incompatible with the results of recent investigations. It would be too harsh and unjustifiable to deny marriage to a woman who has a well compensated valvular lesion. She 181should be informed of the risks of impregnation, but should be warned against marriage only where there exist distinct evidences of incompensation, especially in cases of mitral stenosis. P. 359.
A TEXT BOOK OF OBSTETRICS. Barton Cooke Hirst, M.D.; Professor of Obstetrics in the University of Pennsylvania; Gynecologist to the Howard and Orthopaedic, and the Philadelphia Hospitals, etc. 7th Edition. W. B. Saunders Co., Philadelphia and London. 1912.
Abortion is induced in about 25% of all cases, as the result of placental apoplexies, or of the stimulation of the uterus to contraction by the accumulation of carbondioxid gas in the blood. Pregnancy distinctly increases the danger of the heart lesion. In 58 serious cases, 23 died after premature delivery of the child. In milder cases prognosis is not grave, yet the woman’s condition is by no means free from danger. If the disease be of long standing and serious in character, it appears from statistical studies that about half the women die. P. 423.
PRINCIPLES AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D.; Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital, and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
Abortion and premature labor, especially the latter, occur in cases of dis-compensation, in from 20% to 40%, and stillbirth in 29% to 70%, giving figures collected from various sources by Fellner. P. 489.
THE PRACTICE OF OBSTETRICS. Designed for the use of Students and Practitioners of Medicine. J. Clifton Edgar, Professor of Obstetrics and clinical midwifery in the Cornell University Medical School; Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity and Dispensary; Consulting Obstetrician to the New York Maternity and Jewish Maternity Hospitals. 5th Edition, Revised. P. Blakiston’s & Co., Philadelphia.
Acute Endocarditis not only has an injurious influence upon pregnancy, but it is also apt itself to become extremely grave. Regarding treatment, induced labor will be demanded. P. 310.
BEING WELL BORN. An Introduction to Eugenics. Michael F. Guyer, Ph.D., Professor of Zoology, University of Wisconsin. Bobbs-Merrill Co. Indianapolis. 1916.
Too short an interval between childbirths would also seem to be an infringement on the rights of the child as well as of the mother. Thus Dr. 182R. J. Ewart, (“The Influence of Parental Age on Offspring,” Eugenic Review, Oct., 1911) finds that children born at intervals of less than two years after the birth of the previous child still show at the age of six a notable deficiency in height, weight and intelligence, when compared with the children born after a longer interval, or even with first-born children. P. 166.
FREQUENT PREGNANCIES. The Contributions of Demography to Eugenics. Dr. Corrado Gini, Professor of Statistics at the Royal University of Cagliari, Italy.
If the possibility of generation at any season of the year cannot, as has been shown, have any deleterious effect on the vitality of human offspring, it can none the less have indirect deleterious consequences, in so far as it allows pregnancies to succeed each other at too short intervals. P. 323.
“The deleterious consequences which too short a period after the preceding birth have upon the vitality of the child are indisputable, at least during the first year of life.” P. 323.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch. Rebman Co., N. Y.
“Frequently recurring pregnancies and childbirth, according to Kronig, act as the predisposing cause in the production of neurasthenia.” P. 257.
NEO-MALTHUSIANISM AND RACE HYGIENE, IN “PROBLEMS IN EUGENICS.” Vol. 2. Dr. Alfred Ploetz, President of the International Society for Race Hygiene. London, 1913.
Malthusianism further affects the quality of the offspring by increasing the intervals between single births. In families in which the parents intend to have only a few children, the mother is usually exempt from so frequent child-bearing, and she has ample time for regaining her strength. The greater interval between births has evidently a favorable effect upon the expectation of life of the children that are born. Westergard has stated that in 21,000 births, if the interval between birth is:—
| The percentage of deaths before five years of age is | |
|---|---|
| Less than one year | 20% |
| One to two years | 14% |
| More than two years | 12% |
That means a difference in the mortality between first and last class of 40% in favor of the longer interval. P. 186.
183THE LIFE INSURANCE EXAMINER. A Practical Treatise by Charles F. Stillman, M.S., M.D., Medical Examiner for the Mutual Life Insurance Co.; Clinical Professor of Orthopaedic Surgery in the Women’s Medical College of the N. Y. Infirmary; Orthopaedic Surgeon to the N. Y. Infant Asylum; Member of the Am. Orthopaedic Association; Permanent member of the American Medical Association; Fellow N. Y. Academy of Medicine, etc. 3rd Edition. Spectator Co., N. Y., 1890.
“Postpone (as dangerous insurance risks) all cases of pregnancy; all instances where the mother seems, in the judgment of the Examiner, to have been bearing children too fast.” P. 186.
RASSENVERBESSERUNG. Translated from the Dutch of Dr. J. Rutgers. 2nd Edition. Dresden, 1911.
The combatting of self-induced abortion is one of the problems of Sexual Hygiene. The two causes of most weight in this situation are syphilis and too frequent pregnancy. It is quite evident that both of these causes would be favorably influenced by the use of contraceptive measures. P. 81.
THE MALTHUSIAN, May 15, 1914. Sexual Ethics. A Study of Borderland Questions. Robert Michels, (Review).
Prof. Michels perceives that race control has two aspects; it may be an urgent duty, and it is in any case an inalienable human right. It may be regarded as a duty to actual or potential children, in view of either bad economic conditions,—such as affect the bulk of all European populations,—or defective heredity, and it may also be considered as an obligation of humanity towards the wife and mother. Prof. Michels here speaks with no uncertain voice: “The type of woman continually engaged in child-bearing is a primitive one, out of harmony with the needs and ideas of modern civilized life. Even as few as six pregnancies that go to full term rob a woman of about ten years of her life, and these the best. It is evidently far easier to provide a clear-sighted affection and a wisely conceived and individualized upbringing for two or three children than it is for eight or nine.”
MR. SIDNEY WEBB, in The Times of October 16, 1906.
Assuming, as I think we may, that no injury to physical health is necessarily involved (in the volitional regulation of the marriage state); aware, on the contrary, that the result is to spare the wife from an onerous and even dangerous illness for which in the vast majority of homes no adequate provision in the way of medical attendance, nursing, privacy, rest, and freedom from worry can possibly be made, it is, to say the least of it, difficult on any rationalist morality to formulate any blame of a married couple for the deliberate regulation of their family according to their means and opportunities.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. By Joseph B. De Lee, M.D.
Among diseases incidental to pregnancy must be counted pernicious vomiting. Page 370.
Statistics are uncertain, but out of 118 cases there were 46 deaths. Page 357.
The keynote of treatment is to stop the gestation at a point before either mother or child, or both, are in danger to life or to health. Page 1041.
THE PRACTICE OF OBSTETRICS. By J. Clifton Edgar, M.D., Professor of Obstetrics and Clinical Midwifery in the Cornell University Medical College; Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity and Dispensary; Consulting Obstetrician of the New York Maternity and Jewish Maternity Hospitals, New York City.
Under certain circumstances labor may be much disturbed by pernicious vomiting. The causes comprise actual organic disease of the stomach and functional disturbances from errors in diet. The determining cause of a paroxysm of vomiting is a severe labor pain. The coincidence of labor and vomiting is not unusual in anemic primiparae. Mental emotion is also a cause. As this vomiting may presage the development of eclampsia or some other affection it is best to terminate labor at once. Page 648.
In this chapter it is shown that ignorance of scientific means of preventing conception involves women in harmful practices. The most common is coitus interruptus which results in nervous disorders. Long continued celibacy or unnatural continence leads to sex inversions. When, in spite of these unscientific practices, pregnancy follows, abortion, the greatest disgrace of modern civilization, is the only resort of the harassed mother, unless she will bear unwanted offspring.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch, M.D.
The prevailing practice of coitus interruptus leads, in my experience in consequence of the intense hyperaemia of the uterus and the uterine annexa unrelieved by the occurrence of the orgasm, to a condition of stasis in the female reproductive organs, and this ultimately passes on into chronic netritis, (with relaxation of the uterus, retro-flexion, or ante-flexion, catarrhal diseases of the mucous membrane, erosions and follicular laceration of the portio vaginalis) oophoritis and perimetritis. The evil effects of coitus interruptus for a woman are dependent on the fact that the woman fails to obtain complete sexual gratification, and that this has an important influence on her entire organism. If this ungratifying coitus interruptus is frequently repeated in a voluptuous woman disorders of the reproductive organs ensue, and even more frequently nervous disorders in the form of neurasthenia sexualis. P. 403.
Mantegazza believes that organic disease of the spinal cord may actually result from coitus interruptus.
Hirt considers that even when marital intercourse is carefully regulated with respect to frequency, coitus interruptus may lead to neurasthenic manifestations.
Eulenberg also declares that coitus interruptus is already a frequent cause of sexual neurasthenia in women and that its evil influence in this respect is becoming more and more frequently manifest. P. 405.
Valenta declared that coitus interruptus was one of the chief causes of chronic netritis.
According to Kleinwachter, coitus interruptus is harmful to the woman to an extent by no means trivial, whereas the man in whom ejaculation occurs, suffers comparatively little. P. 407.
186DISORDERS OF THE SEXUAL FUNCTION. By Max Huhner, M.D., Chief of Clinic, Genitourinary Department, Mt. Sinai Hospital Dispensary, New York City.
If the act of coitus is stopped before it is completed, the seminal vesicles have not been able to completely empty themselves, or to empty themselves as completely as during a normal coitus, and are thus left more or less filled. The mucous membrane in the prostalic urethra has not been able to completely deplethorize itself, and thus remains more or less congested after the act. As a result of all this, impulses are sent much sooner from the distended vesicles and the prostatic urethra to the erection center and the cerebrum, so that the desire for coitus is felt sooner than after normal coitus. The seminal vesicles, being never completely emptied during withdrawal coitus, are constantly sending impulses to the erection center, while the mucous membrane of the prostatic urethra, being in a condition of chronic congestion in consequence of repeated acts of withdrawal, is likewise sending continuous impulses to the same center whether coitus is indulged or not. The result of these continued impulses sent from both sources, as well as the repeated demands made upon the center itself from the oft repeated acts of coitus, is, that the erection center does not completely recover itself and finally remains in a state of hyperexcitability.... It must be remembered, however, that all this does not occur as a result of a single act of withdrawal; and it is often only after years of this practice that the harmful effects above described become evident. Page 227.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch, M.D.
Grafe, with reference to the view that if for any reason conception must be avoided this should be done by abstinence from sexual intercourse, remarks, “doubtless the ideal demand, but one which even those with exceptional strength of will are unlikely to satisfy. And the worst of it is that even a single indiscretion will often result in impregnation.” Moreover, it is distinctly contrary to natural conditions that a healthy married couple, united by an intimate affection should live together, abstaining completely from sexual intercourse. The question has already been much discussed, both in speech and writing, and this will continue in the future without altering the fact that the physician will be asked, and will be compelled to give advice regarding the use of means of prevention of pregnancy. P. 399.
The desired goal of artificial sterility will not, however, be reached through advocacy of moderation and continence. P. 400.
187EFFECTS OF ABSTINENCE. Rassenverbesserung. Translated from the Dutch of Dr. J. Rutgers.
And if we could penetrate still more deeply into the recesses of the instincts, and project into the light of day the world of phantasy of those who live in enforced continence, we would draw away in horror from the spectacle of what each individual must conceal from himself and others. We would not then be so eager for the consummation of what is called sexual abstinence. P. 14.
Physiology teaches that every function gains in power and efficiency through a certain degree of control, but that the too-extended suppression of a desire gives rise to pathological disturbances and in time cripples the function. Especially in the case of women may the damage entailed by too long continued sexual abstinence, bring about deep disturbances, all the more because women more often than men misunderstand, or are unaware of this etiological moment, and have not the slightest idea of the true cause of their psychic and somatic injury. P. 15.
The unmarried state is a trying and often injurious condition for a man as well as a woman, when they live in strict continence; and if the latter is not the case and they resort to prostitution, there are even more pain and suffering in store for them. P. 16.
We must not forget that there are always two parties to the situation. What can a physically weaker and spiritually stronger woman do even if she desires continence with her whole soul, but her husband will have none of it? Is it not then her duty to protect herself in order that she may not give birth to a weakly progeny?
HARPER’S WEEKLY. 1915.
When Dr. A. A. Brill, Lecturer in Abnormal Psychology, New York University, and formerly Chief of Clinic in Psychiatry, Columbia University, was asked how he regarded contraception in relation to nervous diseases, he replied emphatically: “You can say that I am for it. It is much better than an abortion. For instance, I have in mind a woman who was discharged from the insane hospital. She had three children and had been three times insane. What chance in life has a child born between two attacks of insanity, whose mother is mentally defective? Even sane women, if they are nervous and emotional, should never bear children against their will. It is foolish to talk about making people have children when they do not want them. It’s bad for the woman and bad for the child. It is very bad for a child to be born into a home where he is not desired. I find that many adult, nervous patients were unwished-for-children, and it was the early attitude of their parents toward them that contributed much to their bent toward nervous invalidism.” 188In reply to the contention of the anti-regulationists that contraception is physically and mentally harmful, he stated that certain methods are injurious, while others are not. He commented on the unfortunate fact that it is the undesirable methods which are employed by the poorer people, because druggists put a high price upon the better means on the plea that they run a risk in selling them at all. Remembering that Dr. Brill was for years connected with Central Islip, he was asked if he did not consider it demanding a good deal to expect a man discharged from an insane asylum and sent home to his wife, to live a sexually abstinent life. He replied: “Only people who know nothing of the sex impulse can make such a demand of a person who has a poor mental organization. Of course it is impossible. It is impossible even for the average normal man, and especially for those who live crowded in two or three rooms.”
THE SEXUAL LIFE. By P. W. Malchow, M.D., Professor of Proctology, and Associate in Clinical Medicine, Hamline University, College of Physicians and Surgeons; member Hennepin County Medical Society, Minnesota State Medical Society, American Medical Association, etc.
There can be no doubt that the influence of prolonged continence upon either the male or female is to dwarf and in many respects destroy that which goes to make a broad and full physical and intellectual personality and that to perform the sexual act whenever there is an existing state of sexual excitement, with the usual marital restrictions, is rather beneficial that otherwise. Page 201.
In cases of nervousness in either sex it may be found that, as a rule, the first indication is a disturbance of the sexual function, following which there will be digestive troubles, then affections of special nerves, of which disorders of sight are the first and most frequent, with neuralgias, etc., later. Observation has shown this to be the general rule, and that is also in accordance with the law of self-preservation. With the conviction that nervousness is first manifested and begins with an alteration in the natural sexual function we may conclude that other functional disorders are a natural sequence. It thus becomes evident that the most prolific cause of nervousness is an inability for natural sexual living. Page 296.
A life of celibacy cannot be said to be a natural one, and when this state of celibacy is combined with propinquity, in which there must of necessity be a source of repeated and more or less constant sexual excitability there is added to one already incomplete life a greater burden of increased tension, which must be a very considerable factor in the causation of unrest or nervousness. Page 155.
How best to circumvent family complications is the burning question of the hour with the average young wife, and a satisfactory solution of this problem would be a boon to society and prevent untold suffering. When confronted with the question, the usual answer is, in effect, “be natural,” which in these days of stress, is no answer at all, as it is not practical. Page 158.
What are the legitimate objects of marriage? We know that many people seek to marry for ends that can scarcely be called legitimate, that men may marry to obtain a cheap domestic drudge or nurse, and that women may marry to be kept when they are tired of keeping themselves. These objects in marriage may or may not be moral, but in any case they are scarcely its legitimate ends. We are here concerned to ascertain those ends of marriage which are legitimate when we take the highest ground as moral and civilized men and women living in an advanced state of society and seeking, if we can, to advance that state of society still further.
The primary end of marriage is to beget and bear offspring, and to rear them until they are able to take care of themselves. On that basis Man is at one with all the mammals and most of the birds. If, indeed, we disregard the originally less essential part of this end,—that is to say, the care and tending of the young,—this end of marriage is not only the primary but usually the sole end of sexual intercourse in the whole mammal world. As a natural instinct, its achievement involves gratification and well-being, but this bait of gratification is merely a device of Nature’s and not in itself an end having any useful function at the periods when conception is not possible. This is clearly indicated by the fact that among animals the female only experiences sexual desire at the season of impregnation, and that desire ceases as soon as impregnation takes place, though this is only in a few species true of the male, obviously because, if his sexual desire and aptitude were confined to so brief a period, the chances of the female meeting the right male at the right moment would be too seriously diminished; so that the attentive and inquisitive attitude towards the female by the male animal—which we may often think we see still traceable in the human species—is not the outcome of lustfulness for personal gratification (“wantonly to satisfy carnal lusts and appetites like brute beasts,” as the Anglican Prayer Book incorrectly puts it) but implanted by Nature for the benefit of the female and the attainment of the primary object of procreation. This primary object we may term the animal end of marriage.
This object remains not only the primary but even the sole end of marriage among the lower races of mankind generally. The erotic idea in its deeper sense, that is to say the element of love, arose very slowly in mankind. It is found, it is true, among some lower races, and it appears that some tribes possess a word for the joy of love in a purely psychic sense. But even among European races the evolution was late. The Greek poets, except the latest, showed little recognition of love as an element of marriage. Theognis compared marriage with cattle-breeding. The Romans of the Republic took much the same view. Greeks and Romans alike regarded breeding as the one recognizable object of marriage; any other object was mere wantonness and had better, they thought, be carried on outside marriage. Religion, which 190preserves so many ancient and primitive conceptions of life, has consecrated this conception also, and Christianity—though, as I will point out later, it has tended to enlarge the conception—at the outset only offered the choice between celibacy on the one hand and on the other marriage for the production of offspring.
Yet from an early period in human history a secondary function of sexual intercourse had been slowly growing up to become one of the great objects of marriage. Among animals, it may be said, and even sometimes in man, the sexual impulse, when once aroused, makes but a short and swift circuit through the brain to reach its consummation. But as the brain and its faculties develop, powerfully aided indeed by the very difficulties of the sexual life, the impulse for sexual union has to traverse ever longer, slower, more painful paths, before it reaches—and sometimes it never reaches—its ultimate object. This means that sex gradually becomes intertwined with all the highest and subtlest human emotions and activities, with the refinements of social intercourse, with high adventure in every sphere, with art, with religion. The primitive animal instinct, having the sole end of procreation, becomes on its way to that end the inspiring stimulus to all those psychic energies which in civilization we count most precious. This function is thus, we see, a by-product. But, as we know, even in our human factories, the by-product is sometimes more valuable even than the product. That is so as regards the functional products of human evolution. The hand was produced out of the animal fore-limb with the primary end of grasping the things we materially need, but as a by-product the hand has developed the function of making and playing the piano and the violin, and that secondary functional by-product of the hand we account, even as measured by the rough test of money, more precious, however less materially necessary, than its primary function. It is, however, only in rare and gifted natures that transformed sexual energy becomes of supreme value for its own sake without ever attaining the normal physical outlet. For the most part the by-product accompanies the product, throughout, thus adding a secondary, yet peculiarly sacred and specially human, object of marriage to its primary animal object. This may be termed the spiritual object of marriage.
By the term “spiritual” we are not to understand any mysterious and supernatural qualities. It is simply a convenient name, in distinction from animal, to cover all those higher mental and emotional processes which in human evolution are ever gaining greater power. It is needless to enumerate the constituents of this spiritual end of sexual intercourse, for everyone is entitled to enumerate them differently and in different order. They include not only all that makes love a gracious and beautiful erotic art, but the whole element of pleasure in so far as pleasure is more than a mere animal gratification. Our ancient ascetic traditions often make us blind to the meaning of pleasure. We see only its possibilities of evil and not its mightiness for good. We forget that, as Romain Rolland says, “Joy is as holy as Pain.” 191No one has insisted so much on the supreme importance of the element of pleasure in the spiritual ends of sex as James Hinton. Rightly used, he declares, Pleasure is “the Child of God,” to be recognized as “a mighty storehouse of force,” and he pointed out the significant fact that in the course of human progress its importance increases rather than diminishes. While it is perfectly true that sexual energy may be in large degree arrested, and transformed into intellectual and moral forms, yet it is also true that pleasure itself, and above all, sexual pleasure, wisely used and not abused, may prove the stimulus and liberator of our finest and most exalted activities. It is largely this remarkable function of sexual pleasure which is decisive in settling the argument of those who claim that continence is the only alternative to the animal end of marriage. That argument ignores the liberating and harmonising influences, giving wholesome balance and sanity to the whole organism, imparted by a sexual union which is the outcome of the psychic as well as physical needs. There is, further, in the attainment of the spiritual end of marriage, much more than the benefit of each individual separately. There is, that is to say, the effect on the union itself. For through harmonious sex relationships a deeper spiritual unity is reached than can possibly be derived from continence in or out of marriage, and the marriage association becomes an apter instrument in the service of the world. Apart from any sexual craving, the complete spiritual contact of two persons who love each other can only be attained through some act of rare intimacy. No act can be quite so intimate as the sexual embrace. In its accomplishment, for all spiritually evolved persons, the communion of bodies becomes the communion of souls. The outward and visible sign has been the consummation of an inward and spiritual grace. “I would base all my sex teaching to children and young people on the beauty and sacredness of sex,” writes a distinguished woman of today; “sex intercourse is the great sacrament of life, he that eateth and drinketh unworthily eateth and drinketh his own damnation; but it may be the most beautiful sacrament between two souls who have no thought of children.” To many the idea of a sacrament seems merely typo for ecclesiastical, but that is a misunderstanding. The word “sacrament” is the ancient Roman name of a soldier’s oath of military allegiance, and the idea, in the deeper sense, existed long before Christianity, and has ever been regarded as the physical sign of the closest possible union with some great spiritual reality. From our modern standpoint we may say, with James Hinton, that the sexual embrace, worthily understood, can only be compared with music and with prayer. “Every true lover,” it has been well said by a woman, “knows this, and the worth of any and every relationship can be judged by its success in reaching, or failing to reach, this standpoint.”
I have mentioned how the Church—in part influenced by that clinging to primitive conceptions which always marks religions and in part by its ancient traditions of asceticism—tended to insist mainly if not exclusively on the animal object of marriage. It sought to reduce sex to a minimum because the pagans magnified sex; it banned pleasure because the Christian’s path on 192earth was the way of the Cross; and though theologians accepted the idea of a “Sacrament of Nature” they could only allow it to operate when the active interference of the priest was impossible, though it must in justice be said that, before the Council of Trent, the Western Church recognized that the sacrament of marriage was effected entirely by the act of the two celebrants themselves and not by the priest. Gradually, however, a more reasonable and humane opinion crept into the Church. Intercourse outside the animal end of marriage was indeed a sin, but it became merely a venial sin. The great influence of St. Augustine was on the side of allowing much freedom to intercourse outside the aim of procreation. At the Reformation, John à Lasco, a Catholic Bishop who became a Protestant and settled in England, laid it down, following various earlier theologians, that the object of marriage, besides offspring, was to serve as a “sacrament of consolation” to the united couple, and that view was more or less accepted by the founders of the Protestant churches. It is the generally accepted Protestant view today.[50] The importance of the spiritual end of intercourse in marriage, alike for the higher development of each member of the couple and for the intimacy and stability of their union, is still more emphatically set forth by the more advanced thinkers of today.
50. It is well set forth by the Rev. H. Northcote in his excellent book, Christianity and Sex Problems, (2nd edition, 1916, F. A. Davis Company, Philadelphia), especially Ch. XIII.
There is something pathetic in the spectacle of those among us who are still only able to recognize the animal end of marriage, and who point to the example of the lower animals—among whom the biological conditions are entirely different—as worthy of our imitation. It has taken God—or Nature, if we will—unknown millions of years of painful struggle to evolve Man, and to raise the human species above that helpless bondage to reproduction which marks the lower animals. But on these people it has all been wasted. They are at the animal stage still. They have yet to learn the A. B. C. of love. A representative of these people in the person of an Anglican bishop, the Bishop of Southwark, appeared as a witness before the National Birth-Rate Commission which, two years ago, met in London to investigate the decline of the birth-rate. He declared that procreation is the sole legitimate object of marriage and that intercourse for any other end was a degrading act of mere “self-gratification.” This declaration had the interesting result of evoking the comments of many members of the Commission, formed of representative men and women with various standpoints,—Protestant, Catholic, and other,—and it is notable that while not one identified himself with the Bishop’s opinion, several decisively opposed that opinion, as contrary to the best beliefs of both ancient and modern times, as representing a low and not a high moral standpoint, and as involving the notion that the whole sexual activity of an individual should be reduced to perhaps two or three effective acts of intercourse in a life-time. Such a notion obviously cannot 193be carried into general practice, putting aside the question as to whether it would be desirable, and it may be added that it would have the further result of shutting out from the life of love altogether all those persons who, for whatever reason, feel that it is their duty to refrain from having children at all. It is the attitude of a handful of Pharisees seeking to thrust the bulk of mankind into Hell. All this confusion and evil comes of the blindness which cannot know that, beyond the primary animal end of propagation in marriage, there is a secondary but more exalted spiritual end.
It is needless to insist how intimately that secondary end of marriage is bound up with the practice of birth control. Without birth control, indeed, it could frequently have no existence at all, and even at the best seldom be free from disconcerting possibilities fatal to its very essence. Against these disconcerting possibilities is often placed, on the other side, the un-esthetic nature of the contraceptives associated with birth control. Yet, it must be remembered, they are of a part with the whole of our civilized human life. We at no point enter the spiritual save through the material. Forel has in this connection compared the use of contraceptives to the use of eye-glasses. Eye-glasses are equally un-esthetic, yet they are devices, based on Nature, wherewith to supplement the deficiencies of Nature. However in themselves un-esthetic, for those who need them they make the esthetic possible. Eye-glasses and contraceptives alike are a portal to the spiritual world for many who, without them, would find that world largely a closed book.
Birth control is effecting, and promising to effect, many functions in our social life. By furnishing the means to limit the size of families which would otherwise be excessive it confers the greatest benefit on the family and especially on the mother. By rendering easily possible a selection in parentage and the choice of the right time and circumstances for conception it is again, the chief key to the eugenic improvement of the race. There are many other benefits, as is now generally becoming clear, which will be derived from the rightly applied practice of birth control. To many of us it is not the least of these that birth control effects finally the complete liberation of the spiritual object of marriage.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. By Joseph De Lee, M.D....
It is said that there is one abortion to eight labors, but in all probability it is more frequent than this. Almost half of the child-bearing women have had a miscarriage before the thirty-fifth year. Statistics are of questionable value because hospital figures do not represent the conditions of private practice. Further, many occur in first weeks and pass under the diagnosis of delayed or profuse menstruation. Finally, many abortions are deliberately concealed. Page 426.
194PRACTICE OF OBSTETRICS. By J. Clifton Edgar, M.D.
Immediate dangers of abortions are: hemorrhage, retention of an adherent placenta, sepsis, tetanus, perforation of the uterus. They also cause: sterility, anemia, malignant diseases, displacements, neurosis, and endometritis. Pages 338–9.
TRUCHTABTREIBUNG UND PRAVENTIVVERKEHR, IN ZUSAMMENHANG MIT DEM GEBURTENRUCKGANG; Eine Medizinische, Juristische und Sozialpolitische Betrachtung von Dr. Max Hirsch. Wurtzburg, Kabitzsch Verlag, 1914.
He who would combat abortion and at the same time assail contraceptive measures may be likened to the person who would fight contagious diseases and forbid disinfection. For contraceptive measures are important weapons in the fight against abortion. The use of contraceptive measures is largely responsible for the fact that the number of abortions does not increase immeasurably. The apprehension is perfectly justified that the prohibition of contraceptive measures would enormously increase the practice of abortion with its dangerous consequences for the life and health of women. P. 131–2.
America has a law since 1873, if I am not mistaken, which prohibits by criminal statute the distribution and regulation of contraceptive measures. It follows therefore, as I have already stated in my introduction, that America stands at the head of all nations in the huge number of abortions. P. 132.
THE DISEASES OF SOCIETY AND DEGENERACY. The Vice and Crime Problem. G. F. Lydston, M.D., Professor of Genito-Urinary Surgery, State University of Illinois; Professor of Criminal Anthropology, Chicago; Kent College of Law; Member of the American Medical Association, etc., etc. The Riverton Press, Chicago, 1912.
The familiar cry of “public demand” would fit the abortion business better than it does some other things. The evil is wide-spread, both in and out of matrimony. Its existence is recognized “under the rose” as a social necessity, yet the law calls it murder. For every man and woman caught in its commission and punished a thousand escape detection.
THE DISEASES OF SOCIETY AND DEGENERACY. G. F. Lydston.
In many instances abortion results directly in the death of the woman. Such are the consequences resulting from ungoverned natural law on the one side, and moral on the other. It must be confessed that an element of sympathy is evoked by the mental distress of the unfortunate woman who is extra-matrimonially pregnant. P. 370.
195SEXUAL PROBLEMS OF TO-DAY. Wm. J. Robinson, Critic and Guide. 1912.
I have gone on record with the statement that about a million abortions are brought about every year in the U. S. Exact statistics are not and never will be available, but I am sure that my estimate is very conservative, and that three million would be nearer the truth. Justice John Proctor Clark stated that 100,000 abortions are performed annually in New York City alone, and if these figures are correct, then the number for the U. S. would be in the neighborhood of two and a half million. P. 158.
There is one measure and one only which will positively do away with the evil of abortion and that is teaching people how to prevent conception. P. 164.
ABORTION AND ECONOMIC NECESSITY. (Hirsch).
According to a report in the Medical Record 80,000 abortions are performed annually in New York and only one case in 1,000 is brought before the authorities.
According to Lewin it has been determined by court investigations that there are at least 200 people in New York who make a profession of performing abortions.
It has been estimated that 2,000,000 abortions are performed annually in the U. S. P. 7.
Bertillon estimates the number of criminal abortions in Paris at 50,000 annually, in Lyons at 19,000. (Le depopulation de la France). P. 8.
We must first attack a very wide-spread fallacy, namely that abortion is more prevalent among unmarried girls than among married women. In other words, that it is concomitant with free sex relations. This fallacy is exploded by practical medical experience as well as by observation and statistics of social conditions. P. 23.
Among the causes of criminal abortion the fear on the part of the woman of the pains and dangers of confinement plays a not inconsiderable role. P. 54.
In marriage the cause for the practice of abortion springs in most cases from economic necessity. Most frequently this necessity is a genuine dire need arising from overcrowded quarters, lack of food and clothing, sickness and lack of employment. P. 33.
This economic need finds its most obvious expression in the congestion of the city populations. P. 34.
The dangers of childbirth are still serious enough to cause a certain 196degree of uneasiness in the woman and the family circle. This foreboding is due partly to our higher valuation upon health and life, and also to a shifting of pre-eminence from a solely generative function in women to other interests in their life. P. 84.
This greater consideration and valuation of woman’s individuality is the expression of continued progress and a higher culture. P. 87.
TRUCHTABTREIBUNG UND PRAVENTIVVERKEHR, In Zusammenhang mit dem Geburtenruckzang; Eine medizinische, juristische und sozialpolitische Betrachtung von Dr. Max Hirsch, Wurtzburg, Kabitzsch Verlag, 1914.
In Chicago six to ten thousand abortions are performed yearly, of which 75–90% are married women. P. 7.
I believe I may say without exaggeration that absolutely spontaneous or unprovoked abortions are extremely rare, that the vast majority—I should estimate it at more than 80% of abortions have a criminal origin. P. 9.
We may affirm that next to sexual diseases, abortion and its consequences are the most important factor in the etiology of chronic genital inflammations and of sterility. P. 9.
Our examinations have informed us that the largest number of abortions are performed on married women. This fact brings us to the conclusion that contraceptive measures among the upper class, the practice of abortion among the lower class, are the real means employed to regulate the number of offspring. P. 32.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch. Translated by M. Eden Paul, M.D. Rebman & Co., New York.
A means of insuring artificial sterility, which in all civilized countries is punishable as a criminal offense, and which is nevertheless very frequently practiced, is the artificial induction of abortion. Especially in North America it would appear that there exist regular professional abortionists. P. 413.
THE FAMILY AND THE NATION. A Study in Natural Inheritance and Social Responsibility. Wm. Cecil Dampier Whetham, M.A., F.R.S. Fellow and Tutor of Trinity College, Cambridge, and Catherine Durning Whetham. Longmans Green & Co., N. Y., Bombay and Calcutta, 1909.
There is no finality, a nation must either be losing or gaining ground, either improving or degenerating. Hence the scientific study of the effect of the existing conditions of any time on the rates of reproduction of different stocks of the nation, should be the chief work of the sociologist, and the control of these conditions the supreme duty of the statesman. P. 5.
In this chapter it is shown that the feeble-minded parent is many times as prolific as the normal parent. A considerable percentage of girls living in prostitution are mentally defective, and if careful statistics were collated it would be found that 95 per cent. of these women come from large families. The feeble-minded should be instructed how to prevent conception, thereby diminishing prostitution and its invariable accompaniment,—venereal disease.
SOME PROBLEMS OF THE SOCIAL EVIL. Hon. Chas. N. Doodnow, Judge of the Morals Court, Chicago. “The Light.” B. S. Steadwell, Editor. Jan.-Feb., 1915.
The Court of Morals conducted an investigation of prostitution along three lines, social, physical and mental. In the first report, April 10th, to December 31st, 1913, 639 cases were examined, representing every race, creed, and nationality. 334 were colored, 298 white, 2 Armenian, 1 Japanese. Occupations: 225 housework, 174 waitresses, 136 laundresses, 83 clerks or cashiers, 6 seamstresses, 4 stenographers, 1 trained nurse, 1 manicurist, 24 scrub women, 110 had no occupation. Venereal disease in infectious stage was diagnosed in 108 cases. 315 showed evidence of having syphilis, and of the remaining 116, had bacteriological tests been made, 50% at least would have been found victims of the disease. As to intelligence, over 400 were mentally deficient, two were found to be insane, and 68 were little more than imbeciles, having mental capacity of less than a seven year old child. Later statistics of 100 women going through the Court were taken showing again that usually their work was of a character which required the least skill and mental effort, and that 97% either were, or had been afflicted with disease, and that the majority were mentally deficient. We did not have any imbeciles, or idiots from the Morals Court, though quite a number of the morons were of the low grade type bordering on the imbecile group. In other words, 89.37% of our cases are feeble-minded, or borderland. If we leave out the borderland cases it shows that 85% of our cases, exclusive of the insane, alcoholics, and drug habitues are distinctly feeble-minded. This finding is interesting since it corresponds to our findings in the Boys’ Court, where we found 84.49% were feeble-minded. It is therefore to be clearly seen here that with the girl defective-delinquent, as with the boy, the basic cause is feeble-mindedness. This is the intrinsic cause, which environment and other causes on the whole, are extrinsic.
198REPORT OF CHICAGO MORALS COURT. December, 1913.
Dr. W. J. Hickson of the Psychopathic Laboratory tested 126 cases excluding insane, alcoholics and drug addicts, for the Chicago Morals Courts, and found 85.83% distinctly feeble-minded.
Of 639 prostitutes examined by a woman physician for the Chicago Morals Court, over 400 were mentally deficient; 2 were found to be insane; 68 were little above imbeciles, having mental capacities of less than a seven year old child.
The State Training School for Girls, at Geneva, Ill., has a population of about 400, of whom a great majority have been committed for sexual immorality. Dr. Olga Bridgman reports that of 118 consecutive cases that were examined upon entry, 105 (or 89%) were graded as feeble-minded. 14 of the 118 had been committed as dependents or uncontrollable. Of the 104 remaining all of whom had been sexually immoral 101 were graded as feeble-minded while only 3 were found normal according to the Binet test.
THE LAW OF POPULATION. Its Consequences and its Bearing upon Human Conduct and Morals. Annie Besant. Asa K. Butts, Publisher. 1879.
The more marriage is delayed the more prostitution spreads. Prostitution is an evil we should strive to eradicate, not to perpetuate, and late marriage, generally adopted would most certainly perpetuate. Marriage is deferred owing to the ever increasing difficulty of maintaining a large family in anything like comfort. Celibacy is not natural to man or to woman, all bodily needs require their legitimate satisfaction, and celibacy is a disregard of natural law. Until nature evolves a neuter sex, celibacy will ever be a mark of imperfection. P. 27–8.
But the knowledge of these scientific checks would, it is argued, make vice bolder, and would increase unchastity among women by making it safe. And if so, are all to suffer, so that one or two already corrupt at heart may be preserved from becoming corrupt in act? Are mothers to die solely that impure women may be held back, and wives to be sacrificed that the unchaste may be curbed. As well say that no knives must be used because throats may be cut, no matches sold because incendiarism may result from them, no pistols allowed, because murders may be committed by them. P. 38.
SLAVERY OF PROSTITUTION. A Plea for Emancipation. Maude E. Miner, Secretary of the New York Probation and Protective Association. McMillan Co., 1916.
The study of young women in prostitution shows that mental deficiency is an important factor in delinquency. 34%, or approximately ⅓ of 577 199delinquent young women at Waverly House were so retarded in mental development as to be considered feeble-minded, and others were mentally retarded enough to need protection and over-sight. Close knowledge of the individual girls convince us that their deficiency facilitates their entrance into prostitution. P. 43.
Explanation of the mental deficiency of these wayward girls which has predisposed them to prostitution is usually found in bad inheritance. P. 44.
A feeble-minded girl was found to be one of 13 illegitimate children to whom her mentally deficient mother had given birth. P. 46.
Over-crowding in rooms, tenements, and neighborhoods is an obvious menace. In congested sections of the lower part of New York, large families, to which these girls belong, were herded into two or three narrow rooms, 12 in three small rooms, seven in two rooms, or a family of five eating and sleeping and living in a single room. P. 55.
Have we realized that every feeble-minded girl is a potential prostitute? Have we realized that feeble-minded mothers give birth to large numbers of children doomed to mental deficiency? Have we realized what this will ultimately mean in deterioration of human stock and in the complication of social problems? To stop the stream which is bringing into prostitution large numbers of mentally deficient girls and women, we must safe-guard these girls and prevent them from having offspring. Evidence presented to the Royal Commission on the Care and Control of the Feeble-minded in Great Britain, and careful studies in America, show conclusively that mental deficiency tends strongly to be inherited, and that feeble-minded mothers are more prolific than normal women. P. 267.
DOWNWARD PATHS. An Inquiry into the Causes which Contribute to the Making of the Prostitute. With a foreword by A. Maude Royden. T. Bell & Sons, Ltd. London.
It is astonishing to find experts denying the element of economic pressure as a factor in the creation of the prostitute. It is an influence constantly present and it is only when we interpret it to mean actual physical starvation that we can say it is rarely a determining factor. Economic pressure does not begin with starvation, it ends there. There is again the long strain of underfeeding and overwork, of the absence of interest, variety and color, and all that makes life worth living to a human being. Poverty often means isolation, and isolation the absence of all those ties which keep us in our place in the social order, and make it worth while to preserve our self-respect. To be without this is to be constantly in danger and it is economic pressure which has thrust many over the brink of the precipice, though few would say their fall was due to actual starvation. P. 10.
200Intimately connected with this aspect of the question is that of home and housing, especially of the child. The age at which children are first corrupted is almost incredibly early, until we consider the nature of the surroundings in which they grow up. Insufficient space, over-crowding, the herding together of all ages and both sexes, these things break down the barriers of a natural modesty and reserve. Where decency is practically impossible, unchastity will follow, and follow almost as a matter of course. There are certainly natural defences in the right instincts of young people brought up in the right kind of home, which we look for in vain among those who have never had space enough for growth, or privacy enough for refinement. P. 11.
We must allot to bad housing and over-crowding a foremost place, not only as undermining the physical health which conduces to normal sexual relationship, but also as a danger to the wholesome innocence of youth. P. 21.
It cannot be too strongly impressed upon persons interested in the housing problem that over-crowding means a violation of childhood in every degree, from the indecencies of mere childish horse-play to complete debauchery. P. 22.
There are two types of feeble-minded girls who are almost inevitably destined to prostitution. There is first the large proportion whose sexual inclinations are abnormally strong, or whose power of self-control over natural impulses is abnormally weak. 2—There is the large class who are non-resistant. They have no active impulse to seek out men, but they will yield to any one who approaches them. There are three important factors that drive the feeble-minded into prostitution by excluding them from other occupations. 1—They often lose their characters at a very early age. A marked characteristic of the feeble-minded is the precocity of their sexual impulse. 2—It is easy enough for any feeble-minded girl to get and keep light, unskilled work at girl’s wages, but not so easy for her to pass like the girl of normal intelligence, from girl’s to woman’s work at the age of 17 or 18, for she is rarely worth woman’s wages. Therefore she finds herself bored by monotonous work and low pay just at the time that she is particularly attractive to man, and her sexual impulses are at their strongest. Very naturally the feeble-minded girl with her incapacity to perceive the consequences turns from her unsatisfying employment to the new life of excitement and easy gain that offers itself. 3—If feeble-minded girls do succeed in getting respectable situations they are very likely to lose them because of their lack of intelligence and general inefficiency. And even if they should discharge their duties in a satisfactory manner they have a curious distaste for staying for any time in one place, and tend to drift from situation to situation. P. 127–128.
Another characteristic of the feeble-minded is their notorious fertility. The superior fertility of the feeble-minded has been proved beyond dispute by statistical inquiry.
201DELINQUENCY AND MENTAL DEFICIENCY. Dr. Olga Bridgman. The Survey, June 13, 1914.
Report of examination of 118 consecutive admissions at the Illinois Training School for Girls at Geneva. Of the 118, 105, or 89%, showed a retardation of three years or more, thus ranking as mentally deficient, 6% were backward, being one or two years retarded, and six, or 5% were graded as normal. According to the Binet tests then, 97% of the children sent to this institution are mentally defective.
COMMERCIALIZED PROSTITUTION IN NEW YORK CITY. George Kneelands. Century Co., New York, 1913. (Chapter by Katherine B. Davis on a Study of Prostitutes Committed from New York City to the State Reformatory for Women at Bedford Hills.)
It is difficult to get at the actual truth as to the number of children the unmarried women have had. The Table shows the admission of 209 women on this point. There are 73 unmarried women who admit having had children, 16 were pregnant at the time of entering, and 18 had previously been pregnant. 428 claimed to have had no children. In this connection it may not be amiss to note the fact that an unmarried woman who has had a child is more apt to belong to the mentally defective class. Of the 647, 20.09% were shown to have hereditary degenerate strains, and 20.56% venereal disease. Page 180.
SOCIAL HYGIENE. March 1915. Vol. 1, No 2. Recent Progress in Social Hygiene in Europe. James B. Reynolds, Counsel, The American Social Hygiene Association.
Recent studies of prostitutes there (in Europe) as here have strikingly brought to light the significant relationship between prostitution and mental defectiveness. A far reaching contribution to the solution of the problems of sex education and prostitution was the Mental Deficiency Act of 1913 for England and Wales. This Act was based on the Report of a Royal Commission on the Care and Control of the Feeble-minded which made a careful and exhaustive study of the entire subject, including the methods of treatment of the mentally defective in all countries. The Commission declares that a great proportion of the evidence unmistakably indicates that mentally defective children are greatly lacking in self-control and peculiarly open to suggestion and hence specially susceptible to the influence of depraving companions. The testimony of numerous experts who appeared before the Commission is highly illuminating on these points. Dr. Kerr, medical officer of the London County 202Council, declared that sooner or later many of these children will be found in the hands of the police, or in maternity hospitals. Dr. Ashby, late medical officer of the Manchester Special Schools stated that the mental defectives tend to an increase of the criminal and immoral classes. Dr. Whittell, Medical Superintendent of the Suffolk County Asylum, argued that the natural and physical evolution of this class is apt to result in various offenses of sexual, or perverted sexual, nature. Dr. Corner, Lecturer on Mental Diseases in the North East London Post Graduate Hospital, said, “One of the most common and dangerous characteristics of the feeble-minded is that they tend to sink socially.” Another expert testified that mentally defective girls in large cities are subject to overwhelming temptations and pressure toward sexual immorality, while still another, looking to the larger aspects of the problem, called attention to the danger resulting from the immoral laxness of mentally defective girls, and the lowering of the mental stamina of the whole nation by the increase of a population of defective intellect. Sir Francis Galton went so far as to declare that mentally defective women commonly become prostitutes. The feeble-minded, as distinguished from idiots, are an exceptionally fecund class, mostly of illegitimate children, and a terrible proportion of their offspring are born mentally deficient. All these experts were in agreement that mentally defective girls are in great danger of becoming immoral, hence prostitutes.
DEGENERACY, ITS CAUSES, SIGNS AND RESULTS. Eugene S. Talbot, M.D. Walter Scott, Ltd., London; Chas. Scribner’s Sons, N. Y. 1898.
Pauline Tarnowsky in her study “Etudes Anthropometriques sur les Prostituées” finds that in Russia prostitution is crime in women taking the line of least resistance. She concludes from her researches, which mine tend to verify, that the prostitute as a rule is a degenerate being, the subject of an arrest of development, tainted with a morbid heredity, and presenting stigmata of physical and mental degeneracy fully in consonance with her imperfect evolution. C. Andronico of Messina, Italy, arrived some time previously at the same conclusions as those of Tarnowsky.
FEEBLE-MINDEDNESS, ITS CAUSES AND CONSEQUENCES. Henry Herbert Goddard, Director of the Research Laboratory of the Training School at Vineland, N. J., for Feeble-minded Boys and Girls. McMillan Co., 1914.
Among the different causes for the social evil feeble-mindedness has been suggested, but nowhere has it been given the prominence that is due it. Anyone who understands feeble-mindedness, especially the moron, cannot expect anything less than that great numbers of these girls will fall into the life of 203prostitution. As to the actual statistics on this subject we have almost none. One very significant record comes from Geneva, Illinois, made by Dr. Bridgman. She found that of 104 girls in the Reformatory who were committed for an immoral life 97% were feeble-minded. This does not by any means indicate that 97% of prostitutes are feeble-minded, because it is only natural to expect that the feeble-minded ones would be the ones to be caught and sent to an institution. These figures, nevertheless, give us some idea of the prevalence of feeble-mindedness in this traffic. Many competent judges estimate that 50% of prostitutes are feeble-minded. Pages 14–15.
The 327 cases here presented constitute a unitary group. They have not been selected. They are of all ages and grades of defect. Page 7.
Our 327 families naturally fall into six fundamental groups, as follows: 4—Accident Group, 57; 5—No Cause, 8; 6—Unclassifiable, 27. Pages 47–48.
The following table gives an idea of the fecundity of these groups of women.
| No. of Mothers | No. of Children | Average | |
|---|---|---|---|
| Hereditary | 139 | 992 | 7.1 |
| Probably Hereditary | 27 | 168 | 6.2 |
| Neuropathic | 36 | 204 | 5.6 |
| Accident | 50 | 258 | 5.1 |
| No Cause | 8 | 258 | 5.7 |
| Unclassified | 27 | 118 | 4.3 |
| ——— | ————— | ——— | |
| 287 | 1,786 | 6.2 |
In addition to the mentality, whether normal or feeble-minded, record has been kept of certain diseases and conditions supposed to be more or less associated with feeble-mindedness in a causal relation. These are the following: 1—Alcohol; 2—Tuberculosis; 3—Sexual Immorality; 4—Paralysis, Insanity, Epilepsy, Neurotic Condition, Syphilis, Criminality, Deafness, Blindness, Migraine, Goitre, Vagrancy. Page 473.
Sexual immorality is closely associated with hereditary feeble-mindedness. Closely connected with the subject of sexual immorality is the one of illegitimacy. Our records show 278 illegitimate children of whom 259, or 93% are in the pure Hereditary group, 12 in the Probably Hereditary group, 3 in the Neuropathic, and 4 in the Accident group. There is nothing new in these facts. They are simply confirmatory of what we have found in other lines. Page 499.
The feeble-minded person is not desirable; he is a social encumbrance, even a burden to himself. In short, it were better, both for him and for Society had he never been born. Should we not then in our attempt to improve the race begin by preventing the birth of more feeble-minded? Page 558.
204THE FEEBLE-MINDED A SOCIAL DANGER. A. F. Tredgold, L.R.C.P., London. M.R.C.S., England. Medical Expert to the Royal Commission on the Feeble-minded, etc. Eugenics Review. Vol. 1, April, 1909. Pub. Eugenics Education Society, London.
In England and Wales on January 1st, 1906 there were a total of 138,529 persons in the country who were defective in mind. This corresponds to 4.03 per thousand population, or to one mentally defective person in every 248. In England and Wales on January 1st, 1906, there were no less than 125,827 insane persons. If we add these to the number of the mentally deficient which I have just stated, we find that in this country there is one person out of every 130 who suffers from severe disease of the mind. P. 98–99.
According to the Registrar General, the average number of births to a marriage in the whole population of this country is 4.6. I have ascertained that the average number of births in these degenerate families is no less than 7.3. It is obvious that if this alarming propagation is not checked, the time must inevitably come when our nation will contain a preponderance of citizens lacking in that intellectual and physical vigor which is absolutely essential to progress. P. 98.
RASSENVERBESSERUNG. Translated from the Dutch of Dr. J. Rutgers. Second Edition, Dresden, 1911.
A not insignificant factor in the use of houses of prostitution is furnished by married men who in the “old fashioned” way wish to “protect” their wives, in order not to be burdened with too many children. Neo-Malthusianism is also the best weapon against this class of supporters of prostitution. P. 73.
MASSACHUSETTS COMMISSION FOR INVESTIGATION OF THE WHITE SLAVE TRAFFIC.
This investigation under Dr. Walter Fernald, included a physical examination study of family and personal history, social reactions, and standards, etc. Out of the 300 prostitutes 154 were feeble-minded (all doubtful were called normal). The 154 were so pronounced as to warrant legal commitment. None of them had the mentality of a normal child of 12 years old. Majority were that of 10 or 9 years old.
INVESTIGATION OF VIRGINIA STATE BOARD OF CHARITIES.
This investigation presents a very high percentage of aments among the prostitute residents of the Richmond red light district. Of 120 persons tested the examiner found 42 or 35% imbeciles and 58 or 48.3% to be morons. That is 100 or 83.3% were mentally defective and only twenty or 16.7% were declared 205normal. Out of this number 93 were found to be between the ages of 20 to 30 and 16 between 30 to 40. All in the child-bearing age, as one will note. That 100 out of the 120 needed institutional care, that they should not reproduce their kind, was of course apparent.
THE MENTALITY OF THE CRIMINAL WOMAN. A Comparative Study of the Criminal Woman, the Working Girl and the Efficient Working Woman in a Series of Mental and Physical Tests. Jean Weidensall, formerly Director of the Department of Psychology, Laboratory of Social Hygiene, Bedford Hills, N. Y. Warnick and York Inc. 1916.
Tests applied to a group of children of working age by the Bureau of Educational Guidance of Cincinnati were also used on a group of 20 maids at Vassar as a norm for testing the women committed to Bedford. 100 reformatory subjects were used for the tests. It is a matter for question whether loss of the parent is the cause of the child’s leaving school and going to work early and of the ultimate unsocial conduct in the case of the Bedford group, or whether loss of parent, retardation, misconduct, etc., are not for the most part but manifestations of the same thing—irresponsibility, mental, physical and social inferiority on the part of both parents and child. The facts at our disposal and eugenic investigations lead us to believe that the latter is in the larger measure true. Out of 100 women recorded 30 had had from one to five illegitimate children. Of the 100 tests for syphilis and gonorrhoea, 45% positive, 4% doubtful, 51% negative, for syphilis. 60% positive, 22% doubtful, 18% negative for gonorrhoea. At best strong character cannot be the rule among individuals ⅔ of whom have less intelligence than that possessed by the average individual among a group of children of 15, (of whom half are themselves retarded), and almost surely not when they have been too untrained industrially and too unschooled socially to have acquired simple every-day habits of restraint and inhibition. Even the more intelligent third of the reformatory subjects differed very obviously and unmistakably in stability and emotional control from the group of Vassar maids.
THE MENACE OF MENTAL DEFICIENCY FROM THE STANDPOINT OF HEREDITY.[51] By Henry H. Goddard, Ph.D., Vineland, N. J. New Jersey Training School.
51. Read before the conference of the Massachusetts Society for Mental Hygiene, Boston, November 19, 1915.
From the standpoint of the child, something can be done to make them a little happier; from the standpoint of society, no amount of mental hygiene can ever render them efficient citizens. Society can, by proper treatment, render them less of a menace than they are naturally, and the ills that we now suffer on account of them can be largely reduced.
206It is estimated that there are from 300,000 to 400,000 mental defectives in the United States. That is based upon the United States census of 1890, in which the question was asked “Whether defective in mind, sight, hearing or speech, or whether crippled, maimed or deformed, with name of defect.” Now if anyone can estimate what proportion of the true number of the feeble-minded would be returned in answer to that question, he will be able to estimate how near the truth is the 200,000 which the census report gives. Three hundred thousand or 400,000 seems to be a conservative estimate.
I am to discuss this topic from the standpoint of heredity. It has not yet been successfully contradicted that two-thirds of this army of 300,000 or 400,000, owe their condition to heredity. A quarter of a million of these people are feeble-minded because their ancestors were feeble-minded. They have inherited the condition just as you have inherited the color of your eyes, the color of your hair, and the shape of your head. There is a tendency in these days to attribute a great deal to heredity. But of this particular thing there seems to be no question. The menace of the problem comes, not from the fact that a quarter of a million inherited their condition, but because they are transmitting that condition to their offspring. Of that quarter of a million feeble-minded persons in the United States, do you know how many are being cared for, guarded and kept from propagating their kind? About 24,000 out of 250,000 are to-day being cared for in such institutions as you have here at Waverley. The rest are living their lives, are raising families, and providing abundant opportunity for the exercise of the charitable impulses of numberless generations to come. And that condition of things is getting worse rather than better.
What shall we do? There have been two answers. Some say, “Segregate, shut them up. Keep the sexes apart.” We are told that if we could do this for a generation our problem would be largely solved. The two-thirds in which the condition is largely hereditary would be eliminated. I want to assure you that the problem is larger than that. In the first place, looked at from the practical standpoint, we do not seem to be able to segregate. We are taking care of 24,000, and there are at least 250,000 to be cared for. If the State of New York cared for its estimated proportion of mental defectives, it would require thirty institutions of 1,000 each. They find it hard to raise money for the three or four institutions they now have. Their appropriations are cut every year. In the State of Massachusetts there are at least 14,000 feeble-minded persons. It would require ten institutions the size of Waverley,—a demand upon the public treasury which we are not willing to meet. I have not found anyone yet who is optimistic enough to think that we shall meet the demand within any reasonable length of time,—a time so short that we can safely rely upon that as a solution of the problem.
I have said that this quarter of a million, this army of feeble-minded people, are propagating. They are propagating a progeny of feeble-minded at somewhere from two to six times as fast as the intelligent people are 207propagating their kind. That is another serious part of the problem. I should like to digress from my particular field for a moment to make a suggestion on the other side. It makes one feel pessimistic when we find that the good stock here in New England—the stock than which there is no better in the world—is gradually disappearing for lack of issue. Of one family after another one reads all too frequently, “The last of his family has passed away.” We are told sometimes that two children in a family are all that can be properly reared; that it is better to rear two children and rear them properly than to rear a larger family and rear them badly. If two children in a family are all that our best and finest and nobler families can properly raise, how many children ought to be raised in a family of these low-grade people? The average in the United States is, for all classes, something less than two, and the average for these defectives is from four to twelve. In that little family that we ran across down in New Jersey, which we call the Kallikaks, you will recall that the good side started from six ancestors. That is to say, Old Martin Kallikak, after he married, had seven children, one of whom died without marrying. From the six who lived and married, sprang all the normal descendants. Martin’s illegitimate son, the child of the feeble-minded girl, was the only one on the bad side, and yet to-day the number of descendants from the illegitimate mating is practically the same as the number descended from the six legitimate children. You can see that it does not take many generations for the progeny of the unrestrained feeble-minded to equal and even outstrip the normal. Our good stock is multiplying very slowly. Our poor stock—the lowest strata of society—multiplies in what might really be called a brutal ratio. If civilization is to advance, our best people must replenish the earth. I think it should be a part of our religion to replenish the world with good, clean people.
We need to know vastly more than we know to-day before we can give definite answers, except in the case of marriage between two feeble-minded persons. Now, that being the case, the argument that I want to make to you is: the propagation of the feeble-minded is going on at an enormous rate. If we could do, and if we did, everything that we wanted to do, and that we knew enough to do, we should be getting only at the surface of the problem, and should be sure in only about one case out of the six possibilities. Now if that is the case, my friends, does it seem that we ought to put off attacking the problem until we cannot stand it any longer? Or does it mean that we had better attack it right away? Is it not best to begin hunting for these defective children wherever they may be found? And they can be found in the school, in our juvenile courts, in our almshouses, in our insane hospitals, in our reform schools, in our homes for cripples, in our asylums for the blind,—in short, wherever there is a dependent group there is an undue proportion of these mental defectives.
Some will say, “If they are in almshouses they are being cared for.” In reality they are being raised and brought to manhood and womanhood and 208then sent out, to propagate their kind. Fifty years ago the problem was not as serious as it is to-day, because these defectives were out in the world by themselves, getting killed by a runaway horse, or falling into machinery, or in some way meeting an untimely death. To-day we are exceedingly careful; we are protecting them in every possible way; we are taking care of them in our institutions and giving them every advantage, and then sending them out into the world—a menace to the rest of humanity.
It would be a dreadful thing if all these problems were solved and we didn’t have any people to give our money and charity to. I suppose we should become hard-hearted if we didn’t have any to befriend. Perhaps we want to keep enough of these unfortunates so that we can still contribute to their safety and welfare. But, my friends, when we realize the suffering, the terrors, the losses of all kinds that these people unintentionally, unwittingly cause us, we have another side of the problem. The menace of the feeble-minded is not a figure of speech. It is no undue sentimentalism that assures us that we need to take care of this group of people. We need to study them very seriously and very thoroughly; we need to hunt them out in every possible place and take care of them, and see to it that they do not propagate and make the problem worse, and that those who are alive to-day do not entail loss of life and property and moral contagion in the community by the things that they do because they are weak-minded.
HEALTH FIRST AND MATRIMONY AFTERWARD. By Edward C. Spitzka, M.D. The Semi-Monthly Magazine Section of the Boston Globe, the Washington Post, the Philadelphia North-American, the Pittsburgh Dispatch, the Chicago Tribune, the St. Louis Globe-Democrat, the Cincinnati Enquirer, etc. May 11, 1913.
We cannot tell men and women how they should mate in order to insure positive types of offspring. But we can state, emphatically, and without reserve, that persons suffering from certain diseases should not enter into the marriage relationship, at peril of the health and happiness of children that may be born to them and the well being of the community at large.
I believe that municipal and state governments should take cognizance of this fact. Eventually it will be regarded as a matter for Federal, perhaps for international action. Every candidate, man or woman, applying for a marriage license should be required to present a physician’s certificate declaring him or her to be free from insanity and certain virulent transmissible diseases.
What then are these diseases? I will list them in the order of importance as menaces to humanity.
1. Constitutional insanity.
2092. The two great forms of constitutional venereal disease: syphilis and gonorrhoea—the former as a source of danger to both the marriage partner and offspring, the latter to the marriage partner only.
3. Deformities that are likely to be associated with the transmission of serious defects of the nervous system, such as cleft palate, hermaphroditism, etc.
4. Epilepsy of the standing of more than one generation.
Medical statistics prove that a proportion of three out of every five children born to imbecile parents are certain to be weak-minded, and that the marriage of such unfortunates is a calamity to the race. Syphilis persists from generation to generation. Any sufferer from this disease who marries before he is certain that it has been eradicated from his system is guilty of a crime against society.
I have hesitated about including epilepsy in this list. It is undoubtedly transmissible to the offspring, though transmission does not occur in every case. A conservative ruling would be that an epileptic who is believed to be the first of his line to contract the disease should be permitted to marry, in the event of his being declared cured. But the epileptic sons and daughters of epileptic parents should, under no circumstances, be licensed to marry.
Note: The late Dr. Spitzka, along with other authorities quoted as being opposed to the marriage of the unfit, was concerned with the diseased offspring which almost invariably result from such marriages. Except in the case of gonorrhoea, which can be transmitted to the marriage partner, he did not object to the union itself, provided the latter remained childless. He would have recommended the use of contraceptives, as the solution of the problem, had he not been prohibited by the law from doing so.
HEREDITARY SYPHILIS IN THE LIGHT OF RECENT CLINICAL STUDIES. Pamphlet. Borden S. Veeder, M.D., St. Louis, Mo. From the American Journal of the Medical Sciences, October, 1916. No. 4, Vol. CXII. P. 522.
In the present state of our knowledge we can summarize the evidence as pointing to the view that in hereditary syphilis the mother is always infected, although very frequently the infection is latent and that true germinal infection does not occur.
Syphilis as a Social Problem. No accurate figures are available as to the incidence of hereditary syphilis. The disease is not reportable, and even if it were it is doubtful if the records obtained in this way would be of any value, as the condition is frequently overlooked, and when recognized would be concealed in many cases because of the stigmata attached. With improved 210methods of diagnosis we are beginning to learn that it is far more common than previously thought, as many conditions in which the etiology was obscure have been found to be the result of a syphilitic infection. Hospital statistics are of little value in this connection. In St. Louis we have been particularly interested in hereditary syphilis, and have admitted many cases to the Children’s Hospital for study which would normally have been cared for in the out-patient clinic, and hence the proportion of syphilis to the total number of admissions is relatively high. We have seen between 300 and 350 children with an hereditary infection in three and a half years and have undoubtedly failed to recognize a number of cases. We have also found many cases of latent syphilis by testing the apparently healthy children of syphilitic families. What is more important is the number of obscure clinical conditions which have been found to be syphilitic in origin.
The importance and cost of syphilis to the family and the community is not generally appreciated. About this point we have collected some interesting information: For a period of about a year an attempt was made to obtain extensive data in regard to the family of every syphilitic child coming to the clinic, to examine all of the other living children as well as the parents, and to test the blood of each member by the complement-deviation method. In this way data was assembled for 100 syphilitic families. Many marriages (10 to 30 per cent.) remain sterile as a result of syphilis and others (13 per cent. according to Haskell) result only in abortions. Our material includes only those families in which a living child came under our direct observation and care.
In these 100 syphilitic families 331 pregnancies occurred which resulted as follows:
| Abortions | 100 or 30.2 per cent. |
| Stillbirths | 31 or 9.3 per cent. |
| Living births | 200 or 60.5 per cent. |
Thus 40 per cent. of the pregnancies terminated in the death of the fetus before term. If the parents had been healthy and of the same social strata we might have expected 30 to 35 deaths before term, or a mortality of 10 per cent. instead of 40 per cent.
Considering next the 200 living births: At the time the data were collected 39 were dead and 161 alive, but 12 of the 161 died during the course of the investigation. Of the 161 examined 107 had both clinical signs of syphilis and a positive Wassermann; 5 were clinically positive but gave negative tests (in all of these the family gave a history of syphilis); 16, although negative as regards clinical manifestations, gave positive reactions, and therefore belong to the group of latent syphilitics. Thus but 33 of the 161 living children were free from the infection, and if we attribute the deaths occurring before term to syphilis, we find that of the 331 pregnancies in 100 syphilitic families 211but 10 per cent. escaped the infection. The toll is summarized in the following table:
| 331 PREGNANCIES IN 100 SYPHILITIC FAMILIES | ||||
|---|---|---|---|---|
| 131 | or 40 per cent. | died before term | } | |
| 51 | or 15 per cent. | died after birth | } | 55 per cent. dead |
| 116 | or 35 per cent. | living but syphilitic | 35 per cent. syphilitic | |
| 33 | or 10 per cent. | living and free from syphilis | 10 per cent. escaped | |
| ——— | ||||
| 331 | ||||
If we add to this record and take into consideration the physical condition of the parents—both of whom were syphilitic in almost all of our cases—we begin to grasp the appalling importance of syphilis from a social standpoint.
In order to show this in another way, studies[52] were made in our clinic in which the waste (total deaths to total pregnancies) occurring in 100 families in which we were treating children with contagious disease, and in 100 families selected at random from our records, were contrasted with the waste in 100 syphilitic families. These groups are designated as C. R. and S. respectively and the data briefly summarized in the following table:
52. Jeans and Butler, Hereditary Syphilis as a Social Problem, Am. Jour. Dis. Child., 1914, viii, 327.
| Group | Total pregnancies | Deaths before birth | Born living now dead | Total | Per cent. waste |
|---|---|---|---|---|---|
| C. | 444 | 46 | 70 | 116 | 26 |
| R. | 442 | 42 | 59 | 101 | 22 |
| S. | 453 | 116 | 104 | 220 | 48 |
The increase in the waste for the syphilitic group of 100 per cent. does not represent the total waste, as it is fair to assume that three-quarters of the living children are syphilitic and many of these defective.
Syphilis. None of the causes supposed to be potent causes of feeble-mindedness is so difficult of investigation, so enigmatical as Syphilis. Not only in the popular mind but in the professional thought, it is given a prominent place, yet of all the causes there is perhaps none for which there is less evidence. This does not necessarily mean it is not a cause, but simply that it is not proved. The terrible nature of the disease, the serious results that it is known to produce, such as miscarriage, deaths in infancy, general paralysis of the insane, the fact that it is one of the two diseases that can be transmitted from the mother to the child because the germs can pass through the chorion cells, the fact of its close connection with sexual immorality, all tend to render it in the minds of most people a horror of which anything can be believed. It is well understood by the medical profession that a mating which shows, first a number of miscarriages followed by deaths in infancy, and finally live offspring, is a picture that means syphilis in one or both of the parents almost without question. In conclusion, there is abundant evidence that syphilis produces miscarriages and early death.
It is claimed that syphilis is responsible for 42 per cent. of abortions and miscarriages, the remaining 58 per cent. embracing all cases of whatever character, artificial or otherwise.
FAMILIAL SYPHILIS. By P. C. Jeans, M.D., “American Journal of Diseases of Children.” January, 1916. Vol. XI. pp. 11–19.
As the result of syphilis numerous families remain sterile. The figures for sterility vary from 10 per cent. to 30 per cent., depending on the material studied. When there is an embryo there is a variety of fates to which it may come. Many marriages result only in abortions (nearly 13 per cent. in Haskell’s material[53]). Since the starting point in our material was a syphilitic child, we have no data bearing on this phase.
53. Haskell: Jour. Am. Med. Assn., 1915, lxiv, 890.
Among our syphilitic patients all the living children of 100 families have been examined, Wassermann tests made and the family history studied. In these 100 families there were 331 pregnancies. Of these 100 (30.2 per cent.) were abortions, 31 (9.3 per cent.) still births and 200 (60.4 per cent.) living births. Of the 200 living births 35 children died early and 4 died late, and 161 remained alive and were examined. Of these, 12 are now dead. Of the 35 who died early, 5 gave an undoubted history of syphilis and a number gave suspicious histories. Of the four who died late, one was an idiot. Of the 161 examined, 107 were clinically positive and had positive Wassermann tests. Five were clinically positive and had negative Wassermann reactions. Sixteen, who showed no evidence of syphilis, gave positive Wassermann reactions. Thirty-three, who gave no clinical proof of syphilis, gave a negative Wassermann reaction.
Of the five who were clinically positive but gave negative Wassermann reactions, one was a young infant who had snuffles and a large spleen. The mother and sister both gave a positive history and a positive Wassermann reaction. Shortly after beginning treatment the baby developed a syphilitic rash. The baby was removed from the hospital and a second Wassermann was not done. The second case was a nursing baby. The mother had active syphilis and was taking treatment. The baby had an active process in the nose. The third case was a 7-year-old girl who had a markedly sunken nose and who for that reason was the starting point for investigating that family. Both the mother and younger brother gave a positive Wassermann. The fourth case was a 4-year-old girl whose mother and younger sister were both positive and the patient had a general rash which was thought to be syphilitic. The fifth case was a 3-year-old boy with a positive history, and who had had some treatment. His mother and younger brother both had syphilis.
A negative Wassermann reaction is obtained in the presence of active syphilis only under certain definite conditions. As had been noted in cases not of this series, very young babies, even with undoubted active syphilis, not infrequently give a negative Wassermann. It has also been noted that even small amounts of mercury tend to cause a positive blood to react negatively.
213H. Boas[54] states that of fifty-seven babies of syphilitic mothers giving negative Wassermann reactions at birth, thirteen during a three months’ period of observation developed syphilitic manifestations and a positive Wassermann, and two others showed syphilitic changes at necropsy, having had no manifestations during life.
54. Quoted by Haberman: Jour. Am. Med. Assn., 1915, lxiv, 1146.
It is seen that 10 per cent., of the children examined had latent syphilis, i.e., a positive Wassermann and no clinical evidence of syphilis. One of these children gave a history of epiphysitis at 3 months. Other than this no early history was acknowledged by any of the mothers. The question naturally arises, Are these children actively infected with syphilis? When we inquire into the history of those showing late manifestations, we frequently find, so far as obtainable history is concerned, that there has been no previous warning that the disease existed. One of our patients developed, as her first known symptom, an interstitial keratitis at 20 years. We know that the spirochete can lie dormant much longer than this and then manifest itself. One patient of this latent group who had taken very irregular treatment for about a year and who had never had previous manifestations, recently developed an active lesion in the throat. Another developed an interstitial keratitis after about two months of anti-syphilitic treatment. A positive Wassermann reaction in these apparently healthy children has the same significance that it does in the parent, and it is our belief that the children in this group are actively infected.
The fact that there are thirty-three children, 10 per cent. of the total pregnancies, who show no evidence of syphilis, and at the same time give a negative Wassermann reaction, is rather hopeful. Yet the pleasure to be taken in this fact is not altogether unalloyed. In this small group there were two mental defectives and an idiot, and it is impossible to say that all of this group are free from syphilitic infection. In one instance, one such negative child returned about a year after his original examination with a tertiary type of lesion and a positive Wassermann. Though no classification of those in this group showing stigmata of degeneration was attempted, it can be truthfully stated that a goodly proportion did show degenerative influences, either physical or mental.
In summing up the total syphilitic infection in these families, we find that where marital relations are uninvolved, all of the fathers and probably all of the mothers have been infected. Presuming that the abortions, stillbirths, all of the early deaths and at least one of the late deaths were due directly or indirectly to syphilitic infection, syphilis among the offspring amounts to 89 per cent. of the total pregnancies, and total syphilis in the family amounts to 93 per cent. of all its members.
It is highly probable that all the mothers of syphilitic children have been infected with syphilis. Of eighty-five mothers of syphilitic children 86 per cent. gave positive Wassermann reactions. All of the remaining cases but six gave a history of infection or treatment, or both. Five of these six patients were examined at least ten years after the birth of their last syphilitic children and the infection is probably dying out.
Eighty-seven per cent. of the mothers deny all knowledge of the infection. The mothers are for the most part infected during the latent stage of the father.
Of 331 pregnancies in 100 families, 30 per cent. were abortions, 9 per cent. stillbirths, 61 per cent. living births. Of the living births 24 per cent. had died. Of those living 80 per cent. had syphilis.
Of the total pregnancies 90 per cent. were presumably syphilitic and although 10 per cent., seem free from syphilis, there is no proof that they all are. The total syphilis in these families amounts to 93 per cent. of the entire family.
For the most part our families followed Kassowitz’s rule; i.e., decreasing grades of infection in the children.
In case of syphilitic mothers bearing non-syphilitic children, it is probable that the infection in the mother is localized in places where it is not readily transmitted.
The idea that there are different strains of spirochetes receives some support from these families.
Transmission to the third generation, though not proved, is distinctly an occasional probability.
OBSTETRICS. A Text-book for the Use of Students and Practitioners. Whitridge Williams, Professor of Obstetrics Johns Hopkins University. Obstetrician-in-Chief to the Johns Hopkins Hospital; Gynecologist to Union Protestant Infirmary, Baltimore, Md. D. Appleton and Co., 1912.
Syphilis is one of the most important complications of pregnancy as it is one of the most frequent causes of repeated abortion, or premature labor. The influence of syphilis upon pregnancy differs materially, and three classes of cases are distinguished, according as infection has taken place: 1—before pregnancy; 2—at the time of conception; or, 3—during pregnancy. When inoculation with the specific poison has occurred before conception the disease nearly always gives rise to abortion or premature labor, more frequently the latter. Le Pileur obtained a striking illustration of the disastrous effects of syphilis from a study of the reproductive histories of 130 women, before 215and after its inception, 3.8 per cent. of the children being born dead before, as compared with 78 per cent. after infection. In premature labor due to syphilis the child is usually dead when it comes into the world; less frequently it is born alive with definite manifestations of the disease. When the mother is suffering from the affection at the time of conception the offspring is always syphilitic. P. 495.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American Authors. Edited by Reuben Peterson, A.B., M.D., Professor of Obstetrics and Gynecology in the University of Michigan, Ann Arbor, Mich.; Obstetrician-in-Chief to the University of Michigan Hospital. Lea Bros. and Co., Philadelphia and New York, 1907.
In marked contrast to the comparatively slight interference of pregnancy with the course of syphilis is the decidedly unfavorable influence of syphilis upon the course of pregnancy. Syphilis, more often than any other infectious disease, is responsible for a great variety of pathological changes in the fetus, placenta and uterus, and for the premature interruption of gestation. Statistics show that the fetal mortality in this disease averages 50%. This figure is lower than that given in the preceding paragraphs for some of the acute infectious diseases, but considering the prevalence of syphilis among all civilized and uncivilized races, it is obvious that the effect of this disease deserves a most careful consideration, not only from the medical, but also from the economic and sociologic point of view. Fournier gives the fetal mortality for cases in which the maternal infection occurs simultaneously with fecundation as 75%, the fetal morbidity being above 91%. Page 347. (Hugo Ehrenfest, M.D.)
A TEXT BOOK OF OBSTETRICS. Barton Cooke Hirst, M.D., Professor of Obstetrics in the University of Pennsylvania; Gynecologist to the Howard and Orthopaedic and Philadelphia Hospitals, etc. W. B. Saunders Co., Philadelphia and London, 1912.
Syphilitis as the most frequent cause of habitual death of the fetus must be excluded before another cause is sought. P. 352.
Of 657 pregnancies in syphilitic women collected by Charpentier 35% ended in abortion, and of the children that went to term a large number were stillborn. Of 100 conceptions in syphilitic women only seven children were alive a year later. P. 333.
PRACTICAL OBSTETRICS. Thomas Watts Eden, Obstetrical Physician and Lecturer on Midwifery and Gynecology, Charing Cross Hospital; Consulting Physician to Queen Charlotte’s Lying-in-Hospital; Surgeon to In-Patient Hospital for Women. 4th Edition. C. V. Mosby Co. 1915.
Of all the systematic causes of abortion however, the most important in 216all respects is syphilis. In all probability more abortions are due to this disease than to any other cause. P. 220.
It will be clear from this enumeration of the conditions which cause it that abortion is not an uncommon event. From some recent statistics presented by Professor Malins to the Obstetrical Society of London it appears that in this country about 16% of pregnancies terminate by abortion, i.e., one abortion occurs to every five births of viable children, and further, it appears that abortion is nearly twice as frequent among the classes from which hospital patients are drawn as among the well-to-do. Women who are the subjects of syphilis or Bright’s disease often sustain a succession of abortions without carrying any pregnancy to term. P. 221.
THE PRINCIPLES AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D., Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital and Dispensary and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
Premature labor is produced by the same factors that bring on abortion, but syphilis plays the most common role here, it being estimated that from 50% to 80% of the cases are thus caused. Next comes nephritis. Habitual abortion means that successive pregnancies are interrupted at the same period of development. Syphilis is usually found as the active factor and more especially in miscarriages of the later months. Each successive abortion occurs at a later period until a living child is born, but it perishes from congenital syphilis, and finally the disease has become so attenuated that a viable child is born. P. 419.
Obstetricians should constantly be on the alert for this protean disease. Its baneful action is often discovered when least expected and it spreads its blight on all three individuals concerned in the procreation of the species, often being transmitted to the second generation. Ricord says that in Paris one in eight is syphilitic, and while in America conditions are better, the disease is not rare and in its lesser manifestations quite common, though often not diagnosed. P. 482.
Interruption of gestation is the commonest symptom (of syphilis) and von Winckel found 61% fetal mortality. P. 483.
THE PRACTICE OF OBSTETRICS. Designed for the use of Students and Practitioners of Medicine. J. Clifton Edgar, Professor of Obstetrics and Clinical Midwifery in the Cornell University Medical College; Visiting Obstetrician to Bellevue Hospital, New York City; Surgeon to the Manhattan Maternity and Dispensary; Consulting Obstetrician to the New York Maternity and Jewish Maternity Hospitals. 5th Edition Revised. P. Blakiston’s & Co., Philadelphia.
This (syphilis) is one of the most common causes of abortion. P. 321.
217The causes of interrupted pregnancy may be placed in three classes. The maternal causes are divisible into systemic and the local. The systemic causes include obesity, marriages of consanguinity, pregnancies in rapid succession, etc., and the toxemia of kidney insufficiency. The local causes include all cases of acute and chronic pelvic congestion. P. 332.
Chief among the paternal causes is syphilis, tuberculosis, extreme youth or old age, great constitutional depression, exhaustion from any cause. P. 333.
MEDICAL GYNECOLOGY. Howard Kelly, A.B., M.D., LLD., F.R.C.S., Professor of Gynecological Surgery in Johns Hopkins University, and Gynecologist to the Johns Hopkins Hospital; Fellow of the American Gynecology Society; Honorary Fellow of the Edinburgh Obstetrical Society; Hon. Fellow Royal Academy of Medicine in Ireland; Fellow British Gynecology Society, etc., etc., etc. D. Appleton & Co., New York and London, 1912.
The susceptibility of syphilis to hereditary transmission is a fundamental character of the disease. It may be transmitted to the offspring directly by the infected sperm of the father, or from the infected ovule of the mother at the time of impregnation, or the infective principle may be conveyed through the medium of the utero-placental circulation during the course of pregnancy. P. 432.
Whether the infection is communicated through the sperm solely, the ovule, or the utero-placental circulation, the uterine death of the fetus is the most habitual expression of hereditary syphilis. Hereditary syphilis is one of the most common causes of abortion. P. 434.
Clinical observation shows most conclusively that certain dystrophies and organic defects in the subjects of hereditary syphilis may be transmitted to the third generation. P. 436.
While we cannot conclude that syphilis is transmitted in its essential nature as a virulent contagious disease, to the third generation, yet it is well known that heredo-syphilis kills the product of conception, or transmits to the survivor an impaired vitality with various dystrophies, and thus constitutes a chief factor in the physical, mental and moral degeneration of the race. From an exhaustive study of heredo-syphilis, Tarnowsky concludes that syphilis has an incomparably more fatal influence upon the species and on society than on the individual. P. 437.
PRINCE A. MORROW, M.D. Eugenics and Racial Poisons. Pamphlet published by the Society of Sanitary and Moral Prophylaxis, 105 W. 40th St., New York. 1912.
Syphilis is the only disease transmitted to the offspring in full virulence, killing them outright, or blighting their normal development. When the 218father alone is infected the mortality is about 38%. When the mother also becomes infected the mortality averages from 60% to 80%. Fully ⅓ of all infected children die within the first six months. Even when the subjects of inherited syphilis successfully run the gauntlet of diseases incident to infancy and childhood they do not always escape the effects of the parental disease. They are subject to various organic defects or stigma of degeneration, as they are termed. A final result of hereditary syphilis is the inability to procreate healthy children. If the subjects of inherited syphilis grow up and marry they are liable to transmit the same class of organic defects to the third generation.
FEWER AND BETTER BABIES, OR THE LIMITATION OF OFFSPRING. Wm. J. Robinson, M.D., Chief of the Department Genito-Urinary Diseases and Dermatology, Bronx Hospital and Dispensary; Fellow of the American Medical Association and of the New York Academy of Medicine.
There are thousands of syphilitic men and women who are perfectly safe as far as their partner is concerned, but are not safe enough to become parents. They cannot infect, but they must not give birth to children for fear that the children may have the taint in them. The use of preventives settles this problem and saves the world from thousands of pitiable hereditary syphilitics. P. 126.
MEDICAL GYNECOLOGY. Howard A. Kelly.
Two fundamental characteristics, contagiousness and susceptibility of hereditary transmission, give to syphilis an altogether special importance in relation to marriage. The statement has been made that syphilis constitutes a far greater danger to Society and the race than to the individual. The chief significance of syphilis as a racial danger comes from its hereditary effects. In addition, hereditary syphilis undoubtedly creates a terrain, or soil, favorable for the reception and germination of tubercle bacilli, and perhaps other bacilli. It does this by impoverishing the organism and diminishing the capacity of resistance against microbic invasion. From the view point of race perpetuation, syphilis is antagonistic to all the family represents in our social system. The essential aim of marriage is not simply the procreation of children, but of children born in conditions of vital health and physical vigor. The effect of syphilis is to so vitiate the procreative process as to produce abortions, or else a race of inferior beings, endowed with defects and infirmities and unfit for the struggle of life. It is this pernicious effect of syphilis upon the offspring which gives to the disease a dominant influence as a factor in the degeneration and depopulation of the race. P. 444.
When a married man has syphilis the first indication is to prevent contamination of his wife, the second is to guard against pregnancy. The interdiction 219of pregnancy should be absolute until time and treatment have exerted an attenuating and curative influence upon the diathesis. P. 448.
A consultation of the works of most authorities shows them to agree that the frequency of abortion to births at full term is from one in five or six to one in ten. P. 453.
SOCIAL DISEASES AND MARRIAGE. Social Prophylaxis. Prince Morow, M.D., Emeritus Professor of Genito Urinary Diseases in the University and Bellevue Hospital Medical College, New York; Surgeon to the City Hospital; Consulting Dermatologist to St. Vincent’s Hospital, etc. Lea Bros. & Co., New York and Phil., 1904.
The influence of inherited syphilis is manifest in the production of various dystrophies, malformations, and lesions of important organs, it seriously compromises the physical development, mental vigor and vital stamina of the descendants and constitutes a harmful factor in the degeneration of the race. The social aim of marriage is not simply the production of children who are to continue the race, but of children born in conditions of vitality and physical health fit to produce a race well-formed and vigorous, not to procreate beings malformed and stamped with physical and mental infirmity, destined to early death, or to drag out a miserable existence of invalidism. P. 21.
The statistics of European observers which have been collected from both private and hospital practice show in a most positive manner the noxious influence of syphilis upon the offspring. An analysis of these statistics taken from all quarters and aspects of the social condition of the parents show that when both parents are infected the mortality is 68 per 100. P. 27.
No other disease is so susceptible of hereditary transmission, so pronounced in its influence, and so fatal to the offspring.
While death in utero may occur as the most habitual expression of hereditary syphilis, its lethal influence is not limited to the period of intra-uterine existence. The child may be born alive, but in many cases the sentence of death is not commuted, it is simply reprieved, it may be for a few months, weeks, or only days. P. 212.
THE WORLD’S SOCIAL EVIL. A Historical Review and Study of the Problems Relating to the Subject. Wm. Burgess. With Supplementary chapter on a constructive policy by Judge Harry Olson, Chief Justice Municipal Court, Chicago. Saul Bros., Publishers, Chicago, 1914.
Based upon statements, experiences and opinions of physicians, public officials and other responsible persons, 50% to 80% of all men between the ages of 18 and 30 years contract gonorrhea. 10% to 18% of the male population contract syphilis. 40% to 60% of all operations upon women for diseases of the generative organs result from gonorrheal infection. 80% of the 220inflammatory diseases peculiar to women are the result of gonorrheal infection. A large per cent., some say one half, of still born and premature deaths of children is due to syphilis. 25% to 35% of all cases of insanity are caused by syphilis contracted years before. 15% to 20% of all blindness is attributed to these diseases. P. 159.
A CONSTRUCTIVE POLICY WHEREBY THE SOCIAL EVIL MAY BE REDUCED. Harry Olson.
The large group of mentally retarded persons who may be included in the term “sub-normal” number in this country, according to the best authorities about 300,000. An important distinction must be made between two groups of the defective classes, those who may, and those who should not enjoy social privileges as members of the community. From a racial and eugenic point of view the inborn, or heredity defectives are by far the most important because the defect is germinal and therefore transmissible to the offspring. This class forms 75% or more of the defective classes. When so many as 75% of the feeble-minded are such by reason of germinal or hereditary taint, and since perhaps 50% of the women of the underworld are sub-normal, it becomes at once apparent that not only in order to reduce the number of women in public prostitution, but also to protect the race itself, we must adopt other methods of eliminating vice than those now employed. P. 358–359.
PROCEEDINGS OF THE NATIONAL CONFERENCE ON RACE BETTERMENT. January 8–12, 1914. Published by the Race Betterment Foundation. Edited by the Secretary.
Statistical Studies. The Significance of a Declining Birth Rate. Frederick L. Hoffman, Statistician of the Prudential Insurance Company, Newark, N. J.
From an economic and social point of view a low birth rate and a low death rate would unquestionably be more advantageous than the opposite condition, which involves much needless waste of human energy and pecuniary expenditure. For reasons which require no discussion, every civilized country desires a normal increase in population, though a high degree of social and economic well-being is not at all inconsistent with even a stationary population condition such as for some years past has prevailed in France. P. 23.
All the available statistical information seems to justify the conclusion that the world’s population in general, and of the more civilized countries in particular is increasing at the present time at a more rapid rate than in earlier years—a condition largely the result of a persistent and considerable decline in the birth rate. P. 28.
221The important causes of death which have increased during the five years ending 1910, as compared with the previous five years, are briefly the following:—Syphilis increased from 4.1 to 5.4, per 100,000 of population. Cancer, and other malignant tumors from 11.5 to 13.7; locomotor ataxia, and other diseases of the spinal cord from 7.3 to 8.4; all diseases of the circulatory system combined from 161.2 to 171.7; ulcers of the stomach from 2.9 to 3.6; diarrhea and enteritis under two years, from 89.0 to 96.2; diseases of the puerperal state considered as a group from 14.2 to 15.5; malformations, chiefly congenital, from 12.2 to 14.9; diseases of early infancy, chiefly congenital debility and premature births, from 73.9 to 75.0. P. 45.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American Authors. Edited by Reuben Peterson, A.B., M.D. Lea Bros. & Co., Phil. and New York. 1907.
The reciprocal relation of gonorrhea and pregnancy is most unfavorable. Gonorrhea exerts a very unfavorable effect upon pregnancy and is responsible for a large number of abortions in the early months. Finally the gonococcus is a great source of danger to the fetus whose eyes may become affected during his passage through the diseased maternal parts. P. 373.
THE PRINCIPALS AND PRACTICE OF OBSTETRICS. Jos. B. De Lee, M.D., Professor of Obstetrics at the Northwestern University Medical School; Obstetrician to the Chicago Lying-in-Hospital and Dispensary and to Wesley and Mercy Hospitals, etc. W. B. Saunders Co. 1913.
Abortion is probably often the result of gonorrhea, acute or chronic. Chronic endometritis is most often the result of gonorrhea. P. 516.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch, Professor of the German Medical Faculty of the University of Prague, Physician to the Hospital and Spa of Marienbad; Member of the Board of Health, etc. Translated by M. Eden Paul, M.D. Rebman Co., New York.
The physician should lend his skilled assistance in producing facultative sterility only when his own special scientific knowledge leads him to consider this urgently necessary. A woman’s life and well being must appear to him of greater importance than the existence, or non-existence of a possible infant. That this view is morally sound is shown by the fact that public opinion justifies the accoucheur in the destruction of a living child when the mother’s life is in danger. P. 395.
222EUGENICS AND RACIAL POISONS. Prince A. Morrow, M.D., Emeritus Professor of Genito Urinary Diseases in the University and Bellevue Hospital Medical College, New York; Surgeon to the City Hospital; Consulting Dermatologist to St. Vincent’s Hospital, etc. Lea Bros. Co., New York and Philadelphia, 1904.
While the gonococcus is not transmissible through heredity it carries with it serious infective risks to the offspring. Fully 80%, and some authorities declare practically all of the blindness of the new born is caused by the gonococcus.
When authorities prohibit marriage for the unfit, they have in mind the probable fruits of such marriage. Women suffering from the diseases mentioned in this chapter give birth to children mentally and physically inferior, likely to sink into pauperism and certain to be in some way a burden upon society. If physicians were free to instruct parents how to prevent conception, the reproduction of their kind by defective and diseased parents living outside of institutions would be eliminated as a social problem.
DR. S. ADOLPHUS KNOPF IN THE SURVEY FOR NOVEMBER, 1916
That insanity, idiocy, epilepsy and alcoholic predisposition are often transmitted from parent to child is now universally admitted and corroborated by every-day experience and by an abundance of statistics. Countless are the millions of dollars expended for the maintenance of these mentally unfit. The state of New York alone spends $2,000,000 annually for the care of its insane. Whether sterilization of these individuals would be the best remedy is a question still open for discussion. The constitutionality of the procedure is doubted by some of our legal authorities. Segregation is resorted to in the meantime with more or less rigor according to state laws. Every year, however, many of the individuals who had been committed to institutions for the treatment of mental disorders are discharged as cured. They are allowed to procreate their kind. Would it not be an economic saving if at least the individuals whose intelligence has been restored were instructed in the prevention of bringing into the world children who are most likely to be mentally tainted and to become a burden to the community?
Of approximately every 500 persons in the United States in 1910, there was one an inmate of an insane asylum.
The exact figures expressed in a recent report (Hill, Joseph A. Report on the Insane in the United States, Bureau of the Census, Department of Commerce) that in a typical community of 200,000 persons, equally divided as to sex, 208 of the males and 200 of the females would be found in the insane asylums. In the course of a year 72 males and 60 females would be admitted to the asylums.
In 1880 the total of inmates in insane asylums in the United States included 22420,695 males and 20,307 females. In 1910, thirty years later, the number of male inmates had increased to 98,695 and the number of female inmates to 80,096. The excess of men among admissions in 1910 indicated a still further increase in the proportion, namely, 128 males to 100 females.
BEING WELL-BORN. An Introduction to Eugenics. Michael F. Guyer, Prof. Zoology, University of Wisconsin. Bobbs-Merrill Co., Indianapolis, Ind. 1916.
The records of the inheritance of insanity, imbecility, feeble-mindedness and other forms of nervous and mental defects are truly startling. Active researches in this field have been in progress now for several years, and as each new set of investigations comes in the tale is always the same. It is questionable if there is a single genuine case on record where a normal child has been born from a union of two imbeciles. Yet the universal tendency is for defective to mate with defective. Davenport gives a list of examples, beginning with such a one as this: “A feeble-minded man of thirty-eight has a delicate wife who in twenty years has borne him nineteen defective children.” Little wonder, in the light of such facts as these, that the number of degenerates is rapidly increasing in what are called civilized countries. But it may be urged, these are exceptional cases, there is surely no considerable number of mental defectives who are married. Let us look at the available facts. In Great Britain in 1901, of 60,000 known feeble-minded, imbeciles and idiots, 19,000 were married, and in the same year, of 117,000 lunatics, 47,000 were married; that is a sum total of 66,000 mentally defective individuals were legally multiplying, or had had the opportunity to multiply their kind, to say nothing of the unmarried who were known to have produced children.
In the State of Wisconsin I note from the tenth Biennial Report of the Board of Control that of 574 patients admitted to the Northern Hospital for the Insane during the year from July 1st, 1908 to June 30th, 1909, 274 were married, and 29 others were known to have been married; this is a total of 303 out of 574, considerably over half. At the Wisconsin State Hospital for the Insane we find the conditions are no better, for out of 499 admitted in the year of 1909–10, 208 were married and 65 others had at some time been married, or a total of 273 out of 499. There is every reason to believe that conditions are approximately similar in other states. P. 231–232.
One of the most disquieting facts in the situation in most states is that many patients—an average of approximately 1,000 a year, in Wisconsin for example—are on parole, subject to recall. This means that although it is recognized that these patients are likely to have to be returned to the asylum or hospital, little or no restraint in the meantime is placed on their marital relations. P. 234.
225SOCIAL ASPECTS. Wm. E. Kellicott.
In the U. S. the census of 1880 reported 40,942 insane in hospitals, and 51,017 not in hospitals, a total of 91,959 known insane. In 1903 the number in hospitals had increased to 150,151. The number not in hospitals was not known and cannot be determined accurately, but it is conservatively estimated as certainly not less than 30,000, and probably it is far greater than this. But taking a total of 180,000 known insane as a conservative figure, the ratio of known insane in the total population was 225 per 100,000 in 1903, as compared with 183 per 100,000 in 1880. P. 33.
The latest census reports for the U. S. give data relative to the dependents and defective in institutions. Insane and feeble-minded, at least 100,000; paupers in institutions 80,000, ⅔ of whom have children and are also physically and mentally deficient: prisoners 100,000; juvenile delinquents 23,000 in institutions; the number cared for in hospitals, dispensaries, homes of various kinds in the year 1904 was in excess of 2,000,000. From these figures we get a rough total of nearly 3,000,000. The foregoing are representative data:—they are published by the volume. It is always the same story—rapid increase of the unfit, defective, insane, criminal, slow increase, even decrease, of the normal and gifted stocks. It is with such conditions in mind that Whetham writes: “This suppression of the best blood of the country is a new disease in modern Europe; it is an old story in the history of nations, and has been the prelude to the ruin of states and the decline and fall of empires.” P. 35.
EUGENICS RECORD BULLETIN. No. 5. A Study of Heredity of Insanity in the Light of the Mendelian Theory. A. J. Rosanoff, M.D., and Florence I. Orr, B.S. Reprinted from American Journal of Insanity. Vol. XXVIII ... 1911. Cold Spring Harbor, N. Y.
In the report of the year ending September 30th, 1909, the New York State Commission in Lunacy gives the number of insane patients in state hospitals and private institutions as 31,540, or one to 276 in the general population. This figure does not include the inmates of institutions for the feeble-minded and for epileptics, it does not include the neuropathic subjects who find their way into prisons, reformatories, almshouses, dispensaries, hospitals for incurables, general hospitals, neurological clinics, etc., and above all, it does not include the many neuropathic subjects whose infirmities are latent, or of such nature as not to incapacitate them for ordinary occupations and life at large. P. 245.
226EUGENICS RECORD OFFICE. Bulletin No. 10 A. Report of the Committee to study and to report on the best practical means to cut off the defective germ-plasm in the American population. The scope of the Committee’s work. By Harry H. Laughlin, Secretary to the Committee. Cold Spring Harbor, N. Y. 1914.
According to the last census, 1910, .914% of the total population, or 841,244 persons, were inmates of institutions in the anti-social and the unfortunate classes in the U. S. Besides these persons who have been committed to institutions, there are many others of equally unworthy personality and hereditary qualities, who have, through the caprice of circumstances never been committed to institutions. In so far as the defective traits of the members of these varieties are inborn, they are to be cut off only by cutting off the inheritance lines of the strains that produce them. This is the natural outcome of an awakened social conscience, which is in keeping, not only with humanitarianism, but with law and order and national efficiency. Society must look upon germ-plasm as belonging to Society, and not solely to the individual who carries it. Humanitarianism demands that every individual born be given every opportunity for decent and effective life that our civilization can offer. Racial instinct demands that defectives shall not continue their unworthy traits to menace Society. There appears to be no compatibility between the two ideals and demands. P. 15–16.
J. H. KELLOGG, LLD., M.D., Superintendent of Battle Creek Sanitarium, Battle Creek, Mich.
A careful study of the returns of the Registrar General of England, according to Dr. Tredgold, an eminent English authority shows that out of every 1,000 children born to-day, as many infants die from “innate defects of constitution” as 50 years ago, and this notwithstanding that the total death rate of infants has been diminished nearly ⅓. The increase of insanity, is cited by Dr. Tredgold, as another evidence of race degeneracy. While the increase of the population of England and Wales in 52 years has been 85.8%, the increase of the certified insane has been 262.2%. At present there is one insane person to 275 of the normal population of England and Wales. Tredgold shows that mental unsoundness, lunacy, idiocy, imbecility and feeble-mindedness may be traced to hereditary influence in 90% of the cases. Mr. David Heron and others have shown that while there has been a marked decline in the birth rate in the population in general, the diminution is almost entirely confined to the healthy and thrifty class. In a section of population numbering a million and a quarter persons, thrifty and healthy artisans, the decline in the birth rate in 24 years, 1889—1904 was over 52%, or three times that in England and Wales as a whole. Study of a large number of families of the working class of incompetent and parasitic character found that the average number of children to the family was 7.4, while in thrifty 227and competent working families, the number was 3.7. In other words, the incompetent and defective classes are multiplying much more rapidly than are the competent and efficient. P. 440.
THE INCREASE OF INSANITY. James T. Searcy, A.B., M.D., LLD., Superintendent Alabama Hospitals for Insane. First National Conference on Race Betterment. January, 1914.
The population of the State of Alabama, according to the census during the ten years which the census includes, insanity increased 16%; the admissions into the insane hospitals increased 45%. These are appalling figures, and we can parallel them all over the U. S., not like them exactly in each state, for they differ. The general population of the U. S. increased 18%, and that of the insane hospitals increased 28% during the years of the census. P. 167.
THE PRACTICE OF OBSTETRICS. Joseph De Lee, M.D.
Epilepsy may practically be regarded as an in-hereditary affection, and children of one subject to this disorder are almost sure to be epileptic. Under no circumstances should parents who are both epileptics bring children into the world.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American Authors. Edited by Reuben Peterson, A.B., M.D., Prof. of Obstetrics and Gynecology in the University of Michigan, Ann Arbor, Mich.; Obstetrician and Gynecologist-in-Chief to the University of Michigan Hospital. Lea Bros. & Co., Phil. and New York. 1907. Chapter XIX.
Marriage should always be discouraged on account of the marked tendency of epilepsy to be transmitted to the offspring. In all grave cases, marriage, or new impregnation, should be prohibited. P. 363. (Hugo Ehrenfest, M.D.)
PARENTHOOD AND RACE CULTURE. An Outline of Eugenics. C. W. Saleeby, M.D., Ch.B., F.Z.S., F.R.S., Edinburgh; Fellow of the Obstetrical Society of Edinburgh; Member of Council of the Eugenics Education Society; of the Psychological Society, and of the National League for Physical Education and Improvement; Member of the Royal Institution and of the Society for the Study of Inebriety, etc., etc. Cassell & Co., Ltd., London, N. Y., Toronto and Melbourne. 1909.
A foremost authority, Dr. F. W. Mott, has independently reached the same conclusion as Dr. Branthwaite, that the chronic inebriate comes as a rule 228of an inherently tainted stock. Dr. Mott, however, reminds us that if alcohol is a weed killer, preventing the perpetuation of poor types, it is probably even more effective as a weed producer. Professor David Ferrier, the great pioneer of brain localisation, in reference to these people speaks of the “risk of propagation of a race of drunkards and imbeciles.” Dr. J. C. Dunlop, Inspector under the Inebriates Act, Scotland, states that his experience leads him to precisely the same conclusion as that of Dr. Branthwaite. Dr. A. R. Urquhart, an Asylum authority, affirms that chronic inebriety is largely an affair of habit, is a symptom of mental defect, disorder, or disease. Dr. Fleck, another authority, says, “It is my strong conviction that a large percentage of our mentally defective children, including idiots, imbeciles and epileptics, are the descendants of drunkards. Mr. McAdam Eccles, the distinguished surgeon agrees; so does Dr. Langdon Down, physician to the National Association for the Welfare of the Feeble-minded; so does Mr. Thos. Holmes, the Secretary of the Howard Association.”
MARRIAGE AND GENETICS. Laws of Human Breeding and Applied Eugenics. Chas. A. L. Reed, M.D., F.C.S.; Fellow of the College of Surgeons of America; Member and former president of the American Medical Association; Professor in the University of Cincinnati. The Galton Press, Cincinnati, Ohio.
The present demand for alcohol is generally the demand of the system for something with which to make up for some persistent defect. In other words, alcoholism is the sign and index of some form of degeneration. Thus the degeneracy that finds expression in alcoholism in one generation may be manifested in the next in the form of epilepsy, feeble-mindedness, insanity, immorality, or criminality. Unfortunately, alcoholism does not seem to lessen the fecundity of its victims. The quality of their progeny is, however, progressively lowered. It is due to the combined influence of transmitted degeneracy and the pernicious effect of environment. As a genetic factor, alcoholism, considered in its immediate relation to the marriage state may be summarised as follows:—
1—The chronic alcoholist generally develops lowered sexual efficiency.
2—General failure of sexual power, associated with strong desire, generally manifested by alcoholics, often results in sexual promiscuity, associated with perversion.
3—Progressive alcoholism destroys the normal psychic type and thus breaks up family ties.
4—Lowered general efficiency of alcoholics tends to pauperism and crime.
5—Lowered general resistance of alcoholics makes them the easier prey of infections and shortens their expectancy of life.
2296—Alcoholism is a germinal defect, the degeneracy underlying which is transmitted in some form to 100% of the progeny of two alcoholic parents.
Marriage with or between degenerates of the alcoholic type is advised against and should be prohibited by law. P. 125–126.
Pauline Tarnowsky in Etudes Anthrope metriques sur le Prostitutees 1887 gives figures derived from measurements of fifty prostitutes in Petrograd in which she found four-fifths of her cases were offspring of alcoholic parents while one fifth were the last survivors of very large families.
THE PRACTICE OF OBSTETRICS. In Original Contributions by American Authors. Edited by Reuben Peterson, M.D.
A chronic state of intoxication may be found in patients (Mothers) with such bad habits as alcoholism, morphinism, cocainism, etc., and in sufferers of trade poisoning, plumbism, nicotism of workers in tobacco factories, etc. Most of these diseases are characterized by a tendency to abortion and a high infantile mortality and morbidity. P. 368.
It is generally admitted that the effect of chronic alcoholism upon pregnancy is most harmful. On account of the frequency with which drunkards are afflicted with venereal diseases, especially syphilis, it is almost impossible to obtain reliable statistics and exact figures, but the fact has been established that chronic alcoholism predisposes the woman to abortion, and that the children of dipsomaniac parents show a strikingly large percentage of malformations and mental abnormalities, especially imbecility and epilepsy. P. 370 (Hugo Ehrenfest, M.D.)
THE PATHOLOGY OF THE FETUS. Aldred Scott Warthin, M.D. (The Practice of Obstetrics, in original Contributions by American Authors, Ed. by Reuben Peterson, M.D.)
Of the antenatal treatment of fetal diseases we at present know little or nothing, but there can be no doubt that a wonderful field is here offered to the medicine of the future. According to our present knowledge such germinal and fetal therapeutics must be chiefly in the line of prevention. We are already in a position to apply some knowledge toward this end. The effects upon the fetus of intoxications, such as plumbism, alcoholism, etc., may be avoided. The production of syphilitic offspring may be restricted, and our knowledge of the later effects upon the fetus of certain diseases, or pathologic states of one or both parents may be utilized toward the bringing into existence of progeny under such conditions as to escape such evils. Our knowledge of heredity, of morbid conditions and predispositions should also be brought to bear upon the question of marriage and fitness to produce 230healthy children. Moral, as well as physical considerations should here be gravely weighed. The health of parents, the hygiene of pregnancy throughout its entire course, etc., are important factors in the improvement of the race, to which the coming civilization and the new medicine must give increasing attention. P. 535.
THE SEXUAL LIFE OF WOMAN IN ITS PHYSIOLOGICAL, BIOLOGICAL AND HYGIENIC ASPECTS. E. Heinrich Kisch. Rebman Co., New York.
A woman with a tendency to alcoholism should under no circumstances be allowed to marry. In the cases, fortunately rare, in which the drink craving exists in women, marriage is even more undesirable than it is in the case of men similarly afflicted, for the female drunkard is in a position in which she can mishandle and neglect her children throughout the entire day. P. 258.
RASSENVERBESSERUNG. Translated from the Dutch of Dr. J. Rutgers. Second Edition. Dresden, 1911.
Pelman examined 709 of the 834 descendants of an alcoholic vagrant, named Ada Inke, who died in 1740. Among these were found 106 illegitimate children, 142 were vagrant beggars, 64 were charity dependents, 181 prostitutes, 96 were tried for various offenses, among these 7 were for murder. These descendants during 75 years cost the State 5,000,000 marks. P. 97.
August Forel, who for years was the psychiatrist at the head of a large insane asylum at Zurich, Switzerland, has this to say about the effects of narcotic poisons and alcohol in particular: “The offspring tainted with alcoholic blastophthoria suffer various bodily and physical anomalies, among which are dwarfism, rickets, a predisposition to tuberculosis and epilepsy, moral idiocy in general, a predisposition to crime and mental diseases, sexual perversions, loss of suckling in women, and many other misfortunes. But what is of much greater importance is the fact that acute and chronic alcoholic intoxication deteriorates the germinal protoplasm of the procreators.”
MICHAEL F. GUYER, Ph.D., Professor of Zoology, University of Wisconsin in “Being Well Born.”
In an investigation on the effects of parental alcoholism on the offspring, Sullivan (Journal of Mental Science, Vol. 45, 1899) gives some important figures. To avoid other complications he chose female drunkards in whom no other degenerative features were evident. He found that among these the percentage of abortions, still-births and deaths of infants before their third year was 55.8% as against 23.9% in sober mothers. In answer to the objection 231that this high percentage may be due merely to neglect, and not to impairment of the fetus by alcoholism, he points out the fact, based on the history of the successive births, that there was a progressive increase in the death-rate of offspring in proportion to the length of time the mother had been an inebriate. P. 169.
A TEXT BOOK OF OBSTETRICS. Barton Cooke Hirst, M.D., Professor of Obstetrics in the University of Penn.; Gynecologist to the Howard, the Orthopaedic and the Phil. Hospitals, etc. 7th Edition. W. B. Saunders Co., Phil, and London, 1912.
The effect of chronic diseases of the mother upon the fetus. Women affected with tuberculosis, cancer, or chronic malarial poisons may give birth to a succession of dead children. P. 353.
Fetal mortality exceeds that of any other period of life. For every four or five labors there is one abortion, and if to this number is added still-births the proportion of fetal deaths to living births is larger. P. 332.
THE DISEASES OF SOCIETY AND DEGENERACY. G. F. Lydston, M.D.
That a multiplicity of children in poverty-stricken families often impels to abortion, is evident. The necessary evils of our prohibitive laws and ethics bearing upon illegitimacy, are obvious; viz:
First, and worst, is infanticide, committed usually before, but only too often after birth. In the latter category I would place abandoned children who die of exposure or starvation, and the bulk of mortalities in foundling asylums and for baby farms. The social ostracism placed upon the mother is a prime factor in this child’s murder. Condemnation and shame are hers if she allows nature to take its course, and the penalty of infanticide stares her in the face if she interferes with the conception. A rarely anomalous state of affairs this.
Second—The brand of infamy placed upon the unborn child, from which only its murder can save it.
Third—The prostitution or suicide of the woman who is found out.
Branded with ignominy from the moment of conception, a burden to society, and a still greater burden to its parent, or parents from the moment of its birth, with no systematic endeavor on the part of society to prevent its growing up a criminal, a drunkard, a pauper, a prostitute, or a physical wreck, what wonder that many a poor woman’s fingers become too tightly entwined around her offspring’s neck. If her motive for the act were always as altruistic 232as its consequences, so far as the child’s welfare is concerned, there are some clear-minded thinkers in the world who could not be brought to judge her harshly. P. 371.
The rights of the unborn will one day be considered. Until they are so considered, and practical efforts made to secure them, we cannot hope for much improvement in the prevention of degeneracy. P. 559.
AMERICAN JOURNAL OF DISEASES OF CHILDREN, November 1914. Vol. 8, pp. 327–335. Question of Hereditary syphilis as a social problem.
Of all deaths of infants in St. Louis in 1913, 1,070 were illegitimate.
Of all deaths in infants due to syphilis 1,550 were illegitimate.
AUGUST FOREL. The Sexual Question. A Scientific, Psychological, Hygienic and Sociological Study. Translated by C. F. Marshall, M.D., F.R.C.S., Late Assistant Surgeon to the Hospital for Diseases of the Skin. London.
The stigma of shame which has branded all illegitimate maternity unfortunately justifies the many cases of abortion, and even infanticide. Things ought to change in this respect, and in the future no pregnancy ought to be a source of shame for any healthy woman whatever, nor furnish the least motive for dissimulation. P. 411.
THE SMALL FAMILY SYSTEM. C. V. Drysdale, D.Sc.
Illegitimacy.—As far as statistics are concerned, the most valuable evidence is that relating to illegitimacy. The Registrar General’s Reports contain a useful amount of information upon this point, and give us the number of illegitimate births per thousand unmarried women within the fertile period, between the ages of 15 and 45. This illegitimacy rate for England and Wales is represented in Fig. 13, and it is noticeable that the fall since the year 1876 has been extremely rapid, much more so in fact than that of the fall in the general birth-rate or in the fertility rate of the married women. While the general birth-rate has fallen from 36.3 to 25.6 (or by 26.5 per cent.), the illegitimate birth-rate has fallen from 14.6 to 7.9 per thousand unmarried women (or by nearly 50 per cent.). This is most striking and satisfactory. An extreme instance is given in the county of Radnorshire, which in 1870–2 had a fertility rate of 308.6 births per 1,000 married women, which sank to 188.7 in 1909, or by 39 per cent. In the same interval the illegitimate birth-rate fell from 41.8 per 1,000 unmarried women to 7.2, or by no less than 83 per 233cent. In Holland a drop of the legitimate fertility from 347 to 315 per 1,000 coincided with a fall of the illegitimate fertility from 9.7 to 6.8 per 1,000, i.e., at a much greater rate. It is true that France, with its low and decreasing fertility rate (from 196 to 158 per 1,000 between 1881 and 1901), has had a comparatively high and increasing illegitimacy rate (from 17.6 to 19.1 per 1,000); and that Ireland, with a somewhat high and slightly increasing fertility (from 283 to 289 per 1,000), has the lowest and a falling illegitimacy rate (from 4.4 to 3.8 per 1,000). But this has been heavily outweighed by Austria with an equally high and steady fertility (from 281 to 284 per 1,000) with the highest illegitimacy rate known (43.4 to 40.1 per 1,000), while Germany comes second with an illegitimacy rate of 27.4 per 1,000 in 1901. Though it cannot be said, therefore, that the lowest birth-rate produces the lowest illegitimacy rate, it most certainly cannot be said that family limitation has had any evil effect in increasing legitimacy. The bulk of the evidence is quite decidedly the other way. In the case of the most notable exception—that of France—we have the authority of Dr. Bertillon for saying that the greatest decency and lowest illegitimacy are found where the birth-rate is lowest. We may also quote from our own Registrar General, who said in his Annual Report for 1909:—
“Except in the cases of the German Empire, Sweden, France, Belgium, and the Australian Commonwealth, the falls shown in illegitimate fertility in Table LXXXIV are greater than the corresponding falls in legitimate fertility.”
So far as the evidence of illegitimacy is concerned, therefore, it may be taken as definitely established that the adoption of family restriction has not led to greater laxity among the unmarried. But it would, of course, be quite unjustifiable to claim that this evidence is final. It may not mean that there is less lax conduct but only that there are fewer results of lax conduct. It is perfectly open for the orthodox moralist to claim that the greater knowledge of preventive methods has permitted an increase of laxity with a reduction of the ordinary effects. This must remain a matter of conjecture. When we find, however, that not only has illegitimacy decreased, but also deaths from abortion and from the diseases ordinarily associated with irregularity, there seems no justification whatever for the contention that chastity has been relaxed. It must not be forgotten in this connection that the encouragement to early marriage afforded by the possibility of avoiding the economic burden of a too early or too large family affords the most likely of all methods for removing the temptations to unchastity and for conquering the hitherto untractable “social evil.” Although the average age of marriage in this country has been rising somewhat lately (probably on account of the increasing cost of living), it is interesting to note that it is lower and fairly steadily decreasing in France. For first marriages the average age at marriage of French men has fallen from 28.6 in 1856 to 27.88 in 1896–1900, and of French women from 23424.25 to 23.5 in the same period. This cannot be regarded as otherwise than a very good sign.
(Note: It is noteworthy in this connection that the French marriage laws are so strict that many thousands of couples live out of wedlock in preference to complying with them.)
We need not dwell upon this question, as the amount of pauperism depends upon a large variety of circumstances. But it is satisfactory to note that pauperism in England and Wales, i.e., the number of persons relieved annually per thousand of the population, has fairly steadily fallen from 34.5 in 1875 to 26.4 in 1910, or by 23.5 per cent. during the period of the declining birth-rate. This is so far reassuring, in that it indicates that the easier circumstances engendered by smaller families do not lead to idleness, as is frequently contended. The industry and saving habits of the French peasantry are world-renowned, and it is worthy of note that France is almost the only country in which the real wages of the working classes have been increasing of late years, while they have dropped 15 per cent. in this country, and nearly 25 per cent. in prolific Germany.
THE REPORT OF THE POOR LAW COMMISSION. By Sir Edward Bradbrook, C.B. Eugenics Review, Vol. 1, April 1909. Eugenics Education Society, London.
The Commissioners throw a strong light upon the ineffectiveness of existing measures when they show that the great and growing expenditure upon education and upon the public health has had no result in reducing pauperism, which is on the contrary of late years deplorably increasing, and that the advance in the rate of wages, and the diminution in the cost of living have been equally ineffectual.
In the words of the Commissioners, children who are brought up in such conditions, surrounded by disease and immorality and drunkenness are almost doomed to pauperism. If relief be given it should be used to check the creation of another generation of paupers. Much that is very instructive is contained in the report on the subject of children who come by one means or another to be under the control of the Guardians of the Poor, and important suggestions are made for reforms in the manner and training of such children. This, however, we need not discuss, as the spread of eugenic principles would tend to reduce their number until the time should come when the children dependent on public care should be few and exceptional. In their discussion of the causes of pauperism, the Commissioners quote a statement from a relief officer of Leeds, that one of the most important causes is early marriage of 235persons dependent upon casual labor. Large families are the rule. Unless we can cut off some of the sources from which that stream is being fed, the attempt to do more constructive work, whether by public assistance or by voluntary charity will continue to be swamped by hopeless cases—men and women ruined by bad habits or disease from infancy who propagate their own misery and hand on another generation of hopeless cases to the future. A great evil justifies strong measures to remedy it. This is true eugenic doctrine. P. 47–50.
THE METHODS OF RACE REGENERATION. C. W. Saleeby, M.D., CH.B., F.Z.S., F.R.S., Edinburgh; Fellow of the Obstetrical Society of Edinburgh; Member of Council of the Eugenic Education Society, of the Psychological Society, and of the National League for Physical Education and Improvement; Member of the Royal Institution and of the Society for the Study of Inebriety, etc., etc. New Tracts for the Times. Cassell & Co., Ltd., London, New York, Toronto and Melbourne. 1911.
At the National Conference on the Prevention of Destitution, held in London at Whitsuntide, 1911, we gathered together in the section dealing with this subject a number of papers by authoritative writers, whose knowledge of the problem is first-hand, and the following is an extract from the paper, the Eugenic Summary and Demand, in which I endeavored to express the substance of the evidence. The mentally defective and diseased, existing in it and as part of it, injure the community in the following ways:
1—They contribute largely to the ranks of chronic alcoholism and inebriety, with all their consequences.
2—They contribute largely to the illegitimate birth rate, that is to say, to the production of children for whose nurture, quite apart from the question of their natural defect, adequate and satisfactory provision is not, or indeed cannot be made.
3—They contribute largely to the ranks of prostitution.
4—They thus contribute largely to the propagation of the venereal diseases, with all their consequences to the present and the future.
5—They are responsible for much crime, major and minor.
6—Both directly, as chronically inefficient, and indirectly, in the ways here cited, they contribute to the number of the destitute, constituting the majority of the naturally, as distinguished from the nurturally unemployable.
7—They contribute largely as parents, married or unmarried, to parental neglect and cruelty to children which is probably more injurious to the adult life of the next generation, than most, or any of us realize.
8—They contribute largely to the ranks of the wastrel and the hooligan. 236In such ways, and to such a degree these persons injure the community. But it is particularly to be noted that therein the community also injures them. The fact is obvious to all of us here. The injury wrought by the present relations between the community and these unfortunate persons is mutual, they injure it and it injures them. And not until we recall the words of Burke, in the light of modern genetics, shall we realize the full measure of this injury, for as that great thinker said, a community is “a partnership, not only between those who are living, but between those who are living and those who are dead, and those who are to be born.” To the foregoing indictment of the present state of things, and remembering that whatever is inherent is transmissible, I therefore add:
9—They become parents and thus contribute incalculably to the maintenance of these evils after we are dead, but not after we are responsible. P. 49–50.
But it does not suffice to pursue positive methods, the encouragement of parenthood on the part of the worthy, and negative methods, the discouragement of parenthood on the part of the unworthy, if there be any agencies in the world which are forever turning worthy stocks into unworthy stocks. If there be such racial poisons, plainly we must stand between healthy stocks and their influence. By the term racial poisons I mean to indicate those agents, whatever they may be which, in greater or less degree, injurious to individuals as individuals, prejudices their subsequent parenthood. The racial poisons are very various, they include substances inorganic, such as lead, organic, such as alcohol, and organized, such as the living causes of certain forms of disease. Circulating in the parental blood, they reach and injure the racial tissues, or germ-plasm. P. 56.
WOMEN AND LABOR. New York Evening World, May 8, 1917.
With American industry preparing to put women into the places of male workers called to the war, it is a rather surprising thing to learn that there already are 7,438,686 women in the United States who earn their own living. Of these no less than one-fourth are married. Here are the figures: Single, 4,401,000; married, 1,890,626; widowed or divorced, 1,147,060.
In 1900 only 4,833,630 women left their homes to work, showing an increase of approximately one-half since then.
In 1890 the married formed 14.3 per cent. of all women sixteen years of age and over engaged in gainful occupations. By 1900 this proportion had increased to 15.9 per cent. From 1900 to 1910 it jumped to the unprecedented proportion of 25.4 per cent. While there were important variations, the great increase was not confined to any one occupation or group of occupations, nor to any one State or group of States. In every occupation examined the married 237formed a larger proportion of all women sixteen years of age and over in 1910 than in 1900.
The proportions were exceptionally high in the South and Arizona—50.8 per cent. in South Carolina, 46.8 per cent. in Georgia, 46.7 per cent. in Florida, 47.4 per cent. in Alabama, 54.2 per cent. in Mississippi, 45.6 per cent. in Arkansas, 40.7 per cent. in Arizona. In contrast, the proportion was only 15.8 per cent. in Connecticut, 15.1 per cent. in Pennsylvania, 13.1 per cent. in Wisconsin, 11.9 per cent. in Minnesota, and 15.7 per cent. in Iowa.
The unusually large proportion of married women engaged outside their homes in the South is explained by the number of negroes living in that section of the country. The total of white women working for a living in the same States is perhaps smaller than in any other part of the United States.
Even more significant than the great increase in the proportion which the married form of all women sixteen years of age and over engaged in gainful occupations is the marked increase in the proportion of all women so employed.
Statistics show that in 1890 just 4.6 per cent. of married women went to work. The figures had expanded to 5.6 per cent. ten years later, and in 1910 had reached 10.7 per cent.
It may be safely assumed that in the years which have elapsed between then and now the increase has more than kept pace with earlier figures. And it is equally certain that once men have been replaced by women under war conditions neither they nor employers will be inclined to restore ante-bellum conditions. The problem is one to give economists grave concern.
MARY ALDEN HOPKINS, Harper’s Weekly, 1915.
“Too many children is as great a danger to family life as too few children,” said Mr. Owen Lovejoy, General Secretary of the National Child Labor Committee. A secretary of this Committee, working for the abolition of child labor, the improvement of the compulsory education laws, and the raising of the standards of education in backward states, Mr. Lovejoy has first knowledge of the condition of children in every state in the Union.
“How many are too many?” he was asked. “I should say any more than the mother can look after and the father earn a living for. There are always too many children in a family if they have to go to work before they get their growth and schooling. It may be that some day the state will help support the children, but under present conditions, as soon as there are too many children for the father to feed, some of them go to work in the mine or factory or store or mill near by. In doing this they not only injure their tender 238growing bodies, but indirectly they drag down the father’s wage. They go to work to help the family, but they really injure it. The wage tends to become an individual wage, the father receiving only enough for his personal maintenance, the mother working both at home and outside, and the children supporting themselves as soon as they can toddle into the cotton fields or hang onto the back of a delivery wagon. Thus the home is dissolved into constituent parts and the burden of the struggle for existence is laid on each. The more that children work, the lower the father’s wages become; the lower the father’s wages become, the more the children must work. So we evolve the vicious circle. The home becomes a mere rendezvous for the nightly gathering of bodies numb with weariness and minds drunk with sleep. No fine spiritual relation can exist between parents and children where the children are an economic asset to the parents. There are people who approve this state of affairs, but no one can who really cares for the welfare of children. We fight this condition with Child Labor Laws. If the children stay out of industry, the fathers have more work and make more money in the end. But one of the strongest factors against getting laws passed or enforced after they are passed, is the families’ immediate need of the children’s pitiful earnings. If there were fewer children in these families, it would be possible to keep them in school and leave the mines and factories to the fathers. There is another aspect to the matter. Not only do these unfortunate children drag down the physique and mentality of the race, but they keep many children of more thoughtful parents from being born at all. Just as long as there are many families that are too large, there will be other families that are too small. Yet these small families are potentially the best families of all. Serious-minded laboring people whose trades are being captured by child laborers are reluctant to bring offspring into a world which cannot promise a life of the simplest comforts in reward for hard labor. Here is the real danger of that race suicide so vigorously condemned by Ex-President Roosevelt and others; for while the man of virtue and strength is deterred from propagating his kind because of the jeopardy in which his children would stand, the vicious and the ignorant, the physically unfit and the discouraged are not deterred by any such consideration, but, regardless of consequences, continue to propagate their kind and swell the proportion of those who will be from birth to death a heavy liability against society. We regard the family—one father, one mother, a group of children to be fed, clothed, and educated during the years that precede maturity—as the fundamental institution of our civilization and the glory, thus far, of all social evolution. One of the causes out of which the family grew has direct bearing upon this matter—that to which Professor Fisk called attention as his chief contribution to the evolutionary theory—the prolonged period of infancy. The evolutionary trend has been to prolong infancy and adolescence, and thus to launch upon society better individuals. This is impossible where the older children in a family are crowded out of the home into the workshop.”
The Child Labor Bulletin, November, 1912, contains special articles on 239the child workers in New York tenement houses. Record after record shows a two-child income supporting a six-child family.
In connection with Mr. Lovejoy’s statement that a high birth rate encourages child labor, it is significant to find from the Galton Laboratories of the University of London, the statement that drastic child labor laws directly lower the birth rate. In “The Report on the English Birth Rate,” from the Eugenics Laboratory, Memoir XIX, Part 1, England, North of the Humber, Ethel M. Elderton, after touching on the influence of the raised standard of decency and comfort, lays the responsibility of the change chiefly upon the lessened economic value of the child to its parents.
Miss Elderton says, “Between 1871 and 1901 the number of children employed largely diminished. Neo-Malthusianism spread and the child ceased largely to be born, because it was no longer an economic asset. The Compulsory Education Act of 1876, the Factories and Workshops Act of 1878, and the Bradlaugh-Besant Trial of 1877 (concerning the lawfulness of publishing pamphlets on contraception) are not unrelated movements; they are connected with the lowered economic value of the child, and with the corresponding desire to do without it.” The relation which Miss Elderton traced between the higher ideals of protection to childhood and the lowered birth rate is the more interesting because she is deeply, passionately alarmed at England’s falling birth rate.
Mr. Lovejoy does not regard the falling birth rate as a wholly undesirable phenomenon. He says: “Children should be born when the parents are in good health, at intervals that will allow the mother to recover her strength, and only as many should be born as the parents can care for. There is no deeper sorrow than to know that a child has died for causes that might have been prevented if the parents had had more wisdom and foresight. The ideals of care and education which we have for our own children should be our ideals for all children. I shall not consider it a calamity if the birth rate falls to a point where every child is so precious to the nation that not one will be allowed to work in a factory or workshop or mine or store under the age of sixteen, and up to that time every one will have proper food and clothes and education. Our race-suicide danger is a danger, nor of quantity, but of quality.”
LATEST OFFICIAL FIGURES ON CHILD LABOR. From United States Census of Occupations, 1910. New York State.
| Age | 10 to 13 years | 14 to 15 years |
|---|---|---|
| Manufacturing and mechanical | 518 | 18,502 |
| Extraction of Minerals | 3 | 47 |
| Agriculture | 1,566 | 5,034 |
| All other occupations | 2,765 | 36,659 |
| Total in all gainful occupations New York State | 4,852 | 60,242 |
| Total in all gainful occupations United States of America | 895,976 | 1,094,249 |
| Total child laborers in the United States of America | 1,990,225 |
240WAGES AND THE COST OF LIVING. Together with its relation to Prevention of Conception. Compiled by C. V. Drysdale, D.Sc.
Apart from the special problems of experts, the great economic question of the day is that of the remuneration of labor and its relation to the cost of living. In Parliament and the press the questions of a minimum or living wage and of the purchasing power of existing wages are continually debated; and it is perfectly evident from the tone of these debates that we are confronted with a most serious difficulty, for which none of the political parties or economic authorities has any satisfactory solution. The recognition of this difficulty is due not to the fact that any new phenomena are present, or that the workers are worse off than at many periods in the past; but to the fact that the compilation of more accurate and official statistics during recent years has brought to light facts which were formerly only surmised, and has made two important conclusions practically indisputable. These are as follows:
A. That the wages of a large fraction of the working classes are insufficient, even when most skilfully employed, for the adequate support of a normal family.
B. That during the last ten or fifteen years of social legislation and of strenuous effort on the part of the working classes and social reformers, the purchasing power of average wages has declined instead of increasing, and this decline shows no definite sign of being arrested.
In order to improve the efficiency of production, it is important that the efficiency of the race should be improved. Hence the reduction of births should be especially encouraged among the poor and those suffering from physical or mental defect or disease, who, it may be noted, should have the strongest personal motives for voluntary restriction.
The restriction of births in proportion to economic or physiological deficiency would steadily improve economic conditions in the following ways:
(a) It would immediately reduce the burden upon the poor with their existing wages.
(b) It would immediately check increased demand, and therefore a further rise in price of food.
(c) It would reduce the burden of charity and taxation.
(d) It would permit the workers to be better nourished and educated.
(e) It would permit the children to be better educated and technically trained.
(f) In course of time it would reduce the number of workers competing and further raise wages.
241(g) The evils of overcrowding, with its serious hygienic and moral dangers, would be rapidly diminished, and the housing problem made easier of solution. A three bedroom house only provides decency for a family not exceeding four children.
(h) It would give better opportunities for thrift among the workers and for their emancipation from the position of “wage slaves.” It would then give them an opportunity of co-operating and owning their own instruments of production.
In support of these statements it may be recalled that in Prof. Thorold Rogers’s Six Centuries of Work and Wages a striking example is given of the continued rise of wages after the Black Death of 1349, despite all efforts of Parliament to fix them.
“It is certain that the immediate consequence of the plague was a dearth of labor, an excessive enhancement of wages, and a serious difficulty in collecting the harvests of those landowners who depended on a supply of hired labor for the purpose of getting in their crops.... The plague, in short, had almost emancipated the surviving serfs.
“I shall point out below what were the actual effects of this great and sudden scarcity of labor. At present I merely continue the narrative. Parliament was broken up when the plague was raging. The King, however, issued a proclamation, which he addressed to William, the Primate, and circulated among the sheriffs of the different counties, in which he directed all officials that no higher than customary wages should be paid, under the penalties of amercement. The King’s mandate, however, was universally disobeyed, for the farmers were compelled to leave their crops ungathered or to comply with the demands of the laborers. When the King found that his proclamation was unavailing, he laid, we are told, heavy penalties on abbots, priors, barons, crown tenants, and those who held lands under mesne lords, if they paid more than customary rates. But the laborers remained masters of the situation. Many were said to have been thrown into prison for disobedience; many, to avoid punishment or restraint, fled into forests, where they were occasionally captured. The captives were fined, and obliged to disavow under oath that they would take higher than customary wages for the future. But the expedients were vain; labor remained scarce and wages, according to all previous experience, excessive.”
Mr. Thorold Rogers tells us of all the expedients employed by Parliament, in the Statute of Laborers, in order to check the rise of wages, and how they broke down and were evaded by the employers themselves. “The rise in agricultural labor is, all kinds of men’s work being taken together, about 50 per cent., of women’s work fully 100 per cent.” Artisans fare equally well. And, despite the rise in price of manufactured articles consequent upon this rise of wages, “there was no corresponding rise in the price of provisions.... The free laborer, and, for the matter of that, the serf, was in his 242way still better off. Everything he needed was as cheap as ever, and his labor was daily rising in value.”
It would, of course, be absurd to apply the lesson of one period of history to another, without consideration of the changed circumstances. But it is equally absurd to pass over such a vivid object lesson as the above without giving it due consideration, especially when it has a sound theoretical basis. Prof. Thorold Rogers was not a disciple of the Malthusian school, and he takes Mill and others to task for the importance they ascribed to the population difficulty. Yet he tells us that the reign of prosperity lasted for some time after the reduction of population by the Black Death, and that a rapid growth of population followed. This is quite in accordance with the doctrine of Malthus, and justifies our belief that, if this increase had been prudentially restricted, prosperity would have been permanently maintained.
A modern illustration of the same principle appears to be given in New Zealand, where the practice of family restriction seems to be almost universal. In the Standard of June 20th, 1912, appeared a note commenting upon the great and increasing prosperity of New Zealand; and it contains the following significant passage:—
“The wages paid to employees and the output of the printing establishments in the country have pretty nearly doubled in the same ten years, rising respectively from £284,605 to £490,246 and £704,285 to £1,377,926. A curious point in connection with the grain mills is that while there were fewer establishments and fewer hands employed in 1910 than in the previous years—although wages are higher—yet the value of the output has almost doubled, being £1,248,001 as against £682,884.”
Some mention should be made of the question of emigration. Strange as it may seem, emigration does not, as a rule, greatly mitigate the population difficulty (though it may have done so to a certain extent in Ireland), and it may even enhance it. The reason for this apparent paradox is not far to seek, and it serves to explain a good many common fallacies as regards the population question. Human beings are not all of equal producing power. Each child born into the world is an immediate consumer, and he remains a consumer without being a producer until his education and training are completed. After that time he becomes a producer, and, if of average talents, he may for a certain period produce enough to support himself and perhaps a wife. It is at the beginning of the effective period that emigration so frequently takes place, so that the old country is burdened with all the consumption of immature children, without any possible return. Emigration can only be a remedy for over-population when it is emigration of non-producers, i.e., children, aged people, tramps, paupers, or lunatics; and it need hardly be said that these are not the types which emigrate, or who are wanted by the colonies. It is quite possible for an already greatly over-populated country to be in great need of further accessions of ready trained workers; but until 243someone discovers how our children may be born at this stage of development it is absolutely absurd to say that such a country is “calling out for population,” in the sense of needing a higher birth-rate. The fact that Ontario, in Canada, has experienced an increase of its death-rate following on an increase of its birth-rate is a vivid illustration of this absurdity.
It is interesting to note, as a confirmation of this theory, that considerable changes in the rate of emigration appear to have had very little influence upon the death-rate. It may be, however, that emigration increases in times of dearth, and thus tends to prevent increased mortality.
NEO-MALTHUSIANISM AND EUGENICS. C. V. Drysdale, D.Sc.
The last few years has been a period of continual persecution of the Neo-Malthusians whenever they try to instruct the poorer classes, and more stringent laws are being framed against them in many countries.
I am glad to say that a recent attempt on the part of the dominant agrarian party in Hungary in this direction has been foiled by a judgment of the Hungarian Medical Senate, which has strongly reported against any attempt to check the practice of family limitation, in the interests of the quality of the race.
WAGES AND THE COST OF LIVING. C. V. Drysdale, D.Sc.
Unlike those of other countries, who, in Lord Morley’s words, have shirked the population question, the statesmen of Holland have been fully alive to it, and have made their country the only one where facilities have been given to the poorer classes to freely obtain knowledge as to the best means of restricting families. The following strong statement by Heer S. van Houten, late Minister of the Interior in the Netherlands (Staats Kundige Brieven, 1899), leaves no doubt as to this difference of outlook:—
“Wage-slavery exists as a consequence of the carelessness with which the former generation produced wage-slaves; and this slavery will continue so long as the adult children of these wage-slaves have nothing better to do than to reproduce wage-slaves. The fault lies in our poorer classes themselves, and also in some clergymen and orthodox pedants who, in their preaching about morality, only permit a choice between an unnaturally lengthened celibacy or an ever-increasing family with the bonds of marriage, and who prevent the acceptance of the higher morality, which finds such easy acceptance among the better classes, of marriage and restriction of the family to the number which the parents can feed and comfortably rear.”
And Heer N. G. Pierson, late Dutch Minister of Finance, has expressed himself equally strongly in his Political Economy, which has just been translated into English:—
“No improvement in the economic situation can be hoped for if the number of births be not considerably diminished.”
Under the ægis of these gentlemen and of Heer Gerritsen, a prominent Councillor of Amsterdam, a Dutch Neo-Malthusianische Bond was formed in 1881, and has carried on an active propaganda among the working classes, with the help of a number of qualified medical men and trained midwives. So great has its success been that it now numbers over 5,000 members, and it was recognised by Royal Decree in 1895 as a society of public utility. An enormous number of practical brochures describing methods of limitation are sent out gratis annually, and poor men and women can get gratuitous advice in every important centre in Holland.
246The result of this work, as indicated by the vital statistics, is clearly seen in Fig. 11. The birth-rate has fallen from 37 in 1876 to 28 in 1912, and with especial regularity and rapidity during the last few years. The death-rate has fallen more regularly and rapidly than in any other country in the world (from a value averaging about 25 per 1,000 to only just over 12 per 1,000 in 1912), and the infantile mortality has similarly shown the most rapid fall on record. It will be observed that, far from this decline in the birth-rate having checked the increase of population, the rate of “natural increase” is now higher than at any previous period, and the highest in Western Europe. This indicates not only that social conditions are rapidly improving, but that the productive efficiency of the population is increasing, instead of diminishing, as in our own country, where the “natural increase” has fallen from 12 to 10 per 1,000. This is explainable on the eugenic ground that in Holland family restriction has taken place among the poor, and has thus tended to eliminate unfitness; while in this and other countries the poor are almost entirely ignorant of restrictive methods. And this view is strikingly confirmed by the paper read by Dr. Soren Hansen at the Eugenics Congress of 1912, in which he stated that the average stature of the Dutch people had increased by four inches within the last fifty years. An examination of the heights of the young men drawn for military service shows that since 1865 the proportion under 5 ft. 2½ in. in height has fallen from 25 per cent. to under 8 per cent., while that of those above 5 ft. 7 in. has increased from 24.5 per cent. to 47.5 per cent. This is a most decided evidence of increased well-being and elimination of unfitness. On the many occasions that I have been in Holland, I have never yet seen any cases of that terrible physical deterioration and economic misery which are so conspicuous in this country. Further, the emigration of the Dutch population is almost infinitesimal.
As regards wages and cost of living, Dutch statistics do not give weighted index numbers to compare with the other figures. But the unweighted mean of money wages of workers in the different government services show the most rapid increase recorded, being about 25 per cent. in Holland between 1894 and 1908, as against 18 per cent. in France and 10 per cent. in England and Wales. (Fig. 12).
As to prices, it is not easy to come to a definite conclusion, as some articles have risen and some fallen in price; but there seems good ground for believing that the cost of living has risen comparatively little in Holland, and that real wages have therefore risen very materially during the period when they have been declining in this and other countries. It is certainly difficult in any case to see how the undoubtedly great advance in health and physique experienced by the Dutch population could have taken place without a great increase in real wages.
According to a diagram given in the Manchester Guardian of August 16th last the cost of living in Holland had gone up by 23 per cent. in 1912. 247An examination of detailed prices, however, showed a relatively small rise up to 1909.
These facts, together with many others which could be adduced, make it clear that in Holland, the only country in which the population problem has been realised and facilities for family limitation been extended to the poor, the expectations of the Neo-Malthusians have been completely justified, and their doctrines have received the confirmation of experience. Amsterdam, in which the first lady doctor in Holland opened a gratuitous clinic for the instruction of poor women in preventive methods, has now the lowest deathrate and infantile mortality of any European capital. And this is in no way attributable to any extension of State help either of a socialistic type, or of that familiar to us in this country, as Holland has been distinguished for its adherence to individualism, and has apparently adopted hardly any measure of State assistance.
DR. S. ADOLPHUS KNOPF IN THE SURVEY, quoting Dr. J. Rutgers, Honorable Secretary to Neo-Malthusian League of Holland.
“All children you now see are suitably dressed, they look now as neat as formerly only the children of the village clergyman did. In the families of the laborers there is now a better personal and general hygiene, a finer moral and intellectual development. All this has become possible by limitation in the number of children in these families. It may be that now and then this preventive teaching has caused illicit intercourse, but on the whole morality is now on a much higher level, and mercenary prostitution with its demoralizing consequences and propagation of contagious diseases is on the decline.
The best test (the only possible mathematical test) of our moral, physiological and financial progress is the constant increase in longevity of our population. In 1890 to 1899 it was 46.20; in 1900 to 1909 it was 51 years. Such rise cannot be equalled in any other country except in Scandinavia where birth limitation was preached long before it was in Holland. None of the dreadful consequences anticipated by the advocates of clericalism, militarism and conservatism have occurred. In spite of our low birth-rate the population in our country is rising faster than ever before, simply because it is concomitant with a greater economic improvement and better child hygiene.”
The good doctor closes his letter by saying: “One must have been a family physician for twenty-five years like myself in a large city (Rotterdam) to appreciate the blessings of conscious motherhood resulting in the better care of children, the higher moral standard. And all these blessings are taken away from you by your government’s peculiar laws, made to please the Puritans.”
Dr. Jacobi, Ex-President of the American Medical Association and the New York Academy of Medicine, said:
248“The future of mankind is conditioned by its children. Unless they be healthy and fit to work physically and mentally, they can not perform any duty in the service of the family, the municipality or the state. Hereditary influences propagate epilepsy, idiocy, feeble-mindedness and cretinism. Such children should not have been permitted to be born. Yet the prohibition of unnecessary and not wanted accessions of human beings is considered criminal.”
Dr. Lydia Allen de Vilbis of the New York State Department of Health, said that among the 25,000 deaths of children under one year of age that occur annually in New York State, half were due to causes with which medical boards could not hope to cope—the defective, the deformed, the crippled, the diseased.
“What are we going to do about these babies who are born only to suffer and die?” she asked. “There are at least 12,000 a year, 1,000 for each month, more than thirty a day. What for? Because we are so stupid that we still believe a pound of cure is better than an ounce of prevention.”
MARY ALDEN HOPKINS. Harper’s Weekly, 1915.
“Last year more than ten thousand children were proposed to the Department of Charities of New York City for commitment to institutions,” writes John A. Kingsbury, Commissioner of Charities in the Department of Public Charities of New York City, in reply to my inquiry concerning his view of the limitation of families. “Poverty or sickness or unemployment has outworn the welcome of more than ten thousand innocent little citizens in their own homes. These children are paying the penalty of the social error of too large families. It is frequently remarked that children are often found in the largest number in those homes which are least equipped to properly provide for them. I believe it is as serious a mistake for parents in adverse circumstances to bring children into the world for whom they are not prepared, as for parents in affluent circumstances to decline to bear children because of the inconvenience or embarrassment to their scheme of living. If contraception can benefit the born by limiting the unborn, without bringing about any physical or moral deterioration in human lives, I am unqualifiedly in sympathy with it.”
JUDGE WM. H. WADHAMS, Court of General Sessions, New York. “The Spreading Movement for Birth Control.” The Survey, Oct. 21, 1916.
In the Court of General Sessions, New York City, Judge Wadhams suspended sentence upon a woman, mother of six children, who had pleaded guilty to a charge of burglary, her second offense. His investigation showed, the judge declared, that the mother had made a hard, but unsuccessful attempt 249to support her children since the father had been driven from his work in garment working five years ago. Meantime, two of the children had been born. Said Judge Wadhams:—
“Her husband is not permitted by the authorities to work because of his being ill with tuberculosis. It would be dangerous for him to work on children’s garments. It might spread consumption to the innocents. There is a law against that. As a result of this law the husband has had no work for four years. Nevertheless, he goes on producing children who have very little chance under the conditions to be anything but tubercular, and, themselves growing up, repeat the process with society. There is no law against that. But we have not only no birth regulation in such cases, but if information is given with respect to birth regulation people are brought to the bar of justice for it. There is a law they violate. The question is whether we have the most intelligent law on this subject we might have. These matters are regulated better in some of the old countries, particularly in Holland, than they are in this country. I believe we are living in an age of ignorance, which at some future time will be looked on aghast.”
LETTER ADDRESSED TO PRESIDENT WILSON BY A GROUP OF NOTABLE ENGLISH WRITERS AND SOCIOLOGISTS, September, 1915.
Sir,—We understand that Mrs. Margaret Sanger is in danger of criminal prosecution for circulating a pamphlet on birth-problems. We therefore beg to draw your attention to the fact that such work as that of Mrs. Sanger receives appreciation and circulation in every civilised country except the United States of America, where it is still counted as a criminal offence.
We, in England, passed a generation ago, through the phase of prohibiting the expressions of serious and disinterested opinion on a subject of such grave importance to humanity, and in our view to suppress any such treatment of vital subjects is detrimental to human progress.
Hence, not only for the benefit of Mrs. Sanger, but of humanity, we respectfully beg you to exert your powerful influence in the interests of free speech and the betterment of the race.
Abortion: As soon as the male sperm has met and joined with the female ova any attempt at removing it or preventing its development or further growth is called Abortion. Abortion is not to be confused with the prevention of conception. The practice of Birth Control, founded on the prevention of conception will eventually do away with the necessity of abortion.
Abortion: the expulsion of the fetus before it is viable.—Dorland’s Medical Dictionary.
Abortion: the arrest of any action or process before its normal completion, as the abortion of pneumonia.—Stedman’s Medical Dictionary.
Birth: the delivery of a child—Gould’s Practitioner’s Medical Dictionary.
Birth Control: a new social philosophy dedicated to conscious and voluntary motherhood, and racial betterment.
Conception: the act of becoming pregnant.—Stedman’s Medical Dictionary.
Conception: the fecundation of the ovum by the spermatozoon.—Gould’s Practitioner’s Medical Dictionary.
Contraception: the prevention of conception.—Stedman’s Medical Dictionary.
Contraceptive: anything used to prevent conception.—Dorland’s Medical Dictionary.
Contraceptive: an agent for the prevention of conception.—Stedman’s Medical Dictionary.
Fecundation: impregnation or fertilization.—Dorland’s Medical Dictionary.
Fetus: the unborn offspring of any viviparous animal; the child in the womb after the end of the third month: before that time it is called the embryo.
Malthusianism: (Thomas Robert Malthus, English political economist, 1766–1834). The doctrine that population increases in geometrical progression; and the teaching, founded on this doctrine, that over-population should be prevented.—Stedman’s Medical Dictionary.
Doctrine of Malthus: the doctrine that the increase of population is proportionately greater than the increase of subsistence.—Gould’s Practitioner’s Medical Dictionary.
Theory of Malthus: that small families will abolish poverty and disease; recommends continence and late marriage to bring about this result.
251Theory of Neo-Malthusians: that small families will abolish poverty and disease; recommends early marriage and use of preventive checks to bring about this result.
Pregnancy: gestation, fetation, gravidity.—Stedman’s Medical Dictionary.
Pregnancy: results from the meeting and fusion of two living cells, the cell furnished by the male (spermatozoon) and that by the female (ovum). To avoid or to prevent conception or pregnancy, then, consists of stopping the male cell from uniting with the female cell.
Prevention of Conception: to prevent the male sperm from meeting the female ova.
Prevention of Conception: the only logical and practical means for eliminating abortions when a child cannot be carried to full term.
Preventive: anything which arrests the threatened onset of disease.—Stedman’s Medical Dictionary.
Modern Art Printing Co., New York.