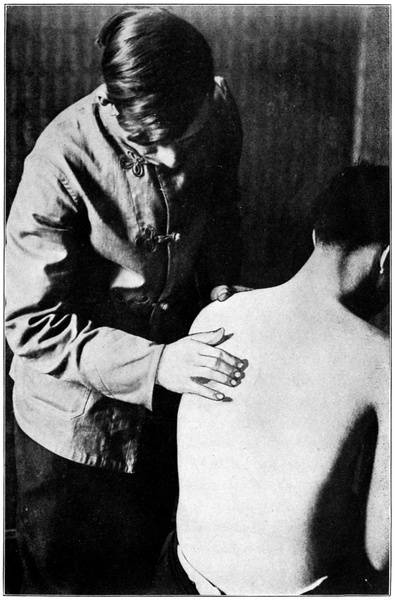
Fig. 1. Position of hands in palpation for record.
Transcriber’s Note: Cover created by Transcriber and placed in the Public Domain.
BY
JOY M. LOBAN, D. C., Ph. C.
Professor of Anatomy and of Theory and Practice of Chiropractic
at the Universal Chiropractic College. Formerly
Professor of Chiropractic Analysis at the
Palmer School of Chiropractic
SECOND EDITION
Revised and Enlarged
PUBLISHED BY
UNIVERSAL CHIROPRACTIC COLLEGE
DAVENPORT, IOWA
1915
Copyright 1915
BY
JOY M. LOBAN
HAMMOND PRESS
W. B. CONKEY COMPANY
CHICAGO
THIS BOOK IS
Dedicated
TO THE GIRL WHO HAS BEEN MY STAFF
AND LANTERN, AIDING AND LIGHTING
ME ON MY WAY IN THIS NEW FIELD
My Wife
| Page | |
| Preface to First Edition | 9 |
| Preface to Second Edition | 11 |
| Introduction | 13 |
| Vertebral Palpation | 15 |
| Definition | 15 |
| General Propositions | 15 |
| Habits of Palpation | 15 |
| Facts Concerning the Spine | 16 |
| Preparation of Patient | 22 |
| Position of Patient | 22 |
| The Record | 23 |
| The Count | 29 |
| Atlas Palpation | 35 |
| The Group Method | 37 |
| The Individual Subluxation | 40 |
| Palpation in Position B | 46 |
| Palpation in Position C | 48 |
| Transverse Palpation | 49 |
| Curves and Curvatures | 53 |
| Difficulties in Palpation | 59 |
| Landmarks | 61 |
| Mental Attitude | 63 |
| Nerve Tracing | 64 |
| Organ Tracing | 64 |
| What Nerves are Traceable | 64 |
| Suggestion | 67 |
| Place in Diagnosis | 67 |
| Technic of Nerve Tracing | 68 |
| Subluxations | 76 |
| Definition—How Produced | 76 |
| Law Governing Location of | 78 |
| Varieties of Subluxations | 80 |
| Technic of Adjusting | 898 |
| General Principles of Adjusting | 89 |
| Special Technic (Thirty-two Moves) | 99 |
| Preferable Adjustments | 155 |
| The Cause of Disease | 165 |
| Simple Subluxation Disease | 184 |
| Secondary Causes | 185 |
| Germ Diseases | 185 |
| Diet | 192 |
| Poisons | 194 |
| Exposure | 198 |
| Bodily Excesses | 201 |
| Inflammation | 202 |
| The Process of Cure | 208 |
| Adjuncts | 215 |
| Spino-Organic Connection | 217 |
| General Discussion | 217 |
| Special Nerve Connections | 235 |
| Table of Diseases and Adjustments | 257 |
| Practice | 276 |
| Office Equipment | 277 |
| Schedule of Examination | 292 |
| Necessity for Correct Diagnosis | 298 |
| Frequency of Adjustments | 302 |
| Specific vs. General Adjusting | 303 |
| Talking Points | 306 |
| Promises to Patients | 308 |
| Retracing of Disease | 309 |
| Limitations of Chiropractic | 312 |
| The Use of Adjuncts | 315 |
| Personality | 319 |
| Chiropractic Prognosis | 322 |
| General Discussion | 322 |
| Practical Prognosis | 323 |
This little work is offered to the profession without apology for its brevity or its form. It has been prepared because of an immediate and pressing need for such a guide in our colleges, and is offered abroad under the impression that many practicing Chiropractors feel the same need.
It is intended for handy reference and clinical use and is arranged as systematically as possible, style being everywhere sacrificed to utility.
The author lays no claim to the origination of any of the subject matter of this book nor to having invented any of the movements described under Technic of Adjusting. The arrangement and phraseology are in the main original. The intention has been merely to condense into practical and convenient form for students and practitioners certain knowledge now held and utilized in our profession.
The author feels himself indebted to the entire profession for the information embodied in this work, and to scientists of all time upon the results of whose infinite and painstaking research are based our present day advancement; to the many friends and co-workers whose valuable criticisms and suggestions have aided in this labor; and to his students, past and present, who have furnished the necessary10 encouragement and inspiration for the achievement of this, the author’s first text-book.
The chief merit of this effort—if merit there be—is its honesty. The author has endeavored to set forth fairly and simply the facts and hypotheses with which we have to deal. Its chief offense, in the eyes of many, will lie in its being just what it purports to be—a book on Chiropractic. Constructive criticism and suggestion are invited from all sources, for by our interchange of thoughts we grow.
J. M. L.
The republication of this book has been made possible by the sustained friendship of the profession for it, and the author’s thanks are due its many buyers and readers who, by their recommendation, have made it both possible and necessary that this book should live and grow.
The new edition has been somewhat enlarged by the introduction of additional matter into each section and by the addition of two entire new chapters on “Preferable Adjustments” and “Chiropractic Prognosis.” New plates have been added and old errors corrected. In every way an attempt has been made to express with conservatism the real advance made by Chiropractic since the first edition was put on the press.
J. M. L.
No two students, approaching for the first time the study of Chiropractic, approach from the same angle. Their viewpoints differ. In order that all may gain as nearly as possible the same viewpoint from which to consider in turn the sections of this book, it will be well if each student reads the entire book before beginning to memorize its parts and convert them into practical working knowledge.
An effort should be made, abandoning all other, to acquire the Chiropractic viewpoint. This accomplished, the rest of the task requires time and patience alone, without waste labor. The section on Vertebral Palpation should be studied step by step, the study of each step being combined with practice in it. Likewise the section on Nerve-Tracing, theory preceding practice. The study of the Technic of Adjusting should occupy those months immediately preceding the commencement of actual adjusting practice and continue during such practice. The chapters on Practice are intended for the student about to enter the field. The table of Spino-Organic Connection can be best understood by those who have studied or are studying the anatomy and physiology of the nervous system.
Let every page be studied with a good medical dictionary14 open at the elbow of the reader. Pass no word without comprehension, no detail without mastery. He who would seek to modify the life processes of the human body must fortify himself against fatal error with every bit of knowledge he can acquire.
Vertebral Palpation consists in the use of the tactile sense to determine the position, relation, size, shape, and as far as possible the condition, of the segments of the spinal column, in order thus to discover the primary causes indicative of disease.
Or, Vertebral Palpation is the name given the manual examination of spinal vertebrae.
Every palpation should be made with the adjustment of the vertebrae in mind. The record of palpation should be a correct guide as to direction of adjustment. No subluxation impossible of adjustment should be recorded.
The two essentials of correct palpation are accurate perception and correct reasoning. To secure the first, a certain approved manner of using the hands is herein laid down and a considerable amount of tactile sense development by practice is required. Correct reasoning depends upon knowledge of all the important facts concerning the spine and of the rules governing palpation.
Absolute concentration is required and to this end many of the following rules are directed.
Every palpater unconsciously forms habits of thought and action. These habits may be good or bad. We deliberately16 form a habit of holding the first three fingers closely together or the habit of using a downward glide, but we should avoid the habit of finding certain subluxations because they are usual and expected rather than because they are actually there. For instance, one may easily form a habit of listing every other vertebra in the spine, his whole record thus depending upon his first choice.
Because of this perfectly natural tendency to establish a routine of thought and action and to follow it precisely, it is best not to attempt palpation without the aid of an experienced teacher until after correct habits have been formed. Once formed, a palpation habit, right or wrong, is very hard to break. Many a teacher has expended himself uselessly in the effort to undo some technical fault acquired by the student in a blundering undirected trial.
The spinal column is composed of twenty-six segments called vertebrae, twenty-four movable and two fixed. The movable vertebrae are divided for convenience in study into three sections. There are seven Cervical vertebrae, twelve Dorsal, and five Lumbar in the normal individual. The number of Dorsals or Lumbars may vary by one in a rare case. These variations occur in about one spinal column in each five hundred and are usually in the Lumbar region, which may contain four or six vertebrae. A prominent first sacral spinous process may be mistaken for an extra Lumbar.
Five vertebrae have special names. The first Cervical is called Atlas; the second Cervical, Axis; the seventh Cervical17 is commonly known as Vertebra Prominens on account of its long and large spinous process, although this long process belongs to the sixth Cervical or first Dorsal instead in 35% of all cases; the large, irregularly fusiform vertebra just below the Lumbars and between the ilia is called the Sacrum; and the smaller one below it, the Coccyx. The latter is occasionally missing.
Each vertebra except the Atlas is composed of a body and an arch; the arch is made up of two pedicles, short, thick plates of bone extending outward and backward from the postero-lateral surface of the body nearer its upper than its lower border, two laminae, thin plates of bone extending backward and inward from their union with the pedicles and joining behind to form the spinous process, and has projecting from it seven processes, two transverse, one spinous, and four articular, two of which are superior and two inferior. The foramen enclosed by the body, pedicles, and laminae is called the neural or vertebral foramen and the canal formed by the connection of these foramina and completed by the ligaments which unite the arches is called the neural, vertebral, or spinal canal. It contains the spinal cord with its membranes and the roots of the spinal nerves. By means of the four articular processes each true vertebra except the first articulates with its fellows above and below.
The body of the vertebra is its largest portion and is joined to its fellows by fibrocartilaginous disks which are sufficiently elastic to permit some torsion and compression. Nine sets of ligaments, including the intervertebral substance18 just mentioned, bind the vertebrae firmly together. Many muscles are attached to the spinal column.
The intervertebral foramina are openings at the sides of the vertebrae, formed by the notching of apposed pedicles. These openings are surrounded by bone, cartilage, and ligaments and vary in shape in different sections of the spine. They permit the exit of the spinal nerves and their sheaths, the re-entrance of some nerve fibres into the neural canal, and the passage of blood-vessels to and from the cord. The entire philosophy of Chiropractic focuses at the intervertebral foramen because there we find the primary cause of all pathological changes in the body.
The spinous and transverse processes merit particular description since they are the levers by which vertebrae are adjusted and nerve impingements at the intervertebral foramina corrected. But it will be found easiest to describe these processes separately in different sections of the spine and before proceeding to this description, a brief picture of the peculiar vertebrae will be presented.
The Atlas is a bony ring composed of two arches, an anterior and a posterior, separated in the recent state by a transverse ligament. Its body is detached and appears as a tooth-like projection upward from the body of the Axis, the odontoid process, which articulates with the anterior arch of the Atlas and around which the Atlas rotates, a ring around a pivot. The Atlas supports the head upon its lateral masses, two wedge shaped bodies between the anterior and posterior arches, thinner internally than externally.19 It has no spinous process but merely a tubercle where the laminae join, so that it can be palpated only from the sides upon the tips of its long transverses. The first Cervical, or suboccipital, nerves emerge by a groove above the pedicles instead of through a foramen.
The Axis, or second Cervical, is distinguished by its large, strong spinous process, which is bifid at its tip, by its superior articular processes which rest upon body, pedicles, and transverses, and by its odontoid process, upreared from the body.
The Seventh Cervical, or Vertebral Prominens, usually has a large spinous process, presents no foramina in its transverse processes, or only one, the left, and shows no facets on body or transverse for the rib articulation, as do the Dorsals.
The Sacrum is the largest vertebra; is curved with its convexity backward; is commonly made up of five fused segments; has only rudimentary spinous and transverse processes except the first; and shows sixteen openings, eight anterior and eight posterior, or four on either side of the median line in front and the same number and arrangement behind. These openings permit the exit of the anterior and posterior primary divisions of the sacral nerves separately.
The Coccyx, usually composed of four fused segments, is a triangular bone which articulates with the Sacrum above and is free at its distal extremity. Its portion of the neural canal is open posteriorly and contains merely the thread-like termination of the cord membranes. It is frequently20 ankylosed to the Sacrum, sometimes in an abnormal position so as to impinge the single pair of coccygeal nerves.
The different regions of the spine show decided differences in structure, though all resemble each other. The Cervicals are smallest, the Dorsals next in size, and the Lumbars largest and strongest of the movable vertebrae. The Dorsals have facets and demi-facets for the articulation of the twelve pairs of ribs with their bodies and intervertebral substance, as well as oval facets upon the anterior aspect of their transverses for articulation with the tubercles of the ribs.
The spinous processes are smallest and usually bifurcated down to and including the fifth. The sixth may show a plain bifurcation, or on any Cervical the bifurcation may be so small as to be imperceptible to touch. The spinous process of the second overlies that of the third so as to make the latter very difficult of detection. Indeed, all cervical spinous processes down to the sixth are harder to palpate than those in other regions, owing to the anterior cervical curve. The processes lie in a groove between prominent muscle ridges.
Dorsal spinous processes are usually single, although the last four, three, two, or one may show plain bifurcation in certain individuals. They are somewhat pointed and overlap, except the lower ones, the obliquity being greatest in the mid-dorsal region and least at the first and last dorsals.
Lumbar vertebrae have broad, flat-tipped spinous processes much larger than the others. The last Dorsal may21 sometimes appear like a Lumbar in shape, so that the change in shape commonly supposed to mark a division between Dorsals and Lumbars is not always an infallible guide.
The transverse processes in the cervical region are very short and lie close in front of the articular processes. They are pierced by foramina for the vertebral artery and vein, except the seventh, which may have one foramen or none. They are difficult of access for palpation because of their shortness and the amount of overlying muscle, but may be reached from the front and side by drawing back the sternomastoid. They increase in length from the second to the seventh.
In the dorsal region the transverses are larger and stronger and more constant in size, shape, and direction, serving to support rib articulations. They extend in a curved direction outward, backward, and slightly upward from the union of laminae and pedicles and terminate in a large subcutaneous club-shaped extremity which may be readily palpated. The eleventh and twelfth dorsal transverses do not articulate with the ribs and must therefore be used with caution or not at all as levers for adjustment. The dorsal transverses are located on a higher level than the spinous processes. In the case of the upper three dorsals the transverse lies in a plane which would cross the mid-spinal line between its own and the next superior spinous. In the mid-dorsal region the transverse is even with the spinous of the vertebra above, though the relation may vary slightly. The lower dorsals return to the same relation as the upper.
The transverse processes of the Lumbars are relatively light compared with the general structure of the vertebrae and are found just even with the interspace between their own and the adjacent superior spinous process. They vary greatly in size, length and strength and may be used as levers for adjustment only when they are large enough to be clearly palpable through the muscle mass which separates them from the body surface.
In all cases where a complete spinal examination is intended the preparation is essentially the same. Have patient arrange clothing so that the spine is exposed to the touch throughout. Avoid bands of cloth across the spine, as these interfere with the necessary continuous gliding movement of the fingers. Advise the patient, if a female, to wear waist or dressing sack, reversed, and have skirts loosened at the waist. If a man, he should strip to the waist and wear coat or coat shirt reversed.
This varies widely according to circumstances but for general purposes use position:
(A) Place patient on stool, feet even on floor and body in an easy, relaxed position. This may be modified by asking him to lean forward and rest elbows on knees, evenly, to facilitate Lumbar palpation. Patient’s head may be erect or flexed forward or backward but should never be rotated or laterally flexed during Cervical palpation except for the purpose of locating some particular transverse process.
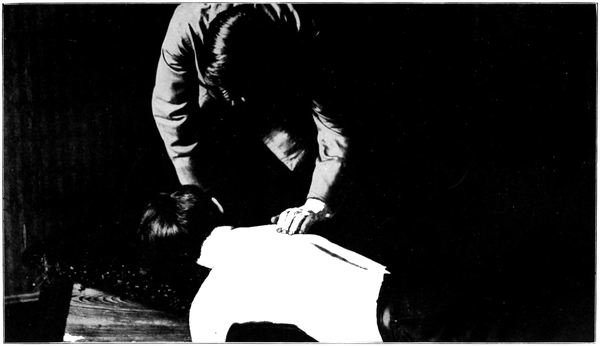
(B) In emergency cases, where haste is urgent or patient is unable to assume a sitting posture, or as a means of re-verifying previous palpation, place the patient on adjusting table prone, face down. (See Fig. 2.) Remember that with the head lying upon its side the upper dorsal vertebrae will assume a curve with its convexity away from the face. Palpation in position (B) should precede every adjustment and, to guard against error, should be considered as a necessary preliminary to the movement of any vertebra.
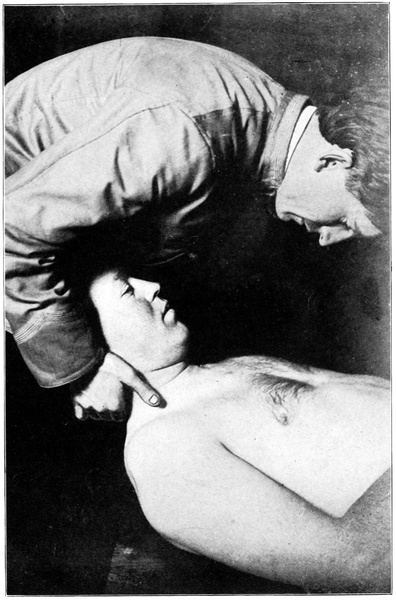
(C) For palpation preparatory to using the Rotary, the Break, and other moves, have patient lying on his back with his head projecting beyond upper end of bench and resting on the hands and wrists of the palpater, or have the patient’s head rest on the bench, a less accessible position.
Each spinal examination should begin with a general survey by which curvatures, marked prominences, etc., may be appreciated. Frequently some very important fact may be noted which would escape attention upon minute examination.
The record of spinal palpation, when completed, should be an accurate history of the irregularities found in the spine and an accurate guide to adjustment. It must be brief and concise as well as readily comprehensible. One should be able to see at a glance any desired point on the24 record, so that it may be used during the adjustment without undue loss of time or attention. Obviously the introduction of any useless mark or sign, such as the inclusion of a number and blank space for each vertebra of the spine, or all possible subluxations with indications as to which do or do not exist in the given case, is a mistake.
The record should contain three parallel columns. In the first column place the number of the vertebra chosen for adjustment. In the second, place the direction of subluxation. In the third, place the word or sign which stands for the indicated movement for correction.
The letter C is used to indicate Cervical, D Dorsal, L Lumbar, and S Sacrum in the record. Immediately following the letter which designates the region, place the number which shows the position in that region occupied by the vertebra in question, the relation of that vertebra to its fellows. For instance, the third Cervical vertebra is C 3, the eleventh Dorsal D 11. To the S for Sacrum append B or A to indicate that the Base or Apex is described as to position. This locates the subluxation. For a record of full spine palpation it is unnecessary to use the letters C, D, or L more than once, as subluxations are recorded in the order of their occurrence from above downward. A dash should always follow the number of the vertebra to separate it from the letters in the second column for convenience in reading.
The directions considered in palpating or recording subluxations are six in number, namely:
| Name | Abbreviation | Meaning |
| Posterior | P | Toward the rear (Dorsad) |
| Anterior | A | Toward the front (Ventrad) |
| Right | R | Toward the right hand |
| Left | L | Toward the left hand |
| Superior | S | Toward the head (Cephalad) |
| Inferior | I | Toward the feet (Caudad) |
As the fingers glide down the spine the posterior vertebra is the one which interposes itself in the path of the fingers, forcing them to describe an outward curve. It is the hill on the automobile road which forces the surmounting of a curved departure from the evenness of the road. It is relatively posterior to its fellows above and below.
The anterior vertebra, to the gliding fingers, means a depression, a valley. It causes the fingers to dip inward from the level of their course.
The right or the left subluxation is appreciated by running the tips of the fingers down the sides of the spinous processes. It really indicates rotation of the whole vertebra more often than any other malposition.
We say that a vertebra is superior when its spinous process is nearer the one above than the one below. It requires a measuring of relative distances. The degree26 to which a vertebra is superior is measured, not by its actual closeness to its fellow, but by the relation between the space above and the space below.
Likewise a vertebra is inferior when it is closer to its fellow below than to its fellow above.
Anterior subluxations are rarely recorded as such, except of the Cervicals or the last Lumbar, because no means of properly adjusting them is known to Chiropractic.
In the second column, that devoted to direction of subluxation, the letter P or A should appear, if at all, as this antero-posterior relation is the first thing to be determined concerning any individual subluxation chosen except the Atlas. With the Atlas the first letter will be R or L. Next the laterality or rotation is indicated by R or L in every case except Atlas subluxation. Finally the S or I indicates the last point to be determined, the approximation of the vertebra to its fellows. This last letter usually shows thinning of intervertebral fibrocartilage, which will be discussed elsewhere.
If you desire to emphasize any direction as being more important than another, underscore the letter which stands for that direction with a single line. If two directions are to be emphasized, one more than another, underscore the one with two lines and the other with one. For example, if a vertebra is found to be quite decidedly posterior, more plainly to the right, and slightly superior, the record will show it thus: P R S.
This is indicated in the third column, separated from the second by a dash, by means of some brief word or words which describe a certain movement used in adjusting. The descriptive words and terms used in this work are all given and explained under Technic of Adjusting. (See p. 89.) Each word or term stands for a definite method of procedure. The best movement for the correction of any subluxation of any vertebra may be found by reference to the section on Preferable Adjustments, p. 155. If other terms are more familiar to the student, or in time replace those which are now common usage in the profession, they will be brief and clear and may be easily substituted for those given.
Palpation, fixing in the mind of the palpater the manner and direction of the subluxation, should also suggest as the obvious correction a movement calculated to reverse the procedure by which the subluxation was first produced. In other words, a certain kind of subluxation stands as the effect of a certain application of force along definite lines determinable by examination. Its correction should be made in a reverse direction along the same lines. By recording with the record of subluxation the desired correction, the adjuster may be reminded daily without new palpation of the movement best fitted to the case. If on trial it is decided that some other movement than the one first indicated will better overcome the abnormality, the record should be changed to correspond to the decision, and thereafter followed.
The completed record in three columns separated by dashes can be conveniently read. It contains no superfluous mark of any kind. It conveys all the necessary information leading to adjustment except diagnosis and case history. This palpation record should be a part of a more comprehensive record concerning the case in full and is best kept on a card, the reverse side of which carries case history. If kept in an indexed card file it may be referred to daily without loss of time and an accurate handling of each case be assured.
Have card perfectly blank on palpation record side. For convenience in reading draw a heavy line beneath the last Cervical subluxation recorded and another beneath the last Dorsal, thus dividing the record as the spine is divided, into three divisions.
Below follows a sample palpation record. It will be seen that here in a very small space may be recorded a great deal of information, for this record contains an accurate list of the primary causes of every disease, weakness, or tendency to disease with which the patient is afflicted, together with the methods for their removal.
| C | 1 | R | Break |
| 4 | P L S | Double Contact | |
| 7 | L I | Rotary | |
| ——————————————————— | |||
| D | 3 | P R | Recoil29 |
| 7 | L S | Pisiform Single Transverse | |
| 10 | P S | Heel Contact | |
| ——————————————————— | |||
| L | 1 | P L I | Recoil |
| 4 | R | Lumbar Single Transverse | |
The above record is made with patient sitting. It is to be used while patient is lying upon the adjusting bench. The most convenient way is to begin palpation in the Dorsal region after patient has been placed for adjustment, in this way. If first subluxation recorded is D 2—P R I, find the vertebra in the region of D 2 which appears P R I to the touch. To avoid error, let the fingers then glide downward to the next recorded subluxation. If this be found to agree in number and direction with the record, it is safe to assume that the first one found was correctly numbered in the palpater’s mind; if not, that an error was made. This can be quickly done. Before each adjustment the vertebra adjusted should be found to agree with the record; by doing this constant accuracy may be assured.
Having described the preparation of the patient and the different positions in which he may be palpated, noted that all records should be made in position A, mentioned that general observation which should immediately precede actual palpation, and interpolated a description of the record to30 be made during the palpation, with its use afterward, we are now ready to consider the technic of the palpation itself. This should begin with a count of the vertebrae and continue with Atlas palpation, general examination of a group of vertebrae, and special examination of individual subluxations in the group. Each of these tasks will be considered in turn.
This depends upon the position of the patient. The letters which follow correspond to the letters describing the position of the patient. q. v.
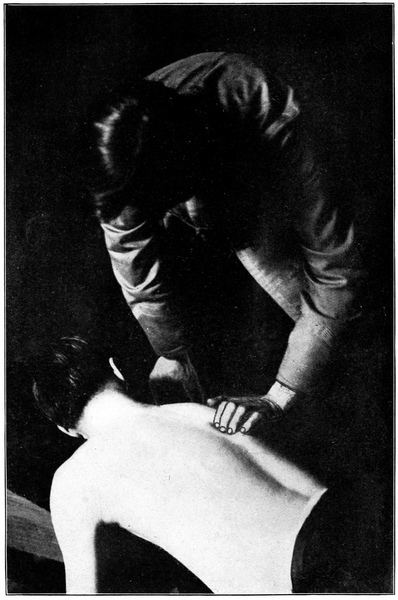
(A) If you desire to palpate with the right hand stand at patient’s left and face toward him with left hand resting on his shoulder or supporting his forehead as you palpate Dorsals or Cervicals respectively. To use left hand stand similarly at patient’s right. Have palpating arm relaxed and easy, extending as nearly as possible so that the forearm and hand make a right angle with the patient’s spine. Let the arm and hand remain close to the patient’s body at all times. Keep the elbow close to your own body and avoid flexion of wrist on forearm, or of forearm on arm at more than a right angle, since such flexion would bring about too great muscular tension for close appreciation of tactile impressions. If necessary lean sidewise and elevate shoulder and palpating arm in order to preserve the proper relation between hand and arm when hand must be elevated as in palpating upper Cervicals.
(B) As above, if you desire to use right hand stand on left side of patient and if left hand stand on right. If the patient lies on a bench so constructed that the head lies on one side, his face must be toward the palpater in order that the same hand may be used in Cervical as in other regions. It is inadvisable to change hands except when absolutely unavoidable. If the patient’s head must be turned from you palpate the Cervicals by standing with feet pointed away from patient and turn your body with one hand resting on patient’s head to hold it steady and the other palpating as if you were standing on the other side. This is difficult and it is rarely necessary to count Cervicals in position B if the record be used as advised on page 29.
(C) Palpation preparatory to the Cervical adjustment will be made in this position or in position A, according as you intend adjusting the Cervicals in the prone or the sitting posture. For the prone position have the patient’s head supported by either hand, while the other hand is applied with the tips of the first three fingers resting on the tips of the spinous processes, from which position they may glide smoothly down, noting deviations from normal in position as well as mentally numbering the vertebrae. While this method of palpation is not so accurate as those given elsewhere, and should be used only as an additional means after record has been made, it will always be necessary to make a count before adjusting any Cervical.
In general it may be stated that the first three fingers of one hand are used with an easy downward gliding movement in which only the tips of the three fingers, evenly placed, are in contact with the patient’s body. This concentrates the attention upon a very small tactile surface which may become extremely sensitive by the concentration. Indeed, it may be said that vertebral palpation only became an art through the application of the principle of concentration in practice. The gliding movement is always downward, because to palpate upward will mass the superficial tissues under the fingers and confuse the palpater. If there is uncertainty in the mind of the palpater, as he proceeds, as to the identity of any vertebra he should go back to the second Cervical, or to any certainly recognizable vertebra previously fixed in mind, and recount.
The use of the hands for Atlas palpation differs from their use elsewhere and will be described under separate head. The use of the hands with the patient lying face upward is also different. If the patient be lying prone, the same three fingers are used and the same downward glide as with patient sitting.
With patient sitting, the palpater should step from side to side, changing hands frequently and usually palpating each vertebra with each hand before reaching a conclusion. There are three reasons for this. More accurate records may be made by combining two different impressions on each vertebra; with frequent change of hands one may33 prevent tiring and consequent loss of sensibility of fingers; this practice develops the tactile organs of both hands equally so that if occasion demand the use of either hand alone it is fitted for the task. To be ambidexterous in all departments of Chiropractic is an invaluable attainment, too often neglected.
Commence at the second Cervical, the first spinous process below the occiput, and let the fingers glide smoothly downward over the tips or along the sides of the spinous processes, without interruption of motion, until they reach the Sacrum. The palpater notes each vertebra passed and its number—mentally—so that when he reaches the Sacrum he knows that he has passed every intervening vertebra and received a touch impression from each. The Sacrum itself may usually be recognized by its peculiar shape and also by its articulations with the ilia.
If the fingers are raised from their contact during the count, the palpater must recommence at the second Cervical. It is impossible to be accurate in replacing the hand, once removed, until the count has been established and the peculiarities of certain vertebrae remembered, together with their numbers.
To determine the location of the fourth Lumbar where, on account of obesity, lipoma, Cervical lordosis, etc., the count of Cervicals or Sacral palpation is difficult, drop on heels behind the patient and place the second finger of34 each hand on the crest of the ileum. Then let the thumbs meet in the mid-spinal line in the same horizontal plane as the two second fingers, which spot should correspond to the interspace between third and fourth Lumbars. This measurement is accurate in about 98% of all cases, when patient sits erect; when it varies it will vary by about half the width of a Lumbar spinous process.
The count should be repeated until the palpater is certain that he is able to palpate every spinous process distinctly or to locate accurately any impalpable one. In making the count, palpater may note the number of some very prominent and easily recognizable Dorsal or Lumbar vertebra to be referred to as a starting point for a recount if confusion arises later. This recounting from some prominent vertebra is permissible only after the first accurate count has been made, but then will save the full count, especially when the patient is in an unfavorable position, as lying on table during adjustment.
The commonest difficulties met with in counting are the following:
Inaccessibility of third Cervical, which lies closely beneath the spinous process of the second and, unless unusually large or somewhat out of its proper position, cannot be readily felt.
An occasional anterior fourth or fifth Cervical which may escape notice unless the head is flexed far toward or the transverse processes examined.
Lipoma or other adipose tissue covering part of the spine.
A missing epiphyseal plate resulting from fracture and absorption, which absence may simulate a wide interspace and be overlooked without careful and detailed observation.
Cervical or Lumbar lordosis. This difficulty may be at least partially overcome by having head bent far forward or body leaning forward with elbows resting on knees and a deliberate attempt on the patient’s part to render the dorsolumbar spine convex backward.
An anterior fifth Lumbar.
The occasional extra vertebra which confuses the palpater.
Finally, the greatest of all difficulties is the imperfect touch of the untrained palpater or the imperfect concentration of the trained. And this is always remediable.
With patient in position A stand behind him and place the tips of the second fingers on the tips of the transverse processes of the Atlas, or first Cervical. It can be felt on each side just anterior and inferior to the mastoid process of the temporal bone. Let the first and third fingers rest respectively above and below the transverses and determine whether the Atlas is subluxated as a whole to the Right or to the Left.
Another convenient method is:
Place first fingers on mastoid processes, second on Atlas36 transverses, and third on angle of jaw. The three fingers of each hand then constitute the points of a triangle. Imagine the base line between the first and third fingers and measure the altitude as a line at right angles to this base line and reaching to the tip of the second finger as the apex of the triangle. The relation of the two altitudes determines the laterality of the Atlas. Thus, if the altitude of the right triangle is less than that of the left, the Atlas is laterally displaced to the Right.
The second matter to determine is the rotation of the Atlas. This is done by using the first and third fingers as probes to determine the amount of space between the transverse and the mandible in front or the mastoid behind. The intention is to compare the laterally prominent side with the other so that the letter A or P on the record will indicate the position of the prominent transverse compared with its fellow.
Next decide as to tipping. Still comparing the prominent transverse with the other, decide whether it is above or below the level of the other by the following method. Placing first three fingers one above the other with the second finger on the tip of the process, note which transverse is highest in the space beneath the ear. List the prominent side as S or Superior, I or Inferior.
Atlas palpation is rendered especially difficult by the special technic and by the interposing tendons of the sterno-cleido-mastoid muscle.
There are three head positions for Atlas palpation. Head erect, face forward; head flexed forward on chest; head flexed backward. Sometimes it is necessary to test in all three positions in order to reach a decision, but ordinarily the first is sufficient.
In general palpation of the spine the author has had the greatest success and attained the greatest accuracy through which is called the Group Method. This consists in dividing the spine mentally into five groups or sections, each of which overlaps its fellows except the end groups. This is of advantage for several reasons.
It limits somewhat the attention of the palpater so that he may examine thoroughly and in detail the various vertebrae without holding his attention so closely to one that he fails to perceive its relation to its surroundings. It furnishes five or six vertebrae at a time for comparison so that one may determine which is most subluxated, and therefore most in need of adjustment, and then allows one to reason upon the remainder of the group with this major subluxation in mind.
The use of the Group Method may best be understood by the study of certain didactic instructions, which follow:
Never record or adjust two subluxations of contiguous vertebrae except in those unusual cases where they are equally subluxated and in the same direction; even then it is wisest to adjust them on alternate days. Let it be understood38 that only in exceptional circumstances should two adjacent vertebrae be listed. The Group Method is chiefly valuable because of this rule, to prevent the overlooking of the most important subluxation by selecting that one first.
Consider the spine as divisible into five groups; in the first group belong the Cervicals below the Atlas; in the second, the seventh Cervical and first five Dorsals; in the third, the vertebrae from the fourth to the eighth Dorsals inclusive; in the fourth, the last five Dorsals and sometimes first Lumbar; and in the last group, all of the Lumbars and the base of the Sacrum. Consider the first Sacral spinous process here rather than the whole Sacrum and remember that this process should seem to complete the regular Lumbar curve. This grouping may be modified somewhat by the exigencies of palpation in any given case, but the group considered should always include from four to seven vertebrae.
In each group proceed in the same manner to select subluxations. Let the fingers glide over the group, first on the tips and then along the sides of the spinous processes, and note that some one vertebra stands out as the sharpest, most abrupt deviation in the group, thus indicating its selection. Remember that neither the one above this nor the one directly below may be adjusted. This narrows your field of observation for this group to two, three, or four remaining vertebrae.
Select then such others in the group as need to be listed39 yet do not conflict with the rule against adjacent subluxations. Proceed to discover and record the exact direction of each. When this is done examine the next lower group in the same way and continue until the whole spine has been palpated.
The Atlas must be considered alone and not as a part of any of the above mentioned groups and its position is judged rather by its relation to the head than to other vertebrae; the Sacrum also requires individual attention, being compared with the Lumbar curve and with the ilia.
The one most pronounced subluxation in a group is often mentioned as the “key” to the group, since its correction would effectually loosen the entire group and sometimes partially correct the apparent abnormalities of the rest. It has also been called “major subluxation” to distinguish it from “minor subluxations” which are the others of less importance in the group. This term is not a good one because it suggests what is not always true, namely, that the mechanically greatest subluxation is more potent than any other. Occasionally a slighter subluxation irritates nerves so as to produce a disease more serious and immediately alarming than the condition following the greater displacement.
If, in the Cervicals, it is noticed upon gliding downward over the spinous processes that the fifth is badly subluxated and must be adjusted, this fact is held in mind for a moment40 while the palpater remembers that he cannot adjust and must not list the sixth or fourth. This leaves only the second, third and seventh for consideration, the Atlas having been separately examined. The seventh may best be included in the next group when such a selection is made, so that the palpater need only decide between the second and third Cervical, providing Atlas has not been chosen, as to which, if either, most requires attention. If Atlas has been listed, then there remains instead only the question as to whether the third is or is not subluxated.
In using the Group Method no preference is given to subluxation in any particular direction, save only that below the Cervicals we discriminate against the anteriors, because we cannot adjust them. The Group Method has to do with determining the points of greatest pressure on nerves and this depends upon one’s impression as to the interrelations between all the members of the group. (See p. 80 under Subluxations.)
Having prepared our patient, surveyed the entire spine, carefully counted the vertebrae to secure a proper orientation, and specially examined the Atlas, then divided the spine into groups and selected the vertebrae to be adjusted with regard to their degree of malposition, let us confine our attention definitely for the first time to the single vertebra below the Atlas.
Reread “Direction of Subluxation” under “The Record,” p. 25. Also read article on “Subluxations,” p. 76.
Bear in mind that each subluxation recorded is intended for adjustment and indicate nothing impossible on your record. For instance, an anterior subluxation in the Dorsal region cannot be corrected and should not be recorded for correction.
Remember the six capital letters used in describing a subluxation.
Use only the downward gliding movement of the three palpating fingers.
Keep in mind the count as you have established it for that particular spine, recalling one or two very prominent and noticeable vertebrae whose numbers you have noted.
Use a light touch. If necessary, change the patient’s position to make the vertebra more accessible instead of pressing with more force.
When in doubt as to direction, change sides and use the other hand. If still in doubt, take a longer glide, covering six vertebrae instead of three or four.
Keep your mind on your work, forgetful of everything else.
And picture to yourself the entire vertebra and its surroundings; its body, pedicles, and laminae, its transverse processes and all articulations; above all, mentally visualize the foramina and nerves. Estimate from the position of each vertebra the pressure at each foramen. Decide whether the vertebra is rotated, tipped, laterally displaced, anterior or posterior, or whether the subluxation partakes of several of these directions.
Decide in what direction movement of the vertebra would release most pressure and list accordingly.
Never hesitate to change your opinion if you discover evidence that you have made a mistake. Keep at all times an open mind in palpation.
The third Cervical, lying under the projecting spinous process of the larger second, may be hard to find, and therefore the full count is always required before listing any vertebra. By requiring the patient, who is in position A, to drop his head forward and rest its weight in the hand which is not palpating, the Cervicals may be more easily palpated. Remember that this posture widens the interspaces and also makes the spinous processes appear more posterior than they really are, this difference being most noticeable at the fourth.
One bifurcation of a Cervical spinous process may be longer than the other and prove confusing unless care be taken always to palpate both bifurcations and note their form. This can almost always be successfully accomplished.
Sometimes the posterior neck muscles and ligaments will be rigid so that they interfere with palpation and at the same time make it impossible for the patient to flex his head forward. Having found that this is due to real contracture and is therefore not susceptible of voluntary relaxation by the patient, support the head in front and push aside the muscles with the fingers, gliding underneath the43 muscle layers as much as possible and close to the spinous processes.
Transverse palpation in the Cervicals is used to verify findings from the spinous processes or to differentiate between rotated and laterally displaced vertebrae and bent spinous processes when the spinous swerves to right or left.
The Dorsals are usually considered in three groups. It must be remembered that the form and obliquity of spinous processes vary considerably in this region. The upper processes are very slightly oblique, slanting downward, the middle Dorsals very oblique, and the inferior ones again only slightly so. There is a form change, most commonly at the eighth Dorsal, which may be mistaken for a posterior subluxation. The process here becomes more horizontal and more blunt.
Among the first four Dorsals a bad lateral or rotated vertebra may be listed as well as a posterior one, since we can readily adjust it. In the middle group either the posterior or rotated vertebra is chosen according to the estimate as to which causes greatest nerve impingement, either being adjustable. In the lower group, however, preference is usually given the posterior vertebra when possible, because rotary subluxations indicate transverse adjustments and it is somewhat dangerous in this region to use the transverses as levers.
The Lumbars and Sacrum are considered in one group. The Lumbars, with patient erect, should curve anteriorly and the first Sacral spinous process should complete the regular curve. This is rarely found, however; the normal is the exception in any part of the spine.
In the Lumbars we usually choose the rotated rather than the posterior vertebra, but solely because rotation here produces the greatest degree of impingement. The laterality of spinous processes, indicating rotation of the whole vertebra around an axis lying in the transverse line between the articular processes, can best be perceived, as a rule, with patient sitting quite erect. If in doubt, have patient lean forward and rest elbows on knees, which posture separates the Lumbars, rendering the individual spinous process easier to discover but the relative position more difficult of determination.
The fifth Lumbar, if anterior, may be so listed, forming an exception to the general rule.
First palpate Sacrum as if part of Lumbar region. Note whether the base (upper portion) is posterior or not. Then stand behind the patient and use both hands to examine the sacroiliac articulations. Use palmar surfaces with the flat hand toward patient’s body, and carefully compare the two sides to detect inequalities, which indicate iliac subluxation, or rotation of Sacrum between the ilia on a transversely45 disposed axis passing through the two articulations, in which case the Sacrum is to be adjusted. Do not mistake a dislocated hip with compensatory tilting of the whole pelvis, or faulty sitting posture with only one tuber ischii supporting the body, for pelvic subluxation.
Be not in undue haste to record pelvic subluxations lest your haste bring its immediate reward in the difficulty of adjustment.
The Coccyx may be detached from the Sacrum by various accidents and later re-ankylosed thereto in an abnormal position so as to impinge upon the rectum or other structures. Impingement of the coccygeal nerves is usually unimportant. Chronic and intractable rectal constipation, with its attendant train of evils, may result from coccygeal displacement with ankylosis. In spite of numerous treatises to the contrary, the writer avers that other symptoms are extremely rare.
To examine the Coccyx use a rubber covering on the second finger. Place patient face down and insert second finger per rectum with the palmar surface upward. If subluxated Coccyx be found, it must usually be fractured with a sharp jerk, in order to relieve the condition. After fracture, it may be absorbed or may re-ankylose to the Sacrum in a better position, or it may remain freely movable.
This is the position for the majority of adjustments, and as the palpation of each vertebra to be adjusted is a necessary preliminary to the adjustment, this method, though not so accurate as the one already described, must also be used.
The use of the first three fingers of each hand and the relation of hands to patient’s body is the same as in Position A, except for palpating Cervicals when the patient’s face is turned away. It will be found very difficult to make a correct full count, especially to count Cervicals, in this position, and is better to use a record already prepared.
Begin at, or near, the first Dorsal to palpate in this position. Find the vertebra which agrees in direction with the first Dorsal subluxation recorded; let the fingers glide downward until they reach the vertebra which, according to the first decision, would correspond in number with the next subluxation on the record. If this also agrees in direction with the record it may safely be assumed that you are accurate in your numbering. Thereafter, during that adjustment, the count can be made or repeated from any prominent vertebra the number and identity of which are easily recognized.
It may be difficult to count or otherwise to palpate the Lumbars in this position because of the increase in the47 normal anterior curve when patient is suspended between the two sections of the bench. This will be obviated if a roll be placed under the thighs or if the bench has an adjustable rear section.
If a solid front bench is used remember the spiral turn in the Cervicals, which occurs because of the resting of the head on one side. The curve due to this rotation of the head is compounded with the ever present anterior curve to make a spiral. Do not expect the vertebrae in this position to agree in apparent direction with a record made with the head straight. It is better to make all decisions as to direction of Cervicals in position A and merely to count them in other positions.
In position B, if the patient’s face be away from the palpater it will be necessary to stand with back toward patient and body twisted, and to change hands for counting, resting the free hand on patient’s head to insure its steadiness.
If there be any apparent disagreement between findings in positions B and A, re-examine carefully in both positions, whereupon that which seemed a disagreement will probably prove to have been an error in one or the other palpation. If apparent disagreement persists after searching examination, position A furnishes the safest guide to48 adjustment because the patient is in his most usual attitude as regards the spinal curves, muscle tension, etc. But it is usually wisest when in grave doubt not to adjust the doubtful vertebra at all.
Since palpation in this position, patient lying on his back with head supported by palpater’s hands, cannot be so reliable as that done in position A, the chief point to be observed is an accurate count. Only the Cervicals below the first can be properly palpated in this position.
Induce the patient to relax the neck muscles as much as may be, and use in palpation the first three fingers of one hand if the count alone is desired or the first three fingers of both hands if you desire to ascertain the direction of any vertebra. In the former case let the fingers press aside the muscles and glide downward from the second Cervical, being careful to lift the head high enough so that the third Cervical is not overlooked beneath the overlapping second. In the latter case let the fingers of both hands glide gently downward while the patient’s head rests upon the palpater’s wrists or knee. Palpate the transverses in much the same manner, paying special attention to their laterality, felt as a prominence on one side lateral to a transverse process and a corresponding depression on the opposite side. Do not be deceived by exceptionally long transverses where both project outward to an equal degree.
Since the greater mass of the vertebra is divided with49 fair equality by the intertransverse line, laterality of transverses indicates laterality of the whole vertebra with the possible exception of the anterior portion of the body. Laterality of a Cervical spinous process may indicate laterality of the entire vertebra or merely rotation around its vertical axis, in which the one articular process is separated from its fellow of the adjacent vertebra while the other remains in partial apposition.
If disagreements appear between palpation made in positions A and C, re-palpate in both positions. If still uncertain call a consultation or follow finding in position A. The Rotary adjustment may sometimes aid in deciding difficult questions if gently attempted and free movement secured. With this adjustment a vertebra will not usually move without rather extreme force unless the articular process on the side sought to be moved has lost its apposition with its fellow of the adjacent vertebra. In any case of disagreement nerve-tracing, the discovery of sensitive nerves on one side only may aid in decision. A knowledge of probabilities, previous experience, and the diagnosis may also serve as partial guides.
Palpation of the transverse processes is easiest in the Cervical and mid-dorsal regions and most difficult in upper Dorsal and Lumbar regions. It has two uses: first, to assist50 in making a record by verifying the work done on the spinous processes; second, to locate a given transverse process in order to use it as a lever for the adjustment of the vertebra.
It will be seen that fulfillment of the first purpose requires careful examination of the direction and position of the transverses as compared with each other and with the spinous process of the same vertebra, while the second requires only the discovery of the exact location of some particular transverse. It will be best to consider the three divisions of the spine separately, excluding from the present chapter Atlas palpation, which has been thoroughly described.
These can be best palpated in the position for Atlas palpation; that is, standing behind the patient and using the palmar surfaces of the fingers of both hands. From the Atlas transverses follow the anterior border of the sternomastoid muscle downward, and opposite each spinous process draw the muscles backward and inward until the tips of the transverses are found with the middle fingers. Their position on the two sides may then be easily compared as well as their relation to those above and below them.
The transverses of the second Cervical may sometimes be so prominent laterally that they are, or one of them is, mistaken for an Atlas transverse. As a rule, however, the51 width of the Cervicals increases from the second downward, the second being narrowest. Chassaignac’s tubercle, on the transverse process of the sixth Cervical and opposite the lower border of the cricoid cartilage, is a prominent point easily felt as a rule. The transverses of the fourth are usually opposite the upper border of the thyroid cartilage.
The Cervical transverses lie very close to the articular processes and the determination of their relation is a better guide to the condition of the articulation than is spinous process palpation. It is also more difficult.
Palpation of Cervical transverses to determine laterality of the vertebra as a whole or its rotation is possible in position C and has been described under that head.
Palpation for direction can be done best in position B. Use three fingers with a gliding movement along the line of the transverses, passing over several to determine which is most posterior. Then repeat the glide on the other side of the spine to determine whether the transverse corresponding to the anterior one is posterior or vice versa, showing that the entire vertebra is merely rotated or is displaced backward. Some palpaters prefer using both hands and palpating both transverses at once and there is no serious objection to this method, if confined to palpation in position B. In many cases, however, it leads to similar palpation of spinous processes, a most execrable habit.
It should be remembered that with the first two Dorsals52 the transverse will be found in a transverse plane which would pass between its own spinous process and that above. This is also true of the last three Dorsals, while in the middle Dorsals the transverse is usually (not always) level with the tip of the spinous process of the next superior vertebra.
Before adjusting, to determine the location of a transverse process in order to direct an adjustment against it, first palpate spinous process and hold it with the tip of the middle finger. Then approximate with the first finger a point even with the tip of the spinous process above and about one inch from the spine—this of course in mid-dorsal. Then let second and third fingers follow the first so that all three rest on or near the transverse to be palpated. Pressing gently, but firmly, move the three fingers until the process can be felt beneath them. Hold the process with the middle finger so as to direct with it the contact of the adjusting hand to a point exactly over the transverse process.
The transverses of a Lumbar vertebra lie just even with the interspace between their own and the adjacent superior spinous process. They are deeply embedded in muscle tissue and very hard to palpate. They may vary considerably in size or length and the last one or two may be absolutely impalpable. It is sometimes advisable to adjust a rotated Lumbar by using the transverse as a lever, but this53 should never be attempted unless the process can be distinctly felt. The method of locating in Lumbar is practically the same as in the Dorsal region.
Palpation of Cervical transverses in position A has been described and is frequently done. Palpation of Dorsal or Lumbar transverses in the same position may sometimes be desirable. It can be done with the same movement as spinous process palpation, and may serve to detect a bent spinous process.
If it is necessary to palpate both transverses at the same time, stand in front of the patient and lean over his shoulder, letting his shoulders rest against your body. Use palmar surface of fingers of both hands and note which transverse is posterior to its fellow, if either, or whether both are posterior to the line of the others above and below them.
It is rarely possible to find if a transverse process be superior or inferior to its normal position, except the Atlas transverses, although this may occasionally be detected. Fortunately this is a rare form of subluxation, or appears rare, although it must be said that this apparent rarity may be due to our comparative inability to detect it in the living subject.
For convenience, curve is used to denote the normal curvilinear deviation from a straight line naturally present in the normal spine or naturally assumed in response to54 the need for equilibrium during the erect position of the body: Curvature means either the abnormal increase of any normal curve or the appearance of any abnormal curvilinear deviation of vertebrae from their normal position. Deviations from normal must contain at least three vertebrae to be considered curvatures.
The general inspection of the spine which precedes the count should bring to light, in addition to prominent subluxations, and general symptoms observable by inspection of the back, any marked curvatures. Their general locality and direction will be noted by this observation and their details left to be discovered by closer examination.
During palpation with a long and rapid glide one may also note these general points with respect to any curvature.
Do not mistake the four normal curves, the anterior Cervical and Lumbar and the posterior Dorsal and Sacral, for curvatures. The normal Lumbar curve is so unusual in practice that a novice has been known to name it a lordosis.
Four varieties of curvature are commonly described. Kyphosis is a curvature with its convexity directed backward, usually, but not always, found in the Dorsal region. Lordosis, the opposite of Kyphosis, is an anterior curvature, usually in the Lumbar in which case it is an accentuation55 of the normal curve. Scoliosis has its convexity directed laterally either to the right or the left. It is commonly also Rotatory, having its vertebrae rotated around their vertical axes so as to make the outer or the inner transverses more prominent than those on the other side.
In a Scoliosis the rotation may swing either the bodies or the spinous processes toward the convex side of the curvature; the latter is much the easier of adjustment while the former furnishes one of the most intricate problems of adjustment.
Without entering here into a discussion of those disturbed metabolic processes—themselves the result of subluxation—which result in curvature by general softening of the bone, as in rachitis or spondylitis deformans, we will simply state the general proposition that almost all curvatures which are in any degree angular result from a single subluxation to be found at the point of the angle. It has been demonstrated in such cases that adjustment at that point will correct the curvature in time but it is usually wiser to hasten matters by selecting other points of attack by a method to be presently suggested.
Long, regular, but not pronounced, Scoliosis, usually in the Dorsal, may be an example of occupation curvature, following the continued use of muscles in a fixed position and not due to subluxation. Another example is the mailman’s Lordosis. These in themselves are not detrimental56 to health and are negligible unless some special point of impingement through individual subluxation exists within them.
The sharp, angular kyphosis of Pott’s Disease, tubercular caries of the vertebrae, the curvature involving three or four vertebrae which are extremely tender to palpation, should warn against adjustment unless one can be very certain that the vertebrae are sufficiently intact. Fracture of a decayed vertebra is easily possible under adjustment. The cause of Pott’s Disease is usually at the angle point, most frequently the tenth Dorsal but possibly any Dorsal from fifth to twelfth.
If it is the purpose of the examiner to straighten the curvature he should choose for adjustment a series of non-adjacent vertebrae which are most prominent in the direction of the curvature; thus in a right scoliosis he should choose only those vertebrae most prominently out to the right, and in a kyphosis only posterior ones. A lordosis as such cannot be properly adjusted except in the Cervicals, but lordosis is usually a compensating curvature (see below) and can be otherwise corrected.
If the patient suffers from some disease which assumes more importance than the curvature and demands attention, select the one vertebra which is causing the disease, without reference to its position in the curvature, and adjust that vertebra into a proper relation with the adjacent ones, even57 though you adjust directly toward the convexity of the curvature. Disease may often be relieved by making a curvature regular more quickly than by eliminating the entire curvature. Sometimes both considerations may influence the selection of vertebrae.
In a curvature there is not necessarily pressure on nerves at every foramen. In fact, such pressure is the exception rather than the rule in curvature and a careful study of the spine must be made in order that adjustments may be accomplished without causing temporary impingement here and there.
A foot-note describing curvature may be appended to the record of palpation. It should contain the special name of the curvature, whether simple or compound, and the numbers of the first and last vertebrae in it. For instance, note may read: “Right rotary scoliosis from D 3 to L 1 inclusive.”
When a primary curvature is present one or two secondary curvatures usually appear to preserve the equilibrium of the body. With a Dorsal kyphosis there is often a Lumbar lordosis and sometimes less marked lordosis in both Cervical and Lumbar. With a primary right scoliosis in the Lumbar there will be a secondary left scoliosis above. The secondary curvature is called compensatory. In selecting vertebrae for adjustment it is well to neglect the compensatory curvature as much as possible, leaving it to right58 itself as the primary one is corrected. If, however, the primary curvature be a lordosis, and not adjustable, work on the secondary curvature may gradually aid in reducing the primary, to a certain extent at least.
This topic is discussed here partly because it is so often associated with curvature.
Ankylosis can be appreciated only by detecting the lack of normal movement between adjacent vertebrae. Place a finger in the interspace between suspected vertebrae and ask the patient to perform the movement calculated to separate the spinous processes in a normally movable spine. If in the Dorsals, ask him to drop the head and shoulders as far forward as possible without bending at the hips. Alternate repetitions of this movement with straightening and the spinous processes should alternately separate and approach each other. Test several successive vertebrae so as to note that all change their position except two.
In the Lumbars have the patient repeatedly bend the body forward from the hips striving to make his spine convex backward. In the Cervicals forward flexion of the head will serve. Occasionally general ankylosis is found with curvature, as in Spondylitis Deformans.
Many Chiropractors mistake failure to move a vertebra with an attempted adjustment for evidence of ankylosis. In nine cases out of ten such failure is due to other reasons, ankylosis being very infrequent. It is a much abused excuse59 for incapability. Free movement between spinous processes is absolute proof that the vertebrae are not ankylosed.
The chief difficulty arises from failure to observe some of the rules herein laid down.
Carelessness or inattention precludes accuracy.
Pain may cause the patient to assume an unnatural or cramped attitude simulating curvature, especially of the Cervicals. More errors occur from this cause in judging the laterality of C 2 than with any other vertebra.
The occasional bent spinous process in Cervical or Dorsal regions may deceive the palpater unless transverse palpation is employed. But the frequency of slightly bent processes in dry spines and a superficiality of reasoning upon the subject have led to great overestimation of their importance. As a matter of fact only a very few maladjustments arise from deception of the palpater in this way, though the profession contains few practitioners who make a routine method of verifying by the transverses. The reason is simple. Bent processes are caused by direct violence applied before the union of shaft and epiphysis is complete. Sufficient force to produce a change of direction usually produces subluxation in the same direction. Adjustment continued until the offending process was quite aligned with its fellows would constitute overadjustment, but adjustment is not usually continued after all symptoms have subsided, so that actually small harm occurs through failure to detect bending.
An epiphyseal plate may be absent, having been broken off by trauma and absorbed. This can be discovered by noting the too-wide space between apparently adjacent vertebrae, and careful palpation will disclose the apparently much anterior vertebra, an appearance not borne out by the position of the transverses. When an epiphysis is absent a patient has a somewhat weak back from lack of muscular attachment.
Lipoma, or the heavy cicatrix following a burn or carbuncle, may render palpation of two or three vertebrae impossible. In such a case only the palpater’s experience and his knowledge of the characteristics of various vertebrae will enable him accurately to number the remainder.
Patients with much adipose tissue may require palpating in several positions in order to permit certainty.
A deep third Cervical which is absolutely impalpable may mislead one, but a careful count which shows one vertebra overlooked indicates the necessity for a careful re-examination of the Cervicals, by which the gap at the third at least may be appreciated. If the Axis is very much inferior the third is especially likely to be overlooked.
Anomalous cases have been found in which there were more or less than the usual number of movable vertebrae, the usual deviation being the presence of twenty-five, and the extra one being most commonly a Lumbar. In one case under my observation there were twenty-five movable vertebrae, apparently thirteen Dorsals according to shape, and only eleven pairs of ribs posteriorly, two pairs being dichotomous61 so that there appeared thirteen pairs anteriorly. Deviations in number occur, in my experience, about once in five hundred cases.
The regional location of vertebrae by means of certain landmarks (so called) in or near the spine, is a much discussed question in the profession. Without discussing the various arguments in favor of this method, chief of which is the inability of the untrained to count vertebrae, let us set forth the principal landmarks used and the facts in regard to them.
The seventh Cervical, called Vertebra Prominens, is usually considered a guide to the count. In over three hundred cases examined for that purpose the seventh Cervical was found to be Vertebra Prominens in about 65%, the other 35% showing the sixth Cervical or first Dorsal to be the prominent one. This method is two-thirds as accurate as counting.
The tubercle (Chassaignac’s) of the sixth Cervical transverse is said to be directly opposite the lower border of the cricoid cartilage and this is a better guide than the above.
The third Dorsal spinous process is said to be on a level with the root of the spine of the scapula, and with arms hanging at sides, the upper angle of the scapula to be on a line between first and second Dorsal spinous process. This is not at all constant.
The inferior angle of the scapula is said by some writers to be on a line with the tip of the seventh Dorsal spine. Others locate it opposite the interspace between seventh and eighth Dorsals. Still others give it as opposite the eighth Dorsal spine. All are correct—sometimes. In truth, the inferior angle may be opposite any part of the spine between the sixth and ninth Dorsals. There is nothing constant about it.
The twelfth rib may be followed to its articulation with the twelfth Dorsal vertebra. This is a good guide, providing that the rib can be palpated. The lower margin of the last rib is usually even with the spinous process of D 12 about one inch and a half from the mid-spinal line. The humor lies in the fact that the patient upon whom the count is so difficult as to require this verification is usually obese and obesity renders the rib impalpable.
The line drawn between the iliac crests falls between the third and fourth Lumbar spinous processes in about 98% of all cases. This is our most reliable landmark. It is used as described under the Count.
All landmarks except the last two show such variance in different individuals as to be quite unreliable. The correct method of numbering spinous processes is the obvious and logical method—count them. The skill and accuracy of touch required for successful counting is invaluable in determining direction of subluxations.
In order to secure that absolute concentration without which it is impossible to appreciate properly those tactile impressions for the very reception of which such continued practice is necessary, the hands should leave the spine as little as possible during palpation; a second person should record subluxations found so that the palpater need only state, and not write, his conclusions; light pressure on the spine should always be used, as a heavy pressure desensitizes nerve-endings in the fingers; and silence should be maintained except for the necessary statement of points to be recorded.
Palpate as rapidly as is consistent with good work. The more rapid the palpation, if concentration is absolute, the more accurate the impressions received.
The end and aim of palpation is to determine the means by which impingement of nerves may be removed with the greatest rapidity and success. Palpation includes such a study of the vertebral column as will fix in your mind a clear thought-picture of the impinged nerves throughout its length.
If you would achieve success in Vertebral Palpation, be persistent. Spare no labor to acquire that accuracy of detail which distinguishes the expert from the amateur. You can make of yourself what you will. There is no limit to the ability which may be acquired. Another may guide your hands but with you lies your success.
Nerve-tracing is that branch of palpation by which the tenderness of irritated spinal nerves is discovered and their paths demonstrated.
Organ-tracing is that branch of palpation which deals with the outlining of the boundaries and surface markings of a tender organ or part.
Palpaters frequently confuse tenderness of one of the parenchymatous viscera for the tenderness of interlaced and branching nerve filaments, especially in the abdominal region. The fact that the tender area takes on the characteristic shape of one of the viscera is conclusive evidence that an organ, and not nerves, have been traced.
Any spinal nerve may be traceable for at least a part of its course. The cranial nerves are made inaccessible to palpation by their location, except the spinal portion of the spinal accessory and the terminal portions of the nerves to the face. Likewise the sympathetic trunks, except perhaps in the neck, are untraceable.
Nerve-tracing is comparatively easy in the upper and lower extremities, neck and back. The superficial nerves of the scalp are hard to follow on account of the hair. The superficial nerves of thorax, abdomen, and pelvis are accessible under the conditions mentioned below; the deep or visceral branches, never.
Of those nerves mentioned as traceable, only such as are irritated and consequently swollen and tender, can be followed. If a nerve is very heavily impinged, especially if the impingement be chronic, it is partially or wholly paralyzed and not traceable. If the heavy impingement be acute, or if there be a light impingement serving as a mechanical irritant, nerve-tracing is a real aid to diagnosis.
About one-half of all the cases which visit Chiropractors for adjustment are susceptible of nerve-tracing. In the remaining half it is absolutely impossible to acquire any information in this way. Of the half who are at all susceptible, it is possible in perhaps four-fifths of all cases to secure some accurate or reliable information.
The patient in whom all accessible nerves seem tender to light palpation is hyperesthetic and unavailable for tracing.
In the usual case one or two nerves will be found easily traceable, while the rest exhibit no tenderness on pressure. Such a case furnishes the most reliable information securable by this method and the tender nerves may be considered as lightly or acutely impinged.
Knowledge of the anatomy of the nervous system is a part of the necessary equipment of the Chiropractor who would trace nerves and this knowledge should be so thorough as to enable the palpater to recognize each tender line found as an anatomically described nerve-path or an error on his part. The examiner must know the paths of all nerves and be able to predict from the first tender points discovered the probable course which the tenderness will follow, so as to direct his search along that probable path.
He must be able to detect unconscious deception on the part of the patient through his knowledge of the anatomical impossibility of the apparent tracing. For instance, if for any reason he may appear to have traced a nerve upward beside the spinal column from D 10 to the eye by way of the vertex, he must know that this is an illusion—because such nerves do not exist and cannot be anatomically demonstrated—or accept the well merited ridicule of any educated person who discovers his absurdity.
Because of the difficulty of determining whether the tender structure found be muscle, nerve, or viscus, and because of the natural suggestibility of both palpater and patient, nerve-tracing cannot be so reliable a guide to nerve-paths as is dissection. It should not be necessary to state this obvious truth but the calm acceptance, by many, of the weird conclusions based upon a belief in the infallibility of nerve-tracing testifies that it is necessary.
Nerve-tracing is valuable only where the nerve-path67 outlined as being tender corresponds to the known path of some nerve.
Paradoxically, knowledge of nerve-paths may lead to error. By the law of expectancy, we are prone to find what we look for and if we hold too strongly to the belief that because we have found one or two points of tenderness we must find a series of points extending along a mentally pictured nerve-path, we may search until we falsely believe that we have found this series.
Likewise the patient, having been carefully informed as to the manner of procedure and knowing what we expect to discover, may unconsciously deceive us by feeling tenderness in response to suggestion, where no real impingement exists.
The value of nerve-tracing in diagnosis has been much overestimated by many, though the tendency of the profession seems to be toward rationalism along that line.
Whereas, in palpation of the spine every real subluxation gives evidence of disease, or tendency to disease, while every normally aligned pair of vertebrae furnish proof that no disease can exist in the area of distribution of the nerve emerging between them, nerve-tracing is much less reliable. If the tender nerve be traceable to a vertebral subluxation it may be taken as additional evidence that the effect of that68 subluxation is disease, rather than tendency to disease, truly an important distinction, but scarcely broad enough to support a diagnosis without aid.
The absence of tenderness from nerves does not negative a disease in any instance, whereas the absence of subluxation does. Like all other expedients for the selection of vertebrae for adjustment without admitting the necessity for first acquiring much skill by much labor, nerve-tracing has a great weakness. Only irritated nerves are tender and the effects of subluxation may be either irritation or paralysis.
If accurately done, sources of error carefully eliminated, and the results of nerve-tracing found to correspond with the condition of the spine and the other symptoms, this method of demonstrating to the patient the connection between the vertebrae and the diseased region of his body is valuable. It aids in convincing him of the validity of the Chiropractic theory.
The palpater, having made his vertebral palpation, may begin at some point in the body indicated by the symptoms as diseased and, finding tenderness, follow the path of a nerve back to the spinal column where the nerve may be fairly presumed to enter the intervertebral foramen.
Or he may use his palpation record as a guide and follow the tender nerves outward to their periphery. This is the better method.
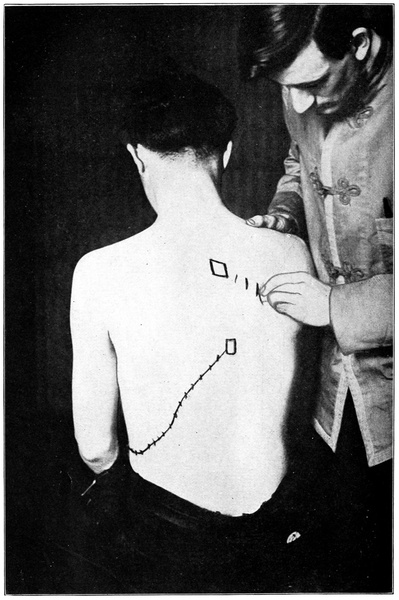
When palpation has been made, remember that the impinged nerve is usually found on the side opposite to the direction of the spinous process in its departure from the median line. With a left subluxation the tenderness is usually, though not always, on the right side. If in the Lumbar, and the subluxation a rotation, the impinged nerve will be found below the transverse process of the subluxated vertebra. In the Cervical and Dorsal regions the tender nerve is usually below, but may be either above or below, the transverse of the subluxated one.
Examine the nerves having exit from the foramina of each subluxated vertebra in turn from above downward. When a tender point is found about an inch from the mid-spinal line, attempt to follow the nerve and palpate until it has been traced as completely as possible.
The region immediately surrounding the spinous process of the subluxated vertebra may be tender because of impingement of the axons of the posterior primary division of that spinal nerve which emerges below the vertebra. Such tenderness is more common with anterior subluxations than with others. It is not to be confused with the soreness which often appears after adjustment and is due to bruising or straining of the tissues.
Nerve tenderness may be discovered at a little distance from the mid-spinal line and at a level slightly lower than70 the emergence of the nerve. If a nerve is irritated, the finger inserted between the ribs near their articulation with the transverse processes will elicit tenderness. The discovery of tender points along the spine is the most important part of nerve-tracing.
Detailed description of the paths of all the spinal nerves may be studied from any standard work on anatomy and will not be included here, but it may be well to remind the reader of certain general tendencies.
The spinal nerves do not cross the median line in front except perhaps fine interlacing fibres.
In the Dorsal region the nerves are usually found following the interspaces until the lower ones debauch upon the abdominal wall anteriorly. There are, however, some Dorsal and lower Cervical nerve bundles which pass obliquely downward and outward to innervate back muscles.
Reference to the section on Spino-Organic Connection will make clear the tissues supplied by each nerve.
Slight deviations from the usual course of nerves are common; marked deviations very infrequent.
Use second finger of either hand for the palpating finger, choosing the hand which can be most conveniently used as determined by the position of patient and the part of the body to be examined. There is no set rule. Reinforce this second finger by the pressure upon it of the first and third and, if desired, by pressing thumb against it. (See Fig. 5.)
Apply the tip of the palpating finger to the nerve with a motion such that it crosses the path of the nerve at right angles back and forth. Meanwhile the probable path of the nerve must be kept in mind. As the finger crosses the nerve-path it makes steady and even pressure upon any structures passing beneath it. The motion of the hand is almost a rolling motion, the finger tip probing, as it were, for a tender spot.
The irritated condition of the nerve which has thus been rolled beneath the finger may be recognized in one of three ways; the patient may involuntarily flinch, betraying the hurt; or he may inform the palpater of the hurt; or the swollen, cord-like nerve may be felt.
The two former are the reliable guides, while the latter is only occasionally possible. In children and in feeble-minded, insane, or mute adults, the first mentioned method must be relied upon entirely. Muscular contraction is the unconscious or reflex response to pain and often occurs independently of the intelligence or state of mind of the subject.
Of all the three methods the one most commonly relied upon is the second—the statements of the patient.
The patient should be informed of your intentions when palpation is begun and should be asked to answer every time you apply your finger, saying, “Yes,” if the spot is tender72 and, “No,” if not. He should speak promptly each time so as to avoid self-deception which might come with reasoning upon his sensations. Occasionally vary the steady rhythm of your movements by omitting one and note if the patient responds mechanically when you do not press.
At times during the tracing, it is well to depart from the probable nerve-path and to touch again a point marked as tender, to see if the patient’s information may be relied upon. Whenever you leave the nerve-path his answer should be, “No,” immediately changing to, “Yes,” when you re-cross the tender line.
At each tender point noted a small mark should be made with an eye-brow pencil or other grease-paint, which leaves a distinct but easily removable mark. These tender points should be noted and marked at intervals of about an inch.
When the entire nerve-path has been traversed in this way, draw a line with the eye-brow pencil, passing through all the marks indicating points of tenderness. This line should be a sufficiently accurate rough outline of the nerve-path to make clear the spinal connection with the diseased area. The significance of this connection will be better understood when the section on Spino-Organic Connection has been studied.
In muscular rheumatism, neuralgia, neuritis, or in case of a local boil or abscess indicating local disturbance of the trophic influence of nerves, clear and definite tracings are common. Muscular spasm, such as wry-neck, usually has a very tender nerve associated. Localized painful disease of any kind is likely to be associated with a very definite nerve tenderness, as is the case frequently with appendicitis, ovaritis, hepatic colic, etc.
The painless disorders, or various disorders of spleen, diaphragm, heart, lungs, etc., though they be of a very serious nature, seldom are discoverable by nerve-tracing unless their serous membranes are involved. Tracings may be made from D 2 or 3 to anterior thoracic walls in heart or lung disease but are not common.
Any spinal nerve may be traceable at times through at least a part of its course.
Several of these have been mentioned, such as the natural suggestibility of both examiner and patient. Among others are: failure in the back, thigh, or leg to reach the really tender nerve because of the interposition of several muscle layers between it and the finger, ignorance of nerve-paths, failure to apply equal pressure to all parts of a nerve, application of such heavy pressure that muscle tissue is bruised and hurt, and failure of full co-operation on the part of the patient. Let us consider these in turn.
If several muscle layers interpose themselves between the searching finger and the nerve, it is proper to push aside the intervening layers, using a twisting and rolling movement until the finger feels underneath the muscles. This done, and a tender nerve found underneath several muscle layers, the same amount of overlying tissue must be pushed aside each time the finger searches for the nerve. Only exhaustive study of the anatomy of the typical nervous system will enable the examiner to know exactly at what point a nerve will become more or less superficial. Unless he does know this it is best to follow the neutral rule that nerves tend to follow the long axes of ribs and limbs and to maintain their depth beneath the surface throughout their course. This statement is too general for accuracy.
Care should be taken that equal pressure be made on all points palpated on one nerve. If the nerve pass over a bone, less force is needed to exert the same pressure than if it overlie muscle or other soft structure. The force used varies constantly as the hand moves from place to place, according to the density and hardness of the structures overlying and underlying a nerve.
Sufficiently heavy pressure will elicit tenderness in all except anaesthetic patients. But if a nerve be irritated it will be tender without heavy pressure, when the finger really makes a close contact with it.
If the patient willfully attempts to deceive the palpater, nerve-tracing might as well be abandoned except in those extreme cases where the patient will flinch against his will on account of extreme sensitiveness.
As far as possible, the second hand is placed opposite the tracing hand and steadily supports the body; its position changes with changes in the position of the first. If the arm is to be examined it had best be held away from the body, and the part to be examined held between the two hands.
For tracing nerves in the neck, back, and upper extremities, the patient should sit easily. For lumbar, abdominal, or pelvic tracing, or for tracing in the lower extremities, have patient lie on side or back. Do not hesitate to change the position of the patient as often as is necessary to secure easy access to the part to be examined and relaxation of the patient’s muscles. Never allow the assumption of a strained position during tracing; the sensation of cramped muscles may be confused with sensations of nerve tenderness.
A vertebral subluxation is a displacement, less than a dislocation, in which the chief element is the partial loss of normal apposition of the articular surfaces of the subluxated vertebra with those of the vertebra above or below, or both. Or, Vertebral subluxation is a permanent partial dislocation.
Subluxations are primarily caused by trauma—falls, blows, strains, etc., being the chief factors. Hereditary weakness in structure of some part predisposes by rendering that portion more easily displaced.
Subluxations are never hereditary but may be congenital through violent or instrumental delivery into the world or may appear hereditary because they occur shortly after birth through the effect of light jars upon the hereditarily weakened segments of the spinal column.
They are always the result of concussions of forces; never of forces acting entirely within the organism. They result from the contact of the body with its environment.
It has been said that muscular action in response to peripheral irritation may produce subluxation. The laws of reflex action render this impossible. Given a normally77 aligned vertebra, and consequently normal nerves and a normal reflex arc in that segment, the ventral horn cells respond to a slight peripheral stimulus by exciting muscular contraction on the same side with the irritation. If the irritation be sufficiently increased, the response occurs on both sides but most strongly on the side from which the irritation comes. Greater irritation merely serves to cause greater distribution of the responsive action. (See any standard physiology on reflex action.) In no case will the difference between the contractions of muscles on the two sides be sufficient to displace a normally aligned vertebra. Nature has provided against that contingency.
Given a subluxated vertebra causing nerve impingement and thus interruption of the normal action of the reflex arc, irritation may result in greater contraction upon the opposite side than upon the side of the irritation. This is an abnormal condition and accounts for the increase of previously existing subluxations under pain or peripheral irritation. But in every instance trauma must and does precede and cause subluxation.
Once produced, however, a subluxation may not cause noticeable effect until it has been increased in degree by the reaction of forces within the body such as poisons, general fever, etc. Thus germs, dietetic errors, exposure to sudden temperature changes, waste of energy through abnormal mental activities, as hate, fear, worry, etc., or through78 physical excess—in fact, all the secondary causes of disease may appear to have produced a subluxation. In fact, they have merely accentuated that which already existed and have done so through the muscular contractions which they induced.
General thinning of intervertebral substance through a condition of disturbed metabolism itself produced through the agency of some one serious subluxation, may narrow all the foramina and increase impingement of nerves at any point where a slight subluxation previously existed. An irritated nerve may become swollen and the nerve impinged at the foramen.
So definite is the law governing the effect of force applied to a given portion of the body upon an associated vertebral segment that the skilled Chiropractor who has studied vertebrate segmentation thoroughly may determine, from the history of a fall or injury, the vertebra which would tend to be subluxated by that injury and the tissues controlled from that part. The rule is this:
Force applied to any body segment tends to subluxate the segmentally associated vertebra. This subluxation tends to produce disease throughout the area of distribution of the subjacent pair of spinal nerves.
The task of explaining this law seems hopeless unless the student is familiar with human embryology and the life history of the vertebrata, as well all the details of human79 anatomy. To such a student the law will be self-evident, so interwoven with the threads of higher organization as practically to form its pattern.
In simple terms we might offer this general statement. Any force applied to the body with sufficient violence will produce subluxation of the vertebra above the spinal nerves supplying the injured area. Thus, the brachial plexus controls the arm and shoulder and connects with the spine by way of the 5, 6, 7, 8, Cervical and 1 Dorsal nerves. Any force striking the arm or shoulder tends to produce subluxation of the sixth or seventh Cervical or first Dorsal vertebra so that all permanent disease conditions resulting will be found in the arm or shoulder or nearby tissues of the neck.
This theme presents a magnificent field for individual study and research but is, per se, beyond the limitations set for this work.
Slight subluxations may exist, because of the adaptation of surrounding parts and the slight play within the intervertebral foramen, without producing noticeable effect. They always, however, evidence a tendency to disease.
The majority of subluxations do produce disease, to some degree, and do so by impinging nerves. Impingement may be either by pressure against a nerve or ganglion or by constriction of a nerve where it passes through an intervertebral foramen; the former occurs in the case of the80 Cervical sympathetic, the sub-occipital nerves, and the sacral nerves; the latter is the commoner form in Dorsal and Lumbar regions of the spine. Probably the most positive constriction of a nerve which can occur within the body is to be found in rotation of Lumbar vertebrae; the body of the rotated vertebra encroaches upon the inferior nerve on the side opposite to the direction taken by the spinous process.
Either variety of impingement produces disease, morbid structure or function, by irritation of the nerve: light impingement irritates, heavy impingement partially or completely paralyzes, the nerve.
According to the abnormal relations between vertebrae subluxations may be variously described as rotated, tipped, anteriorly, posteriorly, or laterally displaced. They commonly combine two or more of these forms, so that the purely rotary or the entirely lateral subluxation is uncommon.
Every vertebra has a vertical axis around which it tends to rotate. This axis is not always the center of mass but depends upon the arrangement of mass, the fixity of cartilages, ligaments, and muscles, which tend to hold some parts of the vertebra more fixed than others, and the apposition of articular processes, which tends to prevent movement in certain directions.
The axis of rotation of the first Cervical is the center of81 the odontoid process of the second Cervical, which articulates with the transverse ligament and anterior arch of the first. A frequent subluxation of the Atlas is a rotation around this process so that the one transverse is permanently posterior to its normal position and the other correspondingly anterior.
The axis of rotation of the Cervicals below the Atlas is in the extreme anterior portion of their bodies. This part remains relatively fixed in rotatory subluxation while the tip of the spinous process describes the greatest arc.
In the Dorsals the axis of rotation lies in the posterior portion of the centrum near the neural canal. When the spinous process appears laterally displaced in rotation the anterior portion of the body is slightly displaced in the opposite direction, twisting and straining the fibres of the intervertebral disk.
In the Lumbar region rotation is the commonest form of subluxation, the axis of rotation being laterally movable upon a transverse line between the articular processes in the beginning and shifting, as soon as the vertebra leaves its normal relations, to the junction of the articular process with that of the adjacent vertebra on the side toward which the spinous process is moving. Thus, in rotation of the vertebra so that the spinous is to the right, the axis will be found on the right side, the superior articular process of the next vertebra serving as a support on which the inferior articular process of the rotating vertebra may turn. The processes are so firmly locked that unless the whole vertebra be quite posterior little lateral movement of the spinous82 process is possible without marked rotation. The body describes the greatest arc because it is further removed from the center of rotation than is the tip of the spinous.
This is a subluxation in which the one transverse process is, or appears to be, superior or inferior to the other. It occurs frequently to the Atlas in combination with lateral subluxation. In fact, the shape of the occipito-atlantal articulations is such that, if the remaining Cervicals maintain their proper relation to each other, the Atlas cannot be laterally displaced without a certain amount of tipping. It will be relatively superior on the prominent side and the head will be tipped toward that side; that is toward the side of the lateral displacement. Thus, on account of the wedge-shaped lateral masses, if the whole Atlas be to the right of its normal position the right side will be superior and the head tipped toward the right. This is only true when the vertebrae below maintain a normal interrelation.
This is a name applied to that condition in which, on account of changes in the intervertebral disks due to subluxation interfering with metabolic processes, the bodies or spinous processes of vertebrae are crowded too closely together.
Occasionally a spine is found in which, on palpation,83 the spinous processes are found to be crowded together in groups, sometimes of two or three, sometimes of five or six; no two interspaces appear equal, a very wide one being succeeded by one or two which are almost inappreciable; the variation in width of the interspaces does not correspond to the known normal variation in those regions where the changing obliquity of spinous processes should modify the relative width of successive spaces. We expect, for instance, to find a wider space between third and fourth Dorsals than between second and third; if we do not find this difference it is doubtless due to cartilage change and the vertebrae are approximated.
In case of general thinning of intervertebral substance unequally divided between different sections of the spine the record will show that almost every vertebra is listed either S or I, and if a system of underscoring is used that these two directions are frequently indicated as most noticeable.
A study of the spine will make clear the fact that if the cartilage between any two Dorsal vertebrae be thinned in front the bodies of the vertebrae will be closer together and the spinous processes more widely separated; the spinous process of the upper vertebra will be crowded against the one superior to it and that of the lower against the one inferior to it. These spinous processes are said to be approximated.
The correction of S or I subluxations, then, depends upon correction of disturbed nutritive processes.
According to the usage of earlier writers on subluxations this term (lateral displacement) included rotation of the vertebra as well as those changes in position in which the whole or nearly all of the vertebra deviates sidewise from its normal position. Since the introduction of the term “rotation” into the description of subluxations, the meaning of the term “lateral displacement” is much more restricted. It refers now to a condition which probably occurs in the strictest sense only in the Cervical region, most frequently with the first and second Cervical, the two being subluxated together.
We have already stated that the most important fact to be determined regarding the Atlas is its lateral displacement, since this produces the greatest impingement of nerves. Lateral displacement of any other Cervical can best be judged by examination of the transverse processes, since by palpation of the spinous process alone it is quite impossible to distinguish between lateral and rotary subluxation.
In the Dorsal and Lumbar regions the R or L used to describe the position of the spinous process most often indicates rotation of the vertebra. While it is perfectly proper thus to describe the subluxation on a record, in the determining of the form of adjustment to be used the position of the whole vertebra must be considered.
Forward displacements may occur anywhere in the spine. In the case of the first Cervical they are usually,85 though not always, forward displacements of only one side—rotation—though the whole Atlas may be anterior if the Axis has moved with it or is tipped so that the spinous process is much superior. This is rare.
Any Cervical may be anterior; usually a series are anterior (if any) amounting to an increase in the Cervical curve—a lordosis. This condition may be corrected by transverse adjustments given from the front and side.
A Dorsal vertebra is only relatively anterior, the adjacent ones being relatively posterior, and the only possible correction at present is the adjustment of the posterior ones. A Lumbar cannot be anterior unless those below it are also anterior, on account of the locking of articulations. Discovery of anterior Lumbars is quite common. The fifth Lumbar may be subluxated anteriorly by slipping forward on the Sacrum; it must be superior at the same time, on account of the shape of the articulating surfaces which face downward and forward. The spinous process is crowded closely against the fourth while the body of the fifth is too widely separated from that of the fourth.
There are many Chiropractors who have always considered the posterior subluxation more than any other, not because it produces greater nerve impingement than others but because it is easiest to detect; it intrudes itself upon the attention of the unskilled examiner most persistently. Nor should its importance be underestimated, though we now86 realize that in some instances a rotated or anterior vertebra may cause more nerve impingement than a posterior one.
The posterior subluxation in the lower Dorsals and Lumbars is the easiest variety to adjust; in this region a posterior displacement of one vertebra tends to bring with that one the next adjacent superior one, the sharpest deviation occurring between the posterior one and the one below it.
Any vertebra may be posterior: the Atlas is rarely so as a whole, and never unless the Axis is also displaced backward; the Cervical and Dorsal regions present frequent variations of this sort, which must not, however, be confused with long, prominent, or overdeveloped spinous processes; the Sacrum may be posterior to the ilium on one side, or to both ilia.
Mention should be made here of a form of subluxation not strictly vertebral—displacement between the condyles of the occipital bone and the lateral masses of the Atlas. This occurs when the head has been moved too violently upon the Atlas so as to cause an immediate nerve irritation and muscle tension sufficient to hold it in its abnormal position. The Cervicals may be quite normal below the Atlas though this, of course, is not the rule. Correction of occipital subluxations is made by applying force to the Atlas and to the skull, sometimes by holding Atlas and rotating the skull.
The relative age of subluxations may be determined, within rather wide limits, it is true, by a study of the form of the spinous process. Newly acquired subluxations are sharply defined, having noticeable edges on the spinous process. In time they tend to become rounded and blunt and appear to cover more surface, just as the mountain range which, when first upheaved, is sharp and rugged, gradually rounds into regular curves through the work of the elements.
In this way Nature protects the subluxated vertebra from further contact with the environment surrounding man, the rounded process offering less opportunity for a blow or shock to affect it.
Bone diseases such as rachitis osteomalacia, etc., and especially Potts’ Disease, or spinal caries, make marked changes in the shape of vertebrae. Also a subluxated vertebra may gradually assume a shape suited to the abnormal position it occupies, the commonest change being the assumption of a wedge shape by the centrum. This is a great obstacle to adjustment, as the abnormal shape of the vertebra makes it tend to settle after each movement into the old abnormal position.
There are few spines without some more or less misshapen vertebrae.
Ankylosis also makes great changes in the shape of88 vertebrae. There are two kinds of ankylosis—true and false. The first is a deposit of bone cells upon bone, often the formation of a bridgelike structure to hold contiguous vertebrae together. This may bind any portions of the vertebrae but most commonly holds the bodies, in which case it can only be appreciated by detecting the lack of movement between normally separable vertebrae. False ankylosis occurs with fever in bone and consists in an exudation of bone substance which sometimes produces remarkable distortions of shape.
Vertebral Adjusting is the art of correcting by hand the malpositions of subluxated vertebrae.
A Vertebral Adjustment, strictly speaking, should mean the complete restoration of normal relation between previously subluxated vertebrae. As used in Chiropractic, it means either a partial or complete restoration of such normal relation.
Maladjustment, as used in the profession, designates any movement of vertebrae by hand which produces or increases subluxation.
It will be well for the student to master first the general rules and principles which govern vertebral adjustment and then to proceed to a detailed investigation of each movement, in turn, before practicing it. The art of adjusting can only be acquired by practice, and a high degree of excellence in it only by long-continued practice. However, the rapidity with which it can be mastered depends largely upon the formation of a clear pre-conception of the work to be done and the manner of its doing.
As the student progresses in the art he finds himself occasionally guilty of errors which mar, in some degree,90 the efficiency of his work. These may arise from unconscious modification of the technic first learned or from unconscious repetition of some necessary modification demanded by a special peculiarity in one or more cases.
This section is intended to furnish the proper pre-conception and also to serve as a monitor to adjusters who, by reference to the precepts herein set down, may discover and remedy their own errors. It is not intended to furnish sufficient education to warrant practice without clinical instruction, which is unwarrantable, but rather to accelerate the education which practice alone can furnish.
The vertebral subluxation being an abnormality of relation between vertebrae, it is obvious that its correction must be a return of normal relation. This can only be accomplished by bringing about a change of relative position. Movement of a section of the spine composed of several vertebrae is not, in the true sense, an Adjustment. It is the single vertebra which must be moved.
The movement should be one calculated to bring the vertebra to its normal position in the most direct manner possible. Such a movement should be used as will reverse the direction of the forces which subluxated the vertebra. It should be applied to the transverse or spinous processes, or to the lamina, as is sometimes done in the case of the Atlas, according to the kind of subluxation. Different subluxations require different handling. Cases vary. Select91 the move best suited to the case. This can be determined most properly by correct palpation which fixes in the mind of the adjuster the position of every part of the vertebra, its relation to its fellows, the points of greatest nerve impingement, etc., all of which should suggest the best method for correction.
The prime object of adjustment is the removal of impingement from nerves.
The movement used in adjusting has been variously described. Many writers and teachers have used the term “thrust” to describe the movement of the hands, and the term is correctly applied to the movement used by many Chiropractors. But a careful study of the methods of applying force in use among the most successful adjusters, those who have attained the greatest results with the slightest percentage of failures and a minimum of pain to the patient, discloses the fact that the chief element of their adjustment is transmitted shock.
The hand is held in close contact with the vertebra to be adjusted and the arms and shoulders describe such movements as to deliver the required amount of force with the slightest possible change in the position of the hands. The vertebra bounds away from the contact hand. In the delivery of a thrust the hand would follow the vertebra, forcing each portion of the movement. The real effect of a thrusting motion, since the hand cannot enter the body as a sharp92 instrument would, is that of pushing. Pushing neither subluxates nor adjusts vertebrae so readily as does a rapidly applied shock.
Let us illustrate with a common experiment in physics. Suspend a number of ivory balls by cords of equal length in such a manner that each is in contact with its fellow and all are in a straight line. When the balls are properly adjusted a straight line should connect their centers. Hold one end ball firmly in the hand or with an instrument which renders it absolutely fixed. Then strike sharply with a light hammer. The balls will all remain stationary except the one on the opposite end which will fly off to a distance exactly measurable according to the force of the blow. How does this occur?
A shock is transmitted through the molecules of the ivory until it reaches the end ball, which is not held back by another. Here the transmitted force is expended in molar motion, the ball leaping away from its fellows as if it had been hung alone and had been struck with the same force.
It is well known that by placing an elbow firmly against a man’s jaw and then sharply striking the closed fist with the other hand, open, a very heavy blow can be given; yet the forearm, through which the shock is transmitted, does not move.
Now ivory is very like human bone. Further, it has been demonstrated that the law illustrated by the above experiment is equally applicable to the movement of vertebrae. The pushing or thrusting movement may move a specific93 vertebra, but it is probable that the chief factor in so doing is the element of transmitted shock contained in the movement and delivered at the instant of release of the hand from the spine at the end of the movement.
On the other hand it is obvious that a pushing or thrusting movement may move several vertebrae in addition to the one directly in contact with the adjusting hand, in consequence of the way in which the spinal segments are closely bound together. If a steady strain is used, in which muscles and ligaments have time to act, one of three results may occur: (a) the specific adjustment; (b) the movement of several vertebrae at one time, which does not constitute an adjustment; (c) the giving way of the spine at its weakest point, which may be some distance from the point of contact with the adjusting hand, the ligaments and muscles having communicated and diffused the strain throughout a large area. In the latter contingency the result is usually a new subluxation or the increase of an old one, instead of an adjustment.
Thus Speed becomes an important factor in correct adjustment.
A good illustration of the value of speed may be taken from a pile of stakes bound together by a cord. If a man with a hammer desires to remove the center stake of the group, and attempts to do so with a slow pushing movement, the result is a change of position of many stakes, which94 adhere to the center stake and to each other. If, on the contrary, he strikes a sharp, quick blow with his hammer, meeting squarely the center of balance of the one stake, it will fly straight from its position leaving the others unmoved. This is exactly what we desire to accomplish with an adjustment. By the speed of the movement we expect to move one vertebra before adhesion or the contraction of muscles or inelasticity of ligaments can diffuse the force.
In order to accomplish the transmitted shock it would seem wisest, at first thought, to draw back the hand and strike the vertebra sharply. On the contrary, it has been found advisable to place the hand carefully in close and immediate contact with the vertebra to be adjusted. Nature herself shows us the way in the delicate shock-transmitting mechanism of the tympanum.
Also the hand of the adjuster will cover much more than merely the spinous or transverse process which is used as a lever and to which it is desired to transmit the shock, unless carefully placed so that only a small portion is in contact; by such a contact diffusion of the shock is prevented and its efficiency within a limited area is increased. A carpenter wishing to countersink a nail places in contact with the nail head a small instrument called a countersink, which he then strikes sharply with a hammer. The contact hand of the adjuster represents the countersink and is used by the two arms as a passive instrument for transmitting shock.
The close contact of the hand, which remains passive, renders the adjustment much less painful to the patient than it would otherwise be, and one of the prime objects in the mind of the adjuster should be the minimizing of pain inflicted, by any means which does not lessen the resulting benefit. Also any drawing back of the hand before the movement warns the patient and tends to induce involuntary muscular contraction which interferes with adjustment.
In an adjustment it is necessary to overcome two kinds of resistance—the passive resistance of inertia, of ligaments, or of superincumbent weight, and the active resistance of muscular contraction. It is important that both forms be minimized.
The first may be lessened through the position of the patient’s body; he is placed so that the vertebra to be adjusted is in the freest possible position. The second is reduced to the least possible quantity, amounting to no more than muscle tonus, by using two methods: (a) Oral Suggestion, and (b) Muscular Suggestion.
Explain to the patient the need for relaxation. Make it clear to him that less force will be required if his muscles are passive. Remind him frequently of this and assume that he desires to relax. A word immediately before the adjustment often induces a temporary relaxation during which96 the adjustment is given. Anything which detracts the attention from the coming shock is an aid. Sometimes asking the patient to inhale and exhale slowly and deeply will sufficiently take his attention from the adjustment. Experience will teach him that he suffers less pain when relaxed and presently relaxation becomes a habit. Instructing patients to think of sleep, turning the eyeballs upward, has been effective with some.
This can only be given by maintaining a state of relaxation in one’s own muscles, which in itself is desirable in most cases, for reasons to be presently explained. In handling Cervical vertebrae move the head gently from side to side with your own hands relaxed as much as possible. The lazy motion suggests relaxation. Then when it is felt that the neck is thoroughly relaxed, vary the motion with a quick adjusting movement.
In Dorsal and Lumbar regions after the hands are in correct position the adjuster should pause a moment both to be sure that the direction of movement and his purpose to move are clearly fixed in his mind and to be certain that both himself and the patient are relaxed. The adjustment is given instantly and from a perfectly lax muscle, as a boxer strikes.
An added advantage is the greater amount of speed and control which may be commanded in this way. The lax arm, being in a neutral state as regards motion, can be contracted97 in any desired direction without loss of force or of time, whereas a taut muscle cannot further effect motion of the arm without relaxation of its antagonistic muscles, which takes time.
Considerable contral over one’s own muscles is necessary in order perfectly to relax arm and shoulder muscles just before the adjustment and then to utilize a measured and determined quantity of force in a desired direction. To acquire this much practice is necessary—practice on the living subject. The desired end may be hastened, however, by acquiring the abstract property of muscular control or by developing control already gained.
Many different forms of exercise will aid in the acquisition of muscular control and the ability to relax and then to follow the relaxation with an instantaneous whiplike contraction in a given direction. The best of these is without doubt bag-punching. The movements employed with a punching-bag, especially the lateral quadruple movement with both elbows and both hands, tend to develop precisely the sort of control needed for correct adjusting. The beginner can do no better than to practice in this way, by which, it must be remembered, only a necessary property, and not by any means the exact movement, may be acquired.
The amount of force used in an adjustment varies so much in different spines and in different parts of the same98 spine that it is quite impossible to state any correct estimate of it in terms of physical units. In general the Cervicals move with least resistance, then the Dorsals, then the Lumbars, and finally the Sacrum and Ilia as hardest of all to displace or replace.
In developing additional force when it is found that the force first used on any vertebra has been insufficient to move it, remember this law: Work equals one-half Mass times the square of the Velocity. In other words, doubling the speed of the movement increases its effectiveness four-fold; tripling it, nine-fold.
The increase in force should never be effected by increasing the weight or pressure upon the patient’s body, for reasons which should be clear from a study of previous pages, but always by increasing the speed of the movement.
The names herein employed to indicate certain movements, each a well-defined method of procedure for the accomplishment of some special end, are the names or descriptive terms which seem to be in the most general use at this time. Few of these movements have arrived suddenly; most of them are the result of gradual growth and evolution: so with the terms by which they are known; they have gradually become a part of the common language of the profession. Usage sanctions them, though some of them are cumbersome, unwieldy, or entirely inappropriate.
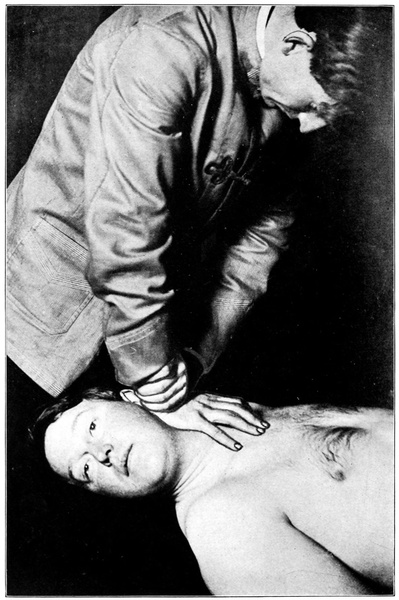
Fig. 7. Morikubo Move. For correction of a lateral and rotated Atlas (L. A.). Pisiform contact with anterior transverse.
A movement for the correction of a lateral and rotated Atlas, indicated for use only when the Atlas is recorded as R. A. or L. A. The position of the patient’s head renders the transverse process inaccessible unless it be anterior on the side from which adjustment is to be given.
Place two sections of the bifid bench together so as to secure the effect of a solid bench with an upward sloping front. Have patient lying on back with back of head resting firmly on bench, chin slightly uptilted. Then turn patient’s head so that it faces sidewise and rests flatly on the side of the least prominent transverse. This exposes the anterior transverse in front of the tendons of the sterno-mastoid muscle.
Stand leaning over head of bench and carefully place the pisiform bone of adjusting hand upon the tip of the transverse process, being careful to push aside the sterno-mastoid tendons if they interpose themselves between the pisiform and the process. The fingers of the adjusting hand extend downward toward the clavicle and rest lightly,100 very lightly, upon the patient’s neck. With the other hand firmly grip the wrist of the adjusting hand, fitting the pisiform of the upper hand into the hollow below the styloid process of the radius.
This is delivered straight downward toward the bench. It should be light and quick and the hand should not follow the process in its movement.
This movement is painful and should not be used if avoidable. When used it requires the utmost care and a careful measuring of force. Err, if at all, on the side of overcaution. The technic will be better understood after study of the more detailed description of “The Recoil”, since the position and use of hands, arms, and shoulders is much the same for both.
Indicated for rotation of a Cervical vertebra in which one transverse process is anterior to its normal position or more anterior than its fellow which may also be somewhat, though less, anterior.
As for the Morikubo Move place the patient in the dorsal recumbent posture with head resting on bench and chin uptilted. Turn patient’s face slightly away from the side of the selected anterior transverse and steady the head with the free hand while palpating.
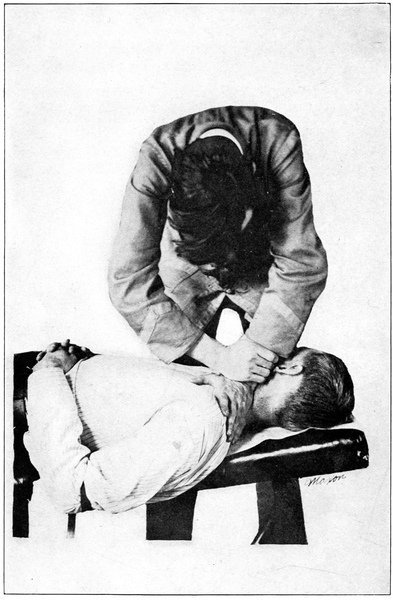
Palpate downward from the Atlas transverse along the posterior margin of the sterno-mastoid, dipping deeply into the neck and exploring with the tips of the first three fingers until the offending process is felt as a nodule of bone plainer to the touch than those above and below. Always reach across the neck to the selected transverse; if it be the right, stand on the patient’s left and use left hand for palpating and for contact hand as well.
Having found the process, gently move aside any tissues which tend to interpose between the finger and the bone, change hands so that the palpating hand is free and the other holds the contact spot clear of interposed tissue and plainly points it out, then place pisiform bone of contact hand gently but firmly against the front of the process so that a mass of bone is felt between the pisiform and the bench when downward pressure is made.
It will be noted here that the head is unstable and tends to rock with slight pressure or movement of the contact hand. Steady the head by placing the knee upon head of bench and against side of patient’s head, not roughly but so that the head cannot move further toward the adjuster.
Now reinforce the contact hand by gripping the wrist with the other, press slightly downward to tighten the contact and avoid slipping, and you are ready for
which is directed sharply downward toward the bench. This move rotates the vertebra around its vertical axis and puts a strain in a backward direction on the whole column at this point.
Care must be used, because the move at best is painful. It is easy to slip across the end of the transverse. Take every precaution to avoid imprisoning a muscle, nerve, or blood-vessel between the contact hand and the vertebra. Rightly used this move is valuable, perhaps most valuable of all anterior Cervical moves, but it requires nice judgment.
This movement differs from the preceding one in two important particulars; the contact hand must be so selected with relation to the side of vertebra adjusted that the fingers will extend upward toward the patient’s head, and the opposing hand supports the head instead of reinforcing the contact hand.
As for preceding move. The head will remain in this position only until the contact is made, after which it will be raised by the supporting hand until a tight contact is felt and the neck muscles drawn fairly taut.
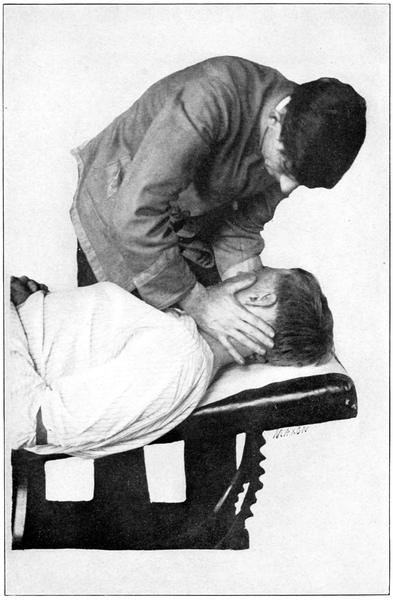
Palpate with left hand if standing on patient’s left to adjust a right, anterior subluxation. Find the offending103 anterior transverse, draw tissues away with middle finger of palpating hand, change to middle finger of free hand which marks and holds the point of contact. Now place (with care) the base of the little finger of the hand which was used for palpating, at a point just below the condyle of the last metacarpal and a little to the palmar side, in direct contact with the front of the transverse. The last finger will be flexed toward the radial side and a shallow depression thus left for the contact.
Hold contact lightly and slip the free hand under the patient’s head, which faces slightly toward the adjuster. Raise the head, bending the neck away from the adjusting hand and toward patient’s chest until it is felt that the contact is secure and that further movement would put the neck upon a strain. You are ready for
which is delivered entirely with contact hand, downward and toward the back of the neck. The delivery is difficult because the force arm is flexed at the elbow and the position awkward. Practice, however, will soon render one adept.
For rotated vertebrae which have one transverse anterior to the other, Cervicals only. This move gives a slightly less advantageous force angle than the preceding, but is less likely to be painful.
Place patient supine on bench so that his head extends beyond the end of bench and is supported by the upraised knee of the palpater. Stand at head of bench so as to face patient’s feet.
Differing from their use in the preceding moves the hands are so placed that the adjusting hand for a right, anterior subluxation will be right hand, for a left anterior the left hand. The opposite hand supports the head after contact is made.
Contact point on hand is second metacarpal at the end of the condyle, or second metacarpo-phalangeal joint. This is placed in front of the offending transverse, the head having been rotated away from that side and other tissues drawn carefully aside from the bone. The back of the hand is downward toward the clavicle, fingers semi-flexed on palm, thumb resting on jaw.
The following position is the correct one for supporting the head in all Cervical adjustments delivered in the above position of patient and adjuster.
Cup the supporting hand slightly and fit the patient’s ear into the cupped palm. Let fingers extend toward the base and back of the neck, the finger position varying according to the amount of rotation of the head so that the fingers are in all cases directly under the head weight. The wrist then flexes on the hand, and wrist and forearm are brought up across the patient’s forehead so that a force delivered from the opposite side cannot cause the head to roll or move upon the supporting hand. After placing both hands draw the head so that the chin is tilted upward until it is felt that contact is snug and tight. This supporting position is invaluable and much neglected by adjusters, who might save themselves much annoyance and many failures by its constant use. In the study of succeeding Cervical moves refer to this description frequently. We shall call it the Hook Support, because the arm and hand resemble a hook which grasps the under side of the head and curves over the upper.
This is delivered entirely with contact hand and in a direction as much posterior as can be achieved without slipping past the end of the process. If the head is sufficiently rotated away from the contact side the angle of force is better than with a straight lateral adjustment, which it somewhat resembles, but not so good for anteriors as either of the two preceding moves. It is chiefly useful when the other two fail.
To move an Atlas so disposed that its one side is posterior while the whole vertebra is laterally displaced in the same direction; to move, for instance, an Atlas R. P.
Have patient lying on back in position C with head projecting beyond bench and supported by adjuster’s knee.
Place the first three fingers of one hand under the most laterally prominent transverse so as to hold it firm, first placing the first finger carefully just behind and against the end of that transverse and then reinforcing it with the second and third fingers, slightly tensed, and resting their tips on the lamina close underneath the occipital bone.
Next place the other hand so that the thumb rests firmly upon the patient’s jaw and the first finger extends backward along the lower margin of the occipital bone.
To complete the position rotate the head gently toward the side of the laterally prominent Atlas, until it rests, face toward the side, and is supported by the three fingers of the one hand and the heel and wrist of the same hand. It will be noted that when the head is rotated the first finger of supporting hand slips to a position directly upon the tip of the transverse process and the other two take its place against the posterior aspect of the tip of the transverse. The Atlas now rests with its intertransverse line almost vertically upward from supporting fingers, which hold it against further rotation.
When the neck muscles have been thoroughly relaxed by slight and gentle movement, throw the upper elbow sharply away from your body, which has the effect of transmitting force through the thumb to the jaw and sharply rotating the head still further, loosening its articulation with the now firmly held Atlas. The condyloid joints thus loosened tend to settle into their proper relations, the weight of the head causing it to slip downward—laterally upon the Atlas.
This is really a movement of the head rather than of the Atlas and is an easy movement when practicable. It requires complete relaxation and will often fail. It is probable that many apparent Atlas subluxations are really subluxations of the head upon that bone which leave Atlas and Axis in normal relation. This move is most used to loosen the Atlas when it resists ordinary adjustments.
The principle involved in this and the three succeeding moves is the same. The contact is made with the end of the laterally prominent transverse process of a Cervical vertebra other than the Atlas, and the movement is directed entirely from side to side. It is to be used only for lateral and not for rotary or anterior or posterior subluxations, a point to108 be remembered as it is just as easy to produce as to correct subluxation with this move.
Have patient lying on back in position C, with head projecting beyond bench and supported by adjuster’s knee. Following a record previously made count downward to a subluxated vertebra and palpate both transverses with the two hands at once to find if one is prominent laterally, remembering that the record indicates merely the position of the spinous process.
Having found the laterally prominent transverse, place the tip of the finger of the corresponding hand on the spinous of the subluxated vertebra; that is, if a right subluxation, use right hand and if a left, use left hand. Then draw the hand around until the middle of the proximal phalanx of the first finger rests against the end of the transverse. The tip of the finger will be freed from the spinous by this movement.
Hold the adjusting hand tense, edgewise to the neck, fingers together and pointing downward. The thumb may rest against the patient’s jaw or may be free; the essential thing is the snug contact of the first finger against the transverse.
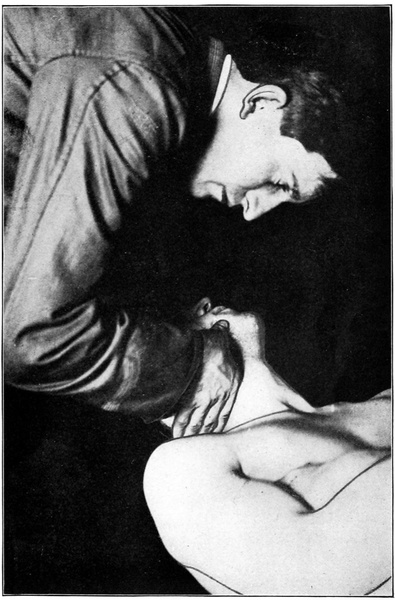
With the hand in position and the head supported by the Hook Support, bend the head laterally, keeping the face upward,109 until it is felt that further movement would strain the muscles.
Deliver the movement in a straight lateral direction, quickly and entirely with the contact hand.
For the Atlas only, and for straight lateral displacement of that vertebra.
Position of patient’s head and of supporting hand exactly as in using Break No. 1. Contact is made with the end of the Atlas transverse on the laterally prominent side. Contact point on hand is second metacarpo-phalangeal joint, or rather, the condyle of the second metacarpal.
As for Break No. 1.
Have patient sitting erect on bench or stool and stand before him. For a right subluxation use left hand and for a left, right hand. Contact point is the middle of the proximal phalanx of the first finger and the fingers reach backward and downward, thumb upward so as to be out of the way.
Force should be applied entirely with the contact hand to avoid the possibility that movement of the head may bring about movement of some other vertebra than the desired one. But in practice the force is usually divided between the head and the vertebra. The Hook Support cannot be used in this position.
The use of this position for the Break avoids the necessity for the patient to lie down again in a new position after having Dorsals and Lumbars adjusted. It is extremely convenient. But on the other hand it is undeniably harder for the patient to relax his muscles when sitting up with head flexed sidewise and a sense of lost equilibrium than when lying down. The Break No. 1 will be found the better for the average case.
Same as Break No. 3 except that adjuster stands behind patient and rests the thumb upon the base of the neck posteriorly while the fingers extend downward and forward toward the clavicle. As with No. 3, the supporting hand rests against the opposite side of the head and forces it sidewise to tighten the contact.
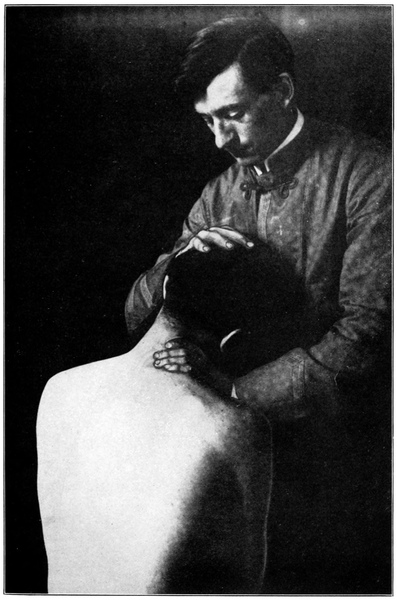
Properly, a quick lateral movement of contact hand while the head is firmly held by the opposing hand.
Note: “The Break” is unfortunately named and it would be well if some less suggestive term were generally substituted.
For the correction of rotation only, and usable in the Cervicals from 2 to 7 inclusive.
A study of the Cervical articulations will make it clear that if a force be applied laterally to the spinous process the probable result will be a rotation of the vertebra, which swings one articular process back from its fellow but leaves the other in close, but modified, contact. Thus the spinous process may appear to the left while the left articular process is fitted firmly against that of the adjacent vertebra, while those on the right are separated. Similar rotation, modified only by the difference in shape of the vertebrae, occurs in the Lumbar region.
A movement applied to the spinous process might correct this condition or might complicate it according to the manner of application. But the most direct line of force for correction is along a line which would pierce the separated articular processes almost in an antero-posterior direction. The Rotary approaches this very closely. It is a setting112 forward of the articular process against its fellow by applying a movement directly to the transverse process, which lies very close to the articular process.
The great safety of the movement lies in the fact that it is impossible with any reasonable amount of force to move the transverse process too far. If the vertebra is not subluxated so as to indicate this movement, gentle attempts to use it will fail. The deceptive bent spinous process may sometimes be detected in this way.
The chief objection to Rotary Nos. 1 and 2 is that the Dorsals and Lumbars cannot be adjusted in this position and the patient must rise from the bench and lie down again to have his Cervicals adjusted. This is obviated if No. 3 is used but the latter position fails to secure the perfect relaxation of muscles of Nos. 1 and 2, and is therefore recommended as an alternative only.
The commonest obstacle to the use of this move is the voluntary or involuntary contraction of the neck muscles. The Hook Support, q. v., will limit this resistance by affording a sense of perfect security to the patient. If muscles are contractured a slight “check” will be felt as the head reaches a certain degree of rotation, and beyond this point it will refuse to move though easily movable within the radius limited by the “check.” It is as if the head were held by an inelastic cord. It is best when contracture is present not to attempt moving the head too far but to deliver the movement with the muscles as much relaxed as possible.
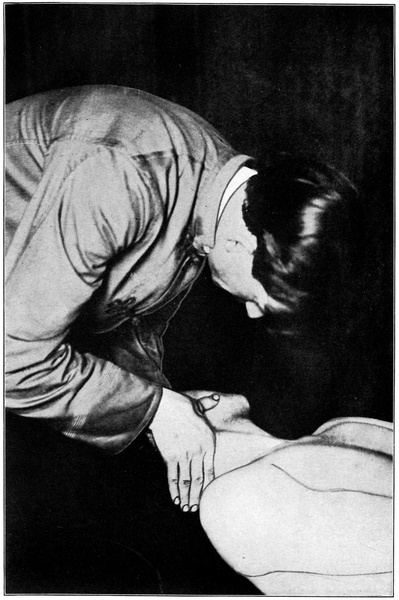
Place patient in position C as described under Technic of Palpation. Stand at head of bench with patient’s head supported by one knee and perhaps also by one hand. Palpate chiefly to discover the numbers of vertebrae, following a record previously made. Finish palpation with the tip of the first finger of either hand resting upon the spinous process of the vertebra to be adjusted.
Consider here which way the vertebra is to be moved; if toward the right use right hand and if toward the left use left hand for adjusting. Draw the adjusting hand straight around until the first finger, about the middle of the proximal phalanx, rests against and behind the transverse process.
It is important that the finger be drawn straight around, and not upward or downward, except with the second Cervical with which the finger may pass slightly upward to the transverse. To insure correct placing of finger let patient’s head be absolutely at rest, supported by the Hook Support with face turned slightly away from the adjusting hand. Reinforce contact finger with the other three fingers held close together behind it. The thumb may or may not be placed against patient’s jaw as desired, but one must be careful not to lose exact contact by drawing adjusting hand upward from a lower Cervical in an attempt to reach the jaw.
Meanwhile the other hand supports the head and holds its weight as described under the Hook Support, q. v.
Next, holding the first finger gently but firmly pressed against the transverse process, turn the head in the direction of the subluxation and away from the adjusting hand. That is, if the vertebra be subluxated to the right turn the face toward the right, the use of the terms “right” or “left” referring to the spinous process.
When the head is drawn around so that the vertebrae are thoroughly separated on the side toward which movement is to be directed, and the patient’s muscles are thoroughly relaxed though it is felt that further rotation of the head would put them upon a tension, give the movement. It consists in a quick throw of the adjusting hand, force transmitted from shoulder through an outward fling of the elbow, directed upward and inward against the transverse process. It replaces the articular process against its fellow, moving one vertebra, smoothly and easily.
All force should be delivered with contact hand. The hand moves through very little space. The principle of the movement is transmitted shock.
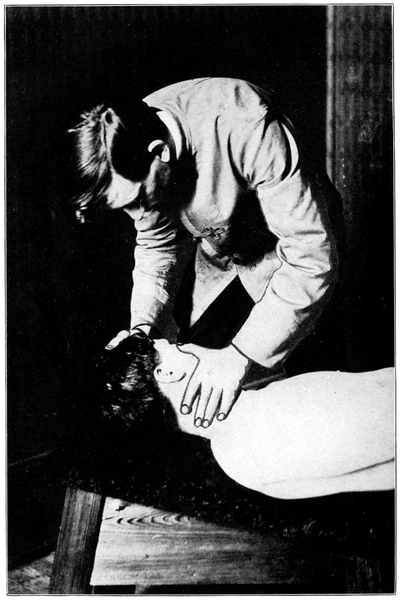
A transition in technic between No. 1 and No. 3.
Patient lies face upward on closed table, head resting upon forward section. Adjuster stands at side of patient, choosing the side according to the subluxation so as to face across the table in the direction toward which spinous process is to move. Palpation is difficult in this position on account of the increase in the curve of the Cervicals, so that it is best to follow a record previously made.
Having found the subluxation make contact as follows.
Reach across patient’s neck with right hand for a right subluxation or left hand for a left, and find spinous process. Then draw the middle finger straight around until the palmar surface of the middle finger just below the second joint fits snugly behind the transverse process. Place the other hand under the head and with both hands working together turn the head toward you, chin upraised, and draw the neck into a greater flexion until it is felt that contact is firm and close.
The movement is a quick drawing toward the adjuster of the second, or contact, finger, which has been, as it were, hooked over the transverse. The transverse is thus drawn116 sharply forward and the vertebra rotates around its vertical axis so that the spinous follows, or tends to follow, the transverse in the same arc of movement.
Patient sitting erect, both feet evenly on floor and hands not braced. Stand in front of the patient but to one side or the other as for Rotary No. 2. Use right hand for adjusting right subluxations and left hand for lefts.
As for No. 2, contact is with palmar surface of second finger but may be shifted to third finger for the lower vertebrae if desired. The thumb is usually placed on the mandible and aids the opposite hand, placed on the other side of the head, in turning and otherwise controlling the head.
Turn the head away from the adjusting hand until the neck muscles feel taut as a result of position and not of contraction. The movement then is given as a sharp jerk of the contact hand forward.
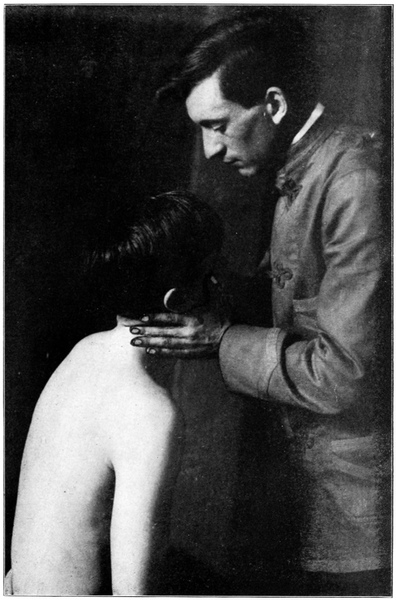
It is held that a vertebra often loses its proper relation with the vertebra below, and consequently with all the vertebrae,117 or the entire column of the spine below, without being disturbed in its relation to the one, or ones, above; that, in other words, the column may be divided into two sections by subluxation, the upper section set askew upon the lower. With this reasoning it would clearly be desirable to so adjust the spine as to move a given vertebra, and with it all vertebra above, so to speak, upon the vertebra below. To do this all vertebrae above the one to which force is applied must needs be firmly anchored to prevent strain between them.
Such a move has been devised by Bunn for Cervical use and is here described from the author’s few observations only. Further study may modify the technic somewhat.
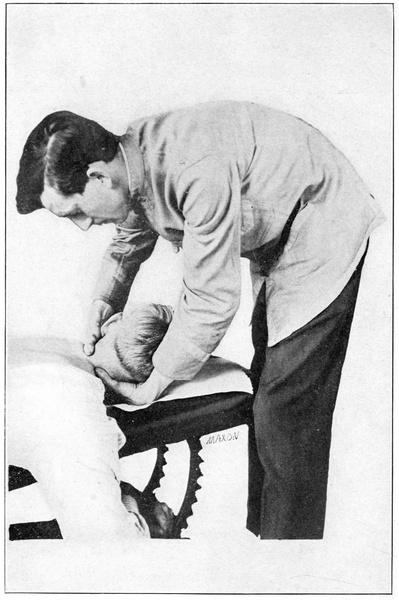
Patient is placed as for Dorsal and Lumbar adjustments in position B. Move is applied to rotated, postero-rotary, and antero-rotary subluxations and face turned toward side from which move is to be made. Adjuster, after palpation which discovers the vertebra to be moved and the direction of movement, stands at the head of table facing patient’s feet.
With the palms of both hands resting against the side of the neck and thumbs extended at right angles to hands, make contact with both thumbs on one vertebra as follows:
If vertebra is to be rotated toward patient’s left, place118 right thumb against spinous process on its left side and left thumb upon right transverse process from behind it. Press firmly with the palm and fingers of each hand against the vertebrae above, gripping around neck and base of skull so as to hold all parts together.
The move is delivered simultaneously with the two hands, forcing spinous process toward the right and transverse in an anterior direction. The head must be raised from the bench and wholly supported by the hands and the head turns with the vertebra.
A powerful comparatively easy move which has the advantage of wide applicability and of avoiding the change of posture of the patient which mars many Cervical moves.
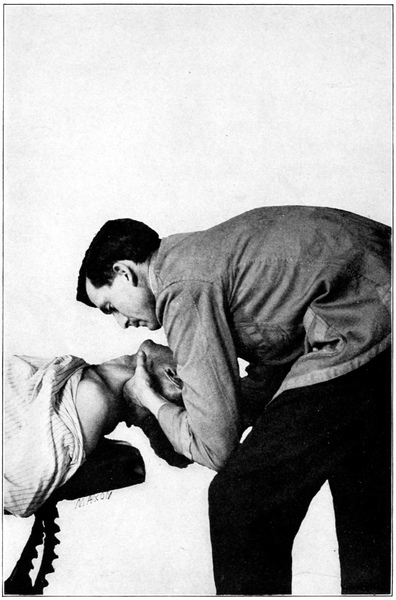
Same as for No. 1.
For a left subluxation to be moved toward the right, place the left thumb upon the right side of the spinous process so that it hooks over the spinous in position to draw or pull the spinous. Place right thumb against the end of119 the left transverse as much on the anterior side as possible so that it may exert a prying force in a posterior direction.
Simultaneous application of force with the thumbs tends to rotate the vertebra as does No. 1, but unlike No. 1 the tendency is to bring the vertebra out in a posterior direction instead of driving it more anteriorly.
This move is applied to rotated Cervicals which are anterior, more on one side than on the other.
For a posterior Cervical below the Atlas. The common and careless practice of moving such a vertebra with the Rotary, or the dangerous practice of using the Recoil may be avoided by this move and much better results obtained.
Patient in position C, head projecting well beyond bench so as to allow for a dropping backward of the head. Palpate as for the Rotary and hold palpating finger on tip of spinous process of posterior vertebra while contact is made.
Contact point is middle of radial surface of first phalanx of first finger and is placed against the tip of the spinous120 process, directly between it and the floor, as the patient lies. Hand is held rigid and edgewise, fingers together so that the contact finger is well supported.
Use the free hand to hold the head with the Hook Support, q. v. Turn the patient’s chin slightly away from the adjusting hand and drop the elbow of adjusting arm down until a straight line could pass through elbow, spinous process, and patient’s chin. It may be well to crouch and rest the elbow against one knee for solidity. Then allow the head to drop backward until chin is elevated and further backward flexion would strain the muscles. You are ready for the movement.
A quick throwing movement upward and inward, or toward patient’s chin. As nearly as may be the force should tend to pass along the spinous process in a direction exactly anterior to the (then) plane of the vertebra.
Note: Either hand may be used with this movement.
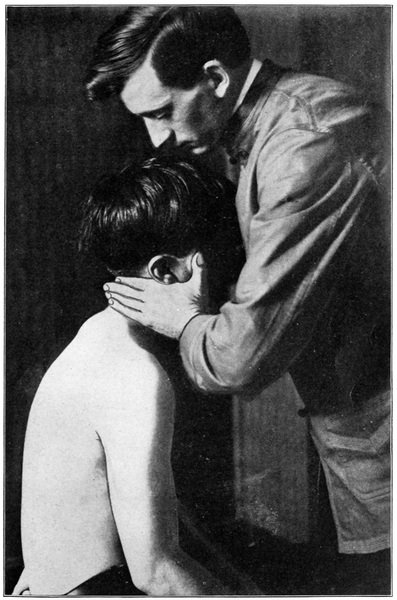
This is indicated for postero-rotary or postero-lateral subluxations. Its line of force is a bisector of the angle between the straight anterior and the straight lateral movement.
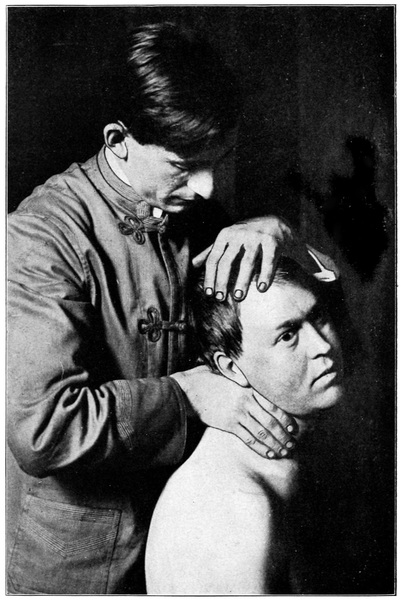
Fig. 18. A movement for Atlas when laterally displaced. Contact: metacarpo-phalangeal joint with end of prominent transverse.
There are two points of contact, both on the first finger, one (first secured) on the radial side of the second phalanx and the other on the radial side of the proximal phalanx. The first contact point is placed against the tip of the spinous, the other behind the transverse process.
Press slightly against the two processes with the finger so as to feel them plainly.
Hold the head with the Hook Support and turn the face away from the adjusting hand (right hand for a P. R., left hand for a P. L.). Drop elbow low and hold it well away from your body so that there appears an obtuse angle between wrist and forearm with the point of the angle toward you. Be careful of this point as the tendency is to make an angle with the point away from you—a weak position.
Drop head backward until firm resistance is felt.
Force is delivered in an antero-lateral direction as above described, entirely with adjusting hand.
For subluxations listed R or L but not Posterior and upon C 6, C 7, D 1, and D 2 only. This movement applies a lateral force to the spinous process so as to correct rotation122 of the vertebra, but I repeat that it is inappropriate for posterior or postero-lateral subluxations.
Patient lying in position B as for Dorsal adjustment. Find the subluxation by following the record and perceiving that the count assumed to be correct permits the subluxations to correspond to those recorded and that a vertebra in this region is R or L, R. A. or L. A., R. S. or L. S., R. I. or L. I. The laterality of the spinous process determines the next step.
For a right subluxation turn the face toward the left and use right hand for contact hand. For a left subluxation turn the face to the right and use left hand for contact hand.
Thumb of contact hand is placed upon and against the side of the spinous process so that it presses firmly. The thumb is extended almost at right angles to the hand which rests upon the patient’s shoulder with fingers extending, and gripping, over the clavicle. Be sure of the solidity of the position.
Next place the other hand upon the patient’s forehead and press the head backward, or toward the side of the contact hand, until the neck is well flexed and the tissues tightened between the now opposing hands.
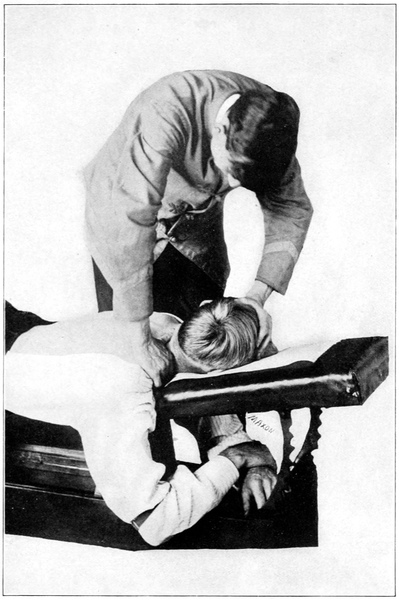
When this tightened condition is reached a quick decisive movement of both hands in opposite directions, but chiefly of the hand applied to the head, will secure an easy movement of the vertebra.
This move is a very valuable adaptation of the old crude and other dangerous “T. M.,” of which No. 2, below, is another, more like the original move but possessing several “safety” features.
The patient sits erect on a flat seat with both feet resting upon the floor as during palpation.
After careful palpation and selection of a vertebra to be adjusted in this way, stand directly behind the patient. If the vertebra is subluxated to the right use right hand for adjusting (or contact) hand, if to the left use left hand. Hold the hand so that the thumb is at right angles to the hand and tense and firm. Place the palmar surface of the end of the thumb against and upon the tip of the spinous process and grasp the neck firmly with the fingers, which extend over the base of the neck and toward the clavicle. The other hand is placed easily on the top of the head.
The completing of position after contact has been made is governed by two considerations; the need for relaxing the124 neck muscles and for so supporting the vertebrae above the contact that movement will take place only at the point of contact. If the neck muscles are contracted the movement is almost always defeated and should always be abandoned to avoid strain.
To secure the desired position ask the patient to relax his muscles and allow you to place his head as desired. If he seeks to place it himself the necessary muscular contraction on his part will defeat the movement. The movements of the head must be passive.
With thumb and remainder of adjusting hand properly placed, use the other hand upon the head as follows: First flex the head forward on the chest as far as possible, then rotate it slightly so that the face is turned a little toward adjusting hand. Then flex the head sidewise until a resisting pull of muscles indicates that they have been stretched taut. It is well during the third movement described to let the forearm swing down at right angles to the hand so that it presses firmly against the ends of all the Cervical transverses, distributing the force among them.
Or, after placing contact hand rest the elbow in the angle at the base of the neck and let the forearm extend upward along the side of the neck. Then flex the wrist until the hand will rest upon the patient’s head and perform the movements of the head as described above.
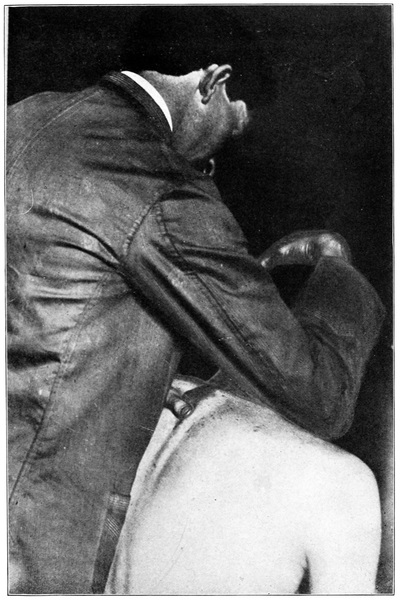
A quick, simultaneous movement of both hands in opposite directions, two-thirds of which is given with the hand125 which holds the head. The thumb in contact with the spinous process moves slightly inward toward the median line but its chief use is to hold the vertebra very firmly. To this end part of its force is directed forward against the shoulder and through the ball of the thumb.
Failure to place the head properly or in securing sufficient flexion of the neck before move is attempted are the chief causes of failure. Force must be delivered quickly and sharply and the best adjustment of this kind is usually the one in which the head and hands move through the least space.
This movement is obviously useful only for the correction of rotation, since the force is directed sidewise against the spinous process.
The “T. M.” was originally intended as a Cervical adjustment, but its greatest use is now from C 6 to D 2 inclusive. Above the sixth its use is questionable because of the possibility of moving more than one vertebra or some other than the one desired.
This movement is best given on bifid bench of the type commonly known to the profession. Place patient on forward section so that its rear edge rests just below the axilla; this may be ascertained by passing a hand under patient’s126 arm after he is in position, when the edge of the bench should be felt about an inch below the hanging arm. The thighs should rest on rear section so that the pubic symphysis is free of the bench. The semicircular pubic cut is an advantage in that it avoids injury without making necessary too great a suspension between sections.
Thus the abdomen and the lower part of the thorax are suspended between sections. Under them an abdominal support may be used but it must have the quality of elasticity in a high degree and must lie always below the plane of the other two sections or it will interfere with a perfect adjustment.
For adjustment of the last two Cervicals or any Dorsal down to the sixth, it is best to turn patient’s head toward the direction of the subluxation. This curves that section of the spine into an arc toward the convex side of which movement may be made more easily than toward the concave.
The patient’s hands may lie under the table, loosely, or may reach back and rest upon the buttocks, palm upward. Whichever position secures best relaxation is to be used in any case.
This movement may be used with the roll. (See Fig. 30 and p. 285.)
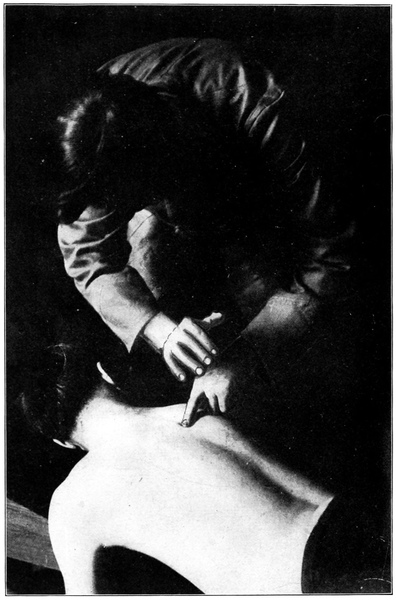
Stand on either side of patient, feet apart for base and poise. The direction of the feet and position of body will127 vary according to the direction of the adjustment, by the following two rules:
Rule 1. For movement of a vertebra away from the side on which you stand, place your arms and hands in such a position that the pisiform bone of adjusting hand, both elbows, and both shoulder joints (shoulders being dropped loosely forward) will fall in the same plane and that the plane of direction in which the vertebra is to be moved. In other words, let the force be applied in a line straight from your body through the vertebra. Always shift your feet to a proper position from which to direct the movement.
Rule 2. To move a vertebra toward the side on which you stand, step close to patient’s body and support yourself with one knee against the adjusting table at the most convenient point. Then place arms so that contact point, elbows, shoulders, and the mid-point of the body’s base, between the feet, are all in the same plane. This insures balance during and after the movement and is the attitude from which the greatest and most carefully measured force can be delivered.
It will be seen that the desire is always to deliver all force in one plane and thus avoid conflict of forces and waste or misdirection through the predominance of one force over the other, and to use both arms with equal facility in the move. There are at least a hundred ways to hinder this movement by varying the preliminary positions. And no one can know the real efficiency of the move who has not become instinctively adept at taking position.
Use of hands for palpation has been described. (P. 46.)
The palpating hand comes to rest with the middle finger on the spinous process of the vertebra to be adjusted. The heel of the hand is raised, the first and third fingers doubled back, and the heel lowered again. Now the middle finger alone is a slender pointer guiding to the contact point.
Place pisiform bone of other hand snugly against the process to be moved. The hand should rest in a slight arch, pisiform against spinous, fingers rigid and flexed on hand, last finger firmly anchored, or pressed into the flesh, to prevent slipping. (Fig. 22 shows the position.)
The anchoring fingers must always extend away from the adjuster. To turn the fingers back across the spine, in moving a vertebra toward you, is always an error, and the price is partial loss of use of one arm.
With the adjusting hand satisfactorily placed, grasp its wrist firmly with the other hand so that the pisiform of the supporting hand rests in the hollow between the wrist and the metacarpal bone of the extended thumb. By this contact force is driven directly through the chain of bones across the wrist and to the pisiform bone without spreading. In grasping the wrist let the thumb extend around the forearm in one direction and the four fingers in the other. Beware of gripping only with thumb and first finger in which case the edge of the supporting hand will rest on the back of the contact hand and spread the delivered force too widely.
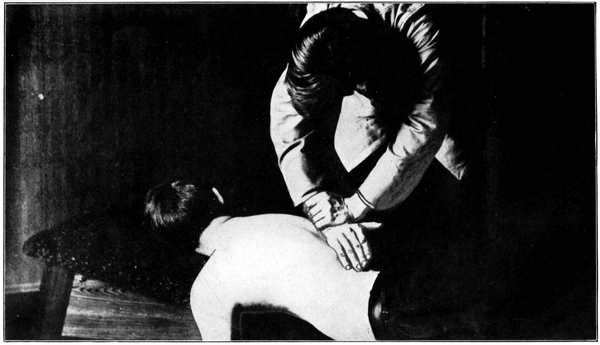
I have said, but have not sufficiently emphasized the command, that the shoulders must be dropped loosely forward. Let me add that just before the movement is given the head should be allowed to sag downward and the muscles to become relaxed. This movement given with stiff shoulders and upraised head becomes a push.
The desired movement is a throwing movement.
Force is released from both shoulders at once, concentrated at the same instant by a slight shifting forward of the elbows, and strikes the spinous process as one force, which is the resultant of the two meeting at the wrist of contact hand and being united there. The two arms use the contact hand as a passive instrument for driving the vertebra.
The objective point, the distance to which the movement is mentally thrown at the instant of delivery, should be the center of mass of the vertebra, varying according to the section of the spine.
The exact contact point of hand with vertebra varies. If the vertebra is to be moved toward the right the pisiform rests against (not upon) the left side of the spinous; if toward the left and inferior, against the right side and just above, in the notch between it and the next superior process. The rule is to so place hand that the spinous process is between130 the pisiform and the direction to which movement is given.
On the hand the contact may be said to vary, according to the direction of subluxation and position of adjuster, so as to describe a circle around the pisiform in the course of the various changes of position necessary to the use of this movement. No error could be greater than to attempt to use always the same face of the pisiform and to adapt the position of hands and arms to this end, when any face or aspect of the little bone is equally good with any other.
When standing on patient’s right use left hand for palpating hand and right hand for contact with the vertebra, using left hand again to grip and reinforce the contact hand. Exception to this is made by introducing an extra change of hands with C 6, or 7, D 1, L 4 or 5, and Sacrum. The change is necessitated by the insecurity of the usual position or the fact that it cramps the wrist of contact hand. To make the change: palpate as usual, hold subluxation with second finger of palpating hand, substitute second finger of other hand and withdraw palpating hand, which is then free to make the contact.
When standing on left side exactly reverse the use of hands. Palpate with the same hand which would be used if patient were sitting. Introduce no unnecessary move into the placing of the hands. This will be found to produce better results than any other technic for this portion of the move.
In using this movement it is perhaps best to deliver nearly equal force with both hands; certainly whatever forces are released by the arms should be simultaneous. It is possible, however, to allow one arm to preponderate in the movement without marring its efficiency, but the amateur adjuster will do well to balance his forces at first.
Speed is a prime essential. By its employment a very ordinary amount of muscular strength can be made to accomplish a large amount of work and very difficult adjustments may be accomplished.
Concentration of mind at the instant of adjustment, so as to secure muscular control and perfect co-ordination of the two arms as well as to direct and concentrate the forces used at a given and strictly limited area, is also essential.
For ordinary adjustments of Dorsal or Lumbar subluxations, excepting the middle four Dorsals, for breaking ankyloses by repeated applications of force, and for overcoming muscular resistance in patients who are unable to relax at all, this form or style of adjusting is probably the best. It is most useful in the Dorsals. In many instances Lumbar vertebrae will move better by application of a slightly slower force, especially if a roll is used. The Recoil may be used with the roll.
While it is easily possible to move any Cervical in this way, making no change in the technic except to use the ulnar side of the fifth metacarpal bone for the contact instead of the pisiform, it is inadvisable in most cases above the sixth, and in some instances absolutely unpardonable. The shock to the nervous system and the danger of moving two or more vertebrae or of subluxating a normal one are too great. In at least one instance hemiplegia instantly followed the use of this move on the Axis, and headaches and nerve exhaustion are frequent sequelae.
For these reasons it is probably best never to use “The Recoil” above the sixth Cervical. For every form of subluxation there is an easier and safer mode of correction.
This has been called “The Recoil” because of a belief that if force be applied to a vertebra in the form of a very rapidly transmitted shock the vertebra will rebound to the shock and settle in its normal position, the intelligence within the body utilizing the force thus blindly applied to bring about this result.
This belief is erroneous. First the vertebra and all surrounding tissues are misshapen to fit their abnormal position and relation and this shape gives them a tendency, if rapidly loosened, to settle into the old abnormal position. Second, there is no such conscious intelligence which has power to replace a subluxated vertebra. If this supposition were correct, then the Innate Intelligence would do well to utilize133 those jars and shocks which ordinarily produce subluxation to bring about normality and keep the spine perfectly aligned.
There is no such internal rebound or recoil as stated above. The chief value of the movement lies in its speed, according to principles equally applicable to other moves, and in accord with the Law of Momentum.
This movement as described above contains many essential principles which follow Parker and Palmer, developers of “The Recoil,” but the technic is considerably modified to suit the author’s own views. It cannot be claimed, therefore, that this is “The Recoil” as now taught by Palmer, since the chief stress is here laid upon the movement of the vertebra in a predetermined direction and not upon the withdrawal of the hands to let “Innate” do the work. The name “Recoil” is really inappropriate for the move as described.
A movement for the adjustment of posterior, postero-superior, or postero-inferior subluxations in the Dorsal region (except middle four) and in the Lumbar. May also be used for postero-laterals when laterality is very slight. Given with patient in position B. Contact point, heel of hand with spinous process.
By the “heel of the hand” is here meant the depression between the scaphoid and pisiform bones. This hollow forms a natural receiver for a spinous process and thus avoids lateral slipping.
The four fingers of adjusting hand are spread out and anchored upon the patient’s body. The wrist is held at a right angle to hand and the arm straightened, the elbow being outrotated until it “locks,” that is until it will move no farther. The other hand grasps the wrist of the adjusting hand.
The rule is to use the right hand for adjusting hand if standing on patient’s right and palpating with left, or to use left hand if on left side and palpating with right. The fingers are to be directed toward the patient’s feet. Exception to this rule is made with the last two Lumbars, where it is more convenient to change hands and direct the fingers toward the head.
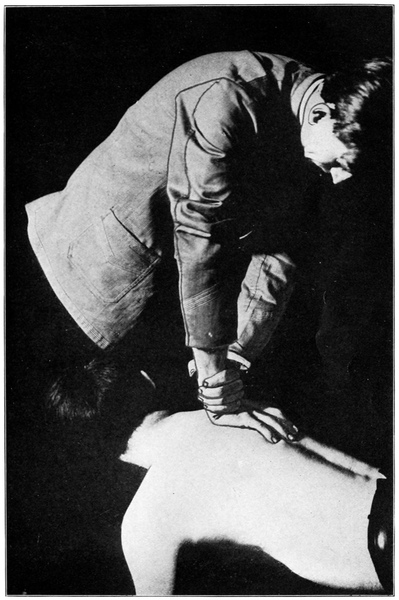
This is given almost entirely with adjusting arm; that is, with the arm whose hand is in contact with the vertebra. The supporting hand serves merely to guide the force to a definite point as if a straight rod were working through a fixed circlet. Indeed, the force in this movement is delivered135 almost straight down from the shoulder. Shoulder should be dropped well out of its socket so as to secure play for a sudden downward movement without raising the hand from its contact. If the shoulder is stiff or the head of the humerus remains in the glenoid cavity the movement cannot be properly given without raising the hand. Movement is quick, sharp, and deep, i. e., directed to the center of mass of the vertebra.
It may be directed straight toward floor to correct a posterior, inclined slightly toward the head or feet to correct approximation, or—as some aver—slightly sidewise to correct a mild degree of rotation.
An adjustment to be used only in the Dorsals from fourth to ninth inclusive, for posterior or postero-rotary subluxations. It is probably best to use this movement only for straight posterior subluxations and to apply either the Pisiform Single Transverse or the Two Finger Double Transverse to the rotary displacements in this region.
Both pisiform bones, each upon a transverse process and both upon the same vertebra.
With patient in position B and the adjuster standing upon his left the contact should be made by the following exact method. Palpate with right hand, which comes to rest upon the spinous process of the subluxated vertebra.136 Note if it be P. R. or P. L., because this fact will govern the next movement. Let the first finger of palpating hand reach outward about one inch and upward to a point opposite the tip of the next superior spinous process, which point will approximate the position of the transverse. This first upon the side of the posterior transverse, which will be the right with a left subluxation or the left with a right one. Let second and third fingers, now abandoning the spinous, follow the first and rest over the assumed position of the transverse.
Now palpate with a deep, limited, massage movement until the club-shaped extremity of the transverse is felt under the middle finger. Hold this point with the middle finger, drawing away the other two, and guide the free hand to an exact contact upon the transverse. Thus if standing on the left, as predicated, the left hand will be first to make contact and with the most posterior transverse, with which most exact contact is necessary.
With pisiform placed, let the fingers extend away from your body; if on the side of the spine opposite you, let them extend downward so as to follow the curve of the rib and to be anchored upon the rib connected with the transverse of contact; if on the same side, let fingers extend downward parallel with the column.
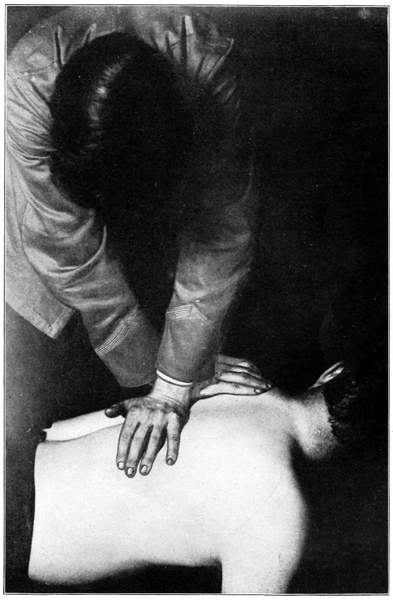
Now—still using the original palpating hand—palpate on the other side from the first contact until the other transverse is discovered. Mark its tip with a quick, deep pressure and a sharp withdrawal of the fingers, so that a spot137 of anaemia appears momentarily. Carefully place the pisiform of the palpating hand in contact, guided by the anaemic spot. If this second contact is on the side on which you stand the fingers will be toward the head; if on the opposite side, they will follow the rib curve outward and downward.
Re-read the above directions carefully. It will be seen that the technic is quite free from unnecessary movements.
The two hands are now placed almost exactly at right angles to each other, arched fingers anchored to prevent slipping.
If you stand on the patient’s right the use of hands is, of course, exactly reversed, the left hand being palpating hand, and making the first contact.
When hands are in position and adjuster standing so as to face directly across the spine, the arms are rotated outward until the elbows “lock.” The adjuster leans over so as to have shoulders directly over the spine, draws the body back from the shoulder girdle to secure freest play in the shoulder joints, and drops head loosely between the shoulders so as to relax the trapezius and prevent any checking of the force.
Directly downward from the shoulders through straight, stiff arms. The force is delivered separately with the two arms and yet simultaneously. If the vertebra is straight138 posterior, equal force must be applied on the two sides; if it is posterior and slightly rotated (P. R. or P. L.), most force must be applied to the more posterior transverse.
Considerable practice and looseness of shoulder are required to use this movement properly. It is a regrettable fact that few adjusters do use it correctly, most of them giving a thrust instead of a transmitted shock.
This modification of the pisiform double transverse move is here described because of its popularity rather than because the author wishes to recommend it. The position is the same as for No. 1, and the uses also, except that it tends to correct postero-inferior subluxations and is not at all adapted for use with superiors.
Both pisiforms below the two transverses (caudad). After palpation which discloses the posterior transverse the hands are placed as follows: Palpating hand rests always on the side of the spine next the operator; opposite hand crosses the spine. Both are slanted upward so that the fingers point toward the head with the axes of the hand slightly diverging above. The wrists are thus crossed in such a way as to force the forearms to be somewhat flexed on the arms and to slant away from the wrists at an obtuse angle. This with the contact below the transverses, renders it impossible not to force the vertebra in an upward (superior) direction when movement is given.
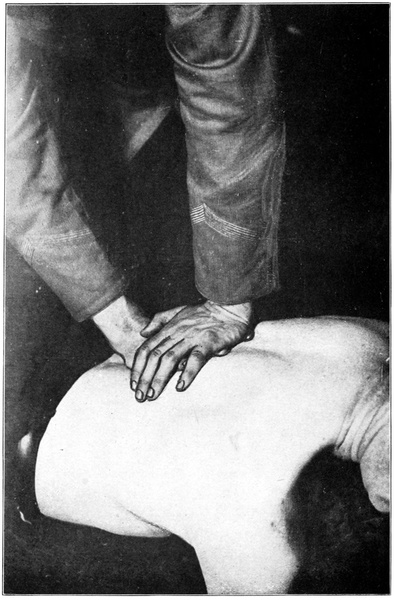
A comparatively slow thrusting movement, which tends to spring the spine. The merit of this method lies in its comparative painlessness. Its technic is not attractive.
A movement for posterior or postero-rotary displacements from fourth to ninth Dorsal inclusive. It serves the same purpose as the Pisiform Double Transverse but is less painful and often easier of delivery. The palmar surface of the fingers, with the flesh of the patient’s back, make a compound cushion which acts as a shock-absorber.
The usual downward gliding movement of left hand if standing on right or of right hand if standing on left will serve for the discovery of the vertebra listed for adjustment. The gliding hand stops with the second finger indicating the spinous process. The first finger reaches upward and outward to the assumed location of the transverse on the side nearest the adjuster; then the second finger reaches to a similar point on the other side, both fingers pointing toward patient’s head. Now the fingers are rolled a little to make sure that they are in contact with the ends of the transverse, the palmar surface of the tip of each finger being the proper contact point. The heel of the contact hand rests near, but not on, the surface of the body over the midspinal line.
The ulnar edge of the free hand is now placed across the tips of the two contact fingers so that it rests directly above the ends of the transverses but separated from them by the finger tips. The upper arm is then straightened and the elbow outrotated until it locks firmly so that the arm makes a straight line directly above the transverses. The body is drawn away from the shoulder girdle, pulling the head of the humerus out of its socket as far as possible to allow free play, for all force is to be given by this straight arm.
If the subluxation is a straight posterior the force is driven directly downward so as to be distributed equally to the two contact points. If it be a postero-rotary, most force is directed to the more prominent (posterior) transverse. Force should be delivered quickly, keeping in mind the principle of transmitted shock.
Contrary to the general belief, as much force can be developed with this move as is needful for any ordinary adjustment. The fact that it is often recommended for use with children or with sensitive or frail patients has led to the belief that it is a relatively ineffective move, whereas its value in such cases lies only in the fact that it inflicts less pain than some others.
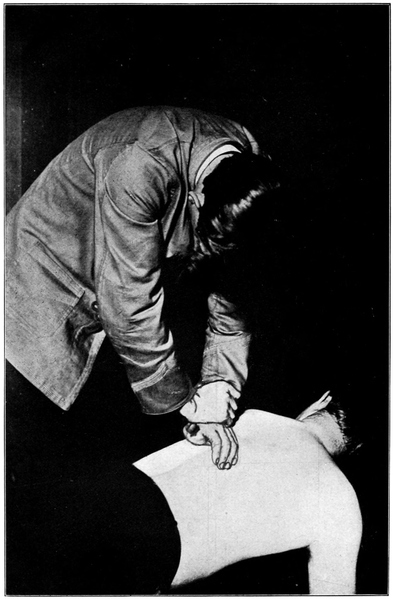
Like the movement just described, this adjustment may be used in the Dorsals from fourth to ninth inclusive. It should be limited to those subluxations which are rotated without being posterior. In such an instance the spinous process appears to be laterally displaced without being posterior, or may appear slightly anterior because it is describing an arc about a fixed center of rotation in the body of the vertebra. One transverse process appears anterior and the other posterior to the line of their fellows.
Palpate as for the Recoil and use the same adjusting hand as in that movement, i. e., right hand if standing on right side and palpating with left, or left hand if standing on left and palpating with right. When the palpating fingers have discovered the subluxated spinous process, the first finger seeks a point even with the tip of the next superior spinous process and about an inch to the side on which is the posterior (prominent) transverse. The second and third fingers follow and, dipping inward with a rolling or massage motion, discover the end of the transverse.
Now the adjusting hand is placed with its pisiform resting directly upon the blunt end of the transverse. If the contact is on the same side of the spine with the adjuster the fingers of adjusting hand extend across the spine and142 are anchored on the other side, the hand arching sharply and fingers extending somewhat downward. If contact is on opposite side of spine the fingers follow the rib curve downward and outward and are similarly anchored. In every case the fingers should extend away from, and never toward, the adjuster’s body. To violate this rule renders one arm almost useless through its position.
At this juncture the palpating hand becomes a reinforcing hand, to grip the wrist of the other and to aid in the movement.
The force is directed in a straight anterior direction, quickly and decisively, as if a spinous process were the lever used. Remember that contact must always be made with the posterior transverse. To drive this anterior is to rotate the vertebra around its vertical axis and to bring the spinous process toward the median line, while the opposite, and more anterior, transverse becomes more posterior, as it should be.
For rotated first or second Dorsals with which, for any reason, the “T. M.” fails. This move involves a use of the head as a lever, as does the “T. M.” No. 2. Inadvisable unless the posterior transverse of the rotated vertebra can be143 palpated—but often used in cheerful disregard of this detail by those sublimely capable adjusters who do not need to find a vertebra before moving it.
Palpate as for No. 1 above. Very deep palpation will be necessary because the spinous process here is nearly horizontal to the body and the transverse is very deeply placed, overlaid with heavy muscles.
When process is found place pisiform bone of free hand upon it, pressing the muscles aside as much as possible to avoid bruising and resting a considerable amount of weight upon the contact hand. Fingers of contact hand may extend across the spine or downward and parallel with the spine. Or, the hands may be changed so that the palpating hand becomes the contact hand and is placed with the fingers gripped over the base of the neck toward the clavicle.
The free hand is now placed upon the forehead and the head, which faces toward the contact hand, is flexed backward until the muscles seem taut.
Is a quick, but fairly gentle, movement of both hands together, so that the head is rocked still further backward at the instant an anteriorly directed force is applied to the144 prominent transverse. The result is rotation of the vertebra—unless there be a loose articulation in the Cervicals which gives way under the force applied to the head.
This movement has various names. The name “Point 2 Contact” is handed down from the days when Palmer used three contact points and three moves and designated the middle of the ulnar side of the fifth metacarpal bone as “Point 2.” The name “Edge Contact” was applied later, during the improvements in its technic when the hooking of the thumbs stiffened its efficiency and made it very valuable. It has since been rediscovered (though in constant use) and re-named “Knife Move.”
A movement which uses the spinous process as a lever and is applicable to D 2, 3, or 4, and to any Dorsal or Lumbar from D 8 down, when posterior, postero-superior, or postero-inferior. It does not correct rotation except insofar as the shape of articular processes may aid an anteriorly directed move in rotating the vertebra.
Some Chiropractors have used the Edge Contact in the Cervicals but this is always improper, as it is practically145 impossible in some, and difficult in all, cases to cover only one spinous process when the head is resting on its side.
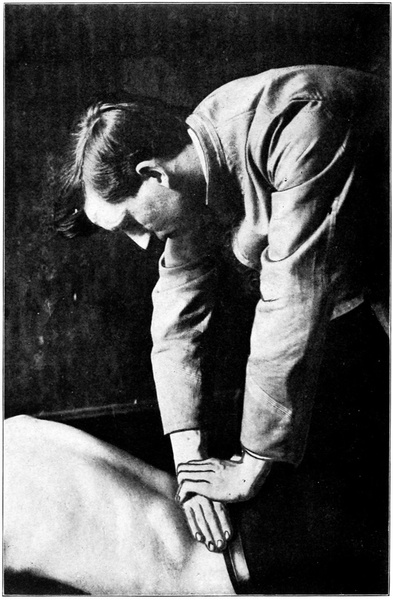
Same as for Recoil or Heel Contact, q. v.
Using the same adjusting hand as for the Heel Contact, place the middle of the ulnar edge of the fifth metacarpal bone in contact with the spinous process. If the vertebra be superior, place the edge of hand above, if inferior, place the hand below. This contact is especially good for S or I vertebrae.
The fingers of adjusting hand cross the spine at a right angle to its long axis. The back of hand will be toward patient’s head except in adjusting the last two Lumbars, with which a change of hands is made necessary by the upward slant of the lower half of the Lumbar curve.
The palpating hand now grips the adjusting hand so that the fingers of the upper hand, held close together, press against and reinforce the lower on its dorsum and just above the contact point. The thumbs are hooked together as shown in Fig. 27, so that the hands may be stiffened and their tendency to roll avoided.
The elbows are outrotated and locked as in the Pisiform Double Transverse Move and both shoulders are loosened.
This is chiefly delivered with the upper arm, using upper hand to drive the lower. Force should be quickly delivered when patient is relaxed. The direction of force should be determined by the direction of subluxation and by the slant of the spinous process. Thus, when patient lies prone upon a bifid bench and sways downward against a lax abdominal support, the spinous processes of the lower dorsal make an acute angle with the plane of the floor. If one be superior, contact above it and force driven straight toward the floor will tend to correct the subluxation. There is a slightly different force angle for every subluxation correctable by this move.
This move is less painful than the pisiform contact and may often be used to advantage, especially in the Lumbar region.
For the correction of a rotated Lumbar. Best used on second and third. This movement should never be attempted unless the transverse process can be palpated. Lumbar transverses are sometimes short or fragile, and unless they can be distinctly felt no force should be applied where they are believed to lie.
Pisiform bone with posterior transverse.
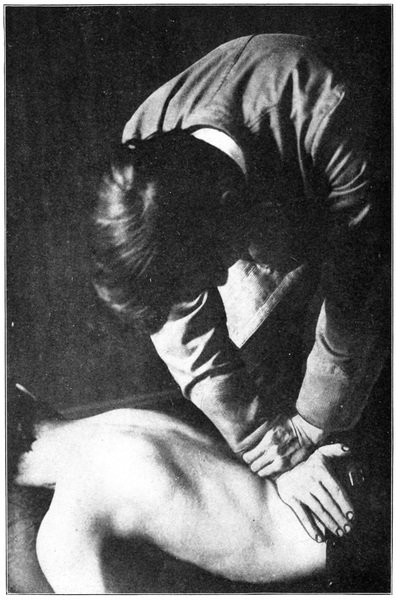
Palpating as if for other movements, pause with the second finger of palpating hand indicating the spinous process of the vertebra to be moved. Note that if the spinous process be to the right of the median line the left transverse will be posterior, if to the left, the right transverse.
The transverse may then be found as in the Dorsals; it should lie even with the interspace above the spinous process, deeply overlaid with strong muscles. When the transverse has been located by a deep, probing movement of the fingers, place adjusting hand, pisiform on transverse, close to the spinous process for greater solidity and fingers extending downward and outward from the midspinal line parallel with the lower rib curve.
If the adjuster stands on the side of the patient opposite to the transverse to be moved the hand opposite the palpating hand becomes the contact hand, as in other moves. But if the posterior transverse is on the same side with the adjuster, a change of hands is made and the palpating hand becomes contact hand. To accomplish this the adjuster must turn and face away from the patient with arm extended straight downward to the contact. After contact is made the remaining hand reinforces the adjusting hand by gripping the wrist.
In making the contact press downward, deeply and firmly, so as to crowd the muscles aside and place the pisiform148 directly upon the transverse. Movement is given after the patient’s body has been swung downward for a considerable distance, and is sharp and decisive, directed straight toward the floor.
A movement sometimes applied to posterior or postero-rotary Lumbars.
From the spinous, find first the more posterior transverse and make contact with it, since most force must be directed there. Stand facing patient’s head and place right hand on right transverse and left hand on left.
Contact point in this move is the tuberosity of the scaphoid with the posterior surface of the transverse. Fingers curve away from median line so as to avoid the rib curve.
After heavy, steady pressure downward, force is delivered with a quick, throwing movement, most force on the posterior side.
Upon the theory that when two forces are simultaneously applied, the one to drive some vertebra cephalad (by its spinous process) and the other to drive some lower vertebra caudad, the intervening vertebrae tend, if anterior, to be149 drawn outward or toward a more posterior position, this move is predicated.
The author does not believe that it accomplishes its purpose, but will briefly describe it for the benefit of those who do.
Patient is placed over a roll which rests under the thighs so as to flex thighs and pelvis on the Lumbar spine, or an adjustable table is so tilted, both sections sloping downward from the middle, as to accomplish the same result.
The usual method, if only a single vertebra is anterior, is to make contact with the vertebrae immediately adjacent, crossing the hands and having fingers of upper hand pointing toward head and of lower hand toward Sacrum. But some adjusters use this move differently, making contact with Sacrum and with the mid-dorsal region in general and applying a slow force with both hands. Contact is with heel of hand upon spinous process.
The adjustment of the comparatively fixed sacrum is difficult at best and requires a very considerable force, violently applied. It is probable that nine-tenths of all attempts to move sacra fail. In children, when sacrum does not articulate properly with the ilia, and in adults in whom the sacrum has been loosened by trauma and remains in150 an abnormal relation to surrounding structures, it can be moved.
The sacrum is described as being posterior at the base or at the apex, and its axis for rotation is believed to be a transverse line through the sacroiliac articulations. Force for its adjustment is applied at right angles to the curve of the sacrum at the point of contact. The best contact is with the heel of the hand against a part of the sacrum, the wrist of the adjusting hand being gripped and reinforced by the other hand. If standing on patient’s left, the right hand becomes adjusting hand for sacrum as for the last two Lumbars, if on the right, the left hand.
Another contact is with the pisiform and adjacent soft part of hand upon the sacral base, the pisiform hooking against the first sacral spinous process.
Do not mistake an anterior fifth Lumbar for a posterior sacral base. Discriminate between iliac and sacral subluxations by noting that with the latter both sacroiliac articulations, and with the former only one seems abnormal.
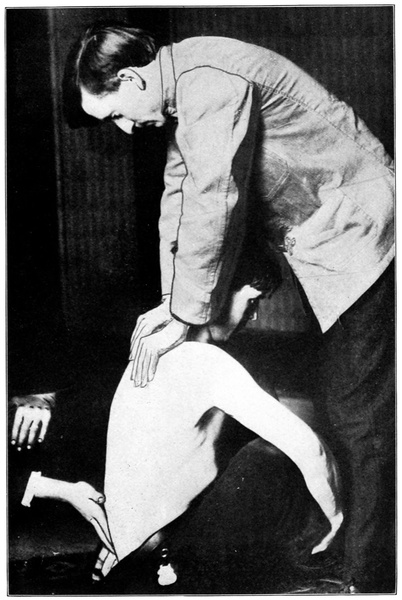
With patient sitting erect on flat surface, feet on floor, stand behind and examine both sacroiliac articulations at once with the palmar surfaces of the fingers of both hands. If the two articulations are similar in every line neither ilium is subluxated, though the sacrum may be rotated on151 its transverse axis between the ilia, so as to be posterior or anterior at base or apex.
But no examination of the ilia is complete without investigating also the lumbosacral articulation. It sometimes happens that though the first sacral spinous process naturally completes the lumbar curve and there is no lumbosacral subluxation the crests of both ilia appear much posterior to their normal relation to the upper part of sacrum: this is a double iliac displacement.
Usually the ilia are both normally articulated; this is one of the most difficult joints to weaken and is seldom affected except by the most extreme force. When iliac subluxation exists one side is affected alone nine times out of ten. The tenth case may show double subluxation.
Nine-tenths of the so-called “iliac adjustments” are quite amusingly ineffective. The force required really to move an ileum (save in joint disease or in children) is tremendous and not to be commanded by the ordinary adjuster. The light jars applied as a routine procedure by so many Chiropractors are in reality nothing more than single percussion strokes which stimulate the sacral nerves.
Place patient in position B and apply the hands to a posterior ilium as to a posterior sacrum, making contact with the most prominent portion of crest or posterior border and driving in a direction which would represent a part of the circumference of a circle of which the transverse sacral152 axis of rotation touches the center, or the center of fixation in the sacroiliac joint.
Place patient on an angle table, i. e., one which rises in the center and slopes away toward either end. Separate the thighs slightly, patient lying face down, and insert the rubber-covered second finger, palmar surface upward, very carefully into the rectum. The tip of the coccyx may then be felt and its movability and position determined. Unless it is immovably fixed in an abnormal position it should not be molested; the movable coccyx responds to mere muscle tension by changes of position and cannot act as a primary cause of nerve impingement.
Usually this examination will be rendered unnecessary by the external palpation which may disclose the movability of the coccyx and at once render further exploration superfluous.
When the coccyx is anteriorly subluxated and ankylosed in that position it may be a factor in producing constipation, hemorrhoids, etc., but its influence in other diseases, especially of the nervous system, has been greatly overrated by those who have not yet fully accepted the doctrine that nerve impingement is the primary cause of all disease.
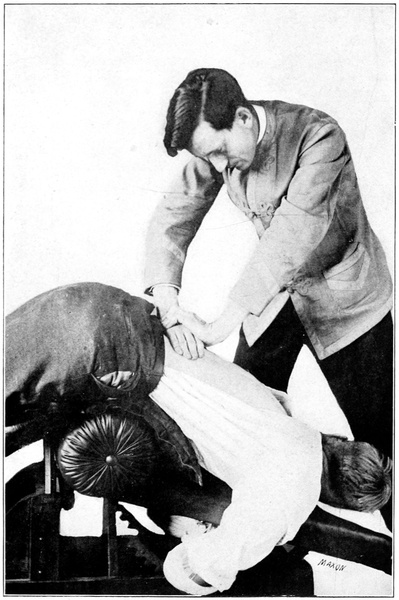
When it has been decided that the coccyx must be moved, the position and use of hand is the same as for the153 palpation. The finger hooks under the tip of the coccyx, draws upon it until a tight contact is secured and then jerks sharply backward upon it with a view to its abrupt fracture. No mitigation of the jerk in the hope of previously loosening or gradually replacing the bone is of value for osseous tissue must be broken before any movement may take place.
This movement is painful and the region of the newly fractured coccyx may remain sore for a period ranging from a few days to several weeks. It is wise to warn the patient of the facts before proceeding.
The fractured coccyx may be absorbed, or may be reankylosed in a proper position or in a new abnormal position, or may remain loose and movable.
We have previously discussed in detail the nature and discovery of curvatures. A few words should be said here about their correction.
If the sole object of the adjustment is to correct the curvature it is best to select for adjustment those vertebrae which are most subluxated in the direction of the curvature. According to the length of the curvature a series of from two to six, separated by some distance, are chosen. These are adjusted until they cease to be the most prominent ones in the curvature and then others, then most prominent, are chosen and adjusted until they in turn cease to be most prominent. In this way the curvature may eventually be154 straightened, or nearly so. It is doubtful if any curvature can be absolutely eradicated, although it may be straightened until unnoticeable except by the expert.
To overcome a curvature it may be necessary to break every rule which governs ordinary adjusting and to invent new ways of placing the hands or of delivering force. No two require exactly the same measures and he is most successful with curvatures who is most adaptable to changing conditions.
One rule may be safely laid down. Do not alternate from day to day, loosening at the same time many vertebrae, but choose the ones most in need of adjustment and follow your choice as long as it is indicated. The chief vertebra is nearly always the one at the angle or point of the curvature.
The sharp, angular curve of Potts’ Disease, involving two or three vertebrae, should warn against adjustment, usually, since in this disease the vertebrae are fragile and easily fractured. If a case has not progressed too far a cure may be effected, but great caution in taking such cases must be exercised. Every Chiropractor should be well informed on the diagnosis of Potts’ Disease, or spinal caries.
Many months are usually required for the straightening of a curvature—how many can scarcely be estimated in advance of the experiment with any case. Often the case which seems simplest requires the longer time, while a very pronounced curvature, as in some cases of rachitis, may yield in a few months.
The selection of the move with which to correct each subluxation depends upon the adjuster’s concept of the kind and direction of the subluxation and of the mechanics of the different corrective moves in his repertoire. The move used should be one in which the application of force is exactly along opposite lines to the lines of force which originally produced the subluxation.
Omitting involved explanations as to the elements of each displacement and the manner of change in bone, muscle, ligament, cartilage, etc., and presupposing a comprehension of the principles of each adjustment named, there follows here a list of possible subluxations of each vertebra in turn, from Atlas down, with a simple statement of the RIGHT MOVE for that subluxation.
In each instance there are other moves than the one listed which would move the vertebra and some which would partially correct it, but none which would quite so definitely tend to correct the displacement. Unfortunately it is not a fact that every movement of a vertebra is an adjustment. If this were true subluxations would not exist, because they could never have been produced. Too often the adjuster uses a move because it is easy, because its use has become habitual with him, rather than because it is indicated by the conditions of the case—then blames Chiropractic because his results are negative or bad.
The move which is suited to a certain kind of subluxation156 of one vertebra may be quite out of place with another, in a different part of the spine. Thus the Recoil is quite proper for a posterior Lumbar and is contraindicated with a posterior middle Dorsal.
If all vertebrae were shaped exactly alike, if all were equal in size, if subluxation were possible only in one direction, then one method of adjustment would be quite sufficient. Diversity of technic is demanded, but a discriminating diversity, with a good reason for every move used.
| First Cervical | |
| Subluxation. | Adjustment. |
| Right—R. | Break, or straight lateral. |
| Right, posterior—R. P. | Rotary lateral. |
| Right, anterior—R. A. | Morikubo. |
| Right, superior—R. S. | Break. |
| Right, inferior—R. I. | Break. |
| Right, posterior, superior—R. P. S. | Rotary lateral. |
| Right, posterior, inferior—R. P. I. | Rotary lateral. |
| Right, anterior, superior—R. A. S. | Morikubo. |
| Right, anterior, inferior—R. A. I. | Morikubo. |
| Left—L. | Break. |
| Left, posterior—L. P. | Rotary lateral. |
| Left, anterior—L. A. | Morikubo. |
| Left, superior—L. S. | Break. |
| Left, inferior—L. I. | Break. |
| Left, posterior, superior—L. P. S. | Rotary lateral. |
| Left, posterior, inferior—L. P. I. | Rotary lateral. |
| Left, anterior, superior—L. A. S. | Morikubo. |
| Left, anterior, inferior—L. A. I. | Morikubo. |
| Anterior (entire Atlas)—A. | Morikubo (both sides). |
| Posterior (entire Atlas)—P. | Rotary lateral (both sides). |
| Note.—All right subluxations adjusted from right side, all left from left side. | |
| Second Cervical157 | |
| Posterior—P. | Posterior Cervical move. |
| Posterior, right—P. R. | Double contact on right side. |
| Posterior, left—P. L. | Double contact on left side. |
| Posterior, right, inferior—P. R. L. | Double contact on right. |
| Posterior, right, superior—P. R. S. | Double contact on right. |
| Posterior, left, inferior—P. L. I. | Double contact on left side. |
| Posterior, left, superior—P. L. S. | Double contact on left side. |
| Right (lateral)—R. | Break (Same if R. I. or R. S.) |
| Right (rotary)—R. | Rotary (Same if R. I. or R. S.) |
| Left (lateral)—L. | Break (Same if L. I. or L. S.) |
| Left (rotary)—L. | Rotary (Same if L. I. or L. S.) |
| Superior—S. | Posterior Cervical move. |
| Inferior—I. | Posterior Cervical move. |
| Anterior (entire Vertebra)—A. | Ventral transverse contact on most anterior side. |
| Anterior, right (lateral)—A. R. | Second metacarpal contact from right. |
| Anterior, right (rotary)—A. R. | Pisiform Ant. Cerv. contact on right. |
| Anterior, left (lateral)—A. L. | Second metacarpal contact from left. |
| Anterior, left (rotary)—A. L. | Pisiform Ant. Cerv. contact on left. |
| Third Cervical | |
| Same as second. | |
| Fourth Cervical | |
| Same as second. | |
| Fifth Cervical | |
| Same as second. | |
| Sixth Cervical158 | |
| Posterior—P. | The Recoil, hands reversed. |
| Posterior, right—P. R. | Recoil, hands reversed. |
| Posterior, left—P. L. | Recoil, hands reversed. |
| Posterior, right, superior—P. R. S. | Recoil, hands reversed. |
| Posterior, right, inferior—P. R. I. | Recoil, hands reversed. |
| Posterior, left, superior—P. L. S. | Recoil, hands reversed. |
| Posterior, left, inferior—P. L. I. | Recoil, hands reversed. |
| Right (lateral)—R. | Break (Same if R. I. or R. S.) |
| Right (rotary)—R. | Rotary (Same if R. I. or R. S.) |
| Left (lateral)—L. | Break, from left (Same if L. I. or L. S.) |
| Left (rotary)—L. | Rotary (Same if L. I. or L. S.) |
| Superior—S. | Edge contact move. |
| Inferior—I. | Edge contact move. |
| Anterior (entire vertebra)—A. | Pisiform Ant. Cerv. contact on most anterior side. |
| Anterior, right (lateral)—A. R. | Second metacarpal contact from right. |
| Anterior, right (rotary)—A. R. | Pisiform Ant. Cerv. contact on right. |
| Anterior, left (lateral)—A. L. | Second metacarpal contact from left. |
| Anterior, left (rotary)—A. L. | Pisiform Ant. Cerv. contact on left. |
| Seventh Cervical | |
| Same as sixth Cervical, except that T. M. may be used on right or left rotary subluxations. | |
| First Dorsal159 | |
| Posterior—P. | Recoil, hands reversed. |
| Posterior, right—P. R. | Recoil, hands reversed. |
| Posterior, right, superior—P. R. S. | Recoil, hands reversed. |
| Posterior, right, inferior—P. R. I. | Recoil, hands reversed. |
| Posterior, left—P. L. | Recoil, hands reversed. |
| Posterior, left, superior—P. L. S. | Recoil, hands reversed. |
| Posterior, left, inferior—P. L. I. | Recoil, hands reversed. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Edge contact. |
| Superior—S. | Heel contact. |
| Inferior—I. | Edge contact. |
| Right—R. | T. M. (Same if R. S. or R. I.) |
| Left—L. | T. M. (Same if L. S. or L. I.) |
| Anterior—A. | No correction. |
| Second Dorsal | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Edge contact. |
| Posterior, right—P. R. | Recoil. |
| Posterior, right, superior—P. R. S. | Recoil. |
| Posterior, right, inferior—P. R. I. | Recoil. |
| Posterior, left—P. L. | Recoil. |
| Posterior, left, superior—P. L. S. | Recoil. |
| Posterior, left, inferior—P. L. I. | Recoil. |
| Left—L. | T. M. (Same if L. S. or L. I.) |
| Right—R. | T. M. (Same if R. S. or R. I.) |
| Anterior—A. | No correction. |
| Third Dorsal160 | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Edge contact. |
| Posterior, right—P. R. | Recoil. |
| Posterior, right, superior—P. R. S. | Recoil. |
| Posterior, right, inferior—P. R. I. | Recoil. |
| Posterior, left—P. L. | Recoil. |
| Posterior, left, superior—P. L. S. | Recoil. |
| Posterior, left, inferior—P. L. I. | Recoil. |
| Right—R. | Pisiform single transverse (on left) (Same if R. S. or R. I.) |
| Left—L. | Pisiform single transverse (on right) (Same if L. S. or L. I.) |
| Anterior—A. | No correction. |
| Fourth Dorsal | |
| Same as third Dorsal. | |
| Note.—While the Recoil is here, the preferred move for posterior and postero-lateral subluxations, the pisiform double transverse or the two finger double transverse may be used if both transverses are palpable. | |
| Fifth Dorsal | |
| Posterior—P. | Double transverse move. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Double transverse. |
| Posterior, right—P. R. | Double transverse. |
| Posterior, right, superior—P. R. S. | Double transverse. |
| Posterior, right, inferior—P. R. I. | Double transverse. |
| Posterior, left—P. L. | Double transverse. |
| Note.—The pisiform double transverse and the two-finger double transverse, apply force in exactly similar directions and may therefore be used interchangeably. The latter is preferable for children. | |
| Posterior, left, superior—P. L. S. | Double transverse.161 |
| Posterior, left, inferior—P. L. I. | Double transverse. |
| Right—R. | Pisiform single transverse (Same if R. S. or R. I.) |
| Left—L. | Pisiform single transverse. (Same if L. S. or L. I.) |
| Anterior—A. | No correction. |
| Sixth Dorsal | |
| Same as Fifth Dorsal. | |
| Seventh Dorsal | |
| Same as Fifth Dorsal. | |
| Eighth Dorsal | |
| Same as Fifth Dorsal. | |
| Ninth Dorsal | |
| Same as Fifth Dorsal. | |
| Tenth Dorsal | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Edge contact. |
| Posterior, inferior—P. I. | Edge contact. |
| Posterior, right—P. R. | Recoil. |
| Posterior, right, superior—P. R. S. | Recoil. |
| Posterior, right, inferior—P. R. I. | Recoil. |
| Posterior, left—P. L. | Recoil. |
| Posterior, left, superior—P. L. S. | Recoil. |
| Posterior, left, inferior—P. L. I. | Recoil. |
| Right—R. | Recoil (Same if R. S. or R. I.)A |
| Left—L. | Recoil (Same if L. S. or L. I.)A |
| Anterior—A. | No correction. |
| A Note.—The use of this move is not quite mechanically correct, but it is advised because of the possible danger of using the transverse processes as levers. | |
| Eleventh Dorsal | |
| Same as Tenth Dorsal. | |
| Twelfth Dorsal162 | |
| Same as Tenth Dorsal. | |
| First Lumbar | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Heel contact. |
| Posterior, right, superior—P. R. S. | Recoil. |
| Posterior, right, inferior—P. R. I. | Recoil. |
| Posterior, left—P. L. | Recoil. |
| Posterior, left, superior—P. L. S. | Recoil. |
| Posterior, left, inferior—P. L. I. | Recoil. |
| Right—R. | Lumbar single transverse move, if transverse is palpable, otherwise Recoil. (Same if R. S. or R. I.) |
| Left—L. | Lumbar single transverse move, if transverse is palpable, otherwise Recoil. (Same if L. S. or L. I.) |
| Anterior—A. | No correction. |
| Second Lumbar | |
| Same as First Lumbar. | |
| Third Lumbar | |
| Same as First Lumbar. | |
| Fourth Lumbar | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Heel contact. |
| Posterior, inferior—P. I. | Heel contact. |
| Posterior, right—P. R. | Recoil, hands reversed. |
| Posterior, right, superior—P. R. S. | Recoil, hands reversed. |
| Note.—The Heel contact may be substituted for the Recoil above if force be carefully directed in the proper direction in delivery. | |
| Posterior, right, inferior—P. R. I. | Recoil, hands reversed.163 |
| Posterior, left—P. L. | Recoil, hands reversed. |
| Posterior, left, superior—P. L. S. | Recoil, hands reversed. |
| Posterior, left, inferior—P. L. I. | Recoil, hands reversed. |
| Right—R. | Lumbar single transverse move, if transverse is palpable, otherwise Recoil. (Same if R. S. or R. I.) |
| Left—L. | Lumbar single transverse, if transverse is palpable, otherwise Recoil. (Same if L. S. or L. I.) |
| Anterior—A. | No correction. |
| Fifth Lumbar | |
| Posterior—P. | Heel contact. |
| Posterior, superior—P. S. | Edge contact. |
| Posterior, inferior—P. I. | Edge contact. |
| Posterior, right—P. R. | Recoil. |
| Posterior, right, superior—P. R. S. | Recoil. |
| Posterior, right, inferior—P. R. I. | Recoil. |
| Posterior, left—P. L. | Recoil. |
| Posterior, left, superior—P. L. S. | Recoil. |
| Posterior, left, inferior—P. L. I. | Recoil. |
| Right—R. | Recoil (Same if R. S. or R. I.) |
| Left—L. | Recoil (Same if L. S. or L. I.) |
| Anterior—A. | “Bohemian” anterior fifth Lumbar move. (Not always advisable.) |
| Sacrum164 | |
| Posterior base—B. of S.—P. | Heel contact on base. |
| Posterior apex—A. of S.—P. | Heel contact on apex. |
| Entire Sacrum posterior Sac. P. | Heel contact between sacroiliac articulations. |
| Coccyx | |
| To be adjusted only when ankylosed in an abnormal position and then by leverage of finger through rectum. | |
Some useful information pertaining to adjustment will be found in section entitled, “Practice,” q. v.
After a careful and painstaking study of the foregoing pages it will still be found that the student is not by any means equipped for the work. He must practice these things to learn them. We learn to do by doing. The chief use of this section will be as a reference and guide during the practice of adjusting.
Disease has been variously regarded as an entity, a process, a condition. It has been mentioned in terms which would almost personalize it, such as, “attacked by pneumonia,” “seized with cramps,” “in the clutches of tuberculosis.” Men have endeavored constantly to discriminate between diseases and to learn the appearance and peculiarity of each, and have resolved each into its peculiar elements only to learn that the merging lines between two diseases or between cases of the same disease are imperceptible. It is no more possible to define any one disease within exact limits and to distinguish it from all others than to consider one function of the human body without studying its interdependence with others.
Disease is a process. It is a natural process. It follows certain well-defined laws and consists in the abnormal performance of function in some bodily organ or organs, or in the untimely performance of some function which would be normal in its proper chronological relation with other functions or at another period of the body’s development. The balance of function of the body is destroyed—some function intensified or diminished—that is all. Every disease, properly studied, reveals its functional base.
Disturbances of the functions of growth, nutrition, and repair produce changes in structure, physical evidences of disease. It is probable that every disease has a certain amount of structural change connected with it; it is hard to conceive of functional derangement without structural change, in a universe in which Nature is eternally building, destroying, or modifying organic peculiarities to meet changing functional demands. But in many instances this structural change is so slight as to be undiscoverable; such diseases are called “functional” to distinguish them from those in which structural pathologic changes are directly discernible, called “organic.”
Recognizing the fact that disease consists in a succession of steps or a series of events, each depending upon the next preceding one and making possible its successor, and desiring to arrest or check this process and correct the damage done, in other words, “to cure disease,” the question arises, “Where does this process begin?”
If we wish merely to check the process or to modify it, as does medicine, the etiology of the disease is less important than the present state. It is then more important that we understand the changes which are taking place in the body at the time of our attempt, the condition of each organ at that time, and the general recuperative or resisting power of the individual.
But if we would correct all the damage done instead of167 merely preventing further damage or building up internal resistance against a still active destructive process; if we would so eliminate the effects of the earlier steps as to make the resumption of the disease process most improbable, we must know each step from the beginning to the present, understand their sequence and relation, and go back to the beginning with our correction, removing the cause.
Since each event in the morbid process depends upon the preceding one and makes possible those which follow, it is possible to stop at any point in the chain of events and declare, “Here lies the Cause of Disease.” This explains the various etiologies adhered to each by a school of intelligent and scientific men, yet each apparently disagreeing most flatly with the others. No matter which step we select as our “ultimate cause” it truly is the cause, or one of the causes, of succeeding steps, which succeeding steps may well stand in our minds as the whole of the disease. Thus the physician, having found a germ, is quite content to look forward from the invasion of the germ and consider that as the primarily necessary requisite for disease production. In retrospect he follows disease back within the body to the time of entrance of the germ and then leaves the body to study the life habits of the germ and its favorite mode of conveyance. He has unwittingly left the direct line of investigation and followed a spur-track.
So with the osteopath who discovers contractured muscles168 drawing a member, or a bone, from its normal position. He proceeds to a study of the effect of such contracture upon other tissues and strives to relieve it by treatment—of the muscle.
The dietist discovers that certain food combinations cannot be properly cared for by an individual and that if taken they tend to develop toxins deleterious to the system. Whereupon he undertakes to discover food combinations which the body can care for and believes that he has solved the question of etiology.
Now it is most important that we find the primary cause, the one which makes possible the operation of all the rest and without which all would be powerless to harm man. This we shall expect to find at the point of entrance of disease into the human organism. The primary cause must be the first step which concerns man, the first change from normal to abnormal, on which all subsequent changes depend. It is useless to pass outside of the consideration of man and those forces which directly affect man, in our search for the cause of disease. We are powerless to affect outside forces or to control or amend the laws of nature through which disease exists.
Let us attempt then to resolve disease into its successive steps and to find the first which concerns man. Correcting that, we shall have corrected, fully and completely, the process which constitutes disease. By striking at the root we may destroy the entire growth.
Irritability is the property of being susceptible to excitement or stimulation. Stimulation is the process of increasing the functional activity of any organ. Inhibition is the act of checking, restraining, or holding back the functional activity of any organ. These definitions, taken from Gould, are here introduced as a necessary preface to an attempt to set forth, without unnecessary reference to, or discussion of, any other theory as to the etiology of disease, the Chiropractic explanation of its presence.
Chiropractic maintains that all the chemical and physical activities of the human organism are controlled, directly or indirectly, through a third form of energy transmitted through the Nerve System; that while all three forms of energy are interdependent and closely related in their ultimate expression, one of the three is the primary and most essential form, and especially indicative of life. We may call this third form Vital Energy.
There are several good reasons for believing that this nerve force is the primary form in which energy is expressed in man and for believing that it controls and directs the others in greater degree than it is controlled and directed by them.
Of the four forms of tissue of which the body is composed—connective, epithelial, muscular, and nervous—the latter is the one damage to which is followed by the greatest and most permanent consequences.
It is a fact that there are several organs whose removal leads to certain death because of their importance in the general economy of the body, but it is also true that section of the nerves leading to these organs just as certainly causes death by the cessation of their functions. There is no organ in the body aside from the nerves themselves which does not immediately cease to act upon withdrawal of its nerve force and at once begin a process of degeneration or atrophy.
Pathologic changes in the Nerve System invariably are followed by pathologic changes in the organs controlled by the diseased segment but the converse is not true. Excitation or inhibition of nerve activity produces corresponding and responsive change in the activity of the organs innervated, but excitation of an organ does not necessarily produce similar changes in the Nerve System. That system possesses the power of inhibiting or permitting responsive action, in other words, the power of choice.
Research in Comparative Anatomy develops the fact that the differences in power of complex action possessed by different organisms are entirely measurable by differences in the structure and complexity of their nerve mechanisms.
Further, by studying the effects of removal or extirpation, or of pathologic changes in various parts of the nerve system it has been demonstrated that the Brain is the center for those higher forms of activity known as psychic, for the power of accelerating or inhibiting the responses of the lower centers of the nerve system to stimulation from without,171 and for the conveyance of authority to act to all the lower centers. The Nerve System is the morphologic, physiologic, and dynamic center of the organism and the Brain the center of the Nerve System. We may, then, logically expect to find in the Brain, or in the channels by which power is distributed from the Brain to lower centers or organs, the initial step in the disease process, which is our present quest.
All nerve tissue in the body is organized and linked together in a complicated aggregation of individual units, communicating by contact, and forming one great Nerve System having its directing center in the Brain. It is said by some writers to consist of two distinct systems—cerebro-spinal and sympathetic—but would better be described as consisting of central organs—brain and spinal cord—and peripheral organs—cranial, spinal, and sympathetic peripheral axons connecting with cells in the central axis and linked together in a net-work improperly separable into separate or distinct divisions, the fibres of different parts being bound together in such a way as to establish an intricate intercommunication, closest on the one hand between the cranial and sympathetic and on the other between the spinal and sympathetic. The sympathetic system may be regarded as nothing more than a medium for proper distribution of impulses originating in the cerebro-spinal system, and a series of reflex centers deriving their power172 to act from the central axis. The proper action of sympathetic ganglia has been demonstrated to depend upon the integrity of the spinal nerve fibres, or rami communicantes, which pass to and terminate in the ganglia with their telodendria (terminal arborizations) in contact with the dendrites (cellulipetal processes) of the ganglion cells.
It will appear that interference with one division or part of the nerve system may be followed by effects partly manifested through a distant part; that excitation or inhibition of a spinal nerve may correspondingly excite or inhibit sympathetic fibres.
Chiropractic has accepted, as a convenient working hypothesis amply justified by years of clinical experiment and anatomical and physiological research, the proposition that all disease in the human body is primarily made possible by injury to (stimulation or inhibition of) some part of the nervous mechanism.
Injury to other tissues, unless the injury also involves nerve tissue, is quickly repaired and the body goes on without disease. Or the injury is sufficient at once to render the body untenable and death ensues. Few pathological changes follow trauma unless nerve tissue be injured.
This theory to be logical must and does include the entire nerve system. Also, since it is noted that each nerve cell presides over the nutrition of its own processes and possesses its own power of repair, it follows that unless an173 injury be of fatal nature or of permanent duration, even injuries to nerves tend toward automatic cure. We must seek a permanently operating interference with nerve tissue.
The brain, enclosed within the comparatively solid cranium, is so well protected that nothing except fracture of the skull, violent concussion, or shutting off of its blood supply from without, will produce permanent change there. Also, unless there be pressure by foreign substance against the brain, an injury will be repaired in time and the body resume its normal functional activity. It has been demonstrated that comparatively few diseases occur in this way. Such as do are called traumatic; i. e., caused by wound or injury.
In the broadest sense all disease is caused by trauma, as we shall presently show.
The upper or cephalic peripheral nerves, called cranial, leave the skull by foramina in its base (except the auditory) and are so protected by the immobility of the bones of the skull as to be comparatively free from direct injury. Peripheral injuries occur to cranial nerves but are repairable; even section of the trigeminal for neuralgia is usually followed after an interval by a reunion of the severed parts. As will be shown later, the special end organs of the cranial nerves are not free from the effects of spinal subluxation and their nuclei (deep origins) often share in morbid changes in the brain tissue due to nutritional disturbances.
The sympathetic portion of the nervous system might be classed with the cranial as regards infrequency of permanent174 interference were it not for the proximity of the great gangliated cord to the transverse processes and bodies of the vertebrae. This proximity renders it liable to sustain permanent impingement in vertebral subluxation.
With the exception of the first pair of Cervical nerves and the Sacral and Coccygeal, all spinal nerves pass through foramina of exit which are composed each of two movable vertebrae. The Chiropractic hypothesis is based upon the discovery that in addition to the part these vertebrae may take in general movements of the spine it is possible that their relation to each other may be changed by the application of force from without, and that this change once produced tends to remain permanently. These permanent vertebral subluxations occur with great frequency, a fact clinically demonstrable by palpation and by the X-Ray.
The discovery of this fact led to the ascertaining of two more, namely,
No disease is ever found without accompanying subluxation.
Since each organ or tissue is connected with some definite and special vertebra, subluxations accompanying disease bear a relation to disease which is controlled by a general law, operative alike on all human organisms.
The latter fact required one other for its complete demonstration; namely, that the removal of the subluxation is always followed by the complete disappearance of the disease.175 Given more perfect methods of correcting subluxations it would follow that proof of the Chiropractic theory would be so complete and overwhelming as to meet at once with general acceptance. The difficulty lies in the fact that with our present methods much time is often required for complete correction of the vertebral displacement and much skill is needed even for successful investigation of the results obtainable. The theory is too often judged by unskilled or imperfect applications of it.
Every school of Chiropractic accepts the presence of the subluxation and has spent much thought and time in the effort to deduce the law governing its connection with disease. Diverse conclusions have been reached owing to the difficulty experienced in completely eradicating the subluxation. When it is accomplished the results are absolutely conclusive. When it is partially or relatively accomplished the results are so good in a great per cent of cases as to lead sometimes to the erroneous belief that the subluxation did not cause the disease since mere partial correction of the subluxation suffices to bring about the apparent total removal of the disease. In every case of thorough experiment the results warrant the recommendation of the subluxation theory as at least a proper working hypothesis.
Without attempting here to review all the various conclusions reached or the methods by which they have been attained, we would simply state our own conclusion, which we believe is the only one compatible with demonstrable facts. It is briefly this: Since every portion of the body is176 connected through the nervous system with the spinal nerves and since it has been proven that this connection is reasonably constant and anatomically demonstrable; since the removal or correction of a subluxation leads in all cases to the complete disappearance of disease from the organs or tissues innervated from the subluxated portion of the spinal column, we conclude that the subluxation is the primary cause of disease.
The final test of the correctness of any theory is the result of its application. Since Chiropractic secures a larger percentage of results than any other known system of healing it is safe to assume, at least, that it has discovered the way to remove the primary cause of disease.
That the Chiropractic theory, or more properly the subluxation theory, does not include all of the etiology of disease is evidenced by the facts of contagion and infection, by the effect upon the organism of the introduction of poison, by the consequences of worry, anger, and other abnormal mental states and conditions. These facts do not in the least invalidate the theory. They merely require explanation which will make clear their relation to the subluxation. That such explanation is abundantly at hand strengthens the position of Chiropractic more than would negation of all other causes save the one we concentrate upon.
The Mentalist who holds that all diseases exist in and are but figments of the mind is as far afield as the Physicist who holds that special nerve energy is nonexistent. The Chiropractor views Man as a complex psycho-physical unit,177 self-operating and internally self-healing until environmental forces disturb the nice adjustment of the machinery.
Disease is produced by, and is, a series of events, chief and most permanent of which is the subluxation. We may consider its etiology according to the order in which the events take place thus:
Concussion of Forces.
Subluxation of Vertebra.
Impingement of Nerve.
Excitation or Inhibition.
Disease—Abnormal Function.
Between the last two steps above, or following the last, are often introduced one or more of the following accessory chains which modify or increase the final effect and are themselves made possible by the first four steps in the direct chain.
Pathogenic germ.
Poisonous excretions from germs.
Tissue destruction by chemical action of such toxins.
Reflex muscular tension tending to increase subluxation and thus augment nerve impingement and its effects.
Or
Dietetic error.
Abnormal chemical action.
Tissue destruction or nerve irritation by chemical poisons.
Reflex motor disturbances which further limit digestive power.
Or
Abnormal mental condition.
Waste of nerve energy with production of toxins.
General metabolic disturbance.
Increased disease wherever disease previously existed.
These are offered merely as illustrations. There are many accessory chains which aid in the production or development of disease and act as secondary causes.
Man was so created, so provided with means for repair, growth, etc., that the body tends to maintain its own functional balance—perfect harmony among all its parts—unless interfered with by some outside agency. There are certain natural laws such as the law of gravitation and the law of momentum and inertia which operate without regard for man or man’s welfare. If man, wittingly or unwittingly, allows himself to come into violent conflict with one of these laws by falling to the ground or in meeting sudden and unexpected opposing force or mass while in motion, that which may be termed a concussion is produced by the meeting of the outside force and the internal bodily resistance.
Many such concussions may occur without serious damage. Some produce wounds or injuries which it is possible179 for the body to heal without causing serious disturbance of function. Other concussions are so violent as to produce displacement of structure which tends to remain permanently. Under Spino-Organic Connection will be found an explanation of the manner in which force applied to various parts of the body tends to affect the spine.
Now the displacement of a bone cannot be corrected by the body without outside aid. No method is provided for such correction. Produced by outside force affecting the body, it can only be reduced by outside force. It is this failure of Nature to make man adaptable to every untoward circumstance which renders him susceptible to disease.
As has been previously stated by no means all concussions of forces produce subluxation. (All subluxations, however, are produced by concussion of forces.) It may be added that not all subluxations impinge nerves and that when they do not so encroach upon nerve tissue they produce no noticeable effect after the first temporary soreness has disappeared.
Every subluxation, however, evidences a tendency to disease. Once moved from its normal position and the poise and symmetry of the body disturbed, there are influences which tend more readily to affect the same vertebra. The subluxated vertebra is more easily disturbed by jars, strains, etc., than the normal one because such jars are less regularly distributed to all its parts. A reflex muscular180 tension due to other and more pronounced subluxations and their disease effects may in turn increase the slight deviations throughout the spine, rendering them in their turn capable of producing disease. When the spine or any part of it has lost its perfect regularity disease is made possible, if not a fact at once. The average number of subluxations in each individual is about nine and one-third. Of this number probably not more than one-third (though no accurate figures are available) are actually productive of conditions nameable as disease at any given time. Discrimination between those which do, and those which do not, produce discoverable symptoms in a given case is a matter which requires a nice technical skill and perfect judgment.
When a vertebra has lost its normal articular relations with its fellows and occupies an abnormal position as a consequence in regard to all surrounding or adjacent tissues it may impinge nerve tissue in two ways, by tension or by constriction. By the displacement of one vertebra of a pair the size and shape of the intervertebral foramen may be altered (occlusion) constricting the nerve which passes through the opening. That this change in the size and shape of the foramina does frequently occur is shown by the frequency with which alterations in the shape of vertebrae appear in dry spines, by post-mortems which have demonstrated the altered foramina in the cadaver and by permanent181 occlusion of the foramina in ankylosed spines so that the occlusion may be preserved. Adding cartilage changes in the intervertebral disks to alterations in bone shape and position, especially the latter, we find full and sufficient reason for all the pathological phenomena which follow the subluxation. Explain it as you will, these morbid results do follow subluxation and can be experimentally produced in animals. Moreover, the disease may be directed to a desired organ or region by selection of the particular vertebra to be displaced.
The suboccipital, sacral, and coccygeal nerves cannot be constricted as they pass through the foramina because they do not emerge through complete rings formed of separate and movable bones. But these nerves may be pressed upon or stretched by displaced bone, as may also the great gangliated cord of the sympathetic, especially the Cervical portion of it. Tension of the Cervical sympathetic cord by subluxation of vertebrae is a very common occurrence.
Whether the impingement be by constriction or by tension the effect is much the same depending upon the degree to which the molecular continuity of the nerve substance is impaired—interference with the function of the organ connected with the nerve and sometimes swelling and pain in the nerve itself followed by degeneration. The effects are chiefly noticeable in peripheral tissues. S. Weir Mitchell says (1872), “A continuous pressure upon a nerve results in the degeneration of the nerve and a disturbance of function of the parts innervated by that nerve.” No clearer statement can be made.
It must not be understood that all nerve impingement is due directly to subluxation of a vertebra. A dislocated shoulder would produce a similar effect of nerve tension. But dislocated shoulders are seldom met with as permanent conditions. Likewise there may be secondary impingement from new growths, themselves due to some primary subluxation. Aneurism of the thoracic aorta often produces hoarseness by impingement of the recurrent laryngeal.
Not all impingement is sufficient to produce noticeable disease. To a certain extent the power of adaptation inherent in the body can overcome its deleterious effects and suppress all signs of its existence until an overtax upon bodily energy lessens this adaptative power. Then disease appears and we say that the overtax caused it.
A slight impingement serves as a mechanical irritant to increase the action of the nerve and the functions of the attached peripheral organs. Such stimulation beyond the normal is always followed by a reaction, or fall to subnormal action.
Heavy impingement, especially the impingement due to marked occlusion of foramina, partly or wholly paralyzes the affected nerves. Often the impingement produces only a latent weakness in some organ, a weakness which may be brought to light only through the introduction of some secondary cause which takes advantage of the susceptibility of the organ to produce some definite disease. As an instance183 of this we may mention typhoid fever. No typhoid case is found without subluxation in the region of the second Lumbar; yet the latent weakness produced by that subluxation may not have been observed until the typhoid germ found a fertile feeding and breeding ground in the weakened tissue and proceeded to multiply there and develop its toxins.
Each nerve cell is trophic to its processes and to the tissue cells to which these processes are distributed. The growth, nutrition and repair of each cell of the body is dependent upon the integrity of the axon which supplies it. The effect of nerve impingement upon the single cell is a weakening of cell structure and a disturbance, slight or great, of the special function possessed by that cell. Dunglisson says of diseases, “All ... are dependent upon modified cell-action.”
Each organ is but an aggregation of cells of some special type or kind. Nerve Impingement usually involves either a whole nerve trunk or many of its fibres and thus weakens either the entire organ or many of its cells and increases or diminishes its special function. Some organs are innervated by more than one nerve and may be injured only in part by a localized impingement.
Alteration of the action of one organ often tends to184 affect the entire body, as in subluxation of the fourth Dorsal interfering with the nerve supply to the liver the secretion of bile becomes altered in character or quantity and the entire system suffers, through deranged digestion, from this alteration in a necessary secretion. Every disease presents symptoms only indirectly referable to the organ which is primarily affected and the problem of the diagnostician is to so discriminate between direct and indirect symptoms as to be able to locate disease.
We have considered a chain of events by which disease is produced without the intervention of any secondary cause. Such a condition may be called, for convenience, a simple subluxation disease. Its existence depends directly upon the subluxation which is the first change manifest in the individual and upon which all the other changes depend.
The two facts that not all subluxations impinge nerves and not all nerve impingements cause demonstrable disease explain why we do not, in practice, find a disease to correspond with each subluxation discovered by palpation. It must be remembered that there may be latent weakness following a subluxation and of importance because it renders the patient susceptible to infection or to the action of other secondary causes.
Among the secondary causes of disease may be mentioned the pathogenic germ, poisons, dietetic errors, abnormal mental states, bodily excesses, exposure to sudden temperature changes, and inhalation of non-poisonous but irritating substances as the most common. Many others might be included but these will suffice for complete illustration of the principle. It will be our endeavor to show how each of these secondary causes operates by virtue of a previous susceptibility, or breaking down of the normal resisting power of the organism caused by subluxation, and how each in turn may bring about increase in subluxation and thus, both directly and indirectly, increase disease.
Bear in mind these two all-important facts. None of these secondary causes can operate without previous subluxation. A subluxation may produce disease without the aid of any secondary cause.
These comprise a large portion of the febrile affections. Most germ diseases are characterized by fever and the presence of circulating toxins with resulting disturbance of the metabolic processes of the body.
It is generally agreed among pathologists that the greater number of varieties of micro-organisms found at times in man are not pathogenic. Some aid in the decomposition of food in the alimentary canal; others have various186 beneficial functions to perform. But some, under proper conditions, feed upon and destroy living tissue. These are the so-called pathogenic germs.
The pathogenic germs are many. They enter the body by various routes, in the air we breathe, the food we eat, the water we drink; sometimes they are communicated by direct contact with other persons or with objects infected with them. The term “contagious” is applied to those diseases whose germs may be carried through the air from one to another; “infectious” refers to those communicable only by contact.
In every healthy individual are found multitudes of germs of both the pathogenic and harmless varieties. We are constantly exposed to the influence of the former yet by no means all bodies into which pathogenic germs find entrance contract disease. This fact has caused much study and among pathologists and bacteriologists generally the conclusion has been reached that the development of colonies of micro-organisms sufficiently to produce disease depends upon what is known as “susceptibility” of the organism. There must be a latent weakness of which the micro-organisms take advantage.
This amounts to the admission that the body contains the inherent property of successfully resisting all germ action. Indeed, the fundamental proposition of Serum-Therapy is that under stress of the presence of dilute germ infusions the body does develop special chemicals which neutralize the germ poisons and kill the germs and which187 remain after the inoculation to guard against any further entrance of germs of the same kind and vulnerable to the same protective chemicals.
This theory is sufficiently correct to have served as an unassailable basis for a most illogical procedure. The truth is that the auto-protective power of the body must be lower than normal and the germs must find a weakened area for development and multiplication before they can develop sufficiently to produce disease. Once they gain a foothold they tend to multiply with great rapidity and to develop alarming symptoms often leading to death.
Only in a few instances does modern science believe that a pathogenic germ can successfully attack a healthy body, but is claimed that there are a few germs, such as the Klebs-Loeffler bacillus (diphtheria producer) and the bacillus of anthrax, which may find lodgment in any organism, healthy or unhealthy, to produce disease.
Now, the susceptibility of the body to germ invasion requires explanation. Merely to say that one is susceptible and another is not leaves too wide a field of possibility for error. It is easy to reason from the fact that all persons are at some time exposed to contagious or infectious diseases while comparatively few contract them that some persons are vulnerable to certain diseases while others are not. It is plain that while a person may be susceptible to typhoid fever because he has a weakness in the intestines, he may be quite immune from pneumonia or tuberculosis or any other infectious or contagious disease. But why this difference? Let us look at the problem from another angle.
Chiropractors find with every contagious or infectious disease certain subluxations whose location with relation to the disease is constant and demonstrable. Thus all cases of pulmonary tuberculosis show a third Dorsal subluxation with only enough exceptions to prove the rule; tonsilitis is invariably accompanied by subluxation of the second, third or fourth Cervical. Correction of the subluxation is, in all except the most fully and virulently developed cases, followed by a radical cure. Indeed, in many of the germ diseases it is possible to abort the fever with improvement of all symptoms in from five minutes to twelve hours. We are so accustomed to checking germ diseases at once that failure to do so leads us to immediate investigation of our palpation and adjustment to discover some technical error in the application of the principles of Chiropractic to the case in question.
It is manifestly impossible by vertebral adjustment to raise the body beyond normal power. Nothing is added to the body; no energy is utilized other than the energy of the body itself which is provided by Nature and released through restoration of the normal carrying capacity of nerves. The highest goal attainable is normality, and it is observed that no matter whether the impingement be in the nature of an excitation or an inhibition of nerve action the effect of a correct adjustment is always in that direction—toward normality. It may be as well to digress here long enough to remark that abnormal change is never the result of adjustment but always of maladjustment, and those189 who claim to be able to produce stimulation by moving a given vertebra one way and inhibition by moving it another are entirely wrong.
It is evident from the results of adjustment in germ disease that the normal body is entirely capable of throwing off the poisons and exterminating the germs, which conclusion quite agrees with science. The fact, not known by other branches of science, and asserted by Chiropractic is simply that the subluxation is the factor which determines susceptibility.
Upon ascertaining that a certain vertebra is in normal alignment we may say with absolute certainty that the organs innervated by the nerves passing through its foramina are not and cannot be the site of any pernicious germ activities. To go further, it has been demonstrated in a number of cases that the subluxation existed before the contagion or infection developed. A man has been known to have a second Lumbar subluxation for many years without effects other than a tendency to constipation and on the appearance of a typhoid epidemic to contract the disease. Correction of the subluxation afforded a cure. Such instances might be cited in great numbers. No person without the necessary subluxation ever contracts a germ disease and the necessary subluxation can be exactly located for the vast majority of such diseases. Unfortunately it is impossible to find a person who has not some subluxations and is not, therefore, subject to some form of contagion or infection.
So far Chiropractic agrees with general knowledge of germ disease and its etiology, simply adding the explanation of susceptibility which all other modes of investigation have failed to afford. In one particular we find apparent disagreement.
We have said that several bacilli are supposed to have power to cause disease in healthy bodies. Diphtheria is a disease caused by one of these. Yet Chiropractic adjustments have rapidly aborted diphtheria, apparently proving that the body has power to react strongly enough to conquer even this germ, providing the nerve channels be opened to allow of exertion of its full activity. It is probable that all diseases fall under the same law and that no germ can find lodgment in healthy tissue. Chiropractic affirms this as a truth and as yet no experience has tended to disprove it; the belief is strengthened by the years.
The experiments which are said to have proven that certain micro-organisms can attack healthy tissue are based upon the supposition that careful examination demonstrated the absence of disease in the animals experimented upon by inoculation. Since these experiments and these examinations were made without any knowledge of vertebral subluxations, and consequently without discovering whether or not there existed latent weaknesses of various organs, we doubt the validity of the experiments. Our own examination of human and animal spines has thus far failed to discover any perfectly normal specimens.
Our clinical experience with diphtheria at least absolutely disproves the conclusions of Pasteur and others in regard to its origin.
It has been observed that in many instances the subluxation which existed previous to infection or contagion is greater and more noticeable during the febrile and active stage of the disease than before, and this fact has led some careless or insufficiently skilled palpaters to assume that the disease caused the subluxation.
The development of germ life is accompanied by the excretion of toxins of greater or less virulence which circulate through the blood and affect the entire body. This poison, irritating sensor nerves, brings about motor reactions in the segments irritated and, since the normal operation of the laws of reflex action is interrupted somewhat by subluxation, and since the muscles immediately around a subluxated vertebra tend to pull upon it with unequal leverage, this motor reaction is likely to increase already existing malalignments, especially in the same body segment in which the poison is generated and in which the irritation is consequently greatest. Thus subluxation is most pronounced during the activity of the disease caused by it and reacting upon it and thus a disease which began as a localized destructive process may manifest systemic effects through its action upon other abnormal spinal segments.
The internal chemistry of the body varies so greatly under changing conditions, the operation of any two different organisms is so hard to compare accurately, that it is impossible to set down any rule for diet which will apply properly to all patients or to all with the same disease or habit of body. In fact, only experiment with an individual can determine the exactly proper diet for him.
Through lack of judgment or of observation of the effects of certain foods upon us we often eat that which our bodies cannot properly digest and assimilate. Sometimes through accident or negligence we partake of food which is proper in kind for us but improper in quality, perhaps partially decomposed. Improper food, when taken into the body, tends to exert a deleterious effect upon health. This fact should not lead us to confine ourselves to reasoning superficially that improper foods cause disease or that dietary measures will cure disease.
Some Chiropractors have held that the hunger of individuals for certain foods is a safe guide to a proper diet. This is manifestly untrue in some cases; the voracious appetite of the convalescent typhoid patient is an example. But it would probably be true if all men were normal. Close observation of a few exceptionally well-developed and normal individuals has disclosed an interesting fact. If a man has no subluxation in that portion of the spine which controls the stomach, the ingestion of decomposing food, even193 though the alteration be so slight as to escape notice on casual examination, induces immediate vomiting followed by no untoward consequences. Only occasionally does one find persons without subluxations in some way affecting the stomach; in such cases the body promptly rejects and expels injurious material.
This carries us to the rather surprising conclusion that the normal person is not susceptible to the influence of bad food. In the majority of individuals, some degree of abnormality existing, improper food has a decidedly bad effect. Passing through the alimentary canal it is improperly digested; toxins are developed; these chemically affect the entire body, perhaps leading only to a congestion and inflammation of some part of the lining of the alimentary tract, perhaps producing a general fever, malaise, diarrhea, and the other effects of a general poisoning.
It has been found that proper adjustment is followed by quick relief in such cases, the commonest effect being the rapid expulsion of the deleterious matter by vomiting and diarrhea with breaking of the fever and lessening of all symptoms.
It has also been observed that during the suffering from dietetic error the subluxation controlling the stomach or some part of the small intestines is often found increased in degree with tension of the adjacent muscles. With adjustment and relief of the other symptoms the muscular tension tends to disappear. This motor reaction from the irritation of food poison undoubtedly serves to increase subluxation194 already existing, thus intensifying effects. But for its primary effect food poison requires a previous subluxation lowering the natural protective power of the body. Food poisoning is often a secondary cause of disease.
When it is found in any specific case that certain foods exert a bad influence upon the progress of the case, that the symptoms are aggravated by the taking of these foods, they must be abandoned. Yet no rigid diet need be prescribed in any case. Every patient will require a different diet, nor is it possible to understand the intimate chemical relations within the body sufficiently to fix a proper diet except by experiment.
A word here about fasting. If improper food were a primary cause of disease, fasting would be an effective, though somewhat radical, removal of the cause of disease and a logical procedure. Since improper food is not a primary cause of disease and since nature requires food for the repair work made possible through adjustments, it would seem unwise for Chiropractors to prescribe fasting. Also it is well to remember that fasting and starvation are synonymous and their symptoms identical.
Any substance taken into the body and not usable as food may be considered poison. Most drugs administered as medicine or used habitually are either directly poisonous and commonly so considered or are poisonous in the sense that they do not build but rather tend to injure the body. Injurious195 substances accidentally taken into the body; certain products included in the preparation of otherwise nutritious foods, alcohol, tobacco, etc., affect the body in varying degrees but in accordance with the same laws. Poisons may be internally generated through the action of pathogenic germs or through the failure of the body to digest food and to prevent injurious chemical changes in it. It has even been said by some that abnormal mental states so affect metabolism as to cause the formation of certain auto-toxins which injuriously affect the entire body.
However poison may make its appearance in the body its presence is associated with certain bad effects. Poison may be corrosive, destroying tissue wherever it touches; it may be stimulating, affecting the nerves so as to increase their activity, following which waste of energy there is a weakening reaction; it may be narcotic, lowering some physiologic process below normal.
If a man without subluxation—and therefore normal—have poison introduced into his body one of two effects will follow. Either the poison will be sufficient to produce death in a short time, and will do so, or the poison will be ejected from the body and the patient recover naturally and without treatment, and recover fully.
This is the statement of the ideal, not the real. The fact is that no person has yet been found without subluxation in some part of the spinal column. Occasional cases have been reported but always by Chiropractors whose statements are open to question on account of imperfect training196 in vertebral palpation or a known habit of unconsidered statement. And in the weakened body, whose natural protective power has been lowered, the effect is different.
The body fails to throw off all the poison normally and some of it remains in the circulation and tends to cause progressively increasing damage. In addition to the direct effect of the poison upon the tissues, the irritation of sensory nerves gives rise to a motor reaction which increases subluxation generally throughout the spine but especially in the segment in which the sensory irritation is greatest. If the poison be taken into the stomach the vertebrae affecting that organ are most affected in the resulting motor disturbances. When vaccine virus is introduced into the arm the greatest influence is upon the last two Cervicals and first Dorsal, causing increased weakening of the nerves to the arm. If the vaccination does not “take” it is because the body is so normal as to be able to take up and rapidly excrete the poison or to neutralize it with an internally generated antitoxin.
This tendency of poisons to increase subluxations already existing has caused many to conclude that new subluxations could be produced by the motor reactions from poison. The laws governing reflex action make this impossible. If a mild stimulus be applied in the segment occupied by a given, and normally aligned, vertebra, the resulting contraction will tend to appear on the same side as the irritation and would—if sufficient to subluxate the vertebra—draw it toward the irritated side. If a stronger stimulus197 were applied the resulting reaction would appear on both sides and with sufficient intensity on the opposite side to the irritation so that the difference between the contractions on the two sides would never be sufficient to overcome the fixity and inertia of the vertebra. If this bit of theorizing be doubted, let me add that if poisons could cause subluxation they would undoubtedly cause drawing of the vertebra toward the irritated side—which is not the way we find them in poisoning cases. Almost without variation, the subluxation is away from the affected side. Such a subluxation produces most impingement on the side of the irritation; the only kind which could follow poisons would produce its effects on the opposite side.
In acute poisoning cases which may possibly proceed to a rapidly fatal termination, while immediate adjustment may be sufficient to cause the expulsion of the poison and the recovery of the patient it is probably wisest to administer an antidote or to call a physician with a stomach pump. Just so, the pulmotor should be summoned for gas asphyxiation; but at least one case was recently encountered in which an adjustment started the heart and artificial respiration movements restored consciousness before the pulmotor could arrive. There are few, if any, acute poisoning cases in which an adjustment will not aid. Sometimes it should be assisted by other measures not strictly within the province of Chiropractic.
Chronic poisoning, such as lead poisoning from paint work, yields well to adjustments providing the secondary198 cause, the persistent inhalation of lead fumes, be discontinued.
Poisons may wound or injure the body whether or not it be normal; in such case they might properly be classed with trauma. But no poison causes disease except through the medium of vertebral subluxation previously produced. Some subluxation which has never been sufficient to produce active disease may be so increased by the action of poisons as to be of serious effect even though the poison has long since been eradicated from the body—for the subluxation is permanent until affected by force outside itself. In considering the etiology of any disease the possibility of its being augmented by medicines, drug habits, or dietetic errors should be weighed with other evidence.
By this term is especially meant exposure to sudden temperature changes. The body may sustain a very high or a very low outside temperature providing the change is gradual enough so that the heat-regulating mechanism may adapt itself properly to protect the body and maintain an even temperature within. A sudden change from a very warm room to a very cold atmosphere; a quick transportation from cold air to a superheated apartment; or a sudden draft of air whose temperature is sharply at variance with surrounding air and therefore with the condition of the body surface may have a very bad effect.
The skin and mucous membranes of the body have become199 accustomed to a certain temperature; the change irritates them. And the immediate result is a motor reaction increasing subluxation in the same body segment in which the irritation is greatest and probably producing first an irritation of the nerves at the spine and then an inflammation of the exposed surface. Thus a “cold” is produced. One who has no subluxation affecting the respiratory tract—a rare degree of normality—may escape coryza, bronchitis, or pneumonia, the most common effects, but may suffer a congestion of the stomach walls or of other parts of the body. It is said that the cold “settled on the stomach.” The fact is that the motor reaction takes advantage of the weak parts of the spine and affects them most, like the pernicious habit of spine-stretching which used to prevail among Chiropractors. This explains why “cold in the head” is so very frequent. The fourth Cervical vertebra is situated at the middle point of the neck and is very freely movable and easily subluxated and, in fact, more often displaced than other Cervicals.
Noxious or poisonous vapors may have an effect identical with that of sudden temperature change. Sleeping in an improperly ventilated room often appears to cause “cold.” Careful study of the part of the body exposed to draft, and of spino-organic connection, will show that in most instances the effect of such exposure is first felt in the same body segment.
It is a well-known fact that not all people are “subject to colds.” One may be “subject to lung colds,” another to200 “cold in the head.” The susceptibility is entirely governed by the condition of the spine, the person having no middle Cervical subluxation being immune from coryza even though subjected to the same exposure which will produce it in others. The pollen of plants produces hay fever in the susceptible in much the same manner that draft produces coryza, both acting as secondary causes.
In this division of secondary causes may be mentioned overwork, continuous loss of sleep, overeating, venereal excesses, etc.
They act in this manner. Wasting and overusing the bodily resources they lower the general vitality. Now, though there be subluxations at various points in the spine there is still transmitted through each impinged nerve a certain amount of Vital Force which to a certain extent maintains the functions of the body and keeps it in a state of activity sufficient for ordinary demands. When the entire stock of vitality is lowered through excess the amount of energy passing through each nerve in the body is lessened, but the effect of such lessening is felt most where there is subluxation. At the high tide of vitality the subluxations are not sufficient, perhaps, to produce serious disease. At low ebb, every organ whose nerve is interfered with suffers keenly. Under such conditions the body is much more subject to adverse influences, to shocks and jars, to contagion or infection, to the action of cold or exposure. Thus bodily excess acts as a secondary cause of disease.
There are many who believe that fear, worry, hate, grief, etc., are in themselves sufficient to produce disease in a normal organism. Shock following the demise of a loved one or some deep disgrace is occasionally alleged as a cause of death or of a rapid decline in health which terminates fatally.
The failure of Suggestive Therapeutics to cure disease except when it is largely imaginary rather argues against this theory. It is also true that proper Chiropractic adjustments not only lead to the cure of disease apparently caused by abnormal mental states but also, restoring proper blood-supply and nutrition to the brain, induce a happier mental state in the patient. Even insanity has been cured in a number of cases by Chiropractic.
We hold that worry, fear, etc., are abnormal; that they arise from the improper expression of Mind through disordered brain-cells. “Diseases of the Mind,” in the strictest sense, cannot occur, but only diseases of the physical medium through which mind is expressed and translated to the physical plane of being—the brain.
A condition of abnormal mental expression or activity, especially worry, fear or anger, probably has a two-fold effect: it rapidly wastes the body energy and, like bodily excess, renders every subluxation more effective; it is possible that it may also really produce auto-toxins, generated by abnormal brain-action and affecting the body metabolism202 adversely. In this way disease appears through the action of abnormal mental states as secondary causes.
They themselves are the result of subluxation of the first or second, sometimes third, Cervical, impinging the nerves which control the blood-supply to the brain and hence its nutrition. Correction of the subluxation causes them to disappear.
Inflammation is a morbid process characterized by the presence of increased temperature and one or more of the symptoms, pain, redness, and swelling. It is distinguished from fever by being confined locally, while fever is a general functional disturbance showing elevation of temperature, increased katabolism, decreased secretion, etc.
Our clinical experience with fevers leads us to accept Metchnikoff’s conclusion that the essential phenomenon of inflammation is hyperaemia. Upon the hyperaemia depend the swelling, pain, and local increase in heat-production. Hyperaemia in turn depends upon disturbance of the vasomotor nerves either as a direct result of some local subluxation or as an indirect consequence of local irritation.
A newly acquired subluxation produces an acute irritation of the pre-ganglionic axons which connect the spinal nerves with the sympathetic ganglia. If these ganglia send out post-ganglionic axons which are vaso-motor in function, an inflammation may be produced without the intervention of any secondary cause. On the other hand, there may be a203 subluxation producing weakness of some part; through injury to that part or the introduction of poisons or irritants such as germ infection, sensory end-organs are affected and the motor reaction which follows increases the subluxation; this slight increase produces acute irritation of the nerve and hyperaemia, with its resultant phenomena, follows. Stated briefly, irritants produce inflammation only by acting through the medium of the spine. If the spine be normal these irritants are insufficient to produce morbid process. Local inflammation tends to develop toxins, especially if it be of bacterial origin, which may in turn affect the entire organism—an effect which will be discussed presently. Exception must be made in those traumatic cases in which hyperaemia is essential to the reparatory process, and which are attended by what may be termed a normally increased heat-production. This beneficent and reparatory condition cannot be termed disease or morbid process.
The normal temperature of the body depends upon the balance maintained between heat-production and heat-expenditure. This balance is maintained through a complicated nerve mechanism consisting of various nidi in thalamus, medulla, spinal cord and sympathetic ganglia, and a network of communicating axons of both the cerebro-spinal and sympathetic systems, controlling the amount of blood passing through any given body area at a given time, the secretion of the perspiratory glands, the internal metabolic processes, etc. Most important are the vaso-motor nerves, directly, but not originally, derived from the sympathetic,204 and governing the size and caliber of all blood-vessels so as to control the amount of blood flowing to and through the surface capillaries on the one hand, or the deep-seated, heat-making organs on the other. More than seventy per cent of the body’s heat expenditure is through the skin by evaporation, radiation, and direct conduction. The major portion of the heat production is in the muscles and the parenchymatous viscera, such as liver, spleen, etc., where metabolism is active.
This mechanism is so delicately adjusted that when the outside temperature is lowered the amount of blood passing to the skin is reflexly lessened while internal heat production is increased and the bodily temperature retained at normal. Conversely, the body perspires freely and the surface is flushed with blood in a high temperature, so that heat production is lessened and its discharge accelerated, again tending to maintain an even and normal temperature.
The nervous mechanism is responsive to many and various forms of stimuli—thermic, emotional, mechanical, physiologic need, toxic. Poisons in circulation may affect the bulbar center and produce general fever. A number of centers in the spinal gray may be stimulated with like result. Or there may be purely local irritation which results in local hyperaemia and inflammation.
It will always be found that the primary cause of any permanent derangement of the mechanism lies in vertebral subluxation impinging some of the nerves and thus throwing the mechanism out of its natural balance and poise. Other205 forms of disturbance are transient and the very nature of the mechanism makes it normally capable of adjusting itself to thermic, mechanic, or emotional stimuli in a short time. Only the subluxation produces permanent elevation of temperature. When such elevation does occur there are many associated changes, increased katabolism, lessening of secretions, anorexia, sometimes mental changes, such as delirium or coma. Fevers vary according to the part of the nerve mechanism affected and the action of any secondary causes.
Fever due to vertebral subluxation alone without any secondary cause operating is very rare. Ordinarily fevers come about in this way. A subluxation occurs which weakens tissue and permits germ invasion; toxins enter the circulation from the germ action and motor reaction increases the original subluxation and causes local inflammation; germ activity is favored by the increasing degree of abnormality and toxins from rapid tissue destruction are added to those already present. The poison-loaded blood then affects the general centers for heat regulation, blood becomes internally engorged, and a chill (internal fever) followed by general increase of temperature occurs. At this juncture any subluxation previously existing is likely to be increased and to add its quota of harm to the rapidly developing picture.
Our problem is to find the original subluxation which controls the site of the original pathologic change and to correct that. In nearly all cases where this is done, even partially, the body is enabled to care for the remainder of the damage and to throw off the accumulated toxins. It is206 not uncommon that the temperature falls two degrees in five or ten minutes after a proper adjustment. We expect always to abort or check a fever in twenty-four hours or less.
There are cases in which the temperature drops after adjustment but presently rises again. This indicates the virulence of the autointoxication or that some other area of poison production is operating than the one our first adjustment would control. A correct diagnosis will enable one to give specific adjustment and check practically any fever except a chronic one with much tissue destruction already accomplished; even some of these yield.
The commonest cause of fever is at the fifth or sixth Dorsal vertebra, long known as Center Place, or Fever Center. Here emerge many pre-ganglionic fibres which distribute their impulses through lower neurons in the sympathetic system to the coeliac plexus and thence to the blood-vessels supplying the major portion of the abdominal viscera. Adjustment here causes a sudden contraction of these abdominal vessels and a forcing of the blood to the surface with rapid cooling.
Often, however, this adjustment is followed by a recrudescence which indicates that some other vertebra must be adjusted. Many fevers, such as typhoid, pneumonia, tonsilitis, etc., yield to specific local adjustment without any involvement of the so-called Center Place.
I have said that we expect to check or abort a fever with spinal adjustments. The facts that we do so and that the207 more rapidly we accomplish the result the more rapid the convalescence and the less likely are complications and sequelae argue loudly against the correctness of any theory which supposes fever to be a beneficial and cleansing process. According to such theory it would be totally wrong and dangerous to abort a fever but wiser to encourage it in taking its course. The exact opposite proves true under Chiropractic. The very fact that fevers do diminish and disappear under proper adjustments is a proof that they are abnormal, since adjustment does not in any case tend to lessen normal processes, but only to restore normality no matter in what way the functions of the body have departed from that condition.
All the clinical evidence gathered by Chiropractors in regard to inflammations and fevers tends to prove the correctness of the theories herein set down. Fever plays a part in so many diseases that it has been considered advisable to consider the subject under a special head.
The vertebral subluxation is the primary cause of all truly pathological conditions. Through its existence the action of a large number of secondary causes becomes possible. Upon no other hypothesis can we explain the remarkable percentage of cures of all known classes of disease through the specific vertebral adjustment.
Nature is the only real curative agent. Neither suggestion, manipulation, adjustment, nor any other known method applied by Man for the eradication of disease has in itself any power to heal. No man possesses power to do more than so arouse the vital energies of the patient that the body heals itself.
We contain within our own bodies the possibilities of perfect normality. Unless interfered with by powerful outside force we should continue normal from birth to death and death itself would only occur through the simultaneous wearing out of all the parts of the human mechanism. The Chiropractor, insofar as his work succeeds in its purpose, assists the body by adjusting displaced structure and affording the body a free and unhindered opportunity for the exercise of its own self-healing powers. It may be interesting and instructive to analyze the process of cure and to study the exact effects of vertebral adjustment as we have studied the exact effects of vertebral subluxation.
An acute subluxation—that is, one resulting entirely from concussion of forces within twenty-four or forty-eight hours prior to the moment of adjustment—rarely produces a condition which could be named as any particular disease.209 The symptoms are those of “wrenched back,” if any. A single adjustment usually suffices to correct such subluxation just as a single movement might correct a dislocated humerus within the same period, and any symptoms promptly disappear. This is probably the maximum benefit to be derived from adjustment and the best time for its administration, because it leaves the spinal column in an exactly normal condition and no more susceptible to further jars or shocks than before the injury. All disease which might have resulted from that subluxation has been fully prevented.
Older subluxations must be dealt with differently because they present a different condition. Adaptative changes have taken place in the shape of the vertebra itself and of every surrounding tissue as they prepare to make the best of their situation. But a vertebra once displaced has lost its poise and broken or modified the reflex arcs through its nerves so that it becomes more likely to respond to further forces applied, or to muscular contractions within the body, by further change of position. Such changes are always followed by further adaptation of the surrounding parts.
The degree of nerve impingement must change to keep pace with the developing malposition and thus, by gradually successive steps, disease develops in the area of peripheral distribution of the nerves. The nerve is under a thumbscrew gradually tightening.
To adjust such a vertebra many successive movements are required. An apparently full and free movement of a subluxation meets the elastic resistance of the solidly packed210 tissues and the pull of the modified intervertebral disk—strains at these tissues—and rebounds so as to settle almost, but not quite, in its old abnormal position. The amount gained in a single adjustment can rarely be appreciated by palpation. To the touch it would appear that no change had been made, except occasionally in the Cervical region. But with repeated adjustments the vertebra will be found to have approached its normal position. Sometimes in a few weeks, sometimes in a few months, the gain becomes palpable and then perhaps visible to the eye in thin subjects.
The relief of impingement then is not usually an instantaneous process, but proceeds by gradual steps. Each movement of the vertebra is accompanied by a shock to the nerve against some part of which the bone is pressing, which may produce some disturbance in the diseased organs and may even appear to have aggravated disease for a time. Some pain and soreness around the vertebra may accompany the necessary adaptative changes of shape which readapt the tissues to their proper shape and relation.
As the impingement of the nerve is gradually relieved the disease is gradually modified and finally disappears. As the course of adjustments nears its conclusion and the impingement has been reduced to a comparatively slight one there may appear a stage of irritation of the nerve which is a reduplication of the first steps which appeared in the development of the disease. As most subluxations appear not all at once but by a series of changes, so disease develops synchronously, passing from stage to stage with the changes211 in the impingement. Often it passes through first an acute and active stage due to irritation and then a chronic and comparatively passive stage due to heavier, inhibiting impingement.
Under adjustment these successive stages tend to reappear in reverse order, the most alarming sometimes appearing last and just before the cure is completed. It must be remembered that from the moment one practitioner administers medicine or other remedy and the other adjusts a vertebra, the clinical courses differ widely. No text-book on medical practice has as yet described the clinical course of the various diseases under Chiropractic adjustment.
In chronic diseases where the nerves are paralyzed there may be a period under adjustment during which no change is apparent. This is followed by a period of rapid gain leading to complete recovery. This may be accounted for by the fact that the nerves are degenerated and must be repaired all along their course before communication is reestablished between nerve centers and peripheral organs. When this repair is sufficiently completed to allow communication, the cure is really well advanced, although evidence of it then first appears. This has been noted especially in locomotor ataxia.
First, under adjustment, the acute or acutely increased impingement is relieved. The caliber of the blood-vessels is at once regulated and the destructive action of fever212 checked. At the same time the vitality of the local tissue in which the germs are active is suddenly increased and there ensues a struggle between the body, as represented by its phagocytes and auto-protective chemicals, and the germs, which if adjustments be continued results in the rapid destruction of the germ colony. Also the elimination of the toxins already in the body proceeds so rapidly that if the fever can be held in check it takes only a short time for the body completely to overcome and eradicate the germs.
Mental diseases—so-called—usually depend upon disturbance of the blood-supply to the brain, controlled by the Cervical sympathetic. Adjustments, relieving the pressure on the sympathetic ganglia or cord and perhaps the direct impingement from the vertebral arteries, restore a normal circulation to the brain. The time required by Nature to effect a cure depends upon the rapidity with which the impingement is removed and the amount and character of the damage to brain tissue which must be repaired. The cure often requires time for a change of materials in brain cells or fibre tracts, by which they are reconstructed and again become capable of expressing normal function.
When the subluxation is corrected, or partially so, the appetite changes and the craving for food becomes more normal. Adjustments may lessen a voracious appetite, increase213 a too capricious one, or abolish a perverted. At the same time the stomach is enabled to digest its contents more properly, the intestines to take it up and continue it, and the tissues to assimilate that which is brought to them. The body eliminates its waste with less effort and in some extreme cases the first effect of the adjustment may be to cause vomiting and diarrhea and thus purge the alimentary tract of materials which have become unusable.
If injurious diet be persisted in the effects of the adjustments will be partly counteracted, the tendency of the poisons generated within the body being to increase subluxation while the tendency of the adjustments is to correct them.
In acute poisoning by way of the alimentary canal and sometimes when poison has been injected hypodermically, the body rids itself of the menace to its integrity by means of vomiting, diarrhea, and increased secretion of urine. Chronic cases tend rather toward the gradual absorption and removal from the body of the poisons and their cure depends upon the cessation of the poisoning; i. e., it is useless to try to cure a morphine case while the patient is still using the drug.
In acute poisoning the muscular contraction often increases subluxation and counteracts the effect of the adjustments, so that it becomes necessary to give very frequent adjustments until relief is had.
After the acute irritation of nerves arising from the exposure and causing irritation has been removed, perhaps by the first adjustment, if the exposure is not repeated the body heals itself with great rapidity, repairing with comparative ease the damage done.
This depends upon the nature of the excess. If it be overeating, perhaps a more moderate diet will of itself and without adjustments enable the body to rid itself of the bad effects and restore general equilibrium. Adjustments will aid and accelerate this process. Venereal excess is most often engendered by an improper state of mind, perhaps demanding attention as a mental disorder, or by an irritation of the genital organs which demands local adjustment for its relief. Normality of the reproductive tract leads to sane forgetfulness and libidinous habits always suggest sexual weakness or disease. Often where a cure would be possible with right habits, no cure can be effected without their correction. A little good sound advice which will arouse the will of the patient to co-operation may aid. Boys with the masturbation habit offer small chance for favorable results in enuresis or nervous disorders unless the secondary cause be understood and overcome.
In this connection the author cannot forbear a reference to the use of other methods to relieve disease in combination with the Chiropractic adjustment. From the foregoing study of the laws governing the cause and cure of disease it will be seen that therapeutical methods have little direct bearing upon the removal of disease. The logical method of effecting the cure is the removal of the cause. The subluxation being always the primary cause, its correction is always the logical method of effecting a cure. Not sometimes but always.
We know that when the subluxation is corrected the body naturally heals itself. Can we accelerate and aid that healing with stimulant or narcotic? Logic says no; experience says no: the use of any method which strikes at the disease beyond its primary cause and operates upon some of the effects of that cause without touching the cause itself is inconsistent with belief in Chiropractic.
Administration of poisonous drugs to the well body is considered poisoning; their administration to the sick body is also poisoning, whose symptoms combine with the disease to produce different outward signs. Fasting is starvation. Massage is stimulation or inhibition. Spondylotherapy means exhaustion of the spinal nerve centers in riotous expenditure of their stored-up energy.
It would require a wisdom beyond the human to improve upon the natural healing processes with which the216 body has been provided. It should be our entire business to remove the obstructions which hinder the full exercise of that healing power—the subluxations—to remove them dexterously and decisively and to interfere in no other way.
Other methods may and do serve to scatter or modify disease but not to cure it—unless they affect subluxations, as they sometimes do without intent. This accidental adjustment factor is valueless in the presence of a scientific and intelligent adjustment.
Let Medicine, Osteopathy, Spondylotherapy, Christian Science, Massage, and Electricity have their field. It is not ours. Nor can any of these methods be rationally combined with Chiropractic. Their basic principles contradict ours; their application interferes with the results of adjustment. If you claim to remove the cause of disease, do so, and do not mar your work by treatment of effects.
It has been said in a previous section that when subluxation and disease are associated the subluxation always precedes the disease and that the former is the cause, the latter the effect. So clearly do we understand this law that we are able to say what subluxation would cause a certain disease and err by only so many cases per centum as there are variations from the usual structure of the spinal column and the nervous system.
But merely to state that a second Dorsal subluxation causes heart disease is not enough. We must know why and how it causes heart disease and whether, perchance, some other subluxation may sometimes have a like effect. We must map out the sphere of malign influence of each possible subluxation so that when our fingers encounter it it at once and inevitably suggests its possible effects, from which, by diagnostic methods, we may choose the one toward which most symptoms point. And we must know the relation of every nerve in the body to peripheral organs and their functions so that when we encounter indubitable evidence of some functional or organic disease we may know exactly where, in the spinal column, to seek for its cause.
We have learned how to discover a subluxation, how to adjust it, and how that adjustment permits a natural cure of its abnormal effects. We must now learn exactly where to218 apply adjustment for any given organ in the body or for any disease. It must be understood in interpreting this statement and all those which follow in this section that it is never proper to adjust a vertebra merely because it is stated to be the cause of a disease believed to exist in a patient. No vertebra should be moved unless palpation determines it to be subluxated. Rather let it be known that as a rule the statements of spino-organic connection here made will prove to be verifiable by palpation. There is no rule in Chiropractic without some exceptions, and mere diagnosis of disease is too notoriously unreliable to serve as a guide to adjustment without the verification of the trained touch.
We wish to know the relation existing between each part of the Nerve System and other parts and between each part and the other organs of the body. Especially we wish to understand the relation between each part of the Nerve System and the spinal column, by which permanent subluxations of the latter interfere with the former’s action and therefore with the peripheral organs.
This requires a general knowledge of anatomy, physiology, and pathology which we shall presuppose the reader to possesses so that we may present only facts to which his attention should be particularly called. Let us begin with the relation of nerve tissue to other tissues where this relation can be most clearly comprehended, namely, with the development of the human embryo.
The complete human organism represents the snarled fusion of a series of similar, yet specialized, somatic segments, each presenting most of the attributes of a simple animal, though the association and co-ordination of all are required for the production of higher animal phenomena.
The embryo is composed of such segments placed with their centers in the same axial line. Each segment contains in association which is morphologic, physiologic, and anatomical, a segment of nerve matter and a somatic (body) segment. The neural segments are arranged end to end so as to form the rudimentary beginning of the complete central nerve axis of the adult human body; the somatic segments blend together with somewhat indefinite lines of cleavage which are to become much more indefinite and obscure by changes in relative form due to differences in the growth rate of different parts or to involuntionary changes following functional inutility at various periods. Gray says, “The intrinsically segmental nature of the spinal cord is expressed by the association of each definite segment with the somatic segment supplied by its nerve.”
Within each segment there may be observed at an early period cell migrations from the walls of the primitive neural tube and amoeboid projection of axonic and dendritic processes from these cells, which serve to bring the other tissues of the segment under the control of the nerve elements; there is an assumption of command, as it were, by220 the nervous system, so that the epithelial, connective, and muscular tissues of each segment are linked in sensomotor and vegetative co-ordination by the contact association of the nerves which ramify them—sensomotor because the nerves are presently to carry the only force capable of inciting activity of any kind in other tissues, vegetative because the functions of growth, nutrition, and repair, in each somatic cell, depend upon the continuity of communication between it and the lowest nerve cell in the nerve pathway which connects it with the higher motor and sensor centers.
Already may be noted a hint and a prophecy of that future segmental organization by which it becomes possible for some spinal vertebra to become displaced and thus begin a morbid process which may diffuse itself throughout an entire body segment, involving neural and somatic elements together. Already the simple organization begins to become rapidly complex and difficult to trace.
Cell masses begin to migrate from the walls of the primitive neural tube to a position laterad to become the spinal ganglia; these send out long dendritic processes which marvellously thread their way to a predetermined peripheral connection which is to bring some cutaneous, or muscular, or joint tissue into sensor relation with the dorsal, or Sensor, portion of the cord and through it with the brain; at the same time they send their axonic processes inward to mingle with and communicate with the dendrites of other sensor221 cells remaining in the central axis to form the gray matter of the cord, and thus, migrating, keep up communication both with the central axis and the periphery. Other cell masses migrate ventrolaterad to form the sympathetic ganglia and they also send out afferent and efferent processes which make a connection on the one hand with the periphery and on the other with the source from which the cells developed, the situation to be occupied by the cord. From this view it is seen that the sympathetic system is merely an offshoot from the same source with all the rest of the peripheral nerve system, merely a mechanism for the proper distribution of nerve impulses from the central organs, and that it retains its connection in all its parts with those organs. Its ganglia, like those of the cord, are always and from the beginning under the domination of the upper or cephalic end of the neural tube.
This cephalic end rapidly expands. Its growth is faster than the rest of the neural tube and from its walls, by proliferation, develop the structures of the cerebrum, mid-brain, and hind-brain. It also gives off ganglionic masses from which grow sensor processes to form the afferent elements of the cranial nerves and contains, like the cord, motor nuclei, or nidi, from which motor axons grow toward the periphery to come into relation with definitely predetermined organs.
Now appear the primitive cartilaginous and membranous elements from which a bony wall is to be built around the central nerve axis, primitive vertebrae, the upper known as cranial and numbering four, and the lower, or spinal, numbering usually thirty-three. These bone structures develop around the brain and spinal cord. Later the cephalic vertebrae fuse into a solid vault, the cranium, completely enclosed except for various foramina for the passage of spinal cord, nerves, and blood-vessels. The succeeding twenty-four vertebrae remain separate and movable upon each other and leave between them the openings for the emergence of the spinal nerves. The last nine segments fuse eventually into two immovable or false vertebrae called Sacrum and Coccyx. These latter also contain foramina from which nerves issue.
When this development and growth of new parts is completed the Nerve System appears as a set of complex organs made of a central axis, brain and spinal cord, and peripheral connections made up of forty-three pairs of directly attached nerves (12 cranial and 31 spinal) with two great gangliated cords and numerous other sympathetic ganglia and communicating cords situated outside the skeletal axis but communicating with it intimately by means of interchange of fibre bundles between the sympathetic and the cerebro-spinal nerves.
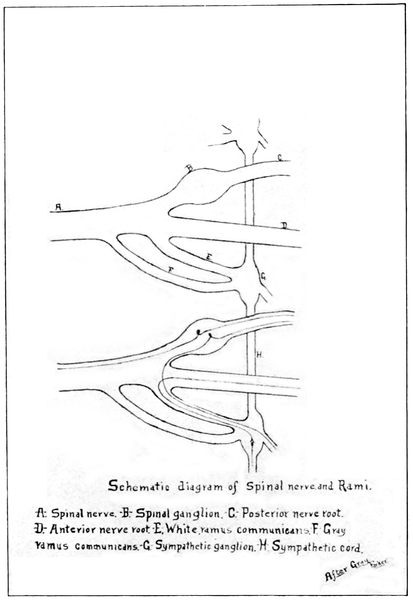
Schematic diagram of Spinal nerve and Rami.
A: Spinal nerve. B: Spinal ganglion. C: Posterior nerve root. D: Anterior nerve root. E: White ramus communicans. F: Gray ramus communicans. G: Sympathetic ganglion. H: Sympathetic cord.
After Gray
Parker
31. Interchange of fibre bundles between spinal and sympathetic nerves.
But we who have viewed the embryonic development even briefly and sketchily, understand that all these complex organs are merely an aggregation of neurons, each neuron made up of a cell body, one or more axons, and dendrites; that the nerve cells are the controlling elements and the axons the centrifugal carriers of nerve energy, while the dendrites are the centripetal processes through which each nerve cell receives communications.
The skull and spinal column, taken together, constitute the bony axis of the body, the center of organization of the skeleton; to these parts are attached other skeletal structures, mandible, ribs and sternum, extremities, classified as the appendicular portion of the skeleton. Likewise are attached, directly or indirectly, the voluntary muscles which move the skeleton, and the vessels and viscera. Any given structure in the body can be traced to a supporting connection with this bony axis.
The bony axis contains the neural axis. Its strength and solidity are such as to preserve the integrity of the most vitally important tissue of the body from every form of injury if such protection be possible. Through openings in the bony axis—foramina—the central nerve organs give off or receive the nerve bundles which bring them into communication with every other structure of the body. And the body has been so arranged that every single part of it is partly or wholly under control of nerves emerging through224 these foramina. Even the brain and spinal cord themselves respond to changes in the blood-vessels which are controlled by nerve impulses which have emerged through the intervertebral or cranial foramina and returned by other routes to supply the muscular coats of the vessels.
Reverting for a moment to the primitive segmental arrangement which is none the less persistent and important because in the completed human the regularity of contour of the segments has been wholly lost and aberrant organs have moved from their original positions carrying their nerve supply with them, let us first state and then illustrate a general law.
Any violence applied to the body tends to affect the spinal column. Such violence does or does not produce permanent displacement of a spinal segment according as it does or does not succeed in overcoming the internal resistance. But whatever effect upon the spine is accomplished will occur most noticeably in the same body segment to which violence was applied. That is, force applied to any body segment tends to subluxate the vertebra which would impinge the nerves controlling that segment. Thus diseases are primarily segmental and later general just as the body is primarily segmental and later co-ordinated into complicated functional systems, all more or less interdependent.
If a man falls so that he strikes first on the point of his shoulder the force will be transmitted almost directly across225 the line of the spine, at right angles, and may subluxate the sixth or seventh Cervical or first Dorsal. If subluxation occurs it is because the law of gravity causes the remainder of the body to keep moving downward after the shoulder strikes and until it too comes to rest. The subluxation which results is a right one if the left shoulder be struck and vice versa. Now the brachial plexus is chiefly controlled by these three vertebrae and a right subluxation tends to impinge most the nerves on the left side, so that if any permanent effect of the fall follow it will be a permanent weakness or disease of the left shoulder or arm, with possible slight extensions along other branches of the same plexus, as to the latissimus dorsi. Also by the internal sympathetic communications from this same region the larynx, trachea, or large bronchi may be affected, occasionally the heart, all structures segmentally associated with the arm.
This law applies throughout the body and can be fully demonstrated by any one having a complete knowledge of nerve connections and body segmentation upon being furnished with a complete and accurate history of any injury to the body. It goes further than this. Toxins or other secondary causes operating within the body tend always to produce their motor reactions and consequent effect upon any subluxated vertebrae in the same body segment with the peripheral irritation, so that if the stomach contain a poison which affects the spine the sixth or seventh Dorsal vertebrae will be most affected and the stomach itself the organ to suffer most.
The spinal column is peculiarly adapted, with its strong ligaments, its cartilage cushions, its perfect flexibility and flexuousness, to withstand jars and shocks. Yet the spine is the door by which disease enters the organism. Concussion of forces, the energy from the environment encountering the bodily resistance, is of no serious effect upon the organism—of no permanent or irreparable effect—unless it affects the spine and brings about vertebral subluxation, disturbance of the normal alignment between vertebrae, and thereby interrupts the perfect healing and controlling influence exerted by the vital part of the segment, the central nerve portion.
When a concussion of forces does produce subluxations, does disturb the perfect poise and balance of that center of structure of the body, its consequences affect an entire body segment, producing, or tending to produce, disturbances through the entire segment.
Disease is the indirect consequence of the contact of man with his environment and is natural but not normal.
The spinal column is a center or a series of centers for disease. In this column will be found the primary cause—the introductory element—by which disease first makes its appearance in a previously healthy body.
The study of Comparative Anatomy is necessary to a complete understanding of the human organism. We may trace in the simplest forms of animal life the beginnings and227 foreshadowings of the same plan of organization. We may follow it through the ascending scale and watch its complexity develop, and by viewing each step in the process we may come fully to realize that the original plan has been preserved throughout, though often in such form that by study of the single species we should fail to recognize it.
We lack space for complete consideration of this subject and shall merely suggest certain facts and phases. No clear analogy can be drawn until we reach the worm, with its rudimentary spinal column and nerves. Roughly speaking, dissection of one spinal segment with its nerves and their controlled area—if this were possible—would separate from the rest a fairly regular layer similar to all the other layers. This is the primitive segmentation.
It is shown much more clearly in the fish but the segments have begun to curve with their periphery directed slightly caudad and some have already shown a preponderating growth over other segments and a change of shape from the original symmetry.
The reptiles and birds show still more complicated segmentation. It is notable that in these lower animals the purely reflex portion of the nervous system is highly developed while the volitional and sensory portions, the cerebral hemispheres, are yet rudimentary. In birds, particularly, the cerebellum is very highly developed because its function of co-ordination of muscles for the maintainence of equilibrium is required in a high degree for flying.
Those land animals which walk on all fours approach still228 closer but their arrangement is much more readily comprehensible than in man. As the animal stands on all fours with head extended, a gigantic cleaver slicing out each vertebra and pair of nerves and slicing straight toward the base of support might be said to divide the body approximately according to the structural and functional arrangement in segments. Yet no segment so separated would exactly correspond to the nerve distribution; there would be enlargement of some organs with extension into the zone previously occupied by their neighbors; enlargement here and atrophy there; invagination of one organ by another and overlapping and intermingling of parts. Even the relation between the spinal cord segments and the vertebrae has departed much from the primitive so that the growth of the vertebrae has exceeded that of the cord and the cord terminates opposite the Lumbar region instead of at the end of the Sacral canal. It may here be remarked that in the human embryo the cord at first occupies the entire length of the neural canal formed within the vertebrae; that in the adult it terminates opposite the lower border of the body of the first Lumbar vertebra and that the nerves, still retaining their original foramina of exit and their relation to the somatic segments, pass downward within the canal to their respective openings and collectively form a brush like mass called “cauda equina.”
The causes of the change in the shape, form, and relation of the different segments are functional: the body changes to meet the changing needs of its environment and the steady progressive functional development from one species to another.
When the animal at last assumes the erect position, doing more intricately and intelligently the bidding of a developing and improving central nervous system, the change of position and the force of gravity bring about a gradual downward, or caudad, tendency of the parts of the somatic segments most remote from the spine and of the nerves which supply them.
The nerves, muscles, and bones of the lower extremities change from almost a right angle to an extremely obtuse angle, less obtuse during infancy and more so in the adult. The forelegs become arms and hang at the sides, extending downward from the part of the spine which controls them. The ribs tend more obliquely downward and outward from the spine and the tendency of all the nerves is downward from their attachment to the spinal cord to their emergence from the intervertebral foramina. In the neck and head alone is this rule varied, the tendency of the nerves and some other structures there being to run from the spine either at right angles or upward.
It seems almost symbolic and indicative of the purpose of creation that the body, which is less strong and vigorous230 in Man than in the lower animals, should tend more and more obliquely downward from its central axis, while the cranium, containing a highly specialized mass of cells and fibres, the organ of Mind, which marks Man’s supremacy in the animal kingdom and is his crowning glory, is reared above the body it dominates.
In all the form changes which mark the growth of the body the organs are arranged to afford the greatest possible economy of space and convenience for use. This perfect and matchless mechanism adapts itself to the changing habits and environments and to the quality and needs of the Mind which inhabits it.
To the practitioner who is fully equipped with an instantly available knowledge of all the nerve connections in the body and to whom palpation of a subluxation at once suggests its somatic sphere of influence as a weakened or diseased area, or to whom mention of a disease immediately calls to mind the organ, or segment, which is primarily affected and its nerve connection with the spine, any tabulation of spino-organic connection or of diseases and adjustments, for reference, is unnecessary. But the ordinary practitioner finds it difficult to acquire and retain such an array of information and much more convenient to refer to reliable and easily read tables which will supply at once any such information desired.
No specific adjustment is possible without knowledge of231 the vertebra which controls the part diseased and toward the healing of which the nerve energy should be directed. Specific adjustment without correct diagnosis is of course impossible. And whenever correct diagnosis has been made it is essential that the mind of the Chiropractor should revert to one certain vertebra which he expects to find subluxated as the primary cause of the disease.
Diagnosis is essential in order to find out what organ is the site of the disease, for all disease is primarily segmental. The location of the disease having been determined, a quick reference to a table showing the spinal connection with that location makes specific adjustment possible. The value of specific, as against general, adjustments will be considered under “Practice.”
One who wishes to determine for himself the proper specific adjustment for a certain disease must, in order to be able to attach any weight to his conclusions or to announce them with any hope of credence by the scientific world, proceed very much after the following method, which sets down what may be termed “standard test conditions” for research into the spino-organic connection.
He must make a correct diagnosis which serves to determine the nature and location of the disease process. In this he may be greatly aided by vertebral palpation and nerve-tracing, especially in differential diagnosis. Any case which affords less than a quite positively correct diagnosis232 should be excluded from the test list because any conclusion based on a doubtful diagnosis must itself be doubtful and may be seriously misleading.
He must then ascertain as far as possible the known anatomical nerve connection between the spine and the diseased part. If several connections are known he must decide according to nervous physiology, by recognizing the morbid functions which constitute the disease and learning which nerves control these functions and which must therefore be deranged in order that the disease may exist. I may say right here that to attempt to answer the problems of Chiropractic on the assumption that standard anatomies are incorrect in their statement of nerve connections is as hopeless as the wail of the schoolboy that the answers in his arithmetic are wrong because his sums fail to come out that way.
The investigator must next be accurate in Palpation, selecting the subluxation which would, from his knowledge of the body segmentation, seem most likely to influence the nerves involved, and positively ascertaining the number of the subluxated vertebra. No one who cannot count vertebrae accurately can positively say which vertebra he has adjusted. More than that, no one who has not counted the vertebrae in the special case in question can say which vertebra he has adjusted. No mere regional localization will suffice for scientific investigation.
Correct and accurate adjustment must follow selection of the single vertebra and the adjuster must know that he233 has used the one special movement, or form of adjustment, which is mechanically right for that kind of subluxation and has so moved the vertebra as to release impingement. Mere movement of a vertebra is not necessarily an adjustment or even a maladjustment; it may be movement without permanent change of relation or release of impingement. (See “Preferable Adjustments,” p. 155.)
There follows the observation of the progress of the case and this must be so careful and accurate that the observer knows to a certainty whether the disease is progressing unfavorably, or favorably, or whether it has been entirely eradicated. He must know the value of every changing symptom, the real meaning of each new development. Every diagnostic method should be at his command for this work. Constant vigilance and constant thought should mark each step of his work.
Finally he must be so cautious and careful in his statements that no doubtful conclusion is allowed to escape from his own mind. We may believe or suspect or hope for proof of our theories but we have no right to state as a fact anything except that which has been proven under the most rigidly guarded scientific test conditions.
Failure to observe any of the precautions mentioned renders worthless the results of investigation. Nothing further than a mere presumption can be based upon research which fails to observe all these rules. It will be readily understood that there are few Chiropractors whose training has been sufficient to enable them successfully to234 accomplish such research. There are thus many things connected with the spino-organic connections which are commonly held as facts but which should be classed as presumptions. And the prevalence of the habit of general adjustment rather than specific makes the future final solution of all these problems remote.
It will be seen that of the three kinds of evidence—Anatomical, Physiological, and Clinical—which are admissible in reasoning upon the connection between the spine and disease, only one form—clinical evidence—has been adduced by Chiropractic. For anatomical and physiological corroboration of our apparent clinical findings we are obliged to turn to standard works on these subjects; fortunately we find it in abundance.
Anatomy, fortified now by research in the morphologic relations of the parts studied and by physiological and pathological experiment which has thrown much light on the proper viewpoints from which to describe structure, contains sufficient data on the nervous system to enable us to explain practically every fact observable in a Chiropractic clinic.
It is true that there are a few statements in the ensuing outlines for which we cannot as yet find the anatomical or physiological proof. But it must be remembered that anatomists and physiologists have never studied the body with a knowledge of the subluxation theory to aid them in gaining perspective and that Chiropractors, as a class, have not235 yet delved deeply enough into anatomy and physiology to extract all the available and illuminating information from them. Ofttimes the facts we value most are most obscure in the texts because to others they seem least important. But they are there. Armed with information concerning Chiropractic facts it is probable that the scientist of the future will corroborate all of our clinical findings of today and emphasize the rational explanations of them.
In the following tables it has been found best to insert in parentheses the capital letter (P) to call attention to any statement in support of which we have gathered less than all three forms of admissible evidence and which is therefore as yet presumptive. It is well, however, for the practitioner to be careful lest he regard too lightly such presumptive statements. Unless there is very strong and reasonable ground for such presumption or a general belief in its correctness all mention of it is omitted. Those labelled presumptive are merely so indicated because they have not yet been proven and not because they have failed to serve as a convenient and useful guide to adjustment. For each presumption offered there is either clinical or anatomical justification but not both.
This section does not purport to state with any degree of completeness the various nerve-paths by which spinal vertebrae come into relation with all, or nearly all, the peripheral organs of the body. It merely points out some of the more236 interesting and important connections, some of the paths which serve to explain the common effects of vertebral adjustment. It is not expected that this resume of the subject will be more than suggestive to the student; certainly it cannot, in so brief a space, be a complete exposition.
Let us begin with the observation that almost every organ of the body, including the central nerve organs themselves, may be adversely affected by spinal subluxation impinging spinal nerve axons at their exit from, or entrance through, intervertebral foramina, or by spinal subluxation producing direct impingement upon some part of the sympathetic system and similarly interfering with its power to functionate.
The Nerve System may be divided into two great divisions, the central axis and the peripheral system which distributes nerve energy from, and brings stimuli to, the central axis. The central axis consists of the brain and spinal cord; the peripheral system of 12 pairs of nerves attached to the brain and having exit (except the eighth) through foramina in the base of the cranium, 31 pairs of spinal nerves emerging through intervertebral foramina whose parts are movable upon each other (except the foramina for sacral and coccygeal nerves), and an intricate system of sympathetic fibres and ganglia arranged in a double chain of ganglia in front and at the sides of the vertebral column, three great prevertebral plexuses, the237 cardiac, coeliac, and hypogastric, and numerous scattered ganglia and communicating cords which bind the ganglia together and connect them with spinal or cranial nerves and with the periphery.
The peripheral system is somewhat complex and numerous intercommunications are established by which nerve impulses originating in the central axis and leaving by one part of the peripheral system may exercise a controlling influence over another part. Plexuses, or intertwinings of nerve axons, are so numerous and complicated that it is difficult to follow each set of nerve stimuli from their origin to their final destination and effect without considerable study.
The spinal nerve axons, taken as a whole, establish paths between the motor gray of the ventral horn of the spinal cord and all voluntary muscles of the body below the head except the trapezius and sternomastoid, partially innervated by the eleventh cranial, and between the sensor cells of the dorsal spinal gray and gracile and cuneate nuclei of the medulla on the one hand and the sensor end organs in skin and mucuous membrane, muscles, tendons, and joints on the other. The ventral cornu receives impulses from the cortico-spinal axons of the direct pyramidal, crossed pyramidal, rubrospinal, and other smaller tracts which bring the spinal gray under the direct voluntary domination of the volitional centers in the brain or of the indirectly voluntary238 pathway through the cerebellum. The spinal nerves are the direct media for motion of the body or its parts in relation to its environment. The sensor gray of the cord is similarly in communication with the conscious sensation area in the cerebrum and with the cerebellum by way of the dorsal tracts of the cord, the lemnisci, and the cerebellar peduncles.
In the main these nerves of motion and sensation are arranged as follows:
The Cervical plexus is composed of the intertwining of axons from the anterior primary divisions of the four upper Cervical nerves. Its branches pass to and innervate many voluntary muscles of the neck and side and back of head, and supply sensor fibres to the adjacent cutaneous areas. Branches also communicate with the last three cranial nerves and one long branch, the Phrenic, or Internal Respiratory Nerve of Bell, passes through the neck and thorax to the diaphragm, as its motor nerve.
The Brachial plexus is made up of the anterior primary divisions of the four lower Cervical nerves and the greater part of the first Thoracic. It is distributed chiefly to the voluntary muscles and integument of the shoulder and arm, forearm, and hand, but sends branches to some muscles of the neck and upper back as well. It, like the Cervical plexus, receives branches from, but gives none to, the Cervical sympathetic.
The Thoracic nerves are not arranged in plexiform fashion like those above but pass separately, for the most239 part, to their destinations. They are distributed to the walls of the thorax and abdomen following the curve of the ribs in direction. The last Thoracic sends one division downward as far as the outer aspect of the ilium.
The Lumbar, Sacral, and Pudendal plexuses are formed of the ventral divisions of the Lumbar, Sacral, and Coccygeal nerves and distribute branches to the integument and voluntary muscles of the lower abdomen, pelvis, and lower extremities. From two of the sacral nerves branches known as “Visceral” pass through the plexus to terminate in the walls of the uterus and rectum.
All of the thoracic nerves and the first and second, sometimes the third and fourth, lumbar give off branches to the sympathetic ganglia, known as white rami communicantes.
The distribution of the 12 pairs of cranial nerves is not so definitely to voluntary muscles and to areas from which conscious sensation is to be derived as is the case with the spinal, although the cranial nerves present many analogies with the spinal and there is abundant reason for considering them as in one series of 43 pairs. There is direct distribution of some cranial nerve fibres to secreting glands, but these fibres are probably merely derived from sympathetic trunks and carried in company with the axons of cranial origin. There is also some direct distribution of cranial nerve axons to visceral walls made of non-striated muscle, as in the case of the vagus distribution to the respiratory and240 alimentary tracts and that of the spinal accessory to the heart. This is a resemblance to the sympathetic.
The cranial nerves carry afferent impressions from the special sense organs, except those of the sense of touch, which function is divided with the spinal nerves.
Various intercommunications exist between the cranial and sympathetic divisions of the peripheral system, by means of which axons starting with one division may be finally distributed with another, or by which an axon of the sympathetic may pass to one of the sensor ganglia of the cranial system and influence its nutrition and condition, and therefore its power to act. There is a limited intermingling of spinal fibres with the lower cranial.
The sympathetic system directly innervates most of the nutritive or vegetative system, the alimentary tract and its accessory organs, the vascular systems, the genito-urinary system, and the ductless glands. To a limited degree it shares this control with the cerebro-spinal and to a much greater degree it brings the central axis into indirect connection with these viscera.
Gray says, “The distinction of the sympathetic system from the cerebrospinal system is made merely for reasons of convenience. The two systems are intimately connected and the sympathetic is morphologically a derivative of the central axis disseminated in connection with the nutritive241 apparatus and establishing relationships among the vegetative organs.”
Most pathways which carry nerve impulses from their origin or inception to the organ in which they are finally expressed as action of some sort or translated into sensation or into stimuli which pass out reflexly over a connected neuron, are composed of more than one neuron. The neurons of a nerve pathway are arranged end to end with the axons all pointing in one general direction so that the nerve energy travels always in the same direction over the entire nerve path. Impulses are transferred from the first neuron in the chain to the second, and from second to third, etc., by contact of the telodendria of the one neuron with the dendrites or receptive processes of the next. Part of the nerve pathway may be within the central axis and part within the trunk of a peripheral nerve.
Several peripheral pathways for afferent impulses may be joined to an efferent pathway so as to complete reflex arcs and the efferent cell be under the controlling influence of some upper neuron coming down from the central axis with the power either to permit or to inhibit the reflex acts which would otherwise take place as a result of peripheral stimuli. Several such lower cells may be under the domination of one upper neuron.
In some instances the nutrition of ganglia or nerve trunks, or of parts of the central axis itself, is under the242 control of sympathetic neurons terminating in connection therewith, so that interruption of the normal action of the sympathetic neuron may be followed by effects manifested through some distant part of the cerebrospinal system. In the following pages we shall discuss nerve pathways with reference to the explanation of diseases caused by vertebral subluxation impinging nerves either by tension or constriction, and therefore our grouping of parts will differ somewhat from any anatomical or physiological grouping with another object in view.
To brain: C 2, 3, or 4 to superior cervical ganglion by direct impingement, through internal carotid nerve to sympathetic plexuses following branch arteries from Circle of Willis. The blood-supply of the brain is under control of the cervical sympathetic and most brain lesions or diseases are due to vascular changes leading to anaemia, hyperaemia, inflammation, or hemorrhage.
To meninges: Loop between first and second cervical nerves to trunk ganglion of vagus and through meningeal branches of vagus (P), or by way of internal carotid nerve to pial sympathetic plexuses. (P) The connection of the first, second, or third cervical with cerebral meningitis is established clinically but there is still doubt as to the explanation.
Eye and Muscles, Retina, Optic Nerve: The external muscles of the eye, the four recti and two oblique with the243 levator palpebrae superioris, are innervated by the Oculomotor, or third cranial, and the fourth and sixth cranial, which receive branches from the cavernous plexus of the sympathetic derived from the internal carotid branch of the superior cervical ganglion. As the ganglion lies in front of the transverse processes of the second, third, and fourth cervical vertebrae, direct impingement upon it by subluxation of one of these vertebrae may cause strabismus or other affection of the external ocular muscles.
The eye-ball receives filaments from the ciliary or ophthalmic ganglion, which in turn is connected with the cervical ganglion by way of cavernous plexus and internal carotid nerve. This pathway controls the radial fibres of the iris and dilates the pupil as a part of the light accommodation reflex mechanism. Loss of pupillary reaction, especially with small pupils, suggests upper cervical subluxation.
The retina, containing the cells of origin of the optic nerve axons and being the special end-organ of the sense of sight has no direct spinal or sympathetic connections but its blood-supply, and therefore its nutrition, is influenced by branches from the sympathetic which enter with the central artery of the retina. Retinal hemorrhage has been cured by cervical adjustment, C 2, 3, or 4.
The conjunctiva is innervated by the sympathetic and by the fifth cranial, or trigeminal.
Olfactory Nerve: Nerve of smell, distributed to the Schneiderian membrane over the upper portion of the nasal244 septum and over the upper lateral wall. There is no known connection by which the trunk of the olfactory nerve can be reached by adjustment but the condition of the special end organs in the membrane and their ability to functionate depend not only upon the integrity of their axons but also upon the nutrition and moisture of the membrane in which they are embedded. This is under the control of the Vidian nerve and of branches from the spheno-palatine, or Meckel’s ganglion, both connected with the carotid plexus of the sympathetic and therefore responsive to adjustment of C 2, 3, or 4. This is also the route by which epistaxis is usually checked.
The external nasal muscles, like those of the rest of the face except some of the muscles of mastication, get their supply from the facial nerve, which connects with the sympathetic plexus on the middle meningeal artery. It may be said parenthetically here that peripheral facial paralysis (Bell’s palsy) yields to adjustment and proves the value of this connection. The nasal integument is under the sensor control of the trigeminal and trophic disturbances may result from its involvement.
Trigeminal Nerve: This is the great sensor nerve of the face and carries a motor division, the inferior maxillary, to some of the muscles of mastication, as the temporal, masseter, and buccinator. It has connected with it four ganglia, which also receive sympathetic roots, and the ganglion of origin of its sensor axons, the Gasserian or semilunar, also receives direct sympathetic communications.245 The importance of this communication is shown by the powerful effect of adjustment of third or fourth Cervical for tic dolouroux.
Ear: The external ear receives branches from the vagus and from the first and second cervical nerves. The middle ear and Eustachian tube are supplied by the tympanic plexus made up of branches from the glosso-pharyngeal, otic ganglion, facial nerve and the small deep petrosal from the sympathetic on the carotid artery. By all these routes communication from the third and fourth cervicals is possible but especially is the latter important. The fourth cervical is the especially frequent subluxation with middle ear disease. To the internal ear and auditory or acoustic nerve there appears to be no direct route from the spine. It has not yet been conclusively established within the writer’s knowledge that adjustments will affect auditory deafness but Meniere’s Disease, inflammation of the semicircular canals, has been cured repeatedly by adjustments of Atlas or Axis, by what route I am unable to state.
Teeth and Gums: It is probable that the only connection between the vertebrae and the teeth is an afferent one by way of the trigeminal. Toothache may be stopped by adjustment of C 3, or C 4, but no evidence is at hand to show that the condition of the teeth is improved or that more than a temporary effect can be had. Trophic changes in the gums may be due to vascular disturbances controlled by the sympathetic.
Tongue: The hypoglossal, motor nerve to both the intrinsic246 and extrinsic muscles of the tongue, receives direct axons from the loop between the first and second Cervical nerves. Sympathetic fibres pass to the blood-vessels and secreting glands of the tongue.
Tonsils: Receive fibres from the spheno-palatine ganglion and by this means are brought under the domination of C 2, 3, and 4. Abundant clinical evidence in tonsilitis, simple, follicular, and suppurative, proves this to be the practically, as well as anatomically, correct nerve connection.
Salivary Glands: The parotid receives branches from the great auricular nerve from the second and third cervical, and from the sympathetic on the external carotid artery, branches from the superior cervical ganglion. The submaxillary and sublingual glands are connected with the submaxillary ganglion, which receives a sympathetic root and which, with the chorda tympani also carrying fibres derived from the sympathetic, controls the secretions of these glands.
Pharynx: The pharyngeal plexus is a mixture of sensory axons from the glosso-pharyngeal, motor components from the vagus and probably sensor from the same nerve, and sympathetic branches from the superior cervical ganglion. All of these may be influenced by the upper cervical adjustment.
Larynx: According to anatomy the larynx is innervated by the superior and inferior, or recurrent, branches of the vagus and by sympathetic branches from the superior cervical ganglion. Clinically the sixth cervical adjustment cures247 laryngitis and aphonia. The explanation probably lies in the fact that the thyroid branches of the middle cervical ganglion, lying in front of the transverses of the sixth, communicate within the thyroid gland with the recurrent laryngeal and with the external laryngeal branch of the superior laryngeal.
Thyroid Gland: “The nerves to the thyroid are amyelinic and are derived from the middle and inferior ganglia of the sympathetic.” (Gray.) The middle cervical ganglia are situated in front of the transverse processes of the sixth cervical vertebra. Clinically, the sixth cervical reaches goitre.
Muscles of Neck: The platysma is supplied by the facial nerve; the sternomastoid by the spinal accessory and cervical plexus; the infrahyoid region by the first three cervical nerves; the suprahyoid region by the facial and the ansa cervicalis; the anterior and lateral vertebral muscles by the cervical nerves from second to seventh inclusive, but especially the second, third, and fourth. It will be seen that muscular disturbance in the neck may result from any cervical subluxation. Torticollis, which usually involves the sternomastoid, yields to the second cervical most frequently.
Lymph Nodes of Head and Face: These lymph nodes are controlled by the cervical sympathetic. Pathological changes in one or more nodes requires careful cervical palpation to determine the presence of a subluxation away from the affected side.
Muscles of Back: The trapezius is innervated by the248 spinal accessory and by the third and fourth cervical nerves; the latissimus dorsi by the sixth, seventh, and eighth cervical through the middle or long subscapular. Occasionally a tender nerve, traceable from the lower reaches of the latissimus to the cervical region has mislead the practitioner into imagining a cervical connection over the back with internal viscera.
The second layer of the back is supplied by the third, fourth, and fifth cervical nerves. The third layer is innervated by the middle and lower cervical and upper three thoracic nerves except the serratus posticus inferior which is supplied by the ninth, tenth, and eleventh thoracic. The fourth and fifth layer are supplied by the posterior primary divisions of the spinal nerves and any given section of these layers may be traced to a vertebra directly above, or cephalad.
Thoracic Walls: The parietal muscles of the thorax are innervated by the intercostal nerves and a very definite segmental association with the spine is traceable.
Diaphragm: Phrenic nerve, which arises from fourth cervical chiefly; lower intercostals, especially eighth and ninth; and phrenic plexus of the sympathetic which may sometimes be reached from the fourth or fifth dorsal vertebrae through the gangliated cord. For motor disturbances of the diaphragm adjust fourth cervical.
Abdominal Muscles: These are supplied by the lower intercostals and the transversalis and internal oblique make connection with L 1 by the iliohypogastric. Cremaster is249 supplied by L 1 and 2 by way of the genital branch of the genitofemoral.
Perineal Muscles: The anterior perineal group are supplied by the perineal branch of the internal pudic which traces to the second, third, and fourth sacral nerves. The posterior perineal and ischiorectal region is also supplied by the sacral and coccygeal nerves.
Trachea and Bronchi: Vagus and sympathetic filaments from first and second thoracic ganglia. The latter receive preganglionic fibres from first dorsal nerve in all probability, as this adjustment reaches the bronchi.
Lungs: The third thoracic ganglia connect with the pulmonary plexus and establish a connection from third dorsal vertebra direct to the lung parenchyma. The Pleurae have a similar connection or may sometimes be reached by the first dorsal.
Heart and Pericardium: In 55% of all heart disease or improper action the second dorsal is responsible; in 40% the first dorsal, and perhaps in the remaining 5% the atlas or axis. The former nerves (T 1 and 2) furnish pre-ganglionic fibres which stream upward through the gangliated cord to terminate in the three cervical ganglia in relation with the dendrites of new neurons (amyelinic) which form the superior, middle, and inferior cardiac nerves and pass into the thorax to mingle with vagal fibres to form the superficial and deep cardiac plexuses, controlling the heart. Probably the upper cervicals occasionally affect the vagus through the loop between the first and second cervical nerves.
Thoracic Aorta: Controlled by sympathetic from first thoracic ganglion or last cervical ganglion, and thus by seventh cervical or first dorsal vertebra.
Abdominal aorta—Coeliac Axis: The upper portion of the abdominal aorta is innervated by the coeliac or solar plexus of the sympathetic. Sub-plexuses from the coeliac accompany the various branches of the aorta and are widely distributed to the blood-vessels and to the glands and non-striated muscle of the abdominal organs. The coeliac plexus receives fibres from the right vagus and from the greater, lesser, and least splanchnic nerves, by the latter route making connection with the thoracic ganglia of the sympathetic from fifth to last. These ganglia receive pre-ganglionic fibres from the thoracic spinal nerves in the form of white rami communicantes, so that it is not incorrect to say that the coeliac plexus and its branches are largely controlled by the condition of the last eight thoracic nerves.
Through this intricate plexus it is difficult to trace the relations of each abdominal organ with the particular vertebrae of which subluxation would produce disease in said organ. By the aid of clinical experimentation covering a period of years and by diligent search among anatomies and physiologies, we have arrived at the conclusions indicated in succeeding statements.
The most important spinal connection with the abdominal blood-vessels is that of the fifth dorsal vertebra, for the fifth dorsal nerve, by its rami, seems greatly to influence the caliber of the aorta and coeliac axis.
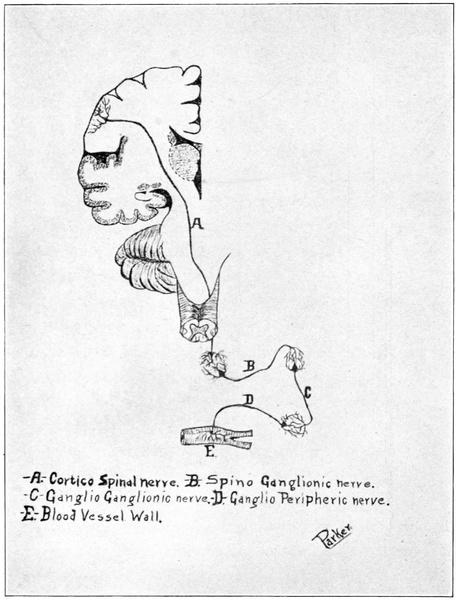
A. Cortico Spinal nerve. B. Spino Ganglionic nerve.
C. Ganglio Ganglionic nerve. D. Ganglio Peripheric nerve.
E. Blood Vessel Wall.
Parker
Fig. 32. Schematic representation of nerve pathway from brain to periphery by way of sympathetic.
Liver: Fourth thoracic nerves (especially the right) to gangliated cord, via great splanchnic nerve to coeliac plexus, by hepatic plexus to interior of liver. The hepatic plexus gives off the cystic plexus which controls the gall-bladder.
Stomach: Sixth and seventh dorsal nerves by white rami to and through the ganglia of the gangliated cord to coeliac plexus. The gastric plexus is an offshoot of the coeliac and gives off Auerbach’s plexus to the muscular coat, and Meissner’s plexus to the submucous and mucous coats of the stomach. The nutrition of the stomach walls, their peristaltic action, and the secretory action of the stomach glands are thus brought under the direct influence of the sixth or the seventh dorsal subluxation.
Pancreas: Eighth dorsal nerve by great splanchnic to coeliac plexus, to hepatic and superior mesenteric plexuses, and by the pancreatico-duodenal branches of the former and pancreatic branches of the latter to the pancreas.
Spleen: The coeliac plexus, the left semilunar ganglion, and the left vagus and right phrenic nerves give off branches which form the splenic plexus. Spinal connection by way of ninth dorsal nerve, by rami communicantes to gangliated cord to great splanchnic nerve to coeliac plexus to splenic plexus. Many nerve pathways like this one are less indirect than they sound; various names have been given to different parts of the same pathway through which, often, the axons pass without interruption. On the way from the cerebral cortex to one of the abdominal viscera there may be only three, sometimes four or five, neurons connected end to end.
Duodenum: Coeliac plexus by way of duodenal branches of hepatic plexus and branches from the superior mesenteric plexus. Spinal connection from eighth dorsal nerve and possibly branches from the upper lumbar ganglia of the sympathetic may join the superior mesenteric plexus, as results in duodenal disease are occasionally reported following specific adjustment of L 1 or 2.
Jejunum and Ileum: Connection same as for duodenum, by superior mesenteric plexus. Adjustment of L 2 in typhoid fever is undoubtedly correct so that it is probable that the lumbar ganglia send branches to this vicinity.
Peritoneum: Nerve supply to the peritoneum is rather general owing to its great extent. It is supplied by the sympathetic from both the lower thoracic and lumbar portions of the gangliated cord through the various abdominal plexuses and in general it may be said that any localized peritoneal disease will yield to the same adjustment as would be made for disease in the immediately subjacent organ.
Suprarenal Capsules: These important glands are supplied by amyelinic fibres derived from the gangliated cord by the lesser splanchnic nerve and connecting with pre-ganglionic fibres from the tenth dorsal nerve. The suprarenal plexus is an offshoot of the coeliac.
Kidneys: Tenth, eleventh, and twelfth dorsal nerves by way of lesser and least splanchnic nerves to renal plexus, an offshoot of the coeliac. McConnell’s experiments and the frequently duplicated clinical feats of Chiropractors prove this to be a vital and dominant nerve pathway in kidney disease.
Ureters: Nerves derived from inferior mesenteric, pelvic, and spermatic plexuses. Most important connection seems to be from first lumbar nerve by lumbar ganglia to inferior mesenteric plexus.
Caecum and Vermiform Appendix: The inferior mesenteric plexus, which supplies these organs probably carries to them chiefly fibres derived from the lumber ganglia which complete a connection with the second lumbar vertebra, especially on the right side.
Colon: Third and fourth lumbar vertebrae, influencing lumbar ganglia and thus inferior mesenteric plexus.
Rectum: Lower lumbar ganglia by inferior mesenteric and plevic plexuses, through superior and inferior hemorrhoidal plexus to rectum. Adjustment L 4 or 5. Visceral branches from the third and fourth sacral nerves also pass directly to the rectal wall and sacral adjustment may affect rectum or anus.
Bladder: The urinary bladder is innervated by the vesical plexus from the pelvic, and by sacral nerve fibres direct. It is said that the vesical plexus contains many spinal nerve fibres which are derived from the second and fourth lumbar nerves especially. Clinically the second or the fourth lumbar will control the bladder much oftener than the sacrum.
Prostate Gland, Seminal Vesicles, Penis, and Urethra: By the vesical and prostatic plexuses derived from the pelvic plexuses, divisions of the hypogastric plexus, which is formed of the abdominal aortic plexus and filaments from254 the lumbar ganglia. The latter receive filaments from the second and third lumbar nerves. There is a connection with the sacral nerves also by the pelvic plexus, though the lumbar adjustment appears the more potent.
Testes and Scrotum: Ilioinguinal from second lumbar, genital branch of genito-femoral from second and third lumbar nerves, internal pudic nerve from the pudendal plexus, and spermatic and pelvic plexuses. The most effective adjustment for scrotal or testicular diseases is L 3.
Uterus and Vagina: Uterovaginal plexus from the pelvic and containing spinal nerve fibres from L 4, L 5, and sacrum.
Ovaries and Fallopian Tubes: The ovarian plexus receives fibres from the abdominal aortic and through it from the lumbar ganglia, influenced by second lumbar adjustment.
Brachial Plexus: The brachial plexus of spinal nerves arises from the nerves from the fifth cervical to the first thoracic inclusive and controls the voluntary muscles of the upper extremity, with its integument. Muscle groups, rather than single muscles, are represented for the most part in the spinal segments giving off these nerves, and the ramification of the nerves within the plexus is such that almost any given muscle might be affected by more than one spinal subluxation. Below are given the principal connections:
Pectoralis Major and Minor Muscles: Sixth or seventh cervical through internal anterior thoracic nerve and first dorsal through external anterior thoracic.
Shoulder Joint: The joint, muscles covering the joint, and integument of this region are innervated by the circumflex nerve which traces through the plexus to fifth and sixth cervical nerves. Sixth cervical adjustment usually affects this joint.
Serratus Magnus Muscle: Sixth cervical by long thoracic, or External Respiratory Nerve of Bell.
Elbow Joint: Sixth cervical vertebra by musculocutaneous nerve.
Anterior Arm Muscles: Sixth cervical.
Posterior Arm Muscles: Seventh cervical and first dorsal.
Lumbosacral Plexus: This plexus, derived from the anterior primary divisions of the lumbar, sacral, and coccygeal nerves, supplies the muscles and integument of the lower extremity, taking with it axons derived from the sympathetic by the lumbar ganglia to supply the blood-vessels, perspiratory glands and sebaceous glands of this region. The latter are responsive to adjustments of the first or second lumbar vertebrae.
Hip-Joint: Third and fourth lumbar nerves by femoral and obturator or accessory obturator nerves and fifth lumbar or first sacral by the nerve to the quadratus femoris or the great sciatic. Fourth lumbar seems the most potent connection and is usually adjusted for hip-joint disease.
Psoas Magnus Muscles: Anterior branches of the second and third lumbar nerves.
Anterior Thigh Muscles: Supplied mostly through the femoral nerve from the second and third lumbar nerves.
Internal Thigh Muscles: Second and third lumbar nerves (chiefly but not wholly) through the obturator, accessory obturator and femoral nerves.
Gluteus Maximus: From the fifth lumbar and first and second sacral nerves through the inferior gluteal branch of the sacral plexus.
Obturator Externus: Second, third, and fourth lumbar nerves through the obturator nerve.
Posterior Thigh Muscles: Fourth and fifth lumbar and sacral nerves through the great sciatic.
Great Sciatic Nerve: This great nerve, direct continuation of the sacral plexus, arises from the fourth and fifth lumbar and first three or four sacral nerves and is widely distributed to muscles and integument of the lower extremity. Sciatica, or sciatic rheumatism, is most commonly relieved by adjustment of fourth or fifth lumbar vertebra; but there is a condition commonly diagnosed as sciatica which is really a sciatic neuritis and due to vasomotor disturbance affecting the blood-supply to the nerve trunk. This responds to adjustment of first or second lumbar because the amyelinic fibres which control these blood-vessels are derived from lumbar ganglia of the sympathetic.
Anterior Leg Muscles: Fourth and fifth lumbar and first sacral nerves through the anterior tibial.
Posterior Leg Region: Fourth and fifth lumbar and first and second sacral through the internal popliteal and posterior tibial.
Knee-Joint: This joint receives branches from the257 great sciatic through both internal and external popliteal, and from the femoral and obturator. It is therefore connected with the lower lumbar and sacrum and with the second lumbar. The latter connection seems oftenest involved in knee joint inflammations.
Foot: Fourth and fifth lumbar and sacral nerves through the great sciatic and its branches.
Sensor Areas of Lower Extremity: In general, any given cutaneous area receives sensor branches from the nerve which supplies the subjacent muscle area. For accurate diagnostic purposes a good chart of sensor distribution may be consulted.
The appended list includes the diseases with which the profession has had experience but is not in any sense a complete list of diseases. It is merely intended for quick and handy reference. In obscure cases or diseases not mentioned it is suggested that the practitioner carefully diagnose the case with reference to the location of the morbid process and then refer to Special Nerve Connections to find the nerve pathway between the spine and the organ indicated as the seat of the disease. Standard works on anatomy and physiology will explain more fully the paths and functions of the nerves but information gleaned from them must be sought out and pieced together from scattered statements and discussions.
| A258 | |
| Disease | Adjustment. |
| Abscess | According to location. |
| Accommodative iridoplegia | C 3 or 4. |
| Acid stomach | D 6 or 7. |
| Acne | D 11 or 12. |
| Acoria | D 6 or 7. |
| Acromegaly | C 1 or 2, D 10, 11, or 12. |
| Addison’s disease | D 10. |
| Adenitis | According to location. |
| Adenoids of pharynx | C 2 or 3. |
| Adiposis dolorosa | D 8 and D 11 or 12. |
| Adrenals, tuberculosis of | D 10. |
| Ageusia | C 1 or 2. |
| Ague | D 4, D 9, D 11 or 12. |
| Albuminuria | D 10, 11, or 12. |
| Albumosuria | D 8, D 10, 11 or 12. |
| Alcoholism | C 1, D 10, 11 or 12. |
| Amenorrhoea | L 4 or 5. |
| Amnesia | C 1 or 2. |
| Amyosthenia | General. |
| Amyloid liver | D 4. |
| Amyloid kidney | D 10, 11 or 12. |
| Anachlorhydria | D 6 or 7. |
| Anaemia | D 4, D 9 and D 11 or 12. Sometimes L 4. |
| Anaesthesia, general | C 1 or 2. |
| Anasarca | D 10, 11 or 12. |
| Aneurism | D 1 or according to location. |
| Angina pectoris | D 2. |
| Aniscoria | C 4. |
| Anorexia nervosa | C 1, D 6 or 7. |
| Anosmia | C 1 or 2, C 4. |
| Anthracosis | D 3.259 |
| Anterior poliomyelitis | C 3 or 4. local zones for permanent paralyses following. |
| Anuria | D 10, 11 or 12. Or L 2 or 4. |
| Aortic stenosis | D 2. |
| Aphasia | C 1 or 2. |
| Aphonia | C 6. |
| Aphthous stomatitis | C 2. |
| Apoplexy | C 2, 3. |
| Appendicitis | L 2. |
| Apraxia | C 1 or 2. |
| Argyll-Robertson pupil | C 1 or 2. |
| Arrhythmia | C 2 or D 2. |
| Arteriosclerosis | D 10, 11 or 12 and local. |
| Arteritis | According to location. |
| Arthritis | According to location. |
| Arthritis deformans | D 10, 11 or 12 and according to location. |
| Ascarides | L 2 or 3. |
| Ascites | D 4. |
| Asphyxia, gas | D 2 or 3, Atlas (First aid only). |
| Asthenia | To correct disease producing same. |
| Asthenopia | C 4. |
| Asthma | D 1. |
| Ataxia, cerebellar | C 1 or 2. |
| Ataxia, locomotor | General adjustment. |
| Athetosis | C 1 or 2. |
| Atrophic cirrhosis of liver | D 4. |
| Atrophy | According to location. |
| Aural discharges | C 1, 2, 3 or 4. |
| B260 | |
| Back, pain in | According to location. |
| Barber’s itch | C 5, D 10, 11 or 12. |
| Bell’s palsy | C 2, 3 or 4. |
| Biliousness | D 4. |
| Blepharitis | C 3 or 4. |
| Blepharospasm | C 3 or 4. |
| Blindness | C 1, 2, 3 or 4. |
| “Blood poisoning” | D 10, 11 or 12 and local. |
| Boils | D 10, 11 or 12 and according to location. |
| Bradycardia | D 1 or 2, possibly C 2. |
| Bright’s disease | D 10, 11 or 12. |
| Bronchitis | D 1. |
| Bronchiectasis | D 1. |
| Broncho-pneumonia | D 1, D 3. |
| C | |
| Caked breast | D 3. |
| Calculi, cystic | L 2 or 4. |
| Calculi, hepatic | D 4. |
| Calculi, renal | D 10, 11 or 12. |
| Cancer | No cure. |
| Cancrum oris | C 2 or 3, D 11 or 12. |
| Canker (mouth) | C 2. |
| Carbuncle | According to location. |
| Carcinoma | No cure. |
| Caries of spine | According to location. See “Prognosis.” |
| Cataract | C 2, 3, or 4. |
| Catarrh, nasal | C 4. |
| Catarrhal gastritis | D 6 or 7. |
| Catarrhal stomatitis | C 2 or 3. |
| Cerebral abscess | C 1 or 2.261 |
| Cerebrospinal meningitis | C 2. |
| Cervical glands, enlargement of | Any cervical. |
| Cervico-brachial neuralgia | C 6. |
| Cervico-occipital neuralgia | C 1 or 2. |
| Chickenpox | C 5, D 10, 11 or 12. |
| Chills | D 5. |
| Chlorosis | D 4, D 9, D 11 or 12. |
| Cholangitis | D 4. |
| Cholecystitis | D 4. |
| Cholelithiasis | D 4. |
| Cholera infantum | D 5 or 6, D 10, 11 or 12, L 2. |
| Chorea | C 1 or 2. |
| Chyluria | D 8, D 11 or 12. |
| Cirrhosis of liver | D 4. |
| Claw hand | C 6 or 7 or D 1. |
| Clubfoot | L 4 or 5. |
| Colic, hepatic | D 4. |
| Colic, renal | D 10, 11 or 12. |
| Colitis | L 2 or 3. |
| Collapse | C 1, D 2, and according to associated condition. |
| Coma | According to cause. |
| Conjunctivitis | C 3 or 4. |
| Constipation | D 4, D 10, or L 3, 4 or 5. |
| Contractures | According to location. |
| Coryza | C 4. |
| Coxalgia | L 4. |
| Cramp | According to location. |
| Croup | C 2 or C 6. |
| Cutaneous eruptions | D 10, 11 or 12. |
| Cyanosis | D 2, D 3 or C 2.262 |
| Cystitis | L 2 or L 4. |
| D | |
| Deafness, catarrhal | C 4. |
| Deafness, central | C 1 or 2 (P). |
| Delirium | C 1 or 2. |
| Dementia | C 1. |
| Dengue | D 5, D 10, 11 or 12 (P). |
| Dentition, disorders of | D 6 or 7. |
| Diabetes insipidus | D 10, 11 or 12. |
| Diabetes mellitus | D 4, D 8, D 11 or 12. |
| Diarrhoea | D 10, 11 or L 2, 3. |
| Dilatation of heart | D 2. |
| Diphtheria | C 2, C 6 and D 11 or 12. |
| Dipsomania | C 1 or 2, D 11 or 12. |
| Dropsy, abdominal | D 4. |
| Dropsy, cardiac | D 2. |
| Dropsy, renal | D 10, 11 or 12. |
| Duodenal ulcer | D 8 or 9. |
| Duodenitis | D 8 or 9. |
| Dysentery | L 2, 3, or 4 and D 11 or 12. |
| Dysmenorrhoea | L 4. |
| Dyspepsia | D 7. |
| Dysphagia | C 2 or D 6 or 7 (P). |
| Dyspnea | D 1 or D 2 or D 3. |
| Dysuria | L 2 or L 4 or sacrum. |
| E | |
| Earache | C 2 or C 4. |
| Ecchymoses | D 11 or 12. |
| Eczema | D 11 or 12 and according to location. |
| Embolism, cerebral | C 2 or 3.263 |
| Emphysema | D 3. |
| Encephalitis | C 1, 2 or 3. |
| Endocarditis | D 2. |
| Enlarged glands | According to location. |
| Enlarged heart | D 2. |
| Enlarged liver | D 4. |
| Enlarged tonsils | C 2 or 3. |
| Enteralgia | D 9 or 10, or L 1 or 2. |
| Enteritis | D 9 or 10, or L 1 or 2. |
| Enterocolitis | D 9 or 10, or L 1, 2 or 3. |
| Enteroptosis | D 9, 10, 11 or L 1, 2, 3. |
| Enterospasm | D 9 or 10, or L 1 or 2. |
| Enuresis | L 2 or 4. |
| Epilepsy | C 1 or 2, sometimes L 3. |
| Epistaxis | C 4. |
| Epithelioma | No cure. |
| Eructations | D 6 or 7. |
| Eruptions, cutaneous | D 11 or 12. |
| Erysipelas | C 5 and D 11 or 12. |
| Exophthalmic goitre | C 6 or 7. |
| F | |
| Facial hemiatrophy | C 1 or 2. |
| Facial paralysis | C 1 or 2. |
| Faecal obstruction | L 2, 3 or 4. |
| Fainting | D 2. |
| False angina | C 1 or 2. |
| Fatty degeneration of heart | D 2. |
| Fatty degeneration of liver | D 4. |
| Fatty infiltration of heart | D 2.264 |
| Fatty infiltration of liver | D 4. |
| Felon | C 6 or 7 or D 1. |
| Fever | D 5. Locate organ of origin. |
| Fibroid tumor | According to location. |
| Follicular tonsilitis | C 2 or 3. |
| G | |
| Gallstones | D 4. |
| Gangrene | According to location. |
| Gastralgia | D 6 or 7. |
| Gastrectasia | D 6 or 7. |
| Gastric neuroses | D 6 or 7. |
| Gastric ulcer | D 6 or 7. |
| Gastritis | D 6 or 7. |
| Gastro-duodenitis | D 7 or 8. |
| Gastroptosis | D 6 or 7. |
| Gland, mammary | D 3. |
| Glaucoma | C 2 or 3. |
| Gleet | L 3 and D 11 or 12. |
| Glossitis | C 2 or 3. |
| Glycosuria | D 4 and D 11 or 12. |
| Goitre | C 6. |
| Gonorrhoea | L 3. |
| Gonnorrhoeal rheumatism | D 11 or 12 and L 3. |
| Gout | D 11 or 12 and L 4. |
| Granulated lids | C 4 and D 11 or 12. |
| H | |
| Hay fever | C 3 or 4. |
| Headache, anaemia | To correct anaemia. |
| Headache, bilious | D 4. |
| Headache, neuralgic | C 1.265 |
| Headache, neurasthenic | C 1 or 2. |
| Headache, ocular | C 2 or C 4. |
| Headache, of constipation | D 4 or D 9 or 10, or L 4 or 5. |
| Headache, toxic | Locate toxin-forming organ. |
| Headache, uterine | L 4 or 5 or sacrum. |
| Hematemesis | D 6 or 7. |
| Hematuria | D 10, 11 or 12. |
| Hemicrania | C 1, 2 or 3. |
| Hemiplegia | C 2 or 3. |
| Hemoptysis | D 3. |
| Hemorrhoids | L 4 or 5 or sacrum. |
| Hepatic hyperemia | D 4. |
| Hepatoptosis | D 4. |
| Hernia, diaphragmatic | C 4 (P). |
| Hernia, femoral | L 4. |
| Hernia, inguinal | L 2 or 3. |
| Hernia, umbilical | D 8. |
| Herpes facialis | C 4. |
| Herpes zoster (shingles) | Vertebra above nerve involved. |
| Hiccough | C 4. |
| Hodgkins’ disease | General adjustment. |
| Hydrocele | D 10, 11 or 12 and L 4. |
| Hydrocephalus | C 2 and D 2. |
| Hydronephrosis | D 10, 11 or 12. |
| Hydropericardium | D 2. |
| Hydrothorax | D 3. |
| Hyperaemia | According to location. |
| Hyperaesthesia, general | C 1 or 2. |
| Hyperchlorhydria | D 6 or 7. |
| Hypertrophy | According to location.266 |
| Hysteria | C 2. |
| Hystero-epilepsy | C 2. |
| I | |
| Icterus | D 4. |
| Icterus neonatorum | D 4. |
| Ileocolitis | L 2, 3 or 4. |
| Impacted gallstones in ducts | D 4. |
| Impotence | L 3 or sacrum. |
| Incontinence of urine | L 2 or L 4. |
| Incompetency, aortic | D 1 or 2. |
| Incompetency, mitral | D 1 or 2. |
| Incompetency, pulmonary | D 1 or 2. |
| Incompetency, pyloric | D 6 or 7. |
| Incompetency, tricuspid | D 1 or 2. |
| Infantile paralysis | C 3 or 4 and according to location. |
| Inflammation, general | D 5. |
| Inflammation of appendix | L 2. |
| Inflammation of bladder | L 2 or 4. |
| Inflammation of bowels | D 9 or 10, L 2, 3 or 4. |
| Inflammation of bronchi | D 1. |
| Inflammation of kidneys | D 11 or 12. |
| Inflammation of larynx | C 6. |
| Inflammation of lungs | D 3. |
| Inflammation of meninges | C 1 or 2. |
| Inflammation of ovaries | L 2 or 3. |
| Inflammation of pharynx | C 2. |
| Inflammation of pleurae | D 3. |
| Inflammation of stomach | D 6 or 7. |
| Inflammation of vertebrae | Next above inflamed one. |
| Inflammation of uterus | L 4 or 5.267 |
| Influenza | C 4, D 1, D 11 or 12. |
| Intestinal neuralgia | D 9 or 10, L 1 or 2. |
| Intestinal neuroses | D 9 or 10, L 1 or 2. |
| Intestinal obstruction | See “Practice.” |
| Intussusception | See “Practice.” |
| Insanity | C 1 or 2, sometimes L 4. |
| Insomnia | C 2. |
| Iritis | C 3 or 4. |
| J | |
| Jaundice | D 4. |
| K | |
| Keratitis | C 3 or 4. |
| Kyphosis | See “Curvatures.” |
| L | |
| Lactation, disorders of | D 3. |
| Lacunar tonsilitis | C 2 or 3. |
| La grippe | C 4, D 1, D 11 or 12. |
| Laryngeal paralysis | C 6. |
| Laryngismus stridulus | C 6. |
| Laryngitis | C 6. |
| Lateral spinal sclerosis | According to location. |
| Lead poisoning | D 4, D 11 or 12. |
| Leucaemia | D 9 and D 11 or 12. |
| Leucorrhoea | L 4. |
| Lipoma | According to location. |
| Lobar pneumonia | D 3. |
| Lockjaw | C 1, 2, or 3. |
| Locomotor ataxia | General adjustment. |
| Lordosis | See “Curvatures.”268 |
| Lumbago | L 3, 4 or 5. |
| Lumbo-abdominal neuralgia | Any Lumbar. |
| M | |
| Malaria | D 4, D 9, and D 11 or 12. |
| Malignant endocarditis | D 2 and D 5 or 6. |
| Mastoiditis | C 1 or 2. |
| Measles | C 5, D 11 or 12. |
| Memory, disorders of | C 1 or 2. |
| Meniere’s disease | C 1 or 2. |
| Meningitis | C 1 or 2. |
| Menorrhagia | L 4. |
| Metrorrhagia | L 4. |
| Migraine | C 1, 2, or 3. |
| Mitral incompetency | D 2. |
| Mitral stenosis | D 2. |
| Monoplegia | According to location. |
| Mouth breathing | C 4 or 5. |
| Movable kidney | D 11 or 12. |
| Mucous colic | D 10 or L 3. |
| Mumps | C 4. |
| Mutism | C 1 or 2 or C 6. |
| Myelitis | According to location. |
| Myocarditis | D 2. |
| Myopia | C 4. |
| Myositis ossificans | According to location, also D 11 or 12. |
| Myxoedema | C 6. |
| N269 | |
| Nephritis | D 10, 11 or 12. |
| Nephrolithiasis | D 10, 11 or 12. |
| Nephroptosis | D 10, 11 or 12. |
| Neuralgia, trigeminal | C 3 or 4. |
| Neuralgia, brachial | C 6 or 7 or D 1. |
| Neuralgia, intercostal | According to location. |
| Neuralgia, of feet | L 4, L 5 or sacrum. |
| Neurasthenia | C 2. |
| Neuritis | According to location. |
| Nodding spasm | C 1 or 2. |
| Nystagmus | C 1, 2, 3 or 4 (P). |
| O | |
| Obesity, pathological | D 8 and D 11 or 12. |
| Obstruction, intestinal | See “Practice.” |
| Oculomotor paralysis | C 2 or 3. |
| Oedema | According to location. |
| Optic atrophy | C 3 or 4. |
| Optic neuritis | C 3 or 4. |
| Orchitis | L 3. |
| Otitis media | C 4. |
| Ovarian disease | L 2. |
| P | |
| Pachymeningitis | C 2. |
| Pallor | D 2 or to correct anaemia. |
| Palpitation | D 2 or C 2. |
| Pancreatic calculi | D 8. |
| Pancreatic hemorrhage | D 8. |
| Pancreatitis | D 8. |
| Paralysis agitans | C 1 or 2. |
| Paralysis, brachial | C 6 or 7 or D 1.270 |
| Paralysis, crural | L 4 or L 5. |
| Paralysis, facial | C 1 or 2. |
| Paralysis, diplegic | C 1 or 2. |
| Paralysis, hemiplegic | C 1 or 2. |
| Paralysis, monoplegic | According to location. |
| Paralysis, sensory | According to location. |
| Parageusia | C 1 or 2. |
| Paratyphoid fever | L 2. |
| Parosmia | C 2 or 3. |
| Parotitis | C 4. |
| Pericarditis | D 2. |
| Perihepatitis | D 4. |
| Perinephric abscess | D 10, 11 or 12. |
| Peritonitis | D 9, 10 and L 2, 3 or 4. |
| Pertussis | C 6, D 1. |
| Pharyngitis | C 2 or 3. |
| Photophobia | C 1 or 2 or C 4. |
| Plantar neuralgia | L 4 or 5. |
| Pleurisy | D 3. |
| Pleurodynia | D 3. |
| Pneumonia | D 3. |
| Priapism | L 3 or sacrum. |
| Proctitis | L 4 or 5. |
| Prolapsed kidney | D 11 or 12. |
| Prolapsed uterus | L 4 or 5. |
| Prostatic disease | L 4 or 5 or sacrum. |
| Ptosis | C 4. |
| Puerperal fever | L 4, D 5, and D 11 or 12. |
| Pulmonary incompetence | D 2. |
| Pulmonary phthisis | D 3. |
| Pulmonary stenosis | D 2.271 |
| Pyelitis | D 11 or 12. |
| Pyelonephrosis | D 11 or 12. |
| Pyaemia | D 5 or 6 and D 10, 11 or 12. |
| Q | |
| Quinsy | C 2 or 3. |
| R | |
| Rabies | C 1 or 2, D 10, 11 or 12. |
| Rachitis | See “Adjustment of Curvatures.” |
| Raynaud’s disease | C 6 or 7 or D 1, or L 4 or 5. |
| Rectal fistula | L 4 or 5. |
| Rectal neuralgia | L 4 or 5. |
| Relapsing fever | D 5, D 9 and D 11 or 12. |
| Renal colic | D 10, 11 or 12. |
| Retinal hemorrhage | C 4. |
| Retinitis | C 4. |
| Retropharyngeal abscess | C 2 or 3. |
| Rheumatic fever | D 5 or 6, D 11 or 12. |
| Rheumatism | D 11 or 12 and according to location. |
| Rhinitis | C 4. |
| Roseola | D 10, 11 or 12. |
| Rubella | C 5, D 6, D 11 or 12. |
| Rubeola | See “Measles.” |
| S | |
| Salivation | C 2, 3 or 4. |
| Salpingitis (Eustachian) | C 4. |
| Salpingitis (Fallopian) | L 2. |
| Sarcoma | No cure. |
| Scarlatina | C 5, D 6, D 11 or 12.272 |
| Scarlet fever | C 5, D 6, D 11 or 12. |
| Sciatica | L 4 or 5, or sacrum. |
| Sclerosis | According to location. |
| Scoliosis | See “Curvatures.” |
| Scrofula | D 11 or 12 and locally. |
| Seminal emissions | L 3. |
| Septicaemia | D 5, D 11 or 12, and for site of entrance of toxins. |
| Smallpox | C 5, D 5, D 10, 11 or 12. |
| Sneezing | C 4. |
| Softening of brain | C 2. |
| Spasm | According to location. |
| Spermatorrhoea | L 3. |
| Splanchnoptosis | Caudad of D 5 according to palpation. |
| Splenic enlargement | D 9. |
| Splenitis | D 9. |
| Splenoptosis | D 9. |
| Spondylitis Deformans | General adjustment. |
| Stenosis | According to location. |
| Stomatitis | C 2, 3 or 4. |
| Strabismus | C 3 or 4. |
| Sudamina | D 10, 11 or 12. |
| Sunstroke | C 2, D 2, D 11 or 12. |
| Suppression of urine | D 11 or 12. |
| Syncope | D 2. |
| Syphilis, primary | According to location of ulcer. |
| Syphilis, secondary | D 5 or 6, D 11 or 12. |
| Syphilis, tertiary | No cure. |
| T273 | |
| Tabes dorsalis | General adjustment. |
| Tapeworm | D 8, 9 or 10, L 2 or 3. |
| Tenesmus | L 4 or 5. |
| Tension, high arterial | D 5. |
| Testicles, pendulous | L 3. |
| Tetanus | C 4, D 5, D 10, 11 or 12. |
| Thrush | C 2 or 3. |
| Tic dolouroux | C 3 or 4. |
| Tinnitus aurium | C 1 or 2. |
| Tonsilitis | C 2 or 3. |
| Toothache | C 4. |
| Torticollis | C 2, 3 or 4. |
| Toxaemia | D 11 or 12 and local according to indications. |
| Toxic gastritis | D 6 or 7. |
| Tricuspid incompetency | D 2. |
| Tricuspid stenosis | D 2. |
| Trigeminal neuralgia | C 3 or 4. |
| Tuberculosis of any organ | See “Special Nerve Connections” to organ diseased. |
| Tuberculosis, general | D 5 or 6, D 11 or 12. |
| Tuberculosis, pulmonary | D 3. |
| Tumor | According to location. |
| Typhoid fever | L 2. |
| Typhus fever | D 5 and L 2 (P). |
| U | |
| Ulceration | According to location. |
| Ulnar neuritis | D 1. |
| Ununited fracture | According to location. |
| Uraemia | D 10, 11 or 12. |
| Urethritis | L 3.274 |
| Urticaria | D 10, 11 or 12. |
| Uterine catarrh | L 4. |
| Uteroversion | L 4. |
| V | |
| Vaccinia | D 5, D 10, 11 or 12 and for site of inoculation. |
| Vaginitis | L 3. |
| Valvular lesions | D 2. |
| Varicella | D 5 or 6, D 10, 11 or 12. |
| Varicocele | L 3. |
| Varicose veins of lower extremities | L 2, 3 or 4. |
| Variola | Same as Smallpox. |
| Varioloid | Same as Smallpox. |
| Vertigo | C 1 or 2. Locally for toxic vertigo. |
| Vomiting, pernicious | D 6 or 7 or C 1. |
| W | |
| Whooping-cough | C 6, D 1. |
| Writer’s Cramp | C 6 or 7 or D 1. |
| Worms, stomach | D 6 or 7. |
| Worms, intestinal | Any Lumbar. |
| Wryneck | C 2, 3 or 4. |
| X | |
| Xerostomia | C 2. |
| Y | |
| Yellow fever | D 4, D 6, D 10, 11 or 12 (P). |
The correct use of the foregoing table depends entirely upon correct diagnosis. Knowledge of the vertebra to be adjusted for the correction of any disease is useless unless the disease be recognized when met. Diagnosis may be, and usually is, aided by Palpation and Nerve-Tracing, which may be considered as divisions of diagnosis since the subluxation and the tender nerve are evidences (symptoms) of disease. But these two divisions can never wholly take the place of a complete diagnosis which calls to the aid of the examiner every harmless method of ascertaining the patient’s condition. The part may not suffice for the whole.
The Chiropractor has an opportunity to become the best of diagnosticians because he has at his command all the usually taught methods and in addition Palpation and Nerve-Tracing, which are especially useful in differential diagnosis. (See “Schedule of Examination.”) The profession is at present lamentably weak in diagnosis and as long as they remain so they will fail to achieve the possible maximum of results from the application of a theory which, per se, is applicable to all disease but which is often imperfectly applied in practice.
The ensuing section is intended rather more for the use of the practitioner than for the guidance of the student but may furnish the student a preconception which will prepare him somewhat, before leaving college, to meet the problems of practice.
Just as too frequently the young Chiropractor overlooks the fundamental logic of Chiropractic which may be epitomized with the terse command, “Adjust the cause,” and considers his practice as requiring him to dabble in every suggested or discovered method of treating effects, so, too frequently, the young Chiropractor is prone to consider that his practice consists solely of the adjustment of vertebrae, that he practices a mechanic art rather than a profession; too frequently he overlooks the thousand details which lead to and surround the adjustment and are essential to its success.
The practice of Chiropractic involves more than correct technic. It includes the use of a vast fund of knowledge; the constant study of diseases and of patients; the art of controlling and directing others sometimes in their very trivial acts. Successful practice requires a proper setting, proper business methods, and a knowledge of psychology.
Anyone entering upon a profession assumes a great moral responsibility and the greatest responsibility of all277 falls upon the doctor, of whatever school. He enters the stricken home at a time when all members of the household are off guard, as it were, at a time when all turn to him as to one of higher knowledge and of greater power for their guidance and often for their strength in affliction; he becomes the repository of their most sacred confidences. He who is unable to meet this responsibility, to realize his influence and his power and to prepare himself with care and conscientious training to acquit himself well, has mistaken his calling. He is unfit for his ministry.
The thorough student wrestles not alone with the technic and the text-book branches necessary in practice but also studies his profession from every possible standpoint, broadening his field of usefulness wherever possible.
This section does not by any means contain all the information not found elsewhere in this book but necessary to the Chiropractor in his practice. It is intended merely to suggest some of the many sides and phases of our work and to open the way for a life study of humanity and of professional life as a Chiropractor.
The patient, upon first entering an office, consciously or unconsciously forms an estimate of the personality and standing in his profession of the occupant of that office. This impression is gathered from the kind and arrangement278 of the furniture and visible equipment, from the neatness or disorder of the room, from countless little things which play each their part in making up the whole appearance. This first estimate is sometimes the only one, for an unfavorable first impression may lead to the loss of a prospective patient. In any case it will play a part in all subsequent judgments which the patient may form concerning the Chiropractor and his work.
Many patients entering our offices have no previous knowledge of our profession; their minds are open and curious, alert for new impressions of some sort. We may impress them as we choose. Every good business or professional man realizes the value of the first impression and strives for a good one. Therefore, upon entering practice, choose for yourself every article which shall have a place in your office. Your surroundings will then truly reflect your personality and will attract those upon whom that personality can work in harmony and understanding. It is of no avail to attract the type of patients you cannot hold, to draw through the borrowed judgment or taste of another surroundings alien to yourself and thus to attract people who will at once sense the incongruity and be repelled by it.
Yet one may aspire. And if you are able to perceive and appreciate truly professional surroundings you may hope to school yourself by association and study to harmonize with them.
In choosing the contents of your office keep in mind good taste, utility, and the psychological effect upon all visitors. Remember that you expect to spend many hours each day in the company of your furniture, and select such things as will contribute to a proper professional state of mind in yourself. A Chiropractor’s profession is in many ways like, yet in many ways unlike, any other. Therefore his office equipment, while following in general the equipment of other professional offices, must be selected with an eye to the special and particular needs of the Chiropractor and his patients. Too little attention has been paid thus far by the profession to the selection of office equipment.
The furnishing of an office depends upon the amount and disposition of the room at your command. One must have at least a waiting room and a private office even if a single rented room must be cheaply partitioned to make the division. A larger suite is a better investment when possible. In the waiting-room should be found easy chairs, library table, hall-rack, mirror, and an easy divan or couch. The floor should be covered with a good rug or carpet and the walls properly and cleanly decorated and hung with restful, pleasant pictures. A book-case filled with carefully selected books is a good addition.
On entering your private office the patient should see your diploma, which hangs in full view of the entrance and280 which bespeaks with no weak voice your fitness to practice, your professional ability. The importance of this point cannot be overestimated. The intelligent visitor expects you to have had careful training and to possess thorough knowledge of your work. If he notes the diploma as evidence of it and of your pride in your college he is assured.
If only two rooms are at your command the second must be at once consulting room, adjusting room, dressing room. As such it should contain your desk, desk chair, chairs for the patient or patients, adjusting table or tables, towel cabinet, lavatory, and a curtained recess for a dressing-table, chair, and hooks for hanging clothing. On the wall hang those charts from which it is at times necessary to explain a part of the human mechanism to the inquirer.
This room should convey a two-fold impression—business and professional. It should contain the special paraphenalia of your profession and some of the suggestive contents of the ordinary business office, such as desk, card-index file, typewriter, etc.
Let us consider these points more in detail.
In your waiting room new patients wait and form their estimate of you before your appearance. They are tired patients, worn perhaps with years of disease, and their comfort must be considered. Some time is theirs for use in some way and the use of their minds during the waiting interval must be studied.
For these reasons first of all the waiting room should be furnished quietly, in perfect taste, but well furnished. A good dark rug for the floor rather than matting or linoleum with their suggestion of bareness, a tinted or papered wall done in a soothing shade, upholstered furniture pleasing to the eye and comfortable for tired, weak bodies, and a library table with proper literature for the occupation of the mind—these are the proper furnishings for a waiting room.
Let the table contain chiefly Chiropractic literature and select that literature with care. Be sure that it reflects the view-point toward your profession with which you wish your patients to be impressed. It must be scientific, well written, not sensational, not dealing coarsely or vulgarly with the revolting diseases or features of disease, but quietly convincing. Your literature must impress with the greatness of Chiropractic without setting forth extravagant claims which your patients will expect you to vindicate. Your selection of books for the book-case must convince all observers of your proper literary taste or the book-case had better be omitted. Likewise the pictures on the walls must suggest pleasant things, restful things, good to contemplate.
When possible secure a high-ceilinged room with good ventilation, plenty of fresh air without drafts. And then let all the articles in the room harmonize. One jarring note in form or color may mar the entire effect, which should be that of comfortable simplicity.
Even more important than the contents of the waiting room is the equipment of your private office. It is in this room that your work is done. There your patients confide to you their weaknesses; there they determine finally whether to trust themselves to your knowledge and skill; in that room they form their judgment as to your cleanliness, your use of system; there they meet you.
Every bit of furniture for the private office having been carefully selected its arrangement should be studied.
When the patient first enters the private office he should be able to see your diploma. He should also sit where he can notice it as he consults you and every other object within his vision during the consultation should be picked so as to avoid attracting his attention to anything foreign to his visit and its purpose.
Two chairs are placed near the desk, one an easy chair for yourself, a revolving chair being preferable, and a straight-backed leather-upholstered chair for the patient. In placing these chairs be careful of two things: let the strongest light shine over your own shoulder and bring the face of the patient out in clear detail; and let your own chair be higher than the patient’s so that he looks slightly upward to meet your direct gaze. For the last mentioned point there is a sound psychological reason; to control any dialogue with another person place yourself on a higher283 level than he and unconsciously he will obey the suggestion and lift his thought to meet yours, offering it rather than commanding with it. The light is arranged for its value in observing, as a matter of diagnosis, every indication in expression, gesture, and skin coloring.
Hanging back of the desk where it may be easily reached but where its gruesome suggestion will not obtrude itself upon the nerves of the sensitive without your deliberate intention, have a vertebral column for demonstration purposes. There are many times when it is necessary to show a subluxation as it would occur.
Beside the desk and within easy reach of your hand should be placed at least a single book-case section containing those reference works which you frequently consult. The contents of this section will be considered later; suffice now to say that they should be well bound and should be so placed that if a doubtful point arise they can be consulted at once without your rising. I am not of the opinion that a pretension of unlimited knowledge is a valuable professional asset. It seems better frankly to seek authoritative information, even in the presence of the patient, than to allow an error to creep into your work, and your more intelligent patients will appreciate your care. Furthermore, this placing of your books is convenient when you are alone and considering the cases which have passed before you during the day. It tempts to study.
The desk should hold a typewriter, significant of business methods, and a card file for case records. Incidentally, you284 should have neat bill-heads and printed stationery for all correspondence, though blank white paper is better than over-ornate design or profuse coloring.
On the wall hang a few good anatomical and physiological charts upon which may be pointed out certain facts for the instruction of patients. It may be suggested that these hang on racks so that the surface charts may be easily changeable and that those ordinarily exposed to view be such as will avoid unpleasant suggestion of any kind. For instance, an X-Ray chart of the body showing the skeleton is but one degree less repugnant to the average person than the bones themselves. Though your college training has robbed the subject of all emotion, for you, take thought for the feelings of your visitors.
For all purposes the best type of bench now on the market is probably that composed of two sections, one fixed and the other—the rear one—sliding on a track. Both sections should be adjustable at various angles to the plane of the base and some of the best tables are made so as to permit changes in the distance from the floor to the entire top or to any part of the top, a great advantage in that the table height may thus be made to suit the height of the adjuster.
An abdominal support is now indispensable but must be so elastic as not to interfere with the adjustment. Leather upholstery is more sanitary than plush and has come into general use.
An opening in the front section such that the face may look downward through it and straighten the cervical and upper dorsal spine for palpation and adjustment has been proven a disadvantage instead of a help and will be entirely unnecessary to one who follows the technic laid down in this book.
A desirable addition to this table is an upholstered roll of quite solid material and about eight inches in diameter. This can be placed under the patient’s thighs on the rear section, thus elevating the thighs and straightening the Lumbar region so as to separate the spinous processes. The roll is especially useful for the adjustment of posterior Lumbar subluxations, being inadvisable with rotation.
With a patient lying on the bifid bench in the ordinary adjusting position the Lumbar spinous processes are crowded together and the bodies separated. In rotation, since the adjustment works by using a short power arm against a long weight arm (distance from contact point to center of rotation against distance from center of rotation to anterior margin of body), and since the heaviest portion of the vertebra—the body—is to be moved most, this position of suspension secures the easiest adjustment. But if the vertebra be posterior and a spinous process contact is used the best adjustment can be secured over the roll or with a table adjustable to an angle equal to that which would be secured with the roll.
Everything in the office should be kept scrupulously clean. A lavatory with towel racks well filled with clean towels is an absolute necessity. If no lavatory is inbuilt in the office a portable one may be secured which will answer every purpose. It will be well if the patient observes that you carefully cleanse your hands before giving an adjustment.
The office should contain a towel cabinet with a stack of clean towels and a compartment for used towels. Or tissue towels may be used to save laundry bills. Before each adjustment a clean towel should be unfolded and placed upon the front section of the bench so that the patient rests head and face upon a perfectly clean surface. When the adjustment is completed toss the towel into the used-towel compartment. This use of towels minimizes the risk of contagion or infection from a germ-infested upholstery, suggests care and cleanliness to your patient, and gives the patient greater trust in you.
A curtained recess separated by a screen from the remainder of the room will serve if no separate room is available for a dressing-room. It is better, if possible, to have a separate dressing-room and better still to have separate dressing-rooms for men and women. If extra rooms are not at your command and you use a curtained recess be sure that it contains good light, a dressing-table with mirror,287 a small chair, and hooks for clothing. Provide also a few dressing-sacks for women though most of them will prefer to furnish their own.
It is a known fact that the patient who can be kept in a quiet, restful, and relaxed state for some time following the adjustment derives the greatest benefit therefrom. Having loosened subluxated vertebrae by adjustment their tendency is to settle in their old abnormal position and every movement of the patient for a time aids this tendency. Quiet permits adaptation of surrounding tissues to the changed position of the vertebra; action facilitates the re-adaptation of the vertebra to the state of surrounding tissues.
If possible a special room should be provided in which patients may lie down in comfort for twenty or thirty minutes following an adjustment. If more than one patient at a time is to rest, separate rooms should be provided for men and women. The rest rooms should have high ceilings and excellent ventilation without drafts. The floors should be carpeted so as to soften footfalls and suggest quiet and rest. Potted plants adorn such a room very well and always afford a pleasant suggestion.
The patients lie on cots, foldable for convenience when not in use, and should lie on their backs as quietly as possible. Some prefer solid cots on rollers so that the cot may be noiselessly rolled beside the adjusting table after the adjustment, the patient may by one turn move himself upon it, and288 it may then be gently rolled into the rest room. This is a more finished, if more expensive, handling of the problem.
It may be well to furnish some occupation for the mind and to this end, since reading in such a position is injurious to the eyes, a good phonograph is a valuable addition. Equip it with a soft parlor needle and select only soothing, restful music. Just as you would avoid doing the walls of the rest room in striking or garish colors, exciting to a diseased mind, so avoid exciting or harsh music. The object of this room is rest for mind and body. Let every thought be directed to that end. With some patients the use of the phonograph or other amusement must be avoided. Study your cases with care.
The trip to the Chiropractor’s office is too often regarded in the light of an unpleasant necessity. If proper care be used in equipping an office and if such means as have been suggested for the rest room be employed, these in addition to the pleasing personality of the Chiropractor may make of the visit a pleasant thing, a part of the day to be anticipated with eagerness.
The number of rooms in a perfectly convenient suite depends upon the approximate number of cases to be handled daily. If it is needful to economize the practitioner’s time a greater number of rooms will be required than would be desirable with a small practice.
A waiting room, a consulting room, two or more adjusting289 rooms, and two rest rooms make probably the best number and employment of rooms. It is desirable if possible that the adjusting room be used for that purpose only and that there be separate rooms for men and women. Each adjusting room can then have its own dressing room or recess. Or in addition to the other rooms named above there may be many small rooms each containing an adjusting table and a rest cot and each serving as the rest room after the adjustment. If a sufficient number be provided as many patients can be handled in this way as time permits, the practitioner need lose no time at all, and each patient may have a room entirely to himself throughout his visit.
This should consist of those standard works to which you will necessarily refer most often. Gray, Morris, or other standard anatomical authority, Brubaker’s or Haliburton’s physiology, Butler or Osier on diagnosis, Delafield and Prudden on pathology, Morat on the physiology of the nervous system, Bing on regional diagnosis of nerve lesions, one or two good works on psychology, gynecology, histology, etc., a good medical dictionary, and any books on Chiropractic in which you have confidence make up an excellent list. Any standard works will suffice and this list is merely suggested for those who may be uncertain as to their own tastes. Always examine a book before buying it, even those named above. Next to works on Chiropractic no single290 book is as necessary or useful as a good medical dictionary, preferably a large and complete one.
Your door should bear a sign in gold or black, setting forth your name and business and perhaps your office hours. It may read, “W. R. Jones, Chiropractor,” or, “Jones & Jones, Chiropractors,” with office hours appended. Avoid repetitions such as “Dr. W. R. Jones, Chiropractor,” or “W. R. Jones, D. C., Chiropractor.”
The word of a satisfied patient to his friend is the best advertisement. Beyond this, considerable diversity of opinion exists as to what constitutes proper, ethical, and wise advertising. I shall make no attempt to settle this question but shall simply suggest that while it is undoubtedly necessary often to explain to the public through various avenues what Chiropractic is and what it can do it is wise to be as reserved and dignified as possible and to avoid offense to any. Thus it is clearly unwise to advertise that your competitor is a fraud, much wiser to convince your readers by the logic and strength of your statements that you are not. Consider good taste and avoid unpleasant references to loathsome or vulgar diseases. Such advertising is associated in the public mind with quackery, with patent medicines and medical institutes, and no matter how sincere and right your motives may be it will be misinterpreted by those you wish to reach.
Consider also the legal side of advertising. Study the laws of your state and avoid any statement which will conflict with the law. In some states it is illegal to advertise with the term “Dr.” unless you hold a medical license. In others to advertise to “treat,” “cure,” or “heal” disease is to practice medicine technically. Such statements miss the truth, in any case, because the Chiropractor administers an adjustment and not a treatment and because Nature alone can cure or heal.
Different communities respond to different collection methods. With one class of patients it may be better never to mention fees except to answer inquiry and simply to submit monthly statements of account to all patients. With another it is necessary to charge in advance. More Chiropractors use this method than any other and many use cards for the purpose.
These cards are best printed with name, address, telephone number, etc., on one side and on the other six or twelve spaces ruled off at one end for punching to indicate adjustments given, and the words, “Good for six (or twelve) Chiropractic adjustments at (office) (residence) when properly countersigned.” A line should be left below for your signature and at the bottom the price of the card should be printed plainly. If desired a space may be left for the patient’s name so that the card may be made non-transferable.
The card is issued at the beginning of a course of adjustments and a duplicate is kept on file. Each time the patient is adjusted he presents his card before leaving and one space is punched out. By this system both the patient and the adjuster may know exactly the number of adjustments given and accounts may be easily kept. Without it, a book entry of some sort must be made for every adjustment.
The best thing about this system is that it reminds the patient that you expect to be paid in advance without the necessity of your saying so, since the words “in advance” follow the statement of price on the card. At the time of payment you give him, as a receipt, a card entitling him to a certain amount of your service at a stipulated place.
This method of procedure for the investigation of new cases is offered as a suggestion to be followed as far as the education of the Chiropractor will permit. If every practitioner adopts some such method of making his own diagnoses he will advance in ability much more rapidly than by accepting the diagnoses given his patients by physicians or others. We should remember, though without arrogance, that our special ability to discover subluxations and our knowledge of their significance as the primary causes of disease renders us better prepared for correct diagnosis than our medical friends, other education being equal.
It should be quite obvious that in attempting the accomplishment293 of any object it is necessary first to have in mind a clear preconception of the things to be accomplished, and second, to have a clear and concise, yet complete, outline of the steps to be taken, their order or sequence, and their relative importance in the accomplishment. These two needs, as regards a Chiropractic diagnosis, we shall endeavor to supply in this section.
Chiropractic Diagnosis properly consists of three parts, Vertebral Palpation, Nerve-Tracing, and Symptomatology, together with the reasoning necessary to properly weigh and summarize the facts ascertained. Of these three divisions two fall properly under the head of Physical Diagnosis and the third, symptomatology, should consist principally of physical diagnosis.
Everywhere the physical or objective sign is given preference over the subjective symptom. Before a single question is asked of the patient relative to the case or its history, every other means of obtaining information properly coming under the head of a Chiropractic diagnosis should be utilized. The questions should come last and be very few and direct. They should serve only to illuminate the few remaining doubtful points in the mind of the examiner, points which perhaps exist only because of some fault or weakness in his methods of examination.
The proper order of examination is as follows:
1. General Observation.
2. Vertebral Palpation.
3. Nerve Tracing.
4. Special Examination.
5. History of Case.
6. Summary.
Observation of the patient with a view to determining any signs of disease should begin with the moment the patient steps into the office. It should continue during your conversation and during the Vertebral Palpation and Nerve Tracing which follow. The mind of the examiner should be constantly on the alert to note any sign on any exposed part of the patient’s body, or any motion which may betray the nature of the disease or diseases with which he suffers.
Before preparing the patient for palpation observe temperament, position and carriage of head, body, and limbs, and facies.
Ask male patients to strip to the waist and female patients to remove all clothing down to the waist except a loose gown or kimono, which is worn reversed so that it opens behind and exposes the spine to direct examination. No greater error can be committed than to attempt examination of the vertebral column through clothing or other covering. Examine with patient seated on a bench or stool with feet evenly placed upon the floor. If the patient is for any reason unable to assume this position the examination may be varied somewhat.
While in this position continue observation of points mentioned above and observe also condition of skin, whether295 abnormal in color, moisture or nutrition, or whether there is flushing, cyanosis, or pallor, roughness, eruption, etc.; the condition of bones and joints other than vertebral; general emaciation or obesity, local malnutrition or hypertrophy; evidences of operation, scars etc.; and action of muscles more in detail than is indicated under position and carriage of parts.
Having observed these things discontinue general observation and all other considerations for the time in favor of Vertebral Palpation.
The primary object of Vertebral Palpation is the location of subluxations, or partial displacements, and the determination of the relative degree and direction of those found. Next comes the recording of subluxations in such a manner that a perusal of your record will enable you to reconstruct at any time a mental picture of the spine, as far as possible. (See Record.) With the making of the record the proper form of adjustment for the correction of each subluxation is decided.
Finally, by failing to find subluxation in certain segments you may safely eliminate those segments from consideration and confine your further attention to the remainder. (See Spino-Organic Connection.) It must be borne in mind that while the finding of a subluxation is not always positive evidence of the necessity for adjustment there, the absence of subluxation of any spinal segment is proof positive296 that no disease exists in the corresponding somatic segment. Differential diagnosis is thus often greatly aided by palpation.
Having thus narrowed the field of operation, trace from spine to periphery every nerve tender enough to be traced, noting the relation of the tender nerves to the subluxations already found by palpation. Whenever it is possible note the degree of tenderness of the various nerves and keep in mind through the remainder of the examination the fact that greater tenderness in some one segment indicated either greater or more acute disease in that segment.
It is best to use great caution about entirely eliminating any segment from consideration because of negative findings in attempted nerve tracing. The fact that no nerve is traceable is not always proof that no impingement exists, but only that no irritation exists. Only light or acute impingement may irritate a nerve. In forty, and possibly fifty, per cent of all cases no nerves are traceable at any time. (See Nerve-Tracing.)
The examiner has by this time formed some concept of the case in hand. He has a clue to the possible nature of the disease and he has narrowed his observation to a few segments of the body or a few organs which demand a more special examination. This may be accomplished by Inspection, Palpation, Auscultation, and Percussion.
Having determined by these methods every fact possible of determination without information from the patient, it becomes necessary to go somewhat into the history of the case. The history of falls, jars, shocks, or injuries of any kind should be taken first and these should be viewed in the light of their bearing upon the previously ascertained condition of the spine. Sometimes the definite history of an accident immediately preceding the development of disease symptoms suggests its connection with the disease and the exact nature of the accident points out to us some one of the several recorded subluxations as the one involved. This in turn may aid a doubtful differential diagnosis. Each step in the process of examination helps to explain and clarify the facts elicited by other steps until the facts marshal themselves into a complete and comprehensible picture.
At this point it will be possible to stop in some cases and rest upon the evidence gathered. If you are able at this time to state clearly the nature of the case, the manner of its cause, the site of disease and of the subluxations causing it, the kind of subluxations, and the chance of recovery under adjustment, it is preferable to do so. You will thus have made a complete diagnosis without recourse to information from the patient except the history of injuries.
Sometimes, however, it will be necessary to go further into the case and ascertain the presence and nature of subjective symptoms. If this be necessary, the examiner should298 confine his questions to the parts indicated as diseased, and thus limit the number of questions and make them all direct and essential. It is important to avoid trivial or irrelevant questioning.
Finally, having ascertained all necessary facts, mentally summarize them all, combining the results of Palpation, Nerve-Tracing, and Symptomatology so as to reach a definite conclusion as to the location and nature of the morbid process, the subluxation producing it, and the exact form of adjustment necessary to correct it.
The examiner should be able at the end of the examination to state exactly what he finds to be the condition of the patient, to give reasons and nerve connections, and to demonstrate a subluxation to back every statement.
The case record should contain all essential information relating to the diagnosis and the correction to be applied.
Diagnosis, in a restricted sense, means merely the naming of diseases. But in the broader and more proper sense it means disease knowing and includes a knowledge of the causal factors, the location and nature of disease, the amount of damage to structure and of functional disturbance, and the probable duration and outcome of the case either with or without Chiropractic adjustments. In this broader sense we use the term hereafter.
The object of diagnosis is correct adjustment. Including as it does palpation, nerve-tracing, and symptomatology, the Chiropractor’s diagnosis of a case should embrace all the knowledge upon which he proceeds with his adjustment.
There are really two all-important questions which constantly recur to confront the busy practitioner. One is, “What is the matter with my patient?” and the other, “What can I do to relieve him?” Practice resolves itself into these two divisions, diagnosis and adjustment.
The real question which should suggest itself to the thinking Chiropractor is not, then, “Should a Chiropractor study diagnosis?” but rather, “From what viewpoint should we study diagnosis? Upon what portions of the subject shall we concentrate our attention?”
Undoubtedly the most important branch of diagnosis to us is vertebral palpation. By its use we discover those facts about the spinal column without which we are entirely unable to proceed as Chiropractors. Knowledge concerning the spine is the most essential part of diagnosis.
Next in order of importance comes the study of physical or objective signs throughout the body—the examination of the body for the discovery of all the changes in the size, shape, position, etc., of organs which indicate disease. This includes nerve-tracing, which in some cases is the most important branch of physical diagnosis after vertebral palpation.
Finally, a certain degree of examination for subjective symptoms may be necessary. But the Chiropractor of the300 future should become, and probably will become, par excellence a physical diagnostician.
For many reasons we should be able to rely upon our own diagnoses. Capability in diagnosis renders us independent of the errors or false beliefs of others. Since it includes a knowledge of subluxations, not included in medical training but still vital to correct interpretation of morbid phenomena, it can be more accurate than any diagnosis which ignores these causal factors. A habit of diagnosing one’s own cases enables one, always resting on his own judgment, to correct and improve himself through all errors, for which he is then alone responsible.
A general knowledge of medical diagnosis, of pathology, bacteriology, etc., enables a Chiropractor to meet the physician on common ground; in fact, it gives the Chiropractor a distinct advantage, since he knows not only what his medical friend knows but also the all-important facts regarding the spine which are unknown to others. Such knowledge and the ability to discuss disease intelligently also furnishes common ground with every patient. Each patient is a specialist in the disease he believes himself to have and he expects from his doctor a greater knowledge than his own.
The recognition of contagious or infectious diseases as such is an absolute necessity in order to obey the laws and safeguard the public health. The exact condition and degree of vitality of the patient and the knowledge of the existence of abscess, gangrene, intestinal obstruction, etc.,301 often warns the Chiropractor that his adjustment would be dangerous to the patient. Much possible injury is avoided by accurate diagnosis. Even the frequency with which adjustments should be given depends upon diagnosis.
There are certain cases which a Chiropractor is powerless to aid and immediate recognition of such cases will save much trouble. In intestinal obstruction from intussusception or from strangulated hernia, for instance, it is best to advise the calling of a surgeon immediately, while in obstruction from volvulus or intestinal paralysis the adjustments may afford relief and should at least be tried first of all.
Any internal abscess presents a possibility of rupture into a serous cavity or the substance of a parenchymatous organ and is therefore dangerous, while a superficial abscess, pointing toward the surface, can best be cared for by adjustment. A badly ulcerated or gangrenous appendix may rupture under adjustment and be followed by diffuse peritonitis. The fragile walls of the ileum in typhoid may perforate under adjustment, while in its earlier stages the disease is easily curable. The rotted vertebral bodies in Potts’ Disease (spinal caries) may be crushed under the heavy hand of an ignorant adjuster.
Intelligent case-taking must include accurate diagnosis.
The frequency of adjustments in practice should be determined entirely by the nature of the case and the circumstances in which patient and adjuster are placed. No hard and fast rules can be laid down but some general advice may be profitable.
Acute fever cases may be adjusted, until the fever is broken, oftener than any other type of cases. The chief object is the regulation of the temperature, after which the body is able properly to repair itself. Sometimes it may be necessary to give from two to six adjustments in a day and in at least one tetanus case the adjustments were given at intervals of about ten minutes for several hours until the fever was under control. After such a series it is wisest to refrain from adjusting again for several days so that the patient may recuperate during the interval, providing the fever does not return. It has been noticed that after a series of adjustments given at short intervals the improvement of the patient often extends over a period of days or weeks.
In ordinary chronic cases, with good vitality and reactive power, the daily adjustment is best at first. Then after a course of from six to twenty-four adjustments according to the judgment of the practitioner, the interval is lengthened and adjustments given on alternate days, a day of rest intervening between each two. In weak patients or those who are extremely sensitive, the shock of the daily adjustment, even at first, and the demand on the body’s recuperative power may be greater than can be met.
In this connection it may be mentioned that the author has encountered several cases of dorsal lordosis produced by too heavy and too frequent adjustments, straining the ligaments faster than they could be repaired and continuing the strain over too long a period. It is possible to over-adjust a patient, producing a weakened spine and other deleterious effects, just as it is possible to establish a “tolerance” for a drug by long continued use.
During a long course of adjustments it is well to allow the patient an occasional week of complete rest, or even more, and it may be wise after a time to reduce the number of adjustments to two per week in some cases.
On the other hand, the practice of giving one adjustment a week from the beginning, as followed by some practitioners who maintain offices in numerous localities and visit each one day per week, is not generally productive of good results and it is the author’s practice to refuse new cases who profess their inability to take more than one adjustment weekly. The interval is so long that all repair work started by each adjustment is completed and an involutionary change sets in before the next.
By specific adjusting is meant the selection and adjustment of the vertebra or vertebrae which are known to be causing definite disease or weakness. The term “specific adjustment” implies that there is a particular reason existing and recognized for every vertebra adjusted.
General adjustment, on the other hand means either the adjustment of all palpable subluxations, or of all the most noticeable ones, or of all found providing that no two successive vertebrae be adjusted, according to the beliefs of different elements in the profession.
Specific adjusting relies upon the diagnosis and requires correct interpretation of disease. General adjusting considers only the condition of the spine and is given upon the principle that if the spine is right the man is right—a perfectly correct principle regardless of whether or not the general adjustment is advisable. Let us consider some of the arguments for and against each method and reach a conclusion if possible.
The use of specific adjustment demands of the Chiropractor an accurate diagnosis and compels him to get his mind into direct contact with the exact condition of the patient in order to select the proper vertebrae. Sometimes the less prominent subluxation causes a more acute or dangerous disease than the more pronounced. Specific adjusting tends to develop more discriminating and accurate palpation.
Specific adjusting weakens and shocks the weak or nervous patient less than general adjusting. It also concentrates the recuperative or reparatory power of the patient on the parts which most need repair. The body possesses only a certain limited capacity for combating disease or building weakened tissue. To scatter this force widely is to weaken its effect in any particular locality.
The habit of specific adjustment and of selecting proper vertebrae enables the Chiropractor to explain definitely at any time just what he is doing and why he is doing it. We assert that in adjusting a vertebra we are removing the primary cause of disease. It is sometimes awkward to be asked if the patient has nine diseases or if it takes nine subluxations to cause one case of acute coryza. A correct answer to either question leaves an embarrassing discrepancy between theory and practice.
In favor of the practice of general adjusting it has been said that errors in diagnosis become unimportant if all subluxations be adjusted; that if the spine be straightened the patient must recover. Against the first statement, which is forceful because diagnosticians are so notably liable to err, it may be said that errors in palpation are almost, if not quite, as frequent as errors in other branches of diagnosis and that one’s tendency to err is less if all possible methods be checked against each other than if one only is used. The second statement is quite true; but it is based upon the assumption that in ordinary practice the spine may be straightened completely. As a matter of fact this rarely, if ever, occurs. It is practically impossible ever to thoroughly “line up” a spine. The best that has been done as yet except in acute subluxations is to so modify subluxations that disease disappears.
We may interject here the statement that no greater or more conclusive betrayal of incompetency can be offered by a Chiropractor than the declaration that he has completely306 “lined up” a spinal column in one, six, or a dozen adjustments, as some have declared. If one be honest in such statements it is proof positive that he is not capable of accuracy in palpation or else lamentably liable to auto-suggestion. Clinicians of proven ability, who have examined more than five thousand spines each, agree that no perfectly normal spine has been discovered, whether the spine has been adjusted or not.
But the chiefest argument against general adjusting is that it scatters the reparatory forces of the body throughout many segments, some of which are not really in need of attention, while the one or two segments which need all possible concentration of energy receive only a diluted share.
If my patient suffers from an acute pneumonia and nothing else and if I require that he submit to a general adjustment including some eight subluxations, two of which are Lumbars, I am unscientific and unwise. What that case demands is an immediate localized improvement.
It is highly probable that the efficient Chiropractor of the future will be a specific adjuster; that every recognized body condition will suggest a definite and scientifically determined corrective measure; and that guesswork will be largely eliminated.
The things which it is most important that the Chiropractor should set before his patient are the theories and307 facts peculiar to Chiropractic, perhaps adduced by Chiropractic investigations alone. These theories and facts have been discussed elsewhere in detail: the subluxation theory, easily demonstratable with a spinal column as an object lesson, the relations between primary and secondary causes of disease, the directness and completeness of the results of vertebral adjustments, these explanations are more convincing than the display of a wealth of knowledge of methods and theories used by other schools of practice. Chiropractic has been builded not by virtue of previously established truths but solely on the vitality of the new principles enunciated by it.
These new ideas cannot hope for full and immediate credence and must be presented carefully, with this fact in mind and with due consideration for the degree of intelligence of the listener. Avoid argumentative discussion with patients, seeking rather to enlighten them about those facts peculiar to Chiropractic and unknown to them than to antagonize them by contradicting their cherished beliefs. It is much wiser to begin with that knowledge of disease which you hold in common with the patient and advance with him, step by step, from that firm foundation to new truths than to begin by attempting to tear down his beliefs. Reason from the known to the unknown. Replace an old idea as to the causation of disease by quietly inserting a new one of greater verity and it will presently and painlessly crowd out the old. This process is much the simplest and easiest.
Nevertheless in presenting Chiropractic we must be gently positive. Chiropractic is known and provable. Always able to fall back upon the clinical test as a final argument with supreme assurance that it will not fail to vindicate our claims, we may present an unshaken front before the most powerful and intelligent attack.
The majority of patients will require from the Chiropractor an expression of his belief in his ability or inability to cure them. They will desire a statement as to the probable time required for a cure. They may even ask a guarantee of success.
These questions are hard to meet truthfully and convincingly, for the truth is that every Chiropractor fails sometimes and is unable to predict that failure in advance and that no one wise enough to predict the length of time which will be required for the cure of any given case has yet arisen. And these truths do not sound reassuring or convincing.
Explain to the patient that nature alone is the curative agent and that the cure depends not alone upon the skill of the adjuster but upon the exact condition of the vertebrae, the exact amount or degree of damage to tissue, the patient’s habits of living, etc. Any accidental interjection of other factors into the case may have an important bearing. You may assure him of the excellent results you have obtained in other cases similar to his, or even cite individual cases if to do so does not violate a professional confidence.309 But you had best avoid a promise to cure or an exact statement of the time which will be needed. State your belief or opinion but do not bind yourself to a promise. Offer your best skill and closest attention; you can do no more.
The patient should rely upon the skill of the Chiropractor as upon the skill of his lawyer or his physician. Neither can honestly promise that he will succeed in his efforts, even though all indications point that way.
From the original concussion of forces which produces a nerve-impigning subluxation to the stage of chronic disease with which the patient usually approaches the Chiropractor for relief, disease develops by a series of gradual steps. Successive changes take place from time to time in the degree of subluxation as it is augmented by further jars, strains, etc., or by the reaction of secondary causes upon it and with these changes come corresponding changes in the development of the disease.
Perhaps the first effect of the bad subluxation is irritation of a nerve and acute functional disturbance such as pain, fever, etc. The later effect may be paralysis and its attendant train of evils.
When the Chiropractor begins adjustment he does not at once return the long-displaced and misshapen vertebra to its normal position. He merely tends to do so, his adjustments making slight and gradual changes from the abnormal back to normal.
Thus it is that the subluxation passes back in reverse order through the successive stages of its development, following a process which may be called the involution of the subluxation. At the same time the morbid process resulting from the subluxation tends to retrace its steps, passing in reverse order through the stages by which it developed. Pains which have not been felt for years may unaccountably return under the reawakening of the long dormant nerves. Headache, long absent but once a prominent feature of the disease, may again make its appearance. The patient feels worse.
These changes, however, take place much more rapidly during the correction than during the development of the disease. To a certain extent they are probably always present, although in many cases they occur so rapidly or are modified so much by changed environment as to be unrecognizable. In many cases it is possible by securing an accurate history and by careful observation of the patient’s progress to observe a definite reappearance, in reverse order, of every important event in the history of the disease. For instance, if the patient has at one time had a severe fever, perhaps lasting many weeks, and has later developed a chronic weakness marking the increase in degree of subluxation, the fever may reappear during adjustments, last a day or two, and disappear forever, having been corrected beyond that stage.
If explained in advance to patients with chronic diseases, the facts of retracing may not cause the patient to311 become discouraged as he would if he failed to understand them. If he knows before your work is commenced that he may expect such phenomena but may possibly escape them he meets them as necessary parts of the process of cure. If they are not explained in advance he is likely to feel that you are doing him injury and to discontinue your service just at the time he most needs them. In fact, it occasionally happens that if adjustments are stopped at some irritant stage of the cure that condition will remain and do great damage.
This theory of retracing has been much abused. Chiropractors have used it to cover a multitude of errors in practice. With some it becomes a habit to call all unfavorable events which occur during adjustments retracing, thus shifting the blame from their own shoulders to Nature’s. This is a pernicious practice because it deceives the patient and also because too frequent repetition of this explanation finally deludes the practitioner into the belief that all such events really are retracing. This view withdraws his attention from his own technic and he ceases to discover his own mistakes by ceasing to look for them.
It is best in the face of any painful or apparently unfavorable development always to examine our own work thoroughly to detect any possible error in diagnosis, palpation, or selection of move for correction. It is always possible for us to err and our cases should be observed at every stage with the most minute care to insure accuracy in detail.
There are many things which can be done better by others than by a Chiropractor. There are others for which the Chiropractor’s training does not fit him at all and to which his methods do not in any sense apply. Knowledge of these limitations is just as essential as acquaintance with the powers of the vertebral adjustment.
Bony dislocations other than vertebral, fractures, wounds causing, or likely to cause, hemorrhage or severe internal injury, should at sight be diverted into the hands of a surgeon. The Chiropractor receives no training in handling such cases and has neither legal nor moral right to attend them. In obstetrics likewise no practical training is given which would prepare the practitioner for delivery and he is unprepared to use necessary asceptic or antiseptic measures.
Some individual cases of disease usually curable will have advanced so far as to require surgical interference. Abscesses or suppurative diseases internally located or having any liability to discharge internally must be avoided. Gangrene, cancer, the advanced stages of tuberculosis (usually) are incurable.
Quarantinable diseases as a class yield readily to adjustment unless some serum treatment has been administered, when the chances of recovery are greatly lessened. But such cases must be reported in conformity with the laws of the state and will probably then be taken out of the hands of the Chiropractor—unfortunately. The laws of the various313 states should be modified to permit Chiropractors, with precautions required of physicians to safeguard the public health, to pass quarantine. Every effort should be put forth to secure such legislation but until it is secured in any state and the Chiropractor’s work is brought under the supervision of the authorities, the laws must be respected strictly.
Syphilis and gonorrhoea, communicable diseases, should be recognized and refused in practice. The former in the primary and secondary stages (not tertiary) and the latter in all stages is corrective by adjustment but the liability of transmission of the disease warns against contact with it unless all precautions known to science be used to avoid possible transmission.
Congenital anomalies of structure do not yield to Chiropractic and are best let alone although no harm is likely to arise through any attempt to correct them by vertebral adjustment.
There are certain other methods which present a superficial resemblance to Chropractic which leads many to believe them closely related. Such methods are Spondylotherapy, Osteopathy, etc. There is a system called Napravit or Naprapathy which may be dismissed with the statement that it is Chiropractic, renamed.
Spondylotherapy, on the other hand, is a system of treating314 disease which takes no account of the vertebral subluxation as its primary cause and seeks to cure disease by stimulating or inhibiting nerve action through the use of mechanical, thermic, or electrical means. Its resemblance is due solely to the fact that most of the treatment is applied to the spine. As well might we say that serum injection for meningitis is Chiropractic because the serum is introduced by lumbar puncture into the spinal canal.
Osteopathy, since the profession has become aware of the superior results obtainable by vertebral adjustment, is rapidly adopting many Chiropractic methods and counterfeiting it as far as possible. Perusal of their literature of various periods clearly shows that this is a new growth and that they have never adopted in theory what they sometimes use in practice. In fact both the above methods treat disease, following the theory of medicine with the use of different remedies only, while Chiropractic adjusts the cause of disease and avoids treatment of any kind. Chiropractic is not a branch of medicine, never can be a branch of medicine because it is inherently and fundamentally antagonistic to the very basic principles of medicine, and no statute can change the fact of such antagonism. But unless we adhere strictly to the fundamental principles of our own practice and limit ourselves to the methods which grow from those principles Chiropractic may become a part of medicine. Which brings us to
There are many methods of treating disease which are more or less beneficial to the patient just as there are some which are always injurious. Shall we employ such of these methods as are beneficial as adjuncts to the practice of Chiropractic? Or shall we adhere to the principle that the treatment of disease is erroneous and the adjustment of its cause the only logical method of procedure? There is much to be said on both sides of this question which has so long agitated the profession.
In the class of beneficial adjuncts may be placed massage, hydrotherapy, spondylotherapy, dietetics, osteopathy, Christian Science, suggestive therapeutics, mechano-therapy, and many others. Each of these has its field of usefulness; each taken alone is productive of some good in some cases at least. Each might possibly augment the results of Chiropractic, or hasten them in some cases, if judiciously used. By judiciously used we mean the avoidance of any method which would in the least interfere with proper vertebral adjustment or its results or which might carelessly cause subluxation. Osteopathy and mechano-therapy frequently cause subluxation because of the ignorance on the part of their users; they need not do so.
Among the pernicious adjuncts, or those which are harmful if combined with adjustments or harmful whenever and however used, may be mentioned drug medicine, serum therapy, and electricity. The first two may sometimes prove the lesser evil if used alone. With Chiropractic they are316 always unnecessary and always tend to lessen the good effect of adjustments. The latter alone is beneficial but in combination with Chiropractic proves a double stimulant to the nerves and should be avoided. The effect of these methods when used with Chiropractic can never be accurately predicted. One can only be certain that some unfortunate effect will follow.
As a secondary consideration the Chiropractor has neither legal nor moral right to practice medicine unless he has received a state license to do so.
Having admitted that the forms of “mixing” indicated as beneficial to the patient may be sometimes justifiable on the score of immediate good to the patient, let us consider another side of the question.
Just as surely as we admit into our practice any method which attacks the disease itself, or which treats any other than the primary cause of the disease, or which seeks to stimulate or inhibit the functions of the body without freeing the natural channels through which the natural healing power of the body should be manifested, just so surely are we adopting the medical theory and making our profession a branch of medicine. Medicine uses many remedies for the cure of disease. Medicine is now broader than the mere administration of drugs. And no matter how we vary the remedy, or what treatment we select, we are denying the truth of the Chiropractic theory and admitting the truth of the medical principle when we use adjuncts in our practice.
Nor are these adjuncts necessary. It has been demonstrated317 by repeated observations that the Chiropractors who use only the vertebral adjustment secure just as high a percentage of results as those who combine one or more other methods with it. This is due to various reasons: the greater perfection attained in Chiropractic by those who apply themselves with concentration to the task of settling every problem by that means; the fact that adjuncts often detract from the effect of adjustment as much as they add results of their own; the tendency of the patient to prefer and to insist upon the easier and less painful methods rather than the adjustment.
The lay patient and the ignorant public are inclined to give credit for results obtained to the best known method used upon them. Thus in spite of the fact that Chiropractic alone obtains a far greater percentage of results than any other combination of methods, the patient is prone to believe that the change of diet or the massage effected a cure and to overlook entirely the least pleasant part of his “treatment,” the adjustment. He does not understand and cannot understand with a mind divided for the consideration of several methods, the connection of the spine with his disease. Often he fails to understand if Chiropractic is used alone but he is forced to conclude that the spine has such connection because adjustment of the spine cured him.
The use of adjuncts has done more to hold back the advance of the profession in the public mind than any other single factor except ignorance within the profession. Furthermore, the Chiropractor who knows that he can rely upon318 various other methods if his adjustment fails does not feel impelled to study his Chiropractic as he should. He weakens in practice, relying more and more upon adjuncts.
It has been repeatedly proven that the Chiropractor who uses only Chiropractic becomes the better practitioner by necessity. It has also proven that the man who is expert in Chiropractic needs nothing else, providing only that he refuses those cases to which Chiropractic cannot apply at all.
The only real problem in Chiropractic is the problem of adjustment. All failures may be attributed either to lack of knowledge and proper application of Chiropractic or to the fact that the patient has not vitality enough to recover from the disease. Do not shift the responsibility for failure upon the system, since with one or two exceptions every known disease has been cured by some Chiropractor, thus proving its possibility. Realize that the work can be done and that its doing depends upon your own skill in diagnosis and technic.
It is inevitable that at some future time Chiropractic will be used in connection with other beneficial methods which will enable us to get results sooner, though not more surely. It is also inevitable that Chiropractic will fail to receive its proper place among healing methods unless we force the world to believe in it as we believe; to know it as we know it. If we develop our system in its purity until it obtains general recognition at its true valuation we shall have accomplished an infinite good for humanity for all time.
We should endeavor to accomplish the greatest good for the greatest number, laboring rather for the ultimate recognition of the subluxation theory and its application at its real value than for immediate slight good or personal gain.
He who would succeed in Chiropractic must have, in addition to a thorough education in his profession, a proper personality. This is the medium through which his education becomes effective, the channel through which he reaches the public, gaining their confidence and approval that he may utilize his knowledge to their good. Many skillful and well-educated practitioners have failed because they lacked the proper personal qualities for attracting patients.
The most essential elements of a proper personality are Courage, Conviction, Confidence, Honesty, Sympathy, and Aggressiveness.
Courage, not recklessness or carelessness but a fearless willingness to assume responsibility—the heavy responsibility of our profession—is indispensable. He who accepts the easy case or the chronic and slowly progressive one and refuses to face the appalling rush of a dangerous and acute malady; he who shrinks through fear for his reputation from a grave risk, has no right in Chiropractic. He has mistaken his calling. While we acquire the knowledge of Chiropractic we acquire also a great responsibility for its320 use; we must utilize it wherever and whenever it is best for the patient, whenever our chances of effecting a cure are the best chances, without regard to ourselves or any personal risk.
By conviction is meant a firm and well-grounded belief in the greatness and efficiency of Chiropractic. Sincerity in one’s practice is a prime requisite for success. A belief grounded in knowledge girds the Chiropractor with an armor so strong that no adversity can pierce it. He who practices Chiropractic without believing in it is in his own mind a cheat and a fraud and cannot expect ultimate prosperity.
Confidence in one’s own ability and knowledge, in one’s power and skill to contest with disease, begets confidence in others. Not conceit, not exaggerated egotism, but a healthy and sane assurance and faith in oneself, engender that steadiness of mind and of hand which make for accuracy and excellence.
Without honesty with oneself, one’s profession, and one’s patients, one forfeits public confidence—and justly. If we promise that which we cannot perform, if we deceive our patients by misleading explanations of untoward events, we deserve failure. It is not intended here to refer to the cheerful and optimistic manner and habit of speech which often aids in the sick room to keep the patient’s mind at rest. This may sometimes deceive the patient as to the gravity of his condition and such deceit may be justifiable; but it should never be extended to the family or to those who have321 a right to know the real condition and cannot be harmed by such knowledge. Strict honesty, whenever harmless to others, should be the fixed policy of all practitioners.
The weak, strained minds of the very ill require and demand sympathy; not the sort which expresses itself in fixed words or phrases of condolence with the unfortunate and at once forgets their needs and sorrows, but the deeper, unspoken feeling of desire to aid, which springs from the heart and finds its best expression in active assistance. If you do not care whether your patient is or is not benefited, if you have no other feeling for him than a business interest in holding a case, you lack the strongest impulse to hard work and study, the desire to aid.
Chiropractic is new. Its principles are yet unknown to the general public. Also this is an age of keen competition and it is our duty to our profession and to the world that instead of hiding our light under a bushel we proclaim our mission to all who will hear. We must be intelligently and wisely aggressive. We must bring ourselves into contact with the public in every legitimate way, compelling it by force of logic and personality to see the reasonableness and greatness of our work.
Question yourself in regard to these things. Examine your own characteristics to discover whether any of these essential elements of personality are lacking. If one be found wanting cultivate it assiduously. Having chosen Chiropractic as a life vocation, work at it not alone for the acquisition of ever-increasing knowledge but for the unfoldment of a powerful and winning personality.
Prognosis is the determining, in advance of the fact, of the probable course, duration, or outcome of a disease. A Chiropractic prognosis is a prediction as to the changes which will take place in a case during and after Chiropractic adjustments.
General Prognosis is an opinion expressed of a disease without reference to any particular case. It is based upon the experience of the profession and the average result obtained with the disease. It furnishes only a basis for consideration of the special prognosis of an individual case. This latter must be based upon the general prognosis of the disease and upon study of every modifying factor present in the case, as general vitality, living habits, facility of adjustment, apparent response to early adjustments, and especially an estimate of the amount and kind of damage done to tissue and the probability of its repair.
Only general prognosis can be set down as a guide to others. To state even this with certainty and safety many precautions must be observed. All cases included as a basis of conclusions must be handled under standard test conditions (see index) as far as may be; in accepting the observations of others one must be sure that they are sufficiently trained and sufficiently careful and veracious to render their statements reliable.
In order to introduce the subject to the literature of the profession and to invite comment and discussion looking toward the ultimate development of a complete Chiropractic prognosis we shall set down, without further preliminary, the general prognosis of those commonly described diseases concerning which we feel qualified to speak. No statement is made without the gathering of reliable evidence.
Abscesses.—Those abscesses which would tend to discharge externally may be adjusted for with success and will rapidly develop, point, and discharge, with quick recovery. Those which might break internally absolutely forbid adjustment because of the almost certain occurrence of peritonitis, pyaemia, or other grave condition.
Acne.—Good, but usually slow.
Addison’s Disease.—Few cases reported, and these slow cures.
Adenoids of Pharynx.—Prognosis so good as to contraindicate operation in every case. The lymphoid growths gradually and slowly absorb under adjustment.
Adiposis Dolorosa.—Only one case seen, the Derkum case. This reduced in six months of adjustment from 360 to 280 lbs. in weight, and was improved in every particular. No final report received.
Alcoholism.—Adjustments greatly aid a cure if alcohol324 be discontinued at once, or if the daily consumption is gradually and steadily decreased. No permanent cure can be secured without the aid of the patient. Acute alcoholic intoxication may be lessened at once by the aid of a single adjustment.
Amenorrhoea.—Prognosis excellent. One to several months required. Conservative amenorrhoea, as in tuberculosis or other wasting disease, disappears only with the occasion.
Anaemia.—If primary, yields slowly but surely. Secondary anaemia depends upon some disease process and its prognosis is that of the disease which produces it.
Angina Pectoris.—A case for careful diagnosis. False angina recovers with general building of nervous system. True angina, usually associated with arteriosclerosis, is frequently fatal and death may occur during any adjustment. If this does not happen most cases recover, though slowly. Let me repeat, there is great danger in handling true angina pectoris.
Anidrosis.—Usually responds to adjustments for the kidneys.
Ankylosis.—Almost any ankylosis, except that in which there is gross deformity of the bones, would yield to repeated applications of force along right lines. Only vertebral ankyloses are amenable to Chiropractic adjustment and those are usually broken in time.
Anterior Poliomyelitis.—Chiropractic experience with325 “infantile paralysis” has been very extensive and gratifying. During the febrile stage the disease may be aborted by one or several adjustments with only slight and transient paralyses resulting. The chronic paralysis which follows an unadjusted case is curable, but restoration of the motor function and trophic tone of the paralyzed members is delayed while the ventral horn cells are regenerated, the axons rebuilt, and the atrophied muscles redeveloped. Often no apparent results will be obtained for one or several months, after which gradual improvement progresses to a complete cure.
Aphonia.—Prognosis excellent. No failures reported.
Apoplexy.—The occasional case in which a premonitory partial paralysis precedes real hemorrhage responds remarkably to adjustment so that with care the hemorrhage may be averted. After hemorrhage the absorption of the clot is slow and tedious, but about 50 per cent recover.
Appendicitis.—In the early stages of the acute form, and in nearly all chronic cases, recovery is almost certain under adjustments. Signs of suppuration indicate immediate operative interference and drainage, and failure to read the signs may lead to rupture, peritonitis, and death. Acute cases yield very quickly as a rule.
Arthritis Deformans.—In well developed cases some almost complete cures have been effected in periods varying from two to four years. Prognosis good as to relief, but poor as to complete recovery.
Ascites.—Fair prognosis, depending upon the nature of the portal obstruction. Cirrhotic ascites does not yield well.
Asthma.—Spasmodic bronchial asthma is almost always curable except in the very aged, but the usual posterior curvature in lower cervicals and upper dorsals requires time and persistent heavy adjustments for its correction. The asthmatic paroxysm may be relieved instantaneously, but will recur at intervals for a long period before the cure is fully established. The cardiac form of asthma depends upon restoration of compensation for a leaking valve, and yields by irregularly progressive diminution.
Blindness.—As a condition, without qualifying terms, blindness offers a bad prognosis. Most cases fail to develop sight under adjustments. Yet some individual cures in optic atrophy, in detached retina, and in other conditions, attest the possibility. Cataract blindness perhaps yields best.
Bradycardia.—If symptomatic, yields as does the disease. If primary, a few adjustments are usually sufficient. In one case the first adjustment increased to 90 a pulse which had been at 60 for fifteen years. In twenty-four hours, without further adjustment, the rate had settled at 69 and there remained.
Bright’s Disease.—Prognosis good, but some cases terminate abruptly with intercurrent disease, such as pneumonia. There is danger until the albuminuria has327 ceased and the strength of the patient markedly improved. Probably the diseased kidney area is simply walled off from the healthy tissue, which then hypertrophies and takes on the work of the entire organ, or pair of organs. If too much damage has been done, the case will terminate fatally in time, even though its progress is checked by adjustments.
Bronchitis.—Acute bronchitis is quickly checked as a rule. Chronic bronchitis may prove intractable, or may require many months for a cure. There are exceptional quick cures of the most chronic cases.
Caked Breast—Mammary Inflammations.—Rapid and positive cure follows proper adjustments.
Cerebral Softening.—Prognosis bad.
Cerebrospinal Meningitis.—Serious always, but no fatalities reported in adjusted cases. Failure to modify fever and cervical retraction within two or three hours, and with one to ten adjustments, is alarming.
Chickenpox.—Like smallpox and the other exanthemata, chickenpox should be modified at once by adjustment and all cases should be light, eruption hastened, and fever quickly broken. Sometimes the rash may be strongly marked and the disease run its usual course in all particulars except fever and prostration, being a febrile with absence of all the consequences of fever.
Cholangitis.—Recovers quickly under adjustment.
Cholecystitis.—Prognosis excellent.
Chorea.—Prognosis excellent in acute and subacute328 cases, less favorable in chronic. No figures are available, but many chronic cases fail to respond at all.
Cirrhosis of Liver.—Doubtful. No statistics have been compiled, but it seems probable that most cases are unmodified by adjustment.
Congestion of Liver.—Prognosis good.
Conjunctivitis.—Readily curable, unless part of a more general infection.
Constipation.—Prognosis usually good, but some cases which have paralyzed the intestines with drugs, or in which atony of the intestinal muscles exists from any cause, are very stubborn. One is led to believe that any case of chronic constipation would respond to proper adjustments in time, but sometimes the time is prolonged more than seems reasonable.
Coryza.—Some cases respond instantly, others persist and run their usual course. Chronic nasal catarrh recovers in favorable climates, and in unfavorable tends to become permanent, though less severe and annoying under adjustment.
Croup.—Always dangerous, but no fatalities reported under adjustments, which are powerfully effective. Croup requires constant attention until all symptoms subside, usually within an hour or two.
Cystitis.—Usually curable, but some chronic cases prove intractable for an unknown reason. There is no way of recognizing the curability of a case before the attempt.
Deafness.—Variable outlook. Deafness due to catarrhal occlusion of the Eustachian tubes is usually curable. That due to middle ear disease sometimes yields. That due to nerve disease is possibly—though not certainly—incurable.
Diabetes Insipidus.—Prognosis excellent. Few cases fail of cure, and no fatalities are reported.
Diabetes Mellitus.—Always necessitating grave and careful consideration, this metabolic disease is marvellously controlled by Chiropractic adjustment. Probably 90 per cent of all cases are curable, and only those presenting impossible problems of adjustment, or those in the very last stages, are hopeless.
Diarrhoea.—Prognosis depends largely upon secondary causes. Adjustments sometimes produce diarrhoea to cleanse the intestinal tract of waste or poisons. Such a diarrhoea, if instituted by Nature without aid, does not cease with adjustments until its purpose is accomplished. Nervous and infective diarrhoeas usually respond well.
Dilatation of Heart.—Compensatory hypertrophy and strengthening of the muscle usually follows adjustment.
Diphtheria.—Under adjustment the false membrane tends to exfoliate and to be coughed out entire within a few hours, with rapid recovery. In children, watch for possible strangulation from loosened membrane. Constant bedside attention is imperative until fever and membrane have disappeared. Convalescence, unless antitoxin330 has been used, is very rapid, and physicians watching the clinical course of diphtheria under adjustment customarily doubt the diagnosis unless culture is made. Antitoxin modifies the prognosis toward gravity, and in spite of adjustments persistent sequelae often follow its use.
Dropsy.—Cardiac or renal dropsy disappears with improvement in the diseased organ.
Dysentery.—In temperate climates death is extremely unlikely. Recovery is often quick and easy, but some cases persist. The tropical amoebic dysentery seems hardest to master and may not improve at all.
Dyspepsia.—Prognosis good.
Endocarditis.—If primary, recovery is the rule. Occurring in the course of some other disease, as rheumatic fever, it renders the prognosis less certain and may terminate fatally. Likely to leave chronic valve weakness or contraction.
Enteritis.—Prognosis generally fair. No figures available.
Enuresis.—The majority recover within a few weeks or months, with occasional exceptions. Failure to get results within a few weeks suggests a change of adjustment.
Epilepsy.—Doubtful. Less than half of all cases recover, and no case can be pronounced cured until all symptoms have been absent for a year. Cases with anterior cervicals offer the poorest chance. It is usually possible to restore consciousness and muscular control331 by an adjustment during the grande mal, in the instant between the tonic and clonic spasms, but such immediate response does not—unfortunately—always mean that a cure will eventually be effected.
Epistaxis.—Nose-bleed usually stops at once following proper adjustment.
Erysipelas.—Cases adjusted early show little spreading of the eruption with but slight constitutional symptoms. After eruption is fully developed it is more difficult to keep down the fever and recovery is slower, but none the less certain unless cardiac or other grave weakness is present.
Exophthalmic Goitre.—Like other forms of goitre this may be reduced, and with its reduction all other symptoms disappear. Many cures are on record.
Friedrich’s Ataxia.—In hereditary cerebellar ataxia (which is probably congenital, rather) cures are limited to 40 per cent or less. History of instrumental delivery, with marked upper cervical subluxation, argue for the natal origin of the disease and increase the probability of cure.
Gallstones.—Prognosis excellent. The calculi absorb under adjustment by a reversal of the chemical process by which their deposit was induced. When small they may pass through the ducts and escape, with slight pain. Adjustment during the painful passage of a gallstone may act upon the duct so as to lessen greatly the pain and hasten the passage.
Gastralgia.—Like other gastric neuroses, is easily curable but may sometimes require correction of a neurotic diathesis, which means time.
Gastric Ulcer.—Usually recovers, but occasionally leaves a fibrous cicatrix which cannot be affected by adjustment and which, if located at the pylorus, may produce stenosis, with consequent incurable dilatation of the stomach. Operation is required for such a condition, but the diagnosis is difficult, and it may be best to test with adjustments for some time.
Gastritis.—Prognosis good. To prevent recurrence adjustments should continue after symptoms subside.
Goitre.—Prognosis good. One large goitre under the author’s observation was reduced in one week so that the neck measurement decreased one inch. Most cases require several months for complete reduction.
Gonorrhoeal Rheumatism.—More stubborn than other forms of rheumatism and sometimes defies adjustment. No percentages are available. It is probable that nothing but a general cleansing of the system will prevent recurrence.
Hay Fever.—Perhaps one-half of all adjusted cases recover fully, some at once and some after several months. By recovery is meant failure of the annual appearance of the attack with no symptoms at any time. No case can be pronounced cured in less than a year. The remaining half are modified little or not at all.
Headache.—Nervous, bilious, ocular, and reflex headaches333 yield well. Toxic headaches, or those accompanying systemic infections, give way slowly with the cleansing of the system.
Hemorrhoids.—Excellent, except when lower lumbars are anterior and defy adjustment.
Hernia.—In all sites and forms of hernia, excepting strangulated hernia, prognosis is good. Strangulation requires immediate surgical interference. Prognosis is better if a truss be used.
Hodgkins’ Disease.—Prognosis theoretically good, but the few cases under adjustment, while benefited, seem to have died of intercurrent disease, so that it is well to suspend judgment.
Hydrocele.—Theoretically hydrocele should respond well, but in practice the author has seen several failures, and no cures.
Hydrocephalus.—If due to cervical twisting at birth, the prognosis is fair; otherwise bad.
Hypertrophy.—Adaptative hypertrophies, those due to overstrain upon an organ, do not and should not disappear until the strain has been relieved. Hypertrophy is sometimes accelerated by adjustment, as in the case of defective heart valves, when thickening of the wall restores and maintains compensation. Other hypertrophies tend to disappear under adjustment.
Hysteria.—Good, but slow. Some extreme cases refuse to respond. Instant recovery from hysterical coma is the rule following adjustment, but the coma tends to recur.
Immunity.—There is no doubt that adjustments often confer immunity from infection and contagion, but it is so difficult to strengthen every part of the body against every possible infection or contagion, and so uncertain that immunity really exists in a given case, that it is best always to assume the possibility of contagion and act accordingly. Adjustments following exposure to known contagion are always wise, but one may never know, if they succeed, that the patient might not have escaped without them.
Impotence.—Variable outlook, according to secondary causes and pathology. Previous venereal disease renders the prognosis most doubtful. Nervous or vascular impotence is likely to respond well. If due to cord disease, the prognosis is to be made on the original disease.
Influenza.—Mortality not more than 2 per cent, and that in the very aged and infirm. Duration varies greatly. May yield at once, first adjustment being followed by disappearance of fever, profuse perspiration, and completed convalescence in from twenty-four to forty-eight hours; or may require several adjustments at frequent intervals to break fever.
Insanity.—No accurate tabulation of results in different forms of insanity has been made. Numerous successes, interspersed with fewer failures, have been reported. The author has both succeeded and failed with acute dementia, but the failure was a twenty-four-hour trial only, and included but three adjustments.
Intestinal Obstruction.—The prognosis of intestinal obstruction from intussusception or strangulated hernia is, under Chiropractic, bad. Such cases are almost surely fatal unless operated. Faecal obstructions or masses of worms, also volvulus, respond quickly and prognosis is good. Careful diagnosis is required before taking a case of apparent complete obstruction.
Irritable Heart.—If purely nervous, recovery is quick and easy. If there is a drug diathesis or organic disease, slow and doubtful.
Jaundice.—Yields readily, but if of the obstructive form the obstruction must first be reduced or removed by adjustments.
Laryngitis.—A few adjustments suffice for simple acute cases. Specific laryngeal infections are more difficult. Laryngitis with ulceration, which is either syphilitic or tubercular, may not recover or may recover after a protracted struggle. Chronic laryngitis of other forms is curable, but requires more time than acute.
Leucorrhoea.—Fair prognosis only.
Lumbago.—Good, unless pain prevents proper adjustment. True lumbago is quick to respond.
Malaria.—Tenacity varies according to climatic conditions. Malarial cachexia always yields slowly, sometimes defies adjustment altogether. No reports are to be had on pernicious malaria. Other forms recover though paroxysms tend to recur several times before checked, but of shorter duration than if no adjustment is given.
Mastoiditis.—Good results in the few cases observed.
Measles.—Excellent. Recovers quickly. Eruption hastened by early adjustment, runs very mild course with little or no fever, catarrhal symptoms disappear early. No sequelae.
Meniere’s Disease.—Labyrinthine disease of this character has been cured, without reported failures, but data is meagre, not more than three or four cases having come under the author’s notice.
Menorrhagia—Metrorrhagia.—Results excellent, and usually quick. One fifty-two-hour intermenstrual hemorrhage from uterus was stopped in one hour by adjustment, with no recurrence.
Migraine.—Migraine, or hemicrania, gives a fair prognosis only. Most cases require a long course of adjustments.
Movable Kidney.—Prognosis good, but change of position and complete fixation slow. No treatment required—merely adjustment.
Myelitis.—Transverse myelitis, if adjusted in the acute stage, may be checked as any other inflammation, and the damage and resulting paralysis will be greatly lessened or altogether prevented. The paralyses which follow myelitis require time for the rebuilding of the degenerated axons whose course is interrupted at the diseased area, but tend to recover.
Myocarditis.—Reports conflict. It is well to consider this a grave condition and one open to investigation.
Myxoedema.—Only one case known to have been under adjustment, and this after several years was markedly improved, but not yet quite cured.
Nephritis.—Prognosis good. Acute cases show rapid, chronic cases slow, improvement.
Neuralgia.—Prognosis excellent in any form. Trophic neuralgias, such as herpes zoster, are slowest as a rule, but occasional cases of tic doloureux will require several months. One may always expect a cure unless the patient, in long cases, becomes discouraged and stops adjustments.
Neurasthenia.—Good, but will be slow unless mental aid be given in the form of freedom from worry or strain.
Neuritis.—Good, but very uncertain as to time; some cases show quick disappearance of all pain and some drag interminably.
Optic Atrophy.—Complete atrophy with total blindness is rarely cured, though occasional partial or complete cures have been reported. Partial atrophy may slowly recover, or recovery may cease at some point short of completion and case remain stationary thereafter.
Ovaritis.—Good, except in suppurative forms. When adhesions have been formed, results are doubtful.
Pancreatitis.—Obscure, hard to recognize, and hard to cure. Prognosis probably bad.
Paralysis Agitans.—Probably in the earliest stages this is curable. Cure of a fully developed case is exceedingly doubtful and the writer has yet to see marked benefit in such a case.
Paralyses.—Prognosis decidedly variable. Apoplectic hemorrhage recovers in about 50 per cent of all cases. Paralyses from central lesions require much more time than peripheral palsies because of the necessity for rebuilding degenerated nerve cells as well as fibres. The paralyses following anterior poliomyelitis are almost certain to be cured if sufficient time is allowed. Most peripheral palsies, except in the very aged, are curable. Any other paralysis but a purely functional one recovers slowly, but this form may yield almost in a day.
Parotitis.—Mumps respond immediately and may be checked at any stage.
Pericarditis.—Usually recovers. Effusions are stubborn and may become purulent, in which case the prognosis is grave.
Peritonitis.—Prognosis grave, but some cases have been reported as cured under adjustment. These are probably localized rather than diffuse inflammations, usually pelvic.
Pertussis, or Whooping-Cough.—Tends to run its course despite adjustments, though some aborted cases are reported. All cases mild under adjustment, with small liability of complications. A nervous cough is likely to persist for months after the infection has passed. Adjustments seem seldom to prevent contagion.
Pharyngitis.—Acute form yields readily. Chronic pharyngitis is more stubborn, but usually curable.
Pleurisy.—Pleurisy, unless purulent or tubercular,339 yields well in varying periods. Purulent and tubercular pleurisy are stubborn and may not recover.
Pneumonia.—The author has had a wide and gratifying experience with pneumonia. At every stage it seems amenable to adjustment, and the usual effect of the first adjustment is a drop of from one to two degrees in the temperature with immediate softening of the consolidated area. Specific adjustments get best and quickest results. Pneumonia should always recover, unless it occurs as an intercurrent event in some chronic and wasting disease, as Bright’s Disease.
Potts’ Disease.—Tubercular caries of the bodies of the vertebrae is curable, within limits. Occasional cases are seen in which Nature has stopped the spread of the disease by walling off the morbid area with exostosis. Such cases should not be adjusted, and the disease may remain latent through a long life. When active the disease proves fatal unless checked, which is possible in the earlier stages, and becomes impossible when the vertebral bodies are too fragile to stand strong adjustments. Discernment in case-taking will avoid any fatalities under adjustment, but by no means all cases of Potts’ Disease are curable.
Pregnancy.—We may correct by adjustment any pathological conditions arising during pregnancy which would be amenable to adjustment under other conditions. A course of adjustments during a normal pregnancy will render delivery easier and lessen, but not abolish, the340 pains. Great care must be exercised in the manner of adjustment.
Prostatic Enlargement.—Varies according to age and recuperative power. Prognosis is bad in the very aged and infirm, but in more vigorous subjects quite good for steady reduction of the hypertrophied gland, with subsidence of attendant symptoms. Venereal history is unfavorable.
Pulmonary Tuberculosis.—In the early stages, where little damage has been done to lung tissue, recovery is rapid and quite certain. In fully developed cases, with characteristic symptoms and marked damage to tissue, prognosis is very grave, and it is usually wisest to advise a trip to the Southwest in preference to adjustments. Tubercular cases should be studied with a view to estimating the exact condition and recuperative power of the patient before taking.
Rachitis.—Prognosis excellent. In a period varying from six months in the best to five to seven years in the slowest cases, all show complete or nearly complete cures. All deformity may be checked in a short time and proper bone nourishment established. Correction of deformities existing prior to adjustment is a growth process. Too many cases become discouraged at the slowness of the work and stop adjustments.
Retinal Hemorrhage.—Prognosis fair. Undoubted cures have been recorded, as well as a few failures. At least one case of hemorrhages followed by partially detached retina has been cured, or nearly so, by adjustments.
Rheumatic Fever.—Hard to adjust because of its painful nature. Results of proper adjustment usually, but not always, good.
Rheumatism.—Muscular rheumatism yields more rapidly than articular. Acute tends to quick recovery, chronic to more or less lengthened and slow improvement. Rheumatic diathesis may require many months of careful adjustment.
Rubella.—Simply and easily checked. Rash slight, and no prostration at all.
Scarlet Fever.—Data on quarantinable cases is meagre, but scarlet fever, or scarlatina, seems to be quickly modified by adjustment. One may expect a drop of from one to two degrees in temperature after first adjustment, followed by steady rise, which will again be checked by the next adjustment. Rash appears early, and all symptoms are mild, but several days are often required to put the patient at ease. Occasional sequelae, such as endocarditis, otitis media, or other inflammations, occur unless case be watched with great care. No fatal terminations under adjustment except in cases which were at first misdiagnosed.
Seminal Emissions.—Prognosis excellent in cases uncomplicated by masturbation or excessive venery; in such cases bad until habits are changed.
Simple Continued Fever.—Always recovers. Usually drops one to two degrees shortly following correct adjustment, with amelioration of all symptoms.
Smallpox.—Infections vary in virulence. In temperate climates all phases are hastened by adjustment and tend to recover without sequelae. The milder smallpox due to infection by vaccination is also amenable to adjustment, and prompt handling will often prevent serious poisoning.
Splanchnoptosis.—Partial or marked relief is usual—and slow. Complete natural replacement of all viscera is the exception rather than the rule.
Splenic Enlargement.—Variable prognosis according to cause. Secondary enlargements due to systematic infection yield with the disappearance of the infection. Primary enlargements yield more readily as a rule, with exceptions. Malarial spleen is slow to reduce.
Splenitis.—Prognosis presumably good, but few authentic cases reported.
Spondylitis Deformans.—Prognosis favorable for slow, slight improvement, but not for complete cure.
Strabismus.—Excellent in young subjects, less than fair in patients over thirty.
Sunstroke.—Theoretically curable, but no experience.
Syphilis.—The primary sore frequently dries under adjustment without the development of any secondary or tertiary stage. If first adjusted during the secondary manifestations symptoms may readily disappear and no tertiary stage ever appear. There are some authenticated cures eight and ten years past without recurrence of any sign. In the tertiary stage the organic lesions do not343 respond. Prognosis is so hopeless in this stage that it seems useless to apply Chiropractic at all.
Tabes Dorsalis.—Posterior spinal sclerosis, commonly called from its chief symptom “locomotor ataxia,” recovers in 40 to 50 per cent of cases adjusted. No accurate pre-judgment can be formed as to the probabilities in any particular case without experiment, nor has any adequate explanation been offered as to why some cases recover and others do not. Those cases which improve at all are likely to recover fully. In any instance, time is required for the regeneration of the dorsal column axons, and while this is going on no improvement may be apparent at all.
Tachycardia.—If symptomatic, as of exophthalmic goitre, tachycardia yields as the disease does. If primary, a few adjustments usually establish a proper pulse rate.
Tetanus.—Only one undoubted case has been brought to the writer’s attention and this one a marvellous cure. Adjustments were given as often as every ten minutes for a time.
Thoracic Aneurism.—Cure exceedingly doubtful, and fatal termination possible at any time. Little information is at hand.
Tonsilitis—Quinsy.—Simple or follicular tonsilitis aborts under adjustment in from a few hours to two or three days. Quinsy, or suppurative tonsilitis, runs its regular course as to duration, but is frequently a febrile after the first day. Spontaneous rupture of the tonsil344 will usually occur and sometimes two or three such ruptures will lengthen the case slightly. Sequalae are wanting, but all forms of tonsilar inflammation tend to recur unless a long course of corrective adjustments is applied to the cervical region.
Torticollis.—Acute spastic or rheumatic torticollis in which permanent contractures have not yet set in may be cured almost invariably in a period varying from a few days to several weeks. Chronic cases with permanent contractures yield very slowly, but prognosis is good for a fairly accurate straightening of the neck. Such cases often leave slight abnormalities even in the most competent hands.
Tuberculosis, Pulmonary.—See Pulmonary Tuberculosis.
Tumors, Benign.—Unlike malignant growths, benign tumors, fatty, fibroid, etc., tend to gradual absorption under adjustment. Perhaps 75 per cent or more may be completely cured. Age is a factor, tumors in young subjects being more readily curable than in the aged or infirm.
Tumors, Malignant.—Prognosis bad. If cancer in any form can be cured proof has escaped the author’s diligent search. It is wisest to refuse all cancerous cases.
Typhoid Fever.—Prognosis excellent if adjustments are commenced during first week of fever, in which case the fever should be aborted at once, followed by one or two mild exacerbations, then permanently checked.345 Doubtful prognosis after first week, because of liability to perforation during adjustment. After second week of fever very grave prognosis under adjustment, and better with nursing alone.
Uteroversion—Prolapsus.—Uteroversions and prolapses are corrected, sometimes rapidly but more often slowly and gradually. Favoring circumstances are freedom from overwork or overlifting. Some extreme cases result in failure.
Valvular Diseases.—These may be grouped for prognosis. No percentages have been compiled, but it may be said that the prognosis is generally good as to relief and restoration of compensation, but poor as to rebuilding of the valves. Many cases of apparent permanent and complete recovery are probably simply cases of excellent compensation. Death occasionally occurs despite adjustments.
Varicocele.—Outlook good for a slow, certain recovery.
Varicose Veins.—Probability favors cure in subjects not beyond middle life, providing they are not greatly overweight or too much on their feet. Cure always slow.
Punctuation, hyphenation, and spelling were made consistent when a predominant preference was found in this book; otherwise they were not changed.
Simple typographical errors were corrected; occasional unbalanced quotation marks retained.
Ambiguous hyphens at the ends of lines were retained.
The hierarchy of the Table of Contents has been used as the guide to the rest of the book, even though the two sometimes differ.
Index not checked for proper alphabetization or correct page references.
Page 26: “P R S” has an underline below “P” and a double-underline below “R”.
Page 34: “flexed far toward” perhaps should be “forward”.
Page 79: “as well all the details” may be missing “as” after “well”.
Page 117: “all vertebra above, so to speak” perhaps should be “vertebrae”.
Page 147: “this move is predicated” was printed as “this more was predicated”; changed here.
Page 158: “Posterior, right, inferior—P. R. I.” was printed as “P. R. L.”; changed here.
Page 187: “but is claimed” probably should be “but it is claimed”.
Page 307: “has been builded” was printed that way.