PLATE SHEWING THE FIRST MORBID APPEARANCE PRODUCED BY THE STAGNATION OF VITIATED BLOOD IN THE CAPILLARIES OF THE LUNGS.
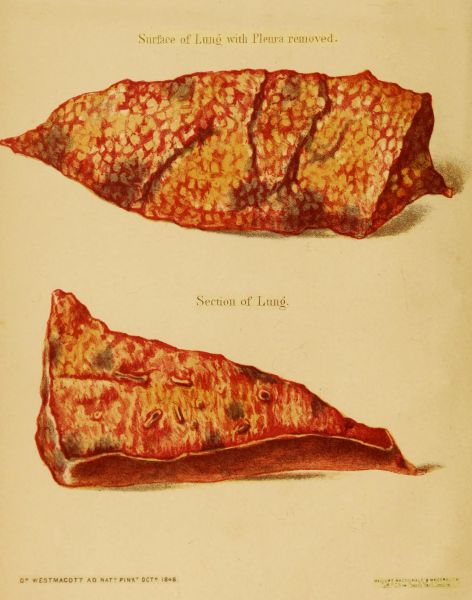
Surface of Lung with Pleura removed
Section of Lung
ON PHLEBITIS.
PLATE SHEWING THE FIRST MORBID APPEARANCE PRODUCED BY THE STAGNATION OF VITIATED BLOOD IN THE CAPILLARIES OF THE LUNGS.
Surface of Lung with Pleura removed
Section of Lung
BY
HENRY LEE, F.R.C.S.
ASSISTANT SURGEON TO KING'S COLLEGE HOSPITAL, ETC.
"There is more to be learnt of the use of the blood in the animal economy from its coagulation
than from its fluidity."—Hunter.
LONDON:
HENRY RENSHAW, 356, STRAND.
1850.
LONDON.
RICHARDS, PRINTER, 100, ST. MARTIN'S LANE.
Since the period when Humoral Pathology fell into merited disrepute, comparatively few attempts have been made, to define with any degree of accuracy, the conditions under which morbid secretions may find their way into the circulation. The diseases produced by the presence of vitiated fluids in the general system, and in parts of the body at a distance from their original source, have received more attention; but they are still far from occupying that position in our systems of medicine and surgery which their importance deserves.
The difficulty of tracing diseased secretions after they have become mingled with the blood, or of recognising their presence in the vessels, has rendered the investigation of their actions often tedious and inconclusive; while, on the other hand, the changes of structure in solid parts, readily appreciated by the senses, have been more calculated to arrest the attention, and to afford that ready solution of the origin of the symptoms which, whether imaginary or real, has a tendency to relieve the mind from farther doubt and suspense. Hence it has happened, that the pathology of the solid parts of the body has received a very disproportionate share of attention.
Most of the observations which have tended to advance our[Pg ii] knowledge of the effects of the introduction of diseased fluids into the blood, have been recorded under the name of Phlebitis or Inflammation of the Veins; and I have retained this title, although it is obviously inadequate to express those constitutional affections which form the most important and characteristic features of these complaints.
The introduction of pus into the system has justly been regarded as the most important of this class of diseases. But the theory of the circulation of pus globules with the blood, supported as it has been by much ingenious reasoning, and most conveniently adapted to explain the formation of purulent deposits, has yet never obtained general belief. The stoppage of the pus globules in the capillary tubes, has appeared to many accustomed to the practical observation of diseases, too mechanical a solution of the origin of these abscesses; and it has become necessary to determine, with more precision than has hitherto been done, the actual conditions under which pus in substance can be received into the circulation.
The simple experiment of mixing some pus with healthy, recently drawn blood, will at once shew that such a combination cannot circulate in the living body. It will be found that the blood coagulates round the globules of pus, and forms a solid mass which will adhere to the first surface with which it comes in contact; and it will be evident, that it is not till the coagulum thus formed is broken up or dissolved, that its elements can circulate with the blood.
It appears not a little surprising that this, perhaps the simplest and the most instructive experiment that can be performed in reference to the subject of the formation of purulent deposits, should not have been resorted to in preference to others which[Pg iii] have been difficult in their execution, and inconclusive in their results.
It has been remarked by Sir Charles Bell, that we can seldom rely upon the answers that are extorted from living animals by experiments which go counter to the natural feeling of mankind; and that it is our duty, if experiments are performed, at all events to prepare for them by the closest previous application of our reason, and so to narrow the question as to be certain that advantage may be gained by our proceedings. Had the simple experiment mentioned above, illustrating the action of pus upon blood out of the body, been duly considered, it might have saved some of the vague and useless experiments which have been performed upon living animals in the investigation of the present subject.
Sept. 1850.
13, Dover Street, Piccadilly.
ON INFLAMMATION OF THE VEINS:
WITH EXPERIMENTS ILLUSTRATING THE EFFECTS OF A VITIATED CONDITION OF THE BLOOD.
I. John Hunter expressed his belief that the blood has "the power of action within itself",[1] and that when it coagulates, it does so in consequence of an "impression" which it receives. Such an impression may be communicated by separation from the living vessels, or from "cessation of natural action"[2] in them. In certain circumstances also the living vessels themselves may be the means of exciting coagulation.[3] In others, the admixture of extraneous substances may either retard or hasten this operation.[4] The experiments made to determine the last point, Mr. Hunter informs us, "were rather imagined than fully carried out; and the subject rather broached and touched upon, than prosecuted".[5] In these experiments, different articles used in medicine were mixed with portions of blood taken from the body; and it was found that, in some cases, they altered both "the time," and "the firmness of the coagulation".[6] The circumstance of medicines being used in such experiments, conveys the idea, that, in instituting these researches, Hunter conceived that substances which would tend to pro[Pg 2]duce such actions out of the body, might likewise produce some effect upon the blood in living animals. In endeavouring to prosecute the idea thus thrown out, I have been led to try the effect of different substances upon the blood, and to consider the changes which may be produced in that fluid, by the admixture of animal secretions. The experiments which will be hereafter detailed, not only confirm Mr. Hunter's notion, that foreign substances may induce actions in the blood when withdrawn from the body, but also show that some of these effects may be produced still more rapidly in the living vessels.
In these experiments, pus was used in preference to any other fluid; first, because the power of coagulating the blood which it was found to possess, enables its influence to be traced within the body; and secondly, because, being an animal secretion, the results obtained are likely to be analogous to those produced by the admixture of other secretions with the blood.
When pus is mixed with blood, fresh-drawn from a healthy animal, it is found in a marked manner to favour coagulation. This effect does not take place immediately, as in the case of the mixture of an acid with the blood; and I have reason to believe, that where the blood has lost its natural power of coagulation, no visible change is produced in it by the addition of pus. It appears, therefore, that this effect depends rather upon a vital than a chemical influence. In some cases, the coagulation takes place in less than two minutes; in others, after a longer period; but in all the experiments made, the influence of pus, when added to blood, in promoting its coagulation, was sufficiently evident. Putrid pus was found to act more rapidly than healthy pus (Exp. 1, b), but the admixture of water was found to retard the operation; the result, in this respect, differing in some degree from the conclusion drawn from a similar experiment performed by Hunter.[7] The causes which usually[Pg 3] favour coagulation out of the body, are rest, and separation of the blood into small quantities. These conditions are, in some degree, brought into play during the circulation of the blood through the capillaries; and when the influence of the admixture of pus with the blood is not sufficient to produce coagulation at once, we should naturally expect the effect to be more readily induced, where these two additional causes concur in favouring such an action. When the pus introduced is in any large quantity, the coagulation of the blood is at once determined, and the entrance of pus into the circulation thereby prevented. The experiments vi, vii, and viii, appear to furnish evidence of the correctness of this opinion, and to show that the result may be produced more quickly in the vessels than elsewhere. In these cases, so sudden was the effect, that the mixture of blood and pus coagulated before it could traverse the jugular vein, as indicated by the induration and cord-like feeling of the vessel.
In Experiment viii, the obstruction formed was sufficient to resist even firm pressure, and in a great measure, if not altogether, to prevent the pus injected from finding its way along the vein. The coagulum was felt in the vessel during the operation, and was there found after death. One effect of the coagulation of the blood thus immediately produced, is necessarily to retain the vitiated blood in the part, and to prevent its being carried in the course of the circulation. This intention may be interfered with, either by accident or design. The coagulum, as in Experiment vi, may be broken up during the process of its formation, or after it has formed, and the parts of which it was composed carried forward with the circulating blood. In such a case, the vein in which the coagulum first formed, is found in its natural condition (except at the part where it may have been mechanically injured), and dark patches of congestion may be found in distant systems of capillaries. If the coagulum be allowed to remain, the vein in which it is formed soon becomes thickened; but, as the experiments cited[Pg 4] prove, this thickening is the effect and not the cause of the stagnation of the vitiated blood in the vessel.
II. When blood coagulates in a serous cavity, a thin pellicle forms upon its surface, and, becoming thickened by deposition from the fibrin of the blood, forms a cyst, which completely circumscribes the effusion. This point has not probably received the attention which it deserves; and as it is believed to be of primary importance in the investigation of the present subject, a short space will be devoted to the purpose of fully establishing it, and tracing its connexion with other and subsequent changes. Every layer of lymph observed upon dissection, has perhaps too generally been considered as the result of inflammation; and hence there has arisen a confusion in the terms employed. That lymph may be derived from the blood directly, and deposited in the form of a membrane, without being secreted by any vessel, has been fully shown by a paper in the Medico-Chirurgical Transactions.[8] Such layers of lymph assume so much the appearance of others, derived by secretion from inflamed capillaries, that they have been described as identical. But the mode of their formation in the two instances is altogether different. In the one case, the process is a local one, confined to the blood itself, and subsequently to the membrane with which it happens to be in contact. In the other case, it is an effort of the constitution, accompanied by constitutional symptoms. The former of these processes was clearly described by Hunter. In describing the process of union by the first intention, "Coagulation", he says, "I imagine to proceed upon exactly the same principle as the union by the first intention. It is particle uniting with particle by the attraction of cohesion, which, in the blood, forms a solid; and it is this coagulum uniting to the surrounding parts which forms the union by the first intention: for union by the first intention is no more than the living parts when separated, whether naturally, or[Pg 5] by art, forming a reciprocal attraction of cohesion with the intermediate coagulum, which immediately admits of mutual intercourse, and, as it were, one interest."[9] "When the blood has coagulated, so as to adhere to both surfaces and to keep them together, it may be said that union has begun."[10] "The uniting medium becomes immediately a part of ourselves, and the parts not being offended at it, no irritation is produced." "If the quantity of blood extravasated be large, the whole will not become vascular, but the surface only, which is in contact with the surrounding parts."[11] The process thus described in general terms may take place in serous cavities. In the third plate at the end of Mr. Hunter's work, is represented a coagulum of blood adhering to the tunica vaginalis. "The adhesion was firm, though it admitted of a separation at one end; when separated, fibres were seen running between it and the testis."
It might seem unnecessary to dwell upon this process further, had not some of the highest authorities in surgery, both here and on the continent, described it as identical with adhesive inflammation. Thus Bichat[12] says, "The cicatrization of wounds in veins after bleeding is a result of inflammation." Now, it is submitted, that when the blood coagulates, either in serous cavities or in veins, the process of union is not usually one of inflammation, or one in which the powers of the constitution are called into increased activity. It is true, that in both cases, inflammation may take place, and lymph, as the result of such inflammation, may be secreted; but this is only when, to use Mr. Hunter's language, the "primary intention" has not been fulfilled.[13]
When a membranous layer of lymph is deposited from effused blood, it adheres with some firmness to the surface with which it is in contact; but, as there is at first no vascular connexion established between them, it may be separated, leaving the part to which it adhered in its natural condition. Lymph derived from adhesive inflammation, on the other hand, when separated, leaves the surface upon which it was formed rough and uneven. Coagulated fibrin, when recently deposited, may thus be distinguished from effused lymph.
The changes which blood undergoes when effused in serous cavities, may likewise take place when it is detained in injured or exposed veins. The coagulation of the blood in such cases (Exp. vii and viii) serves as a bond of union between the sides of the veins (which may be either temporary or permanent), so as to prevent the entrance of any foreign matter into the circulation. When the blood thus coagulates in veins, changes may be produced analogous to those mentioned as occurring in serous cavities. If the quantity of blood be large, a thin pellicle is at first formed upon its surface (see Preparations 1523-25 and 1525-64, in the Museum of Guy's Hospital). This membrane becomes thickened and adheres to the internal surface of the vein (see plate No. 13, Cooper and Travers' Surgical Essays, Part i, and Prep. No. 1736, in the Pathological Museum of the College of Surgeons). It then becomes vascular, and finally so firmly united to a part of the circumference of the vessel as to be inseparable from it, without lacerating its lining membrane.
If the wounded vessel be small, or if the animal be strong and robust, the whole of the blood in the vein may at once coagulate and become united to its sides. The usual economy of nature, however, is here exercised, with a precision proportionate to the strength of the patient. A simple wound in a vein, in healing by the first intention, will not obstruct the circulation through the vessel under ordinary circumstances. A coagulum will form, sufficient to unite together the divided edges, and the circulation of blood through the vessel will be uninterrupted;[Pg 7] but if the wound does not readily heal, coagula may form, which encroach more or less upon the cavity of the vein. There are then three ways in which a coagulum may obstruct the circulation through a vein. 1. By the outer layer of the coagulum forming a membrane, which contains the more fluid parts of the blood. 2. By the whole of the blood contained in the vessel forming a solid coagulum. 3. By a coagulum adhering to the injured side only of the vessel.
In whichever of these ways the process of repair is commenced, it may be interfered with, and the union dissolved. This is practically known to farriers; who, when they want to bleed a second time from the same orifice, break down the "union by the first intention" by a blow upon the vein. During the time that the parts are united only by the fibrin from the blood, any violence must tend to produce the same effect. If the constitution is good, and the coagulating power of the blood unimpaired, the union may be frequently interrupted, and yet be as frequently re-established in the same way. When from any local cause, or from any constitutional peculiarity, the union by the first intention fails at the seat of the injury, it may yet be attempted at some distance up the vein; and then we have coagula formed at different distances along the vessel. If these coagula fill the vein, are firm, and remain undisturbed by violence, the union may be complete, and the vessel sealed at those parts, even although the original wound should suppurate. But it sometimes happens, that the same peculiarity of constitution, or the same local cause, which prevented the union at the original wound, may prevent complete union by the first intention at any other point of the vein; and then its canal is open to any secretion that may be introduced into it. Foreign matter may thus find its way along a vein; but still there is a provision against its being carried the round of the circulation. It has been already shown that the blood, when in a natural condition, has a tendency to coagulate around pus, and, probably, many other fluids, even out of the body (Experiments i, v),[Pg 8] and that this property is exercised in a still more remarkable manner in the living vessels (see Experiments vii, viii). Foreign matter, even after it has got into the veins, may then, by the same means, be prevented from proceeding farther towards the centre of circulation. The process that takes place under such circumstances, is strictly analogous to union by the first intention. The blood may coagulate and adhere to the sides of any part of the vascular system. The union thus formed may be permanent, or the coagulum may be again broken up and carried with the blood in the course of the circulation, as shown in Experiment vi. When this occurs, as is shown in the same experiment, other changes supervene in remote parts of the body. This tendency to coagulate around the foreign matter once impressed upon the blood, cannot be destroyed by the coagulum being mechanically broken up, as indeed is proved by the fact already mentioned, that after one attempt at union in a vein (in consequence of the introduction of foreign matter) has failed, another attempt is made immediately farther up the vessel. Under these last circumstances, we may find a vein partially obliterated at different points, leaving intervals where lymph or pus are secreted. If the purulent matter introduced is allowed to remain a short time only in the vein, no inflammation is produced (Experiment vi). But when any irritating fluid is detained there in consequence of the blood coagulating around it, adhesive, ulcerative, or suppurative inflammation, will be excited (Experiments vii and viii).
The slowness with which veins inflame when cut, tied, or bruised, has been made a subject of comment by different authors; and Mr. Travers, in particular, has endeavoured to reconcile "the infrequency of its occurrence" with the rapid and violent character of the inflammation in certain cases. Although, under ordinary circumstances, a wounded vein does not inflame, yet the annexed experiments show, that pus introduced into its cavity will produce inflammation, in which the system will sympathize. Other fluids besides pus will no doubt produce similar[Pg 9] effects; but those of pus are here particularly noticed, as affording a good illustration of the series of changes produced by the introduction of foreign matter into the blood.
What the symptoms are which characterize the presence of pus, as distinguished from other secretions in the blood, it would probably be difficult to determine in cases as they occur in practice. The examination of the blood in these instances affords no very satisfactory information; for the characters of pus, when the blood has once coagulated round it, are so altered, that I know of no means by which a small quantity can be recognized, when it has once entered the circulation. The conclusions drawn from the different facts now stated are,—first, that inflammation of a vein, or phlebitis, is no essential part of the primary affection which precedes constitutional symptoms, even when morbid matter has found its way into the circulation through a vein. Secondly, that when inflammation of a vein does occur, in some instances at least, it is not the cause, but the consequence of the introduction of diseased or foreign matter into the blood. Thirdly, that although veins are with difficulty inflamed by any mechanical injury, they are susceptible of rapid inflammation, accompanied with constitutional disorder, whenever any irritating fluids are introduced into their cavities.
III. When the principal veins in a part become obstructed, it is natural to suppose that changes should be produced in the smaller veins which supply them. These changes may be expected in a more marked degree, when the obstruction depends upon coagulation of the blood, than when it arises from other causes, inasmuch as the coagulum usually extends to several veins at the same time.
In the experiments that have been made upon animals, it has been a matter of surprise that, while extreme pain was evinced upon the injection of irritating fluids into the veins, comparatively little or no suffering was produced, when similar experiments were performed upon the arteries. The foreign matter introduced in these cases would probably[Pg 10] have the effect of coagulating the blood, as in the instances already mentioned. If this occurred in an artery, the supply of blood below the obstruction would be diminished; but if in a vein, the return of blood would be prevented: in the latter case, the continued influx of blood to the part would necessarily distend the capillaries.
In M. Cruveilhier's[14] experiment, of injecting ink into the veins of dogs, he found, that in thirty-six hours the legs swelled, and a number of bloody patches (foyers apoplectiques) were found in the substance of the muscles and the cellular tissues of the limb. The large veins were distended with adherent coagula of blood, and the smaller veins around the livid patches were also filled with coagulated blood. If the animal were allowed to live, the congested spots suppurated. The appearances thus produced in the muscles and cellular tissue of the limb were evidently not those of inflammatory action propagated along the coats of the veins, for the affection in the capillaries was circumscribed, and terminated in many places abruptly, leaving the veins in the immediate neighbourhood perfectly healthy; still less could the appearance produced depend upon the injected fluid finding its way through the veins (contrary to the course of the circulation) to the capillary system; nor, lastly, could it depend upon the ink finding its way into the general circulation, and producing its effects in its course a second time through the limb; for, not to mention that the capillaries of the lungs and other parts would be equally liable to be affected, one essential condition of the success of the experiment is mentioned to have been, that the fluid injected should not find its way along the vein in the usual course of the blood. We therefore conclude, that it was the coagulation of the blood in the large veins which caused the congestion of the capillaries, those veins remaining unaffected which could discharge their contents by some collateral channel.
In cases of phlegmasia dolens after child-birth, the same principle can sometimes be traced; thus, in a dissection performed by Mr. Lawrence,[15] the external and common iliac veins were filled with a substance like the laminated coagulum of an aneurism. "The tube was completely obstructed by this matter, adhering as firmly as the coagulum does in any part of an old aneurismal sac. In its centre was a cavity containing about a teaspoonful of thick fluid of the consistence of pus, of a light brownish red tint, and pultaceous appearance." The femoral vein was in this case also filled with a coagulum; but, as is observed in the account of the dissection, the red colour of that vein might have been caused by the clot everywhere in contact with it, and therefore cannot be deemed a proof of inflammation.
Mr. Guthrie[16] has published a case of inflammation of the veins after amputation, resembling phlegmasia dolens, in which the veins of the opposite limb, even down to the foot, had become affected. In this case, on the fourteenth and fifteenth days after amputation of the right thigh, the left leg began to swell, and became intolerably painful. "The swelling was elastic, yielding to the pressure of the finger, but not in any manner like an œdematous limb. Upon a careful examination, no pain was felt in the course of the iliac vessels upon that side; the stump looked well, save at one small point, corresponding to the termination of the femoral vein." On examination after death, the termination of the vein on the surface of the stump was open, and in a sloughy condition. At the left groin, the iliac vein was greatly distended with pus. Sir Henry Halford[17] has also mentioned three cases of what he has termed phlegmasia dolens, occurring in the male, in one of which the iliac vein was found obliterated after death. In this case, the patient had suffered, for several years before his death, from swelling of the left[Pg 12] leg and thigh. In the interior of the obliterated vessel there is a coagulum, which has lost its colour, and become firm and completely adherent to the inner surface of the vein. (See Prep. No. 1732, Path. Mus. Coll. of Surgeons.) The rapid swelling and general pain of the limb in such cases, indicate a sudden obstruction to the circulation, while the absence of tenderness in the course of the vessels during the first stages of the disease, tends to show that the contents of the vessels, and not the vessels themselves, are primarily interested in its production.
The foregoing remarks have appeared necessary, in order to explain a circumstance mentioned by Hunter, upon which considerable stress has been laid by subsequent writers. Mr. Hunter observed that the whole side of the head in horses that had been bled would frequently become swollen and inflamed. The explanation of this fact appears very simple, when viewed in relation to the general principle illustrated by the above cases. The horse has only one jugular vein upon each side; and, although in the usual operation of bleeding, its channel is not obstructed, yet if the wound do not readily heal, its contents will coagulate. The circulation will then be obstructed in all the distant branches, and the blood, if long retained, will coagulate in them also. It will then part with its serum, and give rise to all the symptoms of inflammation in the distant vessels; a pulpy elastic swelling, accompanied with great pain, will then be the principal symptom, while the turgescence on the surface will be less than where the superficial veins have been mechanically compressed. It will, however, very frequently happen, that a vein in a part may be felt distended without any symptom of inflammation being present; and, in other cases, the pain and swelling will appear and disappear too rapidly to allow the idea that they depend upon inflammation of the coats of the vein. It has occurred to the author, to feel a vein in the arm and hand distended during life, and after death, to find it empty, and its coats of their natural colour and thickness; in such a case, the coagulum gives way, becomes broken up, and mixed with the circulating blood.
IV. When pus, or other diseased fluid, is confined to the cavity of a vein, the constitutional symptoms produced are comparatively mild, as long as it remains limited and circumscribed by adherent coagula; that is to say, so as to be excluded from the rest of the circulating system. (Compare the frequency of the respiration in Experiments vi and vii.) But the tendency of a clot of blood is to contract; and a time comes when the coagulum is either broken up, or shrinks, so that if no further changes are produced, the current of blood through the vein is re-established.[18] Meanwhile, however, the coats of the veins have undergone changes corresponding to the degree of irritation produced by the contained fluids, and the intention or result to which the inflammation tends. If the coagula have long remained, the coats of the veins are always found thickened, sometimes to three or four times their natural thickness, and sometimes so as to completely obliterate the vessels. The contents of the veins are occasionally found to consist, as far as can be seen, simply of coagulated blood; at other times, they are found filled with soft yellowish coagula, deprived, more or less perfectly, of their colouring matter; more rarely, the cavity of a vein will be found filled with dark-coloured membranous layers, leaving still a channel through the vessel; and occasionally it will be found completely obstructed by "dense, dark-coloured, bluish membranes."
As the coagulum contracts in a vein, if the intention is to obliterate the vessel, its sides are gradually approximated. In the smaller veins, and in the divided extremities of large veins, the sides are soon completely drawn together. But the latter, if not wounded, may for a long[Pg 14] time (see Prep. 1732, Path. Mus., Coll. of Surg.) retain coagulated blood in their contracted, but not completely closed, cavities. In both cases, the coagula which close the veins are liable to be displaced by accident, or to have their adhesions loosened by the changes which they undergo. The position of a vein, and the structure of the organ through which it passes, may be unfavourable to its healthy reparation. The process of repair goes on frequently during a continued flow of blood over the part, and sometimes during the constant action of the muscles in the neighbourhood: at other times, an injured vein will be situated immediately in the bend of a joint, and will be subject to be continually bent and extended with the motions of the limb. In the structure of the bones, the veins lie in unyielding channels, and are consequently deprived of the assistance derived from the approximation of their sides, as in soft parts, during the process of reparation. As the coagula contract in such a case, there is danger lest the union by the first intention should be disturbed, and that the cavities of the injured veins should be left exposed.
Again, in the uncontracted uterus after child-birth, the veins which open upon the placental surface, pass through the firm texture of the organ, and are incapable of contraction independently of the muscular structure which surrounds them. The coagula which close their extremities secure them against the entrance of any foreign matter; but should these coagula be removed before the vessels are otherwise protected, their open mouths are exposed to any secretions that the uterus may happen to contain. In these cases, if a coagulum is not firmly formed, or if it is displaced by violence, it may be broken up, and portions of it mixed with the fluid blood. Subsequent coagula may form in the veins and offer fresh obstructions to the admission of any foreign matter, but these may, as in the first instance, be disturbed, and carried, together with any admixture of the secretions of the part, in the course of the circulation. The period at which the union of a coagulum in a[Pg 15] vein is dissolved, is sometimes marked with great precision. In a case recorded by Dr. Davis,[19] a patient was convalescent from an attack of phlegmasia dolens, when death took place instantaneously, while the patient was in the act of changing the sitting for the recumbent posture; the left external iliac vein was thickened, and its internal tunic was studded in several places with deposits of adherent lymph. The portion most remarkable for this incrustation, as well as for other disease, was immediately beneath Poupart's ligament; the vein, although contracted, was manifestly pervious.
V. It has been shown in the previous sections, that secretions mixed with the blood will alter its properties, and influence the period of its coagulation: that when the blood is thus altered, it may pass through a vessel without leaving any trace of its passage; but that if it coagulates and remains in a vein, the coats of the vessel will then take on increased action. The exciting cause of the inflammation in such cases appears to be conveyed by means of the contents of the vessels to the vessels themselves. But, as in post-mortem examinations, the changes produced in the vessels are much more easily recognized than the alterations in their contents, the former have of late years almost exclusively occupied the attention of pathologists. The cases in which constitutional symptoms follow inflammation of the veins, will be found to divide themselves principally into three large classes. 1. Those in which one of the larger veins has been opened. 2. Those in which some portion of bone has been involved in the original lesion. 3. Those that occur after child-birth.
In each of these three classes of cases, a free communication will be found to exist between the injured part and the general circulation. The natural mode of sealing this communication, when it is no longer proper, is the coagulation of the blood in the veins of the injured part.[Pg 16] When, from some constitutional affection, or from some local peculiarity of structure, this intention is not fulfilled, a ready passage remains open, through which the blood may become infected. When pus has been injected into the veins, it has frequently happened, that no great constitutional disturbance, and no signs of secondary inflammation, have been produced; but this is believed to have depended upon the coagula in the veins having prevented (as probably occurred in Experiments vii and viii) the foreign matter from finding its way along the vessels. But if this obstruction be not offered, or be overcome, then the appearance of secondary inflammation, accompanied by corresponding constitutional symptoms, will be produced.
If water be injected into the cancellous structure of bone, it will find its way out in drops through the apertures of the nutritious vessels. The ready communication which is thus shown to exist between the interior of bones and the veins, has been but too often exemplified by M. Cruveilhier's experiments of introducing mercury into their cancellous structure, and finding it subsequently in the vascular system. This fact assumes peculiar significance, when taken in conjunction with the very large proportion of cases, in which some portions of bone will be found to have been involved in the primary lesion, in those who have died of secondary inflammations. Of fifty-two consecutive cases, occurring in surgical hospital practice, of which I have preserved notes, in no less than forty-one was some portion of the osseous system implicated.
Again, in the third class of cases above-mentioned, if the vena cava be injected after parturition, the injection will very speedily find its way into the uterus.[20] The ready communication which is thus shown to exist between the vascular system and the local affection, in each of the three large classes of cases which usually give rise to subse[Pg 17]quent disease, would of itself afford at least a very remarkable coincidence. But more direct evidence presents itself of the way in which the system becomes contaminated in these affections: thus, after an operation for hæmorrhoidal tumours, an effusion of lymph and pus has been found in the hæmorrhoidal veins,[21] from thence the same appearances have been traced to the inferior mesenteric vein, and the severity of the secondary affection, indicated both by the symptoms and the post-mortem appearances, has fallen upon the liver. These circumstances all tend to point to the venous system as the means by which morbid matter in such instances is introduced: and the still more conclusive facts afforded in the production of secondary disease, by injecting fluids into the veins,[22] allow scarcely a doubt to remain upon the mind, that the unprotected veins are the channels, in a very large proportion of cases, through which the blood becomes infected.
VI. The cancellous structure of bone may be compared to the cellular tissue in soft parts. When inflamed, its intervals become filled up by effusion from the vessels, and an abscess may be as accurately circumscribed in the hard as in the soft structures of the body. In a healthy constitution, the adhesive inflammation will, in this way, always precede the suppurative; but where the inflammation is not circumscribed by adhesion, the secretions may permeate from cell to cell in unadhering parts. In soft structures, a remedy is at hand for allowing the escape of the matter, by a free division of the parts; but in bone, where the same thing takes place, the hard unyielding sides offer an[Pg 18] effectual obstruction to the escape of any effused fluid. The cells of the bone then may become infiltrated, and, unless the veins of the part have been closed, there is nothing to prevent the diseased secretions from finding their way into the circulation.
M. Cruveilhier assures us, that a single drop of mercury introduced into the cancellous structure of living bone, may subsequently be detected in the capillaries of the lung, where it becomes the centre of one or more patches of livid congestion. This experiment appears to afford a perfect illustration of the way in which diseased secretion may be conveyed into the circulation, when the natural processes of repair in bone are abortive. These processes are the same in bone as in the other structures of the body; viz., union by the first intention, and adhesive inflammation. In soft parts, as the fibrin, which forms the bond of union in the first of these, is absorbed, the divided veins collapse, and thus continue closed; but in bony structures, where the injured vessels are held open, as the fibrin which at first closed their extremities becomes removed, their channels may be left as much open to the diseased secretions of the part, as to the globule of mercury in M. Cruveilhier's experiment.
The low degree of organization in bone, and the comparative slowness with which actions are there carried on, render it, in a peculiar degree, liable to interruptions in the process of repair; especially when, as not unfrequently happens, there is reason to believe that the vitality of some portion of the bone has been threatened. The offensive smell of the bone, as well as the appearance of its cancellous structure infiltrated with puriform matter, will frequently show in such cases, that the processes above-named have not followed their natural course.
VII. As a necessary deduction from the accompanying experiments, and those of M. Cruveilhier, alluded to in the previous section, we arrive at the conclusion, that a vitiated condition of the blood may give rise to inflammation of the veins in different parts of the body. The[Pg 19] circumstances which occasionally attend reparation of the uterine veins after child-birth, will be found to lead to the same inference; and the same general proposition will derive fresh support from the consideration of this class of cases.
The veins which terminate upon the placental surface of the uterus are necessarily open when this organ is distended, and become more or less perfectly closed when it contracts. In cases when the contraction is incomplete, innumerable open-mouthed orifices are left bathed in secretions, which are often offensive and undergoing decomposition; the natural protection to the vessels then, is the coagulation of the blood in them. If examined, the uterine veins will be found filled with coagula for some distance. But in cases where this power is impaired, all the uterine veins and arteries recently separated from the placenta may be found bathed in the secretions of the part, under circumstances most favourable for their absorption. The passage of diseased secretions through the vessels cannot always be traced in this, any more than in the other forms of the disease. Many of the substances introduced artificially into the circulation by M. Gaspard, produced no action upon the coats of the veins through which they passed, and yet the general symptoms were precisely similar to those originating from genuine phlebitis. In accordance with this, it may be observed that the uterine veins are often found perfectly healthy when the spermatic, or renal, or still more distant veins are thoroughly disorganized. In either case, the healthy condition of the veins near the original lesion forbids the idea of inflammation having been propagated along the coats of the vessels, while all analogy appears in favour of the disease being transmitted through their contents.
In a certain number of cases no lesion will be found in any of the veins of the body, but the uterine veins will be found to contain some unnatural fluid; at other times coagula of blood, which have lost their elasticity, gritty to the feel, and greyish or light brown in appearance,[Pg 20] will be found filling the veins or leaving intervals in them, where lymph or pus may be recognized. It matters little whether the unnatural fluids, thus found in the uterine vessels, have been absorbed from the cavity of the uterus, or are the product of venous inflammation. The effect upon the blood in either case would be the same.
When obstructions form in the spermatic veins, they are not indicated by any external symptoms; but when the veins opening into the internal iliac are similarly affected, the coagula are liable to extend into its cavity, and even beyond it to the external and common iliac vessels. The free return of the blood from the inferior extremity, will then be prevented. The effects of this have already been described (sec. iii.)
The connection of this form of disease with affections in distant parts of the body, has been noticed by several eminent writers. Legallois has expressed his conviction, that phlegmasia dolens, puerperal fever, and many other puerperal ailments, are solely dependent upon the absorption of pus from the uterine surface. This opinion appears to have been formed upon too hasty a generalization, inasmuch as other fluids besides pus, as evinced by some of the annexed experiments, may produce similar effects upon the blood. But that pus, when absorbed, will determine the coagulation of the blood in the iliac as well as in other veins, must be allowed; and that the symptoms of obstructed venous circulation arising from this cause, will exactly resemble those of phlegmasia dolens, will scarcely be denied.
"Besides depositions of pus in certain portions of the frame," observes Dr. Ferguson, "I have seen two other states of the limb, which are connected with and traceable to the cause originating puerperal fever. In one of these the malady looks like erysipelas...; in the other, the leg is attacked with a disease so exactly resembling phlegmasia dolens, as to leave no doubt in my mind that they are one and the same malady. In this, as in other forms of the disease, there may be a tendency to gangrene of the skin."
The period of the occurrence of what has been described under the name of uterine phlebitis is marked with much precision, and the affection of the system is often general and sudden. It may be stated as the result of all the observations hitherto made, that it occurs most frequently from the 10th to the 20th day after parturition.[23] If the inflammation in such cases were propagated along the vessel only, it would be difficult to account for such an apparently capricious selection of time for its development. This difficulty, however, disappears when the period is observed to be so strictly in accordance with the time at which the same symptoms occur after other local complaints, and to be, moreover, the time at which the coagula formed in the veins, may naturally be expected to shrink.
It has been observed, that inflammation after child-birth usually attacks the spermatic veins alone, and for the most part the one only on that side of the uterus to which the placenta has been attached. The hypogastric veins are comparatively rarely affected. The appearances observed upon dissection in the spermatic vein, usually terminate abruptly at its opening into the vena cava on the right side, or into the renal on the left. This fact is in perfect accordance with that observed by Mr. Arnott, that the coagulum in veins extends usually only to the nearest collateral branch; the explanation appears to be the same in both cases, as illustrated by Experiment vi. If the coagulating blood be left undisturbed, it will form adhesions to the sides of the vessel and produce increased action in its coats; but if mechanically disturbed, it will be carried forward before the process of coagulation is completed, and leave the vein in its natural condition. When any portion of a vein is obstructed, the blood is kept at rest between the obstruction and the next collateral branch; and, if disposed to coagulate, there is nothing to interfere with such an action. But the case is different, as soon as[Pg 22] one vein opens into another. A fresh current of blood is then continually sweeping the orifice of the obstructed vessel; and, even although the blood at this point should have a tendency to coagulate, it is carried on in the course of the circulation, before it can adhere to the sides of the unobstructed vein. The sudden termination of the diseased appearances in these cases, affords an additional proof that the blood is the medium by means of which this affection is transmitted. It is true, in such instances the diseased fluid cannot be always, or even generally, traced in the veins, and very many cases occur where a retained and putrid placenta, or decomposing coagula, remain in contact with the mouths of the uterine veins, without any of the symptoms of local phlebitis being produced; but this is only in accordance with what is observed in cases where purulent or other fluids have been directly injected into the blood. The examination of the blood, or of the vessels, in such cases, will by no means invariably indicate the presence of foreign matter after it has once become thoroughly mixed with the blood, nor will inflammation of the vein through which the fluid passes, be by any means invariably produced.
When a foreign substance is introduced into an artery, any immediate effects upon the blood may naturally be looked for in the system of capillaries which it supplies. If the blood then coagulates, local symptoms alone, will, in the first instance, be produced, and the constitution will remain unaffected. M. Magendie,[24] indeed, asserts that fluids injected into the arteries of animals, return quickly through the corresponding veins, and that this takes place even more rapidly in the living than in the dead body. If this were universally true, it would matter little whether foreign matter were introduced into the arterial or venous system. The effect upon the constitution would be the same in either case. But if, as is now maintained, extraneous matter intro[Pg 23]duced into the blood may, under certain circumstances, produce its coagulation, then the effects will be confined, more or less completely, to the first system of capillaries which the blood meets with in the natural course of its circulation, and the constitution will be affected only in consequence of the changes which then take place. M. Gaspard has shown that greasy fluids, and such as contain sediments, do not find their way readily from the small arteries into the veins. They become entangled in the intermediate capillaries, and there produce, first patches of local congestion, and subsequently serous effusion and abscesses. Some clear fluids, on the other hand, such as solutions of tartar emetic, of opium, and of nux vomica, when introduced into an artery, pass readily in the course of the circulation, and produce their full effect upon the constitution; and in such cases no irritation is manifested in the capillaries through which they pass. The first of these poisons produces vomiting and purging, the second stupor, and the third tetanic rigidity, exactly in the same manner as if they had been introduced into the stomach, or injected into a vein.
There are yet another class of substances differing in their effects from both of the former; and under this head are classed infusion of tobacco, solution of acetate of lead, putrid fluids, etc. These are distinguished from the first class above mentioned, as not offering in themselves any mechanical impediment to the circulation of the blood, and from the second, as not producing the same constitutional symptoms when injected into an artery as when thrown into a vein. M. Gaspard found that, when introduced into an artery, the infusion of tobacco neither produced vomiting nor stupor, the solution of acetate of lead did not act upon the intestines, and the putrid fluids did not produce the evacuations usually observed after their introduction into the system by other means. All these substances, however, were found to produce violent local irritation in the parts to which the branches of the injected artery were distributed, and the constitutional symptoms were those[Pg 24] produced in consequence of the local irritation, and not those which would arise directly from the action of those poisons upon the system.
In Experiment xx, seven or eight cubic inches of common air were gradually injected into the carotid artery of a dog, and half an hour afterwards an ounce of water, to which seventy drops of medicinal prussic acid had been added, was thrown into the same vessel; none of the peculiar effects of the poison followed this operation. At the expiration of another quarter of an hour, an ounce of a saturated solution of nux vomica was likewise injected, still without producing any constitutional symptoms. It is very remarkable in this experiment, that M. Gaspard[25] should have considered that the elasticity of the air contained in the vessels was sufficient to counteract the impetus of the blood, and thus to prevent the progress of the poison along the vessels, especially when we find him stating that, on a post-mortem examination, the smaller vessels appeared to have been obstructed by very hard clots of blood.
(a). On the 25th of September, 1848, having procured four small vessels of equal sizes, I placed in the first some dilute sulphuric acid, in the second some offensive pus, and in the third some water. The fourth vessel was left empty. They were then all equally warmed, and some blood from the jugular vein of a healthy horse was received into each of them so as to fill them to the same level. They were now stirred with separate pieces of wood. At the expiration of two minutes (noted by a watch), the contents of the second vessel had become coagulated into one uniform mass. The contents of the first vessel (containing the acid) were thickened and of a dark brown colour; in the third[Pg 25] and fourth cups the blood was of its natural fluidity, but darker coloured in the cup containing water than in the other. At the expiration of ten minutes, the blood contained in the fourth cup had begun to coagulate; the blood and water still remained fluid. At the expiration of a quarter of an hour, the blood had completely coagulated in the fourth cup, containing blood alone; and had very partially coagulated in the third cup containing the blood and water.
(b). Four vessels were taken, each capable of holding three fluid ounces. In the first was placed half an ounce of cold water, in the second half an ounce of dilute sulphuric acid, and in the third half a drachm of pus, which was quite fresh and sweet. All the vessels were then quickly filled with blood, from the jugular vein of a horse. The contents of each vessel were stirred. The blood and dilute sulphuric acid became thick, and changed in colour almost immediately, as in the first experiment, but did not coagulate. The pus and blood coagulated in six minutes, and the mass was firm in seven. The pure blood coagulated in twelve minutes and was firm in sixteen. The blood and water coagulated in about the same time, but took nineteen minutes to become firm.
The above and the following experiments were made at the suggestion of the author, in conjunction with Mr. T. W. Mayer,[26] veterinary surgeon.
An abscess was opened in the groin and a quantity of pus received into a gallipot; some blood from the divided vessels was also received into the same vessel; they were then stirred together, and in two minutes the mass coagulated. Some blood taken from the same patient in the same manner, but not mixed with pus, coagulated in eleven and a half minutes.
On the 20th of January, 1849, an inflamed and suppurating abscess was opened, and the blood and pus which flowed from it were mixed together. They coagulated in two minutes and twenty seconds. This experiment was repeated several times, with nearly similar results.
In June 1849, a tense inflamed swelling was opened in the perinæum of a patient, who had for years laboured under a very obstinate stricture. A quantity of matter first escaped, and subsequently serum, mixed with shreds of lymph and small quantities of pus and blood, continued to flow for some time. Portions of this mixed fluid were received into separate vessels; they coagulated on an average in about two minutes.
Two ounces and six drachms of blood were taken from a healthy horse, and two drachms of pus were mixed with it. The mass coagulated in three minutes and three-quarters.
A healthy male ass, three years old, was procured, and, with the assistance of Mr. Mayer, was made the subject of the following experiment, on the 23rd of September, 1848. Three drachms of pus were collected from an issue in the chest of a horse, which laboured under inflammation of the lungs. The pus thus obtained was quite pure and sweet, and having been warmed, was injected, by means of a syringe, into the left brachial vein of the ass. The animal lay quiet, till nearly the whole of the pus was injected; it then struggled, and a small quantity of the pus may have been lost. When the operation[Pg 27] was completed, the sides of the vein were brought together with a pin, and the animal was allowed to get up. The vein above the opening could now be felt as a hard, unyielding cord, as high as it could be traced with the hand; but upon gentle pressure being made, so as to propel the blood in the course of the circulation, the hardness completely disappeared. The vein which, immediately after the operation, was hard and prominent, no longer presented anything remarkable to the touch. The animal now moved from side to side, as if inclined to lie down.
Two hours and a half after the operation, the pulse, which naturally was 36, had risen to 60; and the respiration from 12 per minute had increased to 26.
September 24th. Pulse 52; respiration 20; mouth hot; ears cold. In the evening the pulse became 48 and the respiration 16; he coughed occasionally.
25th. Pulse 48; respiration 12; some dullness of countenance, but he is lively and occasionally playful. The left fore-leg is swollen; the ears are very cold. In the afternoon he was killed, and the blood was allowed to flow from the body.
Post-mortem appearances. The wound in the left leg opened directly into the brachial vein, which was filled with lymph and a thin pus for a very short distance, both above and below the external opening; immediately above this, the vein was healthy, nor was there any appearance of disease in any of the other veins of the limb, nor in the veins leading to the heart. The glands in the axilla were swollen. The lungs were found studded irregularly in different parts, with circumscribed spots of livid congestion: these existed both upon the surface and in the substance of the lungs; they were generally about the size of a filbert, but in some places they occupied a single lobule, and were accurately circumscribed by its outline.
On the 23rd of November, 1848, about an ounce of perfectly pure pus (previously warmed) was injected into the right jugular vein of an aged ass; the vein immediately became "corded", and the blood appeared to have coagulated in the vessel. The operation did not much excite the breathing; but the pulse, which naturally was 35 in the minute, rose to 60, and subsequently fell to 55.
24th. The animal dejected; appetite indifferent. The vein can be traced as a thickened cord as far as the sternum. Respiration 12 (the natural standard); pulse 50.
25th. The parts around the vein much infiltrated with serum: pulse 55; respiration 12.
26th. The wound in the neck began to suppurate, and an abscess subsequently formed in the course of the vein, about midway between the opening and the sternum. The general symptoms continued, with very slight variation, until the 4th of December, when the animal was destroyed.
Post-mortem appearances. The jugular vein was found to have become inflamed only in the course of the circulation, and to be obliterated a short distance below the external opening. The surrounding parts were greatly infiltrated with serum and lymph, and several abscesses had formed in the immediate neighbourhood. The lungs did not present any well-defined patches of congestion, as in the last mentioned experiment.
A healthy ass, six years old, was operated on upon the 16th of November, 1848. The respiration was naturally 14 in the minute, and the pulse 38. About two ounces of highly offensive pus, obtained from the frontal sinus of a horse, were injected into the left jugular vein; the pus had unintentionally been mixed with water previous to its being in[Pg 29]jected. The vein became full during the operation, as though the blood in it were in a semi-coagulated state. The pulse now became 60, and the respiration 20 in a minute; slight rigors occurred in two hours.
November 17th. The animal is tranquil; appetite good; pulse 48, small and wiry; respiration 16. In the evening he was rather more excited; the vein was becoming inflamed downwards towards the heart; pulse 60; respiration 20.
November 18th. The vein was more inflamed, and slight suppuration was visible at the orifice of the wound. Respiration 16; pulse 55. From this period to the 23rd, the pulse continued from 55 to 60, and the respiration varied from 12 to 18.
November 26th. The swelling in the situation of the vein is rapidly subsiding; pulse 55; respiration 12.
The animal gradually recovered, and on the 26th of February, 1849, was made the subject of another experiment. The right jugular vein having been opened, two fluid ounces of pure healthy pus were injected, and propelled in the course of the circulation, by pressure upon the vein externally. The vein became tense during the operation, and sensibly resisted the attempts that were made to propel its contents towards the heart. Even forcible pressure was not sufficient to overcome the resistance offered to the return of blood. Soon after the operation, the animal had a rigor; the breathing became laborious, but not accelerated; pulse 57.
After the lapse of seven hours, the animal appeared dejected; he refused to eat or drink; the extremities were cold; breathing 16 in the minute; pulse 60, small and irregular.
February 27th. The vein can be felt thickened as far as the sternum. The general symptoms are the same as on the previous evening.
28th. There appears less constitutional irritation; pulse 60; respiration 14.
March 2nd. Appetite still indifferent; pulse 60; respiration 16.
From this date to the 7th, when the animal was destroyed, the general[Pg 30] symptoms continued much the same, but the induration and swelling around the jugular vein, from the opening to the sternum, became greater.
Post-mortem appearances. The left jugular vein was found completely obliterated. The remains of a firm coagulum obstructed its canal for some distance below the opening which had been made into it, and terminated, below, in an elongated conical portion, which adhered to one side only of the vessel. On the right side, an abscess had formed in the course of the vein; and for two inches, the whole of the parts were imbedded in a confused mass of pus and lymph, in which it was impossible to distinguish the structure of the vein. Both above and below this, for several inches, the vein was filled with coagula, which effectually obliterated it. These coagula extended for several inches in the course of the circulation; but beyond them, in both directions, the vessel was pervious. The lungs presented some slight spots of congestion, but not of the same characteristic kind observed in Experiment vi. The other organs were healthy.
EXPERIMENT IX.[27]
Two drachms of pus, somewhat fetid, derived from a large common ulcer, and diluted with a little water, were injected into the jugular vein of a middling-sized dog. The animal immediately made several convulsive efforts to swallow, and soon became faint. It showed indications of pain, and vomited more than six times in the course of the day. At the expiration of an hour, it appeared slightly relieved by an evacuation, and by passing turbid urine. In the evening, it was very ill; it lay upon its side with its legs extended; had a very feeble pulse and scarcely perceptible respiration. Ten hours after the experiment, it[Pg 31] passed black, liquid, and extremely offensive motions; these were accompanied by immediate relief. The animal regained its appetite, eat and drank freely, and went to sleep. The day following, it appeared nearly well. On the third day, three drachms of the same pus were injected into the opposite vein; after the lapse of a certain time, there occurred, as in the first instance, faintness, vomiting, and frequent desire to pass urine; twelve hours after the injection, frequent liquid, white, and very fetid motions were passed, and the animal died at the expiration of twenty-four hours. On opening the body, no alteration was found either in the intestines or other organs.
The last experiment was repeated on a greyhound with the same results: faintness, fever, vomiting, and repeated evacuations succeeded each other, with recovery after the first experiment, but not after the second. On opening the body, no lesion was observed, except that the inferior lobes of the lungs were gorged and almost hepatized.
Three drachms of recent pus, derived from the same patient as in the last experiments, were injected into the jugular vein of a small emaciated unhealthy dog. After the expiration of three minutes, there was an abundant evacuation of urine, followed by continued vomiting, and repeated ineffectual efforts to pass fæces. For nearly a quarter of an hour, there was a kind of emprosthotonos, rigidity of the limbs, and a death-like condition. Subsequently, fresh vomiting ensued, with very fetid liquid evacuations, which were followed by apparent relief; soon after, however, long continued tenesmus made its appearance, and terminated in death, five hours after the injection of the pus. On opening the body, the mucous membrane of the intestines was found red, swollen, and inflamed, especially in the colon and rectum.
Half an ounce of pus, similar to that used in the preceding instances, but more putrid, in consequence of having been longer kept, was introduced into the veins of a middling sized dog. The animal, as in the other cases, was seized with vomiting, accompanied by violent straining. Subsequently, strongly marked nervous symptoms made their appearance. The eyes wandered; there was extreme sensibility, and involuntary convulsive twitching over the whole body, accompanied by faintness, hiccough, and short piteous cries. The walk was unsteady, staggering, and without apparent object. There was furious delirium, ardent thirst, dyspnœa, palpitation of the heart, etc. This state lasted for nearly two hours, and the animal died in frightful convulsions, without having experienced any critical evacuations, as in the former cases.
Post-mortem appearances. On opening the body, while still warm, the venous blood was found very firmly coagulated, not parting with any of its serum when left at rest; the left ventricle of the heart showed, on its external surface, some stains of the colour of lees of wine, formed by a kind of concrete pellicle, which disappeared only after long rubbing and maceration. The other organs appeared healthy.
Some beef was allowed to decompose in some dog's blood; half an ounce of the fluid resulting from the decomposition, was injected into the jugular vein of a little bitch. Immediately, the animal made several convulsive efforts to swallow, and soon became oppressed, uneasy, and faint. At the expiration of an hour, there was great prostration, accompanied by repeated gelatinous and bloody evacuations, and vomiting of bilious matter. The strength became gradually less, and the animal died three hours after the injection.
Post-mortem appearances. The lungs were found inflamed in a very peculiar manner. They were gorged with blood, of a violet or black[Pg 33] colour, and presented many petechial spots, like small ecchymoses. These spots existed also on the left ventricle of the heart, in the spleen, in the mesenteric glands, in the gall-bladder, and even in the subcutaneous cellular tissue. The peritoneum contained some spoonsful of a reddish serum; but the mucous membrane of the digestive organs was found to have been principally affected. In the stomach it was slightly inflamed. In the intestines, but especially in the duodenum and rectum, it was of a livid colour, presenting many black spots, and covered by a gelatinous and bloody secretion, resembling lees of wine. The tissues in these parts were slightly thickened.
The preceding experiment was repeated, by injecting into the jugular vein of a moderately large dog, an ounce of fluid, derived from the maceration of putrid beef in water. The animal very soon passed extremely offensive, liquid evacuations, with much urine. The breathing became quick and deep, the pulse small and quick. Repeated efforts were made to empty the bowels. There was great depression and want of strength. At the expiration of an hour, a kind of diarrhœa or dysentery made its appearance. Liquid, bloody, and fetid evacuations, continued for an hour and a half, when the animal died.
Post-mortem appearances. Livid, brown, and black patches were found scattered over the lungs. The intestinal canal was filled with a bloody mucous secretion, resembling the matter that had been voided; its mucous membrane was of a livid colour, as in the preceding case.
Two ounces and a half of thick fetid fluid, derived from the maceration of cabbage leaves in an equal quantity of water, for two days, at a temperature of 77 Fah., were injected into the right jugular vein of a moderate sized dog. During the operation, the animal made several[Pg 34] efforts to swallow, and soon became faint, and vomited several times. Some hours afterwards, there was great uneasiness and oppression, with recurrence of the vomiting, and continued faintness during the day. After nine hours, a most copious and very fetid evacuation took place. The discharge was as black as soot, and composed of mucus, with a little fæcal matter, and a large quantity of what appeared to be corrupted blood. Some time afterwards, there was a second evacuation of bloody mucus, exactly resembling the first. On the following day, there was much loss of strength: the animal lay upon its side, or staggered as it walked. There was great and insatiable thirst, with a small feverish pulse. But the most remarkable symptom was the occurrence, at intervals, of palpitation of the heart, accompanied by extraordinary force and sound, resembling that produced by long continued hypertrophy of that organ, in consequence of aneurism[28] of one of the large arteries. On the third and fourth days, the animal was better, but there were still great thirst, fever, and occasional rejection of fluids from the stomach. On the fifth day, the symptoms became aggravated; there was extreme weakness, a tottering gait, excessive thirst, the eyes red and filled with gum; the nostrils were stuffed, swollen, and obstructed with mucus; and the lining mem[Pg 35]brane of the mouth was tumid, and of a violet red colour. In the middle of the day, there was a liquid greyish white evacuation, resembling pus in its odour, consistence, and appearance, mixed with some clots of putrified blood. Death occurred during the following night.
Post-mortem appearances. The mucous membrane of the eyes, nose, and mouth, was red or violet, and covered by a very abundant thick mucus. The lungs were of a dark colour, with some black patches, but still crepitant. The left ventricle of the heart presented several brown stains, resembling ecchymoses, which penetrated into its tissue. Its internal surface was of the colour of lees of wine, offering a singular contrast to that of the right side, which, however, contained a hard fibrinous concretion, two drachms and a half in weight, of a light yellow colour, and resembling grease in appearance. This was of the same consistence throughout, everywhere free, with the exception of a portion of the size of a finger nail, which adhered to an irregular and apparently inflamed spot on the inner surface of the ventricle; no appearance of the injected fluid could be recognized in this clot. It was continued of the same colour and consistence into the pulmonary artery, and into the vena cava, the vena azygos, the axillary, and even the right jugular vein.
The intestinal mucous membrane, especially in the rectum, the duodenum, and a small portion of the small intestines, was of a violet red colour. It was inflamed in longitudinal stripes and in patches, which gave a mottled appearance, even to the outer surface of the intestines, before they were opened. This discolouration was not accompanied by any thickening of the tissues, nor by ulceration, and appeared rather the result of ecchymosis or hæmorrhage. The lining membrane of the rectum was principally affected, and its mucous glands were swollen and very prominent. This intestine contained puriform fluid, resembling the matter evacuated before death. The other intestines contained a very thick greyish white mucus. The mesenteric glands were inflamed, and appeared as if infiltrated with blood. The gall[Pg 36] bladder was mottled on its surface by brown and violet patches, and contained black, thick, ropy bile, resembling melted tar.
Shewing the effects of the introduction of Mercury into an artery.
An ounce and a half of mercury, mixed with water, was injected into the left carotid artery of a sheep. The animal immediately evinced pain, and stood immoveable upon its feet. The head was held down, there was stupor and heaviness, and the eyes were protruded and widely open. The fore legs subsequently became bent, and the head inclined over the right shoulder with a kind of convulsive rigidity, which continued till death. Two hours afterwards, the animal became comatose, with some convulsive motions of the limbs, and the left eye became red and inflamed. Death took place fifty hours after the operation.
Post-mortem appearances. The left eye was found in a state of suppuration, and contained mercury. Many of the branches of the left carotid artery also contained some mercury, which had not penetrated to the capillary system. All the organs supplied with these vessels were red, swollen, and inflamed, in consequence of the presence of the foreign matter. The thyroid gland, the tongue, the cheeks, and the lips, were, however, only affected as far as the median line, leaving the opposite halves pale and in their natural condition.
A drachm and a half of mercury, mixed with some warm water, was injected into the crural artery of a large dog. The animal evinced no pain, and walked resting slightly on the affected limb, which became sensibly colder. After the expiration of an hour, the animal refused its food, became restless, and indicated severe pain in the limb, which was now very hot. On the following day, the leg was swollen and œdematous. On the third day, there was extreme thirst, increased œdema, and great suffering. The animal was killed sixty hours after the operation.
Post-mortem appearances. No disease was found in any organ, ex[Pg 37]cepting the affected limb. This was swollen and œdematous in every part; abscesses of different sizes had formed, which contained sanious fluid, mercury, and pus; some parts were in an incipient state of mortification, and gave out a considerable quantity of air. Globules of mercury were found in different parts, occupying usually the centre of the abscesses, and ran out upon the scalpel when incisions were made into the limb.
Shewing the effect of the injection of Oil into an artery.
Three drachms of olive oil were thrown into the crural artery of a large dog. Slight pain was experienced, and the limb became evidently cold, and the pulse under the tendo-Achillis could no longer be felt. Two hours afterwards, a like quantity of oil was again injected. The leg now began to inflame, and became tender. The following day, the whole limb was œdematous, much swollen, and very painful. Twenty-nine hours after the first experiment, the muscles of the thigh and leg, as well as the cellular tissue, were found in some places gorged with blood, and inflamed in livid patches; in others, infiltrated with yellow serum and gelatinous exudations. No oil could be detected in the affected parts.
An ounce of putrid water, in which some beef had been macerated, was injected into the crural artery of a middling-sized dog. The artery having been tied, the pulse ceased below the tendo-Achillis; the limb, however, preserved its usual degree of heat, offering a contrast in this respect to the last experiment. A considerable degree of fever and restlessness followed the operation; this continued the whole day and the following night, without any vomiting or evacuations, which so constantly followed similar operations upon the veins. The next day the[Pg 38] limb was very painful, but not swollen; there was thirst, with the ordinary secretion of fæces and urine. On the third day, the animal was evidently better; the appetite had become almost natural, and he could walk more easily, although the limb was still very painful. In the night, there were some soft, almost liquid, evacuations. The fourth day, the animal was evidently recovering, when an ounce and a half of very fetid and very concentrated fluid (derived from the maceration of beef), was injected into the crural artery of the opposite limb. The animal immediately evinced pain, accompanied by very violent and remarkable palpitation of the heart. It walked lame, keeping the leg raised, and soon became feverish and uneasy. The symptoms were exactly the same as after the first experiment. The leg became gradually more and more painful, extremely sensitive, but not infiltrated with serum. During the night, there was much expression of pain, and the animal was in continual motion. Death occurred nineteen hours after the second injection. The limb had become swollen only within five or six hours previous to death.
Post-mortem appearances. The limb presented a very large quantity of bloody fluid infiltrated in all the tissues. The superficial muscles were black, and presented more or less the appearances of gangrene. The deep muscles existed as such no longer, but were entirely disorganized, and converted into a putrid pulp, resembling masses of the red lees of wine, extremely fetid, and disengaging a quantity of gas. The limb first injected was still swollen, and presented, in the interior of the adductor muscles, two or three cavities filled with a putrid bloody serum. In the chest, the lungs were healthy, as were also the right cavities of the heart; but the left cavities presented several reddish-black spots, scattered over their external surface. In the left auricle was a firm yellowish-white coagulum, adhering to an inflamed spot on its inner surface. The intestinal canal was filled with a brownish red fluid, resembling altered blood, which, in the stomach and duodenum, was of the colour[Pg 39] of soot. The mucous membrane of these organs, as well as of the jejunum and rectum, were gorged with blood, of the colour of the lees of red wine, but without any inflammatory thickening of their coats.
Shewing the effect of the introduction of Air into an artery.
Seven or eight cubic inches of common air were injected gradually into the crural artery of a large dog. A peculiar rustling noise, depending upon the admixture of the air with the blood, accompanied the operation. No particular symptoms followed; but after some minutes the corresponding vein became distended with frothy blood, which moved with difficulty, and became stagnant in the vessel. The whole limb crepitated upon pressure, but no untoward symptom presented itself for more than half an hour. An ounce of water, to which seventy drops of medicinal prussic acid had been added, was now injected into the same artery. This produced no apparent effect upon the constitution.
A quarter of an hour after, an ounce of saturated solution of nux vomica was injected into the same vessel. This also was followed by no particular symptoms. An hour after the first injection, half an ounce of a weak infusion of tobacco was introduced into the same artery. Excessive pain immediately followed, accompanied by great rapidity of breathing. The animal now appeared as if he were going to die; however, he slowly recovered, appeared giddy and inclined to vomit, and kept himself in a continual state of restlessness. This condition was succeeded by fever, accompanied by extreme sensibility of the limb, and irregularity of the pulse. At the expiration of some hours, he appeared better; the pulse became more regular and less feverish, but the leg continued swollen, and extremely painful upon pressure. During the night, the pain returned, indicated by howling and restlessness. There were several evacuations of fæces and urine. The following morning, there was great prostration with much fever, and[Pg 40] apparent suffering. The limb was slightly emphysematous, swollen, inflamed, and infiltrated with serum.
On the following day, two ounces and a half of water, in which some nux vomica had been boiled, were injected into the crural artery of the opposite limb. The dog expressed no pain; but, at the expiration of ten or twelve minutes, slight convulsive motions became evident, which were gradually converted into violent tetanic spasms. The animal threw himself backwards with his limbs extended, and died, after repeated convulsive attacks, an hour and a half after the last injection.
Post-mortem appearances. On opening the body, no unusual appearances were observed in the limb upon which the last experiment had been tried, but the opposite one was tumid and emphysematous, infiltrated with a greyish red frothy serum of a fetid odour. The small vessels were obstructed by firm clots of blood. The gall-bladder was greatly distended; and the intestinal canal contained a quantity of yellowish mucus.
ON THE INTRODUCTION OF VITIATED FLUIDS INTO THE BLOOD; ITS CONSEQUENCES, AND TREATMENT, WITH CASES.
VIII. The experiments cited in the first part of this essay, illustrate the power possessed by the blood of preventing certain foreign substances from circulating with it. They shew that pus, in particular, has a tendency to coagulate the blood; and that by this means, when introduced into the vessels, its progress is arrested in some part of the circulating system. This fact, which, taken by itself, might appear of little consequence, assumes considerable importance when considered as one of the inherent properties of the blood, at all times ready, under favourable circumstances, to be called into action in the living body. The conditions under which pus will determine the coagulation of the blood, and those under which it will circulate in the living vessels, require to be accurately ascertained, before we can rightly interpret the discordant evidence which we at present have upon this point.
Dr. Sédillot,[29] in a work recently published, mentions, that a great number of cases are met with, in which pus is poured into the general circulation without meeting with any obstruction, and states that, in such instances, he can detect the globules of pus in different parts of the circulating system. He even affirms that he can recognise a disease[Pg 42] caused by purulent infection, by examining, under a microscope, a portion of the blood abstracted from the body.
M. Dance, and, since his time, equally accurate observers, have, on the other hand, failed to detect the characters of pus in the blood, even when that fluid had been injected into the veins of living animals. The results of these different observations may perhaps be reconciled, by considering the influence exercised upon the globules of pus by the blood, before its coagulating power has been impaired. This subject appears not to have hitherto occupied the attention of pathologists.
In all the cases quoted by Dr. Sédillot, in which he detected the globules of pus in the blood, the patients died of the disease; but in the researches instituted by M. Dance and others, the experiments were made upon animals in perfect health. In the latter, the pus cannot enter the circulation, as has already been shewn, or can only do so after the blood has partially or entirely coagulated round it, and the coagulum has subsequently become broken up.
In the act of coagulation under these circumstances, the appearances of the globules of pus are changed,—these being perhaps mechanically compressed by the contraction of the fibrine,—so that the most experienced eye can no longer recognise them.
Pus, mixed with healthy recently drawn blood, out of the body, will entirely lose its characters in this way; and as the coagulation, is by no means retarded in the living vessels, we may, without fear of contradiction, affirm, that globules of pus cannot be detected when introduced into the vessels in small quantities, and mixed with healthy blood.
In cases where, from long-continued disease and the repeated introduction of vitiated fluids into the circulation, the blood has lost its power, there appears no reason to doubt the correctness of Dr. Sédillot's observations; and it is probable that pus-globules may then circulate with those of the blood.
In experiments upon animals, it has always been found that the power of the constitution, in resisting the effects of the injection of pus into the veins, was much greater at the first than at any subsequent operation. This circumstance would appear to associate itself directly with the observations now made, and to afford another illustration of the power of healthy blood in resisting the entrance of some foreign matters into the system.
From the consideration of these facts, and of the experiments previously recorded, it becomes evident, that the introduction of pus into the system through an injured or inflamed vein, can rarely be the first step towards purulent infection of the system. Some change must previously have passed in the blood, by which its coagulating power is impaired, or some unusual mechanical means must have been employed, before the pus can find its way in the course of the circulation. The contradictory statements which have been made by those who have injected pus into the veins, may thus be reconciled, by taking into account the power exercised by the blood in the experiments which have been made. There can be little doubt that, while, in some instances, a portion of the pus has been forced into the general circulation, in the great majority of cases it has been detained in the vein into which it was first introduced, and has never become part of the circulating fluid. We accordingly find some experimenters recording the secondary diseases which they observed, while in other hands these appearances were not produced.
Dr. Sédillot[30] has attempted to prove that the globules, or solid parts[Pg 44] of pus, must be introduced into the system, in order to produce well-marked indications of purulent infection. But this hypothesis would not only appear to be at variance with the oft-repeated experiments of MM. Gaspard and Cruveilhier, in which similar effects were produced by the injection of mercury and of putrid fluids, but would also leave unexplained the mode of the introduction of these globules, where there is evidence that the disease has been communicated through the lymphatic system. The changes which all substances undergo in their passage through the absorbent glands, would at once forbid the idea that globules of pus could be thus introduced unchanged into the circulation; and yet we have direct evidence (Case xxix) that irritating fluids are conveyed in this way into the system, and lead to the formation of secondary abscesses.
Another class of cases, in which there would be difficulty in admitting the doctrine of the introduction of pus in substance into the circulation, presents itself, where, in the primary affections (as in Case VI), no evidence can be obtained of the original lesion having suppurated. The fluids effused in such cases may be serum, lymph, or blood, mixed in different proportions; and yet the constitutional symptoms will be exactly similar to those which follow the formation of pus in other instances. There may exist, both in the primary and in the secondary affection, every intermediate gradation between the healthy secretion of a part, and the formation of pure pus, or pus mixed with blood or lymph, without any of the essential characters of the disease being absent. An inflamed bursa, or a punctured wound, without the formation of pus, (Cases iv and v), may give rise to symptoms as severe, and consequences as fatal, as any that arise from the direct introduction of pus into the system. The secondary affections, in such cases, may run their course and prove as speedily fatal, as where well-formed purulent deposits have taken place. The most severe constitutional symptoms will sometimes be followed by the effusion of bloody fluid only, in one of the serous[Pg 45] cavities (Case xxx). It would be unphilosophical, even were it practicable, to refer such cases to a different disease, merely because the accidental circumstance of the formation of pus is wanting. The origin of the affection in such instances may be as well-marked, the poison can often be traced as distinctly into the system, and the secondary disease may be as clearly connected with the primary, as in any case where pus has been originally formed. In some cases again, the constitutional symptoms which accompany, or are followed by, effusions into distant parts of the body, begin before sufficient time has elapsed to allow the supposition that pus can have been fully formed at the original seat of injury. Such instances occasionally, although rarely, present themselves in extensive burns and scalds, occurring in enfeebled habits, and after amputation of the limbs in scrofulous children.
In nearly all cases, when the origin of the constitutional disease cannot be traced to the introduction of diseased fluid into the system through an open vein, it will be found that the part primarily injured has wanted the degree of vigour, requisite to establish and maintain healthy adhesive inflammation.
Upon another occasion,[31] I have endeavoured to show that, where lymph is effused around a poisoned wound, the virus will find its way less easily along the absorbent vessels, than when no such effusion has taken place; and that when, in such a wound, the effusion of lymph is checked or prevented, as by the administration of mercury, a larger proportion of cases will indicate an affection of the lymphatic system, than when the natural process has not been interfered with. There can be little doubt, that the same principle may be observed with regard to ordinary wounds. The number of cases in which the absorbents inflame, will be in inverse proportion to the number of those in which the original wounds are circumscribed by healthy adhesive inflam[Pg 46]mation. In Case xxvii, it is mentioned, that the surface of a muscle, implicated in the original lesion, was as cleanly dissected as if done with a scalpel, thus showing the total absence of any surrounding effusion of lymph. The absence of, or defect in, the process of adhesion may thus be associated with inflammation of the absorbents, as the want of "union by first intention" has been shown to be connected with inflammation of the veins (Section ii.)
The minuteness of the absorbent vessels, and the changes which their contents undergo in their glands, prevent any unhealthy fluids from being as readily recognised in them as in the veins. But when the progress of inflammation can be traced along these vessels from a wound, towards the centre of the circulation, marked, as it often is, at intervals, by the formation of abscesses, we cannot doubt that an irritating fluid has found its way along their canals: and when the constitutional symptoms, which arise at the same time, terminate in the formation of purulent deposits (as in Case xxix), we cannot but admit that the absorbent vessels are the direct means by which, in such cases, diseased secretions are poured into the blood, and the system becomes infected. It would, therefore, appear that there are two principal conditions, under which local disease may produce a general infection of the system by the direct introduction of vitiated fluids into the blood. The first of these is connected with defective union in injured veins; the second is associated with want of healthy adhesion in inflamed lymphatics.
The period of invasion of the attack differs in some degree in the different classes of cases, but it is generally marked with great precision: even when apparent recovery has been followed by a second attack, the occurrence has in each instance been accurately noted by the sudden appearance of constitutional symptoms (see Case xxxvii).
When one of the large veins has been originally affected, the period which elapses before symptoms of infection of the system manifest[Pg 47] themselves, is comparatively short (Case i). In cases occurring after child-birth, it is usually longer, extending to the end of the second week. After surgical operations or accidents involving some portion of bone, the access of the disease will be marked by a rigor during the third or fourth week; and finally, when the absorbent system is primarily affected, the period of the occurrence of the constitutional symptoms may be much farther removed from that of the original injury (if any such existed), and is by no means so accurately defined.
At the time of the occurrence of the general disturbance of the system, the local injury or wound will generally put on an unhealthy appearance. The skin in the immediate neighbourhood will sometimes assume a dull brownish-red appearance, which will gradually fade into the colour of the surrounding parts. This symptom will usually commence near the termination of the vessels, which are derived from the same trunk as those which supply the injured part. When the original injury is complicated with a wound upon the surface of the body, it will usually become dry and glazed, and the blush upon the skin will commence in its neighbourhood, or a short distance from it, and will usually extend towards the centre of the circulation, without presenting any very defined margin: occasionally it will extend, in the form of erratic erysipelas, over a large part of the body.[32]
IX. The commencement of constitutional disease, after direct infection of the blood, is marked by a sudden change in the manner and appearance of the patient; a severe rigor is usually the most prominent symptom, and is followed by much febrile excitement, or by extreme depression; a very peculiar heat of skin (Case xxii) will sometimes be present, while, at other times, the surface will be covered by a[Pg 48] profuse clammy perspiration. The rigor may be repeated at irregular intervals, but occasionally it will recur about the same hour for three or four days in succession (Case xxxvii); and in a few instances it will not be observed at all.
Great depression frequently accompanies even the first stages of this disease, indicated by a want of tone in the pulse, by an extremely listless manner, and sometimes by a tendency to syncope (Case i). The countenance becomes anxious, the tongue dry and brown in the centre, and red at the edges, or, in other instances, it presents a coating of a pasty yellowish-white colour; a dusky yellow hue frequently pervades the skin, and sometimes the conjunctivæ of the eyes. This may or may not depend upon an accompanying affection of the liver. The pulse varies much in frequency in different cases, and at different times in the same case: generally it is very rapid, especially when accompanied with much heat of skin.
The pain is sometimes severe, and may be referred exactly to the spot which subsequent examination shows to have been the seat of secondary inflammation; at other times it is not confined to any particular situation, but consists of general ill-defined feelings of short duration, and recurring at irregular intervals. The peculiarity of such sensations is best expressed by the terms applied to them by the patients themselves. "Catching pains all over", "soreness of the stomach", and "thrilling in the blood", not unfrequently accompany this disease.
Vomiting may occur, either as a symptom of constitutional disturbance, or as indicative of inflammation of an abdominal organ (Case xxvi). In the latter case, it is extremely obstinate, and the fluid ejected is generally of a green colour. Diarrhœa is a symptom of frequent occurrence, and appears to exercise a considerable influence on the course of the disease. Its appearance will not unfrequently be accompanied by relief of the other symptoms (Case iii); when it occurs, it is gene[Pg 49]rally profuse, and little under the control of medicine, but, if checked, may be followed by a sudden change for the worse in the condition of the patient.
The intellect is seldom affected during the first stages of the complaint; but subsequently, in severe cases, restlessness, delirium, and coma, seldom fail to succeed each other. These symptoms are all peculiar, both in regard to the rapidity with which they make their appearance, and also the sudden manner in which they occasionally disappear. The disease may seem, within a few hours, to leave a part which it has first attacked, and to fall upon a different organ in some remote part of the body.
X. The post-mortem appearances observed in those who die in consequence of the introduction of vitiated fluids into the blood, cannot, for the most part, be distinguished from similar changes produced by other causes; yet there are some effects which are peculiar, and may be directly associated with the reception of foreign matter into the circulation. The most characteristic circumstance, attending the extension of disease to different organs of the body through the medium of the blood, is that several parts of these organs, or even different organs, will be simultaneously attacked. The disease will appear at once in various spots, which will become rapidly disorganized, while the surrounding textures will remain unaltered, either in structure or colour. The appearances observed upon dissection will vary according to the part attacked, and the stage of development in which the disease is found.
The lungs are the organs in which the successive changes may best be observed. When puriform fluid has entered the circulation, the first appearance produced in the structure of the lungs, is that of one or more congested or dilated veins[33] of very small diameter. This[Pg 50] will be followed by a well defined spot, of much darker colour than the surrounding texture. Several of these spots will probably appear at the same time, and each one of them will soon become surrounded by a hard spherical patch of purple congestion. Effusion of lymph will now take place, commencing in the centre of each affected portion, and gradually extending towards its circumference. If the disease continue, each spot will suppurate, and the different parts will become softened and broken down, in the same order in which they were previously solidified.
The liver frequently becomes the seat of secondary inflammation. In the early stage, brownish-red spots may be observed scattered through its substance. These, as they extend, assume a bluish or slate-colour; and the structure of the liver thus affected is found to have lost its consistence, and to be very easily broken down by pressure. Every part affected here, as in the lungs, proceeds rapidly to suppuration; and the usual appearance presented after death, is that of several small circumscribed abscesses, around which the structure of the liver has been condensed only to a very small extent. It sometimes happens, that the larger veins in the liver become inflamed. These vessels, being held open by the firm structure of the part, are not so readily obliterated as in other situations; and it consequently happens, that the lymph and pus poured into them become irregularly mixed with the blood, more or less perfectly coagulated, which they contain: a very peculiar mottled appearance, resembling granite, is thus occasionally produced.
Affections of the spleen, produced by the introduction of foreign matter into the blood, are probably not so readily recognised as similar affections in the lungs and liver. For, although the spleen is often found to be diseased in those who die from infection of the blood, yet it is comparatively seldom that secondary abscesses have been found in it. In the accompanying table, containing twenty-three cases, some morbid appearance, not recognised as peculiarly the result of secondary inflam[Pg 51]mation, was observed in the spleen in no less than eight instances. So large a proportion of cases renders it probable, that the alterations observed have more than an accidental connexion with the disease of which the patient died, although they presented no characters which could be said to be peculiar to that disease. In well-marked cases of secondary affections of the spleen, one or more well defined, but frequently irregular indurations, of a chocolate colour, may be recognised; such patches are usually seen soon after the commencement of the complaint, and in a very short time become softened or broken down. The rapidity with which they lose their original character, may probably account for their being comparatively seldom observed in post-mortem examinations.
Deposits of lymph are sometimes met with in the kidneys; but these are of small extent, of a light colour, and resemble lymph deposited in consequence of ordinary inflammation. The patches of congestion, so characteristic of this disease in other organs, are not here observed. This may depend upon the peculiar disposition of the capillary system of the kidney. The blood has to pass through the Malpigian tufts, and may be purified, or altered in character, before it reaches the proper venous system of the organ.
In cases where purulent infection of the blood has been purposely produced, portions of the kidney will not unfrequently be found inflamed and firmer than natural; but, if the origin of the disease were not known these appearances could not be distinguished from those produced by inflammation of the kidney from other causes.
The skin is liable to be affected in three different forms. (See Cases i, ii, iii, ix, x, and xxxiv). The first of these occurs very rarely, and consists of small deposits of matter in the structure, or upon the surface of the skin, resembling in many respects the pustules of small-pox. The second form is also of rare occurrence, and consists of small congested spots on the surface of the skin. These are generally of a dark purple hue, but I have seen one case in which they were of a bright red[Pg 52] colour. In this instance, a secondary abscess had formed in the knee-joint, and some pustules appeared upon the skin in the neighbourhood. A fortnight before the death of the patient, a number of small bright red spots made their appearance in different parts of the thigh and upper part of the leg; some of these were three or four lines in diameter while others were so small as not to be seen without attention; they appeared in accurately defined spots, of a brighter colour than the mucous membrane of the lips, and continued unchanged in appearance till death. The third form presents itself much more frequently than either of the others, although it has not hitherto much attracted the attention of pathologists, in connexion with purulent or other infection of the blood. It commences very suddenly, and frequently without any particular attention being directed to the part. A large circular patch of congestion, livid or purple in the centre, but becoming of a lighter colour towards the circumference, will form, usually upon some part of the lower extremities. The skin of the calf of the leg is perhaps more frequently attacked than that of any other part. In the centre of the congested portion, mortification very rapidly takes place, and is indicated by the part assuming a black or dull leaden colour. In some cases, it would be difficult to say where the mortification ceases, and the congestion begins; but in other instances, there is a distinct line of demarcation formed: a zone of bright red congestion will then occasionally surround the mortified part.
Some modifications of this third form of affection of the skin may be met with occasionally in the course of the disease. Blotches assuming a livid or dusky red appearance (which gradually fades into the colour of the surrounding skin), will present themselves in different parts (Case xxxvi), and terminate in thick exfoliation of the cuticle, or in small sloughs of the skin. In some instances, the superficial portions only of the skin are destroyed, and the parts beneath appear comparatively unaffected; small circumscribed portions of the outer layer of[Pg 53] the skin will exfoliate, and the subjacent parts will heal without suppuration, by a process similar to that of scabbing (Case iii).
It is remarkable in this disease, that the most vascular parts are those which soonest lose their vitality. Thus, in the case last referred to, portions of the surface of the skin perished, while the deeper layers recovered; again, it is not unusual to observe the whole thickness of the skin destroyed, without any corresponding affection of the cellular membrane beneath. The quantity of blood sent to a part would thus appear to favour mortification in this disease. The reason of this peculiarity will be considered in the next section.
In two of the instances recorded in the Appendix (Cases xxii and xxvi), the lining membrane of the rectum was found of a very dark colour, and in one it had assumed a greenish appearance. This discoloration was at first looked upon as some accidental complication, or as depending upon previous disease. But M. Gaspard has noticed a similar condition, after the artificial introduction of putrid fluid into the blood.[34] In one of the experiments referred to, the mucous membrane of the intestines was everywhere healthy, except in the rectum and duodenum. In the former situation, the rugæ were prominent, and of a violet colour; in the latter, the membrane was of the colour of pale lees of wine. From the coincidence thus observed, we are led to believe that the same condition which produces congestion in the skin, may produce an analogous affection of the mucous membrane. Nor must we omit to note, in connexion with this subject, the fact of the mucous membrane of the vagina being occasionally found of a dark purple colour in those who die of puerperal affections.
In the cellular membrane, serum, lymph, and pus, may be deposited, mixed with each other in various proportions. The surrounding vascularity, in these cases, is unusually small, and the lymph effused not[Pg 54] properly organized; there is, consequently, no natural boundary to the disorganizing process, and the fluid secreted becomes infiltrated in the surrounding parts.
When the muscular structure is affected, suppuration takes place with great rapidity; portions of muscles may be found quite soft, and sometimes pultaceous, in circumscribed patches, around which the fibre is perfectly healthy. Pus is occasionally deposited on the exterior of muscles; and it will be then smeared over the surface, and rather infiltrated in the cellular tissue, than contained in a cyst. In the interior of muscles, there is the same absence of the natural limit to the inflammation; but, owing to the more compact structure of the part, the deposits of matter generally remain circumscribed.
The brain and its membranes frequently present diseased appearances in those who die from secondary inflammation; these, for the most part, may be altogether independent of any peculiar effects of the disease; but, in some cases, it appears probable that they are not altogether unconnected with it. In one of the accompanying cases, the pons Varolii and medulla oblongata were found of a pink colour, in consequence of congestion, where the system had become contaminated by the absorption of diseased secretion; and, in another, a layer of purulent lymph was found within the cavity of the arachnoid, accompanied by marks of inflammatory action in the fourth, and in one of the lateral ventricles.
The serous membranes are peculiarly liable to be attacked by secondary inflammation; and, when affected, suppurate with the greatest readiness. They generally exhibit but a slight degree of vascularity, and sometimes scarcely appear more injected than in their natural condition. In the peritoneal cavity, large quantities of unorganised lymph are frequently poured out, mixed with turbid serum or pus. The synovial membranes of joints, when affected, appear to run directly into suppuration, and will become distended with pus in a very short space of[Pg 55] time. The pleura, on the other hand, will seldom suppurate at first; but lymph will be deposited upon its surface, and its cavity will contain turbid serum, occasionally mixed with blood.
XI. In the first sections, the changes produced in the blood, both in and out of the body, by the admixture of purulent or diseased secretions, were considered; and, in the last section, the post-mortem appearances observed in the different organs of those who have died in consequence of secondary inflammations, have been described. It now remains to connect these two series of observations, and to trace the relation that they bear to each other.
The most direct way in which diseased blood produces disease in the parts to which it is conveyed, is by communicating to them its own condition. Even foreign substances, which have no natural connexion with the body, may, in this way, be conveyed in the blood, and deposited in the organs of the body. Hunter relates a case,[35] in which a house-painter, who had been paralytic in his hands and legs for a considerable time, had his thigh broken, and died, about three weeks after, of the accident: "On examining the body, after death, the muscles, particularly those of the arms, had lost their natural colour; but, instead of being ligamentous and semitransparent, as happens in common paralysis, they were opaque, resembling exactly in appearance parts steeped in a solution of Goulard's extract. From this case it appears, that the lead had been evidently carried along with the blood into the muscles themselves. The blood can thus receive and retain extraneous matter capable of destroying the solids."
If foreign matter may, in this way, be conveyed to different parts of the frame, and there produce its chemical effects, it will readily be admitted, that a mechanical or vital action commenced in the blood,[Pg 56][36] may be continued in it when moved to a different part of the body.
In those who die of secondary inflammations, the result of such actions may frequently be traced from the seat of the primary injury even to the heart itself; and, as it has already been shown that contaminated blood will communicate morbid action to the vessels in which it is contained (section iii), there no longer remains any difficulty in accounting for the sudden way in which this disease may fall upon a particular organ, or the unexpected manner in which the symptoms may shift from one part of the body to another. The conditions of the blood, which may be observed upon dissection, in this disease, so far as they tend to illustrate the present subject, may be included in two general expressions: 1st, those in which the blood has had a preternatural tendency to coagulate impressed upon it; and, 2nd, those in which its coagulating power has, to a greater or less extent, been impaired. In one case, the blood is generally found of a dark colour, with firm, and sometimes adherent coagula in the vessels; in the other, it is thin and fluid.
When a preternatural tendency to coagulate has been impressed upon the blood, it will lodge in different parts of the vascular system, in situations which are most favourable to such an action; when, on the contrary, it has lost its coagulating power, extensive effusions may be expected, or the symptoms included under the term "gangrenous diathesis" may manifest themselves.
As the aggregate diameter of the vessels in the body decreases, the blood in them flows with greater rapidity and force; and when near the heart, it is placed in circumstances unfavourable to coagulation, in consequence of the rapid motion there communicated to it;[Pg 57] and we accordingly find that, although adherent coagula may be formed in the veins leading from the seat of injury, and may be traced thence through other larger vessels, they will usually terminate abruptly, when these open into the vena cava. But when the blood arrives in the cavities of the heart, the tendency to coagulate may again manifest itself. Diseased coagula, presenting a "mottled appearance, partly brown, and partly of a dirty yellow colour", or "dark coloured, and partly composed of a yellowish grey opaque substance", or "with portions inelastic, and of an opaque yellow colour", will be found entangled among the projecting fibres of the auricles and ventricles. In the arteries, the blood is in the most unfavourable circumstances for coagulation during life, in consequence of the comparative smallness of their diameters, and the succession of impulses communicated to their contents; but even here, diseased and adherent coagula may be found in cases of secondary inflammations.
M. Cruveilhier[37] relates an instance in which, after child-birth, the pulmonary artery was found filled with coagula following its divisions. The principal clot had lost its colour, and was adherent to the sides of the vessel, and contained in its centre puriform fluid.
In another case, following the operation for necrosis, the following post-mortem appearances were observed. The left lung presented, in several places, patches of red hepatization, perfectly defined, and resembling so many spots of lobular inflammation. When cut into, these patches presented several puncta of puriform fluid. The veins of the lung contained fibrinous-looking coagula blocking up their cavities; and in the centre of these coagula was a whitish purulent looking fluid.
The diseased condition of the blood may thus be traced visibly from the original wound, through the larger vessels, to the heart, and again from the heart to the capillary system. The disposition to coagulate,[Pg 58] once impressed upon the blood, is not destroyed by that fluid being conveyed to a different part of the body: the action may be retarded by motion in, as well as out of the body, but will nevertheless occur when it is placed under more favourable circumstances.
These circumstances, in the living vessels, are when the blood becomes separated into small quantities, and when it moves slowly along the capillaries. The blood will then coagulate in circumscribed patches,[38] as illustrated in the first characteristic marks of secondary disease which have already been mentioned as occurring in the lungs, the liver, the spleen, and the skin. The accompanying plate is taken from the lung of a donkey in which purulent fluid had been made to circulate with the blood. The stagnation of the blood, when the pus was first introduced, was mechanically prevented, and the livid spots produced by its subsequent coagulation in the capillaries of the lungs has been very faithfully represented. (See Experiment No. vi.)
"Besides the disposition for coagulation," observes Mr. Hunter, "the blood has, under certain circumstances, a disposition for the separation of the red globules, and probably of all its parts; for I have reason to believe, that a disposition for a separation of the red part and coagulation, are not the same thing, but arise from two different principles. This is always observable in bleeding; for if we tie up an arm and do not bleed immediately, the first blood that flows from the orifice, or that which has stagnated for some time in the veins, will soonest separate into its three constituent parts: this circumstance exposes more of the coagulating lymph at the top, which is supposed by the ignorant to indicate more inflammation, while the next quantity taken suspends its red parts in the lymph, and gives the idea that the[Pg 59] first small quantity had been of such service at the time of its flowing, as to have altered for the better the whole mass of blood. Best, therefore, maybe regarded as one of the immediate causes of the separation." Hunter, p. 29.
This disposition of the blood to separate into its constituent parts is evinced in a very marked degree in one class of secondary affections. Extensive effusions of serum, lymph, and pus, mixed in different proportions, will take place in the serous cavities of the body, and become infiltrated in the cellular membrane, accompanied with very slight indications of inflammatory action. The colouring matter of the blood will also sometimes become effused with its other parts; but when this is the case, the blood will be found to have lost its coagulating power: in this respect presenting a direct contrast to the effusion from a healthy wounded vessel. The lymph deposited will be found lying in unorganized flakes, wanting its usual adhesive properties, and very slightly attached to parts, presenting little or no increased vascularity. The rapid manner in which these depositions take place, shows that they are separated from the blood without undergoing any very elaborate process. In this condition of the system, any organ upon which the disease falls, may rapidly become disorganized, or may readily mortify; and, after death, a tendency to rapid decomposition will be manifested. The veins on the surface of the body may frequently be traced as dark blue lines, as though the skin covering them were stained by the colouring matter of the blood. The lungs and other organs may, under these circumstances, be found in every grade of disorganization, till they present all the characteristics of gangrene: even the peculiar fetor which accompanies mortification of the lung, will, in some instances, be present. A tendency to the formation of petechial spots may also be observed in different parts; and even the organs which do not appear to have been the peculiar seat of the disease, will be found to have lost their consistency, and to break down upon comparatively slight pressure.
Mr. Hunter found, that in proportion as the blood retained the power of coagulation, it had the power of resisting putrefaction; and conversely, we observe that, in this class of cases, the deficiency of the former is accompanied in a marked manner by the absence of the latter.
The two conditions of the blood which have now been mentioned, appear to bear a direct relation to the two classes of post-mortem appearances, observed in cases of secondary inflammations: the first being generally connected with congestion of different organs during the first stages of the disease, the second with extensive effusions, accompanied with comparatively little vascularity.
XII. The treatment of secondary inflammations naturally divides itself into local and constitutional, both as regards the primary lesion and the subsequent affections. The circumstances which interfere with union by the first intention in veins, have been shown to be the same as those which precede the formation of purulent deposits, in a large class of cases. Whatever then tends to favour the healthy reparation of a wounded vein, may be regarded as affording security against any subsequent disease; and the chief point in the local treatment is, perhaps, to prevent any accidental circumstances from interfering with the natural process of repair. When the powers of the constitution are enfeebled, even the natural motions of a part may interfere with recovery, and rest sometimes becomes an important object in the treatment. How necessary this is after child-birth, when the divided veins are being closed, every one who has attended such cases practically knows.
Again, after bleeding, the arm will inflame in a much greater proportion of cases, when the patient is obliged to follow his usual occupation, or when, from accidental circumstances (as from the pain experienced in Case i), the arms are kept in motion. It has occurred to me, to see the symptoms of purulent deposits set in, on[Pg 61] the day following prolonged attempts to bring fractured portions of bone into position. In all such cases, any external violence (as in Experiment No. vi), or even the motion of the body, as in Dr. Davis's case (section iv) may loosen the coagula formed, either between the wounded edges, or in the cavities of veins.
In the treatment of the local injury, a valuable hint has been left us by Mr. Hunter, connected directly with the consideration of the pathology of the disease. "The way in which sore arms after bleeding come on, shows plainly that they arise from the wound not healing by the first intention"; and he recommends that the two sides of the vein should be approximated by a compress, until union of the divided edges has taken place.
It has been shown upon very high authority, that the sides of a vein do not unite after venesection (as has sometimes been presumed to be Mr. Hunter's opinion); but that the divided edges only of the vessel are agglutinated by the coagulum, which "serves as a bed to the new membrane." But the case is different, should this first attempt at union fail; the sides of the vessel may then become united, and its cavity for a time obstructed (section iv). The approximation of the sides of the veins would materially facilitate this action, which is the natural security, under the circumstances, against the admission of foreign matter. When an abscess is suspected to have formed in a vein, a similar mode of treatment is recommended by Hunter; the compress, in this case, being placed between the inflamed part and the centre of the circulation. In the pathological museum of the College of Surgeons, one of Mr. Hunter's preparations (No. 1728) exhibits such a case, where, from the imperfect union of a vein, the contents of the abscess had become mixed with the blood.
As the process of reparation has been variously described by authors, so the different theories propounded have led to different kinds of treatment. At the Veterinary College, even within the last few years, it[Pg 62] was publicly taught, that a coagulum in a vein was a foreign substance, and ought to be removed; and the jugular vein in horses which had been bled, was sometimes slit up for several inches, in order to remove the coagula which formed in successive portions of its course.
That a coagulum in a vein may be an irritating substance has been fully proved (sections i and ii); but the irritation depends upon the accidental admixture of foreign matter: and the inflammation of the veins, produced by the contact of impure blood, requires to be carefully distinguished from the natural mode of union by the first intention.
To remove coagula which have formed round purulent secretion (if such could be recognised), might be to remove a cause of irritation; but to remove them in ordinary cases, is to remove the very means prepared by nature for the restoration and safety of the part. In operations involving large vessels, the local conditions which may influence the actions in the veins, appear not to have been fully determined; for while some surgeons regard the tying or cutting of a vein as a serious operation, others are in the habit of doing it without any unusual precaution. In operations upon hæmorrhoidal tumours, the veins involved are of some size, and in two of the instances recorded in the Appendix, a ligature applied to them was followed by purulent deposits. In the usual mode of passing a needle armed with a double ligature through the base of such a tumour, the hæmorrhoidal veins are necessarily sometimes wounded, and there is danger that, in tying the ligatures, the sides of a wounded vein may be drawn asunder. The vessel may thus be held open, and be in a similar condition to the vessels contained in bony structures.
A safe way of performing this operation, when admissible, is to destroy a portion of the mucous membrane with strong nitric acid. The blood in the vessels then becomes charred, and their cavities obstructed, till they are permanently closed by adhesive inflammation. Every means of treating a local injury which tends to produce healthy[Pg 63] union or adhesion, may be considered in some sort as a preventive mode of treatment. Position, topical applications, bandages, and temperature, may all have their influence in producing these healthy actions; but, as the wounds which precede purulent deposits are generally characterized by feeble powers, those conditions which tend to invigorate the parts are principally indicated. "When action is greater than strength, whatever has the tendency to raise the power above irritability should be used: the object of this practice consists in bringing the strength of the constitution and parts as near upon a par with the action as possible, by which means, a kindly resolution, or suppuration may take place, according as the parts are capable of acting." The irritability of a wound frequently appears nothing else than a series of attempts to bring about an action, which it has not the power to accomplish: as soon as that is fulfilled, which the necessity of the parts demands for their healthy condition, irritation will cease. In such cases, everything that will confer strength to carry out the intended action, will prevent inflammation. But no local applications will be sufficient to produce this effect, unless the powers of the constitution are supported at the same time.
A heavy man received a wound in the back of his head from an iron spike; he was kept very low, complaining occasionally of want of food. Repeated hæmorrhage took place at intervals of a day or two, which no local applications could suppress, and he ultimately died from loss of blood. The wound was found to extend through the bone into the lateral sinus, which contained only some fluid blood. No inflammatory action had taken place within the skull, nor had any attempt apparently been made to close the wounded vessel. Any vitiated secretion in contact with the lacerated edges of the vessel would, in such a case, have free access to the circulation.
The constitutional treatment of cases, liable to be succeeded by purulent deposits, is most important; for during the healing of the[Pg 64] primary wound, the system may be influenced by remedies, which may be subsequently quite useless. It is evident, observes M. Cruveilhier,[39] that the treatment of phlebitis ought to be concentrated on the first period of the disease, viz., that of the coagulation of the blood; for as soon as pus has become mixed with the circulating blood, medicine is generally of no avail. When there are indications of the extension of inflammation along a vein, the mode of treatment usually adopted in this country has been the administration of calomel and opium; and, in France, general bleeding, but especially the application of large numbers of leeches. "We may subdue inflammation of veins, whatever their situation, by general blood-letting, and especially by local bleeding, repeated sufficiently often and in sufficient quantities!"[40] It is true that patients recover after such treatment; but the published records of cases not unfrequently terminate with such a description as the following: "The patient was repeatedly bled, and with apparent relief every time, the blood being extremely sizy. Two days, however, previous to death, the vital principle was so exhausted as to need the use of cordials!!"
If the explanation of the mode of adhesion in veins already given be correct, neither the propriety of bleeding, nor of the administration of mercury, as a rule, derives much support from a consideration of the pathology of the disease. Careful comparative experience is still wanting, before we can form a satisfactory judgment of the value of these remedies. The theoretical views upon which they have been adopted, are confirmed neither by the statistical records of cases, nor by the principles of sound physiology. The numerical evidence which we have in some instances, even tends to indicate an opposite plan of treatment.
At a period when puerperal fever was rife, forty cases, attacked with[Pg 65] some form of the disease, "were treated without any bleeding or leeching, or without any attempt to induce the constitutional effects of mercury; and of these, only two died."[41] "In irritable habits, when the inflammation becomes more diffused," says Mr. Hunter, "bleeding should be performed with great caution: even a quick, hard pulse, and sizy blood, are not always to be depended upon as sure indications of bleeding being the proper method of the resolution of the inflammation; more must be taken into the account. The kind of blood is of great consequence to be known; for although it should prove sizy, yet if it lies squat in the basin, and is not firm in texture, and if the symptoms at the same time are very violent, bleeding must be performed very sparingly, if at all; for I suspect, that under such a state of blood, if the symptoms continue, bleeding is not the proper mode of treatment. If we had medicines which, when given internally, could be taken into the constitution, and were endowed with a power of making the vessels contract, such, I apprehend, would be proper medicines. Bark has certainly this property, and is of singular service, I believe, in every inflammation attended with weakness; and therefore, I conceive, should be oftener given than is commonly done."
In bleeding women suffering from puerperal fever during an epidemic, in which the disease frequently terminated in purulent deposits, I have occasionally seen an irregular transparent bluish layer form upon the surface of the blood, almost immediately after the operation; in consequence of this, a repetition of the bleeding was sometimes had recourse to, when the subsequent stages of the disease appeared to indicate that it had not been required. The transparent layer of lymph on the surface of the blood, may, in such instances, be only an indication of its tendency to separate into its different parts, as previously described.[Pg 66] Large bleedings, under such circumstances, inasmuch as they tend to diminish the already enfeebled power of coagulation in the blood, may predispose to the infection of the system, and to the formation of purulent deposits. The influence of mercury upon the system, as illustrated in Case xxvi, may have the same tendency.
The action of mercury, so far as it can be traced upon the surface of the body, is certainly unfavourable both to union by the first intention, and to adhesive inflammation; and, inasmuch as the safety of the patient, after an injury or wound, depends upon the due performance of these processes, its effect upon the system must be regarded as of, at least, doubtful advantage.
When salivation has been induced, serum is poured out, and the texture of the gums is loosened and rendered spongy. When lymph is effused upon the iris, the action of mercury loosens its adhesions, and dissolves its connexions; it cannot, therefore, be supposed that its effect upon the system should render the union of divided vessels stronger, or the newly-formed adhesions in wounds, firmer.
The cases in which purulent deposits usually form, indicate a debilitated state of constitution. They are of much more frequent occurrence in large towns than in the country, and in hospital than in private practice. The depressing influences which give rise to erysipelas, or puerperal fever, will also predispose to the formation of these abscesses; and as scanty diet, loss of blood, debilitating surgical operations, and over-crowded rooms, have been found among the causes of the former, so may they be looked upon as favouring the production of the latter.
The Treatment of Inflammation of the Veins, in which purulent deposits frequently originate, is thus spoken of, after matured observation: "All the experience that I have had on the subject, would lead me to believe that, like erysipelas, it has its origin in a low asthenic state of the system, and that those persons are especially liable to it, who have been much lowered by hæmorrhage at the time of an opera[Pg 67]tion, or by too scanty a diet afterwards. An operation is a shock upon the system, making a great demand upon the vital powers. The effects of this shock are often much aggravated by loss of blood, and a very scanty diet actually makes the patient more liable to some kinds of inflammation. Our mode of practice ought to be rather to sustain his powers by allowing him wholesome nourishment, and not to add to the influence of the other depressing causes, the still worse one of starvation."[42]
The lowering influence of mercury may be considered in a similar way. There can be little doubt that while, on the one hand, it favours the absorption of vitiated fluids, it may, on the other, render the system less able to resist the injurious consequences which they produce.
As many circumstances, besides mere debility, tend to depress the vital powers, so tonic medicines, and a generous diet, must not be looked upon as the only preventive modes of treatment. Each case that occurs in practice may present some peculiarity; in one case, the patient will be found to have previously suffered from diabetes; in another, from disease of the spleen; and in a third, from organic disease of the kidney; and, in each of these, a peculiar mode of treatment may be required.
The general management of this disease, after the formation of purulent deposits has commenced, is probably as little satisfactory as any that come under the notice of the surgeon. The whole character of the affection is characterized by what has been aptly designated as action without power. The excitement of the system will imitate all the acts of genuine inflammation, without any of its healthy results; and loss of energy will appear immediately after, or even arise in conjunction with, the first symptoms of increased action.
In the treatment of such cases, it must be borne in mind, that the[Pg 68] secondary inflammations are not the disease, but the effect of a concealed cause, which may develope itself in any part of the system; and that, while the relief of one organ is sought by depletion or mercurial remedies, additional vigour may be given to the latent evil, so as to render it more ready to develope itself in some other part.
When purulent deposits occur, the sudden congestions, which indicate their commencement, are not accompanied by any reparative actions, and the lymph, which is effused in the second stage of their formation, is not so disposed as to circumscribe and limit the inflammation; there is, therefore, no natural process by means of which such collections of fluid can be evacuated; hence, when situated near the surface, they should be opened as soon as they are detected. It will sometimes happen, that, after the symptoms of secondary inflammation of internal organs have commenced, an abscess will present itself near the surface of the body, and relief will be afforded to the part first affected; at other times, an obstinate and violent diarrhœa will precede recovery. Although the mode of treatment adopted may have little influence either in bringing on, or checking, such salutary actions, it is important to watch their occurrence, and perhaps still more important, to be careful not to mistake a remedial action for a symptom of the disease.
"What treatment," says Cruveilhier, "shall we oppose to purulent infection? To this question experience is as yet dumb, while theory would seem to point to diffusible stimuli and tonics; to ammonia, quinine, and sudorifics; to hot external applications, to the vapour baths, to purgatives, and especially to emetics; to tartarized antimony, in large doses; to vesicatories, and to strong diuretics. Calomel has been extensively employed, to create a fluxion from the intestinal mucous membrane; but all these means have failed as signally in my hands as in those of others; yet, when the injection of putrid matters into the veins of living animals has been followed by abundant and very fetid evacuations, they have usually got well. It is a fundamental fact of pathology, that the[Pg 69] intestinal canal is chiefly affected in diseases caused by miasmata. I am certain that diseases resulting from purulent infection would not be stamped with the seal of incurability, and that nature, seconded by art, would triumph in the majority of cases, if the pus, which is incessantly renewed, did not incessantly renew the sources of infection. As soon as constitutional symptoms manifest themselves, neither general nor local bleeding affords any advantage. A portion of the materies morbi is, no doubt, abstracted with the blood; but, as it is constantly being reproduced, the constitution is only deprived of the power it would otherwise have of resisting the disease."[43] In accordance with this remark, M. Gaspard found that animals, which recovered after the injection of a certain quantity of pus into their veins, often died when the experiment was repeated. The recovery was usually preceded by black, liquid, and extremely fetid evacuations, which often seemed to afford immediate relief. When such evacuations have taken place in other diseases, the gall-bladder has been found distended with black bile;[44] and it appears probable that the liver, in these cases, is one of the principal organs through which the cleansing of the system is attempted. If the supply of morbid matter to the system could be checked, mercurial action, in this stage of the disease, might be of service, by enabling the liver, or other organs, to throw off their vitiated secretions. When patients recover from purulent deposits (Cases iii and xxvii), they are often left in a debilitated and languid state, in which ordinary tonics exercise little influence. The consequences of the disease appear to hang about the system, long after the cause which gave rise to it has ceased. The pulse will sometimes continue irritable, and there will be a tendency to derangement of the secretions of the skin, bowels, and other organs, accompanied by[Pg 70] occasional slight attacks of fever. In this condition, an alterative course of mercury, combined with sarsaparilla, has been found beneficial. These remedies, by stimulating the activity of the excreting organs, may assist the constitution in throwing off the disease; and their mode of action may be the same as in other cases, where the system has been infected by an animal poison.
Case i. William Ford, 33, an apparently healthy man, was seized with the symptom of strangulated hernia, at Harrow, December 28th. He was bled in both arms; but, as the hernia remained unreduced, he was sent to town, in a state of considerable restlessness and suffering. During his journey, the hernia returned of its own accord. He left quite relieved, and remained well till the 31st, when he had a rigor. On the 1st of February, there was a considerable degree of febrile excitement, and the anterior part of the left arm was red, swollen, and painful upon pressure. The tenderness and pain soon extended up the arm, in the course of the cephalic vein: the redness assumed the character of erysipelas. On the 3rd, he suffered from sickness, the matter vomited being green and acid. He had two severe rigors, followed by great heat of skin, and a quick full pulse. The orifice in the left arm discharged a thin serous fluid. On the 4th, he complained of stiffness in the right arm; also of being very feeble and faint. 5th. Wandered much during the night. The right arm was a good deal swollen about the end of the elbow-joint, and presented a patch of a bright red colour above the condyle. The pulse was weak and tremulous; motions of the hands were occasionally observed. He complained of pain in the ring-finger of the right hand, and in the ball of the right great toe. The skin, in both these situations, had assumed a red appearance. 6th. Was delirious during the greater part of the night; countenance expressive of much anxiety; pulse very weak; tongue[Pg 72] covered by a brown dry fur; profuse perspiration; complained of severe pain in the calves of his legs. He died during the following night.
Post-mortem appearances. A small deposit of thick pus was found on the external surface of the left cephalic vein. The blood was coagulated in its cavity, its coats were thickened, and its lining membrane appeared very red. This redness could be traced, though in a less degree, through the whole extent of the vena innominata. On the right side, the cellular tissue, both above and below the elbow-joint, was greatly distended with serum. The cephalic vein of the right arm presented marks of having been inflamed; but not nearly to the same extent as upon the opposite side. The joints in which pain had been experienced during life, were distended with turbid pus; deposits of pus were also found in the anterior mediastinum, and between the œsophagus and trachea. A large gangrenous spot was observed in the skin of the calf of the right leg. The subjacent cellular tissue was much distended with serum.
Case ii. Richard Mason had a small cancerous tumour removed from the lower lip. The operation was performed in the usual way, and the wound appeared to heal by the first intention; a small abscess, however, followed by some ulceration, subsequently appeared in the neighbourhood of the cicatrix. Nine days after the operation, he complained of sore throat and general uneasiness, and three days afterwards he was seized with rigors, followed by cold perspiration and coma.
Post-mortem appearances. A small deposit of matter was found, situated beneath the fascia of the left thigh. The synovial membrane of the left knee was highly inflamed, and contained a large quantity of pus. On the right side, the skin of the whole inferior extremity presented a dark livid appearance, with the exception of that situated upon the fore part of the thigh. The same dark colour was observed in the muscles of the limb, which were infiltrated with blood and serum. The arteries and veins were discoloured, but in other respects presented[Pg 73] nothing remarkable. It was ascertained, that, two years previously, this patient had suffered from diabetes; and upon examining the urine found in the bladder, it was found to contain sugar.
Case iii. Jane Thornton, æt. 32, came under treatment on the 22nd of March. A week previously, her right ancle had become red and painful, and inflammation subsequently extended up the inner side of the leg. When first seen, she was evidently much out of health, although no one organ could be said to be particularly affected. On the 28th of March, she was attacked with severe rigors, and experienced pains in different parts of her limbs: the rigors were repeated for several days in succession. The inflammation of the leg now entirely disappeared, and she complained of pain in the right knee, which was slightly swollen. On the 31st, her bowels became much relaxed; there was great general depression, and much nervous agitation. Both knees were swollen. The general symptoms now became somewhat relieved; but on the 4th April, she was attacked with vomiting, which recurred frequently during the day, and was accompanied with great depression, and severe pain in the epigastrium. On the 5th, the sickness continued, apparently quite uninfluenced by any remedies. She passed considerable quantities of blood by stool: her countenance presented a dusky yellow hue: the pulse was excited, without power, and the sense of depression was greatly increased. On the 7th, the vomiting still continued, and she still passed blood by stool. Some spots of a dark purple colour now made their appearance upon her face. The hands both became slightly swollen; and upon the right one, some small, dark, livid spots, similar to those upon the face, made their appearance. She was much troubled with hiccough. On the 9th, the countenance was very anxious, the complexion more sallow: some more livid spots appeared upon the face and cheeks. The right hand and arm were swollen and painful: some fresh livid spots appeared, upon the knuckles. Complained much of faintness: had extreme debility with occasional hiccough: pulse extremely weak:[Pg 74] the surface of the body was covered with cold perspiration. The sickness had entirely ceased, and there was no blood in the motions: the tongue was rather dry in the centre, but tolerably clean. 10th. She wandered slightly during the night, and vomited once: some blood again appeared in the motions; the right hand and arm were less swollen. 11th. The countenance was anxious, the pulse about 90, and intermitting irregularly. The vomiting recurred several times. The livid spots on the right hand had not increased in size, but appeared like distinct small black superficial sloughs of the skin; these all scabbed off, without suppuration. 12th. The pain and swelling of the arm had nearly subsided. The bowels acted very freely with the aid of medicine, and she expressed herself much relieved. From this time the patient slowly but gradually improved, with one or two slight intermissions, till the beginning of May, when she again complained of pain at the inner part of the right arm, above the elbow. Some hardness could here be felt in the course of the basilic vein. Some small collections of matter were now deposited upon the back of the right hand, resembling, in some respects, the eruption of confluent small-pox. On May 11th, she had regained much of her strength, but still felt some pain in the elbow upon motion. She also complained of the joints of one of her fingers. She now left London for change of air.
B. The following Table is formed of Cases taken consecutively during One Year.
[Pg 75] [Pg 76] [Pg 77] [Pg 78]
C. Case xxvii. George Burton, æt. 22, a stout navigator, was first seen September 18th, 1848. He had an enormous slough of the skin and cellular membrane, covering the lower part of the abdomen on the right side. He gave a most imperfect history of himself, and seemed frequently incapable of comprehending the questions which were put to him. The skin was hot and dry, the pulse 130. For several days, he[Pg 79] remained in the same apathetic condition. The bowels were particularly obstinate, and the purgative medicines which were administered produced no effect whatever.
When the slough separated, the surface of the external oblique muscle was left as clean as if recently dissected. The skin was undermined for some extent, and no attempt was apparently being made to limit the progress of the disease, by the effusion of lymph. Fresh portions of cellular tissue consequently became affected, and the whole surface ultimately exposed was full six inches in diameter. Sept. 25th. Complained of some pain in the chest and upper part of the abdomen; has a constant short cough; perspires very freely. 26th. The pulse has become weaker, but remains of the same frequency (130). It communicates a peculiar jerking sensation to the finger. 28th. Pulse 96, weaker; slight diarrhœa; he vomited several times during the day. 29th. Restless, with delirium. 30th. Passed another restless night, but became better in the course of the day; his appetite returned. Oct. 5th. His appetite again failed; complained of a sense of distension in the abdomen. 8th. An abscess was discovered at the lower and back part of the right leg; the skin over this presented various shades of yellow and brown, giving the appearance of having been extensively bruised. About two ounces of discoloured pus were evacuated, together with a considerable quantity of grumous blood. 10th. Has much improved since the last report; the wound discharges dark semi-coagulated blood. 13th. A second abscess now presented itself in the same leg, and the skin covering it assumed the same discoloured appearance as in the first instance. When opened, it discharged dark-coloured semi-coagulated blood with the matter. He now rapidly improved in health, and at length perfectly recovered.
Case xxviii. Samuel Todd, æt. 58, fell from a wagon fifteen miles from town, and was brought up in an open cart, during a sharp frost. There was a compound fracture of the left leg. Two days afterwards,[Pg 80] he suffered from cellular inflammation around the wound. On the 24th day, he had a slight rigor, and complained of slight stiffness in the right shoulder. He ate and drank well till within two days of his death, which took place on the thirty-fourth day.
Post-mortem appearances. Both lungs contained secondary abscesses, in various stages of formation. The left external iliac and common femoral veins were blocked up with firm coagula, and confined by these was a quantity of purulent-looking fluid; an adherent layer could, for some distance, be peeled off the internal surface of these vessels.
Case xxix. James Howard, æt. 33, had a small abscess in the dorsum of the right foot, which was followed by inflammation of the absorbents; abscesses subsequently formed in the right thigh and groin. Two months after the first appearance of the abscess on his foot, he was seized with rigors, vomiting, and profuse perspiration. He complained also of pain in the lower part of the left lung, and it was said that the respiratory murmur was deficient in this situation. He died on the 23rd day from the appearance of the symptoms of the secondary affection.
Post-mortem appearances. The skin and conjunctivæ were of a light yellow colour; there were incisions in the right groin. In the cavity of the right pleura, were some patches of recently effused lymph, of a yellowish colour. In the lower lobe of the right lung, were several patches of secondary deposit; these were found in different stages of their formation, and some of them were of considerable size; some of the pulmonary veins, in the neighbourhood of those which had suppurated, were found to contain a fluid resembling pus. On the left side was a small abscess, under the pleura costalis. The liver was healthy in structure, rather larger than usual. Kidneys healthy. The veins in the groin presented a healthy appearance.
Case xxx. A gentleman was operated upon for hæmorrhoidal tumours in the usual manner, and died shortly afterwards, with effusion of[Pg 81] bloody serum into one of the pleural cavities. The only peculiarity that could be detected in the appearance of the rectum was, that the blood was still fluid in one of the largest veins. This vein led directly to an ulcer produced by the operation; and, even at its extremity, it contained no appearance of coagulum.
Case xxxi.[45] On the second day after a natural labour, a woman had prolonged rigors, which were followed by abdominal pain and much perspiration. On the fourth day, she was affected with syncope and bilious vomiting, accompanied by extreme prostration. On the fifth day, the abdominal pain, which had subsided, re-appeared with agitation and delirium. On the sixth, she had cold sweats, irregular pulse, rapid breathing, and vomiting. She died on the following morning.
Post-mortem appearances. There was a small quantity of limpid serum in the cavity of the peritoneum. Some of the uterine veins were found to contain a turbid fluid. The heart was half filled with brown blood. The lungs were congested, and the other organs natural.
Case xxxii. A woman, twenty-two years of age, of a nervous temperament, miscarried at the expiration of the first month. She was almost immediately afterwards attacked by rigors and bilious vomiting, accompanied by pains in the loins and in the hypogastrium. On the following day, there was coma, with indications of extreme debility. On the third day, consciousness returned. There was difficult articulation, and moaning. The extremities became cold, the pulse imperceptible, and death occurred upon the same day.
Post-mortem appearances. The peritoneum was slightly injected, and contained a small quantity of reddish serum. The cervix uteri was covered with a layer of pus. Semi-transparent lymph was found in some of the uterine veins. The brain, and other organs, were found healthy.
Case xxxiii. A feeble girl, 21 years of age, was confined at the expiration of the eighth month. On the fourth day, there was shivering and prolonged fainting. The following morning, she had acute abdominal pain, fever, and diarrhœa. On the seventh day, the symptoms had all subsided, but on the eighth the abdominal pain returned, accompanied by syncope. She died two days afterwards.
Post-mortem appearances. The peritoneum was slightly injected, and contained about a pint of red-coloured serum. The uterus was large, white, and firm, its veins half filled with fluid blood; its lymphatics natural; its inner surface lined with a layer of fetid brown blood, but otherwise healthy; the cervix covered with a grey, thin exudation. The lungs, heart, brain, and other organs, were quite sound.
Case xxxiv.[46] Anne Biggs, æt. 39, confined March 18th, 1830, eighth child. On the evening of her confinement, her manner was much excited. On the 19th, she was incoherent, and complained of pain in the calf of the right leg, which was tender on pressure. The pulse being hard, she was bled to eight ounces. On the 28th, the leg was swollen and white; the pain in it much increased: towards evening the calf of the limb became black, while, at the tendo-achillis, the skin was hot, tender, dry, and mottled. The bowels were much opened, the head giddy, the pulse quick and strong. She was again bled, to twenty-six ounces, and twelve leeches were applied to the temple. On the 21st, there was nausea, vomiting, and diarrhœa. On the 23rd, she complained much of the confusion in her head, the leg was tolerably easy,[Pg 83] but the upper and inner part of the thigh was very tender. On the 24th, the diarrhœa continued, and there was increased weakness. A hard swelling, about half as large as an egg, appeared at the wrist, and one of the orifices made by venesection was black and painful. She died in the evening.
Post-mortem appearances. All the ventricles of the brain were dilated with serum, and there was a good deal of effusion into the arachnoid and pia mater. The viscera were perfectly healthy, except the heart and spleen: the latter was very large, and on pressing it, a large quantity of dirty red pulpy matter exuded. The lining membrane of the right auricle and ventricle, when washed, had a dark red hue. The femoral vein, just at the ingress of the saphæna, and the superficial vein in the back of the leg, had their coats much thickened, so as to cut like arteries. Their lining membrane was similar to that of the right cavity of the heart. When they were divided, purulent matter, mixed with thin light-coloured blood, escaped. The cellular tissue forming the sheath of the femoral vessels, and on the calf of the leg, shewed marks of recent inflammation; but there was no appearance of pus in these situations. None of the glands in the groin or ham were enlarged. The inferior vena cava appeared healthy.
Case xxxv. Mrs. Mayhew, æt. 33, was delivered on the 2nd March 1829. On the 5th, there was a discharge of blood from the uterus. From the 6th to the 20th, she made no complaint of uneasiness in any region of the body, though her strength rapidly declined. The countenance was of a dusky yellow hue. The heat of the surface slightly[Pg 84] increased; the respiration hurried, particularly on bodily exertion, and the pulse above 130, and feeble; the tongue pale and glossy, with loss of appetite. The lochial discharge had a peculiarly offensive smell. She died upon the 28th of March.
Post-mortem appearances. When the uterus was laid open, there was found to be a portion of the placenta, about the size of a nutmeg, in a putrid state, adhering to its inner surface. The substance of the uterus, to the extent of an inch around this, was of a peculiarly dark colour, almost black, and as soft as a sponge. On cutting into it, about a teaspoonful of purulent matter escaped from the veins, and a small additional quantity was pressed out from them.... On opening the capsular ligament of the right knee-joint, about six ounces of thin purulent matter escaped, and the cartilages of the femur and tibia were extensively eroded. There was no appearance of inflammation, however, on the exterior of the capsular ligament. The right wrist was swollen, and the cellular membrane around it was unusually vascular, and infiltrated with serum.
Case xxxvi. Mrs. Pope, æt. 40, was delivered, on the 26th of Oct., of her fourteenth child, and appeared to recover favourably until the 3rd of Nov., when she was suddenly attacked with a severe rigor. This was followed by intense head-ache, vomiting, general soreness of abdomen, and suppression of lochia. Nov. 6th. Great prostration of strength; laborious respiration, with pain at the bottom of the sternum, and frequent hacking cough; pulse 135, extremely feeble; skin hot and dry.... Occasional retching and vomiting. Several hard, lumpy cords were found running up in the inside of the thigh, in the direction of the superficial veins. 7th. Delirium; general debility greatly increased; the surface of the body was covered with a yellow suffusion; the middle finger of the left hand was much swollen around the second joint, and the skin covering it was of a dusky red colour.
Case xxxvii. Mrs. Edwards, æt. 35, was suddenly attacked, three[Pg 85] weeks after delivery, with pain in the calf of the right leg, and loss of power in the whole right inferior extremity. On the 5th day from the attack, a considerable swelling, without induration, had taken place from the ham to the foot, and great tenderness was experienced along the inner surface of the thigh to the groin. The extremity became universally swollen, painful, and deprived of all power of motion. The temperature along the inner surface of the limb increased; the integuments were pale and glistening, not pitting upon pressure. The femoral vein, from the groin to the middle of the thigh, was indurated, enlarged, and exquisitely sensible; pulse 80; tongue much loaded; thirst; bowels open. On the 23rd day from the attack, the disease was apparently declining. The femoral vein could no longer be felt, but there was still a sense of tenderness in its course down the thigh, and she experienced considerable uneasiness between the umbilicus and pubes, as well as in the loins. She now, for the first time, began to have rigors, accompanied by a quick pulse, loaded tongue, and thirst. From this period to the 31st day, the swelling of the limb and tenderness in the course of the femoral vessels subsided, but she experienced attacks of acute pain in the umbilical region, loins, and back, which assumed a regular intermittent form. Every afternoon there was a rigor of an hour's duration, followed by increased heat, and profuse perspiration: the skin was hot and dry; pulse 125; tongue brown and parched; bowels open. These febrile attacks gradually declined in severity, and she appeared to recover till the 43rd day, when she had a long and violent fit of cold shivering. The countenance now became expressive of great anxiety, and the pulse extremely weak and feeble. 45th day. Vomiting; pain upon the left side, increased upon taking a deep respiration. 46th day. Another severe and prolonged rigor; skin hot and dry; pulse 140; tongue brown and parched; diarrhœa; respiration hurried, with frequent cough; surface of body presenting a peculiar yellow tinge. The conjunctiva of the right eye now suddenly became of a deep red colour, and so much[Pg 86] swollen, that the eyelids could not be closed. On the day following, the left eye also became red and swollen, the surface of the body was cold and clammy, pulse 140, extremely feeble, with great debility, and repeated attacks of vomiting. From this date, the patient lived nearly three weeks, but for the last fortnight the vision in both eyes was entirely destroyed.
Post-mortem appearances. The left pleural cavity contained upwards of two pints of a thin, purulent fluid. The inferior lobe of the left lung was of a dark colour, and soft in texture. In its centre, about an ounce of thick cream-coloured pus was found deposited in its dark and softened texture. This was not contained in any cyst or membrane, but was infiltrated into the pulmonary tissue. The coats of the vena cava inferior were considerably thickened; its whole cavity was occupied by a coagulum, terminating above in a loose pointed extremity. The left common iliac vein was plugged up, by a continuation of the coagulum from the cava. The coagulum was continued beyond the entrance of the internal iliac, which it completely closed, and terminated in a pointed extremity about the middle of the external iliac. Neither the remainder of the vessel, nor the femoral vein, exhibited any morbid changes. The right common iliac vein was contracted to more than one-half its natural size; it was firm to the touch, of a greyish blue colour; to its internal coat adhered an adventitious membrane of the same colour, containing within it a firm coagulum. The internal iliac was rendered quite impervious by dense, dark coloured bluish membranes; and, at its entrance into the common iliac, it was converted into a solid cord. The contracted external iliac contained within it a soft yellowish coagulum; its coats were three or four times their natural thickness, and lined with dark-coloured membranous layers. The right femoral vein, from Poupart's ligament to the middle of the thigh, was diminished in size, and almost inseparable from the artery. Its tunics were thickened, and its interior[Pg 87] coated with a dense membrane, surrounding a solid purple coagulum strongly adherent to it.
Case xxxviii. George Haydon, ætat. 37, received a wound about half an inch in length over the right radial artery, on March 5th, 1848. The hæmorrhage was arrested by pressure. On the 12th, a small slough formed in the bottom of the wound, the edges of which were inflamed and painful. On the 14th, slight bleeding from the wound occurred, which at first was arrested by the application of cold; but in the evening it recurred in considerable quantity, and again was checked by cold and pressure; during the night, however, profuse hæmorrhage again took place, and was only stopped by the application of the tourniquet above the elbow. On the 15th, the radial artery was tied; but as this did not prevent the hæmorrhage from returning, when the tourniquet was relaxed, the original wound was enlarged. The opening in the radial artery was now with some difficulty discovered; it extended two-thirds round the circumference of the vessel, leaving one-third undivided.
Case xxxix.[47] A middle-aged man received a severe injury of the chest; he lived eleven days after the accident, and during this time he never presented a single inflammatory symptom. The cavity of the left pleura was found completely filled with bloody fluid, and was subdivided into two compartments, by a portion of coloured fibrine, presenting a honey[Pg 88]combed appearance, which passed from the ribs to the lung. The lower compartment was itself subdivided into several others, by layers of coloured fibrine intersecting each other. Large portions of loosely coagulated blood were found in all the cavities; some of these clots were of a rusty colour, others approached nearer to the natural colour of the blood. The lung was compressed against the spine, and the whole surface of the pleural sac was coated by a false membrane, about two lines in thickness, formed by coagulated fibrine. The fibrine which lined the pleura pulmonalis and pleura diaphragmatica, presented on its inner surface a smooth and polished appearance, and in colour exactly resembled the yellowish fibrine found in the clots of the heart of this patient. So uniform was the coating, and so continuous was it throughout its whole extent, that it looked at first merely like thickened pleura; but this appearance was easily destroyed, by peeling off this adventitious membrane from the serous tissue, which there presented the same appearances as the pleura on the opposite side, with the exception of not being quite so smooth: there was neither thickening nor the slightest increase of vascularity in this pleura. A large rent, from which the hæmorrhage had proceeded, was found in the substance of the lung.
Case xl. A man was attacked with diffuse cellular inflammation of the inferior extremity, which terminated in two days with extensive gangrene of the skin. In the superficial and common femoral veins were extensive coagula; these did not completely fill the veins, but slightly adhered at different points to their internal coats. These clots still retained, in some places, the colouring matter of the blood, whilst at others the colourless fibrine alone remained; in both veins, the clots were enveloped in a perfectly transparent, smooth, and polished membrane, presenting the appearance of a serous tissue. In the structure of these membranes were several distinct arborescent vessels, mi[Pg 89]nutely injected;[48] some of these vessels were of sufficient size to allow of the blood being made, by gentle pressure, to circulate through them; but no communication could be traced between these vessels and the coats of the veins. The membranes were easily peeled off from the surface of the clots with which they were in contact. The interior coats of the veins presented their natural colour and polished surfaces, except at the points where the slight adhesions above-mentioned existed.
FINIS.
RICHARDS, PRINTER, 100, ST. MARTIN'S LANE.
[1] Hunter on the Blood. Ed. 1794, p. 21.
[2] P. 25.
[3] P. 24.
[4] P. 97.
[5] P. 94.
[6] P. 98.
[7] Op. cit. p. 98.
[8] Vol. x, p. 45-82.
[9] Op. cit. p. 26.
[10] P. 200.
[11] P. 205.
[12] Anatomie Générale, vol. ii, p. 423.
[13] In speaking of the two principles, I shall use the term by "first intention", to designate that the fibrin is derived from coagulated blood; and restrict the term "adhesive inflammation" to indicate the effusion of lymph from inflamed vessels.
[14] Cruveilhier's Path. Liv. xi.
[15] Medico-Chirurgical Transactions, vol. xii.
[16] Medical and Physical Journal, vol. lvi.
[17] London Medical Gazette.
[18] This remark I have had opportunities of verifying in cases, where needles have been introduced under varicose veins in the lower extremities, and allowed to remain, with a ligature around them, for ten days or a fortnight. The circulation through the vein will in such cases be obstructed; but, in a year or two, will be found to have become completely re-established.
[19] Medico-Chirurgical Transactions, vol. xii.
[20] Dance. Archives Générales de Méd. vol. xviii, p. 480, Dec. 1828.
[21] In cases where pus has been found in veins surrounded by coagula, its presence and detention there have been differently accounted for. M. Cruveilhier appears to have imagined that the loose coagula act as filters, through which the blood passes, while the pus is retained. (Dict. de Méd. et de Chir. t. xii, p. 641.) The true explanation of the way in which coagula form round pus in the veins has already been given.
[22] See M. Gaspard's experiments.
[23] Dr. Lee. Medico-Chirurgical Transactions.
[24] Précis Elémentaire de Physiologie, t. ii, p. 389.
[25] Journal de Physiologie, t. v, p. 328 and 336.
[26] The present mayor of Newcastle-under-Lyme.
[27] This, and the following experiments, are among those recorded by M. Gaspard, referred to in the foregoing dissertation.
[28] I once observed a similar condition in a young woman in St. George's Hospital. Each pulsation of the heart could be heard with great distinctness at a distance of two or three yards from the patient; during the paroxysms, there was the greatest difficulty of breathing; the countenance became anxious and livid, and a distinct thrill was communicated to all the arteries. After death, the countenance and upper part of the body were found livid from venous congestion. The lungs did not readily collapse when the chest was opened. The auricles of the heart were greatly distended with black blood; the inner surface of the left ventricle presented a white patch, of about two square inches in extent; the lining membrane of the aorta, for several inches, was of a bright red colour; this extended round one-third only of the circumference of the vessel. No other structural change could be found in the heart or vessels, which would account for the symptoms observed during life.
[29] De l'Infection Purulente, p. 399.
[30] In deducing general conclusions from experiments upon animals, it must be borne in mind, that in them suppuration is induced with great difficulty. Many of the appearances produced by the injection of putrid fluids (as in Experiment xiv) would, in man, probably have terminated in suppuration. Dr. Sédillot has nevertheless established the fact, that, generally speaking, a different class of post-mortem appearances may be expected from the introduction of decomposed serum, to those produced from fluids containing solid particles.
[31] London Journal of Medicine, vol. i, p. 799.
[32] In a case of fracture of the femur into the knee-joint, I have observed a dark ill-defined erysipelatous blush extend from the affected limb to the body, and thence to the head. Purulent deposits formed in various parts of the body, of which the patient died.
[33] For the knowledge of this fact, I am indebted to Mr. Cæsar Hawkins, of St. George's Hospital.
[34] Journal de Physiologie, t. iv, p. 45.
[35] Op. cit. p. 99.
[36] It may appear unusual to speak of action going on in the blood; but, in so doing, we only illustrate the principle with which we commenced, viz., that "the blood has the power of action within itself."
[37] Op. cit. p. 669.
[38] The term ecchymosis does not appear appropriate to the discoloured condition of parts observed in the commencement of this disease; the blood is not at first extravasated from the vessels, but coagulated in them.
[39] Op. cit. p. 662.
[40] Op. cit. p. 662.
[41] Ferguson (Dr.) On the Diseases of Women. These cases formed one-fifth of the whole number treated.
[42] Brodie (Sir B. C.) Medical Gazette, vol. xxxvii, p. 642.
[43] Op. cit. p. 662.
[44] I have observed this condition after injuries of the spine which proved fatal, by causing inflammation of other parts.
[45] This, and the two following cases, are taken from Tonellé. The author is responsible for the accuracy of all the preceding cases.
[46] Dr. Ferguson.
[47] Med.-Chir. Transactions, vol. xxviii.
[48] Mr. Gray, the Curator of the Museum of St. George's Hospital, has recently shewed me the outer layer of an effusion of blood into the arachnoid cavity, injected from the middle meningeal artery.
Transcriber's Notes
Page 81, Case XXVII. Aug 5th follows September 30th. This has been changed to Oct 5th.