
Title: Duval's artistic anatomy
Completely revised with additional original illustrations
Author: Mathias Duval
Editor: Andrew Melville Paterson
Release date: January 20, 2026 [eBook #77743]
Language: English
Original publication: New York: Funk & Wagnalls, 1905
Other information and formats: www.gutenberg.org/ebooks/77743
Credits: Tim Lindell, Karin Spence and the Online Distributed Proofreading Team at https://www.pgdp.net (This book was produced from images made available by the HathiTrust Digital Library.)
Completely Revised with additional Original Illustrations.
Edited and Amplified by
A. MELVILLE PATERSON, M.D.
LATE DERBY PROFESSOR OF ANATOMY IN THE UNIVERSITY OF LIVERPOOL
FUNK & WAGNALLS COMPANY
New York and London
First published September 1884
Reprinted 1885, 1888, 1890, 1891, 1892, 1894, 1896, 1898, 1899, 1901, 1903, 1904
Revised and Enlarged Edition 1905. Reprinted 1907, 1911, 1914, 1916, 1919
[v]
Few words of preface are needed here. The preface of the original edition still holds good, and sufficiently defines the aims and scope of the book. The first object aimed at is to facilitate the study of artistic anatomy by the demonstration of the meaning of the appearances presented by the various parts of the body. Incidentally it is hoped that through close study the powers of observation will be quickened. By a simple narration of the structure of the body and its mechanism, particularly in relation to surface forms, it is hoped that the student of art may correctly and intelligently appreciate the why and wherefore of the parts which he is called upon to paint or model.
One would reiterate and emphasise the necessity of two additional aids to this end. In his studies the student should have and use the opportunity of seeing and handling the separate bones and also an articulated skeleton; and where possible, he should have access to a fully equipped anatomical museum. He should further take advantage of all means of studying on the living model—on himself, on other[vi] models—and in casts, the movements, attitudes, and gestures of the body, and the resulting surface forms. By these two studies it becomes possible to correlate properly the superficial appearances with the deeper structures, such as bones, joints, and muscles, which are mainly responsible for the characteristic features presented in the living state.
I have to express my indebtedness to my friend Dr. Thurstan Holland for the radiograph (Fig. 25, p. 80) specially prepared by him for this work; and to the publisher of Cunningham’s Text Book of Anatomy for permission to use the figure (p. 315) of the muscles of expression.
A. M. P.
Liverpool, July, 1905.
[vii]
This little work is an epitome of a course of lectures which for about ten years I had the honour of delivering at the École des Beaux-Arts. If during that time I have arrived at a right understanding of the teachings of anatomy, I owe it to the great interest taken in the subject by my listeners of all ages; and my first duty is to thank them for their free interchange of ideas with me, thus enabling me to understand their requirements and the mode of satisfying them. But if the mode of exposition I have adopted is to be rendered clear to a constantly renewed audience, I must, in publishing this work, first explain to the reader how the lectures are to be used, and the principles which guided me in their production.
This summary of anatomy is intended for those artists who, having commenced their special studies, have drawn the human form either from the antique or from the living model—who, in a word, have already what may be termed a general idea of forms, attitudes, and movements. It is intended to furnish them with a scientific notion of those forms,[viii] attitudes, and movements. Thus it is far less a description of the forms of a particular region than the anatomical explanation of those forms, and of their modifications in a state of repose or movement, that we have in view. That is why, instead of proceeding from the surface to the deeper organs and to the skeleton, we take the latter as the starting-point of our studies. In this way alone can we determine the laws which govern the movements of the adjacent segments of the limbs upon each other, and the movements of the limbs with regard to the trunk, as also the reciprocal action of these segments towards each other and in relation to the whole body.
When to these fundamental notions is added a knowledge of the muscular masses which move these bones, the artist will at once be enabled to analyse through the skin, as through a transparent veil, the action of the parts which produce the various forms with their infinite variety of character and movement.
This method of teaching, which may be said to proceed by synthesis, differs from that followed by the generality of works on this subject—books which treat by analysis. We make special allusion to the treatise of Gerdy,[1] which is about the most careful work on plastic anatomy yet published, but which[ix] errs in a somewhat too lengthy description of external form, whilst sufficient space is not devoted to explaining the anatomical reasons of those forms. On the other hand, the remaining anatomical works in the hands of the students in our art schools generally comprise a volume of text and an illustrated atlas.[2] Under these conditions, may I be allowed to remark, somewhat severely, it may be, that our young artists study the atlas by copying and re-copying the plates, but do not read the text? Thus it will be understood why, in this work, a different method has been pursued; and the fact of the plates being intermixed with the text, and in such a way that they cannot well be understood without the aid of the accompanying pages, will in all probability result in the student thoroughly and carefully perusing the text.
Passing on to the manner of using the present work, we must acknowledge that reading anatomical details is at first dry; it will always be so, unless proceeded with in a simple and systematic manner. In the oral courses, the lecturer, handling the objects, and aided by his improvised drawings on the blackboard, can make the most complex parts interesting; and by adroit repetitions and varied illustrations, fix the attention and render the subject[x] comprehensible, whereas it is quite different in a written description. In this case it is the reader who must animate the text for himself by examining and manipulating the parts needful for the elucidation of the descriptions. For this purpose a skeleton and a good plaster cast will suffice. On the cast, with the aid of the plates which accompany the text, it will be easy to follow the course of the muscles; and in this way alone will the study of them become profitable, the student being enabled to examine the model on different sides. By handling the bones, by placing the articulating surfaces in contact, the dry descriptions of the mechanism of the joints will take a tangible form, and will henceforth remain impressed on the memory. For example, notwithstanding our diagrams of the movements of pronation and supination, it is only by handling the bones of the forearm that the student will be enabled to fully appreciate the marvellous mechanism by which the rotation of the radius round the ulna is effected, allowing the hand to present alternately its palmar and dorsal surface; and the same is the case in regard to the skeleton of the foot and head, and the movements of the lower jaw, &c.
The artist will find in this book some pages devoted to the facial angle, to the forms of the head, brachycephalic and dolichocephalic heads, and[xi] to some other questions of anthropology, and will doubtless thank us for having considered here ideas which are daily becoming familiar to the general public.
Our only regret concerning these anthropological studies is that the limits of this volume did not permit us to go deeper into the teachings of the anthropological laboratory, the direction of which was confided to me after the loss of our illustrious master, Broca.
I take this opportunity of expressing my gratitude to my excellent master, Professor Sappey, who allowed me to borrow from his magnificent treatise on anatomy the figures on osteology and myology which constitute the chief merit of this work; and to my friend and colleague, E. Cuyer, whose skilful pencil reproduced the figures from the photographic atlas of Duchenne, as well as the two illustrations of the Gladiator, and the sundry diagrammatic drawings which complete the theoretical explanations of the text.
M. DUVAL.
| CHAPTER | PAGE | |
|---|---|---|
| I. | Introduction to the Revised Edition | 1 |
| II. | Introduction.—Plastic Anatomy: Its History, Importance, and Objects—Order of these Studies—Division of Subject | 7 |
 —THE SKELETON, ARTICULATIONS,
PROPORTIONS. —THE SKELETON, ARTICULATIONS,
PROPORTIONS.
|
||
| III. | Osteology and Arthrology in General—Nomenclature—Vertebral Column | 19 |
| IV. | Skeleton of the Trunk (Thorax)—Sternum—Ribs—Thorax as a Whole | 41 |
| V. | Skeleton of Shoulder—Clavicle—Scapula—Head of Humerus—Shoulder Joint | 55 |
| VI. | Humerus and Elbow Joint | 67 |
| VII. | Skeleton of Fore-Arm—Radius and Ulna—Movements of Pronation and Supination | 77 |
| VIII. | Skeleton of the Hand—Wrist (Carpus)—Hand and Fingers (Metacarpal Bones and Phalanges)—Proportions of the Upper Limb—Egyptian Canon—Brachial Index | 87 |
| IX. | Skeleton of the Hips—Pelvis (Iliac Bones and Sacrum)—The Pelvis according to Sex | 103 |
| X. | The Femur and the Articulations of the Hips—Proportions of the Hips and Shoulders | 116 |
| XI. | The Femur and the Articulation of the Knee Joint; the Shape of the Region of the Knee | 131 |
| XII. | Skeleton of the Leg: Tibia and Fibula, the Malleoli or Ankles—General View of the Skeleton of the Foot; Tibio-Tarsal Articulation | 146 |
| XIII. | Skeleton of the Foot; Tarsus; Metatarsus; Toes and Fingers—Proportions of the Lower Limb—The Foot as a Common Measure | 155 |
| XIV. | Skeleton of the Head: Skull (Occipital, Parietal, Frontal, Temporal Bones); Shapes of the Skull (Dolicocephalic and Brachycephalic Heads) | 164 |
| XV. | Skeleton of the Face: The Orbital Cavities; Lower Jaw; Teeth; Facial Angle of Camper | 173 |
 —MYOLOGY. —MYOLOGY.
|
||
| XVI. | Of the Muscles in General—Muscles of the Trunk: Anterior Region (Pectoralis Major; the Oblique and Recti Muscles of the Abdomen) | 189 |
| XVII. | Muscles of the Back: Trapezius, Latissimus Dorsi, and Teres Major Muscles | 205 |
| XVIII. | Muscles of the Shoulder: Deltoid: Serratus Magnus; The Hollow and Shape of the Arm-pit | 215 |
| XIX. | Muscles of the Arm: Biceps; Coraco-Brachialis: Brachialis Anticus; Triceps; Shape of the Arm | 224 |
| XX. | Muscles of the Fore-Arm and Hand: The Anterior, External, and Posterior Superficial Muscles | 232 |
| XXI. | Muscles of the Fore-Arm and Hand (continued): The Deep Posterior Muscles of the Fore-Arm (Anatomical Snuff-Box); Muscles of the Hand | 244 |
| XXII. | Muscles of the Pelvis; the Gluteal Muscles; Fascia Lata; Muscles of the Thigh; Sartorius, Quadriceps, Adductors, &c. | 252 |
| XXIII. | Muscles of the Leg; Tendo Achillis; Muscles of the Foot | 268 |
| XXIV. | Muscles of the Neck: Sterno-Cleido-Mastoid, Infra-Hyoid, and Supra-Hyoid Muscles | 281 |
| XXV. | Muscles of the Head; Muscles of Mastication; Muscles of Expression: History (Leonardo da Vinci; Humbert de Superville; Duchenne of Boulogne, and Darwin) | 291 |
| XXVI. | Muscles of Expression; Possible and Impossible Combinations of Certain Contractions of the Muscles of the Face | 310 |
DUVAL’S
ARTISTIC ANATOMY
[1]
Artistic Anatomy
In offering instruction in anatomy to artists, one feels compelled at the outset to attempt an answer to the question: Of what use is anatomy, scientifically considered, in the training of the artist?
The artist requires to know his technique, just as an architect or an engineer needs to start with a knowledge of his materials.
Looking backward, we see that science and art have ever progressed side by side. The history of Egypt, of Greece, of the Renaissance, shows glorious traditions of art, along with a full development of learning and philosophy. The advancement of science and of art has always occurred simultaneously, and there never has been a time when they have been divorced from one another.
This is par excellence the age of technical education. There is no questioning the importance of science, or the aid the arts have received from it. We see it in architecture, in the influence of terra-cotta and steel frames; and in art, in the introduction of aniline colours.
Painting and sculpture are the earliest of the arts, and have produced some of the most cherished[2] monuments of history; and originally the chief object portrayed was the human form, in action or repose.
Let us for a moment consider to what extent art has been indebted to anatomy in the production of the masterpieces of the past.
1. Egypt.—Egypt presents the first great School of Art, as of letters and philosophy, and from Egypt knowledge and culture flowed to Greece and Italy.
The vestiges of Egyptian art extant to-day comprise for the most part statues—some of them portraits—coins, sculpture (in low relief), and flat, painted outlines. As a rule, the representations of the human form pretend to no exact representation of detail of form or expression, and for the most part are executed in a formal and stereotyped fashion.
The amount of anatomical knowledge demanded by the art of Egypt could obviously be acquired by direct observation of the nude or semi-nude figures of the living. The history of Egypt, profoundly interesting from all points of view, is of special interest to the anatomist, and centres round the mode of treatment of the dead.
Ascribed usually to a belief in the immortality of the soul, the ceremonial treatment of the body after death was elaborate, and essentially religious. The body was regarded as sacred, and the process of embalming was a religious rite, entrusted to a band of the priesthood—Charhebs or Paraschistes—and no greater detail of anatomical examination was permitted than was deemed necessary for the proper[3] preservation of the body. This band of the priesthood was moreover shunned and outcast, and yet with all these disadvantages some knowledge of anatomical structure must have been obtained.
It was only later, when Greek influence became felt, that a study of anatomy arose in the Medical School of Alexandria. Egypt was the nursing mother of medical teaching, and Alexandria was the first great medical school. Erasistratus (B.C. 285) was the first great anatomist, and he utilised condemned criminals for dissection. Herophilus, a Jew, is said to have dissected 600 bodies.
2. Greece and Rome.—The historical importance of Egyptian art and the Alexandrine School of Anatomy lies in the influence which they exerted upon the culture of Greece and Italy.
Science and art were introduced directly into Greece and Italy from Egypt. Anatomical knowledge in Greece begins with Hippocrates (B.C. 400), who studied in Egypt under Democritus of Abdara. Galen, later (A.D. 131), the great Roman physician, was a Greek by birth, and was taught his anatomy by Heraclianus at Alexandria.
Art in those days had ideals. Its aims were the perpetuation of the godlike, the heroic, the representation of perfect beauty and manly strength. Every reproduction was required to be, if possible, more beautiful than the original—virtually, as Lessing says, a law against caricature. “By no people,” says Winckelmann, “was beauty so highly esteemed as by the Greeks.”
Moreover, the Greek artist was surrounded by a crowd of witnesses, in the masterpieces of[4] sculpture, and in the living active forms of perfect manhood and womanhood. In the games there were ample opportunities for the study of the nude; and every evanescent, subtle movement could be noticed of the lithe and supple frame of the athlete.
Marked attention was given to physical culture; clothing was light, movements free, so that the environment was perfect for the purposes of the sculptor or figure-painter. Prizes were given for beauty, and the artists were the judges.
The work of the artistic anatomist of those days was superficial in a double sense. Cremation was the usual mode of burial, the anatomist dissected apes, and beyond an occasional opportunity of handling human bones, little exact anatomical knowledge was available. But from the artist’s point of view all the anatomy they needed was before their eyes. The best models procurable were before them; and an art that in some respects is perfect owes nothing to the science of anatomy.
3. The Art of the Renaissance.—Egyptian art shows knowledge of form; Greco-Roman art, knowledge of form and proportion; the art of the Renaissance reaches a higher platform, in its portrayal of movement and the expression of emotion.
Three factors combined to give the impetus to art at the time of the revival of learning. In 1315 Mondino di Luzzi made the first public demonstration of the anatomy of the human body. In 1400–1420 the process of wood-engraving, and subsequently the art of printing, were invented. Linked with these two facts, and with the general advance[5] of learning, science, and art, was the great religious revival of that period. The religious sentiment gave the keynote to the artistic pre-eminence of the old masters. Their themes were great, and the result was a grandeur and a power that no merely decorative or realistic school can ever attain.
In the 15th and 16th centuries, artists and anatomists are constantly found in association as fellow-workers and as personal friends. The great work of Andreas Vesalius on Anatomy was illustrated in an exact and artistic manner by Jan van Calcker, Titian’s favourite pupil. Leonardo da Vinci and Della Torre; Michael Angelo and Colombo; Benvenuto Cellini and Da Carpi; and other names might be cited to show the close relations of the artists and anatomists of those days.
There is little doubt that the old masters seized every opportunity of becoming acquainted with anatomical structure. Vasari used to advise his pupils to study “the antique, the nude, and dissections from nature.” Michael Angelo was in the habit of first sketching his figures in the nude condition, and afterwards clothing them with the necessary drapery. Leonardo da Vinci has left few complete pictures; but there are numerous sketches in existence (notably at Milan) in which he has drawn with precision, dissections—e.g., of the knee joint, with bones, ligaments, and muscles in proper position. Ruskin says of him: “We have in this great master a proof of the manner in which genius submits to labour in order to attain perfection.”
4. Modern Art.—For many reasons modern art is more dependent than ever upon anatomical[6] knowledge. Not to dwell upon the ennobling power of religious feeling—notably absent from modern art—the artist of the present day suffers from the plutocratic conditions of modern life, the inartistic fashions of modern dress, and the difficulty of obtaining accurate and well-formed human models; and is compelled to depend more and more upon a scientific knowledge of anatomy.
Among the old masters there is often an excessive exhibition of anatomical structure, and this is liable to occur even more in some of the work of modern artists. A little knowledge is a dangerous thing; and it is of supreme importance that the anatomical knowledge used by the painter or sculptor should be properly applied, so that form, proportion, contour, and expression may all have equal value.
It is too common, unfortunately, for present-day models to be disproportionate in form and deficient in muscular development, and the mistakes of nature are too often reproduced, in the form of defects or exaggerations, in modern sculpture and pictures. The student should seize every opportunity of studying the well-developed living nude form in action in order to obtain an adequate idea of the pattern which he desires to copy.
[7]
Anatomy in general; the anatomy of the external forms of man; physiology of the same.—Origin of the knowledge of the Greek artists of the anatomy of external forms; the influence of gymnastics upon Greek art.—The Renaissance and anatomical study: Mondino di Luzzi (1316).—The anatomical studies of Leonardo da Vinci, Michael Angelo, and Raphael.—Titian and Andreas Vesalius.—The anatomical course of the School of Painting (1648).—What the artist requires in the study of anatomy: proportions, forms (or contours), attitudes, movements.—The order of these studies; divisions of the subject.
Anatomy, as the derivation of the word indicates (from ἀνὰ, across, and τομὴ, section), is the study of the parts composing the body—muscles, bones, tendons, ligaments, various viscera, &c.—parts which we separate one from the other by dissection, in order to examine their shapes and their relations and connections.
This study may be accomplished in various ways: (1) from a philosophical and comparative point of view, by seeking the analogies and differences that the organs present in animals of different species—which is called Comparative Anatomy; (2) from a practical point of view, by seeking out the arrangement of organs, the knowledge of which is indispensable to the physician and surgeon—this is called Surgical or Topographical Anatomy; (3) by examining the nature and arrangement of the organs which determine the external forms of the body—this is Plastic Anatomy, called also the[8] Anatomy of External Forms, the Anatomy of Artists. It is the anatomy of external forms that we shall study here; but the artist ought to know not only the form of the body in repose, or in the dead subject, but also the principal changes of form in the body when in a state of activity, of movement, and of function, and should understand the causes which determine these changes. Plastic anatomy ought to be supplemented by a certain amount of knowledge of the functions of the organs, e.g., muscles and articulations; so that under the title of anatomy of the external forms of man we shall study at the same time the anatomy and the physiology of the organs which determine these forms. We should be contending for what has been long since conceded, were we to endeavour to show to what an extent the studies of anatomy and physiology are indispensable to the artist, who seeks to represent the human form under many and various types of action. Nevertheless, it may be useful to explain how the chefs-d’œuvre of ancient art have been produced with admirable anatomical exactness by men who certainly had not gone through any anatomical studies, and to show what special conditions aided them to acquire, by constant practice, the knowledge that we are obliged to seek day by day in the study of anatomy.
The Greek sculptors have reproduced the human form with marvellous anatomical exactness; in fact, the works of Phidias (the Theseus and the Ilissus), those of Myron (the Discobolus), those of Lysippus and of Praxiteles (the Sleeping Fawn), those of Agasias (the Fighting Gladiator), and other masterpieces[9] given as models in all the schools of art, are such that it is impossible to find fault with them, or to discover in them the least inexactitude, either from an anatomical or a physiological point of view;[3] in fact, not only are the muscles, for example, prominent exactly in their places, but, more than that, these prominences are differently accentuated in corresponding muscles on the different sides, according to the nature of the movement; one side will present the muscles swelled up in a state of contraction, or the muscles may be in repose—that is, relaxed and relatively flattened. At the time when these works of art were produced, the study of anatomy, or even the dissection of the human body, had not yet been attempted; the respect in which the dead body was held was such that the physicians themselves, who should have been able to justify their motives for this study, had never as yet dissected a human body. In order to supply this want of direct knowledge Hippocrates had dissected animals, and had arrived at certain conclusions by the analogy that exists between the organs of quadrupeds and those in man. Galen himself dissected monkeys only, seeking to confine his examination to animals whose anatomical construction might be considered as most closely resembling that of man. Galen never possessed a human skeleton, for in a passage in his anatomical works he states the pleasure that he[10] found in studying at last some human bones that had been deposited in a marshy place by a river which had overflowed its banks. We seem, then, to have a singular contradiction between these two facts, as we know on the one hand that the Greek artists have shown in their works a most rigorous anatomical exactitude, whilst on the other hand neither they nor their contemporary physicians and surgeons had made a study of the anatomy of man by the practice of dissection.
But this contradiction disappears altogether when we examine the conditions which permitted those artists to have constantly before their eyes the nude human body, living and in motion, and so set them to work to analyse the forms, and thus to acquire, by the observation of the mechanism of active muscular changes, a knowledge almost as precise as that which is now obtained by the accurate study of anatomy and physiology. It is sufficient, in fact, to recall to mind the extreme care the ancients gave to the development of strength, and of physical beauty, by gymnastic exercises. In Homer we see the heroes exercising themselves in racing, in quoit-throwing, and in wrestling; later we come to the exercise of the athletes who trained themselves to carry off the palm in the Olympic games; and it is evident, in spite of the ideas that we hold now respecting wrestlers and acrobats, that the profession of an athlete was considered a glorious one, as being one which not only produced a condition of physical beauty and high character, but constituted in itself a true nobility. Thus the life of the gymnast came to exercise a decisive influence[11] on Greek art. The prize of the conqueror in the Olympic games was a palm, a crown of leaves, an artistic vase; but the chief glory of all was that the statue of the victor was sculptured by the most celebrated artist of the time. Thus Phidias produced the handsome form of Pantarces, and these athletic statues form almost the only archives of the Olympiads, upon which Emeric David was able to reconstruct his Greek Chronology. From these works, which became ideals of strength and beauty, the artist had long been able to study his model, which he saw naked every day, not only before his exercises, whilst rubbing himself over with oil, but during the race, or the leaping match, which showed the muscles of the inferior extremities, or during the throwing of the quoit, which made the contractions of the muscular masses of the arm and the shoulder prominent; and during the wrestling matches, which from the infinite varieties of effort, successively brought all the muscular powers into play. Was it then surprising that the images of the gods, destitute of movement and of life, which had so long satisfied the religious sentiment of the people, were succeeded by artistic representations of man in action in statues such as could embody the idea of strength and beauty, studies of the living statues of the gymnasium? Further, we shall see the decline of art proceed side by side with the abandonment of the exercises of the gymnasium. Much later, in the Middle Ages, art awoke and embodied ideas in figures without strength and life indeed, but which nevertheless express in a marvellous manner the mysterious aspirations of the[12] period; but these have not anything in common with the realistic representation of the human form, well developed and active, as seen in Greek art. At the time of the Renaissance, artists not having any longer a living source of study in athletic sports, recognised the necessity of seeking for more precise knowledge in the anatomical study of the human body, in addition to the inspiration drawn from the study of the antique, and thus we see that the revival of the plastic arts occurred simultaneously with the introduction of the practice of dissection. This was not brought about without some difficulty.

Fig. 1.
Reproduction of a drawing of an anatomical study by Leonardo da Vinci. (Choulant’s work, page 8.) This design represents the minute dissection of the muscles of the lateral region of the neck and trunk.]
In the year 1230, Frederic II., Emperor of Germany, and King of the Two Sicilies, passed a law prohibiting the practice of medicine without the practitioners having first studied the anatomy of the human body. In spite of two papal excommunications hurled against the author of this edict, dissections were henceforth regularly pursued in Italy; and one century later—in the year 1316—Mondino di Luzzi was able to write the first treatise on human anatomy, containing descriptions made from studies of the dead body. This treatise was printed in 1478. Artists rivalled physicians in the ardour with which they pursued their anatomical studies; and it may be said that all the painters and sculptors in the fifteenth century gave most careful attention to dissection, or at least studied demonstrations made upon the dead body, for all have left, amongst their drawings, studies that leave no doubt on this head. Among the great masters it may be noted that Leonardo da Vinci (14521519)[13] left thirteen portfolios of various drawings and studies, among which are numerous anatomical studies of remarkable fidelity. The greater number of these were taken from Milan by the French in 1796, and afterwards they were in part restored to Italy; some of them, however, went to enrich the British Museum in London, and were published by[14] Chamberlain.[4] In Fig. 1 is reproduced one of these anatomical drawings. It shows with what care—perhaps with over-scrupulous care—the illustrious master endeavoured to separate by dissection the various fasciculi of pectoral muscle, deltoid, and sterno-cleido-mastoid. It may be noted also that in his Treatise on Painting, Leonardo da Vinci devotes numerous chapters to the description of the muscles of the body, the joints of the limbs and of the “cords and small tendons which meet together when the muscles contract to produce its action,” &c.; and finally, in this same Treatise on Painting, he makes allusion at different times to a Treatise on Anatomy, which he intended to publish, and for which he had gathered together numerous notes. These are fortunately preserved in the Royal Library at Windsor.
Michael Angelo also (1475–1564) made at Florence many laborious studies of dissection, and left among his drawings beautiful illustrations of anatomy, of which several have been published in Choulant’s work, and by Seroux d’Agincourt.[5] Finally, we have numerous drawings by Raphael himself, as proof of his anatomical researches, among which we ought to mention, as particularly remarkable, a study of the skeleton intended to give him the exact indication of the direction of the limbs and the position of the joints for a figure of the swooning[15] Virgin in his painting of the Entombment (Choulant, p. 15). We cannot end this short enumeration without quoting further the names of Titian and Andreas Vesalius, in order to show into what intimate relations artists and anatomists were brought by their common studies. Titian, in fact, is considered the real author of the admirable figures which illustrate the work—“De Humani Corporis Fabrica”—of the immortal anatomist, Andreas Vesalius, justly styled the restorer of anatomy. It is necessary, however, to add that though some of the drawings are by Titian, the greater number were executed by his pupil, Jan van Calcker, as is pointed out in the preface to the edition of the work published at Basle in 1543.
The renaissance of the plastic arts and that of anatomy were therefore simultaneous, and closely bound up one with the other; ever since that time it has been generally recognised that it is necessary to get by anatomical study that knowledge of form which the Greeks found themselves able to embody in consequence of the opportunities they had of studying the human figure in the incessant exercises of the gymnasium. Again, in 1648, when Louis XIV. founded at Paris the Académie de Peinture et de Sculpture, which later on took the title of the École des Beaux-Arts, two sections of study were instituted side by side with the studios properly so called, for imparting to the pupils instruction considered as fundamental, and indispensable to the practice of art. These were the sections of perspective and anatomy.
It is not our place to plead, otherwise than by[16] the preceding historical considerations, the cause of anatomy in its relation to painting and sculpture; but we ought at least to examine what method is likely to prove the most useful for its study. If each anatomical detail does not correspond to an artistic need we are liable in following any treatise written with other than an artistic aim to be entangled in superfluous names and useless descriptions; while at the same time we might neglect details which are to the artist of great importance, although considered of secondary value by authors who have written especially for students in medicine.
We ought, then, to ask ourselves, in the first place, what are the ideas that the artist should seek for in his study of anatomy? To this question all will reply that the ideas of proportion, of form, of attitudes and movements are those in which anatomy is relied upon to furnish precise rules; and as the expression of the emotions, either in painting or sculpture, cannot be reproduced except by various changes in the general attitude of the body, and in the special mechanism of the physiognomy moved by the muscles, we must conclude that our study should deal not only with proportions, form, attitudes and movements, but also with the expression of the emotions and passions. This, then, is the object to be attained. Suppose we try to accomplish it by examining in a first series of studies all that belongs to proportions; afterwards, in a second series, all that has relation to form; in a third, attitudes, &c. Such an order of proceeding, logical though it be, will have the disadvantage[17] of causing numerous repetitions, and the more serious inconvenience of artificially separating parts which in the structure of the body are intimately connected. Thus, form is determined sometimes by osseous prominences, sometimes by the soft parts, which may be muscular or tendinous. Attitudes are determined by the muscles; but these are subject to laws which result from the position and action of the joints; so with movements in the expression of which it is necessary to consider, at the same time, what the conformation of the osseous levers (the direction of the bones and their articulation) allows, as well as that which the muscles accomplish, also the direction of the muscles and the differences of shape produced by their swelling and tension in action, as well as when the antagonistic muscles are relaxed. Proportions themselves cannot be defined without an exact knowledge of the skeleton, for it is the bones alone which furnish us with the landmarks from which to take measurements. A knowledge of the bones and of their articular mechanism is indispensable to us, that we may guard ourselves against being deceived in certain apparent changes of length in the limbs when certain movements take place.
We see, then, that all the ideas previously enumerated as to proportion, form, attitude, movement, depend on the study of the skeleton and muscles. It will thus be easiest and most advantageous to proceed in the following manner:—We will first of all study the skeleton, which will teach us the direction of the axis of each part of the limbs, the[18] relative lengths and proportions of these portions, and the osseous parts which remain uncovered by the muscles, and show beneath the skin the shape and the mechanism of the articulations in their relation to movements and attitudes. We shall then study the muscles, and endeavour to know their shapes, at the same time that, we complete the knowledge we shall have acquired of attitudes and movements. In the third place, we will attempt the analysis of the expression of the passions and emotions; and the study of the muscles of the face, of which the mechanism in the movements of the physiognomy is so special that it would be inconvenient to attempt to treat it with that of the muscles of the trunk and limbs.
[19]
THE SKELETON, ARTICULATIONS, PROPORTIONS.
Osteology and Arthrology.—Anatomical nomenclature: median line; lateral parts; the meaning of terms.—Of the bones in general: long bones (shafts and extremities); flat bones (surfaces, borders); short bones.—Prominences (processes, spines); cavities and depressions of bone (fossæ, grooves).—Bone and cartilage.—The axial skeleton: the vertebral column.—The vertebræ (bodies, transverse processes, spinous processes, &c.).—Cervical, Dorsal, Lumbar vertebræ.—Articulations of the vertebræ.—Movements of the spine.—Movements of the head (atlas and axis).—The curves of the vertebral column.—Relation of the vertebral column to the surface.—Proportions of the parts of the spine.
It is not necessary to emphasise further the importance of a study of the skeleton. By its means we obtain a knowledge of form and proportions; by a study of the several articulations we become acquainted with the complex mechanism by which the whole is knit together, and by which the movements of the various parts of the body occur. Further, the relations of the skeleton to the surface forms of different parts of the body are of fundamental importance. The science of Osteology is the study of bones (ὀστέον, bone; λόγος, description); Arthrology is the study of joints (ἅρθρον, a joint):[22] Myology is the study of muscles (μυς; λογος). The bones are the levers of movement: the articulations represent the fixed points or fulcra of these levers; while the powers which produce motion are represented by the muscles.
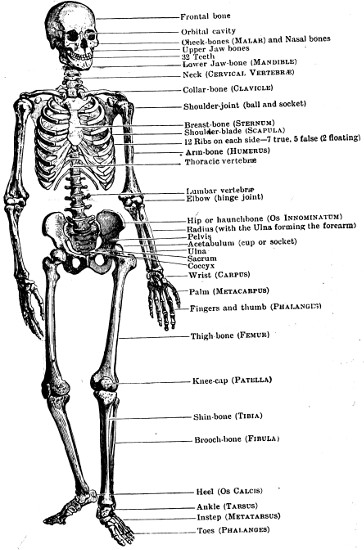
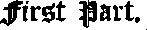
Fig. 2.
Front View of the Skeleton.
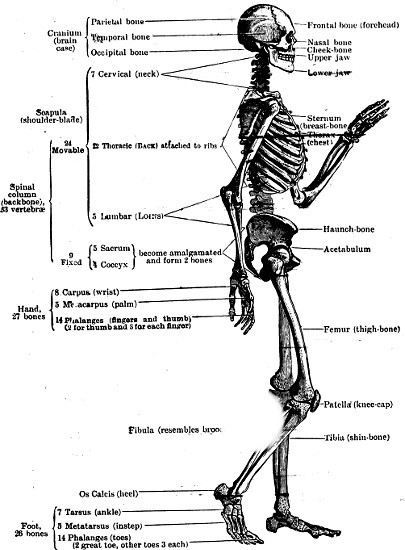
Fig. 3.
Side View of the Skeleton.
Before describing in detail the different parts of the skeleton, it is necessary to consider the method of nomenclature, so that by the employment of proper terms the subsequent descriptions may be more intelligible.
Nomenclature.—In the description of the bones, as of other organs, we have to consider the relation of the portion under consideration to the rest of the body. The figure is always regarded as occupying the erect position, with the face, the palms of the hands, and the toes directed forward. Thus each bone, as well as the other organs or parts, will be found under one or other of two different conditions: either it is median in position, and a vertical plane passing through the longitudinal axis of the body divides it into two similar segments; or else it is lateral in position, and situated outside this median plane. As a type of the first class, we will take the sternum, or breast-bone (see Fig. 11, p. 42). This is a central single bone; it has no fellow, and is composed of two symmetrical portions, one part on the right and one part on the left. As a type of the second class, we will take the humerus (Fig. 18, p. 60), which is a bone situated at the side and one of a pair, inasmuch as there are two, one on the right and one on the left of the median plane. From these two examples it is easy to understand that for the description of each single[23] and symmetrical bone it will be necessary to speak of anterior parts or surfaces directed towards the front of the body, of posterior parts (directed backwards), of lateral portions (right and left), and finally, of parts superior and inferior, looking upwards and downwards (in the case of the sternum a superior and inferior extremity): on the other hand, in the description of a paired and non-symmetrical bone, we shall also have to speak as heretofore of parts superior and inferior, anterior and posterior; but instead of two similar symmetrical portions, one on each side of an imaginary line, it has two dissimilar halves, of which the one looking towards the median plane—towards the axis of the body—is called the internal part, and the other, looking to the outer side (as away from the axis), is called the external part. It is necessary, for brevity and accuracy, to clearly comprehend the meaning of these terms in descriptive anatomy (anterior and posterior, internal and external, superior and inferior) which serve to show the relation of the parts to the skeleton as a whole.
After this first division of bones into single and median, and into double and lateral, if we glance at the skeleton (Figs. 2, 3), it seems at first sight that the various bones present an infinite variety of shape, and defy classification or nomenclature; careful attention, however, will show us that they may be all included in one of the following three classes—viz., long bones, flat or broad bones, and short bones.
Fig. 4.
The Complete Skeleton (in the attitude of “The Fighting Gladiator” of Agasias).
The long bones, which usually act as the axes of the limbs (e.g., the humerus, femur, tibia, &c.),[24] are composed of a central portion, cylindrical or prismatic in shape, called the body, shaft, or diaphysis (διαφύω, to be between), and of two extremities or epiphyses (ἐπιφύω, to be at the end), usually marked by protuberances and articular surfaces. The flat bones (e.g., the shoulder-blade and the hip bone) are formed of osseous plates, on which are various surfaces, borders, and angles.[25] Finally, the small bones, which are found in the vertebral column and in the extremities of the limbs, the hand and foot (carpus and tarsus), present a diversity of form in which cylindrical, cubical, and wedge-like shapes can be made out.
Whether the bone be long, flat, or short, it presents prominences and depressions. The projecting portions of bone are called by various names—tuberosities, protuberances, processes, apophyses, crests, spines, tubercles. To some of these names is added an adjective, which shows, more or less exactly, the form of the process or projection. Thus we speak of a spinous process, mastoid process (μαστὸς, a nipple; εἶδος, form), styloid process, &c. The depressions upon the bones are called by various names—fossa, groove, foramen, sinus, canal, notch, cavity, &c. To these also are added names which indicate their shape, as the digital fossa, from its resemblance to the imprint of a finger; the glenoid cavity (γλήνη, cavity), the cotyloid cavity (χοτύλη, a basin); but more frequently still, the added adjective bears allusion to a connection of the cavity with certain organs, as the bicipital groove, that which contains the tendon of the biceps, or the canine fossa, in relation to the root of the canine tooth.
Structure of Bone.—Bone is characterised by its density, toughness and elasticity. If a long bone, such as the femur, is sawn in two lengthwise, its extremities are found to be composed of a delicate network of cancellous, or spongy bone, in the interstices of which marrow and blood are contained during life; the shaft of the bone is composed,[26] for the most part, of a cylindrical tube of dense, ivory-like compact bone, which encloses the hollow medullary canal of the bone, also filled with marrow during life. The dense bone of the shaft is continuous with a thin sheet of hard bone, which covers over the spongy bone of the extremities.
In the case of the flat and short bones, the structure is like that of the extremities of the long bones. The mass of the bone is composed of cancellous tissue, with a surrounding thinner envelope of compact bone.
If a bone is burnt, it loses one-third in weight, becomes brittle, and loses its organic constituents, retaining its inorganic materials—chiefly calcium phosphate and calcium carbonate. If it is subjected to prolonged soaking in an acid such as hydrochloric acid, its inorganic salts are removed, it becomes soft and pliable, it loses two-thirds of its weight and retains only its organic materials—connective tissues. These in boiling produce glue.
In certain situations bone is found in conjunction with a substance which differs from it in its elasticity, its want of rigidity (it is soft enough to be divided by the scalpel), and in its translucent colour. This substance is known by the name of cartilage. Thus the curved bones termed ribs are prolonged at their anterior extremities by a portion called the costal cartilage, which presents the same form as the ribs properly so called. The bones forming the freely movable joints (like the shoulder, hip and knee joints) are capped by thin layers of hyaline articular cartilage, which forms a pliant elastic cushion in relation to the articulation.
[27]
Most of the bones, at the commencement of their formation, are constructed solely of cartilage, which is gradually transformed into bone as the animal grows by the deposition in it of lime salts; and this transformation of primitive cartilage into bone may be more or less complete according to the species or age of the animal. With advancing age the bones tend to become more and more calcified. Thus we find that in the skeletons of old people the costal and other cartilages may be more or less ossified.
The Subdivisions of the Skeleton.—The human skeleton is characterised by peculiarities due to the assumption of the erect position, the high development of the brain, and the possession of extraordinary manual dexterity. All these factors leave their impress on the bones of the skeleton, as may be seen by comparing the human skeleton with that of such a quadruped as the dog.
The skeleton is subdivided into axial and appendicular parts. The axial skeleton includes the vertebral column, ribs and sternum, and the bones of the cranium and face. The appendicular skeleton comprises the bones of the limbs. In the following pages, for convenience of description, an account will be given of the vertebral column, sternum, and ribs first; of the limbs second; reserving to the last the account of the skeleton of the cranium and face.
The Vertebral Column.—The vertebral column (Figs. 5, 8) is composed of a number of bones named vertebræ, superimposed on one another, and partially separated from one another by a series of intervertebral[28] discs. The column is subdivided into groups of vertebræ, by reason of its connections with other parts of the axial skeleton, or with the skeleton of the limbs.
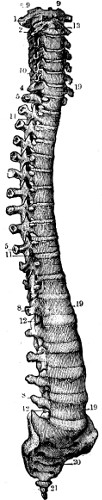
Fig. 5.
The Vertebral Column (antero-lateral aspect).—1, the first cervical vertebra (atlas);—9, 9, its occipital articulating surfaces;—2, the second cervical vertebra, or axis;—13, its body;—4, seventh cervical;—5, 5, transverse processes of the ten first thoracic vertebræ;—8, 8, transverse processes of the lumbar vertebræ;—10, 11, 12, articular processes;—19, 19, bodies of the lumbar vertebræ;—20, the sacrum;—21, the coccyx.
The head is poised on the upper end of the column, and causes the peculiarities, to be described later, in the first two vertebræ (atlas and axis). The attachment of the ribs to the sides of the vertebral column causes the separation of three regions: (1) cervical, belonging to the neck, and comprising seven vertebræ; (2) thoracic (or dorsal), belonging to the thorax, or chest, and comprising twelve vertebræ; and (3) lumbar, belonging to the loin, and comprising five vertebræ. The attachment of the hip bones to the sides of the succeeding vertebræ leads to the fusion of the next five vertebræ together, under the name of the os sacrum, which will be described along with the hip bone and pelvis. Finally, below the sacrum are four small, rudimentary vertebræ, known as the coccyx, forming the attenuated remains of a caudal appendage.
[29]
There are thus, altogether, normally thirty-three vertebræ: seven cervical, twelve thoracic, five lumbar (constituting together twenty-four movable vertebræ); five sacral, and four coccygeal vertebræ (constituting nine fixed vertebræ, which help to form the pelvic basin).
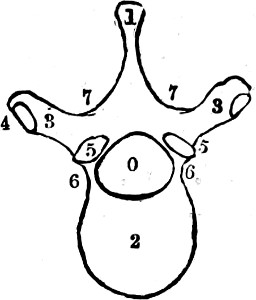
Fig. 6.
Outline of a Vertebra (upper surface).—0, vertebral foramen;—1, spinous process;—2, body of vertebra;—3, 3, transverse process with articulating facets (4, 4) for the tuberosity of the rib (see p. 30);—5, 5, superior articular processes;—6, 6, the parts which connect the body with the base of the transverse and articular processes;—7, 7, vertebral laminæ.
The vertebral column is intended not only to form an axis for the rest of the skeleton, but also to serve as an attachment, direct or indirect, for all the other bony structures; it also forms a bony canal, within which the spinal marrow is contained. It is for this reason that each of the pieces which compose it, called a vertebra, is a sort of bony ring (Fig. 6). The anterior portion of the ring is very thick, representing the segment of a cylinder, and is called the body of the vertebra (2, Fig. 6); and the vertebral column, considered as the median column of support, is essentially constituted by the superposition of these vertebral bodies upon one another, separated by the intervertebral discs. Behind each vertebral body is an arch, the neural arch, which encloses the neural ring. The spinal or neural canal is formed by the combination and connection together of the neural rings. Each neural arch is comparatively slender, but it gives origin to certain projections or processes, three in[30] number, on each side, of which one directed transversely outwards is called the transverse process (3, Fig. 6). In the thoracic region these give partial attachment to the ribs. The other two—directed more or less vertically, one above, the other below—are called the articular processes, superior and inferior. These serve for uniting together the arches of adjoining vertebræ (5, 5, Fig. 6). Finally, the posterior portion of the neural arch is prolonged backwards as a protuberance, more or less pointed, called the spinous process (1, Fig. 6).
Such are the most important parts which we find in each vertebra, but they present particular characters according to the region to which each vertebra belongs. The description of the sacrum and the coccyx, which are formed of vertebræ welded together, and articulating with the hip bones, will be given with that of the pelvis.
The more important features of the movable vertebræ which contribute to give to the whole column its general form are: (1) the size, particularly of the bodies, of the vertebræ; and (2) the characters of the transverse processes. The bodies of the vertebræ are smallest in the upper thoracic region, and increase in size upwards and downwards from the fourth thoracic vertebra. The bodies are largest and most prominent in the loin; in the neck the vertebræ are broad in the transverse diameter, but their antero-posterior diameters are less. The vertebral column is weakest in the upper thoracic and upper lumbar regions, and most mobile in the neck and thorax. Rotary power in the loin[32] is practically prevented by the shape of the lumbar articular processes, which interlock the vertebral arches in this region.
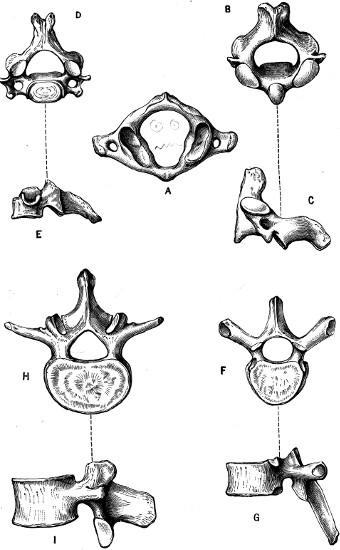
Fig. 7.
The Movable Vertebræ.—A, atlas (upper surface); B C, axis; D E, cervical vertebra; F G, thoracic vertebra; H I, lumbar vertebra.
The spinous processes of the vertebræ, which project more or less obviously in the middle line beneath the skin in different regions, in the cervical region are short and bifid; in the thoracic region they are long, sloped downwards, and “bayonet-shaped”; in the lumbar region they are directed straight backwards, and are “hatchet-shaped.”
Besides these general characters in each region there are certain vertebræ which demand special mention owing to the peculiarities of their shape. These are the first two and the last cervical.
The first cervical vertebra (Fig. 7, A), called the Atlas, because as directly supporting the head, it has been compared to the giant Atlas, supposed by the ancients to support the heavens, is a bony ring with only transverse processes, and on the upper and lower aspects of its lateral portion, two pairs of articular surfaces; the superior articular surfaces are hollow oval surfaces which articulate with the convex condyles of the occipital bone; and by the occipito-atlantoid joints provide for flexion and extension of the head on the spinal column. The inferior articular surfaces are flat and directed downwards to articulate with the axis and form the atlanto-axial joint, which is responsible for the movement from side to side of the head upon the trunk. The axis, or second vertebra (Fig. 7, B C), is so called from the presence on the upper surface of its body of a tooth-like process, the odontoid process (ὀδοὺς, tooth; ἔιδος, form), which projects upwards in an osseofibrous[33] ring formed by a transverse ligament in the anterior part of the ring of the atlas. Ligaments extend from this process to the occipital bone, and it forms a pivot round which the head and the atlas move in the lateral movements of the head upon the spinal column.
In nodding the head the movement occurs primarily at the occipito-atlantoid joint; in shaking the head, the chief movement is between the atlas and axis. These functions, of no moment in the production of surface forms, are of too great an importance in respect of the articulations of the head and trunk to be omitted here.

Fig. 8.
Vertebral Column (lateral view).—1 to 7, bodies of cervical vertebræ;—8 to 19, bodies of thoracic vertebræ;—20 to 24, bodies of lumbar vertebræ;—A, A, spinous processes;—B, B, articular surfaces of transverse processes for the tuberosities of the ribs;—C, auricular surface of sacrum.
The seventh cervical vertebra, or vertebra prominens, is so called because of the extraordinary length of its spinous process, which, except in very stout people, forms a projection easily visible beneath the skin; and this projection is also[34] more conspicuous as it corresponds to that part of the neck where the trapezius muscle, represented only by a fibrous layer—not fleshy—forms a flat surface at the back of the neck. In the centre of this surface the projection of the seventh cervical spine appears on the level of a transverse line passing through the superior border of the shoulder (see Fig. 3). It may be observed that when the model bends the head forward the spinous process of the seventh cervical becomes very prominent. It should also be noted that in the majority of cases the spinous processes of the sixth cervical and first thoracic vertebræ also give rise to superficial projections above and below that produced by the vertebra prominens.
We have been disconnecting the vertebræ in order to account for the construction of the vertebral column; we must next see how the different vertebræ are placed one upon the other—how they articulate in such a manner as to form a column, not rigid, but elastic and curved. The vertebræ are placed one on each other so that the inferior articular processes of one fit exactly on to the superior articular processes of the next beneath, and thus throughout the series we see (Fig. 8) that the bodies of the vertebræ are not in contact one with the other, the space which separates them being filled in the living subject by elastic fibrous discs. These intervertebral discs are very thick in the lumbar region, and become thinner in proportion as we ascend to the superior dorsal and cervical regions. They are thicker in the cervical and lumbar regions than in the thorax; and taken[35] together they form one-seventh of the length of the spinal column. Being compressible and elastic, these fibrous discs give to the column, formed by the placing one on another of the bodies of the vertebræ, a certain degree of flexibility, whereas a column formed of bone alone would have been quite rigid.
In addition to the intervertebral discs, a series of ligaments which join together the posterior portions of the neural arches (laminæ) is of great importance. Composed of yellow elastic tissue to a large extent, they are known as the ligamenta subflava. They consist of two short bands placed on each side of the root of the spinous process, uniting the inferior border of the lamina of one vertebra with the superior border of the lamina situated next below it.
The yellow or elastic tissue which composes these ligaments is similar to a piece of india-rubber; it is elastic—that is to say, it is able to stretch, and to return again by its own reaction to its original size when the cause which extended it has ceased to act: so that each movement of flexion of the column in front results in moving the vertebræ on one another, at the same time stretching these elastic ligaments. When the anterior muscles of the trunk which accomplish this flexion cease to contract, it is not necessary, in order to straighten the column, that the posterior muscles of the back should come into play; the elasticity of the ligamenta subflava suffices for this, as they return to their original dimensions and draw together the vertebral laminæ. We may say, then, that there is at the posterior[36] portion of the column within each vertebra a pair of small springs which keeps the column erect, so that the erect attitude of the trunk is maintained simply by the presence of the elastic ligaments; although more is required when a man supports upon his back any extra weight or burden.
The Ligamentum Nuchæ (paxwax) is a large and powerful ligament composed of yellow elastic tissue. It is highly developed in quadrupeds, and is attached between the spinous processes of the cervical vertebræ and the occipital crest, a vertical ridge on the back of the skull. In man it is a rudimentary structure (as the head is poised on top of the vertebral column) and forms a membranous partition separating and giving partial attachment to the muscles of either side at the back of the neck.
Curves of the Vertebral Column.—The vertebral column is subject to a slight lateral curvature, generally towards the right side. Its chief curves, however, are antero-posterior, and are four in number (Fig. 8): two, the thoracic and sacral curves, concave forwards, are primitive embryonic curves; two, cervical and lumbar, convex forwards, are secondary in their origin. The convexity forwards of the cervical region is to be connected with the raising upwards of the head on the trunk; the convex lumbar curve is due to the straightening of the lower limb, which in the course of development is brought into line with the vertebral axis.
These curves (except the pelvic or sacral curve) are to be associated with a difference in the thickness in front and behind of the vertebral bodies,[37] and of the intervertebral discs in the different regions of the spine.
In most animals the vertebral column has but two curves, one the cervical curve, which is convex inferiorly, the other the dorso-lumbar, which is concave inferiorly.
We have now to examine the influence that the vertebral column has in moulding the external form of the body, and to see if the length of the column can be made use of for a system of proportion.
It is evident, in the first place, that the posterior portions of the vertebræ only can affect the outline of the body, the anterior portions, the bodies of the vertebræ, being deeply hidden in the cavity of the thorax and abdomen. Therefore, in the skeleton the posterior surface of the vertebral column (Fig. 9) presents itself under the aspect of a median crest, formed by a series of spinous processes, the spinal crest, on each side of which is a groove bounded laterally by the series of transverse processes (the vertebral furrow). In the living subject these grooves are filled up by powerful and thick muscles, which project in such a manner that in the erect position the back presents a furrow in the median line bounded on each side by these muscles, at the bottom of which furrow the bony structure of the vertebral column is shown only by a series of projections placed one beneath the other, like the beads of a necklace, each one being formed by the summit or free extremity of a spinous process. These projections are well seen in the thoracic region, in which the curvature of the column is convex backwards, and they show themselves still[38] more clearly when the subject bends forward, and thereby increases this curvature. They are not visible in the cervical region, where the ligamentum nuchæ projects to the surface, and a bed of powerful muscles covers them; but we have seen that the seventh cervical, or vertebra prominens—along with the sixth also in many cases—is remarkable for the projection which its spinous process makes. Finally, in the lumbar region these projections are but little marked, the spinous processes here being short and terminated not by points, but by straight borders (Fig. 8).

Fig. 9.
Vertebral Column (posterior view).—1, 1, cervical transverse processes;—2, 2, thoracic transverse processes;—3, 3, lumbar transverse processes;—7, 8, 9, 10, spinous processes;—11, 11, articular surfaces for occipital bone of skull;—12, odontoid process of the axis;—13, 14, sacrum and coccyx.
The measurements of the vertebral column are useful, on the one hand, as absolute measurements of length and height, and, on the other hand, in giving the ratio of its length to the stature of the subject. The height of the vertebral column in the average adult man is from twenty-three to twenty-four inches, being five for the cervical region, eleven for the thoracic, and seven inches for the lumbar region. But as the length of the vertebral column does not serve as a common[39] measure for the total height of the body or for its different parts, it cannot be used as the basis of a system of proportion. A German zoologist, Carus, has advanced the idea that the length of the column forms one third of the height; but this proposition is not exact. On the other hand, it is not easy to measure the column from the atlas as far as the last lumbar vertebra,[40] without taking account of the sacrum and coccyx. It will be more frequently found that the length of the trunk, from the superior limit of the thorax to the inferior limit of the pelvis, gives a measurement more easy to take, and more useful for comparing the general proportions of the body.
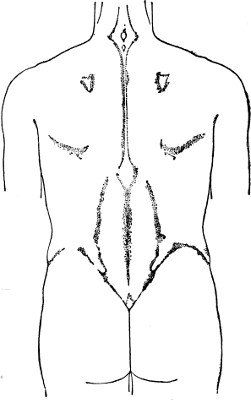
Fig. 10.
Outline of the Back and Shoulders.
It is enough to say here that the proportion of the vertebral column to the height varies according to age and sex, and according as the stature of the individual is very great or very little; the vertebral column is, in fact, in comparison with the height, longer in the infant and in the female than in the adult male; it is also much longer in proportion to the height in subjects of short stature than in tall people. The cause of difference of stature between men and women, infants and adults, long people and short, is principally due to the length of the lower extremities—a question which will be dealt with in a subsequent chapter.
[41]
The Sternum: its three portions—manubrium, gladiolus, xiphoid appendage; position and direction of the sternum; its dimensions, absolute and relative.—The ribs; the true ribs, the false and floating ribs; the obliquity and curvature of the ribs.—Of the thorax in general; its posterior aspect, anterior aspect, and base.
We have already seen that that portion of the vertebral column which is formed by the seven cervical vertebræ is free, and forms of itself the bony structure of the neck. It is the same in the lumbar region, where the five vertebræ alone form the bony structure of the abdomen. The twelve thoracic vertebræ, however, corresponding to the upper two-thirds of the trunk, are in connection with the ribs and sternum, and constitute with these bones the osseous frame-work of the thorax.
The Sternum.—In the front part of the thorax is the sternum, a bone in the middle line, single and symmetrical (Fig. 11). This bone is, in quadrupeds, formed of a considerable number of separate bones jointed together in a linear series. In the human subject it consists of three separate parts, one superior, one in the middle, and one inferior, known respectively as the pre-sternum, meso-sternum, and meta-sternum. The whole bone has been compared in shape to a short Roman sword, of which the pre-sternum represents the handle,[42] or manubrium; the meso-sternum, the longest piece, is the body, or gladiolus; and the meta-sternum, the pointed extremity of the sword, and usually tipped with cartilage, is the ensiform or xiphoid cartilage. Thus constituted, the sternum presents for our consideration an anterior surface, a posterior surface, two lateral borders, an upper and a lower extremity.
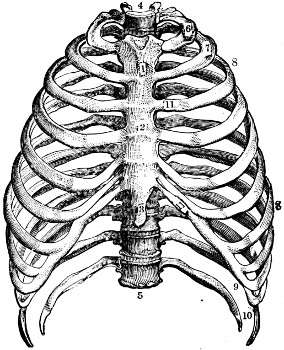
Fig. 11.
Thorax (anterior view).—1, pre-sternum, or manubrium of sternum;—2, meso-sternum, or body;—3, meta-sternum, or xiphoid appendage;—4, body of first thoracic vertebra;—5, twelfth thoracic vertebra;—6 and 7, first and second ribs;—8, 8, the true or sternal ribs;—9, 10, the floating ribs;—11, costal cartilages.
The anterior surface is smooth, but the union of the manubrium with the body of the sternum is marked by a prominent transverse ridge (sternal angle), due to the difference in direction of the[43] two pieces at their junction. This projecting angle is very remarkable in some subjects, and gives a clearly marked convex shape to the superior portion of the anterior surface of the thorax. The posterior surface of the bone, which it is not necessary for artists to study, is generally flat, and presents a returning angle corresponding to the projecting angle of the anterior surface.
The superior extremity of the sternum, forming the broader portion of the bone, is marked by three notches, or depressions: two lateral, one on each side, articulating with the inner end of the clavicle, and one in the middle called the suprasternal, or episternal, notch. This notch, which is easily discerned on the living model, forms the inferior border of the deep depression situated at the lower part of the front of the neck. Its depth is still further increased by the inner ends of the clavicles and by the sterno-cleido-mastoid muscles on either side.
The inferior extremity of the sternum is formed by the meta-sternum, or xiphoid appendage, which remains very frequently in the cartilaginous state, in the form of a plate, thin and tapering. In shape and direction it is very variable, being sometimes pointed, rounded, or bifurcated. It may be situated in a plane corresponding to that of the body of the sternum, or it may be placed obliquely or project forwards or backwards. In a case where it projects in front it may cause a slight elevation of the skin of the region of the pit of the stomach, or epigastrium; but it is a detail of form so irregular that it is not worth reproducing, except in the[44] representation of violent muscular exertion or extreme attenuation.
The lateral borders of the sternum are not vertical, but concave. The sternum is narrowest at the manubrio-sternal junction, the manubrium increasing in size towards its upper end, and the gladiolus, or body of the bone, enlarging towards its inferior part. Each lateral border is marked by seven small notches, or depressions, for the reception of the anterior extremity of each of the cartilages of the first seven ribs. The highest of these depressions is situated on the border of the manubrium just below the clavicular articular surface; the second depression is situated opposite the manubrio-sternal junction, partly on the pre-sternum, partly on the meso-sternum; those following are situated on the edge of the body of the bone, or meso-sternum, and the spaces between the depressions become smaller as they approach its lower extremity, so that the last depressions for the sixth and seventh costal cartilages are almost fused into one. The seventh costal cartilage is usually attached opposite the sterno-xiphoid junction, and is thus connected with both meso-sternum and meta-sternum.
It is necessary also to determine the exact position and direction of the sternum in relation to the other parts of the thorax, in the complete skeleton. The direction of the sternum is not vertical, but very oblique; it forms an angle of fifteen to twenty degrees, with a vertical line passing through the inferior extremity (Fig. 12), and an angle of severity to seventy-five[45] degrees, with a horizontal line passing through the same extremity (Fig. 12). The manubrium is more oblique than the body of the sternum, and the body of the sternum than the xiphoid cartilage. Such is the direction of the sternum in the male; in the female it is less oblique, and approaches the vertical—a disposition which artists are prone to exaggerate by giving a more rounded form to the superior portion of the thorax in the female.
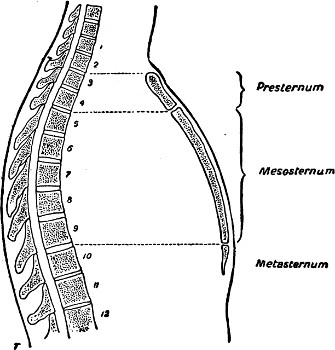
Fig. 12.
Relations of the Sternum to the Vertebral Column.
To compare the relations of the sternum with the rest of the thorax, it is necessary further to determine the level of the parts corresponding to the two extremities in relation to the vertebral column. The upper end of the sternum does not correspond to the first thoracic vertebra, but rather to the disc which separates the second and third, so that the horizontal plane passing through the superior extremity of the sternum strikes the second thoracic vertebra at its lower part (Fig. 12). The horizontal plane passing through the lower end of[46] the sternum strikes the tenth thoracic vertebra; so that, viewing the thorax in profile, the sternum is seen to project between the second and eleventh vertebræ. The exact level of the bone varies with the movements of the chest wall in respiration.
The average length of the sternum in the adult man is eight inches. The pre-sternum, or manubrium, is usually about half as long as the meso-sternum, or body of the bone.
The most important measurement, however, is the length of the sternum without the xiphoid appendage. A measurement equivalent to the length of the sternum is found in various parts of the skeleton, which for the most part are adjacent to the sternum, and the sternal length may be taken as a common measure for constructing a correctly proportioned torso.
As a fact, this measure of the length of the manubrium and body of the sternum is equal to (1) the clavicle, to (2) the vertebral border of the shoulder-blade, and to (3) the distance which separates the two shoulder-blades in the figure when the arms are hanging by the side; further, the length of the sternum is equal to (4) the length of the hand without the third phalanx of the middle finger.
The Ribs.—The thoracic part of the vertebral column and the sternum being known, it is easy to understand the arrangement of the parts which complete the thorax. These parts are the ribs and costal cartilages, arranged somewhat like the hoops of a cask, proceeding from the vertebral column to the sides of the sternum; the ribs articulate posteriorly with the vertebral column, and are connected[47] anteriorly to the sternum or to one another by the costal cartilages. The ribs are twelve in number on each side. They are known as first, second, and third ribs, etc., counting from above downwards; the first seven are the true ribs, or sternal ribs, which have their costal cartilages directly joined to the sternum; the next three (eighth, ninth, and tenth) ribs are the vertebro-costal ribs, as the costal cartilage of each articulates with the cartilage of the preceding rib; the last two, the eleventh and twelfth, are the false, floating or vertebral ribs: they are remarkable for their shortness; they are provided at their extremities with only rudimentary cartilages, which are pointed, and project by free extremities among the muscles of the walls of the abdomen.
In a general sense the ribs are long bones, presenting an external surface and an internal surface, a superior border and an inferior border. They are not horizontal, but oblique, from above downwards and from behind forwards: so that the anterior extremity of a rib is always placed on a lower level than its posterior extremity.
A typical rib possesses three curves. It is bent from behind forwards in a downward direction; it is bent like the hoop of a cask in order to surround the thorax, and presents, therefore, a curve similar to that of a scroll, of which the convexity is turned outwards and the concavity inwards; and, again, it is twisted upon itself as if the anterior extremity had been forcibly carried inwards by a movement of rotation upon its own axis. This curvature of torsion makes the surface, which is really external[48] in the central portion of the rib, become a superior surface in the anterior portion. In order to have a good idea of the torsion of the ribs it is necessary to take a single rib and place it on a horizontal surface, such as a table; it will be then seen that, instead of its being in contact through its entire extent with the flat surface, it touches it only at two points, as if it formed a half-hoop of a cask to which a slight spiral twist had been given.
The ribs vary much in length, in order to correspond to the ovoid shape of the thorax; their length increases from the first to the eighth, which is the longest, and corresponds to the largest part of the thorax; and it gradually diminishes from the eighth to the twelfth.
A typical rib (Fig. 13) consists of the following portions, an indication of which is useful for the study of the shape of the thorax. The posterior extremity is slightly raised, and constitutes the head of the rib. It is shaped like a wedge, and articulates with the bodies of two vertebræ as a rule, and it is received, precisely like a wedge, into the space which separates the bodies of these vertebræ; so that it is in contact by the summit of the wedge with the intervertebral disc, and by the surfaces of the wedge with the vertebra which is situated above and that which is situated below the disc. Beyond the head, the rib presents a portion thin and compressed from before backwards, called the neck of the rib, which is placed in front of the transverse process of the vertebra corresponding to it.
At the external extremity of the neck is a slight enlargement called the tubercle, which corresponds[49] to the level of the external extremity of the transverse process of the vertebra, and which articulates with the corresponding transverse process (Fig. 7, F G). By means of the connections of the head with the bodies of the vertebræ, and of the tubercle of the rib with the transverse process of the thoracic vertebra which corresponds to it, the posterior end of the rib moves on these joints as on a fulcrum, in the act of respiration; the chest cavity being enlarged by the uplifting of the shaft of the rib and by the eversion of the rib simultaneously.
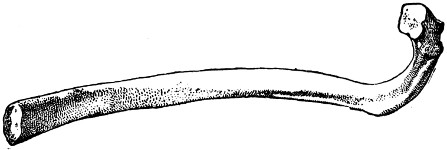
Fig. 13.—A Typical Rib.
Passing on from the tubercle, the shaft of the rib is formed of a bar of bone, which at first is directed outwards and backwards (Fig. 13); then, after travelling some distance, it bends abruptly, so as to be directed forward, describing the characteristic curve of the rib. We give to this bend the name of the angle of the rib. The series of the angles of the ribs shows, upon the posterior aspect of the thorax, a line plainly visible, curved, with its convexity outwards, and having its summit at the level of the eighth rib, which is the longest, and upon which a relatively[50] greater distance separates the angle from the tubercle.
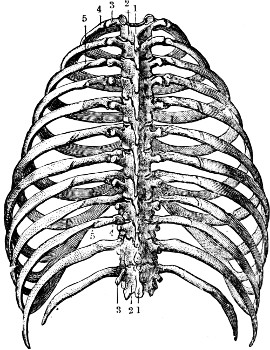
Fig. 14.
Thorax (posterior view).—1, 1, spinous processes of the thoracic vertebræ;—2, 2, vertebral laminæ;—3, 3, series of transverse processes;—4, 4, the parts of the ribs included between the tuberosities and the angles of the ribs;—5, 5, angles of the ribs, becoming more distant from the vertebral column as the rib becomes more inferior.
Such are the characters of ribs in general. For the peculiar characters of the several ribs, after we have spoken of the last two ribs, it will suffice to note the shortness of the upper ribs, and principally of the first, which is flattened from above downward. In other words, it is curved along the borders, and not along the surfaces, and it does not present any twist. The last two ribs, besides being the shortest as a rule (excepting the first rib), are peculiar in their straightness and in the rudimentary nature of[51] the angles; they further have no articulation with the transverse processes of the corresponding vertebræ.
The costal cartilages are attached to the extremities of the ribs in front: these cartilages, in proceeding to join the sternum, follow a course more or less oblique, so that the cartilage of the first rib is oblique from above downwards, and from without inwards; and those following present the same obliquity (Fig. 11), which becomes more accentuated in the cartilages lower down. The spaces which separate these cartilages are wide above, especially between the cartilages of the three first ribs, and become narrower towards the lower part of the chest.
The Thorax as a Whole.—The thorax, the constituent parts of which we have just examined, forms a kind of truncated cone, with its base below and its apex above; but, from an artist’s point of view as to form, it is not necessary to take this into account, as the shape of the summit of the thorax is completely changed by the addition of the osseous girdle constituted by the clavicle and shoulder-blade.
We limit ourselves, then, to a rapid view of the posterior surface, the anterior surface, and the base of the thorax.
The posterior surface (Fig. 14) presents upon the skeleton, in the median line, the series of spinous processes, and on each side, first a row of transverse processes and then the angles of the ribs. As already explained (p. 37), respecting these several details, the summits of the spinous processes, although just[52] under the skin, are scarcely visible, especially in a very muscular subject.
On the anterior surface of the thorax (Figs. 11, 15), in a muscular subject, the osseous details do not show on the external figure, with the exception of the episternal or suprasternal notch (p. 43), and the inner ends of the clavicles, which are more or less visible. The great pectoral muscles form on each side a large fleshy surface, and the median line of separation of these muscles is marked by a narrow depression corresponding to the central portion of the sternum, the only region where this bone becomes subcutaneous; but in less muscular subjects, in the aged and in thin children, all the details of the thoracic frame-work show beneath the skin, and clearly reveal the forms of the costal cartilages with their obliquities, the thin intervals of separation (intercostal spaces) becoming narrower as we get lower down. Moreover, especially in infants, the articulation of the cartilages with the sternum, and the articulation of the cartilages with the anterior extremities of the ribs, are shown by a double row of nodules, as the points of junction of the osseous and cartilaginous portions are slightly elevated. We find therefore a series of chondro-sternal nodules (χόνδρος, cartilage) marking the borders of the sternum, and, on the outer side, a series of chondro-costal nodules, marking the line of junction of the ribs with the cartilages. This chondro-costal line descends obliquely from within outwards; so that, above, it is very near the sternum, owing to the shortness of the cartilage of the first rib, and, below, it is withdrawn from the sternum owing to the[53] greater length of the cartilages of the ninth and tenth ribs.
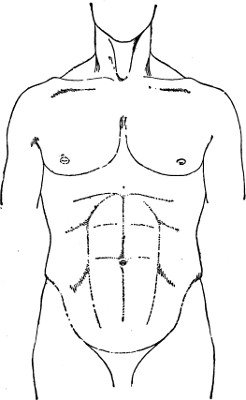
Fig. 15.
Front View of the Chest and Abdomen.
The base, or inferior circumference, of the thorax is
continuous, without distinct limits upon the living subject, with the
abdominal wall behind and laterally; but in front this circumference
presents a depression in the form of an inverted  with the mouth looking downwards (Fig. 11); this depression, limited on
both sides by the cartilages of the lower six ribs, and corresponding
at its apex to the junction of the body of the sternum with its
costo-xiphoid appendage, shows in the living subject a depression of
the same form, called the pit of the stomach, or epigastrium
(ἐπὶ, upon; γαστήρ, stomach). Upon the dead body, or upon a model in a
state of repose, the outlines of the pit may be compared to a pointed
arch; but[54] when the model makes a violent effort, as in taking a deep
inspiration, the elevation of the ribs spreads the cartilages of the
false ribs from the median line, and the pointed arch in question
shortens and tends to take a rounded form. On the other hand, in
very muscular subjects, the great anterior muscles of the abdomen
are sufficiently thick at their superior parts, where they cover
the cartilages of the false ribs, to add their shape to that of the
cartilages, and to give to the epigastric region a more rounded form.
It is this form of a rounded arch that the Greek sculptors have adopted
almost exclusively, and this choice we find justified to some extent
in the fact that they had for their models very muscular athletes,
whom they studied during the wrestling-matches of the gymnasium, when
efforts which dilated the thorax most powerfully were to be observed.
with the mouth looking downwards (Fig. 11); this depression, limited on
both sides by the cartilages of the lower six ribs, and corresponding
at its apex to the junction of the body of the sternum with its
costo-xiphoid appendage, shows in the living subject a depression of
the same form, called the pit of the stomach, or epigastrium
(ἐπὶ, upon; γαστήρ, stomach). Upon the dead body, or upon a model in a
state of repose, the outlines of the pit may be compared to a pointed
arch; but[54] when the model makes a violent effort, as in taking a deep
inspiration, the elevation of the ribs spreads the cartilages of the
false ribs from the median line, and the pointed arch in question
shortens and tends to take a rounded form. On the other hand, in
very muscular subjects, the great anterior muscles of the abdomen
are sufficiently thick at their superior parts, where they cover
the cartilages of the false ribs, to add their shape to that of the
cartilages, and to give to the epigastric region a more rounded form.
It is this form of a rounded arch that the Greek sculptors have adopted
almost exclusively, and this choice we find justified to some extent
in the fact that they had for their models very muscular athletes,
whom they studied during the wrestling-matches of the gymnasium, when
efforts which dilated the thorax most powerfully were to be observed.
[55]
The bones of the shoulder.—The clavicle: its shaft and extremities, sternal and acromial: its proportions.—The shoulder-blade: its situation and relations.—The spine of the scapula: acromion: coracoid process: glenoid cavity.—Proportions of the scapula: the distance which separates the right from the left scapula.—The upper portion of the humerus: the anatomical neck, the surgical neck: the articular head: the tuberosities.—The shoulder-joint: its movements: the increase of mobility assured by the acromio-clavicular and sterno-clavicular articulations the to-and-fro motion of the scapula: the importance of this mechanism with regard to external form.
The shoulder is formed of three bones, of which one is situated in the front, the collar-bone, or clavicle; a second is behind, the shoulder-blade, or scapula; and a third is placed externally, the upper part of the arm-bone, or humerus.
The clavicle (clavicula, diminutive of clavis, a key) is a long bone, placed horizontally at the junction of neck and chest. It connects the breast-bone with the shoulder-blade; and the two clavicles are separated in the middle line by the upper end of the manubrium, or pre-sternum (episternal or suprasternal notch). Its form is that of an italic ∫—that is to say, it describes in a horizontal plane two curves, the internal portion being convex in front, and the outer part convex behind (Fig. 16). It consists of a shaft and two extremities: the shaft, flattened from above down, presents a smooth superior surface, which in the model shows very clearly beneath the skin, and a rough inferior surface[56] for the attachment of a muscle (subclavius), and for the attachment of ligaments connecting it with the first rib internally, and with the coracoid process of the scapula externally (see below); it possesses a posterior and an anterior border, thick and curved: an internal, sternal extremity, thick and triangular, which articulates with the corresponding lateral facet on the manubrium of the sternum: and an outer, acromial extremity, flattened and presenting an oval articular surface for articulation with the acromion process of the scapula. The clavicle thus serves to connect the scapula to the trunk, and by the articulations of its two extremities it increases, as we shall see, the mobility of the shoulder-joint. We find that the clavicle, which is almost horizontal when the arms are hanging in an attitude of repose beside the trunk, becomes oblique in direction when the arms are moved upward and forward, or upward and backward. The length of the clavicle, as we have already said (p. 46), should be equal to that of the sternum without the xiphoid appendix.
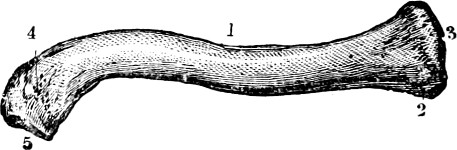
Fig. 16.
Right Clavicle: Upper Surface.—1, body of clavicle;—2, 3, inner or sternal extremity;—4, 5, outer or acromial extremity.
The shoulder-blade, or scapula, is a flat, triangular bone, and consists of a bony plate very thin at certain points, and thickened only along its borders. It is placed on the lateral and posterior aspect of the thorax, and corresponds at its upper border to the second rib: its lower end reaches to the seventh or eighth rib. It is attached by a joint called the[57] acromio-clavicular articulation, which can be felt beneath the skin, to the external extremity of the clavicle. As this joint is the only ligamentous connection of the scapula with the trunk, the bone is capable of great freedom of movement.
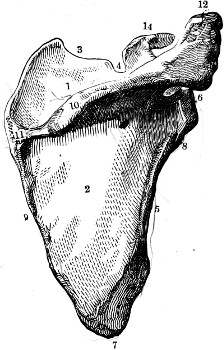
Fig. 17.
Shoulder-blade: Posterior Surface.—1, supra-spinous fossa;—2, infra-spinous fossa;—3, superior border with supra-scapular notch (4);—5, external or axillary border with impression for attachment (8) of the long head of the triceps;—6, glenoid cavity;—7, inferior angle;—9, internal or vertebral border;—10 and 11, spine of shoulder-blade extending into acromion process (12);—14, coracoid process.
The shoulder-blade is described as possessing two surfaces, three borders, three processes, and three angles. The posterior surface, free and visible throughout its entire extent upon the mounted skeleton, is divided into two unequal portions—the upper one, the smaller (supra-spinous fossa) and the lower one, the larger (infra-spinous fossa)—by a bony crest, called the spine of the scapula (10, 11, Fig. 17), which traverses the bone obliquely from within upwards and outwards. It becomes more and more prominent externally, and is afterwards prolonged into a free process, broad and flat, which forms the most elevated and external part of the skeleton of the shoulder (12, Fig. 17), and is known by the name of the acromion process (ἃχρος, summit;[58] ὦμος, the shoulder). It is on the internal or anterior border of this acromion process that the small oval facet is found, by which the scapula articulates with the outer extremity of the clavicle by the acromio-clavicular articulation. The fossa above the spine of the scapula is the supra-spinous fossa (1, Fig. 17), and the larger space below the spine is called the infra-spinous fossa (2, Fig. 17). The anterior surface of the scapula has received the name of the subscapular fossa. It is directed forwards and inwards, and is separated from the ribs and armpit by large muscles. It is but little visible in the articulated skeleton.
Of the three borders of the scapula, one is superior and horizontal; it is the shortest of the three. The second is internal and vertical, parallel to the series of spinous processes of the vertebræ; to this is given the name of the vertebral border. The third, or outer border, is oblique, and is directed downwards and backwards; it corresponds to the region of the armpit, and has received the name of the axillary border. It is particularly to be noticed that the vertebral border is thin; the axillary border, on the contrary, is thick, and presents towards its superior limit a rough space, just below the glenoid fossa, for the attachment of the long head of the triceps muscle (8, Fig. 17). The superior border is remarkable for the presence at its outer extremity of a stout process which projects at first upwards, and is afterwards bent outwards upon itself like a bent finger. It has been likened to the beak of a crow, and has received the name of the coracoid process (κὸραξ, a crow; εἷδος, form). The coracoid process[59] (14, Fig. 17) is placed in front and on the inner side of the acromion, and the two together form an arch over the shoulder-joint, called the coraco-acromial arch, which is completed by a fibrous band proceeding from one process to the other, and called the coraco-acromial ligament. The position of the coracoid process should be particularly noted in relation to the clavicle. It underlies the outer part of the clavicle, from which two important ligaments (conoid and trapezoid ligaments) descend to be attached to its upper surface. These ligaments serve the purpose of slinging the scapula up to the under surface of the clavicle. Of the three angles of the scapula, one only—the superior external angle, which is situated beneath the coraco-acromial arch—deserves a particular description; it is very thick, and becomes enlarged to form an articular surface (6, Fig. 057), which is directed outwards and forwards, and articulates with the head of the humerus. This surface is pear-shaped and is slightly hollowed out, and bears the name of the glenoid cavity. It is much less extensive than the articular head of the humerus, along with which it forms the shoulder-joint.
In regard to the relative proportions of the scapula, it may be noted that the length of the vertebral border is equal to the length of the clavicle, and equal also to the distance which separates the scapulæ behind, when the vertebral borders are vertical, which is the case when the arms are hanging beside the body in a position of relaxation.
The movements of the shoulder-blade, and their effects on external form, will be studied in relation[60] to the articulation of the scapula with the humerus, the scapulo-humeral articulation, or shoulder-joint. We must now pass on to describe the upper portion of the bone of the arm.

Fig. 18.
Left Humerus (anterior surface): 1, body of the bone;—2, articular head;—3, anatomical neck;—4, great tuberosity;—5, lesser tuberosity;—6, bicipital groove;—7, deltoid impression;—11, capitellum;—12, trochlea;—13, external supra-condyloid ridge;—14, condyles;—16, internal supra-condyloid ridge;—17, coronoid fossa.
The arm bone, or humerus, is one of the long bones, and is composed of a shaft, prismatic or nearly cylindrical in form, and of two enlarged extremities, one inferior, which takes part in the articulation of the elbow; the other superior, which takes part in the articulation of the shoulder. We will only concern ourselves for the present with the superior extremity.
The superior extremity of the humerus is large and spherical. It is continuous with the body of the bone by a cylindrical neck, called the surgical neck of the humerus. This extremity is traversed by a circular groove, oblique from above downwards, and from without inwards, called the anatomical neck (3, Fig. 18). This is well marked, and divides the sphere into two parts; the one, situated above, and internal to the anatomical neck, is very regularly rounded, smooth, covered over by a layer of cartilage, and is called the head of the humerus (2, Fig. 18); it is normally in contact[61] with the glenoid cavity of the shoulder-blade, in which it glides in the movements of the arm; the other part of the head, situated below, and external to the anatomical neck, is rough, and divided into two tuberosities by a vertical groove, which is prolonged as far as the upper part of the body of the bone, and which, from its serving to accommodate the long tendon of the biceps, has received the name of the bicipital groove (6, Fig. 18). The tuberosity situated on the outer side of the bicipital groove is large, and is called the great tuberosity (4, Fig. 18); it presents three small surfaces which receive the insertions of the deep muscles of the shoulder—supraspinatus, infraspinatus, and teres minor muscles. The tuberosity situated on the front of the bone, and internal to the bicipital groove, is smaller. It is called the small tuberosity of the humerus (5, Fig. 18), and gives attachment to one muscle only, the subscapularis.
The Shoulder-joint.—The articulation of the shoulder, or scapulo-humeral articulation, may serve as a type of articulations in general. It is necessary in each articulation to consider how the shapes of the bony surfaces in contact correspond to each other. From this we should be able to deduce the nature of the movements permitted by the articulation. It is also necessary to consider the disposition of the ligaments; that is to say, of the fibrous bands which proceed from one bone to the other, and from these we can deduce the limits of the movements of which the joint may be capable.
[62]
The scapulo-humeral articulation is a ball-and-socket joint, formed by the glenoid cavity of the shoulder-blade and the head of the humerus.
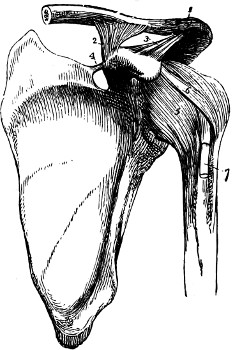
Fig. 19.
Ligaments of Shoulder, with Scapula, Clavicle, and Humerus.—1, Acromio-clavicular ligament;—2, coraco-clavicular ligament;—3, coraco-acromial ligament;—4, supra-scapular ligament;—5, capsule of shoulder-joint;—6, coraco-humeral ligament;—7, tendon of biceps (long head).
Such an arrangement of surfaces in contact with one another permits the head to glide in all directions within the cavity, and consequently the upper limb can be moved in all directions: forwards; backwards; inwards (adduction); outwards (abduction); upwards and downwards. The head of the humerus can also be rotated on the glenoid cavity, either inwards or outwards.
The ligamentous covering of the joint is formed by a fibrous capsule, which is attached on one side to the margin of the glenoid cavity, and on the other side to the anatomical neck of the humerus (5, Fig. 19).
This ligamentous capsule is sufficiently loose to allow the head of the humerus great freedom of movement within the glenoid cavity, without any part of the capsule being put on the stretch, and thus stopping its movement. Thus the movement of the arm forwards is very extensive, as are those[63] backwards and directly inwards, this last being checked only by the meeting of the arm with the lateral surface of the trunk. But the movement of abduction, or of elevation outwards, becomes difficult when the arm approaches the horizontal; here an arrangement comes into play which is of great importance, the study of which shows us that the upper limb, besides the mobility which belongs to the shoulder-joint proper (scapulo-humeral articulation), derives an increase of mobility from the articulations of the shoulder-blade with the clavicle, and of the clavicle with the sternum.
When we apply a humerus to the glenoid fossa of the scapula in such a manner as to draw the arm outwards, we observe that at the moment when the humerus attains the horizontal position, the tuberosities touch the coraco-acromial arch which surmounts the glenoid cavity, and which is completed by the coraco-acromial ligament (3, Fig. 19); in the complete subject, in the living man, when the arm is elevated in carrying it outwards, the same effect of meeting and, so to speak, of contact between the tuberosities of the humerus and the acromial arch is produced, with this result—that the arm, once horizontal, is with difficulty raised higher by the simple play of the scapulo-humeral articulation—that is to say, by the gliding of the head of the humerus in the glenoid cavity. But now a new source of mobility is employed, a new articulation is brought into play—that of the acromio-clavicular joint. The entire scapula moves round the extremity of the clavicle; its inferior angle is carried forward; its external angle—that[64] is to say, the glenoid cavity with the coraco-acromial arch—is carried upwards, and the movement of elevation of the arm is then continued by the play of the shoulder-blade.

Fig. 20.
Outline of Shoulder with the Arm Raised.
As the result is an important change of shape in the shoulder, we ought to particularly examine the shoulder in the region of the back, upon a model in which the arm is raised above the horizontal position. The point of the shoulder is raised, and as this elevation is accompanied by a movement of the shoulder-blade, the vertebral border of this bone does not remain parallel to the spinal column, but while it approaches closer to it at its upper end, it is drawn further away at its lower end, and is obliquely directed from above downwards and outwards (Fig. 20). The inferior angle becomes prominent in the lower part of the armpit, as we may observe in a subject with the arms folded, and shows in a striking manner on a dead crucified body. If the elevation of the arm approaches the vertical, the vertebral border of the shoulder-blade has a tendency to become horizontal, and we observe this change[65] of movement in the model when the bone is seen along the posterior surface of the shoulder and the back, and we should scarcely recognise at first the appearances presented as those we are accustomed to study when it occupies its ordinary situation in the skeleton.
But when the arm is elevated vertically, so that it comes in contact with the side of the head, movement takes place not only at the scapulo-humeral and at the acromio-clavicular joints, but also at the articulation of the internal extremity of the clavicle with the sternum. In that case, in fact, the whole of the shoulder is raised upwards (by the superior fibres of the trapezius muscle), and the clavicle represents the arm of the lever by which this movement is accomplished, while the sterno-clavicular articulation is the hinge. Thus we see the clavicle is changed in its direction, from the horizontal, to become oblique upwards and outwards—that is, its external extremity is raised and carried a little backwards.
The clavicle plays a very important part in the movements of the upper limb. This explains why it is found specially developed in those animals whose fore-limbs possess the most specialised movements—flight, digging, burrowing, striking, or hugging—such as man, the monkey, the bat, the tiger, the mole, etc.; while in those quadrupedal animals which, like the horse, use their fore-limbs for progression only, and in which movements occur only in a plane parallel to that of the body, there is not a trace of clavicle. The part which the clavicle takes in the movements of the arm explains also why the bone presents a variable size in different[66] individuals. It is stronger in the male than in the female; stronger in the working man than in the student; stronger, finally, on the right side than the left, from the habit of using the right arm for the most part in those actions which demand strength and skill. In the left-handed, it is the left clavicle that is stronger than the right. In a word, this bone is, like all the other parts of the skeleton, stronger in proportion as it takes part in active and frequently repeated movements. Thus the breadth of the shoulders is one of the characteristics of athletes; and it is to the strength of the bony structure formed by the clavicle and shoulder-blade, sustained by the first ribs, that the superior portion of the thorax owes its characteristic aspect.
Owing to the presence of the shoulder girdle (scapula and clavicle) the thoracic cage does not present much of the form of a cone at its upper end, or summit; indeed, this region becomes broader in a lateral direction as the clavicle is more developed. It will be enough to contrast the region of the thorax in man with that of such animals as the dog or the horse, which, owing to the absence of a clavicle, have a thorax transversely flattened in the region of the shoulders, and consequently the shoulder-blades more closely applied upon the sides of the thoracic cage.
This is the proper place to discuss the dimensions and proportions of the shoulder; but, as this study consists entirely of a comparison of the transverse diameters of the shoulders with the transverse diameters of the hips, it is better to defer it till after the description of the pelvis.
[67]
The bony structure of the arm and elbow.—The shaft of the humerus.—The axis of the arm and forearm.—Spiral groove of the humerus; the inferior extremity of the humerus; the trochlea and capitellum; the external and internal supra-condyloid ridges.—The superior extremities of the two bones of the forearm; the ulna (sigmoid cavities, olecranon process, coronoid process); radius (head, neck).—The articulation of the elbow; transverse hinge joint.—Movements of flexion and extension; lateral movements.—The external form of the elbow; prominence of the internal condyle and olecranon process.
The shaft of the humerus is prismatic in its upper and middle parts, and flattened from front to back at its lower extremity. Covered over by thick muscles, its outward shape has for us but little interest; it is necessary only to note with regard to its direction that, when the arm is hanging down, the humerus is not altogether vertical, but is tilted slightly downwards and inwards. We shall see that the axis of the bones of the forearm is oblique in the opposite direction; for this reason the arm and forearm form at the elbow a very obtuse angle, looking outwards (Figs. 24, 26).
Among the details to be noted upon the shaft of the humerus, the
bicipital groove is worthy of remark. This vertical groove,
which separates the great from the small tuberosity on the front of
the humerus at its upper end (Fig. 18), is prolonged along the shaft
of the bone, and presents an internal lip slightly prominent, and
an external or anterior lip which is much more marked, which gives[68]
insertion to the broad tendon of the great pectoral muscle. At the
line of junction of the superior with the middle third of the bone,
this lip forms the anterior margin of a rough surface shaped like
the letter
(7, Fig. 18), of which the angle
looks downwards, and which, giving insertion to the deltoid muscle,
has received the name of the deltoid impression. On the back of
the humerus is another groove, broad and shallow, called the spiral
groove of the humerus, which passes downwards and outwards along
the shaft of the bone behind and below the deltoid impression.
The inferior extremity of the humerus deserves to be studied in detail, as its shape gives the key to the movements of the elbow-joint, and explains at the same time several features of the region to be seen in the living model. This extremity is flattened from front to back, and is enlarged into a broad surface which is partly articular, partly non-articular. In the middle are two important articular prominences, smooth and covered with cartilage. Of these the internal portion is called the trochlea (trochlea, pulley). It possesses a groove and two unequal marginal ridges. The internal ridge is more prominent and descends lower than the external one. The other projection (11, Fig. 18), which is situated on the outer side of the trochlea, is rounded in shape, and receives the name of the radial head, or capitellum. It is only obvious when the humerus is looked at from the front or from below: in other words, it does not appear (like the trochlear surface) on the posterior aspect of the lower end of the bone. This surface articulates[69] with the upper end of the radius. There are three depressions, or fossæ, to be seen in relation to the articular surfaces of the lower end of the humerus. On the front of the bone, just above the trochlea and capitellum, are two, which receive the bones of the forearm during flexion of the limb: the coronoid fossa (for the coronoid process of the ulna), above the trochlear surface, and the radial depression for the head of the radius, much shallower, and placed above the capitellum. On the back, above the trochlear surface, is the olecranon fossa, into which the olecranon process is received during extension of the forearm.
The lateral portions of the inferior extremity of the humerus are formed by rough, non-articular projections which give attachment to muscles and ligaments, and are known respectively as the external condyle and the internal condyle of the humerus (14, 14, Fig. 18). Above each condyle is a well-marked bony ridge, which is called the supra-condyloid ridge (external or internal) (13, 13, Fig. 18).
The lower end of the humerus articulates with the upper extremities of the bones of the forearm; and we will next proceed to study the formation of these extremities in order to understand the movements of the elbow-joint and the form of the region.
The forearm is formed of two bones (Fig. 21), which, when the upper limb is hanging beside the body, the palmar surface of the hand being turned forwards, are placed parallel to each other—one on the outer, one on the inner side. The inner bone (1, Fig. 21) is called the ulna, or cubitus,[70] and it is that which by its upper extremity (olecranon) forms the bony prominence of the elbow; the outer bone (10, Fig. 21) is called the radius (from the Latin radius, a spoke of a wheel), and it is by this bone chiefly that the bones of the wrist and hand are carried. For the present we will describe only the upper extremities of these two bones (Figs. 21 and 22).
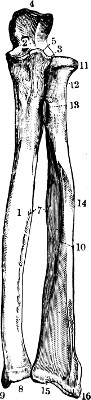
Fig. 21.
The Bones of the Forearm (anterior surface): 1, shaft of ulna;—2, great sigmoid cavity;—3, lesser sigmoid cavity with head of radius;—4, olecranon;—5, coronoid process;—7, interosseous space;—8, inferior extremity of ulna with styloid process (9);—10, shaft of radius;—11, its head;—12, neck;—13, tubercle for biceps;—14, impression for pronator teres muscle;—15, inferior extremity of radius with styloid process (16).
The superior extremity of the ulna presents two processes and two articular cavities. The cavities are the greater and lesser sigmoid cavities; the processes are the coronoid and olecranon processes. The bone articulates with the pulley or trochlea of the humerus by means of the great sigmoid cavity, and with the margin of the head of the radius by the lesser sigmoid cavity. The greater sigmoid cavity (2, Fig. 21) presents in its centre a ridge prominent from before backwards, which corresponds to the groove in the trochlea of the humerus. Below and in front, the great sigmoid cavity is formed (5, Fig. 21) by a bony prominence called the coronoid process (compared to the beak of a crow: κορώνη, a crow; εἶδος, form), which is lodged in the coronoid fossa of[71] the humerus in flexion of the forearm (17, Fig. 18). Above and behind, the great sigmoid cavity is formed by the olecranon process (ὠλενη, the elbow; κάρηνον, the head), a large square projection (4, Fig. 21), which constitutes the prominent point of the elbow, and which accentuates in a high degree the form of the forearm during flexion. During extension of the forearm the olecranon process is lodged partly in the olecranon fossa of the humerus (4, Fig. 23). The lesser sigmoid cavity of the ulna is a small concave surface placed on the outer side of the coronoid process for articulation with the margin of the head of the radius.

Fig. 22.
Figure of the Elbow Joint, right side (anterior view):—1, inferior portion of shaft of humerus;—2, ulna;—3, radius;—4, external condyle;—5, internal condyle;—6, capitellum;—7 and 8, trochlea;—9, coronoid fossa;—10, coronoid process;—11, head of radius.
The superior extremity of the radius forms a small discoidal head (11, Fig. 21) attached by a narrow neck to the body of the bone; this head is flattened at the top and hollowed out to articulate with the capitellum of the humerus (Fig. 22). The margin of the head of the radius revolves in the lesser sigmoid cavity of the ulna.
We see, then, that the articular surfaces of the elbow are formed on the humerus (6, 7, 8, Fig. 22) by a transverse series of projections (the trochlea and capitellum), and on the bones of the forearm by a series of depressions moulded on these projections, so that the whole describes a movement[72] similar to that between two cog-wheels (Fig. 22), a species of transverse hinge. Thus it is easy to understand, à priori, how this disposition of the parts does not permit of any lateral displacement of the bones, or transverse movement; the movements forward and backward are, in fact, the only kind possible in the elbow-joint. The forward movement—that is to say, that by which the anterior surface of the forearm is brought near the anterior surface of the arm—constitutes flexion of the forearm. The movement in the opposite direction constitutes extension.
The disposition of the ligaments—that is, of the fibrous bands or articular capsule which fasten the bones together—modifies very slightly the mechanism we have just deduced from the shape of the articular surfaces; in fact, this capsule is formed on the inner and outer surfaces by ligamentous fibres, very dense and short, called the lateral ligaments, which prevent all lateral movement. On the other hand, the anterior and posterior portions of the capsule are loose, so as not to offer any opposition to the movements of flexion and extension. The only limit to these movements is that resulting from the bony projections of the ulna coming in contact with the humerus. Thus, the movement of flexion can be prolonged until the coronoid process arrives at the coronoid fossa and touches the bottom of that cavity; then the fleshy masses of the forearm come into contact with the anterior surface of the arm, especially if the model is muscular, and flexion is no longer possible. The movement of extension, on the contrary, has a limit which it is important to[73] state precisely, resulting from the beak of the olecranon touching the bottom of the olecranon fossa (Fig. 23); this is produced when the forearm has attained, in the movement of extension, that situation which brings its own axis into direct line with that of the arm. The extension of the elbow cannot therefore exceed the degree which brings the humerus and forearm into the same plane; that is to say, the forearm can never make with the arm an angle facing backwards.
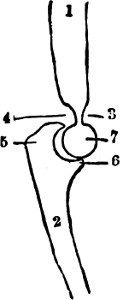
Fig. 23.
Antero-posterior section of the Elbow (through the ulna):—1, humerus;—2, ulna;—3, coronoid fossa;—4, olecranoid fossa;—5, olecranon;—6, coronoid process;—7, section of trochlea.
By comparing the particulars of the mechanism of the elbow with that which we have previously seen of the mechanism of the scapulo-humeral articulation, it will be easy to understand how we may, from the study of the articular surfaces and ligaments, learn the laws of the mechanism of joints. For example, the head of the humerus received into a single concavity may allow to the arm every kind of movement; in the same way the arrangement of a hinge-joint, with a series of projections and depressions, fitted one to the other in a transverse line, renders possible in the elbow-joint only the movements of flexion and extension.
In regard to external form, we learn the following facts from a knowledge of the bones which form the elbow-joint.
1. With respect to the angle which the forearm[74] makes with the arm, if we examine it either upon the skeleton or upon the living subject, the upper limb hanging beside the body, with the palm of the hand turned forward, it is seen that the humerus (page 67) is slightly oblique from above downwards and inwards, while the two bones of the forearm are directed obliquely in the opposite direction—that is, from above downwards and outwards. In other words, the bones of the arm and forearm form at their point of junction—that is, at the level of the elbow—an angle the base of which looks outwards and the apex inwards. This angle only appears in extension of the limb, and is due to the twisted and tilted form of the trochlear surface of the humerus.
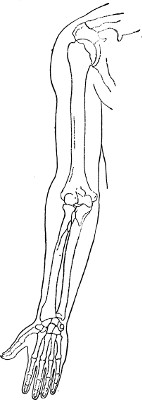
Fig. 24.
Outline of Upper Limb (front view)
2. Concerning the bony prominences which are seen beneath the skin at the elbow (Fig. 24), after studying these osseous structures, we should be able to[75] recognise upon the living model those details of the figure which correspond to the four bony points—namely, the coronoid process in front, the olecranon behind, the external condyle on the outer side, and the internal condyle on the inner side. The coronoid process, covered by muscles, is so buried in the surrounding structure that it does not show externally. It is much the same also with the external condyle, as this projection, not very prominent in the skeleton, disappears completely in the living subject, since this external condyle is situated at the bottom of the angle facing outwards which the forearm makes with the arm, and the mouth of this angle is filled up by the external muscles of the forearm (especially the brachio-radialis, or supinator longus), which take their origin from the external border of the humerus. The external condyle and the external supra-condyloid ridge can be felt beneath the skin; and the former occupies a depression at the back of the elbow on its outer side in extension of the forearm.
On the other hand, the internal condyle, supra-condyloid ridge, and the olecranon process always show clearly beneath the skin, and the olecranon forms that projection, commonly called the point of the elbow, which is so prominent behind during flexion of the forearm, and which follows the movements of the forearm, seeming to rise towards the arm during the extension of the forearm, and to descend during flexion. The internal condyle projects as the apex of the angle formed by the axis of the forearm with that of the arm (Fig. 26, page 81); this is a fixed point placed a little above[76] the line of the elbow-joint, which is useful in measurements.
There is one detail which we must not forget at this stage; in comparing the length of the forearm with that of the arm the olecranon must be excluded, as it projects above the lower end of the humerus; on the other hand, the internal condyle should rather be chosen as a fixed point from which measurements may be taken.
[77]
The bones of the forearm; ulna and radius.—The lower extremities of these bones; their styloid processes; triangular fibro-cartilage of the wrist.—Pronation and supination: change of form and direction of the forearm: and position of the hand.—Prominences of the wrist (styloid processes); the angle which the axis of the hand makes with that of the forearm.
We have already examined the upper ends of the bones of the forearm (radius and ulna) in relation to the elbow-joint. We have still to examine their shafts and lower extremities; and in this chapter we will continue their description, and study the movements of the two bones, and the relation which they bear to the wrist-joint and the hand. In a state of rest the two bones lie parallel, the radius externally, and the ulna internally, separated except at their extremities by a wide interosseous space.
A superficial glance at the bony structure of the forearm (Fig. 21, p. 70) suffices to show that the two bones which compose it offer in many respects a striking contrast to each other. They differ first of all in the relative position which they hold in the forearm. The inner bone is the ulna, which extends upwards beyond the radius by reason of the length of the olecranon process. On the other hand, in the neighbourhood of the wrist, the radius extends beyond the ulna and descends below it. We should also note at the outset that the radius, descending below the ulna, is found to be the only bone of the[78] forearm which articulates directly with the hand and forms the wrist-joint, or radio-carpal articulation. The lower end of the ulna is separated by a wide space from the carpus (cuneiform bone), which is filled up in the living subject by the triangular fibro-cartilage of the wrist-joint. As regards size also these bones present a contrast; the ulna is thick and bulky in its upper part, but becomes thinner as it descends, and its inferior extremity is slender (Fig. 21); the radius, on the other hand, is relatively small at its upper end, and increases in size below, so that its inferior extremity, articulating with the hand, forms a large bony surface.
We need not enter into minute details regarding the shape of the shafts of the two bones.
They are regularly prismatic in form. At the upper end of the shaft of the radius, immediately below the neck, is a tuberosity (13, Fig. 21), directed forwards and inwards, which gives insertion to the tendon of the biceps (bicipital tubercle). From this tuberosity an oblique line passes downwards and outwards, and terminates upon the middle part of the external surface of the bone in a rough space (14, Fig. 21) called the impression for the pronator radii teres, because it gives insertion to the muscle of that name.
With regard to the shaft of the ulna, we need only notice that its posterior border is subcutaneous in its whole extent, and can be felt beneath the skin from the elbow to the wrist.
The lower end of the radius is enlarged and massive. On its inner side it articulates with the ulna. Externally it is prolonged downwards as the[79] styloid process, which forms a well-marked prominence at the outer side of the wrist. The inferior surface is hollowed into a smooth triangular surface for articulation with two of the bones of the wrist (scaphoid and semi-lunar).
The inferior extremity of the ulna is much smaller. It presents a rounded head (8, Fig. 21), which articulates externally with the radius, and below with the triangular fibro-cartilage of the wrist, which intervenes between the ulna and the carpus, and fills the gap between that bone and the cuneiform bone. The ulna is prolonged on its inner side and behind into a styloid process which forms the internal prominence of the wrist. We have already said that the inferior extremity of the ulna does not descend as low as the corresponding portion of the radius; the triangular fibro-cartilage, which lies below the ulna, proceeds from the external border of the inferior extremity of the radius to the base of the styloid process of the ulna; the bones of the wrist articulate with the radius and with this triangular fibro-cartilage, so that the ulna does not take part directly in the articulation of the forearm with the hand (Fig. 28, page 88). The relation of the ulna to the wrist-bones is well shown in a radiograph of the hand, in which the space between the bones at the inner side of the wrist is clearly seen (Fig. 25). This arrangement is of prime importance, as will be seen later, in the movements of the wrist. On account of this space between the ulna and the carpus, the movement of adduction (drawing inwards of the hand) is much freer and more extensive than abduction.
[80]
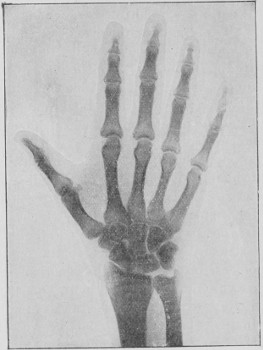
Fig. 25.
The Hand and Wrist: From a radiograph taken specially for this work by Dr. Thurstan Holland, Liverpool.

Fig. 26.
Right Forearm in Supination (the radius and radial half of the hand are shaded by oblique lines): the radius is parallel to the ulna.

Fig. 27.
The Right Forearm in Pronation: the radius (shaded) crosses the ulna, and the radial half of hand (shaded) is placed on the inner side.
Up to the present we have considered the two bones of the arm as placed parallel side by side, and separated by a comparatively broad interval, called the interosseous space (7, Fig. 21). In fact, they are so placed, when the arm is hanging beside the body, in a state of rest, with the palm of the hand directed forwards (Fig. 26), or placed on a flat surface, palm upwards; the hand is then lying on its back, and this position we call supination (supinus, lying on the back). But the hand may be changed in position,[81] turned round so that its posterior surface is directed forward (Fig. 27), or, if the forearm be placed on a flat surface, the back of the hand is turned upwards. In this new position, when the hand lies on its[82] palmar aspect, we speak of it as being in the position of pronation (pronus, lying on the belly).
This change from supination to pronation is accomplished by a change in the relations of the bones of the forearm to one another. They cease to be parallel when the hand is prone, and cross each other; but the two bones do not move similarly in this action; one of them, the ulna, practically remains fixed; the other, the radius, changes its position so as to cross it. On examining the points of contact between the radius and ulna—namely, the superior and inferior articulations of these two bones—we see that the superior radio-ulnar articulation is formed by the circumference of the head of the radius received within the cavity (lesser sigmoid cavity), situated on the outer surface of the coronoid process of the ulna; whilst the inferior radio-ulnar articulation is formed by a sigmoid cavity situated on the internal surface of the inferior extremity of the radius, which articulates with the circumference of the head of the ulna.
The axis of movement may be represented by a line drawn through the centres of the upper end of the radius and the lower end of the ulna. In the superior radio-ulnar articulation, the head of the radius revolves on its own axis and turns in the sigmoid cavity of the ulna; the superior extremity of the radius itself does not change its position; in the inferior radio-ulnar articulation, on the contrary, the radius moves round the head of the ulna, as a wheel round its axle.
These considerations of articular mechanism may be best understood by examining a portion[83] of the skeleton containing the bones of the forearm, which, as is usual in articulated preparations, are connected together by metallic bands that permit the normal movements. In causing the hand to pass from supination to pronation, we see that it is necessary to bring the shaft of the radius across that of the ulna in such a manner that while the upper end of the radius still remains on the outer side, its lower end is entirely altered in position, and is carried to the inner side of the ulna (Figs. 26 and 27). In accomplishing this movement, we perceive that the hand, which articulates only with the radius, must follow the movement of this bone, so that the thumb or radial border of the hand must change from the outer to the inner side; the palm of the hand, which in supination is directed forwards, is turned backwards in pronation, and it is this movement of the radius on the ulna which constitutes the passage from supination (Fig. 26) to pronation (Fig. 27).
The general form of the forearm, irrespective of the details which we shall explain later, regarding the configuration of the muscles, depends directly on the position of these bones, and is changed according as they are parallel or crossed. When the hand is supinated (Fig. 26), the radius being then placed parallel to the ulna and separated from it by a large interosseous space, the form of the forearm is that of the segment of a limb presenting two borders—an external, or radial, and an internal, or ulnar—and two surfaces, one anterior, the other posterior. The forearm, in a word, is slightly flattened from front to back, because the[84] bones are parallel to each other. But when, from the position of supination, the hand passes to that of pronation, the two bones cross each other and come in contact, and the interosseous space practically disappears (Fig. 27). The radius and ulna, taken together, form a single mass, which may be compared to that which two rods assume, placed at first parallel at a certain distance from each other, and which afterwards cross and come into direct contact. Thus in pronation the shape of the forearm becomes completely changed, especially in its lower two-thirds. Instead of a segment of a limb with two surfaces and two borders, it represents a segment rounded and almost cylindrical in its middle part; in complete supination, only the inferior part (wrist) and the superior part (bend of the elbow) preserve the form flattened from front to back.
Artists are usually not sufficiently imbued with these important facts; they are inclined to believe that if a figure has been represented with the forearm in a position of supination, and that for some reason this attitude has been changed to that of pronation, it is enough to change the hand and wrist alone, without altering the model of the forearm in any other detail. On the other hand, the form of the forearm throughout its entire extent and particularly in the middle part, undergoes a change when the hand passes from supination to pronation, and the reverse; and this fact will be still more evident when, in studying the muscles of the region, we see that their direction is completely altered, and this also helps to modify the shape of the limb.
[85]
In the movements of pronation and supination, the forearm changes not only in form, but also in direction. We have previously seen that when the radius and ulna are placed parallel one with the other (supination), the axis of the forearm makes with that of the arm an angle opening outwards. We may again express this fact by saying that if in this case we prolong the axis of the humerus downwards (see the dotted line in Fig. 26), this axis falls internal to the head (inferior extremity) of the ulna, and consequently lies well to the inner side of the radius and interosseous space. But in pronation, the result is that when the radius crosses the ulna at its centre, and is placed internal to it at its lower end, the two crossed bones of the forearm, taken together, make a continuous line with the humerus, the angle at the inner side of the elbow disappears, and the axis of the arm and that of the forearm are almost in the same straight line (Fig. 27).
In order to make the best use of the various details of the bony structures which we have been studying in their application to outward form we will, before commencing the study of the hand, mark once more the prominences which occur at the lower ends of the radius and ulna at the level of the wrist. Of these two projections, which are to the hand what the ankle-bones, or malleoli, are to the feet, one is external, formed by the styloid process of the radius (16, Fig. 21), the other is internal, and is formed by the head of the ulna and its styloid process (9, Fig. 21).
The styloid process of the radius is situated[86] much lower than the styloid process of the ulna.
This position of the bones we may easily verify upon ourselves, without a skeleton, by clasping with the thumb and index-finger of one hand the wrist of the other; we then perceive that the radius descends much lower than the ulna (Fig. 21). Hence the articular line of the forearm with the hand is obliquely directed from above downwards and outwards (the hand being supinated). So that the hand is articulated with the forearm at an angle, due to the downward prolongation of the lower end of the radius: a position which, along with the presence of the articular fibro-cartilage of the wrist, is responsible for the more extensive capacity for adduction than abduction of the hand at the wrist-joint.
In the extended and supine position of the limb the junction of the arm and the forearm forms an angle opening outwards; that of the forearm and hand forms an angle opening inwards.
[87]
The bony structure of the hand.—The wrist, or carpus; eight bones in two rows, superior and inferior.—The radio-carpal articulation, or wrist-joint.—Carpal joints.—The form of the wrist during flexion.—The palm of the hand, or metacarpus; metacarpal bones; their relative lengths (form of the fist).—Carpo-metacarpal articulations; the articulation of the thumb.—The fingers, or phalanges.—Articulations of the phalanges; their movements.—Proportions of the upper limb: the arms extended (the square figure of the ancients); the hand as a common measure; the middle finger and the Egyptian Canon of Charles Blanc.—Brachial index.
The hand is composed of three parts: the wrist, the palm, and the fingers. The bony structure of the wrist is formed by the carpus, that of the palm by the metacarpus (μετὰ, below; καρπὸς, the wrist); the fingers are formed by small bones called phalanges (Fig. 25, page 80).
As the carpus is almost completely hidden by soft parts, fibrous and tendinous, we shall first proceed to enumerate the bones which compose it, and show their articulations.
Notwithstanding its small compass, the carpus is made up of not less than eight bones, which are placed in two transverse rows, one superior, or brachial (next the forearm), the other inferior, or metacarpal (next the metacarpus).
The bones of the two rows are arranged as follows, enumerating them in order from without inwards—that is, from the radial to the ulnar border of the wrist:—The four bones of the first row are:[88] the scaphoid (S, Fig. 28), named from the cavity on the inferior surface being compared to a boat (σκάφη, a boat; εἶδος, form); the semi-lunar (L, Fig. 28); the cuneiform (C, Fig. 28) (whose names indicate their shape); and the pisiform (P, Fig. 28), which, small and rounded, is placed on the anterior surface of the cuneiform bone, and articulates with it alone (Fig. 29). The four bones of the second row, still naming them from without inwards, are (Fig. 28): trapezium, trapezoid, os magnum, and unciform bones (uncus, a hook).
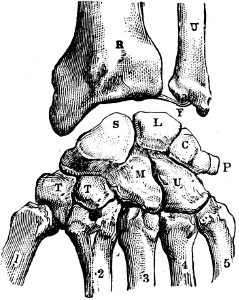
Fig. 28.
The Bony Structure of the Wrist (dorsal surface): R, radius;—U, ulna;—F, triangular fibro-cartilage;—S, scaphoid;—L, semi-lunar;—C, cuneiform;—P, pisiform;—T, trapezium;—T, trapezoid;—M, os magnum;—U, unciform.—Below the carpus: 1, 2, 3, 4, 5, the five metacarpal bones counting from that of thumb (1).
An examination of the bony structure of the carpus as a whole shows that the anterior or palmar surface presents the form of a vertical groove, limited on the inner side by the forward projections of the pisiform and unciform bones, and on the outer side by the projections of the scaphoid and trapezium. This groove is formed into a canal by means of a broad fibrous band (the anterior annular ligament of the wrist), which passes like a bridge across the wrist between the prominences just named. Beneath this bridge, and in the canal thus formed, pass the tendons of the flexor muscles of the fingers, the fleshy bellies of which occupy the forearm, while their[89] tendinous insertions are attached to the phalanges. This explains the fact that these tendons, seen at the lower part of the forearm, are not visible superficially during their passage into the palm of the hand.
The Wrist-Joint.—The radio-carpal joint is formed by the convex upper surface of the carpus, constituted by the scaphoid, semi-lunar, and cuneiform bones, articulating with the lower end of the radius and the fibro-cartilage of the wrist (which lies below the ulna). This articulation permits movements of the hand in four directions: forwards and backwards (flexion and extension); outwards and inwards (abduction and adduction).
Inter-carpal Joint.—The several carpal bones glide upon one another: and there is only a limited movement possible of flexion and extension between the three named bones of the first row (scaphoid, semi-lunar, and cuneiform) and the four bones of the second row; but lateral movements are very limited and practically absent.
It is thus obvious that the movements of flexion and extension of the hand at the wrist-joint are extensive, and amount almost to a right angle, both before and behind, the mobility of the radio-carpal and inter-carpal articulations aiding each other in these movements; on the contrary, the lateral movements of the wrist are more limited, as they are confined to the radio-carpal articulation, and are restricted on the outer side (abduction) by the downward projection of the lower end of the radius. Adduction is a much more powerful movement, rendered freer by the presence of the triangular[90] fibro-cartilage of the wrist, and the separation of the ulna and the cuneiform bones. It should also be noted that in flexion of the hand, when it forms a right angle with the forearm, the posterior surface of the wrist does not present an abrupt curve, but rather a rounded form; the convexity being made up of two series of articulations, the radio-carpal and the inter-carpal articulations.
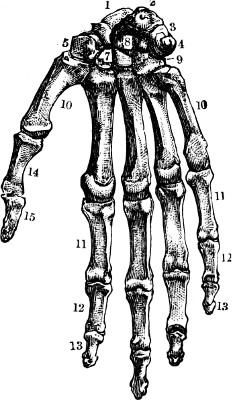
Fig. 29.
Bony Structure of Hand (anterior or palm surface).—1, 2, 3, and 4, the four bones of superior row of carpus:—5, 7, 8, and 9, the four bones of inferior row;—10, 10, the five metacarpal bones;—11, 11, the first phalanges;—12, 12, the second phalanges;—13, 13, the third phalanges;—14 and 15, the two phalanges of the thumb.
The metacarpus (Fig. 29), or skeleton of the palm of the hand, is composed of five slender, long bones—the five metacarpal bones—separated from each other by interosseous spaces. Each metacarpal bone, like the other long bones, is composed of a shaft and two extremities. The shaft is more or less prismatic and triangular; the upper or carpal extremity is cuboid, or wedge-shaped; the lower or digital end is rounded to articulate with the first bone of the finger. The five bones are distinguished by the names, first, second, third, fourth, and fifth metacarpal, counting from the thumb to the little finger; or, again, by the name of the finger to which they correspond (as the metacarpal bone of the thumb, index finger, etc.).[91] The first metacarpal bone, or that of the thumb, is the shortest, and is remarkable for characteristics to which reference will be made later; the second, or metacarpal bone of the index finger, and the third, or that of the middle finger, are the longest. The third is generally longer than the second, so that a line passing through the heads of the series of metacarpal bones describes a curve with its convexity downwards, of which the most prominent part corresponds to the head of the third metacarpal bone. When the hand is firmly closed, and the fingers bent in the palm, it is the head of the third metacarpal bone which forms the most prominent part of the fist.
The metacarpal bones articulate with the carpus by their upper extremities, or bases. In these articulations a very different arrangement is found for the first metacarpal bone when compared with that of the other four.
The articulation of the metacarpal bone of the thumb is formed by a saddle-shaped facet on the trapezium, concave from side to side, and convex from before backwards, and a corresponding facet at the base of the first metacarpal bone. It results, then, that as the rider can move himself on his saddle forwards and backwards, and to either side, so the metacarpal bone of the thumb is equally movable in all directions, and can accomplish the movement of circumduction, by which the extremity of the thumb describes a circle. This mobility permits the thumb to be separated from the other fingers, or to be drawn across the hand, or to touch the tips of the other fingers.[92] This last is called the movement of opposition of the thumb, and it is owing to this property that the thumb possesses of opposing itself to the fingers that the hand of man forms such a wonderful organ for prehension and for performing the most delicate and refined movements. The articulation of the trapezium and metacarpal bone, which is the source of these movements, thus deserves particular mention. The articular surfaces of the two bones are attached to each other by an articular capsule sufficiently loose to allow all the movements of which the first metacarpal bone is capable.
On the other hand, the articulations of the metacarpal bones of the four other fingers do not present any such mobility. In fact, whilst the base of the first metacarpal bone is free, without being connected with that of the second, the bases of the other metacarpal bones are in contact with each other by their lateral surfaces, and are united by dorsal, palmar, and interosseous ligaments. Again, the transverse line of union between the second row of the carpus and the base of these metacarpal bones (carpo-metacarpal line) is irregular, the carpus and metacarpus being dovetailed into each other, especially at the level of the second and third metacarpals, by reason of the projection upwards of the second metacarpal bone, and the projection downwards of the os magnum (Fig. 29). The carpus and the four last metacarpal bones therefore form a series of joints, of which the parts are only slightly movable one on the other, giving a certain elasticity to the whole. The[93] effects of pressure or sudden shock are avoided by the presence of numerous parts united in such a manner as to glide one on the other, at the same time not presenting any independent mobility.
The fingers are formed of a series of slender bones placed end to end, and termed phalanges. Each finger has three phalanges, except the thumb, which has only two. We distinguish the rows of phalanges by the names of the first, second, or third, counting from the base to the free extremity of the fingers; and we give the name of ungual phalanx to the last because it supports the nail. These phalanges, like the other long bones, are made up of a shaft and two extremities. The shaft is semi-cylindrical in shape, rounded behind and flattened in front, where the flexor tendons of the fingers are lodged. The extremities present characters which will be pointed out when the articulations of the fingers are studied.
The articulations of each finger are: the metacarpo-phalangeal articulation, the articulation of the first with the second, and the articulation of the second with the third phalanges (inter-phalangeal articulations).
Each metacarpo-phalangeal articulation is formed by the globular head of the metacarpal bone being received into a glenoid cavity in the base of the first phalanx. Such an adaptation of articular surfaces will permit every kind of movement, and it is easy to understand that each finger can be bent on the metacarpus, straightened, and also inclined to either side (abduction and adduction—the act of separating and bringing together the fingers); but[94] the articular capsule or fibrous band which surrounds each metacarpo-phalangeal joint fixes an exact limit to these movements. Flexion is a much more powerful movement than extension, because the capsules of the joints are deficient behind, their places being taken by a membranous expansion of the extensor tendons which passes over the backs of the joints. Thus extension cannot usually be prolonged further than that position in which the axis of the fingers forms a straight line with that of the metacarpal bones, for just then the anterior portion of the capsule is put on the stretch, and as this part is fibrous, thick, and resisting, it prevents any increase of extension. When the anterior ligament is thinner and more relaxed, as sometimes in the female hand, the fingers can be straightened beyond the straight line, and form an obtuse angle with the metacarpus. On the other hand, this capsule is strengthened on either side by a lateral ligament, which, being inserted at the posterior part of the head of the metacarpal bone, is put on the stretch when the act of flexion is produced, and when this act of flexion arrives at a right angle, the lateral ligaments do not permit it to be carried any farther. It is easy to prove this upon ourselves, as we cannot flex the first phalanx on the metacarpus beyond this point, and we cannot, in any case, bring the anterior surface of the first phalanx of a finger in contact with the palm of the hand, but only the second and third phalanges.
Inter-phalangeal Articulations.—The articulations of the phalanges—that is, those of the first with the second, and those of the second with the third—are constructed on a different plan from the[95] metacarpo-phalangeal articulations. Instead of a head received into a glenoid cavity, we find here, at the inferior extremity of the first and second phalanges, a surface formed like a pulley, or trochlea, with two lateral lips separated by a groove or hollow (Fig. 29); and, on the other hand, on the superior extremity of the second and third we find two cavities corresponding to the lips of the pulley, separated by a median projection which corresponds to the groove. Therefore, given a single phalanx, it will be easy to say whether it is a first, second, or third phalanx, as the first phalanx has at its upper end a single articular cavity, while the second and third have two placed side by side; and again, the third, or ungual, phalanx may be distinguished at the first glance from the second by the shape of its free extremity, which is expanded in front into a rough surface shaped like an arrow-head for the support, not of the nail, but of the pulp of the finger. The inter-phalangeal joints reproduce on a smaller scale the pulley, or trochlea, and joint of the elbow, and present an analogous mechanism permitting only the movements of flexion and extension. In fact, as each of us may prove upon his own hand, while the fingers may be moved from side to side at their metacarpo-phalangeal articulations, the several phalanges can only be flexed and extended at the inter-phalangeal joints; in other words, while the finger enjoys great freedom of movement at its base, it only possesses that of flexion and extension in its component parts. Here again, and for the same reason, flexion is the more powerful movement. The movement of extension of the phalanges is[96] limited, because the anterior portion of the articular capsule put on the stretch by the movement is stout and strong, but we find a great variety in different subjects, and with some, such mobility that the terminal phalanges can be bent backwards. Flexion is limited only by the contact of the soft parts on the anterior surface of a phalanx.
The Proportions of the Upper Limb.—Having examined the skeleton of the upper limb in relation to form and movement, it is necessary next to study its proportions—namely, to inquire, on the one hand, what comparison the length of the limb bears to the height, and, on the other, to compare the length of the different segments of the limb with each other.
The comparison between the upper limbs and the height may be expressed in two ways: first, by examining the two arms outstretched in the horizontal position; the distance which then separates the extremity of one hand from that of the other is termed the span of the upper limbs, and this transverse measure includes not only the length of the arms, but also the breadth of the shoulders; secondly, by examining the upper limb hanging vertically beside the body, and noting to what level on the lower limb the extremity of the hand (nail of the middle finger) reaches.
The relation of the span of the upper limbs to the height has been expressed long since by the formula known as the square figure of the ancients (Fig. 30). If we draw two horizontal lines, one at the soles of the feet (c, d), the other at the summit of the head (a, b), and two vertical lines at right[97] angles to the extremities of the two arms horizontally outstretched, these four lines form by their junction a perfect square; in other words, the man having the arms horizontal is enclosed within a square. This shows that the span of the arms is equal to the height.
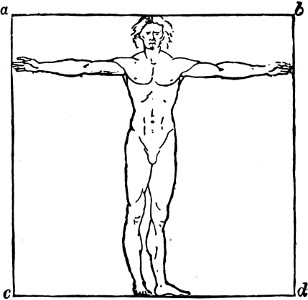
Fig. 30.
Figure in a square, ancient method.
This statement is correct for a man of the Caucasian race of the middle height, but it is not so for the yellow and black races, in whom the span of the arm is greater than the height. If from man we pass on to the anthropoid apes (chimpanzee, gorilla, &c.), we find that the span of the arms in these becomes more and more extended as compared with the height. Thus, in the gorilla, the height being 5 ft. 7¼ in., the span becomes 8 ft. 9¼ in.; and in the chimpanzee, to a height of 5 ft. 5¼ in. the corresponding span is 6 ft. 6 in.
Again, when we examine the upper limbs hanging freely beside the body, we find that in the European of average height the extremity of the middle finger corresponds in general to the middle of the thigh; in subjects of short stature this extremity of the hand descends a little lower than the middle, and, on the other hand, in very tall men it ends at a higher level. In the yellow and[98] black races the extremity of the hand descends much lower than the middle of the thigh; and in the anthropoid apes we find that, in the chimpanzee, the extremity of the hand descends below the knee; in the gorilla it corresponds to the middle of the leg; and, finally, in the orang-outang, and in the gibbon, it reaches almost to the ankle.
If we seek among the various portions of the upper limb a part which would answer as a common measure between them, we cannot find anything satisfactory in this respect. The length of the hand, which would naturally seem to be indicated as a measure, is not contained an even number of times in the length of the bones of the shoulder, arm, or forearm. If, however, we take from the hand the length of the third phalanx of the middle finger, we have a measure equal to that of the vertebral border of the shoulder-blade, or of the clavicle. Under those conditions we may say that the length of the humerus is equal to twice that of the hand, and that of the forearm equal to one and a half the length of the hand; but these proportions are so variable that they cannot be insisted on. We should attach more importance to the rule that takes the hand as a common measure of the entire body in regard to height, taking the height as being equal to ten hands. This is a proportion which often answers in reality, but which presents too many exceptions to be laid down as a law.
We may here state the fact once for all, that there is not an absolute rule for the anatomist, or system of proportions applicable to every class[99] of subject, to those of small as well as those of large stature. If, on the contrary, an ideal proportion is adopted, in which a human figure has been altered, so as to correspond to the abstract conception of beauty, we say that this question of proportion belongs no longer to the domain of anatomy or observation, but that here we rather touch æsthetic doctrines; it is for this reason that we have limited ourselves, when putting forward various ideas of proportion, to indicating, within such limits as direct observation permits, whether a part of a limb might serve as a common measure for this limb or for the total length of the body.
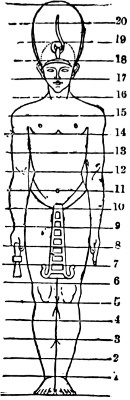
Fig. 31.
The Egyptian Canon.
The Egyptian canon as demonstrated by Charles Blanc, which has a certain historical interest, is that the length of the middle finger, taken as a common measure, should be contained nineteen times in the length of the body. In fact, the “Selection of Funeral Monuments” by Lepsius (Leipzig, 1852) contains the drawing of a very curious Egyptian figure, divided by transverse lines into nineteen parts (not including the head-dress). Now as several passages in different ancient authors seem to indicate that the Egyptian sculptors have taken the finger as the unit of the system, Charles Blanc very ingeniously remarks this fact, that in the figure in question, one[100] of the horizontal lines, the eighth beginning at the soles of the feet, passes exactly at the base of the middle finger in the right hand (closed holding a key), while the seventh touches the extremity of the middle finger of the extended left hand. It seems to him, then, very probable that the distribution of these horizontal lines indicates a system of measuring the figure, and that the space between the seventh and the eighth line measures the length of the middle finger, which thus becomes the standard of this system of proportion. According to the Egyptian rule, the length of the middle finger will be found nineteen times in that of the height (Fig. 31); it may be that this rule was adopted by the Greek artists, and Charles Blanc does not hesitate to think that Polycletus, who has composed a Treatise on Proportions, with a model in marble known by the name of Doryphorus, used no other system but the Egyptian; there has been always found in a number of antique figures this same proportion of nineteen times the middle finger to the height of the body, and in the Achilles, for example, the total height does not exceed by more than ¹⁄₂₀th of an inch the length of the middle finger multiplied by nineteen.
Brachial Index.—An interesting proportion to note is that between the arm and forearm, especially as it has been with anthropologists the subject of important researches, and will familiarise us with the term index, which we must frequently make use of, especially when comparing the transverse and antero-posterior diameters of the cranium. We give, in anthropology, the name index to the number which expresses the proportion of one dimension to some[101] other, this last being represented by 100. Supposing, in fact, that we compare one length, A, equal to one metre, with another length, B, equal to two metres, in this case, the first length being half that of the second, we speak of the index found as 50 (because 50 is the half of 100, and we suppose the second length to be equal to 100). Now the forearm is shorter than the arm; it represents about three-fourths of it; if, then, we take the number 100 to represent the length of the humerus, the number 75, which is three-fourths of 100, would represent the length of the forearm; and then in denoting by the brachial index the proportion of the length (always shorter) of the forearm with that of the arm (always longer) we simply say that the brachial index is represented by 75.
This method of notation, which reduces any numerical proportion to the decimal system, is very valuable, as it permits us to follow without difficulty the degree in which a proportion varies according to the race or species.
Thus we come to speak of the brachial index (proportion of the forearm to the arm) as 75. We have chosen this particular number in order to make the example easy; in reality, in adult European subjects this index is only 74—that is to say, that the forearm is to the arm as 74 is to 100. If we measure the same parts in the adult negro, and reduce to the decimal proportion the numbers obtained, we find the brachial index here is 79—or that the forearm is to the arm as 79 to 100. In the negro, then, the forearm is longer compared with the arm, as 79 is a greater part of 100 than 74.[102] Finally, if we pass on from the human species to the anthropoid apes, we see that the brachial index comes to be 80, and even 100—that is to say, that the length of the forearm becomes equal to that of the arm; and we know, therefore, that the great length of the upper limbs in the anthropoids (page 86) is principally owing to the greater length of the forearm. But the most interesting fact is that in the human race the brachial index is not the same at different ages—thus, in the European infant at birth this index is 80; before the end of the first year it is only 77, and by degrees during childhood it descends until it arrives at 74 in the adult. This clearly shows that the humerus, during the growth of the body, lengthens in proportion more than the bones of the forearm; so that they, which were at first to the humerus as 80 is to 100, come gradually to be as 77 to 100, and finally as 75 or 74 to 100. If we were to glance at comparative osteology we should see that, in such animals as the lion or the horse, the forearm becomes longer in proportion to the humerus, so as to equal, and afterwards to surpass, the length of that bone.
[103]
The bony structure of the hips.—The pelvis; sacrum (five vertebræ welded together); coccyx (the caudal appendage in man and the monkeys resembling man); the innominate bones (ilium, pubis, ischium); the cotyloid cavity; the acetabulum and its notch.—The articulations of the pelvis, sacro-iliac and pubic; sacro-iliac ligaments; ilio-pubic, or Poupart’s ligament (fold of the groin); ligaments of the hip-bones.—The pelvis as a whole.—Comparison of the pelvis in the male and female.
The pelvis is formed by the union of the two hip-bones, one on either side, with the vertebral column, so as to form the pelvic cavity or basin, which is bounded behind by the lower portion of the vertebral column, sacrum and coccyx, laterally by the hip-bones, and in front by the symphysis pubis, the antero-inferior articulation of the two hip-bones together. It completes the trunk and abdomen in their lower parts, and serves to articulate with the thigh-bones (femora) externally. There is a great contrast between the shoulder girdle and the pelvic girdle. The former is freely movable, and has only a slight attachment by the sterno-clavicular joint to the axial skeleton: the latter is immobile, and is firmly adherent to the vertebral column (sacrum) by means of the sacro-iliac joint and powerful accessory ligaments.
The os sacrum (Figs. 5, 8, 32, 35, 38), so called because it was the part of the trunk offered in sacrifice by the ancients to their gods, is formed of five vertebræ (sacral vertebræ) fused[104] together by osseous union, the separate portions of which are easily seen on careful examination. Taken as a whole it forms a pyramid, the base of which (2, Fig. 35) is turned upwards and forwards, corresponding to the body of the first sacral vertebra. This sacral pyramid, being directed obliquely from above downwards and backwards (Figs. 8, 9), presents a surface called antero-inferior, or rather inferior, on which we recognise five united vertebral bodies (Fig. 5, page 28); a postero-superior surface—better called superior—on which we recognise the rudimentary spinous processes (Fig. 9, page 38) and the laminæ of these same five vertebræ, these portions being all united together; and, finally, the lateral surfaces, expanded above to form the auricular surface for articulation with a similar surface on the hip-bone. This surface extends over the sides of the first three sacral vertebræ; and behind it are rough excavations for the attachment of the powerful posterior sacro-iliac ligaments.
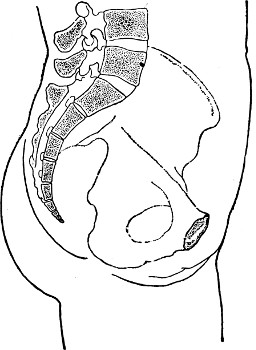
Fig. 32.
Section of the Pelvis.
The coccyx (21, Fig. 5), placed below the sacrum, is a rudimentary caudal appendage, but instead of[105] being, as in the greater number of mammals, free and movable, it is found in man curved towards the interior of the pelvis, whose inferior outlet it contributes to close. Its borders give attachment to powerful sacro-sciatic ligaments, which help to fill up the space between the vertebral column and the hip-bone on each side.
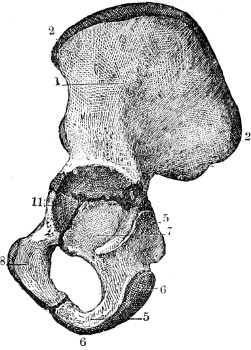
Fig. 33.
The Hip-Bone of an Infant: its three primitive pieces:—1, ilium;—2, its superior border;—5, 6, ischium, its acetabular part (in 7);—8, pubis, its acetabular part (11).
The coccyx is formed of a series of four vertebræ, welded one with the other, and so diminished in size that each of them is reduced to a small osseous nodule, representing a rudimentary vertebral body.
The hip-bones (ossa innominata) are two in number, one on each side, articulating behind with the sacrum, and uniting with each other in front (Figs. 35, 38) to form the symphysis pubis. In order to understand the arrangement of the parts of which a hip-bone consists it is necessary to notice that this bone is made up originally, in an infant, of three distinct parts, which are afterwards joined together as age advances; of these parts, the superior is called the ilium; the two others are inferior; that placed in front is called the pubis, and that behind, the ischium (Fig. 33). The junction of the three parts is effected at the central portion of the bone, at the bottom of the great[106] articular cavity of the hip-joint (acetabulum). The names of almost every part of the hip-bone are derived from its three constituent portions—namely, the ilium, pubis, and ischium.
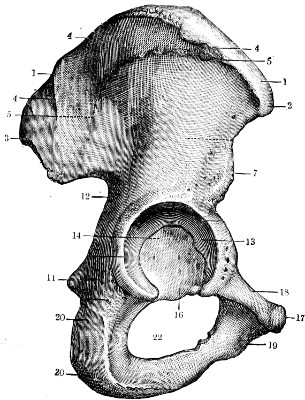
Fig. 34.
Right Hip-Bone (external surface).—1, 1, iliac crest;—2, anterior superior iliac spine;—3, posterior superior iliac spine;—4, superior curved line;—5, inferior curved line;—7, anterior inferior iliac spine;—11, ischial spine;—12, great sciatic notch;—13, acetabulum; and 14, its pit (fovea);—16, its great notch, directed downwards;—17, spine of pubis;—18, horizontal ramus of pubis;—19, body and descending ramus of pubis;—20, 20, tuberosity of ischium;—22, obturator foramen.
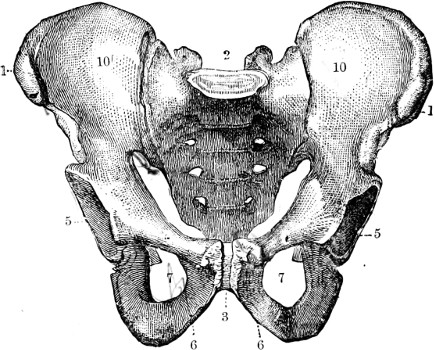
Fig. 35.
Pelvis of the Male.—1, 1, iliac crests;—2, sacrum;—3, symphysis pubis;—5, 5, acetabula;—6, 6, rami of pubes and ischia;—7, 7, obturator foramina;—10, 10, iliac fossa.
Examining first the external surface of the bone, we notice that its upper part is expanded into a large area called the dorsum ilii (5, Fig. 34), which is crossed by three curved lines limiting the attachments of the gluteal muscles (4 and 5, Fig. 34). Below this area the bone is narrowed and presents a circular cavity (13 and 14, Fig. 34), broad and deep, which has received the name of the acetabulum (a vinegar-cup); its use is to form the articular socket of the hip-joint for the reception of the head of the femur. The margin of this cavity is prominent throughout its entire extent, except below, where it is deficient, and gives rise to the notch of the acetabulum; this notch is a valuable starting-point to settle the natural position either of the iliac bone or of the entire pelvis (Fig. 34). If, in fact, this bone of the pelvis is supposed to belong to a figure in the upright position, the acetabular notch should be directed downwards, as shown in Fig. 34. Below the acetabulum the innominate bone is pierced by a large hole, called the obturator or thyroid foramen (22, Fig. 34), bounded by the following parts: behind, by the ischium (20, Fig. 34); in front and above, by the horizontal ramus of the pubis (18); below, by a bony plate formed by a prolongation of the pubis (19) proceeding to join a corresponding prolongation of the ischium. These united bars of bone are called the descending ramus of the pubis and the ascending ramus of the ischium, and they unite to form with[107] those of the opposite side the pubic arch of the completed pelvis. The internal surface of the innominate bone is divided into upper and lower parts by a diagonal line—the ilio-pectineal line—which separates the iliac portion of the bone from the part formed by the ischium and pubis, and also serves to separate in the complete pelvis the upper abdominal part (false pelvis) from the cavity of the true pelvis below. Above this line is the internal expanded surface of[108] the ilium known as the iliac fossa (10, Fig. 35). At its posterior end is the auricular surface of the ilium, for articulation with the sacrum. Below it are, first, a flat surface corresponding to the floor of the acetabulum, and, lower still, the obturator foramen, bounded as we have already described. The borders of the hip-bone are distinguished (Fig. 34) as superior, anterior, posterior, and inferior. The superior border, called the crest of the ilium (1, Fig. 34), is thick and curved like an italic ∫; it is this which marks on the living model the outline of the hip—namely, the limit between the lateral part of the abdomen and the lateral part of the pelvis. It ends in front in the anterior superior spine (2, Fig. 34), and behind in the posterior superior spine of the ilium. The anterior border begins at the anterior superior iliac spine, and presents in succession, from above downwards, a notch, then a prominence called the anterior inferior spine of the ilium (7, Fig. 34), below which is a groove giving passage to the psoas muscle (see later) bounded on its inner side by the ilio-pectineal[109] eminence; finally, this border is continuous with the horizontal ramus of the pubis, and ends internally in the spine and crest of the pubis (17, Fig. 34). The posterior border of the bone is similarly marked by projections and notches. It is limited above by the posterior superior spine of the ilium (3, Fig. 34), and below by the tuberosity of the ischium; and between these are two smaller projections—the posterior inferior spine of the ilium above, and the spine of the ischium below. The ischial spine serves to divide the border into two unequal notches, of which the superior, the larger, is called the great sciatic notch (12, Fig. 34), and the inferior, the smaller, the lesser sciatic notch. Finally, the inferior border is formed by the rami of the pubis and ischium. We will finish the description of this bone by describing its four angles: the antero-superior (2, Fig. 34) is formed by the anterior superior iliac spine; the antero-inferior (17, Fig. 34) by the body of the pubis, which here presents a rough oval surface of considerable extent which articulates with the pubis of the opposite side to form the symphysis pubis; the postero-inferior angle (20, Fig. 34) is formed by the tuberosity of the ischium; and finally, the supero-posterior, thick and flattened, presents on its outer side the posterior iliac spines, and on its inner side the large rough auricular surface, for articulation with the sacrum.
In order to construct the pelvis, the two hip-bones are joined together (at the symphysis pubis), and also join the sacrum (sacro-iliac synarthrosis) by articulations which have nothing in common with those which we have already studied in the[110] limbs—for example, the shoulder or elbow. In those articulations of the limbs the bones were in contact by smooth surfaces, which glided one upon the other without anything interposed between them; such articulations are characterised by their mobility. On the other hand, the sacrum is united on each side to the hip-bones, and the hip-bones themselves articulate in front with each other by rough surfaces, between which are placed plates, more or less thick, of fibro-cartilage (similar to the intervertebral discs), which, in consequence, do not allow them to glide one on the other, but closely join them together. These articulations, which bear the name of synarthroses, or symphyses (σύν, together; φύομαι, to weld), are remarkable not for mobility, but for rigidity. They are characterised by the possession, between the articulating bones, of plates of fibro-cartilage, which act as tough but elastic buffers. Behind, the two sacro-iliac synarthroses support the sacrum, which is firmly wedged in between the two bones of the hip, and is slung between them, while the strong ligaments placed above the joint permit the sacrum to support the weight transmitted to it by the vertebral column. In front and below, the symphysis pubis (3, Fig. 35), besides having fibro-cartilage placed between the bones and adherent to them, is also strengthened by fibrous bands passing superficially from one bone to the other.
These articulations weld the component parts of the pelvis (the sacrum, with the two hip-bones) into a complete basin; but, at the same time, owing to the elasticity of these joints, the pelvis[111] can resist without injury the shocks which are transmitted to it by the vertebral column and the lower limbs. The sacro-iliac and pubic fibro-cartilages break and check the shock which is produced—when, for example, we jump from a height and alight on the soles of the feet.
Besides the sacro-iliac joint and the articulation of the symphysis pubis, the pelvis also possesses other ligaments accessory or special to the hip-bone. The accessory ligaments are those which strengthen the sacro-iliac joint. Above the articulation are the ilio-lumbar ligament, passing from the transverse process of the last lumbar vertebra to the iliac crest at its posterior end, and the sacro-vertebral ligament, passing from the same transverse process to the lateral mass of the sacrum. Below the joint are the two sacro-sciatic ligaments, which, arising together from the side of the sacrum and coccyx in the form of a broad fibrous band, proceed outwards, and, diverging, are attached, one—the great sacro-sciatic ligament—to the tuberosity of the ischium, the other—the lesser sacro-sciatic ligament—to the spine of the ischium. These ligaments convert the sacro-sciatic notches into foramina, through which important muscles pass; and, but for this fact, these ligaments would not need mention here, as they do not appear superficially, being covered by the mass of the gluteal muscles. The special ligaments of the hip-bone are the triangular ligament, which is a membrane partly filling up the pubic arch; the obturator membrane, which almost completely fills the obturator foramen; and Poupart’s ligament (really derived[112] from the aponeurosis of the external oblique muscle of the abdomen, which stretches between the anterior superior spine of the ilium and the spine of the pubis). It is immediately subcutaneous, and corresponds to the fold of the groin. The subcutaneous fascia is attached to the entire length of the ligament, and so creates a depression extending from the spine of the ilium to the pubis. This fold of the groin marks the limit between the skin of the abdomen and that of the thigh. As the deep fascial envelope of the thigh is attached to Poupart’s ligament in its whole length, it pulls on the ligament so as to make it convex downwards in the extended position of the lower limb.
The whole pelvis is expanded above and narrower below, and the lower part of it is, for the most part, concealed from view in the living model. The lower limbs are attached on each side in such a manner that they approach each other at the lower part of the pelvis, so as to leave between them only a narrow interval—the perineum, which corresponds to the genital organs and the parts between the folds of the buttocks. But the upper outline of the pelvis is clearly marked throughout the whole of its extent: on each side the iliac crests, on the superior borders of the hip-bones, form a slightly undulating line, the middle portion of which is most elevated, while its anterior extremity inclines abruptly downwards to terminate at the anterior superior spine of the crest of the ilium, clearly seen in the model when the skin is not loaded with fat; in front, the pelvis presents an extensive curved outline with its concavity upwards, the central parts corresponding to[113] the symphysis pubis, and the lateral parts formed by Poupart’s ligament on each side. This anterior outline of the pelvis forms the lower limit of the abdominal wall. This helps to give the anterior abdominal wall the form of a shield rounded at both upper and lower ends, a form which the ancients seem to have exaggerated in adopting for the epigastric pit a configuration rounded instead of oval, which is the shape it presents in the skeleton. We have previously (page 54) shown how, in numerous cases, the form adopted by the ancient sculptors is sufficiently justifiable.
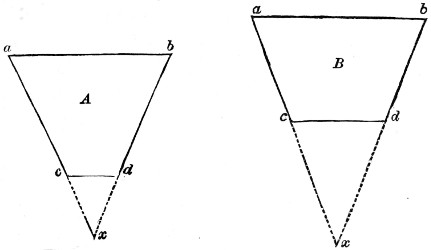
Fig. 36. Fig. 37.
Diagrams showing that the pelvis of the male (A) represents a long segment (a, b, c, d) of a short cone (a, b, x), while the pelvis of the female (B) represents a short segment (a, b, c, d) of a long cone (a, b, x).
After having studied the pelvis with regard to its mechanism and its influence on external form, we ought now to examine it with regard to its proportions—namely, its transverse dimensions; but as the prominence of the hips is formed not only by the superior border of the iliac bones, but also by the great trochanters of the femur, this examination cannot[114] be completed without reference to the relation of the bones of the thigh to the pelvis. For the moment, therefore, we must confine ourselves to the study of the proportions of the pelvis in the male and in the female skeleton.
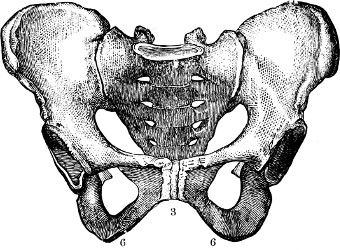
Fig. 38.
Pelvis of the female.
Generally speaking, the pelvis of the female is broader and shorter than that of the male; in the male (Fig. 35) the superior transverse diameter, which is a line that passes through the most prominent portion of the crest of the ilium of one side to the corresponding part of the other, measures from 10 to 12 inches (on the average 11 inches); whilst in the female this line measures from 10¼ to 13¾ inches (on the average 12 inches). On the contrary, the height of the pelvis in man is about 8 inches, whilst it is not more than 7¼ inches in the female. Again, comparing (Figs. 35 and 38) a male with a female pelvis, we see that the first is narrow, the second comparatively broad between the ischial tuberosities.
If we suppose a line drawn at a tangent to the sides of the pelvis, we see that these lines must be prolonged downwards for a considerable distance in order to meet in the female pelvis, but that in the male pelvis they join at a shorter distance from the[115] pelvic outlet. In order to reduce these facts to a simple formula we may say, therefore, that the pelvis of a male represents a long segment of a short cone, while that of the female represents a short segment of a long cone. The student is referred to Figs. 36 and 37, which show this arrangement by means of a simple diagram.
The particular details of shape which distinguish the pelvis in the two sexes are the following:—The thickness of the walls: in the male the bones of the pelvis are stronger, the iliac crests are thicker, more curved, and less expanded, and the different prominences for the insertions of muscles are better marked. The pubic arch, limited above by the symphysis, and on each side by the descending rami of the pubis, is very broad, and has everted edges in the female, in whom it assumes the form of an elliptical arch, while in the male (compare Fig. 35 and Fig. 38 at 3, 6, 6) this same arch is narrow and raised, and takes the form of a pointed arch. For the same reason the tuberosities of the ischium are wider apart in the female than in the male. The spine of the ischium in the female is turned backwards, and appears less obviously in the pelvic cavity. The obturator foramina are wide and triangular in the female, while they are narrow and oval in the pelvis of the male. The sacrum is relatively shorter and broader in the female than in the male.
[116]
The femur: its superior extremity: neck, head, and trochanters.—Hip-joint, or coxo-femoral articulation; movements of the joint; limits of these movements; limits of extension (ilio-femoral ligament); adduction (ligamentum teres); the influence of atmospheric pressure (experiments of the brothers Weber).—The transverse dimensions of the hips and shoulder in the male and female; the various formulæ (ovoid of the ancients, ovoid and elliptical of Salvage); the correct formula; the inter-humeral and inter-trochanteric diameters; the inter-acromial and inter-iliac diameters.—The external form of the region of the hips and great trochanter in particular; the osseous prominences brought into relief on the surface as flat and depressed surfaces.
The femur (Figs. 39 and 43), or bone of the thigh, is one of the long bones. It is the largest bone in the skeleton, and consists, like all the long bones, of a shaft and two extremities (Fig. 39). In this chapter we have to consider its upper end, and its articulation with the hip-bone.

Fig. 39.
Vertical Section Of Femur.—1, 1, 2, 2, the body of the bone with the medullary canal hollowed out;—3, the great trochanter, whence the neck is given off, terminating in the head;—4, inferior extremity of the bone.
The upper extremity of the femur is composed of a head, a neck, and of two tuberosities (the great and small trochanters) placed at the junction of the neck with the body of the bone. The head of the femur (5, Fig. 43) is regularly rounded, and forms three-fourths of a sphere. Its spherical surface, turned inwards, upwards, and forwards, is smooth and covered with cartilage, except at a pit (6, Fig. 43) seen a little below and behind its centre, which gives attachment to the ligamentum teres—a strong fibrous band which connects the femur to the acetabulum.
[117]
The neck of the femur (7, Fig. 43), connecting the head with the shaft, is directed downwards and outwards in the form of a cylinder, flattened a little from front to back, to become attached to the upper extremity of the shaft of the femur at an obtuse angle, looking downwards and inwards (Fig. 39). This angle which the axis of the neck makes with that of the body varies in different individuals. In the adult male it is about 135 degrees; in the female it is less open—that is, it approaches nearer to a right angle. This helps to increase the transverse diameter of the hips in the female. Again, in both sexes this angle approaches gradually to a right angle with the advance of age—a change that assists in shortening the total height in the aged. At the junction of the neck of the femur with the body of the bone are the two tuberosities, or trochanters—one situated above and to the outer side, called the great trochanter (3, Fig. 39; and 8, Fig. 43); the other situated below and to the inner side, at the junction of the neck and the shaft, called the lesser trochanter (10, Fig. 43). The great trochanter is of large size, is quadrilateral in[118] shape, and projects beyond the upper border of the neck. It presents on its surfaces and borders numerous impressions, for the insertion of the muscles of the buttock. The lesser trochanter, on the contrary, is smaller in size, mammillated or conical in shape, and gives attachment to the psoas and iliacus muscles only.
The Hip-joint.—The ilio-femoral or coxo-femoral articulation is formed by the reception of the head of the femur into the cavity of the acetabulum, in which it exactly fits. The edge of the cavity is surrounded by the cotyloid and transverse ligaments, which clasp the head of the femur and serve to deepen the cavity and narrow its orifice. The articulation is a ball and socket joint (enarthrosis). As we should expect from the form of the articular surfaces, every possible description of movement can take place: the head of the femur can glide in all directions in the cavity in which it is received, producing the movement of abduction (the inferior limb being carried outwards, away from the middle line), adduction (towards the middle line), flexion (forwards, the anterior surface of the thigh being brought towards that of the abdomen), extension (backwards), and rotation, of the femur, outwards and inwards. But these movements are variously influenced by the disposition of the ligaments of the joint. Some are limited, others are very extensive.
The ligamentous apparatus of the hip-joint consists of a thick capsule of fibrous tissue, which arises from the margin of the cotyloid cavity and encloses the head and neck of the femur. The[119] disposition of this capsule is very different in front and behind.
The capsule is composed of superficial longitudinal fibres stretching from acetabulum to femur, and thickened, except posteriorly, to form strong ligaments; and deeper, circular fibres, which alone constitute the back part of the capsule—consequently the capsule is thinner and weaker at the back, where the circular fibres appear superficially—constituting the zona circularis, or ligament of Bertini. The posterior portion of the capsule consequently cannot at any time become tense. The movement of flexion, indeed, may be continued as far as possible without causing tension of the back of the capsule of the joint. It is for this reason we speak of flexion of the thigh as unlimited, and, in fact, it may be continued until the anterior surface of the thigh comes in contact with the abdomen.
The other movements of the thigh at the hip-joint are limited by the several longitudinal ligamentous bands of the capsule. In front, the capsule of the joint is put on the stretch when the thigh is carried backwards during extension, and the movement is checked when it arrives at a certain point. This is due to the ilio-femoral, or Y-shaped ligament of Bigelow, which extends from the acetabular margin to the front of the neck of the femur, dividing as it descends into two bands. It is the most important ligament of the hip-joint. Owing to the strength of this ligament, the movement of extension can be limited and checked at any given moment. Now if we try the experiment on ourselves, having flexed the thigh on the abdomen and then gradually[120] extend it, we shall perceive that the movement is arrested at the moment when the axis of the thigh is in a continuous line with that of the body (or if the subject is upright, when the thigh is vertical). If we repeat this experiment on the dissected subject, with the joint prepared, we see that the ilio-femoral ligament is relaxed when the thigh is flexed on the pelvis, and becomes tense in proportion as the bone is extended, and that this tension arrives at its maximum when the femur is found in a line with the trunk, and the ilio-femoral ligament presents an insurmountable obstacle to any further extension.
It is true that a man in the upright position can move his thigh backward; but it is necessary to observe, if, for example, it is the right thigh which is carried backward, it is not in the right hip-joint that the movement takes place, but in the left; in other words, the trunk is flexed upon the left femur. We may therefore state that when the thigh is so extended as to be in the same continuous plane with the trunk, the thigh and trunk form one and the same piece, and the two parts are incapable of further extension; and, consequently, when one thigh is carried behind the vertical line, the trunk must be rotated to an equal extent on the opposite side.
The ilio-femoral band plays also an important part in the maintenance of the erect attitude. Being stretched in extension of the thigh, the head and neck of the femur rest against it, and so the erect position can be maintained without excessive muscular exertion. The ilio-femoral ligament also, aided by the pubo-femoral band of the capsule,[121] presents an obstacle to abduction, or the movement of the thigh outwards, in the upright position, when the ligament is tense. When the thigh is slightly flexed on the pelvis, and the ligament is relaxed abduction of the thigh becomes comparatively easy (Fig. 40).
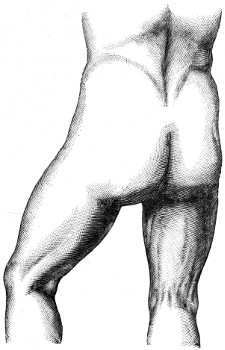
Fig. 40.
Outline of Buttock and Thigh.
The movement of adduction, or bringing of the thighs together, is limited by the ilio-trochanteric[122] band of the capsule, and by the ligamentum teres—a special ligament, not part of the capsule, contained within the joint. This movement becomes very easy if the joint is slightly bent. If we try the experiment on an articulation in which the ilio-femoral ligament is cut, we perceive that in the position of extension the movement of adduction is just as difficult as if the ligament were intact. This is due to the presence of the ligamentum teres. This ligament is attached by one extremity to the rough depression below and behind the head of the femur, and by the other extremity, which is bifurcated, to the margins of the acetabular notch. We have already seen that in the pelvis of a man in the upright position this notch looks directly downwards (page 106); the ligament in this position is also vertical, and is put on the stretch, as the two ligaments, so to speak, help to suspend the pelvis on the heads of the femora. Now, in the upright position, the femur being vertical, the movement of adduction could be produced only by a gliding movement of the head of the femur in the acetabular cavity; but this gliding movement cannot take place, as the head of the femur is kept in position by the tense, round, or suspensory ligament. If, on the contrary, the femur is slightly flexed, the round ligament will be found relaxed; this permits the gliding of the head in the cavity, and at the same time permits of adduction, a movement which may now be accomplished with ease. An experiment which proves these facts without giving an anatomical demonstration of them (obtainable only from[123] a prepared subject) is very easy to accomplish upon oneself. If one stands perfectly upright, rigid, with the body thrown backwards as far as possible, it will be seen that it is almost impossible to bring the two thighs and knees close together. Adduction is almost entirely lost in this position, so that we should be unable to bring the knees together and crush a fragile body, such as an egg, placed between them. But if, on the other hand, we flex the thighs a little, or the trunk is bent on the thighs, adduction becomes extremely easy, and now we can knock the knees together without any difficulty.
The hip-joint is remarkable for the fact that upon it we can most conveniently demonstrate a law which applies also to all the other articulations, but of which we have reserved the explanation until now—namely, the law relative to the influence of atmospheric pressure in maintaining articular surfaces in contact. Up to the present, in studying the articulations, we have spoken of the form of the articular surfaces, and from their outline we have been able to deduce the nature of the movements permitted in the joint; we have spoken of the ligaments which surround the joint, and from their arrangement we have been able to infer the limits imposed upon these movements. But we have not spoken of the conditions which enable one articular surface to glide upon another without separating, and which maintain the surfaces in intimate and permanent apposition. It might be thought that this function devolves on the ligaments, but this would be an error;[124] it is atmospheric pressure which keeps up this contact.
The head of the femur is fitted very exactly into the hollow of the acetabulum. In the first place, the head of the femur is in close contact with the cavity, the non-articular portion of which is filled up by adipose tissue. In the second place, the cotyloid ligament closely encircles the base of the head of the femur, and may be compared to the edges of a cupping-glass. Now, as a vacuum exists between the two articular surfaces, and the air cannot penetrate between them, they adhere very closely to each other, merely allowing one to glide on the other; but if by any means air is allowed to obtain access to the interior of the joint the bones naturally fall apart. The experiments which explain those facts were first demonstrated by the brothers Weber.
We have felt it important to dwell here, once for all, on the important part which atmospheric pressure plays in the mechanism of joints. Analogous experiments show that this pressure plays comparatively the same part in other articulations in maintaining their articular surfaces in contact.
Measurements and Proportions of the Hips.—To return to the study of the region of the hips, we must now examine the transverse dimensions of this region, and the external forms which result from the presence of bony prominences, especially the great trochanter of the femur.
The transverse distance which separates the one great trochanter of the femur from the other should be compared with the distance between the heads[125] of the humeri; in other words, we must compare the diameter of the hips with that of the shoulders.
What strikes us most in this comparison, at the first glance at a series of skeletons, is the great projection which the hips form in the female. In order to express this difference, various formulæ have been proposed. In one such formula the trunk is regarded as a figure more or less regularly oval, of which one extremity corresponds to the shoulders, the other to the hips, and in the two sexes the diameter is greater at one end than at the other. The ancients expressed the formula in the following manner:—In the male and in the female the trunk represents an ovoid—that is to say, an oval similar to that of a figure of an egg having a greater and a smaller extremity. In the male this figure has its greater end above, while in the female the lower is the larger end. According to this formula, in the female the diameter of the hips exceeds that of the shoulders, while in the male it is the diameter of the shoulders which exceeds that of the hips. The formula, as regards the female at any rate, is evidently exaggerated. In fact, Salvage and Malgaigne proposed the following formula:—Allowing that the trunk of the male is an ovoid, with the greater extremity superior, the trunk of the female forms an ellipse—that is to say, a figure in which both extremities are of the same dimensions; so that while in the male the diameter of the shoulders exceeds that of the hips, in the female the diameter of the hips is just equal to it.
Now this last formula also exaggerates the real proportions of the hips in the female. The correct formula is as follows:—In the male, as well as in[126] the female, the trunk represents an ovoid with the greater diameter above; but while in the male the difference between the greater extremity and the smaller is very considerable, in the female this difference is very slight. We can see by actual measurements that in the female the diameter of the hips, though always less, differs very little from that of the shoulders. In the male, the distance from the head of one humerus to the corresponding part on the opposite side (inter-humeral diameter) is on the average 15¼ inches, and the measure taken from one great trochanter to the other (inter-trochanteric diameter) is 12¼ inches; a difference between the two diameters of about one-fifth. In the female, the inter-humeral diameter is on the average 13¾ inches; the inter-trochanteric diameter is 12½ inches; therefore there is between the two diameters a difference of about one-twelfth. These figures also serve to demonstrate that the diameter of the shoulders is greater in the male than in the female (15 to 14), and that inversely the diameter of the hips is greater in the female than in the male (12½ to 12¼); so that, accordingly, if a man and a woman of average stature are supposed to throw their shadow on the same portion of a screen, the shadow of the shoulders of the male would cover a much larger surface than the shadow of the shoulders of the female; and, on the contrary, the shadow of the hips of the woman would exceed the shadow of the hips of the man, but only to a very small extent.
In the foregoing paragraphs we have dealt with[127] the transverse hip-measurements as inter-trochanteric. There is, however, another method of measurement, which justifies to a certain extent the formulæ adopted by the authors previously mentioned; it consists in comparing on the skeleton in both sexes the diameter of the pelvis without the femora with the diameter of the shoulders without the humeri. In this instance the shoulders are represented by the inter-acromial, and the hips by the inter-iliac diameter (from one iliac crest to the other). Under these circumstances the exact measurements show that in the male the inter-acromial diameter is 12¾ inches, and the inter-iliac 11 inches; therefore, as in the other formula, the trunk, deprived of its members, still represents an ovoid, with its greater extremity superior. On the other hand, in the female, the inter-acromial diameter is 11½ inches, and the inter-iliac measurement is 12 inches; so that here the trunk, deprived of its members, represents an ellipse or an ovoid, with its greater extremity below, although the upper extremity differs very little in size from the lower. The fault of this method of measurement is that it does not explain things as they are. The artist does not contemplate the torso as otherwise than complete—that is to say, provided with the upper and lower limbs—and it is absolutely necessary to take into account the part which the head of the humerus and the great trochanter of the femur take in the formation of the contours of the shoulder and hips. We have thought it desirable, however, to demonstrate this mode of measurement, because of the clear illustration which it gives of the greater[128] diameter of the female pelvis as compared with that of the male.
If we arrange in a table the figures given above for the inter-humeral, inter-trochanteric, inter-acromial, and inter-iliac diameters in the male and in the female, or if, better still, we represent those figures by lines intended to express, on the profile of a man and that of a woman, the proportionate value of the diameters of the region of the shoulders compared with the diameters of the pelvis and the hips, we obtain two figures which express in a striking manner all that has been pointed out (Figs. 41 and 42).
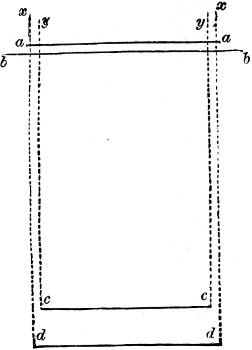
Fig. 41.
Diagram comparing the diameters of the hips with the diameters of the shoulders in the male.
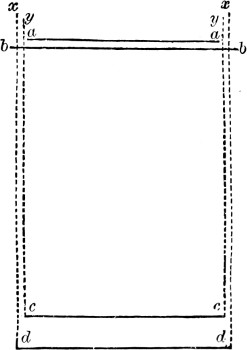
Fig. 42.
Diagram comparing the diameters of the hips with the diameters of the shoulders in the female.
We see, in fact, that in the male subject (Fig. 41) the vertical lines (y and y) passing through the[129] extremities of the inter-trochanteric (d d) and the inter-iliac (c c) diameters, both fall within the extremity of the inter-humeral (b b), and also the inter-acromial diameter (a a); on the contrary, in the female (Fig. 42) we find that these same vertical lines both fall within the extremities of the inter-humeral (b b), but on the outer side of the inter-acromial (a a) diameter.
The Great Trochanter.—A word is necessary concerning the influence of the great trochanter of the femur on the external form of the hip. Looking at the skeleton the great trochanter is seen to stand out so clearly and forms a projection so considerable that we should expect to see on the model a prominence corresponding to its shape. This, however, is not so. The gluteal muscles which proceed from the pelvis to be attached to the great trochanter are numerous and thick, and the fleshy bellies of the more superficial form a projection which is raised above the trochanter; while over the process they are replaced by tendons, more or less flattened, so that the trochanter is marked on the surface by a depression bounded by the muscles—the tensor vaginæ femoris in front, the glutei muscles above and behind. Below, the concave space corresponding to the great trochanter is continuous with the broad, flat surface which occupies the outer aspect of the thigh.
There are many analogous cases where osseous projections are frequently marked on the external figure by a depression, and the reason is always the same as that just explained, that these osseous projections give insertion to muscles, the fleshy bellies of which give place to tendinous expansions at a little[130] distance from them, and form by their thickness a raised surface round the prominence; in a general way, then, we may say that, with a few exceptions (such as the malleoli of the ankle-joints), wherever an osseous surface is covered over only by the skin, the muscles which surround this surface arise above its level, and in consequence the bone is marked by a depression, more or less pronounced as the subject is more or less muscular. Similarly, the middle portion of the sternum is marked superficially by a depression limited on each side by the swelling of the great pectoral muscles, and the internal surface of the tibia forms a long and broad groove when the anterior and posterior muscles of the leg are well developed.
[131]
The bony structure of the thigh and knee.—Shaft of femur: its curvature; oblique direction; linea aspera.—Lower extremity of femur: condyles; inter-condyloid notch; patellar surface.—Patella: ligament of the patella.—Upper parts of the bones of the leg.—Head of the Tibia: tuberosities and tubercle.—Head of fibula.—Articulation of the knee; relation of the bones in flexion and extension.—Ligamentous apparatus; capsule; its laxity and extent in front, whence the facility and extent of movement in flexion; its strength and shortness behind, whence the limit of movement in extension.—Lateral ligaments of the knee: their special mechanism.—Lateral movements of the knee: crucial ligaments.—Form of the region of the knee: surface below the patella; projection of patella; ligament of patella.—Osseous projections on the external surface and the insertion of tendons.—Simplicity of the form of inner surface of the knee.
Having studied the upper extremity of the femur with regard to the articulation, proportions, and contour of the region of the hips, we shall continue the study of this bone by examining its shaft and inferior extremity, and this latter part brings us to the articulation of the knee.
The shaft of the femur is not straight, but is distinctly curved, with its convexity forward and outwards. On the living model this convexity may be recognised in the form of the anterior surface of the thigh, which is distinctly convex in front and on the outer side, the muscles which cover the femur in front being disposed in such a manner as to increase this appearance still more, as their fleshy masses are grouped together in the[132] middle line of the anterior region of the thigh. The outward projection is most marked in cases of excessive muscular development, and is consequently more obvious in the male than in the female, and is best shown in the limbs of athletes. Again, the femur, in the model when standing upright, is not directed vertically, but rather obliquely from above downwards and inwards (Fig. 43), so that the superior extremities of the femur are placed at some distance, comparatively speaking, from each other, while the lower extremities come very near each other at the level of the knees. In the female this obliquity is more clearly marked than in the male, for the upper extremities of the two bones are in the former placed more widely apart, as we have already seen when demonstrating the relative diameter of the hips (inter-trochanteric diameter) in the female.

Fig. 43.
Left Femur (posterior view).—1, 1, linea aspera;—2, 2, its external superior bifurcation;—3, its internal superior bifurcation;—4, 4, its inferior bifurcations;—5, head of femur;—6, depression in the head giving insertion to ligamentum teres;—7, neck of femur;—8, great trochanter;—9, internal surface of great trochanter;—10, small trochanter;—11, external condyle;—12, internal condyle;—13, inter-condyloid notch;—14, 15, tuberosities surmounting each of these condyles.
[133]
The shaft of the femur presents three surfaces—one anterior, one postero-external, and one postero-internal; and three borders, two lateral and one posterior. The two lateral borders are very rounded, not sharp; the posterior border, on the contrary, is very prominent, and forms a rough line, called the linea aspera (1, Fig. 43), which gives insertion to a number of muscles. This linea aspera divides above into two bifurcations slightly diverging, of which the outer one (2, 2, Fig. 43) proceeds towards the great trochanter (gluteal ridge), and the inner one passes towards the lesser trochanter. Below, the linea aspera bifurcates in the same manner, one of its branches going to the inner, the other to the outer condyle of the femur (4, 4, Fig. 43).
The inferior extremity of the femur is widely expanded, both in the transverse and in the antero-posterior diameter. When we examine the posterior aspect of this extremity (Fig. 43) we see that it is formed by two large prominences directed backwards, which are termed the external and internal condyles. These project laterally, and the inner condyle is much more prominent than the outer. The inferior and posterior surfaces of these condyles are smooth and covered with articular cartilage; between them is a deep hollow behind called the inter-condyloid notch (13, Fig. 43). When we examine the anterior surface of the lower end of the femur we see that the condyles are united, and their smooth and continuous articular surface, covered with cartilage, serves to articulate with the knee-cap. This is the patellar surface. This surface presents a[134] depression in the middle line and two lateral lips, of which the external, continuous with the external condyle, is more prominent and rises higher than the internal, which is continuous with the internal condyle. These details are very important, for, as we shall see, the lips of the patellar surface show prominently beneath the skin when the knee is strongly flexed, and we can notice their differences in prominence and height.
In forming the articulation of the knee, the lower end of the femur is in direct contact with the patella and the upper end of the tibia, and is connected (by ligaments) with the upper end of the fibula. We will now consider the patella and the upper extremities of the two bones of the leg.
The patella, which has been compared to a disc (whence its name), is more nearly triangular in shape, presenting an anterior surface longitudinally striated and slightly convex, and a posterior surface moulded on the patellar surface of the femur, and forming an oval articular surface with a median ridge and two lateral hollows. The borders of the patella are three: two lateral oblique borders for the attachment of muscles and ligaments; and a base directed upwards, into which the tendon of the quadriceps extensor (and particularly the rectus femoris) is inserted. The apex of the bone is directed downwards, and attaches a strong ligament which is inserted into the tubercle of the tibia, and is termed the ligament of the patella. Properly speaking, this ligament is a continuation of the tendon of the rectus femoris muscle. The patella should be considered as a sesamoid bone, an[135] osseous nodule developed in the substance of this tendon.

Fig. 44.
The two Bones of Left Leg (anterior view).—1, shaft of tibia;—2, 3, its internal and external tuberosities;—4, spine of tibia;—5, tubercle of tibia;—6, shin;—7, lower end of tibia, with internal malleolus (8);—9, shaft of fibula;—10, its upper end;—11, its lower end or external malleolus.
The leg, like the forearm, is composed of two bones. One, the larger of the two, is placed on the inner side (1, Fig. 44)—the tibia, or shin-bone; the other, much shorter, is situated on the outer side, and a little behind—the fibula (9, Fig. 44). As in the case of the two bones of the forearm, the bones of the leg end at different levels above and below. Above, the tibia rises higher than the fibula, and alone takes a direct part in the articulation of the knee; below, the fibula extends lower than the tibia—so that the outer ankle (external malleolus) descends lower than the inner one. We will now for a moment examine the upper extremities of the two bones.
The upper extremity of the tibia is expanded from side to side, to form the tuberosities (internal and external), surmounted by two articular surfaces, external and internal (2, 3, Fig. 44), for articulation with the corresponding femoral condyles. The non-articular interval between these two surfaces presents in its centre a projection like a bifurcated cone which[136] is known as the spine of the tibia. In front of the spine and behind it are rough triangular surfaces for the attachment of the crucial ligaments.
The circumference of the upper end of the tibia forms a broad rough margin for attachment of the capsule of the knee-joint. In front, it is prolonged downwards into a large triangular surface which ends in a rounded eminence, called the tubercle of the tibia, which gives insertion to the ligament of the patella previously mentioned. On the outer side and back of the external tuberosity is a rounded facet, smooth and covered with cartilage, and directed mainly downwards for articulation with the head of the fibula (10, Fig. 44). Lastly, on the back of the bone is the notch of the tibia, separating the two tuberosities from one another.
The upper end of the fibula forms (10, Fig. 44) an irregular rounded knob. It is situated external to and rather behind the upper end of the tibia, and articulates, as already seen, by its upper surface with the outer tuberosity of the tibia. External to the articular surface is a smooth area for the attachment of the biceps tendon, and the long external lateral ligament of the knee. Behind this area is the styloid process, which gives attachment to the short external lateral ligament of the knee. The head of the fibula can be plainly felt through the skin, below and behind the head of the tibia.
Such are the bony structures which take a direct (femur, tibia, patella) and indirect part (fibula) in the conformation of the knee-joint. In the living model, in the erect posture, the condyles of the femur rest by their inferior surfaces on the upper surface of the[137] tibia, and the apposition of the articular surfaces is rendered more exact by the presence between the articular surfaces of the femur and tibia of two semi-lunar fibro-cartilages, which increase the depth of the tibial surfaces (5, 5, Fig. 46), so that the corresponding condyle of the femur is received into a true articular cavity. At the same time, the patella is closely applied to the confluent anterior surface of the lower end of the femur. When, on the other hand, the model is kneeling, or, more generally, when the leg is flexed (carried backwards), the patella, which is firmly fixed to the tibia by its ligament, glides downwards on the femur, and comes in contact with the lower part of its anterior surface at the same time that the posterior parts of the condyles in turn roll over the upper surfaces of the tibia.
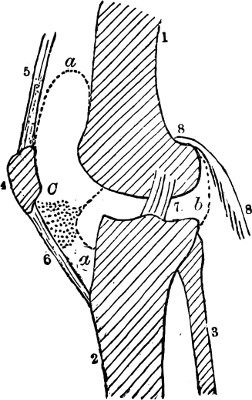
Fig. 45.
The Articular Parts of the Knee (antero-posterior section).—1, femur;—2, tibia;—3, fibula;—4, patella;—5, rectus tendon;—6, ligament of patella;—7, one of the crucial inter-articular ligaments;—8, 8, one of the muscles of the calf;—a, a, anterior part, and b, posterior part of the articular capsule;—C, adipose mass beneath patella.
After this rapid sketch of the bones which enter into the formation of the knee-joint, we have now to study in detail its ligamentous apparatus. The ligamentous apparatus of the knee is essentially composed of a fibrous capsule, attached to the borders of the articular surfaces of the femur, patella, and tibia. It is strengthened on all sides by the[138] tendons of muscles attached to these bones in the neighbourhood of the knee. Without entering into unnecessary detail, we must consider the arrangement of this capsule, and its disposition on its anterior, posterior, and lateral aspects, and then consider how it affects the movements of the knee-joint, rendering some movements easy and extensive, while it limits others or makes them almost impossible.
In front (a a, Fig. 45) the capsule is loose and expanded and is mainly formed by the insertion of the quadriceps extensor muscle into the patella, with its continuation to the tubercle of the tibia as the ligament of the patella. This arrangement accounts for the ease and extent of the movement of flexion. In this movement, the tibia being carried backwards, and drawing with it the patella in the relaxed condition of the quadriceps extensor muscle, the capsule of the joint is put on the stretch. It would curtail the movement of flexion if it were short and compact; but the capsule at this point is so expanded and loose that no increase of movement on the part of the leg can cause any tension. Thus flexion of the knee may be prolonged until the calf of the leg comes in contact with the posterior surface of the thigh.
Behind, the capsule of the joint is short and thick, and consists of a strong posterior ligament. When the leg is flexed on the thigh, this ligament is relaxed; but as the leg passes from flexion to extension it becomes tense, and when extension has arrived at that point which brings the leg in direct continuation with the thigh, no further movement is possible in[139] a forward direction, and the limb is therefore fixed in this position.
There are, moreover, other important ligaments which act, and still more forcibly, in the same manner; namely, the internal and external lateral ligaments of the joint, which must now be considered.
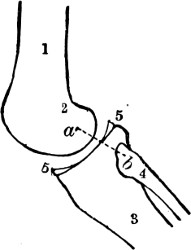
Fig. 46.
The Knee state of the lateral ligaments (a, b) during flexion.—1, femur;—2, condyle of femur;—3, tibia;—4, fibula;—5, 5, section of semi-lunar fibro-cartilage.
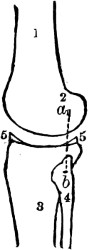
Fig. 47.
The Knee: lateral ligaments tense during extension of the leg on the thigh (the distance, a b, is greater here than in preceding figure); for the lettering, see preceding figure.
The internal lateral ligament is a broad band of fibres, which passes from the inner tuberosity of the femur over the inner tuberosity of the tibia to be attached to the upper part of the shaft of the tibia on the inner side. It helps to form the contour of the inner side of the knee.
The long external lateral ligament is a rounded cord, very strong and quite distinct from the capsule. Its inferior extremity is not inserted into the tibia, but into the head of the fibula between the insertions of the biceps muscle (Figs. 46, 47, a, b). The most[140] remarkable characteristic of these ligaments is that their upper ends, attached to the lateral surfaces of the condyles of the femur, are not inserted at the centre of the curve of the condyles, but at a point situated more posteriorly (a, b, Figs. 46 and 47). During flexion these ligaments are therefore relaxed, but as extension is produced, as the tibia is carried forward on the curved surface of the condyles of the femur, these ligaments gradually become tense, their points of insertion becoming further and further apart, owing to the eccentric insertion of their superior extremities. When the leg reaches that position of extension in which it is in line with the femur, the tension of the lateral ligaments is such as to arrest its movement and completely fix the leg in relation to the thigh. This may be seen by comparing Figs. 46 and 47. We see, then, that owing to the position of the anterior, posterior, and lateral ligaments of the knee-joint, the movement of flexion in this joint is very extensive, while that of extension is limited, as it cannot be prolonged further than the position which brings the leg into direct continuity with the thigh.
These ligaments are also responsible for the amount of lateral movement and rotation possible in the knee-joint. This articulation being formed by two condyles, it is very evident that lateral flexion cannot be produced, for then it would be necessary for one of the condyles to become detached from the corresponding articular surface of the tibia. Lateral movement is thus impossible, but a slight gliding movement under certain conditions takes place between the condyle of the[141] femur and the tibia, a movement produced by a rotatory movement, of which the other condyle forms the centre. These slight movements of rotation, which contribute to the motion by which we direct the point of the foot outwards or inwards, are impossible during complete extension, when the tibia is fixed on the femur by the tension of the lateral ligaments and the posterior part of the capsule, and all the parts have already arrived at their maximum of tension. But when flexion occurs, and especially when the leg is at a right angle to the thigh, as in the seated subject, slight movements of rotation of the leg become possible; they are of small extent, it is true, especially inwards; since it is easier for the knee to take part in the movement which turns the foot outwards, than that which turns it inwards. This difference between rotation inwards and outwards is due to the presence within the joint of two ligaments called the crucial ligaments, of which we will only mention that they arise from the upper end of the tibia, between the two articular surfaces (page 136), and, crossing one another, are attached above to the sides of the inter-condyloid notch of the femur on the corresponding surface of each condyle. This crossing of the two ligaments is increased by the rotation of the tibia inwards, as this movement tends to twist them one on the other, and fix the tibia, so as to prevent rotation of the leg inwards. On the other hand, rotation outwards unwinds these ligaments and renders them more relaxed; so that this movement could be very extensive if the lateral[142] ligaments did not prevent too great displacement between the condyle of the femur and the corresponding surface of the tibia.
There are still in relation to the knee-joint several anatomical particulars which must now be examined in relation to the external form of the living model.
The posterior surface of the knee is covered by numerous muscles and tendons which form the boundaries of the ham or popliteal space; the study of this region will therefore be undertaken along with the description of the muscles of the leg and thigh. On the outer and inner surfaces, and on the front of the knee-joint, however, many details of outward form are caused solely by the osseous and ligamentous parts, to which we must now draw particular attention.
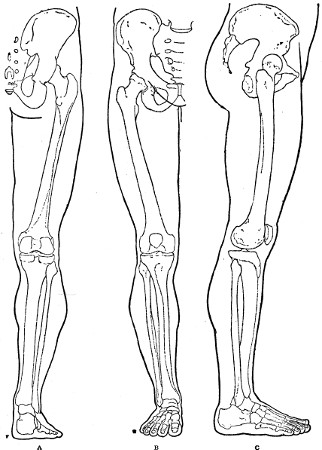
Fig. 48.
Outlines of the Lower Limb.—A, From behind; B, from the front; C, from the outer side.
The anterior surface of the knee alters in shape in the two positions of extension or slight flexion, and in forcible flexion. In forcible flexion we notice particularly the form of the articular lower end of the femur (see page 134). In extension we find on the anterior surface of the knee, in succession from above downwards, a flat triangular space above the patella, corresponding to the tendon of the rectus femoris muscle; next, the prominence of the patella, showing clearly beneath the skin its triangular shape, with the base above and apex below; the two superior angles of the patella are frequently very distinct in the form of two small rounded projections. Below, the ligament of the patella forms a longitudinal eminence in the middle line, reaching to the tubercle of the[143] tibia, which is seen (in semi-flexion) as a large projection. But, again, we frequently perceive on each side of the ligament of the patella a slight, soft eminence, easily depressed, which corresponds[144] to parts not yet mentioned. These are the thin lateral portions of the capsule (lateral ligaments of the patella), which extend from the sides of the patella and patellar ligament to the tibial tuberosities. These portions of the capsule (c, Fig. 45) are thin, and cover a large mass of adipose tissue, which is prolonged into the interior of the joint (as the alar ligaments), and which forms packing for the articulation on either side of the ligament of the patella (6, Fig. 45). When the quadriceps extensor muscle draws forcibly on the patella and its ligament, these compress this adipose mass to a much greater degree, so as to form a bulging on each side, and then the bilateral prominence in question is much more clearly marked.
On the external lateral surface of the knee we note the osseous prominences of the tubercle of the tibia (seen here in profile) and its external tuberosity; behind and below, the head of the fibula; and above, the external condyle of the femur. To certain of these prominences are attached the tendons coming from the thigh, marked on the external surface of the knee by three strong vertical bands; viz.:—in front, the tendon of the patella (seen here in profile); behind, the tendon of the biceps femoris, proceeding to be inserted into the head of the fibula; and between them the part of the aponeurosis of the deep fascia of the thigh, which becomes narrow and thickened, and forms a true tendon—the ilio-tibial band—attached to the outer tuberosity of the tibia.
The form of the internal aspect of the knee is simple. Here the internal condyle of the femur and the corresponding tuberosity of the tibia form[145] together a large regular hemispherical surface. The internal lateral ligament forms a broad band (page 139), which sweeps over the inner tuberosity of the tibia, accompanied by the tendons of the sartorius, gracilis, and semi-tendinosus muscles, to become inserted into the upper portion of the shaft of the tibia. The ligament and tendons soften the outlines of the bones, and give a rounded contour to the inner side of the knee.
[146]
The bony structure of the leg.—Tibia and fibula: tibio-fibular articulation; absence of mobility in the fibula (differences between the leg and forearm: between the foot and hand, also in the quadrumanous monkeys). Inferior extremities of these bones: tibio-fibular articulation; the malleoli: comparison of the internal and external malleoli with regard to length, situation, and form.—The skeleton of the foot: tarsus, metatarsus, and toes.—Importance of the bony structure of the tarsus and its influence on the form of the foot: construction and arrangement of tarsus, posterior half: anterior half.—Articulation of the leg with the foot; movements of the foot.
The two bones of the leg are placed, as we have previously seen (page 135), parallel to each other, the tibia on the inner side, the fibula on the outer side and somewhat behind (Fig. 49). The tibia can be felt beneath the skin in its whole length. Its shaft is triangular in section, and therefore presents three surfaces and three margins (1, Fig. 49): an internal surface covered only by the skin and appearing superficially as a long flat surface, broader above where it looks a little forward, and inclining directly inwards at its inferior part, where it becomes continuous with the prominence of the inner ankle or internal malleolus (Fig. 50, page 150). The external surface is slightly concave in order to lodge the antero-external muscles of the leg, of which the principal is the tibialis anticus; below, this surface inclines forwards, following the course of the tibialis muscle, which, from the antero-external region of[147] the leg, is directed towards the inner border of the foot (Fig. 50, page 150). The posterior surface of the tibia is entirely covered by the strong and numerous muscles of the posterior region of the leg. Finally, of the three margins of the shaft of the tibia the anterior is particularly prominent, and is known by the name of the crest of the tibia or shin (6, Fig. 49).
The fibula appears superficially, as already seen, in the region of the knee, at its upper end. Its lower end is also obviously subcutaneous at the outer ankle, where it forms the external malleolus (9, Fig. 49). The shaft of the bone is long and slender, and is prismatic in form. It is curved from above downwards and forwards, and downwards and inwards. It serves the purpose of a strengthening bar for the tibia, at the same time that it increases the area for the attachment of the muscles of the leg. The shaft of the fibula is surrounded on all sides by these muscles.
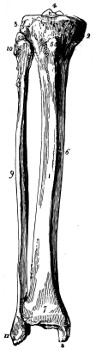
Fig. 49.
Bones of the Leg (front view).
The two bones are separated throughout their entire length by an interval called the interosseous space (Fig. 49), broader above than below, and filled up by a fibrous membrane (interosseous membrane), which, passing from one bone to the other, still further increases the area for attachment of the muscles of the leg. Above, the[148] fibula articulates with the postero-external surface of the superior extremity of the tibia, and this superior tibio-fibular articulation possesses a very slight gliding movement, exercised chiefly through the action of the biceps muscle in external rotation at the knee-joint. Below, the fibula is attached to the corresponding part of the tibia by a strong interosseous ligament, forming a symphysis, or synarthrodial joint. This inferior tibio-fibular articulation has hardly any mobility: it only gives a certain amount of elasticity to the ankle-joint, into which the foot is received. We see, therefore, that there is, with regard to mobility, a great difference between the bones of the leg and those of the forearm; in the forearm the radius is moveable on the ulna, and can turn in such a manner as to cross the latter, and produce the movements of pronation and supination of the hand. Between the fibula and the tibia there is no movement of the kind; the foot is not capable of any movement which may be compared to that which takes place in the hand during pronation and supination. We may say that it is the same with monkeys, in the class called quadrumana; they have not the power of pronation and supination of the foot, which, from this point of view, and also in every other respect, is properly speaking a foot and not a posterior hand, as their ancient name of quadrumana would lead us to suppose.
Ankle-joint.—By their junction the inferior extremities of the tibia and fibula constitute an articular cavity, which forms the ankle-joint, by their articulation with a bone of the tarsus—the astragalus.[149] This tibio-fibular cavity possesses three sides, of which two, the superior and internal, are formed by the tibia, and one only, the external, by the fibula; the two lateral walls correspond to the two osseous parts which form the prominences of the ankles and which are known by the name of malleoli (malleus, a hammer). They are distinguished as the internal or tibial and external or fibular malleoli (Fig. 49, page 147). As the internal ankle or malleolus (8) is of a form and situation very different to that of the external (11), it is important to note here the configuration of the bones by which the subcutaneous prominences are explained.
The malleoli differ in their level, in their situation, and finally in their form (Figs. 50, 51). First, we see at a glance that the external or fibular malleolus (11) descends much lower than the internal malleolus (8). Second, with regard to the transverse plane of the two malleoli, just as the shaft of the fibula is situated behind and to the outer side of the tibia, so the same position is maintained by the inferior extremities of the two bones, and the external malleolus is on a plane posterior to the internal malleolus. A transverse line which passes through the centre of the internal malleolus, passes outwards in front of the anterior border of the external malleolus; and, on the other hand, a transverse line, passing through the centre of the external malleolus, passes inwards behind the posterior border of the internal malleolus. Thirdly, with regard to the differences of form, these are the direct result of the shape of the osseous parts. The malleolar portion of the tibia, or internal malleolus,[150] is square, presenting a horizontal inferior border, and two vertical borders—one anterior, the other posterior. On the contrary, the malleolar portion of the fibula, or external malleolus, is triangular in shape, or rather like the head of a serpent; it terminates below in a pointed extremity, formed by the convergence of the two oblique borders—one anterior, the other posterior—of which the anterior is the more sloping.
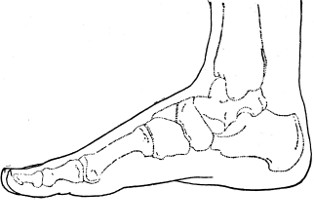
Fig. 50.
Outline of Ankle and Foot (inner side).
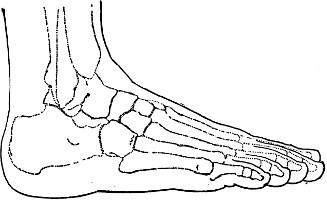
Fig. 51.
Outline of Ankle and Foot (outer side).
[151]
Before entering into a study of the articulation of the leg with the foot, or ankle-joint, we must glance at the bony structure of the foot as a whole, so as to understand properly the significance of the position of one of the bones (astragalus) in relation to this joint.
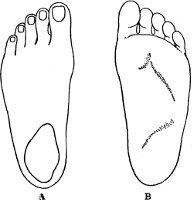
Fig. 52.
Outlines of the Foot (A, Dorsum; B, Sole).
Just as the hand is composed of three sets of bones—the carpus, metacarpus, and fingers—so also the foot is composed of a similar series—the tarsus, metatarsus, and toes; but while in the hand, where the function is principally that of prehension, the fingers are long and the carpus very short, in the foot, which serves as a base of support, the toes are comparatively short, while the tarsus, which corresponds to the carpus, is of considerable size; it forms, in fact, one-half of the length of the foot. In order to understand the form of the foot and its mechanism it is necessary to make a particular study of the bones which compose the tarsus.
As the carpus in the hand is formed by two rows of bones, so also the tarsus is composed of two groups. In the hand the carpal bones are grouped in[152] two more or less transverse rows. In the foot, on the other hand, the rows of tarsal bones are longitudinally arranged; and the inner row overlaps the outer row in relation to the back part of the tarsus. There are two bones in the outer row: the calcaneum or os calcis behind, which forms the prominence of the heel and rests on the ground below: and the cuboid, articulating with it in front and carrying anteriorly the two outer metatarsal bones and the two outer toes. The inner row consists of five bones: (1) the astragalus or talus behind, which articulates with the bones of the leg and helps to form the ankle-joint above, which rests below on the upper surface of the calcaneum, and which articulates in front with the navicular bone; (2) the navicular or scaphoid bone; and in front of this the three cuneiform bones (internal, middle, and external), which lie above and internal to the cuboid bone, and carry the three inner metatarsal bones and the three inner toes.
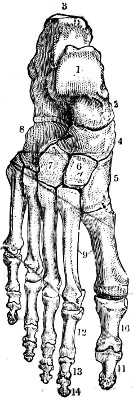
Fig. 53.
The Bones of the Foot, seen from the dorsal surface.—1, astragalus (with its head and neck, 2);—3, calcaneum;—4, scaphoid;—5, internal cuneiform;—6, middle cuneiform;—7, external cuneiform;—8, cuboid;—9, the metatarsus;—10, 11, the two phalanges of the great toe;—12, 13, 14, the first, second, and third phalanges of the other toes.
After this brief sketch of the tarsus, and before entering into the details of the configuration of its parts and the whole taken together, having seen the particular place occupied by the astragalus, we must study its articulation with the tibia and fibula. The part of the astragalus which is received into the cavity between the malleoli, is formed by the posterior three-fourths (1, Fig. 53) of the superior part of the bone, separated from the anterior fourth by a narrow portion called the neck (2, Fig. 53). This articular part is in the form of a pulley, with the antero-posterior groove hardly perceptible, but the lips are prolonged over the sides of the bone,[153] and come in contact with the corresponding parts of the internal and external malleoli. It is readily seen (Fig. 53) that the articular surface of the astragalus is considerably wider in front than behind. The same is seen in the shape of the lower end of the tibia. The tibio-astragaloid articulation permits movement chiefly in the anterio-posterior plane, namely, movement forward (flexion of the foot) and backwards (extension). During flexion of the foot on the ankle the astragalus is received in the malleolar cavity as in a vice, and the result is that no lateral movement is possible. When, however, the foot is extended, and the toes are pointed, the narrower part of the articular surface of the astragalus comes into relation with the wider portion of the inter-malleolar articular surface, and the result is that in this position a certain amount of lateral movement of the foot at the ankle-joint is permitted, aided, it is true, by gliding movements taking place among the tarsal bones themselves. Of the movements of flexion and extension, that of extension is the most free, as it may be continued until the axis of the foot[154] becomes continuous with that of the leg, and here it is arrested by the meeting of the posterior border of the joint with the projections on the posterior border of the astragalus; but the movement of flexion by which the dorsal surface of the foot is brought near the anterior surface of the leg is more limited, for it is impossible to cause the foot to make with the leg an angle less than forty-five degrees, opening upwards and forwards. This is accounted for by the shape of the articular surfaces. In proportion as flexion is produced, the larger part of the articular surface of the astragalus is wedged into the malleolar cavity; thus the movement of flexion is arrested, and the foot is fixed. We cannot carry flexion further without bursting asunder the tibio-fibular joint, just as we should split a piece of wood by driving violently into it a wedge larger than the cavity to be filled.
[155]
Bony structure of the foot.—Union of bones of tarsus; astragalus and calcaneum (canalis tarsi, or tunnel of the tarsus); astragalar articulations, inferior calcaneo-scaphoid ligament; special functions of astragalus in the mechanism of the foot.—The other articulations of the tarsus, and their movements. Metatarsus and Metatarsal bones; importance of fifth metatarsal with regard to form.—The toes and their phalanges.—Skeleton of the foot as a whole; form of the foot.—Plantar arch.—Proportions of the lower limb; the foot as a common measure of the lower limb and the height.
We will now examine briefly the bones of the tarsus, especially with regard to the details which mark their articulations. The inferior surface of the astragalus presents two articular facets, separated by a deep, oblique groove. These two facets correspond with two similarly situated on the upper surface of the calcaneum. The astragalus thus rests upon the calcaneum, but it is supported on the inner side by a projection of the calcaneum, known by the name of the sustentaculum tali; and the anterior facet for the astragalus is to be looked for on the upper surface of this projection (Fig. 53, page 153). The two facets of the calcaneum are also separated by a deep groove. It follows, therefore, that when the astragalus is in its place, the groove of the astragalus and the calcaneum meet and form a kind of tunnel, which is called the cavity of the tarsus, or canalis tarsi. This cavity is filled up during life by a strong[156] ligamentous band, which attaches the astragalus to the calcaneum, and is called the interosseous ligament. Placed between the two calcaneo-astragaloid articulations, one in front of it and the other behind, the ligament forms a sort of pivot, around which the movements between the astragalus and the calcaneum take place. It is round these joints as a centre that the movements take place by which the foot as a whole is turned inwards or outwards, and so that its outer and inner borders are elevated.
We have next to consider the articulations of the calcaneum and astragalus with the other bones of the tarsus. The articulation of the anterior extremity of the calcaneum with the posterior surface of the cuboid presents an interlocked arrangement which is surrounded by strong ligaments, especially on its lower plantar surface (the inferior calcaneo-cuboid ligaments, or long and short plantar ligaments), so that between the calcaneum and the cuboid only a slight gliding movement takes place, and to all intents and purposes these two bones form one elastic piece. The plantar ligaments from their strength have an important influence on the maintenance of the arch of the foot. The cuboid bone articulates in front with the metatarsal bones of the fourth and fifth toes, so helping to complete the outer part of the contour of the foot. On the inner side of the foot the bones completing the tarsus in front of the astragalus are the navicular (or scaphoid), and the three cuneiform bones, internal, middle, and external, which in turn are related to the[157] inner three metatarsal bones. The astragalo-scaphoid articulation deserves the closest attention. The head of the astragalus, so called from its prominent rounded shape, articulates with the navicular bone, which is prolonged internally into a prominent tubercle. Between the sustentaculum tali and this tubercle a very powerful ligament passes, on which a part of the astragalus rests. The ligament is called the inferior calcaneo-scaphoid ligament, or spring ligament, and by its means an articulation is completed between the three bones—the astragalo-calcaneo-scaphoid joint. The whole weight of the body may be supported by the inferior calcaneo-scaphoid ligament, which thus serves an important purpose in supporting the arch of the foot. This is the ligament which gives way in flat-foot. By these articulations the foot possesses the power of lateral movement, by which the toes are carried inwards or outwards, and the outer border of the foot is elevated and the inner border is depressed, or the reverse. On the other hand, the movements of flexion and extension take place chiefly at the ankle-joint, the articulation, previously explained, of the astragalus with the tibia and fibula.
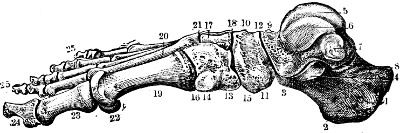
Fig. 54.
Right Foot (internal border).—1, 2, 3, 4, calcaneum;—5, 6, 7, astragalus;—8, posterior calcaneo-astragaloid articulation;—9, head and neck of the astragalus;—10, 11, navicular or scaphoid;—12, astragalo-scaphoid articulation;—13, 14, internal cuneiform;—15, articulation of the internal cuneiform with the scaphoid;—16, the articulation of the internal cuneiform with the metatarsal bone of the great toe;—17, the middle cuneiform;—18, its articulation with the scaphoid;—19, the first metatarsal bone;—20, the second metatarsal bone;—21, the articulation of the second metatarsal bone with the cuneiform bones;—22, sesamoid bone;—23, 24, the phalanges of the great toe; 25, 25, phalanges of the other toes.
The navicular or scaphoid bone articulates in front with the three cuneiform bones, and the cuneiform bones articulate with each other by facets which are flat, but present rough surfaces towards their inferior or plantar portions intended for interosseous ligaments. Similar articulations exist externally between the scaphoid and external cuneiform, and the cuboid bone. It is sufficient to[158] say that in all these articulations a slight gliding movement takes place, just sufficient to give a certain elasticity to the plantar arch, which they contribute to form. We may point out the peculiarities that are to be noted in each of these bones: the scaphoid or navicular bone is concave behind, convex in front, and is prolonged into a prominent tubercle, which can be felt at the middle of the inner border of the foot; the cuboid is quadrilateral or pyramidal in form, and has an oblique groove (14, Fig. 55) on its inferior or plantar surface, which contains the tendon of the long peroneal muscle (see below); finally, the three cuneiform bones are distinguished, counting from within outwards, as the internal, middle, and external cuneiform (Fig. 53, page 153); the middle cuneiform (6) is smaller than the others, and does not extend so far forward, so that in relation to it the line of the tarso-metatarsal joints forms a notch[159] opening into the tarsus, into which the posterior extremity of the second metatarsal bone is received.
In front of the tarsus is found the metatarsus, corresponding to the metacarpus of the hand, while the toes correspond to the fingers. We have only a few words to say about those portions of the skeleton which resemble the corresponding parts of the hand.
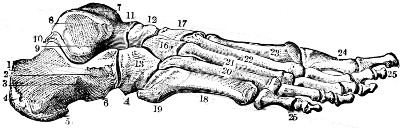
Fig. 55.
Right Foot (external border).—1 to 6, the calcaneum;—7, the tibial surface of the astragalus;—8, the lateral facet of the astragalus for the external malleolus;—9, the tunnel of the tarsus (canalis tarsi);—10, the posterior calcaneo-astragaloid articulations;—11, head and neck of the astragalus;—12, the scaphoid;—13, cuboid;—14, commencement of the groove on the inferior surface of the cuboid (for the tendon of the long peroneus muscle);—16, external cuneiform;—17, middle cuneiform;—18, the five metatarsal bones with their posterior extremities (19);—20, 21, 22, 23, fourth, third, second, and first metatarsal bones;—24 to 25, phalanges of the toes.
The metatarsal bones, five in number, are long bones, each composed of a prismatic shaft and two extremities, one posterior or tarsal, more or less wedge-shaped; the other anterior or digital, forming a rounded, globular head which articulates with the base of a phalanx. The metatarsal bones are placed parallel side by side, but that of the great toe is not markedly shorter than its fellows like the metacarpal bone of the thumb, and the great toe does not possess anything like the same amount of mobility as the thumb. It is further directed straight forward so as to complete the straight line of the inner border[160] of the foot. With regard to particular details, it is necessary to note in the first metatarsal (19, Fig. 54) its large size, in the second (22, Fig. 55), its greater length, for it passes behind the others (in entering into the notch which corresponds to the middle cuneiform), and it also exceeds them in length, so that the second toe is as a rule a little longer than the rest. In the fifth we must note the form of its tarsal extremity, prolonged behind into a process (19, Fig. 55) which appears as a prominence at the middle of the outer border of the foot, and gives insertion to the short peroneal muscle. Lastly, it may be observed that all the metatarsal bones except the first are sloped inwards and forwards, to point as it were towards the great toe.
The phalanges of the toes (Figs. 54 and 55) resemble in number and arrangement the corresponding bones of the hand, only they are much shorter, especially those of the little toe, the two last of which are reduced to small osseous nodules, so that the fifth toe is always much shorter than the rest. The names of the phalanges are the same as in the hand (page 93).
The Foot as a whole.—The skeleton of the foot forms an arch which presents two curves or concavities, one antero-posterior, the other transverse. The sole of the foot forms a hollow which extends from the posterior extremity of the calcaneum to the anterior extremity of the metatarsal bones; but this plantar hollow is much more elevated on the inner side (Fig. 54) than on the outer side (Fig. 55). It is necessary, in other words, in order to understand the general form of the foot, to consider[161] that its dorsal surface looks upwards and outwards, and the sole downwards and inwards. The outer border is thin, and comes almost in contact with the ground, its inner border is thick and is raised from the ground.
The skeleton of a well-articulated foot placed upon a horizontal surface comes in contact with the flat surface only by the posterior extremity (tuberosity) of the calcaneum (heel), and by the heads of the metatarsal bones (the balls of the toes, Fig. 52, page 151). When the foot is covered with its soft parts these points of contact are scarcely changed; for, except at the heel and the balls of the toes, we see that the greater part of the outer border of the foot touches the ground but lightly, unless the subject is carrying a heavy load, which, pressing upon the plantar arch, brings its elasticity into play and slightly flattens it. We shall mention later on the special structures (ligaments and tendons) which act as cords which bend the bow and maintain the plantar arch.
Proportions of the Lower Limb.—As we have already inquired into the ratio of proportions of the hand and upper limb, we shall now see if the foot can furnish any measurements relative to the proportions of the body. We find that we can make the foot, no more than the hand, a common measure for the body in general and for the inferior limb in particular. We must confine ourselves to such measurements as will apply to the average subject. Thus it is easy to perceive upon the skeleton that the distance from the upper margin of the head of the femur to the inferior border of the internal[162] condyle is equal to twice the length of the foot; but this has no practical value—it cannot be used on the living body, as it is difficult to recognise the level of the upper part of the head of the femur. If, instead of the head of this bone, we take the superior border of the great trochanter (a part easily felt beneath the skin), we find that the length from the superior border of the great trochanter to the inferior border of the external condyle scarcely ever measures the length of two feet, as the great trochanter is upon a considerably lower level than the head of the femur.
The leg, including the thickness of the foot, is not as much as twice the length of the foot—that is, the distance from the lower border of the internal condyle of the femur to the ground (or the sole of the foot); but it is interesting to observe that in general the length of the leg, plus the thickness of the foot, is equal to the distance from the great trochanter to the lower border of the external condyle; in other words, the centre point of the lower limb (starting from the great trochanter) corresponds exactly to the line of the knee.
When we compare the length of the foot with the leg, beginning from below upwards, we find a regular proportion, and one of practical interest—viz. that the line from the ground to the middle of the patella usually measures twice the length of the foot.
As a common measure of the height of the body, the foot does not give us a result that can be expressed by an even number. From the numerous researches of Leger on this question, the length of[163] the foot is generally contained 6⅓ times in the total height. However, this number presents an interesting fact when we express this proportion by taking the third part of the foot for a unit; 6⅓ feet forming nineteen thirds of the foot, we see that the height of the body contains nineteen thirds of the foot. It is interesting to observe that the number 19 is precisely that which expresses the proportion that the middle finger bears to the height in the Egyptian canon, according to Charles Blanc.
With regard to the foot itself, we need only say that the tarso-metatarsal line offers, on the skeleton, a simple means of dividing the foot. This line is oblique from within outwards and backwards; its inner extremity at the base of the first metatarsal bone divides the foot into an anterior and posterior half, while its outer extremity, at the base of the fifth metatarsal bone, divides it into a posterior one-third and anterior two-thirds.
[164]
The bony structure of the head; division into cranium and face. Study of the vault, or skull-cap. Occipital bone.—Parietal bone (parietal eminence and temporal ridge).—Frontal bone (frontal eminences, superciliary ridges: nasal eminences: supra-orbital arches).—Temporal bone: mastoid process; zygomatic process.—Sutures of the skull: sagittal suture; lambdoid suture; sphenoidal sutures.—General form of skull: long heads; round heads.—Cephalic indices; dolichocephalic, brachycephalic, and mesaticephalic skulls.
The skeleton of the head is formed of two parts intimately united to each other: one above and behind, formed for the most part of flat bones, simple in form, and called the cranium, containing the brain: the other below and in front, consisting of numerous bones, complex in shape, and constituting the bony structure of the face. The facial bones form the boundaries of the cavities which lodge the principal organs of sense and the apparatus of mastication.
The cranium.—The cranium forms an egg-shaped box with its long axis directed from before backwards. It may be examined from its base, which we need not study here, or from above or from the side. The bones which enter into its construction are eight in number, viz. the sphenoid in the base and side wall, the occipital behind, the frontal in front, the two parietal above, and the two temporal bones on the sides.
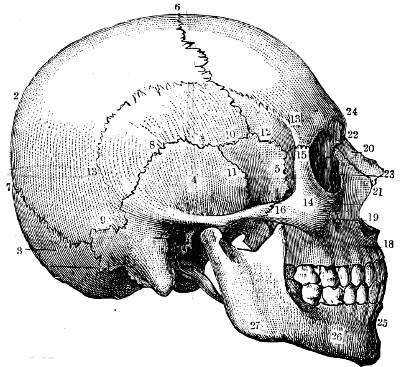
Fig. 56.
The Skull (lateral surface).—1, frontal bone;—2, parietal;—3, occipital;—4, temporal;—5, the great wing of the sphenoid;—6, coronal suture;—7, lambdoidal suture;—8, 9, parieto-temporal suture;—10, spheno-parietal suture—11, spheno-temporal suture;—12, fronto-sphenoidal suture;—13, curved line limiting the temporal fossa;—14, 15, 16, malar bone;—18, the superior maxillary bone, with the infra-orbital foramen (19);—20, 21, 22, the bones of the nose;—23, the lachrymal groove;—24, the nasal eminence;—25, the inferior maxillary bone;—26, the mental foramen;—27, the angle of the jaw.
The occipital bone (3, Fig. 56) forms the whole posterior part of the base and vault of the skull.[165] The bone possesses two distinct parts, inferior and superior. The inferior part is more or less horizontal, and is pierced by a large foramen (foramen magnum) through which the cavity of the cranium communicates with that of the vertebral canal. In front of this foramen is the basilar process of the occipital bone; upon each side are the occipital condyles, by which the skull articulates with the vertebral column—namely, with the lateral masses of the atlas (pp. 31, 32). The superior part (3, Fig. 56), called the squamous or shell-shaped portion of the bone, is more or less triangular in form, with the[166] apex directed upwards. Its borders are hollowed out into numerous irregular denticulations, which work in with similar denticulations on the posterior borders of the parietal bones (7, Fig. 56); and assist in forming the lambdoidal suture. The external or posterior surface is crossed about its middle by a semicircular crest (the superior curved lines) of which the centre forms a prominence called the external occipital protuberance. This prominence is placed below the most projecting point of the back of the skull. The superior curved lines separate the outer or posterior surface of the occipital bone into an upper smooth part, belonging to the vault, which is covered by the scalp, and a lower rough surface, to which the muscles of the neck are attached.
The parietal bones (2 and 13, Fig. 56) are placed on each side of the vault of the skull in front of the occipital bone. Quadrilateral in shape, each bone presents four denticulated borders, of which the superior articulates with the parietal of the opposite side, the posterior with the occipital (7, Fig. 56), the anterior with the frontal (6), and the inferior, which is concave (8, Fig. 56), with the temporal and (slightly) with the sphenoid bone. The parietal bone presents two points for notice on its external surface—1, near its centre a projection called the parietal eminence, better marked in young subjects than in the adult, which represents the place where the ossification of the bone commences; 2, below this prominence a curved line, the temporal ridge, slightly rough (13, Fig. 56), which limits the temporal fossa and gives attachment to the temporal fascia.
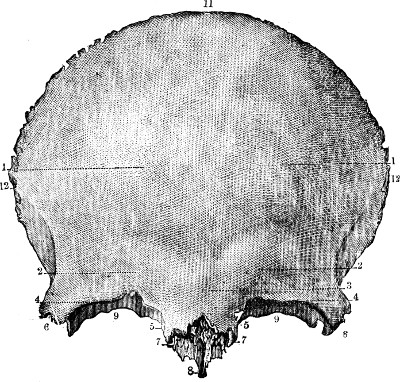
Fig. 57.
Frontal Bone (anterior surface).—1, the frontal eminences;—2, 2, superciliary ridges;—3, nasal eminences;—4, 4, supra-orbital notches;—5, 5, 6, 6, internal and external angular processes;—7, 7, nasal notches;—8, nasal spine;—9, 9, orbital plates;—11, the superior border;—12, the lateral borders.
The frontal bone, a single bone (1, Fig. 56), like[167] the occipital, presents, like it, a vertical and a horizontal part. The latter belongs to the base of the skull and to the face (9, 9, Fig. 57), and forms the roof of the cavity of the orbit (see below). The vertical part forms the anterior and superior wall of the cranium. It has a rounded superior border (11, Fig. 57) which articulates by its denticulated edge with the parietal bones and forms the coronal suture (6, Fig. 56). The anterior superficial surface forms the forehead, and upon it we have to notice the following points:—1, the frontal eminences (1, 1, Fig. 57), better marked in young subjects and in females than in the adult male; 2,[168] below these, the superciliary ridges (2, 2, Fig, 57), which are directed obliquely downwards and inwards, to end in two prominent bosses called the nasal eminences. These prominences are best marked in the adult, and owe their prominence to the fact that the thickness of the bone is hollowed out in this situation into two cavities called the frontal sinuses, which become more developed as the subject advances in age; 3, at the lower border of this part of the bone are the supra-orbital arches (4, 4, Fig. 57), at the margin of the orbit. Curved, with the concavity downwards, each of these arches forms on the outer side an external angular process (6, 6, Fig. 57), which articulates with the malar, or cheek-bone (15, Fig. 56), and on the inner side an internal angular process (5, 5, Fig. 57) which articulates with the nasal process of the upper jaw. Between the two internal angular processes is a median rough space called the nasal notch (7, Fig. 57), into which are received the nasal bones (22, Fig. 56). Each supra-orbital arch presents, at the junction of its middle and inner thirds, a small notch called the supra-orbital notch (Fig. 57).
The temporal bones, one on each side of the skull (4, 11, and 31, Fig. 56), are very complex in shape, but we shall study here only one portion. Each temporal bone is composed of two parts, one belonging to the base, and another belonging to the lateral wall of the skull; the part belonging to the base forming a pyramidal mass of very dense bone, called the petrous portion, which contains the delicate organs of the internal ear; while the part belonging to the lateral wall of the skull (4, Fig. 56) rises up[169] as an irregular osseous disc from the base of the petrous portion of the bone. An orifice, the external auditory meatus which leads into the petrous bone, is found about its centre (31, Fig. 56). Taking this orifice of the auditory canal as a centre, we find on the external surface of the temporal bone—1, behind the auditory canal the mastoid portion of the bone (33, Fig. 56), which articulates with the parietal and occipital bones, and is prolonged downwards as a conical process in the shape of a nipple (μαστός, a nipple) called the mastoid process; 2, above the auditory canal, the squamous portion of the temporal bone (4, Fig. 56), a shell-like bone with a rounded border articulating with the inferior border of the parietal bone (8, Fig. 56). In front is a process (20, Fig. 58) which is directed horizontally towards the face and joins the malar bone (16, Fig. 56). This process, connecting the cranium with the face, is called the zygomatic process (ζυγός, a yoke), and it forms with the corresponding part of the malar bone the zygomatic arch. The zygomatic process rises from the temporal bone by two roots (Fig. 57), of which one sweeps backwards above the orifice of the external auditory canal and helps to form the temporal ridge; the other extends as a rounded ridge transversely inwards towards the base of the skull, and as the eminentia articularis, forms the anterior limit of the glenoid cavity, into which the condyle of the lower jaw is received. Finally, below the auditory canal, the temporal bone gives origin to the styloid process (32, Fig. 56), long and slender, which gives attachment to certain ligaments and muscles of the neck.
[170]
The sphenoid bone is one of the most important in the construction of the cranium, although as it chiefly occupies the middle of the base of the skull, it is not very obvious on the surface. It is the great wing of the sphenoid bone which assists in the formation of the temporal fossa.
The bones of the cranium articulate with one another by denticulated borders, to which the name of sutures is given. As the artist needs to study the skull not only with regard to its superficial form, but also as an object which figures frequently as an accessory in still-life compositions, and as a true representation of these sutures contributes to give to the skull its exact physiognomy, we must not leave the subject without carefully pointing them out. It is necessary for our purpose to examine the skull on its upper and its lateral surfaces.
The upper surface of the skull presents a suture in the middle line, antero-posterior and inter-parietal, called the sagittal suture. Behind, on a level with the superior angle of the occipital bone (7, Fig. 56), this median suture becomes continuous with the occipito-parietal suture to which the name of the lambdoid suture is given-because it resembles the form of a Greek lambda (Λ). In front, the sagittal suture is met by the parieto-frontal suture (6, Fig. 56), which forms a curved line, to which has been given the name of the coronal suture.
On examining the skull on one of its lateral surfaces, we see that
the sutures form in this situation a more complex design, because of
the articulations of the bones entering into the formation of the
temporal fossa (5, 10, 11, 12, Fig. 56). This fossa is[171] formed
by the parietal, squamous portion of the temporal, frontal, and great
wing of the sphenoid bones. It is limited: below by the zygomatic arch
(malar and temporal), and above by the curved line of the temporal
ridge, which marks the temporal, parietal, and frontal bones. The
suture formed within the fossa, at a point called the pterion,
is roughly  or
or
 -shaped, and is occasioned by the
contiguous articulations of the parietal, sphenoid, frontal, and
squamous portion of the temporal bones.
-shaped, and is occasioned by the
contiguous articulations of the parietal, sphenoid, frontal, and
squamous portion of the temporal bones.
We have said that the general form of the skull is egg-shaped, with its greater extremity behind. It is, however, a common observation that the skull may differ remarkably from what may be termed the normal shape. It may be excessively high, or low; excessively prolonged backwards or forwards, or the reverse. One of the best-marked and constant variations is in the ratio of width to length, from which the cephalic index is derived. This may be an individual peculiarity: for instance, of two brothers, one may be round-headed, the other long-headed. Or it may be a racial character: for example, the black races are long-headed, the yellow races are round-headed, and the white races have a cephalic index which may be one or the other, or intermediate between the two extremes.
The cephalic index (index of breadth of the skull) is an important term in physical anthropology.
As we have previously explained, respecting the proportions of the arm and forearm (brachial index, page 100), we understand by the name of index the[172] number which indicates the proportion between a short and a greater length, the latter being considered as equal to 100—that is to say, the figures obtained by direct measurement being reduced to a decimal proportion. We find that in certain skulls the transverse diameter is relatively very short, seeing that it is represented by an index of 75 or less; and such skulls are known as dolichocephalic (δολιχός, lengthened; κεφαλή, head). Others present a transverse diameter which approaches the antero-posterior, since it is represented by an index of 80 or more, the antero-posterior measurement being 100. This cephalic index of 80 or more is called brachycephalic (βραχύς, short). Between these two types are the heads of intermediate form called mesaticephalic, of which the cephalic index is from 75 to 80. The importance of dolichocephalic, mesaticephalic, and brachycephalic types of skull in relation to racial characters has no doubt been exaggerated; but the fact remains that certain races are dolichocephalic, and that certain other races are brachycephalic. A greater difficulty arises in regard to mesaticephalic skulls, which are, after all, in a sense only “averages,” and which, occurring as they do so commonly in the Indo-European race, suggest that either they are due to individual peculiarity or to the mingling of racial characters—in either case weakening the value of skull measurements in the investigation of races.
[173]
The bony structure of the face.—Orbital cavities: margins; cavities.—Nasal fossæ: anterior orifice.—Prominence of the cheek; malar bone and its processes.—Upper jaw.—Lower jaw; body; ramus; sigmoid notch, coronoid process, and condyle: variations with age.—The teeth: parts; names (incisors, canines, premolars, molars), number; relative dimensions of incisors.—Articulation of the lower jaw.—The face and skull as a whole with regard to form.—Facial angle of Camper; its measure; its proper value according to race; its exaggeration in the antique.—Proportions: the head as a common measure: law of eight heads; variations according to the height of the individual; point which corresponds to the middle of the body.
The Face.—Instead of describing the bones of the face separately we will group them together around the cavities which they circumscribe and the prominences which they form. We will therefore study successively the cavity of the orbit, the orifice of the nasal fossæ, the prominence of the cheek-bone, and, lastly, the region of the mouth, along with which we will describe the teeth, the lower jaw, and its articulation with the base of the skull.
The orbits.—The orbits are two cavities situated symmetrically one on each side of the upper portion of the face below the forehead. Each of these cavities is formed like a pyramid with four sides, of which the apex penetrates backwards towards the cranial cavity, and of which the base, turned forwards, forms the orbital opening. This opening, or orbital margin, is of quadrilateral form with rounded angles (Fig. 58), limited by an internal border (7) and an external border, both almost vertical, by a superior[174] border (3) and an inferior border, both oblique, from above downwards and outwards.
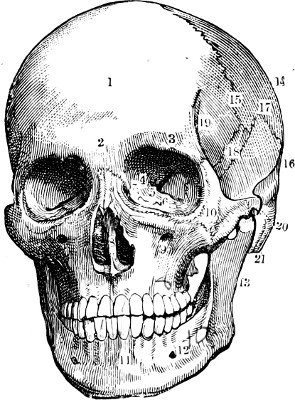
Fig. 58.
The Bony Structure of the Face.—1, the frontal bone;—2, the nasal eminence;—3, supra-orbital notch;—4, the optic foramen;—5, the sphenoidal fissure;—6, the spheno-maxillary fissure;—7, the lachrymal groove;—8, the partition and opening of the nasal fossæ;—9, the infra-orbital foramen;—10, the malar bone;—11, the symphysis of the jaw;—12, the mental foramen;—13, the ramus of the lower jaw;—14, the parietal bone;—15, the coronal suture;—16, the temporal bone;—17, the temporo-parietal suture;—18, the great wing of the sphenoid;—19, the origin of the temporal ridge;—20, the zygomatic arch;—21, the mastoid process.
The superior border is formed by the supra-orbital arch of the frontal bone (3, Fig. 58) previously described, which presents the supra-orbital notch; the inferior border is formed by the superior maxillary and malar bones; a little below its centre is a hole, called the infra-orbital foramen (9, Fig. 58), which is placed in the upper jaw almost in the same vertical line as the supra-orbital notch above the orbit (page 168). The internal border is formed by the junction of the internal angular process of the frontal bone with the ascending (nasal) process of the superior maxilla (Figs. 56 and 58). Behind the inferior part of this border is a deep groove, called the naso-lachrymal groove (7, Fig. 58), for the accommodation of the lachrymal sac (for the tears), which is the commencement of a canal (naso-lachrymal canal)[175] connecting the orbit with the corresponding nasal fossa, and serving to transmit the nasal duct. Finally, the external border is formed by the junction of the external angular process of the frontal with the superior process of the malar bone, or bone of the cheek (10, Fig. 58; 14 and 15, Fig. 56).
The cavity of the orbit has for its walls the osseous plates belonging to the frontal (superior wall) and the several bones of the face we have previously mentioned when describing the orbital opening. We need not enter here into the description of these surfaces and of the several special bones which compose them. We shall only say that the internal wall is directed from before backwards, while the external wall is oblique, from behind forwards and from without inwards. We note, lastly, at the deepest part (towards the apex) of the cavity, three apertures, by which the orbit communicates with deeper cavities; first, a circular orifice called the optic foramen (4, Fig. 58); then, on the outer side of these, two fissures directed outwards, one obliquely upwards (sphenoidal fissure, 5, Fig. 58), and the other obliquely downwards (spheno-maxillary fissure, 6, Fig. 58). The two first communicate with the cranial cavity; the last-named fissure leads into the spheno-maxillary fossa.
The orifice of the nasal fossæ (8, Fig. 58) is situated in the middle of the face below the level of the orbits. It is somewhat heart-shaped (with the base downwards); it is bounded below by the two superior maxillary bones which unite in the middle line and form the anterior nasal spine, upon the sides by the same bones, and above by the two small[176] nasal bones (Fig. 56, page 165) wedged in on each side of the middle line between the nasal processes of the maxillary bones, and articulating above with the nasal notch of the frontal bone.
Below, and to the outer side of each orbit, is the prominence of the cheek formed by the malar bone (10, Fig. 58). This bone is formed like a star with four rays. The superior or orbital process (15, Fig. 56) joins the external angular process of the frontal bone; the anterior process (17, Fig. 56) forms with the superior maxillary the inferior boundary of the orbit; the posterior or zygomatic process (16, Fig. 56) is directed backwards to form by its union with the zygomatic process of the temporal bone, the zygomatic arch; the inferior angle is reduced to a prominent margin which joins with the body of the bone to form the prominence of the cheek. This prominence is due to the projection of a malar process of the upper jaw on which the malar bone is fitted.
There remain now only two bones to examine on the skeleton of the face—namely, the two bones which bound the cavity of the mouth and support the teeth: these are the superior and inferior maxillary or jawbones. The superior maxillary bone (18, Fig. 56) has been in a great measure described already in relation to the orbital and nasal openings. The following points remain to be noticed: 1. The external surface is divided by a ridge descending from the malar process, into two surfaces—one outer, belonging to the zygomatic fossa, and the other anterior, appearing on the face. The facial surface is again subdivided into two smaller fossæ—the canine fossa, in which occurs the infra-orbital foramen, and the incisive fossa, above[177] the incisor teeth—by a ridge (the canine ridge) which is formed by the prominent fang of the canine tooth. 2. The inferior or alveolar border presents a series of cavities for the lodgment of the roots of the upper teeth. The presence of these cavities is marked on the surface of the alveolar border by a series of prominences separated by depressions corresponding to the partitions between the alveoli.
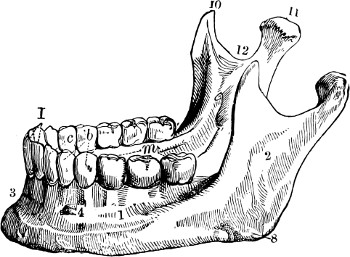
Fig. 59.
The Inferior Maxillary Bone (side view).—1, the body of the inferior maxillary bone and its external oblique line;—2, the ramus;—3, the symphysis of the chin;—4, the mental foramen;—8, the angle of the jaw;—10, coronoid process;—11, the condyle;—12, sigmoid notch;—I, incisor teeth;—c, canine tooth;—b, bicuspid;—m, molar teeth.
The inferior maxillary bone or mandible (Fig. 59) requires more detailed consideration than the other bones of the face, as it takes so direct a share in the surface form that we may say that all the details of its shape are marked in the configuration of the chin and lower parts of the cheeks. It is originally composed of two distinct halves, one right and one left, which are joined together in early life in the middle line of the chin to form the symphysis of the chin, or mental process (11, Fig. 58). It is sufficient to describe one of these halves as we see it in a side view of the skull (Fig. 56).
We see that each half is formed of two strong osseous plates joined together at an angle more or less approaching a right angle, of which the prominence directed downwards and backwards is called[178] the angle of the jaw. The horizontal portion of the bone is called the body; the vertical portion is the ramus.
The ramus consists of a flat external surface, which is continued below into the body of the bone (2, Fig. 59). Its posterior border is thick, and is continued downwards to the angle of the jaw. The anterior border, which is thinner, is grooved, and terminates by joining below the upper alveolar border of the body of the bone. The borders of the groove join the oblique lines on the surfaces of the body of the bone. The superior border is divided by a deep notch (sigmoid notch, 12, Fig. 59) into two very prominent parts. The posterior prominence is thick, and forms the neck, surmounted by the articular head, or condyle, of the jaw (11, Fig. 59), for articulation with the temporal bone; the anterior prominence is in the form of a triangular plate, and bears the name of the coronoid process (10, Fig. 59); it gives insertion to the temporal and masseter muscles.
The body of the lower jaw extends from the angle to the symphysis of the chin (3, Fig. 59); it has an external surface marked by an oblique line, above which is an orifice (12, Fig. 58; and 4, Fig. 59) called the mental foramen, placed in the same vertical line as the supra-orbital notch and the infra-orbital foramen. It is situated about the level of the second premolar tooth. The inferior border of the bone is thick and rounded; its superior alveolar border presents sockets for the teeth, and externally a series of prominences and depressions corresponding to the alveoli and the intervals between them.
The character of the lower jaw changes with[179] age; in the infant, the angle is very obtuse and but slightly prominent: in the adult it becomes almost a right angle: in the aged the form of the jaw is changed by the loss of the teeth and by the absorption of the alveolar border, causing a diminution of height in the body of the bone. In order, therefore, to bring the two jaws in contact with one another, the lower jaw requires to move strongly forwards and upwards, whence occurs a characteristic prominence of the chin in the aged, which seems to project upwards and forwards to meet the prominence of the nose.
The teeth of the adult are altogether thirty-two in number—eight in each lateral half of each jaw. Each tooth is composed of a part fixed in the alveolar cavity called the root, and a free part called the crown. The form of the crown permits the division of the teeth into four distinct classes, which in each half of the jaw are arranged in the following manner, beginning from the median line:—Two incisors (I, Fig. 59), one canine (c, Fig. 59), two premolars, or bicuspids (b, Fig. 59), and three molars (m, Fig. 59)—total, eight. Situated at the most external and posterior portion of the dental arch, the premolar and molar teeth are hidden by the cheeks, and we need only mention that they are characterised by a crown formed of numerous tubercles (two for the premolars, four or five for the molar teeth). On the other hand, the canine and incisor teeth are easily seen when the lips are separated. The canine teeth are characterised by a conical crown with a sharp extremity, which is very large and prominent in the[180] carnivora—e.g., in the dog (whence the name of canines). The incisors present a crown flattened from before backwards, and rectangular in form (square). Their relative size is so constant that it should be stated here. The two largest are the median incisors of the upper jaw; next in order come the lateral incisors of the upper jaw, then the lower lateral, and finally the lower median incisors, which are the smallest. The lower incisors, besides being smaller, are characterised by their chisel-like cutting edge, which is bevelled at the expense of the outer surface.
The articulation of the lower jaw with the skull, or temporo-maxillary articulation, is formed by the articulation of the condyle of the jaw (11, Fig. 59; and 29, Fig. 56) with the glenoid cavity of the temporal bone—a cavity placed in front of the external auditory meatus, and behind the articular eminence—the transverse root of the zygomatic process (page 169). This glenoid cavity, together with the articular eminence, is lined with cartilage, and is separated from the condyle of the jaw by an inter-articular fibro-cartilage. These structures are enclosed in a fibrous capsule which surrounds the articulation, and is strengthened on the outer side by a stout external lateral ligament, attached obliquely from a tubercle at the root of the zygoma downwards and backwards to the outer side of the condyle of the jaw. Therefore, when the jaw is depressed by a movement of rotation of the mandibular condyle upon its axis, this external lateral ligament is made tense, and draws the condyle forward, causing it to leave the glenoid cavity and[181] come in contact with the articular eminence. Thus, when the mouth is widely opened (the lower jaw being greatly depressed) there is a displacement of the condyle of the jaw forwards, which is easily seen in thin subjects, and which should be noted here with its own particular mechanism.
The face, as a whole, presents a special interest when we compare its configuration with that of the cranium, in various individuals and races. In general, the more prominent the skeleton of the face the less the cranium (the forehead) is developed. This was the idea of Camper, a Dutch anatomist and artist, about the middle of the eighteenth century.
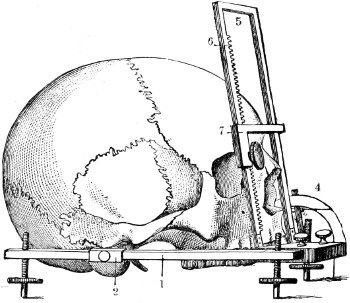
Fig. 60.
The Measurement of the Facial Angle (goniometer applied to a skull).—1, the inferior horizontal plane of the goniometer;—2, movable piece with a pin introduced into the auditory meatus;—4, graduated circle;—5, the oblique plane attached below by a hinge to the horizontal;—6, the rack for placing the bar (7) on the prominent part of the forehead.
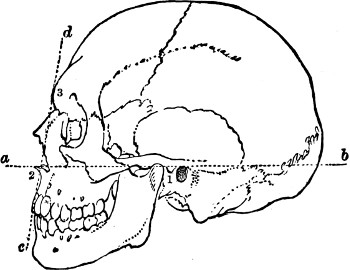
Fig. 61.
The Facial Angle of a Skull of the Caucasian Race (after Camper).—a b and c d, the lines which mark this angle (see the text);—1, the auditory meatus;—2, anterior nasal spine;—3, the most prominent part of the forehead.
Camper proposed to measure the relative proportions of the cranium and face by the angle which the plane of the profile of the face makes with that of the base of the skull. This facial angle has since[182] been the subject of much study on the part of anatomists and anthropologists, who have modified and perfected the process of measurement. It will be sufficient here to show what Camper’s idea was, and that, apart from anatomical considerations, he designed to furnish artists with a means of giving character to the different physiognomies of men and animals. This angle is determined by two planes (upon a head seen in profile, by two lines): one plane, which we may call horizontal, proceeds from the external auditory meatus to the anterior nasal spine, and corresponds to the inferior border of the orifice of the nasal fossa (1, Fig. 60; and a, b, Fig. 61); the other, directed obliquely upwards and backwards, is at a tangent below to the prominence of the incisor teeth, and above to the most prominent part of the forehead (c, d, Fig. 61). Fig. 60 gives an idea of the apparatus with which we measure the facial angle at the present day. It represents the facial goniometer[183] of Jacquart. The mode of measurement here differs from that employed by Camper, in that the inferior or horizontal plane passes forward not by the nasal spine, but by the prominence of the incisor teeth.
Figures 61 and 62, which are reproduced from those of Camper, show on the one hand that while the facial angle is never equal to a right angle, it approaches to it in the best types of the white race.

62.
The Facial Angle of a Negro (after Camper). The figures are the same as in the preceding.
The ancients sought by an exaggeration to idealise the profile of the human face, and by increasing the fulness of the forehead they have given to heads of gods and heroes a facial angle as large as ninety degrees (Fig. 63). These figures show, also, the decrease of the facial angle in proportion as we pass from the white to the yellow and black races:—“The angle which the facial line or characteristic line of the visage makes,” said Camper, “varies from seventy to eighty degrees in the human species. All who raise it higher disobey the rules of art (from imitation of the antique); all who bring it lower fall into the[184] likeness of the monkeys. If I cause the facial line to fall in front I have an antique head; if I incline it backwards I have the head of a negro; if I cause it to incline still further I have the head of a monkey; inclined still more, I have that of a dog; and, lastly, that of a goose.”[6] The figures which explain these ideas are as follows:—The facial angle of Camper averages 80 degrees in the Caucasian race; 75 degrees in the yellow, or Mongol; 60 to 70 degrees in the Negro; 31 degrees in the great monkeys (gorilla); lastly, 25 degrees in the head of a Newfoundland dog.
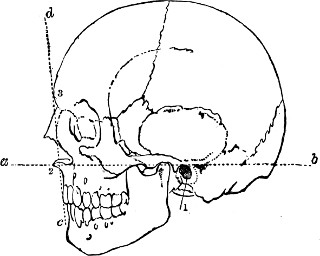
Fig. 63.
The Facial Angle of an Antique Head (Apollo Belvedere)—(Camper).
In our study of the various segments of the limbs we have seen that some of them have been chosen, in different systems of measurement, to serve as a common measure for these limbs, and for the entire body. Thus we have spoken of the canons which respectively take as a unit the hand (contained about ten times in the height of the body), the[185] foot (contained a little more than six times in the total height), the middle finger (contained nineteen times), &c., &c. It is true, also, that the head—i.e., the vertical distance from its summit to the base of the chin—may be taken also as a common measure. This was done long ago. Vitruvius, speaking of the proportions of the human body, states that the height of the head should be the eighth part of the whole body. Leonardo da Vinci, Albert Dürer, and J. Cousin have followed the rule of the Latin author; and the law which makes the head the eighth of the total height has for a long time past become classic in all the schools. The choice of the head as a unit seems sufficiently justified by the two facts that, on the one hand, in every representation of the human body the head is always visible, and forms a part distinct from the rest of the body, and that, admitting that it makes the eighth part of the height, this number is particularly convenient, not being too great; and, on the other hand, it is divisible by two. In this respect it offers, for example, a great advantage over that of nineteen, which represents the proportion of the middle finger to the height.
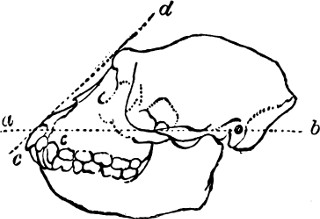
Fig. 64.
The Facial Angle of a Monkey.
(Camper.)
Gerdy, who has adopted the law of eight heads, divides the height of the body in the following way: the first division comprises the head itself; the second extends from the chin to the level of the nipples; the third from the nipples to the umbilicus;[186] the fourth from the umbilicus to the symphysis pubis; the fifth from the pubis to the middle of the thigh; the sixth from the thigh to the knee; the seventh from the knee to the middle of the leg; and, lastly, the eighth, from the middle of the leg to the sole of the foot (Fig. 65).
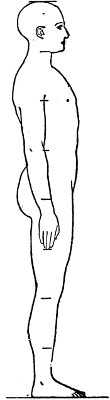
Fig. 65.
Outline of the Human Body (and proportions).
The face itself can further be subdivided into subordinate parts. The classical method of subdivision is to say that the head is the length of four noses: one from the top of the head to the top of the forehead (hair), one each for the forehead and nose, and one for the part below the nose. This is generally, however, incorrect. It is better to divide the face into two portions across the equators of the eyeballs; and subdivide the lower half into two, for the greater part of the nose above, and the lips, mouth, and chin below.
Now, if we submit to experiment the system of the law of eight heads, we see that it is accurate only in subjects of great height—for those who attain seventy-four inches and over; below seventy-two inches the subjects do not measure more than seven and a half, or only seven times the height of their head. In fact, the height of the head is a quantity which varies very little according to the subject; it is on the average, as an absolute measurement, from 8⅔ to 9 inches, and the variations which this value may present do not range below 8¼ inches or above 9 inches. A subject[187] who measures eight heads is very tall (9 × 8 = 72, equal, or superior, to 72 inches); and a subject who only measures seven heads is of short stature (8⅔ × 7 = 61, equal, or more frequently exceeding, 61 inches).
This difference in the number of heads that the body measures in relation to absolute height seems more interesting than the narrow theory which would assign strictly the length of eight heads to each human figure. This absolute system does not agree with that which observation proves correct. Besides, it would be an error to suppose that the ancient sculptors would be slaves to such a system of proportions, since we find in their works precisely the same variations that we do in nature. The Gladiator, it is true, measures eight heads; but at the first glance at this chef d’œuvre we have the impression of a subject of great stature—of a man tall and spare. The Apollo and the Laocoon measure only 7⅔, and the Antinous only 7½ heads.
The variations in height are almost solely caused by the greater or lesser length of the lower limbs. Whether the subject be tall or short, the trunk (with the head and neck) varies comparatively little; but the thighs and legs make the differences of length. Regarding the diversity that we meet with in this question, we see that Gerdy himself has not been exact in indicating the points where the lengths of the head begin and terminate which divide the lower limb, the middle of the thigh, and the lower part of the knee; those points are badly defined, especially as he does not indicate precisely the superior extremity of the thigh. But the looseness and contradiction[188] becomes still more evident when we come to seek, according to the various authors, the intersection between the fourth and fifth head; that is to say, the middle of the body. Without speaking of the singular inconsistency of Vitruvius, who places the middle of the body at the level of the navel, we will note only this fact, that for the passage from the fourth head to the fifth some take the pubis, others some other point.
The centre of height falls lower as the stature of the subject is increased. In subjects of small stature the centre of height corresponds to the symphysis of the pubis; for those of middle height and over, it falls about half an inch below the pubis. But it may be situated at a still lower level, and the artists of antiquity have frequently placed it much lower. In fact, as Professor Sappey says, the taller the stature, the more the centre of the body tends to fall below the symphysis, and the figures of heroes and gods are of tall stature.
We will say, then, in conclusion: 1, that the head, compared with the height, is shorter as the height increases; 2, that to produce a human figure, the absolute dimensions of which would give the impression of a subject of short stature, it would be necessary to give it about 7½ heads, and to cause the centre of the body to fall on the symphysis pubis; while to produce a figure to give the impression of tall stature it would be necessary to give it 8 heads, and to place the centre of the body more or less below the symphysis pubis.
[189]

MUSCLES AND MOVEMENTS.
Of muscles in general.—Muscular contraction: changes of form; movements produced. Composition of muscles; fleshy belly and tendon; aponeurosis. Nomenclature of muscles, their classification into long, broad, and short muscles; their arrangement: superficial and deep. Muscles of the trunk, anterior region.—Great pectoral muscle, its relation to the armpit, its action.—The lesser pectoral.—The breast and nipple.—The external oblique muscle of the abdomen, its fleshy part, its abdominal aponeurosis; linea alba.—Groove and space bounded by the prominence of the external oblique and rectus.—Internal oblique and transversalis muscles.—Rectus abdominis muscle, its aponeurotic sheath, its aponeurotic intersections.—Linea semilunaris; lineæ transversæ.
The form of the body is produced largely by the muscles. Each muscle is formed of a peculiar tissue called muscular tissue or muscular fibre, which has the property of changing its form and of contracting under the influence of nervous action, in most cases controlled by the will. For example, in contracting the biceps muscle on the front of the arm, we see that this muscle, which in a state of repose is fusiform and long, becomes in action (in contraction) short, thick, and rounded; and as it is attached below to one of the bones of the forearm, it draws the anterior surface of[190] the forearm towards the anterior surface of the upper arm and produces flexion of the elbow-joint. This simple experiment, which is easy to repeat at any moment, gives a clear idea of the part which muscles play in the animal economy, and of the part that they take in producing the external form; for it shows that they are the active agents of movements in which the bones are the passive levers, and, at the same time, that a muscle in action presents a very different shape from that which it has in a state of repose, a change which may be stated in a more general manner by saying that in action a muscle becomes shorter, thicker, and more prominent.
Fig. 66.
Diagram of a Contracted Muscle (Biceps).
In general, besides their fleshy mass, the only part which contracts and changes its form, the muscles have extremities more or less slender called tendons, formed of a white fibrous tissue, which are, as it were, actual cords by which the muscle is attached to the bones; during the contraction of muscle these tendons do not change in form, but, as with all tight cords when in a state of tension, they start up, and become more visible and clearly marked beneath the skin (Fig. 66).
Each muscle is enveloped by a fibrous membrane[191] called its aponeurosis, which frequently takes the place of a tendon, if the muscle is broad and thin, so that in these cases the attachment of the muscle, instead of being rounded in the form of a cord, is flattened in the form of a membrane, and the term aponeurosis is at times applied to these membranous tendons. Membranous tendons in the contraction of a muscle give rise to depressions on the surface of the body in the regions where they occur superficially.
The muscles are variously named according to various ideas; sometimes from the region they occupy (pectoral, gluteal, anterior brachial muscles, &c.) or from the direction of their fibres (oblique of the abdomen), or from their dimensions (gluteus maximus, gluteus medius, and peroneus longus, &c.), or again from their form (trapezius, rhomboid, serratus), or from their structure (semi-membranosus, semi-tendinosus). Another mode of nomenclature, which Chaussier attempted to make general, forms the name of a muscle by the association of the names of the bones to which it is attached; in this way we get the sterno-cleido-mastoid muscle, and most of the muscles of the neck. This nomenclature, however, cannot be easily applied to all muscles, for it would make some names of an inconvenient length, owing to the complexity of the bony attachments.
Before we terminate this rapid sketch it may be useful, with regard to plastic anatomy, to point out how the various muscles are classed, according to their form and situation. 1st. With regard to their form we distinguish the muscles as long, broad, and short; the long muscles, consisting in general of a[192] fleshy belly fusiform in shape, and with cord-like tendons, are principally distributed among the great segments of the limbs (arm, forearm, thigh, leg); the broad muscles, with their fibres arranged in broad and thin layers, and with tendons membranous and aponeurotic, are almost exclusively found in the trunk (pectorals, trapezius, latissimus dorsi, &c.); lastly, the short muscles, frequently without tendons, and inserted directly into the bone, are found principally at the extremities of the limbs (hand and foot) and in the face.
2nd. With regard to their situation we distinguish the muscles as superficial and deep. The superficial muscles (Fig. 67) are those which are entirely visible when the subject is stripped of its skin, and of which, accordingly, the fleshy bellies and tendons are marked in their principal details on the external form. These superficial muscles should be carefully studied here with regard to their insertions, forms, and actions. The deep muscles, situated beneath the preceding, form fleshy masses, which are shown externally by the manner in which they fill up the external depressions of the skeleton, and raise up the superficial muscles. It is enough for the artist to know the general indications of these muscular masses, without studying the insertions and forms of each of the muscles composing any given mass.
Under this title we will now study the anterior muscles of the trunk (pectoral and abdominal), and the muscles of the back and the posterior surface of the neck (trapezius and latissimus dorsi). The study[193] of the muscle which covers the lateral wall of the chest (serratus magnus) will be taken after that of the muscles of the shoulder and armpit.
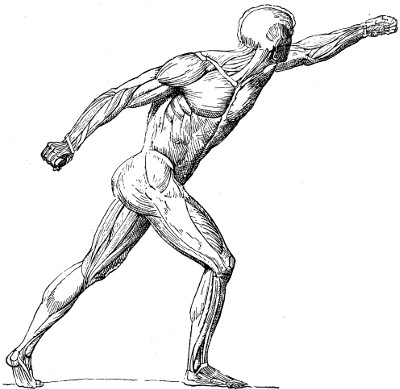
Fig. 67.
General View of the Superficial Muscle (the Gladiator of Agasias with the skin removed. Compare with Figure 4, page 24).
Great pectoral muscle.—The great pectoral muscle (pectoralis major) forms a large fleshy mass (1, Fig. 68) which covers the anterior surface of the thorax, on each side of the middle line of the[194] sternum, and extends outwards as far as the upper part of the arm. This muscle is attached (1st) to the inner half of the anterior border of the clavicle (2, Fig. 68); (2nd), to the whole extent of the anterior surface of the sternum (3, Fig. 68); and (3rd), to the aponeurosis of the external oblique muscle of the abdomen. It arises, also, more deeply from the cartilages of the true ribs (except[195] the first) (9, 9, 9, Fig. 68). From these thoracic origins the muscular fibres are directed towards the arm; the upper fibres pass obliquely from above downwards and outwards; the middle fibres pass transversely outwards, and the inferior, obliquely from below upwards. Towards the insertion of the muscle these different parts cross over each other in a twisted form, so that the upper (clavicular) fibres are placed in front of the inferior (sternal) fibres (7, Fig. 68), which correspond to the anterior margin of the armpit. The muscle is inserted into the outer lip of the bicipital groove of the humerus, the clavicular fibres, known as the portio attollens, being inserted lower down the arm than the external fibres (portio deprimens). The former fibres raise the arm upwards, the latter draw it downwards in relation to the trunk.
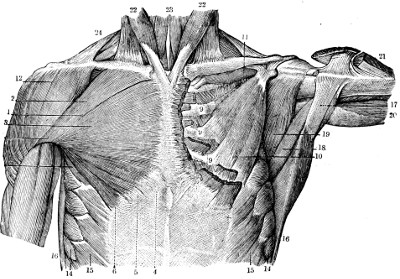
Fig. 68.
The Muscles of the Anterior Surface of the Thorax (to the right the superficial muscles; to the left the deep muscles).—1, the great pectoral muscle;—2, its clavicular fibres;—3, its costo-sternal fibres;—4, 5, 6, its origin from the aponeurosis of the abdomen;—7, its external portion formed by the superposition of the preceding fibres (9, bundles of fibres arising from the cartilages of the ribs; 10, the pectoralis minor);—11, the subclavius;—12, the deltoid;—14, the digitations of the serratus magnus;—15, the digitations of the external oblique of the abdomen;—16, anterior border of the latissimus dorsi, and (17) tendon of the same;—18, teres major muscle;—19, the subscapularis;—20, the long head of the triceps brachialis; 21, the humeral extremity of the deltoid; 22, 22, the sterno-cleido-mastoid;—23, the sterno-hyoid;—24, the trapezius muscle.
When the arm is hanging beside the trunk the great pectoral muscle presents a four-sided square, in which we can distinguish four borders: one supero-external (in contact with the anterior border of the deltoid, 12, Fig. 68), another superior, in the line of the clavicle; the third, internal or sternal, curved with its convexity inwards; and the fourth, infero-external or axillary (forming the anterior boundary of the armpit). But when the arm is horizontal, and especially when it is raised above the horizontal (Fig. 70), the figure of the muscle is represented by a triangle with the base inwards, as the clavicular and supero-external borders then come into line with one another.
The action of the great pectoral muscle is essentially to draw the arm to the trunk; its[196] shape becomes prominent when we carry the arms forward and bring them near each other, as in the attitude of prayer. It also becomes well marked in climbing, for then the muscle takes its fixed point at the humerus and draws the trunk towards it. Acting in a similar manner upon the thorax, with the humerus as a fixed point, this muscle elevates the ribs, and consequently expands the thorax in respiration. Thus we see that the muscle contracts when the inspiratory muscular powers are brought into play as in movements like struggling, anguish, or agony.

Fig. 69.
Outline of the Female Breast.
The breast and nipple.—On the surface of the great pectoral muscle is placed the breast in the female. In the male only the nipple and surrounding areola are found, usually occupying a position at the level of the space between the fourth and fifth ribs on each side. The form of the breast varies in the female with age. In a young woman it is normally round and firm, with its lower aspect more rounded than its upper surface, which is slightly flatter (in the erect position) (Fig. 69).
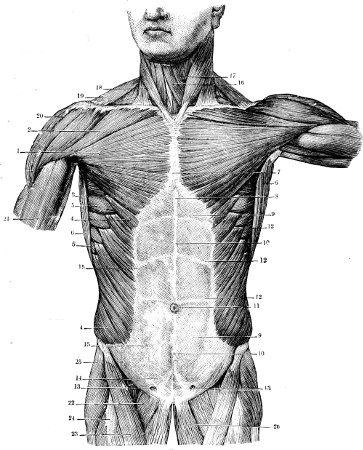
Fig. 70.
The Muscles of the Anterior Wall of the Trunk.—1, 2, 3, the great pectoral;—4, 4, the external oblique of the abdomen;—5, 5, the serratus magnus;—6, 6, the anterior border of the latissimus dorsi;—7, 8, the inferior portion of the sternum;—9, the aponeurosis of the external oblique;—10, linea alba;—11, umbilicus;—12, 12, 12, the tendinous intersections of the rectus abdominis;—13, the inguinal ring;—14, the pyramidalis of the abdomen;—15, the external border of the rectus abdominis;—16, the sterno-hyoid;—17, the omo-hyoid;—18, sterno-cleido-mastoid;—19, the trapezius;—20, the deltoid;—21, the biceps brachialis;—22, the pectineus;—23, the sartorius;—24, the rectus femoris;—25, the tensor of the fascia lata;—26, the adductors.
The great pectoral muscle conceals under its middle third a smaller muscle, the lesser pectoral (10, Fig. 68), which, arising from the third, fourth, and[198] fifth ribs, is directed upwards and outwards, to be attached to the coracoid process of the scapula. This muscle serves to move the scapula by drawing its upper part downwards and forwards. Its outer border becomes obvious when the arm is raised above the head, along the axillary border of the great pectoral muscle.
The external oblique muscle of the abdomen.—The external oblique muscle of the abdomen (Figs. 68 and 70) forms a large sheet half fleshy, half aponeurotic, which covers the lateral and anterior surfaces of the abdomen. The fleshy portion, which forms the outer half of the muscle, is attached to the external surfaces of the lower eight ribs, from which it arises by angular slips or digitations, interlacing with those of the serratus magnus and latissimus dorsi muscles (15, Fig. 68, and Fig. 74). From these costal origins the fibres are carried forwards and downwards; the posterior fibres pass vertically downwards to be attached to the iliac crest (Fig. 74); the others are directed obliquely downwards and forwards, to give origin to a broad membranous tendon (9, Fig. 70) called the aponeurosis of the external oblique muscle. The fibres of this aponeurosis, continuing in the original direction of the muscular fibres, pass in front of the rectus muscle of the abdomen (12 and 15, Fig. 70), where, joining the subjacent aponeuroses of the internal oblique and transversalis muscles, and interlacing with the aponeurotic fibres of the opposite side, it forms a long median raphé, called the linea alba of the abdomen, proceeding[199] from the xiphoid cartilage to the symphysis pubis (10, Fig. 70).
It is important, with regard to external form, to define the direction of the line at which the aponeurotic fibres of the external oblique succeed to the fleshy fibres (Fig. 70). This line descends at first vertically from its origin at the inferior angle of the great pectoral muscle, but its lower part inclines abruptly outwards (4, Fig. 70), towards the anterior superior iliac spine, describing a curve with its convexity downwards and inwards. This line marks the prominence of the anterior or internal border of the muscular fibres; and as, on the other hand, the rectus abdominis muscle forms, by its outer border, another curved line (linea semilunaris), which is at first vertical but inclines inwards below (15, Fig. 70), it follows that this part of the anterior surface of the abdomen is traversed by a narrow vertical groove which opens out below into a large triangular space. This triangular space, bounded above and on the outer side by the external oblique muscle, and on the inner side by the semi-lunar line of the rectus, is limited below by the fold of the groin, or Poupart’s ligament, the line at which the aponeurosis of the external oblique becomes attached to the fascia lata of the thigh (page 111). In the male this part of the aponeurosis of the external oblique is perforated just above the inner end of Poupart’s ligament (13, Fig. 70) by the spermatic cord, which passes obliquely downwards and inwards in the inner part of the groin.
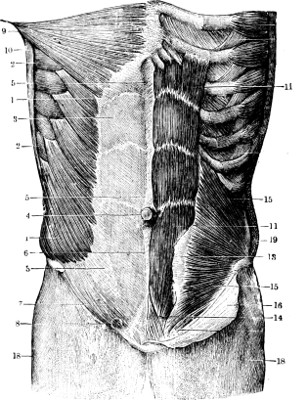
Fig. 71.
The Muscles of the Abdomen (the superficial on the right side, the deep on the left).—1, the external oblique;—2, 2, the serratus magnus;—3, 3, the aponeurosis of the external oblique;—4, the umbilicus;—5, 6, the linea alba;—7, the crural arch or Poupart’s ligament;—8, the inguinal ring;—9, pectoralis major;—10, latissimus dorsi;—11, 11, the rectus abdominis;—13, the anterior portion of its sheath;—14, the pyramidalis;—15, 15, the internal oblique of the abdomen;—16, the inferior portion of the aponeurosis of the external oblique turned downwards;—18, the upper part of the thigh covered by its aponeurotic envelope;—19, a section of the external oblique of the abdomen.
The external oblique muscle draws the ribs downwards[200] and forwards. If the two muscles of that name (that of the right and that of the left side) contract at the same time they bend the body forward; but when one muscle only—e.g., that of the right side—contracts it imparts to the trunk a movement of rotation to the left or opposite side.[201] Generally speaking, whenever we make any great effort the oblique muscles of the abdomen contract, and their prominences, especially the costal digitations[202] and the anterior borders of the muscles, become clearly marked.
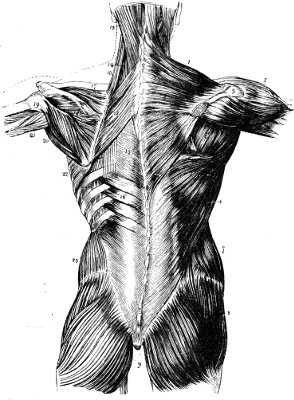
Fig. 72.
The Muscles of the Back.—1, trapezius;—2, its vertebral origin;—3, acromion process;—4, Latissimus dorsi;—5, deltoid;—6, infraspinatus;—7, obliquus externus;—8, gluteus medius;—9, gluteus maximus;—10, levator anguli scapulæ;—11, rhomboid minor;—12, rhomboid major;—13, splenius;—14, transversalis cervicis;—15, vertebral aponeurosis;—16, serratus posticus inferior;—17, supraspinatus;—18, infraspinatus;—19, teres minor;—20, teres major;—21, triceps;—22, serratus magnus;—23, obliquus internus.
The external oblique muscle covers two other muscular layers, which are, passing from without inwards, the internal oblique (15, Fig. 71) and transversalis muscles. The internal oblique muscle is formed by fibres which arise from the fascia of the loin, the crest of the ilium, and Poupart’s ligament. They radiate forwards and for the most part upwards (Fig. 71) to become attached, the superior fibres to the lower six ribs, while the middle and inferior fibres are continued in front as an aponeurosis, or broad flat tendon. The aponeurosis soon becomes united, partly, with that of the external oblique and that of the transversalis beneath. This aponeurosis splits to enclose the rectus abdominis muscle and constitute the sheath of the rectus. The transversalis muscle is formed by fibres directed horizontally, and it terminates in front in an aponeurosis which passes for the most part behind the rectus abdominis, to blend with the aponeurosis of the internal oblique muscle and assist in the formation of the sheath of the rectus abdominis.
The rectus abdominis (11, 11, Fig. 71).—This muscle forms a long, broad, fleshy band on each side of the linea alba, which occupies the middle line of the abdomen. Extending from the epigastric pit to the pubis, it is attached above at its base, which is its widest part, to the cartilages of the filth, sixth, and seventh ribs, and to the ensiform cartilage, and below, at its apex, or narrowest part, by a double tendon to the crest and spine of the pubis. The muscle presents, with regard to form,[203] several remarkable peculiarities. 1st. It is enclosed in a fibrous sheath, formed in front by the aponeuroses of the external and internal oblique muscles (16, Fig. 71), and behind by the aponeuroses of the internal oblique and transversalis; so that in the subject stripped of its skin its shape is half concealed by the aponeurotic lamina which passes in front of it (Fig. 70 and the right half of Fig. 71). 2nd. It is not formed of fleshy fibres proceeding without interruption from the costal cartilages to the pubis, but it is crossed by aponeurotic intersections (Figs. 70, 71), the lineæ transversæ, at the level of which the fleshy fibres are replaced by short tendinous fibres. These aponeurotic intersections are usually three in number, the most inferior being placed at the level of the umbilicus (4, Fig. 71), the other two higher up—one at the level of the ninth rib, the other at the level of the seventh. These intersections adhere to the anterior wall of the sheath of the muscle, and as the muscle is thinner at their level each line is marked on the surface by a transverse groove. 3rd. The portion of the muscle below the level of the umbilicus does not present any aponeurotic intersection, but it rapidly diminishes in breadth from the umbilicus to the pubis, so that the outer border of the muscle slopes from above downwards and inwards. To this arrangement is due the fact, upon which we have already dwelt (page 199), that the narrow groove bounded by the external oblique and the rectus muscles spreads out below the umbilicus into a broad, triangular surface, which is bounded below by the fold of the groin.
[204]
The rectus muscle flexes the trunk; that is, it depresses the thorax and brings it nearer the pubis—a movement which it accomplishes by the flexion of the vertebral column.
The lower part of the rectus muscle is covered by the pyramidalis muscle (14, Fig. 71), of which the contour does not show beneath the skin in the supra-pubic region, as the skin here is always padded by a cushion of fat. This pyramidalis muscle, which is only pointed out here in order that it may be remembered, forms on each side of the middle line a small fleshy triangle, of which the base is attached to the pubis, and the apex forms a short tendon which is inserted into the linea alba, the median fibrous raphé resulting from the interlacing of the aponeuroses of the oblique and transversalis muscles of the abdominal wall.
[205]
Trapezius, attachments and surface form.—Latissimus dorsi.—Deep muscles visible in relation to the trapezius and latissimus dorsi—1, lateral region of neck (splenius and complexus muscles); 2, region of the scapula (rhomboid, infraspinatus, teres major and teres minor muscles).—Deep muscles which are wholly concealed: erector spinæ, etc.
The most superficial muscles of the back are the trapezius and the latissimus dorsi. They form two broad muscular sheets which cover over the whole of the back and the posterior part of the neck, and extend also to the shoulder and arm.
Trapezius muscle.—The trapezius muscle has the following attachments. Its origin is from the middle line of the back, from the inner third of the superior curved line of the occipital bone (13, Fig. 73), the fibrous band of the ligamentum nuchæ between the occipital protuberance and the spinous process of the seventh cervical vertebra, and from the spinous processes of the seventh cervical and of all the thoracic vertebræ. From these origins the muscular fibres are carried outward and converge towards the shoulder, the intermediate fibres passing transversely, the superior obliquely downwards (9, Fig. 74), and the inferior fibres obliquely upwards. The muscle is inserted into the shoulder girdle, to the superior border of the spine of the scapula (Fig. 73), the inner edge of the acromion process, and the outer third of the[206] posterior border of the clavicle (19, Fig. 70; 7–13, Fig. 73).
With regard to external form the trapezius muscle presents this remarkable fact, that in certain regions the muscular fibres are replaced by aponeurotic fibres or tendons, so that in these regions the muscle is thinner and in contraction shows slightly depressed surfaces. These regions are three in number: 1. At the lower part of the neck and the upper part of the back (10, Fig. 73), opposite the level of the seventh cervical spine, the fibres of origin of the muscle are aponeurotic, and form with those of the opposite side a lozenge-shaped or elliptical surface with its long diameter vertical, in the centre of which the spinous processes of the sixth and seventh cervical and first thoracic vertebræ form more or less well-marked projections. 2. At the lower part of the back, at the level of the last thoracic vertebræ, the fibres of origin of the trapezius are also aponeurotic, in a small triangular space; and in the living model, when the trapezius is strongly contracted, its lower angle seems hollowed out, because at that level the muscular fibres are wanting, and in consequence do not swell up when the muscle is in action. 3. At the level of the root of the spine of the scapula, the inferior fibres of the trapezius form at their insertion a small triangular aponeurosis which glides on the bone, and gives rise to a distinct depression at that spot during the contraction of the muscle.
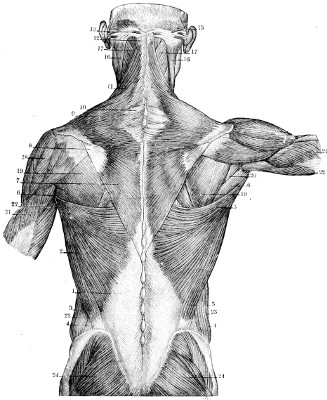
Fig. 73.
The Superficial Muscles of the Back.—1, The lumbo-sacral aponeurosis;—2, the latissimus dorsi;—3, its iliac fasciculus;—4, the space which separates it from the external oblique;—5, the upper portion of the latissimus dorsi;—6, 6, the teres major muscle;—7, the lower portion of the trapezius, with its aponeurotic portion (8) on a level with the spine of the scapula;—9, the central portion of the trapezius, with its aponeurosis (10);—11, 12, 13, the upper portion of the trapezius;—15, the occipito-frontalis muscle;—16, the sterno-cleido-mastoid;—17, the splenius capitis;—18, the deltoid;—19, the infraspinatus;—20, the teres minor;—21, 21, the external head, and 22, 22, internal head of the triceps brachialis;—23, the posterior portion of the external oblique of the abdomen;—24, 24, the gluteus maximus.
Action of the trapezius.—When the shoulder is strongly drawn backwards the whole of the[208] trapezius contracts, and in this case it is the middle portion, of which the fibres are directed horizontally, which shows most prominently beneath the skin. More frequently, however, different parts of the muscle contract separately; thus the superior fibres act, either by taking the shoulder as a fixed point, and bending the head to the corresponding side (as when the face is slightly turned to the opposite side), or by taking their fixed point at the occipital and the cervical origin, and thus raising and supporting the scapula, as when a burden is carried on the shoulder. Under those circumstances the cervical border of the trapezius, that which proceeds from the occipital bone to the clavicle (Fig. 74), becomes prominent in a line nearly parallel to that of the outer border of the sterno-cleido-mastoid (26, Fig. 74); and between these two prominent lines appears a groove (the posterior triangle of the neck), to which we will return in dealing with the deep muscles of this region. Lastly, if the inferior fibres of the trapezius contract alone, they draw the shoulder downwards, and thus we see them become prominent whenever the model causes a dragging with his upper limbs from above downward, e.g., in the case of a bell-ringer who pulls violently and with all his weight on a rope.
The two trapezius muscles (right and left) form together (Fig. 73) a rhomboidal figure with its apex below, which resembles the contour of a monk’s hood. Hence the trapezius has been called by anatomists and artists the cucullary muscle (cucullus, a hood).
[209]
Latissimus dorsi muscle (1, 2, 3, 5, Fig. 73).—This forms a large, somewhat triangular muscular sheet extending from the region of the loins to the upper part of the arm. It arises by means of a broad triangular aponeurosis (vertebral aponeurosis, 1, Fig. 73) from the spinous processes of the lower six thoracic vertebræ, from the spinous processes of the lumbar and sacral vertebræ and the posterior third of the crest of the ilium (3, Fig. 73); the muscular fibres converge from this origin towards the armpit, and the muscle obtains additional origins at its borders. At the outer border of the muscle, three or four fleshy bands join it which arise from the outer surfaces of the last three or four ribs by slips which interdigitate with the fibres of the external oblique muscle of the abdomen (4, 4, Fig. 74). At its upper border, as it crosses the inferior angle of the scapula, the muscle receives a narrow slip of origin from this part of the shoulder-blade. From these origins the muscular fibres are directed upwards and outwards, and converge so as to form a fleshy layer (5, Fig. 73) which, passing over the inferior angle of the scapula and along its axillary border, winds round the teres major muscle (see later), and over the posterior wall of the armpit to reach the upper part of the shaft of the humerus, in which it is inserted by a broad tendon, attached to the floor of the bicipital groove of the humerus (page 61).
This muscle acts first of all like the lower part of the trapezius, but with more energy. It, further, not only depresses the scapula, but also acts on the humerus. It is the contraction of the latissimus[210] dorsi which enables us to bring the arm with force to the side, carrying the upper limb slightly backwards, so that if the contraction is carried very far the arms become crossed behind the back. Indeed, the latissimus dorsi may be called the swimmer’s or golfer’s muscle. It draws the humerus backwards behind the trunk, and at the same time rotates the arm-bone and the whole limb inwards. The prominence formed by the outer border of the latissimus dorsi during contraction (Fig. 74) is principally shown when the muscle accomplishes a powerful effort, such as dragging, or pulling from above downwards, as in pulling on a rope hanging vertically, or in hanging by the arms from a horizontal bar. If in this situation—in the exercise of the trapeze, for example—the model raises himself, and brings the trunk near the bar, the latissimi dorsi muscles become very prominent, for then they take their fixed points at the arms, and act on the trunk by carrying it upwards and forwards.
Among the numerous deep muscles of the back there are not any which are visible on the surface throughout their entire extent, but there are many which appear in part in the spaces which limit the borders of the trapezius, latissimus dorsi, and superficial muscles of the shoulder and neck. These spaces are three in number, one at the side of the neck, one at the level of the lower half of the scapula, and a third over the iliac crest.
The posterior triangle is the name given to the space on the lateral surface of the neck, bounded (Figs. 73 and 74) behind by the supero-anterior border of the trapezius, and in front by the posterior[211] border of the sterno-cleido-mastoid. This space forms a long and superficial groove, extending from the occipital region to the middle of the clavicle. It has a lower part (25, Fig. 74), covered over by the platysma myoides muscle of the neck (to which we will return later), and a superior part, in which parts of one or two powerful muscles of the neck are found. 1st. The muscular fibres which we see (17, Fig. 73) directed obliquely from below upwards and outwards towards the mastoid process belong to the splenius capitis muscle, which arises from the spinous processes of the last cervical and upper four or five thoracic vertebræ, and ascends obliquely outwards to be attached to the mastoid process of the temporal bone beneath the sterno-cleido-mastoid (16, Fig. 73). 2nd. A small fleshy triangle, which may appear above the splenius, at the apex of the posterior triangle, corresponds to a part of a powerful muscle of the neck, called the complexus, which may or may not be completely concealed by the trapezius muscle. It is always responsible for the surface form of the neck, and, along with the other deep muscles, appears as a prominent ridge on each side of the groove formed by the edge of the ligamentum nuchæ.
The space situated in the back at the level of the lower part of the scapula is triangular in form (Figs. 73 and 74). When the arm is hanging beside the trunk the borders of the space are seen to be as follows: Externally, the vertebral border of the scapula; above and internally, the lower edge of the trapezius; and below, the upper[212] edge of the latissimus dorsi. In the floor of the space the greater rhomboid muscle is seen; while external to the triangle are the prominences of the muscles covering the lower part of the dorsal surface of the scapula, the infraspinatus, teres minor, and teres major muscles.
The greater rhomboid muscle (rhomboideus major) arises from the spinous processes of the seventh cervical and upper four or five thoracic vertebræ; its fibres are directed obliquely downwards and outwards, to be inserted into the vertebral border of the scapula. It is only the lower fibres which become superficial, behind the vertebral border of the scapula.
The infraspinatus muscle (19, Fig. 73) rises from the infra-spinous fossa of the scapula. From this origin its fibres ascend and, converging beneath the deltoid (Fig. 74), are inserted by a short tendon into the great tuberosity of the humerus.
The teres minor muscle (20, Fig. 73) rises from the upper part of the thick border of the infra-spinous fossa on the axillary border of the scapula, and ascends along the edge of the infraspinatus and beneath the deltoid, to be inserted into the lowest of three facets on the great tuberosity of the humerus.
The teres major (6, Fig. 73, and 8, Fig. 74) arises from the lower part of the broad axillary border of the infra-spinous fossa; it extends upwards and outwards like the preceding muscles, but it soon leaves the teres minor (5, Fig. 75). Instead of remaining at the posterior part of the shoulder it passes beneath the deltoid, and accompanies[213] the latissimus dorsi muscle (Figs. 17, 18; Fig. 68) to the front of the long head of the triceps, and is finally inserted into the inner lip of the bicipital groove of the humerus. The long head of the triceps is found, therefore, passing between the teres minor, behind, and the upper part of the teres major, in front (Fig. 73, between 20 and 6).
These muscles become more visible and prominent when the arm is raised and arrives at the horizontal position (see the right side of Fig. 73). The space between the edge of the trapezius and the border of the scapular spine above, and the latissimus dorsi below, becomes much lengthened from within outwards, and the deltoid leaves uncovered a greater extent of the infraspinatus, teres major and teres minor muscles; at the same time the scapula, by the elevation of the arm (page 64), being moved so that its inferior angle is drawn away from the vertebral column, a greater part of the rhomboid muscle becomes apparent between the outer border of the trapezius and the upper border of the latissimus dorsi.
Although the other deep muscles of the back are not visible on the subject stripped of its skin, we must not leave the region without giving a few of the names of the powerful fleshy masses which occupy the lumbar region, on each side of the spinous processes, and form two powerful muscular columns, causing a prominence beneath the aponeurosis of the latissimus dorsi (Fig. 73). This mass is formed by muscles in the loin which are closely blended together[214] below, and constitute the erector spinæ. At the lower level of the thorax it separates into an external muscle called the ilio-costalis, which is attached by a series of tendons to the angles of the ribs, and an internal muscle called the longissimus dorsi, which, by a series of tendons, is attached to the ribs and to the transverse processes of the thoracic vertebræ. These muscles are continued through the upper part of the back and the neck by means of smaller slips which need not be particularised. The action of the erector spinæ and its several parts is to straighten the trunk, and maintain it when a burden is borne on the shoulders or back. It is for this reason that their common mass in the lower part of the back is so developed in men who usually carry heavy loads on the shoulders, and forms that powerful muscular mass of the loins, of which the prominence is visible beneath the skin and the aponeurosis of the latissimus dorsi (1, Fig. 73). In the neck, as already stated, the complexus is the most important of the deep muscles in giving rise to the form and contour of this region.
[215]
The deltoid: its form, thickness, actions.—Muscular form of the shoulder as a whole.—The deeper muscles (supraspinatus and subscapularis).—Serratus magnus muscle: its relation to the armpit, its costal digitations; its action in movements of the arm.—Forms of the region of the armpit; prominence of the coraco-brachialis muscle; relations of the biceps and triceps to the armpit.
The upper and outer part of the prominence of the shoulder is formed by a single powerful muscle, called the deltoid. Beneath this are several deep muscles which fill up the fossæ of the scapula (supraspinatus, infraspinatus, and subscapularis). But when the arm is raised and maintained in the horizontal position, the surface below the root of the arm dips into a cavity or pit, corresponding to the external prominence of the shoulder; this cavity, called the armpit, or axilla, has for a roof the skeleton of the shoulder covered by the deltoid, and for its walls—in front, the pectoral muscles, which adjoin the anterior border of the deltoid, and behind, the subscapularis and the latissimus dorsi, separated from the posterior border of the deltoid by the teres major muscle. On the inner side is a muscle applied to the wall of the thorax, the serratus magnus, and on the outer side is the humerus, covered by the biceps and coraco-brachialis muscles. Of the muscles which we have[216] named, some have already been studied in relation to the muscular structure of the trunk (great pectoral and latissimus dorsi); of the others, we will study the deltoid and serratus magnus, in relation to the region of the shoulder and axilla.
Deltoid muscle.—This muscle is so called because it resembles
the Greek letter delta, and is triangular in form; it is short, broad,
thick, and shaped like half a cone to clasp the shoulder-joint. It
arises above from the outer third of the anterior border of the
clavicle (12, Fig. 68), from the acromio-clavicular articulation, from
the convex border of the acromion, and from the entire extent of the
posterior border of the spine of the scapula (18, Fig. 73). From this
origin its fibres are directed downwards, the middle fibres vertically,
the anterior or clavicular fibres downwards and backwards, and the
posterior fibres obliquely forwards, to be inserted into the external
surface of the humerus on a rough -shaped groove, called the deltoid impression (page 68).
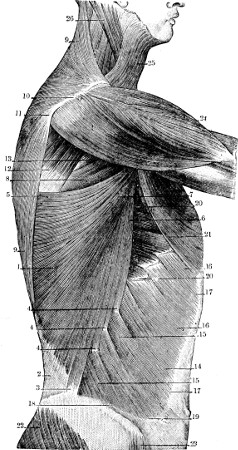
Fig. 74.
The Superficial Muscles of the Shoulder and the Lateral Portion of the Trunk.—1, the latissimus dorsi;—2, the lumbo-sacral aponeurosis;—3, 4, 4, the iliac and costal origins of the latissimus dorsi;—5, 6, 7, the upper portion of the latissimus dorsi;—8, the teres major;—9, 10, 11, the trapezius;—12, the infraspinatus;—13, the teres minor;—14, 15, 16, the external oblique of the abdomen;—17, 18, the anterior and interior border of the same muscle;—19, its inferior internal angle rounded (see page 199);—20, 20, serratus magnus;—21, the pectoralis major;—22, the gluteus maximus;—23, the tensor of the fascia lata;—24, the deltoid;—25, the platysma myoides;—26, the sterno-cleido-mastoid.
This muscle is very thick, and is intersected by a vertical series of strong fibrous bands or septa, which may be seen as depressions beneath the skin in the contracted muscle. The action of the deltoid is to elevate the arm, separating it from the trunk and supporting it in the horizontal position; but while the middle fibres raise the arm directly outwards, the anterior fibres elevate it and carry it forwards, and the posterior fibres carry it backwards. It is necessary to remark that this muscle is never at right angles to the lever which it moves, but it always acts obliquely[218] on the humerus. Hence, although very thick, the deltoid cannot act with great power; therefore the horizontal position of the arm produced by the action of the muscle is one which requires great effort and quickly produces fatigue. In order to understand the unfavourable arrangement of the deltoid with relation to its humeral lever, it is sufficient to compare it with that which the biceps presents relative to the forearm, and to see that the biceps, which acts obliquely on the radius, becomes perpendicular to that bone in proportion as flexion is carried on in the arm; and when the elbow forms a right angle, the biceps muscle is found in the most favourable condition to act with all possible force. In other words, the greatest momentum of a muscle occurs when it is perpendicular to its lever; the deltoid muscle, therefore, does not possess much momentum.
In pointing out the relations which the three borders of the deltoid present, we summarise the various details of the muscular contour of the shoulder:—1st. The superior border of the deltoid, by its origin from the anterior border of the clavicle and the posterior border of the spine of the scapula, repeats the insertions of the trapezius, which is attached to the opposite lip and border of the same bones (Fig. 74). The clavicle, acromion, and spine of the scapula form a species of bony intersection between the trapezius and deltoid, and when the muscles are contracted produce a deep groove between the insertion of the trapezius and the origin of the deltoid. In animals which have no clavicle, and in which the spine of the scapula is not well developed, the fibres[219] of the deltoid and trapezius are directly continuous. We observe an arrangement of this nature in the horse. 2nd. The anterior border of the deltoid is separated from the corresponding border of the great pectoral muscle by a linear interval, very narrow below, but a little broader above, where it forms a small triangle, of which the base corresponds to the middle of the clavicle (Fig. 70). This interval, which becomes visible during the contraction of the two muscles when we endeavour to raise the arm upwards and forwards while it is held behind, as in the act of drawing a load, gives passage to a vein called the cephalic, and under such circumstances this vein becomes prominent and swollen. 3rd. The posterior border of the deltoid forms one of the sides of the triangular space which we have studied in the region of the back, at the level of the infra-spinous fossa (Figs. 73 and 74); and, under its posterior border, pass successively on the one hand the infraspinatus and teres minor muscles, which pass directly beneath the deltoid, and on the other the teres major and latissimus dorsi muscles, which pass more deeply, separated from the deltoid by the long head of the triceps muscle (Fig. 75).
Two muscles of the shoulder remain to be mentioned which are not visible on the model, but must at least be named in order to explain how the fossæ of the shoulder-blade are filled up. These are:—1st. The supraspinatus muscle (11, Fig. 75), which occupies the supra-spinous fossa of the scapula, passes beneath the coraco-acromial arch, and is inserted into the uppermost facet of the great tuberosity of the humerus. 2nd. The infraspinatus muscle occupies[220] the infra-spinous fossa, and is partially concealed by the latissimus dorsi, trapezius, and deltoid. It is also bound down on the back of the scapula by a strong membrane derived from the deep fascia. It is inserted below the supraspinatus into the back of the great tuberosity of the humerus. 3rd. The subscapularis muscle (19, Fig. 68) occupies the subscapular fossa, and is inserted into the lesser tuberosity of the humerus.
The serratus magnus muscle (14, Fig. 68; 5, Fig. 70; 2, Fig. 71; 20, Fig. 73).—This muscle, applied to the lateral part of the thorax, is hidden throughout a great part of its extent by the scapula and the muscles of the chest and shoulder; but it becomes superficial at its lower part, in a series of prominent digitations and muscular bands, which form very characteristic features in the contour of the lateral region of the thorax. At the same time, as the muscle constitutes the inner wall of the armpit, we must describe it here in detail.
The serratus magnus arises by nine fleshy slips from the outer surfaces of the upper eight ribs (an additional slip arising between the first and second ribs). From this origin the muscle, which forms a broad sheet, sweeps backwards round the ribs, to be inserted into the whole length of the vertebral border of the scapula. The five or six upper digitations of the muscle are hidden by the great pectoral muscle (21, Fig. 73), and only its three or four lowest digitations are visible on the side of the thorax between the borders of the great pectoral muscle in front and the latissimus dorsi behind; they interdigitate with the upper slips of origin of the external oblique[221] muscle of the abdomen (20 and 16, Fig. 73). The alternations of origin of the serratus magnus and external oblique are seen when the muscle is contracted, as when the arm is thrust forward. When the arm is hanging loosely, or slightly raised, we see only three digitations of the serratus magnus; but when the arm is strongly elevated the great pectoral frequently leaves another uncovered.
The action of this muscle is to fix the scapula, drawing this bone downwards and forwards, while the rhomboid, on the other hand, draws it upwards and backwards. Fixation of the scapula being necessary to afford a fixed point for the contraction of the muscles of the arm (particularly the biceps), it is easy to perceive that whenever the upper limb accomplishes a powerful effort, the lower digitations of the serratus magnus become clearly visible in the living model, as in a sword-thrust, wrestling, lifting from the ground a heavy body, or in pushing back an adversary, &c.
The serratus magnus muscle forms the inner wall of the armpit or axilla, a cavity of which the anterior wall is represented by the pectoral muscles, and the posterior wall by the subscapularis, teres major, and latissimus dorsi. The cavity forms a triangular pyramid; its summit, directed upwards, corresponds in the skeleton to the interval between the first rib, the clavicle, and the upper border of the scapula. In a dissected subject this cavity is open inferiorly, but in the living model it is closed by the skin which forms the base of the pyramid, and which, in passing from the outer border of the great pectoral muscle to the border of the latissimus dorsi,[222] is hollowed out so as to ascend in the space, into which it is drawn by its attachment to the strong, deep fascia of the axilla.
To complete the description of the axilla we must say a few words concerning its boundaries, and the folds which correspond to the lines of junction of its walls. There is nothing more to add with regard to its anterior limit (formed by the great pectoral muscle) or its posterior limit (formed by the latissimus dorsi and teres major muscles clothing the axillary border of the scapula), but a word must be said of the external limit of the space which corresponds to the root of the arm. This is a comparatively thick surface, and corresponds to the upper part of the shaft of the humerus. The bone is covered by two muscles which descend from the scapula towards the anterior surface of the arm,—the biceps and coraco-brachialis, which we will notice briefly. We will say, first of all, that the form of the coraco-brachialis is clearly visible beneath the skin of the armpit when the arm is strongly raised, as for example in a subject crucified, when it raises the depressed skin in the armpit. The skin is covered with hair more or less abundant, according to the individual, and it is a classic habit to omit this part of the hairy system in every representation of an elevated limb; but the artist should be convinced by the study of anatomy that he should never conform to the habit of tracing on the skin of the hollow of the armpit a fanciful contour, since this skin is smooth and regularly depressed, and only on its external part presents the fusiform muscular prominence of the coraco-brachialis, on the inner side[223] of the anterior surface of the arm. The biceps muscle escapes from under cover of the great pectoral muscle, and lies external to the coraco-brachialis more on the front of the limb.
The triceps muscle of the arm, which, by its long head, takes origin from the scapula, does not pass, like the biceps and coraco-brachialis, through the armpit, but appears behind it on the back of the arm, since, as we have already said, it passes between the teres minor posteriorly and the teres major and latissimus dorsi anteriorly (Figs. 73 and 75).
[224]
1st. Anterior muscles: Biceps, its two heads; its fusiform body; its bifurcation below (aponeurotic expansion and tendon); its action (supinator and flexor of forearm); influence of its aponeurotic expansion on the contour of the forearm.—Coraco-brachialis, brachialis anticus. 2nd. Posterior muscle: Triceps brachialis, its three portions, flat surface formed by its inferior tendon; general contour of the posterior surface of the arm; action of triceps. External form of the arm; external and internal intermuscular grooves.
The muscles of the arm form two distinct fleshy masses, a mass in front formed by the biceps, which occupies the entire length of the arm; by the coraco-brachialis, which occupies only the upper part; and lastly, by the brachialis anticus, which occupies the lower part; and a mass behind, formed by one muscle only, the triceps.
The biceps (12, Fig. 75, and 21, Fig. 70) is so called because it possesses two heads of origin, which are known by the names of the long and short heads. The long head of the muscle presents the form of a long tendon, which arises from the upper limit of the glenoid cavity of the scapula, and descends through the shoulder-joint and the bicipital groove of the humerus to the arm. The short head of the biceps has a less complex course, and arises from the summit of the coracoid process, in common with the coraco-brachialis.
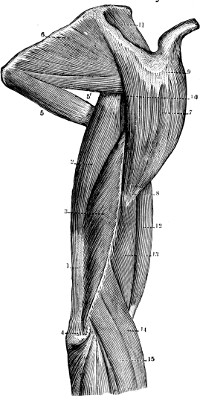
Fig. 75.
The Muscles of the Shoulder and Arm (seen from the external side).—1, the triceps brachialis;—2, its long head;—3, its external head;—4, its attachment to the olecranon;—5, the teres major;—5′, the teres minor;—6, the infraspinatus;—7, 8, 9, 10, the deltoid;—11, the supraspinatus;—12, the biceps brachialis;—13, the brachialis anticus;—14, the supinator longus;—15, extensor carpi radialis longior.
These two tendons (long and short head) descend in the outer wall of the axilla, covered by the great[225] pectoral muscle (Fig. 70, page 197); a little above the lower border of this muscle the fleshy fibres appear and form two cylindrical bellies which descend and become united, at the level of the middle of the anterior surface of the arm, in one large mass, very marked in muscular subjects (12, Fig. 75). A short distance above the elbow-joint, a flat tendon of insertion succeeds to the fleshy muscle; it is at first broad, but soon divides into two parts, one aponeurotic, called the semi-lunar fascia of the biceps; the other, a rounded tendon forming the chief insertion of the muscle. The aponeurotic expansion (2, Fig. 77) of the bicipital fascia is directed downwards and inwards over the common mass of the flexor muscles of the forearm, and soon[226] becomes blended with the aponeurosis of the forearm; the tendon proper (3, Fig. 74) dips down in the hollow of the elbow between the internal and external muscles of the forearm, and is fixed to the bicipital tubercle of the radius (page 78, and Fig. 21), upon which it turns to be inserted into the posterior part of the tubercle.
The biceps muscle is essentially the flexor of the forearm on the arm. This action is evident, and known to all, and it is useless to dwell on it, except to recall the fact that the biceps, in acting on the forearm, is inserted perpendicularly on the lever which it moves, so that it is in the most favourable position for the exercise of all its power. But the contraction of the biceps produces along with flexion of the elbow two other movements to which it is important to direct attention. 1st. If the forearm is in pronation the tendon of the biceps is obviously twisted round the upper part of the radius, since it is inserted into the posterior part of the bicipital tubercle; the first effect produced, therefore, by its contraction is a rotation of the radius outwards, and a movement of supination; the biceps is, therefore, a supinator, and one of the most powerful. 2nd. Besides flexion at the elbow-joint and this movement of supination, the biceps muscle raises and draws inwards the humerus by its action on the shoulder-joint. The three separate movements are found in association with one another in such a movement as the act of raising the hand to the mouth.
During the contraction of the biceps, its aponeurotic expansion is tightened, and binds down the mass of the flexor muscles of the forearm over which[227] it passes; hence it marks on the inner surface of the fleshy part of this portion of the limb, two fingers’ breadth below the internal condyloid ridge, a distinct furrow, during the contraction of the muscle.
The changes of form in the arm which accompany the contraction of the biceps are well known, and it is sufficient to recall the fact that the fleshy belly of this fusiform muscle is lengthened in the state of repose, becoming short and globular during contraction. Nothing is more striking, nor gives a better idea of the change of form in a muscle during contraction, than to examine the biceps in a model, who brings it gradually into action by flexing the forearm on the arm (Fig. 76). We then see on the anterior surface of the arm a kind of fleshy ball becoming more and more clearly marked, which hardens and swells up at the same time, so that it seems to mount up towards the upper part of the arm, to the inferior border of the great pectoral muscle.
The coraco-brachialis muscle forms a narrow fusiform fleshy mass, which occupies the upper part of the inner surface of the arm. It arises from the coracoid process of the scapula (alongside the short head of the biceps), and is inserted into the middle of the internal border of the humerus. When the arm is hanging loosely the lower half only of this muscle is visible on the subject, and its prominence is blended with that of the biceps, while its upper half is hidden within the axillary space, beneath the great pectoral muscle. It becomes visible beneath the skin of the armpit, however, when the arms are raised, as in the position on the cross, and we have[228] already dwelt upon the contour which the fusiform muscular belly of this muscle presents in the outer wall of the axilla. When the coraco-brachialis contracts, its form becomes more prominent, like that of every muscle in contraction; but it is not more visible on this account, for as it draws the arm to the thorax against which it is applied, it conceals by this movement the region in which its prominence is marked.
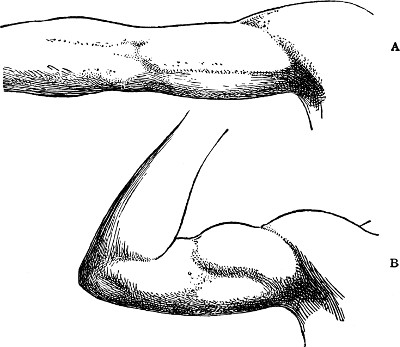
Fig. 76.
A, the arm extended; B, the elbow flexed and the biceps contracted.
The brachialis anticus muscle (13, Fig. 75, and 4, 4, Fig. 77).—Situated beneath the lower half of the biceps, which it overlaps on each side, this muscle is deeply placed, and covers the lower two-thirds of the anterior surface of the humerus, to which it is attached. The fleshy fibres descend almost to the level of the elbow, where they are replaced by a flat[229] tendon, inserted into the front of the coronoid process of the ulna. As the ulna does not exhibit any of the lateral movements comprised in supination and pronation, the brachialis anticus is simply a flexor of the forearm, and when this movement is forcibly accomplished, it may be seen to swell up on each side of the lower part of the biceps.
Triceps muscle.—This muscle (21, 22, Fig. 73; 1, 2, 3, Fig. 75), which forms alone the entire muscular structure of the posterior surface of the arm, has been called the triceps because it arises by three heads, separated above, united below; one central or median, called the long head, and two lateral parts, distinguished as the external and internal heads. The long head (2, Fig. 75), forming a thick and fusiform fleshy belly, arises by a stout tendon from the upper part of the axillary border of the scapula immediately below the glenoid cavity, and passes between the teres major and teres minor muscles to the back of the arm (page 223). At the level of the junction of the middle with the lower third of the arm, the fleshy belly terminates in a broad, flat tendon (1, Figs. 75 and 78) which forms the main insertion of the muscle, and receives the insertions of the two other portions of the muscle. The external head (3, Fig. 75) arises from the upper part of the posterior surface of the humerus (above and to the outer side of the spiral groove), and is directed obliquely downwards and inwards to be attached to the external border of the main tendon almost as low down as the elbow. Lastly, the internal head (22, Fig. 73)[230] arises from the lower part of the posterior surface of the humerus (below and to the inner side of the spiral groove), and is attached to the internal border and deep surface of the inferior common tendon. This tendon is inserted (4, Fig. 75) into the upper surface of the olecranon process of the ulna, and on either side of this it blends with the deep fascia of the forearm.
The form of the posterior surface of the arm is greatly influenced by the presence of the inferior common tendon of the triceps, which, narrow and pointed towards its upper end, forms a large flat surface at the lower part of the arm. This flat surface is overlapped on each side by the prominence of the fleshy parts of the inner and outer heads. Above, in the upper two-thirds of the posterior surface of the arm, two fleshy bellies may be seen side by side, an outer one formed by the outer head, an inner one formed by the long head of the muscle. The inner head, more deeply placed, is only obvious in the lower third of the arm. These various details—viz., the tendinous flat surface above the olecranon, the muscular prominences which bound it on each side, and the two fleshy bellies which ascend above it—become visible in a marked degree when the subject forcibly extends the forearm on the arm, as in struggling against any resistance which causes the position of flexion to be maintained. It is hardly necessary to say that the triceps is essentially the extensor muscle of the forearm on the arm.
It is not only for the purpose of a regular[231] enumeration, but also with regard to the anatomical interpretation of their external forms, that we have classed the muscles of the arm as anterior and posterior. On each side of the arm at both inner and outer borders, a groove runs which separates the anterior from the posterior muscles. In each of these grooves is a fibrous partition called the internal and external intermuscular septum, which extends from the surface to the corresponding supra-condyloid ridge of the humerus, and serves to increase the area of muscular attachment. In muscular contraction, therefore, each septum or aponeurosis is slightly drawn towards the humerus, and on the surface two grooves are clearly seen, each corresponding to an interval, internally or externally, between the anterior and posterior muscles.
The internal groove commences at the inferior extremity of the coraco-brachialis, and descends almost to the inner condyle. Above it is faintly marked, because the numerous nerves and vessels surrounded by cellular tissue fill up the intermuscular space at this level; below it spreads out, and tends to be confounded with the form of the internal part of the brachialis anticus.
The external groove (Fig. 75) is short. It begins at the level of the lower extremity of the deltoid, and does not descend to the external condyle, because the highest muscles of the extensor group belonging to the forearm arise from the lower part of the outer border of the humerus, so that the groove is filled up by these muscles as they curve forwards towards the bend of the elbow.
[232]
Division into groups:—A. Anterior muscles of the forearm. The superficial muscles, or those arising from the inner condyle: pronator radii teres, flexor carpi radialis, palmaris longus, and flexor carpi ulnaris. 2nd. The deep muscles (flexors of the fingers and pronator quadratus). B. Posterior muscles of the forearm. 1st. External muscles: supinator longus (importance with regard to the forms of the external region of elbow); the extensor carpi radialis, longior, and brevior; the supinator radii brevis. 2nd. The posterior superficial muscles: the extensor communis digitorum, extensor minimi digiti, extensor carpi ulnaris, and anconeus.
Muscles of the Forearm.—The two bones of the forearm are covered by a series of muscles with fleshy bellies, generally fusiform, terminating inferiorly in tendons which are frequently very long, and become prominent in the region of the wrist. Some of these muscles move the forearm on the arm, or the radius on the ulna, but the action of the greater number is to move the hand on the forearm and the different segments of the fingers on each other. These muscles are divided into five series, each composed of four muscles, making the total number of muscles in the arm twenty altogether. We shall dwell chiefly upon the superficial muscles, a short mention being sufficient for the deeper ones. We distinguish first of all two groups, anterior and posterior: one on the front, the other on the back of the forearm. The anterior group is divisible into: 1st. An anterior superficial layer, of which[233] each muscle will be studied; 2nd. An anterior deep layer, to which we will briefly refer. The posterior group may be subdivided into three: 1st. An external layer; 2nd. A superficial posterior layer, which we must review in detail; and 3rd. A posterior deep layer, respecting which we shall only say sufficient to enable the reader to understand the shape of the wrist formed by the corresponding tendons.
A. ANTERIOR MUSCLES OF THE FOREARM. I. Anterior superficial muscles.—All these muscles arise by a common tendon from the internal condyle of the humerus; their common origin does not appreciably extend above the level of the condyle, so that at the inner side of the elbow, contrary to what takes place on the outer side, the muscles of the forearm do not ascend on the corresponding side of the upper arm. If from the inner condyle we draw four lines, of which the first goes towards the middle of the radius, the second towards the outer border of the wrist, the third towards the middle, and the fourth towards the inner border of the wrist; these four lines, of which the first is very oblique and the others gradually approach the vertical, will give us the direction of each of these four anterior superficial muscles of the forearm, which are, in the order of the lines, from without inwards, the pronator radii teres, the flexor carpi radialis, the palmaris longus, and the flexor carpi ulnaris.
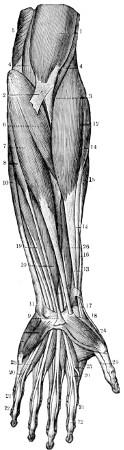
Fig. 77.—The Anterior Muscles of the Left Forearm.—1, the biceps brachialis;—2, its aponeurotic expansion;—3, its tendon;—4, 4, brachialis anticus;—5, the internal head of the triceps;—6, pronator radii teres;—7, flexor carpi radialis;—8, 9, palmaris longus;—10, flexor carpi ulnaris;—11, its attachment to the pisiform bone;—12, 13, supinator longus;—14 and 15, the extensor carpi radialis, longior, and brevior;—16, the abductor longus pollicis;—17, its tendon;—18, tendon of extensor longus pollicis;—19, 20, 21, the superficial flexor of the fingers and its tendons;—22, tendons of the deep flexors;—23, 23, the lumbricales;—24, abductor brevis pollicis;—26, flexor longus pollicis.
The pronator teres (6, Fig. 77) is fleshy throughout the entire extent in which it is visible on the model; arising from the internal condyle, it is directed obliquely downwards and outwards, and[234] disappears beneath the external muscles of the forearm (supinator longus) to be inserted into the radius (around which it is slightly twisted) in the middle of its external surface (impression for the pronator teres, page 78). Contracting, the pronator teres turns the radius forward and inwards, producing pronation. This muscle forms the inner side, very oblique, of a triangular pit, known as the hollow of the elbow, of which the outer side is formed by the supinator longus (12, Fig. 77). In this hollow the tendon of the biceps dips down (3, Fig. 77) along with the brachialis anticus (4, 4, Fig. 77) to be inserted into the bones of the forearm. The upper part of the pronator teres is crossed[235] by the aponeurotic expansion of the biceps (2, Fig. 77), and we have already dwelt on the particulars of external form which result from this arrangement.
The flexor carpi radialis (7, Fig. 77) arises from the inner condyle by a fusiform fleshy belly which descends obliquely to the middle of the forearm. It is replaced by a narrow, strong tendon which gains the outer part of the wrist, and then disappears beneath the annular ligament of the carpus, and, lying in a groove on the anterior surface of the trapezium, is inserted into the bases of the metacarpal bones of the fore and middle fingers. This muscle flexes the hand on the forearm; when it contracts, its tendon becomes very prominent and raises the skin at the lower part of the front of the forearm; it forms the first tendinous prominence that we meet at this level in passing from the radial to the ulnar border, and lies just internal to the groove in which the radial artery pulsates.
The palmaris longus (8, 9, Fig. 77) is much smaller than the preceding muscle; arising from the internal condyle, it forms a short fusiform fleshy belly (8) to which a long slender tendon succeeds. Descending almost vertically to the middle of the wrist, the tendon ends by being inserted into the annular ligament of the carpus and the fascia of the palm (9, Fig. 77). The palmaris longus flexes the hand on the forearm, and its tendon forms in contraction of the muscle a well-marked prominence situated in the middle of the lower part of the front of the forearm on the inner side of the tendon of the flexor carpi radialis. In some subjects this muscle is[236] absent, and it is frequently subject to variations of form.
The flexor carpi ulnaris (10, 11, Fig. 77) arises not only from the inner condyle, like the three preceding muscles, but also (18, Fig. 78) from the posterior border of the ulna (including the olecranon) process; it descends vertically over the ulna, and is inserted by tendinous and fleshy fibres into the pisiform bone of the carpus (11, Fig. 77). As its fleshy fibres continue down to its insertion the form of the muscle is not marked by a prominence such as those produced by the tendons of the preceding muscles; this muscle, therefore, helps to give a rounded form to the whole extent of the inner border of the forearm. It flexes the hand, and at the same time draws it inwards towards the inner side of the wrist.
II. Anterior deep muscles.—These muscles constitute a fleshy mass lying beneath the preceding superficial muscles, and terminate near the wrist in numerous tendons, which pass to the fingers; the tendons of the muscles appear to a slight extent on the model in the grooves between the tendons of the superficial muscles (19, 19, Fig. 77). Lower down the tendons of these muscles lie in the anterior groove of the carpus, bound down by the corresponding annular ligament, and after traversing the hollow of the palm of the hand, they are inserted into the phalanges of the fingers, presenting characteristic features which we will rapidly point out in the enumeration of these muscles.
These deep muscles comprise, 1st, the flexor sublimis digitorum (19, Fig. 77), which divides[237] below into four tendons, one for each finger (except the thumb); 2nd, the flexor profundus digitorum, which also divides into four tendons, one for each finger (except the thumb). On the anterior surface of each finger, therefore, we see two tendons—one superficial (23, Fig. 77) and the other deep. The first (flexor sublimis) presents at the level of the first phalanx (20, Fig. 77) a slit or button-hole, through which the second passes (flexor profundus); owing to this arrangement the tendon of the deep flexor is inserted into the base of the third phalanx (22, Fig. 77). superficial flexor is inserted into the base of the second phalanx (21, There is, indeed, a flexor muscle for each of the phalanges; the first phalanges of the fingers having special flexors in addition, the small lumbricales muscles of the palm of the hand, which arise from the sides of the tendons of the flexor profundus digitorum in the palm of the hand.
3rd. The flexor longus pollicis (26, Fig. 77) arises in the forearm from the radius, and its tendon is inserted into the base of the second or last phalanx of the thumb. It gives no evidence of its existence on the surface. 4th. The pronator quadratus muscle, a quadrilateral fleshy muscle, is disposed in a different manner to the preceding muscles, which must be raised in order to see it. It is formed by transverse fibres placed in the lower fourth of the forearm, and it passes from the anterior surface of the ulna to that of the radius. Its contraction produces pronation, rotating the radius over the lower part of the shaft of the ulna.
B. POSTERIOR MUSCLES OF THE[238] FOREARM. I. External muscles.—These form the fleshy mass which covers the lower third of the outer border of the arm (Fig. 75, page 225) and descends along the outer border of the radius in the forearm. The group comprises four muscles—the supinator longus (brachio-radialis), two radial extensors of the carpus, and the supinator radii brevis.
Of these four muscles, one only is visible on the model throughout its entire extent—viz., 1st, the supinator longus or brachio-radialis (14, Fig. 75; 12, 13, Fig. 77), which arises from the outer supra-condyloid border of the humerus, between the brachialis anticus in front and the triceps behind. It is noteworthy that on this side the muscles of the forearm ascend on the arm almost up to the insertion of the deltoid. The supinator longus enlarges as it descends, so that it presents its greatest size at the level of the external condyle, the prominence of which it completely conceals. It forms the outer vertical boundary (page 234) of the triangular hollow at the bend of the elbow. Just below the middle of the forearm, the fleshy fibres are replaced by a long tendon which lies on the radius, and (13, Fig. 77) is finally inserted into the base of the styloid process of that bone. Notwithstanding its name, this muscle is not essentially a supinator; it acts in this way only when the forearm is in a position of complete pronation, and its proper action in this respect is to bring the forearm into a position between supination and pronation. Its principal function, however, is the flexion of the forearm on the arm, and in this movement its form is clearly shown externally in the form of a prominent band, which rises from the arm, and forms,[239] on the antero-external part of the elbow, a strong fleshy mass, filling up the hollow produced by the flexion of the forearm on the arm. The supinator longus is the most important of the muscles of the forearm with regard to the part it takes in the external form of this region.
The two next muscles (14 and 15, Fig. 77) are partly hidden by the preceding; they are the radial extensors of the carpus (2 and 3), distinguished as the extensor carpi radialis, longior and brevior (15, Fig. 75). They arise from the lower part of the outer supra-condyloid ridge of the humerus and from the outer condyle, and form fleshy masses (3 and 5, Fig. 78), which increase the prominence of the supinator longus, and help to conceal the outer condyle. At about the same level as in the case of the supinator longus, a tendon succeeds the fleshy belly of each of these muscles, and inclines a little backward (Fig. 78); having been crossed by the extensor ossis metacarpi pollicis, by the extensor brevis pollicis (7 and 8, Fig. 78), and by the extensor longus pollicis; each reaches the dorsal surface of the wrist, and is inserted into the base of the metacarpal bone of the index finger (extensor carpi radialis longior), and into the base of the metacarpal bone of the middle finger (extensor carpi radialis brevior, 6, Fig. 78).
4th. Surrounding the upper part of the radius is a small deep muscle, which does not show on the model, and which we mention here only to point out that its presence increases the prominence of the muscular mass on the outer side of the elbow; this is the supinator radii brevis, formed by[240] fibres which, arising from the humerus, elbow-joint, and ulna, are rolled round the back and outer side of the radius, and which acts so as to turn the bone backwards and thus produce supination.
II. Posterior superficial muscles (Fig. 78).—This group comprises the extensor cemmunis digitorum, the extensor minimi digiti, the extensor carpi ulnaris, and the anconeus. These four muscles arise from the external condyle, to which they are attached by a common tendon; from this origin they are directed downwards, the first almost vertically, the last (anconeus) very obliquely backwards and inwards.
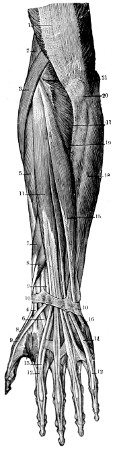
Fig. 78.—The Posterior Muscles of the Left Forearm.—1, the tendon of triceps brachialis;—2, supinator longus;—3 and 4, extensor carpi radialis longior;—5 and 6, extensor carpi radialis brevior;—7 and 8, extensor ossis metacarpi pollicis and extensor brevis pollicis;—9, 9, the extensor longus pollicis;—10, 10, the annular ligament of the wrist (dorsal aspect);—11, 12, the extensor communis digitorum and its tendons;—13, the tendon of the extensor indicis;—14, the tendon of the extensor minimi digiti;—15, 16, extensor carpi ulnaris;—17, anconeus;—18, the flexor carpi ulnaris;—19, the posterior border of the ulna;—20, olecranon;—21, the inner condyle.
1st. The extensor communis digitorum (11, Fig. 78)[241] forms a long fusiform fleshy belly. In the lower third of the posterior surface of the forearm, it gives place to a tendon which soon subdivides into four bands. These remain in contact until they have passed a groove situated in the centre of the inferior extremity of the radius, and separate on the dorsal surface of the wrist, diverging so as to be attached to each of the four fingers. On the back of the hand the tendons of the middle, ring, and little fingers are joined together by two oblique tendinous slips directed obliquely downwards and outwards, from the fourth to the third, and from the third to the second tendon respectively. On the dorsal surface of the first phalanx of each finger (12, Fig. 78) the extensor tendon forms a membranous expansion, and thereafter divides into three slips, a central one inserted into the base of the second phalanx, and two lateral slips which unite again to be inserted into the base of the third phalanx. The tendons cover the backs of the knuckles and of the joints of the fingers.
2nd. The extensor minimi digiti is a small bundle of fleshy fibres lying adjacent to the preceding muscle, but distinctly detached from it. It gives rise to a separate tendon, which passes through a special groove beneath the posterior annular ligament between the lower ends of the radius and ulna. From the wrist it is directed towards the posterior surface of the little finger (14, Fig. 78), where it unites with the tendinous fasciculi from the common extensor tendon for the little finger, and joins in the formation of[242] the membranous expansion on the dorsum of the first phalanx.
3rd. The extensor carpi ulnaris (15, Fig. 78) is a fusiform muscle arising from the external condyle and the posterior surface of the ulna. It is replaced by a tendon in the lower fourth of the forearm (15, Fig. 78). This tendon passes beneath the posterior annular ligament in a groove on the posterior surface of the ulna (10, Fig. 78), and at the inner part of the dorsal surface of the carpus it terminates almost immediately by being inserted into the base of the metacarpal bone of the little finger (16, Fig. 78).
These three muscles are extensors of the fingers and hand. If we examine a living model which has the arm folded on the trunk, the dorsal surface of the forearm being turned forwards, and which quickly moves the fingers and hand, we see clearly the movements of the fingers marked by muscular movements in the upper two-thirds of the posterior surface of the forearm. We can, by following their prominences in contraction, clearly recognise the fusiform bellies of these muscles.
4th. The anconeus occupies the upper part of the posterior surface of the forearm. As its name indicates (ἀγκὼν, olecranon, elbow), it is a muscle of the region of the elbow; it forms (17, Fig. 78) a triangular fleshy mass, of which the apex is attached to the external condyle, and the base is inserted into the external surface of the olecranon, and corresponding part of the ulna (19, Fig. 78). As the ulna does not possess appreciably the movement of rotation, but shares only in flexion and[243] extension of the elbow-joint, the anconeus situated behind the joint has no other action than that of extending the forearm on the arm. When this movement is forcibly produced, we see the anconeus clearly marked by a triangular prominence, of which the upper border, the shortest, is united with the prominence of the triceps; and we have already mentioned the anatomical fact that the inferior portion of the triceps is directly continuous in the forearm with the anconeus muscle.
[244]
3rd. The posterior deep muscles of the forearm; their tendons at the level of the wrist (anatomical snuff-box).—Muscles of the hand;—1st. Muscles of the thumb, or thenar eminence. 2nd. Muscles of the little finger, or hypothenar eminence. 3. Short muscles of the palm (lumbricales and interossei).
III. The deep posterior muscles of the forearm, with regard to external form, are important only in the arrangement of their tendons in the wrist and hand; for this reason we describe them in this chapter along with the muscular structures of the hand and fingers.
As in the other regions, we find in the deep part of the back of the forearm, four muscles. Proceeding from without inwards they are—the extensor ossis metacarpi pollicis, the extensor brevis pollicis, the extensor longus pollicis, and the extensor indicis. The fleshy bellies of these muscles are almost completely hidden beneath the posterior superficial muscles; but their tendons, at least those of the first three, emerge beneath the external border of the common extensor of the fingers, and their form is shown (7 and 8, Fig. 78) by details of great importance on the outer side of the dorsal aspect of the wrist.
[245]
The two first (7 and 8, Fig. 78), the extensor ossis metacarpi pollicis (7) and the extensor brevis pollicis (8), must be described together, as their fleshy parts and tendons are placed together and are almost united throughout the greater extent of their course. These two muscles emerge in the lower third of the forearm, at the outer border of the common extensor of the fingers; and they form at this point, at the junction of the posterior surface with the outer border of the forearm, an oblong eminence, which is soon succeeded by a double tendon. Crossing the tendons of the radial extensors of the wrist, this double tendon is directed towards the outer surface of the lower end of the radius, where it passes through a groove (10) converted into a canal by the posterior annular ligament of the wrist. At the outer border of the wrist these two tendons form a prominence, well marked beneath the skin, when the thumb is separated from the other fingers. Finally, at the base of the metacarpal bone of the thumb these tendons separate, one, that of the extensor ossis metacarpi pollicis, being inserted into the base of the metacarpal bone, while the other, that of the extensor brevis pollicis, passes over the first metacarpal bone to be inserted into the base of the first phalanx of the thumb (8, at the level of the thumb, Fig. 78).
The extensor longus pollicis (9, Fig. 78) emerges, like the preceding tendons, on the outer side of the common extensor, but lower down, on the back of the wrist; its tendon only becomes superficial at this point, and it is directed obliquely downwards through a prominent deep groove on the posterior surface of[246] the lower end of the radius, where it is covered by the posterior annular ligament. On the back of the wrist the tendon is directed obliquely outwards, crossing the tendons of the radial extensors of the wrist, to reach the base of the metacarpal bone of the thumb, where it lies parallel to the tendon of the extensor brevis pollicis. Descending lower than this tendon it is finally inserted into the second or terminal phalanx of the thumb (9, Fig. 78).
The tendons of the extensor ossis metacarpi and extensor brevis pollicis on the one hand, and the extensor longus pollicis on the other, form on the outer part of the back of the wrist a triangular figure, of which the apex corresponds to the upper end of the thumb, and the base to the lower end of the radius. When we separate the thumb strongly from the index finger—that is to say, when we contract the three small muscles which we have been studying—the corresponding tendons mark the borders of this triangle in the form of prominent cords, between which is a deep concavity; to this depression is given the name of the anatomical snuff-box (4, Fig. 78).
The extensor indicis is not visible on the model; it is deeply situated beneath the common extensor of the fingers, and terminates in a tendon (13, Fig. 78) which unites with the tendinous fibres from the common extensor to the index finger. It is to this muscle that the index finger owes its power of extension independent of the other fingers, and of performing the functions which have given it the name of the index or indicating finger. It is to be noted that in separate extension of the index finger (with flexion of the others) the tendon of the extensor[247] communis digitorum in the back of the hand gets curved outwards, by being pulled into line with the extended index finger by the traction of the tendon of the extensor indicis (Macewen).
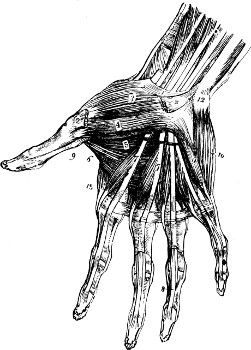
Fig. 79.
Muscles of the Hand (palmar surface).—2, abductor pollicis (cut);—3, opponens pollicis;—4, flexor brevis pollicis;—5, adductor obliquus pollicis;—6, adductor transversus pollicis;—7, deep flexor tendons and lumbrical muscles;—8, flexor tendons on finger;—9, flexor longus pollicis;—10, abductor minimi digiti;—11, flexor brevis minimi digiti;—12, pisiform bone.
Muscles of the hand.—The numerous muscles belonging to the hand form an interesting study in relation to the mechanism of the multiple and delicate movements of the fingers, but as the various details of their complex arrangement do not show very plainly on the surface we may confine our study of them to an enumeration of their principal features.
The dorsal region of the hand (Fig. 78) does not possess any fleshy muscles, but only presents the tendons belonging to the muscles of the forearm. The arrangement of the tendons after passing beneath the posterior annular ligament has already been described (pp. 245–6). Notice should be taken of an arch of veins lying superficial to the tendons. This venous arch receives the veins from the fingers, and is variable in its arrangement and outline.
[248]
On the other hand, the anterior or palmar region of the hand possesses, beside the tendons of the muscles of the forearm, numerous small muscles, which are divided into three groups:—1st, an external group associated with the thumb, forming the fleshy prominence known as the thenar eminence; 2nd, an internal group, belonging to the little finger, forming the hypothenar eminence; 3rd, a middle and deeper group, formed by small muscles belonging to the fingers, and placed deep in the hand beneath the thick palmar fascia, which, occupying the hollow of the palm, fills up the space between the thenar and hypothenar eminences (Fig. 79).
1st. The thenar eminence (2–5, Fig. 79) is of a long ovoid form, with the large superior extremity corresponding to the carpus, and the smaller inferior extremity corresponding to the base of the first phalanx of the thumb. It is formed by six muscles, namely, the abductor pollicis (24, Fig. 77; 2, Fig. 79), which proceeds from the trapezium and annular ligament to the outer side of the first phalanx of the thumb; the opponens pollicis (3, Fig. 79), with a similar origin, inserted into the entire length of the outer border of the first metacarpal bone, so that its contraction draws the whole thumb (phalanges and metacarpal bone) towards the palm of the hand, and thus opposes it to the other fingers; the flexor brevis pollicis (superficial part) (4, Fig. 79), which proceeds from the annular ligament to the base of the first phalanx; the adductor obliquus pollicis (5, Fig. 79), arising from the carpus and heads of the metacarpal bones, and inserted into the inner side of the first phalanx of the thumb; the adductor transversus[249] pollicis (6, Fig. 79), a muscle remarkable for its arrangement, for it arises from the middle of the palm of the hand, from the anterior surface of the third metacarpal bone, and forming a comparatively broad fleshy mass, extends outwards to be inserted along with the adductor obliquus into the inner side of the base of the first phalanx of the thumb; and finally a small muscle deeply placed in the space between the first and second metacarpal bones, and known as the deep part of the flexor brevis pollicis (or the interosseus primus volaris).
2nd. The hypothenar eminence is long and elliptical in form, but smaller than the thenar eminence; it is covered in part by a small muscle which is not shown by any external prominence, but only by the folds which it marks in the skin during its contraction; this is the palmaris brevis, formed of transverse fibres, which, arising from the inner border of the palmar fascia, is inserted into the deep surface of the skin on the inner border of the hand. The contraction of its fibres draws the skin of the part upwards and forms an irregular vertical furrow, so that the prominence of the skin of the upper part of the hypothenar eminence becomes more clearly marked. The hypothenar eminence itself is formed by three small muscles vertically arranged over the fifth metacarpal bone:—1, the abductor minimi digiti (28, Fig. 77; 10, Fig. 79), passing from the pisiform bone to the inner side of the first phalanx of the little finger; 2, the flexor brevis minimi digiti (27, Fig. 77; 11, Fig. 79), passing from the prominence of the unciform bone to the same phalanx; and lastly, 3, the opponens minimi digiti, arising from the unciform[250] bone and inserted into the entire length of the fifth metacarpal bone, so that its contraction slightly draws outwards the whole of the little finger, and opposes it to a certain degree to the thumb.
3rd. The muscles of the middle region of the palm of the hand are in two series. One set is arranged between the tendons of the flexor profundus digitorum muscle (see anterior deep muscles of the forearm, page 237) as small fusiform muscles, which have been compared to the form of a worm—hence their name of lumbricales (7, Fig. 79). The others are arranged in the spaces between the metacarpal bones, and are known as the interosseous muscles.
The lumbricales muscles, as Figure 77 shows (23, 23), are four in number—one for each of the four fingers. Their upper ends are attached to the deep flexor tendons; and from this origin they descend to reach the outer or radial border of the first phalanx of each finger. Sweeping round the knuckle on its outer side, each tendon is inserted into the metacarpo-phalangeal capsule, the outer side of the base of the first phalanx, and into the expansion of the extensor tendon on the dorsum of the first phalanx of each finger. In consequence of this mode of insertion each muscle is a flexor of the metacarpo-phalangeal joint, and in addition, because of its connection with the extensor tendon, it is at the same time an extensor of the inter-phalangeal joints.
The interosseous muscles are seven in number, divided into two series, dorsal and palmar. The dorsal muscles, four in number, are found one in each interosseous space between the metacarpal bones. The three palmar interosseous muscles[251] occupy the three inner spaces. They arise from the sides of the metacarpal bones (the dorsal muscles by double origins, the palmar muscles by single heads from the inner three metacarpal bones); and they are inserted in the same way as the lumbrical muscles into the fingers, so as to act as flexors of the metacarpo-phalangeal, and extensors of the inter-phalangeal joints. The several muscles pass in relation to the sides of the knuckles in a way that need not be detailed here, so as to occupy positions which enable them to act so as to separate or draw together the fingers. The dorsal interossei muscles serve to separate the fingers from each other, while the palmar serve to bring them together; or, to be more precise, the dorsal muscles abduct the fingers from the middle line of the middle finger, while the palmar muscles adduct the fingers on which they act (third, fourth, and fifth) towards the axis of the middle finger.
[252]
The Buttock.—Gluteus maximus, its thickness and form; its relations to the great trochanter.—Gluteus medius.—The subjacent muscles (gluteus minimus, pyriformis, etc.).—Muscles of the thigh; 1st, External region tensor fasciæ latæ (vaginæ femoris), its importance with regard to external form; aponeurosis of fascia lata; 2nd, Anterior region, sartorius, peculiarities of this muscle during contraction; quadriceps extensor (rectus, vastus internus, vastus externus, crureus); 3rd, Internal region, the adductors; 4th, Posterior region, hamstring muscles (biceps, semi-tendinosus, and semi-membranosus).
Muscles of the Pelvis.—The muscles of the pelvis visible on the model are all situated on the posterior surface of that part of the skeleton, and form the buttock, or gluteal region. In front the anterior wall of the abdomen, descending to Poupart’s ligament and the pubis (Fig. 70, page 197), conceals the muscles which proceed from the interior of the pelvis towards the thigh—muscles of which a short sketch will be given along with those of the front of the thigh.
Of the muscles of the gluteal region two only are superficial and well marked on the model—viz., the gluteus maximus and gluteus medius.
The gluteus maximus muscle (Fig. 72, page 201) is the largest and thickest of all the muscles of the body. It is composed of large fleshy fibres directed obliquely from the sacro-iliac region towards the upper part of the femur. Its fibres arise from the posterior extremity of the crest of[253] the ilium (4, Fig. 34, page 107), by an aponeurosis from the back of the sacrum, from the sacrum itself, and from the sacro-sciatic ligament. The coarse fleshy fibres are directed downwards and outwards through the gluteal region (Fig. 67). At the level of the great trochanter these fibres are for the most part inserted into a broad, thick, tendinous lamina, which is continuous with the aponeurosis of the thigh or fascia lata. The lower and deeper part of the muscle is inserted directly into the gluteal ridge of the femur (page 133). The gluteus maximus muscle presents four borders: (1) an internal border, corresponding to its origin, and convex inwards, and (2) an external border, also slightly convex at its insertion. This border corresponds to the line along which the fleshy fibres terminate; it forms a prominence, which curves posteriorly round the great trochanter. When we have enumerated the muscles lying beneath the gluteus maximus, it will be more easy to understand how the muscular structure of the gluteal region as a whole is so prominent that the great trochanter actually forms on the model the centre of a depressed area, bounded behind and above by the prominence of the gluteal muscles, and in front by the tensor muscle of the fascia lata (see Muscles of the thigh). (3) The inferior border of the gluteus maximus is thick, and forms an oblique elevation, beneath which the posterior muscles of the thigh emerge; it is this which helps to form the lower limit of the prominence of the buttock. In the erect position the lower limit of the gluteal region is indicated[254] by a transverse fold (the fold of the nates). This line runs diagonally across the lower border of the gluteus maximus, and is produced not by the edge, but by the weight of the relaxed muscle, and the fat which covers it. (4) The superior border is thin (Fig. 74, page 217), and is continuous with the fascia lata, which covers the gluteus medius, so that its prominence is little marked on the model, being more or less lost in the area corresponding to the position of the gluteus medius muscle.
The gluteus maximus is an extensor of the thigh on the pelvis. In the upright position it supports the pelvis behind and prevents it from inclining forwards. It is by its action that the trunk is raised so as to be in the same line as the upright lower limb. The gluteus maximus is therefore the muscle of the upright position, and we observe the large size which it presents in the human subject compared with its small proportions in animals which do not adopt the biped attitude.
The gluteus medius muscle is situated both above and beneath that of the gluteus maximus—that is to say, the postero-inferior part is covered by the preceding muscle, but its antero-superior part is superficially placed. This latter part (Fig. 74, between 22 and 23) is, however, covered by the thick fascia lata of the thigh, which binds down the muscle to the dorsum ilii. Arising from the anterior three-fourths of the crest of the ilium, and from the dorsum ilii as well as from the fascia over it, the fibres of the gluteus medius descend, converging towards the great trochanter, into the external surface of[255] which they are inserted by a thick aponeurotic tendon. The fleshy fibres cease a little above the great trochanter so as to form a prominence along a curved line with its concavity downwards, which forms the superior boundary of the depression corresponding to the region of the great trochanter, referred to above. The gluteus medius, by its posterior fibres, acts like the gluteus maximus; by its anterior fibres it draws the thigh outwards, acting as an abductor.
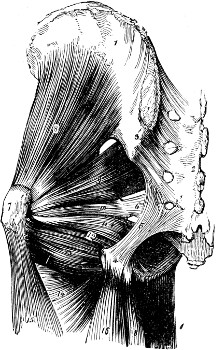
Fig. 80.
The Deep Gluteal Muscles.—1, Dorsum ilii;—2, sacrum;—3, posterior sacro-iliac ligament;—4, tuberosity of ischium;—5, great, 6, lesser sacro-sciatic ligament;—7, great trochanter;—8, gluteus minimus;—9, pyriformis;—10, 11, 12, gemelli and obturator internus 13, quadratus femoris;—14, adductor magnus;—15, vastus externus;—16, biceps and semi-tendinosus—17, gracilis;—18, semi-membranosus.
The gluteus maximus and gluteus medius muscles conceal a series of deep muscles filling up the large space which we observe on the skeleton between the great trochanter and the pelvic wall. These muscles, which we only need to enumerate in order to understand the importance of the prominence of the buttock, are, taking them in order, as follows—the gluteus minimus, which lies exactly beneath the gluteus medius, and proceeds from the dorsum ilii to the superior and anterior border of the great trochanter;[256] the pyriformis, which arises within the pelvis from the anterior surface of the sacrum, escapes from the pelvis through the great sciatic notch, and is directed obliquely towards the great trochanter, into the upper border of which its tendon is inserted; the obturator internus, which proceeds also from the interior of the pelvis, is reflected over the lesser sciatic notch and is inserted into the internal surface of the great trochanter along with two accessory muscles, the gemelli; and finally, the quadratus femoris, formed by short horizontal fibres, which extends from the outer part of the tuberosity of the ischium to the posterior surface of the femur between the two trochanters.
Muscles of the thigh.—The muscles of the thigh are arranged around the femur, and frequently in a direction so oblique that they appear in one portion, for example, on the front, and in another portion on the inner side of the thigh. We can, however, class them in four series—external, comprising the tensor vaginæ femoris (fasciæ latæ); anterior, comprising the sartorius and quadriceps extensor; internal, comprising the adductors; and posterior, comprising the biceps, the semi-membranosus, and the semi-tendinosus.
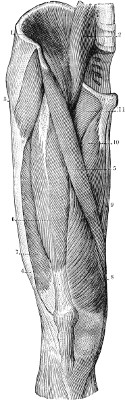
Fig. 81.
The Muscles of the Anterior Surface of the Right Thigh.—1, the iliacus;—2, the psoas;—3, the tensor vaginæ femoris;—4, its tendon (fascia lata);—5, the sartorius;—6, the rectus (long head of quadriceps;—7, vastus externus (the external head);—8, vastus internus (the internal head);—9, the gracilis;—10, the adductor longus;—11, the pectineus.
I. Outer side of the thigh. The tensor vaginæ femoris muscle (3, Fig. 81).—This muscle lies in the plane of the gluteus maximus (23, Fig. 74, page 217), and forms a distinct prominence in front of the great trochanter. It arises from the anterior superior spine of the ilium, and is directed downwards and slightly backwards on the outer side of the thigh, to terminate a short way below the level of the great trochanter by being inserted into the broad and thick aponeurosis—the[257] fascia lata—which covers this region (4, Fig. 81). This aponeurosis is specially thickened by the addition of vertical fibres, which form a tendon of insertion known as the ilio-tibial band. This band descends to the outer side of the knee as a distinct prominent tendon, which is inserted finally into the outer tuberosity of the tibia (see page 135). This muscle rotates outwards the thigh and the whole lower limb, and contributes also to the flexion of the thigh on the pelvis; therefore, when the thigh is extended and not turned inwards, the tensor muscle forms beneath the iliac spine a long muscular elevation, but when it is in action its form becomes short and broad, and forms a characteristic globular mass. This contrast in the form of the tensor muscle in repose and in action has been beautifully shown on[258] the Gladiator, in which there is contraction of the tensor of the right thigh and relaxation of that of the left.
The ilio-tibial band and the aponeurosis of the fascia lata cover, on the outer side of the thigh, the large fleshy mass of the vastus externus (a part of the quadriceps extensor muscle), which belongs to the anterior region of the thigh. This muscle, thus covered in, is shown throughout its entire extent on the surface. Though covered by the fascia lata, it forms a marked convexity on the outer side of the thigh, as a gentle curve in women, and a strongly bowed line in well-developed, muscular men.
II. Front of the Thigh. The sartorius muscle (5, Figs. 81, and 23, Fig. 70, page 197).—This is the longest muscle in the human body. It forms a narrow fleshy band, which arises from the anterior superior iliac spine, and is directed obliquely downwards and inwards. Crossing the front of the thigh obliquely, it descends round the inner side of the knee over the inner condyle of the femur (Fig. 86), describing a curve with the concavity forward. It finally terminates at the upper part of the inner surface of the shaft of the tibia in a flat tendon (19 and 20, Fig. 86) which sweeps forward to be inserted into that bone just below the inner tuberosity in front of and along with the gracilis and semi-tendinosus muscles.
The sartorius flexes and abducts the thigh on the pelvis, and flexes the leg on the thigh; so that it gives to the lower limb a position similar to that of a tailor when seated, hence the name of this muscle (sartor, a tailor). With regard to surface form, this muscle is indicated externally in a peculiar manner. When[259] it contracts, only its superior extremity presents a superficial prominence; throughout the rest of its extent, the presence of the muscle, lying in the depressed groove between the quadriceps extensor in front and the adductor muscles on the inner side, is indicated during contraction by a large shallow furrow, particularly noticeable on the inner side of the thigh, at the junction of the upper two-thirds with the lower third.
Quadriceps extensor (6, 7, 8, Fig. 81).—The quadriceps extensor muscle belongs to the outer and inner regions of the thigh as well as to the front of the limb, but the element of the muscle of most importance in relation to external form—the rectus femoris—is situated anteriorly. The muscle, as its name implies, is composed of four portions: one, the rectus, in the middle; the vastus internus and the vastus externus, on each side; and the crureus, the deepest part, concealed by the other portions of the muscle.
The rectus femoris (21, Fig. 70, and 6, Fig. 81) is long and fusiform in shape—that is to say, larger at its centre than at its extremities. Its superior extremity, the more slender of the two, arises by a double tendon from the anterior inferior iliac spine and the dorsum ilii, and appears on the front of the thigh between the tensor fasciæ femoris and the sartorius muscles. Lying in the angular space which separates these two muscles (Fig. 81), the rectus descends vertically on the front of the thigh, and about four inches above the patella forms a broad tendon (Figs. 81 and 84), the borders of which give insertion on either side to the vastus internus and vastus externus muscles, while its deep surface gives[260] insertion to the crureus muscle, and its base broadens out to be inserted into the patella. From the lower end of the patella a broad ligament—the ligament of the patella—arises (page 134), which is inserted into the tubercle of the tibia; it follows, therefore, that by means of the tendon of the rectus femoris, the patella, and the ligament of the patella, the quadriceps extensor muscle is eventually inserted into the tibia (Fig. 45, page 137).
The vastus internus muscle (8, Fig. 81) is a very large fleshy mass, which covers the inner side of the femur. Arising from the inner lip of the linea aspera of the femur, from the edge of the bone (spiral line) above, and from the internal supra-condyloid ridge below, its muscular fibres are directed downwards and forwards, to be inserted into the deep surface and the inner border of the tendon of the rectus femoris, into the side of the patella, and into the capsule of the knee-joint. It conceals the crureus and partly blends with that muscle. The outline of the vastus internus is easily discernible on the surface, forming a somewhat triangular, convex, and rounded contour; bounded internally by the furrow of the sartorius, externally by a vertical line where it joins the tendon of the rectus femoris, and below by its lower border, it forms a well-marked rounded line sweeping outwards over the internal condyle of the femur to the side of the patella. These details are of great importance in regard to the contour of the region above the patella, and are in marked contrast, as we shall see, with the arrangement presented at the same level by the lower part of the vastus externus.
The vastus externus (7, Fig. 81) lies external to[261] the rectus femoris, and conceals the crureus, with which its deep surface is partially blended. Its origin, which underlies the tensor fasciæ femoris and the ilio-tibial band, is from the upper half of the shaft of the femur, from the outer lip of the linea aspera. Its fibres sweep downwards and slightly forwards to be inserted into the tendon of the rectus, the patella, and the capsule of the knee-joint. The line along which it is inserted into the rectus tendon describes a curve of which the convexity looks towards the supero-external angle of the patella, from which it is separated by a considerable interval (Figs. 81 and 85). Consequently on the surface the flat surface above the patella forms a sort of triangle, of which the borders are very different, the inner border being vertical, the outer one oblique, curved, and higher in position; the base of the triangle corresponds to the patella and the lateral parts of the capsule of the knee-joint; its truncated summit corresponds to the inferior extremity of the fleshy part of the rectus; and the borders of this flat surface, formed by the fleshy insertions of the vasti muscles, become very prominent when the leg is forcibly straightened on the thigh.
The crureus muscle, deeply placed, is the fourth element in the quadriceps muscle. It arises from the upper three-fourths of the shaft of the femur, externally and in front, and forms a thick, fleshy mass, responsible to a great extent for the general contour of the front and sides of the thigh, though it is not actually noticeable directly on the surface. It is almost wholly concealed by the three previous muscles. It is partially blended on each side[262] with the vasti muscles; and it is inserted as well into the deep surface of the tendon of the rectus femoris. It is hardly necessary to point out, since it is clear from its anatomical arrangement, that the quadriceps muscle, passing by means of the patella and the patellar ligament to the tubercle of the tibia, is essentially the extensor muscle of the leg.
It is to be noted that the two vasti muscles have a very different effect in the shaping of the contours of the thigh. The vastus externus has its greatest prominence well above the patella on the outer side: the most prominent part of the vastus internus is formed by its lowest fibres, as they sweep across over the inner condyle of the femur.
III. The inner side of the thigh. The adductor muscles.—We understand by the adductors the numerous muscles that occupy the inner part of the thigh, and which, passing down from the pubis and ischium along the entire length of the femur, fill up the triangular space which appears in the skeleton between the inner surface of the femur and the pubic part of the hip-bone. Some of the muscles of this series take the special name of adductors. We will study in succession three muscles clearly visible on the model—viz. the pectineus, the adductor longus, and the gracilis; afterwards we will mention briefly the muscles almost hidden by the preceding—namely, the adductor brevis and the adductor magnus muscles.

Fig. 82.
The Popliteal Region and Posterior Surface of the Right Leg.—1, internal gastrocnemius;—2, external gastrocnemius;—3, space between gastrocnemii;—4, 5, tendo Achillis;—6, 7, 7, plantaris muscle and its tendon;—8, tendons of deep muscles (common flexor and posterior tibial);—9, peroneus longus;—10, peroneus brevis;—11, soleus;—12, biceps femoris;—13, semi-tendinosus;—14, semi-membranosus;—15, gracilis;—16, sartorius.
The pectineus muscle (22, Fig. 70, and 11, Fig. 81), the first and shortest of the muscles of this region, is a broad fleshy band which extends from the horizontal ramus of the pubis to the upper[263] part of the shaft of the femur (to a rough line passing from the linea aspera to the lesser trochanter). The lower part of this muscle is hidden by the sartorius, and the upper part does not show itself clearly beneath the skin, being covered by the large vessels of the thigh, and also in most cases by a quantity of fat. The pectineus forms the middle part of the floor of a triangular space in the upper third of the thigh, with its apex below, known in surgical anatomy as Scarpa’s triangle, which is bounded externally by the sartorius muscle. The base of the triangle corresponds to the groin, and is formed by Poupart’s ligament. The outer part of the floor of the triangle is formed by a large muscle, of which the greater part is situated in the cavity of the abdomen. This is the ilio-psoas muscle (1 and 2, Fig. 81), which arises from the lateral parts of the lumbar vertebræ (psoas) and from the iliac fossa (iliacus), passes[264] beneath Poupart’s ligament (page 199), and after traversing Scarpa’s triangle is inserted into the lesser trochanter of the femur. This muscle is not visible superficially except just below and internal to the anterior superior iliac spine, where it forms a slight bulging beneath the skin.
The inner part of the floor of Scarpa’s triangle is formed by the adductor longus, triangular in shape (10, Fig. 81); arising by a narrow tendon from the angle of the pubis, it is inserted, beneath the sartorius, into the middle portion of the linea aspera of the femur.
The gracilis is visible throughout its entire length on the inner surface of the thigh (9, Fig. 81). It forms a long slender fleshy band, broader above and narrower below. Arising from the symphysis and descending ramus of the pubis, it descends vertically; a little above the inner condyle of the femur it is replaced by a narrow tendon (15, Fig. 82), which sweeps round the condyle, behind the sartorius, and in front of the semi-tendinosus, to be inserted into the upper part of the inner surface of the shaft of the tibia behind the sartorius and above the semi-tendinosus.
Covered by the preceding muscles and placed more deeply, are the adductors, brevis and magnus, which fill up the space between the gracilis and the femur. The adductor brevis extends from the pubis to the upper part of the linea aspera; the adductor magnus is a thick, fleshy, triangular muscle which arises from the tuberosity and ramus of the ischium, and is inserted into the entire length of the linea aspera of the femur, so that its superior fibres are[265] horizontal and its inferior fibres almost vertical in direction; among these last the most internal, which arise from the ischial tuberosity, form below a distinct tendon, which projects above the inner side of the knee-joint and is inserted into a tubercle (the adductor tubercle of the femur) placed above the inner condyle of the femur.

Fig. 83.
Hamstring Muscles. 1, gluteus medius;—2, gluteus maximus;—3, vastus externus;—4, biceps (long head)—5, biceps (short head)—6, semi-tendinosus;—7, semi-membranosus;—8, gracilis;—9, adductor magnus;—10, sartorius;—11, popliteal space;—12, gastrocnemius.
The action of all the muscles which we have just studied, except the pectineus, is to draw the thigh inwards towards the axis of the body; they also bring the knees close to each other, hence they are called the adductors of the thigh.
IV. The back of the thigh. The posterior muscles of the thigh (hamstring muscles).—These muscles, three in number, arise from the tuberosity of the ischium, and thus their origins are hidden beneath the gluteus maximus. They emerge below the lower border of that muscle and descend vertically; above the posterior surface of the knee (or ham) they divide into two masses, one, the external, formed by a single muscle, the biceps femoris, the other internal, formed by two muscles placed one on the other, the semi-tendinosus and the semi-membranosus.
[266]
The biceps femoris (4, Fig. 83) is so called because, like the biceps in the arm, it is formed above by two heads, a long head which arises from the tuberosity of the ischium, and a short head, more deeply placed, which arises from the linea aspera of the femur. These two heads unite in a stout tendon (12, Fig. 82) which the muscular fibres accompany for the greater part of its length, and which is directed downwards on the outer side of the knee, to be inserted into the summit of the superior extremity of the head of the fibula. This muscle flexes the leg on the thigh, and when it accomplishes this action its tendon becomes very prominent, forming the outer boundary of the region of the ham or popliteal space.
The semi-tendinosus (13, Fig. 82; 6, Fig. 83), visible throughout its entire extent (except at its origin, which is hidden beneath the gluteus maximus), has been so called because in a great part of its length, almost equal to its lower half, it is represented only by its tendon. It arises above from the ischium, and descends parallel to the long head of the biceps, to the inner side of which it is situated; towards the junction of the middle with the lower third of the posterior surface of the thigh, its fleshy belly becomes narrower, and is replaced by a long, thin tendon (13, Fig. 82) which inclines inwards, and passes behind the internal condyle of the femur, describing a slight curve with its concavity forwards behind the tendons of the sartorius and gracilis. With them (pages 258 and 264) it is inserted into the upper part of the internal surface of the shaft of the tibia (24, Fig. 86). This muscle flexes the leg, and in this[267] movement the prominence of its tendon starts out as the internal boundary of the region of the ham.
The semi-membranosus is broader than the semi-tendinosus (7, Fig. 83). It is situated beneath it and projects beyond it on both sides. It is so called because its upper half is formed by a broad membranous tendon arising from the tuberosity of the ischium. The muscular fibres commence below the middle of the thigh and form a large fleshy belly, thick, broad, and short, which passes into a strong tendon (14, Fig. 82) inserted mainly into the posterior surface of the internal tuberosity of the tibia.
The fleshy belly of this muscle projects beyond the tendon of the semi-tendinosus on each side, and reaches to the middle line of the posterior surface of the thigh and knee, forming a large muscular prominence. When the leg is flexed on the thigh, the tendons of the biceps and semi-tendinosus become prominent, bounding a deep pit (the ham or popliteal space) corresponding to the upper part of the posterior surface of the knee, and the fleshy part of the semi-membranosus remains hidden in the bottom of this pit; but when the leg is extended on the thigh there is no longer a hollow, but the posterior surface of the knee presents, on the contrary, a prominent form, produced in the upper part by the fleshy mass of the semi-membranosus, and in the lower part by the muscles of the calf, to be described in the next chapter.
[268]
General arrangement of the muscles with regard to the skeleton.—Anterior muscles of the leg (tibialis anticus and extensors).—External or peroneal muscles; relations of the peroneus longus with the sole of the foot; its influence on the form of the foot.—Posterior muscles; gastrocnemius (details of its composition and form). Soleus muscle, plantaris, tendo Achillis.—Muscles of the foot; 1st, dorsum of foot (extensor brevis muscle); 2nd, muscles of the sole of the foot.
Muscles of the leg.—The arrangement of the skeleton of the leg (tibia and fibula) is such that we might expect a priori to find four muscular masses, one on each of the surfaces of the skeleton, but as the internal surface of the tibia is subcutaneous (2, Fig. 84), is not covered by any muscle, and is overlapped by the anterior and posterior fleshy masses, it forms a long flat surface, slightly hollowed, extending from the inner side of the knee to the internal malleolus. The leg, therefore, presents for our study only three groups of muscles, occupying respectively the anterior or antero-external, the external or peroneal, and the posterior regions of the limb.
I. Anterior muscles (Fig. 84).—Arranged in the space which separates the fibula from the tibia, the muscles on the front of the leg are three in number, called, from within outwards, the tibialis anticus, the extensor proprius hallucis, and the extensor longus digitorum.
[269]
The tibialis anticus (3, Fig. 84) arises from the external surface of the tibia, and from the deep fascia over it (page 146), and descends obliquely downwards and inwards in the form of a prismatic or fusiform fleshy mass, of which the lower end gradually narrows, to be replaced by a strong tendon in the lower third of the leg. This tendon, inclining more and more to the inner side (2, Fig. 86), passes obliquely over the anterior surface of the lower end of the tibia, in front of the internal malleolus. It glides beneath the anterior annular ligament of the ankle, and reaches the inner part of the dorsum of the foot (3, Fig. 86), where it is inserted into the internal cuneiform, and the base of the first metatarsal bone. It flexes the foot on the leg, and inverts it, since it draws the dorsal surface of the foot towards the anterior surface of the leg, while at the same time it turns the foot inwards, and slightly raises its inner border. This muscle, during contraction, shows externally all the details of its shape—in the leg a fleshy mass which slightly overlaps the anterior border of the tibia or shin, and in front of the ankle an oblique cord marking clearly the direction of the tendon.
The extensor proprius hallucis (5, Fig. 84) is concealed at its origin between the tibialis anticus and the extensor longus digitorum. Only its tendon appears superficially (2, Fig. 85) in the lower third of the front of the leg, on the outer side of the tendon of the tibialis anticus. It passes beneath the annular ligament of the ankle and along the inner part of the dorsal surface of the foot (4, Fig. 86), to be inserted into the base of the terminal phalanx of the great toe. When the great toe is forcibly turned up during extension[270] this tendon is clearly shown throughout its entire course. In a normal foot this tendon occupies a straight line from the middle of the ankle-joint to the great toe, and the inner border of the foot and great toe should be parallel to it. In other words, the great toe should be in a line with the inner border of the foot (Fig. 52, page 151).

Fig. 84.
Muscles of the Anterior Region of the Leg.—1, tendon of the rectus femoris;—2, tibia;—3, the anterior tibial muscle;—4, the long extensor of the toes;—5, the proper extensor of the great toe;—6, the peroneus tertius;—7 and 8, the peroneus longus and brevis;—9, the external head of the gastrocnemius;—10, the internal head of the gastrocnemius;—11, extensor brevis digitorum;—12, the superior annular ligament of the dorsum of the foot.
The extensor longus digitorum (4, Fig. 84) arises from the external tuberosity of the tibia, on the outer side of the tibialis anticus, and from the upper three-fourths of the anterior surface of the fibula. It descends vertically, and terminates in a tendon divided into slips, which remain associated together (3, Fig. 85) to pass beneath the anterior annular ligament. Immediately afterwards, these slips spread out like a fan (4, Fig. 85) in the form of four tendons, which pass over the dorsum of the foot to be inserted into the second and third phalanges of the four outer toes. Each tendon behaves like the corresponding extensor tendon in[271] the hand. It forms a membranous expansion on the dorsum of the first phalanx, joined by the tendons of the extensor brevis digitorum, lumbricals, and interossei muscles, and completes the capsule of the meta-tarso-phalangeal joint. Thereafter each tendon splits into three parts—one central and two lateral. The central slip is inserted into the intermediate phalanx, and the two lateral slips, reunited, are attached to the base of the terminal phalanx. Associated with the extensor longus digitorum is the peroneus tertius, an essentially human muscle, which has a common origin with the long extensor. Its tendon accompanies those of the last-named muscle beneath the annular ligament, and is directed outwards on the dorsum of the foot, to be inserted into the base of the fifth metatarsal bone. With the tibialis anticus the long extensor of the toes and peroneus tertius flex the foot on the leg, while at the same time the common extensor extends the toes on the foot. In this action it shows the prominence of its fleshy belly especially at the middle of the leg, and the tendons on the back of the foot are raised up like diverging cords. The peroneus tertius raises the outer border of the foot in such movements as skating and dancing, and it is only then that its prominence shows beneath the skin. Usually it is but little marked.
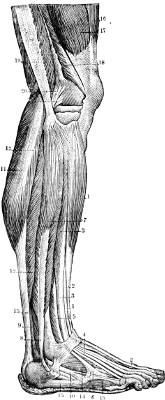
Fig. 85.
Muscles of the Leg (external surface).—1, 1, the anterior tibial muscle;—2, 2, the tendon of the extensor proprius hallucis;—3, 3, the extensor longus digitorum with its tendons (4, 5, and 6);—7, the peroneus longus and its tendon (8);—9, peroneus brevis and its tendon (10);—11, the external head of the gastrocnemius;—12, 12, the soleus;—13, tendo Achillis;—14, extensor brevis digitorum;—15, abductor minimi digiti;—16, the rectus femoris;—17, 18, vastus externus;—19, tendon of the biceps femoris;—20, external lateral ligament of the knee.
II. External muscles (Fig. 85).—These are two in number, placed on the outer side of the fibula, and called the peroneal muscles. They are distinguished as the peroneus longus and peroneus brevis. They completely cover the outer surface of the fibula, the peroneus longus arising from the upper[272] two-thirds, the peroneus brevis from the lower two-thirds of the bone. The peroneus longus is behind and above, the peroneus brevis in front and below. Their tendons descend together and pass beneath the external annular ligament; that of the peroneus brevis lying next the bone and grooving the back of the external malleolus. Winding round the malleolus as on a pulley, they are directed forwards on to the outer border of the foot. Then only the tendons separate from each other, to be inserted into the foot at two points diametrically opposite. One (that of the peroneus brevis) is directed horizontally forwards, on the outer surface of the foot (10, Fig. 85), to be inserted into the base or posterior extremity of the fifth metatarsal bone; while the other, that of the peroneus longus, is directed obliquely forwards and downwards[273] so as to reach the sole of the foot, beneath which it passes, lying in the groove of the cuboid bone; it then runs obliquely across the sole of the foot, from the outer towards the inner border, deeply hidden by the plantar muscles and ligaments, and is finally inserted into the posterior extremity of the first metatarsal bone and the under surface of the internal cuneiform bone.
These two muscles, but especially the peroneus brevis, extend and turn the foot outwards, while at the same time they raise its external border; so that their action is the reverse of that of the tibialis anticus. But the peroneus longus has another important function which explains why the muscle becomes prominent whenever a particular effort is demanded of the foot, as, for example, when it is carried forward in dancing, or in the act of imparting motion to an object. This muscle, owing to the arrangement of its tendon, which passes like the string of a bow across the hollow of the sole of the foot, acts by deepening this hollow; it therefore raises the plantar arch, marked on the dorsal surface by an increase of the curve of the foot.
III. Posterior muscles (Figs. 82, 87).—The back of the leg is thick and fleshy, and is formed by numerous and powerful muscles, divided into two groups: the superficial group, which we shall describe in detail, and the deep group, for which a few words will be sufficient.
The superficial group is formed by the gastrocnemius, plantaris, and soleus muscles.
The gastrocnemius muscle (γαδτήρ, belly; κυήμη, leg) is responsible for the surface form of the[274] prominence of the calf. It consists of two large, fleshy masses known as the inner and outer heads, which arise respectively from the upper part of the inner and outer condyles of the femur on their outer aspect. Overlapped by the insertions of the hamstring muscles, the two heads of the gastrocnemius form the lower boundaries of the popliteal space. They converge at its lower angle to be inserted (separately) into a broad membranous tendon, which forms the beginning of the tendo Achillis (6, Fig. 87). At their origins, each head possesses a tendon which covers its superficial surface. At the insertion the tendon passes upwards for a considerable distance on their deep surfaces. At its insertion into the tendo Achillis, each fleshy head presents a rounded lower border; and it is to be particularly noted that the inner head of the muscle usually descends to a level lower than that of the outer head.
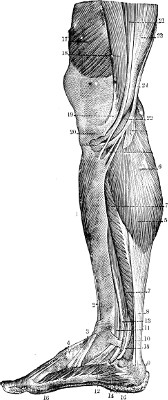
Fig. 86.
Muscles of the Leg (internal surface).—1, tibialis anticus;—2 and 3, its tendon;—4, tendon of the extensor proprius hallucis;—5 and 6, internal head of the gastrocnemius;—7, soleus;—8, tendo Achillis;—9, its attachment to the os calcis;—10, tendon of the plantaris muscle;—11 and 12, tendon of the tibialis posticus;—13 and 14, tendon of the flexor longus digitorum;—15, tendon of the flexor longus hallucis;—16, 16, abductor hallucis;—17, vastus internus;—18, 19, 20, sartorius;—21, 22, gracilis;—23, semi-membranosus;—24, semi-tendinosus.
This muscle bends the knee and extends the foot on the leg. Through the tendo Achillis it acts on the calcaneum or bone of the heel so as to raise the heel and cause the living model, if erect, to rise on the toes. Now the constitution of the muscle is such that its external form is quite different when it is in repose and when it is in contraction. Each head of the muscle, as already stated, possesses at its origin a membranous tendon, which expands over the outer part of the surface, but the inner part of each belly is fleshy. In a state of repose the two halves of the muscle unite in the same rounded and prominent shape, so that we cannot distinguish the part covered by the aponeurotic expansion of tendon[275] from the part formed by free muscular fibres. But when the living model rises on the balls of the toes, or in any other movement produced by a powerful contraction of the muscle, we see the free fleshy part of each head swell up more strongly than the part covered and tied down by the aponeurosis. At that moment, therefore, the whole convex form of the calf presents a slight ovoid surface on each side, and a long vertical prominence in the middle line. This prominence is produced by the mesial muscular parts of the two heads of the muscle, which approach each other during contraction, and unite their double mass in a single median prominence. Fig. 82, by the differences in shading, enables us to distinguish the aponeurotic from the muscular parts, and to observe the important details of shape into the study of which we have entered.[276] The clear or aponeurotic parts correspond to the two flat surfaces already mentioned, and the shaded or fleshy parts correspond to the median prominence, with this difference, that in the calf in contraction, this median prominence is smoother than in Fig. 82, the two halves which compose it being merged into a single mass, except at the angular space above the point where they bound the popliteal space.
We will now return to what we have already said (see page 267) relative to the posterior region of the knee, examined in the living model in extension of the leg. If the model rises on the balls of the toes it is no longer possible to speak of the popliteal space as a hollow at the back of the knee. Under these conditions, the prominences (already studied) of the biceps, semi-membranosus, and gastrocnemius almost join each other, and the plantaris muscle, of which we will speak immediately, helps to fill up the space; the region of the popliteal space forms in reality a prominence, and the posterior surface of the knee is marked in its central portion by a strong muscular projection of which it is not possible to understand the cause except by an attentive study of the muscles named.
The soleus muscle, so called because its form has been compared to that of a sole (Latin—solea), is placed beneath the gastrocnemius, which overlaps it, more on the inner (7, Fig. 86) than on the outer border (12, Fig. 85) of the calf. In its action it is simple. It only acts on the ankle-joint, as a powerful extensor of the foot. Arising from the back of the fibula and from the tibia, its fibres are inserted below into the deep surface[277] of the tendo Achillis to within two inches of the heel.
The tendo Achillis is a strong band of fibrous tissue occupying the lower part of the back of the leg. Membranous above, where it is continued upwards on the deep surface of the bellies of the gastrocnemius muscle, it becomes narrower and thicker below as it approaches the heel. Broadening out slightly at its lower end, it is inserted into the inferior half of the posterior surface of the calcaneum, forming the prominence of the heel. In a muscular leg the fibres of the soleus may be shown superficially, bulging beyond the tendo Achillis at its outer and inner borders, below the outline of the gastrocnemius, and more on the outer than on the inner side (5, Fig. 82, page 263).
The plantaris is a small, insignificant muscle of which the fleshy origin (6, Fig. 82) is from the outer condyle of the femur, under cover of the outer head of the gastrocnemius muscle. Its small fleshy belly is succeeded by a long, thin tendon (7, Fig. 82), which descends obliquely between the gastrocnemius and the soleus to reach the inner border of the tendo Achillis, along which it descends (10, Fig. 86). Sometimes it is united with this tendon early in its course, and sometimes it reaches the calcaneum, or it may join the internal annular ligament at the ankle.
The deep muscles of the back of the leg are not visible on the model except on the inner side above the ankle. Here, on the inner side of the tendo Achillis (8, Fig. 82), is placed a series of tendons, proceeding in the interval between the[278] internal malleolus and the calcaneum to the foot. The muscles are the tibialis posticus, the flexor longus digitorum, and the flexor longus hallucis. The fleshy bellies of these muscles, deeply hidden beneath the superficial muscles, arise from the posterior surface of the tibia, from the fibula, and from the interosseous membrane. Their tendons descend obliquely over the back of the internal malleolus, where those of the tibialis posticus and the common flexor of the toes alone are visible (the tendon of the flexor proprius hallucis being almost entirely hidden beneath the tendo Achillis). From this they are reflected over the internal malleolus and pass into the sole of the foot, bound down on the inner side of the ankle by the dense band of the internal annular ligament. The tibialis posticus is almost immediately inserted by radiating bands into most of the tarsal and metatarsal bones (12, Fig. 86), and the other two tendons reach the toes, where they are inserted in the same manner as we have already described for the tendons of the flexor longus pollicis and the deep flexor of the fingers in the hand.

Fig. 87.
The Muscles of the Calf.—1, biceps;—2, semi-tendinosus;—3, popliteal space;—4, gastrocnemius;—5, 5, soleus;—6, tendo Achillis;—7, os calcis;—8, peroneus longus;—9, tibialis posticus and flexor longus digitorum.
Muscles of the foot.—The muscles of the foot[279] include not only the muscles of the plantar region, corresponding to the palm of the hand, but also the tendons on the dorsum of the foot, and a special extensor muscle, the extensor brevis digitorum.
The tendons of muscles on the dorsum of the foot have already been described (p. 270). The extensor brevis digitorum muscle (11, Fig. 84, and 14, Fig. 85) consists of a short, fleshy belly placed obliquely on the dorsum of the foot, and extending from behind inwards and forwards. It origin is rounded and attached to the upper surface of the calcaneum in the cavity or canal of the tarsus (page 155), external to the astragalus. From this origin it is directed forwards and inwards; becoming broader, it passes beneath the tendons of the common extensor and immediately divides into four muscular slips, each of which has a tendon attached to it. These tendons pass under those of the common extensor, so as to form with them a figure with lozenge-shaped spaces, and proceed to the four inner toes to be inserted, in the case of the great toe, into the base of the first phalanx; uniting, in the case of the second, third, and fourth toes, with the expansions of the extensor tendons on the dorsum of the phalanges. This muscle aids in the extension of the toes, and by its obliquity counteracts the action of the long extensor. When it contracts, the portion of the muscle situated on the outer side of the tendons of the long extensor become very prominent, not being tied down by anything, and this prominence is still clearer because behind it is a depression, more or less evident, corresponding to the calcaneo-astragaloid cavity of the tarsus.
[280]
We will not describe at length the muscles of the sole of the foot with regard to form. The foot derives most of its characteristics from its bony structure; the muscles of the sole round off by their presence the angles of the skeleton and fill up the cavities, but do not modify essentially the bony forms. On the other hand, these numerous muscles are in general but poorly developed, and they are to a large extent united into common masses, which makes it difficult, except for the skilled anatomist, to isolate and recognise distinctly each fleshy belly. It is therefore useless for an artist to enter into a detailed study of these muscles, which reproduce in their general arrangement the distribution of the muscles of the hand. We will content ourselves, then, by saying that the sole of the foot, like the palm of the hand, possesses three muscular masses—1st. An internal group (16, Fig. 86), belonging to the great toe, formed by the abductor hallucis, which arises from the calcaneum, and by the flexor brevis, the adductor transversus, and adductor obliquus hallucis, which arise from the anterior bones of the tarsus and from the metatarsus; 2nd. An external group (15, Fig. 86), belonging to the little toe, formed by the abductor, which arises from the calcaneum, and the flexor brevis, from the cuboid; 3rd. Finally, a central mass, formed by the flexor brevis digitorum, the long flexor tendons, lumbricals, and interossei—which in a sense repeat what we have said regarding the muscles of the same name, more easily studied, in the hand.
[281]
Lateral and anterior regions of the neck.—Sterno-mastoid muscles. The anterior triangle; infra-hyoid and supra-hyoid regions.—Organs contained in the neck (vertebral column, œsophagus, and trachea).—Infra-hyoid muscles—omo-hyoid, sterno-hyoid, sterno-thyroid, and thyro-hyoid.—Supra-hyoid muscles—digastric, stylo-hyoid, and mylo-hyoid.
Muscles of the neck.—We have already, in treating of the trapezius, studied the muscular structure and form of the posterior region of the neck, and the details have been described of the upper part of the side of the neck, and the oblique longitudinal groove between the anterior border of the trapezius and the posterior border of the sterno-cleido-mastoid (pages 208 and 210). It now remains to examine the inferior part of this groove and all the anterior region of the neck. This study should begin with that of the sterno-cleido-mastoid muscles, which have the most important influence on the form of this region, and which by their direction map out on the anterior surface of the neck a muscular interval or space in which it will be easy to study the deeply placed muscles.
The sterno-cleido-mastoid muscles are two in number, one on each side of the neck, extending from the upper limit of the thorax, obliquely upwards and backwards, to the base of the skull (19, Fig. 88). The muscle arises below by two heads—one internal[282] or sternal, which arises by a strong tendon from the front of the first piece of the sternum (18, Fig. 70, page 197), the other external or clavicular, which arises in the form of a thin fleshy band from the inner third of the upper surface of the clavicle, above the origin of the clavicular portion of the great pectoral muscle (Fig. 68, page 194). These two heads are directed upwards and backwards, separated at first by a narrow triangular space, of which the base corresponds to the sterno-clavicular joint (Fig. 68); they then unite to form a single muscle, broad and thick, which ascends obliquely towards the skull, passing behind the angle of the lower jaw and the ear to be inserted into the surface of the mastoid process of the temporal bone and the superior curved line of the occipital bone (16, Fig. 73).
This muscle, being inserted into the skull at a point which is situated behind the axis of the movements of flexion and extension of the head, acts by extending the head on the neck, but to this movement, usually little marked, it adds the power of flexing the neck on the trunk. When both these muscles contract at the same time, they produce extension of the head on the neck and flexion of the neck on the thorax; therefore we see both clearly marked beneath the skin in a person lying down who raises his head (by flexion of the neck). When one muscle only contracts, it turns the face to the opposite side; therefore in the living model whose face is turned to the right the face turns to this side by the contraction of the left sterno-cleido-mastoid muscle, of which the prominence is well shown beneath the[283] skin as a broad band, passing from the sternum to the mastoid process of the temporal bone. There are various attitudes in which this prominence is particularly remarkable, as when we carry the head quickly to one side to answer a question or give an order; or in the act of listening intently, when we concentrate our attention to one side and extend the head a little, turning the region of the ear upwards and forwards, an attitude in which the sterno-mastoid becomes particularly prominent beneath the skin of the neck.
From their insertions and direction we see that these two muscles are very close to each other below and wide apart above. Stretching diagonally across the side of the neck, each muscle forms the interval between two triangular spaces—the posterior triangle behind, bounded by the sterno-mastoid, trapezius, and the clavicle (below); and the anterior triangle in front, bounded by the sterno-mastoid, the middle line of the neck in front, and the lower jaw above. The anterior triangles of the two sides comprise together the space between the two sterno-cleido-mastoid muscles. This space is in the form of a triangle, with its apex below, corresponding to the episternal notch, and its base above, formed by the whole breadth of the lower jaw. This triangle is the anterior region of the neck, divided into two parts by the presence of the hyoid bone—a small bone without direct connection with the rest of the skeleton, and placed transversely above the prominence of the larynx (23, Fig. 88). The lower part forms a vertical plane, oblique downwards and backwards,[284] and sinking behind the sternum; this is the infra-hyoid region, containing the infra-hyoid muscles. The upper part of the area forms a plane approaching more or less the horizontal, proceeding from the hyoid bone to the chin and the circumference of the lower jaw; this is the supra-hyoid region, or that of the chin, containing the supra-hyoid muscles.
Before entering further into the description of these regions we must point out the presence of several organs which, placed in front of the vertebral column, project forwards in the space between the sterno-mastoid muscles. In the middle line of the neck, the region above the hyoid bone corresponds to the floor of the mouth, in which the tongue lies, having on each side large salivary glands partly concealed by the lower jaw; below the depression corresponding to the hyoid bone appear the cartilages of the larynx—the thyroid (pomum Adami), projecting forwards, and more marked in the male than in the female, and the cricoid cartilage, to which the windpipe or trachea is attached. Separating the tongue and larynx from the vertebral column is the cavity of the pharynx, which is continuous below the cricoid cartilage, with the gullet or œsophagus, situated behind the windpipe or trachea. The œsophagus is soft and fleshy, with a cavity effaced when empty. The trachea, which on account of its functions is always open, is formed of incomplete cartilaginous rings, which give it an almost cylindrical form and render it prominent below in the middle line of the neck. Crossing the upper part of the trachea is the median part of a gland known as[285] the thyroid body, which in some cases (especially in the female) may form a slight rounded projection in the infra-hyoid region of the neck.
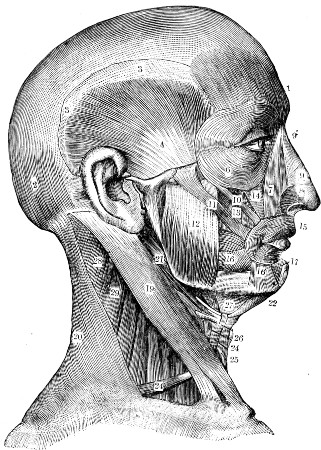
Fig. 88.
Muscles of the Neck and Face.—1, frontal;—2, occipital;—3, aponeurosis of the occipito-frontalis;—4, temporal;—6, orbicularis palpebrarum;—7, levator labii superioris et alæ nasi;—8, dilator naris anterior and posterior;—9, compressor naris;—9′, pyramidalis nasi;—10, zygomaticus minor;—11, zygomaticus major;—12, masseter;—13, levator anguli oris;—14, levator labii superioris;—15, orbicularis oris;—16, buccinator;—16′, depressor anguli oris, or triangularis oris;—17, depressor labii inferioris, or quadratus menti;—19, sterno-cleido-mastoid;—20, trapezius;—21, digastric and stylo-hyoid;—22, anterior belly of the digastric;—24, omo-hyoid;—25, sterno-hyoid;—26, thyro-hyoid;—27, mylo-hyoid;—28, 29, splenius.
The infra-hyoid muscles ascend from the back of the sternum, inside the thorax, towards the lower[286] border of the hyoid bone. They are four in number—two superficial (the omo-hyoid and sterno-hyoid) and two deep (the sterno-thyroid and thyro-hyoid).
The omo-hyoid (24, Fig. 88; 17, 18, Fig. 89) is a small muscle, long and slender, with a very remarkable course. It consists of two fleshy bellies with an intermediate tendon. It arises from the upper border of the scapula near the root of the coracoid process, and is directed at first obliquely forwards and inwards behind the clavicle; after crossing the posterior triangle it turns on itself, and is directed upwards beneath the sterno-mastoid and through the anterior triangle to be inserted into the lateral part of the lower border of the hyoid bone. This muscle, covered at first by the trapezius and then by the sterno-mastoid, is thus visible on the model in only two parts of its course—in front of the sterno-mastoid, where its anterior belly appears over the trachea, and again in the posterior triangle, where its posterior belly occupies the lower portion of the groove which separates the trapezius from the sterno-mastoid. Although deeply placed, this muscle becomes visible beneath the skin, for it is brought into sharp relief during certain actions. Evidently, from its slender form, we cannot expect it to be an important elevator of the scapula; but it serves to depress the hyoid bone. The most important function of the muscle is by its contraction, especially during spasmodic efforts in respiration, as in the strong inspiration in sighing or sobbing; in such cases it prevents the skin and loose aponeurotic tissue from being too strongly depressed in the supra-clavicular[287] fossa by atmospheric pressure. Therefore, if the neck is thin and the fossa well marked, as in an aged female, during the movements of sobbing or abrupt respiration a cord corresponding to the posterior belly of the omo-hyoid muscle may be clearly seen in the supra-clavicular fossa.
The sterno-hyoid (25, Fig, 88; 14, Fig. 89) forms a long, thin, fleshy band, extending from the back of the sternum and clavicle upwards to the lower border of the hyoid bone. Both these muscles are contiguous to each other by their internal borders above, but below, at the deep median fossa corresponding to the episternal notch, they are separated by a narrow angular space, in which appear the trachea and the inner border of the sterno-thyroid muscle.
The two deep muscles of this region (the sterno-thyroid and thyro-hyoid) are continuous with one another. They lie beneath the sterno-hyoid and omo-hyoid muscles, and cover the trachea and larynx in the front of the neck. The sterno-thyroid muscle arises from the posterior part of the first piece of the sternum, and ascends vertically beneath the sterno-hyoid. It appears at the inner border of the sterno-hyoid at the lower part of the neck on each side of the middle line (Fig. 68); reaching the thyroid cartilage, it is inserted into an oblique line on its external surface. The thyro-hyoid muscle arising from this oblique line on the thyroid cartilage ascends to be inserted into the hyoid bone.
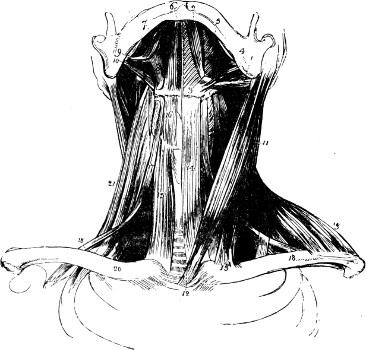
Fig. 89.
The Muscles of the Neck.—1, digastric (posterior belly);—2, digastric (anterior belly);—3, hyoid bone;—4, stylo-hyoid;—5, mylo-hyoid;—6, genio-hyoid;—7, stylo-glossus;—8, hyo-glossus;—9, internal pterygoid;—10, stylo-pharyngeus;—11, sterno-cleido-mastoid;—12, sterno-cleido-mastoid (sternal head);—13, sterno-cleido-mastoid (clavicular head);—14, sterno-hyoid;—15, sterno-thyroid;—16, thyro-hyoid;—17, omo-hyoid (anterior belly);—18, omo-hyoid (posterior belly);—19, trapezius;—20, clavicle;—21, scalenus posticus.
The supra-hyoid muscles proceed from the hyoid bone to the base of the skull and lower jaw, and by their contraction elevate this bone, as can be easily[288] observed in those who bring into action the pharynx or larynx, as in the act of singing or swallowing. The first of these supra-hyoid muscles is the digastric muscle, composed of two fleshy bellies connected together by an intermediate tendon (1, 2, Fig. 89). The posterior belly connects the hyoid bone with the under-surface of the mastoid process; the anterior belly connects the hyoid bone to the lower border of the lower jaw near the chin. Next come two other muscles one behind, lying alongside the posterior belly of the digastric, and called the stylo-hyoid (4, Fig. 89), and another in front, called the mylo-hyoid[289] (5, Fig. 89); this muscle lies underneath the anterior belly, and extends between the hyoid bone and the deep surface of the body of the lower jaw. It thus forms a partition closing in the floor of the mouth on each side of the tongue.
The digastric muscle arises from the under-surface of the mastoid process of the temporal bone. From this origin its fusiform posterior belly descends obliquely downwards and forwards, and near the hyoid bone is replaced by a round tendon. This tendon is attached by a fibrous pulley to the hyoid bone, and, taking its fixed point here, it turns abruptly, so as to be directed obliquely upwards and forwards towards the chin; at the same time this tendon is soon replaced by the anterior belly, also fusiform, which is inserted on the posterior surface of the symphysis of the chin, into a small depression called the digastric fossa. We see that this muscle, with its two bellies, is admirably arranged to raise the hyoid bone, and consequently the whole of the larynx; for the anterior belly carries the hyoid bone upwards and forwards, the other upwards and backwards, and if the two contract at the same time they will raise the hyoid bone directly upwards.
The stylo-hyoid is a small muscular fasciculus which accompanies the posterior belly of the digastric (21, Fig. 88). Arising from the styloid process of the temporal bone, this muscle passes downwards and forwards beneath the posterior belly of the digastric, with which it is closely connected; at the level of the hyoid bone the tendon of the digastric pierces the stylo-hyoid,[290] and the latter terminates by an aponeurotic slip which is inserted into the lateral part of the hyoid bone. On the model the stylo-hyoid and digastric are united in one cylindrical bundle (Fig. 88).
The mylo-hyoid muscle (27, Fig. 88) forms the floor of the cavity of the mouth. It constitutes a quadrilateral fleshy plane, attached by its upper border to the inner surface of the body of the lower jaw in a prominent oblique line; by its inferior border it is inserted into the hyoid bone. Above the hyoid bone the mylo-hyoid muscles are also inserted in the middle line into a fibrous raphe, so that the two muscles, that of the right and left side, form practically a single layer constituting the floor of the mouth. This muscle is covered on its deep surface by the mucous membrane of the mouth and by the fleshy fibres of muscles which are not visible externally, and which, arising from the small tubercles developed on the posterior surface of the symphysis of the chin (genial tubercles), are inserted either into the hyoid bone (genio-hyoid) (6, Fig. 89) or into the tongue (genio-hyo-glossus). The mylo-hyoid muscles, like the previous muscles, assist in raising the hyoid bone and larynx; it is to be noted, too, that the supra-hyoid muscles also act in depressing the lower jaw and opening the mouth.
[291]
1st. Muscles of mastication; masseter, its form, its share in the physiognomy (character of firmness, of violence); temporal muscle. 2nd. Muscles of expression; nature and special mechanism of the muscles of the skin; object of their study (expression of actual passion, momentary and not characteristic of the subject).—History of the question.—Leonardo da Vinci, Le Brun, Camper, Charles Bell, Lavater, Sue, Humbert de Superville.—Particular interest of the drawings given by Humbert de Superville (“Unknown Signs of Art”).—Duchenne of Boulogne and the experimental method applied to the study of physiognomy.—Darwin (physiognomy from the philosophical point of view, and evolution).
The muscles of the head with few exceptions occupy the anterior region of the head and more particularly the face. They are divided into two very distinct classes—1st, the muscles which serve for mastication and move the lower jaw; and 2nd, the muscles which, under the influence of emotion, modify the traits of the countenance and serve for the expression of the emotions. We call these the muscles of expression.
The muscles of mastication present the general arrangement that we have already met with in the various muscles of the trunk and limbs. They are attached to the bones, and they have fleshy bellies, more or less thick, which swell up in contraction, and are marked by prominences, just as the contraction of the biceps is shown by the prominence[292] it produces on the anterior surface of the arm. The muscles of expression, on the contrary, present a different type. These are muscles of the skin, which move the skin and not the parts of the skeleton; therefore their fleshy parts are in general very slender, and their contraction is not marked by any local swelling corresponding to the fleshy body, but only by change in place and form of the folds and membranous structures of the face (eyelids, lips, etc.). We will first study the muscles of mastication.
Muscles of mastication.—The muscles which move the lower jaw are inserted into the ramus and angle of the bone. Those on the inner side of the jaw are the deeply placed pterygoid muscles (so called because they arise from the pterygoid process of the sphenoid bone). We need not dwell on these muscles here, for they are deeply hidden in the zygomatic fossa of the head, and are not visible in any part on the surface. Those on the outer side are inserted either into the ramus and angle of the bone (masseter muscle) or into the coronoid process (temporal muscle).
The masseter muscle is a quadrilateral fleshy mass (12, Fig. 88) of which the upper attachment arises from the zygomatic arch (Fig. 56), and the lower attachment is inserted into the ramus and angle of the jaw. The anterior border of this muscle is thick, and in thin subjects forms a prominence, in front of which the cheeks are sunk so as to produce a more or less marked depression. In contraction the masseter raises the lower jaw and brings it into contact with the upper, against which it presses strongly. It[293] would be superfluous to dwell here on the part this muscle plays in mastication. It is more important to remark that during violent emotions, or even when we accomplish a powerful effort, we involuntarily clench the jaws. Contracting the masseter, therefore, in anger, menace, and in the strong expression which we characterise commonly by saying that the subject grinds his teeth, we see the masseter shown in the form of a quadrilateral prominence on the side of the face. Therefore the accentuation of the form of the masseter contributes to give to the physiognomy an energetic expression, and generally that of brute force.
The temporal muscle (4, Fig. 88) occupies the entire extent of the temporal fossa of the skull (Fig. 56); it arises from the bones that form that fossa and from an aponeurosis which, arising from the borders of the fossa, is attached to the upper border of the zygomatic arch, so as to form a species of cover (temporal fascia) to the fossa in question. From these multiple points of origin the fleshy fibres converge below and form a strong tendon which embraces the coronoid process of the inferior maxillary bone (25, Fig. 56), into which it is inserted. This muscle raises the lower jaw, but as it is shut up, so to speak, in a close space (temporal fossa and aponeurotic cover) it does not show during its contraction a remarkable prominence in the temporal region; nevertheless, in a person performing the movements of mastication we see the skin of the temple, above the zygomatic arch, slightly raised in a series of rhythmical movements; these movements alone show externally the contractions of this muscle during mastication.
[294]
Muscles of expression.—From what we have already said respecting the peculiar arrangement of these muscles of the skin, it is easy to understand that their study must be undertaken in a totally different manner from that of the muscles of the skeleton. We do not seek so much to define the form of the fleshy masses as to trace the direction along which each muscle exercises traction on the skin. Given the bony or cutaneous attachments of the muscle, we must observe the direction in which it acts, and so define the form of the folds or wrinkles which it causes on the skin, and ascertain what facial expression is acquired by these changes. Before we enter into these details, it is necessary to glance rapidly at the history of this particular question of human physiognomy, and then to consider the method by which its study should be undertaken.
First we must remark that we study here, with regard to the muscles of the face, physiognomy in a state of action—namely, the characters that affect the features at a given moment, under the influence of a passionate movement which causes (it may be) the involuntary contraction of one of the numerous muscles of the skin. Indeed, we may almost assert that the muscles of the face might be given names associated with mental states—attention, pain, menace, laughter, sorrow, contempt, disgust, &c. But we cannot pretend to study physiognomy in a state of repose, or to learn by the normal and permanent accentuation of certain of these traits the character of the subject and the passions that most frequently disturb him.
Doubtless, these two studies have numerous points[295] in common; it is easy to admit that, in a subject who is governed by one prevailing or overpowering emotion, such as suspicion, grief, or pain, the permanent or frequently repeated contraction of the muscles which correspond to these emotions can definitely mould the character of the face, so as to leave imprinted on it in a permanent form the sentiments that govern the mind.
But this analysis of the character of a subject is a very delicate study, always very uncertain, and admitting of philosophical developments which would carry us far away from the domain of anatomy. On the other hand, the determination of characteristic expressions impressed upon the face by the contraction of this or that muscle has, from the researches of Duchenne (of Boulogne), become a study which presents all the precision and certainty that we can claim from facts strictly deduced from anatomy.
Before the researches of Duchenne, the majority of books written on expression dealt almost entirely with physiognomy, or the means of recognising the character by the study of the habitual state of the traits of the countenance. We shall, in the first place, mention the works of Le Brun, Camper, Lavater, C. Bell, Humbert de Superville, and Sue, and then we shall refer to the investigations of Duchenne and Darwin.
Long ago, in the drawings of Leonardo da Vinci, we find some valuable indications of the state of the face and neck in the expression of the emotions. This great master, for example, clearly perceived the part that the platysma muscle of the neck takes in the expression of violent passions, and portrayed[296] the transverse folds which then mark it beneath the chin. Le Brun, however, was the first to arrange studies of this character into a doctrinal series. The publications in which his views on this subject have been preserved are numerous.[7] The artist will find there a number of interesting observations, curious comparisons, and ingenious explanations. Le Brun occupied himself principally with the resemblance of certain types of human physiognomies to the heads of animals; in short, he studied physiognomy in relation to character.
Camper, whose works we have already quoted respecting the facial angle (page 181), was an anatomist and an artist. He analysed the action of the facial muscles, and it was he who first laid down this general rule—viz. that the contraction of each muscle of the face produced in the skin one or more folds, of which the direction is always at right angles to that of the muscle, a precept that we shall find to be true with regard to almost every muscle of the face, and especially for the frontalis, the great zygomatic, &c. Besides the exact observations that the artist will meet in the works of Camper, he will find in addition an interesting historical account of the question.
An English anatomist, Sir Charles Bell, celebrated for his studies of the nervous system, also analysed the expressions of the face.[8] But though his work[297] affords picturesque descriptions and admirable illustrations, it is more interesting to the anatomist than the artist.
The title of the work of Lavater (The Art of Knowing Man by his Countenance)[9] indicates the object sought by the author. We find in this work good illustrations, and curious observations especially applicable to the study of physiognomy, but frequently without order, without method, and accompanied by dissertations on whimsical subjects, such as the chapters devoted to imaginations and envies, to warts and beards, and to lines of animality, &c.
In order to have an idea of the manner in which, at this epoch, authors attempted the study of physiognomy, making this delicate analysis a pure affair of sentiment, it is sufficient to mention the work of Sue (Physionomie des Corps Vivants, considéré depuis l’Homme jusqu’à la Plante. Paris, 1797.) In the middle of a long affected treatise on physiognomy and its relation to the passions, this, for example, is how he expresses himself concerning the mouth:—“A mouth delicate and pure is perhaps one of the best recommendations. The beauty of the portal proclaims the dignity of that which passes through. Here also is the voice, the interpreter of the heart and mind, the expression of truth, friendship, and the most tender sentiments.” With regard to the incessant comparison of human physiognomy with that of animals, the author stops at nothing in this singular course, and speaks dogmatically on the physiognomy of fishes, serpents, grasshoppers, and[298] intestinal worms (!), as well as that of man. “Many fishes,” said he, “are wanting in that which gives a character of amenity, kindness, and tenderness.” “The intestinal worms have a very decided physiognomy ... the character of their physiognomy inspires in man sorrow and awe.”
Amidst the works of a more serious, though still empirical character, we must mention in particular one which, although dealing with the countenance only in a secondary degree, yet presents several valuable observations on this subject. We have endeavoured to utilise these investigations in the diagrammatic representation of the action of the muscles of the face. We speak of the treatise of Humbert de Superville (Des Signes Inconscients de l’Art, 1827). The author gives three drawings of the human face, in which the lines represent the eyes, the lower boundary of the nose, and the lips. In one of these drawings (Fig. 90) the lines are all horizontal, in the second (Fig. 91) they are all inclined downwards and outwards (from the median line), and in the third (Fig. 92) they are all inclined upwards and outwards. The author remarks that the first figure (with the lines horizontal) produces an impression of calmness, greatness, and constancy; and he adds that in the same way in nature and architecture horizontal lines give rise to the idea of calmness, stability, and grandeur: the cedar, with its horizontal branches, is of all the trees the one that realises this impression in the highest degree. On the contrary, the second figure (with the lines directed obliquely downwards) gives an impression of sadness, pain, and grief; and the author does not fail to[299] compare the direction of the features of such a countenance with the direction of the architectural lines in tombs and funeral monuments, and that of the branches of the trees which everywhere are planted in preference to others in cemeteries, and whose branches always hang obliquely. Lastly, the third figure (with the lines obliquely upwards) gives rise to the impression of gaiety, laughter, levity, inconstancy; and, to continue the preceding comparison, everyone must acknowledge that Chinese architecture, with its lines oblique and diverging upwards and outwards, can never—at least, in the eyes of a European—produce an impression of grandeur and majesty.
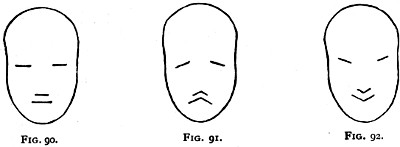
Fig. 90. Fig. 91. Fig. 92.
The Three Figures of Humbert de Superville—(Fig. 90, calmness; Fig. 91, sadness; Fig. 92, gaiety).
These figures, and the remarks that de Superville makes afterwards, but which we have not emphasised here, are strikingly exact, when we consider the features in the state of movement or in a momentary expression of emotion. All the muscles which take part in the expression of pain, sadness, and contempt help to incline the features obliquely downwards and outwards, some by acting on the[300] outline of the eyes, others on that of the mouth, &c. On the contrary, the muscles of laughter, raising its angles, draw the mouth obliquely upwards and outwards, and—for certain reasons that we will analyse further on—seems to give a similar direction to the outline of the eyes. In a word, features, starting from the state of repose, represented by the first figure of Humbert de Superville (Fig. 90), oscillate in two opposite directions, either ascending, to express the scale of gaiety and laughter (in which the features are oblique upwards and outwards, Fig. 92), or descending—sadness, pain, and tears (in which the features are oblique downwards and outwards, Fig. 91). The exactness of the drawings furnished by Humbert de Superville for the general expression of the physiognomy induces us to try, by similar drawings, to represent the action of each muscle separately. Knowing the action of a muscle, and knowing from the photographs of Duchenne the direction that it imparts to a certain feature of the face, either to the line of the eyebrows, the opening of the eyelids, the nostrils, or the lips, we have indicated by a simple stroke or line these changes, either in direction or in the form of one of those lines, and have obtained theoretical figures sufficiently expressive to characterise the emotion geometrically, so to speak, in the manifestation of which this or that muscle is affected. Such are the Figures 96, 98, 100, 102, 103, 104, 106 (page 317 and following), by means of which we will attempt to explain the action of each muscle of expression. We may say that these drawings, without any pretension,[301] are, so to speak, the primer of the language of physiognomy.
We now arrive at the history of the work of Duchenne, to which we owe all that follows. While all his predecessors had been taken up with observation, Duchenne introduced the experimental method into the study of physiognomy. His process, simple in conception, was very delicate in application. His method was to cause the contraction of each muscle singly, and that the expression that resulted might be appreciated not only at the moment of the experiment, but again at any time, and submitted to the judgment of all, he photographed the subject at the moment when the muscle was contracted. This last operation was easily accomplished, but the excitation of a single muscle was a more delicate operation. Everyone knows that by electricity, in placing the two electric needles (the two poles of the current) on the course of a muscle, we can cause the contraction of the muscle beneath the skin. But no subject would lend himself to this experiment. At first he tried on the dead body of an executed criminal a short time after death; but the muscles of the face lose their excitability two hours after death, and then it is only by actual exposure of the muscle and direct stimulation that we can obtain contraction by the application of electricity. On the other hand, if we attempt it on any living subject, we can, it is true, cause a muscle to contract by applying electricity over its site; but the electric current, traversing the skin to reach the muscle, at the same time that it excites the[302] motor nerves of the muscle, excites also the sensory nerves of the skin and produces acute pain. From this fact we see that we produce on the face of the subject, not a simple and characteristic expression, but a true grimace, or an irregular contraction of all the muscles under the influence of the pain.
Duchenne had the good fortune to be able to experiment on a subject in whom a particular infirmity rendered impossible the last inconvenience we have noted. This was an old pensioner of the hospital who had anæsthesia of the face (ἀνα, absence of; αἴσθησις, sensibility), in whom the skin of the countenance was insensible to the most painful excitation; electricity could be applied to the skin without producing any painful reaction, and yet excited the muscles beneath, which had perfectly preserved their contractility, and performed their functions as in a normal subject. He could, therefore, cause this or that muscle to contract alone, and could excite, for example, the action of the great zygomatic, giving to the face the expression of laughter, without the subject having any idea of what his physiognomy reflected; his face, by the action of the electricity, was laughing, while his thoughts might be indifferent or fixed on sad recollections; on the other hand, for example, by the contraction of the superciliary muscle, his countenance might express the most acute pain, while his thoughts might be quite indifferent or borne away by gay and pleasant ideas. In a word, Duchenne was able to realise, under the most precise conditions of experiment, an exact study of the uses of the muscles of expression.
[303]
The work in which Duchenne has given the result of his labours is remarkable particularly for the magnificent atlas of photographs that accompany it, and which have been obtained by the above process. From these photographs have been reproduced as exactly as possible the several figures that accompany the descriptions which follow (Figs. 95, 97, 99, 101, page 316 and following). We cannot enter here into a complete statement of the results obtained by Duchenne, but we will seek at least to show the serious and scientific value of these studies, and to inspire the student to refer to the original work.
These studies have for the artist this important result—namely, to prove to him that frequently the contraction of a single muscle is sufficient to express an emotion, and that it is not necessary to change all the features in order to give to the face the stamp of pain, attention, menace, contempt, disgust, &c., each of these sentiments being expressed by a slight modification, either of the eye alone, or of the lip alone. Each expression has, so to speak, its own exact, precise, and separate mark, produced by a single local modification; but this local modification seems to be reflected throughout the physiognomy, and therefore, from unaided observation, artists had for a long time believed that, for example, attention and pain were shown by the combined action of a number of facial muscles. Now experiment proves that pain may be expressed solely by a muscle which raises and wrinkles the brows, and on a face (Fig. 99) where this muscle alone is contracted (superciliary muscle, page 320) the expression of pain is complete. We[304] naturally believe that the mouth also takes part in it, but if we cover the upper part of the countenance, we perceive that the lower part of the face is in a state of complete repose.
To bring to a close this history, which is not the least interesting part of the subject, we must say that the labours of Duchenne were not at first received with great favour in France. Physiologists as well as artists showed a certain distrust of a work which pretended to give precise rules and scientific laws to a subject about which it had been the custom to make fanciful and sentimental comparisons. Few persons understood the nature of the reason which forced Duchenne to choose as a subject for these experiments a poor man with a physiognomy almost imbecile in repose, and they did not consider that if this face was old, wrinkled, thin, and vulgar, there was the greater reason to be struck with the precision with which the electric excitation enabled the most opposite and characteristic expressions to be taken.
As has been too often the fate of scientific discoveries, the work of Duchenne was neglected in France, and was not appreciated until it had been adopted by a foreign country. It was Darwin who made the results of the French physiologist the basis of his own interesting studies.
It is not necessary to recall the extent and repute of the works of Darwin on The Origin of Species, on the Evolution of Animals and Plants, and on The Descent of Man. What this great naturalist has done for the general morphology of plants and animals he sought to do for the subject of physiognomy. Seeking[305] in the logical chain of natural facts the cause of all biological phenomena, he endeavoured to discover by the attentive study of the movements of expression, and through their origin and development, a series of new arguments in favour of the theory of evolution. In a word, Darwin, by invoking the association of certain useful movements, and comparing the functions with the expressions with which they are associated, sought to explain why one muscle in particular rather than another is affected by the expression of this or that emotion. We cannot here enter further into the analysis of this philosophical work. It is sufficient to remark (having commended the perusal of it as most interesting to the artist[10]) that before we explain anything it is necessary that it should be firmly established. Therefore the explanation of the part that each muscle takes in the expression must be impossible until the fact of the action and the expression associated with the movement of the muscle has been scientifically demonstrated. The philosophical work of Darwin could not have been undertaken if it had not been preceded by the experimental work of Duchenne.
Summarising Darwin’s argument, his thesis may be stated somewhat as follows: that every expression or bodily manifestation of emotion has a physical basis, and an origin in some useful exercise of the particular muscles concerned; that such an action becomes habitual in the individual, and is transmitted from father to son, and from generation to generation;[306] and that the actual physical cause is transferred to a mental condition, so that an action like knitting the brows—primitively for the purpose of actually clearer vision—becomes indicative of a mental state in which the emotion is expressed of a desire for a clearer mental vision, as when a man is engaged in any intellectual problem.
Darwin further enunciated the important principle of Antithesis: which means the employment of exactly the opposite expression (it may be by the relaxation of muscles, or by the contraction of antagonistic muscles), to indicate an opposite or antagonistic attitude of mind. Thus joy is expressed by the contraction of a definite series of facial muscles; grief or dejection is expressed by the relaxation of these and the contraction of opposing muscles. The healthy, alert man holds his head erect; the depressed or miserable has a drooping gait.
A third principle enunciated by Darwin as employed in producing the expression of emotion is the direct action of the nervous system, to a large extent independent of the will, and served mainly through the sympathetic nervous system, such as blushing, trembling, perspiration, &c.
It is important, as Darwin points out, to bear in mind that emotion is expressed not only by facial expression, but by many other agencies as well; by the emission of sounds, by the voice in some cases, by the rattling of the tail quills in the case of the porcupine, &c.; by the inflation of the body, as in the hen who raises up all her feathers in maternal anger, or the dog whose hair stands on[307] end; by gestures, rubbing, licking, caresses, kisses; or by the attitude and movements of the body, head, or limbs.
In his book each emotion and its corresponding expression is carefully analysed, and the physical cause and the particular muscles engaged are pointed out. Thus Darwin says, “Weeping is the result of some such chain as follows: Children wanting food or suffering in any way, cry out loudly as a call to their parents for aid, like the young of most animals. Prolonged screaming leads to the gorging of the blood vessels of the eyes; and this causes first consciously and then habitually the contraction of the muscles round the eyes in order to protect them.” The mouth at the same time is opened widely to allow of a more vigorous scream. The overflow of tears is a consequence of the closure of the eyes.
Again, in regard to the facial expression in laughter, Darwin suggests that as the primitive cause of laughter may have been a practical joke—or, as De Rochefoucauld put it, there is something pleasing in the misfortunes of one’s friends—the expression may be associated with the retraction of the angles of the mouth, and the exposure of the canine teeth, in preparation for self-defence if the victim of the joke should retaliate.
The expression of disdain or disgust in the same way is associated with the contraction of muscles of the eye, nose, and mouth, primitively from purely physical causes, which have become connected with a mental attitude. The head is turned aside, and the eye is half closed to shut out an[308] unpleasant sight; the nostril is raised at the sensation of a disagreeable smell, and the lips are curled in disgust at a nasty taste.
There is not space in which to dwell further on these deeply interesting questions, for a study of which the reader is referred to Darwin’s masterly treatise on the subject.
The figures which illustrate the work of Darwin are in a great measure only reproductions of the photographs published by Duchenne about ten years previously. However, as we have already mentioned, attention has been recalled in France to the works of Duchenne, a more favourable judgment has been passed, and justice has been rendered to him who had opened the way to the experimental study of physiognomy. In 1874 the French began to devote, in the course of anatomy in the School of Fine Arts, several lectures to the account of what we must call the primer or grammar of the expression of physiognomy. Happy in seeing his works included in this classical course of instruction, Duchenne, whom death carried off a few years later, gave to the School of Fine Arts the complete series of large original photographs from which these publications are reduced, and this beautiful collection is to-day one of the most valuable in the French museum of anatomy (Muséum Hugnier).
Although this account may appear long, it is nevertheless very incomplete, being given only with a particular object—that of comparing the works of Duchenne with those preceding him. Those of Duchenne will be made the basis of the studies which follow. We will finish by noting, as interesting[309] and instructive, the works that treat in a more general manner of expression and physiognomy, such as those of Lemoine, Gratiolet, and Piderit.[11]
[310]
Muscles of the upper part of the face: Occipito-frontalis (attention); orbicularis palpebrarum of the eyelids, superior orbital portion (reflection); pyramidalis nasi (menace); superciliary (corrugator supercilii) (pain).—Muscles of the middle region of the face: Great zygomatic (laughter); lesser zygomatic and levator labii superioris (tenderness, sorrow); levator labii superioris alæque nasi (weeping bitterly), compressor naris (lewdness).—Muscles of the lower region of the face: Orbicularis oris; buccinator; depressor anguli oris (contempt); depressor labii inferioris (disgust); platysma muscle of the neck.—Classification into muscles completely expressive and expressive by complement.—Of associations possible and impossible with regard to mechanism and with regard to the nature of the emotions.—Conclusion.
The muscles of the face, which are attached to the skin, move and alter the shape of its folds and apertures. These different cutaneous parts are very complex, but at the same time known to persons who are the greatest strangers to anatomy. For them even it is unnecessary to describe here the eyebrows, the eyelids, the palpebral fissure, the ala or wing of the nose, and the lips. We will only point out, with regard to these parts, the significance of their various anatomical names, the employment of which will be useful in abridging the descriptions that follow.
On the eyebrow we distinguish a broad internal part (towards the median axis of the face) called the head of the eyebrow, and an external part called the tail of the eyebrow, which becomes thinner as it is removed from the middle line.
[311]
On each palpebral fissure, at its inner end, is a small perforated papilla—the lachrymal papilla—the perforation in which is named the punctum lachrymale, carrying the tears from the surface of the eye into the nose by special ducts. Each of the two extremities of the palpebral fissure bears the name of the canthus, or angle. We distinguish, therefore, on the eyelids an external canthus or angle characterised by its pointed form, and an internal characterised by its rounded form, bounding a small oval space called the lachrymal lake, at the bottom of which a rose-coloured fleshy tubercle projects (the caruncula lachrymalis). External to this is a pale fold, the plica semilunaris, a rudiment of the third eyelid (found in birds). We also give the name of commissure (or angle) to each extremity of the buccal aperture (commissure of the lips). The groove extending from the septum of the nose to the centre of the upper lip is known as the philtrum.
Lastly, we must note a fold which normally exists in a more or less marked degree in every subject, and the changes of which take a great part in the expression produced by the various muscles of the cheeks. This is the naso-labial fold, so named because, arising from the region bounded by the cheek and the side of the nose, it is directed obliquely downwards and outwards, passes at a short distance from the posterior border of the wing of the nose, and terminates near the commissure of the lips. In the subject who served for the experiments of Duchenne (Fig. 99, page 320) this fold was strongly marked, as it generally is in all old people.
The human head and face, the features, and[312] the muscles which underlie the skin have, it is supposed, undergone progressive and retrogressive changes in the process of evolution. The cranium has expanded with the evolution of the brain, while the face has become smaller and feebler, and the teeth have shown distinct signs of degeneration and diminution, both in size and number.
Of the soft parts of the face, the apertures of the eyes and mouth have increased in mobility and functional power and refinement of expression; while the nasal apertures and the ears illustrate a retrogression in evolution. The interior of the nasal cavity as well as the nostrils presents a simpler or more degenerate type in man than in the lower animals, in whom the sense of smell is so much more highly developed. The external ear is a good example of a rudimentary organ. Its parts have a definite form, and each wrinkle or corrugation has a separate name (see Fig. 93). It is composed of a mass of elastic cartilage (except in the tip or lobule) which penetrates into the passage of the ear in a tubular form. This cartilaginous pinna is the shrivelled-up remains of the mobile funnel-shaped ear of the lower animals; and the tip of the ear is represented by an angular projection (Darwin’s tubercle) placed on the edge of the rim of the ear (helix).
The lobule is soft, and consists of a mass of fat enclosed in the skin. It is usually free from the neck, but in some cases (as, for example, in the right ear of the poet Byron) the lobule is attached to the skin of the neck, and is not in full relief.[313] The muscles of the nose and ear are also degenerate, and the movements of the nostrils and of the ears are only rudimentary.
In the same way the arrangement of the muscles underlying the skin of the neck and head presents examples of advance or retrogression when compared with the similar muscles of lower animals.
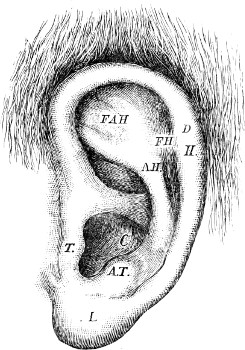
Fig. 93.
The External Ear.—H. helix;—F.H. fossa of the helix;—A.H. anti-helix;—F.A.H. fossa of the anti-helix; C. concha;—T. tragus;—A.T. anti-tragus;—L. lobule;—D. Darwin’s tubercle.
In hairy animals the body is covered all over by a thin layer of muscle which underlies the skin, and is called the panniculus carnosus.
In man the body has become almost denuded of hair, except on the head and face, and at the same time his capacity of facial expression is vastly greater than in one of the lower animals.
The effect of these changes is seen in the condition of the panniculus carnosus. It has degenerated over the hairless trunk, and only remains normally as the platysma myoides of the neck. But, on the other hand, the parts of the panniculus carnosus which have swept over the face and have surrounded the apertures of the eye and mouth in particular, have become differentiated into the complicated series of muscles of expression, rudimentary and[314] feeble on the scalp and in relation to the pinna and the nasal opening, but highly organised in relation to the apertures of the eye and mouth.
It is for the most part these highly differentiated muscles which have to be dealt with in this chapter in connection with the expression of the emotions.
The muscles of expression (Fig. 94) are arranged in three series: one around the eyes and eyebrows, occupying the upper region of the face; the second about the nose; and the third around the aperture of the mouth, occupying the middle and especially the lower region of the face. The first series includes the occipito-frontalis, the corrugator supercilii, and the orbicularis palpebrarum; the second includes the pyramidalis nasi, compressor naris, and dilator alæ nasi; the third set is most numerous, comprising the levator labii superioris alæque nasi, levator labii superioris, zygomaticus major and minor, the levator anguli oris, the orbicularis oris (to which we may add the buccinator), the risorius, depressor anguli oris, and depressor labii inferioris. Finally, in the neck and extending up to the lower jaw is the platysma myoides, which takes a considerable part in certain powerful expressions of the face.
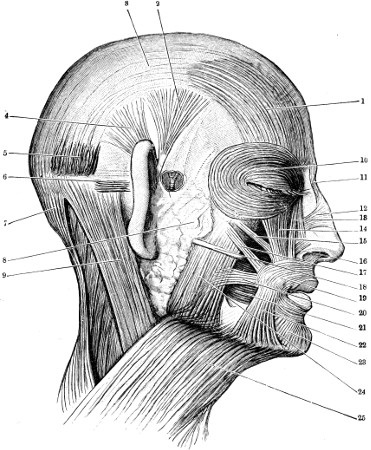
Fig. 94.
(From Cunningham’s “Text Book of Anatomy.”)
The Muscles of the Face.—1, frontalis;—2, attrahens aurem;—3, epicranial aponeurosis;—4, attolleus aurem;—5, occipitalis;—6, retrahens aurem;—7, trapezius;—8, parotid gland;—9, sterno-cleido-mastoid;—10, orbicularis palpebrarum;—11, pyramidalis nasi;—12, compressor naris;—13, levator labii supertoris alæque nasi;—14, levator labii superioris;—15, levator anguli oris;—16, depressor alæ nasi;—17, zygomaticus major;—18, Stenson’s duct;—19, orbicularis oris,—20, risorius;—21, buccinator;—22, depressor anguli oris;—23, depressor labii inferioris;—24, masseter;—25, platysma myoides.
In the study of these muscles we will enter but little into anatomical details, but will content ourselves with pointing out the situation of the muscle, its fixed attachments to the bones of the face, its direction, and, lastly, the point on the skin where it takes its insertion. On the other hand, we must carefully inquire into its mechanism and the manner in which its contraction produces alterations in the[315] skin of the face, and the nature and direction of the folds which it marks thereon. We must ask ourselves[316] what expression results by the occurrence of these alterations in the face. And, lastly, we will endeavour to give a diagram of this expression after the mode of representation employed by Humbert de Superville (page 298).
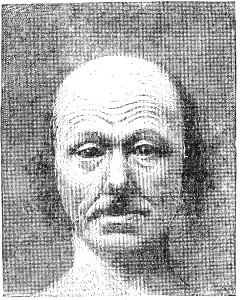
Fig. 95.
Contraction of the Frontal Muscles
(expressions of attention and astonishment).
A.—Muscles of the upper part of the face (forehead, eyebrows, eyelids, and root of nose.)
1st. Occipito-frontalis muscle (muscle of attention).—This muscle (1, Fig. 88, page 285) (Fig. 94) consists of an anterior and a posterior belly, connected by an intermediate membranous tendon covering the scalp. Its anterior belly extends as a fleshy sheet, quadrilateral in form, over each lateral half of the forehead. The muscles of each side are continuous with one another across the middle line. The anterior muscular portion is the frontalis. Its lower border is attached to the skin of the eyebrow, and blends with the orbicularis palpebrarum. From this origin its fibres ascend vertically and parallel to each other towards the region of the roots of the hair, and[317] become continuous, at this level, with the membranous expansion of the epicranial aponeurosis. This aponeurosis, which covers the vault of the skull and is adherent to the skin of the scalp, is prolonged backwards to the occipital region, where it terminates in a bilateral fleshy layer, the occipitalis muscle, attached to the superior curved line of the occipital bone.
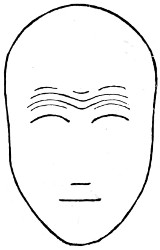
Fig. 96.
Diagram of the frontal muscles (attention).
In order to understand the mechanism of the occipito-frontalis muscle it is necessary to consider it as taking its fixed origin at the posterior part of the skull, through the medium of the epicranial aponeurosis and the occipitalis portion of the muscle; its insertion is its attachment to the deep surface of the skin of the eyebrow and the orbicularis palpebrarum. It has no bony attachment in the region of the forehead. The frontalis, therefore, in contracting, draws the skin of the eyebrow and the upper eyelid from below upwards, and consequently raises the eyebrow, and causes transverse folds to appear in the skin of the forehead.
In examining (Fig. 95) a face in which this muscle is contracted we perceive that it expresses attention; if the contraction of the muscle is very great this expression of attention changes to that of astonishment. In entering into the detail of the changes that the face then presents we see that the eyebrow is raised and its superior convexity is very marked, that the eye is widely opened, clear, and brilliant, and[318] that the forehead is furrowed on each lateral half by curved folds concentric with the curve of the eyebrows, continued more or less from one side to the other, and describing curves in the middle line with the concavity upwards. In a child or young woman, in whom the skin is supple and elastic, it does not give rise to the formation of folds, and the skin of the forehead remains quite smooth during the contraction of the frontal muscle, and then the elevation of the eyebrow, the exaggeration of its curve and the state of the eyes, open and bright, are sufficient to give the expression of attention.
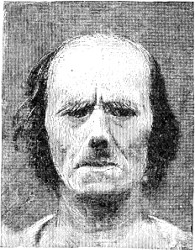
Fig. 97.
The Upper Part of the Orbicularis Palpebrarum (reflection).
Figure 96 is the representation of attention, characterised here solely by the form of the eyebrows and the frontal folds.
2nd. The orbicularis palpebrarum (6, Fig. 88, and 10, Fig. 94).—The orbicular muscle of the eyes is a very extensive muscle which encircles the palpebral orifice. It is composed of numerous portions which can act more or less independently, and which have not all an equal importance in the expression of the face.
a. One part of this orbicular muscle, called the palpebral part, is contained in the thickness of the[319] eyelids, and produces by its contraction the closing of the eyes. If this contraction is moderate it produces only a certain drawing together of the eyelids and reduces the opening of the eyes to the form of a linear slit. This state of the palpebral opening does not constitute by itself an expression, properly speaking, but it may be complementary to various expressions; thus, associated with a slight contraction of the triangular muscle of the lips, which is the muscle of disgust and discontent (page 333), it gives to the countenance the expression of disdain and contempt.
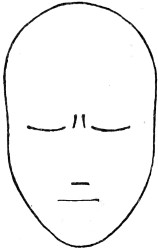
Fig. 98.
Diagram representation of reflection, meditation.
b. A second part of the orbicular muscle is arranged in a circular manner on the outer side of the eyelids, and corresponds exactly to the contour of the orbital orifice of the skeleton (Fig. 58, page 174, and Fig. 88, page 285). This portion, which we may call the orbital portion, is divided into two parts: one, the inferior fibres, the contraction of which moves the lower eyelid slightly upwards and causes a furrow at its junction with the cheek, and without being expressive by itself, completes the expression of laughter by giving to it a character of frankness and truth; and the superior fibres, which merit more detailed study, for they produce by their action a characteristic expression of reflection, meditation, and contemplation.
[320]
This superior orbital portion of the muscle (muscle of reflection) is placed beneath the skin of the eyebrow, and its fibres, like it, describe an arc with the concavity downwards, of which the inner extremity is adherent to the internal border of the orbital opening. The mechanism, therefore, of this muscle is easily foreseen; for, like all curved muscles, more or less fixed at their extremities, it must in contraction straighten its curve. It accordingly acts in this way on the eyebrow, to the skin of which it is adherent, and effaces its curve, rendering it straight transversely; and it depresses, and consequently makes tense, the skin of the forehead, causing its wrinkles to disappear.
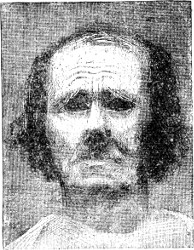
Fig. 99.
Superciliary Muscle (sorrow).
In examining a face in which this muscle is contracted we perceive that it expresses reflection. In Figure 97, owing to the excessive development of the eyebrow, which is greatly lowered, the hairs descend over the eyes, and the expression is rather that of painful reflection or of intense application of the mind pre-occupied with sadness; but we see in every case that this expression is obtained essentially by the lowering and straight direction of the eyebrow,[321] which veils the eye and effaces all wrinkles on the forehead. This alteration in the features is precisely the reverse of that produced by the frontalis muscle, as is shown by the comparison of Figures 95 and 96, and in fact the two states of mind corresponding to the expression given by each of the muscles are precisely the reverse of each other. We cannot be at the same time attentive to an external object and meditating in reflection. Usually the succession of these states of mind and facial expression is as follows:—We are attentive to that on which we are looking, the eye open, brilliant, the eyebrow raised, and the forehead wrinkled (contraction of the frontal muscle); afterwards we reflect on what we have seen, and are, so to speak, abstracted from the external world—the eyebrow is lowered, the forehead smooth, and the eye veiled (by contraction of the superior fibres of the orbicularis palpebrarum), or the eyes may be closed (by contraction of the whole of the muscle).
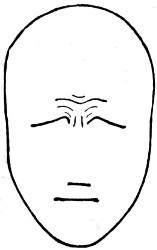
Fig. 100.
Diagram representation of sorrow.
Figure 98 is the representation of reflection, characterised by the absence of the frontal folds, the depression of the eyebrows and the presence of two small vertical folds in the space between the eyebrows, to which the depression of the eyelid gives rise (Fig. 97). This representation of reflection (Fig. 98) does not acquire its full demonstrative significance until we compare it with that of attention (Fig. 96).
[322]
3rd. Pyramidalis nasi muscle (or muscle of menace).—This small muscle, situated in the space between the eyebrows on a level with the root of the nose (11, Fig. 94) (9, Fig. 88, page 285), is formed by short vertical fibres, which is attached by its lower end to a membranous expansion over the nasal bones (Fig. 58, page 174), and by its upper end to the deep surface of the skin of the space between the eyebrows.

Fig. 101.
Great Zygomatic Muscle (expression of gaiety, of laughter).
The contraction of this muscle therefore produces the following result:—Taking its fixed insertion at the nasal bones, it draws downward the skin of the space between the eyebrows, forming short transverse folds, and depressing slightly the inner part of the eyebrow.
In a face in which this muscle is contracted (see the atlas of Duchenne) the expression is that of harshness, menace, and aggression. Looking at the expression of countenance which Duchenne reproduced by this contraction, we can readily believe that if the subject had been represented in full, its attitude would have been one of menace; and the individual would be shaking his fist or brandishing[323] a weapon. Moreover, anything which throws a shadow or a dark look between the eyebrows gives to the physiognomy a character of harshness, as when the contraction of the pyramidalis produces the transverse folds in this region. Therefore, in those persons in whom the eyebrows seem to meet, owing to an exaggerated development of hair in the space between, the physiognomy always presents at first sight the stamp of severity and harshness, which may not agree in the least with the true character of the subject. The expression of the pyramidalis is too delicate, and due to a change of the features too local and slight for us to express it by a drawing, as we have done in the case of the preceding muscles.
4th. Superciliary muscle (corrugator supercilii, or muscle of pain).—This short muscle is deeply hidden beneath the skin of the region of the head of the eyebrow. Its fixed attachment is to the frontal bone, above the superciliary arch; from this origin its fibres are directed outwards and slightly downwards to be inserted into the deep surface of the skin at the middle of the eyebrow.
Its mechanism consists in drawing the eyebrow inwards and slightly upwards, and as it is attached to the middle of the eyebrow it draws it together at this point, namely, towards its inner part. The eyebrow is therefore, so to speak, abruptly hooked upwards and inwards, like a curtain that has been tucked up and attached to a fixed point. It therefore produces on the skin of the forehead folds concentric to this gathering together of the eyebrow and situated in the middle of the forehead, besides[324] producing the vertical furrows, obvious in the figures, between the eyebrows.
Figure 99 represents, after a photograph of Duchenne, the state of the physiognomy caused by the contraction of the superciliary muscle. This physiognomy has an expression characteristic of suffering, and any greater accentuation of the action of the muscle shows in a marked degree the expression of physical or mental agony.
We see that the only parts changed in this expression (compare Fig. 95, page 315) are the inner half of the eyebrow and the region between the eyebrows on the forehead; pain, therefore, is expressed by the raising of this part of the eyebrow and its gathering together abruptly in the middle of the forehead, and by the presence of the short folds immediately above this and the more extended folds occupying the middle region of the forehead.
Figure 100 is a diagrammatic representation of pain, expressed only by changes in the neighbourhood of the inner part of the eyebrow (contrast with Fig. 102 following).
B.—Muscles of the middle region of the face.
5th. The great zygomatic muscle (zygomaticus major, muscle of laughter).—This muscle (17, Fig. 94, and 11, Fig. 88) has its fixed attachment on the cheek-bone; from this origin it is directed obliquely downwards and forwards, to be inserted into the deep surface of the skin near the angle of the mouth.
[325]
6th. Elevator of the angle of the month.—The levator anguli oris is a muscle which largely aids the great zygomatic muscle in its action. It arises from the canine fossa of the upper jaw, and is directed downwards towards the angle of the mouth. It is inserted into the skin, and blends with the orbicularis oris (15, Fig. 94).
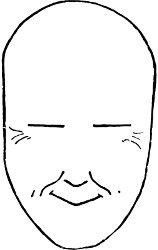
Fig. 102.
Diagram representation of laughter.
The mechanism of these muscles consists in drawing the angle of the mouth upwards and outwards, an action which results in some complex changes in the expression of the countenance. At first the orifice of the mouth is enlarged transversely, and its direction ceases to be straight, so that each lateral half is directed obliquely upwards and outwards. As the naso-labial line (Fig. 95) passes, at its lower end, near the commissure of the lips, this also is carried upwards, describing a slight curve concentric to the commissure of the lips, while the upper part of the line describes a curve with its convexity downwards. The skin of the cheek gathered up towards the cheek-bone becomes more prominent, and forms, below the outer angle of the eye, several radiating folds (commonly called crows’-feet), which throw a slight shadow beneath the external angle of the eye; this makes it appear as if the line of the eyelids is a little raised on the outer side (or oblique upwards).
Figure 101, representing the contraction of the great[326] zygomatic muscle, illustrates in a diagram the frank expression of gaiety and laughter, and we see that the alterations of expression take place only, as we have already said, in the line of the lips, the naso-labial line, and the external angle of the eyes.

Fig. 103.
Diagram representation of the external common elevator (muscle of grief).
Figure 102, giving the representation of laughter according to the preceding description of the great zygomatic muscle, is very similar to the corresponding figure of Humbert de Superville (Fig. 92, page 299), only, in order to express the reality without having regard here to appearances, we have drawn the lines of the eyes horizontal; and, again, the naso-labial furrow has been represented with its form convex downwards and inwards for the upper two-thirds, and with the slight hook which its inferior extremity describes. This naso-labial furrow is of the utmost importance in the expressions produced by all the muscles belonging to the lips, as we shall see in the following description.
7th. The lesser zygomatic (zygomaticus minor) and elevator of the upper lip (levator labii superioris, muscle of grief).—On the inner side of the great zygomatic muscle there exists frequently (10, Fig. 88, page 285), but not constantly, a small muscular fasciculus which arises from the anterior part of the cheek-bone and descends to be inserted into the thickness of the upper lip. This muscle, called the lesser zygomatic, does not take part in the expression[327] of laughter; in fact, it changes the naso-labial furrow in the same manner as the following muscle (the external common elevator), and so expresses, as we shall see, emotion, sadness, and grief.
8th. The elevator of the upper lip (levator labii superioris) arises (14, Fig. 94, and 14, Fig. 88, page 285) from the inferior border of the bony margin of the orbit and descends to the upper lip.
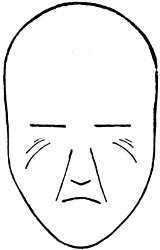
Fig. 104.
Diagram representation of the internal common elevator (muscle of grief with tears).
Its contraction raises the upper lip itself, but not the labial commissure, so that each half of the line of the lips, raised within and remaining depressed at its outer extremity, becomes slightly oblique from above downwards and from within outwards (the reverse of the obliquity produced by the great zygomatic muscle); at the same time the centre of the naso-labial furrow is raised and the furrow becomes curved with its concavity downwards and inwards (the reverse of the curve produced by the great zygomatic).
By means of these changes the countenance takes on the expression of discontent, emotion, and grief (see the atlas of Duchenne).
We give here only one drawing (Fig. 103) in which are shown the two essential changes produced by this muscle (obliquity of the line of the lips and curve of the naso-labial furrow), which seems to us to show in a satisfactory manner the expression of grief in tears. We comprehend the[328] value of this drawing better by comparing it with Figure 102. We see that the changes produced by the muscle of grief (lip and naso-labial furrow) are precisely the reverse of those produced by the muscle of laughter (zygomaticus major), just as the two corresponding emotions are the reverse of each other. We remark also how slight is the distance which separates these two muscles, and how delicate are the shades of anatomical arrangement which separate them, so delicate that authors do not agree as to whether the muscle found between them, the lesser zygomatic muscle, when it exists, should be considered as associated with the great zygomatic or, as we think, with the common elevator of the nose and upper lip. Beyond doubt their anatomical relations should remind us, in the nature of the emotions and their expression, how small a distance there is between laughter and tears.
9th. The elevator of the nose and upper lip (levator labii superioris alæque nasi, muscle of sobbing, of weeping bitterly).—This muscle (13, Fig. 94, and 7, Fig. 88) arises above from the inner border of the orbit; it descends almost vertically to be inserted by some of its fibres into the wing of the nose, and by the majority into the upper lip, not far from its central portion.
It therefore raises the middle part of the lip, the labial commissure remaining fixed, and gives accordingly to each half of the line of the lips a direction oblique downwards and outwards (like the preceding muscle, but in a more characteristic manner); at the same time it dilates the nostril[329] by raising the wing of the nose; lastly, by the traction that it exercises vertically on the skin of the naso-labial furrow, it raises en masse the inner and upper part of this furrow and renders it straight, causing it to form a species of groove wherein the tears flow when they pour abundantly from the inner angle of the eyelids. These changes (see the atlas of Duchenne) give to the countenance the expression of grief with abundant tears, or of weeping bitterly.
The drawing of Figure 104 renders this expression to a certain degree, but it is difficult to realise it with the simple elements we use in these formulæ. We see that all the folds of the face converge towards the inner angle of the eye, or towards the point of attachment of this muscle.
10th. Transverse muscle of the nose (compressor naris, muscle of lasciviousness).—This muscle (12, Fig. 94, and 9, Fig. 88) is attached at its origin to the skin of the cheek on a level with the side of the nose, and is directed transversely forwards over the nose to join a thin aponeurosis which stretches over the bridge of the nose, and receives the insertions of these two muscles, and that of the pyramidalis nasi.
This aponeurosis, which covers the bridge of the nose, forms a fixed point towards which these muscles draw the skin of the cheek and nose, so as to mark on the lateral surface of the nose a series of vertical folds (perpendicular to the direction of the muscle).
Duchenne considered the change produced by these muscles to be characteristic of the expression of lasciviousness. Perhaps this muscle by itself is not[330] sufficiently expressive, but when its contraction accompanies that of certain other muscles, we find very clearly in the physiognomy the element of lewdness pointed out by Duchenne. In his atlas this author gives the photograph of a countenance in which he had produced contraction of the frontalis, the great zygomatic, and the compressor naris; a countenance of which the expression may be directly interpreted as that of an old man in whom the attention (frontalis muscle) is agreeably excited (great zygomatic) by a spectacle arousing lewd ideas (compressor naris); the face produced by Duchenne would be, for example, a study in physiognomy for the head of the old man in the classic subject of Susanna in the bath.
We have not attempted to represent by a drawing an unsatisfactory and perhaps doubtful idea of the expression of this muscle.
C.—Muscles of the lower part of the face.
11th. Orbicularis muscle of the lips (orbicularis oris).—In the substance of the lips, as in the eyelids, a muscle is found, the fibres of which surround the orifice of the mouth—the orbicularis oris (19, Fig. 94, and 15, Fig. 88). This muscle principally possesses functions not primarily pertaining to expression, but to the various uses of the lips—prehension of food, mastication, speech, suction, etc.; the part it takes in physiognomy, although of importance, is secondary to these elemental functions. As in the orbicular muscle of the eyelids, we distinguish in it internal fibres corresponding to the free border of the lips and external[331] fibres more peripherally placed. If the inner fibres only contract (internal orbicular) they close the mouth, and, diminishing the size of the orifice, cause the red surfaces of the lips to be brought closely together in their whole extent. If the outer fibres (external orbicular) contract only, they project the lips forwards and render their surfaces prominent and rounded, as in the expression of pouting or in kissing.
We need not dwell at length on the muscle which constitutes the fleshy layer of the cheeks and forms the lateral walls of the cavity of the mouth. This muscle, called the buccinator (buccinare, to play the trumpet), is a thin sheet of muscle (21, Fig. 94) lining the hollow of the cheek in front of the line of the masseter. It is separated from that muscle posteriorly by a pad of fat (the remains of a suctorial pad), which in the infant is an important aid in suckling, and may be seen projecting into the side of the mouth. It takes a part in movements associated with the actions of the tongue and lips; it plays an important part in mastication by bringing beneath the crown of the teeth the food which passes outside the alveolar arches. It also aids in the articulation of sounds (speech) and in whistling and the playing of wind instruments (whence its name of buccinator), for it is the contraction of this muscle that expels from the mouth the air which inflates the cheeks. By its insertion into the angle of the mouth, where its fibres decussate with those of the orbicularis muscle, the buccinator is able to some extent to assist in the retraction of the mouth, as in grinning or snarling.
12th. The depressor of the angle of the mouth[332] (depressor anguli oris, muscle of contempt).—This muscle belongs to the lower lip. It forms (22, Fig. 94, and 16, Fig. 88) a triangular layer, of which the base is attached to the lower jaw, external to the symphysis of the chin, and from this origin its fibres converge towards the angle of the mouth, where, by its apex, it is inserted into the deep surface of the skin.
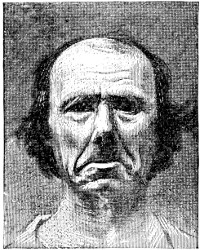
Fig. 105.
Triangular Muscle of the Lips (expression of discontent, of contempt).
This muscle depresses the labial commissure, and therefore renders the line of the lips oblique in a direction downwards and outwards; again, it draws downwards the lower extremity of the naso-labial furrow so as to render this furrow almost straight, except at its lower end, which describes a slight curve embracing the labial commissure.
The expression produced by a slight contraction of this muscle is that of sadness; marked contraction produces the expression of contempt. We have already seen (page 319) that a partial closing of the eyelids usually helps to complete the expression of contempt. Two other movements assist in this expression—a contraction of the common elevator of the nose and upper lip, raising the ala of the nose[333] and curling the lip upwards; and a movement of the head to the opposite side. All these movements may have, as Darwin pointed out, a rational physical basis—the expression of the mouth implying a disagreeable taste, the uplifting of the nose an unpleasant smell, and the aversion of the head a disgusting sight.
Fig. 106.
Diagram representation of the expression of discontent, of contempt.
Figure 105, copied from Duchenne, renders well, by the contraction only of the two triangular muscles of the lips, the expression of discontent and scorn. The depression of the angles of the mouth is characteristic, and the naso-labial furrow, very marked in the subject under experiment, is greatly changed in its direction and in the form of its inferior extremity, according to the mechanism that we have explained.
Lastly, the drawing of Figure 106 gives, so to speak, a diagrammatic formula of contempt by means of the form of the inferior part of the naso-labial furrow, and the concentric folds which it produces below the angle of the mouth.
13th. The depressor of the lower lip (quadratus menti: depressor labii inferioris, muscle of disgust).—This muscle (23, Fig. 94, and 17, Fig. 88), partly hidden by the depressor anguli oris, arises from the anterior part of the body of the lower jaw; from this origin the fibres ascend obliquely upwards and inwards to be inserted into the whole length of the lower lip.
[334]
This muscle’s action is to depress the lower lip, turning it outwards more or less strongly, so as to produce the grimace characteristic of a person who, having introduced into the cavity of the mouth a morsel of food which he does not find to his taste, rejects it forcibly, forming a species of groove with the lower lip turned outwards; if the contraction is less energetic the physiognomy expresses disgust.
We must refer to the atlas of Duchenne for the reproduction of this expression, always more or less rude, and have not attempted a drawing with a simple line as an indication of the labial fissure.
14th. Platysma muscle of the neck (platysma myoides).—In each lateral half of the anterior surface of the neck is a thin muscular sheet situated beneath the skin (25, Fig. 94, and 25, Fig. 74, page 217). This platysma muscle is attached below to the upper part of the chest, from which origin its fibres are directed obliquely upwards and forwards towards the lower jaw, to be inserted into the edge of the jaw, and the skin of the chin, of the lower lip, and the commissure of the lips; the more superior fibres sweep forwards in a horizontal direction across the cheek towards the labial commissure, and constitute the risorius muscle of Santorini (20, Fig. 94).
The platysma, which is not of itself essentially a muscle of expression, adds its contraction to that of various muscles of the face, so as to give to the corresponding expression a character of terrible energy; the risorius muscle does not therefore produce the expression of laughter (of gaiety), but only that of grinning, of forced laughter, threatening or sneering. The platysma in all these cases acts by depressing the[335] lower jaw, slightly opening the mouth, and drawing the labial commissure downwards; it marks at the same time a series of transverse folds on the skin of the neck. These elements are capable of giving to the physiognomy a terrible character, which Leonardo da Vinci has well observed, in his chapter on the mode of representing a person in a state of violent anger, where he says, “it makes the sides of the mouth into a bow, the neck thick and swollen, and marked with wrinkles in front.”
If the characteristic changes produced by the contraction of the platysma of the neck occur along with the contraction of the frontalis muscle, the countenance, as shown in Duchenne’s series of photographs, takes on an expression of attention and astonishment such as might be produced by a terrible spectacle. Associated with the contraction of the superciliary muscle, the expression becomes that of acute pain, as, for example, in a wretch under torture, or a victim torn by a beast of prey. If the contraction of the pyramidalis nasi is accompanied by that of the platysma we have the expression of a savage and barbarous threat.
General considerations.—Associations and combinations.—From the enumeration we have made of the facial muscles from the forehead to the neck, we must perceive that among these muscles there are some which are by themselves completely expressive (e.g., the frontal, superciliary, and great zygomatic), and others which are expressive only in a complementary sense, or intended only to complete or change an expression produced by another muscle (such are the palpebral portion[336] of the orbicularis of the eyelids, and the platysma of the neck), and lastly, others which are almost non-expressive, but yet associated with the true muscles of the expression (e.g. the buccinator). But we have not space here to dwell on these classifications.
A more important question is that of the association of the action of various muscles, and especially of the muscles which are completely expressive by themselves. The expression peculiar to each of these muscles is, so to speak, one of the syllables or words of the language of physiognomy, but, like every other language, physiognomy associates these syllables and words to arrive at its expressions. Now experience shows that usually the associations and combinations are composed of few elements. Usually two suffice; three muscles are sometimes in play simultaneously, hardly ever four.
Again, if we endeavour to realise these combinations theoretically by supposing the contractions of two muscles associated at random, we soon perceive that among the combinations some are easy and ordinary, and this is on account of the nature of emotions which we suppose associated, and the mechanism of the corresponding muscles, while others are impossible for the same reason.
The following is an example of easy combination related at the same time to the emotions and also to the muscular mechanism—viz., the combination of the contraction of the frontalis and of the great zygomatic muscles, as expressive of attention and laughter. On the one hand, attention[337] (frontalis) might be excited by a spectacle which provokes laughter (zygomatic); on the other hand, the frontal muscle and the great zygomatic being situated the one in the forehead and the other in the cheek, acting, one on the eyebrow, the other on the lips, the mechanism of one is independent of that of the other; this, however, from an anatomical point of view, does not prevent the two contracting simultaneously, exactly as the biceps might contract in order to flex the forearm, at the same time that the common extensor of the fingers extends the digital phalanges.
On the other hand, as impossible combinations discordant both to sentiment and muscular mechanism, we may, for example, consider the simultaneous contraction of the frontalis and the superior orbital portion of the orbicularis muscles of the eyelids. The first muscle expresses attention, the second reflection, or two opposite states of the mind, which cannot at the same time be open to external phenomena, and meditating on internal analyses. Again, the first muscle raises, the second depresses the eyebrow, which cannot be at the same time drawn in two opposite directions; just as, to take an example from the muscles of the limbs, the forearm cannot be at the same time flexed by the action of the biceps and extended by that of the triceps.
By submitting them to the same analysis we see that nothing is easier or more concordant to their mechanism and to the emotions than the simultaneous contraction of the frontalis and the depressor anguli oris (attention and contempt), of the superciliary[338] and the depressor labii inferioris (pain and disgust), the pyramidalis and the common elevator of the nose and upper lip (menace and sorrow), etc. On the contrary, for the same double series of reasons we find impossible and discordant associations, such as those of the great zygomatic and the depressor labii inferioris (gaiety and disgust), the pyramidalis and the superciliary (menace and pain), and of the common elevator of the nose and upper lip and the great zygomatic (sorrow and laughter).
There are, however, combinations which at first sight appear discordant to the nature of the passions, but which are found, notwithstanding, not to have any obstacle to their realisation in the mechanism of the countenance. We take, for example, the superciliary and the great zygomatic: one expresses pain, the other laughter—two expressions of an opposite nature; however, as these muscles correspond, one belonging to the head of the eyebrow, the other to the labial commissure, they can act without one counteracting the other, and we may well understand their simultaneous contraction. Now on reflection we find that this association, anatomically possible, is often realised, notwithstanding the apparent incompatibility of the corresponding passions. In the midst of violent physical pain, which causes the involuntary and irresistible contraction of the superciliary, a serene and powerful will finds still the energy to smile. In order to find the realisation in a work of art it is sufficient to study the expression of the countenance of Seneca in the painting by Giordano. A similar example is offered by that of a young woman who has become a mother, and who, though still quivering[339] with the pain of childbirth (superciliary muscle), is divided betwixt the physical pain and the mental joy of seeing the infant to whom she has given birth and at whom she smiles (great zygomatic muscle).
These latter examples show that the anatomical conditions take the lead up to a certain point of those conditions which result from the nature of the emotions, and that a combination of expressions is possible only when it can be realised by the action of the facial muscles.
We will finish here these short studies of the anatomy of the face, happy if we have been successful in showing the artist that in the movements of the face there is neither fancy, caprice, nor inspiration, but that all is subject to exact and precise rules which are the orthography of the language of physiognomy, and that the possible combinations are both large and varied, so that the artist can preserve his liberty of action while conforming to these rules, as the poet observes those of grammar without being on that account embarrassed in the scope of his genius.
[341]

A
B
C
D
E
F
G
H
I
J
K
L
M
N
O
P
Q
R
S
T
U
V
W
X
Y
 -shaped Ligament of Bigelow,
119
-shaped Ligament of Bigelow,
119Z
PRINTED BY CASSELL AND COMPANY, LIMITED, LA BELLE SAUVAGE, LONDON, E.C.4 15719
[1] P. N. Gerdy: “Anatomy of the Forms of the Human Body for Painting, Sculpture, and Surgery.” Paris, 1829.
[2] It is not always thus abroad. Thus in Germany there is the work of E. Harless (“Lehrbuch der Plastischen Anatomie für Akademische Anstalten.” Stuttgart, 1876: 2nd edit.).
[3] We must look for other reasons than ignorance or indifference to explain the fixed scapulæ in pre-Phidian sculpture, or the exaggerated forms given to the extensor brevis of the foot and other muscles. This qualification is necessary to this general statement.—Ed.
[4] See Ludwig Choulant. Gesichte und Bibliographie des Anatomischen Abbildungen. Leipzig: 1852. (A very curious work wherein is found much information respecting the connection of anatomy with the plastic arts.)
[5] Seroux d’Agincourt. History of Art by its Monuments. Paris: 1811. Vol. i., p. 177.
[6] Pierre Camper. “Dissertations sur les différences rúlles que présentent les traits du visage chez les hommes de différents pays et de différent âges.” (Œuvres posthumes. Paris, 1786.)
[7] See especially; Conférences sur l’expression des differents charactères des passions, Paris, 1667. (These essays have been reprinted in the edition of Lavater, by Moreau. Vol. ix., 1820.)
[8] The Anatomy and Physiology of Expression (3rd edition, 1884, published after the death of Sir Charles Bell, and containing his last corrections.)
[9] The edition to consult is that issued in 1820, in ten volumes, by Moreau.
[10] Charles Darwin. The Expression of the Emotions in Man and in Animals.
[11] Albert Lemoine: De la Physionomie et de la Parole. Paris, 1865. Pierre Gratiolet: De la Physionomie et des Mouvements d’Expression. Paris, 1865. Piderit: Wissenschaftliches System der Mimik und Physiognomik. 1867.
Transcriber’s Notes:
1. Obvious printers’, punctuation and spelling errors have been
corrected silently.
2. Some hyphenated and non-hyphenated versions of the same words have
been retained as in the original.