*** START OF THE PROJECT GUTENBERG EBOOK 48341 ***
[Pg 1]
WAR DEPARTMENT :: OFFICE OF THE SURGEON GENERAL
BULLETIN No. 9
OCTOBER, 1915
GUNSHOT ROENTGENOGRAMS
A COLLECTION OF ROENTGENOGRAMS TAKEN IN CONSTANTINOPLE
DURING THE TURKO-BALKAN WAR, 1912-1913, ILLUSTRATING
SOME GUNSHOT WOUNDS IN THE TURKISH ARMY
BY
CLYDE S. FORD
Major, Medical Corps
PUBLISHED BY AUTHORITY OF THE ACT OF
CONGRESS APPROVED MARCH 3, 1915, AND WITH THE APPROVAL OF THE SECRETARY OF
WAR, FOR THE INFORMATION OF
MEDICAL OFFICERS
WASHINGTON
GOVERNMENT PRINTING OFFICE
1916
[Pg 2]
[Pg 3]
TABLE OF ILLUSTRATIONS.
RIFLE WOUNDS. |
| Plate |
Page. |
HEAD. |
| 1. |
Gunshot fracture, skull, lodgment of missile |
12 |
| 2. |
Gunshot fracture, head, lodgment of missile |
14 |
| 3. |
Gunshot fracture, lower jaw, ramus |
16 |
| 4. |
Gunshot fracture, lower jaw, ramus |
18 |
| 5. |
Gunshot fracture, lower jaw, body |
20 |
SPINAL REGION. |
| 6. |
Gunshot wound, spinal region, lodgment of missile |
22 |
| 7. |
Gunshot wound, spinal region, lodgment of missile |
24 |
UPPER EXTREMITY. |
| 8. |
Gunshot fracture, humerus |
26 |
| 9. |
Gunshot fracture, humerus, lodgment of missile |
28 |
| 10. |
Gunshot fracture, humerus, lodgment of missile |
30 |
| 11. |
Gunshot fracture, humerus |
32 |
| 12. |
Gunshot fracture, humerus |
34 |
| 13. |
Gunshot fracture, humerus |
36 |
| 14. |
Gunshot fracture, humerus, lodgment of missile |
38 |
| 15. |
Gunshot fracture, humerus, external condyle |
40 |
| 16. |
Gunshot fracture (a) humerus, (b) ulna |
42 |
| 17. |
Gunshot fracture, elbow |
44 |
| 18. |
Gunshot fracture, elbow |
46 |
| 19. |
Gunshot fracture, elbow |
48 |
| 20. |
Gunshot fracture, elbow |
50 |
| 21. |
Gunshot fracture, radius and ulna |
52 |
| 22. |
Gunshot fracture, radius and ulna |
54 |
| 23. |
Gunshot fracture, radius and ulna |
56 |
| 24. |
Gunshot fracture, radius and ulna |
58 |
| 25. |
Gunshot fracture, radius |
60 |
| 26. |
Gunshot fracture, radius |
62 |
| 27. |
Gunshot fracture, radius |
64 |
| 28. |
Gunshot fracture, radius |
66 |
| 29. |
Gunshot fracture, radius, lower end |
68 |
| 30. |
Gunshot fracture, radius, lower end |
70 |
| 31. |
Gunshot fracture, radius, lower end |
72 |
| 32. |
Gunshot fracture, ulna |
74 |
| 33. |
Gunshot fracture, ulna |
76 |
| 34. |
Gunshot fracture, ulna |
78 |
| 35. |
Gunshot fracture, ulna |
80 |
| 36. |
Gunshot fracture, ulna |
82 |
| 37. |
Gunshot fracture, ulna |
84 |
| 38. |
Gunshot fracture, ulna |
86 |
| 39.[Pg 4] |
Gunshot fracture, ulna |
88 |
| 40. |
Gunshot fracture, ulna |
90 |
| 41. |
Gunshot fracture, wrist |
92 |
| 42. |
Gunshot fracture, wrist |
94 |
| 43. |
Gunshot fracture, metacarpus |
96 |
| 44. |
Gunshot fracture, phalanx |
98 |
CHEST. |
| 45. |
Gunshot wound, chest |
100 |
PELVIS. |
| 46. |
Gunshot wound, pelvis |
102 |
LOWER EXTREMITY. |
| 47. |
Gunshot wound, gluteal region |
104 |
| 48. |
Gunshot wound, thigh |
106 |
| 49. |
Gunshot wound, thigh |
108 |
| 50. |
Gunshot wound, thigh |
110 |
| 51. |
Gunshot wound, thigh |
112 |
| 52. |
Gunshot fracture, femur |
114 |
| 53. |
Gunshot fracture, femur |
116 |
| 54. |
Gunshot fracture, femur |
118 |
| 55. |
Gunshot fracture, femur |
120 |
| 56. |
Gunshot fracture, femur |
122 |
| 57. |
Gunshot fracture, femur |
124 |
| 58. |
Gunshot fracture, femur |
126 |
| 59. |
Gunshot wound, knee |
128 |
| 60. |
Gunshot fracture, tibia and fibula |
130 |
| 61. |
Gunshot fracture, tibia and fibula |
132 |
| 62. |
Gunshot fracture, tibia |
134 |
| 63. |
Gunshot fracture, tibia |
136 |
| 64. |
Gunshot fracture, tibia |
138 |
| 65. |
Gunshot fracture, tibia |
140 |
| 66. |
Gunshot fracture, tibia |
142 |
| 67. |
Gunshot fracture, tibia |
144 |
| 68. |
Gunshot fracture, tibia |
146 |
| 69. |
Gunshot fracture, tibia |
148 |
| 70. |
Gunshot fracture, tibia |
150 |
| 71. |
Gunshot fracture, fibula |
152 |
| 72. |
Gunshot fracture, ankle |
154 |
| 73. |
Gunshot wound, heel |
156 |
| 74. |
Gunshot wound, heel |
158 |
SHRAPNEL WOUNDS. |
HEAD. |
| 75. |
Gunshot fracture, vertex |
160 |
| 76. |
Gunshot fracture, vertex |
162 |
| 77. |
Gunshot fracture, zygoma |
164 |
| 78. |
Gunshot fracture, mastoid process |
166 |
| 79. |
Gunshot fracture, maxilla |
168 |
| 80. |
Gunshot fracture, supra-orbital |
170 |
| 81. |
Gunshot fracture, supra-orbital |
172 |
| 82.[Pg 5] |
Gunshot wound, shoulder |
174 |
| 83. |
Gunshot wound, shoulder |
176 |
| 84. |
Gunshot wound, shoulder |
178 |
| 85. |
Gunshot wound, shoulder |
180 |
| 86. |
Gunshot fracture, clavicle |
182 |
| 87. |
Gunshot fracture, humerus |
184 |
| 88. |
Gunshot fracture, humerus |
186 |
| 89. |
Gunshot fracture, humerus |
188 |
| 90. |
Gunshot fracture, humerus |
190 |
| 91. |
Gunshot fracture, humerus |
192 |
| 92. |
Gunshot fracture, humerus |
194 |
| 93. |
Gunshot fracture, humerus |
196 |
| 94. |
Gunshot fracture, humerus |
198 |
| 95. |
Gunshot fracture, humerus |
200 |
| 96. |
Gunshot fracture, humerus and elbow |
202 |
| 97. |
Gunshot fracture, elbow |
204 |
| 98. |
Gunshot fracture, elbow |
206 |
| 99. |
Gunshot fracture, elbow |
208 |
| 100. |
Gunshot fracture, elbow |
210 |
| 101. |
Gunshot fracture, radius and ulna |
212 |
| 102. |
Gunshot fracture, radius |
214 |
| 103. |
Gunshot fracture, radius |
216 |
| 104. |
Gunshot fracture, ulna |
218 |
| 105. |
Gunshot fracture, metacarpus |
220 |
| 106. |
Gunshot fracture, metacarpus |
222 |
| 107. |
Gunshot fracture, metacarpus |
224 |
| 108. |
Gunshot wound, hand |
226 |
| 109. |
Gunshot wound, multiple, hand and forearm |
228 |
CHEST. |
| 110. |
Gunshot wound, chest |
230 |
| 111. |
Gunshot wound, chest |
232 |
| 112. |
Gunshot wound, chest |
234 |
| 113. |
Gunshot wound, chest |
236 |
| 114. |
Gunshot wound, chest |
238 |
PELVIS. |
| 115. |
Gunshot fracture, ilium |
240 |
LOWER EXTREMITY. |
| 116. |
Gunshot wound, thigh |
242 |
| 117. |
Gunshot wound, thigh |
244 |
| 118. |
Gunshot wound, thigh |
246 |
| 119. |
Gunshot wound, femur |
248 |
| 120. |
Gunshot wound, femur |
250 |
| 121. |
Gunshot wound, femur |
252 |
| 122. |
Gunshot wound, femur |
254 |
| 123. |
Gunshot wound, femur |
256 |
| 124. |
Gunshot wound, femur |
258 |
| 125. |
Gunshot wound, femur |
260 |
| 126. |
Gunshot wound, femur |
262 |
| 127. |
Gunshot wound, femur |
264 |
| 128.[Pg 6] |
Gunshot wound, knee |
266 |
| 129. |
Gunshot wound, knee |
268 |
| 130. |
Gunshot wound, knee |
270 |
| 131. |
Gunshot wound, knee |
272 |
| 132. |
Gunshot wound, knee |
274 |
| 133. |
Gunshot wound, knee |
276 |
| 134. |
Gunshot wound, knee |
278 |
| 135. |
Gunshot wound, leg |
280 |
| 136. |
Gunshot wound, leg |
282 |
| 137. |
Gunshot fracture, tibia and fibula |
284 |
| 138. |
Gunshot fracture, tibia and fibula |
286 |
| 139. |
Gunshot fracture, tibia and fibula |
288 |
| 140. |
Gunshot fracture, tibia and fibula |
290 |
| 141. |
Gunshot fracture, tibia |
292 |
| 142. |
Gunshot fracture, fibula |
294 |
| 143. |
Gunshot fracture, fibula |
296 |
| 144. |
Gunshot fracture, fibula |
298 |
| 145. |
Gunshot fracture, fibula |
300 |
| 146. |
Gunshot fracture, fibula |
302 |
| 147. |
Gunshot fracture, fibula |
304 |
| 148. |
Gunshot fracture, “Pott’s” |
306 |
| 149. |
Gunshot wound, multiple, leg |
308 |
| 150. |
Gunshot fracture, astragalus |
310 |
| 151. |
Gunshot fracture, calcaneus |
312 |
| 152. |
Gunshot wound, heel |
314 |
| 153. |
Gunshot wound, heel |
316 |
| 154. |
Gunshot wound, foot |
318 |
| 155. |
Gunshot wound, foot |
320 |
| 156. |
Gunshot wound, foot, multiple |
322 |
OPERATIVE INTERFERENCE, GUNSHOT WOUNDS. |
157. |
Gunshot fracture, humerus |
324 |
| 158. |
Gunshot fracture, ulna |
326 |
| 159. |
Gunshot fracture, radius and ulna |
328 |
| 160. |
Gunshot fracture, tibia and fibula |
330 |
| 161. |
Amputation, knee |
332 |
| 162. |
Excision, head of humerus |
334
[Pg 7] |
INTRODUCTION
These roentgenograms are not presented as exhibiting a state of
perfection in the art or method by which they were produced, although
they show the results of some of the best and most modern apparatus of
Europe employed in the hands of very skillful operators. Some plates
are included which are indistinct and generally so unsatisfactory from
a technical viewpoint as to be of little interest, if all of them
were not intended to show the general character of the diagnostic
assistance that the roentgenologist rendered the military surgeon in
the base hospitals of Constantinople during the Turko-Balkan War.
The collection of these plates resulted from a systematic visiting
of the hospitals of Constantinople in the winter of 1912-13, during
the course of the first Balkan War, and including all of the military
hospitals of the military zone, with the incidental purpose of
selecting from the roentgenographic plates, which had been prepared
wherever apparatus was installed, such examples of the roentgenography
of gunshot wounds as might show characteristic lesions without
relation to detailed clinical record.
More than 1,500 plates were examined, and from them more than 200 were
selected as exhibiting some lesion that seemed to be characteristic of
some form of gunshot wound, even though the case history could not be
obtained. From these selected plates photographic prints were made. As
some of these photographs displayed somewhat similar conditions, only
162 of them are herewith produced.
As the photographic and reproduction processes have transferred the
rights and lefts of the original negatives several times, the plates
as they appear here are interpreted, for right and left, as though
they were the original photographic plates, which are physically
positive although they are chemically negative; i. e., the right and
left sides of the page should be read as the right and left sides
anatomically. If this distinction be not observed, some confusion may
arise from the habit of roentgenologists in regarding a roentgenograph
as a positive print of a negative plate.
[Pg 8]
I regret that I can not here acknowledge by name my appreciation
and gratitude to the roentgenologists of all hospitals from which
I secured permission to reproduce their plates. To Prof. Wieting
Pasha, the commandant of Gulhané Hospital; to Dr. Ishmael Bey,
the roentgenologist of the Hamedian Hospital; to Dr. Englander,
the roentgenologist of the Austrian Hospital—to all of whom I am
particularly indebted—I wish to acknowledge my thanks.
Projectiles.—The projectiles which figure in the illustrations
were those employed by the nations at war. They are derived (1) from
the Turkish pointed bullet weighing approximately 15.0 grams—it is
fired from the German Mauser and has all the ballistic values of the
projectile from this weapon; (2) the Bulgarian bullet, blunt nosed
or ogival headed and the same as the steel-jacketed bullet of the
Austrian Mannlicher; (3) shrapnel balls and fragments of the shrapnel,
and (4) fragments of steel shells from field artillery.
During the evolution of reduced caliber rifles experiments were made
on cadavers at different ranges. In the published writings of these
workers a great deal was said on the subject of highly destructive
effects which are pretty generally described as explosive effects.
The experimenters were careful to explain that these exaggerated and
highly destructive effects were only seen when firing into cadavers
at close ranges and when the bullet traveling at a maximum velocity
happened to collide with resistant structures like the compact
substance of bone in the diaphysis of the long bones, such as the
femur, tibia, humerus, etc., and the head, as well as organs loaded
with fluid or semifluid masses like the stomach, urinary bladder,
and intestines. In other tissues offering but little resistance like
lung tissues, soft parts generally, and epiphyseal ends of bone,
the wounds inflicted were considered humane in character. Attention
should be called to the infrequency of wounds showing explosive
effects by the rifles of reduced caliber employed in the Turko-Balkan
and Spanish-American wars. The same thing may be said of the
Turko-Italian, Anglo-Boer, and Russo-Japanese wars, all of which were
fought with the new armament.
The reason for the infrequency of the explosive effects in these
wars is due to the fact that the battles were fought in the open at
the ordinary battle ranges beyond the zone of explosive effects.
This fact is all the more emphasized in the present world war, in
which the rifle fire is employed principally in trench warfare at
near-by ranges, and where all the wounds which involve the resistant
structures of the body show the characteristic features usually
described as those of explosive effects.
[Pg 9]
In describing the plates the terms used in connection with range are
as follows:
(1) Close range, from 0 to 100 yards.
(2) Short range, from 100 to 500 yards.
(3) Mid range, from 500 to 1,000 yards.
(4) Long range, from 1,000 to 2,000 yards.
The wound effects of the modern military rifle bullet at various
ranges are usually classified as follows:
(1) Explosive range, from 0 to 500 yards.
(2) Perforating range, from 500 to 1,500 yards.
(3) Penetrating range, from 1,500 to 2,500 yards.
The difficulty in adhering strictly to the last table as far as the
characteristic features of wounds are concerned is this: In battle the
chances of ricochetting of bullets is said to be in the proportion
of one to three. Naturally, the moment a bullet ricochets it loses
more or less of its remaining velocity. The destructive lesion to
be expected from a given shot at a given range against a certain
resistant structure can not be depended upon to occur as it will when
the shot is made with scientific accuracy in the shooting gallery
against cadavers.
Trajectory, or the curved line of flight of a projectile, has
nothing to do with its wound-producing quality, except to increase the
wound-producing frequency when it flattens and approaches the straight
line of sight, because it will then pass through a greater portion of
the space between the gun and the target, which may be occupied by
men, without going over their heads. The greater the velocity, the
flatter the trajectory becomes.
The American, German, and Turkish rifles, with about the same
trajectory, can be fired through a tube 24 inches in diameter at a
range of 500 yards, and the vertical rise of the curve of flight would
not hit the top of the tube. But where the range is increased to 1,000
yards it would be necessary to enlarge the tube to a tunnel, 15 feet
in diameter, in order to fire the bullet through it without striking
the top in its greatly increased curve in flight.
Velocity is the principal factor of the wound-producing power of
the small-caliber bullet, although the latter quality is definitely
related to the cross-sectional area and weight as well as to the hard
metal jacket which preserves its form. The greater the velocity of any
particular bullet the more serious is its wound.
Energy, as the resultant of the components of weight and
velocity, represents the real damaging quality, striking
force, or “punch” of a projectile, with a variation in wound effect as
the energy is distributed over the surface of the body, through the
[Pg 10]
cross-sectional area and the form of the point of the projectile, and
the elements of construction which a affect the preservation of its
shape. As the energy is expressed in the formula,
E = WV2 ,
2g
it is evident that the increase or decrease of the
velocity factor gives greater variation than the increase of weight.
Range is important only as indicating the amount of remaining
energy which may be known to reside in the projectile at any stage
of its flight. Without reference to the ballistic condition (velocity,
weight, form, and construction, etc.) of a particular projectile,
range has no surgical significance. To the military surgeon,
however, it is a term of the greatest interest when these ballistic
conditions are known, as it gives him a very definite indication of
the remaining energy or the damaging effect of a projectile at the
different stages in its flight.
The remaining energy of the American “Springfield,” or German “S”
bullet, for instance, will pass it through the bodies of two men at
2,000 yards and an energy of 8 kilogram-meters, which remains at about
twice that distance, will cause a disabling wound.
Wound infections are more rare in campaign in the more sparsely
settled and rough countries with soldiers of the more primitive class,
simple domestic habits, and greater natural resistance.
Wound treatment should be primarily directed toward the control of
infection with only secondary regard for the correction of deformities
which should follow as a secondary measure after resolution is established.
All treatment should be based on principles applied in the following order:
(1) Life saving.
(2) Restoration of function.
(3) Economy of the patient.
Amputation should be very rare.
Conservation to a degree that seems to be beyond the
experience and conception of the civil surgeon should always be practiced, as
reiterated by Delorme, who says: “In order to avoid the excess of
operative measures which has been seen in recent wars I am urged to
enjoin all potential military surgeons to practice almost uniform conservation.”
[Pg 11]
Weight and muzzle velocity of several projectiles.
|
Weight. |
Velocity. |
| Projectile. |
Grams. |
Grains. |
Meters. |
Feet. |
| American (Springfield) |
9.07 | 150 |
800 | 2,700 |
| French |
12.8 | 197 |
701 | 2,301 |
| German |
10.0 | 154 |
860 | 2,821 |
| Austrian |
15.8 | 244 |
626 | 1,952 |
[Pg 12]
Rifle Wounds
HEAD.
Plate 1.
[Pg 13]
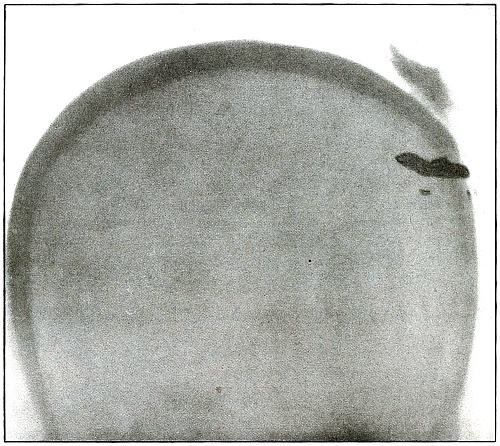
Rifle—Plate 1.
HEAD.
Gunshot Fracture of the Skull,
with Lodgment of the Missile.
The bullet in this case was so badly deformed by ricochet that
part of both core and jacket were lost. While the appearance of the
shadow seems to indicate a direct impact of the nose of the bullet,
the line of contact with the skull must have been tangential, with
some laceration of the scalp; otherwise a cursory examination of the
scalp wound would have revealed the slightly protruding end of the
bullet. The dark shadow above the projectile is due to material used
in dressing. The great thickening of the scalp in the region of the
wound shows a marked cellulitis. Small particles of the lead core of
the bullet can be seen about the wound.
In such cases there is often a marked infection of the scalp
without extension of infection to the cranial cavity, except from
neglect. This is a case, though apparently simple, in which the
radiograph was necessary for correct diagnosis without exploration.
The treatment in such cases is conservative, with removal of
the projectile and care of the superficial infection or subsequent complications.
[Pg 14]
Plate 2.

[Pg 15]
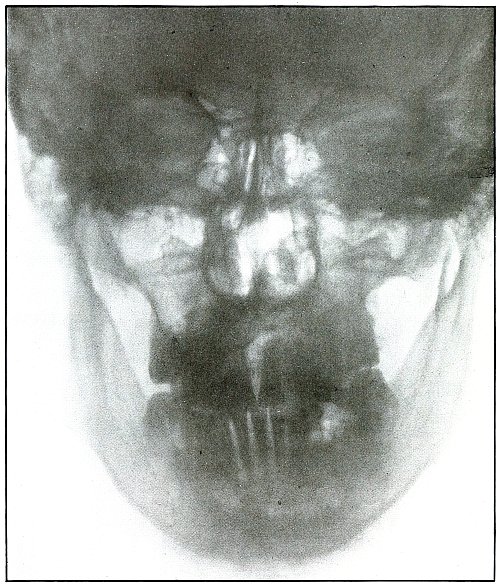
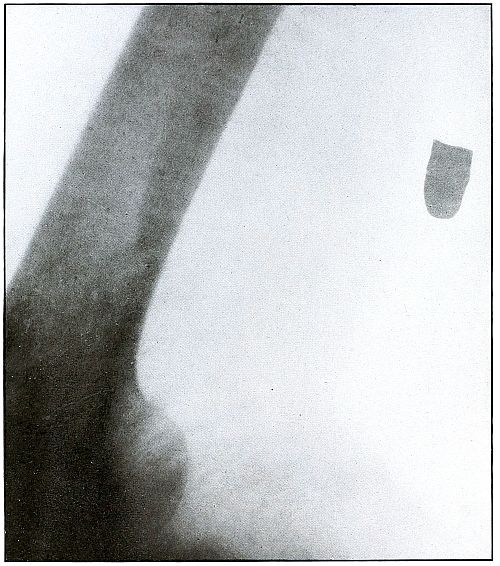
Rifle—Plate 2.
HEAD.
Gunshot Wound of the Head, with Lodgment of the Missile.
Wound of entrance, near outer canthus, with course through eyeball to
ethmoid body.
Wound of exit, none.
The Bulgarian Mannlicher bullet, shown half actual size on the plate,
must be inclined on its long axis, about 30° from the perpendicular,
to the plane of the plate.
The slight penetration of the missile and its normal character show
that, having struck no intervening object, it indicted the wound at
extreme range.
The treatment should meet the indication for removal of missiles in
all superficial or easily accessible locations and when they cause
reaction.
Results to be expected are favorable except for loss of the eye.
[Pg 16]
Plate 3.

[Pg 17]
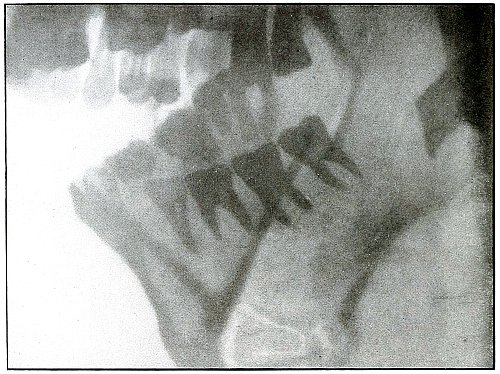
Rifle—Plate 3.
HEAD.
Gunshot Fracture of the Ramus of the Lower Jaw.
Wound of entrance, in the cheek behind the angle of the mouth.
Wound of exit, below the tip of the mastoid.
The course of the bullet was almost tangential to the ramus of the
jaw, anteroposteriorly. The slight fragmentation, which is hardly
more than a splitting of the bone, with little or no displacement,
indicates that the wound was made by a rifle bullet at moderate
velocity and at mid or long range.
Treatment is expectant.
Results are favorable.
[Pg 18]
Plate 4.
[Pg 19]
Rifle—Plate 4.
HEAD.
Gunshot Fracture of the Ramus of the Lower Jaw.
Wound of entrance, over the anterior border of the right ramus.
Wound of exit, beneath the lobe of the ear.
The wound was made by a rifle bullet with the velocity of long range,
because wounds of a shrapnel ball never show such slight injury
without lodgment or without marks of lead.
The damage of the bone was very slight, as only a superficial fragment
was chipped off. There were no signs of primary infection. Reaction
and periostitis suggested the radiograph after infection had rarefied
the fragment, shown but very faintly on the left side of the plate.
The postero-anterior skull radiograph was made with the face
superimposed upon the photographic plate.
Treatment, incision and drainage.
Results, good.
[Pg 20]
Plate 5.
[Pg 21]
Rifle—Plate 5.
HEAD.
Gunshot Fracture of the Body of Lower Jaw,
with Great Fragmentation and Displacement.
Wound of entrance, to the left side of the median line of the lower
jaw below the alveolar process, with course ranging downward and
backward.
Wound of exit, with extensive laceration, beneath lower border of the
bone.
The wound was caused by a rifle bullet at high velocity at or less
than mid range. The fragments are many and rather small, so that much
bone was lost through the wound of exit. This effect was produced by
the splitting due to the relative friability of the bone and to the
imparting of the momentum of the missile to the detached fragments,
which, together with the missile, effected the considerable laceration
of the wound of exit.
Treatment, difficult; guided by septic conditions and surgical means
available.
Results in such cases are favorable to life but topically unsatisfactory.
[Pg 22]
SPINAL REGION.
Plate 6.
[Pg 23]
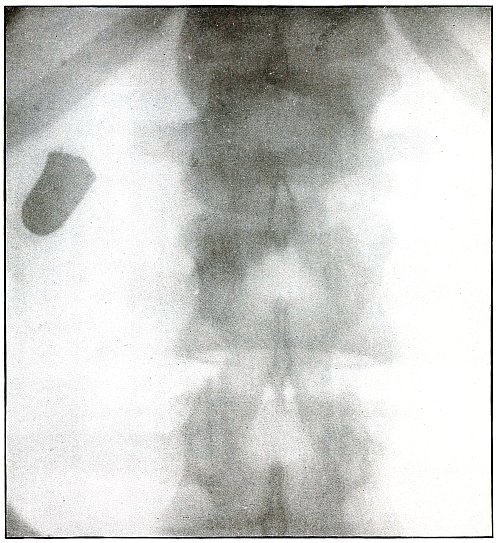
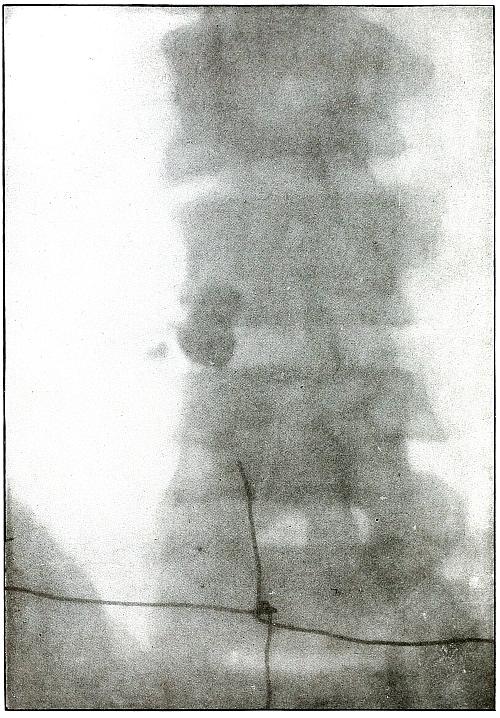
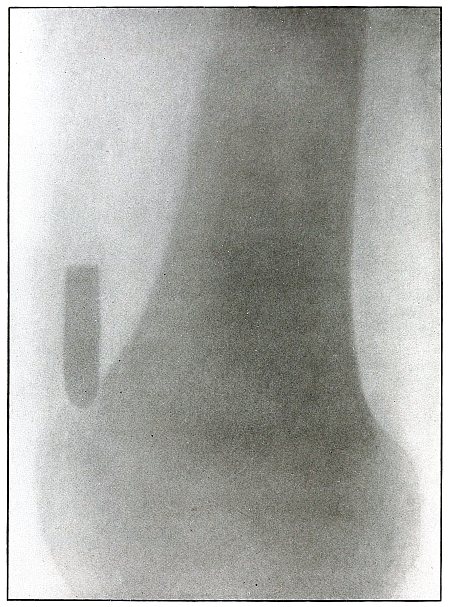
Rifle—Plate 6.
SPINAL REGION.
Gunshot Wound of the Spinal Region—
Lodgment
of the Missile in the Lumbar Muscles.
The bullet is lodged deep in the muscles of the back and not in the
abdomen, as determined by inspection of the plate.
(a) The shadow of the bullet is enlarged laterally, because, while
on the side of the body next to the plate and to the spine, it is at
some little distance from the plate, which accounts for the larger
diameter of the shadow; and it is shortened longitudinally, because
its long axis is inclined at an angle to the plate.
(b) The outline of the shadow is distinct, an evidence that
it is extra-abdominal, as otherwise its outline would be blurred by
the diaphragmatic movement of respiration imparted to the abdominal
viscera during the Röntgen exposure.
[Pg 24]
Plate 7.
[Pg 25]
Rifle—Plate 7.
SPINAL REGION.
Gunshot Wound of the Spinal Region,
with Lodgment of the Missile.
The bullet was either dum-dummed or unjacketed because its soft nose
mushroomed, striking the crest of the ilium, penetrated the lumbar
muscles, and struck the side body of the third lumbar vertebra without
producing fracture.
The exposure, as the spinous processes show, was made with the spine
next to the plate, and the slight shadow, somewhat larger than the
projectile—to judge the size from the undeformed diameter—shows
it to be anterior to the vertebra. The shadow is deep enough to indicate
the location fairly near to the plate, and, almost certainly, not in
the abdominal cavity, where the distance from the plate would have
made the shadow less dense and the movement of respiration probably
would have given it a blurred outline. The shadow of the localizing
cross gives a standard of density to be compared with the shadow of
the projectile in making the estimation.
The treatment is conservative; only pain, paralysis, impaired
function, or sepsis indicate interference.
[Pg 26]
UPPER EXTREMITY.
Plate 8.
[Pg 27]
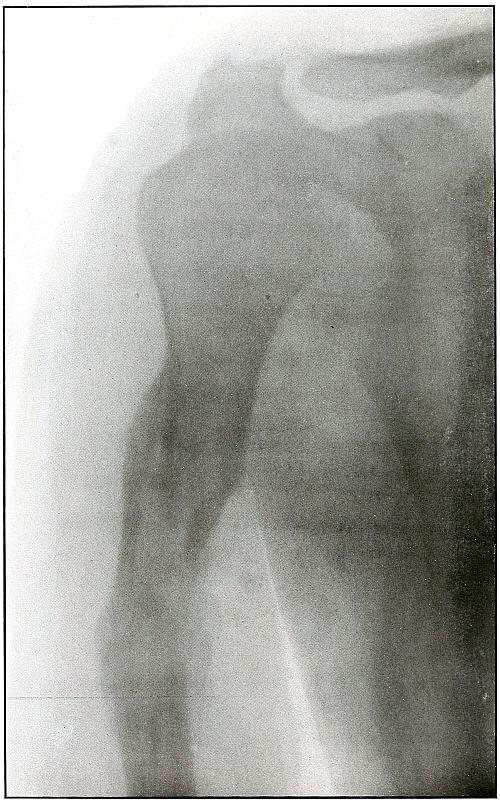
Rifle—Plate 8.
UPPER EXTREMITY.
Compound Fracture of the Humerus
in Advanced State of Repair with Callus Formation.
Wound of entrance, just above middle of anterior aspect of arm.
Wound of exit, about the same height, posteriorly.
The course of the missile was anteroposterior, with high velocity of
short range through the bone with a splitting effect, leaving a few
fragments, large and small, which were not much displaced and caused
but little deformity.
Wound was not infected. The absorption of smaller and the overlapping
of larger fragments caused some shortening.
Treatment, expectant.
Results, favorable.
[Pg 28]
Plate 9.
[Pg 29]
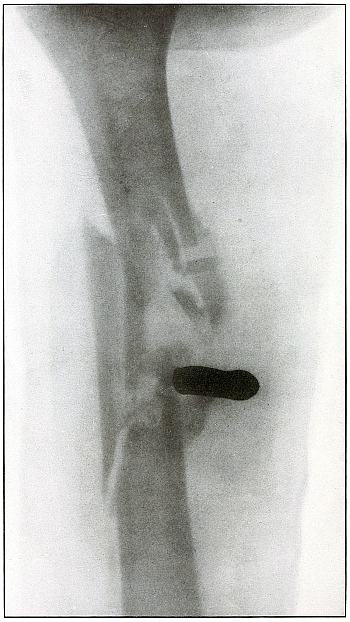
Rifle—Plate 9.
UPPER EXTREMITY.
Gunshot Fracture of the Right Humerus,
with Lodgment of the Missile.
Wound of entrance, antero-external aspect of upper third of arm.
Wound of exit, none.
The missile, deformed by ricochet, struck the bone with greatly
reduced velocity and without sufficient energy to perforate the bone
by which it was deflected slightly from its course and lodged in the arm.
This is something of the same effect that might have been caused by
a shrapnel ball, under the same ballistic conditions with a normal
shrapnel velocity giving about the same penetrating force.
The wound, without infection, is in the first week or two of repair,
before any callus has formed.
Treatment is expectant.
Results favorable.
[Pg 30]
Plate 10.
[Pg 31]
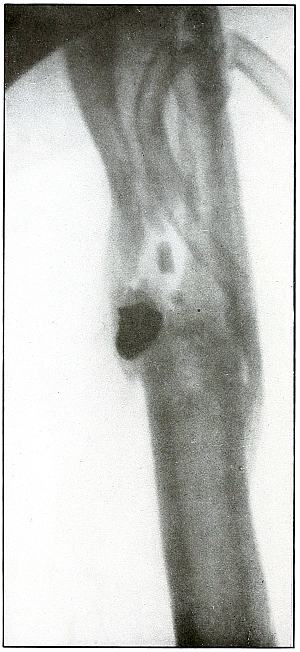
Rifle—Plate 10.
UPPER EXTREMITY.
Gunshot Fracture of the Left Humerus,
with Lodgment of the Missile.
Wound of entrance, anterior surface of upper third of the arm.
Wound of exit, none.
The shadow of the missile shows by its distinct outline and normal
diameter at the tip that the missile lies on the side near the plate;
the shortened length of the projectile indicates that the long axis
lay in an acute angle with a perpendicular to the plate.
The irregular outline of the base of the shadow and the fact of
lodgment shows that the missile was deformed and that it was
incidentally retarded in velocity by ricochet, so that its penetrating
force was not sufficient to carry it through the arm.
The fragments of bone are large and the wound is of the same character
as might have resulted from a shrapnel ball, for the normal ballistic
conditions of the latter simulate the conditions that produced the wound.
The drainage tubes seen in the plate indicate infection.
The conventional treatment in such cases is drainage and other
management of the infection without formal search for the projectile.
Results should be favorable.
[Pg 32]
Plate 11.
[Pg 33]
Rifle—Plate 11.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus.
Wound of entrance, anterior internal aspect of middle and upper third
of arm.
Wound of exit, opposite.
The missile has struck the side of the bone and pursued a course
through the shaft, so that a transverse fracture, as well as the
separation of several medium-sized fragments, resulted from the
splitting effect of the missile.
A larger missile, i. e., a shrapnel ball, with the same striking
energy could have been stopped by the bone, but a wider distribution
of the same energy carried by a larger cross section would have
produced larger fragments.
In this case the location of the shrapnel ball would furnish
unquestioned evidence; or, if a shrapnel ball had produced this
particular bone destruction, its path among the fragments would have
been marked by traces of lead. Two metal fragments indicate that the
lead core of the bullet was exposed.
The wound, not infected, was treated expectantly.
Result in such cases is favorable.
[Pg 34]
Plate 12.

[Pg 35]
Rifle—Plate 12.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus.
The course of the missile was anteroposterior through the middle of
the arm.
The ballistic conditions and lines of force applied to the bone
were somewhat, if not entirely, similar to those producing the
fracture shown in plate 11. The missile struck
the wall of the shaft without passing through the medullary canal, but
a secondary fragmentation of the two large fragments did not follow
except for the breaking of the tip of the distal fragment.
The range was long.
There was little deformity and no infection.
Plaster dressing was applied and the slight outline of callus
formation indicates the process of repair. The lack of contrast in
the shadow of the bone is due to the opacity of the plaster dressing
through which the Roentgen exposure was made.
Treatment in such cases is expectant.
Results should be uniformly good.
[Pg 36]
Plate 13.
[Pg 37]
Rifle—Plate 13.
UPPER EXTREMITY.
Gunshot Fracture of the Right Humerus,
with Lodgment of the Missile.
Wound of entrance, about middle of the anteriorinternal aspect of the arm.
Wound of exit, none.
The course of the missile was from without, downward and inward to a
point of lodgment above the internal condyle. The distinct outline and
normal size of the base of the bullet shows it to be near the plate,
with the internal condyle next to the plate in the exposure.
The bullet mushroomed when it struck the bone with a “soft nose,” in
which the lead was not protected by a tough metal jacket. It may have
been dum-dummed; it is remotely possible that the nose of the jacket
was split by ricochet, or it is more probable that it was of the
unjacketed variety.
The effect is identical with that of a shrapnel ball, striking with
its normal low velocity, which is about the same as that of the
missile in this wound.
The invariable characteristic of a shrapnel wound of a bone, namely,
the small particles of metal marking its course in contact with the
bone, is seen in this plate.
The treatment in such cases is expectant, with due regard to the
character of the infection, and without primary search for the missile.
The results are generally favorable.
[Pg 38]
Plate 14.
[Pg 39]
Rifle—Plate 14.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus,
with Lodgment of the Missile.
The missile was a fragment of a ricocheted rifle ball, with a part of
the lead core carried in a portion of the jacket. The course was from
before, backward, striking the humerus in lower third, and leaving
particles of lead along its trade.
The wound was only slightly infected. Several detached fragments of
bone have been removed.
The treatment in such cases is conservative, with management of the
infection and without formal search for the projectile.
The results in such cases are favorable with some shortening of the bone.
[Pg 40]
Plate 15.
[Pg 41]
Rifle—Plate 15.
UPPER EXTREMITY.
Gunshot Fracture of the External Condyle of the Left Humerus,
with Lodgment of the Missile.
Wound or entrance, internal and posterior aspect of the arm above the
internal condyle.
Wound of exit, none.
The bullet was greatly deformed by ricochet, with the loss of the
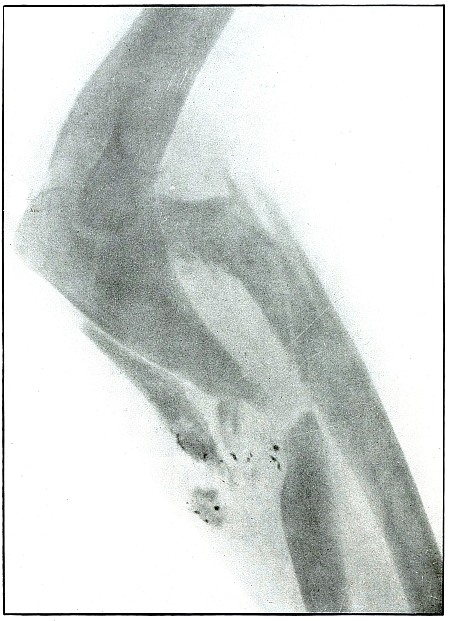
greater part or all of its jacket.
The line of contact of the unprotected lead with the bone is marked by
the same small fragments of lead almost invariably seen in shrapnel
wounds. The ballistic conditions in this case are quite similar to
those of a shrapnel wound, as the projectile has struck the bone
with low velocity. The very slight displacement of a single large
fragment from which the missile is slightly withdrawn indicates that
the striking energy was relatively low and that the elastic tissues,
stretching around the missile at its striking point, contracted after
its energy had been expended and then withdrew the missile from its
farthest point of advance.
The treatment in such cases warrants only the interference suggested
by infection and the interference of the missile with function.
The results expected are most favorable.
[Pg 42]
Plate 16.
[Pg 43]
Rifle—Plate 16.
UPPER EXTREMITY.
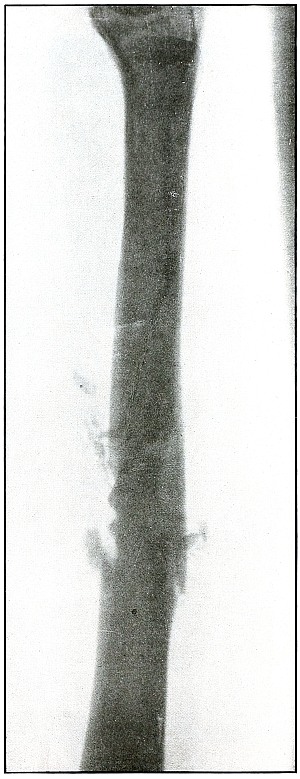
Gunshot Fracture of the Humerus.
The transverse course of the bullet, striking the posterior wall of
the shaft without entering the medullary canal, has fractured the bone
transversely, with a tendency toward splitting off a large fragment
from the distal fragment.
The bullet under these ballistic conditions of high velocity and not
distant range might have bored its way through the cancellous tissue
of the epiphysis of the same bone without any fractures.
Gunshot Fracture of the Ulna.
The transverse course of the bullet in striking the ulna at high
velocity and not distant range has shown a tendency to bore a hole
through the bone. A smaller bullet or a larger bone of the same
structure might easily have provided conditions to permit this effect.
The wounds of exit and entrance in each of these wounds presented
almost identically the same appearance.
The treatment in such cases is that of a simple fracture, as there is
almost always no infection in such wounds.
Results are favorable.
[Pg 44]
Plate 17.
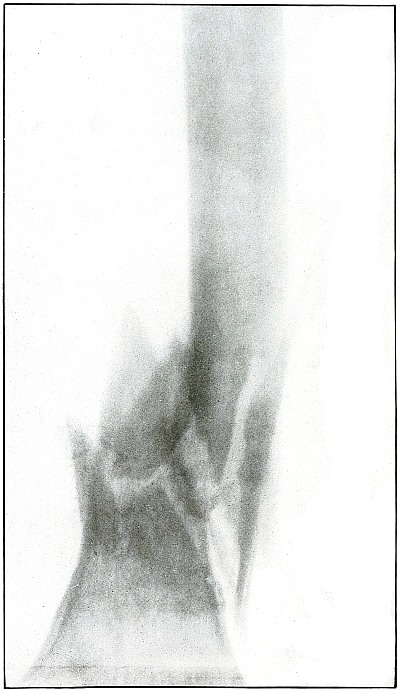
[Pg 45]
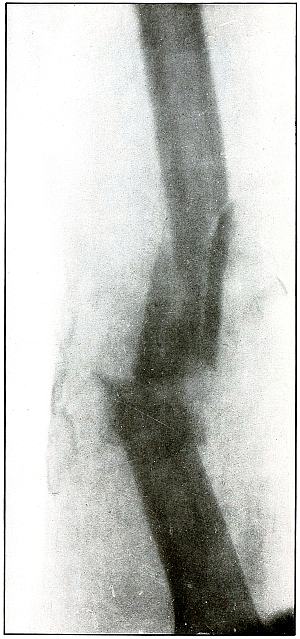
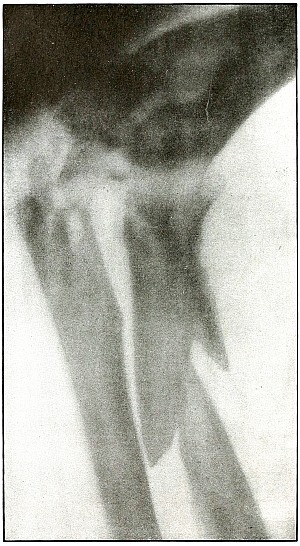
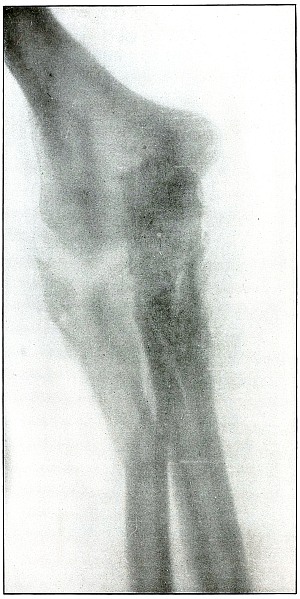
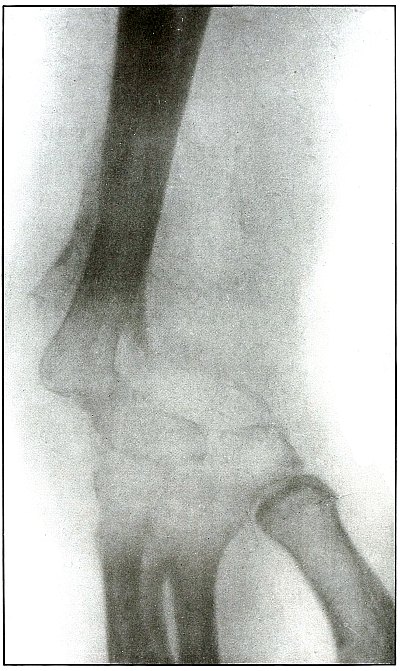
Rifle—Plate 17.
UPPER EXTREMITY.
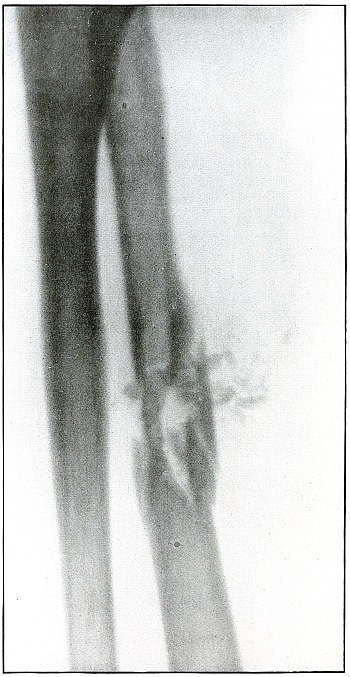
Gunshot Fracture of the Elbow.
The bullet in transverse course and high velocity through both bones
of the forearm struck the head of the radius, thus starting several
splitting lines of fracture and separating large fragments. Smaller
fragments which received some of the energy of the missile have been
carried along with it in turn, striking the ulna and carrying away
smaller fragments from it and causing the laceration which marks the
wound of exit.
Such wounds, with laceration of soft parts and fragmentation of the
bone, are prone to infection, against which treatment is directed. The
indications to be met are much like those of the wound shown in plates
18 and 19. Excision or
immediate methods of bone repair are contraindicated by infection.
Results will depend upon the nature and extent of infection.
[Pg 46]
Plate 18.
[Pg 47]
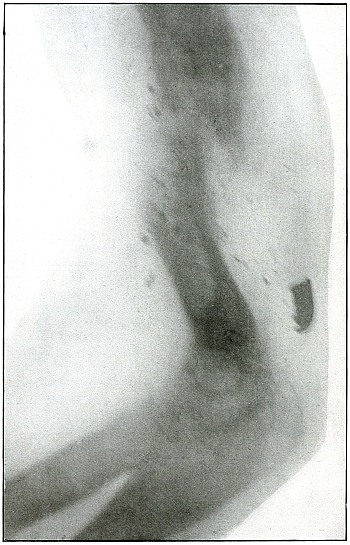
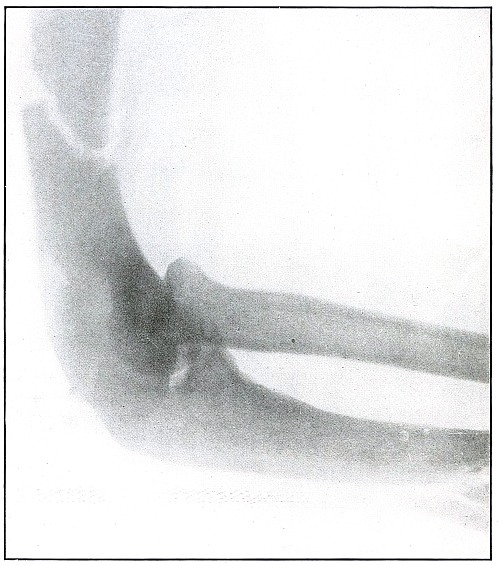
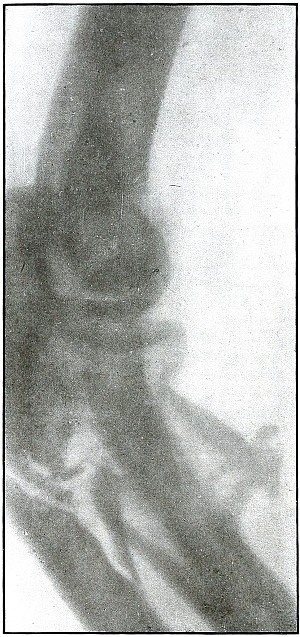
Rifle—Plate 18.
UPPER EXTREMITY.
Gunshot Fracture of the Elbow,
without Injury to the Great Vessels and Nerves.
Wound of entrance, posterior to the external condyle.
Wound of exit, large laceration in front and above the internal condyle.
The wound is an example of the misnamed “explosive” action of a rifle
bullet. The force and direction of the missile, in high velocity,
split the bone into many fragments, and, transmitting its energy to
some of the fragments, carried them through the skin and caused the
large laceration at the point of exit by the simultaneous escape of
the bullet and fragments. The wound was so heavily infected, that a
cellulitis advanced to the shoulder and to the wrist to such extent
that the arm was marked by eminent surgical opinion for amputation.
Free incision, drainage, antisepsis and incidental removal of detached
fragments controlled the infection and brought about slow resolution.
After six months of careful treatment the wound was healed with an
ankylosed elbow with normal function of the forearm, except for
limited rotation.
Treatment indicated in such cases is always conservative. Infections
contraindicate any formal surgical interference. The dangers of
infection in such cases are to be risked to avoid amputation.
Results may be considered favorable even with elbow ankylosis.
[Pg 48]
Plate 19.
[Pg 49]
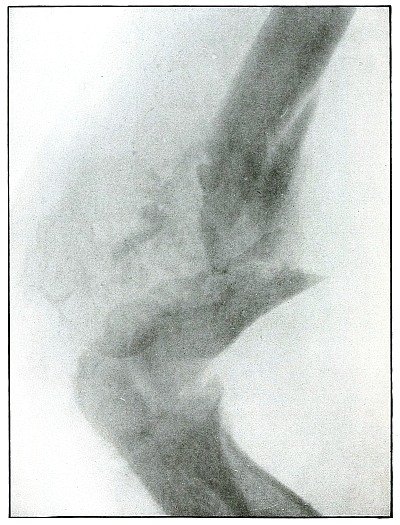
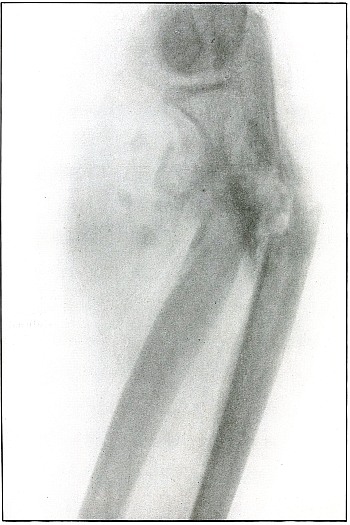
Rifle—Plate 19.
UPPER EXTREMITY.
Gunshot Fracture of the Elbow,
without Injury to the Great Vessels and Nerves.
This is a plate made of the same subject shown in plate 18, when convalescence was several weeks
farther advanced, as is indicated by the removal of fragments and
extensive callus formation.
Both radiographs were made after the apprehension of systemic
infection had passed; the second plate after an additional number of
fragments had been removed.
[Pg 50]
Plate 20.
[Pg 51]
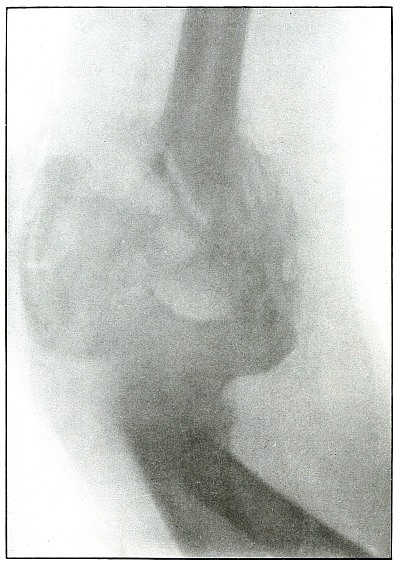
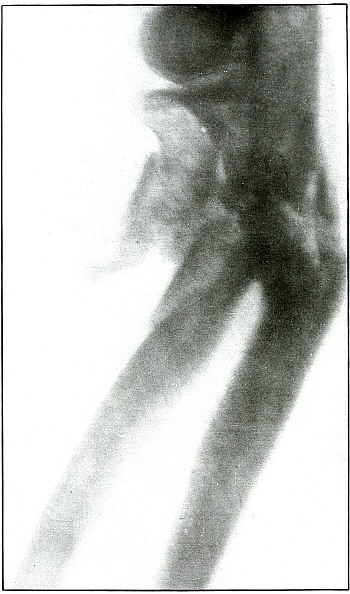
Rifle—Plate 20.
UPPER EXTREMITY.
Gunshot Fracture of the Elbow.
Wound of entrance, posterior aspect of forearm internal to and below
the olecranon.
Wound of exit, external border over head of radius.
The course of the bullet was diagonally anteroposterior from within
outward, striking the posterior border of the upper end of the ulna
and passing through the head of the radius, carrying the fragments
of the latter before it and lacerating the wound of exit. The energy
of impact also fissured the upper end of the shaft of the ulna and
fractured the neck of the radius without detaching the large fragments.
This is the effect of a rifle bullet at short range, or possibly a
ricochet shot at mid range.
The emergency treatment is antiseptic dressing with splint
immobilization.
The subsequent treatment is conservative, whether the wound is clean
or infected. The course of treatment of such an infected wound might
extend from four to six months.
Note.—As the
soldier always escapes the burden of explanation when the wound of
entrance is anterior rather than posterior, it should be remembered
that the forearm may occupy positions in relation to the body which
exposes the anatomically posterior aspect of the forearm to missiles
directed toward the anterior surface of the body; and as the wounds of
the forearm herein presented are described in the anatomical position,
there is no justifiable impeachment of the soldier’s valor in an
inference that he was shot from behind when the wound of entrance
involves the posterior aspect of the forearm.
[Pg 52]
Plate 21.
[Pg 53]
Rifle—Plate 21.
UPPER EXTREMITY.
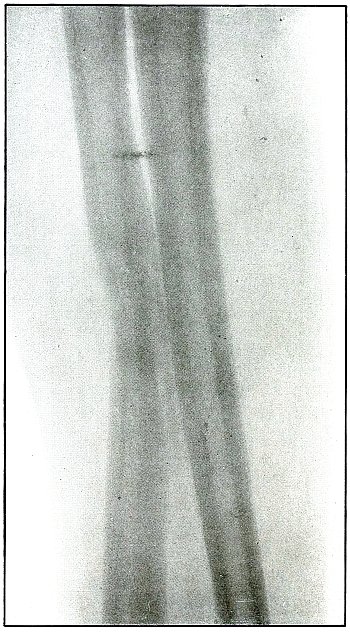
Gunshot Fracture of the Radius and Ulna.
The course of the bullet at short range was transverse through
both of the bones, with a splitting effect and without much small
fragmentation.
The wound of exit in this case was slightly lacerated, but not very
much larger than the wound of entrance.
The treatment should be conservative. Emergency treatment should not
include exploration, and nothing but the conventional iodine dressing
and splints should be applied.
[Pg 54]
Plate 22.
[Pg 55]
Rifle—Plate 22.
UPPER EXTREMITY.
Gunshot Fracture of the Radius and Ulna.
The course of the bullet at short range was transverse through the
upper forearm, striking the radius in the center of the shaft and the
ulna nearer the border. Several small fragments followed the course of
the bullet, but did not emerge with it at the wound of exit to cause a
laceration.
The capitellum was next to the photographic plate and the angular line
of the radius can be seen crossing the straighter line of the ulna.
Further information is obtained from the examination of another
view, plate 23, made of the same subject.
[Pg 56]
Plate 23.
[Pg 57]
Rifle—Plate 23.
UPPER EXTREMITY.
Gunshot Fracture of the Radius and Ulna.
This plate was made from the wound shown in plate 22,
with the arm in greater inward rotation. This position shows the wide separation
of the large fragments of the radius.
Emergency treatment in such cases is antiseptic dressing only, without
exploration, and with fixation by splints for transportation. The
degree of infection determines the subsequent course of conservative
treatment, with operative methods for correction of deformity reserved
for further stage of convalescence and for best surgical facilities.
[Pg 58]
Plate 24.
[Pg 59]
Rifle—Plate 24.
UPPER EXTREMITY.
Gunshot Fracture of the Radius and Ulna in the
Upper Third of the Forearm.
The course of the projectile was from within, outward and diagonally
forward, with a direct impact on the ulna, and a tangential impact on
the radius, with several lines of splitting fracture in the latter
without detaching fragments. Particles of metal, spattered around the
point of first impact, were deposited by the lead core of a bullet,
exposed by a torn jacket, which struck the second bone with its
jacketed surface.
The treatment is always conservative—meeting indications in case of
infection.
Results are good for saving the limb, but not for avoiding deformity.
[Pg 60]
Plate 25.
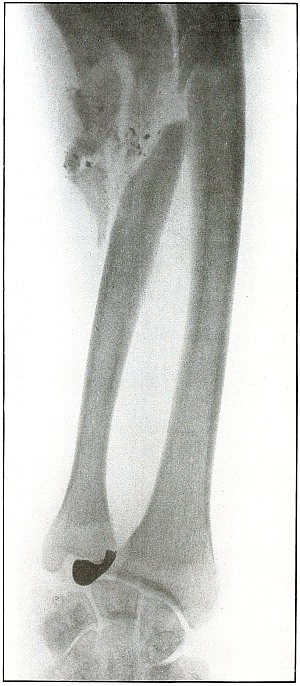
[Pg 61]
Rifle—Plate 25.
UPPER EXTREMITY.
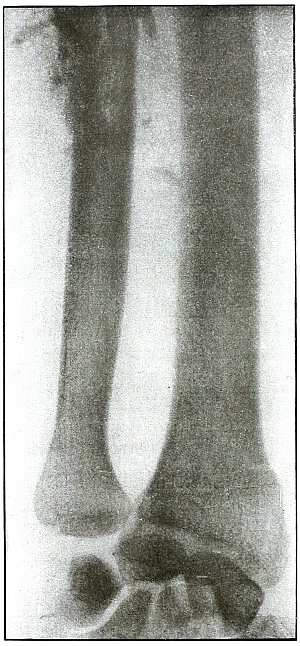
Gunshot Fracture of the Radius.
Wound of entrance, posterior surface of forearm over radius above the middle.
Wound of exit, below and in front of wound of entrance.
The course of the ball in mid range was from behind, forward,
and slightly downward.
While the images of both bones of the forearm are superimposed,
because they both lay in the plane of the projection of the shadow, it
is probable that the radius lay nearer the photographic plate, because
the head of the radius is shown in clearer outline. The fragments of
the fracture can be seen as related to the outlines of the radius.
There is no displacement and only slight fragmentation, so that the
bullet must have almost succeeded in making a punctured wound in the
radius.
The treatment in such cases is regularly that for simple fracture, as
such wounds are almost always aseptic.
The results are uniformly good.
[Pg 62]
Plate 26.
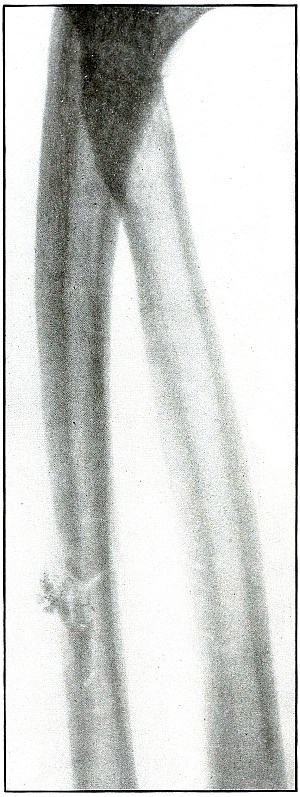
[Pg 63]
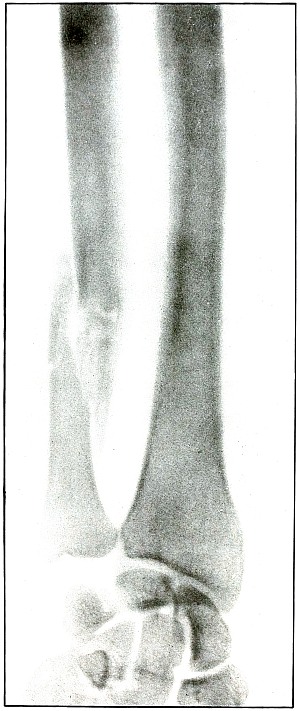
Rifle—Plate 26.
UPPER EXTREMITY.
Gunshot Fracture of the Radius.
Wound of entrance, midway between radius and ulna and midway between
elbow and wrist, anterior aspect of the forearm.
Wound of exit, over radius at point opposite.
The course of the bullet, in the medium velocity of mid range, in
piercing the medullary canal has almost succeeded in drilling the
bone without splitting off several longitudinal fragments. Small
fragments followed the course of the missile, without being energized
sufficiently to lacerate the point of exit by escaping with the
projectile.
The wound of exit in such cases hardly differs enough from the wound
of entrance to be distinguishable. This condition so often obtains
that the great majority of perforating rifle wounds of the forearm
do not show the blow-out or “explosive” effect which seems to be
generally misunderstood as a classic accompaniment.
The bullet was traveling at high velocity of perhaps less than
mid range.
The treatment is usually that of a simple fracture, and warrants no
interference except in case of occasional infection.
Results are almost always good.
[Pg 64]
Plate 27.
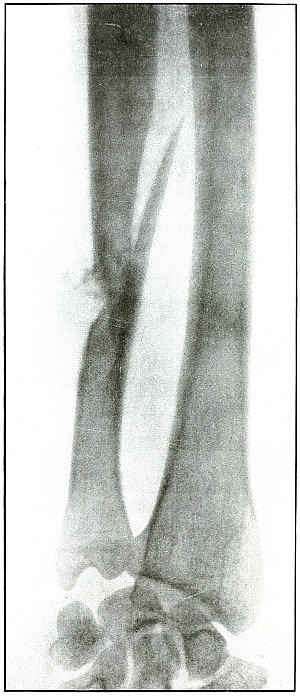
[Pg 65]
Rifle—Plate 27.
UPPER EXTREMITY.
Gunshot Fracture of the Radius.
The course of the bullet, at long range, has been diagonally
anteroposterior through the shaft, causing only a diagonal fracture.
The plate was made after a two-weeks’ convalescence, as is shown by
the beginning of callus formation.
The treatment is that of a simple fracture.
Results are good.
[Pg 66]
Plate 28.
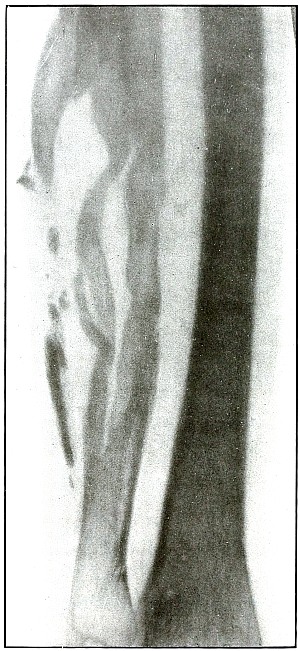
[Pg 67]
Rifle—Plate 28.
UPPER EXTREMITY.
Gunshot Fracture of the Radius.
The course of this bullet was anteroposterior and diagonally from
above downward through the shaft, punching out one side of the shaft
and effecting a diagonal fracture through the bone with only slight
displacement. The wound was infected.
The radiograph was taken during the course of treatment, after the
several small fragments found by the punched-out portion of the bone
were removed. A small drainage tube is in the wound, but the size of
the forearm shows that the reaction is very moderate.
The treatment is that of a simple fracture, except for the indications
to be met in the control of infection.
Results are good.
[Pg 68]
Plate 29.
[Pg 69]
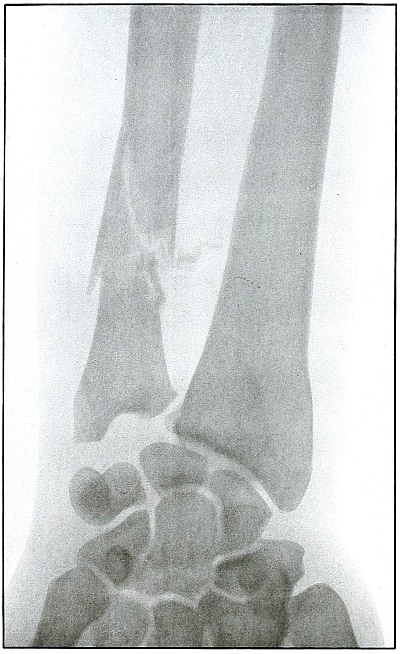
Rifle—Plate 29.
UPPER EXTREMITY.
Gunshot Fracture of the Lower End
of the Radius.
The course of the bullet in long range was diagonally anteroposterior
through the ulnar side of the lower end of the bone, with the wound of
entrance on the anterior and the wound of exit on the posterior aspect
of the wrist. The wound of exit was slightly lacerated by several
small fragments driven off from the ulnar side of the radius. These
fragments were removed through an incision before the radiograph was made.
The emergency treatment of such cases is only antiseptic dressing and
splint immobilization.
When wound is aseptic or after it has closed, a secondary operation
for coaptation, with proper facilities available, might be indicated.
The results as to full restoration of joint function are not favorable.
[Pg 70]
Plate 30.
[Pg 71]
Rifle—Plate 30.
UPPER EXTREMITY.
Gunshot Fracture of the Lower End
of the Radius.
The course of the missile was diagonally transverse, striking the
radius in its lower third.
The projectile in this case is unknown, as it might have been either a
shrapnel ball or a deformed rifle bullet with a torn jacket, exposing
the lead core and marking its course with small particles of lead.
The fissures in the lower fragment and the finer fragmentation at the
seat of impact, indicate a great striking energy, that more often
resides in the high velocity of a rifle bullet than the low velocity
of a shrapnel ball. The wound is therefore classified with rifle wounds.
The treatment is conservative. The course in such cases, without
infection, is very favorable, and not unfavorable even with infection.
Results should be good.
[Pg 72]
Plate 31.
[Pg 73]
Rifle—Plate 31.
UPPER EXTREMITY.
Gunshot Fracture of the Lower End
of the Radius.
Wound of entrance, anterior aspect of wrist, over internal border of radius.
Wound of exit, posterior aspect of wrist between radius and ulna, with laceration.
The range was described as “close”—within a hundred yards—with
the bullet in high velocity. The energy of the projectile, imparted to
small fragments of cancellous tissue, drove them through the wound
of exit, and caused the laceration of the superficial tissues. The
wound was infected (swelling of soft parts clearly shown): resolution
followed extended treatment, with ankylosis of the wrist and radial
displacement of the carpus.
Emergency treatment in all such cases is antiseptic dressing
without exploration or manipulation of fragments, and with splint
immobilization.
Results are unfavorable as to function, depending upon extent of destruction of tendons.
[Pg 74]
Plate 32.

[Pg 75]
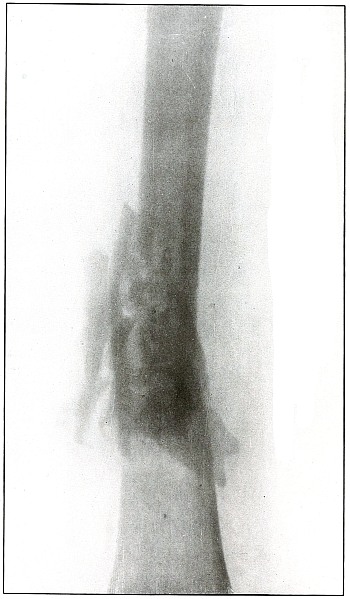
Rifle—Plate 32.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the bullet was transverse through the arm at the
junction of the middle and upper thirds from behind the radial border
externally to the ulnar border internally, striking the wall of the
medullary canal with a punching effect that partly split off short
longitudinal fragments and caused transverse and longitudinal cracks,
without separation or displacement of fragments.
The same ballistic conditions applied to cancellous tissue at the end
of the bone would probably have bored through it without fracture.
This effect is generally seen in wounds of small-caliber bullets
traveling at reduced velocity of long range.
The treatment is that of a simple fracture.
Results, in such cases without infection, could not be bad.
[Pg 76]
Plate 33.
[Pg 77]
Rifle—Plate 33.
UPPER EXTREMITY.
Gunshot Fracture of the Left Ulna.
The course of the missile was from within outward, ranging downward to
the wrist, by deflection, after striking the ulna in its upper half.
The considerable striking energy retained in a small portion of the
mass—consisting of only the nose and a little more of the jacket of
the bullet, but sufficient to fragment a large section of the bone,
and then to traverse more than half the length of the forearm—leaves
no doubt that the shot was fired at very close range, and that the
bullet was broken on a nearly resisting surface, leaving in the nose
of the bullet a striking force equal to that of the entire projectile
at long range.
The posterior surface of the forearm is next to the plate, as the
distinct outline of the styloid process of the ulna and the posterior
border of the articular surface of the radius shows. The radius and
ulna are parallel in the most natural position of supination. The
normal diameter and sharp outline of the nose of the bullet show it to
be next to the plate and on the posterior surface between radius and ulna.
Fragments of the exposed lead core of the bullet have scraped off on
the line of fracture in a manner peculiar to shrapnel wounds, but
never seen in bullet wounds in which the jacket covers all of the lead core.
The treatment is regularly conservative and without interference, as
in this particular wound, which was aseptic.
Secondary treatment may indicate correction of bone deformity.
[Pg 78]
Plate 34.
[Pg 79]
Rifle—Plate 34.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The ballistic conditions of the projectile causing the wound
shown in this plate are substantially those of the wound shown in
plate 32.
The wound of entrance and exit would be practically the same in
chipping off a few small fragments and causing a clean transverse
fracture without any displacement.
The bullet at long range has struck the wall of the medullary canal,
appearance.
Treatment that of a simple fracture.
Results must be good.
[Pg 80]
Plate 35.
[Pg 81]
Rifle—Plate 35.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the bullet at long range has been anteroposterior
through the middle of the forearm, passing through the side of the shaft,
chipping off a few small fragments and causing a long oblique fracture.
The conditions were much the same as those shown in plates
28 and 29,
except that the striking energy of the projectile was somewhat
greater with the velocity of mid range.
The treatment, without infection, is that of a simple fracture.
Results will be uniformly good.
[Pg 82]
Plate 36.

[Pg 83]
Rifle—Plate 36.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the bullet was anteroposterior through the ulna a little
above the middle of the forearm, and fairly through the long axis.
This is a bone effect much similar to those shown in plates
28, 29, and 31,
except that this condition is due to the impact of a missile, with a
still higher velocity of shorter range, imparting its energy to small
fragments of bone, which added their momentum to the destructive force
of the projectile.
No large fragments were carried along with the missile to cause any
more destruction of tissue in exit than in entrance, so that the skin
wounds, under these conditions, are about the same in appearance.
The treatment is conservative and expectant with immobilization.
Results in such cases are uniformly good.
[Pg 84]
Plate 37.
[Pg 85]
Rifle—Plate 37.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the bullet was in an anteroposterior direction at a high
velocity of short range, which, imparting its energy to the fragments,
drove some of them through the tissues as “secondary missiles” and
caused a laceration of the wound to exist.
The longitudinal fragmentation and splitting indicates a considerable
energy of the projectile, which may have been deflected, as its long
axis was turned somewhat from the trajectory at the time of impact.
The emergency treatment is antiseptic dressing and splint immobilization.
The subsequent treatment is conservative with the removal of detached
fragments and with control of infection as the course indicates.
[Pg 86]
Plate 38.
[Pg 87]
Rifle—Plate 38.
UPPER EXTREMITY.
Gunshot Fracture of the Left Ulna.
The course of the bullet was transverse through the middle of the
forearm, striking the posterior border of the ulna.
Small fragments were broken from the posterior wall of the medullary
canal, without destroying the longitudinal continuity of the anterior wall.
The velocity of the bullet was probably that of mid-range, as the
striking energy of the impact was fairly great.
The posterior surface of the forearm lay next to the plate.
The emergency treatment is antiseptic dressing and splint
immobilization.
The subsequent treatment is that of a simple fracture,
as infection is not usual.
[Pg 88]
Plate 39.
[Pg 89]
Rifle—Plate 39.
UPPER EXTREMITY.
Gunshot Fracture of the Left Ulna.
The course of the bullet, with the velocity of long range, was
anteroposterior through the lower third of the forearm, striking the
outer side of the bone. The initial velocity of the projectile was
much reduced, as is shown by the tendency to puncture the bone without
much fragmentation.
There was no displacement of fragments as a direct result of the
impact, although muscular contraction has caused some slight
subsequent overriding.
The wounds of entrance and exit were about the same, if not quite
similar in appearance.
The emergency treatment is the conventional antiseptic dressing with
splint immobilization.
The subsequent treatment is usually that of a simple fracture,
as infection in such cases is rare.
[Pg 90]
Plate 40.
[Pg 91]
Rifle—Plate 40.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the bullet was obliquely anteroposterior through the
lower third of the forearm, striking the radial edge of the bone with
a velocity of long range.
The wounds shown in plates 35 and 39
represent conditions similar to those causing this wound,
except that the ranges were progressively greater.
In this case the projectile exhibited a punching effect at the
point of impact, and although the lines of force are shown in
characteristically divergent fissures, the energy imparted to the
fragments—less than in the preceding cases—has not been sufficient
to separate or to displace the fragments.
The emergency and subsequent treatment is conventionally conservative,
as in the preceding cases.
[Pg 92]
Plate 41.
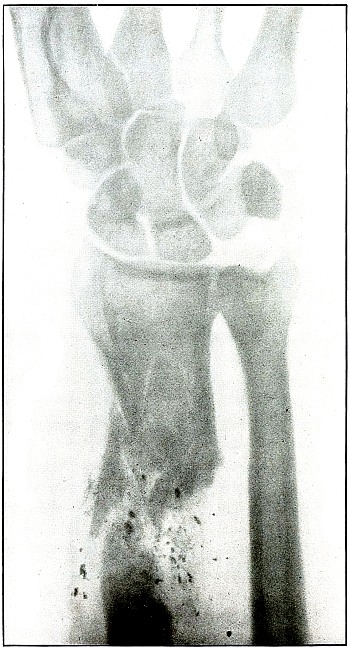
[Pg 93]
Rifle—Plate 41.
UPPER EXTREMITY.
Gunshot Fracture of the Wrist.
Wound of entrance, posterior aspect of forearm over the lower end of
the radius, with the bullet ranging forward and slightly downward to
the wound of exit and covering with great laceration the anterior
aspect of the wrist joint.
The range was close, and the energy of the high velocity of the
missile was imparted to fragments, which, becoming “secondary
missiles,” emerged with the projectile to cause extensive laceration
and destruction of tissue.
The case was received for amputation in the second week, when a grave
degree of infection extended in a cellulitis to the elbow. The ulnar
nerve and vessels were intact, but the flexor tendons were almost
entirely destroyed.
The plate, made after several weeks, when infection was under control
and after the end of the radius and fragments of the carpus had been
informally removed, shows a rarefaction of the carpus and proximal
ends of the metacarpus, due to infection and disuse.
Frequent incisions and extension of drainage, with removal of detached
fragments, was continued for several months. The wound was closed in
the sixth month, with ankylosis and deformity of the wrist,
as shown in plate 42.
[Pg 94]
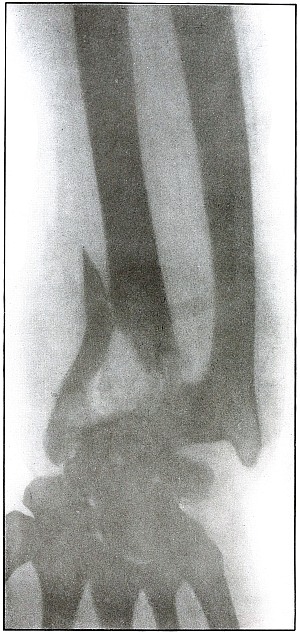
Plate 42.
[Pg 95]
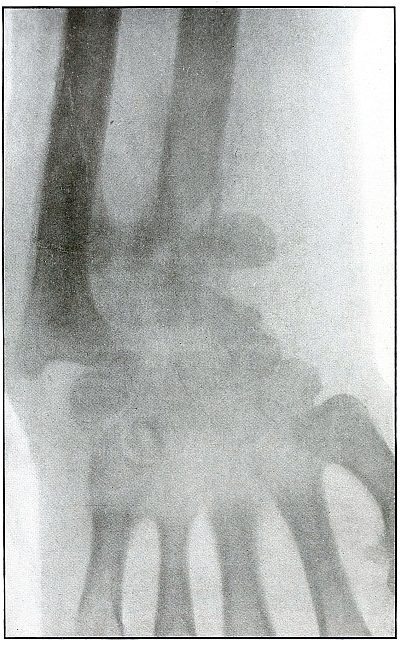
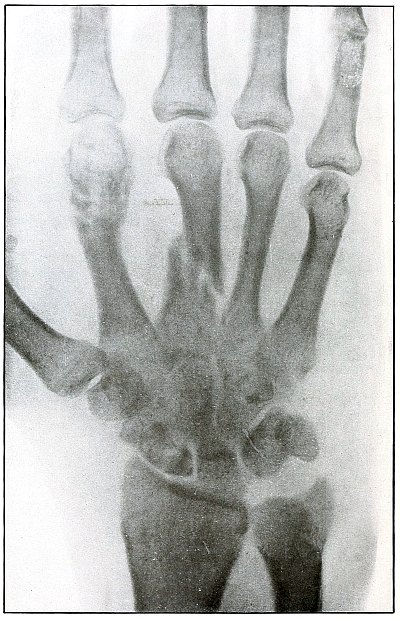
Rifle—Plate 42.
UPPER EXTREMITY.
Gunshot Fracture of the Wrist.
This plate, presenting a lateral view of the wound shown in
plate 41, shows considerable deformity of the
joint, after four months’ treatment, which was even more marked two
months later, when the case was discharged with an ankylosis of the
wrist joint, contracture of the flexor tendons of the fingers, and
slight flexor function of the thumb, permitting apposition with the
first finger.
The result, while leaving much to be desired, preserved a function of
the hand vastly superior to that of a forearm stump.
The treatment in such cases is always courageously conservative, with
amputation only as the extreme measure to save life, with risks of
judgment in favor of conservatism.
Corrective measures may be employed after management if the treatment
of the infection is successful and when the case passes out of the
military category. It is not possible, during a long infection, to
maintain better position in such cases.
[Pg 96]
Plate 43.
[Pg 97]
Rifle—Plate 43.
UPPER EXTREMITY.
Gunshot Fracture of the Metacarpus.
Wound of entrance, inner aspect of the hand over proximal end of the
fifth metacarpal.
Wound of exit, on the outer border of the hand over the distal end of
the second metacarpal.
The velocity of the bullet was in mid or long range, as it displaced
no fragments, and as it made a point of entrance and exit about the
same in appearance.
The wound was infected, which is more frequently the case in the hand
than in the forearm.
The treatment is conservative with free incision and drainage
in the management of infection.
[Pg 98]
Plate 44.
[Pg 99]
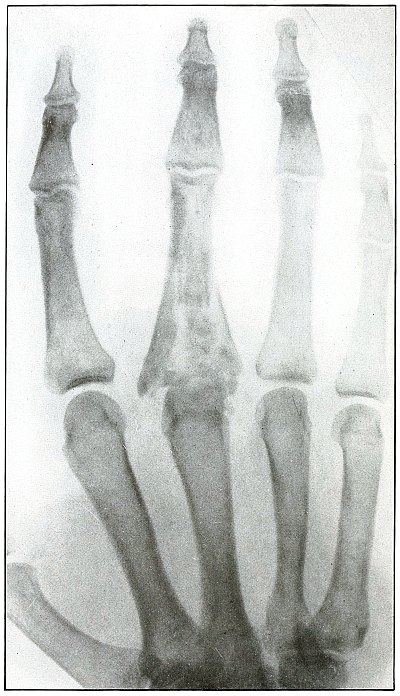
Rifle—Plate 44.
UPPER EXTREMITY.
Gunshot Fracture of the Third Phalanx.
The course of the bullet was anteroposterior through the base of the
proximal phalanx of the middle finger, with a velocity of long range.
It practically punctured the bones and split off a few fragments
without displacement.
The wound of entrance would be much the same as the wound of exit,
with the latter, but a little larger.
Treatment is conservative.
[Pg 100]
CHEST.
Plate 45.
[Pg 101]
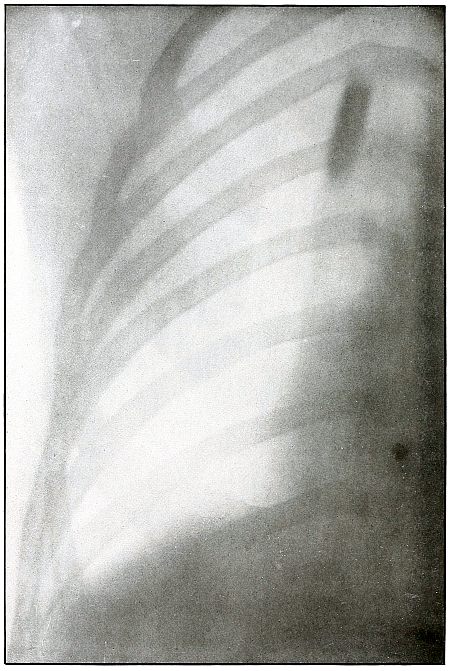
Rifle—Plate 45.
CHEST.
Penetrating Gunshot Wound of the Chest,
with Lodgment of the Projectile Near Posterior Chest Wall.
Point of entrance, pectoral border and fourth rib.
Point of exit, none.
The distinct shadow of the angle of the ribs shows that the posterior
chest wall was next to the photographic plate, and that the larger and
less distinct outline of the anterior portions of the upper ribs was
farther from the plate.
The nearly normal size of the shadow of the projectile shows it to be
much nearer the posterior than the anterior chest wall. The blurred
outline shows it to have moved with respiration. Such conditions
locate its position within the thoracic cavity.
The emergency treatment is antiseptic dressing and rest.
The subsequent treatment depends upon pleural involvement or the
extremely rare infection of the lung.
These cases are nearly all aseptic, and if the great vessels and
nerves of the chest escape injury results are generally favorable.
[Pg 102]
PELVIS.
Plate 46.
[Pg 103]
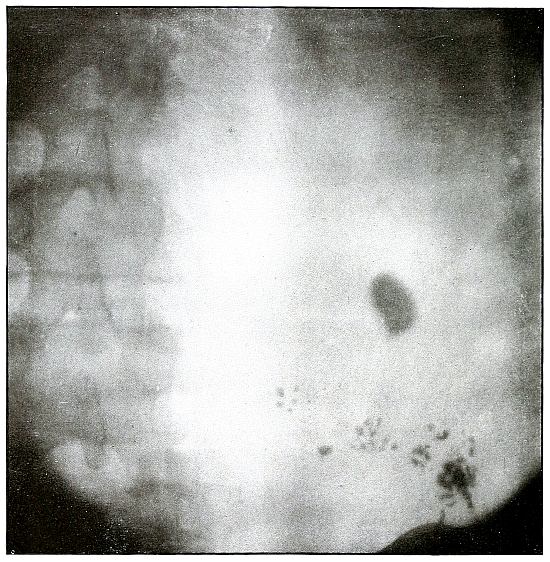
Rifle—Plate 46.
PELVIS.
Gunshot Wound of the Pelvis,
with Lodgment of the Missile in the Abdomen.
The course of the bullet was from behind forward, striking the crest
of the ilium, on which it was deflected, and spattering off some lead
fragments. The slight penetration indicates a velocity of extremely
long range and a striking energy lessened by ricochet.
The irregular outline of the shadow of the projectile shows its
deformity, and the blurred outline indicates intra-abdominal movement
with respiration.
While the missile, as revealed by its shadow, is not a shrapnel ball,
the distribution of lead particles is more suggestive of a shrapnel
than of a rifle projectile, and the ballistic conditions are more
characteristic of the former than of the latter.
There was no abdominal reaction; the invasion of the abdomen was
revealed by the radiograph.
The treatment in such cases is noninterference unless subsequent
developments furnish definite indications.
[Pg 104]
LOWER EXTREMITY.
Plate 47.
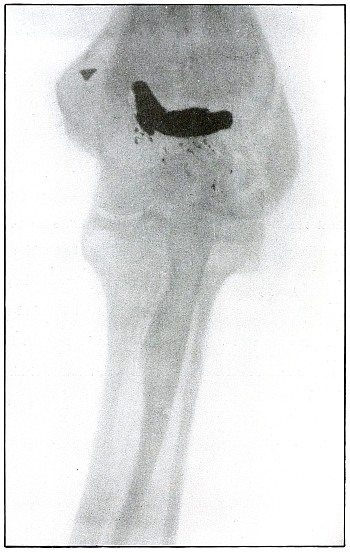
[Pg 105]
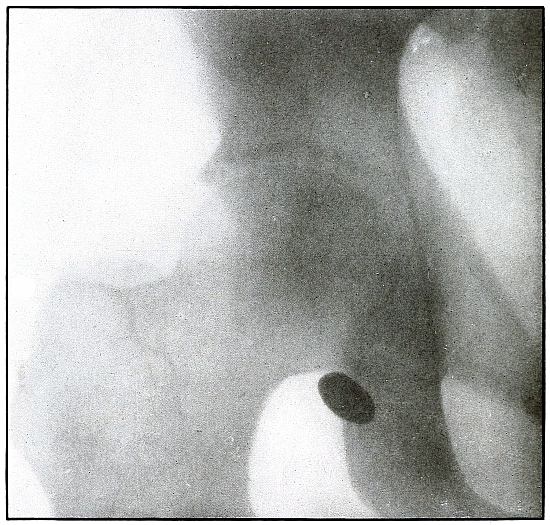
Rifle—Plate 47.
LOWER EXTREMITY.
Gunshot Wound of the Gluteal Region,
with Lodgment of the Bullet Near the Ischium.
Wound of entrance, over gluteal prominence on a transverse line
through the great trochanter.
Wound of exit, none.
There was no bone injury in this case. The bullet, to have lodged in
the soft parts after relatively slight penetration, must have struck
the body at extreme range when its energy was almost spent in flight,
for its normal outline indicates that it was not retarded by ricochet.
The long axis is almost perpendicular to the plate. As the posterior
pelvis was next to the plate, the fairly dense shadow shows the
projectile was not far from the plate and behind the ischium.
The treatment is conservative; infection in such cases is extremely
rare; and only pain or impaired function after many months of
convalescence justifies operation for removal of the missile.
[Pg 106]
Plate 48.
[Pg 107]
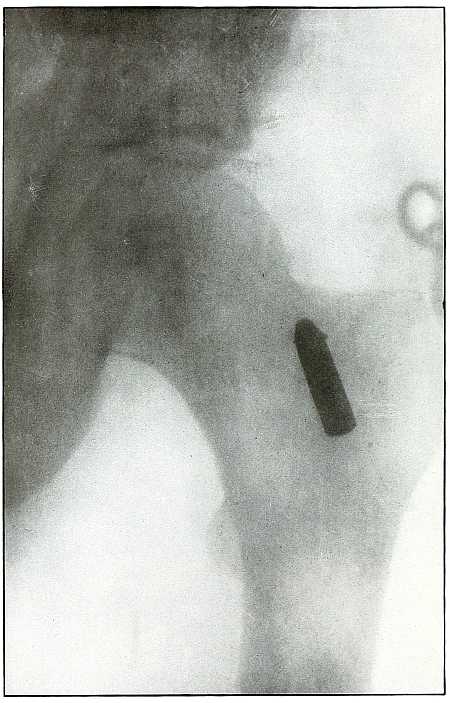
Rifle—Plate 48.
LOWER EXTREMITY.
Gunshot Wound of the Thigh,
with Lodgment of the Bullet.
Wound of entrance, outer aspect of the thigh at the junction of the
upper and middle thirds.
The slight penetration without bone injury and with slight deformity
of the nose of the bullet indicates that the wound was caused by a
ricochet shot at extreme range, after its energy was almost spent.
With the posterior aspect of the thigh next to the plate, the dense
shadow and the nearly normal size of its outline indicate that the
bullet was in the same relative position and that it lay posterior to
the neck of the femur.
As such wounds are rarely infected, the treatment is conservative,
and a search for the missile is only justified by serious infection,
pain, or impaired function.
[Pg 108]
Plate 49.
[Pg 109]
Rifle—Plate 49.
LOWER EXTREMITY.
Gunshot Wound of the Right Thigh,
with Lodgment of the Bullet Behind the Femur.
There is no injury of the bone in this case, as the bullet lodged in
the muscles posterior to the lower third of the femur without striking
the bone. The lighter circular area of the larger end of the shadow
of the projectile shows that its base is farther from the plate than
its nose, which was probably flattened and bent by the ricochet which
reduced its velocity so as to give it but slight power of penetration.
It is not easy to determine from inspection of the plate which side of
the leg lay next to the plate.
With a history of the wound of the right thigh and with the outside
of the leg next to the plate, the projectile must have lain near the
plate on the outside behind the lower end of the femur, midway between
the skin and bone.
The markings seen on the bone are not concerned with the wound, as the
same effect in the plate is seen in the areas beside the bone.
The treatment is conservative; infection is rare.
[Pg 110]
Plate 50.
[Pg 111]
Rifle—Plate 50.
LOWER EXTREMITY.
Gunshot Wound of the Right Thigh,
with Lodgment of the Bullet Behind the Femur.
There is no injury to the bone. The large diameter, shortened length,
and slight density of the shadow show the bullet to be some distance
from and inclining toward the plate and lodged in the muscles behind
the femur, nearer the side away from the photographic plate. It is
difficult to identify the right or left thigh from the radiograph, but
with the history of the wound in the right thigh and the outside of
the leg next to the plate the ball would lie nearer the inside than
the outside of the thigh, nearer the surface behind the femur. As the
shadow shows irregular outline and the location of the bullet low
velocity, the wound was caused by a ricochet shot at very long range.
The treatment is expectant and the course naturally favorable.
[Pg 112]
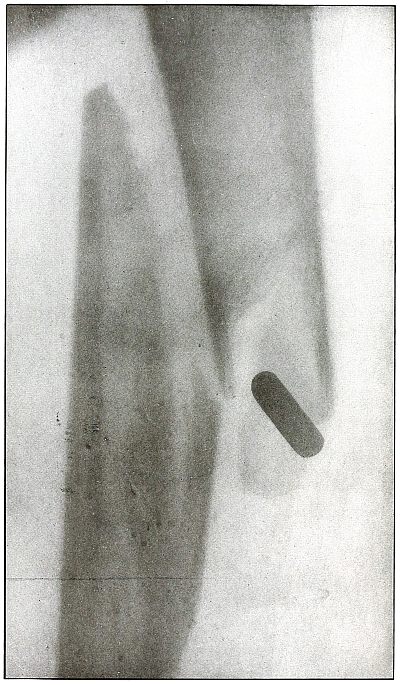
Plate 51.
[Pg 113]
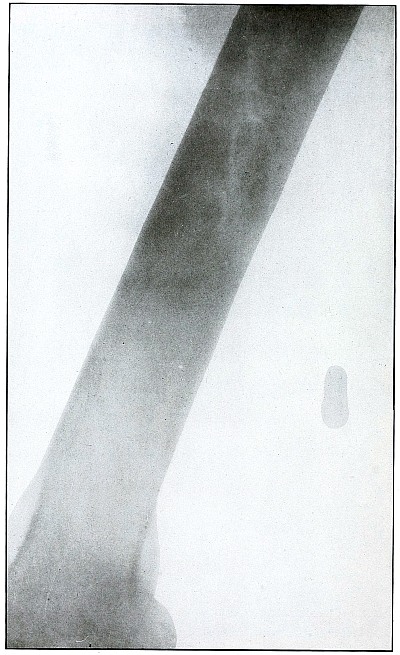
Rifle—Plate 51.
LOWER EXTREMITY.
Gunshot Wound of the Thigh,
with Lodgment of the Missile.
As there is no injury to the bone, the bullet is not deformed. Its
penetrating power was not great enough to carry it through the tissue
so it must have struck the leg at extreme range when its energy was
almost spent.
The actual length of the bullet is 1.25 inches; the length of the
shadow is about 1.50 inches.
The increased length and the relatively slight density of the shadow
indicate the bullet to be some distance from the plate. The case
history places the wound in the right thigh, and the posterior surface
of the leg lay next to the photographic plate. As the density of the
shadow is not greater than the thickest portion of the bone, the
bullet probably lies in front of the border of the outer tuberosity of
the femur.
Although the surgeon’s diagnosis had to be made from the only
available plate, there is something of a speculative element in these
deductions, because if the reaction in the knee joint prevented the
patient from extending the leg the increased length of the bullet
shadow could be accounted for by this position, which would permit the
bullet to lie behind the bone and yet far enough from the plate to
account for the shadow enlargement. The nose of the bullet is at
the epiphyseal line, which is shown in the femur.
[Pg 114]
Plate 52.
[Pg 115]
Rifle—Plate 52.
LOWER EXTREMITY.
Gunshot Fracture of the Upper Shaft of the Femur.
The course of the bullet was anteroposterior and pierced the axis
of the shaft of the femur with three radiating lines of fracture,
resulting from the perforating action of the bullet striking the bone
at long range and with greatly reduced energy.
This plate shows the lateral separation of large fragments,
which is typical of gunshot wounds of long range.
Such wounds are usually not infected.
Emergency treatment is antiseptic dressing and coaptation with
extension and temporary splint, so that it may support the bone for
transportation and may be easily removable at place of continued
treatment.
In these cases with lateral separation of fragments, it is imperative
to supplement extension with pressure in a line perpendicular to the
long axis of the femur.
[Pg 116]
Plate 53.
[Pg 117]
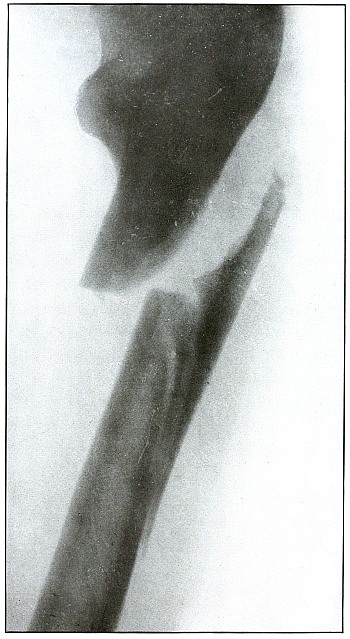
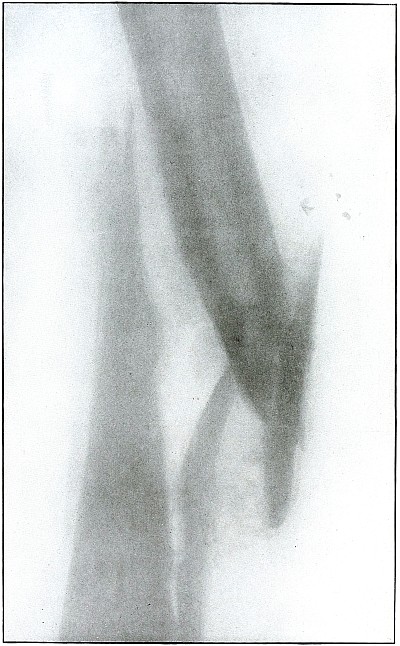
Rifle—Plate 53.
UPPER EXTREMITY.
Gunshot Fracture of the Shaft of the Femur
with Lodgment of the Bullet.
The course of the bullet was antero-posterior and diagonally inward
from the antero-external border of upper third of the thigh. A thin
longitudinal fragment was split off without transverse fracture.
The missile struck the thigh after its energy had been greatly
reduced by ricocheting as a result of striking a resisting object
which flattened its nose and “set up” its body, as shown by the wavy
outlines of the shadows.
The dense and normal-size shadow shows the bullet to be near the plate
and probably in the muscles superficially behind and below the lesser
trochanter.
As the prominent outline of the lesser trochanter shows that the
leg was in external rotation when the negative was made, it is
evident that, with the rotation back to the anatomical position, the
projection of the shadow of the bullet would fall close to or in line
with the shaft of the femur; the position of the bullet is behind the
femur.
The treatment is conservative, with no trouble to be expected from infection.
[Pg 118]
Plate 54.
[Pg 119]
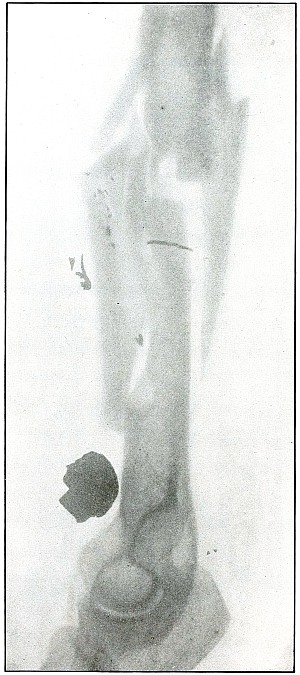
Rifle—Plate 54.
LOWER EXTREMITY.
Gunshot Fracture of the Lower End of the Shaft of the Femur.
The course of the bullet was anteroposterior through the axis of the
femur. Several large fragments which were not displaced were separated
by the force of impact. The separation of the fragments and the
overriding of the ends of the proximal and distal large fragments were
due to bearing bodily weight or to muscular contraction.
The projectile causing the wound was moving with the velocity of mid
range. The wound of exit was not lacerated.
The emergency treatment is antiseptic dressing and temporary splint
immobilization. Permanent dressing, with extension and lateral
compression, is the rule.
Infection in such cases is frequent owing to lack of facilities for
proper dressing on the field.
Results in saving life and limb are generally good.
[Pg 120]
Plate 55.
[Pg 121]
Rifle—Plate 55.
LOWER EXTREMITY.
Gunshot Fracture of the Lower Third of the Shaft of the Femur.
The course of the bullet was diagonally anteroposterior, with a
velocity near mid range, without causing much displacement of fragments.
The wound of entrance and exit would be almost the same in appearance.
Treatment and results would be similar to case shown on plate 54.
Many of these wounds are infected, due, no doubt, to the difficulties
of arranging a clean first-aid dressing and effecting satisfactory
immobilization during the first stage of transportation.
Infection from clothing carried into the wound is rare, as the fairly
high velocity of the bullet causes a spreading of the fibers without
division or punched-out section before the bullet.
As a rule the infected cases of this class recovered without loss of
limb. Amputation was very rare.
[Pg 122]
Plate 56.
[Pg 123]
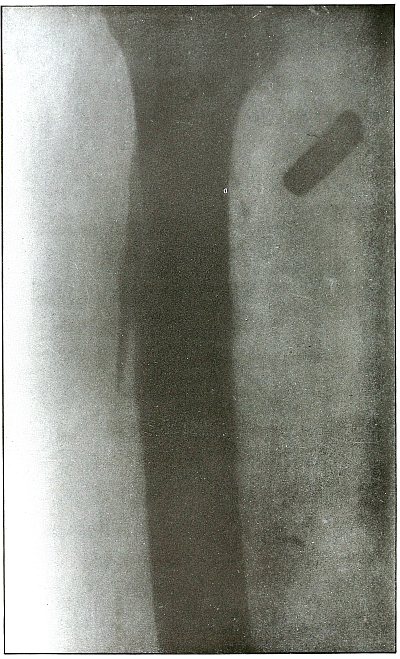
Rifle—Plate 56.
LOWER EXTREMITY.
Gunshot Fracture Below the Middle of the Femur,
with Lodgment of the Bullet Near the Fracture.
The course of the projectile was transverse. The long splitting
fracture, with few large fragments and the lodged undeformed missile,
indicate that the injury to the bone was caused by the missile
striking the bone with large cross section or at an inclined angle so
that all of the remaining energy of the projectile at long range was
absorbed by the bone.
Had the point of the ball struck the bone with the same energy, it
would have produced smaller fragments and might then have passed
beyond the bone. The normal size of the diameter, slightly shortened
length, greater density of the point of the shadow, shows the bullet
to lie behind the bone with its nose pointing slightly backward. The
actual length of the bullet is 1.25 inches: the length of the shadow
is 1 inch.
Treatment and results would be about the same as in
plates 49 and 50.
[Pg 124]
Plate 57.
[Pg 125]
Rifle—Plate 57.
LOWER EXTREMITY.
Gunshot Fracture About the Middle of the Femur,
with Lodgment of the Fragments of a Deformed Bullet.
The course of the missile was transverse. All of the remaining energy
of the retarded velocity of the short range of a ricochet shot was
stopped by the bone with the result of a long splitting fracture, and
the lodgment of one large and a few small fragments of the missile.
The small notched metal fragment lying to the right of the upper
bone fragment is a small bent piece of the jacket, detached from the
greatly deformed lead core, which can be faintly seen lying behind the
lower end of the left side of the upper bone fragment.
The treatment is extension with lateral compression, although this
case, showing by callus formation advancing convalescence, reveals
very bad position.
Results as to life and limb are favorable in such cases, but some
deformity is to be expected.
It should be noted that this is a case from Gulhané Hospital, the best
military hospital in Constantinople, where the surgical service, under
Prof. Wieting Pasha, was skillfully conducted.
[Pg 126]
Plate 58.
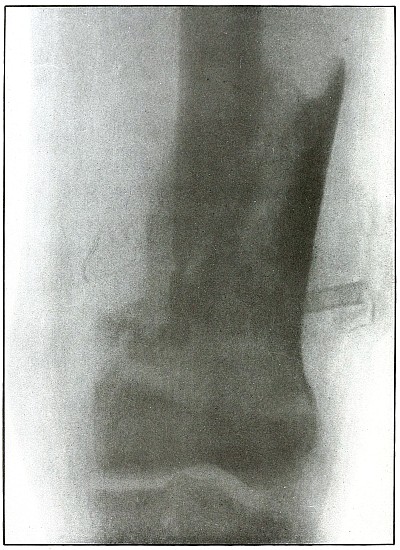
[Pg 127]
Rifle—Plate 58.
LOWER EXTREMITY.
Gunshot Fracture of the Lower End of the Femur.
The course of the bullet was anteroposterior.
The long, oblique, splitting fracture without separate fragments
indicates the long range of the missile in low velocity.
The wound was infected as is indicated by the drainage tubes in place.
The well-advanced callus formation indicates established convalescence.
Results are favorable for recovery with only fair position and some
shortening.
It may be observed that this is also a case from Gulhané Hospital.
[Pg 128]
Plate 59.
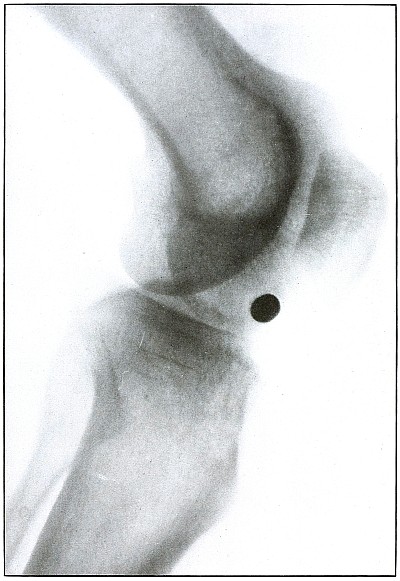
[Pg 129]
Rifle—Plate 59.
LOWER EXTREMITY.
Gunshot Wound of the Left Knee-Joint,
with Lodgment of the Missile in the Joint.
The course of the bullet was transverse, entering the capsule
posterior to the patella without injury to the bone.
As its shadow projection is almost circular, the bullet must be
standing almost on its end pointing toward the plate with its long
axis almost parallel to the line of projection.
As the fibular side of the leg lay next to the plate and as the only
slightly enlarged shadow of the bullet indicates it to be near the
plate, its position is in the joint near the fibular side.
As the bullet is undeformed and its penetrating power very slight, its
velocity was that of extreme range.
The emergency treatment, is, of course, a simple antiseptic dressing
with the leg held in the most comfortable position by muscular action.
The subsequent treatment is removal of the bullet when proper surgical
conditions obtain.
[Pg 130]
Plate 60.
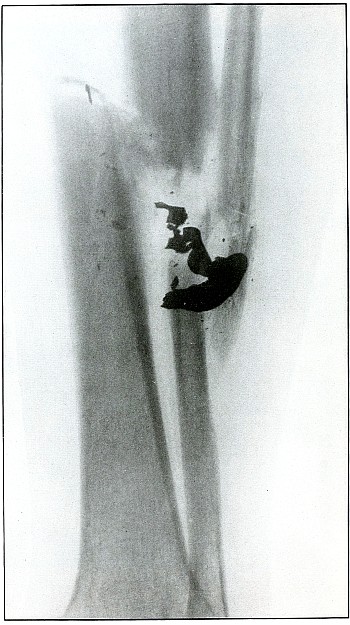
[Pg 131]
Rifle—Plate 60.
LOWER EXTREMITY.
Gunshot Fracture of the Tibia and Fibula,
with Lodgment of the Missile.
The course of the bullet was diagonal from within outward and backward
about the middle of the leg, with the impact tangential on the tibia
and direct on the fibula. The bullet lies just behind the tibia.
It is apparent that the bullet has been greatly deformed and that its
jacket has been badly torn from the core. The force of impact on the
object from which it ricocheted must have been contributed by the
velocity of short range, which reduced the striking energy so greatly
that the bullet was lodged by the resistance of the tibia and fibula.
The wound was not infected, and callus formation shows that repair has begun.
The treatment in such cases, without infection, is noninterference.
The lodgment of the missile need not prejudicate the prognosis, and
certainly the additional damage in the search for the bullet is not
warranted, except under special indications.
[Pg 132]
Plate 61.
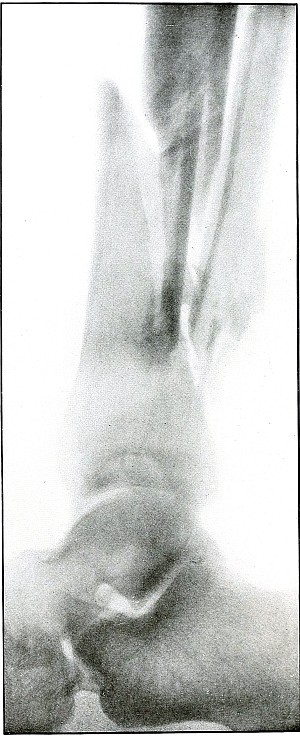
[Pg 133]
Rifle—Plate 61.
LOWER EXTREMITY.
Gunshot Fracture of the Lower Ends of the Tibia and Fibula.
The course of the bullet was transverse, with the velocity of
mid-range.
The fragmentation of the fibula, lying close to the skin, would
produce considerable laceration in the wound of exit.
The treatment is conservative. Infection would depend almost entirely
upon the integrity of the first dressings and immobilization.
Results should be favorable, with care in subsequent treatment.
[Pg 134]
Plate 62.
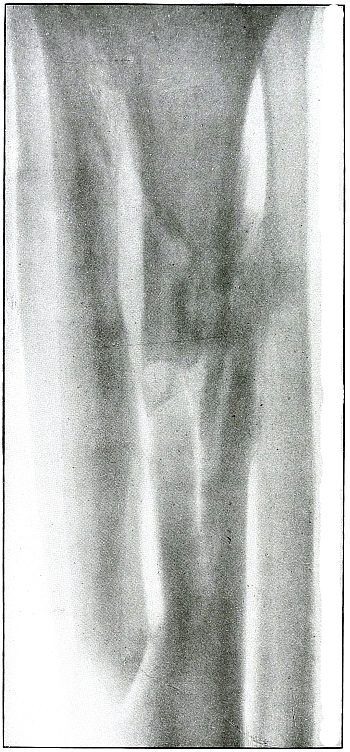
[Pg 135]
Rifle—Plate 62.
LOWER EXTREMITY.
Gunshot Fracture of the Upper Third of the Tibia,
with Large Longitudinal Fragment.
The course of the bullet was anteroposterior and slightly diagonal
from without inward through the shaft of the tibia.
The injury was due to the energy of impact of a bullet, in the high
velocity of short range, striking the axis of the diaphysis, in which
the greater part of its energy was expended in pushing away a wall of
the canal.
Convalescence is well established without infection, as shown by
callus formation.
The treatment in such cases is invariably conservative, with the
removal of such fragments as may be detached by suppuration and sequestration.
[Pg 136]
Plate 63.
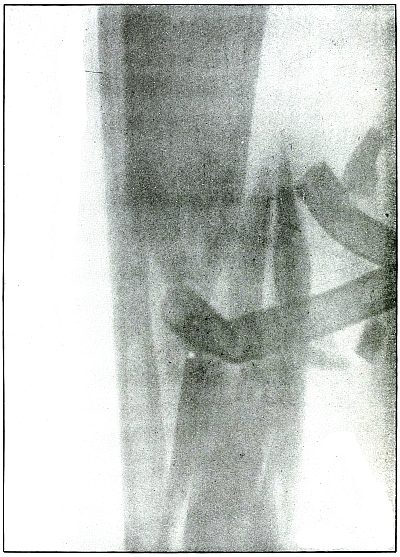
[Pg 137]
Rifle—Plate 63.
LOWER EXTREMITY.
Gunshot Wound of the Middle of the Tibia,
with Few Large Fragments.
The course of the bullet was transverse from without inward.
The direct impact of the bullet, in high velocity of short range, has
produced the typical “X” fracture due to the radiating lines of force.
The wound was infected, as is shown by the drainage tubes in the wound.
The emergency treatment in such cases is simple antiseptic dressing
and temporary splint immobilization.
The subsequent treatment is the management of the infection.
The results in such cases are favorable.
[Pg 138]
Plate 64.
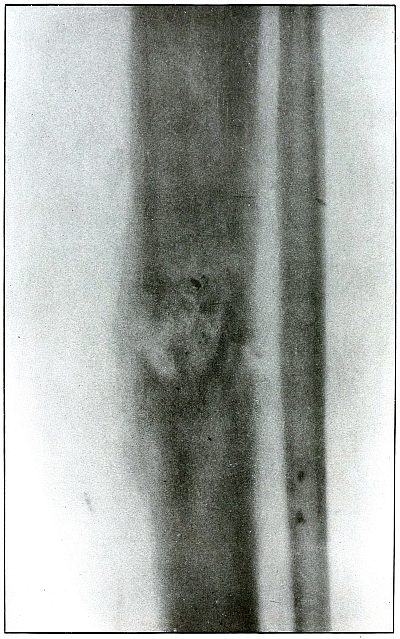
[Pg 139]
Rifle—Plate 64.
LOWER EXTREMITY.
Gunshot Fracture of the Tibia.
The course of the bullet was diagonal, from without inward and from
before backward through the middle of the tibia. Small particles of
metal have lodged at the site of the fracture—a condition which never
occurs in a rifle wound with the jacket of the bullet intact, while it
is the invariable accompaniment of a shrapnel wound of a bone.
It is inferred that the jacket of the bullet in this case was damaged
by ricochet, or that some metal particles from the object against
which the bullet ricocheted were carried into the wound, as some other
small pieces of metal are seen in areas distant from the seat of fracture.
As the fragments are small and not displaced, the velocity of
the missile, at least that of mid-range, was almost sufficient to
perforate the bone without fracture.
[Pg 140]
Plate 65.
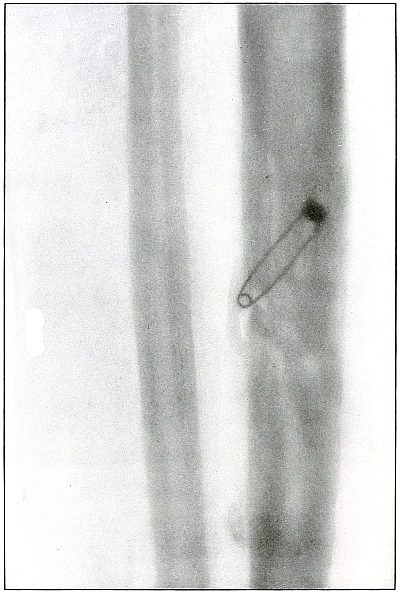
[Pg 141]
Rifle—Plate 65.
LOWER EXTREMITY.
Gunshot Fracture of the Tibia.
The course of the bullet was transverse, from within outward, striking
the bone near the outer border with the velocity of mid or long range,
producing long fissures without separation of fragments.
The safety pin, of course, lies in the dressings and on the side
away from the plate, as shown by its somewhat indefinite outline and
increased length.
The wounds of entrance and exit are practically the same.
The treatment in such cases is that of a simple fracture, except
for the management of an occasional infection, and the results are favorable.
[Pg 142]
Plate 66.
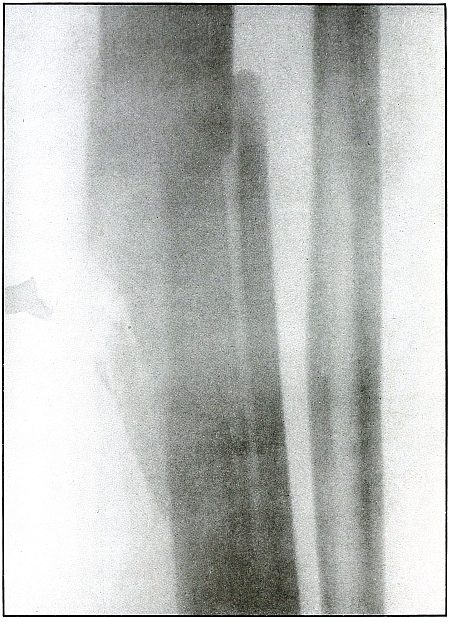
[Pg 143]
Rifle—Plate 66.
LOWER EXTREMITY.
Gunshot Fracture of the Middle of the Tibia,
with Lodgment of the Missile.
The course of the bullet was transverse, from without inward, striking
on the side of the shaft of the tibia.
The bullet was so badly damaged by ricochet that only a portion of it
was the cause of this wound.
The range was short, if not close, as the missile after striking a
resisting object with force enough to break itself retained enough
energy in a fragment of less than half its mass to cause a long
fissure fracture, with the separation of smaller fragments.
The treatment is noninterference, except for infection, which,
contrary to what might be expected from presumable contamination from
the object from which it ricocheted, does not occur more frequently in
ricochet than direct wounds with lodgment of the projectile.
[Pg 144]
Plate 67.
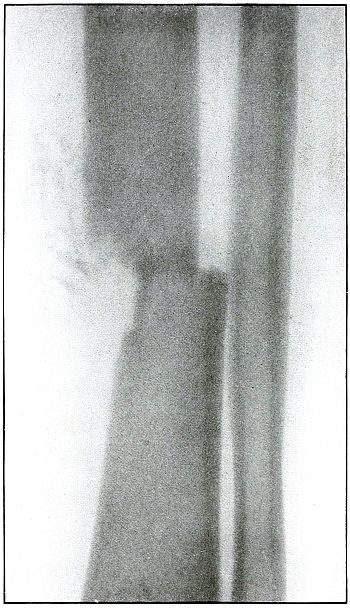
[Pg 145]
Rifle—Plate 67.
LOWER EXTREMITY.
Gunshot Fracture of the Lower Third of the Tibia.
The course of the bullet, with reduced energy of long range, was
anteroposterior, striking the inner border of the bone and punching
out a circular area of small fragments with a single transverse line
of fracture.
The wound of exit was slightly larger than the wound of entrance.
The treatment is conservative. Infection is not probable if emergency
dressing is clean.
[Pg 146]
Plate 68.
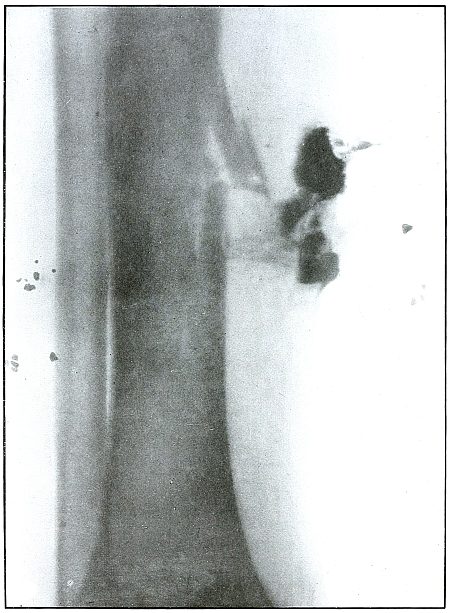
[Pg 147]
Rifle—Plate 68.
LOWER EXTREMITY.
Gunshot Fracture of the Lower Third of the Tibia.
The course of the bullet was diagonally anteroposterior, from without
inward, striking the internal border of the anterior surface of the
bone, and partially splitting off fragments from the side with a
perforating effect.
The range of the shot was long.
The dense and irregular shadows to the right of the fracture are
caused by the material used in dressing and indicate a slight
infection. The small shadows on the tibial side are not a part of the
wound, but are due to opaque material caught in the dressing.
[Pg 148]
Plate 69.
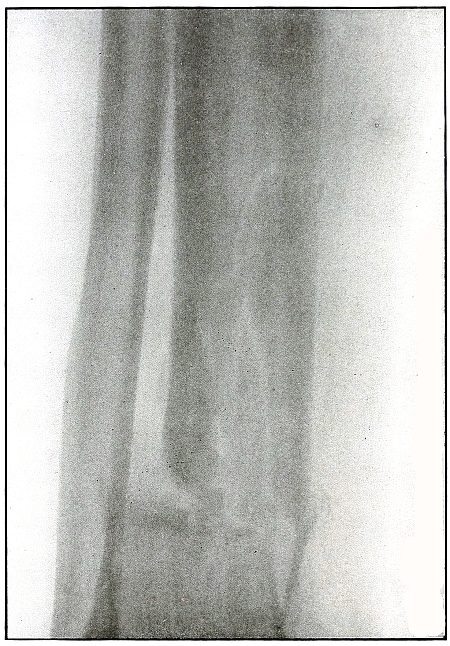
[Pg 149]
Rifle—Plate 69.
LOWER EXTREMITY.
Gunshot Fracture of the Lower End of the Tibia.
The course of the bullet was transverse, from without inward, through
the lower end of the bone, with a piercing effect and a fissuring of
the upper fragment.
The velocity was that of short range.
The wound of exit would be slightly larger than that of entrance, as
some small fragments can be seen extending along the tract of the
missile from the line of transverse fracture toward the internal
border of the leg. There was no laceration of the wound of exit. The
wound was clean.
The treatment is conservative.
Results should be favorable. Infection would depend most probably upon
the asepsis of the first dressing.
[Pg 150]
Plate 70.
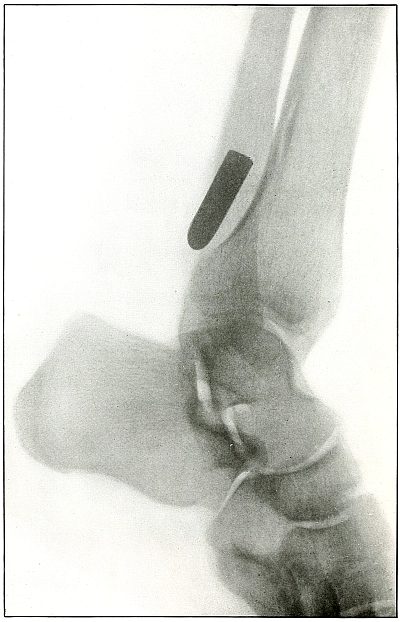
[Pg 151]
Rifle—Plate 70.
LOWER EXTREMITY.
Gunshot Fracture of the Tibia,
with Lodgment of the Missile.
The course of the bullet was from within outward, striking the
posterior surface of the tibia about 2 inches above the ankle, and
causing a slight crack in the bone at the point where its course was
deflected.
The velocity was that of extreme range, as the wholly normal outline
of the projectile and the slight penetration indicates that its energy
was almost entirely lost in flight and not by ricochet.
The sharp outlines of the lower border of the fibula and the external
border of the articular surface of the lower end of the tibia indicate
the position of the fibula as next to the photographic plate.
The bullet lies at a very slight angle with the plate, as is shown
by the curved outline of its base, which condition alone would give a
projection shadow somewhat shorter than the bullet. But as the shadow
is actually somewhat longer than the bullet (about one-eighth inch,
or one-tenth its length), the position of the bullet is some distance
from the plate and most probably lies behind the tibia, at the inside of the fibula.
[Pg 152]
Plate 71.
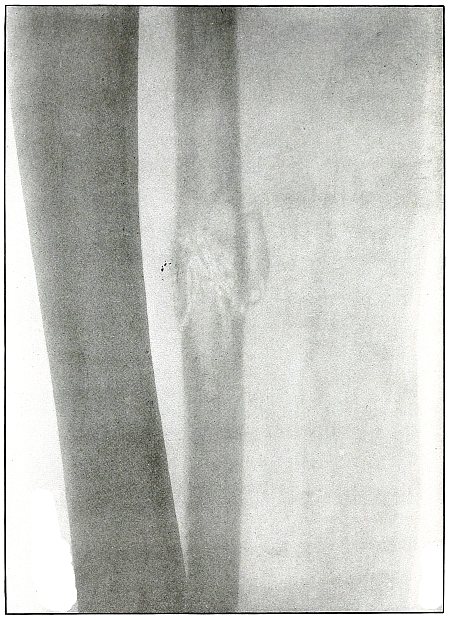
[Pg 153]
Rifle—Plate 71.
LOWER EXTREMITY.
Gunshot Fracture of the Fibula.
The course of the bullet was anteroposterior through the lower third
of the leg, striking the fibula squarely, passing through the bone
with a perforating effect, accompanied by slight fragmentation and
with a reduced velocity of long range.
The wounds of entrance and exit would be almost the same in
appearance. Asepsis in such cases is the almost invariable rule, and
the treatment after the simple dressing is that of a simple fracture.
[Pg 154]
Plate 72.
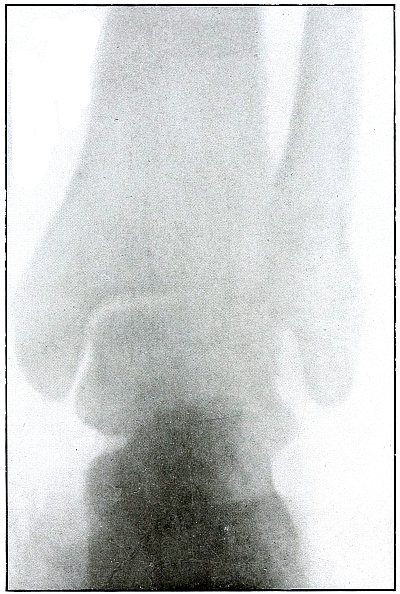
[Pg 155]
Rifle—Plate 72.
LOWER EXTREMITY.
Gunshot Fracture of the Ankle.
The course of the bullet was anteroposterior, striking the fibula
from behind with a velocity of long range, and causing some slight
fragmentation without displacement of the fragments.
The joint architecture is slightly disturbed. The joint mortice is
a bit widened by the external deflection of the external malleolus,
which permits a slight outward rotation of the astragalus.
As the dangers of infection are usually escaped,
the treatment is that for Pott’s fracture.
[Pg 156]
Plate 73.
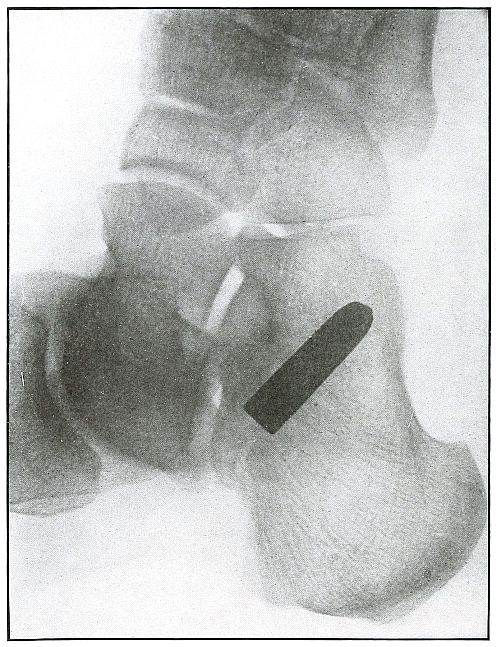
[Pg 157]
Rifle—Plate 73.
LOWER EXTREMITY.
Gunshot Wound of the Heel,
with Lodgment of the Missile.
The course of the bullet was from behind forward through the insertion
of the tendo Achillis and its lodgment along the outer border of the
os calcis.
There was no injury to the bone. The path of the bullet is shown by
the slight mottling above the posterior extremity of the os calcis.
The nose of the bullet is slightly deformed by ricochet at long range.
The very slight penetration and the slight deformity of the nose of
the bullet indicates a velocity of extreme range of both impact of the
ricochet and of the wound.
The sharp outline of fibula and the base of fifth metatarsal shows the
fibula to be next to the plate. The only slight enlargement and square
base of the shadow of the bullet show it to be parallel to the plate,
or at right angles to the line of projection, and thus indicate its
position to be on the fibula side of the os calcis, below the tip of
the external malleolus.
[Pg 158]
Plate 74.
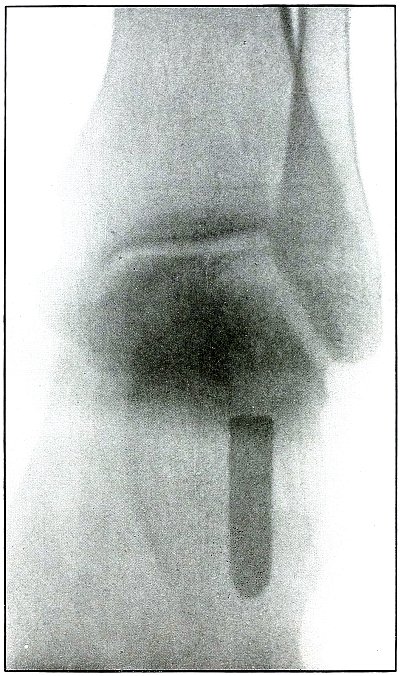
[Pg 159]
Rifle—Plate 74.
LOWER EXTREMITY.
Gunshot Wound of the Heel.
This is the same case as shown in plate 69,
but with the shadow projected from above downward instead of from side
to side, as in the preceding plate. The interpretation of the shadows
in the preceding plate is thus confirmed.
As the heel lay on the plate, the projectile at a sharp angle with the
plane of the plate, several inches farther from the plate than in the
preceding radiograph, and with the line of projection at about right
angles to the long axis of the projectile, the shadow projection is considerably enlarged.
[Pg 160]
Shrapnel
HEAD.
Plate 75.
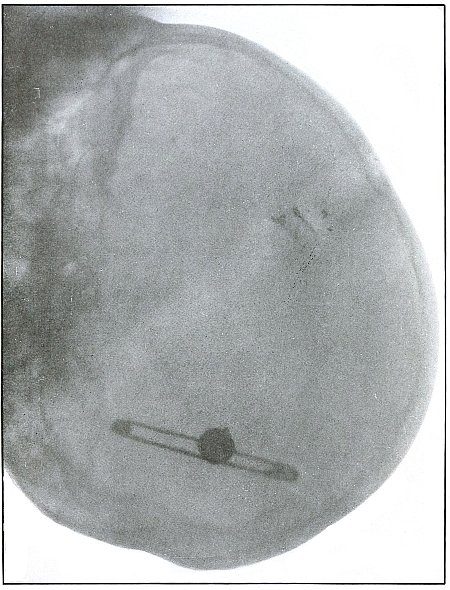
[Pg 161]
Shrapnel—Plate 75.
HEAD.
Gunshot Fracture of the Vertex,
with Intracranial Lodgment of the Missile.
Wound of entrance, left anterior parietal region.
Wound of exit, none.
The missile left a few small fragments spattered on the bone at point
of entrance, with a slight deformation of the ball due to this cause,
as shown in the plate.
The distinct outline and normal size of the ball shows it to be very
near the plate and on the left side of the head, while the enlarged
and blurred image of the safety pin shows its position to be on the
side of the head farther away from the plate.
Emergency treatment is antiseptic dressing only. Subsequent treatment
is directed to fragments and depression, without search for ball.
Septic condition might indicate some later interference.
Results in such cases are favorable if wound is not infected.
[Pg 162]
Plate 76.
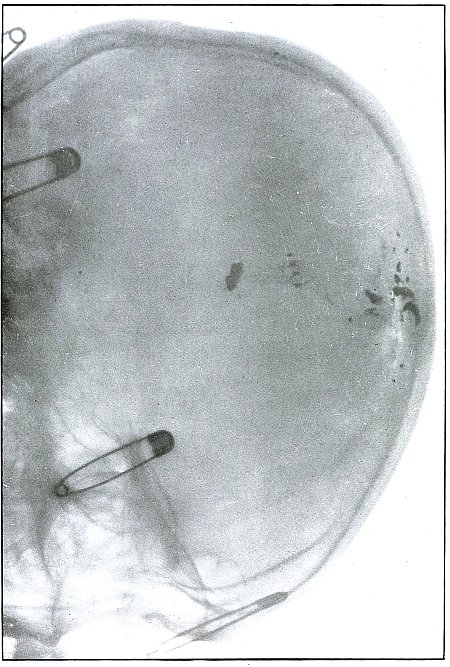
[Pg 163]
Shrapnel—Plate 76.
HEAD.
Gunshot Fracture of the Vertex.
Wound of entrance, upper right and mid-parietal region.
Wound of exit, none.
The missile probably was deformed before striking the skull, upon
which it was fragmented by impact, with several fragments following
the internal contour of the vertex and others remaining spattered
about the wound of entrance.
It is probable that a larger mass of the shrapnel ball, causing the
greater damage to the bone, ricocheted out of the wound.
The distinct outline of the central safety pin and the less definite
image of the shrapnel fragments show the wound to have been farther
from the plate than the safety pin on the left side.
The treatment is expectant, without search for the missile.
Results in such cases are favorable, except for danger of infection.
[Pg 164]
Plate 77.
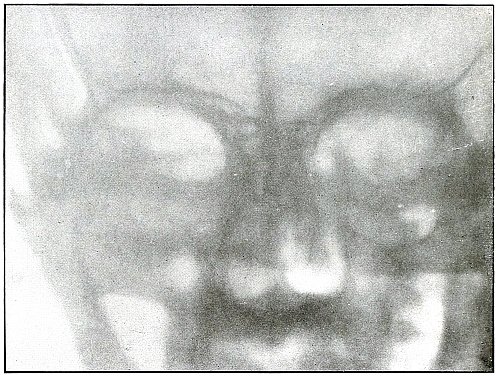
[Pg 165]
Shrapnel—Plate 77.
HEAD.
Gunshot Fracture of Zygoma,
with Lodgment of the Missile in the Zygomatic Fossa.
Wound of entrance, external border of right supra-orbital ridge.
Wound of exit, none.
A few metallic fragments are seen where the missile lodged near the
point of impact with the bone.
The treatment is expectant. Removal of the ball from its superficial
location is indicated if the wound is infected.
Result in such cases is favorable.
[Pg 166]
Plate 78.
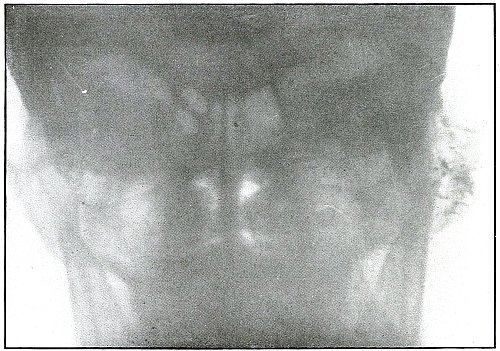
[Pg 167]
Shrapnel—Plate 78.
HEAD.
Gunshot Fracture of the Mastoid Process.
Wound of entrance, upper posterior cheek, in front of the ear.
Wound of exit, posterior to mastoid process, lacerated.
The course of the missile was tangential, with the damage limited to
the outer table of the mastoid. The metal particles scraped off of the
ball by its contact with the bone mark the site of the wound.
Treatment is expectant.
Results are favorable.
[Pg 168]
Plate 79.
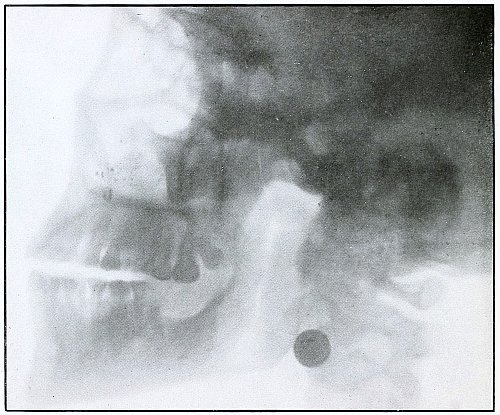
[Pg 169]
Shrapnel—Plate 79.
HEAD.
Gunshot Fracture of the Left Maxilla,
with Lodgment of the Missile in
the
Neck Behind the Angle of the Jaw.
Wound of entrance, below infraorbital ridge, with course through the mouth.
Wound of exit, none.
Missile left a few small metallic fragments spattered on the bone
at the point of entrance. There is slight mark of deformity of the
missile caused by its contact with the bone, shown in its shadow in
the plate.
The distinct outline and normal size of the ball shows it to have been
on the side next to and near the plate.
Treatment indicated is expectant.
Results in such cases are favorable, as seat of probable infection is
readily accessible.
In this particular case, recovery followed with the ball left in
situ, without causing the patient trouble enough to induce him to permit interference.
[Pg 170]
Plate 80.
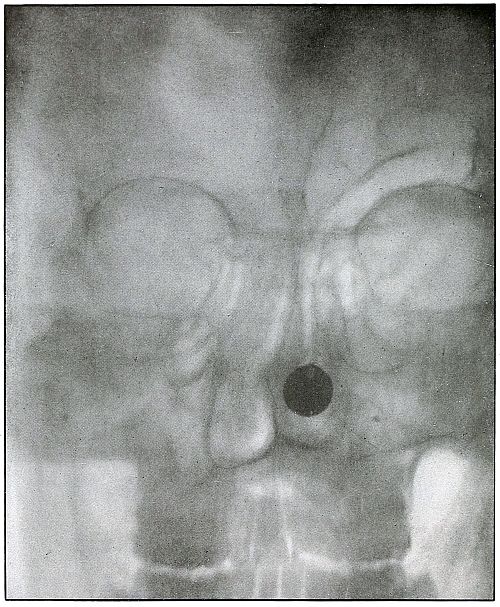
[Pg 171]
Shrapnel—Plate 80.
HEAD.
Gunshot Fracture of the Anterior Table of the Frontal Sinus,
with Lodgment of the Missile in the Posterior Nares.
Wound of entrance, over the left internal super supra-orbital ridge,
with course downward, slightly backward, and slightly to the left
posterior nares.
Wound of exit, none.
The distinct outline and practically normal size of ball shows that
the patient’s face was superimposed on the photographic plate, as the
anterior location of the missile was suspected. The slight deformity
of the ball is due to the impact with the bone. This personal case was
received from the service of Prof. De Page, of the Belgian Red Cross
Mission, at Josh Keshla Hospital, Constantinople, after an operation
for infections of the frontal sinus, in which the anterior table was
entirely removed, with free drainage into the posterior nares, before
the radiograph was made or the exact location of the ball suspected.
The missile is seen in the nares—very near the face—probably in
the middle meatus, in the inferior turbinates, against the septum,
deviated by its lodgment.
Convalescence was finally established and the frontal-sinus wound
practically closed when, without any subjective symptoms, an
obstruction was objectively determined in the left posterior nares,
suggesting the radiograph.
The patient was so entirely free from any symptoms of the lodged
missile that he wisely refused any meddlesome interference. He was
discharged with sinus wound closed very remarkably without indication
for plastic operation and with no symptoms.
[Pg 172]
Plate 81.
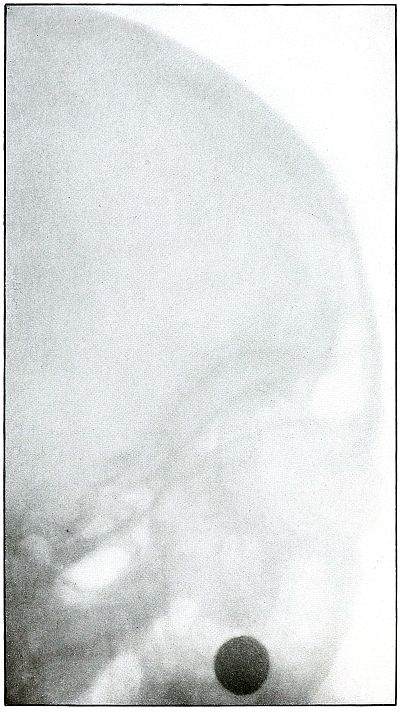
[Pg 173]
Shrapnel—Plate 81.
HEAD.
Gunshot Fracture of Anterior Table of the Parietal Bone
and the Vomer,
with the Lodgment of the Missile in the Posterior Nares.
This plate is a side view of the case in plate No. 80,
showing the antero-posterior location of the ball.
The indefinite outline and enlarged size of the ball shows the ball to
have been farther away from the plate than in plate 80.
[Pg 174]
Plate 82.
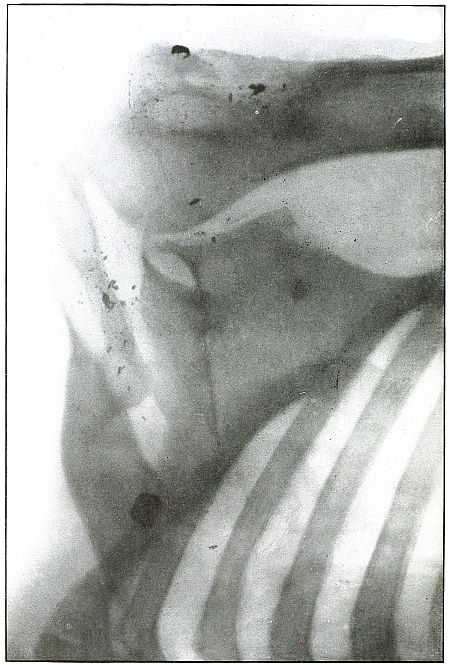
[Pg 175]
Shrapnel—Plate 82.
UPPER EXTREMITY.
Gunshot Wound of the Shoulder,
with Lodgment of the Missile.
The course of the missile was transverse from the posterior surface of
the greater tuberosity of the humerus to the internal border of the
scapula, distributing small metallic fragments along its path.
There is no injury to the bone. The remnant of the ball has passed
behind the scapula and lies near its superior angle.
The treatment in such cases is, of course, conservative, with no
serious consequences expected from infection.
[Pg 176]
Plate 83.
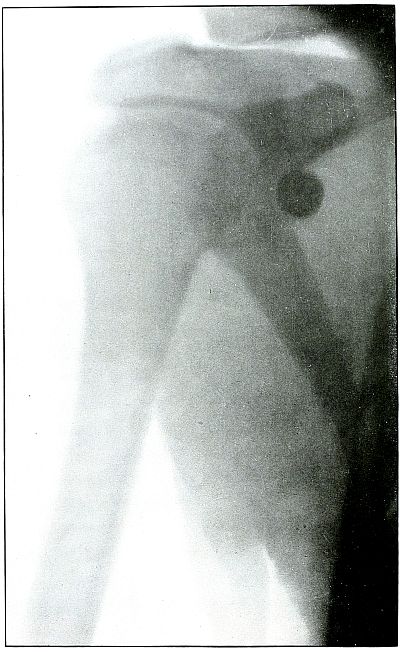
[Pg 177]
Shrapnel—Plate 83.
UPPER EXTREMITY.
Gunshot Wound of the Shoulder,
with Lodgment of the Missile.
The course of the ball was transverse through the posterior border of
the deltoid muscle without contact with the bone, which would have
been revealed by small particles of lead scraped off from the ball.
The actual size, normal outline, and great density of the shadow of
the ball show that it lay next to the plate and that it is, therefore,
lodged posterior and mesial to the glenoid portion of the scapula.
The treatment is noninterference unless removal be indicated by pain,
impairment of function, or infection.
The results should always be good.
[Pg 178]
Plate 84.
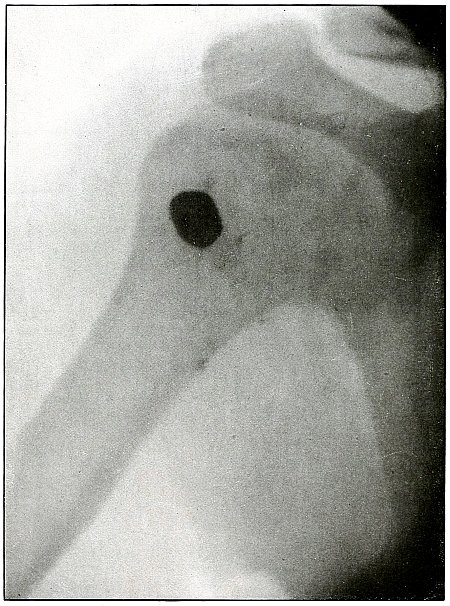
[Pg 179]
Shrapnel—Plate 84.
UPPER EXTREMITY.
Gunshot Wound of the Shoulder,
with Lodgment of the Missile.
The course of the bullet was from before backward and upward through
the deltoid to the anterior surface of the head of the humerus.
The missile is not the conventional shrapnel ball, which is spherical
and about one-half inch in diameter, for the shadow shows a larger
axis in one direction with parallel sides, too symmetrical to be
attributed to deformation. The ballistic conditions are those of
shrapnel.
The missile struck the bone an inch or two below the point of
lodgment. Its path is shown by particles of metal.
Pain or interference with function would be cause for interference in
subsequent treatment, which otherwise would be expectant.
[Pg 180]
Plate 85.
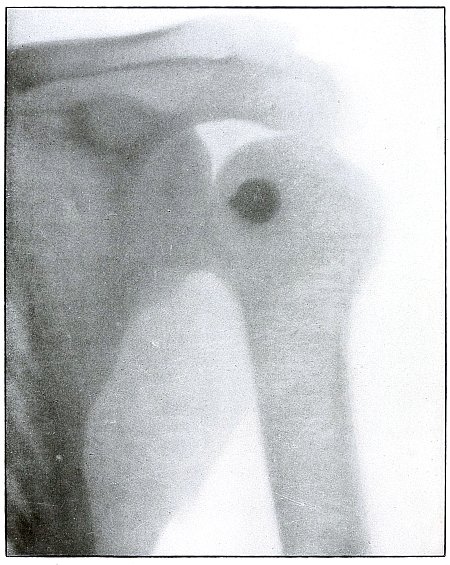
[Pg 181]
Shrapnel—Plate 85.
UPPER EXTREMITY.
Gunshot Wound of the Shoulder,
with Lodgment of the Missile.
The missile lies behind the head of the humerus, under conditions
similar to the cases shown in plates 83
and 84.
The position of the hall is indicated by the outline and depth of
shadow of the normal size of a shrapnel ball. The ball must therefore
be very near the plate and behind the head of the humerus.
There is no injury to the bone. The slight deformity of the ball was
caused by ricochet before it caused the wound, as no particles of lead
are seen on the bone to account for the impact of the missile.
[Pg 182]
Plate 86.
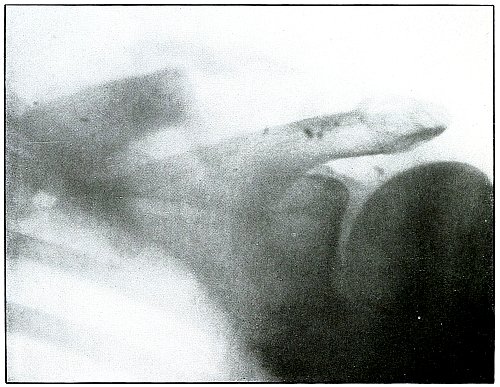
[Pg 183]
Shrapnel—Plate 86.
UPPER EXTREMITY.
Gunshot Fracture of the Clavicle.
The ball ranged from before backward and upward, comminuting the outer
half of the clavicle.
The fragments have been removed. The particles of metal which mark the
path of the ball lie in front of the acromion process of the scapula,
because lack of density and indistinct outline of the shadows show
them to be farther from the photographic plate than the spine of the
scapula which rested on the plate, escaping the imminent danger of
wounding the subclavian vessels.
The treatment is conservative and results are favorable.
[Pg 184]
Plate 87.
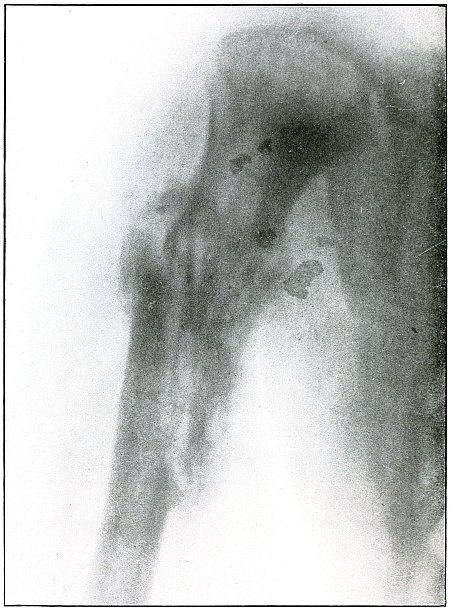
[Pg 185]
Shrapnel—Plate 87.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus.
The missile struck the bone and caused a long, splitting fracture,
with some fragmentation of the proximal fragment.
The wound could have been caused by either a ricocheted rifle bullet
or by a deformed shrapnel ball, either projectile being the low
velocity of long range. These conditions are more common to shrapnel
wounds, but the appearance of the larger metal fragment leads to the
suspicion that it is a piece of the jacket of a rifle bullet.
The wound was not infected, and convalescence is well advanced,
as is indicated by the callous formation.
[Pg 186]
Plate 88.
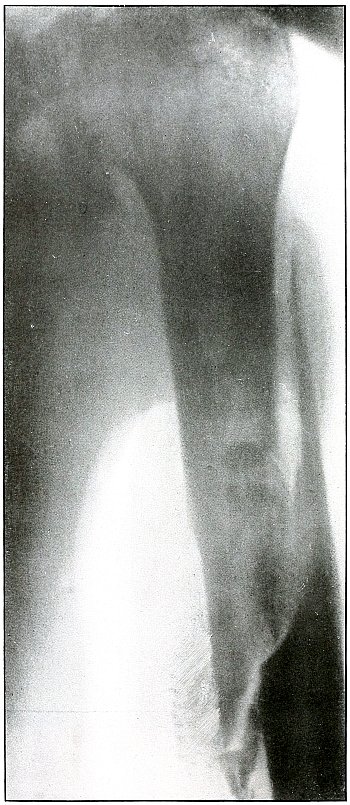
[Pg 187]
Shrapnel—Plate 88.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus,
with Lodgment of the Missile.
The missile struck the shaft of the humerus from an anterior and
external direction and caused a long diagonal splitting fracture with
fragmentation, in which the bone absorbed all of the energy of the
missile at the seat of fracture. The missile lies in the anterior
surface of the humerus, in two fragments; the smaller, much less
distinct, is seen about an inch above the larger.
The wound is not infected, and convalescence is well established,
as is indicated by the callous formation, with overlapping of the
fragments.
The treatment in such cases is conservative and the results are favorable.
[Pg 188]
Plate 89.
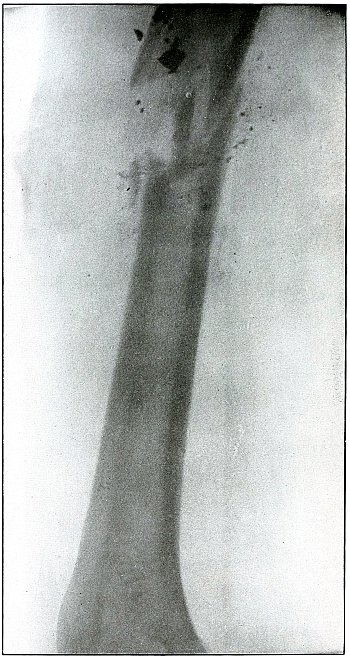
[Pg 189]
Shrapnel—Plate 89.
UPPER EXTREMITY.
Gunshot Fracture of the Humerus.
The course of the missile was from behind forward and outward,
striking the bone on the posterior surface, causing a fracture with
fragmentation, and lacerating the wound of exit with fragments of
bones and with its own deformation.
The wound of exit is indicated in the plate.
The wound is infected.
Fragments of the missile lie on the posterior surface of the bone, as
indicated by their dense shadow and distinct outline. The treatment in
such cases is conservative and the results are favorable.
[Pg 190]
Plate 90.
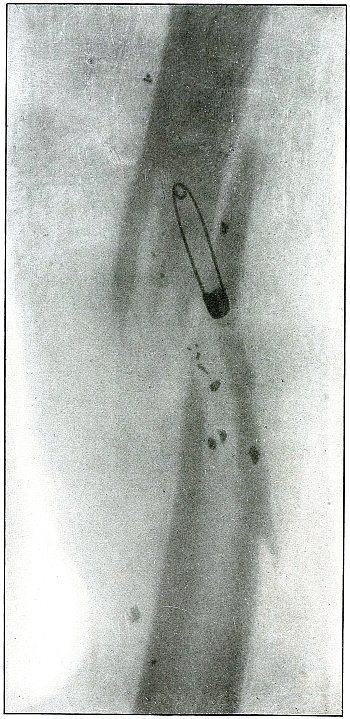
[Pg 191]
Shrapnel—Plate 90.
UPPER EXTREMITY.
Gunshot Fracture of the Left Humerus.
The course of the missile was transverse from without inward, with a
transverse fracture and fragmentation.
This wound might have been caused by either a shrapnel ball or a
deformed rifle bullet, but the distribution of the metallic fragments
rather indicate the course of a shrapnel ball.
The metallic fragments lie farther from the plate than the safety
pin of the dressing, which, therefore, lies behind the bone and the
fragments of the missile lie in front.
The treatment in such cases is conservative and the results are
favorable. The subsequent course may indicate interference for mal-union.
[Pg 192]
Plate 91.
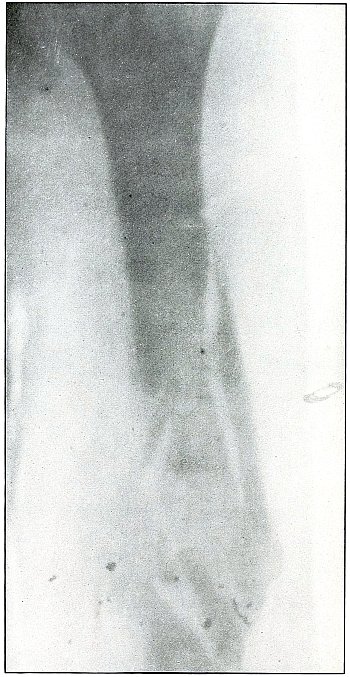
[Pg 193]
Shrapnel—Plate 91.
UPPER EXTREMITY.
Gunshot Fracture of the Left Humerus.
The course of the missile has been from without inward. The fragments
of metal marking the path of the missile lie farther from the plate on
the outer than on the inner side. This would indicate the former to be
in front of the bone and the latter to be behind. The wound could have
been caused by either a deformed rifle bullet or by a shrapnel ball,
but the distribution of metallic fragments along the track of the
missile rather indicates the agent to have been a shrapnel ball.
The case is similar in course and results to that shown in the
preceding plate 90.
[Pg 194]
Plate 92.
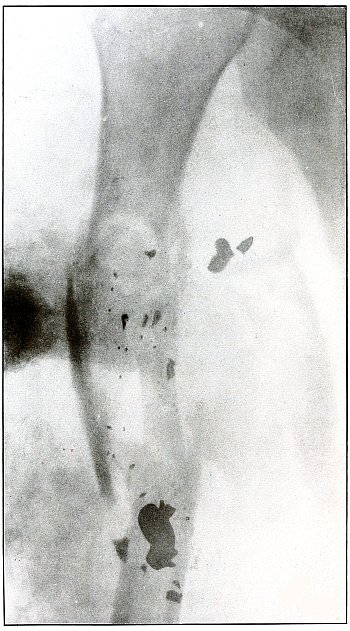
[Pg 195]
Shrapnel—Plate 92.
UPPER EXTREMITY.
Gunshot Fracture of the Right Humerus,
with Lodgment of the Missile.
The missiles, shrapnel balls deformed by ricochet, were multiple, with
a course from without inward and diagonally downward. The streaks
of metal particles along the seat of fracture indicates the path of
a shrapnel ball or fragment from the point of impact to the lower
fragment of the fracture, where several deformed shrapnel fragments
are lodged. Multiple wounds by shrapnel are common.
The wounds of entrance were small. There was no wound of exit. The
wound was not infected. This is another evidence that does not defend
the inference that ricocheted missiles are prone to introduce elements
of infection into a wound.
The plaster dressing does not seem to meet the indications for support
of the fracture.
The treatment is conservative in such cases.
Results are favorable.
[Pg 196]
Plate 93.
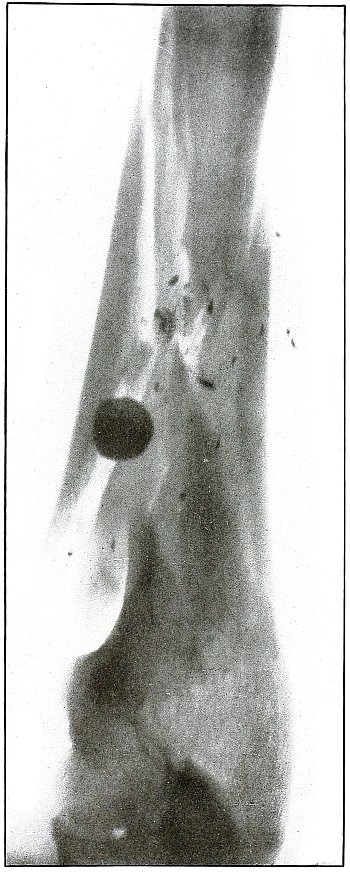
[Pg 197]
Shrapnel—Plate 93.
UPPER EXTREMITY.
Gunshot Fracture of the Right Humerus.
The course of the missile was transverse, from without inward and
downward, striking the shaft of the bone squarely and producing
a characteristic “butterfly” fracture, with a separation of the fragments.
The exposure was made with the ulnar side of the arm next to the
plate, indicated by the clear outline of the internal condyle and the olecranon.
The nearly normal size of the shadow of the shrapnel ball shows it to
be near the plate, and therefore to lie on the inside of the humerus.
The irregular outline of the ball and the metallic fragments spattered
about indicate that the ball was deformed by the detachment of
fragments on direct impact with the bone. The wound is not infected.
The treatment is conservative in such cases and the results are good.
[Pg 198]
Plate 94.
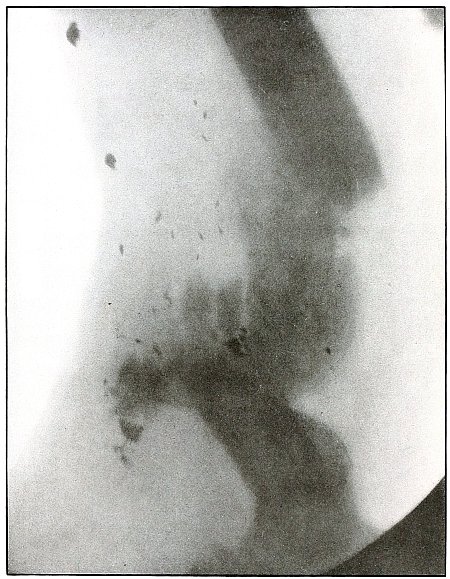
[Pg 199]
Shrapnel—Plate 94.
UPPER EXTREMITY.
Gunshot Fracture of the Right Humerus.
The course of the missile was from behind forward, causing a
transverse fracture of the humerus with some fragmentation.
The wound is in a state of established convalescence, with
considerable separation of the ends of the large fragments and without
infection, shown by the formation of callus and by an attempt at union
in faulty position.
The trail of the metallic fragments of the missile from behind forward
and their location near the anterior surface of the arm indicate the
course of the missile, either a rifle bullet or a shrapnel ball—most
probably the latter, as the lead core of the rifle ball, protected by
the jacket, does not break up into as many small particles as does the
shrapnel ball. The missile was deformed by ricochet before striking
the bone.
The early treatment in such cases is conservative, although the
subsequent course may indicate interference for malposition.
The results are favorable.
[Pg 200]
Plate 95.
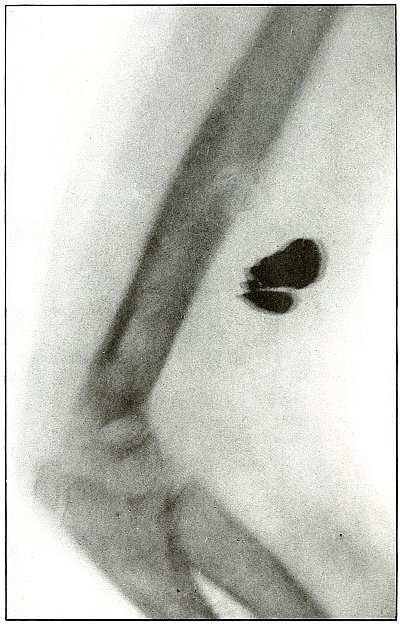
[Pg 201]
Shrapnel—Plate 95.
UPPER EXTREMITY.
Gunshot Wound of the Humerus,
with Lodgment of the Missile.
The course of the missile was from before backward. The missile
consisted of two large fragments of a richocheted shrapnel ball,
almost spent in energy before striking the arm, as its penetration was
just enough to pass through the soft parts and strike the humerus,
causing a fissure without separation of fragments. The wound was clean.
The treatment in such cases is naturally conservative.
[The epiphysis of the olecranon being so distinct
and showing no fusion, indicates the youth of this soldier, whose age
could not have been more than 16 years.]
[Pg 202]
Plate 96.
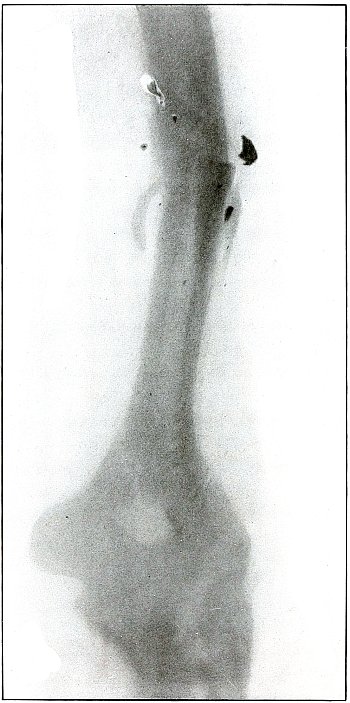
[Pg 203]
Rifle—Plate 96.
UPPER EXTREMITY.
(a) Gunshot Fracture of the Left Humerus—
(b) Gunshot Fracture of the Left Elbow.
The missile was a rifle bullet with the reduced velocity of long
range, passing transversely along the articulations of the elbow,
fragmenting the radius and ulna and fissuring the humerus through both
condyles.
The emergency treatment is antiseptic dressing and immobilization,
with prompt transportation to the base.
Subsequent treatment is conservative, with proper immobilization.
Results as to limb are favorable, with probable loss of function of the elbow.
[Pg 204]
Plate 97.
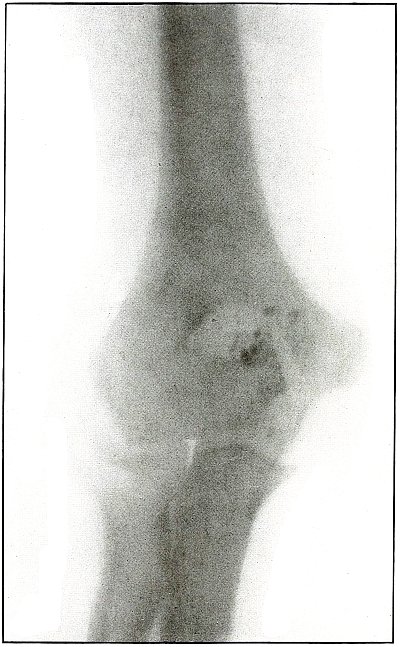
[Pg 205]
Shrapnel—Plate 97.
UPPER EXTREMITY.
Gunshot Wound of the Right Elbow.
The course of the missile was superficial, downward and outward from
above the internal condyle of the right humerus to the wound of exit
over the internal border of the ulna. Metal fragments of the missile
have lodged against the tip of the olecranum, with no fracture
and with no damage to the joint. The low velocity of the missile,
producing so slight a bone injury and the track of lead particles
along the line of contact with the bones determines it to have been a
shrapnel ball.
The wound was not infected.
The treatment in such cases is naturally conservative and the results
are very favorable.
[Pg 206]
Plate 98.
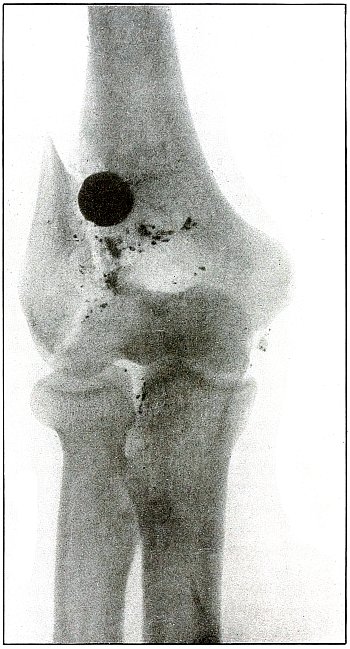
[Pg 207]
Shrapnel—Plate 98.
UPPER EXTREMITY.
Gunshot Fracture of the Right Elbow,
with Lodgment of the Missile.
The course of the ball was from before backward, striking the lower
end of the humerus squarely above and internal to the external condyle
and splitting off the condyles with a line of fracture extending
through the capitellum, without much separation of the fragment.
As the impact was direct, the energy producing such effect was
that of low velocity.
The great radiographic penetration shown in this plate gives the
shadows of the ball great distinctness and definite outline,
especially in the line of fracture, although its opposite border
is not in such sharp contrast. This appearance, together with the
very slight enlargement, leads to the suspicion that the ball lies
posteriorly, but a larger metal fragment, below the ball, is less
clear and suggests a position anterior to the bone. With the posterior
surface of the arm next to the plate and with but little difference
in the distance from the plate to either the anterior or posterior
surface of the bone, it is not easy to determine the location of the
ball in the anteroposterior direction, but it would seem to be on the
anterior surface of the bone.
The wound is not infected. The treatment is conservative and results
favorable.
The subsequent course would probably indicate the removal of a foreign
body from a site so near the joint.
[Pg 208]
Plate 99.
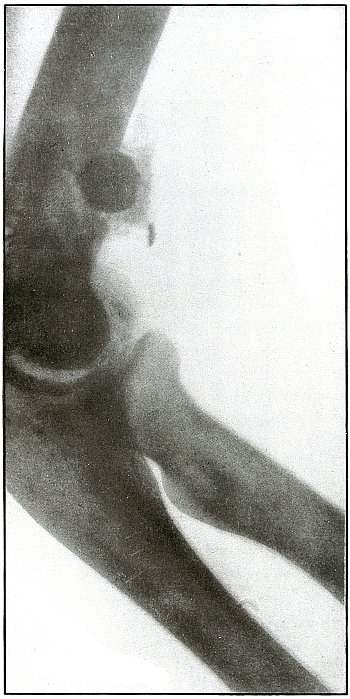
[Pg 209]
Shrapnel—Plate 99.
UPPER EXTREMITY.
Gunshot Fracture of the Right Elbow,
with Lodgment of the Missile.
Same wound as in plate 98.
The sharp holder of the greater sigmoid cavity and the head of the
radius fully obscured by the coracoid process indicate, that in this
exposure, the ulnar side of the arm was next to the plate.
With this condition and the enlarged shadow of the ball, the latter
must lie a little distance away from the plate, and, actually, on the
radial side of the humerus.
The position of the ball in the anteroposterior line is manifest, and
its position confirms the deductions made therefrom in the preceding plate (98).
[Pg 210]
Plate 100.
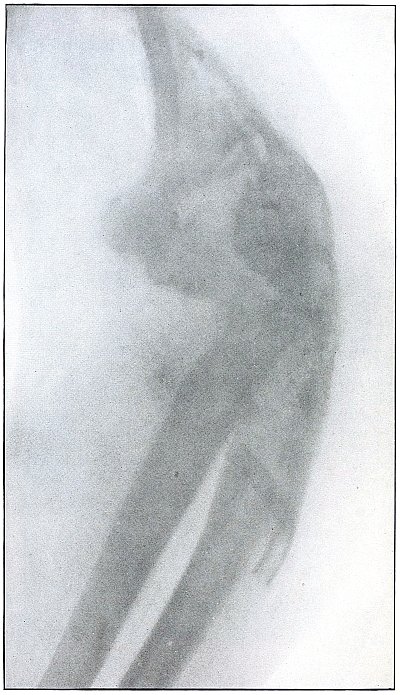
[Pg 211]
Shrapnel—Plate 100.
UPPER EXTREMITY.
Gunshot Fracture of the Elbow.
The primary condition of this wound is not manifest from the
appearance of the plate, which reveals only a destruction of the
joint by fracture and an advanced stage of infection, involving the
fragments and lower end of the shaft of the humerus, as indicated by
the rarefaction of these parts.
Several fragments of the missile are in evidence; it is probable that
others have escaped with drainage.
Drainage tubes are seen in the lower arm and upper forearm. The
primary conservative treatment has been continued through two or
three months.
The case is from Gulhané Military Hospital, where the scientific
character of surgical service already referred to must lead to the
inference that all the surgical indications have been met in the
management of the case.
[Pg 212]
Plate 101.
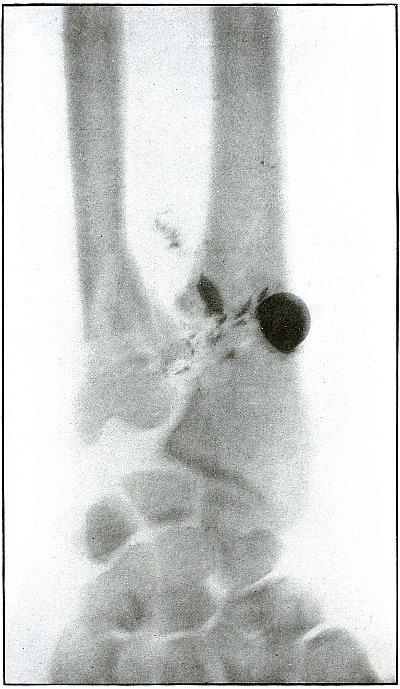
[Pg 213]
Shrapnel—Plate 101.
UPPER EXTREMITY.
Gunshot Fracture of the Left Radius and Ulna,
with Lodgment of the Missile.
The course of the missile was from within outward, striking the ulna a
glancing blow just above the styloid process, fracturing the anterior
surface, and then striking the internal border of the radius and
causing a slight notching fracture with a longitudinal fissure.
The forearm lies in supination, with its posterior surface next to
the plate. As the outline of the missile, as well as of the bone,
is blurred, there is not enough differentiation in the shadows to
indicate the anterior or posterior location of the missile with
reference to the radius.
The shrapnel ball struck the bone with low velocity, as all of its
remaining energy, absorbed by the two small bones, caused little
damage and practically no displacement of fragments. The wound was not
infected.
The treatment in such cases is, of course, conservative.
Results are uniformly good.
[Pg 214]
Plate 102.
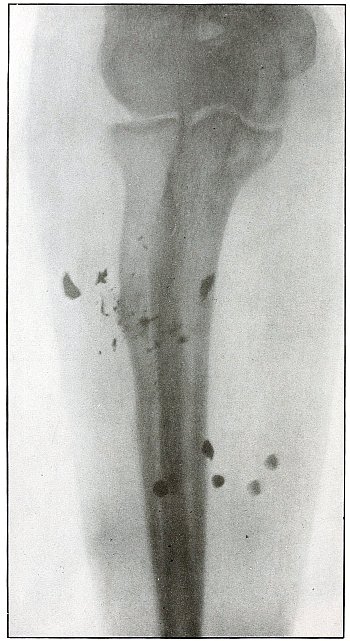
[Pg 215]
Shrapnel—Plate 102.
UPPER EXTREMITY.
Gunshot Fracture of the Right Radius.
A fragmented shrapnel ball, coursing from without inward, struck
the upper third of the shaft of the radius and caused a green-stick
fracture. A fragment of the ball, larger than those seen in the plate,
inflicted the greater damage and escaped through the wound of exit, to
be seen below the large fragment on the left of the plate.
The olecranon process of the right ulna rests on the photographic
plate, with the forearm in semipronation, so that the shadow of the
radius falls nearly in line with that of the ulna. With the forearm
restored to the anatomical position, the spattered metallic fragments,
now seen lying over and to the left of the radius, would then be shown
lying on the outer border of and posterior to the radius, except for
the upper right metallic fragment, now lying over the ulna, which
would be seen lying over the anterior surface of the radius. The six
pellets seen in the lower forearm have not contributed to the injury
of the bone. Their density and indefinite outline indicate a position
in the forearm opposite to the side next to the plate. With the
forearm in supination they would appear in their real position, in
front of the ulna and on the outside of the radius.
[Pg 216]
Plate 103.
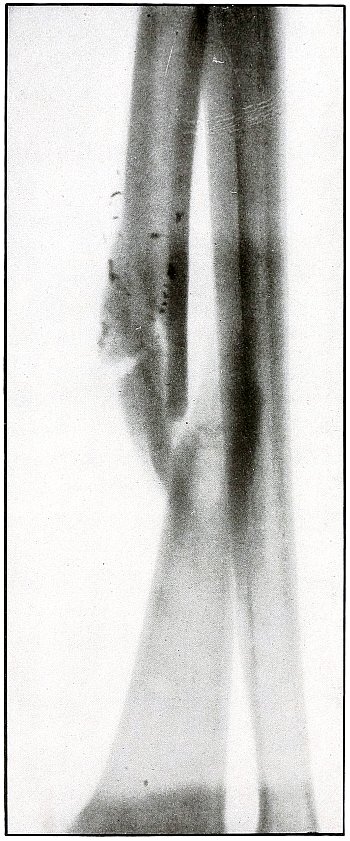
[Pg 217]
Shrapnel—Plate 103.
UPPER EXTREMITY.
Gunshot Fracture of the Right Radius.
The missile in its course from behind forward and from above downward
left a trail of its metal particles along the line of its first
contact until the bone yielded to the pressure in a transverse fracture.
The arm lies in slight pronation with the longitudinal ridges of the
dorsal surface of the ulna, shown distinctly next to the photographic
plate. The upper end of the lower radial fragment, shown as overlying
the ulna, is inclined forward in the anatomical position. The metal
particles are on the outer and posterior border of the radius.
The treatment in such cases is conservative.
Results as to function are uncertain.
[Pg 218]
Plate 104.
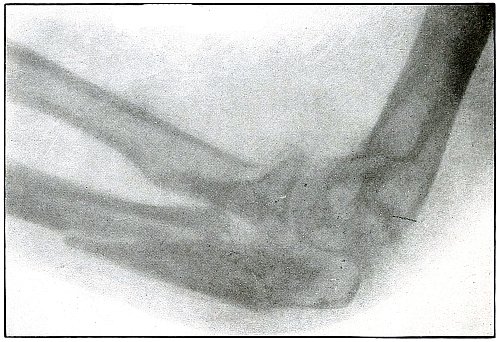
[Pg 219]
Shrapnel—Plate 104.
UPPER EXTREMITY.
Gunshot Fracture of the Ulna.
The course of the missile was tangential along side of the upper end
of the ulna and internal condyle of the humerus, with a splitting
effect on the ulna, which formed three fragments by breaking off the
olecranon, and one lateral fragment from the shaft of the bone without
displacement. The line of metallic particles shows the path of the
ball in its slight contact with the bones, beginning on the side of
the ulna and extending along the side of the internal condyle from
where the ball escaped through the skin. The wound, not infected, was
treated as simple fracture. A few fine lines on the plate above the
fracture are due to scratches on the negative.
Results in such cases should be good.
[Pg 220]
Plate 105.
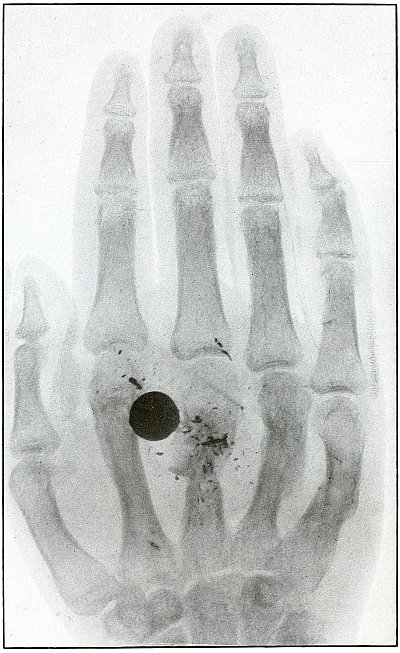
[Pg 221]
Shrapnel—Plate 105.
UPPER EXTREMITY.
Gunshot Fracture of the Right Metacarpus.
The course of the missile was from the outer border of the hypothnear
eminence diagonally downward through the palm, lodging against the
second metacarpal bone with fracture of last four metacarpals.
The metal particles are not seen on the fourth and fifth metacarpals
because the violence at these points was transmitted through soft
parts, but the projectile spent its remaining energy directly against
the second and third metacarpals.
The palm of the hand was next to the photographic plate, as indicated
by the immediate contact of the thumb. The shadow of the bones is not
dense, but in deep contrast with the shadows of the ball and metal
fragments, which are so clearly outlined with the ball of normal size
that the ball is thus shown to lie on the palmar side of the hand.
The treatment is conservative, with judicious interference when
opportunity shall offer for removal of the missile.
[Pg 222]
Plate 106.
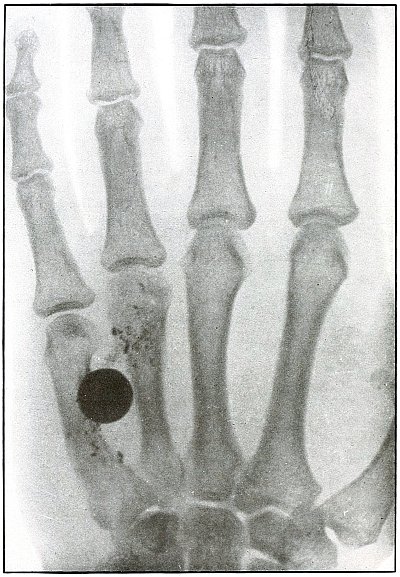
[Pg 223]
Shrapnel—Plate 106.
UPPER EXTREMITY.
Gunshot Fracture of the Left Metacarpus,
with Lodgment of the Missile.
The palm of the hand lies next to the plate. The ball is very slightly
enlarged and the small metal fragments are indistinct, indicating that
they and the ball lie on the back of the hand.
The ball struck the third knuckle and lodged beneath the skin between
the fourth and fifth metacarpals, fracturing both bones without
displacement of fragments. In the recent wound the condition would be
apparent, but after days of inflammatory reaction and infection, the
swelling is too great to make any determination by palpation.
The treatment is removal of the missile. Good results regularly follow.
[Pg 224]
Plate 107.
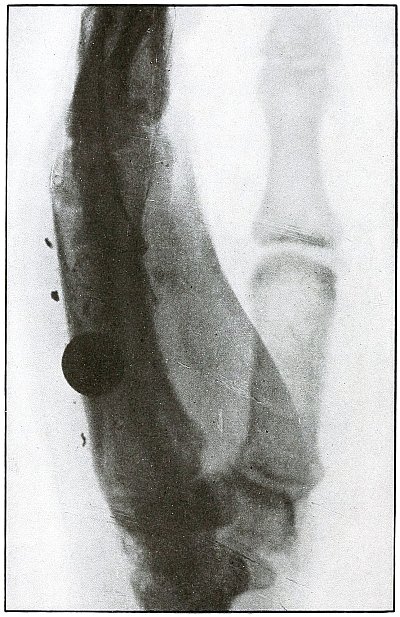
[Pg 225]
Shrapnel—Plate 107.
UPPER EXTREMITY.
Gunshot Fracture of the Left Metacarpus,
with Lodgment of the Missile.
The hand lies with its ulnar side next to the plate, as is indicated
by the sharp outline of the swollen hypothenar eminence, nearer the
plate than the thumb, with the enlarged, poorly defined, and rarefied
shadow of its metacarpal and phalanges.
As the normal size of the balls and the clear outline of the metal
fragments must place them almost in contact with the plate, the ball
is located near the fifth metacarpal. As this is the same case as
is shown in plate 106, the conclusions drawn
from each plate are confirmed by the other.
The wound is infected, as indicated by the swelling of the palm.
The treatment is removal of the missile, with management of the infection.
[Pg 226]
Plate 108.
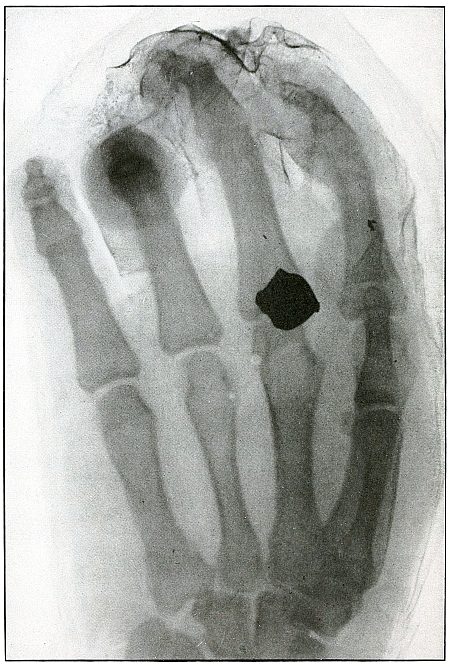
[Pg 227]
Shrapnel—Plate 108.
UPPER EXTREMITY.
Gunshot Wound of the Left Hand,
with Lodgment of the Missile.
The shadow of the hand is shown with the palm next to the plate, as
indicated by the small, well-defined outline of the first metacarpal
lying within the outline of the larger and less-defined shadow of the
second metacarpal. The third finger is flexed at the first phalangeal
joint, and the end of the second phalanx is outlined in deeper shadow,
with its long axis vertical to the plate.
The position raises the first finger from the plate and very
slightly enlarges the size of the shadow of the bullet, although it
retains its sharp outline. The shadow of the ball being very nearly
the normal size, the ball lies on the palmar side of the third
metacarpo-phalangeal joint. It entered the hand on the outer border
of the base of the first finger, and left a fragment of metal on its
slight contact with the bone. The ball was deformed by ricochet before
striking the hand, with almost completely spent velocity. The wound is
infected.
The treatment is the management of infection.
[Pg 228]
Plate 109.
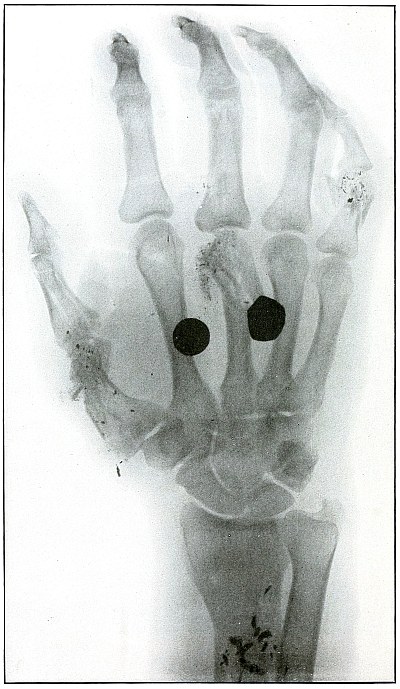
[Pg 229]
Shrapnel—Plate 109.
UPPER EXTREMITY.
Multiple Gunshot Wounds of the Right Hand and Forearm,
with Fracture of the Metacarpus and Phalanges and
Lodgment of the Missile.
The hand lay with the palmar surface next to the plate. The distinct
outline of the small metal fragments and the natural size of the
shadow of the undeformed shrapnel ball show that they lay on the
anterior side of the metacarpus. The arrangements of the metal
particles and bone fragments and the indication of the point of
entrance of one wound on the outer border of the metacarpal of the
thumb indicate the course of the balls to have been from the radial
to the ulna side of the palm. The undeformed ball, then, lies, most
probably, in front of the second metacarpal. The deformed ball shows,
in its enlarged shadow and not so distinct in outline as the normal
ball, that it is on the dorsal surface of the third and fourth metacarpals.
The undeformed ball caused the fracture of the phalanx and metacarpal
of the thumb; the deformed ball fractured the neck of the third
metacarpal; a ball which escaped from the wound and touched the base
of the first phalanx of the middle finger and fractured the first
phalanx of the little finger; and another ball, which glanced along
the anterior surface of the lower end of the shaft of the radius and
left a deposit of metal to mark its course, also escaped from the
ulnar border of the forearm at a point indicated in the plate.
Four balls were concerned with this wound; two of them have lodged
with some damage and two others have escaped, after inflicting a
slight injury. Multiple shrapnel wounds are common. It may be said
that the greater the number of balls lodged in a given area the less
the distance of the plane from the apex of the cone of dispersion of a
shrapnel discharge.
Several shrapnel balls, lodged in a small area without causing much
damage or exhibiting much power of penetration, indicate low velocity
at close range of shrapnel balls on discharge from the shrapnel envelope.
In a personal case, eight shrapnel balls were removed from a forearm.
[Pg 230]
CHEST.
Plate 110.
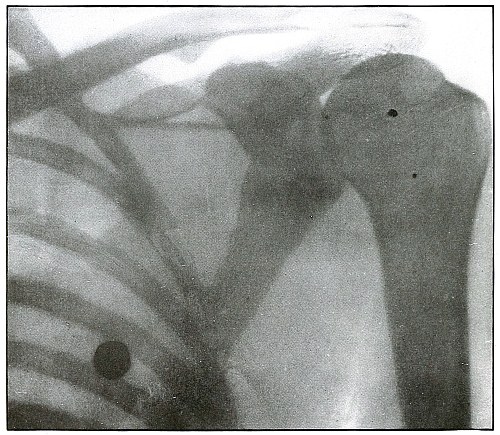
[Pg 231]
Shrapnel—Plate 110.
CHEST.
Gunshot Wound of the Chest,
with Lodgment of the Missile in the Lung.
The posterior chest wall is next to the plate, as the posterior rib
shadows are much more distinct and much smaller than the shadows of
the anterior ribs.
The shadow of the ball is blurred, which shows that it moved with
respiration and is, therefore, probably in the lung. The shadow is
only slightly enlarged and is fairly dense, which indicates it to be
not far from the ribs and, therefore, in the posterior portion of the lung.
The treatment of such cases is conservative; infection is not common;
hæmothorax pleurisy, empyema, pneumonia, and pulmonary abscess
are most frequent complications, named in the order of frequency.
Pulmonary abscess is very rare. Pneumonia was seen in a personal case.
[Pg 232]
Plate 111.
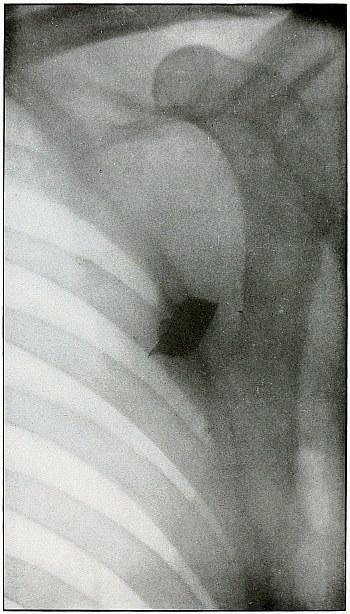
[Pg 233]
Shrapnel—Plate 111.
CHEST.
Gunshot Wound of Chest, with
Lodgment of the Missile Superficially.
While the missile is not a shrapnel ball, it presents similar
conditions and does not need to be separately classified.
The vertebral border of the scapula is distinctly shown in light
shadow, indicating its position near the plate.
The outline of the missile is so distinct and the shadow so dense
that it must lie near the plate, and is located superficially in the
infraspinatus fossa.
[Pg 234]
Plate 112.
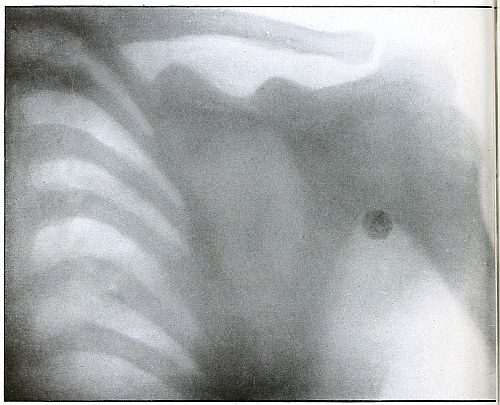
[Pg 235]
Shrapnel—Plate 112.
CHEST.
Gunshot Wound of the Chest, with Fractured Rib
and Lodgment of the Missile in the Axilla.
The back of the patient lay on the plate, as is indicated by the
normal size of the ribs behind and the exaggerated outline in front.
The ball struck the sixth rib behind and caused a fracture at the
angle. It then continued its course to the axilla. The normal size of
the shadow of the ball indicates that it lies superficially behind the
head of the humerus.
The wound of the rib was infected superficially, and the secretion of
the wound carried away the most of the metal particles which the ball
in striking deposited on impact.
[Pg 236]
Plate 113.
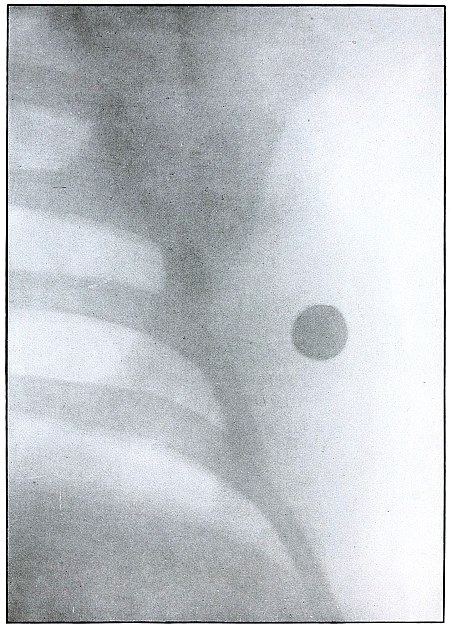
[Pg 237]
Shrapnel—Plate 113.
CHEST.
Gunshot Wound of the Chest, with
Lodgment of the Missile in the Axilla.
There is no wound of the bone.
The ball lies in the axilla, behind, not close to, the plate, because
the density of the shadow is not very great and the size is slightly
enlarged. The distance from the plate is probably that of the mid-axillary line.
The wound is not infected. Pain and impaired movement of the arm
suggested localization of the missile and indicate removal in the
subsequent course of treatment.
[Pg 238]
Plate 114.
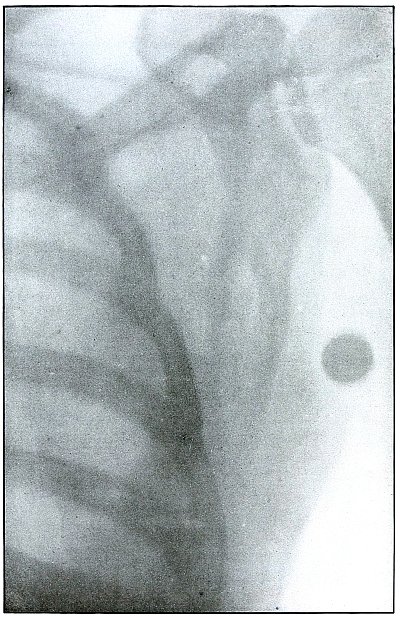
[Pg 239]
Shrapnel—Plate 114.
CHEST.
Gunshot Wound of the Chest, with the
Lodgment of the Missile in the Axilla.
The posterior chest wall lay next to the plate.
The almost normal size of the shadow of the ball indicates that it
lies near the plate, and the blurred outline shows that it has moved
with the chest in respiration. The ball lies, therefore, in the
posterior axilla near the middle of the outer border of the scapula,
imbedded in the thoracic muscles.
The treatment is expectant. Such wounds are rarely infected. Pain or
impairment of function only would indicate removal of the missile from a clean wound.
[Pg 240]
PELVIS.
Plate 115.
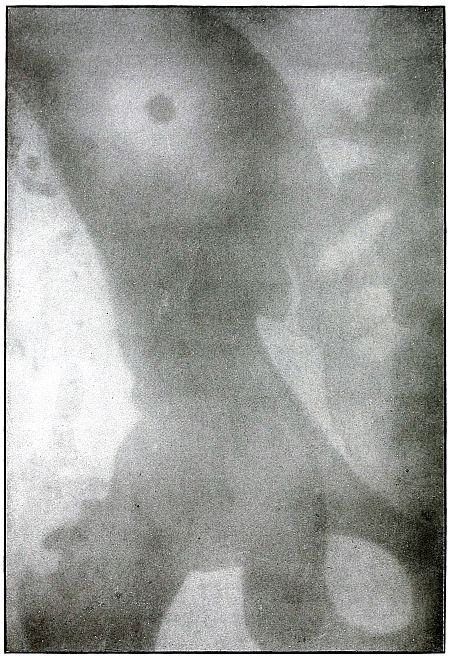
[Pg 241]
Shrapnel—Plate 115.
PELVIS.
Gunshot Fracture of the Crest of the Right Ilium,
with Lodgment of the Missile.
As the wound was received while the soldier was lying prone, the
course of the missile in the body was from above downward, striking
the crest of the ilium, on which it was fragmented, and trailing its
fragments as far down as the great trochanter. The injury to the ilium
was a crushing fracture, with the displacement of small fragments from
the antero-superior spine.
As the sacrum was next to the photographic plate, the missile, judging
from its indistinct shadow, lies farther from the plate and in front
of the bone. The relative distinctness of the large fragment seen on
the wing of the ilium indicates its probable position to be on the
outside of the ilium.
The trail of the smaller metal fragments lies between the
antero-superior spine and the great trochanter, anterior to the plane
of the femur.
The treatment in such cases is always conservative.
[Pg 242]
LOWER EXTREMITY.
Plate 116.

[Pg 243]
Shrapnel—Plate 116.
LOWER EXTREMITY.
Gunshot Wound of the Thigh,
with Lodgment of the Missile.
With the posterior aspect of the thigh lying next to the plate, the
very greatly enlarged shadow of the deformed shrapnel ball indicates
that it lies a relatively great distance from the plate, so that its
location can be determined to be near the internal border of the adductor
muscles, anteriorly, and below the transverse plane of the lesser trochanter.
[Pg 244]
Plate 117.
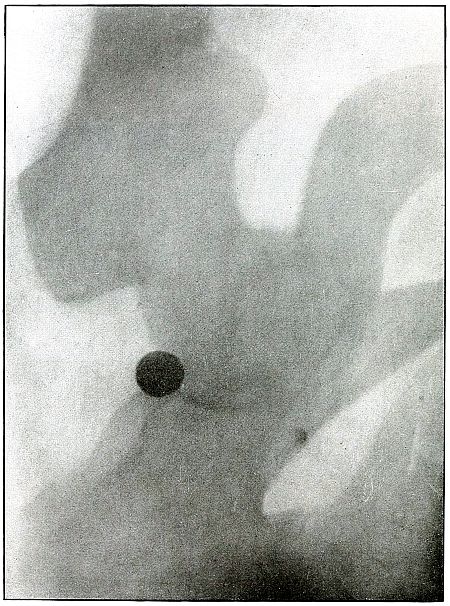
[Pg 245]
Shrapnel—Plate 117.
LOWER EXTREMITY.
Gunshot Wound of the Thigh,
with Lodgment of the Missile.
With the sacrum lying next to the plate, the normal size, clear
outline, and dense shadow of the shrapnel ball indicates its position
to be near the plate. The location can be roughly estimated as the
superficial gluteal region, external to the ramus of the ischium and
near the aerior plane of the upper border of the acetabular cavity.
[Pg 246]
Plate 118.
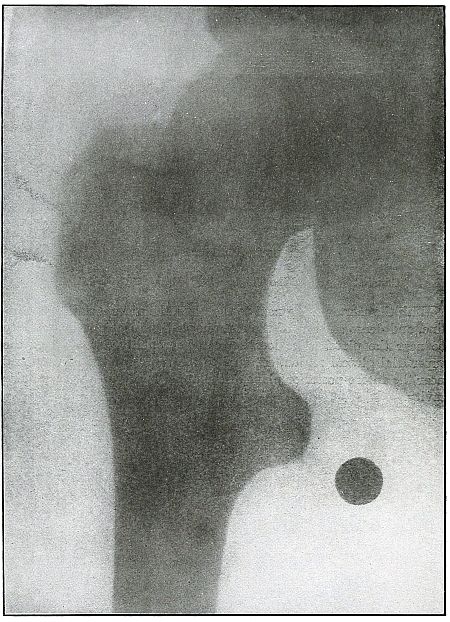
[Pg 247]
Shrapnel—Plate 118.
LOWER EXTREMITY.
Gunshot Wound of the Thigh,
with Lodgment of the Missile.
The normal size, distinct outline, and considerable density of the
shadow of the shrapnel ball show that it lies very near the plate,
posterior to the bone and in the buttocks, quite superficially.
The treatment in such cases is always conservative. Pain or
impairment of function indicate removal after convalescence.
[Pg 248]
Plate 119.
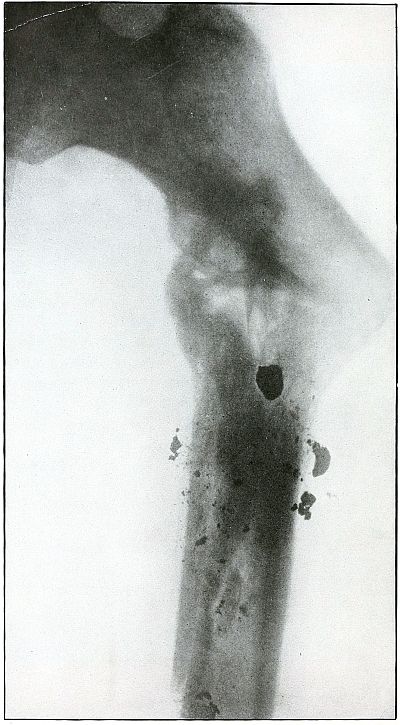
[Pg 249]
Shrapnel—Plate 119.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of the Missile.
The direct subtrochanteric impact disintegrated the missile and
delivered all of its energy to the bone, with a resulting transverse
fracture of the upper end of the shaft of the femur and longitudinal
fragmentation of the shaft. The course of the shrapnel ball was from
behind forward and from above downward, as is shown by the track of
the metal fragments and the lodgment of a larger lead fragment on the
shaft below the seat of fracture. The uppermost large lead fragment,
as shown by the depth of its shadow, lies farther behind the bone and
nearer to the photographic plate than do the other pieces of the ball,
as indicated by their lighter shadows. All of the fragments seem to
lie behind the bone.
The conservative treatment of this wound is justified by the
attempt at repair, as indicated by the callus formation; but it is
manifest, from the extremely faulty position, that the indication for
immobilization and extension in strong abduction were not appreciated.
Proper management of conservative treatment in such cases gives good results.
[Pg 250]
Plate 120.
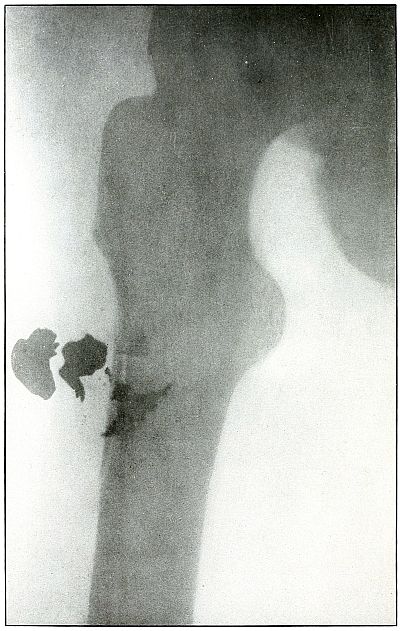
[Pg 251]
Shrapnel—Plate 120.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of Multiple Missiles.
The position of the femur is in outward rotation, as shown by the
full shadow of the lesser trochanter and the vanishing of the greater
trochanter behind the shoulder of the neck. The two larger missiles
lie on the outer side of the bone and the others lie in front on the
seat of fracture. The greatly deformed shrapnel balls and the slight
chipping fracture of the femur indicate that the greater portion of
the striking energy of the missiles was so dissipated in ricochet that
but little force was left for attack on the bone.
The treatment in such cases is expectant and indication rarely arises
for search for and removal of the missiles.
[Pg 252]
Plate 121.
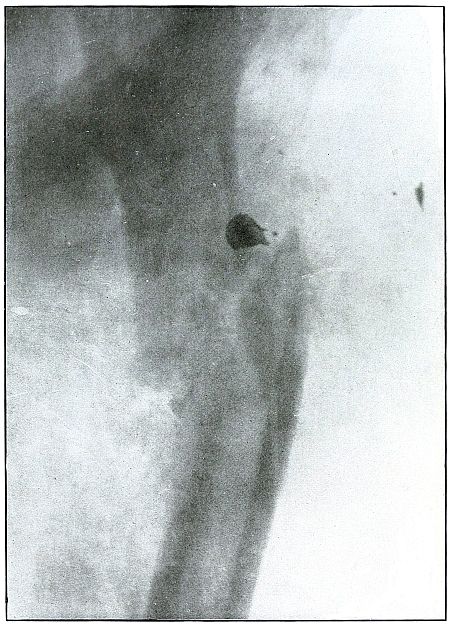
[Pg 253]
Shrapnel—Plate 121.
LOWER EXTREMITY.
Gunshot Fracture of the Shaft of the Femur,
with Lodgment of the Missile.
The course of the shrapnel ball was from within outward, striking the
femur with the energy of high (shrapnel) velocity, with fragmentation
of the missile by impact on the bone. The largest fragment, by the
distinct outline of its shadow, lies close to the plate and behind the
bone; a smaller metal fragment has been carried to the outer border of
the thigh, where it lies superficially; another fragment lies in the
seat of fracture.
The position of fragments is faulty, as the indications for extension
and abduction have not been wholly met, although this is a case from
the well-conducted service of Gulhané Hospital.
The treatment in such cases is conservative and the results are good.
[Pg 254]
Plate 122.
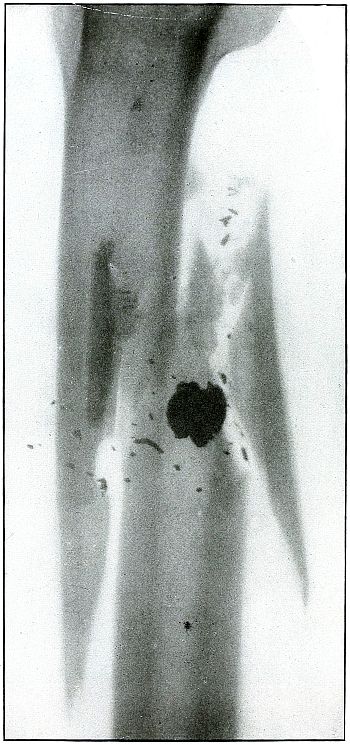
[Pg 255]
Shrapnel—Plate 122.
LOWER EXTREMITY.
Gunshot Fracture of the Shaft of the Femur,
with Lodgment of the Missile.
The shrapnel ball, in its almost directly antero-posterior course from
behind forward, has delivered the energy of high (shrapnel) velocity
to the bone, which had absorbed it all in stopping the missile, with
a resulting approach to a butterfly fracture with displacement of fragments.
The upper end of the lower fragment lies nearer to the plate than to
the lower end of the upper fragment, with the deformed shrapnel ball
lying behind the latter, closer to the plate.
The treatment in such cases is conservative, with good results to
follow except as they may be imperiled by infection.
[Pg 256]
Plate 123.
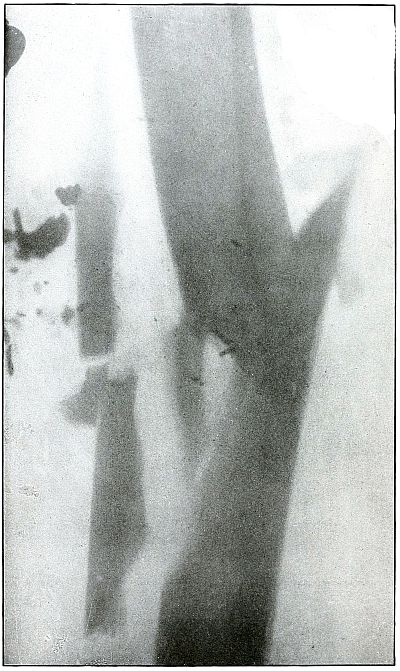
[Pg 257]
Shrapnel—Plate 123.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of the Missile.
While the missile in this case may have been other than a shrapnel
ball, the fracture is one produced by the impact of a missile
delivering great striking energy, with a predominant cross-section
factor in its composition. The fragments are due to the application
of an energy in which the mass was distributed over a relatively
large area on bone, which resulted in the displacement of the large fragments.
The treatment in such cases is conservative.
Results are favorable; infection is generally controlled.
[Pg 258]
Plate 124.
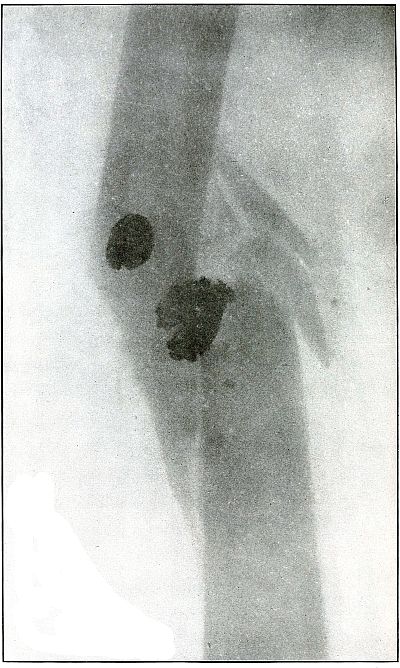
[Pg 259]
Shrapnel—Plate 124.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of Multiple Missiles.
The direct impact of two shrapnel balls, delivering all of their
energy to the femur, resulted in a fracture with large fragments.
The exposure was made through a plaster splint, and shows a faulty
position with progressing repair.
The treatment in such cases is conservative, but with respect for
the indications to maintain proper position of the fragments.
[Pg 260]
Plate 125.

[Pg 261]
Shrapnel—Plate 125.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of the Missile.
The condition shown in the plate is the characteristic result of
direct impact of a projectile of low velocity and great sectional area
in which all of the energy is delivered to the bone against which it lodges.
The distinct outline and dense shadow of the deformed missile
indicates its position to be behind the bone.
The callus formation indicates the favorable progress of repair, but
with the fragments in faulty position.
The treatment in such cases is conservative, with proper respect to
the principles of maintenance of normal relation of the fragments.
[Pg 262]
Plate 126.
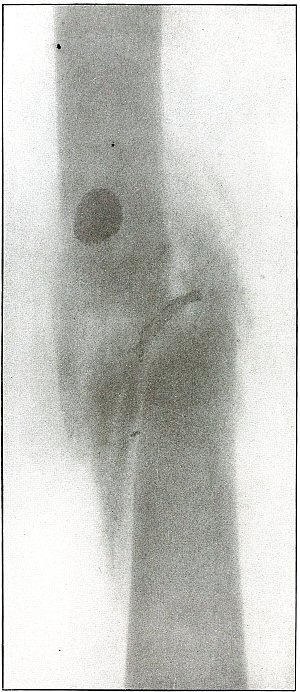
[Pg 263]
Shrapnel—Plate 126.
LOWER EXTREMITY.
Gunshot Fracture of the Femur,
with Lodgment of the Missile.
The course of the shrapnel ball was antero-posterior, with an impact
on the shaft of the femur, which fragmented both the ball and bone
through the imparting or the entire striking energy of the ball to the
bone by the lodgment of the ball. The sharp outline and density of
the shadows of the missile, in contrast with the dense shadows of the
bone, indicate that the missile lies closer to the plate than does the
bone, although the flattened ball does not permit a comparison between
its shadow and the normal size of the ball.
The advanced stage of convalescence is shown by the formation of callous.
The treatment in such cases is conservative and the results are good
if proper position can be maintained.
[Pg 264]
Plate 127.
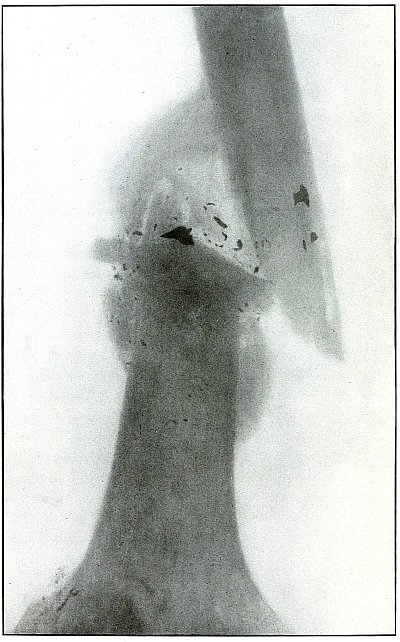
[Pg 265]
Shrapnel—Plate 127.
LOWER EXTREMITY.
Gunshot Fracture of the Shaft of the Femur.
The impact of the missile was delivered with the energy of high
(shrapnel) velocity at close range, as is indicated by the signs of
another shrapnel wound, just above the outer tuberosity (in the lower
left corner of the plate), where a deposit of metallic particle is evidenced.
The fragmentation of the missile, through its contact with the bone,
indicates the great striking force of a missile which ricocheted from
the bone. The general distribution of metallic particles through
a wound of this class indicates certainly that the missile was
unjacketed, and the destructive forces show that its sectional area
was relatively larger, i. e., a shrapnel ball.
The hard metal jacket of a rifle bullet would not give off its
particles in contact with the bone unless it were so greatly deformed
as to have almost entirely lost its jacket. In this state the energy
of a rifle ball must be so greatly reduced, through the violence of
ricochet, that it would not retain enough striking force to cause its
disintegration on impact with the bone. Besides, some particles of the
jacket could be identified, as they are always bent or twisted so that
their character is recognized in the shadow.
[Pg 266]
Plate 128.
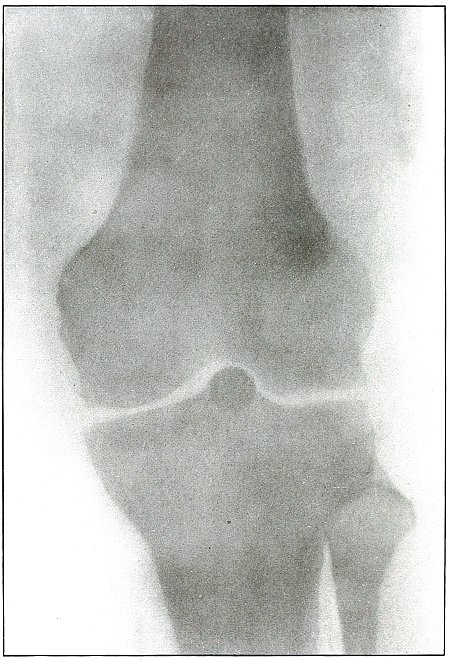
[Pg 267]
Shrapnel—Plate 128.
LOWER EXTREMITY.
Gunshot Wound of the Left Knee,
with Lodgment of the Missile in the Joint.
The slight enlargement and moderate density of the shadow of the
projectile indicates a position a short distance from the plate. A
slight shadow dependent from the external condyle on the outside of
the ball and a metallic marking just outside of the upper contour of
the outer tuberosity indicate an injury to the joint and the path of
the ball from above the outer tuberosity into the joint capsule.
The probabilities are that the ball lies between the head of the tibia
and the patellar notch of the femur, but the absolute certainty of
this deduction must be supported by an exposure in a lateral plane,
which is shown in plate 129.
[Pg 268]
Plate 129.
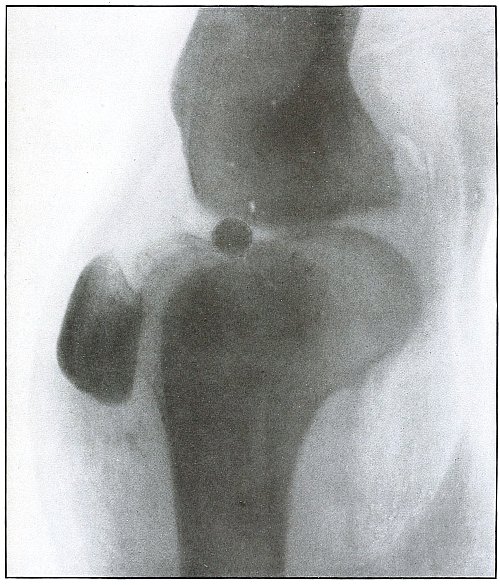
[Pg 269]
Shrapnel—Plate 129.
LOWER EXTREMITY.
Gunshot Wound of the Left Knee,
with Lodgment of the Missile in the Joint.
As the fibular shadow is about the normal size and clearly outlined,
the fibular side of the leg lay next to the plate.
As the shadow of the ball is dense and not much enlarged, it must lie
near the plate. A light shadow in front of the ball, which shows the
anterior crucial ligament, and a metallic marking above the patella,
suggests the path of the ball.
As this is a lateral projection of the same case that is shown in
plate 128 in an antero-posterior projection,
these conclusions are thus verified.
The missile lies in the joint capsule between the head of the tibia,
in front of the spine, and the patellar notch of the femur.
As a foreign body in the knee joint which seriously interferes with
its function, removal is indicated when surgical facilities are at hand.
The results in such cases are usually good.
[Pg 270]
Plate 130.
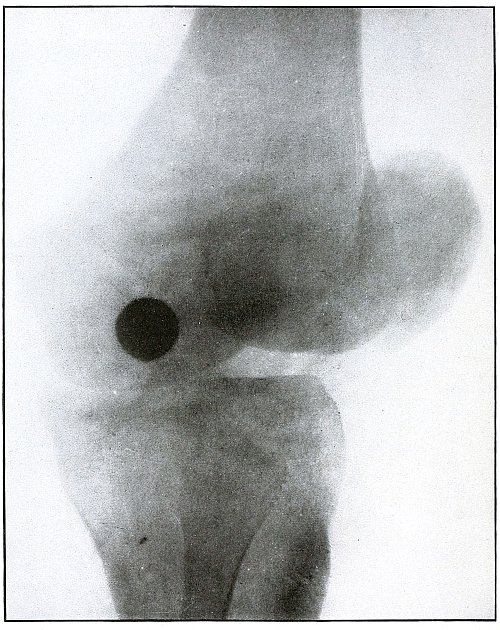
[Pg 271]
Shrapnel—Plate 130.
LOWER EXTREMITY.
Gunshot Wound of the Left Knee,
with Lodgment of the Missile in the Joint.
The line of projection of the shadow is directed obliquely from
behind, focussed on the internal aspect of the knee, with the fibula
next to the plate. As the shadow of the shrapnel ball is much enlarged
and not very dense, the ball must lie some distance from the plate and
away from the fibular side of the joint. As the distances through the
knee joint are about the same in all cases and as shrapnel balls are
approximately the same size, it is evident that the ball lies farther
away from the plate than it does in plate 129,
where it is about the middle of a transverse line through the joint.
It must lie, therefore, superficially between the head of the tibia
and the internal condyle of the femur.
Removal is indicated under favorable surgical conditions. Infection of
the joint may occasionally indicate drainage and removal as emergency treatment.
Results, except for infection, are good.
[Pg 272]
Plate 131.
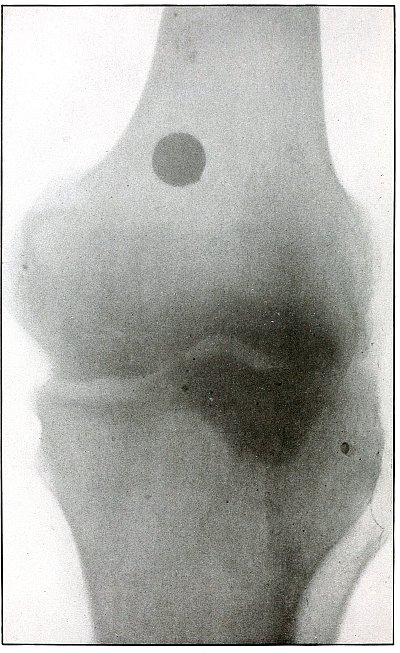
[Pg 273]
Shrapnel—Plate 131.
LOWER EXTREMITY.
Gunshot Wound of the Knee,
with Lodgment of the Missile.
That the knee is not fully extended is shown by the exaggerated
outline of the tibial head.
The enlarged and only fair density of the shadow indicates that the
shrapnel ball lies some distance away from the plate. As the bone is
not injured, the missile must lie either in front of or behind the
femur, and its enlarged shadow shows the position to be in front of
the femur, just above the articular surface, and probably within the
reflection of the capsular ligament.
A comparison with the size of the shadows of the balls shown in plates
128 and 130 will show this
one to be greater than the former and less than the latter, and so
it must bear about the same relation in the distance from the plate.
This would account for the location in front instead of behind the femur.
The treatment is conservative, and removal is indicated when function is disturbed.
[Pg 274]
Plate 132.
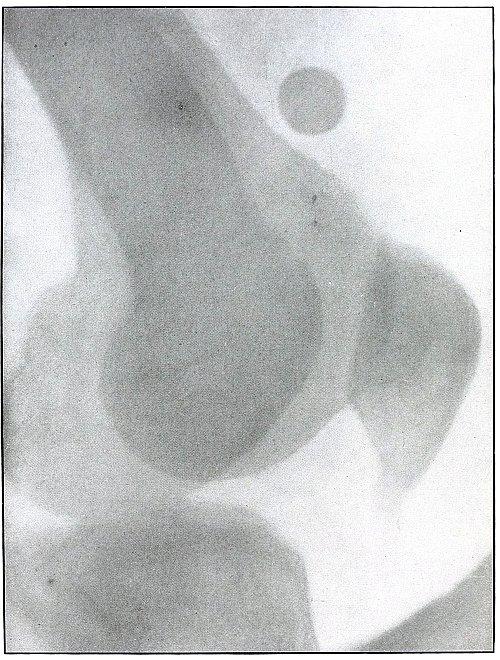
[Pg 275]
Shrapnel—Plate 132.
LOWER EXTREMITY.
Gunshot Wound of the Knee,
with Lodgment of the Missile.
The fibular side of the leg lay next to the photographic plate, as
shown by the enlarged fainter outline of the internal tuberosity.
The shadow of the shrapnel ball is neither as normal in size as that
of the external condyle nor as exaggerated as that of the internal
condyle, and the position is probably neither as close to the plate as
the former nor as far away as the latter.
The missiles lie about the middle of the anterior surface of the lower
end of the femur, above the articular surface.
[Pg 276]
Plate 133.
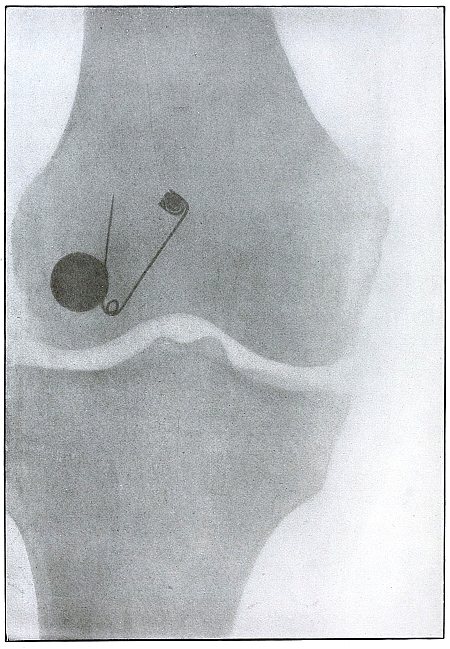
[Pg 277]
Shrapnel—Plate 133.
LOWER EXTREMITY.
Gunshot Wound of the Right Knee,
with Lodgment of the Missile.
The ball struck the outer condyle just above the articular surface
with only enough energy to damage and slightly crack the bone. The
injury to the bone and the metallic mark of the impact can be seen
just above the outer border of the articular cartilage of the outer condyle.
[Pg 278]
Plate 134.
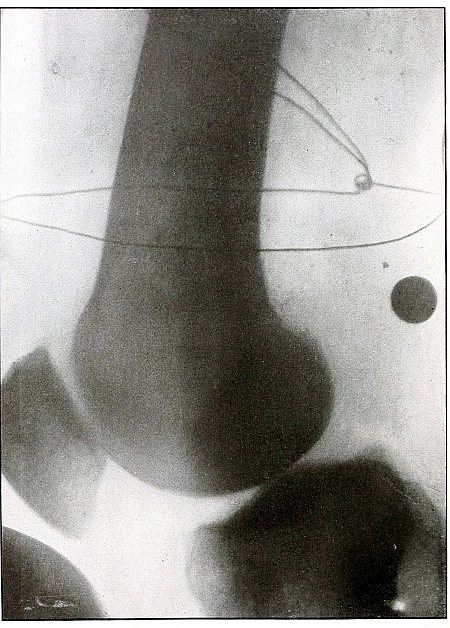
[Pg 279]
Shrapnel—Plate 134.
LOWER EXTREMITY.
Gunshot Wound of the Left Knee,
with Lodgment of the Missile.
The outer tuberosity lay next to the photographic plate, with the knot
in the localizing wire on the inside of the leg and farther away from
the plate.
The line of projection is transversely through the tuberosities.
The shadow of the ball, as it is somewhat enlarged, not sharply
defined, and of medium density, must lie about midway between the
lines of the localizing wire or in the popliteal space just above
and between the tuberosities, much nearer the popliteal surface
than the bone. An accurate localization of the ball in a transverse
line, however, would require an exposure of another plate in an
antero-posterior line, but in this actual case the localization of the
ball had to be made from this single plate, as only one exposure was made.
The ball struck the border of the popliteal space of the femur just
above the tuberosity, without energy enough to cause a fracture,
deform the ball, or even to leave, as a mark of contact, metal particles of the ball.
[Pg 280]
Plate 135.
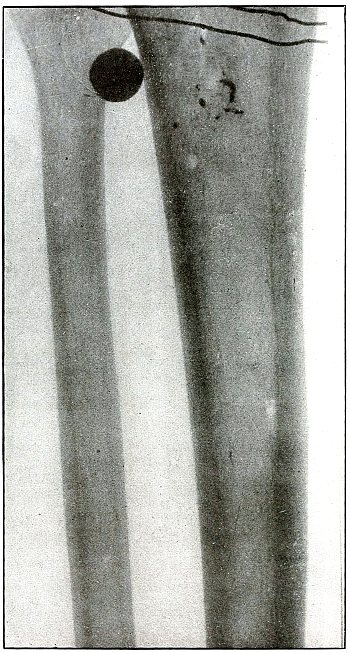
[Pg 281]
Shrapnel—Plate 135.
LOWER EXTREMITY.
Gunshot Wound of the Left Leg,
with Lodgment of the Missile.
The posterior surface of the leg lay next to the plate, as shown by
the outline of the head of the fibula, but any estimate of distance
from the plate, based on depth of the shadows, is of little value
because there is no contrast between localizing-wire shadows in front
of and behind the leg.
The slightly enlarged shadow of the ball indicates it to be farther
from the plate than it would be if it lay behind the fibula. As the
shadows of the metal fragments on the tibia are not sharp enough to
indicate their position to be near the plate, the ball has lodged
anteriorly between the tibia and fibula after ricocheting from the
anterior surface of the tibia. The ball, being undeformed, struck the
tibia with so little force that it barely penetrated the skin.
The reaction of infection in such wounds makes a diagnosis on physical
examination difficult and indicates radiography.
[Pg 282]
Plate 136.
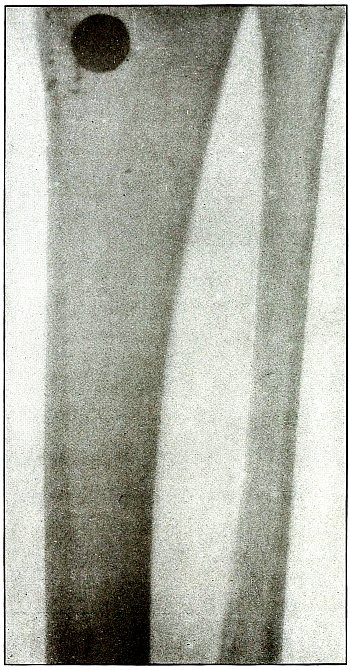
[Pg 283]
Shrapnel—Plate 136.
LOWER EXTREMITY.
Gunshot Wound of the Leg,
with Lodgment of the Missile.
The leg lay with its posterior surface next to the photographic plate.
The enlarged shadow of the ball and the blurred outlines of the
metal fragments require them to be some distance from the plate and
therefore on the anterior surface of the tibia.
The impact has been from within outward with so little energy that the
ball only touched the internal border of the tibia and lodged beneath
the skin.
Without the reaction of inflammation and infection, diagnosis could be
made by palpation, but extensive swelling indicates radiography.
[Pg 284]
Plate 137.
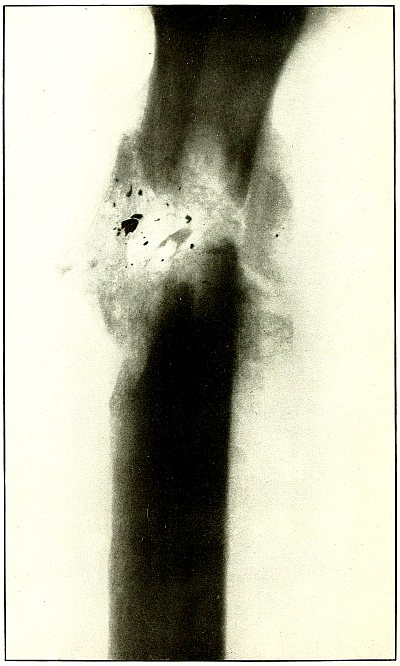
[Pg 285]
Shrapnel—Plate 137.
LOWER EXTREMITY.
Gunshot Fracture of the Tibia and Fibula.
The fibular side of the leg lay next to the plate, as the distinct
and not exaggerated outlines of the fibula can be seen in the dense
shadow of the tibia. The wound, as indicated by the callous tissue, is
shown in a state of repair, after the larger detached fragments of the
fracture had been removed. The wound was caused by a missile carrying
considerable energy. The small particles of metal marking the course
of the missile show it was a shrapnel ball.
[Pg 286]
Plate 138.
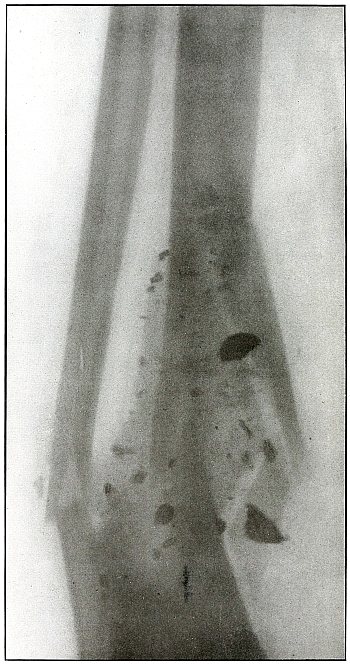
[Pg 287]
Shrapnel—Plate 138.
LOWER EXTREMITY.
Gunshot Fracture of the Right Tibia and Fibula.
This plate shows a type of wound caused by a number of fragments of
a shrapnel ball or other similar missile. The missile was deformed
by a near-by ricochet, from which large and small fragments struck
simultaneously and distributed themselves over a large area. The
larger fragments carried enough energy to fracture the bone by
transmitting all of their energy in lodgment and by possibly breaking
up into smaller fragments.
In this case the energy of the missile was transmitted to the tibia,
with fracture and great fragmentation of the bone. The fracture of the
tibia was secondary, resulting from indirect violence, due to the loss
of the support of the tibia.
[Pg 288]
Plate 139.
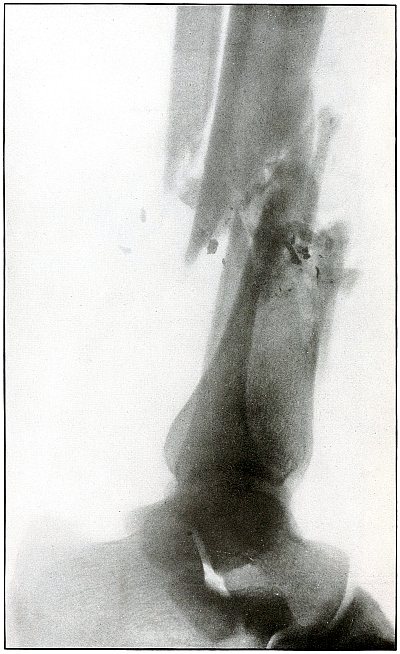
[Pg 289]
Shrapnel—Plate 139.
LOWER EXTREMITY.
Gunshot Fracture of the Right Tibia and Fibula.
The course of the missile was from within outward and from before
backward, striking both the fibula and the tibia, with fragmentation
and displacement of both bones.
The fibula lay next to the plate, as indicated by its distinct normal
shadow and the exaggerated outline of the internal malleolus.
The trail of metal fragments is typical of a shrapnel ball with
the energy of high shrapnel velocity, but any lead missile without a
protective jacket, under like conditions, might have produced the
same effect.
The treatment is conservative until some positive indication
arising in the course of an infection directs interference.
[Pg 290]
Plate 140.
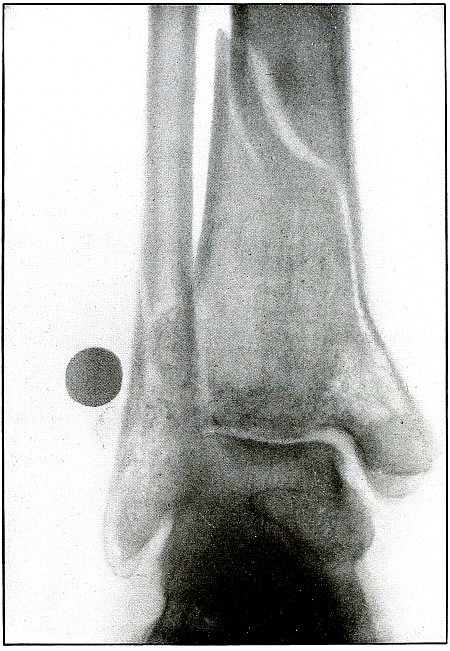
[Pg 291]
Shrapnel—Plate 140.
LOWER EXTREMITY.
Gunshot Fracture of the Left Tibia and Fibula,
with Lodgment of the Missile.
As the heel lay on the plate it is easy to identity the tibia and
fibula of the left leg.
The course of the ball from the internal malleolus across to the
lower end of the tibia and fibula is well marked by the trail of
metal particles left by the contact of the ball with the bones. The
indistinctness of the shadows of the lead particles and of the ball
and the very slight enlargement of the ball indicates a contact with
the anterior surface of the tibia and of the fibula with lodgment
of the ball beneath the skin at the anterior border of the lower
end of the fibula. The remaining energy of the missile was almost
entirely spent on the tibia, causing a long oblique fracture, so that
the contact with the fibula resulted in a crack only, without the
separation of a fragment.
The treatment in such cases is conservative, with the subsequent
removal of the ball from its superficial location.
[Pg 292]
Plate 141.
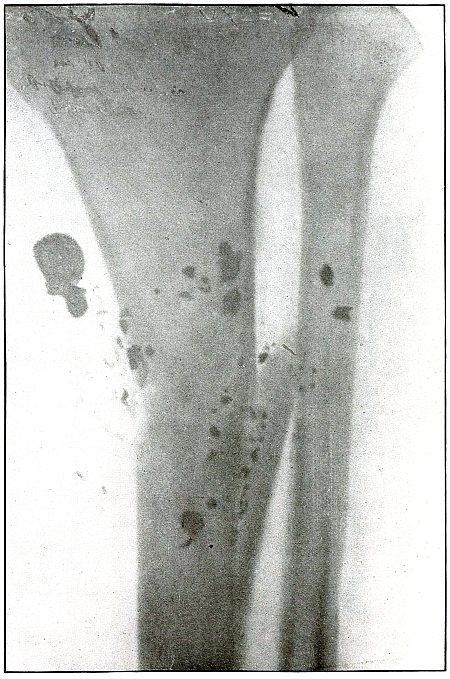
[Pg 293]
Shrapnel—Plate 141.
LOWER EXTREMITY.
Gunshot Fracture of the Left Tibia,
with Lodgment of the Missile.
The course of the ball was from without and behind, ranging upward
and inward, striking the tibia on the outer border, and causing a
splitting fracture without displacement of fragments. The missile
was most probably deformed by ricochet before it struck the bone, as
there is too little bone injury to account for the spattering and wide
distribution of the fragments by the direct impact of an undeformed
ball. Two metallic fragments lying over the fibula were probably
additional missiles detached from the ball as it ricocheted near the wound.
The treatment in such cases would be conservative, while meeting the
indications of infection.
[Pg 294]
Plate 142.
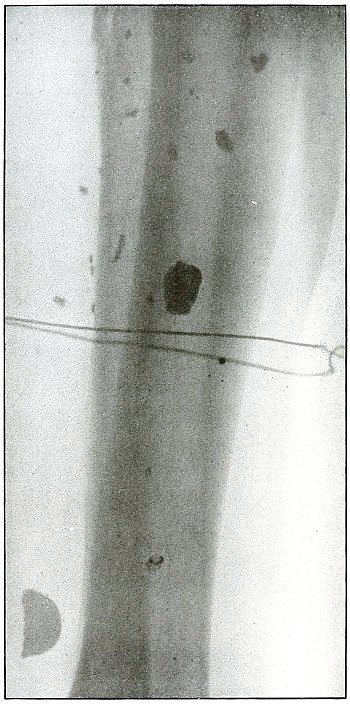
[Pg 295]
Shrapnel—Plate 142.
LOWER EXTREMITY.
Gunshot Fracture of the Left Fibula,
with Lodgment of the Missile.
This plate furnishes another example of the fragmentation of a
shrapnel ball by ricochet on a near-by object before striking the body.
A slight fracture of the fibula is seen (at the top of the plate) with
the lodgment of multiple missiles over a wide area, without other
injury to the bones.
The fragments seen through the shadow of the tibia lie nearer the
plate than the smaller fragments on the fibula. As the largest
fragment, lying below, shows a much enlarged semicircular outline, its
position is not close to the plate and it must lie superficially on
the inner side of the leg.
[Pg 296]
Plate 143.
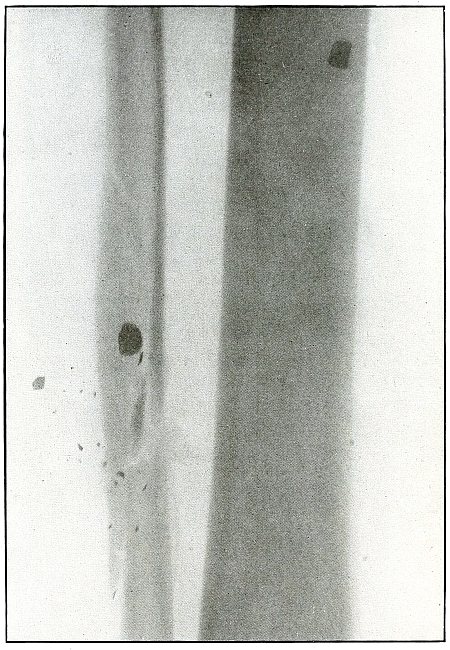
[Pg 297]
Shrapnel—Plate 143.
LOWER EXTREMITY.
Gunshot Fracture of the Right Fibula.
This plate shows the right leg, because the calf always rests on the
plate in the absence of a contraindication, which does not occur in
this case, and because the slight angle of approach of the tibia and
fibula identifies the relation of the lower end of these bones.
The nature of the fracture, without much fragmentation and with no
displacements of fragments, indicates a slight striking energy of the
missile, which was disintegrated by ricochet before striking the bone.
The fragments of a shrapnel ball, spattered on a near-by object,
struck the leg in front over a wide area, as indicated by the
fragments lying over the tibia and smaller ones lying on the inside of
the bone. The larger metal fragment, on the fibula, is some distance
from the plate, and probably lies in front of the bone, while the
smaller ones, seen in sharper outline, lie behind.
[Pg 298]
Plate 144.
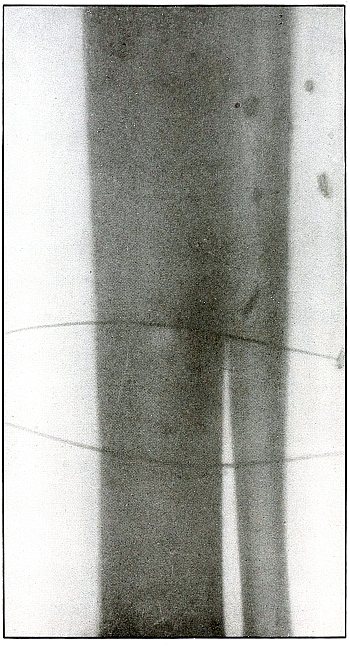
[Pg 299]
Shrapnel—Plate 144.
LOWER EXTREMITY.
Gunshot Fracture of the Left Fibula.
This is another example of the condition, shown in plate 143,
in which a shrapnel hall or similar missile is disintegrated by ricochet before
a fleeting the wound.
By comparison of the shadows of the missiles with the shadows of the
portion of the localizing wire lying nearer the plate (shown more
deeply and distinctly), and with the portion lying in front of the
leg, it can be concluded that the fragments lie superficially in front
of the bones.
A slight fissure fracture of the fibula may be seen in the upper
portion of the plate.
[Pg 300]
Plate 145.
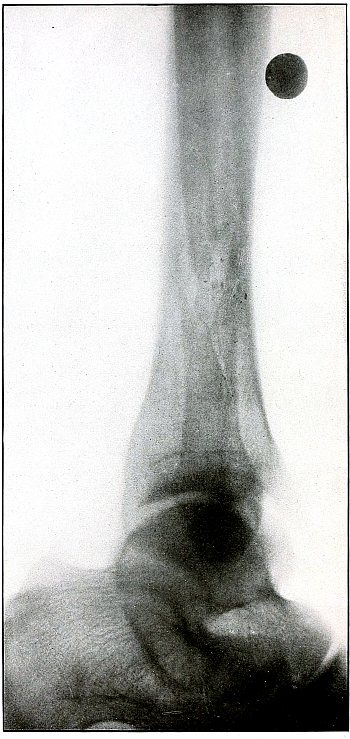
[Pg 301]
Shrapnel—Plate 145.
LOWER EXTREMITY.
Gunshot Fracture of the Fibula,
with Lodgment of the Missile.
The fibular side of the leg lay next to the plate.
The sharp outline, great density, and normal size of the shadow of the
shrapnel ball shows the ball almost in contact with the plate.
The metallic particles marking the contact of the ball and the fibula,
at the seat of a diagonal fracture, without displacement of fragments,
are shown so distinctly that they must also be near the plate.
The course of the ball, therefore, was from without, ranging inward
and upward with the slight energy of long (shrapnel) range. The ball
lies on the fibular side superficially, just in front of the fibula.
[Pg 302]
Plate 146.
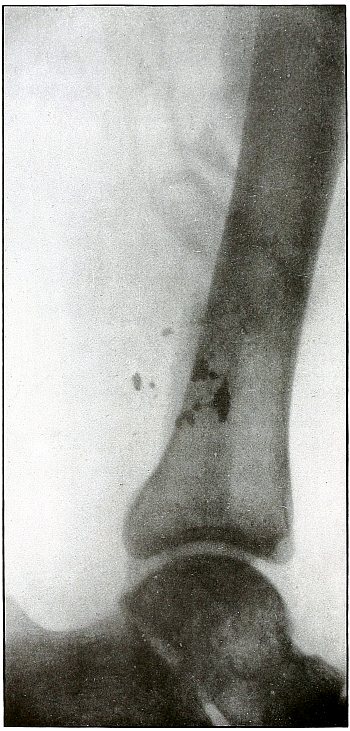
[Pg 303]
Shrapnel—Plate 146.
LOWER EXTREMITY.
Gunshot Fracture of the Right Fibula.
The plate exposed with the tibial side down shows the wound in the
course of treatment, with a drainage tube in position after the
detached fragments of several inches of the fibula have been removed
on account of infection. Several fragments of the missile are shown on
the lower fragment of the fibula.
Conservative treatment is evident and good results should follow.
[Pg 304]
Plate 147.
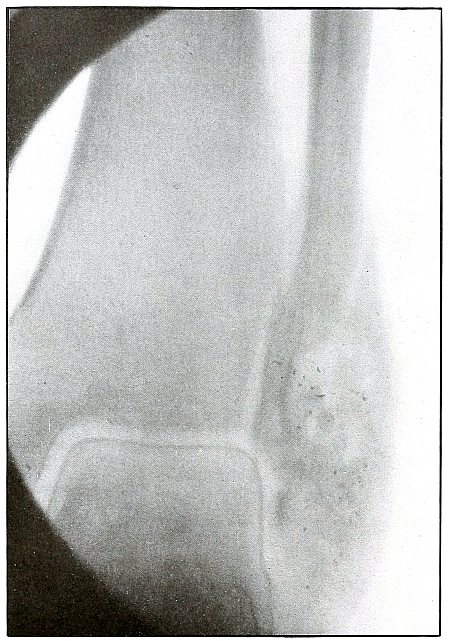
[Pg 305]
Shrapnel—Plate 147.
LOWER EXTREMITY.
Gunshot Wound of the Lower End of the Right Fibula.
As the heel lay next to the photographic plate, the right ankle is
easily identified. The clear shadows of even the very small metallic
particles show them also next to the plate and, therefore, on the
posterior surface of the external malleolus, where a shrapnel ball at
extremely low velocity struck and produced a slight fracture, or more
of a fissure, without separation of fragment.
The joint mortise is intact, as the line of fracture does not extend
to the articular surface.
The shrapnel ball in such cases would lie just beneath the skin or
escape through an adjacent wound.
[Pg 306]
Plate 148.
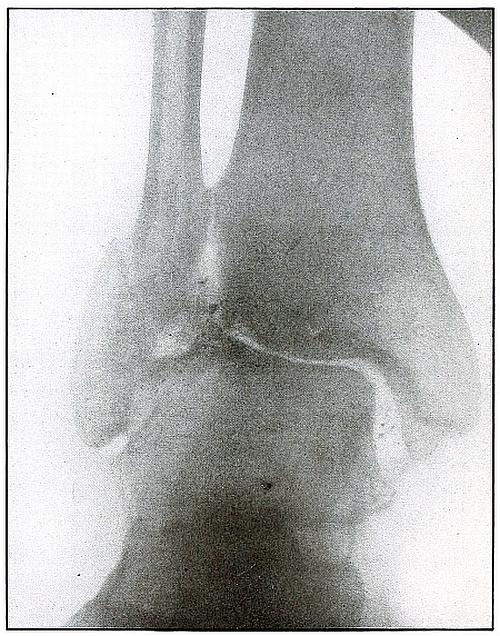
[Pg 307]
Shrapnel—Plate 148.
LOWER EXTREMITY.
Gunshot (Pott’s) Fracture of the Left Ankle.
As the heel lies next to the plate, the left ankle is easily identified.
The course of the missile is shown by a metallic track from the
internal to the external malleolus, and by a point of greater contact
with the internal malleolus at the upper border of its articulation
with the astragulus, resulting in an oblique fracture, separating the
tip of the external malleolus.
At the point of first impact the posterior faciculus of the internal
lateral ligament was severed. The missile therefore passed directly
through the ankle joint, entering just behind the tip of the external
malleolus, coursing over the posterior portion of the superior tibial
articulation of the astragalus in front of the tendo Achillis to
strike the upper articular surface of the external malleolus, with
the resulting fracture. By this mechanism, the joint mortise has been
widened by outward displacement of the external malleolus, while
the rupture of the internal lateral ligament permitted the outward
rotation of the astragulus, thus producing rather faithfully, by
direct violence, a condition which might be called a “simulated Pott’s
fracture” of the first degree.
By the metallic path of the missile it is known that its soft metal
mass was not protected by a hard metal jacket; by the slight damage
done to the bone, which lay directly in its path, its velocity
and consequent energy are revealed as very slight; by the absence
of larger metallic fragments it is shown that the missile was not
deformed nor robbed of its energy through ricochet; and as only these
conditions can be furnished by a lead ball, undeformed and traveling
at low velocity, the missile was a shrapnel ball.
[Pg 308]
Plate 149.
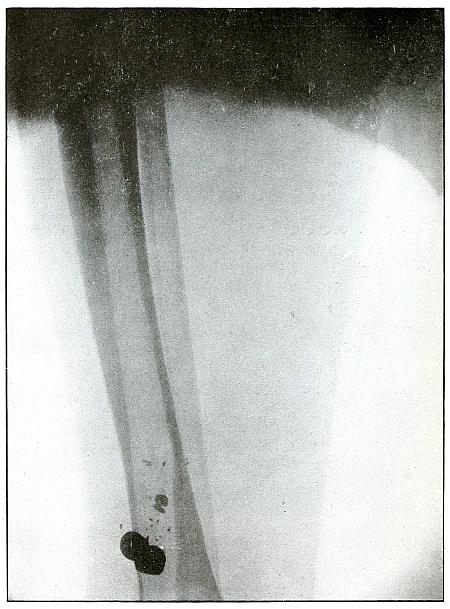
[Pg 309]
Shrapnel—Plate 149.
LOWER EXTREMITY.
Multiple Gunshot Wound of the Leg.
This plate exhibits the characteristic marking of the metal particles
of a shrapnel ball scraped off by contact with the bone, showing the
course of the ball in relation to the bone.
The evidence that two shrapnel balls struck the tibia without
causing a fracture indicates that the velocity of shrapnel balls is,
sometimes at least, very low and that this low velocity may occur at
a comparatively short range from the point where the shrapnel balls
are discharged from the chamber or near the apex of the “cone of
dispersion.” Such multiple wounds are caused before the balls have
been so widely dispersed as when they arrive at the base of the “cone of dispersion.”
[Pg 310]
Plate 150.
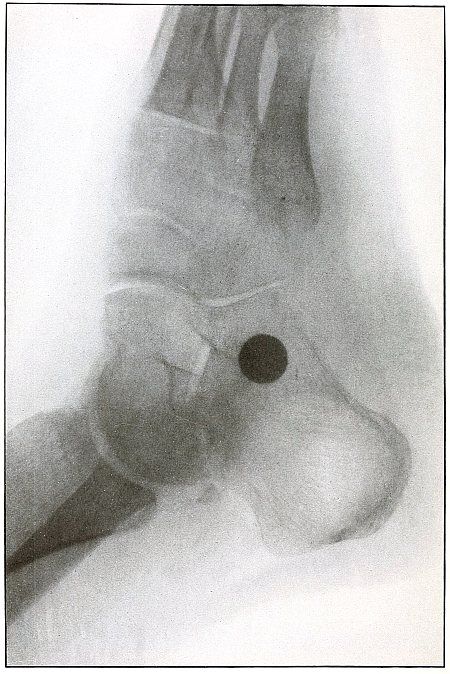
[Pg 311]
Shrapnel—Plate 150.
LOWER EXTREMITY.
Gunshot Fracture of the Left Astragalus,
with Lodgment of the Missile.
The external border of the foot lay next to the plate, as is shown by
the articulation of the cuboid.
A fragment detached from the posterior inferior border of the
astragalus and several small metal particles lying behind the fragment
are in evidence.
The enlarged shadow of the ball indicates that it does not lie close
to the plate, and it must then lie at least as far away as the
internal surface of the calcaneus and at a depth from the sole that
can be measured on the plate.
[Pg 312]
Plate 151.
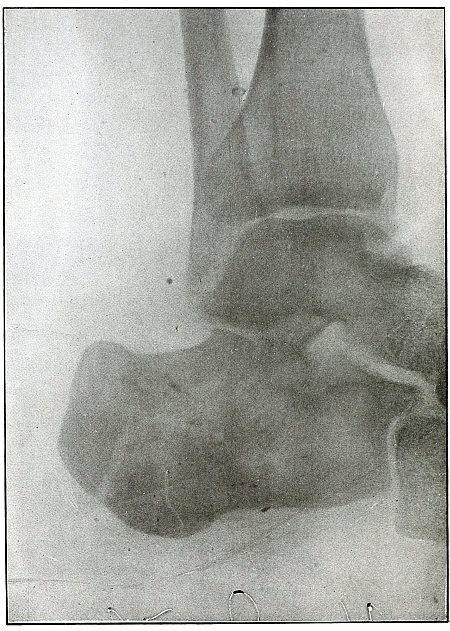
[Pg 313]
Shrapnel—Plate 151.
LOWER EXTREMITY.
Gunshot Fracture of Left Calcaneus.
The fibular side lay next to the plate, as shown by the shadow of the
fibula and the calcaneo-cuboid articulation.
As the metallic particles, showing the path of the missile, appear to
be next to the plate, the course of the missile was from the external
border of the tendo Achillis diagonally downward and forward, causing
only a slight fissure of the calcaneus. A missile, to have done so
little damage and to have left a metallic track showing its contact
with the bone, must have been unjacketed and of low velocity, and
therefore a shrapnel ball.
[Pg 314]
Plate 152.
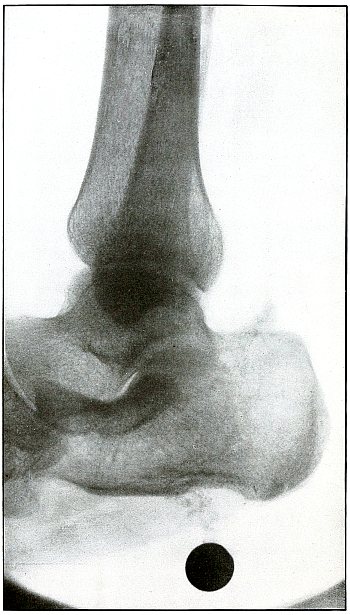
[Pg 315]
Shrapnel—Plate 152.
LOWER EXTREMITY.
Gunshot Wound of the Heel,
with Lodgment of the Missile.
The tibial side of the foot lay next to the photographic plate.
The normal size, great density, and sharp outline of the shadow of
the shrapnel ball show that it lay also close to the plate and about
an inch below the inside of the body of the calcaneus. No metallic
particles mark the track of the ball in this case, because the course
was parallel to the inner surface of the bursa without forceful, or
perhaps any, contact with the bursa, and passing through soft tissue, only.
[Pg 316]
Plate 153.
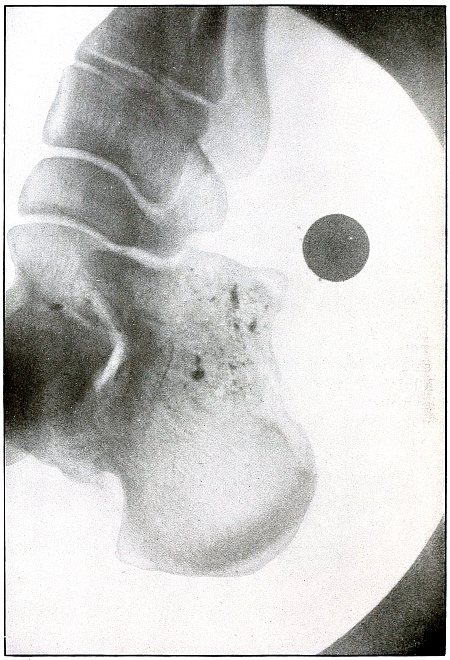
[Pg 317]
Shrapnel—Plate 153.
LOWER EXTREMITY.
Gunshot Wound of the Heel,
with Lodgment of the Missile.
That the inner border of the foot lay next to the plate is shown by
the articulation between astragalus, scaphoid, internal cuneiform, and
first metatarsal.
The metallic particles show the course of the ball from the posterior
calcaneo-astragaloid ligament to below the anterior inferior border of
the calcaneus.
As the shadow of the ball is enlarged and the shadow of the fragments
blurred, their position is not near the plate and their location is therefore
on the external plane of the calcaneus, with the ball lying near the sole.
[Pg 318]
Plate 154.
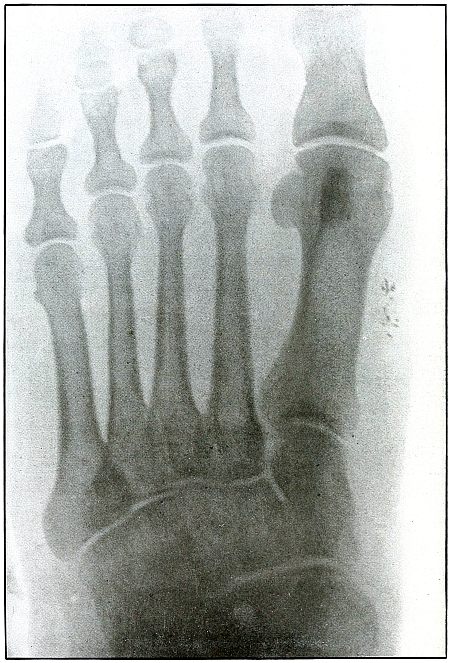
[Pg 319]
Shrapnel—Plate 154.
LOWER EXTREMITY.
Gunshot Wound of the Foot.
The plate shows, in the wound of entrance, the metal particles
deposited by a shrapnel ball which passed out of the sole of the foot
without damage to the bone.
The missile carried some small particles of lead, almost wholly
detached by a ricochet before striking the foot, which were scraped
off as it passed through the skin.
The wound was infected, and radiography was indicated for diagnosis.
[Pg 320]
Plate 155.
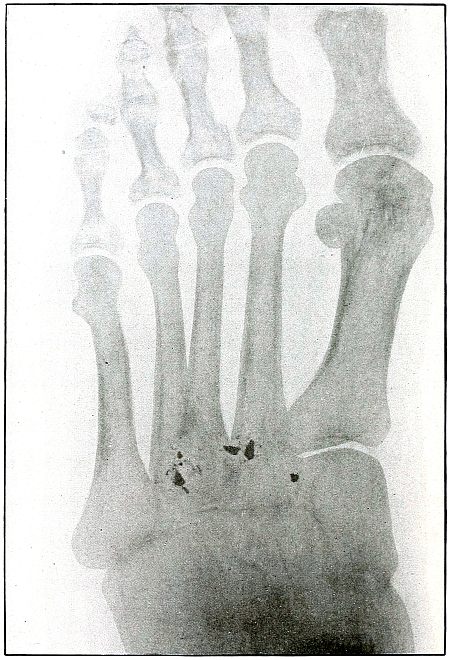
[Pg 321]
Shrapnel—Plate 155.
LOWER EXTREMITY.
Gunshot Wound of the Foot.
The sole of the foot lay next to the plate.
While the very clear, sharp outlines of the metal fragments would seem
to show them very near the plate and consequently at the platen side
of the tarsus, the foot is not of sufficient thickness to make a very
appreciable difference between shadows of such fragments on the dorsal
and on the plantar surfaces of the metatarsus. It is very probable
that the ball struck the convex, rather than the concave outline of
the transverse arch, as the missile has escaped with no fracture
of the bones, which would have been very difficult in mechanical
accomplishment if its course had been along the convex outline.
There is no fracture of the bones, although a shrapnel ball has
passed transversely through the foot, striking the heads of the second
and third metatarsals with only slight injury and leaving a few metal
particles at points of contact.
[Pg 322]
Plate 156.
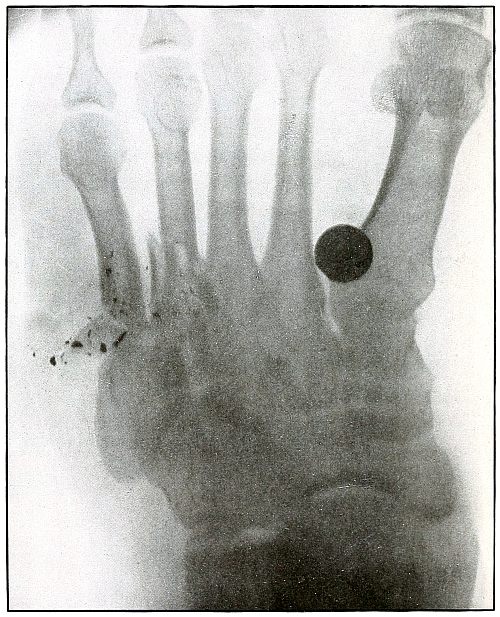
[Pg 323]
Shrapnel—Plate 156.
LOWER EXTREMITY.
Gunshot Wound of the Left Foot by Multiple Missiles,
Fracture of the Metatarsus, and Lodgment of the Missile.
The sole of the foot lay next to the plate.
The normal outline of the shadow of the shrapnel ball shows it to
lie near the plate or at least beneath the plantar surface of the
first metatarsal. The fragments of metal lying near the fourth and
fifth metatarsals lie either in the same relation or on the plantar
side of the metatarsus. The metallic track leads to the wound of exit
of shrapnel ball, other than the one lodged.
Even though the missile has escaped, its identity can be creditably
established by the one remaining, which, it is morally certain, was
the escaped missile’s companion. These shrapnel particles again
demonstrate that the metal deposits seen in other wounds can be
identified as particles of lead scraped off from shrapnel balls in the
contact of the latter with bones.
[Pg 324]
Plate 157.
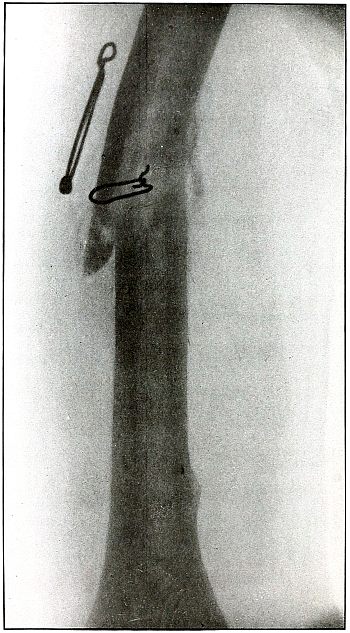
[Pg 325]
OPERATIVE INTERFERENCE IN GUNSHOT WOUNDS.
In the 1,500 radiograph plates from which this collection was
selected, only four were found showing operative interference for the
repair of fractures.
While no data are available from which
to determine accurately the ratio of these operations to the
entire number of fracture cases under treatment, and as, most
certainly, there were some formal amputations, excisions, immediate
immobilization of fractures, and other operative procedures which were
not submitted to radiography, it may nevertheless be justly inferred
from this radiographic evidence that very few such operations were performed.
Operations—Plate 157.
Gunshot Fracture of the Humerus.
This plate shows an attempt to wire a fracture of the humerus, which,
very probably, would have recovered as favorably without interference.
[Pg 326]
Plate 158.
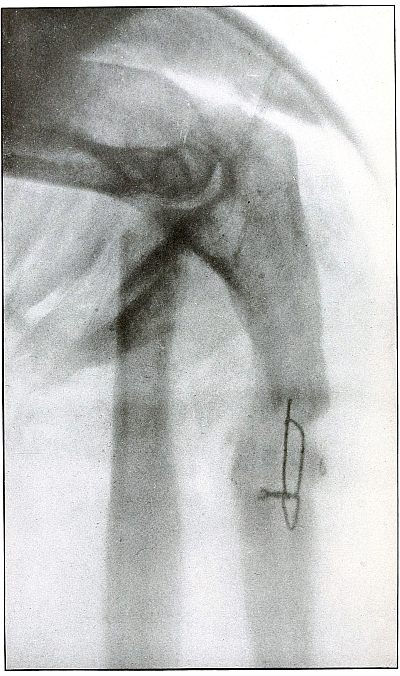
[Pg 327]
Operations—Plate 158.
Gunshot Fracture of the Ulna.
This plate shows an attempt to wire the ulna in a clean wound.
[Pg 328]
Plate 159.
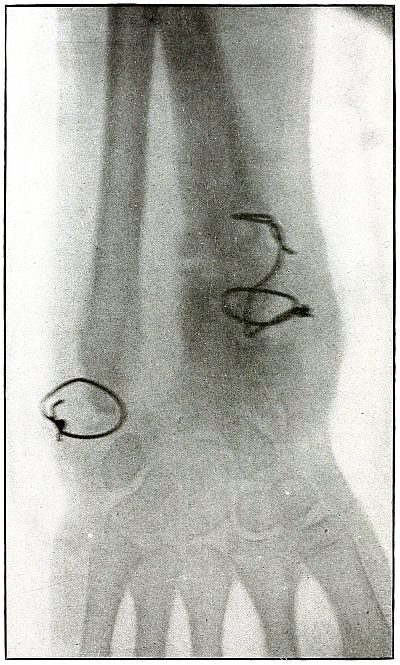
[Pg 329]
Operations—Plate 159.
Gunshot Fracture of the Radius and Ulna.
This plate shows an attempt to wire the radius and ulna where the
indications were rather doubtful.
[Pg 330]
Plate 160.
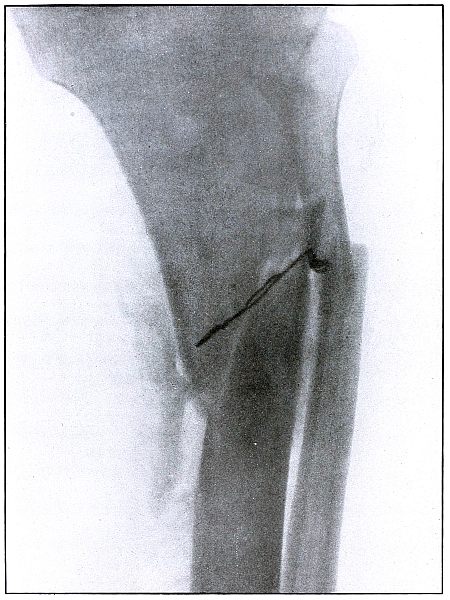
[Pg 331]
Operations—Plate 160.
Gunshot Fracture of the Tibia and Fibula.
This plate shows an attempt at immediate immobilization of the
fragments of the tibia which has failed to meet the mechanical
indications for maintaining correct position.
[Pg 332]
Plate 161.
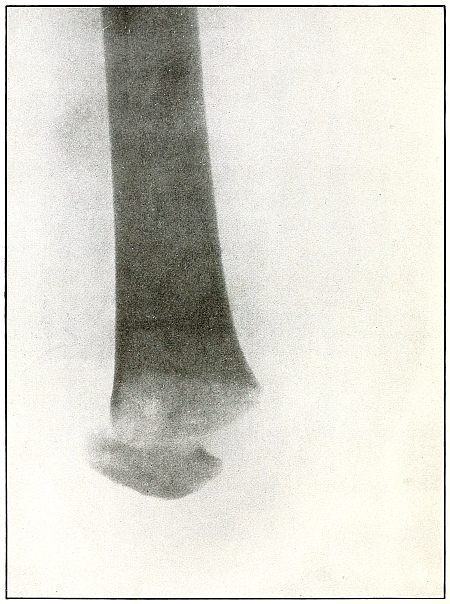
[Pg 333]
Operations—Plate 161.
Amputation at the Knee Joint.
This plate shows a satisfactory result of a secondary amputation at the knee,
after the method of Gritti, following a severe naval shell wound of the leg.
[Pg 334]
Plate 162.
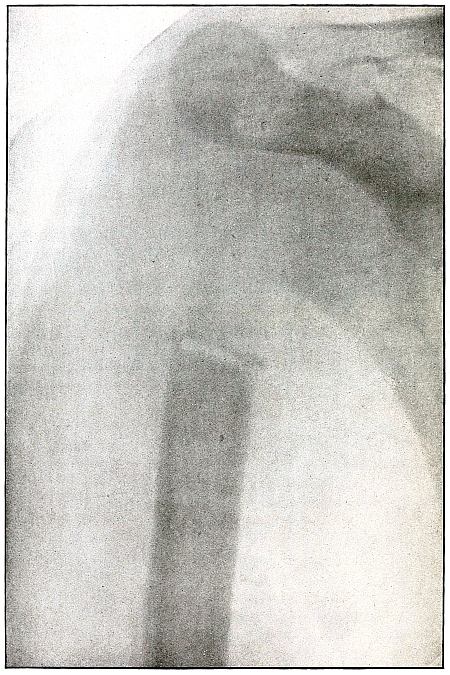
[Pg 335]
Operations—Plate 162.
Excision of the Head of the Humerus.
This plate shows a case of Prof. De Page, of the Belgium Red Cross
Mission at Tash Kishla Hospital, in which the head of the humerus was
excised for extensive comminution of the head of the humerus with infection.
[Pg 336]
Plate 163.
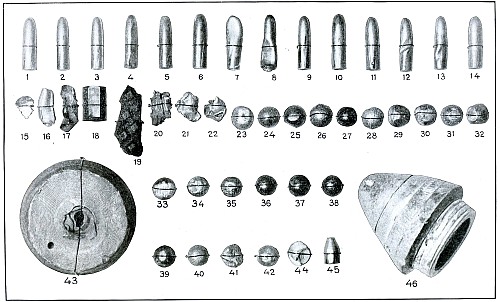
SOME MISSILES REMOVED FROM WOUNDED IN BALKAN WARS.
Figures reduced to two-thirds of natural size.
[Pg 337]
Plate 163.
Of the 46 missiles shown in the illustration, page 336,
1 to 14 are rifle bullets; 15 to 22 are assorted fragments; 23 to 43 and including
44 are shrapnel balls; 45 is an automatic pistol ball, and 43 and 46
are the base and the fuse, respectively, of a shrapnel “nose” or head
of the 75-millimeter field gun.
Four rifle bullets, three shrapnel balls, and Nos. 20 and 27 were
removed from Turkish soldiers admitted to my service at Tash Kishla
Hospital in Constantinople. The remaining missiles, excepting No. 46,
were removed from Bulgarian soldiers on my service at the Etap and the
Queen’s Hospital at Kustendil, Bulgaria. The missile shown as No. 46
was removed by Dr. Tatarcheff, the Bulgarian surgeon in command of a
fixed hospital at Kodemos, Bulgaria, from the upper anterior thigh of
a patient whose history I have and whom I saw and photographed.
Of the fragments, Nos. 15 and 17 are pieces of the nickel jacket of
rifle bullets; No. 16 is the lead “core” of a rifle bullet; No. 22 is
a fragment of the nickel jacket of a rifle bullet which holds a small
portion of the lead core; No. 18 is a brass tube which is carried
in the base of a shell to hold the detonating plunger and fulminate
cap; No. 19 is a piece of a foot plate or step of a gun carriage or
caisson; No. 20 is a shell fragment, and No. 21 is a flattened piece
of a shrapnel ball.
Of the bullets, No. 1 is Bulgarian, removed from a Bulgarian
soldier in an operation for an abdominal wound accidently inflicted
during the firing incident to the celebration attending the
announcement of peace; Nos. 6, 10, 11, and 14 are of the same caliber
as the Bulgarian and were fired from Montenegrin or Servian rifles;
Nos. 2 and 3, slightly smaller in caliber than all the others, are
Greek, and Nos. 4, 5, 7, 8, 9, 12, and 13 are Servian, slightly larger
than the Greek and as much smaller than the Bulgarian. No. 1 is
abraided at the base by the jaws of a forceps by which it was removed
from the wing of the ilium in which it was firmly embedded; Nos. 4, 7,
8, 12, 13, 14 are deformed by ricochet. No. 5 has its nose slightly
abraided by the same cause. No. 8 shows the lead core protruding from
the base of the jacket. Nos. 1, 2, 3, 6, 9, 10, and 11 are normal, as
they struck the body by direct impact. Nos. 2 and 3, which are Greek,
have the nickel jacket worn off on the apex so that the lead core is
exposed, which produces a slight degree of “dum-dum,” but as they
struck the body at very long range and without hitting a bone, they
produced no “dum-dum” effect.
[Pg 338]
Eight of the shrapnel balls were removed from the forearm of one
Bulgarian soldier. (Vide plate 109.)
No. 43 was removed from between the thoracic wall and the
scapula, to which position it passed by destroying the outer half of the clavicle,
penetrating 6 inches from the surface.
The caliber of the missiles.
| Millimeters. |
| Greek |
6.50 |
| Servian |
7.00 |
| Bulgarian |
8.00 |
| Montenegrin |
7.05 and 8.00 |
For comparison it may be observed that the United States
Army rifle bullet is 7 millimeters, equal 30 caliber or 0.30 inch.
The caliber of shrapnel balls varies somewhat, as do the weight and
density, but all of them were approximately ½ inch or 125 millimeters
in diameter.
The caliber of all field guns (of modern type) in the Balkan wars
were 75 millimeters, the “soixante-quinze” of the French, or about 3 inches.
Transcriber Notes:
On Pg 173, the reference to “plate No. 81” was corrected to “plate No. 80”.
On Pg 181, the references to “plates 85 and 86” was corrected to
“plates 83 and 84”.
*** END OF THE PROJECT GUTENBERG EBOOK 48341 ***