| PLATE I |
|
|
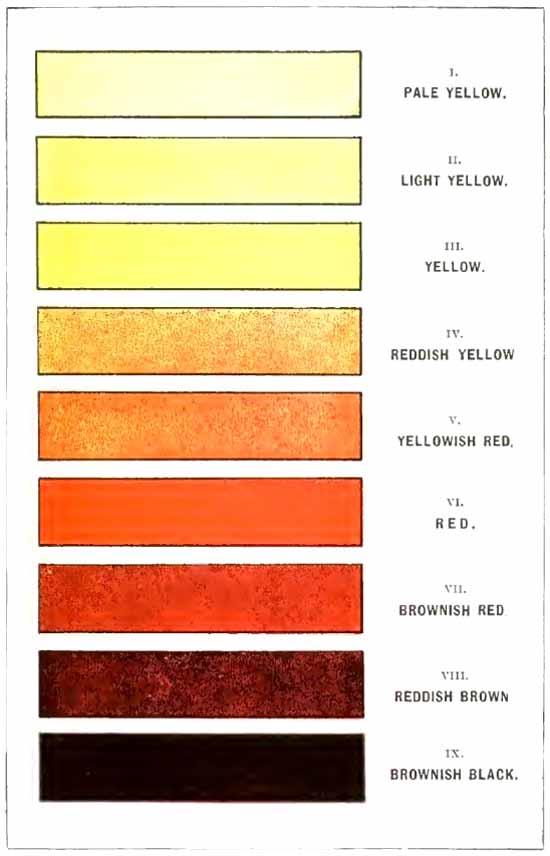
| Scale of urinary colors, according to Vogel. |
This book aims to present a clear and concise statement of the more important laboratory methods which have clinical value, and a brief guide to interpretation of results. It is designed for the student and practitioner, not for the trained laboratory worker. It had its origin some years ago in a short set of notes which the author dictated to his classes, and has gradually grown by the addition each year of such matter as the year's teaching suggested. The eagerness and care with which the students and some practitioners took these notes and used them convinced the writer of the need of a volume of this scope.
The methods offered are practical; and as far as possible are those which require the least complicated apparatus and the least expenditure of time. Simplicity has been considered to be more essential than absolute accuracy. Although in many places the reader is given the choice of several methods to the same end, the author believes it better to learn one method well than to learn several only partially.
More can be learned from a good picture than from any description, hence especial attention has been given to the illustrations, and it is hoped that they will serve truly to illustrate. Practically all the microscopic structures mentioned, all apparatus not in general use, and many of the color reactions are shown in the pictures.
Although no credit is given in the text, the recent medical periodicals and the various standard works have been freely consulted. Among authors whose writings have been especially helpful may be mentioned v. Jaksch, Boston, Simon, Wood, Emerson, Purdy, Ogden, Ewald, Ehrlich and Lazarus, Da Costa, Cabot, Osler, Stengel, and McFarland.
The author wishes hereby to express his indebtedness to Dr. J. A. Wilder, Professor of Pathology in the Denver and Gross College of Medicine, for aid in the final revision of the manuscript; and to W. D. Engel, Ph.D., Professor of Chemistry, for suggestions in regard to detection of drugs in the urine. He desires to acknowledge the care with which Mr. Ira D. Cassidy has made the original drawings, and also the uniform courtesy of W. B. Saunders Company during the preparation of the book.
DENVER, COLORADO,
July, 1908.
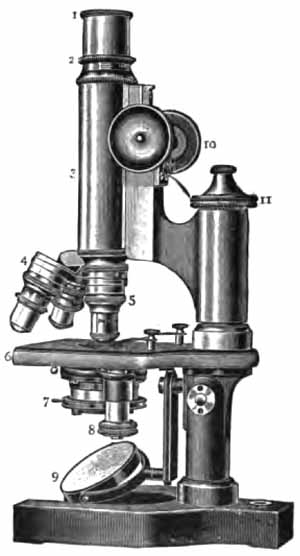
There is probably no laboratory instrument whose usefulness depends so much upon proper manipulation as the microscope, and none is so frequently misused by beginners. Some suggestions as to its proper use are, therefore, given at this place. It is presumed that the reader is already familiar with its general construction (Fig. 1).
|
| FIG. 1.—The microscope: 1, Eye-piece; 2, draw-tube; 3, main tube; 4, nose-piece with objectives attached; 5, objective in position; 6, stage; 7, substage; 8, adjustment of substage; 9, mirror; 10, coarse adjustment; 11, fine adjustment. |
Illumination.—Good work cannot be done without proper illumination. It is difficult to lay too much stress upon this point.
The best light is that from a white cloud. [p. 18] A northern exposure is desirable, since direct sunlight is to be avoided. Good work can be done at night with a Welsbach light. Ordinary gas-light and the incandescent electric light are unsatisfactory, although the latter gives good results when subdued with a heavily frosted globe. The writer uses a frosted electric bulb in a dark-room lantern, and tones the light to the proper degree for low powers by means of frosted-glass plates which slide into the grooves which have held the ruby and orange glasses. One of these plates is made of blue glass, to overcome the yellow of the artificial light. It is not generally advised to do so, but it will be found convenient to use the Abbé condenser for all routine work. With daylight it is best to use the plane mirror: with artificial light, the concave mirror. To obtain best results, the light must be focused upon the object under examination by raising or lowering the condenser.
Illumination may be either central or oblique. Central illumination is to be used for all routine work. To obtain this, the mirror should be so adjusted that the light from the source selected is reflected directly up the tube of the microscope. This is easily done by removing the eye-piece and looking down the tube while adjusting the mirror. The eye-piece is then replaced, and the light reduced as much as desired by means of the diaphragm.
Oblique illumination is to be used only to bring out certain structures more clearly after viewing them by central light: as, for example, to show the edges of a hyaline cast by throwing one of its sides into shadow. Oblique illumination is obtained in the more simple instruments by swinging the mirror to one side, so that the light enters the microscope obliquely. The more [p. 19] complicated instruments obtain it by means of a rack and pinion, which moves the diaphragm laterally. Beginners frequently use oblique illumination without recognizing it. If the light be oblique, an object in the center of the field will appear to move from side to side when the fine adjustment is turned back and forth.
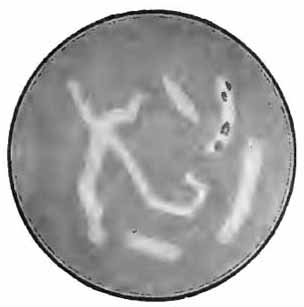
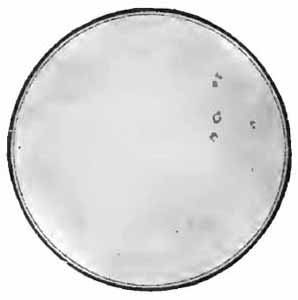
The amount of light is even more important than its direction. It is regulated by the diaphragm. It is always best to use the least light that will show the object well. Unstained objects require very subdued light. Beginners constantly use it too strong. Strong light will often render semitransparent structures, as hyaline casts, entirely invisible (Figs. 2 and 3). Stained objects, especially bacteria, require much greater light.
|
|
| FIG. 2.—Hyaline casts, one containing renal cells; properly subdued illumination (from Greene's "Medical Diagnosis"). | FIG. 3.—Same as Fig. 2; strong illumination. The casts are lost in the glare, and only the renal cells are seen (from Greene's "Medical Diagnosis"). |
If the reflection of the window-frame or other nearby object is seen in the field, the condenser should be lowered a little.
Focusing.—It is always best to "focus up," which saves annoyance and probable damage to slides and objectives. This is accomplished by bringing the objective [p. 20] nearer the slide than the proper focus, and then, with the eye at the eye-piece, turning the tube up until the object is clearly seen. The fine adjustment should be used only to get an exact focus with the higher power objectives after the instrument is in approximate focus. It should not be turned more than one revolution.
There will be less fatigue to the eyes if both are kept open while using the microscope, and if no effort is made to see objects which are out of distinct focus. Fine focusing should be done with the fine adjustment, not with the eye. An experienced microscopist keeps his fingers almost constantly upon one or other of the focusing adjustments. Greater skill in recognizing objects will be acquired if the same eye be always used. To be seen most clearly, an object should be brought to the center of the field.
Magnification.—The degree of magnification should always be expressed in diameters, not times, which is a misleading term. The former refers to increase of diameter; the latter, to increase of area. The comparatively low magnification of 100 diameters is the same as the apparently enormous magnification of 10,000 times.
Magnification may be increased—(a) by using a higher power objective, which is the best way; (b) by using a higher eye-piece; or (c) by increasing the length of tube.
Eye-pieces and Objectives.—The usual equipment consists of one- and two-inch eye-pieces, and two-thirds, one-sixth, and one-twelfth inch objectives. These are very satisfactory for clinical work. It is an advantage to add a one-half-inch eye-piece for occasional use with the two-thirds objective. The one-sixth should have an especially long working distance, otherwise it cannot be used satisfactorily with the Thoma-Zeiss blood-counting [p. 21] instrument, which has a very thick cover-glass. Such a "special one-sixth for blood work" is made by most of the microscope manufacturers.
Objectives are "corrected" for use under certain fixed conditions, and they will give the best results only when used under the conditions for which corrected. The most important corrections are: (a) For tube length; (b) for thickness of cover-glass; and (c) for the medium between objective and cover-glass.
(a) The tube length with which an objective is to be used is usually engraved upon it—in most cases it is 160 mm.
(b) The average No. 2 cover-glass is about the thickness for which most objectives are corrected. Low powers do not require any cover-glass. A cover should always be used with high powers, but its exact thickness is more important in theory than in practice.
(c) The correction for the medium between objective and cover-glass is very important. This medium may be either air or some fluid, and the objective is hence either a "dry" or an "immersion" objective. The immersion fluid generally used is cedar oil, which gives great optical advantages because its index of refraction is the same as that of crown glass. It is obvious that only objectives with very short working distance, as the one-twelfth, can be used with an immersion fluid.
To use an oil-immersion objective a drop of the cedar oil which is prepared for the purpose should be placed upon the cover, and the objective lowered into it and then brought to a focus in the usual way. Immediately after use the oil should invariably be wiped off with lens paper, or a soft linen handkerchief moistened with saliva.
Care of the Microscope.—The microscope is a [p. 22] delicate instrument and should be handled accordingly. It is so heavy that one is apt to forget that parts of it are fragile. It seems unnecessary to say that when there is unusual resistance to any manipulation, force should never be used to overcome it until its cause has first been sought; and yet it is no uncommon thing to see students, and even graduates, push a high power objective against a microscopic preparation with such force as to break not only the cover-glass, but even a heavy slide.
It is most convenient to carry a microscope with the fingers grasping the pillar and the arm which holds the tube; but since this throws a strain upon the fine adjustment, it is safer to carry it by the base. To bend the instrument at the joint, the force should be applied to the pillar and never to the tube or the stage.
Lens surfaces which have been exposed to dust only should be cleaned with a camel's-hair brush. Those which are exposed to finger-marks should be cleaned with lens paper, or a soft linen handkerchief wet with saliva. Particles of dirt which are seen in the field are upon the slide, the eye-piece, or the condenser. Their location can be determined by moving the slide, rotating the eye-piece, and lowering the condenser.
Oil and balsam which have dried upon the lenses and resist saliva may be removed with alcohol or xylol; but these solvents must be used sparingly and carefully, as there is danger of softening the cement. Care must be taken not to get any alcohol upon the brass parts, as it will remove the lacquer. Balsam and dried oil are best removed from the brass parts with xylol.
Measurement of Microscopic Objects.—Of the several methods, the most convenient is the use of a [p. 23] micrometer eye-piece. In its simplest form this is similar to an ordinary eye-piece, but has within it a glass disc upon which is ruled a graduated scale. When this eye-piece is placed in the tube of the microscope, the ruled lines appear in the microscopic field, and the size of an object is readily determined in terms of the divisions of this scale. The value of these divisions in inches or millimeters manifestly varies with different magnifications. Their value must, therefore, be determined separately for each objective. This is accomplished through use of a stage micrometer—a glass slide with carefully ruled scale divided into hundredths and thousandths of an inch, or into subdivisions of a millimeter. The stage micrometer is placed upon the stage of the microscope and brought into focus. From the number of divisions of the eye-piece scale corresponding to each division of the stage micrometer the value of the former in fractions of an inch or millimeter is easily calculated. The counting slide of the Thoma-Zeiss hemocytometer will answer in place of a stage micrometer, the lines which form the sides of the small squares being one-twentieth of a millimeter apart. Any eye-piece can be converted into a micrometer eye-piece by placing a micrometer disc—a small circular glass plate with ruled scale—ruled side down upon its diaphragm.
The principal microscopic objects which are measured clinically are animal parasites and their ova and abnormal blood-corpuscles. The metric system is used almost exclusively. For very small objects 0.001 mm. has been adopted as the unit of measurement, under the name micron. It is represented by the Greek letter µ. For larger objects, where exact measurement is not essential, the diameter of a red blood-corpuscle (7 to 8 µ) is sometimes taken as a unit.
Preliminary Considerations.—The morning sputum or the whole amount for twenty-four hours should be collected for examination. In beginning tuberculosis tubercle bacilli can often be found in that first coughed up in the morning when they cannot be detected at any other time of day. Sometimes, in these early cases, there are only a few mucopurulent flakes which contain the bacilli, or only a small purulent mass every few days, and these may easily be overlooked.
As a receptacle for the sputum a clean wide-mouthed bottle with tightly fitting cork may be used. The patient must be particularly cautioned against smearing any of it upon the outside of the bottle. This is probably the chief source of danger to those who examine sputum.
When the examination is begun, the sputum should be spread out in a thin layer in a Petri dish, or, better, between two small plates of glass, like photographic plates. It may then be examined with the naked eye—best over a black background—or with a low power of the microscope. The portions most suitable for further examination may thus be easily selected.
After an examination the sputum must be destroyed by heat or chemicals, and everything which has come in contact with it must be sterilized. The utmost care must be taken not to allow any of it to dry and become disseminated through the air.
Examination of the sputum is most conveniently [p. 25] considered under three heads: I. Physical examination. II. Microscopic examination. III. Characteristics of the sputum in various diseases. Chemic examination yields nothing of clinical importance.
1. Quantity.—The quantity expectorated in twenty-four hours varies greatly: it may be so slight as to be overlooked entirely in beginning tuberculosis; and it may be as much as 1000 c.c. in bronchiectasis.
2. Color.—Since the sputum ordinarily consists of varying proportions of mucus and pus, it may vary from a colorless, translucent mucus to an opaque, whitish or yellow, purulent mass. A yellowish-green is frequently seen in advanced phthisis.
A red color usually indicates the presence of blood. Bright red blood, most commonly in streaks, is strongly suggestive of phthisis. It may be noted very early in the disease. A rusty red sputum is the rule in croupous pneumonia, and was at one time considered pathognomonic of the disease. "Prune-juice" sputum is said to be characteristic of "drunkard's pneumonia." A brown color, due to altered blood-pigment, follows hemorrhages from the lungs.
Gray or black sputum is observed among those who work much in coal-dust, and is occasionally seen in smokers who "inhale."
3. Consistence.—According to their consistence, sputa are usually classified as serous, mucoid, purulent, seropurulent, mucopurulent, etc., which names explain themselves. As a rule, the more mucus and the less pus and serum a sputum contains, the more tenacious it is.
[p. 26] The rusty sputum of croupous pneumonia is extremely tenacious, so that the vessel in which it is contained may be inverted without spilling it. The same is true of the almost purely mucoid sputum ("sputum crudum") of beginning acute bronchitis, and of that which follows an attack of asthma. A purely serous sputum is fairly characteristic of edema of the lungs.
The portions most likely to contain structures of interest should be very carefully selected, as already described. The few minutes spent in this preliminary examination will sometimes save hours of work later. Opaque, white or yellow particles are frequently bits of food, but may be cheesy masses from the tonsils; small cheesy nodules, derived from tuberculous cavities and containing many tubercle bacilli and elastic fibers; Curschmann's spirals, or small fibrinous casts, coiled into little balls; or shreds of mucus with great numbers of entangled pus-corpuscles.
The sputum should always be examined, both unstained and stained.
The particle selected for examination should be transferred to a clean slide, covered with a clean cover-glass, and examined with the two-thirds objective, followed by the one-sixth. It is convenient to handle the bits of sputum with a wooden toothpick, which may be burned when done with. The platinum wire used in bacteriologic work is less satisfactory because not usually stiff enough.
The more important structures to be seen in unstained sputum are: elastic fibers, Curschmann's spirals, [p. 27] Charcot-Leyden crystals, fibrinous casts, the ray fungus of actinomycosis, and molds. Pigmented cells, especially the so-called "heart-failure cells" (p. 43), are also best studied without staining (Plate II, Fig. 1).
|
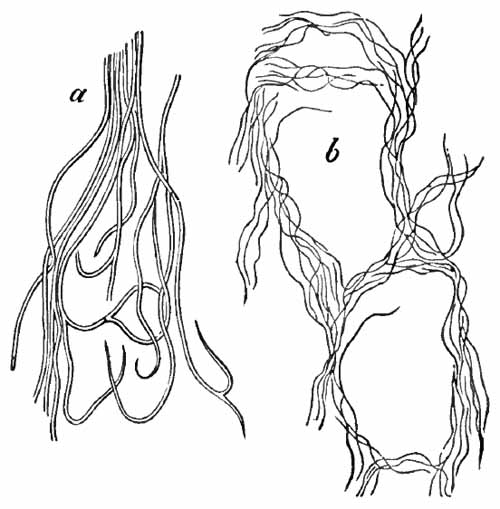
| FIG. 4.—Elastic fibers from the sputum: a, Highly magnified; b, alveolar arrangement, less highly magnified (after Bizzozero). |
1. Elastic Fibers.—These are the elastic fibers of the pulmonary substance (Fig. 4). When found in the sputum, they always indicate destructive disease of the lungs, provided they do not come from the food, which is a not infrequent source. They are found most commonly in phthisis: rarely in other diseases. Advanced cases of tuberculosis often show great numbers, and, rarely, they may be found in early tuberculosis when the bacilli cannot be detected. In gangrene of the lung, where they would be expected, they are frequently not found, owing, probably, to the presence of a ferment which destroys them.
[p. 28] The fibers should be searched for with a two-thirds objective, although a one-sixth is needed to identify them with certainty. Under the one-sixth they appear as slender, highly refractive fibers with double contour and, often, curled or split ends. Frequently they are found in alveolar arrangement, retaining the original outline of the alveoli of the lung (Fig. 4, b). Leptothrix buccalis, which is a normal inhabitant of the mouth, may easily be mistaken for elastic tissue. It can be distinguished by running a little iodin solution under the cover-glass (see p. 37).
To find elastic fibers when not abundant boil the sputum with a 10 per cent. solution of caustic soda until it becomes fluid, add several times its bulk of water, and centrifugalize, or allow to stand for twenty-four hours in a conical glass. Examine the sediment microscopically. [p. 29] The fibers will be pale and swollen. Too long boiling will destroy them entirely.
|
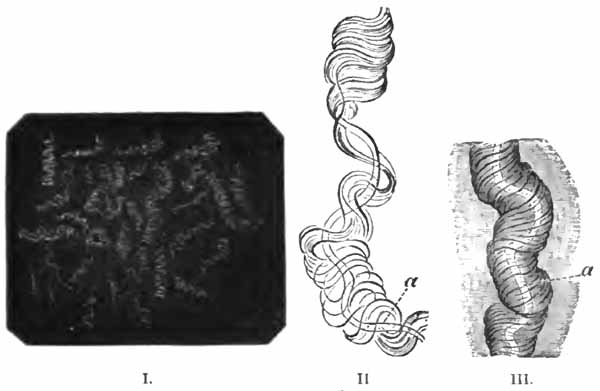
| FIG. 5.—Curschmann's spirals: I., Natural size; II. and III., enlarged: a, central fiber (after Curschmann). |
2. Curschmann's Spirals.—These peculiar structures are found most frequently in bronchial asthma, of which they are fairly characteristic. They may occasionally be met with in chronic bronchitis and other conditions. Their nature has not been definitely determined.
Macroscopically, they are whitish or yellow, twisted threads, frequently coiled into little balls (Fig. 5, I.). Their length is rarely over half an inch, though it sometimes exceeds two inches. Under a two-thirds objective they appear as mucous threads having a clear central fiber, about which are wound many fine fibrils (Fig. 5, II. and III.). Leukocytes are usually present within them, and sometimes Charcot-Leyden crystals. The central fiber is not always present.

|
| FIG. 6.—Charcot-Leyden crystals (after Riegel). |
[p. 30] 3. Charcot-Leyden Crystals.—Of the crystals which may be found in the sputum, the most interesting are the Charcot-Leyden crystals. They are rarely found except in cases of bronchial asthma, and were at one time thought to be the cause of the disease. They frequently adhere to Curschmann spirals. Their exact nature is unknown.
They are colorless, pointed, often needle-like, octahedral crystals (Fig. 6). Their size varies greatly, the average length being about three or four times the diameter of a red blood-corpuscle.
Other crystals—hematoidin, cholesterin, and, most frequently, fat needles—are common in sputum which has remained in the body for a considerable time.
|
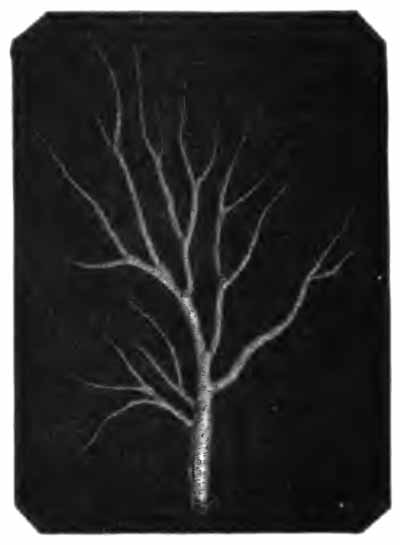
| FIG. 7.—Fibrinous bronchial cast (Sahli). |
4. Fibrinous Casts.—These are fibrinous molds of the smaller bronchi. Their size varies with that of the bronchi in which they are formed. They may, rarely, [p. 31] be three or more inches in length. When large, they can be recognized with the naked eye by floating them out in water; when small, a low power of the microscope must be used. They are easily recognized from their branching, tree-like structure (Fig. 7).
Fibrinous casts are characteristic of fibrinous bronchitis, but may also be found in diphtheria of the smaller bronchi. Very small casts are often seen in croupous pneumonia.
|
| FIG. 8.—Sputum from a case of actinomycosis; stained (Jakob). |
5. Actinomyces Bovis (Ray-fungus).—In the sputum of pulmonary actinomycosis and in the pus from actinomycotic lesions elsewhere small, yellowish, "sulphur" granules can be detected with the unaided eye. The fungus can be seen by crushing one of these granules between slide and cover, and examining with a low power. It consists of a network of threads having a more or less radial arrangement, those at the periphery presenting club-shaped extremities (Fig. 8). This organism, also called Streptothrix actinomyces, apparently stands midway between the bacteria and the molds. It stains by Gram's method.
[p. 32] Actinomycosis of the lung is rare. The clinical picture is that of tuberculosis.
6. Molds.—The hyphæ and spores of various molds are occasionally met with in the sputum. They are usually the result of contamination, and have little significance. The hyphæ are rods, usually jointed or branched (Fig. 58), and often arranged in a meshwork (mycelium); the spores are highly refractive spheres. Both stain well with the ordinary stains.
Structures which are best seen in stained sputum are bacteria and cells.
1. Bacteria.—Only those of some clinical importance will be considered. They are: tubercle bacilli; staphylococci and streptococci; pneumococci; bacilli of Friedländer; and influenza bacilli.
(1) Tubercle Bacillus.—The presence of the tubercle bacillus may be taken as positive evidence of the existence of tuberculosis somewhere along the respiratory tract, most likely in the lung. In laryngeal tuberculosis they are not easily found in the sputum, but can nearly always be detected in swabs made directly from the larynx.
Recognition of the tubercle bacillus depends upon the fact that it stains with difficulty; but that when once stained, it retains the stain tenaciously, even when treated with a mineral acid, which quickly removes the stain from other bacteria. The most convenient method for general purposes is here given in detail:
Gabbet's Method.—(1) Spread suspicious particles thinly and evenly upon a slide or a cover-glass held in the grasp of [p. 33] cover-glass forceps. Cover-glasses are easier to handle while staining. Do not grasp a cover too near the edge or the stain will not stay on it well. Tenacious sputum will spread better if gently warmed while spreading.
(2) Dry the film in the air.
(3) Fix in a flame; i.e., pass the cover-glass rather slowly, with film side up, three times (a slide about twelve times) through the flame of a Bunsen burner or alcohol lamp. Take care not to scorch. Should the film be washed off during future manipulations, fixation has been insufficient.
(4) Apply as much carbol-fuchsin as will stay on, and hold over a flame so that it will steam for three minutes or longer, replacing the stain as it evaporates. If the bacilli are well stained in this step, there will be little danger of decolorizing them later.
(5) Wash the film in water.
(6) Apply Gabbet's stain to the under side of the cover-glass to remove excess of carbol-fuchsin, and then to the film side. Allow this to act for one-fourth to one-half minute.
(7) Wash in water.
(8) If, now, the thinner portions of the film are blue, proceed to the next step; if they are still red, repeat steps (6) and (7) until the red has disappeared. Too long application of Gabbet's stain will decolorize the tubercle bacilli.
(9) Place the preparation between layers of filter-paper and dry by rubbing with the fingers, as one would in blotting ink.
(10) Put a drop of Canada balsam upon a clean slide, place the cover-glass film side down upon it, and examine with a one-twelfth objective. Cedar oil or water may be used in place of balsam for temporary preparations. Smears on slides may be examined directly with an oil-immersion lens, no cover being necessary.
Carbol-fuchsin is prepared by mixing 10 c.c. of a saturated alcoholic solution of fuchsin with 90 c.c. of 5 per cent. aqueous solution of phenol.
[p. 34] Gabbet's stain consists of methylene-blue, 2 gm.; 25 per cent. sulphuric acid, 100 c.c.
Both stains can be purchased ready prepared.
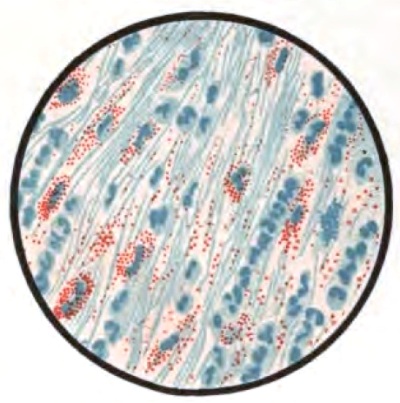
In films stained by Gabbet's method tubercle bacilli, if present, will be seen as slender red rods upon a blue background of mucus and cells (Plate II, Fig. 2). They average 3 to 4 µ in length—about one-half the diameter of a red blood-corpuscle. Beginners must be warned against mistaking the edges of cells, or particles which have retained the red stain, for bacilli. The appearance of the bacilli is almost always typical, and if there seems room for doubt, the structure in question is probably not a tubercle bacillus. They may lie singly or in groups. They are very frequently bent and often have a beaded appearance. It is possible that the larger, beaded bacilli indicate a less active tuberculous process than do the smaller, uniformly stained ones. Sometimes they are present in great numbers—thousands in a field of the one-twelfth objective. Sometimes several cover-glasses must be examined to find a single bacillus. At times they are so few that none are found in stained smears, and special methods are required to detect them. The number may bear some relation to the severity of the disease, but this relation is by no means constant. The mucoid sputum from an incipient case sometimes contains great numbers, while sputum from large tuberculous cavities at times contains very few. Failure to find them is not conclusive, though their absence is much more significant when the sputum is purulent than when it is mucoid.
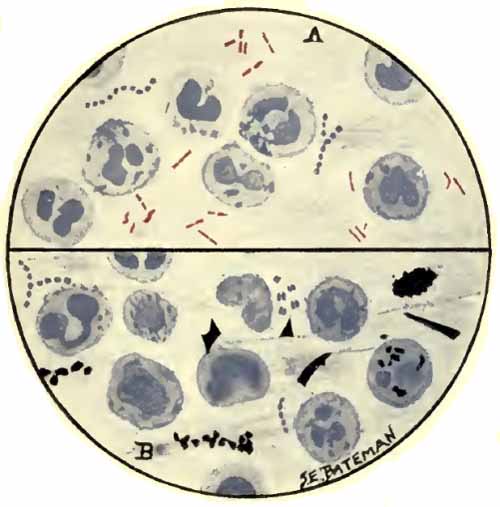
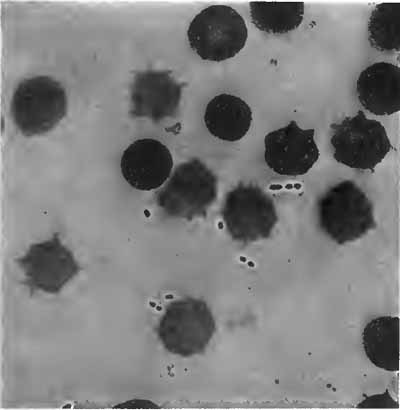
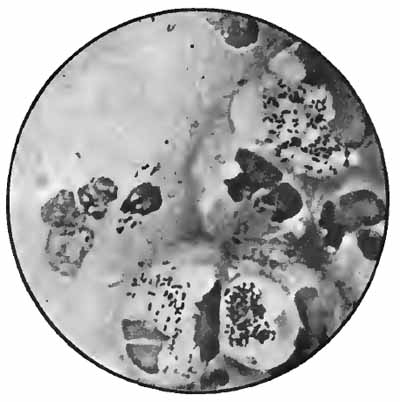
| PLATE II |

|
| FIG. 1.—Heart-failure cells in sputum, containing blood-pigment, from a case of cardiac congestion of the lungs (Jakob). |
|
| FIG. 2.—A, Sputum showing tubercle bacilli stained with carbol-fuchsin and Gabbet's methylene-blue solution (obj. one-twelfth oil-immersion); B, sputum of anthracosis, showing particles of coal-dust stained with methylene-blue (obj. one-twelfth oil-immersion) (Boston). |
When they are not found in suspicious cases, one of the following methods should be tried:
(1) Take a few drams of the sputum in a test-tube, add hot [p. 35] water, and heat until the albumin is coagulated. Let settle for twenty-four hours, or centrifugalize at once, and examine the sediment for tubercle bacilli.
(2) Boil the sputum with just sufficient weak caustic soda solution to render it fluid; neutralize with acetic acid; add several times its volume of water; centrifugalize; and stain the sediment, adding a little of the untreated sputum to make the smear adhere to the cover-glass.
(3) Inoculate guinea-pigs.
There are a number of bacilli, called acid-fast bacilli, which stain in the same way as the tubercle bacillus. Of these, the smegma bacillus is the only one likely ever to cause confusion. It, or a similar bacillus, is sometimes found in the sputum of gangrene of the lung. It occurs normally about the glans penis and the clitoris, and is often present in the urine. The method of distinguishing it from the tubercle bacillus is given later (p. 127).
Other bacteria than the acid-fast group are stained blue by Gabbet's method. Those most commonly found are staphylococci, streptococci, and pneumococci. Their presence in company with the tubercle bacillus constitutes mixed infection, which is much more serious than single infection by the tubercle bacillus. It is to be remembered, however, that a few of these bacteria may reach the sputum from the upper air-passages. Clinically, mixed infection is evidenced by fever.
(2) Staphylococcus and Streptococcus (p. 262).—One or both of these organisms is commonly present in company with the tubercle bacillus in the sputum of advanced phthisis (Plate II, Fig. 2). They are often found in bronchitis, catarrhal pneumonia, and many other conditions.
(3) Pneumococcus (Diplococcus of Fränkel).—The pneumococcus is the causative agent in nearly all cases [p. 36] of croupous pneumonia, and is commonly found in large numbers in the rusty sputum of this disease. It is sometimes met with in the sputum of catarrhal pneumonia, bronchitis, and tuberculosis. It has been found in the saliva in health. Pneumococci are about the size of streptococci. They are ovoid in shape, and lie in pairs, end to end, often forming short chains. Each is surrounded by a gelatinous capsule, which is its distinctive feature (Fig. 9). Diplococci without capsules are common in the sputum, but have no special significance.
|
| FIG. 9.—Diplococcus pneumoniæ in the blood (Fränkel and Pfeiffer). |
Recognition of the pneumococcus depends upon its morphology, the fact that it is Gram-staining, and the presence of a capsule. Numerous methods for staining capsules have been devised, but few are satisfactory. Buerger's method is excellent. It is especially useful with cultures upon serum media, but is applicable also to the sputum. Smith's method usually gives good results, as does also the more simple method of Hiss (p. 263). The sputum should be fresh—not more than three or four hours' old.
[p. 37] Buerger's Method for Capsules.—(1) Mix a few drops each of the sputum and blood-serum on egg-albumin solution (egg-albumin, distilled water, equal parts; shake and filter through cotton). Make thin smears from the mixture and just as the edges begin to dry, cover with Müller's fluid (potassium bichromate, 2.5 gm.; sodium sulphate, 1.0 gm.; water 100 c.c.) saturated with mercuric chlorid (ordinarily about 5 per cent.). Gently warm over a flame for about three seconds. This rapidly fixes the bacteria while still living.
(2) Rinse very quickly in water.
(3) Flush once with alcohol.
(4) Apply tincture of iodin for one to two minutes.
(5) Thoroughly wash off the iodin with alcohol and dry in the air.
(6) Stain about three seconds with weak anilin-gentian-violet freshly made up as follows: Anilin oil, 10; water, 100; shake; filter; and add 5 c.c. of a saturated alcoholic solution of gentian violet.
(7) Rinse off the stain with 2 per cent. solution of sodium chlorid, mount in this solution, and examine with a one-twelfth objective.
Buerger suggests a very useful variation as follows: After the alcohol wash and drying, the specimen is stained by Gram's method (p. 39), counter-stained with aqueous solution of fuchsin, washed, and mounted in water. The pneumococcus holds the purple stain, while all capsules take on the pink counter-stain.
Smith's Method.—This somewhat complicated, but not difficult, method is very useful as a routine stain for the sputum. It brings out well all cells and all bacteria except the tubercle bacillus.
(1) Make thin smears, dry, and fix in a flame in the usual manner.
(2) Apply anilin-gentian-violet a few seconds, gently warming until steam rises.
(3) Rinse in water.
(4) Apply Gram's iodin solution for thirty seconds.
[p. 38] (5) Wash in 95 per cent. alcohol until the purple color ceases to come off.
(6) Wash with equal parts of ether and absolute alcohol, or with ether and absolute alcohol successively.
(7) Apply a saturated aqueous solution of eosin for a minute or two.
(8) Rinse off the eosin with Löffler's methylene-blue, then cover with the methylene-blue, and heat until steam rises.
(9) Wash in water.
(10) Rinse quickly with absolute alcohol.
(11) Apply xylol a half minute or longer.
(12) Mount in balsam.
By this method organisms which stain by Gram's method (staphylococci, streptococci, pneumococci, etc.) are purplish-black; organisms which decolorize by Gram's method (bacilli of Friedländer, influenza bacilli, etc.) are blue; capsules are pink; nuclei of all cells are blue; and granules of eosinophilic cells are bright red.
Anilin-gentian-violet.—Ehrlich's formula is the one generally used, but this keeps only a few weeks. Stirling's solution, which keeps much better and seems to give equal results, is as follows: gentian-violet, 5 gm.; alcohol, 10 c.c.; anilin oil, 2 c.c.; water, 88 c.c.
Gram's Iodin Solution.—Iodin, 1 gm.; potassium iodid, 2 gm.; water, 300 c.c.
Löffler's alkaline methylene-blue is a very generally useful stain for bacteria. It is composed of 30 parts of a saturated alcoholic solution of methylene-blue and 100 parts of a 1:10,000 aqueous solution of caustic potash. It keeps indefinitely.

|
| FIG. 10.—Friedländer's bacillus in pus from pulmonary abscess (obj. one-twelfth) (Boston). |
(4) Bacillus of Friedländer (Bacillus mucosus capsulatus).—In a small percentage of cases of pneumonia, this organism is found alone or in company with the pneumococcus. Its pathologic significance is uncertain. It is often present in the respiratory tract under normal conditions. Friedländer's bacilli are non-motile, [p. 39] encapsulated rods, sometimes arranged in short chains (Fig. 10). Very short individuals in pairs closely resemble pneumococci, from which they are distinguished by the fact that they are Gram-decolorizing.
(5) Bacillus of Influenza.—This is the etiologic factor in true influenza. It is present, often in large numbers, in the nasal and bronchial secretions, and is also found in the local lesions following influenza. Chronic infection by influenza bacilli may be mistaken clinically for tuberculosis, and they should be searched for in all cases of obstinate chronic bronchitis.
Their recognition depends upon the facts that they are extremely small bacilli; that most of them lie within the pus-cells; that their ends stain more deeply than their centers, sometimes giving the appearance of minute diplococci; and that they are decolorized by Gram's method of staining (Fig. 11).
They are stained blue in Gabbet's method for tubercle bacilli, but are more certainly recognized by Smith's method or by Gram's method, followed by Bismarck brown or fuchsin, as follows:
Gram's Method.—(1) Make smears, dry und fix by heat.
(2) Apply anilin-gentian-violet two to five minutes.
(3) Wash with water.
(4) Apply Gram's iodin solution one-half to two minutes.
(5) Wash in alcohol until the purple color ceases to come off.
(6) Apply a saturated aqueous or alcoholic solution of Bismarck brown one-half to one minute, or a weak solution of fuchsin until the film become pink. The latter [p. 40] probably gives a better contrast stain, but there is danger of overstaining.
(7) Wash in water, dry, and mount.
By this method Gram-staining bacteria are purple; Gram-decolorizing bacteria and nuclei of cells are brown or red.
|
| FIG. 11.—Bacillus of influenza; cover-glass preparation of sputum from a case of influenza, showing the bacilli in leukocytes; highly magnified (Pfeiffer). |
2. Cells.—These include pus-corpuscles, epithelial cells, and red blood-corpuscles.
(1) Pus-corpuscles are present in every sputum, and at times the sputum may consist of little else. They are the polymorphonuclear leukocytes of the blood, and appear as rounded cells with several nuclei or one very irregular nucleus (Fig. 8 and Plate II, Fig. 2). They are frequently filled with granules of coal-dust and are often much degenerated. Such coal-dust-laden leukocytes are especially abundant in anthracosis, where angular black particles, both intra- and extra-cellular, are often so numerous as to color the sputum (Plate II, Fig. 2, B). Occasionally mononuclear leukocytes are present.
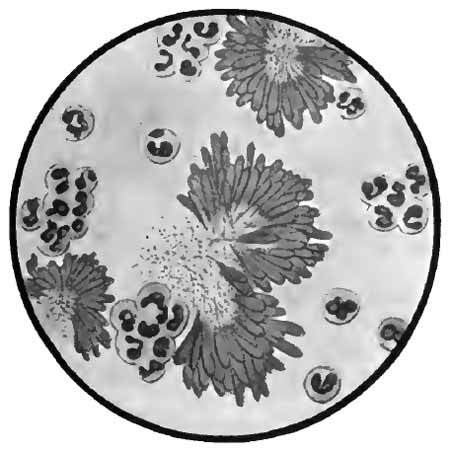
[p. 41] Eosinophilic leukocytes are quite constantly found in large numbers in the sputum of bronchial asthma near the time of the paroxysm, and constitute one of the most distinctive features of the sputum of this disease. They resemble ordinary pus-corpuscles, except that their cytoplasm is filled with coarse granules having a marked affinity for eosin. Large numbers of free granules, derived from disintegrated cells, are also found (Fig. 12).
|
| FIG. 12.—Sputum from a case of asthma showing leukocytes, some containing eosinophilic granules; free eosinophilic granules; and micrococci; stained with eosin and methylene-blue (Jakob). |
Ordinary pus-cells are easily recognized in sputum stained by any of the methods already given. For eosinophilic cells, some method which includes eosin must be used. A simple method is to stain the dried and fixed film two or three minutes with saturated solution of eosin, and then one-half to one minute with Löffler's methylene-blue; nuclei and bacteria will be blue, eosinophilic granules bright red.
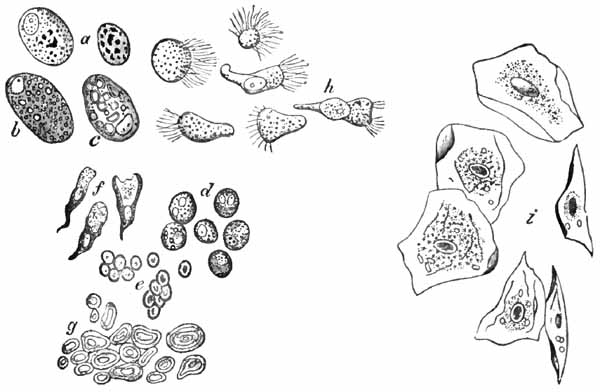
(2) Epithelial cells may come from any part of the [p. 42] respiratory tract. A few are always present. They have little diagnostic value, although a considerable excess would indicate a pathologic condition at the site of their origin. Any of the stains mentioned above will show them, and they can usually be identified in unstained sputum. In general three forms are found:
(a) Squamous cells: large, flat, polygonal cells with a comparatively small nucleus (Fig. 13, i). They come from the upper air-passages, and are especially numerous in laryngitis and pharyngitis. They are frequently studded with bacteria—most commonly diplococci.
|
| FIG. 13.—Different morphologic elements of the sputum (unstained): a, b, c, Pulmonary or alveolar epithelium—a, with normal lung pigment (carbon); b, with fat-droplets; c, with myelin globules; d, pus-corpuscles; e, red blood-corpuscles; f, cylindric beaker-shaped bronchial cells; g, free myelin globules; h, ciliated epithelium of different kinds from the nose, altered by coryza; i, squamous cells from the pharynx (after Bizzozero). |
(b) Cylindric cells from the nose, trachea, and bronchi (Fig. 13, f, h): These are not usually abundant, and, [p. 43] as a rule, they are not identified because much altered from their original form, being often spheric.
(c) Alveolar cells: rather large, round, or oval cells with one or two round nuclei (Fig. 13). Their source is presumably the pulmonary alveoli. Like the leukocytes, they frequently contain particles of carbon (normal lung pigment). In chronic heart disease, owing to long-continued passive congestion, they may be filled with brown granules of altered blood-pigment, and are then called "heart-failure cells" (Plate II, Fig. 1). Alveolar cells commonly contain fat-droplets and, less frequently, myelin globules. The latter are colorless, rounded bodies, sometimes resembling fat droplets, but often showing concentric or irregularly spiral markings (Fig. 13, c, g). They are also found free in the sputum. They are abundant in the scanty morning sputum of apparently healthy persons, but may be present in any mucoid sputum.
(3) Red blood-corpuscles may be present in small numbers in almost any sputum. When fairly constantly present in considerable numbers, they are suggestive of phthisis. The corpuscles when fresh are shown by any of the staining methods which include eosin. They are commonly so much degenerated as to be unrecognizable, and often only altered blood-pigment is left. Ordinarily, blood in the sputum is sufficiently recognized with the naked eye.
Only those conditions which give fairly characteristic sputa are mentioned.
1. Acute Bronchitis.—There is at first a small amount of tenacious, almost purely mucoid sputum, frequently blood-streaked. This gradually becomes more abundant, [p. 44] mucopurulent in character, and yellowish or gray in color. At first the microscope shows a few leukocytes and alveolar and bronchial cells; later, the leukocytes become more numerous. Bacteria are not usually abundant.
2. Chronic Bronchitis.—The sputum is usually abundant, mucopurulent, and yellowish or yellowish-green in color. Nummular masses—circular, "coin-like" discs which sink in water—may be seen. Microscopically, there are great numbers of leukocytes, often much degenerated. Epithelium is not abundant. Bacteria of various kinds, especially staphylococci, are usually numerous.
In fibrinous bronchitis there are found, in addition, fibrinous casts, usually of medium size.
In the chronic bronchitis accompanying long-continued passive congestion of the lungs, as in poorly compensated heart disease, the sputum may assume a rusty brown color, owing to presence of large numbers of the "heart-failure cells" previously mentioned.
3. Bronchiectasis.—The sputum is very abundant at intervals, sometimes as high as a liter in twenty-four hours, and has a very offensive odor when the cavity is large. It is thinner than that of chronic bronchitis, and upon standing separates into three layers of pus, mucus, and frothy serum. It contains great numbers of miscellaneous bacteria.
4. Gangrene of the Lung.—The sputum is abundant, fluid, very offensive, and brownish in color. It separates into three layers upon standing—a brown deposit, a clear fluid, and a frothy layer. Microscopically, few cells of any kind are found. Bacteria are extremely numerous; among them may sometimes be found an acid-fast bacillus probably identical with the smegma bacillus. As before [p. 45] stated, elastic fibers are less common than would be expected.
5. Pulmonary Edema.—Here there is an abundant, watery, frothy sputum, varying from faintly yellow or pink to dark-brown in color; a few leukocytes and epithelial cells and varying numbers of red blood-corpuscles are found with the microscope.
6. Bronchial Asthma.—The sputum during and following an attack is scanty and very tenacious. Most characteristic is the presence of Curschmann's spirals, Charcot-Leyden crystals, and eosinophilic leukocytes.
7. Croupous Pneumonia.—Characteristic of this disease is a scanty, rusty red, very tenacious sputum containing red corpuscles or altered blood-pigment, leukocytes, epithelial cells, usually many pneumococci, and often very small fibrinous casts. This sputum is seen during the stage of red hepatization. During resolution the sputum assumes the appearance of that of chronic bronchitis. When pneumonia occurs during the course of a chronic bronchitis, the characteristic rusty red sputum may not appear.
8. Pulmonary Tuberculosis.—The sputum is variable. In the earliest stages it may be scanty and almost purely mucoid, with an occasional yellow flake, or there may be only a very small mucopurulent mass. When the quantity is very small there may be no cough, the sputum reaching the larynx by action of the bronchial cilia. This is not well enough recognized by practitioners. A careful inspection of all the sputum brought up by the patient on several successive days, and a microscopic examination of all yellow portions, will not infrequently establish a diagnosis of tuberculosis when physical signs are negative. [p. 46] Tubercle bacilli will sometimes be found in large numbers at this stage. Blood-streaked sputum is strongly suggestive of tuberculosis, and is more common in the early stages than later.
The sputum of more advanced cases resembles that of chronic bronchitis, with the addition of tubercle bacilli and elastic fibers. Caseous particles containing immense numbers of the bacilli are common. Far-advanced cases with large cavities often show rather firm, spheric or ovoid masses of thick pus in a thin fluid—the so-called "globular sputum." These globular masses usually contain many tubercle bacilli.
Preliminary Considerations.—The urine is an aqueous solution of various organic and inorganic substances. It is probably both a secretion and an excretion. Most of the substances in solution are either waste-products from the body metabolism or products derived directly from the foods eaten. Normally, the total amount of solid constituents carried off in twenty-four hours is about 60 gm., of which the organic substances make up about 35 gm. and the inorganic about 25 gm.
The chief organic constituents are urea and uric acid. Urea constitutes about one-half of all the solids, or about 30 gm. in twenty-four hours.
The chief inorganic constituents are the chlorids, phosphates, and sulphates. The chlorids, practically all in the form of sodium chlorid, constitute one-half, or about 13 gm., in twenty-four hours.
Certain substances appear in the urine only in pathologic conditions. The most important of these are proteids, sugars, acetone and related substances, bile, hemoglobin, and the diazo substances.
In addition to the substances in solution all urines contain various microscopic structures.
While, under ordinary conditions, the composition of urine does not vary much from day to day, it varies greatly at different hours of the same day. It is evident, [p. 48] therefore, that no quantitative test can be of value unless a sample of the mixed twenty-four-hour urine be used. The patient should be instructed to void all the urine during the twenty-four hours into a clean vessel kept in a cool place, to mix it well, to measure the whole quantity, and to bring four to eight ounces for examination. When it is desired to make only qualitative tests, as for albumin or sugar, a "sample" voided at random will answer. It should be remembered, however, that urine passed about three hours after a meal is most likely to contain pathologic substances. That voided first in the morning is least likely to contain them.
The urine must be examined while fresh. Decomposition sets in rapidly, especially in warm weather, and greatly interferes with all the examinations. Decomposition may be delayed by adding five grains of boric acid (as much of the powder as can be heaped upon a ten-cent piece) for each four ounces of urine. Formalin, in proportion of one drop to four ounces, is also an efficient preservative, but if larger amounts be used, it may give reactions for sugar and albumin, and is likely to cause a precipitate which greatly interferes with the microscopic examination.
Normal and abnormal pigments, which interfere with certain of the tests, can be removed by filtering the urine through animal charcoal, or precipitating with a solution of acetate of lead and filtering.
A suspected fluid can be identified as urine by detecting any considerable quantity of urea in it (p. 66). Traces of urea may, however, be met with in ovarian cyst fluid, while urine from very old cases of hydronephrosis may contain little or none.
[p. 49] Clinical examination of the urine may conveniently be considered under four heads: I. Physical examination. II. Chemic examination. III. Microscopic examination. IV. The urine in disease.
1. Quantity.—The quantity passed in twenty-four hours varies greatly with the amount of liquids ingested, perspiration, etc. The normal may be taken as 1000 to 1500 c.c., or 40 to 50 ounces.
The quantity is increased (polyuria) during absorption of large serous effusions and in many nervous conditions. It is usually much increased in chronic interstitial nephritis, diabetes insipidus, and diabetes mellitus. In these conditions a permanent increase in amount of urine is characteristic—a fact of much value in diagnosis. In diabetes mellitus the urine may, though rarely, reach the enormous amount of 50 liters.
The quantity is decreased (oliguria) in severe diarrhea; in fevers; in all conditions which interfere with circulation in the kidney, as poorly compensated heart disease; and in the parenchymatous forms of nephritis. In uremia the urine is usually very greatly decreased and may be entirely suppressed (anuria).
2. Color.—This varies considerably in health, and depends largely upon the quantity of urine voided. The usual color is yellow or reddish-yellow, due to the presence of several pigments, chiefly urochrome. In recording the color Vogel's scale (see Frontispiece) is very widely used, the urine being filtered and examined by transmitted light in a glass three or four inches in diameter.
The color is sometimes greatly changed by abnormal [p. 50] pigments. Blood-pigment gives a red or brown, smoky color. Urine containing bile is yellowish or brown, with a yellow foam when shaken. It may assume a greenish hue after standing, owing to oxidation of bilirubin into biliverdin. Ingestion of small amounts of methylene-blue gives a pale green; large amounts give a marked blue. Santonin produces a yellow; rhubarb, senna, cascara, and some other cathartics, a brown color; these change to red upon addition of an alkali, and if the urine be alkaline when voided may cause suspicion of hematuria. Thymol gives a yellowish-green. Following poisoning from phenol and related drugs the urine may have a normal color when voided, but becomes olive-green to brownish-black upon standing. Urine which contains melanin, as sometimes in melanotic sarcoma and, very rarely, in wasting diseases, also becomes brown or black upon long standing.
3. Transparency.—Freshly passed normal urine is clear. Upon standing, a faint cloud of mucus, leukocytes, and epithelial cells settles to the bottom. Abnormal cloudiness is usually due to presence of phosphates, urates, pus, blood, or bacteria.
Amorphous phosphates are precipitated in neutral or alkaline urine. They form a white cloud and sediment which disappear upon addition of an acid.
Amorphous urates are precipitated only in acid urine. They form a white or pink cloud and sediment ("brick-dust deposit") which disappear upon heating.
Pus resembles amorphous phosphates to the naked eye. Its nature is easily recognized with the microscope, or by adding a strong solution of caustic soda to the sediment, which is thereby transformed into a gelatinous mass (Donné's test).
[p. 51] Blood gives a reddish or brown, smoky color, and may be recognized with the microscope or by tests for hemoglobin.
Bacteria, when present in great numbers, give a uniform cloud which cannot be removed by ordinary filtration. They are detected with the microscope.
The cloudiness of decomposing urine is due mainly to precipitation of phosphates and multiplication of bacteria.
4. Reaction.—Normally, the mixed twenty-four-hour urine is slightly acid in reaction, the acidity being due to acid salts, not to free acids. Individual samples may be slightly alkaline, especially after a full meal. The reaction is determined by means of litmus paper.
Acidity is increased after administration of certain drugs, and whenever the urine is concentrated from any cause, as in fevers. A very acid urine may cause frequent micturition because of its irritation. This is often an important factor in the troublesome enuresis of children.
The urine always becomes alkaline upon long standing, owing to decomposition of urea with formation of ammonia. If markedly alkaline when voided, it usually indicates such "ammoniacal decomposition" in the bladder, which is the rule in chronic cystitis, especially that due to paralysis or obstruction. Alkalinity due to ammonia (volatile alkalinity) can be distinguished by the fact that litmus paper turned blue by the urine again becomes red upon gentle heating. Fixed alkalinity is due to alkaline salts, and is often observed during frequent vomiting, after the crisis of pneumonia, in various forms of anemia, after full meals, and after administration of certain drugs, especially salts of vegetable acids.
5. Specific Gravity.—The normal average is about [p. 52] 1.017 to 1.020. Samples of urine taken at random may go far above or below these figures, hence a sample of the mixed twenty-four-hour urine should always be used.
Pathologically, it may vary from 1.001 to 1.060. It is low in chronic interstitial nephritis, diabetes insipidus, and many functional nervous disorders. It is high in fevers and in parenchymatous forms of nephritis. In any form of nephritis a sudden fall without a corresponding increase in quantity of urine may foretell approaching uremia. It is highest in diabetes mellitus. A high specific gravity when the urine is not highly colored should lead one to suspect this disease. A normal specific gravity does not, however, exclude it.
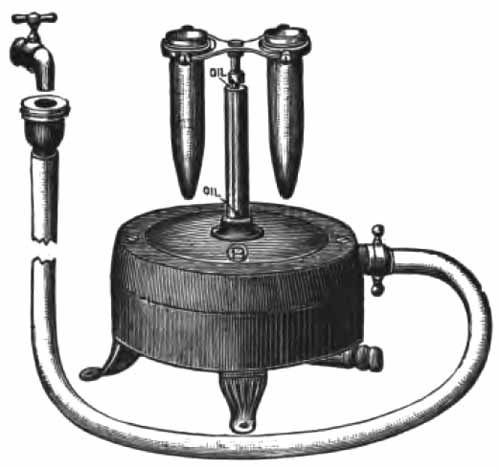
|
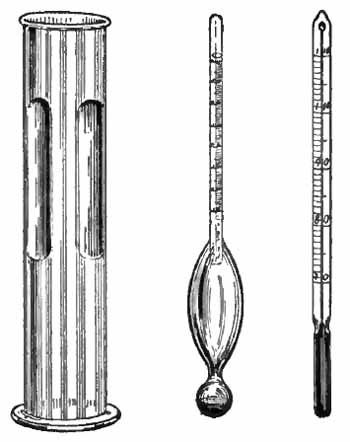
| FIG. 14.—Squibb's urinometer with thermometer and cylinder. |
The specific gravity is most conveniently estimated by means of the urinometer—Squibb's is preferable (Fig. 14). It is standardized for a temperature of 77° F., and the urine should be at or near that temperature. Care should be taken that the urinometer does not touch the side of the tube, and that air-bubbles are removed from the surface [p. 53] of the urine. With most instruments the reading is taken from the bottom of the meniscus.
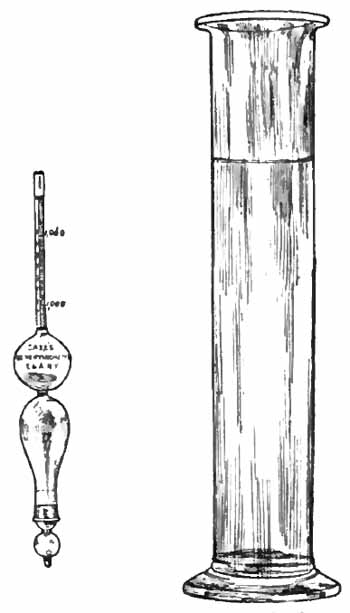
One frequently wishes to ascertain the specific gravity of quantities of fluid too small to float an urinometer. A simple device for this purpose, which requires only about 3 c.c. and is very satisfactory in clinical work, has been designed by Saxe (Fig. 15). The urine is placed in the bulb at the bottom, the instrument is floated in distilled water, and the specific gravity is read off from the scale upon the stem.
|
| FIG. 15.—Saxe's urinopyknometer and jar for same. |
6. Total Solids.—An estimation of the total amount of solids which pass through the kidneys in twenty-four hours is, in practice, one of the most useful of urinary [p. 54] examinations. The normal for a man of 150 pounds is about 60 grams, or 950 grains. The principal factors which influence this amount are body weight (except with excessive fat), diet, exercise, and age, and these should be considered in making an estimation. After about the forty-fifth year it becomes gradually less; after seventy-five years it is about one-half the amount given.
In disease, the amount of solids depends mainly upon the activity of metabolism and the ability of the kidneys to excrete. An estimation of the solids, therefore, furnishes an important clue to the functional efficiency of the kidneys. The kidneys bear much the same relation to the organism as does the heart: they cause no direct harm so long as they are capable of performing the work required of them. When, however, through either organic disease or functional inactivity, they fail to carry off their proportion of the waste-products of the body, some of these products must either be eliminated through other organs, where they cause irritation and disease, or be retained within the body, where they act as poisons. The great importance of these poisons in production of distressing symptoms and even organic disease is not well enough recognized by most practitioners. Disappearance of unpleasant and perplexing symptoms as the urinary solids rise to the normal under proper treatment is often most surprising.
When, other factors remaining unchanged, the amount of solids eliminated is considerably above the normal, increased destructive metabolism may be inferred.
The total solids can be estimated roughly, but accurately enough for most clinical purposes, by multiplying the last two figures of the specific gravity of the mixed [p. 55] twenty-four-hour urine by the number of ounces voided and to the product adding one-tenth of itself. This gives the amount in grains. Häser's method is more widely used but is less convenient. The last two figures of the specific gravity are multiplied by 2.33. The product is then multiplied by the number of cubic centimeters voided in twenty-four hours and divided by 1000. This gives the total solids in grams.
7. Functional Tests.—Within the past few years much thought has been devoted to methods of more accurately ascertaining the functional efficiency of the kidneys, especially of one kidney when removal of the other is under consideration. The most promising of the methods which have been devised are cryoscopy, the methylene-blue test, and the phloridzin test. It is doubtful whether, except in experienced hands, these yield any more information than can be had from an intelligent consideration of the specific gravity and the twenty-four-hour quantity, together with a microscopic examination. They are most useful when the urines obtained from separate kidneys by segregation or ureteral catheterization are compared. The reader is referred to larger works upon urinalysis for details.
Cryoscopy, determination of the freezing-point, depends upon the principle that the freezing-point of a fluid is depressed in proportion to the number of molecules in solution. To have any value, the freezing-point of the urine must be compared with that of the blood, since it is not so much the number of molecules contained in the urine as the number which the kidney has failed to carry off and has left in the blood, that indicates its insufficiency.
[p. 56] In the methylene-blue test of Achard and Castaigne a solution of methylene-blue is injected intramuscularly, and the time of its appearance in the urine is noted. Normally, it appears in about thirty minutes. When delayed, renal "permeability" is supposed to be interfered with.
The phloridzin test consists in the hypodermic injection of a small quantity of phloridzin. This substance is transformed into glucose by the kidneys of healthy persons. In disease, this change is more or less interfered with, and the amount of glucose recoverable from the urine is taken as an index of the secretory power of the kidneys.
In applying these tests for "permeability," "secretory ability," etc., one must remember that the conditions are abnormal, and that there is no evidence that the kidneys will behave with the products of metabolism as they do with the substances selected for the tests, and also that the tests throw unusual work upon the kidneys, which in some cases may be harmful.
The most important are chlorids, phosphates, sulphates including indican, urea, and uric acid.
1. Chlorids.—These are derived from the food, and are mainly in the form of sodium chlorid. The amount excreted normally is 10 to 15 grams in twenty-four hours. It is much affected by the diet.
Excretion of chlorids is diminished in nephritis and in fevers, especially in pneumonia and inflammations leading to the formation of large exudates. In nephritis the [p. 57] kidneys are less permeable to the chlorids, and it is probable that the edema is due largely to an effort of the body to dilute the chlorids which have been retained. In fevers the diminution is due largely to decrease of food. In pneumonia chlorids are constantly very low, and in some cases are absent entirely. Following the crisis they are increased. In inflammations leading to formation of large exudates—e.g., pleurisy with effusion—chlorids are diminished, because a considerable amount becomes "locked up" in the exudate. During absorption chlorids are liberated and appear in the urine in excessive amounts.
|
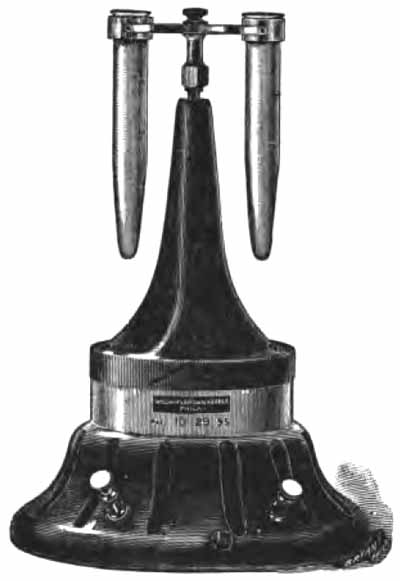
| FIG. 16.—The Purdy electric centrifuge. |
Quantitative Estimation.—The best method for clinical purposes is the centrifugal method.
[p. 58]
|
| FIG. 17.—Water-motor centrifuge. |
Purdy's Centrifugal Methods.—As shown by the late Dr. Purdy, the centrifuge offers an important means of making quantitative estimations of a number of substances in the urine. Results are easily and quickly obtained, and are probably accurate enough for all clinical purposes.
|
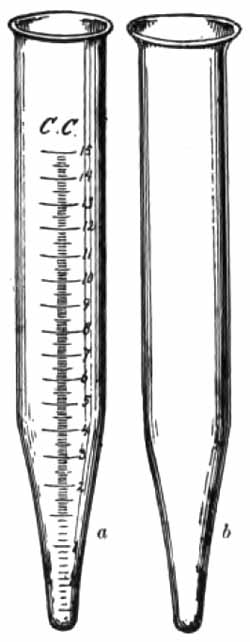
| FIG. 18.—Purdy's tubes for the centrifuge: a, Percentage tube; b, sediment tube. |
In general, the methods consist in precipitating the substance to be estimated in a graduated centrifuge tube, and applying a definite amount of centrifugal force for a definite length of time, after which the percentage of precipitate is read off upon the side of the tube. Albumin, if present, must be previously removed by boiling and filtering. Results are in terms of bulk of precipitate, which must not be confused with percentage by weight. The weight percentage can be found by referring to Purdy's tables, given later. In this, as in all quantitative urine work, percentages mean little in themselves; the actual [p. 59] amount eliminated in twenty-four hours should always be calculated.
The centrifuge should have an arm with radius of 6¾ inches when in motion, and should be capable of maintaining a speed of 1500 revolutions a minute. The electric centrifuge is to be recommended, although good work can be done with a water-power centrifuge, or, after a little practice, with the hand centrifuge. A speed indicator is desirable with electric and water-motor machines, although one can learn to estimate the speed by the musical note.
Estimation of Chlorids.—Fill the graduated tube to the 10 c.c. mark with urine; add 15 drops strong nitric acid and then silver nitrate solution (dram to the ounce) to the 15 c.c. mark. Mix by inverting several times. Let stand a few minutes for a precipitate to form, and then revolve in the centrifuge for three minutes at 1200 revolutions a minute. Each one-tenth cubic centimeter of precipitate equals 1 per cent. by bulk. The normal is about 10 per cent. This may be converted into terms of chlorin or sodium chlorid by means of the table upon page 60. Roughly speaking, the percentage of chlorin by weight is about one-twelfth the bulk-percentage.[p. 60]
| TABLE FOR THE ESTIMATION OF CHLORIDS AFTER CENTRIFUGATION | ||||
| Showing the bulk-percentage of silver chlorid (AgCl) and the corresponding gravimetric percentages and grains per fluidounce of sodium chlorid (NaCl) and chlorin (Cl).—(Purdy.) | ||||
| Bulk-percentage of AgCl. | Percentage NaCl. | Gr. Per Oz. NaCl. | Percentage Cl. | Gr. Per Oz. Cl. |
| ¼ | 0.03 | 0.15 | 0.02 | 0.1 |
| ½ | 0.07 | 0.31 | 0.04 | 0.19 |
| ¾ | 0.1 | 0.47 | 0.06 | 0.28 |
| 1 | 0.13 | 0.62 | 0.08 | 0.38 |
| 1¼ | 0.16 | 0.78 | 0.1 | 0.48 |
| 1½ | 0.19 | 0.93 | 0.12 | 0.57 |
| 1¾ | 0.23 | 1.09 | 0.14 | 0.67 |
| 2 | 0.26 | 1.24 | 0.16 | 0.76 |
| 2¼ | 0.29 | 1.41 | 0.18 | 0.85 |
| 2½ | 0.32 | 1.56 | 0.2 | 0.96 |
| 2¾ | 0.36 | 1.71 | 0.22 | 1.04 |
| 3 | 0.39 | 1.87 | 0.24 | 1.13 |
| 3¼ | 0.42 | 2.02 | 0.26 | 1.23 |
| 3½ | 0.45 | 2.18 | 0.28 | 1.32 |
| 3¾ | 0.49 | 2.35 | 0.3 | 1.42 |
| 4 | 0.52 | 2.49 | 0.32 | 1.51 |
| 4¼ | 0.55 | 2.64 | 0.34 | 1.61 |
| 4½ | 0.58 | 2.8 | 0.35 | 1.7 |
| 4¾ | 0.62 | 2.96 | 0.37 | 1.8 |
| 5 | 0.65 | 3.11 | 0.39 | 1.89 |
| 5½ | 0.71 | 3.42 | 0.43 | 2.09 |
| 6 | 0.78 | 3.73 | 0.47 | 2.27 |
| 6½ | 0.84 | 4.05 | 0.51 | 2.46 |
| 7 | 0.91 | 4.35 | 0.55 | 2.62 |
| 7½ | 0.97 | 4.67 | 0.59 | 2.84 |
| 8 | 1.04 | 4.98 | 0.63 | 3.02 |
| 8½ | 1.1 | 5.29 | 0.67 | 3.22 |
| 9 | 1.17 | 5.6 | 0.71 | 3.4 |
| 9½ | 1.23 | 5.91 | 0.75 | 3.6 |
| 10 | 1.3 | 6.22 | 0.79 | 3.79 |
| 10½ | 1.36 | 6.53 | 0.83 | 3.97 |
| 11 | 1.43 | 6.84 | 0.87 | 4.16 |
| 11½ | 1.49 | 7.2 | 0.91 | 4.35 |
| 12 | 1.56 | 7.46 | 0.95 | 4.54 |
| 12½ | 1.62 | 7.78 | 0.99 | 4.73 |
| 13 | 1.69 | 8.09 | 1.02 | 4.92 |
| 13½ | 1.75 | 8.4 | 1.06 | 5.11 |
| 14 | 1.82 | 8.71 | 1.1 | 5.29 |
| 14½ | 1.88 | 9.02 | 1.14 | 5.49 |
| 15 | 1.94 | 9.33 | 1.18 | 5.67 |
| 15½ | 2.01 | 9.65 | 1.22 | 5.86 |
| 16 | 2.07 | 9.94 | 1.26 | 6.06 |
| 16½ | 2.14 | 10.27 | 1.3 | 6.24 |
| 17 | 2.2 | 10.51 | 1.34 | 6.43 |
| 17½ | 2.27 | 10.87 | 1.38 | 6.62 |
| 18 | 2.33 | 11.2 | 1.42 | 6.81 |
| 18½ | 2.4 | 11.51 | 1.46 | 7.0 |
| 19 | 2.46 | 11.82 | 1.5 | 7.19 |
| 19½ | 2.53 | 12.13 | 1.54 | 7.38 |
| 20 | 2.59 | 12.44 | 1.58 | 7.56 |
| Bulk-percentage to be read on the side of the tube. | ||||
2. Phosphates.—Phosphates are derived largely from the food, only a small proportion resulting from metabolism. The normal daily output of phosphoric acid is about 2.5 to 3.5 gm.
The urinary phosphates are of two kinds: alkaline, which make up two-thirds of the whole, and include the [p. 61] phosphates of sodium and potassium; and earthy, which constitute one-third, and include the phosphates of calcium and magnesium. Earthy phosphates are frequently thrown out of solution in neutral and alkaline urines, and as "amorphous phosphates" form a very common sediment. This sediment seldom indicates an excessive excretion of phosphates.
Quantitative estimation does not furnish much of definite clinical value. The centrifugal method is the most convenient.
| TABLE FOR THE ESTIMATION OF PHOSPHATES AFTER CENTRIFUGATION | |||||
| Showing bulk-percentages of uranyl phosphate (H[UO2]PO4) and the corresponding gravimetric percentages and grains per ounce of phosphoric acid (P2O5).—(Purdy.) | |||||
| Bulk-percentage of H(UO2)PO4. | Percentage P2O5. | Gr. Per Oz. P2O5. | Bulk-percentage of H(UO2)PO4. | Percentage P2O5. | Gr. Per Oz. P2O5. |
| ½ | 0.02 | 0.1 | 11 | 0.14 | 0.67 |
| 1 | 0.04 | 0.19 | 12 | 0.15 | 0.72 |
| 1½ | 0.045 | 0.22 | 13 | 0.16 | 0.77 |
| 2 | 0.05 | 0.24 | 14 | 0.17 | 0.82 |
| 2½ | 0.055 | 0.26 | 15 | 0.18 | 0.86 |
| 3 | 0.06 | 0.29 | 16 | 0.19 | 0.91 |
| 3½ | 0.065 | 0.31 | 17 | 0.2 | 0.96 |
| 4 | 0.07 | 0.34 | 18 | 0.21 | 1.0 |
| 4½ | 0.075 | 0.36 | 19 | 0.22 | 1.06 |
| 5 | 0.08 | 0.38 | 20 | 0.23 | 1.1 |
| 6 | 0.09 | 0.43 | 21 | 0.24 | 1.15 |
| 7 | 0.1 | 0.48 | 22 | 0.25 | 1.2 |
| 8 | 0.11 | 0.53 | 23 | 0.26 | 1.25 |
| 9 | 0.12 | 0.58 | 24 | 0.27 | 1.3 |
| 10 | 0.13 | 0.62 | 25 | 0.28 | 1.35 |
| Bulk-percentage to be read from graduation on the side of the tube. | |||||
Purdy's Centrifugal Method.—Take 10 c.c. urine in the graduated tube, add 2 c.c. of 50 per cent. acetic acid, and 3 c.c. of 5 per cent. uranium nitrate solution. Mix; let stand a few minutes, and revolve for three minutes at 1200 revolutions. [p. 62] The bulk of precipitate is normally about 8 per cent. The percentage of phosphoric acid by weight is, roughly, one-eighty-fifth of the bulk-percentage.
3. Sulphates.—The urinary sulphates are derived partly from the food, especially meats, and partly from body metabolism. The normal output of sulphuric acid is about 1.5 to 3 gm. daily.
Quantitative estimation of the total sulphates yields little of clinical value.
Purdy's Centrifugal Method.—Take 10 c.c. urine in the graduated tube and add barium chlorid solution to the 15 c.c. mark. This consists of barium chlorid, 4 parts; strong hydrochloric acid, 1 part; and distilled water, 16 parts. Mix; let stand a few minutes, and revolve for three minutes at 1200 revolutions a minute. The normal bulk of precipitate is about 0.8 per cent. The percentage by weight of sulphuric acid is about one-fourth of the bulk-percentage.
| TABLE FOR THE ESTIMATION OF SULPHATES AFTER CENTRIFUGATION | |||||
| Showing the bulk-percentages of barium sulphate (BaSO4) and the corresponding gravimetric percentages and grains per fluidounce of sulphuric acid (SO3).—(Purdy.) | |||||
| Bulk-percentage of BaSO4. | Percentage SO3. | Gr. Per Oz. SO3. | Bulk-percentage of BaSO4. | Percentage SO3. | Gr. Per Oz. SO3. |
| 1/8 | 0.04 | 0.19 | 2¼ | 0.55 | 2.64 |
| ¼ | 0.07 | 0.34 | 2½ | 0.61 | 2.93 |
| 3/8 | 0.1 | 0.48 | 2¾ | 0.67 | 3.22 |
| ½ | 0.13 | 0.62 | 3 | 0.73 | 3.5 |
| 5/8 | 0.16 | 0.77 | 3¼ | 0.79 | 3.79 |
| ¾ | 0.19 | 0.91 | 3½ | 0.85 | 4.08 |
| 7/8 | 0.22 | 1.06 | 3¾ | 0.91 | 4.37 |
| 1 | 0.25 | 1.1 | 4 | 0.97 | 4.66 |
| 1¼ | 0.31 | 1.49 | 4¼ | 1.03 | 4.94 |
| 1½ | 0.37 | 1.78 | 4½ | 1.09 | 5.23 |
| 1¾ | 0.43 | 2.06 | 4¾ | 1.15 | 5.52 |
| 2 | 0.49 | 2.35 | 5 | 1.21 | 5.81 |
| Bulk-percentage to be read from graduation on the side of the tube. | |||||
[p. 63] Nine-tenths of the sulphuric acid is in combination with various mineral substances (mineral or preformed sulphates). One-tenth is in combination with certain aromatic substances, mostly products of albuminous putrefaction in the intestine (conjugate sulphates). Among these aromatic substances are indol, phenol, and skatol. By far the most important of the conjugate sulphates and representative of the group is potassium indoxyl sulphate.
Potassium indoxyl sulphate, or indican, is derived from indol. Indol is absorbed and oxidized into indoxyl, which combines with potassium and sulphuric acid and is thus excreted. Under normal conditions the amount in the urine is small. It is increased by a meat diet.
Pathologically, an increase of indican always indicates abnormal albuminous putrefaction somewhere in the body. It is noted in:
(a) Diseases of the Small Intestine.—This is by far the most common source. Intestinal obstruction gives the largest amounts of indican. It is also much increased in intestinal indigestion—so-called "biliousness"; in inflammations, especially in cholera and typhoid fever; and in paralysis of peristalsis such as occurs in peritonitis. Simple constipation and diseases of the large intestine alone do not increase the amount of indican.
(b) Diseases of the stomach associated with deficient hydrochloric acid, as chronic gastritis and gastric cancer. Diminished hydrochloric acid favors intestinal putrefaction.
(c) Decomposition of exudates anywhere in the body, as in empyema, bronchiectasis, and large tuberculous cavities.
[p. 64] Detection of indican depends upon its decomposition and oxidation of the indoxyl set free into indigo-blue.
Obermayer's Method.—In a test-tube take equal parts of the urine and Obermayer's reagent and add a small quantity of chloroform. Mix by inverting a few times; avoid shaking violently. If indican be present in excess, the chloroform, which sinks to the bottom, will assume an indigo-blue color. The depth of color indicates the comparative amount of indican if the same proportions of urine and reagents are always used. The indican in normal urine may give a faint blue by this method. Urine of patients taking iodids gives a reddish-violet color, which disappears upon addition of a few drops of strong sodium hyposulphite solution. Bile-pigments, which interfere with the test, must be removed (p. 48).
Obermayer's reagent consists of strong hydrochloric acid (sp. gr., 1.19), 1000 parts, and ferric chlorid, 2 parts. This makes a yellow, fuming liquid which keeps well.
4. Urea.—From the standpoint of physiology urea is the most important constituent of the urine. It is the principal waste-product of metabolism, and constitutes about one-half of all the solids excreted—about 30 gm. in twenty-four hours. It represents 85 to 90 per cent. of the total nitrogen of the urine, and its quantitative estimation is a simple, though not very accurate, method of ascertaining the state of nitrogenous excretion. Normally, the amount is greatly influenced by exercise and diet.
Pathologically, urea is increased in fevers, in diabetes, and especially during resolution of pneumonia and absorption of large exudates. Other factors being equal, the amount of urea indicates the activity of metabolism. In [p. 65] this connection the relation between the amounts of urea and the chlorids is important. The amount of urea is normally about twice that of the chlorids. If the proportion is much increased above this, increased tissue destruction may be inferred, since other conditions which increase urea also increase chlorids.
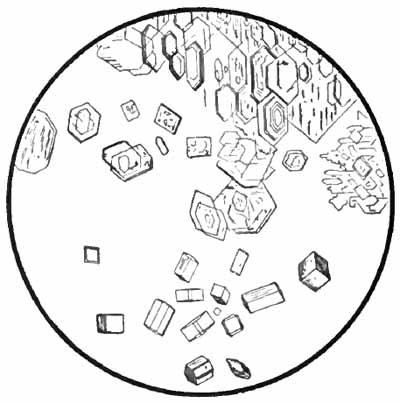
|
| FIG. 19.—Crystals of nitrate of urea (upper half) and oxalate of urea (lower half) (after Funke). |
Urea is decreased in diseases of the liver with destruction of liver substance. It may or may not be decreased in nephritis. In the early stages of chronic nephritis, when diagnosis is difficult, it is usually normal. In the late stages, when diagnosis is comparatively easy, it is decreased. Hence estimation of urea is of little help in the diagnosis of this disease, especially when, as is so frequently the case, a small quantity of urine taken at random is used. When, however, the diagnosis is established, estimations made at frequent intervals under the same conditions of diet and exercise are of much value, provided a sample of the mixed twenty-four-hour urine be used. A steady decline [p. 66] is a very bad prognostic sign, and a sudden marked diminution is usually a forerunner of uremia.
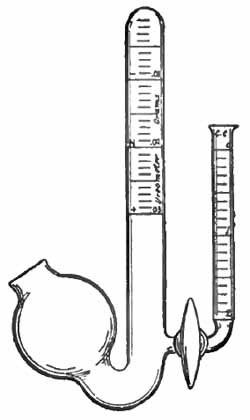
|
| FIG. 20.—Doremus Hinds' ureometer. |
The presence of urea can be shown by allowing a few drops of the fluid to partially evaporate upon a slide, and adding a small drop of pure colorless nitric acid or saturated solution of oxalic acid. Crystals of urea nitrate or oxalate (Fig. 19) will soon appear and can be recognized with the microscope.
Quantitative Estimation.—The hypobromite method, which is generally used, depends upon the fact that urea is decomposed by sodium hypobromite with liberation of nitrogen. The amount of urea is calculated from the volume of nitrogen set free. The improved Doremus apparatus (Fig. 20) is the most convenient.
Pour some of the urine into the smaller tube of the apparatus, then open the stopcock and quickly close it so as to fill its lumen with urine. Rinse out the larger tube with water and fill it and the bulb with 25 per cent. caustic soda solution. Add to this 1 c.c. of bromin by means of a medicine-dropper and mix well. This prepares a fresh solution of sodium hypobromite with excess of caustic soda, which serves to absorb the carbon dioxid set free in the decomposition of urea. When handling bromin, keep an open vessel of ammonia near to neutralize the irritant fumes.
Pour the urine into the smaller tube, and then turn the stopcock so as to let as much urine as desired (usually 1 c.c.) run slowly into the hypobromite solution. When bubbles have ceased to rise, read off the height of the fluid in the large [p. 67] tube by the graduations upon its side. This gives the amount by weight of urea in the urine added, from which the amount excreted in twenty-four hours can easily be calculated. If the urine contains much more than the normal amount, it should be diluted.
To avoid handling pure bromin, which is disagreeable, Rice's solutions may be employed:
| (a) | Bromin, | 31 |
| Potassium bromid, | 31 | |
| Distilled water, | 250. | |
| (b) | Caustic soda, | 100 |
| Distilled water, | 250. |
One part of each of these solutions and two parts of water are mixed and used for the test. The bromin solution must be kept in a tightly stoppered bottle or it will rapidly lose strength.

|
| FIG. 21.—Ruhemann's uricometer. |
5. Uric Acid.—Uric acid is the most important of a group of substances, called purin bodies, which are derived chiefly from the nucleins of the food and from metabolic destruction of the nuclei of the body. The daily output of uric acid is about 0.4 to 1 gm. The amount of the other purin bodies together is about one-tenth that of uric acid. Excretion of these substances is greatly increased by a diet rich in nuclei, as sweetbreads and liver.
Uric acid exists in the urine in the form of urates, which in concentrated urines are readily thrown out of solution and constitute the familiar sediment of "amorphous urates." This, together with the fact that uric acid is frequently deposited as crystals, constitutes its chief interest to the practitioner. It is a very common error to consider these deposits as evidence of excessive excretion.
Pathologically, the greatest increase of uric acid occurs [p. 68] in leukemia, where there is extensive destruction of leukocytes, and in diseases with active destruction of the liver and other organs rich in nuclei. Uric acid is decreased before an attack of gout and increased afterward, but its etiologic relation is still uncertain. An increase is also noted in the uric-acid diathesis and in diseases accompanied by respiratory insufficiency.
Quantitative Estimation.—The following are the best methods for ordinary clinical purposes, although no great accuracy can be claimed for them.
Cook's Method for Purin Bodies.—In a centrifuge tube take 10 c.c. urine and add about 1 gm. (about 1 c.c.) sodium carbonate and 1 or 2 c.c. strong ammonia. Shake until the soda is dissolved. The earthy phosphates will be precipitated. Centrifugalize thoroughly and pour off all the clear fluid into a graduated centrifuge tube. Add 2 c.c. ammonia and 2 c.c. ammoniated silver nitrate solution. Let stand a few minutes, and revolve in the centrifuge until the bulk of precipitate remains constant. Each one-tenth cubic centimeter of sediment represents 0.001176 gm. purin bodies. This amount may be regarded as uric acid, since this substance usually constitutes nine-tenths of the purin bodies and the clinical significance is the same.
Ammoniated silver nitrate solution is prepared by dissolving 5 gm. of silver nitrate [p. 69] in 100 c.c. distilled water, and adding ammonia until the solution clouds and again becomes clear.
Ruhemann's Method for Uric Acid.—The urine must be slightly acid. Fill Ruhemann's tube (Fig. 21) to the mark S with the indicator, carbon disulphid, and to the mark J with the reagent. The carbon disulphid will assume a violet color. Add the urine, a small quantity at a time, closing the tube with the glass stopper and shaking vigorously after each addition, until the disulphid loses every trace of its violet color and becomes pure white. This completes the test. The figure in the right-hand column of figures corresponding to the top of the fluid gives the amount of uric acid in parts per thousand. The presence of diacetic acid interferes with the test.
Ruhemann's reagent consists of iodin and potassium iodid, each 1.5 parts; absolute alcohol, 15 parts; and distilled water, 185 parts.
Those substances which appear in the urine only in pathologic conditions are of much more interest to the clinician than are those which have just been discussed. Among them are: proteids, sugars, the acetone bodies, bile, hemoglobin, and the diazo substances. The "pancreatic reaction" and detection of drugs in the urine will also be discussed under this head.
1. Proteids.—Of the proteids which may appear in the urine, serum-albumin and serum-globulin are the most important. Mucin, albumose, and a few others are found occasionally, but are of less interest.
(1) Serum-albumin and Serum-globulin.—These two proteids constitute the so-called "urinary albumin." They usually occur together, have practically the same [p. 70] significance, and both respond to all the ordinary tests for "albumin."
Their presence, or albuminuria, is probably the most important pathologic condition of the urine. It is either accidental or renal. The physician can make no greater mistake than to regard all cases of albuminuria as indicating kidney disease.
Accidental or false albuminuria is due to admixture with the urine of albuminous fluids, such as pus, blood, and vaginal discharge. The microscope will usually reveal its nature.
Renal albuminuria refers to albumin which has passed from the blood into the urine through the walls of the kidney tubules or the glomeruli. It probably never occurs as a physiologic condition, the so-called "functional albuminuria" being due to obscure or slight pathologic changes.
Renal albuminuria may be referred to one or more of the following causes. In practically all cases it is accompanied by tube-casts.
(a) Changes in the blood which render its albumin more diffusible, as in severe anemias, purpura, and scurvy. Here the albumin is small in amount.
(b) Changes in circulation in the kidney, either anemia or congestion, as in excessive exercise, chronic heart disease, and pressure upon the renal veins. The quantity of albumin is usually, but not always, small. Its presence is constant or temporary, according to the cause. Most of the causes, if continued, will produce organic changes in the kidney.
(c) Organic Changes in the Kidney.—These include the inflammatory and degenerative changes commonly grouped [p. 71] together under the name of nephritis, and also renal tuberculosis, neoplasms, and cloudy swelling due to irritation of toxins and drugs. The amount of albumin eliminated in these conditions varies from minute traces to 20 gm., or even more, in the twenty-four hours, and, except in acute processes, bears little relation to the severity of the disease. In acute and chronic parenchymatous nephritis the quantity is usually very large. In chronic interstitial nephritis it is small—frequently no more than a trace. It is small in cloudy swelling from toxins and drugs, and variable in renal tuberculosis and neoplasms. In amyloid disease of the kidney the quantity is usually small, and serum-globulin may be present in especially large proportion, or even alone. Roughly distinctive of serum-globulin is the appearance of an opalescent cloud when a few drops of the urine are dropped into a glass of distilled water.
Detection of albumin depends upon its coagulation by chemicals or heat. There are many tests, but none is entirely satisfactory, because other substances as well as albumin are precipitated. The most common source of error is mucin. The tests given here are widely used and can be recommended. They make no distinction between serum-albumin and serum-globulin. They are given as nearly as possible in order of their delicacy.
It is very important that urine to be tested for albumin be rendered clear by filtration or centrifugation. This is too often neglected in routine work. When ordinary methods do not suffice, it can usually be cleared by shaking up with a little magnesium carbonate and filtering.
(1) Trichloracetic Acid Test.—The reagent consists of a saturated aqueous solution of trichloracetic acid to which [p. 72] magnesium sulphate is added to saturation. A simple saturated solution of the acid may be used, but addition of magnesium sulphate favors precipitation of globulin, and by raising the specific gravity, makes the test easier to apply.
Take a few c.c. of the reagent in a test-tube or conical test glass, hold the tube or glass in an inclined position, and run the urine gently in by means of a pipet, so that it will form a layer on top of the reagent without mixing with it. If albumin be present, a white, cloudy ring will appear where the two fluids come in contact. The ring can be seen most clearly if viewed against a black background, and one side of the tube or conical glass may be painted black for this purpose.

|
| FIG. 22.—Horismascope: adding the reagent. |
This is an extremely sensitive test, but, unfortunately, both mucin and albumose respond to it; urates when abundant may give a confusing white ring, and the reagent is [p. 73] comparatively expensive. It is not much used in routine work except as a control to the less sensitive tests.
A most convenient instrument for applying this or any of the contact tests is sold under the name of "horismascope" (Fig. 22).
(2) Robert's Test.—The reagent consists of pure nitric acid, 1 part, and saturated aqueous solution of magnesium sulphate, 5 parts. It is applied in the same way as the preceding test.
Albumin gives a white ring, which varies in density with the amount present. A similar white ring may be produced by albumose and resinous drugs. White rings or cloudiness in the urine above the zone of contact may result from excess of urates or mucus. Colored rings near the junction of the fluids may be produced by urinary pigments, bile, or indican.
Robert's test is one of the best for routine work, although the various rings are apt to be confusing to the inexperienced. It is more sensitive than Heller's test, of which it is a modification, and has the additional advantage that the reagent is not so corrosive.
(3) Purdy's Heat Test.—Take a test-tube two-thirds full of urine, add about one-sixth its volume of saturated solution of sodium chlorid and 5 to 10 drops of 50 per cent. acetic acid. Mix, and boil the upper inch. A white cloud in the heated portion shows the presence of albumin.

|
| FIG. 23.—Esbach's albuminometer, improved form. |
This is a valuable test for routine work. It is simple, sufficiently accurate for clinical purposes, and has practically no fallacies. Addition of the salt solution, by raising the specific gravity, prevents precipitation of mucin. Albumose may produce a white cloud which disappears upon boiling and reappears upon cooling.
(4) Heat and Nitric Acid Test.—This is one of the oldest of the albumin tests, and, if properly carried out, one of the best. Boil a small quantity of filtered urine in a test-tube and add about one-twentieth its volume of concentrated nitric [p. 74] acid. A white cloud or flocculent precipitate (which usually appears during the boiling, but if the quantity be very small only after addition of the acid) denotes the presence of albumin. A similar white precipitate, which disappears upon addition of the acid, is due to earthy phosphates. The acid should not be added before boiling, and the proper amount should always be used; otherwise, part of the albumin may fail to be precipitated or may be redissolved.
Quantitative Estimation.—The gravimetric, which is the most reliable method, is too elaborate for clinical work. Both Esbach's, which is very widely used, and the centrifugal method give fair results.
(1) Esbach's Method.—The urine must be clear, of acid reaction, and not concentrated. Always filter before testing, and, if necessary, add acetic acid and dilute with water. Esbach's tube (Fig. 23) is essentially a test-tube with a mark U near the middle, a mark R near the top, and graduations ½, 1, 2, 3, etc., near the bottom. Fill the tube to the mark U with urine and to the mark R with the reagent. Close with a rubber stopper, invert slowly several times, and set aside in a cool place. At the end of twenty-four hours read off the height of the precipitate. This gives the amount of albumin in grams per liter, and must be divided by 10 to obtain the percentage.
Esbach's reagent consists of picric acid, 1 gm., citric acid, 2 gm., and distilled water, to make 100 c.c.
(2) Purdy's Centrifugal Method.—This is detailed in the accompanying table. The percentage by weight is approximately one-fiftieth of the bulk percentage.[p. 75]
| PURDY'S QUANTITATIVE METHOD FOR ALBUMIN IN URINE (CENTRIFUGAL) | |||||
| Table showing the relation between the volumetric and gravimetric percentage of albumin obtained by means of the centrifuge with radius of six and three-quarter inches; rate of speed, 1500 revolutions per minute; time, three minutes. | |||||
| VOLUMETRIC PERCENTAGE BY CENTRIFUGE. | PERCENTAGE BY WEIGHT OF DRY ALBUMIN. | GRAINS PER FLUIDOUNCE DRY ALBUMIN. | VOLUMETRIC PERCENTAGE BY CENTRIFUGE. | PERCENTAGE BY WEIGHT OF DRY ALBUMIN. | GRAINS PER FLUIDOUNCE DRY ALBUMIN. |
| ¼ | 0.005 | 0.025 | 22 | 0.458 | 2.2 |
| ½ | 0.01 | 0.05 | 22½ | 0.469 | 2.25 |
| ¾ | 0.016 | 0.075 | 23 | 0.479 | 2.3 |
| 1 | 0.021 | 0.1 | 23½ | 0.49 | 2.35 |
| 1¼ | 0.026 | 0.125 | 24 | 0.5 | 2.4 |
| 1½ | 0.031 | 0.15 | 24½ | 0.51 | 2.45 |
| 1¾ | 0.036 | 0.175 | 25 | 0.521 | 2.5 |
| 2 | 0.042 | 0.2 | 25½ | 0.531 | 2.55 |
| 2¼ | 0.047 | 0.225 | 26 | 0.542 | 2.6 |
| 2½ | 0.052 | 0.25 | 26½ | 0.552 | 2.65 |
| 2¾ | 0.057 | 0.275 | 27 | 0.563 | 2.7 |
| 3 | 0.063 | 0.3 | 27½ | 0.573 | 2.75 |
| 3¼ | 0.068 | 0.325 | 28 | 0.583 | 2.8 |
| 3½ | 0.073 | 0.35 | 28½ | 0.594 | 2.85 |
| 3¾ | 0.078 | 0.375 | 29 | 0.604 | 2.9 |
| 4 | 0.083 | 0.4 | 29½ | 0.615 | 2.95 |
| 4¼ | 0.089 | 0.425 | 30 | 0.625 | 3.0 |
| 4½ | 0.094 | 0.45 | 30½ | 0.635 | 3.05 |
| 4¾ | 0.099 | 0.475 | 31 | 0.646 | 3.1 |
| 5 | 0.104 | 0.5 | 31½ | 0.656 | 3.15 |
| 5½ | 0.111 | 0.55 | 32 | 0.667 | 3.2 |
| 6 | 0.125 | 0.6 | 32½ | 0.677 | 3.25 |
| 6½ | 0.135 | 0.65 | 33 | 0.687 | 3.3 |
| 7 | 0.146 | 0.7 | 33½ | 0.698 | 3.35 |
| 7½ | 0.156 | 0.75 | 34 | 0.708 | 3.4 |
| 8 | 0.167 | 0.8 | 34½ | 0.719 | 3.45 |
| 8½ | 0.177 | 0.85 | 35 | 0.729 | 3.5 |
| 9 | 0.187 | 0.9 | 35½ | 0.74 | 3.55 |
| 9½ | 0.198 | 0.95 | 36 | 0.75 | 3.6 |
| 10 | 0.208 | 1.0 | 36½ | 0.76 | 3.65 |
| 10½ | 0.219 | 1.05 | 37 | 0.771 | 3.7 |
| 11 | 0.229 | 1.1 | 37½ | 0.781 | 3.75 |
| 11½ | 0.24 | 1.15 | 38 | 0.792 | 3.8 |
| 12 | 0.25 | 1.2 | 38½ | 0.801 | 3.85 |
| 12½ | 0.26 | 1.25 | 39 | 0.813 | 3.9 |
| 13 | 0.271 | 1.3 | 39½ | 0.823 | 3.95 |
| 13½ | 0.281 | 1.35 | 40 | 0.833 | 4.0 |
| 14 | 0.292 | 1.4 | 40½ | 0.844 | 4.05 |
| 14½ | 0.302 | 1.45 | 41 | 0.854 | 4.1 |
| 15 | 0.313 | 1.5 | 41½ | 0.865 | 4.15 |
| 15½ | 0.323 | 1.55 | 42 | 0.875 | 4.2 |
| 16 | 0.333 | 1.6 | 42½ | 0.885 | 4.25 |
| 16½ | 0.344 | 1.65 | 43 | 0.896 | 4.3 |
| 17 | 0.354 | 1.7 | 43½ | 0.906 | 4.35 |
| 17½ | 0.365 | 1.75 | 44 | 0.917 | 4.4 |
| 18 | 0.375 | 1.8 | 44½ | 0.927 | 4.45 |
| 18½ | 0.385 | 1.85 | 45 | 0.938 | 4.5 |
| 19 | 0.396 | 1.9 | 45½ | 0.948 | 4.55 |
| 19½ | 0.406 | 1.95 | 46 | 0.958 | 4.6 |
| 20 | 0.417 | 2.0 | 46½ | 0.969 | 4.65 |
| 20½ | 0.427 | 2.05 | 47 | 0.979 | 4.7 |
| 21 | 0.438 | 2.1 | 47½ | 0.99 | 4.75 |
| 21½ | 0.448 | 2.15 | 48 | 1.0 | 4.8 |
| Test.—Three cubic centimeters of 10 per cent. solution of ferrocyanid of potassium and 2 cubic centimeters of 50 per cent. acetic acid are added to 10 cubic centimeters of the urine in the percentage tube and stood aside for ten minutes, then placed in the centrifuge and revolved at rate of speed and time as stated at head of the table. If albumin is excessive, dilute the urine with water until volume of albumin falls below 10 per cent. Multiply result by the number of dilutions employed before using the table. | |||||
[p. 76] (2) Mucin (Nucleo-albumin).—Traces of the substances which are loosely classed under this name are present in normal urine; increased amounts are observed in irritations and inflammations of the mucous membrane of the urinary tract. They are of interest chiefly because they may be mistaken for albumin in most of the tests. If the urine be diluted with water and acidified with acetic acid, the appearance of a white cloud indicates the presence of mucin.
(3) Albumoses.—These are intermediate products in the digestion of proteids. They have been observed in the urine in febrile and malignant diseases and chronic suppurations, but their clinical significance is indefinite. The following is a simple test: Mix equal parts of the urine, which has been strongly acidified with acetic acid, and a saturated solution of sodium chlorid. A white cloud, which appears upon moderate heating and disappears upon boiling, shows the presence of albumose. If the cloud increases upon boiling, albumin is present and should be removed by filtering while hot. The cloud due to albumose will reappear as the filtrate cools.
2. Sugars.—Various sugars may at times be found in the urine. Glucose is by far the most common, and is the only one of clinical importance. Levulose, lactose, and some others are occasionally met with.
(1) Glucose (Dextrose).—It is probable that traces of glucose, too small to respond to the ordinary tests, are present in the urine in health. Its presence in appreciable amount constitutes "glycosuria."
Transitory glycosuria is unimportant, and may occur in many conditions, as after general anesthesia and [p. 77] administration of certain drugs, in pregnancy, and following shock and head injuries.
Persistent glycosuria has been noted in brain injuries involving the floor of the fourth ventricle. As a rule, however, persistent glycosuria is diagnostic of diabetes mellitus, of which disease it is the essential symptom. The amount of glucose eliminated in diabetes is usually considerable, and is sometimes very large, reaching 500 gm., or even more in twenty-four hours, but it does not bear any uniform relation to the severity of the disease. Glucose may, on the other hand, be almost or entirely absent temporarily.
Detection of Glucose.—If albumin be present in more than traces, it must be removed by boiling and filtering.
(1) Haines' Test.—Take about 1 dram of Haines' solution in a test-tube, boil, and add 6 or 8 drops of urine. A heavy yellow or red precipitate, which settles readily to the bottom, shows the presence of sugar. Neither precipitation of phosphates as a light flocculent sediment nor simple decolorization of the reagent should be mistaken for a positive reaction.
This is probably the best of the copper tests, all of which depend upon the fact that in strongly alkaline solutions glucose reduces copper oxid to lower grades of oxidation. They are somewhat inaccurate, because they make no distinction between glucose and less common forms of sugar; because certain normal substances when present in excess, especially uric acid and creatinin, may reduce copper, and because many drugs—e.g., chloral, chloroform, copaiba, acetanilid, benzoic acid, morphin, sulphonal, salicylates—are eliminated as copper-reducing substances. To minimize these fallacies dilute the urine if it be concentrated, do not add more than the specified amount of urine, and do not boil after the urine is added.
[p. 78] Haines' solution is prepared as follows: completely dissolve 30 gr. pure copper sulphate in ½ oz. distilled water, and add ½ oz. pure glycerin; mix thoroughly, and add 5 oz. liquor potassæ. The solution keeps well.
(2) Fehling's Test.—Two solutions are required—one containing 34.64 gm. pure crystalline copper sulphate in 500 c.c. distilled water; the other, 173 gm. Rochelle salt and 100 gm. potassium hydroxid in 500 c.c. distilled water. Mix equal parts of the two solutions in a test-tube, dilute with 3 or 4 volumes of water, and boil. Add the urine a little at a time, heating, but not boiling, between additions. In the presence of glucose a heavy red or yellow precipitate will appear. The quantity of urine should not exceed that of the reagent.
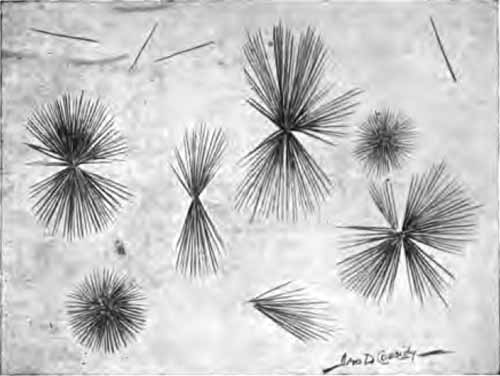
|
| FIG. 24.—Crystals of phenylglucosazone from diabetic urine—Kowarsky's test. X500. |
(3) Phenylhydrazin Test.—Kowarsky's Method.—In a test-tube take 5 drops pure phenylhydrazin, 10 drops glacial acetic acid, and 1 c.c. saturated solution of sodium chlorid. A curdy mass results. Add 2 or 3 cc. urine, boil for at least two minutes, and set aside to cool. Examine the sediment with the microscope, using a two-thirds objective. If glucose [p. 79] be present, characteristic crystals of phenylglucosazone will be seen. These are yellow, needle-like crystals arranged mostly in clusters or in sheaves (Fig. 24). When traces only of glucose are present, the crystals may not appear for one-half hour or more. Best crystals are obtained when the fluid is cooled very slowly. It must not be agitated during cooling.
This is an excellent test for clinical work. It requires slightly more time than Haines' test, but more than compensates for this by increased accuracy. It is fully as sensitive as Haines', and has practically no fallacies excepting levulose, which is a fallacy for all tests but the polariscope. Other carbohydrates which are capable of forming crystals with phenylhydrazin are extremely unlikely to do so when the test is applied directly to the urine by the method just detailed. Even if not used routinely, this test should always be resorted to when Haines' test gives a positive reaction in doubtful cases.
Quantitative Estimation.—In quantitative work Fehling's solution, for so many years the standard, has been largely displaced by Purdy's, which avoids the heavy precipitate that so greatly obscures the end-reaction in Fehling's method. The older method is still preferred by many, and both are, therefore, given. Should the urine contain much glucose, it must be diluted before making any quantitative test, allowance being made for the dilution in the subsequent calculation. Albumin, if present, must be removed by acidifying a considerable quantity of urine with acetic acid, boiling, and filtering. The precipitate should then be washed with water and the washings added to the urine to bring it to its original volume.
(1) Purdy's Method.—Take exactly 35 c.c. of Purdy's solution in a flask or beaker, add twice its volume of distilled [p. 80] water, heat to boiling, and, still keeping the solution hot, add the urine very slowly from a buret until the blue color entirely disappears. Read off the amount of urine added; considering the strength of Purdy's solution, it is readily seen that this amount of urine contains 0.02 gm. of glucose, from which the amount in the twenty-four-hour urine, or the percentage, can easily be calculated. Example: Suppose that 2.5 c.c. of urine discharged the blue color of 35 c.c. of Purdy's solution. This amount of urine, therefore, contains exactly 0.02 gm. glucose, and the percentage is obtained from the equation: 2.5:100 :: 0.02:x, and x equals 0.8 per cent. If, then, the twenty-four-hour quantity of urine were 3000 c.c., the twenty-four-hour elimination of glucose would be found as follows: 100:3000 :: 0.8:x, and x equals 24 gm.
It will be found that after the test is completed the blue color slowly returns. This is due to reoxidation, and should not be mistaken for incomplete reduction.
A somewhat simpler application of this method, which is accurate enough for clinical purposes, is as follows: Take 8¾ c.c. (roughly, 9 c.c.) of Purdy's solution in a large test-tube, dilute with an equal volume of water, heat to boiling, and, while keeping the solution hot but not boiling, add the urine drop by drop from a medicine-dropper until the blue color is entirely gone. Toward the end add the drops very slowly, not more than 4 or 5 a minute. Divide 10 by the number of drops required to discharge the blue color; the quotient will be the percentage of glucose. If 20 drops were required, the percentage would be 10÷20 = 0.5 per cent. It is imperative that the drops be of such size that 20 of them will make 1 c.c. Test the dropper with urine, not water. If the drops are too large, draw out the tip of the dropper; if too small, file off the tip.
Purdy's solution consists of pure crystalline copper sulphate, 4.752 gm.; potassium hydroxid, 23.5 gm.; ammonia (U.S.P.; sp. gr., 0.9), 350 c.c.; glycerin, 38 c.c.; distilled water, to make [p. 81] 1000 c.c. Dissolve the copper sulphate and glycerin in 200 c.c. of the water by aid of gentle heat. In another 200 c.c. of water dissolve the potassium hydroxid. Mix the two solutions, and when cool, add the ammonia. Lastly, bring the whole up to 1000 c.c. with distilled water. This solution is of such strength that the copper in 35 c.c. will be reduced by exactly 0.02 gm. of glucose.
(2) Fehling's Method.—Take 10 c.c. Fehling's solution (made by mixing 5 c.c. each of the copper and alkaline solutions described on page 78) in a flask or beaker, add three or four volumes of water, boil, and add the urine very slowly from a buret until the solution is completely decolorized, heating but not boiling after each addition.
Fehling's solution is of such strength that the copper in 10 c.c. will be reduced by exactly 0.05 gm. of glucose. Therefore, the amount of urine required to decolorize the test solution contains just 0.05 gm. glucose, and the percentage is easily calculated.
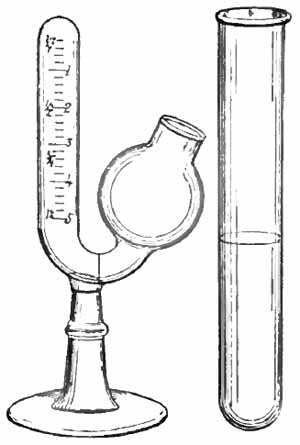
|
| FIG. 25.—Einhorn's saccharimeter. |
(3) Fermentation Method.—This is convenient and satisfactory, its chief disadvantage being the time required. It [p. 82] depends upon the fact that glucose is fermented by yeast with evolution of CO2. The amount of gas evolved is an index of the amount of glucose. Einhorn's saccharimeter (Fig. 25) is the simplest apparatus.
The urine must be so diluted as to contain not more than 1 per cent. of glucose. A fragment of fresh yeast cake about the size of a split pea is mixed with a definite quantity of the urine measured in the tube which accompanies the apparatus. It should form an emulsion free from lumps or air-bubbles. The long arm of the apparatus is then filled with the mixture. At the end of fifteen to twenty-four hours fermentation will be complete, and the percentage of glucose can be read off upon the side of the tube. The result must then be multiplied by the degree of dilution. Since yeast itself sometimes gives off gas, a control test must be carried out with normal urine and the amount of gas evolved must be subtracted from that of the test.
(2) Levulose, or fruit-sugar, is very rarely present in the urine except in association with glucose, and has about the same significance. Its name is derived from the fact that it rotates polarized light to the left. It behaves the same as glucose with all the ordinary tests, and can be distinguished only by polarization.
(3) Lactose, or milk-sugar, is sometimes present in the urine of nursing women and in that of women who have recently miscarried. It is of interest chiefly because it may be mistaken for glucose. It reduces copper, but does not ferment with yeast. In strong solution it can form crystals with phenylhydrazin, but is extremely unlikely to do so when the test is applied directly to the urine.
3. Acetone Bodies.—This is a group of closely related substances—acetone, diacetic acid, and beta-oxybutyric [p. 83] acid. Acetone is derived from decomposition of diacetic acid, and this in turn from beta-oxybutyric acid by oxidation. The origin of beta-oxybutyric acid is not definitely known, but it is probable that its chief, if not its only, source is in some obscure metabolic disturbance with abnormal destruction of fats. The three substances generally appear in the urine in the order mentioned. When the disturbance is mild, acetone only appears; as it becomes more marked, diacetic acid is added, and finally beta-oxybutyric acid appears. The presence of beta-oxybutyric acid in the blood is probably the chief cause of the form of auto-intoxication known as "acid intoxication."
(1) Acetone.—Minute traces, too small for the ordinary tests, may be present in the urine under normal conditions. Larger amounts are not uncommon in fevers, gastrointestinal disturbances, and certain nervous disorders. Occurrence of acetonuria in pregnancy suggests death of the fetus.
Acetonuria is practically always observed in acid intoxication, and, together with diaceturia, constitutes its most significant diagnostic sign. A similar or identical toxic condition, always accompanied by acetonuria and often fatal, is now being recognized as a not infrequent late effect of anesthesia, particularly of chloroform anesthesia. This postanesthetic toxemia is more likely to appear, and is more severe when the urine contains any notable amount of acetone before operation, which suggests the importance of routine examination for acetone in surgical cases.
Acetone is present in considerable amounts in many cases of diabetes mellitus, and is always present in severe [p. 84] cases. Its amount is a better indication of the severity of the disease than is the amount of sugar. A progressive increase is a grave prognostic sign.
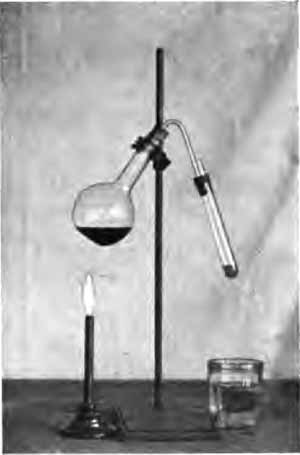
|
| FIG. 26.—A simple distilling apparatus. |
Detection of Acetone.—The urine may be tested directly, but it is best to distil it after adding a little phosphoric or hydrochloric acid to prevent foaming, and to test the first few cubic centimeters of distillate. A simple distilling apparatus is shown in Fig. 26. The test-tube may be attached to the delivery tube by means of a two-hole rubber cork as shown, the second hole serving as air vent, or, what is much less satisfactory, it may be tied in place with a string. Should the vapor not condense well, the test-tube may be immersed in a glass of cold water.
(1) Gunning's Test.—To a few cubic centimeters of urine or distillate in a test-tube add a few drops of tincture of iodin [p. 85] and of ammonia alternately until a heavy black cloud appears. This cloud will gradually clear up, and if acetone be present, iodoform, usually crystalline, will separate out. The iodoform can be recognized by its odor, especially upon heating (there is danger of explosion if the mixture be heated before the black cloud disappears), or by detection of the crystals microscopically. The latter, only, is safe, unless one has an unusually acute sense of smell. Iodoform crystals are yellowish, six-pointed stars or six-sided plates (Fig. 27).
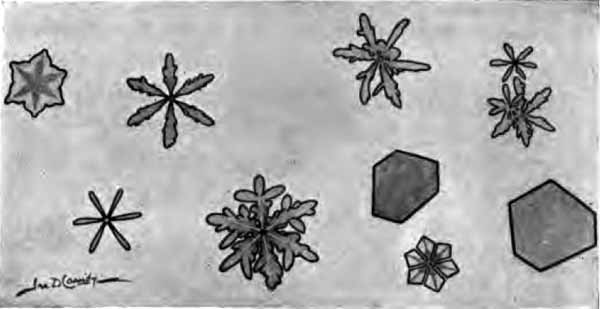
|
|
FIG. 27.—Iodoform crystals obtained in several tests
for acetone by Gunning's method (X about 600). |
This modification of Lieben's test is less sensitive than the original, but is sufficient for all clinical work; it has the advantage that alcohol does not cause confusion, and especially that the sediment of iodoform is practically always crystalline. When applied directly to the urine, phosphates are precipitated and may form star-shaped crystals which are very confusing to the inexperienced.
(2) Lange's Test.—This is a modification of the well-known Legal test. It is more sensitive and gives a sharper end-reaction. To a small quantity of urine add about one-twentieth its volume (1 drop for each 1 c.c.) of glacial acetic acid and a few drops of fresh concentrated aqueous solution of [p. 86] sodium nitroprussid, and gently run a little ammonia upon its surface. If acetone be present, a purple ring will form within a few minutes at the junction of the two fluids.
(3) Trommer's Test.—This new test has proved very satisfactory in the hands of the writer. The urine need not be distilled. Alkalinize about 10 c.c. of the urine with 2 or 3 c.c. of 40 per cent. caustic soda solution, add 10 or 12 drops of 10 per cent. alcoholic solution of salicylous acid (salicyl aldehyd), heat the upper portion nearly to the boiling-point, and keep at this temperature five minutes or longer. In the presence of acetone a purplish-red color appears in the heated portion.
(2) Diacetic acid occurs in the same conditions as acetone, but is less frequent and has more serious significance. In diabetes its presence is a grave symptom and often forewarns of approaching coma. It rarely or never occurs without acetone.
Detection.—The urine must be fresh.
(1) Gerhardt's Test.—To a few cubic centimeters of the urine add solution of ferric chlorid (about 10 per cent.) drop by drop until the phosphates are precipitated; filter and add more of the ferric chlorid. If diacetic acid be present, the urine will assume a Bordeaux-red color which disappears upon boiling. A red or violet color which does not disappear upon boiling may be produced by other substances, as phenol, salicylates, and antipyrin.
(2) Lindemann's Test.—To about 10 c.c. of urine add 5 drops 30 per cent. acetic acid, 5 drops Lugol's solution, and 2 or 3 c.c. chloroform, and shake. The chloroform does not change color if diacetic acid be present, but becomes reddish-violet in its absence. This test is claimed by its advocates to be more sensitive and more reliable than Gerhardt's.
[p. 87] (3) Oxybutyric acid has much the same significance as diacetic acid, but is of more serious import. There is no satisfactory clinical test for it.
4. Bile.—Bile appears in the urine in all diseases which produce jaundice, often some days before the skin becomes yellow; and in many disorders of the liver not severe enough to cause jaundice. It also occurs in diseases with extensive and rapid destruction of red blood-corpuscles. Both bile-pigment and bile acids may be found. They generally occur together, but the pigment is not infrequently present alone. Bilirubin, only, occurs in freshly voided urine, the other pigments (biliverdin, bilifuscin, etc.) being produced from this by oxidation as the urine stands. The acids are almost never present without the pigments, and are, therefore, seldom tested for clinically.
Detection of Bile-pigment.—Bile-pigment gives the urine a greenish-yellow, yellow, or brown color, which upon shaking is imparted to the foam. Cells, casts, and other structures in the sediment may be stained brown or yellow. This, however, should not be accepted as proving the presence of bile without further tests.
(1) Smith's Test.—Overlay the urine with tincture of iodin diluted with nine times its volume of alcohol. An emerald-green ring at the zone of contact shows the presence of bile-pigments. It is convenient to use a conical test-glass, one side of which is painted white.
(2) Gmelin's Test.—This consists in bringing slightly yellow nitric acid into contact with the urine. A play of colors, of which green and violet are most distinctive, denotes the presence of bile-pigment. Colorless nitric add will become yellow upon standing in the sunlight. The test may be applied [p. 88] in various ways: by overlaying the acid with the urine; by bringing a drop of each together upon a porcelain plate; by filtering the urine through thick filter-paper, and touching the paper with a drop of the acid; and, probably best of all, by precipitating with lime-water, filtering, and touching the precipitate with a drop of the acid.
Detection of Bile Acids.—Hay's test is simple, sensitive, and fairly reliable, and will, therefore, appeal to the practitioner. It depends upon the fact that bile acids lower surface tension. Other tests require isolation of the acids for any degree of accuracy.
Hay's Test.—Upon the surface of the urine, which must not be warm, sprinkle a little finely powdered sulphur. If it sinks at once, bile acids are present to the amount of 0.01 per cent. or more; if only after gentle shaking, 0.0025 per cent. or more. If it remains floating, even after gentle shaking, bile acids are absent.
5. Hemoglobin.—The presence in the urine of hemoglobin or pigments directly derived from it, accompanied by few, if any, red corpuscles, constitutes hemoglobinuria. It is a rare condition, and must be distinguished from hematuria, or blood in the urine, which is common. In both conditions chemic tests will show hemoglobin, but in the latter the microscope will reveal the presence of red corpuscles. Urines which contain notable amounts of hemoglobin have a reddish or brown color, and may deposit a sediment of brown, granular pigment.
Hemoglobinuria occurs when there is such extensive destruction of red blood-cells within the body that the liver cannot transform all the hemoglobin set free into bile-pigment. The most important examples are seen in [p. 89] poisoning, as by mushrooms and potassium chlorate, in malignant malaria (blackwater fever), and in the obscure condition known as "paroxysmal hemoglobinuria." This last is characterized by the appearance of large quantities of hemoglobin at intervals, usually following exposure to cold, the urine remaining free from hemoglobin between the attacks.
Detection.—Teichmann's test (p. 202) may be applied to the precipitate after boiling and filtering, but the guaiac test is more convenient in routine work.
Guaiac Test.—Mix equal parts of "ozonized" turpentine and fresh tincture of guaiac which has been diluted with alcohol to a light sherry-wine color. In a test-tube or conical glass overlay the urine with this mixture. A bright blue ring will appear at the zone of contact within a few minutes if hemoglobin be present. The guaiac should be kept in an amber-colored bottle. Fresh turpentine can be "ozonized" by allowing it to stand a few days in an open vessel in the sunlight.
This test is very sensitive, and a negative result proves the absence of hemoglobin. Positive results are not conclusive, because numerous other substances—few of them likely to be found in the urine—may produce the blue color. That most likely to cause confusion is pus, but the blue color produced by it disappears upon heating. The thin film of copper often left in a test-tube after testing for sugar may give the reaction, as may also the fumes from an open bottle of bromin.
6. Diazo Substances.—Certain unknown substances sometimes present in the urine give a characteristic color reaction—the "diazo reaction" of Ehrlich—when treated with diazo-benzol-sulphonic acid and ammonia. This reaction has much clinical value provided its limitations [p. 90] be recognized. It is at best an empirical test and must be interpreted in the light of clinical symptoms. Although it has been met with in a considerable number of diseases, its usefulness is practically limited to typhoid fever, tuberculosis, and measles.
(1) Typhoid Fever.—Practically all cases give a positive reaction, which varies in intensity with the severity of the disease. It is so constantly present that it may be said to be "negatively pathognomonic": if negative at a stage of the disease when it should be positive, typhoid is almost certainly absent. Upon the other hand, a reaction when the urine is highly diluted (1:50 or more) has much positive diagnostic value, since this dilution prevents the reaction in most conditions which might be mistaken for typhoid; but it should be noted that mild cases of typhoid may not give it at this dilution. Ordinarily the diazo appears a little earlier than the Widal reaction—about the fourth or fifth day—but it may be delayed. In contrast to the Widal, it begins to fade about the end of the second week, and soon thereafter entirely disappears. An early disappearance is a favorable sign. It reappears during a relapse, and thus helps to distinguish between a relapse and a complication, in which it does not reappear.
(2) Tuberculosis.—The diazo reaction has been obtained in many forms of the disease. It has little or no diagnostic value. Its continued presence in pulmonary tuberculosis is, however, a grave prognostic sign, even when the physical signs are slight. After it once appears it generally persists more or less intermittently until death, the average length of life after its appearance being about six months. The reaction is often temporarily present in [p. 91] mild cases during febrile complications, and has then no significance.
(3) Measles.—A positive reaction is frequently obtained in measles, and may help to distinguish this disease from German measles, in which it does not occur.
Technic.—Although the test is really a very simple one, careful attention to technic is imperative. Many of the early workers were very lax in this regard. Faulty technic and failure to record the stage of the disease in which the tests were made have probably been responsible for the bulk of the conflicting results reported.
Certain drugs often given in tuberculosis and typhoid interfere with or prevent the reaction. The chief are creosote, tannic acid and its compounds, opium and its alkaloids, salol, phenol, and the iodids. The reagents are:
| (1) | Saturated solution sulphanilic acid in 5 per cent. hydrochloric acid. |
| (2) | 0.5 per cent. aqueous solution sodium nitrite. |
| (3) | Strong ammonia. |
Mix forty parts of (1) and one part of (2). In a test-tube take equal parts of this mixture and the urine, and pour 1 or 2 c.c. of the ammonia upon its surface. If the reaction be positive, a garnet ring will form at the junction of the two fluids; and upon shaking, a distinct pink color will be imparted to the foam. The color of the foam is the essential feature. If desired, the mixture may be well shaken before the ammonia is added: the pink color will then instantly appear in that portion of the foam which the ammonia has reached, and can be readily seen. The color varies from eosin-pink to deep crimson, depending upon the intensity of the reaction. A doubtful reaction should be considered negative.
7. Pancreatic Reaction.—Cammidge has shown that in cases of pancreatitis a substance capable of forming [p. 92] crystals with phenylhydrazin can be developed by boiling the urine with a mineral acid, and has offered the following test as an aid in diagnosis of this obscure condition. The nature both of this substance and the antecedent substance from which it is derived is not known. As originally proposed, the test was complicated and probably not trustworthy, but with his improved and simplified technic, Cammidge has had very promising results. In 200 consecutive examinations in which the diagnosis was confirmed, postmortem or at operation, 67 cases of pancreatitis (65 chronic, 2 acute) gave positive reactions; 4 cases of cancer of the pancreas were positive, 12 negative; 4 cases in which no pancreatitis was found were positive, 113 were negative. Normal urines do not give the reaction. The difficulty and importance of diagnosis in pancreatitis warrant inclusion of the method here even though its true value cannot be definitely assigned. While the test is somewhat tedious, all the manipulations are simple and require no apparatus but flasks, test-tubes, and funnels.
Technic.—Careful attention to detail is imperative. An ordinary routine examination is first made. Albumin and sugar, if present, must be removed: the former, by acidifying with acetic acid, boiling, and filtering; the latter, by fermentation with yeast after the first step of the method proper. An alkaline urine should be made slightly acid with hydrochloric acid.
(1) Forty cubic centimeters of the urine, which has been rendered perfectly clear by repeated filtration through the same filter-paper, are placed in a small flask, treated with 1 c.c. concentrated hydrochloric acid and gently boiled on a sand-bath for ten minutes, a funnel with long stem being placed in the neck of the flask to act as a condenser (Fig. 28). After [p. 93] boiling, the urine is cooled in a stream of cold water and brought to its original bulk with distilled water; 8 gm. of lead carbonate are then added to neutralize the acid. The fluid is allowed to stand a few minutes and then filtered through well-moistened fine-grained filter-paper until perfectly clear.
|
| FIG. 28.—"Pancreatic reaction" flasks fitted with funnel condensers on a sand-bath (Robson and Cammidge). |
(2) The filtrate is shaken up with 8 gm. powdered tribasic lead acetate and filtered. The excess of lead is then removed by passing hydrogen sulphid gas through the fluid or by shaking well with 4 gm. finely powdered sodium sulphate, heating to boiling, cooling to as low a temperature as possible in a stream of water, and filtering as before until perfectly clear.
(3) Ten cubic centimeters of the filtrate are then made up to 17 c.c. with distilled water, and added to a mixture of 0.8 gm. phenylhydrazin hydrochlorate, 2 gm. powdered sodium acetate, and 1 c.c. 50 per cent. acetic acid in a small flask [p. 94] with funnel condenser. This is boiled on a sand-bath for ten minutes, and filtered while hot through filter-paper moistened with hot water into a test-tube with a 15 c.c. mark. Should the filtrate not reach this mark, make up to 15 c.c. with hot distilled water. Allow to cool slowly.
(4) In well-marked cases of pancreatitis a yellow precipitate appears within a few hours; in milder cases, it may not appear for twelve hours. The microscope shows this sediment to consist of "long, light yellow, flexible, hair-like crystals arranged in sheaves, which, when irrigated with 33 per cent. sulphuric acid, melt away and disappear in ten to fifteen seconds after the acid first touches them" (Fig. 29).
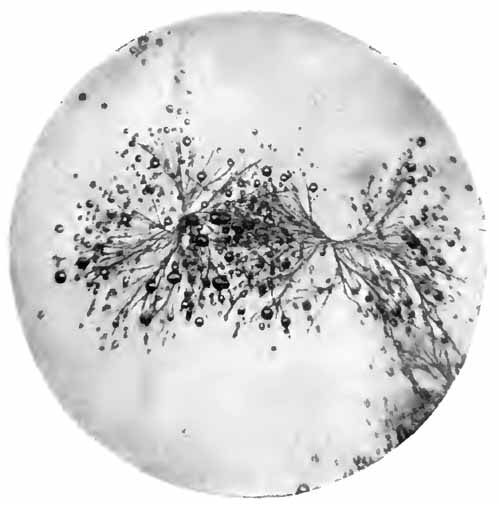
|
| FIG. 29.—Improved "pancreatic reaction." Crystals obtained from a case of chronic pancreatitis with gall-stones in the common duct (X200) (from a photo by P. J. Cammidge). |
(5) To exclude traces of glucose which might be overlooked in the preliminary examination a control test should be carried out in the same manner with omission of step (1).
[p. 95] 8. Drugs.—The effect of various drugs upon the color of the urine has been mentioned (p. 50). Most poisons are eliminated in the urine, but their detection is more properly discussed in works upon toxicology. A few drugs which are of interest to the practitioner, and which can be detected by comparatively simple methods, are mentioned here.
Acetanilid and Phenacetin.—The urine is evaporated by gentle heat to about half its volume, boiled for a few minutes with about one-fifth its volume of strong hydrochloric acid, and shaken out with ether. The ether is evaporated, the residue dissolved in water, and the following test applied: To about 10 c.c. are added a few cubic centimeters of 3 per cent. phenol, followed by a weak solution of chromium trioxid (chromic acid) drop by drop. The fluid assumes a red color, which changes to blue when ammonia is added. If the urine is very pale, extraction with ether may be omitted.
Antipyrin.—This drug gives a dark-red color when a few drops of 10 per cent. ferric chlorid are added to the urine. The color does not disappear upon boiling, which excludes diacetic acid.
Arsenic.—Reinsch's Test.—Add to the urine in a test-tube or small flask about one-seventh its volume of hydrochloric acid, introduce a piece of bright copper-foil about one-eighth-inch square, and boil for several minutes. If arsenic be present, a dark-gray film is deposited upon the copper. The test is more delicate if the urine be concentrated by slow evaporation. This test is well known and is widely used, but is not so reliable as the following:
Gutzeit's Test.—In a large test-tube place a little [p. 96] arsenic-free zinc, and add 5 to 10 c.c. pure dilute hydrochloric acid and a few drops of iodin solution (Gram's solution will answer), then add 5 to 10 c.c. of the urine. At once cover the mouth of the tube with a filter-paper cap moistened with saturated aqueous solution of silver nitrate (1:1). If arsenic be present, the paper quickly becomes lemon-yellow, owing to formation of a compound of silver arsenid and silver nitrate, and turns black when touched with a drop of water. To make sure that the reagents are arsenic-free, the paper cap may be applied for a few minutes before the urine is added.
Atropin will cause dilatation of the pupil when a few drops of the urine are placed in the eye of a cat or rabbit.
Bromids can be detected by acidifying about 10 c.c. of the urine with dilute sulphuric acid, adding a few drops of fuming nitric acid and a few cubic centimeters of chloroform, and shaking. In the presence of bromin the chloroform, which settles to the bottom, assumes a yellow color.
Iodin—from ingestion of iodids or absorption from iodoform dressings—is tested for in the same way as the bromids, the chloroform assuming a pink to reddish-violet color. To detect traces, a large quantity of urine should be rendered alkaline with sodium carbonate and greatly concentrated by evaporation before testing.
Lead.—No simple method is sufficiently sensitive to detect the traces of lead which occur in the urine in chronic poisoning. Of the more sensitive methods, that of Arthur Lederer is probably best suited to the practitioner:
It is essential that all apparatus used be lead-free. Five hundred cubic centimeters of the urine are acidified [p. 97] with 70 c.c. pure sulphuric acid, and heated in a beaker or porcelain dish. About 20 to 25 gm. of potassium persulphate are added a little at a time. This should decolorize the urine, leaving it only slightly yellow. If it darkens upon heating, a few more crystals of potassium persulphate are added, the burner being first removed to prevent boiling over; if it becomes cloudy, a small amount of sulphuric acid is added. It is then boiled until it has evaporated to 250 c.c. or less. After cooling, an equal volume of alcohol is added, and the mixture allowed to stand in a cool place for four or five hours, during which time all the lead will be precipitated as insoluble sulphate.
The mixture is then filtered through a small, close-grained filter-paper (preferably an ashless, quantitative filter-paper), and any sediment remaining in the beaker or dish is carefully washed out with alcohol and filtered. A test-tube is placed underneath the funnel; a hole is punched through the tip of the filter with a small glass rod, and all the precipitate (which may be so slight as to be scarcely visible) washed down into the test-tube with a jet of distilled water from a wash-bottle, using as little water as possible. Ten cubic centimeters will usually suffice. This fluid is then heated, adding crystals of sodium acetate until it becomes perfectly clear. It now contains all the lead of the 500 c.c. urine in the form of lead acetate. It is allowed to cool, and hydrogen sulphid gas is passed through it for about five minutes. The slightest yellowish-brown discoloration indicates the presence of lead. A very slight discoloration can be best seen when looked at from above. For comparison, the gas may be passed through a test-tube containing an equal amount of distilled water. The quantity of lead can be [p. 98] determined by comparing the discoloration with that produced by passing the gas through lead acetate (sugar of lead) solutions of known strength. One part of lead acetate crystals contains 0.54 part of lead. Hydrogen sulphid is easily prepared in the simple apparatus shown in Fig. 30. A small quantity of iron sulphid is placed in the test-tube; a little dilute hydrochloric acid is added; the cork is replaced; and the delivery tube is inserted to the bottom of fluid to be tested.
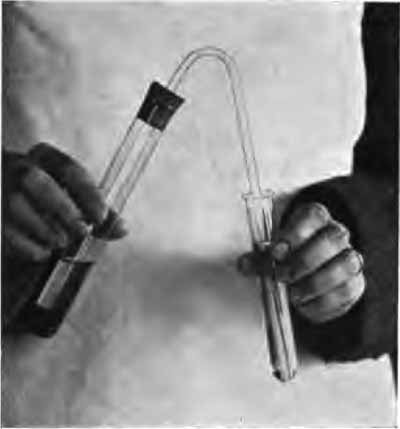
|
| FIG. 30.—A simple hydrogen sulphid generator. |
Mercury.—Traces can be detected in the urine for a considerable time after the use of mercury compounds by ingestion or inunction.
About a liter of urine is acidified with 10 c.c. hydrochloric acid, and a small piece of copper-foil or gauze is introduced. This is gently heated for an hour, and allowed to stand for twenty-four hours. The metal is then removed, and washed successively with very dilute sodium hydroxid solution, alcohol, and ether. When dry, [p. 99] it is placed in a long, slender test-tube, and the lower portion of the tube is heated to redness. If mercury be present, it will volatilize and condense in the upper portion of the tube as small, shining globules which can be seen with a hand-magnifier or low power of the microscope. If, now, a crystal of iodin be dropped into the tube and gently heated, the mercury upon the side of the tube is changed first to the yellow iodid and later to the red iodid which are recognized by their color.
Morphin.—Add sufficient ammonia to the urine to render it distinctly ammoniacal, and shake thoroughly with a considerable quantity of pure acetic ether. Separate the ether and evaporate to dryness. To a little of the residue in a watch-glass or porcelain dish add a few drops of formaldehyd-sulphuric acid, which has been freshly prepared by adding one drop of formalin to 1 c.c. pure concentrated sulphuric acid. If morphin be present, this will produce a purple-red color, which changes to violet, blue-violet, and finally nearly pure blue.
Phenol.—As has been stated, the urine following phenol poisoning turns olive-green and then brownish-black upon standing. Tests are of value in recognizing poisoning from ingestion and in detecting absorption from carbolized dressings.
The urine is acidulated with hydrochloric acid and distilled. To the first few cubic centimeters of distillate is added 10 per cent. solution of ferric chlorid drop by drop. The presence of phenol causes a deep amethyst-blue color, as in Uffelmann's test for lactic acid.
Phenolphthalein, which is now being used as a cathartic under the name of purgen, gives a bright pink color when the urine is rendered alkaline with caustic soda.
[p. 100] Quinin.—A considerable quantity of the urine is rendered alkaline with ammonia and extracted with ether; the ether is evaporated, and a portion of the residue dissolved in about twenty drops of dilute alcohol. The alcoholic solution is acidulated with dilute sulphuric acid, a drop of an alcoholic solution of iodin (tincture of iodin diluted about ten times) is added, and the mixture is warmed. Upon cooling, an iodin compound of quinin (herapathite) will separate out in the form of a microcrystalline sediment of green plates.
The remainder of the residue may be dissolved in a little dilute sulphuric acid. This solution will show a characteristic blue fluorescence when quinin is present.
Resinous drugs cause a white precipitate like that of albumin when strong nitric acid is added to the urine. This is dissolved by alcohol.
Salicylates, salol, and similar drugs give a bluish-violet color, which disappears upon heating, upon addition of a few drops of 10 per cent. ferric chlorid solution. When the quantity of salicylates is small, the urine may be acidified with hydrochloric acid and extracted with ether, the ether evaporated, and the test applied to an aqueous solution of the residue.
Tannin and its compounds appear in the urine as gallic acid, and the urine becomes greenish-black (inky, if much gallic acid be present) when treated with a solution of ferric chlorid.
A careful microscopic examination will often detect structures of great diagnostic importance in urine which seems perfectly clear, and from which only very slight [p. 101] sediment can be obtained with the centrifuge. Upon the other hand, cloudy urines with abundant sediment are often shown by the microscope to contain nothing of clinical significance.
Since the nature of the sediment soon changes, the urine must be examined while fresh, preferably within six hours after it is voided. The sediment is best obtained by means of the centrifuge. If a centrifuge is not available, the urine may be allowed to stand in a conical test-glass for six to twenty-four hours after adding some preservative (p. 48). The "torfuge" (Fig. 31) is said to be a very satisfactory substitute for the centrifuge, and is readily portable.
|
| FIG. 31.—Wetherill's torfuge. |
A small amount of the sediment should be transferred to a slide by means of a pipet. It is very important to do this properly. The best pipet is a small glass tube which has been drawn out at one end to a tip with rather small opening. The tube or glass containing the sediment is held on a level with the eye, the larger end of the pipet is closed with the index-finger, which must be dry, and the [p. 102] tip is carried down into the sediment. By carefully loosening the finger, but not entirely removing it, a small amount of the sediment is then allowed to run slowly into the pipet. Slightly rotating the pipet will aid in accomplishing this. After wiping off the urine which adheres to the outside, a drop from the pipet is placed upon a clean slide. A hair is then placed in the drop and a large cover-glass applied. Many workers use no cover. This offers a thicker layer and larger area of urine, the chance of finding scanty structures being proportionately increased. It has the disadvantage that any jarring of the room (as by persons walking about) sets the microscopic field into vibratory motion and makes it impossible to see anything clearly; and, since it does not allow of the use of high-power objectives, one cannot examine details as one often wishes to do. A large cover-glass with a hair beneath it avoids these disadvantages, and gives enough urine to find any structures which are present in sufficient number to have clinical significance, provided other points in the technic have been right. It is best, however, to examine several drops; and, when the sediment is abundant, drops from the upper and lower portions should be examined separately.
In examining urinary sediments microscopically no fault is so common, nor so fatal to good results, as improper illumination (see Figs. 2 and 3), and none is so easily corrected. The light must be central and very subdued. The two-thirds objective should be used as a finder, while the one-sixth is reserved for examining details.
It is well to emphasize that the most common errors which result in failure to find important structures, when present, are lack of care in transferring the sediment to the slide, too strong illumination, and too great magnification.
[p. 103] In order to distinguish between similar structures it is often necessary to watch the effect upon them of certain reagents. This is especially true of the various unorganized sediments. They very frequently cannot be identified from their form alone. With the structures still in focus, a drop of the reagent may be placed at one edge of the cover-glass and drawn underneath it by the suction of a piece of blotting-paper touched to the opposite edge; or a small drop of the reagent and of the urine may be placed close together upon a slide and a cover gently lowered over them. As the two fluids mingle, the effect upon various structures may be seen.
Urinary sediments may be studied under three heads: A. Unorganized sediments. B. Organized sediments. C. Extraneous structures.
In general these have little diagnostic or prognostic significance. Most of them are substances normally present which have been precipitated from solution either because present in excessive amounts or, more frequently, because of some alteration in the urine (as in reaction, concentration, etc.) which may be purely physiologic, depending upon changes in diet or habits. Various substances are always precipitated during decomposition, which may take place either within or without the body. Unorganized sediments may be classified according to the reaction of the urine in which they are most likely to be found:
In acid urine: uric acid, amorphous urates, sodium urate, calcium oxalate, leucin and tyrosin, cystin, and fat-globules. Uric acid, the urates, and calcium oxalate are [p. 104] the common deposits of acid urines; the others are less frequent, and depend less upon the reaction of the urine.
In alkaline urine: phosphates, calcium carbonate, and ammonium urate.
Other crystalline sediments (Fig. 32) which are rare and require no further mention are: calcium sulphate, cholesterin, hippuric acid, hematoidin, fatty acids, and indigo.
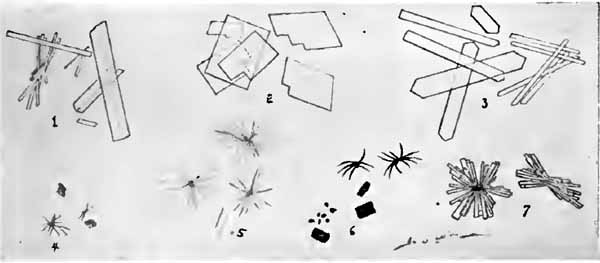
|
| FIG. 32.—Unusual urinary crystals (drawn from various authors): 1, Calcium sulphate (colorless); 2, cholesterin (colorless); 3, hippuric acid (colorless); 4, hematoidin (brown); 5, fatty acids (colorless); 6, indigo (blue); 7, sodium urate (yellowish). |
1. In Acid Urine.—(1) Uric-acid Crystals.—These crystals are the red grains—"gravel" or "red sand"—which are often seen adhering to the sides and bottom of a vessel containing urine. Microscopically, they are yellow or reddish-brown crystals, which differ greatly in size and shape. The most characteristic forms (Plate III and Fig. 33) are "whetstones"; roset-like clusters of prisms and whetstones; and rhombic plates, which have usually a paler color than the other forms and are sometimes colorless. Recognition of the crystals depends less upon their shape than upon their color, the reaction of the urine, and the facts that they are soluble in caustic soda solution and insoluble in hydrochloric or acetic acid. [p. 105] When ammonia is added, they dissolve and crystals of ammonium urate appear.
| PLATE III |
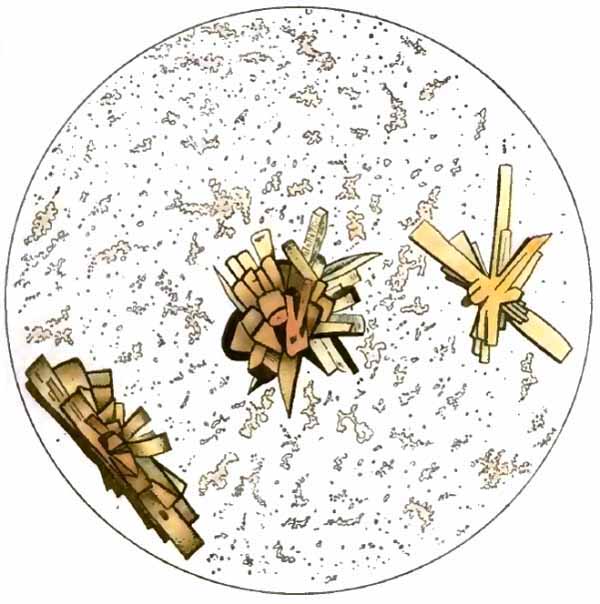
|
| Uric-acid crystals with amorphous urates (after Peyer). |
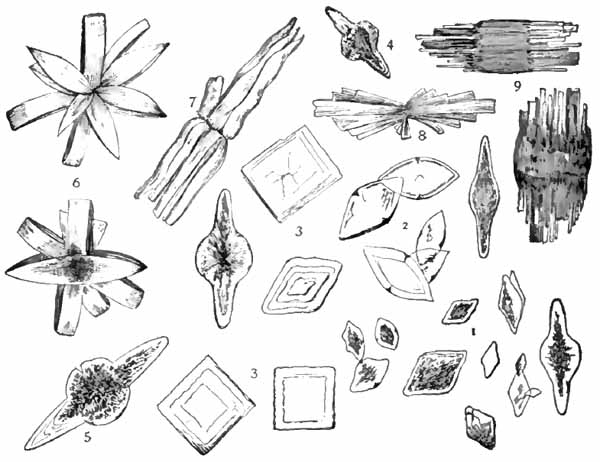
|
| FIG. 33.—Forms of uric acid: 1, Rhombic plates; 2, whetstone forms; 3, 3, quadrate forms; 4, 5, prolonged into points; 6, 8, rosets; 7, pointed bundles; 9, barrel forms precipitated by adding hydrochloric acid to urine (Ogden). |
A deposit of uric-acid crystals has no significance unless it occurs before or very soon after the urine is voided. Every urine, if kept acid, will in time deposit its uric acid. Factors which favor an early deposit are high acidity, diminished urinary pigments, and excessive excretion of uric acid. The chief clinical interest of the crystals lies in their tendency to form calculi, owing to the readiness with which they collect about any solid object. Their presence in the freshly voided urine in clusters of crystals suggests stone in the kidney or bladder, especially if blood is also present (see Fig. 62).
(2) Amorphous Urates.—These are chiefly urates of [p. 106] sodium and potassium which are thrown out of solution as a yellow or red "brick-dust" deposit. In pale urines this sediment is almost white. It disappears upon heating. A deposit of amorphous urates is very common in concentrated and strongly acid urines, especially in cold weather, and has no clinical significance. Under the microscope it appears as fine yellowish granules, often so abundant as to obscure all other structures (Plate III). In such cases the urine should be warmed before examining. Amorphous urates are readily soluble in caustic soda solutions. When treated with hydrochloric or acetic acid they slowly dissolve and rhombic crystals of uric acid appear.
Rarely, sodium urate occurs in crystalline form—slender prisms, arranged in fan- or sheaf-like structures (Fig. 32).
(3) Calcium Oxalate.—Characteristic of calcium oxalate are colorless, glistening, octahedral crystals, giving the appearance of small squares crossed by two intersecting diagonal lines—the so-called "envelop crystals" (Fig. 47). They vary greatly in size, being sometimes so small as to seem mere points of light with medium-power objectives. Unusual forms, which, however, seldom occur except in conjunction with the octahedra, are colorless dumb-bells, spheres, and variations of the octahedra (Fig. 34). The spheres might be mistaken for globules of fat or red blood-corpuscles. Crystals of calcium oxalate are insoluble in acetic acid or caustic soda. They are dissolved by strong hydrochloric acid, and recrystallize as octahedra upon addition of ammonia. They are sometimes encountered in alkaline urine.
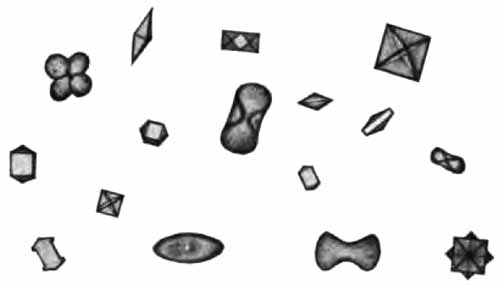
|
| FIG. 34.—Various forms of calcium oxalate crystals (Ogden). |
The crystals are commonly found in the urine after ingestion of vegetables rich in oxalic acid, as tomatoes, [p. 107] spinach, asparagus, and rhubarb. They have no definite significance pathologically. They often appear in digestive disturbances, in neurasthenia, and when the oxidizing power of the system is diminished. Like uric acid, their chief clinical interest lies in their tendency to form calculi, and their presence in fresh urine, together with evidences of renal or cystic irritation, should be viewed with suspicion, particularly if they are clumped in small masses.
(4) Leucin and Tyrosin.—-Crystals are deposited only when the substances are present in considerable amount. When present in smaller amount, they will usually be deposited if a drop of the urine be slowly evaporated upon a slide. They generally appear together, and are of rare occurrence, usually indicating severe fatty destruction of the liver, such as occurs in acute yellow atrophy and phosphorus-poisoning.
The crystals cannot be identified from their morphology alone, since other substances, notably calcium phosphate (Fig. 38) and ammonium urate, may take similar or identical forms.
Leucin crystals (Fig. 35) are slightly yellow, oily-looking spheres, many of them with radial and concentric [p. 108] striations. Some may be merged together in clusters. They are not soluble in hydrochloric acid nor in ether.

|
| FIG. 35.—Leucin spheres and tyrosin needles (Stengel). |
Tyrosin crystallizes in very fine colorless needles, usually arranged in sheaves, with a marked constriction at the middle (Fig. 35). It is soluble in ammonia and hydrochloric acid, but not in acetic acid.
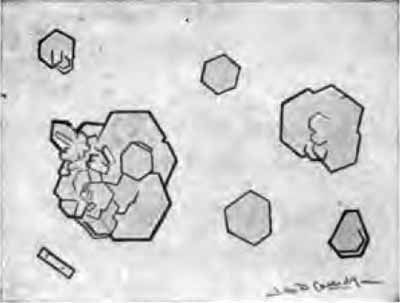
|
| FIG. 36.—Cystin crystals from urine of patient with cystin calculus (X250). |
(5) Cystin crystals are colorless, highly refractive, rather thick, hexagonal plates with well-defined edges. They lie either singly or superimposed to form more or less irregular clusters (Fig. 36). Uric acid sometimes [p. 109] takes this form and must be excluded. Cystin is soluble in hydrochloric acid, insoluble in acetic; it is readily soluble in ammonia and recrystallizes upon addition of acetic acid.
Cystin crystals are very rare, and when found, point to cystin calculus.
(6) Fat-globules.—Fat appears in the urine as highly refractive globules of various sizes, frequently very small. These globules are easily recognized from the fact that they are stained black by osmic acid and red by Sudan III. The stain may be applied upon the slide, as already described (p. 103). Osmic acid should be used in 1 per cent. aqueous solution; Sudan III in saturated solution in 70 per cent. alcohol.
Fat in the urine is usually a contamination from unclean vessels, oiled catheters, etc. A very small amount may be present after ingestion of large quantities of cod-liver oil or other fats. In fatty degeneration of the kidney, as in phosphorus-poisoning and chronic parenchymatous nephritis, fat-globules are commonly seen, both free in the urine and embedded in cells and tube-casts.
In chyluria, or admixture of chyle with the urine as a result of rupture of a lymph-vessel, minute droplets of fat are so numerous as to give the urine a milky appearance. Chyluria occurs most frequently as a symptom of infection by Filaria sanguinis hominis.
2. In Alkaline Urine.—(1) Phosphates.—While most common in alkaline urine, phosphates are sometimes deposited in neutral or feebly acid urines. The usual forms are: (a) Ammoniomagnesium phosphate crystals; (b) acid calcium phosphate crystals; and (c) amorphous phosphates. All are readily soluble in acetic acid.
(a) Ammoniomagnesium Phosphate Crystals.—They are [p. 110] the common "triple phosphate" crystals, which are generally easily recognized (Figs. 37 and 63, and Plate IV). They are colorless, except when bile-stained. Their usual form is some modification of the prism, with oblique ends. Most typical are the well-known "coffin-lid" and "hip-roof" forms. The long axis of the hip-roof crystal is often so shortened that it resembles the envelop crystal of calcium oxalate. It does not, however, have the same luster; this, and its solubility in acetic acid, will always prevent confusion.
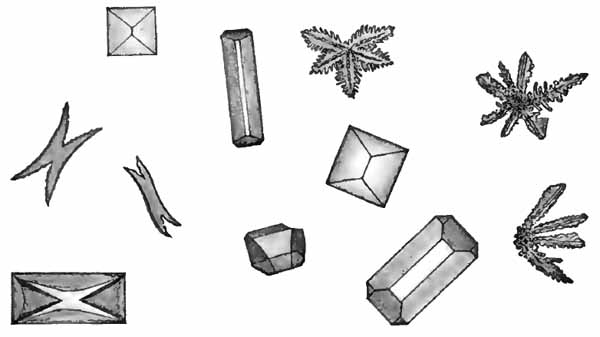
|
| FIG. 37.—Various forms of triple-phosphate crystals (Ogden). |
When rapidly deposited, as by artificial precipitation, triple phosphate often takes feathery, star- or leaf-like forms. These gradually develop into the more common prisms. X-forms may be produced by partial solution of prisms.
(b) Acid Calcium Phosphate Crystals.—In feebly add, neutral, or feebly alkaline urines acid calcium phosphate, wrongly called "neutral calcium phosphate," is not infrequently deposited in the form of colorless prisms [p. 111] arranged in stars and rosets (Fig. 38, 1). The individual prisms are usually slender, with one beveled, wedge-like end, but are sometimes needle-like. They may sometimes take forms resembling tyrosin (Fig. 38, 2), calcium sulphate, or hippuric acid, but are readily distinguished by their solubility in acetic acid.
Calcium phosphate often forms large, thin, irregular, usually granular, colorless plates, which are easily recognized (Fig. 38, 3).
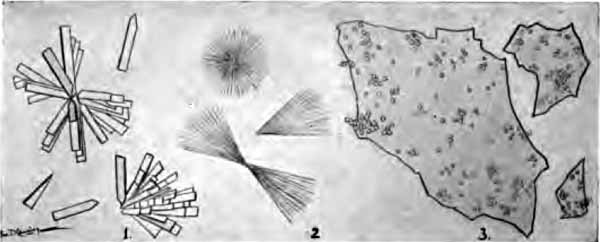
|
| FIG. 38.—Crystals of calcium phosphate: 1, Common form (copied from Rieder's Atlas); 2, needles resembling tyrosin (drawn from nature); 3, large, irregular plates (from nature). |
(c) Amorphous Phosphates.—The earthy phosphates are thrown out of solution in most alkaline and many neutral urines as a white, amorphous sediment, which may be mistaken for pus macroscopically. Under the microscope the sediment is seen to consist of numerous colorless granules, distinguished from amorphous urates by their color, their solubility in acetic acid, and the reaction of the urine.
The various phosphatic deposits frequently occur together. They are sometimes due to excessive excretion of phosphoric acid, but usually merely indicate that the urine has become, or is becoming, alkaline.
[p. 112] (2) Calcium carbonate may sometimes be mingled with the phosphate deposits, usually as amorphous granules, or, more rarely, as colorless spheres and dumb-bells, Fig. 39, which are soluble in acetic acid with gas-formation.

|
| FIG. 39.—Indistinct crystalline sediment (dumb-bell crystals) of calcium carbonate. Similar crystals are formed by calcium oxalate and calcium sulphate (after Funke). |
(3) Ammonium Urate Crystals.—This is the only urate deposited in alkaline urine. It forms opaque yellow crystals, usually in the form of spheres (Plate IV, and Fig. 63), which are often covered with fine or coarse spicules, "thorn-apple crystals." Sometimes dumb-bells, compact sheaves of fine needles, and irregular rhizome forms are seen (Fig. 40). Upon addition of acetic acid they dissolve, and rhombic plates of uric acid appear.
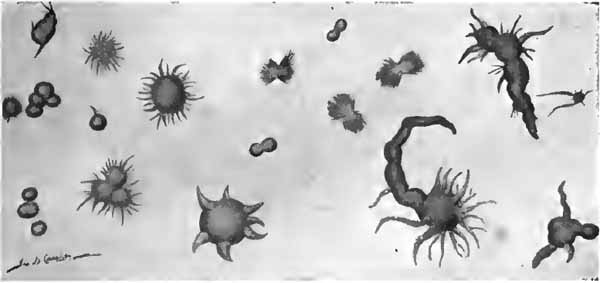
|
| FIG. 40.—Crystals of ammonium urate (one-half of the forms copied from Rieder's Atlas, the others from nature). |
| PLATE IV |

|
| Sediment of alkaline fermentation (after Hofmann and Ultzmann). |
[p. 113] These crystals occur only when ammonia is present in excess. They are generally found along with the phosphates in decomposing urine and have no clinical significance.
The principal organized structures in urinary sediments are: tube-casts; epithelial cells; pus-corpuscles; red blood-corpuscles; spermatozoa; bacteria; and animal parasites. They are much more important than the unorganized sediments just considered.
1. Tube-casts.—These interesting structures are albuminous molds of the uriniferous tubules. Their presence in the urine probably always indicates some pathologic change in the kidney, although this change may be very slight or transitory. Large numbers may be present in temporary irritations and congestions. They do not in themselves, therefore, imply organic disease of the kidney. They probably occur only in urine which contains, or has recently contained, albumin.
While it is not possible to draw a sharp dividing-line between the different varieties, casts may be classified as: (1) Hyaline casts; (2) waxy casts; (3) granular casts; (4) fatty casts; (5) casts containing organized structures—(a) epithelial casts; (b) blood-casts; (c) pus-casts; (d) bacterial casts. As will be seen, practically all varieties are modifications of the hyaline.
The significance of the different varieties is more readily understood if one considers their mode of formation. Albuminous material, the source and nature of which are not definitely known, probably enters the lumen of a uriniferous tubule in a fluid or plastic state. It there hardens into a mold, which, when washed out by the [p. 114] urine, retains the shape of the tubule, and contains within its substance whatever structures and débris were lying free within the tubule or were loosely attached to its wall. If the tubule be small and have its usual lining of epithelium, the cast will be narrow; if it be large or entirely denuded of epithelium, the cast will be broad. A cast, therefore, indicates the condition of the tubule in which it is formed.
The search for casts must be carefully made. The urine must be fresh, since hyaline casts soon dissolve when it becomes alkaline. It should be thoroughly centrifugalized. When the sediment is abundant, casts, being light structures, will be found near the top. In cystitis, where casts may be entirely hidden by the pus, the bladder should be irrigated to remove as much of the pus as possible and the next urine examined. In order to prevent solution of the casts the urine, if alkaline, must be rendered acid by previous administration of boric acid or other drugs.
(1) Hyaline Casts.—Typically, these are colorless, homogeneous, semitransparent, cylindric structures, with parallel sides and usually rounded ends. Not infrequently they are more opaque or show a few granules or an occasional cell, either adhering to them or contained within their substance. Generally they are straight or curved; less commonly, convoluted. Their length and breadth vary greatly: they are sometimes so long as to extend across several fields of a medium-power objective, but are usually much shorter; in breadth, they vary from one to seven or eight times the diameter of a red blood-corpuscle. (See Figs. 2, 41, 42, and 46.)

|
| FIG. 41.—Hyaline casts showing fat-droplets and leukocytes (obj. one-sixth) (Boston). |
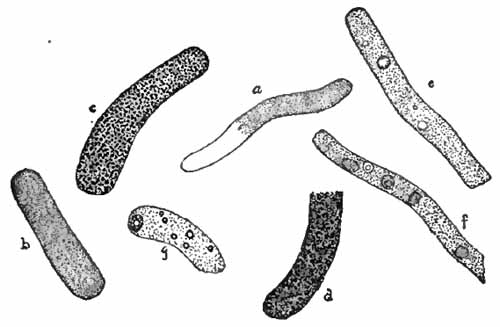
|
| FIG. 42.—Various kinds of casts: a, Hyaline and finely granular cast; b, finely granular cast; c, coarsely granular cast; d, brown granular cast; e, granular cast with normal and abnormal blood adherent; f, granular cast with renal cells adherent; g, granular cast with fat and a fatty renal cell adherent (Ogden). |
Hyaline casts are the least significant of all the casts, [p. 115] and occur in many slight and transitory conditions. Small numbers are common following ether anesthesia, in fevers, after excessive exercise, and in congestions and irritations of the kidney. They are always present, and are usually stained yellow when the urine contains much bile. While they are found in all organic diseases of the kidney, they [p. 116] are most important in chronic interstitial nephritis. Here they are seldom abundant, but their constant presence is the most reliable urinary sign of the disease. Small areas of chronic interstitial change are probably responsible for the few hyaline casts so frequently found in the urine of elderly persons.
Very broad hyaline casts commonly indicate complete desquamation of the tubular epithelium, such as occurs in the late stages of nephritis.
(2) Waxy Casts.—Like hyaline casts, these are homogeneous when typical, but frequently contain a few granules or an occasional cell. They are much more opaque than the hyaline variety, and are usually shorter and broader, with irregular, broken ends, and sometimes appear to be segmented. They are grayish or colorless, and have a dull waxy look, as if cut from paraffin (Figs. 43 and 61). They are sometimes composed of material which gives the amyloid reactions. Waxy casts are found in most advanced cases of nephritis, where they are an unfavorable sign.

|
| FIG. 43.—Waxy casts (upper part of figure). Fatty and fat-bearing casts (lower part of figure) (from Greene's "Medical Diagnosis"). |
Casts which resemble waxy casts but have a distinctly [p. 117] yellow color, as if cut from beeswax (so-called "fibrinous casts"), are often seen in acute nephritis. They have less serious significance than the true waxy variety.
(3) Granular Casts.—These are merely hyaline casts in which numerous granules are embedded (Figs. 42, 44, 46, and 61).
Finely granular casts contain many fine granules, are usually shorter, broader, and more opaque than the hyaline variety, and are more conspicuous. Their color is grayish or pale yellow.
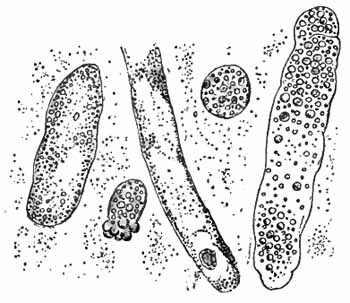
|
| FIG. 44.—Granular and fatty casts and two compound granular cells (Stengel). |
Coarsely granular casts contain larger granules and are darker in color than the finely granular, being often dark brown owing to presence of altered blood-pigment. They are usually shorter and more irregular in outline, and more frequently have irregularly broken ends.
(4) Fatty Casts.—Small droplets of fat may at times be seen in any variety of cast. Those in which the droplets are numerous are called fatty casts (Figs. 43 and 44). The fat-globules are not difficult to recognize. Staining with osmic acid or Sudan (p. 109) will remove any doubt as to their nature.
[p. 118] The granules and fat-droplets seen in casts are products of epithelial degeneration. Granular and fatty casts, therefore, always indicate partial or complete disintegration of the renal epithelium. The finely granular variety is the least significant, and is found when the epithelium is only moderately affected. Coarsely granular, and especially fatty casts, indicate a serious parenchymatous nephritis.
(5) Casts Containing Organized Structures.—Cells and other structures are frequently seen adherent to a cast or embedded within it. (See Figs. 41 and 42). When numerous, they give name to the cast.
(a) Epithelial casts contain epithelial cells from the renal tubules. They always imply desquamation of epithelium, which rarely occurs except in parenchymatous inflammations (Figs. 60 and 61).
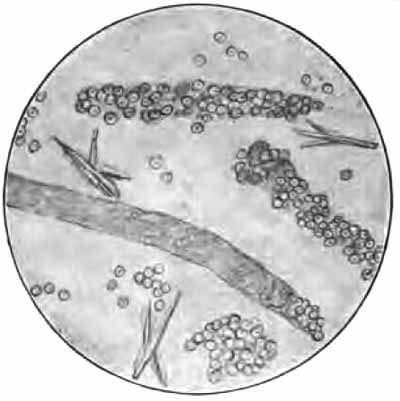
|
| FIG. 45.—Red blood-corpuscles and blood-casts (courtesy of Dr. A. Scott) (obj. one-sixth) (Boston). |
(b) Blood-casts contain red blood-corpuscles, usually much degenerated (Figs. 45 and 60). They always indicate hemorrhage into the tubules, which is most [p. 119] common in acute nephritis or an acute exacerbation of a chronic nephritis.
(c) Pus-casts (see Fig. 62), composed almost wholly of pus-corpuscles, are uncommon, and point to a chronic suppurative process in the kidney.
(d) True bacterial casts are rare. They indicate a septic condition in the kidney. Bacteria may permeate a cast after the urine is voided.

|
| FIG. 46.—Hyaline and granular casts, mucous threads, and cylindroids. There are also a few epithelial cells from the bladder (Wood). |
The structures most likely to be mistaken for casts are:
(1) Mucous Threads.—Mucus frequently appears in the form of long strands which slightly resemble hyaline casts (Fig. 46). They are, however, more ribbon-like, have less well-defined edges, and usually show faint longitudinal striations. Their ends taper to a point or are split or curled upon themselves, and are never evenly rounded, as is commonly the case with hyaline casts.
(2) Cylindroids.—This name is sometimes given to the [p. 120] mucous threads just described, but is more properly applied to certain peculiar structures more nearly allied to casts. They resemble hyaline casts in structure, but differ in being broader at one end and tapering to a slender tail, which is often twisted or curled upon itself (Fig. 46). They frequently occur in the urine along with hyaline casts, and have no definite pathologic significance.
(3) Masses of amorphous urates or phosphates or very small crystals (Fig. 47), which accidentally take a cylindric form, or shreds of mucus covered with granules, closely resemble granular casts. Application of gentle heat or appropriate chemicals will serve to differentiate them. When urine contains both mucus and granules, large numbers of these "pseudo-casts," all lying in the same direction, can be produced by slightly moving the cover-glass from side to side. It is possible—as in urate infarcts of infants—for urates to be molded into cylindric bodies within the renal tubules.

|
| FIG. 47.—Calcium-oxalate crystals, showing a pseudo-cast of small crystals (Jakob). |
(4) Hairs and fibers of wool, cotton, etc. These could be mistaken for casts only by beginners. One can easily [p. 121] become familiar with their appearance by suspending them in water and examining with the microscope (Fig. 57).

|
| FIG. 48.—Renal epithelium from nephritic urine: a, Polyhedral epithelium in nephritis of scarlet fever; b and c, different grades of fatty degeneration in renal epithelium in chronic nephritis (X400) (after Bizzozero). |
(5) Hyphæ of molds are not infrequently mistaken for hyaline casts. Their higher degree of refraction, their jointed or branching structure, and the accompanying spores will differentiate them (Fig. 58).
2. Epithelial Cells.—A few cells from various parts of the urinary tract occur in every urine. A marked increase indicates some pathologic condition at the site of their origin. It is sometimes, but by no means always, possible to locate their source from their form. Any epithelial cell may be so granular from degenerative changes that the nucleus is obscured. They are usually divided into three groups:
(1) Small, round, or polyhedral cells are about the size of pus-corpuscles, or a little larger, with a single round nucleus. Such cells may come from the deeper layers of any part of the urinary tract. They are uncommon in normal urine. When they are dark in color, very granular, and contain a comparatively large nucleus, they probably come from the renal tubules, but their origin in the kidney is not proved unless they are found embedded in casts. Renal cells are abundant in parenchymatous nephritis, especially the acute form. They are nearly always fatty—most markedly so in chronic parenchymatous nephritis, where their [p. 122] substance is sometimes wholly replaced by fat-droplets ("compound granule cells") (see Figs. 44, 48, 60, and 61).
(2) Irregular cells are considerably larger than the preceding. They are round, pear-shaped, or spindle-shaped, or may have tail-like processes, and are hence named large round, pyriform, spindle, or caudate cells respectively. Each contains a round or oval distinct nucleus. Their usual source is the deeper layers of the urinary tract, especially of the bladder. Caudate forms come most commonly from the pelvis of the kidney (see Figs. 49, b, 50, 62, and 63).
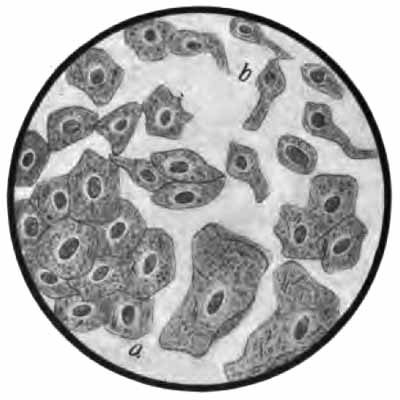
|
| FIG. 49.—Epithelial cells from urethra and bladder: a, Squamous cells from superficial layers; b, irregular cells from deeper layers (Jakob). |
(3) Squamous or pavement cells are large flat cells, each with a small, distinct, round or oval nucleus (Fig. 49, a). They are derived from the superficial layers of the ureters, bladder, urethra, or vagina. Those from the bladder are generally rounded, while those from the vagina are larger, thinner, and more angular. Great numbers of these vaginal cells, together with pus-corpuscles, may be present when leukorrhea exists.
[p. 123]

|
| FIG. 50.—Caudate epithelial cells from pelvis of kidney (Jakob). |
3. Pus-corpuscles.—A very few leukocytes are present in normal urine. They are more abundant when mucus is present. An excess of leukocytes, mainly of the polymorphonuclear variety, with albumin, constitutes pyuria—pus in the urine.
When at all abundant, pus forms a white sediment resembling amorphous phosphates macroscopically. Under the microscope the corpuscles appear as very granular cells, about twice the diameter of a red blood-corpuscle (Figs. 51 and 63). In freshly voided urine many exhibit ameboid motion, assuming irregular outlines. Each contains one irregular nucleus or several small, rounded nuclei. The nuclei are obscured or entirely hidden by the granules, but may be brought clearly into view by running a little acetic acid under the cover-glass. This enables one to easily distinguish pus-corpuscles from small round epithelial cells, which resemble them in size, but have a single, rather large, round nucleus.
Pyuria indicates suppuration in some part of the urinary [p. 124] tract—urethritis, cystitis, pyelitis, etc.—or may be due to contamination from the vagina, in which case many vaginal epithelial cells will also be present. In general, the source of the pus can be determined only by the accompanying structures (epithelia, casts) or by the clinical signs.
A fairly accurate idea of the quantity of pus from day to day may be had by shaking the urine thoroughly and counting the number of corpuscles per cubic millimeter upon the Thoma-Zeiss blood-counting slide.
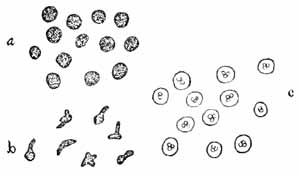
|
| FIG. 51.—Pus-corpuscles: a, As ordinarily seen; b, ameboid corpuscles; c, showing the action of acetic acid (Ogden). |
4. Red Blood-corpuscles.—Urine which contains blood is always albuminous. Very small amounts do not alter its macroscopic appearance. Larger amounts alter it considerably. Blood from the kidneys is generally intimately mixed with the urine and gives it a hazy reddish or brown color. When from the lower urinary tract, it is not so intimately mixed, and settles more quickly to the bottom, the color is brighter, and small clots are often present.
Red blood-corpuscles are not usually difficult to recognize with the microscope. When very fresh, they have a normal appearance, being yellowish discs of uniform size (normal blood). When they have been in the urine any [p. 125] considerable time, their hemoglobin may be dissolved out, and they then appear as faint colorless circles or "shadow cells" (abnormal blood), and are more difficult to see (Fig. 52; see also Figs. 45 and 60). They are apt to be swollen in dilute and crenated in concentrated urines. The microscopic findings may be corroborated by chemic tests for hemoglobin, although the microscope may show a few red corpuscles when the chemic tests are negative.
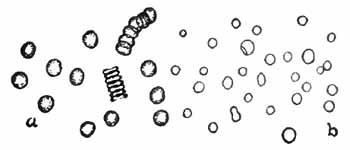
|
| FIG. 52.—Blood-corpuscles: a, Normal; b, abnormal (Ogden). |
When not due to contamination from menstrual discharge, blood in the urine, or hematuria, is always pathologic. Blood comes from the kidney tubules in severe hyperemia, in some forms of nephritis, and in renal tuberculosis and malignant disease. The finding of blood-casts is the only certain means of diagnosing the kidney as its source. Blood comes from the pelvis of the kidney in renal calculus (Fig. 62), and is then usually intermittent, small in amount, and accompanied by a little pus and perhaps crystals of the substance forming the stone. Considerable hemorrhages from the bladder may occur in vesical calculus, tuberculosis, and newgrowths. Small amounts of blood generally accompany acute cystitis.
5. Spermatozoa are generally present in the urine of men after nocturnal emissions, after epileptic convulsions, and in spermatorrhea. They may be found in the urine of both sexes following coitus. They are easily recognized [p. 126] from their characteristic structure (Fig. 53). The one-sixth objective should be used, with subdued light and careful focusing.
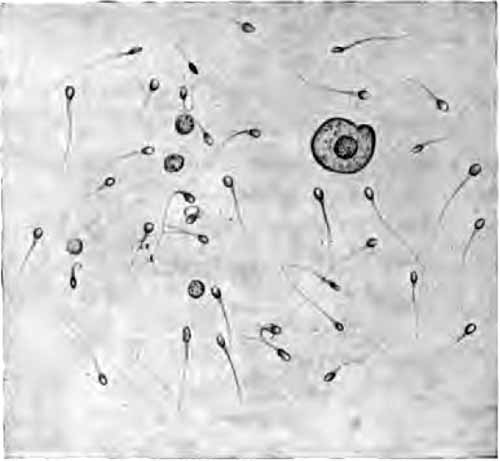
|
| FIG. 53.—Spermatozoa in urine (Ogden). |

|
| FIG. 54.—Micrococcus ureæ (after von Jaksch). |
6. Bacteria.—Normal urine is free from bacteria in the bladder, but becomes contaminated in passing through the urethra. Various non-pathogenic bacteria, notably Micrococcus ureæ (Fig. 54), are always present in decomposing urine. In suppurations of the urinary tract pus-producing organisms may be found. In many infectious diseases the specific germs may be eliminated in [p. 127] the urine without producing any local lesion. Typhoid bacilli have been known to persist for months and even years after the attack.
Bacteria produce a cloudiness which will not clear upon filtration. They are easily seen with the one-sixth objective in the routine microscopic examination. Ordinarily, no attempt is made to identify any but the tubercle bacillus and the gonococcus.
Tubercle bacilli are nearly always present in the urine when tuberculosis exists in any part of the urinary tract, but are often difficult to find, especially when the urine contains little or no pus.
Detection of Tubercle Bacilli in Urine.—The urine should be obtained by catheter after careful cleansing of the parts.
(1) Centrifugalize thoroughly, after dissolving any sediment of urates or phosphates by gentle heat or acetic acid. Pour off the supernatant fluid, add water, and centrifugalize again. Addition of one or two volumes of alcohol will favor centrifugalization by lowering the specific gravity.
(2) Make thin smears of the sediment, adding a little egg-albumen if necessary to make the smear adhere to the glass; dry, and fix in the usual way.
(3) Stain with carbol-fuchsin, steaming, for at least three minutes.
(4) Wash in water, and then in 20 per cent. nitric acid until only a faint pink color remains.
(5) Wash in water.
(6) Soak in alcohol fifteen minutes or longer. This decolorizes the smegma bacillus (p. 35), which is often present in the urine, and might easily be mistaken for the tubercle bacillus. It is unlikely, however, to be present in catheterized specimens. It is always safest to soak the smear in alcohol for several [p. 128] hours or over night, since some strains of the smegma bacillus are very resistant.
(7) Wash in water.
(8) Apply Löffler's methylene-blue solution one-half minute.
(9) Rinse in water, dry between filter-papers, and examine with the one-twelfth objective.
When the bacilli are scarce, the following method may be tried. It is applicable also to other fluids. If the fluid is not albuminous, add a little egg-albumen. Coagulate the albumen by gentle heat and centrifugalize. The bacilli will be carried down with the albumen. Separate the albumen, mix with artificial gastric juice (for preparation of which see test for pepsin, p. 222), and set in an incubator or warm place until digested. Finally, centrifugalize and stain as described above. The bacilli do not stain so well as in the ordinary methods.
A careful search of many smears may be necessary to find the bacilli. They usually lie in clusters (see Plate V). Failure to find them in suspicious cases should be followed by inoculation of guinea-pigs; this is the court of last appeal, and must also be sometimes resorted to in order to exclude the smegma bacillus.
In gonorrhoea gonococci are sometimes found in the sediment, but more commonly in the "gonorrheal threads," or "floaters." In themselves, these threads are by no means diagnostic of gonorrhea. Detection of the gonococcus is described later (p. 264).
| PLATE V |
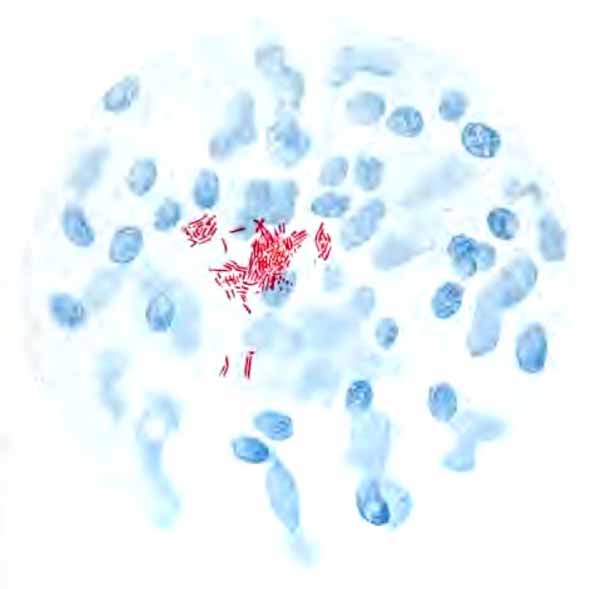
|
| Tubercle bacilli in urinary sediment; X800 (Ogden). |
7. Animal parasites are rare in the urine. Hooklets and scolices of Tænia echinococcus (Fig. 55) and embryos of Filaria sanguinis hominis have been met. In Africa the ova, and even adults, of Distoma hæmatobium are common, accompanying "Egyptian hematuria."

|
| FIG. 55.—1, Scolex of tænia echinococcus, showing crown of hooklets; 2, scolex and detached hooklets (obj. one-sixth) (Boston). |

|
| FIG. 56.—Embryo of "vinegar eel" in urine, from contamination; length, 340 µ; width, 15 µ. An epithelial cell from bladder and three leukocytes are also shown (studied with Dr. J. A. Wilder). |
Other parasites, most of which are described in Chapter VI, may be present from contaminations. A worm [p. 129] which is especially interesting is Anguillula aceti, the "vinegar eel." This is generally present in the sediment of table vinegar, and may reach the urine through use of vinegar in vaginal douches, or through contamination of the bottle in which the urine is contained. It has been mistaken for Strongyloides intestinalis and for Filaria sanguinis hominis. It closely resembles the former in [p. 130] both adult and embryo stages. The young embryos have about the same length as filaria embryos, but are nearly twice as broad and the intestinal canal is easily seen (compare Figs. 56 and 107).
The laboratory worker must familiarize himself with the microscopic appearance of the more common of the numerous structures which may be present from accidental contamination (Fig. 57).
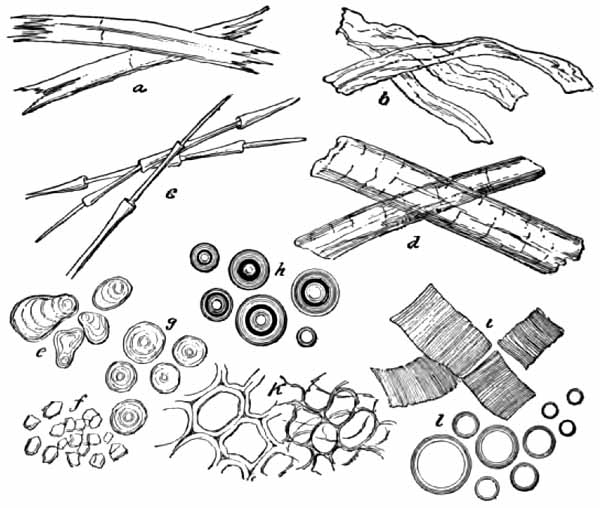
|
| FIG. 57.—Extraneous matters found in urine: a, Flax-fibers; b, cotton-fibers; c, feathers; d, hairs; e, potato-starch; f, rice-starch granules; g, wheat-starch; h, air-bubbles; i, muscular tissue; k, vegetable tissue; l, oil-globules. |
Yeast-cells are smooth, colorless, highly refractive, spheric or ovoid cells. They sometimes reach the size of [p. 131] a leukocyte, but are generally smaller (see Fig. 88, l). They might be mistaken by the inexperienced for red blood-corpuscles, fat-droplets, or the spheric crystals of calcium oxalate, but are distinguished by the facts that they are not of uniform size; that they tend to adhere in short chains; that small buds may often be seen adhering to the larger cells; and that they do not give the hemoglobin test, are not stained by osmic acid or Sudan but are colored brown by Lugol's solution, and are insoluble in acids and alkalis. Yeast-cells multiply rapidly in diabetic urine, and may reach the bladder and multiply there.
Mold fungi (Fig. 58) are characterized by refractive, jointed, or branched rods (hyphæ), often arranged in a network, and by highly refractive, spheric or ovoid spores. They are common in urine which has stood exposed to the air.

|
| FIG. 58.—Aspergillus from urine (Boston). |
Fibers of wool, cotton, linen, or silk, derived from towels, the clothing of the patient, or the dust in the air are present in almost every urine. Fat-droplets are most frequently derived from unclean bottles or oiled catheters. Starch-granules may reach the urine from towels, the [p. 132] clothing, or dusting-powders. They are recognized by their concentric striations and their blue color with iodin solution. Lycopodium granules (Fig. 59) may also reach the urine from dusting-powders. They might be mistaken for the ova of parasites. Bubbles of air are often confusing to beginners, but are easily recognized after once being seen. Scratches and flaws in the glass of slide or cover are likewise a common source of confusion to beginners.

|
| FIG. 59.—Granules of lycopodium (Saxe). |
In this section the characteristics of the urine in those diseases which produce distinctive urinary changes will be briefly reviewed.
1. Renal Hyperemia.—Active hyperemia is usually an early stage of acute nephritis, but may occur independently as a result of temporary irritation. The urine is generally decreased in quantity, highly colored, and strongly acid. Albumin is always present—usually in traces only, but sometimes in considerable amount for a day or two. The sediment contains a few hyaline and finely granular casts and an occasional red blood-cell. In very severe hyperemia the urine approaches that of acute nephritis.
[p. 133]

|
| FIG. 60.—Sediment from acute hemorrhagic nephritis: Red blood-corpuscles; leukocytes; renal cells not fattily degenerated; epithelial and blood-casts (Jakob). |

|
| FIG. 61.—Sediment from chronic parenchymatous nephritis: hyaline (with cells attached), waxy, brown granular, fatty, and epithelial casts; fattily degenerated renal cells; and a few white and red blood-corpuscles (Jakob). |
Passive hyperemia occurs most commonly in diseases of the heart and liver and in pregnancy. The quantity of urine is somewhat low and the color high, except in pregnancy. Albumin is present in small amount only. The sediment contains a very few hyaline or finely granular [p. 134] casts. In pregnancy the amount of albumin should be carefully watched, as any considerable quantity, and especially a rapid increase, strongly suggests approaching eclampsia.
2. Nephritis.—The various degenerative and inflammatory conditions grouped under the name of nephritis have certain features in common. The urine in all cases contains albumin and tube-casts, and in all well-marked cases shows a decrease of normal solids, especially of urea and the chlorids. The characteristics of the different forms are well shown in the table on opposite page, modified from Hill.
[p. 135]| THE URINE IN NEPHRITIS | |||
| PHYSICAL. | CHEMIC. | MICROSCOPIC. | |
| Acute nephritis. | Quantity diminished, often very greatly. Color dark; may be red or smoky. Specific gravity, 1.020 to 1.030. | Urea and chlorids low. Much albumin: up to 1.5 per cent. Reaction acid. | Sediment abundant, red or brown. Many casts, chiefly granular, blood and epithelial varieties. Red blood-cells abundant. Numerous renal epithelial cells and leukocytes. |
| Chronic parenchymatous nephritis. | Quantity usually diminished. Color variable, often pale and hazy. Specific gravity, 1.010 to 1.020. | Urea and chlorids low. Largest amounts of albumin: up to 3 per cent. Reaction acid. | Sediment rather abundant. Many casts of all varieties: fatty casts and casts of degenerated epithelium most characteristic. Blood present in traces: abundant only in acute exacerbations. Numerous fattily degenerated renal epithelial cells, often free globules of fat, and a few leukocytes. |
| Chronic interstitial nephritis. | Quantity markedly increased, especially at night. Color pale, clear. Specific gravity, 1.005 to 1.015. | Urea and chlorids low in well-marked cases. Albumin present in traces (often overlooked), increasing in late stages. Reaction acid. | Sediment very slight. Few narrow hyaline and finely granular casts. No blood except in acute exacerbations. Very few renal cells. Uric acid and calcium-oxalate crystals common. |
| Amyloid degeneration of kidney. | Quantity moderately increased. Color pale, clear. Specific gravity, 1.012 to 1.018. | Slight decrease of urea and chlorids. Variable amounts of albumin and globulin. | Sediment slight. Moderate number of hyaline, finely granular, and sometimes waxy casts. |
3. Renal Tuberculosis.—The urine is pale, usually cloudy. The quantity may not be affected, but is apt to be increased. In early cases the reaction is faintly acid and there are traces of albumin and a few renal cells. In advanced cases the urine is alkaline, has an offensive odor, and is irritating to the bladder. Albumin in varying amounts is always present. Pus is nearly always present, though frequently not abundant. It is generally intimately mixed with the urine, and does not settle so quickly as the pus of cystitis. Casts, though present, are rarely abundant, and are obscured by the pus. Small amounts of blood are common. Tubercle bacilli are nearly always present, although animal inoculation may be necessary to detect them.
4. Renal Calculus.—The urine is usually somewhat concentrated, with high color and strongly acid reaction. Small amounts of albumin and a few casts may be present as a result of kidney irritation. Blood is frequently present, especially in the daytime and after severe exercise. Crystals of the substance composing the calculus—uric [p. 136] acid, calcium oxalate, cystin—may often be found. The presence of a calculus generally produces pyelitis, and variable amounts of pus then appear, the urine remaining acid in reaction.
5. Pyelitis.—In pyelitis the urine is slightly acid, and contains a small or moderate amount of pus, together with many spindle and caudate epithelial cells. Pus-casts may appear if the process extends up into the kidney tubules (see Fig. 62). Albumin is always present, and its amount, in proportion to the amount of pus, is decidedly greater than is found in cystitis.

|
| FIG. 62.—Sediment from calculous pyelitis: numerous pus-corpuscles, red blood-corpuscles, and caudate and irregular epithelial cells; a combination of hyaline and pus-cast; and a few uric-acid crystals (Jakob). |
6. Cystitis.—-In acute and subacute cases the urine is acid and contains a variable amount of pus, with many epithelial cells from the bladder—chiefly large round, pyriform, and rounded squamous cells. Red blood-corpuscles are often numerous.
In chronic cases the urine is generally alkaline. It is [p. 137] pale and cloudy from the presence of pus, which is abundant and settles readily into a viscid sediment. The sediment usually contains abundant amorphous phosphates and crystals of triple phosphate and ammonium urate. Vesical epithelium is common. Numerous bacteria are always present (see Fig. 63).

|
| FIG. 63.—Sediment from cystitis (chronic): numerous pus-corpuscles, epithelial cells from the bladder, and bacteria; a few red blood-corpuscles and triple phosphate and ammonium urate crystals (Jakob). |
7. Vesical Calculus, Tumors, and Tuberculosis.—These conditions produce a chronic cystitis, with its characteristic urine. Blood, however, is more frequently present and more abundant than in ordinary cystitis. With neoplasms, especially, considerable hemorrhages are apt to occur. Particles of the tumor are sometimes passed with the urine. No diagnosis can be made from the presence of isolated tumor cells. In tuberculosis tubercle bacilli can generally be detected.
8. Diabetes Insipidus.—Characteristic of this disease is the continued excretion of very large quantities of pale, watery urine, containing neither albumin nor sugar. The [p. 138] specific gravity varies between 1.001 and 1.005. The daily output of solids, especially urea, is increased.
9. Diabetes Mellitus.—The quantity of urine is very large. The color is generally pale, while the specific gravity is nearly always high—1.030 to 1.050, very rarely below 1.020. The presence of glucose is the essential feature of the disease. The amount of glucose is often very great, sometimes exceeding 8 per cent., while the total elimination may exceed 500 gm. in twenty-four hours. It may be absent temporarily. Acetone is generally present in advanced cases. Diacetic acid may be present, and usually warrants an unfavorable prognosis.
Preliminary Considerations.—The blood consists of a fluid of complicated and variable composition, the plasma, in which are suspended great numbers of microscopic structures: viz., red corpuscles, white corpuscles, blood-platelets, and blood-dust.
Red corpuscles, or erythrocytes, are biconcave discs, red when viewed by reflected light or in thick layer, and straw-colored when viewed by transmitted light or in thin layer. They give the blood its red color. They are cells which have been highly differentiated for the purpose of carrying oxygen from the lungs to the tissues. This is accomplished by means of an iron-bearing proteid, hemoglobin, which they contain. In the lungs hemoglobin forms a loose combination with oxygen, which it readily gives up when it reaches the tissues. Normal erythrocytes do not contain nuclei. They are formed from preëxisting nucleated cells in the bone-marrow.
White corpuscles, or leukocytes, are less highly differentiated cells. There are several varieties. They all contain nuclei, and most of them contain granules which vary in size and staining properties. They are formed in the bone-marrow and lymphoid tissues.
Blood-platelets, or blood-plaques, are colorless or slightly bluish, spheric or ovoid bodies, about one-third or one-half the diameter of an erythrocyte. Their structure, nature, and origin have not been definitely determined.
[p. 140] The blood-dust of Müller consists of fine granules which have vibratory motion. Little is known of them. It has been suggested that they are granules from disintegrated leukocytes.
Coagulation consists essentially in the transformation of fibrinogen, one of the proteins of the blood, into fibrin by means of a ferment derived from disintegration of the leukocytes. The resulting coagulum is made up of a meshwork of fibrin fibrils with entangled corpuscles and plaques. The clear, straw-colored fluid which is left after separation of the coagulum is called blood-serum. Normally, coagulation takes place in two to eight minutes after the blood leaves the vessels. It is frequently desirable to determine the coagulation time. The simplest method is to place a drop of blood upon a perfectly clean slide, and to draw a needle through it at half-minute intervals. When the clot is dragged along by the needle, coagulation has taken place. This method is probably sufficient for ordinary clinical work. For very accurate results the method of Russell and Brodie, for which the reader is referred to the larger text-books, is recommended. Coagulation is notably delayed in hemophilia and icterus and after administration of citric acid. It is hastened by administration of calcium chlorid.
For most clinical examinations only one drop of blood is required. This may be obtained from the lobe of the ear, the palmar surface of the tip of the finger, or, in the case of infants, the plantar surface of the great toe. With nervous children the lobe of the ear is preferable, as it prevents their seeing what is being done. An edematous or congested part should be avoided. The site should be well rubbed with alcohol to remove dirt and epithelial [p. 141] débris and to increase the amount of blood in the part. After allowing sufficient time for the circulation to equalize, the skin is punctured with a blood lancet (of which there are several patterns upon the market) or some substitute, as a Hagedorn needle, aspirating needle, trocar, or a pen with one of its nibs broken off. Nothing is more unsatisfactory than an ordinary sewing-needle. The lancet should be cleaned with alcohol before and after using, but need not be sterilized. If the puncture be made with a firm, quick stroke, it is practically painless. The first drop of blood which appears should be wiped away, and the second used for examination. The blood should not be pressed out, since this dilutes it with serum from the tissues; but moderate pressure some distance above the puncture is allowable.

|
| FIG. 64.—Daland's blood-lancet. |
When a larger amount of blood is required, it may be obtained with a sterile hypodermic syringe from one of the veins at the elbow.
Clinical study of the blood may be discussed under the following heads: I. Hemoglobin. II. Enumeration of erythrocytes. III. Color index. IV. Enumeration of leukocytes. V. Enumeration of plaques. VI. Study of stained blood. VII. Blood parasites. VIII. Serum reactions. IX. Tests for recognition of blood. X. Special blood pathology.
Hemoglobin is an iron-bearing proteid. It is found only within the red corpuscles, and constitutes about 90 per cent. of their weight. The actual amount of hemoglobin is never estimated clinically: it is the relation which the amount present bears to the normal which is determined. Thus the expression, "50 per cent. hemoglobin," when used clinically, means that the blood contains 50 per cent. of the normal. Theoretically, the normal would be 100 per cent., but with the methods of estimation in general use the blood of healthy persons ranges from 85 to 105 per cent.; these figures may, therefore, be taken as normal.
Increase of hemoglobin, or hyperchromemia, is uncommon, and is probably more apparent than real. It accompanies an increase in number of erythrocytes, and may be noted in change of residence from a lower to a higher altitude; in poorly compensated heart disease with cyanosis; in concentration of the blood from any cause, as the severe diarrhea of cholera; and in "idiopathic polycythemia."
Decrease of hemoglobin, or oligochromemia, is very common and important. It is the most striking feature of the secondary anemias (p. 204). Here the hemoglobin loss may be slight or very great. In mild cases a slight decrease of hemoglobin is the only blood change noted. In very severe cases, especially in repeated hemorrhages, malignant disease, and infection by the worms uncinaria and bothriocephalus latus, hemoglobin may fall to 15 per cent. Hemoglobin is always diminished, and usually very greatly, in chlorosis, pernicious anemia, and leukemia.
[p. 143] Estimation of Hemoglobin.—There are many methods, but none is entirely satisfactory. Those which are most widely used are here described.
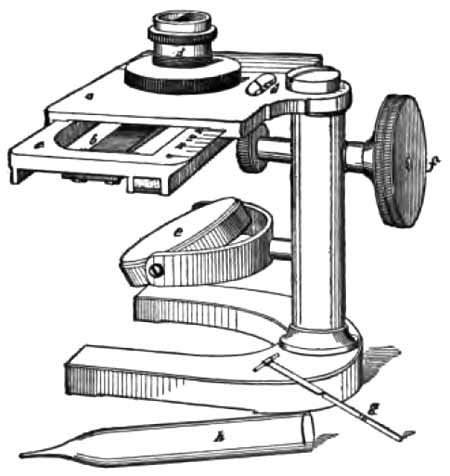
|
| FIG. 65.—Von Fleischl's hemoglobinometer: a, Stand; b, narrow wedge-shaped piece of colored glass fitted into a frame (c), which passes under the chamber; d, hollow metal cylinder, divided into two compartments, which holds the blood and water; e, plaster-of-Paris plate from which the light is reflected through the chamber; f, screw by which the frame containing the graduated colored glass is moved; g, capillary tube to collect the blood; h, pipet for adding the water; i, opening through which may be seen the scale indicating percentage of hemoglobin. |
(1) Von Fleischl Method.—The apparatus consists of a stand somewhat like the base and stage of a microscope (Fig. 65). Under the stage is a movable bar of colored glass, shading from pale pink at one end to deep red at the other. The frame in which this bar is held is marked with a scale of hemoglobin percentages corresponding to the different shades of red. By means of a rack and pinion, the color-bar can be moved from end to end beneath a round opening in the center of the stage. A small metal cylinder, which has a glass bottom and which is divided vertically into two equal compartments, can be placed over the opening in the stage so that one of its [p. 144] compartments lies directly over the color-bar. Accompanying the instrument are a number of short capillary tubes in metal handles.
Having punctured the finger-tip or lobe of the ear as already described, wipe off the first drop of blood, and from the second fill one of the capillary tubes. Hold the tube horizontally, and touch its tip to the drop of blood, which will readily flow into it if it be clean and dry. Avoid getting any blood upon its outer surface. With a medicine-dropper, rinse the blood from the tube into one of the compartments of the cylinder, using distilled water, and mix well. Fill both compartments level full with distilled water, and place the cylinder over the opening in the stage so that the compartment which contains only water lies directly over the bar of colored glass.
In a dark room, with the light from a candle reflected up through the cylinder, move the color-bar along with a jerking motion until both compartments have the same depth of color. The number upon the scale corresponding to the portion of the color-bar which is now under the cylinder gives the percentage of hemoglobin. While comparing the two colors, place the instrument so that they will fall upon the right and left halves of the retina, rather than upon the upper and lower halves; and protect the eye from the light with a cylinder of paper or pasteboard. After use, clean the metal cylinder with water, and wash the capillary tube with water, alcohol, and ether, successively. Results with this instrument are accurate to within about 5 per cent.
A recent modification of the von Fleischl apparatus by Miescher gives an error which need not exceed 1 per cent. It is, however, better adapted to laboratory use than to the needs of the practitioner.
(2) The Sahli hemoglobinometer (Fig. 66) is an improved form of the well known Gowers instrument. It consists of a hermetically sealed comparison tube containing a 1 per cent. solution of acid hematin, a graduated test-tube of the same [p. 145] diameter, and a pipet of 20 c.mm. capacity. The two tubes are held in a black frame with a white ground-glass back.
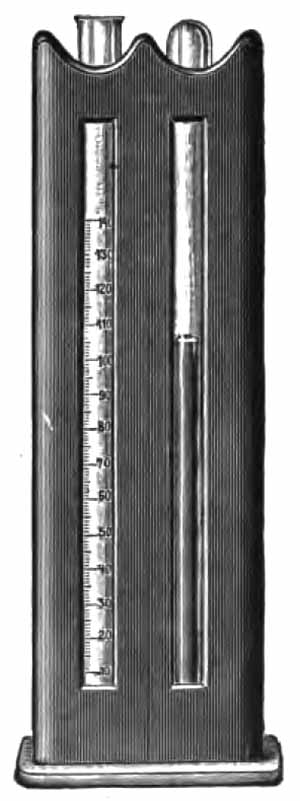
|
| FIG. 66.—Sahli's hemoglobinometer. |
Place a few drops of decinormal hydrochloric acid solution in the graduated tube. Obtain a drop of blood and draw it into the pipet to the 20 c.mm. mark. Wipe off the tip of the pipet, blow its contents into the hydrochloric acid solution in the tube, and rinse well. In a few minutes the hemoglobin is changed to acid hematin. Place the two tubes in the compartments of the frame, and dilute the fluid with water drop by drop, mixing after each addition, until it has exactly the same color as the comparison tube. The graduation corresponding to the surface of the fluid then indicates the [p. 146] percentage of hemoglobin. Decinormal hydrochloric acid solution may be prepared with sufficient accuracy for this purpose by adding 15 c.c. of the concentrated acid to 985 c.c. distilled water. A little chloroform should be added as a preservative.
This method is very satisfactory in practice, and is accurate to within 5 per cent. The comparison tube is said to keep its color indefinitely, but, unfortunately, not all the instruments upon the market are well standardized.
(3) Dare's hemoglobinometer (Fig. 67) differs from the others in using undiluted blood. The blood is allowed to flow by capillarity into the slit between two small plates of glass. It is then placed in the instrument and compared with different portions of a circular disc of colored glass. The reading must be made quickly, before clotting takes place. This instrument is easy to use, and is one of the most accurate.
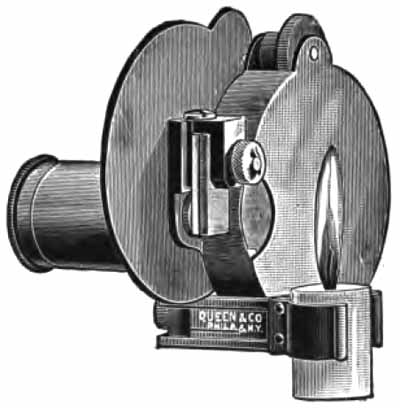
|
| FIG. 67.—Dare's hemoglobinometer. |
(4) Hammerschlag Method.—This is an indirect method which depends upon the fact that the percentage of hemoglobin varies directly with the specific gravity of the blood. It yields fairly accurate results except in leukemia, where the large number of leukocytes disturbs the relation.
Mix chloroform and benzol in a urinometer tube so that [p. 147] the specific gravity of the mixture is near the probable specific gravity of the blood. Add a drop of blood by means of a pipet of small caliber. If the drop floats near the surface, add a little benzol; if it sinks to the bottom, add a little chloroform. When it remains stationary near the middle, the mixture has the same specific gravity as the blood. Take the specific gravity with a urinometer, and obtain the corresponding percentage of hemoglobin from the following table:
| SPECIFIC GRAVITY. |
HEMOGLOBIN PER CENT. |
| 1.033-1.035 | 25-30 |
| 1.035-1.038 | 30-35 |
| 1.038-1.040 | 35-40 |
| 1.040-1.045 | 40-45 |
| 1.045-1.048 | 45-55 |
| 1.048-1.050 | 55-65 |
| 1.050-1.053 | 65-70 |
| 1.053-1.055 | 70-75 |
| 1.055-1.057 | 75-85 |
| 1.057-1.060 | 85-95 |
For accurate results with this method, care and patience are demanded. The following precautions must be observed:
(a) The two fluids must be well mixed after each addition of chloroform or benzol. Close the tube with the thumb and invert several times. Should this cause the drop of blood to break up into very small ones, adjust the specific gravity as accurately as possible with these, and test it with a fresh drop.
(b) The drop of blood must not be too large; it must not contain an air-bubble, it must not adhere to the side of the tube, and it must not remain long in the fluid.
(c) The urinometer must be standardized for the chloroform-benzol mixture. Most urinometers give a reading two or three degrees too high, owing to the low surface tension. Make a mixture such that a drop of distilled water will remain suspended in it (i.e., with a specific gravity of 1.000) and correct the urinometer by this.
(5) Tallquist Method.—The popular Tallquist hemoglobinometer consists simply of a book of small sheets of absorbent paper and a carefully printed scale of colors (Fig. 68).
Take up a large drop of blood with the absorbent paper, [p. 148] and when the humid gloss is leaving, compare the stain with the color scale. The color which it matches gives the percentage of hemoglobin. Except in practised hands, this method is accurate only to within 10 or 20 per cent.
|
| FIG. 68.—Tallquist's hemoglobin scale. |
Of the methods given, the physician should select the one which best meets his needs. With any method, practice is essential to accuracy. The von Fleischl has long been the standard instrument, but has lately fallen into some disfavor. For accurate work the best instruments are the von Fleischl-Miescher and the Dare. They are, however, expensive, and it is doubtful whether they are enough more accurate than the Sahli instrument to justify the difference in cost. The latter is probably the most satisfactory for the practitioner, provided a [p. 149] well-standardized color-tube is obtained. The specific gravity method is very useful when special instruments are not at hand. The Tallquist scale is so inexpensive and so convenient that it should be used by every physician at the bedside and in hurried office work; but it should not supersede the more accurate methods.
In health there are about 5,000,000 red corpuscles per cubic millimeter of blood. Normal variations are slight. The number is generally a little less—about 4,500,000—in women.
Increase of red corpuscles, or polycythemia, is unimportant. There is a decided increase following change of residence from a lower to a higher altitude, averaging about 50,000 corpuscles for each 1000 feet, but frequently much greater. The increase, however, is not permanent. In a few months the erythrocytes return to nearly their original number. Three views are offered in explanation: (a) Concentration of the blood, owing to increased evaporation from the skin; (b) stagnation of corpuscles in the peripheral vessels, because of lowered blood-pressure; (c) new-formation of corpuscles, this giving a compensatory increase of aëration surface.
Pathologically, polycythemia is uncommon. It may occur in: (a) concentration of the blood from severe watery diarrhea; (b) chronic heart disease, especially the congenital variety, with poor compensation and cyanosis; and (c) idiopathic polycythemia, which is considered to be an independent disease, and is characterized by cyanosis, blood counts of 7,000,000 to 10,000,000, hemoglobin 120 to 150 per cent., and a normal number of leukocytes.
[p. 150] Decrease of red corpuscles, or oligocythemia. Red corpuscles and hemoglobin are commonly decreased together, although usually not to the same extent.
Oligocythemia occurs in all but the mildest symptomatic anemias. The blood count varies from near the normal in moderate cases down to 1,500,000 in very severe cases. There is always a decrease of red cells in chlorosis, but it is often slight, and is relatively less than the decrease of hemoglobin. Leukemia gives a decided oligocythemia, the average count being about 3,000,000. The greatest loss of red cells occurs in pernicious anemia, where counts below 1,000,000 are not uncommon.
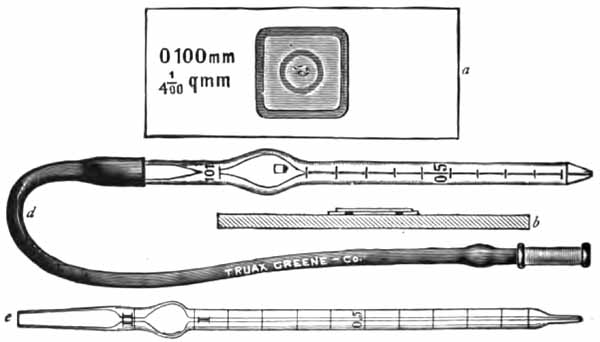
|
| FIG. 69.—Thoma-Zeiss hemocytometer: a, Slide used in counting; b, sectional view; d, red pipet; e, white pipet. |
The most widely used and most satisfactory instrument for counting the corpuscles is that of Thoma-Zeiss. The hematocrit is not to be recommended for accuracy, since in anemia, where blood counts are most important, the red cells vary greatly in size and probably also in elasticity. [p. 151] The hematocrit is, however, useful in determining the relative volume of corpuscles and plasma, and seems to be gaining in favor.
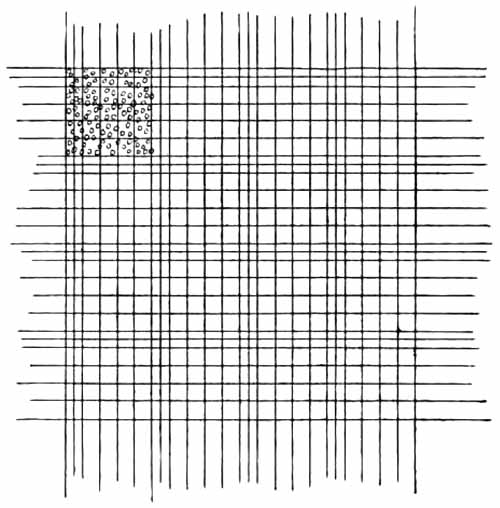
|
| FIG. 70.—Ordinary ruling of counting chamber, showing red corpuscles in left upper corner. |
The Thoma-Zeiss instrument consists of two pipets for diluting the blood and a counting chamber (Fig. 69). The counting chamber is a glass slide with a square platform in the middle. In the center of the platform is a circular opening, in which is set a small circular disc in such a manner that it is surrounded by a "ditch," and that its surface is exactly one-tenth of a millimeter below the surface of the square platform. Upon this disc is ruled a square millimeter, subdivided into 400 small squares. Each fifth row of small squares has double ruling for convenience in counting (Fig. 70). A thick [p. 152] cover-glass, ground perfectly plane, accompanies the counting chamber. Ordinary cover-glasses are of uneven surface, and should not be used with this instrument.
It is evident that, when the cover-glass is in place upon the platform, there is a space exactly one-tenth of a millimeter thick between it and the disc; and that, therefore, the square millimeter ruled upon the disc forms the base of a space holding exactly one-tenth of a cubic millimeter.

|
| FIG. 71.—Method of drawing blood into the pipet (Boston). |
Technic.—To count the red corpuscles, use the pipet with 101 engraved above the bulb. It must be clean and dry. Obtain a drop of blood as already described. Suck blood into the pipet to the mark 0.5 or 1. Should the blood go beyond the mark, draw it back by touching the tip of the pipet to a moistened handkerchief. Quickly wipe off the blood adhering to the tip, plunge it into the diluting fluid, and suck the fluid up to the mark 101, slightly rotating the pipet meanwhile. This dilutes the blood 1:200 or 1:100, according to the amount of blood taken. Except in cases of severe [p. 153] anemia, a dilution of 1:200 is preferable. Close the ends of the pipet with the fingers, and shake vigorously until the blood and diluting fluid are well mixed.
When it is not convenient to count the corpuscles at once, place a heavy rubber band around the pipet so as to close the ends, inserting a small piece of rubber-cloth or other tough, non-absorbent material if necessary to prevent the tip from punching through the rubber. It may be kept thus for twenty-four hours or longer.
When ready to make the count, mix again thoroughly by shaking; blow two or three drops of the fluid from the pipet, wipe off its tip, and then place a small drop (the proper size can be learned only by experience) upon the disc of the counting chamber. Adjust the cover immediately. Hold it by diagonal corners above the drop of fluid so that a third corner touches the slide and rests upon the edge of the platform. Place a finger upon this corner, and, by raising the finger, allow the cover to fall quickly into place. If the cover be properly adjusted, faint concentric lines of the prismatic colors—Newton's rings—can be seen between it and the platform when the slide is viewed obliquely. They indicate that the two surfaces are in close apposition. If they do not appear at once, slight pressure upon the cover may bring them out. Failure to obtain them is usually due to dirty slide or cover—both must be perfectly clean and free from dust. The drop placed upon the disc must be of such size that, when the cover is adjusted, it nearly or quite covers the disc, and that none of it runs over into the "ditch." There should be no bubbles upon the ruled area.
Allow the corpuscles to settle for a few minutes, and then examine with a low power to see that they are evenly distributed. If they are not evenly distributed over the whole disc, the counting chamber must be cleaned and a new drop placed in it.
Probably the most satisfactory objective for counting is the special one-sixth for blood work already mentioned. To [p. 154] understand the principle of counting, it is necessary to remember that the large square (400 small squares) represents a capacity of one-tenth of a cubic millimeter. Find the number of corpuscles in the large square, multiply by 10 to find the number in 1 c.mm. of the diluted blood, and finally, by the dilution, to find the number in 1 c.mm. of undiluted blood. Instead of actually counting all the corpuscles, it is customary to count those in only a limited number of small squares, and from this to calculate the number in the large square.
In practice a convenient procedure is as follows: With a dilution of 1:200, count the cells in 80 small squares, and to the sum add 4 ciphers; with dilution of 1:100, count 40 small squares and add 4 ciphers. Thus, if with 1:200 dilution, 450 corpuscles were counted, the total count would be 4,500,000 per c.mm. This method is sufficiently accurate for all clinical purposes, provided the corpuscles are evenly distributed and two drops from the pipet be counted. It is convenient to count a block of 20 small squares in each corner of the large square. It distribution be even, the difference between the number of cells in any two such blocks should not exceed twenty. Corpuscles which touch the upper and left sides should be counted as if within the squares, those touching the lower and right sides, as outside, and vice versâ.
Diluting Fluids.—The most widely used are Hayem's and Toisson's. Both of these have high specific gravities, so that, when well mixed, the corpuscles do not separate quickly. Toisson's fluid is probably the better for beginners, because it is colored and can be easily seen as it is drawn into the pipet. It stains the nuclei of leukocytes blue, but this is no real advantage. It must be filtered frequently.
| HAYEM'S FLUID. | TOISSON'S FLUID. | |||
| Mercuric chlorid | 0.5 | Methyl-violet, 5 B | 0.025 | |
| Sodium sulphate | 5.0 | Sodium chlorid | 1.000 | |
| Sodium chlorid | 1.0 | Sodium sulphate | 8.000 | |
| Distilled water | 200.0 | Glycerin | 30.000 | |
| Distilled water | 160.000 | |||
[p. 155] Sources of Error.—The most common sources of error in making a blood count are:
(a) Inaccurate dilution, either from faulty technic or inaccurately graduated pipets. The instruments made by Zeiss can be relied upon.
(b) Too slow manipulation, allowing a little of the blood to coagulate and remain in the capillary portion of the pipet.
(c) Inaccuracy in depth of counting chamber, which sometimes results from softening of the cement by alcohol or heat. The slide should not be cleaned with alcohol nor left to lie in the warm sunshine.
(d) Uneven distribution of the corpuscles. This results when the blood is not thoroughly mixed with the diluting fluid, or when the cover-glass is not applied soon enough after the drop is placed upon the disc.
Cleaning the Instrument.—The instrument should be cleaned immediately after using, and the counting chamber and cover must be cleaned again just before use.
Draw through the pipet, successively, water, alcohol, ether, and air. This can be done with the mouth, but it is much better to use a rubber bulb. When the mouth is used, the moisture of the breath will condense upon the interior of the pipet unless the fluids be shaken and not blown out. If blood has coagulated in the pipet—which happens when the work is done too slowly—dislodge the clot with a horse-hair, and clean with strong sulphuric acid, or let the pipet stand over night in a test-tube of the acid. Even if the pipet does not become clogged, it should be occasionally cleaned in this way.
This is an expression which indicates the amount of hemoglobin in each red corpuscle compared with the normal amount. For example, a color index of 1.0 indicates that each corpuscle contains the normal amount [p. 156] of hemoglobin; of 0.5, that each contains one-half the normal.
The color index is most significant in chlorosis and pernicious anemia. In the former it is usually much decreased; in the latter, generally much increased. In symptomatic anemia it is generally moderately diminished.
To obtain the color index, divide the percentage of hemoglobin by the percentage of corpuscles. The percentage of corpuscles is found by multiplying the first two figures of the red corpuscle count by two. This simple method holds good for all counts of 1,000,000 or more. Thus, a count of 2,500,000 is 50 per cent. of the normal. If, then, the hemoglobin has been estimated at 40 per cent., divide 40 (the percentage of hemoglobin) by 50 (the percentage of corpuscles). This gives 4/5, or 0.8, as the color index.
The normal number of leukocytes varies from 5000 to 10,000 per cubic millimeter of blood. The number is larger in robust individuals than in poorly nourished ones, and if disease be excluded, may be taken as an index of the individual's nutrition. Since it is well to have a definite standard, 7500 is generally adopted as the normal for the adult. With children the number is somewhat greater, counts of 12,000 and 15,000 being common in healthy children under twelve years of age.
Decrease in number of leukocytes, or leukopenia, is not important. It is common in persons who are poorly nourished, although not actually sick. The infectious diseases in which leukocytosis is absent (p. 160) often cause a slight decrease of leukocytes. Chlorosis may [p. 157] produce leukopenia, as also pernicious anemia, which usually gives it in contrast to the secondary anemias, which are frequently accompanied by leukocytosis.
Increase in number of leukocytes is common and of great importance. It may be considered under two heads: A. Increase of leukocytes due to chemotaxis and stimulation of the blood-making organs, or leukocytosis. B. Increase of leukocytes due to leukemia. The former may be classed as a transient, the latter, as a permanent, increase.
This term has not acquired a definite meaning. By some it is applied to any increase in number of leukocytes; by others, it is restricted to increase of the polymorphonuclear neutrophilic variety. As has been indicated, it is here taken to mean any increase in number of leukocytes caused by chemotaxis and stimulation of the blood-producing structures; and includes every increase of leukocytes except that due to leukemia.
By chemotaxis is meant that property of certain agents by which they attract or repel leukocytes—positive chemotaxis and negative chemotaxis respectively. An excellent illustration is the accumulation of leukocytes at the site of inflammation, owing to the positively chemotactic influence of bacteria and their products. A great many agents possess the power of attracting leukocytes into the general circulation. Among these are bacteria and many organic and inorganic poisons.
Chemotaxis alone will not explain the continuance of leukocytosis for more than a short time. It is probable that substances which are positively chemotactic also stimulate the blood-producing organs to increased [p. 158] formation of leukocytes; and in at least one form of leukocytosis such stimulation probably plays the chief part.
In general, the response of the leukocytes to chemotaxis is a conservative process. It is the gathering of soldiers to destroy an invader. This is accomplished partly by means of phagocytosis—actual ingestion of the enemy—and partly by means of chemic substances which the leukocytes produce.
In those diseases in which leukocytosis is the rule the degree of leukocytosis depends upon two factors: the severity of the infection and the resistance of the individual. A well-marked leukocytosis usually indicates good resistance. A mild degree means that the body is not reacting well, or else that the infection is too slight to call forth much resistance. Leukocytosis may be absent altogether when the infection is extremely mild, or when it is so severe as to overwhelm the organism before it can react. These facts are especially true of pneumonia, diphtheria, and abdominal inflammations, in which conditions the degree of leukocytosis is of considerable prognostic value.
As will be seen later, there are several varieties of leukocytes in normal blood, and many chemotactic agents attract only one variety and either repel or do not influence the others. These varieties may be divided into two general classes:
(a) Those having active independent ameboid motion. They are able to migrate readily from place to place and to ingest small bodies, as bacteria. From this latter property they derive their name of phagocytes. This group includes all varieties except the lymphocytes. The polymorphonuclear leukocytes are taken as the type of the group, because they are by far the most numerous.
[p. 159] (b) Those having very little or no independent motion—non-phagocytic leukocytes. Only the lymphocytes belong to this class.
By this classification we may distinguish two types of leukocytosis, according to the type of cell chiefly affected: a phagocytic and a non-phagocytic type.
1. Phagocytic Leukocytosis.—Theoretically, there should be a subdivision of phagocytic leukocytosis for each variety of phagocyte, e.g., polymorphonuclear leukocytosis, eosinophilic leukocytosis, large mononuclear leukocytosis, etc. Practically, however, only one of these, polymorphonuclear leukocytosis, need be considered under the head of leukocytosis. Increase in number of the other phagocytes will be considered at another place. They are present in the blood in such small numbers normally that even a marked increase scarcely affects the total leukocyte count; and, besides, substances which attract them into the circulation frequently repel the polymorphonuclears, so that the total number of leukocytes may actually be decreased.
Polymorphonuclear leukocytosis may be either physiologic or pathologic. A count of 20,000 would be considered a marked leukocytosis; of 30,000, high; above 50,000, extremely high.
(1) Physiologic Polymorphonuclear Leukocytosis.—This is never very marked, the count rarely exceeding 15,000 per cubic millimeter. It occurs in the new-born, in pregnancy, during digestion, and after cold baths. There is moderate leukocytosis in the moribund state; this is commonly classed as physiologic, but is probably due mainly to terminal infection.
[p. 160] (2) Pathologic Polymorphonuclear Leukocytosis.—The classification here given follows Cabot:
(a) Infectious and Inflammatory.—The majority of infectious diseases produce leukocytosis. The most notable exceptions are influenza, malaria, measles, tuberculosis, except when invading the serous cavities or when complicated by mixed infection, and typhoid fever, in which leukocytosis indicates an inflammatory complication.
All inflammatory and suppurative diseases cause leukocytosis, except when slight or well walled off. Appendicitis has been studied with especial care in this connection, and the conclusions now generally accepted probably hold good for most acute intra-abdominal inflammations. A marked leukocytosis (20,000 or more) nearly always indicates abscess, peritonitis, or gangrene, even though the clinical signs be slight. Absence of or mild leukocytosis indicates a mild process, or else an overwhelmingly severe one; and operation may safely be postponed unless the abdominal signs are very marked. On the other hand, no matter how low the count, an increasing leukocytosis—counts being made hourly—indicates a spreading process and demands operation, regardless of other symptoms.
Leukocyte counts alone are often disappointing, but are of much more value when considered in connection with a differential count of polymorphonuclears (see p. 181).
(b) Malignant Disease.—Leukocytosis occurs in about one-half of the cases of malignant disease. In many instances it is probably independent of any secondary infection, since it occurs in both ulcerative and non-ulcerative cases. It seems to be more common in sarcoma than in carcinoma. Very large counts are rarely noted.
[p. 161] (c) Post-hemorrhagic.—Moderate leukocytosis follows hemorrhage and disappears in a few days.
(d) Toxic.—This is a rather obscure class, which includes gout, chronic nephritis, acute yellow atrophy of the liver, ptomain poisoning, prolonged chloroform narcosis, and quinin poisoning. Leukocytosis may or may not occur in these conditions, and is not important.
(e) Drugs.—This also is an unimportant class. Most tonics and stomachics and many other drugs produce a slight leukocytosis.
2. Non-phagocytic or Lymphocyte Leukocytosis.—This is characterized by an increase in the total leukocyte count, accompanied by an increase in the percentage of lymphocytes. The word "lymphocytosis" is often used in the same sense. It is better, however, to use the latter as referring to any increase in number of lymphocytes, without regard to the total count, since an actual increase in number of lymphocytes is frequently accompanied by a normal or subnormal leukocyte count, owing to loss of polymorphonuclears.
Non-phagocytic leukocytosis is probably due more to stimulation of blood-making organs than to chemotaxis. It is less common, and is rarely so marked as a polymorphonuclear leukocytosis. When marked, the blood cannot be distinguished from that of lymphatic leukemia.
A marked lymphocyte leukocytosis occurs in pertussis, and is of value in diagnosis. It appears early in the catarrhal stage, and persists until after convalescence. The average leukocyte count is about 17,000, lymphocytes predominating. There is moderate lymphocyte leukocytosis in other diseases of childhood, as rickets, scurvy, and especially hereditary syphilis, where the blood-picture [p. 162] may approach that of pertussis. It must be borne in mind in this connection that lymphocytes are normally more abundant in the blood of children than in that of adults.
Slight lymphocyte leukocytosis occurs in many other pathologic conditions, but is of little significance.
This is an idiopathic disease of the blood-making organs, which is accompanied by an enormous increase in number of leukocytes. The leukocyte count sometimes exceeds 1,000,000 per cubic millimeter, and leukemia is always to be suspected when it exceeds 50,000. Lower counts do not, however, exclude it. The subject is more fully discussed later (p. 208).
The leukocytes are counted with the Thoma-Zeiss instrument, already described. Recently, several new rulings of the disc have been introduced, notably the Zappert and the Türk (Fig. 72), which give a ruled area of nine square millimeters. They were devised for counting the leukocytes in the same specimen with the red corpuscles. The red cells are counted in the usual manner, after which all the leukocytes in the whole area of nine square millimeters are counted; and the number in a cubic millimeter of undiluted blood is then easily calculated. Leukocytes are easily distinguished from red cells, especially when Toisson's diluting fluid is used. This method may be used with the ordinary ruling by adjusting the microscopic field to a definite size, and counting a sufficient number of fields, as described later. Although less convenient, it is more accurate to count the leukocytes separately, with less dilution of the blood, as follows:
[p. 163] Technic.—A larger drop of blood is required than for counting the erythrocytes, and more care in filling the pipet. Use the pipet with 11 engraved above the bulb. Suck the blood to the mark 0.5 or 1.0, and the diluting fluid to the mark 11. This gives a dilution of 1:20 or 1:10, respectively. The dilution of 1:20 is easier to make. Mix well by shaking in all directions except in the long axis of the pipet; blow out two or three drops, place a drop in the counting chamber, and adjust the cover as already described (p. 153).
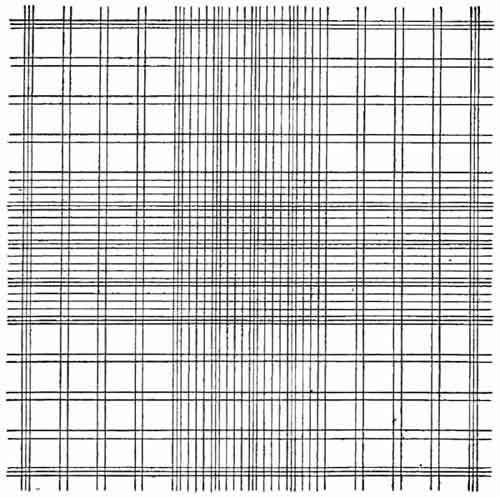
|
| FIG. 72.—Türk ruling of counting chamber. |
Examine with a low power to see that the cells are evenly distributed. Count with the two-thirds objective and a high eye-piece, or with the long-focus one-sixth and a low eye-piece. [p. 164] A one-fourth objective will be found very satisfactory for this purpose.
With the ordinary ruling of the disc, count all the leukocytes in the large square, multiply by 10 to find the number in 1 c.mm. of diluted blood, and by the dilution to find the number per c.mm. of undiluted blood. In every case at least 100 leukocytes must be counted as a basis for calculation, and it is much better to count 500. This will necessitate examination of several drops from the pipet. With the Zappert and Türk rulings a sufficient number can usually be counted in one drop, but the opportunity for error is very much greater when only one drop is examined.
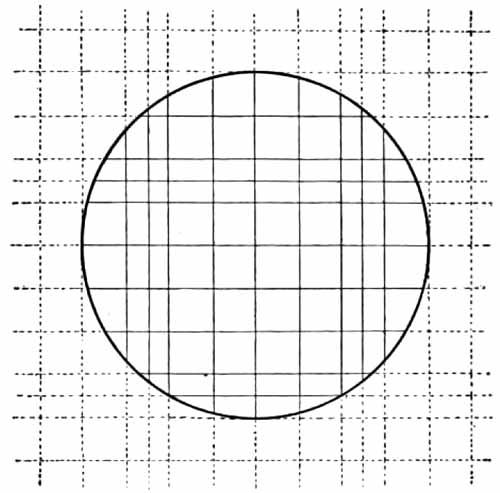
|
| FIG. 73.—Size of field required in counting leukocytes as described in the text. |
In routine work the author's modification of the "circle" method is very satisfactory: Draw out the tube of the microscope until the field of vision has a diameter equal to eight [p. 165] times the side of a small square (Fig. 73). The area of this field closely approximates one-tenth of a square millimeter. With a dilution of 1:20, count the leukocytes in 20 such fields upon different parts of the disc without regard to the ruled lines, and to their sum add two ciphers. With dilution of 1:10, count 10 such fields, and add two ciphers. Thus, with 1:10 dilution, if 150 leukocytes were counted in 10 fields, the leukocyte count would be 15,000 per c.mm. To compensate for possible unevenness of distribution, it is best to count a row of fields horizontally and a row vertically across the disc. This method is applicable to any degree of dilution of the blood, and is simple to remember: one always counts a number of fields equal to the number of times the blood has been diluted, and adds two ciphers.
It is frequently impossible to obtain the proper size of field with the objectives and eye-pieces at hand. In such case, place a cardboard disc with a circular opening upon the diaphragm of the eye-piece, and adjust the size of the field by drawing out the tube. The circular opening can be cut with a cork-borer.
Diluting Fluids.—The diluting fluid should dissolve the red corpuscles so that they will not obscure the leukocytes. The simplest fluid is a 0.5 per cent. solution of acetic acid. More satisfactory is the following: glacial acetic acid, 1 c.c.; 1 per cent. aqueous solution of gentian-violet, 1 c.c.; distilled water, 100 c.c. These solutions must be filtered frequently.
The average normal number of plaques is variously given as 200,000 to 700,000 per c.mm. of blood. The latter figure probably more nearly represents the true normal average, since the lower counts were obtained for the most part by workers who used unreliable methods. Physiologic variations are marked; thus, the number [p. 166] increases as one ascends to a higher altitude, and is higher in winter than in summer. There are unexplained variations from day to day; hence a single abnormal count should not be taken to indicate a pathologic condition.
Pathologic variations are often very great. Owing to lack of knowledge as to the origin of the platelets and to the earlier imperfect methods of counting, the clinical significance of these variations is uncertain. The following facts seem, however, to be established:
(a) In acute infectious diseases the number is subnormal or normal. If the fever ends by crisis, the crisis is accompanied by a rapid and striking increase.
(b) In secondary anemia plaques are generally increased, although sometimes decreased. In pernicious anemia they are always greatly diminished, and an increase should exclude the diagnosis of this disease.
(c) They are decreased in chronic lymphatic leukemia, and greatly increased in the myelogenous form.
(d) In purpura hæmorrhagica the number is enormously diminished.
Blood-plaques are difficult to count owing to the rapidity with which they disintegrate and to their great tendency to adhere to any foreign body and to each other. The method of Kemp, Calhoun, and Harris is practical and is to be recommended:
Wash the finger well and allow a few minutes to elapse for the circulation to become normal. Prick the finger lightly with a blood-lancet, regulating the depth of the puncture so that the blood will not flow without gentle pressure. Quickly dip a clean glass rod into a vessel containing diluting and fixing fluid, and place two or three good-sized drops upon the [p. 167] finger over the puncture. Then exert gentle pressure above the puncture so that a small drop of blood will exude into the fluid. Mix the two by passing the rod lightly several times over the surface of the blended drop. (Some workers first place a drop of the fluid upon the finger and then make the puncture through it, this necessitating less care as to depth of the puncture.) Now transfer a drop of the diluted blood from the finger to a watch-glass which contains two or three drops of the fluid, and mix well. From this, transfer a drop to the counting slide of the Thoma-Zeiss hemocytometer, and cover. An ordinary thin cover will answer for this purpose, and is preferable because it allows the use of a higher power objective. Allow the slide to stand for at least five minutes, and then with a one-sixth or higher objective count the plaques and the red corpuscles in a definite number of squares. At least 100 plaques must be counted. The number of red corpuscles per cubic millimeter of blood having been previously ascertained in the usual manner (p. 152), the number of plaques can easily be calculated by the following equation:
r represents the number of red corpuscles in any given number of squares; p, the number of plaques in the same squares; R, the total number of red corpuscles per c.mm. of blood; and P, the number of plaques per c.mm.
Beginners are apt to take too much blood and not to dilute it enough. Best results are attained when there are only one or two plaques in a small square. With insufficient dilution, the platelets are more or less obscured by the red cells.
The following diluting and fixing fluid is recommended:
| Formalin | 10 c.c. |
| 1 per cent. aqueous solution sodium chlorid (Color with methyl-violet if desired.) |
150 c.c. |
[p. 168] This fluid is cheap and easily prepared, and keeps indefinitely. It fixes the plaques quickly without clumping, and does not clump nor decolorize the reds. It has a low specific gravity, and hence allows the plaques to settle upon the ruled area along with the reds. Fluids of high specific gravity cause the plaques to float so that they do not appear in the same plane with the reds and the ruled lines.
1. Spreading the Film.—Thin, even films are essential to accurate and pleasant work. They more than compensate for the time spent in learning to make them. There are certain requisites for success with any method: (a) The slides and covers must be perfectly clean; thorough washing with soap and water and rubbing with alcohol will usually suffice; (b) the drop of blood must not be too large; (c) the work must be done quickly, before coagulation begins.
The blood is obtained from the finger-tip or the lobe of the ear, as for a blood count; only a very small drop is required.
Ehrlich's Two-cover-glass Method.—This method is very widely used, but considerable practice is required to get good results. Touch a cover-glass to the top of a small drop of blood, and place it, blood side down, upon another cover-glass. If the drop be not too large, and the covers be perfectly clean, the blood will spread out in a very thin layer. Just as it stops spreading, before it begins to coagulate, pull the covers quickly but firmly apart on a line parallel to their plane (Fig. 74). It is best to handle the covers with forceps, since the moisture of the fingers may produce artifacts.
Two-slide Method.—Place a small drop of blood upon a [p. 169] clean slide and push it along with the edge of a second slide held at an angle of 45 degrees to the surface of the first (Fig. 75).
|
| FIG. 74.—Spreading the film: two-cover-glass method. |

|
| FIG. 75.—Spreading the film: two-slide method. |
Cigarette-paper Method.—This gives better results in the hands of the inexperienced than any of the methods in general use, and may be used with either slides or covers. A very thin paper, such as the "Zig-zag" brand, is best. Ordinary cigarette paper and thin tissue-paper will answer, but do not give nearly so good results.
Cut the paper into strips about ¾ inch wide, across the ribs. Pick up one of the strips by the gummed edge, and touch its opposite end to the drop of blood. Quickly place the end which has the blood against a slide or a large cover-glass held [p. 170] in a forceps. The blood will spread along the edge of the paper. Now draw the paper evenly across the slide or cover. A thin film of blood will be left behind (Fig. 76).
|
| FIG. 76.—Spreading the film. Cigarette-paper method applied to cover-glasses. |
The films may be allowed to dry in the air, or may be dried by gently heating high above a flame (where one can comfortably hold the hand). Such films will keep for years, but for some stains they must not be more than a few weeks old. They must be kept away from flies—a fly can work havoc with a film in a few minutes.
2. Fixing the Film.—In general, films must be "fixed" before they are stained. Fixation may be accomplished by chemicals or by heat. Those stains which are dissolved in methyl-alcohol combine fixation with the staining process.
Chemic Fixation.—Soak the film five to fifteen minutes in pure methyl-alcohol, or one-half hour or longer in equal parts of absolute alcohol and ether. One minute in 1 per cent. formalin in alcohol is preferred by some. Chemic fixation may precede eosin-methylene-blue and other simple stains.
[p. 171] Heat Fixation.—This may precede any of the methods which do not combine fixation with the staining process; it must be used with Ehrlich's triple stain. The best method is to place the film in an oven, raise the temperature to 150° C., and allow to cool slowly. Without an oven, the proper degree of fixation is difficult to attain. Kowarsky has devised a small plate of two layers of copper (Fig. 77), upon which the films are placed together with a crystal of urea. The plate is heated over a flame until the urea melts, and is then set aside to cool. This is said to give the proper degree of fixation, but in the writer's experience the films have always been underheated. He obtains better results by use of tartaric acid crystals (melting-point, 168°-170° C.). The plate, upon which have been placed the cover-glasses, film side down, and a crystal of the acid, is heated over a low flame until the crystal has completely melted. It should be held sufficiently high above the flame that the heating will require five to seven minutes. The covers are then removed. Freshly made films of normal blood should be allowed to remain upon the plate for a minute or two after heating has ceased. Fresh films require more heat than old ones, and normal blood more than the blood of pernicious anemia and leukemia.
|
| FIG. 77.—Kowarsky's plate for fixing blood (Klopstock and Kowarsky). |
Fixation by passing the film quickly through a flame about twenty times, as is often done in routine work, is not recommended for beginners.
3. Staining the Film.—The anilin dyes, which are extensively used in blood work, are of two general classes: [p. 172] basic dyes, of which methylene-blue is the type; and acid dyes, of which eosin is the type. Nuclei and certain other structures in the blood are stained by the basic dyes, and are hence called basophilic. Certain structures take up only acid dyes, and are called acidophilic, oxyphilic, or eosinophilic. Certain other structures are stained only by combinations of the two, and are called neutrophilic. Recognition of these staining properties marked the beginning of modern hematology.
(1) Eosin and Methylene-blue.—In many instances this stain will give all the information desired. It is especially useful in studying the red corpuscles. Nuclei, basophilic granules, and all blood parasites are blue; erythrocytes are red or pink; eosinophilic granules, bright red. Neutrophilic granules and blood-plaques are not stained.
(1) Fix the film by heat or chemicals.
(2) Stain about five minutes with 0.5 per cent. alcoholic solution of eosin, diluted one-half with water.
(3) Rinse in water, and dry between filter-papers.
(4) Stain one-half to one minute with saturated aqueous solution of methylene-blue.
(5) Rinse well, dry, and mount. Films upon slides may be examined with an oil-immersion objective without a cover-glass.
(2) Ehrlich's Triple Stain.—This has been the standard blood-stain for many years, and is still widely used. It is probably the best for neutrophilic granules. It is difficult to make, and should be purchased ready prepared from a reliable dealer. Nuclei are stained blue or greenish-blue; erythrocytes, orange; neutrophilic granules, violet; and eosinophilic granules, copper red. [p. 173] Basophilic granules and blood-plaques are not stained (see Fig. 85).
Success in staining depends largely upon proper fixation. The film must be carefully fixed by heat: underheating causes the erythrocytes to stain red; overheating, pale yellow. The staining fluid is applied for five to fifteen minutes, and the preparation is rinsed quickly in water, dried, and mounted. Subsequent application of Löffler's methylene-blue for one-half to one second will bring out the basophilic granules, and improve the nuclear staining, but there is considerable danger of overstaining.
(3) Wright's Stain.—Recently the polychrome methylene-blue-eosin stains, dissolved in methyl-alcohol, have largely displaced other blood-stains for clinical purposes. They combine the fixing with the staining process, and stain differentially every normal and abnormal structure in the blood. Numerous methods of preparing and applying these stains have been devised. Wright's stain is one of the best, and is the most widely used in this country. Directions for preparing it are given in most of the newer large text-books upon clinical diagnosis. The practitioner will find it best to purchase the stain ready prepared. Most microscopic supply houses keep it in stock. The method of application is as follows:
(1) Without previous fixation, cover the blood film with the stain, and let stand one minute.
(2) Add water, drop by drop, until a delicate metallic scum forms upon the surface. Let this mixture remain on the preparation for two or three minutes.
(3) Wash in water until the better spread portions of the film have a pinkish tint.
(4) Dry between filter-papers and mount.
[p. 174] The stain is more conveniently applied upon cover-glasses than upon slides. Films much more than a month old do not stain well. In some localities ordinary tap-water will answer both for diluting the stain and for washing the film; in others, distilled water must be used. Different lots of Wright's fluid vary, and a few preliminary stains should be made with each lot to learn its peculiarities. The principal variation is in the amount of water which must be added to obtain the iridescent scum. Sometimes eight or more drops must be added after the scum appears.
When properly applied, Wright's stain gives the following picture (Plate VI): erythrocytes, yellow or pink; nuclei, various shades of bluish-purple; neutrophilic granules, reddish-lilac; eosinophilic granules, bright red; basophilic granules of leukocytes and degenerated red corpuscles, very dark bluish-purple; blood-plaques, dark lilac; bacteria, blue. The cytoplasm of lymphocytes is generally robin's-egg blue; that of the large mononuclears may have a faint bluish tinge. Malarial parasites stain characteristically: the cytoplasm, sky-blue; the chromatin, reddish-purple.
Jenner's stain, which gives a somewhat similar picture, is preferred by many for differential counting of leukocytes. It brings out neutrophilic granules rather more clearly, but does not compare with Wright's fluid as a stain for the malarial parasite. Unfixed films are stained about three minutes, rinsed quickly, dried, and mounted.
For the physician who wishes to use only one blood-stain, Wright's fluid is undoubtedly the best of those mentioned.
| PLATE VI |
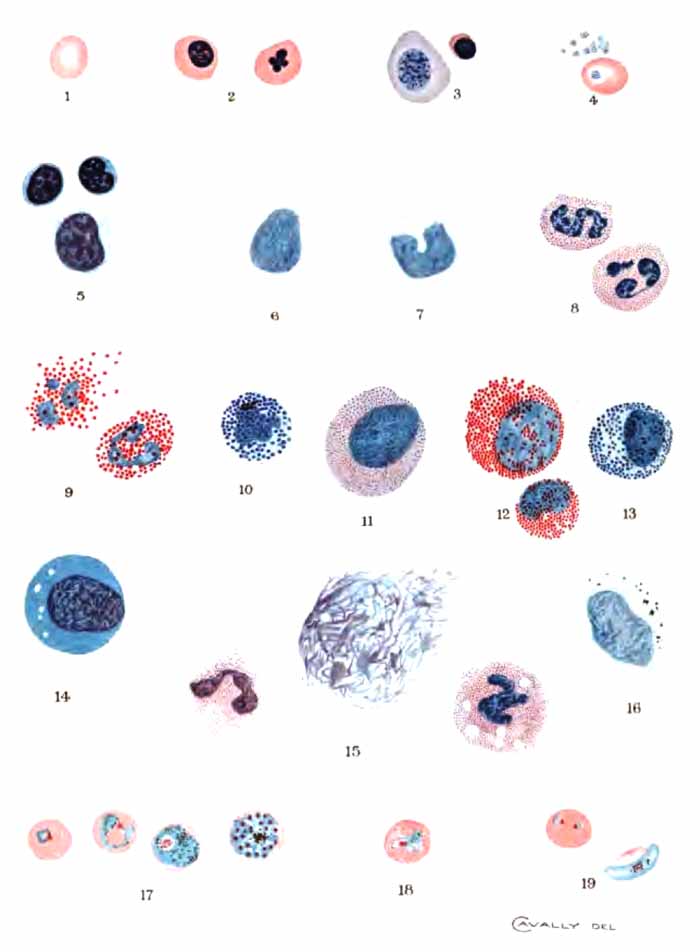
|
| EXPLANATION OF PLATE VI |
|
Stained with
Wright's stain. All drawn to same scale. 1, Normal red corpuscle for comparison; 2, normoblasts, one with lobulated nucleus; 3, megaloblast and microblast. The megaloblast shows a considerable degree of polychromatophilia; 4, blood-plaques, one lying upon a red corpuscle; 5, lymphocytes, large and small; 6, large mononuclear leukocyte; 7, transitional leukocyte; 8, polymorphonuclear neutrophilic leukocytes; 9, eosinophilic leukocytes, one ruptured; 10, basophilic leukocyte; 11, neutrophilic myelocyte. The granules are sometimes less numerous and less distinct than here shown; 12, eosinophilic myelocytes; 13, basophilic myelocyte; 14, "irritation" or "stimulation" form, with small vacuoles; 15, degenerated leukocytes: two polymorphonuclear neutrophiles, one ruptured, one swollen and vacuolated; and a "basket cell" composed of an irregular meshwork of nuclear material; 16, large mononuclear leukocyte containing pigment-granules: from a case tertian malaria; 17, four stages in the asexual cycle of the tertian malarial parasite: the second and fourth were drawn from the same slide taken from a case of double tertian; 18, red corpuscle containing tertian parasite and showing malarial stippling; 19, estivo-autumnal malarial parasites: two small ring forms within the same red cell, and a crescent with remains of the red corpuscle in its concavity. |
Much can be learned from stained blood-films. They furnish the best means of studying the morphology of the blood and blood parasites, and, to the experienced, they give a fair idea of the amount of hemoglobin and the number of red and white corpuscles. A one-twelfth-inch objective is required.
1. Erythrocytes.—Normally, the red corpuscles are acidophilic. The colors which they take with different stains have been described. When not crowded together, they appear as circular, homogeneous discs, of nearly uniform size, averaging 7.5 µ in diameter (Fig. 84). The center of each is somewhat paler than the periphery. The degree of pallor furnishes a rough index to the amount of hemoglobin in the corpuscle. They are apt to be crenated when the film has dried too slowly.
Pathologically, red corpuscles vary in size and shape, staining properties, and structure.
(1) Variations in Size and Shape (See Plate VIII and Fig. 84).—The cells may be abnormally small (called microcytes, 5 µ or less in diameter); abnormally large (macrocytes, 10 to 12 µ); or extremely large (megalocytes, 12 to 20 µ).
Variation in shape is often very marked. Oval, pyriform, caudate, saddle-shaped, and club-shaped corpuscles are common. They are called poikilocytes, and their presence is spoken of as poikilocytosis.
Red corpuscles which vary from the normal in size and shape are present in most symptomatic anemias, and in the severer grades are often very numerous. Irregularities are particularly conspicuous in leukemia and pernicious anemia, where, in some instances, a normal erythrocyte [p. 176] is the exception. In pernicious anemia there is a decided tendency to large size and oval forms, and megalocytes are rarely found in any other condition.
(2) Variations in Staining Properties (See Plate VIII).—These include polychromatophilia, basophilic degeneration, and basophilic stippling. They are probably degenerative changes, although polychromatophilia is thought by many to be evidence of youth in a cell, and hence to indicate an attempt at blood regeneration.
(a) Polychromatophilia.—Some of the corpuscles partially lose their normal affinity for acid stains, and take the basic stain to greater or less degree. Wright's stain gives such cells a faint bluish tinge when the condition is mild, and a rather deep blue when severe. Sometimes only part of a cell is affected. A few polychromatophilic corpuscles can be found in marked symptomatic anemias. They occur most abundantly in malaria, leukemia, and pernicious anemia.
(b) Basophilic Granular Degeneration (Degeneration of Grawitz).—This is characterized by the presence, within the corpuscle, of small basophilic granules. They stain deep blue with Wright's stain; not at all, with Ehrlich's triple stain. The cell containing them may stain normally in other respects, or it may exhibit polychromatophilia.
Numerous cells showing this degeneration are commonly found in chronic lead-poisoning, of which they were at one time thought to be pathognomonic. Except in this disease, the degeneration indicates a serious blood condition. It occurs in well-marked cases of pernicious anemia and leukemia, and, much less commonly, in very severe symptomatic anemias.
(c) Basophilic Stippling.—This term has been applied [p. 177] to the finely granular appearance often seen in red corpuscles, which harbor malarial parasites (Plate VI). It is commonly classed with the degeneration just described, but is probably distinct. Not all stains will show it. With Wright's stain it can be brought out by staining longer and washing less than for the ordinary blood-stain. The minute granules stain reddish purple.
(3) Variations in Structure.—The most important is the presence of a nucleus (Plates VI and VIII and Fig. 84). Nucleated red corpuscles, or erythroblasts, are classed according to their size: microblasts, 5 µ or less in diameter; normoblasts, 5 to 10 µ; and megaloblasts, above 10 µ. Microblasts and normoblasts contain one, rarely two, small, round, sharply defined, deeply staining nuclei, often located eccentrically. Occasionally the nucleus is irregular in shape, "clover-leaf" forms being not infrequent. The megaloblast is probably a distinct cell, not merely a larger size of the normoblast. Its nucleus is large, stains rather palely, has a delicate chromatin network, and often shows evidences of degeneration (karyorrhexis, etc.). In ordinary work, however, it is safer to base the distinction upon size than upon structure. Any nucleated red cell, but especially the megaloblast, may exhibit polychromatophilia.
Normally, erythroblasts are present only in the blood of the fetus and of very young infants. Pathologically, normoblasts occur in severe symptomatic anemia, leukemia, and pernicious anemia. They are most abundant in myelogenous leukemia. While always present in pernicious anemia, they are often difficult to find. Megaloblasts are found in pernicious anemia, and with extreme rarity in any other condition. They almost invariably [p. 178] exceed the normoblasts in number, which is one of the distinctive features of the disease. Microblasts have much the same significance as normoblasts, but are less common.
2. The Leukocytes.—An estimation of the number or percentage of each variety of leukocyte in the blood is called a differential count.
The differential count is best made upon a film stained with Wright's, Jenner's, or Ehrlich's stain. Go carefully over the film with an oil-immersion lens, using a mechanical stage if available. Classify each leukocyte seen, and calculate what percentage each variety is of the whole number classified. For accuracy, 500 to 1000 leukocytes must be classified; for approximate results, 200 are sufficient. Track of the count may be kept by placing a mark for each leukocyte in its appropriate column, ruled upon paper. Some workers divide a slide-box into compartments with slides, one for each variety of leukocyte, and drop a coffee-bean into the appropriate compartment when a cell is classified. When a convenient number of coffee-beans is used (any multiple of 100), the percentage calculation is extremely easy.
The actual number of each variety in a cubic millimeter of blood is easily calculated from these percentages and the total leukocyte count. An increase in actual number is an absolute increase; an increase in percentage only, a relative increase. It is evident that an absolute increase of any variety may be accompanied by a relative decrease.
A record is generally kept of the number of nucleated red cells seen during a differential count of leukocytes.
The usual classification of leukocytes is based upon their size, their nuclei, and the staining properties of the granules [p. 179] which many of them contain. It is not altogether satisfactory, but is probably the best which our present knowledge permits.
(1) Normal Varieties.—(a) Lymphocytes.—These are small mononuclear cells without granules (Plate VI and Fig. 86). They are about the size of a red corpuscle or slightly larger, and consist of a single, sharply defined, deeply staining nucleus, surrounded by a narrow rim of protoplasm. The nucleus is generally round, but is sometimes indented at one side. Wright's stain gives the nucleus a deep purple color and the cytoplasm a pale robin's-egg blue in typical cells. Larger forms of lymphocytes are frequently found, especially in the blood of children, and are difficult to distinguish from the large mononuclear leukocytes.
Lymphocytes are formed in the lymphoid tissues, including that of the bone-marrow. They constitute, normally, 20 to 30 per cent. of all leukocytes, or about 1000 to 3000 per c.mm. of blood. They are more abundant in the blood of children.
The percentage of lymphocytes is usually moderately increased in those conditions which give leukopenia, especially typhoid fever, chlorosis, pernicious anemia, and many debilitated conditions. A marked increase, accompanied by an increase in the total leukocyte count, is seen in pertussis and lymphatic leukemia. In the latter, the lymphocytes sometimes exceed 98 per cent.
(b) Large Mononuclear Leukocytes (Plate VI).—These cells are two or three times the diameter of the normal red corpuscle. Each contains a single round or oval nucleus, often located eccentrically. The zone of protoplasm surrounding the nucleus is relatively wide. With [p. 180] Wright's stain the nucleus is less deeply colored than that of the lymphocyte, while the cytoplasm is very pale blue or colorless, and sometimes contains a few reddish granules. The size of the cell, the width of the zone of cytoplasm, and the depth of color of the nucleus are the points to be considered in distinguishing between large mononuclears and lymphocytes. When large forms of the lymphocyte are present, the distinction is often difficult or impossible. It is then advisable to count the two cells together as lymphocytes. Indeed, they are regarded by some hematologists as identical.
Large mononuclear leukocytes probably originate in the bone-marrow or spleen. They constitute 2 to 4 per cent. of the total number of leukocytes: 100 to 400 per c.mm. of blood. An increase is unusual except in malaria, where it is quite constantly observed, and where many of the cells contain ingulfed pigment.
(c) Transitional Leukocytes (Plate VI).—These are essentially large mononuclears with deeply indented or horseshoe-shaped nuclei. A few fine neutrophilic granules are sometimes present in their cytoplasm.
They are probably formed from the large mononuclears, and occur in the blood in about the same numbers. The two cells are usually counted together.
(d) Polymorphonuclear Neutrophilic Leukocytes (Plate VI).—There is usually no difficulty in recognizing these cells. Their average size is somewhat less than that of the large mononuclears. The nucleus stains rather deeply, and is extremely irregular, often assuming shapes comparable to letters of the alphabet, E, Z, S, etc. (Fig. 86). Frequently there appear to be several separate nuclei, hence the widely used name, "polynuclear [p. 181] leukocyte." Upon careful inspection, however, delicate nuclear bands connecting the parts can usually be seen. The cytoplasm is relatively abundant, and contains great numbers of very fine neutrophilic granules. With Wright's stain the nucleus is bluish-purple, and the granules, reddish-lilac.
Polymorphonuclear leukocytes are formed in the bone-marrow from neutrophilic myelocytes. They constitute 60 to 75 per cent. of all the leukocytes: 3000 to 7500 per c.mm. of blood. Increase in their number practically always produces an increase in the total leukocyte count, and has already been discussed under "phagocytic leukocytosis." The leukocytes of pus, pus-corpuscles, belong almost wholly to this variety.
A comparison of the percentage of polymorphonuclear cells with the total leukocyte count yields more information than a consideration of either alone. With moderate infection and good resisting powers the leukocyte count and the percentage of polymorphonuclears are increased proportionately. When the polymorphonuclear percentage is increased to a notably greater extent than is the total number of leukocytes, no matter how low the count, either very poor resistance or a very severe infection may be inferred. In the absence of acute infectious disease a polymorphonuclear percentage of 85 or over points very strongly to gangrene or pus-formation. On the other hand, except in children, where the percentage is normally low, pus is uncommon with less than 80 per cent. of polymorphonuclears.
Normally, the cytoplasm of leukocytes stains pale yellow with iodin. Under certain pathologic conditions the cytoplasm of many of the polymorphonuclears stains [p. 182] diffusely brown, or contains granules which stain reddish-brown with iodin. This is called iodophilia. Extracellular iodin-staining granules, which are present normally, are more numerous in iodophilia.
This iodin reaction occurs in all purulent conditions except abscesses which are thoroughly walled off or purely tuberculous abscesses. It is of some value in diagnosis between serous effusions and purulent exudates, between catarrhal and suppurative processes in the appendix and Fallopian tube, etc. Its importance, however, as a diagnostic sign of suppuration has been much exaggerated, since it may occur in any general toxemia, such as pneumonia, influenza, malignant disease, and puerperal sepsis.
To demonstrate iodophilia, place the air-dried films in a stoppered bottle containing a few crystals of iodin until they become yellow. Mount in syrup of levulose and examine with a one-twelfth objective.
(e) Eosinophilic Leukocytes, or "Eosinophiles" (Plate VI).—The structure of these cells is similar to that of the polymorphonuclear neutrophiles, with the striking difference that, instead of fine neutrophilic granules, their cytoplasm contains coarse granules having a strong affinity for acid stains. They are easily recognized by the size and color of the granules, which stain bright red with Wright's stain.
Eosinophiles are formed in the bone-marrow from eosinophilic myelocytes. Their normal number varies from 50 to 400 per c.mm. of blood, or 1 to 4 per cent. of the leukocytes. An increase is called eosinophilia, and is better determined by the actual number than by the percentage.
Slight eosinophilia is physiologic during menstruation. [p. 183] Marked eosinophilia is always pathologic. It occurs in a variety of conditions, the most important of which are: infection by animal parasites; bronchial asthma; myelogenous leukemia; scarlet fever; and many skin diseases.
Eosinophilia may be a symptom of infection by any of the worms. It is fairly constant in trichinosis, uncinariasis, filariasis, and echinococcus disease. In this country an unexplained marked eosinophilia warrants examination of a portion of muscle for Trichina spiralis (p. 255).
True bronchial asthma commonly gives a marked eosinophilia during and following the paroxysms. This is helpful in excluding asthma of other origin. Eosinophiles also appear in the sputum in large numbers.
In myelogenous leukemia there is almost invariably an absolute increase of eosinophiles, although, owing to the great increase of other leukocytes, the percentage is usually diminished. Dwarf and giant forms are often numerous.
Scarlet fever is frequently accompanied by eosinophilia, which may help to distinguish it from measles.
Eosinophilia has been observed in a large number of skin diseases, notably pemphigus, prurigo, psoriasis, and urticaria. It probably depends less upon the variety of the disease than upon its extent.
(f) Basophilic Leukocytes or "Mast-cells" (Plate VI).—In general, these resemble polymorphonuclear neutrophiles except that the nucleus is less irregular and that the granules are larger and have a strong affinity for basic stains. They are easily recognized. With Wright's stain the granules are deep purple, while the nucleus is pale blue and is nearly or quite hidden by the granules, so that its form is difficult to make out. These granules are not colored by Ehrlich's stain.
[p. 184] The nature of mast-cells is undetermined. They probably originate in the bone-marrow. They are least numerous of the leukocytes in normal blood, rarely exceeding 0.5 per cent., or 25 to 50 per c.mm. A notable increase is limited almost exclusively to myelogenous leukemia, where they are sometimes very numerous.
(2) Abnormal Varieties.—(a) Myelocytes (Plate VI).—These are large mononuclear cells whose cytoplasm is filled with granules. Typically, the nucleus occupies about one-half of the cell, and is round or oval. It is sometimes indented, with its convex side in contact with the periphery of the cell. It stains rather feebly. The average diameter of this cell (about 15.75 µ) is greater than that of any other leukocyte, but there is much variation in size among individual cells. Myelocytes are named according to the character of their granules—neutrophilic, eosinophilic, and basophilic myelocytes. These granules are identical with the corresponding granules in the leukocytes just described. The occurrence of two kinds of granules in the same cell is rare.
Myelocytes are the bone-marrow cells from which the corresponding granular leukocytes are developed. Their presence in the blood in considerable numbers is diagnostic of myelogenous leukemia. The neutrophilic form is the less significant. A few of these may be present in very marked leukocytosis or any severe blood condition, as pernicious anemia. Eosinophilic myelocytes are found only in myelogenous leukemia, where they are often very numerous. The basophilic variety is less common, and is confined to long-standing severe myelogenous leukemia.
(b) Atypical Forms.—Leukocytes which do not fit in [p. 185] with the above classification are not infrequently met, especially in high-grade leukocytosis, pernicious anemia, and leukemia. The nature of most of them is not clear, and their number is usually so small that they may be disregarded in making a differential count. Among them are: (a) Border-line forms between polymorphonuclear neutrophiles and neutrophilic myelocytes; (b) small neutrophilic cells with a single round, deeply staining nucleus: they probably result from division of polymorphonuclear neutrophiles; (c) "irritation forms"—large non-granular mononuclear cells, whose cytoplasm stains fairly deep purple with Wright's stain, and intense brown with Ehrlich's: they appear in the blood under the same conditions as myelocytes; (d) degenerated forms: vacuolated leukocytes, or merely palely or deeply staining homogeneous or reticulated masses of chromatin (Plate VI).
3. Blood-plaques.—These are not colored by Ehrlich's stain, nor by eosin and methylene-blue. With Wright's stain they appear as spheric or ovoid, reddish to violet, granular bodies, 2 to 4 µ in diameter. When well stained, a delicate hyaline peripheral zone can be distinguished. In ordinary blood-smears they are usually clumped in masses. A single platelet lying upon a red corpuscle may easily be mistaken for a malarial parasite (Plate VI).
Blood-platelets are being much studied at present, but, aside from the facts mentioned under their enumeration (p. 165), little of clinical value has been learned. They have been variously regarded as very young red corpuscles (the "hematoblasts" of Hayem), as disintegration products of leukocytes, as remnants of extruded nuclei of erythrocytes, and as independent nucleated bodies. The most probable explanation of their origin seems to be that of [p. 186] J. H. Wright, who, from his recent studies, regards them as detached portions of the cytoplasm of certain giant-cells of the bone-marrow and spleen.
A study of blood bacteriology is useful, but is hardly practicable for the practitioner. Most bacteria can be detected only by culture methods. The spirillum of relapsing fever can be identified by the method for the malarial parasite in fresh blood. The blood must be taken during a paroxysm. The organism is an actively motile spiral thread, about four times the diameter of a red corpuscle in length. The movements which its active motion causes among the corpuscles render it conspicuous. It can also be seen in stained preparations (Fig. 78). The disease has rarely been seen in the United States.

|
| FIG. 78.—Spirillum of relapsing fever (Karg and Schmorl). |
Of the numerous animal parasites which have been [p. 187] found in the blood, three are especially interesting clinically: Plasmodium malariæ, Filaria sanguinis hominis, and Trypanosoma hominis.
1. Plasmodium Malariæ.—This organism is one of a large group, the hemosporidia (p. 247), many of which live within and destroy the red corpuscles of various animals. Three varieties are associated with malarial fever in man—the tertian, quartan, and estivo-autumnal malarial parasites.
(1) Life Histories.—There are two cycles of development: one, the asexual, in the blood of man; and the other, the sexual, in the intestinal tract of a particular variety of mosquito.
(a) Asexual Cycle.—The young organism enters the blood through the bite of the mosquito. It makes its way into a red corpuscle, where it appears as a small, pale "hyaline" body. This body exhibits ameboid movement and increases in size. Soon, dark-brown granules derived from the hemoglobin of the corpuscle make their appearance within it. When it has reached its full size—filling and distending the corpuscle in the case of the tertian parasite, smaller in the others—the pigment-granules gather at the center or at one side; the organism divides into a number of small hyaline bodies, the spores or merozoites; and the red corpuscle bursts, setting spores and pigment free in the blood-plasma. This is called segmentation. It coincides with, and by liberation of toxins causes, the paroxysm of the disease. A considerable number of the spores are destroyed by leukocytes or other agencies; the remainder enter other corpuscles and repeat the cycle. Many of the pigment-granules are taken up by leukocytes. In estivo-autumnal fever segmentation occurs in the [p. 188] internal organs and the segmenting and larger pigmented forms are not seen in the peripheral blood.
The asexual cycle of the tertian organism occupies forty-eight hours; of the quartan, seventy-two hours; of the estivo-autumnal, an indefinite time—usually twenty-four to forty-eight hours.
The parasites are thus present in the blood in great groups, all the individuals of which reach maturity and segment at approximately the same time. This explains the regular recurrence of the paroxysms at intervals corresponding to the time occupied by the asexual cycle of the parasite. Not infrequently there is multiple infection, one group reaching maturity while the others are still young; but the presence of two groups which segment upon the same day is extremely rare. Fevers of longer intervals—six, eight, ten days—are probably due to the ability of the body, sometimes of itself, sometimes by aid of quinin, to resist the parasites so that a number sufficient to cause a paroxysm do not accumulate in the blood until after several repetitions of the asexual cycle. In estivo-autumnal fever the regular grouping, while usually present at first, is soon lost, thus causing "irregular malaria."
(b) Sexual Cycle.—Besides the ameboid individuals which pass through the asexual cycle, there are present with them in the blood many individuals with sexual properties. These are called gametes. They do not undergo segmentation. Many of them are apparently extracellular, but stained preparations usually show them to be surrounded by the remains of a corpuscle. In tertian and quartan malaria they cannot easily be distinguished from the asexual individuals until a variable time after the blood leaves the body, when the male gamete sends out [p. 189] one or more flagella. In estivo-autumnal malaria the gametes take distinctive ovoid and crescentic forms, and are not difficult to recognize. They are very resistent to quinin and often persist in the blood long after the ameboid forms have been destroyed, but are probably incapable of continuing the disease until they have passed through the cycle in the mosquito.
When a malarious person is bitten by a mosquito, the gametes are taken with the blood into its stomach. Here a flagellum from the male unites with the female, which soon thereafter becomes encysted in the wall of the intestine. After a time it ruptures, liberating many minute rods, or sporozoites, which have formed within it. These migrate to the salivary glands, and are carried into the blood of the person whom the mosquito bites. Here they enter red corpuscles as young malarial parasites, and the majority pass through the asexual cycle just described.
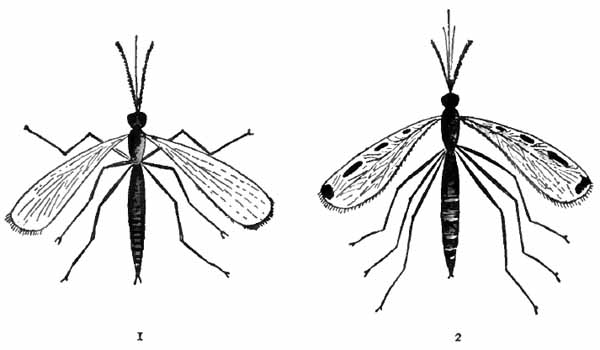
|
| FIG. 79.—Mosquitos—Culex (1) and anopheles (2) (Bergey). |
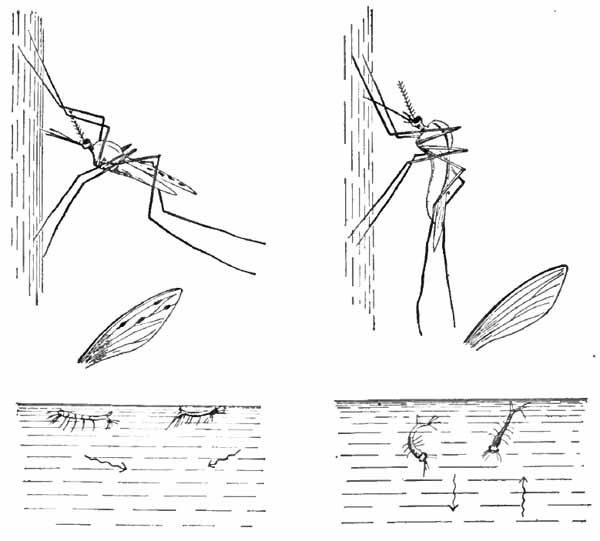
|
| FIG. 80.—Showing, on the left, anopheles in resting position, its dappled wing, and the position of its larvæ in water; on the right, culex in resting position, its plain wing, and the position of its larvæ in water. The arrows indicate the directions taken by the larvæ when the water is disturbed (Abbott). |
The sexual cycle can take place only within the body of one genus of mosquito, anopheles. Absence of this mosquito from certain districts explains the absence of [p. 190] malaria. It is distinguished from our common house-mosquito, culex, by the relative lengths of proboscis and palpi (Fig. 79), which can be seen with a hand-lens, by its attitude when resting, and by its dappled wing (Fig. 80). Anopheles is strictly nocturnal in its habits; it usually flies low, and rarely travels more than a few hundred yards from its breeding-place, although it may be carried by winds. These facts explain certain peculiarities in malarial infection; thus, infection occurs practically only at night; it is most common near stagnant water, especially upon the side toward which the prevailing winds blow; and the [p. 191] danger is greater when persons sleep upon or near the ground than in upper stories of buildings. The insects frequently hibernate in warmed houses, and may bite during the winter. A mosquito becomes dangerous in eight to fourteen days after it bites a malarious person, and remains so throughout its life.
(2) Detection.—Search for the malarial parasite may be made in either fresh blood or stained films. If possible, the blood should be obtained a few hours before the chill—never during it nor within a few hours afterward, since at that time (in single infections) only the very young, unpigmented forms are present, and these are the most difficult to find and recognize. Sometimes many parasites are found in a microscopic field; sometimes, especially in estivo-autumnal infection, owing to accumulation in internal organs, careful search is required to find any, despite very severe symptoms. Quinin causes them rapidly to disappear from the peripheral blood, and few or none may be found after its administration. In the absence of organisms, the presence of pigment granules within leukocytes—polymorphonuclears and large mononuclears—may be taken as presumptive evidence of malaria. Pigmented leukocytes (Plate VI) are most numerous after a paroxysm.
(a) In Fresh Unstained Blood (Plate VII).—Obtain a small drop of blood from the finger or lobe of the ear. Touch the center of a cover-glass to the top of the drop and quickly place it, blood side down, upon a slide. If the slide and cover be perfectly clean and the drop not too large, the blood will spread out so as to present only one layer of corpuscles. Search with a one-twelfth-inch objective, using very subdued light.
[p. 192] The young organisms appear as small, round, ring-like or irregular, colorless bodies within red corpuscles. The light spots caused by crenation and other changes in the corpuscles are frequently mistaken for them, but are generally more refractive or have more sharply defined edges. The older forms are larger colorless bodies containing granules of brown pigment. In the case of the tertian parasite, these granules have active vibratory motion, which renders them conspicuous; and as the parasite itself is very pale, one may see only a large pale corpuscle in which fine pigment-granules are dancing. Segmenting organisms, when typical, appear as rosets, often compared to daisies, the petals of which represent the segments, while the central brown portion represents the pigment. Tertian segmenting forms are less frequently typical than quartan. Flagellated forms are not seen until ten to twenty minutes after the blood has left the vessels. As Cabot suggests, one should, while searching, keep a sharp lookout for unusually large or pale corpuscles, and for anything which is brown or black, or in motion.
| PLATE VII |
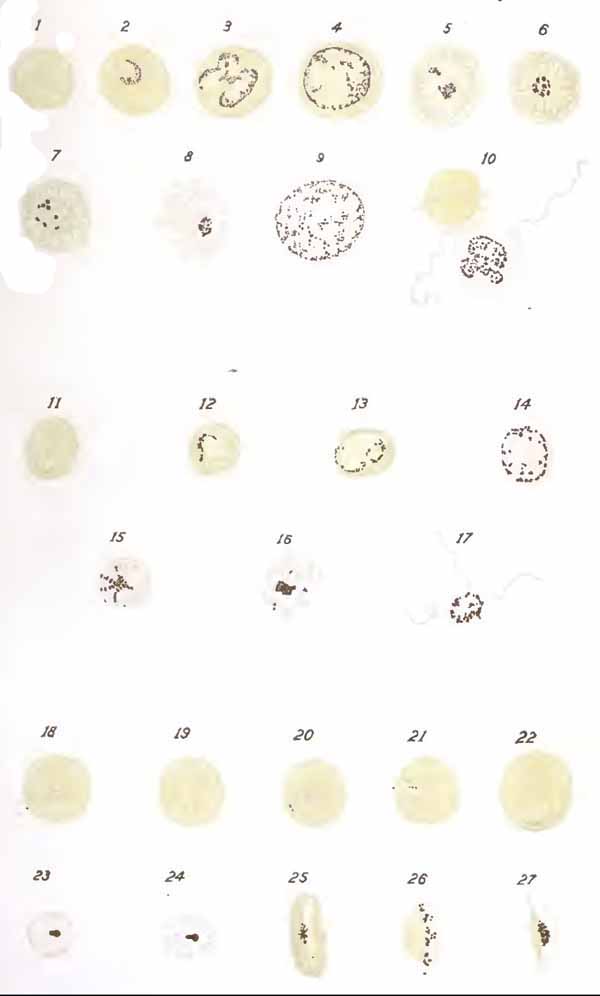
|
| EXPLANATION OF PLATE VII |
|
Various forms of
malarial parasites (Thayer and Hewetson). 1 to 10, inclusive, Tertian organisms; 11 to 17, inclusive, quartan organisms; 18 to 27, inclusive, estivo-autumnal organisms; 1, young hyaline form; 2, hyaline form with beginning pigmentation; 3, pigmented form; 4, full-grown pigmented form; 5, 6, 7, 8, segmenting forms; 9, extracellular pigmented form; 10, flagellate form; 11, young hyaline form; 12, 13, pigmented forms; 14, fully developed pigmented form; 15, 16, segmenting forms; 17, flagellate form; 18, 19, 20, ring-like and cross-like hyaline forms; 21, 22, pigmented forms; 23, 24, segmenting forms; 25, 26, 27, crescents. |
(b) In Stained Films (Plate VI).—Recognition of the parasite, especially the young forms, is much easier in films stained by Wright's or some similar stain than in fresh blood. When very scarce, they may sometimes be found, although their structure is not well shown, by the method of Ruge. This consists in spreading a very thick layer of blood, drying, placing for a few minutes in a fluid containing 5 per cent. formalin and 1 per cent. acetic acid, which removes the hemoglobin and fixes the smear, rinsing, drying, and finally staining. If Wright's stain be used in this method, it is recommended that the [p. 193] preparation be subsequently stained for a half-minute with borax-methylene-blue (borax, 5; methylene-blue, 2; water, 100).
In films which are properly stained with Wright's fluid the young organisms are small, round, ring-like or irregular, sky-blue bodies, each with a very small, sharply defined, reddish-purple chromatin mass. Many structures—deposits of stain, dirt, blood-plaques lying upon red cells, etc.—may simulate them, but should not deceive one who looks carefully for both the blue cytoplasm and the reddish-purple chromatin. A plaque upon a red corpuscle is surrounded by a colorless zone rather than by a distinct blue body. Young estivo-autumnal parasites commonly take a "ring" form (the chromatin mass representing the jewel), which is infrequently assumed by the other varieties. The older tertian and quartan organisms show larger sky-blue bodies with more reticular chromatin, and contain brown granules of pigment, which, however, is less evident than in the living parasite. The chromatin is often scattered through the cytoplasm or apparently outside of it, and is sometimes difficult to see clearly. Typical "segmenters" present a ring of rounded segments or spores, each with a small, dot-like chromatin mass. With the tertian parasite, the segments more frequently form an irregular cluster. The pigment is collected near the center or scattered among the segments. In estivo-autumnal fever usually only the small "ring bodies" and the crescentic and ovoid gametes are seen in the blood. The gametes are easily recognized. Their length is somewhat greater than the diameter of a red corpuscle. Their chromatin is usually centrally placed, and they contain more or less coarse pigment. The remains of the [p. 194] red cell often form a narrow rim around them or fill the concavity of the crescent.
While the parasites are more easily found in stained preparations, the varieties are more easily differentiated in fresh blood. The chief distinguishing points are included in the following table:
| VARIETIES OF THE MALARIAL ORGANISM | ||
| TERTIAN. | QUARTAN. | ESTIVO-AUTUMNAL. |
| Asexual cycle, forty-eight hours. | Seventy-two hours. | Usually twenty-four to forty-eight hours. |
| Substance pale, transparent, comparable to hyaline tube-cast. | Highly refractive, comparable to waxy tube-cast. | Highly refractive. |
| Outline indistinct. | Distinct. | Distinct. |
| Ameboid motion active. | Sluggish. | Active. |
| Mature asexual form large; fills and often distends corpuscle. | Smaller. | Young forms, only, in peripheral blood. |
| Pigment-granules fine, brown, scattered throughout. Very active dancing motion. | Much coarser, darker in color, peripherally arranged. Motion slight. | Very few, minute, inactive. Distinctly pigmented forms seldom seen. |
| Segmenting body rarely assumes typical "daisy" form. 15 to 20 segments. | Usually typical "daisy." 6 to 12 segments. | Not seen in peripheral blood. |
| Gametes resemble asexual forms. | Same as tertian. | Appear in blood as distinctive ovoids and crescents. |
| Red corpuscles pale and swollen. | Generally darker than normal. | Dark, often bronzed. |
2. Filaria Sanguinis Hominis.—Of the several varieties of this worm, Filaria nocturna is most common and [p. 195] most important clinically. The adults are thread-like worms about 8 to 10 cm. long. They are rarely seen. They live in pairs in the lymphatic channels and glands, especially those of the pelvis and groin, and often occur in such numbers as to obstruct the flow of lymph. This is the most common cause of elephantiasis. Infection is very common in tropical countries, especially in Samoa, the West Indies, Central America, and the Isthmus of Panama. It is said that in Samoa 50 per cent. of the natives are infected.
The female is viviparous, and produces vast numbers of embryos, which appear in the circulating blood. These embryos are very actively motile, worm-like structures, about as wide as a red corpuscle and 0.2 to 0.4 mm. long (Fig. 107). They are found in the peripheral blood only at night, appearing about 8 P.M. and reaching their maximum number—which is sometimes enormous—about midnight. If the patient change his time of sleeping, they will appear during the day. Infection is carried by a variety of mosquito, which acts as intermediate host.
Diagnosis rests upon detection of embryos in the blood. They can be seen in stained preparations, but are best found in fresh unstained blood. A rather large drop is taken upon a slide, covered, and examined with a low power. The embryo can be located by the commotion which its active motion produces among the corpuscles. This motion consists almost wholly in apparently purposeless lashing and coiling movements, and continues for many hours.
3. Trypanosoma Hominis.—Various trypanosomes are common in the blood of fishes, amphibians, birds, and [p. 196] mammals (Fig. 81). They live in the blood-plasma and do not attack the corpuscles. In some animals they are apparently harmless; in others they are an important cause of disease.
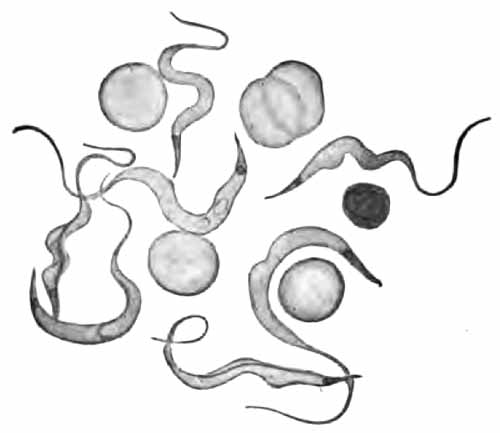
|
| FIG. 81.—Trypanosomes from blood of gray rat (Boston). |
Trypanosoma hominis is an actively motile, spindle-shaped organism, two or three times the diameter of a red corpuscle in length, with one end terminating in a long flagellum. It can be seen with medium power objectives in either fresh or stained blood. Human trypanosomiasis is common in Africa. As a rule, it is a very chronic disease. "Sleeping sickness" is a late stage when the organisms have invaded the cerebrospinal fluid. Infection is carried by a biting fly, Glossina palpalis.
1. Agglutination.—In the blood-serum of persons suffering from certain infectious diseases there exist soluble bodies, called agglutinins, which have the property of [p. 197] rendering non-motile and clumping the specific micro-organism of the disease, and have little or no influence upon other bacteria. This "agglutination" takes place even when the blood is greatly diluted. Undiluted normal blood can agglutinate most bacteria, but loses this power when diluted to any considerable degree. These facts are taken advantage of in the diagnosis of several diseases.
When applied to the diagnosis of typhoid fever, the phenomenon is known as the Widal reaction. As yet, it is the only agglutination reaction which has any practical value for the practitioner.
Either blood-serum or the whole blood may be used. Serum is the better. To obtain it, it is convenient to use little vials, such as can be made by breaking off the lower half-inch of the tubes which have contained peptonizing powder. They must, of course, be well cleaned. One of these is filled to a depth of about one-fourth inch from a puncture in the finger, and is set aside for a few hours. When the clot has separated, it is picked out with a needle, leaving the serum. One drop of the serum is then added to nine drops of normal salt solution, making a dilution of 1:10. Distilled water may be used for dilution, but is more liable to cause error. The dilution can be more accurately made in the leukocyte pipet of the Thoma-Zeiss instrument. When the whole blood is used, it can be secured in the pipet and at once diluted with the salt solution. When it must be transported a considerable distance, dried blood is most convenient. A large drop is allowed to dry upon a clean slide or unglazed paper. It will keep for months without losing its agglutinating power. When ready to make the test, the dried stain is dissolved in ten drops of normal salt solution, care being [p. 198] taken that the drops are about the same size as the original drop of blood.
The reaction can be detected either microscopically or macroscopically:
Microscopic Method.—(1) The blood or serum having been obtained and diluted 1:10 as just described, mix it with a bouillon culture of the typhoid bacillus to any desired dilution. One drop of each makes a blood-dilution of 1:20, etc. The culture should be between eighteen and twenty-four hours old, and the bacilli must be actively motile. A stock agar culture should be kept at room temperature, and bouillon tubes inoculated the day before the examination is to be made. Agar cultures can be purchased from dealers in biologic products. They must be renewed monthly.
Instead of the bouillon culture, McFarland recommends the use of a suspension made by removing some of the growth from the surface of a fresh agar culture and mixing it well with a little sterile water. It is then necessary to examine the suspension microscopically to make sure that there are no natural clumps.
(2) Place a few drops of the mixture of blood and culture upon a perfectly clean slide and apply a cover-glass. The cover may be ringed with vaselin to prevent evaporation, but this is not usually necessary.
(3) Examine at intervals with a high dry lens—a one-sixth will answer very well. The light must be very subdued. At first the bacilli should be actively moving about. If the blood be from a case of typhoid, they will gradually lose their motion and gather together in clumps (Fig. 82). The clumps should be large, and the few bacilli remaining isolated should be motionless. Pseudo-reactions, in which there are a few small clumps of bacilli whose motion is not entirely lost, together with many freely moving bacilli scattered throughout the field, should not mislead. As a control, a drop [p. 199] of the culture should always be examined before making the test.

|
| FIG. 82.—Showing clumping of typhoid bacilli in the Widal reaction. At one point a crenated red blood-corpuscle is seen (Wright and Brown). |
Normal blood may produce clumping if time enough be allowed. The diagnostic value of a positive reaction is, therefore, impaired unless clumping takes place within a limited time. With dilution of 1:20 the time limit should not exceed one-half hour; with 1:40, one hour. Tests based upon lower dilution than 1:20 are probably not reliable.
Macroscopic Method.—The principle is the same as that of the microscopic method. Clumping of the bacilli causes a flocculent precipitate, which can be seen with the naked eye. A dead culture gives the same results as a living one. This method is as reliable as the microscopic and is more convenient for the practitioner, although it requires more time.
Dead cultures, together with apparatus for diluting the blood, are put up at slight cost by various firms under the names of typhoid diagnosticum, typhoid agglutometer, etc. Full directions accompany these outfits.
[p. 200] The Widal reaction is positive in over 95 per cent. of all cases of typhoid fever. It may, rarely, be positive in other conditions, owing, sometimes at least, to faulty technic. It appears often as early as the sixth or seventh day; usually during the second week. It remains during the whole course of the disease, and frequently persists for years.
2. Opsonins.—That phagocytosis plays an important part in the body's resistance to bacterial invasion has long been recognized. According to Metchnikoff, this property of leukocytes resides entirely within themselves, depending upon their own vital activity. The recent studies of Wright and Douglas, upon the contrary, indicate that the leukocytes are impotent in themselves, and can ingest bacteria only in the presence of certain substances which exist in the blood-plasma. These substances have been named opsonins. Their nature is undetermined. They probably act by uniting with the bacteria, thus preparing them for ingestion by the leukocytes; but they do not cause death of the bacteria, nor produce any appreciable morphologic change. They appear to be more or less specific, a separate opsonin being necessary for phagocytosis of each species of bacteria. There are, moreover, opsonins for other formed elements—red blood-corpuscles, for example. It has been shown that the quantity of opsonins in the blood can be greatly increased by inoculation with dead bacteria.
To measure the amount of any particular opsonin in the blood Wright has devised a method which involves many ingenious and delicate technical procedures. Much skill, such as is attained only after considerable training in laboratory technic, is requisite, and there are many sources [p. 201] of error. It is, therefore, beyond the province of this work to recount the method in detail. In a general way it consists in: (a) Preparing a mixture of equal parts of the patient's blood-serum, an emulsion of the specific micro-organism, and a suspension of washed leukocytes; (b) preparing a similar mixture, using serum of a normal person; (c) incubating both mixtures for a definite length of time; and (d) making smears from each, staining, and examining with a one-twelfth objective. The number of bacteria which have been taken up by a definite number of leukocytes is counted, and the average number of bacteria per leukocyte is calculated; this gives the "phagocytic index." The phagocytic index of the blood under investigation, divided by that of the normal blood, gives the opsonic index of the former, the opsonic index of the normal blood being taken as 1. Simon regards the percentage of leukocytes which have ingested bacteria as a more accurate measurement of the amount of opsonins than the number of bacteria ingested, because the bacteria are apt to adhere and be taken in in clumps.
Wright and his followers regard the opsonic index as an index of the power of the body to combat bacterial invasion. They claim very great practical importance for it as an aid to diagnosis and as a guide to treatment by the vaccine method. This method of treatment consists in increasing the amount of protective substances in the blood by injections of normal-salt suspensions of dead bacteria of the same species as that which has caused and is maintaining the morbid process, these bacterial suspensions being called "vaccines." The opinion of the majority of conservative men seems to be that while vaccine therapy is undoubtedly an important addition to our [p. 202] methods of treatment of bacterial infections, particularly of those which are strictly local, yet the value of the opsonic index in measuring resisting power or as an aid to diagnosis and guide to treatment is still sub judice.
1. Guaiac Test.—The technic of this test has been given (p. 89). It may be applied directly to a suspected fluid, or, better, to the ethereal extract. Add a few cubic centimeters of glacial acetic acid to about 10 c.c. of the fluid; shake thoroughly with an equal volume of ether; decant, and apply the test to the ether. In case of dried stains upon cloth, wood, etc., dissolve the stain in distilled water and test the water, or press a piece of moist blotting-paper against the stain, and touch the paper with drops of the guaiac and the turpentine successively.

|
| FIG. 83.—Teichmann's hemin crystals (Jakob). |
2. Teichmann's Test.—This depends upon the production of characteristic crystals of hemin. It is a sensitive test, and, when positive, is absolute proof of the presence of blood. A number of substances—lime, fine [p. 203] sand, iron rust—interfere with production of the crystals; hence negative results are not always conclusive. Dissolve the suspected stain in a few drops of normal salt solution upon a slide. If a liquid is to be tested, evaporate some of it upon a slide and dissolve the residue in a few drops of the salt solution. Let dry, apply a cover-glass, and run glacial acetic acid underneath it. Heat very gently until bubbles begin to form, replacing the acid as it evaporates. Allow to cool slowly. When cool, replace the acid with water, and examine for hemin crystals with two-thirds and one-sixth objectives. The crystals are dark-brown rhombic plates lying singly or in crosses, and are easily recognized (Fig. 83). Failure to obtain them may be due to too great heat or too rapid cooling. If not obtained at first, let the slide stand in a warm place, as upon a hot-water radiator, for an hour.
The more conspicuous characteristics of the blood in various diseases have been mentioned in previous sections. Although the great majority of blood changes are secondary, there are a few blood conditions in which the changes are so prominent, or the etiology so obscure, that they are commonly regarded as blood diseases. These will receive brief consideration here.
This is a deficiency of hemoglobin, or red corpuscles, or both. It is either primary or secondary. The distinction is based chiefly upon etiology, although each type presents a more or less distinctive blood-picture. Secondary anemia is that which is symptomatic of some other [p. 204] pathologic condition. Primary anemia is that which progresses without apparent cause.
1. Secondary Anemia.—The more important conditions which produce secondary or symptomatic anemia are:
(a) Poor nutrition, which usually accompanies unsanitary conditions, poor and insufficient food, etc.
(b) Acute infectious diseases, especially rheumatism and typhoid fever. The anemia is more conspicuous during convalescence.
(c) Chronic infectious diseases: tuberculosis, malaria, syphilis, leprosy.
(d) Chronic exhausting diseases, as heart disease, chronic nephritis, cirrhosis of the liver, and gastro-intestinal diseases, especially when associated with atrophy of gastric and duodenal glands. The last may give an extreme anemia, indistinguishable from pernicious anemia.
(e) Chronic poisoning, as from lead, arsenic, and phosphorus.
(f) Hemorrhage—either repeated small hemorrhages, as from gastric cancer and ulcer, uterine fibroids, etc., or a single large one.
(g) Malignant tumors: these affect the blood partly through repeated small hemorrhages, partly through toxic products, and partly through interference with nutrition.
(h) Animal Parasites.—Some cause no appreciable change in the blood; others, like the Uncinaria and Bothriocephalus latus, may produce a very severe anemia, almost identical with pernicious anemia. Anemia in these cases is probably due both to toxins and to abstraction of blood.
The blood-picture varies with the grade of anemia. [p. 205] Diminution of hemoglobin is the most characteristic feature. In mild cases it is slight, and is the only blood change to be noted. In very severe cases hemoglobin may fall to 15 per cent. Red corpuscles are diminished in all but very mild cases, while in the severest cases the red corpuscle count is sometimes below 2,000,000. The color index is usually decreased.
Although the number of leukocytes bears no relation to the anemia, leukocytosis is common, being due to the same cause.
Stained films show no changes in very mild cases. In moderate cases variations in size and shape of the red cells and polychromatophilia occur. Very severe cases show the same changes to greater degree, with addition of basophilic degeneration and the presence of normoblasts in small or moderate numbers. Megaloblasts in very small numbers have been encountered in extremely severe cases. Blood-plaques are usually increased.
2. Primary Anemia.—The commonly described varieties of primary anemia are pernicious anemia and chlorosis, but splenic anemia may also be mentioned under this head.
(1) Progressive Pernicious Anemia.—It is frequently impossible to diagnose this disease from the blood examination alone. Severe secondary anemia sometimes gives an identical picture. Remissions, in which the blood approaches the normal, are common. All the clinical data must, therefore, be considered.
Hemoglobin and red corpuscles are always greatly diminished. In none of Cabot's 139 cases did the count exceed 2,500,000, the average being about 1,200,000. In more than two-thirds of the cases hemoglobin was [p. 206] reduced to less extent than the red corpuscles: the color-index was, therefore, high. A low color-index probably indicates a mild type of the disease.
The leukocyte count may be normal, but is commonly diminished to about 3000. The decrease affects chiefly the polymorphonuclear cells, so that the lymphocytes are relatively increased. In some cases a decided absolute increase of lymphocytes occurs. Polymorphonuclear leukocytosis, when present, is due to some complication.
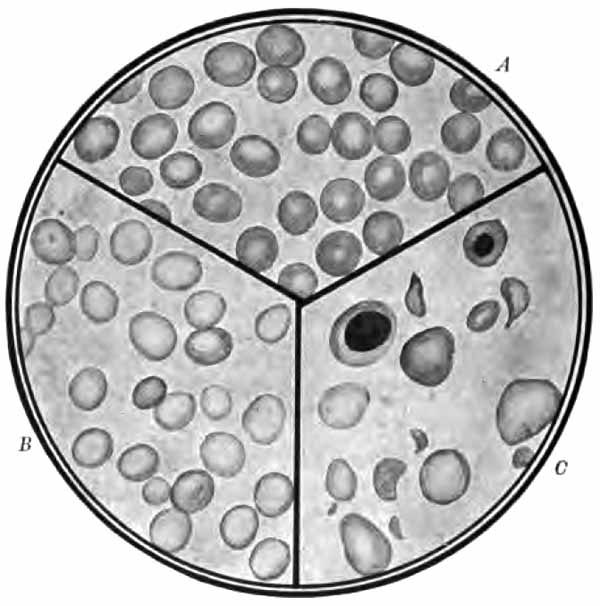
|
| FIG. 84.—A, Normal blood; B, chlorosis; C, pernicious anemia. The plate shows the sharp contrast between cells rich in hemoglobin and the pale cell of chlorosis, and also the poikilocytosis and marked variations in size noted in pernicious anemia. A normoblast and megaloblast also appear. Stained smears (from Greene's "Medical Diagnosis"). |
| PLATE VIII |
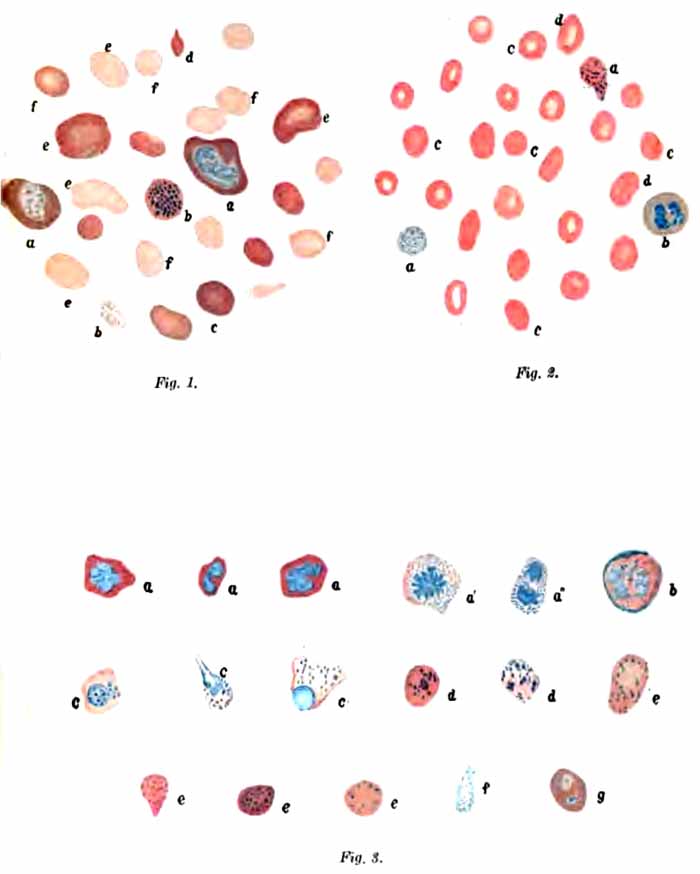
|
| EXPLANATION OF PLATE VIII. |
|
Fig. 1.—Preparation from an advanced case of progressive pernicious
anemia from unknown cause: a, Megaloblasts or gigantoblasts; the
protoplasm shows marked polychromasia; b, stained granules in
erythrocytes with normally stained protoplasm; c and d,
polychromatophilic degeneration; e, megalocytes; f, normocytes. Fig. 2.—Preparation from the same case taken some time later while the patient was subjectively and objectively in perfect health: a, Punctate erythrocytes with normal and anemic degenerated protoplasm; b, polynuclear leukocyte; c, normal red blood-corpuscles; d, somewhat enlarged erythrocytes. Fig. 3.—Series of cells from a case of severe progressive pernicious anemia of unknown etiology; preparation made two days antemortem: a, Nucleated red blood-corpuscles characterized as normoblasts by the intense staining of the nuclei; a' and a", karyokinetic figures in erythrocytes; the protoplasm finely punctate; b, beginning karyolysis in a megaloblast; c, erythroblasts with coarse granulation of the protoplasm; d, nuclear remains (?) and fine granulation of the protoplasm; e and f, finely punctate red blood-corpuscles; g, megalocyte with two blue nuclei; nuclear remains (?) in the polychrome protoplasm. |
| (Nothnagel-Lazarus.) |
The red corpuscles show marked variation in size and shape (Plate VIII and Fig. 84). There is a decided [p. 207] tendency to large oval forms, and despite the abundance of microcytes, the average size of the corpuscles is generally strikingly increased. Polychromatophilia and basophilic degeneration are common. Nucleated red cells are always present, although in many instances careful search is required to find them. In the great majority of cases megaloblasts exceed normoblasts in number. This ratio constitutes one of the most important points in diagnosis, since it is practically unknown in other diseases. Blood-plaques are diminished.
The rare and rapidly fatal anemia which has been described under the name of aplastic anemia is probably a variety of pernicious anemia. Absence of any attempt at blood regeneration explains the marked difference in the blood picture. Red corpuscles and hemoglobin are rapidly diminished to an extreme degree. The color index is normal or low. The leukocyte count is normal or low, with relative increase of lymphocytes. Stained smears show only slight variations in size, shape, and staining properties of the red cells. There are no megaloblasts, and few or no normoblasts.
(2) Chlorosis.—The clinical symptoms furnish the most important data for diagnosis. The blood resembles that of secondary anemia in many respects.
The most conspicuous feature is a decided decrease of hemoglobin (down to 30 or 40 per cent. in marked cases), accompanied by a slight decrease in number of red corpuscles. The color-index is thus almost invariably low, the average being about 0.5.
As in pernicious anemia, the leukocytes are normal or decreased in number, with a relative increase of lymphocytes.
[p. 208] In contrast to pernicious anemia (and in some degree also to secondary anemia) the red cells are of nearly uniform size, are uniformly pale (Fig. 84), and their average diameter is somewhat less than normal. Changes in size, shape, and staining reactions occur only in severe cases. Erythroblasts are rarely present. The number of plaques is generally decreased.
(3) Splenic Anemia.—This is an obscure form of anemia associated with great enlargement of the spleen. It is probably a distinct entity. There is decided decrease of hemoglobin and red corpuscles, with moderate leukopenia and relative lymphocytosis. Osler's fifteen cases averaged 47 per cent. hemoglobin and 3,336,357 red cells. Stained films show notable irregularities in size, shape, and staining properties only in advanced cases. Erythroblasts are uncommon.
Except in rare instances, diagnosis is easily made from the blood alone. Two types of the disease are commonly distinguished: the myelogenous and the lymphatic. Atypical and intermediate forms are not uncommon. Pseudoleukemia, because of its clinical similarity to lymphatic leukemia, is generally described along with leukemia.
1. Myelogenous Leukemia.—This is usually a chronic disease, although acute cases have been described.
Hemoglobin and red corpuscles show decided decrease. The color-index is moderately low.
Most striking is the immense increase in number of leukocytes. The count in ordinary cases varies between 100,000 and 300,000. Counts over 1,000,000 have been [p. 209] met. During remissions, the leukocyte count may fall to normal.
While these enormous leukocyte counts are equaled in no other disease, and approached only in lymphatic leukemia and extremely high-grade leukocytosis, the diagnosis, particularly during remissions, depends more upon qualitative than quantitative changes. Although all varieties are increased, the characteristic and conspicuous cell is the myelocyte. This cell never appears in normal blood; extremely rarely in leukocytosis; and never abundantly in lymphatic leukemia. In myelogenous leukemia myelocytes usually constitute more than 20 per cent. of all leukocytes. Da Costa's lowest case gave 7 per cent. The neutrophilic form is generally much more abundant than the eosinophilic. Both show considerable variations in size. Very constant also is a marked absolute, and often a relative, increase of eosinophiles and basophiles. Polymorphonuclear neutrophiles and lymphocytes are relatively decreased.
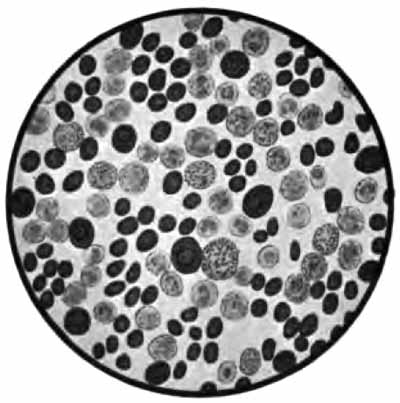
|
| FIG. 85.—Blood from a case of splenomedullary leukemia, stained with Ehrlich's triple stain (Jakob). |
[p. 210] The red cells show the changes characteristic of a severe secondary anemia, except that nucleated reds are commonly abundant; in fact, no other disease gives so many. They are chiefly of the normoblastic type. Megaloblasts are uncommon. Blood-plaques are generally increased.
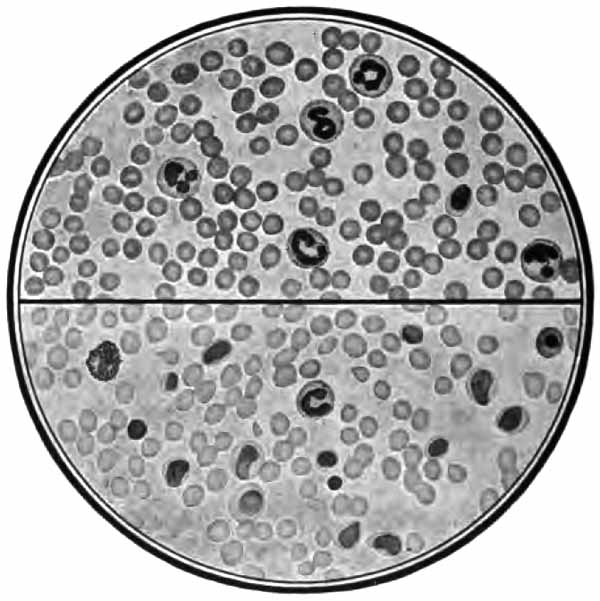
|
| FIG. 86.—Blood: Lymphatic leukemia (lower section); marked leukocytosis (upper section). Stained smears. Compare types of leukocytes with Fig. 85 (from Greene's "Medical Diagnosis"). |
2. Lymphatic Leukemia.—This form may be either acute or chronic. There is marked loss of hemoglobin and red corpuscles. The color-index is usually moderately low.
The leukocyte count is high, but lower than in the myelogenous type. Counts of 100,000 are about the average, but in many cases are much lower. This high [p. 211] count is referable almost wholly to increase of lymphocytes. They generally exceed 90 per cent. of the total number. In chronic cases they are chiefly of the small variety; in acute cases, of the large form. Myelocytes are rare.
The red corpuscles show the changes usual in severe secondary anemia. Erythroblasts are seldom abundant. Blood-plaques are decreased.
3. Pseudoleukemia (Hodgkin's disease) resembles lymphatic leukemia in that there is marked and progressive enlargement of the lymph-nodes. There is, however, no distinctive blood-picture. The changes in hemoglobin and red cells resemble those of a moderate symptomatic anemia, with rather low color-index. The leukocytes are commonly normal in number and relative proportions.
4. Anæmia Infantum Pseudoleukæmica.—Under this name von Jaksch described a rare disease of infancy, the proper classification of which is uncertain. There is enlargement of liver and spleen, and sometimes of lymph-nodes, together with the following blood-changes: grave anemia with deformed and degenerated red cells and many erythroblasts of both normoblastic and megaloblastic types; great increase in number of leukocytes (20,000 to 100,000), and great variations in size, shape, and staining of leukocytes, with many atypical forms and a few myelocytes.
The table on the following page contrasts the distinctive blood-changes in the more common conditions.
[p. 212]| DIFFERENTIAL DIAGNOSIS OF BLOOD DISEASES | |||||
| SECONDARY ANEMIA. | PERNICIOUS ANEMIA. | CHLOROSIS. | MYELOGENOUS LEUKEMIA. | LYMPHATIC LEUKEMIA. | |
| Hemoglobin. | Diminished according to degree of anemia. | Diminished. | Greatly diminished. | Decidedly diminished. | Markedly diminished. |
| Red Corpuscle Count. | Normal in mild cases; diminished in all others. | Greatly diminished. | Slightly diminished. | Decidedly diminished. | Markedly diminished. |
| Color-index. | Normal or slightly diminished. | High. | Low. | Usually slightly diminished. | Usually slightly diminished. |
| Leukocyte Count. | Not necessarily affected; leukocytosis common. | Normal or diminished. | Normal or diminished. | Extremely high. | Very high. |
| Red Corpuscles on Stained Films. | Variations in size and shape in moderate cases; variations in staining reactions and normoblasts in severe cases. | Marked variations in size, shape, and staining reactions. Average size increased. Tendency to large oval forms. Erythroblasts always present; megaloblasts exceed normoblasts. | Nearly uniform size and shape; average size decreased; pale centers. Erythroblasts very rare. | Similar to secondary anemia, except normoblasts generally very numerous. | Similar to secondary anemia. Erythroblasts not numerous. |
| Leukocytes on Stained Films. | Normal proportions or increase of polynuclears. | Lymphocytes relatively, sometimes absolutely, increased. | Lymphocytes apt to be relatively increased. | Large numbers of myelocytes (average, 20 per cent.). Absolute increase of eosinophiles and basophiles. Relative decrease of polynuclears and lymphocytes. | Lymphocytes exceed 90 per cent. Other varieties relatively decreased. |
Laboratory methods may be applied to the diagnosis of stomach disorders in: I. Examination of the gastric contents removed with the stomach-tube. II. Certain other examinations which give information as to the condition of the stomach.
Stomach digestion consists mainly in the action of pepsin upon proteids in the presence of hydrochloric acid and in the curdling of milk by rennin.
Pepsin and rennin are secreted by the gastric glands as zymogens—pepsinogen and renninogen, respectively—which are converted into pepsin and rennin by hydrochloric acid. Hydrochloric acid is secreted by certain cells of the fundus glands. It at once combines loosely with the proteids of the food, forming acid-albumin, the first step in proteid digestion. Hydrochloric acid, which is thus loosely combined with proteids, is called "combined" hydrochloric acid. The acid which is secreted after the proteids present have all been converted into acid-albumin remains as "free" hydrochloric acid, and, together with pepsin, continues the process of digestion.
At the height of digestion the stomach-contents consist essentially of: (1) Water; (2) free hydrochloric acid; (3) combined hydrochloric acid; (4) pepsin; (5) rennin; [p. 214] (6) mineral salts, chiefly acid phosphates, of no clinical importance; (7) particles of undigested and partly digested food; (8) various products of digestion in solution. In pathologic conditions there may be present, in addition, various microscopic structures and certain organic acids, of which lactic acid is most important.
A routine examination is conveniently carried out in the following order:
(1) Give the patient a test-meal upon an empty stomach, washing the stomach previously if necessary.
(2) At the height of digestion, usually in one hour, remove the contents of the stomach with a stomach-tube.
(3) Measure and examine macroscopically.
(4) Filter. A suction filter is desirable, and may be necessary when much mucus is present.
(5) During filtration, examine microscopically and make qualitative tests for—(a) free acids; (b) free hydrochloric acid; (c) lactic acid.
(6) When sufficient filtrate is obtained, make quantitative estimations of—(a) total acidity; (b) free hydrochloric acid; (c) combined hydrochloric acid (if necessary).
(7) Make whatever additional tests seem desirable, as for blood, pepsin, or rennin.
Gastric juice is secreted continuously, but quantities sufficiently large for examination are not usually obtainable from the fasting stomach. In clinical work, therefore, it is desirable to stimulate secretion with food—which is the natural and most efficient stimulus—before attempting to collect the gastric fluid. Different foods stimulate secretion to different degrees; hence for the sake of uniform results certain standard "test-meals" have been [p. 215] adopted. Those mentioned here give practically the same results.
1. Test-meals.—It is customary to give the test-meal in the morning, since the stomach is most apt to be empty at that time. If it be suspected that the stomach will not be empty, it should be washed out with water the evening before.
(1) Ewald's test-breakfast consists of a roll (or two slices of bread) without butter and two small cups (300 to 400 c.c.) of water or weak tea without cream or sugar. It should be well masticated. The contents of the stomach are to be removed one hour afterward. This test-meal is used for most routine examinations. Its disadvantage is that it introduces, with the bread, a variable amount of lactic acid and numerous yeast-cells. This source of error may be eliminated by substituting a shredded whole-wheat biscuit for the roll.
(2) Boas' test-breakfast consists of a tablespoonful of rolled oats in a quart of water, boiled to one pint, with a pinch of salt added. It should be withdrawn in forty-five minutes to one hour. This meal does not contain lactic acid, and is usually given when detection of lactic acid is important, as in suspected gastric cancer. The stomach should always be washed with water the evening previous.
2. Withdrawal of the Contents.—The Boas stomach-tube, with bulb, is probably the most satisfactory form. It should be of rather large caliber, and have an opening in the tip and one or two in the side near the tip. When not in use, it should be kept in a vessel of borax solution, and should be well washed in hot water both before and after using.
It is important confidently to assure the patient that introduction of the tube cannot possibly harm him; and [p. 216] that, if he can control the spasm of his throat, he will experience very little choking sensation. When patients are very nervous, it is well to spray the throat with cocain solution.
The tube should be dipped in warm water just before using: the use of glycerin or other lubricant is undesirable. With the patient seated upon a chair, his clothing protected by towels or a large apron, and his head tilted forward, the tip of the tube, held as one would a pen, is introduced far back into the pharynx. He is then urged to swallow, and the tube is pushed boldly into the esophagus until the ring upon it reaches the incisor teeth, thus indicating that the tip is in the stomach. If, now, the patient cough or strain as if at stool, the contents of the stomach will usually be forced out through the tube. Should it fail, the fluid can generally be pumped out by alternate compression of the tube and the bulb. If unsuccessful at first, the attempts should be repeated with the tube pushed a little further in, or withdrawn a few inches, since the distance to the stomach is not the same in all cases. The tube may become clogged with pieces of food, in which case it must be withdrawn, cleaned, and reintroduced. If, after all efforts, no fluid is obtained, another test-meal should be given and withdrawn in forty-five minutes.
As the tube is removed, it should be pinched between the fingers so as to save any fluid that may be in it.
The stomach-tube must be used with great care, or not at all, in cases of gastric ulcer, aneurysm, uncompensated heart disease, and marked arteriosclerosis. Except in gastric ulcer, the danger lies in the retching produced, and the tube can safely be used if the patient takes it easily.
[p. 217]Under normal conditions, 30 to 50 c.c. of fluid can be obtained one hour after administering Ewald's breakfast. More than 60 c.c. points to motor insufficiency; less than 20 c.c., to too rapid emptying of the stomach, or else to incomplete removal. Upon standing, it separates into two layers, the lower consisting of particles of food, the upper of an almost clear, faintly yellow fluid. The extent to which digestion has taken place can be roughly judged from the appearance of the food-particles.
The reaction is frankly acid in health and in nearly all pathologic conditions. It may be neutral or slightly alkaline in some cases of gastric cancer and marked chronic gastritis, or when contaminated by a considerable amount of saliva.
A small amount of mucus is present normally. Large amounts, when the gastric contents are obtained with the tube and not vomited, point to chronic gastritis. Mucus is recognized from its characteristic slimy appearance when the fluid is poured from one vessel into another.
A trace of bile may be present as a result of excessive straining while the tube is in the stomach. Larger amounts are very rarely found, and generally point to obstruction in the duodenum. Bile produces a yellowish or greenish discoloration of the fluid.
Blood is often recognized by simple inspection, but more frequently requires a chemic test. It is bright red when very fresh, and dark, resembling coffee-grounds, when older.
Particles of food eaten hours, or even days, previously, may be found, and indicate deficient motor power.
[p. 218] Search should always be made for bits of tissue from the gastric mucous membrane or newgrowths. These, when examined by a pathologist, will sometimes render the diagnosis clear.
A routine chemic examination of the gastric contents involves qualitative tests for free acids, free hydrochloric acid, and organic acids, and quantitative estimations of total acidity, free hydrochloric acid, and sometimes combined hydrochloric acid. Other tests are applied when indicated.
1. Qualitative Tests.—(1) Free Acids.—The presence or absence of free acids, without reference to the kind, is easily determined by means of Congo-red.
Congo-red Test.—Take a few drops of a strong alcoholic solution of Congo-red in a test-tube, dilute with water to a strong red color, and add a few cubic centimeters of filtered gastric juice. The appearance of a blue color shows the presence of some free acid (Plate IX, B, B'). Since the test is more sensitive to mineral than to organic acids, a marked reaction points to the presence of free hydrochloric acid.
Thick filter-paper soaked in Congo-red solution, dried, and cut into strips may be used, but the test is much less delicate when thus applied.
(2) Free Hydrochloric Acid.—In addition to its digestive function, free hydrochloric acid is an efficient antiseptic. It prevents or retards fermentation and lactic-acid formation, and is an important means of protection against the entrance of pathogenic organisms into the body. It is never absent in health.
[p. 219] Amidobenzol Test.—To a little of the filtered gastric juice in a test-tube, or to several drops in a porcelain dish, add a drop of 0.5 per cent. alcoholic solution of dimethylamido-azobenzol. In the presence of free hydrochloric acid there will at once appear a cherry-red color, varying in intensity with the amount of acid (Plate X, C). This test is very delicate; but, unfortunately, organic acids, when present in large amounts (above 0.5 per cent.), give a similar reaction.
Boas' Test.—This test is less delicate than the preceding, but is more reliable, since it reacts only to free hydrochloric acid.
In a porcelain dish mix a few drops of the gastric juice and the reagent, and slowly evaporate to dryness over a flame, taking care not to scorch. The appearance of a rose-red color, which fades upon cooling, shows the presence of free hydrochloric acid (Plate IX, 1).
Boas' reagent consists of 5 gm. resublimed resorcinol, and 3 gm. cane-sugar, in 100 c.c. alcohol. The solution keeps well, which, from the practitioner's view-point, makes it preferable to Günzburg's phloroglucin-vanillin reagent (phloroglucin, 2 gm.; vanillin, 1 gm.; absolute alcohol, 30 c.c.). The latter is just as delicate, is applied in the same way, and gives a sharper reaction (Plate IX, 2), but is unstable.
(3) Organic Acids.—Lactic acid is the most common, and is taken as the type of the organic acids which appear in the stomach-contents. It is a product of bacterial activity. Acetic and butyric acids are sometimes present. Their formation is closely connected with that of lactic acid, and they are rarely tested for. When abundant, they may be recognized by their odor upon heating.
Lactic acid is never present at the height of digestion in health. Although usually present early in digestion, it disappears when free hydrochloric acid begins to appear. [p. 220] Small amounts may be introduced with the food. Pathologically, small amounts may be present whenever there is stagnation of the gastric contents with deficient hydrochloric acid, as in many cases of dilatation of the stomach and chronic gastritis. The presence of notable amounts of lactic acid is significant of gastric cancer, and is probably the most valuable single symptom of the disease. In the great majority of cases detection of more than 0.1 per cent. (see Strauss' test) warrants a diagnosis of malignancy.
As already stated, the Ewald test-breakfast introduces a small amount of lactic acid, but rarely enough to respond to the tests given here. In every case, however, in which its detection is important, Boas' test-breakfast should be given, the stomach having been thoroughly washed the evening before.
Uffelmann's Test for Lactic Acid.—Thoroughly shake up 5 c.c. of filtered stomach fluid with 50 c.c. of ether for at least ten minutes. Collect the ether and evaporate over a water-bath. Dissolve the residue in 5 c.c. water and test with Uffelmann's reagent as follows:
In a test-tube mix three drops concentrated solution of phenol and three drops saturated aqueous solution of ferric chlorid. Add water until the mixture assumes an amethyst-blue color. To this add the solution to be tested. The appearance of a canary-yellow color indicates the presence of lactic acid (Plate IX, A, A').
Uffelmann's test may be applied directly to the stomach-contents without extracting with ether, but is then neither sensitive nor reliable.
| PLATE IX |
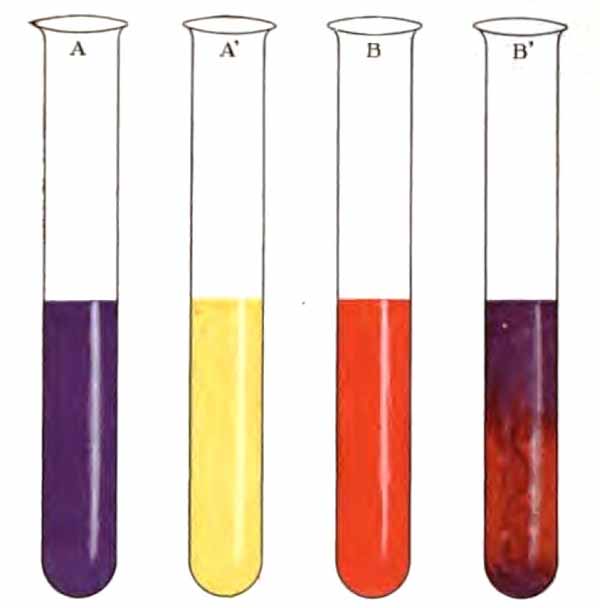
|
| A, Uffelmann's reagent; A', A after the addition of gastric fluid containing lactic acid; B, water to which three drops of Congo-red solution have been added; B', change induced in B when gastric fluid containing free hydrochloric acid is added (Boston). |
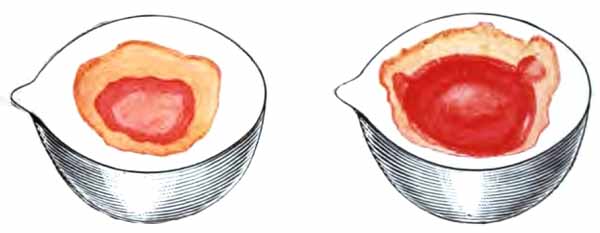
|
| 1, Resorcin-test for free hydrochloric acid; 2, Günzburg's test for hydrochloric acid (Boston). |

|
| FIG. 87.—Separatory funnel for Strauss' lactic acid test (Sahli). |
Strauss' Test for Lactic Acid.—This is the best test for clinical work, since it gives a rough idea of the quantity present. Strauss' instrument (Fig. 87) is essentially a separating funnel with a mark at 5 c.c. and one at 25 c.c. Fill to the 5 c.c. mark [p. 221] with filtered stomach fluid, and to the 25 c.c. mark with ether. Shake thoroughly for ten or fifteen minutes, let stand until the ether separates, and then, by opening the stop-cock, allow the liquid to run out to the 5 c.c. mark. Fill to the 25 c.c. mark with water, and add two drops of tincture of ferric chlorid diluted 1:10. Shake gently. If 0.1 per cent. or more lactic acid be present, the water will assume a strong yellowish-green color. A pale green will appear with 0.05 per cent.
(4) Pepsin and Pepsinogen.—Pepsinogen itself has no digestive power. It is secreted by the gastric glands, and is transformed into pepsin by the action of a free acid. Although pepsin digests proteids best in the presence of free hydrochloric acid, it has a slight digestive activity in the presence of organic or combined hydrochloric acids.
The amount is not influenced by neuroses or circulatory disturbances. Absence or marked diminution, therefore, indicates organic disease of the stomach. It is an important point in diagnosis between functional and organic conditions. Pepsin is rarely or never absent in the presence of free hydrochloric acid.
Test for Pepsin and Pepsinogen.—With a cork-borer cut small cylinders from the coagulated white of an egg, and cut these into discs of uniform size. The egg should be cooked very slowly, preferably over a water-bath, so that the white may be readily digestible. The discs may be preserved in glycerin, but must be washed in water before using.
[p. 222] Place a disc in each of three test-tubes.
Into tube No. 1 put 10 c.c. distilled water, 5 grains pepsin, U.S.P., and 3 drops of the official dilute hydrochloric add.
Into tube No. 2 put 10 c.c. filtered gastric juice.
Into tube No. 3 put 10 c.c. filtered gastric juice and 3 drops dilute hydrochloric acid.
Place the tubes in an incubator or warm water for three hours or longer. At intervals, observe the extent to which the egg-albumen has been digested. This is recognized by the depth to which the disc has become translucent.
Tube No. 1 is used for comparison, and should show the effect of normal gastric juice.
Digestion of the egg in tube No. 2 indicates the presence of both pepsin and free hydrochloric acid.
When digestion fails in tube No. 2 and occurs in No. 3, pepsinogen is present, having been transformed into pepsin by the hydrochloric acid added. Should digestion fail in this tube, both pepsin and pepsinogen are absent.
(5) Rennin and Renninogen.—Rennin is the milk-curdling ferment of the gastric juice. It is derived from renninogen through the action of hydrochloric acid. Lime salts also possess the power of transforming renninogen into the active ferment.
Deficiency of rennin has the same significance as deficiency of pepsin, and is more easily recognized. Since the two enzyms are almost invariably present or absent together, the test for rennin serves also as a test for pepsin.
Test for Rennin.—Neutralize 5 c.c. filtered gastric juice with very dilute sodium hydroxid solution; add 5 c.c. fresh milk, and place in an incubator or in a vessel of water at about 104° F. Coagulation of the milk in ten to fifteen minutes shows a normal amount of rennin. Delayed coagulation denotes a less amount.
[p. 223] Test for Renninogen.—To 5 c.c. neutralized gastric juice add 2 c.c. of 1 per cent. calcium chlorid solution and 5 c.c. fresh milk, and place in an incubator. If coagulation occurs, renninogen is present.
(6) Blood.—Blood is present in the vomitus in a great variety of conditions. When found in the fluid removed after a test-meal, it commonly points toward ulcer or carcinoma. Blood can be detected in nearly one-half of the cases of gastric cancer. The presence of swallowed blood must be excluded.
Test for Blood in Stomach-contents.—To 10 c.c. of the fluid add a few cubic centimeters of glacial acetic acid and shake the mixture thoroughly with an equal volume of ether. Separate the ether and apply to it the guaiac test (p. 89); or evaporate and apply the hemin test (p. 202) to the residue. When brown particles are present in the fluid, the hemin test should be applied directly to them.
2. Quantitative Tests.—(1) Total Acidity.—The acid-reacting substances which contribute to the total acidity are free hydrochloric acid, combined hydrochloric acid, acid salts, mostly phosphates, and, in some pathologic conditions, the organic acids. The total acidity is normally about 50 to 75 degrees (see method below), or, when estimated as hydrochloric acid, about 0.2 to 0.3 per cent.
Töpfer's Method for Total Acidity.—In an evaporating dish or small beaker (an "after-dinner" coffee-cup is a very convenient substitute) take 10 c.c. filtered stomach-contents and add three or four drops of the indicator, a 1 per cent. alcoholic solution of phenolphthalein. When the quantity of stomach fluid is small, 5 c.c. may be used, but results are less accurate than with a larger amount. Add decinormal solution [p. 224] of sodium hydroxid drop by drop from a buret, until the fluid assumes a rose-red color which does not become deeper upon addition of another drop (Plate X, A, A'). When this point is reached, all the acid has been neutralized. The end reaction will be sharper if the fluid be saturated with sodium chlorid. A sheet of white paper beneath the beaker facilitates recognition of the color change.
In clinical work the amount of acidity is expressed by the number of cubic centimeters of the decinormal sodium hydroxid solution which would be required to neutralize 100 c.c. of the gastric juice, each cubic centimeter representing one degree of acidity. Hence multiply the number of cubic centimeters of decinormal solution required to neutralize the 10 c.c. of stomach fluid by ten. This gives the number of degrees of acidity. The amount may be expressed in terms of hydrochloric acid, if one remember that each degree is equivalent to 0.00365 per cent. hydrochloric acid.
Example.—Suppose that 7 c.c. of decinormal solution were required to bring about the end reaction in 10 c.c. gastric juice; then 7 X 10 = 70 degrees of acidity; and, expressed in terms of hydrochloric acid, 70 X 0.00365 = 0.255 per cent.
Preparation of decinormal solutions is described in text-books on chemistry. The practitioner will find it best to have them made by a chemist, or to purchase from a chemic supply house.
| PLATE X |
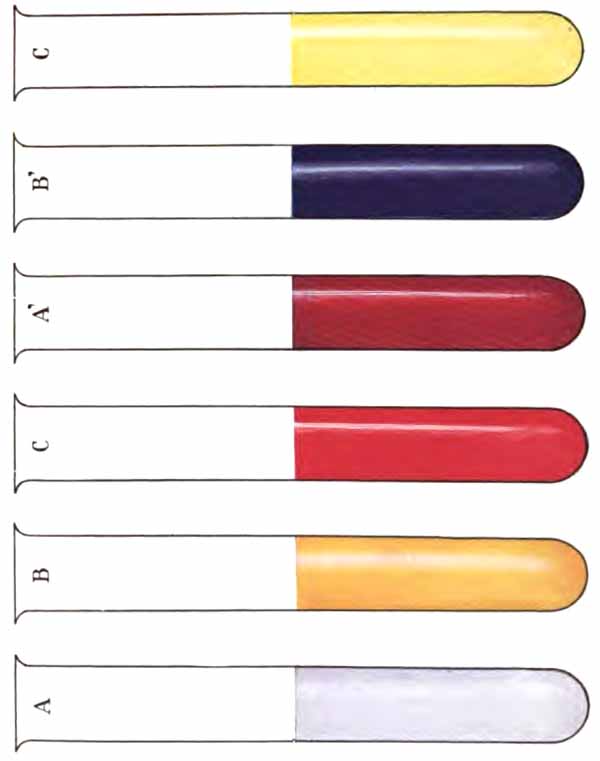
|
| A, Gastric fluid to which a 1 per cent. solution of phenolphthalein has been added; B, gastric fluid to which a 1 per cent. solution of alizarin has been added; C, gastric fluid to which a 0.5 per cent. solution of dimethylamido-azobenzol has been added; A', A after titration with a decinormal solution of sodium hydroxid; B', B after titration with a decinormal solution of sodium hydroxid; C', C after titration with a decinormal solution of sodium hydroxid (Boston). |
(2) Hydrochloric Acid.—After the Ewald and Boas test-breakfasts, the amount of free hydrochloric acid varies normally between 25 and 50 degrees, or about 0.1 to 0.2 per cent. In disease, it may go considerably higher, or may be absent altogether.
When the amount of free hydrochloric acid is normal, organic disease of the stomach probably does not exist.
Increase of free hydrochloric acid above 50 degrees [p. 225] (hyperchlorhydria) generally indicates a neurosis, but also occurs in most cases of gastric ulcer and beginning chronic gastritis.
Decrease of free hydrochloric acid below 25 degrees (hypochlorhydria) occurs in some neuroses, chronic gastritis, early carcinoma, and most conditions associated with general systemic depression. Marked variation in the amount at successive examinations strongly suggests a neurosis. Too low values are often obtained at the first examination, the patient's dread of the introduction of the tube probably inhibiting secretion.
Absence of free hydrochloric acid (achlorhydria) occurs in most cases of gastric cancer and far-advanced chronic gastritis, in many cases of pernicious anemia, and, sometimes, in hysteria.
The presence of free hydrochloric acid presupposes a normal amount of combined hydrochloric acid, hence the combined need not be estimated when the free acid has been found. When, however, free hydrochloric acid is absent, it is important to know whether any acid is secreted, and an estimation of the combined acid then becomes of great value. The normal average after an Ewald breakfast is about 10 to 15 degrees.
Töpfer's Method for Free Hydrochloric Acid.—In a beaker take 10 c.c. filtered stomach fluid and add four drops of the indicator, a 0.5 per cent. alcoholic solution of dimethylamido-azobenzol. A red color instantly appears if free hydrochloric acid be present. Add decinormal sodium hydroxid solution, drop by drop from a buret, until the last trace of red just disappears, and a canary-yellow color takes its place (Plate X, C, C'). Read off the number of cubic centimeters of decinormal solution added, and calculate the degrees, or [p. 226] percentage of free hydrochloric acid, as in Töpfer's method for total acidity.
When it is impossible to obtain sufficient fluid for all the tests, it will be found convenient to estimate the free hydrochloric acid and total acidity in the same portion. After finding the free hydrochloric acid as just described, add four drops phenolphthalein solution, and continue the titration. The amount of decinormal solution used in both titrations indicates the total acidity.
Töpfer's Method for Combined Hydrochloric Acid.—In a beaker take 10 c.c. filtered gastric juice and add four drops of the indicator, a 1 per cent. aqueous solution of sodium alizarin sulphonate. Titrate with decinormal sodium hydroxid until the appearance of a bluish-violet color which does not become deeper upon addition of another drop (Plate X, B, B'). It is difficult, without practice, to determine when the right color has been reached. A reddish-violet appears first. The shade which denotes the end reaction can be produced by adding two or three drops of the indicator to 5 c.c. of 1 per cent. sodium carbonate solution.
Calculate the number of cubic centimeters of decinormal solution which would be required for 100 c.c. of stomach fluid. This gives, in degrees, all the acidity except the combined hydrochloric acid. The combined hydrochloric acid is then found by deducting this amount from the total acidity, which has been previously determined.
Example.—Suppose that 5 c.c. of decinormal solution were required to produce the purple color in 10 c.c. gastric juice; then 5 X 10 = 50 = all the acidity except combined hydrochloric acid. Suppose, now, that the total acidity has already been found to be 70 degrees; then 70 - 50 = 20 degrees of combined hydrochloric acid; and 20 X 0.00365 = 0.073 per cent.
(3) Organic Acids.—There is no simple direct quantitative method. After the total acidity has been [p. 227] determined, organic acids may be removed from another portion of the gastric filtrate by shaking thoroughly with an equal volume of neutral ether, allowing the fluids to separate, and repeating this process until the gastric fluid has been extracted with eight or ten times its volume of ether. The total acidity is then determined, and the difference between the two determinations indicates the amount of organic acids.
(4) Pepsin.—No direct method is available. The following is sufficient for clinical purposes:
Hammerschlag's Method.—To the white of an egg add twelve times its volume of 0.4 per cent. hydrochloric acid (dilute hydrochloric acid, U.S.P., 4 c.c.; water, 96 c.c.), mix well, and filter. This gives a 1 per cent. egg-albumen solution. Take 10 c.c. of this solution in each of three tubes or beakers. To A add 5 c.c. gastric juice; to B, 5 c.c. water with 0.5 gm. pepsin; to C, 5 c.c. water only. Place in an incubator for an hour and then determine the amount of albumin in each mixture by Esbach's method. Tube C shows the amount of albumin in the test-solution. The difference between C and B indicates the amount of albumin which would be digested by normal gastric juice. The difference between C and A gives the albumin which is digested by the fluid under examination. It has been shown that the amounts of pepsin in two fluids are proportionate to the squares of the products of digestion. Thus, if the amounts of albumin digested in tubes A and B are to each other as 2 is to 4, the amounts of pepsin are to each other as 4 is to 16.
Certain sources of error can be eliminated by diluting the gastric juice several times before testing.[p. 228]
A drop of unfiltered stomach-contents is placed upon a slide, covered with a cover-glass, and examined with the two-thirds and one-sixth objectives.
Under normal conditions little is to be seen except great numbers of starch-granules, with an occasional epithelial cell, yeast-cell, or bacterium. Starch-granules are recognized by their concentric striations and the fact that they stain blue with iodin solutions.
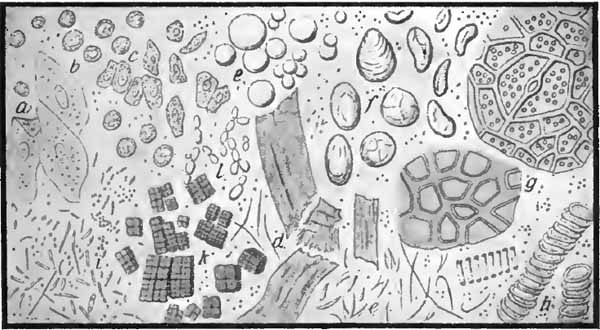
|
| FIG. 88.—General view of the gastric contents: a, Squamous epithelial cells from esophagus and mouth; b, leukocytes; c, cylindric epithelial cells; d, muscle-fibers; e, fat-droplets and fat-crystals; f, starch-granules; g, chlorophyl-containing vegetable matters; h, vegetable spirals; i, bacteria; k, sarcinæ; l, budding (yeast) fungi (Jakob). |
Pathologically, remnants of food from previous meals, red blood-corpuscles, pus-cells, sarcinæ, and excessive numbers of yeast-cells and bacteria may be encountered (Fig. 88).
Remnants of food from previous meals indicate deficient gastric motility.
Red Blood-corpuscles.—Blood is best recognized by the chemic tests already given. The corpuscles [p. 229] sometimes retain a fairly normal appearance, but are generally so degenerated that only granular pigment is left.
Pus-cells.—Pus is rarely encountered in the fluid removed after a test-meal. Considerable numbers of pus-corpuscles have been found in some cases of gastric cancer. Swallowed sputum must always be considered.
Sarcinæ.—These are small spheres arranged in cuboid groups often compared to bales of cotton. They frequently form large clumps and are easily recognized. They stain brown with iodin solution. They signify fermentation. Their presence is strong evidence against the existence of gastric cancer, in which disease they rarely occur.
Yeast-cells.—As already stated, a few yeast-cells may be found under normal conditions. The presence of considerable numbers is evidence of fermentation. Their appearance has been described (p. 130). They stain brown with iodin solution.
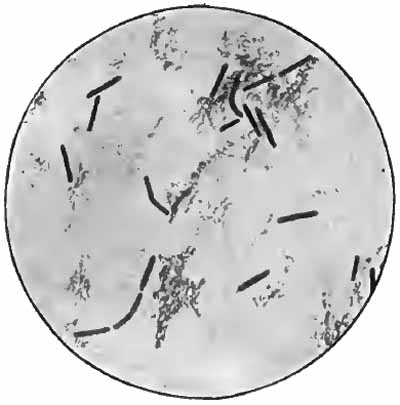
|
| FIG. 89.—Boas-Oppler bacillus from case of gastric cancer (Boston). |
Bacteria.—Numerous bacteria may be encountered, especially in the absence of free hydrochloric acid. The Boas-Oppler bacillus is the only one of special significance. [p. 230] It occurs in the majority of cases of cancer, and is rarely found in other conditions. Carcinoma probably furnishes a favorable medium for its growth.
These bacilli (Fig. 89) are large (5 to 10 µ long), non-motile, and usually arranged end to end in chains. They stain brown with iodin solution, which distinguishes them from Leptothrix buccalis (p. 270), which is not infrequently found in stomach fluid. They also stain by Gram's method. They are easily seen with the one-sixth objective in unstained preparations, but are best recognized with the one-twelfth, after drying some of the fluid upon a cover-glass, fixing, and staining with Löffler's methylene-blue or by Gram's method.
A few large non-motile bacilli are frequently seen; they cannot be called Boas-Oppler bacilli unless they are numerous and show something of the typical arrangement.
In the diagnosis of stomach disorders the practitioner must be cautioned against relying too much upon examinations of the stomach-contents. A first examination is especially unreliable. Even when repeated examinations are made, the laboratory findings must never be considered apart from the clinical signs.
The more characteristic findings in certain disorders are suggested here.
1. Dilatation of the Stomach.—Evidences of retention and fermentation are the chief characteristics of this condition. Hydrochloric acid is commonly diminished. Pepsin may be normal or slightly diminished. Lactic acid may be detected in small amounts, but is usually absent when the stomach has been washed before giving the [p. 231] test-meal. Both motility and absorptive power are deficient. The microscope commonly shows sarcinæ, bacteria, and great numbers of yeast-cells. Remnants of food from previous meals can be detected with the naked eye or microscopically.
2. Gastric Neuroses.—The findings are variable. Successive examinations may show normal, increased, or diminished hydrochloric acid, or even entire absence of the free acid. Pepsin is usually normal.
In the neurosis characterized by continuous hypersecretion (gastrosuccorrhea), 40 c.c. or more of gastric juice can be obtained from the fasting stomach. Should the fluid contain food-particles, it is probably the result of retention, not hypersecretion.
3. Chronic Gastritis.—Free hydrochloric acid may be increased in early cases. It is generally diminished in well-marked cases, and is often absent in advanced cases. Lactic acid is often present in traces, rarely in notable amount. Secretion of pepsin and rennin is always diminished in marked cases. Mucus is frequently present, and is very significant of the disease. Motility and absorption are generally deficient. Small fragments of mucous membrane may be found, and when examined by a pathologist, may occasionally establish the diagnosis.
4. Achylia Gastrica (Atrophic Gastritis).—This condition may be a terminal stage of chronic gastritis. It is sometimes associated with the blood-picture of pernicious anemia. It gives a great decrease, and sometimes entire absence of hydrochloric acid and ferments. The total acidity may be as low as 1 or 2 degrees. Small amounts of lactic acid may be present. Absorption and motility are usually not affected.
[p. 232] 5. Gastric Carcinoma.—As far as the laboratory examination goes, the cardinal signs of this disease are absence of free hydrochloric acid and presence of lactic acid and of the Boas-Oppler bacillus. These findings are, however, by no means constant.
It is probable that some substance is produced by the cancer which neutralizes the free hydrochloric acid, and thus causes it to disappear earlier than in other organic diseases of the stomach.
The presence of lactic acid is the most suggestive single symptom of gastric cancer. In the great majority of cases its presence in notable amount (0.1 per cent. by Strauss' method) after Boas' breakfast, the stomach having been washed the evening before, warrants a diagnosis of malignancy.
Carcinoma seems to furnish an especially favorable medium for the growth of the Boas-Oppler bacillus, hence this micro-organism is frequently present.
Blood can be detected in the stomach fluid by the chemic tests in nearly one-half of the cases, and is more common when the newgrowth is situated at the pylorus. Blood is present in the stool in nearly every case.
Evidences of retention and fermentation are the rule in pyloric cancer. Tumor particles are sometimes found late in the disease.
6. Gastric Ulcer.—There is excess of free hydrochloric acid in about one-half of the cases. In other cases the acid is normal or diminished. Blood is often present. The diagnosis must be based largely upon the clinical symptoms, and where ulcer is strongly suspected, it is probably unwise to use the stomach-tube.
1. Absorptive Power of the Stomach.—This is a very unimportant function, only a few substances being absorbed in the stomach. It is delayed in most organic diseases of the stomach, especially in dilatation and carcinoma, but not in neuroses. The test has little practical value.
Give the patient, upon an empty stomach, a three-grain capsule of potassium iodid with a glass of water, taking care that none of the drug adheres to the outside of the capsule. At intervals test the saliva for iodids by moistening starch-paper with it and touching with yellow nitric acid. A blue color shows the presence of an iodid, and appears normally in ten to fifteen minutes after ingestion of the capsule. A longer time denotes delayed absorption.
Starch paper is prepared by soaking filter-paper in boiled starch and drying.
2. Motor Power of the Stomach.—This refers to the rapidity with which the stomach passes its contents on into the intestine. It is very important: intestinal digestion can compensate for insufficient or absent stomach digestion only so long as the motor power is good.
Motility is impaired to some extent in chronic gastritis. It is especially deficient in dilatation of the stomach due to atony of the gastric wall or to pyloric obstruction, either benign or malignant. It is increased in most conditions with hyperchlorhydria.
The best evidence of deficient motor power is the detection of food in the stomach at a time when it should be empty, e.g., before breakfast in the morning. When more than 60 c.c. of fluid are obtained with the tube one hour after a Ewald breakfast, deficient motility may be inferred.
[p. 234] Ewald's salol test is scarcely so reliable as the above. It depends upon the fact that salol is not absorbed until it reaches the intestine and is decomposed by the alkaline intestinal juices.
The patient is given 15 grains of salol with a test-breakfast, and the urine, passed at intervals thereafter, is tested for salicyluric acid. A few drops of 10 per cent. ferric chlorid solution are added to a small quantity of the urine. A violet color denotes the presence of salicyluric acid. It appears normally in sixty to seventy-five minutes after ingestion of the salol. A longer time indicates impaired motor power.
3. To Determine Size and Position of Stomach.—After removing the test-meal, while the tube is still in place, force quick puffs of air into the stomach by compression of the bulb. The puffs can be clearly heard with a stethoscope over the region of the stomach, and nowhere else.
If desired, the patient may be given a dram of sodium bicarbonate in solution, followed immediately by the same amount of tartaric acid, also in solution; or he may take the two parts of a seidlitz powder separately. The carbon dioxid evolved distends the stomach, and its outline can easily be determined by percussion.
As commonly practised, an examination of the feces is limited to a search for intestinal parasites or their ova. Much of value can, however, be learned from other simple examinations, particularly a careful inspection. Anything approaching a complete analysis is, on the other hand, a waste of time for the clinician.
The normal stool is a mixture of—(a) Water; (b) undigested and indigestible remnants of food, as starch-granules, particles of meat, plant-cells and fibers, etc.; (c) digested foods, carried out before absorption could take place; (d) products of the digestive tract, as altered bile-pigments, mucus, etc.; (e) products of decomposition, as indol, skatol, fatty acids, and various gases; (f) epithelial cells shed from the wall of the intestinal canal; (g) harmless bacteria, which are always present in enormous numbers.
Pathologically, we may find abnormal amounts of normal constituents, blood, pathogenic bacteria, animal parasites and their ova, and biliary and intestinal concretions.
The stool to be examined should be passed into a clean vessel, without admixture of urine. The offensive odor can be partially overcome with turpentine or 5 per cent. phenol. When search for Amoeba coli is to be made, the vessel must be warm, and the stool kept warm until examined; naturally, no disinfectant can be used.
1. Quantity.—The amount varies greatly with diet and other factors. The average is about 100 to 150 gm. in twenty-four hours.
2. Frequency.—One or two stools in twenty-four hours may be considered normal, yet one in three or four days is not uncommon with healthy persons. The individual habit should be considered in every case.
3. Form and Consistence.—Soft, mushy, or liquid stools follow cathartics and accompany diarrhea. Copious, purely serous discharges without fecal matter are significant of Asiatic cholera, although sometimes observed in other conditions. Hard stools accompany constipation. Rounded scybalous masses are common in habitual constipation, and indicate atony of the muscular coat of the intestine. Flattened, ribbon-like stools result from some obstruction in the rectum, generally a tumor or stricture from a healed ulcer, most commonly syphilitic. When bleeding piles are absent, blood-streaks upon such a stool point to carcinoma.
4. Color.—The normal light or dark-brown color is due chiefly to altered bile-pigments. The stools of infants are yellow, owing partly to their milk diet and partly to the presence of unchanged bilirubin.
Diet and drugs cause marked changes: milk, a light yellow color; cocoa and chocolate, dark gray; various fruits, reddish or black; iron and bismuth, dark brown or black; hematoxylin, red; etc.
Pathologically, the color is important. A golden yellow is generally due to unchanged bilirubin. Green stools are not uncommon, especially in diarrheas of childhood. The color is due to biliverdin, or, sometimes, to [p. 237] chromogenic bacteria. Putty-colored or "acholic" stools occur when bile is deficient, either from obstruction to outflow or from deficient secretion. The color is due less to absence of bile-pigments than to presence of fat. Similar stools are common in conditions like tuberculous peritonitis, which interfere with absorption of fats, and in pancreatic disease.
Notable amounts of blood produce tarry black stools when the source of the hemorrhage is the stomach or upper intestine, and a dark brown or bright red as the source is nearer the rectum. When diarrhea exists, the color may be red, even if the source of the blood is high up. Red streaks of blood upon the outside of the stool are due to lesions of rectum or anus.
5. Odor.—Products of decomposition, chiefly indol and skatol, are responsible for the normal offensive odor. A sour odor is normal for nursing infants, and is noted in mild diarrheas of older children. In the severe diarrheas of childhood a putrid odor is common. In adults stools emitting a very foul stench are suggestive of malignant or syphilitic ulceration of the rectum or gangrenous dysentery.
6. Mucus.—Excessive quantities of mucus are easily detected with the naked eye, and signify irritation or inflammation. When the mucus is small in amount and intimately mixed with the stool, the trouble is probably in the small intestine. Larger amounts, not well mixed with fecal matter, indicate inflammation of the large intestine. Stools composed almost wholly of mucus and streaked with blood are the rule in dysentery, ileocolitis, and intussusception. In the so-called mucous colic, or membranous enteritis, shreds and ribbons of altered mucus, sometimes representing complete casts of the bowel, are passed.
[p. 238] 7. Concretions.—Gall-stones are probably more common than is generally supposed, and should be searched for in every case of obscure colicky abdominal pain. Intestinal concretions (enteroliths) are rare.
Concretions can be found by breaking up the fecal matter in a sieve (which may be improvised from gauze) while pouring water over it. It must be remembered that gall-stones, if soft, may go to pieces in the bowel.
8. Animal Parasites.—Segments of tape-worms and the adults and larvæ of other parasites are often found in the stool. They are best searched for in the manner described for concretions. The search should be preceded by a vermicide and a brisk purge. Patients frequently mistake vegetable tissue (long fibers from poorly masticated celery or "greens," cells from orange, etc.) for intestinal parasites, and the writer has known physicians to make similar mistakes. Even slight familiarity with the microscopic structure of vegetable tissue will prevent the chagrin of such errors.
Complicated chemic examinations are of little value to the clinician. Certain tests are, however, important.
1. Blood.—When present in large amount, blood produces such changes in the appearance of the stool that it is not likely to be overlooked. Traces of blood (occult hemorrhage) can be detected only by special tests. Recognition of occult hemorrhage has its greatest value in diagnosis of gastric cancer and ulcer. It is constantly present in practically every case of gastric cancer, and is always present, although usually intermittently, in ulcer. Traces of blood also accompany malignant disease of the [p. 239] bowel, the presence of certain intestinal parasites, and other conditions.
Detection of Occult Hemorrhage.—Soften a portion of the stool with water, treat with about one-third its volume of glacial acetic acid, and extract with ether. Should the ether not separate well, add a little alcohol. Apply the guaiac test to the ether as already described (p. 89).
In every case iron-containing medicines must be stopped, and blood-pigment must be excluded from the food by giving an appropriate diet, e.g., bread, milk, eggs, and fruit. At the beginning of the restricted diet give a dram of powdered charcoal, or 7 grains of carmin, so as to mark the corresponding stool.
2. Bile.—Normally, unaltered bile-pigment is never present in the feces of adults. In catarrhal conditions of the small intestine bilirubin may be carried through unchanged. It may be demonstrated by filtering (after mixing with water if the stool be solid) and testing the filtrate by Gmelin's method, as described under The Urine.
Care must be exercised in selection of portions for examination. A random search will often reveal nothing of interest. A small bit of the stool, or any suspicious-looking particle, is placed upon a slide, softened with water if necessary, and pressed out into a thin layer with a cover-glass. A large slide—about 2 by 3 inches—with a correspondingly large cover will be found convenient. Most of the structures which it is desired to see can be found with a two-thirds objective. Details of structure must be studied with a higher power.
[p. 240] The bulk of the stool consists of granular débris. Among the recognizable structures met in normal and pathologic conditions are: remnants of food, epithelial cells, pus-corpuscles, red blood-corpuscles, crystals, bacteria, and ova of animal parasites (Fig. 90).
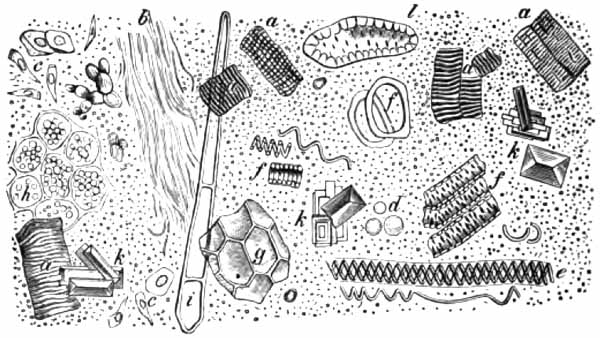
|
| FIG. 90.—Microscopic elements of normal feces: a, Muscle-fibers; b, connective tissue; c, epithelial cells; d, white blood-corpuscles; e, spiral vessels of plants; f-h, vegetable cells; i, plant hairs; k, triple phosphate crystals; l, stone cells. Scattered among these elements are micro-organisms and débris (after v. Jaksch). |
1. Remnants of Food.—These include a great variety of structures which are very confusing to the student. Considerable study of normal feces is necessary for their recognition.
Vegetable fibers are generally recognized from their spiral structure; vegetable cells, from their double contour and the chlorophyl bodies which many of them contain. These cells are apt to be mistaken for the ova of parasites. Starch-granules sometimes retain their original form, but are ordinarily not to be recognized except by their staining reaction. They strike a blue color with Lugol's solution when undigested; a red color, when slightly digested. Muscle-fibers are yellow, and sometimes appear as short, [p. 241] transversely striated cylinders with rather squarely broken ends. Generally, the ends are rounded and the striations faint, or only irregularly round or oval yellow masses are found. Curds of milk are especially important in the stools of children. They must be distinguished from small masses of fat. The latter are soluble in ether, and stain red with Sudan III.
Excess of any of these structures may result from excessive ingestion or deficient intestinal digestion.
2. Epithelial Cells.—A few cells derived from the wall of the alimentary canal are a constant finding. They show all stages of degeneration, and are often unrecognizable. A marked excess has its origin in a catarrhal condition of some part of the bowel. Squamous cells come from the anal orifice; otherwise the form of the cells gives no clue to the location of the lesion.
3. Pus.—Amounts of pus sufficient to be recognized with the eye alone indicate rupture of an abscess into the bowel. If well mixed with the stool, the source is high up, but in such cases the pus is apt to be more or less completely digested, and hence unrecognizable. Small amounts, detected only by the microscope, are present in catarrhal and ulcerative conditions of the intestine, the number of pus-cells corresponding to the severity and extent of the process.
4. Blood-corpuscles.—Unaltered red corpuscles are rarely found unless their source is near the anus. Ordinarily, only masses of blood-pigment can be seen. Blood is best recognized by the chemic tests (p. 239).
5. Bacteria.—In health, bacteria constitute about one-third of the weight of the dried stool. They are beneficial to the organism, although not actually necessary [p. 242] to its existence. It is both difficult and unprofitable to identify them. The great majority belong to the colon bacillus group, and are negative to Gram's method of staining.
In some pathologic conditions the character of the intestinal flora changes so that Gram-staining bacteria very greatly predominate. As shown by R. Schmidt, of Neusser's clinic in Vienna, this change is most constant and most striking in cancer of the stomach, owing to large numbers of Boas-Oppler bacilli, and is of considerable value in diagnosis. He believes that a diagnosis of gastric carcinoma should be very unwillingly made with an exclusively "Gram-negative" stool, while a "Gram-positive" stool, due to bacilli (which should also stain brown with Lugol's solution), may be taken as very strong evidence of cancer. A Gram-positive stool due to cocci is suggestive of intestinal ulceration. The technic is the same as when Gram's method is applied to other material (p. 40), except that the smear is fixed by immersion in methyl-alcohol for five minutes instead of by heat. Fuchsin is the best counter-stain. The deep-purple Gram-staining bacteria stand out much more prominently than the pale-red Gram-negative organisms, and one may be misled into thinking them more numerous even in cases in which they are much in the minority. The number of Boas-Oppler bacilli can be increased by administering a few ounces of sugar of milk the day before the examination.
Owing to the difficulty of excluding swallowed sputum, the presence of the tubercle bacillus is less significant in the feces than in other material. It may, however, be taken as evidence of intestinal tuberculosis when clinical signs indicate an intestinal lesion and reasonable care is [p. 243] exercised in regard to the sputum. Success in the search will depend largely upon careful selection of the portion examined. A random search will almost surely fail. Whitish or grayish flakes of mucus or blood-stained or purulent particles should be spread upon slides or covers and stained by the method given upon p. 127. In the case of rectal ulcers, swabs can be made directly from the ulcerated surface.
6. Crystals.—Various crystals may be found, but few have any significance. Slender, needle-like crystals of fatty acids and soaps (Fig. 32) and triple phosphate crystals (Fig. 90) are common. Characteristic octahedral crystals of calcium oxalate (Fig. 47) appear after ingestion of certain vegetables. Charcot-Leyden crystals (Fig. 6) are not infrequently encountered, and strongly suggest the presence of intestinal parasites. Yellowish or brown, needle-like or rhombic crystals of hematoidin (Fig. 32) may be seen after hemorrhage into the bowel.
7. Ova of Parasites.—The stool should be well mixed with water and allowed to settle. The ova will be found in the upper or middle portions of the sediment. Descriptions will be found in the following chapter.
Animal parasites are common in all countries, but are especially abundant in the tropics, where almost every native is host for one or more varieties. Because of our growing intercourse with these regions, the subject is assuming increasing importance in this country. Many parasites, hitherto comparatively unknown here, will probably become common.
Some parasites produce no symptoms, even when present in large numbers. Others cause very serious symptoms. Only those which have clinical interest will be considered here. The illustrations will give a better idea of their appearance than any description. They belong to three classes: I. Protozoa. II. Vermes. III. Arthropoda.
1. Amoeba Coli Dysenteriæ.—This organism is found, often in large numbers, in the stools of tropical dysentery and in the pus and walls of hepatic abscesses associated with dysentery, and is generally regarded as the cause of the disease. It is a colorless, granular cell, 20 to 40 µ in diameter (Fig. 91). It contains one or more distinct vacuoles; a round nucleus, which ordinarily is obscured by the granules; and frequently red blood-corpuscles and bacteria. When at rest, its shape is spheric; but upon a warm slide it exhibits the characteristic ameboid motion, [p. 245] constantly changing its shape or moving slowly about. This motion is its most distinctive feature. Other amebæ, resembling the pathogenic variety but smaller (10 to 15 µ in diameter), are sometimes found in normal feces.

|
| FIG. 91.—Amoeba coli in intestinal mucus, with blood-corpuscles and bacteria (Lösch). |
When the presence of amebæ is suspected, the stool should be passed into a warm vessel and kept warm until and during the examination. A warm stage can be improvised from a plate of copper with a hole cut in the center. This is placed upon the stage of the microscope, and one of the projecting ends is heated with a small flame. Amebæ are most likely to be found in grayish or blood-streaked particles of mucus. Favorable material for examination can be obtained at one's convenience by inserting into the rectum a large catheter with roughly cut lateral openings. A sufficient amount of mucus or fecal matter will usually be brought away by it.
2. Trichomonas Vaginalis.—The acid discharge of catarrhal vaginitis sometimes contains this parasite in [p. 246] abundance. It is oval or pear-shaped, one to three times the diameter of a red blood-corpuscle in length, and has a cluster of flagella at one end (Fig. 92). It is not unlike a pus-corpuscle in size and general appearance, but is actively motile. When in motion the flagella are not easily seen. No pathogenic significance is ascribed to it. Other varieties of the genus have been found in the feces, the urine, and the sputum.

|
| FIG. 92.—Trichomonas vaginalis (after Kölliker and Scanzoni). |
A similar but somewhat smaller organism, Cercomonas hominis (Fig. 93), has been found in the feces in a variety of diarrheal conditions and in from 10 to 25 per cent. of healthy persons in tropical regions.
|
| FIG. 93.—Cercomonas hominis: A, Larger variety; B, smaller variety (Davaine). |
In urine or vaginal discharges these organisms might be mistaken for spermatozoa by one who is entirely unfamiliar with the appearance of either.
3. Paramoecium Coli (Balantidium Coli).—This parasite is an occasional inhabitant of the colon of man, and sometimes produces diarrhea. It is an oval organism, about 0.1 mm. long, is covered with cilia, and contains [p. 247] a bean-shaped nucleus, two contractile vacuoles, and variously sized granules (Fig. 94).
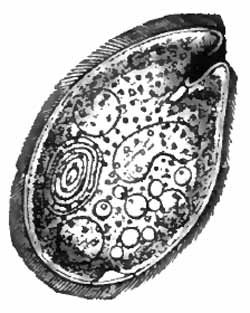
|
| FIG. 94.—Balantidium (Paramoecium) coli (Eichhorst). |
4. Hemosporidia.—This is a large group of parasites with two life-cycles: one in the blood-corpuscles or plasma of a vertebrate host—man, mammals, birds, reptiles; the other in the body of some insect. The malarial parasite, already described; the organism (Pirosoma bigeminum) producing Texas fever in cattle; and the questionable parasite (Piroplasma hominis), which has been described as the cause of "tick fever" of Montana, belong to the group.
5. Trypanosomes have been mentioned (p. 195).
1. Cestoda.—Tape-worms are very common parasites of both man and the animals. The most important are Tænia saginata, Tænia solium, Bothriocephalus latus, and Tænia echinococcus. They all pass a larval stage in the body of an intermediate host. In the adult stage they consist of a linear series of flat, rectangular segments (proglottides), at one end of which is a smaller segment, the scolex or head, especially adapted for attachment to the host. The series represents a colony, of which the [p. 248] scolex is ancestor. The proglottides are sexually complete individuals, derived from the scolex by budding. With exception of the immature segments near the scolex, each contains a uterus filled with ova. The three tape-worms first mentioned are distinguished from one another mainly by the structure of the scolex and of the uterus (Fig. 100). The scolex should be studied with a low-power objective. The uterus is best seen by pressing the segment out between two plates of glass.
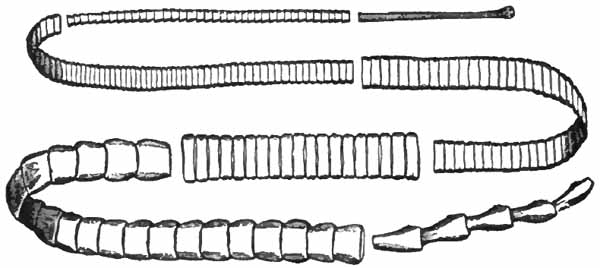
|
| FIG. 95.—Tænia saginata (Eichhorst). |
(1) Tænia Saginata or Mediocanellata (Fig. 95).—This, the beef tape-worm, is the common tape-worm of the United States. Its length sometimes exceeds twenty-five feet. The middle segments measure about one-fourth by one-half inch. The scolex is about the size of a pin-head, and is surrounded by four sucking discs, but has no hooklets (Fig. 96). The uterus extends along the middle line of the segment and gives off about twenty branches upon each side (Fig. 100). The larval stage is passed in the muscles of various animals, especially cattle, where it lies encysted (cysticercus stage).
The larva is ingested with the meat, its capsule is [p. 249] dissolved by the digestive juices, and it attaches itself to the intestinal wall by means of its suckers. It then develops into the mature worm.
The ova are present in the stools of infected persons, often in great numbers. They are spheric or ovoid, yellow in color, and have a thick, radially striated shell (Fig. 101). Their greatest diameter is 30 to 40 µ (about four or five times the diameter of a red blood-corpuscle). Vegetable cells, which are generally present in the feces, are often mistaken for them.
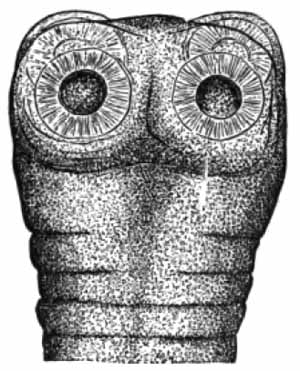
|

|
|
FIG. 96.—Head of Tænia saginata (Mosler and Peiper). |
FIG. 97.—Head of Tænia solium (Mosler and Peiper). |
(2) Tænia solium, the pork tape-worm is very rare in this country. It is usually much shorter than Tænia saginata. The scolex is surrounded by four sucking discs, and has a projection, or rostellum, with a double row of horny hooklets (Fig. 97). The uterus has only seven to ten branches (Fig. 100).
The ova closely resemble those of Tænia saginata, but are a little smaller (Fig. 101).
(3) Bothriocephalus latus, the fish tape-worm, is the largest parasite of man, sometimes reaching fifty feet in [p. 250] length, although generally not more than half so long. It is common in some countries of Europe and in Japan, but is very rare in this country. The head is not unlike the bowl of a spoon in shape. It is unprovided with either suckers or hooklets, but has two longitudinal grooves which serve the same purpose (Fig. 98). The uterus, which is situated in the center of the segment, is roset-shaped (Fig. 100).

|
| FIG. 98.—Head of Bothriocephalus latus: a, a, Bothridies; b, neck (Blanchard). |
The larval stage is found in fish, especially the pike.

|
| FIG. 99.—Egg of Bothriocephalus latus, showing lid and yolk granules (photograph by F. C. Wood). |
The ova are characteristic. They measure about 45 by 70 µ, are brown in color, and are filled with small spherules. The shell is thin, and has a small hinged lid at one end (Fig. 99).
[p. 251] Bothriocephalus latus is interesting clinically because it often causes a very severe grade of anemia.
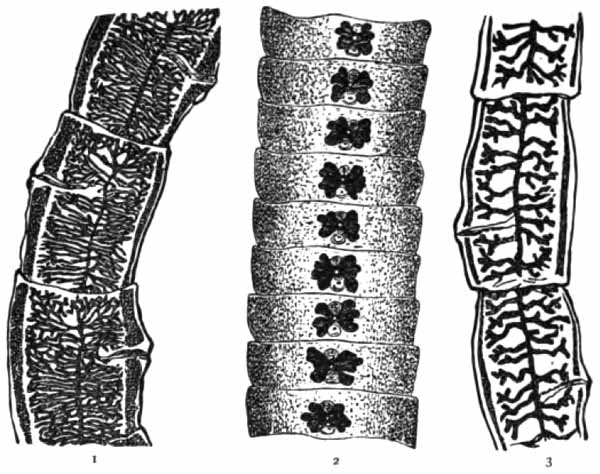
|
| FIG. 100.—Segments of—(1) Tænia saginata; (2) Bothriocephalus latus; (3) Tænia solium, showing arrangement of uterus. |
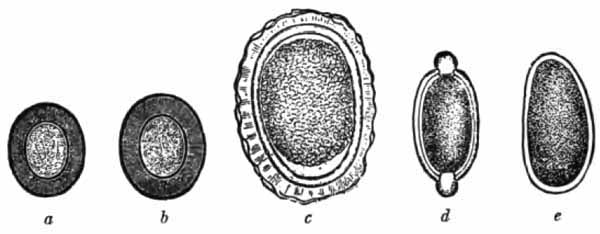
|
| FIG. 101.—Comparative size of eggs of intestinal parasites: a, Tænia solium; b, Tænia saginata; c, Ascaris lumbricoides; d, Trichocephalus dispar; e, Oxyuris vermicularis (after Strümpell). |

|
| FIG. 102.—Tænia echinococcus; enlarged (Mosler and Peiper). |
(4) Tænia Echinococcus.—The mature form of this tape-worm inhabits the intestine of the dog and wolf. The larvæ develop in cattle and sheep ordinarily, but are [p. 252] sometimes found in man, where they give rise to echinococcus or "hydatid" disease. The condition is unusual in America, but is common in Iceland and Australia.
The adult parasite is 2.5 to 5 mm. long, and consists of only four segments (Fig. 102). It contains many ova. When the ova reach the digestive tract of man, the embryos are set free and find their way to the liver, lung, or other organ, where they develop into cysts, thus losing their identity. Other cysts, called "daughter cysts," are formed within these. The cyst-wall is made up of two layers, from the inner of which develop larvæ which are identical with the head, or scolex, of the mature parasite. These are ovoid structures about 0.3 mm. long. Each has four lateral suckers and a rostellum surmounted by a double circular row of horny hooklets. The rostellum with its hooklets is frequently invaginated into the body.
Diagnosis of echinococcus disease depends upon detection of scolices, free hooklets, or particles of cyst-wall, which is characteristically laminated and usually has [p. 253] curled edges. These can be found in fluid withdrawn from the cysts, or, less frequently, in the sputum or the urine when the disease involves the lung or kidney (Figs. 55 and 103).
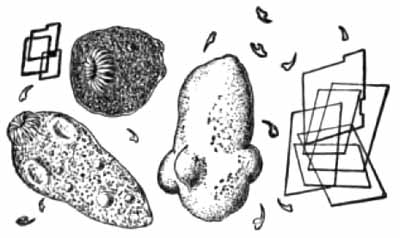
|
| FIG. 103.—Contents of echinococcus cyst, showing hooklets, scolices, and cholesterin crystals (Wood). |
The cyst-fluid is clear, between 1.002 and 1.010 in specific gravity, and contains a notable amount of sodium chlorid, but no albumin.
2. Nematoda.—(1) Ascaris Lumbricoides.—The female is 20 to 40 cm. long and about 6 mm. thick; the male, a little more than half as large. Their color is reddish or brown. They are the common "round-worms" so frequently found in children. Their habitat is the small intestine. Large numbers are sometimes present.
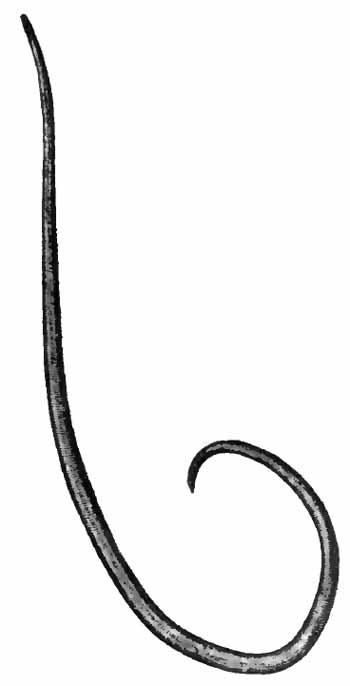
|
|
FIG. 104.—Ascaris lumbricoides (female) (Mosler and Peiper). |
The diagnosis is made by detection of the worms or ova in the feces. The latter are generally numerous. They are elliptic, measuring about 50 by 70 µ, and have an unsegmented protoplasm (Fig. 105). The shell is thick, and is surrounded by an uneven gelatinous envelop which is often stained with bile.
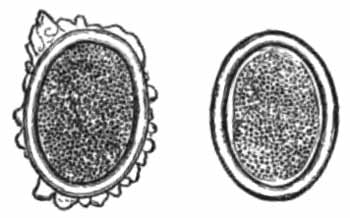
|
|
FIG. 105.—Eggs of Ascaris lumbricoides (Mosler and Peiper). |
(2) Oxyuris Vermicularis.—This is the "thread-worm" or "pin-worm" which inhabits the colon and rectum, especially of young children. Its presence should [p. 254] be suspected in all unexplained cases of pruritus ani. The female is about 1 cm. long; the male, about 0.6 cm. (Fig. 106).
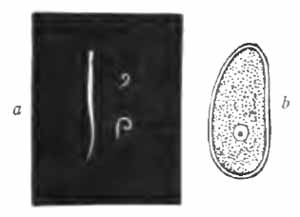
|
| FIG. 106.—Oxyuris vermicularis and egg: a, Natural size; b, egg (after Heller). |
The worms are not infrequently found in the feces; the ova, rarely. The latter are best found by scraping the skin at the margins of the anus, where they are deposited by the female. They are asymmetrically oval, about 50 µ in length, and often contain a partially developed embryo.
(3) Filaria Sanguinis Hominis.—A description of this worm will be found in the chapter upon the Blood, p. 194. The embryos are sometimes found in urine and chylous fluids from the serous cavities. Their motion is then usually less active than when in blood. That shown in Fig. 107 was alive sixty hours after removal of the fluid. Embryos were present in the blood of the same patient.
[p. 255]

|
| FIG. 107.—Filaria sanguinis hominis (embryo) in chylous hydrocele fluid; length, 300 µ; width, 8 µ. A number of red blood-corpuscles also appear (studied through courtesy of Dr. S. D. Van Meter). |

|
| FIG. 108.—Trichinella spiralis (larvæ) from head of right gastrocnemius muscle; seventh week of disease (two-thirds objective; eye-piece 4) (Boston). |
(4) Trichina (Trichinella) Spiralis.—This is a very small worm, not exceeding 3 mm. in length when fully developed. Infection in man occurs from ingestion of insufficiently cooked pork, which contains encysted embryos. These reach maturity in the small intestine. The female produces great numbers of young, which [p. 256] migrate to the voluntary muscles, chiefly near the tendinous extremities, and there become encysted.
Trichiniasis is generally accompanied by a marked eosinophilia. The diagnosis is made by teasing out upon a slide a bit of muscle, obtained preferably from the outer head of the gastrocnemius, the insertion of the deltoid, or the lower portion of the biceps. The coiled embryos can easily be seen with a two-thirds objective (Fig. 108).
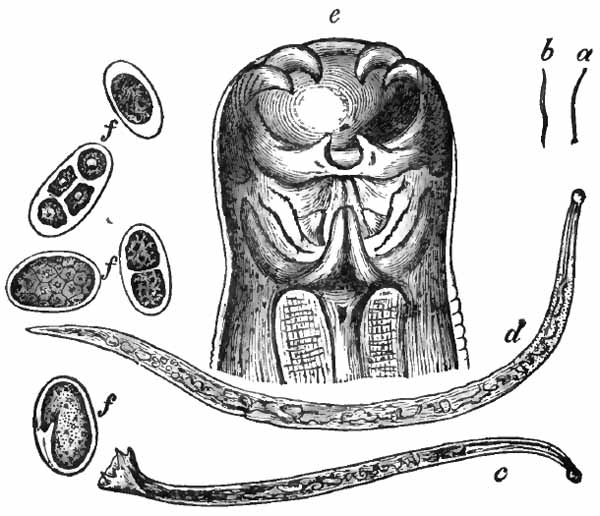
|
| FIG. 109.—Uncinaria duodenalis: a, Male (natural size); b, female (natural size); c, male (enlarged); d, female (enlarged); e, head; f, f, f, eggs (after v. Jaksch). |
(5) Uncinaria.—The two varieties of this worm, Uncinaria duodenalis and Uncinaria Americana, are among the more harmful of the animal parasites. They inhabit the small intestine, usually in great numbers, and commonly produce a severe and often fatal anemia. Infection is common in subtropical regions, notably in Egypt, in some European countries, and, especially, in Porto Rico and the West Indies, where about 90 per cent. of the rural population is infected. It is much more [p. 257] common in the United States than was formerly supposed.
The adult worms are seldom found in the feces, but may appear after a dose of thymol followed by a brisk purge. They resemble Oxyuris vermicularis to the naked eye. Ova are usually present in enormous numbers. Those of Uncinaria duodenalis measure about 30 by 50 µ; of Uncinaria Americana, somewhat more. They have a thin, smooth, transparent shell, and their protoplasm is divided into 2, 4, 8, or more rounded segments (Fig. 110).
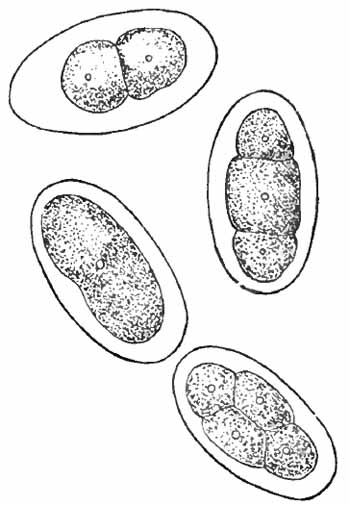
|
| FIG. 110.—Four eggs of the New World hook-worm (Uncinaria Americana), in the one-, two-, and four-cell stages. The egg showing three cells is a lateral view of a four-cell stage. Greatly enlarged (after Stiles). |
(6) Strongyloides Intestinalis.—Infection with this worm is by no means so rare in this country as the few clinical reports would indicate. It is very common in subtropical countries, notably in Italy and in southern China. It seems probable that the parasite is the cause [p. 258] of "Cochin China diarrhea," although some authorities regard it as harmless.
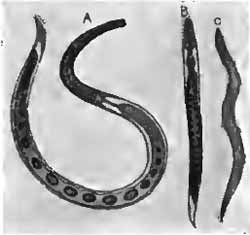
|
| FIG. 111.—Strongyloides intestinalis: A, Mature female; B, rhabditiform larva; C, filariform larva (after Braun). |
The adult worm, which reproduces by parthenogenesis, is about 2 mm. long. It inhabits the upper portion of the small intestine, but neither it nor the ova appear in the stool unless an active diarrhea exists. Ordinarily the eggs hatch in the intestine, and when infection is severe, embryos can be found in the feces in large numbers. These are the "rhabditiform embryos," which measure about 0.40 by 0.02 mm. They are actively motile, and are best found by making a small depression in the fecal mass, filling it with water, and standing in a warm place (preferably an incubator) for twelve to twenty-four hours. The embryos will collect in the water, and can be easily found with a two-thirds objective.
Outside the body the rhabditiform embryos develop into a free-living, sexually differentiated generation. The young of this generation are the more slender "filariform embryos" (Fig. 111). Infection can occur either through these embryos of the free-living generation, or by direct transformation of rhabditiform into filariform embryos and these into the parthenogenic parasitic adult.
(7) Trichocephalus Dispar (T. Trichiurus).—This, [p. 259] the "whip-worm," is 4 or 5 cm. long. Its anterior portion is slender and thread-like, while the posterior portion is thicker (Fig. 112). It is widely distributed geographically, and is one of the most common of intestinal parasites in this country. It lives in the large intestine, especially the cecum, with its slender extremity embedded in the mucous membrane. Whip-worms do not, as a rule, produce any symptoms, although gastro-intestinal disturbances, nervous symptoms, and anemia have been ascribed to them. They, as well as many other intestinal parasites, are probably an important factor in etiology of appendicitis, typhoid fever, and other intestinal infections. The damage which they do to the mucous membrane favors bacterial invasion.
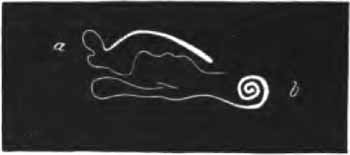
|
| FIG. 112.—Trichocephalus dispar; a, Female; b, male (natural size) (Heller). |
The number present is usually small. The worms themselves are rarely found in the feces. The ova, which are not often abundant, are easily recognized. They are brown, ovoid in shape, about 50 µ long, and have a button-like projection at each end (Fig. 101).
Most of these are external parasites, and the reader is referred to the standard works upon diseases of the skin for descriptions. The itch-mite (Acarus scabiei) and the louse (Pediculus capitis, corporis, vel pubis) are the more common members of the group.
[p. 260] A number of flies may deposit their ova in wounds or in such of the body cavities as they can reach, and the resulting maggots may cause intense irritation. Ova may be swallowed with the food and the maggots appear in the feces. Probably most important is the "screw worm," the larva of Compsomyia macellaria, infection with which is not rare in some parts of the United States. The ova are most commonly deposited in the nasal passages, and the larvæ, which may be present in great numbers, burrow through the soft parts, cartilage, and even bone, always with serious and often with fatal results.
Pus contains much granular débris and numerous more or less degenerated cells, the great majority being polymorphonuclear leukocytes—so-called "pus-corpuscles." Eosinophilic leukocytes are common in gonorrheal pus and in asthmatic sputum. Examination of pus is directed chiefly to detection of bacteria.
When very few bacteria are present, culture methods must be resorted to, but such methods do not come within the scope of this work. When considerable numbers are present, they can be detected and often identified in cover-glass smears. Several smears should be made, dried, and fixed as described under Sputum (p. 32). One of these should be stained one-fourth to one-half minute with Löffler's methylene-blue, rinsed well with water, dried, mounted, and examined with an oil-immersion lens. This will show all bacteria except the tubercle bacillus, and often no other stain is necessary for their identification. In many cases special stains must be applied.
Gram's method (p. 40) is a very useful aid in distinguishing certain bacteria. The more important organisms react to this staining method as follows:
[p. 262]|
GRAM STAINING (Deep purple). |
GRAM DECOLORIZING (Colorless, unless a counterstain is used). |
| Staphylococcus. | Gonococcus. |
| Streptococcus. | Meningococcus. |
| Pneumococcus. | Bacillus of influenza. |
| Bacillus diphtheriæ. | Typhoid bacillus. |
| Bacillus tuberculosis. | Bacillus coli communis. |
| Bacillus of anthrax. | Spirillum of Asiatic cholera. |
| Bacillus of tetanus. | Bacillus pyocyaneus. |
| Bacillus aërogenes capsulatus. | Bacillus of Friedländer. |
| Koch-Weeks bacillus. | |
| Bacillus of Morax-Axenfeld. |
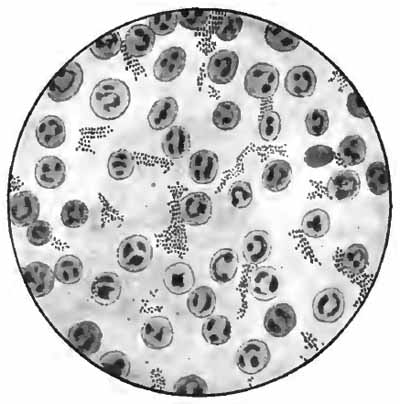
|
| FIG. 113.—Staphylococcus pyogenes albus from an abscess of the parotid gland (Jakob). |
The most common pus-producing organisms are staphylococci and streptococci. They are both cocci, or spheres, their average diameter being about 1 µ. Staphylococci are commonly grouped in clusters, often compared to bunches of grapes (Fig. 113). There are several varieties, which can be distinguished only in cultures. Streptococci are arranged side by side, forming chains of variable length (Fig. 114). Sometimes there are only three or four individuals in a chain; sometimes a chain [p. 263] is so long as to extend across several microscopic fields. Streptococci are more virulent than staphylococci, and are less common.
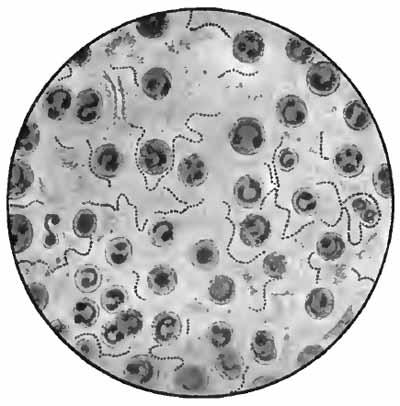
|
| FIG. 114.—Streptococcus pyogenes from a case of empyema (Jakob). |
Should bacteria resembling pneumococci be found, Buerger's method (p. 37) should be tried. When it is inconvenient to stain before the smears have dried, capsules can be shown by the method of Hiss. The dried and fixed smear is covered with a stain composed of 5 c.c. saturated alcoholic solution gentian-violet and 95 c.c. distilled water, and heated until steam rises. The preparation is then washed with 20 per cent. solution of copper sulphate, dried, and mounted in Canada balsam.
Pneumococci may give rise to inflammations in many locations. When they form short chains, demonstration of the capsule is necessary to distinguish them from streptococci.
If tuberculosis be suspected, the smears should be stained by one of the methods for the tubercle bacillus (pp. 32 and 127), or guinea-pigs may be inoculated. [p. 264] The bacilli are generally difficult to find in pus, and bacteria-free pus would suggest tuberculosis.

|
| FIG. 115.—Diplococcus pneumoniæ from ulcer of cornea (obj. one-twelfth oil-immersion) (study through courtesy of Dr. C. A. Oliver) (Boston). |
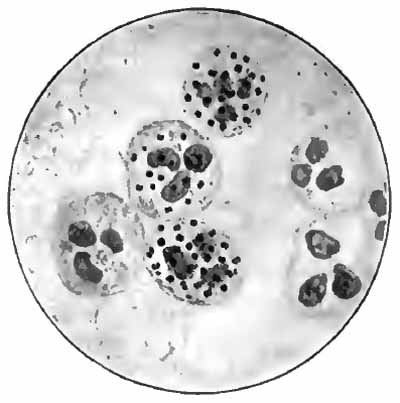
|
| FIG. 116.—Gonococci in urethral pus (McFarland). |
Gonococci, when typical, can usually be identified with sufficient certainty for clinical purposes in the smear stained with Löffler's methylene-blue. They are coffee-bean-shaped cocci which lie in pairs with their flat surfaces together (Fig. 116). They lie for the most part within pus-cells, an occasional cell being filled with them, while the surrounding cells contain few or none. A few are [p. 265] found outside of the cells. It is not usual to find gonococci when many other bacteria are present, even though the pus is primarily of gonorrheal origin. Whenever the identity of the organism is at all questionable, Gram's method should be tried. In rare instances it may be necessary to resort to cultures. The gonococcus is distinguished by its failure to grow upon ordinary media.
Gonococci are generally easily found in pus from untreated acute and subacute gonorrheal inflammations,—conjunctivitis, urethritis, etc.,—but are found with difficulty in pus from chronic inflammations and abscesses, and in urinary sediments.
The serous cavities contain very little fluid normally, but considerable quantities are frequently present as a result of pathologic conditions. The pathologic fluids are classed as transudates and exudates.
Transudates are non-inflammatory in origin. They contain only a few cells, and less than 2.5 per cent. of albumin, and do not coagulate spontaneously. The specific gravity is below 1018. Micro-organisms are seldom present.
Exudates are of inflammatory origin. They are richer in cells and albumin, and tend to coagulate upon standing. The specific gravity is above 1018. Bacteria are generally present, and often numerous. The amount of albumin is estimated by Esbach's method, after diluting the fluid. Bacteria are recognized by cultures, animal inoculation, or stained smears.
Exudates are usually classed as serous, serofibrinous, seropurulent, purulent, putrid, and hemorrhagic, which [p. 266] terms require no explanation. In addition, chylous and chyloid exudates are occasionally met, particularly in the peritoneal cavity. In the chylous form the milkiness is due mainly to the presence of minute fat-droplets, and is the result of rupture of a lymph-vessel. Chyloid exudates are milky chiefly from proteids in suspension, or fine débris from broken-down cells. These exudates are most frequently seen in carcinoma and tuberculosis of the peritoneum.
Cytodiagnosis.—This consists in a differential count of the cells in a transudate or exudate, particularly one of pleural or peritoneal origin.
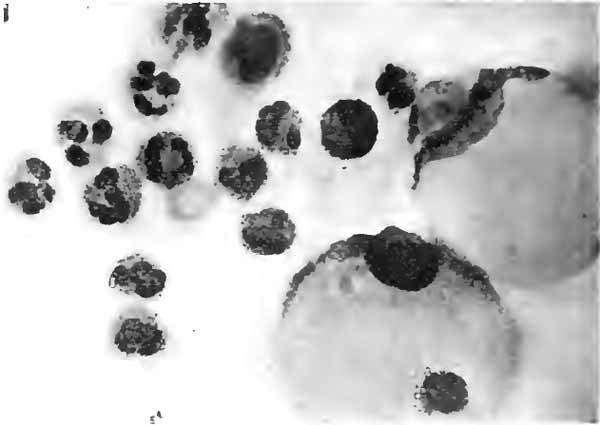
|
| FIG. 117.—Cytodiagnosis. Polymorphonuclear leukocytes and swollen endothelial cells from acute infectious non-tuberculous pleuritis (Percy Musgrave; photo by L. S. Brown). |
The fresh fluid, obtained by aspiration, is centrifugalized for at least five minutes; the supernatant liquid is poured off; and cover-glass smears are made and dried in the air. The smears are then stained with Wright's blood-stain, to which one-third its volume of pure methyl-alcohol has [p. 267] been added. Cover the smear with this fluid for one-half minute, then dilute with eight or ten drops of water, and let stand about two minutes. Wash gently in water, and [p. 268] dry by holding the cover-glass between the fingers over a flame. Mount in balsam and examine with a one-twelfth objective.
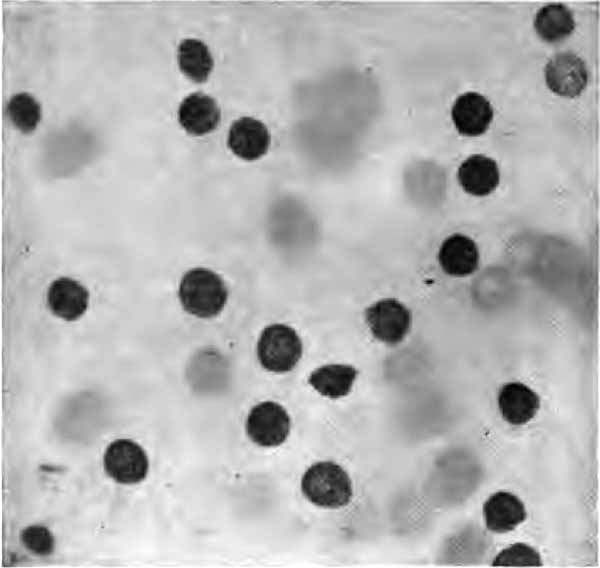
|
| FIG. 118.—Cytodiagnosis. Lymphoid cells from pleural fluid; case of tuberculous pleuritis (Percy Musgrave; photo by L. S. Brown). |
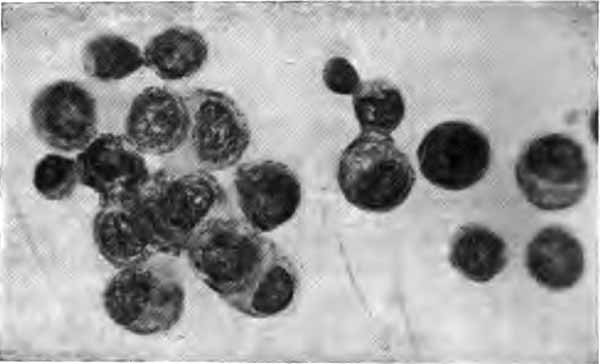
|
| FIG. 119.—Cytodiagnosis. Endothelial cells from transudate or mechanical effusion (Percy Musgrave; photo by L. S. Brown). |
Predominance of polymorphonuclear leukocytes (pus-corpuscles) points to an acute infectious process (Fig. 117).
Predominance of lymphocytes (Fig. 118) generally signifies tuberculosis. Tuberculous pleurisy due to direct extension from the lung may give excess of polymorphonuclears owing to mixed infection.
Predominance of endothelial cells, few cells of any kind being present, indicates a transudate (Fig. 119). Endothelial cells generally predominate in carcinoma, but are accompanied by considerable numbers of lymphocytes and red blood-corpuscles.
Examination of the fluid obtained by lumbar puncture is of value in diagnosis of certain forms of meningitis.
Tubercle bacilli can be found in the majority of cases of tuberculous meningitis. The sediment, obtained by thorough centrifugalization or by coagulation and digestion (p. 128) is spread upon slides and stained by one of the methods already given. A considerable number of smears should be examined. In doubtful cases, inoculation of guinea-pigs must be resorted to.
The Diplococcus intracellularis meningitidis is recognized as the cause of epidemic cerebrospinal fever, and can be detected in the cerebrospinal fluid of most cases, especially those which run an acute course. Cover-glass smears from the sediment should be stained by the method for the gonococcus. The meningococcus is an intracellular diplococcus which often cannot be distinguished [p. 269] from the gonococcus in stained smears (Fig. 120). It, also, decolorizes by Gram's method. The presence of such a diplococcus in meningeal exudates is, however, sufficient for its identification.

|
| FIG. 120.—Diplococcus intracellularis meningitidis in leukocytes. X2000 (Wright and Brown). |
Various organisms have been found in other forms of meningitis—the pneumococcus most frequently. In some cases no micro-organisms can be detected even by culture methods.
Inoculation of animals is one of the most reliable means of verifying the presence of certain micro-organisms in fluids and other material.
Clinically, it is applied almost exclusively to demonstration of the tubercle bacillus when other means have [p. 270] failed or are uncertain. The guinea-pig is the most suitable animal for this purpose. When the suspected material is fluid and contains pus, it should be well centrifugalized, and one or two cubic centimeters of the sediment injected by means of a large hypodermic needle into the peritoneal cavity or underneath the loose skin of the groin. Fluids from which no sediment can be obtained must be injected directly into the peritoneal cavity, since at least 10 c.c. are required, which is too great an amount to inject hypodermically. Solid material should be placed in a pocket made by snipping the skin of the groin with scissors, and freeing it from the underlying tissues for a short distance around the opening. When the intraperitoneal method is selected, several animals must be inoculated, since some are likely to die from peritonitis caused by other organisms before the tubercle bacillus has had time to produce its characteristic lesions.
The animals should be killed at the end of six or eight weeks, if they do not die before that time, and a careful postmortem examination should be made for the characteristic pearly-gray or yellow tubercles scattered over the peritoneum and through the abdominal organs, particularly the spleen, and for caseous inguinal and retroperitoneal lymph-glands. The tubercles and portions of the caseous glands should be crushed between two slides, dried, and stained for tubercle bacilli. The bacilli are difficult to find in the caseous material.
Micro-organisms are always present in large numbers. Among these is Leptothrix buccalis (Fig. 121), which is especially abundant in the crypts of the tonsils and the [p. 271] tartar of the teeth. The whitish patches of pharyngomycosis leptothrica are largely composed of these fungi. They are slender, segmented threads, which generally, but not always, stain violet with Lugol's solution, and are readily seen with a one-sixth objective. At times they are observed in the sputum and stomach fluid. In the former they might be mistaken for elastic fibers; in the latter, for Boas-Oppler bacilli. In either case, the reaction with iodin will distinguish them.

|
| FIG. 121.—Gingival deposit (unstained): a, Squamous epithelial cells; b, leukocytes; c, bacteria; d, Leptothrix buccalis (Jakob). |
Thrush is a disease of the mouth seen most often in children, and characterized by the presence of white patches upon the mucous membrane. It is caused by the thrush fungus, Oïdium albicans. When a bit from one of the patches is pressed out between a slide and cover and examined with a one-sixth objective, the fungus is seen to consist of a network of branching segmented hyphæ with numerous spores, both within the hyphæ and in the meshes between them (Fig. 122). The meshes also contain leukocytes, epithelial cells, and granular débris.
[p. 272]

|
| FIG. 122.—Thrush fungus (Oïdium albicans) (Jakob). |
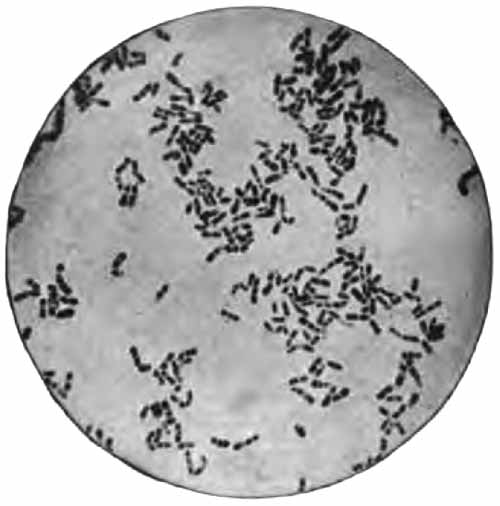
|
| FIG. 123.—Bacillus diphtheriæ, from culture on blood-serum. X1000 (Fränkel and Pfeiffer). |
Acute pseudomembranous inflammations, which occur chiefly upon the tonsils and nasopharynx, are generally caused by the diphtheria bacillus, but may result from streptococcic infection. In many cases diphtheria [p. 273] bacilli can be demonstrated in smears made from the membrane and stained with Löffler's methylene-blue or 2 per cent. aqueous solution of methyl-green. They are straight or curved rods, which vary markedly in size and outline, and stain very irregularly (Fig. 123). A characteristic form is a palely tinted rod with several deeply stained granules (metachromatic bodies), or with one such granule at each end. They stain by Gram's method. It is generally necessary, and always safer, to make a culture upon blood-serum, incubate for twelve hours, and examine smears from the growth.

|
| FIG. 124.—Bacillus and spirillum of Vincent, from case of ulcerative stomatitis. Stained (obj. one-twelfth oil-immersion; X1000) (Boston). |
Vincent's angina is a chronic pseudomembranous and ulcerative inflammation of pharynx and tonsils. It is probably caused by two micro-organisms living in symbiosis—one a fusiform bacillus, the other a long spirillum (Fig. 124). They can readily be demonstrated in smears stained with Löffler's methylene-blue. The bacillus is spindle shaped, more or less pointed at the [p. 274] ends, and about 6 to 12 µ long. The spirillum is a very slender, wavy thread, about 30 to 40 µ long.
Tuberculous ulcerations of mouth and pharynx can generally be diagnosed from curetings made after careful cleansing of the surface. The curetings are well rubbed between slide and cover, and the smears thus made are dried, fixed, and stained for tubercle bacilli. Since there is much danger of contamination from tuberculous sputum, the presence of tubercle bacilli is significant only in proportion to the thoroughness with which the ulcer was cleansed. The diagnosis is certain when the bacilli are found within groups of cells which have not been disassociated in making the smears.
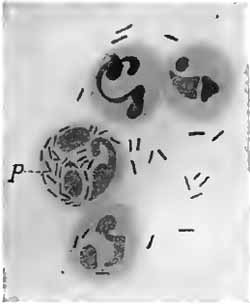
|
| FIG. 125.—Conjunctival secretion from acute contagious conjunctivitis; polynuclear leukocytes with the bacillus of Weeks; P, phagocyte containing bacillus of Weeks (one-twelfth oil-immersion; ocular iii) (Morax). |
Staphylococci, pneumococci, and streptococci are probably the most common of the bacteria to be found in nonspecific conjunctivitis and keratitis. The usual cause of acute infectious conjunctivitis, especially in cities, seems to be the Koch-Weeks bacillus. This is a minute, slender rod, which lies within and between the pus-corpuscles (Fig. 125), and is negative to Gram's stain. In smears it cannot be [p. 275] distinguished from the influenza bacillus, although its length is somewhat greater. The diplobacillus of Morax and Axenfeld gives rise to an acute or chronic blepharo-conjunctivitis without follicles or membrane, for which zinc sulphate seems to be a specific. It is widely distributed geographically, and is common in many regions. The organism is a short, thick diplobacillus, is frequently intracellular, and is Gram-negative (Fig. 126). A delicate capsule can sometimes be made out.

|
| FIG. 126.—The diplobacillus of Morax and Axenfeld (from a preparation by Dr. Harold Gifford). |
Early diagnosis of gonorrheal ophthalmia is extremely important, and can be made with certainty only by detection of gonococci in the discharge. They are easily found in smears from untreated cases. After treatment is begun they soon disappear, even though the discharge continues.
Pseudomembranous conjunctivitis generally shows either streptococci or diphtheria bacilli. In diagnosing diphtheric conjunctivitis, one must be on his guard against the [p. 276] xerosis bacillus, which is a frequent inhabitant of the conjunctival sac in healthy persons, and which is identical morphologically with the diphtheria bacillus. The clinical picture is hence more significant than the microscopic findings.
Various micro-organisms—bacteria, molds, protozoa—have been described in connection with trachoma, but the specific organism of the disease is not definitely known.
By far the most frequent exciting causes of acute otitis media are the pneumococcus and the streptococcus. The finding of other bacteria in the discharge generally indicates a secondary infection, except in cases complicating infectious diseases, such as typhoid fever, diphtheria, and influenza. Discharges which have continued for some time are practically always contaminated with the staphylococcus. The presence of the streptococcus should be a cause of uneasiness, since it much more frequently leads to mastoid disease and meningitis than does the pneumococcus. The staphylococcus, bacillus of Friedländer, colon bacillus, and Bacillus pyocyaneus may be met in chronic middle-ear disease.
In tuberculous disease the tubercle bacillus is present in the discharge, but its detection offers some difficulties. It is rarely easy to find, and precautions must always be taken to exclude the smegma and other acid-fast bacilli (p. 35), which are especially liable to be present in the ear. Rather striking is the tendency of old squamous cells to retain the red stain, and fragments of such cells may mislead the unwary.
Favus, tinea versicolor, and the various forms of ring-worm are caused by members of the fungus group. To demonstrate them, a crust or a hair from the affected area is softened with a few drops of 20 per cent. caustic soda solution, pressed out between a slide and cover, and examined with a one-sixth objective. They consist of a more or less dense network of hyphæ and numerous round or oval refractive spores. The cuts in standard works upon diseases of the skin will aid in differentiating the members of the group.
A large number of analyses of human and cow's milk are averaged by Holt as follows, Jersey milk being excluded because of its excessive fat:
| HUMAN MILK. | COW'S MILK. | |||
| Normal variations, per cent. |
Average, per cent. |
Average, per cent. |
||
| Fat | 3.00 to | 5.00 | 4.00 | 3.50 |
| Sugar | 6.00 to | 7.00 | 7.00 | 4.30 |
| Proteids | 1.00 to | 2.25 | 1.50 | 4.00 |
| Salts | 0.18 to | 0.25 | 0.20 | 0.70 |
| Water | 89.82 to | 85.50 | 87.30 | 87.00 |
| 100.00 | 100.00 | 100.00 | 100.00 | |
The reaction of human milk is slightly alkaline; of cow's, neutral or slightly acid. The specific gravity of each is about 1.028 to 1.032. Human milk is sterile when secreted, but derives a few bacteria from the lacteal ducts. Cow's milk, as usually sold, contains large numbers of bacteria. Microscopically, human milk is a fairly homogeneous emulsion of fat, and is practically destitute of cellular elements.
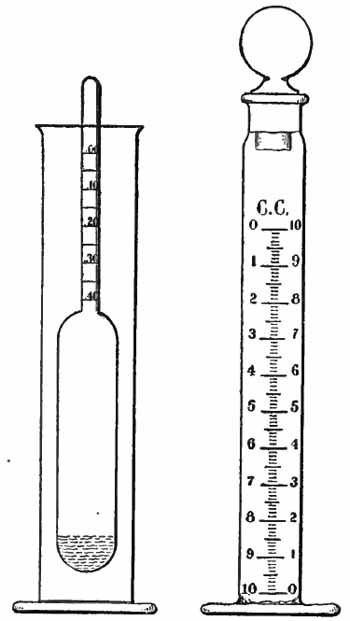
|
| FIG. 127.—Holt's milk-testing apparatus. |
Chemic examination of milk is of great value in solving [p. 278] the problems of infant feeding. The sample examined should be the middle milk, or the entire quantity from one breast. The fat and proteid can be estimated roughly, but accurately enough for many clinical purposes, by means of Holt's apparatus, which consists of a 10 c.c. cream gage and a small hydrometer (Fig. 127). The cream gage is filled to the 0 mark with milk, allowed to stand for twenty-four hours at room temperature, and the percentage of cream then read off. The percentage of [p. 279] fat is three-fifths that of the cream. The proteid is then approximated from a consideration of the specific gravity and the percentage of fat. The salts and sugar very seldom vary sufficiently to affect the specific gravity, hence a high specific gravity must be due to either an increase of proteid or decrease of fat, or both, and vice versâ. With normal specific gravity the proteid is high when the fat is high, and vice versâ. The method is not accurate with cow's milk.
For more accurate work the following methods, applicable to either human or cow's milk, are simple and satisfactory.

|
| FIG. 128.—Tube for milk analysis. |
Fat.—Leffmann-Beam Method.—This is essentially the widely used Babcock method, modified for the small quantities of milk obtainable from the human mammary gland. The apparatus consists of a special tube which fits the aluminum shield of the medical centrifuge (Fig. 128) and a 5 c.c. pipet. Owing to its narrow stem, the tube is difficult to fill and to clean. Exactly 5 c.c. of the milk are introduced into the tube by means of the pipet, and 1 c.c. of a mixture of equal parts of concentrated hydrochloric acid and amyl-alcohol is added and well mixed. The tube is filled to the 0 mark with concentrated sulphuric acid, adding a few drops at a time and agitating constantly. This is revolved in the centrifuge at 1000 revolutions a minute for three minutes, or until the fat has separated. The percentage is then read off upon the stem, each small division representing 0.2 per cent. of fat.
[p. 280] Proteids.—T. R. Boggs' Modification of the Esbach Method.—This is applied as for urinary albumin (p. 74), substituting Boggs' reagent for Esbach's. The reagent is prepared as follows:
| (1) | Phosphotungstic acid | 25 gm. |
| Distilled water | 125 c.c. | |
| (2) | Concentrated hydrochloric acid | 25 c.c. |
| Distilled water | 100 c.c. |
When the phosphotungstic acid is completely dissolved, mix the two solutions. This reagent is quite stable if kept in a dark glass bottle.
Before examination, the milk should be diluted according to the probable amount of proteid, and allowance made in the subsequent reading. For human milk the optimum dilution is 1:10; for cow's milk, 1:20. Dilution must be accurate.
Lactose.—The proteid should first be removed by acidifying with acetic acid, boiling, and filtering. Purdy's method may then be used as for glucose in the urine (p. 79); but it must be borne in mind that lactose reduces copper more slowly than glucose, and longer heating is, therefore, required; and that 35 c.c. of Purdy's solution is equivalent to 0.0268 gm. lactose (as compared with 0.02 gm. glucose).
It is frequently desirable to detect formalin, which is the most common preservative added to cow's milk. Add a few drops of dilute phenol solution to a few cubic centimeters of the milk, and run the mixture gently upon the surface of some strong sulphuric acid in a test-tube. If formaldehyd be present, a bright-red ring will appear [p. 281] at the line of contact of the fluids. This is not a specific test for formaldehyd, but nothing else likely to be added to the milk will give it.

|
| FIG. 129.—Spirochæte pallida: a and b, Typical pallida; c and d, atypical curves in pallida; e, thick pallida, apparently splitting into three; f, two pallida partly so closely coiled as to resemble thick portion of e (X1800) (Goldhorn). |
In 1905 Schaudinn and Hoffmann described the occurrence of a very slender, spiral micro-organism in the lesions of syphilis. This they named Spirochæte pallida, because of its low refractive power and the difficulty with which it takes up staining reagents. Its etiologic [p. 282] relation to syphilis is now almost universally admitted. It is not found in tertiary lesions.

|
| FIG. 130.—Spirochæte refringens (X1800) (Goldhorn). |
Spirochæte pallida is an extremely slender, spiral, motile thread, with pointed ends. It varies considerably in length, the average being about 7 µ, or the diameter of a red blood-corpuscle; and it exhibits three to twelve, sometimes more, spiral curves, which are sharp and regular and resemble the curves of a corkscrew (Fig. 129). It is so delicate that it is difficult to see even in well-stained preparations; a high magnification and careful focusing are, therefore, required. Upon ulcerated surfaces it is often mingled with other spiral micro-organisms, which adds to the difficulty of its detection. The most notable of these is Spirochæte refringens, which is distinguished by being coarser and having fewer curves of wider and less sharp contour (Fig. 130).
Spirochæte pallida is most easily demonstrated in chancres and mucous patches, although the skin lesions—papules, pustules, roseolous areas—often contain large numbers. Tissue-juice from the deeper portions of the lesions is the most favorable material for examination, because the organisms are commonly more abundant than upon ulcerated surfaces and are rarely accompanied by other micro-organisms. After cleansing the surface a superficial incision with a scalpel or sharp needle is made at the edge of a lesion, or the surface is gently scraped away with a curet, and a drop of blood and serum is expressed. The less blood the better, because the [p. 283] corpuscles may hide the spirochæte. Very thin cover-glass smears are then made.
Goldhorn's stain gives very good results. It can be purchased ready prepared from E. Leitz, New York. The unfixed smear is covered with the stain for four or five seconds. The excess of stain is poured off, and the preparation introduced slowly, with the film side down, into distilled water. It is held in this position for four or five seconds, and is then washed by shaking about in the water. By this method the Spirochæte pallida appears of a violet color, which can be changed to bluish black by flooding with Gram's iodin solution for fifteen or twenty seconds. The preparation is then washed, dried, and mounted.
Absence of spermatozoa is a more common cause of sterility than is generally recognized. In some cases they are present, but lose their motility immediately after ejaculation.
Semen must be kept warm until examined. When it must be transported any considerable distance, the method suggested by Boston is convenient. The fresh semen is placed in a small bottle to the neck of which a string is attached. This is then suspended from a button on the trousers so that the bottle rests against the skin of the inguinal region. It may be carried in this way for hours. When ready to examine, place a small quantity upon a warmed slide and apply a cover. The spermatozoa are readily seen with a one-sixth objective (Fig. 53). Normally, they are abundant and in active motion.
Detection of semen in stains upon clothing, etc., is [p. 284] often important. The finding of spermatozoa, after soaking the stain for an hour in normal salt solution or dilute alcohol and teasing in the same fluid, is absolute proof that the stain in question is semen, although it is not possible to distinguish human semen from that of the lower animals in this way.
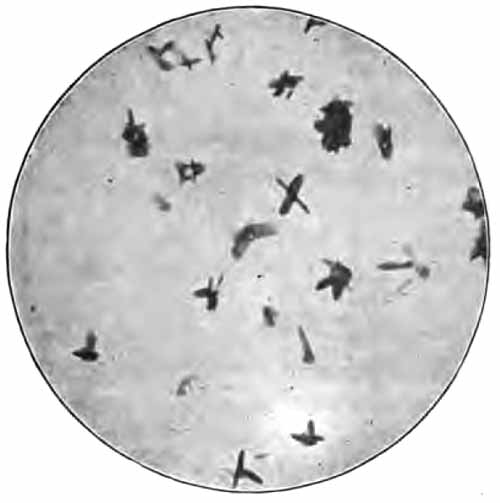
|
| FIG. 131.—Seminal crystals (medium size) (X750) from a stain on clothing. A single thread one-eighth inch long was used in the test, the stain being three years and four months old (Peterson and Haines). |
Florence's Reaction.—The suspected material is softened with water, placed upon a slide with a few drops of the reagent, and examined at once with a medium power of the microscope. If the material be semen, there will be found dark-brown crystals (Fig. 131) in the form of rhombic platelets resembling hemin crystals, or of needles often grouped in clusters. These crystals can [p. 285] also be obtained from crushed insects, watery extracts of various internal organs, and certain other substances, so that they are not absolute proof of the presence of semen. Negative results, upon the other hand, are conclusive, even when the semen is many years old.
The reagent consists of iodin, 2.54 gm.; potassium iodid, 1.65 gm.; and distilled water, 30 c.c.
The apparatus and reagents listed here are sufficient for all the tests described in the text. Those in smaller type are less frequently required. For ordinary routine work a much smaller list will suffice.
Beakers and flasks, several sizes, preferably of Jena glass.
Blood lancet, or some substitute (Fig. 64).
Bunsen-burner or alcohol lamp.
Buret, 25 c.c. capacity; preferably with Schellbach stripe.
Buret and filter-stand combined.
Centrifuge—hand, electric, or water-power (Figs. 16 and 17). With the last two a speed indicator is desirable. Radius of arm when in motion should be six and three-fourth inches. Plain and graduated tubes accompany the instrument; milk-tubes (Fig. 128) must be purchased separately. When sedimentation only is desired, the torfuge (Fig. 31) is a cheap and convenient substitute.
Cigaret-paper, "Zig-zig" brand, or some similar thin paper.
Corks, preferably of rubber, with one and two holes.
Cover-glasses, No. 2 thickness—seven-eighth-inch squares are most convenient.
[p. 287] Cover-glass forceps.
Esbach's tube (Fig. 23).
Evaporating dish.
Filter-paper: ordinary cheap paper for urine filtration; "ashless" quantitative filter-paper for chemic analyses.
Glass funnels.
Glass rods and tubing of sodium glass: for stirring rods, urinary pipets, etc.
Glass slides: the standard 1- by 3-inch size will answer for all work, although a few larger slides will be found convenient; those of medium thickness are preferable.
Graduates, cylindric form, several sizes.
Granite-ware basin.
Hemoglobinometer: see pp. 143 to 147 for descriptions of the different instruments.
Hemocytometer: either Türk or Zappert ruling is desirable (Figs. 69, 70, and 72).
Labels for slides and bottles.
Litmus paper, red and blue, Squibb's preferred.
Microscope (Fig. 1): should have Abbé condenser, 1- and 2-inch eye-pieces, and two-thirds, one-fifth, or long focus one-sixth and one-twelfth inch objectives. A one-half inch eye-piece, a micrometer eye-piece, and an attachable mechanical stage are very useful additions.
Petri dish or cleaned photographic plates for sputum examination.
Stomach-tube.
Test-glass, conic, one side painted half white, half black.
Test-tubes, rack, and cleaning brush.
Ureometer, Doremus-Hinds' pattern (Fig. 20).
Urinometer, preferably Squibb's (Fig. 14).
[p. 288] Blood-fixing oven, or Kowarsky's plate (Fig. 77).
Copper-foil and gauze.
Holt's cream gage and hydrometer (Fig. 127).
Horismascope (Fig. 22).
Pipets, graduated, 5 c.c. to 50 c.c. capacity.
Ruhemann's tube for uric-acid estimation (Fig. 21).
Saccharimeter (Fig. 25).
Strauss' separatory funnel for lactic-acid test (Fig. 87).
Suction filter.
Urinopyknometer of Saxe (Fig. 15).
Widal reaction outfit: either living agar cultures of the typhoid bacillus, or the dead cultures with diluting apparatus, which are sold under various trade names.
Water-bath.
All stains and many reagents are best kept in small dropping bottles. Formulæ are given in the text.
Acid, glacial acetic. Other strengths can be made from this as desired.
Acid, hydrochloric, concentrated (contains about 32 per cent. by weight of absolute hydrochloric acid). Other strengths can be made as desired.
Acid, nitric, strong, colorless.
Acid, nitric, yellow. Can be made from colorless acid by adding a splinter of pine, or allowing to stand in sunlight.
Acid, sulphuric, concentrated.
Alcohol, ethyl (grain-alcohol). This is ordinarily about 93 to 95 per cent., and other strengths can be made as desired.
Aqua ammoniæ fortior (sp. gr. 0.9).
Bromin or Rice's solutions (p. 67), for urea estimation.
[p. 289] Chloroform.
Diluting fluid for erythrocyte count (p. 154).
Diluting fluid for leukocyte count (p. 165).
Dimethyl-amido-azobenzol, 0.5 per cent. alcoholic solution.
Distilled water.
Esbach's reagent (p. 74).
Ether, sulphuric.
Ferric chlorid: saturated aqueous solution and 10 per cent. aqueous solution.
Haines' (or Fehling's) solution (p. 78).
Lugol's solution (Liquor Iodi Compositus, U.S.P.). Gram's iodin solution (p. 38) can be made from this by adding fourteen times its volume of water.
Obermayer's reagent (p. 64).
Phenylhydrazin, pure.
Phenol.
Phenolphthalein, 1 per cent. alcoholic solution.
Purdy's (or Fehling's) solution (p. 80).
Robert's reagent (p. 73).
Sodium chlorid (table-salt), saturated aqueous solution.
Sodium hydroxid (caustic soda), 40 per cent. solution; other strengths can be made from this as desired.
Sodium hydroxid, decinormal solution. This is best purchased ready prepared.
Sodium nitrite, 0.5 per cent. solution for diazo reaction. Must be freshly prepared.
Sulphanilic acid solution for diazo reaction (p. 91).
Stains:
Carbol-fuchsin (p. 33).
Eosin, saturated aqueous solution.
Gabbet's stain (p. 34).
[p. 290] Löffler's alkaline methylene-blue solution (p. 38).
Stain for fat: Sudan III, saturated solution in 70 per cent. alcohol; or 1 per cent. aqueous solution osmic acid.
Wright's stain for blood.
Tincture of guaiac, diluted to a light sherry-wine color (keep in a dark-glass bottle).
Turpentine, "ozonized" (p. 89).
Acid, boric, for preserving urine (p. 48).
Acid, oxalic.
Acid, salicylous (salicyl aldehyd), 10 per cent. alcoholic solution.
Alcohol, amylic.
Alcohol, ethyl, absolute.
Alcohol, methyl (pure).
Barium chlorid mixture (p. 62).
Benzol.
Boas' reagent or Günzburg's (p. 219).
Boggs' reagent (p. 280).
Calcium chlorid, 1 per cent. solution.
Canada-balsam in xylol: necessary only when permanent microscopic preparations are made.
Carbon disulphid.
Charcoal, animal.
Chromium trioxid.
Congo-red, strong alcoholic solution.
Copper sulphate.
Diluting fluid for blood-platelet count (p. 167).
Egg-albumen discs in glycerin (p. 221).
Ether, acetic, pure.
Florence's reagent (p. 285).
Formalin (40 per cent. solution of formaldehyd gas).
[p. 291] Iodin crystals.
Iron sulphid.
Lead acetate (sugar of lead); used in 10 per cent. solution to clarify urine.
Lead acetate, tribasic.
Lime-water.
Magnesium carbonate.
Müller's fluid saturated with mercuric chlorid (p. 37).
Pepsin, U.S.P.
Phenylhydrazin hydrochlorid.
Potassium ferrocyanid, 10 per cent. solution.
Potassium persulphate.
Ruhemann's reagent (p. 69).
Silver-nitrate crystals; also dram to the ounce aqueous solution, and "ammoniated" solution (p. 68).
Sodium alizarin sulphonate, 1 per cent. aqueous solution.
Sodium carbonate.
Sodium chlorid, 2 per cent. solution; from this, normal salt solution (0.8 per cent.) can be made as desired.
Sodium hyposulphite.
Sodium nitroprussid.
Sodium sulphate.
Stains:
Anilin-gentian violet (p. 38).
Bismarck-brown, saturated aqueous or alcoholic solution.
Ehrlich's triple stain for blood.
Eosin, 0.5 per cent. alcoholic solution for blood.
Fuchsin, weak solution; can be made when desired by adding a little carbol-fuchsin to a test-tube of water.
Gentian-violet, saturated alcoholic solution.
Goldhorn's spirochæte stain (p. 283).
Methylene-blue and borax solution (p. 193).
Methylene-blue, saturated aqueous solution for blood.
Sulphur, powdered.
[p. 292] Trichloracetic acid solution (p. 71).
Uranium nitrate, 5 per cent. aqueous solution.
Xylol.
Zinc, arsenic free.
| Meter (unit of length): | Millimeter (mm.) | = 1/1000 | meter. |
| Centimeter (cm.) | = 1/100 | meter. | |
| Kilometer | = 1000 | meters. | |
| Micron (µ) | = 1/1000 | millimeter. | |
| Gram (unit of weight): | Milligram (mg.) | = 1/1000 | gram. |
| Kilogram (kilo.) | = 1000 | grams. | |
| Liter (unit of capacity): | Cubic Centimeter | = 1/1000 | liter. Same as milliliter (ml.). |
| 1 Millimeter | = | 0.03937 (1/25 approx.) in. 1000 microns. |
| 1 Centimeter | = | 0.3937 (2/5 approx.) in. 0.0328 feet. |
| 1 Meter | = | 39.37 in. 3.28 feet. |
| 1 Micron (µ) | = | 1/25000 in. 0.001 millimeter. |
| 1 Gram | = | 15.43 grains. 0.563 dram (Avoir.). 0.035 ounce (Avoir.). 0.0022 pound (Avoir.). 0.257 dram (Apoth.). 0.032 ounce (Apoth.). 0.0027 pound (Apoth.). |
| 1 Kilogram | = | 35.27 ounce (Avoir.). 2.2 pound (Avoir.). |
| 1 Liter | = | 1.056 (1 approx.) quart. 61.02 cu. inches. 1000 cu. centimeters. |
| 1 Sq. Millimeter | = | 0.00155 sq. in. |
| 1 Sq. Centimeter | = | 0.1550 sq. in. |
| 1 Sq. Meter | = | 1550 sq. in. 10.76 sq. feet. |
| 1 Cu. Millimeter | = | 0.00006 cu. in. |
| 1 Cu. Centimeter | = | 0.0610 cu. in. 0.001 liter. |
| 1 Cu. Meter | = | 35.32 cu. feet. 61025.4 cu. in. |
| 1 Inch | = | 25.399 millimeters. |
| 1 Sq. Inch | = | 6.451 sq. centimeters. |
| 1 Cu. Inch | = | 16.387 cu. centimeters. |
| 1 Foot | = | 30.48 centimeters. |
| 1 Sq. Foot | = | 0.093 sq. meter. |
| 1 Cu. Foot | = | 0.028 cu. meter. |
| 1 Ounce | = | 437.5 grains. 16 drams. |
| 1 Pound | = | 16 ounces. |
| 1 Grain | = | 0.065 (3/50 approx.) grams. |
| 1 Dram | = | 1.77 (1¾ approx.) grams. |
| 1 Ounce | = | 28.35 (30 approx.) grams. |
| 1 Pound | = | 453.59 (500 approx.) grams. 27.7 cu. inches. 1.215 lb. Troy. |
| 1 Dram | = | 60 minims. |
| 1 Ounce | = | 8 drams. |
| 1 Pint | = | 16 ounces. |
| 1 Gallon | = | 8 pints. |
| 1 Dram | = | 3.70 cu. centimeters. |
| 1 Ounce | = | 29.57 cu. centimeters. |
| 1 Pint | = | 473.1 cu. centimeters. |
| 1 Gallon | = | 3785.4 cu. centimeters. 231 cu. inches. |
| 1 Scruple | = | 20 grains. |
| 1 Dram | = | 3 scruples 60 grains. |
| 1 Ounce | = | 8 drams 480 grains. |
| 1 Pound | = | 12 ounces. |
| 1 Grain | = | 0.065 grams. |
| 1 Dram | = | 3.887 grams. |
| 1 Ounce | = | 31.10 grams. |
| 1 Pound | = | 373.2 grams. |
| To convert |
minims fluidounces grains drams cubic centimeters cubic centimeters grams grams |
into |
cubic centimeters cubic centimeters grams grams minims fluidounces grains drams |
multiply by |
0.061 29.57 0.0648 3.887 16.23 0.0338 15.432 0.257 |
| CENTIGRADE. | FAHRENHEIT. | CENTIGRADE. | FAHRENHEIT. |
| 110° | 230° | 37° | 98.6° |
| 100 | 212 | 36.5 | 97.7 |
| 95 | 203 | 36 | 96.8 |
| 90 | 194 | 35.5 | 95.9 |
| 85 | 185 | 35 | 95 |
| 80 | 176 | 34 | 93.2 |
| 75 | 167 | 33 | 91.4 |
| 70 | 158 | 32 | 89.6 |
| 65 | 149 | 31 | 87.8 |
| 60 | 140 | 30 | 86 |
| 55 | 131 | 25 | 77 |
| 50 | 122 | 20 | 68 |
| 45 | 113 | 15 | 59 |
| 44 | 111.2 | 10 | 50 |
| 43 | 109.4 | +5 | 41 |
| 42 | 107.6 | 0 | 32 |
| 41 | 105.8 | -5 | 23 |
| 40.5 | 104.9 | -10 | 14 |
| 40 | 104 | -15 | +5 |
| 39.5 | 103.1 | -20 | -4 |
| 39 | 102.2 | —— | —— |
| 38.5 | 101.3 | 0.54° | = 1° |
| 38 | 100.4 | 1 | = 1.8 |
| 37.5 | 99.5 | 2 | = 3.6 |
| 2.5 | = 4.5 |
To convert Fahrenheit into Centigrade subtract 32 and multiply by 0.555.
To convert Centigrade into Fahrenheit multiply by 1.8 and add 32.