Transcriber’s notes:
In this transcription, hyperlinks are indicated by a black dotted underline (and a teal highlight when the mouse pointer hovers over them). A red dashed underline indicates the presence of a transcriber’s comment; scrolling the mouse pointer over such text will reveal the comment. Footnote markers in the text are hyperlinked to the footnotes located at the end of the book. Page numbers are shown in the right margin.
Cross-references to tables, figures and pages within this volume have been hyperlinked, but cross-references to the other three volumes of the publication have not been hyperlinked because they are not yet available in html format.
The table of contents contains a mix of italicised and non-italicised entries that generally correspond to different heading levels in the body of the text, but the correspondence is inaccurate and not all headings are listed. No attempt has been made to correct these anomalies.
Where appropriate, illustrations have been repositioned close to their first reference in the text, and their page locations have been adjusted in the list of illustrations at the beginning of the book.
The text contains several archaic symbols representing measures of weight that were used by apothecaries. Modern browsers display the symbols correctly with Times New Roman or Lucida Sans Unicode fonts. The main symbols are ‘ʒ’ representing the drachm unit of weight, and ‘℥’ representing the ounce unit of weight (8 drachms = 1 ounce). The third symbol does not have an exact computer equivalent and has been represented in this transcription by the character ‘ɱ’, which can signify ‘minim’ (a measure of volume equal to 1/60th of a fluid drachm), ‘drop’, or ‘part by volume’. If the symbols are not displayed correctly, try using a different font or a different browser, or click on ‘minim’, ‘drachm’ or ‘ounce’ to see images of what they look like. Roman numerals x, v, i and j (i and j both represent 1) indicate the quantities associated with these symbols.
Various inconsistencies of spelling and hyphenation occur throughout the text; some are simple typographical errors but most are probably variations attributable to the book's multiple authorship. Words with variable spellings that occur with similar frequency (e.g. trocar / trochar, aneurism / aneurysm) have not been changed, but most other spelling inconsistencies have been ‘corrected’ to the predominant form (e.g. Caesarian --> Caesarean, turbinate --> turbinal). Omitted letters have been corrected by inserting the missing letters in square brackets (e.g. sella turc[ic]a). Simple typos such as uretha (urethra) and polpyus (polypus) have been corrected silently, and likewise with missing punctuation such as commas omitted from the index and the table of contents. An apostrophe is used inconsistently with the proper noun Bruening or Bruenings.
Inconsistencies of spacing and hyphenation have been treated similarly. For example, spaces have been removed from the abbreviations i.e. e.g. and from percentage values. Compound nouns that occur equally often with/without hyphens, have not been changed, e.g. bone forceps / bone-forceps, attic wall / attic-wall, whereas those that are more often either hyphenated or not hyphenated, have been standardised accordingly, e.g. punch forceps --> punch-forceps, heart-failure --> heart failure.
| HENRY FROWDE | HODDER & STOUGHTON |
| Oxford University Press | Warwick Square, E.C. |
Great as have been the advances made in Surgery during the last fifteen years, there is no direction in which they have been more noticeable than in the elaboration of those comparatively small but important details of operative technique which do so much to ensure a low mortality and a successful result.
These improvements have been developed simultaneously throughout the whole of the vast field covered by modern Surgery, and it has become increasingly difficult for any single writer to deal with such an important subject as Operative Surgery in an authoritative and efficient manner. The scope of the subject is so wide that it is difficult to ensure that the work when published shall be thoroughly up to date, while a second and even greater difficulty is for any one, however great his ability and experience, to deal equally exhaustively and authoritatively with all of the many branches of which he would have to treat.
To avoid both of these difficulties and thus to make sure that the work shall reflect faithfully the present position of British Operative Surgery, the plan has been adopted of securing the co-operation of a number of prominent British Surgeons. Each writer deals with a branch of the subject in which he has had special experience, and upon which, therefore, he is entitled to speak with authority.
Besides the two important points just referred to, a third equally important one has been kept in view throughout. Particular care has been taken to make the work of as much practical utility to the reader as possible. Not only are the various operations described in the fullest detail and with special reference to the difficulties and dangers and the best methods of overcoming and avoiding them, but the indications for the individual operations are described at length, and the after-treatment and results receive adequate notice.
It is therefore hoped that the work will be useful alike to those who are about to operate for the first time, and to those surgeons of experience who desire to keep themselves informed as to the progress that has been made in the various branches of Operative Surgery.
The division of the work into a number of sections each written by a different author, necessarily involves some overlapping of subjects and some diversity of opinion upon points of technique. Efforts have been made to prevent overlapping of subjects as far as possible by care in their distribution and by conference between the authors concerned, but no attempt has been made to harmonize conflicting views. Each author supports his individual opinions by the weight of his authority, and any discrepancies may be taken to represent the absence of unanimity on various minor points that is well known to exist among surgeons of all countries.
The task of editing a work contributed to by so many writers might well appear to be an onerous one, but, owing to the promptitude, courtesy, and forbearance of all concerned, it has been a source of great pleasure, and the Editor’s most cordial thanks are tendered to all those who have devoted so much time and trouble to the work.
Every effort has been made to keep this volume strictly within the definition of a work upon Operative Surgery—a somewhat difficult task in the case of certain of the special subjects with which it deals. In some cases methods of examination or manipulation have been described that are not strictly operative in nature, but their inclusion has been justified upon the ground that many of them are essential in operations upon the regions concerned, and all require special manipulative skill and dexterity.
The Index to this volume has been arranged in five parts, one part for each Section comprised in it. In this way it has been possible to economize space and, it is hoped, to render the task of reference easier.
In the Section on Vaginal Gynæcological Operations, instrument blocks have been kindly supplied by Messrs. Montague, Down Bros., and Griffin. The remaining illustrations are from original sketches by the author.
In the Section on Ophthalmic Operations, Messrs. Weiss have kindly supplied the instrument blocks. The remainder of the illustrations are original. Mr. Mayou desires to thank Mr. W. H. McMullen for valuable help in reading the proof sheets.
In the Section on Operations upon the Ear, all the illustrations, with the exception of the instrument blocks kindly supplied by Messrs. Mayer and Meltzer and a few illustrations from Tod’s Manual of Diseases of the Ear, are original.
In the Section on Operations upon the Nose, the instrument blocks have been supplied by Messrs. Mayer and Meltzer, who have also furnished them in the Section on Operations upon the Throat. Mr. F. A. Rose has kindly read the proof sheets of the latter Section, for which Mr. Harmer desires to thank him.
JOHN BLAND-SUTTON, F.R.C.S. (Eng.)
Surgeon to the Middlesex Hospital, and Senior Surgeon to the Chelsea Hospital for Women, London
Abdominal Gynæcological Operations
JOHN PHILLIPS, M.A., M.D. (Cantab.), F.R.C.P.
Professor of Obstetric Medicine, King’s College, London; Obstetric Physician and Gynæcologist to King’s College Hospital
Vaginal Gynæcological Operations
M. S. MAYOU, F.R.C.S. (Eng.)
Assistant Surgeon to the Central London Ophthalmic Hospital; Ophthalmic Surgeon to the Children’s Hospital, Paddington Green
Ophthalmic Operations
HUNTER F. TOD, M.A., M.D. (Cantab.), F.R.C.S. (Eng.)
Aural Surgeon to the London Hospital
Operations upon the Ear
W. DOUGLAS HARMER, M.C. (Cantab.), F.R.C.S. (Eng.)
Surgeon to the Throat and Nose Department, St. Bartholomew’s Hospital
Operations upon the Larynx and Trachea
StCLAIR THOMSON, M.D., F.R.C.P. (Lond.), F.R.C.S. (Eng.)
Professor of Laryngology and Physician for Diseases of the Throat, King’s College Hospital, London
Operations upon the Nose and its Accessory Cavities
SECTION I
OPERATIONS UPON THE FEMALE GENITAL ORGANS
PART I
ABDOMINAL GYNÆCOLOGICAL OPERATIONS
By JOHN BLAND-SUTTON, F.R.C.S. (Eng.)
Surgeon to the Middlesex Hospital and Senior Surgeon to the Chelsea Hospital for Women, London.
CHAPTER I
PAGES
| CŒLIOTOMY | |
| Preparation of Patient, 3. Basins, Dishes, and Instruments, 4. Suture and Ligature Material, 5. Dabs, 5. Gloves, Operating Table, Anæsthesia, 6. The Incision, 7. Misplaced Viscera, 8. Closure of Wound, 8 | 3–9 |
CHAPTER II
| OVARIOTOMY | |
| The Operation, 10. Cysts of the Broad Ligaments, 14. Spurious Capsules, 15. For Carcinoma of Ovary, 15. Incomplete Ovariotomy, 16. Anomalous Ovariotomy, 16. Ovariotomy followed by Hysterectomy, 17. Repeated Ovariotomy, 17. Pregnancy after Bilateral Ovariotomy, 17. Ovariotomy at Extremes of Life, 18. Ovariotomy in Old Age, 19. Mortality, 19 | 10–20 |
CHAPTER III
| OÖPHORECTOMY | |
| Operation, 22. Abdominal Hysterectomy after Bilateral Oöphorectomy and Ovariotomy, 25. Mortality, 25. Operation for Primary Cancer of the Fallopian Tube, 26 | 21–28 |
CHAPTER IV
| OPERATIONS FOR EXTRA-UTERINE GESTATION | |
| Indications, 29. Operation, 29. Concurrent Intra- and Extra-uterine Pregnancy, 33. Results of Operative Treatment, 34 | 29–35 |
CHAPTER V
| HYSTERECTOMY AND MYOMECTOMY | |
| Indications, 36. Subtotal Hysterectomy, 36. Total Hysterectomy, 40. Mortality, 44. Risks of Abdominal Hysterectomy, 45. Abdominal Myomectomy, 46 | 36–49 |
CHAPTER VI
| ON THE RELATIVE VALUE OF TOTAL AND SUBTOTAL HYSTERECTOMY | |
| Cancer of the Body of the Uterus and Fibroids, 52. Sarcoma, 53. Cancer of the Uterus after Bilateral Ovariotomy, 55. Adenomyoma of the Uterus, 56. Fate and Value of Belated Ovaries, 56 | 50–60 |
CHAPTER VII
| HYSTERECTOMY FOR PRIMARY CARCINOMA OF THE UTERUS | |
| For Cancer of the Cervix, 61. For Cancer of the Body of the Uterus, 63 | 61–65 |
CHAPTER VIII
| OPERATIONS FOR DISPLACEMENT OF THE UTERUS | |
| Ventro-suspension for Retroflexion of the Uterus, 66. Ventro-fixation for Prolapse of the Uterus, 67 | 66–68 |
CHAPTER IX
| OPERATIONS UPON THE UTERUS DURING PREGNANCY, PARTURIENCY, AND PUERPERY | |
| Cæsarean Section, 69; Immediately after the Death of the Mother, 72. Ovariotomy and Hysterectomy during Pregnancy and in Labour, 73. Ovariotomy during the Puerperium, 76. Fibroids and Pregnancy, 77. Pregnancy with Cancer of the Cervix, 82. Concurrent Uterine and Tubal Pregnancy, 82. Pregnancy with Tumours growing from the Pelvic Walls, 83. Operations for Puerperal Sepsis, 83 | 69–85 |
CHAPTER X
| OPERATIONS FOR INJURIES OF THE UTERUS | |
| Gynæcological, 86. Obstetric, 87; to the Pregnant Uterus, 89; to the Gravid Uterus in the course of an Abdominal Operation, 89. Bullet Wounds of the Pregnant Uterus, 90. Stab-wounds of the Pregnant Uterus, 91 | 86–92 |
CHAPTER XI
| THE AFTER-TREATMENT, RISKS, AND SEQUELÆ OF ABDOMINAL GYNÆCOLOGICAL OPERATIONS | |
| After-treatment of Abdominal Operations, 93. Complications of Abdominal Gynæcological Operations—Metrostaxis, 95; Bed-sores, 95; Post-anæsthetic Paralysis, 95; Giving way of the Wound, 96; Hæmorrhage, 97; Intrapelvic Hæmorrhage, 98; Pneumonia, 99; Parotitis, 99; Thrombosis, 101; Pulmonary Embolism, 101; Foreign Bodies left in the Abdomen, 105; Tetanus, 107; Injury to the Intestines, 109; Intestinal Obstruction, 110; Perforating Ulcer of the Stomach and Small Intestine, 111; Injuries to the Bladder, 111; to the Ureter, 112. The fate of Ligatures, 117. Post-operative Kraurosis, 120. The Cicatrix, 120 | 93–122 |
PART II
VAGINAL GYNÆCOLOGICAL OPERATIONS
By JOHN PHILLIPS, M.A., M.D. (Cantab.), F.R.C.P.
Professor of Obstetric Medicine, King’s College, London; Obstetric Physician and Gynæcologist to King’s College Hospital.
CHAPTER XII
| PREPARATION OF THE PATIENT FOR PERINEAL AND VAGINAL OPERATIONS: OPERATIONS FOR INJURIES TO THE PERINEUM AND PELVIC FLOOR | |
| Preparation of the Patient, 125. Operations for Repair of a Complete Laceration of the Perineum, 127. Operation for Laceration of the Pelvic Floor, 132 | 125–133 |
CHAPTER XIII
| OPERATIONS UPON THE URETHRA AND BLADDER | |
| Extirpation of a Urethral Caruncle, 134. Operations for Incontinence following Labour, 134; for Vesico-vaginal Fistula, 135; for Recto-vaginal Fistula, 139; for Cystocele, 140 | 134–141 |
CHAPTER XIV
| OPERATIONS UPON THE VULVA AND VAGINA | |
| Operations upon Bartholin’s Glands, 142. Operations for Atresia of the Hymen and the Vagina, 143. Dilatation of the Vulval Orifice, 143. Colpotomy, 144; Anterior, 145; Posterior, 147; Lateral, 148 | 142–148 |
CHAPTER XV
| OPERATIONS UPON THE UTERUS | |
| Passage of the Uterine Sound, 149. Reposition of a Chronic Uterine Inversion, 151. Curetting the Uterus, 152. Dilatation of the Cervix, 156—Rapid Dilatation, 157; Gradual Dilatation, 159. Operations for Hypertrophy of the Cervix, 160. Trachelorrhaphy, 161. Vaginal Fixation, 164 | 149–164 |
CHAPTER XVI
| OPERATIONS FOR NEW GROWTHS OF THE UTERUS | |
| For Uterine Fibro-myomata, 165—for Pedunculated Tumours, 165; for Sessile Tumours, 166; for Interstitial Tumours, 167. Vaginal Hysterectomy, 167—for Carcinoma, 168; for Fibroids, 173 | 165–173 |
SECTION II
OPHTHALMIC OPERATIONS
By M. S. MAYOU, F.R.C.S. (Eng.)
Assistant Surgeon to the Central London Ophthalmic Hospital; Ophthalmic Surgeon to the Children’s Hospital, Paddington Green.
CHAPTER I
| GENERAL CONSIDERATIONS APPLICABLE TO OPERATIONS UPON THE EYE | |
| General Preliminaries to an Operation, 177. Local Preparation of the Patient, 80. Making and Healing of Wounds in the Globe, 182—Purification of Hands, 182; of Instruments, 183; Direction of Incision, 183; Position of Incision, 184; Dressings, 186; Bandaging, 186 | 177–186 |
CHAPTER II
| OPERATIONS UPON THE LENS | |
| Surgical Anatomy, 187. Discission or Needling, 189—for Cataract, 189; for High Myopia, 190. Capsulotomy, 192. Evacuation, 194. Evulsion of the Capsule, 195. Extraction of the Lens, 195. Modifications, 201; Delivery of the Lens by Irrigation, 203; Extraction of the Lens in its Capsule, 204; Subconjunctival Extraction, 204. Couching, 209 | 187–210 |
CHAPTER III
| OPERATIONS UPON THE IRIS | |
| Iridotomy, 211. Alternative Methods—Kuhnt’s Operation, 212; Ziegler’s, 213. Iridectomy—Optical Iridectomy, 214; Glaucoma Iridectomy, 217—for small Growths of the Iris, 225; for Prolapse of the Iris, 225. Transfixion of the Iris, 226. Division of Anterior Synechiæ, 227 | 211–227 |
CHAPTER IV
| OPERATIONS UPON THE SCLEROTIC | |
| Anterior Sclerotomy, 228. Cyclo-dialysis, 229. Sclerectomy, 231. Posterior Sclerotomy, 232. Paracentesis of the Anterior Chamber, 233. For Penetrating Wounds of the Globe, 234. Electro-magnet Operations—with Small Magnet, 237; with Giant Magnet, 238 | 228–239 |
CHAPTER V
| OPERATIONS UPON THE CORNEA AND CONJUNCTIVA | |
| Removal of a Foreign Body from the Cornea, 240. Cauterization of the Cornea, 240. Operations for Conical Cornea, 241. Removal of Tumours involving the Cornea, 243. Tattooing the Cornea, 243. Scraping Calcareous Films, 243. Operations upon the Conjunctiva—Removal of Foreign Bodies, 244; for Pterygium, 244; Expression, 245; Conjunctivoplasty, 245; Removal of Tarsal Cysts, 246 | 240–246 |
CHAPTER VI
| OPERATIONS UPON THE EXTRA-OCULAR MUSCLES | |
| Squint Operations, 247. Tenotomy, 248. Advancement, 251 | 247–254 |
CHAPTER VII
| ENUCLEATION OF THE GLOBE AND ALLIED OPERATIONS | |
| Enucleation, 255. Evisceration, 257. Mules’s Operation, 259. Frost’s Operation, 259. Operations upon the Socket after Removal of the Eye—Paraffin Injection, 260. Operations for Restoration of a Contracted Socket—Skin-grafting, 261; Inclusion of Flaps (Maxwell’s Operation), 261 | 255–262 |
CHAPTER VIII
| OPERATIONS UPON THE EYELIDS | |
| Surgical Anatomy, 263. Suture of Wounds of the Eyelids, 263. Operations for Ankyloblepharon, 264; for Symblepharon, 264. Upon the Palpebral Aperture, 265—Canthoplasty, 265; Canthotomy, 265; Canthorrhaphy, 265; Tarsorrhaphy, 266. Ptosis Operations, 267; Shortening the Eyelid by Excision of a portion of the Tarsal Plate, 267. Attachment of the Lid to the Occipito-frontalis Muscle, 268. Advancement of the Levator Palpebræ Muscle, 272. Grafting a portion of the Superior Rectus into the Lid, 273 | 263–274 |
CHAPTER IX
| OPERATIONS FOR ENTROPION, REPAIR OF THE EYELIDS, TRICHIASIS, AND ECTROPION | |
| Electrolysis, 275. Skin and Muscle Operation, 275. Rectification of a Faulty Curvature of the Tarsus—Burow’s Operation, 276; Streatfield’s Operation, 277. Transplantation of the Lash-bearing Area—Arlt’s Operation, 278. Ectropion Operations, 279—for Passive Ectropion, 280; Snellen’s Suture Method, 280; Fergus’s Operation, 281; Kuhnt’s Operation, 281; Argyll Robertson’s Operation, 282. For the Active or Cicatricial Form, 284; VY Operation, 284; Denonvillier’s Operation, 285; Fricke’s Operation, 285; Thiersch’s Skin-grafting, 287. Repair of large Losses of Substance from the Eyelids, 287; De Vincentiis’ Operation, 287; Dieffenbach’s Operation, 288 | 275–289 |
CHAPTER X
| OPERATIONS UPON THE LACHRYMAL APPARATUS | |
| For the Relief of Lachrymal Obstruction, 290—Dilatation of the Canaliculus, 290; Slitting the Canaliculus, 291; Syringing the Lachrymal Duct, 292; Probing the Lachrymal Duct, 292; the Insertion of Styles, 293. For Obliteration of the Canals, 294; Obliteration of the Canaliculi, 294; Excision of the Lachrymal Sac, 294. Opening a Lachrymal Abscess, 297. Operations upon the Lachrymal Gland—Removal of the Palpebral Portion, 298; Removal of the Orbital Portion, 299. Operations upon the Orbit—Exploration of the Orbit (Krönlein’s Method), 299; Evisceration of the Orbit, 301; Opening an Orbital Abscess, 301 | 290–301 |
SECTION III
OPERATIONS UPON THE EAR
By HUNTER F. TOD, M.A., M.D. (Cantab.), F.R.C.S. (Eng.)
Aural Surgeon to the London Hospital.
CHAPTER I
| EXAMINATION OF THE EAR: GENERAL CONSIDERATIONS WITH REGARD TO OPERATIONS | |
| Examination of the Ear, 305—Sources of Illumination, 305; Technique of Examination, 306; Method of cleansing the Ear, 307. General Considerations with regard to Operations—Preliminary Surgical Toilet, 309; Anæsthesia, 310. Position of Patient and Surgeon, 313 | 305–313 |
CHAPTER II
| OPERATIONS UPON THE EXTERNAL AUDITORY CANAL | |
| Operations for Furunculosis, 314. Removal of Exostoses from the External Meatus, 316. Removal of Foreign Bodies—by Syringing, 322; by Instruments, 323; by Post-aural Incision, 326; by Operation upon the Mastoid, 327. Operations for Stenosis of the External Meatus, 328. Operations for Atresia, 330; for Aural Polypus, 331 | 314–334 |
CHAPTER III
| OPERATIONS UPON THE TYMPANIC MEMBRANE AND WITHIN THE TYMPANIC CAVITY | |
| Surgical Anatomy of the Tympanum, 335. Paracentesis, 336. Artificial Perforation of the Tympanic Membrane, 340. Division of the Anterior Ligament, 341. Division of the Posterior Fold, 341. Intratympanic Operations, 342; Division of Adhesions, 342; Tenotomy of the Tensor Tympani, 346; Tenotomy of the Stapedius, 347. Removal of Granulations from the Tympanic Cavity, 348. Operations upon the Ossicles—Direct Mobilization, 349; Removal of the Ossicles, 351 | 335–363 |
CHAPTER IV
| OPERATIONS UPON THE EUSTACHIAN TUBE | |
| Catheterization, 364. Passing of the Eustachian Bougie, 369. Washing out the Tympanic Cavity through the Eustachian Tube, 372 | 364–372 |
CHAPTER V
| OPERATIONS UPON THE MASTOID PROCESS:
WILDE’S INCISION AND SCHWARTZE’S OPERATION | |
| Surgical Anatomy, 373. History of the Mastoid Operation, 375. Wilde’s Incision, 377. Schwartze’s Operation, 378. Treatment of Special Conditions—in an Infant, 389; Subperiosteal Abscess, 389; Bezold’s Mastoid Abscess, 389; Necrosis, 390; Osteomyelitis, 390 | 373–390 |
CHAPTER VI
| THE COMPLETE MASTOID OPERATION | |
| Methods of Operation, 392; Küster-Bergmann (Schwartze-Stacke) Operation, 393; Wolf’s Operation, 396; Stacke’s Operation, 397; Preservation of the Ossicles and Tympanic Membrane, 399. The Formation of Post-meatal Skin Flaps, 401. Closure of the Wound, 404. Skin-grafting after the Mastoid Operation, 405. After-treatment of the Case, 410. Difficulties and Dangers of the Operation, 412. Results, 415 | 391–416 |
CHAPTER VII
| OPERATIONS UPON THE LABYRINTH | |
| General Considerations, 417. Indications, 417. Surgical Anatomy, 420. Methods of Operating, 421; Curetting a Localized Lesion of Wall, 421; Opening the Vestibule, 422; Removal of the Cochlea, 424; Extirpation of the Labyrinth, 425 | 417–428 |
CHAPTER VIII
| OPERATIONS FOR EXTRA-DURAL ABSCESS AND MENINGITIS OF OTITIC ORIGIN | |
| On Intracranial Complications in General, 429. Operations for Extra-dural Abscess, 430. Operations for Meningitis of Otitic Origin, 433 | 429–438 |
CHAPTER IX
| OPERATIONS FOR LATERAL SINUS THROMBOSIS OF OTITIC ORIGIN | |
| General Considerations, 439. Exposure of the Lateral Sinus, 440. Opening of the Lateral Sinus, 442. Ligature of the Jugular Vein, 446. Exposure of the Jugular Bulb, 454 | 439–458 |
CHAPTER X
| OPERATIONS FOR INTRACRANIAL ABSCESS OF OTITIC ORIGIN | |
| Indications, 459. Operation, 460. After-treatment, 469. Complications, 469. Prognosis and subsequent Progress, 470. Recurrence of Symptoms, 471 | 459–471 |
SECTION IV
OPERATIONS UPON THE LARYNX AND TRACHEA
By W. DOUGLAS HARMER, M.C. (Cantab.), F.R.C.S. (Eng.)
Surgeon to the Throat and Nose Department, St. Bartholomew’s Hospital.
CHAPTER I
| ENDOLARYNGEAL OPERATIONS | |
| Indications, 475. Operation by Indirect Laryngoscopy, 477. Operation by Direct Laryngoscopy, 479 | 475–486 |
CHAPTER II
| EXTRA-LARYNGEAL OPERATIONS | |
| Thyrotomy, 487. Hemi-laryngectomy, 495. Anatomy of the Laryngeal Lymphatics, 496. Total Laryngectomy, 498. Comparative Results of Extra-laryngeal Operations, 502. Infrathyreoid Laryngotomy, 510 | 487–516 |
CHAPTER III
| OPERATIONS UPON THE TRACHEA | |
| Tracheotomy, 517; in Diphtheria, 526; in Conditions other than Diphtheria, 544. Tracheo-fissure and Resection of the Trachea, 546 | 517–548 |
CHAPTER IV
| INTUBATION OF THE LARYNX | |
| Intubation v. Tracheotomy in Diphtheria, 549. Indications, 552. Operation, 553. Difficulties, 555. After-treatment, 556. Complications, 557 | 549–558 |
CHAPTER V
| TRACHEOSCOPY AND BRONCHOSCOPY | |
| Indications, 559. Tracheoscopy, 560. Upper Bronchoscopy, 562. Lower Bronchoscopy, 562. Complications, 563. Results, 566 | 559–566 |
SECTION V
OPERATIONS UPON THE NOSE AND ITS ACCESSORY CAVITIES
By StCLAIR THOMSON, M.D., F.R.C.P. (Lond.), F.R.C.S. (Eng.)
Professor of Laryngology and Physician for Diseases of the Throat, King’s College Hospital, London.
CHAPTER I
| GENERAL CONSIDERATIONS
IN REGARD TO OPERATIONS UPON THE NOSE AND NASO-PHARYNX | |
| Sources of Illumination, 569. Local Anæsthesia, 572. Local Ischæmia, 573. Bleeding and its Control, 574. The Protection of the Lower Air-passages from the Descent of Blood, 576. Shock, 577. Sepsis and other Complications, 577. Asepsis, 578. After-treatment, 578. Cleansing the Nose, 579. After-results, 580 | 569–580 |
CHAPTER II
| OPERATIONS FOR INJURIES, DEFORMITIES, FOREIGN BODIES,
AND RHINOLITHS: OPERATIONS UPON THE TURBINALS: OPERATIONS IN SYPHILIS AND LUPUS | |
| Operations for Injuries to the Nose—Fractures of the Nasal Bones and Septum, 581. For Congenital Occlusion of the Nostrils, 582. Removal of Foreign Bodies, 584; of Rhinoliths, 586. Operations upon the Turbinals, 586; upon the Inferior Turbinal, 587; upon the Middle Turbinal, 592. For the Results of Syphilis—Sequestrotomy, 594; Post-syphilitic Adhesions of the Velum, 595. For Tuberculosis, 596 | 581–596 |
CHAPTER III
| OPERATIONS UPON THE NASAL SEPTUM | |
| For Deformities—Removal of Spurs, 597; Perforating the Septum, 598. For Simple Deviation, 598; Gleason-Watson Operation, 599; Asch’s Operation, 599; Moure’s Operation, 599. For Combined Bony and Cartilaginous Deformity—Submucous Resection, 601. Complementary Operations, 610. For Perforation of the Nasal Septum, 611. For Abscess, 612. For Hæmatoma, 612 | 597–612 |
CHAPTER IV
| OPERATIONS FOR REMOVAL OF NASAL GROWTHS THROUGH THE NOSTRILS: OPERATIONS FOR OBTAINING DIRECT ACCESS TO THE NASAL CAVITIES AND NASO-PHARYNX | |
| Removal by the Snare, 613. Removal by Forceps and Curettes, 615. Lateral Rhinotomy (Moure’s Operation), 618. Rouge’s Operation, 622. Combination of Moure’s and Rouge’s Operations, 625. Extension of Rouge’s Operation to allow of Access to the Maxillary Antrum, 625. Other Methods, 625 | 613–625 |
CHAPTER V
| OPERATIONS UPON THE ACCESSORY NASAL SINUSES | |
| Operations upon the Maxillary Sinus—Catheterizing the Maxillary Sinus, 626; Puncturing from the Nose, 626; from the Alveolar Margin, 628. Operation through the Canine Fossa only, 631; the Caldwell-Luc Radical Operation, 631; Drainage through the Nasal Wall only, 637. Operations upon the Frontal Sinus—Catheterizing and Washing out the Frontal Sinus, 638; Opening the Frontal Sinus in Acute Suppuration, 642; Killian’s Operation, 642; the Ogston-Luc Operation, 651; Kuhnt’s Operation, 653. Operations upon the Sphenoidal Sinus, 653; Sounding and Washing out, 653; Opening the Sphenoidal Sinus, 656. Operation in Multiple Sinus Suppuration, 659 | 626–660 |
CHAPTER VI
| OPERATIONS INVOLVING THE NASO-PHARYNX: OPERATIONS FOR RETROPHARYNGEAL ABSCESS: OPERATIONS FOR NASO-PHARYNGEAL ADENOIDS | |
| Methods of obtaining Access to the Naso-pharynx through the Nose, 661; through the Mouth, 662. Retropharyngeal Abscess, 664. Removal of Naso-pharyngeal Adenoids, 665 | 661–672 |
| FIG. | PAGE | |
| 1. | Secondary Cancer of the Ovary | 15 |
| 2. | Secondary Cancer of the Ovary in Section | 15 |
| 3. | An Infected Fallopian Tube | 23 |
| 4. | A Tuberculous Fallopian Tube and Ovary: Entire and in Section | 24 |
| 5. | Primary Cancer of the Fallopian Tube | 27 |
| 6. | A Section of Primary Cancer of the Fallopian Tube | 27 |
| 7. | A Gravid Fallopian Tube | 30 |
| 8. | A Gravid Fallopian Tube, containing Twins | 32 |
| 9. | A Diagram to show the Arterial Supply of the Uterus | 37 |
| 10. | A Fibroid growing near the Right Uterine Cornu | 38 |
| 11. | The Mattress Suture | 40 |
| 12. | The Stump after Subtotal Hysterectomy | 40 |
| 13. | A Bicornate Uterus | 42 |
| 14. | A Bicornate Uterus shortly after Delivery | 43 |
| 15. | Villous Disease of the Uterus | 45 |
| 16. | An Adenomyomatous Uterus | 55 |
| 17. | An Adenomyomatous and Tuberculous Uterus | 56 |
| 18. | Uterus with the Decidua in situ | 58 |
| 19. | Cancer of the Uterus | 64 |
| 20. | The Fundus of a Uterus | 68 |
| 21. | Portion of Ovary and Fallopian Tube | 71 |
| 22. | A Uterus distorted by Fibroids | 76 |
| 23. | A Gravid Uterus in Sagittal Section | 79 |
| 24. | Diagram representing a Gunshot Injury of the Uterus | 91 |
| 25. | The Pulmonary Artery and Adjacent Part of the Lung and Trachea | 103 |
| 26. | A Pair of Pressure Forceps | 106 |
| 27. | The Relation of Parts after Ricard’s Operation of Uretero-cysto-neostomy | 114 |
| 28. | A Uterus in Sagittal Section | 119 |
| 29. | Patient prepared for Operation | 126 |
| 30. | Complete Laceration of the Perineum | 127 |
| 31. | Long-handled Sharp-pointed Scissors curved on the flat | 128 |
| 32. | Complete Laceration of the Perineum | 128 |
| 33. | Complete Laceration of the Perineum | 129 |
| 34. | Laceration of the Pelvic Floor | 132 |
| 35. | Repair of a Lacerated Perineum, with Non-union of the Sphincter Ani, before a Plastic Operation | 133 |
| 36. | Repair of a Laceration of the Perineum after a Plastic Operation | 133 |
| 37. | Auvard’s Self-retaining Speculum | 136 |
| 38. | Knives for freshening the Edges of a Vesico-vaginal Fistula | 136 |
| 39. | Toothed Forceps for use in Vesico-vaginal Fistula | 136 |
| 40. | Emmett’s Hook | 136 |
| 41. | Sims’s Operation for the Repair of a Vesico-vaginal Fistula | 136 |
| 42. | Simon’s Operation for the Repair of a Vesico-vaginal Fistula | 136 |
| 43. | Repair of a Vesico-vaginal Fistula by Dédoublement | 137 |
| 44. | Repair of a Vesico-vaginal Fistula. Sims’s Operation | 137 |
| 45. | Stoltz’s Operation for Cystocele | 140 |
| 46. | Sims’s Vaginal Rest | 144 |
| 47. | Pozzi’s Retractors | 145 |
| 48. | Anterior Colpotomy | 146 |
| 49. | Martin’s Trochar for Pelvic Abscess | 147 |
| 50. | The Passage of the Uterine Sound. Introduction of the point into the external os uteri | 149 |
| 51. | The Passage of the Uterine Sound. Commencement of the tour de maître | 149 |
| 52. | The Passage of the Uterine Sound. Completion of the tour de maître | 150 |
| 53. | The Passage of the Uterine Sound. Entry of the sound into the uterine cavity | 150 |
| 54. | Chronic Uterine Inversion | 151 |
| 55. | Volsella for fixing the Cervix | 154 |
| 56. | Hegar’s Dilators (three sizes) for dilatation of the Cervix Uteri | 154 |
| 57. | Metal Bougies for dilatation of the Cervix | 154 |
| 58. | Bozemann’s Double-channelled Tube | 154 |
| 59. | Budin’s Celluloid Catheter | 154 |
| 60. | Murray’s Flushing Curette; Blunt Curette | 154 |
| 61. | Dilatation of the Cervix | 158 |
| 62. | Marckwald’s Operation for Congenital Hypertrophy of the Cervix | 160 |
| 63. | Hegar’s Operation for Supravaginal Elongation of Cervix | 160 |
| 64. | Emmett’s Scissors (left) for Trachelorrhaphy | 162 |
| 65. | Trachelorrhaphy | 162 |
| 66. | Pedunculated Fibroid Polypi in various Stages of Extrusion | 165 |
| 67. | Wire Écraseur | 166 |
| 68. | Submucous Fibro-myomata, capable of Treatment by Morcellement | 166 |
| 69. | Galabin’s Broad-ligament Needle (right) | 171 |
| 70. | Jessett’s Broad-ligament Needle | 171 |
| 71. | Vaginal Hysterectomy | 171 |
| 72. | Vaginal Hysterectomy. Final stage | 172 |
| 73. | Schauta’s Needle-holder | 172 |
| 74. | Window of the Operating Theatre, King’s College Hospital | 179 |
| 75. | Bull’s-eye Electric Hand-lamp | 180 |
| 76. | Lang’s Eye Speculum | 182 |
| 77. | Undine for washing out the Conjunctival Sac | 182 |
| 78. | Cataract Extraction | 183 |
| 79. | Sympathetic Ophthalmia | 184 |
| 80. | Cystoid Scar after Glaucoma Iridectomy | 185 |
| 81. | An Eye Bandage | 186 |
| 82. | A Pressure Bandage | 186 |
| 83. | A Lens Three Weeks after Needling | 187 |
| 84. | Anatomy of the Anterior Segment of the Eye | 189 |
| 85. | Eye Speculum | 191 |
| 86. | Fixation Forceps | 191 |
| 87. | Secondary Cataract | 192 |
| 88. | Capsulotomy. The method of incising the capsule | 193 |
| 89. | Capsulotomy. The method of dividing a dense band | 194 |
| 90. | Iris Forceps | 195 |
| 91. | Iris Scissors | 195 |
| 92. | A Vectis | 195 |
| 93. | Pagenstecher’s Spoon | 195 |
| 94. | Lens Extraction | 196 |
| 95. | The Knife entering the Anterior Chamber in Cataract Extraction | 197 |
| 96. | Making the Counter-puncture in Cataract Extraction | 197 |
| 97. | Incision and Iridectomy in Cataract Extraction | 198 |
| 98. | Opening the Capsule with Forceps in Cataract Extraction | 199 |
| 99. | Cataract Extraction | 200 |
| 100. | McKeown’s Irrigation Apparatus for washing out the Anterior Chamber | 203 |
| 101. | Subconjunctival Extraction | 204 |
| 102. | Iridotomy | 211 |
| 103. | Iridotomy | 211 |
| 104. | Iridotomy by Ziegler’s Method | 213 |
| 105. | Iridotomy by Ziegler’s Method | 213 |
| 106. | Iridotomy by Ziegler’s Method | 213 |
| 107. | Optical Iridectomy | 216 |
| 108. | Optical Iridectomy | 216 |
| 109. | Optical Iridectomy | 217 |
| 110. | The Normal Angle of the Anterior Chamber | 217 |
| 111. | The Angle of the Anterior Chamber from a Case of Recent Glaucoma | 218 |
| 112. | The Angle of the Chamber in a Case of Chronic Glaucoma | 219 |
| 113. | Iridectomy for Glaucoma | 219 |
| 114. | Iridectomy for Glaucoma | 221 |
| 115. | Iridectomy for Glaucoma | 221 |
| 116. | Iridectomy for Glaucoma | 222 |
| 117. | Glaucoma Iridectomy | 223 |
| 118. | Prolapse of the Iris through a Punctured Wound of the Cornea | 226 |
| 119. | Cyclo-dialysis Operation | 229 |
| 120. | Cyclo-dialysis Operation | 231 |
| 121. | Lagrange Operation for the Production of a Cystoid Scar in Chronic Glaucoma | 232 |
| 122. | Lagrange Operation for Chronic Glaucoma | 232 |
| 123. | Hollow Needle used for Paracentesis of the Anterior Chamber | 234 |
| 124. | Author’s Chair for the Localization of Foreign Bodies in the Eye by the X-rays | 236 |
| 125. | Small Electro-magnet for extracting Pieces of Steel from the Eye | 237 |
| 126. | Large Electro-magnet | 239 |
| 127. | Electro-cautery | 241 |
| 128. | Tattooing Needles | 243 |
| 129. | Graddy’s Forceps | 245 |
| 130. | Tenotomy | 249 |
| 131. | Tenotomy by the Open Method | 250 |
| 132. | Prince’s Forceps for Advancement | 252 |
| 133. | Advancement by the Three-stitch Method | 253 |
| 134. | Enucleation | 257 |
| 135. | Mules’s Operation. First step | 258 |
| 136. | Mules’s Operation. | 258 |
| 137. | Maxwell’s Operation for Contracted Socket. First step | 262 |
| 138. | Maxwell’s Operation. Final step | 262 |
| 139. | Canthorrhaphy | 266 |
| 140. | Harman’s Operation for Ptosis | 270 |
| 141. | Ptosis Operation. Panas’ | 271 |
| 142. | Ptosis Operation. Advancement of the Levator Palpebræ | 273 |
| 143. | Ptosis Operation. Advancement of the Levator Palpebræ | 273 |
| 144. | Treacher Collins’s Entropion Forceps | 275 |
| 145. | Lid Clamp | 277 |
| 146. | Streatfield’s Entropion Operation | 278 |
| 147. | Arlt’s Operation for Trichiasis | 278 |
| 148. | Snellen’s Sutures | 280 |
| 149. | Fergus’s Operation for Slight Ectropion of the Lower Lid | 281 |
| 150. | Modified Kuhnt’s Operation for Severe Ectropion. Second step | 282 |
| 151. | Modified Kuhnt’s Operation. Fourth step | 282 |
| 152. | Argyll Robertson’s Operation for Ectropion. Second step | 283 |
| 153. | Argyll Robertson’s Operation for Ectropion. Final step | 283 |
| 154. | VY Operation for Ectropion of the Lower Lid due to a Scar. First step | 284 |
| 155. | VY Operation for Ectropion. Final step | 284 |
| 156. | Denonvillier’s Operation for Ectropion of the Lower Lid. First step | 285 |
| 157. | Denonvillier’s Operation for Ectropion | 285 |
| 158. | Fricke’s Operation | 286 |
| 159. | De Vincentiis’ Operation to replace the Loss of the Inner Portion of the Lower Lid | 288 |
| 160. | De Vincentiis’ Operation completed | 288 |
| 161. | Modified Dieffenbach’s Operation to replace the Loss of the whole Lower Lid. First step | 288 |
| 162. | Modified Dieffenbach’s Operation. Third step | 288 |
| 163. | Canaliculus Dilator | 290 |
| 164. | Canaliculus Knife | 291 |
| 165. | Lachrymal Syringe | 292 |
| 166. | Muller’s Retractor for Excision of the Lachrymal Sac | 294 |
| 167. | Axenfeld’s Retractor for Excision of the Lachrymal Sac | 294 |
| 168. | Excision of the Lachrymal Sac | 295 |
| 169. | Excision of the Lachrymal Sac | 295 |
| 170. | Excision of the Palpebral Portion of the Lachrymal Gland | 298 |
| 171. | Clar’s Lamp | 305 |
| 172. | Gruber’s Aural Speculum | 306 |
| 173. | Angular Spring Forceps | 306 |
| 174. | Examination of the Ear | 307 |
| 175. | Aural Forceps holding Cotton-wool | 307 |
| 176. | Milligan’s Intratympanic Syringe | 308 |
| 177. | Neumann’s Syringe for Subcutaneous Injection | 311 |
| 178. | Burkhardt-Merian’s Aural Instrument | 314 |
| 179. | Crocodile Forceps | 324 |
| 180. | Imray’s Scoop for extracting a Foreign Body | 325 |
| 181. | Aural Probe | 332 |
| 182. | Wilde’s Aural Snare | 332 |
| 183. | Wilde’s Snare being passed round an Aural Polypus | 332 |
| 184. | Wilde’s Snare gripping the Neck of Polypus | 332 |
| 185. | Polypus arising from the Attic Region | 332 |
| 186. | Anatomical Preparation of the Middle Ear | 335 |
| 187. | Paracentesis Knife held in position in the Hand | 337 |
| 188. | Tympanic Membrane showing Incision in Acute Suppuration of the Middle Ear | 338 |
| 189. | Line of Incision in Acute Suppuration of the Attic | 338 |
| 190. | Lines of Incisions in Intratympanic Operations | 341 |
| 191. | Cutting through Intratympanic Adhesions | 344 |
| 192. | Free Edge of Tympanic Membrane cut through | 344 |
| 193. | Sexton’s Instrument | 344 |
| 194. | Method of using Siegle’s Speculum | 345 |
| 195. | Division of Intratympanic Adhesion with Excision of Handle of Malleus | 346 |
| 196. | Schwartze’s Tenotomy Knife | 347 |
| 197. | Lucae’s Probe | 350 |
| 198. | To show Sites of Perforation in Attic Suppuration and Caries of the Ossicles | 352 |
| 199. | Removal of the Malleus by Wilde’s Snare. First position | 354 |
| 200. | Removal of the Malleus by Wilde’s Snare. Second position | 354 |
| 201. | Delstanche’s Ring-knife | 354 |
| 202. | Removal of Malleus by Delstanche’s Ring-knife | 355 |
| 203. | Ludwig’s Incus Hook | 356 |
| 204. | Zeroni’s Incus Hook | 356 |
| 205. | Removal of Incus by Zeroni’s Hook | 356 |
| 206. | Pfau’s Attic Punch-forceps | 357 |
| 207. | Removal of the Outer Attic-wall with Forceps | 357 |
| 208. | Diagrammatic Section to show Correct and Wrong Positions of Incus Hook | 360 |
| 209. | Eustachian Catheter | 365 |
| 210. | Passing the Eustachian Catheter | 365 |
| 211. | Passing the Eustachian Catheter | 365 |
| 212. | Passing the Eustachian Catheter | 366 |
| 213. | Passing the Eustachian Catheter | 366 |
| 214. | Author’s Graduated Eustachian Bougie | 370 |
| 215. | Left Temporal Bone, showing Anatomy of the Middle Ear and Mastoid Process | 373 |
| 216. | Diagram showing Position of Sink Incisions in Post-aural Operations | 380 |
| 217. | Schwartze’s Operation | 381 |
| 218. | Schwartze’s Operation | 382 |
| 219. | Schwartz’s Seeker | 383 |
| 220. | Schwartze’s Operation completed | 384 |
| 221. | The ‘Radical’ Mastoid Operation | 393 |
| 222. | Stacke’s Protector | 394 |
| 223. | The ‘Radical’ Mastoid Operation | 395 |
| 224. | Pfau’s Curette for the Eustachian Tube | 396 |
| 225. | The ‘Radical’ Mastoid Operation completed | 396 |
| 226. | Wolf’s Operation | 397 |
| 227. | Stacke’s Operation | 398 |
| 228. | Post-meatal Skin Flaps | 401 |
| 229. | Post-meatal Skin Flaps | 401 |
| 230. | Closure of Wound after ‘Radical’ Mastoid Operation | 401 |
| 231. | Körner’s Post-meatal Flap | 402 |
| 232. | Panse’s Post-meatal Flap | 402 |
| 233. | Stacke’s Post-meatal Flap | 402 |
| 234. | Skin-grafting of Mastoid Wound Cavity after Operation | 406 |
| 235. | Ballance’s ‘Stopper’ for pushing in the Graft | 406 |
| 236. | Pipette for sucking Air and Fluid from beneath the Graft | 406 |
| 237. | Skin-grafting of Mastoid Wound Cavity after Operation | 407 |
| 238. | Skin-grafting of Mastoid Wound Cavity after Operation | 407 |
| 239. | Posterior Portion of Skin Graft covering Outer Surface of Wound Cavity | 408 |
| 240. | Diagram to show Exposure of the Semicircular Canals | 423 |
| 241. | Operation upon the Labyrinth | 424 |
| 242. | Extirpation of the Labyrinth | 425 |
| 243. | Method of Removal of Bone by the Forceps | 434 |
| 244. | Diagram to show the usual Points at which the Lateral Sinus is primarily infected | 442 |
| 245. | The Lateral Sinus exposed and opened | 444 |
| 246. | Incision for Exposure of the Internal Jugular Vein | 448 |
| 247. | Exposure of the Internal Jugular Vein high up | 449 |
| 248. | Ligature of the Internal Jugular Vein low down in the Neck | 450 |
| 249. | Free Exposure of the Lateral Sinus, which has been incised, with Ligature of the Internal Jugular Vein | 451 |
| 250. | Method of suturing the Open End of the Internal Jugular Vein in the Neck | 452 |
| 251. | Topography of the Auditory Region of the Skull | 462 |
| 252. | Exploration for a Temporo-sphenoidal Abscess | 463 |
| 253. | Exploration for a Cerebellar Abscess | 467 |
| 254. | Skiagram showing a Tumour of the Larynx | 476 |
| 255. | Horsford’s Instrument for transfixing the Epiglottis | 478 |
| 256. | Multiple Papillomata of the Larynx | 479 |
| 257. | Tube-spatulæ used for Laryngoscopy | 481 |
| 258. | Removal of Multiple Papillomata by Direct Laryngoscopy | 482 |
| 259. | Intrinsic Tumour of the Larynx | 487 |
| 260. | Extrinsic Tumour of the Larynx | 487 |
| 261. | Thyrotomy | 490 |
| 262. | Total Laryngectomy | 498 |
| 263. | Total Laryngectomy. Gluck’s Method | 501 |
| 264. | Infrathyreoid Laryngotomy | 510 |
| 265. | Instruments for Laryngotomy | 512 |
| 266. | Laryngotomy Canula fitted with Inner Tube | 513 |
| 267. | Skiagram showing an Angular Tracheotomy Tube in the Trachea | 518 |
| 268. | Anatomy of the Larynx and Trachea and the Position of Incisions for the Operations in this Region | 525 |
| 269. | Tubes for Tracheotomy | 527 |
| 270. | Trachea showing Ulceration caused by a Badly Fitting Tube | 537 |
| 271. | Stenosis following Tracheotomy | 539 |
| 272. | Tubes used in the Treatment of Stenosis of the Larynx | 539 |
| 273. | Trachea showing Ulceration into the Innominate Artery after Tracheotomy | 542 |
| 274. | Aneurism of the Aorta perforating the Trachea | 542 |
| 275. | Sarcoma of the Trachea | 546 |
| 276. | Instruments for Intubation of the Larynx | 553 |
| 277. | Instruments for Bronchoscopy | 560 |
| 278. | Instruments for Bronchoscopy | 562 |
| 279. | Upper Bronchoscopy with the Patient in the Dorsal Position | 564 |
| 280. | Lower Bronchoscopy with the Patient in the Dorsal Position | 565 |
| 281. | Laryngoscope Lamp | 570 |
| 282. | Clar’s Electric Light | 570 |
| 283. | Frontal Search-light | 571 |
| 284. | Meyer’s hollow Vulcanite Nasal Splint | 581 |
| 285. | Krause’s Trochar and Canula | 583 |
| 286. | Nasal Punch-forceps | 583 |
| 287. | Post-nasal Forceps | 584 |
| 288. | Nasal Dressing Forceps | 585 |
| 289. | First Step in removing the Anterior End of the Inferior Turbinal, which is seen to have undergone Polypoid Degeneration | 587 |
| 290. | Nasal Scissors | 588 |
| 291. | Amputation of the Posterior End of the Inferior Turbinal | 590 |
| 292. | Nasal Spokeshave | 592 |
| 293. | First Step in the Removal of the Anterior End of the Middle Turbinal | 594 |
| 294. | Second Step in the Removal of the Anterior End of the Middle Turbinal | 594 |
| 295. | Cresswell Baber’s Nasal Saw | 597 |
| 296. | The Gleason-Watson Operation for Deformity of the Septum | 599 |
| 297. | Asch’s Cutting Scissors | 599 |
| 298. | Lake’s Rubber Splint | 599 |
| 299. | Bayonet Knife | 604 |
| 300. | Incision for Submucous Resection of the Septum | 605 |
| 301. | Making the Incision from the Convex Side in Submucous Resection of the Septum | 605 |
| 302. | Dull-edged Detacher | 605 |
| 303. | Denudation of the Septum in Submucous Resection | 606 |
| 304. | Complete Denudation of the Deviated Septum | 606 |
| 305. | Ballenger’s Swivel Septum Knife | 606 |
| 306. | The Method of employing Ballenger’s Swivel Septum Knife | 607 |
| 307. | Submucous Resection of the Septum | 607 |
| 308. | Submucous Resection of the Septum | 608 |
| 309. | Submucous Resection of the Septum | 608 |
| 310. | Semi-diagrammatic Transverse Section of the Nose | 610 |
| 311. | Operation for Perforation of the Septum | 612 |
| 312. | Nasal Snare | 613 |
| 313. | Luc’s Nasal Forceps | 616 |
| 314. | Tongue Clip | 617 |
| 315. | Incisions for Lateral Rhinotomy (Moure’s Operation) | 619 |
| 316. | The Area of Bone removed in Lateral Rhinotomy | 619 |
| 317. | Lateral Rhinotomy | 620 |
| 318. | Rouge’s Operation. First stage | 622 |
| 319. | Rouge’s Operation. Second stage | 623 |
| 320. | Catheterizing the Maxillary Sinus | 626 |
| 321. | Lichtwitz’s and Moritz Schmidt’s Antrum Needles | 627 |
| 322. | Puncturing the Maxillary Sinus | 627 |
| 323. | Antrum Drills | 629 |
| 324. | Solid Rubber Obturators | 629 |
| 325. | Antrum Nozzle | 629 |
| 326. | Washing out the Maxillary Sinus from an Alveolar Opening | 630 |
| 327. | The Incision in the Caldwell-Luc Operation upon the Maxillary Sinus | 632 |
| 328. | The Caldwell-Luc Operation upon the Maxillary Sinus | 632 |
| 329. | Opening the Maxillary Sinus from the Nose | 633 |
| 330. | Carwardine’s Punch-forceps | 634 |
| 331. | The Opening into the Maxillary Sinus from the Inferior Meatus of the Nose | 635 |
| 332. | Denker’s Operation | 637 |
| 333. | Catheterizing the Frontal Sinus | 639 |
| 334. | Radiograph to show the Value of the Röntgen Rays | 639 |
| 335. | Radiograph showing Canula in the Frontal Sinus | 639 |
| 336. | Killian’s Operation upon the Frontal Sinus | 644 |
| 337. | Killian’s Operation upon the Frontal Sinus | 644 |
| 338. | Periosteal Elevators | 645 |
| 339. | Killian’s Triangular Curved Chisel | 645 |
| 340. | Citelli’s Bone-forceps | 645 |
| 341. | Hajek’s Bone-forceps | 645 |
| 342. | Killian’s Operation upon the Frontal Sinus | 646 |
| 343. | Radiograph of the Sphenoidal Sinus | 653 |
| 344. | Radiograph of the Sphenoidal Sinus | 653 |
| 345. | Catheterizing the Sphenoidal Sinus | 654 |
| 346. | Killian’s Long Nasal Speculum | 655 |
| 347. | Radiograph showing a Probe in the Sphenoidal Sinus | 657 |
| 348. | Sphenoidal Punch-forceps | 657 |
| 349. | Adenoid Curette | 667 |
| 350. | The Removal of Naso-pharyngeal Adenoids | 667 |
| 351. | Removal of Naso-pharyngeal Adenoids | 668 |
When the abdomen is opened for the purpose of removing a diseased viscus, the operation receives a specific name, such as nephrectomy, gastrectomy, splenectomy, and so forth. In many instances the abdomen is occupied by a tumour which defies the skill of the surgeon to localize to any particular organ until it is exposed to view through an incision; it is usual to apply the term cœliotomy to an operation of this kind, and it merely implies that the belly is opened by a cut. Cœliotomy is a useful expression, because many abnormal conditions arise in the abdomen which require treatment through an incision in its walls which do not lend themselves to an expressive term, for example, the removal of omental cysts, the evacuation of pus, blood, or the removal of foreign bodies, &c. It is true that a cœliotomy performed on an uncertain diagnosis may become a colectomy, ovariotomy, hysterectomy, &c., and the preliminary step to the performance of the operations to be described in this section is an abdominal incision, or cœliotomy. For whatever purpose a cœliotomy is required in the treatment of diseases of the female pelvic organs, the preparation of the patient and the initial steps are alike; it will therefore be convenient to describe the manner of carrying them out.
The preparation of the patient. It rarely happens that an operation is so urgent as to leave little time for a thorough preparation of the patient. It is desirable that the preliminaries should occupy two days at least. During this time the patient is kept in bed and the bowels are freely evacuated, either by calomel at night, with a saline draught in the morning, or by an ounce of castor oil.
On the morning of the operation the large bowel is thoroughly emptied by a soap and water enema, care being taken to use soft soap, to avoid producing a pimply eruption known as the ‘enema rash’.
It is well known that injuries to the abdominal organs, whether by accident or in the course of a surgical operation, are liable to be followed by septic parotitis. Recent writers attribute this complication to microbic infection of the ducts of the salivary glands (see p. 99); its occurrence may be avoided by including careful cleaning of the teeth among the preliminaries advisable for an abdominal operation. It is such a simple and comfortable ordinance that there is no reason for not following it.
The preparation of the skin needs to be very thoroughly carried out. After a warm bath the hair is shaved from the abdomen, pubes and vulva, and the skin is well washed with warm soapy water and swathed in gauze compresses wrung out of a solution of perchloride of mercury, 1 in 5,000. These compresses remain for twelve hours. The abdomen is again washed, and a second compress is applied which remains on until the operation.
Occasionally patients object to have the abdomen and pubes shaved. In such cases the hair can be easily removed by a depilatory. I have found a powder prepared according to the following formula useful:—
Sodium monosulphide, 1 part; calcium oxide, 1 part; starch, 2 parts; sufficient water is added to make a stiff paste, which is spread over the parts. After five minutes it is washed off by means of a dab of cotton-wool and the skin freely washed with warm water. This preparation is only efficacious when freshly prepared.
The washing and application of compresses require care on the part of the nurse, for some patients have skin so tender that it is easily blistered, and a crop of small pustules is a source of inconvenience, and leads to stitch-abscesses. In certain cases over-preparation may be worse than no preparation.
When patients are advanced in years it is extremely necessary to protect them from being chilled by undue exposure. It is well to clothe their lower limbs in warm flannel garments or drawers made out of Gamgee tissue. No open doors or windows should be permitted; though in summer this is comfortable to the surgeon it may be disastrous to the patient. In winter the temperature of an operating-room should not be below 65°F. In this way ether pneumonia is best avoided.
In operations, such as oöphorectomy, ovariotomy and hysterectomy, it is the rule not to operate during menstruation; experience has taught me that operations performed during this period are not followed by evil or untoward consequences, and for many years I have disregarded it.
Immediately before the patient is placed on the table the bladder should be emptied naturally, or by means of a sterilized glass catheter.
In all pelvic operations it is a great advantage to employ nurses who have had a special training in ‘abdominal nursing’.
Basins and dishes. All receptacles such as basins, pots, instrument dishes and the like should be boiled. Mere rinsing or washing in warm water is insufficient.
Instruments. These should be constructed of metal throughout, as this enables them to be thoroughly sterilized by boiling. Needles and scalpels may be enclosed in perforated metal boxes. Forceps and the handles of scalpels are nickelled, and this keeps them bright. The following instruments are necessary: Scalpel, twelve hæmostatic forceps, dissecting forceps, two fenestrated forceps which are also useful as sponge-holders, a volsella, six curved needles of various sizes, two straight needles, silks of various thickness, and six dabs.
The surgeon should make a practice of employing a definite number of instruments and dabs for all occasions, as it will save him much anxiety in counting them at the end of the operation.
During the operation the instruments and silks are immersed straight from the sterilizer in warm sterilized water.
Suture and ligature material. The most useful material at present employed in pelvic surgery is silk. This material has a wide range of usefulness, as it is employed to secure pedicles, for the ligature of blood-vessels, and for sutures; it can be obtained of any thickness, and is easily sterilized by boiling without impairing its strength. In abdominal surgery there are four useful sizes, No. 1, 2, 4, and 6, of the plaited variety of silk. The thread is wound on a glass spool and boiled for one hour immediately before use. If any silk is left over from the operation it may be reboiled once or twice without impairing its strength. (The fate of silk ligatures is discussed on p. 117.) Many surgeons employ catgut and hold it in high esteem. I regard it as an unsatisfactory and dangerous material; moreover it cannot be boiled, which is the simplest and safest method of making ligatures sterile.
Dabs. Nothing is so convenient for removing blood from a wound as sponges; their absorbent property and softness are excellent, but they are difficult to sterilize; therefore they are highly dangerous, and on this account should be banished from surgery. An excellent substitute is absorbent cotton-wool enclosed in gauze (Gamgee tissue). This material can be cut to any size or folded into any shape, and is easily sterilized by heat, or by boiling, without damage to its absorbent properties.
For a cœliotomy six dabs are prepared of various sizes, according to the nature of the case. These are boiled for one hour and then immersed in sterilized warm water and washed from time to time in the course of the operation.
I always employ six dabs, then there is no difficulty at the end of the operation concerning their number. The dabs at the completion of the operation are destroyed.
Many serious consequences have arisen from dabs and instruments accidentally left in the peritoneal cavity after pelvic operations. This subject is considered on p. 105.
The operator should remember that his responsibility in this matter is determined by a decision in a Court of Law.
The employment of dry gauze dabs in abdominal operations is objectionable because it is harsh and irritating to the peritoneum and leads to the formation of adhesions.
Gloves. Increasing experience proves that gloves are most valuable in securing freedom from sepsis. It is a very important matter that the surgeon, the assistant, and the nurses who help at the operation should wear rubber gloves boiled immediately before the operation for ten minutes.
The wearing of gloves diminishes the mortality of the operation, and minimizes its unpleasant and often dangerous sequelæ, such as suppuration around sutures, septic emboli, tympanites, and the like. Care must be taken to impress upon all who take part in an operation that it is as essential to thoroughly wash and disinfect the hands before inserting them in gloves as when no gloves are worn. It is also necessary to warn nurses that the smallest hole in a glove renders it useless.
To the operator thorough disinfection of the hands is of the highest importance, for he may puncture or tear the gloves during the operation; or a difficulty may arise in the course of it which will render it advantageous for him to remove one or both gloves to overcome it. It is with me a rule that if in the course of an operation it is necessary to remove the gloves, I resume them for the final stages, and particularly for the insertion of the sutures. The use of rubber gloves marks a most important advance in operative surgery.
The operating table. In many cases of cœliotomy a table such as is employed for the ordinary operations of surgery answers very well, but for hysterectomy, oöphorectomy, and similar procedures it is a great convenience to use a table on which the patient can be placed in the Trendelenburg position, that is, with the pelvis raised, and the head and shoulders lowered: this allows the intestines to fall towards the diaphragm and leave the pelvis unencumbered. There are many varieties of tables employed for this purpose. As these tables are made of metal, it is necessary before the table is tilted to fix the patient’s arms parallel with her trunk, otherwise they fall across the edge of the table, and in some instances a troublesome paralysis of the muscles of the upper limb has been the consequence.
It is worth while pointing out that most of the examples have happened in the course of long operations (see Post-anæsthetic paralysis, p. 95).
Anæsthesia. The majority of surgeons employ a general anæsthetic, such as ether, chloroform, or a mixture of chloroform and ether, in pelvic operations. The most usual practice in London is to render the patient unconscious with nitrous oxide gas and maintain the anæsthesia with ether. It is a method which has given me the greatest satisfaction. As a rule, it is wise whenever possible to employ an experienced anæsthetist and trust to his judgment in regard to the selection of the anæsthetic.
In exceptional cases pelvic operations such as ovariotomy and hysteropexy have been successfully performed with the aid of intradural injections of a solution of eucaine, novocaine, or stovaine.
The incision. The operation-area is isolated by sterilized towels and the pelvis well tilted and so arranged as to face a good light. When the patient is completely unconscious, the operator (standing usually on the right side with the assistant opposite him) freely incises the wall of the abdomen in the middle line between the umbilicus and the pubes (this incision is conveniently termed the median subumbilical incision; its length varies with the necessities of the case, but is usually 7 to 10 centimetres). The first cut generally exposes the aponeurotic sheath of the rectus; any vessels that bleed freely require seizing with hæmostatic forceps. The linea alba is then divided, but as it is very narrow in this situation, the sheath of the right or left rectus muscle is usually opened. Keeping in the middle line, the posterior layer of the sheath is divided and the subperitoneal fat (which sometimes resembles omentum) is reached; in thin subjects this is so small in amount that it is scarcely recognizable, and the peritoneum is at once exposed, and, as a rule, the urachus comes into view. In order to incise the peritoneum without damaging the tumour, cyst, or intestine, a fold of the membrane is picked up with forceps and cautiously pricked with the point of a scalpel; air rushes in, destroys the vacuum, and generally produces a space between the cyst (or intestines) and the belly-wall; the surgeon then introduces his finger, and divides the peritoneum to an extent equal to the incision in the skin.
It is important to remember that the bladder is sometimes pushed upward by tumours, and lies in the subperitoneal tissue above the pubes; it is then liable to be cut.
On entering the peritoneal cavity, the surgeon introduces his hand, and proceeds to ascertain the nature of any morbid condition that he sees or feels, or he evacuates any free fluid, blood, or pus which may be present. Occasionally he finds that attempts to remove a tumour would be futile or end in immediate disaster to the patient; then he desists and closes the wound, and the procedure is classed as an exploratory cœliotomy. Should a removable tumour, such as an ovarian cyst, an echinococcus colony in the omentum, or the like be found, it is removed.
Before suturing the incision, the surgeon usually spreads the omentum over the small intestine; occasionally he will be surprised to find this structure, even in well-nourished women, represented by a mere fringe of fatty tissue attached to the lower border of the transverse colon.
The recesses of the pelvis are then carefully mopped in order to remove fluid, blood, or pus; the dabs and instruments are counted, and preparations made to suture the incision.
Misplaced viscera. In addition to tumours and normal enlargement of the uterus due to pregnancy, or an overfull bladder, there are certain malformations as well as displacements of normal viscera the surgeon may encounter in the pelvis which will, in some cases, cause him a certain amount of embarrassment, such, for example, as a bifid uterus or a spleen which has elongated its pedicle, or even twisted it, and, falling so low in the abdomen as to occupy the pelvis, may even cause prolapse of the uterus. In some of these cases it drags the tail of the pancreas with it. The cæcum and the vermiform appendix often occupy the true pelvis; in middle-aged and elderly women the transverse colon sometimes forms a loop (the omega-loop), the extreme convexity of which often reaches to the pelvis. I have seen the right lobe of the liver extend into the pelvis, and come in contact with the unimpregnated uterus. It is important to remember that a kidney sometimes occupies the hollow of the sacrum; such a misplaced kidney has been removed under the impression that it was a tumour. When a kidney occupies the pelvis it lies behind the peritoneum as when it occupies its normal position in the loin. A horseshoe kidney is a fertile source of divergent opinion in diagnosis. A very large hydronephrosis simulates very closely an ovarian cyst until exposed through an abdominal incision; in such a contingency the operator performs nephrectomy; when the kidney is large enough to resemble an ovarian cyst it can easily be removed through the median incision.
A very distended stomach will reach the hypogastrium and has many times been mistaken for an ovarian cyst; such a distended stomach has received a thrust from an ovariotomy trocar and the operator has been astonished to see food issue through the opening.
Tumours of the pelvic organs are often complicated with abnormal and diseased conditions of the intestines, large and small; it is therefore necessary for any one undertaking gynæcological abdominal operations to be prepared to perform resections of the colon, enterorrhaphy, gastro-jejunostomy, and the like when necessary.
Transposition of the viscera is a rare anomaly to encounter in the course of an abdominal operation. I met with it once in 3,000 cœliotomies; the condition was recognized before operation.
Closure of the wound. There are about fifty methods known and advocated for the closure of the median subumbilical incision, and the following is a list of materials used by surgeons for this purpose: silk, silkworm-gut, catgut, linen thread, and horsehair; silver, iron, aluminium, bronze, and platinum wire, and Michel’s metal clips. The object of these various methods and materials is to obtain a firm scar.
The first requisite for securing an unyielding scar is perfect asepsis; but even the most perfectly healed abdominal scar may yield. Nature in her great operation of uniting the lateral halves of the belly-wall in a median cicatrix, the linea alba, cannot secure a non-yielding scar, it is therefore presumptuous of the surgeon to think he can always ensure it.
The method which has given me the best results is a simple one. The peritoneum, sheath of the rectus, and rectus muscle are carefully approximated by interrupted sutures of No. 4 silk carefully sterilized and inserted with the hands covered with rubber gloves. The sutures are inserted at intervals of rather less than 2 centimetres apart. Care must be taken to include the peritoneum in these sutures. The skin is then brought together by a continuous suture of No. 2 silk. When the operation has been undertaken for a septic condition, such as pelvic peritonitis, suppuration of an ovarian cyst, an acute pyosalpinx, or the like, then it is useless to introduce buried sutures for the muscular and aponeurotic layers, as they will quickly become infected. In such conditions the abdominal walls are brought together by interrupted sutures involving all the layers.
Those who are curious in regard to the various methods of closing median cœliotomy wounds should consult a brochure published in 1904 on The Closure of Laparotomy Wounds as practised in Germany and Austria, by Walter H. Swaffield. This little book contains the detailed methods and views communicated to him by more than fifty leading surgeons.
In Great Britain there is plenty of variety in the methods and material employed for the closure of the incisions in abdominal operations, but at the present time there is a marked tendency to return to the older and simpler methods. The most dangerous and unreliable suture material for the abdominal incision is catgut (see p. 96).
In studying the details of such operations as ovariotomy and hysterectomy from books, it should be remembered that it is merely the principles that can be explained. There are so many details in every operation that can only be learned from watching, or, what is far better, assisting a skilful and experienced surgeon in their performance. This is true of all forms of surgical procedure. No man can become a navigator without going to sea, however thoroughly he masters the principles of seamanship from books, so no surgeon can acquire the art of operating from merely reading descriptions of surgical operations. If a surgeon can bring to bear upon abdominal gynæcological operations, in addition to mere surgical dexterity, a competent knowledge of the pathology of the organs, he will find it of the greatest assistance. I would warn him particularly to take little heed of the sneers of those eminently practical surgeons who affect to despise pathology.
Ovariotomy signifies the removal through an abdominal incision of cystic and solid tumours of the ovary, and parovarian cysts.
The history of this operation is of great interest to surgeons because it was the forerunner, so to speak, of all abdominal gynæcological operations; they followed as a natural consequence on the establishment of ovariotomy, and operations on the abdominal viscera generally are to be regarded as an extension of pelvic surgery.
It is usual to state that ovariotomy was first performed by Ephraim McDowell, of Kentucky, 1809: this is of historical interest only, for it had no effect whatever in drawing attention to the feasibility of removing ovarian cysts: it was in fact a still-born operation. The pioneers of this operation were undoubtedly Baker Brown and Spencer Wells in London, Thomas Keith in Edinburgh, and Clay in Manchester. These surgeons brought the operation out of a ‘slough of despond’ and placed it on firm ground. Spencer Wells and Keith were fortunate later in their work in receiving guidance from Lord Lister’s discovery of antisepsis: this, combined with the introduction of the short ligature, firmly established the operation.
The improvement in securing the pedicle has played an important part in the development of ovariotomy. McDowell tied the pedicle, but left the ligature hanging out of the wound. Doran, who has written an excellent review of this matter, ascribes the intraperitoneal method of dealing with the pedicle to the systematic advocacy of Tyler Smith. The method has been followed by brilliant results.
Baker Brown used to sear the pedicle with a cautery, and this method was adopted with great success by Thomas Keith. The method of ligature is so simple and safe that the cautery for this purpose has been long abandoned.
The operation. The preliminary preparation of the patient and the necessary instruments are described on p. 5. The Trendelenburg position is not so necessary for the removal of large ovarian tumours as the smaller examples which are apt to be firmly adherent to the floor of the pelvis. In cases where the abdomen contains free fluid, ascitic or due to the bursting of a cyst, or pus, it is a wise precaution to conduct the early stages of the operation with the patient in the horizontal position, otherwise the tilting will cause the fluid to gravitate towards the diaphragm. As soon as the fluid has been removed the pelvis may be raised if it be likely to facilitate the operation.
In the early days of ovariotomy it was the custom to tap the cyst, or, in the case of multilocular tumours, to force the hand into the mass and break down the septa of contiguous loculi and allow the viscid material to escape. These devices were recommended because it was regarded as a method making for safety to extract the cyst through a small abdominal incision. Occasionally it is possible to extract the wall of a large single-chambered parovarian cyst, after tapping, through an incision 7 centimetres in length. When the tumour is multilocular, or malignant, or full of grease or pus, it is difficult and extremely dangerous to tap it, as the material may infect the peritoneum either with septic matter or with malignant particles, and end disastrously.
Cases have been reported in which, after traumatic rupture, or tapping, of a dermoid, the epithelial contents escaped into the belly. Subsequently the peritoneum was found dotted over with minute nodules furnished with tufts of hair growing among the visceral adhesions. When a woman with an ovarian cyst contracts typhoid fever, the cyst may become filled with pus which contains the bacillus typhosus. Such a case occurred in my practice in 1907.
For many years I have abandoned the use of clumsy trocars of all kinds and remove the tumour entire, although it may require an incision from the ensiform cartilage to the pubes. These large incisions heal quickly, and are no more prone to hernia than the short incisions. This is the only way of ensuring the safety of the peritoneum from being contaminated by the harmful, dirty, and often malignant contents of the cysts. In dealing with burst cysts a free incision enables the surgeon to thoroughly and gently clean the peritoneal cavity.
The abdominal cavity is opened by a median subumbilical incision (see p. 7). Occasionally a difficulty may be encountered on reaching the peritoneum, for, if the cyst has been infected, the peritoneum and cyst wall may be so intimately adherent that they cannot be separated. In these circumstances it is a wise plan to extend the incision upwards and enter the abdominal cavity above the tumour. It is also to be borne in mind that when the tumour adheres to the abdominal wall it is extremely probable that a coil of intestine may be adherent also. When a tumour is impacted in the pelvis it may push the bladder high in the abdomen; in such an event this viscus is apt to be opened in making the incision. If the surgeon has any doubt concerning the position of the bladder, he should instruct an assistant to introduce a sound into it through the urethra.
In a typical case, when the peritoneum is opened the surgeon at once recognizes the bluish-grey glistening surface of the ovarian cyst, and gently sweeps his hand over it in order to ascertain its relations and to learn whether the cyst wall be free from adhesions. It is of the utmost importance to be satisfied as to the nature of the tumour, especially when the operator follows the unsatisfactory practice of tapping, for if he plunge a trocar into a uterine tumour, or into a pregnant uterus, he will involve himself in anxious difficulty. Decomposing fluid, tenacious mucus, or blood-stained fluid may obscure the parts, and should be sponged away: they indicate a ruptured cyst, a malignant tumour, or a twisted pedicle. Much free blood may be due to the bursting, or abortion, of a gravid tube. When the surgeon has satisfied himself that the cyst or tumour is free to be removed he lifts it out of the abdominal cavity, and if in this process the wall be so thin that it is likely to burst, or actually leaks, the weak spot may be freely incised with a knife over a convenient receptacle.
Adhesions. Although the surgeon may have had reasons to suspect the presence of adhesions, frequently he finds none, and on other occasions when he least expects them there are many. The most frequent adhesions are omental, and fortunately they are the least important: they should be detached and tied with thin silk. Adherent epiploic appendages require the same treatment. Intestinal adhesions require care and patience. When the intestines are adherent by strands and bands, these may be cautiously snipped with scissors; when the adhesions are sessile and soft the gut may be gently detached by means of a moist dab; but if very firm it may be necessary to dissect off a piece of cyst wall and leave it on the gut. The vermiform appendix requires especial care, for it may be mistaken for an adhesion and divided. When intestines are accidentally opened in the course of an ovariotomy they require the most careful attention. Wounds in the colon may be safely sutured. Holes in adherent small intestine may sometimes be sutured, but if the gut has been extensively involved it may be necessary, and often judicious, to resect a few centimetres and join the cut ends by a circular enterorrhaphy.
Adhesions to the parietal peritoneum are as a rule easily detached with the finger. The most serious adhesions are those which occur in the depths of the pelvis, involving the uterus, bladder, or rectum, and the separation of these may involve such accidents as wounds opening the rectum or bladder, and injury to the ureters and iliac veins. The treatment of such misfortunes will be considered later.
The pedicle. When the tumour is withdrawn from the belly the pedicle is easily recognized: the Fallopian tube serves as an excellent guide to it. The pedicle consists of the Fallopian tube and adjacent parts of the mesometrium containing the ovarian artery, pampiniform plexus of veins, lymphatics, nerves, and the ovarian ligament. When the constituents of the pedicle are unobscured by adhesions, the round ligament of the uterus is easily seen and need not be included in the ligature.
In transfixing the pedicle the aim should be to pierce the mesometrium at a spot where there are no large veins, and tie the structures in two bundles, so that the inner contains the Fallopian tube, a fold of the mesometrium, and occasionally the round ligament of the uterus; whilst the outer consists of the ovarian ligament, veins, the ovarian artery, and a larger fold of peritoneum than the inner half.
Pedicles differ greatly; they may be long and thin, or short and broad. Long thin pedicles are easily managed. The assistant gently supports the tumour, whilst the operator spreads the tissues with his thumb and forefinger, and transfixes them with the pedicle needle armed with a long piece of silk doubled on itself. The loop of silk is seized on the opposite side and the needle withdrawn. During the transfixion care must be taken not to prick the bowel with the needle. The loop of silk is cut so that two pieces of silk thread lie in the pedicle. The proper ends of the thread are now secured, and each is firmly tied in a reef-knot; for greater security the whole pedicle may be encircled by an independent ligature, taking care that it embraces the pedicle below the point of transfixion. (I use No. 4 plaited silk for transfixing the pedicle, and a piece of No. 6 silk for surrounding it.)
After the operator has gained some experience in this simple mode of tying the pedicle, he may, if he thinks it desirable, practise other methods.
After securely applying the ligature the tumour is removed by snipping through the tissues on the distal side of the ligature with scissors. Care must be taken not to cut too near the silk, or the stump will slip through the ligature; on the other hand, too much tissue should not be left behind. The stump is seized on each side by pressure forceps, and examined to see that the vessels in it are secure; it is then allowed to retreat into the abdomen. Should it begin to bleed it must be caught with forceps, drawn up, retransfixed, and tied below the original ligature.
Occasionally a pedicle will be so broad that it is unsafe to trust to this simple form of ligature. Broad pedicles will require three or more ligatures. When several ligatures are required it is important to remember that the ovarian artery lies in the outer fold of the pedicle and the uterine artery at the inner end, and it is often possible to secure these vessels separately with a thin piece of silk. The pedicle can then be secured with a series of interlocking ligatures.
When an ovarian tumour has undergone axial rotation and has tightly twisted its pedicle, the ligature should be applied to the torsioned area: a single ligature is then sufficient.
It is impossible to frame absolute rules for ligaturing the pedicle. In this, as in all departments of surgery, common sense must be exercised, and at the present day, when ovariotomy is practised so widely, no one would think of performing this operation without assisting at, or watching its actual performance by an experienced surgeon.
Having satisfied himself that the pedicle is secure, the surgeon examines the opposite ovary, and if obviously diseased it should be removed.
The operator then sponges up any blood or fluid which may have collected in the recesses of the pelvis. Whilst employed in this way he gives instructions to have the dabs and instruments counted.
When the operator limits the number of dabs to six he can easily have them displayed before him. The incision is sutured in the manner described on p. 9.
Cysts of the broad ligaments. Occasionally the surgeon on opening the abdomen finds that the cyst or tumour is situated between the layers of the broad ligament. Sessile cysts of this kind are removed by what is known as enucleation. The peritoneum overlying the cyst is cautiously torn through with forceps until the cyst wall is exposed; then by means of the forefinger the surgeon proceeds to shell the cyst out of its bed, taking care not to tear the capsule or any large vein in its wall; it is also necessary to exercise the greatest care to avoid injury to the ureter. It is not uncommon, after enucleating a cyst in this way, to find the ureter lying at the bottom of the recess. (For treatment of an injured ureter see p. 112.)
When the enucleation is completed the walls of the capsule are carefully examined for oozing vessels which require ligature. The capsule can often be closed in such a way as to bring its walls into apposition and thus obliterate its cavity; it then requires no further attention. When there is much oozing the capsule is treated on the plan known as marsupialization. The edges of the capsule are brought to the lower angle of the abdominal wound and secured with sutures, and a drain, either of gauze or a rubber tube, is introduced, and the remainder of the wound closed in the usual manner.
Enucleation is usually accompanied by more loss of blood than simple ovariotomy; this, and the prolonged manipulation, is often responsible for severe shock.
Spurious capsules. It is necessary for the surgeon to remember that an ovarian cyst, and especially an ovarian dermoid, is sometimes invested by a spurious capsule. It is now well known that slow effusions of blood, tuberculous exudations (Fig. 4), hydatid cysts, and ovarian cysts become enclosed by capsules of fibrous tissue formed by the organization of the peritoneal exudation which their presence excites. These capsules are often so firm, and so completely encyst the fluid exuded into the pelvis in cases of tubal tuberculosis, that such encapsuled collections of fluid resemble, and are often mistaken for, ovarian cysts. It is also necessary to mention that true ovarian cysts project from, but never invade the layers of the broad ligament. From time to time cases are reported in which ovarian cysts, especially dermoids, have been found between the layers of the broad ligament: such are in all probability instances in which a false capsule has formed around the cyst, and the surgeon committed an error of observation in regarding it as a layer of the broad ligament.
Ovariotomy in carcinoma of the ovary. When an operation is undertaken for the removal of solid or semi-solid tumours of the ovary, and especially when bilateral and accompanied by vomiting, it is incumbent on the surgeon to make a careful examination of the gastro-intestinal tract, for in many of these cases cancer will be found either at the pylorus, or in the cæcum, or the colon, and particularly in the sigmoid flexure. In such circumstances the ovarian masses are secondary to the cancerous focus in the gastro-intestinal tract.
Bilateral malignant tumours of the ovaries are sometimes secondary to primary cancer of the gall-bladder and the breast. Some of these secondary cancerous tumours of the ovaries form masses as big as the patient’s head.
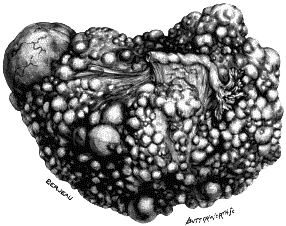 Fig. 1. Secondary Cancer of the Ovary. An ovary converted into a solid
mass of cancer secondary to a focus in the sigmoid flexure of the colon:
it weighed 5 lb. Two-fifths size.
Fig. 1. Secondary Cancer of the Ovary. An ovary converted into a solid
mass of cancer secondary to a focus in the sigmoid flexure of the colon:
it weighed 5 lb. Two-fifths size.
|
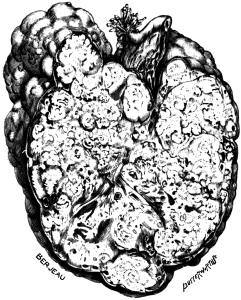 Fig. 2. Secondary Cancer of the Ovary in Section. This is a section of
the ovary represented in the preceding figure. Half size.
Fig. 2. Secondary Cancer of the Ovary in Section. This is a section of
the ovary represented in the preceding figure. Half size.
|
In such conditions the ovaries and sometimes the uterus should be removed even for the purpose of making the patient comfortable. When the primary disease is in the cæcum, colon, or sigmoid flexure, and is operable, the growth should be resected and the cut ends of the bowel united by circular enterorrhaphy. In one instance, where the cancer occupied the ileo-cæcal valve, I succeeded in making a lateral anastomosis between the ileum and ascending colon, after performing bilateral ovariotomy. The woman survived the operation two years.
Incomplete ovariotomy. The surgeon may start on an operation and, after opening the abdomen, may find many adhesions, yet he feels that the removal of the tumour is possible. He sets to work and overcomes many of the difficulties, but finds at last such extensive pelvic adhesions that it is imprudent to proceed further. In such cases he evacuates the contents of the cyst and stitches the edges of the opening in the cyst to the margins of the abdominal wound, and drains the cavity. This mode of dealing with a cyst is usually termed ‘incomplete ovariotomy’.
An incomplete ovariotomy is a very different condition to an enucleation. The cavity left after enucleation closes completely, but when the wall of an ovarian cyst or adenoma is left the tumour gradually grows again, or it may suppurate so profusely that the patient slowly dies exhausted. There are few things sadder in surgery than the slow, miserable ending of an individual who has been subjected to an incomplete ovariotomy.
Anomalous ovariotomy. In a few instances, generally under an erroneous diagnosis, surgeons have removed ovarian tumours through an opening other than the classical one known as the median subumbilical incision. Under the impression that the tumour was splenic, an ovarian tumour of the right side has been successfully removed through an incision in the left linea semilunaris (R. W. Parker). An ovarian tumour, supposed to be a renal cyst, has been successfully extracted through an incision in the ilio-costal space (Le Bec). Strangest of all, a small ovarian dermoid has been removed through the rectum under the impression that it was a polypus of the bowel (Stock, Peters).
Hysterectomy after bilateral ovariotomy. After the removal of both ovaries for cysts or tumours, the uterus is a useless organ: it is fast becoming the practice under such conditions to remove it. There is much to be said in favour of this procedure, especially if the uterus be large and flabby, because it tends to fall backwards into the pelvis. In such circumstances it is better surgery to remove it than to perform hysteropexy. The risk of intestinal obstruction after bilateral ovariotomy is greater than after hysterectomy. Cases are known in which cancer has attacked the uterus years after bilateral ovariotomy and oöphorectomy (see p. 55).
Repeated ovariotomy. Very many cases are known in which women have been twice submitted to ovariotomy. Thus it is the duty of the surgeon when removing an ovarian tumour to examine carefully the opposite ovary. So many examples are known of women who have borne children after unilateral ovariotomy (twins and even triplets) that this alone is sufficient to prohibit the routine ablation of both glands.
A second ovariotomy is not attended with more risk than a first ovariotomy. The abdominal incision must be made with extra caution, because intestine may be adherent to it and runs a risk of being wounded. In some instances the cicatrix is very thin, and the surgeon cutting through it is liable to cut the intestine before being aware that the knife has entered the abdomen.
Some surgeons recommend that in a second ovariotomy the opening may with advantage be made a little to one side of the original incision.
Cases have been reported in which patients have been thrice submitted to ovariotomy: in such instances it is probable that one of the tumours was a sessile broad ligament cyst.
Pregnancy after bilateral ovariotomy. It is an interesting fact that several cases have been carefully reported in which women who have had bilateral ovariotomy have subsequently become pregnant. This event has been explained by assuming that in some of the patients a portion of at least one ovary has been left. This meets with more favour than the idea of the existence of a supernumerary ovary. The cases have been collected by Doran.
In order to afford some notion of the relative frequency of the various cysts and tumours classed as ovarian, a list of one hundred consecutive examples which I removed at the Chelsea Hospital for Women is appended:—
| Fibromata | 2 | Dermoids | 15 | |
| Sarcomata | 2 | Papillomata | 2 | |
| Carcinomata | 1 | Parovarian | 5 | |
| Simple cysts | 45 | Tubo-ovarian | 3 | |
| Adenomata | 25 |
The case classed as a carcinoma was secondary to cancer of the pylorus; both ovaries were affected. The three classed as tubo-ovarian were probably exceedingly large examples of hydrosalpinx; one was so big that it came in contact with the liver.
I have compared this table with the experience of other surgeons, and although there is much variation in them it represents a fair average of the proportions of the different ovarian operations usually classified under the head of ovariotomy.
Ovariotomy at the extremes of life. Cysts and tumours arise in the ovary during intra-uterine, and at all periods during extra-uterine life, even in extreme old age: they also attain such dimensions in infants and old women as to demand the aid of the surgeon, and with excellent results. Many years ago I collected the recorded cases and tabulated one hundred instances in which ovariotomy had been performed in infants and girls under fifteen years of age. These tumours fall into three groups:
| Simple cysts and adenomata | 41 | with | 3 | deaths. |
| Dermoids | 38 | " | 5 | " |
| Sarcomata | 21 | " | 7 | " |
In the case of simple cysts, adenomata, and dermoids, the results are encouraging. It is possible that some of the cases described as sarcomata belonged to the deadly group now known as malignant teratomata.
Ovarian tumours sometimes attain large dimensions in children, and Keen reported a case in which he removed an ovarian tumour from a girl which weighed 44 kilogrammes: the girl weighed 27 kilogrammes after the operation. An ovarian cyst with a twisted pedicle has been found in a fœtus at birth (Otto von Franque).
The subjoined table shows cases in which ovarian tumours have been removed from infants under three years of age. It is often stated that Professor Chiene performed ovariotomy on an infant of three months. This is an error; it was an ovary occupying the sac of an inguinal hernia.
Ovariotomy in Infants
| Reporter | Age | Result | Nature of Tumour | Reference | |
|---|---|---|---|---|---|
| 1 | D’Arcy Power | 4 months | R. | Dermoid | Trans. Path. Soc., xlix. 186. |
| 2 | MacGillivray | 11 months | R. | Cyst | Lancet, 1907, i. 1487. |
| 3 | Roemer | 1¾ years | R. | Dermoid | Deutsche Med. Woch., 1883, ix. 762. |
| 4 | Péan | 2 years | R. | Dermoid | Clin. Chir., 1887–8, 8th series. |
| 5 | Hooks | 2½ years | D. | Dermoid | Am. J. of Obst., 1886, xix. 1022. |
Ovariotomy in old age. In 1891 I was able to find twenty-two records of successful ovariotomy in women over seventy years of age. Since that date Howard A. Kelly and Mary Sherwood made a collective investigation, and succeeded in obtaining notes of one hundred cases of ovariotomy performed on women over seventy years of age: the death-rate amounted to 12%.
The subjoined table concerns itself with ovariotomy performed on women after the age of eighty years, and the results are remarkable, notwithstanding the circumstance that these women of eighty years and upwards must have been blessed with a stronger constitution than their contemporaries.
Ovariotomy in Women of Eighty Years of Age
| Reporter | Age | Result | Reference | |
|---|---|---|---|---|
| 1 | Owens | 80 | R. | Brit. Gyn. Soc. Journal, iv. 88. |
| 2 | Richardson | 80 | R. | Brit. Med. Journ., 1894, i. 523. |
| 3 | Heywood Smith | 81 | R. | Lancet, 1894, i. 1618. |
| 4 | Spencer | 82 | R. | Brit. Med. Journ., 1893, ii. 1271. |
| 5 | Homans | 82 | R. | Bost. Med. and Surg. Journ., 1888, 454. |
| 6 | Edis | 81 | R. | Brit. Med. Journ., 1892, i. 860. |
| 7 | Bush | 84 | R. | Ibid., 1894, ii. 67. |
| 8 | Remfrey | 83 | R. | Trans. Obstet. Soc., xxxvii. 152. |
| 9 | Kraft | 84 | R. | Hospitalstidende, Copenhagen. |
| 10 | Owens 1 | 87 | R. | Lancet, 1895, i. 542. |
| 11 | Thornton | 94 | R. | Trans. Obstet. Soc., xxxvii, 158. |
| 12 | Bland-Sutton | 85 | R. | Middlesex Hospital. |
| 1 A second operation on patient No. 1 in the list. | ||||
Mortality. The death-rate after ovariotomy is hard to estimate, especially as surgeons differ widely in the classification of the cases. In the simple and uncomplicated forms of ovarian cysts and tumours the operation should be almost free from risk. Many surgeons, excluding malignant conditions, have had lists of a hundred operations with no deaths.
If all kinds of tumours are included as represented in the table on p. 17, a 5% mortality in experienced hands would be regarded as a good result. In general hospital work it is probably as high as 10%. With less experienced surgeons who do not perform many operations the death-rate will vary from 10 to 15%.
The risks and after-consequences of ovarian operations are set forth in Chapter XI.
Doran, A. On complete Intraperitoneal Ligature of the Pedicle in Ovariotomy. St. Bartholomew’s Hospital Reports, 1877, xiii. 195.
—— Pregnancy after the Removal of Both Ovaries for Cystic Tumour. Trans. Obstetrical Society, 1902, xliv. 231.
Bland-Sutton, J. On Secondary (metastatic) Carcinoma of the Ovaries. Brit. Med. Journal, 1906, i. 1216.
—— On Cancer of the Ovary. Ibid., 1908, i. 5.
Le Bec. Ovariotomie double; un des kystes enlevé par la région lombaire, l’autre par le devant de l’abdomen; adhérences totales; guérison. Gaz. des Hôpitaux, 1887, 290.
Stocks. Prolapse of an Ovarian Cyst. Brit. Med. Journal, 1857, ii. 487.
Peters, H. Ovariotomie per anum. Wiener Klin. Wochensch., 1900, xiii. 110.
Oöphorectomy signifies the removal through an abdominal incision of an ovary and Fallopian tube for affections mainly inflammatory.
The evolution of this operation is of great interest to surgeons. The removal of ovaries as a surgical operation was introduced independently by Hégar in Germany and Battey in Georgia, for the relief of pelvic pain and dysmenorrhœa, in 1872. In the same year Lawson Tait performed his pioneer operation and removed an ovary and tube for the relief of pain due to disease of the ovary. Subsequently he advocated bilateral oöphorectomy for the purpose of inducing an artificial menopause in women with uterine fibroids. From these beginnings the operation began to be performed for the relief of a variety of conditions connected with the generative organs, such as—
Pyosalpinx and tubo-ovarian abscess, hydrosalpinx, tuberculous ovaries and tubes, sarcoma and carcinoma of the Fallopian tubes, gravid Fallopian tubes, ovarian abscess, ovarian pregnancy, prolapse of the ovary; finally bilateral removal of the ovaries has been practised for the relief of inoperable cancer of the breast.
Bilateral oöphorectomy is occasionally performed for osteomalacia (a rare disease in Great Britain), as it arrests pain and the excessive output of phosphates in the urine, which is a marked feature of this affection. This extension of the operation we owe to Fehling of Bâle (1887).
Time and experience have considerably modified surgical opinion in regard to oöphorectomy. Removal of the ovaries is no longer practised for the relief of hæmorrhage due to fibroids: it is easier, safer, and affords greater relief to the patient to remove the uterus (see p. 36). When dysmenorrhœa is so severe as to need radical operation, hysterectomy is the only certain method, with conservation of at least one ovary. The removal of both ovaries in certain forms of insanity is now abandoned, and this is true of bilateral oöphorectomy for the relief of mammary cancer.
In other directions the operation has undergone extension, for in some chronic diseases of the Fallopian tubes it is difficult to completely extirpate the affected tissues without removing the uterus. These will be considered in describing the actual operation.
Apart from the many modifications in the details of the operations some operators prefer to remove the ovaries and tubes through an incision in the vaginal fornix. This is known as Colpotomy, or Vaginal Cœliotomy.
Some writers attempt to subdivide the various modifications of oöphorectomy and apply to them special terms: for example, the removal of the ovary and tube would be termed salpingo-oöphorectomy. Removal of the tube would be called salpingectomy, and the excision of the ovary, oöphorectomy. This terminology may be precise, but it is certainly clumsy. A few writers designate these operations as ‘removal of the uterine appendages’; this phrase, though comprehensive, is neither precise nor elegant.
Operation. The patient is prepared in the same manner, and the same instruments are required, as for ovariotomy. In many of these operations the Trendelenburg position is of the greatest advantage.
In a case of prolapse of the ovary, or a gravid tube or ovary in the earliest stages, the operation presents no difficulty and can be carried out with the ease and safety of the simplest ovariotomy; but there are many cases where the tubes and ovaries contain pus and are distended into cysts as big as a fist, or even as large as the patient’s head, which are adherent to bowel, uterus, bladder, indeed everything with which they come in contact; this renders their removal tedious and exacting for the surgeon and dangerous to the patient. Although a suppurating ovarian cyst adheres to surrounding organs, its removal is simpler than in the case of a large pyosalpinx, because the Fallopian tube is intimately enclosed within the folds of the broad ligament, and these connexions serve to bind it firmly in the pelvis.
In undertaking the removal of such enlarged tubes the surgeon’s first duty is to expose the parts by a free incision, and then carefully isolate the intestines and upper parts of the abdomen with dabs in order to prevent them from being contaminated with pus. He will quickly recognize in the majority of cases that he has to deal with tubal disease, because the distended uterine section of the tube will lie on the more globular outer portion of the tube and assume the familiar shape of a chemical retort. With the fingers the adherent omentum and bowels are carefully detached, and the adhesions between the distended tube or ovary and the rectum are carefully broken through with the finger, and the parts withdrawn from the pelvis. With great care it is usually possible to carry this out without bursting the tube. This is important as it prevents the universal spread of pus in the pelvis. When the tube bursts in the process of removal it is useful to swab it up with some strips of gauze and thus keep the ‘Gamgee dabs’ clean for the final stages.
As soon as the diseased parts are extracted, a dab is pressed into the hollow to check the oozing: the pedicle is clamped with forceps and the tube and ovary detached.
It is the common practice in dealing with inflamed and septic ovaries and tubes to transfix and ligature the pedicles as in a simple clean ovariotomy. The consequences of this practice are not satisfactory, for the pedicles being infected often give rise to trouble, because the silk acts as a seton, an abscess forms which may open up through the abdominal wound, the rectum, or perforate into the bladder, and leads to the establishment of a sinus which persists for many months until the ligature is extruded. There are several methods of avoiding this: for example, the arteries in these broad pedicles may be ligatured separately with thin silk, and the edges of the peritoneum drawn together by two or three mattress sutures (Fig. 11, p. 40).
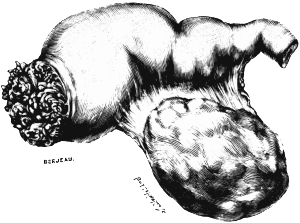 Fig. 3. An Infected Fallopian Tube. The cœlomic ostium of the tube is
unoccluded and is in the process of slowly engulfing the fimbriæ.
Removed from a woman in the acute stage of salpingitis. Three-quarter
size.
Fig. 3. An Infected Fallopian Tube. The cœlomic ostium of the tube is
unoccluded and is in the process of slowly engulfing the fimbriæ.
Removed from a woman in the acute stage of salpingitis. Three-quarter
size.
In cases where the Fallopian tube is thickened quite up to the uterine angle, it may be exsected from the uterus: in such cases the uterine artery will be tied and the flaps at the uterine angle can be brought into apposition by a mattress suture.
In acute cases of salpingitis the cœlomic ostium is open and the infective material can be seen leaking from it (Fig. 3). In chronic cases this ostium is firmly occluded (Fig. 4). Acute cases are dangerous as they are apt to cause post-operative peritonitis. Chronic cases are difficult on account of visceral adhesions.
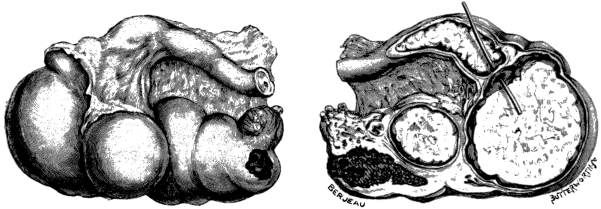 Fig. 4. A Tuberculous Fallopian Tube and Ovary: Entire and in
Section. Caseous matter has exuded through the cœlomic ostium of the tube
and become encapsuled. Natural size.
Fig. 4. A Tuberculous Fallopian Tube and Ovary: Entire and in
Section. Caseous matter has exuded through the cœlomic ostium of the tube
and become encapsuled. Natural size.
The most serious complication likely to arise in the enucleation of a pyosalpinx, especially on the left side, is a firm adhesion to the rectum; this may be occasionally anticipated when the patient gives a clear history of one or more sudden discharges of pus from the anus. An accidental tear of the rectum through comparatively healthy tissues may be repaired by interrupted sutures, but when the injury is in tissues altered by chronic suppuration, the only course open to the surgeon is to drain with a wide rubber tube, and it is surprising as well as gratifying to know that a fistula of this kind low in the rectum will often close in a week or ten days. It is important to bear in mind that an undetected tear into the rectum, if the abdomen be closed without drainage, will, in all probability, lead to fatal peritonitis.
It has happened that a surgeon in removing a pyosalpinx tore a hole in the rectum; he was unaware of the accident, and a few hours after the operation ordered 10 ounces of saline solution to be injected into the bowel. This fluid passed through the rent in the gut direct into the pelvis with fatal consequences.
After removing the diseased parts and securing the large vessels directly concerned in the pedicles, attention is directed to the oozing from the torn tissues in the floor of the pelvis. Any vessel which is bleeding should be ligatured with thin silk, and then the recesses of the pelvis may be firmly plugged with a dab wrung out of hot water: this is a valuable measure of hæmostasis. This dab is removed in two or three minutes, and any vessel which is bleeding is quickly seen and ligatured.
In cases where the enucleation of adherent and inflamed tubes leaves large raw and slightly oozing surfaces in the pelvis, drainage is a wise precaution. After a trial of a variety of measures for this purpose I find the simplest to be a narrow rubber drainage tube reaching to the bottom of the pelvis and emerging at the lower extremity of the abdominal incision. It is rarely required for more than forty-eight hours. Some surgeons are opposed to drainage, and one writer compares it to ‘defending oneself against the sparks of Vulcan with an umbrella’; his mortality is high.
In simple cases the incision is closed according to the method described on p. 9; but after the removal of suppurating ovaries and tubes it is better to unite the wound by a single layer of sutures through all the tissues of the abdominal wall: buried sutures in such conditions nearly always give trouble.
Abdominal hysterectomy after bilateral oöphorectomy and ovariotomy. After the complete removal of the ovaries and tubes the uterus is a useless organ, and when the ‘appendages’ have been removed for inflammatory lesions, acute or chronic, it may become a troublesome organ. In some instances a uterus devoid of its appendages has been attacked by cancer. In a few instances in which patients have undergone bilateral oöphorectomy, or bilateral ovariotomy, successful conception has followed the operation (see p. 17).
The most annoying consequences which follow bilateral oöphorectomy for salpingitis, acute or chronic, are hæmorrhage, pain, or a purulent discharge. Every surgeon with an ordinary experience of this class of surgery has probably had to remove the uterus on several occasions as a sequel to bilateral oöphorectomy.
It is advised by many surgeons, when they find the appendages so hopelessly diseased that they must be removed, to perform subtotal hysterectomy at the same time. My own practice in this matter is to perform subtotal hysterectomy when it is necessary to remove the uterus as well as the appendages in chronic disease; and total hysterectomy when it is deemed advisable to remove the uterus with the appendages in acute infective conditions. The reasons for this modification are obvious, because in chronic conditions there is little liability for the stump to become infected, for experience teaches that though the distended tubes contain pus in chronic cases, yet on bacteriological examination this pus is sterile. In the acute cases the pus swarms with micro-organisms—bacillus colli, staphylococcus, and occasionally streptococcus; these infect the stump, set up suppuration, infect the ligatures, and establish a chronic sinus. To cure this condition it is necessary to remove the stump by the vaginal route.
In cases of tuberculous infection of the Fallopian tubes it is not necessary to remove the uterus unless it is obviously implicated by the disease. In several patients I have left an ovary without any subsequent ill consequences.
Mortality. In order to estimate the risks of oöphorectomy it is necessary to classify the heterogenous conditions for which this operation is required. In the majority of cases the chief cause is inflammatory (septic) affections of the Fallopian tubes: other causes are tubal and ovarian pregnancy, and prolapse of the ovary. Tubal pregnancy is considered in a separate chapter, and as prolapse of the ovary is so often associated with retroflexion of the uterus it is dealt with in the chapter on Hysteropexy.
In order to give some notion of the relative frequency of the infective conditions of the tubes and ovaries usually classed in Hospital Reports as ‘diseased uterine appendages’, I chose one hundred consecutive operations from my case-reports at the Chelsea Hospital for Women. They are classed thus:—
| Salpingitis | 49 |
| Pyosalpinx | 31 |
| Hydrosalpinx | 10 |
| Tuberculous | 8 |
| Ovarian abscess | 2 |
In order to give some idea of the risks of unilateral and bilateral oöphorectomy, I gathered the following facts from the Hospital Reports, prepared by the Registrar. During the years 1903–7 (both years inclusive) the staff performed the operation of oöphorectomy for diseased uterine appendages on 287 women. Of these four died. During the thirteen years I have filled the post of surgeon to this hospital I have performed on an average twenty oöphorectomies yearly for the diseased conditions set forth in the above table. I lost one patient during the whole of this period, and that was in 1902. The chief risks of oöphorectomy for inflammatory conditions are undetected injury to bowel, especially the rectum, and septic peritonitis when the streptococcus is present in the tubes in acute cases.
Operation for primary cancer of the Fallopian tube. This disease is rarely diagnosed before operation. The treatment adopted in the cases first reported was oöphorectomy, but in the majority of patients the disease quickly returned and destroyed them in a few months.
It subsequently became the practice to remove the uterus as well as the tubes and ovaries, but a quick recurrence in these circumstances is the rule.
The really favouring factor in the case is the condition of the cœlomic ostium of the tube. When this remains open, the cancerous cells escape freely and implant themselves on the pelvic peritoneum and adjacent organs. In very rare instances the cœlomic ostium is occluded: in this happy circumstance a fairly long freedom from recurrence may be hoped for.
The relation between the condition of the cœlomic ostium of the Fallopian tube and the recurrence of cancer is illustrated by the following cases:—
A woman, fifty-seven years of age, had a large submucous fibroid in the uterus. At the operation the cœlomic ostium was not only patent, but the carcinoma protruded through it and nodules of growth could be seen on the wall of the rectum at the point where the tube rested on the bowel. The patient recovered from the operation and enjoyed good health for eleven months, then signs of recurrence became manifest and she died a few weeks later.
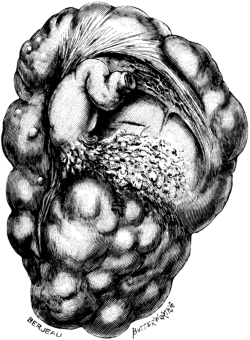
Fig. 5. Primary Cancer of the Fallopian Tube. An ovarian cyst associated
with primary cancer of the corresponding tube. The cœlomic ostium is
open and the cancerous material has leaked out on to the cyst wall. Half
size. |
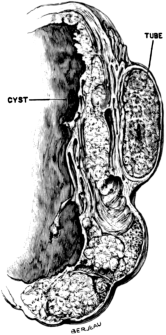
Fig. 6. A Section of Primary Cancer of the Fallopian Tube. This is the
cyst wall and cancerous tube represented in the preceding drawing: it
shows the cancerous infiltration of the cyst wall. Half size. |
A woman, forty-nine years of age, had a large fibroid in her uterus and a Fallopian tube stuffed with cancer, but the cœlomic ostium was completely occluded. The uterus, ovaries, and tubes were removed. The patient subsequently remarried and was in good health three years later.
Primary cancer of the Fallopian tube is almost invariably unilateral and its association with fibroids of the uterus is unusual. It is necessary for the surgeon to remember that a cancerous Fallopian tube may lead to complications with an ovarian cyst. Our knowledge of primary cancer of the Fallopian tube has grown up within the last twenty years, and some of the recorded cases puzzled the reporters because the disease was associated with a cyst, sometimes of a large size.
In Fig. 5 I have represented an instructive specimen, which is an ovarian cyst complicated with primary cancer of the corresponding Fallopian tube. In this instance the cyst was as big as a cocoa-nut and multilocular: the ampulla of the tube is stuffed with cancer, but the ostium is patent and a ‘stream’ of cancerous material has flowed over the wall of the cyst. In addition, the cancerous material has infiltrated the wall of the ovarian cyst. The patient recovered from the operation, but a year later she had an extensive recurrence.
The primary mortality of simple oöphorectomy, or oöphorectomy combined with hysterectomy for primary cancer of the Fallopian tube, is about 5%, and this is low in comparison with abdominal hysterectomy for cancer of the cervix; it is due to the fact that tubal cancer does not so readily become septic (Doran).
Doran, A. A table of over fifty complete cases of Primary Cancer of the Fallopian Tube. Journal of Obst. and Gyn. of the British Empire, 1904, vi. 285.
Bland-Sutton, J. Tumours Innocent and Malignant, 4th Ed., 1906, 400.
—— On Cancer of the Ovary, Brit. Med. Journal, 1908, i. 5.
The systematic surgical treatment of extra-uterine gestation we owe to the genius of Lawson Tait. His first operation for this condition was performed in 1883. Tait wrote that he conceived and carried out this operation in obedience to the canon of surgery relating to the arrest of hæmorrhage, and which is valid in other regions of the body.
Many surgeons (even a butcher) had removed living, dead, and putrescent extra-uterine fœtuses from the abdomen of living women, but Tait was the first to attempt the operation in those early stages of tubal gestation in which the tube bursts, or expels (tubal abortion) the products of conception through the cœlomic ostium or a rent in the gestation-sac, into the abdominal cavity, accompanied by an escape of blood so abundant that it may destroy life in a few hours.
Indications. The operative treatment of extra-uterine gestation depends mainly on the stage at which it is required.
When a gravid tube is detected before rupture, the operation is practically that of oöphorectomy: and is simple and safe.
When the operation is required in consequence of the bursting, or abortion, of an early gravid tube, great promptness is often required on the part of the surgeon to prevent the patient dying from hæmorrhage, and although the operation in these circumstances is really an oöphorectomy, it often has to be performed in the patient’s room as an emergency operation and without the elaborate surroundings of a modern operating theatre.
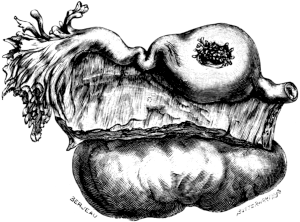 Fig. 7. A Gravid Fallopian Tube. There is a hole in the gestation-sac,
and tufts of villi project through it. The patient was in the seventh
week of her tenth pregnancy when she was seized with abdominal pain and
died in ten hours from hæmorrhage. (Museum of St. Bartholomew’s
Hospital.) Natural size.
Fig. 7. A Gravid Fallopian Tube. There is a hole in the gestation-sac,
and tufts of villi project through it. The patient was in the seventh
week of her tenth pregnancy when she was seized with abdominal pain and
died in ten hours from hæmorrhage. (Museum of St. Bartholomew’s
Hospital.) Natural size. There are few accidents which test the skill, nerve, and resource of a surgeon more than cœliotomy for a suspected intraperitoneal hæmorrhage from a gravid tube, and few operations are attended with such brilliant results. Surgeons are often astonished to find a large amount of blood in the pelvis due to a small perforation in a gestation-sac no bigger than a cherry (Fig. 7).
Operation. In removing tubes of this kind it is necessary to apply the ligature on the uterine side of the rent in cases of rupture of the tube, but when the rent involves the wall of the uterus the opening will require the application of a mattress suture for its complete closure. In some rare instances of the interstitial variety of tubal pregnancy, the uterus has been so involved that in order to effectually control the bleeding it has been found necessary to remove the uterus.
After the pedicle has been safely ligatured and the blood removed, the abdominal incision is sutured as described on p. 9. When the shock due to the bleeding and operation has been great, it is sometimes judicious to pour one or two pints of saline solution at the temperature of 102° F. direct into the abdominal cavity.
The majority of cases of internal bleeding from gravid tubes in the early stages are submitted to operation at periods varying from a few hours, days, weeks, or even months, after the primary bleeding.
When the tube bursts, the hæmorrhage may not be so profuse as to induce death; and the woman, recovering from the shock, does not manifest such grave symptoms as to demand surgical aid. The consequence is that the patient sometimes remains for several weeks under palliative treatment (unless a renewal of bleeding kills her), and at last she seeks surgical advice. Appreciation of the true nature of the case leads to operation.
In such cases, when the abdomen is opened, the free blood in the abdominal cavity is easily removed by sterilized dabs of absorbent material. The damaged tube and ovary are removed as in oöphorectomy. When there is much free blood care must be taken that no clots are left in the iliac fossæ. When the blood has remained in the belly for several weeks after rupture, it is judicious to insert a small drain for a few days. The importance of removing blood and blood-clot from the peritoneal cavity is demonstrated on p. 98.
Where a tubal pregnancy progresses beyond the third or fourth month and invades the broad ligament before giving trouble from internal bleeding, an operation may be necessary at any moment. At this period the operation consists in exposing the parts by a median subumbilical incision, and then opening the gestation-sac, turning out the fœtus, placenta, and clot, and controlling the bleeding by firmly packing the cavity with dabs. The edges of the sac are then stitched to the lower end of the wound; the upper part of the incision is closed, and the sac is drained with a rubber tube of suitable size and allowed to gradually heal.
In cases where the pregnancy continues beyond the fourth month to full time an operation may be required at any moment. Up to the fourth month it may be even possible, in some cases, to remove the embryo, placenta and gestation-sac on the same plan as an ovarian cyst. This is occasionally possible even when the gestation runs to term, but in the majority of cases, when the gestation has passed the fourth month and the fœtus is alive, the surgeon cannot expect to deal with the sac in this summary manner, (unless it be a cornual pregnancy) he has to reckon with the placenta.
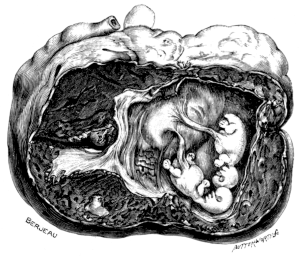 Fig. 8. A Gravid Fallopian Tube, containing
Twins. (McCann’s case. Museum R. College of Surgeons.)
Full size.
Fig. 8. A Gravid Fallopian Tube, containing
Twins. (McCann’s case. Museum R. College of Surgeons.)
Full size.
In operating for the removal of a gravid tube in the early weeks, the surgeon may be exercised in his mind in regard to the opposite tube, for a careful study of the literature of this subject clearly shows that the patient is liable to conceive in the opposite tube, and in some instances this has happened within a few weeks of the removal of its fellow. The liability of a repeated tubal pregnancy may be fixed at 5 per cent. Moreover, in operating for tubal pregnancy, the opposite tube should be carefully examined, because both tubes may be gravid, though, as a rule, the pregnancies are of different dates. To spare a woman a recurrence of tubal pregnancy it has been urged that the surgeon should remove the opposite tube, but men of ripe experience and judgment are averse to such a proceeding, for it is an established fact that uterine pregnancy is not uncommon after unilateral tubal gestation. My own experience is in harmony with this. In some cases of unilateral tubal abortion the operator has cleared out the tubal mole and clot, and left the tube. This is not good practice: I think a tube which has once been pregnant should be removed. If the opposite tube is obviously diseased, and this happens in a small proportion of patients, it should be removed.
The method of dealing with the sac of an extra-uterine gestation after the fifth month depends in a great measure upon whether the fœtus is alive or dead. The gestation-sac after this date consists usually of the expanded tube closely incorporated with the tissues of the broad ligament, which may be thick in some parts and very thin in others. To the walls of the sac, coils of the intestine, and particularly the rectum, adhere. Experience decides that the safest plan, after exposing the gestation-sac through an abdominal incision, is to cut into it and remove the fœtus and placenta. When the fœtus is dead there will be little trouble from the placenta. The edges of the incision are stitched to the margin of the abdominal wound and drained.
In those rare cases where the amnion erodes the tube and invades the belly (ventral pregnancy), the gestation-sac, with its contents, has been successfully removed by merely transfixing its base with silk ligatures.
The great danger of operations for extra-uterine gestation after the fifth month, when the fœtus is alive, or only recently dead, is the furious bleeding which accompanies the detachment of the placenta. It may be stated that an operation for tubal pregnancy after the fifth month of gestation, with a quick placenta, is the most dangerous in the whole range of surgery. About two-thirds of the patients die. The greatest danger is hæmorrhage, and the other is sepsis when the placenta has been left to slough. It cannot be urged with too much force that when it is fairly evident that a woman has an extra-uterine gestation, it should be dealt with by operation without delay: and my experience of the operation leads me to believe that it is a wise plan to remove the placenta at the primary operation. Fortunately very few extra-uterine fœtuses survive to term.
In cornual pregnancy, or, as it is often termed, ‘pregnancy in the rudimentary horn of a so-called unicorn uterus,’ the removal of the uterus is often necessary; there is, however, a variety of this form of pregnancy in which the fully developed cornu may be spared, namely, that in which the rudimentary but gravid cornu is connected with it by a distinct and usually solid pedicle. Many such have been observed and very carefully described.
In nearly all varieties of tubal pregnancy the uterine tissues are sometimes so torn that it is difficult to arrest the hæmorrhage: in this case it is now and then a wise practice to remove the uterus.
Concurrent intra- and extra-uterine pregnancy. The operative treatment of this condition requires consideration under three headings:—
1. Tubal and uterine pregnancy coexist, but the complication is recognized in the early stages. In this condition the signs are those of an early tubal rupture or abortion (Fig. 7); in the majority of the reported cases operation has been undertaken with the impression that the trouble was simply due to tubal pregnancy, the intra-uterine gestation being detected, or in some cases merely inferred from the size of the uterus, in the course of the operation.
In these circumstances the operation is carried out as for a simple tubal pregnancy, care being taken to disturb the uterus as little as possible. In many instances such an operation has been followed by brilliant consequences, for the intra-uterine pregnancy has remained undisturbed and the patients have become the happy mothers of living children.
Occasionally the operation has been followed by miscarriage and other untoward results, but, speaking generally, a gravid uterus is very tolerant of interference.
2. Uterine and extra-uterine pregnancy running concurrently to term. (Compound pregnancy.) This may be described as the most dangerous combination to which child-bearing women are liable. In order to show what a disastrous conjunction it is to women with two ‘quick’ children—one intra- and the other extra-uterine—I have arranged some recorded cases in the table on p. 35. Fortunately this form of compound pregnancy is rare, but a rarer combination has been recorded by Menge, in which the extra-uterine fœtus occupied the ovary and ran nearly to term. When the woman came into labour, the ovarian pregnancy was regarded as an obstructing tumour, and preparations were made for performing cœliotomy. The intra-uterine child was born in the meantime. When the supposed tumour was extracted, to the surprise of all it contained a living fœtus. The mother and both children survived.
3. Uterine pregnancy complicated with a sequestered extra-uterine fœtus. This is a very rare condition, but some cases have been very carefully recorded (Leopold, Stonham, Worrall).
The physical signs are those of a pelvic tumour incarcerated by a gravid uterus. The nature of the swelling may be sometimes accurately inferred before operation, as in Worrall’s remarkable case. The sequestered fœtus should be removed by cœliotomy.
After the death of the fœtus the operative treatment of extra-uterine gestation is, as a rule, a simple proceeding, the fœtus and placenta can be easily and safely removed. We have no certain means of deciding when an extra-uterine fœtus is dead, nor do we know exactly how long after the death of the fœtus the placental circulation ceases, but we do know that in course of time, if the fœtus is retained, the placenta disappears, because in cases where the fœtus is in the condition known as lithopædion there is usually no placenta. When a retained extra-uterine fœtus is wholly or partially converted into adipocere, the tissues have a strong tendency to adhere to the walls of the sac. This is especially marked in connexion with the hairy scalp.
Although a sequestered extra-uterine fœtus is uncommon, yet a surgeon may stumble on one when he least expects it: these bodies may remain undisturbed in the pelvis many years, even fifty, and be only discovered in the post-mortem room, but they are always liable to be infected from the adjacent bowel or bladder; then suppuration is inevitable. In some instances the pus makes its escape at the umbilicus, and as the sinus persists the surgeon explores it, and, on laying it open, is surprised when he extracts the fœtus, sometimes entire.
This is sometimes referred to as ‘navel delivery’, and of this several examples have been recorded. In one such case a fœtus was extracted by a butcher: the woman recovered, and the account of this remarkable case ends thus: ‘She had a navel rupture, owing to the ignorance of the man in not applying a proper bandage’ (Phil. Trans., Abridged Edition, 1805, vol. viii, p. 517). This is a good instance of professional bias in the apportioning of blame.
Usually, when pathogenic micro-organisms gain access to the gestation-sac the fœtus decomposes, and fistulæ form, by which pus, accompanied by fragments of fœtal tissue and bones, finds an exit and affords evidence of the nature of the case. These fistulæ may open into the rectum, bladder, vagina, uterus, or some spot on the anterior abdominal wall below or near the umbilicus. The treatment is simple, and consists in dilating the sinus and extracting all the fragments. If this be thoroughly carried out the sinus quickly closes. Partial operations are useless: if but a bit of a bone remain, a troublesome sinus will persist. It is bad practice to attempt to extirpate the sac in such condition; such an operation usually terminates fatally.
In a case of old-standing lithopædion it is unusual to find any trace of the placenta. J. W. Smith operated on a woman in whom a lithopædion had caused intestinal obstruction. The fœtus had probably been retained 15½ years, and the placenta was represented by a calcified encapsuled ball, with an average diameter of 6 cm.
Results of operative treatment. In order to afford some notion of the risks attending the surgical treatment of extra-uterine gestation, as well as to give an idea of its relative frequency in hospital practice, the following figures will serve. From 1896 to 1907, both years inclusive, 116 operations were performed for extra-uterine gestation in the Chelsea Hospital for Women. During this period all the varieties of tubal pregnancy were encountered (ampullary, isthmial, tubo-uterine), including the rare condition of a full-time living fœtus free among the intestines, and the more uncommon condition of a full-time cornual pregnancy. There were four deaths in the series, one in 1897, 1902, and two in 1905. Death in the fatal cases was attributed to pulmonary embolism, peritonitis, and in two to heart failure.
A Table showing Cases of Concurrent Intra- and Extra-uterine Pregnancy (Compound Pregnancy) running to Term, with the Fate of the Mother and Children.
| Recorder. | Year. | Fate of Mother. | Intra-uterine Child. | Extra-uterine Child. |
|---|---|---|---|---|
| Cooke | 1863 | Died | Died | Died |
| Sale | 1871 | Died | Lived | Lived |
| Wilson | 1880 | Died | Died | Lived |
| Galabin | 1881 | Died | Died | Died |
| Franklin | 1893 | Died | Lived | Died |
| Matthewson | 1894 | Lived | Lived | Killed 1 |
| Ludwig | 1896 | Lived | Lived | Lived |
| Allardice | 1905 | Lived | ? | Dead 2 |
| Menge | 1907 | Lived | Lived | Lived |
1 This fœtus was killed by means of a stilette passed through the abdominal wall of the mother into its thorax. The patient had two subsequent confinements without difficulty. In 1898 the ‘lump’ had shrunk, but was movable and caused no difficulty. Pacific Medical Journal, September, 1898.
2 Intra-uterine child born naturally at the seventh month. Extra-uterine fœtus died, set up septic changes, and was removed by cœliotomy some weeks later.
Leopold. Ovarialschwangerschaft mit Lithopädionbildung von 35-jähriger Dauer. Arch. f. Gyn., 1882, Bd. xix. 210.
Menge. Eine reine Ovarialschwangerschaft mit bebendem Kinde. Vide Fränkische Gesellschaft für Geburtshülfe and Frauenheilkunde. Münch. med. Wochensch., 1907, liv. 2452.
Smith, J. W. Jour. of Obstet. and Gyn. of the British Empire, 1908, xiii. 180.
Stonham, C. Lithopædion, Trans. Path. Soc., 1887, xxxviii. 445.
Worrall. Ectopic Gestation complicating Normal Pregnancy. Abdominal section. Recovery. Med. Press and Circular, 1891, i. 296.
Hysterectomy is the name applied to the surgical operation for the removal of the uterus.
Indications. Hysterectomy is mainly required in the radical treatment of fibroids and malignant disease (carcinoma, sarcoma, and chorion-epithelioma). It is occasionally required for injury, and certain morbid states due to acute and chronic sepsis; and for a condition but little understood, termed generically fibrosis. Hysterectomy is also carried out for such conditions as diffuse adenomyoma of the uterus, hæmato-metra, tuberculous endometritis, and on rare occasions for chronic inversion of the uterus and inveterate dysmenorrhœa.
The presence of fibroids in the uterus is a common cause for which hysterectomy is required, and the history of this operation is full of interest.
The uterus may be removed by two methods. In one, access is obtained to the uterus through an incision in the belly-wall; this is termed abdominal hysterectomy. In the other, the whole uterus is extirpated through the vagina, and on this account it is termed vaginal hysterectomy or colpo-hysterectomy.
The abdominal method of removing the uterus may be performed in two ways:—
In one the body of the uterus and a portion of its neck is removed; this is called subtotal hysterectomy (or supravaginal hysterectomy). In the other the body of the uterus and the whole of its neck are excised: this is total hysterectomy (or panhysterectomy). The ovaries and Fallopian tubes may, or may not, be removed, according to the disease for which the operation is undertaken. This is a matter which will receive ample consideration later on (see p. 56).
For the satisfactory performance of abdominal hysterectomy the Trendelenburg position is necessary.
The abdomen is opened by the median subumbilical incision; but when the operation is performed for the removal of large tumours it will frequently require extension above the umbilicus. The operator should never allow himself to be embarrassed by a small incision. As soon as the peritoneal cavity is reached, the surgeon introduces his hand and carefully makes out the nature of the case, the presence or otherwise of adhesions, other tumours, and the relation of the fibroid to the uterus, and determines whether it is impacted in the pelvis. The uterus is then carefully lifted out through the incision, or drawn out with the assistance of a volsella; the intestines and omentum are isolated from the pelvis with a large warm dab.
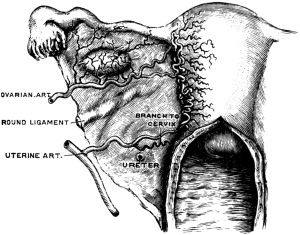 Fig. 9. A Diagram to show the Arterial Supply of the Uterus.
Fig. 9. A Diagram to show the Arterial Supply of the Uterus.
In a simple case the broad ligaments are seized with hæmostatic forceps; if the ovaries and tubes are healthy and the surgeon wishes to preserve them, the forceps are applied between the ovary and the uterus; but if they are obviously diseased and must be sacrificed, the forceps are applied to the broad ligaments near the brim of the pelvis beyond the outer pole of the ovary. In some instances the round ligament of the uterus can be seized with the same forceps, but in many cases it is necessary to clip it separately. It is an advantage to secure the round ligament at this stage, for the forceps controls its artery and prevents the stump of the ligament unduly retracting the peritoneum. The broad and round ligament on each side are divided, and the uterine artery is exposed on each side of the uterus and caught with forceps: a peritoneal flap is then fashioned on the anterior wall of the uterus at its junction with the neck, taking care not to injure the bladder; and a similar flap is cut on the posterior wall. The uterus is then detached at a point well below the junction of the cervix with the body of the uterus: if the forceps are correctly applied to the vessels the detachment of the uterus is an almost bloodless proceeding: a small vessel here and there will perhaps require the application of a pair of forceps.
The principle involved in this part of the operation may be explained by reference to the diagram (Fig. 9). The blood-supply of the uterus follows four routes; two of these are the ovarian arteries which traverse the broad ligaments to reach the cornua of the uterus, where they anastomose with the terminations of the uterine arteries; the latter come into relation with the uterus near the junction of the body and cervix, and then ascend the sides of the uterus to the cornua. No large vessels are found on the anterior or posterior surface of the uterus. An arterial twig runs along the round ligament, bringing the ovarian artery into relation with the deep epigastric artery. If the surgeon thoroughly appreciates the distribution of the ovarian and uterine vessels he will at once perceive that if the four forceps are properly applied to the vessels the blood-supply is under absolute control: indeed, in many cases a subtotal hysterectomy can be performed without the loss of more than an ounce of blood. When the broad ligament is clamped and detached there is a spurt of blood from the uterine cornu which lasts until the corresponding uterine artery is caught with the forceps, and the cessation of the bleeding at the uterine cornu is a sign that the artery is securely clipped. It must be remembered that with a small tumour in the uterus the vessels follow their normal courses and can be easily found, but when the uterus is deformed by huge tumours, the vessels are not so easily seen, and they are of large size and give rise to furious bleeding when divided. In dealing with large and vascular uterine fibroids another factor has to be reckoned with, namely, the enormous veins in the pampiniform plexus, interspersed with lymphatics which in some cases are as thick as the index-finger; it is not an uncommon thing to meet with lymphatics in this situation a centimetre in diameter and filled with straw-coloured lymph.
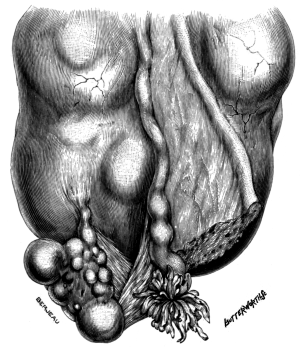 Fig. 10. A Fibroid growing near the Right Uterine Cornu. It separates
the ovarian ligament, Fallopian tube, and round ligament of the uterus
from each other. Full size.
Fig. 10. A Fibroid growing near the Right Uterine Cornu. It separates
the ovarian ligament, Fallopian tube, and round ligament of the uterus
from each other. Full size.
The surgeon now secures the vessels. The ovarian pedicles are transfixed and ligatured with silk as in ovariotomy: the round ligament is usually included in the ovarian pedicle. It occasionally happens that a fibroid situated near the uterine cornu will grow in such a manner that it widely separates the ovarian ligament, the Fallopian tube, and the round ligament from each other as shown in Fig. 10. In such a condition it is impossible to save the ovary without risk, and also inadvisable to attempt the inclusion of the round ligament in the pedicle containing the ovarian vessels. In these circumstances the round ligament is easily secured by a mattress suture, which should include both layers of the corresponding broad ligament.
When the surgeon decides to leave an ovary and the corresponding Fallopian tube, these structures are carefully examined to determine if they are healthy and free from any suspicious fluid. When the endometrium is septic or cancerous both ovaries and tubes should be removed. When the surgeon decides to leave an ovary and its corresponding Fallopian tube, he should take care in securing the ligatures to include the ligament of the ovary: it is very liable to slip out of the encircling loop of silk. It is often convenient to include the round ligament of the uterus in the pedicle, but it is not a disadvantage when it is tied separately.
The uterine arteries are ligatured with thin silk; these vessels as they run up the sides of the uterus are accompanied by veins, so that there is a vascular tract at the point where the cervix is divided. If after the uterine vessels are secured there is oozing from these veins, it is easily controlled by a mattress suture. This kind of suture is so useful that the mode of inserting it may be given in more detail. In the diagram (Fig. 11) the silk is represented in position before it is tied, and in that particular instance it is represented as being passed through the peritoneal flaps from before backwards, and this is usually the most convenient route; occasionally the reverse direction is easier. It will be noticed in the diagram that this suture not only controls oozing from the tissue in the immediate neighbourhood of the uterine vessels, but it also embraces the main vessels, and thus serves as an additional security against hæmorrhage; it also brings the peritoneal flaps into apposition.
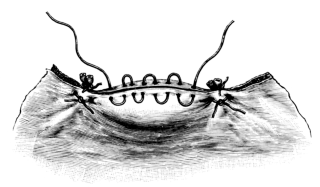 Fig. 12. The Stump after Subtotal Hysterectomy.
To show the method of applying the continuous suture.
Fig. 12. The Stump after Subtotal Hysterectomy.
To show the method of applying the continuous suture.
As soon as the oozing of blood has been controlled, the cervical canal is examined to ascertain if it be free from polypi or cancer. Should the condition of the cervix be in the least degree suspicious of cancer it must be extirpated. When it is healthy, then the flaps are brought together by one or two interrupted sutures, and the edges more carefully approximated by a continuous suture of thin silk. In suturing the flaps it is necessary to avoid puncturing the bladder, which is quite close to, and often forms part of, the anterior flap. Care must also be taken in passing the needle (especially when it has sharp edges) in the neighbourhood of the stumps of the uterine arteries, or they will be pricked, and then free bleeding will cause delay in the operation.
When this operation is properly performed, there should be no projecting stump on the floor of the pelvis; the sutured edges of the peritoneum merely appear as a thin line below the base of the bladder.
The pelvis is now cleared of blood and clot; the dabs and instruments are counted, and it is also useful to examine the condition of the vermiform appendix, and if grossly diseased it should be removed.
The abdominal incision is then sutured in the way described on p. 9.
This operation differs from the preceding in the fact that the neck of the uterus is removed as well as its body. The abdomen is opened in the usual way and the uterus is withdrawn from the abdomen and the arteries controlled by forceps, and the broad ligaments divided exactly as in the case of the subtotal operation. Unless the uterus be very big it is drawn well out of the abdomen and the bladder peeled off its anterior aspect. The surgeon then feels for the extremity of the cervix and opens the vagina with the scalpel and carefully detaches it from the neck of the uterus, taking great care to keep close to the cervix in order to avoid wounding the bladder or the ureters. As soon as the uterus is detached, the cut edge of the vagina is seized with the volsella to prevent it retracting. In some instances the body of the uterus may be removed as in the subtotal operation, and the cervix detached separately; occasionally the surgeon begins his operation with the intention of performing the subtotal operation, but finds the cervix unhealthy or cancerous, and removes it.
As soon as the uterus is removed and all bleeding under control, then the blood-vessels are secured with ligatures; the ovarian artery and vein are secured on each side in the usual manner. The chief point in this operation is the method of dealing with the vaginal opening. In the subtotal operation the vessels concerned in the stump are the uterine arteries, but in the total operation the territory of the vaginal arteries is invaded, and these vessels are apt to bleed when the patient is returned to bed, unless care is taken to secure them in the course of the operation. The parts which require most attention are the lateral angles in the immediate neighbourhood of the uterine arteries; these angles may be secured by a mattress suture involving the anterior and posterior wall of the vagina; any oozing on the anterior or posterior wall is commanded by a mattress suture involving these walls separately, so as not to completely close the vaginal opening. Bleeding from the cut edges of the vagina may also be readily controlled by means of a continuous suture of thin silk. The peritoneum is sutured over the cut ends of the vagina, so that when the operation is completed a thin seam is seen lying under the base of the bladder.
In cases where the uterus is removed for septic conditions, such, for example, as an infected or gangrenous fibroid, or when cancer of the corporeal endometrium and a submucous fibroid coexist, I modify the last stages of the operation. After the ovarian and uterine arteries are ligatured, the cut edges of the vagina are secured in the following way: the cut edge of the peritoneum covering the bladder is stitched to the cut edge of the anterior wall of the vagina, and in the same way the peritoneum in relation with the posterior vaginal wall is stitched to the corresponding cut edge of the vagina. The flaps at the lateral angles of the vaginal opening are drawn together with a suture and the intervening segment is left with merely the cut edges in apposition: this affords a route for the escape of pus if required.
Whether the peritoneum is sutured over the vaginal opening, or whether the edges are merely left in apposition, the recesses of the pelvis are thoroughly cleared of fluid and clot. The dabs and instruments are counted, and the wound sutured as recommended on p. 9. In septic conditions the abdominal incision should be closed with a single row of through and through sutures. Before the patient leaves the operating table it is useful to examine the vagina and mop out any blood which has found its way there in the course of the operation. It is also useful to pass a glass catheter and withdraw any urine that has accumulated during the operation.
If there is evidence of free oozing it is most likely to come from the cut edges of the vaginal wall in a case of total hysterectomy: under such conditions it is easy to apply a pair of fenestrated forceps to the oozing area and leave them on for thirty-six hours. They will cause the patient trifling inconvenience. Care must be taken not to fix the blade too far on the anterior flap, or it will lead to subsequent sloughing of the bladder.
When there is free oozing of blood from the cervical canal after subtotal hysterectomy, it is easily and safely controlled by applying a pair of fenestrated forceps on each side of the cervix, but not too deeply, or the ureters may be nipped. These should be left on for thirty-six hours.
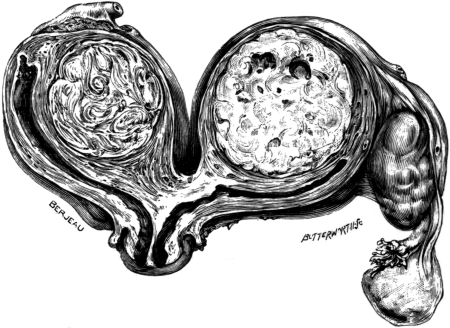 Fig. 13. A Bicornate Uterus. This uterus is shown in coronal section;
each cornu contains a fibroid. Removed from a spinster aged 32 on account
of acute pain probably caused by the axial rotation of one cornu. Two-fifths size.
Fig. 13. A Bicornate Uterus. This uterus is shown in coronal section;
each cornu contains a fibroid. Removed from a spinster aged 32 on account
of acute pain probably caused by the axial rotation of one cornu. Two-fifths size.
The details of the operation set forth in this account refer to a simple or uncomplicated hysterectomy, and under these conditions it cannot be described as a difficult operation to any surgeon accustomed to abdominal operations, but the complications not infrequently met with in connexion with uterine fibroids are occasionally very formidable, and tax the skill and resource of the boldest; e.g. fibroids which are inflamed and adherent to the colon, rectum, or small intestines; fibroids associated with unilateral or bilateral pyosalpinx, or a suppurating ovarian cyst incarcerated in the pelvis by the enlarged uterus; fibroids complicated by cancer in the neck of the uterus; or a cervix fibroid firmly incarcerated in the pelvis by a big fibroid in the fundus of the uterus, and pushing the bladder upwards in front of the tumour.
Cervix fibroids. The operative treatment of this variety needs separate consideration because these tumours do not lend themselves to any routine method.
When the uterus with the tumour in its cervix can be raised out of the pelvis far enough to allow the necessary manipulations, then total hysterectomy can be performed easily and quickly. Occasionally the tumour is wide and so fixed in the pelvis that it will be necessary to split the uterus longitudinally and to enucleate the fibroid from its bed; then an ordinary subtotal or total hysterectomy can be carried out. The enucleation of a large impacted cervix fibroid requires to be conducted carefully, without undue display of force, or so much shock is produced that the patient’s life will be placed in the gravest peril.
 Fig. 14. A Bicornate Uterus shortly after Delivery. The pregnancy
occurred in the left half. The vesico-rectal ligament is well shown.
Fig. 14. A Bicornate Uterus shortly after Delivery. The pregnancy
occurred in the left half. The vesico-rectal ligament is well shown.
On hysterectomy when the uterus is double. Fibroids and cancer arise in malformed uteri, as well as in those of normal shape (Fig. 13). When the body of the uterus is double (bicornate) and the surgeon stumbles upon it in the course of a pelvic operation he may be puzzled if he is not familiar with the anatomical conditions associated with this malformation.
When the body of the uterus is bicornate the rectum lies in the middle line of the pelvis, and a median vertical fold of peritoneum, the ligamentum vesico-rectale passes, from its anterior aspect through the gap between the uterine cornua to become continuous with the peritoneum covering the posterior surface of the bladder (Fig. 14). That portion of the vesico-rectal ligament which lies between the rectum and the neck of the uterus divides the recto-vaginal fossa into a right and a left half. This peritoneal ligament requires careful treatment, or the surgeon may accidentally open the rectum or the bladder. In closing the peritoneum over the cervical stump it is sometimes necessary to bring the edges of the abnormal fold into apposition vertically by a continuous suture.
In a case of this kind in which I performed total hysterectomy for cancer of the neck of the uterus the extensive peritoneal connexions were somewhat troublesome, and when the uterus was removed it seemed as if the floor of the pelvis had been stripped of its serous covering. The bifid nature of the uterus had been anticipated before the operation, as an imperfect vertical septum was known to exist on the posterior vaginal wall. The patient made an excellent recovery.
Experience teaches that bicornate uteri cause more difficulties in diagnosis than in technique, but the presence of the vesico-rectal ligament would probably bar the removal of the uterus by the vaginal route. The existence also of a median longitudinal septum, partial or complete, in the vagina would be another difficulty.
Mortality. In order to give some idea of the great improvement which has taken place in the operation of abdominal hysterectomy for fibroids in London the following figures will be found of great interest.
In the year 1896 the results of abdominal hysterectomy for fibroids in the hospitals of London may be inferred from the following table:—
| St. Bartholomew’s | 7 | with | 3 | deaths |
| St. Thomas’s | 5 | " | 2 | " |
| St. George’s | 1 | " | 0 | " |
| Middlesex | 6 | " | 1 | " |
| University College | 3 | " | 0 | " |
| Samaritan | 17 | " | 4 | " |
| Soho (for women) | 1 | " | 0 | " |
| Chelsea Hospital for Women | 9 | " | 1 | " |
| 49 | " | 11 | " |
In these hospitals and the New Hospital for Women the returns in 1906 are as follow:—
| St. Bartholomew’s | 26 | with | 4 | deaths |
| St. Thomas’s | 40 | " | 2 | " |
| St. George’s | 8 | " | 0 | " |
| Middlesex | 50 | " | 0 | " |
| University College | 21 | " | 1 | " |
| Samaritan | 37 | " | 2 | " |
| Soho (for women) | 60 | " | 1 | " |
| Chelsea (for women) | 80 | " | 1 | " |
| New (for women) | 26 | " | 0 | " |
| 348 | " | 11 | " |
 Fig. 15. Villous Disease of the Uterus. The uterus is shown in sagittal
section. The cavity is dilated and occupied by a villous tumour growing
from its posterior wall. Successfully removed from a multipara aged 83.
Full size.
Fig. 15. Villous Disease of the Uterus. The uterus is shown in sagittal
section. The cavity is dilated and occupied by a villous tumour growing
from its posterior wall. Successfully removed from a multipara aged 83.
Full size.
The returns during 1906 and 1907 from my service at the Chelsea Hospital for Women and the Middlesex Hospital, as verified by the Registrars, were 101 abdominal hysterectomies for fibroids; all the patients recovered. Of these 101 operations, 7 were total and the remainder subtotal hysterectomy.
The risks of abdominal hysterectomy. The dangers of hysterectomy are those common to cœliotomy, such as sepsis, peritonitis, shock, and the risks of the anæsthetic. There are certain special dangers, such as hæmorrhage; injury to the vesical segments of the ureters, and especially the bladder; injury to the intestines, especially the rectum; acute intestinal obstruction; thrombosis and pulmonary embolism. These risks and dangers are considered fully in their relation to all forms of abdominal gynæcological operations in a special chapter (see Chap. XI).
Among the rarer forms of death after hysterectomy may be mentioned acute perforation of the stomach or the small intestine, cerebral hæmorrhage, lobar pneumonia, thrombosis of the right auricle, embolism of the femoral artery ending in gangrene of the leg, suppression of urine, and acute mania. These are fatal conditions which follow any major operation in surgery, and have no special connexion with hysterectomy.
The removal of the uterus has been rendered so safe that even in advanced age it has been employed with success, as the subjoined table shows:—
Table of Cases in which Hysterectomy was performed on Women of Seventy Years and upwards.
| Reporter. | Age. | Nature of Operation. | Result. | Reference. |
|---|---|---|---|---|
| Bland-Sutton | 73 | Subtotal for Fibroid 28 lb. | R. | Trans. Obstet. Soc., 1900, xli. 300. |
| Stewart McKay | 70 | Subtotal for Fibroid 19 lb. | R. | Australian Med. Gaz., 1907, 14. |
| Bland-Sutton | 83 | Vaginal Hyst. for Villous disease. Fig. 15. | R. | Trans. Obstet. Soc., 1906, xlix. 46. |
| Malcolm | 74 | Total for Fibroids. | R. | Brit. Med. Journal, 1907, ii. 1571. |
Under this general term it is usual to include operations for the removal, through an abdominal incision, not only of pedunculated subserous fibroids, but also sessile and interstitial (intramural) fibroids of the uterus.
The earliest operations of this kind were performed by Spencer Wells (1863); but little attention was given to this matter until the advantages of abdominal myomectomy were strongly advocated by A. Martin (1880) and Schroeder (1893). The operation has been practised by many surgeons and gynæcologists imbued with conservative ideals in regard to the uterus. In its early days the operation was attended with a very high mortality, but the great improvements in hysterectomy have limited very materially the scope of abdominal myomectomy.
Abdominal myomectomy. This signifies the removal of one or more pedunculated subserous fibroids through an incision in the abdominal wall, preserving the uterus, Fallopian tubes, and the ovaries.
Abdominal enucleation. In this operation a sessile fibroid is shelled out of its capsule: the uterus, ovaries, and tubes are preserved.
Hysterotomy. In this operation a submucous fibroid is removed, through an incision in the wall of the uterus, which opens the uterine cavity.
The preliminary steps for each of these procedures is the same as for ovariotomy, and the Trendelenburg position is of great advantage.
After opening the abdomen the intestines are carefully protected by a warm dab, and the tumour carefully examined.
When the stalk is narrow it may be transfixed and secured with silk thread, like the pedicle of an ovarian cyst. When the pedicle is short and broad the tumour should be shelled out of its capsule, and any obvious blood-vessel is easily secured with forceps and ligatured with silk. The opposite flaps of the capsule are brought into apposition by mattress sutures, and the redundant portions of the capsule cut away and the free edges carefully brought together by a continuous suture of thin silk.
When a fibroid is embedded in the wall of the uterus, the tumour is exposed by cutting through its capsule and seizing it with a volsella; as a rule, it shells out quite easily. This is followed by free bleeding. The vessels are then seized with forceps and ligatured with thin silk. In order to completely control the oozing, mattress sutures are passed through the wall of the capsule on each side, their number varying with the size of the tumour.
In some instances a uterus contains ten or more fibroids, and each must be enucleated and the capsule secured with ligatures, as described above.
Sometimes the oozing is difficult to control, and the surgeon sutures the edges of the capsule to the lower angle of the incision, and stuffs the cavity or bed of the tumour with gauze.
In removing a large submucous tumour through an incision in the wall of the uterus, the surgeon necessarily opens the uterine cavity (hysterotomy). After controlling the bleeding the walls of the uterine incision are closed, as in Cæsarean section.
In many instances in which the surgeon attempts to carry out myomectomy or enucleation, he has such difficulty in controlling the oozing that he is driven to remove the uterus.
It is admitted by most writers that the ideal method of dealing with fibroids requiring removal by cœliotomy is to remove them either by ligature or by enucleation. In actual practice this ideal operation of removing the tumours and leaving the uterus and ovaries intact can only be carried out in a small proportion of cases, probably in less than 10 per cent., and it is fair to state that enucleation and hysterotomy are often more troublesome and serious operations than hysterectomy; also the preservation of the uterus is not always an advantage to the patient.
When a woman is submitted to hysterectomy for fibroids we can assure her that the tumours will not recur, but after a myomectomy or enucleation in a woman in the reproductive period of life we cannot give her this assurance, for she may have in her uterus many ‘seedlings’ or ‘latent fibroids’ and one or several of these may grow into formidable tumours.
There are three conditions in which myomectomy and enucleation are legitimate procedures:—
1. A young woman contemplating marriage, or a married woman anxious for offspring, if her tumour be single and admits of myomectomy or enucleation, may have her uterus spared. Although I have carried out these measures on many occasions, I only know of five patients who have subsequently borne children.
2. Occasionally in pregnancy (see p. 82).
3. Myomectomy is a very safe undertaking in patients at, or after, the menopause, where a stalked fibroid gives trouble by twisting its pedicle, or by shrinking to such a size that it falls into the true pelvis and becomes impacted; or, more rarely, the pedicle of such a tumour entangles a loop of small intestine and obstructs it.
In order to give the matter a statistical basis I have drawn up an analysis of ninety-five consecutive cases of myomectomy and enucleation out of my practice, with the subsequent history of some of the patients. This experience covers a period of twelve years.
Of these ninety-five patients three died as the result of the operation—two from pneumonia in the fourth week after operation, and one a few days after operation: in this case there is reason to believe that the tumour was complicated with cancer of the body of the uterus.
Six of the women were submitted to myomectomy during pregnancy, and in four cases the operation was undertaken under the impression that the tumour was an ovarian cyst which had undergone axial rotation. These cases occurred in the days before I recognized that ‘red degeneration’ of fibroids complicating pregnancy caused them to be painful and tender (see p. 78). In one patient this complication was clearly recognized. In the sixth patient the tumour was regarded by some capable gynæcologists, who examined her, as a tubal pregnancy complicating a gravid uterus. Five of these patients went to term and were delivered of living children. The sixth miscarried two months after the myomectomy.
Of the ninety-two successful myomectomies, five subsequently became pregnant and had living children, but in each instance the fibroids were subserous. I have not known a patient to become pregnant after abdominal myomectomy for a submucous fibroid, large or small. In calculating the probability of pregnancy from these statistics it must be mentioned that the patients fall into three categories:—
1. Forty women were in the child-bearing period of life and married; many of them were multiparæ.
2. Twenty were single women and probably capable of bearing children in a favouring environment.
3. The remainder were spinsters or barren wives.
A significant feature in the after-history of ten of these women is the fact that some years later other fibroids grew in the uterus, and hysterectomy became a necessity on account of menorrhagia in seven of them; of these, two died from the operation, which was difficult and tedious. One patient was operated upon two years after the myomectomy, and had borne a child in the interval, and the other seven years.
The last fact to mention is that one patient, from whom a submucous fibroid had been enucleated from the cavity of the uterus (hysterotomy), died four years later from cancer arising in the body of the uterus (see p. 51).
Olshausen has recently considered this question, and indicates that the chief objection to the abdominal enucleation of uterine fibroids is its high mortality.
He furnishes a table of 563 cases, collected from twelve operators, including himself; of these 59 patients died, representing a mortality of 10.5 per cent. Olshausen, in the years 1900–5, performed enucleation on 124 patients with 14 deaths. Eight of the patients subsequently came under notice with recrudescence of fibroids. Christopher Martin has performed abdominal myomectomy 73 times with 1 death.
The question of myomectomy, when fibroids complicate pregnancy and labour, or give trouble after labour, is considered in detail on p. 78.
Bland-Sutton, J. Fibroids in a Unicorn Uterus. Clin. Journ., Lond., 1901–2, xix. 1.
Bland-Sutton, J. Case of Fibroids in both halves of a Bicornate Uterus. Proc. R. Soc. of Medicine, 1908. Obstet. and Gyn. Sect., ii. 95.
Czerwenka. Uterus bicornis unicollis, &c. Centralbl. f. Gyn., Leipz., 1900, xxiv. 207.
Doran, A. The Removal of a Fibroid from a Uterus Unicornis in a Parous Subject. Brit. Med. Journ., 1899, i. 1389.
Gow, W. J. Cystic Intraligamentous Myoma with Double Uterus. Trans. Obstet. Soc., Lond. (1898), 1899, xl. 134.
Heinricius. Ein Fall von Myoma im rudimentaren Uterus bicornis unicollis. Monatschr. f. Geburts. u. Gyn., Berl., 1900, xii. 419.
Kamann. Uterus bicornis unicollis with a Myoma in the Left Horn; Subtotal Extirpation of the Left Horn. Centralbl. f. Gyn., 1905, xxix. 795.
Martin C. The Ingleby Lectures. On the Dangers and Treatment of Myoma of the Uterus. Lancet, 1908, ii. 1682.
Olshausen, R. In Veits’ Handbuch der Gynäkologie, Wiesbaden, 1907, Bd. ii, p. 607.
Routh, A. Fibroid of One-horned Uterus. Trans. Obstet. Soc., 1888, xxix. 2 and 57, with a good drawing.
The great success which followed the use of the short ligature in ovariotomy induced several surgeons to apply the same principle to the cervical pedicle when removing the uterus for fibroids. The result was dismal failure. Matters improved somewhat after Koeberlé introduced the serre-nœud, and this continued the safest method until 1892. In the meantime antisepsis had begun to take effect in pelvic surgery, and attempts were made by Bardenheuer (1881), Polk, and other surgeons to avoid the dangerous difficulties connected with the treatment of the stump by removing the cervix as well as the uterus (total hysterectomy), and they attained an encouraging measure of success. Nevertheless, other surgeons (Goffe, Milton, Heywood Smith, and Stimson) felt that the enucleation of the cervix was not always necessary, and sought to find a way of avoiding it. The credit of solving this difficulty fell to Baer of Philadelphia (1892), for he showed that it is dangerous to constrict the neck of the uterus with ligatures, it is only necessary to secure the arteries.
Baer’s method of supravaginal hysterectomy, or, as it is now commonly termed, the subtotal operation, soon supplanted the total method of Bardenheuer. The publication of Baer’s paper had great consequences; it came at a time when the attention of gynæcologists was centred on improvements in hysterectomy. The method was promptly tested and adopted in London. The effects of this improvement in technique in a few years revolutionized the surgical treatment of uterine fibroids, as the statistical results set forth on p. 44 amply prove.
The great advantage of Baer’s method is its simplicity and safety; but there is a disposition on the part of a few surgeons to prefer the total operation, mainly on the ground that the cervical stump left after subtotal hysterectomy is liable to become attacked by cancer.
As far as I can ascertain, Dr. M. Mann, of Buffalo, was the first to draw attention to the occurrence of cancer in the neck of the uterus after the body of the organ had been removed. He stated in 1893 that he ‘removed an ovarian tumour and the body of the uterus, by accident, along with it; the cervix was left’. The patient recovered. ‘Six months afterwards cancer developed in the cervix, from which she died.’
When cases of cancer supposed to arise in the stump left after subtotal hysterectomy come to be critically analysed, they fall into four groups:—
1. The disease existed in the neck of the uterus at the time of the primary operation, but was overlooked.
2. Cancer attacked the cervical stump subsequent to subtotal hysterectomy.
3. The fibroid which necessitated the hysterectomy was really a sarcomatous tumour of the uterus.
4. The suspected growth on the cervix is not malignant, but a granuloma.
Each of these postulates requires separate consideration.
Many observations have been published which show beyond dispute that surgeons have performed subtotal hysterectomy in ignorance that the cervix was already cancerous, and the hæmorrhages of which the patients complained before the operation were due as much to the cancer in the neck of the uterus as to the fibroids. This should serve as a warning that, in cases where the surgeon contemplates performing a subtotal hysterectomy, he should carefully examine the cervix beforehand; at the time of the operation he should also critically examine the cut surface of the cervix, and if it be in the least suspicious he should remove the neck of the uterus. It is necessary to remember that cancer attacks any part of the cervical endometrium, therefore an early cancerous ulcer in the middle of the cervix will run a great chance of being missed by a surgeon who is content with a subtotal hysterectomy.
It is certain that cancer does occasionally attack a cervical stump left after subtotal hysterectomy at such an interval after the operation as to make it certain that the cancer did not exist at the time of the operation. Such a case occurred in my practice. I performed subtotal hysterectomy in 1901 on a woman forty-two years of age, mother of one child; eighteen months later there was a cancerous ulcer on the cervix; the whole of the cervical stump was promptly removed and the nature of the disease established microscopically. In 1908 the patient was in excellent health.
In another case under my care I performed total hysterectomy for fibroids in ignorance that the patient had cancer of the cervix. Some months after the operation cancer recurred in the vaginal vault and scar of the hysterectomy; the neck of the uterus had been preserved by the doctor, and on examination the cancer was found. In this instance, although total hysterectomy was performed, it had no effect in staying the course of the disease.
It is necessary to utter a caution in regard to the occurrence of cancer of the cervix after subtotal hysterectomy. I removed a uterus containing a large globular submucous fibroid from a barren married woman forty-five years of age. Six years later she came under my observation with a large granulating and bleeding growth on the cervix uteri. I had no doubt from the naked-eye characters that this was a primary carcinoma, although it surprised me to find it there, especially as the woman had never been pregnant. On my urgent representations she allowed me to remove the cervix. On microscopic examination the suspected cancer turned out to be a granuloma. Two years later the patient was in good health. Polk has recorded a similar experience. These facts show that caution is necessary in accepting reports of cancer of the uterine stump after subtotal hysterectomy.
Cancer of the body of the uterus and fibroids. In deciding between total and subtotal hysterectomy for fibroids the probable presence of cancer requires consideration in another aspect. Although uterine fibroids do not predispose to cancer of the neck of the uterus, many writers in recent years have expressed their suspicions that the presence of a submucous fibroid favours the development of cancer in the corporeal endometrium. Piquand, in 1905, drew attention to this matter and emphasized what other observers had pointed out, namely, that a submucous fibroid is often associated with changes in the mucous membrane of the uterus, which not only causes excessive bleeding, but sets up inflammatory conditions giving rise to leucorrhœa, salpingitis, pyosalpinx, and morbid changes in the endometrium, rendering it susceptible to cancer. His statistics support his conclusions, for they represent that in one thousand women with fibroids fifteen will probably have cancer of the body of the uterus. My own observations support this opinion. This complication is found most frequently between the fiftieth and the sixtieth year of life. If we narrow the ages of the patient and exhibit the liability in its most emphatic form it would run thus: that in patients submitted to hysterectomy for fibroids over the age of fifty years, about ten per cent of them will have cancer of the corporeal endometrium.
In 1906 I looked through the case-notes of five hundred patients who had been submitted to operation for uterine fibroids under my care. Of these sixty-three patients had attained the age of fifty years and upwards. Among these sixty-three women there were eight cases of cancer of the corporeal endometrium; the nature of the disease in each case was verified by careful microscopic examination.
Consequently, in performing subtotal hysterectomy for fibroids in women of fifty years and upwards, the surgeon should have the uterus opened immediately after its removal and assure himself that the endometrium is free from cancer. If there be any suspicion in this direction he should remove the cervix.
Sarcoma. The most insidious danger which besets the surgeon in dealing with fibroids of the uterus is the occurrence of an encapsuled sarcoma in the guise of an innocent fibroid. I have for some years dropped the name of myoma for these common uterine tumours, preferring to apply the term fibroid in a generic sense to all encapsuled tumours of the uterus. Every histological condition is found in them, from the hard calcified body looking like a block of coral to a soft diffluent collection of œdematous connective tissue, and tumours composed of tissue indistinguishable from spindle-celled sarcomata.
I have elsewhere recorded briefly a case in which I removed the uterus from a woman forty years of age, which contained a fibroid as big as an ostrich’s egg. On section it appeared to be a moderately firm fibroid, with its tissue whorled as is usual in hard fibroids and enclosed in a complete capsule. Some months later the patient complained of pain, and on examination a hard mass occupied the floor of the pelvis; a portion of this was excised and submitted to three competent histologists, who reported the growth to be an innocent fibroid. The patient died fourteen months after the primary operation with her pelvis filled with recurrent growth. The tumour was a spindle-celled sarcoma.
Much has been written regarding the sarcomatous degeneration of fibroids. In this matter I have maintained an attitude of active scepticism. My experience amounts to this: the case which I have briefly described is the only example in a thousand cases of hysterectomy in which an encapsuled sarcoma in the guise of an innocent fibroid has come under my observation, therefore I come to the conclusion that it is an uncommon event, and on turning to the literature of the subject it will be found that unequivocal examples are few.
From a careful study of the question, I have formed the opinion that if a woman with fibroids and concomitant cancer of the neck of the uterus seeks advice on account of hæmorrhage, and the cancer has attacked the vaginal portion of the cervix, the nature of the case will be appreciated. The cases likely to be overlooked are those where the cancer is situated somewhat higher in the cervical canal than usual, so that it is not easily detected by the examining finger, and so low in the cervix that the disease is not exposed when the body of the uterus is amputated in the course of a subtotal hysterectomy. A knowledge of this, as well as the fact that cancer of the cervix is almost exclusively a disease of women who had been pregnant, should make the surgeon particularly careful in performing subtotal hysterectomy for fibroids in women who have had children, in order to assure himself that it is not cancerous.
In addition to the liability of the stump left after subtotal hysterectomy to become cancerous, it is stated by some surgeons that the patient is more liable to intestinal obstruction than after the total operation. This objection is easily met, because a perusal of their writings shows clearly that they do not perform the operation properly. In subtotal hysterectomy, performed according to Baer’s instructions, there should be no stump projecting from the pelvic floor, but merely a thin seam underlying the base of the bladder.
I have dealt in detail with these two methods of hysterectomy, because when it can be performed subtotal hysterectomy is, as a rule, a simpler operation than total hysterectomy. There are conditions in which it is imperative to remove the whole of the cervix, especially when the canal is very patulous and perhaps septic; when it is large and hard, or large and spongy; and especially if there is the least suspicion of malignancy in the cervix, or in the body of the uterus.
It must, however, be borne in mind that cancer has attacked the scar left in the vagina after a total hysterectomy (Quénu). At the present time the subtotal method enjoys the greatest favour in London, but it must be remembered that where the total operation is most indicated, it is often difficult of execution. Although I have a decided preference for the subtotal operation, especially in spinsters and barren wives, I have performed total hysterectomy in more than 200 patients, so that I am in no way blind to its merits.
Cancer of the uterus after bilateral ovariotomy. The uterus, after complete removal of both ovaries, is not only a useless organ, but it may become attacked by cancer. Blacker reported a case in which a woman, thirty-nine years of age, underwent bilateral oöphorectomy for a uterine fibroid: eight years later cancer attacked the neck of the uterus and destroyed the patient.
In 1902 I performed abdominal myomectomy on a woman forty-seven years of age, and removed both ovaries and Fallopian tubes; the latter contained pus. Four years later this patient came under observation with extensive cancer of the cervix.
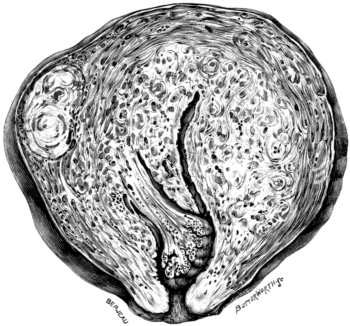 Fig. 16. An Adenomyomatous Uterus. The organ is shown in sagittal
section in order to display the great thickening of the endometrium. From
a spinster aged 43 years. Two-thirds size.
Fig. 16. An Adenomyomatous Uterus. The organ is shown in sagittal
section in order to display the great thickening of the endometrium. From
a spinster aged 43 years. Two-thirds size.
In 1901 a patient had bilateral ovariotomy performed; five years later she complained of severe uterine hæmorrhage. I removed the uterus by the abdominal route (total hysterectomy). The corporeal endometrium was cancerous throughout. The patient survived the operation six months. Similar cases have been recorded by Martin, Butler-Smythe, and Playfair.
Adenomyoma of the Uterus. This disease has not received adequate recognition at the hands of British surgeons, yet it is a condition which occasionally causes much doubt in the surgeon’s mind in the course of hysterectomy. This adenomyomatous change affects the endometrium and is, in some cases, associated with interstitial and subserous fibroids: it causes often great enlargement of the uterus, and under these conditions the fundus can be felt high in the hypogastrium. The patients are often profoundly anæmic as the result of long-continued menorrhagia. The physical and clinical signs of the disease are those present in patients with a large degenerating submucous fibroid. Indeed the surgeon often removes the uterus under this impression, and, after the operation is completed, when he divides the uterus expecting to see the usual encapsuled tumour, to his surprise finds a uterus with greatly thickened walls (Fig. 16).
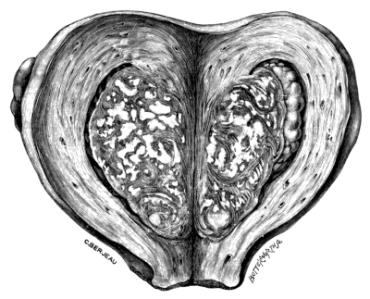 Fig. 17. An Adenomyomatous and Tuberculous Uterus. The uterus is
opened by a vertical incision in its posterior wall. The anterior wall is occupied
by a mass of tuberculous adenomatous tissue. The patient, a spinster aged 46,
was in excellent health four years after the operation. Two-thirds size.
Fig. 17. An Adenomyomatous and Tuberculous Uterus. The uterus is
opened by a vertical incision in its posterior wall. The anterior wall is occupied
by a mass of tuberculous adenomatous tissue. The patient, a spinster aged 46,
was in excellent health four years after the operation. Two-thirds size.
Microscopically the adventitious material is made of irregular tracts of endometrium containing glands and strands of unstriped muscle tissue.
It is important for the surgeon to recognize these cases because, contrary to the rule with simple uterine fibroids, these adenomyomatous uteri are often adherent to the adjacent bowel and to the bladder: in connexion with this fact several observers have pointed out that uteri affected with this disease are often associated with inflammatory affections of the Fallopian tubes, and there are good reasons for the belief that the adenomyomatous change has a microbic origin. In this connexion it is worth mention that adenomyomatous uteri are sometimes tuberculous (Fig. 17). Some examples of this disease have been mistaken for cancer of ‘the body of the uterus’.
In this disease subtotal hysterectomy gives admirable results, immediate and remote.
The only improvement of any importance made in Baer’s operation of subtotal hysterectomy concerns the ovaries. These Baer removed with the Fallopian tubes, but in 1897 I advocated, at the Obstetrical Society, London, that they were of great value to the patient, and pointed out that their conservation, when healthy, spared the patient the annoyance of that curious vaso-motor phenomenon, known to women as ‘flushings’, which is the only obtrusive sign of the menopause.
It is now admitted by those surgeons in London who have had much experience of hysterectomy for fibroids, that the immediate results of preserving at least one healthy ovary in this operation are admirable, especially in women under forty years of age, for the retention of an ovary is of striking value ‘in warding off the severity of an artificial menopause’ (Crewdson Thomas).
Although I have left one or both ovaries in the performance of abdominal hysterectomy for fibroids in more than 300 patients, in only two instances have I found anything detrimental in the practice. In these two patients it was necessary to remove one of the ovaries. Since 1906 I have modified the method by leaving only one ovary, even when both were healthy, and find that the immediate good consequences of the operation are in no way impaired. There is reason to believe that whatever good effects follow the practice of leaving a belated ovary (that is, an ovary divorced from the uterus and left in the pelvis), they are temporary, for in the course of a few years the ovarian tissue disappears and the patients experience the usual symptoms of the menopause. It is possible that the rate of atrophy of the secreting tissue of a belated ovary depends on the age at which a patient is submitted to hysterectomy.
In 1898 I performed subtotal hysterectomy on a woman, thirty-one years of age, for fibroids, conserving the right ovary. Nine years later (1907) I operated again for intestinal obstruction, and found this ovary healthy and functional, for a ripe corpus luteum was visible on its surface. Even a portion of an ovary, if it contain follicles, will maintain menstruation.
In performing abdominal hysterectomy for fibroids, there are three points which require consideration in relation to the subsequent comfort of the patient, and they depend mainly on the conservation of a healthy ovary. These three points relate to: (a) the patient’s comfort in securing freedom from flushings; (b) if she be married, her marital relations; and (c) if single, her nubility.
In regard to marital relations in women with a belated ovary, nothing trustworthy is forthcoming, but I believe the retention of an ovary is an additional factor in promoting domestic bliss. The question of nubility is interesting; I am able to state that women who have had subtotal hysterectomy performed, with conservation of one ovary, have married and lived happily with their husbands; and I am of opinion that the preservation of the vaginal segment of the neck of the uterus is an important factor, as it leaves the vagina intact, and though such women are sterile, they are certainly nubile.
Without overstating the case it may be said that a belated ovary is a very precious possession to a woman under forty years of age, whether she be married or single.
In regard to the fate of such ovaries, in the present condition of our knowledge it may be stated that:—
In a woman under the fortieth year of life, a belated ovary remains active and discharges ova.
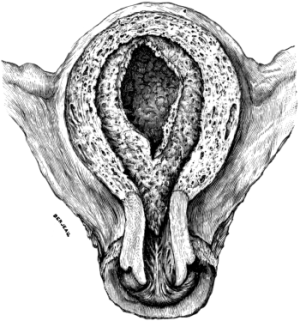 Fig. 18. Uterus with the Decidua in Situ.
The parts of the uterus occupied by the decidua represent
the menstrual area of the uterus.
Fig. 18. Uterus with the Decidua in Situ.
The parts of the uterus occupied by the decidua represent
the menstrual area of the uterus.
An ovary belated after the fortieth year of life atrophies, and menopause symptoms will often ensue in the course of a few months after the operation. The retention of an ovary minimizes the menopause disturbances, and they are never so acute and prominent under these conditions as they are when an acute menopause is induced by the sudden and complete removal of all ovarian tissue. Some experienced observers maintain that an ovary is a valuable possession to any woman who menstruates, even at the age of fifty years, the persistence of menstruation being obtrusive evidence that this gland is functional. Experimental evidence, obtained from rabbits, proves that the removal of the whole uterus has no deterrent effect on ovulation, and it does not prevent the occurrence of œstrus and ovulation at periodically recurring intervals. There is no necessity to appeal to experiments on animals in this matter, as clinical observations on women are most eloquent in proclaiming the great value of a conserved ovary when the uterus is removed on account of troublesome and dangerous fibroids.
In reference to the value of ovarian tissue after hysterectomy for fibroids, attention should be drawn to a modification of this operation known as the Abel-Zweifel method, by which a small segment of the menstrual area of the uterus is left as well as one or both ovaries: this permits menstruation to continue in a subdued form.
Doran has particularly studied this method and practised it, but I cannot express any opinion as to its value, never having had the courage to perform it.
My aim in performing hysterectomy for fibroids is to abolish as completely as possible the menstrual area of the uterus (Fig. 18), and up to the present my efforts have been successful, and I have no complaint from any patient that this disagreeable phenomenon has manifested itself, although I have been at great pains by my own exertions, as well as by the kind efforts of those who have been associated with me in my hospital work, to keep in touch with women who have been so unlucky as to require such a serious operation as the removal of the uterus.
Baer, B. F. Supra-vaginal Hysterectomy without Ligature of the Cervix in Operation for Uterine Fibroids. A new method. Transactions of the American Gynæcological Society, 1892, xvii. 235.
Bardenheuer. Die Drainierung der Peritonealhöhle. Im Anhang: Thelen: Die Totalextirpation wegen Fibroid. Stuttgart, 1881, 271.
Goffe, I. Riddle. This surgeon furnishes an interesting account of the development of Total and Subtotal Hysterectomy for Fibroids, in The Transactions of the American Gynæcological Society, 1893, xviii. 372.
Koeberlé, E. Documents pour servir à l’histoire de l’extirpation des tumeurs fibreuses de la matrice par la méthode suspubienne. Gaz. med. de Strasbourg, 1864, xxiv. 17; 66; 158. 1865, xxv. 78; 118.
Pozzi, S. Traité de Gynécologie, 1905, i. 424. This contains an interesting review of the serre-nœud and clamp period of hysterectomy. He states that Tillaux, in a communication to the Academy in 1879, proposed the use of the word Hysterectomy.
Doran in his Harveian Lectures, London, 1902, gives an admirable critical summary of this important question up to that date.
Bland-sutton, J. Essays on Hysterectomy, 1905, 2nd Ed., 60.
—— Journal of Obs. and Gyn. of Gt. Britain, 1904, v. 434.
Mann, M. Trans. Am. Gyn. Soc., 1893, p. 123.
Polk. Am. Journ. of Obstetrics, 1906, liv. 78.
Quénu. Rev. de Gyn. et de Chir. Abdom., 1905, Sept.–Oct., ix. 720.
Richelot. La Gynécologie, 1903, viii. 399.
Turner, G. Brit. Med. Journ., 1905, ii. 953.
Blacker, G. F. Uterus with Fibroids and Carcinoma of the Cervix. Trans. Obstet. Soc., 1896, xxxvii. 213.
Bland-sutton, J. A Clinical Lecture on Adenomyoma of the Uterus. Brit. Med. Journal, 1909, 1.
Butler-Smythe. Carcinomatous Uterus removed eighteen and a half years subsequent to Double Ovariotomy. Trans. Obst. Soc., 1901, xliii. 214.
Playfair. Carcinoma of Uterus. Ibid., 1897, xxxix. 288.
Martin, A. Die Krankheiten der Eierstöcke und Nebeneierstöcke, 1899, s. 907.
Bland-Sutton, J. Abdominal Hysterectomy for Myoma of the Uterus, with brief notes of twenty-eight cases. Transactions of the Obstetrical Society, 1897, xxxix. 292.
—— The Value and Fate of Belated Ovaries. The Medical Press and Circular, 1907, ii. 108.
Bond. An Inquiry into some Points in Uterine and Ovarian Physiology and Pathology in Rabbits. British Medical Journal, 1906, ii. 121.
Doran, A. Subtotal Hysterectomy: after history of sixty cases. Transactions of the Obstetrical Society, 1905, xlvii. 363.
Thomas, G. C. The after histories of one hundred cases of Supravaginal Hysterectomy for Fibroids. Lancet, 1902, i. 294.
The modern operation of hysterectomy as a radical measure for the relief of cancer of the uterus has a somewhat curious history. In 1878 Freund extirpated the uterus for carcinoma of the cervix through an abdominal incision; his method was quickly practised by other surgeons, but the great mortality of the operation soon caused it to be abandoned for the vaginal route advocated by Czerny and supported by Schroeder, Olshausen, Martin, and Péan amongst other gynæcologists. This method, however, has been abandoned, for, although the operative mortality of vaginal hysterectomy for cancer of the uterus has fallen to 5 per cent., the operation has disappointed expectation, as it can only be employed on early cases of the disease with anything like a hopeful prospect of curing the patient, and, even when performed on carefully selected cases, the risks of recurrence are so great and often follow so rapidly on the operation that surgeons have lost confidence in the method. This has induced gynæcologists to turn their attention again to the abdominal route. The cancerous uterus is now subjected to what is known as ‘radical abdominal hysterectomy’, a method with which the names of Ries, Mackenrodt, Dührssen, and Wertheim are closely associated.
Hysterectomy for cancer of the cervix. The greatest obstacle to the success of vaginal hysterectomy in the radical treatment of cancer of the neck of the uterus is the limitations which the anatomical environment imposes on the surgeon, for as soon as the disease overruns the cervix it implicates the vagina, the bladder, the vesical portions of the ureters, and the rectum. The ‘radical abdominal operation’ enables the operator not only to remove the uterus and its neck, but the broad ligament, the ovaries, Fallopian tubes, infected lymph glands, and the infected para-uterine connective tissue, and by affording the operator free access to the floor of the pelvis the proceedings may be carried out with a free exposure of the operating field, thus allowing important structures like the ureters to be dissected out of implicated tissue. Indeed it has even been recommended, in cases where the bladder has been extensively involved, to resect this viscus and engraft the ureters into the rectum.
The primary object of these extensive operations is not only to facilitate the wide removal of connective tissue around the cervix in early cases of carcinoma, but also to allow the advantages of operative treatment to be extended to patients to whom it would be otherwise absolutely barred.
One great danger which attends operations for the removal of cancerous organs is what may be called ‘post-operative cancer-infection’, that is, in the course of the operation tracts of connective tissue are opened up and become soiled with cells, which engraft themselves on this tissue and on the peritoneum, and give rise to extensive masses of cancer which are often described as recurrent cancer. This accident often causes the patient to die quicker than if the primary cancer had been left untouched. In the radical operation it is one of the essentials to avoid soiling the wound with cancer cells. This rule, of course, applies to operations for cancer in any part of the body.
Operation. The steps of the radical abdominal operation advocated by Wertheim are as follows:—
As a preliminary, the cancerous cervix is treated by scraping, cauterizing, and disinfectants. It is an advantage to carry out these measures a few days before the main operation. The Trendelenburg position is indispensable and the abdomen is opened by a free median subumbilical incision. After isolating the intestines with dabs, the ureters are exposed by incising the posterior layer of the broad ligament; they are then traced to the parametrium. It is necessary to avoid too free a disturbance of their vascular network or they will slough.
The bladder is then separated from the uterus. The infundibulo-pelvic, the broad, and the round ligaments are ligatured and divided. The particular order in which they are dealt with is not a matter of consequence. The uterine vessels are secured in the following manner:—The index finger is pushed along the ureter through the parametrium towards the bladder, until the tip of the finger appears there; the vessels are then raised on the finger, which covers the ureter so as to protect it whilst the vessels are ligatured and divided. As soon as the uterine vessels are divided the vesical segments of the ureters are exposed, cleaned if necessary, and separated from the cancerous cervix.
The posterior layer of the peritoneum is divided and the rectum separated from the vagina: at this stage the uterus is sufficiently isolated from the surrounding structures to allow of removal. This is effected in the following way:—
The two layers of the parametrium are taken off as close as possible to the pelvic wall, and the vagina closed with bent clamps and divided below them: the clamps are used to prevent soiling the operation-area with cancerous cells.
In order to extirpate the lymph glands, the peritoneum is divided upwards and the iliac vessels laid bare, and every enlarged gland from the division of the aorta to the obturator foramen is removed and the oozing vessels carefully secured.
The wound is treated in the following way:—
The cavity created by the removal of the uterus is filled in loosely with iodoform gauze, which extends to the vulva. An exact closing of the peritoneal cavity over this gauze is effected by the sewing up of the anterior and posterior flaps of peritoneum. The final step is the closure of the abdominal incision.
After-treatment. This is relatively simple. The strips of iodoform gauze are removed through the vagina in from five to ten days successively. The patient gets up on the fifteenth day. The bladder requires very careful attention, as it is usually paralysed for some days.
Mortality. The immediate mortality of these extensive abdominal operations for cancer of the neck of the uterus is very high, more than 20%, but recent statistics (1909) show that this death-rate is being considerably improved with increased experience on the part of the operators.1
Dangers. The chief risks of the operation are sepsis, cancer-infection, and injury to the ureters.
The ureters have proved a fertile source of trouble because they are deliberately exposed in the course of the operation, and they are sometimes accidentally divided. It is not uncommon to find a ureter completely blocked by cancer, and occasionally the ureter, after being bared by the operator, undergoes necrosis a few days later.
Wertheim points out that in some instances ureteral fistulæ due to necrosis may be induced to close by the application of iodine or sulphate of copper. It is, however, unfortunately true that many patients with ureteral fistulæ after the radical operation have been obliged to undergo nephrectomy (see p. 112).
The ‘radical operation’ for cancer of the neck of the uterus is on its trial in Great Britain. The operative mortality is very high, and no reliable returns concerning the remote results are at present available.
Hysterectomy for cancer of the body of the uterus. The most satisfactory method of dealing with cancer arising in the corporeal endometrium consists in performing total abdominal hysterectomy (see p. 40), removing not only the uterus and its neck, but both ovaries, Fallopian tubes, mesometria, and any enlarged lymph glands that are detected. In the course of the operation the surgeon should avoid any undue handling of the uterus, and, in withdrawing it from the pelvis, care should be taken not to infect the operation area with any fluid or semi-fluid stuff which is liable to escape from the cervical canal.
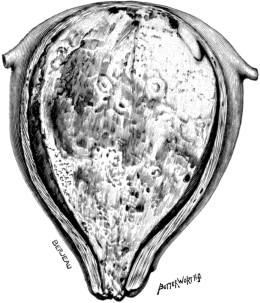 Fig. 19. Cancer of the Uterus. Coronal section through a uterus affected
with primary cancer of the corporeal endometrium. The mass measured 10
centimetres transversely and 12 centimetres vertically. Removed by
abdominal hysterectomy. Two-thirds size.
Fig. 19. Cancer of the Uterus. Coronal section through a uterus affected
with primary cancer of the corporeal endometrium. The mass measured 10
centimetres transversely and 12 centimetres vertically. Removed by
abdominal hysterectomy. Two-thirds size.
There is a rare variety of cancer of the corporeal endometrium, namely, that which attacks small atrophic uteri. These small uteri may sometimes be extirpated by the vagina, but often the narrowness of the vagina in aged spinsters compels the surgeon to resort to the abdominal route.
Cancer of the body of the uterus occasionally causes such enlargement of this organ as to render its removal by the vaginal route difficult as well as undesirable. When this form of cancer is complicated with fibroids, as a rule, vaginal hysterectomy is impracticable.
Cancer of the body of the uterus is more frequent in spinsters and barren wives than in multiparæ; for this reason the cancer often assumes the massive form, because the cervical canal being narrow, pathogenic micro-organisms do not obtain such free ingress as in the case of women with a patulous canal. In some instances the cancerous mass will expand the uterine cavity and lead to thinning of the walls as in Fig. 19.
Clinically, cancer of the corporeal endometrium is a more insidious disease than cancer of the neck of the uterus, but since its frequent association with fibroids has been recognized (see p. 52) mainly as a consequence of the vulgarization of hysterectomy, many cases are detected fairly early and with improved results for the patients.
Mortality. The risk to life in abdominal hysterectomy for cancer of the body of the uterus is somewhat greater than after removal of the uterus for fibroids. This is due to the fact that when the cancer ulcerates and sloughs, the risk of sepsis is therefore increased; this also makes convalescence slower.
The remote results vary greatly; these depend in a large measure on the extent of the disease at the time of the operation. When the cancerous mass is compact, as in Fig. 19, good results may be expected. When the growth has perforated the uterine wall and small bud-like processes project on the serous surface, the disease may be expected to recur rapidly in the abdomen. Cancer of the uterus remains an opprobrium to operative gynæcology.
Hysteropexy is a term applied to an operation for fixing the uterus, by means of sutures, to the anterior abdominal wall.
This procedure was advocated as a definite surgical operation for displacements of the uterus independently by Olshausen and Kelly (1886).
The operation when employed for severe retroflexion of the uterus is now known as ventro-suspension of the uterus; when carried out for prolapse it is termed ventro-fixation of the uterus. When care is taken in the selection of patients, hysteropexy is an operation which is followed by satisfactory consequences.
The preliminary preparation and the instruments required as those used for a simple cœliotomy (see p. 5).
Operation. The patient is placed in the Trendelenburg position, and the abdomen is opened as for ovariotomy, except that the incision is shorter; the operator then determines with his fingers the position and condition of the body of the uterus. If it be free, it is then straightened, and the condition of the ovaries and the tubes ascertained.
In many patients, where retroflexion of the uterus is accompanied by pain, the distress is often due to a prolapsed ovary, incarcerated in the pelvis by the retroflexed fundus of the uterus; in another set of cases the retroflexion is produced by a tumour in the ovary, such as a small dermoid, but more often the body of the uterus is drawn backwards by a small fibroid in the fundus of the organ. In these conditions an operation embarked upon as a simple hysteropexy may become an oöphorectomy, an ovariotomy, or a myomectomy, according to the necessity of the case. When the enlargement of the ovaries is due to œdema from incarceration, they should be left, as the swelling will quickly subside when the misplacement of the uterus is corrected.
The uterus is fixed to the abdominal wall in the following way:—
A curved needle armed with a silk thread (No. 4) which has been carefully boiled is passed through the aponeurosis and adjacent peritoneum on one edge of the wound, then through the anterior surface of the uterus near the fundus, and finally through the peritoneum and aponeurosis on the opposite edge of the incision; when this suture is tightened, it will be found to draw the uterus to the anterior abdominal wall, and at the same time approximate the edges of the wound. Two sutures should be introduced. In patients who have had children care should be taken not to pass the needle so deeply into the uterus that the suture traverses the superficial parts of the endometrium and becomes infected: this will lead to a suture sinus. The rest of the wound is then closed according to the method described on p. 9.
Operation. When hysteropexy is needed for a large, bulky, and prolapsed uterus, the steps of the operation are the same as for retroflexion, but it is necessary to introduce a greater number of retaining sutures. Further, as the uterus tends to slip downward into the vagina, it is an advantage, as soon as the fundus of the uterus is drawn into the wound, to transfix it with a stout suture, in order that the assistant may use it as a tether to keep the uterus in position whilst the surgeon introduces the main sutures. In some cases, where the uterus is very large, it may be requisite to employ four, five, or even six sutures to secure it to the abdominal wall.
In all cases of hysteropexy the uterus is of necessity sutured to the lower angle of the wound, and is therefore in close relation to the bladder. It facilitates the operation to introduce the lowest sutures first and then gradually work up to the fundus. The wound is then closed and dressed as described for cœliotomy.
After-treatment. This is conducted on the same lines as after ovariotomy.
Risks. Hysteropexy, when performed by surgeons experienced in pelvic surgery, is such a simple operation that it should have no mortality. At the Chelsea Hospital for Women, from 1904 to 1906, both years inclusive, this operation was performed on 190 patients, all of whom recovered from the operation.
Many of these operations were complicated with oöphorectomy, ovariotomy, or myomectomy. A wide study of operation returns show that hysteropexy is not absolutely free from risk, as deaths from sepsis, lung complication, and intestinal obstruction have been reported.
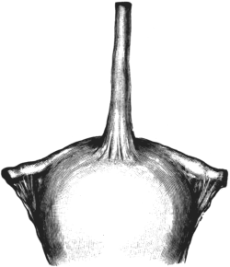 Fig. 20. The Fundus of a Uterus. A long fibrous cord arises from the
fundus as a result of hysteropexy performed nearly five years previously
for inveterate retroflexion. Full size.
Fig. 20. The Fundus of a Uterus. A long fibrous cord arises from the
fundus as a result of hysteropexy performed nearly five years previously
for inveterate retroflexion. Full size.
The remote consequences of hysteropexy are of interest. When the uterus has been enlarged by previous pregnancy its fundus can be brought without undue strain into contact with the anterior abdominal wall, so that when it is secured by sutures there is little or no strain on them. When hysteropexy is performed on spinsters or barren married women in whom the uterus is small, there is, in many instances, a strain on the sutures. The effect of this strain is twofold. When the uterus is attached to the abdominal wall by an aseptic suture, lymph is exuded from the surfaces of the peritoneum in contact with the retaining sutures. This effused lymph organizes into a tenacious tissue, and the strain of the uterus, when the operation is performed on virgins, or the weight of the organ when it is done for prolapse, will cause the sutures to erode their way out of the uterine wall, but the plastic material effused around the silk threads slowly stretches as the uterus descends into the pelvis, producing a tendon-like structure which may be called the ‘artificial fundal ligament’ (Fig. 20).
In patients in whom the length of the uterus allows its fundus to come in contact with the abdominal wall without strain, the union may be so secure that the woman may pass through one or more pregnancies successfully without disturbing the union, or even stretching it. This I have proved in twelve instances where some subsequent trouble such as appendicitis, gall-stones, ovariotomy, cancer of the colon, or the like has led to a repeated cœliotomy, and has afforded me an opportunity of examining the condition of the uterus.
In one remarkable case where a small uterus had been securely fixed by its fundus to the abdominal wall by means of ten thick sutures (the operation had been performed in a cottage hospital in Yorkshire), the patient complained of persistent pain, and was sent to me on this account. I found the sigmoid flexure of the colon caught in one of the sutures, which accounted for some of the woman’s trouble, but the uterus was so firmly fixed to the abdominal wall and had been so dragged upon that it had become a rounded sausage-like organ. Its removal was followed by immediate relief. Among rare accidents which have followed this simple operation is tetanus when catgut and wallaby tendon has been used for the retaining sutures (see p. 107).
Kelly, H. A. Hysterorrhaphy. American Journal of Obstetrics, 1887, xx. 33.
Olshausen. Ceber ventrale Operationen bei Prolapsus und Retroversio Uteri. Centralblatt für Gynäkologie, 1886, x. 698.
Pregnancy is apt to be complicated with tumours growing in the walls of the uterus, e.g. fibroids, cancer of the neck of the uterus, or cysts and tumours of one or both ovaries; morbid conditions of the Fallopian tubes, e.g. pyosalpinx, tubal pregnancy; tumours and cysts in the broad ligament; displaced viscera occupying the pelvis, e.g. the spleen or the kidney; tumours arising in the pelvic bones, e.g. osteoma, enchondroma, or sarcoma; and echinococcus cysts and colonies growing in the omentum, but occupying the pelvis, or arising in the pelvic tissues.
This is a formidable list, and any one of them may so complicate the pregnancy that it may be necessary to remove the tumour, and in some instances to perform Cæsarean section, or even hysterectomy.
This signifies the removal of a fœtus and placenta from the uterus through an incision involving the abdominal and uterine walls.
This operation is required when the outlet of the pelvis is too narrow to permit the transit of a viable child, as in rickets and osteomalacia; when the vagina is malformed; when the pelvic outlet is narrowed by tumours growing from the pelvic wall. Occasionally the passage of a fœtus is barred by tumours growing from the uterus, especially a large cervix fibroid, or a fibroid growing from the lower segment of the uterine wall. An ovarian cyst, especially a dermoid incarcerated by the uterus, may render this operation necessary. The rarest causes are cancer of the neck of the uterus and cancer of the rectum.
This operation is advocated by some obstetricians in certain cases of eclampsia and placenta prævia.
Operation. When it is known some days beforehand that the patient will be submitted to this operation, she should be prepared as for ovariotomy. Often it happens that the operation is undertaken after labour has commenced, and in circumstances which make time very precious. Even then the abdomen, pubes, and vulva can be shaved and thoroughly washed with warm soap and water, and lightly rubbed with ether and cotton wool.
The instruments required are those given on p. 5.
When the patient is under the influence of ether and the bladder emptied with the catheter, an incision is made in the linea alba from the umbilicus to the pubes. The belly-wall of a woman advanced in pregnancy is very thin, and, unless the surgeon be cautious, the knife will come in contact with the uterus before he is aware of it.
The uterus lies just under the incision, and the operator ascertains that it lies centrally (often the uterus is somewhat rotated to the right or left), and then makes a free incision through the uterine wall and extracts the fœtus and placenta; as the uterus contracts, he slips his left hand behind the fundus, and grasps the uterus near the cervix, and effectually controls the bleeding. The assistant passes a large warm flat dab into the belly to restrain the intestines and omentum. The uterine cavity is sponged out, and the finger passed through the os uteri into the vagina in order to ensure a free passage for blood and serum.
The incision in the uterine wall may be closed either by a double or a single set of silk sutures. When two layers of sutures are employed, the first set involve the mucous and adjacent half of the muscular layer[;] these sutures should be fairly close together, for they not only bring the parts into apposition, but they restrain the bleeding. A second row of silk sutures is now inserted, including the serous coat and adjacent half of the muscular layer. These threads should not be tied too tightly, as the tissues of a gravid uterus are soft and easily tear. In closing the uterine incision the surgeon should not spend time vainly in endeavouring to stanch the bleeding from the edges of the incision; this is best effected by dexterously inserting and securing the sutures.
The recesses of the pelvis are carefully cleaned by gentle sponging, and the parietal incision is closed as after ovariotomy.
The dressing varies with the fancy of the operator; a piece of sterilized gauze and a square of Gamgee tissue held in position by a many-tail of flannel firmly applied is all that is necessary.
Although Cæsarean section is one of the simplest operations that can be performed on the pelvic organs, it formerly had a very high mortality; but since the principles of asepsis have been thoroughly established the death-rate from this operation has been so reduced that it varies from 4 to 10% according to the skill of the operator; indeed the results are so good in the hands of careful and skilful men that on recovery from the operation the patient may reconceive, and there are conditions in which the patient is desirous to produce more children with the knowledge that they must be extricated by Cæsarean section. There are many instances on record of women being submitted to this operation twice, and some thrice; and at least two patients have undergone this operation four times (Sinclair). In view of the fact that a woman after being submitted to Cæsarean section may reconceive, it has been urged (especially by Sinclair) that the anterior surface of the uterus should be attached to the abdominal wall in such a manner as to promote the formation of adhesions, so that when the patient needs to be submitted to ‘repeated Cæsarean section’, the adhesions resulting from the primary operation will so shut off the operation area from the general peritoneal cavity, that the uterus may be opened and the fœtus and placenta extracted by a practically extraperitoneal operation. This question has been discussed in an able and comprehensive paper by Wallace, and also by Sinclair.
There is one great danger which women run by becoming pregnant after Cæsarean section, namely, rupture of the uterus. Some cases illustrating this accident have been reported. This accident has been discussed by Wallace.
Although a few writers, particularly Wallace, consider that all Cæsarean sections should be performed with a view to ulterior pregnancy, this is not the opinion of the majority, for there are many women who, having passed such an ordeal once, have no desire to do so again, and ask for something to be done to prevent its possibility in the future. This involves what is known as ‘sterilization’.
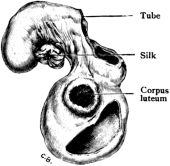 Fig. 21. Portion of Ovary and Fallopian Tube. The parts were removed a
year after a supposed complete oöphorectomy had been performed to induce
an artificial menopause. This fragment of ovary maintained menstruation
regularly. Full size.
Fig. 21. Portion of Ovary and Fallopian Tube. The parts were removed a
year after a supposed complete oöphorectomy had been performed to induce
an artificial menopause. This fragment of ovary maintained menstruation
regularly. Full size.
Sterilization after Cæsarean section. When Cæsarean section is performed the uterus is preserved, and after convalescence the woman is in a position to reconceive. There are conditions in which she is most anxious to produce more children even with the risk of having them extracted by this operation. On the other hand, some women, knowing the risks, ask that steps may be taken to prevent a recurrence of what they consider a catastrophe. This appears a simple matter, but it is not so in reality, for in many instances in which the operator had been under the impression that he had effected this by ligature of both Fallopian tubes in continuity, he has been surprised when the woman has again come under his notice well advanced in pregnancy.
This has happened even when each tube has been ligatured in two places and a segment of the tube exsected between the ligatures. Bilateral oöphorectomy has been recommended, but on the whole, when the patient and her husband wish that further risks should be avoided, the wisest plan is to perform subtotal hysterectomy instead of Cæsarean section; moreover it is a difficult matter to completely remove healthy ovaries, and it needs only a small portion to maintain menstruation (Fig. 21).
The whole of this matter is one that is really a question of ethics, and the extreme views are represented by Wallace and Sinclair in the papers to which reference has already been made. The difficulty of effectively sterilizing women by simply relying on bilateral oöphorectomy is shown by the well-established cases in which patients have successfully conceived after bilateral ovariotomy and oöphorectomy.
The youngest patient on whom Cæsarean section has been carried out with success to the mother and child was thirteen years of age. The operation was performed by Gache in Buenos Ayres on account of smallness of the pelvis. Women have recovered after a self-inflicted Cæsarean section.
Doran, A. Pregnancy after Removal of both Ovaries for Cystic Tumour. Journal of Obstetrics and Gynæcology of the British Empire, 1902, 11, i.
Gache, S. Opération césarienne sur une fille de 13 ans: Guérison. Annales de Gynécologie, 1904, p. 601.
Harris, R. P. Six self-inflicted Cæsarean Operations with recovery in five cases. Am. Journ. of the Medical Sciences, 1888, xcv. 150.
Sinclair, Sir William. Cæsarean Section successfully performed for the Fourth Time on the same Woman, with remarks on the production of Utero-parietal Adhesions. Journal of Obstetrics and Gynæcology of the British Empire, 1907, xii. 335.
Wallace, Arthur J. On Repeated Cæsarean Section. Ibid., 1902, ii. 555.
It occasionally happens that a woman in whom the course of pregnancy is nearly complete dies suddenly from disease, such as hæmoptysis, hæmatemesis, cardiac trouble, or uterine hæmorrhage in the preliminary stage of labour; or is killed by accident. In some such circumstance attempts are sometimes made to rescue the unborn child, by performing Cæsarean section. It is true that such efforts are rarely attended with success, but in cases where death is very sudden and the surroundings such as to enable the operation to be performed without delay, the child may be extracted from the uterus and survive. Successful cases of this kind are published from time to time.
In order to show how necessary it is to act promptly the following case may be mentioned:—
A woman in the eighth month of pregnancy was found to be suffering from cancer of the neck of the uterus. The child was alive. I decided to perform hysterectomy. The uterus was exposed through a free incision in the abdominal wall and quickly detached from its cervix. The uterus with the fœtus inside was handed to an assistant, who quickly extracted the child. Although the time which elapsed from the complete etherization of the mother until the extraction of the child from the uterus was 2½ minutes, it required the display of some energy to induce the child to breathe. This is the first record as far as I know of a child being delivered alive from a uterus detached from its mother. The woman died on the fourth day after the operation, and the child on the fourteenth.
Möglich had a successful case. A patient aged forty-one years, with placenta prævia, died from hæmorrhage, and an asphyxiated fœtus was promptly extracted by cœliotomy. Prolonged efforts at artificial respiration were successful, and the child was well five weeks later (see also Sippel).
Hugier, M., and Monod, M. Cæsarean Operation immediately after the death of the Mother. Lancet, 1829–30, i. 899.
Möglich. Ueber Kaiserschnitt an der Toten. Münchener med. Wochensch., 1908, lv. 202.
Sippel. Sectio Cæsarea in mortua. Monats. f. Geb. u. Gyn., 1907, xxvi. 618.
Although the directions in surgical writings are clearly laid down concerning the course to be pursued when pregnancy and labour are complicated by an ovarian tumour, the difficulty which often confronts the operator when he is face to face with the actual case is uncertainty regarding the nature of the tumour. Although he may begin the operation under the impression that he has to deal with an ovarian tumour, it may turn out to be a fibroid, a tumour of the pelvic wall, a misplaced spleen or kidney, a tubal pregnancy, a sequestered extra-uterine fœtus (lithopædion), or a calcified hydatid cyst. Thus an expected ovariotomy may terminate as a Cæsarean section, or as a hysterectomy. In many cases the surgeon must rely on his own judgment and experience, but it may be useful to furnish some directions which may help him. It may be useful also to mention what unexpected conditions are sometimes found. Thus an experienced gynæcologist like Prof. Olshausen once removed a gravid uterus under the impression that it contained a cystic fibroid which would obstruct delivery. When it was examined after removal, the suspected fibroid proved to be a large sacral teratoma growing from the fœtus.
Ovarian tumours and pregnancy. Before the fourth month of pregnancy, single and double ovariotomy is attended with a low rate of mortality, and the risk of disturbing the pregnancy is small. The removal of a parovarian cyst during pregnancy is more liable to be followed by abortion than single or double ovariotomy. After the fourth month the risk is that of an ordinary ovariotomy, but the chances of abortion increase with each month. It is also a fact that ovariotomy may be safely carried out between the eighth and ninth months of gestation without precipitating labour, even when the tumour is incarcerated in the pelvis.
In many cases in which ovariotomy is urgently indicated during pregnancy, the pedicle will be found twisted.
When the tumour is situated above the uterus there is rarely any difficulty in dealing with it, as the pedicle is usually long, but it will require extra care in applying the ligature, as the tissues, being unusually vascular and soft, are easily lacerated. Occasionally the tumour lies in the pelvis below the uterus: in this case the surgeon carefully insinuates his hand between the pelvic wall and the uterus, and then gently withdraws the tumour from its incarcerated position.
Cases in which Ovariotomy has been performed near the End of the Ninth Month of Pregnancy
| Surgeon. | Result to Mother. | Result to Child. | Reference. |
|---|---|---|---|
| Pippingsköld | R. | Stillborn | Am. J. of Obstet., 1880, xiii. 308. |
| Bland-Sutton | R. | Lived | Brit. Med. Jour., 1895, i. 461. |
| Morse | R. | Lived | Trans. Obstet. Soc., xxxviii. 221. |
In operating for ovarian cysts complicating pregnancy, the surgeon should, after removing the cyst, carefully examine the other ovary, for twin tumours may be present. Berry Hart performed ovariotomy on a woman in the fifth month of pregnancy, and removed a dermoid of the left ovary ‘enlarged to about the size of a man’s brain by recent hæmorrhage due to the twisting of a pedicle’. The patient died on the ninth day. A frozen section was made of the pelvis, and on inspecting the cut surface the right ovary, converted into a dermoid, was found incarcerated by the gravid uterus.
Many cases have been published in which ovariotomy has been undertaken during the late months of pregnancy, or shortly after delivery, and the surgeons have been astonished to find both ovaries converted into tumours; in very many instances they were dermoids. Cases of this kind have been recorded by Knowsley Thornton, F. Page, Cullingworth, Berry Hart, Malcolm Campbell, and others, including myself. These observations demonstrate that a woman may have both her ovaries occupied by dermoids, yet the glands are capable of yielding fertilizable ova.
Campbell relates that Brewis, in performing an ovariotomy during pregnancy, attempted to conserve some ovarian tissue by resecting the dermoids; this proved impracticable, and both ovaries were excised. Miss Ivens records a case in which a woman thirty-five years of age was five months pregnant and required ovariotomy on account of an incarcerated ovarian dermoid. In the course of the operation both ovaries were found to contain dermoids. A tumour was successfully excised from each. Pregnancy continued undisturbed.
Campbell, M. Case of Bilateral Ovarian Dermoid Tumour associated with Pregnancy. Lancet, 1907, ii. 1760.
Cullingworth, C. J. Three cases of Suppurating Dermoid Cyst, of or near the Ovary, treated by Abdominal Section. St. Thomas’s Hospital Reports, 1887–9, xvii. 139.
Hart, Berry. See Clarence Webster’s Researches in Female Pelvic Anatomy, Edin., 1892, p. 124.
Ivens, Miss F. Pregnancy complicated by Bilateral Ovarian Dermoid Cysts. Brit. Med. Journal, 1908, i. 625.
Page, F. Acute Peritonitis after Confinement; abdominal section; Dermoid Disease of both Ovaries; removal; recovery. Lancet, 1893, ii. 250.
Thornton, K. A case of removal of both Ovaries during Pregnancy. Trans. Obstet. Soc., London, xxviii. 41.
Ovariotomy during labour. When an ovarian tumour is discovered during labour and it impedes delivery, ovariotomy should be performed.
In this condition it follows that the tumour lies in the pelvis; when the tumour is tightly impacted by the contracting uterus it has happened that the surgeon has been unable to reach the tumour until he has emptied the uterus by Cæsarean section. Several operators have had this difficulty, myself among them. I have added a list of reported cases drawn from British sources. For this I hope not to be accused of what is sometimes perhaps facetiously called ‘insularity’. The enormous population of these islands should furnish material enough to settle the principles of treatment which should govern these terrible cases of obstructed labour.
One of the commonest conditions met with in ovariotomy during pregnancy and labour is to find that the cyst has undergone axial rotation and twisted its pedicle. The technique in these circumstances is very simple.
Ovariotomy for Tumours obstructing Labour at Term
| Operator. | Nature of Tumour. | Result to Mother. | Fate of Child. | Reference. |
|---|---|---|---|---|
| Williams | Cyst | R. | No record | Trans. Obstet. Soc., xxvi. 203. |
| Spencer | Dermoid | R. | Lived | Ibid., xl. 14. |
| Boxall 1 | Dermoid | R. | Lived | Ibid., xl. 25. |
| Bland-Sutton 1 | Dermoid | R. | Lived | Lancet, 1901, i. 382. |
| Sinclair 1 | Cyst | R. | Lived | Lancet, 1901, i. 158. |
| Favell 1 | Dermoid | R. | No record | Brit. Med. Journal, 1901, i. 894. |
1 In these cases it was necessary to perform Cæsarean section in order to extract the tumour from the pelvis.
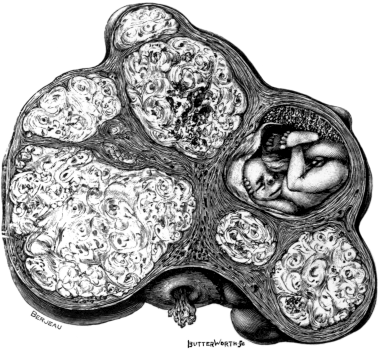 Fig. 22. A Uterus distorted by Fibroids. It contains a fœtus of four
months’ development. Removed by the subtotal operation from a primigravida,
aged 42. Half size.
Fig. 22. A Uterus distorted by Fibroids. It contains a fœtus of four
months’ development. Removed by the subtotal operation from a primigravida,
aged 42. Half size.
Ovariotomy during the puerperium. It occasionally happens that a woman may go through her pregnancy and labour with an unrecognized ovarian tumour in her abdomen; during the puerperal period it may cause symptoms which lead to its recognition, because in the course of the labour the cyst may burst, undergo axial rotation, or suppurate. When a puerperal woman possesses an ovarian tumour which gives rise to unfavourable signs, ovariotomy should be resorted to without delay. The operation in these circumstances is comparatively simple, and such adhesions as may be present are usually recent and easily overcome.
Single and even double ovariotomy can be performed during puerpery without in any way interfering with involution of the uterus or lactation.
In 1896 I was able to collect fifteen recorded cases of double ovariotomy during pregnancy, and sixteen in which ovariotomy was performed during the puerperium, or shortly after abortion. Since this date McKerron has collected the statistics relating to the whole question of pregnancy and ovarian tumours in a very comprehensive manner.
Bland-Sutton. Surgical Diseases of the Ovaries, &c., London, 1896, 2nd Ed. pp. 180–91.
—— The Surgery of Labour and Pregnancy, complicated with Tumours, Lancet, 1901, i. 382, 452, 529.
McKerron, R. G. Pregnancy, Labour, and Childbed with Ovarian Tumour, London, 1903.
Fibroids and pregnancy. In a large number of instances in which operations have been undertaken when fibroids complicate pregnancy, they have been performed on an erroneous diagnosis. The tumours when small and placed laterally simulate ovarian cysts; when large and lying high in the abdomen they have been mistaken for renal tumours, and when low in the pelvis they have been regarded as incarcerated ovarian cysts. The variety of fibroid most likely to lead to operation, under the impression that it is an ovarian cyst, is an interstitial fibroid which becomes painful in consequence of undergoing red degeneration. The difficulty which faces the surgeon in this condition is to decide on a safe course.
When the tumour is not likely to cause difficulty it may be wise to close the abdomen. If the tumour is pedunculated and incarcerated, he may be able to extract the tumour and ligature the pedicle without disturbing the pregnancy; a big fibroid invading the broad ligament may be enucleated; a large cervix fibroid will render delivery impossible, and will necessitate hysterectomy.
A study of many recorded cases in which hysterectomy has been performed on account of fibroids complicating pregnancy shows that the operation had been undertaken on account of a great increase in the size of the tumours, the concurrent pregnancy not being discovered until the parts were examined after removal.
Hysterectomy may be necessary at any time during pregnancy; after labour has begun; and during puerpery on account of fibroids. During pregnancy it is a straightforward operation, the subtotal operation being preferable. When it is needed during puerpery it is for septic complications, and there is no greater difficulty in performing hysterectomy then than during pregnancy, but the risk to the patient from sepsis is much greater: therefore total hysterectomy with drainage is advisable.
Fibroids have many times been enucleated from the gravid uterus and the pregnancy has gone successfully to term.
When pregnancy complicated with fibroids goes to term and the tumour occupies the neck or the lower segment of the uterus so as to offer an impassable barrier to the passage of the fœtus, abdominal hysterectomy is a necessity.
Red Degeneration. Among the new things which the surgical treatment of uterine fibroids has brought to light is a knowledge of that change to which these tumours are liable, known as ‘red degeneration’.
This increase in our knowledge of the pathology of fibroids is extremely useful in diagnosis, for red degeneration is especially liable to occur in fibroids lodged in a pregnant uterus, and, as I pointed out in 1904, it has the effect of rendering them painful.
One of the most striking features of a uterine fibroid is its insensitiveness, and equally remarkable is its painfulness and tenderness when in a state of red degeneration, but these signs are only exhibited by such fibroids when associated with pregnancy.
Red degeneration, even in an extreme degree, in fibroids occupying the walls of a non-gravid uterus is, as a rule, painless. It is also curious that a gravid uterus may contain four or five fibroids, the size of large potatoes, in its walls, yet only one will exhibit this red degeneration and become acutely painful, whilst its companions remain as insensitive as apples. In the early stages of this change the fibroid exhibits the colour in streaks, but as the pregnancy advances it permeates the whole tumour. Occasionally in the mid-period of pregnancy this necrotic change may be so extreme that the central part (sometimes the whole) of the tumour is reduced to a red pulp.
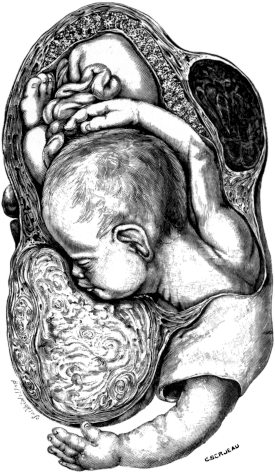 Fig. 23. A Gravid Uterus In Sagittal Section.
Fig. 23. A Gravid Uterus In Sagittal Section.
The woman miscarried at the seventh month: delivery was obstructed by a cervical fibroid. The parts were removed by total hysterectomy. The small fibroid is in the condition of red degeneration (Museum, R. College of Surgeons). Half size.
The suddenness with which this pain comes on may be illustrated briefly by the following case:—A primigravida, aged 30, two months pregnant, was seized with sudden pain during a railway journey. Her condition became so alarming that she left the train at an intermediate station and placed herself under the care of a doctor whom she knew. A large, tender, and increasing swelling was found in the abdomen. The doctor regarded the patient’s trouble as being due to rupture of a tubal pregnancy. He asked me to see the patient, and I found a large swelling on the right side of the abdomen reaching as high as the liver. I considered that some change had taken place in this tumour consequent on the pregnancy: it was also probable that it might be an ovarian cyst which had twisted its pedicle. The swelling was very tender. On opening the abdomen the tumour proved to be a large subserous fibroid undergoing red degeneration. The gravid uterus contained several fibroids of the interstitial variety: it was removed. These fibroids exhibited the red change in streaks.
It is a curious and noteworthy fact that many of the operations tabulated on pp. 81 and 82 were undertaken on an erroneous diagnosis. In some the acute pain and tenderness of which the patients complained led the surgeons to believe that the troubles were due to an ovarian cyst which had twisted its pedicle, or to the bursting (or abortion) of a gravid Fallopian tube.
Practitioners and obstetricians are now becoming familiar with the fact that when a pregnant woman, who has also fibroids in the uterus, complains of sudden acute pain, it may be due to one of the fibroids undergoing red degeneration.
The cause of this change is unknown. Lorrain Smith and Fletcher Shaw, after an examination of four specimens, three of which were associated with pregnancy, believe that the change is due to thrombosis of the vessels of the fibroid. In two tumours they isolated micro-organisms, e.g. staphylococci in one and diplococci in another: the patients with these tumours exhibited toxic symptoms.
In my early investigations of this disease I often took the tumours to the bacteriological laboratory with the hope of finding some micro-organism which would account for the degeneration. The results were so persistently negative that the search was abandoned. Since learning that Smith and Shaw had found micro-organisms in two cases I had the next specimen which came to hand examined, and it happened to be the fibroid obtained from the acute case described on p. 79. From the softened parts Mr. Somerville Hastings succeeded in obtaining staphylococcus pyogenes aureus in pure culture.
The views here expressed in regard to the red degeneration of fibroids are founded on an examination of thirty-four recent examples.
Bland-Sutton, J. The Inimicality of Pregnancy and Uterine Fibroids. Essays on Hysterectomy, 1905, 76.
Fairbairn, J. S. A Contribution to the Study of one of the Varieties of Necrotic Changes in Fibro-myomata of the Uterus. Journ. of Obstet. and Gyn. of the British Empire, 1903, iv. 119.
Smith, J. L., and Shaw, W. F. On the Pathology of the Red Degeneration of Fibroids. Lancet, 1909, i. 242.
Cases of Hysterectomy performed on Patients in Labour in which the Obstruction was due to Fibroids
| Operator. | Result to Mother. | Fate of Child. | Nature of Operation. | Reference. |
|---|---|---|---|---|
| Spencer | R. | L. | Cæs. Sect., Subtotal Hyst. | Trans. Obstet. Soc., xxxviii. 389. |
| Bland-Sutton | R. | D. | Total Hyst. See Fig. 23. | Trans. Obstet. Soc., xlvi. 238. |
| Morison | R. | D. | Cæs. Sect., Total Hyst. | Northumberland and Durham Medical Journal, July, 1904. |
| Acland | R. | ? | Cæs. Sect. and Subtotal Hyst. | Lancet, 1904, ii. 948. |
| Spencer | R. | L. | Cæs. Sect., Total Hyst. | Trans. Obstet. Soc., 1906, xlviii. 240. |
| Spencer | R. | D. | Cæs. Sect., Total Hyst. | Trans. Obstet. Soc., 1908. |
| Pollock | R. | L. | Cæs. Sect., Subtotal Hyst. | Trans. Obstet. Soc., 1908. |
The aim of the surgeon is to save the life of the child as well as that of the mother. To this end, when the operation is carried out and the uterus exposed the child is extracted by Cæsarean section. Then in the majority of cases total or subtotal hysterectomy is performed. This is sometimes clumsily termed Cæsarean hysterectomy. In some instances the operator has been content merely to perform Cæsarean section in the hope that the patient may wish to reconceive.
In order to afford some notion of the frequency with which fibroids cause trouble to pregnant and parturient women, I have collected thirty-six cases which have been reported to the London Obstetrical Society from 1900 to 1908 (both years inclusive), and arranged them in the subjoined tables: they show in an unmistakable way that pregnant women with fibroids do often require aid from surgery, and that such efforts are rewarded with success. There is no condition which simplifies hysterectomy so much as pregnancy.
A Table of Cases in which Abdominal Hysterectomy was performed for Pregnancy complicated with Fibroids
These cases are recorded in the Transactions of the Obstetrical Society, 1900–8, both years inclusive.
| Recorder. | Age of Patient. | Period of Pregnancy. | Result to Mother. | Reference to Volume. |
|---|---|---|---|---|
| Horrocks | ? | 5th month | ? | 1900, xlii. 242. |
| Routh | 33 | 33 weeks | R. | Ibid., 244. |
| Doran | 40 | 5th month | R. | 1901, xliii. 178. |
| Donald | 43 | 9th month | R. | 1901, xliii. 180. |
| Donald | 34 | 4th month | R. | Ibid. |
| Donald | 34 | 4th month | R. | Ibid. |
| Donald | 41 | 4th month | R. | Ibid. |
| Routh | ? | 8½ months | R. | 1902, xliv. 41. |
| Doran | 39 | ? | R. | 1904, xlv. 119. |
| Doran | 30 | 4th month | R. | Ibid. |
| Doran | 30 | ? | R. | Ibid. |
| Boyd | 42 | 8th month | D. | Ibid., 106 |
| Boyd | 40 | 3rd month | R. | Ibid. |
| Fairbairn | 22 | 5th week post partum | R. | Ibid., 194. |
| Doran | 38 | 4th week post partum | R. | 1904, xlvi. 274. |
| Taylor | 33 | 3rd month | R. | 1905, xlvii. 333. |
| Andrews | ? | 3rd day post partum | R. | Ibid., 4. |
| Lea | 39 | 7th week post partum | R. | Ibid., 1 |
| Boyd | 42 | 4th month, total | R. | 1907, xlix. 49. |
| Bland-Sutton | 39 | 4½ months | R. | 1907. |
| Dauber | 31 | 3rd month | R. | 1908. |
| McCann | 25 | 4½ months | R. | Ibid. |
| Spanton | 33 | 2½ months | D. | Ibid. |
Table of Cases in which Abdominal Myomectomy was performed during Pregnancy
From the Transactions of the Obstetrical Society, 1900–8, both years inclusive.
| Recorder. | Age of Patient. | Stage of Pregnancy. | Result. | Reference. |
|---|---|---|---|---|
| Donald | 31 | 3rd month | R. | 1901, xliii. 194. |
| Walls | ? | ? | R. | Ibid., 195. |
| Routh | ? | 5th month | R. | 1904, xlvi. 279. |
| Spencer | 41 | 9th month | R. | Ibid., 122. |
| Malcolm | 32 | 7th week post partum | R. | Ibid., 15. |
| Doran | 28 | 2nd month | R. | 1905, xlvii, 426. |
| Vaughan | ? | 4th month | R. | Ibid., 427. |
| Vaughan | ? | 3½ months | R. | Ibid. |
| Swayne | 40 | 5th month | R. | 1908, l. |
| Swayne | 35 | 4½ months | R. | Ibid. |
| Williamson | 32 | 7th month | R. | Ibid., 73. |
| Scharlieb | 37 | 4½ months | R. | Ibid. |
| Scharlieb | 39 | 3½ months | R. | Ibid. |
Pregnancy complicated with cancer of the cervix. When a pregnant woman comes under observation with cancer of the neck of the uterus in an operative stage in the early months, hysterectomy should be performed: in some instances the cervix has been amputated without disturbing the pregnancy.
In the later stages good consequences follow the induction of labour and the immediate performance of hysterectomy. Surprising as it may seem, a uterus immediately after labour can be safely extirpated through the vagina.
When the cancer is so advanced as to be inoperable, the pregnancy should be allowed to go to term, and if the cancerous mass offer an impassable barrier to delivery, Cæsarean section should be performed. This operation has been found necessary to extract a dead fœtus.
Most surgeons in dealing with operable cases of this complication of pregnancy remove the parts through the vagina, because in the abdominal operation the septic cervix is withdrawn through the abdomen; this makes it extremely difficult to avoid soiling the pelvic peritoneum.
Concurrent uterine and tubal pregnancy. This condition may require operation in three different circumstances:—
1. Tubal and uterine pregnancy occur simultaneously and the complication is recognized in the early months. Here the operation would be that of oöphorectomy, and the uterine pregnancy may continue undisturbed to term.
2. Intra- and extra-uterine gestation with living fœtuses runs concurrently to term. This is an exceedingly dangerous, though a rare, combination. The table on p. 35 shows how deadly a compound pregnancy is to the mother: it sets forth also the fate of the children.
3. Uterine pregnancy is complicated by the presence of a quiescent (sequestered) extra-uterine fœtus. Many cases have been reported in which a fœtus of this character has occupied the pelvis, yet the woman conceived and the child was safely delivered at term; but a sequestered fœtus may constitute an impassable barrier and require removal (Operations for Compound Pregnancy, see p. 33).
Pregnancy complicated by tumours growing from the pelvic walls. When the pelvis is occupied by a chondroma, osteoma, or a sarcoma growing from the innominate bones or the sacrum, or from the fascia of the pelvis and displacing the gravid uterus, the proper course is to perform subtotal hysterectomy. If the obstruction is not detected until the child is viable, and there is no especial call for urgency, interference should be postponed until near term; the child can then be saved by Cæsarean section, and the uterus removed.
The operation in such circumstances calls for the exercise of judgment, but it is rarely difficult. Among interesting tumours complicating labour and obstructing delivery, special mention may be made of dermoids and teratomata lying in the hollow of the sacrum. Skutsch has collected the chief German records.
Echinococcus cysts (hydatids) have grown in the pelvic connective tissue and obstructed labour. Cases have been reported by Knowsley Thornton, Küstner, Blacker, and others.
Blacker, G. F. Clinical Lecture on Uterine Fibroids complicating Pregnancy. The Clinical Journal, 1908, xxxi. 309.
Küstner. Kaiserschnitt wegen eines Echinokokkus im Becken. Zentralbl. f. Gynäk., 1907, xxxi. 1390.
Skutsch, F. Ueber die Dermoidcysten des Beckenbindegewebes. Zeitsch. f. Geburts. and Gynäk., 1899, xl. 353.
Thornton, J. K. Removal of Hydatids of the Omentum and from the Pelvis. Medical Times and Gazette, 1878, ii. 565.
Acute septic infection (puerperal) of the uterus, too frequent even in this antiseptic epoch, is a desperate condition, but attempts have been made to deal with it by two methods—either hysterectomy, or the ligature and excision of the thrombosed ovarian veins.
So far as hysterectomy for this condition is concerned, it may be stated that it has been tried, but with no encouraging measure of success; it is a very desperate proceeding, and has been occasionally successful by the abdominal, as well as by the vaginal route. It is possible that vaginal hysterectomy may now and then be a wise operation in acute puerperal infection, but better results have been attained by ligature of the thrombosed pelvic veins, and by drainage of the pelvic cavity. Some interesting operations, with brilliant results, have been published by Trendelenburg, Michels, Cuff, Bumm, and others.
In some cases of puerperal pyæmia a careful examination of the patient’s abdomen has enabled the surgeon to feel the thrombosed ovarian vein, and in others the vein has been exposed by an incision running from the tip of the eleventh rib to the spine of the pubes, parallel with Poupart’s ligament. The muscles are divided and the peritoneum reached; this is reflected until the thrombosed ovarian vein is exposed and separated from the ureter. About half an inch below its junction with the renal vein or the vena cava, as the case may be, it is securely ligatured and divided; the vein is then slit up and the clot turned out. The operation, when carried out in this way, is extraperitoneal. In some instances successful ligature of the thrombosed ovarian vein has been effected by the usual median incision into the peritoneal cavity.
The object of ligaturing the thrombosed ovarian vein is to prevent the pathogenic micro-organisms in the clot from entering the circulation. Bumm reported five cases in which he ligatured these veins. Three of the patients recovered.
It is more than probable that if operative interference be carried out on thrombosed ovarian veins before the condition of the patients become desperate, more of them might be rescued. Success has been attained even in desperate conditions; for example, Friedemann ligatured these veins in a woman whose general condition was not only bad, but who also had extensive bed-sores. She recovered.
T. G. Stevens reported the details concerning a woman who died, of acute septicæmia, eleven days after a subtotal hysterectomy (by Galabin) for fibroids. The right ovarian vein was thrombosed from the ligature in the pelvis to its entrance into the vena cava, and he isolated from the clot and produced in cultures the bacillus pyocyaneus. He also stated that ‘the vein could have been easily dissected out, and possibly the fatal result might have been averted’.
This operation rests on sound principles, for the ligature of the ovarian veins prevents the septic blood entering the circulation, thereby setting up, among other things, endocarditis and pulmonary embolism.
The great difficulty in dealing with this condition is the selection of suitable cases. Experience teaches that acute cases are unsuitable. The best results have been attained in the chronic forms of the disease where the thrombosis was limited. There is great uncertainty in a given case as to the extent of the thrombosis and the number of veins implicated. As has already been mentioned, there are two routes for gaining access to the thrombosed vessels—the extraperitoneal and the intraperitoneal. I prefer the intraperitoneal route (cœliotomy), for it enables the surgeon to deal with the vessels, iliac or ovarian, of both sides, as well as allowing a thorough examination of the pelvic organs, and it permits the drainage of any collection of serum or pus found in the pelvis. From a study of the reported cases it is clear that the best results are obtained by cœliotomy. The ligature of thrombosed ovarian veins in chronic puerperal pyæmia promises good results for the future, but it needs further experience to teach us the kind of case in which it is likely to be successful.
Bumm, E. Zur operativen Behandlung der puerperalen Pyämie. Berliner Klin. Wochensch., 1905, xlii. 829.
Cuff, A. A Contribution to the Operative Treatment of Puerperal Pyæmia. Journ. of Obstet. and Gyn. of the British Empire, 1906, ix. 517.
Ferguson, J. Haig. Abdominal Hysterectomy for Acute Puerperal Metritis and Acute Salpingitis. Obstet. Transactions, Edin., 1906, xxxi. 123.
Friedemann, G. Die Unterbindung der Beckenvenen bei der pyämischen Form des Kindbettfiebers. Münchener Med. Wochensch., 1906, liii. 1813.
Lendon, A. A. Puerperal Infection, Thrombosis: Ligature of the Right Ovarian Vein. Australian Medical Journal, 1907, xxvi. 120.
Michels, E. The Surgical Treatment of Puerperal Pyæmia. Lancet, 1903, i. 1025.
Stevens, T. G. The Bacteriological Examination of a Thrombosed Ovarian Vein (following Hysterectomy). Trans. Path. Soc., li. 50.
Trendelenburg, F. Ueber die chirurgische Behandlung der puerperalen Pyämie. Münchener Med. Wochensch., 1902, xlix. 513.
Injuries of the uterus fall into six groups:—
1. Gynæcological injuries.
2. Obstetric injuries.
3. Injuries to the pregnant uterus.
4. Injuries to the pregnant uterus in the course of abdominal operations.
5. Bullet-wounds of the pregnant uterus.
6. Stab-wounds of the pregnant uterus.
Gynæcological injuries. The simplest and certainly the commonest accident is perforation of the uterus with a sound, dilator, or forceps in the operation of curetting. Many cases are known in which the uterus has been perforated by clean instruments of this class and the patients have suffered no inconvenience.
On the other hand, when the sound or the uterus is septic, perforation of the uterus has been followed by a rapidly fatal peritonitis; indeed, some of these injuries may prove as lethal as a snake-bite.
Occasionally very serious consequences follow simple perforations by dilators and curettes; this has induced some gynæcologists to urge that if, in the course of dilatation and curettage of the uterus, a rupture or perforation of the uterine wall occurs, it is better to perform a cœliotomy and assure oneself of the safety of the patient than to hope that no untoward result will ensue.
This advice is too sweeping. When the perforating instrument is clean, and there is little or no bleeding, the case may be left to itself; if untoward signs arise, cœliotomy should be performed. Sometimes a pelvic abscess occurs as a sequence to the accident, and will require evacuation through the vaginal fornix, or, perhaps, by means of an incision in the flank. Verco found a piece of a curette, 2¾ inches long, in an abscess cavity behind the uterus. The patient had been curetted two weeks previously.
A perforation, or a rent in the uterine wall, in the course of curetting, is a serious accident when the operator is unaware that such has happened, and proceeds to flush out the uterine cavity with poisonous antiseptic solutions, especially perchloride of mercury. Cases are known in which, under these conditions, the woman has died in the course of a few hours.
Injuries, in the course of instrumentation of the uterus, are not always mere perforations; some are wide rents—and this is an especial danger in removing sessile submucous fibroids (vaginal myomectomy). A serious complication of tears or rents of the uterine wall, whether the uterus is gravid or non-gravid, is extrusion or prolapse of the intestine. It is also remarkable that in several reported cases the practitioner has mistaken the intestines for ‘secundines’, even in unimpregnated uteri, and has withdrawn them, and even cut lengths of intestine away, before recognizing his error.
In one case of this kind, where a practitioner had withdrawn and removed several feet of intestine through a rent in the course of a curettage, I performed cœliotomy, closed the hole in the uterus, joined the cut ends of the bowel with sutures, resected the mesentery belonging to the removed bowel, and thus saved the patient’s life. In another case, where a practitioner had torn the uterus during curettage and intestine appeared in the vagina, there was such free bleeding that I found it prudent to perform subtotal hysterectomy. This patient also recovered. Successful operations of this kind have also been performed by Werelius and Nixon Jones.
Palmer Dudley relates that on one occasion, in curetting a recently gravid uterus, he tore the posterior wall without being aware of it, and withdrew eight inches of intestine, thinking it to be secundines; he recognized the error, and pushed the intestine back through the opening in the uterine wall. The patient recovered, and subsequently had two successful pregnancies.
These cases show how impossible it is to recommend any hard and fast lines of treatment. Much depends on the circumstances of the case, the character of the injury, and above all on the experience and resourcefulness of the practitioner.
Ruptures or tears of the uterus in the process of instrumental dilatation or curettage are by no means rare, and they have a high mortality. Jakob of Munich collected 141 instances of such injuries, and of these twenty-three died chiefly from septic peritonitis. Among these injuries seventy-three were inflicted with the curette, nineteen with the sound, fourteen with forceps (Ausräumungszangen), and six were due to flushing catheters.
Obstetric injuries. The uterus is liable, during labour, to be torn, as a result of its own expulsive efforts, especially when the transit of the fœtus is hindered or obstructed by narrowness of the pelvic outlet, tumours, or undue size of the child. This form of injury is called spontaneous rupture, to distinguish it from the rupture due to midwifery implements. The uterus is frequently torn in the obstetric manœuvre known as ‘turning’.
The literature relating to this accident is abundant, and the reports issued from lying-in institutions deal with extensive figures, but unfortunately the reporters are not in harmony on the principles of treatment.
There are three methods of dealing with rupture of the uterus:—
1. Treating the patient conservatively, which means at most lightly packing the part with antiseptic gauze.
2. Performing cœliotomy and stitching up the rent in the uterus.
3. Hysterectomy, preferably by the abdominal route, as this enables the peritoneal cavity to be cleared of clot.
The only point in which there is any semblance of agreement among obstetricians is this: in cases of complete rupture, in which the fœtus and membranes are extruded from the uterus into the belly, cœliotomy is clearly indicated.
Admirable reports have been published by Walla, Klien, Ivanoff, and Munro Kerr.
Klien’s is a critical and very valuable study, based upon 347 cases of rupture of the uterus published in the preceding twenty years. Of these cases 149 were operated upon, with a mortality of 44 per cent.; 198 were not operated upon, 96 recovered and 102 died—a mortality of 52 per cent. Among the unoperated cases some were not treated in any way, and in these the mortality was 73 per cent., whilst in those treated by drainage, plugging and irrigation, the mortality was only 37.5 per cent.
When there is dangerous bleeding Klien advises immediate operation. Lacerations of the vagina make the prognosis unfavourable, and especially injury of the bladder.
During the last ten years hysterectomy has been so much improved and the technique so simplified, that the operative treatment of complete rupture of the gravid uterus will be more frequently undertaken in the future than it has in the past, and with every prospect of reducing the heavy bill of mortality at present associated with this grave accident.
Donaldson (1908) reports a remarkable case in which the uterus ruptured during forceps delivery; 12½ feet of small intestine, detached from the mesentery, were extruded with the fœtus. Cœliotomy was performed, the detached intestine cut away, and the proximal end of the bowel anastomosed into the cæcum. A long rent in the posterior wall of the uterus was closed with sutures. The patient survived the accident ten days, and died from sepsis; ‘the entire uterus seemed to be a sloughing mass.’ Donaldson states that, had he removed the uterus at the time he operated on the intestine, the patient would probably have survived.
Injuries to the pregnant uterus. Some of the most remarkable injuries inflicted on the gravid uterus are the consequences of attempts to induce what is technically called criminal abortion, especially when the abortion is self-induced. Kehr has recorded an example of a desperate effort of this kind:—A widow, twenty-nine years of age, when in the fifth month of an illicit pregnancy, fired a revolver bullet into the uterus through the anterior abdominal wall. Cœliotomy was performed, and the wound in the uterus closed by suture. The woman aborted on the fourteenth day, but recovered.
A gravid uterus in the later months of pregnancy is a big organ, and, like the abdominal viscera generally, may be severely damaged by blows, kicks from horses or brutal men, butts from animals, such as a calf or a goat, falls upon the belly, or a fall downstairs, or the woman may be run over. The treatment to be adopted in these conditions varies widely with the circumstances. As a general rule it may be stated that the most satisfactory mode of treatment is cœliotomy; this permits a thorough examination of the organ, and facilitates removal of effused blood. In the late stages of pregnancy accidents of this kind entail Cæsarean section.
Among the most curious injuries of this group are those known as horn-rips: these are cases in which the pregnant uterus is torn open by the horn of a bull. An interesting collection of cases illustrating this accident has been made by Robert P. Harris. Even after very severe injuries, in some of which the intestines protruded, women have recovered, and several children survived this terrible mode of delivery.
Injury to a gravid uterus in the course of an abdominal operation. In spite of every care it has happened on many occasions that a pregnant uterus has been mistaken for an ovarian cyst, the abdomen has been opened and a trocar plunged into the uterus. In some instances a uterus in which the pregnancy has advanced as far as the sixth month has been removed under the impression that it was a large ovarian cyst, and this accident has happened with a pregnant uterus greatly enlarged in the somewhat rare condition known as hydramnios. A pregnant uterus is also liable to be stabbed by an ovariotomy trocar when the condition is complicated with unilateral or bilateral ovarian cysts. The gravid uterus has very thin walls and, occasionally, resembles so very closely an ovarian cyst as to deceive an inexperienced operator.
When the surgeon finds that he has injured a pregnant uterus in the course of an abdominal operation three courses are open to him, each of which has been practised with success by surgeons of renown:—
1. Sew up the incision in the uterus.
2. Perform Cæsarean section.
3. Remove the uterus (subtotal hysterectomy).
Several cases have been reported in which injury to a gravid uterus during ovariotomy has terminated fatally, especially when the surgeon followed the plan of sewing up the wound in the uterus.
A careful consideration of the reported cases indicates that the best results follow for the patient when the surgeon performs Cæsarean section, as the following record shows:—
Sir Spencer Wells had removed a large, multilocular ovarian cyst from the left side of the patient, when he felt what was supposed to be a cyst of the right ovary. When tapped it was found to be a gravid uterus, in which pregnancy had advanced to near the fifth month. Cæsarean section was at once performed and the patient recovered.
Injuries of this kind are rarely likely to happen now, for the clumsy ovariotomy trocar is passing out of use.
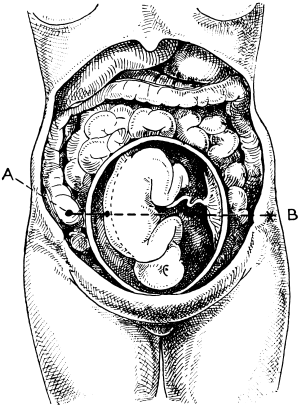 Fig. 24. Diagram representing a Gunshot Injury of the Uterus. The woman
was aged 28, and in the seventh month of pregnancy. The bullet was
extracted from under the skin on the left side, four inches behind the
anterior superior spine of the ilium. The line A B represents the track
of the bullet. (British Medical Journal, 1896, vol. i, p. 332.)
Fig. 24. Diagram representing a Gunshot Injury of the Uterus. The woman
was aged 28, and in the seventh month of pregnancy. The bullet was
extracted from under the skin on the left side, four inches behind the
anterior superior spine of the ilium. The line A B represents the track
of the bullet. (British Medical Journal, 1896, vol. i, p. 332.)
Bullet-wounds of the pregnant uterus. These are very rare, and, like rupture of the uterus, liable to be complicated with injury of the intestines; it is for this reason that the canon of surgery applicable to penetrating wounds of the abdomen should be practised in these circumstances, and the patient submitted to cœliotomy.
When the gravid uterus is penetrated by a bullet there may be little bleeding on account of the contracting property of the uterine tissue. In some instances amniotic fluid stained with blood escapes. In operating, the anterior as well as the posterior surface of the uterus should be carefully examined in order to determine if the bullet passed through this organ. In some instances the fœtus has been injured by the bullet. When free bleeding follows a bullet-wound of the gravid uterus the hæmorrhage is usually due to damage of blood-vessels connected with the intestines.
The best method of dealing with the uterus in such conditions is undetermined, but a study of the few reported cases indicates that the best results follow cœliotomy, with suture of the perforated intestine and the hole or holes in the uterus. The patients usually abort. In Prichard’s case (Fig. 24) hysterectomy was performed, but the patient died.
Even in some apparently desperate cases good consequences follow the conservative operation, as the following reports demonstrate:—
In a case under the care of Albarran, the patient was aged nineteen years and in the fifth month of pregnancy when shot. There were four perforations of the small intestines, and the mesenteric artery was wounded. He resected 20 centimetres of small intestine. A loop of umbilical cord protruded through the bullet-hole in the uterus; this was resected and the ends of the cord tied. The patient miscarried a few hours after the operation, but recovered.
Baudet reported a case in which there were four perforations of the small intestine: he sutured the wounds in the uterus and the holes in the bowel; the woman aborted some hours after the operation, but recovered.
In a case under Robinson’s care the bullet entered the uterus and penetrated the right shoulder of the fœtus. The patient, who was in the eighth month of pregnancy, quickly miscarried. The bullet was found in the débris. The patient not only recovered, but reconceived, and gave birth to another child in the following year.
Stab-wound of the pregnant uterus. Examples of this kind of injury are rare, but some of the recorded cases are remarkable. Guelliot has recorded the details of a case in which a pregnant woman was stabbed in the buttock. The knife passed through the great sciatic notch, and penetrated the uterus and the child’s skull. The woman miscarried of a dead fœtus next day. The great sciatic nerve was injured, but the woman recovered, though she remained lame.
Steele recorded an example where a woman, six and a half months pregnant, stabbed herself in the lower abdomen with a knife; she was taken to a hospital and kept at rest until the wound healed. Six weeks after the injury the woman was delivered of a live male child, normally developed, but much of the child’s large and small intestines protruded through an opening in the abdomen. The jejunum was completely severed as a result of the stab. Steele attempted to deal with this extraordinary lesion surgically, but the child died a few hours later.
Albarran. Plaies multiples de l’intestin et de l’utérus gravide par balle de revolver. Bull. et Mém. de la Soc. de Chirurgie de Paris, 1895, xxi. 243.
Baudet, R. Plaies de l’intestin et de l’utérus gravide par balle de revolver. Bull. et Mém. de la Soc. de Chir. de Paris, 1907, xxxiii. 779.
Bland-Sutton, J. A Clinical Lecture on the Treatment of Injuries of the Uterus. The Clinical Journal, 1908, xxxi. 289. On two cases of Abdominal Section for Trauma of the Uterus. The Am. Journal of Obstetrics, 1907, lvi.
Braun-Fernwald, R. von. Über Uterusperforation. Zentralbl. f. Gyn., 1907, xxxi. 1161.
Congdon, C. Abdominal Section for Trauma of the Uterus. The Am. Journal of Obstetrics, 1906, liv. 618.
Donaldson, H. J. An unusual Obstetric Complication, causing the removal of 126 inches of Small Intestine. Surgery, Gynæcology, and Obstetrics, 1908, vi. 417.
Dudley, P. Discussion on Accidental Rupture of the Non-parturient Uterus. Trans. Am. Gyn. Soc., 1905, xxx. 21.
Guelliot. Coup de couteau ayant pénétré à travers l’échancrure sciatique jusqu’à l’utérus gravide et jusqu’au fœtus, &c. Société de Chirurgie, 1886, xii, 337.
Harris, R. P. Cattle-horn Lacerations of the Abdomen and Uterus of Pregnant Women. The Am. Journal of Obstetrics, 1887, xx. 673.
Ivanoff, N. De l’étiologie, de la prophylaxie et du traitement des ruptures de l’utérus pendant l’accouchement. Annales de Gynécologie, 1904, 449.
Jakob, J. Gefahren der intra-uterinen instrumentalen Behandlungen. Zentralbl. für Gyn., 1906, xxx, No. 19, 561.
Jarman, G. W. Accidental Rupture of the Non-parturient Uterus, with report of cases. Trans. of the Am. Gyn. Society, 1905, xxx. 15.
Kehr, H. Über einen Fall von Schussverletzung des graviden Uterus. Centralbl. für Chir., 1893, xx. 636.
Kerr, Munro. On Rupture of the Uterus. Brit. Med. Journal, 1907, ii. 445.
Klien. Die operative and nichtoperative Behandlung der Uterusruptur. Arch. f. Gyn., 1901, lxii. 193.
Prichard, A. W. A case of Bullet-wound of the Pregnant Uterus. Brit. Med. Journal, 1896, i. 332.
Robinson, W. S. Death of Fœtus in utero from Gunshot-wound: Recovery of the Mother. Lancet, 1897, ii. 1045.
Steele, D. A. K. Stab-wound of Fœtus in utero. Surgery, Gynæcology, and Obstetrics, 1908, vi. 293.
Verco, W. A. The Australian Med. Gazette, 1908, 681.
Walla, A. von. Ruptura uteri completa, abdominale Totalextirpation. Heilung. Centralb. für Gynäk., 1900, xxiv. 497.
The performance of ovariotomy, hysterectomy, and allied procedures is attended by several risks, immediate and remote, which may spoil the best-planned and most carefully executed operation. Some of these may be avoided by careful attention to the details embraced by the phrase ‘after-treatment’.
The patient is returned to the bed with gentleness and usually lies on her back, but many anæsthetists prefer to turn the patient on one or other side for an hour, until there is a fair return to consciousness. The patient then lies on her back and a pillow is placed under the knees. Hot-water bottles should not be placed in the bed with the patient until she is completely conscious, and they are rarely needed. The healing of blisters caused by hot-water bottles is a slow process. During the first twelve hours the patient complains of pain, thirst, and vomiting.
The thirst is in a measure relieved by administering six or eight ounces of normal saline solution by the rectum an hour after the patient returns to bed, and repeating it in three or four hours. The patient may wash her mouth out frequently with water, hot or cold, according to her fancy, and if there is no vomiting she may swallow a little hot water from time to time. As a rule, it is better for her to abstain from swallowing anything for the first eighteen hours; the best way to avoid vomiting after an anæsthetic is to keep the stomach empty.
There is always some pain after an abdominal operation, partly due to tension on the sutures, and colic. The injection of normal saline solution (a teaspoonful of salt to a pint of water) by the rectum often controls this, but occasionally the pain is so severe that it is necessary to give a quarter of a grain of morphine hypodermically, or in a suppository, about twelve hours after the operation, in order to procure sleep. The routine use of morphine after these operations is injudicious and rarely necessary.
At the end of twenty-four hours small quantities of barley-water, tea, or milk and water are given, and if retained they may be taken in increasing quantities. On the fourth day an enema is given to clear the bowel, and then the patient will take fish, chicken, &c., and soon get on to convalescent diet.
When vomiting is very troublesome, it is sometimes necessary to keep a patient on rectal feeding two or three days.
When there is abdominal distension, this may be relieved by the passage of a rectal tube at intervals of three hours, and if this fails a turpentine enema should be given.
Patients should always be encouraged to empty their bladder naturally: many are unable to pass water whilst lying on their backs. In these cases the urine is drawn from the bladder by a carefully sterilized glass catheter. Before passing the catheter, the nurse carefully wipes away the mucus from the urethral orifice. Cleanliness and care with the catheter must be enforced: cystitis causes much misery. During the first few days the quantity of urine passed by the patient is measured, and recorded in the notebook.
The temperature should be observed every four hours during the first week and recorded. The first record after the operation is usually subnormal, and in twelve hours it rises to normal or beyond. During the first twenty hours it may rise to 100° without causing alarm; beyond this, if accompanied by a rapid pulse, an anxious face, and distended belly, it will cause anxiety to the surgeon. A temperature of 101° or 102° unaccompanied by other unfavourable symptoms is not a cause for alarm, unless maintained.
The state of the pulse is a valuable guide and more trustworthy than the temperature. When the pulse remains steady and full there is no cause for alarm. When it increases in frequency to 120 or 130 beats per minute, and is thin and thready, then there is danger, even if the temperature is only slightly raised.
On the seventh or eighth day the sutures will require removal. Occasionally a hæmatoma forms in the wound; and in patients in whom the operation has been performed for septic conditions, stitch abscesses will occur. In septic cases the sutures require to remain a few days longer, to allow the wound to unite more securely.
When oöphorectomy, ovariotomy, or hysterectomy is followed by a non-febrile convalescence the patient may be allowed to leave her bed on the fourteenth day, and at the end of another week she may return to her home or go to the seaside according to circumstances. When the wound has healed by primary union, and this is usual where aseptic methods have been followed and buried sutures employed for the fascial and muscular layer, an abdominal belt is unnecessary. When suppuration has taken place in the wound and healing has been retarded, especially in a patient in whom operations have been performed for septic conditions, it is a useful precaution to advise her to wear a well-made belt. This is more necessary for women who have to get their living by hard work.
Metrostaxis. After ovariotomy and oöphorectomy, unilateral or bilateral, blood sometimes escapes from the uterus in the course of the first week, and simulates menstruation: it sometimes occurs within forty-eight hours of the operation, and is usually ushered in with a rise of temperature (100°-101°).
Bed-sores. These sometimes give trouble when operations are performed on elderly or enfeebled patients, especially when they are thin and have incontinence of urine. With due watchfulness and care on the part of the nurse a bed-sore ought rarely to occur.
Post-anæsthetic paralysis. Paralysis following operations on the pelvic organs occurs in connexion with the upper and lower limbs; it is an awkward and avoidable complication. Some of the simplest cases are those which arise from the pressure upon an individual nerve, such as the ulnar, circumflex, or musculo-spiral, due to the arm coming in contact with the sharp edge of a metal operating table. When the patient’s legs are flexed across the sharp edge of the table and fixed, as in the Trendelenburg position, during a long operation, the external popliteal nerve is liable to be pressed upon by the condyles of the femur. This will lead to paralysis of the muscles supplied by it. In some instances the paralysis is bilateral. Paralyses of this kind are identical with what are known as ‘sleeping palsies’. The more serious paralyses are directly due to the Trendelenburg position, in which there is a great tendency for the arms to be displaced over the head and hang downwards or abducted, as this position causes the clavicle to compress the nerves of the brachial plexus upon the first rib, or the scalenus anticus muscle, and perhaps, as some observers believe, between the clavicle and the transverse processes of the fifth and sixth cervical vertebræ.
Most of the writers on this subject attribute the paralysis more particularly to drawing the head to one side when the patient lies in the Trendelenburg position with abducted upper limbs, as it tends to stretch the lower cervical nerves of the opposite side, especially the fifth. This stretching is probably a greater factor in producing paralysis than pressure.
The form of paralysis produced in this way is that known as Erb’s palsy, and the muscles particularly concerned are the deltoid, brachialis anticus, biceps, and the supinator longus. Sometimes the spinati are involved. Occasionally the paralysis is bilateral. A case has been reported in which there was a total lesion of the brachial plexus, including the muscles of the shoulder girdle.
The following facts serve to show that stretching rather than pressure is responsible for this class of paralyses. A patient had undergone a vaginal operation in the crutch position, when the assistant drew her along the table by means of his fingers hooked in the axillæ over the folds of the pectoral muscles: next morning both upper limbs were found to be paralysed, and they remained in this condition many weeks.
In some of the lighter forms the paralysis passes off in a few days, but cases are known in which it has persisted for many months, and as it renders the limb useless for a time it is a serious matter.
Halstead refers to a case of bilateral peroneal paralysis following salpingectomy in the Trendelenburg posture which disabled a patient for six months.
On the whole prognosis is favourable, and recovery the rule.
Büdinger has described a case in which the upper limb was paralysed after an abdominal operation. The patient died some weeks later, and a clot of blood was found pressing on the surface of the brain at a spot corresponding to the arm centre.
Büdinger. Über Lähmungen nach Chloroformnarkosen. Archiv f. klin. Chir., 1894, Bd. xlvii. 121.
Cotton, F. J., and Allen, F. W. Brachial Paralysis—Post-narcotic. Boston Med. and Surg. Journal, 1903, cxlviii. 499.
Halstead, A. E. Anæsthesia Paralysis. Surgery, Gynæcology, and Obstetrics, 1908, vi. 201.
Turney. Post-anæsthetic Paralysis. Clinical Journal, 1899, xiv. 185.
Giving way of the wound. After cœliotomy the patient runs a risk of the wound being burst open, and this accident seems particularly liable to happen in cases where catgut has been selected for the suture material. Accidents of this kind belong to two categories:—
1. Many cases occur in patients from violent coughing or vomiting, as the straining causes the knots of the sutures to slip.
2. In feeble patients, and those debilitated by anæmia, diabetes, &c., and especially in septic wounds, the union of the edges of the incision unite very slowly; if the sutures are taken out on the eighth day, as is the custom, the wound is liable to burst asunder. This accident is prone to occur in patients whose abdominal wall has been greatly distended by a large tumour, and especially by pregnancy. On the whole the accident is more prone to complicate Cæsarean section than any other operation on the pelvic organs, and cases have been reported in which there has been a repetition of the accident. The largest collection of case-reports in which the wound has burst open after cœliotomy has been made by Madelung; a perusal of his paper shows that it is an accident with a high mortality. It is a fact that cases of this kind are rarely published, and from inquiries I find that it is of common occurrence. It has certainly diminished since surgeons have widely adopted the method of securing the wound with buried suture, but this is not always a preventative. The complication which makes the accident so unfortunate for the patient is the protrusion of the intestines.
In dealing with this condition the surgeon carefully and gently cleans the extruded intestines and omentum with sterilized water, returns them into the abdomen, and resutures the wound.
Madelung, O. Ueber den postoperativen Vorfall von Baucheingeweiden. Verhandlung. d. Deutschen Gesellsch. f. Chir., Berlin, 1905, xxxiv, 2. Theil, p. 168.
Hæmorrhage. However carefully an operation may be conducted or whatever material may be employed for ligatures, there is a liability of bleeding after the patient has been returned to bed. Severe internal bleeding is usually due to the slipping of a ligature from an ovarian pedicle, or a uterine artery: it may come from a vaginal artery, especially in total hysterectomy, and occasionally from a vessel in an adhesion which has been missed in the course of the operation, for oozing which is scarcely appreciable when a patient is collapsed may become very free when reaction occurs.
Severe internal bleeding is manifested by very obvious signs: pallor, cold skin, rapid but feeble pulse, restlessness, and sighing respiration. When these symptoms are manifested the wound must be reopened, the blood and clot removed, and the bleeding point secured. It often happens, where the bleeding is due to the slipping of a ligature from the uterine or ovarian artery, that by the time the surgeon reopens the wound the patient is so bloodless that there is difficulty in determining the source of the bleeding. In very bad cases it is a wise plan to arrange for an assistant to perform the intravenous infusion whilst the surgeon deals with the bleeding vessel. (See Vol. I, p. 405.)
Intravenous injection is the best method of treating patients when the loss of blood has been great. It is unwise to transfuse more than three pints into the veins, or the lungs will become waterlogged and the patient will be later in great peril. When the loss is moderate in amount and the patient is not greatly enfeebled, a pint or more of saline solution may be poured into the abdomen before closing the incision, and this may be supplemented by the administration of six or more ounces of the solution by the anus at two-hourly intervals until the force of the circulation is restored.
In some instances the subcutaneous injection of normal saline solution may be employed. A suitable region is the loose tissue under and around the breasts. When this method is adopted the skin should be rendered antiseptic, otherwise troublesome abscesses and cellulitis will arise in the subcutaneous tissue at the situation where the saline solution has been injected.
Intrapelvic hæmorrhage. For many years I have maintained that two factors which have enabled hysterectomy to vanquish oöphorectomy in the treatment of uterine fibroids are rigid asepsis and perfect hæmostasis. In the early days of intrapelvic surgery there used to be much discussion on the subject of free blood in the pelvic cavity: some practical surgeons urged that it was harmful and would induce peritonitis, and others took the opposite view. From my own observations I came to the conclusion that effusions of blood in the abdomen were often quickly absorbed, but that this was not invariable; and that post-operative collections of blood were very liable to become septic, especially when drainage was employed. I also pointed out that the large effusions of blood in the abdomen due to tubal abortion, or to the rupture of a gravid tube, are often attended with fever, and in some instances the temperature rises to 103°. In such cases, when operative interference is undertaken, the deliquescent clot present in the pelvis often gives off a musty odour. Much light has been thrown on this condition by Dudgeon and Sargent, who have specially investigated the bacteriology of intraperitoneal effusions. These observers have isolated from intraperitoneal effusions of blood a white staphylococcus, which makes its appearance in the blood within a few hours of being effused, and they are of opinion that the febrile disturbances so frequently found after effusions of blood into the peritoneal cavity are due to the presence of this organism.
Apart from the pathological importance of these observations there is a point of practical value connected with them. The white staphylococcus will infect sutures and give rise to stitch-abscesses in the wound; in view of this fact it behoves the surgeon who has to deal with a stale effusion of blood in the pelvis and evacuates it by an incision through the abdominal wall, that in closing the incision he should employ through and through sutures, and not attempt to suture it layer by layer. I have noticed the same tendency to stitch-abscess in cases of diffuse pelvic inflammation due to infection by the gonococcus.
Pneumonia. This is a serious and not infrequent sequel of cœliotomy, especially when it concerns diseased conditions in the upper half of the abdomen: pneumonia occurs frequently as a sequel to ovariotomy, hysterectomy, and allied operations, and occasionally has a fatal ending. It may arise from inhalation, or may be due to the dorsal position (hypostatic pneumonia), or it may arise from infection.
Inhalation pneumonia is not uncommon, and although it is often attributed to the anæsthetic, especially ether, it is doubtless due to a combination of causes, such as a cold room, undue exposure of the body, septic teeth, the chilling effects of ether on the tissues of the lung, and occasionally to a dirty face-piece belonging to the ether or chloroform apparatus.
Hypostatic congestion of the lungs is liable to occur in the aged and in debilitated patients; it is a complication in such cases always to be guarded against.
Embolic pneumonia is the most serious form, and occurs as a sequel to operations for septic conditions, such as pyosalpinx, suppurating ovarian cysts, septic fibroids, and post-operative sepsis; it is also associated with thrombosis, especially when the pelvic veins contain septic clot.
In the preceding section attention was drawn to the appearance in intra-abdominal blood-effusions of a white staphylococcus: such collections of blood are prone to decompose and cause the temperature to rise.
On several occasions in which blood has been effused freely into the pelvic cavity, either as a consequence of tubal pregnancy, or as a sequel to an operation, such as an abdominal myomectomy, and the blood has been allowed to remain, or it has been inefficiently drained, the patients have died from septic pneumonia.
In cases of septic thrombosis the patients run a definite risk from pulmonary embolism. When the embolus is large the patient sometimes dies in a few minutes (see p. 101); but even in cases where the embolus is too small to promptly destroy the patient’s life, its lodgment in the lungs entails in some instances a very serious illness, and occasionally a fatal termination.
Parotitis. Septic parotitis, or, as it is sometimes called, symptomatic or secondary parotitis, to distinguish it from mumps, is an occasional sequel to abdominal operations of all kinds. Careful observations have shown that parotitis is more common after operations for septic conditions, and, although it occasionally occurs after operations which run an afebrile course, the conditions underlying it are mainly septic in character.
Septic parotitis is distinguished from mumps in the following points:—
It occurs as a complication of some other affection, is in itself non-contagious, and occasionally suppurates. There are two views held in regard to its etiology: some hold that it is due to direct infection of the duct (Stenson’s) of the parotid gland by micro-organisms from the mouth, whilst others maintain that the path of infection is mainly by the blood-stream.
Two able investigations have recently been published in regard to this condition, in which one writer (Bucknall) supports the view that it is an ascending affection from the mouth, and the other (Tebbs) brings forward evidence that the elements of infection reach it by the blood-stream.
Lequeu has seen many cases of post-operative parotitis, and at his suggestion Verliac and Morel investigated the condition in the laboratory. They came to the conclusion that this variety of parotitis originates in the ducts of the gland.
When parotitis complicates post-operative convalescence, it is almost entirely confined to septic cases: it may occur within two days of the operation or as late as the thirtieth day. It is more common between the sixth and tenth days, and its advent is accompanied by much disturbance. The parotid swells and becomes painful and tender; the skin over it is red and often brawny. These signs are accompanied by fever, malaise, and depression of spirits. In mild cases they subside in a few days, but in severe cases rigors occur, with high fever and suppuration.
The mild cases are best treated with warm fomentations, frequently changed. If suppuration occurs, the pus will need to be evacuated by a scalpel, but incisions in a suppurating parotid gland should be carried out with careful regard to the branches of the facial nerve (pes anserinus), and the large vessels intimately associated with it.
The surgeon need not be in a great hurry to use the scalpel in these cases, for it seems occasionally as if the skin would slough, and yet when it is incised no pus escapes. This septic parotitis is deceptive in the red and brawny appearance of the skin covering the swollen gland, and the misleading sense of fluctuation. In many instances the inflammatory products escape by way of the parotid duct.
Septic parotitis is an unpleasant and painful complication of an abdominal operation, but it is rarely dangerous and has only had a fatal termination in very exceptional cases.
Thrombosis. After operations on the pelvic organs, thrombosis occasionally occurs in the iliac, femoral, and saphena veins, accompanied by fever, pain, especially in the course of the long saphenous vein, and œdema of the limb. It is noticed most frequently about the twelfth day after operation.
In some patients the thrombosis is confined to the superficial veins of the calf and thigh, but when the femoral and internal iliac veins and the associated lymphatics are involved, the œdema is of a solid kind. Apart from the danger which ensues from the detachment of a fragment of clot and its arrest in the pulmonary artery, this complication is often very serious for the patient, for it entails a long confinement to bed, a tedious convalescence, and the œdema of the limb will sometimes persist for many weeks or months, in spite of topical applications, careful bandaging, or judicious massage.
Post-operative thrombosis was formerly fairly common after hysterectomy for fibroids and in the later stages of malignant disease of the uterus. Its frequency after operations for fibroids was attributed to the profound anæmia in patients who had severe and exhausting metrorrhagia. I am convinced that it is due to sepsis. In several instances I have caused the clot found in thrombosed veins to be examined bacteriologically, and pathogenic microscopic organisms have been isolated. I am also satisfied that in some cases of thrombosis of the veins of the thigh, especially those limited to the saphenous veins, the clotting spreads from the superficial veins of the hypogastrium which are infected from the abdominal incision.
Pulmonary embolism. In perusing the clinical histories of a series of cases of ovariotomy, hysterectomy, myomectomy, and, indeed, after almost any surgical operation, here and there a record may be read to this effect: ‘The patient appeared to be doing well after the operation, when she sat up, laughed and chatted with the nurse, then suddenly fell back and died in a few minutes.’
Anything more tragic than this it is difficult to conceive, and, as a rule, after such a sad occurrence, the relatives are so distressed that they rarely permit an examination of the body. Death in such circumstances is usually attributed to embolism of the pulmonary artery. In some instances this is an assumption, but there are many in which an embolus has been demonstrated, and a few in which the source has been detected.
Post-operative embolism of the pulmonary artery is an important matter for surgeons interested in the operative treatment of uterine fibroids, for it follows such operations more frequently than any other. In order to afford some notion of the relative liability of patients to this accident after subtotal and total hysterectomy for fibroids, I have gathered the following statistics, which are interesting as showing an extraordinary variation in the practice of different operators:—
Baldy ascertained that among 366 operations for fibroids in the Gynecean Hospital, Philadelphia, there were thirteen sudden deaths attributed to pulmonary embolism.
In the Middlesex Hospital between the years 1896 and 1906 (both years inclusive) there were 212 abdominal hysterectomies performed for fibroids. Three of the patients died from pulmonary embolism. Spencer, in eighty-five total hysterectomies, had two deaths from pulmonary embolism. R. Lyle, in eight cases of subtotal hysterectomy, had one sudden death.
Mallet collected the records of 1,800 cœliotomies: there were six deaths attributed to embolism, and of these, three followed operations for uterine fibroids. Chas. P. Noble, in forty-two vaginal myomectomies, lost two patients, one from septic endocarditis, the other from embolism; in the latter case the fibroid was gangrenous.
Olshausen, from the year 1896 to the end of 1905, performed 366 hysterectomies for fibroids; twenty-seven of these patients died. Five of the fatal cases were due to embolism.
Since 1894 I have performed more than a thousand operations of various kinds for fibroids, and have lost one patient from pulmonary embolism. This happened in 1900. The woman was forty-five years of age and profoundly anæmic from profuse and long-continued menorrhagia. Twelve days after subtotal hysterectomy she asked to be pillowed up in bed; this was done, when she suddenly slipped down the bed in agony and died in fifteen minutes. At the post-mortem examination the right pulmonary artery was found plugged with a thick clot. No thrombosed vessels were found in the pelvis.
The symptoms of pulmonary embolism may occur at any period from the hour of the operation up to the thirtieth day. In the majority of patients embolism happens about the twelfth day. The symptoms supervene with great suddenness and seem to be preceded by movement, such as sitting up, getting out of bed, and especially straining during defæcation. Withrow tells of a patient who was attacked whilst ‘putting on her clothes to leave the hospital’. She died in twelve hours. Reclus, at a meeting of the Société de Paris, 1897, mentioned that a patient quitting the hospital, apparently convalescent from hysterectomy, fell dead in the courtyard from pulmonary embolism. In one remarkable instance a patient complained of sciatic pain fifteen days after hysterectomy. In order to afford relief the surgeon flexed the patient’s thigh on her abdomen and then suddenly extended it. This dislodged a clot, and the woman was seized with the symptoms of pulmonary embolism and died in forty-seven minutes. At the post-mortem examination the pulmonary artery was found occluded with clot and the ovarian vein contained a thrombus (Byron Robinson).
It is important to note that these fatal cases of pulmonary embolism occur when they are least expected, and it is an unusual sequence in patients with obvious thrombosis of the femoral and saphenous veins.
The most constant symptoms are urgent dyspnœa accompanied by great distress; in some instances the patient becomes pallid and in others cyanotic. Death may follow in a few minutes; in less severe cases it is delayed several hours, the patient remains conscious, but suffers severe mental agony.
A pulmonary embolism is not necessarily fatal, for a woman after a pelvic operation may complain of sudden pain in the chest, urgent dyspnœa, exhibit great mental distress, and in a short time spit up sputum mixed with blood. In a few hours the urgent symptoms subside and in two or three days pass away, and the patient recovers. I have seen five examples of this mild form of pulmonary embolism after hysterectomy. One of the patients appeared to suffer from a succession of small pulmonary emboli.
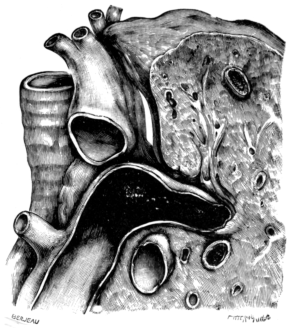 Fig. 25. The Pulmonary Artery and Adjacent Part of the Lung and Trachea.
The artery is completely occluded by a clot derived from a thrombus in
the right auricle. (Museum of the Middlesex Hospital.) Three-quarter
size.
Fig. 25. The Pulmonary Artery and Adjacent Part of the Lung and Trachea.
The artery is completely occluded by a clot derived from a thrombus in
the right auricle. (Museum of the Middlesex Hospital.) Three-quarter
size.
Somerville Hastings refers to a woman thirty-six years of age, anæmic from profuse, long-continued menorrhagia due to a uterine fibroid, who, whilst waiting in the hospital for hysterectomy, was seized with pulmonary embolism and died three hours later. An embolus occupied the pulmonary artery, resembling a blood-clot found in the left common and internal iliac veins. Hastings also states that in a patient who died from pulmonary embolism, after an operation, a thrombus occupied the right cardiac ventricle, and he thought it possible that this intraventricular clot furnished the embolus (Fig. 25).
We must bear in mind that individuals apparently in good health die suddenly in the street, in the armchair, in a bath, or even during sleep: it is a fair assumption that some of the instances of sudden death occurring during convalescence from surgical operations may be due to failure of the heart absolutely unconnected with the operation. It is, however, undeniable that thrombosis of the pelvic veins after ovariotomy, or hysterectomy, is a source of fatal emboli. At present there is very little evidence available as to the cause of the thrombosis, but it can scarcely be doubted that sepsis, it may be only of a mild type, is responsible for some of the cases.
A careful consideration of the matter reveals beyond any doubt that pulmonary embolism occurs much more frequently after hysterectomy or fibroids than after any other operation, and it is especially liable to happen in women who are profoundly anæmic from profuse and prolonged menorrhagia. This indicates that long-continued and irregular losses of blood induce some change in the composition of this important fluid, which favours its coagulation.
It has been suggested that the practice of keeping patients strictly confined to bed for two or three weeks after hysterectomy and allied operations is responsible for the thrombosis which is the source of these fatal emboli. Some American surgeons act on this suggestion and insist on their patients getting out of bed a few days after such operations. This method does not commend itself to British surgeons. In my own practice I make it a rule, even in the most favourable conditions, to keep the patients confined to bed for two weeks. No patient is allowed up until her temperature has been normal for at least three days. The consequences of this practice appear to be justified, for in more than a thousand hysterectomies, only one of my patients lost her life in consequence of pulmonary embolism.
In cases of embolism of the pulmonary artery, death does not always occur immediately, but may be postponed for an hour or more after the lodgment of the embolus.
Trendelenburg is of opinion that it might be possible to remove this clot by direct surgical intervention. After careful consideration of the matter he carried out this operation on a woman aged sixty-three years; he raised an osteoplastic flap on the left side of the thorax, exposed the conus arteriosus, and intended to withdraw the clot, by means of a specially constructed pump, through a slit in its walls. The patient died from excessive bleeding before the clot could be extracted; the operation was hindered by an adherent pericardium.
Trendelenburg has carried out this operation on a man forty-five years of age. This patient was tabetic and sustained a spontaneous fracture of the femur. One month later he was seized with urgent dyspnœa and signs clearly indicating the lodgment of an embolus in the pulmonary artery. Trendelenburg exposed the heart, opened the pulmonary artery, and by means of polypus forceps succeeded in withdrawing 34 centimetres of clot. The incision in the artery was carefully closed with sutures. The man improved considerably as the result of the operation, but died thirty-seven hours later. At the post-mortem examination the left and right branches of the pulmonary artery contained an embolus. From the surgical point of view there are no reasons why such a bold example should not be repeated with success.
When patients who are profoundly anæmic from menorrhagia due to fibroids undergo hysterectomy, it is a useful measure to give them twenty grains of citrate of sodium twice daily in order to diminish the abnormal tendency of the blood to coagulate in the vessels. Certainly this drug should be administered if there is the least evidence of thrombosis.
Foreign bodies left in the abdomen. Every writer on ovariotomy and kindred operations insists on the importance of exercising the utmost personal vigilance in counting instruments and dabs before, and immediately after, an abdominal operation in order to avert the dangers which ensue when instruments, dabs, gauze, or drainage tubes are accidentally left in the abdominal cavity. Before the era of antiseptic surgery nearly all the patients in whom foreign bodies were left in the abdominal cavity died. In several instances the surgeon has discovered, on counting the sponges and instruments after the operation, one or more to be missing, and, failing to find them in the room, has reopened the wound and recovered the missing article. In many lucky cases, a sponge or compress has given rise to an abscess, and, the wound reopened, the sponge presented at the opening. Often a compress of cotton-wool or gauze has slowly ulcerated into the rectum and been discharged through the anus.
When things of this kind are left in the abdomen the risks are not so great now as in pre-antiseptic days, but they cause much discomfort and anxiety as well as suffering: moreover, such an accident entails reopening the wound and occasionally a serious operation for the removal of the missing article, and as a recent decision in a Court of Law fixes the responsibility on the operator, there is always the possibility of an action at law with all its vexations and the liability of being mulcted in damages.
The behaviour of foreign bodies left in the abdomen is curious and also interesting from the great length of time which metal instruments will sometimes remain without causing very urgent symptoms, and the tendency they exhibit to penetrate adjacent viscera.
Among the early cases Sir Spencer Wells reported one in which a pair of forceps was found in a patient’s bladder who died a month after ovariotomy. Olshausen mentions that a pair of forceps was passed by the rectum nine months after ovariotomy, and Terrillon tells of a pair of pressure forceps which remained eight months in the belly and came out close to the navel. One of the most remarkable instances is recorded by MacLaren, in which a pair of forceps was left in the abdomen in the course of a hysterectomy. Two years later, a swelling formed in the right iliac region; this was explored through an abdominal incision, and the hæmostatic forceps represented in Fig. 26 was found embedded in the omentum; the forceps had ulcerated into the cæcum and the blades were lodged in the vermiform appendix. The patient recovered.
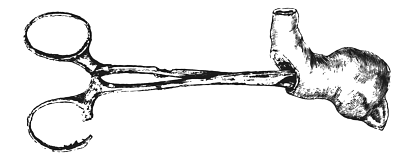 Fig. 26. A Pair of Pressure Forceps: this instrument had remained in
the abdomen two years after hysterectomy. The forceps had ulcerated into the
cæcum and the blades had lodged in the vermiform appendix. (After MacLaren.)
Fig. 26. A Pair of Pressure Forceps: this instrument had remained in
the abdomen two years after hysterectomy. The forceps had ulcerated into the
cæcum and the blades had lodged in the vermiform appendix. (After MacLaren.)
In order to illustrate the diminished risks run by patients when the instruments and dabs used in operations are thoroughly sterilized, reference may be made to a case recently reported by J. E. F. Stewart (Australia), in which he removed a pair of pressure forceps which had remained in the abdomen for ten years and a half. The patient, who had been more or less an invalid since the primary operation, had suffered from attacks of acute pain, constipation alternating with diarrhœa, and pains in the lower limbs. The instrument, which measured 5 inches long and 2½ across the handles, was lying point downwards in the pelvis, and the ring handles could be felt through the belly-wall before the operation: it had made its way into the small intestine.
The tendency for a foreign body, whether hard like forceps, or soft like gauze pads, to erode its way into the intestine is very remarkable. Thus Gifford operated on a patient with intestinal obstruction; an impacted mass was felt in the ileum, it was extracted through an incision in the gut and proved to be a pad of cotton-wool enveloped in gauze. She recovered. Three months previously this woman had undergone abdominal myomectomy.
Another source of risk to patients is the practice or habit of packing the pelvic recesses with strips of gauze temporarily, either with the hope of controlling oozing, or to serve as a drain. I have long abandoned this habit. The disadvantage of gauze stuffing which needs consideration in this section is the risk that some portion, or the whole of it, is sometimes left in the wound. Examples are known where long strips of ‘gauze stuffing’, sometimes amounting to a yard or more, have been passed through the anus a year after the operation. Many intractable sinuses have had a forgotten piece of gauze as the cause of their persistence.
A woman had cœliotomy performed for peritonitis, the consequence of criminal abortion; she had a long convalescence due to an intractable sinus. Eventually the patient was thought to have tuberculous disease of the appendages, and a mass, formed mainly by the Fallopian tube, was removed. The walls of the tube were intact, but when slit open the tube was found to contain a small gauze tampon (Kouwer).
The isolated records relating to foreign bodies left in the abdomen are very numerous. Thus Wilson in 1884 was able to collect twenty-eight cases from periodical literature and personal reports from friends. An interesting discussion took place on the reading of a paper on this subject before an American gynæcological society, by R. W. Waldo, and the number of cases related by the members is astonishing and refer to such things as sponges, dabs, forceps, a strip of iodoform gauze ‘a yard wide and two yards long’, a pair of spectacles, and ‘an operating-room towel’, which were left in the abdominal cavity.
The most comprehensive collection of records relating to foreign bodies left in wounds of all kinds has been made by F. von Neugebauer; they amount to 195.
Gifford, G. T. British Medical Journal, 1907, ii. 1042.
Kouwer, Prof. Zentralbl. für Gynäk., 1907, xxxi. 1447.
MacLaren, A. Annals of Surgery, 1896, xxiv. 365.
Neugebauer, F. v. Monatsschriften für Geburtsh. u. Gyn., 1900, Bd. xi, 821, 933. Zentralbl. für Gynäk., 1904, xxviii. 65.
Stewart, J. E. F. Australian Medical Gazette, 1906, xxv. 446.
Waldo, R. W. American Journal of Obstetrics, 1906, liv. 553.
Wilson, H. P. C. Trans. American Gynecological Society, 1884, ix. 94.
Tetanus. This dread complication of wounds occasionally occurs after ovariotomy, and during the ‘reign of the clamp’ it was especially frequent in Germany (Olshausen). Cases have been reported in England, and tetanus has been noticed to affect patients who have been ovariotomized in rooms recently plastered.
Since Kitasato demonstrated the bacillary origin of tetanus poison, and showed that the bacillus can be transported by dust, knowing its liability to attack suppurating wounds, we can understand that when the pedicle of an ovarian cyst was secured by a clamp and allowed to slowly slough away, more or less exposed to air and dust, it offered a nidus for the tetanus bacillus.
Tetanus, however, has not quite disappeared as a sequel to operations on the pelvic organs, for in 1902 a case was reported by Dorsett in which a patient died of this disease after hysteropexy, and the tetanus bacillus was detected in some wallaby tendon employed to suspend the uterus. Tetanus has also been traced to infected catgut employed in cholecystotomy (1905).
Ed. Martin reported the occurrence of tetanus after vaginal fixation of the uterus and colporrhaphia anterior. Cumol-catgut was employed.
Menzer has recorded a similar case which occurred in Dührssen’s Klinik (1901). The ligatures were of catgut.
Mallet refers to two post-operative deaths from tetanus. One patient had undergone an operation for bilateral pyosalpinx and the other had a fibroid of the uterus complicated with an ovarian cyst. There was an interval of eighteen months between the two fatal cases. Catgut was employed as the ligature material.
In practice it is important to remember that tetanus arises from infection: hence all instruments which have been in contact with this disease must be sterilized, and this should be effected by submitting them to prolonged boiling.
Tetanus occurs as a rare sequel to miscarriage and normal labour. Kraus and von Rosthorn have reported some carefully investigated cases of this kind.
Dorsett, W. B. Two fatal cases of Tetanus following Abdominal Section due to Infected Ligatures, &c. Am. Journ. of Obstet., 1902, xlvi. 620.
Mallet, G. H. Some Unusual Causes of Death following Abdominal Operations. Ibid., 1905, li. 515.
Martin, Ed. Postoperativer Tetanus (with references). Zent. f. Gyn., 1906, xxx. 395.
Meinert. Drei gynäkologische Fälle von Wundstarrkrampf. Arch. für Gyn., 1893, xliv. 381.
Menzer. Tetanus Infection after Vaginal Fixation of the Uterus. Zeitsch. f. Geb. u. Gyn., 1901, xliv. 517.
Olshausen, R. Tetanus nach Ovariotomie Billroth-Lücke’s. Handb. der Frauenkrankheiten, 1877–9, ii. 367.
Taylor, H. Tetanus after Hysterectomy. Am. Journ. of Obstet., 1908, lvii. 574.
Injury to intestines. Intestines great and small are very liable to injury in the performance of intrapelvic operations. Unless care is taken in opening the abdomen, the intestines are apt to be cut, especially when there has been chronic peritonitis, as in tuberculous and gonococcal infections, which cause the small intestine to adhere to the parietal peritoneum investing the anterior abdominal wall. Where cœliotomy is being performed a second or third time, through or near the original cicatrix, it is necessary to proceed with extreme caution for fear of cutting an adherent coil of gut.
Intestine is also liable to be torn in separating adhesions from the tumour, and great care is necessary when cysts are firmly adherent to the floor of the pelvis, for in separating them the rectum runs a great risk of being damaged.
In removing tumours to which the vermiform appendix adhered it is necessary to be careful and avoid mistaking it for an adhesion, for there is reason to believe that this structure has been divided and its nature overlooked; an accident of this sort leads usually to fatal peritonitis.
It has happened, in the course of removing very adherent ovaries and tubes from the floor of the pelvis, that in transfixing the pedicle a coil of ileum has also been transfixed with the needle and tied to the stump. This accident is not likely to happen now that the Trendelenburg position is almost universally employed.
In sewing the abdominal incision the intestines have been pricked with a needle, and in some instances the bowel has been accidentally included in the sutures and sewn to the abdominal wall. On one occasion while securing a very long incision with through and through sutures, while passing the needle through the abdominal wall, it broke, and the broken end came with great force against the anterior wall of the stomach and tore a hole in it. This I secured at once with suture and the accident had no bad consequences.
An unrecognized wound of the bowel in the course of a pelvic operation is almost certainly fatal. Accidental injuries, such as punctures and cuts, require immediate suture, and I have never known any harm follow. On the other hand, ragged tears in thickened and inflamed bowel require careful consideration in order to spare patients the inconvenience and distress of fæcal fistulæ.
In regard to small intestine a very small opening may occasionally be safely secured with fine silk, but in most cases it is wiser, if the bowel is thickened and inflamed around the hole, to resect well wide of the damaged portion and join the cut ends (circular enterorrhaphy).
Holes low down in the rectum are difficult to suture securely. These should be treated by drainage, using a wide rubber drain; the convalescence will be tedious, but the fistula will close.
It is useful to remember that if the rubber tube be too long it may enter the hole in the bowel and thus maintain the fistula. On one occasion I was asked to close a fæcal fistula which had followed an oöphorectomy. This fistula persisted five years. At the operation I found a hole in the sigmoid flexure with its margins adherent to the opening in the parietes, so that the tube passed directly into the bowel. The gut was detached and the opening closed with sutures, and it gave no further trouble.
If, in the course of an ovariotomy or hysterectomy, the surgeon discovers a cancerous stricture in the colon or cæcum he should resect the affected section, if it permits of this treatment; otherwise lateral anastomosis should be performed. (See Vol. II.)
Intestinal obstruction. It is difficult to estimate with any approach to accuracy the relative frequency of intestinal obstruction after operations on the uterus and its appendages; nevertheless the danger is real. The obstruction may be acute or chronic: it may occur within thirty hours of the operation or be delayed for months or years. The causes may be arranged under five headings:—
1. Adhesions to the abdominal wound.
2. Adhesions to the pedicle, stump, or a raw surface in the pelvis.
3. Strangulation around an adventitious band.
4. Obstruction due to an overlooked cancer in the colon.
5. Strangulation in a sac formed by a yielding cicatrix.
The form of intestinal obstruction with which we are most concerned here arises shortly after the operation and in the course of convalescence; it may be caused by adhesions to the abdominal incision, the pedicles, raw surfaces in the pelvis left after the removal of adherent cysts and tumours, and the cervical stump of a subtotal hysterectomy.
The subject is one of importance, for the complication is fairly common in the practice of some surgeons, and is one which it is very necessary to recognize, for, unless measures of relief are undertaken promptly, the patient surely dies.
From a careful study of the matter I have come to the conclusion that acute intestinal obstruction is more frequent after ovariotomy than after hysterectomy, and this is due to the fact that the stump or pedicle left after the removal of an ovarian tumour lies higher in the pelvis, and in closer relation to ileum and jejunum, than the cervical stump left after the removal of the uterus. This view also receives support from the fact that acute intestinal obstruction following hysterectomy is more frequent in the practice of those surgeons who perform subtotal hysterectomy improperly, and leave a large piece of the neck of the uterus sticking up like a median post in the floor of the pelvis. As far as I can judge from the scanty records relating to this complication after hysterectomy, it is the sigmoid flexure of the colon which is most commonly adherent to the cervical stump. The best way of avoiding this accident is to remove the supravaginal cervix so freely that, when the peritoneum is closed over the incision in the floor of the pelvis, there is nothing visible except a narrow thin line of suture at the base of the bladder.
The only rational method of treating acute intestinal obstruction following operations in the pelvis, is to promptly reopen the abdomen and set free the adherent coil of gut. Operations of this kind after hysterectomy are more often successful than when they are a sequel to ovariotomy, and this is, I think, due to the fact already mentioned, that when intestinal obstruction follows ovariotomy or oöphorectomy, the obstruction arises in the small intestine and is usually very acute and more dangerous; whereas after hysterectomy the obstruction affects, as a rule, the sigmoid flexure of the colon, and though it may be fairly acute, is not nearly so dangerous, and gives far better results to operative treatment.
Perforating ulcer of the stomach and small intestine. A rare cause of death after ovariotomy or hysterectomy is a perforating ulcer of the stomach or jejunum. Since 1887 I have seen three cases. In each instance the patient died from septic peritonitis. Rosthorn lost a patient from perforating ulcer of the stomach after hysterectomy. Olshausen states that he has seen at least four examples of this accident.2
Injuries to the bladder. This viscus has been injured in a variety of ways during operations on the pelvic organs. An overfull bladder has been mistaken for an ovarian cyst and been punctured with a trocar before the mistake was discovered. When tumours are impacted in the pelvis the bladder is often pushed up into the hypogastrium; this happens with bilateral ovarian tumours, incarcerated fibroids, and especially with large cervix fibroids. When the bladder is pushed up, care should be exercised in making the abdominal incision, or it will be cut. Punctures and incisions in the bladder should be immediately closed with sutures of fine silk.
The bladder is liable to be injured in the performance of subtotal and total hysterectomy, especially in the latter operation when separating it from the neck of the uterus. In the subtotal operation the risk arises chiefly in suturing the peritoneal flaps over the cervical stump, for the bladder is liable to be punctured with the needle as it lies close to the anterior flap.
Injuries to the ureter. Since the vulgarization of hysterectomy, injuries of the ureters have become common; nearly all are inflicted in cases where the neck of the uterus is removed, as in total abdominal hysterectomy, and in vaginal hysterectomy, because the vesical segments of these ducts come into close relationship with it.
British surgical and gynæcological periodical literature contains very little that concerns ureteral injuries, but it is only necessary to look into the pages of the Zentralblatt für Gynäkologie to find ample evidence that the integrity of the ureters is frequently sacrificed to modern pelvic surgery.
Blau published statistics from Chrobak’s Klinik in Vienna showing that in the interval January, 1900, to January, 1902, the ureters were injured fifteen times. In total hysterectomy seven times; in the course of ovariotomy on three occasions.
Sampson stated that from August, 1889, to January, 1904, the uterus was removed 156 times for cancer of its neck at the Johns Hopkins Hospital, Baltimore, and the ureters were injured nineteen times. The injuries were of various kinds, such as ‘ligating, clamping, cauterizing, cutting.’
In abdominal hysterectomy for fibroids the risk of injuring a ureter is not great. Thus Deaver writes that in the course of 250 abdominal hysterectomies he injured the ureter once, but the accident entailed the death of the patient.
I have performed hysterectomy on 1,000 occasions and injured the ureter once; my patient had a narrow escape for life and lost a kidney.
I have been present on five occasions when a ureter was injured. Four of the operations were for the removal of the uterus on account of fibroids, and one was an ovariotomy. Four of the patients died.
The injuries to which the ureters are liable in the course of hysterectomy are as follows:—
1. One or both ureters have been included in the ligatures applied to the uterine arteries.
2. One or both ureters have been cut or completely divided with scissors, or knife, in removal of the uterus.
3. A segment of a ureter 7 centimetres in length has been accidentally exsected.
4. One or both ureters have been compressed by clamps applied to restrain bleeding in the course of vaginal hysterectomy, and subsequently sloughed.
5. Ureters exposed in the course of ‘radical’ operations for cancer of the neck of the uterus often slough.
6. A ureter is sometimes transfixed by a needle and thread when sewing the layers of the broad ligament together in the course of a subtotal hysterectomy.
The most dangerous injury to the ureters occurs in the course of a subtotal hysterectomy, especially if it is not recognized at the time of the operation. In such circumstances the urine will slowly leak into the connective tissue of the broad ligament and form an extravasation extending into the loin.
In some cases the fluid will leak directly into the pelvis, and a sinus will form in the abdominal wound and allow the urine to escape; this may be the first intimation that a ureter has been injured, whereas when a ureter has sustained damage in the course of a total abdominal or a vaginal hysterectomy, the leakage of urine along the vagina will quickly apprise the surgeon of the accident.
There is another form of injury to the ureter which should be mentioned. Occasionally a fibroid, but more often a cyst or tumour arising from the base of the broad ligament, will involve the corresponding ureter and carry it upwards in such a way that, when the layers of the broad ligament are reflected, the ureter will be found crossing the crown of the tumour like a strap. In such a case the pressure has usually exerted a banal influence on the kidney, and it is often in the condition known as sacculation. In a case under my own care in which I attempted to remove a malignant tumour of the broad ligament, and in which the ureter ran over its upper pole in this way, thinking it was an adhesion, traction was made upon it, and the ureter came away with a portion of the renal pelvis. At the post-mortem examination the kidney was merely a thin-walled sac with purulent contents.
In all cases in the course of an abdominal hysterectomy it is useful for the surgeon to inform himself of the condition of the kidneys. Whilst performing a subtotal hysterectomy, one of the fibroids burrowed deeply between the layers of the left broad ligament; when all the bleeding was checked, I looked carefully to determine that the ureter was safe, and found it kinked by the ligature applied to the corresponding uterine artery; it was at once removed. On palpating the kidneys I found the right kidney small, and shrunken, and useless. Fortunately the woman recovered.
The method of treating an injured ureter varies greatly and will depend not only on the extent of the damage, but also on the time at which it is recognized. For example, if the surgeon recognizes the injury in the course of the operation, he will be able to deal with it at once. This we may term immediate treatment. The more difficult cases are those in which the injury is unrecognized at the time of the operation and only becomes obvious in the course of convalescence; the treatment in such circumstances may be called secondary.
The primary treatment of an injury to a ureter in the course of a pelvic operation will depend in a large measure on the ability, judgment, and experience of the surgeon, as well as on the extent of the injury. For example, if the ureter be partially divided, the opening may be closed with sutures of thin silk; when the duct is completely divided, the cut ends may be invaginated, the upper into the lower, and retained in position by suture. When five or more centimetres of the ureter have been accidentally exsected, none of these methods is applicable; in such circumstances several plans have been tried. Of these the simplest is ligature of the proximal end with the hope of inducing atrophy of the kidney; in several recorded instances this has proved successful. The surgeon who adopts this method should satisfy himself that the patient has another kidney, and that it is, as far as he can ascertain at the time, healthy. Some surgeons who have divided a ureter have promptly removed the corresponding kidney; others have secured the proximal end in the upper angle of the abdominal incision and removed the kidney subsequently.
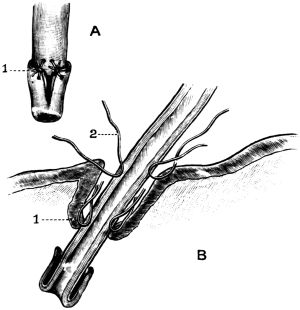 Fig. 27. The Relation of Parts after Ricard’s Operation of
Uretero-cysto-neostomy (after Lutaud). A, the proximal end of the ureter
with the mucous membrane reflected. B, the walls of the bladder, showing
the mode of fixing the ureter to its walls. 1 and 2, sutures.
Fig. 27. The Relation of Parts after Ricard’s Operation of
Uretero-cysto-neostomy (after Lutaud). A, the proximal end of the ureter
with the mucous membrane reflected. B, the walls of the bladder, showing
the mode of fixing the ureter to its walls. 1 and 2, sutures.
It has been suggested that when a portion of a ureter has been resected and the proximal end cannot be engrafted into the wall of the bladder, it should be turned into the cæcum or the sigmoid flexure, according to its position, and thus preserve to the patient the kidney and save her the distress of a urinary fistula. This method has not found favour with practical surgeons. The most promising procedure consists in engrafting the proximal end of the cut ureter into the bladder. This is known as uretero-cysto-neostomy, an operation which has been made the subject of a valuable thesis by Dr. Lutaud. This thesis appears to have been inspired as a result of two successful operations performed by Ricard. The principle of this method is as follows: —
The abdomen is opened by the usual median subumbilical incision, and the peritoneum covering the damaged duct is incised and its proximal end exposed: the mucous membrane of the ureter is reflected like a cuff. An opening is made in the bladder wall in a situation convenient for making the junction, and two centimetres of the ureter are allowed to project freely into the vesical cavity, ‘à la façon d’un battant de cloche.’ The ureter is secured by sutures to the vesical mucous membrane, and to the muscular coat of the bladder. The sutures should be of thin catgut and must not perforate the bladder or the ureteral walls. The bladder itself near the junction should be attached by sutures to the adjacent peritoneum to prevent dragging (Fig. 27).
Lutaud significantly points out that we know little of the subsequent fate of ureters which have been engrafted into the bladder. The immediate results have been successful, but there is good reason to believe that when a ureter has been engrafted into the bladder, its walls become sclerosed by a chronic ureteritis, and its lumen is gradually stenosed. These changes take place slowly and cause little or no discomfort in connexion with the kidney or the bladder, so that they pass unnoticed.
If the opinion expressed by Lutaud, that the ureter becomes stenosed after uretero-cysto-neostomy, is found to be a constant, or even a frequent, sequel to the transplantation of a ureter into the bladder, it will cause surgeons to be careful, and not follow too literally the advice given by some writers to the effect that in performing the ‘radical operation’ for cancer of the cervix, if the ureters are implicated these ducts may be divided and their proximal ends engrafted into the bladder.
Lockyer, in removing a burrowing fibroid, wounded the bladder and divided the right ureter; he sutured the vesical incision and removed the right kidney. During the twenty-four hours following the operation there was anuria. The abdomen was reopened and then it was found that the left ureter had also been divided. The proximal end of this ureter was engrafted into the bladder through the wound which had been already sutured. Convalescence was disturbed by a urinary fistula. The woman recovered and reported herself in good health three years later.
It has happened that after nephrectomy for the cure of a ureteral fistula, the sequel of a ‘radical operation’, the remaining ureter became thoroughly blocked by recurrent growth and the patient died from anuria.
In the cases where the injury to a ureter has been overlooked in the course of the operation many difficulties arise before the true conditions are appreciated. In some instances they soon become obvious; for example, Purcell in 1898 performed an abdominal hysterectomy, next day the patient had complete anuria. The abdomen was reopened fifty-eight hours later; a distended ureter was easily recognized behind the ligatures applied to the right and left uterine artery respectively. The ligatures were removed, the swelling quickly subsided, and urine reached the bladder. The woman recovered.
When a ureter is injured in the performance of total hysterectomy, urine escapes by the vagina, and at first there may be some doubt whether the leak is due to an injury to the bladder or to the ureter. In such conditions the quantity of urine voided from the bladder is compared with that which escapes from the vagina; if the quantities are equal, or nearly equal, the leak is in a ureter. A more reliable method is to inject a solution of methylene blue into the bladder through the urethra. If the coloured fluid escapes from the vagina, the leak is in the bladder; if not, it is in the ureter. When a vaginal leakage occurs a few days after a vaginal hysterectomy, it is probably due to necrosis and sloughing of a ureter, or the duct may have been included in a ligature which has separated by sloughing.
Noble, in 1902, published an interesting series of injuries to the ureter. One of these is of great value, because it proves that a ureter may be accidentally ligatured and give rise to no symptoms.
A woman of thirty-three years of age was submitted to vaginal hysterectomy for cancer of the neck of the uterus, complicated with pregnancy. She died four days after the operation, and at the post-mortem examination the left ureter was found occluded with a ligature. The ureter and pelvis of the kidney were distended with urine.
The urine voided during the four days amounted on the first day to 480 c.c. (16 oz.); second day, 780 c.c. (26 oz.); third day, 1,440 c.c. (48 oz.); fourth day, 960 c.c. (32 oz.). These quantities would lull suspicion in regard to any patient, but the facts of the case are sufficient to raise suspicions of another kind, namely, that it is possible and probable that a ureter has been ligatured in the course of an operation, and the patient has recovered without any one having any suspicion that such an accident has happened.
As soon as the surgeon clearly establishes the existence of a ureteral fistula he is beset with the necessity of deciding which duct is the seat of damage. Some years ago, when it was the practice to remove the kidney for a persistent ureteral fistula, the decision involved the surgeon in a grave responsibility, for the removal of the wrong kidney could only be regarded as a catastrophe for the patient. Morris has recorded a case in which this actually happened. A woman had total hysterectomy performed for a cervix fibroid by a gynæcologist; in the course of the convalescence a ureteral fistula was recognized, and as this failed to close spontaneously, a surgical colleague performed nephrectomy, and next day found to his chagrin that he had removed the kidney belonging to the uninjured ureter. Serious accidents of this kind are less likely to happen now, because the surgeon can avail himself of the cystoscope and ureteral catheter; with these instruments it is possible, not only to decide with certainty which ureter is injured, but also to determine the position and extent of the damage. See also Vol. III.
It is important to remember that every ureteral fistula does not require an operation. It is always advisable, when it has been clearly established that a woman has a leaking ureter, to wait a little, certainly six weeks, for many fistulæ of this kind will gradually close. In describing such a case, Jonas draws attention to a cystoscopic sign of some value. He performed a total hysterectomy for fibroids, and on the tenth day the nurse reported the escape of urine by the vagina. The daily output of urine from the bladder, which had averaged 50 ounces, fell to 25 ounces. On cystoscopic examination, urine could be seen issuing from the right ureteral orifice; at first the left orifice could not be seen, but on careful watching a movement was detected similar to the contraction of a ureter discharging urine, but no fluid came from the opening. This is known as leergehen (empty contraction), and it indicates that there is a lateral opening, but not complete interruption in the continuity of the ureter. Such a case should have an opportunity of healing spontaneously. This happened in Jonas’s patient.
Weibel states that a ureteral fistula due to necrosis after a radical operation for cancer of the uterus usually occurs in the second week. The earliest day is the seventh, and the latest the eighteenth day after operation. The majority of these fistulæ heal in from three to twelve weeks. If a fistula persist for more than three months spontaneous healing is not to be expected. A ureteral fistula is a serious matter for the patient. Blacker has had three cases after total hysterectomy. In one the kidney was removed on account of septic changes. The second had an attack of suppression of urine lasting twenty-four hours; it passed off, the patient recovered and the fistula healed. The third died eight weeks after the hysterectomy with symptoms of pyæmia; a small abscess had formed near the site of the fistula.
The fate of ligatures. When a ligature is satisfactorily applied to a pedicle the tissue on the distal side of the ligature is isolated from the circulation. The fate of this tissue and of the ligature has been the subject of much speculation.
It is a matter of common observation that when animal tissues are cut off from the circulation, they atrophy; but if pathogenic micro-organisms gain access to such parts, suppuration ensues. In due course, through the activity of the living cells, the dead tissues are detached from the living, a process termed sloughing.
When a piece of healthy tissue is removed from the body and immersed in a sterile solution, and absolutely isolated from the atmosphere, decomposition is indefinitely postponed, but as soon as unsterilized air is allowed access to it, putrefactive changes ensue. The pedicle after ovariotomy is in an air-tight chamber, and if the tissues included by the ligature are healthy, and the silk employed for the purpose is absolutely aseptic, this pedicle, when returned into the abdomen, resembles the piece of tissue isolated from contact with the atmosphere. No septic changes occur, but aggressive leucocytes attack the silk and may, in course of time, effect its removal, even the knots. For this desirable result three conditions require to be fulfilled: (1) the ligatured tissue must be aseptic; (2) the ligature should be absolutely sterile; and (3) air or intestinal contents must be excluded.
These conditions may be prevented in many ways. The tissues included in the ligature are not always free from infective organisms, especially the Fallopian tube, which is usually included in the ligature, and this structure, especially in cases where oöphorectomy is performed for inflammatory diseases, often contains septic microbes; this endangers the ligature and leads to the formation of pus, with its complications, sloughing of the pedicle and abscess. The tissues may be healthy and aseptic, but the ligature may have been imperfectly sterilized, or become contaminated by assistants, or even by the hands of the surgeon during its application.
The operation may have been conducted aseptically and the tissues be healthy, but the ligature becomes infected by the admission of air as a result of drainage, or implication of the bowel or bladder.
I made a careful study of the fate of silk sutures employed in pelvic surgery extending over many years, and came to the conclusion that, even under favourable conditions, silk ligatures disappear very slowly. The silk used to secure an ovarian pedicle may, in very favourable circumstances, disappear in twelve months, but the knots require nearly double that time. The piece of silk which encircles the Fallopian tube is apt to behave in a curious way; in 1898 I removed an ovarian cyst the size of a fist, and tied its slender pedicle with thin silk. Although the recovery was uneventful, the patient complained during many weeks of cramp-like pains on the side from which the cyst was removed. These pains gradually subsided, and ten months later, during menstruation, the patient noticed on the napkin a tiny loop of silk, which she saved. This was the loop of silk which secured the Fallopian tube; it had ulcerated into the tube and been conducted into the uterus and escaped. I have since had a like condition, the loop making its appearance three weeks after an ovariotomy. It has been established by experiments on the long uterine cornu of rabbits, that an encircling ligature will ulcerate through, leaving the lumen of the cornu intact. Clinical observations regarding ligatures applied to Fallopian tubes in the performance of Cæsarean section for the purpose of preventing pregnancy prove that this is a useless measure (see p. 71), for these tubes in many instances have recovered their patency, and pregnancy has recurred. It is a fair inference that the ligature ulcerates into the lumen of the tube, which then heals behind it, without stricture of the canal. A similar condition of things sometimes arises after Cæsarean section, especially when the uterine incision is closed by two layers of sutures. Those sutures which involve the endometrium will ulcerate into the uterine cavity and cause irregular slight losses of blood until they escape.
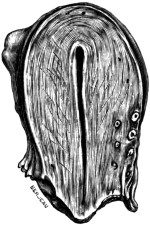 Fig. 28. A Uterus in Sagittal Section. Showing silk ligatures which had
been introduced in the operation of Cæsarean section four years
previously. (Museum, Royal College of Surgeons.) Full size.
Fig. 28. A Uterus in Sagittal Section. Showing silk ligatures which had
been introduced in the operation of Cæsarean section four years
previously. (Museum, Royal College of Surgeons.) Full size.
It is important to emphasize the fact that silk sutures in uterine tissue will, in some instances, remain unabsorbed for many years. A patient who had been submitted to Cæsarean section in 1903 came under my care four years afterwards for the removal of the tumour which caused obstruction; the sutures used to close the uterine incision were visible, and a microscopic examination showed that each silk suture was enclosed in a fibrous tissue sheath (Fig. 28).
The fact that silk sutures will resist absorption for such a long period has an important practical bearing, because so long as pathogenic micro-organisms are denied access they remain inert, but if any septic condition arises in their neighbourhood, and these sutures become involved, they will give rise to abscesses and sinuses as surely as if they had been buried but a few days.
Patients often suffer great distress and annoyance on account of abscesses and sinuses due to septic ligatures, and a sinus will persist as long as the ligature remains. Abscesses and sinuses resulting from troublesome ligatures may escape in many directions; the most common spot is at the lower angle of the abdominal incision; the rectum is another channel of escape, and also the bladder. When a ligature makes its way into the bladder it will set up cystitis and serve as a nucleus for a vesical calculus. In an unusual case recorded by Edebohls, double oöphorectomy was performed for uterine fibroids; a year later the ligature on the left side escaped through the vagina; six months later he performed abdominal hysterectomy. The vermiform appendix was adherent to the stump on the right side; it was removed, and a silk ligature tied in a complicated knot was found in it, making its way towards the cæcum.
On one occasion a woman, who had been submitted to subtotal hysterectomy in the Antipodes, suffered from frequent micturition and fœtid urine; she came under my care. On dilating the urethra, it was found that the cervical stump had ulcerated through the posterior wall of the bladder and projected freely into the vesical cavity, bristling with thick silk ligatures encrusted with phosphatic deposit. The ligatures were removed, the urine soon became acid, and the vesical discomfort quickly subsided, in spite of the anomalous position of the cervical stump.
Until surgeons fully realized the importance of thoroughly sterilizing the silk employed for the pedicles in ovariotomy, it was quite common for the silk loops to ulcerate through the bladder wall and set up cystitis.
Many cases have been reported in which a loop of silk, effecting an entrance into the bladder in this fashion, has formed the nucleus of a phosphatic calculus.
Post-operative kraurosis. In a small proportion of patients (perhaps not more than one per cent.) who have undergone bilateral ovariotomy, oöphorectomy, or hysterectomy, the vulva undergoes the peculiar atrophic changes which are characteristic of the condition known as kraurosis vulvæ. This change, so far as my observations go, is chiefly seen in patients who have been submitted to these operations after the fortieth year of life. The cause of these changes is unknown. The condition is troublesome and inconvenient in married women, but spinsters rarely complain of it. Post-operative kraurosis is as rebellious to treatment, and its causation as inexplicable, as kraurosis occurring independently of operation.
The cicatrix. Although the employment of buried sutures has made abdominal incisions more secure in the process of healing, and renders them firmer after union, and thus reduces the chances of a yielding scar, and saves the patient the inconvenience of an abdominal hernia or the annoyance of wearing an abdominal belt, it renders the patient liable to another discomfort, namely, stitch-abscess. This complication arises from a variety of causes—for example, imperfect sterilization of the suture material, or of the patient’s skin preceding the operation. The sutures may be soiled by the hands of nurses and assistants, or the fingers of the surgeon. All these things may be safeguarded, but the operation may have been required for the removal of infected cysts, or pelvic peritonitis: in these cases it is wise not to bury sutures.
Troublesome buried sutures should be removed. In many instances this is easy of accomplishment, and in others it requires patience and often perseverance, even when the patient is under an anæsthetic. The simplest implement for removing a buried suture is a crochet-hook.
The disadvantage of stitch-abscesses, apart from the inconvenience they cause patients during their convalescence, is that they often cause the scar to yield at that spot, and necessitate the wearing of an abdominal belt. If the hernia is of small extent, and especially when it is situated near the lower angle of the scar, it is difficult to fit a belt which will restrain it without the use of perineal bands or straps. In such cases a truss, on the principle of those employed for inguinal hernia, is more satisfactory than a belt.
Occasionally a scar forms a raised hard red keloid band, and causes some anxiety to the patient. These keloid scars shrink and whiten in the course of a year or eighteen months.
Cancer of the cicatrix. Several cases have been recorded in which, after the removal of an ovarian adenoma, a new growth, described as ‘cancer of the cicatrix’, has formed in the scar. These growths are probably due to the soiling of the wound at the time of operation with epithelial fragments from the tumours.
After abdominal hysterectomy for cancer of the body of the uterus, or its cervix, the abdominal wound may become infected with this disease, and in cases where exploratory cœliotomy has been performed for diffuse cancerous disease of the peritoneum the cicatrix is liable to become permeated by malignant disease also.
Baldy, J. M. The Mortality in Operations for Fibroid Tumour of the Uterus. Trans. Am. Gynæcological Association, 1905, xxx. 450.
Bartlett, W., and Thompson, R. L. Occluding Pulmonary Embolism. Annals of Surgery, 1908, xlvii. 717.
Blacker, G. F. Lancet, 1909, i. 395.
Bland-Sutton, J. Hunterian Lecture on Thrombosis and Embolism after Operations on the Female Pelvic Organs. Lancet, 1909, i. 147.
Blau, A. Ueber die in der Klinik Chrobak bei gynäkologischen Operationen beobachteten Nebenverletzungen. Beiträge f. Geb. u. Gyn., 1903, Bd. vii. 53.
Bucknall, R. The Pathology and Prevention of Secondary Parotitis (with Literature). Med.-Chir. Trans., 1905, lxxxviii. 1.
Deaver, J. B. Hysterectomy for Fibroids of the Uterus. Am. Journ. of Obstetrics, 1905, lii. 858–74.
Hastings, S. A Preliminary Note on Embolism in Surgical Cases. Archives of the Middlesex Hospital, 1907, xi. 78.
Jonas, E. Temporary Uretero-vaginal Fistula after Panhysterectomy for Fibroid of the Uterus. Am. Journ. of Obstetrics, 1907, lvi. 731.
Lequeu. Sur les parotidites post-opératoires. Bull. et Mém. de la Soc. de Chir. de Paris, 1907, T. xxxiii. 1044.
Lutaud, P. Sur un procédé d’urétéro-cysto-néostomie dans le traiment des fistules urétéro-vaginales et urétéro-cervicales. Paris, 1907.
Lyle, Ranken. A Series of Fifty Consecutive Abdominal Sections. Journal of the British Gynæcological Society, 1906–7, xxii. 120.
Mallet, G. H. Am. Journ. of Obstetrics, 1905, li. 516.
Morris, H. Lectures on the Surgery of the Kidney. British Medical Journal, 1898, i. 1039.
Noble, C. P. Clinical Report upon Ureteral Surgery. American Medicine, 1902, iv. 501.
—— Myomectomy. New York Medical Journal, 1906, lxxxviii. 1008.
Olshausen, R. Veit’s Handbuch der Gynäkologie, 1907, 2nd Ed., Bd. i. 715.
Purcell, F. A. The Risks to the Ureters when performing Hysterectomy, &c. Journ. Brit. Gyn. Soc., 1898–9, xiv. 174.
Robinson, B. Sudden Death, especially from Embolism, following Surgical Intervention. Medical Record, 1905, lvii. 47.
Spencer, H. R. Discussion at Exeter on Uterine Fibroids, &c. British Medical Journal, 1907, ii. 452.
Tebbs, B. N. Symptomatic Parotitis. Med.-Chir. Trans., 1905, lxxxviii. 35.
Trendelenburg, F. Zur Herzchirurgie. Zentralbl. für Chir., 1907, No. 44, 1302.
—— Ueber die chirurgische Behandlung der puerperalen Pyämie. Münchener Med. Wochenschr., 1907, xxxiv. 1302.
Weibel, W. Das Verhalten der Ureteren nach der erweiterten abdominalen Operation des Uteruskarzinoms. Zeitsch. f. Geb. u. Gyn., 1908, lxii. 184.
In operations upon the perineum and vagina, the same scrupulous precautions against sepsis should be taken as in abdominal section. Before proceeding to practical details, it will be useful to consider a few points regarding the distribution of bacteria in these parts. Not only the ordinary bacteria of the skin, but also those from the rectum, and, under certain conditions, from the urine and the vaginal secretion abound on the perineal and vulval surfaces. The healthy virgin vagina may be considered free from pathogenic organisms, harbouring only the harmless vaginal bacillus of Döderlein. After sexual congress the vagina contains pathogenic organisms, and in conditions such as carcinoma of the cervix and body of the uterus, and in all forms of vaginitis, many varieties of bacteria are present in great numbers.
The normal uterus is germ-free; in fact the external os uteri may be said to divide the bacteria-free from the bacteria-containing area of the genital canal. But in carcinoma and in the various forms of septic endometritis, the uterus not only contains many pathogenic bacteria, but acts also as a continual source of infection to the vagina and external genital organs. It follows, therefore, that this area may be exceedingly difficult to render sterile, and in certain conditions this is indeed impossible. None the less, every effort should be made to attain this object; for even if the organisms cannot be entirely removed, yet their numbers can be considerably reduced, and it must be remembered that the action of septic organisms is, to a great extent, directly proportionate to their numbers.
The same general principles apply to the preparation of patients for operations on the perineum and vagina as for operations on other parts of the body. Very particular attention, however, must be paid to the bowels; nothing is more prejudicial to the success of an operation, or more annoying to the operator, than to have the area of operation soiled by an escape of fæcal matter from an imperfectly emptied lower bowel. The aperient should be given at least 24 hours before the time of operation. A copious soap-and-water enema should follow after the usual interval, and, an hour or two beforehand, the lower bowel should be thoroughly washed out with a gentle stream of warm water.
 Fig. 29. Patient prepared for Operation. In lithotomy position with
crutch applied, Auvard’s speculum inserted, and volsella attached to the anterior
lip of the cervix uteri. Kelly’s pad is omitted for sake of clearness. (From a
photograph.)
Fig. 29. Patient prepared for Operation. In lithotomy position with
crutch applied, Auvard’s speculum inserted, and volsella attached to the anterior
lip of the cervix uteri. Kelly’s pad is omitted for sake of clearness. (From a
photograph.)
The external genitals should be shaved, and washed with ethereal soap solution and hot water the day before the operation, then douched with a 1–2,000 solution of perchloride of mercury, and a compress, soaked in the same solution, laid over the vulva. After the enema has acted, and after the final wash-out, the washing and douching should be repeated and a fresh compress applied.
If there is any vaginal discharge, the vagina should be douched out three times a day for two or three days previous to the operation, with an antiseptic such as 1–4,000 perchloride of mercury, or 1% formalin. The healing of a perineal wound is considerably impaired if it be continually bathed in an unhealthy vaginal discharge.
When the patient is on the table and under the anæsthetic, the external parts should again receive a thorough final disinfection, and, in addition, the vagina should be thoroughly swabbed out with ethereal soap solution, by means of swabs on holders. A final douching with 1–2,000 perchloride of mercury completes the process.
In all cases of vaginal hysterectomy for carcinoma, particular attention must be paid to the preliminary disinfection of the vagina by means of douching for two or three days before the operation. The vagina is swarming with various kinds of bacteria, and by careful attention to these principles the risk of sepsis will be materially diminished.
After the above preparations have been carried out, the patient is anæsthetized and placed on the table in the lithotomy position, the legs being kept well apart and fixed by means of a crutch. The buttocks are brought well to the edge of the table, and a Kelly’s pad may be placed beneath them. The legs should be encased in sterilized towels or linen stockings, and towels placed on the hypogastrium (Fig. 29).
Under the term colporrhaphy (suture of the vagina) is included any operation in which denudation and subsequent suturing of one or both walls of the vagina is carried out. Anterior colporrhaphy includes the various operations devised for cystocele; posterior colporrhaphy, the procedures carried out for incomplete rupture of the perineum (colpo-perineorrhaphy), prolapse of the pelvic floor, and to produce narrowing of the vagina.
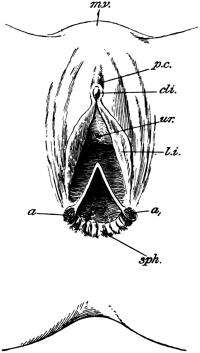 |
Fig. 30. Complete Laceration of the Perineum. (From a photograph.)
a, a'. Ends of torn sphincter ani. |
The appearance of the parts in this condition is quite characteristic (Fig. 30); the laceration of the recto-vaginal septum appears as a triangular space with its apex upwards, its sides equal, and its base formed by the retracted sphincter ani (Fig. 32). The separated ends of the sphincter are seen as two slightly depressed circular spots at the base of each side of the isosceles triangle a, a'. The object of the operation is to adapt these two ends, repair the recto-vaginal rent, and re-form the perineal body. There is often much irregular scar tissue about the opening, which may cause additional difficulty at the operation.
 Fig. 31. Long-handled sharp-pointed Scissors curved on the flat.
Fig. 31. Long-handled sharp-pointed Scissors curved on the flat.
The instruments necessary are six Spencer Wells artery forceps, long dissecting forceps with hooked points, a pair of sharp-pointed angular and a pair of sharp-pointed curved scissors (see Fig. 31), flat curved needles and Schauta’s needle-holder (Fig. 73).
The preparatory treatment consists in regular gentle purgation daily for a week, dieting, rest in bed for three days, and antiseptic vaginal douches of lysol (1 drachm to the quart).
Operation. The patient is placed in the dorsal position on a Kelly’s pad, and after the usual purification, denudation is commenced. The skin over the circular depressions corresponding to the ends of the severed sphincter (Fig. 30, a, a') is seized with the dissecting forceps and slightly raised. This portion of skin on either side is removed by means of the scissors, thus baring the ends of the sphincter and opening up the cellular tissue.
The point of one blade of the scissors is now buried in the cellular tissue at this bared spot on the operator’s right side, and is carried along the free torn edge of the recto-vaginal septum between the deep and superficial tissues until the apex of the laceration is reached. A similar incision is made on the opposite side.
The triangles of the vaginal flap are now raised by means of catch-forceps and the scissors passed carefully into the cellular tissue, and the recto-vaginal septum is split transversely, producing a raw surface somewhat the shape of a butterfly in outline (Fig. 33). A median extension of the denudation is made in an upward direction for another inch in length to form a supporting column. This flap may, if the tissues are sufficiently redundant, be removed along the line running at its base. The raw surface should be swabbed over carefully, and any bleeding points secured by ligatures. Large venous sinuses are very often opened, and, should the bleeding recur after the adaptation of the flaps, the operation will inevitably fail.
Closure of the recto-vaginal rent is first carried out by interrupted sutures, as is seen in the semi-diagrammatic drawing (Fig. 32). The threaded needle in a holder is passed from the rectal side of the flap through the flap on to the raw surface, then over the rent on to the raw surface of the other side; it finally finds its exit again on the rectal side of the flap. Four or more sutures may be passed in this way, a final one bringing the cut ends of the sphincter ani together. Each suture should be tied and the ends cut short before the next one is inserted, and the knots will lie just beneath the mucous membrane of the rectum.
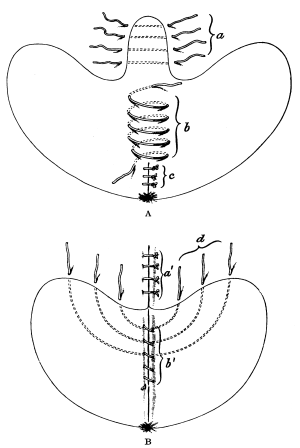 Fig. 33. Complete Laceration of the Perineum. In A the ‘butterfly’
surface has been denuded and the recto-vaginal rent repaired (c).
Fig. 33. Complete Laceration of the Perineum. In A the ‘butterfly’
surface has been denuded and the recto-vaginal rent repaired (c).
a. Sutures passed through the sustaining column, but not tied.
b. The ‘buried’ spiral suture passed but not tied.
In B is shown the oval raw surface left to be brought together by sutures (d) after the buried suture (b') has been tied. (Diagrammatic.)
We have now a large butterfly raw surface to deal with. The extension corresponding to the head is first of all dealt with by four or more separate sutures (Fig. 33, a). The large raw surface is now reduced in size by the passage of a deeply buried suture (Fig. 33, b); those used in the preceding manœuvres are best of silk. The buried suture should be catgut, and is passed in a spiral direction, as is seen in the diagram; the area of the raw surface is very much reduced by it (Fig. 33, b').
The parts to be brought together will now present the appearance shown in Fig. 33, B, and they are approximated by means of silk sutures, which are entered on the skin surface on one side, passed beneath the raw surface, and made to emerge on the skin surface on the opposite side. Four to six of these may be inserted.
Great care must be taken to see that no bleeding points are left unsecured, and a current of hot 1 in 4,000 perchloride solution should be allowed to play over the surface, after which the sutures are tied. Each suture should be left about an inch and a half long in order to facilitate removal later on. A gauze drain should be passed into the vagina and an antiseptic gauze pad placed over the perineum.
After-treatment. The patient’s knees should be tied together, the urine drawn off by a catheter every six hours for the first 48 hours, and the wound kept as dry as possible. Throbbing and pain in the perineum with slight rise of temperature are generally indicative of suppuration taking place either between the flaps or along the sutures. A smart purge should be given on the morning of the third day and daily afterwards. If there are any scybala left in the rectum it is better to inject a little warm olive oil into it through a catheter before the bowels are expected to act.
The patient should be allowed to get up on the twenty-first day. There should be proper control of flatus and motions from the date of operation.
The objects of this operation are twofold: first, to secure the torn ends of the levator ani to the lateral vaginal sulcus and perineum; and, secondly, to draw up or lift the pelvic floor, which is more or less depressed.
 |
Fig. 34. Laceration of the Pelvic Floor.
The double triangular surface has been denuded. (Semi-diagrammatic,
from a photograph.)
The sutures, 1–5, on the operator’s right side are passed and tied; those on the left are passed but not tied.
a. Anus c. Cervix h. Site of hymen. The arrow denotes the direction in which the sutures are passed. |
The patient is placed in the lithotomy position and a retractor is inserted in the anterior cul-de-sac in order to elevate the anterior vaginal wall: Fig. 34 shows the appearances then seen. The left forefinger or some gauze packing is placed in the rectum and a double triangular space is denuded by means of sharp-pointed scissors, the base line of the double triangle being formed by the hymen. Two tenacula are inserted as indicated in the drawing (Fig. 34, t, t). The mucous membrane is now removed from the M-shaped space, great care being taken to penetrate deeply into the lateral sulci. After all bleeding has been arrested in the usual manner, the sutures should be passed. On the left-hand side of the figure these are indicated as inserted, not tied, whereas on the right they are tied and cut. Subsequently the somewhat quadrilateral raw surface which is left is brought together by five deep sutures, and the operation is complete. A Y-shaped cicatrix will be the result.
Cases in which the perineum is apparently intact, but in which the sphincter is not united (Figs. 35, 36).
These are the cases in which a complete laceration of the perineum is apparently completely healed after operation, but the patient finds that she has incontinence both of flatus and fæces.
On inspection of Fig. 35 this will be well explained. The patient is lying on her back in the lithotomy position: a represents the sphincter which has been torn through; the two cut ends, b and c, are represented by two dark circular, somewhat depressed spots. The rectal orifice gapes; there is no sphincteric power present. The perineum anterior to the anus is firmly healed.
Operation. The most certain and effectual method in these cases is to split up the healed perineum antero-posteriorly and treat the case as one of complete laceration of the perineum (see p. 128). This has been carried out in the case represented in the illustration (Fig. 35), and Fig. 36 shows the result: the patient entirely recovered power over the sphincter ani and the sustaining power of the pelvic floor was much improved.
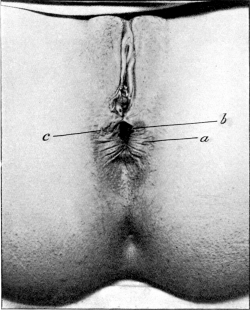 Fig. 35. Repair of a Lacerated Perineum, with Non-union of the Sphincter
Ani, before a Plastic Operation. (From a photograph.)
Fig. 35. Repair of a Lacerated Perineum, with Non-union of the Sphincter
Ani, before a Plastic Operation. (From a photograph.)
a. Ununited sphincter ani. |
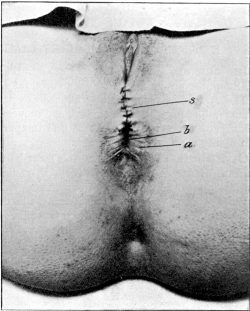 Fig. 36. Repair of a Laceration of the Perineum after a Plastic Operation. (From a photograph.)
Fig. 36. Repair of a Laceration of the Perineum after a Plastic Operation. (From a photograph.)
a. Repaired sphincter ani. |
Indications. A urethral caruncle is a bright red, tender tumour, usually on the posterior portion of the urethral orifice.
The symptoms requiring interference are pain on micturition, dyspareunia, bleeding and discomfort on movement, and, occasionally, retention of urine which is probably due to apprehension of pain rather than to any mechanical obstruction.
Operation. To be effectual this must be thorough, and may take the form of deep cauterization with a Paquelin’s cautery, or excision. The latter operation consists in excising a wedge-shaped piece of the posterior wall of the urethra containing the caruncle. Free bleeding will usually take place, which must be controlled by means of hæmostatic forceps. The edges of the wound are brought together by fine silk or catgut sutures, which must be passed completely through the raw surfaces to prevent recurrent hæmorrhage.
The after-treatment consists in keeping the wound as clean and dry as possible.
This is probably due to injury to the pelvic floor and the anterior fibres of the levator ani, producing a backward displacement of the urethra.
Operation. The operation recommended by Dudley consists of first denuding the vaginal mucous membrane over a horseshoe-shaped space between the clitoris and the urethral orifice and then drawing the urethra forward with sutures passed through the anterior portion of the orifice and inserted near the clitoris. It will then be seen that the urethra is carried forward nearly an inch. The raw edges are brought together in the usual manner by catgut or silk sutures.
The author’s experience of this operation has been unsatisfactory on the whole, and he has obtained better results by the wearing of a ring pessary.
For simple vesico-vaginal fistula. This condition is fortunately very rare at the present time. Many operations have been devised for this condition, but the original one recommended by Sims, with subsequent modifications, appears to the author to be most efficient and applicable to the large majority of varieties of this condition.
Preparatory treatment. The chief object is to obtain a healthy condition of the fistulous edges, which are nearly always inflamed, thickened, and covered by urinary deposits, usually of a phosphatic character. These are best removed by means of a soft sponge or cotton-wool, and the raw edges treated with a weak solution of nitrate of silver (gr. ij to the ounce). Hot vaginal douches of lysol solution (ʒj to a quart) should be given night and morning, and the parts freely smeared with vaseline to protect them from the action of the irritating urine. Any cicatricial tissue which may be present around the fistula should be treated by submucous division.
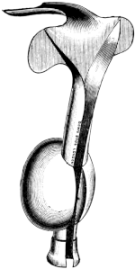 |
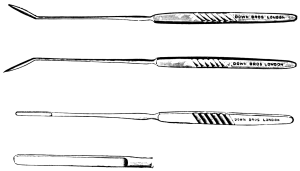 Fig. 38. Knives for freshening the Edges of a Vesico-vaginal Fistula.
Fig. 38. Knives for freshening the Edges of a Vesico-vaginal Fistula.
|
 Fig. 39. Toothed Forceps for use in Vesico-vaginal Fistula.
Fig. 39. Toothed Forceps for use in Vesico-vaginal Fistula.
|
Operation. The instruments necessary are: a Sims’s or Auvard’s (Fig. 37) speculum; two flat spatulæ; three long-handled knives (Fig. 38), one with a long haft and a short straight narrow blade, and the others with angular blades (right and left); two long-handled, sharp-pointed, curved scissors (right and left); an Emmett’s hook for making counter-pressure (Fig. 40); toothed forceps (Fig. 39) and tenaculum; six Spencer Wells’s forceps; Schauta’s needle-holder (Fig. 73) with short curved needles.
The patient is placed in the lithotomy position. A strip of mucous membrane is then removed from the whole of the vaginal edge of the fistula by means of an angular knife. In the original operation Sims (Fig. 41) made the surface oblique, but Simon (Fig. 42) considered the raw surface should be at right angles to the mucous membrane. The blade of the knife should not wound the vesical mucous membrane.
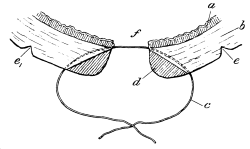 Fig. 41. Sims’s Operation for the Repair of a Vesico-vaginal Fistula.
Fig. 41. Sims’s Operation for the Repair of a Vesico-vaginal Fistula.
a. Bladder mucous membrane. |
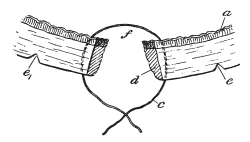 Fig. 42. Simon’s Operation for the Repair of a Vesico-vaginal
Fistula. Letters as in the preceding figure.
Fig. 42. Simon’s Operation for the Repair of a Vesico-vaginal
Fistula. Letters as in the preceding figure.
|
After the bleeding has ceased, the sutures, which may be of silk or catgut, are passed by means of the needle through the pared edge of the fistula on one side, passing across the fistula, and piercing the raw surface on the opposite side. The entry of the needle should be made about 1/4 – 1/3 of an inch from the raw edge (Fig. 44). Emmett’s hook, shaped like a button-hook, is useful to produce counter-pressure against the needle point. The sutures are tied, and milk is injected into the bladder to test the accuracy of the union.
As a rule, fistulæ are bounded by rather scanty and inelastic walls, owing to the presence of cicatricial tissue; it is therefore more advantageous not to remove any tissue in order to produce a raw surface, or as little as possible. To fulfil this condition, the method of dédoublement or flap-splitting, as practised by Walcher, may be carried out (Fig. 43, A, B, and C).
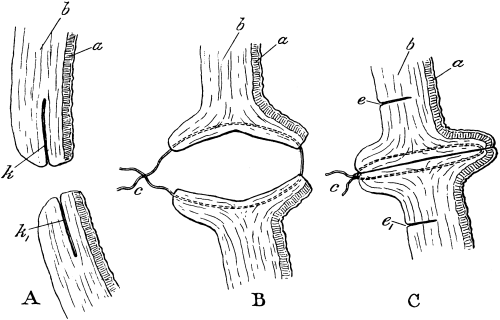 Fig. 43. Repair of a Vesico-vaginal Fistula by Dédoublement.
Fig. 43. Repair of a Vesico-vaginal Fistula by Dédoublement.
A. The flap-splitting stage.
B. The flaps separated and the suture passed.
C. Suture tied, approximating the flaps.
a. Bladder mucous membrane.
b. Vaginal wall.
c. Suture.
e, e'. Liberating incisions.
k, k'. Flap-splitting incisions.
In A the flap-splitting is seen in section (k, k'); in B the flaps have been everted towards the bladder and vagina respectively and the suture passed. In C this suture has been tied; liberating incisions, e, e', have been made on the vaginal surface to prevent tension in the wound.
The patient is placed, as before, in the lithotomy position, and the cervix is pulled down, while the edges of the fistula are kept steady by a volsella on either side. The margin of the orifice is then split all round to a depth of from a quarter to half an inch. Vesical and vaginal mucous membrane flaps are thus produced, giving a large raw surface without any loss of substance. The sutures are passed as shown in Fig. 43, C.
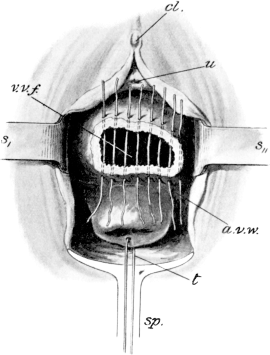 |
After-treatment. This is very simple: if the patient is able, she should pass water, either in the dorsal or genu-pectoral position, otherwise a catheter should be passed every six hours.
Modifications of this operation have been devised, more especially for the larger fistulæ: they will be briefly mentioned.
1. Repair by turning up vaginal flaps to form the base of the bladder is recommended by A. Martin of Berlin. He first frees the adherent edges of the fistula and then raises the flaps from the vaginal wall and brings them over the opening, suturing them carefully together. By this method the mucous membrane of the vagina forms the new lining to the bladder, and the exposed raw surface a new anterior vaginal wall. The edges of this latter denuded surface are united by sutures, as in the operation of colporrhaphy.
2. Closure of the fistula by detaching the bladder from the vagina and suturing it independently is described and practised by Mackenrodt.
The patient is placed in the lithotomy position, and the fistula is exposed: the cervix is drawn downwards and backwards by means of a wire loop or tenaculum, and the urethral prominence held with a pair of hooked forceps. An incision is then made in the median line extending across the fistula and through the vaginal walls down to the bladder, in this way exposing the entire base of the bladder. The edges of the fistula are then split so that the bladder and the vaginal walls are separated. The two vesical flaps are now carefully and separately sutured by catgut and the edges of the vaginal wound are brought together as much as possible: if necessary, the fundus of the uterus may be used to assist in closing the opening.
For vesico-utero-vaginal or juxta-cervical fistula. In this affection the cervix is involved, and it must therefore be carefully differentiated from the vesico-vaginal variety, in which the cervix is intact.
In operating upon such cases the chief difficulty will be found in denuding the surfaces necessary for the introduction of the sutures, owing to the density of the cicatricial tissues, which are always present. This is best overcome by drawing the cervix forcibly downwards and backwards and incising the anterior cul-de-sac; the bladder wall with its fistulous opening is then dissected off the anterior surface of the cervix and carefully sutured independently of the cervical laceration; the latter is treated by suture in the usual way (see p. 128). In the deeper forms of juxta-cervical fistula, the above technique is impossible, and suprapubic incision and suture of the bladder must be substituted.
This condition may be defined as an opening between the rectum and vagina through which flatus, or fæces, or both, may pass from the former into the latter; it is chiefly the result of an imperfect union subsequent to an operation for complete perineum laceration. It may also be caused by the rupture of a pelvic abscess or by the spread of primary malignant disease of the rectal wall.
Operation. If the sphincter ani is incompletely united, it will be found much the most satisfactory proceeding to divide the healed portions of the perineum and make a complete perineal laceration; this may then be treated as described above (see p. 128).
If, however, the sphincter is intact and serviceable the fistula should be pared and the edges brought together by silk sutures. It is not infrequently necessary to perform a temporary colostomy (see Vol. II) in order to divert the fæcal contents of the bowel during the process of healing.
In cystocele there is prolapse of the anterior vaginal wall and the corresponding area of the posterior bladder wall. Cystocele often complicates rectocele and prolapsus uteri, and operation upon it is often carried out in combination with colpo-perineorrhaphy.
Operation. The operation for the cure of this affection is very simple, and may be performed:—
(1) By denuding an oval space over the swelling and bringing the raw edges together.
(2) By Stoltz’s operation, which is really purse-string suture.
The instruments necessary are a bladder sound, two tenacula, sharp-pointed angular scissors, a needle-holder and fine silk.
(1) The parts are exposed with a Sims’s or Auvard’s speculum and a volsella, or silver wire is passed through the cervix, by means of which traction downwards and backwards may be exerted. The cystocele itself is fixed by tenacula, and, with the sound in the bladder, an oval incision is carried completely round the base of the cystocele. The whole area contained in this incision is denuded by knife or scissors, care being taken to avoid wounding the bladder mucous membrane.
Any bleeding having been controlled, a spiral buried suture, as in the operation for perineorrhaphy (see p. 128), is passed antero-posteriorly, thus reducing the size of the raw area and making a solid support in the median line. The raw edges are then brought together by sutures. The catheter should be passed every eight hours for three days, and then the patient should be allowed to micturate on her hands and knees.
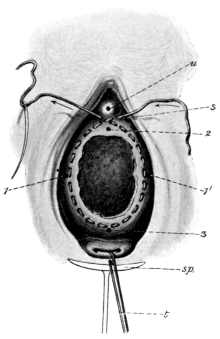 |
Fig. 45. Stoltz’s Operation for Cystocele. The oval surface has been
denuded and the circumferential suture passed but not tied.
1,1',2,3. The four points first selected as boundaries for denudation. |
(2) Stoltz’s operation. The instruments necessary are: a No. 8 male bladder sound; two tenacula; hooked forceps; sharp-pointed angular scissors, and a needle-holder (Schauta’s for preference).
The patient is placed in the lithotomy position and the parts are exposed by means of an Auvard’s speculum. A silver wire or tenaculum is passed through the posterior lip of the cervix, by means of which downward and backward traction may be exerted. Four points must be selected: two lateral (Fig. 45, 1, 1'), fixing the external boundaries of the surface to be denuded; one immediately behind the orifice of the urethra (2); and a fourth in front of the cervix (3). These four points should be capable of close approximation. They are carefully joined by curved incisions so that the area to be denuded is almost oval in shape. The bladder sound is now passed, and the mucous membrane of the vagina kept on the stretch by pressure on its point. The process of denudation should be carried out with a scalpel or pointed curved scissors. It will be found that bleeding rarely gives any trouble. The point of the needle threaded with silk is inserted on the operator’s right side of the urethral orifice and a little below it; it pierces the mucous membrane on the left side of the median line, and again appears upon the surface. By an in-and-out stitch all the way round the circle which has been pared, the point finally issues on the operator’s left side of the urethra and below it: by traction on these two ends the edges of the denuded surface are drawn together and the prolapsed bladder is sutured in its normal situation. A puckered cicatrix results. This method is valuable for prolapsus uteri when combined with the operation of posterior colporrhaphy.
The glands of Bartholin, or the vulvo-vaginal glands, are two racemose structures about the size of a pea, lodged between the layers of the triangular ligament, one on each side of the orifice of the vagina. Their ducts open a little in front of the fossa navicularis, on each side of the vaginal orifice, in the groove between the attached border of the hymen and the labium minus.
Removal of a cyst of Bartholin’s gland. These cysts really arise in the ducts rather than in the gland itself. The orifice of the main duct is very liable to become blocked from inflammation of the vulva, and leads to the formation of a single cyst varying in size from a cherry to an orange. Less common is the blocking of the secondary ducts, wherefrom a collection of small cysts results. The cyst forms a characteristic tense ovoid or pyriform swelling in the posterior third of the labium majus. The chief symptoms the patient complains of are discomfort in walking and pain on coitus.
Operation. The best procedure is complete excision of the cyst. A longitudinal incision is made over its cutaneous surface, and the cyst carefully dissected out, together with the gland itself: care must be taken not to perforate the vaginal mucous membrane stretched over the inner surface of the cyst. Brisk bleeding from vessels at the base of the cyst, usually follows from the cavity which contained the cyst and this must be carefully arrested, otherwise a large hæmatoma may result. The cavity is closed by five or six interrupted catgut sutures, passing deeply through its sides and floor, so as to ensure complete closure. A gauze drain may be inserted and retained for twenty-four hours.
The method of incising the cyst, swabbing its interior with undiluted carbolic acid, and packing it with gauze is not to be recommended, for cure is neither so rapid nor so certain as in excision.
Incision of an abscess of Bartholin’s gland. Abscesses arise by infection passing into the gland along the ducts, and are a very frequent accompaniment of gonorrhœa. The orifice of the duct can usually be seen red and prominent, and may exude pus if pressure be made over the abscess-sac. Sometimes the abscess bursts and spontaneous recovery may follow, but it is very liable to recur, for infection lurks among the smaller ducts and is carried to a fresh part of the gland, and the process may continue until the whole gland has been thus destroyed.
Operation. The abscess must be freely incised and all pockets and septa broken down. It is stuffed with iodoform gauze, which is changed daily, and the cavity is allowed to granulate up from the bottom. If the abscess recurs, or if it consists only of a small collection of pus surrounded by brawny œdema, the whole gland should be excised.
Occlusion of the hymen is the commonest form observed. The vagina becomes slowly distended with blood, forming an elastic pelvic swelling (hæmato-colpos) upon which the uterus is, so to speak, perched. Later in the course of the disease, this organ itself (hæmato-metra) and the Fallopian tubes (hæmato-salpinx) may become affected similarly.
Indications. In atresia of the hymen symptoms only commence after puberty; there is then congenital amenorrhœa with periodic pelvic pain and gradual formation of a pelvic swelling. On inspection the hymen is distended and the blood-tumour above it gives a bluish tint to its surface.
Operation. After administration of an anæsthetic, careful palpation of the tubes should be made per rectum: if they are distended it is better to open the abdomen, ligature and remove them; if not, the hymen should be incised by means of a crucial opening and the characteristic tarry fluid allowed to escape: no hypogastric pressure should be used.
Irrigation and packing with gauze may be resorted to as after-treatment, but are considered unnecessary by a large number of operators.
Atresia of the vagina may be congenital or acquired. In the latter case the condition results from contraction of adhesions developed from damage done during labour; or it may follow acute septic vaginitis, the introduction of acids or irritating materials to produce abortion, or as a sequel to typhoid fever.
Treatment is by slow dilatation with Hegar’s bougies over an extended period of time; relapse is common.
Indications. This is done for vaginismus due to a pathological spasm of the levator ani and resulting in more or less complete obstruction to coitus.
 Fig. 46. Sims’s Vaginal Rest.
Fig. 46. Sims’s Vaginal Rest.
Operation. Under an anæsthetic the vulval orifice should be thoroughly dilated by means of the thumbs, and for some days subse quently graduated Sims’s ‘vaginal rests’ (Fig. 46) should be inserted twice daily and worn for twenty minutes at a time. This treatment may be necessary for a fortnight or longer. In many cases of dyspareunia the cause will be found to be due to a thick, fleshy, and unruptured hymen or to tenderness about the remnants of that organ. Under these circumstances, exsection is the better plan to pursue. The hymen is seized with a pair of toothed forceps and removed with curved scissors along its entire base of attachment. Free bleeding often occurs from the raw surface, which must be controlled by ligatures. The two almost parallel cut edges must then be carefully brought together either by continuous or interrupted suture.
By colpotomy is meant making an opening into the peritoneal cavity through the vagina; the operation is known as anterior or posterior colpotomy, according to whether the opening is made through the anterior or posterior fornix.
Colpotomy has certain advantages over abdominal section. There is less interference with the peritoneum and intestines, and therefore less shock; if pus is present, there is less risk of infecting the general peritoneal cavity, and better drainage; there is no abdominal scar, and therefore no risk of hernia; lastly, there are certain pathological products which can be more easily reached by this route. The operation is difficult in a nullipara, where the vagina is narrow, and easier in a multipara, where the vagina is more capacious, and it is still easier if the cervix can be drawn down as far as the vaginal orifice.
A serious disadvantage is that, during the course of the operation, it may be found impossible to deal adequately with the conditions for which the operation is being performed; in the case of a tumour, for instance, its size, position, or the presence of adhesions may render it necessary to complete the operation by the abdominal route. Further, in more than one instance, the abdomen has had to be opened after the completion of the operation on account of bleeding, the source of which could not be dealt with by the vagina.
Therefore, before deciding upon the removal of a tumour by colpotomy, all the above points must be taken into consideration.
Indications. When the above conditions are fulfilled, colpotomy is suitable for:—
(i) The evacuation of collections of pus or blood in Douglas’s pouch.
(ii) The removal of fibro-myomata, ovarian tumours of small size, and early tubal pregnancies.
(iii) The drainage of collections of pus or the removal of the appendages in cases of acute inflammation where immediate operation is necessary.
(iv) Conservative operations upon the Fallopian tubes or ovaries.
(v) A preliminary to the performance of vaginal hysteropexy.
(vi) Those cases in which the patient’s general condition is unfavourable to the performance of exploration by the abdominal route.
Anterior colpotomy is more suitable for removing small tumours growing from the anterior wall of the uterus, or for conservative operations on the ovaries. Posterior colpotomy is more suitable for removing inflamed appendages, and for evacuating collections of pus or blood from Douglas’s pouch.
 Fig. 47. Pozzi’s Retractors.
Fig. 47. Pozzi’s Retractors.
Posterior colpotomy has been used for many years for the opening of abscesses and hæmatoceles in Douglas’s pouch. The anterior operation is of more recent date, and its relative advantages and disadvantages and the indications for its use have not yet been definitely agreed upon by the majority of gynæcologists. Taking all things into consideration, the disadvantages of colpotomy seem to outweigh its advantages, and, except for the evacuation or drainage of collections of blood or pus behind the uterus, the operation may be said to have few indications.
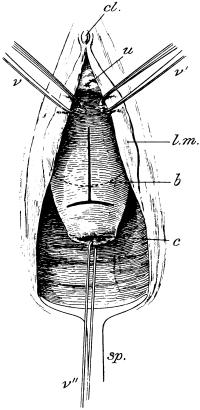 Fig. 48. Anterior Colpotomy.
Fig. 48. Anterior Colpotomy.
The patient is in the lithotomy position, the speculum is passed and the cervix pulled down by a tenaculum. The T-shaped incision has been made.
b. Outline of bladder.
c. Cervix.
cl. Clitoris.
l.m. Labium minus.
sp. Speculum.
u. Urethral orifice.
v,v',v''. Volsella.
Anterior colpotomy. A posterior Pozzi’s (Fig. 47) or Péan’s retractor is passed into the vagina, and the cervix is seized with a volsella and drawn downwards and backwards. A sound passed into the bladder defines its lower limit. A T-shaped incision is now made through the vaginal mucous membrane, the transverse portion just below the point to which the bladder has been found to extend (Fig. 48, b). This incision should pass completely through the vaginal mucous membrane, but no further, and should extend across the whole width of the anterior surface of the cervix. Some operators use a simple longitudinal or a transverse incision. The vaginal mucous membrane is now carefully pushed upwards with the pulp of the finger until the lower limit of the bladder is defined. Great help is gained at this stage by the use of the bladder sound. On pushing up the vaginal mucous membrane still further the peritoneum is reached, and is recognized by its white glistening appearance, and by the fact that its two opposed surfaces glide freely over one another under the finger. The next step is to open the peritoneum: it is picked up with catch-forceps, and a small transverse incision is made into it with a pair of scissors; the finger is passed through, and the incision is extended on either side, care being taken not to pass too far outwards for fear of injuring the ureters or uterine vessels.
After the peritoneum has been opened, the pelvic organs can be carefully examined with the fingers, and the purposes for which the operation has been undertaken can be proceeded with. The next step usually consists in drawing out the fundus of the uterus, by which much more room and much better access to the pelvic organs is gained. To accomplish this, the uterus is caught with a volsella in the middle line, as high up as possible, and drawn downwards and forwards. If necessary, a second volsella is applied above the first, and so on, until the uterus is delivered. A very complete examination of the appendages can now be made, for the tubes and ovaries can be drawn out of the wound and examined directly.
When the object of the operation has been attained, and all the blood has been carefully removed by swabs, the next and final step consists in closing the peritoneal and vaginal wounds. The uterus is replaced, and the peritoneal incision is closed by a single layer of catgut sutures; the vaginal incision is similarly dealt with. The vagina is cleared from blood-clot and gently irrigated with an antiseptic solution. A gauze plug is inserted lightly, and the patient is put back to bed. The catheter should be used every six or eight hours for the first twenty-four hours.
Posterior colpotomy. A posterior speculum is passed and the cervix drawn downwards and slightly forwards with a volsella. A transverse incision is then made through the vaginal mucous membrane at the junction of the posterior fornix with the cervix. This exposes the peritoneum more or less easily, and this structure is picked up with catch-forceps, and a transverse incision made into it with scissors; a finger is passed through this, and the incision is extended on either side. The pelvic organs can now be explored and the tubes and ovaries drawn down and examined. The peritoneal and vaginal incisions are then closed by separate layers of catgut sutures.
To open a collection of pus in Douglas’s pouch, the best method is to pass a pair of sinus-forceps, with the blades closed, into the most prominent part of the swelling. The blades are then opened and the forceps withdrawn. The finger passed into the abscess cavity gently breaks down any adhesions. The cavity is then irrigated with hot salt solution and a drainage tube inserted, which projects just outside the vulva: the lower end of the tube should be carefully packed around with cyanide gauze. The tube should be changed every day and the vagina douched with an antiseptic. Another method is to plunge a Martin’s trochar (Fig. 49) into any softened spot in the swelling and then withdraw the needle, leaving a blunt dilating forceps to extend the opening.
 Fig. 49. Martin’s Trochar for Pelvic Abscess.
Fig. 49. Martin’s Trochar for Pelvic Abscess.
In opening an abscess, the most stringent precautions against sepsis should be observed. The vagina must be most carefully prepared beforehand, by rubbing over with swabs and ethereal soap, and by a subsequent copious douche of 1 in 1,000 perchloride of mercury: otherwise continual reinfection of the abscess cavity occurs, and healing is much delayed.
Lateral colpotomy—Paravaginal section.
Indications. The object of the operation is to increase the amount of room in the vagina in certain cases of vaginal hysterectomy in elderly virgins, or in women who have a small vagina.
Operation. The same preliminaries are carried out as before. The incision is carried completely round the cervix at its junction with the vagina. The lateral margin of the vulva is then held tense, and an incision is made, beginning at the circumcervical incision running down the lateral vaginal wall, through the margin of the vulva and on to the skin externally, ending at a point midway between the perineum and the ischial tuberosity, i.e. about 1½ inches to the side, and in front of the perineum; the incision may be lateral only or bilateral. In sewing up, it is important to reunite the cut edges of the levator ani, or pelvic weakness will result.
This is an operation which is much less frequently resorted to than formerly, owing partly to the risks of sepsis attending its performance and partly to the greater perfection of the bimanual examination. Passing the uterine sound should always be looked upon as a surgical operation. The facts learnt by the use of the sound are: (1) the length and direction of the uterine cavity; (2) the condition of the endometrium: bleeding as a rule follows withdrawal in fibro-myomata and endometrial disease; (3) whether a fibroid growth is projecting into the uterine cavity, and if so, how much.
 Fig. 50. The Passage of the Uterine Sound. Introduction of
the point into the external os uteri.
Fig. 50. The Passage of the Uterine Sound. Introduction of
the point into the external os uteri.
|
 Fig. 51. The Passage of the Uterine Sound. Commencement
of the tour de maître.
Fig. 51. The Passage of the Uterine Sound. Commencement
of the tour de maître.
|
The sound may be passed in the dorsal position (Fig. 61), the cervix being held by a volsella and exposed by means of a posterior speculum, or in the left lateral position, the method usually adopted in the consulting room. In the latter the right index-finger is passed up to the anterior lip of the cervix, the sterilized sound is taken in the left hand with its concavity backwards and its bulbous end is slid gently along the palmar surface of the finger in the vagina until the os uteri externum is reached; through this it should be passed for about a quarter of an inch (Fig. 50). The instrument should now be steadied by the thumb and the two distal joints of the second finger of the right hand, and its subsequent movements controlled by the left (Fig. 51).
If the uterus is in a state of retroversion, the bulbous end will gradually enter the uterine cavity by pressing the handle of the sound forward and at the same time giving an upward and slightly backward impulse to its tip; the rough surface of the handle will be found to be looking towards the sacrum. Should the uterus be anteverted, the handle is held in the left hand as before and passed through an arc of a circle by raising the handle and turning it forward until it lies beneath the symphysis pubis, in the median line (tour de maître) (Fig. 52). The rough surface of the handle now looks anteriorly and the bulbous end is pressing against the internal os uteri; now bring back the handle directly to the perineum and it will glide into the uterine cavity (Fig. 53).
 Fig. 52. The Passage of the Uterine Sound. Completion of
the tour de maître.
Fig. 52. The Passage of the Uterine Sound. Completion of
the tour de maître.
|
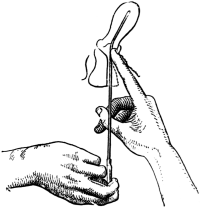 Fig. 53. The Passage of the Uterine Sound. Entry of the sound
into the uterine cavity.
Fig. 53. The Passage of the Uterine Sound. Entry of the sound
into the uterine cavity.
|
Difficulties to be met with will be: (1) An acutely anteflexed uterus; if traction is made on the cervix with a volsella the canal is straightened and the difficulty overcome. (2) Spasmodic contraction of the internal os uteri; this soon passes off with a little steady pressure. (3) A fibroid may project into the lumen of the canal. (4) Congenital or acquired stenosis of the external os uteri.
When there is a septic discharge from the vagina, the sound should be passed in the dorsal position and through a speculum.
Indications. Chronic inversion of the uterus, with severe hæmorrhage and bearing-down pain. The uterine fundus presents in the vagina and simulates a fibroid polypus in process of extrusion.
Operation. This is most likely to be successful if continuous pressure be brought to bear against the inverted fundus while an attempt is made simultaneously to dilate the contracted cervix.
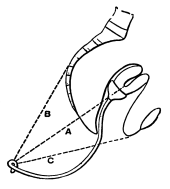 Fig. 54. Chronic Uterine Inversion. Aveling’s
repositor in place with elastic cords A, B, and C, in action.
Fig. 54. Chronic Uterine Inversion. Aveling’s
repositor in place with elastic cords A, B, and C, in action.
The patient is placed under an anæsthetic in the dorsal position and the whole hand is passed gradually into the vagina. The tips of the fingers and thumb should be pressed into the circular space at which the flexion of the walls of the body on the cervix has occurred. With the palm of the hand upward pressure is made, counter-pressure being exerted by the other hand over the lower hypogastrium. Reduction usually begins by a slight dimpling of the inverted fundus.
A more scientific method of exerting continuous pressure is by the application of Aveling’s sigmoid repositor and elastic cords (Fig. 54). This instrument consists of a vulcanite cup into which is secured a steel S-shaped rod terminating below in a loop. The cup is made of various sizes and should always be smaller than the inverted fundus over which it fits.
After it has been applied, the instrument is carefully packed round with gauze to keep it in place. Two elastic bands in front and two behind are fastened by one end to the steel loop and by the other end to an abdominal belt. By this means constant and direct pressure is obtained on the fundus uteri in the direction of the pelvic axis.
Pain is usual and must be relieved by morphine. The cup usually elevates the fundus and corrects the inversion in about twenty-four hours, but as much as three days has been occupied in the process.
The term ‘curetting’ is applied to the operation of scraping away the lining membrane of the uterus, either for the relief of some pathological condition or for diagnostic purposes.
The endometrium is not removed in its entirety by curetting, for the uterine glands dip down to a slight extent between the muscle fibres of the uterine wall. The endometrium is removed as far down as the muscular coat, and, consequently, those parts of the glands lying amongst the muscular fibres are left intact.
Indications. These may be divided into the cases in which the operation is (1) Remedial and (2) Diagnostic in nature.
The diseased states of the endometrium are many and their exact pathology is still under discussion. It is, therefore, more practical to consider the remedial indications for curetting from the point of view of symptoms.
(i) Uterine hæmorrhage is the chief symptom which calls for curetting. The causes of the hæmorrhage may be certain forms of endometritis. Thus hæmorrhage is a prominent symptom of the so-called ‘hypertrophic glandular endometritis’, a diffuse overgrowth or adenomatous condition of the endometrium, probably the after-result of a previous inflammation. There is one form which gives rise to specially profuse hæmorrhage—the ‘polypoid’ or ‘villous’ form, which arises usually in women over forty years of age.
The hæmorrhage from fibro-myoma of the uterus may require removal of the endometrium in order to relieve the bleeding temporarily at any rate. When milder measures fail, curetting is of great service in arresting the profuse menorrhagia which so often accompanies subinvolution of the uterus.
Certain cases in which the actual cause of the hæmorrhage is not evident are relieved by curetting; amongst these are such conditions as arterio-sclerosis of the uterine vessels.
(ii) A leucorrhœal discharge is another symptom for which curetting is sometimes indicated.
It may be called for when the endometrium is congested and œdematous from such conditions as displacements of the uterus and chronic subinvolution.
It is better not to curette for a purulent uterine discharge; extension of the infection may be caused and give rise to pyosalpinx.
(iii) Sterility. Curetting should follow dilatation, in the hope that the new endometrium formed may afford a better nidus for the ovum.
(iv) Frequent abortion in the early months. Curetting often cures this by removing the diseased endometrium.
(v) Inoperable carcinoma of the cervix. Removal of the redundant portions of the growth by the curette, followed by cauterization or other measures, relieves the hæmorrhage and foul discharge. Great caution must be exercised, lest the peritoneum or bladder be opened into by the curette and the sufferings of the patient thereby increased. Cells of the disease may also be pushed into the pelvic lymphatics; considerable febrile disturbance may also follow the operation. In this condition a blunt curette (Fig. 60, B) may be gently used; the same instrument is safest in abortion up to the eighth week of pregnancy; after this date it is better to use the fingers only.
Fragments removed by the curette are subjected to microscopical examination for diagnostic purposes. The various conditions which may have to be diagnosed are:—
1. Carcinoma of the body of the uterus.
2. Retained products of conception.
3. Tuberculosis of the endometrium.
4. Chorio-epithelioma malignum.
Operation. The following instruments are required: a volsella (Fig. 55); a self-retaining weighted speculum (Fig. 37); uterine dilators (Figs. 56, 57); a uterine sound; a Bozemann’s tube (Fig. 58); Budin’s celluloid catheter (Fig. 59); and one or other flushing curettes.
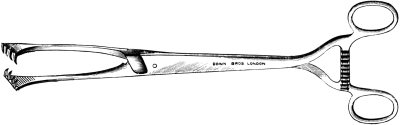 Fig. 55. Volsella for fixing the Cervix.
Fig. 55. Volsella for fixing the Cervix.
|
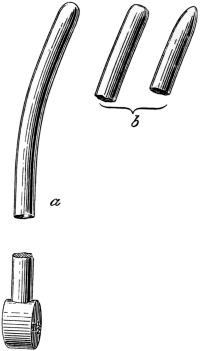 Fig. 57. Metal Bougies for dilatation of the Cervix.
Fig. 57. Metal Bougies for dilatation of the Cervix.
a. As used by the author. |
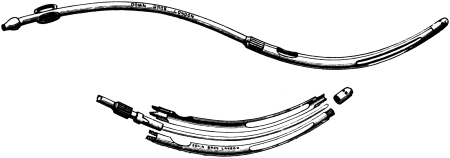 Fig. 58. Bozemann’s Double-channelled Tube.
Fig. 58. Bozemann’s Double-channelled Tube.
 Fig. 59. Budin’s Celluloid Catheter.
Fig. 59. Budin’s Celluloid Catheter.
There are many varieties of curettes, and each has its own adherents. The most generally useful is Murray’s sharp flushing curette, which has a groove for the recurrent flow (Fig. 60, A). There are many varieties of blunt curettes. The model depicted in Fig. 60, B, enables the operator to clear out the uterine cornua and is of the best shape.
The patient is placed in the lithotomy position and the various antiseptic precautions already described are carried out. A speculum is passed and the cervix is steadied by a volsella applied to the anterior lip.
The cervix is first dilated up to a suitable degree for the passage of the curette; up to No. 12 Hegar is usually sufficient. The curette is now taken and passed into the uterus. In performing the operation a definite plan should always be followed so as to ensure that no part of the uterine cavity is missed. The curette is passed up to the top of the fundus uteri with its cutting edge directed to the posterior wall. It is then drawn downwards with steady pressure to just below the internal os. It is then again passed upwards and the manœuvre repeated with just sufficient change of direction to ensure the curette passing over fresh tissue. This is repeated until the whole of the posterior wall has been thoroughly dealt with from side to side. The anterior wall and sides of the uterus are then treated in turn in the same way. Finally the fundus is curetted by a lateral movement of the instrument, especial attention being paid to the Fallopian tube angles, which are very apt to escape the curette.
A rasping or grating sound indicates that the endometrium over a given part has been removed and that the muscular walls have been reached. In spite of the most careful attention it is very difficult to remove the endometrium completely. If a uterus be scraped, as it is thought, thoroughly, and be examined post mortem, strips of mucous membrane will often be found untouched, showing the difficulties of complete removal.
After the operation an intra-uterine douche of 1 in 2,000 perchloride of mercury or some other suitable antiseptic is given with a Bozemann’s tube or Budin’s catheter. If a flushing curette has been used, this of course has already been done. After the douche, some application may be made to the interior of the uterus: the best is iodized phenol (liquid carbolic acid, 2 parts; tincture of iodine, 1 part). To do this the interior of the uterus is first dried with a Playfair’s probe armed with cotton-wool; another similar probe is then taken, dipped into the solution, and passed into the uterus. The vagina is protected by inserting a plug of cotton-wool into the posterior fornix. The uterus is then lightly packed with ribbon gauze. If there is hæmorrhage, the packing should be firmer, and a vaginal tampon should be placed in below the cervix. The packing should be removed in twenty-four hours. The patient may get up at the end of a week and resume her ordinary duties in a fortnight.
Indications. Dilatation may be performed:—
| (i) | As a means of diagnosis. |
| (ii) | As a preliminary to the use of the curette or to removal of intra-uterine growths. |
| (iii) | As a method of cure for spasmodic dysmenorrhœa. |
Contra-indications to the rapid method of dilatation of the cervix are very few: a recent attack of peri- or parametritis would certainly be one, but when the effects of a salpingitis have quieted down there seems very little reason against its use. Where carcinoma of the body of the uterus is known to exist, and in old age, it should only be resorted to with the greatest caution, if at all.
Methods:—
(a) Rapid dilatation by means of graduated metal bougies.
(b) Gradual dilatation by means of tents.
(c) Combined gradual and rapid dilatation.
In a large majority of cases rapid dilatation is the operation selected. Its one disadvantage is that when a great degree of dilatation is necessary, or when the operation is performed too rapidly, the cervix is liable to be torn, an event which is especially liable to occur when the tissues of the cervix are rigid. These lacerations are longitudinal in direction and in the neighbourhood of the internal os uteri. They sometimes result in hæmorrhage, which can easily be controlled by plugging the cervical canal. Unless strict asepsis be maintained, these lacerations of course form a channel for infection of the pelvic cellular tissue.
It is obvious that dilatation will be easier to perform, and laceration less liable to occur, if the cervix is in a softened condition—a physiological state which is always present during pregnancy and labour. Efforts should therefore be directed, when possible, to ensure a soft state of the cervix before performing rapid dilatation.
Immediately after the cessation of a period, the cervix is soft and somewhat patent, and advantage may be taken of this fact. The introduction of a glycerine tampon two hours beforehand produces a certain amount of softening. But nothing ensures so much softening as the introduction of a tent into the cervix about twelve hours previous to the rapid dilatation.
It is therefore recommended in all cases, where possible, to perform dilatation by this latter means, viz. a combination of the gradual and rapid methods.
Rapid dilatation by means of graduated metal bougies. Hegar’s original dilators (Fig. 56) were solid vulcanite bougies, graduated from 1 to 26, the numbers corresponding to the diameter of the bougie in millimetres. Each was 5¼ inches in length, the handle measuring 1½ inches and the bougie the remainder. The bougie formed a slight curve and tapered off to a blunt point.
These bougies were rather short and too sharply pointed, and they could not be sterilized by boiling. To overcome these disadvantages, uterine dilators are now made about the same length as a male catheter, with a sharper curve than Hegar’s original one, and a blunter point; the larger sizes are of hollow metal for the sake of lightness. There are many varieties of dilator, each with minor differences as to length, curve, handle, and shape of the point.
The author uses metal bougies. These have somewhat the shape of the ordinary uterine sound, are thirty-five in number, and graduated in size. Like the sound, the upper portion is bent at an angle of about 160° with the solid handle, a circular shallow depression indicating the 2½ inch mark in the smaller numbers; in the larger this is not considered necessary.
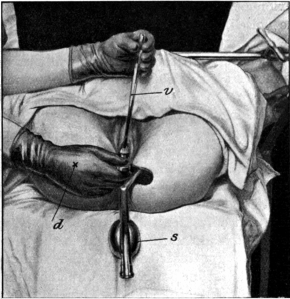 Fig. 61. Dilatation of the Cervix. The patient
is in the lithotomy position. Auvard’s speculum has
been inserted, a volsella attached to the anterior
cervical lip and a bougie passed. (From a photograph.)
Fig. 61. Dilatation of the Cervix. The patient
is in the lithotomy position. Auvard’s speculum has
been inserted, a volsella attached to the anterior
cervical lip and a bougie passed. (From a photograph.)
d. Right hand inserting bougie.
s. Speculum.
v. Volsella.
Operation. Instruments: an Auvard’s self-retaining weighted flushing speculum; a volsella; a Bozemann’s tube or Budin’s catheter; a uterine sound; and a set of dilators.
The patient is anæsthetized and placed in the lithotomy position with the legs supported by a crutch. Strict asepsis must be observed; the labia must be shorn of long hairs; this is followed by cleansing of the vagina and a vaginal douche, and finally the vulva is washed with antiseptic lotion. The speculum is passed and held by an assistant, but if self-retaining, as in Fig. 61, the assistant is not necessary: a sound is then inserted to ascertain the length and direction of the uterine cavity. If anteflexion be present, the anterior lip of the cervix should be seized with the volsella and fixed by slight traction. If retroversion or retroflexion be present, then the posterior lip should be fixed. Traction by the volsella tends to straighten out the uterine canal, and thus makes the passage of the bougies easier. The bougies are now passed in order, commencing with the size which will pass easily. The bougie is passed by means of the right hand into the cervical canal until the internal os uteri is reached; resistance will now be felt. Firm and continuous pressure in the proper direction must be made, and in a short time the resistance gives way, and the bougie will pass into the uterine cavity. An interstitial fibroid produces a tortuous channel and much difficulty will often be experienced in passing a bougie in such a case. It will be found on attempting to withdraw the instrument that it is grasped by the internal os uteri; in the course of one to five minutes this spasm will relax, and only then should the bougie be withdrawn. The next in size should be ready and introduced in the same manner, and the succeeding ones are inserted until the required dilatation is produced. Sterilized vaseline or glycerine of perchloride of mercury may be smeared over the point of the dilator to facilitate its passage. Each succeeding bougie should increase in size by not more than 1 mm.: occasionally a case is met with where this seems too large a difference, and it is really better to have them made with a ½ mm. difference. As a preliminary to the use of the curette, dilatation up to No. 12 Hegar is necessary. The index-finger can be introduced into the uterine cavity after the passage of No. 19 or 20 Hegar, while full dilatation up to No. 26 is required for any operation with scissors or the écraseur on intra-uterine growths.
It is evident that the degree of dilatation for exploratory purposes will be governed by the diameter of the operator’s finger, or rather of its second joint, and this varies very much in different people. By means of the finger a uterus can be explored in which the cavity is much longer than the operator’s finger, if the viscus be forced down on to the finger by the pressure of the other hand above the symphysis pubis. The operator must not be satisfied until he has felt the whole extent of the uterine wall, especially the two cornua, which are favourite seats of disease. After completion of the operation it is well to give an antiseptic intra-uterine douche by means of a Bozemann’s tube. The uterus and cervix should be lightly packed with sterile ribbon gauze, 1 inch wide; the free end is left projecting through the os uteri. The packing should be removed in twenty-four hours, and an antiseptic douche given.
Difficulties and dangers. The difficulty due to non-dilatability is overcome by means of the preliminary use of a tent. The complication produced by a fibroid, altering the direction of the uterine canal, has been mentioned. Extreme anteflexion or retroflexion gives trouble during the passage of the earlier numbers, but as dilatation is effected this disappears.
The dangers are:—
1. Laceration of the cervix.
2. Rupture of the uterus.
3. Sepsis and its sequelæ.
4. Hæmatoma between the layers of the broad ligament.
Laceration of the cervix has been referred to: it begins as a rule at the internal and extends towards the external os uteri; it may be deep or superficial, and is recognized as a sulcus into which the finger can be passed from above downwards: rarely, laceration into the peritoneum may take place.
Rupture of the uterus is liable to occur when the uterine wall has been weakened by the changes which accompany the completion of the menopause, or has been infiltrated by carcinoma, or, more rarely, by vesicular mole.
Sepsis may occur from absorption through a laceration if asepsis has not been maintained: it may lead to an attack of pelvic cellulitis or even septicæmia.
If the uterus is fixed or not freely mobile, and the condition is complicated by any tubal or ovarian disease, great care must be exercised in manipulation.
Gradual dilatation by tents. There are three varieties of tents—sponge, laminaria, and tupelo.
Sponge tents should never be used, for they are extremely difficult to render sterile.
The commonest and the safest to use, because they can be most easily sterilized, are laminaria tents, made from sea-tangle (Laminaria digitata). These are cylindrical rods, which expand evenly, from imbibition of moisture. Tupelo tents are larger than laminaria and expand more rapidly.
To use tents that are not absolutely sterile is to court disaster, and in former times they were responsible for many fatalities from sepsis. The best way to keep laminaria and tupelo tents is in a solution of 1 in 1,000 corrosive sublimate in absolute alcohol. They may be kept in this for an indefinite period, and so are always ready for use.
Contra-indications. All septic states of the uterus and cervix, for the retention of pent-up discharges is very likely to lead to local or general infection. Tents should never be used then in such conditions as carcinoma of the body of the uterus, sloughing polypus, acute endometritis and cervicitis.
Method of introduction of a tent. The patient is placed in the lateral or lithotomy position and a vaginal douche given. A Sims’s speculum is passed and the cervix seized and drawn down with a volsella so as to straighten the cervical canal. The direction and length of the uterine cavity is ascertained by passing the sound. The most suitable size of tent is now selected, and, being held in a special form of tent introducer or suitable pair of forceps, is passed into the cervical canal, well past the internal os uteri. The end should project slightly into the vagina. The vagina should then be douched again and lightly packed with sterilized gauze. The patient must remain in bed.
The tent should be left in position for twelve to fifteen hours, when it will have exerted its full action. The action of tents is twofold: it causes (1) dilatation, and (2) softening of the cervix, the softening being accompanied by an abundant secretion of mucus from the cervical glands.
Method of removal. Tents are removed by traction on the silk thread attached to the vaginal end. The part of the cervical canal which exerts the greatest resistance to the dilating action is the internal os uteri, and after the tent has been removed a well-marked constriction is always to be seen at this point. If there is much resistance to removal by reason of the tent being gripped at the internal os, it should be taken in a pair of forceps and gently pulled and levered out.
This is a congenital condition and there is no thickening of the mucous membrane and underlying tissues; hence the diameter of the cervix is not increased. The operation best adapted for the treatment of this condition is the wedge-shaped incision, recommended by Marckwald (Fig. 62).
Operation. The cervix is split bilaterally into an anterior and posterior portion by means of scissors, and out of each portion is excised a wedge-shaped piece of tissue, leaving a deep groove. The sutures are passed as in Fig. 62, and the raw surfaces are brought together.
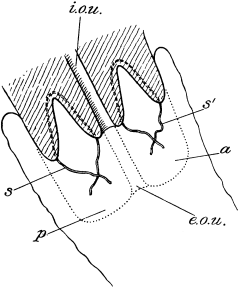 Fig. 62. Marckwald’s Operation for Congenital Hypertrophy of the Cervix.
The wedge-shaped portions have been excised and the sutures passed but
not tied.
Fig. 62. Marckwald’s Operation for Congenital Hypertrophy of the Cervix.
The wedge-shaped portions have been excised and the sutures passed but
not tied.
a,p. Anterior and posterior lip of cervix before exsection. |
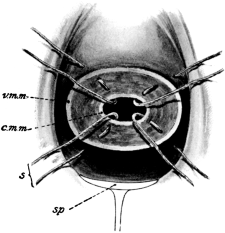 Fig. 63. Hegar’s Operation for Supravaginal Elongation of Cervix. The
cervix has been removed and four sutures passed but not tied.
Fig. 63. Hegar’s Operation for Supravaginal Elongation of Cervix. The
cervix has been removed and four sutures passed but not tied.
c.m.m. Cervical mucous membrane. |
Circular amputation, as carried out by Hegar, is more suitable for supravaginal elongation of the cervix, the result of prolapsus uteri.
The patient is anæsthetized and placed in the lithotomy position and the cervix is pulled down by a volsella and amputated transversely by a knife or scissors. A certain amount of retraction of the stump takes place, producing an inversion of the vaginal wall. The raw surface remaining must be covered by uniting the vaginal and cervical mucous membranes. Sutures are passed in the following manner: a short stout, straight needle, threaded with a loop of silk, is passed from the vaginal mucous membrane, across and beneath the raw surface of the stump, and emerges on the mucous membrane of the cervix (Fig. 63). From eight to ten of these sutures are passed at regular intervals and tied. The sutures are removed on the tenth day and the patient should be kept in bed for fourteen days.
Indications. This operation is performed for the repair of certain forms of laceration of the cervix. It was formerly practised in every case in which a laceration occurred: it is now only permissible in cases in which there is extroversion of the mucous membrane with certain symptoms, such as hæmorrhage or free leucorrhœal discharge accompanied by backache on exertion and general ill health. It was formerly considered that there was a direct relation between cervical laceration and cancer, but further inquiry has failed to corroborate this view.
The instruments required are: a Sims’s or Auvard’s speculum; long-handled, angular-bladed knives (right and left); Emmett’s scissors (right and left) (Fig. 64); toothed dissecting forceps; short stout needles with sharp triangular points, straight or very slightly curved.
 Fig. 64. Emmett’s Scissors (left) for Trachelorrhaphy.
Fig. 64. Emmett’s Scissors (left) for Trachelorrhaphy.
Operation. As it is usually found that subinvolution is present and kept up by the laceration, it is best to perform a preliminary curettage (see p. 154) before proceeding to the operation proper.
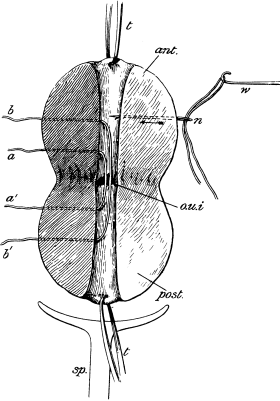 Fig. 65. Trachelorrhaphy. The patient is in the lithotomy position. The
left half of the cervix has been denuded and two sutures, a, a' and
b, b', passed. The right half is intact, but the method of passing
the needle n is indicated.
Fig. 65. Trachelorrhaphy. The patient is in the lithotomy position. The
left half of the cervix has been denuded and two sutures, a, a' and
b, b', passed. The right half is intact, but the method of passing
the needle n is indicated.
ant. Anterior lip of cervix.
post. Posterior lip of cervix.
t,t. Tenacula.
o.u.i. Os uteri internum.
sp. Speculum.
w. Wire.
The patient is placed in the lithotomy position and an Auvard’s speculum is inserted. A piece of stout silver wire or a tenaculum is passed deeply through the anterior and posterior lips of the cervix; steady traction can be made through these and the uterus kept fixed while denudation and suturing are carried out. Should marked extroversion be present, with hypertrophy of the cervical glands, the curette should be freely applied to the diseased surface.
The uterine sound is passed to mark the situation of the internal os uteri, and an antero-posterior linear piece of lining membrane, about a quarter of an inch in breadth, must be allowed to remain untouched. This is necessary to prevent total occlusion of the cervical canal when the denuded flaps are sutured (Fig. 65).
Denudation. The right half of the anterior and posterior lips of the cervix (upper and lower from the operator’s point of view) are first pared by means of the angular knives and scissors, great care being taken to see that the deep angle of the reflexion is not overlooked. The other side is then treated in a similar manner. The tissues will be found extremely hard and resistant, especially if there be much cicatrization about the angle of the laceration.
The passage of the sutures (Fig. 65). The short stout, triangular-pointed needle is first doubly threaded with silk or stout chromicized catgut so that a loop of three to four inches in length is produced. The needle and the silk suture are passed as in Fig. 65, two on either side.
The triangular-pointed needle must be held in Schauta’s specially strong holder (Fig. 73), and should be made to pierce the cervix near the raw surface on one lip, and pushed through the tissues immediately below this to emerge on the strip of unpared cervix already mentioned. It is then carried across the sulcus and is made to emerge through the opposite lip of the cervix. A stout wire is now hooked into the loop and pulled through the needle track. When the two wire sutures are inserted on either side, the flaps are brought together and the wires twisted together.
Results. Primary union is the rule, and the wire sutures may be removed at the end of the tenth or twelfth day. The cervix has the appearance observed in the nullipara, and may lead to complications in any ensuing labour from difficulty of dilatation.
Dührssen modifies Emmett’s operation by a flap-splitting procedure which, however, does not appear to possess sufficient advantages to warrant its general introduction.
This operation consists in the fixation of the retroverted fundus uteri in an anteverted position, by suturing it to the anterior vaginal cul-de-sac.
Indications. These are somewhat uncertain, and the field of utility of the operation is rapidly becoming more limited. Advocates of this procedure recommend it for backward displacement of the uterus with or without adhesions. It is considered specially applicable to cases in which slight retroversion is complicated by moderate prolapsus. The results which have so far obtained do not appear to be so good as those resulting from the use of a well-fitting pessary.
Operation. The technique recommended by Dührssen appears to be the most satisfactory, and is as follows: The patient is anæsthetized and placed in the dorsal position with the knees supported by a Clover’s crutch. After purification of the parts (see p. 126) the cervix is pulled down as far as possible by means of a volsella: a curettage is then carried out as a preliminary measure (see p. 154). If cervical hypertrophy is present, amputation by Marckwald’s method (see p. 160) should be performed, as an elongated cervix acts as a preventive to satisfactory anteversion of the uterus. A transverse or T-shaped incision is now made as in vaginal hysterectomy (see p. 169), and the cellular tissue pushed up by the index-finger until the peritoneum is reached. The peritoneum is now seized with a volsella and cut through, and the edges sutured to the lips of the vaginal wound. The uterine fundus is then anteverted by means of a sound: by pressing the handle of the instrument towards the perineum the fundus is brought into the wound. By means of a rectangular curved needle a stout silk suture is passed through the anterior wall of the fundus as high up as possible: the vaginal flaps are not included, as the suture is to be used for traction only. The uterus is now forcibly pulled down and two other sutures are introduced in the same manner higher up. Three sutures of catgut are passed through the uterine wall, including the vaginal and peritoneal flaps. The silk traction sutures are now withdrawn and the permanent ones tied. The vaginal wound is carefully sutured by means of fine silk.
Difficulties and dangers. The risks of the operation are peritonitis and wounding of one or both ureters or the bladder wall. Absolute rest for fourteen days is necessary and no local after-treatment is called for.
Uterine growths include primary malignant disease and fibro-myomata; the former should be treated by exploration and subsequent vaginal hysterectomy (see p. 168), while the latter should be dealt with according to their relations and attachments to the uterine wall.
Fibro-myomata may present themselves to the operator in one of the following forms:—
1. As a fibroid polypus still intra-uterine or presenting through a naturally dilated and thinned-out cervix (submucous pedunculated).
2. As sessile growths presenting by their lower segments at the os uteri, which may be closed, or may be in varying degrees of dilatation (submucous sessile).
3. As tumours incorporated in the uterine wall (interstitial).
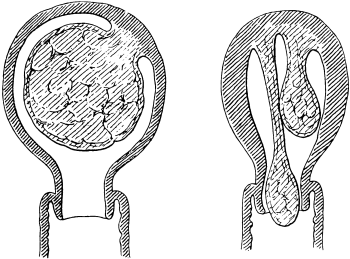 Fig. 66. Pedunculated Fibroid Polypi in various Stages of Extrusion.
(From drawings made at time of operation.)
Fig. 66. Pedunculated Fibroid Polypi in various Stages of Extrusion.
(From drawings made at time of operation.)
Operations for pedunculated tumours. If a fibroid polypus be still intra-uterine (Fig. 66) the proper treatment is to dilate the cervix (see p. 156), and, if the pedicle be sufficiently thin, to seize the growth with a pair of stout polypus forceps and twist it off by a slow rotary movement of the handles. Should the pedicle be thicker than the finger, the use of the wire écraseur is advisable. This is a scientific snare, with a loop of pianoforte wire and a handle or wheel by which it can gradually be tightened, causing the wire to slowly cut through the stalk of the growth (Fig. 67).
 Fig. 67. Wire Écraseur.
Fig. 67. Wire Écraseur.
The cervix is steadied with a volsella and the loop of the écraseur is shaped and bent to the size and position of the fibroid. The instrument is then passed into the uterine cavity and the noose pushed over the tumour up along the pedicle. The wire loop is then tightened up by means of the handle or wheel, and the wire cuts its way through and separates the growth from the uterine wall. It is somewhat dangerous to put any traction on the tumour before its separation, as is recommended by some writers, as the uterine wall itself may become somewhat inverted and the wire loop may cut through into the peritoneal cavity.
If the fibroid polypus has passed through the external os uteri, treatment is more simple. Slight traction may be made upon it by means of forceps, and the pedicle severed with scissors; no hæmorrhage takes place, owing to the retraction of the stump.
Operations for sessile tumours. In submucous sessile fibroids (Fig. 68) in which the lower segment of the uterus is somewhat thinned out and dilated, operative interference may be as follows: Preliminary dilatation of the cervix by bougies may be necessary. The capsule of the tumour is then incised with a sickle-shaped knife and the growth is enucleated by means of the finger or a blunt spoon. In some cases mere incision of the capsule is sufficient, and the uterus expels the growth later on.
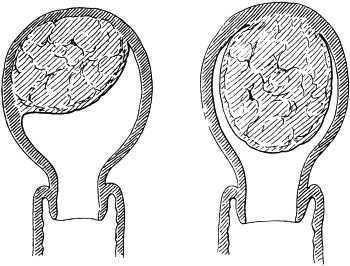 Fig. 68. Submucous Fibro-myomata, capable of Treatment by Morcellement.
(From drawings made at time of operation.)
Fig. 68. Submucous Fibro-myomata, capable of Treatment by Morcellement.
(From drawings made at time of operation.)
Another method of treating these cases is by the operation of morcellement, which consists in removing the tumour piecemeal by means of specially made forceps.
The instrument used by the author consists of a strong pair of forceps somewhat like those used in lithotomy, with the two distal ends notched with sharp teeth like a volsella. A portion of the tumour is seized between these two blades, and partly cut and partly twisted off. With patience and care the whole tumour may be thus removed. In one case the author was enabled to remove two large growths, each filling a pint measure. This operation is specially suitable in women in whom an abdominal operation is to be avoided.
Operations for interstitial tumours. Interstitial fibroid tumours, if not above the size of a small fœtal head, should be treated by vaginal hysterectomy (vide infra); if large, by hysterectomy by the abdominal route (see p. 36).
Vaginal hysterectomy. By vaginal hysterectomy is meant removal of the whole uterus by the vagina, with or without the appendages. The advantages that the vaginal operation possesses over abdominal hysterectomy are, there is less disturbance of peritoneum and intestines, less shock, and no abdominal scar or risk of subsequent hernia. The operation is limited to uteri not exceeding in size the head of a full-time fœtus.
Indications. (i) Malignant disease of the uterus (fundus or cervix) in an early stage: chorio-epithelioma malignum.
(ii) Certain cases of fibro-myoma of the uterus.
(iii) Certain cases of inflammatory disease of the uterine appendages complicated by recurrent attacks of local perimetritis.
(iv) Other conditions, such as intractable uterine hæmorrhage, usually due to uterine myo-fibrosis, and, as a last resort, severe dysmenorrhœa.
It has also been advised for irreducible chronic inversion of the uterus, and for severe procidentia uteri. No case of the former has occurred in the author’s experience in which the operation was found necessary. In the latter condition the operation is not to be recommended, the almost certain result of the procedure being prolapse of the vaginal walls and the intestines (enterocele).
Vaginal hysterectomy for carcinoma. The only cases suitable for operation are early ones, in which the disease is still confined to the uterus itself, which should be freely mobile in all directions. No signs of infection of the surrounding cellular tissue and vaginal walls should be present. It cannot be too strongly insisted that all cases should be thoroughly examined under anæsthesia to settle this point before operation is decided upon. Rectal examination is most important to estimate the condition of the sacro-uterine ligaments, the cervix being pulled down so as to place them on the stretch.
Occasionally, cases of carcinoma of the cervix are seen, in which the cellular tissue immediately surrounding the cervix is apparently free from disease, but if search be made further outwards, a hard, fixed mass is found plastered, as it were, on to the side of the pelvis, indicating advanced disease of the lymphatic glands, or cellular tissue at the outer part of the broad ligaments. Such cases are hopeless for operation.
If the disease is in the sloughing stage, and there is foul discharge, Paquelin’s cautery should be applied to the diseased surface, followed by vaginal douches of formalin (ʒj to the pint), or some other efficient antiseptic, given three times a day for three days prior to operation. The operation consists of three main stages:—
| (a) | Separation of the cervix from the vagina, pushing up of the bladder and ureters, and opening the anterior and posterior peritoneal pouches. |
| (b) | Removal of the uterus by ligaturing and dividing the broad ligaments. |
| (c) | Treatment of the peritoneal and vaginal flaps thus left. |
First of all, the growth, if of the cervix, should receive careful preliminary attention, for it constitutes a continuous source of infection, not only by means of septic organisms, but also of cancer cells, which may become implanted in the wound and cause early recurrence. The cervix is drawn down with a volsella and all visible growth is burnt away with the Paquelin cautery, until apparently healthy tissue only is left. The cervix is then completely closed by the application of a volsella or three or four stout silk sutures, passing through both anterior and posterior lips. The ends of the sutures may be left long if preferred and serve as tractors.
After these preliminary measures against infection have been completed, the removal of the uterus is proceeded with. A posterior speculum, Auvard’s or Pozzi’s, is passed, and the cervix is drawn downwards and somewhat backwards by traction on the volsellum or the long ends of the silk sutures. A sound is passed into the bladder to define its lower limit. A transverse or T-shaped incision (Fig. 48) is now made through the vagina at the level of the cervico-vaginal junction in front. This constitutes the anterior incision, and the transverse portion should extend completely across the anterior aspect of the cervix, passing through the whole thickness of the vagina, but no further.
The knife is now laid aside, and the operator proceeds to push up the vagina and bladder from the anterior aspect of the cervix with the index-finger or a winged director, until the anterior peritoneal pouch is reached. This is at once recognized by its glistening white appearance and by the manner in which its opposing surfaces glide over one another.
This part of the operation must be conducted very cautiously for fear of injury to the bladder: the pulp of the finger only must be used in the separation. The frequent use of the bladder sound is very useful at this stage, as it is quite easy to wound this viscus laterally. Bleeding from the divided twigs of the vaginal vessels often obscures the field of operation and renders the separation of the bladder troublesome: it well repays the operator to stop all bleeding after making the vaginal incision.
The peritoneum is next picked up and opened with scissors. The anterior fold of peritoneum may sometimes be more easily reached after the bases of the broad ligaments have been ligatured and divided, thus allowing the uterus to be drawn down more readily, and making the peritoneum more accessible. An anterior retractor is then passed to keep the bladder out of the way.
A second incision similar to the first is now made across the posterior aspect of the cervix at the level of the cervico-vaginal junction, more or less cellular tissue is traversed, and the posterior peritoneal pouch is opened. By joining the ends of these two incisions the cervix is completely separated from the vagina.
 Fig. 69. Galabin’s Broad-ligament Needle (right).
Fig. 69. Galabin’s Broad-ligament Needle (right).
 Fig. 70. Jessett’s Broad-ligament Needle.
Fig. 70. Jessett’s Broad-ligament Needle.
The uterus is now suspended in the pelvis by the attachments of the broad ligaments only; the next step consists in ligaturing and dividing these. The cervix is drawn over towards the patient’s right side by an assistant, so as to expose the base of the left broad ligament. Additional space is gained by drawing aside the left wall of the vagina by means of a retractor. By passing the left index-finger behind the broad ligament the tube and ovary can be easily felt, and if necessary the bent finger can pull them down for inspection; the finger is then placed beside the cervix below and behind the base of the broad ligament. A Galabin’s or Jessett’s (Fig. 70) needle, carrying a stout silk suture, is passed through the ligament from before backwards, on to the tip of the finger (Fig. 71).
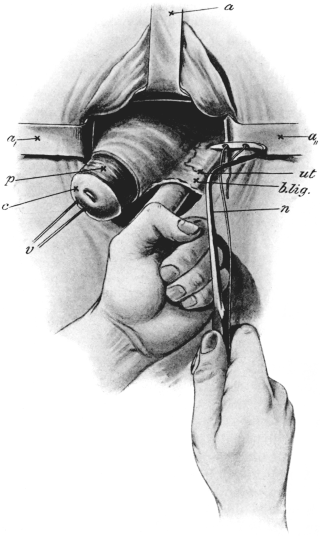 |
Fig. 71. Vaginal Hysterectomy. The patient is in the lithotomy position,
the vaginal incisions have been made and the peritoneal cavity opened. The left
broad ligament is exposed, and a Galabin’s needle threaded with silk is being passed
from before backwards on to the index-finger of the operator’s left hand inserted
into the peritoneal cavity. (Semi-diagrammatic, from a photograph.)
a, a', a''. Retractors. |
The ligature should be passed about one-third of an inch up the broad ligament. It is then tied tightly and the ends left long and drawn aside. The segment of broad ligament included in the ligature is divided as near the uterus as is justifiable; in carcinoma of the cervix at least half an inch from the disease should be allowed. Care must be taken at this stage to avoid injury to the ureters; these lie about one inch distant from the cervix; consequently all ligatures must be passed as near the cervix as possible compatible with being clear of the disease.
A second ligature is now passed through the broad ligament above the first and then a third, and more if necessary. The second generally includes the uterine artery, which can always be recognized by its strong pulsation under the finger; the third ligature will control the Fallopian and ovarian arteries. After the arteries on the left side have been secured and divided, attention is directed to the right broad ligament. The cervix is drawn over to the left side, the fundus delivered, and the upper portion of the right broad ligament is dealt with in a similar manner, but from above downwards. If the ovaries and tubes are diseased, they can now be removed by piercing the pedicle and tying the stump in the usual way.
The uterus having been extirpated, the next step consists in dealing with the wound. First, all bleeding is stopped, and the wound is swabbed clean and dry. The ligatures on either side are tied in two bunches and the ends cut off just within the vagina (Fig. 72). The anterior and posterior flaps of peritoneum are united with a few catgut sutures passed by means of Schauta’s needle-holder (Fig. 73); the walls of the vaginal vault are treated in a similar fashion, leaving a circular orifice in the median line into which gauze can be inserted for the purpose of drainage.
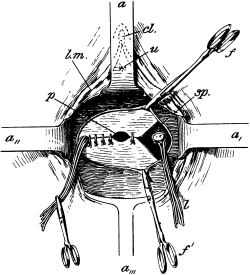 |
Fig. 72. Vaginal Hysterectomy. Final stage. The uterus has been
removed, and the peritoneal flaps are in process of suture.
a, a', a'', a'''. Retractors. |
Some operators prefer to control the vessels in the broad ligaments by means of hæmostatic forceps instead of ligatures. Each broad ligament is clamped in three or more portions and the tissue between them and the uterus cut through. They must be allowed to remain in position for at least forty-eight hours, as recurrent hæmorrhage is possible if they are removed earlier. The only advantages of the forceps appear to be the rapidity with which the operation can be carried out, and the good drainage. The disadvantages are, that it is a somewhat unsurgical proceeding; there is often much pain from the nipping of the broad ligaments, and inconvenience from the presence of the handles between the labia; the intestines may be damaged; sloughing and risk of sepsis must be reckoned with.
After-treatment. The catheter should be used at first four times daily; the author recommends that the gauze should be removed at the end of twenty-four hours, but some operators retain it longer. The ligatures should be pulled upon a little daily after the seventh day, and they gradually cut their way through the tissues in their grasp. No vaginal douching should be administered until after the expiration of a week.
Vaginal hysterectomy for fibroids. This is not often called for. The operation is necessarily limited to fibroid uteri not exceeding in size a fœtal head. Uterine fibroids of such a size can usually be treated in other ways, either temporarily by curetting, or, if submucous, permanently by enucleation through the vagina. The operation is most suitable for uteri containing many small fibroids causing severe hæmorrhage which cannot be controlled by more palliative measures.
The vagina must be large enough to admit of delivery of the uterus through its lumen. Therefore, in virgins and nulliparæ, the abdominal operation is always to be preferred. In any case, if the vagina be too narrow, additional room may be gained by lateral vaginal section (see p. 148) or episiotomy.
The operation does not differ in technique from the removal of the uterus for carcinoma, already described. In some cases it may be preferable to bisect the uterus in the sagittal plane before removing it, after the cervico-vaginal attachments have been separated and the peritoneal pouches opened.
Operations upon the eye differ so widely from general surgical operations that it is necessary to say something of the preparations for them before passing on to their actual performance. Although not formidable in themselves, they require great accuracy and presence of mind; slight mistakes, such as too small an incision, may cost the patient his sight, which sometimes may be almost more important than life itself.
Most intra-ocular operations are performed without general anæsthesia; it is therefore important that the patient should be given confidence by talking to him during the operation, so that he may follow the instructions of the surgeon during its performance; loss of self-control on the part of the patient, movement of the head, screwing up of the eyes, &c., may lead to disastrous results, however well performed the operation itself may be.
The urine should always be examined, especially in cases of cataract, as not infrequently this disease is associated with diabetes, and it is often advisable to treat the general condition before operation.
The bowels should be opened by an aperient the night before the operation, as it is desirable to keep them confined for the first two days afterwards, so as to avoid straining. During the first week after a major operation, when the patient is confined to bed, they should be evacuated in the supine position.
The best time for operating, if possible, is the morning, as the patient has had a night’s rest and is less likely to lose self-control. Usually there is some pain after the cocaine has gone off, and the patient is better able to stand it during the daytime.
Anæsthetics. General anæsthesia should be induced in all patients with congested eyes, in small children, patients who are deaf, and those who show a want of self-control. Chloroform should be used for all intra-ocular operations, and should be given to the full surgical degree. It should be given on a towel or an inverted mask specially made for the purpose, a Junker’s inhaler being used during the time the actual operation is being performed. As the surgeon usually stands at the head of the patient, the anæsthetist should stand on the side away from the eye being operated on. The local use of cocaine in addition to general anæsthesia is indicated when operating on patients to whom it is advisable to give as little anæsthetic as possible.
Local anæsthesia is obtained by the use of a 4% solution of cocaine instilled four or five times before the operation at intervals of three minutes; a drop of the solution should also be instilled into the eye which is not being operated on, to prevent an accidental reflex stimulation of the conjunctiva and screwing up of the eyes. Adrenalin (1–1,000) may be used in conjunction with the cocaine; it is especially useful in squint operations, as it lessens the hæmorrhage. Eucaine and stovaine have been used, but are not nearly so satisfactory. Under ordinary circumstances the only pain felt during an intra-ocular operation is during removal of the iris; this is obviated to a great extent by instilling the cocaine at least 15 minutes before the operation is performed, so as to allow time for its diffusion into the anterior chamber. The patient should be warned when to expect the pain, so that he may not move; his self-control may be tested beforehand by pricking the nose with a pin.
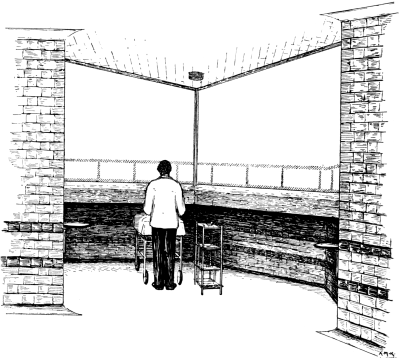 Fig. 74. Window of the Operating Theatre, King’s College Hospital.
The windows are fitted with outside blinds so that either can be used separately,
or the surgeon may stand in the angle and operate with his back to the light.
A recess beneath the window allows the patient’s face to be brought close to the
light on dark days.
Fig. 74. Window of the Operating Theatre, King’s College Hospital.
The windows are fitted with outside blinds so that either can be used separately,
or the surgeon may stand in the angle and operate with his back to the light.
A recess beneath the window allows the patient’s face to be brought close to the
light on dark days.
The theatre. The theatre should possess, as far as possible, all the modern improvements found in an up-to-date general surgical operating-room. The light should proceed from a single large window, which, if possible, should face the north. The window should consist of a single pane of glass or of two panes forming the angle of the theatre; it should begin about 5 feet from the floor and should extend to the ceiling (Fig. 74). The advantage of an angular window is that it allows the operator to stand with his back to the light in the angle, and so enables onlookers to see. No top light should be allowed, as it produces a corneal reflection which may prevent the operator from seeing the position of his knife in the anterior chamber. Beneath the window there should be a recess for the end of the operating table, so that the patient’s face can be brought close to the window if necessary (Fig. 74). This recess is formed by building the main wall of the theatre further out than the window, which has to be supported by a transverse girder.
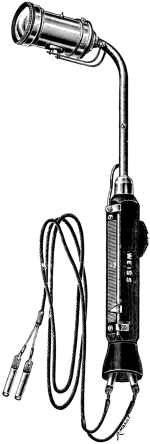 Fig. 75. Bull’s-eye Electric Hand-lamp. For use when artificial
illumination is required.
Fig. 75. Bull’s-eye Electric Hand-lamp. For use when artificial
illumination is required.
The window should be fitted with outside blinds so that the theatre can be easily darkened for the operations, such as capsulotomy, which require the use of artificial light. The best artificial light is a small enclosed electric hand-lamp fitted with a bull’s-eye, by means of which the operation field can be brilliantly illuminated while the surrounding area is left in comparative darkness (Fig. 75). Failing this, a single powerful lamp with a ground-glass globe, placed in front of the patient, will serve, the rays of light being brought to a focus on the eye by means of a large convex lens of about + 10 D.
For squint operations it is desirable to have a light fixed to the ceiling, directly over the head of the operating table, for testing the position of the eyes either by the reflection of the light from the surface of the cornea or by the Maddox rod test.
The operating table should be provided with a means of adjusting its height and the position of the head-piece, so that the patient’s head can be brought to about the level of the operator’s elbows when the latter is standing upright with his arms at his side.
After operation the patient should be warned to lie still and not to strain in any way; he should be carried to bed and should lie on his back if possible. If a patient cannot sleep on his back it is better that he should lie on the sound side than be without rest. A length of bandage should be fastened round the wrist of the hand on the same side as the eye which has been operated upon, and should be attached to the bed so as to prevent the hand being put up to the eye during sleep. After major operations, such as those for cataract and glaucoma, the patient is confined to bed for ten days, during the first four of which the head should not be raised from the pillow, the bowels being evacuated while the patient is in the supine position; but old patients with a tendency to bronchitis or hypostatic pneumonia must be propped up in bed and allowed to get up earlier: in these patients it is better to perform the operation in the summer if possible. In old people and patients with a tendency to melancholia the mental condition must be carefully watched, as frequently they cannot stand the confinement to bed and darkness.
When operating upon the eye, a surgeon has to face the great difficulty that he is operating in an area which is not always aseptic, since it is practically impossible to render the conjunctival sac sterile. At the same time, the conjunctiva has been shown to be sterile in health in 25% of cases, pyogenic organisms (principally the staphylococcus albus) being found only in 15%; but, although these are usually not of a very virulent character, they are by far the most frequent cause of sepsis; ten cases of suppuration after operation which the author has examined were all due to this organism. After the methods of purification given below, this percentage is considerably reduced, so that, if due precautions are taken, the risk of sepsis is comparatively small. On the other hand, if conjunctivitis or lachrymal obstruction be present, the risks are enormously increased, especially in the latter condition owing to the frequent presence of the pneumococcus in the discharge, unless special precautions are taken. It is, therefore, of the utmost importance that every case should be examined for lachrymal obstruction before operation. Care should be taken also to see that there is no purulent discharge from the nose or any septic sores about the face.
Sepsis after intra-ocular operations manifests itself in one of two forms: either by suppuration, which usually ends in a rapid and complete destruction of the eye (panophthalmitis), or more rarely in less virulent cases by recurrent attacks of hypopyon associated with acute irido-cyclitis; or by a plastic irido-cyclitis, which may lead to slow disorganization of the eye, with always the possibility of destruction of the other eye by sympathetic cyclitis (sympathetic ophthalmia). Although these conditions are comparatively rare, owing to the improvement in modern aseptic and antiseptic methods, every surgeon of experience will meet with these disastrous complications; indeed it has been suggested that immunization with staphylococcus vaccine should be carried out before major intra-ocular operations, since infection is generally due to this organism.
The methods of purifying the eye before operation. On the second night previous to the operation the eye should be bandaged and examined the following morning for conjunctival discharge. If any be present, an examination for organisms should be made, and the operation postponed until the conjunctival condition has improved. In the event of the case being extremely urgent, the conjunctiva should be swabbed over with nitrate of silver (10 gr. to the oz.) immediately before the operation; some surgeons prefer 1–2,000 perchloride of mercury. If lachrymal obstruction be present, the sac should be thoroughly washed out with boric lotion and protargol (10%) injected. The canaliculi may be temporarily occluded subsequently (see p. 294). If the lashes be very long they should be cut short. Epilation is performed by some Continental surgeons, but is not practised in this country. Various forms of specula are made to keep the lashes out of the field of operation; of these, a modification of Lang’s is perhaps the best (Fig. 76).
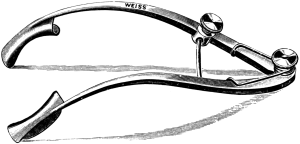 Fig. 76. Lang’s Eye Speculum. Designed to hold the lashes away
from the field of operation.
Fig. 76. Lang’s Eye Speculum. Designed to hold the lashes away
from the field of operation.
On the morning of the operation the lids should be thoroughly cleansed with soap and water, followed by 1–2,000 solution of perchloride of mercury, special attention being paid to the lid margins and lashes. The conjunctival sac should be washed out with boric lotion and a pad of cyanide gauze applied over the closed lid.
It has already been pointed out that the great danger in intra-ocular operations is sepsis. It is the aim and object of every ophthalmic surgeon to make such wounds into the globe as will become rapidly shut off from the conjunctival sac. Delay in the healing tends to the formation of a fistulous opening into the globe. This aperture in the continuity of the globe may lead either directly on to the surface or beneath the conjunctiva, subsequent inflammation in which may spread to the interior of the eye.
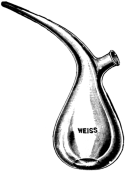 Fig. 77. Undine for washing out the Conjunctival Sac.
Fig. 77. Undine for washing out the Conjunctival Sac.
Cocaine and other solutions used at the time and subsequently to operation should be sterilized. To ensure this the solutions should either be boiled immediately before use, or put up in drop bottles made in one piece with a long tapering neck, which is sealed off, and can be broken immediately before use. These bottles can be kept in an aseptic solution so as not to soil the hands of the surgeon.
The hands of the surgeon are purified. After the dressings have been removed, the patient’s head and the area surrounding the operation are covered with sterilized towels. In operations such as advancement, where sutures are used, it is desirable that the face should be covered with sterile muslin, with a hole cut in it for the eye, so as to prevent the sutures being contaminated from the skin of the face. The eyelids are again washed in 1–2,000 perchloride of mercury lotion, and the conjunctival sac is washed out with a strong stream of boric lotion or normal saline by means of a sterilized irrigator or an undine (Fig. 77) which has been kept in a bowl of lotion.
Instruments. Non-cutting instruments are boiled for 15 minutes in distilled water and placed in a tray of 1–80 carbolic lotion. Some surgeons prefer to place the instruments in the tray without lotion on sterile wet lint, as this excludes infection from the surgeon’s hands due to the lotion running off them on to the instrument. Failing distilled water, a small quantity of soda may be added to the water used for boiling, but this has the disadvantage that a deposit is liable to form on the instruments. This may be obviated to a certain extent by not placing them in the solution until it is boiling. Cutting instruments should be sterilized by dipping them in liquefied carbolic acid (crystals dissolved by heating with 10% of water) for half a minute immediately prior to use and then into absolute alcohol to remove the acid; they are then placed in the tray. The greatest care should be taken to see that cutting instruments and needles do not touch the side of the dish. The edges and points should always be carefully tested immediately before sterilization on a drum covered with fine kid specially made for the purpose. The points should pass through the drum by the weight of the instrument held flat on the open palm; the cutting edge should also be tested. Scissors are best tested by cutting wet cigarette paper, special care being taken to see that the edges are good near the points. Immediately after operation the instruments should be boiled, and dried whilst hot in order to prevent rust.
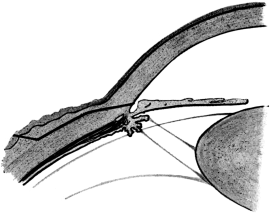 Fig. 78. Cataract Extraction. The drawing shows the line of incision.
Note the conjunctival flap.
Fig. 78. Cataract Extraction. The drawing shows the line of incision.
Note the conjunctival flap.
The direction of an incision into the globe should be as oblique as is consistent with the object of the operation, so as to allow larger healing surfaces to come into apposition. With this object in view it is desirable that a conjunctival flap should be formed to all wounds wherever possible (Fig. 78). Further, owing to the extreme vascularity of the conjunctiva, as has been shown elsewhere,3 wounds in it become firmly united after 48 hours. As a rule sutures are best avoided and are seldom required.
Position of the incisions. Corneal incisions are to be avoided, if possible, for the following reasons: firstly, the cornea being free from blood-vessels heals comparatively slowly; secondly, the wound is liable to become fistulous owing to the rapidity with which the epithelium grows down the side of the wound. On the other hand, incisions situated from 3 to 6 millimetres behind the limbus are liable to injure the ciliary body, and, in addition to irido-cyclitis being set up by the trauma, the iris or ciliary body will prolapse into the wound and prevent the union of its edges, with the result that sepsis may spread into the globe along the prolapsed portion of the uveal tract and set up an irido-cyclitis which may not only ruin the eye affected but may also cause a sympathetic irido-cyclitis in the other eye (Fig. 79).
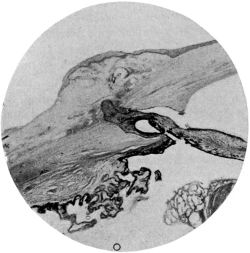 Fig. 79. Sympathetic Ophthalmia. The exciting eye of a case following
cataract extraction. The section shows the incarceration of the iris in
the wound.
Fig. 79. Sympathetic Ophthalmia. The exciting eye of a case following
cataract extraction. The section shows the incarceration of the iris in
the wound.
The site of election of an incision into the anterior part of the globe is therefore about 1 millimetre behind the limbus; that is to say, as near the cornea as is consistent with obtaining a good conjunctival flap to cover the wound in the globe (Fig. 78). When possible it is advisable to make all incisions in an upward direction for the following reasons: They are more easily performed; any deformities, such as an iridectomy, are hidden by the upper lid; more perfect rest is obtained, as the wound is not exposed in the palpebral aperture, the eye being turned upwards when the lids are closed.
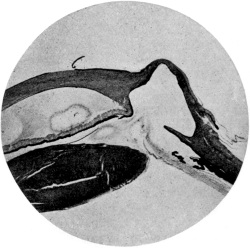 Fig. 80. Cystoid Scar after Glaucoma Iridectomy.
Fig. 80. Cystoid Scar after Glaucoma Iridectomy.
The immediate danger of the passage of a knife into the anterior chamber of the eye is the wounding of the lens. To avoid this the point of the knife should be always kept superficial to the iris if a clear lens be present in the eye. After operation the chief danger is prolapse of the iris into the wound. This is best avoided at the time of operation by carefully replacing the iris with the spatula at the end of the operation, but unfortunately prolapse not infrequently occurs during the first few days owing to the reaccumulation of the aqueous in the anterior chamber and its sudden escape through the imperfectly healed wound as the result of straining or of some movement on the part of the patient; the iris may be carried into the wound with the escaping aqueous, and a fistulous opening or a scar may form subsequently (Fig. 80).
The less manipulation used consistent with the object of the operation the less likelihood is there of cyclitis following it. All instruments should be held lightly in the fingers, which should be as far as possible responsible for the fine manipulation required. The part of the hand not actually holding the instrument should be steadied on the face before the instrument is brought in contact with the eye.
When more than one operation has to be performed on the same eye it is desirable that all ciliary injection after the first operation should have disappeared before the second is undertaken.
Dressings. A pad of sterilized wool, with a few layers of cyanide gauze moistened with 1–6,000 perchloride of mercury lotion next the closed eyelid, held in position by a bandage, is all that is necessary.
Bandaging. The bandage is started on the forehead over the affected eye and is carried in a direction away from the eye to be covered. A complete turn is made to encircle the head and is fixed with a pin. The bandage is then brought up beneath the ear and over the eye and fixed with pins on the forehead (Fig. 81). When absolute rest is desired, it is necessary to bandage both eyes. After intra-ocular operations this is desirable for the first three days. When pressure is desired, a figure-of-eight bandage should be used (Fig. 82). A useful bandage (Moorfield’s bandage) for occlusion of both eyes is made from stockinette, which fits closely over the eyes and nose and is fastened with tapes.
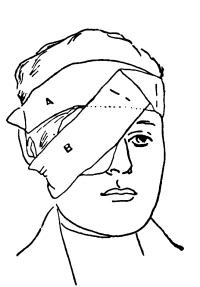 Fig. 81. An Eye Bandage. The first turn, A, encircles the head and is
fixed with a pin. This portion of the bandage can be put on before the
operation and obviates movement of the head. The turn B is then brought
up below the ear and fixed with pins.
Fig. 81. An Eye Bandage. The first turn, A, encircles the head and is
fixed with a pin. This portion of the bandage can be put on before the
operation and obviates movement of the head. The turn B is then brought
up below the ear and fixed with pins.
|
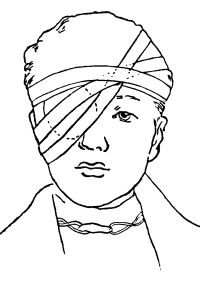 Fig. 82. A Pressure Bandage. The first turn of a 1½-inch bandage
encircles the head. It is then carried beneath the ear and over the head
in a figure-of-eight. The final turn goes round the head and is fixed by
a pin at the point of crossing of the previous turns.
Fig. 82. A Pressure Bandage. The first turn of a 1½-inch bandage
encircles the head. It is then carried beneath the ear and over the head
in a figure-of-eight. The final turn goes round the head and is fixed by
a pin at the point of crossing of the previous turns.
|
The dressings should not be disturbed for at least 24 hours. The lids are then cleansed with 1–6,000 perchloride of mercury lotion, and the lower one is pulled down so as to allow the escape of tears and to see if any discharge be present. The upper lid should not be touched. If no discharge be present the eye is re-dressed. If discharge be present the conjunctival sac should be washed out carefully with boric lotion. Most wounds with conjunctival flaps are shut off in 48 hours, after which time it is advisable to wash out the conjunctival sac twice a day with boric lotion. Great care should be taken to see that no undue pressure is made on the globe. The patient should be warned not to screw up the eyes or strain whilst the dressing is being performed.
Surgical anatomy. The lens consists of fibres which are developed from cells originating in an inclusion of the fœtal epiblast. A normal lens is surrounded by a capsule, the anterior half of which is lined with a single layer of epithelial cells on its inner surface. In fœtal life the cells which line the posterior half of the capsule go to form the lens fibres, so that after birth the lens capsule is lined by cells only on its anterior surface. The lens capsule, which is deposited from the epithelial cells lining it, consists of a highly elastic membrane; small wounds in its continuity, therefore, gape widely. Throughout life the cells lining the capsule continue to become new lens fibres, but at the same time the bulk of the lens does not increase markedly. This is due to the fact that the lens fibres become more closely packed together and lose some of their watery constituents (sclerosis). The older central part of the lens is the first to undergo this process, with the result that a definite hard nucleus is found in the lenses of people about the age of thirty to thirty-five and upwards.
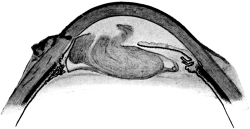 Fig. 83. A Lens Three Weeks after needling. The section shows the
swelling and breaking up of the lens in the anterior chamber. The iris
has become adherent to the needle puncture.
Fig. 83. A Lens Three Weeks after needling. The section shows the
swelling and breaking up of the lens in the anterior chamber. The iris
has become adherent to the needle puncture.
Chemically the lens fibres are composed of crystallin, which is closely allied to a serum globulin and is therefore soluble in salt solution. When the lens capsule has been opened, by operation or accident, the saline aqueous is admitted to the lens, which becomes opaque, swells up, and is gradually absorbed (Fig. 83). In those under the age of thirty, therefore, a simple incision into the capsule is all that is required to cause it to be absorbed. But, as has already been pointed out, the lens develops a hard nucleus after that age and will not then be absorbed satisfactorily by simply opening its capsule; to remove it, as is done in senile cataract, the hard nucleus must be extracted from the eye.
The lens is held in position by the suspensory ligament, which consists of interlacing fibres attached on the one hand to the ciliary process and on the other to the capsule at the lenticular margins (Fig. 84). Prolapse of the vitreous after cataract extraction is prevented by the integrity of this ligament and the posterior capsule of the lens, together with the hyaloid membrane of the vitreous. The tension on the fibres of the suspensory ligament, in addition to keeping the lens in its place, also exercises traction on the lens capsule. In dislocated lenses there is a gap in the suspensory ligament either as the result of injury or of congenital malformation; when such cases require operation there is some difficulty in producing a sufficient gap in the capsule to promote their absorption, owing to the mobility of the lens and the want of traction on the incision in the capsule.
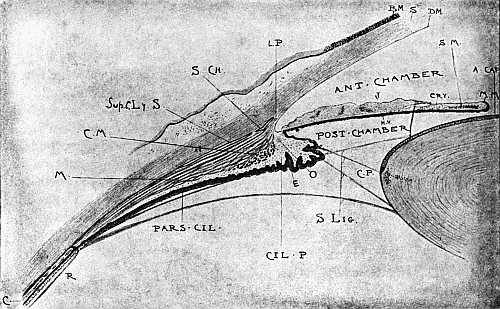 Fig. 84. Anatomy of the Anterior Segment of the Eye.
Fig. 84. Anatomy of the Anterior Segment of the Eye.
| Cil. P. Ciliary process. | S. Ch. Canal of Schlemm. | ||
| L. P. Lig. pectinatum, between the fibres of which are the spaces of Fontana. | |||
| Sup. C. Ly. S. Suprachoroidal lymph-space which extends backwards between the choroid and sclerotic. | |||
| M. Longitudinal portion | } of the ciliary muscle. | ||
| C. M. Circular portion | |||
| O. Circulus arteriosus. | S. Lig. Suspensory ligament of the lens. | ||
| E. Epithelium covering the ciliary process. | |||
| Pars Cil. Pars ciliariis retinæ. Pars plana of the ciliary body. | |||
| R. The retina. | } The junction of these with the pars plana is known as the ora serrata. | ||
| C. The choroid. | |||
| J. Iris. | S.M. Sphincter muscle. | Cry. Crypt. | |
| M. M. Pigment epithelium. | S. Cornea. Substantia propria. | ||
| B. M. Bowman’s membrane. | D. M. Descemet’s membrane. | ||
| A. Cap. Anterior capsule of the lens. | C. P. Canal of Petit. | ||
Discission of the lens has for its object the tearing open of the anterior capsule, so that the lens substance may be broken up and absorbed.
Indications. This operation will be required:
(i) For cataract in patients under the age of about thirty. The forms of cataract for which these operations are usually performed are: (i) complete congenital cataract, in which the whole lens is opaque and consists of little more than a shrunken capsule which may have to be extracted if discission is unsuccessful; (ii) lamellar cataract, of sufficient density to interfere seriously with vision; (iii) posterior polar cataract in rare instances; (iv) traumatic cataract, to complete the absorption of the lens by breaking up its fibres.
Before operating on any form of cataract the following facts must be ascertained as far as possible:—
(a) Vision. It must be remembered that in children a defective eye retaining the power of accommodation is often more useful than an eye which sees better but has to wear different glasses for different distances. Vision must be reduced to less than 6/18 in both eyes after correction with glasses before the operation should be undertaken. In rare cases, in children, and in traumatic cataract where the cataract is very dense and confined to one eye, it may be removed partly to improve the personal appearance and partly to enable the patient to see large objects.
An eye without a lens (aphakia) will not work with an eye with a lens even if the former be corrected with glasses.
If the patient be unable to see letters, he should have a ready and quick perception of light, no cataract, however dense, being sufficient to prevent this.
(b) A patient should have a good projection of light; that is to say, he should be able to locate the light when thrown into the eye with a mirror whatever direction it comes from. Children generally turn the head towards the light, provided that they can see it and that the eye is not defective from other causes.
(c) Note whether the pupils are equal and active. In children most useful information can often be obtained as to the condition of the fundus by means of the pupil, which often will not react when the patient is unable to appreciate light.
(d) The condition of the fundus of the other eye, if observable, should be taken into account, as many diseases of the fundus, such as choroiditis and myopia, are bilateral, and would influence the prognosis considerably.
(e) The lachrymal sac and conjunctiva should be free from all signs of inflammation (see p. 181).
(ii) For the removal of a lens for high myopia. In selected cases operation gives very satisfactory results with great improvement of vision; indeed full normal distance vision has been obtained without glasses. The operation, however, is only justifiable under certain circumstances, the chief of which are:—
| (a) | The amount of myopia should exceed 18 D. |
| (b) | Distance vision should be defective—less than 6/18 with glasses. |
| (c) | Ophthalmoscopically the macular region should be sound. |
| (d) | Binocular vision should be absent. |
| (e) | The patients should be children or young adults. |
| (f) | If there is some serious reason why the patient is unable to wear glasses. |
In emmetropia, if the lens be removed, a glass of + 11 D. has to be placed before the eye for distance vision and + 14 D. for near vision. It is impossible to predict the exact amount of correction of myopia which will be produced by the removal of the lens, owing to the surgeon’s inability to estimate the refractive power of the lens associated with the distortion of the posterior pole of the globe. Usually a patient with about 22 D. of myopia is rendered emmetropic by the operation.
There are two main objections which have been raised to the operation: first, that there is a slight risk of septic infection, sympathetic ophthalmia even having been known to occur; secondly, that retinal detachment seems rather more common after operation than in ordinary myopia of the same degree. As a rule it is only advisable to perform the operation on one eye, the patient using the other for reading purposes, but under certain circumstances, as when the operation has been successful for a considerable period of time, it would be justifiable to perform it on the other eye. The operation should never be performed on patients having only one eye.
Instruments. Speculum (Fig. 85), fixation forceps (Fig. 86), discission needle.
 Fig. 85. Eye Speculum.
Fig. 85. Eye Speculum.
Operation. First step. The operation is best performed by artificial light. The pupil having been dilated with atropine and the eye anæsthetized with cocaine (a general anæsthetic being necessary, however, for young children), the speculum is inserted by first drawing up the upper lid, making the patient look down, and inserting the top blade, and then drawing down the lower lid, making the patient look up, and inserting the lower blade. The speculum is opened to its full width without undue strain on the canthus and is kept in position by tightening the screw. The eye is steadied by fixation forceps held in the left hand, which grasp the conjunctiva as close to the cornea as possible directly opposite to the spot at which the puncture is to be made; the puncture is made directly behind the limbus and the needle is passed into the anterior chamber.
Second step. Using the shaft of the needle lying in the cornea as a fulcrum on which to rotate the needle, an incision is made in the anterior capsule of the lens, and the lens fibres are broken up by a stirring movement. The needle is then rapidly withdrawn in the same plane in which it was inserted so as to avoid making a crucial incision in the cornea with the spear-like end and thereby losing the aqueous. The best way to make sure of this is to mark one side of the handle so that it may be inserted and withdrawn in the same position. A pad and bandage are then applied.
After-treatment. The pupil should be kept dilated subsequently by the use of atropine twice a day until the lens has become absorbed. The bandage may be removed about the fourth day and dark glasses worn.
The effect of the operation on the lens varies considerably. It may swell up so rapidly that the tension of the eye becomes increased, in which case an evacuation may have to be performed; in other cases, especially in the cases of a patient with high myopia, several needlings may be required before absorption is complete.
Capsulotomy is the division of the opaque capsular membrane left after a cataract has been removed.
 Fig. 87. Secondary Cataract. Opaque capsule
after cataract extraction.
Fig. 87. Secondary Cataract. Opaque capsule
after cataract extraction.
Indications. After a cataract has been removed, either by discission or extraction, an opaque membrane is usually left. This is due to the proliferation of the cells in the anterior capsule of the lens while attempting to lay down new lens fibres. Although the posterior capsule is clear and free from cells, those from the anterior capsule may spread to it and so render it opaque. A fibrinous exudate may also organize and help to thicken the membrane (Fig. 87). For these reasons and also because the soft matter may not have absorbed entirely, it is not advisable to operate too soon after a cataract has been removed. There should be at least six weeks’ interval after an extraction has been performed. A few surgeons operate earlier than this, the idea being that the membrane is then softer and more easily divided.
Although the operation of discission for after-cataract (capsulotomy) is simple it is not to be undertaken lightly. The patient’s vision should be less than 6/18. In former days the operation was looked upon as attended with as much risk as the extraction, owing to the frequency with which it was followed by inflammation. The reasons for this seem to have been want of proper antiseptic precautions, the passage of the needle through the non-vascular corneal tissue instead of through the conjunctiva, and also the use of a badly made needle, often resulting in prolapse of the vitreous into the wound. A proper discission needle should have sufficient width in its spear-like point to cut a hole large enough to admit the shaft freely; hence needles which have been sharpened several times should be discarded. It need hardly be said that there should be no signs of cyclitis (keratitis punctata) present when the operation is undertaken.
Instruments. These are the same as for discission, with the addition of a needle with a long cutting edge.
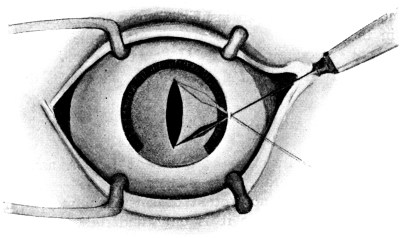 Fig. 88. Capsulotomy. The method of incising the capsule. The fulcrum
of movement of the needle is where the shaft lies in the sclerotic.
Fig. 88. Capsulotomy. The method of incising the capsule. The fulcrum
of movement of the needle is where the shaft lies in the sclerotic.
Operation. Capsulotomy is best performed by artificial light under cocaine. The cutting needle is inserted into the anterior chamber as in the previous operation. The point is then thrust through the membrane below (but it should not penetrate deeply, otherwise the vitreous will be torn) and an incision is made in an upward direction. This incision usually gapes sufficiently to give a clear pupil (Fig. 88). Those surgeons who operate early try to cut out a triangular portion of the membrane. When a dense band is present which gives before the needle and cannot be divided, a second or ordinary discission needle should be passed into the anterior chamber from the limbus opposite to the cutting needle. The discission needle is made to pass behind the band whilst the cutting needle lies in front of it. By a rotary movement of the discission needle around the cutting needle the band is carried against the edge of the latter and so divided. The needles are then withdrawn (Fig. 89).
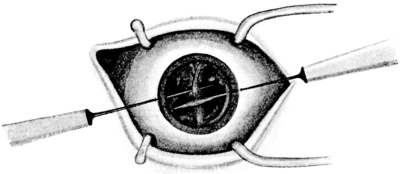 Fig. 89. Capsulotomy. The method of dividing a dense band.
This is done with two needles.
Fig. 89. Capsulotomy. The method of dividing a dense band.
This is done with two needles.
Results. These are good as a rule, but the operation may have to be performed again owing to an insufficient or non-central opening being obtained in the membrane, or to a fresh membrane forming; this is liable to take place if any irido-cyclitis follow the operation.
After-treatment. This should be carried out as described for needling.
Indications. (i) In cases of increased tension associated with soft lens substance in the anterior chamber.
(ii) To accelerate the absorption of soft lens matter from the anterior chamber. As a rule it is only undertaken for the former condition.
Instruments. Speculum, fixation forceps, bent broad needle, curette.
Operation. Under cocaine.
First step. An incision is made behind the limbus, usually in an upper segment of the cornea, by means of a bent broad needle. The point of the instrument is passed into the anterior chamber immediately behind the limbus with the handle at right angles to the cornea; directly the anterior chamber has been entered the handle is depressed so that the point of the instrument shall turn forwards and avoid injuring the iris. The blade is passed on into the anterior chamber until the point reaches about the centre of the pupil. It is then either withdrawn directly, or, if a larger incision be desired, lateral pressure is made so that in withdrawing the blade the wound is enlarged.
Second step. Evacuation. With the rush of aqueous which follows the incision some soft matter is usually evacuated; then a curette may be introduced, if necessary, and the lens fragments removed by gentle manipulation. Occasionally the iris may prolapse into the wound; if this happens it should be replaced, but if it occur more than once the prolapsed portion should be removed. Suction apparatus has been used for removing the soft lens matter, but it is not to be recommended in most cases, owing to the difficulty of sterilization and the trauma which it may cause. After-treatment as for needling should be carried out.
Indications. (i) In congenital cataract when the lens consists of little more than a dense capsular mass.
(ii) In dense capsular membranes following removal of a lens by discission in which a cutting needle cannot make a hole.
Instruments. Speculum, fixation forceps, keratome, capsule forceps, discission needle.
Operation. A general anæsthetic is usually desirable.
First step. The pupil is previously dilated with atropine. In the case of congenital cataract a discission needle is first passed into the mass to estimate its consistency. If it consist of little more than capsule an incision is made at the limbus with the keratome as described for evacuation.
Second step. The blades of the capsule forceps are then inserted closed, opened, and the opaque capsule grasped and withdrawn from the eye. The speculum is then removed and a pad and bandage applied. The pupil should be kept dilated with atropine subsequently, as a certain amount of irido-cyclitis following the operation is not infrequent. Occasionally the iris may become entangled in the wound, and it should then be removed.
Indications. (i) For all forms of cataract in patients over thirty years of age.
(ii) For cases of high myopia over the same age.
(iii) For lenses containing foreign bodies.
(iv) For displacement of the lens causing irritation.
Probably no operation in surgery has so many modifications, many of which possess advantages and disadvantages which counterbalance each other so nearly that the individual surgeon must decide for himself which is the most satisfactory to carry out. The opinion of many surgeons, including the author, is that the ideal operation is one which can obtain sight for the patient at one sitting. The operation described below is carried out with this object in view, the various modifications and the indications for their use being subsequently discussed.
Instruments. Speculum, two pairs of fixation forceps, a Graefe’s knife, iris forceps (Fig. 90), iris scissors (Fig. 91), capsule forceps, cystotome, curette or spoon, iris spatula, vectis (Fig. 92), or lens spoon (Fig. 93).
 Fig. 90. Iris Forceps. Care should be taken to see that the teeth
dovetail properly.
Fig. 90. Iris Forceps. Care should be taken to see that the teeth
dovetail properly.
 Fig. 91. Iris Scissors. Their cutting power should be tested on wet
cigarette paper before use.
Fig. 91. Iris Scissors. Their cutting power should be tested on wet
cigarette paper before use.
 Fig. 92. A Vectis. It should be made of stiff steel.
Fig. 92. A Vectis. It should be made of stiff steel.
 Fig. 93. Pagenstecher’s Spoon. It is an advantage to bend the shaft near
the spoon to a right angle.
Fig. 93. Pagenstecher’s Spoon. It is an advantage to bend the shaft near
the spoon to a right angle.
Operation. The operation is performed under cocaine and is divided into five steps:—
1. Incision.
2. Iridectomy.
3. Opening the lens capsule.
4. Delivery of the lens.
5. Toilet of the wound.
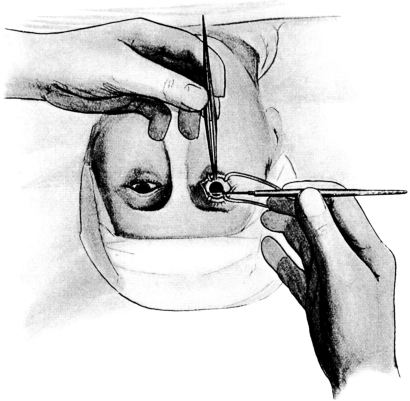 Fig. 94. Lens Extraction. Showing the position of the hands when
making a section upwards with a Graefe’s knife.
Fig. 94. Lens Extraction. Showing the position of the hands when
making a section upwards with a Graefe’s knife.
First step. The incision. The surgeon, standing behind the patient’s head and holding the knife with the edge directed upwards, in the right hand for the right eye and in the left hand for the left, fixes the eye with a pair of forceps held in the other hand, by grasping the conjunctiva below and to the inner side as close to the limbus as possible (Fig. 94). Most continental surgeons stand in front of the patient and cut upwards. The point of the knife is then passed on the flat into the anterior chamber from the outer side, 1.5 millimetres behind the corneo-sclerotic junction.
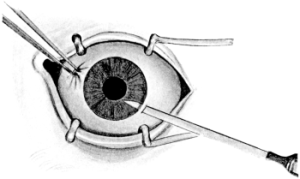 Fig. 95. The Knife entering the Anterior Chamber in Cataract Extraction.
The point of the knife is directed downwards and inwards.
Fig. 95. The Knife entering the Anterior Chamber in Cataract Extraction.
The point of the knife is directed downwards and inwards.
|
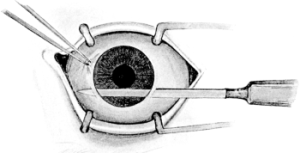 Fig. 96. Making the Counter-puncture in Cataract Extraction. The
counter-puncture is shown completed.
Fig. 96. Making the Counter-puncture in Cataract Extraction. The
counter-puncture is shown completed. |
It is first directed downwards and inwards until the chamber is penetrated (Fig. 95). The knife-point is then directed horizontally and passed across the anterior chamber in a line parallel with an imaginary tangential line across the top of the cornea. The counter-puncture is then made, the knife emerging 1 millimetre behind the corneo-sclerotic junction (Fig. 96). In making the counter-puncture the beginner is apt to go too far back in the sclerotic owing to the angle of the chamber being placed behind the limbus; he should therefore aim for a point about 1 millimetre inwards from the limbus. The knife is next made to cut upwards by a sawing movement so that a flap is formed of corneal tissue about 3 millimetres in breadth (a breadth and a half of a new Graefe’s knife), the upper margin being at the corneo-sclerotic junction. When the corneal flap has been made, the knife should lie beneath the conjunctiva, from which a flap about 3 or 4 millimetres in length should be formed. The knife-edge is then turned forward and made to cut its way out. In making the section, care must be taken not to prick the patient’s nose or eyelid with the point of the knife, as it may cause him to move his head with disastrous results. This is more likely to happen with patients who have sunken eyes.
 Fig. 97. Incision and Iridectomy in Cataract Extraction.
Fig. 97. Incision and Iridectomy in Cataract Extraction.
Second step. Iridectomy. The patient is made to look downwards. A pair of iris forceps are inserted, closed, into the anterior chamber, opened, and the iris grasped near its root, and withdrawn. The piece of iris is then removed with the iris scissors, dividing it parallel with the incision as close to the eye as possible (Fig. 97). If the conjunctival flap hinders the insertion of the iris forceps into the anterior chamber, it may be turned forward over the cornea with the point of the closed forceps.
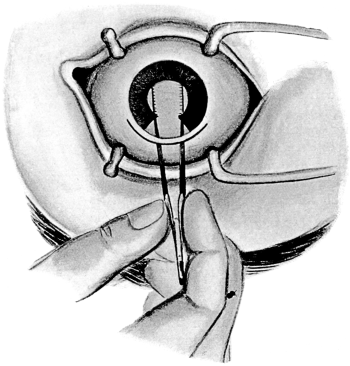 Fig. 98. Opening the Capsule with Forceps in Cataract Extraction.
The forceps are inserted closed, brought in contact with the lens, opened, and the
capsule grasped between the blades and withdrawn by a gentle side-to-side movement.
Fig. 98. Opening the Capsule with Forceps in Cataract Extraction.
The forceps are inserted closed, brought in contact with the lens, opened, and the
capsule grasped between the blades and withdrawn by a gentle side-to-side movement.
Third step. The capsule of the lens is opened. This is done in order to allow the lens nucleus and soft matter to escape. Since the anterior capsule becomes opaque after the removal of the lens, owing to the multiplication of the cells in their attempt to lay down new lens fibres, it is desirable to remove a portion of the anterior capsule from the pupillary area. This may be performed (a) by means of capsule forceps which are inserted closed, and when in position over the lens are opened as widely as possible without entangling the iris, then pressed down on to the anterior capsule of the lens and closed; in this manner the portion of the capsule thus included is removed by a slight lateral movement (Fig. 98); (b) by means of a cystotome, the lens capsule being opened by a triangular or T-shaped incision over the pupillary area; (c) by the point of the knife as it passes across the anterior chamber; (d) by a discission needle before the section is made. When the capsule of the lens has been opened properly the lens nucleus is usually seen to come forward. The advantage of the capsule forceps over the other methods is that they remove a larger portion of the capsule and leave no tags which may become incarcerated in the wound. On the other hand they are somewhat more difficult to use; more pressure on the lens is required, and therefore dislocation of the lens in its capsule may result. It is, therefore, not advisable to use them in cases in which a fluid vitreous is suspected. If the teeth of the forceps are not well made they will not grasp the capsule; it is therefore always advisable to have the cystotome in readiness. The cystotome also should be used when the anterior chamber becomes filled with blood so that the margin of the iris cannot be seen and there is a risk of the iris being grasped by the forceps.
The method of opening the capsule with the point of the knife or needle is useful in cases of extraction without iridectomy; the pupil should be dilated before the operation.
Fourth step. Delivery of the lens is performed by a gentle pressure, combined with massage, on the extreme lower margin of the cornea with a curette or spoon, until the upper margin of the lens presents in the wound, when the pressure is gradually made upwards over the cornea until the lens is delivered. Delivery of the lens may be prevented by—
(a) Imperfect opening of the capsule, which is usually the result of using a blunt cystotome; if capsule forceps are used this difficulty hardly ever arises.
(b) Too small an incision. The margin of the nucleus may present and not be able to pass the wound. The wound must then be enlarged with the iris scissors and the lens delivered in the ordinary way. Only by experience can the amount of pressure required for the delivery of the lens be gauged.
(c) A sticky consistency of the cortex is not infrequently found in cases of immature cataract. When the lens presents and cannot be delivered readily it may be helped out by means of the cystotome plunged into its substance, pressure being used on the cornea at the same time.
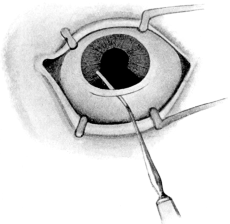 Fig. 99. Cataract Extraction. Replacing the iris, and any tags of
capsule which may be in the wound, with an iris spatula.
Fig. 99. Cataract Extraction. Replacing the iris, and any tags of
capsule which may be in the wound, with an iris spatula.
If from these or any other causes the suspensory ligament rupture and the vitreous present in the wound, the lens should be removed with the vectis. The vectis, which should be made of stiff steel, is passed vertically into the incision and behind the lens nucleus by depressing the handle; with a steady gentle pressure forwards it is then withdrawn together with the nucleus. The forward pressure should be such as to prevent the instrument slipping on the nucleus, for if it does so the accident is nearly always followed by a rush of vitreous. A Pagenstecher’s spoon may be used instead of the vectis, and is to be preferred in cases where a small nucleus is suspected, since the latter may slip through the loop of the vectis and fail to be delivered.
Fifth step. Toilet of the wound. After the nucleus has been extracted, all the soft matter should be removed as far as possible by gentle expression with the spoon. The angles of the coloboma in the iris should be replaced by stroking it inwards on its anterior surface with the iris spatula, paying particular attention to the angles of the wound (Fig. 99). The spatula should also be passed throughout the extent of the wound so as to free it from any capsule which may have prolapsed into it. The conjunctival flap is then placed in position by stroking it upwards with the iris spatula.
After-treatment. Atropine is instilled either at the time of operation or at the first dressing, and continued until all signs of redness of the eye have disappeared. The patient should remain in bed for at least ten days, both eyes being bandaged during the first four days. The eye that has been operated on should be covered for at least two weeks; subsequently a shade or dark glasses should be worn.
Modifications. The operation may be modified in various ways.
The incision. The position of the incision has undergone many modifications. The one described above is now in general use.
The size of the incision should be increased when (a) a large nucleus is expected, as in old people; (b) an immature cataract is to be extracted; or (c) a fluid vitreous is suspected, so that the lens may be delivered with as little pressure as possible.
The iridectomy may be omitted. Extraction without iridectomy is undoubtedly the ideal operation; it leaves the pupil unbroken and the eye looking normal to external appearance. Further, the pupil reacts more strongly to light than if an iridectomy has been performed. The presence of the iris further prevents the prolapse of any capsule into the wound. At the same time it is attended with considerable risk of prolapse, which, as has been pointed out, is a very great danger to the eye. With proper care this probably only occurs in about 5% of the patients operated upon, but is so serious that the opinion of most surgeons is in favour of the combined method (iridectomy and extraction); but at the same time it is the practice of many surgeons to omit the iridectomy under the following circumstances: first, if the patient be young and the deformity will interfere with his getting employment; secondly, if extraction of the lens in its capsule be performed the unbroken circle of the iris will help to prevent the prolapse of the vitreous which is otherwise so liable to take place.
Eserine (gr. ii ad ℥i) should be used to prevent prolapse of the iris after the extraction has been performed, and should be continued once a day until a good anterior chamber is present, which is usually in about twelve to twenty-four hours, when atropine should be substituted. If the iris betray any liability to prolapse after the operation, as shown by the drawing upwards of the pupil, an iridectomy should be performed before the patient leaves the table. In any case the eye should be examined on the evening of the operation, and, if prolapse has occurred, that portion of the iris should be removed. If a prolapse of the iris occurs and is not discovered until the wound has healed, the conjunctiva should be dissected off the surface in the form of a flap and the iris tissue drawn out of the wound and removed, the angles caught in the scar being freed if possible. The opening in the globe is subsequently closed by replacing the conjunctival flap in position, or, if it has not been possible to preserve the conjunctiva over the cicatrix, by raising a flap from the ocular conjunctiva in the neighbourhood and stitching it down over the opening in the globe. Not infrequently this operation is followed by an attack of acute iritis, which usually subsides under treatment.
Preliminary iridectomy. The iridectomy may be performed at a previous operation. It has the advantages that the surgeon learns how the patient will behave under operation, and how the eye will react to such an operation. There is an absence of bleeding at the second operation, which makes it easier, and there is less liability for the iris to become adherent to the capsule. The disadvantages, which seem to outweigh the advantages, are that there is a double chance of sepsis, and that the patient has to submit to two operations when one is sufficient. It is only performed by the author in cases in which there is a tendency to increased tension in the eye due to swelling of the lens in the early stages of the cataract. When a preliminary iridectomy is performed a keratome may be substituted for the Graefe’s knife in making the incision for the iridectomy, a much smaller one being necessary.
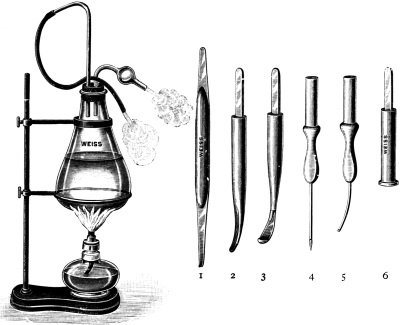 Fig. 100. McKeown’s Irrigation Apparatus for washing out the Anterior
Chamber. The second and third terminals are the most useful.
Fig. 100. McKeown’s Irrigation Apparatus for washing out the Anterior
Chamber. The second and third terminals are the most useful.
Delivery of the lens by irrigation. McKeown removes the soft lens matter by a process of irrigation into the anterior chamber, a practice not yet much adopted, but of considerable service in removing the soft matter after the extraction of the nucleus, especially in immature cataract. It is also probable that the thorough removal of the soft lens matter by this method reduces the number of cases of cyclitis following the operation, since the soft matter forms a suitable medium for the growth of organism. The apparatus used is shown in Fig. 100, nozzle No. 2 being the most useful; it is inserted into one angle of the wound and a stream of sterilized normal saline solution at 39°C. (in the flask) is allowed to flow into the anterior chamber; this stream is obtained by raising the flask until sufficient pressure is obtained. An undine may be substituted for the flask. Care should be taken that there is a free return of fluid from the anterior chamber; irrigation should be continued until as much as possible of the soft matter has been removed.
Extraction of the lens in its capsule. This operation is frequently performed in India, where patients will often not return for needling of secondary cataract (capsulotomy). Although the method undoubtedly yields good results, the percentage of eyes damaged by loss of the vitreous must be higher than when the posterior capsule of the lens is left intact. The operation may be performed with or without an iridectomy, the lens being removed by pressure on the cornea with a large strabismus hook. If the vitreous should present, the lens should be removed with the vectis.
Extraction of the lens in its capsule is also performed when the lens is dislocated and causing irritation. If the lens be in the anterior chamber immediate extraction is called for, as glaucoma is a usual complication. Eserine is first instilled in order to contract the pupil and prevent the lens passing back into the posterior chamber; an incision is then made as for a cataract extraction and the lens removed by means of the vectis. Complete dislocation of the lens into the vitreous rarely requires operation, as the patient is able to see. Partial dislocation (luxation) occasionally calls for extraction, the vectis usually being employed for delivering the lens, but before undertaking the operation an attempt should be made to get the lens into the anterior chamber by dilating the pupil and making the patient lie face downwards; if this is successful eserine should be instilled to contract the pupil behind the lens and so retain it in the anterior chamber, from whence it can more easily be extracted. Some surgeons prefer to fix the lens with a needle passed through the sclerotic behind the ciliary body before making the incision.
Subconjunctival extraction. In order to diminish the risks of sepsis, more especially in cases in which the conjunctiva is affected with trachoma, some continental surgeons deliver the lens into a pocket beneath the conjunctiva, whence it is subsequently removed. The operation has the additional advantage of a better blood-supply to the corneal flap, which is also held in better position after the operation.
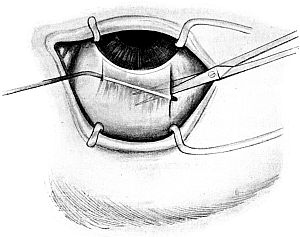 Fig. 101. Subconjunctival Extraction. The section in the sclerotic being
completed with a Graefe’s knife, the figure shows the method of undermining the
conjunctiva to form a pocket into which the lens is delivered and from which it
is subsequently removed.
Fig. 101. Subconjunctival Extraction. The section in the sclerotic being
completed with a Graefe’s knife, the figure shows the method of undermining the
conjunctiva to form a pocket into which the lens is delivered and from which it
is subsequently removed.
Operation. A section upwards is made with a Graefe’s knife as in the ordinary method of extraction previously described, the lens capsule being opened with the point of the knife as it is passed across the anterior chamber. When the section through the sclerotic has been completed and the knife lies entirely beneath the conjunctiva it is withdrawn.
The wound in the conjunctiva on the outer side is then enlarged upwards with scissors, and an iris spatula is passed beneath the conjunctiva from the small wound on the inner side and the point made to appear in the wound on the outer side; by this means the conjunctiva is raised on the spatula, and by means of sharp-pointed scissors a pocket is made in an upward direction by undermining the conjunctiva (Fig. 101). Delivery of the lens is then performed into this pocket, from which it is subsequently removed, the conjunctival wound on the outer side being closed with a stitch. The advantage of this form of subconjunctival extraction over other forms which have been devised is that if difficulty is met with in delivering the lens, &c., the operation can be readily converted into an ordinary extraction by completing the division of the conjunctival flap.
Complications. These may be immediate or remote.
Immediate. 1. If the knife-point become entangled in the iris as it is passed across the anterior chamber it should be slightly withdrawn, if this can be done without loss of aqueous, the iris being thereby disengaged.4
2. Loss of the aqueous before the section is complete may result in the entanglement of the iris as before described, or the iris, owing to the presence of the aqueous in the posterior chamber, may bulge forward in front of the knife-blade. The latter complication is more likely to occur if the section be made too rapidly. The iris may sometimes be disengaged by depressing the handle of the knife towards the patient’s chin and raising the blade towards the cornea so as to allow the aqueous in the posterior chamber to escape. If this cannot be accomplished, the section should be completed and the iris, which may be divided by the knife, removed subsequently when doing the iridectomy.
3. Avulsion of the iris due to movement of the patient’s head. This is more liable to take place if the eye has not been properly cocainized some time before the operation. The grasping of the iris by the forceps is always felt by the patient to a certain extent, and he should be warned not to move. Avulsion is usually not complete and only results in a larger iridectomy than was intended.
4. Dislocation of the lens. (a) When opening the capsule, either from too great pressure of the capsule forceps, or from the patient moving his head. The lens must then be delivered by the vectis. (b) If, in delivering the nucleus, the upper edge is not made to present by pressure on the lower part of the cornea, the nucleus, especially if it be small, is liable to be dislocated upwards beyond the incision. It must then be removed with the vectis. In cases where a small nucleus is suspected, pressure should be made on the sclerotic above the incision with a curette, as well as on the lower part of the cornea, so as to make the nucleus present in the wound.
The lens may be dislocated backwards into the vitreous; if this should happen and the lens cannot be delivered, the flap must be replaced in position and the eye bandaged. Unfortunately this complication is usually followed by irido-cyclitis and loss of the eye.
5. Loss of the vitreous. There are two chief phenomena which may indicate that loss of vitreous is about to take place after the extraction of the lens.
(a) The wound gapes unnaturally after the expulsion of the lens, and the clear vitreous may be seen presenting in the wound in the still unruptured hyaloid membrane.
(b) There may be an apparent deepening of the anterior chamber owing to the fluid vitreous making its way forward through the ruptured hyaloid into that cavity.
If the vitreous presents in the wound before the lens has been removed, the latter should be delivered as rapidly as possible by the vectis, as has previously been described.
If the vitreous be lost or one of the phenomena previously mentioned occurs after the delivery of the lens, the speculum should be removed from the eye and the conjunctival flap replaced in position as quickly as possible. The eyelid is then carefully raised from the surface of the eyeball by means of the lashes held in the finger and thumb and carried downwards over the globe until it is in the closed position, and a bandage is then applied.
As little manipulation as possible should be carried out when once the vitreous has shown itself about to present, and unless the iris be obviously in the wound no attempt should be made to replace it.
Loss of vitreous may be the result of subchoroidal hæmorrhage, which may only make itself manifest after the patient has been put back to bed.
Loss of vitreous is frequently accompanied by hæmorrhage into the vitreous, as is seen subsequently by the floating opacities therein. As a rule these clear, and useful vision is obtained.
Detachment of the retina may follow loss of vitreous even months after operation. This complication seems more liable to occur if the vitreous which is lost in the first instance be normal and not of the fluid type.
6. Intra-ocular hæmorrhage (see Glaucoma Iridectomy, p. 224).
Remote. 1. Panophthalmitis is a result of infection of the wound. It usually makes its appearance about the third day and must be treated by evisceration. Occasionally the purulent material is limited to the line of the incision or even to the anterior chamber; in the latter instance the wound should be opened up and the anterior chamber washed out with peroxide of hydrogen solution (10 vols. %). Microscopic examination of the pus should be made and a vaccine prepared and administered; in two cases so treated by the author a good recovery resulted.
2. Escape of the aqueous beneath the conjunctiva usually occurs about the third day, owing to the conjunctival wound having healed without the opening into the globe being properly shut off. This is accompanied by considerable pain, with chemosis and some œdema of the upper lid. It is usually distinguishable from acute iritis by the pupil being evenly dilated and discoloration of the iris being absent. The condition usually subsides in three or four days, when the wound in the globe has become shut off.
3. Acute iritis not infrequently occurs after extraction. It usually comes on about the third day and may be accompanied by hypopyon. It may settle down under atropine, leeching, and dry heat, but may also pass on into the more chronic form; adhesion of the iris to the capsule, however, frequently results. More rarely the disease may not make its appearance till two or three weeks after the operation (latent sepsis), the patient suffering from recurring attacks of hypopyon. In these cases in which the hypopyon persists, washing out the anterior chamber with peroxide of hydrogen (10 vols. %) and the administration of a vaccine is of service.
4. Chronic irido-cyclitis is usually primary, but may occasionally follow an acute attack of iritis. Of all the disastrous complications, this is by far the worst. It may not only destroy the sight of the eye on which the operation has been performed, but may set up sympathetic ophthalmia in the other eye. The eye does not settle down well after the operation, there being usually some prolapse of the iris or capsule into the wound. It remains injected or flushes up on exposure to light. After a time (usually about the end of the third week) keratitis punctata makes its appearance, and the tension of the eye may become decreased or occasionally increased. The disease may resolve or go on to shrinking of the globe. Energetic treatment with atropine and hot fomentations locally, with the internal administration of iron, is indicated. The administration of staphylococcus vaccine causes only temporary improvement in most instances. In six cases so treated by the author the improvement was only temporary, in spite of the fact that there was a definite local reaction to the vaccine and in two cases the staphylococcus albus was isolated from the fluid in the anterior chamber. If at the end of two months the eye be red and well-marked keratitis punctata be present, and if the pupil be beginning to be drawn up and the eye shows no tendency to improve, enucleation should be seriously considered; this is especially advisable if the projection of light has become defective, showing that the retina is probably detached. If any signs of sympathetic irritation, such as mistiness of vision, ciliary flush, or photophobia, appear in the eye which has not been operated on, the exciting eye should be enucleated. On the other hand, if well-marked inflammation has developed in the sympathizing eye, which may also be cataractous, and the other eye has a fair amount of vision, it becomes extremely questionable whether it is advisable to enucleate the exciting eye. Every case must be judged on its own merits according to the extent and severity of the disease. In a few cases in which the incarceration of the capsule in the wound leads to a very chronic cyclitis, its division with a cutting needle will sometimes lead to subsidence of the inflammation. It is most important that every eye that has been operated on should be examined for the presence of keratitis punctata, especially before allowing the patient to use the eye or before another operation is performed on it.
5. Glaucoma following extraction occurs as a result of (a) soft lens matter blocking the angle of the anterior chamber. As a rule the tension will usually subside under eserine, but evacuation of the anterior chamber (see p. 233) may have to be performed; on the whole the results are satisfactory. (b) The incarceration of the capsule in the wound, pulling forward the iris and blocking the angle of the anterior chamber. Division of the lens capsule is usually sufficient to make the tension subside. Failing this, sclerotomy should be performed; the prognosis is not nearly so good when the increased tension is due to this cause.
6. Striate keratitis usually makes its appearance on the second or third day after operation. The cornea near the line of incision presents a grey striped appearance with the striæ arranged at right angles to the wound. Pathologically the condition is due to an infiltration of the deeper layers of the cornea, the striped appearance being caused by wrinkling of Descemet’s membrane; the condition probably arises from septic infection. As a rule the affection subsides without giving rise to further trouble, but occasionally local suppuration and even panophthalmitis may follow.
A grey horizontal line about the centre of the cornea is sometimes seen after an eye has been too tightly bandaged; this always disappears when the bandage is removed.
7. Erythropsia (red vision) occasionally follows the extraction of the lens, and is probably due to bleaching of the visual purple following the admission to the eye of an unusual amount of light; it usually disappears in a few weeks.
8. Defective vision. Glasses have to be worn after removal of the lens. Usually patients who were previously emmetropic require about + 11 to see clearly for distance and + 15 for near vision.
The section produces some flattening of the corneal curvature at right angles to the line of the incision; this usually amounts to about two diopters.
Couching is the removal of the lens from the pupillary area by depressing it backwards into the vitreous. It is rather a relic of the past than a present-day operation, although it is extensively practised by quacks in India. Under certain circumstances the operation still seems justifiable; it is very simple, and is followed by immediate restoration of vision, but the subsequent risks of irido-cyclitis, retinal detachment, and glaucoma are so great, that, according to some authorities, couching should only be undertaken in preference to extraction when the latter operation has only a chance of one in three of giving satisfactory vision.
Indications. The chief indications for its performance are:—
(i) The presence of a fluid vitreous, the patient having had the lens of the other eye extracted with bad results.
(ii) In the insane, where it would be impossible to carry out the after-treatment of extraction satisfactorily.
Operation. The operation is usually done under cocaine; in the case of the insane a general anæsthetic is usually necessary. It has been performed by simple depression of the lens backwards into the vitreous with a needle passed through the cornea (anterior route). This operation yields unsatisfactory results owing to the lens being liable to return into the pupil; this can be partly overcome by sweeping the needle round the periphery of the lens so as to divide the suspensory ligament, but the operation is not so satisfactory as when the needle is passed in from behind the ciliary body and the lens pressed down from behind (posterior route), to which the following description applies. The capsule of the lens should be torn freely, so that some absorption may subsequently take place and diminish the risk of complications.
Instruments. Speculum, fixation forceps, needle.
First step. The pupil should be dilated with atropine. The patient’s head should be well raised on the table. The needle is passed through the sclerotic about 5 millimetres behind the limbus to the outer side. The posterior capsule of the lens is then freely divided by a sweeping movement.
Second step. The needle is next made to appear in the lower part of the pupil by carrying it round the lower and outer border of the lens. The anterior capsule is then freely divided.
Third step. The shaft of the needle is laid flat on the surface of the lens towards its upper part, and by raising the handle of the needle the lens is displaced backwards into the vitreous. The tearing of the suspensory ligament on the inner side may be assisted by the cutting edge of the needle during depression.
Complications. Immediate. Difficulty may be experienced in making the lens lie at the bottom of the vitreous, and it is only by frequent depression of the lens backwards and downwards, with a sweeping movement of the needle to divide the suspensory ligament, that the desired effect can be obtained.
Remote. The lens nucleus may prolapse through the pupil into the anterior chamber. If this should happen, the patient should be placed on his back and the pupil dilated with atropine; if the nucleus does not go back into the vitreous chamber it should be depressed by means of a needle passed through the cornea.
Glaucoma may result from the dislocation of the nucleus into the anterior chamber and should be treated as described above. It may also be present with a lens which is dislocated backwards. This condition is very liable to end in loss of sight. Probably the only hope of relieving the tension is by the use of eserine or the performance of a cyclo-dialysis.
Cyclitis and retinal detachment may also follow, and usually end in blindness.
Indications. Iridotomy is an operation which is performed when the iris has become drawn up after a cataract extraction, so that there is no pupil, or the pupillary area is covered by the upper lid. A long interval should elapse between the extraction and the iridotomy, since these cases have usually suffered from cyclitis following the operation. Iridotomy should not be performed for at least six months after all signs of cyclitis have disappeared, for the frequent failure of the operation is due to the fact that the opening made in the iris and underlying capsule becomes filled with fibrous exudation as the result of cyclitis, which is frequently set up again by the operation if undertaken before a sufficient time has elapsed for the eye to settle down after the inflammation. The ideal operation, therefore, is to make an artificial pupil with the least amount of trauma to the ciliary body.
Instruments. Speculum; fixation forceps; a long, narrow, bent ‘broad needle’; Tyrrell’s hook, iris scissors, iris forceps, and spatula.
Operation. Many operations have been devised for this most troublesome condition, but the following is the one that the author has found to be successful.
The operation is usually performed under a general anæsthetic, but this is not essential.
 Fig. 102. Iridotomy. Showing the incision with a long, bent broad
needle.
Fig. 102. Iridotomy. Showing the incision with a long, bent broad
needle.
|
 Fig. 103. Iridotomy. Showing the method of withdrawing the band of iris
and capsule with a Tyrrell’s hook.
Fig. 103. Iridotomy. Showing the method of withdrawing the band of iris
and capsule with a Tyrrell’s hook.
|
First step. The surgeon stands facing the patient on the same side as the eye to be operated on. The long, bent, broad cutting needle is passed into the anterior chamber from the limbus downwards and inwards, and is driven directly through the iris and underlying capsule. The needle is then made to pass in an upward and outward direction behind the iris into the pupillary area above, or if no pupil be present, again through the iris (Fig. 102). The bent broad needle is made to cut laterally by slightly deflecting the handle so as to produce a band of iris and capsule; the cutting needle is then withdrawn.
Second step. A Tyrrell’s hook, bent to the correct angle, is passed beneath the band (Fig. 103), which is drawn into the wound and removed with iris scissors. A large opening is thus obtained with a minimum amount of trauma. If the hook should slip, the band may be seized with iris forceps, withdrawn from the wound, and removed.
Alternative methods. The following methods have been practised:—
Simple incision across the fibres of the iris by means of Graefe’s or Knapp’s knife.
Division with scissors through a wound of the limbus.
By these two methods the opening produced is small, and is very liable to be closed by the subsequent cyclitis. The following operation yields more satisfactory results.
Kuhnt’s operation.
Instruments. Speculum, fixation forceps, Graefe’s knife, iris forceps and scissors.
First step. The surgeon, standing facing the patient, enters the anterior chamber about 2 millimetres inwards from the limbus at the junction of the middle and lower third of the cornea with a Graefe’s knife, the cutting edge directed downwards. The knife is then made to penetrate the iris and underlying capsule, and to travel beneath this to a similar point on the other side, where it is made to come back again into the anterior chamber by again penetrating the iris, and finally out again through the cornea. The knife is then made to cut out in a downward direction.
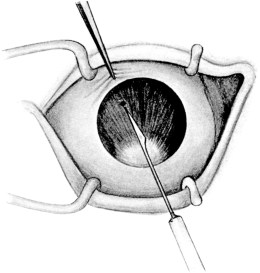 Fig. 104. Iridotomy by Ziegler’s Method. Showing the shape of the knife
and the position of the first puncture in the iris; the cutting is
performed by a sawing movement.
Fig. 104. Iridotomy by Ziegler’s Method. Showing the shape of the knife
and the position of the first puncture in the iris; the cutting is
performed by a sawing movement.
Second step. Iris forceps are inserted and the flap of iris and capsule is withdrawn and as much of it removed as possible. A more or less triangular opening usually results.
Ziegler’s operation.
Instruments. Ziegler’s knife needle, speculum, fixation forceps.
The object of the operation is to cut a V-shaped flap in the iris and underlying capsule, folding the flap backwards on its base so as to form a triangular opening in the iris membrane to serve as a pupil.
First step. The knife needle is entered at the corneo-sclerotic junction with the blade turned on the flat and is passed completely across the anterior chamber to within 3 mm. of the apparent iris periphery. The knife is then turned edge downwards, and carried 3 mm. to the left of the vertical plane (Fig. 104).
Second step. The point is now allowed to rest on the iris membrane, and with a dart-like thrust the membrane is pierced. Then the knife is drawn gently up and down with a saw-like motion, without making much pressure on the tissue to be cut, until the incision has been carried through the iris tissue from the puncture in the membrane to just beneath the corneal puncture. This movement is made wholly in a line with the long axis of the knife, the shank passing to and fro through the corneal puncture, loss of the aqueous being avoided in the manipulation (Fig. 105).
Third step. The pressure of the vitreous will now cause the edges of the incision to bulge open immediately into a long oval. The knife-blade is raised until it is above the iris membrane, and is then swung across the anterior chamber to a corresponding point on the right of the vertical plane. Owing to the disturbance in the relation of the parts made by the first cut, this point is somewhat displaced and the second puncture must be made 1 mm. further over.
 Fig. 105. Iridotomy by Ziegler’s Method. Showing the first incision
and the position of the second.
Fig. 105. Iridotomy by Ziegler’s Method. Showing the first incision
and the position of the second.
|
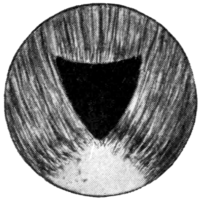 Fig. 106. Iridotomy by Ziegler’s Method. Final step; the triangular
flap of iris attached at its base is turned downwards.
Fig. 106. Iridotomy by Ziegler’s Method. Final step; the triangular
flap of iris attached at its base is turned downwards.
|
Fourth step. With the knife-point again resting on the membrane, a second puncture is made and the incision is carried rapidly forward by the sawing movement to meet the extremity of the first incision at the apex of the triangle, thus making a V-shaped cut. Care must be taken that the pressure of the knife-edge on the tissue shall be most gentle, and that the second incision shall terminate a trifle inside the extremity of the first, in order that the last fibres may be severed and thus allow the apex of the flap to fall down behind the lower part of the iris membrane (Fig. 106). When the operation has been completed the knife is turned on the flat and withdrawn.
The operation of iridectomy differs widely in its performance, according to the different conditions for which it is used. Hence it is better to prefix the condition for which it is employed, thus: preliminary iridectomy, optical iridectomy, glaucoma iridectomy.
Apart from being one of the stages of removal of a cataract, already described, it is performed as an independent operation in the following conditions:—
1. For optical purposes (optical iridectomy).
2. For the relief of glaucoma, primary and secondary (glaucoma iridectomy).
3. For small growths at the free margin of the iris.
4. For prolapse of the iris through a wound.
Indications. Iridectomy for optical purposes is performed for a centrally situated nebula of the cornea and in some very rare cases of small central opacities in the lens. In the latter condition it is rarely of much value, as nearly all the rays which enter the eye pass through the central portion of the lens. Further, in this condition the lens may be removed and better sight obtained with glasses. Optical iridectomy should always be performed opposite a clear portion of the cornea, the lower segment of the eye being chosen, otherwise the coloboma may be subsequently covered by the upper lid. The site of election for the operation is downwards and inwards, but in all cases the patient should be carefully examined in the following ways: (1) the vision is tested, any refraction being corrected without a mydriatic; (2) the pupil is then dilated, and the best situation for the iridectomy determined by means of a stenopaic slit. The vision must be definitely improved by the use of these before operation can be advised. The disadvantage of an iridectomy is that it allows more light to enter the eye, and, if the periphery of the lens be uncovered, spherical aberration may result. For both these reasons, therefore, it is advisable to make the iridectomy as small as possible. Tattooing of the central scar in the cornea will often diminish the amount of light entering the eye, but before undertaking the latter operation, the eye should be cocainized and the area covered with a piece of black paper to see if the vision is improved thereby.
Instruments. Speculum, fixation forceps, bent broad needle or small keratome, Tyrrell’s hook, iris forceps, scissors, and spatula.
Operation. The operation is usually performed under cocaine.
First step. The eye is fixed by grasping the conjunctiva directly opposite the spot at which the incision is to be made. The incision is then made by means of a keratome or bent broad needle directly behind the limbus, and enlarged laterally if desired (Fig. 107).
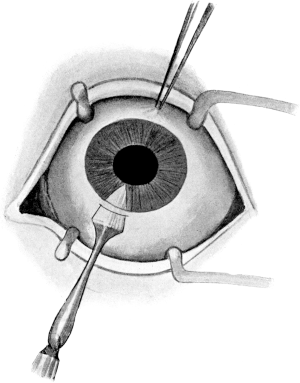 Fig. 107. Optical Iridectomy. The incision being
made with a keratome.
Fig. 107. Optical Iridectomy. The incision being
made with a keratome.
|
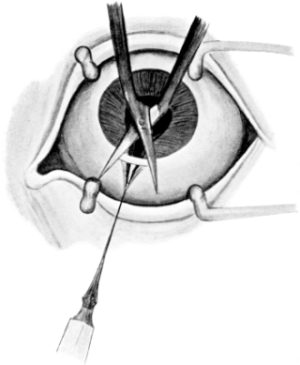 Fig. 108. Optical Iridectomy. Method of removing the iris to produce
a small coloboma.
Fig. 108. Optical Iridectomy. Method of removing the iris to produce
a small coloboma.
|
Second step. A Tyrrell’s hook, bent at the correct angle, is passed on the flat into the anterior chamber. When the margin of the iris is reached the handle is rotated and the hook is made to engage the free border of the iris, which is then withdrawn from the wound; a small portion is removed with scissors, which should be held at right angles to the wound when dividing the iris (Fig. 108).
Third step. The iris should be carefully replaced and the pupil kept under the influence of eserine until the anterior chamber has re-formed, when atropine should be substituted.
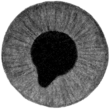 Fig. 109. Optical Iridectomy. Showing the coloboma.
Fig. 109. Optical Iridectomy. Showing the coloboma.
Care must be taken to see that the Tyrrell’s hook presents no sharp angle, and great care is required in its manipulation, otherwise the lens capsule may be damaged, and traumatic cataract will result. If the iris slips from the grasp of the Tyrrell’s hook, iris forceps should be used, the iris being grasped near its free margin and as small a portion as possible withdrawn.
Brudenell Carter’s method. The ordinary optical iridectomy divides the sphincter iridis and so inhibits the activity of the pupil. With the idea of obviating this, Brudenell Carter removed a small portion of the iris (button-hole), leaving the pupillary margin intact. On the whole the results of the latter operation are no more satisfactory, and the operation is more dangerous to perform owing to the likelihood of wounding the lens, and to the fact that monocular diplopia occasionally results.
The pupil should be under the influence of eserine. The incision is made as in the previous operation. De Wecker’s iris scissors are inserted open into the anterior chamber, closed, and the piece of iris which bulges up between the blades cut off; this can usually be withdrawn with the scissors; or if not, it should be removed subsequently by forceps.
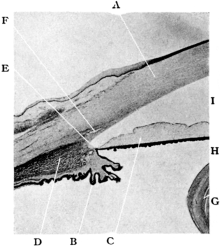 |
Fig. 110. The Normal Angle of the Anterior Chamber.
A. Cornea. |
Surgical and pathological anatomy. The fluid in the anterior and posterior chambers of the eye is secreted from the ciliary body by a process of modified filtration. The fluid passes partly direct into the posterior chamber and partly behind the suspensory ligament of the lens, making its way forward into the posterior chamber through the fibres of the suspensory ligament. From the posterior chamber it passes into the anterior through the pupil; from the anterior it filters at the angle of the anterior chamber through the ligamentum pectinatum into the canal of Schlemm; thence it is carried into the blood-stream by the venous anastomosis in that region (Fig. 110).
The essential change found in all cases of primary glaucoma is the blocking of the angle of the anterior chamber owing to the root of the iris being applied to the back of the cornea, and thus preventing the filtration of the fluid into the canal of Schlemm, as a result of which the tension of the eye is raised, either acutely (acute glaucoma) or slowly from time to time (chronic glaucoma) (Fig. 111). The aim of every operation for the permanent relief of glaucoma is the opening up of Schlemm’s canal at the angle of the anterior chamber or the creation of a new lymph channel between the anterior chamber and the subconjunctival tissue (filtrating cicatrix). Although this latter condition is not unattended by the risk of the spread of inflammation from the conjunctiva to the interior of the globe, it is not an inadvisable condition to obtain in some cases of chronic glaucoma if the scar be small and free from iris tissue; in this disease the opening up of the canal of Schlemm by iridectomy is often impossible. (See Sclerectomy, p. 231.)
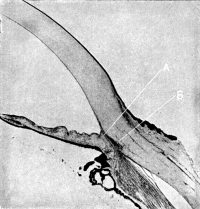 |
Fig. 111. The Angle of the Anterior Chamber from a Case of Recent
Glaucoma. Showing its occlusion by the base of the iris, A, being
adherent to the posterior surface of the cornea, so preventing
filtration of the aqueous into the canal of Schlemm, B.
|
Indications. Since the days of von Graefe, who first performed iridectomy empirically for the relief of glaucoma, the operation has held the first place in its treatment.
(i) In primary glaucoma. Iridectomy should be undertaken as early as possible in the disease. In acute cases, unless the tension is relieved, the disease ends in rapid destruction of the sight. Operation should always be undertaken as quickly as possible, provided the patient has not lost his perception of light for longer than about ten days.
Whilst waiting for the operation, the pupil should be put under the influence of eserine (2 to 4 grains to the oz.) with the idea of reducing the tension by contraction of the pupil. Some surgeons, in addition to using eserine, perform a posterior scleral puncture with the idea of temporarily reducing the tension and allowing the acute symptoms to subside, and do the iridectomy some twenty-four to forty-eight hours later. This method is extremely useful (a) in cases where a general anæsthetic is inadvisable, since the reduction of tension allows cocaine to diffuse into the eye; (b) in cases liable to subsequent intra-ocular hæmorrhage, a more gradual reduction of tension being obtained, rupture of a choroidal vessel is less likely to occur; (c) a deeper anterior chamber is often obtained, and hence there is less risk of wounding the lens during the operation; (d) in cases where the operation has been performed in one eye and the lens has been subsequently extruded on the dressings.
In chronic cases early iridectomy is desirable, since the root of the iris applied to the posterior surface of the cornea becomes atrophic, so that when an iridectomy is performed the iris tears off at the anterior part of the atrophic portion, leaving the angle of the chamber still occluded by its root (Figs. 112 and 113). It is especially in these cases that a filtrating cicatrix, which sometimes follows iridectomy or sclerotomy, is desirable, and indeed some surgeons (Herbert and Lagrange, see p. 231), have recently performed operations with this idea in view, and it is probable that this operation or cyclo-dialysis will prove to be of use in these cases.
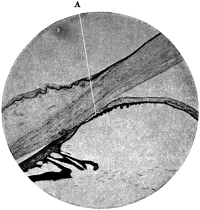 Fig. 112. The Angle of the Chamber in a case of Chronic Glaucoma. The
iris, A, has become atrophic at its root. An iridectomy in this case
would not free the angle of the chamber, as the iris would separate at
the point A.
Fig. 112. The Angle of the Chamber in a case of Chronic Glaucoma. The
iris, A, has become atrophic at its root. An iridectomy in this case
would not free the angle of the chamber, as the iris would separate at
the point A.
|
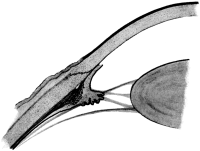 Fig. 113. Iridectomy for Glaucoma. Failure to relieve the tension owing
to the iris not tearing off at its junction with the ciliary body, due
to atrophy from prolonged contact with the cornea.
Fig. 113. Iridectomy for Glaucoma. Failure to relieve the tension owing
to the iris not tearing off at its junction with the ciliary body, due
to atrophy from prolonged contact with the cornea.
|
Operation is only contra-indicated in a few very rare cases in which the tension is controlled by the use of eserine.
(ii) In congenital glaucoma (bup[h]thalmos). In this affection the results of iridectomy vary. Without doubt, the tension has been relieved by iridectomy in some cases, and either this operation, sclerectomy, or cyclo-dialysis should be tried if the disease be not too far advanced.
(iii) In secondary glaucoma. For obvious reasons the predisposing causes should always be taken into consideration. Thus it would be of no use to perform an iridectomy in the case of a growth in the choroid. On the other hand, an iridectomy would be unjustifiable for soft lens matter in the anterior chamber, which merely requires evacuation. An early iridectomy in cyclitis is not likely to influence the course of the disease favourably; at the most a paracentesis is required. As the early stages of cyclitis may give rise to tension, it is essential that every case of glaucoma should be examined for keratitis punctata before operation.
In iris bombé and total posterior synechiæ an iridectomy is indicated more to re-establish the communication between the anterior and posterior chambers than to clear the angle, and therefore it need not be so extensive. In cases of iris bombé where iritis is still present, and in cases of cysts of the iris, transfixion is all that is necessary.
It is very doubtful if iridectomy in glaucoma following thrombosis of the central vein is justifiable, for as a rule the tension is not permanently relieved thereby. In secondary glaucoma following cataract extraction or anterior synechiæ, division of the capsule or the anterior synechiæ will often relieve the tension.
Instruments. Speculum, fixation forceps, Graefe’s knife (with a short, stiff, narrow blade), iris forceps, scissors, and spatula.
Operation. With the idea of opening up the angle of the anterior chamber by removing the iris as near its root as possible, the incision should be made somewhat further back behind the corneo-sclerotic junction than in cataract extraction. At the same time, if the incision be placed too far back the ciliary body is liable to prolapse into the wound. The old idea of opening up the canal of Schlemm by dividing it has been abandoned, as to do so would certainly result in prolapse of the ciliary body; and even if this did not happen, no good would result, since the canal would become closed subsequently by cicatricial tissue.
Although von Graefe used a keratome for making the incision, most British surgeons of the present day use a Graefe’s knife, as it gives an incision that is less shelving and more irregular, thus predisposing to the formation of a filtrating scar; a good conjunctival flap is obtained with it and there is less risk of wounding the lens.
When performing the iridectomy it is practically impossible to cut the iris with scissors at its attachment to the ciliary body, and it is better to rely on tearing it off from the ciliary body, as it is in this situation that the iris is thinnest and most likely to give way, provided it has not become atrophic by prolonged contact with the cornea.
In acute cases and in cases of secondary glaucoma where there are many adhesions a general anæsthetic is desirable.
First step. The incision. The position of the surgeon is as for cataract extraction. The eye is fixed by grasping the conjunctiva close to the limbus downwards and inwards. If the patient be under an anæsthetic, two pairs of fixation forceps should be used, one being held by an assistant. Occasionally in glaucoma the conjunctiva tears very easily, and in these cases scleral forceps are of use, or, if the knife be already in the eye, grasping the insertion of the superior or inferior rectus. The Graefe’s knife should be directed downwards and inwards towards the point of fixation, the point being passed through the sclerotic 1.5 mm. behind the limbus to the outer side. Directly the anterior chamber is entered, the handle is depressed towards the patient’s chin. The knife-point is kept superficial to the iris and is passed very slowly across the anterior chamber, close to its periphery until the position of the counter-puncture is reached. The counter-puncture should be situated about 1 mm. behind the limbus in a direct line with the original puncture. Care must be taken in making the counter-puncture that the knife-point does not slip back on the sclerotic and so emerge further back in the eye than is desired. The knife is then made to cut out upwards and a good conjunctival flap is obtained. The incision should be carried out slowly, so that the aqueous escapes gradually, as sudden reduction in the intra-ocular tension is liable to lead to intra-ocular hæmorrhage.
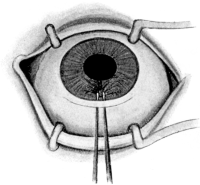 Fig. 114. Iridectomy for Glaucoma. Showing the position in which the
iris should be grasped with forceps.
Fig. 114. Iridectomy for Glaucoma. Showing the position in which the
iris should be grasped with forceps.
|
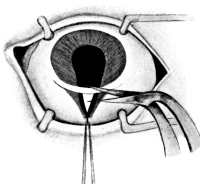 Fig. 115. Iridectomy for Glaucoma. Showing the irido-dialysis produced
before division.
Fig. 115. Iridectomy for Glaucoma. Showing the irido-dialysis produced
before division.
|
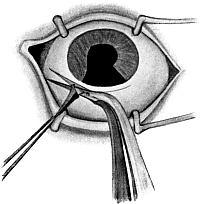 Fig. 116. Iridectomy for Glaucoma. Division of the iris to form the
inner angle of the coloboma. The iris is pulled out as far as possible
before removal.
Fig. 116. Iridectomy for Glaucoma. Division of the iris to form the
inner angle of the coloboma. The iris is pulled out as far as possible
before removal.
Second step. The iridectomy. The iris forceps are inserted closed into the anterior chamber, opened, and made to grasp the iris near the periphery (Fig. 114) towards the side of the wound on which the iris is first to be divided; then with a slight side-to-side movement of the forceps the iris is withdrawn from the wound until its peripheral attachment to the ciliary body, near where it is held by the forceps, is felt or seen to give way (irido-dialysis) (Fig. 115). The iris is then drawn a little further out from the wound, and one side of the dialysis is divided with the scissors as near the scleral wound as possible. The iris held in the forceps is then pulled over to the other angle of the wound, and as much of it as possible is pulled out and divided close to the scleral incision (Fig. 116). The angles of the incision are freed from iris by means of the spatula and the conjunctival flap is replaced in position. Both eyes are then bandaged.
After-treatment. The patient should be kept in bed for a week, and during the first four days should not be allowed to raise the head from the pillow. After that time the eye not operated upon may be uncovered; eserine should have been instilled into it before the operation and at subsequent dressings to prevent the possible onset of glaucoma owing to the dilatation of the pupil which follows the application of the bandage to the eye. It is not necessary to use any mydriatic or myotic for the eye which has been operated upon.
Complications. These may be immediate or remote.
Immediate. 1. In passing a Graefe’s knife into the anterior chamber to make the section, care must be taken that the cutting edge is directed upwards. If by accident it should be inserted with the cutting edge directed downwards the knife should be withdrawn and the operation postponed for a day or two until the anterior chamber has re-formed.
Care must be taken that the cutting edge is kept on the same plane as the upper edge of the back of the knife, otherwise the incision is liable to pass further back than is intended.
2. Splitting the cornea. The anterior chamber often being little more than a potential space, the knife may be passed between the lamellæ of the cornea and may not enter the anterior chamber at all. The indication that the knife-point is not in the anterior chamber is that there is no diminished resistance, such as is usually felt when the knife enters the chamber; if its point be slightly depressed, the cornea will be seen to dimple in over the position of it, showing that the point is not free in the anterior chamber.
3. Locking of the knife. This is due to the fact that the puncture and counter-puncture are not made in the same plane, the knife being twisted. It is much more liable to occur if a knife be chosen with a blade which is not sufficiently stiff. As a rule the blade can be made to cut out, but failing this, the knife should be withdrawn sufficiently to allow a fresh counter-puncture to be made, or else withdrawn altogether and the operation postponed.
4. Wound of the lens. The great safeguard against wounding the lens is to keep the point of the knife always superficial to the iris and in the periphery of the anterior chamber. If the lens be definitely wounded at the time of the operation it should be extracted immediately after the iridectomy. If the wound be only subsequently discovered (usually about the third or fourth day), provided the lens be not presenting in the wound, the eye should be allowed to settle down and the traumatic cataract extracted some time after the tenth day.
 Fig. 117. Glaucoma Iridectomy. Failure
to relieve the tension owing to displacement of the lens.
Fig. 117. Glaucoma Iridectomy. Failure
to relieve the tension owing to displacement of the lens.
5. Presentation of the lens in its capsule. The lens may present in its capsule at the time of the operation or be found subsequently on the dressings. In the latter instance it is very liable to carry iris into the wound, and a cystoid cicatrix results. This accident is usually due to increased tension in the vitreous chamber; a large incision, especially if placed rather far back in the sclerotic, will also favour its occurrence. If the accident should happen to one eye, and acute glaucoma be present in the other, it is advisable to do a posterior scleral puncture before the iridectomy is performed. Partial dislocation of the lens forward may occur after the wound has healed, leaving the tension of the eye not reduced. This is a condition extremely difficult to recognize, and it is usually only discovered pathologically; if recognized clinically, extraction of the lens should be performed (Fig. 117).
6. Intra-ocular hæmorrhage. Hæmorrhage into the anterior chamber occurs at the time of the operation and is readily absorbed; occasionally it may persist for a considerable time in cases of glaucoma of long standing.
After the operation hæmorrhage may also occur from the cut margin of the iris, which never heals, viz. never becomes covered with endothelium. The hæmorrhage may occur as late as two weeks after the operation and may recur from time to time; it is especially liable to occur in old people with arterio-sclerosis. It is usually absorbed without giving rise to any trouble beyond delay in the convalescence.
Retinal hæmorrhages are frequent and usually small, but a considerable hæmorrhage may take place into the vitreous. As a rule these clear up satisfactorily unless the macular region be involved.
Subchoroidal hæmorrhage. Of all the immediate complications which follow an intra-ocular operation this is by far the worst. The hæmorrhage is due to the giving way of a large choroidal vessel following the sudden reduction of tension, with the result that the choroid and retina are stripped up from the sclerotic, and, with the lens, may be partially extruded from the wound in the globe, from which the hæmorrhage then proceeds. It may occur whilst the patient is still on the operating table, or it may be discovered only after he has been put back to bed, the blood being seen coming through the dressings. Patients who have this condition complain of pain in the ‘corner of the eye’ at the time of the operation. The treatment consists in evisceration or enucleation. It is probable that limited extravasation of blood may also occur, which need not end in disintegration of the eye, but may cause vitreous opacity and defective vision for some weeks after the operation.
Remote. 1. The tension is not reduced by the iridectomy. In acute cases the prognosis with regard to the reduction of the tension and the improvement of vision is very satisfactory. The same cannot be said of chronic cases, especially those which have been operated on rather late in the disease. If iridectomy, which may be repeated downwards or extended from the previous coloboma, fail to reduce the tension, one or more of the following measures should be adopted:—
(a) The use of eserine.
(b) Sclerotomy.
(c) Cyclo-dialysis.
(d) Sclerectomy.
(e) Post-scleral puncture.
It is probably in this order that they should be tried.
2. Prolapse of the iris and irido-cyclitis should be treated as already indicated under cataract extraction (see p. 208).
3. The onset of glaucoma in the other eye may be induced by the dilatation of the pupil caused by bandaging, and is best avoided by the use of eserine. If it should occur, an iridectomy should be performed.
4. Astigmatism produced by the incision is corrected with glasses. This astigmatism is very marked, often amounting to six or eight diopters or more.
Indications. This is performed—
| (i) | As a diagnostic measure. |
| (ii) | As a curative measure. |
In the latter instance it is obvious that the growth must be very small and situated at the free margin of the iris to yield a satisfactory result, especially if it be of a malignant character.
Operation. The operation is performed under cocaine, eserine having been previously instilled in order to contract the pupil.
First step. An incision should be made with a narrow Graefe’s knife in the limbus in a position most suitable for removing the growth. The incision should be as large as possible so as to avoid wiping off any portions of the growth into the anterior chamber.
Second step. The iris should be seized well in the periphery so as to avoid breaking up the growth; it is then withdrawn with the growth, and the latter removed.
This operation is usually performed for prolapse of the iris following a wound of the cornea or limbus, and may be attempted up to about the third day after the original injury.
Operation. A general anæsthetic is usually desirable. The prolapsed iris should be seized with the forceps and withdrawn from the wound. A second pair of forceps is used to take a fresh hold on the iris, which can usually be drawn out further (Fig. 118). It is then divided as close to the corneal wound as possible. The iris usually flies back into the anterior chamber clear of the corneal wound by its own elasticity, but if it does not do so it should be freed with a spatula. The pupil should be kept subsequently under atropine.
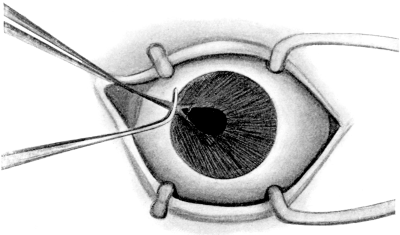 Fig. 118. Prolapse of the Iris through a Punctured Wound of the
Cornea. Method of withdrawing the iris by two pairs of iris forceps before removal.
Fig. 118. Prolapse of the Iris through a Punctured Wound of the
Cornea. Method of withdrawing the iris by two pairs of iris forceps before removal.
Indications. This operation is undertaken in cases of iris bombé when iritis is still present and when an iridectomy would subsequently lead to a drawn-up pupil. It is also of service to evacuate the contents of cysts of the iris (local iris bombé).
Instruments. Speculum, fixation forceps, Graefe’s knife (narrow).
Operation. The knife is entered at the limbus from the outer side directly opposite the occluded pupil. The apex of the iris bombé is transfixed and the point of the knife made to appear above the pupillary area; the iris bombé on the other side of the pupil is then transfixed and the knife is withdrawn.
Indications. Anterior synechiæ rarely require division unless they are likely to cause tension or the adherent iris is considered a source of danger to the eye on account of its liability to septic infection. If the synechiæ are causing tension, the method of division described under sclerotomy is probably the most satisfactory; otherwise the following method devised by Lang can be used.
Instruments. Speculum, fixation forceps, Lang’s knives—one with a sharp point, and one blunt.
Operation. Under cocaine. The incision is made at the limbus in a favourable situation for the division of the synechia. The sharp-pointed knife is introduced into the anterior chamber and then rapidly withdrawn so as not to lose the aqueous. The blunt knife is then inserted through the incision and, partly by cutting and partly by tearing, the synechia is divided in a direction from the periphery towards the pupil.
The operation is not at all easy to perform, since the iris gives before the knife. Great care should be taken to avoid evacuating the aqueous, as the operation is thereby rendered much more difficult or even impossible.
Indications. Sclerotomy is an operation undertaken for the relief of increased intra-ocular tension. It is performed—
(i) Usually as a secondary operation when iridectomy has failed.
(ii) As a primary operation for the division of anterior synechiæ causing tension.
A few surgeons prefer the operation to iridectomy, especially in cases of bup[h]thalmos. When practised after an iridectomy which has been done upwards, the sclerotomy is sometimes performed in a downward direction; otherwise the section is usually made upwards. The intra-ocular tension is probably relieved by the formation of a filtration cicatrix, and it is therefore probable that it may be largely superseded by the operations of cyclo-dialysis and sclerectomy.
When performed for the division of anterior synechiæ the position of the incision should be planned according to the situation of the synechia to be divided.
Instruments. Speculum, fixation forceps, Graefe’s knife with a narrow blade.
Operation. The operation is done under cocaine. Eserine should have been previously instilled in order to contract the pupil and prevent prolapse of the iris.
Graefe’s knife should be passed across the anterior chamber in the same manner and position as for a glaucoma iridectomy (see p. 221). In the complete method the knife is made to cut out through the sclerotic, leaving a band of conjunctiva to hold the flap in position. In the incomplete method a band of sclerotic is left in the periphery. If the operation is done in a downward direction, it is better for the surgeon to stand on the opposite side of the patient to the eye on which the operation is to be performed, operating across the patient.
Complications. Any of the complications which follow an iridectomy for glaucoma may occur (see p. 222). Prolapse of the iris is probably the most frequent.
Indications. This operation has only recently come into general use in this country, so that statistical results have at present by no means been worked out, but most satisfactory results have been obtained from it in individual cases; according to German authorities about 30 per cent. are permanently cured. Although at present its performance is largely limited to blind eyes and to eyes that have undergone previous operations for glaucoma, it is probable that it may come into further use as a primary operation in the treatment of chronic glaucoma and bup[h]thalmos. It is also of service in cases of dislocation of the lens backwards, associated with increased tension, where iridectomy would certainly be followed by loss of the vitreous.
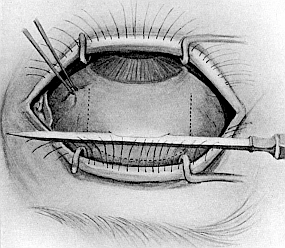 Fig. 119. Cyclo-dialysis Operation. Showing the method of commencing
the incision in the sclerotic; it is subsequently deepened with the point of the knife.
The dotted lines mark the incision for turning forward the conjunctival flap.
Fig. 119. Cyclo-dialysis Operation. Showing the method of commencing
the incision in the sclerotic; it is subsequently deepened with the point of the knife.
The dotted lines mark the incision for turning forward the conjunctival flap.
The operation has for its object the separation of the ligamentum pectinatum from its attachment to the sclerotic, with the probable result that the ciliary body and iris root become retracted by the ciliary muscle, so that the canal of Schlemm is opened up and again communicates with the anterior chamber. It also opens up a free communication between the anterior chamber and the suprachoroidal lymph-spaces. The reduction of tension is often not fully manifest for about ten days after the operation.
Instruments. Speculum, fixation forceps, Graefe’s knife, fine pair of straight iris forceps, fine pair of sharp-pointed straight scissors, iris spatula.
Operation. The operation is best performed under a general anæsthetic, as it is attended with considerable pain, although cocaine and adrenalin are frequently used and are always advisable, since the hæmorrhage from the scleral vessels renders it difficult to gauge the depth of the wound in the sclerotic.
First step. By means of the straight iris forceps and sharp-pointed scissors a semilunar conjunctival flap is first raised over the site for the scleral incision. The incision in the sclerotic should be situated about 5 mm. behind the corneo-sclerotic junction over the ciliary region, the outer and upper quadrant of the eye being the easiest position for subsequent manipulation (Fig. 119).
Second step. With a Graefe’s knife the fibres of the sclerotic are carefully divided in an oblique direction forward until the suprachoroidal lymph-space is opened for about 3 mm. The first part of the incision is performed with the blade and completed with the point of the knife, the anterior flap of sclerotic being held forward by straight iris forceps. Heine uses a keratome, dividing the fibres of the sclerotic with the point by stroking it along the line of the incision. The depth of the incision should be carefully gauged from time to time with the iris spatula; the pigment of the ciliary body is usually seen in the bottom of the wound when the sclerotic has been penetrated.
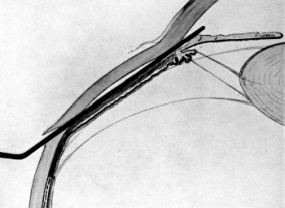 Fig. 120. Cyclo-dialysis Operation. Showing the spatula separating the
ciliary body and ligamentum pectinatum from the sclerotic.
Fig. 120. Cyclo-dialysis Operation. Showing the spatula separating the
ciliary body and ligamentum pectinatum from the sclerotic.
Third step. The iris spatula is directed forwards and inserted between the sclerotic and the ciliary body, keeping close to the former. With a gentle side-to-side movement the spatula is made to separate the ciliary body from the sclerotic for about one-eighth of its whole circumference; then the ligamentum pectinatum is detached from the sclerotic for about the same distance by gently passing the spatula forwards and making the latter appear in the anterior chamber (Fig. 120). If it be desired to evacuate the anterior chamber, the spatula is slightly rotated so as to allow the escape of the aqueous. As a rule this is not necessary or even advisable. The spatula is then withdrawn and the conjunctival flap is replaced in position. Eserine should be instilled.
Complications. (1) Unless the incision be carried carefully through the sclerotic, or the manipulations with the iris spatula be very gentle, loss of vitreous is liable to take place. As a rule, this, if not great, is of little consequence. (2) In passing the iris spatula forward to separate the ligamentum pectinatum the point may pass between the layers of the cornea; this is recognized in the resistance offered to the side-to-side movement of the spatula, which should be withdrawn slightly and the point depressed so as to engage the ligamentum pectinatum. (3) Subchoroidal hæmorrhage has been known to occur after the operation.
The object of the operation is the production of a filtration cicatrix free from iris tissue for the relief of intra-ocular tension in chronic glaucoma.
Instruments. As for glaucoma iridectomy, with the addition of a small curved pair of scissors.
Operation. Under cocaine.
First step. The incision is performed as for glaucoma iridectomy (see p. 221), except that the incision should be rather smaller and should be carried more obliquely through the sclerotic, so that a long scleral flap is obtained. A large conjunctival flap is very essential to cover the wound.
Second step. An iridectomy is usually performed as for glaucoma; this may be omitted.
Third step. After all the bleeding has ceased, the conjunctival flap is turned forwards on to the cornea so as to expose the scleral flap; with small curved scissors made for the purpose, an elliptical portion is removed from the sclerotic by a single snip (Figs. 121 and 122), and the conjunctival flap is replaced in position. As a result, a hole is made into the anterior chamber, which thus communicates with the subconjunctival tissue, which is bulged forwards in the form of a clear vesicle by the escaping aqueous when the wound has healed.
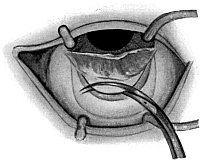 Fig. 121. Lagrange Operation For the Production of a Cystoid Scar in
Chronic Glaucoma. Showing the method of removing a piece of the
sclerotic.
Fig. 121. Lagrange Operation For the Production of a Cystoid Scar in
Chronic Glaucoma. Showing the method of removing a piece of the
sclerotic.
|
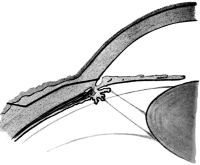 Fig. 122. Lagrange Operation For Chronic Glaucoma. Showing the piece of
sclerotic removed by the scissors (black lines).
Fig. 122. Lagrange Operation For Chronic Glaucoma. Showing the piece of
sclerotic removed by the scissors (black lines).
|
The immediate results of this operation are satisfactory provided that enough sclerotic be removed to produce a filtration cicatrix. As yet sufficient time has not elapsed for any statistical results to be obtained, but the cases in which the operation has been performed are reported as satisfactory.
Indications. Posterior scleral puncture is performed—
(i) For the relief of tension, the indications for which have already been described under the indications for iridectomy in glaucoma (see p. 218).
(ii) For the evacuation of fluid behind a detached retina.
The operation in the latter instance, although not yielding very satisfactory results with regard to the reattachment of the retina, may be carried out with some hope of success in certain cases. Before performing the operation the pathological cause of the detachment should be carefully investigated, for it is obvious that it would be useless to perform the operation in a case of detachment due to a choroidal tumour or if definite bands of fibrous tissue could be seen in the vitreous pulling off the retina. Undoubtedly it should be undertaken as soon as possible after the detachment has occurred and the puncture should enter the space filled with subretinal fluid. Whether the puncture should penetrate the overlying retina is still a disputed point.
After the operation a pressure bandage should be applied and the patient should be kept on his back and not allowed to raise his head from the pillow for at least three weeks. This latter part of the treatment is most essential; indeed as good results may be obtained with complete rest as by performing scleral puncture. Unfortunately, recurrence is very liable to take place whichever method be used, even if reattachment of the retina be obtained.
Instruments. Speculum, fixation forceps, Graefe’s knife.
Operation. Under cocaine. If no special position be indicated the puncture is best made upwards and inwards. The patient is made to look outwards and downwards. The conjunctiva over the sclerotic, well behind the ciliary body, is drawn down so that when released it shall form a valvular opening to the scleral wound. The Graefe’s knife is driven through the conjunctiva and sclerotic, the incision being made antero-posteriorly in the direction of the fibres of the sclerotic to avoid wounding the choroidal vessels. It is probably better to enlarge the wound when withdrawing the knife than to turn the latter at right angles before it is withdrawn, as has been recommended by some surgeons. A bead of vitreous usually escapes under the conjunctiva. If the tension be not lowered, gentle massage of the globe through the lid should be employed.
Indications. Evacuation of the contents of the anterior chamber is performed for several conditions:—
(i) To reduce the tension of the eye when due to an altered consistency of the aqueous, as for instance in cyclitis.
(ii) To evacuate pus from the anterior chamber following metastatic infection.
(iii) To evacuate the anterior chamber in bad corneal ulceration, especially when associated with hypopyon and tension.
(iv) To examine the aqueous for organisms in cases of cyclitis following operation or of metastatic origin.
(v) To evacuate soft lens matter (see p. 194).
 Fig. 123. Hollow Needle Used for Paracentesis Of the Anterior Chamber.
This is used when it is desired to examine the aqueous
bacteriologically. Care should be taken to see that the cutting blade is
sufficiently wide to take the shaft of the needle.
Fig. 123. Hollow Needle Used for Paracentesis Of the Anterior Chamber.
This is used when it is desired to examine the aqueous
bacteriologically. Care should be taken to see that the cutting blade is
sufficiently wide to take the shaft of the needle.
The operation is usually performed through an incision directly behind the limbus. In the case of corneal ulceration it is sometimes performed by dividing the base of the ulcer with a Graefe’s knife (Sämisch’s section). When collecting the aqueous for bacteriological examination, a sterile hollow needle with a point similar to a discission needle, attached to a hypodermic syringe, should be passed into the anterior chamber at the limbus and the fluid withdrawn into the syringe by an assistant (Fig. 123). The spot through which the needle is passed is first touched with the electro-cautery to ensure asepsis.
Instruments. Speculum, fixation forceps, bent broad needle, iris spatula.
Operation. Under cocaine. The puncture is usually made upwards and outwards unless there be some other special indication for its position, such as a mass of pus in the lower angle of the anterior chamber. The eye is fixed opposite the spot at which the puncture is to be made, and the bent broad needle is passed into the anterior chamber through an incision directly behind the limbus. The needle is then withdrawn and is usually followed by a rush of aqueous. The remainder of the aqueous is then evacuated by pressing the lower margin of the wound with an iris spatula. In some cases where a very tenacious hypopyon is present it may be withdrawn with the iris forceps. The only complication liable to occur is prolapse of the iris into the wound, which should be replaced with the spatula, or failing that, removed.
Indications. Of all the conditions which a surgeon is called upon to see, penetrating wounds of the globe may present the most difficult problems as to treatment. The most important factors in their treatment and prognosis are—
1. The time at which the patient presents himself for treatment and the condition of the wound are all-important in the prognosis. Thus in the case of a wound which is obviously septic and going to terminate in panophthalmitis the eye should be eviscerated.
2. The position and extent of the wound. Formerly it was taught that if the ciliary body were wounded the eye should be excised. The reason for this was that these injuries were so frequently followed by sympathetic ophthalmia owing to prolapse of the iris and ciliary body. It is now generally recognized that sympathetic ophthalmia only follows if the wound becomes septic, irido-cyclitis with keratitis punctata being present, and it is only after the latter symptom manifests itself that the eye should be excised, provided that the wound be not so extensive as to preclude all chance of recovery from the outset.
In wounds of the sclerotic all portions of the uveal tract and vitreous which prolapse should be removed, and the wound closed with sutures passed through the superficial episcleral tissue. Unless the wound be small the prognosis is not good, as it is liable to be followed by irido-cyclitis, or, if this does not occur, detachment of the retina may ensue, following on organization of the exudates in the vitreous.
Wounds of the cornea usually result in prolapse of the iris, which should be removed in the manner described under iridectomy (see p. 208).
3. If the lens be injured. Unless the wound amounts to little more than a punctured wound of the globe involving the lens, the prognosis is bad. The wound in the lens capsule and the breaking up of the lens mean the presence of soft matter in the anterior chamber—a condition which favours sepsis and is liable to produce increased tension from blocking the angle of the chamber. In patients under thirty the pupil should be dilated with atropine and the lens allowed to absorb—assisted at a later date by needling, when the eye has entirely settled down after the original injury. If the patient be over thirty it is often extremely difficult to decide whether extraction of the lens should be undertaken at the time of the injury or at a later date. The results of both procedures are very unsatisfactory, and the surgeon should be guided partly by the position and extent of the wound. Given these in a fairly favourable position, it is probable that immediate extraction will give the best result.
4. If the eye contain a foreign body. Usually these are pieces of metal or glass. The following points should be investigated to determine whether the foreign body be in the eye:—
(i) The history of these accidents is usually the same. The patient is chipping with a hammer and chisel, and a piece flies off and strikes the globe. In the case of glass it is usually a mineral-water bottle which bursts.
(ii) The position and nature of the wound in the cornea and sclerotic.
(iii) The condition of the anterior chamber—whether evacuated or not.
(iv) The tension of the eye, which may be lowered.
(v) The presence of a hole in the iris.
(vi) The presence of traumatic cataract.
(vii) Whether the foreign body is visible with the ophthalmoscope or by focal illumination.
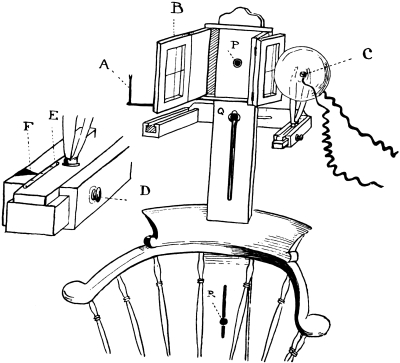 Fig. 124. Author’s Chair for the Localization of Foreign Bodies in The
Eye by the X-rays. A is a rifle sight for centring the anode, C, on the cross wire,
B, behind which the photographic plate is subsequently placed. P is the screw
clamping the head-piece on to the patient’s head. Q is the screw for regulating the
height of the tube and the distance from the patient. R is the screw for regulating
the height of the head-piece. The inset shows the arm carrying the tube more
highly magnified. E is the sliding arm carrying the tube for lateral displacement
marked for stereoscopic photographs. F is the pointer for marking the position
of the anode. D is the screw for clamping when in position.
Fig. 124. Author’s Chair for the Localization of Foreign Bodies in The
Eye by the X-rays. A is a rifle sight for centring the anode, C, on the cross wire,
B, behind which the photographic plate is subsequently placed. P is the screw
clamping the head-piece on to the patient’s head. Q is the screw for regulating the
height of the tube and the distance from the patient. R is the screw for regulating
the height of the head-piece. The inset shows the arm carrying the tube more
highly magnified. E is the sliding arm carrying the tube for lateral displacement
marked for stereoscopic photographs. F is the pointer for marking the position
of the anode. D is the screw for clamping when in position.
(viii) The localization of the foreign body by the X-rays. The latter is the most important factor of all, since the foreign body may pass right through the globe and be embedded in the orbit.
Operative treatment. If the injury be a recent one and the foreign body a metal of magnetizable properties, it is best removed by an electro-magnet after localization by the X-rays (Fig. 124). Sideroscopes have been used, but are not so satisfactory. If the foreign body be non-magnetizable, such as a piece of copper cap or manganese steel, an attempt may be made to remove it with forceps after localization. If the foreign body be embedded in the lens it is often advisable to extract the lens together with it. If the foreign body be of glass, and it be only small, it is usually best left alone, unless capable of easy removal, e.g. if it be situated in the anterior chamber; the eye will often tolerate the presence of glass provided it be aseptic.
The eye should be removed—
(i) If the wound be obviously septic.
(ii) If the wound be very large, more especially if the lens be injured.
(iii) If the foreign body be a large piece of metal and cannot be extracted.
(iv) If the eye does not settle down after one of the operations described below, especially if irido-cyclitis with keratitis punctata should have supervened.
If the injury be of long standing. It is of little use as a rule attempting to extract a foreign body from the eye after three days, unless it be loose in the vitreous or embedded in the lens, as it becomes surrounded by lymph. Under these circumstances it is better to leave it alone, or, if it be causing signs of irritation, to enucleate the eye.
Magnets for the removal of magnetizable foreign bodies from the eye are of two types—(1) a small magnet, which is inserted into the globe, (2) a giant magnet, which is used to attract the foreign body in the eye from the outside.
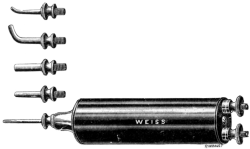 Fig. 125. Small Electro-magnet for extracting Pieces of Steel from the Eye. It
is made to work direct off the electric main.
Fig. 125. Small Electro-magnet for extracting Pieces of Steel from the Eye. It
is made to work direct off the electric main.
Surgeons differ as to which is the best method to employ. The statistical results of both are about the same. Many surgeons in this country, and with them the author, prefer the small magnet, especially of the recent more powerful type (Hirschberg), which runs off the main electric current, for the following reasons: it is more accurate (after localization by the X-rays), there is less trauma to the globe involved, it is more portable, and, when the foreign body is in the anterior or the posterior chamber, it is much easier to extract it with a small magnet than with a large one.
With the small magnet. Instruments. Beer’s knife, fixation forceps, magnet (Fig. 125), and suture. The points of the magnet, which are detachable, are sterilized by boiling.
Operation. The foreign body is first localized accurately by means of the X-rays. If it lies near the wound of entrance the magnet point is inserted, the electric circuit completed, and the foreign body withdrawn, the wound of entrance being enlarged if necessary. If the foreign body lies at some distance from the wound, as for instance in the vitreous, an antero-posterior incision is made in the sclerotic, as near to it as possible, by plunging the knife through the conjunctiva and the sclerotic, the former having previously been drawn to one side so as to form a valvular opening. The size of the incision should be such that it will admit the point of the magnet and allow the foreign body to come out, the size of the foreign body being judged by the X-ray photograph. After the knife has been withdrawn, the point of the electro-magnet is inserted and the circuit closed, the magnet being withdrawn with the foreign body attached to it. The conjunctival wound is closed by a suture if necessary. If the foreign body be situated in the anterior or posterior chamber or the lens, an incision should be made into the anterior chamber with a keratome, the point of the magnet inserted, and the foreign body withdrawn. In cases in which the foreign body is deeply embedded in the lens, more especially in patients over thirty years of age, extraction of the lens together with the foreign body should be performed.
Complications. Immediate. Failure to extract the foreign body may arise from—
1. The foreign body being embedded in lymph. It is therefore of the utmost importance that the operation should be performed as soon as possible after the injury.
2. The foreign body being deeply embedded in the sclerotic so that the magnet will not exert sufficient traction to withdraw it.
3. The foreign body being non-magnetic (all steel is not magnetic).
4. Too small a wound being made for its extraction, the metal being wiped off on the edges of the wound as the magnet is withdrawn.
5. Insufficient power in the magnet.
Remote. 1. Panophthalmitis, which must be treated by evisceration.
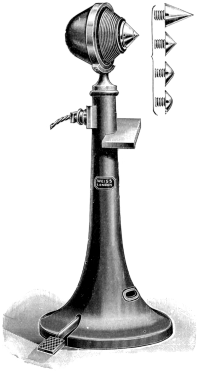 Fig. 126. Large Electro-magnet.
The current is turned on by means of the foot pedal.
Fig. 126. Large Electro-magnet.
The current is turned on by means of the foot pedal.
2. Irido-cyclitis; if this be prolonged, and keratitis punctata appear, enucleation should be performed.
3. Traumatic cataract; this may subsequently require needling.
4. Detached retina as the result of organization in the vitreous; this may occur months after the original injury.
With the giant magnet. The foreign body should have been previously localized by the X-rays, and its position and size determined, so that it may be removed by the shortest possible route and with the least amount of injury to the eye.
Instruments. Giant magnet (Fig. 126), steel spatula. (Watches and magnetizable metal should be removed from both the patient and the surgeon.)
Operation. Under atropine and cocaine. The patient is at first seated in a chair some three feet in front of the magnet, the eyelids being held apart by the surgeon; the electric circuit is closed. The patient’s head is next gradually advanced towards the magnet. If a foreign body be present in the eye and be magnetizable, the patient will usually withdraw his head or cry out with pain, and the foreign body may be seen bulging forward the iris from the posterior chamber. From this position it may be removed by manipulating the head and eye in relation to the magnet so as to withdraw it into the anterior chamber, from whence it is removed through the entrance wound or an incision at the limbus either by the giant magnet directly applied to the wound or by magnetizing a steel spatula which is inserted into the anterior chamber and connected with the magnet by a flexible steel cable. The small magnet previously described may be used, or the foreign body removed by means of iris forceps.
A piece of steel in the vitreous always travels round the posterior surface of the lens and through the suspensory ligament, and does not injure the lens capsule.
Complications. These are similar to those described under the small magnet operation.
Removal of a foreign body from the cornea requires a good light (focal illumination). The use of a binocular lens is also of service. Foreign bodies lodged on the surface of the cornea can be removed easily under cocaine with a spud. If the foreign body be deeply embedded in the cornea a fine sterile discission needle should be used. When a foreign body, such as a chip of iron, is deeply embedded, the needle should be inserted slightly to one side of the entrance wound and passed beneath the foreign body so as to lift it from its bed. When the foreign body has partially penetrated the anterior chamber but still lies in the cornea, an incision should be made with a keratome at the limbus and the foreign body pushed back through the entrance wound with the aid of an iris spatula. If the foreign body be iron, the electro-magnet may be of use, and in this case should be tried before resorting to an incision in the anterior chamber. A stain is left frequently after the removal of foreign bodies; this should be removed as far as possible. Subsequently the eye should be bandaged for a few days and bathed with boric lotion. Atropine should be instilled if there be any signs of infiltration around the wound.
Either a chemical or the actual cautery may be used.
Indications. Corneal ulceration. The cornea being extremely dense, organisms do not penetrate very deeply into its substance, so that destruction of the bacteria is effected by cauterization of the spreading portion of an ulcer; the albumin is also coagulated and so a barrier is presented to their advance.
Operation. The eye is thoroughly cocainized, and the spreading portion of the ulcer is first defined by staining with fluorescine, washing away the excess of stain with boric lotion.
By a chemical caustic. Liquefied carbolic (carbolic acid crystals liquefied in 10 per cent. of water) is applied upon a sharpened match. Any excess should be removed so as to prevent its running on to the cornea. A speculum is inserted and the cornea is dried by blotting with cigarette paper; the stained area is lightly touched with the point of the stick, particular attention being paid to the spreading margin. A dense white plaque is the result; this usually clears up in a few days. Atropine ointment is applied daily to the conjunctival sac.
 Fig. 127. Electro-cautery.
Fig. 127. Electro-cautery.
By the actual cautery. The electro-cautery (Fig. 127) point should be extremely fine and only raised to a dull red heat. The stained area should be touched lightly with the point.
The actual cautery is best for serpiginous corneal ulcers, carbolic acid being more satisfactory for those of the vesicular type.
Indications. Since the operation for conical cornea is not without serious risks, it should only be undertaken when the vision cannot be improved with glasses to 6/18; high + or - cylinders will often yield satisfactory results. The object of all forms of operation is the flattening of the cone.
Operation. This may be carried out either by excision of the apex of the cone or by cauterization.
Excision of the apex of the cone is probably the more satisfactory method, although it is somewhat more difficult to perform. The object of the operation is to remove an elliptical portion of the whole thickness of the cornea from the apex of the cone, the long axis of the ellipse being placed horizontally. It leaves the eye with only a minute scar as compared with the nebula produced by the cautery, which is often so great as to require an optical iridectomy to restore vision.
Instruments. Speculum, fixation forceps, a narrow Graefe’s knife, straight iris forceps, and scissors.
The operation is done under cocaine, atropine having been previously instilled.
First step. The apex of the cone is transfixed by the Graefe’s knife with the blade directed slightly upwards and forwards, the knife being made to cut out. The cornea in this situation is extremely thin, being often not more than 1 mm. in thickness. The length of the incision should not exceed 2 mm.
Second step. The flap of corneal tissue thus made is seized with the straight iris forceps and removed with iris scissors, producing a small elliptical opening. The chief difficulty of the operation is the seizing of the corneal flap, which is most difficult to hold; care must be taken not to injure the lens capsule with the iris forceps or scissors when the cornea has collapsed as the result of the evacuation of the anterior chamber. The eye should be firmly bandaged subsequently, and the patient kept in bed until the anterior chamber has re-formed.
Complications. Slow re-formation of the anterior chamber. The anterior chamber will often take two or three weeks to re-form, owing to the hole in the cornea not closing. During this time the eye is open to septic infection and therefore the greatest care should be taken to keep it aseptic when dressing it. For this reason and also because the following complications are due to the same cause, it is desirable to remove as little corneal tissue as possible in performing the operation. It is probable that conjunctivoplasty (see p. 245) would considerably facilitate the rapid closure of the wound.
Anterior polar cataract may result from prolonged contact of the lens with the wound in the cornea. As a rule this seldom interferes much with vision.
Anterior synechiæ from incarceration of the iris in the wound occasionally result and may require subsequent division.
Acute glaucoma is by no means an infrequent complication—indeed the author has seen four successive cases of conical cornea, operated on both by excision and by the cautery, followed by this complication. It is probably due to adhesion of the root of the iris to the back of the cornea during the time the anterior chamber is empty. It can usually be relieved by an iridectomy.
The electro-cautery operation. The operation generally adopted is known as the target operation. It consists in surrounding the apex of the cone with two rings of cautery marks, the outer made at a dull red heat, the inner with the point slightly brighter, whilst the apex is cauterized at a red heat, so that rings of different depth are obtained. Cauterization of the apex should stop just short of perforation, the inner ring being deeper than the outer. With this method secondary glaucoma and anterior synechiæ are not so liable to occur. On the other hand, an optical iridectomy has to be performed more frequently. A few surgeons still cauterize the apex of the cone until a perforation is produced. This latter operation seems to have the disadvantages of both methods and the advantages of neither.
Tumours which involve the cornea are usually secondary to tumours occurring at the limbus. The chief of these are: simple—dermoid patches, moles of the limbus; malignant—sarcoma, endothelioma, epithelioma. Dermoid patches should be shaved off as close to the cornea as possible; the white area left after their removal can be improved by tattooing.
Malignant tumours in very early stages may be removed locally with scissors and forceps, the cautery being applied to their base, since they do not tend to invade the sclerotic deeply.
Indications. (i) To do away with the blinding effects of light through a scar after iridectomy has been performed (see p. 215).
(ii) To simulate a pupil on a white scarred cornea.
The operation is not without risks, as it may light up old inflammation in a previously quiet eye. Panophthalmitis and sympathetic ophthalmia have both been known to follow it. The pricking of the needle may carry in epithelium and implantation dermoids may arise.
Instruments. A fine single needle is generally used, occasionally a bundle of needles (Fig. 128).
Operation. Under cocaine. Chinese ink, sterilized and prepared by rubbing up with 1–6,000 perchloride of mercury, is smeared over the area to be tattooed. Multiple punctures in an oblique direction are then made into the cornea over the area desired. More paste is then rubbed in over this area. The cornea should be intensely black after the operation, as a certain amount of the ink is carried away by phagocytosis and shedding of the epithelium. Subsequent reaction may be reduced by means of an iced compress. Atropine should be instilled.
Calcareous films, when not associated with active irido-cyclitis, may be removed with advantage to the vision. Care should be taken to see that no keratitis punctata is present before the operation is undertaken.
Instruments. Speculum, fixation forceps, a spoon which should have rather a blunt edge.
Operation. Under cocaine. The area is very lightly scraped with the spoon. The calcareous changes are in the deeper layers of the epithelium and Bowman’s membrane and hence are easily removed. The scraping should be carried well beyond the apparent margin of the film. The epithelium often takes some time to regenerate. As a rule the results are satisfactory, although the film is apt to recur in the course of years, but it may be removed again if necessary.
Foreign bodies lodged in the conjunctival sac, unless embedded in the conjunctiva, are usually found by the surgeon under the upper lid, the sulcus subtarsalis being a favourite situation. They are easily removed with a spud or needle, after the instillation of a drop of 4% cocaine solution. Subsequently the eye should be bandaged for a few hours until the effect of the cocaine has passed off, as in wiping the eye the patient may wipe off the epithelium of the cornea whilst it is insensitive from the cocaine.
In order to evert the upper lid the patient is made to look strongly down, the eyelashes are seized between the thumb and forefinger of the left hand, the skin of the upper lid is pushed down above the tarsal cartilage with the thumb of the right hand, and the lid is everted by pulling it upwards against the point of the thumb.
Indications. Pterygium should be removed when advancing across the cornea, especially when the pupillary area is becoming involved. The operation of ablation is the one now generally in use.
Instruments. Speculum, straight iris forceps, small sharp-pointed scissors.
Operation. Under adrenalin and cocaine the neck of the pterygium is seized with the forceps and the body and neck are carefully dissected from the conjunctiva. The body and neck should be very carefully separated right up to the corneal margin by means of forceps and scissors. The head is then stripped off the cornea with a sharp pull. The wound in the conjunctiva should be subsequently closed with fine sutures, otherwise the disease will certainly recur. In stripping the head from the cornea some of the epithelium may be torn off with it. This usually regenerates without impairing the vision.
This is an operation for the removal of follicular formations in the conjunctiva, and is used more especially in trachoma.
Instruments. Graddy’s forceps (Fig. 129), fixation forceps.
 Fig. 129. Graddy’s Forceps.
Fig. 129. Graddy’s Forceps.
Operation. The operation may be performed under cocaine and adrenalin, a little solid cocaine being rubbed into the area to be expressed. In severe cases in which both eyes are affected, and in small children, a general anæsthetic may be necessary.
Although a number of instruments are in use, perhaps the best, and certainly the least painful, is Graddy’s forceps. In the case of the upper lid it is everted, one blade of the forceps being passed into the fornix, the other being placed over the upper surface of the everted lid. A gentle steady pressure is applied, and the lid is drawn out between the blades. In this way as much of the conjunctiva is gone over as is necessary. The lower fornix is best expressed by picking up the loose fold of the fornix with ordinary forceps and then expressing with Graddy’s.
If only one or two follicles be present they can be picked up with the ordinary fine dissecting forceps and expressed, but when situated on the tarsus the follicles are best enucleated with a spud; a solution of 1 in 50 perchloride of mercury in glycerine is then rubbed into the conjunctiva. The operation may have to be repeated several times as new follicles form.
Conjunctivoplasty is an operation for the transplantation of a flap of conjunctiva to cover some loss of substance or defect in the continuity of the globe.
Indications. The operation may be necessary—
(i) To close large recent wounds of the cornea.
(ii) To close the wound made by the excision of a cystoid scar.
(iii) To facilitate the healing of a clean ulcer such as Mooren’s ulcer, or to cover the aperture made by an ulcer that has perforated.
(iv) In the treatment of conical cornea by excision of the apex of the cone, it might facilitate the rapid closure of the wound and assist in flattening of the cornea.
Operation. First method. Under cocaine. A flap of conjunctiva is raised from around the limbus, having its base as near the area to be covered as possible; its breadth should be one and a half times the width of the area to be covered. This flap is drawn across the defect in the cornea and stitched to the conjunctiva on the other side; the wound made in raising the flap should be allowed to heal by granulation.
The stitches holding the flap in position cut through in two or three days, but by that time their purpose will have been served. If the flap be still adherent to the wound its base may be divided and any superfluous tissue removed; the remainder will disappear rapidly.
Second method. The conjunctiva is dissected up all round the cornea as close to the limbus as possible, and backwards as far as the insertion of the recti. A purse-string suture is then inserted around its margins and drawn tight so that the whole cornea is covered by conjunctiva. The operation is suitable for cases in which large areas have to be covered.
The Meibomian glands being embedded in the tarsal plate, cysts in them present both on the conjunctival surface and towards the skin, but the contents are always evacuated from the former.
Instruments. Walton’s iris knife, sharp spoon.
Operation. Under adrenalin and cocaine. The eyelid is everted and a drop of the solution is injected into the cyst with a hypodermic syringe. A vertical stab is made into the cyst with the knife and the contents are then evacuated with a sharp spoon.
Difficulty may arise in fixing the cyst whilst making the incision; this is best obviated by holding the everted lid between the finger and thumb.
In some cases, when the cyst has persisted for a considerable time, the sac-wall becomes so thickened that it has to be dissected out before the mass in the lid will disappear.
Indications. Operations upon eyes with concomitant squint are undertaken for two purposes:—
(i) For cosmetic reasons, to remedy a deformity due to a squinting eye which is amblyopic.
(ii) To rectify the muscular equilibrium in alternating or latent squints, so that binocular vision may be regained.
When the operation is performed for the latter reason the adjustment will naturally have to be much more accurate than for the former, so as to bring about the superimposition of the images falling on each macula. The muscular balance is interfered with by the administration of a general anæsthetic, and therefore the results cannot be gauged accurately. Thus it is desirable that operations upon the ocular muscles should be performed under local anæsthesia. This is usually possible, except in the case of very small children.
During and after the operation muscular equilibrium is tested by means of an electric light fixed to the ceiling immediately over the head of the patient (see Fig. 74). The room is darkened and the patient is made to look at the light. In a case with an amblyopic eye the reflection of the light should appear in the middle of each cornea if the eye be properly adjusted. In cases where good vision is present in both eyes the Maddox rod test should be used, the rod being placed before the eye not being operated on; the bar of light produced by the rod should pass through or within a few inches of the light if the adjustment has been performed accurately.
The tendons of the recti muscles are inserted into the globe at the following distances from the corneo-sclerotic junction: internal, 5 mm.; inferior, 6 mm.; external, 7 mm.; superior, 8 mm. Each muscle is held in place by expansions on either side of the tendon as well as by the tendinous insertions. Division of these expansions allows a greater retraction of the muscle and is, therefore, to be undertaken when a considerable degree of squint has to be overcome. On the other hand, there will be a danger that the muscle may not regain a proper attachment to the globe if division be too freely performed, and a squint in the opposite direction may result; proptosis also may be caused thereby. It is, therefore, better to combine tenotomy with advancement in high degrees of squint over twenty degrees convergent and in all cases of constant divergence. This is usually better than performing a tenotomy in the other eye, as there still remains the muscle of the other eye in reserve to tenotomize if necessary, if the advancement be insufficient to correct the squint. Further, it is much easier to rectify a muscular error by accurate tenotomy than by advancement. Division of the tendon of the internal rectus only, without its expansion, will usually rectify cases of latent convergent strabismus with a deviation of about 12° prism (Maddox test). Cases of latent divergent strabismus of about 8° prism (Maddox test) require complete division of the tendon of the external rectus, and, in some cases, of the expansion as well. Tenotomy of the superior rectus for hyperphoria should only be undertaken in bad cases; that is to say, of over 12° prism, any lateral deviation being first corrected, as occasionally the correction of the lateral deviation, especially when this is due to the faulty insertion of a muscle, will sometimes correct the hyperphoria present.
Partial tenotomies are performed by some surgeons for the correction of latent muscular errors, but the experience of most in this country is that little benefit is gained unless the tendon be completely divided. Tendon-lengthening by various methods has been performed, but has not come into general use.
After all operations upon the ocular muscles both eyes should be occluded to keep the eyes at rest whilst the muscle is gaining its fresh attachment to the globe; this usually takes about seven days, after which time both eyes should be uncovered, and if there is a tendency to convergence atropine should be used. Glasses correcting any error of refraction should be worn.
Tenotomy may be performed by (1) the open, or (2) the subconjunctival method.
Instruments. Speculum, straight blunt-pointed scissors, strabismus hook, needle and silk, needle-holder.
Operation. The operation is performed under adrenalin and cocaine.
1. By the open method. The surgeon stands on the right side facing the patient when dividing the right external or the left internal rectus, but at the head of the table when dividing the right internal or the left external rectus.
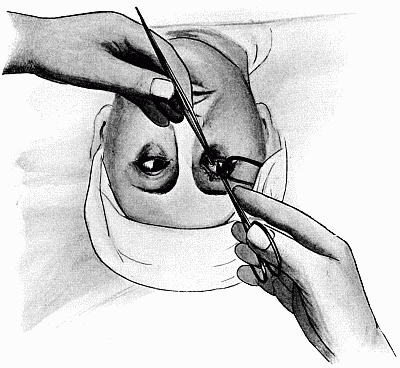 Fig. 130. Tenotomy. Showing the method of holding the scissors and the
position of the hands.
Fig. 130. Tenotomy. Showing the method of holding the scissors and the
position of the hands.
First step. The speculum is inserted and the patient is made to look away from the muscle to be divided. The conjunctiva is freely divided vertically with scissors directly over the insertion of the tendon into the globe (see Fig. 130) and dissected backwards.
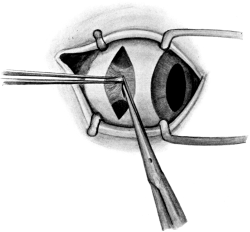 Fig. 131. Tenotomy by the Open Method. The tendon is first button-holed
about its centre and the expansions are then divided upwards and downwards
to the required extent.
Fig. 131. Tenotomy by the Open Method. The tendon is first button-holed
about its centre and the expansions are then divided upwards and downwards
to the required extent.
Second step. The tendon of the muscle is then seized with fixation forceps and button-holed about its centre as close to the globe as possible (Fig. 131). The lower blade of the scissors is then passed through the hole in the tendon, and the rest of the tendon and its expansions are divided upwards and downwards to the extent required to bring the eye straight as tested by its appearance or by the Maddox rod test. The strabismus hook may be inserted, both upwards and downwards, to see that the tendon is properly divided, but all pulling on the muscle with a hook should be avoided, as it is painful and disturbs the muscular equilibrium. The conjunctiva is then brought together with a fine silk suture. If the squint be over-corrected by the tenotomy, a deep hold should be taken with the stitch so as to draw the eye back into position.
2. By the subconjunctival method. This is unsatisfactory in that accurate adjustment by division of the expansion of Tenon’s capsule is not possible. It is painful, and is sometimes followed by a troublesome hæmorrhage into the capsule of Tenon. Occasionally it may be of use in some cases of amblyopic eyes where a small wound is desirable. The conjunctiva is button-holed below the tendon, and separated from the surface of the muscle. The capsule of Tenon is then opened below the tendon, a strabismus hook is passed through the opening with its concavity against the globe, and is then rotated upwards beneath the tendon, which is subsequently divided between the hook and the globe.
Complications. These may be immediate or remote.
Immediate. 1. Hæmorrhage into the capsule of Tenon, leading to intense proptosis, only occurs when the subconjunctival method is adopted. As a rule the hæmorrhage ceases on the application of pressure, but occasionally it may be necessary to open up the wound and turn out the blood-clot.
2. Perforation of the globe has been known to occur during the division of a tendon in an obstreperous patient. It should be treated as a wound of the sclerotic (see p. 235).
3. Tenonitis very rarely occurs, but may lead to matting down of all the extra-ocular muscles and defective movements of the globe. Panophthalmitis has been known to follow this condition.
Remote. 1. Failure to correct the muscular error. If the error be large it must be rectified by tenotomy of the corresponding muscle of the other eye or by the advancement of the opposing muscle of the same eye. This should not be undertaken until five or six weeks have elapsed since the previous operation.
2. Over-correction of the muscular error at the time of the operation may be remedied by stitching the tenotomized muscle forward to the extent required to bring the eye straight. Advancement of the tenotomized muscle should be performed if the over-correction be only discovered after the operation. In cases with binocular vision lesser degrees of deviation may be corrected with prisms if they are causing symptoms, while small errors of over-correction, of about 3° prism, often disappear after the first few weeks.
3. Defective movement in the tenotomized muscle is usually present for the first week or two after the operation, but recovery usually takes place after the muscle has regained its attachment to the globe; it may persist, however, to a slight extent; this is most liable to occur after free division of the tendon and its expansion (more especially in the case of the external rectus), or because the tendon has not been divided close enough to the globe. In patients with previous binocular vision diplopia is present after the operation on turning the eyes towards the same side as the tenotomized muscle, but this usually disappears.
4. A granulation may form at the site of the tenotomy wound. It may be due to a tag hanging from the wound or to a portion of a stitch that has been imperfectly removed. It should be snipped off with scissors and the conjunctiva drawn together over its base.
5. Proptosis may result from too free a division of a tendon.
6. Retraction of the caruncle is best avoided by closing the conjunctival wound with a stitch, and thus pulling the caruncle forward.
Advancement is an operation undertaken to rectify a squint by forming a fresh attachment for one of the ocular muscles nearer the cornea, and at the same time shortening it. There are three main types of operation performed:—
1. The capsulo-muscular, in which the tendon, together with the attachment of the capsule of Tenon to it, is advanced.
2. The tendon only is isolated, shortened, and advanced.
3. The tendon is shortened by folding it upon itself.
The first operation is by far the most satisfactory of these, owing to the fact that a broader new insertion of the muscle is obtained, which is less likely to yield subsequently; it is the operation usually performed in this country.
The chief cause of unsatisfactory results after advancement operations is the cutting through of the sutures holding the tendon in position. The various operations, which are some fourteen in number and have mostly their respective surgeon’s name attached, differ principally in the method of insertion of these sutures. Whichever method of inserting sutures be used, the main factors which aim at preventing the stitches from cutting out are (1) that the stitches should take a good hold in the scleral and episcleral tissues on the corneal side of the wound, for the passing of which it is most essential that the needles should be sharp; (2) that complete rest of the muscles should be ensured by bandaging both eyes for the first seven days after the operation; (3) that the opposing muscle should be tenotomized so as to prevent traction on the sutures.
Of the many operations that have been devised the capsulo-muscular advancement or some modification of it is most frequently used.
Instruments. Speculum, straight scissors, fixation forceps, Prince’s advancement forceps (Fig. 132), four sharp needles and strong silk, needle-holder.
 Fig. 132. Prince’s Forceps for Advancement. Care should be taken to
see that the spring catch holds satisfactorily.
Fig. 132. Prince’s Forceps for Advancement. Care should be taken to
see that the spring catch holds satisfactorily.
Operation. Under adrenalin and cocaine. First step. The patient is made to look away from the side on which is the muscle to be advanced, and the conjunctiva over the muscle is freely divided with scissors, by a curved incision with the convexity towards the cornea, and dissected back.
Second step. The capsule of Tenon is button-holed by a small incision well above or below the tendon. A tenotomy hook is passed beneath the tendon and its expansion and brought out through a small hole in Tenon’s capsule on the opposite side of the tendon. The smooth blade of Prince’s forceps is then inserted in place of the hook, and the tendon with its expansion is grasped between the blades. The forceps are given to an assistant, who should avoid all traction on the muscle. The eye is then rotated in the direction of the muscle to be advanced, and tenotomy of the opposing muscle is performed by the open method.
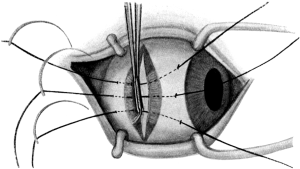 Fig. 133. Advancement by the Three-stitch Method. Showing the sutures
in position. A firm hold on the sclerotic to the corneal side of the wound is essential
to the success of the operation.
Fig. 133. Advancement by the Three-stitch Method. Showing the sutures
in position. A firm hold on the sclerotic to the corneal side of the wound is essential
to the success of the operation.
Third step. The muscle to be advanced and its expansion, which are clamped between the blades of Prince’s forceps, are separated from the globe with the scissors and given again to the assistant to hold. Three strong silk sutures are passed in the following order, middle, upper, and lower, first through the conjunctival and episcleral tissue on the corneal side of the wound and then as far back as possible through the muscle and out through the conjunctiva near the cut margin on the other side of the wound (Fig. 133). Care should be taken that the middle stitch is passed through the episcleral tissue exactly opposite the horizontal plane of the cornea and the central portion of the tendon. The portion of the tendon and capsule within the grasp of the forceps is then removed with scissors by cutting close to the blades of the Prince’s forceps, taking care not to cut the sutures.
Fourth step. The middle suture should be first tightened to the extent required to bring the eye straight. The upper and lower sutures are then tied.
If, on testing with the Maddox rod, the error be found to be slightly over-corrected by the advancement, the eye can be drawn back by taking a firm hold with the conjunctival stitch over the tenotomy wound. The conjunctival stitch may be removed on the fourth day, but the stitches holding the advanced muscle in position should not be removed till after the tenth day. Atropine in both eyes is desirable, especially when there is any tendency to convergence. Glasses should be worn on uncovering the eyes.
Complications. 1. The eyes may not be straight after the operation. No further operation for rectification should be undertaken for at least two or three months. If there be a tendency to convergence, glasses should be worn and atropine used. Small latent errors may be corrected by prisms. If the muscular error be insufficiently corrected tenotomy may be performed on the other eye. If the muscular error be over-corrected it may also require tenotomy on the other eye, the adjustment by tenotomy being more accurate than that by advancement.
2. Thickening over the site of the advanced muscle usually disappears in a few months.
Other complications as described under tenotomy may occur (see p. 250).
The principal substitutes for simple enucleation are evisceration, Mules’s and Frost’s operations.
Enucleation is the removal of the globe from Tenon’s capsule.
Indications. Enucleation should be performed in preference to Mules’s operation in—
| (i) | Malignant tumours. |
| (ii) | Injuries followed by cyclitis. |
| (iii) | Painful blind eyes. |
In malignant tumours enucleation should only be performed when there are no signs of extra-ocular extension. If extra-ocular extension be present, evisceration of the orbit should be performed, provided there be no evidence of general metastasis. In cases of glioma of the retina it is especially desirable that the optic nerve should be cut as far back as possible and the cross-section carefully examined for gliomatous tissue, since the disease spreads to the brain along this structure.
In injuries followed by non-suppurative cyclitis enucleation or Frost’s operation is preferable to Mules’s operation, since cases have been recorded of sympathetic ophthalmia following the latter operation, and it is these cases of non-suppurative cyclitis which are especially prone to give rise to that disease.
Blind painful eyes, especially when affected with glaucoma, are best removed, as occasionally the underlying cause, when not known, may prove to be an intra-ocular growth.
Instruments. Speculum, fixation forceps (two pairs), straight scissors, strabismus hook, strong curved scissors.
Operation. Before the anæsthetic is administered the forehead should be marked over the eye to be enucleated, so as to guard against the accident of removing the wrong eye. It is usual, at any rate in the case of hospital patients, to get their written consent for the operation.
First step. The speculum is inserted. In the case of the right eye the conjunctiva is seized with the fixation forceps downwards and outwards, or in the case of the left eye, downwards and inwards. The straight scissors being held with the right thumb and ring finger, the conjunctiva is divided freely all the way round, as close as possible to the cornea, and dissected back.
Second step. The capsule of Tenon is opened below the external rectus by grasping it with forceps and buttonholing it with the scissors. The strabismus hook is passed through the opening made in Tenon’s capsule with its concavity against the globe, turned upwards beneath the tendon, and the latter is pulled well forward and freely divided from above downwards between the hook and the globe. The superior and inferior recti are treated in a similar manner. In dividing the internal rectus a small portion should be left attached to the globe, so that subsequently it can be grasped with forceps to rotate the globe outwards when dividing the optic nerve.
Third step. The globe is dislocated between the lids by opening the speculum widely and pressing it backwards. If the globe will not dislocate, it is either because the tendons are imperfectly divided, or the palpebral aperture is too small to allow of its delivery; the latter is liable to be the case in small children or in those with a staphylomatous globe. In such cases the palpebral fissure should be enlarged by dividing the outer canthus.
The fourth step is the division of the optic nerve. The globe is rotated strongly outwards, either by pulling on the tendon of the internal rectus or by pulling the globe outwards with the finger; the optic nerve is felt for by passing the strong curved scissors behind the globe. When the nerve is defined the blades are opened widely, pressed backwards, and the nerve divided. The globe is then pulled forward with the finger, and the oblique muscles and remaining attachments divided. Hæmorrhage is easily controlled by pressure and the use of adrenalin.
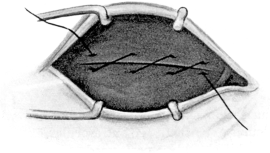 Fig. 134. Enucleation. Method of suturing
the conjunctiva; the suture requires no knot.
Fig. 134. Enucleation. Method of suturing
the conjunctiva; the suture requires no knot.
Fifth step. When the bleeding has ceased, the conjunctival wound is united in a horizontal direction by means of a thick silk suture running over and over; no knot is required and the ends are left long, so that it may subsequently be removed easily (Fig. 134). The usual dressings are applied with a firm pressure bandage for the first six hours. The suture should be removed at the end of the seventh day. No artificial eye should be worn for at least six weeks after the operation, and then only for a few hours at a time until the conjunctiva becomes accustomed to it. It should always be taken out at night.
Complications. These may be immediate or remote.
Immediate. Cutting into the globe. This may occur during the division of the optic nerve, and is usually due to imperfect dislocation of the globe. Although of little consequence as a rule, it may be extremely serious, as for instance in the case of an intra-ocular growth, when it is conceivable that a portion of it might be left behind. If this accident should happen, the portion of the sclerotic and choroid left behind should be carefully sought for and removed.
Adhesion of Tenon’s capsule. Eyes that have been the subject of acute inflammation are much more difficult to enucleate, owing to adhesion of the surfaces of Tenon’s capsule. In these cases the globe has practically to be dissected out of that structure.
Remote. Hæmorrhage into the stump may occur, leading to proptosis of the conjunctiva and extravasation into the eyelids and beneath the skin of the face. The use of a firm pressure bandage and the omission of the suture is usually sufficient to prevent this occurring, but the blood-clot may have to be turned out and the bleeding point sought for and ligatured.
Granulations and polypi in the socket are usually the result of leaving some tag of tissue between the margins of the wound, and are therefore more likely to occur when no suture is used to close the wound. They should be removed with forceps and scissors.
Polypoid masses sometimes form in a socket as the result of an imperfect artificial eye causing an œdematous condition of the conjunctiva. They should not be removed, owing to the contraction caused thereby, but the artificial eye should be left out, when they will often disappear.
Contracted socket is usually the result of an imperfectly performed enucleation or loss of large portions of the conjunctiva; for the operations for its relief, see p. 261.
Evisceration is the removal of the intra-ocular contents.
Indications. It is the ideal operation for a suppurating globe; in these cases enucleation is contra-indicated because the lymph-space round the optic nerve is opened up by the division of the latter and the inflammation may spread directly to the meninges.
Instruments. Speculum, fixation forceps, Beer’s knife, scissors, scoop and stitches.
Operation. A general anæsthetic is necessary.
First step. The eye is transfixed about 4 mm. behind the corneo-sclerotic junction with a Beer’s knife, which is made to cut out upwards (Fig. 135). The flap of corneal and scleral tissue is then seized with forceps and the cornea removed entirely by completing the incision in the sclerotic round it with scissors (Fig. 136).
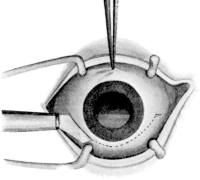 Fig. 135. Mules’s Operation.
Fig. 135. Mules’s Operation.First step. Excision of the cornea. |
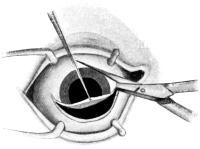 Fig. 136. Mules’s Operation. The completion
of the excision of the cornea with scissors.
Fig. 136. Mules’s Operation. The completion
of the excision of the cornea with scissors.
|
Second step. The contents of the globe are then eviscerated by means of a spoon, and the cavity flushed out with 1 in 4,000 perchloride of mercury lotion. Great care should be taken to remove all portions of the uveal tract; this is best ensured by visual inspection after the hæmorrhage has ceased. The interior of the sclerotic should appear perfectly white.
Third step. Although not absolutely necessary, and inadvisable in the case of a septic globe, a single suture may be passed through the centre of the wound in the conjunctiva and sclerotic.
Complications. As the operation is not infrequently performed for panophthalmitis, much swelling of the lids and discharge from the socket may take place after the operation; these symptoms usually subside in the course of a few weeks without further trouble. The interval which must elapse before an artificial eye can be worn is considerably longer than after enucleation.
Mules’s operation is the insertion of a celluloid globe into the sclerotic after evisceration, followed by closure of the scleral wound over it. In both this and Frost’s operation a better stump is formed, so that more movement may be obtained in the artificial eye which is subsequently worn over the inserted globe.
Indications. (i) The operation is especially suitable for anterior staphyloma following ophthalmia neonatorum. In young children the presence of the ball in the orbit assists the development of that structure.
(ii) It is also suitable for large, recently made, fairly aseptic wounds in the globe.
Operation. The first two steps are the same as for evisceration.
Third step. A glass or, better, a celluloid or gold-plated ball is inserted into the sclerotic, which is closed over it by two rows of interrupted sutures, one of catgut passing through the sclerotic, the other of silk closing over the conjunctival wound. To facilitate the closure of the conjunctival wound it is advisable to dissect the conjunctiva back from the limbus before excising the cornea. The ball inserted in the sclerotic should fit the cavity loosely.
Complications. In about 17% of the cases the ball is not retained; this is not infrequently due to too large a size being used, or to the wound being imperfectly closed by the sutures. If two rows be used, as described above, extrusion of the ball is far less frequent than if one only be inserted. If the globe be extruded the patient is in the same position as if he had had evisceration performed.
In this operation the eye is enucleated, a celluloid globe is inserted into Tenon’s capsule, and the conjunctiva is closed over it by means of sutures passing through Tenon’s capsule and the conjunctiva.
Operation. The first four steps in the operation are similar to those described under enucleation.
Fifth step. A small, loosely-fitting glass globe is inserted into Tenon’s capsule. A purse-string suture of strong catgut is then inserted into the cut margin of Tenon’s capsule, taking care to include in the sutures the cut ends of the tendons of the recti muscles. The suture is drawn tight and tied so that Tenon’s capsule and the muscles are thereby drawn over the globe. The conjunctival wound is closed over this by a separate suture of silk.
The advantage of this operation over the other substitutes for simple enucleation is that it can be used after any enucleation. The chief disadvantages are that the globe is sometimes extruded unless the wound be carefully closed by sutures, and occasionally it may become dislocated from Tenon’s capsule beneath the conjunctiva, thus preventing an artificial eye from being worn, and requiring removal. These disadvantages are largely done away with if the method of suture described above be used.
Indications. Occasionally after an eye has been removed the movements in the socket are not communicated sufficiently to the artificial eye which is placed over it, so that the glass eye has a fixed, staring appearance. As a rule, this can be remedied by the use of a Snellen’s improved eye, which has a rounded posterior surface and fits well on to the stump. If this be not satisfactory, the injection of paraffin into the stump will often improve the movements considerably. The injection should be made by what is known as the ‘cold method’.
The ‘cold method’ of paraffin injection is by far the most satisfactory, for the following reasons:—
(a) The temperature need not be so high, and no damage is therefore done to the tissues.
(b) It is more easily regulated (see Vol. I, p. 682).
(c) Embolism is less likely to occur.
Instruments. Fixation forceps, tenotomy knife, speculum, a large paraffin syringe, and a short needle having a big bore.
Operation. This may be performed under adrenalin and cocaine.
First step. The stump is drawn forwards with forceps. A tenotomy knife, inserted well to the outer side of the stump, is then swept freely round and a pocket is formed in the centre of the orbit into which the injection can be made. The tenotomy knife is then withdrawn.
Second step. The sterile melted paraffin (melting-point 115° F.) should be poured into the syringe, which should have been previously kept in a hot-water bath. The paraffin is then allowed to cool slowly until it just becomes opalescent. The injection should be made through the hole made by the tenotomy knife, sufficient paraffin being inserted to obtain the desired result. The operation is usually followed by considerable swelling of the tissues, which will subside in three or four weeks.
As the result of wearing badly-formed artificial eyes or of subsequent inflammation in the conjunctival sac, the socket not infrequently becomes so contracted that the prosthesis cannot be retained. Enlargement of the sac may be obtained by two methods:—
(a) Skin-grafting (Thiersch’s method).
(b) Transplantation of skin from the surrounding structures (Maxwell’s operation).
Indications. This procedure is especially suitable for cases in which the base of the socket opposite the palpebral aperture has to be enlarged, and it is usually performed prior to Maxwell’s operation for the restoration of the fornices in severe cases.
Instruments. Scalpel, speculum, skin-grafting razor, probes, and a piece of thick style wire.
Operation. First step. The base of the socket is freely divided in a horizontal direction opposite the palpebral aperture so as to produce a gaping wound.
Second step. This gaping wound is put on the stretch in the following way: A thick piece of style wire is bent round to fit into the fornices of the socket, the ends being brought out over the lid at the inner canthus. The circle of wire is opened out as far as possible so as to put the wound at the bottom of the socket on the stretch to its fullest extent.
Third step. Skin grafts are then cut from the inner surface of the arm (see Vol. I, p. 670), applied by means of probes, and pressed down on to the raw surface. No dressings should be applied directly to the grafts, but a watch-glass may be placed over the palpebral aperture and dressings applied over it. The style wire should be removed on the fourth day.
Indications. It is especially useful for the enlargement of the socket by the formation of new fornices. As a rule it is performed for the reproduction of the lower fornix, as it is frequently due to the obliteration of this cul-de-sac that the artificial eye cannot be retained. The operation, however, may be modified and applied to the formation of both the upper and outer culs-de-sac.
Instruments. Scalpel, forceps, scissors, and sutures.
Operation. A general anæsthetic is required.
First step. An incision is made in the lower fornix throughout its whole length and carried downwards for a distance of about half an inch (Fig. 137, A).
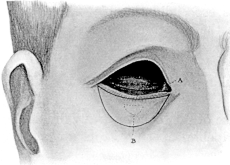 Fig. 137. Maxwell’s Operation for Contracted Socket. First step. A is
the incision through the conjunctiva. The flap of skin from the outer
surface of the lower lid is entirely raised from the subcutaneous
tissue, except for the pedicle B which holds the new fornix in position.
Fig. 137. Maxwell’s Operation for Contracted Socket. First step. A is
the incision through the conjunctiva. The flap of skin from the outer
surface of the lower lid is entirely raised from the subcutaneous
tissue, except for the pedicle B which holds the new fornix in position.
|
 Fig. 138. Maxwell’s Operation. Final step. Showing the flap of skin
from the outer surface of the lower lid turned in to form the new lower
fornix. The surface wound has been closed by sutures.
Fig. 138. Maxwell’s Operation. Final step. Showing the flap of skin
from the outer surface of the lower lid turned in to form the new lower
fornix. The surface wound has been closed by sutures.
|
Second step. A crescentic piece of skin is marked out on the lower lid by two incisions which have their concavity directed upwards. The upper one is parallel with the margin of the lower lid and about 5 millimetres below it. This crescentic flap is then dissected up from the deeper tissues all round, except for a small pedicle at its centre (Fig. 137, B).
Third step. The incision forming the upper margin of the crescentic piece of skin is deepened until it meets the incision made in the fornix, so that the lower lid is converted into a band of tissue attached only at each end.
Fourth step. The upper margin of the incision in the fornix is stitched to the upper margin or concavity of the crescentic piece of skin after the latter has been displaced upwards beneath the band of tissue carrying the lashes, and the lower margin of the crescentic piece of skin is stitched to the conjunctival edge of the band, so that the crescentic piece of skin is folded on itself and forms the new lower fornix, being held down in its position by the pedicle (Fig. 138). The sutures should be of catgut, as their subsequent removal is somewhat difficult.
Fifth step. The surface wound is closed by silkworm-gut sutures. The socket should be packed with gauze, or else a piece of style wire should be inserted, as in the previous operation, so as to maintain the groove in the new lower fornix.
The eyelids consist of well-marked planes of tissue, which are, from without inwards—
1. Skin with very little subcutaneous fat.
2. Orbicularis muscle.
3. Tarsal plates, which are attached to the orbital margins by the palpebral ligaments and which thereby form a barrier to the passage of infection backwards into the orbit.
4. Subconjunctival tissue and conjunctiva.
It is most important for successful results that flaps and incisions should be made accurately down to and in the correct layer of the lid.
Along the lid margin, between the eyelashes and the posterior border of the eyelid, is a white line (intermarginal line) formed by the edge of the tarsal plate. In the many operations in which the lid is split the incision is carried along this line.
The blood-supply to the eyelids is derived from arterial arches—two in the top lid, and one in the lower—which run parallel to the margins. As far as possible, therefore, flaps should be planned with their bases at right angles to the course of the vessels. The extreme vascularity of the lid, together with the small amount of subcutaneous fat, allows of almost complete detachment of flaps of skin without fear of necrosis, but at the same time every care should be taken to avoid injuring these flaps when manipulating them. Hæmorrhage is controlled during the operation by means of clamps or by direct pressure of the lid between the finger and thumb. As a rule a general anæsthetic is required for most of the operations.
Wounds which involve the skin only are brought together in the ordinary way with a few fine sutures. In wounds of the upper lid care should be taken to suture the levator palpebræ, if divided, as otherwise traumatic ptosis may result.
Suture of wounds involving the lid margin.
(a) In simple division the margins of the lids are brought together by means of a fine suture; the conjunctival surface is first approximated, and then the skin by a deep suture which includes the tarsal cartilage. Accurate apposition of the lid border is very essential. Unfortunately a certain amount of ectropion frequently follows, which may require for its relief one of the operations given below (see p. 284).
(b) Occasionally the lid margin carrying the lashes may be torn off. As a rule, the strip remains attached to the lid. It should then be accurately sutured in position, taking care that the lashes take their correct turn outwards. In cases where the strip is torn off entirely, the skin and conjunctiva should be sutured together. When large portions of the lid are lost, some form of plastic operation, such as is performed for making a new lid, is required (see p. 287).
(c) When the canaliculus has been divided the end attached to the lachrymal sac should be sought for and divided for a short distance inwards from the wound (see p. 291), the entrance being kept open daily by a probe to prevent traumatic stricture.
Fusion of the eyelids together is either a congenital condition or the result of injury, and may take the form of bands or firm fibrous union. It is rarely complete and is often associated with symblepharon. The union should be divided on a director, or by careful dissection, taking care not to wound the underlying globe. The raw surfaces are kept apart by daily dressing until they are covered by epithelium. No externa[l] dressing should be applied.
Partial adhesion of the lid to the globe in which a few bands pass from the lid to the globe are best treated by division followed by union of the ocular conjunctiva over the raw surface; no external dressing should be applied. Any tendency to fresh adhesion may be prevented by daily inspection.
In extensive adhesion of the lid to the globe, where the lids are entirely adherent to the globe and the cornea is destroyed, interference is inadvisable. In less extensive adhesion, the lid is first separated from the globe, reunion being prevented by covering the denuded area on the globe with a flap of bulbar conjunctiva transplanted from an area that does not come in contact with the raw surface on the eyelid (Teale’s operation), or by Thiersch’s grafts from a situation where there are no hairs; or by grafting mucous membrane from the mouth of the patient or a frog. Teale’s operation, or some modification, is by far the most satisfactory, but unfortunately it cannot always be carried out when the loss of conjunctiva is large.
Indications. In contraction of the palpebral aperture, either due to a congenital condition, or the result of a wound, trachoma, or other cicatricial contraction.
Instruments. Speculum, forceps, scissors, and three sutures.
Operation. The speculum is inserted and opened as widely as possible. One blade of the scissors is passed into the cul-de-sac at the outer angle of the lid and the palpebral aperture enlarged by dividing the outer canthus horizontally. The external tarsal ligament which is split longitudinally is then cut across with scissors passed into the upper and lower wound. The conjunctiva is drawn up into the wound and stitched to the skin at the margin to prevent reunion. The stitches should be removed about the sixth day.
Canthotomy is simple division of the outer canthus without stitching the conjunctiva into the wound. It is useful in some cases of blepharospasm associated with fissure at the outer canthus.
Union of the eyelids, usually at the outer canthus.
Indications. (i) When the eyelids do not cover the globe as the result of—
(a) Cicatricial contraction of wounds, burns, &c., about the lid.
(b) Long-standing facial paralysis.
(c) Exophthalmic goître.
(ii) To help maintain the lid in position after ectropion operations.
Instruments. Beer’s knife, fixation forceps, spatula, and sutures.
Operation. First step. The position for the new external canthus is determined by holding the lids together at the outer canthus, and is marked on the upper and lower lids. From these points incisions are carried outwards to the external canthus along the intermarginal line in the top and bottom lids. These incisions are deepened to about 5 millimetres.
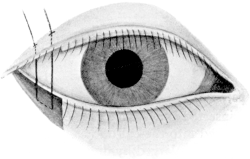 Fig. 139. Canthorrhaphy.
Fig. 139. Canthorrhaphy.
Second step. From the inner end of the incision in the lower lid a vertical one is made downwards for about 5 millimetres, and is then carried out to the external canthus. The tissue thus marked out, bearing the lashes, is then removed.
Third step. A corresponding, slightly larger, area is similarly removed from the under or conjunctival surface of the upper lid (Fig. 139).
Fourth step. These two areas are brought into apposition by means of a strong suture passed through their centre. The suture should have a needle at either end, and these should be passed from the conjunctival surface and brought out through the middle of the raw area in the lower lid, about 2 millimetres apart, and then through the middle of the raw area in the upper lid and out through the skin. The suture is tied so that the two raw areas are brought into accurate apposition. The margins of the wound may then be brought together by sutures if necessary. The main suture should be left in for at least ten days.
Indications. (i) Complete union of the eyelids may be required when an eye has been removed and for some reason an artificial one cannot be worn.
(ii) Partial union is effected in cases of paralysis of the first division of the fifth nerve when corneal ulceration threatens. A similar union is also useful in keeping the lower lid in position during the process of cicatrization in many of the operations for ectropion described below. The adhesions produced can be subsequently divided when contraction has ceased.
Instruments. Knife, forceps, scissors, spatula.
Operation. Complete. As narrow a strip of tissue as possible is removed from the lid borders behind the eyelashes. This is best performed by everting the upper lid and shaving off the posterior margin with a sharp knife; the lower lid is then treated similarly. The raw areas are brought into apposition with fine sutures.
Partial. When only a temporary adhesion is required, as after ectropion operations, it is sufficient to make raw corresponding areas of about 2 millimetres on the posterior margins of the top and bottom lids on either side of the central position of the cornea and unite them with sutures, which may be removed about the end of the first week.
The following operations are usually only undertaken for congenital ptosis, but they are occasionally required for the paralytic and traumatic varieties. All the operations are far from satisfactory, and should only be undertaken when the lid covers the pupil completely or so nearly that the head has to be thrown back to see objects directly in a line with the eyes. The relative value of the various operations apart from their indications is a matter of opinion amongst ophthalmic surgeons; therefore the various types of operations which are performed are given below.
There are four types of operation, which respectively aim at—
1. Shortening the eyelid by excision of a portion of the tarsal plate.
2. Attachment of the lid to the occipito-frontalis muscle.
3. Advancement of the levator palpebræ muscle.
4. Grafting of part of the superior rectus muscle into the lid to take the place of the levator palpebræ superioris.
Fergus’s operation (modified). The object of this operation is to shorten the eyelid by removing the upper portion of the tarsal plate, the cut margin of which is subsequently sutured to the tendon of the levator palpebræ and the palpebral ligament.
The results of the operation are satisfactory, especially in cases in which there is some movement in the eyelid. The author, who has performed most of the ptosis operations on several occasions, has had most uniform results by this method, the modification of which was first suggested to him by Mr. Treacher Collins.
It has the advantage that the amount of retraction required may be more easily estimated, the corneal complications are of much rarer occurrence, and the resulting scar forms a natural fold in the lid. It is obviously not applicable to cases in which the eyelid is already short, as in the cases of ‘Chinese eye’ in which little can be done beyond enlarging the palpebral aperture.
Instruments. Spatula, scalpel, artery and dissecting forceps, scissors, and sutures.
Operation. First step. The spatula is inserted into the superior fornix. A curved incision is made directly below the orbital margin throughout its whole length. The skin and orbicularis muscle are divided and dissected downwards so as to expose the upper surface of the tarsal plate. A suture is then passed through this flap so that it may be drawn down by an assistant.
Second step. A narrow strip about 3 millimetres broad is excised from the whole length of the tarsal plate; in doing this care must be taken not to button-hole the conjunctiva or flap of skin.
Third step. The cut margin of the tarsal plate is sutured to the levator palpebræ and palpebral ligament by two sutures passed in the following manner: A thick catgut suture armed with a curved needle is passed through the upper cut margin of the orbicularis palpebrarum, palpebral ligament, and levator palpebræ (if the latter be present) at about the junction of the middle and inner thirds of the wound, a firm hold being taken on these structures. The needle is then passed through the tarsal cartilage parallel to the lid border for a distance of about 3 millimetres and out again on to its anterior surface. The needle is then again carried through the levator palpebræ, palpebral ligament, and orbicularis in the upper part of the wound. A similar suture is passed about the junction of the middle and outer thirds of the wound. When both sutures are in position they are tied sufficiently tightly to produce the retraction of the lid desired, slight over-correction being necessary. The skin wound is then closed with sutures.
There are three chief methods of affecting this attachment:—
(a) By cicatricial bands (e.g. Hess’s operation).
(b) By a suture left permanently in position (e.g. Harman’s operation).
(c) By the attachment of the skin of the lid to the muscle (e.g. Panas’ operation).
Indications. In the majority of the cases of congenital ptosis the levator palpebræ is completely absent, as shown by the want of upward movement in the lid, and it is for this condition that one of the operations of this type is performed. In rare cases the occipito-frontalis muscle is also absent or imperfectly developed, and in these cases these operations should not be undertaken.
Hess’s operation. The object of this operation is to insert silk stitches between the eyelid and the occipito-frontalis muscle, and to leave them in long enough for a fibrous band of union to form along the stitch tracks.
Instruments. Scalpel, dissecting forceps, needle and holder, spatula, artery forceps.
Operation. First step. The eyebrow having been shaved, an incision 2 inches long is made about in the line of the brow, and the skin is dissected down almost to the lid margin.
Second step. Three sutures are passed, one in the middle, and one at each end of the lid; each suture carries two needles. The needles are inserted in the intermarginal line of the lid about 3 millimetres apart and brought out into the wound above, so that the lid margin is held by the loops. These threads are then carried deeply beneath the upper edge of the wound into the substance of the occipito-frontalis muscle, brought out through the skin well above the eyebrow and tied over a piece of drainage tube. The sutures should be drawn tight enough to produce an undue amount of retraction of the lid, as this tends to drop again after removal of the sutures. The skin wound is then closed and a small dressing is applied to cover the drainage tube on the forehead. The eye itself should be covered with a celluloid shield, as it is usually impossible for the patient to close the palpebral aperture, and the cornea is liable to be injured by exposure. The deep sutures should be left in for at least three or four weeks, so that they may bring about a fibrous band between the muscle and the eyelid by their irritation. The immediate result of the operation is usually excellent, but the lid is very apt to drop again in the course of six months or a year after removal of the stitches.
Harman’s operation. The aim of this operation is to insert a fine metal chain between the occipito-frontalis and the lid, the chain being left permanently in position. The operation has not yet been performed sufficiently often to allow any definite statement about the final results to be made.
The results have not been very satisfactory in three cases in which the author has performed this operation.
Instruments. A 4-inch straight surgical needle, to which is attached the fine wire chain such as is used by spectacle makers to attach glasses to the dress. It measures about O.75 millimetre in diameter. It is attached to the needle by a soldered ring or by means of a piece of silk doubly looped through the needle without a knot.
Operation. Under a general anæsthetic. ‘The method of implanting the chain will be followed readily by reference to Fig. 140. The chain-needle is inserted above the external angular process at A, is passed inwards, and with a slightly upward inclination deeply beneath the tissues of the forehead, to be withdrawn at B; as much of the chain is drawn through as desired. The needle is reinserted at B, passed beneath the brow close to the orbital margin and through the tissues of the lid to C, where it is withdrawn and the chain after it. In like manner it is passed from C to D through the substance of the tarsus and withdrawn. It is now returned from D to E above the brow and withdrawn, and a final length embedded above the brow from E to F, which is just above the internal angular process. The chain should be buried completely and stretched evenly between the points A, B, C, D, E and F; and by traction the loop BCDE should be adjusted at B and E; when the lid is at the desired height the slack at B and E is taken up by traction on A and F.
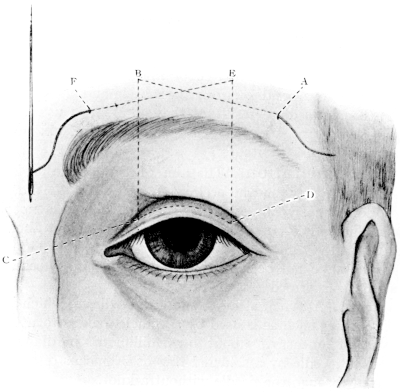 Fig. 140. Harman’s Operation for Ptosis.
Fig. 140. Harman’s Operation for Ptosis.
‘The position of the points E and B is of importance; they must be situated in the region of the most effective elevation of the brow by contraction of the frontalis muscle, as determined by experiment before the commencement of the operation (and they should be placed well above the eyebrow).
‘The lengths of chain lying buried above the brows from A to B and E to F, and the angles A B C and D E F, are arranged so that there is sufficient holding power to prevent the subsequent drop of the lid, but will not prevent adjustment to forcible traction on the lid until the links of the chain have become interwoven and surrounded by the growth of connective tissue. This growth should be sufficiently vigorous by the end of a week to securely fix the chain against all the force of traction of the orbicularis muscle. (In one case in which the author removed the chain after two weeks there was no connective tissue in the links and it was easily withdrawn.) Until this time the free ends of the chain should be turned towards each other over the skin of the brow and cemented in position by a cotton-wool and collodion dressing, after which time the free ends, A and F, are cut off and the free extremities pushed beneath the skin.’
Panas’ operation. In this operation a direct adhesion of the skin of the lid to the occipito-frontalis muscle is aimed at.
Instruments. Lid spatula, scalpel, dissecting forceps, scissors, sutures.
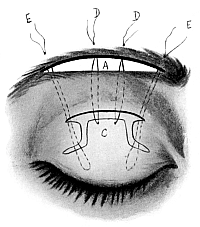 Fig. 141. Ptosis Operation. Panas’.
Fig. 141. Ptosis Operation. Panas’.
Operation. Under a general anæsthetic.
First step. An incision, 2 inches long, is made in the line of the brow, and an incision of a similar length is made into the skin of the lid about half an inch below it. The tissue between these two incisions is undermined so as to produce a band of skin and subcutaneous tissue. From the ends of the lower wound vertical incisions are made into the lid, running slightly outwards and inwards respectively towards the outer and inner canthus (Fig. 141).
Second step. The flap, C (Fig. 141), thus produced is raised, and doubly armed sutures, D D, are passed through its upper margin and are carried beneath the band of skin and subcutaneous tissue. The needles are then carried deeply beneath the upper margin of the wound A into the substance of the occipito-frontalis muscle and brought out on to the forehead. Outer and inner sutures, E E, are passed deeply into the substance of the tarsus both ends are then passed beneath the band and brought through into the upper wound, whence they are passed beneath the upper margin of the wound into the occipito-frontalis muscle and are tied over a piece of drainage tube. They hold the lid in position during the process of cicatrization. Considerable over-correction should be employed as the lid tends to drop subsequently. No dressings should be applied over the open palpebral aperture. The stitches are removed on the tenth day. A small depression is usually seen where the skin of the lid passes beneath the band.
This is especially suitable for cases in which the levator palpebræ has some power, that is to say, when there is some movement of the lid present. It is also suitable for cases of traumatic and paralytic origin. The movement of the lid by the levator palpebræ is best estimated by eliminating the action of the occipito-frontalis by holding down the brow and asking the patient to raise the lid.
Instruments. Lid spatula, knife, forceps, scissors, sutures.
Operation. Under a general anæsthetic.
First step. A spatula is inserted into the upper conjunctival fornix. An incision is made just below the eyebrow over the upper margin of the tarsal plate throughout its length. The skin, especially of the lower margin of the wound, is dissected up and the orbicularis muscle divided, the tarsal plate, with the superior palpebral ligament attached to it, and the orbital margin being exposed. The superior palpebral ligament is then divided carefully high up near the orbital margin and directly below, in a small quantity of fat, will be found the tendon of the levator palpebræ superioris. The tendon can usually be distinguished from the palpebral ligament by the fact that it is elastic when pulled on.
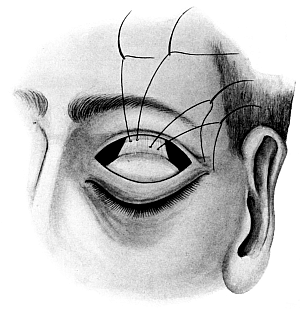
Fig. 142. Ptosis Operation. Advancement of the Levator Palpebræ.
Showing the suture passed through the tendon; the difficulty of the operation is
to find it. (Diagrammatic.)
|
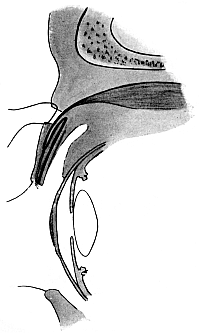
Fig. 143. Ptosis Operation. Advancement of the Levator Palpebræ.
Showing the sutures in position. The tendon is shortened by folding it
on itself.
|
Second step. The advancement of the muscle is then performed in one of the three following ways: (a) by excising a portion of the tendon and suturing the divided ends together; (b) detaching the tendon from the tarsal plate and bringing it from behind forward through a hole made in the upper margin of that structure and suturing it on its anterior surface towards the lower margin; (c) by folding the tendon on itself. The last method is the one most usually performed. Two sutures with a needle at each end are passed through the substance of the muscle and tied (Fig. 142). The ends of these sutures are then carried downwards between the tarsal cartilage and the orbicularis palpebrarum and out in the intermarginal line of the eyelid. The sutures are then tied tightly so as to secure rather more than the amount of retraction required (Fig. 143). The palpebral ligament and orbicularis palpebrarum are then united and the wound in the skin is closed.
Motais’ operation. Indications. This operation is performed for cases of ptosis in which there is partial or complete loss of upward movement of the lid. In cases of congenital ptosis the superior rectus is not infrequently absent or imperfectly developed, as is shown by the defective upward movement of the eye. It need hardly be said that it is most important to see that the superior rectus is well developed before undertaking the operation. Vertical diplopia always follows the operation, and therefore it is advisable only to undertake it when the ptosis is bilateral, a similar operation being performed on both sides. Another somewhat hypothetical objection is that during sleep the eyelids are rolled upwards by the superior recti so that the lids are slightly open, but this occurs in almost all successful ptosis operations. Occasionally there is some defective upward movement of the eye after the operation.
Instruments. Speculum, straight strabismus scissors, lid retractor, needle holders and stitches.
Operation. A general anæsthetic is desirable in all cases.
First step. The superior rectus is exposed through a horizontal incision in the conjunctiva, as in the first stage for advancement. The tendon is defined in the wound and a strabismus hook passed beneath it; its middle portion is isolated and two silk sutures, with a needle at each end, are passed through it and tied.
Second step. The speculum is removed and the eyelid everted and pulled upward by means of a retractor or two silk stitches passed through the substance of the lid. Starting from the middle of the wound the conjunctiva of the fornix is divided backwards and the under surface of the tarsal plate is exposed.
Third step. An incision is carried through the tarsal plate parallel to and near its upper border well into the substance of the orbicularis muscle on the other side. The needles on each end of the doubly armed sutures holding the isolated portion of the superior rectus muscle are passed through the hole in the tarsal plate and are carried downwards between the orbicularis muscle and the tarsal plate to near the lid margin, where they are brought out through the skin and tied over a piece of drainage tube. The conjunctival wound is closed by sutures.
Complications. Ulceration of the cornea is more likely to occur after those operations in which the lid is much over-retracted, such as Hess’s, Panas’ operation, and the advancement of the levator palpebræ. It usually affects the lower corneal margin and may be merely roughening and opacity of the epithelium or deep septic ulceration. If the ulceration be severe, the sutures holding the lid in position should be taken out and the eye treated as for corneal ulceration; on the other hand, slight abrasion of the epithelium will often heal without taking out the sutures.
Sepsis. The difficulty of keeping the wound aseptic after these operations is considerable, and not infrequently inflammation may take place; provided it does not go on to suppuration, the final result is improved thereby; should suppuration take place the sutures must be removed.
The operations commonly performed for entropion and trichiasis are of three types:—
1. Operations for the destruction of the individual hair follicles.
2. Rectification of a faulty curvature of the tarsus.
3. Transplantation of the lash-bearing area.
Indications. In cases of trichiasis where a few eyelashes turn in on the conjunctiva or cornea they may be removed by this method.
Operation. A platinum electrolysis needle (negative pole) is passed alongside each lash into the follicle, and a constant current of about 5 milliampères allowed to pass for a half to one minute. There is usually some bubbling seen around the hair, which will fall out when touched if the operation has been properly performed. It is a comparatively painless operation and free from scarring if the hair follicle be not penetrated by the needle. This is best ensured by using a rather blunt point and not turning on the current until the needle is in position.
Indications. This operation is especially suitable for the senile or spastic forms of entropion of the lower lid, not infrequently seen after much bandaging in old people, which has failed to yield to treatment by pulling the lid outwards with strapping.
Instruments. Straight scissors, fixation and entropion forceps.
 Fig. 144. Treacher Collins’s Entropion Forceps.
Fig. 144. Treacher Collins’s Entropion Forceps.
Operation. Adrenalin and cocaine solution is injected beneath the skin of the lower lid. A horizontal strip of skin as near the lid margin as possible is seized with the entropion forceps (Fig. 144) and removed by one snip of the scissors. The underlying orbicularis muscle is then removed over the same area and the wound closed with sutures. If a more pronounced result is required, a vertical piece of skin is removed at the outer end of the previous wound and allowed to granulate.
Burow’s operation. The object of this operation is to restore the inverted tarsal edge of the lid by dividing the cartilage from the conjunctival surface, and it is especially suitable for those cases in which the whole of the upper lid border is buckled inwards to a slight extent owing to cicatricial contraction such as is often seen in the late stage of trachoma and occasionally as a congenital deformity in the lower lid.
Instruments. Lid spatula and Beer’s knife.
Operation. The operation is performed under a general anæsthetic.
First step. The lid is everted over the lid spatula. An incision is then made along the white line, the result of cicatricial contraction, seen in the sulcus subtarsalis about 3 millimetres behind the upper lid margin; the incision should extend throughout the whole length of the lid and completely divide the tarsal plate. Care should be taken that the cut is made at right angles to, and not obliquely through the tarsal cartilage. When the eyelid is replaced the lid margin will be found to lie in its proper position.
Second step. If the skin of the upper lid be very lax or a more marked result be desired an elliptical piece of skin may be removed from the upper lid above the site of the underlying incision and the wound stitched together so as to exaggerate the outward curve of the lashes; this is usually desirable in most cases, since there is a strong tendency for the lid to become inverted again owing to the contraction of the wound, which is allowed to heal by granulation.
Streatfield’s operation. The object of this operation is the removal of a wedge-shaped piece of the tarsal cartilage directly behind the lashes throughout the length of the upper lid. The division is made from the outside, and the wound is subsequently sutured so that the margin of the lid is everted. It has the advantage over the previous operation that no granulating area is left to cicatrize; it is especially suitable for cases in which there is much buckling inwards of the upper tarsal plate, and yields most satisfactory results even when the deformity is great.
 Fig. 145. Lid Clamp.
Fig. 145. Lid Clamp.
 Fig. 146. Streatfield’s Entropion Operation.
Fig. 146. Streatfield’s Entropion Operation.
Instruments. Beer’s knife, fixation forceps, lid clamp (Fig. 145), spatula, and sutures with a glass bead threaded on each.
Operation. The operation is performed under a general anæsthetic.
First step. The lid is fixed in a clamp. The surgeon makes an incision in the skin directly above the lash-bearing area throughout the whole length of the lid and parallel to its margin. A second incision is made about 3 millimetres above this, and its extremities are curved downwards to join the first. The piece of skin and orbicularis muscle between them is removed and the tarsal cartilage is exposed.
Second step. A wedge-shaped strip is removed from the tarsal cartilage throughout the whole length of the lid, the apex of the wedge reaching just through the cartilage, but not the conjunctiva on its under surface.
Third step. Mattress sutures are then inserted. Each suture should have a needle at either end. A bead may be threaded on the stitch to prevent it cutting into the lid margin. The needles are passed from the margin of the lid directly above the eyelashes, about 3 millimetres apart, and brought out through the lower margin of the wound. They are then passed from within outwards through the tarsal plate and the upper margin of the wound, being brought out through the skin about half an inch above it and tied (Fig. 146). A few points of suture in the skin may be added if necessary.
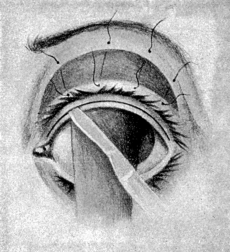 Fig. 147. Arlt’s Operation for Trichiasis.
Fig. 147. Arlt’s Operation for Trichiasis.
Arlt’s operation. Indications. The operation is suitable for cases of trichiasis in which part or the whole of the lashes of the upper lid turn inwards and rub on the surface of the cornea.
Instruments. Beer’s knife, forceps, scissors, sutures, lid clamp.
Operation. First step. A lid clamp is applied to the upper lid. An incision is made in the intermarginal line and the tarsal cartilage is split behind the lash-bearing area for a depth of about 5 millimetres throughout the whole extent of the lid (Fig. 147).
Second step. An incision through the outer surface of the lid above the lashes is made to meet the other at right angles, so that the lashes are carried on a band of tissue attached at each end.
Third step. A semilunar piece of skin is then removed by a curved incision above the last, joining it at the outer and inner ends, and the band carrying the lashes is stitched to the upper margin of this incision; the line of the incision along the intermarginal zone behind the lashes is allowed to heal by granulation. The subsequent contraction caused thereby pulls down the band carrying the lashes to a certain extent. It is, therefore, desirable to pull the band of lashes upwards at the time of operation to a greater extent than is required for the final result in order to overcome this tendency for the condition to re-form as a result of cicatricial contraction of the granulating area. In order to obviate the cicatricial contraction some surgeons cover the area with a graft of mucous membrane.
Ectropion may affect the upper lid, but it occurs far more frequently in the lower. Operations undertaken for its relief vary very considerably for the following reasons:—
1. The cause of the ectropion. The active or cicatricial form requires different and more extensive operations than the passive form, such as occurs after facial paralysis, senile ectropion, or that occurring after blepharitis.
2. The degree of ectropion, whether it is partial, affecting merely the lid margin; or complete, affecting the whole lid.
Ectropion of the lower lid is always accompanied by epiphora, owing to the want of application of the canaliculus to the lacus lachrymalis. The canaliculus is also apt to become obliterated as the result of marginal blepharitis. Before undertaking any of the operations described below this condition must be remedied, either by dilating the canaliculus or by slitting it inwards for a short distance (see p. 290), otherwise, even if the operation be successful in restoring the deformity, the overflow of tears causes the patient to pull down the lower lid constantly in wiping them away, and this tends to reproduce the condition.
After many of the operations a temporary tarsorrhaphy is required to keep the lid in position during the process of cicatrization. The temporary bands produced by this operation are so placed on either side of the cornea as not to interfere with vision altogether. Canthorrhaphy is also desirable in some cases, especially when the ectropion affects the outer end of the lid.
The deformity to be overcome in ectropion is not only the turning outwards of the lid; in cases which have existed for any length of time the lid border becomes permanently elongated and requires to be shortened before it will keep in position. The exposed conjunctiva, especially in cases secondary to blepharitis, becomes thickened near the lid margin, and, though it may regain a more or less normal appearance after the lid has been replaced in position, the thickened margin frequently prevents the proper apposition of the canaliculus, and in these cases it is often desirable to remove this tissue (see Fergus’s operation).
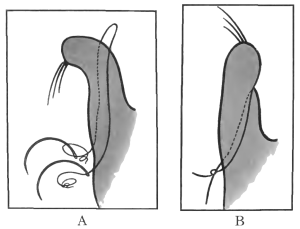 Fig. 148. Snellen’s Sutures.
Fig. 148. Snellen’s Sutures.
A. A suture in position.
B. The suture tightened.
Snellen’s suture method. The object of this operation is to pass sutures through the lower lid from rather above the apex of the eversion out on to the cheek, so that when tightened they draw the lid up into position. The inflammation which occurs around the sutures leaves a permanent band of cicatricial tissue which continues the action of the sutures after they have been removed.
Indications. Snellen’s sutures are useful in moderate degrees of the senile form of ectropion in which there is not much thickening of the lid margins. Although the results are satisfactory in carefully selected cases, the operation is attended with considerable pain and is very liable to be followed by a marked inflammation along the stitch tracks; indeed, the final results are not very satisfactory unless some inflammation does occur.
Instruments. Two, and occasionally three, sutures of thick silk armed at either end with 3-inch straight needles.
Operation. A general anæsthetic is desirable, although not absolutely necessary. The needles belonging to each stitch are inserted about 3 millimetres apart, from the conjunctival surface above the apex of the everted lid, and after passing deeply near the lower cul-de-sac on the posterior surface of the tarsus, they are brought out on the cheek low down and tied over a piece of drainage tube. The loops, when drawn tight, draw the lid margin inwards (Fig. 148). Two of these sutures are usually required at such a distance apart as to divide the lower lid into thirds. They should be left in place some two or three weeks.
 Fig. 149. Fergus’s Operation for Slight Ectropion of the Lower Lid. Showing
the lines of the incision.
Fig. 149. Fergus’s Operation for Slight Ectropion of the Lower Lid. Showing
the lines of the incision.
Fergus’s operation. This operation consists in excision of the apex of the everted lid.
Indications. It is a most satisfactory operation for cases in which the lid margin has undergone thickening from blepharitis and for cases of slight senile ectropion.
Instruments. Beer’s knife, fixation forceps, and sharp-pointed scissors.
Operation. Under adrenalin and cocaine, a little solid cocaine being rubbed into the conjunctiva. A strip of thickened conjunctiva and subconjunctival tissue corresponding to the apex of the eversion is removed along the whole length of the lid (Fig. 149). The wound produced is united with sutures. The pull of the conjunctiva, which is stitched to the lid margin, is sufficient to draw that structure inwards into position.
Kuhnt’s operation (modified). The object of this operation is the removal of a triangular piece of conjunctiva and tarsal cartilage from the centre of the lower lid, the base of the triangle being placed towards the free margin of the lid so as to produce sufficient shortening of the elongated lid border to hold it in position. The skin of the lid is also shortened by removal of a triangular portion at the external canthus.
Indications. It is especially suitable for cases of paralytic ectropion (lagophthalmos) and severe degrees of senile ectropion of the lower lid.
Instruments. Lid spatula, Beer’s knife, scissors, forceps and sutures.
Operation. A general anæsthetic is required.
First step. The lower lid being held between the finger and thumb is split in the intermarginal line along the outer two-thirds of its length, and the incision deepened till the lower border of the tarsus is reached. For this purpose some surgeons use a broad keratome instead of a Beer’s knife.
Second step. A triangular piece of conjunctiva and the whole thickness of the tarsus are removed from the centre of the lower lid, the base of the triangle being towards the free margin of the lid and being of sufficient length to produce the shortening desired to bring the lid up into position (Fig. 150); this is best estimated by making the incision forming the inner limb of the V and overlapping the outer flap until the lid is pulled upwards into position.
Third step. A triangular piece of skin with its base upwards is excised from the outer canthus in the following manner (Fig. 150). An incision is made outwards and slightly upwards from the canthus. A vertical incision, twice the length of the preceding one, is made directly downwards from its outer end to the outer canthus, and the lower end of this is then joined by an incision completing the triangle. The skin marked out by this triangle is then dissected up and removed. The undermining of the flap formed by the skin and subcutaneous tissue of the outer part of the lid is continued inwards until the flap, when pulled up into place, restores the lid to its proper position.
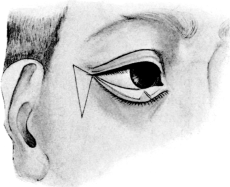 Fig. 150. Modified Kuhnt’s Operation for Severe Ectropion. Second
step. The outer half of the lid is split and a V-shaped portion of the
tarsal plate removed. The triangular piece of skin at the outer canthus
is entirely removed.
Fig. 150. Modified Kuhnt’s Operation for Severe Ectropion. Second
step. The outer half of the lid is split and a V-shaped portion of the
tarsal plate removed. The triangular piece of skin at the outer canthus
is entirely removed.
|
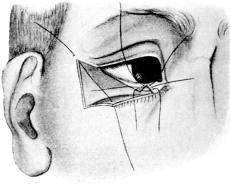 Fig. 151. Modified Kuhnt’s Operation. Fourth step. Showing the sutures
in position. The outer part of the lid has been undermined and dissected
up. The V-shaped gap in the tissues is sutured first.
Fig. 151. Modified Kuhnt’s Operation. Fourth step. Showing the sutures
in position. The outer part of the lid has been undermined and dissected
up. The V-shaped gap in the tissues is sutured first.
|
Fourth step. The lid is sutured into position. The V-shaped wound in the conjunctiva and tarsus is sutured, the knots being placed on the conjunctival surface with the exception of the suture at the lid border, which is turned the other way, the ends being brought out through the skin of the outside flap, after the latter has been sutured in position, and the two ends tied over a bead. The outside flap of skin is brought up into position by a suture at its upper angle. As the result of this a few eyelashes project beyond the outer canthus; these should be excised. Additional sutures to hold the flap in position are then inserted. Both eyes should be bandaged after the operation, otherwise the knots in the conjunctiva may rub on the cornea.
Argyll Robertson’s operation. The operation aims at shortening the border of the lower lid and at the same time pulling it upwards into position by means of a strap of skin and subcutaneous tissue cut from the outer side, the attached end of the strap being formed by the outer portion of the skin of the lower lid.
Indications. It is especially useful for paralytic cases, and as a subsequent measure to the VY operation described below for cicatricial ectropion. The operation is likely to be successful if a marked reduction in the deformity is effected by pulling the skin at the side of the outer canthus upwards.
Instruments. Scalpel, dissecting forceps, artery forceps, scissors, sutures.
Operation. First step. An incision, 2 millimetres below the lid margin and opposite its outer third, is carried through the skin parallel to the border of the lower lid outwards to the canthus; having reached this point the direction of the incision is changed and it is carried more upwards and outwards till the upper end is on a level with the upper orbital margin. The incision is then carried outwards for about 6 millimetres and again downwards, slightly diverging from the former incision, until it is opposite the lower orbital margin. This flap of skin and subcutaneous tissue is dissected up from above downwards (Fig. 152).
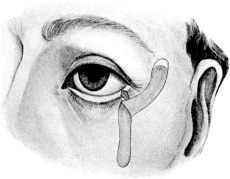 Fig. 152. Argyll Robertson’s Operation for Ectropion. Second step.
Showing the method of shortening the lid and the strap of skin
reflected. The upper convex line shows the piece of skin to be removed
so that the lid may be pulled upwards into position.
Fig. 152. Argyll Robertson’s Operation for Ectropion. Second step.
Showing the method of shortening the lid and the strap of skin
reflected. The upper convex line shows the piece of skin to be removed
so that the lid may be pulled upwards into position.
|
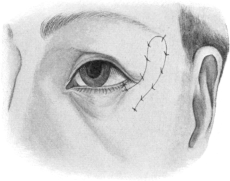 Fig. 153. Argyll Robertson’s Operation for Ectropion. Final step. The
strap of skin has been sutured in position after pulling it upwards
sufficiently to reduce the deformity and enlarging the raw area upwards
to allow this to be done.
Fig. 153. Argyll Robertson’s Operation for Ectropion. Final step. The
strap of skin has been sutured in position after pulling it upwards
sufficiently to reduce the deformity and enlarging the raw area upwards
to allow this to be done.
|
Second step. A V-shaped portion is removed from the margin of the lower lid near the outer canthus, the base of the V being of sufficient length to produce the shortening of the lid required when the edges of the incision are brought together.
Third step. The strap of skin is pulled upwards to the extent required to replace the lid in position, and sutured there. The raw area must be enlarged upwards so as to accommodate the upper end of the strap. It is better to do this than to shorten the strap, since a firm hold is thus obtained (Fig. 153).
The numerous operations which have been devised for this condition are divided into two groups: (1) the transplantation of flaps in the neighbourhood of the lesion, and (2) the grafting of skin flaps from other parts of the body. The latter method is usually only undertaken when the employment of flaps from the neighbourhood of the deformity is impossible, as the cicatricial contraction which follows the grafting of flaps from other parts of the body is usually attended by considerable shrinkage and therefore does not yield such satisfactory results.
VY operation (Wharton Jones). Indications. This operation is useful for cases of ectropion affecting the middle parts of the lower lid, generally due to a scar such as would result from a healed sinus after tuberculous periostitis of the lower orbital margin.
Instruments. Dissecting forceps, scalpel, artery forceps, sutures.
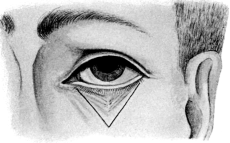 Fig. 154. VY Operation for Ectropion of the Lower Lid due to
a Scar. First step. Showing incision.
Fig. 154. VY Operation for Ectropion of the Lower Lid due to
a Scar. First step. Showing incision.
|
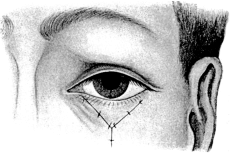 Fig. 155. VY Operation for Ectropion.
Final step. Showing the lid in position.
Fig. 155. VY Operation for Ectropion.
Final step. Showing the lid in position.
|
Operation. The operation is performed under a general anæsthetic. A V-shaped incision, with the apex downwards, is made to embrace the whole margin of the lower lid. The upper ends of the V should skirt the outer and inner canthus and roughly lie over the lower orbital margin, enclosing the scar, the apex of the V falling rather below the orbit. The incision should include the skin and subcutaneous tissue. The V-shaped flap is dissected up and the lid liberated from the underlying scar tissue. The incision is then sewn up in the form of a Y (Fig. 155). Temporary tarsorrhaphy (see p. 266) is always desirable. Subsequent shortening of the lid margin by the Argyll Robertson method is sometimes necessary.
Denonvillier’s operation. This procedure is useful to remedy an ectropion of the outer portion of the lower lid by the transposition of flaps at the outer canthus.
Instruments. Scalpel, dissecting and artery forceps, scissors, sutures.
Operation. The operation is performed under a general anæsthetic.
First step. An oblique incision (Fig. 156), starting from below the inner end of the deformity, A, is carried outwards and slightly upwards for 12 mm. to the point B. From the point B a curved incision B C is carried upwards to and along the orbital margin. This marks out a triangular flap. From C the incision is carried outwards and downwards in a curved direction to D, which is situated about 2 cm. from the external canthus, thus marking out another triangular flap B C D.
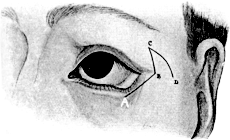 Fig. 156. Denonvillier’s Operation for Ectropion of the Lower Lid. By
reversed flaps at the outer angle. First step. The flap B C D is
brought down to form the outer part of lower lid.
Fig. 156. Denonvillier’s Operation for Ectropion of the Lower Lid. By
reversed flaps at the outer angle. First step. The flap B C D is
brought down to form the outer part of lower lid. |
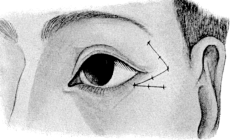 Fig. 157. Denonvillier’s Operation for Ectropion. Showing the operation
completed after transposition of the flaps.
Fig. 157. Denonvillier’s Operation for Ectropion. Showing the operation
completed after transposition of the flaps.
|
Second step. Both flaps are dissected up, and, when all bleeding has ceased, the apices of the triangles are transposed and sutured in position, the incision thus forming a Z-like figure (Fig. 157). A canthorrhaphy is generally required.
Fricke’s operation. This has for its object the transplantation of flaps from the side of the forehead or face into the lid to remedy a loss of tissue resulting from operation or cicatricial contraction.
Indications. The operation is usually performed for cicatrices about the upper lid, the flap being turned down from the side of the forehead. A flap may be turned in from the inner side in addition if necessary. The operation may also be applied to ectropion of the lower lid.
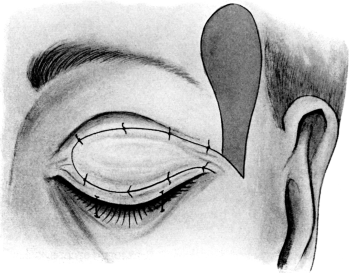 Fig. 158. Fricke’s Operation. To replace the loss of portions of the skin
of the upper lid.
Fig. 158. Fricke’s Operation. To replace the loss of portions of the skin
of the upper lid.
Operation. When planning the flaps the following points must be taken into account:—
(i) The flap must be cut so that its base contains the main blood-supply of the part made use of.
(ii) It should be at least one-third larger than the area to be covered. This is estimated by cutting a piece of protective the size of the area to be covered and laying it on the skin before the flap is cut.
(iii) The base of the flap should consist of a considerable amount of subcutaneous tissue as well as skin, but the apex may be little more than the skin itself.
(iv) The direction of the subsequent contraction should be taken into account so as to assist the final result.
First step. The lid is first freed by dividing all the cicatricial bands, or, if only a small cicatrix be present, by excising that. The lid is then pulled down into position and put fully on the stretch. This is best performed by stitching the margin of the lid to the cheek.
Second step. The flap is marked out at least one-third larger than the size required to cover the raw area. The base of the flap should be placed a little below the raw area to be covered, so that the rotation of the flap into position is easily performed without danger of constriction to the base (Fig. 158).
Third step. The flap having been raised and all bleeding stopped, it is rotated and sutured in its new position, the wound made by the removal of the flap being brought together by sutures or, if it be too large for this, covered by skin grafts (see Vol. I, p. 670).
Indications. As has already been pointed out, this method is not so satisfactory as the method by flaps described above, but it is frequently the only one available when the surrounding skin has been destroyed, as after extensive lupus of the face.
Instruments. Scalpel, forceps, skin-grafting razor, probes.
Operations. First step. As for the previous operation.
Second step. Grafts are cut from a situation free from hairs, such as the inner side of the upper arm (see Vol. I, p. 671).
Third step. After all bleeding has been stopped, the grafts are applied, straightened with probes, and pressed firmly down on to the raw surface. The edges of each graft should slightly overlap the one next to it. Great care should be taken in applying the dressings not to disturb the grafts (see Vol. I, p. 673).
If the whole thickness of the skin be used (Wolff’s method), care should be taken to see that the under surface is free from fat.
Losses of portions of the lid margins usually result from operations for malignant growths. When the loss is in the upper lid, some modified form of Fricke’s operation is the best method of remedying the deformity. When a large area is to be covered, transplantation of a flap from the arm by the Tagliacotian method has to be performed (see Vol. I, p. 679).
Fricke’s operation is also applicable to the outer portion of the lower lid. When the inner end of the lower lid is affected, De Vincentiis’ operation yields satisfactory results. When the whole lower lid has been lost, a modified Dieffenbach’s method with the use of the ear cartilage is indicated.
De Vincentiis’ operation. The operation aims at shifting the remains of the lid bodily inwards to cover the gap left by the removal of the growth.
Instruments. Scalpel, dissecting forceps, artery forceps, scissors, sutures.
Operation. First step. The portion of the whole thickness of the lid together with the growth is excised by a V-shaped incision (Fig. 159).
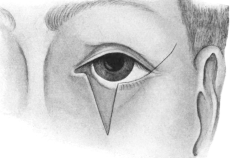 Fig. 159. De Vincentiis’ Operation to replace the Loss of the Inner
Portion of the Lower Lid. Showing the inner portion of the lid removed
by a V-shaped incision and the relief incision made outwards from the
external canthus.
Fig. 159. De Vincentiis’ Operation to replace the Loss of the Inner
Portion of the Lower Lid. Showing the inner portion of the lid removed
by a V-shaped incision and the relief incision made outwards from the
external canthus.
|
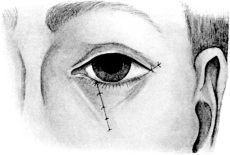 Fig. 160. De Vincentiis’ Operation Completed. The lower lid has been
pulled inwards and united to the opposite side of the gap left by the
V-shaped incision. The incision outwards from the outer canthus, now
much diminished in length, is also sutured.
Fig. 160. De Vincentiis’ Operation Completed. The lower lid has been
pulled inwards and united to the opposite side of the gap left by the
V-shaped incision. The incision outwards from the outer canthus, now
much diminished in length, is also sutured.
|
Second step. The outer canthus and orbito-tarsal ligament are divided with the scissors. The incision is then carried outwards and upwards with a scalpel, in a line with the lower margin of the lid, the incision being long enough to free the lower lid sufficiently to slide it inwards and to enable the edges of the V-shaped wound to be united (Fig. 160).
Dieffenbach’s operation (modified with the use of ear cartilage). This operation consists in shifting inwards a flap of skin and subcutaneous tissue derived from the outer side of the face to take the place of the eyelid which has been removed, the conjunctiva and tarsal plate being represented by a piece of skin and cartilage taken from the posterior surface of the ear and stitched to the inner surface of the flap.
Operation. First step. The growth, together with the eyelid, is first removed by a V-shaped incision, the base of the V being formed by the margin of the lower lid.
Second step. An incision is carried directly outwards from the external canthus. The length of this incision should be 1¼ times the length of the lid margin. An incision is then carried downwards from its outer end parallel to the outer limb of the V by which the lower lid has been excised. This flap is then raised freely (Fig. 161).
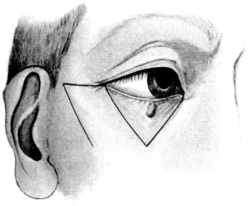 Fig. 161. Modified Dieffenbach’s Operation to replace the loss of the
whole lower lid. First step. The whole lower lid, together with the
growth, is removed by the V-shaped incision and the flap to form the new
lid is dissected up from the outer canthus. The diagram shows the
incision marking out the flap.
Fig. 161. Modified Dieffenbach’s Operation to replace the loss of the
whole lower lid. First step. The whole lower lid, together with the
growth, is removed by the V-shaped incision and the flap to form the new
lid is dissected up from the outer canthus. The diagram shows the
incision marking out the flap. |
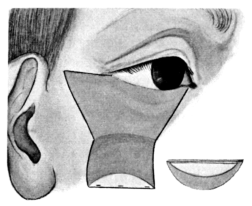 Fig. 162. Modified Dieffenbach’s Operation. Third step. Showing the
flap turned down, to the free border of which is attached the flap of
skin and ear cartilage. The inset shows the proportion of skin and
cartilage (light area) to be removed from the back of the ear.
Fig. 162. Modified Dieffenbach’s Operation. Third step. Showing the
flap turned down, to the free border of which is attached the flap of
skin and ear cartilage. The inset shows the proportion of skin and
cartilage (light area) to be removed from the back of the ear.
|
Third step. The ear is turned forward and a semilunar portion of the skin is marked out and deepened down to the cartilage. The base of this semilunar portion should be equal in length to the upper margin of the flap that is to form the new lid (Fig. 162). The skin is then dissected up for about 3 millimetres from the crescentic part of the incision back towards the straight one forming the base of the semilune. When this part of the skin has been raised the cartilage is divided, first by a curved incision, 3 millimetres behind that through the skin, and then along the straight incision joining the ends of the curved one. It is separated from the skin on the anterior surface of the ear, and the semilunar piece of skin and cartilage is thus removed. The portion of cartilage removed with the skin is smaller than the latter; the two portions coincide in length along their straight margins, but the depth of the crescent of cartilage is considerably less than that of the skin (Fig. 162). The cartilage is usually too thick to form the new tarsus and must be pared down until the right thickness is obtained. It is then applied to the inner surface of the flap to form the new lid, the skin surface being directed inwards to help to form the lower conjunctival sac. It is fixed firmly by sutures at its margin, which are passed through the whole substance of both flaps, and tied on the outer surface of the new lid.
Fourth step. The flap forming the new lower lid is sutured in position. The surface from which the flap is taken is closed as far as possible with sutures after undermining the edges, any raw area being covered by skin grafts taken from the arm.
Operations upon the lachrymal apparatus are divided into—
| I. | Operations upon the lachrymal canals. |
| II. | Operations upon the lachrymal gland. |
The majority of operations are undertaken for the relief of obstruction to some portion of the canal which leads from the conjunctival sac to the nose, obstruction to which causes an overflow of tears (epiphora)—a condition which must be distinguished from hypersecretion (lachrymation).
The obstruction may occur in any part of the canal, that is to say, in the puncta, canaliculi, lachrymal sac or duct; and it is most important to determine the cause and position of the obstruction in every case before undertaking an operation for its relief. Hence it need hardly be said that the nose should be carefully examined in every case unless the cause is obvious. The operations are divided into two classes:—
1. Those which are undertaken for the relief of the obstruction.
2. Those which are undertaken for the obliteration of the canals.
Except under exceptional circumstances, the latter operations are only undertaken when a cure cannot be brought about by the former.
The presence of a septic focus, such as a distended lachrymal sac, apart from the irritation and increased lachrymal secretion caused thereby, is a source of grave danger to the eye if not relieved, as it is a frequent cause of serpiginous corneal ulceration.
Indications. (i) Contraction of the puncta following marginal blepharitis, especially when associated with ectropion.
(ii) Preparatory to syringing or probing.
(iii) To dilate a stricture of the canaliculus.
Instruments. Nettleship’s canaliculus dilator (Fig. 163).
Operation. The operation is performed under adrenalin and cocaine, a little solid cocaine being rubbed in over the canaliculus.
The lid is slightly everted and put on the stretch by pulling it downwards and outwards with the thumb. The depression caused by the punctum is seen on the top of a small elevation. The point of the dilator is entered vertically into the punctum and then turned parallel with the lid margin and passed onwards with a steady pressure. At the same time it should be rotated between the finger and thumb, until the inner bony wall of the lachrymal sac is felt. The only difficulty which may be experienced is in entering the dilator into the punctum, owing to the small size of the latter. For this reason the fine point of Nettleship’s dilator is more suitable than the form modified by Lang. Even Nettleship’s dilator is too large in a few cases, and here a large sharp-pointed pin is sometimes of use in defining the punctum before using Nettleship’s dilator.
Indications. To enlarge the punctum and direct the entrance to the canaliculus inwards. This is especially desirable before ectropion operations and for the removal of concretions (leptothrix) from the duct. In former days the canaliculus used to be slit with the idea of passing very large probes down the lachrymal duct; this has now been abandoned, since slitting the canaliculus throughout its whole length, as is required for this treatment, does away with the capillary attraction.
Instruments. Dilator, canaliculus knife (Fig. 164), straight iris forceps, sharp-pointed scissors.
Operation. It is usually performed on the lower canaliculus. The eye is cocainized as in the previous operation and the patient is made to look up.
First step. The canaliculus is first dilated. The knife is inserted for a short distance with the handle parallel to the lid margin. The lower lid being held on the stretch by the thumb, the handle of the knife is raised towards the brow, thus dividing the canaliculus. The blade of the knife should be directed upwards and slightly backwards.
Second step. As the lips of the wound are liable to reunite, it is better to remove the posterior lip of the groove. This is performed by seizing the latter with forceps and dividing it with scissors. The entrance to the canaliculus should be kept open by means of the dilator passed twice a week for a month.
Indications. (i) To test whether the lachrymal canals are patent.
(ii) By constantly cleansing the sac and washing away all purulent discharge the mucous membrane may regain a more healthy condition, and so an obstruction due to an alteration in the mucous lining may be relieved. In cases with a purulent discharge a small quantity of protargol (10% solution) may be left in the sac after syringing.
(iii) The injection of adrenalin and cocaine into the sac before its excision.
 Fig. 165. Lachrymal Syringe.
Fig. 165. Lachrymal Syringe.
Operation. The eye is cocainized and the patient made to look up. The punctum is everted by pulling down the lower lid. The canaliculus is then dilated. The nozzle of the lachrymal syringe (Fig. 165) should be passed until it is felt to impinge on the bony outer wall of the sac. Withdraw the syringe slightly and apply gentle pressure to the piston. The fluid will either regurgitate through the upper canaliculus or, if the duct be patent, pass down into the nose and so into the throat.
Complications. If too forcible syringing be used extravasation of the fluid may take place. This is accompanied by pain and swelling in the lachrymal region. It usually subsides under hot fomentations, but suppuration and even cellulitis of the orbit have been known to occur.
Indications. (i) In cases of congenital lachrymal obstruction due to débris blocking the duct.
(ii) When syringing has failed to bring about a cure, a probe may be passed once or twice to see if dilatation causes any improvement. It is especially useful in children.
(iii) As a preliminary to the insertion of styles.
Various forms of probes are employed, those of Bowman being in general use. Too fine a probe should not be used, otherwise a false passage is liable to be made.
Operation. This is performed under adrenalin and cocaine, which should be injected into the lachrymal sac.
The lower punctum is dilated and the probe passed parallel to the lid margin until it is felt to impinge upon the lachrymal bone. Keeping the point applied to the bone, the handle of the probe is rotated upwards through rather more than a quarter of a circle and passed by a gentle pressure downwards and slightly outwards into the duct, keeping the point of the probe close to the bone the whole way. The direction of the probe after entering the duct should be downwards, outwards, and backwards in the direction of the first molar tooth on the same side. The backward direction of the duct is much more marked in young children than in adults.
Complications. A false passage may be made into the antrum of Highmore. If such an accident should occur, no further attempt should be made to pass a probe for a few days until the wound has healed.
A few surgeons still insert styles into the lachrymal duct with the idea of continuous dilatation. The hollow styles used by Bickerton are the ones most frequently employed.
Instruments for dilating, slitting the canaliculus, probing, and styles. Also Stilling’s knife.
Operation. A general anæsthetic is desirable.
First step. The canaliculus is dilated and slit up, the posterior lip being removed (see p. 29).
Second step. The duct is dilated by probing (vide supra) or enlarged by passing Stilling’s knife down it.
Third step. A style is passed down the dilated duct. The lower end of the style should rest upon the floor of the nose, otherwise there is a tendency for the style to slip into the duct and disappear. Care should be taken that the upper end does not rub on the globe. Styles should generally be left in position from three to six months. A style should at first be made of lead wire and moulded until a suitable pattern is obtained, from which a hollow gold style can be made subsequently.
Complications. 1. Dacrocystitis may follow the insertion of a style, which should then be removed until the inflammation has subsided.
2. The style may slip down the duct. If this should occur an attempt should be made to grasp it through the slit canaliculus. The lower end may present in the nose and the style can then be withdrawn with forceps. Occasionally styles lodge in the antrum of Highmore, in which case they must be removed after localization by the X-rays through an opening from the mouth above the canine tooth.
When syringing and probing have failed to relieve the lachrymal obstruction, one of the following operations for the obliteration of the lachrymal passages may be employed.
Indications. In cases of lachrymal obstruction in which an immediate operation upon the globe is required.
Operation. Under cocaine. Fine sutures armed with a small curved needle are passed beneath both the upper and lower can[al]iculus and tied so as to include them in the ligature. Permanent obliteration may be caused by the destruction of the lining membrane with the actual cautery.
Indications. (i) For mucocele in cases of lachrymal obstruction which have failed to yield to other treatment.
(ii) In all cases of tuberculous disease of the sac.
(iii) For a recurrent lachrymal abscess after subsidence of the acute inflammation.
(iv) For hypopyon ulcer associated with lachrymal obstruction.
(v) Before operation on the globe in cases of lachrymal obstruction.
(vi) For lachrymal fistula.
Instruments. Small scalpel, forceps, Muller’s speculum (Fig. 166), Axenfeld’s retractor (Fig. 167), straight scissors, horsehair sutures.
 Fig. 166. Muller’s Retractor for Excision of the Lachrymal Sac.
Fig. 166. Muller’s Retractor for Excision of the Lachrymal Sac.
|
Operation. Hæmorrhage is the most troublesome part of this operation; it is best controlled by injecting adrenalin (made from the dried gland, ʒj, and ℥j of water) and cocaine, 10%, into the sac a quarter of an hour before operating. Swabs on the end of a glass rod dipped in adrenalin and cocaine may also be used during the operation. A general anæsthetic is desirable, but many surgeons perform the operation under local anæsthesia, produced by injecting 5% cocaine with 1 in 1,000 adrenalin into the tissue surrounding the sac; but the latter plan has the disadvantage that the mixture may cause severe toxic effects, and the patient usually experiences some pain while the upper portion of the incision is being made and the lower end of the sac is being divided.
First step. The internal tarsal ligament is first defined by putting the lids on the stretch. An incision should be made, 15 millimetres in length (5 millimetres of which should fall above the tarsal ligament), backwards and inwards directly over the lachrymal sac. Muller’s retractor is then inserted to retract the wound laterally, the hooks being made to engage the margins of the incision by means of forceps. The superficial fascia and the fibres of the orbicularis muscle are then divided. The internal tarsal ligament in the upper part of the wound, together with the glistening deep fascia, is exposed and divided carefully so as not to injure the lachrymal sac, which is found directly beneath it (Fig. 168).
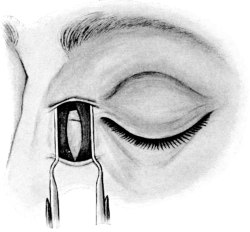 Fig. 168. Excision of the Lachrymal Sac. Showing the internal tarsal
ligament in the upper part of the wound with the sac lying beneath.
Fig. 168. Excision of the Lachrymal Sac. Showing the internal tarsal
ligament in the upper part of the wound with the sac lying beneath.
|
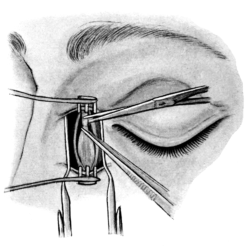 Fig. 169. Excision of the Lachrymal Sac. Showing the method of defining
the upper end of the sac. The internal tarsal ligament has been divided
and the sac is well pulled forward with forceps.
Fig. 169. Excision of the Lachrymal Sac. Showing the method of defining
the upper end of the sac. The internal tarsal ligament has been divided
and the sac is well pulled forward with forceps.
|
Second step. With scissors the sac-wall is then separated from the deep fascia which encloses it, first externally and then internally, the canaliculi being divided. Axenfeld’s retractor is then inserted in the longitudinal axis of the wound (Fig. 167). The middle of the sac is grasped with forceps and pulled forward, and the top of the sac is defined and detached. This is frequently difficult owing to the troublesome hæmorrhage which often occurs. The sac is pulled well forward, and the posterior wall is separated, the neck of the sac being divided as far down the duct as possible by means of scissors. A large probe is passed down the duct into the nose. Some surgeons remove the periosteum of the lachrymal bone as well as the sac, which is unnecessary. The wound is closed by three sutures, the middle one including the divided ends of the internal tarsal ligament. A firm dressing should be applied so as to keep the walls of the cavity in contact. In tuberculous cases it is desirable to curette the lower end of the duct after removal of the sac. The stitches are removed on the seventh day.
Complications. These may be immediate or remote.
Immediate. 1. Inability to find the sac. This may happen to a beginner, and is generally due to the fact that the dissection is carried too much inwards towards the nose. It should not occur if the guides to the sac carefully borne in mind, namely, the internal tarsal ligament and, on the inner side, the lachrymal crest, which can easily be felt with the finger or forceps in the wound.
2. Opening the conjunctival sac. This may take place when dividing the canaliculi. It is more likely to occur if the deep fascia has been imperfectly divided before carrying out the dissection to the inner side. As a rule the opening heals readily.
3. Opening of the orbit, due to the division of the fascia attached to the posterior lip of the lachrymal groove. It is recognized by the fact that orbital fat presents in the wound, and for this reason it makes the operation more difficult. It is most likely to happen when the lower end of the sac is being divided. It lays the orbit open to the possibility of septic infection. The internal rectus has been divided, no doubt due to the fact that the fascia, which passes from the outer surface of this muscle, is attached to the posterior lip of the lachrymal groove, and the muscle has been thereby pulled up into the wound; with ordinary caution such an accident is impossible.
4. Injuries to the cornea. Corneal abrasions by the clumsy insertion of retractors may lead to severe corneal ulceration.
Remote. 1. Epiphora. Normally the lachrymal secretion is largely removed from the conjunctival sac by a process of evaporation. It is only when the hypersecretion of tears takes place that the lachrymal apparatus is called much into use. As a rule, patients who have had the lachrymal sac excised do not complain of epiphora, except in a cold wind. Occasionally this epiphora may be so troublesome that removal of the palpebral portion of the lachrymal gland is desirable for its relief. There is no fear of the conjunctival sac becoming dry after this operation, since there are numerous accessory lachrymal glands (glands of Waldeyer and Krause) opening on to the superior fornix.
2. A sinus. The wound may break down and a sinus may form at the site of the incision. These cases are nearly always of tuberculous origin and not infrequently have underlying bone trouble. They can usually be made to heal by the use of iodoform and scraping.
3. Recurrence of the mucocele or lachrymal abscess. Occasionally the mucocele may re-form, or an abscess result after removal of the sac. This is due either to a piece of sac-wall being left behind, or to the relining of the cavity with epithelium from the cut end of the duct. It is particularly liable to occur in cases of a tuberculous nature. Firm pressure with the dressings after the operation is the best method of preventing the cavity relining with epithelium. If the condition has arisen, the pseudo-sac should be excised.
Indications. Lachrymal abscess is due to an inflammation around the sac-wall through which infection of the cellular tissue has taken place. The abscess should not be opened until pus is present, as even considerable swelling and œdema will often subside without suppuration; this is usually about the end of the third day. Further, if the opening be made too soon, the inflammation takes considerably longer to subside.
Instruments. Beer’s knife, forceps, and probe.
Operation. Usually performed under gas. An incision is made over the lachrymal sac and is carried downwards and inwards to the bone by a single puncture of the knife. The pus is evacuated, and the cavity stuffed with gauze, which should be changed daily for the first three days. Hot fomentations should be applied. As soon as the swelling has subsided, the lachrymal obstruction should be treated by one of the methods previously described.
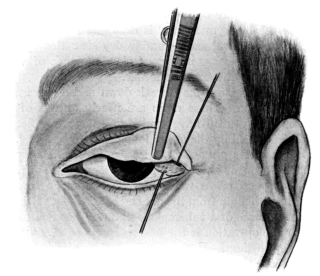 Fig. 170. Excision of the Palpebral Portion of the Lachrymal Gland.
The lid is doubly everted and the gland is dissected out from within outwards.
Fig. 170. Excision of the Palpebral Portion of the Lachrymal Gland.
The lid is doubly everted and the gland is dissected out from within outwards.
Indications. For obstinate epiphora after removal of the lachrymal sac.
Instruments. Fixation forceps (two pairs), two sharp hooks, strabismus scissors, suture.
Operation. Usually performed under adrenalin and cocaine.
First step. The upper lid is doubly everted. The eversion is best carried out by holding the singly everted lid between forceps and then re-everting it; the forceps are then given to an assistant to hold. With a syringe a few drops of 5% cocaine are injected through the conjunctiva into the area to be operated upon.
Second step. The gland is seen beneath the conjunctiva at the outer part of the upper fornix, seized with forceps, and drawn forwards. A horizontal incision is made with scissors through the conjunctiva, which is dissected backwards. The edges of the wound are then held apart by means of sharp hooks (Fig. 170).
Third step. The gland, which is seen as a nodule, is drawn forward with forceps. By means of the scissors the gland is separated from its attachments along its whole length, starting on the inner side, the wound being subsequently closed with a few points of catgut suture.
Indications. It is usually undertaken for tumours (endotheliomata, &c.) and retention cysts.
Instruments. Knife, artery and dissecting forceps, retractors, ligatures.
Operation. Performed under a general anæsthetic.
First step. An incision, three inches long, is made through the skin immediately below the outer third of the orbital margin. The underlying orbicularis palpebrarum is divided, and the orbital fascia covering the gland is defined and incised.
Second step. The gland is first separated from the periosteum of the depression in the bone in which it lies, and is drawn forward and carefully dissected out from the lid. The wound is then closed with sutures.
An abscess in the lachrymal gland should be opened by an incision similar to, but not so long as that in the above operation.
In this operation the bony outer wall of the orbit is divided above and below, and turned outwards so as to expose the orbital contents without interfering with the globe; the bony wall, being kept attached to the overlying tissue, can be replaced subsequently without fear of necrosis.
Indications. The operation is performed in cases of a suspected tumour of the orbit, which, if small and non-malignant, can be removed, the eye being left in situ. If doubt exists as to the nature of the tumour a piece can be removed and examined microscopically, either at the time of the operation or later. It is especially suitable for tumours of the optic nerve and for orbital cysts behind the globe.
Instruments. Scalpel, dissecting forceps, artery forceps, scissors, periosteum detacher, chisel and hammer, or preferably, a motor rotary saw, and retractors.
Operation. Performed under a general anæsthetic.
First step. A slightly curved incision with the convexity forwards is made so as to expose the outer margin of the orbit and carried down to the bone. The periosteum is separated from the inner surface of the outer wall of the orbit by means of a periosteum detacher and divided horizontally, the finger is inserted, and the orbit explored. If a small tumour or cyst be found it can sometimes be shelled out through this incision without enlarging the wound further.
Second step. The eye and orbital contents are carefully protected with a large flat retractor. The bone is first divided above, by means of either a chisel or a saw. The upper incision should pass through the base of the external angular process of the frontal bone, and run backwards and slightly downwards to the posterior end of the spheno-maxillary fissure. The lower incision should run directly backwards from the lower orbital margin into the spheno-maxillary fissure. The triangular wedge of bone attached by its outer surface to the soft tissues in the temporal fossa is then forced outwards. In doing this care must be taken not to fracture the orbital wall anteriorly, otherwise the space to work in will be much reduced.
Third step. Consists in the removal of the tumour. Care must be taken to displace the external rectus to one side so as to avoid injury to it as much as possible. If the case should be one of an optic nerve tumour, for which the operation is most frequently performed, the optic nerve is divided close behind the globe. The tumour is freed from the surrounding ciliary nerves and the ophthalmic artery and brought up into the wound as much as possible. The optic nerve is then divided at the apex of the orbit and the tumour removed. The wound in the periosteum of the outer wall of the orbit is closed with a catgut suture, the bone, together with the soft parts, replaced in position and the skin wound closed by sutures. A drainage tube should be inserted for at least twenty-four hours.
Complications. 1. Proptosis. The operation is liable to be followed by great proptosis as the result of hæmorrhage into the orbit. If the optic nerve has been removed, the globe may be dislocated forwards between the lids and come in contact with the dressings.
2. Corneal ulceration. As the cornea is frequently anæsthetic from division of the ciliary nerves, ulceration is very liable to follow. It is, therefore, desirable in many cases to stitch the lids together after closing the skin wound.
3. Defective outward movement in the globe is of frequent occurrence, owing either to injury of the external rectus or the sixth nerve, or to involvement of them in the scar tissue. Stitching the periosteum together obviates the latter to a certain extent.
4. As the wound cicatrizes a certain amount of enophthalmos is very liable to result.
Indications. This operation is usually performed for some form of new growth originating either in the eye or the orbit.
Operation. This may be modified (1) according to the position of the growth. In severe cases of rodent ulcer and sarcomatous growths, which involve the lids, it is desirable that the lids should be removed with the tumour; but in cases of tumour of the optic nerve, or disease situated far back in the orbit, and not involving the lids or conjunctiva, these structures may be retained, since a much better socket is thus obtained. (2) The nature of the growth. In simple tumours, such as nævi and some cases of arterio-venous aneurism which have failed to yield to other treatment, the incomplete method, in which the lids are retained, is all that is necessary, but in malignant cases they should be removed.
The Complete Method. An incision down to the bone is first made, completely encircling the orbital margin and including any growth that may be involving the skin. The periosteum is then separated completely, as near to the optic foramen as possible. Care must be taken in dealing with the periosteum over the lachrymal bone, as the bone is liable to be fractured and an opening made into the nose if undue force be used. The apex of the cone formed by the periosteum is divided, as far back as possible, with curved scissors, and the whole orbital contents are removed. The wound is packed with gauze, and skin-grafting is subsequently performed when the bone has become covered with granulations; this usually occurs about the end of the second week.
The Incomplete Method. The globe is first enucleated and the outer canthus divided. The lids are well retracted and an incision is carried down to the bone along the orbital margins. The periosteum is then stripped up from the walls of the orbit and the apex of the cone divided as far back as possible, as in the previous operation. The conjunctiva and outer canthus are then united with sutures. As a rule, skin-grafting is not necessary after this operation.
Orbital abscesses should be incised where they point. In the upper lid care should be taken not to divide the levator palpebræ muscle; the incision should be placed well to one side. In making an incision over the inner side of the orbit care should be taken not to detach the pulley of the superior oblique. The cause of the abscess should be ascertained if possible. Suppuration in the ethmoidal sinuses coming through from the nose is the commonest cause, and should be treated appropriately (see Section V).
In order to perform successfully the various operations upon the ear, it is essential that the surgeon should be familiar with the technique of its examination, which, for the sake of convenience, will first be briefly described.
 Fig. 171. Clar’s Lamp.
Fig. 171. Clar’s Lamp.
For this purpose it is necessary to make use of certain instruments in order to obtain a clear view of the deeper parts of the auditory canal and tympanic membrane. Most important amongst these are the following:—
Mirror. A head-mirror, such as the ordinary laryngological mirror with a focus of eight inches, is to be preferred to the hand-mirror, as it leaves both hands free for manipulation.
Sources of illumination. Although the light reflected from the sky on a bright cloudless day is excellent, it can seldom be made use of, and so for practical purposes the source of light is usually artificial. It is wiser always to use the same kind of light—for instance, electric—as in this way a more accurate comparison can be made of the various pathological conditions seen on examination. In the consulting room, the lamp recommended by Dr. Greville Macdonald, furnished either with a thirty-two candle-power frosted burner or with a Nernst light, is most suitable. As a portable lamp, it is useful to have an electric bull’s-eye lamp, run off from a dry-celled battery: it can be held in the position of the ordinary lamp, the light being reflected into the ear by means of the head mirror. The ordinary surgical head-lamp, although not well adapted for inspection of the deeper parts of the auditory canal, is eminently suited for obtaining good illumination during the performance of the mastoid operations; or in its stead a head-mirror with lamp attached may be used, as recommended by Clar (Fig. 171).
Aural specula. Of the various aural specula employed, Gruber’s is very good (Fig. 172). A special speculum in which a portion has been removed from the narrow end is sometimes useful in order to facilitate operative procedures within the external meatus.
Forceps. The best are angular spring forceps with bulbous points (Fig. 173).

Fig. 172. Gruber’s Aural Speculum.
|
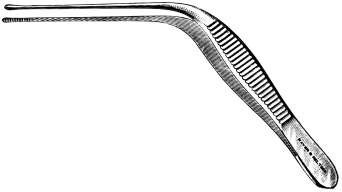 Fig. 173. Angular Spring Forceps.
Fig. 173. Angular Spring Forceps.
|
Position of the patient. The patient should sit upright in a chair with the side to be examined turned towards the surgeon. To prevent movement, the head should be supported by an assistant or by a head-rest fixed to the back of the chair. The lamp is placed a little behind and to the left of the patient’s head, on a level with the head of the examiner.
Technique of examination. To convert the external meatus into a straight canal, the auricle has to be pulled backwards and downwards in an infant, backwards in a child, and backwards and upwards in an adult. The speculum should be warmed and inserted gently into the meatus by the thumb and index-finger of the left hand, whilst the pinna is held between and pulled back by the second and third fingers (Fig. 174). This leaves the right hand free for manipulation. The largest possible speculum should be used, in order to give the maximum amount of room and illumination. It should only be introduced into the meatus as far as the adaptable cartilaginous portion permits—about half an inch in the adult—and not forced into the bony portion. The utmost gentleness is essential in order to obtain the confidence of the patient; this is absolutely necessary for the performance of the various small operations upon the auditory canal and tympanic cavity under local anæsthesia.
 Fig. 175. Aural Forceps holding Cotton-wool.
Fig. 175. Aural Forceps holding Cotton-wool.
|
Method of cleansing the ear. Except when the auditory canal is completely blocked by inspissated pus, cerumen, or epithelial débris, it is sufficient to mop out the ear with small pledgets of cotton-wool. To prevent injury to the walls of the meatus and to the tympanic membrane, the pledget is held between the blades of the forceps in such a fashion that it partially projects beyond its points (Fig. 175). The forceps is passed through the lumen of the speculum along the auditory canal and then quickly withdrawn. This is repeated with fresh pledgets until the meatus is cleansed. If there is much purulent discharge, only a brief moment may be given (after the withdrawal of the forceps) in which to inspect the deeper parts. Such a view, however, should always be obtained in order to form an accurate diagnosis. If this method fails to cleanse the ear, syringing becomes necessary.
Technique of syringing. The patient should be sitting down, as syringing may cause giddiness. The fluid should be aseptic, and at a temperature of 100° F. The patient’s head is inclined to the affected side, and the auricle is pulled upwards or backwards. The syringe is inserted a short distance within the meatus, and applied to the upper posterior wall so that the stream of lotion flows along the roof of the canal to the drum, and returns along the floor, thus washing out the contents. The best syringe is one with a metal plunger, as it can be easily sterilized. After syringing, the auditory canal should be dried and again inspected. If the inspissated pus or epithelial débris cannot be removed by simple syringing, an ear-bath of warm hydrogen peroxide (10 vols. %) should be given, and the ear again syringed after ten minutes.
 Fig. 176. Milligan’s Intratympanic Syringe.
Fig. 176. Milligan’s Intratympanic Syringe.
Syringing out of the attic. In certain cases of chronic attic suppuration, it is advisable to syringe out the attic. For this a special syringe is necessary. It consists of a fine canula whose point is turned up almost at right angles to its shaft (known as Hartmann’s canula), to which is fitted a piece of india-rubber tubing and a ball syringe. Milligan’s modification of this instrument is now generally used, as it permits of the canula being held in the hand, and instead of having a ball syringe, is connected by rubber tubing to a small irrigator (Fig. 176).
The patient sits upright in a chair in the ordinary position for examination of the ear; a speculum is inserted into the meatus, and held in position with the left hand; the canula, together with the ball syringe (if Hartmann’s is used), is held in the right hand. Under good illumination the canula is passed inwards along the auditory canal, and its point inserted through the perforation. By gently pressing on the syringe, the fluid is forced into the attic, which is thus washed out.
With Milligan’s instrument, the irrigator is fixed about two feet above the level of the ear. While the canula is being inserted, the escape of lotion is prevented by compressing the tube against the shaft of the instrument by means of the thumb. After the canula has been inserted into the opening, relaxation of this pressure permits of flow of the lotion. Milligan’s method is better than Hartmann’s, as the surgeon has more control over the instrument. Pain due to the introduction of the canula may be greatly minimized by previously inserting within the margins of the perforation either a pledget of cotton-wool soaked in a saturated solution of cocaine, or a crystal of cocaine.
After the cavity has been thoroughly washed out, the auditory canal is carefully dried as a final step, gentle inflation by Politzer’s method may be performed in order to expel any fluid still remaining within the attic.
In this connexion two points must be borne in mind: (1) The surgeon must have a good view of the part operated upon. For this reason when operating upon the auditory canal, the tympanic membrane, and tympanic cavity, he will usually require to work by reflected light.
(2) There must be no movement of the patient’s head during the operation. If the operation is performed under a local anæsthetic, it is therefore very important that the patient’s head should be kept fixed by means of an assistant.
Preliminary surgical toilet. If there be no existing suppuration, the ear should be cleansed, some twelve hours before the operation, by first giving an ear-bath of hydrogen peroxide lotion. This is done by making the patient incline the head to the opposite side so that the affected ear is uppermost. The warm solution is then poured into the meatus. After ten minutes the ear is syringed out with a 1 in 5,000 aqueous solution of biniodide of mercury, and a strip of sterilized gauze is then inserted into the auditory canal. The auricle and surrounding parts should also be surgically cleansed, and afterwards protected by a simple aseptic compress. If, as in furunculosis of the external meatus, syringing or cleansing of the ear is very painful, drops of a 10% solution of carbolic acid in glycerine may be instilled frequently into the meatus instead. If there is an existing otorrhœa, it is obviously impossible to render the field of operation absolutely aseptic. The ear, however, should be cleansed, but the auditory canal should not be plugged with gauze. The existence of a purulent discharge is no excuse for lack of cleanliness. Failure of such precautions may lead to disaster; for example, to perichondritis of the auricle as a sequel of the mastoid operation.
Before the actual operation takes place, if necessary after the anæsthetic has been given, the ear and surrounding parts should again be carefully cleansed, and the auditory canal syringed out with biniodide of mercury solution.
In intrameatal operations the head should be wrapped in a sterilized towel, and a square of sterilized lint, having an aperture in the centre so as to expose only the auricle and meatus, should be placed over the side of the head and face. In operations on the mastoid process, and in those involving a post-auricular incision, the head should also be shaved for at least two or three inches beyond the region of the ear.
Anæsthesia. Both local and general anæsthesia are used. Unless contra-indicated for some special reason, and unless the operation is a very trivial one, it is wiser to give a general anæsthetic. Of these, chloroform is the most suitable in adults and infants, and the A. C. E. mixture in children. Ether, although it may be safer, is frequently a source of annoyance to the operator, as it tends to increase the hæmorrhage.
In order to produce local anæsthesia two methods may be employed: (1) The instillation of fluids into the meatus; (2) subcutaneous injection of fluids beneath the lining membrane of the meatus and into the surrounding parts of the auricle.
The solution usually employed is a sterilized aqueous solution of cocaine hydrochloride in varying strengths up to 20%, to which may be added equal parts of 1 in 1,000 adrenalin chloride solution; the latter not only increases its analgesic properties, but also acts as a powerful hæmostatic.
Instillation. As the auditory canal and the tympanic membrane are lined with epithelium which is very resistant to the absorption of fluids, complete anæsthesia is almost impossible to obtain. This method, therefore, is practically limited to such trivial operations as the curetting away or snaring off of granulations or polypi from the external or middle ear. To render anæsthesia more complete, the affected part may be finally rubbed over with a crystal of solid cocaine hydrochloride just before the operation—is begun. On the other hand, if the raw surface is large—for example, the wound left after a recently performed complete mastoid operation—the cocaine employed should not be stronger than a 5% solution in order to minimize the risk of poisoning. Gray of Glasgow has suggested, as a more penetrating anodyne solution, a mixture consisting of a 10% solution of cocaine hydrochloride in equal parts of aniline oil and absolute alcohol, a solution which he especially advocates in order to produce anæsthesia of the tympanic membrane before doing paracentesis.
Subcutaneous injection. This is a modification of Schleich’s method, and was first introduced by Neumann of Vienna. It consists in injecting a very weak solution of cocaine and adrenalin chloride subcutaneously beneath the periosteum lining the auditory canal. By this method even the complete mastoid operation has been performed, and in certain clinics it is used continually in the minor operations of paracentesis of the tympanic membrane, division of intratympanic adhesions, extraction of polypi, and ossiculectomy. A solution of beta-eucaine or novocaine may be used in preference to cocaine, as being less dangerous. According to Neumann, three solutions are necessary: (a) a 1 in 2,000 solution of adrenalin chloride containing a 1% solution of beta-eucaine; (b) a 1 in 3,000 solution of adrenalin chloride containing a 1% solution of cocaine; (c) a 20% solution of cocaine.
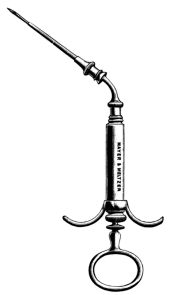 Fig. 177. Neumann’s Syringe for Subcutaneous Injection.
Fig. 177. Neumann’s Syringe for Subcutaneous Injection.
The syringe for injecting the solution has a capacity of 1 cubic centimetre, and for convenience its needle is fixed at an obtuse angle to the body of the syringe (Fig. 177). The technique of the injection depends on whether the operation is to be limited to the auditory canal and tympanic cavity, or is to involve the mastoid process.
If the complete mastoid operation is going to be performed, the needle of the syringe, now filled with the eucaine solution, is thrust through the skin about the middle point of the mastoid process, and a few drops of the solution are injected. The needle is then forced upwards towards the temporal ridge, at the same time being thrust in deeply until it touches the bone, so that a syringeful of the solution is injected beneath the periosteum. The needle is then withdrawn and reinserted at the same point, but in a backward direction, the solution being injected along the posterior portion of the mastoid process; in a similar manner the solution is injected downwards towards the tip of the mastoid. The ear being now pulled well forward, the needle is made to pierce the fold between the auricle and the mastoid process, just above the posterior ligament, and is pushed inwards between the anterior border of the mastoid process and the cartilage of the meatus, and a further syringeful of the solution is injected. A large speculum is now inserted into the ear, so that by pressing it against the wall of the meatus the skin, at the termination of the cartilaginous portion, is made to project in folds. The needle of the syringe, filled with cocaine solution, is pushed into this fold, and a few drops of the solution injected. By degrees the needle is still further pushed inwards, keeping it in close contact with the bony wall so that the fluid is injected beneath the periosteum. If the injection has been successful, a white bulging of the superior wall of the auditory canal will be noticed. To render anæsthesia complete, further injections may be made into the inferior and anterior walls of the auditory canal. Finally, a pledget of cotton-wool soaked in a 20% solution of cocaine is pushed into the tympanic cavity.
In the case of simple opening of the mastoid, subcutaneous injections into the auditory canal are not necessary. On the other hand, if the operation is limited to the auditory canal and tympanic cavity, the injections into the mastoid process are not required, but a primary injection of a small quantity of eucaine solution into the auriculo-mastoid fold considerably diminishes the pain produced during the act of injection into the auditory canal. Fifteen minutes should be allowed to elapse before the operation is begun. The anæsthesia lasts about half an hour.
Difficulties. It is by no means easy to inject fluid beneath the periosteum of the auditory canal, owing to its close adherence to the bone. The needle by mistake may repierce the skin at a point farther in, so that the fluid, instead of being injected beneath the periosteum, is injected into the auditory canal itself. In these cases anæsthesia will not be obtained, and the operator may possibly blame the principle of subcutaneous injection, rather than his own faulty technique.
In favour of subcutaneous injection it is urged that most of the minor operations within the tympanic cavity, including ossiculectomy, may be performed with the patient sitting up in the chair in the consulting room, and further, that the patient can afterwards go home; that the operation is rendered more easy owing to there being practically no bleeding; and that in the case of the more severe operations, such as opening of the mastoid antrum, the surgeon, in a case of emergency, may make use of this method if he cannot possibly obtain the services of an anæsthetist.
Against subcutaneous injection is the pain of the injection, which may be so great that the patient will not submit to it, and in consequence the proposed operation may have to be postponed.
In the case of the mastoid operation, it is difficult to believe that local anæsthesia, however efficient, will be looked upon with favour either by the surgeon or by the patient, except when a general anæsthetic is absolutely contra-indicated. The discomfort produced by retraction of the parts, the jarring caused by chiselling, and the consciousness of what is taking place, are far more unpleasant and more of a shock to the patient, than a general anæsthetic carefully given. Further, it is not always possible to foretell the extent of the operation, and if repeated injections become necessary, there is danger of eucaine or cocaine poisoning being produced.
Position of the patient and the surgeon
1. In the minor operations the patient may be operated on whilst in the sitting posture, whether a local anæsthetic or a general one of gas and oxygen is employed. The relative positions of the patient and the surgeon are then the same as for the ordinary routine examination of the ear. Special care, however, should be taken that the patient’s head is supported by the anæsthetist or assistant in order to prevent involuntary movements.
2. If the patient is operated on in the recumbent position, the head may rest comfortably on an ordinary pillow, but if chiselling is going to take place, the best support is a loosely filled sand-bag. The head should be turned towards the opposite side so that the affected ear is uppermost, and the surgeon stands at the side to be operated on. The lamp, the source of reflected light, should be held about six inches above the patient’s shoulder on the opposite side.
The operative treatment consists in incising the furuncles and, if necessary, curetting out their contents.
Indications. (1) If, in spite of palliative treatment for two days, the pain be so intense as to prevent sleep, and be accompanied by pyrexia.
(2) If there be accompanying œdema of the auricle and surrounding parts.
(3) If the furuncles occur during the course of a middle-ear suppuration, and occlusion of the external meatus prevents free drainage of the purulent secretion.
When possible, it is always preferable to operate under a general anæsthetic, such as gas and oxygen. If, however, the patient objects to a general anæsthetic, it should be explained that, in spite of the application of anodynes, the operation, although of momentary duration, will be excessively painful.
Operation. After the ear has been thoroughly cleansed, a large aural speculum is inserted within the meatus and the auditory canal dried with pledgets of cotton-wool.
The instrument usually used for this operation is a small and narrow sharp-pointed knife known as Hartmann’s furunculotome (Fig. 178, C). Equally suitable, however, is a fine bistoury; or, if necessary, a small tenotome or the ordinary paracentesis knife.
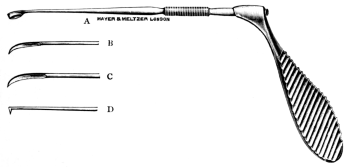 Fig. 178. Burkhardt-Merian’s Aural Instrument.
Fig. 178. Burkhardt-Merian’s Aural Instrument.
A. Curette. B. Myringotome. C. Furunculotome.
D. Hook for removal of foreign body.
The surgeon holds the speculum in position within the meatus with the left hand, and with the right inserts the knife through the lumen of the speculum along the meatus until its point passes the innermost limit of the furuncle. It is then quickly withdrawn, at the same time incising the furuncle freely down to its base. Another method is to transfix the furuncle by passing the knife through its base and making it cut outwards through the skin. In a similar manner any other furuncles that may be present are incised or transfixed.
If the inflammatory process, instead of being localized as a furuncle, extends to the subcutaneous tissues, and especially if it is accompanied by much pain, pyrexia, and occlusion of the external meatus, linear scarification may become necessary.
After incision, the contents of the furuncle are rapidly scooped out with the curette (Fig. 178, A). Slight hæmorrhage may occur, but can be arrested at once by plugging the meatus for a minute with a strip of sterilized gauze. The auditory canal is finally syringed out with a warm aqueous 1 in 5,000 solution of biniodide of mercury and firmly plugged with gauze soaked in a 10% solution of carbolic acid in glycerine; a hot fomentation being afterwards applied to the side of the head.
If the operation has been performed under a local anæsthetic (and this should only be done if a solitary furuncle is present), the pain is usually too great to permit of firm packing of the auditory canal. This after-packing, however, should be carried out, if possible, for the following reasons: firstly, it presses out the contents of the furuncle; secondly, it prevents auto-infection from one hair follicle to another; and thirdly, it tends to dilate the auditory canal.
After-treatment. If the furuncles have occurred during the course of a middle-ear suppuration, the gauze plugging must be removed within a few hours after the operation. The ear is then syringed out once or twice daily with a warm solution of lysol or carbolic acid, a small wick of gauze soaked in a 10% solution of carbolic acid in glycerine being afterwards inserted along the meatus.
If there be no accompanying middle-ear suppuration, the packing should not be removed for at least twenty-four hours. The pain produced by the first dressing may be severe, but can be usually avoided by first soaking the gauze with 5% solution of cocaine for a few minutes before removal and then gently withdrawing it whilst the ear is being syringed with a warm aseptic lotion. For the next two or three days it is sufficient to insert a drain of gauze soaked in a 1 in 3,000 alcoholic solution of perchloride of mercury.
Results. Although cure may be expected, it is not uncommon for further furuncles to occur in crops at repeated intervals. This is due to auto-infection of the hair follicles, which to a large extent may be prevented by painting the surface of the auditory canal daily, for at least two or three weeks, with an oil containing a drachm of nitrate of mercury to the ounce.
In the case of diffuse inflammation, although relapses are uncommon, superficial necrosis of a portion of the bony meatus may afterwards occur as a result of involvement of its periosteal lining. If this takes place, stenosis of the auditory canal may afterwards occur from subsequent cicatrization.
Dangers. With ordinary precautions no accident should occur, but the following may be mentioned: (1) if the furuncles are deeply placed, the tympanic membrane may be incised inadvertently, and a middle-ear suppuration may result; (2) a too violent incision may cut through the meatal cartilage posteriorly, and, as a result of septic infection, may give rise to perichondritis of the auricle. This, fortunately, is rare.
Indications. The indications vary, depending on whether there is a coexisting middle-ear suppuration or not.
If there be no middle-ear suppuration. Operation is not urgent, but is justifiable under the following conditions:—
(i) When one ear only is affected. (a) If there be complete deafness due to obstruction of the auditory canal. The question of operation, however, should be decided by the patient, because it may be postponed indefinitely so long as no symptoms occur.
(b) If there be recurring attacks of discomfort or of pain in the ear as a result of eczema, of otitis externa, or of actual pressure of the growth itself. The patient may desire operation to obtain permanent relief.
(c) If there be deafness of the opposite side from other causes, and the presence of the exostoses is causing deafness of the functionally good ear.
(ii) When both ears are affected. In addition to the indications already given, operation is advisable on the worse side if there be almost complete obstruction on both sides, accompanied by recurrent attacks of deafness, owing to the narrowed passage of the auditory canal becoming repeatedly blocked from accumulation of cerumen or epithelial débris.
Operation is contra-indicated if previous examination indicates that the deafness is due to a chronic middle-ear catarrh or internal-ear disease, as in these cases restoration of hearing, which is the primary object of the operation, will be impossible.
If middle-ear suppuration be present operation is generally advisable.
(i) In acute middle-ear suppuration operation is urgent if there are signs of retention of pus, provided it is impossible to dilate the lumen of the auditory canal. Before resorting to operation an attempt should always first be made to obtain free drainage, as the obstruction may be due merely to inflammatory swelling of the tissues lining the auditory canal. With cessation of the acute inflammation, this swelling may subside and the lumen of the auditory canal again become patent; and if recovery with healing of the tympanic membrane takes place the hearing may again become normal, rendering the operation no longer necessary.
(ii) In chronic middle-ear suppuration operation is always indicated if there are symptoms of retention of pus. It is also advisable as a prophylactic measure, although not urgent, even although no acute symptoms are present.
Operation. When there is no middle-ear suppuration.
The operation may be performed either (a) through the external meatus or (b) by reflecting the auricle forward by a post-auricular incision.
Through the external meatus. This method is only indicated if the exostosis is situated at the entrance of the meatus and is pedunculated.
A general anæsthetic is given, the patient being in the recumbent position. The surgeon works by reflected light. After the ear has been thoroughly cleansed a large-sized aural speculum is inserted into the meatus and the outlines of the exostosis are defined with a probe. A small gouge or chisel is used. It is inserted into the meatus in such a fashion that its point presses between the pedicle of the exostosis and the wall of the bony meatus. With successive sharp taps of the mallet, the gouge is made to cut through the pedicle, care being taken that the instrument is not driven in too deeply, on to the tympanic membrane.
The growth, which can now be felt to be movable within the meatus, can usually be removed by grasping it between the blades of forceps, or can be expelled by syringing the ear. After its removal the auditory canal should be plugged for a few minutes with a solution of cocaine and adrenalin chloride. This checks all hæmorrhage, and at the same time enables the surgeon to get a good view of the deeper parts to see if further growths are situated more deeply within the meatus. Such growths, provided they are pedunculated and do not abut on the tympanic membrane, can sometimes also be removed by the same method; much depends on their shape and situation. If sessile or too deeply placed, the operation may have to be completed by reflecting forward the auricle. Before terminating the operation a clear view of the tympanic membrane should always be obtained.
The meatus is finally syringed out with a 1 in 5,000 aqueous solution of biniodide of mercury and dried, a strip of sterilized gauze being inserted into the auditory canal. A simple dressing is then applied to the side of the head.
Other methods of operation through the external meatus.
(a) Perforation of the exostosis, or enlargement of the small passage existing between multiple exostoses, by means of the burr.
Although successful results have been recorded, this method is not advised, as cicatricial tissue almost invariably causes closure of the opening made. To keep the opening patent it is necessary to insert a small lead or silver canula, frequently a source of great discomfort.
(b) If the exostosis has a very fine pedicle, it may be possible to nip through its base with a pair of forceps, but it is not so sure a method as the employment of a gouge and mallet.
(c) Such methods as attempts to destroy the growth by means of the galvano-cautery or by the pressure of laminaria tents should be avoided; they are useless and unsurgical.
By reflecting the auricle forward. This is indicated if the exostoses are multiple, have a broad base, and are deeply situated.
The position of the patient, and the anæsthetic, are the same as in the previous operation. Reflected light may not be necessary.
The ear and the surrounding parts are carefully cleansed and the head is shaved for a short distance over and beyond the mastoid process. A curved incision is made close behind the auricle (Fig. 226), beginning at the upper level of its attachment and extending downwards along the retro-auricular fold. The incision goes down to the bone. The auricle is reflected forward and the soft tissues are separated from the bone until Henle’s spine and the posterior upper margin of the auditory canal are brought into view. Any bleeding, chiefly from branches of the posterior auricular artery, is at once arrested by pressure forceps, ligatures being afterwards applied. The assistant’s duty is to hold the auricle well forward and at the same time to keep the wound dry by swabbing.
The fibrous portion of the canal is carefully separated from the bony portion with the periosteal elevator, the growth, if possible, being exposed without tearing through the thin layer of skin which covers it.
The method of procedure now depends on the character and number of the exostoses present.
(a) If situated superficially, they are removed by chiselling through their base with a gouge. They should be thoroughly removed, if necessary cutting through the normal bone well behind their base.
(b) If deeply placed, they are more easily removed by first chiselling away a part of the upper posterior wall of the external meatus. This is done in the same manner as in the early stage of the complete mastoid operation (see p. 397). If possible the antrum should not be exposed, and care should be taken not to cut too deeply for fear of injuring the tympanic membrane.
(c) If the exostoses spring from the anterior wall, it is necessary to make a T-shaped incision through the posterior membranous portion of the auditory canal in order to bring them into view clearly. This is done with a tenotomy knife, the flaps being held apart by means of forceps. The growths can now be removed by means of the gouge and mallet.
(d) If the obstruction is due to multiple small exostoses forming an annular stricture within the bony canal, it is better to separate the membranous portion completely from the bony meatus. In doing so the skin over the exostoses tears through, so that the membranous portion can be reflected outwards as a finger-like process. To give greater room for the operation, the auricle and fibrous portion are pulled well forward by means of a loop of gauze passed through the lumen of the cartilaginous meatus.
If necessary, reflected light should now be used. To reach the exostoses it may be necessary, as in the previous case, to remove part of the posterior bony wall. With the gouge and mallet the exostoses are carefully chiselled away. They frequently abut on the tympanic membrane, so that their removal without injuring it may be well-nigh impossible. It is of the utmost importance that the field of operation should be kept dry, if necessary by repeatedly mopping out the canal with pledgets of cotton-wool soaked in adrenalin solution. The chief difficulty is to determine the situation of the tympanic membrane. A fine probe is used to discover any existing chink between the growths; this will be a guide to show the direction in which to work. As soon as a small passage has been made, sufficient to allow of a view of the deeper-lying parts, the ear should be syringed out and dried, and a thorough inspection made. The tympanic membrane can usually be seen as a greyish-blue membrane; at other times it can be recognized by touching it with a probe. After making certain of the position of the membrane, the rest of the operation is easy. A small seeker (Fig. 219), such as is used in the mastoid operation, is passed through the opening already made, and with it the deeper limits of the exostoses can be felt. The opening is gradually enlarged by removing the growths piecemeal with the chisel or gouge.
Although the burr is contra-indicated when operating through the external meatus, it is frequently of great service in these cases in rendering the walls of the canal smooth. The disadvantages of using a burr are, that it is less easy to control (unless the surgeon has had considerable experience in using it), and that it destroys all the epithelial lining of the auditory canal with which it comes in contact. It should, therefore, only be used in those cases in which there is a complete ring of exostoses, but should be avoided if the exostoses are limited and if it is still possible to leave untouched a portion of the epithelial lining of the auditory canal.
When the surgeon considers he has successfully removed the obstruction, he should verify this fact by syringing out and drying the ear, and again obtaining a clear view of the tympanic membrane.
The fibrous portion is now replaced by inserting a finger into the cartilaginous meatus and pressing it back into the bony canal, the auricle being meanwhile pulled back into its normal position. The edges of the posterior wound are sutured together and the auditory canal is gently packed with gauze which should be inserted right down to the tympanic membrane. It is not necessary to make special meatal skin flaps, as careful packing of the auditory canal should be sufficient to keep the parts in apposition.
When middle-ear suppuration is present. In acute middle-ear suppuration the chief difficulty is to decide what operation to perform. As operation is only indicated if there is retention of pus, it is wiser to open the mastoid antrum; the exostosis, if superficial and pedunculated, can also be removed at the same time. If, however, the obstruction is due to multiple and deeply placed exostoses, this part of the operation should be deferred to a later date, that is, after the acute symptoms have subsided.
In chronic middle-ear suppuration the only operation to be recommended is the complete mastoid operation (see p. 392).
After-treatment. The after-treatment is practically the same whatever operation has been performed. The first dressing need not be done until the third day. The gauze plugging is then withdrawn and the auditory canal is syringed out and dried. If only a single exostosis has been removed the wound surface is small, and it is usually sufficient to puff in some boracic powder and again insert a piece of gauze. This may be repeated every second day, healing usually taking place within two or three weeks. In the case of deeply situated multiple exostoses, especially if removed from the anterior wall, considerable swelling of the soft parts lining the auditory canal may occur as a result of the manipulations. In such cases, after syringing out any existing blood-clots, some cocaine and adrenalin solution should be instilled into the meatus. An aural speculum is then gradually worked into the auditory canal, which is gently mopped out with small pledgets of cotton-wool, and the deeper parts are carefully inspected. Sometimes the torn ends of the fibrous portion, instead of covering the bony walls, are found to project into the auditory canal and to cause considerable narrowing of its lumen. By careful manipulations with the probe or by stroking the edges with tiny pledgets of cotton-wool, these rough surfaces may be smoothed down. It is very important, in the early days of the after-treatment, to prevent any narrowing at the site of the operation. This is one of the chief causes of subsequent failure. The gauze should always be reinserted right down to the tympanic membrane, and if there is not much secretion it should be packed firmly against the posterior and outer portion of the canal in order to prevent subsequent stenosis from the tendency of the cartilage to prolapse forward owing to the soft parts having been separated from the bony canal at the time of the operation.
The wound behind the ear heals very quickly and the stitches can generally be removed on the third or fourth day. Subsequent treatment consists in preventing the formation of granulations over the wound area. This is best accomplished by keeping the auditory canal aseptic and dry. If granulations occur they should be touched from time to time with a saturated solution of trichloracetic acid. If healing has not taken place within two weeks, it will frequently be advantageous to discontinue the gauze packing and, in its stead, to instil drops of pure rectified spirit.
If a middle-ear catarrh with secretion of fluid occurs, owing to the tympanic membrane having been injured, it may be impossible to continue the gauze packing. In these cases only a fine drain of gauze should be inserted into the meatus, the dressing being changed as frequently as may be necessary.
Provided asepsis is maintained, the middle-ear inflammation usually subsides rapidly with healing of the membrane. After healing has taken place, inflation of the middle ear is recommended twice a week, for two or three weeks, in order to aid recovery and to prevent adhesions forming within the tympanic cavity.
Dangers. 1. If the exostoses be deeply situated, the tympanic membrane may be injured.
2. If much of the anterior wall of the auditory canal be removed, the temporo-maxillary joint may be opened.
3. It is possible that the tympanic membrane may not be recognized, and, by working too deeply, the labyrinth or the facial nerve may be injured.
Prognosis. Provided no accident has occurred during the operation, a successful result should be obtained. Stenosis, however, may occur from cicatricial contraction if the operation has been incompletely performed.
Before considering the question of removal of foreign bodies, the following points cannot be emphasized too forcibly:—(1) No attempt should be made to remove a foreign body until it is certain that one really exists. (2) Provided there is no middle-ear suppuration, a foreign body left in the ear will very rarely cause any immediate harm. (3) The most serious complications are due almost invariably to ill-advised haphazard attempts to remove the foreign body; as a rule from working blindly in the dark without making use of reflected light.
If a foreign body be suspected, the surgeon should first carefully examine the auditory canal in order to determine its character and position and the condition of its walls. On this will depend the treatment to be employed.
If the object be a living insect it should be killed at once by the instillation of warm oil, rectified spirit, or chloroform. This will cause immediate relief of the intense pain and tinnitus which may have been set up by its movements against the sensitive tympanic membrane.
The methods employed for the removal of a foreign body are syringing, extraction by instruments through the external meatus, and removal by operation by making a post-auricular incision and reflecting forward the auricle.
By syringing. In the vast majority of cases syringing is successful, and therefore should always be tried except under the following conditions:—(a) If the foreign body be of such a nature that it may be driven inwards; for example, a percussion cap for a toy pistol, lying with its concavity outwards.
(b) If there be much inflammation and swelling of the walls of the external meatus, unfortunately frequently due to previous unsuccessful attempts at extraction by instruments. In such cases forcible syringing may cause considerable pain, and in addition immediate removal of the foreign body may be impossible owing to the temporary occlusion of the meatus.
Unless urgent symptoms of retention of pus behind the foreign body are present, it is wiser to wait for a few days until the inflammation has subsided, in order that the canal may become more patent and permit of a more favourable opportunity for removal of the foreign body. The auditory canal, in the meanwhile, may be mopped out two or three times a day with pledgets of cotton-wool, and a 1 in 5,000 alcoholic solution of biniodide of mercury afterwards instilled into the ear.
The method of syringing has already been described (see p. 308). The syringe should be a large one with its tip protected by some india-rubber tubing. The point is inserted within the meatus up against the foreign body and the stream of lotion is directed towards any chink which may exist between it and the auditory canal. It may be necessary to use many syringefuls with considerable force before the foreign body can be expelled, but the syringing should be stopped if pain or giddiness are caused.
If the foreign body cannot be removed at the first attempt, drops of rectified spirit may be instilled into the ear several times a day, provided there are no urgent symptoms. This will tend to diminish any swelling of the soft tissues of the external meatus and of the foreign body if it is a vegetable substance. The ear should again be syringed after two or three days. In many cases this will now be successful; if not, the foreign body may be moved gently with a probe (using a speculum and reflected light), great care being taken not to push it further into the auditory canal, and another attempt may be made to remove it by prolonged syringing. If this fails it may be left in situ for a still longer period, provided there are still no symptoms requiring its immediate removal. In some cases, instead of the instillation of alcohol, a 5% solution of carbolic acid in glycerine or olive oil proves more effectual.
In the case of a hard substance, repeated attempts may be made to dislodge it before resorting to further measures; but in the case of a soft vegetable substance like a pea, it must not be forgotten that moisture tends to make it swell and perhaps will necessitate almost immediate extraction by instruments.
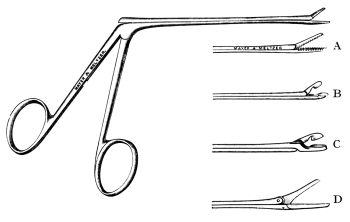 Fig. 179. Crocodile Forceps. Two-thirds size.
Fig. 179. Crocodile Forceps. Two-thirds size.
A, Points of crocodile forceps, full size.
B and C, Aural punch-forceps.
D, Aural scissors.
Extraction by instruments.
Indications. (i) If inspection shows that the foreign body can at once be removed by a suitable instrument: for example, a percussion cap the edge of which may be grasped by a pair of forceps (Figs. 179 and 193); or a small boot button whose shank, if it faces outwards, may be caught by a small hook.
(ii) If repeated attempts have failed to remove the foreign body by syringing.
(iii) If previous attempts by others have failed, and the foreign body has been pushed in beyond the isthmus, and cannot be removed after prolonged syringing.
(iv) If syringing produces violent giddiness, showing the probable presence of a perforation of the tympanic membrane.
(v) If there be symptoms of acute inflammation of the middle ear or of pus being pent up behind the foreign body.
Operation. An anæsthetic may not be necessary in adults if the foreign body is not too deeply placed within the ear, if its removal appears to be a simple matter, and if the patient is of a placid temperament. Otherwise, unless contra-indicated for some special reason, a general anæsthetic should always be given in children, and it is also preferable in adults for the following reasons:—(1) Inability to remove the foreign body after repeated attempts by syringing usually means that its extraction by instruments will be a somewhat difficult matter. (2) The risk of injury to the meatal walls or tympanic membrane from involuntary movements of the patient during the operation is far greater than the risk of the anæsthetic. (3) If the foreign body cannot be removed through the meatus by means of instruments, the post-meatal operation is indicated. This, if necessary, can be done at once if the patient is under a general anæsthetic.
If no anæsthetic is given the patient may sit up in a chair; otherwise, the recumbent position is advised.
It is usually necessary to use an aural speculum, but if the foreign body be situated near the entrance of the meatus a sufficient view may be obtained by pulling the tragus forward and the auricle backward. Good illumination is essential.
(i) If the body be a soft substance, such as a pea, the core of an onion, or a fragment of wood, it is best removed by fixing into it some form of sharp hook (Fig. 178, D). These hooks vary in shape. They may be curved, or shaped like a crochet-hook, or have the sharp point placed at right angles to the shaft of the instrument.
In the case of a round substance like a pea, especially if it is tightly impacted within the meatus, its removal is sometimes facilitated by first slicing it into pieces by means of a small bistoury.
As a rule, the foreign body is impacted at the junction of the cartilaginous and bony portion of the auditory canal; sometimes, however, it is more deeply situated within the osseous meatus, usually the result of previous attempts to extract it.
In the former case, the instrument is passed along the upper posterior wall of the canal between it and the foreign body, the point of the hook being kept upwards or downwards so as not to project into the auditory canal. The instrument is first passed well beyond the foreign body, and then the shaft is twisted round so that the hook projects into the auditory canal. With a quick movement it is drawn outwards a short distance so that the point of the hook pierces the impacted substance. Gentle traction is now used and in the majority of cases the foreign body can be extracted.
If this fails, a slightly curved fenestrated scoop (Fig. 180) or curette should be passed, if possible, between the foreign body and the anterior wall of the auditory canal. The hook already fixed into the foreign body prevents it from being driven further within the meatus, whilst the scoop, if it can be got beyond the foreign body, can usually lever it out.
If the foreign body has been pushed in beyond the isthmus and lies deeply within the osseous canal, it is better to pass the hook along the anterior inferior wall of the meatus, because owing to the inclination of the tympanic membrane its anterior inferior margin is much more deeply placed than its upper posterior part.
(ii) In the case of a hard substance, such as a piece of stone, coal, or a bead, blunt hooks may be used instead of sharp ones. They should be passed into the meatus beyond the foreign body in the manner already described.
(iii) In other cases, depending on its shape and position, the foreign body is better removed by means of a snare, the loop of which is manipulated round it and then drawn tight in the same manner as in the extraction of a polypus.
The chief points to observe in these manipulations are (a) not to push the foreign body farther in and (b) not to injure the walls of the meatus or the tympanic membrane.
Other methods of extraction are—(1) Drilling through the foreign body, if it is a hard substance, and then inserting a fine hook into the opening so made. (2) The agglutinative method, which consists in dipping a small paint-brush into a concentrated solution of seccotine or glue and then inserting it into the meatus until it comes in contact with the foreign body. The brush is left in this position for several hours in the hope that it may become adherent to the foreign body; if so, on withdrawing the brush from the ear, the foreign body should be extracted with it. This method can only be used provided the ear is kept dry.
These procedures, although said to be successful in a few cases, are not recommended.
After-treatment. If the tympanic membrane and auditory canal have not been injured, it is sufficient to dry the meatus and puff in a little boracic powder. If there be abrasions of the canal, a small strip of gauze should be inserted and changed as frequently as it becomes moist with secretion, the meatus, if necessary, being also syringed out with an aseptic lotion. If there be acute inflammation of the walls of the canal, accompanied by much swelling and purulent discharge, drops of glycerine of carbolic (1 in 10) may be instilled frequently. After the inflammation has subsided, an alcoholic solution of 1 in 3,000 biniodide of mercury may be employed. If the tympanic membrane has been injured, either from the presence of the foreign body itself or from the attempts at extracting it, the treatment is similar to that for an ordinary middle-ear suppuration.
Removal by operation. This may be done in the following ways:—
By means of a post-aural incision.
Indications. (i) If prolonged attempts to remove the foreign body by instruments have failed. This operation becomes imperative if there are signs of retention of pus within the middle ear.
(ii) If the foreign body has been pushed into the tympanic cavity and cannot be removed otherwise. In such cases, if the perforation is large and the foreign body is small, an attempt may first be made to dislodge the substance by injecting fluid into the middle ear through the Eustachian tube by means of the catheter and syringe (see p. 372). This method, however, is rarely successful.
Operation. The procedure is the same as for the removal of exostoses (see p. 318). After separating the fibrous from the bony portion of the canal, an incision is made through it and the cut edges are held aside with forceps. Usually the foreign body can now be seen lying within the canal. It is best removed by passing a small fenestrated curette beyond it and levering it out. In some cases one of the hooks already mentioned will be found to be more suitable. Forceps should not be used, as they may inadvertently push the foreign body farther in. If the foreign body be very deeply placed, removal of the upper posterior portion of the bony meatus may be necessary. The subsequent steps of the operation and its after-treatment are similar to that already described in the case of an exostosis.
By means of an operation upon the mastoid.
Indications. (i) If the above measures fail to remove the foreign body.
(ii) If there be symptoms of inflammation of the mastoid process, or of internal-ear or of intracranial suppuration.
(iii) If there be facial nerve paralysis the result of pressure from the foreign body.
Operation. The operation performed depends on the condition found. Simple opening of the mastoid antrum may be sufficient in a case of recent middle-ear suppuration, although it is usually necessary also to remove a considerable portion of the posterior wall of the auditory canal before the foreign body can be extracted. If these measures fail, an attempt may be made to dislodge the foreign body by forcibly syringing through the aditus, or by the insertion of a probe through it, into the tympanic cavity. If this likewise ends in failure, it will then be necessary to perform the complete operation. These cases fortunately are rare.
If it be certain that chronic middle-ear suppuration already exists, the complete mastoid operation is indicated.
If it becomes necessary to operate on the mastoid process, owing to other means having failed to dislodge the foreign body, it is wiser, as a rule, to perform the complete operation at once, because, under these circumstances, irreparable destruction must have taken place within the tympanic cavity.
The technique of these operations and their after-treatment are described in the chapter on operations upon the mastoid process (see p. 390).
Stenosis, or stricture of the auditory canal, is practically always the result of traumatism or inflammatory conditions; it is only very rarely congenital.
Indications. (i) If there be deafness of the other ear, and the functionally good ear periodically becomes deaf from obstruction of the narrow passage by cerumen or epithelial débris, and the patient is weary of conservative treatment.
(ii) If there be recurrent attacks of otitis externa.
(iii) If there be retention of pus, the result of inflammation of the external or middle ear, which is not relieved by conservative treatment.
The operation is contra-indicated if there is accompanying deafness, due to chronic middle-ear or to internal-ear disease, provided there is no suppuration within the external or middle ear.
Operation. The method of operation depends on whether the stricture is membranous, fibrous, or bony in consistence, or whether it is limited or is causing a general narrowing of the auditory canal. It may take one of the following forms:—
Dilatation. This method is not very satisfactory, and is limited to recent cases of membranous or fibrous stricture of the annular variety. After cleansing the meatus, a small laminaria tent is inserted through the stricture, and if the pain is not too severe it is left in situ for at least twenty-four hours and then withdrawn. The ear is again carefully cleansed, and if possible a larger laminaria tent is substituted. This procedure is repeated until the maximum amount of dilatation has been obtained.
Incision of the stricture. This also is limited to membranous or to fibrous strictures of the annular variety.
The operation, if necessary, may be performed under a local anæsthetic, produced by subcutaneous injections, although usually a general anæsthetic is preferable.
The ear and surrounding parts are surgically cleansed by the ordinary methods. The surgeon works by reflected light. The patient may be in either the sitting or the recumbent position, depending on whether a local or general anæsthetic is given. In the latter case the auditory canal should be filled with cocaine and adrenalin solution before the anæsthetic is administered in order to diminish bleeding as far as possible.
The ear having been dried, a conveniently large aural speculum is inserted, and with a tenotome or a furunculotome radiating incisions are made through the stricture. One of the small flaps thus made is grasped with a fine pair of tenaculum forceps, and the surgeon cuts through its base, keeping the knife as close as possible to the wall of the auditory canal. Each flap is treated in a similar fashion. Instead of making radiating incisions, the tissue forming the obstruction may be transfixed through its base, the knife being made to cut in a circular fashion right round the auditory canal, keeping as close as possible to its wall.
On completion of the operation, a piece of india-rubber tubing, of as large a size as possible, is inserted into the dilated canal. It should only be removed for the purpose of cleansing and should be at once reinserted. A silver canula, if necessary, can afterwards replace the india-rubber tubing. This canula may have to be worn for months.
This operation is often most unsatisfactory, as the stricture, instead of being annular as first supposed, may be found, on operation, to extend a considerable distance along the auditory canal and, in addition, to be partially due to a general thickening of the underlying bone.
Excision of the stricture. The auricle is reflected forward and the preliminary steps of the operation are performed as already described for removal of a deep-seated exostosis (see p. 319). The surgeon makes a transverse incision with a knife through the fibrous portion of the auditory canal, just external to the stricture, and carries it right round the meatus, thus separating the outer portion of the membranous from the bony canal. The fibrous portion is now pulled outwards by means of a retractor, and the thickened tissue, forming the stricture, is peeled off from the surrounding bony meatus with a small periosteal elevator and so removed. If the stenosis is partially due to thickening of the walls of the canal itself, it may also be necessary to chisel away a considerable portion of its upper posterior part. After completion of the operation a clear view of the tympanic membrane should be obtained.
In this operation a considerable portion of the bony canal is denuded of its epithelial lining membrane, so that there is a special tendency to the re-formation of cicatricial tissue. To prevent this taking place two methods may be employed:—(1) If much of the upper posterior wall of the bony meatus be removed, a post-meatal flap should be made and kept in position by means of a catgut suture carried through the skin behind the auricle. The formation of such a flap is described as a step in the complete mastoid operation (see p. 401).
(2) If no bone be removed, the membranous portion is replaced in situ, the posterior auricular wound closed, and as large an india-rubber tube as possible is inserted into the meatus. A week or ten days later, as soon as granulations begin to form, skin-grafting may be undertaken (see p. 410).
If grafting be not successful, the india-rubber tube or silver canula must be kept constantly within the meatus (only being removed for cleansing purposes) until healing takes place.
The complete mastoid operation is indicated in the case of stenosis occurring in chronic middle-ear suppuration if symptoms of retention of pus occur.
In acute middle-ear suppuration, however, every attempt should be made to avoid operation, as the lumen of the auditory canal may again become patent after the acute inflammation has subsided.
Atresia of the external meatus may be either congenital or acquired.
Indications. (i) In congenital cases operation is only justifiable if the atresia is due to a membranous web situated in the outer part of the auditory canal and if, as a result of tuning-fork tests and of inflation through the Eustachian tube, it is fairly certain that the middle ear is normal.
Operation is contra-indicated in cases of bony atresia. Although attempts have been made to make an artificial canal in order to restore the hearing power, a successful result has not yet been obtained. Apart from the difficulty of retaining the patency of any canal so made, the accompanying malformation of the middle ear renders a successful result impossible (Paper by author, Journal of Laryngology, &c., March, 1901). Although the tympanic membrane is said to have been exposed by operation in a few cases, experience has shown that the supposed tympanic membrane was really the capsule of the temporo-maxillary joint.
(ii) In acquired cases operation is indicated if the other ear is deaf; if the site of the occlusion of the auditory canal is in its outer part and is due to membranous or fibrous tissue, and if there is no previous history of middle-ear disease, and if the labyrinth is still intact.
Operation is not advised if the other ear is normal, unless the patient particularly desires it.
Operation is contra-indicated if there is internal-ear deafness on the affected side and if the other ear is normal; or if there is a definite history of the closure of the auditory canal having been the result of a previous middle-ear suppuration. In the latter case the destructive changes within the tympanic cavity will be so marked that the chances of improving the hearing will be very slight in spite of the most successful operation.
Operation. If the obstruction be due to a fibrous band, an attempt may be made to remove it by excising it by the intrameatal method. In other cases the post-auricular method is necessary.
The chief point to remember is to make a large opening. For this reason the post-auricular method is to be preferred, as a considerable portion of the upper posterior wall can be removed and a large meatal flap fashioned (see p. 401).
Results. If the stricture or point of occlusion of the auditory canal is limited and composed of membranous and fibrous tissues, a good result can be usually obtained, and there is no reason why complete recovery of hearing should not take place if the labyrinth and tympanic cavity are normal.
Unfortunately, as in all cases of stricture, there is a tendency for it to recur.
In this section only the aural polypi which project from the tympanic cavity into the external auditory meatus will be considered; whereas the treatment of granulations, and with them the minute polypi which are still limited to the tympanic cavity, will be discussed in the chapter on operations within the middle ear.
Indications. An aural polypus should always be removed because, apart from the fact that it is a symptom of underlying disease, it may obstruct free drainage of the purulent discharge, and therefore become a source of danger.
Operation. The simplest and the best method is removal by the snare.
In the case of small and soft polypi, the polypus is removed by traction—formerly called avulsion—after the snare has been tightened round its pedicle; with a large, tough, fibrous polypus considerable force may be required to tear through its pedicle. This procedure in the case of polypi arising from the region of the tegmen tympani has been known to give rise to fatal meningitis. In such cases the pedicle of the polypus should be cleanly cut through by the snare—so-called excision.
As aural polypi are always associated with suppuration, it is especially necessary that the ear should be thoroughly cleansed before operation.
A local anæsthetic (see p. 310) is sufficient in the case of smaller polypi, but if the polypus be large and tough, it is wiser to give a general anæsthetic, such as gas and oxygen. Or a 3% solution of cocaine may be injected into the growth, which, according to Frey of Vienna, renders removal absolutely painless; this, however, has not always been my experience.
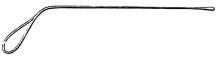 Fig. 181. Aural Probe.
Fig. 181. Aural Probe.
The size of the polypus and the origin of its pedicle should be determined before operating, if necessary by using a probe (Fig. 181); also it must be diagnosed from a bulging congested tympanic membrane, or from the inner surface of the tympanic cavity, which may be exposed to view owing to complete destruction of the membrane having already occurred.
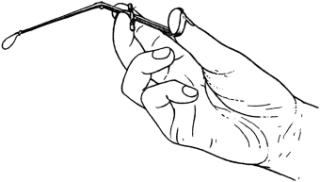 Fig. 182. Wilde’s Aural Snare. The snare is held in
the usual position for extraction of a polypus.
Fig. 182. Wilde’s Aural Snare. The snare is held in
the usual position for extraction of a polypus.
|
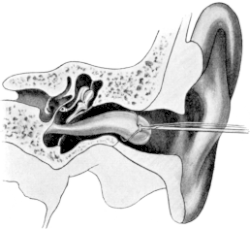 Fig. 183. Wilde’s Snare being passed
round an Aural Polypus. (Semi-diagrammatic.)
Fig. 183. Wilde’s Snare being passed
round an Aural Polypus. (Semi-diagrammatic.)
|
A Wilde’s snare is generally used. It is a fine angular snare fitted with soft copper wire. The loop of the snare should be bent downwards and forwards and should be of such a size as to just surround the growth. The snare is held between the thumb and the first and second finger of the right hand (Fig. 182). Under good illumination, and using the speculum and reflected light if necessary, the shaft of the snare is passed along the upper portion of the auditory canal until the edge of the polypus is reached. The loop is made to encircle the polypus (Fig. 183), the snare is gradually pushed inwards with a gentle sinuous movement until it reaches the point of attachment of the growth. The loop is then tightened until it firmly grasps the neck of the polypus (Fig. 184). The friable tissue is torn through by gentle traction and the polypus is withdrawn in the snare. Care must be taken not to injure the tympanic membrane through which the polypus may be projecting; it is for this reason that the loop is bent at an angle to the shaft of the snare so that it may lie parallel to the tympanic membrane whilst in the act of grasping the polypus. If the polypus be very small its pedicle may be clearly defined before operation, and the snare passed round it directly (Fig. 185).
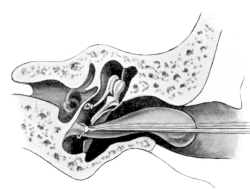 Fig. 184. Wilde’s Snare gripping the Neck of Polypus. (Semi-diagrammatic.)
Fig. 184. Wilde’s Snare gripping the Neck of Polypus. (Semi-diagrammatic.)
|
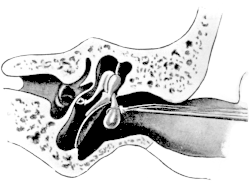 Fig. 185. Polypus arising from the Attic Region. The snare is in
position for the extraction of the polypus. (Semi-diagrammatic.)
Fig. 185. Polypus arising from the Attic Region. The snare is in
position for the extraction of the polypus. (Semi-diagrammatic.)
|
If the polypus be very large and tough, the snare is made to cut clean through its pedicle as near to its attachment as possible, instead of employing traction. The snare is then withdrawn, the polypus being afterwards grasped and removed by means of forceps. In this latter case it may be necessary to use a stronger snare fitted with piano steel wire instead of the ordinary copper wire. On removal of the polypus there may be considerable hæmorrhage. After it has ceased the ear is syringed out and dried. The auditory canal is then inspected, and if it is found that the growth has not been removed completely, this can be done now by reapplication of the snare.
After final cleansing of the meatus, a strip of gauze is inserted, and the ear protected with a pad of cotton-wool and a bandage.
After-treatment. The dressing should be removed within twenty-four hours, and the ear cleansed by syringing. After mopping it dry drops of rectified spirits should be instilled.
On removal of the first dressing, any polypoid tissue which remains may be cauterized under cocaine anæsthesia by the actual cautery, or by a bead of chromic or trichloracetic acid (see p. 348).
Further treatment consists in keeping the ear clean and dry. For the first few days it should be syringed daily, dried, and spirit drops instilled. As the secretion becomes less the syringing should be diminished. If the perforation be large, instead of instilling drops, some finely powdered boric acid may be puffed in.
Other methods of removal. These are not recommended, but merely mentioned for the sake of completeness.
By forceps. The rough and ready method of extracting a polypus forcibly from the ear by means of forceps, although practised formerly, has now been discarded as being unsurgical and dangerous.
Ligation. The operation consisted in passing a snare over the polypus and grasping it tightly as near to its base as possible. The snare was then twisted round its axis in order to tighten the loop further and so obliterate the blood-supply of the growth, the wire of the snare being afterwards cut through with pliers and the snare withdrawn. After a few days the polypus became gangrenous from want of blood-supply, and separated from its deep attachments.
Curetting. This method, which should only be made use of in the case of small multiple polypi within the tympanic cavity, will be considered when discussing the treatment of granulations within the middle ear (see p. 398).
Dangers. Hæmorrhage is seldom profuse, but if it is, it can always be arrested by packing the meatus with cocaine and adrenalin solution.
The chief dangers are injury to the contents of the tympanic cavity, such as dislocation or removal of the ossicles; or subsequent meningitis. These mishaps are usually the result of forcible extraction, or of blindly curetting the ear after this has been done. Meningitis, however, has been known to occur, in spite of every precaution being taken, if, owing to caries of the tegmen tympani, the polypus has its origin from the dura mater of the middle fossa.
Prognosis. If the polypus be single and of recent origin, the result probably of acute inflammation of the middle ear, its removal may cause complete recovery and cessation of the middle-ear suppuration.
In the case, however, of multiple polypi associated with chronic middle-ear suppuration and usually signifying underlying bone disease, recurrences may be frequent and further operations may become necessary.
It may here be emphasized that a polypus in itself is not a disease, but merely a symptom of disease.
After removal of a large polypus, the patient should always be kept under observation for a day or two in case of symptoms of acute inflammation of the mastoid process arising and necessitating further operation.
The tympanic membrane. The chief points to notice when operating on the tympanic membrane are its inclination and its relation to the inner wall of the tympanic cavity.
The normal membrane is inclined obliquely downwards and forwards so that it forms an obtuse angle of 140 degrees with the roof and an acute angle of 27 degrees with the floor of the external meatus. In infants the inclination is even greater.
Its relation to the tympanic cavity varies in its different parts. It lies nearest to the inner wall in the region of the umbo, being only 2 millimetres distant from the promontory, and is furthest from it in the posterior quadrant.
Running backwards, just below the posterior fold, is the chorda tympani nerve, which may be cut through in the act of paracentesis and in division of the posterior fold.
The tympanic cavity. For the purpose of description the portion of the tympanic cavity above the level of the tympanic membrane is known as the attic or epitympanic cavity; whilst the part below its level is called the cellar or hypotympanic cavity (Fig. 186).
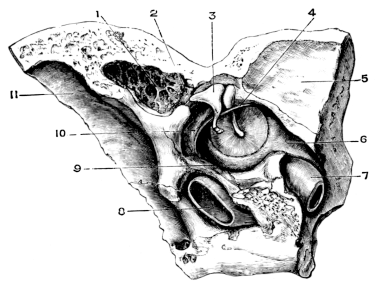 Fig. 186. Anatomical Preparation of the Middle Ear. 1½ nat. size.
1, Antrum; 2, Aditus; 3, Attic, containing head of malleus and body of
incus; 4, Chorda tympani nerve; 5, Middle fossa of intracranial cavity;
6, Eustachian tube; 7, Carotid canal; 8, Jugular vein in jugular fossa;
9, ‘Cellar’ or floor of tympanic cavity; 10, Canal of facial nerve; 11,
Sigmoid groove for lateral sinus. (From the Author’s Diseases of the
Ear.)
Fig. 186. Anatomical Preparation of the Middle Ear. 1½ nat. size.
1, Antrum; 2, Aditus; 3, Attic, containing head of malleus and body of
incus; 4, Chorda tympani nerve; 5, Middle fossa of intracranial cavity;
6, Eustachian tube; 7, Carotid canal; 8, Jugular vein in jugular fossa;
9, ‘Cellar’ or floor of tympanic cavity; 10, Canal of facial nerve; 11,
Sigmoid groove for lateral sinus. (From the Author’s Diseases of the
Ear.)
The attic contains the head of the malleus and the body and short process of the incus, and communicates posteriorly with the antrum by a variable sized opening—the aditus. Its roof, the tegmen tympani, a plate of bone frequently of extreme thinness, separates the cavity of the middle ear from the middle fossa of the cranium. The facial canal extends backwards along the inner and upper border of the tympanic cavity, passing above the vestibule and the fenestra ovalis to curve downwards posteriorly beneath the external semicircular canal, which at this point forms the inner and inferior boundary of the aditus.
The ossicles form a movable chain fixed at three points: namely, the attachment of the handle of the malleus to the tympanic membrane; the posterior ligament of the incus, a feeble structure, binding its short process to the entrance of the antrum; and the strong annular ligament connecting the footplate of the stapes to the margins of the fenestra ovalis.
In addition, the anterior, external, and superior ligaments of the malleus also tend to keep it in position and limit its movements.
The tensor tympani muscle, extending from the processus cochleariformis, crosses the tympanic cavity to be inserted into the inner margin of the neck of the malleus; and the stapedius muscle emerging from the apex of the eminentia pyramidalis is inserted into the head of the stapes.
These ligaments and muscles partially divide the cavity into smaller compartments, such as the outer attic and Prussak’s space, so that in some cases inflammation may be limited to only a part of the tympanic cavity; a fact to be remembered in considering the question of operative procedures.
Indications. The chief object of paracentesis (myringotomy or simple incision) is to permit of escape of fluid from the tympanic cavity.
(i) In acute inflammation of the middle ear, if the acute symptoms continue in spite of palliative treatment, and the following conditions are present:—(a) An increasing congestion and bulging of the tympanic membrane, especially if accompanied by earache and pyrexia. (b) The obvious presence of pus within the tympanic cavity, shown by a circumscribed, angry red or yellow protuberance on the tympanic membrane. (c) Accompanying cerebral symptoms, such as drowsiness, vomiting, vertigo, and convulsions. (d) Tenderness over the mastoid process. (e) Paroxysms of pain acute enough to prevent sleep.
Paracentesis should be done early in infants and in specific fevers. In the former case even a slight middle-ear inflammation may give rise to all the cardinal symptoms of meningitis, which frequently subside rapidly as the result of simple paracentesis; in the latter, there may be rapid destruction of the drum, which a timely incision may possibly prevent.
(ii) In middle-ear catarrh with exudation. Paracentesis is justifiable in order to remove the secretion, if the hearing does not improve after a month’s treatment, owing to the existence of exudation within the tympanic cavity.
(iii) As a preliminary to intratympanic operations.
Operation. The auricle and surrounding parts are surgically cleansed (see p. 309), the preliminary toilet, if possible, being carried out at least half an hour before the operation is performed.
Although apparently a trivial matter, it is of the utmost importance to render the auditory canal as aseptic as possible in order to prevent secondary infection of the tympanic cavity from without.
 Fig. 187. Paracentesis Knife held in position in the Hand.
Fig. 187. Paracentesis Knife held in position in the Hand.
It is wiser to give a general anæsthetic, such as gas and oxygen, as the pain of the operation may be intense. If this is refused, local anæsthesia by Gray’s solution (see p. 310) or by a subcutaneous injection of cocaine and adrenalin may be employed. In infants an anæsthetic is not necessary.
The patient may be sitting up or lying down. If a general anæsthetic has not been given, the patient’s head must be held firmly by an assistant in order to prevent sudden movement. The surgeon works by reflected light in order to obtain a clear view of the tympanic membrane.
The point of election for the incision is through the posterior part of the membrane, excepting when it is obvious from the bulging and appearance of the membrane that the incision must be made in the anterior inferior quadrant.
The incision is made by means of a paracentesis knife, which is shaped like a tiny bistoury set at an angle to its handle (Fig. 187). The double-edged spear-shaped knife is now seldom used, as with it there is a tendency to puncture rather than to incise the membrane.
The tympanic membrane is pierced by the paracentesis knife at its inferior posterior margin. With a quick movement the drum is incised freely, the incision being carried in an upward direction midway between the malleus and the circumference of the membrane posteriorly, until it reaches Shrapnell’s membrane (Fig. 188). In making this incision the inclination of the membrane must not be forgotten. Owing to its lower margin being more deeply placed than the upper, there is a tendency for those who have not had much practice in doing a paracentesis to begin their incision too high up, as they fail to realize the greater depth of the canal at this point. The soft tissues of the upper posterior wall of the external meatus close to the membrane, if much congested, may be incised also in the act of withdrawing the knife. In doing this the chorda tympani nerve may perhaps also be cut, resulting in loss of taste on the affected side for a time; this is a matter of no importance. As a result of this free incision, drainage is given to the contents of the tympanic cavity, attic, and antrum.
In order to prevent rapid closure of the perforation and to give better drainage, some authorities advise making a flap-shaped incision. To do this, the membrane is incised upwards, nearly to its upper border; the knife is then carried backwards and downwards before it is withdrawn from the wound.
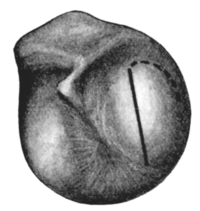 Fig. 188. Tympanic Membrane showing Incision in Acute Suppuration of the
Middle Ear. Usual line of incision; dotted line shows continuance of
incision to make a flap opening for drainage.
Fig. 188. Tympanic Membrane showing Incision in Acute Suppuration of the
Middle Ear. Usual line of incision; dotted line shows continuance of
incision to make a flap opening for drainage.
|
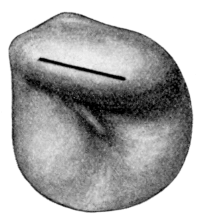 Fig. 189. Line of Incision in Acute Suppuration of the Attic.
Fig. 189. Line of Incision in Acute Suppuration of the Attic.
|
Occasionally the acute inflammation is limited to the attic, Shrapnell’s membrane appearing deeply congested and bulging outwards so as to cover the processus brevis, whilst the rest of the membrane may be only slightly injected. In such cases it is sufficient to incise the bulging area, beginning the incision just above the region of the processus brevis and carrying it horizontally backwards to its posterior extremity (Fig. 189).
After-treatment. In acute middle-ear inflammation, after the first rush of blood and discharge has been mopped away, a small drain of sterilized gauze should be inserted into the auditory canal and the ear protected with a pad of sterilized gauze. The dressing and gauze drain should be changed as often as may be necessary, depending on the amount of discharge. The ear should not be syringed out unless the discharge becomes very profuse and thick.
In acute middle-ear catarrh with exudation, a Siegle’s speculum (Fig. 194) should be inserted into the meatus after free incision of the membrane, and as much fluid as possible extracted by suction. In addition, gentle inflation by means of Politzer’s method will help to expel from the middle ear the fluid, which should then be mopped out of the external meatus. This should be repeated daily.
Difficulties and dangers. The usual fault is to mistake the congested posterior wall of the external meatus for the membrane.
If the patient is not under an anæsthetic, the incision may be made too timidly, the membrane being only scratched. The pain thus inflicted will cause the patient to jerk away the head and probably prevent the membrane from being incised freely. The incision, therefore, must be made in a bold and rapid manner. It is better to make the incision too free than too small.
Care must be taken not to plunge in the knife too deeply for fear of wounding the mucous membrane of the inner wall of the tympanic cavity. This may result in adhesions between it and the membrane.
Further, cases have been recorded in which a too violent incision has injured or dislodged the ossicles, or in which severe hæmorrhage has occurred, presumably from puncturing the bulb of the jugular vein, which was projecting abnormally through the floor of the tympanic cavity.
The two chief causes of failure are insufficient drainage from too small an incision, which may necessitate a further operation, and secondary infection from without.
Results. In the majority of cases, provided free drainage is established, the discharge ceases and healing of the membrane takes place from within a day or two to four weeks, depending on the character of the case. If the symptoms continue it may become necessary to perform the mastoid operation (see p. 373).
The object of the operation is to equalize the pressure within the tympanic cavity and external meatus so as to enable vibrations of sound to be transmitted more readily by the membrane and chain of ossicles to the inner ear.
Indications. (i) In the case of an extremely calcified membrane which apparently cannot vibrate.
(ii) To relieve tinnitus or vertigo which appears to be due to an alteration of tension within the tympanic cavity, the result of an impermeable stricture of the Eustachian tube.
(iii) As a means of diagnosis. If the hearing be improved or the subjective symptoms relieved as a result of the artificial opening, then, if the perforation closes (as it probably will do), the surgeon is in a position to suggest some more radical measure, such as ossiculectomy (see p. 351).
Operation. Two methods are employed: (i) The knife; (ii) The galvano-cautery. The perforation should be made in the postero-inferior quadrant.
In favour of the galvano-cautery is the fact that the perforation does not tend to close so rapidly. On the other hand, considerable damage may be done unless it is applied with extreme care. For this reason it is wiser to operate under a general anæsthetic, such as gas and oxygen.
If the paracentesis knife be used it is not sufficient to make a simple incision; a small triangular flap must be excised. The operation should be performed under good illumination. The paracentesis knife is inserted boldly through the membrane a little behind and above the umbo. The membrane is incised in an upward and slightly backward direction towards its margin; then downwards parallel to its posterior border; then horizontally forward, meeting the original point of the incision. The excised portion of the membrane is removed by seizing it with a fine pair of crocodile forceps, or by means of a fine snare, if it has not been completely detached.
The galvano-cautery is applied cold; when it is in contact with the drum, the circuit is closed so that the point of the cautery becomes red-hot. After the membrane has been burnt through it is withdrawn rapidly so as not to scorch the surrounding tissues. In using the cautery care must be taken to push it only just through the membrane for fear of injuring the inner wall of the tympanic cavity.
After-treatment. The after-treatment consists in protecting the ear by a strip of gauze, which is changed as often as may be necessary.
Indication. It is advised by Politzer in those cases of marked retraction of the drum in which inflation causes an immediate improvement in hearing, which, however, only lasts a short time. In several cases Politzer found the cause of this to be due to tension of the anterior ligament causing retraction of the malleus.
Operation. The anterior fold is divided with the paracentesis knife just in front of the processus brevis of the malleus. The knife is then introduced 2 millimetres inwards through the incision and made to cut in an upward direction as far as Shrapnell’s membrane (Fig. 190, C). This should divide the ligament.
If the operation be successful, improvement in hearing and also diminution of the subjective noises should take place.
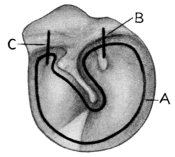 Fig. 190. Lines of Incisions in Intratympanic Operations. A, Removal of
membrane in ossiculectomy; B, Division of posterior fold; C, Division of
anterior ligament.
Fig. 190. Lines of Incisions in Intratympanic Operations. A, Removal of
membrane in ossiculectomy; B, Division of posterior fold; C, Division of
anterior ligament.
Indication. The same as for the anterior ligament. Owing to the increased tension of the upper posterior quadrant of the tympanic membrane, it is assumed that the movements of the malleus are diminished, and with this the hearing power. Seeing, however, that the prominence of the posterior fold is due to the projection outwards of the processus brevis as a result of the handle of the malleus having become indrawn with the membrane, it is difficult to understand how its division can possibly be a means of restoring the retracted membrane to its normal condition.
On the few occasions on which I have performed this operation, no improvement has followed. Others, however, maintain that it may do good in certain cases. This, perhaps, may be possible if it is combined with other intratympanic operations, such as division of the anterior ligament or of the tensor tympani muscle.
Operation. The paracentesis knife is inserted through the most prominent part of the fold and is made to cut through it from above downwards (Fig. 190, B). If this is successful, gaping of the cut edges takes place and the membrane assumes a less retracted position, and increased hearing and diminution of the subjective symptoms should occur on inflation and rarefying of air within the external ear.
General considerations with regard to intratympanic operations and their results. The chief difficulty, from a clinical point of view, is to determine beforehand the exact pathological changes which already exist within the tympanic cavity. For this reason the indications given with regard to operation are of necessity somewhat empirical. For example, retraction of the tympanic membrane may be due to closure of the Eustachian tube; to adhesions between it and the promontory; to contraction of the tensor tympani, of the anterior ligament, or of the posterior fold. An operation to remove only one of these causes may, therefore, be insufficient; the difficulty is to know what to do. Even if further operations are performed, the result may be negative owing to adhesions having taken place already between the ossicles themselves, or from binding down of the incudo-stapedial joint or of the stapes to the inner wall of the tympanic cavity. And apart from this, even if temporary benefit is obtained, the final result may be worse than that which existed before operation owing to the natural tendency for adhesions to re-form.
The prognosis is better in the case of post-suppurative conditions than in the non-suppurative ones.
Improvement by operation may be hoped for if a temporary increase in the hearing power, with diminution of the subjective symptoms, is obtained as a result of inflation; especially in those cases in which the malleus is only locally adherent to the promontory.
Generally speaking, however, these operations are not recommended, owing to the impossibility of being able to give a good prognosis, and therefore they can only be considered as experimental.
These operations are contra-indicated—(1) If there be internal-ear deafness.
(2) If the stapes (as shown by tuning-fork tests and Gellé’s test) be ankylosed within the fenestra ovalis, especially in the case of otosclerosis.
(3) If the membrane be completely adherent to the inner wall at its upper posterior quadrant, especially if this is of long standing, as the stapes will almost certainly also be fixed by adhesions.
The position and extent of the intratympanic adhesions vary exceedingly, and may be the result either of middle-ear catarrh or suppuration. The following conditions may be found:—
(i) Adhesion of the handle of the malleus to the promontory, the rest of the tympanic membrane being movable.
(ii) Adhesions between other parts of the tympanic membrane and the inner wall of the tympanic cavity, either by bridles or bands of fibrous tissue, or by the membrane itself being adherent over a large area.
(iii) Adhesion of the edge of a perforation to the inner wall.
(iv) Adhesions surrounding the articulation between the incus and stapes, and the stapes itself.
Indications. Operation is justifiable in the case of adhesion of the malleus to the promontory if the rest of the membrane is freely movable; if the membrane bulges outwards and there is temporary improvement in hearing on inflation; and if examination shows that the labyrinth is intact. This operation is all the more indicated if there is marked deafness on both sides: it should then be attempted on the worse side. If, however, the intratympanic adhesions are extensive, it is very doubtful whether an attempt to separate the free part of the membrane from the part adherent to the inner wall is worthy of consideration.
It must also be remembered that adhesions in the region of the stapes cannot be seen, unless a large perforation of the membrane already exists. Operation is then only justifiable as a last resource if there is extreme deafness accompanied by distressing subjective symptoms.
Operation. Unless the patient is very sensitive or nervous, local anæsthesia is sufficient. It is more convenient for the patient to be sitting up in a chair than to be in the recumbent position. The surgeon works by reflected light. Before the operation is begun, the ear must be surgically cleansed and carefully dried.
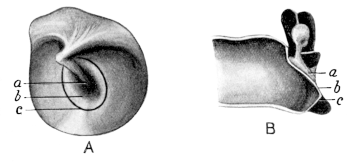 Fig. 191. Cutting through Intratympanic Adhesions. The malleus is
adherent to the promontory. A, Surface view; B, Vertical section. a, Handle of
the malleus; b, Membrane adherent to the promontory; c, Line of incision to cut
through the membrane.
Fig. 191. Cutting through Intratympanic Adhesions. The malleus is
adherent to the promontory. A, Surface view; B, Vertical section. a, Handle of
the malleus; b, Membrane adherent to the promontory; c, Line of incision to cut
through the membrane.
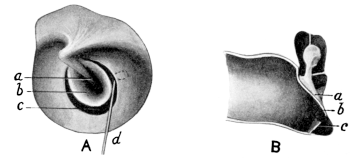 Fig. 192. Free Edge of Tympanic Membrane cut through. A, Surface
view; B, Vertical section. a, Malleus adherent; b, Membrane adherent; c, Free
edge of membrane; d, Spatula freeing membrane.
Fig. 192. Free Edge of Tympanic Membrane cut through. A, Surface
view; B, Vertical section. a, Malleus adherent; b, Membrane adherent; c, Free
edge of membrane; d, Spatula freeing membrane.
(i) Adhesion of the handle of the malleus to the promontory. With a paracentesis knife the membrane is incised round the handle of the malleus (Fig. 191). A small sickle-shaped knife, fixed at right angles to its shaft, is then inserted through the incision (in front of or behind the malleus as may be most convenient to the operator) and is made to cut through the adhesions between the malleus and the promontory (Fig. 192). In order to make sure that this has been accomplished, a small ring-knife, such as is used in the operation of ossiculectomy, is passed round the tip of the malleus, between it and the inner wall of the promontory, and slight traction is then exerted in order to pull the handle of the malleus outwards from the inner wall.
Provided asepsis has been maintained, this small operation seldom gives rise to any inflammatory reaction. The after-treatment consists in inserting a strip of gauze into the auditory canal; if it becomes moist with secretion, it should be changed.
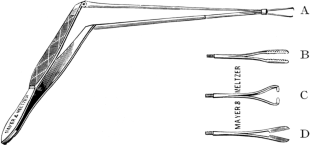 Fig. 193. Sexton’s Instrument. A, For removal
of a foreign body; B and C, For removal of the malleus;
D, Scissors.
Fig. 193. Sexton’s Instrument. A, For removal
of a foreign body; B and C, For removal of the malleus;
D, Scissors.
Many methods have been devised to prevent recurrence of adhesions, but few are successful. Amongst these are daily inflation of the ear by means of Politzer’s method or the catheter; the injection of oil into the middle ear; and the insertion of small pieces of celluloid between the malleus and inner wall of the promontory according to the method of Gomperz. Another method is to resect the handle of the malleus (Fig. 195). After being freed from the promontory as above described, the manubrium is cut through with a pair of fine scissors (Fig. 174) just below the processus brevis, and the lower fragment is removed by means of Sexton’s forceps (Fig. 193).
(ii) Adhesion between the membrane and the inner wall of the tympanic cavity. Siegle’s speculum should be used to determine the position and extent of the adhesions (Fig. 194).
There are two methods of operation:—
(a) In the case of bands forming a bridle between the tympanic membrane and inner wall, an attempt may be made to cut through them. This is done by incising the membrane with a paracentesis knife in front of or behind the adherent portion, and then inserting through this incision the sickle-shaped knife. By rotating it upwards or downwards, as the case may be, the bands forming the adhesions are cut through. If this has been successfully performed, and if the retraction of the membrane was solely due to these bands, the tympanic membrane will be found to be freely movable on diminishing the pressure of air within the external meatus by means of Siegle’s speculum.
(b) If the adhesions be extensive, the only method affording a chance of success is to separate the free portion of the tympanic membrane from the part adherent to the inner wall, leaving the latter in situ. To do this the membrane is incised with a paracentesis knife just beyond the margin of the adherent portion, the incision being carried right round the affected part. A tiny spatula, bent at right angles to its shaft, is then inserted through the incision and passed round beneath the movable portion of the membrane so as to free it completely (Fig. 192).
(iii) Adhesion of the edge of a perforation to the inner wall. If the middle-ear suppuration has only recently ceased, it may be sufficient to divide the adhesion with a small knife curved on the flat and afterwards force the tympanic membrane outwards by means of inflation through the Eustachian tube, and by rarefaction of the air within the external meatus. In the majority of cases, however, it is necessary to excise the adhesion, especially in the more chronic conditions. This is done by cutting through the movable part of the membrane just beyond the adherent portion (vide supra).
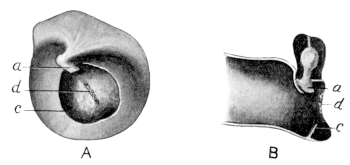 Fig. 195. Division of Intratympanic Adhesion with Excision of Handle
of Malleus. A, Surface view; B, vertical section. a, Remains of malleus (handle
already excised); c, Free edge of membrane; d, Scar tissue on promontory, at
which point malleus and membrane were previously adherent.
Fig. 195. Division of Intratympanic Adhesion with Excision of Handle
of Malleus. A, Surface view; B, vertical section. a, Remains of malleus (handle
already excised); c, Free edge of membrane; d, Scar tissue on promontory, at
which point malleus and membrane were previously adherent.
(iv) Adhesions surrounding the articulation between the incus and stapes, and the stapes itself. These adhesions can only be observed if a large perforation involves the upper posterior quadrant. Even then it may be anatomically impossible to see the stapes. The operation should only be performed if definite bands of adhesions can be seen. Sometimes, although rarely, it happens that such adhesions are present. If the incudo-stapedial joint be fixed to the inner wall of the tympanic cavity, the adhesions are separated from it by passing the knife between the joint and the inner wall. In order to cut through adhesions surrounding the base of the stapes, a small horizontal incision should be made along its upper margin, and also along the lower, if this is in view. This operation, however, is seldom of any value.
Indication. The chief indication for this operation is marked retraction of the tympanic membrane, in a case of middle-ear deafness, in which there are no adhesions between the membrane and the inner wall of the middle ear, and in which it is assumed that the retraction is due to shortening of the tensor tympani muscle.
Operation. The first step of the operation is to incise the tympanic membrane with a paracentesis knife in a vertical direction just behind the margin of the malleus. At the same time the posterior fold can be cut through, if required, by continuing the incision upwards. Through the incision thus made Schwartze’s tenotomy knife (a very fine blunt-pointed instrument curved on the flat (Fig. 196)) is inserted, its point being directed upwards. The knife is pushed upwards until its shaft is on a level with the processus brevis. The handle is then rotated in a forward direction so that the sharp edge of the knife, which is kept close to the posterior border of the neck of the malleus, makes a circular movement forwards and downwards and thus cuts through the tendon of the muscle. If the knife has been too deeply inserted, the attempt to rotate the shaft forwards will be resisted by the projecting processus cochleariformis. To overcome this difficulty the shaft of the instrument is rotated backwards so as to raise the point of the tenotomy knife and thus free it; the instrument is then withdrawn slightly and the shaft again rotated forwards. The division of the tendon can be distinctly felt, and may be accompanied by a slight crackling noise; after this has been effected, the knife is rotated backwards and withdrawn through the incision in the tympanic membrane.
After-treatment. There is usually a slight effusion of blood within the tympanic cavity, but no special treatment is required beyond keeping the ear aseptic. Absorption takes place rapidly.
The result of the operation is disappointing. There is seldom any improvement with regard to hearing; a few cases, however, have been reported in which the attacks of vertigo have diminished in intensity.
Indications. They are limited.
(i) As the result of middle-ear suppuration the malleus and incus may become exfoliated. The theory has been advanced that the unopposed action of the stapedius muscle prevents free movement of the stapes in these cases, and for this reason tenotomy of its tendon is advocated.
This operation, however, should only be performed provided that the edge of the membrane is not adherent to the inner wall of the tympanic cavity, and there is no internal-ear deafness.
(ii) The operation is also performed as a preliminary measure to removal of the stapes (see p. 361).
Operation. The operation is simple, as the head of the stapes and the tendon of the stapedius muscle are usually within view in consequence of the destruction of the tympanic membrane. The ear is cleansed and dried, and the part rendered insensitive by the previous application of a pledget of cotton-wool soaked in cocaine solution. The tiny tendon is severed with a snick of the paracentesis knife, cutting through it from above downwards under good illumination.
Results. These vary; usually there is no improvement, but sometimes marked increase of hearing occurs. As the operation can do no harm and can be done without any inconvenience to the patient, it may be attempted subject to the restrictions given above.
Indications. Granulations should always be removed if conservative treatment fails.
Operations. (a) Cauterizing; (b) Curetting. The former method is employed when the granulations are very small and localized; the latter when they are multiple and larger.
Cauterization. The tympanic cavity is cleansed and rendered anæsthetic (see p. 310). The auditory canal and tympanic cavity are then carefully dried. This is of importance in order to prevent scalding of the surrounding tissues during the act of cauterization. The ordinary electric cautery is used; only a weak current is necessary as the point of the cautery, of necessity, is very small. Under good illumination, the cautery is inserted cold along the auditory canal until it just touches the granulation. The circuit is then closed, and on the point of the cautery becoming white-hot, it is pressed against the granulation and then rapidly withdrawn from the ear. The current should not be shut off until the cautery is withdrawn, otherwise it will adhere, on cooling, to the tissues with which it is in contact, and on withdrawal will cause bleeding.
Instead of the electric cautery, the granulations may be touched with a bead of chromic acid fused on to a probe, or with a saturated solution of trichloracetic acid. The galvano-cautery has the greatest effect. Chromic acid has the disadvantage that unless it is very accurately applied it tends to affect a larger area than was possibly intended. Trichloracetic acid, although more localized in effect, is not so potent.
After-treatment consists in blowing in a slight amount of boric acid powder and keeping the ear dry.
Curetting. This is performed by means of small ring-knives (Fig. 178) or sharp spoons. They vary in size, and are either straight or bent in different directions to the shaft of the instrument. The instrument selected depends on the position and size of the granulation.
To minimize the hæmorrhage, adrenalin may be added to the cocaine solution. The curette is made to encircle the granulation and cuts through its attachment with a firm movement, limited to the area of the granulation. Curetting should not be done in a haphazard fashion, but deliberately under good illumination. If bleeding occurs it must be arrested before further curetting takes place.
After-treatment. The ear is syringed out to remove any fragments of granulation tissue or blood-clot. It is then dried and a strip of sterilized gauze inserted. After twenty-four hours this is removed and drops of rectified spirits, if necessary containing ten grains of boric acid or a drachm of the perchloride of mercury lotion to the ounce, may be instilled into the ear three or four times a day.
Dangers. With due care none should occur. The following mishaps, however, have occurred from too violent curetting: (1) Injury or displacement of the ossicles; (2) internal-ear suppuration from dislodging of the stapes or injury to the promontory; (3) facial paralysis; (4) meningitis from injury to the tegmen tympani; (5) acute inflammation of the mastoid process.
Results. Provided that the granulations are localized and due to inflammation of the mucous membrane, a good result may be anticipated. If, however, there be underlying bone disease of the tympanic walls, or if the mastoid process be already affected, recurrences are usual, and further operative treatment may become necessary.
The object of the operation is to improve the hearing by breaking down the fibrous adhesions with the tympanic cavity, which diminish the mobility of the ossicles.
Direct massage of the malleus. Indications. (i) As a therapeutic measure. If the malleus be adherent to the promontory and there is no improvement on inflation, but perhaps slight improvement as a result of pneumatic massage.
(ii) As a means of diagnosis. If temporary improvement takes place it may be assumed that the stapes is not absolutely fixed, and that the deafness is partly due to adhesions preventing movements of the ossicles, a condition which may point to the advisability of performing ossiculectomy in suitable cases.
Operation. The ear is rendered insensitive by means of cocaine or Gray’s solution (see p. 310).
The manipulation is carried out with a Lucae’s probe (Fig. 197). Within its handle is a spring to render its movements resilient; and at its tip is a cuplike depression to embrace the point of the processus brevis of the malleus. The tip of the probe may be covered by a fine layer of cotton-wool or india-rubber.
The probe is inserted, under good illumination, into the auditory meatus and is applied to the processus brevis of the malleus. The vibrations are given by the rapid movements of the hand from the wrist, the arm being kept fixed. This procedure, which may be painful, should not last longer than one minute. Frequently there is considerable reaction, shown by congestion about the processus brevis and Shrapnell’s membrane. It is therefore wiser not to repeat the procedure at shorter intervals than one week.
Results. It is difficult to foretell what the result will be, as it is chiefly dependent on the extent of the adhesions already existing within the tympanic cavity and on the mobility of the stapes within the fenestra ovalis. If the latter is already fixed, then improvement is impossible. If, however, the adhesions are limited, a better result may be obtained by this method than by pneumo-massage and inflation. The surgeon must be guided by the extent and duration of the improvement as to how long to continue the treatment. Unfortunately, relapses are not uncommon, though temporary benefit may be obtained.
Massage of the stapes. This is only done as a last resource in the hope of obtaining some improvement in hearing.
Indications. (i) In cases in which mobilization of the malleus has caused no improvement, and it is hoped, from the history of the case, that this is due to fibrous adhesions fixing the stapes within the fenestra ovalis. This condition must be carefully distinguished from otosclerosis or bony ankylosis of the stapes, in which latter conditions any such procedure is absolutely contra-indicated.
(ii) Direct mobilization may be undertaken as a preliminary step previous to removal of the stapes itself. If the stapes is movable and slight improvement occurs, then its removal may be justifiable under certain conditions. If, however, the stapes is fixed and no improvement occurs, then its removal will be attended with such difficulty as to almost negative this being attempted.
Operation. If a perforation of the upper posterior quadrant be present, a small pledget of cotton-wool soaked in a 20% solution of cocaine is brought into contact with the inner wall of the tympanic cavity. After a few minutes Lucae’s probe is placed in position against the head of the stapes and the vibratory movements are carried out. If no perforation of the drum exists, then it is first necessary to excise a flap in the upper posterior quadrant of the membrane.
Difficulties. The chief difficulty is anatomical. Projection forward of the upper posterior part of the tympanic ring or a deeply placed niche of the fenestra ovalis may prevent a view of the stapes.
If the membrane has to be incised, the slight amount of bleeding may also prevent a good view being obtained.
There is no actual danger in the operation, but if the stapes is fixed or if much force is used, it is by no means difficult to fracture the crura of the stapes.
Except under the most rare conditions only the malleus and incus are removed; the stapes, if possible, being left undisturbed.
These operations will therefore be considered separately.
Removal of the malleus and incus. This operation was first proposed by Schwartze in 1873, and later by Kessel, Ludewig, Sexton, and Zeroni.
Indications. The indications for operation may be considered with regard to (1) chronic middle-ear suppuration and (2) non-suppurative middle-ear disease, whether the result of a previous middle-ear suppuration or of a chronic middle-ear catarrh.
In chronic middle-ear suppuration, the chief object of the operation is to ensure drainage and if possible to remove the cause of the suppuration; in non-suppurative conditions, to improve the hearing.
 Fig. 198. To show Sites of Perforation in Attic Suppuration and Caries
of the Ossicles. 1. Perforation in front of malleus. 2. Perforation
behind malleus. 3. Perforation involving posterior attic region and
upper posterior part of membrane. (From the Author’s Diseases of the
Ear.)
Fig. 198. To show Sites of Perforation in Attic Suppuration and Caries
of the Ossicles. 1. Perforation in front of malleus. 2. Perforation
behind malleus. 3. Perforation involving posterior attic region and
upper posterior part of membrane. (From the Author’s Diseases of the
Ear.)
It may here be mentioned that the position of the perforation in the attic region is frequently of importance when considering the question of treatment. If situated in front of the malleus, the disease is probably limited to the outer attic region and malleus; if just behind the malleus, then probably both the malleus and incus are affected; but if the perforation extends farther back, involving the upper posterior quadrant of the drum, especially its bony margin, it suggests disease not only of the ossicles together with the walls of the aditus and antrum, but perhaps also of the mastoid process (Fig. 198).
(i) In chronic middle-ear suppuration. Before operation is considered, it is presumed that conservative measures, such as syringing, instillation of astringent and antiseptic drops, and washing out of the attic by means of Hartmann’s canula with various solutions, have been given a thorough trial and failed.
(a) If the suppuration be limited to the attic region (although the main portion of the tympanic membrane is intact), provided there is marked deafness and there are symptoms of lack of free drainage indicated by recurrent attacks of headache, a feeling of heaviness or giddiness, or pain radiating up the head on the affected side.
(b) If there be caries of the malleus and incus, and the outer attic wall, with recurrence of granulations after repeated removal, especially if accompanied by cholesteatomatous formation, provided there is no evidence of disease of the mastoid process itself.
(c) Although the general symptoms and the condition found on examination justify the complete mastoid operation, yet if the patient refuses to have this operation performed, the simpler operation of ossiculectomy may be undertaken if desired. This will permit of free drainage and diminish the risk of future intracranial complications. It should, however, be clearly explained to the patient that no guarantee can be given with regard to effecting a permanent cure as a result of this operation.
(ii) In non-suppurative conditions.
(a) If there be marked middle-ear deafness, the result of adhesions, and the malleus is fixed to the promontory. Operation is justifiable if it is found that after each inflation of the middle ear, improvement of hearing is obtained which, however, is not permanent but only temporary.
(b) If, as the result of artificial perforation, made under the conditions already laid down, improvement takes place temporarily, but a relapse occurs from closure of the perforation (see p. 340).
(c) If tinnitus and attacks of vertigo, due to marked retraction of the membrane, are temporarily relieved by inflation. In this case operation should only be carried out as a last resource after all other measures have failed to cure and if the symptoms are very severe and distressing.
(d) If there be marked middle-ear deafness with extensive adhesions on both sides and evidence points to the stapes being freely movable. The operation is justifiable, as an experiment, on the worse side.
Operation. The only operation to be considered is the intrameatal one. Stacke originally suggested a post-auricular incision, and reflecting the auricle forward, and, after removing the ossicle, to remove also the outer attic-wall by means of the chisel. This method, however, has now been given up as being too radical, but will be mentioned later on in connexion with the mastoid operation (see p. 397).
Unless contra-indicated, a general anæsthetic should be given, as it is not always possible to foretell whether the operation will be difficult or easy. In addition it may be necessary to curette out granulations and also to remove the outer wall of the attic. Unless the patient is very insensitive, this is almost impossible under local anæsthesia (see p. 311).
Before the anæsthetic is given, the ear should be filled with a 5% solution of cocaine containing a 1 in 2,000 solution of adrenalin chloride in order to diminish the bleeding during the operation.
The field of operation is isolated from the surrounding parts by covering the head with a sterilized towel having an opening cut in it just sufficient to expose the auricle and meatus.
The following are the steps of the operation: (1) freeing the malleus from its attachments to the tympanic membrane, and from the inner wall of the middle ear, if adherent to it; (2) cutting through the tendon of the tensor tympani muscle; (3) removal of the malleus; (4) removal of the incus; (5) removal of the outer wall of the attic; (6) curetting out of granulations, if present. The method of operation varies slightly according to the condition found.
Removal of the malleus. In post-suppurative and non-suppurative conditions the chief cause of failure is the recurrence of adhesions, so for this reason it is wisest to remove the membrane as completely as possible.
With a paracentesis knife, the membrane is incised below and behind the malleus. The incision is then carried upwards along its posterior border to the posterior fold, then round the complete margin of the tympanic membrane and along the anterior fold and border of the malleus, so as to meet the original point of the incision. The knife is then reinserted just in front of the processus brevis and cuts through the anterior ligament in an upward direction; in a similar fashion the posterior fold is also cut through (Fig. 190).
The next step is tenotomy of the tensor tympani muscle (see p. 345).
The malleus thus freed can easily be removed by seizing its handle with a pair of Sexton’s (Fig. 193) or crocodile forceps (Fig. 179). In removing the malleus it is necessary to remember that its head is situated within the attic and therefore cannot be pulled out directly, but must first be drawn downwards until it is seen within the tympanic cavity. If this precaution be not taken, the neck of the malleus may be broken, leaving the head behind. If this takes place its extraction may be a matter of difficulty.
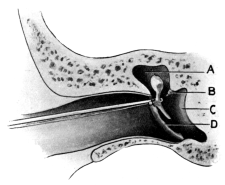 Fig. 199. Removal of the Malleus by Wilde’s Snare. First position.
After cutting through the tensor tympani muscle by Schwartze’s method.
Fig. 199. Removal of the Malleus by Wilde’s Snare. First position.
After cutting through the tensor tympani muscle by Schwartze’s method.
|
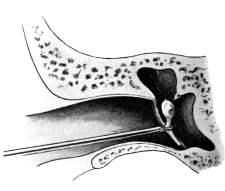 Fig. 200. Removal of the Malleus by Wilde’s Snare. Second position.
Malleus pulled down from attic—about to be withdrawn from auditory
canal.
Fig. 200. Removal of the Malleus by Wilde’s Snare. Second position.
Malleus pulled down from attic—about to be withdrawn from auditory
canal.
|
Instead of using Sexton’s forceps, the malleus may be removed by means of Wilde’s snare. This is the method advocated by Schwartze. After cutting through the tensor tympani muscle, the loop of the snare is threaded over the head of the malleus and guided upwards until it embraces its neck. The loop is then drawn tight so as to hold the malleus firmly in its grasp. The ossicle is extracted by first pulling it downwards (Fig. 199), so as to dislodge it from the attic, and then outwards (Fig. 200).
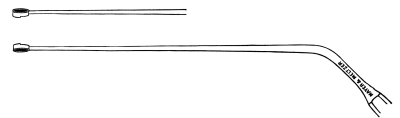 Fig. 201. Delstanche’s Ring-knife.
Fig. 201. Delstanche’s Ring-knife.
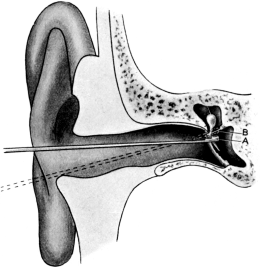 Fig. 202. Removal of Malleus by Delstanche’s
Ring-knife. A, Curette inserted round
handle of malleus; B, Curette pushed upwards,
in act of cutting through tendon of tensor tympani muscle.
Fig. 202. Removal of Malleus by Delstanche’s
Ring-knife. A, Curette inserted round
handle of malleus; B, Curette pushed upwards,
in act of cutting through tendon of tensor tympani muscle.
Another method of extracting the malleus, and in my opinion the one to be preferred, is by Delstanche’s ring-knife (Fig. 201). This instrument differs from the ordinary ring-knife in that the upper border of its anterior part is especially sharpened so as to form a fine cutting surface. After the malleus has been freed from the membrane by means of the paracentesis knife, Delstanche’s ring-knife is made to encircle its handle. It is then pushed gradually upwards, keeping as close to the posterior border of the malleus as possible, until it cuts through the attachment of the tensor tympani. In doing this the instrument will embrace the neck of the malleus (Fig. 202). This permits of sufficient leverage to extract the malleus by gentle traction in a downward and outward direction without danger of fracturing its shaft. If much resistance be felt, probably the tensor tympani muscle has not been cut through, and another attempt should be made to do this before trying further extraction. The advantage of this instrument is, that once the knife has encircled the malleus it should be possible not only to cut through the tensor tympani, but to extract the bone itself without the use of any other instrument. If Schwartze’s tenotomy knife be used, two tenotomy knives are required, one for the right and one for the left ear. Delstanche’s ring-knife is equally good for either ear.
Extraction of the incus. Although it is frequently stated that extraction of the incus is more difficult than that of the malleus, in reality it is the easier part of the operation as, unlike the malleus, it has no firm attachments.
After removal of the malleus all hæmorrhage must be arrested and a view obtained of the inner wall of the tympanic cavity. If it be possible to see the long process of the incus and its articulation with the head of the stapes, the articulation should be cut through with a small sickle-shaped knife. The knife is inserted just in front of the long process of the incus and, keeping close to it posteriorly, is made to cut downwards and backwards, thus separating its connexion with the stapes. Frequently the long process cannot be seen, or it may indeed have already disappeared as a result of caries. Theoretically this delicate manœuvre is performed in order to prevent injury or dislodgment of the stapes during the act of removal of the incus. From a practical point of view, however, it does not appear to make any difference whether the incudo-stapedial articulation is cut through or not.
A variety of instruments have been described for the purpose of removal of the incus. Ludewig’s incus hook (named after Ludewig, who was one of the first to draw attention to this operation) is still recommended by many as being the best. It consists of a solid curved hook, having a length of 5 millimetres and a width of 2 millimetres, bent at right angles to its shaft (Fig. 203). A pair of these are necessary, one for each ear; also several sets of different sizes may be required owing to the variation in depth, height, and roof of the attic region. I, however, prefer Zeroni’s (Fig. 204). This hook, instead of being solid, consists of a steel eyelet having a backward curve similar to that of Ludewig’s.
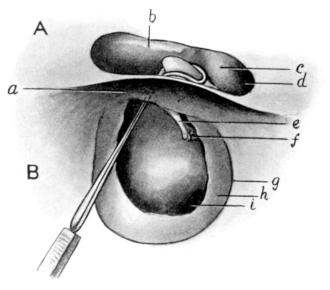 |
Fig. 205. Removal of Incus by Zeroni’s Hook. A, Diagrammatic section
showing opening in tegmen tympani: b, processus cochleariformis; c,
external semicircular canal; d, aditus and antrum. B, Diagrammatic
section, through the auditory canal, just beyond the tympanic membrane:
e, long process of incus; f, incudo-stapedial joint; g, tympanic
ring; h, remains of the tympanic membrane; i, fenestra rotunda;
above it is the promontory.
|
The technique is the same whichever pattern is employed. The instrument is inserted in such a fashion that the hook is directed upwards, having its concavity backwards. It is passed into the attic at the point previously occupied by the head of the malleus. The shaft of the instrument is then rotated backwards so that the hook passes over the body of the incus (Fig. 205). As the rotatory action is continued downwards and finally forwards, the incus is dislodged from its position and forced into the tympanic cavity. It can now be seized by a pair of Sexton’s or crocodile forceps and removed. If it falls into the floor of the tympanum, it can usually be dislodged by syringing, or else by means of a small hook passed in circular fashion along the floor of the cavity.
Removal of the outer wall of the attic. In the majority of cases of chronic middle-ear suppuration, it is advisable to remove the outer wall of the attic in addition to performing the simple operation of ossiculectomy. If granulations be present they should first be removed, in order to give a clear view of the inner wall of the tympanic cavity, which can usually be obtained, owing to the fact that a large perforation of the membrane is probably present. The malleus and incus are then removed.
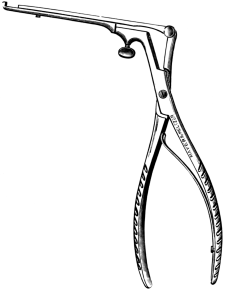 Fig. 206. Pfau’s Attic Punch Forceps.
Fig. 206. Pfau’s Attic Punch Forceps.
|
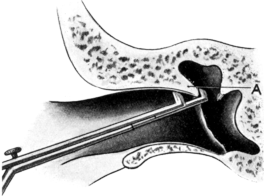 Fig. 207. Removal of Outer Attic-wall with Forceps. A, Outer attic-wall.
Fig. 207. Removal of Outer Attic-wall with Forceps. A, Outer attic-wall.
|
To remove the outer wall of the attic a small but strong pair of punch-forceps is required (Fig. 206). The instrument is directed along the roof of the auditory canal, its cutting edge held upwards and the blades kept slightly open, until the outer blade is felt to pass over the outer wall of the attic. The handle is then depressed so that the end of the forceps is forced upwards and embraces the outer wall between its points (Fig. 207). This is confirmed by attempting to withdraw the forceps, which the outer bony wall of the attic will now prevent. The position of the forceps being assured, its blades are brought together by pressure on the handle, and in this manner a small portion of the bone is punched out. In this way the outer wall of the attic is gradually cut away in small fragments. Sometimes this is extremely easy, owing to the auditory canal being large and the outer wall of the attic being thin and easily cut through. In other cases, owing to the thickness of the bony walls or to the narrowness of the canal, it is extremely difficult. If the outer wall of the attic has been completely removed, a fine probe, whose point is bent upwards, can be inserted into the attic and then withdrawn without encountering any obstruction, owing to the roof of the attic and outer wall of the auditory canal being now continuous. In some cases this part of the operation may not be necessary, as the outer wall of the attic may have already disappeared as a result of the caries.
Into the larger opening thus made, small curettes are passed upwards and backwards and any granulations in the region of the aditus and entrance to the antrum are curetted away. Finally the cavity is thoroughly swabbed out with the pledgets of cotton-wool soaked in a 1 in 2,000 alcoholic solution of biniodide of mercury. The cavity is then dried and a small drain of sterilized gauze inserted within the auditory canal, the ear being afterwards covered with a pad of gauze kept in position by a bandage.
After-treatment. In cases of non-suppuration there is rarely any pain, and if asepsis has been maintained, there is seldom much discharge beyond slight sanious oozing. Unless there is considerable discomfort the dressing need not be changed for two or three days. If possible the ear should not be syringed, but merely mopped out with pledgets of cotton-wool moistened with boric lotion and then dried, the gauze drain being afterwards inserted. This process may be repeated daily until healing is complete.
In middle-ear suppuration there may be considerable pain, owing to the forcible bruising of the tissues of the inner part of the auditory canal during the act of removal of the outer wall of the attic. Sometimes, indeed, there is much swelling of the lining membrane of the canal, with the occurrence of furuncles as the result of septic infection.
If there be no pain, the after-treatment is the same as above described, excepting that it may be necessary to syringe out the ear at each dressing owing to the discharge. If there be much pain, with swelling of the canal, the gauze drain should be removed and a 10% solution of carbolic acid in glycerine frequently instilled into the meatus. Subsequently drops of rectified spirit may be substituted.
Difficulties. 1. If the auditory canal be very small there may not be sufficient room to insert the instruments through the speculum. In such cases, if there be no middle-ear suppuration, it is wiser to leave the condition alone. If, however, suppuration exists, either the conservative treatment must be continued or the complete mastoid operation recommended.
2. Hæmorrhage, especially on curetting away the granulations, may be sufficient to prevent a view of the deeper parts. It can, however, usually be arrested quickly by plugging the auditory canal with gauze soaked in adrenalin and cocaine solution. Even if the surgeon has to wait a few moments, this must be done, as it is very necessary to obtain a clear view of the field of operation.
3. Extensive adhesions between the membrane and inner wall may render it difficult to separate the shaft of the malleus without fracturing its neck.
4. In old-standing cases in which there is a large perforation of the membrane, the malleus may be so retracted as not only to be difficult to see but difficult to seize. In this particular case, division of the tensor tympani with Schwartze’s tenotome and then extraction of the malleus by means of Sexton’s forceps is a better procedure than trying to encircle its shaft with Delstanche’s ring-knife.
5. Removal of the incus by the ordinary instruments may be rendered impossible owing to the narrowness of the attic posteriorly from chronic thickening of its walls. In these cases a seeker, such as Schwartze uses in the mastoid operation (Fig. 219), may be employed with advantage. It is passed over the incus in the same manner as an incus hook.
Accidents. 1. Fracture of the handle of the malleus. This is the result of too forcible extraction. If a Delstanche’s ring-knife has been used, this may be due to the tensor tympani not having been cut through; this should now be done. The head of the malleus is then removed either by means of a small hook or some form of curette bent at right angles to its shaft, depending on what is most suitable for the case in question.
2. Failure to extract the incus. In the course of a chronic middle-ear suppuration, the incus may become exfoliated or gradually disappear as the result of caries. It does not therefore always follow that inability to extract the incus means that the surgeon has failed in his manipulations, although frequently this is the case, the instruments failing to extract the incus, or perhaps dislodging it into the mastoid antrum, a fact which is difficult to determine and may only be discovered if the subsequent performance of the complete mastoid operation becomes necessary.
3. Facial paralysis. This accident is usually due to the incus hook not being inserted high enough up, so that, instead of entering the attic, it presses on the inner upper border of the tympanic cavity, and on being rotated in a backward and downward direction, it follows the line of the facial canal (Fig. 208). If much force be employed the frail wall of the facial canal will be fractured or pressed in on the underlying facial nerve. It is very rarely, however, that the nerve is completely crushed or torn through, and therefore recovery almost invariably takes place.
The facial nerve may also be injured whilst curetting away granulations in the upper posterior part of the tympanic cavity.
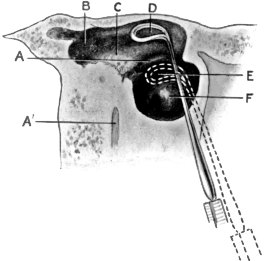 |
Fig. 208. Diagrammatic Section to show Correct and Wrong Positions of
Incus Hook. A, Facial nerve canal; A', Facial nerve, in section; B,
Antrum; C, External semicircular canal; D, Incus hook in its correct
position in the attic, above facial canal; E, Incus hook in wrong
position, about to press on facial canal; F, Promontory.
|
4. Injury to or removal of the stapes. This very rarely occurs during the act of removal of the incus, but is generally the result of too violent curetting. If only the crura be broken off, it does not matter; but if the stapes itself be dislodged from the fenestra ovalis, the subsequent symptoms may be attacks of vertigo, nausea, and vomiting. As a rule these symptoms subside. If, however, the internal ear becomes infected (although judging from literature and my own experience this is of very rare occurrence), complete deafness or even meningitis may occur as the result of labyrinthine inflammation or suppuration.
Results. (a) With regard to arrest of the disease. If the disease be limited to the ossicles themselves and to the anterior and outer part of the attic, a favourable prognosis may be given. Complete cessation of the discharge and scarring over of the affected part may take place within a month, or after a much longer period.
If, however, the disease be more extensive and involves the walls of the attic posteriorly and the region of the aditus, as shown by the presence of a fistula or granulations, the prognosis is uncertain and continuance of the discharge and recurrence of the granulations may eventually necessitate the complete mastoid operation.
(b) With regard to hearing. In the case of chronic attic suppuration the hearing power may be increased to a distance of 12 feet off for conversation, provided the internal ear is not affected and the stapes is not fixed within the fenestra ovalis; occasionally the result is much better. On the other hand, the hearing power may be made worse.
In post-suppurative conditions, the prognosis is not so favourable, as frequently the stapes is already bound down by adhesions; this is the more probable in the case of chronic middle-ear catarrh. In both these conditions the operation should never be performed without first explaining to the patient that it is practically experimental. The chief cause of failure is the recurrence of adhesions, which even the most complete and careful operation cannot always prevent.
Removal of the stapes. This operation is still in its infancy and it is, as yet, impossible to express an opinion with regard to its success or failure, and therefore the indications laid down are only tentative.
The objects of the operation are: (1) to improve the hearing in cases of deafness presumably due to fixation of the stapes within the fenestra ovalis, and (2) to relieve symptoms of tinnitus and vertigo due to the same cause.
Before this operation is advised careful examination must be made in order to determine whether the labyrinth is intact, especially if the operation is undertaken with the view of improving the hearing.
Indications. (i) If there be ankylosis of the stapes on both sides, accompanied by marked deafness and distressing subjective symptoms, operation is justifiable on the worse side.
(ii) In a one-sided affection provided the subjective symptoms of noises and giddiness are so oppressive as to render the patient’s life unbearable. The operation, of course, must not be attempted unless every other form of treatment has failed.
Operation. The operation may be performed either through the meatus, or by reflecting forward the auricle by means of the post-aural incision, and chiselling away the upper posterior part of the bony meatus in the manner suggested by Stacke (see p. 397).
The choice of the operation depends principally on the existing anatomical and pathological conditions.
If the meatus be very narrow the intrameatal method may fail to bring the stapes into view. If, on the other hand, the meatus be wide and there be a large perforation, the result of previous middle-ear suppuration, the incudo-stapedial joint or the head of the stapes itself may be actually within the field of operation.
The intrameatal method. The patient should be fully anæsthetized and the operation performed under good illumination. A portion of the tympanic membrane in its upper posterior quadrant is excised in order to bring into view the incudo-stapedial joint. The incision is begun just behind the handle of the malleus and is carried upwards and backwards in a circular fashion through the tympanic membrane along the posterior fold, and then downwards for a little distance along its margin. The flap so made either falls downwards, or can be pressed downwards so as to expose to view the inner wall of the tympanic cavity. With a small knife, curved on the flat, the incudo-stapedial joint is cut through. With a fine hook the long leg of the incus is dislocated forwards or backwards from the stapes. The head of the stapes will now be seen, with the tendon of the stapedius muscle running horizontally backwards. With a paracentesis knife, the tendon is cut through close to its attachment to the stapes.
A fine, blunt-pointed hook is now inserted between the crura of the stapes. If the stapes be not firmly ankylosed it can usually be removed by slight traction. If, however, it be firmly fixed, its crura will probably be broken. To determine whether the stapes is ankylosed or not, direct pressure of the probe on the head of the stapes may be necessary. If the head of the stapes cannot be seen, it is advisable, as suggested by Dench of America, to punch out part of the upper posterior margin of the attic-wall with the attic forceps (see p. 357).
The post-aural method. The preliminary steps of the operation are the same as have been already described for removal of an exostosis (see p. 318).
After separating and reflecting forward the membranous from the bony portion, the upper posterior part of the tympanic ring is chiselled away until a view of the stapes can be obtained. The incus is then disarticulated from the stapes.
If the stapes be ankylosed by fibrous adhesions to the margins of the fenestra ovalis, an attempt may be made to free it by cutting through the adhesions with a fine bistoury. If this be impossible, a sharp hook may be fixed into the margin of the plate of the stapes in the hope of forcibly extracting it. Some authorities advise chiselling away of the margins of the fenestra ovalis. If an opening can be made into the vestibule by this means, it is hoped that the resulting scar tissue will form a membrane more resilient than the ankylosed stapes, and, in this way, permit vibrations of sound to enter the labyrinth. This operation, however, necessitates the complete mastoid operation in order to freely expose the region of the fenestra ovalis.
After-treatment. It is sufficient to protect the ear with a small gauze drain. Occasionally there may be considerable vomiting and vertigo as an immediate result of the operation; this usually passes off within two or three days. Meanwhile the patient should be kept in a recumbent position and, if necessary, given small subcutaneous injections of morphine.
Difficulties. The chief difficulty is to obtain a good view; even if this be obtained it is difficult to extract the stapes without fracture of its crura.
Dangers. As a result of opening up the labyrinth, one would expect considerable risk of infecting the internal ear. Judging from recorded cases, this, however, seldom occurs.
Results. The chief advocate of the removal of the stapes is Jack of Boston (Boston Med. and Surg. Journ., January, 1895), who again in 1902 (Archives of Otology, vol. xxxi, p. 407) stated: (1) that removal of the stapes did not destroy the hearing but sometimes improved it; (2) that the operation upon cases of moderate deafness might give brilliant results but was also attended with some risk to the hearing; (3) that the operation on the profoundly deaf was not advisable, as usually the stapes could not be removed owing to surrounding adhesions, and even if it were, no improvement was likely to occur owing to the sound-perceiving apparatus having probably already undergone irremediable changes.
Blake (Archives of Otology, vol. xxii), on the other hand, states emphatically that stapedectomy is harmful rather than beneficial.
The question, therefore, of removal of the stapes from the point of view of hearing is purely experimental. If there be bony ankylosis, it will be found impossible to remove the bone, and an attempt to do so will result in fracture of its crura. If, on the other hand, it be not ankylosed but movable, probably massage or, in cases of perforation of the tympanic membrane, direct mobilization of the bone will give results as good as those following stapedectomy.
The most favourable results are to be expected in those cases in which the operation is performed to relieve symptoms the result of previous middle-ear suppuration. In otosclerosis no benefit is ever obtained, and therefore the operation is absolutely contra-indicated.
On the other hand, there is ample evidence that the hearing power, in spite of removal of the stapes, may be retained. As an example may be quoted a case in which the stapes was removed accidentally in curetting out the ear after the removal of the malleus and incus, and in which I afterwards performed the complete mastoid operation owing to the continuance of the middle-ear suppuration. In spite of this, whispering could be heard at a distance of 20 feet (Journal of Laryngology, &c., vol. xxii, p. 33).
Under this heading may be considered manipulations requiring special technical knowledge and skill: (1) Catheterization; (2) passing of bougies; and (3) washing out the tympanic cavity through the Eustachian tube.
Indications. (i) As a means of diagnosis in order to determine (a) the amount and character of the obstruction within the Eustachian tube; (b) the condition of the mucous membrane and whether any exudation is present within the middle ear.
(ii) For the purpose of treatment. (a) In order to instil medicated drops or vapours into the Eustachian tube and tympanic cavity; (b) as a preliminary measure to the passage of bougies into the Eustachian tube or to washing out the tympanic cavity through the Eustachian tube.
(iii) Catheterization is preferable to Politzer’s method if only one ear is affected. Politzer’s method, on the other hand, is preferable to catheterization (a) in small children; (b) in the case of slight middle-ear catarrh if both ears are affected; (c) if the passing of the catheter is very difficult and causes pain owing to nasal obstruction; (d) in nervous individuals who object to the catheter; (e) if the sudden inflation by means of Politzer’s method is more effectual than by catheterization.
Points to notice before inflation. 1. Care must be taken that the lumen of the catheter is not obstructed, and that the compressed air bag and auscultation tube are also in working order.
2. The nose must be cleansed of all secretion; if filled with crusts or in a septic condition, inflation must be avoided.
3. The patient should be sitting. Sometimes on inflation of the ear, especially for the first time, an attack of giddiness or faintness may occur.
4. The nose should always be examined to see that the passage is free. If it be obstructed catheterization may be impossible, or some special manipulation will be required in order to pass the catheter through the nose.
5. In order to prevent muscular contraction of the palatal muscles, which may grip the end of the catheter and so prevent its entrance into the orifice of the Eustachian tube, the patient should be told to breathe quietly and keep the eyes open.
 Fig. 209. Eustachian Catheter.
Fig. 209. Eustachian Catheter.
A short silver or plated catheter is usually used. It is 5 inches in length and curved at its extremity. To indicate the position of the point of the catheter in the post-nasal space, a ring is attached to its outer and wider extremity corresponding with the concavity of the curvature of its beak (Fig. 209). The size of the catheter varies in diameter from Nos. 1 to 4 English size, that is, the same scale as used for urethral catheters. The source of compressed air used for the inflation is usually a Politzer bag having an india-rubber tube attached. At its end is a vulcanite pointed nozzle which accurately fits into the wider extremity of the catheter.
Technique. The patient is seated facing the surgeon, the head being supported by a prop or by an assistant. If the patient be at all sensitive, it is wiser to spray a very small quantity of a 2 or 5% solution of cocaine or eucaine into the nose, or, better still, to pass gently a probe tipped with a small pledget of cotton-wool soaked in the cocaine solution along the inferior meatus. This will effectively anæsthetize the region of the pharyngeal orifice of the Eustachian tube, which is the most sensitive part.
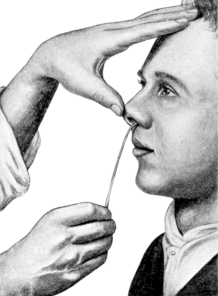 Fig. 210. Passing the Eustachian
Catheter. Introduction of the catheter within the nostril.
Fig. 210. Passing the Eustachian
Catheter. Introduction of the catheter within the nostril.
|
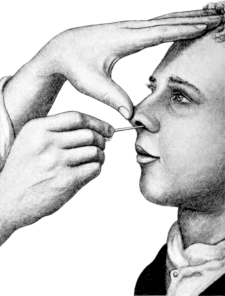 Fig. 211. Passing the Eustachian Catheter. Passage of the catheter along
the floor of the nose.
Fig. 211. Passing the Eustachian Catheter. Passage of the catheter along
the floor of the nose.
|
The surgeon stands in front of the patient. The larger extremity of the catheter is held lightly between the thumb and first finger of the right hand, its beak being turned downwards, whilst the tip of the nose is tilted up by the thumb of the left hand (Fig. 210). In introducing the catheter into the nostril, the right hand is kept low down so that the stem of the catheter is almost in a vertical position. In this way the tip passes over the floor of the vestibule. As the catheter is gently pushed through the nose the right hand is raised so that the instrument assumes the horizontal position and passes backwards between the septum and the inferior turbinal, its beak being kept in close contact with the floor of the nose (Fig. 211). As the beak of the catheter enters the post-nasal space, it will be felt to glide over the soft palate.
With regard to the best method of introducing the beak of the catheter into the orifice of the Eustachian tube, opinions vary. Of the many methods advised only two will be given.
The first is more suitable to those who have not had much experience in using a catheter; the second is the one naturally adopted by an expert.
The first method. The catheter is pushed backwards until it is felt to impinge against the posterior wall of the naso-pharynx. The beak, which at this stage is directed downwards, is next rotated a quarter of a circle inwards so that it points horizontally towards the opposite side; the position is shown by the ring at its outer extremity (Fig. 212). The catheter is now gently withdrawn until the beak is felt to catch against the posterior edge of the vomer. During these procedures the stem of the catheter should rest on the floor of the nasal cavity. The manipulations are carried out with the right hand whilst the outer extremity of the catheter is kept fixed in position by means of the thumb and finger of the left hand.
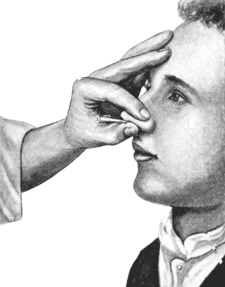 Fig. 212. Passing the Eustachian Catheter. Beak of the catheter in the
post-nasal space. The catheter is turned to the opposite side so that
its beak impinges against the posterior border of the septum.
Fig. 212. Passing the Eustachian Catheter. Beak of the catheter in the
post-nasal space. The catheter is turned to the opposite side so that
its beak impinges against the posterior border of the septum.
|
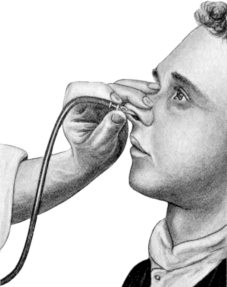 Fig. 213. Passing the Eustachian Catheter. Catheter in position; act of
inflation.
Fig. 213. Passing the Eustachian Catheter. Catheter in position; act of
inflation.
|
The catheter is next pushed a short distance backwards to free it from the soft palate and rotated downwards, and finally round in an outward direction until the ring points to the outer canthus of the eye on the side to be catheterized (Fig. 213).
The point of the instrument should now engage the Eustachian tube; if, however, inflation shows this not to be the case the probability is that the catheter has been pushed too far backwards and rests on its posterior lip. This can be remedied by drawing it a little further outwards.
The second method. The catheter, with its beak turned downwards, is passed gently and rapidly along the inferior meatus of the nasal cavity, and at the same time rotated slightly outwards against the inferior turbinal bone. Whilst the catheter is within the nose, this outward rotation is prevented by the narrowness of the inferior meatus, but as soon as the beak of the catheter has passed behind the level of the inferior turbinal into the free post-nasal space, it will revolve outwards and upwards and in so doing will enter the Eustachian tube, which lies just behind and above the posterior end of the inferior turbinal bone.
Provided there be no abnormal obstruction within the nose, this method is an exceedingly simple one. With the practised hand the manipulation can be carried out so smoothly and quickly that the catheter will be in position before the patient has had time to realize the fact.
Difficulties. 1. Irritability of the mucous membrane. The passing of the catheter through the nose may set up a violent spasm of sneezing or coughing. When the beak has entered the post-nasal space, the irritation may cause such intense contraction of the palatal muscles that the point of the catheter may become fixed and its movement rendered impossible. If this takes place, the catheter should be withdrawn and the part anæsthetized by means of cocaine and eucaine solution, which is best applied locally on a pledget of wool at the end of a probe.
2. Partial nasal obstruction. On inspecting the nose the obstruction is usually found to be due to a deviated septum or spur, or to adhesions situated at its anterior part. Sometimes a passage can be effected by simply diminishing the curve of the catheter. At other times the obstruction can be overcome by introducing the catheter with its stem held upwards and outwards, so that on entering the nose the beak dips in beneath the anterior end of the inferior turbinal. As the catheter is pushed gently inwards its outer extremity is brought round with a circular movement so that it gradually assumes the horizontal position. No force must be used. As the catheter is pushed farther in, it may rotate to a varying degree according to the formation of the nasal cavity. Sometimes, indeed, the catheter may make a complete rotation during its passage through the nose. At other times, after the obstruction is passed, the catheter is best pushed through the nose with the beak pointing directly upwards. The great point is gentleness; the catheter should be allowed to take whatever position suits it best, but after the beak has entered the post-nasal space the stem should lie horizontally along the floor of the nose and its beak should point downwards.
3. Complete nasal obstruction. If the obstruction be one-sided, then the catheter must be introduced into the nasal space through the opposite side.
This is performed in the ordinary manner, except that the catheter must be longer and possess a larger curvature. On reaching the post-nasal space, its beak is turned round so as to point towards the outer canthus of the eye on the affected side. It may be necessary to alter the curve more than once in order to get the point of the catheter to exactly engage into the orifice of the Eustachian tube.
If both sides be completely obstructed, the only method to adopt is catheterization from the mouth. The ordinary catheter is used. It is passed into the mouth, its beak being directed upwards, until it reaches the posterior wall of the pharynx. The catheter is then pushed directly upwards until its stem impinges against the soft palate. The beak is then turned outwards until it lies almost horizontally. In this position it should enter Rosenmüller’s fossa. The catheter is now withdrawn a little and should be felt to pass over a slight obstruction—the posterior lip of the Eustachian orifice. By gently pressing the beak slightly outwards, it should engage within the entrance of the Eustachian canal.
4. Obstruction within the post-nasal space. A common error in introducing the catheter is to push it too far backwards, so that on rotation of the beak outwards it passes behind the Eustachian tube and lies in Rosenmüller’s fossa. In this position the sounds referred to the examiner’s ear through the auscultation tube during the act of inflation differ from the normal sounds in that they are soft and distant. In a case of doubt inflation should again be practised with the catheter in varying positions. If the catheter be in the correct position, the patient should be able to talk without discomfort, and there should be no tendency to retching or coughing. If, however, the beak lies in Rosenmüller’s fossa, considerable irritation is caused, and on inflation the patient feels the air in the throat and not in the ear.
Catheterization may be rendered difficult by the presence of a large pad of adenoids or of a tumour; or inflation of air into the Eustachian tube may be quite impossible owing to the occlusion of its pharyngeal orifice, the result of scarring.
Mishaps. 1. Rupture of the tympanic membrane. With a normal membrane this is difficult to produce, in spite of even forcible inflation. Such an accident usually occurs at the site of some previous scar or atrophic patch in the membrane. If it occurs, there may be a temporary feeling of giddiness, noises, and pain in the ear. Inflation, of course, should be stopped at once and the ear protected for a day or two by plugging the meatus with a piece of cotton-wool.
2. Severe epistaxis. This is usually the result of trying to force the catheter through an obstructed nose, but it may also take place, though rarely, when manipulations have been carried out in a gentle fashion.
3. Syncope. This is fortunately of rare occurrence and usually only happens on the first occasion that the catheter is passed. For this reason the patient should always be in a sitting posture, and on the slightest appearance of pallor or faintness the catheter should be withdrawn. The attack invariably passes off, but for the moment it is very unpleasant.
4. Surgical emphysema. If the point of the catheter lacerates the mucous membrane, the air may be forced into the submucous tissue. This mishap, however, rarely occurs as the result of simple catheterization, but is more likely to follow forcible attempts to pass a bougie into the Eustachian tube.
Indications. This may be done for the following reasons:—
(i) As a means of diagnosis, to demonstrate the existence and position of a stricture.
(ii) To dilate a stricture.
(iii) As a therapeutic measure, to treat the mucous membrane of the Eustachian tube by means of a medicated bougie.
Bougies are made of various materials, but for ordinary purposes the gum-elastic is the best. They are about 7 inches in length with a slightly bulbous point.
In the adult the length of the Eustachian tube is approximately 1½ inches, of which 1 inch forms the cartilaginous and ½ inch the osseous portion. The narrowest part of its lumen is known as the isthmus, and is situated at the junction of its cartilaginous and bony portion. On passing the bougie through the catheter into the Eustachian tube, it is essential to know how far its point is projecting beyond the point of the catheter. For this purpose the bougie may be marked at its outer extremity. Five inches from the point of the bougie, that is, the same length as the catheter, is a black band a centimetre in length; a centimetre farther up is another black band; and again after an intervening space of a centimetre is a third black band (Fig. 214).
Technique. The catheter is introduced in the ordinary way, and its position within the entrance of the Eustachian orifice is verified by means of inflation. It is kept fixed with the left hand, and the bougie is pushed into the catheter until the beginning of the first mark on the former just reaches the outer extremity of the latter; the tip of the bougie will now be flush with the point of the catheter. If there be no pain and no resistance, the bougie is very gently pushed on until the beginning of its second black band just enters the catheter. Its point will now project 2 centimetres within the Eustachian tube; that is, to about the region of the isthmus. If the bougie has been successfully introduced into the Eustachian tube, the patient generally states that the instrument is felt within the ear itself. No force should be used for fear of making a false passage, and with gentle manipulation it is very rare for actual pain to occur. On reaching the isthmus resistance may be met with, but by the exercise of slight pressure the bougie can usually be made to pass through it; if there be much resistance the bougie should be withdrawn and a finer one substituted. After passing through the isthmus, the bougie may be pushed in another centimetre, but no further, in case it may actually enter and injure the contents of the tympanic cavity.
After the tip of the bougie has passed through the isthmus the surgeon will hear its movements through the auscultation tube as a rub or crackling sound. It is left in position for five or ten minutes and then withdrawn. The ear should then be gently inflated, when the air entry into the tympanic cavity will probably be found to be much more free.
As the passage of the bougie causes a certain amount of reaction, it should not be passed oftener than once a week. Although no force should ever be employed, the largest possible bougie should be passed at each successive sitting until complete dilatation has been obtained.
Difficulties. 1. If the catheter be not in position, the bougie may pass behind the tip of the Eustachian orifice and enter Rosenmüller’s fossa. This can usually be felt by the patient as a pricking sensation in the throat, and may produce retching and coughing.
2. A stricture of the Eustachian tube may be so great as to prevent entrance of the bougie.
Dangers. (a) Surgical emphysema. If the mucous membrane be lacerated by the bougie, air may be forced into the subcutaneous tissues on inflation, after its withdrawal. In some cases the surgical emphysema is so considerable as to involve the side of the neck and face, and indeed has been known to necessitate the performance of laryngotomy.
The best treatment is to make the patient suck ice and to forbid all attempts at blowing the nose and coughing. Sometimes it is also necessary to scarify the pharynx and soft palate with a small bistoury. Recovery may be hastened by gentle massage of the neck and face. Inflation should not be attempted again for at least a week.
(b) The bougie may be pushed in too far and cause injury to the contents of the tympanic cavity.
(c) The tip of the bougie may break off whilst in the Eustachian tube. With a gum-elastic bougie this is very rare, but it is more likely to occur if the brittle celluloid bougies are used. To prevent this unfortunate disaster the bougie should be carefully examined before passing it, to see that it is not cracked nor broken. If such an accident does happen it is wiser to do nothing, because as a rule the fragment is afterwards expelled spontaneously.
Results. If the obstruction be fairly recent and limited to the pharyngeal end of the Eustachian tube, excellent results may be obtained by using either the simple bougie or the catgut variety moistened with a 5% solution of silver nitrate.
Owing to the general thickening of the tube, there is a marked tendency for further stricture to take place in the more chronic cases, even if a temporary improvement is obtained, and for this reason the use of the bougie is seldom to be recommended.
Indications. (i) In chronic middle-ear suppuration in which the perforation is situated in the anterior inferior quadrant and the continuance of the otorrhœa is apparently due to the secretion not being able to drain from the tympanic cavity. This method may be employed to effect drainage and in order to cleanse the tympanic cavity thoroughly before the instillation of medicated drops. In these cases the floor of the tympanic cavity is usually at a considerable depth beneath the lower limit of the membrane (Fig. 186).
(ii) In order to remove a small foreign body lying on the floor of the tympanic cavity which cannot be expelled by syringing. The operation is only tentative and is seldom successful.
Contra-indications. (i) If there be acute middle-ear suppuration; (ii) if the perforation be very small, as there will be a considerable risk of the fluid being driven into the mastoid antrum and further infecting it.
Technique. A catheter of wide calibre is passed in the ordinary manner. Inflation is practised to see if it is in the right position. The left hand fixes the outer extremity of the catheter at its entrance within the nose and keeps it in position. The patient inclines the head over to the affected side and holds a receiver beneath the ear. A small brass syringe whose nozzle accurately fits the outer extremity of the catheter is used. Slight force may be required during the act of syringing, but must not be sufficient to cause pain within the ear. A certain amount of fluid always escapes into the throat although the catheter is in its right position, and this may set up an attack of retching and coughing. To avoid this the patient should incline his head slightly forward as well as to the affected side and breathe gently with the mouth open. If the manipulation be successful the fluid will trickle out of the external meatus.
A foreign body is rarely expelled by this method, as the force of fluid syringed into the Eustachian tube is seldom sufficient, and it is not wise to use too great pressure. In order to expel all the fluid from the tympanic cavity, the ear is afterwards inflated by Politzer’s method, and at the same time the fluid is mopped out of the ear by means of pledgets of cotton-wool.
Results. If the continuance of the middle-ear suppuration has been chiefly due to the retention of the purulent secretion in the lower part of the tympanic cavity, this method of treatment is frequently most satisfactory. In other cases no benefit is obtained owing to the suppuration being due to other causes.
Dangers. The chief danger is the infection of the mastoid cells.
With few exceptions the conditions requiring operative procedures on the mastoid process are the result of some suppurative lesion which has originated within the tympanic cavity.
The object of such operations is to arrest or eradicate the disease which, by further extension through the bony walls of the temporal bone, might eventually cause death by giving rise to some suppurative intracranial complication.
For their successful performance a knowledge of the anatomical relationships of the mastoid process is essential. It is sufficient here to remind the reader of the main surgical points in this connexion (Fig. 215).
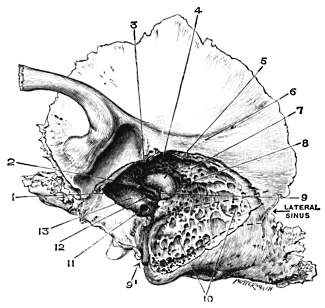 |
Fig. 215. Left Temporal Bone, showing Anatomy of the Middle Ear and
Mastoid Process. 1, Anterior wall of external meatus, partly removed; 2,
Canal for tensor tympani muscle, ending in processus cochleariformis; 3,
Attic; 4, Aditus; 5, External semicircular canal; 6, Posterior root of
zygoma; 7, Tegmen tympani; 8, Antrum; 9, Fallopian canal for facial
nerve; 9', Stylo-mastoid foramen; 10, Mastoid cells; 11, Fenestra
rotunda; 12, Fenestra ovalis; 13, Promontory. Dotted line shows outline
of sigmoid groove for lateral sinus.
|
The mastoid antrum. At birth the mastoid antrum is almost fully developed. In infancy it is situated superficially and at a much higher level in relation to the auditory canal than in the adult. In the infant, also, the petro-squamous and the squamo-mastoid suture are still patent. As the mastoid cells develop, the antrum gradually becomes more deeply placed, so that in the adult it is from half to three-quarters of an inch from the surface.
Its roof, the tegmen tympani, is continuous with that of the attic. Anteriorly it is separated from the external auditory meatus by the posterior wall of the auditory canal, whose innermost margin forms the outer wall of the aditus. On its inner wall lie the semicircular canals, whilst posteriorly the lateral sinus is separated from it by an intervening layer of mastoid cells or compact bone. Between the semicircular canals and the lateral sinus is a small area composed of a thin layer of bone, separating the antrum from the posterior fossa of the cranial cavity.
The mastoid process. In the infant this is undeveloped and is merely represented by a small bony protuberance. By the fourth year it has practically reached the adult type.
Anatomically the mastoid process can be subdivided into three chief types: (1) the pneumatic, in which the cells are few and large; (2) the diploic, containing numerous small cells; and (3) the compact, in which the bone is extremely dense. Mixed types are frequently found, the cortex, as a rule, being more dense than the deeper portion. Occasionally it is uniformly sclerosed, almost of the consistence of ivory, but in these cases the condition is usually pathological, the result of chronic inflammation of the mastoid process.
The mastoid cells converge towards the antrum and may be divided into two groups: (1) those extending vertically downwards to the tip of the mastoid process; and (2) those lying between the antrum and the sigmoid process of the lateral sinus. In addition to these two groups, it must not be forgotten that cells may extend in other directions; for instance, (a) anteriorly, along the root of the zygoma; (b) posteriorly, communicating with the cells of the occipital bone; (c) inferiorly, between the floor of the tympanic cavity and the jugular fossa; (d) internally, spreading inwards towards the apex of the petrous bone and surrounding the labyrinth; or (e) enveloping the orifice of the Eustachian tube.
The facial nerve, after dipping beneath the external semicircular canal, passes vertically downwards through the mastoid process to emerge at the stylo-mastoid foramen. Entering this foramen and running along the canal are the stylo-mastoid branches of the posterior auricular artery. These vessels, if cut through by the chisel, may bleed in a marked manner, thus drawing the attention of the operator to the fact that he is in close proximity to the facial canal and nerve.
Surface anatomy. Although it is impossible to foretell with certainty before operation what the anatomical structure of the mastoid process may be, yet some information may be gathered from the formation of the skull.
In the dolichocephalic type, the mastoid process is broad and frequently contains large cells, especially at its tip and round the lateral sinus, which is usually deeply placed. In the brachycephalic type, on the other hand, there is a greater tendency for the mastoid process to be narrow and to consist of dense bone, for the middle fossa to extend low down and to overlap the outer wall of the antrum, and for the lateral sinus to project forward and superficially, even to within 2 or 3 millimetres of the posterior border of the external meatus.
The posterior root of the zygoma may be considered approximately the line of demarcation between the roof of the antrum and mastoid process, and the floor of the middle fossa of the skull. This, however, is only a rough guide, as in some cases, especially of the brachycephalic type, the middle fossa may dip below this point. If this ridge is not well marked, then Reid’s base-line must be taken as the guide.
Just behind the auditory meatus, at its upper posterior margin, is the spine of Henle, which forms the anterior boundary of the suprameatal triangle. Macewen, who first described this triangle, gave it as a guide for the exposure of the antrum. Experience, however, has shown that no reliance can be placed on this as a landmark, as, if the bone is chiselled through at this point, it is by no means uncommon to expose the dura mater of the middle fossa. A point 10 millimetres (two-fifths of an inch) behind the spine of Henle corresponds to the anterior border of the sigmoid sinus. Behind the suprameatal triangle and beneath the zygomatic ridge is the body of the mastoid process, which has a smooth surface and is perforated by small foramina through which pass tiny vessels.
The antrum, in the adult, is situated at a slightly higher level than the tympanic membrane, its floor roughly corresponding with a line drawn horizontally backwards through the middle of the posterior wall of the bony meatus.
Although opening of the mastoid process as an operative measure dates back to the eighteenth century, yet Schwartze, in 1873, was the first to establish the operation as a practical procedure.
Schwartze’s operation consisted in the simple opening of the antrum and mastoid cells, leaving the middle ear untouched. This procedure was carried out no matter whether the disease was recent or long standing. It soon became recognized, however, that this operation did not effect a cure in all cases, more especially in those in which the disease involved the walls of the tympanic cavity.
Küster, in 1889, suggested removal of the posterior wall of the external auditory meatus, and about the same time von Bergmann advocated removal of the outer attic-wall. The Küster-Bergmann operation, first practised by Zaufal, may therefore be considered to be the origin of the complete mastoid operation.
Stacke’s name is frequently though wrongly mentioned in association with the complete operation, which is sometimes termed the Schwartze-Stacke operation. Stacke’s operation was devised with a view to removal of the ossicles and outer wall of the attic in those cases in which the bone disease was limited to these regions. This operation, however, is occasionally of service in the performance of the complete mastoid operation (see p. 397).
Thus the year 1889 may be considered as the starting-point of the complete mastoid operation. Since that date many modifications have been introduced, the majority of which are not worthy of reference.
After the technique of the operation had been developed and practised for some time, more careful attention was directed to the after-treatment. In the earlier days of the radical operation it was the rule to leave the wound open and to plug it with gauze, or to insert a drainage tube which was carried through the membranous portion of the external meatus.
The next step was the making of post-meatal skin flaps, with closure of the posterior incision and packing of the wound through the auditory canal; and the names most prominently associated with this are Panse, Körner, and Stacke.
Still more recently, in order to shorten the after-treatment, the wound cavity has been skin-grafted by the method first suggested by Siebenmann and afterwards amplified by Charles Ballance.
The operations which will be considered are:—
1. Wilde’s incision.
2. Opening of the mastoid process and antrum.
3. The complete or radical mastoid operation.
Although definite indications for the above operations will be given, it must be remembered that in many cases the extent of the operation will depend very largely on the pathological condition found during the course of the operation itself, as frequently the clinical symptoms are not sufficient to determine beforehand what operation is indicated.
In comparing the simple opening of the mastoid cells and antrum with that of the complete or radical operation, the fundamental difference is that in the former the tympanic cavity and its contents are not interfered with, whereas in the complete operation the middle ear, antrum, and mastoid cells are converted into one large cavity. In consequence, complete recovery of hearing may take place in the former case; in the latter, however, this is not possible.
Although these operations, especially in the more acute conditions, are performed from the point of view of saving the life of the patient, due regard must also be given to the preservation or restoration of the hearing power, if this indeed is possible. If the hearing power be very poor, that is, if conversation cannot be heard more than 12 feet off, and especially if the deafness be partially due to changes having already taken place within the labyrinth, then the complete operation is to be preferred if it be doubtful whether Schwartze’s operation will be sufficient to eradicate the disease. If, on the other hand, the hearing power of the affected ear be fairly good, and with this there is deafness of the opposite side, then, unless it is absolutely essential that the complete operation should be performed, an attempt should be made to effect a cure by the simpler operation, provided it is first explained to the patient that it may perhaps be necessary to perform the complete operation afterwards.
In cases of acute inflammation of the mastoid process or of a subperiosteal abscess lying over it, Wilde made a post-aural incision, incising the tissues down to the bone. The indications for doing this are now considered to be very few, but it must be remembered that in Wilde’s day the mastoid operation had not been developed.
Indications. (i) In infants it is sometimes justifiable, as the pus may have escaped to the surface of the mastoid process either through the squamo-mastoid suture or along the posterior wall of the auditory canal, between the periosteum and bone, without there being any actual disease of the bone.
(ii) As a temporary measure, to permit of drainage of a subperiosteal abscess, if the operation on the mastoid process cannot be performed for twenty-four hours or more.
(iii) In acute middle-ear suppuration a free incision down to the bone may relieve the pain if there are symptoms of periostitis of the mastoid process; it is, however, rarely necessary.
Contra-indications. In older children and adults (with the above exceptions) this operation is not sufficient, as the periostitis or subperiosteal abscess over the mastoid process is secondary to underlying bone disease which can only be eradicated by an operation on the mastoid process itself. Although healing may apparently take place, fistulæ or other evidences of mastoid disease almost invariably occur afterwards.
Operation. In an infant a general anæsthetic is not necessary, but in an adult gas anæsthesia is advisable. The mastoid region is surgically cleansed; the auricle is pulled forward and a free incision is carried down to the bone, in a curved direction downwards over the mastoid process. Originally Wilde made a vertical incision; but it is better, if possible, that the incision should be the same as would be made in performing the mastoid operation, which indeed will probably have to be carried out afterwards. After the hæmorrhage has ceased and the purulent contents of the abscess, if present, have drained away, fomentations should be applied and changed frequently during the first twenty-four hours. After this a simple dry dressing is sufficient.
Results. Except in the case of tiny infants, this procedure is seldom successful in curing the condition, and must be considered as only a temporary measure.
(Opening of the mastoid process and antrum)
Indications. (a) In acute middle-ear suppuration. (i) If, in spite of free drainage, earache, pyrexia, and tenderness over the body of the mastoid do not abate within three days. This is all the more urgent if the condition is the result of scarlet fever or influenza, as in these cases the disease may spread with extreme rapidity.
(ii) If there be an obvious abscess over the mastoid process; except in infants, in whom Wilde’s incision may be attempted as a tentative measure, although it is not recommended.
(iii) If there be symptoms of meningeal irritation.
(iv) If a profuse otorrhœa has continued for over four weeks and is accompanied by sagging downwards of the upper posterior wall of the external meatus, a definite sign that the antrum is involved.
(v) If a profuse otorrhœa has continued for over eight weeks, with no sign of abatement, even although the temperature may be normal and although there may be no symptoms of inflammation of the mastoid process. The continuance of the otorrhœa is presumably due to accumulation of pus in a large antral cavity. The object of the operation is to permit of free drainage and to prevent involvement of the mastoid process itself. The question of operation, however, must be considered very carefully. There is no doubt that in many cases conservative measures may effect a cure even although the suppuration has already existed for many months.
(b) In chronic middle-ear suppuration. Although the complete mastoid operation is usually indicated, yet the simple opening of the mastoid antrum may be advised under the following conditions, provided there are no symptoms of inflammation of the mastoid process nor signs of disease of the bony walls of the tympanic cavity:—
(i) If the perforation, however large, be surrounded by a rim of tympanic membrane (showing that there is no disease of its bony margins), and if the malleus be not adherent to the inner wall of the tympanic cavity.
(ii) If the hearing be good, that is, if speech is heard farther off than 12 feet, especially if the other ear (from whatever cause) be quite deaf.
Politzer, among others, still maintains that there is frequently no communication between the affected mastoid cells and the antrum if the mastoid abscess is the result of acute middle-ear suppuration. For this reason he considers that the antral cavity should only be opened if there be definite evidence of bone disease between the abscess cavity and the antrum, or if symptoms of extra-dural abscess or some intracranial complication be present. It is, however, difficult to believe that some communication, however microscopic, does not always exist between the antrum and the mastoid cells, seeing that the latter originally developed as outgrowths from the antrum itself, and must have become infected by direct extension from it. At the same time there is no doubt that complete recovery takes place in a certain number of cases in which the antrum has not been opened.
In my opinion, however, it is always wiser in such cases to open the antrum. Politzer considers that if this be done, healing does not take place so rapidly as in those cases in which the antrum has not been opened. On the other hand, if the antrum be not opened, the main object of the operation, that is, free drainage of the contents of the aural cavity, is not attained.
Operation. Preparation of the patient. The head should be shaved for a space of 2 inches around the mastoid region, twenty-four hours before the operation if possible. In women the hair in front of the ear, instead of being shaved off, should be combed forward and plastered down with carbolic soap. By doing this the hair can be arranged so as to cover the bald area during convalescence, a matter of great satisfaction to the patient.
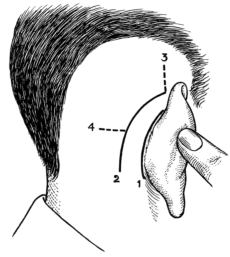 Fig. 216. Diagram showing Position of Skin Incisions in Post-aural
Operations. 1, For removal of foreign bodies or exostoses, or for
excision of a stricture within auditory canal; 2, Usual incision for the
mastoid operation; 3, Prolongation of incision upwards for exposure of
temporo-sphenoidal lobe; 4, Extension of incision backwards, for
exposure of lateral sinus or cerebellum.
Fig. 216. Diagram showing Position of Skin Incisions in Post-aural
Operations. 1, For removal of foreign bodies or exostoses, or for
excision of a stricture within auditory canal; 2, Usual incision for the
mastoid operation; 3, Prolongation of incision upwards for exposure of
temporo-sphenoidal lobe; 4, Extension of incision backwards, for
exposure of lateral sinus or cerebellum.
The area of the operation and surrounding parts should be thoroughly washed with ethereal soap solution and afterwards protected with a compress of 1 in 2,000 solution of biniodide of mercury. After the patient has been anæsthetized, the cleansing process should be repeated, and the auditory canal syringed out with the lotion. The head is then covered with a sterilized towel drawn tightly over the ear and scalp, a portion of the towel being afterwards cut away so as to expose only the field of operation. The patient should be in the recumbent position, the head resting on some hard substance, such as a partially-filled sand-bag, and turned over to the opposite side, so that the affected ear is uppermost.
In addition to the ordinary instruments, those specially required for this operation are a well-balanced mallet and several gouges and chisels of varying size, one or two sharp spoons, a seeker, and a malleable blunt-pointed silver probe. They should be sterilized in the ordinary manner.
The incision. The surgeon stands at the side to be operated upon, facing the patient’s head. The auricle is pulled forward. An incision is made through the skin, beginning just above the pinna, and is carried downwards in a curved direction towards the tip of the mastoid process, lying about half an inch behind the insertion of the auricle (Fig. 216). Before making the incision, the tip of the mastoid process should be determined. Care must be taken not to let the knife slip at the end of the incision and so incise the neck tissues. The line of incision should correspond to what will afterwards be the middle of the wound cavity in the bone. If the incision be made too far forwards or too far backwards, one of the edges of the skin incision may afterwards tend to overlap the opening in the bone and in this way hinder the dressing and perhaps lead to the formation of a sinus. If there be much thickening of the soft tissues and periosteum, it may be necessary to make the incision longer than usual in order to expose the field of operation sufficiently.
In the upper angle of the incision the temporal fascia and the underlying temporal muscle will be exposed. Except in very muscular subjects, in whom the muscle comes low down into the wound and has to be cut through, it is better to push the lower border of the muscle upwards by means of a periosteal elevator. The incision is now carried right down to the bone throughout its length.
If there be an abscess over the mastoid process, its purulent contents should be allowed to drain away, the abscess cavity being then irrigated with a weak solution of biniodide of mercury (see p. 389).
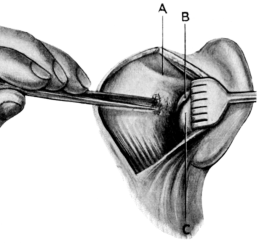 Fig. 217. Schwartze’s Operation. Showing field of operation with
anatomical landmarks and gouge in position for opening of antrum.
Fig. 217. Schwartze’s Operation. Showing field of operation with
anatomical landmarks and gouge in position for opening of antrum.
A, Zygomatic ridge; B, Spine of Henle: behind and above it is the suprameatal triangle; C, Fibrous portion of cartilaginous meatus, not separated from bony. (In this and the following diagrams the gouge or chisel is drawn small. In actual practice they may be much larger.)
Exposure of the field of operation. The periosteum and overlying soft tissues are then reflected forwards and backwards with a rugine, until the following points are brought into view: namely, the upper posterior margin of the bony meatus (taking care not to separate the fibrous from the bony portion of the meatus) and Henle’s spine in front, the zygomatic ridge above, and the fibres of the sterno-mastoid muscle below (Fig. 217). The tip of the mastoid process should just be seen. To do this it may be necessary to cut away some of the fibres of the sterno-mastoid muscle.
If the surgeon has two assistants, the duty of one of them is to hold apart the edges of the wound by means of retractors, whilst the other is employed in keeping the wound dry. If there be only one assistant, the edges of the wound may be held apart by metal retractors.
Careful examination of the field of operation should now be made. There may be no external signs of disease. As a rule, however, as a result of the inflammatory process having already extended to the surface, the periosteum is found to be much thickened, with extreme vascularity of the underlying bone, or there may be a subperiosteal mastoid abscess of varying size.
Excepting in infants, in whom pus may escape through the squamo-mastoid suture, a subperiosteal abscess is always secondary to a fistula in the bone, which is usually situated over the body of the mastoid process just behind the suprameatal triangle. It may, however, occupy some other position.
In the case of Bezold’s mastoid abscess (see p. 389), although no fistula may be seen on the surface of the bone, pus may be found to well up from beneath the mastoid process on cutting through the fibres of the sterno-mastoid muscle. In other cases there may be actual necrosis of the bone, as a rule involving the lower margin of the squamous portion of the temporal bone (see p. 390).
The method of opening the antrum in a straightforward case will first be described.
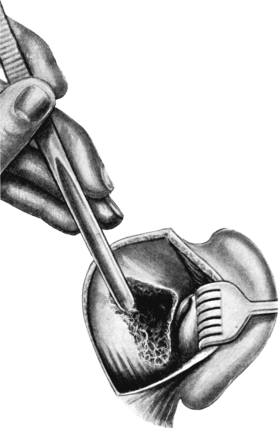 Fig. 218. Schwartze’s Operation. Showing exposure of the antrum. Note
sloping position of gouge in removal of bone in region of lateral sinus.
Fig. 218. Schwartze’s Operation. Showing exposure of the antrum. Note
sloping position of gouge in removal of bone in region of lateral sinus.
Opening the antrum. The approximate surface marking of the antrum is the suprameatal triangle and the region just behind it, which, however, as has been mentioned, is an uncertain guide. It is wiser, therefore, in all cases of operation on the mastoid process to assume that the case is one in which the lateral sinus extends far forward and is superficial, and that the middle intracranial fossa is low lying.
The area of bone to be removed depends on the age of the patient; in the adult it is about half an inch square, having as its boundaries the zygomatic ridge above and Henle’s spine in front.
The bone should be removed by short decided taps of the mallet on the gouge or chisel, held in contact with the bone in a sloping direction (Fig. 217). This precaution is specially indicated whilst in the act of removing the bone from above downwards and from behind forwards, in order to prevent injury to the middle fossa, which may be low lying, or the lateral sinus, which may project abnormally far forward (Fig. 218).
To permit of better control over the instrument, the hand holding it may rest lightly against the patient’s head, which is now covered with a sterilized towel. This control should always be sufficient to prevent the chisel or gouge being driven unexpectedly too far inwards, an accident which may easily happen if, by chance, there is a sudden diminished resistance to the stroke owing to unexpected softening of the bone or the inadvertent exposure of the dura mater. It is this accidental slipping of the instrument which is often responsible for injury to the lateral sinus or the facial nerve. With regard to choice of instruments, I prefer the gouge, as it is safer than the chisel, owing to it having rounded edges.
On removal of the superficial part of the cortex, the mastoid process may be found to be sclerosed, or to consist of small or large cells filled with granulations or purulent secretion.
(a) If the bone be sclerosed. The operation may be extremely difficult, as the antrum is frequently of small size and very deeply placed. As the tympanic cavity must not be interfered with, it is not permissible to insert the seeker along the auditory canal into the attic in order to determine the position of the aditus. The only guides, therefore, are the anatomical landmarks.
The best method is to chisel away the bone close to and parallel to the upper posterior margin of the external meatus. In chiselling along the upper wall of the opening, the gouge, instead of being directed downwards, as was the case in removal of the outer portion of the cortex, is now directed inwards and at the same time slightly upwards and forwards. In enlarging the lower part of the opening, the bone is chiselled away obliquely inwards and upwards. The strokes of the gouge are made alternately from above and below, so that gradually a funnel-shaped opening is formed, having its point directed towards the aditus.
Anteriorly, the bone is removed as close to the posterior wall of the auditory canal as possible, including the suprameatal spine. Above, the line of chiselling must not extend beyond the zygomatic ridge, whilst below sufficient bone should be removed towards the tip of the mastoid process to permit of inspection of the deeper parts of the wound.
From time to time the operator makes use of the seeker (Fig. 219). This is a blunt-pointed probe whose tip is bent at right angles to its shaft. With it any opening is probed carefully to see whether it is merely a mastoid cell, or dura mater covering the outer wall of the lateral sinus, or the middle cranial fossa, or if indeed it is the antrum itself. The chief mistake is to work too low down. If the antrum be small it may be missed, and the bone may be chiselled away too deeply in endeavouring to discover it and the facial nerve or the external semicircular canal injured. It is wiser, therefore, to work high even if the dura mater of the middle fossa is exposed by doing so. This should not lead to any harmful result provided the dura mater is not injured.
As soon as the antrum is reached, pus will be seen to ooze through the opening made, especially if it is under tension. The probe or seeker can now be passed into a cavity of varying size. The antrum is recognized by its smooth surface, which has quite a different appearance to that of the mastoid cells.
(b) If the mastoid be not sclerosed. The pathological condition found on removal of the superficial cortical layer depends on the anatomical structure and on the extent and virulence of the inflammatory process. Only a few cells may be involved, or on the other hand the whole mastoid process, if it be of the pneumatic type, may be converted into a mere shell of bone, forming a large cavity filled with masses of septic granulation tissue, carious bone, and pus. Sometimes, indeed, owing to the tegmen tympani or bony wall of the sigmoid sinus being already destroyed, the dura mater above or the lateral sinus posteriorly may be found already exposed within the cavity. If this is the case the pus may pulsate if present in large quantity. Any patches of soft carious bone or granulation tissue should be removed with the curette.
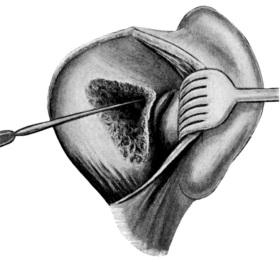 Fig. 220. Schwartze’s Operation completed. The seeker is being passed
through the aditus into the attic. Note the posterior border of the
external semicircular canal which forms the inner and lower margin of
the aditus.
Fig. 220. Schwartze’s Operation completed. The seeker is being passed
through the aditus into the attic. Note the posterior border of the
external semicircular canal which forms the inner and lower margin of
the aditus.
If the disease be limited to a few superficial mastoid cells, it is sufficient, according to those who do not always explore the antrum, to expose and curette the cavity freely and to do nothing further. This, however, should only be done if the bone surrounding the abscess cavity is hard and apparently normal, and if there is no tract of granulations leading from it in any direction. If an opening be found leading directly into the antrum, it should be enlarged with the curette or gouge. The extent of the antrum is next defined with the seeker, any overlapping ledges of bone being removed by the gouge until the whole of its inner surface is exposed.
The region of the aditus is now inspected under good illumination, using a head-light if necessary. It is recognized as a small opening at the anterior inner part of the antrum, on the floor of which may be seen the posterior border of the external semicircular canal, standing out as a whitish rounded eminence. Bone may be removed from its upper inner margins, but the lower portion should not be interfered with for fear of injuring or displacing the incus. To confirm the opening into the aditus, a blunt-pointed curved probe may be passed for a short distance through the aditus into the attic (Fig. 220).
With the curette all granulations should be removed.
Treatment of the mastoid process. The question now arises as to how much bone to remove. This depends on the condition found; the chief point is to make certain of removing all the infected cells.
In the case of marked sclerosis, the opening need not be large because, if the bone between the cortex and the antrum be solid, it is hardly probable that infection can spread through it to any outlying cells in the tip of the mastoid or elsewhere.
In the diploic and pneumatic varieties, the seeker must be used constantly in order to discover any outlying cells, which are then opened freely. If this be done systematically, infected cells may be found some distance away from the antrum itself, although an area of apparently healthy bone lies between them and the antrum. It must not be forgotten that cells may extend posteriorly as far as the occipital bone, or anteriorly along the zygomatic process, or even into the upper posterior part of the auditory canal itself (see p. 374). If such infected cells be not discovered, healing will be prevented.
However small or large the opening may be, all rough corners must be removed, so that at the end of the operation a smooth funnel-shaped cavity exists. To obtain this a burr may be used, worked either by the electric motor or, if a portable one, by an assistant. The burrs are of various sizes and of the cross-cut variety recommended by Ballance. Some operators perform the operation by burring throughout. Personally, during the earlier stages of the operation, I prefer to use the gouge and mallet. If the operator has not had much experience in the use of the burr there is always a slight risk, if it be not kept sufficiently under control, and especially if too great pressure be used, of it being driven through the dura mater above or into the lateral sinus posteriorly, or of it injuring the contents of the tympanic cavity. As a means of finishing the operation no instrument could be better. In private practice, however, few surgeons keep one. For this reason it is advisable to become accustomed to the chisel and gouge.
Removal of part of the posterior wall of the auditory canal. This may be necessary if the anterior wall of the antrum and mastoid process be affected. The fibrous portion of the auditory canal is partially separated from the bony portion and held forward by means of a retractor. The upper posterior portion of the bony meatus can now be removed either by means of punch-forceps or by the chisel, to what extent does not matter so long as its innermost portion, ‘the bridge,’ is not interfered with, that is, so long as the tympanic cavity and aditus are not encroached upon.
Exposure of the dura mater and lateral sinus. This may have already occurred before the operation, as a result of extension of the bone disease, or it may be necessary to do so during the course of the operation. Owing to the fact that an extra-dural abscess is a frequent complication of acute inflammation of the mastoid process, Victor Horsley and Körner advocate the exposure of the dura mater and the lateral sinus in every case, especially if a tract of carious bone leads in their direction. No harm is done in exposing these structures, and it precludes missing an extra-dural abscess.
It is better to expose the dura mater than to leave it covered with infected bone and septic granulations.
Final step of the operation. In order to make certain that a free opening exists between the antrum and the tympanic cavity, some warm boric lotion should be syringed through the opening of the aditus. A small syringe is used, having a fine piece of india-rubber tubing fixed on to its point. The end of the tubing is pushed into the entrance of the aditus. The fluid is then syringed through and should emerge from the external meatus. This is also beneficial in order to cleanse the tympanic cavity of its purulent secretion. To expel all the fluid from the middle ear the syringe is emptied and the piston withdrawn to its full extent. Its point is again placed within the entrance of the aditus and the piston pressed home, so that air is forced through and so drives out any remaining fluid from the tympanic cavity into the external meatus, which in its turn should be carefully dried. If there be no perforation, or if it be very small, the membrane should be freely incised before fluid is syringed through the aditus.
Immediate treatment of the wound cavity. The wound cavity is lightly packed with sterilized ribbon gauze, half an inch in width. Care must be taken to introduce the gauze right down to the aditus and to pack the cavity evenly.
The wound should be left open for a few days until the acute inflammation of the soft tissues has subsided, after which the upper and lower angles of the wound can be partially closed by sutures. A strip of gauze is also inserted into the auditory canal and a light dressing of plain sterilized gauze and a pad of cotton-wool covers the ear and surrounding parts. The bandage should be passed round the head and not beneath the chin, as the latter method is often a source of great discomfort to the patient during the stage of vomiting following the anæsthetic.
Blake of America has suggested that the wound should be allowed to fill with blood-clot on the supposition that the subsequent organization of the clot will result in a rapid closure of the wound. This method cannot be considered seriously owing to the impossibility of keeping the wound sterile.
After-treatment. There is seldom any shock, but there may be considerable pain during the next twenty-four hours.
If there has been no subperiosteal abscess, the dressing need not be removed for forty-eight hours. If an abscess has been present the dry dressing should be removed after twenty-four hours, and if there is much œdema and inflammation of the surrounding region, a compress of wet boric lint, kept in position by a few turns of a bandage, should be substituted, and changed every four hours.
Drainage tubes should be shortened and removed as soon as possible. The gauze within the wound cavity should be changed every second day, or daily if there be much secretion. If there be much discharge and the condition be very septic, an ear-bath of hydrogen peroxide may be given at each dressing and the cavity syringed out with a weak solution of biniodide of mercury; otherwise it is sufficient to use boric acid lotion.
If the operation has been successful, the purulent discharge from the tympanic cavity rapidly diminishes, frequently ceasing before the third day. The auditory canal is then firmly packed with gauze, especially in its outer part, in order to prevent stenosis of its lumen, which is liable to occur if the posterior fibrous portion of the canal has been separated from the bony meatus during the operation. Granulations very quickly block the aditus and so separate the antrum and mastoid cavity from the tympanic cavity. The wound can now be treated as an ordinary deep surgical wound, care being taken that it is packed from the bottom at each dressing.
If all the diseased bone has been removed, smooth healthy granulations will cover the wound. The continuance of pus from any spot, or the local growth of exuberant granulations, suggest the presence of an infected cell or a fragment of carious bone. Under cocaine anæsthesia, the part should be inspected carefully, and, if necessary, curetted freely. In other cases the local application of chromic or trichloracetic acid is sufficient.
After the second week the wound becomes shallower, actual healing of the wound depending on the size of the cavity.
Unless a very large amount of bone had to be removed, the resulting deformity is not great and usually only consists of slight sinking in of the skin. In some cases the final result is only a fine scar, which can generally be concealed by the hair.
The difficulties and dangers of the operation are considered in the next chapter (see p. 412).
Results. 1. If the operation has been successful (and this is usually the case), pyrexia and pain rapidly disappear, the patient experiencing remarkable relief from the head symptoms, so that within twenty-four hours he feels almost well. Healing of the wound is usually complete within six weeks, and before this date the hearing power will probably have been restored to normal.
2. The operation may not have been successful and the following unfavourable symptoms may occur:—
(a) The pyrexia may continue irregularly for a few days. If there be no other symptoms, this is probably due to septic absorption from the wound and need not cause very great alarm. If accompanied by pain, it may either mean that all the infected mastoid cells have not been opened, or suggest the onset of osteomyelitis of the temporal bone. If, in addition, such symptoms as rigors, delirium, optic neuritis, headaches, or vomiting occur, they indicate some intracranial complication.
In cases of doubt it is wiser to explore the wound under a general anæsthetic and then to determine what operation will be necessary.
(b) The general condition of the patient may be excellent, but otorrhœa or a fistula over the mastoid process may persist. Continuance of otorrhœa, in spite of healing of the wound posteriorly, means that although the disease involving the mastoid process has been eradicated, yet the walls of the tympanic cavity are themselves involved. This will probably necessitate the subsequent performance of the complete mastoid operation.
On the other hand, the suppuration may cease from the middle ear with complete recovery of hearing, and yet a fistula of the mastoid may remain. This means that all the diseased bone has not been removed. This should now be done.
In an infant. In an infant under two years of age the incision should be somewhat higher than usual. In making it, too much pressure should not be used, as the bone is frequently thin at this age, and if carious it may be so soft that the knife may possibly enter the intracranial cavity. In exposing the area of operation, it must be remembered that the posterior root of the zygoma and the antrum lie at a much higher level than in the adult. The opening into the antrum, therefore, is made almost above rather than behind the margin of the auditory canal. In these cases a fistula is usually present, and the bone is so soft that it can generally be removed by means of a sharp spoon or curette. At the same time, however, the aditus should be exposed and the opening made funnel-shaped in order to allow of proper dressing.
Subperiosteal abscess. The treatment depends on the extent of the abscess. If it be small, the lining membrane may be dissected away, the wound being afterwards treated in the ordinary manner. If the abscess cavity extends upwards towards the parietal region, or forwards along the temporal fossa, then drainage tubes should be inserted, their ends being brought out into the mastoid wound. It is rarely necessary to make counter-incisions. The completion of the operation is seldom difficult, as the fistula actually leads into the antrum. If the fistula be a large one and the bone is carious a sharp spoon may be used; otherwise a gouge is necessary.
Bezold’s mastoid abscess. If the lower portion of the mastoid process be composed of large cells, the abscess within the mastoid may break through the bone at its inner surface in the region of the digastric fossa. In consequence of this the pus may infiltrate the neck tissues beneath the fascia of the sterno-mastoid muscle and form a large abscess recognized clinically as a hard and painful swelling situated below the mastoid process instead of over it. This condition was first described by Bezold.
After exposing the antrum in the ordinary way, the tip of the mastoid process is opened freely. It is usually found to contain large cells filled with pus. Any granulation tissue is curetted away and the cavity dried. The inner surface of the bone is then inspected carefully in order to find the opening, which usually leads into the digastric fossa. The margins of the fistula should be curetted freely and the opening enlarged, if necessary. If the deep-lying cervical abscess be large, the finger may be passed into the abscess cavity behind the mastoid process, between it and the cut fibres of the sterno-mastoid muscle. In this way the limits of the cavity can be made out, and any septa forming pockets within it can be broken down. A counter-incision should be made through the tissues of the neck at the lower limit of the abscess. The opening should be sufficiently large to permit the insertion of a large drainage tube into the cavity. If the abscess be small it may not be necessary to make a counter-opening, but merely to insert a drainage tube into it, passing it from above downwards along the passage made by the finger.
Necrosis. In children necrosis of the temporal bone is not uncommon, especially if the middle-ear suppuration occurs in the course of a specific fever or is the result of tuberculous infection.
The part usually affected is the lower margin of the squamous portion of the temporal bone and the tympanic ring. Sometimes, however, the necrosis is very extensive, involving a large area of the petrous bone, including the labyrinth. These cases are always grave, and if a fatal result occurs it is usually in consequence of meningitis.
In adults necrosis is rare excepting as a localized patch usually situated superficially in the cortex of the mastoid process. Partial necrosis of the labyrinth, more especially of the vestibule and the portions of the semicircular canals, is also met with occasionally. When the necrosed area is superficial, such as the squamous portion of the temporal bone or the cortex of the mastoid process, it should be removed. If, however, it be situated more deeply, forcible removal should not be attempted until the sequestrum becomes loose, the wound cavity being meanwhile kept as aseptic as possible.
Osteomyelitis. In children, as the result of acute inflammation of the mastoid process, the bone may be found riddled with small points of pus, sometimes termed osteomyelitis. As a result of free opening of the mastoid cavity recovery, as a rule, takes place in the ordinary manner.
Distinct from this is another condition in which thrombosis of the diploic veins occurs. It is, fortunately, a rare complication of mastoid disease. It may occur before operation or be the result of infection of the bone as a result of operation. The infection tends to spread in every direction, more especially upwards along the parietal region and towards the occiput. With this, localized areas of necrosis or abscesses may occur, giving rise to painful swellings on the head, and usually are accompanied by cellulitis of the scalp, pyrexia, and intense headaches.
The only chance of recovery is to expose the affected area freely, and thoroughly remove all the diseased bone. To do this it may be necessary to lay bare the dura mater over a considerable area. If, however, the disease be not quickly eradicated, death will eventually occur as a result of extension of the septic infection to the larger veins, or from some other intracranial complication.
Before considering the question of the radical operation, it is assumed that conservative treatment has been attempted and has failed, and that the middle-ear suppuration has existed for a considerable period.
Indications. (i) As a prophylactic measure. If there be merely a perforation of the tympanic membrane and no evidence of disease of the ossicles nor the walls of the tympanic cavity, the probability is that the continuance of the suppuration is due to an affection of the mucous membrane rather than of the underlying bone; for example, to a chronic empyema of a large antrum cavity which, owing to its anatomical structure, will not drain freely.
In such cases the complete mastoid operation is only indicated if the deafness is extreme, the bone conduction diminished, and the high tuning-forks not well heard, or if the ossicles are bound down by adhesions to the inner wall of the tympanic cavity, as it is then obvious that the hearing power cannot be restored completely.
It must, however, be remembered that in many cases a slight discharge may exist for years without giving rise to any complications. If the patient be made aware of the slight danger which exists in every case of middle-ear suppuration, and be in a position to obtain medical attention if retention of pus occurs, then operative measures may be deferred indefinitely. If, on the other hand, the patient intends going to some remote country where medical attendance is impossible, then it is probably wiser to submit to the complete operation rather than risk future trouble.
(ii) If there be recurrent attacks of giddiness, nausea, or headaches radiating up the affected side which are not arrested by the ordinary methods of treatment. These symptoms of retention of pus within the antrum and mastoid process should be considered as danger signals. In this case also it is assumed that the hearing cannot be restored, and in consequence there is no object in performing Schwartze’s operation.
(iii) If there be recurrence of polypi and granulations within the tympanic cavity in spite of curetting, especially if the operation of ossiculectomy has already been performed.
(iv) If there be symptoms of retention of pus due to want of free drainage in the case of stenosis of the external meatus, whether due to fibrous contraction of its soft parts, or from the presence of exostoses.
(v) If cholesteatomatous formation be present. Even if there be no symptoms necessitating immediate interference, operation is usually indicated owing to the fact that cholesteatoma is the commonest predisposing cause of intracranial suppuration and septic thrombosis of the lateral sinus.
(vi) If there be a fistula of the bony wall of the mastoid process, whether it extends anteriorly into the auditory canal or externally through the skin over the region of the mastoid process. It must not be forgotten, however, that simple opening of the antrum and mastoid cells will be quite sufficient if the condition is the result of a recent and acute inflammation of the mastoid process.
(vii) If there be facial paralysis occurring in the course of a chronic middle-ear suppuration. This may mean either that there is bone disease involving the facial canal, or that the inflammatory process has spread through the Fallopian canal towards the inner ear. In either case operation is indicated.
(viii) As a preliminary step in intracranial suppurative lesions of otitic origin.
(ix) In tuberculosis of the middle ear. If the patient’s general condition permits of it, and if the pulmonary disease be slight or arrested, the complete operation should always be done. The difficulty is to remove all the diseased bone. If this can be done the wound will heal quite well.
(x) In acute inflammation of the mastoid process occurring in the course of chronic middle-ear suppuration, the complete mastoid operation should be performed, as in these cases the attic, aditus, and antrum are always involved.
(xi) Amongst the rarer conditions for which the complete operation may be necessary are removal of a foreign body which has been pushed inadvertently into the region of the attic and aditus and cannot otherwise be removed; and actinomycosis of the temporal bone.
The actual method of carrying out this operation varies. For those who have not had great experience the best method is first to open the antrum, as in Schwartze’s operation, and then to remove the ‘bridge’ of bone between it and the tympanic cavity (Küster-Bergmann operation, sometimes called the Schwartze-Stacke operation). Instead of doing this, the upper posterior part of the auditory canal may be chiselled away simultaneously during the act of exposing the antrum (Wolf’s operation). On the other hand, the mastoid and antrum may be exposed from within outwards by removing the outer attic wall and working backwards (Stacke’s operation).
The Küster-Bergmann (or Schwartze-Stacke) operation. The preliminary preparation, the position of the patient, and the instruments required are the same as in opening the antrum.
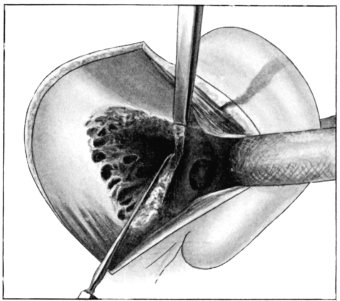 Fig. 221. The ‘Radical’ Mastoid Operation. To show removal of the
‘bridge’ from above. The seeker, inserted into the aditus, acts as a
protector to the underlying external semicircular canal and facial
nerve.
Fig. 221. The ‘Radical’ Mastoid Operation. To show removal of the
‘bridge’ from above. The seeker, inserted into the aditus, acts as a
protector to the underlying external semicircular canal and facial
nerve.
The incision is begun just above the upper insertion of the pinna, and is carried downwards in a curved direction behind the auricle along the margin of the skin and scalp. Some authorities prefer to make the incision close behind or even along the post-auricular fold. In favour of the incision being placed far back is the concealment of the scar by the hair. Also, as it is situated on healthy bone somewhat posterior to the actual wound cavity, it should heal by primary union and with no after-displacement of the auricle. In addition, if it be necessary to expose the lateral sinus, this can usually be done by simple retraction of the soft parts.
The exposure of the field of operation is the same as in the simple opening of the antrum, excepting that the soft tissues should be separated a little further forwards and above the external bony meatus, as in this operation the upper posterior wall has to be removed.
The antrum is opened as already described (see p. 382).
The fibrous portion of the external meatus is separated carefully from the posterior wall of the bony meatus by means of a periosteal elevator, and is pulled forward by a retractor. The external portion of the posterior wall is now removed in a wedge-shaped fashion by alternate strokes of the chisel from above downwards (Fig. 221) and from below upwards. The upper level of the bone to be removed corresponds with the zygomatic ridge. After a small portion has been removed, a pair of forceps is passed into the auditory meatus and its point made to project into the wound posteriorly through the end of the now detached fibrous portion of the auditory canal. With the forceps a piece of gauze is drawn through the auditory meatus in the form of a loop. By its means the auricle and fibrous portion are pulled well forward, thus exposing to view the tympanic cavity. Two openings are now seen: one, the auditory canal and tympanic cavity, in front, and the other, the antrum and mastoid cavity, behind. Between them is the ‘bridge’; that is, the innermost portion of the posterior wall of the auditory canal.
Any granulations present are curetted away gently from the tympanic cavity. The seeker is next passed into the tympanic cavity, and its point directed upwards and backwards into the aditus, so that it rests on the floor of the latter, or its point may be inserted into the aditus through the mastoid wound. Beneath it lies the eminence of the external semicircular canal and the facial nerve. This is a most important landmark. Provided the seeker is kept in this position, all the bone lying superficially to it can be removed without injury to the semicircular canal or facial nerve.
 Fig. 222. Stacke’s Protector.
Fig. 222. Stacke’s Protector.
In this connexion may be mentioned Stacke’s probe or ‘protector’ (Fig. 222). Although historically an instrument of importance, I do not make use of it. It is so large and of such sharp outline that, unless used with extreme care, it is itself very liable to injure the facial nerve. For this reason I prefer the seeker, a much finer and more delicate instrument, which will serve the purpose without the same risk (Fig. 219).
The ‘bridge’ is now carefully removed by the gouge or chisel, frequent use being made of the seeker meanwhile. As the roof of the antrum, aditus, and attic is a continuous one, the bone to be removed is necessarily at a higher level than the roof of the bony meatus. This is a point which must not be forgotten, as the great fault of the beginner is to remove the bone too low down.
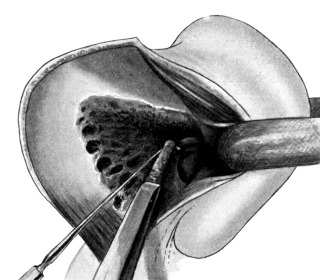 Fig. 223. The ‘Radical’ Mastoid Operation. Showing removal of the
remains of posterior wall of the auditory canal; the seeker acting as a
protector.
Fig. 223. The ‘Radical’ Mastoid Operation. Showing removal of the
remains of posterior wall of the auditory canal; the seeker acting as a
protector.
As the aditus is approached, the strokes of the chisel must be very gentle. If too much force be used, the chisel, on breaking through the innermost portion of the ‘bridge’, may injure the deeper-lying parts, more especially the facial nerve.
Some authorities advocate removal of the ‘bridge’ by means of bone forceps. This, however, is not so sure a method as by the chisel or gouge.
After removal of the bridge, the tympanic cavity, antrum, and mastoid will form a continuous cavity. As a rule the outline of the external semicircular canal appears as a well-marked white eminence, and projecting beyond it are the remains of the posterior wall of the auditory canal. In removing this ridge good illumination is essential. The bone is removed in layers with the chisel, beginning at the tip of the mastoid process, and working parallel to the auditory canal and the underlying facial canal. If necessary the seeker may be used as a guide, its point being allowed to rest on the floor of the aditus, superficial to the semicircular canal (Fig. 223).
The amount of bone removed should be such that at the end of the operation the auditory canal is only separated from the main cavity of the mastoid antrum by a slight eminence, the remainder of the posterior wall, which is continuous with that of the external semicircular canal.
Occasionally the facial canal and the stylo-mastoid canal are abnormally superficial. Provided the bone be removed in the manner just described, the facial nerve should not be injured, even though it may be exposed inadvertently. A warning of this occurrence is given by bleeding from the vessels within the canal (see p. 374).
If the malleus and incus be still in situ, they can now be seen and can usually be removed by the curette. No force must be used. Removal of the incus is a matter of no difficulty. In the case of the malleus there may be some resistance owing to the attachment of the tendon of the tensor tympani muscle. If so, the malleus should be grasped by a fine pair of forceps and the tendon severed by means of Schwartze’s tenotomy knife.
The overhanging edge of the outer wall of the attic can now be felt by means of the seeker. It is best removed by gentle taps of the chisel or small gouge. Especial care must be taken not to drive the gouge too far inwards. If this be done inadvertently, the transverse portion of the facial nerve passing along the inner wall of the tympanic cavity may be injured. As a safeguard some surgeons use an attic punch-forceps or a burr, others a Stacke’s protector which should be inserted into the attic before chiselling away its outer wall.
After the outer attic wall has been removed, the roof of the auditory canal and the attic should be continuous. This is verified by inserting the seeker, with its point turned upwards, within the attic, and then withdrawing it; no ridge of bone should now prevent its withdrawal.
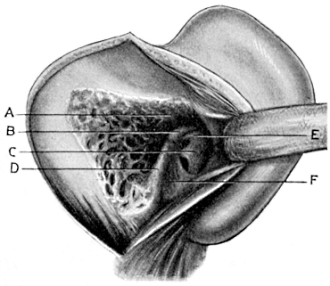 Fig. 225. The ‘Radical’ Mastoid Operation completed. A, Attic and
antrum; B, External semicircular canal; C, Promontory and inner wall of
tympanic cavity; D, Remains of posterior wall of auditory canal; E,
Facial nerve canal; F, Floor of auditory canal.
Fig. 225. The ‘Radical’ Mastoid Operation completed. A, Attic and
antrum; B, External semicircular canal; C, Promontory and inner wall of
tympanic cavity; D, Remains of posterior wall of auditory canal; E,
Facial nerve canal; F, Floor of auditory canal.
Granulations or the epithelial lining of cholesteatomata should be removed from the recesses of the tympanic cavity with a small curette. Care must be taken not to injure the surface of the promontory, or the region of the fenestra ovalis and fenestra rotunda. It is especially important to curette away the mucous membrane from the orifice of the Eustachian tube in order that scar tissue may obliterate its lumen and so prevent reinfection of the middle ear from the naso-pharynx. For this purpose a narrow curette is necessary (Fig. 224).
Removal of the innermost portion of the floor of the auditory canal is not always necessary. Sometimes, however, the ‘hypotympanum’ is well marked, and in order to ensure a good result it is wiser to remove this projecting piece of bone. If the ridge of bone be removed piecemeal, and if the gouge or chisel be kept parallel to the floor of the canal, there should be no danger of wounding the bulb of the jugular vein. Cases, however, have been recorded in which this has occurred.
The final step is to see that no pockets nor overhanging ledges or ridges of bone remain, and that all the diseased area has been removed. The cavity, although irregular in outline, should be a continuous one with a smooth surface (Fig. 225).
Wolf’s operation. This slight modification of the Küster-Bergmann operation requires merely a note of description. The position of the patient and the preliminary steps of the operation are the same as in the former operation.
In this operation, instead of first exposing the antrum cavity and afterwards removing the posterior wall of the external meatus, this procedure is performed in one step.
The chisel or gouge is first brought into contact with the bone just behind the upper posterior margin of the auditory canal. The bone is removed in layers by chiselling it away in a forward direction and in such a manner that each stroke of the chisel is carried directly into the auditory canal (Fig. 226). With each successive stroke, begun a little more posterior and inferior to the one preceding it, more bone is removed until at length the antrum is exposed. There should be no risk of injuring the external semicircular canal nor the facial nerve, owing to the fact that the outer wall of the antrum lies superficial to the tympanic cavity and aditus.
After the antrum has been exposed, the technique of the operation is the same as that already described in the Schwartze and Küster-Bergmann operation.
Advantages. 1. If the surgeon be experienced it saves much time, as the preliminary steps of the operation can be carried out very rapidly.
2. If the mastoid be sclerosed and there are no landmarks, the antrum, however small, is bound to be reached by making use of this method, by keeping high up, and, if necessary, exposing the dura mater. To verify the depth to which the bone may be removed and also the position of the antrum, the seeker should be inserted occasionally through the tympanic cavity into the aditus.
Disadvantages. If the surgeon be not experienced, it is not so safe a method as that of first exposing the antrum.
Stacke’s operation. After exposure of the field of operation, as in the Küster-Bergmann operation, the fibrous portion of the auditory canal is separated posteriorly from the bony portion.
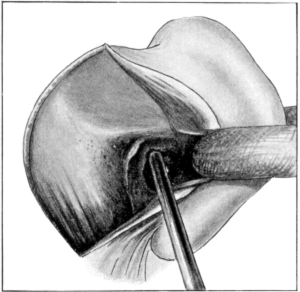 Fig. 227. Stacke’s Operation.
Fig. 227. Stacke’s Operation.
Any granulations, together with the malleus and incus, are removed from the tympanic cavity (see p. 353). Under a good illumination, using a head-lamp if necessary, the surgeon passes a seeker along the auditory canal, its point being made to project into the attic in order to define its limits and that of the aditus. The innermost portion of the upper posterior wall of the auditory canal, that is, the outer wall of the attic, is now removed piecemeal by means of a small gouge (Fig. 227). By working backwards the aditus is approached, the bone being removed carefully in small fragments. The seeker is inserted repeatedly into the entrance of the aditus so as to rest on the external semicircular canal, in order that the position of the latter and the underlying facial nerve may be kept constantly in mind. More bone above and external to this point is removed in small fragments, until at length the upper and innermost portion of the antral wall is removed and its cavity thus exposed. The cavity is gradually enlarged by removing still more bone in a backward and outward direction, until finally it resembles that left after the complete operation. Stacke originally devised this method in those cases in which he considered that the disease was limited to the ossicles, the walls of the attic, aditus, and innermost portion of the antrum. It was, indeed, merely a more radical method of performing ossiculectomy.
Advantages. Although this operation has practically been abandoned as a method of performing ossiculectomy, yet under the following conditions it may be adopted during the performance of the complete operation:—
1. If the mastoid be very sclerosed and if the antrum cannot be exposed, although the bone has been removed to a depth corresponding to its usual position.
2. If there be difficulty in exposing the antrum in the performance of the radical operation owing to the lateral sinus projecting far forwards and the middle intracranial fossa overlapping it externally.
Disadvantages. The chief disadvantage is that it is more difficult and tedious to begin the operation within the depth of the wound, and if the meatus is very deep and narrow it may be almost impossible to carry out.
Preservation of the ossicles and tympanic membrane after performing the complete mastoid operation.
This method of operation is well known and has been performed for some years, especially by Jansen of Berlin, and in America.
The only indication for this modification of the complete mastoid operation is disease involving the antrum and mastoid process so extensively as to require complete removal of the posterior wall of the auditory canal, without there being any coexisting bone disease of the walls of the attic or of the ossicles.
As the complete mastoid operation is only performed for some condition due to chronic middle-ear suppuration, it is difficult to imagine that the ossicles and attic region could remain unaffected when the extent of the disease necessitates the complete operation.
In my opinion, if it be necessary to remove the ‘bridge’ it is also necessary to remove the outer wall of the attic and with this the malleus and incus. If, on the other hand, there be no bone disease of the attic region or of the ossicles, Schwartze’s operation, or some modification of it, should be sufficient. The majority of aurists agree that, excepting in those cases in which the continuance of the suppuration is due to an empyema of the antral cavity, the ossicles are almost invariably carious to a greater or lesser extent in chronic middle-ear suppuration. This view is supported by Grunert’s researches (Archiv für Ohrenheilkunde, Band 40), who found that the ossicles were only normal in five cases in a series of 113 cases in which the complete operation had been performed.
Although removal of the ‘bridge’ may eradicate the disease within the mastoid process and antrum, yet, if the ossicles are left, post-suppurative adhesions will almost certainly afterwards bind them down and so cause a greater deafness than if they had been removed originally. Still, a few isolated cases have been reported in which hearing to the extent of 20 feet or more has been obtained as the result of this operation. The same results, however, frequently occur after the performance of the complete operation with removal of the malleus and incus. Until we have a large and consecutive series, recording the results of this particular operation in detail, together with information regarding the duration of the symptoms, the previous treatment, and the condition of the ear before operation, it is impossible to judge the value of this method.
This is done for two reasons: firstly, to prevent stenosis of the auditory canal; and secondly, to aid the growth of the epithelium over the wound surface, so that the latter will heal as rapidly as possible.
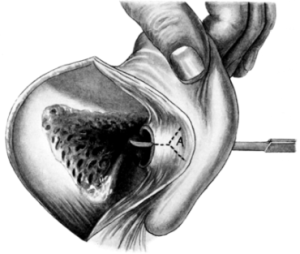 Fig. 228. Post-meatal Skin Flaps (Author’s method). Bistoury incising the
posterior fibrous portion of the auditory canal. The dotted line shows the line of
incision. A is the Y-shaped flap afterwards sutured to the skin behind the
auricle.
Fig. 228. Post-meatal Skin Flaps (Author’s method). Bistoury incising the
posterior fibrous portion of the auditory canal. The dotted line shows the line of
incision. A is the Y-shaped flap afterwards sutured to the skin behind the
auricle.
|
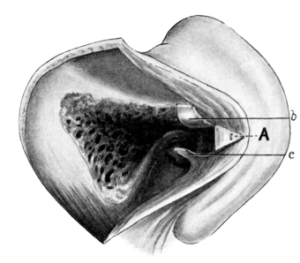 Fig. 229. Post-meatal Skin Flaps (Author’s
method). Flaps cut: A, Y-shaped flap sutured to
the skin; b, Superior flap; c, Inferior flap.
Fig. 229. Post-meatal Skin Flaps (Author’s
method). Flaps cut: A, Y-shaped flap sutured to
the skin; b, Superior flap; c, Inferior flap.
|
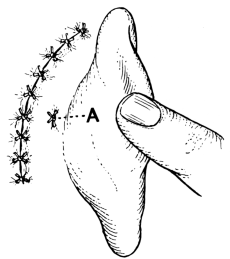 Fig. 230. Closure of Wound after ‘Radical’ Mastoid Operation. A is the
point at which the Y-shaped meatal flap is sutured to the skin.
Fig. 230. Closure of Wound after ‘Radical’ Mastoid Operation. A is the
point at which the Y-shaped meatal flap is sutured to the skin.
These flaps may be formed in several different ways. The following is the technique I adopt: A long, narrow, curved bistoury is passed down the auditory meatus so that it projects through the detached end of the fibrous portion, its point being directed backwards. The auricle is held well forward and the fibrous portion of the meatus cut through posteriorly, from within outwards, for a short distance (Fig. 228). The edge of the bistoury is then directed in a slanting direction upwards and outwards, and the incision continued as far as the cartilaginous portion of the meatus, care being taken not to cut into the concha. The bistoury is then withdrawn and reinserted at the point at which it was first made to turn upwards. It is now directed downwards and outwards and, in a similar manner, the incision is made in a slanting direction towards the inferior margin of the cartilaginous meatus. In carrying out these manipulations care must be taken that the outer portion of the bistoury does not injure the tragus or other portion of the auricle, a mistake which can easily occur. The fibrous portion of the meatus is thus divided by a Y-shaped incision into three small flaps; namely, a posterior or external V-shaped flap, and a superior and an inferior flap (Fig. 229).
The outer flap is fixed to the skin behind the auricle by means of a catgut suture (Fig. 230), and the auricle is then pulled back into its normal position. By inserting the tip of a finger into the meatus, the upper and lower flaps are pressed upwards and downwards against the roof and floor of the mastoid cavity, and can be kept in position afterwards by suturing the flaps to the subcutaneous tissue or by packing the cavity through the meatus with a strip of ribbon gauze.
Amongst other methods the following may be mentioned:—
Körner’s method (Fig. 231). Two parallel incisions are made in a longitudinal direction through the fibrous portion of the posterior wall of the meatus and are prolonged outwards as far as the concha. On the auricle being restored to its normal position, this posterior flap is pressed backwards and so covers a large area of the posterior wound surface. The chief objection to it is that, owing to involvement of the concha, there is considerable enlargement of the meatal opening and therefore subsequent disfigurement.
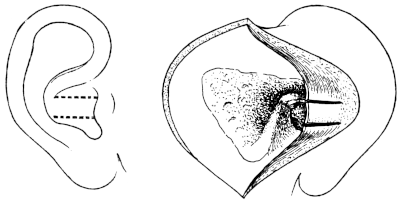 Fig. 231. Körner’s Post-meatal Flap.
Fig. 231. Körner’s Post-meatal Flap.
Panse’s method (Fig. 232). A transverse incision is carried through the posterior margin of the meatus, at the junction of the concha and auditory canal posteriorly. With a pair of scissors or knife, the posterior wall of the fibrous portion of the canal is now split by a longitudinal incision. In this way two flaps are formed, a superior and inferior one. They are fixed into position by catgut sutures through the subcutaneous tissues at the upper and lower angles of the wound.
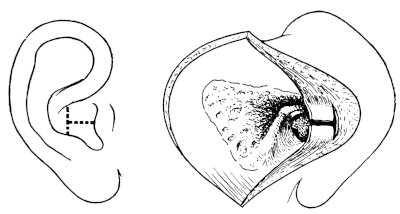 Fig. 232. Panse’s Post-meatal Flap.
Fig. 232. Panse’s Post-meatal Flap.
Stacke’s method (Fig. 233). This consists of a large inferior flap, formed by making a longitudinal incision along the posterior upper border of the fibrous portion of the auditory canal and a transverse incision meeting it at right angles, the latter cutting through the fibrous portion of the meatus at its junction with the concha.
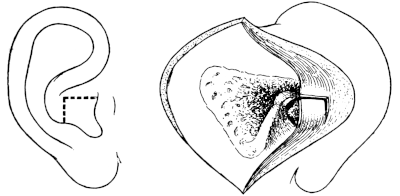 Fig. 233. Stacke’s Post-meatal Flap.
Fig. 233. Stacke’s Post-meatal Flap.
In order that these flaps may be thinner and more adaptable, the subcutaneous tissue should be cut away. Of these flaps the Y-shaped one is the most practicable, as it is suitable whether the posterior wound is closed or left open.
Körner’s method has the objection that there is subsequent disfigurement owing to the large meatal opening formed by cutting into the concha. It has the advantage, however, that the large posterior flap will cover the posterior surface of the wound cavity to a considerable extent, and also that it will permit a good view of the surface.
Panse’s flap is only of service if the posterior wound is left open and if there is not sufficient tissue left to make a posterior flap owing to previous destruction of the posterior wall of the auditory canal.
Stacke’s method is good if skin-grafting is afterwards employed.
Excepting under the conditions mentioned below, the posterior wound is closed by bringing together the edges of the skin incision with fine silkworm-gut sutures (Fig. 230). Before this is done, the wound cavity should be irrigated with a weak solution of biniodide of mercury, dried, and the deeper parts of the wound plugged with a strip of gauze inserted through the external meatus. This will not only arrest the hæmorrhage and keep the inner part of the wound dry, but at the same time will keep the skin flaps in position. After the wound has been closed, firm pressure should be applied in front and behind the ear to press out any blood from the cavity.
As a final step the gauze which has been inserted into the meatus is removed, and the cavity again packed evenly and lightly from the bottom of the wound with a fresh strip. The ear and surrounding parts are protected with a pad of sterilized gauze covered with cotton-wool and kept in position with a bandage.
The posterior wound should be left open under the following circumstances:—
1. If there be an abscess over the mastoid process. Although it may be possible to excise the whole of the lining membrane of the abscess cavity, it is wiser to leave the wound open for the first few days. The innermost portion of the wound cavity is packed through the external meatus, only the superficial part being packed through the posterior wound incision. As healthy granulations appear, the posterior packing is diminished, so that the edges of the incision gradually come together. If necessary, the edges of the wound can also be freshened and brought together by silkworm-gut sutures under cocaine anæsthesia.
2. If there be extensive disease of the bone, especially if the dura mater and lateral sinus are covered with septic granulations.
3. If there be bone disease of the anterior and inferior parts of the tympanic cavity. The after-treatment of packing or the curetting away of granulations can be carried out more easily through the posterior wound than through the external meatus, as it gives a better view of these regions.
4. In young children it is frequently advisable to leave the posterior wound open owing to the difficulty of packing the wound cavity through the small external meatus.
In order to shorten the duration of healing, a large Thiersch’s skin graft may be transplanted into the wound cavity. If this procedure be adopted it may be carried out in several ways. The skin may be transplanted in one large piece or in several small portions, and it may be introduced into the wound cavity either immediately after the completion of the mastoid operation or from seven to ten days later.
There is considerable diversity of opinion as to whether skin-grafting should be employed or not, and also when it should be done.
This may be partially accounted for by the fact that although, theoretically, the application of skin grafts is easy, yet, practically, the technique is difficult. Those who favour skin-grafting point to the fact that healing of the wound may take place within five weeks, whereas, if grafting be not undertaken, cicatrization of the cavity, even under favourable conditions, can hardly be expected to occur before eight to twelve weeks.
The skin-grafting operation as suggested by Charles Ballance is generally performed as a second stage, some ten or more days after the primary operation. This, from the patient’s point of view, is a serious matter; and the disappointment caused by the grafting not being always successful has induced many to give it up and to be content with what seems to be a more certain, though more prolonged, after-treatment.
More recently, however, it has been shown that in suitable cases skin grafts, if applied at the time of the completion of the primary operation, will take just as well as at a later date. This altogether alters the aspect of the case. If at the end of the primary operation it be certain that all the diseased bone has been removed and the cavity has been rendered aseptic, there can be no objection to the immediate application of skin grafts. If the result be successful, the period of after-treatment is considerably curtailed. If, on the other hand, it be not successful, the patient, beyond having a raw surface on his arm or leg for a few days, is no worse off than if the graft had not been applied.
Skin-grafting, however, cannot be done in every case. Two conditions are necessary for its success: firstly, that all the diseased bone has been removed; and secondly, that the wound cavity is aseptic.
Immediate skin-grafting, therefore, should not be employed if, in addition to the chronic disease, there be acute inflammation of the mastoid process, or of the subcutaneous tissues covering it; nor should it be done if it has been necessary to expose the dura mater over a large area, nor if there be any possibility of some subsequent intracranial complication. In such cases it may be justifiable to do skin-grafting after the acute symptoms have subsided. If, however, the case be progressing satisfactorily, the advisability of submitting the patient to a second operation should be a matter of careful consideration.
Disease of the inner wall of the tympanic cavity, or around the orifice of the Eustachian tube, is also a contra-indication against grafting, as the graft, if applied, will not take over these areas. The author’s opinion with regard to skin-grafting is that, if it can be applied immediately after the completion of the primary operation (and the conditions justifying this are limited), it may be done. If, however, the conditions be such that they will not permit of this, it should not be done at all.
Technique. When the grafting is done at the completion of the mastoid operation. The first step is to see that the mastoid wound cavity is rendered thoroughly aseptic and dry. All bleeding points in the soft tissues are arrested by means of pressure forceps. The mastoid cavity is then filled with hydrogen peroxide lotion, which is afterwards syringed out with a warm saline solution, the cavity being dried with sterilized strips of gauze, and finally packed from the bottom with a fresh strip.
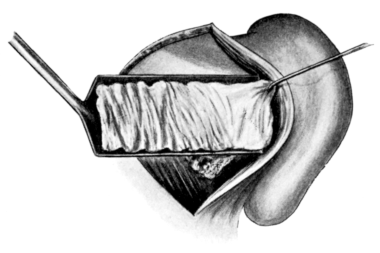 Fig. 234. Skin-grafting of Mastoid Wound Cavity after Operation. Skin
graft being transferred from the spatula to the mastoid cavity.
Fig. 234. Skin-grafting of Mastoid Wound Cavity after Operation. Skin
graft being transferred from the spatula to the mastoid cavity.
The size of the graft, which is usually taken from the thigh, should be at least 2 inches in width and 4 inches in length. The skin is cleansed by washing it with soap and water, then with ether, and finally with normal saline solution, the part being afterwards dried with a sterilized towel. It does not matter what type of razor is used to remove the graft, so long as it is sharp. The chief point to observe, in order to secure success, is to see that the skin is kept uniformly stretched—the tighter the better. The technique of removal of grafts is described elsewhere (see Vol. I, p. 670). The graft taken from the leg is transferred to a large spatula and smoothed out over its surface. The auricle is now pulled forward, and the gauze strip is removed from the mastoid cavity. The spatula is laid across the surface of the cavity so that it rests on the anterior margin of the wound surface (Fig. 234). With a sharp probe the edge of the graft, which just overlaps the spatula, is held in position at this point, the spatula being gently retracted so as to leave the graft stretched across the surface of the wound cavity. With a ‘stopper’ (Fig. 235), the graft is now pushed inwards towards the tympanic cavity.
 Fig. 235. Ballance’s ‘Stopper’ for pushing in the Graft.
Fig. 235. Ballance’s ‘Stopper’ for pushing in the Graft.
 Fig. 236. Pipette for sucking Air and Fluid From beneath the Graft.
Fig. 236. Pipette for sucking Air and Fluid From beneath the Graft.
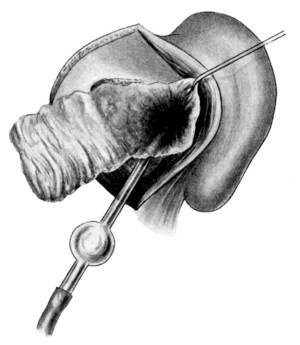 Fig. 237. Skin-grafting of Mastoid Wound
Cavity after Operation. Skin graft in the act
of being sucked into position by the pipette.
Fig. 237. Skin-grafting of Mastoid Wound
Cavity after Operation. Skin graft in the act
of being sucked into position by the pipette.
A glass pipette (Fig. 236), having a curved beak, is then passed inwards beneath the graft until its point, directed downwards, lies within the tympanic cavity (Fig. 237). Any blood which has accumulated between the bone and the graft is now sucked out, and in doing this the graft becomes closely applied to the bone surface (Fig. 238). After removing the pipette, any part of the graft which is not adherent to the bone is smoothed out over its surface. The tympanic cavity and the innermost portion of the mastoid cavity are then plugged with sterilized pellets of cotton-wool wrapped in gauze and dusted with aristol powder. The outer portion of the cavity is filled up with a strip of gauze, its end being brought out through the external auditory meatus.
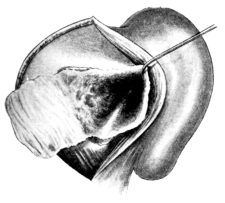 Fig. 238. Skin-grafting of Mastoid Wound Cavity after Operation. Skin
graft in position.
Fig. 238. Skin-grafting of Mastoid Wound Cavity after Operation. Skin
graft in position.
|
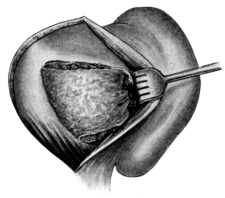 Fig. 239. Posterior Portion of Skin Graft covering Outer Surface of
Wound Cavity.
Fig. 239. Posterior Portion of Skin Graft covering Outer Surface of
Wound Cavity.
|
The posterior part of the graft, still projecting beyond the posterior margin of the wound, is now turned forwards so as to form a covering over the gauze filling up the wound cavity (Fig. 239). On the auricle being restored to its normal position, this portion of the graft is brought into contact with the subcutaneous tissues of the skin forming the post-aural flap, which now forms the outer wall of the mastoid cavity. The posterior incision is closed with sutures and a dry dressing and bandage are applied to the ear.
If skin-grafting be performed a week or more after the primary operation. The post-aural wound, now healed, has to be reopened. In doing so there may be considerable bleeding, which must be arrested. The mastoid cavity is usually found to be covered with a fine layer of granulations. They are curetted away carefully, special attention being paid to the region of the Eustachian tube and the floor of the tympanic cavity. After removal of the granulations, the bone should appear uniformly smooth though somewhat vascular. If any points of carious bone be found they should be removed freely with the gouge or burr. Considerable time may have to be spent in arresting the oozing from the surface of the bone cavity. This is best done by washing out the cavity with hydrogen peroxide solution and then plugging it tightly for a few moments with adrenalin solution. The gauze is withdrawn in a few moments. If there be still oozing, the pressure will have to be repeated until it ceases. The method of applying the graft is the same as already described.
After-treatment. The outer dressing may be changed every second day, but the wound itself is not interfered with until the eighth day. If asepsis has been obtained, the posterior wound has usually completely healed, so that the stitches can be removed at the first dressing. Owing to the secretion from within the cavity there may be a certain amount of odour, and as a rule some purulent discharge from the meatus. Under good illumination the strip of gauze is gently removed through the meatus and afterwards the small pellets of cotton-wool. In order to make certain that all are removed, a note should be made at the time of transplanting the graft as to how many were inserted in the wound cavity. The ear is now syringed out gently with a weak solution of hydrogen peroxide and afterwards dried by mopping it out with small wicks of cotton-wool.
A speculum is next inserted into the meatus and the cavity thoroughly examined. Any portions of the graft not in absolute contact with the bone or which overlap the skin of the meatus will have died, and can be removed by forceps. Care, however, must be taken not to pull off these portions too forcibly, as in doing so other pieces of the graft may be torn away. The external meatus is then plugged with a tiny piece of gauze and a dry dressing applied. If the graft has not taken and has died, it will be expelled at the first dressing on syringing.
Further treatment consists in syringing and afterwards drying the cavity daily. From day to day the outer layer of the graft will gradually come away piecemeal. At the end of the second week the patient can usually go home and carry out the treatment for himself, but he should be seen by the surgeon at least once a week until complete healing has taken place. If the graft has not taken uniformly over the surface of the bone, small patches of granulations may be seen covering these areas. Under cocaine anæsthesia these patches should be curetted. If the granulations recur repeatedly, it means that there is some underlying carious bone, and that healing will not take place until the tiny fragment is eventually exfoliated.
Results. Statistics vary. There is no doubt that the results are better according to the experience of the surgeon with regard to grafting. If it be only applied in those cases in which it is certain that all the diseased bone has been eradicated at the primary operation, then the percentage of success with relation to failure is very high. If, however, skin-grafting be adopted as a matter of routine, the ultimate result is probably not so good as in a similar series of cases in which grafting has not been done.
Skin-grafting through the external meatus. This has been advised chiefly in order to avoid a second operation.
The technique of applying the graft is practically the same as that for transplanting a large graft. The same care must be taken to get the interior of the mastoid cavity aseptic and dry. To avoid a general anæsthetic, the small grafts may be removed from the arm or leg under local anæsthesia produced by a subcutaneous injection of Schleich’s solution. The graft is transferred from a small spatula to the edge of the meatus and then coaxed into position within the cavity by means of probes. The grafts are kept in position by small pellets of cotton-wool covered with gauze. If successful, the grafting may shorten the duration of the after-treatment. It is not, however, so satisfactory a procedure as applying a large graft directly through the post-aural wound.
In order to keep the grafts in position, Drew has suggested laying the graft on sterilized gold-beater’s skin, and in this way applying it to the interior of the mastoid cavity.
More recently, Stoddart Barr of Glasgow has introduced an ingenious method of getting the grafts into position. The graft is manipulated over the end of a suitably-bent glass tube, having attached to the other end a piece of rubber tubing with a glass mouthpiece or small rubber bag. The graft at the end of the tube is passed through a wide speculum to the inner wall of the tympanum, when, by blowing air through the tube, the graft is spread out over the inner surface, including the tympanic walls, aditus, and antrum.
If the posterior wound has been closed. Provided the temperature keeps normal and there be no pain and no head symptoms, the first dressing need not take place until the fifth or sixth day. By this time the edges of the skin incision have usually united, so that the stitches can be removed, although occasionally the wound may have to be opened up to permit of drainage on account of septic infection. The withdrawal of the gauze from the auditory canal may cause considerable pain, which, however, can be prevented by continuous irrigation of the ear before and during its removal (see p. 315).
After the gauze has been removed, the ear is mopped out with pledgets of cotton-wool. To relieve the pain a few drops of a sterilized 1% solution of cocaine may be instilled and left within the ear for a few minutes.
Under good illumination, the largest possible speculum is inserted into the meatal orifice. The cocaine solution is mopped out, and the cavity dried, in order that careful inspection of the deeper parts may be made. The chief point is to see that the flaps are in position. There may be slight oozing from the surface of the wound, but as a rule the bone appears almost white, owing to the fact that granulations have not yet begun to form. The wound is then packed gently and evenly with gauze and the ear protected again with an external dressing and bandage.
Until the first dressing has taken place, the patient should be kept in bed. After this, provided the condition be satisfactory, he may be allowed to get up for a few hours every day, the period being gradually increased; by the tenth day or so he is practically well. In an uncomplicated case there is seldom any shock or discomfort after the operation, so that frequently the patient is anxious to be up and about even before the first dressing has been performed. It is wiser, however, to insist on rest for the first few days.
The subsequent dressings should be done every second or third day, depending on the condition found. If the wound cavity be clean, and if there be no odour, it is sufficient to irrigate it with a simple saline or boric lotion. Granulations begin to cover the bone about the tenth day, when there may be some purulent discharge necessitating daily dressings. To keep the parts sweet, an ear-bath of hydrogen peroxide (10 vols. %) may be given, the ear being subsequently irrigated with a 1 in 5,000 solution of biniodide of mercury.
Provided the patient be doing well there should be no temperature, pain, nor headaches. If any of these symptoms occur, or if the patient feels ill, or has attacks of sickness and becomes drowsy, the surgeon should at once be suspicious of some impending intracranial complication.
If the case be progressing favourably and all the diseased area of bone has been completely removed, granulations do not become exuberant, but form a fine smooth layer over the wound surface, the last portion to become covered being the region of the external semicircular canal and the ridge forming the remains of the posterior wall of the bony meatus. Exuberant granulation tissue is significant of underlying bone disease. If patches be observed, a 10% or stronger solution of cocaine should be applied to the part, which should afterwards be curetted. This process may have to be repeated on several occasions until, perhaps, a small spicule of bone is removed, after which granulations usually cease. As a rule the bone is completely covered with granulations by the fifth or sixth week. Meanwhile, owing to the growth of epithelium from the edges of the flaps, the raw surface within the wound cavity gradually becomes smaller, and with this there is diminished secretion.
The gauze packing can usually be discontinued about this period, or considerably earlier, perhaps even by the third week. In its stead an aqueous solution containing 50% of rectified spirit with 10 grains of boric acid to the ounce may be instilled into the wound cavity after it has been cleansed and dried.
Complete cicatrization of the cavity should take place within two or three months, depending on the size of the cavity.
If the posterior wound has been left open, the first dressing should be done on the second or third day.
The subsequent treatment depends on each individual case. If the wound has been left open on account of its septic condition, or owing to the dura mater having been exposed and found covered with granulations, its edges may be brought together by sutures after a period of ten days or so, when the wound cavity looks clean, and the packing carried out through the meatus.
On the other hand, if the wound has been left open on account of bone disease involving the inner wall of the tympanic cavity or region of the Eustachian tube, the packing should be continued through the posterior opening until the patches of carious or necrosed bone heal or are exfoliated. In these cases the granulation tissue tends to become fibrous in character in consequence of the necessary curettings, and eventually to form a thickened pad covering the inner wall.
After complete healing has taken place, the patient, before being dismissed, should be warned to visit the surgeon at least once in three months. Owing to the large cavity being lined with epithelium, desquamation takes place to a greater or lesser extent, so that the wound cavity may gradually become filled with masses of epithelial débris or cerumen. In consequence the cavity may become septic, and on removal of the epithelial débris underlying ulceration may be found. This can usually be cured by aseptic treatment, but if granulations have already occurred, curetting and the application of trichloracetic and chromic acid may be necessary.
Anatomical difficulties. The chief difficulties are due to a middle fossa overlapping the antral cavity, a lateral sinus projecting far forwards and lying superficially, and a sclerosed mastoid having no landmarks to indicate the way into the antrum. Unfortunately these conditions are frequently associated.
Formerly it was advised that it was wiser not to proceed further if the antral cavity could not be discovered after chiselling to a depth of three-quarters of an inch. This advice, however, is no longer reliable, as by the combination of the Stacke, Wolf, or Küster-Bergmann method any anatomical difficulties should certainly be overcome.
An inexperienced operator may mistake a large mastoid cell for the antrum and in this way may get into difficulties. The opening into the antrum, however, can always be identified by passing a bent malleable silver probe in an inward and forward direction into the aditus. If only a large cell has been opened, the probe will show that it is a limited cavity.
Hæmorrhage. In the majority of cases this is more of an inconvenience than a danger, being chiefly due to a general oozing from the soft tissues. It is, however, very necessary that the surgeon should have a clear view of the deeper parts whilst operating. If he works blindly in a pool of blood he courts disaster.
The hæmorrhage is best prevented by first curetting away any granulation tissue and then packing the cavity firmly with a strip of gauze. If this be not sufficient, it may be again packed with gauze containing adrenalin solution. It will repay the surgeon to have a good assistant to keep the field of operation dry. Troublesome bleeding, coming from a small vessel in the bone, may be arrested by the local application of a small fragment of Horsley’s sterilized wax (see Vol. I, p. 437).
Wound of the lateral sinus. This is a serious matter for two reasons: firstly, it may prevent completion of the operation; and secondly, it may lead to infection of the sinus.
If the sinus has already been exposed before the accident occurs, the surgeon promptly arrests the hæmorrhage by placing the forefinger of his left hand directly over the wound in its wall and exerts sufficient pressure to completely obliterate the sinus at this point. With his finger kept in this position, the wound cavity is carefully dried, and, if there be sufficient room, a piece of sterilized gauze is then packed between the bone and the outer wall of the sinus, both above and below the site of the injury. If there be not enough room to do this, then the surgeon with his right hand, or the assistant, should punch away more bone by means of bone forceps. After the lumen of the sinus has been obliterated above and below the injured area, the finger may be removed. If the packing has been successful, there will be no bleeding; if there be still slight bleeding, it can be controlled by further pressure. If possible, this method should always be carried out, as it practically excludes any chance of after-infection of the sinus.
If the injury takes place before the sinus has been sufficiently exposed to permit of direct pressure with the finger, then the only thing to do is to press in a small strip of gauze and plug the opening. As to what should be done next is a matter of opinion. Some surgeons are content to leave the gauze in situ. The author prefers to expose the sinus further, as in the former case, and to make certain that it is obliterated above and below the injured area. No doubt, if the injury be slight, the pressure of the strip of gauze covering the puncture will be sufficient to control the hæmorrhage, and the patency of the sinus may be maintained on healing. At the same time infection of the sinus has been known to take place, although the symptoms of this may not occur for ten days or two weeks after the operation.
If the sinus projects far forwards the gauze plugs may so inconvenience the operator as to prevent him completing the operation, which therefore may have to be delayed for at least a week. If, however, the sinus be injured at an early stage of the operation and the symptoms for which it is being performed are urgent, then, in spite of all difficulties, the antrum, at any rate, must be opened to permit of drainage, the operation being completed at a later date.
Injury to the facial nerve. The nerve may be injured in any part of its course within the tympanic cavity, or in its vertical course through the stylo-mastoid canal. To avoid this injury, curetting of the tympanic cavity should always be performed gently, and care should be taken not to chisel too low down,—the usual fault of the inexperienced.
Twitching of the face means that the nerve has been touched. If the patient be under deep anæsthesia, it is difficult to say whether the nerve has been injured or divided. In a case of doubt, it is wiser to discontinue the anæsthetic until the conjunctival reflex returns, when it can easily be demonstrated whether the facial nerve is affected or not.
If the injury be the result of curetting, it is wiser to do nothing. Recovery almost invariably takes place, owing to the fact that the paralysis has been caused by slight injury of the nerve. If, however, the nerve has been chiselled through, and the injury has occurred in its lower portion, it should be freely exposed over this area. The severed ends of the nerve should then be approximated and left in situ. In this case permanent paralysis is possible.
The after-treatment consists in avoidance of pressure in packing, the giving of strychnine internally, and faradism or galvanism to keep up the tone of the facial nerve and the muscles it supplies. Careful testing of the electrical reaction will show whether nerve regeneration is taking place or not. If the paralysis has existed for six months, and if in addition there be a definite reaction of degeneration, then the question of anastomosing the peripheral portion of the facial nerve to the spinal accessory, or what is more advisable, to the hypoglossal nerve, may be considered (see Vol. I, p. 452).
Injury to the labyrinth. Of the semicircular canals the external is the more liable to injury. The cochlea may also be injured from violent curetting of the promontory, or infected from dislodgment of the stapes; or it may even happen that a careless operator may inadvertently chisel through the promontory itself. In consequence of these accidents, vertigo, vomiting, and nystagmus may persist for several days, but as a rule they gradually diminish and disappear.
The treatment is expectant. As a result of pyogenic infection, suppuration of the labyrinth may occur. Even if this does not take place, complete deafness may result.
Injury to the dura mater. The subsequent danger is meningitis, fortunately a rare occurrence. The immediate treatment is to irrigate the part with weak biniodide of mercury solution, and then to remove more bone over the site of the injury. The intracranial pressure will keep the dura mater in close contact with the bone, so that if subsequent infection occurs there will be free drainage. The site of injury should be carefully isolated from the general mastoid wound cavity by covering it with sterilized gauze. If signs of meningeal irritation occur, the wound should be inspected, and if there be any evidence of localized meningitis, it should at once be surgically treated.
With regard to life. If, at the time of the operation, the disease be limited to the mastoid cavity, there should be no immediate danger to life.
With regard to recovery. (i) The operation is successful. Roughly speaking this occurs in at least 80% of the cases, complete healing taking place within eight to twelve weeks. If skin-grafting has been successfully performed the duration of healing may be considerably shorter. If the bone disease has been eradicated with complete healing of the cavity, the possibility of intracranial complications in the future can be excluded. On this account the patient may be considered as a healthy individual from an insurance point of view.
(ii) The after-treatment may be prolonged. The chief causes of delay in healing and continuance of the suppuration are sepsis and caries of some part of the bony wall, usually the promontory or floor of the tympanic cavity, or around the orifice of the Eustachian tube. In the former case the use of ear-baths of hydrogen peroxide or of rectified spirit, or frequent syringing of the cavity with a weak biniodide of mercury solution, and afterwards drying it and protecting it with gauze, may be sufficient to effect a cure. In the latter case the local condition must be treated.
Another condition delaying cure is reinfection from the throat through a patent Eustachian tube. In this case, although the mastoid cavity becomes lined with epithelium, mucous membrane may still cover not only the region around the Eustachian orifice, but the main portion of the tympanic cavity. The chief object in these cases is to close the orifice of the Eustachian tube. Sometimes this can be done by curetting under cocaine; in other cases by actual cauterization. After closure has been obtained, the cavity should be dried and gently packed with gauze impregnated with boric acid or aristol powder.
Again, cholesteatomatous formation may be the immediate cause of relapses. In these cases it is very difficult to remove all the diseased tissue. Even although the patient may apparently be cured, yet, unless kept under close observation, recurrence of cholesteatomatous masses take place, and frequently cause further caries of the underlying bone.
Finally, delay in healing may be due to careless after-treatment: if the cavity has not been properly packed, granulations spring up in the region of the aditus and gradually form a partition between the mastoid and tympanic cavities. If this takes place, further disease of the bone may occur owing to the retention of the secretion.
(iii) Symptoms may occur pointing to some intracranial complication, and further operation may become necessary.
With regard to hearing. The hearing power depends not only on the condition before operation, but also on the result of the after-treatment. The average hearing power after the removal of the malleus and incus is about 12 feet off for ordinary conversation. The same result should be obtained after the complete mastoid operation, provided there be no internal-ear deafness and provided the stapes be not already ankylosed within the fenestra ovalis. If the patient before operation hears conversation at a greater distance than 12 feet he should be told that the hearing power may be reduced to this amount. If, however, there be considerable deafness, due to polypi or granulations blocking up the tympanic cavity and auditory canal, the hearing power may be improved by the operation. The ultimate hearing depends on the condition of the stapes within the fenestra ovalis: if it remains freely movable, the hearing power may be extremely good. The great object, therefore, of the after-treatment is to prevent the inner wall of the tympanic cavity becoming covered with granulations which may become organized later into a fibrous pad covering the inner wall of the tympanic cavity, and thus prevent movement of the stapes and, in consequence, marked deafness. The prevalent idea that the hearing power is destroyed irrevocably, as a result of the complete operation, is quite wrong: equally so is the harmful statement that, as a result of this operation, complete restoration of the hearing can be obtained.
Labyrinthine suppuration usually occurs in the course of a chronic middle-ear suppuration; more rarely, as the result of tuberculous disease of the temporal bone, or in consequence of an acute middle-ear suppuration. In the latter case, however, it is a matter of experience that, although symptoms of labyrinthine suppuration may be present, they almost invariably subside as a result of drainage of the middle ear and mastoid. This is an important point which should be remembered, as otherwise the labyrinth may be explored unnecessarily at a considerable risk to the patient’s life.
The most frequent paths of extension of the pyogenic infection from the middle ear to the internal ear are through the external semicircular canal, the promontory, and the fenestra ovalis, the result of cholesteatomatous erosion, caries, or necrosis. Hinsburg, in 198 cases of labyrinthine suppuration, traced the infection in 61 cases. In 27 cases the infection had entered through the external semicircular canal, in 17 through the fenestra ovalis, in 7 through a fistula of the promontory, in 5 through the fenestra rotunda and ovalis, and in 5 through a fistula in the posterior or superior semicircular canal (Archives of Otology, 1902, vol. xxxi, p. 116).
Although operations on the labyrinth are practically limited to suppurative disease, yet under certain conditions they are justifiable when no suppuration is present.
These operations may consist in partial or complete opening of the semicircular canals, or of the vestibule, or in removal of the cochlea, or complete extirpation of the labyrinth.
(i) In non-suppurative labyrinthitis.
(a) To relieve vertigo. This operation is only justifiable if the condition cannot be cured by other methods, and is so distressing as to render the patient’s life unendurable.
In such cases it is first essential to make certain that the attacks of vertigo originate from some lesion within the semicircular canals. For this reason the other forms of vertigo must be excluded, and, in addition, there should be evidence of definite involvement of the labyrinth, such as falling over of the patient to the affected side, internal-ear deafness, or post-suppurative changes within the middle ear, suggestive that the internal ear has also become affected. It must, however, be remembered that it is possible, though extremely rare, for a lesion, limited to the semicircular canals, to produce marked vertigo without any deafness being present, in which case the operation will be limited to extirpation of the semicircular canals.
(b) To relieve tinnitus. If the tinnitus be unbearable and all other measures have failed to cure it, the question of extirpation of the cochlea, in order to destroy the nerve-terminals, may be discussed. This operation, so far, has not been completely successful, and therefore it cannot be recommended.
In this connexion it may be mentioned that, instead of attacking the cochlea, it has been proposed to divide the auditory nerve before it enters the internal meatus. Charles Ballance has recently described such a case.
The difficulty of this latter operation and the very slight chance of cure which it offers, owing to the tinnitus probably being central, are sufficient to raise the question as to whether such an operation is really justifiable.
(ii) In suppurative labyrinthitis. The object of the operation is to remove the infective focus and, by permitting drainage, to prevent further complications, such as meningitis or intracranial suppuration.
Before deciding the question of operation every means available should be used to determine: (1) whether the symptoms are merely the result of disturbance of the labyrinthine function in consequence of suppuration still limited to the tympanic and mastoid cavities; (2) whether the labyrinthine lesion is localized or general; (3) whether the labyrinthine suppuration is associated with some intracranial complication, more especially meningitis or cerebellar abscess.
Suggestive of labyrinthine suppuration are vertigo, vomiting, spontaneous nystagmus, and disturbances of the equilibrium. In the more acute cases there may be loud tinnitus, pyrexia, rapid onset of deafness (with inability to hear high tuning-forks and loss of bone conduction), facial paralysis, and deep-seated pain.
In addition much information may be gained by determining the character of the spontaneous nystagmus, if present, or whether nystagmus can be elicited by Bárány’s caloric tests.
(a) If the ear be normal, there is no spontaneous nystagmus.
If, however, the ear be syringed with water above or below the body temperature, a rotatory nystagmus will be obtained if the patient’s head is kept in the erect position, or a horizontal nystagmus if the patient is lying in the horizontal position with the face upwards.
Syringing with hot water causes a nystagmus directed towards the ear syringed; syringing with cold water, away from the ear.
(b) If there be a localized labyrinthine lesion, and the function of the labyrinth is still maintained, the same results will be obtained on syringing. Care, however, must be taken that the syringing is not forcible, otherwise the caloric tests will be unreliable, as in these cases nystagmus may be produced on even slight increase of pressure within the external auditory canal, and with this there may be a sensation of giddiness and nausea.
Spontaneous nystagmus, however, will probably be present, and will be directed towards the affected side. This spontaneous nystagmus is greatly modified by the caloric tests, being strongly exaggerated on syringing with hot water, and weakened or arrested on syringing with cold water.
(c) If the function of the labyrinth be destroyed, as in suppurative labyrinthitis, nystagmus will not be produced as a result of the caloric tests, but the spontaneous nystagmus, if present, will be directed towards the opposite, the normal side.
These various tests must be taken in combination with the symptoms, and frequently are of extreme value in deciding whether operation is indicated or not.
The chief difficulty is to exclude the possible existence of a cerebellar abscess (see p. 460). In favour of labyrinthine inflammation is complete internal-ear deafness, although this in itself does not exclude an accompanying intracranial lesion.
1. Immediate exploration of the labyrinth is indicated (provided there is internal-ear deafness):—
(a) If symptoms of acute labyrinthine suppuration occur in the course of a middle-ear suppuration, even although at the time of opening of the mastoid no definite fistula of the labyrinthine wall can be discovered.
(b) If symptoms of involvement of the labyrinth be present and a definite fistula is found on operation.
(c) If symptoms of a cerebellar abscess or of meningeal irritation be present in addition to those suggestive of a labyrinthine affection.
2. Opening of the labyrinth should be delayed if Bárány’s and other tests show that the labyrinth is not yet destroyed:—
(a) If, in spite of clinical symptoms pointing to involvement of the labyrinth, pus be found under tension within the tympanic cavity or the mastoid process.
(b) If the symptoms before operation consist only of attacks of vertigo and nystagmus, and on operation merely an erosion of the outer wall of the labyrinth (usually the external semicircular canal) is discovered.
In the above cases, if the symptoms be due to irritation of the labyrinth, a rapid recovery is to be expected as a result of the mastoid operation. If, however, they continue or become progressively worse, then the wound cavity must be reopened and the labyrinthine wall carefully examined and further operation undertaken.
The reader may again be reminded that although exploration of the labyrinth is indicated when it is certain that a suppurative lesion exists, yet it is a very serious mistake to open up a labyrinth not yet infected.
Although a great advance has been made in the last few years with regard to operations on the labyrinth, yet there is still much to be learnt, not only with regard to the indications for operation but the result obtained by operation. Now that operations on the labyrinth have become universal, the general tendency is to operate on the immediate occurrence of symptoms of labyrinthine irritation without waiting to see whether simple opening of the mastoid process will not be sufficient—a matter much to be regretted.
Surgical Anatomy. The facial canal, it will be remembered, extends horizontally backwards above the promontory, and passes downwards superficially to the inferior portion of the vestibule which lies between the fenestra ovalis below and ampullary ends of the external and superior semicircular canals above. The nerve then extends directly downwards towards the stylo-mastoid foramen, being situated deeply within the posterior meatal wall.
Of the semicircular canals the external is the most prominent, and the only one visible during the performance of the ordinary mastoid operation; its outer border forms the inner and lower boundary of the aditus, and can usually be recognized as a white eminence. The superior semicircular canal can only be seen on careful removal of the overlying bone; its ampullary end is found lying just above that of the external canal. It forms the highest point of the labyrinth, becoming fused with the innermost portion of the tegmen tympani, and is in such close relationship with the upper surface of the petrous bone as to cause a smooth elevation on its surface. It is at this point in the operation of removal of the semicircular canal that the greatest risk is encountered of breaking through the petrous bone and of injuring the dura mater.
The posterior semicircular canal lies at right angles to the external canal, and is best exposed by careful removal of bone just posterior to the latter (see Fig. 240).
The outer half of the first whorl of the cochlea is formed by the promontory. Anteriorly it is in close relationship with the carotid canal, whilst below it lies the dome of the jugular fossa. Medially the modiolus is only separated from the internal auditory meatus by a very fine rim of brittle bone, which can easily be broken; a mishap which may permit of escape of the cerebro-spinal fluid, and also of possible infection of the meninges through the internal meatus.
These operations may be divided into: (1) simple curetting away of a localized lesion of the labyrinthine wall; (2) opening up of the vestibule with removal of the semicircular canals; (3) opening of the cochlea; (4) a combination of these methods—extirpation of the labyrinth.
Curetting away of a localized lesion of the labyrinthine wall. It has been already stated that, provided the labyrinth be not yet destroyed, it is not justifiable to explore it on the mere discovery of an erosion of the semicircular canal. At the same time, if a definite fistula from which granulations protrude is present, a small fragment of bone may be chipped away, the granulations being afterwards removed by the curette. Unless pus is found to exude from the labyrinth, it is not necessary to do anything further at the present moment. If, however, at a later period, symptoms of labyrinthine infection occur, then it is necessary to further explore the semicircular canal and vestibule, the extent of the operation depending on what is discovered at the time of the operation.
Sometimes an examination of the tympanic cavity may be prevented before operation owing to the auditory canal being filled with polypi or granulations. On performing the complete mastoid operation and curetting away these granulations and polypi, a fistula may be found in the promontory, and carious bone may be felt on probing. Not infrequently these cases are tuberculous in origin and are accompanied by facial paralysis. Provided there be no labyrinthine symptoms, it is sufficient to curette out the granulations, but only gently. Violent curetting may break through the barrier between the infected area and the internal meatus and so lead to meningitis. It is wiser to curette too little than too much.
A further condition which may be met with is necrosis of a portion of the promontory, or of the walls of the vestibule, or of the semicircular canals. If the sequestrum be not quite loose at the time of operation, it should be left in situ, provided there be no intracranial symptoms. In fact, there is less danger in leaving the sequestrum than in attempting to remove it. After the operation, the wound cavity is kept open, so that the sequestrum can be removed at a later date after it has separated from the living bone.
Opening the vestibule (with partial or complete removal of the semicircular canals). This may be performed by one of the following methods:—
Above and behind the facial nerve through the semicircular canals. The complete mastoid operation is performed first. The chief difficulty is to expose the field of operation so as to obtain sufficient room for the necessary manipulations. To do this the following steps should be carried out: The tip of the mastoid process and the remains of the posterior wall of the auditory canal are removed to their extreme limit without injury to the underlying facial nerve. The floor of the auditory canal is also chiselled away until the lower level of the tympanic cavity is brought freely into view, the amount of bone removed depending on the anatomical condition found. To expose the anterior portion of the tympanic cavity, the skin incision is extended slightly forwards, but not far enough to wound the temporal artery, the soft tissues being then separated from the bone and the auricle pulled still further forwards and downwards.
Skin meatal flaps are now fashioned—either the Y-shaped flap or Stacke’s flap (see p. 403)—and are afterwards kept in position by means of sutures. Good illumination is necessary, and for this reason a head-light should be used. One assistant is employed to retract the soft tissues from the wound, another to keep it as dry as possible.
The exposed portion of the external semicircular canal is first identified. If the bone be soft, the arches of the semicircular canal should be defined (Fig. 240). The posterior canal will be discovered by gouging away the bone just posterior to the arch of the external semicircular canal, and the superior, by working inwards and upwards towards the roof of the attic. If the outline of the canals can be made out, the further steps of the operation are rendered very much easier. Unfortunately, the bone is sclerosed in the majority of cases, rendering anatomical exposure of the canals an impossibility.
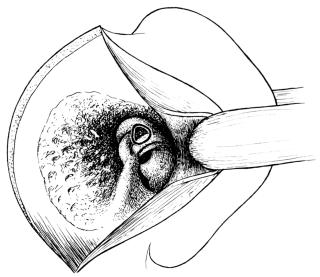 Fig. 240. Diagram to show Exposure of the Semicircular Canals. The
‘black ring’ shows the area at which the semicircular canals and
vestibule may be opened.
Fig. 240. Diagram to show Exposure of the Semicircular Canals. The
‘black ring’ shows the area at which the semicircular canals and
vestibule may be opened.
The next step is to remove the eminence of the horizontal semicircular canal. This is best done by means of a small gouge and mallet. Some prefer a burr, specially constructed to cut vertically; others a chisel. I prefer a fine gouge. As the facial canal runs along the lower anterior portion of the external semicircular canal, the gouge should be directed in a backward direction in removal of the outer wall of the latter, so as to cut away from the facial canal.
The surgeon should be content to remove the bone piecemeal, as, owing to its brittleness, it is very apt to splinter, or the point of the gouge itself may slip and so injure the facial nerve.
After an opening has been made into the canal, it should be enlarged by following the canal forward until its ampulla is reached. After this has been done, a fine probe, bent at a right angle (Schwartze’s seeker will do very well), is passed into the opening, and the limits of the vestibule made out as far as possible. The bone is then removed in an upward direction until the ampulla of the superior canal is reached. The opening may then be extended backwards so as to remove the outer wall of the vestibule, that is, the portion of bone which lies between the ampullæ of the superior and external canals.
If the bone be sclerosed, so that it is impossible to find the superior and posterior canals, then, after opening the exposed portion of the external semicircular canal, the bone should be chiselled away at the area marked out in Fig. 240. By this means the vestibule will certainly be reached, and from this point its opening can be extended in any given direction. A sufficient opening should be made so that the inner portion of the vestibule can be seen (Fig. 241). During each step of the operation a clear view must be obtained.
Not infrequently the facial nerve is exposed or pressed upon in chipping away the outer wall of the external semicircular canal, as will be shown by sudden twitchings of the face. If the surgeon be careful, and works in a direction away from the nerve, it should not be injured. If possible, the outer margin of the horizontal semicircular canal, together with the Fallopian canal, should be left intact as a bridge crossing the vestibule. If necessary, the external and superior canals can be removed in their entirety. A fine probe is inserted into the lumen of the canal so as to tell its direction, and its outer wall is then burred away. For this particular purpose a burr should be used as soon as the surgeon has got beyond the region of the facial nerve. After a view of the interior of the vestibule has been obtained, the ampullary nerves may be destroyed by means of the curette or with pure carbolic acid at the end of a probe. Removal of the posterior canal is best effected by opening it just behind the external semicircular canal and following it out in an upward direction until it meets the superior, and then downwards until it enters the vestibule. This extensive operation is one of extreme difficulty and seldom necessary.
Posterior to the semicircular canals: Neumann’s method. Neumann enters the vestibule posteriorly. The bone forming the inner wall of the antrum is removed by means of bone forceps or gouge and mallet until the posterior semicircular canal is opened. By this means the posterior surface of the petrous bone can be exposed as far inwards as the internal auditory meatus.
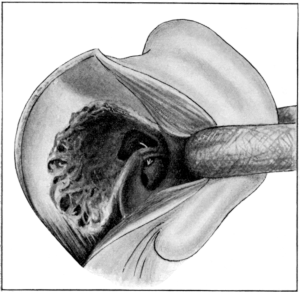 Fig. 241. Operation upon the Labyrinth. To show the opening into the
vestibule above the facial nerve with partial or complete removal of the
semicircular canals. The arrow passes behind the facial canal between
the vestibule and the fenestra ovalis.
Fig. 241. Operation upon the Labyrinth. To show the opening into the
vestibule above the facial nerve with partial or complete removal of the
semicircular canals. The arrow passes behind the facial canal between
the vestibule and the fenestra ovalis.
Below and anterior to the facial nerve through the promontory. The preliminary steps of the operation having been performed and the field of operation freely exposed, the stapes, if still present, is extracted by means of a small hook passed between its crura. The bridge of bone between the fenestra ovalis and fenestra rotunda is then cut through by light taps on a very fine gouge. The bone is removed by attacking the lower limit of the fenestra ovalis, and working downwards until the fenestra rotunda is reached. With a fine curette or scoop the loosened fragments of bone are removed. Care must be taken not to work above the region of the fenestra ovalis or the facial nerve will probably be injured. After a sufficient opening has been made, a bent probe can be passed through the opening in the promontory in an upward and backward direction behind the facial nerve into the inferior and anterior portion of the vestibule (Fig. 241).
Removal of the cochlea. If necessary, the first turn of the cochlea can now be removed by gouging away the promontory from behind forwards. If the anterior wall of the external auditory canal interferes with this being done, it may be partially removed by means of the gouge and mallet. After the first half-turn of the cochlea has been opened, its contents may be curetted out, care, however, being taken to avoid the carotid canal, which lies in close relationship with its anterior inferior portion. If the bone be carious only gentle curetting is necessary. If, however, this be not the case, simple curetting may not be sufficient, and the gouge and mallet may have to be used. To destroy the cochlear nerve, the whole of the cochlea should be removed. This is sometimes a difficult matter to determine. If the operation be done for the relief of tinnitus, then, after as much as possible of the cochlea has been removed, the interior may be swabbed out with strong carbolic acid solution, which should set up sufficient inflammatory reaction to destroy the nerve-terminals.
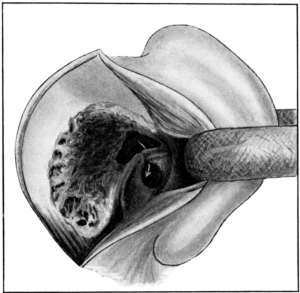 Fig. 242. Extirpation of the Labyrinth. The vestibule is freely opened
and the greater portion of the semicircular canals and cochlea is
removed.
Fig. 242. Extirpation of the Labyrinth. The vestibule is freely opened
and the greater portion of the semicircular canals and cochlea is
removed.
Extirpation of the labyrinth. This consists in the removal of the semicircular canals, and opening of the vestibule and cochlea, the steps of which have already been described in the above operations.
Before the operation is completed, the inner wall of the vestibule and the cochlea should be carefully examined for fistulæ, and in order to see if any pus enters these cavities from within. If this be the case it means that, in addition to labyrinthine suppuration, there is presumably an extra-dural abscess of the posterior intracranial fossa, drainage of which is essential in order to obtain a recovery.
After the operation has been completed, the cavity should be filled with hydrogen peroxide, then gently syringed out with weak biniodide solution, and finally dried and lightly packed with sterilized gauze.
Even although the operation may have been performed in a non-suppurative case, it is wiser to leave the posterior wound open for the first few days in order to permit of free drainage.
After-treatment. If the suppuration has been limited to the internal ear, a successful result may be expected if the symptoms subside rapidly as a result of the operation. If there be complete destruction of the labyrinth before operation its performance should give rise to no symptoms of shock nor further disturbance of equilibrium.
In the majority of cases, however, owing to the nerve-terminals being still in a state of activity, the irritation set up as a result of the operation may cause increased attacks of nystagmus, vertigo, and vomiting. The vomiting is the first symptom to disappear, and then the nystagmus; but complete recovery of equilibrium may not occur for a considerable period, during which time the patient, though otherwise well, may still have a slightly staggering gait.
If the operation has been limited to the external semicircular canal, and the hearing power still exists, the after-treatment should be carried out as already described in the complete mastoid operation. If, on the other hand, the cochlea has been interfered with, or if it be certain that there is no longer any hearing power, then there is no object in trying to preserve the patency of the tympanic cavity, which in this case may be allowed to granulate up from its depth like an ordinary surgical wound.
The immediate anxiety of the surgeon after the operation is the possible onset of meningitis or the presence of a cerebellar abscess, which will necessitate further operation unless otherwise contra-indicated (see p. 460).
Comparison of the operations. Opening of the vestibule above the facial nerve is limited to those cases in which the lesion is situated within the semicircular canals and to the posterior portion of the vestibule; that is, either in non-suppurative cases in which the operation is performed in the hope of curing vertigo, or in suppurative cases in which the function of hearing still exists.
Opening of the vestibule below the facial nerve is to be preferred as a rule, especially if the function of hearing is already destroyed, because it permits of drainage from the inferior part of the vestibule; in addition, by working forwards, the outer wall of the cochlea can be removed and any disease within it can be tracked out to its limits.
If there be suppuration within the cochlea, sufficient drainage will not be obtained by merely opening the vestibule through the semicircular canals, but the cochlea itself must be opened. Again, if the lower portion of the vestibule and cochlea be first explored and found filled with purulent secretion, it is wiser to complete the operation by also opening the vestibule from above,—that is, to completely extirpate the labyrinth, which is now functionally useless and almost certain to be infected throughout its whole extent.
Intracranial complications. If, in addition to the labyrinthine suppuration, intracranial suppuration be suspected, the labyrinth should be explored first; but when possible the operation should be arrested at this point to see if the symptoms subside. If they continue, the exploration of the intracranial cavity can then take place through the internal ear, after a delay of twenty-four hours or more.
Of the intracranial complications, meningitis is most frequent, and next in order cerebellar abscess. In addition, thrombosis of the bulb of the jugular vein may take place from infection through one of the smaller tributary veins; or a localized extra-dural abscess may be found situated along the posterior portion of the petrous bone in consequence of direct extension of the infection through the internal auditory meatus, or as a result of empyema of the endolymphatic sac. This latter condition is almost impossible to diagnose, but may be discovered accidentally if the vestibule is opened by the posterior route according to Neumann’s method.
Difficulties. The chief difficulties are anatomical, and the inability to obtain a clear view owing to general oozing of blood.
The first is generally due to insufficient removal of bone; the second can usually be controlled by means of good assistants and the frequent employment of hydrogen peroxide or of adrenalin solution.
Dangers. Injury to the facial nerve. This, as might be expected, is not infrequent. If a burr be used, the nerve may be completely torn across and permanent paralysis may result. If, however, the gouge and mallet be employed, complete recovery usually takes place, as the injury seldom consists in complete destruction of the nerve.
Opening up of the internal meatus. This may be accompanied by a gush of cerebro-spinal fluid. There is nothing to be done except to try and keep the part as clean as possible and see that there is free drainage. Undoubtedly, as a result of this mishap, death has afterwards occurred in consequence of septic meningitis.
Injury to the internal carotid or bulb of the jugular vein. These are possibilities which, however, should not occur if ordinary care is taken.
Prognosis. The prognosis of labyrinthine suppuration is always grave, owing to the frequency of intracranial complications.
The most favourable cases are those in which the disease is localized and is of chronic duration. The most unfavourable are those in which acute suppurative labyrinthitis is accompanied by extensive bone disease.
According to statistics, the mortality is about 50% in cases not operated upon. As a result of operation, this has been reduced to less than 20%, and in the majority of these cases the ultimate fatal result cannot be put down to the operation itself. The patient is frequently seen too late, that is, after intracranial complications have already occurred. There is no doubt that the death-rate will diminish proportionately according as the necessity of operating early becomes more and more recognized.
With regard to hearing, extensive operations upon the labyrinth lead to complete deafness; nor, indeed, can recovery of hearing be expected except in those cases in which the disease and operations have been limited to the semicircular canals and to the posterior portion of the vestibule, and even then recovery of hearing is exceptional.
As the intracranial complications of otitic origin are due to direct extension of the pyogenic infection through the temporal bone to the cranial cavity, it follows that they will depend on the extent of the disease within the temporal bone, the direction in which it has spread, and the virulence of the infection. For this reason, also, the site of the intracranial lesion is always in close relationship with the area of the diseased bone. Thus, if the infection spreads upwards through the attic and tegmen tympani, it may lead to extra-dural abscess or to meningitis of the middle fossa, or to a temporo-sphenoidal abscess. Similarly, disease of the mastoid cells posteriorly may give rise to a perisinuous abscess, to meningitis of the outer surface of the posterior fossa, to lateral sinus thrombosis, or to a cerebellar abscess situated superficially and involving the outer portion of its lateral lobe just behind the lateral sinus; or caries of the floor of the tympanic cavity may give rise to thrombosis of the jugular bulb; or internal-ear suppuration to an extra-dural abscess occupying the posterior surface of the petrous bone, to meningitis of the posterior fossa, or to an abscess of the cerebellum deeply placed in its anterior inferior angle.
Operation is always imperative unless the patient is seen too late and it is obvious that the condition is hopeless.
Before operation is decided on the following points must be carefully considered: (1) Is it possible that the symptoms simulating the intracranial lesion are due to suppuration still limited to the temporal bone? (2) What is the character of the lesion? and (3) What is its situation?
As a rule, so long as the suppurative process is limited to the middle ear and to the mastoid region, the symptoms are those of a local septic infection. At the same time it must be remembered that in infants and in young children it is not uncommon for retention of pus within the middle ear to produce a clinical picture closely simulating an intracranial suppurative lesion. The ear, therefore, should always be inspected in every case. Sometimes a bulging membrane is discovered or the existing perforation is found to be insufficient for drainage. In such cases the symptoms may subside on free drainage being obtained by the simple act of paracentesis of the tympanic membrane.
If, however, free drainage already exists, the mastoid operation should be performed at once.
If the intracranial symptoms be still somewhat indefinite, and there is no apparent urgency, the intracranial cavity should not be explored immediately unless this is found to be imperative at the time of operation. This can be done later, if the symptoms do not subside.
Although exploration of the intracranial cavity is always urgent when it is certain that an intracranial suppurative lesion is present, yet to explore with a negative result is a grave misfortune, owing to the possibility of infecting the intracranial cavity.
Although the surgeon may be certain that an intracranial lesion is present, yet it may be very difficult to determine its character or whether several lesions coexist. The surgeon must therefore be prepared to act according to what he finds at the time of operation.
Thus, if exploration of the temporo-sphenoidal lobe be negative, and yet the cardinal symptoms point to an intracranial abscess, the cerebellum must also be explored. Again, if the diagnosis of intracranial abscess be doubtful before operation, and if, during the operation, lateral sinus thrombosis be discovered, it is wiser to limit the operation to tying of the jugular vein and removal of the septic thrombus. The bone, however, should be removed above and behind the sinus so as to expose the dura mater covering the temporo-sphenoidal lobe and the cerebellum.
In such cases, if the symptoms of intracranial suppuration still continue, it is an easy matter to explore the temporo-sphenoidal lobe or cerebellum at a subsequent operation.
Although under exceptional circumstances (see p. 461) it may be justifiable to open an intracranial abscess by directly trephining the skull over it, yet free opening of the mastoid process should be the first step in the operation, as the primary focus of the disease exists within the temporal bone. In addition, much information may thus be gained in a doubtful case with regard to the situation of the intracranial lesion.
This is far more common as a sequel of acute than of chronic disease of the mastoid process.
Indications. Operative interference is indicated in order to permit of drainage. An extra-dural abscess is frequently discovered accidentally, especially if the surgeon follows out the golden rule to trace any patch of carious bone to its limit. In doing so he may suddenly meet with a gush of purulent discharge coming through an opening in the bone in the region of the tegmen tympani or sigmoid sulcus.
Although an extra-dural abscess may give rise to no special symptoms, the following are suggestive:—
1. If, in spite of opening up the mastoid cells and antrum, pyrexia and headache persist, especially if the headache be localized to the affected side and accompanied by tenderness on pressure above the ear or behind the mastoid process.
2. If, before operation, there be a very profuse discharge from the ear, apparently too copious to come from the tympanic cavity or mastoid antrum.
3. In children an extra-dural abscess may give rise to symptoms of cerebral irritation or compression if it extends upwards from the tegmen tympani along the parietal region; or, if situated in the posterior fossa, to retraction and stiffness of the neck.
Although such symptoms may be also associated with an intracranial abscess or meningitis, yet, if on exploration of the intracranial cavity a large extra-dural abscess be discovered, further operation may be postponed (unless its extension is obviously necessary) until time is given to see whether the symptoms will subside or not.
Operation. If the mastoid process has not been opened already, the simple or the complete operation is performed, according to whether the suppuration is recent and acute, or is of long standing.
If, however, this has been done, the wound is reopened, all granulations are curetted away, and the cavity is cleansed and dried.
The antrum and mastoid cavity are then thoroughly examined. If a fistula in the bone already communicates with the abscess, pus may be seen to ooze through it. If not, careful search is made for any carious tract of bone, which is now followed up until the dura mater is reached.
After the pus has drained away more bone is removed so as to expose the dura mater fully over the infected area, which is usually vascular or covered with granulations. The latter, however, should be left severely alone. If the abscess be situated in the middle fossa above the tegmen tympani, the bone is best removed by chiselling upwards until the lower margin of the squamous portion of the temporal bone is reached. Then, with a pair of bone forceps, more bone can be punched away quickly until a sufficient opening is obtained (Fig. 243).
Exploring with the probe and curetting away of granulations should be avoided as far as possible for fear of injuring the sinus. If its wall be already inflamed, it may be torn through, and the resulting hæmorrhage may render the further steps of the operation a matter of extreme difficulty.
Before completion of the operation, a blunt-pointed seeker should be passed round the edge of the opening in the bone to see that its margin is smooth and even, and all sharp edges of bone bordering on the dura mater should be removed. If this precaution be neglected, a splinter may get pressed inwards and injure the dura mater, and thus set up meningitis.
If possible the bone should be removed until the healthy dura mater is reached. If the extent of the abscess prohibits this, its limits, however, should be ascertained. This can be done by pressing the dura mater inwards with a spatula so as to separate it from the overlying bone.
The final step is to irrigate the cavity with warm boric or saline solution and to insert drains of gauze or of fine india-rubber tubing between the dura mater and bone. The wound cavity is then lightly packed with gauze and a simple dry dressing applied.
After-treatment. Provided there be no other intracranial symptoms, recovery should be as rapid as in the case of simple inflammation of the mastoid process. In the after-dressings, however, special care should be taken not to press in the gauze roughly or tightly against the still inflamed dura mater, in case of injuring its surface and causing further extension of the pyogenic infection to the meninges or lateral sinus. The dressings should be changed daily. It is sufficient to irrigate the wound with some mild aseptic lotion and afterwards to repack it lightly. If Schwartze’s operation has been performed, the after-treatment is similar to that already described (see p. 387). In the case of the complete operation, after the purulent discharge has practically ceased and the surface of the wound appears healthy, the packing of the cavity may be carried out through the meatus, instead of through the posterior wound, the latter being then allowed to close.
Intracranial complications. Infection of the lateral sinus is the most frequent complication, but meningitis, ulceration of the surface of the brain, or intracranial abscess may also occur.
One or more of these complications may already exist at the time of operation, but may not be sufficiently marked to warrant further exploration of the intracranial cavity. It is wiser, therefore, to give a guarded prognosis during the first few days after the operation, not only with regard to recovery, but also to the possibility of further operative procedures becoming necessary.
Formerly the onset of symptoms of meningitis was a distinct contra-indication to operation. More recently, however, this view has become modified, especially as it has been shown definitely by Macewen, Jansen, Brieger, and others that recovery is possible if operation is undertaken sufficiently early before the inflammation of the cerebral membrane has become diffuse.
In this connexion must be mentioned—(1) Serous meningitis: a name given to an increase of the cerebro-spinal fluid within the subdural or subarachnoid space, or the ventricles, the hypersecretion being probably caused, as Merkens suggests (Deutsche Zeitsch. für Chir., vol. lix), by the toxic infection induced by the suppurative focus in contact with the external surface of the dura mater. The symptoms of serous meningitis may closely simulate an intracranial abscess or a purulent meningitis, except that frequently there is no pyrexia. (2) Purulent meningitis, which may be diffuse or localized. (3) Pseudo-meningitis: that is, a condition simulating meningitis but in reality due to irritation of the meninges as a result of suppuration still confined within the temporal bone—for example, the result of acute middle-ear suppuration in infants.
Clinically it is often difficult to determine before operation which variety is present.
Indications. Operation is indicated as soon as the onset of meningitis has been diagnosed and should be performed without delay. Waiting for all the cardinal symptoms of meningitis to occur will never save life. The only possibility of doing so is to operate while the inflammatory process is still localized. At the same time it must be recognized that whenever symptoms of meningitis occur the prognosis is most serious.
Lumbar puncture should always be performed as an aid to diagnosis. If the cerebro-spinal fluid be clear and sterile, diffuse meningitis can usually be excluded, although at the same time it must be remembered that it does not negative a localized meningitis without increased intracranial pressure. Increased flow of cerebro-spinal fluid indicates increased intracranial pressure, perhaps the result of serous meningitis. Slight turbidity suggests early purulent meningitis, especially if bacteria are present, but not necessarily that the case is hopeless. If the fluid be definitely purulent, operation may be considered out of the question; a case, however, has been recorded in which recovery took place.
The value of cytological examination of the fluid is still doubtful. Marked increase of polynuclear cells is said to point to acute and intense inflammation, whereas an abatement of the polynucleosis may be taken as a sign of diminution of the meningeal irritation. With this, increased leucocytosis, increasing as recovery progresses, may be looked upon as a hopeful sign.
If it be obvious that the patient is dying, not only from the local infection but also on account of general septic absorption, operation, of course, is excluded. Similarly, at the present time, post-basic meningitis of infants is rightly deemed inoperable.
Operation. Although no set operation can be described, the principles of the operation are to expose the infected area widely so as to allow of free drainage and, at the same time, to relieve intracranial pressure. The extent of the operation will therefore depend largely on what is found during the course of the operation itself.
1. In an infant or young child, if the symptoms develop in the course of an acute otitis media, the tympanic membrane should first be inspected to see if there is sufficient drainage. If not, it should be freely incised, and opening of the antrum and mastoid may be delayed for at least twelve hours.
2. In an adult, immediate exploration of the mastoid and antrum is indicated on the onset of meningeal symptoms, even although they occur during the course of an acute middle-ear suppuration.
If the symptoms of meningitis in these cases be as yet indefinite, and if pus be found under tension within the mastoid cavity, or if an extra-dural abscess exists, the dura mater should not be incised at once, but a delay of twenty-four hours should be advised; in many cases complete recovery will take place. If, however, the symptoms continue, intracranial exploration will be necessary.
3. In chronic middle-ear suppuration, meningitis is usually secondary to, or accompanies, other intracranial complications or internal-ear suppuration, the symptoms of which it may mask.
After performing the mastoid operation any tract of carious bone is followed out to its limits.
According to what he finds, the surgeon may first expose the dura mater covering the lower portion of the middle fossa (Fig. 243), or of the posterior fossa behind and in front of the lateral sinus; these are the usual sites of infection. The removal of bone must be free, in order to get well beyond the limits of the infected area, if possible. The dura mater is incised to the limits of its exposure either crucially or by cutting it through in the form of a large flap.
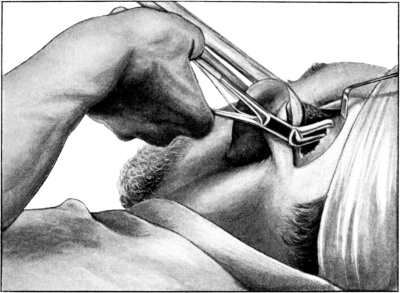 Fig. 243. Method of Removal of Bone by the Forceps. In this instance the
bone is being removed above the tegmen tympani in order to expose the lower
portion of the middle fossa.
Fig. 243. Method of Removal of Bone by the Forceps. In this instance the
bone is being removed above the tegmen tympani in order to expose the lower
portion of the middle fossa.
The dura mater is usually congested, but if an extra-dural abscess or lateral sinus thrombosis be present, it may be thickened and of a leathery appearance; or in the latter case almost gangrenous.
The further steps depend on the conditions met with on incision of the dura mater.
1. In serous meningitis a certain amount of clear fluid may escape and the brain surface may be only slightly congested. After removal of the bone and of the dura mater over the infected area the surface of the brain should be scarified in various directions to make certain that the pia-arachnoid has been incised, and fine drainage tubes should be inserted between the latter and the dura mater. In these cases a hernia seldom occurs, although the brain surface may bulge slightly into the wound.
2. In purulent meningitis the surface of the brain is usually covered with turbid fluid or purulent lymph, which may be localized to the site of the diseased bone, or may have spread from this point to a varying extent over its surface.
If the limit of the infection cannot be reached, in spite of removal of a considerable extent of bone and dura mater, all that can be done is to irrigate the exposed area with warm saline solution and to insert fine drainage tubes between the brain and dura mater, at the same time (as in the case of serous meningitis) incising the meninges in various directions.
3. Purulent lepto-meningitis is usually accompanied by encephalitis. If localized by adhesions an accumulation of pus may occur, forming an abscess on the surface of the brain, which also may be superficially ulcerated or necrosed. If there be intracranial pressure from encephalitis, the brain tissue usually protrudes as a dark, hæmorrhagic friable mass, in which shreds of necrotic brain tissue will be seen. In other cases, if there be no increased intracranial pressure and if the condition be quite localized, no hernia may occur, but the surface of the brain may be rough or eroded.
Any purulent secretion should be removed by irrigation, care being taken not to disturb the brain more than is necessary, so as to diminish the risk of breaking down the surrounding adhesions. A hernia may or may not form immediately. If no hernia takes place, it is wiser to do nothing further; that is, provided sufficient bone and dura mater have been removed to reach the limits of the infected area. Some authorities, however, consider that the necrosed portion of the brain should be curetted out. Although in other parts of the body the removal of necrosed tissue is a proper procedure, yet in the case of the brain there is considerable risk of setting up further œdema or septic cerebritis, the progress of which may have become arrested at the time of the operation.
If the inflamed brain tissue protrudes to an excessive degree during the operation itself, the opening in the skull should be enlarged, if it be not already of considerable magnitude, and the dura mater incised to the full limits of the opening. The protruding mass may then be cleanly excised by means of a scalpel. If, however, the brain tissue continues to prolapse, the wound cavity should be simply cleansed and protected by a dressing of sterilized gauze. If the encephalitis subsides, the hernia will not increase in size, and if the wound cavity be kept aseptic, it may gradually shrink.
After-treatment. This consists in covering the wound surface lightly with gauze so as to permit of free drainage, and changing the dressing as often as may be necessary.
In serous meningitis a large quantity of cerebro-spinal fluid may escape, and the dressings must be changed frequently. If recovery be going to take place, the temperature gradually becomes normal and the symptoms of meningitis disappear. In involvement of the posterior fossa, the head retraction gradually diminishes and after a few days free movement is noticed. Adhesions form rapidly, binding together the surface of the brain, meninges, and the overlying bone. For this reason the drainage tubes, already inserted between the dura mater and brain, can be removed within a day or two. The exposed dura mater usually becomes covered with granulations from which a certain amount of purulent discharge may be secreted. The duration of the after-treatment depends on the extent of the operation and the size of the wound. Eventually the skin flaps grow together and cover the brain, which afterwards may be felt pulsating through the scar. In these cases it is usually necessary to provide the patient with some protection, such as an aluminium plate.
If, however, a hernia forms and gradually increases in size, the brain should be explored again to see if another abscess can be discovered; or the lateral ventricle itself may be tapped in case of it being distended with fluid. Both these operations, however, must be looked upon as extreme measures.
If the patient otherwise recovers and a hernia still persists, the question arises what to do. Conservative treatment should first be employed, aseptic dressings being maintained, and slight pressure applied with compresses soaked in rectified spirits. If these measures fail, then the projecting portion of the hernia may be excised (see Vol. III).
Other methods. In addition, the following methods of treatment have been suggested. Although many failures have occurred in proportion to the few successful cases published, yet they show the possibility that something can be done by operative measures, and that considerable advance has been made in recent years in this direction.
(i) Repeated lumbar puncture. In a few cases of serous meningitis this has proved successful in that it has relieved intracranial pressure. It is, however, only of value if free communication still exists between the spinal theca and subarachnoid space.
(ii) Continuous drainage from the spinal canal. Friedrich, of Kiel, has suggested a counter-opening in the spinal canal by means of laminectomy in order to permit of drainage of the entire dural sac.
(iii) Puncture of the lateral ventricle. The temporo-sphenoidal lobe is pierced with a trocar, just above the zygomatic ridge, until the ventricle is reached; this has been performed frequently in order to relieve intracranial pressure. I know of only one recorded instance in which recovery has taken place in spite of there being pyogenic infection of the lateral ventricle; a fact which was proved by tapping the ventricle and removing from it a drachm and a half of purulent fluid (Archives of Otology, vol. xxxv, p. 535).
(iv) Drainage through the internal ear. West and Scott have recently described a case of meningitis which occurred after having curetted the inner wall of the tympanic cavity. They then opened up the labyrinth and inserted a wire drain through the internal auditory meatus, at the same time making a counter-opening in the lumbar region, through which they drained the spinal canal. The patient, a child, ultimately recovered.
Prognosis and after-results. Unless saved by operation, meningitis is almost uniformly fatal. Even if the patient recovers, whether as the result of operation or not, deaf-mutism or mental deficiency frequently occurs. In a few cases, however, complete recovery has taken place.
The sigmoid portion of the lateral sinus is the part usually infected. Thrombosis, however, may occur primarily in the region of the jugular bulb from direct extension of the pyogenic infection through the floor of the tympanic cavity; this, though less frequent than involvement of the sigmoid sinus, is not so rare as has hitherto been supposed.
Operative treatment is imperative as soon as septic thrombosis of the sinus has been diagnosed. This, however, is not always an easy matter. Sometimes, indeed, there are no clinical symptoms, the condition perhaps only being discovered whilst performing the complete mastoid operation as a prophylactic measure. The sinus is generally exposed accidentally whilst following out a tract of carious bone, and, to the surprise of the surgeon, pus or granulations may be seen to exude or protrude from an opening in its outer wall. On further exposure of the sinus on each side of the thrombus, the dura mater may appear to be of a dark colour for a short distance, but beyond this to be of normal appearance.
Seeing that there are no symptoms, the presumption is that the sinus is occluded on each side of the septic thrombus by a non-infective clot. It is, therefore, sufficient in such cases to simply excise the sinus wall over the septic area. If the case be so treated, it is essential that the sinus should only be curetted gently over the exposed opening, but otherwise left undisturbed. Also this limited operation should only be performed if the surgeon is satisfied that the septic focus is surrounded on each side by an organized normal clot—the condition in fact being treated as a simple abscess.
To secure free drainage, only the depth of the mastoid wound should be packed with gauze, the surface being protected by a simple dry dressing. The after-treatment is the same as that already described for the complete mastoid operation in which the posterior wound has been left open.
In other cases, if there be an acute inflammation of the mastoid process and if only one rigor has occurred, it may not necessarily mean that thrombosis of the sinus has taken place, as the rigor may be due simply to septic absorption. In such cases it is justifiable to delay opening the sinus if it is found to be exposed within the wound cavity and to be covered with granulations.
The bone, however, should be freely removed until the normal dura mater is reached, and the cavity afterwards rendered as aseptic as possible by syringing it out with hydrogen peroxide lotion. In a large proportion of cases a favourable result occurs, the pyrexia and head symptoms disappearing and an uneventful recovery taking place. On the other hand, gradually increasing pyrexia or a sudden rigor may occur, perhaps not until ten days or so after the primary operation, showing that the sinus has become infected after all. It should then be opened at once, but before doing so the jugular vein should be tied (see p. 448).
In a typical case, however, there is a history of repeated rigors, and in addition there may be attacks of vomiting and headache localized to the affected side, with pain and tenderness on pressure behind the mastoid process, and optic neuritis. In the more severe cases there may also be evidence of thrombosis of the jugular vein or cavernous sinus. It must, however, be remembered that a high and intermittent pyrexia, especially in children, may take the place of rigors. The principles of surgical treatment are to expose the sinus and remove the infective clot completely.
In connexion with this operation two points cannot be impressed too forcibly on the reader:—
1. The operation must be performed at once. The greater the experience of the surgeon the more he realizes that expectant treatment is nearly always fatal, and that a successful result depends largely on early and complete operative measures.
2. Before the sinus is interfered with in any way it is essential to obliterate its lumen below the thrombus in order to prevent any portion of it being swept into the circulation during its removal.
Indications. (i) In doubtful cases to decide whether thrombosis exists or not.
(ii) As a preliminary to opening the sinus with or without ligature of the jugular vein.
Operation. The first step is to perform the complete mastoid operation, except in the case of acute inflammation of the mastoid process, when Schwartze’s operation will be sufficient.
To expose the field of operation more freely, an incision an inch or more in length is made horizontally backwards, beginning at the mid-point of the posterior margin of the primary incision (Fig. 216), the soft parts being reflected upwards and downwards from the bone, and the flaps so formed being then retracted. Above, the bone should be exposed beyond the level of Reid’s base-line, which roughly corresponds to the line of the transverse sinus; below, the tip of the mastoid should be cleared until the mastoid vein is reached. If it be thrombosed it may be assumed that the lower part of the lateral sinus is also thrombosed. Bleeding from the bone at this point may be arrested by temporarily plugging the foramen with a fragment of sterilized wax.
The condition found on opening the mastoid process varies considerably. If the result of acute inflammation of the mastoid process, the mastoid cells surrounding the sigmoid sinus usually contain pus or granulations, on removal of which a fistula may be seen to communicate with the outer wall of the sinus; or the bone around the sigmoid groove may already be destroyed, with free exposure of the sinus within the wound. With this there is frequently an extra-dural abscess. In other cases, if the infective process has been very virulent, evil-smelling pus, sometimes intermixed with bubbles of gas, may escape on chiselling through the mastoid cortex. This is a sure sign of extensive disease, the sinus wall often being gangrenous and the bone surrounding it necrosed and discoloured.
If occurring in the course of a chronic middle-ear suppuration, very little disease of the mastoid process may be found except along the path by which the infection has spread.
After the sinus wall has been reached, sufficient bone should be removed to expose its outer surface for at least half an inch above and below the supposed infected area.
The decision as to whether thrombosis exists or not may have to be made during the operation itself, and is based partly on the appearance of the sinus wall and partly on the symptoms, the relative value of each varying in each individual case.
Normally the sinus pulsates and is of a bluish-grey colour. If thrombosed, the wall of the sinus may be of a yellow or dark colour and may not pulsate, but neither discoloration nor the absence of pulsation is an absolutely reliable sign of thrombosis. Again, if the sinus be covered with granulations or purulent lymph, it is sometimes impossible to say whether it is thrombosed or not, especially if the clot is limited and parietal. Further, the thrombus may be situated low down towards the jugular bulb, so that if it has not extended very far upwards the exposed portion of the lateral sinus may still be normal in appearance. Palpation of the sinus with the finger or aspiration with a hollow needle is sometimes advised as an aid to diagnosis. These procedures, however, are extremely unwise, owing to the risk of dislodging a small fragment of the infected clot, which may easily occur if the latter does not obliterate the sinus completely. As a means of diagnosis the withdrawal of blood by the aspirating needle is of no value, as it does not negative the presence of a parietal thrombus, owing to the possibility of the needle passing through it into the free lumen of the sinus.
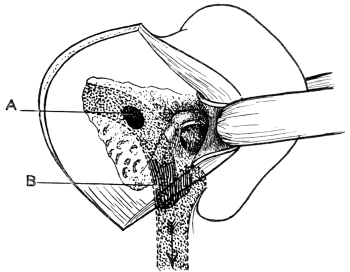 Fig. 244. Diagram to show the usual Points at which the Lateral Sinus is
primarily infected. A, High up; from the posterior mastoid cells. In
this case it may not be necessary to tie the jugular vein. B, Low down;
involving the jugular bulb. This necessitates ligature of the vein.
Fig. 244. Diagram to show the usual Points at which the Lateral Sinus is
primarily infected. A, High up; from the posterior mastoid cells. In
this case it may not be necessary to tie the jugular vein. B, Low down;
involving the jugular bulb. This necessitates ligature of the vein.
Indications. The sinus should always be opened as soon as it is certain that septic thrombosis has occurred.
Contra-indications. The only contra-indication for opening the sinus and removing the thrombus is the certainty that either the patient’s general condition will not permit of the operation being performed, or that the septic thrombosis has spread beyond the region from which it is possible to remove it.
For this reason, operation is unjustifiable if the patient is already suffering from septic pneumonia, pericarditis, or acute septicæmia; or, on the other hand, if there are symptoms of cavernous sinus thrombosis on both sides, or general meningitis. If, however, the patient’s general condition be good, operation may be attempted as a last resource even although a pulmonary empyema or a one-sided cavernous sinus thrombosis already exists.
Operation. After exposure of the lateral sinus, the next point to determine is the site and extent of the infected area (Fig. 244). On this will depend whether it will be necessary or not to tie the jugular vein in the neck.
The sinus is first exposed towards the jugular fossa until its surface appears normal for at least half an inch. It is wiser, however, always to expose the sinus as low down as possible. A strip of sterilized gauze is then pressed in between the bone and the outer wall of the sinus so as to obliterate its lumen at this spot. Instead of removing the bone from above downwards, the sinus may be exposed first at its lowest limit by chiselling directly through the tip of the mastoid process. In this way it can be obliterated by a strip of gauze before attacking the area of infection. The overlying bone is afterwards removed from below upwards until the thrombosed area is reached.
In removal of the bone from above downwards there is a certain risk of small particles of clot being dislodged into the circulation, or, if the sinus wall is injured, of hæmorrhage taking place if the thrombus at this particular point does not completely occlude the sinus. If, however, the sinus be first exposed and obliterated at its lowest limit, these risks are greatly minimized. There is no special technique in removing the bone beyond that already given in the description of the complete mastoid operation.
The next step is to expose the lateral sinus behind the infected area and follow it backwards until the dura mater appears normal for at least three-quarters of an inch. If necessary, the skin incision must be prolonged still farther backwards, in order to permit of removal of the bone overlying the transverse sinus, which may, perhaps, have to be exposed even to the torcular Herophili.
In removing the bone overlying the infected thrombus, the gouge and chisel should be used rather than the bone forceps or burr. With the latter there is greater risk of dislodging particles of clot into the circulation, owing to pressure of the instrument on the sinus wall.
After the sinus has been exposed well beyond the region of the thrombus, the bone forceps may safely be used, especially in exposure of the transverse sinus; and this is a much more rapid method than removing the bone by means of the gouge and mallet. To prevent the inner blade of the forceps from nipping the sinus wall between it and the bone, the dura mater forming the outer wall of the sinus should be separated from the overlying bone by means of a dura mater separator. In the region of the infected area the sinus wall may be adherent to the bony wall as a result of the inflammatory adhesions, and, in addition, may be extremely friable and so easily torn through.
In exposure of the sinus two points should be remembered: firstly, that it is sometimes difficult to differentiate it from the dura mater covering the temporo-sphenoidal lobe above and the cerebellum below; and secondly, that the transverse sinus is a very much broader vessel than is imagined, being even half an inch in width. Not much force is required to obliterate its lumen, but care must be taken to pack the gauze evenly across its whole width.
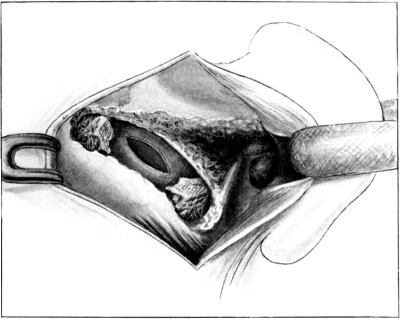 Fig. 245. The Lateral Sinus exposed and opened. The lumen of the sinus is
obliterated above and below the region of the infected thrombus by plugs of ribbon
gauze pressed in between the sinus wall and the overlying bone. In this case it is
not necessary to tie the jugular vein.
Fig. 245. The Lateral Sinus exposed and opened. The lumen of the sinus is
obliterated above and below the region of the infected thrombus by plugs of ribbon
gauze pressed in between the sinus wall and the overlying bone. In this case it is
not necessary to tie the jugular vein.
After the sinus has been occluded above and below the area of infection, it should be incised with a small knife along its whole length between the obstructing plugs of gauze (Fig. 245). If there be bleeding, it may be due to the sinus being obliterated incompletely, or it may come from the superior petrosal sinus. To find out where the bleeding comes from, the finger should be pressed upon the sinus at its upper and lower limits, close to the obstructing plugs of gauze. If the bleeding stops, it shows that the sinus has not been obliterated completely; this can now be done by further plugging with gauze. If, in spite of this, bleeding still continues, it presumably comes from the petrosal sinus.
All clot and granulations are now rapidly curetted out and the lateral sinus plugged with gauze. After a moment the gauze is withdrawn and another small piece is pressed into the lateral sinus at the point of entrance of the petrosal sinus. After the bleeding has been arrested, the outer wall of the lateral sinus is excised by cutting it away with blunt-pointed scissors. The interior of the sinus is then inspected, special attention being given to the lower portion to see if its lining is normal. If this be not the case, even if there be no signs of thrombosis, it means that the surgeon has failed to get well below the infected area, and therefore the internal jugular vein must be ligatured. If, however, it be normal, the gauze plug already placed between the sinus wall and the overlying bone is left undisturbed.
If there be no bleeding from the sinus (excepting a slight amount from the blood contained within the isolated portion), the thrombus is curetted out and the inner surface of the sinus inspected. After excising the outer wall, search is made for the superior petrosal sinus, which presumably is thrombosed, although perhaps only by normal clot. To expose this tributary, which enters the lateral sinus at the point at which it turns downwards to form the sigmoid sinus, bone must be removed in front of the lateral sinus along the angle forming the roof and inner wall of the mastoid and antrum; that is, along the superior margin of the petrosal bone. If the inner surface of the lateral sinus in its neighbourhood be normal, nothing need be done. If, however, the sinus wall be infected, the petrosal sinus should be followed out, if possible, its outer wall being incised and the clot removed, bleeding being afterwards arrested by pressure.
As a final step, the gauze plugging which still obliterates the lumen of the sinus in its upper part is removed. If the sinus be normal at this point, free hæmorrhage will occur; this is arrested at once by again introducing a strip of gauze between the sinus and the bone. Although during the earlier stages of the operation the inner lining of the posterior portion of the sinus may have seemed to be normal, yet it occasionally happens that hæmorrhage does not at once occur on removing the plug of gauze; but after a moment or two a long smooth clot, gradually tapering at its end, may be shot out from the opening within the sinus, being followed by a gush of blood. The terminal portion of this clot is non-infective and of recent formation. Its appearance is always a matter of satisfaction, as it means that the sinus has been freely exposed and opened behind the infected area.
If on exposure of the sinus it be found that the clot extends so low down that it will be impossible to obliterate the sinus well below the infected area, the jugular vein should be ligatured at once before interfering further with the sinus from the mastoid wound.
Attempts to remove the clot from the jugular bulb by curetting out the sinus from above are only referred to to be condemned. The surgeon who believes in this method hopes that all the infected portion of the clot will be swept out by the flow of blood. It is not, however, always possible to introduce a curette into the jugular fossa, and if the clot extends beyond this region it cannot be curetted away completely. The result of the operation does not depend so much on the skill of the surgeon as on whether the terminal portion of the clot be infected or not. Recovery is most likely to take place if a non-infective clot already extends beyond the region of the curette and so obliterates by natural means the lumen of the vein below the point reached by the surgeon. If, on the other hand, free hæmorrhage occurs as a result of the curetting, it means that the lumen of the vein has been restored, but there is no guarantee that all the clot has been completely removed. If any infective portion remains, a fatal result will almost certainly occur eventually as the result of pyæmia.
Indications. Unfortunately, opinion is not unanimous with regard to this matter. The chief arguments raised against ligature of the jugular vein are: (1) That it favours extension of the thrombus along the veins communicating with it, especially along the inferior petrosal and condyloid veins, which enter the jugular bulb. (2) That it in no way prevents the spread of infection along other paths, owing to the freedom with which its tributaries communicate with one another. (3) As a result of obstruction in the circulation, acute inflammation of the cerebellum may take place.
Since the jugular vein should only be ligatured if the symptoms point to the onset of a general infection of the circulation and if it be found impossible at the time of operation to obliterate the sinus below the infected thrombus, and since this vein is the chief route by which this infection takes place, it seems a matter of common sense that it should be ligatured. At the same time, as many as possible of its tributaries above the point of ligature should also be ligatured well beyond the point at which they may be thrombosed.
Although extension of the infection may take place along other veins after ligature of the jugular vein, it is impossible to say whether the result is post or propter hoc. Against ligature, statistics have been quoted to show that in a series of cases in which the jugular vein has not been tied the percentage of recoveries is just as high as in those in which it had been ligatured. This argument is not quite sound, because there is no doubt that in the cases in which ligature of the jugular vein is justified the chances of recovery, owing to the extension of the thrombus downwards, must be less than in the less serious cases in which it is admittedly unnecessary to tie the vein. It is also impossible to say how many cases would otherwise have ended fatally if ligature had not been performed.
In the majority of cases the vein is ligatured after exploration of the lateral sinus. In a few cases, however, the symptoms warrant it being performed as a primary step of the operation, even before the mastoid process has been opened.
After exposure of the lateral sinus. (i) If the clot extends so low down that it is impossible to obliterate the lumen of the sinus below its lower limit.
(ii) If there be thrombosis of the bulb of the jugular vein. This condition is sometimes difficult to diagnose. There may be no symptoms excepting, perhaps, rigors occurring during the course of chronic middle-ear suppuration, as even the lower portion of the sinus may be quite normal in appearance owing to the clot being limited entirely to the jugular bulb. The probability of the diagnosis being correct is strengthened by the presence of granulations or carious bone on the floor of the tympanic cavity. It is better to risk tying a normal vein than to fail to tie one already infected.
(iii) If the sinus was obliterated above the jugular bulb at the primary operation and rigors occur subsequently, showing that the sinus is infected still lower down.
Before exposure of the lateral sinus. (i) If there be thrombosis of the jugular vein. In addition to the ordinary signs of lateral sinus thrombosis, there may also be infiltration of the tissues, or tenderness along the anterior border of the sterno-mastoid muscle. The prevalent idea that a thrombosed jugular vein can be felt on palpation as a hard cord extending down the neck is erroneous. If anything be felt it is probably some enlarged cervical glands lying along the line of the vein. In any case it is bad practice to palpate the internal jugular, as by doing so there is considerable risk of dislodging particles of the septic clot.
(ii) If, as a result of septic infection, the general condition of the patient be so serious that a prolonged operation seems unjustifiable. In such cases, the lateral sinus is rapidly exposed and incised after tying the internal jugular, its contents are curetted out and the wound cavity lightly plugged; the completion of the operation, consisting of the opening up of the mastoid cells and antrum, and possibly also exploration of the intracranial cavity, may be performed next day or later.
(iii) If it be doubtful whether septic thrombosis of the sinus has already occurred, it is justifiable in certain cases merely to expose the sinus freely and not to open it (see p. 440). If rigors subsequently occur in these cases and it becomes evident that the sinus has become infected after all, then it is wiser to tie the jugular vein as a primary step of the operation before opening up the sinus itself.
The writer’s reason for doing so is, that at the second operation he has always found the clot to be extensive, or, at any rate, to be situated so low down as to prevent the sinus being obliterated below the infected area.
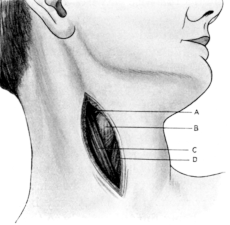 Fig. 246. Incision for Exposure of the Internal Jugular Vein. The
illustration shows the superficial structures. A, Common facial vein;
B, Fascia covering the hyoid bone; C, Anterior border of the
sterno-mastoid muscle; D, Omo-hyoid muscle.
Fig. 246. Incision for Exposure of the Internal Jugular Vein. The
illustration shows the superficial structures. A, Common facial vein;
B, Fascia covering the hyoid bone; C, Anterior border of the
sterno-mastoid muscle; D, Omo-hyoid muscle.
Operation. Formerly it was considered sufficient to divide the vein between two ligatures and to leave it in situ. Now, however, the upper portion of the vein is brought out through the wound in the neck after this has been done.
The patient lies in the recumbent position with the affected side close to the edge of the table. The head and shoulders should rest on a hard pillow in such a fashion that the neck is slightly extended, the chin being drawn upwards and the head turned a little to the opposite side so that the anterior border of the sterno-mastoid muscle can be clearly defined throughout its whole length. The surgeon stands at the side to be operated on. The neck is carefully cleansed, but in doing so care should be taken not to rub the neck too violently, nor should any attempt be made to palpate the line of the jugular vein in the hope of feeling it. There is no object in doing so, and if it is thrombosed a portion of the clot may be dislodged.
An incision, at least three inches in length, is made along the anterior border of the sterno-mastoid muscle, the mid-point of the incision corresponding to about the level of the cricoid cartilage. On cutting through the skin and platysma some small veins may be met with: they should be clamped with forceps and divided. If, however, the anterior jugular vein be exposed, it should be drawn to one side, if possible, and not divided. The anterior border of the sterno-mastoid muscle is clearly defined, until the upper border of the omo-hyoid muscle is reached (Fig. 246). Its edge is then drawn slightly outwards by means of a retractor and separated from the underlying deep fascia. Beneath this fascia is the carotid sheath, which encloses not only the carotid artery but the internal jugular vein and the vagus nerve. The vein is external and somewhat superficial to the artery, and the vagus nerve lies behind. A vein of varying size will be seen crossing obliquely downwards and outwards to pierce the deep fascia at a level corresponding to the cornua of the hyoid bone; this is the common facial vein about to enter the internal jugular (Fig. 247). If the surgeon has not had much experience and has difficulty in finding the jugular vein, a certain method of doing so is to find the facial vein and then follow it down until it enters the jugular. The carotid sheath should be opened about this point, and the position of the vein ascertained by feeling the pulsations of the carotid artery. The sheath of fascia covering the jugular vein is picked up with a pair of fine forceps and cut through with a sharp scalpel, which should be inclined obliquely outwards so that the flat of the knife is held towards the vessel. Any enlarged lymphatic glands lying over the vein must be removed.
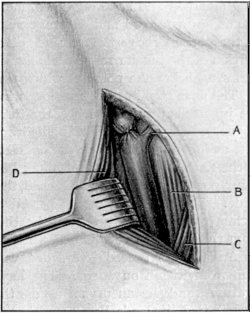 |
Fig. 247. Exposure of the Internal Jugular Vein high up. A, Common
facial vein; B, Sterno-hyoid muscle; C, Omo-hyoid muscle; D, Anterior
border of the sterno-mastoid muscle retracted outwards. A ligature is
placed around the jugular vein just above the common facial vein. When
the jugular is ligatured at this spot it is not necessary to tie the
facial vein. In actual practice the vein, of course, would be tied and
cut between two ligatures, the upper portion of the vein being brought
out into the neck.
|
When the vein has been identified, a blunt dissector is passed between its outer wall and the sheath, so as to separate the two. The sheath is incised upwards and downwards until the vein is freely exposed. If the vein be patent, it will be of a bluish colour, expanding and diminishing in volume with each act of respiration. If it be thrombosed, there is usually accompanying periphlebitis which may make the separation of the sheath from the vein and the surrounding tissues difficult. If there be no periphlebitis, the thrombosed portion may be purplish, or, if the clot be of long standing and breaking down, more of a yellowish colour; the vein stands out as a cord and does not pulsate. If the thrombus be limited to the portion above the entrance of the common facial vein, the upper portion of the jugular may be small and collapsed, only becoming full and pulsating below the point at which the facial joins it.
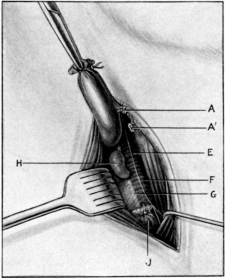 Fig. 248. Ligature of the Internal Jugular Vein low down in the Neck.
The upper portion of the vein is dissected out and brought into the
neck. A, A', Cut ends of the ligatured facial vein; E, Descendens noni
nerve; F, Carotid sheath and internal carotid artery; G, Vagus nerve;
H, Gland; J, Lower end of the internal jugular vein. The hook pulls
aside the omo-hyoid muscle.
Fig. 248. Ligature of the Internal Jugular Vein low down in the Neck.
The upper portion of the vein is dissected out and brought into the
neck. A, A', Cut ends of the ligatured facial vein; E, Descendens noni
nerve; F, Carotid sheath and internal carotid artery; G, Vagus nerve;
H, Gland; J, Lower end of the internal jugular vein. The hook pulls
aside the omo-hyoid muscle.
The next step in the operation is to get well below the point at which the jugular is thrombosed. If the thrombus be practically limited to the jugular fossa the vein may be ligatured above the common facial; if not, as low down the neck as possible. In ligaturing the vein low down in the neck, the skin incision must be extended downwards, and as the lower portion of the neck is reached, the omo-hyoid will have to be pulled aside. The probe should be passed all round the vein so as to make certain that it is freed from its sheath, and especially that it is separated from the vagus nerve which lies behind it.
An aneurysm needle threaded with silk is now passed around the vein from within outwards. The loop of silk is cut so as to form two ligatures, and the aneurysm needle then withdrawn; the lower ligature is first tied, its ends being cut short. The upper ligature is then tied a short distance above it, but in this case the ends are left long. The vein is raised from its bed by slight traction on this ligature and is cut across between the two, the lower portion being allowed to sink back into the wound. The upper portion is then carefully separated for some distance upwards. Lying behind the vein may be seen the vagus nerve (Fig. 248). Any tributaries are clamped between two forceps, cut across, and ligatured, the upper end of the vein being brought out into the upper angle of the wound. Care must be taken that enough of the vein is dissected out to allow of this being done, especially if the ligature is applied above the level of the common facial; in this case the facial need not be tied.
If there be no periphlebitis, inflammation of the soft tissues, or thrombosis of the vein itself in the neck, the wound may be closed by means of silkworm-gut sutures, excepting at its upper angle through which the open end of the jugular vein projects. If, however, the vein be thrombosed, and especially if there be periphlebitis, the wound should be left open, except perhaps at its lower angle, and should be lightly packed with gauze, as in these cases cellulitis of the neck may afterwards occur.
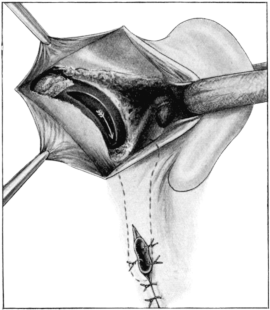 Fig. 249. Free Exposure of the Lateral Sinus, which has been incised,
with Ligature of the Internal Jugular Vein. The lateral sinus is
obliterated posteriorly by a plug of gauze pressed in between its outer
wall and the underlying bone. The sinus is freely exposed almost down to
the jugular fossa. The vein has been ligatured and its upper portion
sutured to the skin wound in the neck. The arrow shows the direction
along which the sinus and vein are syringed.
Fig. 249. Free Exposure of the Lateral Sinus, which has been incised,
with Ligature of the Internal Jugular Vein. The lateral sinus is
obliterated posteriorly by a plug of gauze pressed in between its outer
wall and the underlying bone. The sinus is freely exposed almost down to
the jugular fossa. The vein has been ligatured and its upper portion
sutured to the skin wound in the neck. The arrow shows the direction
along which the sinus and vein are syringed.
After completion of the operation in the neck the surgeon turns to the mastoid process. If the ligature of the vein has been the primary step, the mastoid operation is now performed and the lateral sinus is freely exposed for a considerable distance behind the thrombus. If, however, the mastoid operation has been the first stage, and the jugular has been tied as soon as exposure of the sinus showed it to be thrombosed, the operation on the mastoid is now completed and the sinus opened as already described (see p. 444). The next step is to incise the sinus freely from above downwards towards the jugular fossa and curette out the thrombus.
If there be considerable hæmorrhage, it means that the thrombus is probably parietal and situated within the jugular bulb, the bleeding presumably coming from the inferior petrosal sinus or other tributaries which enter the bulb or upper portion of the jugular vein. If the bleeding be excessive, the sinus is plugged after a moment or two, by inserting a piece of gauze into its lumen towards the jugular bulb.
In this case the portion of the vein brought into the neck is usually also filled with blood. After isolating it from the deeper tissues by packing strips of gauze round it, the vein is deliberately opened just above the ligature. The bleeding usually stops after a moment or two, but if it cannot be controlled, the lumen of the vein must again be closed by a ligature, the end of the vein being allowed to project on to the neck.
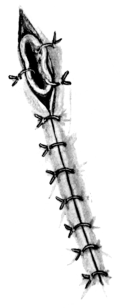
If there be no bleeding from the lower portion of the lateral sinus and jugular bulb, it means that the vessel is completely thrombosed at this point. The clot should now be removed by curetting through the sinus from above downwards towards the jugular bulb, and also from below upwards through the open end of the jugular vein.
The venous channel is afterwards syringed through from above downwards. To do this, a piece of rubber tubing is inserted into the opening in the lateral sinus and some warm saline solution is injected through it with a syringe. If the clot be not firmly adherent it can usually be washed out through the opening in the vein. No force should be used. If gentle syringing be not sufficient to expel the clot, the attempt must be given up. The chief objection against syringing is the possibility of particles of the septic thrombus being forced into the veins communicating with the jugular bulb. A small drainage tube is inserted within the sinus.
In order to keep the lumen of the vein in the neck open, it should be stitched to the edge of the wound surface by several catgut sutures (Fig. 250). If the bleeding necessitated plugging of the lower end of the sinus and retention of a ligature on the vein in the first instance, syringing should be postponed until the first dressing; the portion of the vein left protruding through the skin wound in the neck is then cut across, and the edge of the vein sutured to the margin of the wound under cocaine.
The mastoid cavity is lightly plugged with gauze and a dry dressing applied. The wound in the neck is similarly treated.
After-treatment and progress of the case. There is frequently considerable shock after the operation, especially if exposure of the jugular bulb has been undertaken, partly owing to the duration of the operation and to hæmorrhage. If the patient be very collapsed, a continuous saline injection, to which some brandy may be added, may be given per rectum according to Moynihan’s method. After the primary shock has passed off, the immediate result is usually satisfactory.
If the jugular vein has not been ligatured, the first dressing should be performed within forty-eight hours, the gauze packing being removed, the wound syringed out, and afterwards repacked. The plugs of gauze, which were pressed in between the outer wall of the sinus and the overlying bone in order to obliterate the lumen of the latter, should not be interfered with for at least six days. If the case progresses favourably, the temperature becomes normal within a day or two, the patient feels well, and the wound assumes a healthy appearance. If, on removal of the gauze plugging, hæmorrhage takes place, then the plugging must be renewed and not touched again for three or four days. After it is possible to remove these plugs, the wound is treated as has already been described in Schwartze’s operation or in the complete operation in which the posterior wound was left open.
If the jugular vein has been ligatured, the sinus and vein should be syringed through daily, and this should only be stopped after all secretion has ceased, usually a matter of a week or ten days.
When the sinus, jugular bulb, and vein have been exposed throughout their length the wound is treated as an ordinary surgical one, being packed until it granulates up from the bottom (vide infra).
Apart from intracranial and pyæmic complications, the progress of the case may be delayed owing to the enfeebled and septic condition of the patient, and also from the occurrence of abscesses in the neck, or region of the mastoid itself. These abscesses are the result of septic thrombosis occurring in some tiny vessel. The first sign of their occurrence is an attack of pyrexia, shortly followed by a painful swelling at the affected spot. Any collection of pus should be drained at once. Although it is quite good practice to close the incision in the neck in a clean case, yet there must be no hesitation to open it up on the slightest sign of it becoming septic.
The case may appear to progress favourably for the first week or ten days, and then an intermittent and increasing pyrexia may occur for no obvious reason. This is usually due to extension of the infection along the petrosal sinuses, or perhaps along the transverse sinus.
Symptoms of involvement of the cavernous sinus may arise, perhaps even with formation of a peri-orbital abscess; or, on the other hand, the patient may gradually sink in consequence of septic toxæmia; or the end may come more suddenly with the onset of basal meningitis. Unfortunately, these cases are almost hopeless from the first, as very little can be done from a surgical point of view owing to the fact that they are not seen soon enough.
In thrombosis of the cavernous sinus the only hope of recovery lies in its exposure and incision of its wall. The sinus may be approached by tracking forwards the superior petrosal sinus—a matter of considerable difficulty, and seldom justifiable. Recently Charles Ballance has suggested the adoption of the Hartley-Krause route for extirpation of the Gasserian ganglion, and says he has found the operation easy and effectual. If pus be evacuated from the sinus he considers it advisable to adopt the recommendation of Voss, who cuts away the zygoma and removes more bone from the basal aspect of the skull so as to get direct drainage (Allbutt and Rolleston’s System of Medicine, 1908, vol. iv, Part ii, p. 495).
This may be performed either by following the sinus downwards or through the floor of the auditory canal and tympanic cavity. The former method was first described by Grunert (Archiv für Ohrenheilkunde, 1902, vol. liii, p. 287); the latter by Piffl (Archiv für Ohrenheilkunde, 1903, vol. lviii, p. 76).
Indications. The object of the operation is to remove the septic clot situated within the jugular bulb in the hope of preventing extension of the infection along the veins leading into it, more especially the inferior petrosal sinus. This indeed has been known to occur even after the lateral sinus has been curetted out, the jugular vein ligatured, and the venous channel syringed through.
Grunert’s operation. After free opening of the mastoid process and exposure of the outer wall of the lateral sinus, the skin incision is extended downwards beyond the tip of the mastoid. The soft tissues are then separated from the bone forwards and backwards so as to expose completely not only the mastoid process, but also the digastric fossa and base of the skull immediately behind it, up to the outer bony margin of the jugular foramen. Unless care is taken, the forcible traction forwards of the soft tissues necessary to expose the field of operation may injure or tear the facial nerve as it emerges from the stylo-mastoid foramen.
The tip of the mastoid process is removed first. The lateral sinus is then freely exposed to its lowest possible limit by removing the overlying bone. In doing this it must be remembered that the sinus becomes horizontal just before it ends in the jugular fossa, so that at this point the skull forms its floor instead of its outer wall.
After having exposed the sinus as freely as possible, the ‘bridge’ of bone separating it from the outer wall of the jugular foramen is removed in small pieces by nipping it away with narrow biting forceps until the jugular bulb is exposed from its outer surface. The facial nerve should not be injured, as it lies in front and external to the portion of the bone to be removed.
In performing the later stages of the operation, the patient’s head should be turned well over to the opposite side in order to get a good view of the parts lying behind and beneath the mastoid process; and in tracking the sinus downwards, the probe should be used carefully in order to try and define the exact position of the jugular fossa.
Piffl’s operation. Owing to the anatomical difficulty of reaching the jugular bulb by following the sigmoid sinus downwards, especially in those cases in which the sinus lies far forwards and in which, at the same time, there is a very well-developed jugular fossa, Piffl recommends exposure of the jugular bulb from above through the auditory canal. The object of this method is to prevent injury to the facial nerve, which he states is almost certain to occur in Grunert’s operation, if carried out in cases such as those just mentioned.
After the complete mastoid operation has been performed, the skin incision is extended downwards and forwards in order that the soft tissues may be freed from the floor and anterior surface of the bony portion of the auditory canal as far forward as the Glaserian fissure. The soft tissues are pulled forward with a blunt hook to give sufficient room. The lower portion of the tip of the mastoid is removed by means of the gouge, as far as can be done without injuring the facial nerve, which in this operation is pulled backwards with the soft tissues at the posterior inferior margin of the wound. The lower bony margin of the auditory canal, now freely exposed, is removed by means of a pair of fine biting forceps until the floor of the tympanic cavity is reached. If there be not sufficient room, the bone may be clipped away as far as the styloid process, which also may be removed by bone-forceps after the muscles attached to it have been dissected off.
In freeing the styloid process, its posterior surface must be approached with caution for fear of injuring the facial nerve, which here lies in close connexion with it. In the front of the wound the capsule of the temporo-maxillary joint may be exposed, but must not be interfered with.
After removal of the styloid process, the uppermost portion of the external jugular vein should be seen emerging from the jugular fossa. This is followed upwards by careful removal of the bone between it and the floor of the auditory canal and tympanic cavity, until the jugular bulb is brought into view. This part of the operation must be proceeded with very cautiously, the bone being nibbled away in small fragments with gouge forceps which are of sufficient strength to nip through the bone without having to wrench it away. The amount of bone to be removed and the difficulty of the operation depend largely on the anatomical condition found.
Whether Grunert’s or Piffl’s operation has been employed, the operation may be completed either by incising the outer wall of the sinus and jugular bulb, then curetting out the thrombus, and finally washing through the lower portion of the vein from above downwards, or by the more radical method of also exposing the upper portion of the jugular vein throughout its whole length. To do this the post-aural incision is continued downwards until it joins the one previously made in the neck. To obtain room, the neck must be somewhat extended and the jaw pulled well forward and the sterno-mastoid muscle backwards. The jugular vein is then dissected upwards towards the bulb.
The nearer the jugular fossa is approached the deeper and more difficult becomes the exposure of the vein. Passing in front of it may be found the stylo-pharyngeal, stylo-hyoid, and digastric muscles. In Grunert’s operation they need not be cut through as the vein will lie posterior to them. In Piffl’s operation these muscles probably have been already reflected forward, after removal of the styloid process.
Particular care must be taken not to injure the nerve trunks, which are in such close relationship with the vein. Lying immediately behind the vein is the vagus nerve; the spinal accessory passes downwards and outwards behind it, and the glosso-pharyngeal and hypoglossal nerves forwards between the vein and the internal carotid artery.
After the vein, the jugular bulb, and the sigmoid sinus have been exposed throughout their course, their outer wall is cut through with a pair of blunt-pointed scissors along its whole length, so as to convert the venous canal into an open gutter. The thrombus is then curetted out and the dissected portion of the jugular vein cut off as high up as possible. Any bleeding from the inferior petrosal sinus or condyloid veins, which may not be thrombosed, should be arrested by direct pressure of a strip of gauze over the bleeding points. The wound cavity is then washed out with a weak biniodide solution and dried.
The lower portion of the incision in the neck may be closed with sutures and a small drainage tube inserted at its lower angle. The upper portion of the wound, now directly continuous with that of the mastoid cavity, is left open and packed lightly with gauze, which is inserted into the remains of the venous channel.
Comparison of operations for lateral sinus thrombosis. Except when the thrombus is limited to the upper part of the sigmoid sinus, it is undoubtedly wiser to tie the jugular vein than to be content with curetting out the clot after obstructing the sinus above and below by means of gauze plugs. Exposure of the jugular bulb is so difficult an operation and requires so much time, especially if the whole length of the upper portion of the jugular vein is also dissected out, that it is seldom advisable to perform it; nor will it often be justifiable owing to the condition of the patient, who is seldom strong enough to undergo such a prolonged operation. The records of this particular operation are so few that it is impossible as yet to determine its value.
If the sinus be exposed as low down as possible, and the jugular vein dissected out and brought out into the neck, and the venous channel afterwards syringed through, the chances of recovery should be almost as good as in the case of free exposure of the jugular bulb.
If the inferior petrosal sinus be already infected before the operation, it does not matter whether the operation performed is that of syringing through the jugular bulb or freely exposing it, as in either case the inferior petrosal sinus cannot be followed out.
Curetting of the lower portion of the sinus without previous ligature of the jugular vein should never be done.
Difficulties and dangers of the operation. The chief difficulty in these operations is anatomical; the chief danger is hæmorrhage.
If the hæmorrhage be due to accidental tearing of the wall of the sinus in the earlier part of the operation, and if it be impossible to obliterate the sinus below this point by pressing in gauze between its wall and the underlying bone, then the jugular vein should be tied before anything else is done.
Extreme vascularity of the bone is not unusual after ligature of the jugular vein. In these cases the surgeon must rely on the cleverness of the assistants in keeping the field of operation clear by careful swabbing.
In exposure of the jugular vein there may be difficulty in finding the vessel, especially if the cervical glands are enlarged, or if there be matting together of the tissues in consequence of periphlebitis or cellulitis. In these cases the best plan is to identify the common facial vein and then trace it down to its entrance into the jugular vein.
With regard to the sinus, the chief danger is injury of its inner wall whilst curetting out its contents: this may afterwards give rise to meningitis or a cerebellar abscess. Accidental pricking of a non-thrombosed jugular vein may allow of entry of air into the vein and so cause death: this is a catastrophe I have not yet met with. Also, if the operator be careless or inexperienced, he may injure the carotid artery or vagus nerve; in the former case the only thing to do is to ligature the artery above and below the wound.
Complications. The chief intracranial complications are meningitis and cerebellar abscess; the former usually from extension of the septic thrombosis along the petrosal sinuses. If, at the time of operation, it be doubtful whether intracranial suppuration already exists or not, the surgeon should content himself with removing the septic thrombus from the sinus and await further symptoms. At the time of the operation, however, sufficient bone should be removed to expose the dura mater over the cerebellum. If, in addition to the clinical symptoms, the appearance of the dura mater, the increased intracranial tension, and the absence of palpation suggest the presence of an abscess, the cerebellum should then be exposed and explored (see p. 467). Before doing this, the wound should be made as aseptic as possible and a fresh set of sterilized instruments used.
The complications resulting from general septic infection are pyæmia and septicæmia.
Prognosis. The prognosis depends entirely on whether the septic focus can be completely removed or not. Failure to do this is frequently due to the operation not having been sufficiently extensive. It is a matter of experience that if a second operation has to be performed recovery seldom takes place. For this reason the first operation must be thorough.
If such cases could be operated on in the earliest stage whilst the infective thrombus was still limited, without doubt a higher percentage of recoveries would be obtained. Unfortunately, the surgeon may not be summoned until too late, owing to the seriousness of the condition not having been realized.
In any individual case it is impossible to tell for the first few days after the operation what the ultimate result will be. Without operation a fatal termination is practically certain. As a result of operation about one-third of the cases may be expected to recover.
An intracranial abscess, the result of disease of the temporal bone, is usually situated close to the surface of the brain, and is in close relationship with the diseased area of bone through which the infection has taken place. The actual track of the infection can frequently be traced through the bone to the dura mater and brain substance itself; sometimes, indeed, a fistula is found to pass through the bone and to communicate with the intracranial abscess. On the other hand, though rarely, the surface of the bone to all appearances is normal and there are no adhesions between it and the dura mater and underlying brain substance, and the abscess may be situated deeply within the brain.
With regard to the comparative frequency of temporo-sphenoidal and cerebellar abscess, in 100 cases collected from the records of the London Hospital the writer found that in children under ten years of age temporo-sphenoidal abscess occurred in 87% and cerebellar only in 13%, whereas in adults cerebral abscess occurred in 65% and cerebellar in 35%; and that a cerebral and cerebellar abscess occurred together only in 5% of the cases.
These statistics are practically the same as Körner’s (Die otitischen Erkrankungen des Hirns, der Hirnhäute und der Blutleiter). Ballance, on the other hand, considers cerebellar abscess a more frequent occurrence than temporo-sphenoidal.
Multiple abscesses may be met with, usually the result of pyæmia.
Indications. An intracranial abscess must always be opened and drained.
Indications pointing to such a condition are persistent headache, purposeless vomiting, a slow pulse, a subnormal temperature, and optic neuritis. With this there is usually some change in the mental condition, especially in the case of a temporo-sphenoidal abscess. In the early stages there may be attacks of simple forgetfulness or mental aberration, or, on the other hand, that of extreme mental excitement. Owing to the intracranial pressure caused by the increase in size of the abscess, the mental state becomes impaired and the condition known as slow cerebration or the ‘dream state’ may be observed.
It must, however, not be forgotten that the same clinical picture may be produced by other conditions, such as an intracranial tumour: in the case of a middle-ear suppuration, however, an intracranial abscess may be diagnosed unless this can otherwise be excluded.
Before operation is decided on, the site of the lesion must be determined. This can only be done if certain localizing symptoms are present.
In a temporo-sphenoidal abscess, if the cortical region be affected, there may be paralysis or paresis of the opposite side, beginning with the face and then spreading to the arm and leg; or in the opposite order if the internal capsule be involved.
If the left temporo-sphenoidal lobe be the site of the lesion, aphasia may be met with, and if the abscess extends backwards, word-blindness may occur. If the centre of hearing be affected there may be complete deafness of the opposite side owing to its destruction; or tinnitus or hyperacusis if the centre be only irritated by the proximity of the abscess; or if the anterior extremity be involved anosmia or parosmia may be noticed. Another important sign, occurring in conjunction with the above symptoms, is a fixed pupil on the affected side.
In a cerebellar abscess the symptoms are less marked, or may even be absent, so that the abscess may remain undiagnosed during life and only be discovered at the autopsy, which may perhaps have been performed on account of the sudden and unexpected death of the patient from rupture of the abscess itself. In walking, in addition to a peculiar staggering gait, there is a tendency for the patient to direct his course gradually towards the affected side. Lateral nystagmus, if present, is usually directed towards the affected side and has to be differentiated from that due to internal-ear disease. If a cerebellar abscess be associated with a labyrinthine suppuration and the latter is explored by operation, the nystagmus will still remain directed to the affected side. If, however, no cerebellar abscess be present the labyrinthine operation will be followed by nystagmus strongly directed to the opposite side. Optic neuritis and vomiting usually are more severe than in temporo-sphenoidal abscess. Headache, if present, may be referred to the occipital region, and there may also be slight retraction of the neck or pain behind the mastoid region as a result of localized and early meningitis of the posterior fossa. If the abscess be very large, there may be paresis or paralysis of the facial nerve and perhaps also of the upper extremity. The deep reflexes may also be altered, the knee-jerk being frequently absent on the affected side. The patient in the late stage usually lies curled up in bed on the side opposite to the lesion, with the knees flexed.
Methods of operation. Two methods may be employed:—
1. Trephining directly over the area of the abscess (rarely necessary).
2. First performing the mastoid operation and then following out the route of infection (usual method).
In the case of middle-ear suppuration, trephining has practically been abandoned, and rightly so, since it has become recognized that the intracranial abscess is due to direct extension of the pyogenic infection from the middle-ear and mastoid cavities.
The only circumstances in which trephining may be advised are—(1) If the diagnosis be certain and the operator has no experience of aural surgery. In a case of emergency he is wiser, perhaps, to trephine and drain the abscess, leaving the mastoid to be dealt with afterwards by someone competent to do so. (2) If, after performing the mastoid operation, the situation of the abscess be doubtful. In order to diminish the risk of infection of the brain by an exploratory puncture which may prove negative, the bone may be trephined a little beyond the mastoid wound, either above or behind, according as a temporo-sphenoidal or cerebellar abscess is suspected. If, however, it be considered advisable to make a fresh opening in the bone beyond the septic wound cavity, the aural surgeon will probably prefer to do so by means of the gouge and bone-forceps, to which he is more accustomed.
Trephining has also been advised if the patient is so ill that a prolonged operation is impossible; or if there is cessation of respiration during the operation itself, which may occur in a cerebellar abscess as a result of pressure on the medullary respiratory centres. To those accustomed to perform the mastoid operation, the opening of this cavity and the necessary removal of bone can be done more rapidly by the gouge or bone-forceps than by the trephine.
For whatever reason trephining is done, it is afterwards essential to perform the mastoid operation and to remove the primary focus of the disease, otherwise one of the fundamental principles of surgery will be neglected.
Operation. The preliminary preparation of the patient is the same as for the mastoid operation, only the head should be shaved over a wider area. The exposure of the field of operation is the same whether the brain is explored through a trephine opening or from an extension of the mastoid operation.
In the case of the temporo-sphenoidal lobe, it is necessary to extend the incision behind the auricle vertically upwards for an inch or more (Fig. 252); whereas if the cerebellum has to be explored, an incision is carried backwards at right angles to the post-aural incision, just below its mid-point (Fig. 253). In the former case, on reflecting the soft tissues from the underlying bone, the squamous portion of the temporal bone, immediately above the zygomatic ridge, will be exposed; in the latter, the base of the skull behind and below the mastoid process and lateral sinus will be laid bare.
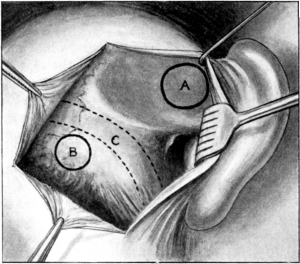 Fig. 251. Topography of the Auditory Region of the Skull. A, Point of
trephining for a temporo-sphenoidal abscess; B, For a cerebellar
abscess; C, Dotted line marking a portion of the lateral sinus.
Fig. 251. Topography of the Auditory Region of the Skull. A, Point of
trephining for a temporo-sphenoidal abscess; B, For a cerebellar
abscess; C, Dotted line marking a portion of the lateral sinus.
1. Trephining. The trephine used should be three-quarters of an inch to one inch in diameter according as the patient is a child or an adult. Either the hand trephine or Macewen’s improved pattern mounted with a guard may be used. If available, the trephine may be worked by a motor, but in this case it should be remembered that the bone will be pierced more quickly than by the hand instrument.
Trephining for a temporo-sphenoidal abscess. The object of the operation is to expose the lowest portion of the middle fossa just above the roof of the antrum and tympanic cavity. The trephine, therefore, should be placed so that it is situated just above the suprameatal spine, its lowest margin being slightly above the zygomatic ridge (Fig. 251). After the disk of bone has been removed the exploration of the abscess is then carried out.
Trephining for a cerebellar abscess. The point at which the bone is trephined must be behind and below the curve formed by the transverse and sigmoid portion of the lateral sinus; that is, behind the mastoid process and below Reid’s base-line.
If the mastoid operation has not been performed, the centre pin of the trephine should be placed at a point 1¼ to 1½ inches behind the centre of the external auditory meatus, and an inch below Reid’s base-line (Fig. 251). If, however, the mastoid has already been opened and the lateral sinus exposed, the trephine should be placed so that its anterior border is just behind the sinus and its upper border well below Reid’s base-line.
2. After performing the mastoid operation. If this has been done already, the wound is reopened, and cleansed by filling it with hydrogen peroxide. After gently curetting away any granulations the wound cavity is irrigated and then packed in order to dry it. Under good illumination, careful inspection is made to see if a fistula or a tract of diseased bone extends in any direction. Whether the middle or posterior fossa should first be explored depends not only on the clinical symptoms but also on the condition found on opening the mastoid cavity.
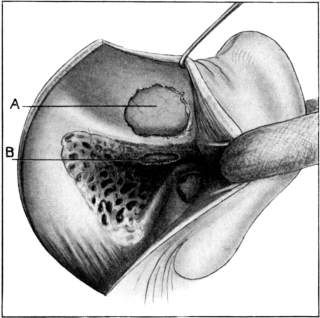 Fig. 252. Exploration for a Temporo-sphenoidal Abscess. A, Above the
tegmen tympani; B, Through the tegmen tympani. Occasionally these
methods are combined; the bone between the openings being also removed.
Fig. 252. Exploration for a Temporo-sphenoidal Abscess. A, Above the
tegmen tympani; B, Through the tegmen tympani. Occasionally these
methods are combined; the bone between the openings being also removed.
Opening of a temporo-sphenoidal abscess. A temporo-sphenoidal abscess may be explored either through its lowest point, that is, through the roof of the antrum and floor of the middle fossa, or through its outer wall just above the zygomatic ridge. To obtain a view of the roof of the antrum and mastoid cavities, the head of the patient should lie almost flat on the operating table and be turned well over to the opposite side. The bony roof of the antrum and mastoid is removed by means of the gouge and mallet, and so expose the dura mater covering the floor of the middle fossa (Fig. 252). If a fistula communicates with the antrum cavity and the middle fossa, the bone surrounding it is first attacked. In removing the bone, it must be remembered that the tegmen tympani is exceedingly thin, and unless care is taken pieces of bone may be pressed inwards on to the overlying dura mater. Sufficient bone should be removed to determine whether the dura mater is normal or not. To do this it may be necessary to chisel away the tegmen tympani outwards until the squamous portion of the temporal bone is reached, after which a pair of bone forceps may be used until a sufficient opening is obtained.
The condition found on examination of the dura mater varies. In many cases it is congested or covered with granulations at the site of the infection, and usually it is adherent to the underlying bone. At other times it seems normal.
Increase of the intracranial pressure, as shown by the bulging outwards of the dura mater, and absence of pulsation are suggestive of an abscess. These signs, however, are not conclusive, as on the one hand increased intracranial pressure may be due to other causes and on the other it is quite possible to have pulsation if the abscess be small and deeply placed.
If an extra-dural abscess be present, the intracranial cavity should not be explored at once unless this is absolutely necessary, but this step of the operation should be delayed for at least twenty-four hours. If, however, immediate operation be necessary, special precautions must be taken to render the part as aseptic as possible, and a fine layer of gauze should be packed between the margin of the bone and the dura mater in order to prevent further infection of the brain or meninges. In an uncomplicated case only sufficient bone should be removed to permit of the insertion of a large drainage tube; that is, the dura mater should not be exposed over a larger area than the size of a shilling.
If there be disease of the tegmen tympani and the symptoms point to a temporo-sphenoidal abscess, the brain should be explored through this opening in the bone (Fig. 252), as the abscess is thus not only drained through its most dependent part, but also through its stalk.
If, however, the diagnosis be doubtful, the temporo-sphenoidal lobe may be explored through a fresh opening, just above the tegmen tympani. This will diminish the risk of septic infection from the mastoid cavity. After the dura mater has been exposed sufficiently a small incision is made in it, taking care to avoid wounding any of the vessels. With a pair of forceps the cut edge of the dura mater is drawn outwards and the incision is prolonged in each direction with a pair of blunt-pointed scissors. Similarly, the dura mater is cut through at right angles to the primary incision, so that four small flaps are made and turned back so as to expose the outer surface of the brain.
As a rule the dura mater, arachnoid, and pia mater are fused together by inflammatory adhesions, so that from a practical point of view they need hardly be considered as separate structures. Similarly, at the site of infection, the point of the so-called stalk of the abscess, the cerebral membranes are adherent to the underlying brain, especially if there has been any localized meningitis. For this reason it is sometimes necessary to peel away the dura mater from the brain, in order to expose the latter.
As a rule, very little fluid escapes: if present in considerable quantity, and if it escapes from between the dura mater and brain, it is an unfavourable sign, as it generally signifies early meningitis.
If meningitis be present, purulent lymph or secretion may be seen on the surface of the brain, either localized or spreading from the site of the infection.
If the intracranial pressure be great, the brain will bulge through the opening in the dura mater. If the abscess be very large and situated superficially, the thin layer of brain substance forming its outer wall may rupture as soon as an opening has been made in the dura mater. Sometimes, indeed, the pus may be seen to ooze through an opening in the dura mater, which may be found to communicate with the abscess cavity.
The next step is to open the abscess. Formerly a trocar and canula were used. This method is no longer in favour for the following reasons:—If the wall of the abscess cavity be very thick, it may not be pierced; secondly, the trocar may pass through the abscess cavity and enter the brain substance beyond without draining it; and thirdly, even if the trocar enters the abscess cavity the pus may be so thick as to plug its lumen. For these reasons a fine pair of Lister’s sinus-forceps or a narrow-bladed bistoury is recommended. In the ordinary case Lister’s forceps can be used.
The direction in which the brain is explored depends upon the point at which this is done. Thus, if the procedure be carried out through the tegmen tympani, the brain is explored in an upward direction. The forceps are made to pierce the brain for about an inch; the blades are then slightly dilated and the forceps partly withdrawn. If a large abscess exists, the cavity is usually opened at once and pus flows out along the track of the forceps. If the abscess be small and deeply placed, its cavity may not be entered on the first thrust of the forceps. In this case they are closed and withdrawn. The brain is then explored by thrusting the forceps first upwards and forwards, then upwards and backwards, and finally upwards and inwards; in the latter case it is unwise to pierce the brain for more than an inch and a quarter for fear of entering the lateral ventricle.
If the brain be explored through the outer wall of the temporo-sphenoidal lobe, the first direction in which this is carried out is directly inwards. If this be not successful, the brain is further explored in a direction forwards, upwards, or backwards, the exploratory instrument at the same time pointing slightly inwards.
If exploration proves negative, it may also be necessary to explore the cerebellum. If, however, the surgeon be still convinced that a temporo-sphenoidal abscess exists, he may next pierce the brain with the bistoury, in case the forceps has failed to enter the abscess cavity, perhaps owing to its walls being very thick. If all efforts fail to find the abscess, the little finger may be inserted into the brain itself to see if the resistant wall of an abscess can be felt. This procedure, however, should be avoided if possible, as by doing so it causes destruction of a certain amount of brain tissue.
If an abscess be opened a varying quantity of pus escapes, usually evil smelling. In the more chronic cases it is thick and greenish; in the acute cases it may contain shreds of necrosed brain tissue or be intermixed with bubbles of gas. Sometimes there is also an escape of turbid cerebro-spinal fluid, which if excessive is suggestive either that the lateral ventricle has been opened inadvertently or that the abscess has already burst into it. In these cases the patient is usually comatose or in the state of muttering delirium at the time of the operation.
After the abscess has been opened, the forceps or bistoury should be retained in position until the pus has drained away. A large tube is then pushed into the abscess cavity along the line of the forceps or bistoury. It is only permissible to withdraw the instrument with which the abscess has been opened after the end of the tube is well within the cavity. The outer end of the tube should be flush with the surface of the wound. To prevent it slipping too far into the brain, it may be anchored to the edge of the skin wound by a silkworm-gut suture. If the abscess be drained through the tegmen tympani, it will be difficult to bring the tube out into the wound without kinking it. For this reason I prefer to incise the brain substance slightly outwards after the abscess cavity has been reached, so that a tube can be inserted obliquely upwards and inwards at a point corresponding to the angle between the tegmen tympani and the squamous portion of the temporal bone. If the exploratory puncture has been made above the tegmen tympani and an abscess discovered, the question arises whether another drainage tube should not also be inserted into the brain through an opening in the roof of the antrum so as to drain the abscess from below. This, however, I do not think necessary.
In addition to the rubber tube, many varieties of drainage tubes have been suggested, such as decalcified chicken bone, as originally used by Macewen, and glass or silver tubes; the object of the latter being to resist the pressure of the brain, which may compress a rubber tube. The rubber tube is the simplest form of drainage, and if sufficiently thick it should be employed. To make more certain of free drainage, some surgeons use two tubes placed side by side. I think, however, one large tube (half an inch in diameter) is better than two small ones.
Irrigation of the abscess cavity is still a matter of opinion. If the abscess be small and circumscribed, the best method is to open it with as little disturbance as possible to the surrounding parts, insert a large drainage tube, and to do nothing further.
If, however, the abscess be large and irregular in shape, so that the drainage is not free, and especially if it be very septic and contains necrosed brain tissue, irrigation is justifiable if gently carried out. The best method is to insert a fine tube along the lumen of the large one and allow some warm saline solution to flow slowly along it into the abscess cavity, the fluid returning along the larger tube. If two tubes have already been inserted into the abscess cavity, the fluid injected through one will escape by the other. Whatever method is employed, care must be taken that there is free exit for the fluid, as otherwise the abscess cavity may become over-distended, and in consequence rupture of a portion of its wall may take place, especially the inner, which perhaps only consists of a thin layer of brain tissue separating the abscess from the lateral ventricle. During the act of irrigation there is a risk of some of the fluid, now loaded with septic particles, escaping between the surface of the brain and the dura mater and thus setting up a secondary meningitis.
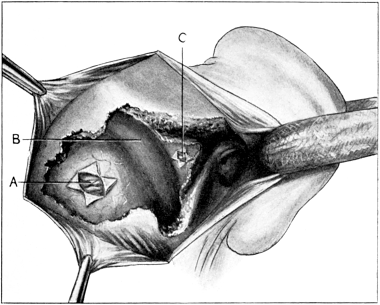 Fig. 253. Exploration for a Cerebellar Abscess. A behind, and C in front
of the lateral sinus; B, Lateral sinus.
Fig. 253. Exploration for a Cerebellar Abscess. A behind, and C in front
of the lateral sinus; B, Lateral sinus.
Opening of a cerebellar abscess. The cerebellum may be explored from two different points, either in front or behind the lateral sinus. The posterior route is adopted if the abscess is superficial in the outer portion of the lateral lobe, usually the result of lateral sinus thrombosis or disease of the posterior mastoid cells. The anterior route is indicated if it is thought that the abscess is deeply placed in the anterior inferior portion of the cerebellum, that is, in those cases in which it is apparently a complication of labyrinthine suppuration, or the result of disease of the inner wall of the antrum and mastoid cavities (Fig. 253).
(a) Behind the lateral sinus. After exposure of the lateral sinus the bone is removed either by means of the gouge and mallet or by bone-forceps, until a considerable area of the dura mater is exposed behind and below the curve of the sinus (Fig. 253). The dura mater is then incised as already described.
The cerebellum is explored by thrusting the instrument inward for about an inch. As a rule the abscess is found at once. If it be not discovered at the first attempt, the instrument should be directed forwards, upwards, and inwards towards the posterior surface of the petrous bone. Care, however, must be taken that it is not pushed in too far, otherwise it may pierce the anterior upper margin of the cerebellum, and if an abscess be present, the meninges may thus become infected. If the surgeon has exposed the dura mater by trephining, it is necessary to push the exploratory instrument at least two inches inwards and forwards in order to reach an abscess situated in the anterior inferior portion of the cerebellum. In such cases it is by no means difficult to miss a small abscess, and further, drainage is frequently incomplete when an abscess is discovered. For this reason, if the cerebellum be explored first behind the lateral sinus and no abscess is discovered, it should further be explored by the anterior route in front of the lateral sinus. If the cerebellar abscess be secondary to lateral sinus thrombosis, and if there be no doubt as to the diagnosis, the inner wall of the sinus should be made as aseptic as possible, and the dura mater forming it incised freely; the cerebellum being thus explored through the site of infection.
(b) In front of the lateral sinus. The lateral sinus is first exposed (Fig. 253). The triangular area of bone situated in front of it, between it and the semicircular canals, and forming the inner boundary of the antrum and mastoid cavities, is now removed with the gouge and mallet or with a suitable pair of forceps. If it be certain that internal-ear suppuration exists, or if the operation be secondary to opening of the labyrinth, the posterior wall of the petrous bone may be removed until the internal auditory meatus is almost reached. If, however, the labyrinth be intact, care must be taken not to chisel away too much bone for fear of encroaching on the posterior semicircular canal. On exposure of the dura mater an extra-dural abscess may be met with, usually the result of internal-ear suppuration. Even if no pus be seen, it is always a wise precaution, if internal-ear suppuration coexists, to separate the dura mater from the posterior wall of the petrous bone by means of an elevator in order to prevent any deeply situated extra-dural abscess being missed. After the dura mater has been exposed sufficiently it is opened by a crucial incision. In this region absence of increased tension within the brain and lack of bulging outwards of the cerebellar tissue do not necessarily imply the absence of an abscess; the cerebellum to all appearances may appear normal and flaccid, although a small abscess may be present.
The cerebellum is explored in various directions to a distance of not more than one inch. After the pus has been evacuated a tube is inserted as described above. In the majority of cases this method is far superior to opening the cerebellum behind the lateral sinus, especially as it is now recognized that the chief cause of cerebellar abscess is internal-ear suppuration.
After-treatment. This is similar to that of any ordinary abscess, but care must be taken that free drainage is maintained. The main part of the mastoid wound is lightly plugged with gauze, the tube inserted into the brain abscess being brought flush with the surface of the skin. The gauze filling the wound cavity should be arranged around the tube so that it rests comfortably within the wound and is not kinked. If the drainage tube be in its proper position, pus should be seen to ooze out of it.
Although the mastoid cavity itself need not be dressed daily, if necessary the outer dressings may be removed twice a day, in order to see that drainage of the abscess is continuous. After the first two or three days, the tube is gradually shortened. If the abscess be a recent one and not encapsuled, it becomes rapidly obliterated by pressure of the surrounding brain tissue, so that the tube may be forcibly ejected within a few days. On the other hand, if the abscess has existed for a considerable period and is bounded by a thick wall, which may be extremely resistant, the purulent discharge may continue for many days and necessitate the continuance of drainage. Generally speaking, the tube may be shortened every second or third day, and can usually be dispensed with by the end of the second week, if not before. It is, however, very necessary that the tube should not be withdrawn until it is certain that the abscess cavity has been obliterated completely.
The general treatment of the case in no way differs from that already described for the mastoid operation in which the wound has been left open posteriorly.
Complications. (i) On turning back the flaps of the dura mater, a hernia, consisting of friable congested brain tissue, may occur at once. This is extremely rare as a result of a simple abscess of the brain, but is significant of encephalitis frequently associated with meningitis (see p. 436). If an abscess be suspected, the brain should be explored as already described. If, however, no abscess be discovered, the treatment consists in removal of more bone and further incision of the dura mater, in order to permit of free drainage and to relieve tension.
(ii) Opening into the lateral ventricle. This may be due to rupture of its wall owing to the sudden diminution of pressure from too rapid drainage of the abscess cavity, or it may occur accidentally from thrusting in the exploratory instrument or drainage tube too deeply. Its occurrence is evidenced by the sudden gush of cerebro-spinal fluid. The ultimate danger is subsequent infection of the cavity, which, unfortunately, frequently occurs.
(iii) Cessation of breathing. This is more likely to occur in a cerebellar abscess in consequence of direct pressure on the medullary respiratory centres. The immediate treatment is to do artificial respiration and to open the cerebellar abscess by the quickest method possible. If this be successful, respiration probably will be restored.
Prognosis and subsequent progress. In an uncomplicated case a favourable prognosis may be expected, provided the abscess is successfully opened and drained without much disturbance of the surrounding parts. Many factors, however, may lead to a fatal result. With regard to recovery: in 100 cases taken from the records of the London Hospital during the last ten years, recovery took place in 20% operated on for cerebral and 10% for cerebellar abscess. Other statistics give a much higher percentage of recovery, but it must be remembered that in hospital patients a large number of the cases are only seen by the surgeon at a very late stage, when the brain abscess is complicated by other intracranial or suppurative lesions, and the patient is in an almost moribund condition; so that the operation may only be undertaken as a forlorn hope.
If the operation is going to be successful, the head symptoms quickly disappear. Even if the patient was comatose before operation, the recovery may be so rapid that his mental condition may be almost normal within twenty-four hours. In many cases, if the abscess be a large one, convalescence will be tedious or prolonged; sometimes, indeed, complete restoration of the mental faculties, in spite of a most successful operation, will not be obtained. The chief relief to the patient is the cessation of the terrible headaches from which he has been suffering.
Unfavourable symptoms are the sudden onset of pyrexia accompanied by delirium usually the result of diffuse meningitis, or of infection of the lateral ventricles. In the latter case there is a rapid termination in drowsiness, coma, and death.
Although the brain abscess may be draining freely, the patient for some days may lie in a semi-comatose condition as a result of œdema or inflammation of the surrounding brain tissue; in such cases prognosis is difficult, but hope of recovery may be entertained if the pulse and temperature keep practically normal.
Recurrence of symptoms. This may take place within the first few days after the operation as a result of infective cerebritis, the presence of another abscess, or faulty drainage; or at a much later period, owing to the formation of another abscess or to a cyst within the brain at the site of the former abscess.
1. If the recurrence of the symptoms appears immediately after the operation, the wound should be inspected carefully, if necessary under an anæsthetic. If drainage be not free, the tube should be removed and a pair of forceps inserted along the track leading into the abscess, their blades being then slightly opened and withdrawn. On doing this an accumulation of pus may escape. The cavity may then be irrigated gently with saline solution and a larger tube inserted.
If, however, this procedure does not give a satisfactory result, the finger may be inserted into the brain to feel if the abscess is loculated. By this means any existing septa may be broken through; or if a feeling of resistance suggests the presence of another abscess, this part of the brain can also be explored. It must also be remembered that although a temporo-sphenoidal abscess has been opened successfully and is draining well, the continuance of the symptoms may be due to a coexisting abscess of the cerebellum, or vice versa; in other cases, in spite of all care, the patient gradually sinks, partly from exhaustion and partly from general toxæmia, the result of infective cerebritis.
2. Recurrence of symptoms at a later period. The occurrence of a fresh abscess is usually owing to the fact that the primary focus of the disease has not been completely removed at the first operation; for instance, if the surgeon only trephined and drained the abscess without performing the mastoid operation.
A cyst is usually the result of the abscess having been encapsulated and its wall not having been removed at the first operation. If a cyst be discovered on exploring the brain in consequence of these symptoms, its wall should be removed if possible.
Apart from symptoms of intracranial pressure, the patient may suffer from attacks of Jacksonian epilepsy from time to time, presumably due to the post-operative adhesions. If they continue in spite of conservative treatment, it may become necessary to operate in order to remove this source of irritation (see Vol. III).
Indications. (i) Tumours. Tumours of the larynx are more often innocent than malignant. Sir F. Semon5 collected 12,297 cases seen between 1862 and 1888 by 107 laryngologists, and of these 10,747 (or 88%) were benign and 1,550 (or 12%) were malignant. Of the innocent forms, papilloma, either simple or multiple, occurred in 39%; fibroma, sessile or pedunculated, was next in frequency; cystic tumours were not nearly so common; and other forms, including myxoma, angeioma, adenoma, lipoma, and enchondroma, were rare. The period during which these tumours are most common is between the ages of 20 and 40 years, but they are also frequent during childhood.
Malignant growths occur at a later age, mostly between the ages of 40 and 60, and attack males more than females. Carcinoma is far more common than sarcoma, and is generally of the squamous-celled variety. Endothelioma has not often been discovered.
The importance of distinguishing innocent from malignant tumours is greater now than in former years, since it is agreed that endolaryngeal operations are preferable for the eradication of the former, while the latter are better treated by extra-laryngeal methods. Moreover, the differential diagnosis has steadily improved, owing to the more general use of the laryngoscope and the introduction of recent methods of examination. Thus, by direct laryngoscopy it is possible to investigate children as easily as adults. Microscopical examination of fragments removed with laryngeal forceps is of great value in confirming the clinical diagnosis; the sections can be made by freezing, or in paraffin, the latter method requiring, with recent improvements, not more than twenty-four hours. Semon, who has done more than any other man to improve the early diagnosis of malignant disease of the larynx, is strongly in favour of such examinations. It must be remembered, however, that the result is sometimes inconclusive, for it is difficult to be certain that the actual growth has been removed. In cases that are thought to be malignant, it is better to open the thyreoid6 cartilage than to rely upon endolaryngeal operation, as there is a danger of stimulating the growth to greater activity, especially by repeated interference. When the thyreoid cartilage has been opened, the whole disease can be explored thoroughly and a fragment selected from which to make a frozen section. In the majority of cases a definite diagnosis can thus be arrived at, and even when it is necessary to examine several fragments the amount of time lost is small.
As regards the value of skiagraphy, Walsham and myself have found that photographs can be made of tumours of the larynx which in some instances determine accurately the position and extent of the disease.
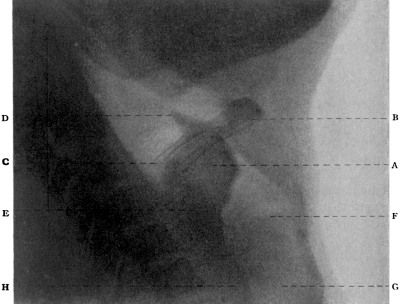 Fig. 254. Skiagram showing a Tumour of the Larynx. A, Tumour; B, Body
of hyoid; C, Greater cornu of hyoid; D, Epiglottis; E, Posterior plate of cricoid;
F, Vocal cord; G, Trachea; H, Œsophagus.
Fig. 254. Skiagram showing a Tumour of the Larynx. A, Tumour; B, Body
of hyoid; C, Greater cornu of hyoid; D, Epiglottis; E, Posterior plate of cricoid;
F, Vocal cord; G, Trachea; H, Œsophagus.
Fig. 254 is a photograph showing a cancer of the upper opening of the larynx, lying above the vocal cords, the position of which was proved to be accurate by later operation upon the patient. It is, however, doubtful whether the method will eventually assist in the differential diagnosis between innocent and malignant growths.
(ii) Tuberculosis. Endolaryngeal operations are successfully performed for chronic conditions such as ulceration or tumour, and, rarely, in acute forms such as abscess, necrosis, and the like. Removal of a portion of the epiglottis occasionally gives great relief to a patient who is suffering from dysphagia.
(iii) Strictures resulting from trauma, from the ulcerations of syphilis, diphtheria, and other inflammatory diseases, or caused by congenital webs.
(iv) Foreign bodies impacted in the larynx.
(v) Œdema of the mucous membrane due to trauma or inflammation, local abscess, necrosis, and other allied conditions, in which obstruction is likely to supervene.
The operation may be performed either by indirect or by direct laryngoscopy.
It being essential that the patient should be tolerant, this method is chiefly applicable in the case of adults. The operation may require a course of instruction, but this presents no difficulty if given with discretion. The employment of cocaine, novocaine, and adrenalin is of the greatest importance to both surgeon and patient. Cocaine, which is generally to be preferred, may be used in strong solutions—10 or even 20%—if applied to the mucosa by a small swab of wool; but, if used as a spray, weaker solutions are employed (4%). With neurotic patients cocaine must be applied cautiously, as a sense of suffocation is sometimes produced. It is necessary first to treat the soft palate, the uvula, base of the tongue, pharynx, and epiglottis; secondly, with the help of a laryngeal mirror, the interior of the larynx must be cocainized; this can be accomplished by expelling a few drops of the solution from a laryngeal syringe or by means of a swab attached to a suitable wool-carrier. Fifteen to twenty minutes must be allowed to gain the full effect of anæsthesia. The patient must be instructed on no account to swallow the saliva. The secret of successful intralaryngeal operations lies in the thorough application of these principles, and in not attempting the operation until the patient is able to tolerate the presence of an instrument within the larynx. The surgeon must be experienced in the use of laryngeal instruments, and must be provided with a complete equipment, including forceps (Mackenzie’s, Whistler’s, Grant’s, &c.), which must be of different lengths to suit the patient, snares, galvano-cautery, curettes, probes, and other instruments for the application of drugs. Proper illumination is also very important.
 Fig. 255. Horsford’s Instrument for transfixing
the Epiglottis.
Fig. 255. Horsford’s Instrument for transfixing
the Epiglottis.
When removing an intralaryngeal growth, the surgeon sits facing the patient. The mouth is opened to the fullest extent, and the tongue drawn well forward and held by the patient’s right hand. The mirror is introduced in such a way that the tumour is distinctly seen. If the epiglottis overhangs, it can be drawn forward with the forceps; or, in rare instances, a special instrument (Fig. 255) can be used for transfixing its upper margin with a thread, the latter being grasped by a pair of pressure forceps, which, being allowed to hang, will automatically raise the obstruction.
The forceps, having been warmed, are taken in the right hand when the tumour is on the right side of the larynx and in the left hand when the tumour is on the left, thus allowing a clearer view than when the same hand is employed irrespective of the position of the disease. It is introduced as follows: firstly, the handle is directed towards the patient’s left ear until the point of the forceps has passed beyond the back of the tongue and lies behind the epiglottis; secondly, the instrument is quickly rotated so that the handle lies below the chin; thirdly, the hand is raised so that the point is directed forwards; fourthly, the whole instrument is quietly lowered and the beak of the forceps directed towards the growth. This manipulation is made more difficult by the laryngeal image being reversed in an antero-posterior direction.
When the point is seen to rest upon the growth, the instrument is opened, and the tumour grasped and avulsed: with careful manipulation there is little danger of wounding the normal mucosa, and hæmorrhage is insignificant. When dealing with multiple growths the patient must understand that it may be necessary to repeat the operation, either immediately or after an interval. Given suitable instruments, sufficient experience, and a tolerant patient, it is possible to remove, with the help of cocaine, the majority of simple tumours. Operations upon cysts, the scarification of mucous membrane with a guarded knife, the curettement of tuberculous ulcers, and cauterization of the larynx, are all conducted upon similar lines. Foreign bodies can generally be removed with forceps; thus, F. A. Rose7 reported a case in which part of the breastbone of a chicken, measuring 1 inch in length and over ¾ of an inch in width, was removed after having been impacted in the larynx for nearly forty-eight hours. In rare instances such an operation is not successful; e.g. with a foreign body firmly impacted, multiple papillomata, or an intolerant patient, general anæsthesia may be required, and removal may have to be effected through a tube-spatula or by external incision.
After-treatment. Intralaryngeal wounds generally heal well, but every effort should be made to prevent infection of the parts, to allay any inflammation that may arise, and to avoid catarrh and swelling of the mucosa. It is advisable to order complete vocal rest until the redness has subsided, and the patient should refrain from coughing; the sucking of ice, or the inhalation of benzoin or other medicated steam, has a sedative action upon the parts. If the larynx becomes septic or filled with irritating discharge, the use of sprays or powders is indicated; in such a case the patient may be given a parolein spray, with menthol, eucalyptus, or other antiseptic, for constant use; or a powder such as orthoform, the latter being sucked into the larynx through a warmed glass tube (Leduc’s insufflator), or applied by the surgeon. In the later stages the patient may be treated by the local application of caustic fluids, or by galvano-cautery, as occasion requires. The success of such operations depends largely upon the skill of the surgeon; if attention be given to the after-treatment the results are very good, and the voice is generally recovered. As Semon has shown conclusively, there is no practical danger of the occurrence of malignant degeneration through the influence of instrumentation.
(Killian’s Method)
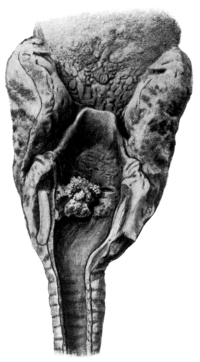 Fig. 256. Multiple Papillomata of the Larynx. (From Specimen No. 1647
in the Museum of St. Bartholomew’s Hospital.)
Fig. 256. Multiple Papillomata of the Larynx. (From Specimen No. 1647
in the Museum of St. Bartholomew’s Hospital.)
Indications. (i) Multiple papillomata. These tumours occur most commonly during the early years of life, and operations for their removal present great difficulties, first, in their removal, and, secondly, owing to their inveterate tendency to recurrence whatever operation is performed; moreover, in some instances operation seems to stimulate the growths to greater activity. The case reported by Stoker is a well-known instance. He was consulted by a man thirty years of age who had suffered from papilloma for twenty-three years, during which period one surgeon had performed 100, and a second 120 operations.
(ii) Benign tumours other than papillomata, which are not amenable to operation by indirect laryngoscopy.
(iii) Foreign bodies. Direct laryngoscopy is advised for patients who are intolerant (e.g. young children), or when the object is firmly impacted, or when other methods of treatment have failed. Thus in one of my cases a man presented himself with a long pin impacted transversely above the vocal cords; it was found impossible to remove it by indirect laryngoscopy without serious injury to the parts. An anæsthetic was therefore given and a large tube-spatula passed into the larynx: with strong forceps the pin was bent upwards and removed with ease.
(iv) Granulations, ulcers, necrosis, and other inflammatory conditions such as are caused by diphtheria, tubercle, syphilis, and many other diseases.
(v) For diagnostic purposes. There can be little doubt that direct laryngoscopy has a great future before it as a means of determining the nature of doubtful laryngeal conditions. If the upper parts of the larynx be swollen, if there be any stenosis such as follows ulceration, or if the patient be intolerant, the air-passages cannot be thoroughly examined with the laryngoscope alone. With the newer method many of these difficulties have disappeared, and it is now possible for the surgeon to diagnose with certainty many conditions which would otherwise have remained doubtful.
The apparatus required consists of:
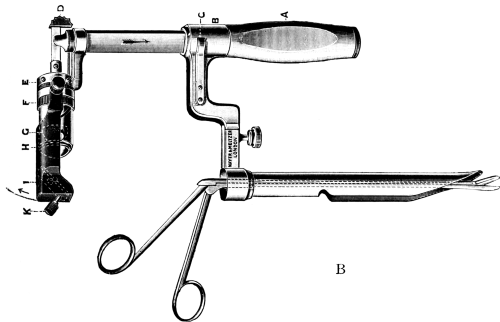
(a) The tube-spatulæ. The tube originally suggested by Killian was made of straight metal and circular in section, the distal end being cut obliquely with the projecting portion fashioned like a spatula. A strong handle, at right angles to the tube, was used for manipulation. Different sizes were required for children and adults. Various modifications of these tubes are now in use, notably those of Mosher and Bruenings: the instrument recommended by the latter is easier to manipulate and gives a better view than the earlier forms described.
(b) The lamp for illumination. Different forms of head-lamp (Killian’s, Kirstein’s) and hand-lamp (Caspar’s) have been devised for illumination from the outside, and Chevalier Jackson has invented a lamp which is sufficiently small to pass to the distal end of the tube, where it lies in a compartment of its own lest it should be broken and fall into the trachea. Recently these electroscopes have been improved upon by Bruenings, in whose instrument (Fig. 257) the lamp is more powerful and is attached to the handle in such a manner that it can be easily swung into position when required. A condensing lens has also been added and the light can be focused to any desired distance. If preferred, an ordinary forehead-mirror reflecting the light from a powerful Nernst lamp (100 c.p.) can be employed.
(c) The instruments for operation. Various forms of forceps for removal of tumours have been devised by Killian, von Eicken, Bruenings, Patterson, and others. In any form that is employed it is necessary, in order to allow of clear vision, that the handle should be set at an angle with the shaft. For foreign bodies, hooks of different shapes are also useful. Other requirements include a gag for opening the mouth, a tongue depressor, tongue forceps, suitable cotton-wool carriers, the requisites for tracheotomy, and a darkened room.
Operation. The operation can be performed with local or general anæsthesia. With patients who are intolerant chloroform is more reliable, and is preferable to other drugs, which tend to excite secretion. Chloroform should always be employed for children. It should be given slowly and in the smallest possible quantity, the head of the patient being kept lower than the body to allow blood and mucus to drain away from the trachea. To make the parts more tolerant, cocaine can also be applied to the vocal cords, or a dose of morphine (codeine is advised in children) can be given half an hour before the operation. The importance of a skilled anæsthetist cannot be too strongly emphasized. With chloroform, the patient should lie upon the back or right side, with the head projecting beyond the end of the table, so that the neck can be extended as required. With cocaine the upright position is often preferred, and the patient should sit on a low stool facing the surgeon. When the patient is recumbent, the surgeon should sit or kneel behind the head (Fig. 258). He should observe the strictest antiseptic precautions, and should introduce no instrument which has not been properly sterilized; further, the tubes should be previously warmed to prevent ‘fogging’, and oiled with sterilized liquid paraffin before introduction. There should be two assistants, one (the chloroformist) to support the head and watch the respiration and pulse, the other to help with instruments.
 Fig. 258. Removal of Multiple Papillomata by Direct Laryngoscopy
Fig. 258. Removal of Multiple Papillomata by Direct Laryngoscopy
In order to examine the larynx, the mouth is opened by a gag, and the tube-spatula is passed to the upper border of the epiglottis; when this has been inspected the spatula is pushed behind it, and the upper portion of the cricoid plate is examined; the tongue is then pulled forward and the tube tilted so that the larynx can be seen. The examination should be methodical, and should include the vocal cords, ventricular bands, and openings of the ventricles. The whole manipulation can be performed with great delicacy, and is entirely guided by the eye, so that there is little fear of injury even in young children.
In this and the further technique the chief difficulties are caused by: (a) The prominence of the upper teeth. This may seriously interfere with the easy passage of a straight tube, even when the neck is fully extended. The difficulty can be overcome by turning the head laterally, so that the tube passes through the opposite angle of the mouth. (b) The mucus, which collects in the tube and obstructs the vision. This must be overcome by using a secretion aspirator, by frequent sponging, or, as suggested by Ingals, by giving a previous dose of atropin[e]. (c) Intolerance of the parts, which can be counteracted by the judicious use of cocaine (10%). It may be noted that this combination of chloroform and cocaine is not dangerous, even in young children, so long as the cocaine is prevented from running into the pharynx.
The condition of the larynx having been thoroughly examined, the operation can proceed. The method of removing multiple papillomata will first be described. In some cases it will be found that better exposure of the tumours is obtained if the end of the tube is placed above the epiglottis rather than in the larynx itself. The position of the growths having been determined, a suitable forceps is selected and introduced through the tube. The papillomata are seized and avulsed separately, without injury to the normal tissues. To arrest the bleeding it may be necessary to apply cocaine and adrenalin mixture, and to raise the foot of the table so that the blood drains away from the field of operation. As far as possible, all the growths should be removed; it may be difficult to attack those which are situated in the anterior commissure or subglottic region, but this difficulty may be overcome by the use of specially devised instruments; thus, von Eicken has invented a tube which is long enough to pass through the larynx and into the trachea, the portion lying in the larynx being provided with a lateral window which can be turned in any direction, so that a growth can be made to project into the tube, where it can be easily removed.
At any moment during this operation the surgeon may be called upon to perform tracheotomy.
After-treatment. This must be carried out upon the same lines as those already suggested; everything must be done to relieve congestion and irritation. Killian advises internal administration of arsenic for a period of several months, and, if this fails, potassium iodide in large doses. It should be remembered that in some instances syphilis seems to play an important part in the causation of these conditions. Ingersole suggests that X-rays prevent recurrence, and may even cause shrinkage of existing growths.
Recurrence occurs in most cases in some degree, and requires further operation; this may be carried out after an interval of a week or longer, according to the case. At these secondary operations it may not be necessary to use the forceps; local applications such as absolute alcohol, salicylic acid in absolute alcohol (2–10%), solutions of silver nitrate or chromic acid, and many other drugs, have been advised by different surgeons. Wylie is strongly in favour of the galvano-cautery, and is of opinion that the technique is more reliable and the liability of local infectivity diminished. If the latter method be employed, very little should be done at one sitting, otherwise great inflammatory reaction may be set up, entailing tracheotomy. A tracheotomy tube may be required for a short time while such treatment is being carried out; some surgeons, with whom the author does not agree, always perform preliminary tracheotomy, and claim that the papillomata are less likely to recur if complete rest is thus given to the larynx.
Results. In discussing the value of the above method it is necessary to refer to the results obtained by other operations, such as—
(i) Tracheotomy (see p. 522). This operation has been advocated as a method of curing papillomata. It has been noted that by giving rest to the larynx the congestion is relieved, the papillomata decrease in size, and in some cases completely disappear. Mackenzie8 published seven cases which he had had under observation for a minimum of two years, with four recoveries, the canula having been worn for periods varying from six to fifteen months. He also mentioned thirteen other cases in which good results had been obtained by other surgeons, and was of opinion that the method was most successful with ‘virgin’ cases. There are, however, many objections to this form of treatment. For instance, it is often necessary to retain the tube for a prolonged period, two years or longer, and even then the result is doubtful; moreover, the prolonged use of a canula is disastrous to the larynx, not only in retarding development, but also in the production of stenosis; there is also a danger of bronchitis, of broncho-pneumonia, and possibly of tuberculosis. In regard to the last, G. A. Wright,9 in reporting a case in which tubercle supervened, argues that ‘presumably there is more risk of this happening to the wearer of a tracheotomy tube than when breathing in a normal way through the mouth or nose’. Further, the line of treatment is difficult to enforce on account of the aversion shared by most parents to the performance of tracheotomy.
(ii) Laryngo-fissure (see p. 487). Under this head are included thyrotomy, or complete division of the thyreoid cartilage; partial thyrotomy, where a small portion of the upper or lower part of the thyreoid cartilage is left intact (an operation which does not give a good exposure of the larynx); infrathyreoid laryngotomy, which is only applicable to adults; cricotomy, with division of the cricoid cartilage and crico-thyreoid membrane; and subhyoid pharyngotomy. Of the above, thyrotomy is the most satisfactory operation, because it gives the best exposure of the parts and facilitates removal of the growths; recurrence, however, is frequent, permanent injury to the voice is common, and stenosis may result.
The results of these operations, especially during childhood, are by no means satisfactory. In the statistics carried up to 1896, collected by Rosenberg and von Bruns,10 laryngotomy was performed 143 times on 109 children; 11 were operated upon twice, 3 children three times, and 1 child seventeen times. 52 of the children were under four years of age; 20 died, principally from suffocation with recurrent papillomata; 43 showed recurrences after repeated operation; 40 were cured (i.e. 36%), and of these 10 showed disturbance of voice.
It must be admitted that operations for the treatment of papillomata do not meet with any great measure of success. It seems probable, however, that the results obtained by endolaryngeal removal are better than those obtained by either tracheotomy or laryngo-fissure. To quote Killian11: ‘Formerly, and especially from the standpoint of the surgeon, laryngotomy for laryngeal papillomata was very frequently done in little children in whom removal was impossible by endolaryngeal methods. In my judgment, direct laryngoscopy renders such a surgical procedure unnecessary. We can in all cases, with the aid of a tube-spatula under narcosis, remove papillomata, and the operation can be repeated as often as seems necessary.’ These remarks express the general feeling of the present day, and the most important factor in determining the success of operative treatment is early diagnosis. Such diagnosis divides the cases into two classes: those in which the growths are localized, and those in which they are diffuse. The first class is easy to treat by endolaryngeal methods, and, given careful after-treatment, the prognosis is satisfactory. The second class is serious, and far more difficult to treat; when Killian’s method fails the prognosis is very bad. Finally, it must be borne in mind that, as recurrence may not occur for several months, a guarded prognosis must be given in every case.
The removal of other benign tumours and of foreign bodies, and the treatment of granulations, are conducted upon similar lines, and are attended with excellent results.
Indications. This operation is performed for two purposes:
(i) To obtain access to the cavity of the larynx when the diagnosis is uncertain, or as a preliminary to other operations.
(ii) As a method of eradicating certain diseases, of which the following are important:—
1. Malignant tumours, both carcinoma and sarcoma, in which an early diagnosis has been made, and so long as they remain intrinsic.
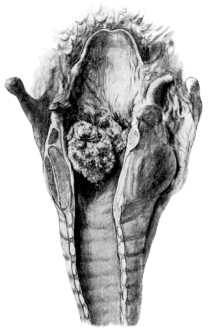 Fig. 259. Intrinsic Tumour of the Larynx. (From Specimen No. 1649 in
the Museum of St. Bartholomew’s Hospital.)
Fig. 259. Intrinsic Tumour of the Larynx. (From Specimen No. 1649 in
the Museum of St. Bartholomew’s Hospital.)
|
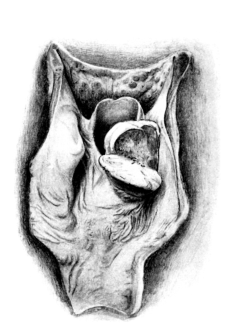 Fig. 260. Extrinsic Tumour of the Larynx. (From Specimen No. 1653 in
the Museum of St. Bartholomew’[s] Hospital.)
Fig. 260. Extrinsic Tumour of the Larynx. (From Specimen No. 1653 in
the Museum of St. Bartholomew’[s] Hospital.)
|
It is advisable to follow Krishaber in the separation of all forms of laryngeal cancer into two classes, the Intrinsic and the Extrinsic. The term ‘intrinsic’ implies a growth springing from the vocal cords, the ventricular bands, the ventricles, or the subglottic space, and the growth must lie entirely within the laryngeal cavity. ‘Extrinsic’ is the term used for a growth affecting the arytenoids, the posterior part of the cricoid cartilage, the aryteno-epiglottidean fold, or the epiglottis. Such a growth is not entirely limited to the larynx, but also involves some part of the pharynx.
2. Extrinsic localized malignant tumours which are attached to the epiglottis, or to the aryteno-epiglottic fold.
3. Innocent tumours which are too extensive for endolaryngeal operation or of a doubtful character. In either of these cases it is justifiable to perform an external operation, which may be thyrotomy, or occasionally, an atypical operation: thus Semon12 removed a large fibromatous tumour of the larynx by submucous resection, without opening the cavity of the larynx.
4. Stenosis following syphilis, trauma, acute exanthemata, scleroma, and other rare diseases. C. Jackson has reported twenty-four cases falling under this head, nineteen of which lived for more than a year after the operation with useful voices. If the surgeon is satisfied that the disease is quiescent, he should point out to the patient that it may be possible to cure the obstruction by thyrotomy. It must, however, be remembered that tertiary syphilitic lesions may again become active as the result of operative interference. It is probable that slight cases of stenosis can be treated better by intubation than by thyrotomy. Thyrotomy has also been suggested to relieve stenosis caused by double abductor paralysis of the vocal cords, but such cases are better treated by tracheotomy or intubation.
5. Foreign bodies. Thyrotomy is rarely necessary, and should be reserved for irregular or sharp-pointed bodies, such as tooth-plates or bones, which are so firmly jammed that removal by other methods is impracticable. If there has been much laceration of the soft parts, a tracheotomy tube should be retained for a few days until the swelling has subsided.
6. Tubercle. Thyrotomy has been successfully performed in such cases, mostly under the impression that the disease was malignant. The differential diagnosis between tuberculous and malignant growths is sometimes very difficult until the tumour has been explored. In cases that are known to be tuberculous, the feeling prevails that thyrotomy is not to be recommended. It should be remembered that the external wound is liable to become tuberculous.
Instruments. Scalpel, curved scissors, dissecting forceps, pressure forceps, aneurism needles, double hook retractors, bone shears (Waggett’s) or bone scissors, tenaculum forceps, needles on handles, catgut in various sizes, a Hahn’s tube, and tracheotomy equipment. A head-light is required for illumination of the deeper parts during removal of tumours.
Operation. In England, owing to the fact that the administration has been in skilled hands, chloroform is not considered dangerous, and the operation is well tolerated even for three or four hours (e.g. in laryngectomy). On the Continent, however, Kocher, von Bruns, and others advocate local anæsthesia with cocaine or novocaine. Jackson suggested rectal etherization as an alternative, but this has many dangers. In my opinion a general anæsthetic should be given, as it enables the operation to be performed more thoroughly and is followed by less shock. It must nevertheless be borne in mind that, if the growth is intrinsic and of large size, it is difficult to administer chloroform, and the patient is liable to suffer from urgent dyspnœa. In such a case i[t] is advisable to perform preliminary tracheotomy with novocaine alone (see p. 544).
As regards the operation, the important question arises whether tracheotomy ought to be performed several days prior to the main operation, in order to accustom the patient to the tube and the new method of breathing. The following reasons are advanced in favour of this: the main operation is shortened, and relief is given to the larynx and lungs, so that congestion subsides and broncho-pneumonia is less likely to supervene. The objections are also important, namely, that there are two operations instead of one, and perhaps two anæsthetics (though this can be avoided if local anæsthesia is used for the tracheotomy); that the tracheotomy wound becomes septic, and infection of the trachea and bronchi is apt to occur, with consequent bronchitis; that the air which passes into the lungs is devoid of moisture and heat; that the trachea becomes surrounded by adhesions; and that it is altogether unnecessary. The objections in my opinion outweigh the advantages claimed; it is better to perform tracheotomy as a first stage in the operation of removal, except in cases where there is great laryngeal obstruction, where dyspnœa is present, or where bronchitis fails to yield to other forms of treatment. In such cases tracheotomy should be performed first, and the second operation should be carried out a week or ten days later when all the conditions are favourable.
When operating upon the larynx the surgeon must use every precaution to prevent blood from running into the lower air-passages, and this may be accomplished by a tampon in the trachea or by keeping the head of the patient lower than the body. The former method appears to me to be more reliable than the latter; and I prefer to use a Hahn’s canula, although the sponge requires from ten to fifteen minutes to swell. This canula is more reliable than Trendelenburg’s, whose inflated bag is apt to slip or collapse suddenly. As soon as the thyreoid cartilage has been opened, a second sponge should be inserted above the canula, and by this means the air-passages are completely blocked.
If an ordinary tracheotomy tube be used, the operation must be performed either with the head lower than the body (Rose’s position), or with the whole body inclined (Trendelenburg’s position), or with a combination of the two; and in any case a sponge should be placed in the upper part of the trachea after the thyreoid has been opened. Many surgeons prefer the combined method. Under no conditions must blood be allowed to pass below the tube. Whatever form of canula is used, it should be fitted with a Hahn’s tube and funnel (Fig. 266), so that the anæsthetist can give the chloroform without interfering with the surgeon. The patient should lie upon the back on a flat table, the head extended slightly over a small cushion in the position for tracheotomy.
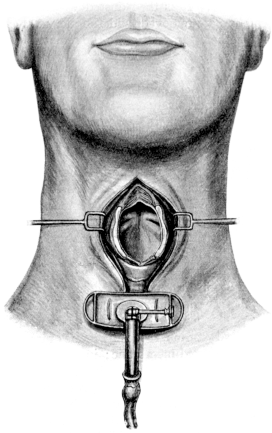 Fig. 261. Thyrotomy. Showing exposure of the
larynx, and tube for the anæsthetic.
Fig. 261. Thyrotomy. Showing exposure of the
larynx, and tube for the anæsthetic.
First stage. A vertical incision is made in the middle line from the hyoid almost to the sternum, so as to expose the thyreoid cartilage and the pretracheal muscles; these are retracted, so that the anterior aspect of the trachea is exposed; the isthmus of the thyreoid gland is completely divided, and search made for bleeding points until the wound is quite dry. A large opening is made accurately in the middle line of the trachea; this will be at least two rings below the cricoid cartilage in order that the tube may be well away from the region of the growth. In adults, if a Hahn’s tube be employed, the section should include at least three rings of the trachea.
Second stage. The anterior aspect of the thyreoid cartilage, and the crico-thyreoid membrane, are freely exposed, the infrahyoid muscles being separated by at least one inch and, if necessary, retracted. Ten minutes after the tube has been inserted, the crico-thyreoid membrane is punctured, exactly in the middle line, in order to admit the inner blade of the bone forceps; the latter is pushed upwards, slowly and without force, between the posterior portions of the vocal cords, until the whole length of the thyreoid cartilage is included between the blades; the forceps are then forcibly closed, great care being taken that the outer blade is cutting exactly in the middle line. By quickly opening the cartilage in this manner, there is practically no danger of destroying the anterior attachments of the vocal cords, or cutting through the substance of one of them. The two halves of the larynx are forcibly separated and retained in this position by hooked retractors, so that the interior of the larynx is exposed. In order to give a free exposure, it is necessary, as a rule, to divide with a knife the crico-thyreoid membrane; but the thyreo-hyoid membrane should not be touched, nor should the attachments of the epiglottis be disturbed. The separation must be performed carefully in order to avoid a fracture of the cartilages. The pharynx is plugged with gauze, so that no saliva can enter the wound, and after all secretion has been removed from the larynx a small sponge or plug is inserted into the upper end of the trachea. Cocaine, 20%, is freely applied with a swab of wool to every part of the larynx in order to constrict the vessels; persistent hæmorrhage can be controlled by plugging the cavity with wool soaked in cocaine; ‘this fully suffices . . . and the employment of adrenalin, as I have personally experienced in one case, increases the risk of secondary parenchymatous hæmorrhage’ (Semon). Further, and this is of importance, by the use of cocaine the irritability of the larynx and the laryngeal reflex are destroyed. The tumour can now be inspected; it must be thoroughly exposed by cutting through the soft or hard structures (cricoid if necessary) so that its limits can be determined, thus enabling the surgeon to decide whether it is possible to obtain a satisfactory result by local removal.
Third stage. In the words of Butlin13: ‘an incision is carried around it (the tumour) with knife or scissors, including more than half an inch of the surrounding apparently healthy tissues, without respect to the after use of the voice or any other consideration except the complete removal of the disease. The included area is cut out right down to the cartilage, which is laid bare and finally scraped absolutely bare with Volkmann’s sharp spoon.’ The cavity is then plugged for a few moments until the bleeding has been controlled. The hæmorrhage is never serious, and can be controlled by catgut ligature if necessary. The wound must be completely dry. It is then dusted with a powder such as orthoform; the retractors are removed, and the alæ of the thyreoid cartilage allowed to fall together. In relation to the removal of the tumour, Butlin has shown that there is ‘little liability of malignant disease infiltrating the cartilage of the larynx’, so that, as a general rule, the latter can be left if all the soft tissues, including the perichondrium, are removed from its surface; this is comparatively easy to accomplish in the case of the thyreoid, but more difficult with the arytenoids and cricoid cartilage. C. Jackson has criticized the use of a sharp spoon as likely to cause infection of the cartilage.
Fourth stage. In some instances it is possible partially to unite the divided mucous membrane, and so to lessen the granulating area: when this is done it is of the utmost importance that the lumen of the larynx should not be constricted, as any constriction will increase the danger of stenosis. In many instances it is not advisable to attempt to repair the wound that has been produced.
In suturing the external wound the alæ of the thyreoid are brought accurately into the position which they occupied before division, in order that the anterior attachments (if left) of the vocal cords should heal at their proper level. In some instances the cartilages fall naturally into the desired position, especially if one or two catgut sutures are inserted into the thyreo-hyoid membrane; in other cases it may be advisable to insert one or two similar sutures through the cartilage itself and thus obtain correct apposition. These sutures should lie on the outer aspect of the mucosa, so as not to traverse the cavity of the larynx itself. In cases where only the anterior portion of a vocal cord has been removed, Semon recommends that the divided end be sutured to the ventricular band; it is reasonable to suppose that, by attention to this detail, a better voice will be afterwards obtained. The infrahyoid muscles are approximated with one or two catgut sutures in the upper part of the wound; the skin is united with a continuous silk suture, as far downwards as the lower part of the thyreoid cartilage. The lower part of the wound is left open, to procure free drainage through the crico-thyreoid and tracheal openings. The whole of this lower wound is packed very loosely with gauze, so that discharges are not retained. It is necessary to emphasize the importance of not plugging the cavity of the larynx. The Hahn’s tube is removed as soon as the operation is completed, and replaced by a tracheotomy canula; the whole wound is covered by a loose pad of antiseptic gauze, which is kept in position by tapes or loosely applied bandages. No dissection for removal of lymphatic glands is required.
The above may be called the typical operation for malignant disease in which the growth is intrinsic; it gives a better exposure of the parts than other operations such as transverse laryngotomy (division of the thyreoid cartilage at the level of the ventricles), subhyoid pharyngotomy, partial thyrotomy, cricotomy, and crico-tracheotomy; the removal of tumours is therefore easier, and better after-results are obtained. If the growth be found more extensive, it may be necessary to modify the procedure. For example:
(a) When the epiglottis is involved, an extensive dissection of the thyreo-hyoid membrane can be made in order to expose and remove the growth thoroughly together with any soft parts or cartilage which appear to be involved. Branches of the superior thyreoid arteries, or the hyoid branch of the lingual artery, will be ligatured. The superior laryngeal nerves should always be preserved whenever possible, as loss of sensation increases the liability of food passing into the larynx.
(b) When the aryteno-epiglottidean fold is involved, a transverse incision can be made through the thyreo-hyoid membrane, immediately above the thyreoid cartilage on the same side, and the wound enlarged until the tumour is exposed. In this manner I was able to remove the large carcinoma shown in Fig. 254, including the soft parts of the right half of the larynx, the right half of the epiglottis, the right arytenoid, and the wall of the pharynx in relation to the right pyriform fossa: the lymphatic glands were not removed. One year later the patient continued to enjoy good health with no signs of any recurrence. In this connexion it is important to emphasize that when the disease is very extensive, and particularly when the posterior portion of the cricoid and arytenoids is involved, such an operation is useless, and the surgeon must decide whether partial or complete laryngectomy should be performed. In rare instances the operation should be abandoned in favour of tracheotomy (palliative).
(c) When the tumour extends downwards into the subglottic region, it is necessary to split the cricoid anteriorly and divide the upper rings of the trachea, after which the tumour can be removed with as much of the structures as may be desirable.
(d) When the growth extends across the middle line in the anterior commissure, or when a second growth is situated directly opposite on the other side of the larynx, the whole disease must be removed regardless of damage to the tissues which are not affected.
(e) When the operation is performed for stenosis, it is necessary to remove freely all the fibrous tissue without attempting to preserve any part that is diseased. The hæmorrhage is generally severe and necessitates preliminary plugging of the trachea with a Hahn’s canula.
After-treatment. This must be conducted so as to prevent the chance of broncho-pneumonia and sustain the strength of the patient. With Butlin’s method the patient is placed on his side, or face downwards, with the head low and with only a small pillow, so that all secretions pass out of the air-passages through the external wound. This undoubtedly gives better drainage to the wound, and is less exhausting than the upright position during the early stages of convalescence. The dressings on the wound must be changed, especially in the early days, as often as they become soaked; it is also an advantage to insufflate an orthoform powder, or an antiseptic parolein preparation, with the object of cleansing the larynx. The tracheotomy tube should be retained, usually from ten to twenty days, until the patient can swallow well and as long as there is a flow of pus from the wound.
‘During the day of the operation nothing is swallowed, although fragments of ice may be kept in the mouth for the comfort of the patient. If there is fear of collapse and the patient is feeble and very old, brandy and beef-tea may be administered by the rectum. On the following morning the first attempt is made to swallow. The patient leans far forwards with the head down, and the dressing is taken off the wound, beneath which a basin is placed. Cold water is drunk out of a glass. If the experiment is successful, all the water passes down into the stomach; if it is only partially successful, some escapes into the larynx; but the posture of the patient ensures that the liquid runs out through the wound and does not pass into the air-passages. As soon as water can be readily swallowed, milk, beef-tea, and other liquids may be drunk, for the fear of “Schluck-pneumonie” is practically at an end. The wound is generally closed within ten or twelve days of the operation, and the patient is rarely confined to the house for more than ten days’ (Butlin). It is probable that the healing by this, which is called the ‘open’ method, is as rapid as with Moure’s, in which the whole length of the incision is closed; the open method would also appear to be safer and less often attended by complications.
Complications. (1) Broncho-pneumonia is most to be dreaded. Death from shock or collapse, from hæmorrhage, from septic conditions of the wound, or from iodoform poisoning, is now rarely met with and can more easily be prevented. Even pneumonia is uncommon, owing to more scientific methods of treatment. It is still to be feared in very old patients; in those who already suffer from bronchial catarrh at the time of the operation; in alcoholics; and in cases with old-standing renal, pulmonary, or heart affections. The improvement in this direction is due to greater antiseptic precautions, and to the prevention of aspiration of blood and septic secretion during and after the operation by free drainage of the wound.
(2) Stenosis. It sometimes happens that a considerable mass of granulation tissue appears in the anterior commissure, or upon the surface of the cartilage that has been bared by the operation; if this be left untreated it may gradually enlarge in size until a prominent cushion is produced, which reaches to the opposite side and thus causes stenosis with definite laryngeal obstruction. Such a swelling may be mistaken for recurrence, but is nearly always of inflammatory character. It is by no means certain what is the causation of this condition, which appears to occur more with some surgeons than with others; it has been suggested that the presence of sutures in the region of the anterior commissure may cause an irritation, especially if silk is used. It appears to me, having in mind similar conditions in other surgical wounds, that the cause is to be found in some form of sepsis, and that it can be prevented to a great extent by precautions at the operation and by proper after-treatment. If there be any obstruction to breathing, the larynx is inspected and the projecting granulations are removed by intralaryngeal forceps. The remainder of the mass generally shrinks and disappears. If the stenosis be troublesome (chiefly in syphilitic cases), the prolonged use of a laryngo-tracheal canula (p. 540), or of an intubation tube, or dilatation with bougies, may be necessary. In rare instances a permanent tracheotomy tube is required, with a valve to encourage expiration through the mouth.
This operation is suitable for certain cases of malignant disease which is strictly limited to one half of the larynx. The requirements and first and second stages of the operation are similar to those for thyrotomy (see pp. 490, 491).
Third stage. A transverse incision is made on the side affected along the upper border of the thyreoid cartilage, through the skin and fasciæ; and, if necessary, a second transverse incision is made at the level of the lower border of the cricoid so that a skin flap can be turned back. The affected half of the larynx must now be considered as a tumour to be removed. The infrahyoid muscles are dissected away from the ‘tumour’ and retracted; the upper part of the lateral lobe of the thyreoid gland (the isthmus having been previously divided) is displaced outwards by blunt dissection, and the soft tissues above the thyreoid are similarly treated: the larynx should be pulled well over to the opposite side while this is being effected, great care being necessary to avoid wounding the carotid artery in the deeper part of the dissection. The branches of the superior thyreoid artery, the crico-thyreoid artery, and the veins of this region are ligatured with catgut. In some instances, when the growth has not perforated the cartilage, the separation can be performed subperiosteally. Superiorly, the thyreo-hyoid membrane is completely divided on the same side, and the mucosa is cut through above the upper limit of the growth. If the growth extends upwards, the epiglottis may be removed either totally or partially. Inferiorly, a transverse incision must be made through the crico-thyreoid or crico-tracheal membrane, or lower in the trachea. The inferior constrictor of the pharynx is divided as close to the attachment to the thyreoid as possible, and the cavity of the pharynx is opened behind the growth. The cricoid plate is split with bone scissors in the interarytenoid interval, and the final attachments are rapidly divided with a few touches of the knife.
In this operation, as with other operations for cancer, the main thought of the surgeon must be to remove the tumour thoroughly, including the soft tissues of the neck when these are diseased, the lateral wall of the pharynx, and the cervical glands upon the same side, whether they are known to be affected or not. In this respect the operation differs materially from thyrotomy; and I agree with Semon that, if hemi-laryngectomy is necessary, the lymphatic glands of the same side should in all cases be removed. The two dissections may be accomplished at the same time, or one may be performed later at a second operation; in the latter event an incision along the anterior border of the sterno-mastoid muscle is preferred. The operation must be very complete in order to be successful, and requires a knowledge of the anatomy of the lymphatics.
The following description is Cuneo’s14 and has been confirmed by de Santi.15
The lymphatics which drain the mucous membrane of the larynx are divided into two distinct regions, namely, the supraglottic and the infraglottic zones. These regions are separated by the inferior vocal cords, and injection of the cords themselves generally passes into the upper zone. The upper region is most densely supplied, and covers the epiglottis, the aryteno-epiglottidean folds, the superior vocal cords, and the ventricles.
The lymphatics communicate freely in the posterior wall of the larynx (not in the anterior commissure), but though an injection into one half of the larynx easily passes into the mucous membrane of the other side, it is exceptional for it to pass as far as the corresponding glands of that side. The lymphatics of the larynx anastomose to a large extent with the networks of the adjacent organs (tongue, pharynx, trachea).
The supraglottic lymphatics perforate the thyreo-hyoid membrane where the superior laryngeal arteries enter, and end in (1) a substerno-mastoid gland under the posterior belly of the digastric; (2) glands on the internal jugular vein opposite the bifurcation of the carotid artery; and (3) glands on the same vein opposite the middle of the lateral lobes of the thyreoid gland. The glands in the front of the thyreo-hyoid membrane receive lymphatics from the pharynx, but none from the larynx.
The subglottic lymphatics perforate the crico-thyreoid membrane in two places (a) anteriorly, near the middle line, ending in (1) a prelaryngeal gland which lies in the V-shaped space between the crico-thyreoid muscles or under one of the same (a gland above the isthmus of the thyreoid gland is rarely present), and (2) a pretracheal gland (or glands) below the isthmus; (b) laterally, to end in (1) the glands which lie parallel to the recurrent laryngeal nerve, from which trunks run to (2) the substerno-mastoid group and (3) the supraclavicular glands.
It is important also to consider the question from the clinical aspect. With ‘intrinsic’ growths, involvement of glands is very uncommon unless the posterior (cricoid) zone is affected; it seems to be equally rare with tumours of both supra- and infraglottic zones; extension to the lymphatics of the opposite side is likewise improbable. With ‘extrinsic’ growths, the glands are rapidly involved; tumours that were originally intrinsic follow this rule as soon as they begin to affect the cartilages and extrinsic lymphatics of the larynx. These facts must be remembered because palpation of the neck may be quite misleading in early stages of the disease. On the other hand, in many advanced cases, such as those requiring palliative tracheotomy, the glands become massive and form definite tumours. The substerno-mastoid chain is, clinically, the situation that is specially affected; and any of its glands, from the digastric muscle above to the supraclavicular region below, may be involved. The prelaryngeal gland is rare, as are likewise the pretracheal and recurrent forms; nevertheless, the recurrent glands become attacked by advanced disease, affecting the upper part of the trachea.
Indications. This operation is performed for malignant tumours which have affected (a) the whole of the interior of the larynx, including the cartilages, or (b) the posterior portion of the larynx, including the arytenoid cartilages and pharyngeal aspect of the cricoid plate. In other words, it is employed in cases of extrinsic cancer in which the growth is not too advanced to render the prospect of its eradication hopeless. The operation should not be performed for tuberculosis.
It is essential that the patient should be in good health; one who is emaciated or who has organic disease, especially incurable bronchitis, is quite unsuitable for laryngectomy. On no account ought the operation to be undertaken unless the diagnosis of malignant disease has been confirmed, and unless the growth is known to be too extensive for thyrotomy. In many instances, therefore, thyrotomy is the first stage in the operation of total laryngectomy.
Operation. The instruments, anæsthetic, and position require the same consideration as with thyrotomy (see p. 489).
First stage. A vertical incision is made, in the middle line, from the hyoid to a point one inch above the sternum, and the anterior aspects of the thyreoid cartilage and trachea are exposed, with complete division of the isthmus of the thyreoid gland. The infrahyoid muscles are dissected from the larynx and widely retracted. By blunt dissection the upper part of the lateral lobes of the thyreoid gland is separated and bleeding arrested. The trachea, having been isolated in this manner, is divided obliquely from the front, upwards and backwards, as close to the cricoid cartilage as the disease allows without injury to the œsophagus; the lower end is carefully freed from the œsophagus, and two strong catgut sutures are passed through it with which the divided stump can be drawn forwards. If possible, a small transverse incision is made through the skin immediately above the suprasternal notch and made to communicate with the upper incision; the trachea is brought beneath the bridge of skin into the button-hole thus formed, and firmly attached by means of sutures. In some cases the trachea is sewn into the lower part of the original incision. A tracheotomy tube is inserted, through which the anæsthetic is continued. By this means the lower air-passages are completely cut off from the region of the tumour, and no blood or septic matter can pass into the lungs.
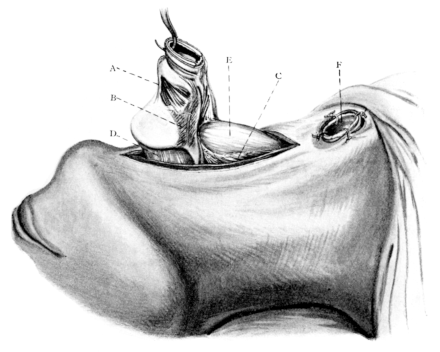 Fig. 262. Total Laryngectomy. A, Crico-thyreoid muscle; B, Attachment of
inferior constrictor of pharynx to thyreoid cartilage; C, Cut edge of inferior constrictor;
D, Thyreo-hyoid membrane; E, Œsophagus; F, Trachea.
Fig. 262. Total Laryngectomy. A, Crico-thyreoid muscle; B, Attachment of
inferior constrictor of pharynx to thyreoid cartilage; C, Cut edge of inferior constrictor;
D, Thyreo-hyoid membrane; E, Œsophagus; F, Trachea.
Second stage. The lateral aspect of the larynx is freely separated so that the attachment of the inferior constrictors is defined. The superior laryngeal artery is ligatured on each side, and divided, together with the internal laryngeal nerves. The thyreo-hyoid membrane is transversely divided, and the pharynx is opened so as to expose the upper limit of the growth; this may necessitate a transverse incision through the skin, or a vertical division of the hyoid bone in the middle line with retraction of its two halves. The larynx having been isolated above, below, and laterally, its removal can be completed according to the situation of the growth, in most cases from below. The lower end of the larynx is hooked forward, and dissected away from the œsophagus by means of scissors or a sharp scalpel (Fig. 262). While this is being effected, the extent of the growth must be constantly examined by inspection and palpation, so that the whole mass is removed, including, if necessary, the pharynx and upper part of the œsophagus. It is important not to drag upon the œsophagus; C. Jackson has shown experimentally that this causes severe shock by affecting the depressor fibres of the vagus, which may result in death. It follows, therefore, that this part of the operation, though easy in the dead body, requires the utmost care and detailed technique. The division of the constrictors should be as close to their attachment as possible, and the final division of the pharyngeal mucosa should be half an inch beyond the limit of the growth. The epiglottis should generally be removed.
Third stage. The toilet of the pharynx and œsophagus remains to be decided. In order to restore the cavity of the pharynx, the upper end of the œsophagus is brought upwards whenever possible and accurately united to the pharynx in the region of the hyoid bone, this being accomplished by a double layer of catgut sutures uniting the mucous membranes. The infrahyoid muscles are then brought together by a vertical row of stitches, so as to cover and support the line of union. The wound having been thoroughly packed with gauze, the skin is sutured, excepting the lower end, which remains open for drainage. In cases where the pharynx is thus completely closed, a tube must be passed previously through the nose into the œsophagus, and retained for purposes of feeding. This is preferable to sewing the tube into the wound itself, and is rarely troublesome if the tube is sufficiently stiff to prevent its displacement by retching. At the conclusion of the operation the tracheotomy tube is replaced by an ordinary silver canula, and the wounds are lightly dressed.
After-treatment. This is conducted upon similar lines to those adopted in the after-treatment of thyrotomy. During the first ten days, until the pharyngeal wound is firm, the patient must be fed through the tube and by rectal administration. Sterilized water may be sucked uphill, and, as swallowing improves, food may be administered by the mouth. In most cases a pharyngeal fistula results, which may require a later plastic operation. A second operation is necessary for the removal of lymphatic glands, probably on both sides of the neck.
The complications are similar to those following thyrotomy (see p. 494).
Modifications. The above operation, which in the main has been planned by surgeons in America (S. Cohen, Keen, &c.), is preferable to the numerous modifications, of which the following may be mentioned as examples:—
Gluck’s operation. In this there is no preliminary tracheotomy. A large rectangular flap is turned to one side to expose the front of the larynx and trachea, the latter being isolated laterally and the thyreoid isthmus divided. A transverse incision is made through the thyreo-hyoid membrane in order to expose the upper aperture of the larynx thoroughly. By plugging the pharynx and adopting a low position for the head, saliva and blood are prevented from running into the air-passages. The interior of the larynx having been cocainized, a tracheotomy tube is inserted between the vocal cords. This is sutured in position in such a manner that the cavity of the larynx is completely shut off from the pharynx. If a general anæsthetic be employed, it can be continued through the canula by a Hahn’s adjustment (Fig. 266). The larynx, and any part of the pharynx or œsophagus which is diseased, are separated from above downwards, the trachea being severed transversely as a final stage and sewn into a button-hole immediately above the sternum. A soft rubber tube having been introduced through the nose into the œsophagus, the walls of the latter are united over the tube by a double row of catgut sutures, completely isolating the gullet. The cavity is covered with gauze, and the skin flap is partially sutured into its original position. An ordinary canula is placed in the trachea and the wounds are dressed.
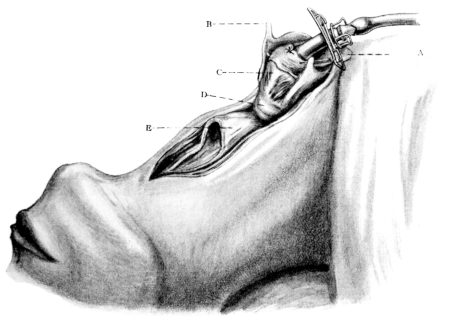 Fig. 263. Total Laryngectomy. Gluck’s Method. Tracheotomy canula
with rubber tube for Hahn’s adjustment tied into the upper opening of the larynx.
A, Epiglottis; B, Superior cornu of thyreoid cartilage; C, Posterior surface of
cricoid with crico-arytenoid muscles; D, Trachea; E, Œsophagus.
Fig. 263. Total Laryngectomy. Gluck’s Method. Tracheotomy canula
with rubber tube for Hahn’s adjustment tied into the upper opening of the larynx.
A, Epiglottis; B, Superior cornu of thyreoid cartilage; C, Posterior surface of
cricoid with crico-arytenoid muscles; D, Trachea; E, Œsophagus.
In cases where the pharynx has been extensively removed a fistula remains, but Gluck has devised a plastic operation by means of which this can afterwards be closed. In some cases this fistula may be obliterated by the natural falling in of the parts, without further operation, and in the meantime the patient is provided with a funnelled tube for feeding, placed in the œsophagus with the upper end below the base of the tongue.
The advantages claimed by Gluck for this operation are the avoidance of preliminary tracheotomy, the prevention of blood from passing into the trachea, the complete separation of the trachea from the gullet, and the early feeding through the mouth. These, however, are chiefly met by the former operation.
Chiari and le Bec perform the operation in two stages. In the first, the trachea is isolated and divided transversely, the lower end being sutured above the sternum. The second operation, undertaken one or two weeks later, consists of a complete removal of the disease.
Föderl suggests the possibility of uniting the lower end of the trachea (after laryngectomy is completed) to the tissues beyond the hyoid bone, and thus restoring the air-passages; but the method is not free from danger, and the trachea is apt to slough.
S. Handley16 performed a complete transverse resection of the pharynx, with laryngectomy, for malignant growth in the following manner: Preliminary gastrostomy was performed; a week later, when the patient had recovered, a low tracheotomy was effected, the trachea being plugged with gauze above the tube. The whole of the larynx and a complete section of the pharynx were then removed as described in Gluck’s method; and, the trachea having been brought into the lower part of the wound, the pharynx and œsophagus were closed by sutures. The patient recovered with a pharyngeal fistula through which the saliva passed, the latter being led to the stomach through the gastrostomy opening. In a second similar case the result was fatal. ‘The patient died on the table, apparently from irritation of the vagus, after the operation was practically complete.’ Handley believed that the failure was due to a defect in his technique, and that, if he had frozen the two vagi below the point at which he was working, death would not have occurred.
In order to obtain a trustworthy idea of the value of the various operations for malignant disease, it is necessary to refer to the history of the operations.17 Czerny, in 1870, was the first to demonstrate by experiments on dogs the possibility of removing the entire larynx, and various attempts were afterwards made by different surgeons, notably by Billroth, to accomplish the same in man. In 1881 Foulis was able to collect twenty-five cases of total laryngectomy, and found that not one of them was alive twelve months after the operation. Partly in consequence of this, thyrotomy was given a trial, and in 1887 P. Bruns collected nineteen cases, with two deaths and sixteen local recurrences. He therefore concluded that ‘attempts to extirpate the disease by means of thyrotomy have shown themselves to be altogether insufficient and useless’; and so it came about that all external operations, at this date, were considered by most authorities to be unsatisfactory. Much attention was, however, drawn to the subject by the illness of the German Emperor, and Semon particularly emphasized the great importance of early diagnosis. The result of this was marvellous. The importance of Krishaber’s division of carcinoma of the larynx into two forms, intrinsic and extrinsic, was recognized by Butlin, to whom the greatest credit is due for having first shown that thyrotomy ought to be reinstated. Butlin and Semon have since perfected this operation, which has rightly been described as the English operation. It is now recognized throughout this country as the operation which gives perfectly ideal results, so long as it is restricted to early stages of intrinsic malignant disease (in which an early diagnosis is indispensable) and is thoroughly carried out. As Semon concludes, ‘if these demands be complied with, the position of thyrotomy, as being the operation in the early stages of malignant disease of the larynx, will remain impregnable, so long as we have to fight malignant disease by operation.’ That this is true will be seen by the results mentioned later.
It is also necessary to refer to the other side of the question, namely, the position of laryngectomy. Many well-known surgeons in Europe and the United States have been convinced that laryngectomy, partial or complete, is the only possible treatment for cancer in this region. Gluck18 says:
‘As showing the progress that has been made during the last fifteen years in this subject, I may mention that in my first series of ten cases only two were successful, and in nine cases of another series I had four deaths. Since then I have performed many operations with ever improving results. Thus in one series of thirty-five hemi-laryngectomies I had three deaths: one twenty-four days after the operation, of heart failure, when the wound was already healed; another independently of the operation, of phlegmon of the right gluteal muscle; the third of pneumonia five days after operation.
‘My most recent results show a series of twenty-two complete laryngectomies with one death, that of a man of seventy, who died on the eleventh day of iodoform poisoning. Of the partial extirpations of the larynx and pharynx, generally combined with removal of infected glands, I can point to a series of twenty-seven cases with only one death. This was a case in which the carotid had been tied, and death occurred from hemiplegia five days after the operation.
‘At present I could show you thirty-eight living patients who have been cured by these operations; the oldest case was operated on thirteen years ago. Of those already dead, a number have lived 11, 8, 6½, 5½, 4½ and 3½ years after the operation in good health, and some have died of other illnesses, not of recurrence. One man, nine years after hemi-laryngectomy, had recurrence in the other half of the larynx and in the glands; after the second operation he lived over two years, and died at seventy-six. The operations lengthened his life for eleven years.
‘A man of seventy-six had the larynx and pharynx extirpated, and lived 11½ years after the operation. Twice I have performed complete laryngectomy for tubercle; one case died in spite of that of consumption; the other was done four years ago and the patient is perfectly well.
‘In all I have performed 125 of these operations since the year 1888, and the record is one of great progress, both in technique and also in the elaboration of plastic operations and mechanical appliances for the improvement of the post-operative condition.’
Many large operations of this description have undoubtedly been performed because of the statement that it is impossible to obtain a lasting cure by performance of thyrotomy. Even at the present day this opinion holds its ground, and so long as there is a general grouping of the cases, progress cannot be made.
Thyrotomy. I shall attempt to show that thyrotomy is the best operation for early malignant disease, whether carcinoma or sarcoma, so long as it remains intrinsic. No attempt will be made to separate the different forms of these diseases. The points to be considered are the following:—
The mortality of the operation itself has been greatly reduced; von Bruns19 states that ‘between 1890 and 1898 there was an immediate fatality of 15%’ in sixty cases collected by Schmiegelow and himself. In comparison with these figures, the recent results of English surgeons have been very favourable. Thus Butlin and Semon have performed forty-eight thyrotomies for malignant disease since 1890 with only two deaths. In Butlin’s case the patient was over seventy years of age, very obstinate, very intractable, and persisted in sitting up from the time of the operation. He died, in the course of three or four days, of septic pneumonia. The results of other surgeons have been excellent, but are not included for three reasons: There is still considerable confusion in the selection of cases suitable to this operation; the operation is often performed by those who are not conversant with the difficulties and dangers that may arise; and it has sometimes to be undertaken for a patient who is also suffering from bronchitis or constitutional disease. Moreover, the above figures are sufficient to show that the immediate mortality from this operation under favourable circumstances is not large.
Recurrence, in Semon’s cases, occurred in 13.6%, which is not a large proportion. It usually occurs early or not at all. Semon and Jackson noted that none of their patients suffered from recurrence after the lapse of the first year. This is a point of great importance; and in this connexion Semon points out, as an additional advantage of thyrotomy, ‘that even in the cases in which either the operation has not been complete, or in which unfortunately genuine recurrence has taken place, the operation does not bring us to the end of our resources; but that, on the contrary, by a repetition of the operation, or by hemi-laryngectomy, or by total extirpation of the larynx, a lasting cure may still be obtained, where the minor operation has failed.’
Cures. I hope it will soon become generally recognized that the radical operation of thyrotomy for removal of early intrinsic malignant disease is attended by a remarkable number of complete cures, and compares favourably with almost any other operation for similar conditions in other parts of the body. Butlin (see Table, p. 507), Semon, and C. Jackson have all obtained, in recent years, from 60 to 80% of lasting cures. In Semon’s twenty-five cases,20 one died of the operation, three cases recurred within a year, and one was too recent to be included, the remaining twenty were cured for varying periods, namely:
1 case over 15 years.
4 cases between 10 and 15 years.
4 cases between 5 and 10 years.
2 cases over 4 years.
3 cases over 3 years.
2 cases over 2 years.
1 case just 2 years.
1 case 1 year and 10 months.
1 case died 5 years after operation from pulmonary embolism.
1 case died 4 years after operation from pneumonia.
In both the last cases recurrence was excluded.
The condition of the patient after thyrotomy. The voice results are often surprisingly good even when a free excision of soft parts, including one or both vocal cords, has been required. In from 40 to 60% of cases that are cured, the voice is practically normal, though rough and reduced in volume and range. Of the remainder, the majority recover sufficiently to produce a considerable whisper, and only a few suffer complete loss of voice. The causes of a complete loss of voice, when it occurs, are chronic inflammation, cicatricial contractions, or improper union of the cartilage. Further, a loss of voice is probable in the event of a recurrence of the growth.
The breathing is not affected unless the operation is followed by stenosis. The power of swallowing is soon regained, and the general condition of those who are cured is one of complete happiness and general excellence of health.
These results may now be briefly compared with those obtained by laryngectomy, whether partial or complete.
Hemi-laryngectomy. The immediate mortality of this operation also has been greatly reduced. Sendziak collected 108 cases, up to 1894, showing a mortality of 26.3%; von Bruns 106 cases, between 1890 and 1898, with a mortality of 17%; Gluck has performed thirty-five such operations with only three deaths—8.1%. The number of cases reported in England is too small to be of value, chiefly because thyrotomy or total extirpation has been considered better. Taking, therefore, the best published results, it appears that the mortality is at least twice as great as with thyrotomy.
The danger of recurrence is also greater, partly because the glands are affected. Statistics show that recurrence occurs in at least one-fourth of the cases, possibly more, and is generally fatal. It is impossible to give a prognosis as to cure in the early stages after operation, but there are instances of life being prolonged for many years; a case of Gluck’s lived for eleven years.
The after-condition is not unsatisfactory. The permanent wearing of a tracheotomy tube is rarely necessary. Swallowing is soon recovered, and the voice is often good.
Total laryngectomy. Although the mortality of this operation has been greatly reduced by many improvements in recent years, it still remains higher than that of thyrotomy. As far as can be judged from the small number of cases that have been reported by English surgeons, there seems to be a direct mortality of at least 20% from these operations. C. Jackson21 has, however, performed eight consecutive total laryngectomies without a death in the first thirty days. He writes: ‘Of eight total laryngectomies done by me, three were hemi-laryngectomies followed by recurrence and the total operation. Of the eight laryngectomies, one lived seven years. I felt justified in claiming a cure, but upon inquiry a few weeks ago I was informed by relatives that he died of cancer of the stomach. One case lived three years without recurrence, dying of cerebral hæmorrhage, and one eight months, dying of alcoholism. Of the remaining five, three recurred within a year, one apparent cure was lost to observation after a year, and one is too recent to record: one of the three prompt recurrences had metastases in the lungs, liver, and pancreas. Thus, of eight laryngectomies, no absolute ultimate cures can be claimed, though three were apparent cures at the end of one year.’
Butlin has performed total laryngectomy upon seven patients, only one of whom died from the operation. He says: ‘I first removed a large mass of glands on both sides, and later took out the larynx, which was so diseased, that the surrounding parts were infiltrated for a considerable distance. He lived six weeks after the second operation, and then died of double pneumonia, which was attributed to an attack of influenza when he was up and about his room. I do not know whether the pneumonia was due to that cause or to sepsis of the lungs, for we had on several occasions some difficulty in feeding him, and in getting a tube properly down his œsophagus.’
The following is a table showing Butlin’s operations since the year 1890, from a paper which was read at the Second Congress of the International Surgical Society at Brussels in 1908:—
| Operations. | |||||
| Number and type of operation | Type of operation | Number of patients | |||
| 23 | Thyrotomy 1 | 21 | patients | ||
| 1 | Hemi-laryngectomy | 1 | patient | ||
| 7 | Laryngectomy 2 | 6 | patients | ||
| — | — | ||||
| 31 | operations on | 28 | " | ||
| Died of the operation (1 thyrotomy, 1 laryngectomy) | 2 |
| Died of recurrence | 4 |
| Died of intrathoracic disease, probably cancerous glands, within 2 years | 1 |
| Died of cancer of tongue 3 | 1 |
| Lost sight of after operation | 1 |
| Alive after operation for recurrence | 2 |
| Well within 3 years | 3 |
| Died of other disease after 3 years | 1 |
| Well after 3 years 4 | 13 |
| — | |
| 28 |
1 In two patients the operation was repeated.
2 In one patient thyrotomy was followed by laryngectomy, but the patient was included amongst the thyrotomies only.
3 This was regarded as a second attack of cancer, for the disease of the tongue was some distance from the larynx, and there was no sign of cancer of the intervening parts. Also more than a year elapsed before he began to suffer from cancer of the tongue.
4 Periods during which patients remained well lasted from 3 to 15 years.
Recurrence after laryngectomy is, therefore, more frequent than after thyrotomy, and it is difficult to estimate the proportion of cases that are cured by this operation. Butlin writes: ‘Of the six patients who survived the operation, one died of probable cancerous glands in the mediastinum, one had inoperable recurrence in the cervical glands, three were alive within three years, and one was well three years after the operation.’ He says: ‘I began to perform laryngectomy three years ago on account of Gluck’s success, and of the excellent modification due to Solis Cohen. I wish I had begun to perform it earlier. I am sure that several of the cases on which I performed thyrotomy were much better fitted for laryngectomy, and I cannot help thinking I might have saved one or two patients in whom recurrence took place if I had then removed the larynx. I think the glands ought to be removed in every case in which there is extensive carcinoma of the larynx, even if it be intrinsic, unless the disease is limited to the middle zone of the interior of the larynx. Even in these cases it would probably be a wise precaution to remove the glands. I have never removed the glands and the larynx at one sitting.’ Von Bruns,22 from statistics of all total operations since 1890, gives the following proportions:—
| Cure, over 3 years | 8.6% |
| Cure, 1 to 3 years | 17.4% |
| Cure, under 1 year | 32.0% |
| Recurrence | 23.4% |
| Death due to operation | 18.5% |
The voice after laryngectomy. Many efforts have been made to replace the lost voice. The artificial larynx, as first devised by Gussenbauer, consisted of three distinct parts: a tube for the trachea through which the patient inspired; a tube communicating with the pharynx so as to allow of expiration through the mouth; and a phonation canula which fitted into the former. This canula was supplied with a valve which closed during expiration so as to allow of breathing through the mouth, and a phonation apparatus for production of the voice. A large number of modifications of this larynx have been made at different times but have rarely been successful. The irritation and pain caused by the pharyngeal portion, the difficulty in swallowing and in keeping the tubes clean, and the exhaustion caused by prolonged use, have combined to make the apparatus unsatisfactory.
As the result of recent improvements in laryngectomy, most surgeons isolate the trachea as already described, and thus entirely shut off all communication with the mouth. The patient then has a choice of two methods—(1) the bucco-pharyngeal voice, or (2) a phonetic apparatus such as that described by Gluck, consisting of (a) an external tracheotomy canula for breathing, (b) an internal canula, possessing a valve which closes during expiration and causes the air to pass upwards to another compartment containing a small rubber band or tongue, the vibration of which forms the voice, and (c) a third tube of rubber, which is easily fitted to the upper part of the inner canula and is of sufficient length to reach the mouth. When the patient wishes to speak, the upper end of the last-mentioned tube is either placed in the angle of the mouth or passed through the nose to the back of the pharynx, and the air which has been made to vibrate in the inner tube is thus carried to the mouth. This instrument is easy to adjust and clean, produces remarkable phonetic effects, and is much the most ingenious and serviceable device that has so far been invented. In some cases, however, a patient can make himself understood without an instrument of any kind. ‘A whispered voice remains even after the pharynx has been completely shut off from the air-passages and, as shown by experience, may be developed by practice until it is quite sufficient for the demands of the patient. Hans Schmidt’s case has become more or less celebrated, in which, under conditions of this sort, a loud though rough and monotonous voice was developed. One of Mikulicz’s patients was even able to sing. Gottstein explains the development of a pseudo-voice by the formation of an air-chamber in the pharynx and œsophagus, which is voluntarily inflated and emptied by the patient’ (von Bruns).
Swallowing after laryngectomy is satisfactory, and the general health in many cases improves. The mental condition of the patient is often disappointing. ‘Even in favourable cases, when the tumour does not recur after laryngectomy, the patient finds himself in such a condition of inferiority to his fellows, that he may, with some reason, ask himself (at least in certain cases) whether death would not have been preferable to such an existence as is left to him’ (Moure23). With recurrence of the disease the patient’s life is terribly sad.
It must therefore be admitted that laryngectomy is at present an operation of necessity, suitable for certain cases only, capable of prolonging life, and, rarely, of curing the patient. It is difficult to foreshadow the future of this operation; but, in the words of Gluck, ‘our first object must be to save life; our next, to leave the patient in such a physical condition that the life so saved is worth living.’
The above statistics are sufficient to show that the results of laryngectomy for extrinsic disease compare unfavourably with the results obtained by thyrotomy in intrinsic forms of cancer. In this country there have not been sufficient cases to estimate accurately the percentage of recoveries. The disease may recur at any period after the operation, and the prospect of a cure is always doubtful.
It is, however, to be hoped that, with improved methods of examination, earlier diagnosis, and a careful selection of the cases, better results will in future be obtained. Authorities such as Butlin and Semon support this view, and agree that further attempts must be made to make this operation successful.
In order to avoid confusion with other operations included under laryngotomy, this term is used to denote the operation in which the larynx is opened through the crico-thyreoid membrane. The operation is an easy one in adults, but in children the crico-thyreoid space is so small that it is almost impossible to introduce a tube without division of the cricoid cartilage (see Crico-tracheotomy, p. 529).
A tube introduced through the crico-thyreoid membrane lies in the subglottic space well below the vocal cords, and the latter should not be injured when the operation is performed with care. If inflammation supervenes, there may be a swelling of the subglottic region, making the tube difficult to manipulate; and for this reason the operation is particularly suited to cases which require a tube for a short period only, such as—
Indications. (i) Sudden laryngeal obstruction due to impaction of food or other foreign body. This is more common in adults: in children dyspnœa is rarely so urgent as to necessitate an operation.
(ii) Sudden œdema of the larynx caused by trauma, fracture, or acute inflammation, when the equipment for tracheotomy is not obtainable; or,
(iii) As a preliminary to major operations upon the upper air-passages, in order to prevent blood from passing down into the trachea.
This last method of treatment marks a distinct advance in the surgery of the throat. Attention was first directed to it by Bond24, who has used the method for the past sixteen years with intent to make such operations less dangerous to life, and to increase, therefore, the number of cases that could be operated upon. His objects were to prevent respiration through the pharynx, thus obviating the coughing and struggling due to imperfect anæsthesia and making the anæsthetic easier and safer to administer; to shorten the operation and make it easier for the surgeon; and to get rid of preliminary tracheotomy whenever possible.
The value of this practice is well recognized by many surgeons. Butlin writes: ‘I do not know how many times I have employed this preliminary laryngotomy, but certainly more than a hundred times, so that I am now in a position to urge the importance of it on the profession.’ It has now been adopted at many of the hospitals in England before removal of tumours in the naso-pharynx, the upper and lower jaw, the tongue, palate, floor of mouth, and tonsil, in those cases where bleeding is likely to be severe.
In order to ascertain the feeling of my colleagues on this subject I have collected, with the assistance of Mr. Boyle, all the major operations performed upon the upper air-passages during the last six years at St. Bartholomew’s Hospital. These are tabulated below.
Table showing Operations upon the Upper Air-passages during the Years 1902–7 inclusive at St. Bartholomew’s Hospital
| With Laryngotomy. | Without Laryngotomy. | |||
|---|---|---|---|---|
| Cases. | Deaths. | Cases. | Deaths. | |
| Excision of Tongue | 20 | 03 | 13 | 2 |
| " " half Tongue | 25 | 02 | 46 | 1 |
| " " Floor of Mouth | 13 | 13 | 01 | |
| " " Tongue and Floor of Mouth | 05 | 01 | 01 | 1 |
| " " Palate | 08 | 01 | ||
| " " Upper Jaw | 12 | 13 | ||
| " " Lower Jaw | 01 | 09 | ||
| " " Tumour of Gums | 01 | |||
| " " Tonsil | 02 | 01 | ||
| " " Naso-pharyngeal Tumour | 03 | |||
| Total | 90 | 06 | 97 | 5 |
This table shows that nearly half the cases were treated by laryngotomy. In sixty-three of these, where the tongue or floor of the mouth was concerned, no preliminary ligature of the lingual artery was performed; of the seventy-three similar cases treated without laryngotomy there was preliminary ligature of one lingual in thirty-one cases (42.5%), and of both arteries in twelve cases (16.4%).
From this it is apparent that lary[n]gotomy has to some extent taken the place of preliminary ligature of one or both linguals. The operation is simple, rapid in execution, and meets all requirements; it is not surprising to find, therefore, that in recent years the number of laryngotomies has proportionately increased.
Table showing Operations as performed in different Years
| Year. | Cases. | With Laryngotomy. | Without Laryngotomy. |
|---|---|---|---|
| 1902 | 039 | 19 | 20 |
| 1903 | 035 | 05 | 30 |
| 1904 | 031 | 16 | 15 |
| 1905 | 032 | 18 | 14 |
| 1906 | 029 | 18 | 11 |
| 1907 | 021 | 14 | 07 |
| Total | 187 | 90 | 97 |
Operation. In cases of extreme emergency the operation can be performed with almost any kind of knife, but the following instruments are preferred: a sharp-pointed bistoury or tenotome, a sharp-pointed dilator (Fig. 265, B), a tube and introducer. The tube should be small, short, with a fixed collar, and made of silver; an introducer such as Butlin’s is a great advantage (Fig. 265, A). As bleeding may occur, it is necessary to prepare dissecting forceps, retractors, pressure forceps and catgut.
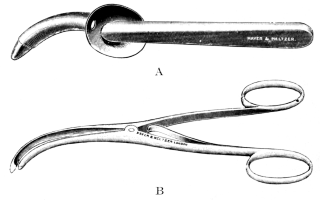 Fig. 265. Instruments for Laryngotomy. A, Tube
and introducer (Butlin’s); B, Sharp-pointed dilator
(Bailey’s).
Fig. 265. Instruments for Laryngotomy. A, Tube
and introducer (Butlin’s); B, Sharp-pointed dilator
(Bailey’s).
A general anæsthetic is usually employed when infrathyreoid laryngotomy forms the first stage of the main operation, but it should be remembered that the amount of chloroform required is less when given through a tube.
The preparation of the skin and the position of the body are the same as for tracheotomy. A transverse incision one inch in length is recommended, and this should lie directly over the crico-thyreoid interval, which is easy to determine in the adult. The incision can be made quickly by pinching up a vertical fold of skin, transfixing immediately above the cricoid, and cutting outwards: with this method the anterior jugular veins are rarely wounded, but if any vessel has been pricked it should be seized and tied at once.
The sharp dilator, placed exactly in the middle line immediately above the cricoid, is pushed backwards between the infrahyoid muscles until the resistance caused by the crico-thyreoid membrane is reached. It is then firmly stabbed into the larynx and widely dilated so as to tear open the membrane: the dilator having been withdrawn, the tube, with tapes attached and mounted upon the introducer, is rapidly inserted, a proceeding which is made easier by first smearing the instrument with a small amount of glycerine. The whole operation can be performed in less than a minute, and is rarely attended by serious hæmorrhage; moreover, when the original puncture is immediately above the cricoid there is less danger of wounding the crico-thyreoid artery. The operation is attended by few difficulties, and is superior to one in which dissection or cutting is employed.
At this stage a prolonged period of apnœa is usually encountered, and this symptom is more marked than with tracheotomy; when seen for the first time it may be alarming, and it is therefore of practical importance. In a few moments, however, the patient settles down to the altered conditions of respiration; coughing may be excited but soon disappears. When the breathing becomes regular, the tapes are tied round the neck and a rubber tube is attached (Fig. 266) similar to that used with Hahn’s apparatus, and through the tube the chloroform is continued. This method has the following advantages: it gives far more room to surgeon and anæsthetist, and enables the latter to manipulate the laryngotomy tube and to prevent it from tilting in such a way that the lower end impinges against the front of the trachea with consequent obstruction; further, the opening into the larynx is completely blocked, blood and lotion being unable to enter from outside.
As soon as true anæsthesia with regular automatic breathing has been obtained, the lower part of the pharynx should be plugged with a soft marine sponge to which a piece of tape or silk is attached, this being pushed down behind the tongue and firmly wedged in position; it is advisable to use a large sponge, as this blocks the pharynx and pushes forward the tongue, an advantage to the surgeon when operating upon that structure. If the mouth be obstructed by a tumour, the same result can be obtained by two or more smaller sponges passed in succession; or, as suggested by Bond, a small sponge may be pulled down into the larynx. As soon as the pharynx has been completely shut off, the main operation can proceed, and those who have once used this method can appreciate how much more quickly it can be performed and how much more comfortably for all concerned.
At the conclusion of the operation, when all bleeding has been controlled, the laryngotomy tube should be removed. The wound should not be sutured or plugged, and only a light dressing should be applied: the latter can be kept in place by a bandage, which, however, must on no account be tight, owing to the danger of emphysema.
Complications may arise—(a) During the operation. There may be troublesome bleeding owing to pricking of a vein, superficial or deep, or of the crico-thyreoid artery; this occurred in eight of the cases mentioned above, and in four was severe. In one of the latter the bleeding continued for thirty minutes before the vessel was finally secured. The condition is simple to treat: the wound must be enlarged, and the infrahyoid muscles separated so that the crico-thyreoid membrane is thoroughly exposed; the bleeding vessel can then be seized and tied, after which the tube is inserted. This is preferable to attempting to stop the bleeding by the introduction of the tube.
Difficulty in introducing the tube may occasionally occur. It may be due to imperfect division of the membrane; thus in one case the tube was passed down between the coats of the larynx and not within its cavity; and another case is recorded where the mucous membrane was similarly pushed backwards owing to the dilator having split the cricoid cartilage. Care must be taken, therefore, that the membrane is properly punctured, and that the opening is thoroughly dilated before any attempt is made to introduce the tube. Replacement of the tube was necessary in only one case, on the second day, owing to recurrence of bleeding from the wound in the mouth.
(b) After the operation. Emphysema occurred in six of the ninety cases; in two it was slight; in three it was extensive and involved the chest, neck, and face; and in one, where death supervened twelve hours after the operation, there was emphysema of the mediastinum. In two of these cases the laryngotomy wound had been sutured; in two others the operation was attended with severe hæmorrhage, and the mouth was plugged with gauze to control it. It is probable that emphysema is more likely to occur if there is any obstruction to breathing through the mouth after the operation, such as may be caused by the falling back of the remaining part of the tongue. The following precautions should be observed to prevent it: The laryngotomy wound must always be left open, and covered by a loose piece of gauze which does not press upon the neck; the patient must be nursed on his side, not upon the back; suturing the remaining part of the tongue is not sufficient; if plugging is left in the mouth, the tube must be temporarily retained, and removed after a few hours when breathing is not obstructed; early removal, however, is preferred.
Bronchitis is mentioned in two of the cases already quoted, pneumonia in one case, pneumonia and empyema in one, and purulent mediastinitis in one, with three deaths in all. Of these five cases, four had operations upon the tongue. On the other hand, without laryngotomy, bronchitis was rather more common (seven cases) and broncho-pneumonia occurred in two, both of which died. In order to throw more light upon the subject, we have examined the charts of all the cases after the operation, and have found that in most of them there was a rise of temperature to 99° F., or slightly higher, which lasted for periods varying from one to seven days; the pulse and respiration were little affected. In laryngotomy cases there were only eighteen instances of temperatures of over 100° F., as against twenty-five where no laryngotomy had been performed. Here again the pulse and respiration were only slightly affected, so that the condition was probably due to local inflammation and not to involvement of the lung. The results are by no means conclusive, but justify the general feeling that laryngotomy does not increase, but probably diminishes, the danger of infection of the lungs.
Healing of the wound may take place in normal conditions in about five days, but the period is frequently longer—from ten to twenty days; suppuration is uncommon, and was only mentioned in two instances where the wound had been sutured. The scar left after laryngotomy is often depressed for several months, but eventually becomes loosened and is then scarcely noticeable.
Death occurred in six cases, but there was no evidence to show that there was any connexion with the laryngotomy; on the contrary, the operations were more severe, and infrathyreoid laryngotomy was performed partly for the very reason that the condition of the patients was less favourable.
From my experience, the advantages which were originally claimed by Bond, Butlin, and others have been completely upheld; the larger operations upon the upper air-passages are easier to perform and can be more thoroughly completed; and it is very possible that the after-results may be improved by the greater facility which is thus afforded. I would strongly urge laryngotomy in all large operations of this region; the tube should be removed early, and the wound should not be sutured.
There is evidence to show that this operation was known to the ancients, and that it has been practised during at least two thousand years chiefly for the treatment of foreign bodies in the air-passages. From the sixteenth century to the present time it has been frequently performed, and the discovery of diphtheria in 1881 by Bretonneau opened up a new field for the operation.
It is uncertain when tubes were introduced in the after-treatment of tracheotomy, but Dr. George Martin in 1730 was the first to describe a double tube which allowed of the removal of the inner part for purposes of cleaning. The movable collar was invented by Luer, and the angular tube now generally used is associated with the name of R. W. Parker, to whose research we owe many of the recent improvements in connexion with this operation.
Indications. Obstruction to respiration is the most important, and must be distinguished carefully from the dyspnœa which is due to pulmonary affections, disease of the heart, or organic lesions in other parts of the body. Laryngeal obstruction may be due to—
(i) Diphtheria. The extent to which diphtheritic obstruction has to be taken into account is shown by the following table:—
Table showing the Number of Cases admitted to the Fever Hospitals of London (M.A.B.) during the Years 1902–7, inclusive25
| All forms of Diphtheria. | Laryngeal Cases. | Tracheotomy Cases. | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases. | Deaths. | Mortality per cent. | Cases. | Deaths. | Mortality per cent. | Cases. | Deaths. | Mortality per cent. | |
| 1902 | 06,839 | 0741 | 10.8 | 0639 | 134 | 20.9 | 0264 | 086 | 32.5 |
| 1903 | 05,422 | 0504 | 09.3 | 0560 | 102 | 18.2 | 0223 | 067 | 30.0 |
| 1904 | 04,639 | 0464 | 10.0 | 0659 | 116 | 17.6 | 0247 | 079 | 32.0 |
| 1905 | 04,224 | 0346 | 08.2 | 0706 | 116 | 16.4 | 0255 | 072 | 28.2 |
| 1906 | 04,937 | 0444 | 09.0 | 0702 | 127 | 18.1 | 0275 | 101 | 36.7 |
| 1907 | 05,674 | 0544 | 09.6 | 0981 | 169 | 17.2 | 0432 | 129 | 29.9 |
| 31,735 | 3,043 | 09.6 | 4,247 | 764 | 17.9 | 1,696 | 534 | 31.5 | |
An examination of the above figures shows that in recent epidemics 13% of the cases developed symptoms of laryngeal affection; that about 40% of these laryngeal cases were treated by tracheotomy (in some cases preceded by intubation); and that the mortality in all the cases of tracheotomy was 31.5%. Tracheotomy in diphtheria, therefore, must still be regarded as a serious operation.
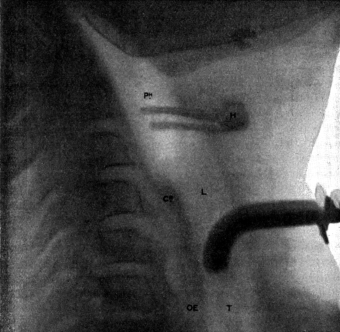 Fig. 267. Skiagram showing an Angular Tracheotomy Tube in the Trachea.
H, Body of hyoid; PH, Pharynx; CR, Posterior plate of cricoid; L, Larynx;
OE, Œsophagus; T, Trachea.
Fig. 267. Skiagram showing an Angular Tracheotomy Tube in the Trachea.
H, Body of hyoid; PH, Pharynx; CR, Posterior plate of cricoid; L, Larynx;
OE, Œsophagus; T, Trachea.
The operation is required chiefly during the early years of life, namely, from one to six (see table on p. 543). Although the larynx cannot be inspected in children, it is easy to determine whether mechanical obstruction is present; for inspiration is noisy and accompanied by stridor, the voice is lost or reduced to a whisper, and attempts to cough are frequent. The alæ nasi are dilated, the extra muscles of respiration are called into action, and laryngeal excursion is seen. On examining the chest, recession is evident; and during inspiration the supraclavicular fossæ, the intercostal spaces, and the epigastrium are all indrawn. The amount of recession depends more upon the muscles of the chest than upon dyspnœa, and is marked in weakly children. When dyspnœa becomes urgent the restlessness increases, and this is an important indication that an operation is required. In very serious cases the face is drawn, livid, or extremely pale; respiration is deficient, and the chest expansion feeble. An examination of the lungs shows the air entry to be imperfect; the bases are dull to percussion, and all sounds absent. The action of the heart is feeble, rapid, or intermittent; no nourishment can be swallowed. It is always difficult to determine how much of this collapse is due to toxin; but by relieving the obstruction the most distressing feature of the disease is removed, better aeration of the blood is obtained, and the heart is relieved from strain. The operation also drains the trachea, and the amount of poison absorbed is thus diminished. There is abundant evidence to show that the best results are obtained by early operation, especially in young children, in whom the larynx is comparatively small. It should be remembered that dyspnœa is often worse at night, and that at any moment there may be spasm.
(ii) Infectious diseases, such as (a) secondary diphtheria, by no means uncommon in the fever hospitals of London: in the five years 1902 to 1906, thirty cases are recorded, with sixteen deaths (53%), a very high mortality; (b) scarlet fever or measles, which provided 118 cases in which tracheotomy was performed, with eighty-seven deaths (74.3% mortality); (c) erysipelas, small-pox, typhoid fever, influenza and whooping-cough, which occasionally cause dyspnœa, calling for tracheotomy.
(iii) Acute laryngitis (other forms) in which œdema supervenes as the result of septic infection, or of the inhalation of steam, boiling water, or irritating chemicals, or as the result of trauma with or without fracture of the cartilages, or in the course of renal or heart disease. Brandy in excess, and certain drugs such as iodide of potassium, may also cause œdema of the larynx, and two cases are recorded by Fournier where death occurred before tracheotomy could be performed, as the result of taking iodides.
For conditions such as these tracheotomy is better than intubation, and, as the swelling may extend into the trachea, the high operation is not advised. Although the operation should not be undertaken until other treatment has been tried, it is well to remember that collapse of the lung, broncho-pneumonia, and complications, are likely to arise when the obstruction is allowed to persist.
(iv) Syphilis. In the tertiary stages of either acquired or congenital syphilis (rare) the larynx may be affected, and in long-standing cases of over ten years, when the mucosa is much thickened, there is a danger of obstruction. Even when energetic antisyphilitic treatment has been advised the disease may become acute. Tracheotomy may be necessary for the relief of (a) œdema, likely to occur suddenly with necrosis, perichondritis, or the breaking down of gummata; (b) fibrous stenosis, which may cause a gradual increase of dyspnœa or become suddenly acute from spasm or œdema (iodides?); (c) adhesions, whether simple bands or webs; or (d) fixation of the vocal cords in the middle line, resulting from inflammation of the laryngeal joints or from paralysis of the abductor muscles.
(v) Tubercle. This rarely causes true laryngeal obstruction, excepting in those acute cases where subglottic œdema, abscess, or sequestrum is present. Tracheotomy was at one time used in certain cases in order to give complete rest to the larynx, but this has been abandoned as unsatisfactory; it should not be performed unless there is urgent laryngeal obstruction, since ‘it has many and grave disadvantages. It materially diminishes the efficiency of the cough, the secretion from the lungs is apt to accumulate in the bronchi and alveoli, and set up miliary tuberculosis. Again, the patient can often ill withstand even this slight operation; his power of speaking is diminished or lost and his mental anxiety is increased. Not rarely also, the tracheotomy wound becomes infected with tubercle. For these reasons tracheotomy should never be performed in phthisis except for severe dyspnœa’ (Lack26).
(vi) Certain nervous diseases, such as abductor paralysis. Urgent dyspnœa may occur in (a) advanced bilateral abductor paralysis, or (b) unilateral abductor paralysis associated with pressure upon the trachea by tumours. In the bilateral form it is difficult to determine when to operate; but the danger of suffocation, increased during the night, makes it necessary to overrule the objections of the patient. Tracheotomy (or intubation) may be performed merely as a temporary relief where the paralysis results from diphtheria, syphilis, toxic neuritis, &c.; in more serious cases the tube must be worn permanently, unless total recurrent paralysis supervenes (as it may do, though rarely in tabes) accompanied by cadaveric position of the cords and the restoration of free breathing. This latter condition can be induced by total division of both recurrent laryngeal nerves, but the operation, which has been performed on one or two occasions, has not been attended with satisfactory results. In cases of long duration the tube may be plugged during the day, or a valve may be added to the canula, so that the patient can speak by expiration through the larynx.
(vii) Tracheal compression by tumours of the neck or mediastinum, of the thyreoid or thymus, or by aneurism, or by tuberculous bronchial glands. In these conditions inspiration and expiration are equally affected, and if the obstruction is low down, a long canula (such as König’s, Kocher’s, or Salzer’s) will be required in order to relieve the dyspnœa. The pressure of such tubes may cause ulceration of the wall of the trachea, and hæmorrhage may occur. This danger is especially to be feared when an aortic aneurism presses upon the trachea (see p. 542).
Tracheotomy should, therefore, be reserved for extreme cases, where it is impossible to remove the cause of the obstruction: on the other hand, dyspnœa caused by tumours of the neck which are removable (e.g. thyreoid tumours) should be relieved by radical operation without tracheotomy.
(viii) Congenital laryngeal stridor, glottic spasm, laryngismus stridulus, epilepsy, congenital webs and diseases of the crico-arytenoid joint such as ankylosis (true or false) or luxation. In these cases tracheotomy is rarely necessary, but when the operation is advisably undertaken the dyspnœa may require a permanent tracheotomy tube or prolonged intubation unless a radical removal of the disease can be effected.
(ix) Cut-throat. Tracheotomy is advised as a preliminary to further plastic operations in all cases where any part of the air-passages has been opened, in order to avoid the danger of suffocation and to prevent hæmorrhage into the trachea.
(x) Fracture of either the hyoid, thyreoid, or cricoid cartilage, that of the thyreoid being the most common, and of the cricoid the most serious. These fractures are always associated with hæmorrhage and œdema of the mucous membrane, sometimes with emphysema; and the swelling thus caused within the larynx may be so great that tracheotomy or laryngotomy becomes urgently necessary for the relief of dyspnœa. Theoretically it is advisable to expose the fracture, so that it may be sutured or wired in its proper position, but, even in those instances where this is attempted, it is advisable to retain the tracheotomy tube for a few days until all swelling has subsided.
(xi) Sudden dyspnœa during surgical operations, due to—
(a) Mechanical obstruction to respiration, such as is caused by impaction of foreign bodies within the larynx (tooth-plates, teeth, blood, pus, vomited food, &c.), by faulty position of the head or falling backwards of the tongue, by a swollen condition of the larynx, by tumours or abscesses (retropharyngeal) which obstruct the air-way, by cicatricial contraction of the pharynx or larynx, by paralysis of the vocal cords, or by spasm of the muscles of the jaws so often associated with a similar condition of the glottis and auxiliary muscles of respiration. In a case reported by Boyle, a well-nourished muscular man was anæsthetized for the operation of internal urethrotomy; considerable difficulty was encountered with his breathing, and only towards the end of the operation was it discovered that he had well-marked stenosis of the upper opening of the larynx.
The entrance into the larynx of vomited food or blood is certainly dangerous, and may occur during the simplest operations even when properly performed, as, for instance, during removal of tonsils or adenoids. It is more likely to occur if the patient has not been prepared for an anæsthetic, or if the latter be badly administered, if the laryngeal reflex be lost, if the patient be in a bad position or suddenly moves, or if the surgeon allows too much blood to collect in the pharynx.
(b) Failure of respiration from an overdose of chloroform or other anæsthetic. To remedy such conditions it is essential that the air should be expelled from the chest as rapidly as possible. Artificial respiration can only be successful when the air passes freely both into and out of the lungs: in rare instances there may be so much difficulty in maintaining a free passage that tracheotomy should be performed.
(xii) Multiple papillomata of the larynx. Here tracheotomy is required for the relief of dyspnœa and as a preliminary to other operations. It has also been suggested as a method of curing the papillomata by giving rest to the larynx. After the performance of tracheotomy the congestion is relieved and the growths decrease in size; in some cases they completely disappear, but the treatment is uncertain and not to be recommended (see p. 485).
(xiii) Malignant disease of the pharynx or larynx which is too advanced for other forms of treatment. Palliative tracheotomy may be employed in order to relieve dyspnœa or as a means of giving rest to the larynx. It is most commonly used for cases of extrinsic carcinoma of the larynx: thus C. Jackson reported twenty-nine such cases, in twenty-one of which he advised palliative tracheotomy and in only eight laryngectomy. Of the former, tracheotomy was actually performed in nine, but none of the patients lived for more than thirteen months. It seems doubtful whether tracheotomy has any marked effect in retarding the course of malignant disease, though it sometimes gives relief.
(xiv) Foreign bodies in the air-passages. It makes no difference what views are held as to the advisability of tracheotomy in the treatment of these cases. The fact remains that the first essential is the safety of the patient, and, if the dyspnœa is urgent, relief must be afforded. When a foreign substance has been inhaled the surgeon must always be prepared for tracheotomy, and it is not advisable for him to leave the patient, even for a short interval, without proper supervision. In addition, the operation has been advocated as the proper treatment for all cases of foreign bodies in the lower air-passages: nevertheless, removal by Killian’s method gives far better results (see p. 559).
(xv) As a preliminary to operations upon the upper air-passages tracheotomy is rarely necessary, its place having been taken by infrathyreoid laryngotomy: it is, however, often performed before undertaking the larger operations upon the larynx (see p. 489).
Anatomy. The length of the trachea of an adult is about 4½ inches, of which 2½ inches lie above the level of the sternum; the cervical portion, which consists of eight or more rings, extends from the cricoid cartilage above to the suprasternal notch below. In order to determine the upper limit of the trachea it is advisable to palpate the following structures, which lie in the middle line, from above downwards: namely, the hyoid bone with its greater cornua, the thyreoid cartilage which forms the greatest prominence on the front of the neck, and the cricoid cartilage; in this manner it is possible to detect whether there is any deflexion of the trachea from the middle line as the result of a tumour lying in one side of the neck.
The anterior border of the sterno-mastoid muscle on each side is also an important landmark; the two muscles approach each other as they descend to their attachments to the sterno-clavicular joints, thus forming an angle the position of which corresponds to the notch in the manubrium sterni. By drawing a line transversely across the cricoid cartilage to the anterior borders of the sterno-mastoid muscles, a triangular space is marked off which may be described as the tracheotomy triangle (Fig. 264).
Beneath the skin and superficial fascia lie the two anterior jugular veins; these run from above downwards, to communicate with a branch which crosses the middle line of the neck, commonly in the lower part of the tracheotomy triangle, and there is an interval between them which is, in most cases, sufficiently large to prevent their being injured by a central incision. The pretracheal muscles, namely, the sterno-hyoids and sterno-thyreoids, are closer together; but the interval can be recognized by the greater thickness of the deep fascia which passes between them. When the latter is incised, these muscles can be separated, and the trachea is exposed, together with the structures that lie on its anterior aspect. These are the following:—
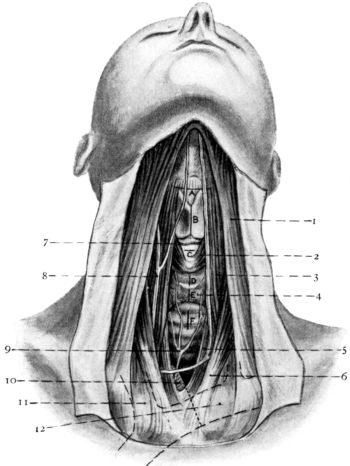 Fig. 268. Anatomy of the Larynx and Trachea and the Position of Incisions
for the Operations in this Region. A, Subhyoid pharyngotomy; B, Thyrotomy;
C, Infrathyreoid laryngotomy; D, ‘High’ tracheotomy; E, ‘Median’ tracheotomy;
F, ‘Low’ tracheotomy; 1, Platysma; 2, Crico-thyreoid muscle; 3, Sterno-hyoid
muscle; 4, Isthmus of thyreoid gland; 5, Sterno-thyreoid muscle; 6, Sterno-mastoid
muscle; 7, Crico-thyreoid artery; 8, Anterior jugular vein; 9, Inferior thyreoid vein;
10, Innominate artery; 11, Right innominate vein; 12, Left innominate vein.
Fig. 268. Anatomy of the Larynx and Trachea and the Position of Incisions
for the Operations in this Region. A, Subhyoid pharyngotomy; B, Thyrotomy;
C, Infrathyreoid laryngotomy; D, ‘High’ tracheotomy; E, ‘Median’ tracheotomy;
F, ‘Low’ tracheotomy; 1, Platysma; 2, Crico-thyreoid muscle; 3, Sterno-hyoid
muscle; 4, Isthmus of thyreoid gland; 5, Sterno-thyreoid muscle; 6, Sterno-mastoid
muscle; 7, Crico-thyreoid artery; 8, Anterior jugular vein; 9, Inferior thyreoid vein;
10, Innominate artery; 11, Right innominate vein; 12, Left innominate vein.
(a) The isthmus of the thyreoid gland, which varies greatly in size. It may be either a thin band with few vessels of importance, covering the second, third, and fourth tracheal ring; or hypertrophied and vascular, extending higher in the neck even to the front of the cricoid or thyreoid cartilage. This condition also results when a pyramidal lobe is present.
(b) The pretracheal fascia, which encloses the isthmus of the thyreoid gland and, when traced upwards, finds attachment to the anterior aspect of the cricoid cartilage, thus forming the suspensory ligament of the isthmus. Passing downwards it covers the anterior surface of the trachea, and, though somewhat indefinite, can easily be traced behind the sternum as far as the pericardium, with which it blends. This is a point of great practical importance in determining the extension of inflammation into the mediastinum.
(c) Veins. Small transverse branches of the superior thyreoid veins run upon the upper border of the isthmus between the layers of the fascia which surround this structure. The inferior thyreoid veins, larger in size, run from the lower border of the isthmus vertically downwards in front of the trachea to communicate with the left innominate; in their upper part they may consist of several small veins which join together to form two main branches, of which the left may lie directly in the middle line; small communicating branches of these veins run transversely across the lower border of the isthmus. The left innominate vein crosses the front of the trachea somewhat obliquely, and may lie at least half an inch above the suprasternal notch.
(d) Arteries. The crico-thyreoid artery runs transversely across the crico-thyreoid space, being placed in front of the suspensory ligament, and gives off numerous branches, which enter and supply the interior of the larynx, as well as small descending branches which run to the isthmus of the thyreoid gland. A small branch of the inferior thyreoid artery is also constantly found behind the isthmus, and in rare instances a thyreoidea ima branch of the innominate, varying greatly in size, may pass upwards in front of the trachea.
In young children the same relations are found, but with certain differences. Owing to the larynx being relatively high in the early years of life, the length of the cervical portion of the trachea is almost 2 inches when the head is extended, and the bifurcation is considerably higher than in the adult; further, the trachea is more movable and is smaller in diameter. The laryngeal cartilages are difficult to distinguish, but a mass composed of the thyreoid and cricoid cartilages can always be felt, and its position determined by careful inspection. It is very important to remember that, even when the head is extended, the cricoid cartilage lies rather less than 2 inches above the upper margin of the sternum. In very young children it is common to find two transverse creases in the skin, of which the upper usually lies over the upper border of the thyreoid and the lower over the cricoid cartilage. The lower crease thus assists in determining the upper limit of the trachea.
The anterior jugular veins in young children are comparatively large; the infrahyoid muscles are less defined and more difficult to recognize; and the isthmus of the thyreoid gland is very broad, appears to be part of the lateral lobes, and occupies a higher position in the neck, often passing in front of the crico-tracheal membrane as well as the first and second tracheal rings. The inferior thyreoid veins are larger, more numerous, and more difficult to separate; the left innominate vein is somewhat higher in the neck; the thymus gland, which gradually decreases in size with the increase of age, may extend into the neck, in front of the trachea, and may even reach as high as the isthmus of the thyreoid; the fasciæ are softer and less definite, and the fascia which covers the trachea is easily stripped from its surface.
Operation. As local anæsthetics are of little practical value in the case of children, the surgeon must decide whether a general anæsthetic shall be used; for any nervousness on his part increases the danger of death upon the table. A general anæsthetic is not necessary, but undoubtedly has certain advantages: the operation is easier and can be performed more rapidly; the patient is more likely to fall asleep; and any vomiting that occurs is beneficial rather than harmful. On the other hand, children suffering from diphtheria are apt to die suddenly under chloroform; and it should never be administered when there is any sign of heart failure, when obstruction is very marked, when cyanosis is present, or when the patient is prostrate. The danger has probably been exaggerated, and depends more upon the experience of the anæsthetist than upon the actual disease; in my opinion it is as a rule safer to employ a small quantity of chloroform, which should be given on the operating table after everything has been prepared. The child should be allowed to choose its own position, generally curled up on one side, and the administration must be slow. By observing these precautions it usually happens that the child becomes quiet, and that with the loss of consciousness the breathing improves; the child can then be placed in the proper position, and the more difficult part of the operation can be completed before restlessness returns.
The instruments required are: a small scalpel, scissors, two dissecting forceps, three or more fine-pointed pressure forceps, two double hook retractors, one blunt hook, an aneurysm needle, and a suitable dilator for the wound; some form of aspiration apparatus may also, in rare instances, be necessary (Fig. 278). Three or four tracheotomy tubes such as described by Parker, and a small tube containing sterilized catgut, which is eminently suitable for the tying of vessels, and for that purpose preferable to silk, should also be in readiness. All the instruments should be kept together in a metal case, as well for private as for hospital practice, so as to be ready in case of emergency. They should be boiled for at least twenty minutes both before and after each operation, and should be laid out separately upon a dry sterilized towel in the position selected by the surgeon.
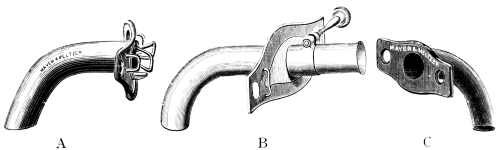 Fig. 269. Tubes for Tracheotomy. A, Parker’s; B, Durham’s; C, Baker’s
rubber tube.
Fig. 269. Tubes for Tracheotomy. A, Parker’s; B, Durham’s; C, Baker’s
rubber tube.
Tracheotomy tubes may be made of silver, rubber, vulcanite, celluloid, or a gum-elastic material, but most surgeons prefer a silver tube in the early stages of treatment. An angular form should be used, for ‘with the ordinary quarter circle tube, the lower extremity tends to impinge on the anterior wall of the trachea, and this is attended with many inconveniences and even with grave risks’ (Parker27). A movable shield is equally important, and this should be flush with the neck in order to avoid the possibility of its being removed by the patient. Further, the tube should consist of two parts—an outer tube to which the shield is attached, and an inner tube which projects slightly beyond the outer and can be removed for purposes of cleaning. To encourage breathing through the larynx, a window may be added in the upper part of the tubes. Parker’s tube, which meets all the above requirements, is the one most commonly used in England. When longer tubes are necessary, either Durham’s or Stewart’s is recommended: in these, the position of the shield can be altered, and the length of the tube arranged, to suit the patient. In cases of long duration the use of rubber tubes such as Morrant Baker’s is indicated. An introducer is rarely necessary except for rubber or long tubes. As taper and bivalve tubes are liable to injure the trachea, their use is not advised. The tube chosen should fit loosely, and should project far enough into the trachea to be secure from slipping out during coughing or struggling. Short tubes are preferable, and the wider the tube the easier the breathing and the better the drainage. The approximate diameter of the trachea varies at different ages, and the size of tube suitable in each case varies chiefly according to the trachea, but partly also according to the fatness of the neck. The accompanying table indicates the appropriate dimensions.
Table showing Size of Trachea and of Tube required at Different Ages
| Age. | Approximate diameter of trachea. | Approximate diameter of tube. | Number of tube. | |
|---|---|---|---|---|
| Parker’s | Durham’s | |||
| 6 months | 4 mm. | 04 mm. | 16 | — |
| 1½–2 years | 6–8 mm. | 07 mm. | 20 | 1 |
| 2–4 years | 8–10 mm. | 08 mm. | 24 | 2 |
| 4–10 years | 10–12 mm. | 09 mm. | 28 | 3 |
| 10–20 years | 12–19 mm. | 10 mm. | 30 | 4 |
Tracheotomy, even under favourable circumstances, is attended by many difficulties; the urgency of the case, the restlessness of the patient, the movements of the larynx, the frequent absence of a proper operating table and equipment, the importance of a good light, of sensible assistants, of a trained nurse, and, above all, of a calm disposition, make this one of the most anxious and difficult operations in surgery, yet there is no medical man who may not be called upon to perform it.
It is important to make the best possible preparations. A table of suitable height can usually be improvised and placed in a good light. If the operation be at night, gas lamps or candles can be used, and the illuminant should be placed in a definite position rather than held by the parents. The child should be wrapped in a large towel in order to control the movements of the arms, body, and legs, and should then be placed upon the table; it is advisable to leave him in ignorance of the operation, whatever his age, until the last moment. The skin of the neck should be rapidly washed or sponged with ether, and the head extended over a small pillow or rolled towel. The operation must never be commenced until the proper position is obtained; on the other hand, extension of the head should not be too great for fear of increasing the dyspnœa. Three assistants are preferred—one to hold the head firmly in the middle line so that the point of the chin is exactly in line with the suprasternal notch (this is probably the anæsthetist), a second to hold the body at the opposite end of the table, and a third to assist the surgeon with sponges or retractors. It should be the duty of the last named to prevent any membrane or pus from being coughed over the principals after the trachea has been opened.
There are four varieties of the operation, viz.:
1. Crico-tracheotomy (with division of the cricoid cartilage).
2. High tracheotomy (involving section of the trachea above the isthmus of the thyreoid gland).
3. Low tracheotomy (section of trachea below the isthmus of the thyreoid gland).
4. Median tracheotomy (section of trachea through the isthmus of the thyreoid gland).
Crico-tracheotomy is an easy operation owing to the superficial position of this portion of the air-passage, but is inadvisable for the following reasons:—
(1) The larynx being narrower than the trachea, a smaller tube is required; (2) the swelling of the mucosa often extends downwards and causes constriction of this region; (3) the tube is not well tolerated; (4) pressure ulcers, necrosis of the cricoid, and granulations are frequent complications; and (5) retained tube is more common than with other operations, this really being the most important consideration. The comparative value of the remaining operations is largely a matter of opinion.
It is not uncommonly stated that tracheotomy is better done by touch than by sight: the object to be achieved is to find the trachea, and there are two methods of doing this. The first is the deliberate method, suitable for patients in good condition when there is no urgent dyspnœa; it can be performed entirely by sight, and the greater the experience of the surgeon the fewer his difficulties. In such cases skilful technique is of far greater value than haste. The high operation is preferred, because the trachea is more superficial, less movable, and easier to find; it has less complicated relations, the blood-vessels are less numerous, the fasciæ are not so loose, the tube is easier to fit and unlikely to slip out, healing of the wound is more rapid, and complications seldom occur. In cases where the isthmus is very broad or highly placed, so that the upper parts of the trachea and cricoid are covered, a median operation is recommended. Low tracheotomy is rarely necessary.
The second is the rapid method, to be applied in cases of emergency. Turner, of the South Eastern Hospital, strongly advocates such an operation without an anæsthetic. The incision made is from ½-5/8 of an inch in length, this being repeated without attention to the bleeding until the trachea is reached. The latter is opened in the usual manner. The tip of the finger is placed in the wound in order to control the hæmorrhage, and as a guide to the dilators. When these have been introduced, the child is at once drawn beyond the end of the table so that the head hangs downwards. The bleeding usually ceases in a few moments, though in some cases the tube is inserted to control it. The advantages claimed for this method are that the operation is quicker, and that no distinction between ‘high’ and ‘low’ is required. The wound is smaller, there is less danger of sepsis, and the eventual scar is hardly visible; no hooks or retractors are used, so that the trachea cannot be displaced. If the wound be in the middle line it is impossible to miss the trachea. This operation is performed entirely by touch, and the bleeding is not considered. Its adoption may be necessary to save the patient’s life, but in the hands of an inexperienced surgeon the operation is attended with great difficulties.
High tracheotomy. The incision must be exactly in the middle line; this can be accomplished easily if the surgeon keeps in mind two important landmarks, namely, the point of the chin, and the suprasternal notch. To determine the upper end of the incision, a point is chosen midway between the anterior borders of the sterno-mastoid muscles at the level of the cricoid cartilage. The thyreoid cartilages being steadied between the fingers and thumb of the left hand, a bold incision is made from the upper point, 1½ inches in length, extending in a young child almost to the suprasternal notch. A long incision is generally preferable, and, when the neck is fat, should commence over the middle of the thyreoid cartilage. The skin and superficial fascia are divided between the two anterior jugular veins, and any bleeding is controlled. The incision is repeated so as to divide the deep fascia lying between the sterno-hyoid muscles, close to one another in the upper part of the incision, and these are separated with the knife. It is now advisable to pause and to seize the bleeding points, allowing the pressure forceps to fall on both sides of the wound to act as retractors. The infrahyoid muscles are separated by at least an inch, and, if retractors are necessary, care must be taken that the muscles alone are included and that the retraction is equal on the two sides. If there has been no ‘tailing’ of the wound the following structures are then exposed from above downwards: the lower border of the thyreoid cartilage, and the front of the cricoid, both easily seen or felt; and a vascular mass, namely, the isthmus of the thyreoid gland, covered by fascia and completely concealing the trachea. The landmark that is required at this stage is the cricoid arch; this should be found, and a small transverse incision should be made along its lower border to divide the suspensory ligament; the handle of the scalpel or a blunt hook is introduced beneath the pretracheal fascia, and the isthmus dragged downwards into the lower portion of the wound, an operation which can be accomplished easily if done without hesitation. The upper rings of the trachea are now exposed; and, unless the superficial veins have been divided, there should be no bleeding. The trachea should not be opened until it has been exposed completely and all bleeding has been arrested. It is unnecessary to ligature the vessels at this stage unless the forceps have been so placed as to interfere with the part of the trachea chosen for section, or an artery of considerable size is encountered; in the latter instance there is a danger of subsequent hæmorrhage if the ligature is applied close to the tube. While the trachea is being opened, it is necessary to overcome the movements of the larynx by grasping the cricoid with the finger and thumb of the left hand. The scalpel should be gently stabbed into the middle of the trachea to ensure puncturing the mucous membrane as well as the outer wall, and the opening should be quickly enlarged in an upward direction until three rings have been divided, preferably the first, second, and third. It is imperative that this incision should be in the middle line, should not be too small, and should only pass through the anterior tracheal wall; if force be used there is danger of puncturing the œsophagus, or even of striking the bodies of the vertebræ.
At the moment when the trachea is opened there is a sudden rush of air out of the lungs. This is reassuring to the surgeon, and at this point the dilator should be introduced and the anæsthetic abandoned. Temporary cessation of breathing is common after the first inspiration, but the great improvement in colour shows that there is no cause for alarm; with the return of consciousness the child begins to cough, and this has two results, partly clearing the tubes of mucus, pus, or membrane, and partly promoting deeper inspiration and better expansion of the lungs. Cyanosis is thus speedily removed, unless membrane is abundant; and even where this is the case, it is advisable to encourage coughing in order to dislodge the membrane, which can be grasped with forceps or caught with a sponge as it appears in the wound. The use of a feather or a soft rubber catheter for irritation of the trachea to promote coughing should be abandoned, as such instruments often displace the membrane downwards. As soon as breathing is regular and the cough allayed, the vessels can be ligatured.
A tube of suitable size having next been selected, the opening in the trachea is widely dilated and the point of the canula quickly inserted into position, the outer tube alone being used, with tapes for tying attached. Unless the tube ‘sits’ well without tilting, different sizes should be tried until the breathing becomes easy, a sure sign that the lower opening of the canula is pointing in the right direction. The tapes are tied firmly on the right side of the neck, after which the inner tube is introduced and fixed in position.
The wound remains to be treated. Various methods have been recommended to guard against infection: the use of antiseptic watery solutions, such as perchloride of mercury, chloride of zinc, carbolic acid, and perchloride of iron, is dangerous; insufflation of powders, on the other hand, such as orthoform, aristol, and the like, is certainly effective in keeping the wound clean, and is better than the employment of an oil emulsion; suturing the wound is unnecessary and is not recommended. A dry antiseptic gauze is applied to the wound and kept in position by the pressure of the shield. Lastly, a thin covering of gauze is placed over the front of the neck, and the patient returned to bed.
Low tracheotomy. The incision should be rather longer than in the ‘high’ operation and should reach almost to the suprasternal notch. The fasciæ, anterior jugular veins, and infrahyoid muscles are treated as before, and there must be no ‘tailing’ of the wound. The landmark required is the isthmus of the thyreoid gland, and its lower border must be determined and dragged upwards by a blunt hook. It is important to remember that the lower part of the trachea lies deeper in the neck and is more difficult to expose owing to the blood-vessels that lie anterior to it; the thymus gland, also, may extend upwards and require to be retracted. Whereas in high tracheotomy practically the whole operation is best done by clean cutting, in the lower operation this is more dangerous, and the deep dissection must be performed partly with forceps or blunt director; if an artery be divided or venous bleeding occurs, it should be controlled immediately. No attempt should be made to perform this operation rapidly owing to the relations of the parts; nor should the trachea be opened before its rings are exposed thoroughly, as complications may arise after imperfect division of the pretracheal fascia. In the opening of the trachea and the further stages, the operation is similar to high tracheotomy.
Median tracheotomy. The child being placed in the required position as before, an incision is made, from the lower border of the thyreoid cartilage almost to the sternum, through the skin and superficial fascia. With a series of cuts, exactly in the line of the original incision, the fascia lying between the pretracheal muscles is divided; the bleeding points are seized with pressure forceps, and retractors are introduced to expose the isthmus. The isthmus itself is treated in one of two ways: in urgent cases it is boldly divided by one or two cuts of the knife; but if time can be spared, a threaded aneurysm needle may be passed under it, first on one side and then on the other, after which the needle is withdrawn, and the two ligatures can be tied so as to leave between them a space of one-third of an inch in which a cut can be made without hæmorrhage. The tracheal rings are thus exposed and can be divided as before.
Accidents. The accidents that occur are less numerous than might be expected when it is considered how often this operation is performed by those who are quite unpractised in surgery; many of them are the direct result of inexperience or arise because the operator becomes confused. If the patient be in a bad position, or if a wrong incision be made, the trachea is difficult to find, and it is better to expose the thyreoid cartilage and prolong the incision downwards until the windpipe has been discovered.
Hæmorrhage, however, is the chief difficulty, and is sometimes unavoidable; it may be arterial or venous. The arteries of this region are generally small, being branches of the superior or inferior thyreoids, and this accounts for the fact that severe arterial bleeding is rare. Nevertheless, the smaller vessels may at times be very troublesome: for instance, the crico-thyreoid artery or one of its branches may be divided, in which case the cut ends will retract and will be difficult to seize; and if the trachea has been opened, blood may continue to enter in sufficient quantity to cause troublesome coughing. Abnormal arteries, such as the thyreoidea ima, are not of great practical importance.
Venous hæmorrhage is far more common, and, taking into account the anatomical relations of the veins, and their great size (increased by cyanosis) in children, it seems remarkable that bleeding is so seldom fatal; in desperate cases a very small amount of blood is sufficient to cause suffocation. Venous bleeding will stop only when respiration becomes free, and this is not possible so long as blood is being sucked into the air-passages. Every effort should be made, therefore, to prevent blood from passing into the trachea, either by hanging the head over the end of the table as soon as the dilators have been introduced, or by introducing a canula against which the walls of the trachea can be compressed.
Failure to breathe, after an opening has been made, is due to either obstruction or collapse and requires rapid treatment. The trachea must be widely dilated, and forceps used to remove any membrane which presents itself in the wound; the assistant must then slowly compress the ribs two or three times to empty the chest and encourage respiration. If consciousness returns, the patient begins to cough and mucus or membrane is expelled from the air-passages. On the other hand, it is useless to continue artificial respiration if the obstruction is not relieved; aspiration must be employed if special instruments are at hand. The fact that a number of surgeons have lost their lives as the result of sucking through a catheter in the attempt to save the child is sufficient to condemn this practice; but good results have been obtained by passing a catheter low down into the trachea and blowing through it with a syringe or even with the mouth. As soon as the trachea has been emptied by one of these methods, artificial respiration should be continued, and collapse treated by injections of strychnine, brandy, or ether. No attempt should be made to introduce a canula until the breathing is restored. As Turner remarks: ‘Heart failure during operation generally recovers with artificial respiration, and twelve hours later the condition is indistinguishable from that of a case who has not so closely approached death. The real remedy against such an accident is never to postpone operation until the heart is exhausted.’
After-treatment. Although this is a subject which has produced a great deal of discussion, there is a widespread impression among the younger members of the profession that it is of little importance. Much has been said about the dangers of interference, and any suggestion put forward has been criticized by those who have had large experience, with the result that confusion is prevalent. As a matter of fact, the subject is one of the greatest importance, for there is no operation in surgery in which the after-treatment can be neglected. Care should be exercised in choosing a nurse who has special knowledge of children and of the after-treatment of tracheotomy. Great discretion is required in the management of such cases, and there is little doubt that harm may result where too much attention is shown. At many of the hospitals a special nurse is appointed for attendance on the more desperate cases only. The main duty of the nurse is to watch the child, for any difficulty in breathing requires immediate attention. It is necessary that she should understand the proper management of the tube; she must see that the inner tube never becomes clogged, and if the tube slips out of the trachea it must be reintroduced or a dilator inserted; she must also be responsible for the feeding of the child. The difficulties that arise during the first few days after operation call for much tact and experience.
It is unnecessary to enter here into the discussion about food, stimulants, or general treatment, except to point out that swallowing may be very difficult. The food must be nourishing, fluid being in most cases preferred; occasional sips of water should be administered to find out whether coughing is produced, in which case nasal feeding can be advised without hesitation. A short rubber catheter should be passed through the nose at regular intervals according to the nature of the case. As a general rule a small quantity of nourishment should be given every two hours, studying, as far as possible, the likes and dislikes of the patient. By the observance of these principles the child soon becomes tolerant, and proper nourishment can be administered, thus removing one of the great difficulties of after-treatment.
The atmosphere of the room. The value of steam for producing warmth and moisture is undoubted; the amount required depends on the case. The main object to be kept in view is to encourage secretion from the mucous membranes, and so to prevent the formation of crusts. When secretion is scanty a large amount of moisture is required, and vice versa; also, when much pus is present, extra moisture is of value to prevent it from becoming dried and to allow it to be expectorated. The value of disinfectants is doubtful, but on general principles it may be said that the more septic the secretion the greater the indication for their use: tincture of benzoin, oil of eucalyptus, and thymol act as sedatives; carbolic acid, creosote, and numerous other drugs are useful disinfectants; soda and potash, recommended by R. W. Parker, tend to liquefy the exudations. Steam, however, is more important than all these, and should be advised as being likely to encourage the quicker healing of the wound: even in catarrhal conditions improvement is more rapid when this practice is adhered to.
The most important point in the after-treatment, however, as far as the surgeon is concerned, is to prevent recurrence of the obstruction. Obstruction is most often due to the blocking of the inner tube by secretions, a condition easy to recognize from the symptoms which are produced. The inner tube should be removed, thoroughly cleaned, and reintroduced. This usually suffices to allow the child a period of quiet breathing, and sleep may be obtained. To keep the tube free it is very necessary to repeat the removal at regular intervals. In those cases where the secretion is tenacious, the tube constantly becomes blocked, but it is better to remove it again than to allow a feather to be passed. Nothing is gained by attempting to hurry the separation of crusts, and the passage of a feather tends to force downward far more than can be extracted, and so to increase the danger of broncho-pneumonia. If dyspnœa continues after removal of the inner tube, a spray should be used, or a small amount of fluid should be dropped into the trachea to moisten the secretions.
Changing the outer tube rarely presents any difficulty because the tissues of the neck soon become matted together, a funnel being thus produced along which the canula is introduced with ease. A new tube should be prepared before removal of the old, and dilators should be at hand for use if the child is frightened, struggles, or coughs: the canula should be introduced quickly and without hesitation, sufficient force being employed to overcome any obstruction. Unless the original opening in the trachea was too small, it should be possible to introduce a tube equal in size to that which was removed. Frequent changing of the outer tube should be avoided.
The time for removing the outer tube. In every case of diphtheria there is a certain amount of catarrh, with swelling of the mucosa, increased secretion, and some difficulty of breathing. In addition, the habit of breathing through a canula is difficult to alter; the child shows an aversion to breathing through the natural air-passages, and is often frightened or bad-tempered. As soon as the secretion becomes small in amount and serous rather than purulent in consistence, an attempt should be made to discard the tube: the canula should not be retained a day longer than is necessary, the usual period varying from five to fifteen days. Various methods may be adopted:—
1. If the outer tube be provided with a window, the tip of the finger can be placed on the opening to compel the child to breathe through the larynx; breathing may be difficult, but by this means an indication can be obtained as to whether it is advisable to persist.
2. If the above method be successful, the tube may be removed. A small pad of gauze is placed over the wound and the child further encouraged to breathe through the larynx. Expiration is generally easier than inspiration, and older children should be encouraged to blow out a candle or to sound a whistle, this process being continued so long as the child can endure it, but not to the stage of exhaustion. It is often possible to remove the tube at the first attempt.
3. The canula may be plugged with a cork which the nurse removes when necessary: it is often possible to replace the plug while the child is asleep without his becoming conscious of the fact, thus showing that the dyspnœa is largely mental.
4. In some children breathing is easy so long as the tube is simply plugged and is not removed; in such cases the canula can be replaced by a shield and a plug which does not pass into the trachea. This may completely deceive the child.
5. The silver tube can be changed for one of rubber, and this can be shortened daily until nothing remains but the shield.
If these various methods have been tried with no success it is probable that the case is abnormal, but before this can be conceded it is necessary to repeat that, in the large majority of cases, the difficulty of removing the tube is due not so much to definite stenosis of the larynx as to the bad habit acquired by the patient.
Complications arising after tracheotomy and preventing removal of the tube:—
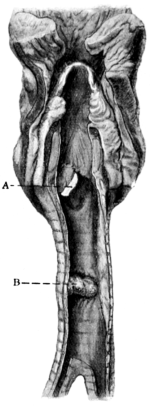 Fig. 270. Trachea showing Ulceration caused by a Badly Fitting Tube.
A, Tracheotomy opening; B, Ulcer caused by the end of the tube. (From
Specimen No. 1659a in the Museum of St. Bartholomew’s Hospital.)
Fig. 270. Trachea showing Ulceration caused by a Badly Fitting Tube.
A, Tracheotomy opening; B, Ulcer caused by the end of the tube. (From
Specimen No. 1659a in the Museum of St. Bartholomew’s Hospital.)
1. Wound infection. This rarely occurs at the present time, and diphtheritic wounds are seldom seen. Some inflammation of the wound is natural under the conditions, and may be associated with œdema of the surrounding tissues; this generally yields to antiseptic treatment in a few days. In very weakly children suffering from a virulent form of disease the healing of the wound may be slow, and septic conditions are apt to arise ending in cellulitis of the neck or even typical erysipelas. Owing to the disposition of the fasciæ there is a tendency for the infection to spread in a downward direction, and for mediastinal inflammation or suppuration to occur: this appears to be more common after low tracheotomy. The prognosis in such cases is not good, and every endeavour should be made to prevent the possibility of their occurrence by absolute cleanliness at the operation and by suitable after-treatment of the wounds.
2. Septic conditions of the trachea are less common since the introduction of antitoxin, but occur in cases where false membrane is abundant. There may be swelling of the mucosa, or copious discharge which persists for long periods.
3. Ulceration may be due to sepsis or to pressure from a badly fitting tube, especially when the latter has been worn for a protracted period (Fig. 270). It may cause perforation and localized abscess either in front of the trachea or in the neighbourhood of the œsophagus, and may result in a communication with the latter. In the region of the cricoid, ulcers are liable to cause necrosis. The signs of such ulceration are: continuance of purulent discharge, discoloration of the tube, bleeding from the wound, and, above all, difficulty in removing the tube.
At the first indication of ulceration the cause of irritation should be removed. It is advisable to discard a metal in favour of a rubber tube, or, if possible, to remove the tube altogether. Strenuous efforts must then be made to disinfect the trachea by the insufflation of antiseptics, either as powders or in solution. The healing of such ulcers is very slow, and granulations are apt to form resulting in obstruction and preventing removal of the tube. In later stages contraction of fibrous tissue causes stenosis; this is more common in the neighbourhood of the cricoid, especially when the latter has been divided at the time of the operation.
4. Granulations. The possible presence of granulations must always be borne in mind. I believe this condition is far less common than is generally supposed, and that in many cases the granulations are entirely limited to the neighbourhood of the wound, where they can be seen. It is doubtful whether they are responsible for the dyspnœa which occurs. Great ingenuity and patience are required for the treatment of this condition. The wound must be kept scrupulously clean and all source of irritation removed. A rubber canula should be substituted in place of a metal one; if it were possible it would be advisable to discard the tube altogether, but as yet no form of dilator has been devised which will take the place of the canula. If the granulations be large they should be removed either with a sharp spoon or with suitable forceps, the area having been anæsthetized previously by a small quantity of the novocaine and adrenalin mixture. When small, the use of silver nitrate is preferable. It may be necessary to repeat this after a few days, and as soon as seems advisable a further attempt should be made to dispense with the tube. At this stage time must be allowed for the various tissues to regain their normal condition. Should this treatment prove unsuccessful, a thorough investigation must be made under chloroform. The wound is enlarged as far upwards as the cricoid, bleeding being arrested with the mixture just described. By throwing a strong light into the wound, the condition of the mucous membrane can be inspected and granulations removed. If there be no granulations in the trachea, a tube speculum can be passed through the mouth to ascertain the condition of the larynx (see p. 480). Such a method of procedure is preferable to the passage of probes, forceps, sponges, and other articles through the larynx, in the hope that any obstruction may be removed. If ulceration or necrosis of cartilage be discovered, it is impossible to relieve the condition by surgical means without prolonged treatment with tubes and the constant use of antiseptics. Under these conditions it is advisable to consider the removal of the tracheotomy tube in favour of intubation. In the hands of many foreign authorities the use of intubation tubes covered with gelatine, in which antiseptic is introduced, has been attended with such conspicuous success that further attempts should be made in this country; there is little doubt that, as our knowledge of the treatment of such wounds improves, better results are daily attained. Whatever treatment is considered it is important first of all that the actual cause should be distinguished. This is now possible owing to the great advances made in methods of examining the larynx.
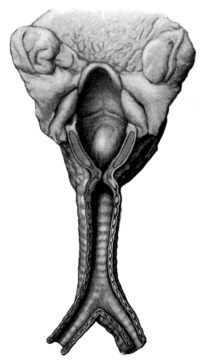 Fig. 271. Stenosis following Tracheotomy. (From Specimen No. 1659d in
the Museum of St. Bartholomew’s Hospital.)
Fig. 271. Stenosis following Tracheotomy. (From Specimen No. 1659d in
the Museum of St. Bartholomew’s Hospital.)
5. Stenosis of the larynx or trachea occurs in old-standing cases, as the result of ulceration, after some cases of crico-tracheotomy, and especially where a tube has been worn for a very protracted period. Breathing through a tube, if continued for a long time, interferes with the natural growth of the air-passage above it. The child grows, but the larynx remains stationary. This condition is aggravated by the fact that some inflammation is constantly present, especially in the neighbourhood of the wound, so that the tissue become fibrous and hard. The fibrous tissue contracts and stenosis is caused. According to von Bruns, Kohl,28 and others, constrictions of the trachea may in rare instances result from some kinking of its wall. Such conditions as a bulging of the posterior wall due to the approximation of the posterior ends of the cartilage secondary to the spreading of the anterior portions, inversion of the tracheal margins from too small an incision, overlapping of the tracheal wound, and cicatricial union between the thyreoid and cricoid, must be exceedingly rare. Here, again, a definite diagnosis can always be made by proper investigation, but treatment is more difficult. Dilatation must be attempted by either continuous or intermittent methods. If preferred, a short piece of rubber tubing can be passed upwards from the tracheotomy wound into the larynx and kept in place for several hours by two silk sutures, one passing out of the tracheal wound, the other out of the mouth; or a stenosis canula can be inserted with some form of hollow plug which passes upwards into the larynx (Fig. 272). The question whether the tracheotomy wound should be kept patent is difficult to answer. When stenosis is extreme there is no alternative, and the open wound allows of the constant passage of graduated bougies, which is more easily accomplished from below than from above. If treatment be persistent the prospect of a good result is not unfavourable, and there is every reason to believe that in the future the number of cases which require a permanent tracheotomy tube will be reduced to a minimum.
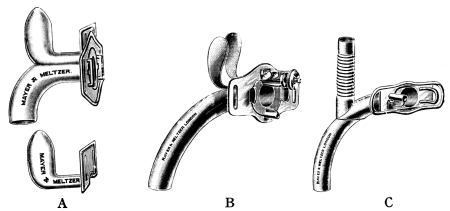 Fig. 272. Tubes used in the Treatment of Stenosis of the Larynx.
A, Lack’s; B, Störk’s; C, Schimmelbusch’s.
Fig. 272. Tubes used in the Treatment of Stenosis of the Larynx.
A, Lack’s; B, Störk’s; C, Schimmelbusch’s.
6. Paralysis. In the larynx there may be paralysis of the sensory or of the motor nerves. In the former case food may enter into the trachea and cause troublesome coughing and possibly ‘Schluck-pneumonie’. When the motor nerves are affected, the paralysis is commonly abductor and may be unilateral or bilateral, the latter associated with inspiratory dyspnœa. ‘Complete paralysis of the recurrent laryngeal nerve may also occur, but is nearly always confined to one side’ (C. A. Parker29). Such paralyses may last from a few days to several months, and are very troublesome when associated with the passage of food into the trachea; when severe, nourishment should consist of fluids which can be administered by a nasal tube.
Further complications arising during the after-treatment of tracheotomy:
7. Broncho-pneumonia. This occurs in the worst forms, and is accompanied by high temperature with definite signs in the lungs. The absence of septic discharge, the restlessness of the patient, and the rapidity of the breathing (in many instances accompanied by ‘recession’ not caused by obstruction in the tube) make the condition easy to recognize. There is no satisfactory treatment for septic broncho-pneumonia which has already developed, but it may be prevented. Within recent years it has become less common. This is due to better technique in the operation, and to careful attention during the after-treatment. The habit of passing feathers into the trachea has been abandoned with advantage to the patient. When possible the child should be removed from septic influences which are liable to infect the throat, for the occurrence of tonsil[l]itis as a sequel to tracheotomy is always to be feared in wards containing septic cases.
8. Emphysema may occur in the neighbourhood of the wound, or in rare cases may be extensive and involve the whole of the face, neck, and chest. Champneys30 was the first writer to call attention to this complication of tracheotomy. After a large number of observations and experiments, he was of opinion that emphysema of the anterior mediastinum occurs in a certain proportion of tracheotomies and is of frequent occurrence in cases that are fatal; that it may be associated with pneumothorax; and that the conditions which favour its production are a low division of the deep cervical fasciæ in the neighbourhood of the sternum, combined with obstruction of the air-passages and strong inspiratory efforts; artificial respiration, especially if improperly performed; and want of skill on the part of the operator; further, that the dangerous period of the operation is between the division of the deep cervical fascia and the efficient introduction of the tube. To this may be added those cases in which the tube slips out of the trachea into the cellular tissue above the sternum and thus causes more or less obstruction to breathing. It seems probable that the air is sucked into the cellular tissues beneath the pretracheal fascia, rather from the outside than from the trachea, and that with forced expansion of the chest it finds its way beneath the fascia into the mediastinum.
9. Hæmorrhage may occur as the result of slipping of a ligature during an attack of vomiting or struggling after the operation; it is usually venous and requires nothing but passing notice. Secondary hæmorrhage may result from ulceration into one of the larger arteries or veins. Kocher31 states that ‘the number of cases recorded is now about eighty-seven, of which fifty-six are associated with the innominate artery. Unfortunately it is not known how often in these cases inferior tracheotomy had been performed. Low tracheotomy was performed in my case because an excision of the larynx for cancer had been undertaken. Doubtless the danger of these fatal complications is much greater with inferior tracheotomy owing to the pressure of the canula.’ Von Bruns32 also agrees that ‘the vast majority of fatal hæmorrhages were in cases of inferior tracheotomy. Of thirty-six cases in which the source of hæmorrhage was given, twenty-eight were traced to the innominate vein, two to the right carotid, and one each to the superior thyreoid, the left innominate, the right jugular and the left jugular.’ Bleeding is also recorded in cases of aneurism of the aorta, in which tracheotomy has been performed, as the result of erosion of the tracheal wall and the bursting of the sac. Further, troublesome oozing may take place from the mucous membrane of the trachea when this is inflamed, or when granulations are present, or when there is much sloughing of tissues, and especially after a metal tube has been worn for a considerable period. Hæmorrhage from an enlarged thyreoid isthmus is also described. When due consideration is given to the septic condition of the wounds and the close relation of large vessels, it is surprising to find that hæmorrhage proves so seldom fatal.
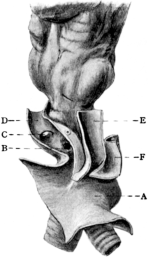
Fig. 273. Trachea showing Ulceration into the Innominate Artery after
Tracheotomy. (From Specimen No. 1622a in the Museum of St.
Bartholomew’s Hospital.) A, Aorta; B, Ulcer; C, Right subclavian; D,
Right common carotid; E, Left common carotid; F, Left subclavian.
|
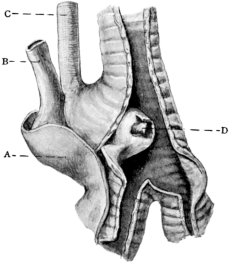
Fig. 274. Aneurism of the Aorta perforating the Trachea. (From Specimen
No. 1500 in the Museum of St. Bartholomew’s Hospital.) A, Aorta; B,
Left subclavian; C, Left common carotid; D, Ulcer in sac of the
aneurism.
|
10. Cardiac paralysis may also complicate tracheotomy. When supervening in the acute stages of the disease, the patient becomes prostrate and vomiting is persistent, while the heart gradually fails. In other cases death occurs suddenly and unexpectedly, in mild as well as in severe disease; this may happen at any period, during the first days or later, during convalescence. Heart failure is more common in diphtheria than in any other infectious disease which is met with in this country.
Prognosis. It may be said that all cases of laryngitis caused by diphtheria are of a serious nature, and especially those which require tracheotomy (see Table, p. 517). The mortality amongst tracheotomized patients during five years was 31.5%, and the variations in each separate year were slight. Such results are far from satisfactory, but it must be remembered that in pre-antitoxin days less than 30% recovered after tracheotomy (Goodall33). The use of antitoxin, first suggested by Behring, is undoubtedly responsible for this remarkable decrease in the mortality. The sooner the serum is injected the better the prognosis with tracheotomy. A large dose should be given, 8,000 to 18,000 units, irrespective of age, and the dose may be repeated on the second day if required. Improvement generally commences between twelve and twenty-four hours after injection; the swelling of the mucosa subsides, and secretion is diminished; false membrane is not so copious, and rarely extends to the trachea and bronchi; crusts become less adherent, and are expelled by the patient. In this manner the whole area of the disease becomes clean, and there is less absorption of toxins. It is now generally agreed that serum should be used in all suspicious cases, and some authorities inject at once not only the patient, but also other children living in the same house. It is hoped by early injection to avoid the necessity for tracheotomy.
The age of the patient is very important, as the following table shows:
Table showing Total Diphtheria Tracheotomies performed at the Fever Hospitals in London during 1902–6, including those in which Intubation was previously performed and those in which no Antitoxin was used
| Age. | Times. | Deaths. | Percentage of Deaths. |
|---|---|---|---|
| Under 1 | 0062 | 040 | 64.5 |
| 1–2 | 0256 | 123 | 48.0 |
| 2–3 | 0272 | 087 | 31.9 |
| 3–4 | 0231 | 054 | 23.3 |
| 4–5 | 0196 | 045 | 22.9 |
| 5–6 | 0119 | 019 | 16.0 |
| 6–7 | 0067 | 018 | 26.9 |
| 7–8 | 0022 | 005 | 22.7 |
| 8–9 | 0012 | 003 | 25.0 |
| 9–10 | 0009 | 003 | 33.3 |
| Over 10 | 0016 | 006 | 37.5 |
| Total | 1,262 | 403 | 31.9 |
From these figures it is apparent (1) that children less than one year of age rarely recover after tracheotomy; this is especially true of diphtheria, although in other forms of laryngeal obstruction cases of recovery have been reported in children of six months; (2) that in the early years of life tracheotomy is most commonly needed, especially between the ages of one and five years; (3) that the death-rate gradually decreases between the ages of one and six years, after which there is a rise.
In explanation of these facts it appears probable that after five years of age the larynx and trachea are increased in size, so that obstruction is only met with where there is a large amount of membrane, namely, in the worst cases; in patients over ten, the age which marks the change to the adult type of larynx, the air-passages become so large that obstruction seldom occurs even when much membrane is present; dyspnœa, in these cases, points to extension of the disease to the smaller tubes, and tracheotomy is unable to give the same relief.
In considering the prognosis, not only must the symptoms peculiar to the case be taken into account (as for instance the pulse, temperature, respiration and general condition), but also any complications that arise. It must be borne in mind that tracheotomy does not cure, although it can relieve, the patient; that nearly one-third of the cases die; that the disease, and not the operation, is responsible for most of the deaths. Moreover, the amount of toxæmia depends upon the virulence of the infection, which is variable in different epidemics; upon the area of mucous membrane infected; and upon the constitution of the patient. In so-called hæmorrhagic diphtheria the result is always fatal.
The effect on after-life. It was stated by Landouzy at the Berlin Tuberculosis Congress in 1899 that, judging by the rarity of the scar, few tracheotomized children reach adult life, but inquiries in Germany showed that this was incorrect. H. W. L. Barlow, in reviewing the literature of the subject, concludes that ‘in the large majority of cases the cure is permanent and complete’. In cases where a tracheotomy tube has been retained for a long period, however, complications are liable to arise; these include stenosis of the larynx or trachea, bronchitis, pneumonia, and possibly tuberculosis (see p. 485).
The indications for tracheotomy in conditions other than diphtheria have already been described. Although local anæsthetics are of little practical value in children, their use is much preferred where adults are concerned. The three drugs most commonly used at the present time are eucaine, cocaine, and novocaine, and of these novocaine is unquestionably to be preferred for subcutaneous injection as being less toxic, less irritant to the tissues, and at least as efficient in producing anæsthesia. Whichever drug is chosen, a small quantity of chloride of sodium should be added in order to make the solution isotonic with the blood serum, and thus to render it practically non-irritant. Many surgeons add adrenalin to contract the vessels in the injected area and so to prevent the drug from being absorbed into the general circulation: owing to the large size of the vessels and their proximity to the heart this is important, but it must also be remembered that with strong solutions there is great contraction of vessels, and that when the effects have disappeared there is a slight danger of recurrent hæmorrhage. Semon has drawn attention to this danger in connexion with operations upon the larynx, and after minor operations in other regions of the body it is not uncommon to find a small hæmatoma which necessitates reopening the wound.
In order to ensure the full effects of local anæsthesia with the least possible disadvantage, the drug should be used in weak solution, and the injection should be made at least a quarter of an hour before the operation is commenced. It is only necessary to prick the skin at one point, namely, at the upper end of the proposed incision; a small quantity of the fluid should be expelled, after which the needle may be withdrawn. After a short interval it is possible to reinsert the needle (or a larger one if preferred) and to push it deeper, until the whole length of the incision has been injected, without distress to the patient.
The following solution will be found effective:
| ‘Novocaine, 4% solution | ɱ x = 1.3% |
| ‘Sodium chloride, 4% solution | ɱ vj = 0.8% |
| ‘Adrenalin, 1–1,000 | ɱ i = 0.003% |
| ‘Distilled water to | ɱ xxx |
‘These local anæsthetics are all, more or less, rapidly decomposed and rendered inactive in the presence of even traces of an alkali or alkaline carbonate. If boiling is resorted to in order to sterilize the syringe, great care must be taken that no soda is present.’—Lang.
Moreover, the finished solution cannot be boiled without decomposing the adrenalin, and it is customary therefore to add thymol or Ol. Gaultherii (0.1%), which keeps the solution antiseptic without being irritant.
The operation, which is often required in adults, must be carried out upon the lines already described. The enlargement of the thyreoid and cricoid cartilages, the small amount of fat, the small size of the thyreoid isthmus and of the pretracheal vessels after puberty, make the trachea easy to find. Difficulties, however, arise and are determined by the urgency of the case and the nature of the disease. Thus, with inflammation, the neck may be so swollen that the trachea is many inches from the surface; with tumours the trachea may be displaced, or the obstruction may be in the thorax. Under such conditions it is important to note the probable position of the trachea before the operation is commenced, and to be prepared for serious hæmorrhage.
The after-treatment also corresponds to that which is adopted in diphtheria. It is important to keep the tube clean and to prevent it from irritating the trachea. The time for removal of the canula varies according to the condition. Thus, when tracheotomy is performed for a foreign body, the tube may be removed as soon as the object has been extracted; on the other hand, when treating stenosis of the larynx it may be necessary to advise permanent wearing of the canula.
Complications are less common than with tracheotomy for diphtheria. Under favourable conditions there is little danger of pneumonia unless the wound becomes infected, as may happen when the operation is undertaken for the relief of septic inflammations.
Although tracheotomy is in itself a slight operation, it should be reserved for cases that demand it. The mortality of the operation under favourable conditions is probably very small; on the other hand, in acute septic conditions and in patients suffering from bronchitis there are grave dangers of complications.
Although these operations are very rarely performed, advance has been made in their technique during recent years.
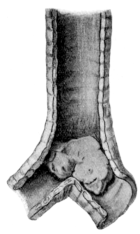 Fig. 275. Sarcoma of the Trachea. (From Specimen No. 1658a in the
Museum of St. Bartholomew’s Hospital.)
Fig. 275. Sarcoma of the Trachea. (From Specimen No. 1658a in the
Museum of St. Bartholomew’s Hospital.)
Indications. (i) Tumours of the trachea. These are uncommon. Thiesen34 in 1906 collected from literature 135 cases, of which 89 were innocent and 46 malignant. The majority of the former were papilloma (25), fibroma (24), enchondroma (17), and intratracheal struma (10). Of the latter, carcinoma (28) was more common than sarcoma (18). More than half of these tumours were situated high up in the trachea. These cases were collected from a period covering seventy-five years, which proves that they are extremely rare as compared with tumours of the larynx.
(ii) Stenosis due to previous inflammation. Stenosis may be caused by diphtheria or other fevers, syphilis, the presence of a foreign body, or the inhalation of corrosive acids or chemical fumes. Such cases are generally treated by endotracheal methods (see p. 559).
(iii) Cut-throat, or injury. An operation may be necessary after crushing or bullet wounds, or, in later stages, owing to the development of stenosis.
The diagnosis of these conditions is now comparatively easy, and with the help of direct laryngoscopy and X-ray photography the exact condition can, in many cases, be determined. In some instances the tumour may be removed by endotracheal operation, especially if the growth is innocent.
Tracheo-fissure is more reliable, and should always be performed when there is any suspicion of malignancy. The preliminary stages are similar to those of tracheotomy. A section of the trachea is first made in the region of the tumour, and the opening is enlarged so that the growth can be thoroughly explored; this can be better accomplished when the trachea is illuminated by a good electric lamp, in some instances a Killian’s tube being required. When possible, a tampon canula is inserted into the lower part of the trachea. When the growth is low down, the patient is placed in the Trendelenburg position in order to prevent the inspiration of blood. Should the diagnosis be uncertain, a portion of the tumour can be excised and a frozen section made. If proved to be innocent, the growth can then be freely excised with scissors or galvano-cautery. The bleeding is arrested, and the tracheotomy tube is retained for several days. The after-treatment must be conducted on lines similar to those laid down for laryngectomy, the patient being turned on the face in order to prevent pneumonia. ‘Up to the present time about two dozen operations of this sort have been reported. The author has removed in this manner four intratracheal thyreoids with permanent result’ (von Bruns).35
Resection. If the tumour be malignant, the surgeon must first decide whether its removal is practicable or whether palliative tracheotomy is preferable. In the former case the trachea is isolated laterally and divided transversely well below the growth. Whenever possible the lower end is then brought outwards and temporarily attached to the lower part of the incision above the sternum. The resection of the trachea is then carried out, so that the growth is freely removed, care being taken to preserve the recurrent laryngeal nerves. ‘Where the section of the trachea to be removed is limited to 4 centimetres or less, the two ends can generally be approximated and united, restoring the calibre of the tube and normal mouth respiration’ (Brewer).36 This is accomplished by numerous catgut sutures some of which include the entire thickness of the tube. The muscles can be approximated so as to cover the incision, and the wound can be drained freely. On the other hand, the lower end of the trachea may be permanently fixed in the wound as described under laryngectomy (see p. 498). Von Bruns has removed a cancer on the posterior wall of the trachea with six tracheal rings, thus giving the patient six years of life. He remarks: ‘operative treatment in tumours of the trachea shows brilliant results. Untreated the condition leads to death from suffocation. In seven cases operated upon by me, the results were all favourable.’
Intubation, or ‘tubage’, was first recommended by Loiseau and Bouchut in France; in 1880 attention was drawn to the subject by Sir W. Macewen in England, and soon afterwards O’Dwyer37 of New York published articles which resulted in its being extensively tried in America; since that time it has continued to be popular in that country for the treatment of laryngeal diphtheria. ‘The good results which American physicians have secured by intubation may be explained, perhaps, by the circumstance that according to their reports diphtheria takes a milder form in America’ (Tillmanns).38 Intubation has been extensively used in Europe, especially in Germany, but never to the same extent as tracheotomy, and in England it has been practised at only a small number of hospitals; thus, of the nine M. A. B. fever hospitals in London only three used it regularly during 1906–7, and none of them so often as tracheotomy.
Intubation versus Tracheotomy in Diphtheria. Since the introduction of the newer method of treatment in 1880 the subject has been widely discussed in America, on the continent of Europe, and in England. There is no evidence to show that treatment with antitoxin has been beneficial to one operation more than to the other.
The advantages claimed for intubation are:
1. No anæsthetic is required.
2. Consent of friends is easily obtained.
3. No cutting: great rapidity.
4. No wound to heal.
5. Tube worn more easily than the tracheotomy tube.
6. Breathing through natural passages, so that warmth and moisture are added to the air.
7. Its earlier performance.
8. Its better results in children under five.
9. Recovery is quicker.
The practical disadvantages are:
1. Quite unsuitable except at special hospitals, as great dexterity and constant practice are necessary.
2. Respiration is interfered with during introduction, so that celerity is indispensable, accidents are frequent, and failure is common.
3. Tube may be coughed up (28%, Goodall39), blocked (12%, Goodall), and does not provide good drainage for secretions.
4. Swallowing difficult.
5. Complications common: Broncho-pneumonia, ulceration, cicatrization.
6. After-treatment difficult and constant watching required.
7. Necessity for secondary tracheotomy (32.6%), which has a greater mortality (death in 46.1%, see table below).
8. Retained tube.
In considering the above it is the obvious duty of the surgeon to advise what he considers the better operation for the case, and this must depend largely upon the amount of his experience; the argument that the operation is superior because it can be previously practised on the cadaver is a bad one, and implies a failure to realize the many difficulties which will be encountered in the selection of cases, the operation itself, and its after-management.
I am strongly of opinion that the operation ought not to be tried indiscriminately by those who have no knowledge of these difficulties. In the hands of an expert it is a justifiable method of treatment which is suitable for selected cases, and it is one which can be used early; tracheotomy, on the other hand, is naturally delayed, or used for serious cases and those which have not derived relief from intubation.
Although intubation has received extensive trial, the published results show great variations and do not prove that intubation is superior to tracheotomy, but rather the reverse.
Table showing Details of Cases during 1906 and 1907 at the M. A. B. Hospitals where Intubation is favoured
| Intubation only. | Both operations. | Tracheotomy only. | Total operations. | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases. | Deaths. | %. | Cases. | Deaths. | %. | Cases. | Deaths. | %. | Cases. | Deaths. | %. | |
| Eastern | 78 | 04 | 05.1 | 44 | 19 | 43.1 | 030 | 13 | 43.3 | 152 | 036 | 23.6 |
| Western | 25 | 07 | 28.0 | 10 | 04 | 40.0 | 126 | 41 | 32.5 | 161 | 052 | 32.2 |
| Park | 31 | 03 | 09.7 | 11 | 07 | 63.6 | 016 | 11 | 68.7 | 058 | 021 | 36.2 |
| Total | 134 | 14 | 10.4 | 65 | 30 | 46.1 | 172 | 65 | 37.7 | 371 | 109 | 29.3 |
Certain points in the table deserve attention:
1. In cases treated by intubation only, the results are excellent, namely, death in 10.4%.
2. In cases where tracheotomy was afterwards performed the mortality is high, i.e. 46.1%.
3. Where tracheotomy was the original operation the mortality is also high, i.e. 37.7%.
4. The total operations at these hospitals taken together show a rather higher mortality than appears in the table below.
As regards the first three points, the facts are the same as in any published statistics dealing with the relative advantages of the two operations. I wish to emphasize that the results obtained by intubation depend very largely upon the selection of the cases and I agree with Turner and Cuff that, in order to arrive at any conclusion in the matter, it is necessary to compare the total results of those hospitals where intubation is favoured with those of the hospitals where tracheotomy is chiefly employed.
Table showing Comparative Results at ‘Intubation’ and ‘Tracheotomy’ Hospitals
| Three ‘Intubation’ Hospitals. | Six ‘Tracheotomy’ Hospitals. | Total Cases. | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases. | Deaths. | Mortality per cent. | Cases. | Deaths. | Mortality per cent. | Cases. | Deaths. | Mortality per cent. | |
| 1902 | 076 | 023 | 30.2 | 0222 | 071 | 32.0 | 0298 | 094 | 31.5 |
| 1903 1 | |||||||||
| 1904 | 156 | 047 | 30.1 | 0173 | 047 | 27.1 | 0329 | 094 | 28.5 |
| 1905 | 157 | 046 | 29.3 | 0184 | 040 | 21.7 | 0341 | 086 | 25.2 |
| 1906 | 166 | 058 | 34.9 | 0188 | 051 | 27.1 | 0354 | 109 | 31.5 |
| 1907 | 205 | 051 | 24.8 | 0289 | 086 | 29.7 | 0494 | 137 | 27.8 |
| Total | 0760 2 | 225 | 29.6 | 01,056 3 | 295 | 27.9 | 1,816 | 520 | 28.7 |
1 No return.
2 Of these more than 400 were intubations.
3 Of these 23 or more were intubations.
From these figures it will be seen that the total result for five years is a mortality of 27.9% as against 29.6%, in favour of tracheotomy. This serves, in my opinion, to strengthen the position of those hospitals which rely upon tracheotomy. Upon a comparison of this sort it would certainly appear that the results of intubation, at any rate in England, are not so good as has been stated. I am aware that this opinion is not shared by many authorities and that Stack40 writes, ‘taking everything into consideration, my impression is that under the most favourable conditions of operating, nursing, &c., the mortality is almost halved by doing intubation as a routine instead of tracheotomy.’
It has been claimed that intubation gives better results in children under five. This question has been worked out by H. W. L. Barlow,41 who concludes that ‘the younger the child, the longer will it require the tube, and the more frequently, therefore, has the latter to be inserted’, and ‘from the mortality alone, there is no indication that one operation is better suited for certain age periods than another, but since secondary tracheotomy appears to be rarest at three years old and the intubation fatality is least between four and six years, it follows that children from three to six are best adapted for intubation’.
Conclusions. Intubation is justifiable for diphtheria of a mild type if sufficient experience can be obtained and if the after-treatment can be personally carried out. The success of the operation depends largely upon a proper selection of the cases; in other words, it is not suitable for the worst types of this disease. It should never be performed upon a patient in whose case the question of tracheotomy does not arise.
In my opinion it is not a good operation for those general hospitals where there is constant change among the resident officers; it seems probable that it will remain the treatment of a small number of physicians who have frequent opportunities of practising their art.
Indications. (i) In diphtheria, intubation is justifiable when the disease is of a mild type without great toxæmia, where early diagnosis has been made, and antitoxin has been administered. It is not recommended when there is great pharyngeal inflammation, or in cases with bronchitis or pneumonia, or when the patient is prostrate, nor for severe obstruction caused by excessive swelling or false membrane in the larynx or trachea. In the last-mentioned condition intubation is difficult to perform, and the patient may be choked by false membrane which has been pushed down: intubation should be abandoned in favour of tracheotomy when immediate relief is not obtained.
(ii) In other forms of septic laryngitis, there is evidence to show that with intubation the mortality is higher than with tracheotomy; in œdematous laryngitis, such as follows the inhalation of steam, every effort should be made to prevent laryngeal obstruction by other forms of treatment, for intubation is difficult to perform owing to the swollen condition of the tissues; moreover, injuries are common, and there is a danger that the upper opening of the tube will become obstructed. Again, the tube may be expelled by coughing, and the child suffocated without relief.
(iii) In chronic stenosis, intubation is now extensively employed. Fibrous contraction such as follows some cases of thyrotomy, or syphilis and other inflammatory diseases, can be treated successfully by this method. Short light tubes, of vulcanite or similar material, are inserted and retained in position for long periods, three months or longer; with the pressure so exerted the amount of fibrous tissue appears to be diminished, and the lumen of the larynx is dilated.
Operation (in diphtheria). The apparatus required consists of a gag for opening the mouth, a set of tubes with a gauge showing the size for each age, an instrument for intubation and extubation, and equipment for tracheotomy.
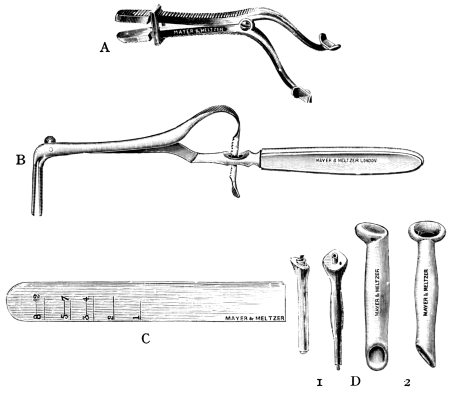 Fig. 276. Instruments for Intubation of the Larynx. A, Gag (O’Dwyer’s);
B, Forceps for intubation and extubation (Thorner’s); C, Gauge; D, Tubes: 1,
O’Dwyer’s; 2, Thorner’s.
Fig. 276. Instruments for Intubation of the Larynx. A, Gag (O’Dwyer’s);
B, Forceps for intubation and extubation (Thorner’s); C, Gauge; D, Tubes: 1,
O’Dwyer’s; 2, Thorner’s.
The tubes recommended by O’Dwyer are of gilded bronze, but other materials such as vulcanite or hard rubber are sometimes used. The tubes have undergone frequent modifications and those designed by Bayeux are shorter, lighter, and a great improvement (Goodall). In Thorner’s type (Fig. 276) the lower end has been cut off at an angle, so that it may pass more easily between the vocal cords; the intubator and extubator have been replaced by a single pair of beaked forceps with a ratchet attached to the handles, so that, when the beaks are separated, the tube is gripped firmly and cannot be disengaged until the trigger of the ratchet has been pulled; with these forceps the tube is not obstructed while it is being taken in and out of the larynx, and there is less need for hurry; further, the top of the tube has a funnel-shaped opening ‘which greatly facilitates the introduction of the beaks when the tube is in the larynx, inasmuch as it allows the beak to glide from any point of the rim almost automatically into the opening, and what this means can be appreciated by those who have had experience with the old extractor’ (Kyle).42
No preparation of the patient is required, but a blanket must be wrapped round the arms, body, and legs to control the struggling. Two assistants are required, one to hold the patient, the other to steady his head and manipulate a gag. The upright position is preferred by many surgeons because the patient is less frightened, and the breathing is easier; but the child may be laid upon a table, with the head slightly extended and exactly in the middle line of the body, or the head may be allowed to hang over the end of the table and the tube passed from behind, in a manner similar to that used for direct laryngoscopy. No anæsthetic is necessary. The first assistant or nurse should sit on a low chair with the child on his knee, holding him so that he directly faces the surgeon; a second assistant stands behind with a gag in his hand. A tube of suitable size, with a thread attached, and mounted on the introducer, is taken in the right hand; the assistant introduces the gag, opens the mouth to the fullest extent, and steadies the head with his two hands; the surgeon now passes the left index-finger over the back of the tongue, so that the tip of it passes behind and below the epiglottis until the cricoid is felt; this is the most important landmark, and as soon as it is located the finger is drawn upwards and forwards in order to hook up the epiglottis, and the introducer and tube are rapidly passed over it; the method of introduction being that used for all laryngeal instruments. As soon as the end of the tube is level with the end of the finger, the handle of the introducer is raised so as to throw the point as far forward as possible; the instrument is then bodily lowered, so as to drive the tube downwards through the larynx until it rests firmly and securely against the ventricular bands, which prevent further passage of the collar; the tube is now held in place with the left index-finger until the introducer is removed. The whole operation in experienced hands should take from three to five seconds only, and must be performed without force.
If the tube has been properly introduced, it is usual for the child to begin coughing, and this may continue for a short time, accompanied by noisy and rattling inspiration; the cough gradually disappears and breathing becomes easy. The tube causes temporary aphonia, which may persist for a few days after its removal, but is otherwise well tolerated; the patient is not conscious of the presence of the canula unless it becomes blocked.
The operation is simple in the hands of those who are accustomed to the use of laryngeal instruments; in a normal larynx there is no difficulty in introducing a tube, but in diphtheria the parts are inflamed and obstruction is present. Children are often intolerant or frightened; they are liable to retch or choke during introduction, but the latter can sometimes be accomplished by waiting for an inspiratory effort; if the struggling is very troublesome a small quantity of chloroform (cocaine in adults) may be given with safety.
Difficulties of the operation. The difficulty of passing the tube over the base of the tongue can be avoided by pulling the tongue downwards and forwards and passing the introducer through the mouth with the hand to the left of the patient’s face and rotating downwards when the point is in the pharynx. Failure to find the opening of the larynx is often due to not keeping the instrument exactly in the middle line. The tube may be too large (even when it corresponds to the age of the child) owing to swelling either in the larynx or in the subglottic region; in such a case a smaller tube must be tried, and it is essential that no force should be used to drive the tube into place, or dangerous complications may arise. Even a smaller tube may not be passed on the first occasion, and the surgeon has to decide whether he will try the same tube again or one that is smaller; the latter may not be suitable for the age. The tube may be too small, and this may be recognized by the ease with which it passes; as a result, the first strong cough expels it out of the larynx, and another must be introduced. A tube of correct size may be in the larynx without relieving the dyspnœa; this may be due to one of the following causes: (a) some membrane may have been pushed in front of the tube, an event which is evidenced by the noisy and difficult respiration, and which requires that the tube shall be withdrawn with the thread and again introduced, after an interval; (b) the tube itself may become blocked with membrane, with the result that it is at once coughed out; or (c) the child may be asphyxiated so that tracheotomy becomes a necessity. This last is a point that must always be remembered: intubation should never be performed unless everything has been prepared for opening the trachea. The tube may pass into the œsophagus in spite of all care, and this may increase the dyspnœa by pressing upon the posterior part of the larynx, in which case it must be withdrawn by the thread and a further attempt made. It has frequently happened that the tube with its thread has passed down the œsophagus into the stomach, an accident which ought to be avoided. No serious consequences are likely to occur, as the tube will be passed per rectum, or in rare instances vomited.
The question arises as to how many attempts should be made before intubation is abandoned. This varies in each case and depends upon the amount of distress caused by the previous attempts. With each further trial the child becomes more and more restless, and if the third attempt fails, it is better to desist, or to allow at least an interval of half an hour. When the dyspnœa becomes urgent there must be no hesitation, and either the tube must be reintroduced or tracheotomy performed; both operations are difficult under these circumstances, and the surgeon should choose the method of which he has the greater experience.
It is very important to remember that tracheotomy is required in nearly a third of the cases at one stage or another; at the M. A. B. fever hospitals of London during 1902–6 there were 429 cases of intubation for diphtheria, and of these 117 required tracheotomy later, i.e. 27.2%. As Goodall says: ‘Every case that was intubated four or more times came to tracheotomy. I therefore lay down the rule that if three insertions, each of several hours’ duration, fail to cure the laryngeal obstruction, tracheotomy should be performed. Frequent expulsion of the tube by coughing a few minutes after its insertion is also an indication for tracheotomy.’
After-treatment. A case of intubation requires more personal attention than one of tracheotomy. It is essential that the doctor should remain within easy call, as the tube may be blocked or coughed out at any moment. This danger is not so great as it appears; when the tube is coughed out there is no immediate asphyxia, and a fatal result is uncommon; an interval of at least twenty minutes usually occurs before the dyspnœa becomes urgent, in which time the doctor can be called; it may even happen that the tube is not required again, and that the obstruction has disappeared. When the tube becomes blocked, the state is more serious; in most cases it will be coughed out of the larynx, but if the child is very weak or the tube very firmly fixed, the obstruction must be at once relieved. It is for this reason that some surgeons prefer to leave a thread attached so that the nurse can extract the tube, but the latter has a disadvantage, namely, that the child may pull the tube out. This can be prevented by tying up the hands of the child while the tube is being worn, but even then the child may bite the string; the general practice therefore is to remove the thread, and the tube is then expressed by lateral pressure on the sides of the trachea, or by passing the finger below and behind the larynx and so pushing out the tube. The method is termed ‘enucleation’,43 and where it fails the extubator must be used. A nurse must be chosen who has had previous experience of intubation; she must understand the symptoms which necessitate interference with the tube, and the feeding of the child. Swallowing is often difficult, and liquids tend to pass through the canula into the trachea; the patient chokes and may cough up the tube. The danger of pneumonia is also increased. To overcome the dysphagia the patient should be made to suck uphill through a tube, or semi-solids may be tried: in other cases nasal or rectal feeding can be ordered: temporary removal of the tube has also been recommended for purposes of feeding, but vomiting often occurs with reintroduction immediately after a meal. In very troublesome cases there is distinct danger in repeated intubation; tracheotomy should be performed if the child is becoming exhausted from want of nourishment.
Changing the tube. O’Dwyer recommends that the tube should be retained for forty-eight hours without change, after which it should be removed once a day: it must, however, be remembered that while the tube is retained coughing is greatly impeded, so that septic material collects in the trachea and is liable to cause pneumonia.
Extubation by the thread and by enucleation has already been mentioned, but these methods are not applicable in every case. Extubation is difficult to perform, especially if respiration is obstructed and the patient struggling; whenever necessary, chloroform should be given. The preparation required is similar to that for intubation; a table and tracheotomy instruments are made ready; the upright position is preferred, and two assistants are required to hold the child and the gag; expanding forceps are introduced as if intubation were being done, and the tube is grasped securely and rapidly extracted, the whole operation being carried out as quickly as possible and without any suggestion of force. In experienced hands no danger is to be feared, but if two or three attempts are unsuccessful, tracheotomy should be performed. The time for removal of the tube varies from a few hours to four or five days in favourable cases. The main object is to dispense with the tube as soon as possible, and to err on the side of too early removal even in spite of the fact that reintroduction may be necessary.
Complications may occur, but there is no evidence that they are more numerous than with tracheotomy. Injury to the larynx is liable to result, especially from inexperience of the method, and this may be followed by hæmorrhage, emphysema, or abscess. In rare instances a false passage has been made, generally through the ventricle of the larynx: pressure ulcers may form, there may be necrosis of the cartilage, peritracheal abscess, or cicatricial contraction; or, as with tracheotomy, subglottic swelling may persist and granulations may be formed. When urgent dyspnœa follows the removal of the tube, one of these conditions must be suspected. O’Dwyer maintains that ‘the cause of persistent stenosis following intubation in laryngeal diphtheria can be summed up in a single word—traumatism,’ but ‘paralysis of the vocal cords may possibly furnish an occasional exception to this rule’ (Jacobson).44
‘Retained tube,’ which is the term applied to cases of more than five days’ duration, is certainly more common after injury, but does not occur more frequently than with tracheotomy; many cases have been reported where intubation tubes were used for long periods with ultimate recovery, but the method is uncertain unless the exact condition of the larynx can be determined (see p. 480).
Pneumonia. It has been shown that large numbers of bacilli are present in the lungs, where they may cause inflammation quite apart from any operation; in laryngeal cases the danger is increased owing to the obstruction which causes deficient aeration of, and improper expectoration from, the lung. Where tracheotomy is performed the dyspnœa is relieved and the expectoration easy; with intubation, on the other hand, there is no stage of apnœa after introduction, which seems to indicate that the air does not pass so easily through the smaller tube; coughing is more difficult and the amount of expectoration less; mucus, pus, or membrane in small pieces, can all be expelled through the tube, but not so freely as through the larger canula, and are more likely to be swallowed. For these reasons it would appear that pneumonia is less to be feared after tracheotomy; there is, however, considerable difference of opinion on this point, and statistics have not proved of great value.
Indications. (i) Foreign bodies. Accidental inhalation of foreign bodies is more common in children than in adults in the proportion of about two to one. The character of the foreign body should be considered before treatment is advised, and for this purpose the inhaled bodies may be divided into three classes:
| (a) | Pointed; such as bones, needles, teeth, nails, &c. | ||
| (b) | Rounded; | i. | Hard, such as coins, stones, or buttons. |
| ii. | Soft (in some cases capable of swelling), such as meat, beans, peas. | ||
| (c) | Fluid; such as blood, pus, or vomited food. | ||
To these may be added pieces of necrosed cartilage from the larynx, trachea, or bronchi; and calcareous concretions from bronchial glands, which occasionally perforate the walls of the air-passages.
Any of the above may become impacted in the trachea or fall into one of the bronchi: the right bronchus is affected nearly twice as often as the left owing to its larger size, its direction (which is more nearly that of the trachea), and the inclination of the septum to the left of the middle line.
(ii) Tumours of the trachea (see p. 546).
(iii) Stricture of the trachea resulting from previous inflammation or trauma. Tracheoscopy is useful both for accurate diagnosis and for treatment of such conditions. The following case may be quoted as an illustration: A boy of 17 was admitted to my hospital on account of dyspnœa, caused by obstruction in the lower air-passages. The chest was examined and a skiagram taken, the latter showing a definite shadow in the position of the bifurcation of the trachea. This was possibly an enlarged gland which pressed upon the trachea. I decided to give the boy an anæsthetic and perform tracheoscopy. On passing the tube a stricture was found in the trachea at the level of the suprasternal notch, which was so small that a large probe completely blocked its lumen, thus causing cessation of breathing. Under the condition it was impossible to dilate the stricture by endotracheal methods. The trachea was therefore exposed, but appeared to be normal. An opening was made into it above the stricture, and it was then seen that the latter was caused by a thickening of the anterior and lateral walls, involving two rings of the trachea and apparently of inflammatory nature. As no history of inflammation had been obtained the tissue was examined microscopically, and this confirmed the diagnosis. Division of the stricture completely relieved the dyspnœa, and after a few days the wound was allowed to heal. Three months later there was some return of the dyspnœa, and tracheoscopy was again performed. The stricture had to some extent returned, but was easily dilated through the tube, and two months later there had been no further dyspnœa. By the passage of bougies through a bronchoscope a stricture of the bronchus has been relieved in a similar manner.
(iv) For diagnostic purposes alone, to determine the cause of pressure upon the air-passages; as in tumours of the mediastinum, aneurism, and the like.
The instruments required correspond in the main to those used for direct laryngoscopy (see p. 480). The special instruments include (a) bronchoscopes, which are long circular tubes of dimensions suitable to the patient:
Length and Size of Tube required in Upper Bronchoscopy (Killian)
| Adults. | Children. | |
| Length | 30–40 cm. | 20–30 cm. |
| Diameter | 9–14 mm. | 5–7 mm. |
These should be marked externally in centimetres, measured from the distal end of the tube, and should be provided with a lateral window to allow of free breathing through the opposite bronchus when the tube is introduced into the one which is obstructed; of the various forms in use, the sliding tube of Bruenings appears to me superior; (b) instruments for extraction, including forceps and hooks according to the nature of the body to be removed; (c) aspirator for removal of mucus, and sponge-holders, the length of the bronchoscope.
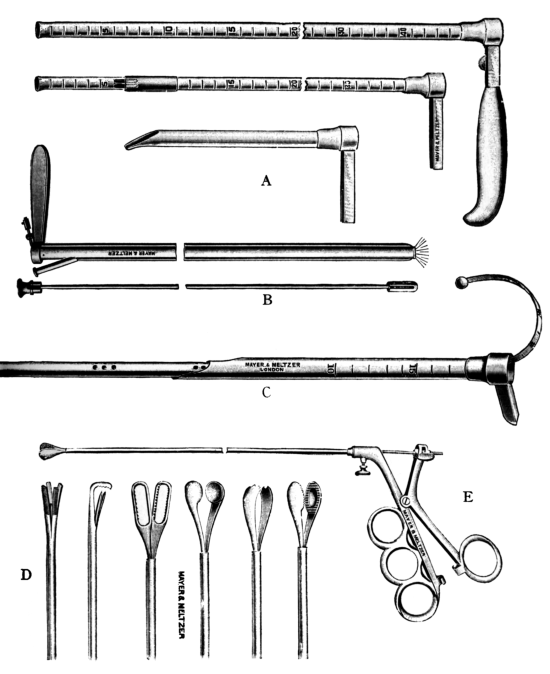 Fig. 277. Instruments for Bronchoscopy. Bronchoscopes: A, Killian’s;
B, Jackson’s; C, Bruening’s. D, Instruments for extraction. E, Handle (Watson
Williams’s).
Fig. 277. Instruments for Bronchoscopy. Bronchoscopes: A, Killian’s;
B, Jackson’s; C, Bruening’s. D, Instruments for extraction. E, Handle (Watson
Williams’s).
Operations (see also p. 481). As regards the anæsthetic, chloroform is preferable in children, but in adults cocaine may suffice. The operations are best performed in a room which can be made dark.
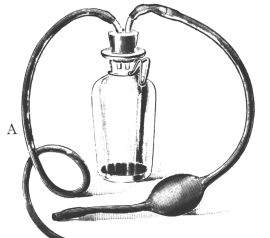
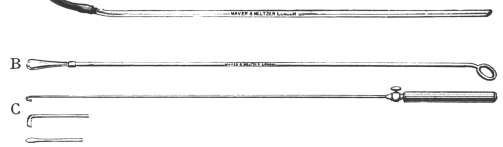
Tracheoscopy. The preliminary stages are similar to those of direct laryngoscopy. If the larynx be found normal, a smaller tube can be passed through the tube-spatula between the vocal cords, and the spatula can then be divided and removed in separate halves. In Bruening’s instrument the inner tubes are so constructed that they can be pushed through the outer tube and made to project like a telescope to any desired distance. In this way the subglottic region and trachea can be explored.
Upper bronchoscopy. The tubes are passed through the mouth, and the inner one is projected until the bifurcation of the trachea is visible. In order to avoid injury to the tissues, the operation should be performed entirely by sight and with great care. Three cases have been recorded where tracheotomy was needed for the relief of dyspnœa caused by œdema of the larynx which had followed traumatism.
The tube having been passed, cocaine (10%) is applied to the bifurcation of the trachea, and mucus is removed by sponging or by an aspirator. If the secretion be excessive, the foot of the table should be raised so that the mucus drains away from the part to be explored.
It is the duty of the anæsthetist or some competent assistant to note that normal respiration is maintained, and the necessity for tracheotomy or artificial respiration must always be borne in mind.
If the operator be experienced, bronchoscopy can be performed without endangering the patient’s life even in the case of a young child. A baby of eight months has been successfully treated by this method.
Lower bronchoscopy. Preliminary tracheotomy (median or low) having been performed, a wide tube is introduced into the bronchus through the wound in the trachea. This method has the following advantages: It is easier to perform, and the surgeon requires less experience of technique; the tube, being wider, is more readily illuminated; there is little danger of asphyxia; in passing the tube no organisms are introduced from the mouth, and there is less danger of pneumonia. If these advantages are weighed, it becomes apparent that the lower operation is preferable for surgeons without experience. In all cases with urgent dyspnœa preliminary tracheotomy is practically essential.
By a combination of the above methods the diagnosis of foreign bodies can be positively determined in the majority of cases. As Killian said in 1902: ‘We have now reached a position in which, in many cases at least, one can not only obtain a positive result but with confidence can assert that the foreign body is not present.’ In support of this statement numerous cases have been reported, especially in Germany and America. Von Eicken, in 1904, collected 42 cases of bronchoscopy, in 35 of which a definite diagnosis of a foreign body was made; in 4 it was shown that none was present; and in 3 only were negative results obtained. Since that time the results have been equally good, for in 1907 Killian increased this number to 164 reported cases in which a foreign body had been actually discovered.
As soon as the foreign body is clearly seen, a pair of forceps is selected and introduced through the tube. The object is grasped and drawn through the tube, if this be possible, or the tube and forceps may be withdrawn together from the trachea. If the foreign substance be broken the operation can be repeated until all of it has been removed. If the patient becomes collapsed it may be necessary to postpone the continuation of the treatment until the following day. A second attempt is often successful when the first has proved a failure.
Bronchoscopy is comparatively easy to perform (a) when the foreign body lies in the trachea or main bronchus; (b) when the foreign body has been accurately located; or (c) when the operation can be performed early, before inflammation has supervened. In the rare instances where the body lies in one of the secondary or tertiary bronchi, or has penetrated the substance of the lung, the difficulties are much increased, and in such conditions the question of the advisability of lower bronchoscopy should be considered.
Complications seldom occur after removal of foreign bodies by these methods if the surgeon is careful to avoid injury when passing the tubes. There may be temporary hoarseness owing to congestion of the mucous membrane. Ingals has reported two cases in which death occurred soon after the operation, with symptoms like those of delayed poisoning from an anæsthetic, and has raised the question whether it is advisable to use cocaine or atropin[e] in these operations. Delavan, on the other hand, suggests that injury to the pneumogastrics may account for such collapse. As stated above, the combination of chloroform and cocaine does not appear to be dangerous if used with discretion.
 Fig. 279. Upper Bronchoscopy with the Patient in the Dorsal Position.
Fig. 279. Upper Bronchoscopy with the Patient in the Dorsal Position.
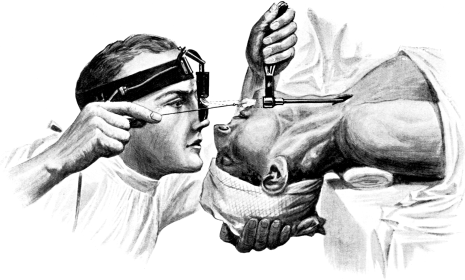 Fig. 280. Lower Bronchoscopy with the Patient in the Dorsal Position.
Fig. 280. Lower Bronchoscopy with the Patient in the Dorsal Position.
Results. Removal of foreign bodies by bronchoscopy gives far better results than the older methods of treatment such as tracheotomy, bronchotomy, and thyrotomy. With the last-named operations more than one-third of the cases have been fatal: while on the other hand, taking the 164 cases45 collected by Killian, it is found that in 159 (leaving out 5 with unknown result) only 21 (or 13%) died, viz. 2 from cocaine; 2 because it was impossible to remove the object on account of bronchial stenosis; 1 from suffocation in spite of upper and lower bronchoscopy; and the remaining 16 of pulmonary complications—5 with the foreign body in the lung, and the others in spite of its removal. Upper bronchoscopy was fully successful in 54 cases, and lower bronchoscopy in 63. The result of the remaining 21 operations is not stated.
Speaking of his own cases, Killian writes: ‘My own statistics give perhaps a better judgment for the future of cases of foreign bodies in the deeper air-passages than the general, since I have gradually acquired a larger experience and more practice. Nevertheless, I have the impression that in many cases my technic has not reached the highest mark, and I hope to obtain better results in the future. As shown by the list of cases, only one death resulted in the eighteen cases, and this was six months after the removal of the foreign body, caused by severe lung complication due to its long sojourn in the air-passages. In only two cases was I unable to find the foreign body and in only one was I unable to remove it on account of its being coughed up.
‘Upper bronchoscopy was performed in twelve cases, upper and lower in five, and lower tracheo-bronchoscopy in one. However, I hope in the future, with improved technic, to be successful with the upper method at the first sitting and to use the lower only in the severest cases.’
To Killian of Freiburg is due the chief credit for having introduced a safe method of treatment, the value of which is at last beginning to be generally recognized in England. As Paterson46 says, ‘it is earnestly to be hoped that the time has now come when workers in this country will recognize its enormous advantages.’
An intimate knowledge of the surgical anatomy of the nose is an important factor in successful treatment. It is sufficient to recall the close relations of the nasal chambers and their accessory sinuses with the cavities of the orbit and the cranium, and to remember that the shape and size of these air-spaces may vary considerably within physiological limits.
The arrangements of the vascular, lymphatic, and nervous supplies, and their connexion with neighbouring parts and the body generally, have also to be kept in mind.
In planning and carrying out operative procedures it is also well to keep in mind the important physiological functions of the nose.
Disease in the nose involves both medical and surgical treatment. The general progress of surgery, improved technique, local anæsthesia, and the control of hæmorrhage we now possess, have all tended to replace local medication by surgical measures. But in many affections of the nose—such as syphilis, or diphtheria—surgical relief is quite secondary to medical treatment. In any case the surgeon cannot dispense with a knowledge of suitable topical applications and the principles on which they are founded.
A good source of illumination is the first necessity for satisfactory operations on the upper air-passages. The natural sources at our disposal are sunlight and diffuse daylight. They have the great advantage of not altering the natural colours of the parts examined. Reflected sunlight forms a perfect illuminant, if we are careful not to bring the rays to an exact focus on the mucous membrane, as this might produce a burn.
Diffuse daylight is too feeble for the examination of the cavities of the nose and larynx, but it can be used for inspecting the mouth, pharynx, and ear. Direct daylight is particularly serviceable for examining suspicious rashes or patches in the mouth and pharynx, and eruptions on the skin.
Some form of artificial light is indispensable. That furnished by an ordinary paraffin lamp or a gas flame is sufficient for examination. The flame should have its flat side towards the observer, and be enclosed in a glass chimney, without a globe or shade. If neither of these lights be available, an ordinary candle, or, better still, three candles tied together, will suffice.
For use in the study a paraffin reading-lamp or a gas standard is equally suitable. The latter is rendered more effective by the adoption of an Argand burner or a Welsbach mantle. The oxy-hydrogen limelight is the most perfect of artificial illuminants, but it is bulky and expensive. The most convenient light is that given by a 32 or 50 candle-power electric light in a frosted globe, and with the filament waved. The Nernst electric burner gives increased brilliancy.
The electric light has the further advantage that it is unnecessary to maintain it constantly vertical. When enclosed in a bull’s-eye, the lamp can be rotated so as to direct the pencil of light-rays either upwards or downwards, as well as from side to side.
 Fig. 281. Laryngoscope Lamp.
Fig. 281. Laryngoscope Lamp.
|
Whichever light is employed the rays can be concentrated and rendered more powerful by enclosing it in a dark chimney with a bull’s-eye condenser. The light must also be provided with some arrangement by which it can be raised and lowered (Fig. 281). For operating the Clar light is useful (Fig. 282).
In all these methods the light is reflected, but the direct rays of the electric light can be used in a small lamp fixed on the forehead, and fed from an accumulator or direct from the street current through a suitable resistance. It is better than reflected light in operations on the nose and throat, and the portable accumulator and frontal photophore (Fig. 283) are convenient for use in the patient’s own home.
The lamp should be placed on a stand or table so that the light is on a level with the patient’s ear, and 3 or 4 inches distant from it. In Continental schools it is customary to place the light on the patient’s right hand. In this country the lamp is usually placed close to the patient’s left ear, i.e. on the observer’s right hand. As practitioners will often be called to see patients who are confined to a bed which can only be approached from one side, it is desirable that they should accustom themselves to work equally well with the light on either side, and the frontal mirror over either eye.
Cocaine. It is often desirable to secure a slight degree of local anæsthesia to facilitate complete exploration of the nose. Many operations can be carried out by rendering the nasal mucosa absolutely insensitive with cocaine.
Applied in the nose cocaine is (a) an anæsthetic, (b) a powerful vaso-constrictor, and, consequently, it (c) produces local anæmia. Hence cocaine is of great value in nasal surgery, not only because it renders the mucous membrane insensitive, but also because it retracts the tissues and reduces the hæmorrhage.
Methods of use. A small area can be anæsthetized by placing a few crystals of hydrochlorate of cocaine on the required spot, where the mucus will dissolve it in situ. A 2 to 5% solution may be sprayed into narrow nostrils, to facilitate examination. It is a better plan to moisten pledgets of cotton-wool or ribbon gauze with a 10% solution, and place them in direct contact with the part to be operated on. The addition of a little suprarenal extract will not only facilitate examination and treatment by its hæmostatic action, but, for the same reason, will tend to prevent the cocaine being absorbed and producing its toxic effects.
For the more complete anæsthesia required for operation the following plan is advised. Equal parts of a 20% solution of cocaine and the standard 1–1,000 extract of suprarenal gland are mixed together. Short strips of 1-inch wide ribbon gauze are moistened with this solution and laid flat in close contact with the nasal area to be operated on. They are left in place for at least half an hour, and even at the end of one hour local anæsthesia will only be more marked. While the final preparations are being made for operation a fresh layer of moistened gauze may be applied. Finally, if there should still remain the slightest degree of sensation over the spot to be treated, a few cocaine crystals will render it quite numb.
Submucous injection of cocaine. Great caution is necessary in making intracellular injection of cocaine, as the drug is intensely toxic in this form, and, fortunately, only a small dose is required. It is a good plan never to exceed 1 centigramme (1/6 grain) of the salt. As the hæmostatic effect of suprarenal gland extract is required at the same time, the two are combined; 1/6 grain of cocaine, 2 drops of adrenalin, 1/6 grain of sodium chloride, and 1/50 grain of morphia are dissolved in 60 minims or more of sterilized water, and slowly injected below the mucosa. At least 20 minutes must elapse to secure full effects.
Substitutes for cocaine. For submucous injection it is better to substitute eucaine or novocaine. Eucaine can be kept in a ready and portable form in small glass ampoules in the dose of 1/6 grain with 1/2000 grain of adrenalin, and tablets are sold containing 1 centigramme (1/6 grain) of either of these drugs in combination with adrenalin and chloride of sodium. One of these tablets is dissolved in 60 minims or more of water and boiled. It is reported that as much as 1 grain of novocaine may be injected at one sitting, but I prefer to keep to the limit of 1/6 grain, and have always been able to obtain complete local anæsthesia with it.
Eucaine is much less toxic than cocaine, and novocaine is said to be still safer. They act just as well for submucous injection, but, applied to the mucous surface, the anæsthesia is not so complete, and the vaso-constrictor effect is less. Still, for susceptible subjects, either is to be preferred to the more toxic cocaine.
Adrenalin. The delicate manipulations of intranasal surgery have been greatly facilitated by the employment of the extract of the suprarenal gland under various names—adrenalin, adrenine, adrin, perinephrin, adnephrin, epinephrin, suprarenalin, suprarenin, epirenin, paranephrin, renaglandin, hemesine, hæmostasine, vasoconstrictine, renostypticin, &c. These liquids are generally of the strength of 1 in 1,000, and can be used undiluted on mucous surfaces. But they can be diluted with normal saline solution, solutions of cocaine, or other drugs. If kept in well-stoppered, tinted glass bottles the solution can be preserved for many weeks. The solid extract is useful for those who only employ it occasionally, and in this form it is conveniently made up with cocaine, eucaine, or novocaine, so that solutions of the desired strength are prepared as required.
Applied to a mucous surface adrenalin produces a local ischæmia by contracting the blood-vessels, so that the surface becomes pale and shrunken. At least 20 minutes are required to secure this effect and it is only more marked at the end of an hour. An extensive operation, such as submucous resection of the septum, can then be performed without the loss of more than a trifling amount of blood in most cases. The vaso-constrictor action is followed by a stage of dilatation, disposing to secondary hæmorrhage, which, according to some authorities, may be ‘violent and sometimes serious’.47 I have been fortunate in not meeting with this occurrence. Its possibility can generally be guarded against, and need never prevent the employment of the drug when indicated.
Adrenalin has no anæsthetic power, but its constricting action lessens the tendency of cocaine to be deeply absorbed, increases the latter’s local effect, and allows of a weaker solution being employed.
Another secondary result is the very irritating rhinitis which is sometimes induced. It passes off in 24 to 48 hours.
Uses. The addition of a small quantity of adrenalin to a cocaine solution mitigates the toxic action of the latter, and its use appears to check tendency to collapse, either from shock or chloroform, during serious operations on the nasal cavities. Its chief use is to check hæmorrhage and allow us to perform practically bloodless operations in the nose.
Methods. Adrenalin is employed as described for cocaine. Disappointment in the result obtained is nearly always due to neglect in recognizing that its full effect cannot be obtained in less than 20 to 60 minutes.
Bleeding in the nose cannot be controlled as easily and directly as in the operations of general surgery, and there is always the risk of blood passing into the lower air-passages.
Causation. Hæmorrhage is apt to be not only more free, but also more serious, in young children and in patients over 60. The tendency is increased with menstruation or pregnancy, and hæmophilia is to be particularly looked for. In the nose the vascular turbinals bleed freely; a small varicose vessel on the septum is the commonest source of epistaxis,—often very copious. Many vascular growths are met with, and malignant ones are apt to bleed profusely.
Secondary hæmorrhage may occur between the third and eighth day, when clots or crusts become detached.
The prevention of local hæmorrhage. The patient should be prepared more carefully than usual for an operation. Hæmophilia should be inquired after, and if there is any suspicion of it lactate of calcium is administered for three days beforehand, in doses of 15 to 30 grains twice a day. If the patient be an undoubted hæmophilic, an operation should be avoided if possible. It is well to suspend the use of alcohol and tobacco for at least three days beforehand. Many risks are avoided if the operation can be carried out in the home or hospital where the patient has slept, and if he can remain there afterwards.
The arrest of local hæmorrhage. The preliminary use of adrenalin will diminish bleeding in many cases (see p. 573). When it does occur, unless the hæmorrhage is serious, it is well not to be too precipitate in efforts to arrest it. Such attempts, by stimulating the patient, detaching blood-clots, or exciting reflexes, may even maintain it. The clothing should be loose, the operating-room should be well aired and cool, and iced water should always be at hand. If freely sluiced over the face, behind the ears, and round the neck, cold water has such a remarkable reflex vaso-constrictor action that it alone is sufficient to arrest hæmorrhage in the majority of operations on the nose and throat. Its stimulating effect on the respiration and circulation is always agreeable to the patient, and may be very valuable when he is under a general anæsthetic.
If operated upon under a local anæsthetic, the patient’s head should be inclined forwards, so that the blood can drip from the nose. The first formed clots may be expelled, but then he should avoid sniffing, sneezing, or coughing, and sit with the head forward and the nostrils completely closed with his thumb and forefinger. Five to ten minutes in this position will arrest the bleeding in most cases of epistaxis. A slight oozing of blood may be allowed to go on for a few hours in certain cases. If the bleeding persists, ice should be applied externally and held in the mouth, the nose may be syringed with very cold or with very warm salt and water (ʒi to the pint), and the horizontal position assumed.
If this fails, a pledget of cotton-wool is dipped in peroxide of hydrogen solution (10 vols. %) and introduced into the bleeding nostril, the orifice of which is then closed by the surgeon’s thumb. This may be repeated more than once, the patient lying on his side, face downwards, and pinching both nostrils. If a galvano-cautery be available, and the bleeding comes from a limited and visible point, it can be sealed with a touch of the cautery point.
If these methods fail, plugging must be resorted to. With the nasal speculum and good illumination, the bleeding area is cleansed with cocaine and adrenalin and a strip of 1-inch ribbon gauze is carefully packed on to the spot, the end being left just within the vestibule, so that the patient can remove it for himself at the end of 12 or 24 hours. It is better to use a single strip of gauze, instead of cotton-wool, as portions of the latter might be detached and left behind. If there be fear of the gauze strip becoming adherent, it can be well smeared with plain sterilized vaseline.
If the bleeding comes from far back in the nose, or from the post-nasal space, it may become necessary to plug the latter cavity. A sterilized sponge, about the size of a Tangerine orange, is squeezed very dry and tied round its centre with a piece of tape or a stout silk ligature, leaving two free ends of about 12 inches in length. A soft rubber catheter is passed along the floor of the nose till it appears below the soft palate, when the end is seized with forceps and drawn through the mouth. To this end one of the tapes is made fast, so that when the catheter is withdrawn from the nose, the sponge is pulled up into the post-nasal space; the other end hangs out of the mouth. The two tapes are tied together over the upper lip. The anterior part of the nostril can then be packed with gauze, if necessary. If the patient be under chloroform, one tape can be dispensed with; the soft palate is simply held forward with the forefinger of one hand, while the other passes the compressed sponge up into the naso-pharyngeal space.
Plugs in the nose should be avoided. They are painful, interfere with repair, prevent drainage, and may be followed by septic troubles in the nose, accessory sinuses, middle ear, or cranial cavity. Bleeding often recurs on their removal. In any case they should not be left unchanged for more than 24 or, at the most, 48 hours. Removal is facilitated by soaking them well with peroxide of hydrogen, and detaching them slowly and gently. Ligature of the external carotid (see Vol. I, p. 384) may be necessary in extreme cases.48
When operated upon under local anæsthesia the patient is able to prevent blood descending from the nose or throat into the larynx or trachea. In this he is assisted by throwing the head forwards.
When the patient is under a general anæsthetic other measures must be taken to guard against the descent of blood into the windpipe and lungs. The most important is to see that the anæsthesia is never so deep as to abolish the swallowing or coughing reflexes. Fortunately these are amongst the last to go, yet in many cases it is well to let the patient come partly round, so as to expel blood and mucus by coughing. If the frontal sinus is being operated upon, the nose is carefully packed beforehand. When the ethmoidal labyrinth is being cleared, or the sphenoidal sinus opened, a sponge may be placed in the post-nasal space as described above until the operation is completed. During the operation upon the maxillary sinus through the canine fossa, a sponge placed between the last molar teeth and the cheek on the same side, and frequently renewed, will keep any blood from entering the pharynx. In operations upon the naso-pharynx, it is a wise precaution, when much bleeding is anticipated, to perform a preliminary temporary laryngotomy and plug the pharynx with a sponge (see p. 510).
In many proceedings security is attained by rolling the patient well over to one side, so that the blood runs out of the corner of the mouth, of blood is also swallowed. This may be vomited as consciousness returns; if not, an aperient should be given within 24 hours to prevent gastro-intestinal sepsis.
The descent of blood into the trachea and lungs, if sudden and copious, may cause immediate asphyxia; or, if less abundant, it may cause septic pneumonia. When it occurs, the anæsthesia should be stopped, and the patient rolled well over on to his face or inverted, until the breathing is quite unobstructed. After all nose and throat operations it is a wise precaution for the patient to be kept on his side, the head on a low pillow, and face downwards, while the body is arranged in the gynæcological position.
Shock, particularly in operations on the nose, is apt to be marked in young children and in elderly persons. It is for this reason that we try to avoid the removal of adenoids in patients under 3 years of age, or of polypi in those over 60; and that in all cases we endeavour to operate as rapidly as possible.
This possibility of shock is guarded against and treated in the usual way. The use of cocaine and adrenalin—even in patients under a general anæsthetic—helps to avoid it,49 and anæsthesia should never be too deep or prolonged. When operating under local anæsthesia it is sometimes wiser not to attempt too much at one sitting, e.g. to treat only one side of the nose at a time. In certain conditions, and when a general anæsthetic is employed, it may be safer to try and complete treatment at one operation.
Deaths have been recorded after the simple use of the galvano-cautery, or the removal of nasal polypi, and of course are more to be feared after major operations, such as the radical cure of sinus suppurations.
Septic infection from nasal operations may spread to the accessory sinuses, meninges, ear, eye, tonsils, glands, gastro-intestinal tract, bronchi, and lungs. From the naso-pharynx, the ears and the lower food and air tracts are chiefly threatened. The orbit may be invaded in operations on the ethmoid; the external muscles of the eye may be injured in the frontal sinus operation; and optic atrophy may be due to plugging of the ophthalmic vein.
While these accidents may sometimes be directly due to operation, it is well to remember that in treating such septic conditions as are entailed by nasal suppuration, the complications may only be precipitated by traumatism and may also be purely coincident. It is not to be forgotten that latent infection—of influenza, erysipelas, measles, scarlatina, diphtheria, or other disease—may develop immediately after an operation upon the nose or throat, and until its true character is recognized the operation is often unjustly blamed. Septic infection, in these necessarily exposed wounds of the air-passages, may be traced to insanitary surroundings.
The field of operation in rhinology can never be rendered completely sterile, and in many cases is particularly septic. Wounds through the mucous membrane cannot be protected with dressings in the usual way; so that the local methods of repair require particular study.
In the nose, when there is no suppuration, it is safer to make no attempt to purify the cavity, beyond cleansing the vibrissæ and vestibules. The Schneiderian membrane will not tolerate any antiseptic lotion of such a strength as to be effective, and weaker solutions only interfere with the action of the cilia, the protective power of the mucus, and other defensive arrangements of the nose. If pus, scabs, or foreign bodies exist in the nose, it should be well washed with a simple tepid alkaline solution.
But every care should be taken to purify the surgeon’s hands, sterilize all instruments, and see that no contamination takes place during the operation. This is assisted by having the patient’s head surrounded by a carbolized towel, and his face, moustache, and beard well washed, for the surgeon’s hands and instruments come in frequent contact with these parts.
After all intranasal operations everything should be avoided which interferes with the drainage, ventilation, and natural repair of the region. Protective dressings cannot be employed, and we have in most cases to aim at healing under a blood-clot. Tags of semi-detached tissue and loose clots of blood are removed, but otherwise the parts are disturbed as little as possible. For the first two or three days the nose may be left alone, and if there be no bleeding the patient is encouraged to breathe through it. When there is much formation of thick mucus, or blood-clots or sloughs are loosening, a tepid alkaline lotion can be used. The pain of stiffness or dryness in the nose is relieved by an ointment or an oily spray.
Adhesions are apt to form between the septum and the outer wall when opposing surfaces are injured by the galvano-cautery. They may occur in narrow cavities after cutting operations. If an adhesion be seen to be threatening in the first few days, it should be broken down with a probe, and strips of gauze or plates of white celluloid introduced daily until healing takes place. If it forms later, it is wiser to wait until the fleshy bridge becomes less vascular and contracts, when it may be divided with a knife or the galvano-cautery at a white heat, and the opposing surfaces are then kept apart as described.
All post-operative conditions in the nose and throat will heal more rapidly and pleasantly if the patient be freely exposed, day and night, to abundance of fresh air; and while fatigue is generally to be avoided, the sooner the patient is out of bed and in the fresh air, the better for him. Our inability to operate under aseptic conditions should make us more careful to raise the resistance of the individual by general care, and to protect him from external dangers.
The simplest and safest method of cleansing the nose is by blowing it,—one nostril at a time. Sometimes it is required to hawk any discharge backwards and expel it through the mouth.
Watery lotions are frequently required to assist in cleansing the nose. Strong antiseptics and astringents must be avoided. All nose lotions should be alkaline, and isotonic with the blood plasma. These requirements are met by prescribing one or more alkalis (bicarbonate of soda, borax, salt, &c.), in the strength of about 5 grains to the ounce. They may be rendered more pleasant by the addition of white sugar or glycerine. The addition of a small amount of some mild antiseptic—menthol, thymol, oil of eucalyptus, carbolic, sanitas, listerine, &c.—may give a pleasant flavour. But all antiseptics have a slight irritant action which is disagreeable if there be an intact mucosa, although they may be more helpful in certain cases of ulceration or intranasal sepsis. When the Schneiderian membrane is more or less damaged, when there are foreign bodies, sloughs, necrosis, &c., in the nasal chambers, these or similar antiseptics can be employed, though always with an alkaline basis.
All nose lotions should be employed tepid. They may be sniffed, irrigated, sprayed, or syringed into the nostrils. Crusts, scabs, and sloughs may have to be removed from the nose with forceps, after its sensitiveness has been deadened with cocaine; peroxide of hydrogen will help to detach them.
Incomplete operation may be unsatisfactory in many ways. Thus, nasal obstruction may be unrelieved: foci of suppuration may be left in the accessory sinuses: portions of adenoid growth or tonsils left behind may continue to give trouble: malignant growths may not be extirpated freely enough. On the other hand, operations may fail to relieve, or even produce a worse state of affairs, if too much tissue be sacrificed. This is important as regards the nose, owing to the important respiratory and defensive function of its mucous membrane. It is a good rule to injure the inferior turbinal as little as possible, otherwise a condition of crusting rhinitis may be set up, with secondary atrophy in the pharynx and larynx.50
Much judgment is required in adapting the suitable operation to each case. While in some instances one or more small interventions are all that is required, in another a well-planned and more extensive operation may be indicated. In any case, the advice of Semon should be kept in mind, viz. that the magnitude of an operation should not exceed the gravity of the symptoms calling for relief.
The external injuries of the nose belong to general surgery. It might be well to recollect that the fleshy end of the nose may be completely detached, and yet, if carefully and promptly replaced, perfect union will occur.51
Setting a recent fracture. One or both nasal bones may be displaced, causing a flat bridge with a sharp ridge on either side.
In the septum fracture generally takes place in the quadrilateral cartilage, or displacement occurs at its junction with the vomer or superior maxilla. It may be accompanied by a hæmatoma (see p. 612), and the occurrence of epistaxis shows that it is really a compound fracture. Care should therefore be taken not to infect the wound in the nose, and the patient should be warned on the subject.
The application of cocaine and adrenalin may allow of careful inspection of the septum. But, as the exact condition of things is marked by swelling, it is nearly always advisable to administer a general anæsthetic. Crepitus can rarely be made out. A hæmatoma is dealt with as directed (see p. 612). If there be any displacement of the septum—and it generally takes place towards the side on which there is already some convexity or depression of the nasal bones—the parts should be raised into place by manipulation with the little finger in the nostril. A flat-bladed forceps, like those of Adams, may be used. One blade in each nostril will straighten the septum and, at the same time, raise the whole nose into place. Small pencils of sterilized cotton-wool, smeared with vaseline (see p. 608), are then carefully packed up into the roof of the nose and kept there by Meyer’s vulcanite tube (Fig. 284). They are changed every 24 or 48 hours, for a week or so. The vomer is rarely fractured, although much callus is often thrown out in the displacements which occur between it and the cartilage.
Recent cases require no splints. In fact, if the displacement be promptly reduced—under general anæsthesia—the restored parts will generally maintain their position.
Elevating an old fracture. In neglected cases it may be necessary to re-fracture the nasal bones, and when these are replaced an external splint may be necessary. This can be made of plaster of Paris; or the outside of the nose may be covered with a piece of heavy adhesive plaster, and outside that a shield of tin, copper, or, preferably, aluminium.52
Fracture of the ethmoid is, fortunately, rare. When it occurs it is apt to run into the cribriform plate, and be associated with the escape of cerebro-spinal fluid and other indications of fracture of the anterior fossa of the skull.
Operation for congenital occlusion of the anterior nares. If the web obstructing the nostril be thin and membranous, and of low vitality, a simple and effective method is to destroy it with the galvano-cautery. It is best to spread the treatment over several sittings, so as to diminish the local reaction. The application of cocaine may not be sufficient to numb the pain, as the tissue of the obstructing web is more allied to skin than to mucous membrane. It should therefore be punctured quickly in two or three places, with a sharp cautery point raised nearly to a white heat. If the patient be nervous it may be well to administer nitrous oxide gas.
After the operation the nasal orifice is kept distended until healing has taken place by wearing Meyer’s vulcanite tube in it or short lengths of full-sized rubber drainage tube, well smeared with boric, aristol, zinc, or similar ointment. These simple nasal dilators are changed once or twice daily, and the nostril is well cleansed on each occasion.
If the web obstructing the anterior naris be more fleshy in character (and it is more apt to be of this nature when it is incomplete), it may be necessary to remove it with a knife. So as to leave as much epithelial tissue as possible, and avoid retraction, the operation is done as follows, under local or general anæsthesia: A narrow, sharp-pointed instrument, such as a Graefe’s or other ophthalmic knife, is used to puncture the web from before backwards, and it is then made to sweep round the obstructing diaphragm, while gradually cutting its way towards the central lumen. The tongue of skin thus formed can be used as a graft to cover most of the raw surface. The restored anterior naris is kept patent, as already described, till healing takes place.
In some cases the following operation has been shown to be easy and effective: An incision is made at the junction of the web with the septum, keeping close to the latter and passing straight down to the floor of the nose. On the outer side a similar incision is made, but sloping somewhat outwards. The flap formed between these two incisions is not cut off, but is bent backwards and fastened to the floor of the nose by a single horsehair stitch.53
Operation for congenital occlusion of the posterior choanæ. If the obstruction be not freely and completely removed it tends to re-form. A general anæsthetic is required. Unless the operator is ambidextrous he will find it most convenient to stand on the patient’s left hand, and to introduce his own left forefinger into the post-nasal space. This enables him to guide any straight, sharp instrument, such as an antrum drill (Fig. 323), Krause’s trochar (Fig. 285), or a surgical bradawl, from the front of the nose until it presses against and breaks through the obstructing diaphragm in two or more points. If preferred, an electric trephine can be used, and often pressure with the tip of a pair of nasal punch-forceps will be sufficient. The latter, either straight or tip-tilted (Fig. 286), are then inserted through the nostril, and, still guided by the left forefinger in the post-nasal space, are employed to clip away all the obstruction. To prevent any possibility of this reforming it is recommended by some surgeons that a small piece should be nipped out of the posterior margin of the bony septum. This can be done with the beaked punch-forceps of Grünwald (Fig. 286), passed through the nose, or with a pair of Loewenberg’s post-nasal forceps (Fig. 287) introduced through the mouth. In either case their action is controlled and directed by the operator’s left forefinger in the post-nasal space.
No special after-treatment is required. The patient should be ordered a tepid alkaline nose lotion, and should be encouraged to make use of the nasal air-way and acquire the habit of blowing the nose.
It might be helpful to remember that foreign bodies not only enter the nasal cavities (1) through the anterior nares, but also (2) through the posterior choanæ, or (3) by penetration through the walls. They may also arise (4) in situ, as in the case of sequestra and rhinoliths. The last group will be considered separately.
A foreign body, if small, may form the centre of a rhinolith.
Operation. Great care and gentleness are required in the removal of foreign bodies from the nose. The extraction should never be attempted blindly, or forcibly, or hurriedly. A little delay to make necessary arrangements does no harm. If a child will not submit to examination it is much better to employ a general anæsthetic so as to complete examination and, if found necessary, extraction at the one sitting. If the nose be not well illuminated and opened with a nasal speculum, groping about in the dark will only do further damage and result in disappointment.
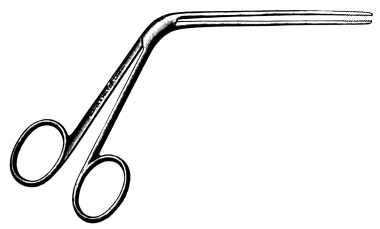 Fig. 288. Nasal Dressing Forceps.
Fig. 288. Nasal Dressing Forceps.
In adults removal can generally be carried on under cocaine. The nostril is cleaned with cotton-wool, and if the extremity of the probe used for detecting the presence of a foreign body be curved to a right angle, it will also serve for gently levering or displacing it forwards. With a small pair of nasal dressing forceps (Fig. 288) it can generally be firmly seized and gently extracted, care being taken not to include any of the mucosa nor to drag the foreign body out regardless of the sinuosities of the cavity. Lister’s ear hook is a most useful instrument. Sometimes a nasal snare will help to extract the substance or to tilt or drag it into a better position.
Unless coated with solid accretions there is never any need to break up a foreign body; anything small enough to slip into the nose is small enough to be extracted entire. If it should be found impossible to remove the body through the anterior nares, it may be pushed backwards into the post-nasal space, where the forefinger of the left hand is in readiness to prevent its falling into the gullet or larynx.
The usual warm alkaline lotion may be used to clear the nose, but liquid should never be forcibly injected into the nostril with the idea of thus expelling the foreign body. If the lotion be sent up the nasal chamber on the same side it will only drive the intruding substance further in; if injected on the opposite side there is risk of otitis media.
In the case of small children it is sometimes recommended that a piece of muslin should be placed over the mouth, and that the practitioner should then apply his lips to those of the patient and by blowing forcibly through the mouth drive out the foreign body by the blast of air from the post-nasal space. Or the same principle may be applied by insufflating the air from a Politzer’s bag through the opposite nostril. Both plans are alarming and seldom effective.
The after-treatment consists of some simple cleansing lotion and soothing ointment.
These concretions are almost unknown in children, in whom foreign bodies are met with most frequently. A general anæsthetic is, therefore, not so often required, otherwise the remarks on the removal of foreign bodies will be found to apply to the extraction of calculi. With the help of cocaine and good illumination they can easily be removed with a strabismus hook, Lister’s ear hook, or a pair of fine probe-pointed nasal forceps with serrated extremities. In some cases where the calculus has sent prolongations into the recesses of the meatus, it might first be necessary to crush it. In that event a general anæsthetic may be required.
The after-treatment consists in simple cleansing measures. Subsequent syringing of the nose should be done from the opposite side.
Indications. In many cases of hypertrophic rhinitis it is necessary to remove portions of redundant turbinal tissue. It is never desirable—and it can only rarely be necessary—to remove the whole of the inferior turbinal. ‘Turbinotomy,’ or amputation of the whole inferior turbinal, was recognized as an operation some years ago. But it was never generally accepted, as it was always realized that the highly important physiological functions of the lower spongy bone could not be spared. Improved technique, particularly in being able to correct deformities of the septum without the sacrifice of any mucous membrane (see p. 603), now enables us to rectify nasal stenosis with the sacrifice of much less turbinal tissue.
The middle turbinal is not of so much importance in the physiology of the nose, and the whole of this body is not infrequently removed. This may be done not only because it is diseased, but even a healthy middle turbinal may require amputation in order to approach the accessory sinuses or diseases in the deeper regions of the nose. Part of the healthy inferior turbinal may also require removal—as in the radical operation on the maxillary sinus.
As these operations will be referred to frequently later on, and as their performance enters into different groups of operation, they will be described first.
Amputation of the anterior end. Indications. The amputation may be required:
(i) On account of polypoid degeneration of the anterior extremity of the turbinal.
(ii) To allow of access to the antro-nasal wall (see p. 633).
(iii) To avoid operation on the septum by relieving nasal stenosis.
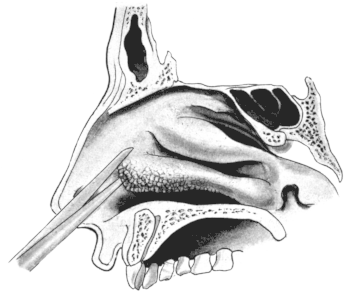 Fig. 289. First Step in removing the Anterior End of the Inferior Turbinal,
which is seen to have undergone Polypoid Degeneration.
Fig. 289. First Step in removing the Anterior End of the Inferior Turbinal,
which is seen to have undergone Polypoid Degeneration.
Operation. The local application of cocaine and adrenalin (see p. 573) is sufficient.
Anæsthesia. With the patient sitting upright in a chair, and the nostril well illuminated, a pair of nasal scissors (such as Heymann’s, Walsham’s, or Beckmann’s) are made to grasp as much of the anterior extremity as it is desired to remove, generally the anterior third (Fig. 289). The scissors are pressed very firmly against the outer nasal wall, so as to divide the base of the turbinal as close as possible to its attachment. If the scissors slip off the bone it should be divided with Grünwald’s punch-forceps. The semi-detached extremity is then surrounded with a nasal snare, carrying a No. 5 piano wire, and cut through (Fig. 291).
It is well not to seize and twist off the anterior extremity, as this might lead to the ripping out of a larger portion than was intended. Besides, it might cause fracture of the base of the remaining piece of the inferior turbinal bone and this might become displaced inwards so as to block the air-way more than ever.
After-treatment. It is well to check the hæmorrhage without the use of plugging. Some antiseptic powder—europhen, xeroform, formidine, aristol, &c.—if lightly insufflated over the wounded area, will assist in the formation of a protective scab. This should not be disturbed for some days, during which the nose is made comfortable by some menthol and boric ointment, or a paroleine spray. When the scab begins to break down its removal is assisted by warm alkaline lotions (see p. 579). The stump may require a few applications of nitrate of silver or other silver salt. There is no danger in this operation. Healing, as in other intranasal operations, takes from three to six weeks.
Amputation of the lower margin. Indications. This is not infrequently necessary when there is a general hypertrophy—as in the compensatory hypertrophy of septal scoliosis (Fig. 310)—or when the whole lower and outer margin is occupied by papillary hypertrophies (Fig. 289).
Operation. The operation can be carried out under the local application of cocaine and adrenalin, but is frequently performed as part of some other operation under a general anæsthesia.
The steps have to be varied according to the degree and extent of the hypertrophic tissue requiring removal. When this is principally along the lower border of the turbinal it can be removed with one cut of a stout pair of nasal scissors (Fig. 290). Under good illumination a blade is insinuated along the concavity, while the other passes between the convexity and the septum. Care should be taken that the direction of the scissors is parallel to the axis of the turbinal body, and that the cut embraces only that portion of the lower area to be removed. The severed portion should be quickly seized with a pair of punch-forceps and lifted out, or the patient, if only under local anæsthesia, may be requested to blow it forward into a tray. Otherwise it is apt to become obscured in the outpouring of blood, and, if the patient is unconscious, to be sucked backwards out of sight. If, as not infrequently happens, the lower margin remains attached at its posterior extremity, a wire snare is threaded along over it so as to cut this through. When the papillary hypertrophy is more diffuse it is apt to be concealed in the concavity of the turbinal. From this hiding-place it can be partially dislodged with a probe and then cut off with a snare.
The after-treatment is similar to that for removal of the anterior end.
Removal of the posterior end. Indications. The posterior extremity of the inferior turbinal is very subject to a moriform hypertrophy, and some delicacy and skill are required in removing it.
Operation. The interior of the nose on the affected side should be treated with a weak solution of cocaine and adrenalin. The most disagreeable part of the operation is the introduction of the operator’s finger into the post-nasal space. Hence the fauces should be freely sprayed with a 5% solution of cocaine. This will deaden painful sensation, but it will not prevent the discomfort nor the nausea often induced.
It is well to avoid as much as possible the direct application of cocaine or adrenalin to the moriform hypertrophy itself, for it is an extremely vascular growth, and if much contracted it is more difficult to ensnare.
The operation may also be carried out under a general anæsthetic, when one is given for other surgical measures in the nose. In that case it is best to defer the removal of the moriform hypertrophy until the end—practically until the patient is commencing to recover consciousness—on account of the sharp hæmorrhage which is apt to accompany it.
The chief difficulty of the operation lies in the fact that the part to be operated on cannot be kept in view, either directly or indirectly, and that therefore success depends a good deal on delicacy of touch.
A nasal snare—such as that of Blake, Krause, or Badgerow—is threaded with No. 5 piano wire, and a loop left out a little larger than sufficient to grasp the growth. This loop is then bent over smartly towards the side to be operated on, and a slight kink is given to it. The loop is then slightly withdrawn within the barrel, and this again brings it into a straight line. If now the snare be passed along the floor of the nose until the end of it is opposite the posterior extremity of the turbinal, and if the looped wire be slightly projected from the barrel, the loop will tend to curve outwards to the side on which it was kinked. In this way it will be felt to surround the moriform growth, which can then be cut off.
It must be confessed that this is not always successful, that there is no means of making sure that the snare is applied to the root of the growth, and that once the bleeding is started posterior rhinoscopy fails to reveal if any of it still remains. It is better therefore to introduce the purified forefinger of the left hand into the post-nasal space, so as to define the growth and guide the loop of the snare over it. The nail of the same finger then keeps the wire close to the base of the hypertrophy, while the loop is drawn home (Fig. 291). The patient may then be relieved of the discomfort of the operator’s finger in his throat, and may be given time to clear away the collected mucus. A little delay is advantageous, as it allows coagulation to take place in the large veins of the moriform growth. Some surgeons recommend that once the growth is strangled the snare should be left in situ for 10 or more minutes. This is irksome and unnecessary, and bleeding is seldom excessive if the snare be not employed for cutting off the hypertrophy, but is used as follows: Once the loop is drawn firmly home so as to embrace the growth tightly, a few minutes’ rest is given. Then, steadying the patient’s head with the now disengaged left hand, the snare is plucked from the nose with a quick movement. This brings away the mulberry hypertrophy in its grasp, and frequently a strip of mucosa from the lower margin of the turbinal. No bone is removed in this operation. The bleeding may be very sharp at first, but generally ceases under the usual measures (see p. 574). Occasionally it is extremely troublesome, and as the bleeding surface overhangs the post-nasal space the only local pressure which is available is that of a post-nasal plug.
After-treatment. As secondary hæmorrhage is apt to be met with the patient should be advised to leave his nose alone, neither blowing nor clearing it, nor using any cleansing measures for 48 hours. After that time he can employ the usual warm alkaline nose lotion. He should be warned against the habit of hawking backwards, as this would tend to a recurrence of the hypertrophy.
Prognosis. Great relief can generally be promised within a few days. There is no danger in the operation. The hæmorrhage may be troublesome, especially in men. The precautions described in the previous chapter are well worth observing (see p. 574).
Complete turbinotomy. Indications. As already remarked it must be extremely rare for this operation to be required. Papillary hypertrophy chiefly attacks the lower and posterior parts of the turbinal, and these can be removed as described above, so that if the entrance of the nostril is made free by anterior turbinectomy, there will still be left a sufficient area of functionally active mucosa. If, however, almost the entire inferior turbinal be degenerated, or if it be replaced by malignant growth, it can be removed in the following way.
 Fig. 292. Nasal Spokeshave.
Fig. 292. Nasal Spokeshave.
Operation. Anæsthesia may be local or general. If no other operative procedure be required at the same time, the anæsthesia of nitrous oxide gas or chloride of ethyl will be long enough. Owing to the vascularity of the part adrenalin should be applied for at least 30 minutes beforehand.
Removal of the turbinal is easily and quickly carried out with Carmalt Jones’s or Moure’s spokeshave (Fig. 292). This is introduced, passed as far as the posterior extremity of the turbinal, and the edge is guided in place with the operator’s left forefinger in the post-nasal space. With a sharp pull the spokeshave is then drawn forwards and the detached body can be lifted out with a pair of punch-forceps. Owing to the slope of the attached border it is seldom that the whole of the turbinal is removed. Those who are skilled in the use of this instrument can manipulate it so as to leave a good part of the attached margin of the turbinal, and the spokeshave can be used instead of the scissors for removal of the inferior margin. But its action is apt to be uncertain, and as it may unexpectedly rip out more than was intended, it is seldom employed nowadays.
After-treatment. After the removal of such a large portion of secreting surface the nasal secretion may dry into adhering crusts and scabs for some weeks—possibly for six or even eight. The scabs should be softened by the use of ointment or oily sprays, and removed by the fere use of warm alkaline lotions. The even healing of the granulating surface requires watching; its progress should be inspected from time to time, as the surface may require touching with a weak nitrate of silver solution.
Indications. Amputation of the anterior end may be required for (1) simple hypertrophy, (2) cyst or empyema in the anterior extremity, (3) to gain access to the ostia of the various accessory sinuses, (4) as a first step to uncover the ethmoidal cells, and (5) as a first step in removal of ethmoidal polypi.
Operation. Local anæsthesia with cocaine and adrenalin is sufficient, and the operation can be carried out with the patient sitting in the examination chair. It frequently forms part of some other intranasal operation which is performed under a general anæsthetic, but the preliminary application of cocaine and adrenalin should still be carried out (see p. 572). If the pieces of gauze soaked in the cocaine-adrenalin mixture be carefully tucked up on each side of the head of the turbinal, the part to be removed is generally well exposed. With a pair of Grünwald’s punch-forceps (Fig. 286) or Panzer’s scissors (Fig. 290), the anterior attachment to the outer wall is cut through (Fig. 293) so as to free the end, around which a cold wire snare can be passed and the extremity removed (Fig. 294.) In cases where it is difficult to introduce the punch-forceps under the attachment of the middle turbinal the blades may be applied to the lower margin, about half an inch from the anterior extremity so as to bite out a wedge. Into this the loop of the wire snare is inserted and the head of the turbinal can easily be snared off.
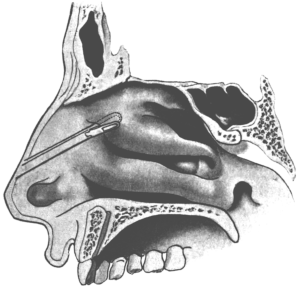 Fig. 293. First Step in the Removal of the Anterior End of the
Middle Turbinal.
Fig. 293. First Step in the Removal of the Anterior End of the
Middle Turbinal.
|
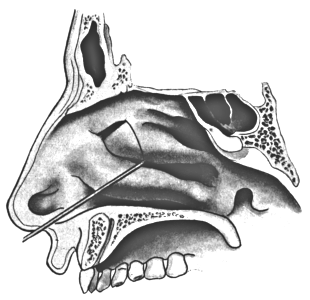 Fig. 294. Second Step in the Removal of the Anterior End of the
Middle Turbinal.
Fig. 294. Second Step in the Removal of the Anterior End of the
Middle Turbinal.
|
The snare is generally recommended as being safer than the punch-forceps. There is certainly a risk attending any slip in manipulating the latter in this region, more so, indeed, than in the deeper ethmoidal regions, for in the anterior part of the nasal roof the cerebral floor dips down lower than it does posteriorly, and the nasal fossa in the anterior part of the middle meatus is very narrow, so that if the forceps slipped they might impinge on the cribriform plate.
But when the middle turbinal is softened and broken down by disease it is as safe, and it is certainly more convenient, to take out a wedge from its centre, as directed above, and then with a pair of Grünwald’s or Luc’s forceps to twist out not only the anterior extremity, but also the posterior half. The latter part can also be removed with a spokeshave, as directed for the inferior turbinal (see p. 591).
After-treatment. There is not the same tendency to crusting as occurs after operation on the inferior turbinal. Hæmorrhage is also less troublesome. Plugging is therefore the less likely to be required, and should always be avoided if possible, since it would interfere with drainage from the various accessory sinuses, and this operation is frequently required when their contents are particularly septic. The best plan is to leave the nose severely alone for 48 hours, and then to clear it gradually with the help of warm alkaline lotions.
Sequestrotomy. The discovery of a syphilitic sequestrum always calls for active treatment.
Operation. If the sequestrum be not loose we must wait until it is movable. Its detachment will be expedited by mercurial inunctions or injections, and suitable local cleansing and disinfecting measures. As soon as any movement can be detected in the dead mass we can proceed, under cocaine, to detach it. Various forms of polypus forceps and bone-pliers may be required, and the necrosed bone has to be raised from its bed by a variety of lever and to-and-fro movements. Several sittings may be necessary, but this is inevitable, as any violent measures are soon arrested by hæmorrhage. When the necrosed bone has been mobilized it may be too large for extraction through the nares; such a mass as the greater part of the body of the sphenoid has sometimes necrosed en bloc. In such cases the dead bone must be broken up in situ and then removed piecemeal through either the anterior or posterior nares. Very rarely Rouge’s operation may be required (see p. 622).
Operations for post-syphilitic adhesions of the velum. So long as there is an adequate passage for nasal respiration it is best to leave any slight degree of stenosis alone. When there is complete atresia, and when mouth-breathing, deafness, or other consequences develop, some effort at relief should be made.
Operation. Under chloroform, and with the hanging head, W. G. Spencer54 separates the soft palate from its adhesion to the posterior pharyngeal wall, draws it forwards, and fixes it by two silk sutures to the muco-periosteum of the hard palate. Tilley carries out the same principle by threading the soft palate on both sides with strong silver wire and anchoring it to the incisor teeth. The wires cut out in 10 to 14 days, but by this time considerable healing will have taken place over the raw surfaces from which the adhesions had been separated.55
After freeing the soft palate, H. B. Robinson prevents it from again uniting by the following method: ‘A piece of lead plate is cut the full breadth of the naso-pharynx and bent so that one arm rests on the dorsal surface of the soft palate, and the lower one on the buccal surface, the cut margin being received between the plates and apposed to the bend, and so kept away from the pharyngeal wall.’ The piece of lead is kept in place by silk threads attached to the four corners, two passing forward through the nostrils and two through the mouth. The lead plate is not removed for a fortnight.56
Whatever method is employed to enlarge the stricture, dilatation must be kept up for some time by the frequent passage of the forefinger, a palate hook, or a dilatable bag.
Results. Stenosis of the passage from the naso-pharynx to the meso-pharynx, caused by syphilitic adhesions between the soft palate and the posterior pharyngeal wall, is one of the most difficult affections in this neighbourhood to operate on with satisfactory results. The cause of disappointment lies in the low vitality of specific scars and their well-known tendency to contract.
Surgical measures are sometimes required for the damage left by syphilis during the healing process.
The saddle-back deformity of the external nose is best corrected by subcutaneous injection of paraffin (see Vol. I, p. 681).
Perforations in the hard or soft palate may require operation to close them (see Vol. I, p. 717).
Tuberculosis only occurs in the nose in the mitigated form of lupus. Surgical interference is frequently called for, generally in the form of curettage or the application of caustics.
The most satisfactory caustic is the galvano-caustic point, applied under cocaine, and at repeated sittings.
Curettage is required in more advanced cases. Chloroform is always required. Not only should all soft and diseased tissue be scraped away with a Volkmann’s spoon, but the curettage should be carried on vigorously until a healthy and resistant area has been reached. It is rare for too much tissue to be removed, whereas recurrences are only too frequent.
Indications. A spur or ledge, uncomplicated with deviation of the septum, occasionally requires removal. It will generally be found in the lower meatus, at the junction of the quadrilateral cartilage and ethmoid with the superior maxillary crest and vomer.
Operation. The operation can be carried out painlessly and bloodlessly under cocaine and adrenalin. The galvano-cautery, trephine, and spokeshave should be avoided. An incision is made from behind forwards along the summit of the projection, and the muco-perichondrium is turned upwards and downwards. (For particulars as to reflecting these flaps see p. 605.) A straight, fairly stout nasal saw (Fig. 295) is inserted below the projection, and, while the patient’s head is steadied with the left hand, the saw is carried inwards and upwards with short, swift movements. During the first of these the cutting edge should be directed obliquely towards the opposite nostril so that the saw gets a good bite into the base of the spur. Otherwise, if simply directed vertically the resistance it meets with is likely to send it obliquely outwards, and the obstruction will be imperfectly removed. This defect will be the more apparent later on, when some heaping up of scar tissue is sure to take place over any trace of projection. In other words, in order to remove a spur flush with its base it is necessary to cut deeper than the base. At the same time it is important to avoid buttonholing the septum by cutting into the opposite nostril.
When the spur lies close along the floor of the nose it may be necessary to direct the saw from above downwards. The result is not so satisfactory, and the removal may have to be completed by seizing and twisting off the semi-detached spur with a pair of polypus forceps, or stripping it forwards with a spokeshave.
After-treatment. The reflected flaps of muco-perichondrium are replaced and maintained in position for 48 hours with plugs of cotton-wool. Subsequently a warm alkaline nasal lotion and a little ointment may be required.
Perforating the septum. It will be seen that if a spur is associated with a convexity of the septum to the same side it will be very difficult to remove the projecting obstruction adequately without cutting into the concave side of the septum, and so producing a perforation. Some surgeons even recommend that this should be done intentionally, and maintain that the resulting perforation seldom gives any trouble. This may be true in some cases, and the result is sometimes fairly good. But we have more completely satisfactory methods at our disposal; the perforation method does not relieve the majority of cases, and it interferes with the subsequent performance of more perfect operation. It can therefore only be approved of when the surgeon has not acquired the technique of the submucous resection operation (see p. 603).
Operation. When it has been decided to produce a perforation it is carried out with the nasal saw, as described for the removal of spurs (see p. 595). The saw is introduced so as to embrace as much as possible of the projection.
After-treatment. The drying and scabbing of discharge along the margin of the perforation is apt to give trouble for some weeks. This inconvenience is the more marked the nearer the perforation approaches to the anterior nares. It must be met by careful and repeated cleansing and lubrication of the nasal chambers. Any scabs should be carefully softened with hydrogen peroxide, lifted off the edge of the perforation, and any underlying ulceration treated with applications of nitrate of silver, argyrol, &c.
It is very rare to find a deviation of the nasal septum without some accompanying spur or ledge. It is still more rare to meet with a deviation which is entirely limited to the cartilaginous septum; there is nearly always some bony formation in the deformity, contributed by the nasal spine of the superior maxilla, the vomer, or the perpendicular plate of the ethmoid, or by all three. Hence the limited field of application for the various operations which have been designed for ‘straightening the cartilaginous septum’. In the few cases where the deformity is almost entirely cartilaginous these operations are only partially successful in overcoming its resiliency. They will therefore be only briefly considered.
Gleason-Watson operation. For a thorough performance this operation requires a general anæsthetic. The scheme of the operation is to make a U-shaped incision around the convexity, leaving it attached above. The flap of cartilage is then pushed through the U-shaped opening into the concave side. As its bevelled edge is larger than the button-hole in the septum it will be to some extent prevented from slipping backwards (Fig. 296). This tendency may also be combated by an attempt to snap through the base of the flap of cartilage, and by careful packing of the formerly obstructed nostril. The operation is performed with a nasal saw, carried from below upwards, and maintained carefully in the antero-posterior axis of the septum.
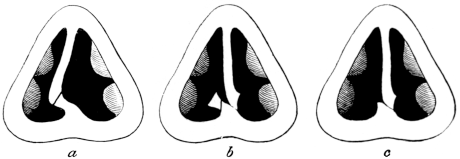 Fig. 296. The Gleason-Watson Operation for Deformity of the Septum.
a shows the incision made from the stenosed nostril, and below the convexity;
b represents the septum as pushed into the free nostril; and c shows the result
after subsequent removal of the spur.
Fig. 296. The Gleason-Watson Operation for Deformity of the Septum.
a shows the incision made from the stenosed nostril, and below the convexity;
b represents the septum as pushed into the free nostril; and c shows the result
after subsequent removal of the spur.
Asch’s operation. The resiliency of a deviated cartilaginous septum is more completely overcome by this method of operating. It requires a general anæsthetic.
 Fig. 297. Asch’s Cutting Scissors. Employed in the operation upon
the septum.
Fig. 297. Asch’s Cutting Scissors. Employed in the operation upon
the septum.
By means of appropriate cutting scissors (Fig. 297) a crucial incision is made over the summit of the convexity of the deviation, so that we have four triangular flaps meeting at the point of greatest stenosis. By means of the finger introduced into the obstructed nostril, or suitable septal forceps, these four flaps are snapped across at their bases so as to overcome their tendency to spring back.
 Fig. 298. Lake’s Rubber Splint.
Fig. 298. Lake’s Rubber Splint.
Into the formerly obstructed nostril is introduced a Meyer’s vulcanite hollow splint (Fig. 284), a Lake’s rubber splint (Fig. 298), or a gauze packing. This should be retained for 48 hours. Afterwards it will require daily changing and cleansing, possibly for several weeks. In the opposite nostril a lighter support will serve to keep the ends of the fragments in situ.
Moure’s operation. According to its author this operation can be carried out under local anæsthesia, but it is generally advisable to employ some such general anæsthetic as nitrous oxide or chloride of ethyl. By means of suitable scissors one incision is made through the septum parallel to the bridge of the nose and above the prominence of the deviation, and by another parallel to the floor of the nose the septum is divided below the deviation. This is now only fixed at its anterior and posterior extremities, but has been rendered more movable from side to side. By means of a specially designed dilator and splint the septum can be moulded into a good position, and maintained there until healing takes place.
The conditions in which any of these operations can prove suitable are rarely met with. In the worst forms of stenosis from septal deformity they are useless. At the best they can never completely remove it. In one of them a perforation is made on purpose, and in the others it not infrequently is produced unintentionally. The objections to a perforation have been described (see p. 598). Hæmorrhage, shock, and prolonged and painful after-treatment are important drawbacks. A dry scabby condition of the septum may be produced, and the patient may complain more of this than of his previous nasal stenosis; indeed, he may find that the stenosis is unrelieved and that a constant source of irritation has been added to it.
The perforation operation should only be employed when the patient is in circumstances where a complete submucous resection cannot be carried out. The Gleason-Watson operation is unsuitable where the deviation reaches high up. It should be avoided if it is seen that the perforation will have to be brought close forward to the anterior nares.
Another objection is that any of these operations, particularly the production of a perforation, will greatly increase the difficulties and diminish the benefits of the subsequent complementary operations which are only too often required.
Asch’s operation is easily carried out, and may be practised by those who have not mastered the technique of submucous resection (see p. 603). Moure’s operation is easily and quickly performed, and where a well-marked deviation of the anterior part of the cartilaginous septum is met with, it will give considerable relief.
Submucous Resection (Window operation)
This is the most perfect operation we at present possess for the cure of deformities of the nasal septum. It has largely supplanted those already outlined; it is suitable for the most extreme degree of deformity: and it will secure complete relief to the symptoms produced, whether they consist of stenosis of the air-way, obstruction to discharge, or reflex effects.
The design of the operation is to excise all obstructing cartilage and bone, with any projecting spurs or ledges, while preserving intact the mucous membrane on each side. It has been brought to its present degree of perfection chiefly by the work of Killian and Freer.57
Indications. The special indications of this operation would appear to be:—
1. Cases where it is desirable to establish normal nasal respiration and remove mouth-breathing, with its numerous consequences.
2. Correction of the disfigurement caused by the lower end of the quadrilateral cartilage projecting into one nostril.
3. Cure of headaches or reflex neuroses of nasal origin.
4. The relief and treatment of Eustachian catarrh.
5. Facility for treating nasal polypi and affections of the accessory sinuses.
Objections to the operation. (a) That the excision of a large part of the septum may lead to flattening or deformity of the nose. This objection is groundless. A strip of septal cartilage is always left above, beneath the crest of the nose. Falling in of the bridge of the nose could only be consequent on entire removal of this ‘bowsprit’ of cartilage, or from its destruction through the wound becoming septic. No deformity has occurred in my hands in over 200 operations. On the contrary, the appearance of the nose is generally much improved.
(b) That the operation entails greater risks from any subsequent blows on the nose. This objection has been met by the experience of Otto Freer in four cases where severe blows, causing epistaxis and occurring even within a week of operation, did not result in any damage to the fleshy septum, nor to the external appearance of the nose.58
(c) That the operation is long and tedious. The duration of the operation depends on the nature of the case, the skill of the surgeon, and the difficulties met with—chiefly in the way of hæmorrhage. A simple deviation of the cartilaginous septum can be removed by this method in 10 to 20 minutes. Many beginners are apt to be content with such a partial removal. More time is required in completely removing bony deformities. Many cases take 30 minutes, and none need exceed an hour when once the necessary dexterity has been acquired. More time is taken up if fresh applications of cocaine or adrenalin have to be made, if bleeding be troublesome, and if one of the flaps should be punctured.
(d) That the operation requires special skill. This is a real objection to the popularization of the operation. It does not seem probable that it can ever pass out of the hands of those who are kept in daily practice in rhinological technique.59
(e) That the operation is unsuitable for children. Owing to the small size of the nasal chambers the operation presents greater technical difficulties before the age of sixteen. My own practice formerly was to await this age, and Killian used to advise that children under twelve were not fit subjects. But Freer held that the operation is proper for children at all ages, although with them the deformity tends to recur unless every vestige of it has been removed. Killian has lately adopted this view, and agrees that the operation may be performed on children even as young as four years of age.60
Advantages of the operation. These may be summarized as follows:—
1. A general anæsthetic is not inevitable.
2. Hæmorrhage gives no trouble.
3. Absence of pain and shock.
4. No reaction. The post-operative temperature seldom rises above 99° F.
5. Absence of sepsis, with its possible extension to ears, sinuses, or cranial cavity.
6. No splints are required, and no plugs after the first 48 hours.
7. Rapid healing, without crust formation.
8. No risk of troublesome adhesions.
9. Short after-treatment.
10. Speedy establishment of nasal respiration.
11. Suitability for every variety of deformity of cartilage or bone in the septum which may require treatment.
12. No ciliated epithelium is sacrificed.
13. Accuracy of result can be depended on; the prognosis is, therefore, the more definite.
14. If the external appearance of the nose be altered at all it is in the way of improvement.
It will be seen that the above advantages cancel most of the drawbacks which were formerly so annoying in nasal surgery.
Contra-indications. 1. Elderly people are so accustomed to their nasal obstruction, and its secondary consequences are generally so fully established, that the benefits would be much less marked than earlier in life.
2. Serious or progressive organic disease. This does not apply to quiescent or arrested tuberculosis.
3. Active syphilis.
4. Lupus.
5. The operation should be postponed if the patient shows any symptoms of influenza, or of acute or infectious catarrh.
Operation. Submucous resection can be completely carried out under local anæsthesia, as described on p. 572. Killian and others secure local anæsthesia by submucous injection of cocaine and adrenalin (see p. 572), but I have found this method alarming to the patient, apt to produce disagreeable palpitation, and not superior to the method of superficial application already described, particularly if sufficient time is allowed for the mixture to act, and if a few cocaine crystals are allowed to dissolve over the site of incision some minutes before starting it.
In nervous subjects it is better to administer chloroform, not so much because of any pain they suffer, but because of the mental strain they are apt to feel in watching the various manipulations.
Position. The operation is best done with the patient horizontal on an operating table, with the head and shoulders well raised. His nose is then almost on a level with the eye of the surgeon, who is armed with a frontal search-light or Clar’s mirror (see p. 571), although he can also operate successfully with an ordinary forehead reflector.
 Fig. 299. Bayonet Knife.
Fig. 299. Bayonet Knife.
The incision. This can be made with a narrow scalpel, but a much shorter instrument mounted on a bayonet handle cutting all round the point will be found more satisfactory (Fig. 299). The incision is made from the side of the convexity, just anterior to it, and generally about half a centimetre behind the junction of the skin and mucous membrane (Fig. 300). It is started high up in the attic of the nose, and carried downwards to the floor. Sometimes it curves a little backwards below, but it is quite unnecessary to convert it into an L-incision by a second cut backwards. The incision, in its whole extent, divides the mucous membrane and cartilage at one cut, but without puncturing or wounding the mucosa of the opposite (concave) side. In doing this the operator’s forefinger in the opposite nostril serves as a useful guide (Fig. 301). In those cases where the lower free end of the quadrilateral cartilage is displaced from behind the septum cutaneum into one nostril— commonly but erroneously described as ‘dislocation of the septum’—the incision is made directly over the exposed extremity (Fig. 300, b-a).
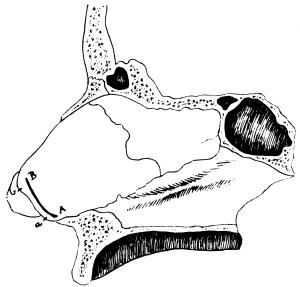 Fig. 300. Incision for Submucous Resection of the Septum. The incision
is made, on the convex side, from B to A. If the free end of the
quadrilateral cartilage is displaced from behind the septum cutaneum,
and presents in one nostril, then the incision is made from b to a.
Fig. 300. Incision for Submucous Resection of the Septum. The incision
is made, on the convex side, from B to A. If the free end of the
quadrilateral cartilage is displaced from behind the septum cutaneum,
and presents in one nostril, then the incision is made from b to a.
|
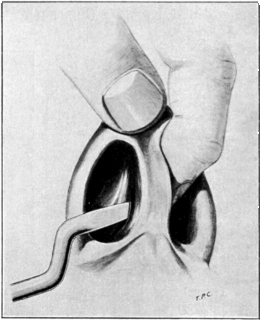 Fig. 301. Making the Incision from the Convex Side in Submucous
Resection of the Septum. The forefinger of the left hand acts as a guard
in the opposite nostril.
Fig. 301. Making the Incision from the Convex Side in Submucous
Resection of the Septum. The forefinger of the left hand acts as a guard
in the opposite nostril.
|
Raising the convex flap. With a small sharp elevator the muco-perichondrium is raised along the posterior edge of the incision. Great care must be taken not to pass the raspatory between the mucous membrane and the closely adhering perichondrium. The dead white, slightly roughened surface of the bare cartilage should be distinctly visible, and should not be coated with any soft, smooth, or pinkish perichondrium. Once the flap is well started a dull-edged detacher (Fig. 302) will readily undermine it by sweeping movements gradually advancing upwards and backwards. If possible the limits of the convexity should be passed, but it is well not to attempt to go round sharp projections, as it is there that perforations are apt to take place. It is easier at a later stage to strip the flap off crests or spurs.
Incision through the cartilage. If the cartilage has not already been completely cut through at the first incision it is now divided in the same extent as the cut in the muco-perichondrium, great care being taken not to button-hole the mucosa of the concavity.
Raising the concave flap. The sharp elevator, followed by the dull-edged detacher, is introduced from the incision on the convex side. The muco-perichondrium of the concavity is now raised in the same way and with the same precautions already used on the convexity, the sharp elevator and then the dull-edged detacher being introduced through the incision in the obstructed orifice, and manœuvred between the cartilage and the concave flap without puncturing the latter (Fig. 303).
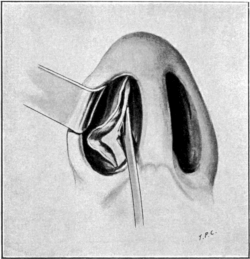 Fig. 303. Denudation of the Septum in Submucous Resection. The
muco-perichondrium has been raised from the convex side of the septum,
and the cartilage has been cut through (from A to B in Fig. 300). The
dull-edged detacher is shown separating the mucous membrane from the
concavity of the deflexion.
Fig. 303. Denudation of the Septum in Submucous Resection. The
muco-perichondrium has been raised from the convex side of the septum,
and the cartilage has been cut through (from A to B in Fig. 300). The
dull-edged detacher is shown separating the mucous membrane from the
concavity of the deflexion.
|
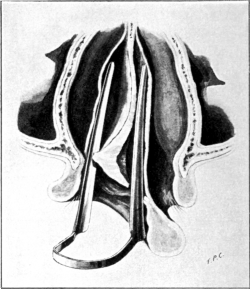 Fig. 304. Complete Denudation of the Deviated Septum. Semi-diagrammatic
drawing of a transverse section of the nose, viewed from above. The
deviated septum has been divided in front, and its muco-perichondrium
has been stripped up on each side. The nasal speculum is introduced
through the convex nostril, and a blade is inserted on each side of the
septum, between it and its mucous covering.
Fig. 304. Complete Denudation of the Deviated Septum. Semi-diagrammatic
drawing of a transverse section of the nose, viewed from above. The
deviated septum has been divided in front, and its muco-perichondrium
has been stripped up on each side. The nasal speculum is introduced
through the convex nostril, and a blade is inserted on each side of the
septum, between it and its mucous covering.
|
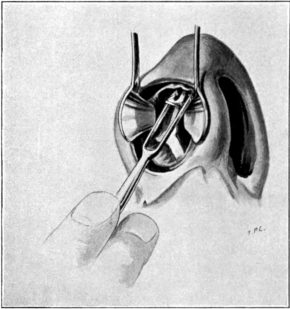 Fig. 306. The Method of employing Ballenger’s Swivel Septum Knife. The
knife is shown cutting out the cartilaginous deviation.
Fig. 306. The Method of employing Ballenger’s Swivel Septum Knife. The
knife is shown cutting out the cartilaginous deviation.
Excision of the deviated cartilage. A long Killian’s nasal speculum (Fig. 346), or the long Thudichum’s speculum I have had made, is now introduced through the obstructed nostril, one blade being inserted on each side of the now denuded septum (Fig. 304). It is easy to see if the mucous membrane has been sufficiently stripped off. If not, it can be carried further with a few sweeps of the raspatory. Ballenger’s swivel septum knife61 (Fig. 305) is then placed astride the anterior cut surface of the cartilage, pushed upwards and backwards below the roof of the nose until it comes in contact with the ethmoid, then downwards and backwards to the angle between the ethmoid and the vomer, and, finally, pulled forwards along the upper margin of the vomer (Fig. 306). The excised cartilage is thus removed en bloc, and may measure an inch by one and a half inches.
The empty pocket between the two separated and flaccid mucous membranes is wiped out and the two fleshy curtains are allowed to fall together. With a nasal speculum each nasal chamber is next carefully inspected to see that the thoroughfare is completely restored. As a rule deeper obstructions, formerly invisible, will come into view, and the mucosæ are again separated with a long nasal speculum and more of the septum is shaved off with Ballenger’s knife or clipped away with Grünwald’s punch-forceps, which also serve to remove portions of the vomer and of the perpendicular plate of the ethmoid.
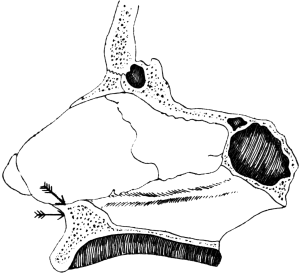 Fig. 307. Submucous Resection of the Septum. The arrows indicate the
points where the chisel may be applied when exostosis of the nasal
maxillary spine requires removal.
Fig. 307. Submucous Resection of the Septum. The arrows indicate the
points where the chisel may be applied when exostosis of the nasal
maxillary spine requires removal.
Excision of bony spurs and ledges. It has been pointed out that it is extremely rare to find a deviation limited entirely to the cartilaginous septum. I have never yet met a case in which it was not desirable to remove some of the bony septum.
When the deformity of the septum is principally composed of bone the operation is started as already described. It is then easier to lay bare any thickening or deviation of the nasal process of the superior maxilla, or of the chondro-vomerine suture—the usual sites of bony obstructions. When the main mass of deviated cartilage has been cut out with Ballenger’s knife free access is obtained from above to these deformities, and the fleshy muco-perichondrium can be peeled off on each side with much less risk of a tear or puncture. Still, much care is required in working round sharp corners, and, when the spurs lie low, the flaps frequently require to be reflected right down to the floor of the nose. Once well exposed, the maxillary spine is attacked with strong punch-forceps or chisel and hammer, and as pieces of it are prised up they are twisted off with forceps. Once the obstructing maxillary spine is cleared away it is easier to deal with any vomerine deformity.
A great deal of the success of an operation depends on the complete removal of these spurs and ledges, and as they may have to be followed back nearly to the posterior choanæ this part of the operation may be the most difficult, as it is the most necessary (Figs. 307–9).
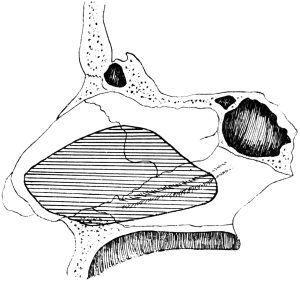 Fig. 308. Submucous Resection of the Septum. The shaded area indicates
the extent of the bony and cartilaginous septum usually requiring removal.
Fig. 308. Submucous Resection of the Septum. The shaded area indicates
the extent of the bony and cartilaginous septum usually requiring removal.
|
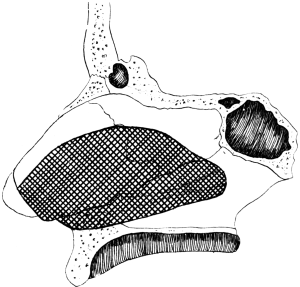 Fig. 309. Submucous Resection of the Septum. The shaded portion
indicates the extent of cartilage and bone removed in marked deformity, when the
free end of the quadrilateral cartilage projects into one nostril.
Fig. 309. Submucous Resection of the Septum. The shaded portion
indicates the extent of cartilage and bone removed in marked deformity, when the
free end of the quadrilateral cartilage projects into one nostril.
|
The pocket between the two flaps is again carefully wiped free of blood-clot and chips of bone and cartilage, and when the two mucous membranes are allowed to fall together they should hang perfectly plumb in the middle line and allow of an uninterrupted view through each nasal chamber, right back to the post-nasal space.
Stitches. With a small Trélat’s needle the incision is closed with one or two catgut stitches.
Dressing. Plain sterilized cotton-wool is tightly rolled into pencils about 3 inches long, and well smeared with sterilized vaseline. These are carefully packed into each nostril. The nose should not be tightly plugged, our object being to keep the two mucous membranes in apposition, but at the same time entirely occluding nasal respiration.
After-treatment. The patient remains quiet for the rest of the day. Ice may be given to suck and an iced cloth laid across the bridge of the nose. At the end of 48 hours the plugs are removed and will be found to come away very easily. The patient should be warned against blowing his nose, but may suck blood-stained mucus backwards and hawk it out through the mouth. Any discomfort may be soothed by spraying the nostrils with liquid vaseline, or introducing a piece of menthol and boric ointment into each nostril morning and evening.
The relief to the former state of nasal obstruction may at once be appreciable. If there be any local reaction it may take 3 or 4 days for the obstruction to subside. In 7 to 10 days the patient begins to enjoy the benefit of the operation, but it is only after 3 weeks that the full advantage of it is established.
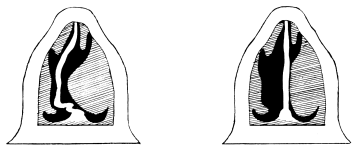 Fig. 310. Semi-diagrammatic Transverse Section of the Nose. Shows
the compensatory hypertrophy of the inferior turbinal in the unobstructed nostril.
Part of this frequently requires removal after the septum has been straightened.
Fig. 310. Semi-diagrammatic Transverse Section of the Nose. Shows
the compensatory hypertrophy of the inferior turbinal in the unobstructed nostril.
Part of this frequently requires removal after the septum has been straightened.
Complementary operations. As a rule the formerly patent nostril is found after this operation to be the more obstructed of the two. The reason of this is readily explained by a reference to Fig. 310. The now redundant hypertrophy in the formerly good nasal chamber is removed—according to its degree and extent—by one of the methods described on p. 587.
From long disuse marked alar collapse may interfere with the good results of the operation.
Difficulties. Insufficient illumination is a difficulty that can easily be provided against by using a frontal photophore or Clar’s mirror (see p. 571).
Hæmorrhage presents no difficulty if patients are prepared as directed (see p. 574), unless one happens unexpectedly on a patient with a hæmophilic tendency. In one such case I had no trouble at the time of operation, but bleeding gave great annoyance for a fortnight afterwards.
The incision I have described has always proved sufficient. In some cases this straight incision is unintentionally converted into an L-shaped one, when the flap is torn over a sharp low-lying spur. Beginners may find it easier to start with an L-shaped incision, but it is unnecessary and does not leave so small and clean a wound.
The perichondrium should be raised with great care, for it is more easy than one would think to leave it adhering to the septum, while separating only the mucous membrane.
Previous operations always increase the difficulties of the proceeding. The old-fashioned ‘shaving off’ of spurs often removed the entire thickness of the cartilage at one part, without perforating the concave mucosa. The submucous resection (window operation) is not infrequently not carried far enough. In either of these circumstances we are confronted with the great difficulty of trying to separate the two muco-perichondria—now closely united to one another.
When a perforation of the nasal septum is situated at some distance within the nasal orifice it seldom gives any trouble. A perforation may also be situated close to the anterior nares without even making its presence known. But in some cases—no matter what the original cause of the perforation—constant annoyance is given to the patient by the crusting and bleeding which takes place along its margin. When these crusts have been carefully removed inspection will show that the cause of the trouble is the projecting free edge of the cartilage which prevents the edges of mucous membrane from each nostril from closing over it. When this circular edge is healed over smoothly, secretions cease to adhere to it, and the patient is not troubled by the annoying crust formation.
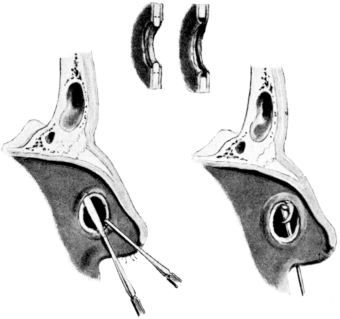 Fig. 311. Operation for Perforation of the Septum. The muco-perichondrium
is reflected for some distance round the opening so as to allow of the
projecting rim of cartilage being removed. The exposed edge is then covered
over by the mucous surfaces falling together.
Fig. 311. Operation for Perforation of the Septum. The muco-perichondrium
is reflected for some distance round the opening so as to allow of the
projecting rim of cartilage being removed. The exposed edge is then covered
over by the mucous surfaces falling together.
This desirable condition can be brought about in crusting perforations by means of the following operation designed by Goldstein.62 After preparation with cocaine and adrenalin (see p. 573), the muco-perichondrium is reflected on each side along the whole circumference of the perforation for a distance of about a quarter of an inch from the free margin. Over the greater part of the circumference this can be done with Freer’s sharp elevator, or with the small sharp elevator employed in submucous resection of the septum. In dissecting the anterior part of the circumference the same kind of elevator can be used, but with the operating edge bent forward at an acute angle (Fig. 311). A slit in the elevated mucous membrane, posterior to the perforation, will relieve tension. With a Ballenger’s single-tine swivel septum knife a rim of cartilage is then cut away around the perforation, so that the two mucous surfaces from opposite nostrils can come in contact and overlap the circular edge of cartilage. This smooth surface will prevent any further sticking and crusting of discharge. It is kept in situ for 48 hours by vaselined cotton-wool plugs, similar to those used in the submucous resection of the septum (p. 608).
A free incision is made into it, under cocaine or nitrous oxide anæsthesia. A horizontal cut should extend right across the swelling, and as low in it as possible, to prevent the pocketing of pus. It is sufficient to make it on one side, as the pus from the other side can be pressed across through the defect in the cartilage. Any loose fragments of cartilage should be probed for and removed. The lips of the incision are kept apart by loosely tucking in a small piece of ribbon gauze. This promotes drainage of the lower part, and is changed daily. Afterwards healing takes place under simple cleansing measures.
If the hæmatoma be small and not in a suppurating nose, evaporating lotions are applied externally and the swelling is left alone, being carefully inspected daily for early symptoms of suppuration. If the swelling be large and tense, it is safer to incise it freely as described above for abscess of the septum.
Indications. Operation with the snare is indicated in cases of simple mucous polypi, if only a few polypi are present, and no sinus suppuration is suspected. It is a suitable method for the removal of papilloma, fibroma, and bleeding polypus of the septum. The snare is also serviceable in the removal of enchondroma, osteoma, and growths, if of limited size, after they have been detached from their bases or broken up with a chisel or bone forceps.
Instruments. The surgeon will employ the pattern of snare to which he is accustomed. The simpler models, such as those of Krause, or some modification of Blake’s instrument, such as that of Badgerow, when threaded with No. 5 piano wire will be found sufficient in most cases (Fig. 312). For tougher growths, or those with a thicker pedicle, the snare of Lack can be recommended. It is threaded with heavier wire, and by a screw arranged in the handle the loop can be slowly and steadily contracted.
Operation. The nose is carefully prepared with cocaine and adrenalin (see p. 573), remembering that any growth or polypus is itself insensitive. The anterior part of the nasal cavity, and particularly the septum, should be thoroughly anæsthetized.
Under good illumination the snare is introduced with the loop vertical, and passed alongside the growth,—between it and the septum or to the outer side, as space permits. It is then swept round a half-circle, so as to bring any tumour within the loop, and by a to-and-fro movement the snare is worked upwards towards its base. The attachment of the ordinary mucous polypus is generally in the region of the middle meatus. The wire loop is thus threaded on to the growth or polypus. The loop is now steadily tightened until it is felt that the pedicle is grasped,—it is seldom visible. By a quick movement of avulsion the tumour is then torn from its attachment. This will bring away some of the œdematous tissue on the distal side of the loop, and there will be less tendency to recurrence than if the root were simply cut across. With the removal of a first polypus others come into view and they must be treated in the same manner. The number which can be removed at one sitting will depend on how well the patient is able to bear the manipulations and how much bleeding there is. If both nostrils be affected it is well to treat them on alternate weeks.
When the growth slips, or is pushed backwards, it can be brought forward into the field of operation by asking the patient to blow down the nose, with the opposite nostril closed. Or the presenting part of a polypus may be seized with a pair of toothed catch-forceps and the wire loop slipped over this.
If the growth be hanging backwards, and presents in the post-nasal space, as it often does when it originates from the mucosa of the maxillary antrum, it may be necessary for the surgeon to introduce his left forefinger behind the palate,—as described on p. 590 (compare Fig. 291),—so as to steady the growth and at the same time slip the wire loop around it. If there be no space for the latter manipulation, the left forefinger is used to steady the mass while a pair of polypus forceps is guided along the floor of the nose until the growth can be seized between the blades so as to tear it from its attachment and pull it out through the anterior nares.
After-treatment. The bleeding will generally cease spontaneously, assisted by cold ablutions to the face, or pinching the end of the nose until a clot forms (see p. 575). If bleeding persists, a piece of gauze, moistened with peroxide of hydrogen, should be packed in lightly and removed as soon as the patient can lie down quietly. It is best to avoid the use of any plug. It was to plugging that Luc attributed the loss of a patient from meningitis consequent on the removal of polypus.63
If the entrance to the nose be tender, it may be smeared with a little menthol and boric ointment; ice-cold cloths may be kept across the bridge of the nose; and pain or sensitiveness can be relieved by a few doses of phenacetin or some similar anti-neuralgic.
Insufflations of antiseptic powder are useless, and the nasal cavity should be left alone for 24 or 48 hours. A nose lotion should then be used two or three times a day, until the local condition is again inspected at the end of a week.
Any attempt to destroy the roots of polypi by the galvano-cautery is useless and dangerous.
Indications. This operation is indicated in all cases of recurring polypi and extensive caries of the ethmoid, but the plan of operation is also suitable for the removal of some cases of papilloma, fibroma, enchondroma, or osteoma.
It can also be employed in certain cases of malignant disease in the nose. When the growth appears to be limited to the nasal fossæ, and particularly in cases of sarcoma, the above operation may be indicated. Even when glands are present this may still be the preferable operation, as glands can be removed at a separate sitting.
Possibly a better method of deciding the case of malignant intranasal disease suitable for this operation will be founded on the discovery of the original attachment of the growth. If located towards the front of the nose in the anterior part of the middle meatus, removal can be carried out on the lines described.
Contra-indications. If there be any mental symptoms suggesting that intracranial inflammation has taken place already, the patient should be carefully examined before operation is embarked on. It is unsuitable for debilitated and elderly subjects. In patients over 60 with recurrent polypi it is wiser to secure relief by a series of small operations under cocaine.
Many neoplasms and inflammatory hypertrophies, such as mucous polypi, can be removed satisfactorily per vias naturales by the method to be described. Naturally the details will vary with the situation and extent of the disease to be removed. The following description applies particularly to growths or hypertrophies springing from the ethmoidal region:—
Operation under cocaine. The nose is carefully prepared with adrenalin and cocaine, the strips of moistened ribbon gauze being carefully tucked in between the septum and the ethmoidal region, as well as between this latter and the outer wall. The inferior turbinal and the front of the nasal cavity should be similarly prepared, so as to diminish vascularity, retract the healthy tissue, and thus increase the space for operating in, while lessening the risk of wounding the septum and so causing adhesions. At least one hour should be given for the solution to act. The operation is done with the patient sitting upright in the ordinary examination chair, with the body craned forward somewhat, and the head supported and held in focus by an assistant. Ready to the surgeon’s hand should be some lengths—about a yard—of 1-inch to 2-inch ribbon gauze, and a vessel of cold sterilized water into which it is easy to shake off the growths as they are removed with the forceps.
If the middle turbinal has not already been removed it may have to be amputated, as described on p. 592. In many cases of ethmoidal caries it is easily removed with nasal forceps.
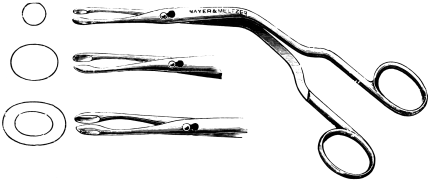 Fig. 313. Luc’s Nasal Forceps.
Fig. 313. Luc’s Nasal Forceps.
The instrument I recommend is Luc’s forceps64 (Fig. 313), supplemented by Grünwald’s punch-forceps (Fig. 286). The former are introduced vertically, so that one blade passes between the ethmoid and the septum and the other passes under cover of the middle turbinal. By insinuating them carefully, and gradually working them upwards and outwards, a large mass of tissue or carious ethmoid can be grasped, twisted off, and shaken from the forceps into the vessel of water. Before any marked flow of blood has taken place it will be possible to make a second or third introduction of the forceps, and seize the successive masses of growth which come into view. When the bleeding obscures the field of operation one of the strips of gauze can be picked up quickly in the forceps and used for plugging that side of the nose, while a similar operation is carried out in the opposite nasal chamber, if it is affected.
Hæmorrhage may require the plug being left in situ for a few minutes, so as to get a clear view of the depths of the nose. This is better secured if the end of the gauze strips are first soaked in either adrenalin or a 10% solution of hydrogen peroxide. In this way the main mass of the ethmoid can be completely cleared away, the posterior ethmoidal cells opened up, and the front wall of the sphenoidal sinus broken down. Not infrequently the surgeon finds afterwards that this latter cavity has been quite inadvertently, though successfully, opened.
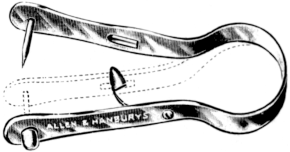 Fig. 314. Tongue Clip. Keeps the tongue drawn forwards to allow of
general anæsthesia, when the post-nasal space is plugged.
Fig. 314. Tongue Clip. Keeps the tongue drawn forwards to allow of
general anæsthesia, when the post-nasal space is plugged.
Operation under general anæsthesia. Under a general anæsthetic this operation can be even more satisfactorily carried out, but the surgeon has to keep well in view the anatomical relations of the parts, and the altered relationship to the horizontal position compared with what he is more accustomed to with the patient sitting in the examination chair. When chloroform is employed the interior of the nose is prepared in the same way beforehand with adrenalin and cocaine; the patient is placed horizontal on an operating table with his head and shoulders slightly raised; the post-nasal space is plugged with a sponge (see p. 575); and the tongue is drawn forward with a clip (Fig. 314) so that the administration of the anæsthetic through the mouth is quite uninterrupted. This method allows the surgeon to operate deliberately, generally with the hæmorrhage under easy control, the field of operation well illuminated, and no anxiety in regard to the anæsthetic.
The removal of polypoid ethmoid can thus be completely carried out. With this method I have removed at one sitting a mass of diseased ethmoid which weighed four ounces.65 It also permits the introduction of the operator’s little finger to some distance, so as to detect polypoid or carious surfaces.
With a ring-knife any irregular spicules or projections can be smoothed down. The ring-knife—or a Volkmann’s spoon—is carefully introduced behind a mass of growth, and then pulled briskly out through the nose while hugging its outer wall. The nasal roof should be diligently respected.
When the operation has been completed the post-nasal plug is removed, and it is well to pass the forefinger of the left hand well up into the posterior choanæ to detect and push forwards any masses of growth which may have been driven backwards.
Hæmorrhage generally ceases with the usual remedies (see p. 576). It is better to avoid all plugs.
Dangers and complications. This operation in careless or inexperienced hands is not free from risks. The chief danger is from injury to the cribriform plate, as any damage in this area, occurring in the septic conditions which generally call for operation, is generally followed by fatal meningitis.
In addition to the usual precautions, particular attention should be paid while manœuvring in the anterior part of the space between the septum and the outer nasal wall. Here the punch-forceps are not directed backwards against the main mass of the sphenoid, but, as the head has to be extended in order to approach the anterior area, they follow an obliquely upward direction which brings them into dangerous proximity with the floor of the cranial fossa—which dips down lower in front than it does posteriorly. Great care, therefore, is taken to avoid any thrusting or boring movements with the forceps. They are first made to press outwards as much as possible the opposing walls of this narrow region, so that polypoid masses can fall between the blades under good inspection.
Occasionally the os planum is perforated, resulting in emphysema of the eyelids or an ecchymosis like a ‘black eye’. An orbital abscess may follow (Lack).
Direct inspection and treatment of the deeper regions of the nose, the naso-pharynx, the ethmoidal labyrinth, and the neighbouring area of the maxillary sinus, is well secured by the following operation, which has been fully described by Moure of Bordeaux.66
Indications. This operation is particularly suitable for malignant growths originating in the upper or inner walls of the maxillary sinus, the ethmoidal labyrinth, the deeper regions of the nose, the naso-pharynx, or the sphenoid. It might be required for very vascular naso-pharyngeal fibromata with extensive prolongations. It is very suitable for necrosis—generally syphilitic—of the sphenoid when threatening the base of the brain.
For malignant growths in the regions mentioned, this route is particularly suitable, if, of course, the limitation of the growth and the absence of secondary infection justify intervention. The large space formed by throwing the nose and antrum into one cavity gives a freer field than removal of the superior maxilla, without the disfigurement and tendency to recurrence so apt to be associated with this latter operation, since it seldom includes removal of the ethmoid, which is the usual seat of origin of the disease. In Moure’s operation the functions of the eye, and of the nerves and muscles of the face, are not interfered with, nor are there those difficulties with phonation and deglutition which are left by removal of the upper jaw.
The interior of the nose is prepared with adrenalin and cocaine (see p. 572), chloroform is administered, and a sponge is packed into the naso-pharynx (see p. 575).
Operation. An incision is made from the inner border of the eyebrow, along the side of the nose, until it enters the lower margin of the nasal orifice. A second incision, starting from the same spot above, is next carried round the lower margin of the orbit and outwards as far as the malar eminence (Fig. 315).
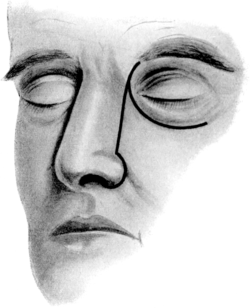 Fig. 315. Incisions for Lateral Rhinotomy (Moure’s Operation).
Fig. 315. Incisions for Lateral Rhinotomy (Moure’s Operation).
|
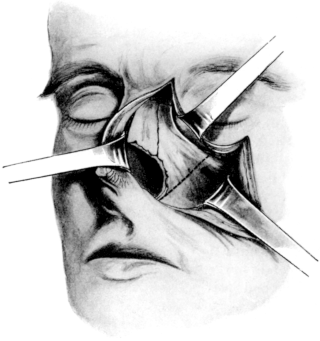 Fig. 316. The Area of Bone removed in Lateral Rhinotomy. The flaps have
been retracted, and the dotted lines show where the bones are chiselled through.
Fig. 316. The Area of Bone removed in Lateral Rhinotomy. The flaps have
been retracted, and the dotted lines show where the bones are chiselled through.
|
The lobule of the nose is then detached, so that the fleshy parts of the nose can be thrown over to the opposite side, while a triangular flap is turned downwards and outwards. With a raspatory the nasal process of the frontal bone, the nasal bone, the ascending process of the superior maxilla, and the canine fossa are next exposed. The lachrymal sac is carefully defined and retracted. A chisel is first driven through the superior maxilla, close to its junction with the malar bone, but avoiding the infra-orbital nerve, and the section is carried downwards across the canine fossa until it reaches the alveolar border (Fig. 316). From the lower extremity of this incision—which of course enters the maxillary sinus—the bone which separates it from the pyriform fossa is broken through with stout forceps. In this way the antro-nasal wall is detached close to the floor of the nose, and can be removed together with the inferior turbinal. The nasal bone itself is next removed, together with part of the lachrymal bone and the nasal process of the frontal. Finally the middle turbinal and lateral mass of the ethmoid are removed with punch-forceps (Grünwald’s or Luc’s), Volkmann’s sharp spoons, or a ring-knife.
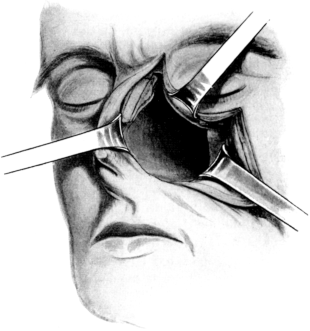 Fig. 317. Lateral Rhinotomy. The side of the nose has been removed, and
direct access obtained to the upper and deeper nasal regions.
Fig. 317. Lateral Rhinotomy. The side of the nose has been removed, and
direct access obtained to the upper and deeper nasal regions.
A gouge, or Killian’s eye protector (Fig. 342), is then slipped inwards and downwards at the upper part of this opening until it comes in contact with the body of the sphenoid. An assistant holds it closely parallel to the cribriform plate, where it acts as a protector. With a large sharp spoon, acting from above downwards and forwards, the ethmoidal labyrinth can be cleared away with any tumour which may have infiltrated it. The os planum, if not already destroyed, can be removed, so as to obtain access to the orbit. Direct approach is given to the sphenoidal sinus. The septum can be readily resected, but an endeavour should always be made to preserve a strip of cartilage under the bridge of the nose to prevent any external deformity (see p. 609). It is needless to say that great care must be taken while working close to the cribriform plate.
A malignant tumour can then be removed with forceps, sharp spoons, and the fingers, any prolongations being followed into the naso-pharynx, the maxillary sinus, the sphenoidal sinus, the lateral mass of the ethmoid, or even into the pterygo-maxillary fossa. Success largely depends on the care with which this curettage is carried out. It should be followed by the application of caustics or Paquelin’s cautery.
Bleeding is generally abundant at first. It can be controlled with tampons and the use of hydrogen peroxide. When the whole of the malignant growth has been removed, hæmorrhage generally stops spontaneously. Firm packing of the wound is therefore unnecessary and is best avoided. The large cavity is filled with one long strip of 1-inch ribbon gauze, which is left projecting from the nostril, and the skin incisions are carefully brought together with silkworm-gut sutures. Healing takes place by first intention. There may be a little flattening of the side of the nose, but there is no disfigurement, and a few months afterwards it is difficult to detect any trace of the operation. The strip of gauze is removed in 24 to 48 hours, and simple intranasal cleansing measures are then instituted (see p. 579).
No special instruments are required for this operation. Full illumination—with a Clar’s mirror or frontal search-light (see p. 571)—is particularly necessary.
In addition to the usual preparations, the mouth, teeth, and gums should be purified as much as possible beforehand.
General anæsthesia, preferably with chloroform, is required.
Indications. With the progress of rhinology the occasions for invading the nasal chambers otherwise than by the natural orifices have steadily diminished. Rouge’s operation was formerly employed in dealing with deformities of the septum, in the treatment of ozœna, in lupus of the nose, for the removal of simple mucous polypi, in operations on naso-pharyngeal fibromata, or as a simple method of exploration. In all these circumstances it is now uncalled for, as we are possessed of simpler, safer, and more effective methods.
In more modern times it has been advocated as a route of approach to the accessory cavities of the nose by some authors, but this proposition has not met with general support.
The chief indications for Rouge’s operation are as follows:—
1. Very large sequestra. The majority of syphilitic sequestra can be removed through the natural orifice. In some cases they can be broken up after being mobilized and then removed through the nostrils. If still impossible of extraction Rouge’s operation is indicated.
2. Osteomata are sometimes too large to be extracted through the natural orifice, and as they are much too hard to break up in situ, this operation is clearly indicated.
3. Malignant growths.
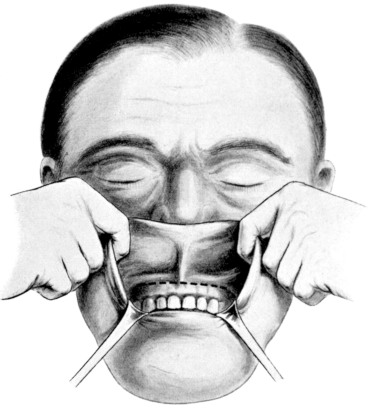 Fig. 318. Rouge’s Operation. First stage. The upper lip is everted and
retracted by an assistant standing behind the patient’s head. The dotted line
indicates the line of incision.
Fig. 318. Rouge’s Operation. First stage. The upper lip is everted and
retracted by an assistant standing behind the patient’s head. The dotted line
indicates the line of incision.
Operation. Standing behind the head of the patient, an assistant seizes the extremities of the upper lip between the forefinger and thumb of each hand, so as to turn it up against the nostrils and present its mucous surface. A small packet of loose gauze is placed at each corner of the mouth, to be handy for stanching any bleeding. An incision is then made across the gum, a little below the gingivo-labial fold, from the first upper molar on one side to the other (Fig. 318). This is carried right down to the bone.
With a raspatory the soft parts can be easily and rapidly separated up, so as to bring the orifice of each nasal chamber into view. With a pair of scissors curved on the flat the cartilage of the septum is next detached from the nasal maxillary spine, or the latter can be detached with a chisel and hammer (Fig. 319). The assistant is now able to pull the everted lip with the fleshy parts of the nose further up on to the face, fully exposing the pyriform orifice of the nasal chambers, with part of the anterior wall of the superior maxilla exposed on each side.
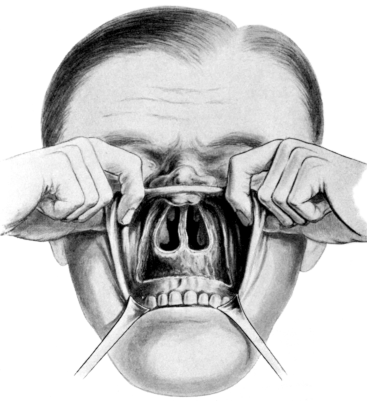 Fig. 319. Rouge’s Operation. Second stage. The soft parts are retracted.
Fig. 319. Rouge’s Operation. Second stage. The soft parts are retracted.
The conditions met with are then dealt with as required. Hæmorrhage gives little trouble, and can generally be checked by pressure with strips of gauze, possibly supplemented by the use of peroxide of hydrogen. When the operation has been completed the everted lip is turned down, and falls into place, where it can be secured by a few catgut sutures.
After-treatment. Two pads of cotton-wool over the upper lip, to right and left of the nasal openings, will give relief and secure healing of the wound by first intention. The mouth should be kept as clean as possible, and cleansing measures to the nasal chambers will be required in proportion to the amount of destruction of its self-cleansing mucous membrane.
Advantages. This operation has several advantages:—
(a) It is not difficult of execution, and can be carried out with a scalpel and a raspatory.
(b) It gives a free access to the floor of the nose and the anterior part of the nasal fossæ. The vestibule, the natural orifice of the nose, only measures 20 millimetres by 7 to 8 millimetres. Rouge’s operation exposes an orifice measuring 3½ centimetres by 2 centimetres. The posterior margin of the septum, instead of being 8 centimetres distant from the outside, is now brought within a reach of 5 centimetres. The floor of the nose lies on a lower level than that of the vestibular entrance, and is wider some distance in than it is at the orifice. By means of this operation the whole floor comes into clear view, and the exit from the nasal chambers becomes the widest part of the nose.
(c) The bones of the face are not interfered with, and the amount of traumatism is slight.
(d) Bleeding, which is so apt to be troublesome in operations through the skin of the face, is less and is easily controlled.
(e) The patient can be assured that there will not only be no disfigurement, but not even the slightest scar on the face.
(f) The operation can be repeated without any disfiguring scars. In operations upon the nose through the face the cicatrix becomes more marked with each intervention.
The two methods above described can be combined if necessary. This would be called for particularly in growths so large that they could not be attacked through the narrow vestibule of the nose, and for those in which the attachment is evidently in the ethmoidal region. This combination might be called for in any large innocent or malignant growth.
When the growth involves both the nasal cavity and the maxillary sinus Rouge’s operation can be extended so as to form part of the Caldwell-Luc operation (see p. 631).
The latter operation is modified as suggested by Denker (Fig. 332), i.e. the opening through the canine fossa is extended forwards until the nasal cavity is opened through the pyriform opening. This will give free access to the large cavity formed by throwing the antrum and the nasal chamber on the same side into one easily inspected space (Fig. 332). Hæmorrhage gives no cause for anxiety, there is no disfigurement, the original root of the implantation can be eradicated, and, if necessary, the operation can be repeated without difficulty. If the growth extends upwards and inwards to the ethmoidal region this infralabial opening can be combined with Moure’s operation.
Indications. This operation is suitable for any form of growth invading both the antrum and nasal cavities, and is therefore generally called for in malignant growths.
The other methods for obtaining access to the nasal cavity through the face—described as the methods of Hippocrates, Syme, Dupuytren, Langenbeck, Lawrence, Ollier, &c.—are now only of historical interest. They all leave a scar on the face; bleeding is troublesome; they do not give a greatly enlarged field; and most of them do not bring the seat of disease any closer. With the advances made by rhinology the necessity for intervention through the face has become more infrequent.
It is rarely possible to enter the antrum through its natural ostium. The attempt may be made after the local use of cocaine and adrenalin (Fig. 320).
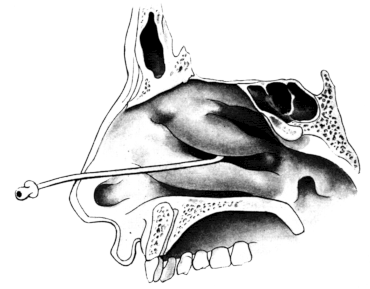 Fig. 320. Catheterizing the Maxillary Sinus.
Fig. 320. Catheterizing the Maxillary Sinus.
Indications. It is chiefly employed as a diagnostic test. As a curative measure it is seldom successful except in comparatively recent infection. If the case be uncomplicated by suppuration in other cavities, if the teeth in the upper jaw on the same side be intact, and if the patient be anxious to avoid more severe measures and be willing to undergo the discomfort of a daily puncture, lavage has been reported as successful when repeated 27 times, even in a case with a history of 17 years’ duration.67 But under the circumstances just mentioned it is wiser to recommend the establishment of an antro-nasal communication (see p. 637).
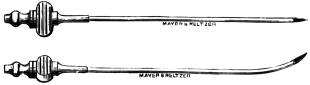 Fig. 321. Lichtwitz’s and Moritz Schmidt’s Antrum Needles.
Fig. 321. Lichtwitz’s and Moritz Schmidt’s Antrum Needles.
Operation. This is done under local anæsthesia from the inferior meatus. One pledget of cotton-wool, soaked in cocaine and adrenalin, is carefully tucked under the inferior turbinal on the affected side, and another is applied to the septum. At the end of 20 minutes a straight Lichtwitz’s or curved Moritz Schmidt’s (Fig. 321) hollow needle is passed under the inferior turbinal and introduced upwards and outwards as near as possible to the centre of its attachment. The handle of the needle is tilted against the cartilaginous septum, while the point is directed towards the malar eminence. When it is felt to encounter the thin, membranous part of the antro-nasal wall it is easily thrust through (Fig. 322).
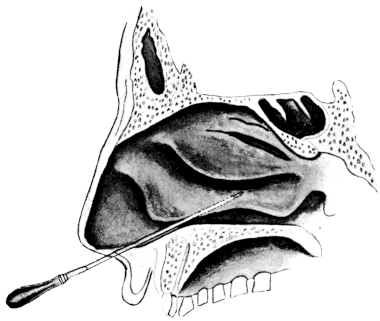 Fig. 322. Puncturing the Maxillary Sinus. The dotted part represents
the portion of the exploring needle which passes under cover of the inferior
turbinal.
Fig. 322. Puncturing the Maxillary Sinus. The dotted part represents
the portion of the exploring needle which passes under cover of the inferior
turbinal.
While the nasal cavity is kept under inspection, air is blown through the needle, and any secretion can be observed escaping from under the centre of the middle turbinal. This douche of air is then followed by an irrigation of warm normal saline solution. In an acute case this lavage can be repeated daily until the symptoms of tension are relieved, or until the secretion begins to escape spontaneously.68
Puncturing the maxillary sinus from the middle meatus incurs a greater risk of striking the orbit and is not so likely to reveal a small amount of thick secretion on the floor of the cavity.
This is one of the oldest methods of drainage. It is less frequently employed nowadays, partly because carious teeth and empty sockets are not so commonly met with, and partly because the results have not proved very satisfactory.
Indications. The operation is useful as a diagnostic or palliative measure. In cases of unilateral multi-sinusitis, if a suitable tooth socket be available, the alveolar operation serves both to determine the condition of the maxillary sinus and to establish drainage, while the other cavities are being investigated or treated. In patients who are too old or feeble to endure more radical measures, or who decline them, the obturator may be left in indefinitely. In that case, if the neighbouring teeth be intact, a solid gold plug should be fitted to the denture bearing the false first molar. During the night this is exchanged for the soft rubber plug. If several teeth be missing it is more comfortable to have the obturator and denture separate—the latter being made with a setting to receive the flange.
An anæsthetic should always be given. Nitrous oxide gas or chloride of ethyl are generally recommended for this short operation, but in cases that present any difficulty it is better to follow the nitrous oxide with ether, or the chloride of ethyl with chloroform.
 Fig. 324. Solid Rubber Obturators. Used in alveolar drainage of the
maxillary sinus.
Fig. 324. Solid Rubber Obturators. Used in alveolar drainage of the
maxillary sinus.
| |
 Fig. 325. Antrum Nozzle.
Fig. 325. Antrum Nozzle.
|
Operation. The most suitable tooth socket is that of the first molar, but if this be not available, that of the second bicuspid or second molar may be employed. If a tooth in one of those situations be carious, or be suspected as the cause of the sinusitis, its extraction and the drilling of the alveolus may be carried out under the same anæsthetic. The patient can be recumbent on an operating table, or lying back in a dentist’s chair. A small antrum drill (Fig. 323) is grasped in the hand as a bradawl is held, with the forefinger lying along it to within 1 to 1½ inches from the end, where it acts as a stop to prevent the instrument from plunging too deeply into the sinus. The drill is held vertically against the alveolar border, and with a few quick, rotatory thrusts is pushed into the cavity. The inner of the tooth sockets is selected. If required, the hole can be enlarged by a similar instrument of a larger bore. A plug, which fits firmly into the opening, is introduced, and nothing further is required for that day. A solid vulcanite obturator is recommended. It should be left in situ for two or three days, when it is removed to allow of the cavity being syringed through, and is then replaced by a solid, soft rubber plug, of a somewhat smaller diameter (Fig. 324). The vulcanite obturator is better for establishing the canal; if removed too soon it may be difficult to replace it, and manipulation may set up severe neuralgia. A small size—No. 6 or 7—is quite sufficient.
 Fig. 326. Washing out the Maxillary Sinus from an Alveolar Opening.
Fig. 326. Washing out the Maxillary Sinus from an Alveolar Opening.
At the end of two or three days lavage of the cavity is gradually instituted. A pint of warm sterile normal saline solution is sent through the cavity by a Higginson’s syringe, fitted with a suitable nozzle (Fig. 325). As the stream issues from the nose it is received in a black vulcanite tray, which readily demonstrates the colour, quality, and quantity of antral secretion (Fig. 326). When the pint of liquid is finished, air is blown through, so as to leave the sinus as dry as possible. The patient should be advised to replace the rubber obturator, properly cleaned and purified, as soon as possible. If this be neglected—for even as short a time as 5 minutes—the soft tissues may obstruct the channel so as to render the reintroduction painful and perhaps impossible. Another useful warning is not to wear a plug so long as to allow of the flanges being worn away, and so risk the penetration of the rubber tube into the cavity.
The syringing should at first be daily, even twice a day if necessary, and then gradually diminished in frequency, until after the lapse of a week it is found that the maxillary sinus is quite free of any pus or flocculent mucus. By changing the obturator daily the patient can readily tell whether a washing out is required. When three to six months have passed without any trace of secretion, the empyema may be considered cured. This is the more likely if a formerly obscure sinus becomes translucent, and if the patient passes through a ‘cold’ without suppuration beginning in it again. A trifling amount of discharge is sometimes kept up by the mere presence of the obturator.
If the saline solution fails to arrest the discharge permanently, I have rarely found that any other lotion is more effective. Strong antiseptic solutions are too irritating; milder ones, like boric lotion, permanganate of potash, weak mercurial lotions, &c., are without effect. If the discharge remain thick and offensive, peroxide of hydrogen may be added to the salt solution in the proportion of 2 vols. %. As an astringent, sulphate or chloride of zinc may be tried, in the proportion of 1 grain to the ounce; or the cavity may occasionally be washed out with a 2% solution of argyrol or nitrate of silver.
In cases where a cure has been obtained, the obturator is first discontinued during the night and is then exchanged for one of smaller size. The opening in nearly all cases will close spontaneously. Occasionally the track may be stimulated with nitrate of silver, pure carbolic acid, or a small curette.
Results. This method of treatment is only curative in uncomplicated cases limited strictly to the maxillary sinus. If all suppuration has not disappeared before the end of three months, a complete cure is not to be expected by persevering longer.
Desault’s operation. Previously to the introduction of the Caldwell-Luc operation it was customary to make an opening into the maxillary sinus from the canine fossa, and to curette, drain, pack, and carry out all subsequent treatment through the buccal orifice. The reinfection of the cavity from the mouth was, of course, inevitable: the treatment was prolonged and unpleasant: and the results were so unsatisfactory that the method has now been abandoned in favour of one or other of the operations to be described.
Indications. This is the favourite operation in well-marked chronic empyema of the antrum.
The mouth, teeth, and gums are purified as thoroughly as possible. The face, with any moustache or beard, should also be well cleansed. The nose on the affected side is prepared with cocaine and adrenalin (see p. 572).
On the Continent this operation is sometimes carried out under local anæsthesia, but chloroform is generally employed. When the patient is unconscious, a sponge is packed in the post-nasal space (see p. 575), the tongue is drawn forward with a tongue clip (Fig. 314), and the chloroform administered from a Junker’s apparatus.
Operation. The surgeon, armed as usual with a forehead electric search-light or Clar’s mirror (Figs. 282, 283), stands on the affected side. In addition to the post-nasal sponge, another is inserted far back between the molars on the side to be operated. This cheek sponge prevents any blood from running down into the pharynx and requires changing frequently.
The cheek being well retracted by an assistant, an incision is made half a centimetre below the gingivo-labial fold, extending from the first molar to the canine tooth (Fig. 327). It is carried down to the bone, so that the muco-periosteum can quickly be separated upwards, exposing the canine fossa. With hammer and chisel a circular piece of the wall is then cut through, measuring about half an inch across, and the opening is enlarged with bone-forceps or burr sufficiently to admit the surgeon’s little finger.
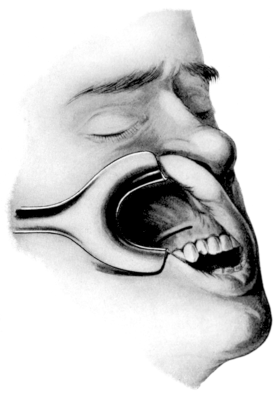 Fig. 327. The Incision in the Caldwell-Luc Operation upon the Maxillary Sinus.
Fig. 327. The Incision in the Caldwell-Luc Operation upon the Maxillary Sinus.
|
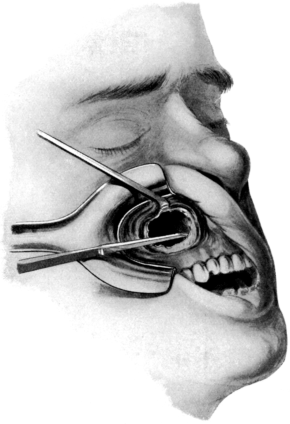 Fig. 328. The Caldwell-Luc Operation upon the Maxillary Sinus. Breaking
through the antro-nasal wall below the level of attachment of the
inferior turbinal. The opening has been purposely represented coming too
far forward in order to include the view of the antro-nasal wall.
Fig. 328. The Caldwell-Luc Operation upon the Maxillary Sinus. Breaking
through the antro-nasal wall below the level of attachment of the
inferior turbinal. The opening has been purposely represented coming too
far forward in order to include the view of the antro-nasal wall.
|
The first opening of the sinus is frequently accompanied by free bleeding. This soon ceases, particularly if the cavity is packed for a little while with a strip of 2-inch ribbon gauze. During the operation, pieces of this gauze, 1 to 1½ yards long, prove very useful in checking any oozing and allowing a clear inspection of the walls of the sinus. They may be dipped in adrenalin, or, if the bleeding is sharp, in a 10% solution of peroxide of hydrogen, and left in place for a few minutes, while iced water is freely applied to the face and neck. As soon as the bony wall has been removed, the diseased mucous membrane presents in the opening in irregular, polypoid, bluish-greyish masses, bathed in pus which may be highly fœtid. The diseased mucous membrane should be carefully plucked out of the cavity with a pair of Grünwald’s forceps, supplemented by the use of a small ring curette, and guided by the eye and the touch of the operator’s little finger. Some surgeons recommend that the whole mucous lining of the sinus be carefully and completely removed, and the walls scraped down until they are white and bare. Unless the whole mucosa is diseased, this hardly seems necessary, particularly if a free opening be made into the nose. Polypoid masses and degenerate mucous membrane are chiefly met with on the floor of the antrum (in the crevices between the cusps of the teeth), on the inner wall in the neighbourhood of the ethmoid, and in the recess in the malar region, and it is to these areas that attention should be directed.
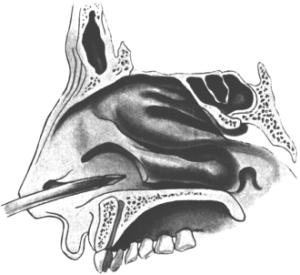 Fig. 329. Opening the Maxillary Sinus from the
Nose. This is done with a Krause’s trochar and canula,
after removal of the anterior end of the inferior turbinal.
Fig. 329. Opening the Maxillary Sinus from the
Nose. This is done with a Krause’s trochar and canula,
after removal of the anterior end of the inferior turbinal.
The next step is the making of a free communication with the nose. If the inferior turbinal is hypertrophied on the affected side, or comes so low as to obstruct any access to the antro-nasal wall, its anterior extremity should first be removed (see p. 587 and Fig. 289). It is better to have done this a few weeks previously under cocaine. The antro-nasal wall lying below the attachment of the inferior turbinal is next attacked with a chisel, hammer, and punch-forceps (Fig. 330). This can be done from the antral aspect, but I have always found it useful to break it through first from the nose with Krause’s curved trochar and canula. When the end of this makes its appearance in the sinus, it forms a useful landmark (Fig. 329).
This antro-nasal opening should be made as large as possible, particular care being taken to bring it well forward and to smooth down the remains of the ridge separating the nose from the sinus. The opening should allow of the surgeon’s little finger passing freely from the antrum into the floor of the nose, and vice versa (Fig. 328).
Whenever the ethmoid is diseased, as it often is in maxillary sinusitis, that part of it which bounds the inner antral walls should be punched away. The middle turbinal, in that case, will probably have been already removed.
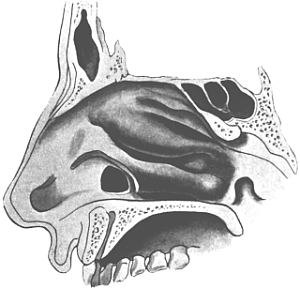 Fig. 331. The Opening into the Maxillary Sinus from the Inferior Meatus
of the Nose. The anterior extremity of the inferior turbinal has been
amputated. The opening can be extended backwards, level with the floor
of the nose, and under cover of the inferior turbinal.
Fig. 331. The Opening into the Maxillary Sinus from the Inferior Meatus
of the Nose. The anterior extremity of the inferior turbinal has been
amputated. The opening can be extended backwards, level with the floor
of the nose, and under cover of the inferior turbinal.
Some surgeons recommend that the infected corners of the antrum be now wiped out with a solution of chloride of zinc (40 grains to ℥j), and the cavity packed with a strip of gauze which is led out through the nostril, whence it is removed at the end of 24 to 48 hours. The use of this irritant seems inadvisable. The sinus may be syringed out with warm saline solution, and temporarily packed with a long strip of iodoform gauze, while the operation is being completed. The wound in the cheek can be closed with a couple of catgut sutures; but if there has been no destruction of the bony alveolus, this is unnecessary: the soft parts will fall into natural and complete apposition. The post-nasal sponge is removed, the iodoform ribbon gauze is withdrawn through the nostril, and the patient is put back to bed with the affected side uppermost.
After-treatment. A large pad of cotton-wool, bound firmly to the cheek over the region of the canine fossa, will relieve pain and help to keep the edges of the wound together. Nourishment should be fluid for the first three days, and taken from a feeding-cup from the opposite corner of the mouth. As a rule, there is no reaction, and the temperature seldom rises above 100° F. A little puffiness below the orbit will soon subside, and pain is relieved by a few doses of phenacetin, aspirin, pyramidon, or some similar anti-neuralgic. The patient is frequently up and out in a few days.
As a rule, the less the local after-treatment the better. The nose may require to be cleansed with the usual alkaline lotion (see p. 579). If secretion hangs about the antro-nasal opening, or collects in the cavity, the latter should be washed out once or twice daily until it ceases. A short length (4½ in.), but large bore, silver Eustachian catheter is passed from the nose into the maxillary sinus, and a pint of warm saline solution is sent through it with a Higginson’s syringe. The patient soon learns to do this for himself, and it may have to be continued for a few weeks. If the discharge persists, the cavity may be painted over with a solution of nitrate of silver, or a strip of ribbon gauze can be moistened with argyrol solution (25%) and passed through the antro-nasal opening into the sinus, where it is left for a few hours.
Results. In cases of chronic empyema of the maxillary sinus this operation is very successful. Failure may be due to overlooking stumps of teeth within the cavity, and from leaving detached pieces of the carious wall within it. If the pyogenic polypoid mucous membrane be not carefully removed, suppuration may persist. The corner which is difficult to reach is the acute anterior one. At the same time, an unnecessary denudation of the cavity will delay healing, and the scar tissue which more or less occupies the sinus will then tend to be irregular and dry, instead of being smooth and moist. Removal of too much of the inferior turbinal is apt to induce a scabby condition.
But persistence of nasal suppuration after this operation is generally found to be due to overlooked disease in some other sinus. The ethmoid is so frequently affected that it should always be carefully explored, and treated either before or at the time of the operation upon the maxillary sinus. Any suspicious-looking cells can be cleared away under cocaine during convalescence. Suppuration in the frontal sinus will have generally been excluded beforehand. It is perhaps more common for reinfection from the sphenoidal sinus to be overlooked.
Dangers. Operation upon this sinus is generally regarded as quite free from the risk of cerebral infection. This undeniably is so, when the antral empyema is uncomplicated by suppuration in other cavities, but the operation is not free from risk if they are also infected. An operation upon one maxillary sinus has been known, even in the most skilful hands, to cause death by meningitis or diffuse septic osteomyelitis of the cranium. Post-mortem examinations show that this disaster was due to infection spreading upwards from an infected ethmoid, frontal, or sphenoidal sinus, when local resistance had been diminished, or the virulence of the organisms has been increased by the surgical traumatism of the maxillary sinus.
Such risks are best avoided by determining the condition of all the sinuses before commencing treatment of nasal suppuration. If a tooth socket be available, the maxillary sinus should first be drained through it, so as to diminish the septic intensity of the affection. The ethmoid region, if diseased, is next treated (see p. 615). The sphenoidal orifice should be enlarged if that cavity be diseased, and the frontal sinus, if suppurating, should be operated on before the maxillary. If no tooth socket be available, both frontal and maxillary sinuses can be operated upon at the same sitting. Plugs are best avoided; communication should be made as free as possible; stitches need not be employed; and everything should be done to avoid retention and secure free drainage.
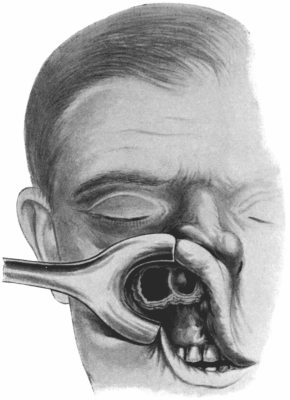 Fig. 332. Denker’s Operation. This is an operation for gaining access to
the maxillary antrum and the lower part of the nasal cavity on the same
side. The incision through the mucous membrane, and the steps of the
operation, are a combination of the operations of Rouge and
Caldwell-Luc.
Fig. 332. Denker’s Operation. This is an operation for gaining access to
the maxillary antrum and the lower part of the nasal cavity on the same
side. The incision through the mucous membrane, and the steps of the
operation, are a combination of the operations of Rouge and
Caldwell-Luc.
Modification. In the above operation the region which generally requires to be denuded of mucous membrane is the rough floor—the irregular surface lying over the cusps of the teeth. The ridge of the antro-nasal opening is a situation in which secretion is apt to lodge and dry into scabs. To overcome this drawback it has been suggested by Bönninghaus that the muco-perichondrium of the outer part of the nasal floor and the interior surface of the antro-nasal wall should be carefully preserved in the form of a flap which is then laid down over this bare area, and fixed there by a stitch and packing.
Another drawback of the Caldwell-Luc operation is that, although inspection and treatment of the greater part of the maxillary sinus is secured, still there are two corners which are not well exposed. They are both on the floor of the antrum, the round posterior corner and the narrow acute corner in front. The antro-nasal wall corresponding to these two situations is not removed, and hence the corners are apt to escape inspection at the time of the operation and free drainage afterwards.
To avoid this Denker has proposed that the opening in the canine fossa should be carried forward into the nose, and the opening in the antro-nasal wall extended forwards to meet it. This allows of much more complete inspection and treatment of the sinus cavity, and abolishes the anterior angle. The flap of muco-perichondrium proposed by Bönninghaus can also be much more easily manipulated. It is said that there is no fear of disfigurement from the cheek falling in (Fig. 332).
It was long ago proposed by John Hunter, and later by Mikulicz and Krause, that an opening should be made into the maxillary sinus from the nose. This operation has latterly been developed by Claoué and Réthi, and now has many supporters.
Operation. On the Continent it is frequently carried out under local anæsthesia, but chloroform is generally required. If the inferior turbinal comes down close to the floor of the nose, the anterior third or half should be removed (see p. 587 and Fig. 289). The antro-nasal wall lying below the attachment of the inferior turbinal is then broken through with chisel and hammer, or a Krause’s trochar (Fig. 285), and the opening enlarged with punch-forceps (Fig. 286). For the anterior margin of the opening—the one most difficult to remove—special forceps which cut forwards have been designed (Fig. 330).
The opening is large enough to allow the introduction of curettes and of the application of treatment from the nose. The patient soon learns to wash out the sinus for himself, with a silver Eustachian catheter and Higginson’s syringe, as after the Caldwell-Luc operation.
Results. The advantages claimed for this operation are that it is simple, quicker, and as effective as the one with the opening from the canine fossa. But, of course, it does not allow any inspection, and only a partial removal, of the diseased contents of the sinus.
Still the results obtained are so satisfactory,69 that it seems advisable to try it in the majority of cases as a necessary first step, even if the Caldwell-Luc operation has to be completed later. But where the case has a long history; marked obscurity on transillumination; a foreign body in the sinus; or where the Streptococcus pyogenes is the virulent organism, or where the streptococcus is associated with the presence of squamous epithelium and lymphocytes,70 it adds little to the gravity or complexity of the procedure if the canine fossa be opened at the same time, the diseased cavity inspected, and everything completed under the one anæsthesia.
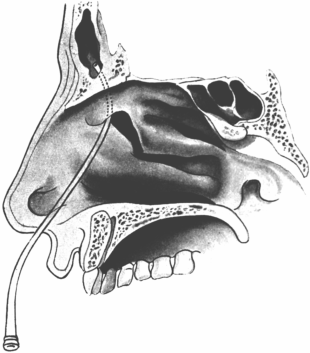 Fig. 333. Catheterizing the Frontal Sinus.
The anterior end of the middle turbinal has been removed.
Fig. 333. Catheterizing the Frontal Sinus.
The anterior end of the middle turbinal has been removed.
Indications. This method is indicated—
(i) As a first step in diagnosis and treatment.
(ii) To diminish the risk of retention and decrease virulence in those patients where an external operation is not indicated or is declined.
(iii) It is rarely required for acute frontal sinusitis, although it might be used in acute exacerbation of a chronic suppuration.
Operation. It is very seldom that it is possible to sound a frontal sinus, unless the anterior ethmoidal cells have been broken down by disease. When this has occurred—or when the anterior extremity of the middle turbinal has been removed, as described on p. 592—the anterior region of the middle meatus is well anæsthetized. Under good illumination a thin silver canula is then introduced until it reaches the middle meatus with its beak lying below and in front of the bulla ethmoidalis. By depressing the hand the point of the instrument is then directed upwards, forwards, and slightly outwards, until it slips into the frontal cavity (Fig. 333). No force should be employed. The end of the catheter is bent to suit the conditions met with. A bead of pus exuding from the hiatus semilunaris will often serve as a useful guide. If there be any uncertainty as to the catheter having entered the frontal sinus, its exact situation can be determined by the Röntgen rays (Figs. 334, 335).
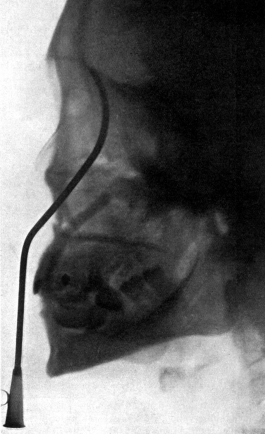 Fig. 334. Radiograph to show the Value of the Röntgen Rays. The
canula might be thought to have entered the frontal sinus, whereas the X-rays
show that its point has only penetrated an ethmoidal cell. Compare with the following
figure.
Fig. 334. Radiograph to show the Value of the Röntgen Rays. The
canula might be thought to have entered the frontal sinus, whereas the X-rays
show that its point has only penetrated an ethmoidal cell. Compare with the following
figure.
|
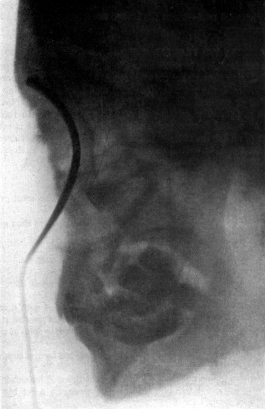 Fig. 335. Radiograph showing Canula in the Frontal Sinus.
Fig. 335. Radiograph showing Canula in the Frontal Sinus.
|
A Politzer’s inflation bag is now connected with the end of the frontal canula, and air is blown through it. This will be heard gurgling through the sinus, and if the anterior region of the middle meatus is at the same time kept under observation, thick mucus or pus will be seen to be driven out by it. The Politzer’s bag is then replaced by a syringe, and a pint of warm sterile normal saline solution (ʒj to Oj) is sent into the sinus, and as it returns is received in a black vulcanite tray. The latter readily shows up the presence of any flakes of mucus or pellets of pus. If successful, the above proceeding can be repeated twice daily.
When the cavity can be catheterized from the nose it should be washed out daily with liquids similar to those indicated for suppuration in the maxillary antrum (see p. 630).
Results. I am very doubtful if a permanent cure is ever effected by this treatment in a case of established chronic suppuration. In a case in which I was certain that the suppuration was not of more than four months’ duration intranasal treatment was a failure, although carried out most carefully on 44 successive days.71
The cause is very apparent whenever these sinuses come to be opened; the cavity itself is generally stuffed with fungating mucosa, and the fronto-ethmoidal cells—where the lavage never penetrates—are affected in the same way.
It is rare for this to be necessary. The contents of the cavity generally make their way through the natural ostium, before any of the bony walls give way. Still, the posterior (cerebral) wall may yield, giving rise to meningitis or cerebral abscess. The treatment of this complication is given on p. 650. The orbital wall may be penetrated, with the formation of an orbital abscess which should be evacuated. It is most uncommon of all for the anterior wall to give way. When this does occur the abscess should be opened through an incision designed on the principle given later on for chronic empyema (see p. 652).
At the present time the Killian operation is the one most generally employed.
Indications. The indications for this operation are thus given by Killian himself:—
1. Failure of other operations.
2. Presence of fistula or abscess, or indications of necrosis.
3. Symptoms of intracranial complications.
4. When in a case of chronic purulent frontal sinusitis there is pain and fever with a fœtid discharge.
5. Persistent headache, particularly when associated with discomfort in the region of the eye, and not relieved by intranasal treatment.
6. When the discharge from the sinus remains foul, in spite of repeated irrigations.
7. When recurring groups of polypi are produced by the suppuration in the frontal and ethmoidal cells.
8. When a simple purulent discharge is not relieved by careful intranasal treatment, and the patient desires permanent relief by radical operation.
A radiograph is taken and is an extremely useful help to indicate the size and extent of the frontal sinus, and to prepare the surgeon for meeting with troublesome orbito-ethmoidal cells.
As the ethmoid is diseased in nearly all cases it should be cleared away at previous sittings, under cocaine or chloroform (see p. 615). Even when healthy, the anterior extremity of the middle turbinal should be amputated (see p. 592). If the antrum be also suppurating and a suitable tooth socket be available, the alveolus will have been drilled at one of these preliminary treatments. If the sphenoidal sinus be suppurating, its orifice will have been enlarged.
One hour before the operation the strips of ribbon gauze, soaked in adrenalin with the addition of 5% cocaine, are carefully laid all over the mucous membrane of the nose on the affected side. The face, moustache, and beard are well purified. When the patient is under chloroform three pencils of tightly rolled cotton-wool are introduced into the nose; one along the middle meatus, a second in front of the inferior turbinal upwards towards the bridge of the nose, and the third in the inferior meatus. The first two pledgets are useful afterwards for anatomical definition, and the third keeps them in place. A sponge is inserted in the post-nasal space (see p. 575).
Operation. There is no advantage in shaving off the eyebrow. It can be thoroughly purified and helps to locate the skin incision; if removed, it takes some time to grow again, and is apt not to correspond in size with the eyebrow of the opposite side. The skin incision is first defined by scratching through the cutis with the tip of the knife. It starts at the outer end of the eyebrow, passes inwards along the very centre of the eyebrow itself, and then sweeps downwards and outwards over the side of the nose, to end on the cheek (Fig. 336). When the whole extent has been marked out three or four cross scratches are made. The object of this is to ensure correct coaptation of the flaps, and to avoid any risk of disfigurement. Returning to the outer extremity of the incision, it is now carried down through all the soft tissues till it meets the periosteum. The flaps are retracted a little upwards and downwards, while the free hæmorrhage is met with pressure forceps. The periosteum incisions are now carefully planned. Starting again from the outer corner the knife is drawn inwards parallel to, and slightly above, the upper margin of the supra-orbital arch; but, instead of curving round the inner end of the orbit, in the track of the skin incision, it is kept straight along under the upper flap to end over the glabella. The periosteum can now be reflected from the front of the sinus, and pushed upwards with the skin on to the forehead. The lower skin flap is detached and retracted downwards, until the inner third of the supra-orbital arch is defined. The periosteal covering is next cut through by carrying the knife along the lower border, but instead of passing inwards parallel to the first periosteal incision this second one sweeps down on to the side of the nose, in the track formed by the skin incision (Fig. 337).
 Fig. 336. Killian’s Operation upon the Frontal Sinus.
Shows the skin incision, with the
transverse scratches made to ensure correct coaptation of the flaps.
Fig. 336. Killian’s Operation upon the Frontal Sinus.
Shows the skin incision, with the
transverse scratches made to ensure correct coaptation of the flaps.
|
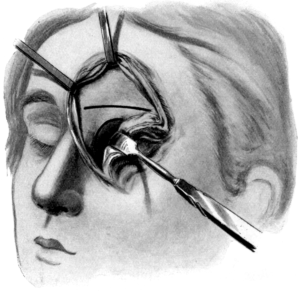 Fig. 337. Killian’s Operation upon the Frontal Sinus. The thick lines
indicate the incisions through the periosteum.
Fig. 337. Killian’s Operation upon the Frontal Sinus. The thick lines
indicate the incisions through the periosteum.
|
The periosteum is carefully peeled off the nasal process of the superior maxilla, and turned down from the inner third of the supra-orbital arch, exposing a triangular area of bone. The periosteum must be carefully preserved over the inner part, to avoid the risk of necrosis of the arch, which is converted into a bridge, the ‘Killian bridge’, by the opening in bone below and above it.
The upper flap of soft parts, with the periosteum, is well retracted up on to the forehead. The radiograph will have given an idea of the extent to which the front wall of the sinus must be laid bare. With a chisel and hammer the sinus is opened at its inner extremity. A good plan is to employ Killian’s triangular curved chisel (Fig. 339) and to cut a trench in the bone along the upper margin of the bridge. This trench is gradually deepened at the inner end until the sinus is entered. The entry is generally announced by the bulging upwards of the blue, polypoid, pyogenic membrane into which the thin white delicate mucosa of the cavity has been converted. The anterior wall is now completely removed with hammer, chisel, and forceps. Those of Lombard, Horsley, Hajek (Fig. 341), Jansen, Citelli (Fig. 340), or similar models enable us to bevel down the margins of the cavity carefully as it slopes up on to the forehead.
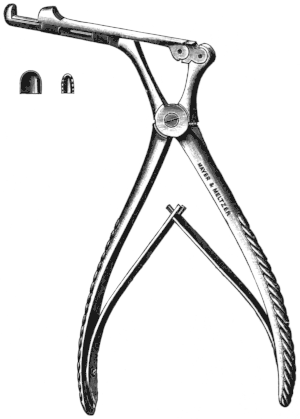 Fig. 340. Citelli’s Bone-forceps.
Fig. 340. Citelli’s Bone-forceps.
|
 Fig. 341. Hajek’s Bone-forceps. |
The pyogenic membrane is now carefully plucked away with a pair of Grünwald’s forceps. I never find it necessary to curette the cavity, which must always be a risky proceeding. Small pledgets of ribbon gauze, if gently rubbed along the surface and into the corners, will detach every scrap of diseased mucosa.
The septum separating the two frontal sinuses may be found to be defective. The opening through the eyebrow on one side may open into a cavity which communicates only with the nasal cavity of the opposite side—one sinus being very large and extending far beyond the middle line, while the other is quite small. Or only one frontal cavity may be present. An extensive acquaintance with the surgical anatomy of the region is required to prepare the surgeon for encountering these and other irregularities, and the systematic use of radiography will prevent him from being taken by surprise.
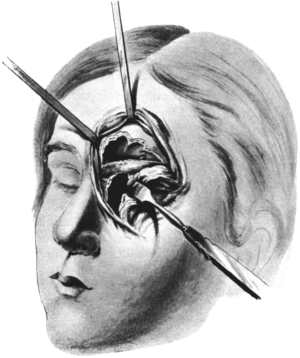 Fig. 342. Killian’s Operation upon the Frontal Sinus. The periosteum
has been preserved on the bridge. Above this the frontal sinus is exposed: at
its inner (nasal) extremity the frontal bulla is indicated, mounting up into the
cavity; at the outer extremity an arrow indicates the orifice of a fronto-orbital
cell which should be opened up. The periosteum lying above the bridge has been
retracted up with the soft parts on to the forehead. Below the bridge is the opening
to the ethmoidal region. The curved retractor is protecting the eyeball.
Fig. 342. Killian’s Operation upon the Frontal Sinus. The periosteum
has been preserved on the bridge. Above this the frontal sinus is exposed: at
its inner (nasal) extremity the frontal bulla is indicated, mounting up into the
cavity; at the outer extremity an arrow indicates the orifice of a fronto-orbital
cell which should be opened up. The periosteum lying above the bridge has been
retracted up with the soft parts on to the forehead. Below the bridge is the opening
to the ethmoidal region. The curved retractor is protecting the eyeball.
The next step is to make the opening below the bridge. The exposed surface of the nasal process of the superior maxilla is cut through with the triangular chisel. The opening is enlarged with bone-forceps until free access is obtained to the anterior ethmoidal cells. The pledgets of cotton-wool placed in the nose at the beginning of the operation now come in to help as guides. The periosteum is further elevated from the lachrymal bone above its groove, from the orbital plate of the ethmoid as far back as the anterior ethmoidal vessels, and from the orbital plate of the frontal bone below the bridge and extending outwards to the trochlear attachment and the supra-orbital notch. During this proceeding the contents of the orbit are protected from pressure by several folds of gauze, and are carefully retracted outwards by Killian’s protector. The area of bone which can now be clipped away comprises parts of the lachrymal, of the lamina papyracea, and of the floor of the frontal sinus. The whole of the floor of the sinus must be removed, either from above the bridge or from below. If this cannot be done without anxiety as regards the attachment of the pulley of the superior oblique, it is better to risk this than to leave pus-secreting pockets of orbito-ethmoidal cells cut off from drainage in the roof of the orbit. But the pulley of the superior oblique should never be divided from its attachment to the rim of the orbit. It is much safer to reflect the periosteum further outwards and downwards from the lower border of the Killian bridge. In doing this the pulley of the superior oblique is detached with it; any diplopia, most noticeable on looking downwards and outwards, is generally temporary; and as a rule it will disappear when the swelling subsides and the periosteum gets back to its anchorage (Fig. 342).
It is this part of the operation which is the most delicate, tedious, and important. It is very common to meet with irregularities. The orbital recess of the frontal sinus itself may run back in the roof of the orbit nearly as far as the foramen opticum. One or two galleries may be met with in the roof of the orbit—prolongations of orbito-ethmoidal cells—passing outwards as far as the temporal end of the eyebrow. Their presence can only be revealed after removal of the floor of the frontal sinus proper, and in this way two or three bony dissepiments may have to be removed before the orbital fat arises, as it should do, to occupy the lower part of the exposed frontal sinus. In this part of the operation much help is obtained by the careful use of a probe, by frequently securing a field free from bleeding by pressure with adrenalin or peroxide, and by the knowledge previously gained by skiagraphy.
If the Röntgen rays have shown that the frontal sinus does not extend above the level of the bridge, or if radiography be not available and there is any uncertainty as to the extent of the cavity, this lower opening should be made first.
In the inner part of the large orifice which has been made below the bridge the deeper ethmoid cells can be treated, and the sphenoidal ostium is much nearer than when viewed from the introitus narium, so that it is easy to enlarge it and deal with the contents.
Now, as throughout the operation, great care must be taken to shield the eyeball with gauze pads and the protector. The hanging pressure forceps are apt to be pushed against the globe.
The whole area of operation is next carefully cleaned with warm normal saline solution. Any projecting corners or loose spicules of bone are removed. If any point of pus should show up it must be carefully followed to its source. The cotton-wool pledgets are removed from the nose. The pressure forceps are twisted off, and any vessels that require it are ligatured. A strip of ribbon gauze is loosely packed in the lower part of the enlarged fronto-ethmoidal space, and the end is led down to the nasal orifice. The flaps are brought together, and care is taken that the reflected periosteum is pulled back with them. Formerly Killian in the majority of cases used to sew up the whole wound at once. He now agrees that it is safer to leave the external angle with a small drainage tube running inwards and downwards to the area of the fronto-ethmoidal cells. The inner part of the incision in the eyebrow, and all the part lying below the bridge, can be closed. Killian employs aluminium-bronze wire, and a metal suture seems preferable, as the contamination of the wound edges makes stitch-abscess not uncommon.
Secondary suture—on the second or third day—is reserved by Killian for cases when (1) the history or appearance of the mucosa indicates a recent exacerbation, (2) there is a history of erysipelas, (3) the pus is very fœtid, (4) there is any history of a tendency to wound complications, or (5) there is marked invasion of the diploë in the frontal bone.
Double cyanide gauze, rung out of boric lotion and covered with a good supporting pad of cotton-wool, is then put on. But when there is any question of intracranial complication, when the pus is fœtid or there is any necrosis, and when the surgeon is forced to operate during an acute exacerbation, it is better to apply warm boric fomentations and leave the upper and outer supra-orbital part of the incision freely open.
After-treatment. The patient is put to bed on the sound side, so as to assist drainage. He is advised not to blow the nose, but to hawk as much of the secretion as possible backwards and then expectorate it. The gauze drain is removed from the nose at the end of twenty-four hours, and is not renewed. The drainage tube at the temporal end of the incision is changed at the end of forty-eight hours, and afterwards is removed and cleansed daily. The dressing is also changed daily, after the first forty-eight hours, so as to keep a careful watch for any retention. On the fifth day the sutures can be removed, and soon afterwards the dressing can be discontinued and the eye left uncovered. Intranasal treatment should be avoided for a while. But after two or three weeks the granulating surface behind the bridge is painted occasionally with a 2 to 3% solution of nitrate of silver. Any crusts are removed after soaking with peroxide of hydrogen.
Complications and dangers. The operation is not free from danger. Latent cerebral trouble connected with the sinus may be roused into activity by the local traumatism, however skilfully effected. The shock, or the lowered local resistance, may stimulate a latent infection in neighbouring sinuses, and also weaken the lines of defence protecting the cranial cavity.
In 1905 Logan Turner collected the record of twenty-four deaths which had occurred after operation on the frontal sinus.72 This number has been exceeded by the fatalities since published and the much greater number which have never been recorded.73 The chief dangers are (1) a spreading septic osteomyelitis, (2) meningitis, and (3) abscess in the frontal cerebral lobe.
Infection of the bone is indicated chiefly by a puffy, tender swelling on the forehead or temple, adjoining the upper flap. There may be little or no rise of temperature, and little complaint on the part of the patient. But no time should be lost in laying the wound freely open, searching for any shut-off focus of pus, and applying hot boric fomentations diligently. Once infection is established in the bone it may be impossible to stay its progress, even by the most thorough removal of diseased tissue: but the effort should be made.74
Meningitis is an equally dangerous complication. It may arise without direct injury to the cerebral wall of the sinus. If, during removal, the anterior end of the middle turbinal be damaged too high up, the lymph channels around the olfactory nerve may be opened so freely that infection spreads along them to the meninges. Or the cerebral wall may sometimes be broken through without a serious result, if the dura mater be left intact behind it. But if there be any damage done to the wall in the neighbourhood of the crista galli or cribriform plate, the dura mater is almost inevitably injured at the same time, and a rapid and fatal meningitis may be expected. The infection is generally streptococcal, and surgery is powerless to stop its progress.
Abscess in the frontal cerebral lobe may arise from operation on the frontal sinus. In my experience it is more apt to occur independently of interference with the sinus, to remain latent, and then to be simply roused into activity by the local traumatism. The symptoms are, unfortunately, very vague. Rise of temperature, headache, irritability, drowsiness, and optic neuritis may be present. On the occurrence of these symptoms the sinus should be freely reopened, and the posterior (cerebral) wall carefully inspected for any necrosing area. In any case it should be removed and the frontal lobe explored in all directions.75
These dangerous complications, in many cases, were no doubt due to a failure to recognize that the complicated group of ethmoidal cells were involved in all cases of chronic frontal suppuration, and that previous to the introduction of the Killian operation our operative methods were very apt to dam up suppuration in dangerous corners. Finally, it was only when rhinologists first began to investigate frontal sinusitis that it was recognized what a dangerous region this is. To be convinced of this it is only necessary to compare the anxiety inspired by our regard for the cerebral wall of the frontal sinus with the calmness with which we regard an opening into the middle fossa, or through the dura mater, in mastoid operations.
We are not yet in possession of definite evidence in regard to the proportionate number of deaths which are due directly or indirectly to pus in the frontal sinus. Some observers hold that more deaths have occurred from operation than from neglected cases. Molinié has followed the history of fifteen private patients with frontal sinusitis, and not operated on, for ten years. Only one has died, and that was from another cause.76 In any case we may still accept Lermoyez’s dictum: ‘Avoir une sinusite chronique est chose moins grave qu’on ne croit: opérer une sinusite frontale est chose plus sérieuse qu’on ne le dit.’77
Doubtless the dangers have been diminished since the more general adoption of the Killian operation, but accidents may occur in the most skilful hands. This must be kept in mind when drawing up the indications for interference.
Results. In uncomplicated cases, successfully operated on, the results are most satisfactory. The preservation of the Killian bridge quite prevents any really unpleasant disfigurement. The depression which may form above it is proportionate to the size and depth of the cavity. No man need decline the operation on account of the scar left. In women we are able, with the help of a radiograph, to form an idea beforehand as to the degree of depression which may be left. This, if required, can be remedied by the injection of paraffin (see Vol. I), but, fortunately, the frontal sinus in women is not, as a rule, so deep as in men.
As regards cessation of purulent discharge the result will depend on the extent of the sinus, the presence of complicated orbito-ethmoidal cells, and the skill of the operator. If the ethmoidal labyrinth has not been completely dealt with, one or two cells may continue to secrete. It may be wiser to leave them alone. In very deep sinuses a ‘dead space’ between the back of the Killian bridge and the posterior (cerebral) wall of the sinus remains open, and may continue to secrete if not cicatrized over evenly.
But secretion is no longer pent up in the fronto-ethmoidal group of cells, and the patient is relieved of headache, depression, and other symptoms of septic absorption.
This operation was first described by Ogston,78 but was independently conceived by Luc.79 Its principle is to make a fairly free opening into the frontal sinus, and then establish a large communication with the nasal cavity. The inner part of the supra-orbital rim is sometimes destroyed. But the operation does not provide for the treatment of orbito-ethmoidal cells, the anterior ethmoidal region and the sp[h]enoidal wall are not exposed, and if there be a large orbital recess to the frontal sinus it cannot be satisfactorily dealt with.
Indications. But the Ogston-Luc procedure, or some modification of it, is still suitable in (1) exploratory openings of the frontal sinus, (2) when the sinus requires opening for a recent and acute infection80, and (3) for mucoceles and suppurating mucoceles.81
Operation. A general anæsthetic is required. It is not necessary to shave the eyebrow, but the surrounding skin should be well purified. A curved incision is made through the eyebrow down to the bone along the inner third of the supra-orbital ridge, reaching from the supra-orbital notch to opposite the inner canthus. In the latter direction it can be extended if the ethmoidal region is chiefly affected, and if the ethmoid only requires exposing the incision is placed lower down.
With a raspatory the soft parts are turned upwards and downwards so as to expose the anterior wall of the sinus, which is opened with chisel and hammer. A probe will indicate its depth and direction. The opening is enlarged with bone-forceps sufficiently to allow inspection of the interior of the cavity, and permit of the passage into the nose being enlarged with forceps, curettes, or burrs. The polypoid mucosa occupying the sinus and the fronto-ethmoidal cells along the passage to the nose are carefully plucked away. A drainage tube or wick of gauze is inserted from the sinus down into the cavity of the nose, so that it can be withdrawn from the anterior nares at the end of twenty-four hours. The drainage tube is replaced by some surgeons. The frontal wound is sometimes closed at the time of the operation, and sometimes left open.
Results. These are variously given by different observers. Thus one author states that it will effect a cure in 85% of cases,82 while another operated by this method in eleven cases, of which two died and not one was completely cured.83
The subject does not require further discussion, as most operators have now given this operation up in favour of the improvements wrought in it by Killian. Luc himself has abandoned it in favour of the Killian operation. The latter is undoubtedly to be preferred in all cases of well established chronic purulent sinusitis with fungating mucosa and involvement of the ethmoidal cells.
In this operation the entire anterior wall of the frontal sinus is chiselled away, so as to allow of the soft parts covering it being pressed down into the cavity until they are applied to the posterior wall. This, naturally, effects a complete obliteration of the cavity, but in order to secure it the orbital ridge has frequently to be removed to such an extent that a frog-like prominence is given to the eye, and the resulting disfigurement is very marked. Besides, this operation does not deal with the orbital recess of the sinus, or the orbito-ethmoidal cells—the most important part of the operation. In fact, the only advantage of this operation—complete obliteration of the sinus—is secured by Killian’s operation, which also allows these regions to be dealt with, permits free drainage into the nose, and avoids disfigurement.
 Fig. 343. Radiograph of the Sphenoidal Sinus. The beak of a
punch-forceps is seen in a posterior ethmoidal cell (which has been
opened) and pressing against the anterior wall of the sphenoidal cavity.
Fig. 343. Radiograph of the Sphenoidal Sinus. The beak of a
punch-forceps is seen in a posterior ethmoidal cell (which has been
opened) and pressing against the anterior wall of the sphenoidal cavity.
Surgical Anatomy. In operating on this sinus there are many anatomical and pathological points which it is desirable to remember. Only a few of them can be recalled.
The cavity is seldom absent, although it may be quite small. Its size and conformation may be irregular. Thus in one instance it may extend far out into the wing of the sphenoid, while in another it may be even smaller than a posterior ethmoidal cell invading the body of the sphenoid bone and lying above it.
While the sphenoidal sinus on one side is very small the opposite one may be so large that it comes in relation with the optic groove of the opposite side.
The anterior wall of the sphenoidal sinus can be opened with safety. The roof comes into close relation with the structures round the sella turc[ic]a. The outer wall is close to many large blood-vessels which might cause troublesome hæmorrhage if wounded. The upper outer wall may be as thin as paper.
There may be deficiencies present in the bony walls, so that, for instance, the mucous membrane of the sinus and the dura mater may be in direct contact.
The Röntgen rays give such valuable information as to the size and relations of the cavity, as well as to diseases in its cavity or walls, that a radiograph should be taken in all cases (Figs. 343 and 344).
 Fig. 344. Radiograph of the Sphenoidal Sinus. This is a sequel to the preceding
illustration. The front wall of the sinus has been broken through, and the
beak of the forceps is now shown inside the sphenoidal cavity.
Fig. 344. Radiograph of the Sphenoidal Sinus. This is a sequel to the preceding
illustration. The front wall of the sinus has been broken through, and the
beak of the forceps is now shown inside the sphenoidal cavity.
Indications. Lavage alone may be sufficient for acute or recent cases, but in chronic forms of suppuration a larger and permanently patent ostium must be established, both to allow of more effective drainage and of treatment of the interior of the cavity.
When the interior of the nasal chamber is in a normal condition it is only possible to catheterize this cavity in a limited number of cases. The region of the middle turbinal and olfactory cleft is carefully prepared with cocaine and adrenalin. A pledget soaked in the mixture is inserted between the middle turbinal and the septum, and pushed backwards until it reaches the anterior wall of the sinus.
A canula is then inserted in a sloping direction inwards and upwards diagonally across the plane of the middle turbinal until it impinges on the nasal surface of the sphenoid, in the neighbourhood of the ostium (Fig. 345). The latter is found by feeling with the tip of the catheter. The opening is never visible in health. It may lie a little external to the direction of the olfactory cleft—about 5 millimetres from the middle line.
If this plan be not successful, the ostium sphenoidale can more certainly be discovered in the following way. A more complete and prolonged application of cocaine is carried out, particularly in the neighbourhood of the olfactory cleft and the spheno-ethmoidal recess. Killian’s long nasal speculum (Fig. 346), sterilized and warmed, is inserted between the middle turbinal and the septum. By separating the blades of the speculum the passage is dilated, so that the instrument can be slipped further in, and so, by alternating movements of expansion and advance, the front wall of the sinus is brought into view. During this procedure the middle turbinal is crowded outwards, and no alarm need be caused if a slight cracking sound shows that its attachment has been fractured.
The mouth of the sphenoidal sinus is often indicated by the muco-pus oozing from it or pulsating in harmony with the pulse. If discharge be not escaping the ostium may be only a potential and not an actual orifice—like that of the meatus urinarius—and has then to be more carefully sought for and detected with a probe. If there be difficulty in finding the ostium, the front wall should not be broken through until the presence and size of the sinus has been demonstrated by means of a radiograph (Figs. 343 and 344). The sinus is washed out, as described for the frontal and maxillary cavities.
Indications. Profuse purulent post-nasal catarrh, persistent headache, orbital or ocular or intracranial symptoms, call at once for relief. Not infrequently suppuration in other cavities will not cease, even though operated on, until the sphenoidal sinus has been treated.
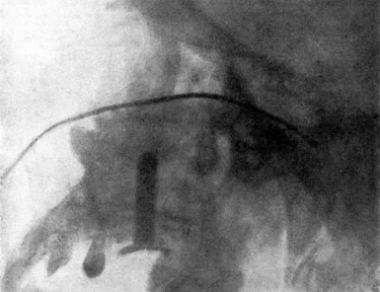 Fig. 347. Radiograph showing a Probe in the Sphenoidal Sinus.
An india-rubber obturator is in the maxillary antrum.
Fig. 347. Radiograph showing a Probe in the Sphenoidal Sinus.
An india-rubber obturator is in the maxillary antrum.
Operation. Unless long-standing suppuration or ozœna have produced such atrophy of the middle turbinal that the front wall of the sphenoidal sinus is easily inspected from the front, it will be necessary to remove the greater portion of the middle turbinal. If the anterior end has had the typical amputation performed (see p. 592), then the rest can be removed with the punch-forceps of Grünwald, the wire snare, or, under nitrous oxide anæsthesia, the spokeshave.
This will bring the anterior wall of the sinus with its ostium into view. Killian’s long nasal speculum (Fig. 346) may still be necessary. With the help of cocaine the ostium can then be enlarged with various instruments. Hajek’s hook can be inserted into the orifice and the front wall torn away. I have not found this satisfactory. It is much simpler to insert the beak of a small Grünwald’s forceps into it, or a small ring-knife, and by a series of boring and screwing motions to render the ostium patent. It is then easy to introduce a beaked Grünwald’s or some such punch-forceps as those of Cordes (Fig. 348) and cut away as much of the front wall as may be required. This can be done freely in an inward and downward direction, and an opening as large as the tip of the little finger, and sufficient for drainage and treatment, is thus established.
 Fig. 348. Sphenoidal Punch-forceps.
Fig. 348. Sphenoidal Punch-forceps.
When describing the removal of posterior ethmoidal cells (see p. 616) it was pointed out that the tip of the forceps not uncommonly breaks through the thin portion of the anterior sphenoidal wall.
If the natural ostium sphenoidale be not visible it would be risky to make an artificial opening without first determining by radiography the presence and size of the sinus. When this has been ascertained, palpation with a pair of sinus-forceps or a Lichtwitz’s trochar and canula will generally detect a thin spot where firm pressure is sufficient to penetrate into the cavity. The opening is then enlarged as described.
In all these procedures care must be taken that the instrument does not burst suddenly through the front wall with such force that it impinges on and damages the posterior wall.
The opened sinus must be dealt with according to the conditions met with. Necrosed portions of bone may require to be removed, but they rarely occur, except in syphilitic cases. Polypoid masses of mucous membrane, obscuring the opening, may be carefully lifted out with forceps or curette, so as to facilitate drainage; but it is never necessary to think of curetting the interior generally, and particular regard should be paid to the posterior wall.
After-treatment. Profuse hæmorrhage has sometimes occurred after opening the sinus. In a case of Gleitsmann’s the bleeding did not take place until seven days after the operation,84 and in one of C. R. Myles’s cases profuse hæmorrhage occurred on the ninth day and required ligature of the external carotid.85 It is possible that the bleeding in such cases may come from a branch of the internal maxillary artery, or even from the cavernous sinus. It can be met by firm plugging with a long strip of 1-inch ribbon gauze, of which the end is soaked in adrenalin or peroxide of hydrogen. Hæmorrhage is not a complication that I have ever met with, after having opened a large number of sphenoidal cavities, and I do not think it is to be dreaded if the opening be made as directed.
The sinus is washed out with a warm normal saline solution. The addition of peroxide of hydrogen may be useful. The condition of the mucous membrane may be improved by cleansing the sinus with iodoform emulsion, or plugging it for twelve or twenty-four hours with iodoform ribbon gauze. Any pigment can be kept in contact with the walls for some time by dipping the end of a piece of ribbon gauze into a solution of argyrol (25%) or nitrate of silver (2%) and packing it into the cavity. The other end of the strip is left just within the vestibule of the nose, so that the patient can withdraw it himself.
But if a sufficient opening has been made into the cavity to allow of natural ventilation and drainage, it is well to abstain from too much local medication—particularly if there be neither polypus, necrosis, nor foreign body in the sinus, and if it be not subject to reinfection from the suppuration in the posterior ethmoidal cells. It is remarkable how, under such conditions, suppuration will cease in a sphenoidal sinus if left alone, when, if frequently treated, secretion will continue indefinitely. In my experience the sphenoidal sinus is one of the most satisfactory of the accessory sinuses to treat.86
Other methods. The sphenoidal sinus can also be opened and treated during Killian’s operation on the frontal sinus (see p. 648).
It has been proposed to approach the sphenoidal sinus by first traversing the maxillary antrum. Such a complicated route, involving extensive destruction of tissue, has no advantage over the direct and simple method described. Attempts to reach the sphenoidal sinus from the naso-pharynx are not practical. This is easily seen by observing the thickness of the floor of the cavity depicted in Fig. 345.
Before starting treatment in a case of multi-sinusitis a complete examination should be formulated. The importance of making the differential diagnosis as complete as possible cannot be overestimated.
In initiating treatment attention should be directed first to the ethmoidal region. The ethmoid should be attended to in all cases of suppuration in the frontal sinus. It is generally necessary, in any case, to clear it away to gain access to the sphenoidal orifice. It is well to remove it before or during operation on the maxillary sinus. The sphenoidal sinus should be catheterized, and, if infected, the orifice will require enlarging and the cavity treating. A frontal sinus should be washed out several times before deciding on a radical operation. It not uncommonly ceases to secrete after the ethmoid has been cleared.
The radical operation on the frontal sinus should not be embarked on until the ethmoid and sphenoid have been attended to. A radical frontal operation should take precedence of the maxillary, unless both cavities are operated on at the same time.
Many growths in the naso-pharynx, whether originating in the space or descending into it from the posterior choanæ, can be removed by the following method.
Indications. This operation is indicated for the ordinary mucous polypus of the nose when presenting in the post-nasal space. Polypoid masses of the ethmoid may project through the posterior cavity and are removed in the same way. A naso-pharyngeal polypus (also called choanal polypus, post-nasal polypus, or benign pharyngeal polypus) is easily removed by this procedure. Innocent tumours of the post-nasal space, such as papilloma, adenoma, fibroma, and cysts, can be removed by the same method.
Under cocaine. Cocaine and adrenalin (see p. 572) should be carefully applied to the septum and turbinals, as it is the passage of the instrument from the front which is often the most painful part of the proceeding. The pharynx should be lightly sprayed with a 5% solution of cocaine so as to check reflex action.
While the patient is seated in the ordinary examination chair the surgeon stands at his left hand and introduces a looped snare (Fig. 312, p. 613) through the nostril most suitable for approaching the root of the growth. When the snare has reached the post-nasal space, the surgeon introduces the purified forefinger of the left hand through the mouth and up behind the soft palate, as in Fig. 291. Here it serves to manipulate the loop over the growth, and holds it close to the root of the pedicle while the snare is pulled home.
A few minutes should be allowed to elapse to permit the patient to recover from the unpleasant manipulation, and also to allow of coagulation of the strangulated blood-vessels. The growth should not be cut through, as it is wiser to pluck it from its attachment by a quick movement of avulsion.
The growth may come away with the snare through the nostril, or may fall into the pharynx and be expectorated.
In fairly roomy nostrils a stout polypus forceps can be used instead of the snare.
Under chloroform. In nervous subjects the same method should be carried out under a general anæsthetic, care being taken that the growth does not cause embarrassment by occluding the larynx.
Under chloroform, of course, more extensive operations can be carried out on the post-nasal space. The pedicle can be attacked with a pair of scissors with long handles, short blades, and slightly curved on the flat. These are introduced through that nostril which appears to be in most direct line with the pedicle, to act as a raspatory, and then cut through the base of the growth. In some cases an instrument such as Langenbeck’s elevator (Fig. 338) will prove useful if introduced through the nostril. The growth is then removed through the mouth by a twisting movement with a strong volsella.
Many growths in the naso-pharynx can be removed through the mouth, without preliminary operations through the face or through the hard or soft palate.
Indications. The following method of access to the naso-pharynx is chiefly called for in true fibroma of the naso-pharynx, otherwise called naso-pharyngeal polypus, fibroid tumour of the base of the skull, fibroid tumour of the naso-pharynx, retro-maxillary polypus, or juvenile sarcoma of the naso-pharynx.
It is also a plan of procedure which may be called for in any very large, innocent tumours of the naso-pharynx, particularly in cases where nasal stenosis prevents access from the nostrils. It would be a suitable method in any operable cases of malignant disease of the post-nasal space.
Operation. The patient is chloroformed and placed in the position of Rose (hanging head). The mouth being propped open, and the tongue drawn forward, the tumour is first explored with the forefinger, to detect and detach any secondary adhesions. A raspatory which works laterally is next passed from one side of the naso-pharynx to the other above the growth. A rugine which works in a sagittal plane is then introduced below the tumour and made to pass upwards behind it—the reverse movement of Gottstein’s curette in the removal of adenoids (Fig. 350). This movement is facilitated by securely gripping the tumour and dragging it forwards with a stout pair of alligator or volsella forceps. The tumour can thus be so liberated that, with some twisting movements, it can sometimes be extracted entire—often dragging down with it through the naso-pharynx any prolongations thrown forward into the nose.
It is useless to attack such growths as true fibroma of the naso-pharynx with an ordinary wire snare, or such an instrument as a pair of adenoid forceps. For these firm tumours, specially powerful forceps have been designed by Doyen and Escat.
Hæmorrhage is apt to be sudden and copious, but the more rapidly and completely the growth is removed the sooner will bleeding cease—even spontaneously. After complete removal firm pressure with a marine sponge will generally check it. A post-nasal plug should be avoided, and is not usually required. Incomplete operations not only start hæmorrhage but may start septic absorption.
Modifications. (a) Preliminary laryngotomy. A preliminary laryngotomy, strongly recommended by J. W. Bond and extensively adopted by Butlin, adds nothing to the dangers of the case. It allows of the laryngo-pharynx being packed, so that there is no anxiety in regard to the descent of blood into the lungs, and it permits the steady administration of the anæsthetic through the laryngotomy canula. The surgeon is thus relieved of two great anxieties, and can devote himself without embarrassment to more deliberate operation.
The laryngotomy tube can be removed as soon as the patient recovers consciousness and all hæmorrhage has ceased.
(b) Division of the soft palate. In addition to the operation of laryngotomy, the following procedure will allow of more deliberate removal.
The soft palate and uvula are carefully divided in the middle line, and a silk ligature is placed through each lateral half so that they can be held forward out of the way. This gives more direct access to the post-nasal tumour, and if then found to crowd the cavity too closely to allow of manipulation, the posterior part of the hard palate can be chiselled away in the middle line. At the conclusion of the operation the divided palate is carefully united in the middle line (see Vol. II).
Selection of method. In some cases operation through the mouth may have to be combined with a second operation from the front—such as the method of Moure (see p. 619) or that of Rouge (see p. 622).
Rapidity of operation is important, as, once the pedicle has been cut through, or the body of the tumour removed, the hæmorrhage tends to subside spontaneously, or is quickly controlled by packing.
The hanging head (Rose) or the Trendelenburg position is generally recommended.
The preliminary laryngotomy seems desirable in all cases. The division of the palate should be avoided if possible. It may not always unite, and is less likely to do so if subsequent operations are required. The soft palate is very elastic, and in some cases it can be tied out of the way by means of a soft rubber catheter passed along the floor of the nose, and out through the mouth.
Ligature of the external carotid, strongly recommended by Chevalier Jackson87, is not necessary unless the patient is very anæmic or weak from former hæmorrhages. It should then be only a temporary ligature (see Vol. I, p. 383).
Hæmorrhage, as already remarked, is chiefly guarded against by rapid and complete operation. The preliminary use of adrenalin and cocaine, the administration of lactate of calcium, and the other methods recommended for the prevention of bleeding (see p. 574) should be carefully attended to. But in every case preparation should be made beforehand for ligature of the external carotids and for saline infusion.
Indications. The disease is serious, and when not diagnosed almost inevitably ends in death. Before the abscess bursts death may result from spasm of the glottis, laryngeal œdema, or asphyxia. The affection runs its course in 5 to 10 days, and if the abscess opens spontaneously death almost inevitably results—either from suffocation, or septic pneumonia, or cardiac failure.
Operation. When the diagnosis is settled intervention should be prompt. It is not necessary to wait for distinct fluctuation. The pus focus may be so difficult of manipulation in an infant, and the pharyngeal muscle may be so thick and indurated, that it is practically impossible, even in the later stages of retropharyngeal abscess, to detect the presence of pus by palpation.88
The evacuation of the abscess through the mouth was formerly looked upon as dangerous, owing to the difficulty of drainage, the fear of pus burrowing behind the œsophagus, and the risk of flooding the larynx with pus. The more difficult plan of opening it from the neck was generally recommended. The majority of cases can be opened through the mouth with perfect safety.
No general or local anæsthetic is administered, but everything necessary for an immediate tracheotomy should be ready at hand. No gag should be employed, a tongue depressor or the operator’s left forefinger being sufficient both to keep the mouth open and act as a guide. The infant is swaddled in a shawl so as to completely control the movements of the extremities and is then laid on its side on a low pillow, and held by a trustworthy assistant. The sinus-forceps used for opening a peritonsillar abscess are thrust into the most prominent part of the swelling, and the opening enlarged by separating the blades as they are withdrawn. A slender sharp-pointed bistoury, guarded and guided by the index-finger, may be used instead of the forceps. The pus will pour out through the nose and mouth. The incision of the pharynx should be free, deep and long, and directed against the posterior wall of the pharynx and as close to the median line as possible, so as to avoid any chance of wounding the internal carotid.
The surgeon may feel more security if, with the same precautions and with the patient in the same position, he first aspirates the pus cavity.
If more accustomed to it, he may also prefer to have the child flat on its back, with the head overhanging the edge of the table.
Suffocation may be so imminent when the patient is first seen that a preliminary tracheotomy is required.
The external operation, which leaves a certain scar, is reserved for some rare cases—as when the abscess is too low to be easily reached through the mouth, when the spasm of the masseters cannot be overcome, when a large pulsating vessel is noticed in front of the abscess, and when the abscess points towards the neck. It is also the suitable one for the chronic and generally tubercular form of abscess more commonly met with in older patients.89
The external operation is made through an incision along the posterior border of the sterno-mastoid muscle, and the dissection is carried behind the large vessels of the neck and in front of the prevertebral muscles.
After-treatment. The after-care of the patient will require consideration, since the disease is generally met with in the feeble and ill nourished.
If the abscess be opened in good time the patient is at once relieved and begins to recover rapidly.
Indications. The removal of naso-pharyngeal adenoids is not called for simply because they are accidentally discovered to be present, nor does the need of operation depend solely on the size of the growths or the nasal obstruction they produce. Adenoids require removal whenever the symptoms attributable to them call for relief. These symptoms may be arranged in three groups, according as they are those (i) of nasal stenosis, (ii) of secondary septic infection, or (iii) of reflex effects.
(i) Amongst the first are mouth-breathing and all the numerous sequelæ, including facial, buccal, dental, and thoracic deformities. It must not be forgotten that mouth-breathing may never be present, and yet deformities of the chest or septic or reflex results can be produced by a small amount of growth in the post-nasal space.
(ii) Amongst secondary septic infections are catarrhal conditions of the Eustachian tube and otitis media, and catarrhal infection of any part of the air-passages. Cervical glands and so-called ‘glandular fever’ occur in this group, as do septic gastritis and other conditions caused by the conveyance of sepsis to more distant parts.
(iii) Various reflex effects are sometimes attributable to naso-pharyngeal adenoids. Laryngismus stridulus, reflex cough, chorea, convulsions, night-terrors, enuresis nocturna, and aprosexia are some of the ailments which may justify operation on Luschka’s tonsil.
As it is chiefly in children that this operation is required it is important to see that they are free from indication of infectious fevers. The operation should be postponed until any acute catarrh has subsided. If there be otorrhœa the ears should receive suitable cleansing treatment for a week or two beforehand. The condition of the teeth requires attention.
The operation is so frequently carried out in private houses that it is well to make inquiries into the health of the members of the household, recent illness, and sanitation. When possible, a large, airy room with a south aspect should be chosen.
Operation. In adults it is possible to carry out the operation under cocaine. On the Continent, particularly in hospital practice, it is often done without any anæsthetic at all. In this country general anæsthesia is almost the universal custom. Opinion is divided as to which is the safest and most suitable anæsthetic to employ.
When the removal of tonsils or other operation is not carried out at the same time, an anæsthesia of less than a minute is sufficient. In adults, and in children over 10 years of age, nitrous oxide does excellently. Younger children are apt to be alarmed by the face-piece and apparatus necessary for nitrous oxide, and this gas does not seem so suitable for them as for adults. In younger children chloride of ethyl is extensively employed on the Continent, but has not met with general favour here.
When the tonsils require removal, or any other operation on the upper air-passages is carried out at the same time, and in young children generally, an anæsthesia allowing of more deliberation is desirable. For this, some operators employ ether,—preceded or not by nitrous oxide. But the well-known objections to pure ether in the surgery of the air-passages have caused the preference to be given to chloroform, or to one of the mixtures of chloroform and ether.
The patient should lie quite flat on the operating table, with only a low pillow or folded towel under the head. The anæsthetist, who takes charge of the gag and flexes or rotates the head as directed, stands at the end of the table. At the patient’s right hand stands the surgeon, and within easy reach are his instruments, sponges, and iced water. Standing on the same side and behind him is the nurse. Her duty is to soothe the patient while passing into unconsciousness, and later on to roll him well over on to his right side as the operation finishes.
The operation can be carried out more correctly, rapidly, safely, and comfortably if the surgeon be armed with an electric forehead search-light (see p. 571). Failing this, the table should be brought close up and parallel to a window, with the patient’s right hand next the light.
Surgeons differ as to the degree of anæsthesia desirable. Some like it to be quite light, so that the patient is all the time in the struggling stage and requires his hands to be controlled by the nurse. I think this is quite as dangerous as when the anæsthesia is pushed until the patient is relaxed, with the corneal reflex just abolished, and the swallowing and coughing reflexes still present.
 Fig. 349. Adenoid Curette. StClair Thomson’s modification.
Fig. 349. Adenoid Curette. StClair Thomson’s modification.
When the anæsthetic is administered steadily, with plenty of air, a degree of unconsciousness is generally secured which will allow of an operation lasting two or three minutes without any further adminis[t]ration. Should the patient show signs of recovering consciousness more chloroform can be given from a Junker’s apparatus.
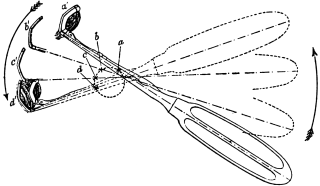 Fig. 350. The Removal of Naso-pharyngeal Adenoids. Semi-diagrammatic
illustration to show how the curette revolves around an axis which moves
from a, through b and c, to d. The growth is pressed into the fenestra of the
instrument in the a' position, and when the sweeping movement has brought
it to d', it is detached and caught in the cage.
Fig. 350. The Removal of Naso-pharyngeal Adenoids. Semi-diagrammatic
illustration to show how the curette revolves around an axis which moves
from a, through b and c, to d. The growth is pressed into the fenestra of the
instrument in the a' position, and when the sweeping movement has brought
it to d', it is detached and caught in the cage.
The anæsthetist then opens the mouth with a suitable gag, such as Doyen’s or Mason’s, and maintains the patient’s head exactly in the middle line of the body. Directing the electric search-light into the pharynx, the surgeon depresses the tongue with a spatula in the left hand, while with the right he holds the adenoid curette—some modification of the original Gottstein model (Fig. 349). This is best seized firmly dagger-wise (Fig. 351). It is then introduced along the tongue and slipped up into the post-nasal space. Once safely behind the soft palate and kept straight in the middle line, no harm can be done. Dropping the tongue depressor, the surgeon depresses the handle of his instrument until the beak of it is felt in contact with the posterior free margin of the septum. Pressing the cutting blade firmly and steadily along this it is swept upwards, backwards, and downwards along the vault of the naso-pharynx, while the curette revolves around an imaginary centre in its shaft (Fig. 350). As the instrument is withdrawn from the pharynx, its cage will be found to contain the adenoid growth, removed en bloc and generally complete (Fig. 351). Should the growth slip from the cage, or remain semi-detached from the posterior pharyngeal wall, it can be seized and lifted from the throat with a pair of post-nasal forceps (Fig. 287).
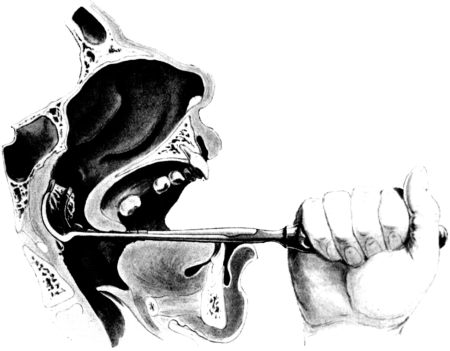 Fig. 351. Removal of Naso-pharyngeal Adenoids. The growth is shown
as partially removed from its attachment, and bulging into the cage of the instrument
which opens to receive it.
Fig. 351. Removal of Naso-pharyngeal Adenoids. The growth is shown
as partially removed from its attachment, and bulging into the cage of the instrument
which opens to receive it.
The rush of blood which now takes place is met by rolling the patient well over to his right side, with his face over the edge of the table, so that the blood can run into the right cheek and so out through the mouth. With the patient on his side there is no anxiety of asphyxia from descent of blood or fragments of growth into the trachea, and the surgeon can more deliberately explore the post-nasal space and, with a simple adenoid curette, remove any lateral remains of growth which may have escaped the caged curette.
Sponges are merely used to cleanse the mouth and pharynx in order to make sure that no semi-detached fragments are left behind. If present, tonsils can be conveniently removed at this stage.
Bleeding, which may be very free for a minute or two without any cause for anxiety, is promptly arrested by freely sluicing the patient’s face and neck with ice-cold water.
After-treatment. The patient is put back to bed, lying well over to one side. He should not be allowed to lie on his back, or left unattended, until consciousness has returned. Collapse may occur at this time, generally as a precursor of vomiting, or blood may be vomited and then, owing to the patient’s semi-conscious condition, may be drawn into the trachea.
Ice may be sucked. After a few hours, if there be no vomiting, barley-water, lemonade, tea, thin beef-tea, or beef jelly can be given. Milk and milky food should be avoided. An aperient should be given the same evening, as any foul breath or feverish condition is more likely to be due to blood and mucus in the stomach than to local sepsis. The mouth is kept cleansed with the tooth-brush and an alkaline wash.
It is best to avoid local treatment for the nose. At the end of a few hours the patient is encouraged to clean the nose, and if he be supplied with abundance of fresh air through freely opened windows, the wound in the post-nasal space will heal promptly without any local or general reaction. Occasionally an alkaline nose lotion is required if there has been much secondary rhinitis, or if the child be kept in vitiated air.
One day in bed is generally sufficient, and a child may be allowed out in two or three days, though fatigue should be avoided for a week. Suitable after-treatment in the way of breathing exercises, gymnastics, speech correction, and tonics is often needed. Relief of nasal stenosis may require completion by attention to the condition of the turbinals and septum.
The operation in adults is performed under nitrous oxide. This can be carried out in exactly the same way as that already described, but some surgeons prefer to have the patient sitting up in a dentist’s chair. In that case, after the removal of the mass of growth, the patient’s head is thrown forward between his knees.
Difficulties and dangers. It may be said that the operation itself, carried out with usual care and in a patient who is not a hæmophilic, is free from danger. The chief anxiety is from the anæsthetic, and no inconsiderable number of deaths from this cause have been reported. When possible, it is well to secure the services of an expert anæsthetist who is well used to laryngological work, and accustomed to the operator’s particular methods.
Hæmorrhage may be brisk, even profuse, for a few minutes, but as a rule it promptly ceases if the operation be completed, the patient well rolled to one side, the air thoroughfare left clear so as to allow free breathing and avoid congestion, and the gag removed to permit swallowing and diminish pharyngeal reflexes. The more rapidly and completely the operation is executed, the less will be the bleeding. It not infrequently originates from semi-detached fragments of growth. Even when the hæmorrhage is profuse it is better to push on and complete the removal of growth before attempting to check it. The value of free applications of ice-cold water cannot be exaggerated (see p. 574). In many cases bleeding is maintained by the surgeon’s anxious efforts to stop it with sponging, pressure, or the application of styptics. The greatest danger arises in the case of hæmophilics. If this diathesis be undoubtedly present, the operation should be avoided. If only suspected, more care than usual should be taken in preparing the patient for operation, and lactate of calcium in 15 to 30 grain doses twice a day might be given for two or three days beforehand.
When bleeding persists it is met by keeping the patient very quiet and free from alarm, in a cool and well-ventilated room, and only lightly covered with clothes. Ice is given to suck and applied on each side of the neck, while iced cloths are applied to the face and forehead. Clots are blown out of the nose so as to permit the access of fresh cold air to the post-nasal space. With a pipette, or a pledget of cotton-wool, a few drops of adrenalin can be trickled into the nostril and allowed to run backward. If these measures fail—as they rarely do—the post-nasal space must be plugged (see p. 575). When hæmorrhage takes place after the removal of adenoids and tonsils, it will generally be found that the source of it is in the tonsillar area.
The uvula may retract strongly at the moment of introducing the curette and then get crushed against the posterior pharyngeal wall: or it may be seized by mistake with the post-nasal forceps and be torn away. The same instrument has sometimes been responsible for fracturing the posterior margin of the septum, injuring the Eustachian cushion, and tearing off strips of mucosa from the pharynx. These complications are avoided by using a frontal search-light, operating deliberately, and abandoning the forceps in favour of the curette. This latter instrument can be manipulated without these risks if it be first guided safely behind the uvula and then used more like a carpenter’s adze than a curette. The stroke with the caged curette should be carried through in one movement and exactly in the middle line of the body, but always on the posterior wall. There is no need to attempt removal of adenoid tissue on the lateral walls. This atrophies if the main mass is removed, and the fossa of Rosenmüller can be cleared out with the forefinger.
Local sepsis rarely follows if the precautions described be observed, and local douching is avoided. Any local fœtor—if not arising from the stomach—is generally traceable to some semi-detached fragment which can be removed from the posterior wall with a wire snare (Fig. 312) or a pair of forceps (Fig. 287).
Deafness, earache, and otitis media will sometimes follow the operation, even when the use of a nasal douche has been carefully avoided. They are best met by warm applications, disinfection of the ear with carbolic lotion (5%), and early incision of the drum under nitrous oxide gas.
Other methods of operation. Removal through the nasal chambers—the route originally used by Meyer for his ring-knife—is not to be recommended.
Treatment of the growth with the galvano-cautery, introduced through the mouth, is difficult, risky, and unsatisfactory.
The use of Loewenberg’s forceps, or some modification (Fig. 287), is generally abandoned by any one who has become accustomed to the Gottstein’s curette. A small pair of forceps is, however, very serviceable in quite young children in whom the post-nasal space may be so small as to prevent the manœuvring of any form of curette.
The position with the extended head over the end of the table—Rose’s position—increases the congestion and hæmorrhage, and by throwing forward the cervical vertebræ makes the approach to the roof of the naso-pharynx more difficult.
OPERATIONS UPON THE FEMALE GENITAL ORGANS
ABDOMINAL
gynæcological operations, 1
after-treatment of, 93
complications following, 95
hysterectomy, 36
risks of, 45
myomectomy, 46
ABSCESS OF BARTHOLIN’S GLANDS
incision of, 142
ADENOMYOMA OF UTERUS, 56
ADHESIONS IN OVARIOTOMY, 12
ANÆSTHETIC FOR CŒLIOTOMY, 6
ANTERIOR COLPOTOMY, 145
ATRESIA OF HYMEN AND VAGINA
operations for, 143
AUVARD’S SPECULUM, 136
AVELING’S SIGMOID REPOSITOR, 151
BARTHOLIN’S GLANDS
operations upon, 142
BED-SORES AFTER CŒLIOTOMY, 95
BELATED OVARIES
fate of, 56
BLADDER
injuries during hysterectomy, 111
operations upon, 134
BROAD-LIGAMENT CYSTS
removal of, 14
CÆSAREAN SECTION, 69
CANCER
of body of uterus, abdominal hysterectomy for, 63
vaginal hysterectomy for, 168
and fibroids, 52
cervix with pregnancy, 82
cicatrix after cœliotomy, 121
Fallopian tube, operation for, 26
ovary, ovariotomy for, 15
uterus after bilateral ovariotomy, 55
CAPSULES
spurious, in ovariotomy, 15
CARCINOMA (see Cancer)
CARUNCLE, URETHRAL
extirpation of, 134
CERVIX
cancer of, in pregnancy, 82
dilatation of, rapid, 156
gradual, 159
fibroids, hysterectomy for, 42
hypertrophy of, operations for, 160
CHRONIC UTERINE INVERSION
reposition of, 151
CICATRIX
after cœliotomy, 120
cancer of, 121
CŒLIOTOMY, 3
COLPOTOMY, 144
anterior, 145
posterior, 147
COMPLETE LACERATION OF PERINEUM, 127
COMPOUND PREGNANCY, 33
CURETTAGE, 152
CYST
of Bartholin’s glands, removal of, 142
broad ligament, 14
CYSTOCELE
operations for, 140
DABS FOR CŒLIOTOMY, 5
DÉDOUBLEMENT
Walcher’s, 137
DILATATION
of cervix, 156
vulval orifice, 143
DILATORS, HEGAR’S, 153
DUDLEY
operation upon perineum, 134
DÜHRSSEN
trachelorrhaphy, 163
EMBOLISM, PULMONARY
after abdominal section, 101
EMMETT’S
hook, 136
scissors, 162
trachelorrhaphy, 161
ENUCLEATION OF FIBROIDS, 46
EXTIRPATION OF URETHRAL CARUNCLE, 134
EXTRA-UTERINE GESTATION
operation for, 29
results of operation, 34
FALLOPIAN TUBE
operation for cancer of, 26
FIBROIDS
abdominal hysterectomy for, 61
cancer of uterus and, 52
cervix, hysterectomy for, 42
enucleation of, 46
hysterectomy for, 61, 173
interstitial, vaginal removal of, 167
pedunculated, vaginal removal of, 165
and pregnancy, 77
red degeneration of, 78
sessile, vaginal removal of, 166
vaginal hysterectomy for, 173
FISTULA
juxta-cervical, operation for, 139
recto-vaginal, operation for, 139
vesico-utero-vaginal, operation for, 139
FOREIGN BODIES LEFT IN ABDOMEN, 105
GALABIN’S
broad-ligament needle, 169
GASTRIC ULCER
perforating after cœliotomy, 111
GESTATION, EXTRA-UTERINE
operations for, 29
GLANDS, BARTHOLIN’S
operations upon, 142
GYNÆCOLOGICAL
operations, abdominal, 1
vaginal, 125
uterine injuries, operations for, 86
HÆMORRHAGE AFTER CŒLIOTOMY, 97
HEGAR’S
dilators, 153
operation for hypertrophy of cervix, 160
HYMEN
operation for atresia of, 143
HYPERTROPHY OF CERVIX
operations for, 160
HYSTERECTOMY, ABDOMINAL, 46
subtotal, 36
total, 40
in bifid uterus, 44
after bilateral ovariotomy, 17
for adenomyoma, 56
for cancer of body of uterus, 63
cervix, 61
for fibroids, 61
Wertheim’s operation, 62
HYSTERECTOMY, VAGINAL
for cancer, 168
fibroids, 173
HYSTEROPEXY
abdominal, 66
vaginal, 164
HYSTEROTOMY, 46
INCISION OF ABSCESS OF BARTHOLIN’S GLANDS, 142
INCONTINENCE OF URINE FOLLOWING LABOUR
operations for, 134
INJURIES OF UTERUS
operations for, 86
INJURY
to bladder during pelvic operations, 111
gravid uterus during abdominal operations, 89
intestines during gynæcological operations, 109
ureter during pelvic operations, 112
INTERSTITIAL UTERINE FIBROIDS
vaginal removal of, 167
INTESTINAL OBSTRUCTION
after pelvic operations, 110
INTESTINES
injuries to during gynæcological operations, 109
INTRAPELVIC HÆMORRHAGE
after cœliotomy, 98
JESSETT’S
broad-ligament needle, 169
JUXTA-CERVICAL FISTULA
operations for, 139
KRAUROSIS, POST-OPERATIVE, 120
LACERATIONS
of pelvic floor, repair of, 132
perineum, repair of, 127
LATERAL COLPOTOMY, 148
LIGAMENT, BROAD (see Broad ligament)
LIGATURES
fate of, in pelvic operations, 117
MACKENRODT
vesico-vaginal fistula operation, 138
MARCKWALDT
operation for hypertrophy of cervix, 160
MARTIN’S
trochar, 147
vesico-vaginal fistula operation, 137
MENSTRUATION AND PELVIC OPERATIONS, 4
METROSTAXIS
after gynæcological operations, 95
MYOMECTOMY
abdominal, 46
vaginal, 167
OBSTETRIC UTERINE INJURIES
operations for, 87
OÖPHORECTOMY, 21
hysterectomy after bilateral, 25
OPERATING TABLES, 6
OVARIAN TUMOURS
and pregnancy, 74
removal of (see Ovariotomy)
OVARIES, BELATED
fate and value of, 56
OVARIOTOMY, 10
adhesions in, 12
anomalous, 16
for cancer of ovary, 15
at extremes of life, 18
incomplete, 16
in infants, 18
during labour, 75
mortality of, 19
pregnancy after, 17
during puerperium, 76
repeated, 17
spurious capsules in, 15
OVARY, REMOVAL OF (see Oöphorectomy)
PARALYSIS, POST-ANÆSTHETIC, 95
PARAVAGINAL SECTION, 148
PAROTITIS
following abdominal operations, 99
PASSAGE OF UTERINE SOUND, 149
PÉAN’S RETRACTOR, 145
PEDICLE IN OVARIOTOMY
treatment of, 12
PELVIC FLOOR
repair of laceration of, 132
PELVIC OPERATIONS
complications during, 111
PELVIC TUMOURS
during pregnancy, 83
PERINEUM
repair of lacerations of, 127
PNEUMONIA
after abdominal operations, 99
POST-ANÆSTHETIC PARALYSIS, 95
POSTERIOR COLPOTOMY, 147
POZZI’S RETRACTOR, 145
PREGNANCY
after bilateral ovariotomy, 17
bullet wounds of uterus during, 90
with cancer of cervix, 82
compound, operations for, 82
and fibroids, 79
injury to uterus during, 89
operations upon uterus during, 69
and ovarian tumours, 74
and pelvic tumours, 83
PREPARATIONS FOR VAGINAL OPERATIONS, 125
PUERPERAL SEPSIS
operations for, 83
PUERPERIUM
ovariotomy during, 76
PULMONARY EMBOLISM
after abdominal operations, 101
RECTO-VAGINAL FISTULA
repair of, 139
RED DEGENERATION IN FIBROIDS, 78
REPOSITION OF CHRONIC UTERINE INVERSION, 151
RETRACTOR
Péan’s, 145
Pozzi’s, 145
RICARD
uretero-neo-cystostomy, 114
SARCOMA OF UTERUS
hysterectomy for, 53
SEPSIS, PUERPERAL
operations for, 83
SIGMOID REPOSITOR, AVELING’S, 151
SIMS’S
speculum, 136
vaginal rest, 144
SOUND, UTERINE
passage of, 149
SPECULUM
Auvard’s, 136
Sims’s, 136
SPURIOUS CAPSULES IN OVARIOTOMY, 15
STABS OF PREGNANT UTERUS, 91
STERILIZATION
after Cæsarean section, 71
STOLTZ
cystocele operation, 140
SUBTOTAL HYSTERECTOMY, 36
relative value of, 50
SUTURES FOR CŒLIOTOMY, 5
SWAFFIELD
closure of wounds, 9
TAIT, LAWSON
oöphorectomy, 21
operation for extra-uterine gestation, 29
TENTS
dilatation of cervix by, 160
TETANUS
after gynæcological operations, 107
THROMBOSIS
after abdominal section, 101
TOTAL HYSTERECTOMY, 40
relative value of, 50
TRACHELORRAPHY
Emmett’s, 161
Dührrsen’s, 163
TUMOURS
ovarian, during pregnancy, 74
pelvic, during pregnancy, 83
ULCER
gastric perforating, after cœliotomy, 111
URETER
injury to during pelvic operations, 112
URETERO-NEO-CYSTOSTOMY, 114
URETHRA, FEMALE
operations upon, 134
URETHRAL CARUNCLE
extirpation of, 134
UTERINE SOUND
passage of, 149
UTERUS
operations upon (see individual operations)
adenomyoma of, 86
bullet wounds of pregnant, 90
cancer of body with fibroids, 52
after ovariotomy, 55
chronic inversion of, reposition of, 151
compound pregnancy, 82
fibroids and pregnancy, 77
fibro-myomata, operations for, 46, 165
gynæcological injuries to, 86
pregnant, injuries to, 91
wounds of, 89, 91
VAGINA
atresia of, operations for, 143
operations upon, 142
VAGINAL
cœliotomy, 144
gynæcological operations, 125
hysterectomy, for cancer, 168
fibroids, 173
hysteropexy, 164
myomectomy, 167
rest, Sims’s, 136
VENTRO-FIXATION OF UTERUS, 67
VENTRO-SUSPENSION OF UTERUS, 66
VESICO-UTERO-VAGINAL FISTULA
repair of, 139
VESICO-VAGINAL FISTULA
repair of, 135
VISCERA, MISPLACED
in cœliotomy, 8
VULVA
operations upon, 142
dilatation of, 143
WALCHER
dédoublement, 137
WERTHEIM
hysterectomy, 62
WOUNDS OF PREGNANT UTERUS, 90
OPHTHALMIC OPERATIONS
ABSCESS
lachrymal, incision of, 297
orbital, 301
ACTIVE (CICATRICIAL) ECTROPION
operations for, 284
ADRENALIN
in ophthalmic operations, 178
ADVANCEMENT
of levator palpebræ, 272
ocular muscles, 251
AFTER-TREATMENT OF OPERATIONS IN GENERAL, 180
ANÆSTHETICS, 177
ANKYLOBLEPHARON
operations for, 264
ANTERIOR
chamber, evacuation of, 194
paracentesis of, 233
sclerotomy, 228
synechiæ, division of, 227
APERTURE, PALPEBRAL
operations upon, 265
ARGYLL ROBERTSON
ectropion operation, 282
ARLT
entropion operation, 278
ATTACHMENT
of lid to occipito-frontalis, 268
BANDAGES, EYE, 186
BRUDENELL CARTER
iridectomy, 217
BUROW
entropion operation, 276
CALCAREOUS FILMS
scraping, 243
CANAL, LACHRYMAL
operations upon, 290
CANALICULI
dilatation of, 290
incision of, 291
obliteration of, 294
CANTHOPLASTY, 265
CANTHORRHAPHY, 265
CAPSULE OF LENS
evulsion of, 195
CAPSULOTOMY, 192
CATARACT
needling of, 189
secondary, operations for, 192
CAUTERIZATION OF CORNEA, 240
CHAMBER, ANTERIOR (see Anterior chamber)
CICATRICIAL ECTROPION
operations for, 284
COCAINE
sterilization of, 182
CONGENITAL GLAUCOMA
iridectomy for, 219
CONICAL CORNEA
operations for, 241
CONJUNCTIVA
expression of, 245
removal of foreign bodies from, 244
CONJUNCTIVOPLASTY, 245
CONTRACTED SOCKET
operations for, 260
CORNEA
cauterization of, 240
conical, operations for, 241
operations upon, 240
removal of foreign bodies from, 240
tattooing the, 243
tumours, removal of, 243
CORNEAL TUMOURS
removal of, 243
COUCHING, 209
CYCLO-DIALYSIS, 229
CYSTOID SCAR
after iridectomy, 184
CYSTS, TARSAL
removal of, 246
DE VINCENTIIS’ OPERATION, 287
DENONVILLIERS
ectropion operation, 285
DIEFFENBACH’S OPERATION, 288
DILATATION OF CANALICULI, 290
DISCISSION OF THE LENS, 189
DIVISION
of anterior synechiæ, 227
tarsal cartilage for entropion, 276
DUCT, LACHRYMAL
probing and syringing, 292
ECTROPION OPERATIONS, 279
ELECTRO-CAUTERY OPERATION FOR CONICAL CORNEA, 242
ELECTROLYSIS FOR TRICHIASIS, 275
ELECTRO-MAGNET OPERATIONS, 237
ENTROPION OPERATIONS, 275
ENUCLEATION
of the globe, 255
EVACUATION
of the anterior chamber, 194
EVISCERATION
of the globe, 257
orbit, 301
EVULSION
of the lens capsule, 195
EXCISION
of apex of conical cornea, 241
lachrymal sac, 294
EXPLORATION
of the orbit (Krönlein’s), 299
EXPRESSION
of the conjunctiva, 245
EXTRACTION
of foreign bodies from conjunctiva, 244
from cornea, 240
globe, 237
lens, 195
EXTRA-OCULAR MUSCLES
operations upon, 247
EYELIDS
operations upon, 263
EYE-SOCKET
contracted, operations upon, 261
paraffin injections into, 260
FERGUS
ectropion operation, 281
plastic operation upon eyelid, 267
FILMS
calcareous, scraping, 243
FIXATION FORCEPS, 190
FLAPS
transplantation of for ectropion, 284
FOREIGN BODIES
in conjunctiva, 244
cornea, 240
globe, 237
FRICKE
plastic eyelid operation, 285
FROST’S OPERATION, 259
GIANT ELECTRO-MAGNET OPERATIONS, 238
GLAND, LACHRYMAL
excision of, 298
GLAUCOMA
iridectomy for, 217
GLOBE
direction of incisions in, 183
enucleation of, 255
evisceration of, 257
Frost’s operation upon, 259
Mules’s operation upon, 259
operations for penetrating wounds of, 234
wounds in, 182
GRAFTING SUPERIOR RECTUS INTO LID, 273
HANDS
sterilization of, 182
HARMAN
ptosis operation, 269
HEINE
cyclo-dialysis, 229
HESS
ptosis operation, 268
INCISION
of the canaliculi, 291
into the globe, 183
INJECTION
of paraffin into eye-socket, 260
INSERTION OF STYLES, 293
INSTRUMENTS
sterilization of, 183
IRIDECTOMY, 214
for glaucoma, 217
growths of iris, 225
optical, 214
Brudenell Carter’s, 217
for prolapse of iris, 225
IRIDOTOMY, 211
Kuhnt’s, 212
Ziegler’s, 213
IRIS
iridectomy for growths of, 225
operations upon, 211
prolapse of, iridectomy for, 225
transfixion of, 226
IRRIGATION
delivery of lens by, 203
KRÖNLEIN
exploration of orbit, 299
KUHNT
ectropion operation, 281
iridotomy, 299
LACHRYMAL
abscess, opening of, 297
canals, obliteration of, 294
operations upon, 290
duct, probing, 292
syringing, 292
gland, operations upon, 298
sac, excision of, 294
LANG’S SPECULUM, 181
LASH-BEARING AREA
transplantation of, 278
LENS
capsule, evulsion of, 195
delivery of, by irrigation, 203
discission of, 189
extraction of, 195
operations upon, 187
surgical anatomy of, 187
LEVATOR PALPEBRÆ
advancement of, 272
LID MARGIN
suture of wounds of, 264
LIDS
operations upon, 263
LOCAL PREPARATION OF PATIENT FOR OPERATION, 180
MCKEOWN
removal of lens, 203
MAGNET, ELECTRO-, OPERATIONS, 237
MAXWELL
contracted socket operation, 261
MOTAIS
ptosis operation, 273
MULES’S OPERATION, 259
MUSCLES, EXTRA-OCULAR
operations upon, 247
MYOPIA
discission of lens in, 190
NEEDLING OF THE LENS, 189
OBLITERATION
of the canaliculi, 294
lachrymal canals, 294
OCULAR MUSCLES
advancement of, 251
tenotomy of, 248
OPERATING
tables, 180
theatres, 179
OPERATIONS
general preliminaries, 177
OPTICAL IRIDECTOMY, 214
ORBIT
abscess of, 301
evisceration of, 301
exploration of, 299
operations upon, 299
plastic operations upon, 260
ORBITAL
abscess, opening, 301
portion of lachrymal gland, removal of, 299
PAGENSTECHER’S SPOON, 196
PALPEBRAL
aperture, operations, upon, 265
portion of lachrymal gland, removal of, 298
PANAS
ptosis operation, 271
PARACENTESIS
of anterior chamber, 233
PARAFFIN INJECTIONS
into eye-socket, 260
PASSIVE ECTROPION
operations for, 280
PENETRATING WOUNDS
of the globe, 234
PLASTIC OPERATIONS
upon the eyelids, 287
orbit, 260
POSTERIOR SCLEROTOMY, 232
PREPARATIONS FOR EYE OPERATIONS, 177
PRIMARY GLAUCOMA
iridectomy for, 218
PROBING LACHRYMAL DUCT, 292
PROLAPSE OF IRIS
iridectomy for, 225
PTERYGIUM
operations for, 244
PTOSIS OPERATIONS, 267
PURIFICATION OF EYE, 181
RECTIFICATION
of faulty curve of tarsus, 276
REMOVAL
of eye, operations upon socket after, 260
foreign bodies from conjunctiva, 244
from cornea, 240
globe, 236
SAC, LACHRYMAL
excision of, 294
SCLERECTOMY, 231
SCLEROTOMY
anterior, 228
posterior, 232
SCRAPING CALCAREOUS FILMS, 243
SECONDARY
cataract, operations for, 192
glaucoma, iridectomy for, 219
SEPSIS
after intra-ocular operations, 181
SKIN-GRAFTING
for contracted socket, 261
ectropion, 287
SKIN AND MUSCLE ENTROPION OPERATION, 275
SNELLEN’S SUTURES, 280
SOCKET, CONTRACTED
operation for, 261
operations upon after removal of eye, 260
SPECULUM, LANG’S, 181
SQUINT OPERATIONS, 247
STREATFIELD’S OPERATION, 277
STERILIZATION
of cocaine, 182
instruments, 183
STYLES
insertion of, 293
SURGICAL ANATOMY
of glaucoma, 217
lens, 187
SUTURE OF WOUNDS OF LIDS, 263
SUTURES, SNELLEN’S, 280
SYNECHIÆ, ANTERIOR
division of, 227
SYMBLEPHARON OPERATIONS, 264
SYRINGING
lachrymal duct, 292
TARSAL CARTILAGE
division of, for entropion, 276
TARSAL CYSTS
removal of, 246
TARSORRHAPHY, 266
TATTOOING THE CORNEA, 243
TENOTOMY
of ocular muscles, 248
THEATRES, OPHTHALMIC, 179
THIERSCH
skin-grafting for ectropion, 287
TRANSFIXION
of the iris, 226
TRANSPLANTATION
of the lash-bearing area, 278
TRICHIASIS
operations for, 275
TUMOURS
corneal, removal of, 243
UNDINE, 182
VECTIS, 196
VY OPERATION FOR ECTROPION, 284
WHARTON JONES
ectropion operation, 284
WOUNDS
of eyelids, suture of, 263
globe, 234
ZIEGLER
iridotomy, 213
OPERATIONS UPON THE EAR
ABSCESS
extra-dural, operations for, 431
Bezold’s mastoid, operations for, 389
cerebellar, opening of, 467
cerebral, opening of, 459
intracranial, operations for, 459
subperiosteal mastoid, operation for, 389
temporo-sphenoidal, opening of, 463
ADHESIONS, INTRATYMPANIC
division of, 342
ANÆSTHESIA
in aural operations, 310
ANÆSTHETIC SOLUTIONS
Neumann’s, 311
ANATOMY
of the labyrinth, 420
mastoid area, 373
ATRESIA
of the external auditory canal, operations for, 330
ATTIC
syringing out of the, 308
AUDITORY CANAL, EXTERNAL
operations upon, 314
for atresia, 330
stenosis, 328
removal of exostoses from, 316
foreign bodies from, 322
polypi from, 331
AURAL
instrument, Burkhardt-Merian’s, 315
mirror, 305
polypus, removal of, 333
specula, 306
BEZOLD’S MASTOID ABSCESS
operation for, 389
BOUGIE, EUSTACHIAN
passage of, 369
BULB
jugular, exposure of, 454
BURKHARDT-MERIAN’S AURAL INSTRUMENT, 315
CANAL, AUDITORY (see Auditory canal)
CANULA
Hartmann’s, 308
Milligan’s, 308
CATH[ET]ERIZATION
of Eustachian tube, 364
CAUTERIZATION
of granulations in tympanum, 348
CEREBELLAR OTITIC ABSCESS
opening of, 467
CEREBRAL OTITIC ABSCESS
opening of, 459
CLAR’S LAMP, 305
CLEANSING OF EAR, 307
COCHLEA
removal of, 424
COMPLETE MASTOID OPERATION, 391
CURETTING
of aural polypi, 334
labyrinth, 421
tympanic granulations, 348
DILATATION
of external meatus, 328
DIVISION
of anterior tympanic ligament, 341
intratympanic adhesions, 342
posterior tympanic fold, 341
EAR
cleansing of, 307
EUSTACHIAN BOUGIE
passage of, 369
EUSTACHIAN TUBE
catheterization of, 364
lavage of tympanum through, 372
EXAMINATION OF EAR
methods of, 305
EXCISION
of stricture of external meatus, 329
EXOSTOSES
removal of from external meatus, 316
EXPOSURE
of the jugular bulb, 454
vein, 448
lateral sinus, 440
EXTERNAL AUDITORY CANAL (see Auditory canal, external)
EXTERNAL MEATUS
operations for stenosis of, 328
removal of exostoses from, 316
EXTIRPATION OF LABYRINTH, 425
EXTRA-DURAL ABSCESS
operations for, 431
FOREIGN BODIES
in ear, removal of, 322
FURUNCULOSIS
of ear, operations for, 314
GALVANO-CAUTERY PERFORATION
of tympanic membrane, 340
GENERAL ANÆSTHESIA
in aural operations, 310
GRANULATIONS
in tympanum, removal of, 348
GRUNERT
operation on the jugular bulb, 454
HARTMANN’S CANULA, 308
ILLUMINATION
in aural examinations, 305
INCISION
of external auditory meatus, 328
Wilde’s mastoid, 377
INCUS
removal of, 351
INTRACRANIAL OTITIC ABSCESS
operations for, 459
after-treatment of, 469
complications of, 469
prognosis and results in, 470
recurrence of symptoms after, 471
INTRATYMPANIC OPERATIONS, 342
JUGULAR BULB
exposure of, 454
JUGULAR VEIN
ligature of, 446
KNIFE
paracentesis, 340
KÖRNER
post-meatal flaps, 402
KÜSTER-BERGMANN
mastoid operation, 393
LABYRINTH
operations upon, 417
curetting, 421
extirpation of, 425
surgical anatomy of, 420
LABYRINTHITIS
non-suppurative, operation for, 417
LAMP, CLAR’S, 305
LATERAL SINUS THROMBOSIS
operations for, 439
comparison of operations, 457
complications following, 458
difficulties and dangers in, 457
exposure of jugular bulb, 454
exposure of sinus, 440
Grunert’s operation for, 454
ligature of jugular vein for, 446
Piffl’s operation for, 455
opening of sinus, 442
prognosis in, 458
LAVAGE OF TYMPANUM, 372
LIGAMENT, ANTERIOR TYMPANIC
division of, 341
LIGATURE
of aural polypus, 333
jugular vein, 446
LOCAL ANÆSTHESIA, 310
MALLEUS
direct massage of, 349
and incus, removal of, 351
MASSAGE
direct, of malleus, 349
stapes, 350
MASTOID
abscess, Bezold’s, 389
subperiosteal, 389
area, anatomy of, 373
necrosis of, operation for, 390
operation, the complete, 391
closure of the wound after, 404
history of the, 375
in an infant, 389
Küster-Bergmann method, 393
post-meatal flaps, use of, 401
preservation of ossicles and tympanic membrane after, 399
for removal of foreign bodies from ear, 327
Schwartze’s method, 378
skin-grafting after, 405
Stacke’s method, 397
for stenosis of external auditory canal, 330
for subperiosteal abscess, 389
Wilde’s incision in, 377
Wolf’s method, 396
process, operations upon, 373
osteomyelitis of, 390
MEATUS, EXTERNAL (see External meatus)
MEMBRANE, TYMPANIC (see Tympanic membrane)
MENINGITIS, OTITIC
operations for, 433
after-treatment of, 436
prognosis and results, 438
MILLIGAN’S CANULA, 308
MIRROR, AURAL, 305
MOBILIZATION OF THE OSSICLES, 349
NECROSIS
of mastoid, operation for, 390
NEUMANN’S
anæsthetic solutions, 311
method of opening vestibule, 424
syringe, 311
OPENING OF LATERAL SINUS, 442
OSSICLES
operations upon the, 349
massage of the, 349, 356
mobilization of the, 349
preservation of the, after mastoid operation, 399
removal of the, 351, 361
OSTEOMYELITIS OF MASTOID
operation for, 390
PANSE
post-meatal flaps, 402
PARACENTESIS TYMPANI, 336
knife for, 340
PIFFL
operation upon the jugular bulb, 454
POLITZER
division of anterior tympanic ligament, 341
POLYPUS, AURAL
operations for, 331
POST-AURAL OPERATION (see Mastoid operation)
POST-MEATAL FLAPS, 401
REMOVAL
of the cochlea, 424
ossicles, 351, 361
foreign bodies from the ear, 322
SCHWARTZE
mastoid operation, 378
SINUS, LATERAL (see Lateral sinus)
SKIN FLAPS
post-meatal, 401
SKIN-GRAFTING
after mastoid operation, 405
SNARE, WILDE’S, 332
SPECULA, AURAL, 306
STACKE
mastoid operation, 397
post-meatal flaps, 402
STAPEDIUS
tenotomy of, 347
STAPES
massage of, 350
STENOSIS OF EXTERNAL MEATUS
operations for, 328
SUBPERIOSTEAL MASTOID ABSCESS
operations for, 389
SURFACE ANATOMY
of mastoid process, 375
SURGICAL
anatomy of labyrinth, 420
mastoid area, 373
tympanic cavity, 335
toilet of ear, 309
SYRINGING
out of attic, 308
ear, 308
for removal of foreign bodies, 322
TEMPORO-SPHENOIDAL ABSCESS
opening, 463
TENOTOMY
of tensor tympani, 346
stapedius, 347
TENSOR TYMPANI
tenotomy of, 346
THROMBOSIS OF LATERAL SINUS
operations for (see Lateral sinus thrombosis)
TOD’S POST-MEATAL FLAPS, 401
TREPHINING
for otitic cranial abscess, 462
TUBE, EUSTACHIAN (see Eustachian tube)
TYMPANIC CAVITY
lavage of, 372
operations within, 335
surgical anatomy of, 335
TYMPANIC FOLD
posterior, division of, 341
TYMPANIC GRANULATIONS
curetting of, 348
TYMPANIC MEMBRANE
artificial perforation of, 340
division of anterior ligament of, 341
post. tympanic fold, 341
paracentesis of, 336
preservation of after mastoid operation, 399
surgical anatomy of, 335
TYMPANUM (see Tympanic cavity)
VEIN, JUGULAR (see Jugular vein)
VESTIBULE
opening the, 422
WILDE
mastoid incision, 377
snare, 332
WOLF
complete mastoid operation, 396
OPERATIONS UPON THE THROAT
ANÆSTHESIA
for direct laryngoscopy, 482
laryngotomy, 512
thyrotomy, 489
tracheotomy, 544
ANATOMY
of laryngeal lymphatics, 496
the trachea, 523
BRONCHOSCOPY
lower, 562
upper, 562
BUTLIN
after-treatment in thyrotomy, 494
laryngectomy operations, 507
CHIARI
total laryngectomy, 502
CRICO-TRACHEOTOMY, 529
CUNEO
anatomy of laryngeal lymphatics, 496
CURES AFTER THYROTOMY, 505
DIPHTHERIA
tracheotomy for, 517, 526
DIRECT LARYNGOSCOPY
Killian’s method, 479
ENDOLARYNGEAL
operations, 475
removal of multiple papillomata, 485
EXTRA-LARYNGEAL OPERATIONS, 487
FEEDING AFTER THYROTOMY, 494
FÖDERL
total laryngectomy, 502
GLUCK
total laryngectomy, 500
HANDLEY
total laryngectomy, 502
HEMI-LARYNGECTOMY, 495
mortality after, 506
recurrence after, 506
HIGH TRACHEOTOMY, 530
INDIRECT LARYNGOSCOPY, 477
INFRATHYREOID LARYNGOTOMY, 510
INTUBATION, 549
of the larynx, 549
v. tracheotomy in diphtheria, 549
KILLIAN
direct laryngoscopy, 479
LAMP
for direct laryngoscopy, 480
LARYNGEAL LYMPHATICS
anatomy of, 496
LARYNGEAL STENOSIS
after tracheotomy, 538
LARYNGECTOMY, TOTAL, 498
Butlin’s cases, 507
Chiari’s cases, 502
Föderl’s cases, 502
Gluck’s operation, 500
Handley’s cases, 502
Le Bec’s cases, 502
mortality after, 506
recurrence after, 507
swallowing after, 509
voice after, 508
LARYNGO-FISSURE
for removal of multiple papillomata, 485
LARYNGOSCOPY
direct, 479
indirect, 477
LARYNGOTOMY
infrathyreoid, 510
LARYNX
intubation of, 549
LE BEC
total laryngectomy, 502
LOW TRACHEOTOMY, 532
LOWER BRONCHOSCOPY, 562
LYMPHATICS, LARYNGEAL
anatomy of, 496
MEDIAN TRACHEOTOMY, 532
MORTALITY
after hemi-laryngectomy, 506
total laryngectomy, 506
thyrotomy, 504
PAPILLOMATA, MULTIPLE
removal of, 484
PRELIMINARY TRACHEOTOMY, 523
RECURRENCE
after hemi-laryngectomy, 506
total laryngectomy, 507
thyrotomy, 505
REMOVAL OF TUBE AFTER TRACHEOTOMY, 535
RESECTION OF TRACHEA, 547
SKIAGRAPHY
in endolaryngeal operations, 476
STENOSIS
after tracheotomy, 538
SWALLOWING
after total laryngectomy, 509
THYROTOMY, 487
complications in, 494
cures after, 505
feeding after, 494
mortality after, 504
recurrence after, 505
TOTAL LARYNGECTOMY, 498
TRACHEA
anatomy of, 523
operations upon, 517
resection of, 547
TRACHEO-FISSURE, 547
TRACHEOSCOPY
indications for, 558
TRACHEOTOMY, 517
accidents during, 533
after-treatment of, 534
complications of, 536
for diphtheria, 517, 526
high, 530
intubation v., 549
local anæsthesia for, 544
low, 532
median, 532
preliminary, 523
for removal of multiple papillomata, 485
stenosis after, 538
TUBE SPATULÆ
for direct laryngoscopy, 480
TUBE, TRACHEOTOMY
removal of, 535
TUMOURS, ENDOLARYNGEAL, 475
UPPER BRONCHOSCOPY, 562
VOICE AFTER TOTAL LARYNGECTOMY, 508
OPERATIONS UPON THE NOSE AND NASO-PHARYNX
ABSCESS
retropharyngeal, 664
of septum, operation for, 612
ADENOIDS
removal of, 665
ADRENALIN
in nasal operations, 573
AFTER-RESULTS OF OPERATIONS, 580
AIR-PASSAGES, LOWER
protection of during operations, 576
AMPUTATION
of anterior end of inferior turbinal, 587
lower margin of inferior turbinal, 588
posterior end of inferior turbinal, 589
ANÆSTHESIA
for complete turbinotomy, 591
local, 572
for removal of posterior end of inferior turbinal, 589
ANTRUM, MAXILLARY (see Maxillary sinus)
ASCH
operation upon the septum, 599
ASEPSIS, NASAL, 578
BLEEDING
control of, 574
BÖNNINGHAUS
operation upon the maxillary sinus, 637
BOND
preliminary laryngotomy in naso-pharyngeal operations, 663
BUTLIN
preliminary laryngotomy in naso-pharyngeal operations, 663
CALDWELL-LUC
operation upon the maxillary sinus, 631
CANINE FOSSA
operation through, 631
CATHETERIZING
frontal sinus, 638
maxillary sinus, 626
CHOANA, POSTERIOR
congenital occlusion of, 583
CLAR’S LAMP, 570
CLEANSING THE NOSE, 579
COCAINE
submucous injection of, 572
substitutes for, 573
COMPLETE TURBINOTOMY, 591
COMPLICATIONS FOLLOWING OPERATIONS, 577
CONGENITAL OCCLUSION
of nostrils, 582
posterior choana, 583
DEFORMITIES OF SEPTUM
operations for, 597
DENKER
operation upon the maxillary sinus, 625, 637
DESAULT
operation upon the maxillary sinus, 631
DEVIATION, SIMPLE, OF NASAL SEPTUM
operations for, 598
DIVISION OF THE SOFT PALATE
for removal of naso-pharyngeal growths, 663
ELEVATING OLD NASAL FRACTURES, 582
EUCAINE ANÆSTHESIA, 573
EXAMINATION OF NOSE
methods of, 569
FOREIGN BODIES
removal of, 584
FOSSA, CANINE (see Canine fossa)
FRACTURES, NASAL
operations for, 582
FRONTAL SINUS
catheterizing and washing out, 638
Killian’s external operation, 642
Kuhnt’s external operation, 653
Ogston-Luc external operation, 651
operation for suppuration in, 638
GLEASON-WATSON
operation upon the septum, 599
GROWTHS, NASAL
removal of, 616
HÆMATOMA OF SEPTUM
operation for, 612
HÆMORRHAGE
control of in nasal operations, 574
ILLUMINATION
for nasal operations, 569
INJURIES, NASAL
operations for, 581
ISCHÆMIA, LOCAL, 573
KILLIAN
frontal sinus operation, 642
KUHNT
frontal sinus operation, 653
LAMP, CLAR’S, 570
LARYNGOTOMY, PRELIMINARY
in naso-pharyngeal operations, 663
LATERAL RHINOTOMY (see Rhinotomy, lateral)
LOCAL
anæsthesia, 572
ischæmia, 573
MAXILLARY ANTRUM (see Maxillary sinus)
MAXILLARY SINUS
operations upon, 626
Bönninghaus’s operation upon, 637
Caldwell-Luc operation upon, 637
canine fossa, operation through, 631
catheterizing, 626
Denker’s operation upon, 625, 637
Desault’s operation upon, 631
operation through nasal wall, 637
puncturing, 626
radical operation upon, 631
MIDDLE TURBINAL
operations upon, 592
MOURE
lateral rhinotomy, 618
operation upon the septum, 599
NARES, ANTERIOR
congenital occlusion of, 582
NASAL BONES
operations for fracture of, 582
NASAL GROWTHS
removal of, 613
NASAL SEPTUM
abscess of, 612
deformities of, 597
hæmatoma of, operation for, 612
operations upon, 597
Asch’s operation, 599
Gleason-Watson’s operation, 599
Moure’s operation, 599
perforating the, 598
perforation of, operation for, 611
removal of spurs from, 597
simple deviation, operations for, 598
submucous resection of, 601
NASAL SYPHILIS
operations for the results of, 594
NASO-PHARYNX
adenoids, removal of, 665
examination of, 569
operations for direct access to, 618, 661
post-syphilitic affections of, 595
sequestrotomy in, 594
NOSE
methods of examining, 569
NOSTRILS
congenital occlusion of, 582
NOVOCAINE ANÆSTHESIA, 573
OCCLUSION OF NOSTRILS
congenital, 582
OGSTON-LUC
frontal sinus operation, 651
OPENING SPHENOIDAL SINUS, 656
PALATE, SOFT (see Soft palate)
PERFORATING THE SEPTUM, 598
PERFORATION OF THE SEPTUM
operation for, 611
POST-SYPHILITIC AFFECTIONS OF NOSE AND NASO-PHARYNX, 595
PROTECTION OF AIR-PASSAGES DURING OPERATIONS, 576
PUNCTURING
the maxillary sinus, 626
RADICAL OPERATION UPON THE MAXILLARY SINUS, 631
REMOVAL
of foreign bodies from nose, 584
nasal growths, 613
rhinoliths, 586
spurs from the nasal septum, 597
RESECTION OF THE SEPTUM
submucous, 601
RETROPHARYNGEAL ABSCESS, 664
RHINOLITHS
removal of, 586
RHINOTOMY
combined lateral and sublabial, 625
lateral, Moure’s, 618
sublabial, Rouge’s, 622
ROBINSON
operation for post-syphilitic affections of nose, 595
SEPSIS AFTER NASAL OPERATIONS, 577
SEPTUM (see Nasal septum)
SEQUESTROTOMY IN NOSE AND NASO-PHARYNX, 594
SHOCK DURING OPERATIONS, 577
SINUS, FRONTAL (see Frontal sinus)
SINUS, SPHENOIDAL (see Sphenoidal sinus)
SOFT PALATE
division of, for removal of naso-pharyngeal growths, 663
SOUNDING SPHENOIDAL SINUS, 653
SPENCER
operation for post-syphilitic affections of nose, 595
SPHENOIDAL SINUS
opening, 656
sounding and washing out, 653
SPURS OF SEPTUM
operations for, 597
SUBLABIAL RHINOTOMY
Rouge’s, 622
SUBMUCOUS
injection of cocaine, 572
resection of the septum, 601
SUPPURATION IN FRONTAL SINUS
operation for, 638
SYPHILIS, NASAL
operations for results of, 594
TILLEY
operation for post-syphilitic affections of nose, 595
TUBERCULOSIS OF THE NOSE, 596
TURBINALS
operations upon, 586
inferior, amputation of inferior end, 587
lower margin, 588
removal of posterior end, 589
middle, operations upon, 592
TURBINOTOMY, COMPLETE, 591
OXFORD: HORACE HART
PRINTER TO THE UNIVERSITY
1 Comyns Berkeley and Bonney have published the best immediate results of this operation which have been obtained in England. British Medical Journal, 1908, ii. 961, and Lancet, 1909, i. 320.
2 Bland-Sutton, J. On Perforation of the Stomach and Small Intestine as a Sequel to Ovariotomy and Hysterectomy. Journ. of Obstet. and Gyn. of the British Empire, 1909, xv.
3 Mayou, Hunterian Lectures, 1905.
4 For the other complications which may arise in passing a Graefe’s knife across the anterior chamber, see Glaucoma Iridectomy, p. 222.
5 Internat. Centralblatt für Laryngol., Jahrgang v u. vi, 1888–9, ‘Die Frage des Ueberganges gutartiger Kehlkopfgeschwülste in bösartige, speciell nach intralaryngealen Operationen.’
6 [The spelling of this word has been adopted in conformity with the Basle Anatomical Nomenclature.—Ed.]
7 Proc. Roy. Soc. Med. London, vol. i, No. 2, Laryn. Sect., p. 5.
8 Brit. Med. Journ., 1901, vol. ii, p. 883.
9 Ashby and Wright, Dis. of Child., 4th ed., p. 350.
10 Bergmann, E. von, Sys. Pract. Surg., vol. ii, p. 231.
11 Trans. Amer. Laryng. Assoc., 1907, p. 127. Discussion of paper by C. G. Coakley on ‘Removal of papillomata of larynx by direct instrumentation with the aid of Killian’s tubes.’
12 Brit. Med. Journ., 1905, vol. i, p. 6.
13 Op. Surg. Malig. Dis., 2nd ed., p. 191.
14 Poirier and Cuneo, Lymphatics, Eng. ed., 1903, p. 286.
15 De Santi, Malignant Disease of the Larynx, 1904, p. 10.
16 Proc. Roy. Soc. Med., London, vol. i, No. 4, 1908, Clin. Sect., p. 66.
17 An account of the history of these operations will be found in a paper by Sir F. Semon, Brit. Med. Journ., 1903, vol. ii, p. 1113.
18 Brit. Med. Journ., 1903, vol. ii, p. 1123.
19 Bergmann, E. von, Sys. Prac. Surg., vol. ii, p. 245.
20 Trans. Med. Soc., London, 1907, vol. xxx, p. 130.
21 Brit. Med. Journ., 1906, vol. ii, p. 1480.
22 Bergmann, E. von, Sys. Pract. Surg., vol. ii, p. 245.
23 Brit. Med. Journ., 1903, vol. ii, p. 1148.
24 Brit. Med. Journ., 1907, vol. i, p. 7.
25 Metropolitan Asylums Board’s Ann. Rep., Med. Supplement, 1902–1907.
26 Cheyne and Burghard, Manual of Surg. Treat., 1901, Pt. v, p. 449.
27 Tracheotomy in Laryngeal Diphtheria, 2nd ed., p. 42.
28 Bergmann, E. von, Sys. Pract. Surg., vol. ii, p. 270.
29 Nose and Throat, 1906, p. 94.
30 Trans. Med. Chirurg. Soc., vol. lxv, p. 85; vol. lxvii, p. 102.
31 Chirurg. Operat., 1907, p. 631.
32 Bergmann, E. von, Sys. Pract. Surg., vol. ii, p. 265.
33 Brit. Med. Journ., 1899, vol. i, p. 199, ‘On the Value of the Treatment of Diphtheria by Antitoxin.’
34 Trans. Amer. Laryng. Assoc., 1906, p. 264, ‘Tumours of the Trachea.’
35 Bergmann, E. von. Sys. Pract. Surg., vol. ii, p. 249.
36 Keen’s Surgery, 1908, p. 510.
37 New York Med. Journ., 1885, vol. xlii, p. 145.
38 Text Book of Surgery, 1900, vol. ii, p. 625.
39 Edin. Med. Journ., 1902, p. 235, ‘Observations on Intubation of the Larynx.’
40 Allbutt and Rolleston, Sys. of Med., 1905, vol. i, p. 1025.
41 Metropol. Asylums Board’s Ann. Rep., Med. Supplem., 1904, p. 319.
42 Diseases of the Nose and Throat, 1907, p. 726.
43 For a description of this method see Metropol. Asylums Board’s Ann. Rep., Med. Supplem., 1898, p. 187.
44 Operations of Surgery, 5th ed., vol. i, p. 640.
45 Trans. Amer. Laryng. and Otol. Soc., 1907, p. 80, ‘The Treatment of Foreign Bodies in the Respiratory Tract and Esophagus.’
46 Brit. Med. Journ., 1906, vol. ii, p. 357, ‘The Direct Examination of Œsophagus and Upper Air-passages.’
47 C. A. Parker, Diseases of the Nose and Throat, London, 1906.
48 Chevalier Jackson, Transactions American Laryngological Association, 1907.
49 G. W. Crile, Journal Amer. Med. Assoc., June 17, 1905.
50 W. H. Stewart, Proc. Laryngol. Soc. Lond., March 5, 1898, p. 57.
51 J. M. Renton, Brit. Med. Journ., December 16, 1905.
52 T. A. de Blois, Trans. Amer. Laryn. Association, 1900, p. 12.
53 G. K. Grimmer, Proc. Royal Soc. of Med. (Laryngol. Section) April, 1908.
54 Proc. Laryngol. Soc., London, vol. v, November, 1897, p. 4.
55 Ibid., vol. x, March 6, 1903, p. 81.
56 Ibid., vol. xiv, June, 1907, p. 106.
57 For bibliography and more detailed description, see StClair Thomson, Med.-Chir. Trans., vol. lxxxix, 1906; Lancet, July, 1906; and Brit. Med. Journ., vol. ii, 1906.
58 Annals of Otology, Rhinology, and Laryngology, June, 1905.
59 ‘As all operators who know it will confess, the Fensterresektion of the septum belongs to the most extremely difficult intranasal operations.’ Zarniko, Die Krankheiten der Nase, 1905, p. 300.
60 Beiträge zur Anatomie, &c. des Ohres, der Nase, und des Halses, Hefte 1–4, 1908.
61 The Laryngoscope, vol. xv, June, 1905, No. 5, p. 417.
62 The Laryngoscope, xvi, 1906, p. 879.
63 Revue hebd. de Laryn., 1903, xxiv, Nr. 46, November 14, p. 597.
64 La Tribune Médicale, 1905.
65 Proc. Laryn. Soc. Lond., 1907, xiv, p. 106.
66 Moure, Revue hebdomadaire de Laryngologie, October 4, 1902; Duverger, ibid., September 2, 1905.
67 Koenig. Soc. paris. de Laryn., 1905, 30 juin.
68 Logan Turner, Edinburgh Medical Journal, August, 1906, p. 152.
69 C. A. Parker, Brit. Med. Journ., October 10, 1908, p. 1099.
70 Logan Turner, ibid., p. 1096.
71 Proc. Royal Soc. Med., 1907, December.
72 Logan Turner, Edinburgh Medical Journal, 1905, March.
73 Die Komplikationen der Stirnhöhlenentzündungen, von P. H. Gerber, Berlin: S. Karger, 1908.
74 H. Tilley, Lancet, 1899, August 19, p. 534, and Edinburgh Medical Journal, 1905, March, in paper of Logan Turner’s.
75 A successful case is reported, Proc. Roy. Soc. of Med., Lond., 1908, June meeting, by L. V. Cargill, William Turner, and the writer.
76 Annales des Maladies de l’Oreille, 1905, juillet, ii. 72.
77 Ibid., 1904, XXX. vi. 579.
78 Ogston, The Medical Chronicle, 1884, December.
79 Luc, Société Française d’Otologie, Paris, 1896, mai.
80 StClair Thomson, The Practitioner, 1906, July.
81 Logan Turner, Edinburgh Medical Journal, 1907, November and December.
82 Lermoyez, Annales des Maladies de l’Oreille, 1902, novembre.
83 H. L. Lack, Edinburgh Medical Journal, 1902, June, p. 542.
84 Transactions of the American Laryngological Association, 1895, p. 91.
85 Ibid., 1903, p. 241.
86 Proceed. Royal Society of Medicine, Meeting of June, 1908.
87 The Laryngoscope, xiv, 1904, p. 267.
88 M. A. Goldstein, ibid., xviii, January, 1908, p. 46.
89 George E. Waugh, The Lancet, September 29, 1906.
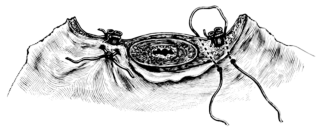
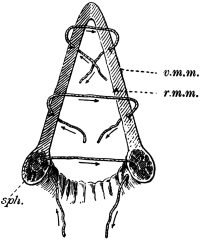

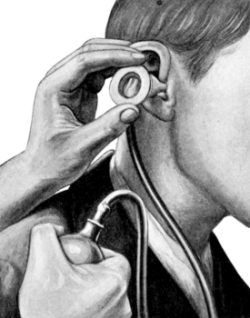
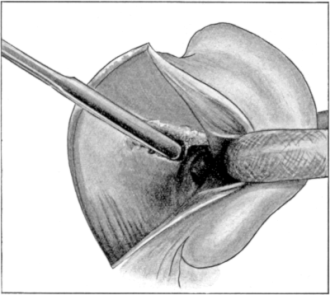
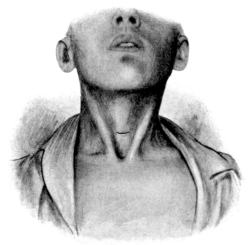

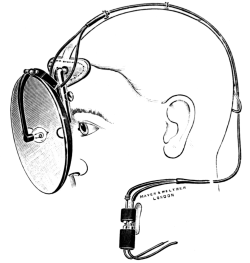
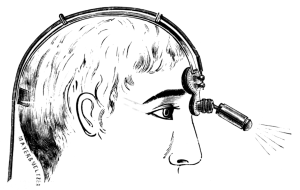

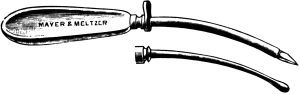
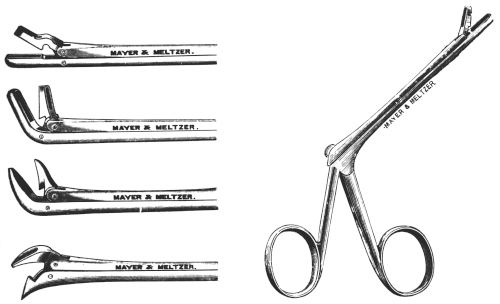
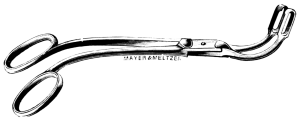
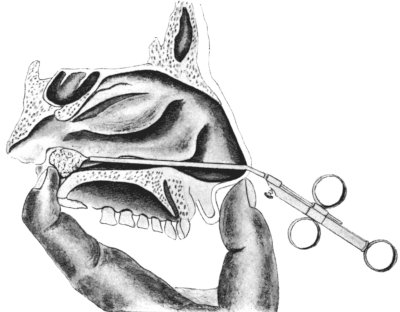

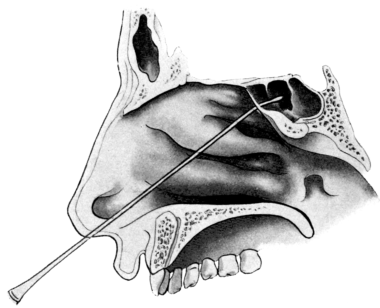

{kind=link}
{kind=link}
{kind=link}