Transcriber’s notes:
In this HTML version, page numbers are listed in the right margin,
hyperlinks are indicated by a dotted underline, and transcriber comments
are marked by a red dashed underline; scrolling the mouse over such
words will reveal the original text. Footnote markers in the text are
hyperlinked to the footnotes located at the end of the book.
The book contains numerous spelling inconsistencies. No change has been
made to those representing archaic spellings (e.g. somethimes, urin,
feavers, joynts) and those occurring in quotations. Spelling
variants occurring with similar frequency have been left in their
original form (e.g. Röntgen/Roentgen, rachitic/rhachitic,
albumen/albumin – the correct spellings is used for egg albumen
but both are used randomly for serum/urine albumin). Most other spelling
inconsistencies have been changed to the more-frequent or more-accurate
form (e.g. twofold→two-fold, guinea pig→guinea-pig,
oedema→edema, neuroedema→neuredema, gm.→g.,
Luborsch→Lubarsch, Bauman→Baumann,
McCluggage→McClugage, Eijkmann→Eijkman). Although the
spelling of 'fæces' and its adjective 'fecal' is not consistent, the two
spellings are used consistently throughout the book and therefore have
not been altered. Similarly 'hemorrhage' and 'hemoglobin' are
consistently spelt thus, while other words pertaining to blood
consistently use the æ ligature, e.g. 'hæmatemesis', 'hæmatoma',
'hæmaturia', 'leukæmia', 'hyperæmia'.
Wrong or missing French accents and typos have been corrected where
necessary. German expressions in the bibliography contain various
apparent inconsistencies that have not been changed because of my
unfamiliarity with the language and what was perhaps legitimate at the
time of writing (e.g. Moeller-Barlow'sche Krankheit,
Moeller-Barlow'scher Krankheit, Moeller-Barlowscher Krankheit and
Barlow'schen Krankheit; Muench. med. Woch., Muenchn. med. Woch. and
Muenschner med. Woch.; Beiträge z., Beitraege zur, Beitrag zur). The
term Gernest-mark on p. 108 should probably be geruestmark (or
perhaps gerüstmark) as used elsewhere in the book (pp. 96, 107, 108 and
128).
The book also contains numerous hyphenation inconsistencies. Some of
these have been altered to conform with the most common usage in the
text, but most have not been changed because hyphenation is notoriously
variable and subject to fashion.
Subheading use is somewhat inconsistent; for example, under the
subheading Alimentary Tract in chapter IV, there appear various
non-alimentary items, and in the same chapter Microscopic Pathology
appears as a stand-alone subheading whilst its equivalent Gross
Pathology is relegated to an in-line paragraph introduction.
The bibliography contains two very similar references attributed to Gee.
The second appears to be a duplicate of the first, but it is probable
that the title is incorrect because the publication details (1889, XXV,
85) relate to a different paper by Gee entitled ‘Bloody Urine the
Only Sign of Infantile Scurvy’, and although there are several
comments in the book about scurvy and haematuria (blood in the urine),
e.g. p. 204, none cite Gee's paper.
The second entry for Morse, J. L. in the bibliography should be numbered
as (2) and the source should be Boston Med. and Surg. Journal, 1914,
CLXX, 504. (not Jour. Am. Med. Assn.)
Inconsistent punctuation in the bibliography list has been corrected
(e.g. semicolon→colon).
CLINICAL PROFESSOR OF PEDIATRICS, UNIVERSITY AND BELLEVUE HOSPITAL
MEDICAL COLLEGE, NEW YORK CITY
ILLUSTRATED
PHILADELPHIA AND LONDON
J. B. LIPPINCOTT COMPANY
COPYRIGHT, 1920, BY J. B. LIPPINCOTT COMPANY
PRINTED BY J. B. LIPPINCOTT COMPANY
AT THE WASHINGTON SQUARE PRESS
PHILADELPHIA, U. S. A.
Interest in scurvy has been stimulated in the last few years as the result of a new and broader conception of nutrition. It has come to be realized that in addition to the substances heretofore recognized as of essential importance in the dietary—the proteins, fats, carbohydrates and the salts—there is still another group, termed “vitamines,” “accessory food factors” or “food hormones,” which must be included in order to render the diet complete and adequate. It has become increasingly evident that the attention of physiologists and of clinicians has been focussed too sharply and too narrowly on the caloric value of foodstuffs. At the same time we have begun to appreciate the existence of a group of nutritional disorders which depend largely on a deficiency of these illusive vitamines or food factors, and which evidently are of vital importance to the welfare of the individual and of mankind. Scurvy is one of this newly-constituted group, and due to this association has acquired a fresh and broader significance. It is in this light that the intensive research work must be interpreted, which has been applied within the past few years, both in this country and abroad, to problems relating to this disorder. It is clear that the subject is in its infancy, and is destined to participate in a consideration of many of the nutritional and infectious diseases of the adult and the child.
The World War has tended also to demand a renewed consideration of scurvy. This disorder has played a rôle in all wars—in the campaigns of the Cæsars, the pilgrim ages of the Crusaders, and the numerous wars of the last century. In the recent war it existed among the various armies, particularly those in the East, to an extent greater than at first was realized. In Mesopotamia it is stated to have been one of the decisive factors in forcing the surrender of the British at Kut. Its incidence, however, was not limited to the military forces. Reports from England and the continental countries clearly indicate that scurvy prevailed among the civilian population during the past few years to a degree unknown in peace times. This was especially true of infants and children.
For the past seven years I have been engaged in an investigation of scurvy both in the laboratory and in the clinic, and have treated various aspects of the subject in a large number of articles published in various medical journals. In the course of these studies there has been ample opportunity for a comprehensive review of the widely-scattered literature. No treatise on scurvy has been published in English since the classical work of Lind in 1772. The time, therefore, seemed opportune to gather into one volume the recent advances in this field and to offer to the clinician, to the hygienist, and to the biological chemist a presentation of the existing status of this important nutritional disease.
It is with pleasure that I acknowledge my obligation to Dr. Lester J. Unger, who has assisted in carrying out much of the work described in this volume. Thanks are due also to Dr. Charles Gottlieb for the radiographs which are here reproduced, and to Dr. Gertrude McCann for seeing the work through the press. To my associates in the clinic who shared in the observations, and to friends who read various chapters in the course of their preparation, I wish to express my appreciation.
Alfred F. Hess.
New York,
August, 1920.
| PAGE | |
| Preface | iii-iv |
| CHAPTER I | |
| History of Scurvy | 1 |
| (a) Outbreaks on Land; (b) Outbreaks at Sea; (c) Infantile Scurvy; (d) Scurvy in the World War | |
| CHAPTER II | |
| Pathogenesis and Etiology | 23 |
| Pathogenesis: Theories; Potassium Deficiency; Acidosis; Toxic; Bacterial; Vitamine (Accessory Factor) | |
| Etiology: Breast-Fed Infants | 35 |
| Artificially Fed Infants: Pasteurized Milk; Boiled and Sterilized Milk; Dried Milk; Condensed Milk; Proprietary Foods (Effect of Alkalization) | 40 |
| Age, Season and Climate; Economic Status; Psychic Element; Predisposition; Effect of Other Food Constituents; Exciting Factors | |
| CHAPTER III | |
| The Antiscorbutic Vitamine | 62 |
| Characteristics: Relation To Heat, Drying, Aging, Ultra-Violet Rays, Shaking | 65 |
| Mode of Action—(a) Direct: As a Nutriment; Antitoxin; Catalyzer; (b) Indirect: Endocrine Action | 69 |
| Fate in the Body: Storing; Content in Blood; Excretion; Fate in Gastro-intestinal Tract; Effect on Digestive Processes | 74 |
| Irregularities of Action; Effect on Growth | |
| CHAPTER IV | |
| Pathology | 81 |
| (a) Gross: General Appearance; Hemorrhages; Anasarca; Heart; Lungs; Alimentary Tract and its Glands; Urinary Tract; Lymph Nodes; Organs of Internal Secretion; Brain and Spinal Cord; Bones; | |
| (b) Microscopic: Skin; Muscles; Blood-vessels; Lungs; Heart; Intestinal Tract and its Glands; Kidney; Adrenals; Pancreas; Thymus; Central Nervous System; Peripheral Nerves; Retina; Bones | |
| CHAPTER V | |
| Experimental Scurvy | 111 |
| Historical Review | |
| Pathogenesis | 116 |
| Pathology: Effect on the Fœtus; Scurvy in the Monkey; Microscopic Pathology; Bones; Teeth; Nerves; Blood Vessels; Interpretation of Bacteria in the Tissues | 122 |
| Symptoms | 135 |
| CHAPTER VI | |
| Antiscorbutic Foods | 143 |
| Historical Review | 143 |
| Milk: Raw; Pasteurized; Dried | 150 |
| Fruits and Fruit Juices: Dried | 153 |
| Vegetables: Cabbage; Effect of Heating. Potato. Swede | 158 |
| Dehydrated Vegetables: Canned Foods (Tomatoes) | 166 |
| Germinated Cereals and Pulses; Meat and Eggs; Beer And Alcoholic Beverages; Miscellaneous | |
| Conclusions | 173 |
| CHAPTER VII | |
| Symptomatology and Diagnosis | 176 |
| In Adults | 176 |
| In Infants: (a) Acute; (b) Subacute; (c) Latent.—hemorrhage Of Gums; Subperiosteal Hemorrhage: Skin; Mucous Membranes and Subcutaneous Tissues; Hemorrhages of Internal Organs; Nails and Hair; Eczema; Edema; Tenderness; Beading of Ribs; Separation of Epiphysis; “White Line” Cardiovascular System; “Cardiorespiratory Syndrome” Nervous System; Urinary System; the Blood and Blood-vessels; Nutrition and Growth; Fever; Complications; Epidemic Form | 183 |
| Differential Diagnosis: Rheumatism; Purpura; Congenital Syphilis; Bone Tumors; Osteomyelitis; Poliomyelitis, etc. | 219 |
| CHAPTER VIII | |
| Prognosis | 225 |
| CHAPTER IX | |
| Treatment | 230 |
| Preventative; Curative | |
| Non-dietetic | |
| CHAPTER X | |
| Metabolism | 241 |
| In Adults: Body Exchanges | 241 |
| In Infants: Body Exchanges; Analysis of Organs; Chemistry of Blood | 242 |
| In Animals: Monkey; Guinea-Pig | 245 |
| CHAPTER XI | |
| Relation of Scurvy to Other Diseases | 248 |
| Beriberi; Ship-beriberi; Pellagra; Rickets; Osteogenesis Imperfecta; Osteomalacia; Hunger Edema; “mehlnaerschaden” Exudative Diathesis; Diseases Due to a Food Excess | |
| Appendix: Lind’s Recipes for Preparing Stable Antiscorbutics | 259 |
| Bibliography | 261 |
| FIG. | PAGE | |
| 1. | Dependence on potato as antiscorbutic | 7 |
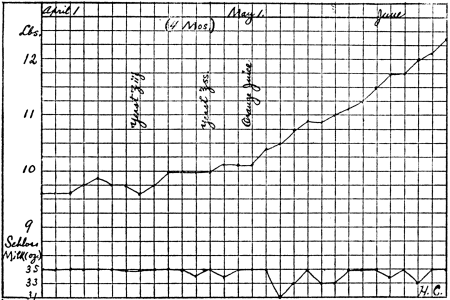
| 2. | Weight curve of scorbutic baby. Effect of alkalization of milk | 51 |
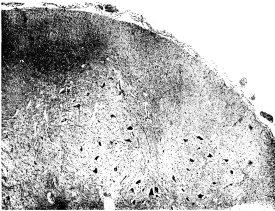
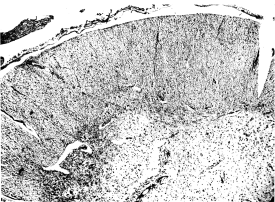
| 3. | Lumbar cord in case of scurvy | 105 |
| 4. | Lumbar cord in case of scurvy. Focal degeneration | 105 |
| 5. | Bone in scurvy. Microscopic pathology | 108 |
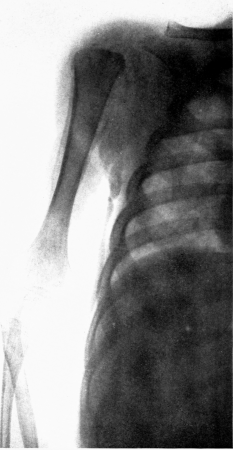
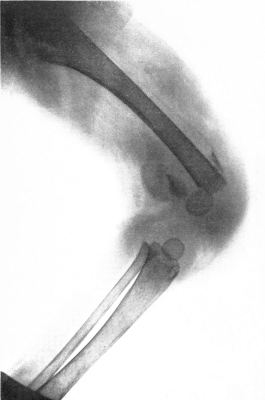
| 6. | Subperiosteal hemorrhage and separation of epiphysis. Roentgenogram | 109 |
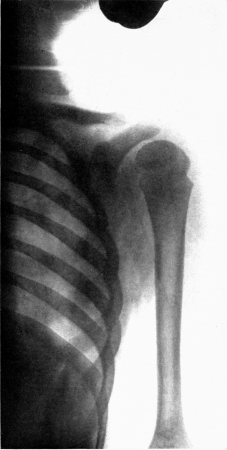
| 7. | Complete restitution of epiphysis without deformity. Roentgenogram | 109 |
| 8. | Curve of fecal excretion in scurvy | 121 |
| 9. | Diagrammatic representation of guinea-pig scurvy | 130 |
| 10. | Loss of weight in guinea-pig scurvy | 139 |
| 11. | Dried milk as an antiscorbutic | 140 |
| 12. | Dehydrated vegetables as a cause of scurvy | 164 |
| 13. | Cure of scurvy by addition of canned tomato | 166 |
| 14. | Failure of yeast as prophylactic | 171 |
| 15. | Temperature, pulse, and respiration in scurvy | 186 |
| 16. | Subperiosteal hemorrhage and separation of epiphysis. Roentgenogram | 192 |
| 17. | Periosteal “tags” and “streamers.” Roentgenogram | 193 |
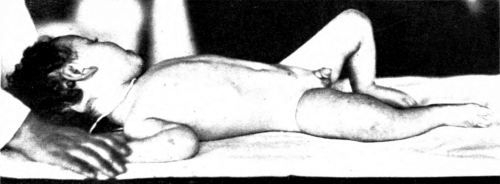
| 18. | Infant with marked scurvy. Characteristic position | 198 |
| 19. | Scorbutic beading of ribs. Roentgenogram | 198 |
| 20. | “White line.” Roentgenogram | 199 |
| 21. | Cardiac enlargement. Roentgenogram | 200 |
| 22. | Electrocardiogram showing “cardiorespiratory syndrome” | 201 |
| 23. | Stationary weight during cure of scurvy. Oliguria followed by polyuria | 206 |
| 24. | Development of scurvy in spite of normal gain in weight | 214 |
| 25. | Retardation of growth in length when no orange juice was given and supergrowth when given once more | 216 |
TABLES | ||
| TABLE | PAGE | |
| 1. | Fecal flora of scorbutic infants | 29 |
| 2. | Necropsy reports of scurvy | 82 |
| 3. | Relative distribution of the antiscorbutic factor in the commoner foodstuffs | 157 |
| 4. | Platelets and other blood cells in scurvy | 209 |
| 5. | Data of epidemic of scurv | 218 |
| 6. | Duration of treatment before marked improvement was noticed | 237 |
Outbreaks on Land.—Like many other diseases, the life history of scurvy shows several distinct phases. We hear of it first as a plague, infesting armies and besieged towns; then as a dread disease, decimating the sailors of the navy and of the mercantile marine, and, since the end of the last century, more often as a nutritional disturbance, endangering the health of infants. Very recently it has acquired an entirely new interest, as the representative of a class of disorders which has revealed the essential importance to man of unknown dietary factors.
It is difficult, as may be imagined, to define with precision the earliest description of scurvy, as the older references are so vague as to be open to individual interpretation. The reference of Hippocrates to a large number of men in the army who suffered from pains in the legs and gangrene of the gums, which was accompanied by loss of teeth, seems sufficiently definite to be identified as this disease. The Greek, Roman and Arabian writers do not seem to have been acquainted with scurvy. This is as we should expect, for fruits and vegetables grew in such plenty in these southern countries that scurvy must have been a disorder of rare occurrence.
An interesting early description of scurvy, and one which is quite convincing, is that of de Joinville, who accompanied the Crusaders in their invasion of Egypt under St. Lewis, about the middle of the thirteenth century. He refers to the lividity and spongy condition of the gums, and describes how “the barber surgeons were forced to cut away the dead flesh from the gums to enable the people to masticate their food” he describes their debility, their tendency to faint, and the black spots on their legs. The disease broke out in Lent, during which time the soldiers partook of no meat, but consumed a species of eel which they believed “ate the dead people” and therefore led to this loathsome disease.
It is probable that scurvy existed in the northern parts of Europe and Asia ever since they were settled by man. We should hardly expect to have records of this condition, in view of the low educational status of the people, their greatly restricted literature, and their lack of intercourse with the people in the southern countries. In the sixteenth century, with the development and spread of education, we begin to hear of scurvy from various sources. Claus Magnus, in his “History of the Northern Nations,” published in 1555, described the disease which he tells us flourished among the soldiers in the camps and in the prisons. About this time Ronsseus, Echtius and Wierus wrote special treatises on this disease, and recommended many dietary measures which we recognize to-day as most efficacious. The number of monographs on this subject multiplied with great rapidity in the course of the next twenty-five or fifty years; none of them, however, added anything essential to our knowledge. In 1645 the Faculty of Medicine at Copenhagen published a “consilium” for the benefit of the poor, treating of the causes, prevention and cure of this disease, which was prevalent among the Danes and other northern nations.
The colonists of the northern part of America were sorely afflicted with scurvy. It is said that the French met with such high mortality during the severe winters in Canada, that they frequently debated the wisdom of abandoning this settlement. This was true also in regard to the English and their settlement in Newfoundland. Indeed, it was scurvy which forced the early settlers in Hudson Bay to discontinue their intentions of colonizing that region.
In an essay published in the eighteenth century (1734), Bachstrom described an epidemic of scurvy which occurred in 1703 during the siege of Thorn, in Prussia, by the Swedes, which caused the death of 5000 of the garrison, in addition to a large number of the inhabitants. It is interesting to note that this epidemic took place in the middle of the summer, and not in the cold season. From this time on we meet with many descriptions of scurvy in connection with the wars at various periods. For instance, in the Russian armies, in the war between the Austrians and the Turks in 1720; in the English troops who had taken Quebec from the French in 1759; among the French soldiers in the army of the Alps in the spring of 1795. It is unnecessary to review these accounts in detail. This period is distinguished rather by the appearance of a great classic on Scurvy, the work of the English naval hygienist, Lind (1752). This book has intrinsic value to-day, and, at the time it appeared, served to crystallize the conception of scurvy, which had been stretched out of all proportions to include an ever-increasing conglomeration of clinical conditions. Scurvy had become the Alpha and Omega of professional routine, the catchword of the day, the asylum ignorantiæ of the practical man. Into this chaos, as Hirsch expresses it, “the first beams of light fell when Lind’s classical work appeared.”
It will be of little value to consider the great number of epidemics of scurvy which occurred from this time to the present day. They may be found in tabular form in the excellent survey of scurvy by Hirsch. The literature of this long period may likewise be found in a work of encyclopædic character, that of Krebel, which gives the titles, with a summary of the various articles on this subject, appearing to the year 1859. If we look over the chronological table compiled by Hirsch, we note a remarkable similarity regarding the incidence of the recurring epidemics. In almost all cases they broke out among troops, whether in Russia, in India, in Africa, or in our United States. The epidemics which are not attributable to military life or campaigns are found to have taken place generally in prisons, insane asylums, poorhouses or houses of refuge and correction. It would seem that no war is omitted from this list of sickness and death. There are in all 143 land epidemics between 1556 and 1877, two occurring in the sixteenth century, four in the seventeenth, 33 in the eighteenth, and 104 in the nineteenth century. The marked increase in the nineteenth century occurred in institutions, in asylums and prisons, rather than in the armies. This fact may be ascribed to altered social conditions which led to a great multiplication of eleemosynary institutions.
Coming down to more recent times, we learn that scurvy occurred extensively during the Crimean War, and that it was prevalent also among the troops in our own Civil War. In the “Medical and Surgical History of the War of the Rebellion,” we find the following statements:
“A scorbutic tendency was developed at most of our military posts during the winter season, after the troops had been confined to the use of the ordinary ration with the desiccated vegetables. The latter in the quantities failed to repress the disease. At posts which could be readily supplied with potatoes only the taint was manifested, on account of a want of liberality in the issues.” And again: “Among the white troops during the five and one-sixth years covered by the statistics, 30,714 cases of scurvy were reported; and 383 deaths were attributed directly to that disease.”
Munson writes: “It (scurvy) prevailed among our troops during the Civil War and its recognition was a surprise and shock to professional ideas preconceived from practice in civil life.”
As is well known, the besieged in Paris during the Franco-Prussian War in the winter of 1870–71 suffered severely from scurvy. The accounts of their pitiable condition have been portrayed for us by numerous French writers (Delpech, Hayem, Lasèque and Legroux). The people lived mainly on rice and bread, with an occasional addition of potatoes or horse meat. The winter was exceptionally severe, which was supposed to have intensified the scorbutic condition. Not only were the inmates of the prisons on the Seine attacked, numbering about one thousand, but even the patients in the military hospitals developed the disease. It is of interest to remember that the siege lasted but little over four months, from September 17th to January 27th, the date of the armistice.
In the Russo-Japanese War, after the siege of Port Arthur, it was found that one-half of the garrison of 17,000 men had scurvy.
Although there are certain parts of the world where scurvy is of frequent occurrence, no country has been entirely free from it. As might be expected, it has been particularly prevalent in the North, where vegetation is scanty—in Greenland, Alaska, Russia and the Baltic States. It has likewise prevailed in the tropics when the crops have failed. India has been conspicuous for its large number of epidemics; some years ago scurvy occurred in Arabia among the English troops stationed at Aden, both among the British and the native troops. A recent communication from Aruba, a small island of Dutch Guiana, lying north of Venezuela, illustrates how devastating scurvy still is in some parts of the world. This account tells of 3000 cases of this disease which occurred in 1915 among a population of less than 10,000, owing to the fact that the crops had failed almost entirely during the years 1912, 1913 and 1914.
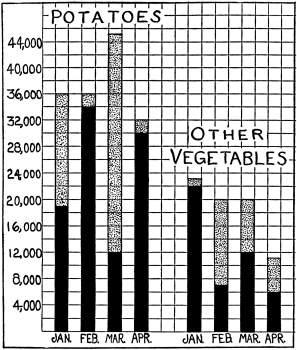 Fig. 1.—A comparison between the requisitioned quantity (in thousand pound units) of
potatoes and other vegetables, and the quantity received per month by an institution in
which more than 200 cases of scurvy occurred at the beginning of April, 1916. The total
height of column represents the amount needed and requisitioned; the solid black portion
the amount received. The number of inmates in the institution remained approximately
the same.
Fig. 1.—A comparison between the requisitioned quantity (in thousand pound units) of
potatoes and other vegetables, and the quantity received per month by an institution in
which more than 200 cases of scurvy occurred at the beginning of April, 1916. The total
height of column represents the amount needed and requisitioned; the solid black portion
the amount received. The number of inmates in the institution remained approximately
the same.It is important for us to realize that we are still dependent on the annual crops for our protection from scurvy; in other words, the world is leading a hand-to-mouth existence in regard to its quota of antiscorbutic food. The truth of this condition has been realized for Ireland, sadly illustrated by numerous epidemics, notably the great epidemic of 1847 reported by Curran. It was demonstrated by the outbreaks of scurvy in Norway in 1904 and 1912, and was brought to the attention of many in the United States in the spring of 1916. In this year our potato crop fell far below the normal, with the result that scurvy appeared in various parts of the United States, especially in institutions (Fig. 1).
The fact that scurvy may occur in any land and climate, even in the garden spots of the world, is strikingly shown by the epidemics reported from Algiers, and the ravages of this disease among the gold seekers in California in 1849. Nothing could be more incongruous than the occurrence of a deficiency disease in this land of plenty.
Outbreaks at Sea.—It is doubtful, however, whether attention would have been focussed so early and so sharply on scurvy, had it not been for the voyages of exploration undertaken in the sixteenth century. These long trips on sailing vessels, where for many months little or no fresh vegetable or animal food was obtainable, were almost as if designed to make a test of the dietetic origin of scurvy. The result was inevitable—five to six months after the ships were out of touch with land, the majority of the crew frequently were incapacitated by this disease, thereby wrecking many an expedition.2
The earliest account of the outbreak of scurvy at sea is that of Vasco de Gama, who in 1497 discovered a passage to the East Indies by way of the Cape of Good Hope. The narratives of subsequent explorers, especially those of Cartier and of Drake, are replete with descriptions of the ravages of scurvy. The expedition of Lord Anson in 1740 is always cited as a memorable example of an undertaking which foundered as the result of scurvy. After a cruise of four years, this expedition had lost from this disease more than four out of five of the original number of its crews. In striking contrast to this picture, and to that furnished by the voyages of earlier navigators, is that of Captain Cook, who in 1772 undertook a voyage lasting over three years, sailing from 52° north to 71° south, with a loss of but one of his crew from disease, and that not from scurvy. This remarkable feat, more than any other, centered attention on the feasibility of preventing scurvy, and resulted in measures tending to eradicate it from the navy. Captain Cook attributed the absence of scurvy among his crew to “sweetwort,” an infusion of barley, which he prepared fresh and served liberally. He also prized the antiscorbutic value of sauerkraut.
We find accordingly in 1795, at the instance of Sir Gilbert Blaine, that improvements were introduced in the victualling of the fleet. As the result of a regular ration of lemon juice, the incidence of scurvy fell precipitously. It is due largely to this provision that between the years 1779 and 1813, according to the statistics of Sir Jay Barrow, the morbidity and the mortality in the British Navy was decreased by 75 per cent.
It has been shown that it took a generation after the efficacy of antiscorbutics had been demonstrated in various expeditions, for an antiscorbutic to be included in the ration of the navy. The merchant marine of England was far more conservative, and for many years after scurvy had been eradicated from the navy we still read of its occurrence on the vessels making voyages to India, China and Ceylon. Gradually, however, its incidence became less and less. Its toll of death, before preventive measures were employed, may be appreciated from the fact that it has been estimated that scurvy destroyed more sailors than all other causes incidental to sea life, including the great slaughter of naval warfare. Sir R. Hawkins stated in the latter part of the sixteenth century that he could give an account of 10,000 mariners who had been destroyed by scurvy during the twenty years that he had been at sea.
As is well known, scurvy has played an important rôle in Arctic and Antarctic explorations, and has been the cause of the failure of many of these expeditions. It is now realized that the development of scurvy is quite preventable, that if a sufficient quantity of meat (especially raw meat) is consumed, explorers can be entirely independent of a supply of fresh vegetables. This fact was brought out by the Arctic Survey Committee (British), who “were appointed to enquire into the causes of the outbreak of scurvy in the recent Arctic expedition” (1877), and who reported that it may result from an absence of fresh meat. That this conclusion was sound has been proved by the experiences of Nansen and of Johansen, who wintered safely in Franz-Josefsland on a diet of meat and bacon. More recently Stefánsson has carried out successful Arctic explorations, depending entirely on fresh meat as antiscorbutic foodstuff and making no provision whatsoever for vegetable food.
Infantile Scurvy.—Glisson, to whom we owe the first description of rickets, likewise was the first to recognize scurvy in infants. In his classic treatise on rickets, written in 1668, he writes as follows:
“The scurvy is sometimes conjoyned with the affect. It is either hereditary, or perhaps in so tender a constitution contracted by infection, or lastly, it is produced from the indiscreet and erroneous Regiment of the infant, and chiefly from the inclemency of the air and climate where the child is educated.”
“The scurvy complicated with this affect hath these signs: 1. They that labor under this affect do impatiently indure purgations; but they who are only affected with the Rachites do easily tolerate the same. 2. They are much offended with violent exercises, neither can they at all endure them. But although in this affect alone, there be a kind of slothfulness and aversation from exercise, yet exercise doth not so manifestly, at least not altogether so manifestly hurt them, as when the scurvy is conjoyned with the Rachites. 3. Upon any concitated and vehement motion they draw not breath without much difficulty, they are vexed with diverse pains running through their joynts, and these they give warning of by theyr crying, the motion of the Pulse is frequent and unequal, and somethimes they are troubled with a Palpitation of the Heart, or threatened with a Lypothymie, which Affects are for the most part soon mitigated, or altogether appeased by laying them down to rest. 4. Tumours do very commonly appear in the Gums. 5. The urin upon the absence of the accustomed feavers is much more intense and increased.”
Glisson’s description of scurvy was entirely lost sight of, overshadowed by his description of rickets, so that for over two hundred years no word of infantile scurvy is to be found either in the English or other literature. There is no doubt that from time to time cases must have occurred, but they were looked upon probably as rickets or as a manifestation of one of the hemorrhagic diseases.
In 1859 Moeller described some cases which evidently were scurvy, but which he termed “acute rickets.” He realized that they presented a novel clinical picture but failed to recognize that they represented a disorder quite distinct from rickets.3 This article was followed within the next few years by reports of other German writers (Bohn, Steiner, Foerster) who, accepting Moeller’s point of view, considered these cases merely as an acute form of rickets. They were led to this erroneous conclusion chiefly on account of the lack of marked involvement of the gums, which they considered an essential sign, influenced by their conception of adult scurvy. This viewpoint has pervaded the German literature even to the present day, when it is still considered necessary to bring further evidence that infantile scurvy in its pathogenesis and pathology is identical with adult scurvy.
In 1871 Ingerslev, an assistant of Hirschsprung in Copenhagen, wrote a paper on “A Case of Scurvy in a Child,” which is quite convincing. Two years later Jalland, an English physician, reported a similar case of “Scurvy in a Ten-Months-Old Infant.” In 1878 Cheadle reported three cases of infantile scurvy with typical tumefaction of the gums, and obscure tenderness of the legs, and followed this paper by two others, which appeared in 1879 and 1882. Cheadle clearly recognized the disease as scurvy. However, as the title of his first paper—“Three Cases of Scurvy Supervening on Rickets in Young Children”—indicates, he considered it a condition engrafted upon rickets. About this time (1881) Gee presented a brief but accurate account of five cases of scurvy which he termed “osteal or periosteal cachexia.”
In 1883, Barlow published his classical paper on this subject, the first to furnish anatomical proof that this disorder of infants presented the pathological changes characteristic of adult scurvy. Previous to this publication there had been but one autopsy report, that by Moeller, which had been incorrectly interpreted. The work of Barlow was accepted remarkably quickly in England and in America, but less promptly on the Continent. This was probably due to the fact that infantile scurvy was occurring far more frequently in these two countries, and that the subject was open therefore to more prompt investigation. This increased prevalence of infantile scurvy in the two great English-speaking nations has continued to the present time, and no doubt is due to the extensive employment of artificial feeding and of proprietary foods. In 1894 not less than 106 cases were reported to the Academy of Medicine of New York City by various physicians, and in 1898 the comprehensive investigation of the American Pediatric Society appeared, which was based on 379 cases.
It was soon evident that infantile scurvy occurred to a greater or less degree throughout the civilized world. In France, Monfalcon had reported a case in 1820 which is sometimes referred to as the earliest case of infantile scurvy mentioned in the literature. It relates, however, to an older child and was published as a case of scorbutic rickets. Netter was one of the first in France to recognize the true nature of the disorder, and published several papers in 1898 describing typical cases. Infantile scurvy was, however, almost unknown in that country until what is termed “lait maternisé” and “lait fixé” came into vogue. This is apparent from a table prepared by Lecornu, which gives a list of all cases in the French literature between 1894 and 1904, and of the diets on which they came about. The former of these milk preparations is subjected to various manipulations and then heated to a temperature above the boiling point; the latter is shaken violently in a machine to render the fat globules smaller, and is then sterilized by one of the usual methods.
Switzerland has undergone an experience similar to that of France. Previous to 1903 only five cases of infantile scurvy had been published from that country. In this year Stoos published an additional five. In 1907 Bernheim-Karrer reported nine cases, all of which had developed on homogenized milk, a process very similar to that employed by the French to break up the fat globules. The increase of infantile scurvy in Switzerland may be judged by the fact that a commission was formed in the following year to investigate its occurrence.
In Germany there was for many years continued discussion as to the true nature of scurvy. Some believed it to be a form of rickets, others a form of scurvy; still others a combination of scurvy and rickets. Some thought it merely hereditary syphilis, and not many years ago Naegeli looked upon it as an entity distinct from scurvy on rickets. The subject attained additional importance through an epidemic of infantile scurvy, which broke out in Berlin in 1898, among infants who received milk from one of the largest dairies. The episode led to prolonged discussion in the Berlin Medical Society, and to several excellent papers, among which that by Neumann deserves particular mention.
The disorder has been reported in Holland by DeBruin, who recorded numerous cases; in Denmark, by Hirschsprung, who refused to recognize its scorbutic nature; in Italy, by Concetti, and by others. It was not long before there were reports of cases from almost every part of the world, including Australia (Money) and East India (Nichols).
In view of the fact that scurvy is endemic among adults in Russia, we should also expect to find infantile scurvy widespread in that country. In point of fact, quite the contrary seems to be the case. In connection with the great scurvy epidemic in Russia (1898–99), Tschudakoff personally examined over 10,000 persons and found 11.11 per cent. of the people sick with this disease. He states that in the course of this large experience he did not meet with a single case under the age of five years. Fuerst writes that Filatow, the great Russian children’s specialist, declared that he knew of no case of Barlow’s disease described in the Russian literature. This is not literally correct, as Doepp described an epidemic of scurvy in the St. Petersburg Foundling Asylum occurring in 1831. It serves to emphasize, however, the paucity of cases among infants in this great land of endemic adult scurvy. Lyabmow, in referring to the scurvy in Kazan, tells us that among 28,000 cases only a few infants were affected, and Rauchfuss made the statement at the International Congress at Copenhagen, in 1884, that although he had seen a great many cases of scurvy, he had never seen it in children one to two years of age. We shall not, in this place, comment on this interesting and apparently paradoxical situation, but shall have occasion to refer to it in considering the pathogenesis. It may be added that in Norway and Sweden, where scurvy is to some extent also endemic among the adult population, there is a similar lack of scurvy among infants.
Scurvy in the World War.—The greatest advance in medicine during the past generation has been in the fields of hygiene and preventive medicine. One might therefore have expected that the World War would have differed from previous wars in a notable absence of scurvy among the troops and the civilian population. This is true to a limited degree only. Reports which have been published in the course of the war, and especially since hostilities have ceased, show that the troops who were incapacitated by scurvy must have numbered many thousands. As was to be expected, scurvy occurred most often in Russia, where it is endemic. The largest number of cases was reported by Boerich, who as director of a Red Cross Central Station in Russia saw 1343 cases. Other German physicians who had charge of caring for the Russian prisoners give accounts of the occurrence of some hundreds of cases of scurvy. An article by Much and Baumbach gains added interest from the novel suggestion that scurvy is transmitted by means of vermin. That scurvy must have reached large proportions is shown by the fact that in July, 1916, a medical commission was sent by the Germans to investigate the scurvy in a Russian army corps, and that it was necessary to establish for this disease in every division a sanatorium comprising 100 beds. Hoerschelman, who wrote an account of this investigation, blames the bad hygienic surroundings, the lack of sleep, the overexertion, as well as the deficiency of food, for the occurrence of the epidemic. As usual, very few cases occurred among officers. He describes a number of instances where scurvy was feigned by rubbing the gums and making them bleed, or by irritating them with the juice of tobacco. These reports on scurvy in Russia bring us little new from a purely medical standpoint. They emphasize the occurrence of night-blindness as an early and frequent symptom. It is difficult to judge whether this manifestation was due entirely to the scurvy, or was in part the result of other deficiencies in the diet. For instance, Hift states that the night-blindness was cured by cod liver oil, or by the water in which beef liver had been cooked. This would point rather to a deficiency of the fat-soluble vitamine, as these substances could have little effect in curing scurvy. The cases reported by Wassermann, where neuritic pains in the legs played a considerable rôle, evidently are also not simple scurvy, but may well be the result of more than one food deficiency or a complicating ostitis. In the same way some reports show clearly that “hunger edema” complicated scurvy.
Scurvy occurred next in frequency among the nations neighboring Russia. Speyer tells us that a German sanitary commission was sent to Bulgaria largely with the object of investigating scurvy in that country. The excellent monograph on the pathology of scurvy just written by Aschoff and Koch was founded on an experience in Roumania among Turkish, German and Austrian soldiers. Added to its other woes the Servian army was visited by scurvy. Wiltshire gives us a description of this disease based on an observation of 3000 cases in the first half of the year 1917. In regard to scurvy in this part of the world, Morawitz writes that when he reached Roumania he was surprised to find scurvy the most prevalent disease in the army, and that since the spring of 1917 it was widely disseminated among the German troops. Lobmeyer writes of scurvy among the Turkish troops, and Disqué reports 500 cases among prisoners captured in Turkestan.
Along the Western front very few cases are described. There is an account by Korbsch of 51 cases in this area in 1915. Schreiber describes 30 cases among the German prisoners of war captured in the beginning of 1917, which were diagnosed as purpuric rheumatism. Arneth recounts that sporadic cases of scurvy occurred among the German troops, especially among the older soldiers, and that in many cases this was combined with the hunger edema. He attributes the scurvy to a dependence on dehydrated vegetables in the ration.
From all these accounts it is evident that scurvy played an important rôle in the general nutrition of the troops on the Eastern front. Probably it was of the latent variety, which is exceedingly difficult to diagnose, but which increases the susceptibility to infection, and intensifies the severity of all medical or surgical diseases. Von Niedner takes this point of view, stating that although scurvy had been largely prevented in this war, the obscure rudimentary type had not been eradicated. He remarks upon a fact, noted in our Civil War and other wars, that under these conditions eruptions assume a hemorrhagic character in typhoid fever, cerebrospinal fever, rheumatism and other infections. Pick made a similar observation at a medical meeting in Vienna in reference to scurvy in the Austrian army, drawing attention to the hemorrhagic diathesis existing among the troops and expressing the opinion that scurvy was occurring in this war as in previous wars.
Very little scurvy seems to have broken out among the British troops in Europe. Thirty-two cases were reported as occurring in the middle of 1915 at a divisional rest station in France. It made marked inroads, however, on the health of the Colonial troops in Mesopotamia. In the report of the Mesopotamia Commission we read that 7500 men were lost to the force in 19 weeks as a result of scurvy, and that this happened in the summer of 1916 although additions had been made to the ration in the previous spring. A conception of the extent of the scurvy may be formed from the accompanying table, published by Willcox:
| Scurvy (Indians) | Beriberi (British) | |
|---|---|---|
| 1916 (July 1—Dec. 31) | 11,445 | 104 |
| 1917 | 2,199 | 84 |
| 1918 | 825 | 51 |
It will be noted that thousands of cases occurred among the Indian troops. This was due to the fact that the British ate more potatoes and fresh meat. In his official report of the outbreak of scurvy among Indian troops, Colonel Hehir writes: “The only vegetable now allowed is 2 ounces of potatoes and the only fresh meat 28 ounces a week. It is very doubtful whether this authorized ration, if not supplemented by other vegetables and more meat, is sufficient to prevent scurvy.” In the account which this officer gives of the medical conditions during the siege of Kut-el-Amara, it is stated that there were 1050 admissions for scurvy, fully developed, incipient and latent. It is remarked that those Indians who ate horseflesh were decidedly less affected. From the fact that special hospitals for scurvy were established in June, 1916, at Bagdad, Amora and Basrah, it is evident that a large number of cases must have been encountered. Most significant in this connection, however, are the preventive measures which were instituted by the British government. A body of 256 men, designated as the Madras Gardener’s Corps, were dispatched to Mesopotamia to plant gardens all over the country and to supply packets of seeds to various units. At Bagdad alone their output of vegetables was over 400,000 pounds. This certainly constitutes a remarkable innovation in the hygiene of armies.
The French army was not entirely spared from scurvy. In 1917 Harvier, an army surgeon, was surprised to discover that 95 per cent. of the 800 troops of which he had charge suffered from scurvy; he tells us that other epidemic centres were recognized later outside this sector. Elsewhere we read of the occurrence of scurvy in France, involving 40 per cent. of the 1700 men of the South African Labor Corps, and that this disorder was still more serious in another company owing to the fact that it was not recognized (Dyke).4 Benoit reported 63 cases which he discovered in 1917 among 300 laborers. According to his account, all these laborers received the same food, and those with scurvy recovered quite independently of any change in the dietary.
There are many accounts of scurvy among the Italian troops. Vannutelli gives a description of an epidemic of some 200 cases of infectious purpura with manifestations of hemorrhagic scurvy. Another writer informs us that in June, 1916, scurvy broke out among some Italian troops stationed at an altitude of 1500 to 2000 metres (Gingui). Vallardi gives an account of 180 cases among Italian troops in Macedonia, accompanied by slight jaundice and enlargement of the glands.
The American soldiers seem to have been practically spared from scurvy. This was due probably to their ample ration and to the fact that they were in the field for a comparatively short period. The Surgeon-General’s report to date, which has been kindly furnished me, showed but 5 cases in 1917 occurring in Europe and the United States, and but 15 cases reported during the year 1918.
The civilian population of the various warring countries was by no means spared. There are no reports from Russia to indicate the extent of scurvy, but from what is known of the food conditions prevailing there toward the end of the war, one can be certain that the number must have been large. The greatest amount of scurvy has been reported from Austria, more particularly from Vienna. Previous to the war scurvy was a rare disease in this city, both among adults and infants. During the war, however, as the result of a lack of fresh food and the dependence on dehydrated vegetables, a large number of cases developed. Tobler reports over 200 cases in children between the ages of two and fifteen years, which occurred in 1917 in child-caring institutions where the milk supply was markedly deficient, where fresh vegetables were lacking, and the supply of potatoes gave out about Christmas, 1916. A conception of the deficiency of the milk supply may be gained from the statement that there were but sixteen quarts a day for about 1500 people. Some of these children were undergoing fresh-air treatment and were out of doors in the “sun stations” day and night. For the cure of these children a simple decoction of fir-tops was used, a therapeutic procedure stated by Lind to have been of value in the Russo-Swedish War of 1708.
That scurvy must have occurred extensively among the infants in Vienna may be gathered from the report of Erdheim, who records 31 autopsies on infants under the interesting title of the “Barlow Heart.” In Berlin scurvy occurred also in the foundling asylums, as reported by Eric Mueller and by Brandt. This was caused by a diet of pasteurized milk and dehydrated vegetables. In an article bearing the suggestive title of “On a Marked Increase in Barlow’s Disease in the Years of the War 1917–1918,” Epstein states that in Prague there had been an endemic increase of infantile scurvy since August, 1917. The only information regarding scurvy among the adult civilian population of Germany is that furnished by Morawitz, who states that this disorder occurred sporadically. Here again it is probable that there were many latent or rudimentary cases which were not recognized.
In Great Britain there are reports which show that scurvy manifested itself in institutions caring for the poor. In Glasgow we learn of 50 cases developing in the Poor Law Hospital in the course of fifteen months, and in Newcastle of 16 cases appearing in the Poor Law Infirmary in the course of three months.
It is probable that when more detailed reports are available, it will be found that there was far more scurvy than was appreciated during the course of the war. It will be impossible, however, to gain even an approximate knowledge of the extent to which this disorder prevailed, as in many instances it was inextricably interwoven with other nutritional diseases. The situation which Enright describes in Cairo among the Turkish prisoners suffering from war edema, where there was “evidently a scorbutic factor involved,” probably held true for many other parts of the world. War and scurvy must still be regarded as associated evils, for war is closely linked with famine and food deprivation—the dominant factor in the production of scurvy.
At the outset it may be stated that there is no longer any reason to doubt that adult scurvy and infantile scurvy are one and the same disease, having an identical pathogenesis. For many years, far longer than the facts warranted, there was discussion whether Barlow’s disease was true scurvy or merely a form or a complication of rickets, or perhaps a distinct hemorrhagic disease. This question may be relegated to the past, so that we may proceed to consider the pathogenesis of scurvy in the infant and in the adult under a common heading.
There is no need of studying all the theories which have been advanced to account for scurvy. They have been manifold and most of them have died a natural death. For many years the potassium deficiency theory, suggested by Garrod, gained wide acceptance. That scurvy should be attributed to a lack of this salt is readily comprehensible in view of the abundance of potassium in the antiscorbutic foodstuffs, the fruits and the vegetables. It was not long before it was evident that this was not the correct solution, as the salts of potassium served neither to prevent nor to cure scurvy. This theory was accordingly modified to include only organic potassium. Experiment, however, failed to support the validity of this hypothesis, and it was gradually abandoned.
Another theory which had a short but popular career was the citric acid theory, which was maintained vigorously by Netter. This explanation seemed logical in view of the marked potency of the citrous fruits, and particularly when it was shown that human milk contains a greater percentage of the salts of citric acid than cow’s milk, and that some of these salts are lost in the course of heating. This hypothesis withstood neither the practical test nor chemical investigation. It was found that the various salts of citric acid, either singly or in combination, are unable to cure scurvy. This treatment has been employed repeatedly on man and on animals with little or no success; we also have resorted to it in vain. It was shown, furthermore, that it rested on an insecure chemical basis, as boiled milk contains but 0.1 g. per litre less citric acid than raw milk—an amount which is negligible from a therapeutic point of view.
Before considering what may be termed the prevailing theories, a few lines must be devoted to the acidosis theory championed by Sir Almroth Wright. According to this writer scurvy is due primarily to an excess of acid compared with alkaline food.5 A theory of this nature was open to verification, and soon collapsed when put to the test. It was found, in the first place, that an addition of alkali was unable to cure experimental scurvy. It may be added that we have found it of no value in infantile scurvy. Holst and Froelich pointed out that potatoes and peas, two excellent antiscorbutic vegetables, have an alkaline and not an acid ash; that adding hydrochloric acid to dandelion juice improves rather than diminishes its potency; that 1 g. of cabbage, which suffices to protect a guinea-pig from scurvy, does not contain sufficient alkali to neutralize an acid state; and, finally, that scurvy is not encountered in the well-established acidosis of diabetes.
Let us turn to some of the current theories of the etiology of scurvy. For years many have held to the toxic theory, believing that poisons either were consumed in the food or formed in the intestine by means of bacterial action. At present this view is held by the minority. The situation in this respect may be compared to that of beriberi, about which there is also no consensus of opinion, a minority attributing it to the action of an unknown toxin.
A consideration of the clinical course of scurvy sheds but little light on this aspect, and can be interpreted as well for as against the action of a toxin. The nervous system, which is well known to be particularly vulnerable to toxins, is but slightly affected—the cardiorespiratory phenomena (indicating an involvement of the pneumogastric nerves), the occasional changes in the optic disks, and the abnormality of the tendon reflexes constitute the aggregate. In a general way it may be stated that the symptoms resemble those brought about by poisons of various kinds—the cottonseed poisoning in swine, the toxic products of the wheat embryo, or even mercurial poisoning in man.6 The nervous symptoms, especially the irritability of the heart, remind one of the enterogenous intoxication or enterotoxic polyneuritis described by Von Noorden. Such analogies are interesting and suggestive, but can be accorded little weight in deciding the question at issue.
If a toxin is to be regarded as the proximate cause of infantile scurvy, the question naturally arises as to the nature of the toxin. Is it exogenous or endogenous? There is sound basis for believing that the hypothetical poison is not introduced preformed in the food. In the first place, infantile scurvy frequently develops in babies who receive milk of the very best grade indeed, in contradistinction to rickets, this is not preëminently a disease of the poor. Furthermore, there is no relation between the concentration of the food mixture and its liability to induce scurvy. For example, if among a large number of infants receiving pasteurized milk from a common source, some are given the milk diluted by one-half, others given it diluted by one-third, and still others whole milk, the last group will show the least tendency to scurvy, which we should not expect were the poison contained in the food. Nor is it at all uncommon to encounter scurvy in an infant which has been fed with a very dilute milk mixture. Another side of this question should, however, be mentioned—stale pasteurized milk is more apt to produce scurvy than the freshly pasteurized, but here again the injury is in inverse ratio rather than in direct ratio to the amount consumed. There are reports of adult scurvy having been occasioned by decomposed food, such as Torup’s investigation of Nansen’s polar expedition, but the diet had not been faultless in other respects. The experiments of Jackson and Harley, who produced scurvy in monkeys by feeding tainted tinned meat, cannot be unreservedly accepted, as they are substantiated by no pathological examination of the bones, and the diarrhœa and the blood and mucus in the stools do not suggest simple scurvy.
Of those who held to the toxic origin of scurvy the majority had in mind an endogenous toxin, although the conception of the nature of this poison varied greatly. The minority report of the American Pediatric Society states that “scurvy appears to be a chronic ptomaine poisoning due to the absorption of toxins.” Neumann considered scurvy a chronic poisoning, formed probably from the albumin of the milk, and considered the fact that the infant refused to take the harmful food as weighty evidence of its toxic nature. Kohlbrugge included scurvy in his group of “fermentive diseases,” due to the overgrowth of harmful bacteria in the intestine, which are normally restrained by the acid reaction of the chyme. McCollum and Pitz, on the basis of a study of experimental scurvy, suggested that as the result of a break in the metabolism it might be due to the retention of fæces and consequent absorption of toxins. Still more recently Gerstenberger suggested that as the result of the break in the metabolism of carbohydrates, a defunctioning substance, possibly oxalic acid, is produced, which has a strong affinity for calcium.
It is of no avail to discuss these various hypotheses—the formation of intestinal toxins—except where they are based on observations which can be tested and controlled. This is true solely of the relation of constipation to scurvy, and we shall confine ourselves therefore to a consideration of this aspect of the question.
There can be no question whether retention of fæces of itself can bring about scurvy; this is excluded by the marked instances of constipation frequently encountered among thriving babies. The majority of bottle-fed babies and a large number of the breast-fed suffer from a greater or less degree of constipation. On looking over our records of infantile scurvy from this point of view, and comparing them with non-scorbutic infants, we have not been able to note a characteristic distinction. Some of the infants had normal stools, others suffered from constipation, while the records of a great number showed occasional loose stools. Furthermore, in cases of latent or subacute infantile scurvy, it was of no moment whether a laxative was given or whether constipation was induced by means of opium. The report of the American Pediatric Society shows that the majority have had a similar experience; the bowels were regular in seventy-four instances, irregular in fifteen, constipated in one hundred and twenty-six, and diarrhœal in seventy-seven. In this connection, it may be pointed out that the preparation termed “malt soup,” the diet which in our experience has been most frequently associated with scurvy, is essentially laxative, and, on the other hand, that one of the most potent antiscorbutics is potato, which has no definite laxative property. It may be added, as noted elsewhere, that scurvy developed in infants in spite of their receiving cod liver oil or olive oil for long periods. It is evident, therefore, that the retention of fæces is not the essential factor in the etiology of scurvy. Its secondary rôle, especially after scurvy has developed, will be considered later in this chapter.
| Infant. | Diet. | Date. | Scorbutic condition. | Source of material. | Types of bacteria. | Remarks. |
|---|---|---|---|---|---|---|
| M. | Malt soup and cereal | Dec. 1 | Subacute | Rectum | B. acidoph. B. bifidus M. ovalis B. coli | {Normal infant’s flora. {Gram + bac. predominant. {No spore-bearing or putrefactive types. {B. acidoph. about 40% viable bact. |
| Do. | Dec. 4 | Do. | Do. | Do. | Do. | |
| Same, also 20 c.c. liquid petrolatum, one week | Dec. 11 | Subperiosteal hemorrhage | Do. | Do. | {Relatively more B. coli. {Many B. bifidus {No putrefactive bact. | |
| Same diet, oil stopped, orange juice 10 days | Dec. 21 | Markedly improved | Do. | Do. | Normal infants’ flora. Bacteria as above. | |
| K. | Malt soup and cereal | Dec. 11 | Subperiosteal hemorrhage | Rectum | Streptococci B. coli M. ovalis | {Gram - bacteria predominant. {B. coli gram + diploc. numerous. {B. acidoph. few. |
| Do. + orange juice (60 c.c.), 8 days | Dec. 21 | Markedly improved | Do. | B. bifidus B. coli Streptococci | {Gram + bac. predominant. {Many B. bifidus {Streptoc. unchanged. | |
| S. | Formula: Cream, water, flour, sugar, also cereal | Dec. 21 | Mild scurvy | Rectum | B. lact. aerog. B. coli M. ovalis B. bifidus B. welchii | {Gram + and - bact. about equal. {Many lact. aerog. {Putrefactive bact. in minority. |
| Malt soup and cereal | Feb. 11 | More marked | Do. | B. lact. aerog. M. ovalis B. bifidus Dipheroids | {Gram + bact. in great majority (B. bifidus). {Spore bearers very few. {Flora not at all putrefactive. |
In order to elucidate this question Torrey and Hess made a study of the relation of the intestinal flora to the scurvy of guinea-pigs and of infants. In guinea-pigs they found in the intestinal tract merely such bacteria as are encountered on the oats and hay fed these animals. The bacteria were few in number and hardly any were actively proteolytic. Furthermore, there was no change in the flora on adding antiscorbutic food, although the scorbutic symptoms disappeared. Recently Givens and Hoffman, as the result of a similar study, have come to the same conclusion. The investigation of infants led to similar results, and is illustrated in Table 1. It will be seen that the infants were all on a high carbohydrate diet, and that in two instances the flora was compared, not only during the active scorbutic process, but after orange juice had been given for a week or more. The bacteria were such as one should expect on a diet rich in carbohydrates; putrefactive organisms were present only in small numbers; and in the case in which they were most numerous (S), they had disappeared upon the subsequent examination, although the scurvy had become more marked. It is evident, therefore, that in the scurvy of infants as well as of guinea-pigs there is no overgrowth of putrefactive bacteria in the intestinal tract, and therefore no basis for the hypothesis of ptomaine or similar intoxication. Other poisons may, however, be absorbed from the intestine as the result of a prolonged deprivation of an essential vitamine.
There are those who believe that scurvy is of bacterial origin, some going so far as to regard it as a communicable disease. This viewpoint was maintained by the famous Boerhaave and supported with all the weight of his authority by Villemin in the seventeenth century. It is a view held by many, if not by the majority, of physicians in Russia to-day, and recently has been advanced by European army surgeons. This question illustrates in an interesting manner how the trend of the day influences medical thought—it has been suggested lately by Much and Baumbach that the scurvy microörganism may be carried by means of lice. But clinical experience points absolutely against the infectious nature of scurvy. Indeed, the only episode which lends any support to this opinion is its widespread and seemingly epidemic character; the fallacy of such deductions has been well illustrated in regard to beriberi, which for many years was regarded as an infectious and communicable disease. The fact that whenever scurvy occurs among a body of troops the officers are spared, constitutes convincing evidence against its communicability. This peculiarity of incidence was noted by Hoerschelman and others in the recent World War, and is referred to in the Report of the War of the Rebellion. Many of the earlier writers, in discussing the occurrence of ship scurvy, drew attention to the paucity of cases among the officers.
When we turn to bacteriological studies we find that some years ago Ausset claimed to have isolated “a pasteurella type of organism” from a case of infantile scurvy, and suggested it as the causative agent of this disorder. On the other hand, Hart, Rehn, Hirschsprung, von Starck, Schmorl, and recently Boerich, have failed to find bacteria in the blood, although the total number of cultures must be admitted to have been small. Czerny and Keller report negative bacterial growth from fluid aspirated from affected joints.
The only articles considering this important question from the experimental side are those of Jackson and Moody, and of Moore, who conclude tentatively that scurvy may be a bacterial infection. Jackson and Moody cultivated a diplococcus from the tissues of scorbutic animals after death, reproduced hemorrhages by inoculating cultures of these microörganisms into the circulation, and recovered the bacteria from the tissues some weeks later. Their results are open to the criticism that bacteria were found only after death, and that all blood cultures during life proved negative. An article by Moore, however, which has just appeared from this same laboratory, states that “an organism of the streptococcus viridans type was isolated from the blood” in a case of adult scurvy. In one instance we recovered an organism of this type from the blood of an infant suffering from scurvy. It is highly important that more blood cultures should be carried out in the course of human or animal scurvy, and that particular note should be made of the stage of the disorder when they are taken.
There is no doubt that invasion of the blood-stream does occur readily in the course of scurvy, but this takes place generally after the disease has developed and must be regarded as a secondary phenomenon and therefore unessential from an etiologic standpoint. Indeed one of the striking and important symptoms of scurvy is the marked susceptibility to infection (furunculosis, nasal diphtheria, “grippe,” etc.), which comes about as the result of the nutritional disturbance. An excellent example of this interrelationship is the “epidemic” of hemorrhagic scurvy described in the chapter on symptomatology. Hemorrhages coming about in this way should be regarded as focal complications rather than as truly scorbutic. It should be realized that, at the present time, it is not possible to distinguish between local symptoms which are truly nutritional or scorbutic in nature, and those which are bacterial and of secondary origin.
The newest theory, and the one at present most widely accepted, is the vitamine (accessory factor) theory. It was evident to Lind in the seventeenth century that scurvy could be prevented and cured by means of fruits or vegetables, a fact which became increasingly clear to succeeding generations. Until the latter part of the nineteenth century, however, this miraculous virtue of plants stimulated little inquiry and no research. As far back as 1841 Budd realized that “the explanation depended on the study of organic chemistry, and the experiments of physiologists,” but until recently it was not perceived that the solution of the problem involved the introduction of a new chemical factor. This view suddenly took shape after Eijkman in 1897 showed the nature of polyneuritis in fowl, and Hopkins in 1906, going a step farther, demonstrated the necessity of one or more unidentified food factors for the normal nutrition of the rat. The work which established this novel theory on a scientific basis in relation to scurvy was the classic investigation of Holst and Froelich, referred to so frequently in connection with experimental scurvy. These investigators showed that the mere drying of vegetables was sufficient to deprive them of their antiscorbutic power, although from a chemical standpoint they seemed unaltered; that high degrees of heat had generally the same effect; that under certain conditions these foods withstood prolonged heating, demonstrating that the antiscorbutic factor was not a ferment; that acids and alkalies played no essential rôle in the etiology; that fats, proteins and carbohydrates were not significant factors; that as little as 1.0 g. of cabbage suffices to afford protection to a guinea-pig. In other words, by a process of exclusion they showed that it is a disorder due to the lack of an unidentified food factor.
Subsequent studies, carried out within the past few years, have served only to strengthen this viewpoint. For example, an “artificial orange juice” composed of the various salts, citric acid, and sucrose in the proportions in which they are found in the natural juice, failed, in the experience of Hess and Unger, to protect or to cure guinea-pigs—demonstrating that this preparation did not contain the essential factor. In the same way, Harden and Zilva were able to protect animals from scurvy with a preparation of lemon juice which had been almost entirely deprived of its salts. It is needless to multiply these examples. It is sufficient to state that there has been no investigation during the last years of intensive study of scurvy, which has tended to weaken the vitamine hypothesis. It may be stated, therefore, that experiments have demonstrated that scurvy is due essentially to the lack of a specific vitamine. It is unwise to proceed farther and place it in the group of so-called “deficiency diseases,” including beriberi, pellagra, etc., unless the reservation is made that these several diseases may present marked differences. It is quite possible that one may be what might be termed a simple deficiency disease, whereas another may have important additional etiologic factors. At any rate, unless it is realized that there has been no proof that all are due to similar deficiencies, we may, by stamping them all alike and by grouping them together, be misled into taking their close relationship for granted. In regard to scurvy, there may well be other etiologic factors, but they are of a secondary character. Bacterial invasion has been referred to in this connection, and it is possible that toxins are absorbed from the intestine after nutrition has been disturbed. Diarrhœa and digestive disturbances may play a rôle. Whether the total intake of food or the correlation of its constituents—protein, carbohydrate, fat and salts—affects the action of the vitamine, is one which has not been well studied clinically or experimentally. In regard to beriberi, it is claimed that there is a direct ratio between the quantity of carbohydrate ingested and the amount of vitamine required. No such interrelationship exists in regard to scurvy. This was evident a few years ago (1917) when some infants receiving pasteurized milk, prepared with the addition of 3 per cent. flour, did not tend to develop scurvy more readily than others receiving simple pasteurized milk. A consideration of the antiscorbutic vitamine will be postponed for a subsequent chapter.
Etiology.—In considering infantile scurvy we are concerned almost entirely with the artificially-fed baby. It is true that in the literature we meet with scattered reports of scurvy in breast-fed babies and that these cases seem to constitute a noteworthy group; in point of fact, they are comparatively few. The collective investigation of the American Pediatric Society includes ten infants who had been given breast milk exclusively, and Concetti adds another ten in his compilation of 682 cases.7 In spite of their paucity these cases require separate consideration because they represent an important aspect from an etiologic standpoint. How are we to explain the fact that human milk may lead to rather than protect against this disorder? On investigating more closely it is found that these cases differ in several important respects from the group which has been artificially fed. They are of a different age; instead of being in the second half year of life they are generally but a few months old. Furthermore, the signs are not the same. The hemorrhages involve the upper extremities fully as frequently as the lower extremities, and often appear at unusual sites—for example, on the scalp or as large subcutaneous effusions at various parts of the body. In many instances it has been noted that the nursing mothers were suffering from some debilitating disease such as tuberculosis or syphilis, or had an insufficient supply of milk, or that there had been some other unusual factor, as Freund has shown in an article devoted to this particular aspect. It is not necessary, however, to fall back on these attendant circumstances to exclude from consideration many of the cases. For example, Crandall’s case of “scurvy in an infant of six weeks” should be invalidated, not because, as Freund suggests, the mother had rheumatism and insufficient milk, but because of the age of the infant, and the course of the disease; first one arm was involved, then the other, then hemorrhages appeared on the skin, and finally it was cured by giving a teaspoonful of fresh cream before each nursing. Had the baby really suffered from scurvy it could not have been cured by this means. Southgate’s case must also be rejected, not because the mother was tuberculous but in view of the symptoms—the arms and legs were pseudoparetic, “the legs, feet and hands were double their normal size,” and moderately large hemorrhages were present on the back and chest. It seems hardly necessary to discuss in detail the score of cases which comprise this group, as, in general, the same criticism applies to all. Some evidently were congenital syphilis, still more must be regarded as sepsis, and others as unknown toxic conditions. Apart from these cases the question must be considered whether scurvy can occur in a breast-fed infant. Personally, we have never met with a case of this kind, and, as Finkelstein aptly remarks, there has been “no necropsy of a breast-fed case or conclusive X-ray picture.” It seems possible only if an infant, for a period of months, has obtained a scanty supply of milk, or when the milk has been exceedingly deficient in the antiscorbutic vitamine. Even under such conditions it does not seem possible for scurvy to become manifest in six weeks (Crandall’s case), or in four weeks, as in a case reported by the American Pediatric Society, unless we believe that the infant suffered also from a certain degree of intrapartum or congenital scurvy. In view of the fact that an infant requires about one pint of milk to furnish it with an adequate daily quota of the antiscorbutic factor, it is theoretically possible, under extreme conditions, for it to become scorbutic, in spite of being nursed at the breast. Such an occurrence must be regarded as exceedingly rare, far more so than the current statistics illustrate, for considerably less than a pint of milk a day will prevent the appearance of manifest scurvy for a period of several months. Some of the reported cases may have been latent scurvy, rendered acute by a complicating bacterial infection.
It might be expected that by ascertaining the occurrence of infantile scurvy in countries where it is endemic, we could learn under what conditions and how frequently breast-fed babies develop this disorder. Approaching the question from this angle, it is found that the available data is meagre and not entirely convincing. Peculiarly enough infantile scurvy has rarely been reported from Russia, where scurvy is, in many sections, endemic. For example, although Tschudakoff, who personally examined over 10,000 persons, in connection with the great scurvy epidemic in Russia (1898–99) found 11.11 per cent. of the people suffering from this disease, he did not meet with a single case under the age of five years. Fuerst writes that Filatow, the celebrated Russian children’s specialist, declared that he knew of no instance of Barlow’s disease described in the Russian literature.8 Shortly after the recent war scurvy broke out among the wet-nurses in an infant asylum in Vienna. A very few of the infants nursed by these women developed the disorder, far fewer than might have been expected (personal communication). Hopkins recently wrote a communication to the effect that in the island of Aruba, in the Dutch West Indies, they had been unable to grow any crops in 1912, 1913, 1914, that 3000 cases of scurvy had developed there during the year 1915, and that in 1917 it was again being noted. In answer to a personal inquiry regarding the occurrence of scurvy among the infants of Aruba, he wrote that “infantile scurvy is very rare,” although “most all of the babies are breast-fed for about a year.”9
On the other hand, descriptions of the coincidence of scurvy in mother and nursling are even more fragmentary; in fact, we have been able to find but two reports of this kind. The one most frequently cited is that of Cheadle, which consists merely of the following bald statement: “With the exception of one or two doubtful cases, of which the details of breast-feeding and diet are imperfectly given, the only instances of scurvy arising in sucklings are those when the nursing mother has been suffering from scurvy at the time.” The other report has been gleaned from a recent editorial in the British Medical Journal, which refers to the above mentioned outbreak of scurvy in Vienna, affecting in some cases both mothers and breast-fed infants.
It is difficult to pass judgment on this question in view of the paucity of data. In the near future, probably, when we learn in detail about the epidemics of scurvy which occurred during and immediately following the war, we shall be in a better position to weigh its pros and cons. In view of the above data it does not seem that nursing infants readily develop scurvy, even though their mothers do not obtain a full quota of antiscorbutic vitamine in their food. This appears to be the clinical result, whatever its interpretation may be. It cannot be explained on the assumption that human milk contains a particularly large quota of this factor. In a test carried out to elucidate this question it was found that eight ounces a day of breast milk was insufficient to alleviate the symptoms in a case of scurvy, and that twelve ounces barely sufficed. This milk was from a woman who was on a liberal diet containing an adequate supply of vegetables. It had been previously demonstrated that sixteen ounces of cow’s milk is sufficient to cure infantile scurvy, so that it is evident that human and cow’s milk do not differ essentially in this respect. There are, however, other factors to be considered—for example, the incomparable freshness of the milk suckled from the breast, which may endow it with additional potency, or the possibility that the lack of vitamine may be compensated for by the large quantity of milk consumed. It also may not be entirely immaterial whether the vitamine is supplied in one dose, as, for example a daily feeding of orange or tomato juice, or whether this factor is furnished to the infant in frequent small quantities in the mother’s milk throughout the day. In this connection we cannot help contrasting the relation of beriberi to breast feeding. As is well known, infants which develop beriberi are almost always nursed and not bottle-fed, and show signs of this disorder, although the mothers are in apparent health, and give no clinical evidence of disease.
Turning to a consideration of the artificially-fed infant, there exists a somewhat similar situation in regard to the occurrence of scurvy on a diet of raw cow’s milk. In almost all reports of this kind the quantitative viewpoint is entirely disregarded, and little or nothing is stated to indicate how much milk the infant consumed. And yet this factor is of essential importance in interpreting the cause of the nutritional failure. It is clear, for example, that if a baby receives but eight ounces daily of raw milk—one-half the requisite amount—it may well develop scurvy, notwithstanding the fact that the milk has not been heated. In addition to the quantity, there are other factors which play a greater or less rôle in the relation of raw milk to the etiology of scurvy. It is no doubt of consequence whether the fodder of the cows was rich or very poor in the antiscorbutic factor, and, accordingly, whether the baby received what may be termed an “antiscorbutic-rich” or an “antiscorbutic-poor” milk. Furthermore, the age of the milk must be borne in mind, for we have found that even raw milk loses some of its potency on becoming stale.10
One of the mooted questions relative to the etiology of scurvy is the rôle of heated milk, and more particularly of pasteurized milk. In view of the vogue which pasteurization has acquired in the large municipalities, especially in the United States, this aspect has assumed increasing importance, and deserves detailed investigation. Pasteurization has achieved so much in limiting the infectious diseases, especially the diarrhœal disorders of infancy, that it has come to be looked upon as heresy to deprecate its virtues in any regard.
It has become increasingly evident that in the course of pasteurization milk loses an important measure of antiscorbutic vitamine. The term pasteurization, when employed in this connection, is not meant to be synonymous merely with the heating of milk to 140° to 165° F., but embraces the entire commercial process—the heating, handling, subsequent cooling, aging and all other factors involved. There can be no doubt that milk which has undergone this elaborate treatment has suffered in its antiscorbutic property. In 1914 Hess and Fish reported mild cases of scurvy occurring among infants who had received milk heated to a temperature of 165° F. for thirty minutes. This degree of heat is claimed by many physicians and hygienists, including the National Commission on Milk Standards, not to destroy its chemical constituents. Nevertheless typical cases of scurvy supervened after this diet had been followed for a period of six to nine months. Subsequent experience, published by Hess in 1917, with milk heated to only 145° F., served to confirm the previous observations. That these cases were true scurvy was proved by the fact that a cure resulted when raw milk was substituted. A similar experience in Berlin reported by Neumann and others was convincing, but was not heeded in this country. In 1901 one of the largest dairies in that city established a pasteurizing plant where all milk was raised to a temperature of about 60° C. After an interval of some months infantile scurvy began to be reported from various sources throughout the city. Neumann depicts the situation as follows: “Whereas, Heubner, Cassel and myself had seen only thirty-two cases of scurvy from 1896 to 1900, the number of cases suddenly rose from the year 1901, so that the same observers—not to mention a great many others—treated eighty-three cases in 1901 and 1902.” At a spirited meeting held by the Berlin Medical Society in 1903 to discuss this subject, Heubner was able to report 65 cases. An investigation was made, and the pasteurization discontinued. The result was almost immediate, the cases decreasing just as suddenly as they had increased. These reports and others demonstrate that unless additional antiscorbutic food is given, a diet of pasteurized milk will lead to the development of scurvy. As the antiscorbutic vitamine is not entirely destroyed by pasteurization, the severity of the disorder will be in inverse ratio to the amount of milk which is consumed.
It has been our experience that milk pasteurized in the home or institution did not lead to scurvy to the same extent as that which was commercially pasteurized. Babies fed on home-pasteurized milk did not develop manifest scurvy. The difference in the two processes consists mainly in the amount of handling during the process of heating and the subsequent aging which the milk undergoes. An interval of forty-eight hours usually elapses between commercial pasteurization and the delivery of the milk to the consumer. In New York city most of the better-grade milk is pasteurized at the farm, so that it is subjected to a longer period of aging than the poorer grade, which is not pasteurized until it reaches the city. Although our results indicated the effect of freshness or staleness on milk which had been heated, they showed also that other factors must be involved, for home-pasteurized milk which is forty-eight hours old is superior to the commercial product of the same age. This difference we believe is due to the handling which the milk undergoes, to the mechanical processes involved in commercial pasteurization.
In considering this aspect of the development of infantile scurvy on a diet of heated milk, it is of interest to refer to the experience of Switzerland and of France. In 1907 Bernheim-Karrer reported nine cases of scurvy which occurred on “homogenized” milk. This milk is forced between rapidly-rotating surfaces at a temperature of 55° to 65° C. at a pressure of 150 atmospheres. This process had been introduced the year previous by a large dairy which was well known for its excellent grade of milk. Before this innovation, milk usually had been boiled for a long while before being fed to infants. In France a similar epidemic of scurvy followed the introduction of the use of homogenized milk (lait fixé). Lecornu gives an interesting account of this episode, remarking on the large number of cases of scurvy occurring on this milk compared with sterilized milk, which was employed so much more extensively. These experiences furnish excellent examples of the harmful effect of industrial methods on milk, especially on its antiscorbutic vitamine. Lecornu also emphasized the scorbutic influence of “lait maternisé,” which is similar to the German Gaertner milk, and is subjected to dilution, centrifugation, and sterilization.11 He states that before this preparation was introduced scurvy was practically unknown in France. Lecornu attributes the deleterious effect of the “lait maternisé” and the “lait fixé” to bacterial contamination, as does Bernheim-Karrer. We believe, rather, that its loss of potency is due to the mechanical processes to which it has been subjected.
Boiled and, more particularly, sterilized milk, is regarded as a common cause of infantile scurvy and figures prominently among the foods held accountable for this disorder. It has been pointed out, however, that thousands of infants, especially in Europe, receive milk of this kind, and do not develop scurvy. Statistics such as those of Variot, who has distributed in his out-patient department, during a period of twelve years, 400,000 quarts of sterilized milk (heated in half-litre bottles and hermetically sealed at the farm) without observing a case of scurvy, must be accorded weight in this connection.12 Escherich, some years previously, stated that he did not meet with scurvy in Graz, although he was accustomed to feed babies on sterilized milk. Budin, the celebrated French children’s specialist, writes: “As for the so-called infantile scurvy which is alleged to follow the use of sterilized milk, I have heard a very great deal about it during the last few years, but I am still looking for my first case.” Evidence from such sources cannot be summarily cast aside, but must be given due consideration. It is evident that the mere heating or sterilization of milk, although it reduces the antiscorbutic vitamine, does not do so to a degree sufficient to lead to the production of clinical scurvy. Our experience accords with that of the above observers. Some years ago we fed infants with milk which had been boiled for five minutes, and, at another time, made use of home-made evaporated milk which had been heated for a period of seventeen hours, until it had been reduced to one-eighth its volume. This evaporated milk was well borne for months, although slightly caramelized in the course of heating, and did not lead to any signs of scurvy. Clearly there are other factors involved in this question besides the mere subjection to heat. We believe that every step in the process is important—the freshness of the milk, whether or not it is agitated and exposed to the air, whether it is sealed carefully and used soon after sterilization,13 and, finally, whether the baby receives a sufficient quantity. If this milk, which has certainly lost some of its vitamine content, is given in small amount, it will not supply an adequate amount of the antiscorbutic factor.
Neumann, Czerny, and others state that they have even cured infantile scurvy by giving boiled milk obtained from a different source. In the Berlin epidemic, Neumann laid particular emphasis on the fact that the milk which induced scurvy had been doubly heated, having been pasteurized commercially and later boiled in the home before it was fed to the baby. Plantenga has also laid stress on the influence of two-fold heating, citing an interesting experience with scurvy in his clinic. When the milk was pasteurized one day and boiled for five minutes on the subsequent morning, 23 cases of infantile scurvy developed among the 200 infants attending his dispensary. The following year when the procedure was altered so that the milk was merely pasteurized, no case of this disorder developed. There can be no doubt that milk which has been heated twice must have lost more of its antiscorbutic properties than milk which has been heated but once, and that aging also must contribute to this loss. Whether there is what may be termed a peculiar sensitization of milk following pasteurization, has not been definitely shown.
Up to the present time dried milk has played an insignificant rôle in the etiology of infantile scurvy. One of the factors which has hindered the general acceptance of dried milk by physicians and laymen has been the fear that its use might lead to the development of Barlow’s disease. It is therefore important to consider this aspect of the subject, especially as dried milk seems destined to be used to an increasing extent. A recent report to the Local Government Board by Coutts states that “Millard and Naisch in England confirmed the testimony of Miele in Belgium, and Gautier and Genevoix in France, that scurvy is not to be feared” from this foodstuff. This coincides with our experience, namely, that dried milk not only does not lead to scurvy, but may contain sufficient antiscorbutic vitamine to cure this disorder. Recently a scorbutic baby was fed with milk which had been dried by the so-called Just-Hatmaker process—whereby it is subjected on a drum for a few seconds to about 230° F.—with the result that the hemorrhages of the gums began to be absorbed in about three days, and all symptoms to disappear shortly thereafter. This infant received dried milk to the equivalent of 24 ounces of fresh milk, and this preparation had been dried and canned somewhat over three months before it was used. Recently two infants, suffering from marked scurvy, were treated with milk which had been dried six months previously. The one received only sixteen ounces a day and the other a quart; both recovered within a few days after this food had been substituted for malt soup. Not long ago, as reported elsewhere in a paper by Unger and myself, after curing a baby of scurvy by means of this milk, it was maintained in health for a subsequent period of three months on a diet which contained no additional source of antiscorbutic vitamine. These results are emphasized as illustrating the peculiar relationship of drying and of the application of heat to the antiscorbutic vitamine, and because recently several reports have appeared, for example, that of Barnes and Hume in England, and of Hart, Steenbock and Smith in this country, to the effect that dried milk is devoid of antiscorbutic value. The difference of opinion is due to the assumption that dried milk is a uniform product and has identical antiscorbutic properties. For milk to retain its antiscorbutic value, notwithstanding drying, it must have been rich in vitamine before desiccation, it must have been dried quickly, and packed within the shortest possible interval in air-tight, preferably hermetically sealed, containers. As in relation to the heating of milk, so in regard to its drying, it is not the degree of heat to which it is subjected which is all important, but rather the associated conditions. The merits of each process will have to be tested individually and perhaps even each particular brand of milk.14
In the foregoing, the dictum has been accepted without comment that fresh milk may be either rich or poor in antiscorbutic vitamine. This point of view has recently gained general acceptance, on the assumption that the milk of the stall-fed cow is markedly deficient in this factor. Recent work by Hart, Steenbock and Ellis gives evidence that “summer pasture milk is much richer in this nutritive factor than dry feed milk or winter produced milk, involving the use in the ration of corn silage or sugar mangels.” In some experiments (unpublished) we have found that dried milk shows similar variations, being a much more potent antiscorbutic when obtained from cows fed on fresh fodder than a similar milk from the same cows on fodder containing a minimum amount of antiscorbutic vitamine. The supposition of a direct quantitative ratio between the antiscorbutic intake in the food and output in the milk needs confirmation, especially as it does not quite coincide with the experience among human beings in countries where adult scurvy is endemic. In such countries—for example, Russia—nursing infants do not develop scurvy to the extent that would be expected, and it is possible that this exemption is due in part to a selective secretion of antiscorbutic vitamine into the milk.
As is well known, a diet of condensed milk leads to scurvy. This is not surprising, considering the prolonged heating to which this milk has been subjected. It is probable that many cases of mild scurvy developing on this food and characterized by beading of the ribs (rosary) and other indefinite manifestations, have been erroneously diagnosed as rickets.
It is hardly necessary to discuss separately the various kinds of milk which have led to scurvy in the course of infant feeding.15 The principles laid down in the preceding discussion hold good for milk of all kinds. Heat will destroy a certain amount of vitamine, and, if the heating is followed by aging, still more will be lost. If an interval elapses and a second heating ensues, there will be further loss of vitamine. It should never be forgotten in considering foods in their relation to the causation of scurvy, that the amount of food given must not be overlooked. For example, a pint of ordinary pasteurized milk will lead to scurvy, whereas a quart in most cases will be sufficient to tide the baby over until the period of mixed feeding. No general rule can be laid down, however, as may be judged from the fact that dried milk which has been subjected to almost all the influences which are deleterious to the antiscorbutic vitamine—heating, drying, aging, all carried out in a neutral medium—nevertheless retains its specific potency.
Infantile scurvy has always been far more prevalent in England and in America than in Europe, notwithstanding the fact that on the continent practically all milk for babies is boiled or sterilized. This has been ascribed, and probably rightly so, to the widespread usage of proprietary foods in the English-speaking countries. Among the cases reported by the American Pediatric Society about 60 per cent. had been given foods of this description. How is this relationship to be explained? These preparations in general may be stated to consist of cereals, sugar, with occasionally a small amount of dried milk; they are mixed with varying proportions of water and milk and then cooked. It is evident that two important causative factors of scurvy are thus furnished, namely, a small and inadequate quota of milk and the application of heat. In most instances not more than sixteen to twenty ounces of milk are used to make up the day’s feeding, and frequently this has been previously pasteurized. But there is an additional factor which comes into play in this connection, one to which we have recently drawn attention in treating of “The Deleterious Effect of the Alkalization of Infants’ Food.” It has been shown that the antiscorbutic vitamine is peculiarly sensitive to the faintest alkaline reaction, in which medium it rapidly undergoes deterioration, and even total destruction if heat is applied. Proprietary foods, with but few exceptions, are alkaline, having been rendered so by the addition of potassium carbonate or bicarbonate, in order to prevent acid fermentation of the fat and to counterbalance the relative poverty of potassium in cow’s milk. Little or no regard has been paid to this reaction; the textbooks on children’s diseases give this point no consideration whatsoever, expressing the salt content merely in terms of total ash. By this means ideal conditions are furnished for the destruction of a large part of the vitamine, and if this factor is not present in excess, scurvy will readily develop. It is to these various circumstances—the deficiency of milk, the alkalinity and the heating—that the scorbutic quality of proprietary foods is to be ascribed.
The most flagrant example of an infant’s food leading to scurvy is “malt soup”—an alkaline preparation of malt, which is prepared with flour and a small amount of milk.16 This food brings about scurvy almost invariably unless an antiscorbutic is added to the dietary. That this effect is due to the alkaline potassium carbonate was shown by a recent test which is illustrated in chart. (Fig. 2). Here we see that in a case of scurvy, when the food was altered and prepared with the same amount of milk and alkali, the disorder did not abate (although the carbohydrate had been discontinued), but when the potassium carbonate was omitted a gain in weight ensued, and, we may add, the symptoms disappeared.
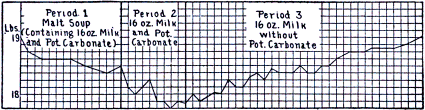 Fig. 2.—Human scurvy: weight curve of a baby that developed scurvy on a diet of malt
soup (period 1). During period 2 the flour and malt soup were omitted from the diet, the
same amount of milk and potassium carbonate being continued. The disorder did not abate.
The only change in period 3 was a discontinuation of the potassium carbonate. This brought
about a gain in weight and cure, showing the destructive effect of the alkali on the vitamine.
Fig. 2.—Human scurvy: weight curve of a baby that developed scurvy on a diet of malt
soup (period 1). During period 2 the flour and malt soup were omitted from the diet, the
same amount of milk and potassium carbonate being continued. The disorder did not abate.
The only change in period 3 was a discontinuation of the potassium carbonate. This brought
about a gain in weight and cure, showing the destructive effect of the alkali on the vitamine.
A test of this kind once more raises the question whether carbohydrates lead to the development of scurvy. As previously stated, there are many who believe that the carbohydrates, especially starch, have this harmful effect by requiring a large amount of the various vitamines for their metabolism. This relationship was first brought forward by Bradden and Cooper in regard to beriberi. It is a suggestion which cannot be disregarded in view of the great amount of scurvy which comes about on diets rich in carbohydrates, especially those containing malt sugar. We do not believe, however, that the harmful effect which this foodstuff exerts can be explained on the above hypothesis, as experience has shown that infants may receive for many months equally large amounts of carbohydrates—cane sugar, flour, or a combination of both—and nevertheless not manifest a similar tendency to develop scurvy.
Age Incidence.—Scurvy may occur at any age if the diet does not furnish sufficient antiscorbutic factors. As a matter of fact, it is encountered most often among infants and adults, not because these two age-groups are particularly susceptible, but because there are peculiar attendant circumstances. In the case of the infant, it is due to the fact that for almost the entire first year of its life it is dependent entirely upon milk, a foodstuff poor in antiscorbutic vitamine, and containing, under favorable conditions, barely enough to meet its requirement. If, therefore, the potency of the milk is weakened, or if an insufficient quantity is fed, and more particularly when both of these factors are involved, a scorbutic condition will ensue. The reason why older children, those over one and a half or two years of age, do not develop scurvy is largely due to their varied and liberal diet, which is amply provided by the mother or guardian, so that even in times of want they receive more than their due share of the available food supply.17
From a clinical standpoint scurvy may be said to occur in infants during the second half year of their lives. There is general agreement on this point; it is borne out by the investigation of the American Pediatric Society and by the statistics of various individuals. On the basis of a large experience, Still states that nearly eighty per cent. of the cases appear between the ages of six and ten months, and that in no case did the disorder occur before the age of five months. It is of importance from both the etiologic and the therapeutic standpoint to distinguish clearly between the age when infantile scurvy is commonly diagnosed, and the earlier stage when it appears as a general nutritional disorder. We must remember that scurvy generally takes from six to nine months to become manifest, this developmental period varying mainly in proportion to the degree of the dietary deficiency. It is evident, therefore, that there must be a prolonged period of nutritional failure which precedes the diagnosis. This stage consists of two early phases, the first months where the faulty diet causes no apparent change and seems to have no deleterious effect on the infant, and the second, of latent and subacute scurvy. The “latent” condition is one merely of unsatisfactory nutrition and retarded growth, which it is not possible to interpret; “subacute scurvy,” which develops subsequently, is distinguished by characteristic signs and symptoms. We shall not review their symptomatology, as it is given in the chapter devoted to this topic. The subject is brought forward in this connection to emphasize the fact that the scorbutic condition occurs far earlier than is generally realized, and furthermore, that if the earlier and more subtle symptoms of scurvy were comprehended, the age incidence would fall earlier than the current figures indicate. The earliest instance of this disorder which we have seen occurred in a baby four and a half months of age.
Age does not seem to play a definite rôle in regard to the incidence among adults. Scurvy frequently has been encountered among old men, and is of common occurrence among the most vigorous of the nation, the young soldiers and sailors. Some have stated that it takes place less often among soldiers in the twenties than among those in the thirties, but this has not been demonstrated. The fewest cases have been reported among children over two years of age. It was due to the apparent immunity of this age-group that, until very recently, German writers doubted the identity of infantile and adult scurvy. The exclusion of children of this age is merely fortuitous and, moreover, is by no means absolute. One of the earliest cases of scurvy in children, reported by Montfalcon, occurred in a child six years old. Bateman in America described a case in a child of about this age. Barlow, in one of his first articles, reported scurvy in a small group of older children. The case so frequently quoted by German authors in this connection is that of Fraenkel, who described both clinically and pathologically a case of scurvy in a boy eight years of age. These cases by no means exhaust the number which are reported. Recently, Tobler has given us an account of scurvy, occurring during the war, in a Viennese foundling asylum which harbored children between the ages of two and fourteen.
Season and Climate.—Many of the older writers laid great stress on the influence of season on the occurrence of scurvy, which they believed broke out particularly in the cold and damp months of the fall, winter and early spring. It is true that most of the epidemics have occurred at these seasons of the year. This is merely what should be expected, considering that the disease depends mainly upon the supply of fresh fruits and vegetables. Where conditions are abnormal, as in war, there have been notable exceptions to this seasonal incidence. In the “Report of the War of the Rebellion” there is an instructive graph illustrating the occurrence of scurvy in our Civil War and in the Crimean War, which shows that this disease prevailed to the greatest extent during the winter months in the former, whereas in Crimea, the season of greatest frequency was the summer time. One of the severest outbreaks of scurvy on record is that which occurred at the siege of Thorn in Germany in the year 1703. During the months of July and August, when the weather was excessively hot, scurvy ravaged the besieged army. There are, furthermore, many reports of scurvy in the tropics during the dry season. In the island of Aruba, in the Dutch West Indies, which has been visited by scurvy year after year, and which is referred to elsewhere, the disease is endemic during the dry, hot season. Formerly it broke out on the men-of-war and vessels of the mercantile marine while they were in southern waters. As regards infantile scurvy, it has always seemed to us that season played a slight rôle; that cases which occurred in the summer tended to be less severe and to be characterized by periods of intermission rarely observed in the winter time.
The effect of climate has been accorded a variable place in the etiology of scurvy. Lind believed that a damp, cold climate, such as that of the Low Countries, was conducive to scurvy. On the other hand, since it is realized that diet is the essential element, all other factors have been regarded as of no moment whatsoever. It is difficult to pass judgment on this question, since scurvy is now endemic in such a limited area of the world. It seems quite possible that a damp, cold climate, which depresses the various functions of the body, may exert an influence where the quota of antiscorbutic foodstuff is not quite adequate. Exposure to infection is also greater under such climatic conditions.
Economic status has to be considered in connection with infantile scurvy. Numerous writers have drawn attention to the fact that scurvy is seen relatively more frequently among the infants of the well-to-do and the rich than among those of the poor. This curious and paradoxical situation is due to the zealous care which the former receive—the extreme precautions in sterilizing the milk, the addition to the formulas of expensive proprietary foods, the watchfulness to avoid the child’s obtaining a chance bit of fruit or vegetable. Since the popularization of commercially-pasteurized milk in the larger municipalities, and the advertising propaganda for the sale of “baby foods” which has extended their use among the masses, this distinction in the social status has been largely obliterated.
Sex seems to play no part in the etiology of scurvy. Several writers have claimed, however, that there is a certain degree of racial immunity. For example, Sheppard reports that the Zhob Kakai seldom develops scurvy, although he naturally excludes vegetables from his diet, and Boerich noted among the prisoners of war that the Slavs, especially the White Russians, were more susceptible.18 Of course a lack of susceptibility of this nature can be merely relative. Such a racial distinction may seem far-fetched, but if we admit that disposition and habits of life can play a rôle, it is quite possible for races to vary in their predisposition to this disorder. Moreover, we shall see that individuals differ markedly in this respect. Lind and others repeatedly emphasize the fact that the indolent and slothful sailor was stricken with scurvy far oftener than the one who was active, and claimed that physical exercise even tended to bring about a cure.19 Those who have had a large experience with scurvy in adults are almost unanimous in believing that a psychic element enters into its etiology. In this way, in a measure, they account for the frequency of scurvy among defeated troops, in besieged armies, and among men depressed by homesickness, fatigue, and discouragement. This point of view cannot be lightly disregarded, bearing in mind that depressed mental states alter the functions of the organs and markedly affect secretion. The many cases and epidemics in institutions for the insane cannot, however, be attributed to this cause, but are probably almost entirely due to a want of supervision of the dietary. Among infants, the question of the influence of race and of the mental state needs but little consideration.20 For some time we have carefully observed the course of scurvy among happy and contented infants compared with those of an unhappy and fretful disposition; in some instances the former, although the diet was similar, seemed to develop scurvy less readily than the latter.
There can be no doubt that there is predisposition to scurvy, as there is, probably, to every nutritional disorder. Among soldiers and sailors a certain number develop scurvy on the same ration which does not harm others. Some years ago when scurvy developed among a group of infants fed on pasteurized milk, this idiosyncrasy was noted. The distinction, however, is rarely sharply defined. Careful clinical investigation will generally show that the infants which seem to be spared are not thriving quite normally; they are somewhat pale, and do not gain in weight as they should, and their appetite is poor. The most interesting experience of this kind is the following which is frequently cited: In a family where the first child developed scurvy, Finkelstein took the precaution, in the case of the second child, to have the milk boiled for as short a time as possible, and to begin mixed feeding early. In spite of these precautions this boy also developed scurvy. Finkelstein states that once before he had met with a similar mishap. An experience which he relates, regarding a foster-mother, an excellent nurse, who had three infants in succession develop scurvy in spite of preventive measures, is also of interest in this connection. The latter occurrence evidently cannot be attributed to hereditary or family predisposition, and serves to emphasize the inherent difficulties of the subject. v. Starck’s report of an instance where twins were fed on similar milk mixtures and one developed scurvy, whereas the other thrived satisfactorily, is a striking illustration of the rôle of idiosyncrasy. This case, as well as many others, fails to be absolutely convincing in view of the fact that the daily intake of milk is not recorded.
A predisposition to scurvy cannot be ascribed to a condition of general malnutrition. For example, among infants it has never seemed that those suffering from marasmus or atrophy were particularly prone to develop scurvy. Whether syphilis, tuberculosis or malaria tends to precipitate the onset of this disorder cannot be stated.21 In view of the fact that prematurity is such an important factor in the pathogenesis of rickets, it would be of interest to know whether a similar relationship exists between infantile scurvy and prematurity. The only clinical condition which we have found predisposing to scurvy is the “exudative diathesis” of Czerny, a term which implies a tendency to develop exudations of the skin or of the mucous membranes. Probably it is not without significance that in this diathesis the blood-vessels may evince a decided weakness, an increased permeability, as demonstrated by the “capillary resistance test.” (See Symptomatology.)
Nothing whatsoever is known regarding the possible influence of the fat, protein, carbohydrate and salt content of the diet on the development of scurvy. Is it entirely immaterial whether one or another food element largely predominates, or is the antiscorbutic factor to some extent modified by other components of the food? Influences of this kind, which at most are secondary, cannot be ascertained by the biologic test which at present has to be relied on to measure the development of scurvy and the potency of antiscorbutics. It is quite possible that the course of scurvy may be affected by the character of gastric and intestinal digestion, by the activity of the glands which pour their secretions into these organs, by the destruction or elimination of the antiscorbutic factor in the food. The frequent association of dysentery and scurvy noted during the recent war and referred to by many previous writers, shows the effect of intestinal disorders. These hypotheses are tentatively advanced because it is evident that some factor exists, apart from the mere antiscorbutic value of the diet, which at times exerts a potent influence on the development of scurvy. Cases developing in spite of a moderate amount of antiscorbutic food, and others not responding to the addition of vegetables or fruit to the diet—although not numerous—have occurred too frequently and have been reported by too experienced observers to be brusquely disregarded. For example, Neumann, one of the keenest clinical students of scurvy, stated that he had met with four instances of this nature. Hess and Fish reported two similar experiences.
The secondary etiologic factors are mainly predisposing; a few words, however, must be added concerning what may be termed exciting factors. Infection is the most important condition which may suddenly and precipitously induce scurvy. This fact was brought to our attention in 1912 in connection with the outbreak of scurvy among infants receiving pasteurized milk. Its explanation was not clear at the time, but was elucidated by subsequent experience, and was described in 1917 as follows: “Latent scurvy was prematurely changed to florid scurvy by the presence of a ward infection; an epidemic of ‘grippe’ precipitated an epidemic of scurvy exceptional in its hemorrhagic tendency.” The association of scurvy and infection has been recently emphasized by McCarrison and others, and seems to hold good for the other so-called deficiency diseases. In this connection one other exciting cause of scurvy may be mentioned, namely, trauma. The older writers noticed that following a fall or an accident, a sailor frequently developed scurvy, and Barlow in 1894 remarked on the influence of trauma in connection with infantile scurvy. As might be inferred, its effect is mainly to induce premature rupture of the weakened blood-vessels; in infants we have seen this occasioned by pressure exerted on the lower end of the thigh to ascertain the presence of tenderness. Viewing the situation broadly, it must be acknowledged that except for the realization that scurvy is due to a new food factor—a vitamine—our fundamental understanding of its pathogenesis has advanced but little, in spite of the employment of experimental methods and the availability of modern technic.
It is doubtful whether mere clinical studies will contribute in a large measure to the solution of the pathogenesis of scurvy. Much may, however, be learned by investigations of the metabolism in human scurvy—an aspect of the problem which, as will be brought out in a subsequent chapter, hardly has been explored. By this means may be acquired a clearer understanding of the effect of an antiscorbutic deficiency on the tissues and on cellular activity. Much may be expected from physiologic and pharmacologic studies of the specific vitamine, although it is not yet available in a pure state. Finally, it is probable that the solution of similar questions relating to the pathogenesis of cognate disorders—a study which is engaging the best efforts of so many workers throughout the world—will shed light on this particular disease.
We shall not discuss the subject of vitamines in general, but confine ourselves to the more limited field of the antiscorbutic vitamine. The recognition of the “accessory” dietary factors is of such recent date, however, that it will be well to consider briefly how attention came to be directed to them and how their existence was ascertained. As in the case of so many scientific discoveries, it is difficult to point to the exact time when the advance was made. On looking back we find that Lunin, in 1881, noting that mice were unable to live on a diet consisting of protein, fats, carbohydrates, salts and water, came to the conclusion “that other substances indispensable to nutrition must be present in milk besides caseinogen, fat, lactose and salts.” This work did not stimulate similar investigations, nor did Lunin, as might have been expected, allude to scurvy. The work which focussed attention on this novel aspect of dietetics was the report of Eijkman, in 1897, to the effect that when fowl are fed decorticated rice, they develop a disease resembling beriberi, and that the paralytic symptoms disappear on feeding them rice polishings or its alcoholic extract. Here, for the first time, was a positive rather than a negative experiment, and one capable of simple verification. The subject was placed on a scientific basis by the classic investigation of Hopkins, who experimented with purified food substances, and demonstrated how diets which were deficient could be rendered adequate. As early as 1906 he wrote “the animal body is adjusted to live either upon plant tissues or other animals, and these contain countless substances other than the proteins, carbohydrates and fats.” “In diseases such as rickets, and particularly in scurvy, we have had for long years knowledge of a dietetic factor, but though we know how to benefit these conditions empirically, the real errors in the diet are to this day quite obscure.” The work of Osborne and Mendel, and McCollum and Davis in this country, of Schaumann, Funk, Stepp and others, all led to the conclusion that purified diets are unable to satisfy the nutritive requirements of rats or mice, and that extracts of the natural foods suffice to render the diet adequate.
The same rule holds for man, who, when deprived of these vitamines, develops the so-called deficiency diseases—typically modern disorders. Regarded as a group, they are a consequence of our altered mode of life and peculiar civilization. They follow naturally upon the development of immense cities housing millions of people, who necessarily must receive perishable foodstuffs produced at a great distance. To even a greater extent they are the product of countless ingenious methods devised mainly to render foods stable—drying, heating, the addition of preservatives—most of which accomplish their object, but incidentally rob the food of its essential vitamine.
None of the vitamines has been isolated in a pure state. The nearest approach to this desired end has been the work of Funk, who obtained the water-soluble vitamine in a state of such concentration that about 3 mg. sufficed to cure a pigeon of polyneuritis. In considering the attributes of the antiscorbutic vitamine, it must be borne in mind that this factor is referred to as it exists in various foods; for example, in orange juice or in cabbage, and furthermore, that the method of ascertaining its presence or concentration is limited to the crude biological test of animal feeding.
The antiscorbutic factor is distinguished by being the most sensitive of the three vitamines, the most unstable, the least resistant to physical or chemical processes. It may be regarded as one of the most delicate indicators of the biological integrity of foodstuffs; however, as Falk and his co-workers have shown, the enzyme property of living matter is still more readily destroyed. The antiscorbutic vitamine is soluble in water, and therefore is termed by some the “water-soluble C” factor. It is also soluble in alcohol, as shown by the experiments of Hess and Unger and of Harden and Zilva, and the therapeutic tests on infants of Freise and of Freudenberg.23 It possesses, therefore, the solubility of the water-soluble vitamine. Some have suggested that it may be derived from this vitamine, others that instead of one there may be a series of antiscorbutic factors—suggestions based on pure hypothesis. Holst and Froelich showed that this vitamine passes, without appreciable loss, through dialyzing parchment, and Harden and Zilva (2) that it can pass through a porcelain filter. The latter, using the method of Seidell, demonstrated that this vitamine is not adsorbed by fine precipitates such as fuller’s earth, differing in this respect from the water-soluble vitamine; and that in a mixture of equal volumes of autolyzed yeast and orange juice, the antiscorbutic vitamine remained unaffected, whereas the water-soluble A was entirely removed.
One of the most distinctive characteristics of the antiscorbutic factor is its sensitiveness to even moderately high degrees of heat. In this respect it differs markedly from the water-soluble or so-called “antineuritic vitamine” which withstands exposure to high temperature. The reaction of the antiscorbutic vitamine in this regard is not a simple one, and cannot be expressed by a mere statement of the degree of heat and the length of exposure. Numerous other factors, especially the reaction of the medium, but also the physical environment, must be taken into consideration—for example, cabbage is more resistant to the action of heat than its juice. An understanding of the relation of antiscorbutics to heat may perhaps best be obtained by considering the subject in connection with some definite foodstuffs. The most exhaustive study from a quantitative standpoint is that of Delf. She showed that when cabbage is subjected for an hour to a temperature of 80° to 100° C., 90 per cent. of its antiscorbutic vitamine is lost, and that 80 per cent. is lost when a temperature of 90° to 100° is maintained for twenty minutes, or a temperature of 60° for a period of sixty minutes. This experiment shows that the destructive influence of heat is enhanced to a comparatively slight degree by a rise of temperature, only about threefold when it is raised from 60° C. to the boiling point. This result points to a temperature coefficient of about 1.5 to 10° C. of temperature. It is suggested by Delf that this low coefficient of destruction is opposed to the enzyme or protein-like theory of the nature of the vitamine, and suggests a simpler constitution. On the other hand, we must bear in mind that the proteins which have been used in experiments and found to possess a high coefficient of heat, have been tested in the pure state, whereas the vitamine of the cabbage is bound up in the cell.
Experiments with this vitamine as found in milk accord with the above investigation, demonstrating that intensity of heat is not as destructive as prolonged heating. This agrees with the clinical experience that milk which has been boiled for a few minutes does not induce scurvy as readily as pasteurized milk which has been heated for 45 minutes to 140° or 165° F. (Hess and Fish).
As demonstrated by tests with orange and with lemon juice, the antiscorbutic vitamine is greatly protected from the destructive effect of heat when it is associated with an acid. This was shown first by Holst and Froelich and has been confirmed by numerous observers. An excellent example of marked thermostability conferred on a food by its acid reaction is furnished by the tomato, which is strongly antiscorbutic even after it has been subjected to the canning process. Conversely, Harden and Zilva have shown that the vitamine is destroyed by alkali even when dilute (one-fiftieth normal sodium hydrate) and kept in contact at room temperature; this alteration does not take place at once, but in the course of several hours.
It is true that the antiscorbutic factor is peculiarly sensitive to drying, but there are exceptions to this rule, so that it is incorrect to state, as does the British Report of the Medical Research Committee, that “it may be regarded as an axiom that dry or dried foodstuffs will not prevent scurvy.” We have shown that fresh milk dried by the Just-Hatmaker process may retain by far the greater moiety of its virtue. In this regard rapidity of desiccation and subsequent protection from oxidative processes are important factors. The general rule holds true, however, that this vitamine, in contradistinction to the “water-soluble” vitamine, is readily damaged and destroyed by drying.
This vitamine is peculiarly sensitive to aging, especially when it is present in an alkaline or neutral medium; but even in an acid medium its potency soon diminishes. Harden and Zilva found this to be the case with lemon juice stored for a fortnight in the cold room, and our experience has been similar in regard to orange juice kept in the refrigerator under a layer of liquid petrolatum. In milk the antiscorbutic factor diminishes with age, especially following pasteurization, in the course of which most of the acid-forming bacteria have been destroyed. Aging has the least effect when the food with which the vitamine is associated has been dried. This is true not only of lemon and of orange juice as demonstrated experimentally and clinically, but even of milk, which even after it has been dried and stored for months, may still possess marked curative value.24
Experiments by Harden and Zilva showed that exposure of lemon juice to ultra-violet rays for eight hours does not influence its antiscorbutic activity, that exposure of autolyzed yeast for the same length of time likewise does not impair its “antineuritic” potency, but that under identical conditions the fat-soluble factor in butter becomes inactivated. Similar tests carried out by the author with orange juice led to the same result. It thus appears that one of the vitamines—not the most unstable—manifests a peculiar sensitiveness to a certain form of physical or chemical action.
In view of the fact that shaking partly destroys pepsin and rennin, as shown by Shaklee and Meltzer, it would be of interest to ascertain whether this process brings about any impairment of the antiscorbutic vitamine. Particular interest is attached to this question because it is generally recognized that milk loses some of its potency in the course of handling—whatever may be comprised by this term. In experiments on the fat-soluble vitamine Steenbock and his co-workers found that “somewhere in the course of the manipulation to which the butter fat had been subjected, factors had been introduced which were responsible for a vitamine destruction.”
Before discussing the question of the manner in which the antiscorbutic vitamine functionates, it may be well to state briefly the type of the disturbance which its deficiency occasions. The chief manifestation is damage to the integrity of the endothelium of the vessels, resulting in hemorrhage—whether from diapedesis or from rhexis or both of these conditions, the microscope does not inform us. Nor can it be stated positively that the endothelium has not been injured by a secondary toxic or bacterial factor. However this may be, the end result of the deficiency is endothelial damage, a pathologic condition which may be demonstrated clinically in scurvy by the “capillary resistance test” (chapter VII). The other marked functional alteration in scurvy is increased susceptibility to infection; but how a vitamine deficiency induces this vulnerability cannot be explained. Clinical tests show that the blood contains sufficient antitoxin (diphtheria) to afford protection. Harden and Zilva found that “guinea-pigs fed on an unrestricted mixed diet, on a quantitatively restricted mixed diet, and a scorbutic diet showed no differentiation in amboceptor and agglutinin titres, and in the complement activity of the blood.” If this is to be interpreted as indicating that the protective substances of the body undergo but little alteration, we must consider whether susceptibility to infection, as well as tendency to hemorrhage, is not due largely to alteration in the cement substance of the endothelial and epithelial membranes.
The Mode of Action of the Vitamine.—One of the most interesting as well as puzzling questions in regard to the antiscorbutic vitamine concerns the manner in which it prevents or cures scurvy. It is a subject which at present is in a state of flux, hardly having emerged from the realm of hypothesis, so that detailed consideration will profit little. At first the modus operandi was explained and accepted as enzyme action, but it was soon evident, in view of the thermostability of the vitamine, that it could not be classed as a ferment or enzyme in the generally-accepted sense of this term. In general, it may be stated that there are two main views: one that the vitamine acts directly, and the other that it acts indirectly through the function of the endocrine glands. Direct action, furthermore, may be accomplished in at least one of three ways. The vitamine may (1) serve as a source of nutriment for the tissues, (2) exert an antitoxic effect on toxic products, or (3) function as a catalyzer. The first interpretation is evidently the simplest and conforms to the long-established knowledge of caloric food factors. That such small amounts as 2 c.c. of orange juice daily should suffice to protect an animal from nutritional disaster runs counter, however, to former conceptions of food nutrition. Further than this there is little against this viewpoint. In its favor is the fact that, up to a certain point, antiscorbutics act in direct ratio to the amount given; for example, 2 c.c. of canned tomato juice is insufficient to prevent scurvy in guinea-pigs, 3 c.c. will protect some but not all of a series, whereas when the amount is increased to 4 c.c. daily all animals will be saved. As we are considering new food factors it is manifestly unwise to judge them by old standards, and to decide offhand that they cannot possess such a high degree of nutritive power. This question must be regarded as still open.
The antitoxic theory suffers from the fact that the toxic origin of scurvy cannot be established. Before this is possible, it is clear that it will be difficult to bring forward convincing evidence of a neutralizing substance. Against this theory is the fact that elimination therapy is of no avail in the treatment of infantile scurvy. Hess and Unger (1919) failed to alleviate the symptoms by means of catharsis, diuresis, sweating and repeated intravenous injections of normal salt solution. In its favor it may be advanced, in a general way, that the vitamine, in many characteristics, resembles an antitoxin—in its extreme lability, its destruction by heat, aging and alkalies. On the other hand, antitoxins also are readily destroyed by acid which, as has been shown, exerts a protective influence on the antiscorbutic factor. The rapidity of action of the vitamines, one of the most impressive phenomena, calls to mind the neutralizing action of an antitoxin, and probably has given rise to the analogy. Williams suggests that the vitamines have “a general, non-specific, antitoxic or eliminative action” on toxic substances resulting from the metabolic decomposition of food.
The theory has been advanced that the action of the vitamines is catalytic. Although this viewpoint has been taken regarding the water-soluble rather than the antiscorbutic vitamine, it will be well to review briefly the work on which it is based. Among the first to suggest this hypothesis were Vedder and Clark, who noted a relationship between the amount of vitamine required by fowls and their carbohydrate intake. Funk in 1913 made a similar observation in regard to beriberi, and in the following year, with von Schoenborn, showed that a vitamine-free diet led to hyperglycæmia, with diminished amount of hepatic glycogen, and that the addition of water-soluble vitamine diminished the hyperglycæmia and increased the liver glycogen. The work of Burge and his co-workers on the catalase content of tissue led to a similar conclusion. Their results may be summarized by the statement that the oxidative processes are hampered and fail to balance the autolytic changes, and, furthermore, that a relationship exists between the catalase activity, acidosis and normal oxidative processes. This theory would presuppose that scurvy is due to the formation of toxins which are normally in process of continual destruction in the body. According to some, these catalyzed toxic substances are metabolic in character, originating from incompletely oxidized food; according to another interpretation, they are the product of autolyzed tissue cells (tissue toxins). The difficulty with this explanation is that scurvy cannot be prevented or cured by a diet containing food of high catalytic power. For example, wheat embryos which, according to recent investigations of Crocker and Harrington, have a high catalytic activity, were found of no therapeutic value in relation to infantile scurvy (Hess, 3).
This problem has been approached from quite a different angle. As is well known, certain bacteria require serum, blood, milk, etc., in order to grow satisfactorily on artificial culture media. It has been established recently, primarily by the work of Lloyd, that this peculiarity in the cultivation of microörganisms is due largely to their requirement of vitamine. She found a relationship of the inverse order between the amount of amino acid present in the culture medium and the amount of vitamine required to stimulate the growth of strains of meningococcus. Reasoning from this experience, she suggests that the action of the accessory growth factors is to increase the reaction velocity of the proteolytic metabolism. Here we find the vitamines once more regarded as catalyzers. This author, however, associates their activity with proteolytic rather than with carbohydrate metabolism. Interesting and suggestive work of similar nature has been carried out in relation to the growth of protozoa and of yeasts (Eddy). Investigations of this kind, dealing with unicellular organisms propagated on a simple food, have the advantage of greatly simplifying the problem.
The recent work of Dutcher falls under this caption, differing merely in the fact that he attributes to the vitamines an indirect action. He has demonstrated that the tissues of polyneuritic birds show a decrease in catalase activity to a point 56 per cent. below normal, and that this activity is largely restored when the birds are cured with vitamine. According to this writer the vitamine functions as a metabolic stimulant, and its lack results in a depression of the body oxidations with an accompanying formation of toxic metabolic products, injurious to the nervous system. The action is regarded as coming about in an indirect manner, being accomplished through the hormone action of the vitamines on one or more glands of internal secretion.
The endocrine hypothesis, suggested by Funk in his monograph, is not without some corroborative evidence. In testing the pharmacologic action of the water-soluble vitamine, Uhlmann found that it stimulated the various glands of the digestive tract, in this respect acting like pilocarpine. Some years ago Albert expressed the opinion that the action of this vitamine was “vagotropic” like atropine, and recently Dutcher has reported definite relief and cessation of polyneuritic symptoms by means of pilocarpine (0.5 mg. subcutaneously). He claims equally good results from thyroxin, the hormone of the thyroid gland, from desiccated thyroid and from tethelin (pituitary). Voegtlin and Myers conclude, as the result of experiments with brewers’ yeast, that the chemical and physical properties of secretin and vitamine are identical.
The early work of Funk and Douglas, which showed that various glands of internal secretion diminish in size and undergo degenerative changes when the diet is vitamine-free, the newer work of McCarrison and of Dutcher to the same effect, clearly point to an intimate relationship between some of the endocrine glands and the vitamines. As regards scurvy, the only work is that of Rondoni, McCarrison and of LaMer and Campbell on the adrenal glands, which were found by all to be enlarged in guinea-pigs suffering from this disorder. These investigations must be regarded as tentative rather than conclusive until confirmed by similar necropsy reports in man. In this connection it should be noted that thyroid, parathyroid or suprarenal extract is of no avail in the treatment of scurvy. This failure may, however, be explained by the fact that the normal balance of glandular activity was not established. We must bear in mind, however, that although the vitamines may influence the secretion of the glands of internal secretion, this explanation does not satisfactorily account for the symptoms of the “deficiency diseases.” These disorders do not in the slightest respect resemble the clinical pictures which we are accustomed to associate with a lack of activity of the glands of internal secretion. If the polyneuritis of beriberi and the hemorrhages of scurvy are attributable to a diminished secretion of the endocrine glands, then it will be necessary to revise present conceptions of their physiologic functions.
The Fate of the Vitamine in the Body.—One of the most important questions in relation to the antiscorbutic vitamine, quite apart from its chemical nature, physiologic function, and its source, is its fate in the human body after it has reached the alimentary canal or been carried to the tissues. It can be readily appreciated that our knowledge of this aspect is very meagre. We shall endeavor, however, to detail what little is known of this subject, conscious of the fact that investigations of the next few years may contradict our present viewpoints.
Most of the constituents necessary for the construction of tissue or for carrying on its functions can be synthesized by the animal body from the basal foodstuffs. It has been ascertained within the past decade that certain constituents—for example, some amino-acids of the protein molecule—are building-stones which cannot be primarily elaborated by the cells, but must be supplied by the food. At present the vitamines—including the antiscorbutic vitamine—are included in this new and essential group of substances which the human organism cannot manufacture. Animal experiments seem to bear out this conception of the vitamine whether we regard them as dynamic or as indispensable tissue elements in the structural sense.
A closely-related but less fundamental question is that of the ability of man to store vitamines—whether the tissues can hoard an excess of these factors, or whether, in this respect, we are carrying on a precarious hand-to-mouth existence in regard to cellular nutrition. It is of course clear that at all times the various organs and tissues must contain a certain amount of the vitamines. This has been shown for the water-soluble or “antineuritic vitamine” by the fact that even the organs of birds which have died of polyneuritis contain an appreciable quantity of the specific vitamine, although an insufficiency of this very factor has led to their death. That such is the case is demonstrated for the antiscorbutic vitamine by the fact that muscle tissue contains sufficient antiscorbutic to protect individuals subsisting largely on a diet of which raw meat constitutes the sole antiscorbutic agent (Stefánsson). It is very probable that some organs contain more of the vitamines than others; this has been proved for the “antineuritic” factor, and seems to hold good for the antiscorbutic—the liver being particularly rich. No quantitative study has been carried out from this point of view regarding the antiscorbutic vitamine, and it would be well worth our while to ascertain the relative antiscorbutic potency of the various organs of the body. Some time ago we undertook experiments to determine whether the guinea-pig is capable of storing this vitamine. One series of guinea-pigs was fed daily 6 c.c. of orange juice for a period of two weeks, whereas another series, of about the same weight, was given, in addition to the basal ration, only 3 c.c. per capita (the minimal protective dose). After this preliminary period both series were placed on a diet containing practically no antiscorbutic. Both groups came down with scurvy after about the same interval, leading to the conclusion that there could have been little if any storing of the excess vitamine by those which received twice the “minimal protective dose.” The experiments of Harden and Zilva, who fed a concentrated lemon juice, showed that this potent agent also was unable to provide against a subsequent period of antiscorbutic deficiency. It should be realized that the results of these tests on guinea-pigs cannot be applied to man without tests on other species.
It might be thought that the blood—the purveyor of the vitamines to the tissues—would be particularly rich in these essential factors. Such, however, was not our experience in respect to the antiscorbutic vitamine. The blood possibly varies greatly in this respect according to the diet of the individual, or even according to the interval elapsing after the ingestion of antiscorbutic food. Our opinion is based on the surprisingly poor therapeutic effect of blood transfusion in the treatment of scurvy. To illustrate: An infant weighing about fifteen pounds received six intravenous injections of citrated blood—one of 200 c.c., given by the direct method, and a month later five smaller transfusions with citrated blood, which aggregated 205 c.c.25 In spite of this addition of blood, the hemorrhage and congestion of the gums did not disappear, nor the general condition improve, as would have happened had 50 or 75 c.c. of orange juice been given by mouth. It seems probable that small quantities of vitamine are being transmitted at all times by the blood and supplied to the cells, but that its normal content of this factor is not great. The antiscorbutic potency of blood may perhaps be compared to that of milk. Animal investigation may show that various vessels—for example, those supplying or draining certain glandular organs—differ in the antiscorbutic quality of the blood which they carry. It is evident, therefore, that many transitory factors may influence the vitamine content of the blood, and that—as in the case of milk and fruits and vegetables—we are not dealing with a constant and unvarying agent.
Nothing whatsoever is known concerning the excretion of the antiscorbutic vitamine. No attempts have been made to recover it from the urine, or to ascertain if, when large amounts are ingested, the excess is thrown off by the body. This suggests the question—a corollary of that raised in connection with the vitamine content of the blood—whether it is immaterial if the vitamine is taken frequently in small amounts, or is provided only occasionally and at longer intervals in larger amounts. Is it of no moment whether the infant receive its quota of antiscorbutic every few hours through the medium of the breast milk, or only once a day in the form of orange juice or tomato? If we turn to studies on the other vitamines for enlightenment as to the possibility of excretion, we find that Muckenfuss recovered the water-soluble factor from ox bile and from human urine.26 In this article he proposes the interesting question of a possible variation in the vitamine output under pathological conditions, which may be responsible for the development of functional disturbances in children.
It would be of interest to know the fate of the antiscorbutic vitamine in the gastro-intestinal tract. How is it affected by a lack of the acid gastric juice, or by the alkaline intestinal secretions, or by the bacteria in the lumen of the gut? From which part of the intestine is it largely absorbed? May an appreciable amount undergo destruction before this is accomplished? None of these questions can be answered satisfactorily in the present state of our knowledge, but they suggest that the mere fact that an adequate quota of antiscorbutic vitamine is provided in the food does not necessarily insure an adequate supply for the tissues. If in addition to the question of intake we must take into account that the vitamines may suffer various vicissitudes, it may come to pass that pathological conditions at times destroy or render them partially inactive. In this way we may account for irregularities in the clinical course of disorders associated with vitamine deficiency.
Of prime importance, however, is the effect of the vitamines on the glands of the alimentary tract and on the digestive processes. A diminution of gastric juice, or in some instances a total absence, has been observed in adult scurvy, and noted by us in two cases of infantile scurvy. As mentioned elsewhere, some consider the function of the water-soluble vitamine analogous to that of secretin. In applying this hypothesis to scurvy it must be borne in mind that the sequence may be reversed, that the lack of vitamine may not lead to the gastric achylia, but that the achylia may come about secondarily as the result of the malnutrition.
We have referred to “irregularities” in the course of the “deficiency diseases.” A careful perusal of the literature leaves one with the impression that the most experienced observers are not entirely satisfied with the exclusively etiologic relationship of the vitamine to its respective nutritional disorder. In regard to scurvy, more particularly, there are numerous scattered reports where the disorder did not yield to antiscorbutic foods as might have been expected, or where, on the other hand, it suddenly and inexplicably retrogressed, although there had been no alteration in the dietary.27 These instances are not common, but they occur from time to time, and their occurrence must be accounted for. In relation to beriberi and avian polyneuritis improvement of this kind has frequently been explained on the theory of a sudden mobilization of vitamines from the tissues. There is, however, no data on which to base such explanations, and it may be that a lack of parallelism between vitamine intake and the clinical course may be due at times to processes taking place in the alimentary tract.
The fat-soluble vitamine has been termed by some the growth vitamine. All the vitamines, however, are closely associated with the function of growth, which their deficiency tends to inhibit. In the chapter on symptomatology, it will be pointed out that infants suffering from scurvy fail to grow normally both in length and in weight. To a certain extent this may be due to a loss of appetite, which is one of the characteristic phenomena accompanying the scorbutic condition. On the other hand, this anorexia may be secondary and not primary to the impairment of the growth impulse, which may lead to a dysfunction of various body processes.
It is of little value to look ahead and try to foresee what the next decade will bring forth in regard to the nature of the vitamines. Investigation has broadened remarkably during the past few years and now embraces the chemical field—chemical and adsorption methods, the large realm of biology, including studies in physiology and pharmacology; and recently pathology has once more been called upon to aid in the solution of the problem. Probably additional vitamines will be discovered. From time to time it has been suggested that a specific growth vitamine exists quite distinct from the three which are recognized, and recently Mellanby has suggested still another food factor—a specific “rachitic vitamine.” When we reflect that the characteristic functions of the various organs—the kidneys, liver, etc.—must depend on essential differences in chemical structure, the complexity of the entire problem of unidentified factors becomes evident.28
Physicians have had a general knowledge of the pathology of scurvy for a great many years. Lind, in his “Treatise on the Scurvy,” published in 1772, included a chapter on “dissections” and a postscript on “Appearances on Dissections of Scorbutic Bodies,” based on a large, although indefinite, number of postmortem examinations. In the century which followed, there are to be found many reports of scurvy, especially in connection with the frequent wars, but it is surprising how little detailed pathologic information they furnish. Barlow’s publication in 1883, establishing the identity of the scurvy of adults and of infants, must be regarded as the modern milestone in the study of the pathology of this disorder. This work did not contribute richly to the data of the subject, or suggest novel interpretations, but directed attention to a new source of material—the increasing number of cases of infantile scurvy—at a critical moment when the opportunity for the study of scurvy in the adult was rapidly becoming less. At the time of Barlow’s exposition of the true nature of “acute rickets,” scientific medicine was concentrating its interest on pathology. Tissues were being carefully studied by means of the microscope, and scurvy was subjected to this new method of investigation. As a result of intensive application of this technic, a lesion of the bones was identified and established as characteristic of scurvy. Study was focussed so exclusively on the bones, that for many years, indeed until very recently, the other organs of the body were neglected. This is true of the gross as well as of the microscopic anatomy. Protocol after protocol gives a hasty account of the appearance of the various organs, merely as a routine introduction to a careful and often minute study of the bones (Table 2). As the result of this myopic vision, enlargement of the heart, for example, which should have been noted many years ago, was, until recently, unobserved—indeed, the heart is but occasionally mentioned in the protocols.
| Number of Cases | Author | Date | Gross | Microscopic |
|---|---|---|---|---|
| Adults | ||||
| Many | Lind | 1772 | Brief summaries | |
| 51 | von Himmelstein | 1843 | Brief summaries | |
| 8 | Hayem | 1871 | Résumé | Brief résumé. |
| 7 | Lasèque & Legroux | 1871 | Fairly detailed | |
| 7 | Charpentier | 1871 | Brief summaries | |
| 13 | Sato & Nambu | 1908 | Fairly detailed | Fairly detailed. |
| 2 | Urizio | 1917 | Brief summaries | Brief summaries. |
| 1 | Feigenbaum | 1917 | Brief summary | Brief summary. |
| 23 | Aschoff & Koch | 1919 | Very complete | Very complete. |
| Infants and Children | ||||
| 1 | Smith | 1876 | Brief report | |
| 3 | Barlow | 1883 | Fairly detailed | Bones, brief report. |
| 1 | MacKenzie | 1883 | Brief summary | |
| 1 | Northrup | 1892 | Brief report | |
| 1 | Cassel | 1893 | Brief report | |
| 2 | Sutherland | 1894 | Fairly detailed | Brain and liver, 1 case. |
| 1 | Reinert | 1895 | Very complete | Fairly complete. |
| 1 | Hirschsprung | 1896 | Summary | |
| 3 | Meyer | 1896 | Fairly detailed | |
| 1 | Baginsky | 1897 | Fairly detailed | Brief, bones more in detail. |
| 1 | Naegeli | 1897 | Fairly detailed | Bones only. |
| 1 | Manz | 1899 | Summary | |
| 5 | Schoedel & Nauwerk | 1900 | Very complete | Very complete. |
| 1 | Jacobsthal | 1900 | Very complete | Very complete. |
| 1 | Stoos | 1903 | Fairly complete | Bones only. |
| 1 | Looser | 1905 | Summary | |
| 1 | Hoffmann | 1905 | Summary | Bones only. |
| 1 | Stoeltzner | 1906 | Bone only | Bone only. |
| 22 | Fraenkel | 1908 | Résumé | Bones only. |
| 1 | Nobécourt et al | 1913 | Brief report | Bone only. |
| 3 | Ingier | 1913 | Brief report | Bones, very complete. |
| 1 | Bahrdt & Edelstein | 1913 | Complete | Bones, brief report. |
| 31 | Erdheim | 1918 | Brief summaries | Brief résumé. |
| 1 | Epstein | 1918 | Very detailed | |
A new era in the pathology of scurvy was inaugurated by the availability of experimental scurvy and also by the stimulation occasioned by the recent conception of vitamines and the so-called deficiency diseases. In endeavoring to elucidate this fascinating problem, it has gradually been realized that pathology may be of service—for example, in relation to the involvement of the endocrine glands. Accordingly, studies of the minute pathology of the various organs have been undertaken in many laboratories throughout the world (Italy, India, England, Germany and the United States). An additional stimulus to investigation in pathology has been furnished by the recent war, which, as shown elsewhere, led to a great increase in scurvy among both the military and civilian population. The excellent report of Aschoff and Koch from Roumania was made possible by this catastrophe, and will no doubt soon be followed by others of similar character.
Gross Pathology.—General Appearance.—The skin usually is pale, livid, and dotted with numerous petechiæ. These vary in size from the tiniest pin-points, barely recognizable to the naked eye, to ecchymoses of moderately large size. The most frequent site is the lower extremities. The trunk is always less affected, hemorrhages tending to occur along the mid-line and especially around the umbilicus. There may be also larger superficial hemorrhages, showing great differences in color, from the redder tone of the more recent, to the blues, browns and greens of the older lesions. Bleeding from the nose and mouth is not uncommon in fatal scurvy, and occasionally exophthalmos is present, usually unilateral, and due to subperiosteal hemorrhage of the orbital plate of the frontal bone. Rigor mortis is generally slight, and, according to Lind and to von Opitz, decomposition takes place rapidly.
There may be great emaciation, especially where secondary infection has supervened. General wasting occurs, however, in uncomplicated scurvy due to starvation—the result of lack of appetite or a deficiency of the general food supply. Children, especially infants, are undersized, as illustrated in treating of the symptomatology, and their bones may be decidedly smaller than normal. Generally there is some edema about the ankles, and in children a somewhat characteristic puffiness about the eyes. General anasarca also occurs, in some cases associated with renal involvement. Peculiar boggy, “tumor-like” masses of localized edema may be present, which were considered by the earlier writers (Lind) to be one of the typical lesions of this condition.
Hemorrhages.—Hemorrhage is such a striking manifestation that it is not surprising to find it was regarded by the older writers as the pathognomonic sign of scurvy. The bleeding may take place into almost any organ, and vary from small petechiæ to very extensive extravasations. The hair follicles and sweat glands are particularly susceptible, as Lasèque and Legroux noticed in cases occurring in the French prisons. Aschoff and Koch, during the recent war, noted the same peculiarity of involvement, calling attention also to the fact that previous skin diseases such as keratosis or seborrhea seemed to predispose to this localization.
Trauma plays a very important rôle in determining the location of the deeper as well as of the superficial hemorrhages. In adults, especially in soldiers, in whom the greater number of cases have been recorded, the lower extremity is the commonest site, between the knee and ankle, the area most exposed to blows as well as acted upon by static congestion. In infants, the inner aspect of the thighs is a frequent site due to the trauma of the diaper.
The most characteristic hemorrhage, the subperiosteal, will be fully discussed when considering the bone lesions. The deeper hemorrhages may be very extensive. They tend to follow the connective-tissue strata, and in the muscles are usually limited by the muscle sheaths. The blood surrounds the muscle fibres, which appear quite intact. The neighboring blood-vessels are congested and may contain thrombi, both venous and arterial. Such thrombi are found also in areas where extravasation has not taken place, and conversely, hemorrhages occur where no thrombi are demonstrable, so that a mutual causal relationship cannot be proved. Further evidence in regard to the mechanism of these extravasations is presented in the discussion of the minute anatomy. Brownish pigment, undoubtedly derived from the blood, is frequently found in the neighborhood of the hemorrhagic areas. New connective tissue also grows in these areas, so that in healing cases a marked formation of scar tissue will be found. Bizarre forms of hemorrhage at times have given rise to confusion in diagnosis; hemorrhage involving the right lower abdominal quadrant may simulate appendicitis; when occurring in the region of the transverse colon it has been mistaken for an epigastric new-growth.
Certain parts of the body seem less predisposed to hemorrhage. The central nervous system is often spared, notwithstanding extensive bleeding elsewhere, the meninges being somewhat more frequently involved. Hemorrhage of the lungs is also less common than might be expected, and it is probably true as Lasèque and Legroux suggested, that previous pulmonary disease, particularly tuberculosis, is an important predisposing factor.
Anasarca.—This comprises the second characteristic lesion found in scurvy at necropsy and was referred to in the earliest records of the disease. In the account of his dissections Lind writes: “The breast, belly and several other parts of the body were filled with this water or serum,” mentioning also the pericardium and ventricles of the brain. He also noted that all the tissues seemed to contain an excessive amount of fluid, a condition which may be so striking that the muscles appear bathed in serum. In one of his first cases with postmortem verification, Barlow described this appearance as follows: “The muscular walls of the thorax were pale yellow and watery, as though they had been bathed in serum.” In many cases this edema is most marked in the neighborhood of the hemorrhages, for example, in the muscles of the thigh when subperiosteal hemorrhage has taken place; less frequently it is produced by venous thrombosis.
Any or all of the serous cavities may be involved in this hydrops, the order of frequency being pericardium, pleuræ, peritoneum, and joint surfaces, especially the knee. The fluid is clear and straw-colored, or, in the event of secondary infection, becomes cloudy and fibrino-purulent. Later the exudate may become organized so that the entire cavity is filled with a solid mass, which binds the organs together and obliterates the cavity. The exudate may be blood-stained or apparently consist entirely of clotted blood.
Heart.—In the protocols of most necropsies, the heart is passed over with scant mention. For example, Lind’s only statement in this regard is that “all those who died suddenly, without any visible cause of their death, had the auricles of their heart as big as one’s fist, and full of coagulated blood.” Barlow accords it no attention, nor do most of the writers who immediately followed him. The first careful description of the heart is to be found in the excellent work of Schoedel and Nauwerk, which contains the following record in regard to three of the five necropsies on infantile scurvy: (1) Pericardial fluid somewhat increased, both ventricles moderately dilated, the right somewhat hypertrophic. (2) The heart showed a hypertrophy of the right and left ventricles, as well as dilatation of the right ventricle. (3) The right ventricle is dilated and slightly hypertrophied, the muscles pale and tough. There is no word of comment relative to these cardiac changes, which evidently were considered fortuitous. The same observation holds true in regard to a necropsy on an eight-year-old child reported by Ingier, which showed a moderate hypertrophy of the left ventricle. We look in vain, likewise, for information on the subject in the work on guinea-pig scurvy by Holst and Froelich, and that on scurvy in the monkey by Hart and Lessing. The first linking of cardiac enlargement with scurvy is found in a paper by Darling, who described “right-sided hypertrophy and degenerative changes in the vagus and all its branches.” Hess described and demonstrated by means of roentgenograms the enlarged heart in infantile scurvy. Recently Erdheim, in an article entitled “Das Barlowherz,” reported the occurrence of enlargement of the heart, especially of the right ventricle, in 21 out of 31 necropsies of infantile scurvy, and concluded that a direct ratio exists between the degree of enlargement and the intensity of the disorder. These reports gain added interest in view of the enlargement of the right heart so frequently encountered in beriberi, and described by Andrews in infants dying of this condition. In addition to the definite statement of Darling regarding adults, mention may be made of the observation of Aschoff and Koch, that in two cases of uncomplicated scurvy there were fatty degeneration and dilatation of the heart. Fatty degeneration of the muscle is frequent, brown atrophy exceptional. Sato and Nambu also found hyperæmia and atrophy with increase of connective tissue between the muscle fibres.
The pericardial cavity contains almost invariably an increased quantity of fluid, which may be so great as to impede the heart’s action. Adhesive pericarditis has been described. The cardiac valves are normal, unless previously damaged.
Lungs.—The lungs are almost always congested, but apart from this are remarkably free from abnormality. Smaller or larger hemorrhages are described occasionally, which are usually considered truly scorbutic; Andrews, however, found similar lesions in beriberi. In the necropsy of Stephen Mackenzie’s case, described by Barlow, these small hemorrhages are stated to have resembled small red tubercles scattered throughout the lung. There may be pulmonary infarcts. Edema of the lungs is not uncommon, as we should expect, especially as a terminal condition. Pneumonia, lobular or lobar, is one of the most frequent complications and causes of death. Active tuberculosis is a not uncommon secondary manifestation.
Subserous hemorrhages are almost the rule; if infection supervenes, the pleuræ become thickened and covered with an exudate of pus and fibrin.
Alimentary Tract.—The lesions of the gums so well recognized clinically are fully discussed under symptomatology. The remarkable fact that these hemorrhages do not appear in edentulous gums has been the centre of the controversy as to the identity of adult scurvy and Barlow’s disease. This same lack of involvement is noted in adults whose teeth have been extracted. Where teeth are present, the gums are swollen and edematous, often of a livid, reddish color; less frequently, pale and pouting. Hemorrhage is seen at the edge of the gum adjacent to the teeth. In advanced cases the gums are enormously swollen, fungous, ulcerated and covered with a foul, greenish, necrotic mass, which may extend widely over the buccal mucous membrane. The teeth become loosened and fall out. Secondary infection undoubtedly plays the chief rôle in producing this condition, for the most severe forms are found only where caries and pyorrhœa preëxisted. This seat of infection may serve as the source of dissemination throughout the body, giving rise to many of the lesions found at postmortem, especially in the lower part of the intestinal tract.
The stomach shows no characteristic changes. Congestion of the mucosa is frequent, at times associated with small superficial erosions; the latter gain added interest in view of their occurrence in guinea-pig scurvy. Hemorrhages occur here also and may involve any of the mural coats.
The duodenum shows often intense congestion. This occurs with sufficient frequency to demand attention, especially as a similar condition has been described in other disorders grouped with scurvy. Willcox and others found congestion of the duodenum and of the lower intestine in beriberi, and Andrews described not only congestion but even minute hemorrhages. Small duodenal ulcers are by no means infrequent both in human and in guinea-pig scurvy (Holst and Froelich). The presence of such marked congestion surrounding the papilla of Vater would lead us to expect the occurrence of catarrhal jaundice associated with scurvy. But, on the contrary, icterus has rarely been noted in scurvy. Urizio has described jaundice in this connection, but it is difficult to decide whether his cases were true scurvy, as they occurred in an epidemic of jaundice and no histologic examination of the bones was carried out.
The intestine may present a variety of lesions.29 The mucosa is frequently congested and swollen, and the solitary follicles and Peyer’s patches enlarged. These changes may progress to necrosis and extensive ulceration. In an outbreak of scurvy occurring in this country in 1917, in a large institution for epileptics, ulceration was a frequent lesion at necropsy.30 Dysentery, a frequent complication of scurvy in some epidemics, may add to this ulceration and lead to even complete sloughing of the inner lining of the intestine. Hemorrhages are found in the mucous, serous or muscular layers. Here, as elsewhere, the hemorrhages vary in size from petechiæ to large infiltrations of blood. A very striking picture is sometimes presented by the pale, edematous intestinal wall dotted or streaked with vivid red.
Liver.—The liver is frequently congested, as would be expected in view of the involvement of the right heart. Erdheim found congestion, however, in only nine among thirty-one necropsies, although enlargement of the heart was present twenty-one times. There may be hemorrhages in the glandular tissue or under the peritoneum. “Cloudy” and fatty degenerations occur occasionally, and in some cases an early cirrhosis. Lind found abscess of the liver, and wrote that in a few instances “the matter or corruption was hardened, as it were, into a stone.”
Spleen.—This organ is usually somewhat enlarged and congested. Charpentier, in the Paris epidemic of 1871, found it often three to four times the normal size and very soft, and Lind tells us that “the spleen was three times bigger than natural, and fell to pieces, as if composed of congealed blood.” It must be remembered that the pathologic as well as the clinical picture of the scurvy of Lind and his time was generally complicated by infection. The enlargement is usually by no means so great, and no doubt is due in part to intercurrent infections. On section, it is found frequently to contain much reddish-brown pigment. Hemorrhage may also occur. In beriberi, Andrews observed frequent congestion of the spleen and also a loss of normal markings.
Pancreas.—There is but one reference to a lesion of the pancreas in scurvy, that of Sato and Nambu, who encountered hemorrhage of this organ in one case among the necropsies performed in the course of the Russo-Japanese War.
Kidneys.—Here again, congestion and hemorrhage are the two lesions most commonly found. The kidneys also may show any of the forms of nephropathy ordinarily recognized, but these must be regarded as complicating conditions and not a part of the true scurvy.
Small hemorrhages may be found in the uterus, bladder or urethra. They are especially common in the bladder, both in man and in the guinea-pig, and in some instances may be the cause of the hæmaturia noted during life.
Lymph-nodes.—General enlargement of the lymph-nodes has been described, but occurs probably only in advanced cases where a general infection has been superadded. As a rule the enlargement is confined to nodes draining areas where hemorrhage has occurred. On section these nodes are reddish or brownish as the result of the pigment which they contain, the “black and red spots of different sizes” mentioned by Lind. Following infection they may become purulent, resulting in the inguinal buboes so frequently mentioned by the older authors,31 or in the purulent mesenteric nodes associated with intestinal ulceration.
Organs of Internal Secretion.—Until recently these organs have received but little attention. It is probable, however, that in the near future they will be the object of close study and that new information will be acquired as to their condition in this disorder. Hemorrhages are commonly seen in the adrenals, enlarging them greatly and giving them a deep red color; the hemorrhage generally involves mainly the medullary portion.32 It is probable that careful scrutiny will disclose hemorrhages in the other glands of internal secretion. The question of the involvement of these glands will be again considered under the microscopic anatomy, and has been taken up from a functional standpoint in treating of the possible indirect action of the vitamines.
The brain and the spinal cord likewise have been but little studied. It is hardly to be expected that much will be learned from an investigation of the gross pathology of these organs, but the microscopic anatomy offers a promising field of research. Hemorrhage may occur into the brain substance, into the cord or the membranes surrounding them. Pachymeningitis hemorrhagica interna has been described frequently (Meyer, Hayem, Sutherland, Sato and Nambu) and may give rise to the symptoms of meningitis. Sutherland reports an instance where thrombosis of the basal artery was found postmortem. In one case, that of Feigenbaum, hemorrhage of the cord was diagnosed during life and confirmed at necropsy.
The peripheral nerves may be the seat of hemorrhages, the blood lying between the nerve trunk and its sheath. This is particularly well illustrated in the recent work of Aschoff and Koch.
Bones.—Palpation of the body will often reveal distinct lesion of the bones, such as fractures, either ununited or healed with the formation of large calluses; subperiosteal hemorrhages, especially of the distal end of the femur or of the tibia, may be evident to the eye as well as to the touch. Crepitation of the bones may serve to further establish the break in continuity of the bones. This lesion was well known to the older writers. Lind writes that “in some, when moved, we heard a small grating of the bones. Upon operating those bodies the epiphyses were found entirely separated from the bones; which, by rubbing against each other, occasioned this noise.” “All the young persons under 18 had in some degree their epiphyses separated from the body of the bone, this water having penetrated into the very substance of it.” Poupart was also struck by this phenomenon in young adults.
Another bony alteration which is readily palpable is “beading” of the ribs, the counterpart of the rhachitic rosary. This has not been considered a sign of scurvy, and when noted clinically or at postmortem has been passed over without comment, just as has been the case with cardiac hypertrophy. In infants the beading has been attributed to rickets, and this error has been largely responsible for the general opinion that almost all infants suffering from scurvy suffer also from rickets. If we scan the literature with this question in mind, we find numerous casual references to beading of the ribs in scurvy. Fraenkel’s frequently cited case of a child of seven who died of acute scurvy, showed beading of the ribs during life as well as after death. The true scorbutic character of these enlargements was substantiated by microscopic examination. In their pathologic studies on scurvy among soldiers, Aschoff and Koch frequently describe beading of the ribs, which they attribute to an infraction of the costochondral junctions.33 There may be fracture at this junction, or a separation of the cartilages from the sternum, as described by Lind.
This beading of the ribs, which involves mainly the middle tier, was described by Holst and Froelich in their classic report of guinea-pig scurvy, and has been noted by all subsequent investigators in this field. It has usually been called “rhachitic” or “pseudo-rhachitic” in spite of the fact that this junction is the site of typical scorbutic microscopic lesions. Hart and Lessing refer to the “rhachitic rosary” in monkeys, likewise not realizing that it is the product of scurvy.
The subperiosteal hemorrhage has long been recognized as a lesion characteristic of scurvy.34 It occurs exceptionally in the upper extremities, and most commonly at the lower end of the femur; it may, however, involve almost any of the bones, and has been described in connection with the scapula, cranial vault, orbital plate of the frontal bone, ribs, etc. It varies greatly in its size, being confined to a small area or extending a long distance on the shaft of the bone. It rarely is as large as one would expect from external appearance, as much of the swelling is due to edema and hemorrhage into the soft parts. The periosteum rarely becomes separated at the line of junction of the epiphysis and diaphysis. The underlying blood coagulates rapidly, and the periosteum begins to calcify within a few weeks, as shown by the X-ray.
The most frequent site of fracture, or separation of the epiphysis, is the lower end of the femur. This may be accompanied by local swelling, or be discovered at necropsy, or during life by means of the X-ray in cases in which it has not been suspected. An interesting fracture reported by the author, and also mentioned by Kaufmann and by Schoedel, is that of the head of the femur leading to the development of coxa vara. In the author’s case, the condition was found in a scorbutic infant who had never stood on its feet. Schoedel suggests that scurvy may at times be the etiologic factor in coxa vara as well as in some cases diagnosed as congenital dislocation of the hip.
On sectioning the bones longitudinally the cortex is noted to be exceedingly thin, a mere shell and very brittle. The trabeculæ are so thin and reduced in number that the bone has become a very fragile structure. The marrow is no longer deep red at the ends of the long bones, but yellowish, frequently presenting a patchy appearance. It has a gelatinous consistency. This “Geruestmark” is one of the characteristic anatomical changes of scurvy, and will be fully described in considering the microscopic picture. Hemorrhages can be clearly distinguished in the marrow, and are of varying shades denoting their irregular occurrence. These hemorrhages were considered by Looser to be the cause of the connective-tissue formation in the marrow, but do not occur with sufficient constancy to warrant this interpretation. Moreover, this “frame-work marrow” is found where there is no evidence of previous hemorrhage.
Skin.—As pointed out by Aschoff and Koch, examination of skin which to gross appearance was the seat of typical small hemorrhages, showed various lesions. In some, perhaps the most typical forms, there had been a fresh extravasation of red blood-cells. This condition is found usually in the subepidermal layers, especially in the papillary stratum. These small hemorrhages occur very frequently about the hair follicles and sweat glands, especially when they have been diseased. Where the bleeding has been of long standing, dark brownish pigment deposits are found and all blood-cells may have disappeared. Phagocytic cells are almost always present and may be of the “wandering” or of the more fixed connective-tissue type. Many round cells may be seen in these areas lying between the connective-tissue strands or around the blood-vessels. Rheindorf, as quoted by Tuechler, has called attention to this round-celled reaction, which in many instances gives a picture analogous to the granulomas, and which leads him to infer an infectious origin for these lesions. Other areas which appeared to be the seat of hemorrhage are shown by the microscope to be small abscesses or new connective tissue often loaded with pigment and detritus, apparently representing the final stage of these lesions. Aschoff and Koch have found that suitably-stained preparations frequently show a loss of elastic fibres, which Rheindorf states constitutes one of the earliest changes of this disorder. The blood-vessels in the vicinity of the hemorrhages are congested, especially the capillaries and small venules.
The muscles also present a similar diverse picture of old and recent hemorrhages, pigment deposit and round-celled infiltration. Increase of connective tissue is usually found between the fibre bundles and in some cases where the hemorrhages are apparently of long standing, as evidenced by loss of contour of the red cells and pigmentation of the surrounding areas, this scar tissue formation is very marked. Changes in the muscle fibres themselves have not been encountered by all observers. Hayem describes widespread fatty degeneration and a deposit of pigment within the fibres, Leven a loss of sarcolemma, while Lasèque and Legroux found fatty changes which were equally marked in muscles showing no hemorrhage. On the other hand, Aschoff and Koch, in their careful studies, did not find noteworthy fatty change of the fibres, but observed often that the fibres within the hemorrhagic areas seemed shrunken and were stained abnormally deep with eosin.
In monkeys dying of experimental scurvy, Hart and Lessing describe granules in the muscles, which, judged by their staining affinities, evidently contained calcium and were similar to those found in the adrenal glands.
Blood-vessels.—A similar difference of opinion obtains in regard to the changes in the walls of the blood-vessels, especially of those in hemorrhagic areas. This question is of particular interest because of its bearing on the problem of the mechanism involved in the escape of the blood. Since it has been demonstrated that neither the clotting time nor the viscosity of the blood is markedly changed in scurvy but that weakness of the vessel walls exists, as demonstrated by “the capillary resistance test,” it is natural that we should seek an explanation in the microscopic pathology of the vessels. So far no change has been found. The application of some of the newer stains, such as those for mitochondria and other cell granules, has not been resorted to for this study, and might furnish valuable information.
Hayem found fatty infiltration of the walls of the small veins and capillaries, and believed this to play an important rôle in the etiology of these bleedings. Lasèque and Legroux also found occasional fatty changes. Other authors have failed to demonstrate similar lesions, or have considered them due to postmortem change. Koch searched in vain for “rents” in the vessel walls to account for the escape of blood. Hyaline degeneration has also been described, but is believed to result from secondary infections and not to be an intrinsic lesion of scurvy (Sato and Nambu, Aschoff and Koch).
Thrombosis of vessels is found both in the neighborhood of hemorrhage and elsewhere, the thrombi at times completely occluding the vessels and giving rise to typical wedge-shaped infarcts. The lung often shows areas of this kind.
Lungs.—Hemorrhages of various size occur in the tissue of the lung or in the air spaces. Hemorrhagic infarcts also have been described, and Sato and Nambu report hyaline degeneration of the blood-vessel walls. Secondary pneumonias, usually broncho-pneumonic in type, are of common occurrence, and in many epidemics constitute the prevailing cause of death. Tuberculous lesions are also frequently present, and are stated to assume fresh activity as the result of the nutritional disorder. Edema occurs frequently, the fluid in the acini often containing red blood-cells. Subpleural hemorrhages, thickening of the pleura, purulent or fibrinous pleurisy are common lesions.
Heart.—Although hypertrophy and dilatation of the heart have been noted by several observers, microscopic changes have rarely been recorded. Meyer, and also Leven, report fatty degeneration of the muscle fibres, which, however, was found by Aschoff and Koch in only one case. Sato and Nambu described an increase of connective tissue, and others anemia and pigmentation. Thickening of the pericardium and subserous hemorrhages also occur.
Gums.—Where it has been possible to examine the gums of early cases, where swelling, redness or bluish discoloration are the chief symptoms and before secondary infection has set in, the microscopic picture is very similar to that of the skin. Small hemorrhages, round-celled infiltration, increase of connective tissue, clumps of pigment containing cells, or a diffuse deposit of brownish granules complete the picture. Congestion and edema are usually evident. The changes are most pronounced in the deeper layers of the submucosa and about the muscles, leaving the superficial layers strikingly intact, beneath an apparently normal epithelium. In the later stages, erosion of the mucosa occurs, and the upper layers of submucosa become involved. Polynuclear cells appear in great numbers, abscesses and ulcers are formed, which with proper staining can be shown to harbor the various types of mouth bacteria, cocci, spirillæ, etc. The pigmentation becomes intense, and a marked increase of the newly-formed connective tissue takes place.
The lesions of the stomach are neither characteristic nor, as a rule, very striking. Hemorrhages occur, the larger ones generally in the subperitoneal layers, the smaller ones in any of the coats. Thickening of the wall follows or accompanies these hemorrhages. Superficial erosions of the mucosa or even ulcers may be seen.
The striking congestion of the duodenum has been fully discussed in considering the gross pathology. At any level in the intestinal tract hemorrhage may take place, with the resulting pigmentation and scar tissue formation. The lymphoid structures—solitary follicles and Peyer’s patches—are usually intensely congested and often the seat of hemorrhage. They constitute the sites of predilection for ulcerative processes of the gut. Bacteria can be demonstrated at times in the submucous layers; however, no type has been found to predominate, the flora being composed of the usual intestinal forms. Aschoff and Koch have demonstrated in these ulcers the spirilla and fusiform bacilli so commonly found in the mouth. These follicular ulcers may be found in any part of the intestine, and may be shallow erosions, or extend through the follicle into the deeper tissues. Hemorrhages are commonly located about the follicles. The epithelial layer is edematous, often showing an increased number of cells.
The lymph-nodes may be congested, or edematous and hemorrhagic. Pigment is usually present and in some cases the peripheral sinus is distended with pigment-loaded cells. Where secondary infection has occurred, extensive necrosis of the glands is seen. This is found frequently in mesenteric nodes where severe intestinal lesions are present. The nodes lying in the drainage paths of hemorrhagic areas, especially the inguinal nodes, show active resorption of blood and blood pigments, and, as noted above, may be the seat of infection.
Liver.—In this organ, likewise, no change is found with sufficient regularity to warrant its acceptance as a distinctive lesion of scurvy. Fatty infiltration is, however, very common in the centre as well as in the periphery of the lobules. It is frequently associated with congestion, which may be so great as to lead to atrophy. In one case of Aschoff and Koch the picture resembled that of primary liver atrophy. The organ frequently contains extravasated blood or depositions of old blood pigment. It should be noted that Boerich described early cirrhosis in several of his cases, and that Aschoff and Koch record that one of their severe, acute cases showed “a recent cellular cirrhosis.” An exceptional lesion is reported by Reinert—a “leucocytic” infiltration of the liver and spleen occurring in a three-year-old child, and resembling that seen in pseudoleukæmia. Finally, it should be remembered in this connection that Hart and Lessing found calcium deposits not only in the muscles and adrenal glands of their monkeys, but also in the liver.
The spleen shares the general congestion of the internal organs. Sato and Nambu invariably found large numbers of pigment granules in this organ. Hirschsprung noted many Malpighian corpuscles, Reinert describes a true hyperplasia of the splenic pulp, and others mention infarcts and subcapsular hemorrhages.
The kidneys are often normal. On the other hand, various forms of nephritis are found, with cloudy swelling or interstitial change—a not infrequent complication of scurvy. More typical of the primary disease are congestion and hemorrhages, the bleedings occurring either under the capsule, into the interstitial tissues, or into the lumina of the tubules. Hayem found fatty infiltration of this organ and Aschoff and Koch a slight change of this kind in one case.
Adrenals.—A new interest in the study of the adrenals in diseases of the “deficiency” group has been created by the recent work of McCarrison. This author found the adrenals increased in size and weight in guinea-pigs dying of scurvy, whereas the adrenalin content of these glands was markedly decreased. On section there was hemorrhagic infiltration, “usually circumscribed in extent and situated around the periphery of the adrenal cortex.” This was seen even in early cases before hemorrhage had occurred elsewhere in the body. He describes also “degenerative changes in the cellular elements of cortex and medulla” consisting of vacuolation and disintegration of the cells with disappearance or loss of staining reactions of their nuclei. Rondoni, some years previously, had called attention to this increase in size and hyperæmia of the adrenals in guinea-pigs fed exclusively cereal diets. He, as well as McCarrison, noted an increase, though much less marked, as the result of starvation. LaMer and Campbell recently have confirmed McCarrison’s report of an augmentation in the weight of the adrenal glands in guinea-pigs fed on diets deficient in the antiscorbutic factor.
Comparable lesions have as yet not been found in human scurvy. These glands have been found normal by Jacobsthal, Schoedel and Nauwerk, Ingier and Epstein. In the cases of Aschoff and Koch no abnormality was noted except an almost constant increase in lipoid content. In those of Boerich the glands were normal in all but one case; in this instance the medulla was somewhat increased in size. In passing, we may repeat that Hart and Lessing found calcium deposits in the adrenals of four of their five monkeys, a lesion which has never been recorded in man.
It is valuable in this connection to compare the adrenal in scurvy with that of beriberi. In this disorder, Albert found the adrenal normal in one case, and Andrews describes only congestion in his eighteen necropsies. Ono found an increased adrenalin content in nine fatal cases, and states that the medulla appeared “fatter” than normal. More data will have to be obtained before it can be determined whether characteristic changes occur in scurvy, and how to interpret the hypertrophy described by several authors as common to guinea-pig scurvy.
Pancreas.—Sato and Nambu appear to be the only investigators who have described lesions in the pancreas. They found hemorrhages in one case among thirteen.
Thymus.—This organ has rarely been examined. Aschoff and Koch found no abnormalities in adults, nor did Jacobsthal in a case of infantile scurvy. Boerich noted enlargement in one instance.
Other Organs of Internal Secretion.—Very little attention has been paid to these organs. Aschoff and Koch state that the thyroids and hypophyses were normal in their cases.
Generative Organs.—No abnormalities have been described.
Central Nervous System.—The most frequent abnormality of the central nervous system is, as would be expected, hemorrhage; this has been discussed in the section dealing with gross pathology. No specific changes have been found in nerve-cells or fibres of the brain.
In a case of fatal scurvy in an infant a “focal degeneration of the lumbar cord” has been described, extending for a distance of about a quarter of an inch (Hess). The lesion differed from that of poliomyelitis in the absence of round-celled infiltration and of the characteristic changes in the anterior horn cells (Figs. 3 and 4). The outstanding feature was a loss of cells in the lateral groups of the left anterior horn; there were also fewer nerve fibres in this region, but this diminution was less striking. No definite interpretation of this case can be made as the data are insufficient to permit a conclusion as to whether the lesion was truly scorbutic or the result of an associated process. Schoedel and Nauwerk found no change in the spinal cord stained by Marchi’s method.
Peripheral Nerves.—The sheaths of the large nerves as well as those of the vessels are very often invaded by hemorrhage. The extravasated blood is found to lie around but rarely among the nerve fibres, which do not show any pathological alteration. Ingier is one of the very few to describe a degeneration of the nerve fibres. In one guinea-pig in which scurvy was induced she found “many marked degenerated fibrillar bundles of both sciatic and peroneal nerves, slight degeneration of the phrenic nerves and one vagus and its cardiac branch.” Another animal is referred to as having shown “very marked and well-developed degeneration of the nerves of the lower extremities.” It is open to question whether starvation played a rôle in the causation of these lesions. Schoedel and Nauwerk, and Aschoff and Koch examined these nerves but failed to find any lesions; the latter directed their attention especially to the vagus of twenty-two cases.
Retinal hemorrhages were found by Jacobsthal, and by Kitamura, who records “decided edema of the retina, marked bleeding and circumscribed hypertrophy of the nerve fibres” such as is found in albuminuric retinitis. These changes are considered again under the symptomatology of scurvy.
Bones.—Our knowledge of the minute pathology of the bones is far more complete and detailed than that of any other structure. This was to be expected in view of the fact that this is the only tissue in which the lesions are diagnostic. In considering the microscopic pathology it must be remembered that all the bones are rarely affected by scurvy, and that those that are involved show the scorbutic changes to a varying degree. One of the peculiarities of the lesion is that it involves the end of the diaphysis or rather the junction of the diaphysis and the cartilage. The bones most apt to show typical changes are the ribs; we shall therefore describe a section made through a costochondral junction.
The costochondral junction is generally swollen, somewhat beaded, and when cut longitudinally shows on gross examination a transverse yellowish bar, corresponding to the area of disorganization which will be described below. Under the microscope the line of juncture is not sharp and straight as is normally the case, but presents a wavy or irregular contour, the cartilage jutting into the bony end of the rib, instead of abutting in neat apposition to it. The bone is hollowed out and irregularly concave, whereas the cartilage presents a convex appearance. At the site of the junction is the Truemmerfeld area, where the normal tissue is splintered and fragmented. Everything in a state of disorder—trabeculæ of bone of various shapes and sizes lie scattered about, the cells irregularly arranged and much distorted, signs of recent hemorrhage, unrecognizable detritus. The picture is that of weakened bone having been crushed by the pressure of the more compact cartilage. Higher magnification shows that there are few osteoblasts (generally associated with the deeper fragments of bone), a varying number of intact red cells, according to the occurrence of hemorrhage, and occasional spindle- and star-shaped connective-tissue cells. Covering this mass of detritus there is frequently, as Aschoff and Koch have emphasized, more or less protective fibrin which has undergone some hyaline or connective-tissue organization.
The cartilage is also not normal. Its cells do not present an orderly arrangement, the proliferating columns having disappeared in the central convex portion, and being present to a varying extent near the periosteal borders. If we judge from sections of early scurvy in guinea-pigs, this disturbance of the columnar formation of the proliferating cartilage is one of the early signs of scurvy, and is associated with an unevenness and irregularity in shape and size of the bone trabeculæ. In young individuals, where cartilage activity is great, these changes are most marked and the entire zone of active cells may be somewhat widened.
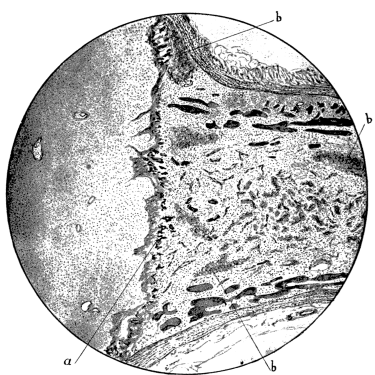 Fig. 5.—Infantile scurvy. Epiphyseal junction of lower end of femur: (a) calcified cartilage at
“Truemmerfeld” (b) hemorrhage in the fibrous marrow (Gernest-mark). Bone cortex and
trabeculae abnormally thin. McCallums’ Text Book of Pathology. W. B. Saunders Co.
Fig. 5.—Infantile scurvy. Epiphyseal junction of lower end of femur: (a) calcified cartilage at
“Truemmerfeld” (b) hemorrhage in the fibrous marrow (Gernest-mark). Bone cortex and
trabeculae abnormally thin. McCallums’ Text Book of Pathology. W. B. Saunders Co.
Below the Truemmerfeld is the Geruestmark or framework marrow, another distinguishing feature of scurvy. This extends for about 5 to 10 mm. toward the lymphoid marrow, where it ends more or less abruptly. It is composed of a loosely-constructed fibrillar tissue on a gelatinous-appearing groundwork, of sparsely scattered cells, and bony trabeculæ which are markedly thin and weak. Here and there are hemorrhages and blood pigment, especially adjacent to the “Truemmerfeld.” Another feature which strikes one at first glance is that the entire marrow area is incompletely filled by the thin and greatly-depleted trabeculæ of the spongiosa. The question has been raised whether this rarification is to be considered entirely of scorbutic origin. It is due evidently to a lack of function of the osteoblasts, which are diminished in number, and are represented by a layer of shrivelled spindle cells along the walls of the atrophied bony columns. They may fail almost entirely, as may its osteoid border, which is significant of active bone tissue. The lack of bony structure and rarification clearly is not due to an increase in the number or the function of the osteoclasts, for these do not appear in excess. It is mainly the result of normal bone resorption with a lack of normal bone regeneration. Aschoff and Koch suggest that the framework marrow may be able to manufacture bone, but cannot accomplish this because there is a lack of material from which to make osteoid tissue. This, they believe, constitutes the primary deficiency—a lack or faulty development of cement substance, which in turn may depend on an alteration of colloid material. Regarded in this light, the lesions of the bones resulting in fracture and those of the blood-vessels resulting in rupture and hemorrhage are dependent on a deficiency of the same basic material.
Hemorrhage occurs in the bone as elsewhere; it is almost never lacking. It appears either as large hemorrhages in the spongiosa, especially where the normal marrow joins either the Geruestmark or the Truemmerfeld, or merely as scattered cells, possibly the result of diapedesis. The blood-vessels in these areas are narrow and extremely thin-walled. The most typical site of hemorrhage is beneath the periosteum, a lesion widely known on account of its clinical significance (Fig. 16). Here the blood may extend for a considerable distance along the shaft, but rarely beyond the epiphyseal line. The clot forms readily, demonstrating that the nature of the hemorrhage is not a defect in coagulation, and in its midst may be seen fibrin, pigment, granulation tissue, and more or less firm connective tissue—constituting the callus. The inner surface of the periosteum is frequently lined with newly-formed bone and with a more or less dense deposition of lime salts, which becomes heavier in the course of the healing process, and is readily observed in radiographs. This periostitis ossificans may result in the clot being surrounded by a perfect shell of bone, with bony columns penetrating the deeper layers.
As the result of the lack of bone formation and the consequent weakening of the corticalis and the spongiosa, frequently a separation of the diaphysis from the epiphysis results. This lesion should not be regarded as a true separation, for, as Barlow pointed out, the line of cleavage is not at the junction, but below it, involving the uppermost region of the diaphysis. It is therefore correct to speak of a fracture or infraction. This lesion is generally accompanied by a deformity of the surface contour of the junction, due to a displacement of the cartilage, as a result of which “angular beading” of the rib is brought about. In some instances the cartilage is “telescoped” into the crushed end of the bone. To a varying extent fibrin covers the end of the fractured bone; the angles adjacent to the periosteum contain blood which becomes organized into dense connective tissue, thus serving as a splint for the fractured parts. In the course of healing a large number of foreign body giant-cells appear, blood-vessels sprout from the periosteum as well as the bony surface, and the necrosed tissue gives place to an active formation of callus, which generally leads to complete regeneration and restitution. It is remarkable how quickly and perfectly an epiphysis may become reunited to its shaft (Figs. 6 and 7). Sometimes, however, this takes place with resulting deformity, as in the development of coxa vara of the femur.
As Czerny and Keller have stated, it is difficult to define sharply the relation of bone fragility to scurvy. Histologically there is great similarity between the “osteotabes infantum” described by Ziegler and conditions sometimes found in infantile scurvy. The main distinction is that in the latter disorder the lesion is less generally distributed throughout the skeleton, and is particularly marked in a limited area of the bones (epiphyses). In considering this question it should be borne in mind that, experimentally, osteoporosis and scurvy can be brought about by diets which are absolutely dissimilar. For example, Bartenstein showed that young guinea-pigs develop osteoporosis and multiple fractures on a diet of raw milk containing an adequate quota of antiscorbutic vitamine.
Rickets and infantile scurvy are commonly found associated, although they bear no causal relationship to each other. The distinctive characteristic of rickets is the broad area of osteoid tissue which is formed at the epiphyseal junction, a broad band of incompletely calcified cartilage not found in scurvy. In the latter disease osteoblastic bone growth is greatly inhibited, but what growth does take place occurs in a normal and orderly manner. The osteophytes, for example, which so commonly develop at right angles to the axis of the bone in the subperiosteal hemorrhages, are composed of apparently normal bone. Another marked distinction between the two conditions is the paucity of blood-vessels in the cartilaginous area and in the marrow in scurvy, compared with the increased vascularity so generally encountered in rickets. It is evident, therefore, that although these two nutritional disorders bear a superficial resemblance to each other pathologically, they are radically different and almost antithetical.
There is no mention whatsoever of scurvy in animals previous to 1895, when Theobald Smith wrote: “When guinea-pigs are fed with cereal (it has been observed for some years in this laboratory), with bran and oats mixed, without any grass, clover, or succulent vegetable, such as cabbage, a peculiar disease, chiefly recognizable by subcutaneous extravasations of blood, carries them off in from four to eight weeks.” Smith did not pursue the subject further.
Coincident with the appreciation of the value of experimental methods, one would have expected attempts to produce scurvy in animals. The disorder had been recognized for a great many years, the fact that it was occasioned by a dietary deficient in fresh food was widely known, so that it would seem natural for clinicians or laboratory workers to have tried to induce the disease in animals by a similar restricted diet. There is, however, no suggestion of such an experiment in the voluminous literature on scurvy. The explanation of the neglect of an experimental study of scurvy appears to be that this was considered a disorder which required little investigation—its etiology, its prevention and its cure seemed thoroughly understood. It is strange that the mere fact that such a severe disturbance responded, as if by magic, to the administration of simple foodstuffs should not have awakened curiosity as well as wonder, and stimulated inquiry into the nature and significance of the curative agent.
In 1903 Bolle published the results of experiments on guinea-pigs which had been fed for various periods on raw or sterilized milk. He reported that the animals developed a marked fragility of the bones, varying in intensity in proportion to the degree of heat to which the milk had been subjected. These changes Bolle interpreted as typical scurvy, but it is difficult to decide whether the disorder was actually true scurvy, in view of the indefinite description of the bone lesions.
Bartenstein repeated Bolle’s work and described in detail the changes in the bones. From his work we learned that it was of little moment whether the animals were fed raw or sterilized milk—their nutrition failed within about the same length of time, and they died within a month. The chief pathologic change was a marked fragility of the bones, leading to spontaneous fractures, or to breaking of the bones in the course of ordinary manipulation. Bartenstein described the disorder as “beginning with the degeneration of the marrow, and secondarily leading to an atrophy of the bone due to increased absorption and deficient new formation of bone, especially at the endochondral lines of ossification. As the result of the osteoporosis, spontaneous fractures occur without noticeable hemorrhagic diathesis.” He found a deficiency of calcium in the bones of animals suffering from even a mild degree of this disorder. Hart and Lessing are of the opinion that we cannot accept Bartenstein’s diagnosis of scurvy. They compare this disorder to that described by Ziegler as “osteotabes infantum,” in which there is a more or less pronounced “jelly marrow” which has replaced the lymphoid cells in scattered areas. They sum up their analysis of the question with the statement that “the primary marrow changes in the diaphysis, the marked lacunar absorption by osteoclasts, the absence of subperiosteal hemorrhages, do not indicate typical scurvy.” Schmorl produced comparable lesions in dogs and came to the conclusion that the disorder was one “very similar” to scurvy but not identical with it, the essential difference being that in all animals there was a most marked absorption of bone by osteoclasts.
Similar results were obtained by others. In 1904 Peiper and Eichloff attempted to produce scurvy in dogs by means of a diet composed exclusively of raw or of sterilized milk. The following year we find a report by Esser of feeding goats on sterilized milk. None of these studies hits the mark; a condition of fragilitas ossium was produced rather than typical scurvy.
In 1907 the first systematic and convincing experimental study of scurvy appeared. In this year Holst and Froelich published a preliminary account of their classic work, undertaken in an endeavor to fathom the nature of “ship beriberi,” a disorder which disabled so many of the sailors in the Norwegian navy. We must remember that until recently attention has been focussed on the infectious diseases, and little thought given to the investigation of nutritional disorders. Although experimental investigation in this field may be stated to have been initiated by this work, it in turn had been stimulated by a conception of dietary diseases which had just begun to be realized. This new viewpoint was the result of the work of Eijkman. As has been mentioned in considering the pathogenesis of human scurvy, Eijkman demonstrated that hens developed polyneuritis, a disease resembling beriberi, when fed on polished rice, and that the simple change to a diet of unpolished rice, or the addition of rice polishings to the dietary, sufficed to protect or to cure. This work had been repeated and substantiated. It was evident to those who considered the question that the old lines of thought in regard to food and dietetics inadequately explained remarkable phenomena of this kind. It was also clear that nutritional disorders were subject to experimental investigation in a way similar to the infectious diseases, which were absorbing the interest of the various laboratories. It is unnecessary to review the rapid rise of investigative work in this field. It may be stated, in general, that during the past few years the investigations of scurvy have become so numerous that an established research technic may be said to have developed in connection with its study.
Attempts have been made to produce scurvy in various animals, but it has been brought about regularly only in the guinea-pig and in the monkey. Experiments on the dog are as yet too few to justify our regarding this animal as definitely available for this study. The nutrition of rats, mice, rabbits, hogs, pigeons, fowl, receiving a diet identical with that which regularly occasions scurvy in guinea-pigs, either progresses normally or a state of malnutrition develops which cannot be identified with scurvy. Recently Hart, Steenbock and Smith have reported that cattle can be reared to maturity on a diet which will produce scurvy in the guinea-pig in four to five weeks. We are therefore confronted with the remarkable and inexplicable phenomenon, a fact concurred in by almost all investigators, that a diet induces either normal nutrition or malnutrition, according to the experimental animal employed. A diet of polished rice, or other decorticated grain, will lead to the development of scurvy in the guinea-pig, to polyneuritis in the pigeon or fowl, or, according to Holst and Froelich, to a combination of these disorders in the hog.35 The basis of these divergent results cannot be surmised, and is worthy of the most thorough investigation. It may well be that the elucidation of this problem—for example, why we are able to bring about scurvy in the guinea-pig but not in the rabbit, will shed light on the pathogenesis of this disorder. Are we to conclude that some of these animals have the power to synthesize the vitamine whereas others must depend upon the food for it, or are we to presuppose an ability to maintain normal life and function without any or with a minimal amount of this vitamine? The difference between these two groups, the susceptible and non-susceptible animals, probably is not as absolute as we have been wont to regard it. Recently Harden and Zilva have shown that although rats are able to thrive on a diet free from antiscorbutic vitamine, they show an appreciable gain in weight when this factor is added to the dietary. If such be proved to be the case, we must regard the non-susceptibility of the rat, the rabbit, etc., as relative rather than absolute.
From time to time a doubt has been raised as to whether we should accept guinea-pig scurvy as the counterpart of human scurvy. This question can be answered only by comparing the disorder in the one species with that in the other—as to mode of production, pathology, symptomatology, means of cure and all other phenomena. Viewed from these standpoints it is found that in almost every respect the disorder is identical in man and in the guinea-pig. The outstanding distinction is the difference in the length of time elapsing before the development of symptoms. In the child or in the adult it takes about six months of the deficient diet before clinical symptoms are manifest and a diagnosis can be established; in the guinea-pig the disorder can be recognized two weeks after restricting the diet. In the one instance we seem to be dealing with a nutritional disorder which is chronic or at least subacute, and in the other with a markedly acute condition. This distinction is open, however, to certain qualifications. In the first place, we must consider the duration of life of the two species, the comparatively short span of the guinea-pig compared with that of man. It must be borne in mind, furthermore, that the guinea-pig is placed on a diet absolutely devoid of all antiscorbutic vitamine, whereas this rarely obtains in human beings. For example, the diet which is most markedly scorbutic for infants is the “malt soup” previously mentioned, but even this food contains an amount of the antiscorbutic factor which is not negligible. But after taking these differences into consideration, it is nevertheless evident that the guinea-pig is far more sensitive to scurvy than man. This does not indicate that the guinea-pig is an unsuitable experimental animal, any more than the fact that the pigeon is more susceptible to polyneuritis than man indicates that it is unsuited to investigations of beriberi. It merely prevents our carrying out delicate quantitative experiments, and cautions against drawing too finely-spun deductions. In all nutritional investigations it should never be forgotten that conclusions drawn from experiments on animals are merely provisional, and must await substantiation on man, and, furthermore, that where differences in reaction are noted, the clinical data should be accorded full consideration.
Pathogenesis of Guinea-pig Scurvy.—From a pathogenetic point of view guinea-pig scurvy and human scurvy show remarkable points in common. Any diet that leads to the development of scurvy in man likewise brings it about in the guinea-pig, and contrariwise, any food which cures the disorder has the same beneficent effect on both species. This similarity extends so far that, as will be shown in the chapter on antiscorbutics, the relative potency of the various foods is approximately the same for man and for the guinea-pig. The parallelism generally is striking. The dietary which has been commonly employed in experimental scurvy has been that first suggested by Holst and Froelich, namely, oats, hay and water. Recently, however, this dietary has been enlarged in order to make it more complete, so as to include adequate protein, water-soluble and fat-soluble vitamine, and inorganic salts. To this end the group of workers at the Lister Institute (Chick and co-workers, Harden and Zilva) place their animals on a basal diet of one part of crushed oats and two of wheaten bran, and a daily ration of 50 to 60 c.c. of milk autoclaved for one hour at 120° C. This milk still retains a small amount of antiscorbutic vitamine. Cohen and Mendel have employed, apparently with good result, a “soy bean cracker,” containing soy bean flour which has been heated for 30 minutes at 15 pounds’ pressure (120° C.), 3 per cent. of sodium chloride, the same percentage of calcium lactate and of dried brewers’ yeast, and raw milk sufficient to supply 5 per cent. of butter-fat.
The use of raw milk was introduced by Jackson and Moore, and adopted by McCollum and Pitz and again by Pitz in a series of interesting experiments. The milk was given ad libitum. The results of these investigations were puzzling at first, until it was shown by Chick, Hume and Skelton that the dietary on which they were based contained a fundamental error which accounted for their lack of consistence. Although milk is not rich in the antiscorbutic factor, it possesses it in moderate degree, so that the outcome will be quite different according to whether a guinea-pig takes, for example, 50 c.c. or 100 c.c. daily. It is quite evident, therefore, that a food of this kind cannot be offered ad libitum, and that if this rule is not observed, most disconcerting results will follow.36 This basic error in framing the dietary has made it impossible to accept the deductions of these authors. The conclusions of McCollum and Pitz are so striking and have led to such wide discussion, that they require consideration, in spite of the fact that the error in the dietary is now recognized. These authors found that the cæcum of their animals was greatly distended with putrefying fæces. As the cæcum is extraordinarily large and delicate in this species, they drew the deduction that the development of scurvy in the guinea-pig was due principally to the retention of fæces. “An impacted cæcum, the seat of putrefaction, may cause injury to the cæcal wall, sufficient to permit the invasion of the tissues by bacteria, or the animals may perhaps be injured primarily by the absorption of toxic products of bacterial origin.” Accessory dietary factors or vitamines, according to this theory, are supposed to play no part in the disorder, and antiscorbutics, such as orange juice, are considered to owe their efficacy mainly to their laxative properties, and to be replaceable by other laxatives such as phenolphthalein or oleum petrolatum. The efficacy of orange juice is supposed to be due to its content of citrates, and to be replaceable by what was termed “artificial orange juice,” a mixture composed of the various salts, citric acid and sucrose, in the proportions in which they are found in the natural juice.
These reports stimulated renewed interest in experimental scurvy, suggesting new aspects, and therefore directing attention to points requiring investigation. There were no data at hand on the consistency of the contents of the bowel in guinea-pigs, so that it was necessary to make appropriate observations in normal and in scorbutic animals. It was soon reported by various workers, Rappleye, Cohen and Mendel, Hess and Unger, and others, that there was no definite relationship between the occurrence of scurvy and impaction of the cæcum. In Fig. 8 we see portrayed the stool output of a guinea-pig during the period in which it was developing scurvy, and during a subsequent period when it was being cured by means of orange juice. It is clear that there was no significant variation in the output during these divergent periods. A similar conclusion was arrived at by those who examined the cæcums of animals postmortem. Cohen and Mendel write: “Summarizing our experience with nearly one hundred scorbutic animals, we conclude that actual impaction of the fæces in the cæcum occurred in about one-quarter of the cases, and visible damage to wall, i.e., congestion or hemorrhage, or impaction, or both, was found in perhaps half of the cases. It should be noted that this statement covers all the diets we have tried.” We concur in this conclusion. Not infrequently we found the cæcums of markedly scorbutic pigs to contain semi-fluid fæces, the consistency of its contents depending on the character of the diet, quite apart from its adequacy and lack of the antiscorbutic factor. For example, a diet rich in milk, containing 100 c.c. or more, led to the formation of rather solid fæces; if oats were added to the milk diet the fæces in the cæcum were found to be still more solid, and this portion of the gut more often impacted. This condition could be detected by palpation even during life. Just as we encountered scorbutic animals on an oat, hay and water diet, who had semi-fluid fæces in the cæcums, so we met with others which were on a milk diet, and showed no signs of scurvy, although their cæcums were impacted with fæces of a putty-like consistence. Guinea-pigs do not seem to be able to tolerate a diet containing a large quantity of the fat of cow’s milk. Such a diet leads to impaction of the large intestine resulting in death, but does not induce scurvy. Jackson and Moore produced a condition of this kind by feeding pigs with cream containing 26 to 28 per cent. fat. “In every case,” they write, “the large intestine was distended with light mustard-colored semi-solid fæces.” This pathological condition is not understood, but is quite distinct from scurvy, and remarkable in view of the fact that the milk of the guinea-pig contains as high as 25 per cent. of fat. It is an interesting illustration of the marked biological difference in the butter-fat of various species.
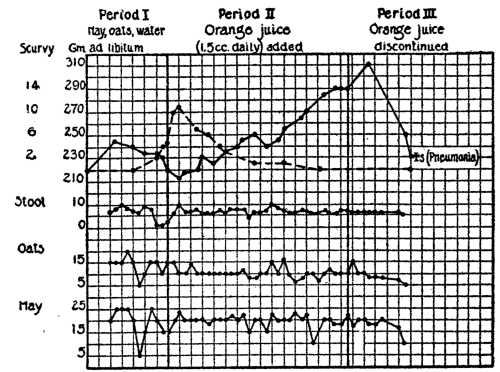 Fig. 8.—Shows a period with the development of scurvy, and one where it was
cured by giving orange juice. It will be noted that there was no marked constipation
while the animal had scurvy. During a period of a few days the amount
of stool was scanty, corresponding to the decreased intake of oats and hay on
the days preceding. Broken line represents clinical course of scurvy.
Fig. 8.—Shows a period with the development of scurvy, and one where it was
cured by giving orange juice. It will be noted that there was no marked constipation
while the animal had scurvy. During a period of a few days the amount
of stool was scanty, corresponding to the decreased intake of oats and hay on
the days preceding. Broken line represents clinical course of scurvy.
Nor was it found, as McCollum and Pitz claimed, that antiscorbutics were replaceable by laxatives in the diet. Without entering into the details of this aspect of the subject, which will be considered in the chapter on symptomatology, it may be stated that attempts to prevent the occurrence of scurvy or to cure it by means of laxatives invariably failed. Chick, Hume and Skelton, as well as Hess and Unger, gave oleum petrolatum to a series of pigs without the slightest favorable effect. Hart, Steenbock and Smith recently reported that they had administered 1 c.c. of this oil on alternate days to one series of pigs, and 2 mg. of phenolphthalein on alternate days to another series, without relieving the scurvy. Cohen and Mendel, in order to test the adequacy of their diet as to roughage, supplemented it with additions of considerable filter paper and sawdust, “without averting the appearance of scurvy.” It is evident, therefore, that constipation does not play an essential rôle in the pathogenesis of scurvy in the guinea-pig, and that antiscorbutics are by no means synonymous or interchangeable with laxatives. These results accord with observations on infantile scurvy.
The Pathology.—The pathology of guinea-pig scurvy is essentially that of human scurvy. Hemorrhages and separations of the epiphyses or fractures of the long bones dominate the macroscopic picture. The hemorrhages are found rarely in the gums, but are common about the joints, in the muscles of the jaw or in those of the hind legs. They may be subcutaneous and appear as bluish discolorations at various parts of the body, especially if the disorder has resulted in death or if infection has been superadded. On stripping the skin we often note hemorrhages in the intercostal muscles, and beading of the ribs at the site of the costochondral junctions, least marked in the upper and in the floating ribs. This has been frequently described in connection with guinea-pig scurvy; its similarity to the rosary of human rickets has been drawn attention to recently by Jackson and Moore. It should not be regarded as “pseudo-rhachitic,” but as typically scorbutic, from a microscopic as well as a macroscopic viewpoint. On closer examination a yellowish-white transverse line may be seen at the epiphyseal junction of the ribs, and frequently some subperiosteal hemorrhage. Beading of this character has been reported by Ingier also in the “snuffles” of hogs and as the result of trauma. A similar enlargement of the chondral junctions of the sternum may be found on examining its posterior surface.
The joints of the body always show some changes. The epiphyses are enlarged to a variable degree, resembling the epiphyses typical of human rickets. As in infants, this change is met with most commonly at the wrist joint, involving the ulna and the radius. The knee-joint is likewise often involved, especially the ends of the tibia; the elbow, ankle, and the shoulder may also show an articular swelling of the bones. About these joints hemorrhages in the subcutaneous tissues may be seen, or edema extending along the extremities. Not infrequently a fracture of one of the long bones is found, which may or may not have been diagnosed during life. The common site of fracture is the lower part of the tibia or fibula. Much more frequent than fractures are separations of the epiphyses, which long since have been recognized as typical of infantile scurvy. Even gentle handling in the course of performing the necropsy may occasion a lesion of this kind—of the tibia at the knee, of the radius or ulna at the wrist, or indeed at any of the epiphyseal junctions. The infracted ends occasionally may be seen held insecurely by a delicate band of periosteum. The shafts of the bones are brittle, rarefied, and easily broken.
On opening the chest, slight hemorrhages may be noted in the pericardium and in the visceral and costal pleuræ. The heart is frequently enlarged, and the pericardial sac contains an excess of serum; the right ventricle, however, is not found disproportionately hypertrophied. Pneumonia is met with very frequently and constitutes a common terminal infection.
On opening the abdomen we may note subperitoneal hemorrhages of the muscular wall or of the coils of intestine. The liver and spleen are generally normal, as is the pancreas. The kidney frequently shows minute hemorrhages beneath the capsule and on section.
The adrenals not infrequently are large. This fact was first brought out by Rondoni and Montagnani, and is of added interest in view of its confirmation by McCarrison as well as by LaMer and Campbell. Its significance is discussed at length in the consideration of the adrenal gland in human scurvy. In view of the fact that fasting leads to a similar hypertrophy, and that guinea-pig scurvy frequently is complicated by fasting, these observations should be extended. In all investigations of this kind, bacterial cultures should be taken of the adrenals, or other organs, to be certain that there is no complicating infection.
There have been no reports as to the effect of scurvy on the size of the testicles, ovary, thymus, thyroid or parathyroid glands in the guinea-pig, such as have been made by McCarrison in relation to avian polyneuritis.
The alimentary tract occasionally shows macroscopic changes similar to the lesions found in man. The entire canal is frequently very empty, especially the stomach and the small intestine, due to the lack of appetite for some days previous to death. In the stomach we may find areas of congestion or numerous small superficial ulcers surrounded by congestion and covered with mucus; occasionally these ulcers are somewhat larger and deeper. The larger ulcers are more frequently situated in the first part of the duodenum, often proximal to the papilla of Vater. Holst and Froelich described this lesion in one of their early communications. More common than ulceration of the duodenum is a diffuse congestion of its upper part. This lesion is of note because it has been described frequently in the protocols of human necropsies, and is found in beriberi, in avian polyneuritis, and in pellagra in man. Its significance is unknown, and has indeed never been discussed.
Lower down in the bowel there are occasionally areas of congestion and ulceration, but no section seems particularly predisposed to these lesions. The contents of the bowel, especially of the cæcum, as mentioned above, depend more on the character of the food than on the existence of scurvy. If the diet has consisted of milk and oats, the cæcum will be found full and perhaps impacted, whereas if hay and oats have been fed, the cæcum will be less full and its contents semisolid.
In view of the fact that many of the animals have taken very little food for some days previous to their death, it will be well to describe briefly the macroscopic picture of simple starvation in guinea-pigs. When guinea-pigs are given only water they live about one week; if orange juice is added to this water diet they succumb a little later to starvation. Under all these conditions the striking pathologic change—absent in scurvy—is edema. It is true that the limbs may show slight edema in scurvy, and that the pericardial and the pleural sacs, and even the peritoneal cavity, occasionally contain a small quantity of serum, but it is comparatively an insignificant amount. Moreover it is difficult to decide to what extent this edema is due to scurvy, and to what extent to starvation. In typical starvation, on the other hand, such as occurs on the limited diets enumerated above, we find marked subcutaneous edema, sometimes a true anasarca, and frequently also ascites. We are reminded of the “war edema” and its frequent association with starvation. Another distinction between the two conditions is the fact that the marrow in starvation is yellow and not red as in scurvy. In passing, it may be mentioned that the ascites was greater when orange juice had been given than where the animal received only water.
In perusing the literature but one study has been noted on the effect of a scorbutic diet on the fœtus. This investigation was carried out on a large series of guinea-pigs by Ingier (1915). The following comprise her conclusions:
“1. Pronounced cases of Barlow’s disease may be produced in the fœtus as early as ten to fifteen days after the commencement of dieting pregnant guinea-pigs with oats and water. There are wide individual variations. The scorbutic changes in the skeleton are greatest in the earlier embryonic stages. The fœtuses of that period, with practically no exceptions, die and show marked traces of impeded growth.
“2. Fœtuses from the later period of pregnancy are born alive, and apparently fully developed, with comparatively slight changes in the osseous system.
“3. Even a short extension of the period of extra-uterine dieting on milk from scorbutic mothers, and later on oats and water, is sufficient to change the latent scurvy into a highly-pronounced case.
“4. The fœtus cannot be kept alive longer than the adult animal, about twenty-eight days, either by intra-uterine dieting alone or by combined intra- and extra-uterine dieting.
“5. The mothers show signs of the disease at an early period and are more severely attacked than non-pregnant animals. Death also occurs comparatively often in the first period of gestation.”
In these experiments intra-uterine fractures, premature births and still-born litters are frequently mentioned. This suggests naturally an inquiry as to whether similar occurrences have been observed in human scurvy. In considering the pathogenesis of human scurvy, we have remarked on the meagreness of the data on this most interesting aspect of this disorder. In view of the similarity between human and guinea-pig scurvy, we should expect not only miscarriages and still-births to result, but cases of congenital scurvy, especially of the latent or rudimentary type.
Scurvy Has Been Induced Also in the Monkey.—The most extensive investigation of this kind is that of Hart and Lessing, who brought about scurvy in several young Macaci Rhesi which had been fed for some months on boiled condensed milk with the addition of cooked rice and pig-nuts. Typical scurvy resulted in all but one instance, and in this case an old animal was used and a different pathological picture developed. These experiments require brief reviewing, as the clinical signs and gross pathology in monkeys differ somewhat from those encountered in guinea-pigs, and particularly as these distinctions render scurvy in monkeys and in infants practically identical.
Apart from general listlessness and lack of activity, the first sign is hemorrhage of the gums, the characteristic sign of infantile scurvy. This is stated to be constant; in the guinea-pig it is most exceptional. Another sign characteristic of infantile scurvy is the subperiosteal hemorrhage, which in the guinea-pig may be found as a small effusion near one of the larger joints or the costochondral junctions, but in the monkey consists of large effusions, similar to those described by Barlow. Subperiosteal hemorrhages of the cranial bones were constantly seen, and not infrequently involvement of the scapula and of the maxilla. Hemorrhage into the orbit leading to exophthalmos and to hemorrhagic discoloration of the upper lid—a lesion not infrequent in human scurvy—is also described; in guinea-pigs we have met with exophthalmos only in two instances. In all other respects scurvy in the monkey resembles that in the guinea-pig, even to the extent of the scorbutic rosary of the lower true ribs. Hart and Lessing describe the presence of the “white line” of Fraenkel, which is referred to at length in treating of the symptomatology of human scurvy. This is a shadow, seen by means of the X-ray, traversing the long bones near their epiphyses—a definite “shadow band” associated with a narrow light zone lying just beneath it. This “white line” has been noted likewise by Talbot, Dodd and Peterson in the scurvy of monkeys.
Microscopic Pathology.—Turning to the microscopic pathology, we find that the changes are similar to those described elsewhere in connection with human scurvy. It will be unnecessary, therefore, to give more than a general survey of the typical alterations. Little has been added to the description of lesions so carefully depicted in the first report of Holst and Froelich (1907). The bone marrow at the ends of the diaphyses in proximity to the epiphyseal junction loses its normal lymphoid character and is replaced by a reticular or fibrillated substance, the so-called “framework” marrow (Geruestmark of Schoedel and Nauwerk) containing a homogeneous mucoid tissue and only a few osteoblasts and marrow cells. The number of blood-vessels is considerably reduced and fresh hemorrhage or blood pigment is frequently seen. The osseous tissue itself shows marked changes, corresponding to the rarification and brittleness noted on gross examination. The osseous trabeculæ are fewer in number and those which remain are slender and irregular, and frequently appear as isolated islets. The cortical substance also becomes very thin. There are marked alterations in the intermediate cartilages, especially of the ribs.37 Instead of the cells being arranged in orderly rows, they are irregularly placed, and frequently greatly reduced in size and number. The bone trabeculæ on which they abut are not well formed or of equal length, and do not present an even and transverse plane, but are misshapen, small, so that the line of junction with the cartilage is zigzag. In cases of marked scurvy the junction may be entirely disorganized and deformed, showing fractures of the rarefied bone and hemorrhages in the neighborhood. This leads frequently to a macroscopic deformity of bone, a bulging of the surface at the costochondral junction—the scorbutic “beading” or “rosary” of the ribs. Recently Delf and Tozer have described these changes, classifying them as those occurring in “incipient,” “definite,” “acute,” “chronic definite,” and “chronic acute” scurvy. Fig. 9 shows these types in diagrammatic form. In this figure we see how varied may be the manifestations of this nutritional disorder, according to whether it has existed for a shorter or a longer time; in some instances the picture is very puzzling. The “incipient scurvy” corresponds to what we have termed clinically “latent scurvy” in infants, a condition which cannot be diagnosed and is manifested merely by a faulty nutrition which responds promptly to the addition of an antiscorbutic to the diet. There have been no histologic examinations in man at this incipient stage, but we may infer that they are similar to the bony changes found in the guinea-pig. When the scurvy has become chronic in an animal which has lived for months on a quota of antiscorbutic food sufficient to preserve life but insufficient to prevent the development of scurvy, we find a microscopic picture at the costochondral junction differing widely from that seen in the acute stage. Not only are the columns of cartilage cells represented merely by misshapen vestiges, but an ossified band (Fig. 95) is seen at the junction. It is probable that this is frequently the cause of the marked cessation of growth which has been described in connection with this type of scurvy in infants. Delf and Tozer interpret this ossified band at the junction as “an attempt to strengthen the junction in an abnormal manner, the normal process having broken down.” If the animal is again deprived of antiscorbutic food the ossified band breaks down, the junction becomes deformed and disorganized, and a condition of “chronic scurvy (acute)” is stated to have developed.

1. Diagram of normal rib-junction.
2. Diagram of rib-junction to illustrate “Incipient Scurvy.” This rib-junction is very nearly normal, but shows what may be regarded as the first recognizable signs of the onset of the disease; these are: (a) An appearance of general abnormality (when compared with the normal). (b) Unevenness of the junction and slight disorganization of the rows of cartilage cells. (c) Shortening of the length of the rows of cartilage cells. (d) Shortening, and decrease in number of the trabeculæ. (e) Increased amount of blood in the marrow cavity.
3. Diagram of rib-junction to illustrate “Definite Scurvy.” Histological signs vary considerably in these cases (according to the severity of the disease), and may approach in appearance those characteristic of the “Acute” condition. The rows of cartilage cells may be almost normal, but are more often noticeably shortened and usually somewhat disorganized or arranged in circular groups. The trabeculæ are usually about half the normal length and have a truncated appearance. The junction as a whole may present an uneven, slightly disorganized appearance and there is sometimes a certain amount of macroscopic deformity.
4. Diagram of rib-junction to illustrate “Acute Scurvy.” In these cases the junction and rows of cartilage cells are often completely disorganized, causing a marked macroscopic deformity of the bone. The bone of the shaft is frequently fractured. The marrow is no longer in contact with the edge of the junction and the space is filled with a mass of connective tissue; this is very characteristic in cases of fracture. A condition in which the trabeculæ have almost disappeared and the rows are much shortened is also found in “Acute Scurvy,” in those ribs in which no fracture of the shaft has occurred; usually, however, there is little or no ossification across the junction. There is frequently hemorrhage into the marrow cavity.
Diagrams 5 and 6 illustrate types of “Chronic Scurvy.”
5. May be described as “Chronic Definite Scurvy.” The rows are much shortened but not disorganized and an ossified band extends across the junction.
6. May be described as “Acute Chronic Scurvy.” The junction is deformed, and the rows are very disorganized; the trabeculæ have disappeared and an ossified band extends across the junction. There is no connective tissue to be seen and no existing, or recent, fracture.
It has been noted by many investigators that changes in the teeth take place in the course of scurvy. They become somewhat yellow and lose their glistening appearance, and occasionally break off. The molars commonly become loosened, so that they can readily be removed from their alveolar sockets; less frequently this is true of the incisors. Until recently, however, this subject has not been studied in detail, and no significant histologic changes in the teeth have been described. Jackson and Moore showed that with marked changes in the teeth there was often “great dilatation of the veins in the pulp attended by more or less hemorrhage into the pulp,” and that “in guinea-pigs fed on oats and hay there was almost complete necrosis of the pulp of the incisor teeth, also more or less necrosis in the pulp of the molars.”
Recently an intensive study of this subject has been made by Zilva and Wells, which is of special interest because it describes the first beginnings of these lesions, and particularly because we have no knowledge whatsoever of the dental changes which occur in human scurvy. These investigators found a fibroid degeneration of the pulp of the teeth, a pulpar fibrosis. “It is clear at once,” they write, “and it is an important fact that no trace of cellular organization, no trace of cell nuclei, no trace of interstitial cement substances can be found anywhere. Nerves, cells, blood-vessels, and odontoblasts have all shared the process of fibrication and are no longer recognizable.” These radical changes in the teeth, brought about by a deficiency of antiscorbutic vitamine, were demonstrated not only in guinea-pigs but also in monkeys. In some instances they were found where a histologic examination of the costochondral junctions showed nothing abnormal. “Profound changes were recorded where the scorbutic changes during life were so slight as to be almost unrecognizable,” and, they continue, “the mildest degree of scurvy which could just be discovered at the postmortem examination produced well-defined changes in the structure of the teeth.” If this work is confirmed, we must consider the teeth as one of the first tissues of the body to be affected by scurvy. The authors quite rightly raise the question whether the teeth of young children may not likewise be injured by a deficiency of antiscorbutic vitamine, whether this may not play a rôle in the dental caries so prevalent among civilized communities. It is evident, they state, that such transient conditions of infantile scurvy as have been described by Hess as “subacute” or “latent” scurvy, may occur more often than is usually suspected, and may reasonably be expected to influence dentition. It seems quite possible that the caries of the permanent teeth is due not only to infantile rickets but also to infantile scurvy.
Besides the typical histologic changes in the bones there are alterations in other organs which require mention. All investigators have found a degeneration of the muscles, showing a loss of their striations, swelling of the fibres, and the presence of irregularly-distributed vacuoles and granules. The interstitial tissue frequently is permeated with edema, as we should expect from gross appearances. Holst and Froelich have reported a fatty degeneration of the heart muscle, as well as of the epithelium of the mucous membrane of the glands of the stomach and of the intestine. Hart and Lessing, in their protocols of necropsies on monkeys, describe an interesting lesion associated with the degenerated muscle fibres—a collection of granules staining deep blue with hæmatoxylin and dissolving on the addition of acid. These granules, interpreted as being composed of calcium, were found in the muscles of the limbs, of the tongue, and in the heart. It is reasonable to attribute their formation to an absorption of bone throughout the body. Similar calcium deposits were seen frequently in the adrenal glands, in their cortex, or at the border of the cortex and medulla. This lesion gains special interest in view of the calcium deposits described so frequently in connection with mercurial poisoning, more particularly as the symptoms of scurvy and of this toxic condition have marked clinical resemblances.
There has been but little histologic investigation of the nerves in experimental scurvy. In fact, the only systematic study of the kind is that of Holst and Froelich, whose attention was drawn to this field in an attempt to solve the relationship between scurvy and ship beriberi. These writers found a true Wallerian polyneuritis in only two pigs, one of which had been fed on wheat bread made with yeast, and the other on decorticated barley. In many instances, however, there was extensive degeneration of the axis cylinders without degeneration of the sheaths. They do not, however, attribute great importance to these changes, as the same lesions were found in the nerves of animals fed on cabbage and fresh potatoes. In view of the confusing reports on the nerves of birds in experiments on polyneuritis, one cannot be too careful in drawing conclusions from histologic studies of this kind.
In the study by Jackson and Moore on experimental scurvy in guinea-pigs, the histology of the blood-vessels is carefully considered. “Marked thinning of the wall” was found and depicted; “the wall as a whole had partially melted away, leaving few traces.” These parts of the wall contained many small round bodies resembling cocci, which were stained a deep blue by the Wright and the Giemsa methods. These bodies were present also in the lumen of the vessel and in the inner layers of the more normal portions of the wall. In addition to such changes in the veins, “lesions having the shape, location, and characteristics of infarcts, were found in the ends of the diaphyses of the long bones.” As a result of this pathologic picture the authors are of the opinion that they may have been dealing with a mild infection. This is quite possible, as scurvy tends to render the tissues less resistant to the entrance of bacteria. We believe, however, that even if such were the case, the phenomenon must be regarded merely as secondary in its relation to the pathogenesis of scurvy.
Following the study on the pathology of experimental scurvy, Jackson and Moore undertook to determine primarily whether the small stained bodies seen in the sections of the scurvy lesions were bacteria. This investigation has been cited frequently as presenting cogent evidence in favor of the infectious nature of scurvy, so that it will be necessary to consider it fully; the general question of whether scurvy is a bacterial infection is discussed under the consideration of etiology.
As is well known, Morpurgo, a generation ago, claimed to have produced rhachitic lesions in young rats by means of artificial infection with a gram-positive diplococcus. Pappenheimer brought about similar lesions in rats by the injection of a suspension of bone marrow from a rhachitic animal. Koch injected a streptococcus longus intravenously into young dogs, occasioning gross bony changes of the epiphyses and costochondral junctions, and microscopic changes resembling scurvy—an irregular line of ossification and “a framework” marrow, which, however, showed regions of osteoid. Jackson and Moody were able to isolate from the crushed tissue of their guinea-pigs “a diplococcus of low virulence with a tendency to form chains and produce green (color) on blood agar.” Pure strains of these organisms inoculated into the circulation of guinea-pigs and rabbits, living under ordinary conditions (a mixed diet consisting of green vegetables, hay and oats), gave rise in most instances to hemorrhagic and other lesions in the bones, joints, muscles, lymph-glands or gums. Hemorrhages were found beneath the periosteum in the region of the lower incisor teeth and the acetabulum and ribs. These results are far from constituting evidence in favor of the microbic origin of scurvy. They show merely that the tissues of scorbutic animals frequently harbor bacteria, and that injections of these bacteria will bring about hemorrhages which may be subperiosteal in character. They are open to the specific criticism that scurvy was produced readily in the rabbit, an animal which otherwise does not develop scurvy, and, furthermore, they differ from feeding experiments in inciting scurvy notwithstanding the fact that the animals were receiving an antiscorbutic diet (green vegetables). Cultures of the hearts’ blood of the affected animals were sterile in every instance; a result obtained likewise by Holst and Froelich.
Further studies of this kind should be carried out and should include cultures of the blood and tissues of guinea-pigs in the various stages of scurvy, especially the early stage. In addition, a histologic study should be made of the bones of animals injected with bacteria (preferably streptococci), in order to ascertain whether notwithstanding an unrestricted diet, typical lesions can be produced by this means.
For further details of the pathology of scurvy, the reader is referred to the chapter on human pathology.
Symptoms.—Let us consider the symptomatology of guinea-pig scurvy. In the course of an observation of many hundreds of animals we have been struck by the striking uniformity of the signs and symptoms. The animals made use of were almost invariably of moderate size, weighing from 200 to 300 grams. Where heavier pigs were employed the disease progressed less rapidly, but the signs were the same; they were, however, more difficult to elicit, owing to the subcutaneous fat. Most of the animals were on a diet of hay, oats and water ad libitum, but there was no variation in symptoms where fat and fat-soluble vitamine were supplied by an addition of egg yolk or of cod liver oil, or where egg albumen was fed to render the protein adequate, or where the inorganic salts were supplemented by additions of sodium or calcium chloride.
There is a variability in the sign which signalizes the onset of the disorder—sometimes it consists of a flattening of the weight curve, at others of an inordinate excitability of the animal, or frequently of a tender joint, generally a wrist. The joints almost invariably become tender early in the disease, causing the animal to wince and cry when it is examined. Accompanying this tenderness there is often slight swelling due to edema, or perhaps some hemorrhage, which alters the sharp, clean-cut contour of the joint. This edema may extend upward along the tendon sheaths. Soon the animal becomes lethargic rather than nervously active, and may look ill, as manifested by a roughness of its coat and its unnatural posture. Frequently it sits on three legs with the tender hind leg drawn upward and outward so as to escape pressure—a posture termed by Chick, Hume and Skelton (1918, 2) “the scurvy position,” and indicative of hemorrhage into the joints or muscles. At times it lies curled up, with the side of its face resting on the floor, as if to support its painful or sensitive jaw; this they have termed the “face-ache position.” The two diagnostic signs, however, are the hemorrhages about the joints and the loosening of the teeth. The diagnosis frequently can be established by the twelfth to the fourteenth day; the earliest diagnosis was made on the eighth day. Hemorrhages appear somewhat later than tenderness, and are situated at the joints, most frequently at the knee, which may be markedly swollen and show a bluish or reddish discoloration, extending upward or downward for some distance. Other joints are often involved, frequently the wrist, the ankle or the shoulder. In other cases hemorrhages into the muscles are noted, especially of the leg or of the thigh, and later, especially toward the end, hemorrhages from the bowel. Fractures or separations of the epiphyses may be found on examination or may be occasioned by the physical examination. A frequent site of this lesion is at the wrist or at the knee, involving the head of the tibia or the lower end of the femur. These fractures knit rapidly when an antiscorbutic is given, but result at times in deformity.
Loosening of the teeth is another typical sign. It is, however, one which does not appear early and is somewhat difficult to elicit. The molar teeth are generally involved, especially those of the upper jaw, which may be so completely separated from their alveolar sockets that they can readily be removed by forceps. It is, however, impossible to examine the molar teeth satisfactorily during life. Far less frequently an incisor tooth becomes loosened; more often it loses its glistening appearance and looks dull and yellowish. Occasionally an incisor tooth fractures. The gums are rarely altered sufficiently to aid diagnosis; not infrequently they are congested or bluish, rarely hemorrhagic, and never ulcerous or spongy. This is the chief difference between the symptomatology of scurvy in the guinea-pig and in man, and probably is the result of lesser susceptibility of the former to infection by pyogenic bacteria. In general, however, the disorder in the guinea-pig bears a closer analogy to infantile than to adult scurvy; due to the fact, possibly, that young pigs are generally used for the experiments.
A sign of great interest, although not of diagnostic importance, is the “beading” of the ribs noted by many observers, and emphasized by Jackson and Moore. It has been described also in monkeys by Hart and Lessing. This is an enlargement or swelling of the costochondral junctions of the ribs, especially of the lower true ribs. It corresponds clinically to the “beading” and the “rosary” so characteristic of infantile rickets and mistakenly termed the “rhachitic rosary.” As pointed out, in discussing the symptomatology and pathology of human scurvy, this sign must be regarded as truly scorbutic in animals as well as in infants. The “rosary” is difficult to palpate in pigs which have considerable subcutaneous tissue; in thin animals, however, its course can be followed, the gradual development and subsequent disappearance. In this connection the enlargement of the epiphyses must be mentioned, another sign supposed to be characteristic of rickets in infants. Marked swelling of the wrists is frequently encountered in guinea-pigs suffering from scurvy—a bony enlargement involving the lower epiphyses of the ulna and of the radius. This is met with far more commonly in chronic scurvy than in the usual acute case. Where the disorder has existed for a long period, these bony knobs may persist indefinitely, constituting the sole residual sign of a former scorbutic condition.
The relation of loss of weight to the development of the scurvy requires consideration. In experiments carried out on rats to test the diets in respect to the water-soluble and the fat-soluble vitamines, the weight curve is used as the main criterion to judge whether the foodstuff is adequate. In guinea-pigs we cannot employ the weight curve as a criterion. Not infrequently an animal develops scurvy, and nevertheless does not lose in weight, but even gains slowly and steadily. This occurs when the appetite remains good, and the dietary is complete except for antiscorbutic vitamine. The same holds true for human scurvy, as we have noted in connection with the symptomatology. We have attempted to make up for this defect by adding to the charts a curve representing the clinical course (Fig. 10). Although this curve is computed on an empirical basis, it gives a comparatively true picture of the disease and is far more exact than attempting to portray the disease by means of a weight curve.38 Indeed, when we rely on the latter method it is impossible frequently to illustrate graphically the reaction of guinea-pigs to various influences. Another disadvantage of the weight curve is that it is influenced by factors having no direct relation to scurvy, especially infections of various types which retard the gain.
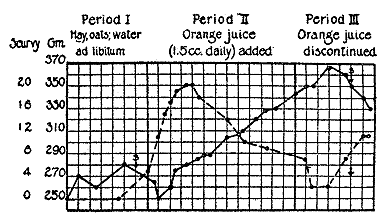 Fig. 10.—Hay, oats, and water ad libitum during period I
resulted in a lack of gain in weight, and in a development of
scurvy. During period II, 1.5 c.c. of orange juice were given
daily, and as will be seen there was a marked gain in weight
and disappearance of the scorbutic signs, although, as is generally
the case, they continue to develop for a short while after
an antiscorbutic is given. When the orange juice was discontinued
in the third period, the weight once more fell and the
scurvy redeveloped. The broken line represents the course of
the scurvy, and is a composite formed on the basis of the
aggregate of the scorbutic signs. Each square represents a
2-day interval.
Fig. 10.—Hay, oats, and water ad libitum during period I
resulted in a lack of gain in weight, and in a development of
scurvy. During period II, 1.5 c.c. of orange juice were given
daily, and as will be seen there was a marked gain in weight
and disappearance of the scorbutic signs, although, as is generally
the case, they continue to develop for a short while after
an antiscorbutic is given. When the orange juice was discontinued
in the third period, the weight once more fell and the
scurvy redeveloped. The broken line represents the course of
the scurvy, and is a composite formed on the basis of the
aggregate of the scorbutic signs. Each square represents a
2-day interval.
Guinea-pigs generally die of scurvy after having lost about one-third of their body weight; occasionally the loss is greater, reaching almost 50 per cent. This loss is due partly to the scorbutic condition, but to a greater extent to starvation occasioned by a marked lack of appetite. In this connection it may be noted that guinea-pigs frequently lose for a few days following the addition of an antiscorbutic to the dietary (Fig. 11). This reaction is evident from a perusal of the weight charts of other investigators, and occurs likewise in human scurvy. This loss is accompanied, as Gerstenberger has pointed out, by diuresis, which may be so marked that it is evident to the casual observation of those caring for the animals.
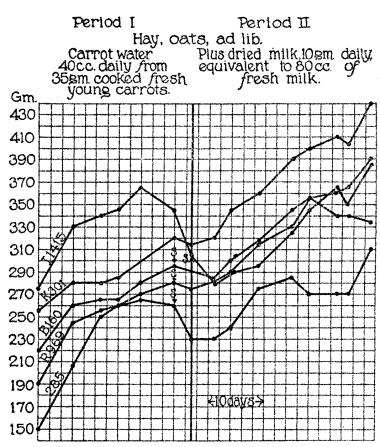 Fig. 11.—These guinea-pigs developed scurvy in spite of
receiving a large quantity of the water in which young
carrots had been cooked for only 20 minutes. It will be
noted, however, that although the pigs developed scurvy
they did not lose weight, as is usually the case. After they
had developed definite scurvy they were given in addition
the equivalent of 80 c.c. of a dried milk prepared by being
heated to about 116° C. for a few seconds. The addition
of this milk to the diet cured the scurvy, showing that it
had largely retained its antiscorbutic vitamine.
Fig. 11.—These guinea-pigs developed scurvy in spite of
receiving a large quantity of the water in which young
carrots had been cooked for only 20 minutes. It will be
noted, however, that although the pigs developed scurvy
they did not lose weight, as is usually the case. After they
had developed definite scurvy they were given in addition
the equivalent of 80 c.c. of a dried milk prepared by being
heated to about 116° C. for a few seconds. The addition
of this milk to the diet cured the scurvy, showing that it
had largely retained its antiscorbutic vitamine.
Exophthalmos may be mentioned again in this connection as a very rare sign of guinea-pig scurvy. Hæmaturia also occurs at times; it is not known how frequently it is present, whether it is an early manifestation in the guinea-pig as in the infant, or whether the source of the blood is the kidney or the bladder.
The superficial lymphatic glands are frequently palpable in scurvy, especially those in the inguinal region. This sign is emphasized by some pathologists. It has seemed to us attributable less to the nutritional condition than to the infections which so frequently complicate the disorder.
According to Jackson and Moore a rise of temperature does not accompany scurvy in the guinea-pig. As the result of an examination of nine guinea-pigs they conclude that “experimental scurvy is a non-febrile disease in the majority of affected animals.” Nor did they find a leucocytosis, the average leucocyte count of eight scorbutic pigs being about 8000.
As the data are meagre, a consideration of the chemical alterations associated with the scurvy of guinea-pigs and monkeys will be taken up in conjunction with the metabolism of human scurvy. The therapy of animal scurvy will also be deferred (chapter VI), as the reaction to dietetic measures is practically the same in man and in animals. In concluding this chapter we would call attention to the following interesting statement contained in the recent paper by Delf and Tozer: “In other experiments, however, where a liberal supply of an antiscorbutic was given and where the fat-soluble A growth factor was known to be deficient, the resulting histological changes in the rib-junctions of the animals examined were found to resemble closely those of ‘Definite’ or of ‘Definite Chronic’ scurvy. In these test cases the antiscorbutic chosen was, we believed, deficient in the fat-soluble A growth factor (for example, orange juice). This fact is mentioned because in the case of an animal not receiving an adequate supply of fat-soluble A the resulting changes in the junctions are not dissimilar from, and are likely to be confused with, those caused by scurvy alone.” If this observation is confirmed, it emphasizes the necessity in nutritional experiments, of constructing a dietary which is complete in every respect except the one under investigation; it also suggests the development of new pathologic entities in relation to other nutritional disorders resulting from a lack of the accessory food factors.
Historical Review.39—It is impossible to state when and how the knowledge of the value of antiscorbutic foodstuffs came to be appreciated. It is probable that the potency of herbs and fruits in scurvy was known empirically to individuals and groups of people long before the fact gained general recognition. A most interesting history of antiscorbutics is given in the excellent work of Hirsch and in our great classic on scurvy by Lind. The first realization of the value of lemons and oranges seems to have been the result of a chance discovery. Budd tells us that in the sixteenth century sailors of a Dutch sailing vessel laden with these fruits were attacked with scurvy, and that, when they partook of the lemons and oranges in the cargo, a miraculous cure resulted. He narrates also the following striking incident, which is mentioned likewise by Lind:
In the year 1600 four sailing vessels left England for the East Indies. The sailors on three of these ships did not receive lime juice, whereas those on the fourth received their daily quota. The men of the first three ships suffered severely from scurvy, but those on the fourth escaped.
In an excellent work on “Scorvey,” published in 1685, Harvey wrote: “Wherefore most acids, especially spirit of salt marine, juice of sorrel, limons, citrons, etc., are so deservedly extolled in some scorbutic distempers and seconded with good success.” Thus we see that even at this early date it was taken for granted that citrous fruits possessed virtue in curing scurvy. Bachstrom (Observationes circa Scorbutum, 1734) evidently was well-acquainted with the antiscorbutic value of scurvy grass, and relates the story of a sailor severely disabled from scurvy who was put ashore to perish on Greenland, and crawled on the ground, grazed on scurvy grass like a beast of the field, and was able to return home perfectly recovered. (Cited from Lind.)
The credit for forcing a general acceptance of the antiscorbutic value of fresh food belongs to Lind. He did not, however, have an easy task, and in 1747, in order to convince those who still were skeptical, he resorted to an experiment on human beings. Twelve patients in his hospital were given the same diet, except that some received sea-water in addition to their dietary, others vinegar, or elixir of sulphuric acid, or a daily portion of cider, or oranges and one lemon daily. The last two groups, as we should expect, recovered quickly; one man who received cider improved, but in no other case was any alleviation noted.
Lind extols the value of lemons and oranges, of berries, of sour cabbage, of cider, and of all fresh fruits and vegetables. In spite of the fact, however, that Lind’s teaching was based on an experience with thousands of patients suffering from scurvy in the naval hospital, his ideas did not take root. It required an event which came directly under the official eye to bring about radical changes in the diet of the sailors. In 1795 the English Fleet suffered from a severe epidemic of scurvy, which was finally controlled by giving the sailors fresh vegetables and fruit. This therapeutic result was so convincing that thenceforth a daily ration of lime juice was ordered for the sailors and a regular issue provided for the navy. This marks the cessation of scurvy as a scourge of the British navy. From this time the disease appeared only sporadically. The sharp decrease in the incidence can be appreciated by Budd’s statement that 1457 cases of scurvy were admitted to the Royal Naval Hospital in 1780, whereas in 1810 an English physician reported that in the seven preceding years he had not treated a single patient in this hospital suffering from scurvy. In another marine hospital, between the years 1806 and 1810, only two cases of scurvy were admitted.
Nothing was done for the British merchant service until over half a century later, although scurvy continued to make its appearance among the sailors with varying severity. Smith states in the article on this subject in Allbutt’s System of Medicine: “In 1864 it was pointed out by Doctor Barnes that during the twelve years following 1851, 1058 cases of scurvy had been admitted into the hospital ship Dreadnought.” In 1854 a law was passed requiring every vessel to carry an adequate supply of lime juice. This law, however, failed in effect, due to the fact that a large part of the lime juice was adulterated. A new shipping-act was passed, therefore, in 1867, with the object of preventing adulterations, at the same time increasing the daily quota for each seaman from half an ounce to one ounce.
It may be of interest to add a few words concerning certain antiscorbutics which have been under discussion or recognized for so many years that they have acquired an historical aspect. One of these foodstuffs is sauerkraut, which was recognized by Lind in 1772 as having particular potency in this disease. It is interesting to note, in this connection, that this writer appreciated the close relationship of acidity to antiscorbutic virtue. “One quality,” he writes, “entering the most perfect antiscorbutic composition is a vegetable accescency.” He prized sauerkraut for its inherent value, and particularly, because he found that “sour cabbage will keep for an East-India voyage.”
The famous navigator Cook, whose voyages were remarkable for the freedom from illness which his sailors enjoyed and the absence of scurvy, always kept a large supply of sauerkraut on hand. It was believed by many that the immunity of the Dutch seamen to scurvy was due to their large consumption of this vegetable. As the result of this empirical knowledge, the English navy in 1780 introduced the use of sauerkraut into its ration. As just noted, however, this antiscorbutic was supplanted some few years later by an issue of lime juice.
It is common knowledge that outbreaks of scurvy follow closely upon a failure of the potato crop. This has been particularly the case in Ireland, where it was especially evident in relation to the great epidemic of scurvy in 1847. Holst and Froelich inform us that “all scurvy epidemics in Norway in the nineteenth and beginning of this century followed failure of the potato crop.” Nor is this danger past. In an article entitled “The Rôle of Antiscorbutics in Our Dietary,” the author recently reported that the partial failure of the potato crop in the eastern part of the United States led to the development of scurvy in numerous institutions, in one of which over 200 cases of definite scurvy developed in the spring (1916).
The occurrence of scurvy in the navy and on sailing vessels has been associated in the minds of many with the large amounts of salted meat which necessarily was included in the dietary. It was evident that meat that was salted had no antiscorbutic value, but the query has been raised whether eating a considerable amount of salted meat did not induce scurvy. Lind mentions “flesh long salted” as leading to the development of scurvy. The question of the value of meat as an antiscorbutic is of importance at the present time, chiefly in connection with Polar expeditions and army rations. As the result of an outbreak of scurvy in the Polar expedition of 1875–6, a British Arctic Survey Committee was appointed to make an investigation. In 1877 it reported that “although the scurvy was due to the absence of lime juice from the sledge dietaries, meat in large amounts is able to prevent the disease.” Stefánsson also emphasized the value of meat in preventing scurvy in the Polar regions. In his expeditions he has found that raw meat, if taken in sufficient quantity, is able to afford complete protection. Jackson, who lived for some years among the Samoyeds, tells us that this tribe, owing to the fact that they consumed considerable reindeer meat, never suffered from scurvy in spite of the fact that they ate no vegetables or fresh fruit during the winter.
The following account, a personal communication from Dr. Harrison J. Hunt, who spent four years in the Arctic regions, is of interest in this connection:
“For some four years I was with the Smith Sound Eskimos, on the northwest coast of Greenland. These people get nothing but animal food normally, and have lived that way for many generations, yet are healthy, of good physique, and are normal in other ways. Scurvy was unknown to them as far as I could ascertain; certainly there was none while I was among them. Much of their meat is eaten raw, and the rest only partly cooked; that is, ‘rare done.’
“Whalers who were accustomed to winter in Hudson Bay practically always had scurvy in the crew. It was common knowledge among the captains that fresh meat was curative of scurvy, and it was their practice to obtain meat from the Eskimos whenever possible for that purpose. The last English expeditions to the South Polar regions were afflicted with scurvy which was entirely and quickly eradicated by the use of fresh seal meat in the place of salt meats and canned foods. They do not state that this meat was eaten raw or even rare cooked. On the Danish coast of Greenland, during seasons poor in game, scurvy is quite common, but the natives there live largely on breadstuffs (very coarse rye bread). Personally, during my four years in the Arctic, I took no fresh vegetables whatever, or other commonly-called antiscorbutics, relying solely on rare or raw meat. I never was stronger or more healthy in my life. I did have dried fruits and vegetables, and usually plenty of fresh bread. Usually the Eskimos eat their raw meat in a frozen condition, and I can attest that it is extremely palatable in that condition.”
We do not wish to discuss, in this place, the value of meat as an antiscorbutic; in passing, however, it may be said that, as in the case of the other antiscorbutics, its efficacy will depend largely upon the amount consumed. The British Mesopotamia Commission Report of 1917 shows that scurvy can develop on a ration which includes 28 ounces of meat a week. We must remember, however, that this refers to cooked meat, whereas in the Polar expeditions meat generally was eaten in a raw state.
Recently an historical inquiry has appeared in an article by Chick, Hume and Skelton as to the antiscorbutic virtue of limes and lemons. This sketch is of exceptional interest because it treats of the oldest and most cherished antiscorbutics, and particularly because it has unearthed a peculiar fallacy in their connection. As they state, there would appear to be every reason for believing “that the use of so-called lime juice was responsible for the disappearance of scurvy from the British navy in the first decade of the nineteenth century.” It would seem, however, that the lime juice which gained this great reputation in the navy some 125 years ago was in reality lemon juice, and that it was not until about 50 years ago that lime juice was really used. These authors show—by one of those striking human experiments which, occasionally, is available—that in a Polar exploration which was organized in 1850 lemon juice was issued to each man, and that no case of scurvy developed, whereas in a similar expedition which went out in 1875 lime juice was issued and scurvy developed the following spring with great severity among the sledge crews. This investigation, therefore, seems to prove that lime juice, the prototype of antiscorbutics, has been accorded a false position; that in reality the sailors of the past have been protected by lemon juice.
Antiscorbutic Foods.—As far as has been ascertained, the antiscorbutic food factor exists in all fresh vegetable and animal tissues, being present to a far greater degree in the former than in the latter. It is distinguished by being associated in nature with cells which are the seat of active metabolism, just as the water-soluble vitamine is associated mainly with cells which are in an inactive or dormant state. Vegetables or fruits may be mildly or highly antiscorbutic; there is indeed a remarkable difference in their content of antiscorbutic factor or vitamine. They vary widely also in the degree to which their potency is affected by physical or chemical conditions. In this chapter the most common animal and vegetable antiscorbutic foodstuffs will be considered and the effect which processes such as drying, canning, change of reaction, etc., exert on their specific value. Their therapeutic application in the prevention and cure of scurvy will be considered in a subsequent chapter. Until recently our knowledge of this subject was empirical and inaccurate; as the result of scientific work, however, carried out during the past few years in different parts of the world, quantitative and comparative figures of antiscorbutic food values have been evolved.
Milk.—It is important to have as accurate an idea as possible of the value of milk as an antiscorbutic, as the infant depends on it during the first months of its life for a supply of this essential factor. Considerable attention has been paid to this question in the last few years, and recent reports tend to confirm the former estimations which had been overlooked and forgotten. In 1847 Curran wrote that in the Irish epidemic of this year they had admitted to the Dublin Union Hospital 80 cases of scurvy which had been on a diet which included one pint of milk daily, but was deficient in vegetables. From this experience he realized that milk was not rich in the principles which protect against scurvy. In the following year Parkes came to the same conclusion, stating that 500 to 750 c.c. of raw milk did not always suffice to prevent scurvy. In addition to these opinions concerning adults, similar conclusions have been drawn from clinical experience with infants. Barlow (1894) realized that a small amount of milk was insufficient to protect against scurvy. Still writes: “The antiscorbutic power of fresh, unboiled milk is evidently slight.” In 1914 Hess and Fish pointed out that “milk must not be considered as having potent antiscorbutic properties.” Nevertheless, when this question was raised recently by the experimental work of Jackson and Moore, and that of McCollum and Pitz, it was not appreciated that, like other antiscorbutics, milk must be regarded from a quantitative standpoint, and that, as it is a weak antiscorbutic, its effect must depend largely on the quantity consumed.
The first laboratory work on this subject was that of Froelich in 1912, who showed that guinea-pigs could be protected by an exclusive diet of fresh milk, and that raw milk is more effective than heated milk. In his work, the amount of milk taken by the animals was not measured, so that it is impossible to glean from it more than these general conclusions. In the following year, as a result of some quantitative experiments, Funk stated that he was able to protect guinea-pigs with 50 c.c. of fresh milk in addition to an oat diet. This estimate, as subsequent workers showed, is too low. Chick, Hume and Skelton were the first, however, to investigate the antiscorbutic potency of milk in a systematic and convincing manner. They demonstrated that if the daily consumption of fresh milk was less than 50 c.c., a guinea-pig died almost as quickly as if it received no milk; if the daily quota varied from 50 to 100 c.c., a greater or less protection from scurvy was observed, varying proportionately with the amount consumed; if 100 to 150 c.c. were taken daily, which practically amounts to a complete milk diet, satisfactory growth and development occurred, and no symptoms of scurvy were observed. This represents in a general way the present conception of the antiscorbutic power of milk. In passing, it may be remarked that it is not altogether clear why 50 c.c. of milk do not afford partial protection, and prolong the life of the animal for a definite length of time. The authors conclude that “milk is evidently a food poor in the antiscurvy accessory factor, and a ration large in comparison with that of other antiscorbutic materials is necessary to afford satisfactory protection from scurvy.” The error must be avoided, however, of regarding milk as a standard article of diet containing a definite and specific amount of vitamine per cubic centimetre. It will be shown later that this point of view cannot be taken in regard to vegetables, and it is probable that it cannot be assumed for milk.
A general conception of the antiscorbutic potency of cow’s milk may be gleaned from the fact that it requires a minimum of about sixteen ounces (500 c.c.) daily to protect an infant from scurvy or to cure it. Twelve ounces have failed to effect a cure in several instances, although the milk was raw and of the best grade. If it is pasteurized, a larger quantity is required, depending upon various conditions connected with the heating process and upon the age of the milk, circumstances fully discussed in relation to etiology. Thus it becomes evident that pasteurized milk assumes a two-fold rôle, acting as an antiscorbutic if little of its vitamine content has been destroyed and if a large quantity is consumed, or leading to the development of scurvy when one or both of these conditions is unfavorable. The same holds true for milk which has been boiled for a short period. If the milk has been heated twice, it tends to produce scurvy; if it is condensed, the greater part of its antiscorbutic value is destroyed.
It seems necessary to emphasize again the important fact that dried milk may possess marked antiscorbutic potency, depending on the method of preparation (Fig. 11). As stated, sixteen ounces of milk dried by the Just-Hatmaker process cured scurvy promptly, in spite of the fact that the milk had been dried six months previously. Here, therefore, is a food of high caloric value, compact, antiscorbutic, and stable. The fact that milk, in spite of drying, retains this labile vitamine for so long a period, demonstrates that it is available in the most remote parts of the world, and that the possibilities of its transportation are unlimited.
Little is known regarding the antiscorbutic content of the milk of the various domestic animals. Some claim that goat’s milk is notably rich in this particular, but experiments with it are too few to warrant conclusions. Lind writes: “Goats, of all animals, afford the richest whey, possessed of the greatest antiscorbutic virtue . . . which in a singular manner restores the constitution when weakened and impaired by scurvy.” Human milk possesses about the same potency as cow’s milk, as mentioned in the discussion of the occurrence of infantile scurvy in countries where the adult form is endemic. Twelve ounces of human milk, from a woman on a liberal and varied diet, barely sufficed to alleviate the symptoms of a case of moderate intensity.
Orange and Lemon Juice.—The most thoroughly studied antiscorbutic foods are orange and lemon juice, which have been singled out because they contain the antiscorbutic factor in the highest concentration. It has been ascertained through the work of various investigators that guinea-pigs require about 3 c.c. daily of either of these juices to protect them from scurvy, but that about half this amount is sufficient to prevent the manifestation of clinical signs.
Both of these juices withstand heat remarkably well. Orange juice can be boiled for 10 minutes without noting any diminution of its antiscorbutic value, and lemon juice heated to 110° C. without appreciably losing its efficacy. However, orange juice undergoes some change as the result of being heated in an autoclave for 45 minutes at a temperature of 110° under 10 to 15 pounds pressure. Although 6 c.c. of this heated preparation were able to prevent the development of scurvy, the guinea-pigs did not gain nearly as well as those which received 3 c.c. of the unheated juice. It seemed as if there was a destruction of some factor apart from the antiscorbutic principle.
In spite of the fact that these juices withstand heat well, they are sensitive to some other conditions. Orange juice which had been stored in the cold for three months was unable to protect guinea-pigs in the dosage of 3 c.c. per animal, resembling in its action the autoclaved juice. When this orange juice was six months old, double this quantity failed to protect; throughout this period it was kept in the ice-box and covered with a layer of oleum petrolatum to avoid the access of air or possible contamination. Harden and Zilva met with a similar experience, and state that “after storing treated (concentrated) lemon juice for about a fortnight in a cold room, a marked loss can be observed in its potency.”
These authors reported also that when orange juice is rendered slightly alkaline it loses its antiscorbutic potency. This question was investigated in relation to canned tomato juice, as well as to orange juice, and it was found that shortly after having been rendered 0.05 N alkaline to phenolphthalein, neither of these foods had lost an appreciable amount of its antiscorbutic factor. Five cubic centimetres per capita daily of freshly-alkalized orange juice were able to cure a group of pigs which had developed scurvy on another diet. If, however, 24 hours were allowed to elapse instead of only one-half to one hour, between the alkalization and the feeding, then a considerable amount of the antiscorbutic factor was lost. The same general rule seems to hold for alkalization as for heating, i.e., the length of time the antiscorbutic food is subjected to the deleterious influence is fully as important as the intensity of the process. Advantage has been taken of the fact that freshly-alkalized orange juice retains its potency, in using it intravenously in the treatment of infantile scurvy.
Subcutaneous injections of neutralized orange juice failed to cure scurvy in guinea-pigs; Harden and Zilva were equally unsuccessful with large doses of their concentrated lemon juice. This is of interest in view of the marked therapeutic result which Shiga obtained with subcutaneous injections of the water-soluble vitamine in pigeons suffering from polyneuritis. It should be added that Holst and Froelich (1912) failed to cure scurvy in guinea-pigs by intraperitoneal inoculations of orange juice.
Lemon juice or orange juice may be dried and lose little of its antiscorbutic power. In their paper of 1912 Holst and Froelich reported the efficacy of lemon juice evaporated in a vacuum, and recently Harden and Zilva published experiments which proved that “by evaporating the treated lemon juice to dryness in an acid medium an active dry residue is obtained.” Still more recently Givens has shown that orange juice reduced to a powdered form by means of a spraying process has lost little of the antiscorbutic factor. These results prove that under certain conditions the antiscorbutic factor withstands drying; one of these favorable influences is an acid reaction, and another, rapidity of desiccation.40
Lime Juice.—Recently an investigation of lime juice has been carried out by Chick, Hume and Skelton. They were “unable to detect any significant protection in a daily ration of from 5 to 10 c.c. of preserved lime juice which was several months or a year or more old.” Crude lime juice of various ages had slight antiscorbutic value, affording only partial protection in a daily ration of 5 c.c. Even fresh juice was found not to be very efficacious compared with lemon juice. The authors conclude that “the relative value of these two fruit juices deduced from the trials with monkeys is therefore in accord with that obtained in the experiments with guinea-pigs, i.e., the value of fresh lemon juice is approximately four times that of fresh lime juice.” Holst and Froelich in 1907 carried out a similar but less extensive investigation. They also found that lime juice was unable to protect guinea-pigs from scurvy. Fuerst, a co-worker of Holst, continued this work, and in his article of 1912 stated that guinea-pigs should not be protected by a daily addition to their ration of 25 g. of lime juice; these guinea-pigs received a mixed diet consisting of dry vegetables, butter, almonds and malt extract. These two reports of the Norwegian investigators on this interesting subject should have attracted attention.
Other Fruits.—A word may be said in regard to some other fruits. The antiscorbutic potency of raspberries was tested by Holst and Froelich (1912) and found comparable to oranges and to lemons. The juice was also highly resistant to heat, so that 10 c.c. of freshly-pressed juice were of protective value, even after it had been subjected to 100 or 110° C. for one hour. Guinea-pigs which were thus treated showed no microscopic signs of scurvy in any of the ribs, in the tibiæ or the femora.
| Classes of Foodstuffs | Antiscorbutic Factor | Classes of Foodstuffs | Antiscorbutic Factor |
|---|---|---|---|
| Meat, Fish, Etc.: | Vegetables and Fruits: | ||
| Lean meat (beef, mutton, etc.) | + | Cabbage, fresh | +++ |
| Liver | + | Cabbage, cooked | + |
| Tinned meats | 0 | Cabbage, dried | Very slight |
| Beef juice | + | Swede, raw expressed juice | ++ |
| Lettuce | ++ | ||
| Milk, Cheese, Etc.: | Carrots, fresh raw | + | |
| Milk, cow’s, whole raw | + | Carrots, dried | 0 |
| Milk, cow’s, skim raw | + | Beetroot, raw, expressed juice | Less than + |
| Milk, cow’s, dried | + | Potatoes, raw | . . . . |
| Milk, cow’s, boiled | Less than + | Potatoes, cooked | + |
| Milk, cow’s, pasteurized | Less than + | Potatoes, dried | 0 |
| Milk, cow’s, condensed (sweetened) | Less than + | Beans, fresh, raw | ++ |
| Onions | ++ | ||
| Eggs: | Lemon juice, fresh | +++ | |
| Fresh | ?0 | Lemon juice, preserved | ++ |
| Dried | ?0 | Lime juice, fresh | ++ |
| Lime juice, preserved | Very slight | ||
| Cereals, Pulses, Etc.: | Orange juice | +++ | |
| Wheat, maize, rice, whole grain | 0 | Raspberries | ++ |
| Wheat germ | 0 | Grapes | + |
| Wheat, maize, bran | 0 | Apples | + |
| White wheaten flour, pure corn flour, | Bananas | Very slight | |
| polished rice, etc. | 0 | Tomatoes (canned) | ++ |
| Linseed, millet | 0 | ||
| Dried peas, lentils, etc. | 0 | Miscellaneous: | |
| Soy beans, haricot beans | 0 | Yeast, autolyzed | 0 |
| Germinated pulses or cereals | ++ | Meat extract | 0 |
| Beer | 0 | ||
| Cod liver oil | 0 | ||
| Olive oil | 0 | ||
| Human blood | + | ||
| * This table is a modification of one prepared by the Medical Research Committee | |||
These authors also reported that they found banana and apple poor in antiscorbutic power, 30 g. daily being insufficient to protect a guinea-pig (Table 3). This was our experience with banana in the treatment of infants suffering from mild scurvy. The banana has been shown by Sugiura and Benedict to be poor also in the water-soluble vitamine. It would be of interest to determine the difference in vitamine content between the fully ripe and the unripe fruit.
In view of the fact that grapes are used considerably in the treatment of infantile scurvy, it is of importance to realize that they are poor in the antiscorbutic principle. Chick and Rhodes found that three of four guinea-pigs receiving 20 g. daily developed scurvy; they rated the potency as ten times less than that of orange juice.
It is everyday knowledge that fresh vegetables are of great value in the protection from, and cure of, scurvy. The first experimental investigation of this subject was that of Holst and Froelich, published in 1907, and continued in a series of papers extending to 1916. These investigators tested the potency of a large number of vegetables by feeding them in varying quantities to guinea-pigs. They found that all vegetables have antiscorbutic value but to a markedly varying degree. Cabbage, sorrel leaves, endive, head salad, and dandelion leaves, were found to be of most avail in protecting against scurvy, whereas carrots, cooked potatoes and cooked turnips, and cauliflower proved to be of less value. In general, it may be stated that the leafy vegetables have more antiscorbutic power than the roots or the tubers. This generalization, we shall see, is not without exception, e.g., the swede. Similar experimental work has been recently carried on by a group of investigators at the Lister Institute, who have added considerably to our knowledge in this field. In all this experimental work cabbage has been found to be the most potent of the vegetables, and therefore experiments have centered about it just as in considering fruits the work has centered about orange juice or lemon juice. We shall, therefore, discuss in detail its reaction to heat and dehydration.
Cabbage.—Holst and Froelich found that 1 g. daily of fresh cabbage afforded nearly complete protection to guinea-pigs, and Delf has corroborated this work. This amount is sufficient to prevent the development of manifest scurvy, although it does not induce satisfactory growth. In this respect it is comparable to giving 1.5 c.c. of orange juice daily. If guinea-pigs take only 0.5 g. of raw cabbage, scurvy will develop; whereas 2 g. or more will promote satisfactory growth and no scorbutic changes will be found on microscopic examination.
Effect of Heating.—Vegetables are of decidedly less antiscorbutic value when cooked than raw; cabbage, for instance, on being boiled is weakened about one-half. Heating to 110° C. for an hour destroys almost all of its antiscorbutic factor. Delf’s tests did not show so great a loss. She came to the conclusion, of theoretical and practical value, that slow cooking at a low temperature is much more deleterious than rapid cooking at a higher temperature. Hess and Unger found that carrots lost much of their antiscorbutic power after boiling, and that this was the result of a true destruction, the vitamine not having been merely dissolved in the water of boiling; for if guinea-pigs consumed 40 c.c. per capita of this water, they were not protected against scurvy (Fig. 11). Acidulating the water with 10 per cent. vinegar did not reduce the loss, an experience similar to that of others using citric acid or lemon juice.
Vegetables cannot be considered from an antiscorbutic standpoint as a standard and uniform foodstuff, as they vary in their content of this factor according to their freshness and age. This was demonstrated by means of feeding experiments with carrots. For example, 35 g. of old carrots, such as were used for feeding the laboratory animals, afforded but little protection after having been cooked in an open vessel for about 45 minutes, whereas the same amount of young carrots cooked this way protected the guinea-pigs. It is obvious that this distinction is of importance in evaluating the antiscorbutic content of the various foods, and in considering whether individuals and groups of individuals are receiving an adequate quota of antiscorbutic vitamine. It will be noted later that it is also of importance in connection with the potency of dehydrated vegetables. Recent experiments indicate that not only age, but the degree of ripeness must be considered in appraising the food value of vegetables. Feeding experiments showed that tomatoes which were fully ripe were more potent than those which were slightly green. Probably many other factors play a rôle in determining the richness of vegetables in vitamine. It may not be immaterial whether they are allowed to ripen on the vine or shrub, or mature subsequently. The nature of the soil may also affect the antiscorbutic quality of the vegetables or fruit. So that it is evident that we must not be schematic in considering this question, and must realize that a table of antiscorbutic values, such as accompanies this text (Table 3), does not furnish definite and inflexible values.
There is a marked difference between vegetables and vegetable juices in keeping quality, and in their reaction to heat and to acid. In general, it may be stated that the juices are much more sensitive. Holst and Froelich brought out this point in 1912 and enlarged upon it in their publication of 1916. The different juices vary greatly in this respect; for example, dandelion juice is acutely sensitive to heat, whereas sorrel leaves withstand high temperatures very well. In regard to these differences an analogy may be drawn to the fruit juices. Lemon, orange and raspberry juices are markedly thermostable, but lime juice is weakened markedly by heat. Many of these juices are protected by the addition of acid—5 per cent. of lemon juice increasing the thermostability of cabbage juice—whereas, as we have stated, little is gained by cooking vegetables in an acid medium.
Potato.—The civilized world is dependent for its quota of antiscorbutic foodstuff largely upon the potato. It might be thought, therefore, that this would signify that the potato is endowed with great antiscorbutic power. Such is not the case, however, as demonstrated both by laboratory tests and clinical experience. Considering its importance, there have been surprisingly few feeding experiments carried out with potato. Holst and Froelich (1912) found that 17 g. of potatoes, steamed at 100° C. for 30 minutes, afforded but slight protection, and that it required 20 g. to fully protect a guinea-pig. Givens and Cohen failed to ward off scurvy by means of cooked potatoes fed to the equivalent of 5 g. of the raw vegetable (guinea-pigs will not eat raw potatoes). There are no accurate figures as to the quantity of potatoes needed to protect a human being from scurvy. The statement of Doctor Guy, however, who after careful study of convicts’ diets, concluded that 14 ounces daily would protect them from scurvy (if the ration included one ounce of other fresh vegetable and 4 ounces of meat), is probably close to the mark.41 With the experience that potatoes play such a significant rôle in the prevention of scurvy, how are we to interpret the fact that they are only mildly antiscorbutic? Potatoes are consumed in very large amounts; in the Temperate Zone probably twice as many pounds of potatoes are consumed during the winter as of all other vegetables combined (Fig. 1). It is evident, therefore, that in a practical evaluation of antiscorbutic foodstuffs, not only the intrinsic antiscorbutic potency must be considered, but also the quantity of the vegetable or fruit consumed.
Swede.—We cannot leave the consideration of vegetable antiscorbutics without adding a few words as to the value of swede juice,42 which has been recently highly recommended by Chick and Rhodes, who found it comparable to the cabbage and the onion, and even to orange juice. For example, 25 c.c. of raw swede juice were equivalent to 1.5 g. of raw cabbage. It is, therefore, more potent than the juice of raw carrot, and far more efficacious than the juice of the beetroot (Table 3). Tests carried out with this antiscorbutic in infant feeding seemed to show that it is of value in this field. The authors believe that the potency of vegetables is closely associated with certain botanical species, and that in this way the marked virtue of the swede can be explained, as it belongs to the natural order of Cruciferæ, which includes also the cabbage, the scurvy grass and the cresses. If, however, this is a rule of nature, it is difficult to explain the marked difference between the lime and the lemon, which are both varieties of Citrus Medica.
Dehydrated Vegetables.—For hundreds of years fresh vegetables have been dried to serve as food during the winter months and have fulfilled a useful purpose on account of their small bulk and great food value. The question for us to consider, however, is whether dehydrated vegetables still retain their antiscorbutic quality and can be counted on to supply this factor in the dietary. At present this subject is engaging the attention of laboratory workers as well as of practical dietitians and food hygienists. The experience of the past is not happy in this regard. In the Medical and Surgical History of the War of the Rebellion we read as follows: “A scorbutic tendency was developed at most of our military posts during the winter season, after the troops had been confined to the use of the ordinary ration with desiccated vegetables. The latter in quantities failed to repress the disease.” In spite of this and similar military experiences43 the employment of dehydrated vegetables was urged recently for rationing our soldiers, the claim being made that “by simply soaking in water and boiling in the same water these vegetables are brought back to the condition of fresh vegetables.” Both in this country and in England there was strong propaganda during the war to dehydrate vegetables on an enormous scale and to substitute them for the fresh food.
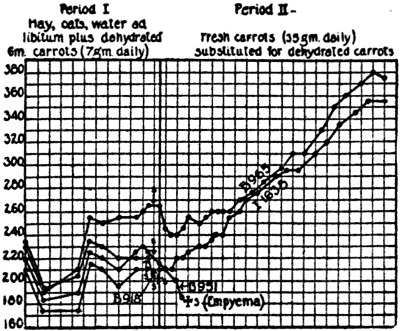 Fig. 12.—Hay, oats, water ad libitum, and 7 g. of dehydrated
carrots dried at a room temperature of about 130° F.
about 1 month previously. All animals developed scurvy.
The marked gain in weight when an equivalent amount of
fresh carrots was substituted for the dehydrated vegetable
corresponded to the disappearance of scorbutic signs.
Guinea-Pig B 951 did not receive fresh carrots, as it was
evidently ailing at the time the second period began.
Fig. 12.—Hay, oats, water ad libitum, and 7 g. of dehydrated
carrots dried at a room temperature of about 130° F.
about 1 month previously. All animals developed scurvy.
The marked gain in weight when an equivalent amount of
fresh carrots was substituted for the dehydrated vegetable
corresponded to the disappearance of scorbutic signs.
Guinea-Pig B 951 did not receive fresh carrots, as it was
evidently ailing at the time the second period began.
Experimental investigation on this subject may be summarized as showing that vegetables dried according to present methods lose their antiscorbutic value as the result of dehydrating (Fig. 12), and that they become still more impoverished as the result of aging. We should not sweepingly condemn the principle of dehydration, as very possibly some slight modifications in the process may be devised which will counteract the deteriorating influence. In their paper of 1912, to which reference has been made so often, Holst and Froelich reported that potatoes, carrots, peas, lentils and almonds have practically no protective value after they are thoroughly dried. In two reports—one giving the results of feeding various brands of dehydrated carrots to guinea-pigs, and the other of an attempt to cure scurvy in babies by means of these carrots—we also came to the conclusion that the antiscorbutic factor had been almost completely destroyed. Givens and Cohen (1918) found that even cabbage dried at a low temperature retained only a small amount of its potency after a month, and Delf and Skelton came to practically the same conclusion, also noting that the cabbage on being kept, steadily lost what little of the antiscorbutic factor had survived the drying process. The same was true of the fat-soluble factor. These authors made an observation which may prove of value in helping to solve this problem, namely, that “the residual amount is distinctly greater if the cabbage is plunged into boiling water before drying.” This protective action of heat they suggest may indicate that: “Some at least of the destruction may be due to the activity of an enzyme or other body originally present in the living tissue.”
Another observation which may prove of practical value in rendering dehydrated vegetables the nutritional equivalent of the fresh vegetable is that when the carrots selected for dehydration are young and fresh a product is obtained which possesses decided antiscorbutic power. In this connection the following statement by Falk and his co-workers in a study of the enzyme action of vegetables and the effect of dehydration is significant: “In considering these enzyme results, it may be pointed out that the state of ripeness and the age of the vegetable undoubtedly influence the activities.”
The most promising dehydration experiment has been conducted by Holst and Froelich and was published in 1916 in a paper which has passed unnoticed. They dried white cabbage so that it retained its antiscorbutic properties, and, to a large extent, its color and taste, for a period of two years. This result was accomplished by keeping out all moisture and preventing hydrolysis,44 a method which is employed in preserving antitoxins, toxins and agglutinins. It is by far the most encouraging test reported, and should be made the basis of further work by those actively interested in perfecting dehydration.
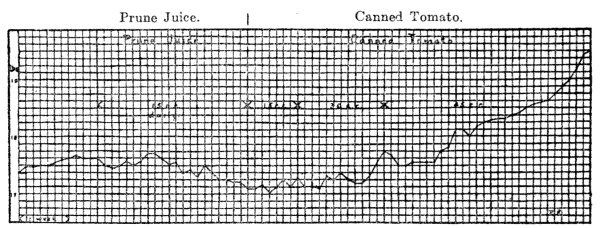 Fig. 13.—Cure of scurvy by the addition of canned tomato. In this case, as frequently,
the alleviation of symptoms preceded the gain in weight.
Fig. 13.—Cure of scurvy by the addition of canned tomato. In this case, as frequently,
the alleviation of symptoms preceded the gain in weight.
Canned Food (Tomatoes).—In the course of canning, as in dehydrating, most vegetables and fruits lose their antiscorbutic properties. A general denunciation, however, of all canned foods is incorrect, as there are exceptions to this rule. It has been shown by Hess and Unger that canned tomatoes possess a high degree of antiscorbutic power (Fig. 13), and it is probable that most of the acid fruits and vegetables are able to withstand the canning process. It was found, in an experiment embracing many series of guinea-pigs, that 4 c.c. daily of strained, canned tomato are sufficient to afford protection, even when a lot was used which had been prepared a year previously. This is indeed remarkable, considering that the food undergoes a two-fold heating in the course of canning, during one of which (“processing”) the temperature is raised to fully 230° F. Tomatoes have another advantage over most other vegetables in that they are richly endowed with the water-soluble vitamine, as shown by our tests on pigeons suffering from polyneuritis, and by the experiments on rats of Osborne and Mendel, who found tomatoes far superior in this respect to turnips, onions, beetroots or beans. They are also rich in the fat-soluble vitamine. In view of the availability of canned tomatoes and their excellent keeping quality they are well suited to an extended use as an antiscorbutic. In the subsequent chapter we shall discuss their employment in infant feeding and in the army ration.
Germinated Cereals and Pulses.—In 1912 Fuerst reported that although the resting seed—the cereal grain, the pea, bean and lentil—are poor in antiscorbutic vitamine, they develop this principle as soon as they germinate. They possess, in other words, latent antiscorbutic properties, and are potentially antiscorbutic. This observation is not only of scientific interest but of practical value, as these pulses are well suited for transport and do not readily deteriorate. For this reason, Chick and her co-workers at the Lister Institute, who were searching for an antiscorbutic foodstuff for the army, directed their attention to the utilization of the pulses. In the course of a thorough investigation (1919) they found that although it required 30 to 40 g. daily of dry green peas to prevent scurvy in the guinea-pig, a consumption of 10 g. of the germinated peas afforded satisfactory protection.45 The soaked seeds have an antiscorbutic value comparable to many of the fresh vegetables; by no means as great as cabbage, but somewhat greater than that of carrots. As the result of cooking, their potency was found to be reduced about 75 per cent. We shall have occasion to refer to this antiscorbutic food in the chapter on treatment in connection with the rationing of armies.
Meat and Eggs.—As has been stated, animal tissues are distinctly inferior to fruits and vegetables in the antiscorbutic principle. As there has been no accurate evaluation of these foods—the only test being one by Chick, Hume and Skelton, where 10 c.c. of raw beef juice failed to protect guinea-pigs—we have to depend upon clinical experience for our knowledge. Beef juice is highly rated by physicians in the prevention of infantile scurvy, but it is probably far less potent than vegetables or fruit juices. The Arctic explorers, and many who have lived in the Arctic regions, agree that the inhabitants are protected from scurvy during the winter months by their diet of fresh meat and fish. The Admiralty Enquiry on the outbreak of scurvy in the Arctic Expedition of 1875 reported that a large ration of meat is necessary to afford protection. Curran (1847) described three cases admitted to the hospital in the great Irish epidemic of that year, where the diet previously had included three-quarters of a pound of meat on five days of the week. From these and similar experiences the conclusion is manifest that the divergence of opinion regarding the value of meat is based upon quantitative differences in the rations. Evidently, if sufficient meat is provided, the development of scurvy will be obviated. Another factor which must be borne in mind is that those who refer to meat in the Arctic regions refer to fresh raw meat, which is a far more valuable antiscorbutic than the ordinary cooked meat.
There is almost no experimental data on the antiscorbutic value of eggs. Hard-boiled eggs were fed to guinea-pigs and it was found that 9 g. per capita daily was insufficient to protect them. An attempt was also made to cure infantile scurvy with a daily addition of one raw egg to the dietary, but without avail. It is possible that fresh raw eggs have an antiscorbutic value comparable to meat, but the large quantity required makes dependence upon them impracticable.
Beer and Alcoholic Beverages.—For generations beer has been highly regarded as an antiscorbutic. Captain Cook prized it greatly and always supplied his men with a freshly-made infusion of malt called “sweetwort.” Lind writes: “Beer and fermented liquors of any sort will be found the best antiscorbutic remedies” (p. 76). He refers at different times to the value of spruce beer, ale, wine and other vinous liquors. In his excellent book on “Military Hygiene,” Munson writes: “Good beer and wine have decided value, also vinegar.” On the other hand, recent scientific experiment has shown that beer has practically no antiscorbutic value. There is but one study on this subject, that of Harden and Zilva, which is quite convincing. They found that guinea-pigs and monkeys developed scurvy in spite of the fact that they received, respectively, 50 c.c. and 180 c.c. of beer daily. They conclude, as a result of their experiments, that “bottled ale and stout and fined beer as brought on to the market, are lacking both in antineuritic and antiscorbutic accessory factors, and that kilned material is also wanting in these two principles.” The apparent contradiction between practical experience and laboratory investigation in regard to beer is due to a difference in the process of brewing. Cook and Lind and the older authors refer to freshly-made beer, whereas the modern beer which was tested in the laboratory was made from “high-dried” material. The antiscorbutic potency of beer as formerly used was due to its preparation from freshly-germinated grain and its consumption shortly after brewing. Dyke tells us of an interesting incident illustrating the importance of this distinction. In the recent war an outbreak of scurvy occurred among the Kaffir labor battalion in France. At home these natives consume a large amount, as much as three gallons a day, of Kaffir beer, which is made from freshly-germinated corn, and is consumed shortly after it is made. The French prepared a similar fermented beverage for their South African laborers, the sole difference in preparation being that the process of germination had been omitted for reasons of convenience. Scurvy resulted, a disorder which is practically unknown among the natives at home.
Miscellaneous Foodstuffs.—During the past few years a great many different kinds of foods have been tested in the laboratory for their antiscorbutic value. It will be well for completeness’ sake to say a word about them, although they have been found to possess little or no antiscorbutic properties. The studies of Holst and Froelich showed definitely that all the cereals—oat, barley, rye, maize, and preparations made from the bran or from the endosperm—are devoid of antiscorbutic vitamine. Cohen and Mendel added 3 per cent. of calcium lactate or sodium chloride, or 5 per cent. of butter, without enhancing the value of oats in this respect.
As is well known, yeast possesses the water-soluble vitamine in marked concentration. It is natural, therefore, that its antiscorbutic power was put to the test, especially as it has been accorded therapeutic value. Hess and Unger showed that autolyzed yeast was of no value in the cure of infantile scurvy (Fig. 14); Chick and Hume (1917) and Cohen and Mendel (1918) came to the same conclusion in regard to guinea-pig scurvy, making use of autolyzed yeast, yeast extract and dried brewers’ yeast.
In view of the fact that cod liver oil is practically a specific for human rickets, Hess and Unger tried the effect of this oil both in infantile scurvy and in that of guinea-pigs. It proved to have no protective or curative value. The animal experiments were confirmed by Cohen and Mendel. The use of olive oil also proved futile.
Pitz in 1918 reported that in animal experiments he had found that lactose was able to protect against scurvy, and attributed this result to its power to alter the intestinal flora. We shall not enter into a detailed discussion of this question, as the study was carried out on a ration embodying unlimited and uncontrolled amounts of milk, and it has since been shown that the apparent cure was due to an increased consumption of milk by the animals in the progress of the experiment. Cohen and Mendel, Harden and Zilva, Hart, Steenbock and Smith (1919) all failed to protect or to cure their animals with lactose when they were placed on a ration which was definitely measured and limited. Hess and Unger failed to cure infantile scurvy by means of lactose.
It has been suggested that scurvy is due to a lack of secretion of the endocrine glands, a question which will be referred to again in considering the relation of scurvy to other “deficiency diseases.” With this idea Ingier added thyroid, hypophysis, thymus and parathyroid to the food of guinea-pigs, or gave it parenterally. She was unable to observe any beneficial results. Jackson and Moore met with the same result on feeding desiccated thyroid gland. We may add that we gave dried thyroid and also parathyroid glands in the treatment of infantile scurvy without effect.
Any consideration of the question of antiscorbutic foodstuffs brings into sharp relief the difference between empiricism and scientific investigation. For well over a hundred years it was generally known that scurvy could be cured by fruits or vegetables, and yet no further progress was made toward a more complete understanding of the value of these foodstuffs. As far back as 1847 Budd ascribed the action of antiscorbutic foods “to an essential element, which, it is hardly too sanguine to state, will be discovered by organic chemistry or the experiments of physiologists in a not far distant future.” Busk, in giving his testimony in 1877 before the British Scurvy Commission, said that it was his belief “that scurvy was due to the fact that the diet was lacking in a peculiar and as yet little-understood factor.” The question remained in this hypothetical and inactive state until it was attacked recently by experimental methods. Decided advance has been made only in the past few years, since these foodstuffs have been studied from a quantitative viewpoint.
The antiscorbutic factor is abundant in fresh foods, especially in vegetables and fruits, and to a considerably less extent in animal foods, such as milk, meat and fish. Among the vegetables there is a marked distinction in potency. A beginning has been made in standardizing these various foodstuffs, in grading them approximately according to their antiscorbutic efficacy (Table 3). It should be remembered, however, that the importance of an antiscorbutic food depends not only on its intrinsic content of the antiscorbutic factor, but quite as much on the amount of the food which is eaten. For example, although potatoes possess only moderate virtue compared with orange juice, they are of greater practical value in view of the large quantities which are consumed and their availability when green vegetables are lacking. Furthermore, the fact recently brought out that the various vegetables, and perhaps the fruits as well, have considerably more value when they are fresh and young than when they are old, warns us not to carry our quantitative standardization too far.
Fruits and vegetables which are dehydrated have been found to have lost their antiscorbutic properties. This generalization is not without its exception, for it has been found that cabbage and tomato withstand drying well, and that if milk is dried under favorable conditions it retains a very large part of its antiscorbutic value. It may be stated that the outlook is bright in regard to dehydration, as the problem has not yet been thoroughly studied, and the process may be so improved that there will be little difference in the nutritional value between the fresh and the dehydrated food.
The study of antiscorbutic values points a lesson in regard to the methods of cooking vegetables. It has demonstrated that short cooking, associated with a high degree of temperature, is less deleterious than longer cooking at a low degree. In other words, that less damage is brought about by boiling or by steaming vegetables than by stewing them. Here age and freshness again play a rôle; in fact, a double rôle, as the older and tougher vegetables contain not only less antiscorbutic, but require more prolonged cooking.
In general, the belief is correct that canning destroys the antiscorbutic value of foods, but once more an exception must be made, for it has been found that acid foods, such as the tomato, withstand the canning process with but little loss of potency.
The field of antiscorbutic foodstuffs is one which is fertile for future investigation. The antiscorbutic status of milk heated to various heights of temperature and subjected to various degrees of aging furnishes problems of great practical importance. A lack of growth has been noted when antiscorbutics are given which have been subjected to a high degree of heat (e.g., autoclaved orange juice). Whether this is due to the destruction of some other growth factor is a question which has been raised by several experimental studies and requires an answer.
It is quite possible that we shall find useful antiscorbutic foods which at present are unknown or unappreciated. The recent introduction of the swede, of the canned tomato and of germinated pulses suggests and even renders this probable. On the other hand, the recognition of the comparative poverty of the antiscorbutic factor in lime juice shows the importance of putting each foodstuff to the experimental test.
The identity of scurvy in the infant, in the young child and in the adult is thoroughly established and requires no further substantiation. There are, however, sufficient differences between the symptoms of adult scurvy and those of Barlow’s disease to render it advisable to consider them separately. These distinctions are due largely to the fact that the former disorder affects mature tissues, whereas the latter is engrafted upon tissues which are in the process of rapid growth and development. The symptomatology is influenced also by the striking differences in environment—the passive, shielded existence of the infant, contrasted with the active and exposed life of the adult. Although we shall, therefore, treat adult and infantile scurvy separately, it should be borne in mind that, from an etiologic and pathologic viewpoint, such a division is artificial and is resorted to merely for purposes of clarity.
Adult Scurvy.—The earliest sign of scurvy is usually a change in the complexion of the individual. His color becomes sallow or muddy, an aspect difficult to describe, but one which is characteristic, and constitutes an important danger signal to the eye of the experienced physician. About the same time the patient loses his accustomed vigor, seemingly becomes indolent and complains of tiring quickly, and of breathlessness. He may experience fleeting pains in the joints and limbs, especially in the legs, symptoms which are frequently attributed to rheumatism. At this early stage the appetite may still be normal, there is usually no loss in weight, but merely a general malaise which is significant, although in no way distinctive. Very soon the gums become sore, bleed readily, and are found to be congested, spongy, and somewhat hemorrhagic at their edges. Absolute reliance must not, however, be placed on this sign for early diagnosis, as at times it does not appear until later. Careful examination at this stage will disclose petechial spots on the body, more especially on the legs, at the site of the hair follicles, or even larger ecchymoses, depending upon the hemorrhagic tendency of the individual, his exposure to bruising, the adequacy of his diet, and secondary infection. Less frequently bleeding from the nose occurs early, or the eyelid suddenly becomes swollen and purple, or the urine shows the presence of blood.
These signs progress steadily with a varying degree of rapidity. The complexion becomes more dingy and somewhat brownish, the weakness increases so that the slightest exertion causes breathlessness and palpitation, and the gums become spongy and even fungous. If there is infection of the gums and the teeth are carious, the breath is extremely foul—a sign long associated with scurvy. Later the teeth become loose and may fall out, and the alveolar process undergoes necrosis. The surface hemorrhages increase in severity, large effusions appearing on the trunk, on the extremities, and less often beneath the mucous membrane of the mouth. A bloody diarrhœa may take the place of the constipation which is generally noted earlier in the disease. There are at this time hemorrhages into the muscles and deeper tissues, especially into the calves of the legs, giving rise to hard, brawny, tender swellings which have been termed “scurvy sclerosis.” This is sometimes the earliest sign noted by the patient and may puzzle the physician who has not met with it before. The swelling may be found in the popliteal space or at the site of the tendo Achilles, and result in lameness and contracture of the neighboring joint. Frequently there is slight edema of the ankles associated with a glossiness of the extensor surfaces of the legs. This infiltration differs from ordinary edema in being firm and not pitting on pressure. The skin is dry and rough, the follicles being unusually elevated;46 the hair likewise is dry and loses its lustre. Not infrequently subperiosteal hemorrhages occur, giving rise to exquisitely tender swellings, especially of the tibia or of the femur, or of the ramus of the lower jaw, as has been noted in connection with guinea-pig scurvy. If there are wounds or ulcers they assume a hemorrhagic aspect, the edges becoming bluish or livid and showing no tendency to heal; even scars which have existed for many years change in color and show an altered state of nutrition, and ulcers long healed break out afresh.
Nowadays, the disease usually does not reach this stage, and rarely progresses further. If, however, the patient remains untreated, he becomes progressively weaker and more lethargic; there is frequent palpitation, shortness of breath, and increasing loss of weight. The pains in the limbs render him helpless and an object of pity. Marked edema may be added to the picture as the result of starvation, so that the legs become swollen, and even the face becomes bloated. Hemorrhages into the skin as large as the palm of the hand appear on different parts of the body. The gums swell to such an extent that they overlap and may even hide the teeth and protrude from the mouth as foul fungoid growth. Death comes about in various ways. Frequently sudden and fatal syncope occurs, due to heart weakness or to the pouring out of fluid into the pleural or the pericardial cavities. Another frequent cause of death is secondary infection, resulting in pneumonia, which finally ends the suffering of the patient. The fatal outcome is thus described in the narrative of Lord Anson’s voyage:
“Many of our people, though confined to their hammocks, ate and drank heartily, were cheerful, and talked with much seeming vigor, and in a loud, strong tone of voice; and yet, on their being the least moved, though it was only from one part of the ship to another, and that in their hammocks, they have immediately expired; and others, who have confided in their seeming strength, and have resolved to get out of their hammocks, have died before they could well reach the deck. And it was no uncommon thing for those who could do some kind of duty, and walk the deck, to drop down dead in an instant, on any endeavor to act with their utmost vigor; many of our people having perished in this manner during the course of this voyage.”
The disease may develop and progress in various ways. It may remain latent for a long period and be cured by some accidental change of diet, or, as more frequently occurs, it runs a moderately acute course, and is promptly cured by means of antiscorbutics. In the days when scurvy was common and widespread it sometimes became chronic, developing into the “inveterate scurvy” of the older authors, which was notably resistant to treatment. Harvey, in his treatise published in 1685, states that “a mild scurvy may continue or be protracted to ten, twenty, or thirty years.”
In addition to the general picture of the disease which we have presented, mention should be made of other less common symptoms. As is well known, one of the characteristic signs of scurvy is hemorrhage. Indeed, in many of the systematic treatises of medicine it is classified as a hemorrhagic disease. Besides the bleeding into the gums, skin and bones, hemorrhage into the stomach may take place, giving rise to hæmatemesis, or there may be hemorrhage into the eye, under the conjunctiva or into the anterior chamber, leading to the destruction of the eyeball. A very unusual form is meningeal bleeding, giving rise to symptoms of apoplexy. It may be stated in general that hemorrhage dominates the picture of scurvy. Eruptions which in normal individuals are simply macular or papular, assume a hemorrhagic character when occurring in a scorbutic individual. This phenomenon was noted in the recent war in connection with the eruption of typhus fever, and has been observed by military and naval surgeons in numerous expeditions.
Scurvy reduces the nutritional state of probably all the cells and tissues of the body. If the resistance is still further lowered by exposure, nutritional disturbances will result more readily than where the tissues are normal and well nourished. For this reason we believe that scurvy may predispose to frostbite. Reports of congelations occurring in the trenches in the course of the World War tend to confirm our opinion that scurvy was a predisposing factor in many of these cases. This has been true in other wars. For example, Munson writes that “during the Crimean War the temperature was never very low and a report of the times suggests that the large number of congelations observed among the soldiers might well be regarded as gangrene owing to a scorbutic tendency exaggerated by the cold.”
In connection with the involvement of the gums, another typical symptom of scurvy, it should be remembered that this sign may appear late and therefore fail to be of value for early diagnosis, and that it occurs also in purpura and thus may lead to error. This is especially the case if there is pyorrhœa. As is well known, hemorrhages of the gums appear only where teeth are present, and are absent in the edentulous gums of old people as well as in babies who have no teeth. Immerman is probably correct in believing that an injury is always necessary to produce a hemorrhagic lesion in scurvy, and that this explains the early involvement of the gums and also their non-implication in the absence of teeth.
It is a common belief that separation of the epiphyses occurs only in infants and young children, and not in the scurvy of adults. This, however, is not correct, as in severe adult scurvy there is frequently a separation of the epiphyses of the long bones of the lower extremities or of the ribs, the latter resulting in a sinking of the sternum.
The pulse is sometimes slow and feeble, having been recorded as low as 40 beats per minute, but more frequently is rapid, in the neighborhood of 140. It is, however, almost invariably unduly excited by emotion or by mild physical activity. Frequently there is a low type of fever, which has been termed “scorbutic fever,” but which probably should be regarded as a complication of the disease rather than as an intrinsic symptom.
There is little tendency to the formation of pus. Although the lymphatic glands are frequently enlarged and effusions into the tissues and into cavities of the body are by no means uncommon, they show little tendency to become purulent. In the severe cases described by the older authors, the breaking down of the glands in the inguinal region—buboes—is frequently noted. The urine is apt to be scanty, becoming much more profuse following treatment. Perspiration is also retarded.
A peculiar symptom reported in connection with numerous epidemics of scurvy, both on sea and on land, is nyctalopia or night-blindness. The patients can see fairly well during the day, but have very little vision as soon as darkness develops. This phenomenon has puzzled many observers, as nothing abnormal has been found on examination of the eyes. Recently O’Shea, who met with many cases of this nature among soldiers, has reported that in an ophthalmic examination of 22 cases the only abnormality was pallor of the optic disc in 3 cases. This weakness of sight is due to the general nutritional weakness and has been reported in connection with other exhausting and nutritional diseases—for example, hunger edema. More rarely there is day-blindness.
As a complication, dysentery may be mentioned. This has been described by Schreiber and others in scurvy epidemics occurring in the course of the World War. Jaundice may appear, and might be expected to occur more often in view of the marked congestion of the upper duodenum found so frequently at necropsy.
Pericarditis, hydrothorax, pleurisy with effusion, pneumonia, are common complications of severe forms of scurvy. Lind reports that the dominant complication varies in different epidemics; that on one cruise many cases of diarrhœa would occur and on another many pulmonary infections.
O’Shea reports the exceptional case of a man who was operated upon for acute appendicitis. A large hemorrhage in the wall of the cæcum was found, as well as some other hemorrhages in the peritoneal cavity. This report is interesting, not so much from a diagnostic standpoint as because “contrary to what might have been expected, scorbutic cases when operated upon showed no particular tendency to hemorrhage.”
Infantile Scurvy.—The stereotyped picture of infantile scurvy and the one which this term commonly suggests, is that of the acute form of the disease. In acute infantile scurvy we have to do generally with a poorly-nourished, pale infant with a peculiarly alert and worried expression. As we approach its bed it whimpers or cries out in terror. Frequently its posture is characteristic, as it lies quietly on its back with one thigh everted and flexed on the abdomen. Examination shows that one or even both thighs are swollen and exquisitely tender, or that there is merely tenderness, the baby shrieking at the slightest pressure upon the lower end of the femur. If teeth are present, the adjacent gums are red, swollen and bleed readily. This is the syndrome which the medical student is taught to carry away to guide him in his everyday practice. It is the acute, florid type, and presents a striking picture, but must not be regarded as the common form of the disorder. If we are to diagnose infantile scurvy early and not overlook its more subtle manifestations, the classic textbook description must be augmented by portrayals of types of the disorder which are less crude and more difficult to recognize—of “subacute” and of “latent” scurvy.
The commoner form, which we have termed “subacute infantile scurvy,” comprises a large number of symptoms which are inconclusive individually, and frequently escape correct interpretation. The affected baby is usually in the second half of the first year of life, and does not gain in weight or gains but slightly for weeks. It may be fairly well nourished, but is pale or sallow, with perhaps slight edema of the upper eyelids. The mother or nurse complains that the child is irritable and peevish, and that the appetite is poor or capricious. The gums show a lividity or slight peridental hemorrhage, which on subsequent examination may be no longer visible, and may have consisted merely of a rim of crimson edging the borders of the upper gum, perhaps behind an upper incisor, as Still pointed out. On closer examination it may be observed that the papillæ of the tip of the tongue are markedly congested, and that a petechial spot is to be seen on its frenum, on the palpebral conjunctiva, or here and there on the surface of the body, more especially where there are erosions, eczema or other skin lesions. Attention may be called to tenderness of the lower thighs, which in some instances is definite, in others so ill-defined and fleeting that it is impossible to convince oneself of its significance or even reality. There may be slight edema over the crests of the tibia, of a kind which does not pit on pressure. The knee-jerks are almost always markedly exaggerated. The urine is diminished in volume but is generally normal or contains a trace of albumen and red and white blood-cells. The pulse is frequently rapid, and becomes markedly rapid and irregular on the slightest excitement. The respirations are also rapid (Fig. 15).
These symptoms do not constitute a rigid entity, but are subject to manifold variations. The syndrome may be rendered less typical and clear by the fact that the infant has gained steadily rather than lost in weight, as is sometimes the case if the food has been insufficient during the first few months of life. Roentgenograms of the bones may show the “white line” at the epiphyses first described by Fraenkel (Fig. 20) or a thickening of the periosteum. However, too great reliance should not be placed on these signs in making an early diagnosis of this disorder, as neither is invariably present.
An instance of subacute scurvy, which in many respects is typical, is the following:
I. F., girl, was seen when 3 months old, weighing somewhat over 8 pounds. She was given Schloss milk, 4 ounces, and then 5 ounces every three hours, and did well, weighing 11¼ pounds two months later. As she failed to gain for some weeks, although getting 6 ounces of food, it was thought that this might be due to the fact that she was getting pasteurized milk and had never received an antiscorbutic. Autolyzed yeast had been tried as a prophylactic antiscorbutic, but failed to bring about a gain. When, however, orange juice was substituted for the yeast, a prompt growth-reaction resulted, a gain of 1¼ pounds in four weeks. Accompanying this lack of gain in weight there were many of the other symptoms enumerated above; irritability, pallor, slight tenderness of the lower ends of the femora, albumin and a few red and white cells in the urine. The pulse- or heart-beat was frequently over 150, and the respiration 60 (Fig. 15). The diagnosis of subacute scurvy was substantiated by the prompt subsidence of all symptoms when orange juice was administered.
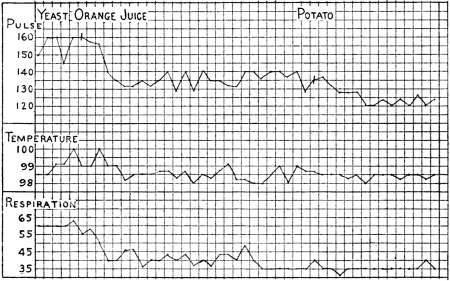 Fig. 15.—Chart of I. F., aged 7 months, showing a prompt effect on pulse, respiration and
temperature of substitution of orange juice (30 c.c.) for autolyzed yeast (30 c.c.) and a further
response when the former was replaced by potato (15 g.).
Fig. 15.—Chart of I. F., aged 7 months, showing a prompt effect on pulse, respiration and
temperature of substitution of orange juice (30 c.c.) for autolyzed yeast (30 c.c.) and a further
response when the former was replaced by potato (15 g.).
Infantile scurvy may be dormant for a long time. The diagnosis of latent scurvy is based mainly on the reaction to specific therapy, on the marked improvement when orange juice, tomato, potato or other antiscorbutic food is given. The symptoms themselves are suggestive, and do not enable an absolute diagnosis to be made. In our experience with many cases of this kind the usual course has been as follows: The infant has been generally from 6 to 9 months of age, and fed for a considerable period on pasteurized milk, which may or may not have been prepared with cereal decoction. Nor has it been material whether gruels also had been given. When about 6 months of age the baby ceased to thrive, to gain satisfactorily, to look healthy, and to feed as it should. The most careful investigation or physical examination has failed to solve the difficulty. On the other hand, the history of a diet of heated milk, especially if the quantity was not large, considered in conjunction with the pallor and poor appetite, the increased knee-jerks, and perhaps a rapid pulse and respiration (the cardiorespiratory syndrome), has awakened suspicion. Orange juice or canned tomato, prescribed in such cases with a view to diagnosis as well as to treatment, frequently brings about a magic result. The following case, the weight chart of which is reproduced (Fig. 14), is fairly typical of this abnormal nutritional state:
H. S., boy, born December 15, 1915, was artificially fed until January 4, 1916, when he weighed 6½ pounds. He was given 28 ounces of Schloss milk a day. (This was prepared from pasteurized milk which was not heated a second time. It contains per litre (quart) 140 c.c. of whole milk, 140 c.c. of 20 per cent. cream, 50 g. of dextrimaltose, 5 g. of plasmon, 0.2 g. of potassium chlorate, and 700 c.c. of water.) By March 1 he weighed 9 pounds, and gained three-quarters of a pound more in the course of this month. During April he gained only 4 ounces. As will be seen from the chart, there was almost a cessation of gain from April 10 to May 3, although yeast was added to the diet. May 2, orange juice was given. The weight advanced at once, the color and the general appearance improved, and an eczematous condition of the face rapidly healed. It will be noted from the chart that the gain occurred, although the food intake remained the same.
Epicrisis: A baby 4 months old with latent scurvy, which existed since he was at least 3 months of age.
This condition of latent scurvy is probably the commonest type of the disorder, especially in the larger cities where almost the entire milk supply for infants is pasteurized. It usually passes unrecognized. Most infants fortunately are given orange juice by the time they are 6 months of age, and may receive a small amount of vegetable or potato before they are much older, so that they are protected from serious harm in this way. But there is no doubt a considerable number, especially those peculiarly susceptible, who quite unbeknown to anyone pass through the state of latent scurvy.
If this large group of cases were included in the incidence of infantile scurvy, we should not look upon it as a disorder which occurs rarely during the first six months of life.
When scurvy goes unrecognized or untreated for a long time, or the antiscorbutic content of the food is exceptionally small, or the patient unusually susceptible, the disorder may progress and resemble the advanced cases described in connection with the adult type of this disease. Happily such instances are rare. One of the most typical and vivid descriptions of an extreme case of infantile scurvy is that reported by Vincent:
The infant lay in its bed extremely apathetic and barely conscious. Its face was ashy gray in color, the respirations were extremely frequent, the pulse-rate was 144 per minute, and the temperature 103.2°. When touched it moaned feebly, and made no attempt at movement. The mouth was kept open, the lower jaw hanging away from the face. There was a complete absence of muscular tone, so that the infant appeared to be quite incapable of voluntary movement.
The mouth presented a horrible appearance. No sign of the teeth could be discovered, though it was stated that several had appeared. All that could be seen was a purple mass, which was so extensive that on superficial inspection it was difficult to distinguish between the upper and lower jaws, despite their wide separation. Scattered over this purple mass were areas of necrosing tissue, the odor of which was extremely unpleasant.
Petechial hemorrhages were distributed over the back and limbs, and a large patch of extravasated blood was found in the region of the left hip.
Tenderness was present in all the limbs, as manifested by moaning and by the facial expression. There was a general enlargement over both humeri throughout their length; the ulna and radius did not appear to be thus affected, but the index-finger of the right hand was enlarged, especially at the junction of the metacarpal bone with the first phalanx, the enlargement being at each side of the joint. In the legs the signs were extreme. At both knee-joints the skin was tightly stretched over the swollen epiphyses; the tenderness also was greater than at any other part.
Bleeding from the gums and nose had occurred; no history of hæmaturia could be obtained. The motions were semisolid, green, and offensive. During the last twenty-four hours the infant had refused food.
The baby was given large amounts of lemon juice and subcutaneous injections of salt solution and the necrosing surfaces of the gums were scraped and swabbed with boracic solution. By the third day the pulse was 100, the temperature 99.8°, the odor from the mouth scarcely noticeable, and the general condition distinctly improved. It continued to improve and to gain in weight and when seen at the end of the sixth week of treatment it was doing well and was quite happy.
It will be well to consider in detail the signs and symptoms which may develop in the course of scurvy.
Hemorrhage.—Hemorrhage of the gums is one of the characteristic signs of scurvy. For a reason not clearly understood it involves first and foremost the tissues about the upper incisors. If, however, we fix our attention too narrowly to this region we may be led into error; in several instances we have first encountered hemorrhages about the molar or the canine teeth, which had been overlooked because the anterior part of the gums had been found normal. Where teeth are absent or not in the course of eruption hemorrhages do not appear. At the onset the gums may be merely deep red or bluish red, especially if they overlie upper incisors which are close to the surface. Hemorrhage is particularly apt to occur where the edges of the teeth have just broken through the mucous membrane. In this connection the question arises as to whether every hemorrhage of the gums in infants is to be considered a sign of scurvy. This is a matter of some diagnostic importance. We have seen hemorrhages of the gums at the site of erupting molar teeth where, as prolonged observation proved, not even latent scurvy existed. This sign should not, therefore, be regarded as pathognomonic. In two infants entirely free from scurvy we have noted slight hemorrhage of the gums overlying incisor teeth. It should be well understood that such an occurrence is most exceptional; it is to be attributed probably to bacterial invasion or to a constitutional hemorrhagic condition. One of these cases was the following:
The infant was 8½ months old. It had been nursed by the mother up to this time and was well nourished, but when first seen had some fever, probably due to a grippe infection. About ten days later distinct linear hemorrhages of the gums were noted over the two upper incisor teeth. No treatment was instituted for this condition, and it healed within a week. There was no subsequent sign of similar hemorrhage or of other scorbutic manifestation in the months that the baby was under observation.
The localization of the hemorrhage in the gums is due largely to trauma, occasioned by the sharp contact of the jaws or of the nursing-bottle. Local infection plays almost no rôle in infants, although in the adult where there is caries of the teeth it frequently incites hemorrhage. Dental caries and gingival infection may lead to local hemorrhage, even where the nutritional conditions are normal.
Subperiosteal hemorrhage is a sign distinctive of infantile scurvy, although it must be borne in mind that it may take place in the scurvy of adults. It involves most frequently the lower end of the femur and the tibia, but occurs in connection with the humerus, the mandible, the scapula and other bones.47 The hemorrhage usually manifests itself as a swelling which appears suddenly at the lower end of the femur or femora. It is brought about by trauma, at times in the course of diapering, or by manipulation in testing for local tenderness. The swelling is very tender, and varies in size from an enlargement which is difficult to appreciate, to one which renders the leg fully twice its normal circumference (Fig. 18). It may involve merely a small part of the long bone or extend up or down the shaft for a long distance. As might be supposed from the nature of this lesion, the enlargement persists for weeks, frequently long after the gums and the general symptoms have disappeared. During this period it becomes harder and less tender, and may develop the consistency of bone; it is in this stage that such swellings have been diagnosed as new growths, and that incision or even amputation of the leg has been resorted to. In subacute cases the swelling—which must be regarded as hemorrhagic rather than scorbutic—may be absorbed gradually in spite of the fact that no antiscorbutic food has been given. This has led to the mistaken conclusion that the scurvy has been cured without dietetic treatment.
Subperiosteal hemorrhage may be clearly seen by means of the fluoroscope or in X-ray photographs (Figs. 16 and 17). The shaft of the bone appears surmounted by an elongated blood-clot, which is more or less distinct according to its age and density. It may become calcified, as clearly seen in figures. More often the periosteum undergoes calcification or ossification, especially near the site of the separation of the epiphysis. This gives rise to a bizarre radiographic picture which may be difficult to interpret—the opaque strip or streamer being almost unrecognizable as periosteum (Fig. 17).
Hess and Unger observed that in several instances where subperiosteal hemorrhage had been diagnosed, X-ray examination disclosed that the swelling of the thigh was due mainly to infiltration of the muscles and subcutaneous tissue. It is surprising how an infiltration of serum gives rise to a swelling which resembles in appearance and consistency the classical subperiosteal tumor.
The skin, mucous membranes and subcutaneous tissues are frequently the sites of hemorrhage. There is a difference of opinion as to how frequently petechial hemorrhages occur in scurvy, particularly as to whether they are encountered early in this disorder. Great variation in this regard may be noted in individuals and in groups of cases occurring at different times. In the cases reported in 1914 by Hess and Fish, petechial hemorrhages were frequently an early sign, to such an extent that they led to a study of the blood and blood-vessels in this disorder. The hemorrhages in this “scurvy epidemic” were the result of a complication of scurvy with an infectious disease. It is not necessary, however, for infection to exist to bring about a rupture of the small vessels. The idiosyncrasy of the individual has to be considered as well as the fact that infants have a tendency to develop minute skin hemorrhages, especially such as have an exudative diathesis. In the course of scurvy, petechiæ may be found not only in the skin, but in the mucosa of the mouth, especially overlying the hard palate, and also in the palpebral conjunctiva, identical with the minute petechiæ so significant of general sepsis. In addition to these minute hemorrhages larger ones are not infrequently found in various parts of the body, especially in the neighborhood of the joints. They appear as discolorations of various intensities and shades, and are often interpreted as being merely the result of bruises. These have been encountered most often about the knee-joint, on the forehead, or in the concha of the external ear, where they may best be seen by means of transmitted light.
A form of hemorrhage which must be especially mentioned, although it is very infrequent, is that taking place into the orbit, leading to a proptosis of the eyeball, usually the left (Still). This sign should be borne in mind, as it occurs occasionally before other symptoms have rendered the diagnosis clear, and may lead to a diagnosis of tumor.
As mentioned above, hemorrhages into the muscles or between the muscle planes are very common in adults, leading to hard swellings, the typical “scurvy sclerosis.” Such effusions occur much less frequently in infants, due probably to their lack of activity. In addition to these hemorrhages there are serous effusions of the muscles similar to those which are found in the pleural and pericardial cavities. These effusions are very striking at necropsy, when one incises the muscles—for example, the muscles of the thigh. During life they are frequently mistaken for subperiosteal hemorrhages.
Less frequently there are hemorrhages into the internal organs. These, however, play a comparatively insignificant rôle in the symptomatology of this disease. At postmortem examination we find numerous hemorrhages of the pleura, pericardium and peritoneum, which rarely produce symptoms during life. Still records a case with marked abdominal pain and swelling, which he believed to have been due to hemorrhage into the wall of the intestine. As previously mentioned, O’Shea met with a case of hemorrhage into the cæcum which was mistakenly operated upon for appendicitis. Hæmothorax and hæemopericardium occur, especially associated with local inflammatory processes of tuberculous nature. The clinical aspect of hemorrhage of the gastro-intestinal and the genito-urinary tracts will be considered elsewhere.
In the scurvy of adults as well as that of infants, the nails and the hair are altered by the nutritional condition. Mention has been made of the hyperkeratosis recently emphasized by Wiltshire as an early sign, occurring especially on the thighs and legs. The skin is frequently dry, the so-called “goose skin” that is seen in some poor nutritional states. The nails are thin, brittle and lined; at times small hemorrhages will be noted beneath them. The hair also becomes thin and dry, and there is a tendency for petechial hemorrhages to develop at the roots.
In a paper on the therapeutic value of yeast and of wheat embryo the author called attention to the fact that eczema may occur in connection with infantile scurvy, and be cured by means of orange juice. We have met with eight cases of eczema in infantile scurvy, which, in almost every instance, have yielded promptly to an antiscorbutic, thus proving their scorbutic nature. A case of this kind is the following:
M. L., seven months old, was getting “Molkenadaptierte” milk, and in addition autolyzed yeast. On May 25th it developed nasal diphtheria, but soon afterward did well. On June 9th it was gaining, but its pulse was 160 and respirations 80. A few days later it developed marked eczema about the neck and to a less extent on the back and buttocks. The “capillary resistance test” was negative. Cardiographic tracings showed merely a simple tachycardia. A few days later petechial spots appeared at the site of the eczema. On June 17th orange juice was given. The appetite improved, the cardiorespiratory syndrome disappeared, and the child began to gain. The eczema also cleared up rapidly without any local treatment.
We wish to draw particular attention to this skin condition, as it is generally not mentioned, or has been regarded merely as a chance occurrence. The report of the American Pediatric Society includes two cases of eczema as a complicating condition. This symptom is of special interest in view of the fact that a similar skin lesion constitutes one of the typical signs of pellagra. In a case of infantile scurvy we have seen an eruption at the nape of the neck which was symmetrical and greatly resembled that of pellagra. Andrews refers to the occurrence of eczema in his description of infantile beriberi.
In a paper published a few years ago attention was drawn by Hess and Fish to the fact that infantile scurvy frequently is associated with the exudative diathesis of Czerny, a pathological condition which predisposes to the development of exudations of the skin and the mucous membranes. Infants suffering from this condition—intertrigo, eczema, recurrent bronchitis—seem to be particularly susceptible to scurvy and to develop it more quickly than others.
As is well known, edema constitutes a not infrequent symptom of adult scurvy. It has not, however, been accorded any place in the symptomatology of infantile scurvy. We do not refer to the edema in connection with subperiosteal hemorrhage or separation of the epiphyses of the long bones, but a mild and peculiar form which is seen early in the disease. It involves most regularly the upper eyelids, and the legs—especially the skin covering the lower part of the tibiæ. In the latter site it differs from edema as usually encountered, in that it does not pit on pressure; it is firm, tense, causing some glossiness of the overlying skin, which is rendered difficult to wrinkle or to pinch between the fingers. Not infrequently the skin is slightly reddened, a sign of interest, in view of a similar, although much more intense, hyperæmia seen in pellegra.
In addition to this very mild edema there may be marked swelling, resulting in what might be called, following the terminology of beriberi, “wet scurvy.” The legs, body and even the face may be swollen. This has been frequently described in adult scurvy, and occasionally in infantile scurvy. The first case of infantile scurvy described in America, that of Northrup, had marked edema of the scrotum. Edema is frequently met with in “ship beriberi,” a disorder considered by some writers to be a combination of beriberi and scurvy.
The symptom leading to the diagnosis of scurvy most often is tenderness or swelling of one of the extremities, as the antecedent clinical signs, comprising latent scurvy, are generally overlooked. These manifestations involve usually the distal end of the thigh or thighs. The tenderness is elicited most readily by pressure just above the knee, which causes the baby to wince, and to quickly flex the thigh, a reaction termed by Heubner “the jumping-jack phenomenon.” As a result of pain and tenderness, the leg lies often immobile in a state of pseudo-paralysis (Fig. 18). There may be tenderness elsewhere than in the long bones. Kerley refers to two cases showing tenderness of the spine, and we have seen a similar case. Not infrequently there is tenderness of the chest wall, the earliest symptom noted by nurse or mother being unaccountable crying whenever the baby is lifted by the thorax. This is largely due to the sensitiveness of the ends of the cartilage and bone which are pressed together at their junction.
An early sign of infantile scurvy is beading of the ribs—the development of a “rosary” similar to that characteristic of rickets (Fig. 19). This has recently been described by Hess and Unger in an article devoted to this subject. That this rosary is truly scorbutic and not rhachitic is proved by the fact that it recedes rapidly when antiscorbutic foodstuff is given, and that it remains uninfluenced by treatment with cod liver oil. A similar scorbutic rosary occurs in guinea-pig scurvy, but has been termed “pseudo-rhachitic.” It is important that this sign should be recognized, as it is probable that much of the confusion regarding the relationship and frequent association of these two diseases is due to considering the beading rhachitic. The interpretation of infantile scurvy as “acute rickets,” the view held previous to the writings of Barlow, was based largely on the development of the rosary. To-day the error is made of regarding early scurvy as chronic rickets; the rickets supposed to be occasioned by a diet of condensed milk is probably more often scurvy. This beading differs generally from the round knobby “rosary” usually encountered. It is more angular, the junction taking on a step-like form, as if the abutting ends of the cartilage and the bone were of unequal size, and not well fitted to each other. In the accompanying radiograph (Fig. 19) it will be noted that the “beads” present an irregular appearance.
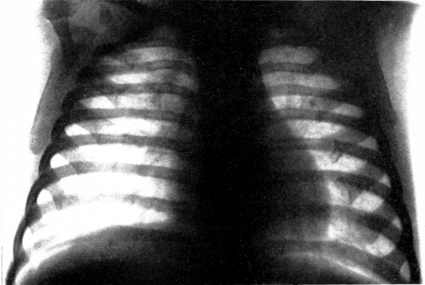 Fig. 19.—Same infant as in figure 17. Scorbutic beading of the ribs (rosary). This developed
on a diet which included cod liver oil, and decreased when an antiscorbutic was given.
Note peculiar ragged appearance of “beads.”
Fig. 19.—Same infant as in figure 17. Scorbutic beading of the ribs (rosary). This developed
on a diet which included cod liver oil, and decreased when an antiscorbutic was given.
Note peculiar ragged appearance of “beads.”
In Figs. 6, 16 and 17 will be seen illustrations of a separation of the epiphyses of the head of the humerus, and of partial and of complete separation of the lower ends of the femora. This is a frequent lesion of fully developed scurvy in infants, children, and even in young adults. It is most frequent at the lower end of the femur, the upper end of the tibia, the head of the humerus, and the costochondral junctions. It is to these epiphyseal separations that the term fracture or infraction usually refers. Union is remarkably perfect even where no splint has been employed, and nature has effected the cure (Fig. 7). Occasionally there is some deformity, as when coxa vara develops. The callus is often remarkably large; an old callus sometimes undergoes destruction in the course of scurvy.
 Fig. 20.—Radiograph. Infant 14 months of age, showing “white line” at wrist some
months after cure of scurvy.
Fig. 20.—Radiograph. Infant 14 months of age, showing “white line” at wrist some
months after cure of scurvy.
We have referred to use of röntgenograms in connection with separation of the epiphyses, subperiosteal hemorrhage, cardiac enlargement and beading of the ribs. In addition to its application in these connections, the X-ray may be of service to show a peculiar alteration of the ends of the long bones—the white line of Fraenkel. This is portrayed in Fig. 20. It is best seen at the lower ends of the radius and femur, and appears as a white, transverse, somewhat irregular band. Its diagnostic value has been greatly exaggerated, as it is frequently not present when the disease is advanced (observe radiographs illustrating separation of the epiphyses). This sign should therefore not be relied on for establishing the diagnosis. Furthermore, changes may be seen in connection with rickets (cases receiving antiscorbutic diet) which are very difficult to differentiate from the “white line.” It cannot be employed as a criterion of the progress of the case, as it may persist for months after all other signs and symptoms have disappeared.
The joints may be involved in scurvy. In most instances, however, where swelling of the joints is diagnosed, the lesion is periarticular. An effusion of serum or of blood does occur occasionally into the joints and has been found at operation, at necropsy, and by puncture. If these effusions are allowed to go undisturbed, to be absorbed as a result of antiscorbutic treatment, they rarely suppurate. Czerny and Keller report the articular fluid as invariably sterile.
The cardiovascular system has been given but scant attention in connection with scurvy. Adults complain not infrequently of palpitation and pain over the pericardium, or rather of a tightness or oppression in the chest. Little information is given regarding the size of the heart. Darling described enlargement of the heart, especially a right-sided hypertrophy, which he thought was pathognomonic of the Rand type of scurvy. The pulse is described in some cases as slow, and in others as rapid. In descriptions of infantile scurvy the entire subject is generally passed over without mention—for example, in the excellent report of the American Pediatric Society nothing whatsoever is stated regarding the heart’s action or the pulse. Barlow wrote: “There is nothing to note regarding the heart and lungs.”
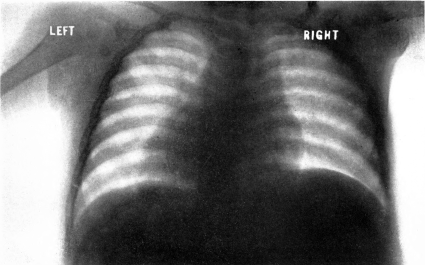 Fig. 21.—Radiograph. Scorbutic infant 14 months of age, showing cardiac enlargement and broadening of shadow at base of heart.
Fig. 21.—Radiograph. Scorbutic infant 14 months of age, showing cardiac enlargement and broadening of shadow at base of heart.
In a paper written a few years ago, it was pointed out by the author that there is frequently enlargement of the heart, and more especially of the right heart. This can be elicited at the bedside and has been substantiated in numerous cases by means of the Röntgen-ray, which demonstrates not only enlargement of the heart, but also a marked broadening at its base, at the site of the large vessels (Fig. 21). These phenomena resemble closely the description of Reinhard in cases of beriberi.
Necropsy protocols usually are incomplete and unsatisfactory in their descriptions of the heart. The excellent monograph of Schoedel and Nauwerk, however, which reports five careful necropsies, contains the following data regarding three:
1. Pericardial fluid somewhat increased, both ventricles moderately dilated, the right somewhat hypertrophic.
2. The heart showed a hypertrophy of the right and left ventricles, as well as dilatation of the right ventricle.
3. The right ventricle dilated and slightly hypertrophied, the muscles pale and tough.
In addition to this enlargement of the heart, or perhaps associated with it, there is a combination of signs which has been termed “the cardiorespiratory syndrome” (Hess). It will be noted in the above description of a case of subacute scurvy, that the pulse- or heart-beat was frequently over 150, and the respiration 60. These phenomena were noted in several instances before their significance and intimate relationship to scurvy were realized. The heart-beat not infrequently is found to be 200 per minute, and to be characterized by marked lability—increasing to an astonishing degree as the result of slight exertion or excitement. A mild febrile disturbance causing a rise of temperature to little more than 100° F. will send the pulse-rate up 30 beats. It must not be thought that this refers to severe cases; the babies we have in mind are similar to the one cited as an instance of subacute scurvy. Apparently they are not ill, but show merely some tenderness of the thighs, pallor, and the other minor signs described. The cardiographic tracings showed a simple tachycardia with an exceptionally tall T-wave in some tracings, such as is commonly seen in exophthalmic goitre (Fig. 22).
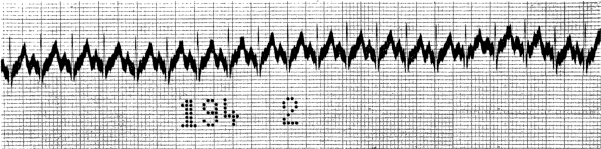 Fig. 22.—Electrocardiogram in case showing cardiorespiratory syndrome. Tachycardia with exceptionally tall T-wave.
Fig. 22.—Electrocardiogram in case showing cardiorespiratory syndrome. Tachycardia with exceptionally tall T-wave.
The rapidity of respirations is perhaps a more delicate indicator of this disturbance than the pulse and has been found to be markedly affected when the latter was merely slightly increased in rate. For example, in one instance the respirations were 64, 60 and 64 on three successive days, while the pulse was 124, 141 and 136; in other words, there was a 2:1 instead of the normal 4:1 pulse-respiration ratio. The accompanying chart (Fig. 15) illustrates the phenomenon in all its details better than a verbal description. There is one point in connection with it, to which especial attention should be called. This is a reaction evident at a glance at the chart—the sharp drop in the pulse and in the respiratory rate when orange juice was given. It is the essence of the phenomenon; a therapeutic response which proves that the rapidity is scorbutic in nature.
The main involvement of the respiratory system in scurvy is the polypnœa just described in connection with the cardiorespiratory syndrome. There is no aphonia, a sign so typical of adult and of infantile beriberi, although at times the voice is abnormal and whining. The lungs frequently show some dullness posteriorly, which may be due to engorgement or to the pressure of the enlarged heart. Pneumonia is a frequent complication and edema a terminal event. Hydrothorax associated with hydropericardium is of frequent occurrence, and was noted in the early description of this disease in adults and in the first account of Barlow. These effusions rarely progress to what may be termed the clinical degree and under antiscorbutic treatment are rapidly absorbed.
It is commonly thought that scurvy does not involve the nervous system; that this is a feature which distinguishes it sharply from beriberi, another “deficiency disease.” This view is incorrect, for the nervous system is probably affected in many cases of scurvy. The rapidity and lability of the pulse, combined with the rapid respirations, would seem to be due to a disturbance of the vagus mechanism. It is true that in beriberi the vagus is involved to a still greater extent, especially its recurrent laryngeal branch which brings about the characteristic aphonia. In scurvy the knee-reflexes are generally increased. Very rarely they are absent in infantile scurvy, as described in adults. It is impossible to judge whether the pain and tenderness in infants are due in part to a sensitiveness of the nerve trunks as well as of the periosteum. Careful studies in adult scurvy should furnish an answer to this question. No methodical examination for areas of anæsthesia or paræsthesia, signs which occur so frequently in connection with beriberi, has been carried out in scurvy. In certain epidemics, however, pains in the limbs have been prominent symptoms.
The optic discs are generally pale in both infants and in adults, with occasional signs of neuredema. Nyctalopia, so frequently encountered, must be regarded as a circulatory symptom rather than as one of nervous origin.
In a recent paper the author described a focal degeneration of the lumbar cord in a case of infantile scurvy, the lesion involving mainly the anterior horn cells (Figs. 3 and 4). In view of this report it would be well to watch for corresponding clinical signs of involvement of the spinal cord. Herpes has been described in connection with both adult and infantile scurvy. In one of the early cases in the American literature Fruitnight reported a case with herpes in a girl five years of age. In considering the rôle of the nervous system, mention should be made of cases where sweating constituted an important symptom. Finkelstein lays particular stress on this symptom in infantile scurvy. We have not met with it frequently; possibly it is due in part to complicating rickets.
As would be expected, the nervous system is at times the site of hemorrhage. Such lesions cannot, however, be considered essentially nervous. For instance, hemorrhage into the meninges may occur, as in the case of Sammis, where there was “a general clonic convulsion” before death, and a blood-clot 2½ inches long by ½ inch wide was found at necropsy between the dura and arachnoid. Fife reported a similar case. Finkelstein also has drawn attention to the occurrence of meningeal hemorrhage, and Hess and Fish reported obtaining bloody cerebrospinal fluid from a case with meningeal symptoms. Recently Aschoff and Koch have depicted hemorrhages in the sheath of the sciatic nerve, which undoubtedly must have given rise to symptoms during life.
In view of many of these symptoms, especially those involving the vagus, scurvy must be looked upon as a disorder which may seriously affect the nervous system. Furthermore, when we note the marked reaction brought about by the antiscorbutic vitamine—for example, the sharp fall in the rate of respirations and of pulse, as shown in Fig. 15, after giving orange juice, we must conclude that the antiscorbutic vitamine functions, at least indirectly as an antineuritic vitamine—that it must possess this character to allay the various nervous signs of this disorder.
The urinary system is frequently involved in the course of scurvy. Among 38 cases Still reports that 89 per cent. gave evidence of urinary changes and that 60 per cent. showed hæmaturia. Finkelstein found urinary signs in at least a third of his cases. Our figures, the result of a study of subacute and mildly acute cases, correspond more nearly with those of Finkelstein.
The occurrence of pronounced renal hemorrhage as a first symptom of scurvy is emphasized in many descriptions of this disease, and has impressed itself in the minds of physicians. It is true that this occurs sometimes at the onset, as does hemorrhage into or about the joints, or hemorrhage behind the eyeball. It is well to bear these possibilities in mind, but they must be regarded as very exceptional early signs of this disorder. We have encountered frank hæmaturia but once in the early stage of infantile scurvy. The blood emanates generally from the kidneys, although the submucous hemorrhages of the bladder as well as in the urethra, described both in man and in guinea-pigs, indicate that the blood in the urine may have its origin lower down in the tract. This bleeding should be regarded not as a sign of nephritis, but rather as a hemorrhagic manifestation. It is less frequent in adults than in infants. O’Shea reports some degree of hemorrhage in 15 per cent. of his cases (adults).
A true nephritis, however, may occur in connection with scurvy. There may be albumen and many casts, or a urine loaded with casts and cylindroids. These peculiar casts may appear suddenly, as in the alimentary intoxication of infants, and disappear just as rapidly when antiscorbutic treatment is given. The urine may contain a large number of pus cells as in pyelitis. This condition may be accompanied by irregular fever, but in two instances we have encountered it where the temperature was normal. It is to be regarded, probably, merely as one of the manifestations of secondary infection so commonly associated with scurvy. Some pus cells may continue to be present in the urine for a period of months. This is likewise true of the red cells. We have under observation at present an infant which had subacute scurvy almost three years ago and still has red blood-cells in the urine.
Oliguria is a common symptom of both adult and infantile scurvy. Lind mentioned this symptom, and in this connection remarks on the beneficent effect of antiscorbutic treatment. Charpentier called attention to the fact that in a case of scurvy the urine decreased from 1250 g. to 800 g. The report of the American Pediatric Society mentions scanty urine in 9 cases and suppression of urine in one. This sign, however, was not emphasized until recently, when Gerstenberger, and Hess and Unger drew attention to its frequent occurrence in infants. It has some diagnostic significance and should be borne in mind where a decreased excretion of urine is reported. A counterpart of this symptom is the sudden outpouring of urine frequently noted after antiscorbutic treatment has been instituted. This polyuria accounts for the loss of weight or lack of gain which sometimes accompanies unmistakable general improvement, and which is difficult otherwise to understand (Fig. 23). It is interesting to learn that oliguria occurs commonly in both adult and infantile beriberi.
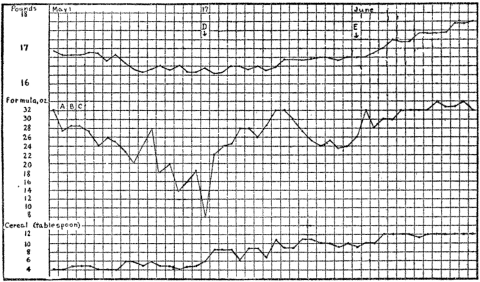 Fig. 23.—Joseph G., aged 9 months. Chart showing stationary weight (due to oliguria
followed by diuresis) in spite of marked variation of fluid intake. A=Schloss milk; B=cod
liver oil; C=egg yolk; D=1 ounce of orange juice; E=potato (orange juice stopped).
Fig. 23.—Joseph G., aged 9 months. Chart showing stationary weight (due to oliguria
followed by diuresis) in spite of marked variation of fluid intake. A=Schloss milk; B=cod
liver oil; C=egg yolk; D=1 ounce of orange juice; E=potato (orange juice stopped).
One of the earliest, as well as one of the most constant symptoms of scurvy, is a lack of appetite. It is a typical sign of latent scurvy, although occasionally we have met with cases where the appetite remained unimpaired until the hemorrhagic stage was reached. In adults there is sometimes bulimia and a marked capriciousness of the appetite. Anorexia is a true scorbutic symptom, disappearing with remarkable rapidity when antiscorbutic food is given, and not capable of alleviation by tincture of gentian or other vegetable bitters. Whether it depends upon a lack of secretions in the gastro-intestinal tract is not known, as there has been no thorough study of this aspect of the disorder. The hydrochloric acid generally is deficient in cases of scurvy. Recently McCarrison has laid emphasis on the importance of the impairment of the digestion and assimilative function in scurvy. This subject gains added interest in view of the recent reports of Uhlmann as well as of Voegtlin, showing that water-soluble vitamine acts as a stimulant for the various secretions of the gastro-intestinal tract.
As a result of McCollum’s statement that scurvy is due mainly to constipation, marked attention has been directed recently to the action of the bowels in this disorder. This question has been discussed in the chapter on etiology, and, therefore, will be referred to in this place merely from the clinical viewpoint. In our experience the activity of the bowel varies greatly in cases of latent or subacute scurvy. In a great many instances it has been normal; more often there has been slight constipation, and exceptionally there has been irregular diarrhœa. In other words, no causative relationship or parallelism could be observed between the emptying of the intestinal tract and the development of scurvy. This in general has been the experience of others. In the report of the American Pediatric Society the bowels are stated as having been regular in 74 cases, irregular in 15, constipated in 126, and diarrhœal in 65. It may be added that we were unable to cure scurvy by means of liquid petrolatum or phenolphthalein, either in infants or in guinea-pigs, and likewise unable to protect guinea-pigs from scurvy by means of various laxatives. On the other hand, opium given in the form of the camphorated tincture did not lead to an intensification of the symptoms, although, in one case, the bowels did not move for over three days.
As complications involving the gastro-intestinal tract may be mentioned the vomiting of blood, which is stated in the above report as occurring in 2 of the 361 cases, as well as bleeding from the bowel, which was noted in 37 cases, in 12 of which there was bloody diarrhœa. However, these are late symptoms, and correspond to the mycotic ulcers which are so frequently found, especially in the large intestine, in cases of scurvy. Mention may again be made of the fact that hemorrhages may occur under the peritoneum and give rise to symptoms simulating appendicitis or general peritonitis.
Jaundice has been described in connection with certain epidemics of scurvy. To our knowledge it has not been reported in infants.
The presence of worms has been frequently reported in the bowel or in the stool of patients suffering from beriberi. There have been no similar investigations in relation to scurvy. It would be interesting to inquire into this question, as it is quite possible that a lack of antiscorbutic foodstuff may favor the presence of parasites in the intestinal canal.
Before closing this consideration of the involvement of the alimentary tract, we would call attention to the relation of stomatitis to scurvy. Among adults this is a common complication. In infants it is uncommon, due to the absence of carious teeth and secondary infection; we have encountered it in but two instances. Stomatitis is of importance in this connection, as it frequently develops on the basis of malnutrition, scurvy being one of the disorders which may constitute the substratum. Such may be the case where stomatitis occurs in epidemic form —for example, among large bodies of troops. It may be remarked that stomatitis at times was a very common disease among the soldiers in the recent war.
| Name | Date | Platelets | Leukocytes | Erythrocytes | Hmgl. % (Sahli) | Remarks |
|---|---|---|---|---|---|---|
| M. H. | 5/ 3 | 280,000 | ...... | ......... | .. | |
| 5/ 4 | 248,000 | 10,000 | ......... | .. | ||
| 5/ 5 | ....... | ...... | ......... | .. | Boiled orange juice given. | |
| 5/ 8 | ....... | ...... | 4,300,000 | 35 | ||
| 5/16 | ....... | 15,900 | ......... | .. | ||
| 7/ 2 | ....... | 6,800 | 5,456,000 | 40 | Well but pale. | |
| A. L. | 5/ 3 | 300,000 | ...... | ......... | .. | |
| 5/ 5 | ....... | 21,000 | ......... | .. | ||
| 5/ 9 | ....... | ...... | 5,480,000 | .. | ||
| 5/11 | 320,000 | ...... | ......... | .. | ||
| 5/13 | ....... | ...... | ......... | 65 | ||
| 5/16 | ....... | 11,500 | ......... | .. | ||
| H. C. | 5/ 8 | 320,000 | 20,000 | ......... | .. | |
| 5/ 9 | ....... | ...... | 5,340,000 | .. | ||
| 5/13 | ....... | ...... | ......... | 70 | ||
| 5/16 | 362,000 | ...... | ......... | .. | ||
| B. B. | 5/ 4 | 496,000 | 21,000 | ......... | .. | A severe case. |
| 5/13 | 585,000 | 14,000 | 3,200,000 | 70 | ||
| 5/18 | ....... | 17,600 | ......... | .. | ||
| 7/13 | ....... | 40,000 | 7,672,000 | 82 | Has gained well lately. | |
| 7/15 | ....... | ...... | 7,640,000 | 88 | ||
| H. Y. | 5/15 | 560,000 | ...... | ......... | .. | |
| 5/16 | 424,000 | ...... | ......... | .. | ||
| 7/ 9 | ....... | ...... | 5,750,000 | 45 |
Scurvy is associated with an alteration of both the blood and the blood-vessels. The characteristic pallor, which is one of the most common as well as earliest symptoms, is due in a large measure to the anemia. This anemia is of the secondary type, but has definite peculiarities, and does not resemble that encountered in the course of tuberculosis, rickets or marasmus. The hemoglobin is greatly diminished, far out of proportion to the decrease in the number of the red cells. Not infrequently we will find a hemoglobin index of 0.5. Table 4, above taken from the article on this subject by Hess and Fish (1914), brings out the details of the blood-picture. It shows that there may be a polycythemica, which may persist after the other signs of the disorder have disappeared. Brandt has recently made similar observations, reporting in one instance over ten million red cells two months after treatment. In soldiers suffering from scurvy Wassermann has encountered cases where, during convalescence, the red-cell count has risen to over six or seven millions and the hemoglobin to 110 or 120 per cent. Under the microscope the red cells show poikilocytosis, anisocytosis and a lack of hemoglobin; they are slightly enlarged, with the occasional occurrence of exceptionally large cells resembling the “dropsical cells” described in connection with chlorosis. Sometimes a few nucleated red cells and myeloblasts are seen; megaloblasts are also reported.48 The blood-picture bears a remarkable similarity to that of chlorosis, a point of interest, in view of the fact that both scurvy and chlorosis have been attributed to a disordered function of the endocrine glands. The “dropsical cells” suggest a disturbance of the salt balance in the plasma. In some cases we have found a decreased fragility of the red cells, which also has been described in chlorosis.
The total number of leucocytes is slightly increased. In our cases the mononuclear cells have averaged 66 per cent., which is somewhat high even for infants. This has been the experience of Labor, who, however, also describes an eosinophilia during convalescence, a phenomenon which we have not encountered. Some describe a marked increase in the polynuclear cells, which, probably, is to be regarded as the reaction to secondary infections. There is indeed a marked difference of opinion in regard to the morphology of the blood in scurvy in adults as well as in infants. Some found a large number of one type of cell—for example, nucleated red cells, myelocytes, eosinophiles—whereas others have failed to observe an increase of these cells. The divergent reports probably should be attributed to the fact that the investigators are describing scurvy of various grades of severity, of different stages of development, or complicated by intercurrent disease.
Nobécourt, Tixier, and Maillet have questioned whether there is always complete recovery from this anemia, which is severe from the standpoint of hemoglobin and iron. The older authors reported instances where men have been weakly and ailing for the remainder of their lives after an attack of scurvy. In some infants pallor and anemia may persist for months after apparent cure; however, this is the exception rather than the rule.
In view of the fact that scurvy frequently is classed as a hemorrhagic disease, and that hemorrhages play such an important rôle in its symptomatology, a consideration of the factors concerned in the coagulability of the blood is of interest. In an investigation (Hess and Fish) it was found that the oxalated plasma (of blood taken directly from a vein) showed a slightly delayed coagulation time—eight to fourteen minutes. The “bleeding time” carried out according to the simple method of Duke was slightly increased. Holt reports a case where a child bled to death following incision into an epiphyseal swelling at the lower end of the femur. The number of blood platelets is increased, running parallel, as is usually the case, with the number of red cells (Table 4). This increase in the blood-platelets, recently confirmed by Tobler and by Brandt, is a very exceptional phenomenon, and was not anticipated in connection with a disorder characterized by hemorrhage. The antithrombin content of the plasma is normal.
The investigation was directed to a study of the integrity of the blood-vessels in order to account for the hemorrhages. To this end the “capillary resistance test” was devised.49 In the majority of cases this was found to be “positive” (the blood-vessels showing an increased permeability) and to become negative when antiscorbutics were given and the symptoms disappeared. This shows that the cellular structure of the vessels is altered in the course of scurvy, and indicates probably that this is an important cause of the hemorrhages. The edema of the face and ankles, the outflow of serum into the body cavities and into the muscles (Barlow) must be regarded as other evidences of the inadequacy of the vessel walls. The tendency of children with exudative diathesis to develop scurvy is perhaps still another manifestation of vascular weakness. This point of view has been strengthened recently by the pathological studies of Aschoff and Koch, who regard scurvy as a nutritional disorder in which there is a lack of some colloidal substance needed for the normal structure of the vessels.
When one makes a subcutaneous puncture in infants suffering from scurvy, a small hemorrhage very often develops at the site of the puncture wound. This is not the case when one makes a hypodermic puncture in a normal person or in a hemophiliac, although it does occur in cases of purpura. This “stick test” is not a constant sign of scurvy, but, like the capillary resistance test, was found in many cases and disappeared with the subsidence of the disorder. It shows that the cells of the skin and subcutaneous tissues are affected, and possibly that their thromboplastic power is diminished.
Nutrition and Growth.—The general nutrition suffers in scurvy as the disease progresses. It is a mistake, however, to picture the scorbutic individual, either adult or infant, as in a state of malnutrition. Not infrequently he appears well nourished, an appearance which is heightened by the slight edema of the face. Infants generally for a period of weeks or months preceding the onset maintain a stationary weight. This may be the only sign of the scorbutic condition. For example:
An infant seen in 1915 gained about one-half a pound during the months of February, March, April and May. At this time it was somewhat over 9 months of age and had never received raw milk or other antiscorbutic food. In June it was given orange-peel juice, and gained 2 pounds within a month. There were no other scorbutic signs or symptoms, and no loss of appetite during the months of February and March, although the baby was suffering from a progressive scurvy.
The growth impulse of the body throughout an attack of scurvy remains unimpaired, being merely in an inactive or quiescent state. Fig. 14 shows this very well, demonstrating that when an antiscorbutic food is added to the dietary the gain may be abnormally great—there may be supergrowth. Generally such marked increases are due to an increase in the consumption of food, following the stimulation of the appetite. However, decided gain in weight may follow the giving of orange juice or other antiscorbutic despite the fact that the intake of food is maintained at the same level.
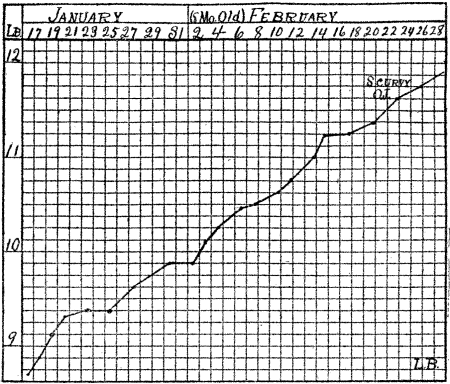 Fig. 24.—Development of scurvy in spite of normal gain in weight in a baby who had been
underfed since birth.
Fig. 24.—Development of scurvy in spite of normal gain in weight in a baby who had been
underfed since birth.
Although it may be stated as a principle that the development of scurvy is accompanied by a failure to gain in weight, there are exceptions to this rule. Under certain conditions the weight may follow a perfectly normal course during the entire period. Fig. 24 illustrates this clinical paradox:
A baby was seen in January, when it was 7½ months of age. Toward the end of February, in spite of constant and normal gain in weight, he manifested unmistakable signs of scurvy—peridental hemorrhage over the upper incisor teeth, which were erupting, and tenderness of the lower ends of the femora. The scorbutic nature of these signs were substantiated by their prompt subsidence on the administration of orange juice. We explain the phenomenon as follows: This baby had been starved in a two-fold sense throughout the first months of its life—it had received a diet lacking in caloric value as well as deficient in antiscorbutic vitamine. Its growth impulse had been held in abeyance for months by both of these factors. When sufficient calories were supplied in the dietary, growth was no longer repressed, and a steady gain resulted in spite of the continued inadequacy of the antiscorbutic factor.
It has been shown that during the period of infancy undernourishment must be extreme to occasion stunting of growth in length. In animals Aron demonstrated that lack of nutrition led to a decrease of the fat and of the muscle of the body, but that the skeleton nevertheless continued to grow, and the ash content of the body to increase. In marasmus, or infantile atrophy, the baby usually grows in length, although its weight remains stationary or decreases. In scurvy we have shown that there is frequently a definite retardation of growth in length, an observation which has been recently confirmed by Epstein in babies which developed this disorder in the foundling asylum of Prague during the war. This fact shows how profoundly the metabolism must be disturbed by this disorder. Figure 25 portrays this retardation in growth and the sharp reaction when orange juice was added to the dietary. It also demonstrates that the growth impulse remains unimpaired and capable of quick response when the essential food factor is furnished.
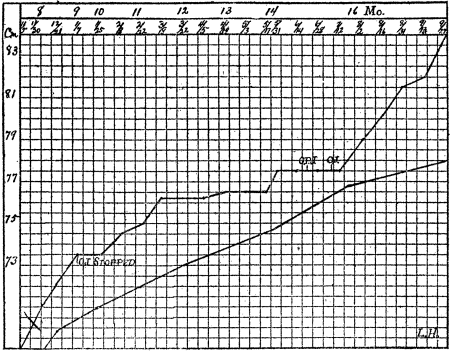 Fig. 25.—Showing retardation of growth in length during the period when no orange juice
was given and supergrowth when it was given once more, O. J.=orange juice. O. P. J.=
orange-peel juice. Lower curve represents the normal.
Fig. 25.—Showing retardation of growth in length during the period when no orange juice
was given and supergrowth when it was given once more, O. J.=orange juice. O. P. J.=
orange-peel juice. Lower curve represents the normal.
Fever.—Fever frequently accompanies scurvy. It is generally of a low grade, ranging between 100° and 101°, as may be seen in Fig. 15. There is a difference of opinion as to whether the rise of temperature should be considered as truly scorbutic in nature, as “scorbutic fever,” or regarded merely as a condition grafted upon the nutritional disturbance. A phenomenon which might seem to argue for its essential scorbutic character is the sharp subsidence on giving antiscorbutic food. On the other hand, this may quite as well be interpreted as due to a secondary reaction, checking the absorption of toxins or bacteria. High temperatures—for example, fever of 103° or over—are attributable to a complicating infection and should lead to careful examination for the source of the trouble; pyelitis should particularly be borne in mind. In a recent case fever of uncertain origin disappeared following the transfusion of blood.
We have already considered numerous complications of scurvy, and shall therefore not go over this ground again. Many of them are due to hemorrhages or to serous effusions in various parts of the body. Another large group in adults as well as in infants are the result of infection. The respiratory tract is particularly susceptible, pneumonia constituting the most common cause of death. In infants we meet with frequent attacks of “grippe,” widespread occurrence of nasal diphtheria, furunculosis and torpid ulcers of the skin, pyelitis, otitis, adenitis, etc. We have encountered nasal diphtheria—with typical bloody mucous discharge—so frequently in connection with scurvy, that where this local infection occurs among a group of infants they should be carefully examined for latent or mild scurvy. Aschoff and Koch recently have laid emphasis on the frequency with which diphtheria complicated scurvy among adults (soldiers). Dysentery is another complication resulting from an invasion of bacteria. Local infections occur more often in adults than in infants—cervical adenitis following gingival pyorrhœa, “bubo” of the groin following infection of the lower extremity, abscess of the calf of the leg following hemorrhage into this region.
Scurvy sometimes occurs in epidemic form, especially in the army, but also, as in Russia, among the civilian population. This results when a large group of individuals have been maintained on a limited and inadequate ration, and especially where this nutritional condition is complicated by intercurrent infection. It should not be interpreted as evidence of the bacterial origin of scurvy. A few years ago the author reported an epidemic of scurvy in connection with an outbreak of grippe in an infant asylum. Twelve infants in one ward were affected. The signs were atypical—an undue degree of hemorrhage occurring at atypical sites (Table 5). It will be noted from the table that the ages of the infants, the distribution of the hemorrhages, the development of signs (in some instances) in spite of antiscorbutic treatment, the sharply defined epidemic character, distinguish these cases from the scurvy commonly seen. This is an instance where latent scurvy was prematurely changed to acute scurvy by an intercurrent ward infection; an epidemic of grippe precipitated a pseudo-epidemic of scurvy. It is important, especially for army surgeons, to bear in mind that where latent scurvy exists a bacterial invasion will lend the disorder a hemorrhagic character. This has been noted during the recent war in connection with typhus fever on the Eastern front, and was remarked upon during the Crimean War and our War of the Rebellion. Some years ago Wherry made a similar observation in the course of experiments with the plague bacillus—guinea-pigs fed on a cereal diet developed far more hemorrhages subsequent to infection than those which received cabbage in addition.
| Case | Age, Mos | Weight | Site of Hemorrhages | Date | Diet | Remarks |
|---|---|---|---|---|---|---|
| lbs. oz. | ||||||
| 1. J. H. | 6½ | 9 6 | Humerus, tibia, face. | Apr. 19 | Breast milk (1 week); pasteurized milk previously. | Grippe since end of February; nephritis; v. Pirquet negative. |
| 10 4 | Upper eyelid | May 9 | ||||
| 2. L. S. | 5 | 12 14 | External ear, parietal bones, vertebral column, abdominal wall | May 4 | Pasteurized milk formula; orange juice 1 oz. daily since April 22. | Twitchings and convulsions; signs of intoxication; red blood cells in urine fever to 101° F.; v. Pirquet negative. |
| 3. A. R. | 10 | 12 8 | Femur | Apr. 19 | Pasteurized milk formula; vegetables for a month; orange juice longer; getting orange juice and vegetables. | Grippe end of January; again in April; fever until April 17; v. Pirquet positive; gums negative. |
| Femur again swollen and tender. | June 4 | |||||
| 4. D. E. | 5 | 7 | Both ears; parietal bones. | Apr. 29 | Breast milk since April 19; May 30, changed to pasteurized milk. | Grippe throughout March; intoxication; nephritis; no relapse although no orange juice given. |
| 5. T. K. | 10 | 15 13 | Ear and face | Apr. 27 | Pasteurized milk, cereal, vegetable, soup; orange juice since April 15. | Two teeth; gums negative; v. Pirquet negative. |
| 6. P. G. | 4 | 8 4 | Tibia | May 8 | Pasteurized milk formula. | Grippe end of February and first half of March gained 20 oz. during last month; v. Pirquet negative. |
| 7. I. P. | 2 | 6 4 | Abdomen | Mar. 7 | Breast milk for past week; pasteurized milk previously. | Grippe; probable source of epidemic. |
A correct and early diagnosis of scurvy is the more important in view of the fact that we possess a specific remedy, and that the disorder is not self-limited. Recognition generally presents little difficulties for those who have seen cases, but is a stumbling block where the symptomatology has been gleaned merely from the textbooks. It has been our experience that medical students who were conversant with scurvy from a theoretical standpoint failed to diagnose a case presented to them in the clinic. Where diagnosis is uncertain, the most important aid is an exact knowledge of the previous diet, and observation of the reaction of the patient to antiscorbutic treatment. These diagnostic points should be constantly remembered in relation to the discussion which follows, and will not be reiterated in the differentiation of scurvy from the various other diseases.
The scurvy of adults and of infants are very similar. The main difference is the subjective symptoms in the adult—pains in various parts of the body—and the fact that the gums are frequently the site of infection and ulceration, as well as of hemorrhage. It might be thought that when scurvy occurs in epidemic form it would be readily recognized, but experience shows that for months it may permeate the ranks of troops or the inmates of almshouses, and pass as rheumatism. This is the cardinal diagnostic error in adult as well as in infantile scurvy—time and again, and in spite of urgent and repeated warnings, patients continue to be treated for rheumatism. Holt writes: “In fully four-fifths of the cases which have come to my own notice this (rheumatism) has been the previous diagnosis.” Such has been our experience. The diagnosis should not be difficult. In sporadic cases, the individual has limited his diet usually on account of indigestion, or diarrhœa, or following some dietetic whim or medical advice given months previously. Where scurvy occurs en masse it may follow an inability to obtain fresh food—as during war, on shipboard, in the Tropics or in the Arctic regions—or be the result of a misplaced reliance on some article of food—for example, dehydrated vegetables. More careful investigation will disclose that the “rheumatic” pains and tenderness are not in the joints but in the muscles and tendons. The calf muscles are frequently painful and excessively tender and somewhat swollen or infiltrated; the hamstring tendons or the tendo Achilles may be sore and slightly swollen and the site of slight subcutaneous hemorrhages. In some cases there is bone tenderness, pain on percussion of the shins or of the sternum. These signs may be accompanied by, or even precede, hemorrhages in the gums. The diagnosis of rheumatism in infants indicates a lack of knowledge of pediatrics, as this disease is hardly ever encountered in babies under a year and a half of age.
It is not always easy to differentiate scurvy from purpura. In either disease the gums may be hemorrhagic and swollen, there may be scattered subcutaneous hemorrhages and pains in the limbs. Occasionally, as in a case seen a few years ago, we may be forced to resort to the dietetic test. A close inquiry into the previous diet, however, a history of previous attacks of purpura, the number, and especially the large size, of the subcutaneous hemorrhages, and above all, the diminished number of blood-platelets, should make diagnosis possible. In scurvy the platelets are almost always over 300,000 per cubic millimetre, whereas in purpura they are reduced to less than 200,000.
In the army it may be difficult to distinguish scurvy from beriberi, especially if they occur side by side as in the recent English campaign in Mesopotamia. There may be a combination of the two diseases, a picture similar to ship-beriberi, regarded by Nocht as a hybrid of these diseases. The diagnosis is rendered more difficult, as at times scurvy is associated with signs of neuritis. We shall have to depend on the involvement of the gums and the hemorrhages in scurvy, and on the hyperæsthesia, paræsthesia, and anæsthesia in beriberi; marked edema points to the latter disease.
We have thus far had in mind frank and outspoken cases of scurvy. When we come to consider latent or early cases, the diagnosis is more difficult and may have to be merely tentative. All that need be added, in view of the clinical picture sketched above, is that this condition should not be forgotten in treating adults who have malaise and indefinite “rheumatic” pains and, more particularly, in relation to infants who fail to gain, whose appetite is capricious, whose disposition has become fretful and who have developed the sallow scorbutic complexion. This warning is particularly opportune at present in the United States, where pasteurized milk is fed so extensively to infants, and an antiscorbutic food is not always given.
In addition to the symptoms just enumerated, tenderness of the bones, especially of the distal ends of the femora, should be sought for, the urine should be examined carefully for red blood-cells, and perhaps the ends of the long bones radiographed for “the white line” of Fraenkel.
The experience of Comby with infantile scurvy is illuminating. Among the fifty-five cases which he has seen, the diagnosis was erroneous in forty-five, and among thirteen cases recently met with, the physician failed to recognize the disorder in all but two. The infants had been given sodium salicylate, had been treated with electricity and massage for the supposed acute poliomyelitis, or given mercury for syphilis, or incisions or trephining had been carried out for acute osteomyelitis. Some had been put into plaster casts for coxalgia or for Potts’ disease. This experience requires little comment. It should be added, however, that in the course of an epidemic of poliomyelitis, such mistakes are apt to happen, and, to our knowledge, did occur in the recent epidemic.
In regard to “the pseudo-paralysis” of congenital syphilis diagnosed as scurvy, it should be remembered that this lesion occurs almost always before the fifth month of life. A history of previous papular eruption, the bilateral enlargement of the epitrochlear glands, and the Wassermann test should suffice to establish the correct diagnosis.
Besides the clinical conditions enumerated above, we may add the following, which have been confused with scurvy: Neuritis, hemorrhagic nephritis, calculus of the urinary tract, renal tumor, orbital tumor, appendicitis, peritonitis, pleurisy and pneumonia. Holt writes as follows: “I have known two cases to be operated upon by eminent surgeons, once with a diagnosis of sarcoma and once of ostitis of both tibiæ. Not until the subperiosteal hemorrhages and epiphyseal separations were discovered was the nature of the trouble suspected.” Recently we saw a case of fracture of the distal end of the femur diagnosed as infantile scurvy; the baby had caught its thigh between the bars of the crib and snapped the bone in trying to extricate itself. Finkelstein adds acute endocarditis, hemorrhagic septicæmia with multiple bone swellings, and leukæmia as having been confused with scurvy.
In an interesting account of scurvy in the Russian army during the recent war, Hoerschelman states that tired soldiers at times feign scurvy. They produce a “pseudo-scurvy” by means of scratching the gums with their nails or rubbing them with tobacco, and at the same time bring about hemorrhages of the skin by means of trauma.
Scurvy in the breast-fed infant has been fully considered under etiology. We wish merely to state again that one cannot be too cautious in venturing this diagnosis in a nursing baby. The great majority of reported cases are not scurvy, but bacterial infections, syphilis, or various forms of intoxication. In establishing a diagnosis the same principles hold as in the case of bottle-fed infants.
The most important consideration in the diagnosis of scurvy is to keep in mind the heterogeneous character of its symptoms, and the manifold diseases with which it may be confused. Surgeons should be alert to this danger when about to perform operations for osteomyelitis or bone tumor. The mistakes occur because cases are infrequently seen and because the signs, being dependent largely upon hemorrhage, occur in such varied locations of the body. Where diagnosis cannot be made from the signs or symptoms, the most important aid is a thorough acquaintance with the previous diet of the individual and observation of his reaction to antiscorbutic treatment.
The outcome of scurvy, as we encounter it in peace time in the Temperate Zone, is generally favorable, so that it plays but an insignificant rôle in our mortality statistics. This results from the fact that we are abundantly provided with a specific remedy, so that if the diagnosis is made early and treatment is prompt and thorough, the patient will rapidly recover and suffer no physical disability. Where antiscorbutic foodstuffs are not procurable, however, this disease constitutes a terrible scourge, causing many deaths and spreading among an army, a ship’s crew, or among the civil population with the rapidity of an epidemic. For example, the ships of the East India Company in their voyages round the Cape often lost nearly one-half of their crews, and in Lord Anson’s famous voyage round the world 380 out of 510 seamen perished from the disease. Moreover, if the antiscorbutic treatment is inadequate or the patient goes untreated for a long period, the cure may be incomplete, a condition of malnutrition and weakness developing, which may persist for years. To appreciate this clinical condition we must refer to the account of physicians who saw thousands of cases of severe and untreated scurvy among the sailors, who were of necessity deprived of aid until they reached land. Lind laid stress on a type of this disease which developed under these circumstances and which he termed “obstinate scurvy.” He writes: “I have met with numerous instances not only among the common seamen, but of officers, with whom it had taken such deep root in the constitution as to prove a lasting affliction to them during a great part of their lives. . . . Persons are likewise subject in different periods of their life afterwards to habitual rheumatism, pains and stiffness in their joints; and sometimes eruptions on the skin.” In his treatise on scurvy, published in 1685, Harvey refers to this chronic nutritional disorder as “inveterate scurvy.” He pictures patients who had gone untreated for a long time as “molested with vagrant, ambulative, distending, creeping, vellicating or lancinating pains of several parts of the body. . . . They are often loose and subject to falling into violent fluxes of the belly, diarrhœa and lienteries.”
Infants as well as adults usually recover rapidly and completely from scurvy, the result depending largely upon the early recognition of the disease. We must always bear in mind, however, that from a histologic standpoint the cure is not simultaneous with the magic disappearance of the clinical symptoms, but that months probably elapse before the tissues return to their normal state. It is difficult to give reliable mortality statistics for infantile scurvy, for so many cases are of the rudimentary form that percentages are necessarily misleading. Still writes that in 5 out of 64 cases the disease proved fatal by diarrhœa and exhaustion. The American Pediatric Society reports 29 deaths out of 397 cases, which gives a similar mortality percentage. When infantile scurvy was not so generally recognized by physicians the mortality was much higher, and we find that Barlow encountered 7 deaths in his first series of 31 cases.
Even when the child recovers it may not regain its normal health if it has continued for a prolonged period in a state of chronic scurvy. It may remain pale and fail to gain in weight in spite of a liberal and well-balanced diet. Cases of this kind are not infrequent. In this connection it is worthy of note that 4 of the 41 cases of “cœliac disease,” an interesting intestinal condition described by Still, had scurvy just before or during the onset of the disease. This observation conforms to the experience that chronic bowel disorders often follow in the wake of adult scurvy.
In adults the heart may be weakened by scurvy, and death may result from cardiac failure. Cardiac disturbances occur also in infantile scurvy. This involvement might be expected, in view of the tachycardia (cardiorespiratory phenomenon) which is so frequent a symptom of infantile scurvy. The heart may be rapid for months or even for years after the disorder, and tachycardia may develop on the occasion of even a mild infectious disease. For example, a fever of 101°, due to a common coryza, may cause the heart-beat to rise to perhaps 180 a minute. Children so affected succumb readily to infection, especially to pneumonia, which may lead to sudden collapse followed by death.
An important factor in the prognosis of scurvy, as in that of other disorders due to a lack of vitamines, is the marked susceptibility to infection. Even latent or subacute scurvy causes a peculiar susceptibility to diphtheria (especially the nasal type), to coryza, bronchitis, and pneumonia. A perusal of the literature shows that this susceptibility was noted by the older authors in relation to adults.
The local signs usually disappear quickly without leaving any trace. The hemorrhages are absorbed and the eczema heals within a few days. The fractures unite promptly with the formation of an unusually large callus. The urine, which may have contained red blood-cells or have been markedly hemorrhagic, quickly becomes normal and, in our experience, gives no further evidence of renal damage. Still reports, however, the case of a frail child who had a trace of albumen in the urine two years after an attack of scurvy. A rare local injury, which may lead to death, is cerebral hemorrhage. Recently Sammis reported a case of this kind, which was characterized by convulsions during life, and in which subdural hemorrhage was found at necropsy.
If we acknowledge an individual idiosyncrasy to scurvy we should expect a tendency to a recurrence of the disease. Lind was of this opinion, stating that “by observations made on this disease, it appears that those who are once afflicted with it, especially in so high a degree as that squadron was, are more subject to it afterwards than others.” It is difficult at the present day to express a personal opinion on this matter, as clinical experience is meagre and the scurvy of guinea-pigs is so acute that it cannot be used for comparison. Some of the recurrences have been due probably to the fact that the patient had not been completely cured of his first attack. We have met with two cases of recurrences in infants, one of which is of particular interest as it happened in spite of giving lemon juice in the intervening period. The history was as follows:
In September, 1914, one month after the baby was admitted to the institution, it developed scurvy of a moderate grade. It was then six months of age and weighed 10¼ pounds. It was put on a simple mixture containing from 24 to 30 ounces of pasteurized milk and was given in addition ½ ounce of lemon juice a day. It improved, but during the winter had bronchitis, otitis, enteritis, and later furunculosis. In spite of the fact that it had been receiving an antiscorbutic for almost this entire period, it developed scurvy once more in February, at the age of 11 months, and when it weighed 14½ pounds. It was evident that this baby was peculiarly susceptible to scurvy. It may be added that the second attack was complicated by nasal diphtheria.
In this connection attention should be drawn to a peculiar and puzzling clinical phenomenon, which we have noted several times. Even if the antiscorbutic treatment is carried out incompletely and only for a short period, recrudescences may not take place. We have seen cases where orange juice was given for merely ten days or two weeks—that is, only until all scorbutic signs had disappeared,—and yet the scurvy did not return, the infants thrived for months thereafter, but were merely somewhat pale and undernourished. In the case of two babies which we have in mind, the diet remained absolutely unchanged, with the exception of the short period of antiscorbutic treatment, but this seemed sufficient to bring about a diminished susceptibility.
“Seek the cure of scurvy neither in the armamentarium of the physician nor in the apothecary shops. The druggist will be of as little aid to you as the art of the surgeon. On the other hand, employ fresh vegetables, the juice of fresh antiscorbutic plants, oranges and lemons or the juice of those fruits preserved with sugar; in this way without other means you will be able to overcome this terrible disease.” This reads like the advice of some modern therapeutist; it is, however, the conclusion of a physician (Kramer) who wrote on scurvy almost two hundred years ago, and shows that the treatment of scurvy has undergone no fundamental change in the intervening years. Our resources, however, have been amplified by an increased knowledge of the relative value of antiscorbutic foodstuffs and by the introduction of some new ones.
Prevention.—In the Temperate Zone, under ordinary conditions, the adult population consumes sufficient antiscorbutic foodstuff to protect it from scurvy. Under exceptional circumstances, however—for example, when the potato crop fails, or, in the case of individuals, when the diet has been unduly restricted, scurvy will be encountered. This disorder is still an important problem, however, in relation to the health of adults in the Tropics, in military expeditions and in Polar explorations. From what has been stated in the preceding chapter, it is evident that, at the present time, no reliance can be placed on dehydrated vegetables as a protective agent. The recent suggestion of using germinated dried pulses and seeds, under circumstances where fresh food is not available, is practical and probably will be resorted to in the future. To this end the pulses (beans, peas, lentils) are soaked in water for 24 hours, and then kept moist with access of air for about 48 hours at room temperature. During this period they sprout and develop small radicles. They are cooked in the usual way and have been found to possess an antiscorbutic value comparable to that of most vegetables. An individual should receive about four ounces a day of these sprouted seeds. In the treatment of some Serbian soldiers suffering from scurvy, Wiltshire found that this amount of germinated beans brought about a cure. There are, however, two drawbacks to their general use. The prolonged cooking necessary for their preparation reduces their antiscorbutic potency, and they have been found indigestible when consumed in sufficient quantity.
Under similar conditions canned tomatoes can be employed; they have the disadvantage of greater bulk, but are a more potent antiscorbutic, require no preparation whatsoever, and are readily digested. They form part of the present ration of the United States Army, in which they can be given “in lieu of an equal quantity of potatoes not exceeding twenty per cent. of the total issue.”50 The necessity of including an antiscorbutic in the army ration has been recognized only in recent years; during our Civil War and for thirty years thereafter there was no such provision. It was stated at that time that a general scorbutic taint pervaded the troops—a mere euphemism for the widespread existence of subacute or latent scurvy. Even to-day the ration of the French and of the Italian armies makes no definite provision in this regard and the Russians provide merely for a variable quantity of vegetables.
Recently it has been shown that lemon and orange juices (Givens and McClugage) can be dried and still preserve their antiscorbutic value. It is quite possible that concentrated preparations of this kind will be serviceable for army use and in regions where fresh fruit or vegetables cannot be obtained.51
Lind makes numerous ingenious suggestions for preparing antiscorbutic remedies (Lind, pp. 7, 8 and 9) which have a practical as well as historic interest. (Appendix 1.) One of these includes a formula for the preparation of orange and lemon juice which may be preserved for years; another gives a method for the preservation of berries and other fruits which are to be picked when partly ripe and put up in earthen pots; still another gives the recipe for preparing a simple decoction of fir tops, which was found by the Swedes efficacious in preventing the development of scurvy among their soldiers. It is interesting that a similar practice was resorted to in Vienna during the recent war and recommended as a prophylactic for scurvy in children (Tobler).
The prevention of infantile scurvy, especially in its rudimentary form, is of great practical importance, because of its frequent occurrence. There is no question but that breast milk and raw cow’s milk furnish sufficient antiscorbutic vitamine, but there is a difference of opinion as to whether pasteurized milk, or milk that has been brought just to the boiling-point, or even sterilized milk, is adequate in this respect. Much of this divergence of opinion is due to the fact that the various clinicians have not considered or stated the quantity of milk which they have found sufficient to protect, and also because milk itself differs in its antiscorbutic value according to its freshness and probably also according to the fodder of the cows.52 Without entering once more into a discussion of this question, it may be stated that unless the cow’s milk is raw, the infant should receive additional antiscorbutic foodstuff. Moreover, this supplement to the dietary should be made as soon as possible, so as not to allow the vitamine deficiency and inadequate diet to exist for even a short period. In our experience there is no contra-indication to the giving of orange juice or of strained canned tomato, the two antiscorbutics with which we have had a large experience, to babies one month of age or even younger. The common practice, however, is to wait until the infant is five or six months of age, which certainly must allow a rudimentary scorbutic condition to develop. At the age of a month one teaspoonful of orange juice may be given; it should be diluted with water and sugar added if it is tart. This may be administered notwithstanding the fact that a baby has a tendency to looseness of the bowels, as orange juice, as recently pointed out by Gerstenberger, has practically no laxative action. Occasionally babies regurgitate orange juice, but the reaction usually ceases after a day or two. If it does not, a small amount of an alkali—for example, limewater or sodium bicarbonate—may be added just previous to feeding; in this state the juice will be better tolerated.53 The amount of orange juice should be increased so that when the baby is three months of age it receives one tablespoonful.
A few years ago Hess and Fish recommended the use of an infusion of orange peel in infant feeding. The peel was finely grated, soaked overnight in water (1 ounce of the peel to 2 ounces of water), and a small amount of sugar added to this liquid. Animal experiments showed that this preparation possessed decided antiscorbutic value. This decoction may well be used for the sake of economy, and even when the orange juice is employed the infusion of the peel may be added.
An antiscorbutic which vies with orange or with lemon juice in adaptability for infant feeding is canned tomatoes, as recently suggested by Hess and Unger. Tomatoes are not in good repute among food experts in view of the small amount of calories which they contain—only about 100 to the pound—and are regarded with suspicion amounting almost to superstition by mothers and nurses as a food for children. In spite of this fact, it may be stated without hesitation that they are fully as well borne by infants a few weeks or months of age as orange or lemon juice. In considering antiscorbutics, it has been shown that notwithstanding the canning process and subsequent aging, they preserve their potency. The dose is two tablespoonfuls for babies over three months of age. The tomatoes are merely strained through a colander and warmed (not cooked). To illustrate their innocuous character, it may be added that as much as 6 and 8 ounces a day of this juice have been given to a baby under one year of age without producing untoward symptoms. This antiscorbutic should have wide applicability, especially in the United States.54
Another antiscorbutic which can be used in a routine way to prevent infantile scurvy is swede juice, prepared by grating the raw vegetable and squeezing the pulp in muslin. Chick and Rhodes report that this juice has been adopted for use in some of the English infant-welfare centres. It should be given in about the same dosage as the tomatoes, and seems applicable where the swede can be readily obtained.
For babies over six months of age, reliance may be placed on the ordinary household vegetables—potatoes, spinach, carrots, squash, etc. Attention should be paid to the amount which is taken, as one or two teaspoonfuls of a vegetable which is poor in antiscorbutic power, such as carrots or beets, will be insufficient to protect against scurvy. Especially is this true if the vegetables are old and stale and are cooked for a long period;55 some years ago two infants under our care developed scurvy in spite of a small daily ration of vegetables.
Potato in the amounts usually consumed is a valuable antiscorbutic. It is not an exaggeration to state that it is the main antiscorbutic bulwark of man. In giving baked potato to children it is commonly advised to use the floury part just beneath the peel; this should be put through a sieve and mixed thoroughly with boiled milk so as to constitute a cream; for younger babies it can be prepared with water to form a diluent similar to the barley water so commonly employed to dilute cow’s milk (1 tablespoonful of potato to a pint of milk, cooked for 15 minutes). Little reliance should be placed on beef juice in the usual dosage and none on eggs.
Cure.—There is almost nothing in the realm of therapy which is so striking as a scorbutic patient’s prompt reaction to antiscorbutic treatment. It is all the more marvelous as the cure is effected by means of foodstuffs with which we are accustomed to associate no specific virtue. A magic result is seen frequently within 24 or 48 hours. A baby which has had a poor appetite, has been irritable and exquisitely tender, suddenly regains its appetite, is no longer fretful, and can be handled without occasioning crying. Within a week, if the case is mild, all definite symptoms of scurvy may have disappeared, and soon thereafter the infant is thriving and apparently cured. A table is here reproduced (Table 6) from the report of the American Pediatric Society showing the duration of treatment before marked improvement was noticed:
| Days | Cases | Weeks | Cases | Months | Cases |
|---|---|---|---|---|---|
| 1 | 19 | 1 | 47 | 1 | 6 |
| 2 | 58 | 2 | 27 | 2 | 4 |
| 3 | 46 | 3 | 8 | 3 | 4 |
| 4 | 26 | 4 | 1 | ||
| 5 | 19 | 5 | 1 | ||
| 6 | 1 | 6 | 1 | ||
| 7 | 2 | ||||
| 8 | 2 | ||||
| 9 | 1 | ||||
| 10 | 7 | ||||
| 12 | 2 |
In most instances a gain of weight accompanies improvement. In not a few instances, however, there is a temporary loss or cessation of weight, due in part to an increased excretion of urine. Occasionally there is observed a short exacerbation of the symptoms following the giving of an antiscorbutic—a swelling of the thigh or hemorrhage of the gums. A similar phenomenon has been noted in relation to the treatment of polyneuritis in birds and of beriberi in man.
In the cure of scurvy the same dietetic remedies are employed as in its prevention. Orange juice is the sovereign remedy, and should be given in a dosage of about 2 ounces a day.56 Canned tomato is also most efficacious. If these changes in the dietary are carried out, it is not absolutely necessary to alter the food, although it is advisable to do so. Some writers, for example Neumann and Czerny, treat the disorder by giving milk which has been scalded or brought to the boiling-point. Others lay particular stress on changing the source of the milk supply, believing that the sameness of the diet leads to the occurrence of scurvy. Such, however, cannot be the case, as otherwise breast-fed babies would be highly subject to this disease. In the report of the American Pediatric Society one case developed on condensed milk and was cured by sterilized milk, and another developed on pasteurized milk and was cured by sterilized milk and broths. These results are explicable; large amounts of milk were given to effect the cure. It may be said in general that in addition to giving fruit or vegetable juices the milk should be either raw or heated to as low a degree as possible (duration of heating as well as height of temperature). Furthermore, the antiscorbutic treatment should be continued for a period of months, as the clinical improvement far outstrips the restoration of the bones and other tissues. It seems necessary again to call attention to the fact that too great reliance has been placed on the use of beef juice, which has been shown, both in experiment and in the clinic, to possess comparatively weak antiscorbutic properties.
Orange juice may be given intravenously. This method may be resorted to where the patient is in an advanced stage of the disease or where food cannot be tolerated by mouth; for example, in cases such as that mentioned by Cheadle, where death took place owing to the fact that the antiscorbutic could be taken only sparingly, on account of the extreme prostration of the patient. For this purpose the orange juice is obtained in as sterile a manner as possible, boiled for about five minutes and is rendered neutral or slightly alkaline just previous to its injection by the addition of normal sodium hydroxide. Hess and Unger report three cases where this procedure was carried out without the slightest untoward reaction. In one instance, improvement was noted 16 hours after the injection. In view of the novelty of this treatment it may be of interest to cite a case:
A baby 16 months old had hemorrhage of the gums and tenderness of the legs, which were held in the characteristic flexed and everted position. Eliminative treatment was tried without avail; Dover’s powder and warmth to promote perspiration; caffeine to promote diuresis; and 2 tablespoonfuls of liquid petrolatum three times a day to increase elimination from the bowels. Intravenous injections of salt solution also proved of no value.
Four intravenous injections of orange juice were given—6 c.c., 12 c.c., 6 c.c., and 35 c.c. As was stated, improvement was noted 16 hours after the first injection. The infant was less irritable, the gums no longer hemorrhagic, and the “capillary resistance test” (that is to say, the development of petechial spots on the forearm when a tourniquet was applied for 3 minutes to the upper arm) changed from positive to negative.
Harden, Zilva and Still have recommended the use of a concentrated lemon juice for the cure of scurvy, constituting a form of “intensive” treatment. In four cases this proved to be of clinical value. Freise has made use of an alcoholic extract of turnips, and Freudenberg of a similar extract of carrots. These preparations did not seem to be markedly potent, and therefore possess no particular therapeutic advantages.
Non-dietetic Therapy.—There is little to be done for the patient in addition to the giving of sufficient antiscorbutic. No one has reported success with any drug. We have tried the use of atropin, adrenalin, thyroid and parathyroid extracts, cod liver oil, autolyzed yeast, lactose, sodium chloride, calcium chloride, etc., without noting any improvement. Mercurials are stated to be positively harmful, especially when ulcers are present. The patient should be kept in bed, and exertion not allowed on account of the involvement of the heart, which has led to sudden collapse and death. The gums may be treated with nitrate of silver stick or tincture of myrrh. If there is fracture of the long bones with displacement, splints should be applied. Under no circumstances should hemorrhagic effusions in or about the joints be incised. The patient should be placed in a room which is well aired and lighted, and should be handled and dressed as infrequently as possible, so as to avoid discomfort and pain. It is particularly important that intercurrent infections should be avoided by shielding patients from contact with those who have infectious diseases, especially respiratory infections.
Studies of the chemical exchanges in scurvy have been surprisingly few. It is a field that should repay investigation, promising to afford a clearer insight into the intermediary metabolism in this disorder. One of the first to touch upon this question was Garrod, who in 1848 reported that there was a diminution of potassium salts in the urine and in the blood of scurvy patients. In 1877 Ralfe confirmed the potassium deficiency in the urine, but denied its importance from an etiologic standpoint, as he was unable to benefit scurvy patients by administering potassium nitrate. He reported an increase of uric acid in the urine, a diminution of the total acidity, and a reduction of the alkaline phosphates. Litten found the analyses of the urine very contradictory in respect to potassium, but stated that beyond a doubt its uric acid content is increased at the height of the disease, although this diminishes rapidly with convalescence. These few and scattered articles comprise the sum of metabolic studies up to the last decade, and even during the succeeding period they have been very few—so few, indeed, that they furnish insufficient data from which to draw conclusions.
The first careful study of the mineral metabolism in a case of scurvy is that of Baumann and Howard, published in 1912. Its conclusions are not very definite. They may be summed up by their statement that “chlorin and sodium were retained during the fruit-juice period, but excreted in excess of the intake during the preliminary period,” and that “more potassium, calcium and magnesium were retained during the fruit-juice period.”
This same year Lust and Klocman published the first metabolism study of a case of infantile scurvy. The baby was 18 months old and the metabolic changes were investigated during the active, convalescent, and “the healing stage” of the disorder. This study seems to have been carefully carried out. The fact, however, that the infant received 800 c.c. daily of slightly-boiled milk during the active stage, and was improving at this time, may also have had a beneficial effect on the metabolism in respect to scurvy. The results of these writers are surprising—quite different from what they expected or what we should have expected. They write: “The balance of the mineral metabolism, including the total ash, the calcium, phosphorus and chlorin during the florid stage of the disease must be regarded not only as not damaged, compared to that of the healthy child, but indeed as somewhat increased.” “All the more striking, on the contrary, are the results found during the stage of convalescence. Here the balances were all markedly negative, and only after a lapse of weeks was the tendency manifested to a return to normal conditions.” The authors regard these results as indicating a sort of washing out of “dead material” during convalescence—of material which had gathered during the florid stage of the disease. According to their interpretation the disease is due, not to a primary or secondary salt deficiency, but to a disturbance in salt elimination, and in the first place, of a calcium excretion. This is shown by the fact that even in the “stage of healing,” when the total ash and the phosphorus balance once more had become positive, the calcium balance nevertheless remained somewhat negative. The metabolism of infantile scurvy, they believe, far from showing a resemblance to rickets, manifests quite the contrary tendency. The study of this case of infantile scurvy and that of Baumann and Howard of a case of adult scurvy, comprise the total investigation of the metabolism in human scurvy.
In the course of a recent discussion on rickets before the Medical Society of Vienna, Moll states briefly that in a case of infantile scurvy, at the height of the disease, he found a positive calcium balance, which became poor and later negative on giving fruit juice; in other words, a partial confirmation of the work which has just been cited.
In 1913 Bahrdt and Edelstein reported the analyses of the organs of an infant almost nine months old who died of scurvy; an examination of the tissues, especially of the bones, should be most valuable in checking up determinations of the metabolism during life. This investigation runs absolutely contrary to that of Lust and Klocman. The bones showed a decrease of ash, especially of calcium and of phosphorus, and also a lack of calcium in the muscles, but normal amounts in the liver and in the kidneys. These conditions resemble the deficiency of ash and of lime commonly associated with rickets, and it seems quite possible that this infant had rickets as well as scurvy, and that in this way the discrepancy between the two reports is to be explained. The fact that the water content of the bones was two to three times the normal, also lends emphasis to this interpretation. In any metabolism study of infantile scurvy, great care will have to be exercised that the disorder is not complicated by rickets, and the issue thereby confused. It will be very difficult to avoid this pitfall, for there is no test by which early rickets can be diagnosed. The danger of this complication may be realized when we bear in mind that the majority of infants have rickets to some degree. An investigation of the chemistry of adult scurvy has an advantage from this point of view.
Chemical examination of the blood has yielded such valuable information regarding metabolic diseases, that it might be expected to shed light on the disturbances of scurvy. The only investigation from this standpoint is that of Hess and Killian, who have reported estimations of the urea, creatinine, sugar, CO2 combining power, diastase, cholesterol, chlorine and calcium.57 The urea content was normal, varying between 12 and 14 mg. per 100 c.c. of blood; this is the average of twenty-one tests on ten cases of infantile scurvy. (In severe cases of beriberi Yano and Nemoti have recently reported that the blood contains an increase of urea, and that its excretion is frequently disturbed.) The creatinine was estimated in two cases and was found to be 2.0 mg. and 1.7 mg. per cent., respectively,—also normal figures. The blood sugar varied from 0.12 to 0.14 per cent. and was examined in almost all the cases in which urea was estimated; these figures are at the upper level of normality (no attention was paid to the interval elapsing between the feeding and the withdrawal of the blood). The diastatic activity was likewise normal. The CO2 combining power showed figures under 40 to 45, according to the Van Slyke method, and indicated therefore a mild degree of acidosis. In six cases the chlorides were estimated, the figures being remarkably constant at about 0.42 or 0.43. Cholesterol was a little below normal in the four cases examined. Contradictory results were obtained in regard to calcium. Earlier tests showed a definite deficiency of this salt, but those carried out more recently have generally yielded normal results. Further studies of the blood calcium are highly desirable to ascertain whether it varies in amount in the circulation, and especially in different stages of the disease. This aspect is worthy of particular attention in view of the positive calcium balance noted by Lust and Klocman during the active stage of scurvy, and the negative balance during the period of convalescence.
It is evident from the limited data concerning the blood chemistry of scurvy that it is a field which has been inadequately explored and will repay more intensive study. Investigations of this kind have recently been made possible by the introduction of accurate methods requiring only small quantities of blood.
Studies of the metabolism of animals suffering from scurvy are almost as few as those on man. The work of Morgan and Beger, which is frequently quoted in this connection, is not applicable, as it concerns rabbits, which do not develop scurvy. They found that rabbits fed solely on oats and water suffered in their nutrition (loss of appetite, emaciation, paralysis of hind legs), and could be cured by the addition of sodium bicarbonate to the dietary. In 1916 Lewis and Karr published a paper on the constituents of the blood and the tissues of guinea-pigs fed on an exclusive oat diet. They found the urea content several times greater than normal, but that it fell to normal once more if cabbage or orange juice was given. From the standpoint of scurvy, this investigation is open to the criticism that the diet was too incomplete, and also, as the authors suggest, that the animals suffered from partial starvation and a lack of water.
In the following year Karr and Lewis published a paper on a different phase of this subject, and came to the following conclusions: “No changes in urinary elimination of phenols, nor in the degree of conjugation of the phenols, were observed, provided the factor of partial starvation was ruled out. This is believed to indicate that no increased bacterial action occurs in the intestine of scorbutic guinea-pigs despite the difficulty of evacuation of the fæces.” These results are in harmony with the bacteriological study of Torrey and Hess, who found that there was no increase in the proteolytic flora of the intestine in infants or in guinea-pigs suffering from scurvy.
In 1917 Baumann and Howard published the only metabolism study which has been carried out on guinea-pigs suffering from scurvy, and they are of the opinion that this disorder has a profound effect on the mineral metabolism of this animal. The calcium was excreted in notably large amount; potassium was also lost, and to a greater extent than sodium; the only element which was consistently retained during the active stage as well as during the period of recovery, was magnesium. This study was followed shortly by one from the same laboratory, by Howard and Ingvaldsen, carried out on a monkey suffering from scurvy. It was inconclusive, not conforming to the experiments on the guinea-pigs; the authors state that the “changes in the mineral excretion of the monkey during the scorbutic period were not sufficiently significant to admit of easy interpretation.” “The marked loss of the various mineral substances encountered in experiments with man and guinea-pig was not observed in the present series.” It should be remembered, however, that the diets of the guinea-pigs and the monkeys were quite different, the former consisting mainly of oats, and the latter of condensed milk. It is quite possible that the basic diet may play a rôle in the metabolism of this disease, although, as stated elsewhere, its effect cannot be noted clinically. Special attention should be paid to this factor in metabolic studies, in view of the widely-held opinion that the carbohydrates exert a potent influence in the development of beriberi.
The investigations of the nitrogen metabolism in man and in animals have been most unsatisfactory. The two on human beings—an infant and an adult—were negative; that on guinea-pig scurvy cannot be utilized on account of the restricted diet of oats, which contained insufficient nitrogen, whereas the one on the monkey showed some loss of nitrogen, which led the authors to suggest an increased nitrogenous catabolism in scurvy. This comprises the total data on this subject.
Summarizing the results of these few metabolic studies, it may be stated that they harmonize on one point only—the positive balance of calcium during the active stage of the disease. The investigation of Baumann and Howard on adult scurvy, of Lust and Klocman and of Moll on infantile scurvy, and of Howard and Ingvaldsen on the monkey, are all in agreement in this important conclusion.
In the foregoing there has been frequent reference to the close relationship between scurvy and the incidence of the infectious diseases—to the fact that a scorbutic condition increases the susceptibility to infection. This is indeed one of the most characteristic, as well as one of the most important phenomena associated with scurvy and other disorders resulting from vitamine deficiency. Mention has been made of the special susceptibility to the diphtheria bacillus, and to the organisms leading to coryza and the respiratory diseases, but no doubt this applies also to invasion by other bacteria. We wish, however, to confine ourselves to the nutritional disorders, first in their relationship one to the other, and second, as a group of deficiency diseases, due to a lack of vitamines of various kinds. As is well known, in addition to scurvy, this group generally includes beriberi, a disease attributed to a lack of the water-soluble vitamine, and xerophthalmia, an eye condition which recently has been brought about in rats by placing them on a diet free from fat-soluble vitamine. These, however, form only the nucleus of the disorders which commonly are included in this category. Schaumann, the first to formulate this classification, illustrated his conception of the interrelationship by depicting the various members as spokes of a wheel surrounding a central hub. He included scurvy, rickets, osteomalacia, typical beriberi, ship-beriberi, pellagra and mehlnaerschaden. Funk made a similar classification of disorders which he termed the “avitaminosen.” There is a tendency to enlarge rather than to decrease the membership of this class, and recently war or hunger edema, infantile atrophy and diarrhœa, sprue, cœliac disease, leprosy and others have been proposed as suitable candidates. At the present time it is impossible to determine which and how many of this motley company should be associated with scurvy. Some, possibly, are the result of a lack of vitamine, but for the present it will be well to bear in mind that three vitamines only have stood the test of experiment, and only these three therefore can be definitely connected in a causal relationship with pathologic conditions. In addition to this consideration of the interrelationship of the “deficiency diseases,” the kinship of allied disorders—more particularly of rickets—must be discussed.
Although at first thought beriberi and scurvy would seem far apart from a clinical point of view, they have some important features in common. In both there is a tendency to a rapidity of the heart’s action and a marked lability of the pulse, to an enlargement of the cardiac ventricles, to an involvement of the vagus, and to an exaggeration of the deep reflexes. It is unnecessary to describe these signs and symptoms in detail, as they have been fully considered under symptomatology. It has been recorded from time to time that under certain circumstances scurvy has developed in man where one should have expected beriberi, and vice versa. Darling, who has had a large experience in this field, writes: “A deficient dietary in a tropical African negro mine laborer causes severe scurvy, in a Cape Colony African mine laborer, mild scurvy, and in some African negroes a diet that causes scurvy in one set of men causes neuritis in others.” Possibly some minor differences in the dietary can explain this difference in reaction—for we do not know all the sources of the water-soluble vitamine, but such an experience deserves to be cited as it is not an isolated instance. It is all the more worthy of attention because it harmonizes to a certain extent with the everyday experience of animal investigation. As has been stated elsewhere, a diet of decorticated grain will lead to scurvy in the guinea-pig, to polyneuritis in the pigeon, and to a combination of these diseases in the hog! Results of this kind show that there must be a relationship between the etiologic factors of scurvy and of beriberi. It is unwise at present to attempt to define the relationship more precisely. The remarkable observation, first made by Fuerst, and since confirmed by numerous investigators, that seeds and legumes are devoid of antiscorbutic potency but acquire this power on sprouting, constitutes another link in the evidence of their kinship. Funk has suggested that the antiscorbutic vitamine can be formed from the “antineuritic” vitamine, a theory which is very attractive but needs confirmation and experimental proof. It is quite evident that this change does not usually occur in animals, in view of the specificity of the vitamines for their respective diseases—of the antiscorbutic for scurvy and the water-soluble for beriberi.
It will be noted that “ship-beriberi” is included in this group of diseases. Very little is known about this condition, except what is contained in the investigation of Nocht (1903) and that of Holst and Froelich. It is a very rare condition but of interest because it is characterized by spongy, hemorrhagic gums and other signs encountered in scurvy. The feature which differentiates it sharply from scurvy, however, is an anæsthesia of the extremities. Ship-beriberi is generally regarded as a combination of beriberi and scurvy. Where these two disorders occur concomitantly, the beriberi manifests itself some months before the scurvy, as the latter takes much longer to develop.
In considering the vitamines in connection with diseases of the nervous system, mention may be made of “central neuritis” and the “peripheral neuritis” which has been reported from the West Indies. This bears only a partial resemblance to beriberi, as there is no edema, nor dyspnœa, and its course is more chronic. Judging from the report of Edwards from Jamaica, the cases more closely resemble pellagra, terminating after many years. A degeneration of the cells of the spinal cord was found and “in some isolated patches of the cerebellum and in the roots of the optic and auditory nerves.” The disease occurs among the poor classes whose diet is inadequate chiefly in nitrogen.
Eijkman was the first to draw an analogy between beriberi and pellagra, and thus to suggest that the latter might be a disease due to an unidentified factor; he compared the pernicious effect of a diet of polished rice with that of decorticated corn. Of recent years, largely as the result of the investigations of Goldberger and his co-workers, pellagra has come to be regarded as a dietetic disorder primarily due to a lack of adequate protein, rather than to a lack of a specific vitamine. Its relationship to scurvy cannot, therefore, at the present time, be discussed from an etiologic viewpoint. Apart, however, from the question of etiology, the two diseases have certain clinical symptoms in common. Weston states that “distinguished physicians, who were really astute observers, have mistaken pellagra for scurvy, eczema, various kinds of intestinal troubles, syphilis, and many other diseases.” In the chapter on symptomatology, attention has been directed to the fact that an eczema which yields to antiscorbutic treatment may occur in scurvy; at times it presents the symmetrical arrangement so typical of pellagra. In other cases a fleeting erythema may be observed, another sign noted frequently in pellagrins. In some instances congestion of the gums has been recorded. In describing a little girl of three who had pellagra, Weston writes: “The gums are also red and swollen, suggesting scurvy.” This child had eaten large amounts of turnips, so that there could have been no question of complicating scurvy. Lombroso and some of the earlier authors drew attention to the fact that fragility of the bones, of the ribs and of the long bones, was often associated with pellagra. These various clinical similarities should not be construed as evidence in favor of the “avitamine” nature of pellagra. They indicate, rather, that in nutritional disorders, whatever may be their underlying cause, the vessels, the bones, and other tissues may suffer and lead to similar—but not identical—clinical pictures.58
The relation between scurvy and rickets is a subject which was discussed by Glisson. With the renewed interest in infantile scurvy which followed Barlow’s work toward the end of the last century, children’s specialists ranged themselves into opposing camps on the question of the interrelationship and interdependency of these two diseases. Some accepted Barlow’s dictum that infantile scurvy is an absolutely distinct and separate entity; others, for example, Hirschsprung, declared that the so-called scurvy was merely a form of rickets; whereas a third group considered it a combination of rickets and scurvy. This last viewpoint was actively maintained by Cheadle on the clinical side, and later by Schoedel and Nauwerk on the pathologic side—the latter declaring that rickets is “an inseparable component of infantile scurvy,” and that the entire disease should be regarded merely as “an episode in the course of rickets.” Even Barlow, in a paper published in 1894, wrote: “Rhachitic changes already present may act as a physiological determinant of the sites in which scurvy becomes manifest” and “rickets as a basis plus inadequate food gives the simplest explanation of the typical case” (of scurvy).
We had an exceptional opportunity to test this thesis in 1914, in an institution where scurvy broke out among infants who were on a diet of pasteurized milk. All these infants were receiving cod liver oil daily, as prophylactic treatment against rickets. Many infants have been seen since that time, who in spite of receiving cod liver oil developed scurvy, and others in whom large doses of this oil failed to mitigate the scurvy, although it prevented rickets. The same failure has been encountered in the treatment of scurvy in guinea-pigs. This experience has been without exception, both from a prophylactic and a curative standpoint.
Confusion between the two diseases has resulted from the fact that the majority of infants in the Temperate Zone have some degree of rickets. Thus the two diseases have been found very frequently associated in pathologic examination of the bones, leading some to infer that they are in some way interdependent. They have been also confused clinically, as mentioned in another connection, owing to the fact that beading of the ribs—the rhachitic rosary—has been mistakenly regarded as a pathognomonic sign of rickets, whereas it is also a sign common to scurvy. It is important to bear in mind that from the pathologic viewpoint scurvy and rickets present strikingly dissimilar pictures—the former is characterized by an almost complete cessation of activity of bone-forming elements, whereas the latter is distinguished by a hyperplastic condition leading to a marked overgrowth of cartilage and of abnormal bone. Viewed from the pathologic, etiologic and clinical standpoint, we believe that there is no basis for assuming an interrelationship between the two disorders, and that scurvy will develop as readily and as rapidly where rickets is absent as where it is present.59
It is premature to discuss the relationship of these two disorders from the vitamine standpoint. In 1910 Schaumann suggested that rickets was due to a lack of a specific food factor, and somewhat later Funk included it among the “avitaminosen.” Recently Mellanby, as the result of experiments on dogs, has affirmed that the fault lies in a lack of the fat-soluble or a closely-related vitamine. Investigations of the near future will probably decide the merits of this contention; our experience is that rickets develops in infants even where the diet contains adequate fat-soluble vitamine. If rickets is proved to be a disorder depending on a vitamine, it belongs, naturally, in the same group as scurvy. This would indicate relationship, but not interrelationship. Just as the mere fact that a lack of vitamines leads to scurvy and to beriberi does not signify, in theory or in practice, the existence of pathogenetic interrelationship. However, as stated, this is a subject which does not as yet rest on a secure foundation.
Osteogenesis imperfecta and osteomalacia are disorders of dietetic or metabolic origin characterized by fragility of the bones. The latter has developed new significance and importance due to its increased occurrence in almost epidemic form in the Central Empires at the close of the World War. The etiology of both disorders is most obscure. In the future in considering their pathogenesis it will be well to draw a sharp distinction between them. Osteogenesis imperfecta is a disease in which an injury occurs to the fœtus without any manifest illness in the mother, which seems to indicate a primary lesion of the fœtus (perhaps metabolic); osteomalacia, on the other hand, attacks the mother who gives birth to an apparently healthy fœtus. The latter gains added interest because it is a disease of the bones which is attributed to dysfunction of the endocrine glands, to a disturbance especially of the parathyroid. If this observation is confirmed, it furnishes another anatomical basis for associating the glands of internal secretion with pathologic conditions of the bones.
One cannot survey the various diseases of the bones—scurvy, rickets, osteoporosis, osteogenesis imperfecta, osteomalacia, etc.,—without realizing that this group is at present in a state of great confusion and will have to be rearranged and winnowed. The differentiation between some of these diseases is not in every instance clear morphologically—for instance, early cases of scurvy and osteoporosis—so that it is difficult to consider them satisfactorily from the standpoint of pathogenesis. Clinical differentiation is still more difficult and uncertain. It seems probable that new entities will be established, as has happened in the past. It is not so long since rickets included almost all the bone diseases of infants. Gradually congenital syphilis, scurvy, and achondroplasia were segregated as distinct diseases. Probably a similar separation of other pathologic conditions, now so entangled as to be indistinguishable, will be evolved.
Among the diseases which have been attributed to a vitamine deficiency are “war or hunger edema,” sprue, the “mehlnaerschaden” of infants, and the “exudative diathesis” described by Czerny and Keller. Future investigation will disclose whether any of these disorders belong in the group with scurvy. The hunger edema, noted in the late war and in previous wars, seems to be a complex condition, quite dissociated from scurvy, as many of the sufferers consumed comparatively large quantities of potatoes or other vegetables. The “mehlnaerschaden” resembles scurvy and the other vitamine disorders in its tendency to produce hydremia and susceptibility to infection. It also develops in spite of a liberal supply of antiscorbutic foodstuff in the dietary. As its name implies, it comes about on a diet containing large quantities of carbohydrate, of the cereal paps so commonly fed to infants. It is conceivable that an unbalanced diet of this kind may not provide a sufficiency of all the vitamines.
It does not seem probable that exudative diathesis, a term which implies a predisposition to develop exudations or denudations of the skin and mucous membranes, is the result of a lack of vitamine. This condition does, however, predispose to scurvy. The association was very evident in the group of cases reported by Hess and Fish in 1914. It is not without significance that the blood-vessels in exudative diathesis also show a decided weakness, an increased permeability, as judged by the “capillary resistance test.” In both scurvy and in exudative diathesis eczema and petechial hemorrhages are encountered.
There may be nutritional diseases due to an excess of food rather than to a deficiency. A superfluity may be harmful by hindering the proper utilization of the food, or may possibly lead to the formation of deleterious products. Disturbances of this kind do occur. For example, it is by no means uncommon for an infant which has been overfed with milk to show the typical signs of rickets. Young guinea-pigs which are fed liberal amounts of cow’s milk develop a disease characterized by fragility of the bones. The experience of Lubarsch, who produced osteogenesis imperfecta in rabbits by means of a diet consisting mainly of liver, or adrenal gland, is of interest, especially as this condition did not come about when they were fed muscle tissue.
From what has been stated, it must be evident that this subject not only is in a state of flux but that it is in a state of great confusion. This applies not only to the relationship of vitamines to these disorders, but to their identification and demarcation pathologically as well as clinically. During the past few years we have begun to regard these diseases from a new viewpoint, which no doubt will be helpful, but it is probable that they will not be sharply defined and their relationships determined until it is possible to bring about each disease definitely and regularly in an experimental animal. Until this time we should proceed slowly, and not bring about “confusion worse confounded” by yielding to the vogue, and grouping together heterogeneous and little-understood clinical conditions under the caption of deficiency diseases. There is a growing danger of attributing every unexplained nutritional disorder to the new, overworked, but ill-defined vitamines—of their sharing with the secretions of the endocrine glands the fate of becoming the dumping-ground for every unidentified disorder.
Extract from “Treatise on Scurvy,” by James Lind, London, 1772.
(a) Recipe for preparing a stable orange or lemon juice. Let the squeezed juice of these fruits be well cleared from the pulp and purified by standing for some time; then poured off from the gross sediment; or, to have it still purer, it may be filtrated. Let it then be put into any clean open vessel of china or stone-ware, which should be wider at the top than bottom, so that there may be the largest surface above to favor the evaporation. For this purpose a china basin or punch-bowl is proper, and generally made in the form required; all earthen glazed vessels are unfit, as their glazing will be dissolved by the acid. Into this pour the purified juice, and put it into a pan of water, upon a clear fire. Let the water come almost to a boil, and continue nearly in that state (with the basin containing the juice in the middle of it) until the juice is found to be of the consistence of a thick syrup when cold. The slower the evaporation of the juice the better; and it will require at least twelve or fourteen hours continuance in the bath heat before it is reduced to a proper consistence.
It is then, when cold, to be corked up in a bottle for use. Two dozen good oranges, weighing five pounds four ounces, will yield one pound nine ounces and a half of pure juice; and when evaporated, there will remain about five ounces of rob, or extract; which in bulk will be equal to less than three ounces of water. So that thus the acid, and the virtues of twelve dozen lemons or oranges, may be put into a quart bottle, and preserved for several years.
I have now some extract of lemons which was made four years ago.
Those who intend this extract for making punch may infuse some of the fresh peel of the oranges or lemons into the spirit before it is used.
But for this purpose I find it is sufficient to add a very small quantity of the outer peel to the extract a little before it is taken off the fire, and there will be all that is requisite to make it entirely equal to the freshest fruit.
(b) How to preserve berries and other fruits for long periods. And it may be proper to acquaint them that most berries, and several fruits, when gathered two-thirds ripe on a dry day, while the sun shines, if put into earthen pots, or rather in dry bottles, well corked, and sealed up, so that no air or moisture can enter, will keep a long time, and at the end of a year, be as fresh as when new pulled.
(c) Method of preparing an antiscorbutic decoction from fir-tops, leaves, bark, etc. When the Swedes carried on a war against the Muscovites, almost all the soldiers of their army were destroyed by the scurvy, having putrid gums, rigid tendons, etc. But a stop was put to the progress of this disease by the advice of Erbenius, the King’s physician, with a simple decoction of fir-tops, by which the most deplorable cases were perfectly recovered, and the rest of the soldiers prevented from falling into it.
I am inclined to believe by the description given by Cartier of the ameda tree, with a decoction of the bark and leaves of which his men were so speedily recovered, that it was the large swampy American spruce tree.
A simple decoction of the tops, cones, leaves or even green bark and wood of these trees is an excellent antiscorbutic medicine; but it will, I am apt to think, become much more so when fermented, as in making spruce beer. By carrying a few bags of spruce or its extract to sea, this wholesome drink may be prepared at any time. But where it cannot be had the common fir-tops used for fuel in the ship should be first boiled in water, and the decoction afterwards fermented with molasses in the common method of making spruce beer; to which a small quantity of wormwood and horse-radish root (which it is easy to preserve fresh at sea) may be added. The juice of the cocoanut tree was experienced to be of very great benefit to several persons afflicted with the scurvy.
Albert, J.: A Case of Infantile Beriberi with Autopsy Report, Phillip. Jour. of Sci., Sec. B, 1908, III, 345.
American Pediatric Society: Collective Investigation on Infantile Scurvy in North America, Arch. of Ped., 1898, XV, 481.
Andrews, V. L.: Infantile Beriberi, Phillip. Jour. of Sci., 1912, VII, 67.
Anson, Lord: Walter and Robins, Voyage Round the World, London, 1848.
Arneth: Ueber Skorbut im Felde, Deutsch med. Woch., 1918, XLIV, 509.
Aron, H.: Biochemie des Wachstums des Menschen and die hoeheren Tiere, Jena, 1913, Gustav Fischer, 58.
Aschoff, L., and Koch, W.: Der Skorbut, Jena, 1919, Gustav Fischer.
Ausset, E.: (1) La Maladie de Barlow, Annal. de med. et chir. Inf., 1904, VIII, 289.
Ausset, E.: (2) Un cas de maladie de Barlow chez un enfant nourri exclusivement avec du babeurre frais, Bull. Méd., 1910, XXIV, 675.
Bachstrom: Observationes circa Scorbutum, 1734.
Baginsky, A.: Demonstration von anatomischen Praeparaten eines Falles von Barlowscher Krankheit, Berl. klin. Woch., 1897, XXXIV, 324.
Bahrdt, H., and Edelstein, F.: Organanalysen bei Barlowscher Krankheit, Zeitschr. f. Kinderheilk., 1913, IX, 415.
Barlow, T.: (1) On Cases described as Acute Rickets, Med. Chir. Trans., 1883, LXVI, 159.
Barlow, T.: (2) Infantile Scurvy and Its Relation to Rickets, Lancet, London, 1894, II, 1075.
Barnes, K. E., and Hume, E. M.: Relative Antiscorbutic Value of Fresh, Dried and Heated Cow’s Milk, Biochem. Jour., 1919, XIII, 306.
Barrow, Sir Jay: Supplement to Encyclopedia Britannica, article “Navy,” cited by Budd.
Bartenstein, L.: Beitraege z. Frage des kuenstlichen Morbus Barlow bei Tieren, Jahrb. f. Kinderheilk., 1905, LXI, 6.
Bateman: Scurvy in a Child, Birmingham Med. Review, 1886, Abstr. Arch. Ped., 1886, III, 304.
Baumann, L., and Howard, C. P.: (1) Metabolism of Scurvy in an Adult, Arch. Int. Med., 1912, IX, 665.
Baumann, L., and Howard, C. P.: (2) Mineral Metabolism of Experimental Scurvy of the Guinea-pig, Am. Jour. Med. Sci., 1917, CLIII, 650.
Benoit, A.: Une Épidémie de Scorbut, Paris Méd., 1919, IX, 469.
Bernheim-Karrer: Saeuglingskorbut bei Ernaehrung mit Homogenisierter Berner Alpenmilch, Korrespondenzbl. f. Schweizer Aerzte, 1907, XXXVII, 593.
Blane, Sir Gilbert: Observations on the Diseases Incident to Seamen, 1789, London, J. Murray.
Boerhaave: Cited by Lind.
Boerich, R.: Ueber Skorbut, Archiv. f. Klin. Med., 1919, CXXX, 151.
Bohn: Acute Rachitis, Jahrb. f. Kinderheilk., 1868, II, 201.
Boldyreff, W. N.: Quelques Considerations sur les Causes étiologiques du Scorbut, Comp. rend. soc. de biol., 1917, LXXX, 911.
Bolle, C.: Zur Therapie der Barlowschen Krankheit, Ztschr. f. diaetet. u. physik. Therap., 1902–03, VI, 354.
Bradden, W. L., and Cooper, E. A.: The Influence of the Total Fuel Value of a Dietary upon the Quantity of Vitamine Required to Prevent Beriberi, Brit. Med. Jour., 1914, I, 1348.
Brandt, H.: Blutuntersuchungen bei Barlow’scher Krankheit, Archiv. f. Kinderheilk., 1919, LXVII, 395.
Budd, G.: Tweedies’ System of Pract. Med., Phila., 1841, Lea and Blanchard, 99.
Budin, P.: The Nursling, London, 1907, Caxton Pub. Co.
Burge, W. E., and Neill, A. J.: (1) The Effect of Starvation on the Catalase Content of the Tissues, Am. Jour. Phys, 1917, XLIII, 58.
Burge, W. E., and Neill, A. J.: (2) The Normal Mechanism for the Control of Oxidation in the Body, Am. Jour. Phys., 1918, XLVI, 117.
Busk, G.: Report of Committee on Scurvy, etc., London, 1877.
Caillé, A.: Minority Report, Amer. Ped. Soc. Collective Investigation (see above).
Carel: Un Cas de Scorbut imputable au Lait Stérilisé, Bull. de la Soc. de Pédiat. de Paris, 1910, XII, 79.
Cassel: Ein Fall von Skorbut, Arch. f. Kinderheilk., 1893, XV, 350.
Charpentier, P.: Étude sur le Scorbut, Paris, 1871, A. Delahaye.
Cheadle, W. B.: Infantile Scurvy, Allbutt’s System of Med., 1901, V, 64.
Chick, H., and Delf, E. M.: The Antiscorbutic Value of Dry and Germinated Seeds, Biochem. Jour., 1919, XIII, 199.
Chick, H., and Hume, M.: The Distribution Among Foodstuffs (especially those suitable for the rationing of armies) of the Substances required for the Prevention of (a) Beriberi and (b) Scurvy, Trans. Soc. Trop. Med. and Hyg., 1917, X, 141.
Chick, H., and Skelton, R. F.: (1) An Estimate of the Antiscorbutic Value of Milk in Infant Feeding, Lancet, London, I, 1918, 1.
Chick, H., and Skelton, R. F.: (2) The Relative Content of Antiscorbutic Principle in Limes and Lemons, Lancet, London, 1918, II, 735.
Chick, H., and Rhodes, M.: An Investigation of the Antiscorbutic Value of the Raw Juices of Root Vegetables, Lancet, London, 1918, II, 774.
Cohen, B., and Mendel, L. B.: (1) Diet and Roughage in Relation to the Experimental Scurvy of Guinea-pigs, Proc. Soc. Exp. Biol. and Med., 1918, XV, 122.
Cohen, B., and Mendel, L. B.: (2) Experimental Scurvy of the Guinea-pig in Relation to the Diet, Jour. Biol. Chem., 1918, XXXV, 427.
Comby, J.: (1) Twelve New Cases of Infantile Scurvy, Arch. de Méd. des Enfants, 1917, XX, 337.
Comby, J.: (2) Infantile Scurvy, Presse Médicale, 1918, XXVI, 480.
Concetti, L.: Sopra due casi di morbo di Barlow, Rev. di clin. pediat., Firenze, 1909, VII, 225.
Coplans, M.: (1) On the Etiology of Scurvy, Lancet, London, 1904, I, 1714.
Coplans, M.: (2) On the Etiology of Scurvy, Jour. Trop. Med., London, 1904, VII, 99.
Coutts, F. J. H.: Upon an Inquiry as to Dried Milks, etc. Report to the Local Govt. Board, 1918, New Series No. 116, 31.
Couvy: Une Épidémie de Beriberi et de Scorbut, Annales d’Hygiène de Méd. Coloniales, 1911, XIV, 97.
Crandall, F. M.: Scurvy in an Infant of Six Weeks, Arch. of Pediat., 1899, XVI, 851.
Crocker, W., and Harrington, G. F.: Catalase and Oxidase Content of Seeds, Jour. Agricult. Research, Wash., D. C., 1918, XV, 137.
Curran, J. O.: Observations on Scurvy, etc., The Dublin Quart. Jour. Med. Sciences, 1847, IV, 107.
Czerny A., and Keller, A.: Handbuch des Kindes Ernaerung, etc., Leipzig, 1907, II, 93.
Darling, S. T.: The Pathologic Affinities of Beriberi and Scurvy, Jour. Am. Med. Assn., 1914, LXIII, 1290.
Delf, E. M., and Skelton, R. F.: The Effect of Drying on the Antiscorbutic and Growth-Promoting Properties of Cabbage, Biochem. Jour., 1918, XII, 448.
Delf, E. M., and Tozer, F. M.: The Antiscorbutic and Growth-Promoting Properties of Raw and Heated Cabbage, Biochem. Jour., 1918, XII, 416.
Delpech, M. A.: Le Scorbut pendant le Siège de Paris, Annales d’Hyg., 1871, XXXV, 2nd S.
Disqué, L.: Enstehung and Verlauf des Skorbuts im Jahre, 1916, Med. Klinik, 1918, XIV, 10.
Duke, W. W.: Pathogenesis of Purpura Hemorrhagica, Arch. Int. Med., 1912, X, 445.
Dutcher, R. A.: Nature and Function of the Antineuritic Vitamine, Proc. Nat. Acad. of Sci., 1920, VI, 10.
Dyke, H. W.: An Outbreak of Scurvy in the South African Native Labour Corps, Lancet, London, 1918, II, 513.
Eddy, W. H.: Further Observations on Pancreatic Vitamine, Proc. Soc. Exper. Biol. and Med., 1917, XIV, 164.
Editorial: Deficiency Diseases in Vienna, Brit. Med. Jour., 1920, I, 477.
Edwards, C. R.: Peripheral Neuritis in Jamaica, Jour. Trop. Med. and Hyg., 1916, XIX, 53.
Eijkman, C.: Eine beriberiaehnliche Krankheit der Huehner, Virchow’s Archiv., 1897, CXLVIII, 523.
Enright, J. I.: War Edema in Turkish Prisoners, Lancet, London, 1920, I, 314.
Epstein, A.: Ueber eine Auffaellige Haeufung der Barlow’schen Krankheit im den Kriegsjahren, 1917–1918, Jahrb. f. Kinderheilk, 1918, LXXXVIII, 237.
Erdheim, J.: Ueber das Barlowherz, Wien. klin. Woch., 1918, 1293.
Escherich, T.: (1) Skorbut. Verhandl. d. Gesellsch. f. Kinderheilk., 1898, XV, 77.
Escherich, T.: (2) Zur Kenntnis der Unterschiede zwischen den natuerlichen und kuenstlichen Ernaehrung des Saeuglings, Wien klin. Woch., 1900, XIII, 1185.
Esser: Blut-und Knochenmarksveraenderungen bei Ernaehrungsschaden, Verhandl. deutschen Naturforsch. u. Aerzte, Abt. f. Innere Med., 1908, 86.
Falk, K. G., Mcguire, G., and Blount, E.: The Oxidase, Peroxidase, Catalase and Amylase of fresh and dehydrated vegetables, Jour. Biol. Chem., 1919, XXXVIII, 229.
Feigenbaum, D.: Ein Beitrag zur Kenntnis der Rückenmarkblutungen beim Skorbut, Wien. klin. Woch., 1917, XXX, 1455.
Fife, C. A.: Pathology of Infantile Scurvy, N. Y. Med Jour., 1910, XCI, 1322.
Filatow: Cited by M. Schubert, Beriberi und Skorbut, Deutsch. Arch. f. klin. Med., 1905, LXXXVI, 79.
Finkelstein, H.: Lehrbuch der Saeuglingsk., II, Berlin, 1912.
Fischer, Th.: Zur Kenntnis der hereditaeren Syphilis, Muenchn. med. Woch., 1890, XXXVII, 621.
Foerster, R.: Ein Fall von acute Rachitis, Jahrb. f. Kinderheilk, 1868, I, 444.
Fraenkel, E.: Fortschritte a. d. Gebiete der Roentgenstrahlen, 1904, VII, Nos. 5 and 6; 1906, X, No. 1; 1908, Ergaensungsbd., XVIII.
Freise, E.: Der Alkoholextract aus Vegetabilien als Traeger. Barlowheilende Stoffe, Monatschr. f. Kinderheilk, 1914, XII, 687.
Freudenberg, E.: Beitrag zur Frage des Barlow-Schutzstoffes. Monatschr. f. Kinderheilk, 1914, XIII, 141.
Freund, G.: Zur Kenntnis der Barlow’schen Krankheit (Brust Kind) Arch. f. Klin. Med., 1905, LXXXVI, 129.
Froelich, T.: Experimentelle Untersuchungen ueber den infantilen Skorbut, Ztschr. f. Hyg. u. Infektionskrankh., 1912, LXXII, 155.
Fruitnight, J. H.: Infantile Scurvy, Especially its Differential Diagnosis, Arch. of Pediat., 1894, XI, 486, 573.
Fuerst, L.: Infantiler Scorbut oder Haemorrhagische Rhachitis, Berl. klin. Woch., 1895, XXXII, 389.
Fuerst, V.: Weitere Beitraege zur Aetiologie des experimentellen Skorbuts des Meerschweinchens, Ztschr. f. Hyg. u. Infektionskrankh. 1912, LXXII, 121.
Funk, C.: (1) On the Chemical Nature of the Substance which Cures Polyneuritis in Birds, Jour. Physiol., 1911, XLIII, 395.
Funk, C.: (2) Die Vitamine, Wiesbaden, 1914, J. F. Bergman.
Funk, C., and Douglas, M.: Studies on Beriberi, VIII, Jour. Physiol, 1914, XLVII, 475.
Funk, C., and von Schoenborn, E.: The Influence of a Vitamine Free Diet on the Carbohydrate Metabolism, Jour. Physiol., 1914, XLVIII, 328.
Garrod, A. B.: On the Nature, Cause and Prevention of Scurvy, Month. Jour. Med. Sci., 1848, Vol. VIII, 457.
Gee: (1) On Osteal or Periosteal Cachexia, St. Bart. Hosp. Rep., 1881, XVII, 9.
Gee: (1) On Osteal or Periosteal Cachexia, St. Bart. Hosp. Rep., 1881, Rep., 1889, XXV, 85.
Gerstenberger, H. J.: Pathogenesis of Infantile Scurvy, an Hypothesis, Am. Jour. Med. Sci., 1918, CLV, 253.
Gingui, F.: Riforma Med., 1918, XXXIV, 22.
Givens, M. H., and Hoffman, G. L.: Preliminary Observations on the Relation of Bacteria to Experimental Scurvy in Guinea-pigs, Jour. Biol. Chem., 1920, XLI, 33.
Givens, M. H., and McClugage, H. B.: The Antiscorbutic Property of Fruits, Am. Jour. Dis. Child., 1919, XVIII, 30.
Glisson: Treatise on the Rickets, London, 1651.
Goldberger, J.: Studies on Pellagra, Hyg. Lab. Bull’s., 1914–1920.
Guerrero and Quinto: Cited by Vedder, Beriberi, p. 259.
Harden, A., and Zilva, S. S.: (1) Note on the Etiology of Scurvy in Guinea-pigs, Biochem. Jour., 1918, XII, 270.
Harden, A., and Zilva, S. S.: (2) The Differential Behavior of the Antineuritic and Antiscorbutic Factors Towards Adsorbents, Biochem. Jour., 1918, XII, 93.
Harden, A., and Zilva, S. S.: (3) The Antiscorbutic Factor in Lemon Juice, Biochem. Jour., 1918, XII, 259.
Harden, A., and Zilva, S. S.: (4) Accessory Factors in the Nutrition of the Rat, Biochem. Jour., 1918, XII, 408.
Harden, A., and Zilva, S. S.: (5) An Investigation of Beer for Antineuritic and Antiscorbutic Potency, Jour. of the Institute of Brewing, 1918, XXIV, 197.
Harden, A., and Zilva, S. S.: (6) The Susceptibility of the Antiscorbutic Principle to Alkalinity, Lancet, London, 1918, II, 320.
Harden, A., Zilva, S. S., and Still, G. F.: Infantile Scurvy, Antiscorbutic Factor of Lemon Juice in Treatment, Lancet, London, 1919, I, 17.
Harlan, G. P.: Land Scurvy in England, Brit. Med. Jour., 1917, II, 46.
Hart, C.: Der Skorbut der kleinen Kinder (Moeller-Barlow’sche Krankheit) Nach Experimentellen Untersuchungen, Jahrb. f. Kinderheilk, 1912, LXXVI, 507.
Hart, C., and Lessing, O.: Der Skorbut der Kleinen Kinder, Stuttgart, 1913, Ferdinand Enke.
Hart, E. B., Steenbock, H., and Ellis, N. R.: Influence of Diet on the Antiscorbutic Potency of Milk, Jour. Biol. Chem., 1920, XLII, 383.
Hart, E. B., Steenbock, H., and Smith, D. W.: Effect of Heat on the Antiscorbutic Properties of Some Milk Products, Jour. Biol. Chem., 1919, XXXVIII, 305.
Harvey, G.: A New Discourse of the Smallpox and Malignant Fevers with an Exact Discovery of the Scurvy, London, 1685.
Harvier, P.: Épidémie de Scorbut, Paris Méd., 1917, VII, 394.
Hawkins, Sir R.: Voyage to the South Sea, A. D. 1593, in Purchas’s “Pilgrim,” Vol. IV.
Hayem, M. G.: Note sur l’Anatomie Pathologique du Scorbut, Gazette Méd. de Paris, 1871, XXVI, 126.
Hess, A. F.: (1) Infantile Scurvy: II. A New Aspect of the Symptomatology, Pathology and Diet, Jour. Am. Med. Assn., 1915, LXV, 1003.
Hess, A. F.: (2) Infantile Scurvy: III. Its Influence on Growth (Length and Weight), Am. Jour. Dis. Child., 1916, XII, 152.
Hess, A. F.: (3) Infantile Scurvy: IV. The Therapeutic Value of Yeast and of Wheat Embryo, Am. Jour. Dis. Child., 1917, XIII, 98.
Hess, A. F.: (4) Subacute and Latent Infantile Scurvy, The Cardiorespiratory Syndrome (a New Sign), Jour. Am. Med. Assn., 1917, LXVIII, 235.
Hess, A. F.: (5) Infantile Scurvy: V. A Study of Its Pathogenesis, Am. Jour. Dis. Child., 1917, XIV, 337.
Hess, A. F.: (6) The Rôle of Antiscorbutics in Our Dietary, Jour. Am. Med. Assn., 1918, LXXI, 941.
Hess, A. F.: (7) Focal Degeneration of the Lumbar Cord in a Case of Infantile Scurvy, Jour. Infect. Dis., 1918, XXIII, 438.
Hess, A. F., and Fish, M.: Infantile Scurvy: The Blood, the Blood-Vessels, and the Diet, Am. Jour. Dis. Child., 1914, VIII, 386.
Hess, A. F., and Killian, J. A.: Chemistry of the Blood in Scurvy, Proc. Soc. Exp. Biol. and Med., 1918, XVI, 43.
Hess, A. F., and Unger, L. J.: (1) Experiments on the Scurvy of Guinea-pigs, Proc. Soc. Exp. Biol. and Med., 1918, XV, 82.
Hess, A. F., and Unger, L. J.: (2) The Scurvy of Guinea-pigs: I. The Experimental Dietary, Jour. Biol. Chem., 1918, XXXV, 479.
Hess, A. F., and Unger, L. J.: (3) The Scurvy of Guinea-pigs, II, Experiments on the Effect of the Addition of Fruits and Vegetables to the Dietary, Jour. Biol. Chem., 1918, XXXV, 487.
Hess, A. F., and Unger, L. J.: (4) Experiments on Antiscorbutics, Report of an Antiscorbutic for Intravenous Use, Proc. Soc. Exp. Biol. and Med., 1918, XV, 141.
Hess, A. F., and Unger, L. J.: (5) Canned Tomatoes as an Antiscorbutic, Proc. Soc. Exp. Biol. and Med., 1918, XV, 96.
Hess, A. F., and Unger, L. J.: (6) Scurvy: VIII, Factors Affecting the Antiscorbutic Value of Foods, Am. Jour. Dis. Child., 1919, XVII, 221.
Hess, A. F., and Unger, L. J.: (7) The Scurvy of Guinea-pigs: III. The Effect of Age, Heat and Reaction on Antiscorbutic Foods, Jour. Biol. Chem., 1919, XXXVIII, 293.
Hess, A. F., and Unger, L. J.: (8) The Deleterious Effect of the Alkalization of Infants’ Food, Jour. Am. Med. Assn., 1919, LXXIII, 1353.
Hess, A. F., and Unger, L. J.: (9) Scorbutic Beading of the Ribs, Am. Jour. Dis. Child., 1920, XIX, 331.
Heubner, O.: Ueber die Barlowsche Krankheit, Berl. klin. Woch., 1903, XL, 285.
Hift, R.: Beobachtungen ueber Skorbut and Hemeralopie, Abstract, Deutsch. med. Woch., 1918, XLIV, 100.
Himmelstein, von S.: Beobachtungen ueber den Skorbut, Arch. f. d. gesammte Med., 1843, V, 490.
Hirsch, A.: Handbook of Geographical and Historical Pathology, London, 1885, New Sydenham Society.
Hirschsprung, H.: Die Moellersche Krankheit. Jahrb. f. Kinderheilk, 1896, XLI, 1.
Hoerschelman, E.: Zur Klinik der Skorbuts in der russischen Armee, Deutsch. med. Woch., 1917, XLIII, 1617.
Hoffmann: Untersuchungen eines Falles von Barlow’scher Krankheit, Beitraege z. path. Anat., 1905, Suppl. VII, (Festschrift fer Arnold).
Holst, H., and Froelich, T.: (1) Experimental Studies Relating to Ship Beriberi and Scurvy, Jour. of Hyg., 1907, VII, 634.
Holst, H., and Froelich, T.: (2) Ueber experimentellen Skorbut, Ztschr. f. Hyg. u. Infektionskrankh., 1912, LXXII, 1.
Holst, H., and Froelich, T.: (3) Scorbutus and its Prophylaxis, Norsk. Mag. f. Laegevidensk., 1916, LXXVII, 989.
Holt, L. E.: Diseases of Infancy and Childhood, New York and London, 1919, Appleton.
Hopkins, F. G.: (1) The Analyst and the Medical Man, Analyst, 1906, XXXI, 395.
Hopkins, F. G.: (2) Feeding Experiments Illustrating the Importance of Accessory Factors in Normal Dietaries, Jour. of Physiol., 1912, XLIV, 425.
Hopkins, G. R.: The Etiology of Scurvy, Jour. Am. Med. Assn., 1917, LXIX, 1641.
Howard, C. P., and Ingvaldsen, T.: The Mineral Metabolism of Experimental Scurvy of the Monkey, Johns Hopkins Hosp. Bull., 1917, XXVIII, 221.
Hutchison, R.: Some Disorders of the Blood and Blood-Forming Organs in Early Life, Lancet, London, 1904, I, 1253.
Ingier, A.: (1) Beitraege zur Kenntnis der Barlowschen Krankheit, Frankfurt. Ztschr. f. Path., 1913, XIV, 1.
Ingier, A.: (2) A Study of Barlow’s Disease Experimentally Produced in Fetal and Newborn Guinea-pigs, Jour. Exper. Med., 1915, XXI, 525.
Jacobsthal, H.: Zur Pathologie der Knochenerkrankungen bei Barlowscher Krankheit, Beitraege z. path. Anat., 1900, XXVII, 173.
Jackson, F., and Harley, V.: An Experimental Inquiry into Scurvy, Lancet, London, 1900, I, 1184.
Jackson, L., and Moody, A. M.: Bacteriologic Studies on Experimental Scurvy in Guinea-pigs, Jour. Infect. Dis., 1916, XIX, 511.
Jackson, L., and Moore, J. J.: Studies of Experimental Scurvy in Guinea-pigs, Jour. Infect. Dis., 1916, XIX, 478.
Jalland, W. H.: Med. Times and Gazette, London, 1873, I, 248.
Johanneson, A.: Ueber die Sterilization der Milch. Jahrb. f. Kinderheilk, 1901, LIII, 251.
Karr, W. G., and Lewis, H. B.: Phenol Excretion of Guinea-Pigs Maintained on an Exclusive Oat Diet, Am. Jour. Physiol., 1917, XLIV, 586.
Kaufmann, E.: Lehrbuch der Speziellen Pathologischen Anatomie, Berlin, 1911, Georg Reimer.
Kerley, C. G.: Practice of Pediatrics, Phila., 1918, Saunders & Co.
Kitamura, S.: Ein Beitrag zur Kenntnis der Netzhautveraenderungen beim Skorbut, Deutsch. med. Woch., 1910, XXXVI, 403.
Koch, J.: Untersuch. uber die Lokalisation d. Bakterien, etc., Zeitschr. f. Hyg., 1911, LXIX.
Kohlbrugge, J. H.: Die Gaerungskrankheiten, Centralbl. f. Bakt. etc., Orig. 1911, LX, 223.
Korbsch, R.: Ueber Skorbut im Felde, Deutsch. med. Woch., 1919, XLV, 185.
Kramer: Medicina Castrensis, 1721, Cited by Charpentier (see above).
Labor, M.: Eine Beobachtung ueber das Blutbild des Skorbuts, Wien. klin. Woch., 1916, XXIX, 912.
LaMer, V. K., and Campbell, H. L.: Changes in Organ Weight Produced by Diet Deficient in Antiscorbutic Vitamine, Proc. Soc. Exper. Biol. and Med., 1920.
Lasèque, Ch., and Legroux, A.: L’Épidémie de Scorbut dans les Prisons de la Seine et a l’Hôpital de la Pitié, Arch. Gén., 1871, II, 5, 680.
Lecornu, P.: Les Laits Industriels, Thèse de Paris, 1904.
Leven, M.: Une Épidémie de Scorbut observée a l’Hôpital Militaire d’Ivry pendant le Siège de Paris, 1871.
Lewis, A. B., and Karr, W. G.: Changes in the Urea Content of the Blood and Tissues of Guinea-pigs Maintained on an Exclusive Oat Diet, J. Biol. Chem., 1916, XXVIII, 17.
Lind, J.: Treatise on Scurvy, London, 1772.
Litten, M.: Nothnagel’s Handbuch der Spec. Path. u. Therap., 1901, VIII, 3, 277.
Lloyd, D. J.: On Vitamines, Amino Acids, and Other Chemical Factors Involved in the Growth of the Meningococcus, Jour. of Path., 1916–17, XXI, 118.
Lobmeyer, G.: Kriegschirurgische Bedeutung des Skorbuts, Abstracted in Deutsch. med. Woch., 1918, XLIV, 557.
Looser, E.: Ueber die Knochenveraenderungen beim Skorbut, Jahrb. f. Kinderheilk., 1905, LXII, 743.
Lubarsch, O.: Ueber alimentaere Schlagaderverkalkung, Muench. med. Woch., 1910, Nr. 30, 1577.
Lunin, N.: Ueber die Bedeutung der Anorganischen Salze fuer die Ernaehrung des Thiers, Ztschr. f. physiol. Chem., 1881, V, 31.
Lust, F., and Klocman, L.: Stoffwechselversuche bei Barlow’sche Krankheit, Jahrb. f. Kinderheilk., 1912, LXXV, 663.
Lyabmow: Aerztl. Gesellschaft zu Kasan, 1900, Cited from M. Schubert, Beriberi und Skorbut, Arch. f. klin. Med., 1905, LXXXVI, 79.
McCarrison, R.: (1) The Pathogenesis of Deficiency Disease, Indian Jour. Med. Research, 1919, VI, 275.
McCarrison, R.: (2) The Influence of the Scorbutic Diet on Adrenal Gland, Indian Jour. Med. Research, 1919, VII, 188.
McCollum, E. V., and Davis, M.: The Necessity of Certain Lipins in the Diet during Growth, Jour. Biol. Chem., 1913, XV, 167.
McCollum, E. V., and Pitz, W.: The Vitamine Hypothesis and Deficiency Diseases, A Study of Experimental Scurvy, Jour. Biol. Chem., 1917, XXXI, 229.
MacKenzie: Reported by Barlow, 1883.
Marfan, A. B.: Maladies des Os, Paris, 1912.
Manz, R.: Beitraege zur Kenntnis der Moeller-Barlow’scher Krankheit. Inaug. Addr., Heidelberg, 1899.
Medical and Surgical History of the War of the Rebellion: 1888, Washington, I, Part 3, Chap. 8.
Mellanby, E.: An Experimental Investigation of Rickets, Lancet, London, 1919, I, 407.
Meyer, E.: Ueber Barlow’sche Krankheit, Arch. f. Kinderheilk, 1896, XX, 202.
Moeller: (1) Acute Rachitis, Koenigsberg. med. Jahrb, 1859, I.
Moeller: (2) 2 Faelle von acuter Rachitis, Koenigsberg. med. Jahrb. 1862, III.
Moll, L.: Stoffwechsel in Barlow’sche Krankheit, Mitteil. d. Gesellsch. f. innere Med. u. Kinderheilk. in Wien, 1919, XVIII.
Monfalcon: Rachitis, Dictionnaire des Sciences, 1820, XLVI.
Money: Three Cases of Infantile Scurvy, Intercolon. Med. Jour. of Australia, 1897.
Moore, J. J.: Experimental Studies in Diet Deficiency Diseases, Proc. Inst. of Med. of Chicago, 1918, 254.
Morawitz, P.: (1) Echter und Falscher sporadischer Skorbut, Muench. med. Woch., 1918, LXV, 339.
Morawitz, P.: (2) Der Skorbut und verwandte Krankheiten, Jahresb. f. aerztl. Fortbildung, March, 1919, 15.
Morgan, A., and Beger, C.: Zeitschr. Physiol. Chem., 1915, XCIV, 324.
Morpurgo, B.: Ueber eine Infectioese Form der Knochenbruchigkeit bei weissen Ratten, Verhandl. d. deutsch. patholog. Gesellsch., 1900, III, 40.
Morse, J. L.: (1) Infantile Scorbutus (50 cases), Jour. Am. Med. Assn., 1906, XLVI, 1073.
Morse, J. L.: (1) Infantile Scorbutus (50 cases), Jour. Am. Med. Assn., CLXX, 504.
Much, H.: Skorbut, Muench. med. Woch., 1917, LXIV, 854.
Mueller, E.: Ueber ein gehaeuftes Auftreten von Skorbut bei Kindern, Berlin klin. Woch., 1918, LV, 1024.
Muckenfuss, A. M.: The Excretion of Vitamines, Arch. of Pediat., 1919, XXXVI, 80.
Munson, E. L.: Military Hygiene, New York, 1901.
Murlin, J. R.: Some Problems of Nutrition in the Army, Boston Med. and Surg. Jour., 1918, CLXXIX, 396.
Naegeli, O.: Zur pathologischen Anatomie und zum Wesen des Morbus Barlow, Centralbl. f. allg. Path. u. path. Anat., 1897, VIII, 687.
Nansen and Johansen: Cited by Holst and Froelich (see above).
Netter: Le Scorbut Infantile, La Semaine Médicale, 1899, No. 8.
Neumann, H.: Bemerken ueber Barlow’sche Krankheit, Deutsch. med. Woch., 1902, XXVIII, 628.
Nichols: Infantile Scurvy, Brit. Med. Jour., 1896, I, 25.
Von Niedner: Hæmorrhagische Exantheme, Med. Klinik, 1918, XIV, 333.
Nobécourt, P., Tixier, L., and Maillet: Hematologie et Altérations osteo-médullaires dans la Maladie de Barlow, Compt. Rend. de l’Assoc. de Pédiatrie, 1913–15, 123.
Nocht, B.: Festschrift zum 60 Geburtstage v. R. Koch, 1903, 203.
Van Noorden, C.: Ueber enterogene Intoxicationen, Berl. klin. Woch., 1913, L, 51.
Northrup, W. P.: Scorbutus in Infants, Arch. of Pediat., 1892, IX, 1.
Ono, S.: Adrenalin Content of Suprarenal, Taiwan Igakuku Zasshi, Tokio, 1916, CLXX, 1014.
Osborne, T. B., and Mendel, L. B.: (1) The Relations of Growth to the Chemical Constituents of the Diet, Jour. Biol. Chem., 1913, XV, 311.
Osborne, T. B., and Mendel, L. B.: (2) The Distribution of Water Soluble Vitamine, Jour. Biol. Chem., 1919, XXXIX, 29.
O’Shea, H. V.: Scurvy, The Practitioner, 1918, Oct.-Nov.
Pappenheimer, A.: Further Experiments upon the Extirpation of the Thymus in Rats, Jour. Exper. Med., 1914, XX, 477.
Parkes: Med.-Chir. Rev., 1848, Art. VIII.
Peiper and Eichloff: Korrespondenzbl. d. Verein d. Aerzte, Stralsund, 1904.
Pick, F.: Skorbut, Deutsch. med. Woch., 1916, XLII, 1402.
Pickens, R. M.: A Death from Scurvy, Lancet, London, 1917, II, 21.
Pitz, W.: Studies of Experimental Scurvy, Jour. Biol. Chem., 1918, XXXIII, 471.
Plantenga, B. P.: Rohe Milch als Saeuglingsnahrung, Arch. f. Kinderheilk., 1912, VIII, 155.
Poupart: Étranges Effets du scorbut arrivés à Paris en 1699, Hist. de l’Acad. Royale des Sci., 1699.
Ralfe, C. H.: Inquiry into the General Pathology of Scurvy, Lancet, London, 1877, I, 868; II, 81.
Rappleye, W. C.: A Note on Experimental Scurvy in the Guinea-pig, Boston Med. and Surg. Jour., 1918, CLXXIX, 98.
Rauchfuss: Cited from Heubner, O., Lehrbuch f. Kinderheilk., Leipzig, 1903, I, 698.
Rehn, H.: Ein Fall von Skorbut, Berl. klin. Woch., 1889, XXVI, 11.
Reinert, E.: Ein Fall von Barlow’scher Krankheit, Muenschner med. Woch., 1895, XLII, 370.
Reinhard, P.: Roentgenbefunde bei beriberiartigen Erkrankungen, Arch. f. Shiffs-u. Tropenhyg., 1916, 20.
Report of Mesopotamia Commission: London, 1917.
Richard, R., and Lloyd, G. W.: Early Signs of Scurvy, Brit. Med. Jour., 1920, I, 329.
Rondoni, P.: Remarks on the Pathogenesis of Deficiency Diseases and on Pellagra, Brit. Med. Jour., 1919, I, 542.
Salant, W.: The Importance of Diet as a Factor in the Production of Pathological Changes, Jour. Am. Med. Assn., 1917, LXIX, 603.
Sammis, J. F.: A Case of Scurvy with Cerebral Hemorrhage, Arch. of Pediat., 1919, XXXVI, 274.
Sato, T., and Nambu, K.: Zur Pathologie und Anatomie des Skorbuts, Virchow’s Arch., 1908, CXCIV, 151.
Schaumann: Die Aetiologie der Beriberi unter Beruchsichtigung des gesammten Phosphorstoffwechsels, Beihefte z. Arch. f. Schiffs-u. Tropenhygiene, 1910, XIV, 325.
Schmorl, G.: (1) Ueber Stoerung des Knochenwachstums bei Barlow’scher Krankheit, Centralbl. f. allg. Path. u. path. Anat., 1899.
Schmorl, G.: (2) Zur Path. Anatomie der Barlowschen Krankheit Beiträge z. path. Anat., 1901, XXX.
Schmorl, G.: (3) Ueber die Pathogenese der bei Moeller-Barlowscher Krankheit auftretenden Knochenveraenderungen, Jahrb. f. Kinderheilk, 1907, LXVI, 50.
Schoedel, J., and Nauwerk, C.: Untersuchungen ueber die Moeller-Barlow’sche, Krankheit, Jena, 1900.
Schreiber, G.: Scorbute et Dysenterie, Paris Médical, 1918, VII, 508.
Schreiber, G., and François, M.: Scorbut Infantile chez un enfant de quatre ans nourri au lait homogénéisé, Arch. de Méd. des Enfants, 1914, XVII, 610.
Seidell, A.: Vitamines and Nutritional Diseases, U. S. Public Health Reports, 1916, XXXI, 364.
Senator, H.: Ueber lymphadenoide und aplastische Veraenderungen des Knochenmarks, Zeitschr. f. klin. Med., 1904, LIV, 1.
Shaklee, A. O., and Meltzer, S. J.: (1) The Mechanical Destruction of Pepsin, Am. Jour. Physiol., 1908, XXIII, 29.
Shaklee, A. O., and Meltzer, S. J.: (2) The Influence of Shaking upon Trypsin and Rennin, etc., Proceed. Soc. Exp. Biol. and Med., 1908, VI, 103.
Sheppard, A. L.: Scurvy in Zhob, Baluchistan, Indian Jour. Med. Research, 1916, IV, 340.
Smith, T.: Hemorrhagic Periostitis of the Shafts of Several Long Bones with Separation of the Epiphyses, Trans. Path. Soc., London, 1876, XXVII, 219.
Smith, Th.: Bacilli in Swine Disease, U. S. Dept. Agric., Bureau Animal Industry, Ann. Rep. 1895–96, 172.
Smith, W. J.: Scurvy, Allbutt’s System of Med., 1901, V, 586.
Southgate, F. H.: A Case of Scurvy in a Breast-Fed Infant, Arch. of Pediat., 1893, X, 505.
Speyer: Waden-Abszesse bei Skorbut, Deutsch med. Woch., 1918, XLIV, 626.
Von Starck: Quoted from Czerny and Keller (see above).
Steenbock, H., Boutwell, P. W., and Kent, H. E.: Fat-Soluble Vitamine, J. Biol. Chem., 1918, XXXV, 517.
Stefánsson, V.: Observations on Three Cases of Scurvy, Jour. Am. Med. Assn., 1918, LXXI, 1715.
Steiner: Kompendium der Kinderkrankheiten, Leipzig, 1878, F. C. W. Vogel.
Stepp, W.: (1) Experimentelle Untersuchungen ueber die Bedeutung der lipoide fur die Ernaehrung, Zeitschr. f. Biol., 1911, LVII, 135.
Stepp, W.: (2) Weitere Untersuch. ueber d. Unentbehrlichkeit d. Lipoide, etc., Zeitschr. f. Biol., 1912, LIX, 366.
Still, G.: (1) Common Disorders and Diseases of Childhood, 1915, London, 3rd Ed.
Still, G.: (2) Cœliac Disease, Lancet, London, 1918, II, 163.
Stoeltzner, W.: Ein Anatomisch untersuchter Fall von Barlow’scher Krankheit, Jahrb. f. Kinderheilk., 1906, LXIII, 36.
Stoos, M.: Barlowsche Krankheit, Correspondenzbl. f. Schw. Aerzte, 1903, XXXIII, 497.
Sugiura, K., and Benedict, S. R.: The Nutritive Value of the Banana, Jour. Biol. Chem., 1918, XXXVI, 171.
Sutherland, G. A.: On Hæmatoma of the Dura Mater Associated with Scurvy in Children, Brain, 1894, XVII, 27.
Talbot, F. B., Dodd, W. J., and Peterson, H. O.: Experimental Scorbutus and the Röntgen Ray Diagnosis of Scorbutus, Boston Med. and Surg. Jour., 1913, CLXIX, 232.
Tobler, W.: Der Skorbut in Kindesalter, Zeitschr. f. Kinderheilk., 1918, XVIII, 63.
Torrey, J. C., and Hess, A. F.: The Relation of the Intestinal Flora to the Scurvy of Guinea-pigs and of Infants, Proc. Soc. Exp. Biol. and Med., 1918, XV, 74.
Torup: Report of the Committee Appointed to Inquire into the Causes of the Outbreak of Scurvy in the Recent Arctic Expedition, London, 1877.
Trop. Dis. Bull.: 1918, XII, 257.
Tschudakoff: Cited from Heubner, O.; Lehrbuch. f. Kinderheilk., Leipzig, 1903, I, 698.
Tuechler: (Quotes Rheindorf) Ueber Skorbut, Med. Klin., 1918, XIV, 112.
Uhlmann, F.: Beitraege zur Pharmakologie die Vitamine, Zeitschr. f. Biol. 1918, XLVIII, 419, 457.
Urizio, L.: Skorbut und nicht-spirochaetogener Icterus epidemicus, Wien. klin. Wochenschr., 1917, XXX, 1449.
Vallardi, C.: Riforma Med., 1918, XXXIV, 793.
Vannutelli, F.: Un Epidemia di Porpora Infettiva con Manifestazione Emorragico-scorbutiche tra le Truppe Combattenti, Il Policlinico, Sez. Pratica, 1917, XXIV, 873.
Variot, G.: Du Lait Stérilisé, Compt. rend. de l’Acad. d. Sci., 1905, CXXV, 1002.
Vedder, E. B.: Beriberi, New York, 1913, Wm. Wood & Co.
Vedder, E. B., and Clark: A Study of Polyneuritis Gallinarum, Phillip. Jour. Sci., 1912, VII.
Villemin: Cause et Nature de Scorbut, Bull. d. l’Acad. de Med., 1874, 680, 739.
Vincent, R.: The Nutrition of the Infant, New York, 1904, Wm. Wood & Co.
Voegtlin, C.: The Effect of Alkali on Vitamines, Proc. Amer. Soc. Biol. Chem., 1916, 24.
Voegtlin, C., and Myers, C. N.: A Comparison of the Influence of Secretin and the Antineuritic Vitamine on Pancreatic Secretion and Bile Flow, Jour. Pharm. and Exp. Therap., 1919, XIII, 301.
Wassermann, S.: (1) Ueber Hochwertige Erythrozyten and Hemoglobinbefunde bei Kriegern, Muench. med. Woch., 1918, LXV, 927.
Wassermann, S.: (2) Ueber eine mit Schwellung und Roetung der Beine verbundene Knochenschmerzhaftigkeit bei Kriegern, Wien klin. Woch., 1918, LXVIII, 968.
Weston, W.: Pellagra in Early Childhood, Am. Jour. Dis. Child., 1914, VII, 124.
Wherry, W. B.: The Influence of Scurvy on Hemorrhages in Plague. Jour. Infect. Dis., 1909, VI, 564.
Willcox, W. H.: Treatment and Management of Diseases Due to a Deficiency of Diet, Scurvy and Beriberi, Brit. Med. Jour., 1920, I, 73.
Williams, R. R.: Some General Aspects of the “Vitamine” Problem, Amer. Med., 1916, N. S. XI, 756.
Wiltshire, H.: Hyperkeratosis of the Hair Follicles in Scurvy, Lancet, London, 1919, II, 564.
Wright, A. E.: The Causation and Treatment of Scurvy, Lancet, London, 1908, II, 725.
Yano, K., and Nemoti, T.: Studies of the Blood in Beriberi, Arch. Int. Med., 1917, XX, 103.
Ziegler, E.: Ueber Osteotabes infantum u. Rachitis, Centralb. f. allgem. Path. u. patholog. Anat., 1901, XII, 865.
Zilva, S. S.: (1) Action of Ultra Violet Rays on the Accessory Food Factors, Biochem. Jour., 1919, XIII, 164.
Zilva, S. S.: (2) Influence of Deficient Nutrition on the Production of Agglutinins, Complement and Amboceptor, Biochem. Jour, 1919, XIII, 172.
Zilva, S. S., and Wells, F. M.: Change in the Teeth of the Guinea-pig Produced by a Scorbutic Diet, Proceed. of the Royal Soc., 1919, B. XC, 505.
A
Acid, effect on keeping qualities of antiscorbutics, 66, 161
Adrenals, 102
in guinea-pig scurvy, 122
Adult, scurvy in, history of, 1
Age incidence, 51
Aging, effect on antiscorbutics of, 67
Agglutinins, effect of scurvy on, 68
Alimentary tract, gross pathology, 89
microscopic pathology, 100
Alkalization, effect on milk of, 50
on orange juice of, 66, 154
Amboceptor, effect of scurvy on, 68
Animals, scurvy in, 114
Anorexia, 206
Antiscorbutics, and antiscorbutic foods, 143, 149, 157
history of use of, 9, 143
Antitoxin, effect of scurvy on, 68
Appendicitis, confused diagnosis, 183
Appetite, 206
Apple, antiscorbutic value of, 158
Army, use of canned tomatoes in ration of U. S., 231
B
Bacteria, fecal, in scurvy, 28
as etiological factor in scurvy, 134
in tissues, 133
Bacterial theory of scurvy, 30
Banana, antiscorbutic value of, 158
Beading of ribs, 197
in guinea-pig, 129, 137
pathology of, 94
Beef juice, 236
Beer, antiscorbutic value of, 20, 169
Beriberi, differential diagnosis, 221
relation to scurvy, 249
Berries, antiscorbutic value of, 156
Blindness, 182
Blood cells, changes in, 209–211
Blood cells, chemistry of, 244, 245
coagulability of, 211
Blood vessels, changes in, 68, 98, 209
in guinea-pigs, 133
Blood, vitamine content of, 76
Bones, gross pathology, 93
microscopic pathology, 105
Brain, pathology, 93
Breast fed, scurvy in, 35
C
Cabbage, antiscorbutic value of, 159
dehydrated, 165
effect of heat on, 159
Calcium, deposits of, 98, 102, 103
metabolism, 241–247
“Capillary resistance test,” 212, 257
“Cardiorespiratory syndrome,” 200
Cardiovascular system, 199
Carrots, antiscorbutic value of, 159, 160
Central nervous system, gross pathology, 93
microscopic pathology, 104
Cereals, antiscorbutic value of, 170
germinated, 167
Cerebrospinal fluid, 203
Chlorides, 242–247
Citric acid theory, 23
Climate, 55
Complement, effect of scurvy on, 69
Complexion, characteristic change in, 176, 184
Complications of scurvy, 182, 202, 205, 217
Constipation, 27, 118–122, 207
Cord, spinal, pathology, 93, 104
Creatinine, 244
Cure, 236
D
Deficiency diseases, general discussion, 63, 248
Diastase, blood content of, 244
Diet, general, 59
Digestive disturbances, 78
Diphtheria, antitoxin in blood, 68
as complication of scurvy, 217
Drying, effect on vitamines of, 66
Duodenum, pathology, 89
E
Economic status, 55
Eczema, 195
Edema, 178, 184, 196
hunger, 256
war, 256
Eggs, antiscorbutic value of, 168
Endocrine organs, gross pathology, 92
microscopic pathology, 104
extracts of, as preventive, 172
theory of vitamine action, 72
Epiphyses, separation of, 96, 181, 198
Etiology, 35
exciting factors in, 60
Excretion of vitamine, 77
Expeditions, scurvy in Arctic, 10
Experimental scurvy, 111
pathogenesis, 116
pathology, 122
symptoms, 135
Eyeball, proptosis, 193
F
Familial tendency, 58
Fats, in diet, effect on scurvy, 59
Fœtus, effect of scorbutic diet on, 125
Food, excess of, 257
Foods, antiscorbutic, 143, 149
proprietary, 49
Fractures, 95
Frost-bite, 180
Fruit juices, 153
Fruits, fresh, 144
G
Generative organs, pathology, 104
Glands, endocrine, 72
changes in, 73, 92, 104
Glucose, blood content of, 244
Grapes, antiscorbutic value of, 158
Growth in scurvy, 213
Guinea-pig pathogenesis, 116
pathology, 122
relation to human, 115
symptoms, 135
Gums, 177, 181, 184
in infantile scurvy, 189
pathology of, 89, 100
H
Hair, changes in, 194
Heart, 200
gross pathology, 87
microscopic pathology, 99
Heat, effect on vitamine of, 65
Hemorrhages, 180, 189
as early symptoms, 178
distribution of, 84
gastric, 208
orbital, 193
subperiosteal, 95, 191
urinary, 204
History of scurvy, 1
Hog, effect of scorbutic diet on, 115
Hypophysis, 104
I
Infantile scurvy, history, 10
in artificially fed, 40
in breast-fed, 35
increase during World War, 21–22
relation to epidemic scurvy of adults, 15, 37
relation to rickets, 11, 110, 252
symptomatology, 183
Infection, as exciting factor, 60, 218
increased liability to, 68
effect on prognosis, 227
Intestines, gross pathology, 90
microscopic pathology, 100
Intravenous use of orange juice, 238
Irregularities in course of deficiency diseases, 78
J
Jaundice, 208
Joints, lesions of, 199
K
Kidneys, gross pathology, 91
microscopic pathology, 102
L
Laxatives, failure to cure with, 28, 207
Lemon juice, antiscorbutic value of, 153, 234
dried, 155, 232
ration in British Navy, 9, 144
Lentils, value as antiscorbutic, 167, 231
Lice, theory of transmission of scurvy by, 30
Lime juice, antiscorbutic value of, 156
fallacy in regard to, 149
use in British Navy, 144
Liver, gross pathology, 91
microscopic pathology, 101
Lungs, gross pathology, 88
microscopic pathology, 99
Lymph-nodes, gross pathology, 92
microscopic pathology, 101
M
Malnutrition, general, 58
Malt soup, 50
Marrow, changes in, 107
Meat, fresh, 147, 168
salt, 146
“Mehlnaerschaden” of Czerny, 256
Metabolism in scurvy, 241–247
Milk, alkalized, 50
amount necessary to prevent scurvy, 49, 117, 150
boiled, 44, 65
condensed, 48
dried, 46, 66, 152
effect of industrial methods on, 43
evaporated, 45
pasteurized, 40, 65
home vs. commercial, 42
sterilized, 44
breast, amount necessary to prevent scurvy, 36, 39, 153
as cause of beriberi, 39
cows, antiscorbutic value of, 40, 152
goats, antiscorbutic value of, 153
Mineral metabolism in scurvy, 241–247
Monkey, scurvy in, 114, 127
pathology, 128
Muscles, pathology, 97
N
Nails, changes in, 194
Necropsy reports, 82
Nephritis, 205
Nerves, peripheral, in guinea-pig
scurvy, 132
pathology, 105
Nervous system, effect of scurvy on, 202
Nutrition, general, in scurvy, 58, 59, 213
Nyctalopia, 182
O
Orange juice, antiscorbutic value of, 153, 234
“artificial,” 33
dried, 155
effect of alkalization of, 154
intravenous use of, 238
subcutaneous use of, 155
peel, antiscorbutic value of, 234
Osteogenesis imperfecta, 255
Osteomalacia, differentiation of, from scurvy, 255
Osteomyelitis, differentiation of, from scurvy, 222
Osteoporosis, differentiation of, from scurvy, 255
Osteotabes infantum, 109
P
Pains, as early symptom, 176
Pancreas, gross pathology, 91
microscopic pathology, 104
Pasteurized milk, 40
Pathogenesis of scurvy, theories of, 23
Pathology of scurvy in guinea-pig, 122
in man, gross, 83
microscopic, 96
in monkey, 128
Peas, antiscorbutic value of, 167, 231
Pellagra, 251
Phenols, excretion of, 245
Phosphate metabolism, 241–247
Pigeon, effect of scorbutic diet on, 114
Pneumonia, 202
Posture, characteristic, in guinea-pig, 136
Posture, characteristic, infant, 183
Potassium deficiency theory, 23
metabolism, 241–247
Potatoes, antiscorbutic value of, 6, 7, 146, 161, 235
Prevention of scurvy, 230
Prognosis, 225
Protein in diet, effect on scurvy, 59
Psychic element in scurvy, 57
Purpura, differential diagnosis, 221
Pyorrhœa, relation to lesion of gums, 181
R
Racial immunity, 56
Rats, effect of scorbutic diet on, 114, 115
Recurrent scurvy, 228
Respirations, 201
Retina, hemorrhages in, 105
Rheumatism, confusion with scurvy, 176, 220
Ribs, beading of, 197
pathology, 94
in guinea-pig, 129, 137
Rickets, relation of, to scurvy, 11, 110, 252
S
Sauerkraut, antiscorbutic value of, 145
Season, effect on incidence, 54
Sex, effect on incidence, 56
Shaking, effect on antiscorbutic factor, 68
Ship beriberi, 250
Skin, pathology, 96
Spleen, gross pathology, 91
microscopic pathology, 102
Sprue, 256
Starvation, pathology of, 125
Stomach, gross pathology, 89
microscopic pathology, 100
Storage of vitamine in body, 74
Streptococcus in blood in scurvy, 134
Subacute form of scurvy, 184
Subcutaneous use of antiscorbutics, 155
Swede, antiscorbutic value of, 162, 235
Symptomatology, in adult, 176
in infant, 183
Syphilis, congenital, differential diagnosis, 222, 223
T
Teeth, in guinea-pig scurvy, 130, 137
in human scurvy, 177
Temperature, in guinea-pig scurvy, 141
in human scurvy, 181, 216
Thymus, pathology of, 104
use of gland in treatment, 172
Thyroid, pathology of, 104
use of gland in treatment, 172
Tomatoes, canned, antiscorbutic value of, 166, 231, 234
in U. S. Army ration, 231
Toxic theory of pathogenesis of scurvy, 25
Treatment of scurvy, 230
duration of, 237
non-dietetic, 239
U
Ultra-violet rays, effect on antiscorbutics, 67
Urea content of blood, 244
of tissues, 245
Urine in scurvy, 204–206
V
Vegetable juices, keeping qualities of, 161
Vegetables, antiscorbutic value of 144, 158
canned, 166
dehydrated, 163
effect of heat on, 159
fresh, 144, 158
ripeness of, effect on antiscorbutic value, 160
Vitamine, antiscorbutic, general discussion of, 62
action of, 68, 69
as antitoxin, 69
as catalytic agent, 70
as nutriment, 69
blood content of, 76
effect of heat on, 65
of ultra-violet ray on, 67
excretion of, 77
Vitamine, experimental evidence for, 62
fate in body, 74, 77
relation to water-soluble factor, 65, 67
relation to antineuritic vitamine, 67
resistance to chemical and physical processes, 64
storage in body of, 74
theory of scurvy, 32
W
“White line” of Fraenkel, 128, 198
World War, scurvy in, 15
X
X-ray in diagnosis of scurvy, 128, 192, 198
Y
Yeast, antiscorbutic value of, 171
1 The best historical review of scurvy is to be found in Hirsch’s Handbook of Geographic and Historical Pathology, from which account we have drawn many facts.
2 The fact that crews of vessels which set sail in winter were more subject to scurvy than those which set out in the summer must be attributed to the existence of latent scurvy among the sailors at the time of sailing, rather than to the season of the year.
3 Infantile scurvy is frequently termed “Die Moellersche Krankheit.” There seems to be no occasion for giving Moeller credit for discovering this disease, as he believed that he was dealing with rickets merely in an acute form. He recognized the clinical similarity to scurvy, but in one of his cases sharply differentiates it from adult scurvy by the fact that “lemon juice and fresh vegetables” were of no avail in the treatment.
4 The writer adds that he believes that the health of the natives at home is protected by Kaffir beer, which they consume even to the amount of 3 gallons a day, and which is made from germinated Kaffir corn. This cereal is germinated by steeping it in water for forty-eight hours and is then dried in the sun. Only enough is prepared for one brew. The French prepared a similar fermented beverage for these South African laborers; the sole difference in its mode of preparation was that the corn had not been germinated.
5 The cases on which Wright based his theory were soldiers who developed scurvy during the siege of Ladysmith. It is probable that the men were suffering from starvation, purpura and dysentery. That they did not have scurvy is proved by the fact that they were cured by giving lactate and bicarbonate of soda.
6 In chronic mercurial poisoning the following suggestive symptoms occur: anemia, bleeding and spongy gums, loosening of the teeth, a quickened pulse, ulcers of the extremities. At times mercury attacks the nervous system, producing palsy. The resemblance is heightened by the fact that calcium metastases have been found in the muscle in experimental scurvy (Hart and Lessing) comparable to those characteristic of mercurial poisoning.
7 These figures constitute an irrefutable argument against the statement frequently made that a monotonous diet leads to scurvy. It is only when the monotonous diet does not contain an adequate quantity of antiscorbutic vitamine that it is to be feared.
8 This is not literally correct, as Doepp described an epidemic of scurvy in the St. Petersburg Foundling Asylum occurring in 1831.
9 During 1919 in Aruba there were 293 births and 30 deaths under one year, most of these deaths being due to intestinal diseases. The mothers subsist mainly on maize or guinea small corn, with some goat and sheep meat, and a little fresh fish, but no vegetables or fruit. The water is brackish.
10 Moore raises the interesting question as to whether a diseased condition of the cow may decrease the vitamines of the milk—whether a certain outbreak of scurvy among guinea-pigs might have been due to their having been fed on the milk of a cow suffering from experimental streptococcus mastitis. If such proves to be the case, it would have an important bearing on the question of scurvy and pseudo-scorbutic conditions in nursing infants.
11 In the case of the “lait maternisé,” which is a milk of high fat content, the dilution of the preparation also must have been a factor. Ounce for ounce, cream is poorer in antiscorbutic vitamine than an equal quantity of milk. It is also possible that the mere dilution of milk—quite apart from the absolute amount consumed—is not immaterial in affecting this highly sensitive vitamine.
12 It is to be noted, however, that Variot remarks that these infants frequently develop anemia unless additional diet is given, so that it must be considered open to question whether some of these babies did not have latent scurvy. Of course, unless it is certain that these infants were receiving only sterilized milk, and absolutely no other food, for a period of at least six months, they cannot be considered apposite to the question.
13 Carel reports an interesting case which points to the importance of staleness. A baby was taken to the country with a supply of sterilized milk sufficient to last for some weeks. At the end of this time it did not thrive, but regained its health when a fresh supply of milk was used. When this second supply became stale the infant again developed the same signs, and the condition was diagnosed as scurvy.
14 In making tests of dried milk particular attention should be paid to the age of the milk before it is desiccated. Investigators should also be certain that the milk has not undergone heating previous to the drying process. Some well-known brands of dry milk have been not only pasteurized, but subsequently evaporated before drying.
15 Ausset reports a definite case of scurvy developing in a baby nine months old, which had received buttermilk almost since birth. At the time of admission to the hospital it was getting 900 c.c. a day. This case is interesting on account of the acid nature of the food.
16 Malt soup is prepared by dissolving the alkaline malt soup extract in water, and mixing wheat flour with milk. These two mixtures are then boiled together for about three minutes. According to some directions, 11 ounces of milk are used; in our formula 16 ounces were employed.
17 It would seem, however, that the growing infant requires relatively more antiscorbutic vitamine than does the adult. We know that its caloric requirement is fully a quarter to a third greater. In regard to vitamine, judgment cannot be based on experimental evidence, but on comparative figures. For example, unless we take this viewpoint, we must believe that, as an infant of six months weighing 15 pounds requires 15 c.c. of orange juice daily to furnish its antiscorbutic quota, an adult weighing 160 pounds requires 180 c.c. daily—the juice of three good-sized oranges. On this basis the adult would require six quarts (6000 c.c.) of fresh milk daily, twelve times the minimum requirement for an infant, which is one pint (500 c.c.) a day. These figures are manifestly too high.
18 It would be of interest to know whether the negro infant is more susceptible than the white baby, in view of its markedly heightened susceptibility to rickets. There are, however, no reports or statistics to enlighten us on this point.
19 “Where the indisposition is but beginning, and even when the gums have been pretty much tainted, there have been numerous instances of a perfect recovery without having the benefit of fresh vegetables; provided the patient is able to use due exercise. . . . When it is advanced to what I have called the second stage it is hardly to be cured without their (fruits and vegetables) assistance.” (Lind.)
20 Caillé has described a case of scurvy in an infant suffering from Mongolian idiocy, and we have also seen a similar case.
21 Many of the older authors believed that mercurial drugs were especially prejudicial in cases of scurvy.
22 Vitamine is used throughout this monograph as synonymous with “accessory food factor” or “food hormone” as a convenient descriptive term, without any intention of connoting a definite chemical substance.
23 Freise cured a case of infantile scurvy by giving about 2 c.c. of an extract obtained from turnips by means of absolute alcohol. Seven weeks were necessary to cause a disappearance of symptoms. Freudenberg employed an extract of carrots, prepared with 96 per cent. alcohol, and effected a quicker cure.
24 Reference is made to a milk dried by the Just-Hatmaker process, containing about 3 per cent. of moisture. The clinical data on which this conclusion is based are given in the previous chapter.
25 The dates and quantities of the transfusions were as follows: March 26th, 200 c.c.; April 27th, 30 c.c.; April 28th, 35 c.c.; April 29th, 30 c.c.; May 2nd, 75 c.c.; May 3rd, 35 c.c.
26 This investigation was carried out by means of activating fuller’s earth with these fluids. This method is inapplicable to the antiscorbutic vitamine, which is not adsorbed by this material. An attempt to feed concentrated human urine to guinea-pigs resulted in their death.
27 Neumann, for example, writes that he has seen at least four children whose condition was not improved, although in addition to the milk, they took asparagus, spinach, and other vegetables or apple sauce. Some years ago we had a similar experience. It has likewise happened that infantile scurvy did not recur, although the diet was the same as that which originally led to the disorder.
28 For recent and comprehensive reviews of the vitamines the reader is referred to papers by A. B. Macallum (Trans. Royal Canadian Institute, Toronto, 1919) and by W. H. Eddy (Abstracts of Bacteriol. 1919, Vol. iii, 313.)
29 For details regarding the intestinal lesions in infantile scurvy, the reader is referred to Barlow’s description of the case of Stephen Mackenzie, to one necropsy report by Theodor Fischer, one by Hirschsprung, one by Meyer, and five by Schoedel and Nauwerk. The prevailing lesions are hemorrhages, pigmentation, follicular ulceration, and enlargement of the mesenteric glands.
30 The potato crop largely failed this year, and there was considerable scurvy in the spring, as described in the chapter on antiscorbutics.
31 Lind writes: “In the months of July and August I opened near seventy large swellings in the groin, proceeding entirely from scurvy.” . . . “We found the glands under their arm-pits much enlarged and surrounded with purulent matter, as well as the muscles of their arms and thighs.” . . . “The glands of the mesentery are generally obstructed and swelled. Some of these were found partly corrupted and imposthumated.”
32 In view of the report of Hart and Lessing of calcium deposits in the adrenal glands of monkeys suffering from scurvy, special attention should be given to this point in necropsies on human beings.
33 The beading may have the usual, rounded, smooth, knobby character. There may be, however, what one might term “angular beading,” the junction taking on a step-like form, as if the abutting ends of the cartilage and the bone were of unequal size and not well fitted to each other. The cartilage overtops the bone, so that on palpating the joint there is a precipitous fall as we run the finger outward from the surface of the cartilage, or a sudden elevation on palpating the rib from without inward toward the sternum.
34 There seems to be some misconception as to the pathogenesis of the subperiosteal hemorrhage in scurvy. In most reports this lesion is described as if it resulted from a hemorrhage burrowing its way beneath the periosteum and raising it from the subjacent bone. In point of fact, such an event is impossible, as will be fully realized when one experiences the great difficulty in separating periosteum from normal bone. Scurvy involves a periosteum which is not normal; it is insecurely attached to the shaft of the bone, so that it is readily stripped off by hemorrhage.
35 Hogs fed on 1.5 kg. of rye bread and 0.5 kg. of meat heated to 100° or 110° C. for a half hour showed the hemorrhages, loosening of the teeth and affections of the gums characteristic of scurvy, as well as the paralysis and neuritis typical of polyneuritis.
36 A guinea-pig requires about 80 to 100 c.c. of fresh milk per diem to protect it from manifest scurvy, if this constitutes its sole antiscorbutic quota. There is, however, a great difference in the amount of milk which individual animals consume, so that if we furnish it ad libitum our results will be irregular, one animal developing scurvy and another remaining well, according to individual appetite. Frequently guinea-pigs take very little milk at first, learning gradually to drink more and more, so that it comes to pass that only after some weeks, if at all, they take sufficient to afford protection. Under these circumstances, if any addition is made to the dietary after the experiment has progressed, the lack of development or cure of the scurvy may mistakenly be attributed to this newly introduced factor, whereas, in point of fact, it is due to an increased consumption of milk.
37 These changes are not found in every specimen, so that in order to be able to exclude scurvy definitely, it is necessary to examine a considerable number of ribs; several may be normal, only one or two showing the characteristic microscopic changes.
38 A maximum count of 35 was formulated, representing the highest degree of clinical scurvy. This includes three grades of beading of the ribs, four of tenderness of each knee and wrist joint, and four of swelling of each of these joints. It is apparent from the clinical curve (Fig. 10) that an animal may have developed a marked degree of scurvy (20 points), and gained rather than have lost in weight.
39 It is of interest that John Hall, the son-in-law of Shakespeare, and a prominent physician of Warwickshire, was one of the first to urge the use of antiscorbutics. In a quaint work entitled, “Select Observations on English Bodies, or Cures both Empericall and Historical” (1657 London), he describes how he cured scurvy by means of brewing a beer or ale from “Scorbutick hearbs, viz.: scurvy grass, water-cresses and brook lime.” This book, which ran through at least two editions, has not achieved the popularity of the works of the father-in-law.
40 Preserved mulberries which had been sugared and cooked for one-quarter to one-half an hour were found by Holst and Froelich (1912) to possess good antiscorbutic power three months later.
41 Dr. Guy’s evidence, Report of the Lords Commissioners of the Admiralty on the Outbreak of Scurvy in the Recent Arctic Expedition—1877 (cited from Chick and Hume).
42 The swede is a root vegetable of the natural order Cruciferæ. It is grown to a large extent in England, but is practically unknown in the United States.
43 “We find the College of Physicians at Vienna sent to Hungary great quantities of the most approved antiscorbutic herbs dried in this manner; which were found to be of no benefit. Many of these would have their virtues as little impaired by drying as spinage, e.g., marsh trefoil. Kramer tried almost every species of dried herbs to no purpose.” (Treatise on The Scurvy. James Lind, London, 1772, p. 143.)
44 The cabbage was subjected to a preliminary drying for 8 days at 37° C. It was then put in an air-tight desiccator which contained a dish of phosphorus pentoxid. (The pentoxid was replaced for several weeks until it ceased to liquefy.) It was then placed in cylinders which had been rendered air free by means of a suction pump and which contained phosphorus pentoxid. This was kept at 37° C. and examined after 10, 18 and 26 months. A similar result was not obtained when calcium chlorid was employed, the temperature held at 37° C. and the cabbage was kept in an air-tight cylinder rather than in a vacuum. However, under these conditions if the cabbage was placed in the ice-box at a temperature of 4°, 10° or 12° C. the antiscorbutic property was conserved after boiling.
45 The pulses, after having been soaked in water for 24 hours, were kept moist, with access of air, for about 48 hours at room temperature, and during this time germinated, developing a radicle usually about 1 cm. in length.
46 As the result of an experience with thousands of cases of scurvy in the Serbian army, Wiltshire has recently laid great emphasis on this follicular hyperkeratosis. He states that the earliest recognizable sign of scurvy is an enlargement of the hair follicles of the inner and anterior aspects of the thigh and upper leg, which show numerous conical elevations about the size of a pin’s head. A hair, broken or unbroken, frequently pierces the follicle.
47 There seems to be some misconception as to the pathogenesis of the subperiosteal hemorrhage in scurvy. In most reports this lesion is described as if it resulted from a hemorrhage burrowing its way beneath the periosteum and raising it from the subjacent bone. In point of fact, such an event is impossible, as will be fully realized when one experiences the great difficulty in separating periosteum from normal bone. The scorbutic process involves the periosteum so that it is no longer normal but becomes insecurely attached to the shaft of the bone, and is readily stripped off by hemorrhage.
48 Senator regarded the marrow in scurvy as being aplastic. Nobécourt, Tixier and Maillet report postmortem examinations where the marrow showed an increased number of myelocytes and nucleated red cells of various kinds. They consider the typical blood change an intense myeloid reaction of the blood.
49 A blood-pressure band, or tourniquet, is placed about the arm, and the pressure increased until the forearm becomes cyanosed and the radial pulse is almost obliterated. The pressure is then maintained at this level for 3 minutes. The principle of this test consists in subjecting the capillaries and venules to increased intra-vascular pressure to observe whether this strain results in the escape of blood. In infants the pressure was usually raised to 90 mm.; in some cases it had to be raised higher in order to entirely obstruct the return flow of the blood.
The test is considered to be “positive” when the forearm shows many petechial spots. In normal infants petechiæ were almost always absent, or there were few to be seen. This is not a specific test for scurvy, but demonstrates a weakness of the vessel walls, whatsoever may be the cause. It is found to be positive in the majority of cases of scurvy.
50 We have been unable to ascertain through inquiries from the Surgeon-General’s Office the nature of the experience which led to their incorporation in the ration, and whether they were added specifically as an antiscorbutic. They appear for the first time in the revision of the Army Regulations of 1895. The only reference to the antiscorbutic property of canned tomatoes which we have been able to find in the literature is in the excellent treatise by Munson on Military Hygiene.
51 Since the above was written, an article has appeared by P. W. Bassett-Smith (Scurvy: With Special Reference to Prophylaxis in the Royal Navy. Lancet, London, 1920, I, 1102) showing that lemon juice can be prepared in tablet form and preserve its efficacy for at least three months. Each tablet contained the equivalent of 24 c.c. of lemon juice, and less than one-fifth of a tablet was sufficient to protect a guinea-pig from scurvy. This therapeutic procedure seems of great promise in providing an antiscorbutic ration for the navy or the army.
52 It is not possible to say exactly how much raw milk a baby needs to protect it against the development of scurvy. We may, however, reach an approximate estimation of this figure. We know that it takes about 2 c.c. of orange juice to protect a guinea-pig against manifest scurvy, and about 10 c.c. to protect a baby. The ratio, therefore, between the guinea-pig and the infant in this regard would seem to be about 5 to 1. We also know that it takes about 80 to 100 c.c. daily of fresh cow’s milk to protect a guinea-pig for long periods. If we assume the ratio of 5 to 1, it would therefore seem that it would require about 500 c.c. or a pint, of fresh raw milk daily as a minimum to protect the baby. (It is quite possible that a slight negative balance of the vitamine may exist unless a still greater amount is given.)
53 Orange juice undergoes a decided color change as soon as it has become neutral or very slightly alkaline, assuming a more translucent and far deeper yellow or amber color. This change may be utilized by the attendant in determining the reaction, thus rendering titration or other time-consuming methods unnecessary.
54 There is no relation whatever between the acidity of canned vegetables and their possible contamination with tin. Experiments carried out to determine this question demonstrated, for example, that a “sample of red kidney beans showing the highest acidity contained the least tin,” and that those samples containing the most tin were all relatively low in acidity. (Report of Conn. Agric. Station Bull. 200, 1917, J. P. Street.)
55 Salant, in experiments on rabbits, found that old or winter carrots did not have the same protective action against tartrates as young carrots, although their diuretic action is the same.
56 It is difficult to state the exact dosage of orange juice which is necessary. One teaspoonful daily has failed to cure, and rapid cures have been accomplished by giving one tablespoonful. It is well, however, to give a larger amount if it is tolerated.
57 Almost all of these cases were receiving liberal daily amounts of cod liver oil, which should exclude the possibility of complicating rickets.
58 There is no adequate reason for placing in this group “cœliac disease,” a nutritional disorder of children recently described by Still, and suggested by McCarrison as belonging to the category of the vitamine deficiency diseases. A case of this kind has come to our attention which resembled pellagra in many respects. It showed the bright red, denuded tongue, the intestinal symptoms, the occasional edema, marked loss in weight, and evanescent erythema—all symptoms of markedly disturbed nutrition but not distinctive of a lack of vitamines.
59 The only evidence in favor of a true interrelationship is furnished by a necropsy report of Hart and Lessing on one of five monkeys fed on a scorbutic diet. This animal died of disseminated tuberculosis, and the bones showed “the classic picture of severe rickets.” This occurrence cannot be explained, although illness and lack of exercise no doubt played a rôle. Until similar cases are reported, the incident must be regarded merely as interesting and suggestive.