The Project Gutenberg EBook of Schweigger on Squint, by C. Schweigger
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
Title: Schweigger on Squint
A Monograph by Dr. C. Schweigger
Author: C. Schweigger
Editor: Gustavus Hartridge
Translator: Emily J. Robinson
Release Date: March 20, 2011 [EBook #35639]
Language: English
Character set encoding: ISO-8859-1
*** START OF THIS PROJECT GUTENBERG EBOOK SCHWEIGGER ON SQUINT ***
Produced by Ian Deane, Josephine Paolucci and the Online
Distributed Proofreading Team at https://www.pgdp.net.

LONDON
J. & A. CHURCHILL
11, NEW BURLINGTON STREET
1887
The subject of Squint is so interesting that we venture to think an English rendering of this exhaustive monograph will be acceptable to many ophthalmic surgeons and students.
While adhering as far as possible to the spirit and style of the original we have not hesitated here and there to give a somewhat free translation. This has been partly necessitated by the difficulty of finding an exact equivalent in English for all the terms used in the original text.
In the German Edition the old system of inches is used. We have (with the consent of the author) altered these to the dioptric system.
E. J. R.
G. H.
Amicus Plato, amicus Socrates, magis amica veritas. May my friends and colleagues, whose views differ from mine, read the following observations without prejudice. A fact, which does not agree with the system, is generally worth more than theory, still it is very difficult for even the most important fact to find recognition if it contradicts received opinion. For theories and dogmas are narcotics, which are necessary to men; some flatter themselves by composing them, while others content themselves by satisfying their own craving for a creed. Reasonably applied, they may be useful, but the boundary line is only too easily over-stepped. It is the task of science to observe also whether theories correspond with the progress of facts. The present reigning theory on strabismus will have to submit to various limitations; on the other hand, we are ready to leave to the scholastic science of medicine and its followers certain dogmas which remain unproved and which have nothing but the fact of their existence to recommend them.
The small compass of the following treatise proves that it was not intended to exhaust the rich literature on the subject; I have only referred to the same where it appeared to me necessary for the interest of the work in hand.
Above all, it has been my endeavour to treat the subject of[Pg viii] this treatise (which occurs so frequently in practice) in a way intelligible to every physician, at the same time, however, to bring sufficiently into notice those facts and views which are of value to my special colleagues.
C. SCHWEIGGER.
Berlin.
Introduction. PAGES
Ordinary use of the word squint and its meaning. Apparent
squint. Paralytic and typical squint. Law of association.
Squint angle and linear measure of the deviation.
Permanent, periodic, latent, monolateral, and alternating
squint 1-8
Convergent Squint.
Donders' theory and the test of it by statistics. Limits
of error in the subjective and objective determination of
hypermetropia. Statistics of convergent squint. Hypermetropia
and favouring circumstances. Participation
of the accommodation. Preponderance of the interni
and insufficiency of the externi. Nebulæ of the cornea. 9-26
Periodic Convergent Squint.
In myopia, emmetropia, and hypermetropia. Intermittent
squint. Accommodative squint 27-35
Convergent Squint in Myopia 36-38
Squint From Paralysis of the Abducens 39-40
Hysterical Squint 41-43
Divergent Squint.
Absolute and relative divergence. Statistics of divergent
squint. Causes 44-49
Dynamic Squint, Insufficiency of the Interni And
Muscular Asthenopia.
Diplopia and power of overcoming prisms. Facultative
divergence. Dynamic absolute divergence. Parallel
strabismus. Relative divergence in myopia. Muscular
asthenopia. Dynamic relative divergence. Treatment
[Pg x]of muscular asthenopia 50-63
Binocular Vision in Squint.
Single vision in squint. Theory of exclusion. Forms of
binocular vision in squint 64-74
Visual Acuteness of the Squinting Eye.
The trial of vision and its results. Appearance, diagnosis.
Peculiarities and statistics of congenital defective vision.
Relation of the same to defective vision in squint 75-104
Cure of Squint.
Spontaneous cure. Voluntary loss of the habit. Cure of
convergent squint by means of convex glasses. Strabotomy.
Tenotomy. Advancement. Result of the
operation and choice of methods. After-treatment by
means of influence on the ocular muscles and on the
accommodation. Aim of more extended results of the
operation. Artificial strabismus. Operation for periodic
convergent squint. Strabotomy in homonymous diplopia.
Operation for squint after paralysis of the abducens.
Operation for divergent squint and for periodic divergence.
Degree of the result of the operation. Determination
on the age best suited for operation 105-141
By squinting, in the German vocabulary, is understood every oblique direction of the visual axes. We prefer that the eyes which turn towards us should do so in a straight line, and feel it to be something ugly and out of harmony, if anyone squints at us. Æsthetic feeling is, however, too individual and uncertain a guide to be laid down as a foundation for the decision of questions of medicine. Parents have repeatedly brought to me children said to squint, when frequent and careful examination of them showed normal position of the eyes and perfect binocular vision; the over-anxious parents had taken mere physiological convergence or side glances for squinting.
On the other hand, cases appear in which such a strong semblance of squinting is present, that at the first glance one cannot say whether absolute fixation takes place or not. A very simple examination suffices to determine these doubts:—Cause the patient to gaze at a certain point on the horizon and cover first one eye and then the other. If the covered eye remains stationary, no squint exists, but if it is observed that when giving one eye its freedom and covering the other, the first must make a movement in order to fix the object to[Pg 2] be looked at, it is only a question of discovering whether the squint does not simply ensue from the covering up of the eye. We will return to these cases at greater length, in order to occupy ourselves now with the fact, that the examination above referred to proves the non-existence of strabismus, while appearance still allows us to suspect its existence.
This apparent contradiction finds its explanation in the fact that the scientific notion of squinting is determined by the direction of the visual axes. Strabismus is present when one eye only is directed to the fixed point, while the visual line of the other eye deviates from it.
But we cannot see the direction of the visual line, we can only judge of it from the position of the cornea. It is exactly that line which joins the point fixed with the centre of the fovea centralis. We can determine the position of the cornea by a perpendicular line passing through the centre of the cornea; this does not coincide with the visual line but deviates from it about 5° outwards. In the case of parallel lines of vision the corneæ are directed slightly outwards, a position which we are accustomed to consider as the normal one. If the angle formed by the above-mentioned perpendicular and the visual line is larger than usual, i. e. if the corneæ move further outwards than usual, the unusual appearance strikes us, and gives us the impression of a divergent squint. The enlargement of this angle, which is usually indicated as Angle a, is a peculiarity of the hypermetropic eye; and where we have an apparent divergent squint we may expect to find also hypermetropia, while an apparent convergent squint occurs occasionally in myopia of high degree.
If we turn now to those cases in which a real deviation of the visual line occurs, we must first consider the cause, and afterwards distinguish it from paralysis of the ocular muscles. The faulty position may be constantly present or it may only occur when the paralysed muscle is called into action. It is[Pg 3] almost invariably combined with double vision; sometimes the latter is the prevailing symptom, whilst the faulty position of the eye is in no way obtrusive, and can only be proved by careful investigation.
In contrast to paralysis of the ocular muscles stands the typical concomitant squint, in which the squinting eye normally accompanies the movements of the other. Transitional forms may thus be brought about, in some of which the paralysis recovers, with complete or almost complete restoration of movement, but with continuance of the squint. On the other hand, in concomitant strabismus, restriction of movement towards the opposite side not unfrequently develops itself.
This impairment of movement has its origin generally in a want of use. Those who squint have less need for movement, since one of their eyes is already directed obliquely. In divergent strabismus this is apparent, but in convergent strabismus the squinting eye governs the field of vision on the side to which it turns. When the fixing eye is turned towards the side of the squinting eye in convergent strabismus, the latter, it is true, makes a concomitant movement, which does not, however, bring it by a long way to the limit of the movement of which it is capable. The defect of motion is therefore generally present in both eyes, and is usually most marked in the squinting eye. Often, indeed, there is present at the same time a congenital or acquired insufficiency of the antagonistic muscle, but that want of use has also much to do with it, is shown by the improvement of mobility that often follows even short practice.
From the law of equal innervation, which governs the movements of the eyes, it follows that the fixing eye lapses into the associated deviation as soon as the squinting eye is directed straight forwards. If, for example, a convergent squinting eye is put into fixation, an innervation of the external rectus, with which just as strong an associated contraction of the[Pg 4] internal rectus of the other eye, is called forth; the direction of the squint then, as well as the degree of deviation, is transferred from one eye to the other. It is naturally the same with divergent squint.
Squinting upwards or downwards seldom occurs as a symptom by itself; more frequently it is associated with convergent or divergent squint.
According to the law of associated movements, when an eye squinting upwards is put into fixation, the other eye should make a movement downwards, as normally both eyes move together up and down, yet this is not always the case. For example, when an upward deviation is present in convergent squint, it not uncommonly follows that the secondary deviation of the eye which usually fixes is also inwards and upwards; only exceptionally in cases of deviation in height of the squinting eye does the sympathetic movement take place without change of height. Sometimes with deviation of height, I found combined a distinct rotation of the eye, generally thus, that together with the movement upwards was combined a rotation of the vertical meridian outwards and vice versâ; in fixing the eye a rolling inwards was combined with the movement downwards. The other eye then usually showed a similar rotation (thus the meridian of both eyes rotated simultaneously to the right or left), but the deviation in height was not always the same.
The law of equal innervation requires in alternate fixation, first with one eye, then with the other, that the same degree of deviation be transferred to the non-fixing eye. When exceptions appear, and the deviation in the two eyes is unequal, it is (provided the inequality has not been caused by attempted operation, or is the result of paralysis), usually to be explained by the fact, that an accommodative movement takes place when we are expecting an associated one. For example, if there is convergent squint and hypermetropia in both eyes,[Pg 5] but more hypermetropia in one than the other, in alternate fixation it will be found that the least hypermetropic eye always undergoes the greatest deviation, because in fixation with the more hypermetropic eye a stronger effort of accommodation unites itself with a corresponding innervation of the internal rectus, which is transferred equally to the other and non-fixing eye. Thus it happens frequently in divergent strabismus, when one eye is myopic, the other emmetropic. If the latter fixes an object stationed near the "far point" of the myopic eye, the internal recti and the accommodation act simultaneously; on the other hand if the myopic eye fixes, it wants no accommodation and the emmetropic eye sinks into divergence.
With regard to the immutability of the squint; it must not be understood that the squint angle always remains the same with the same individual; in most cases the amount of deviation varies, the squint is now less, now greater; it is desirable however, to know the bounds within which it fluctuates.
To determine the degree of the squint one can either ascertain the angle of the squint, or use v. Graefe's so-called linear measure of deviation.
The squint angle is that angle, which the visual line of the squinting eye encloses with the direction it ought normally to take—it may be measured with the aid of a perimeter. The patient's head is so placed by means of a chin rest, that the axis of the squinting eye is in the centre of the arc of the perimeter; a distant point in the centre of the field of vision is fixed. Behind the patient is a candle, the reflection of which is thrown into the squinting eye by means of a plane mirror; now slide the mirror along the arc of the perimeter, till the reflection on the cornea stands in the centre of the pupil of the eye which is under observation. The point which the mirror occupies on the arc of the perimeter, indicates the squint angle. In deviation in height of the squinting eye,[Pg 6] bring the arc of the perimeter into the corresponding direction and so measure at the same time the degree of deviation in height. Were the method more exact than it is, one would be able to measure the angle formed by the visual line and the axis of the cornea.
To find the linear measure of the deviation, cover the fixing eye and allow the squinting eye to fix. Hold a millimetre measure close to the under lid, so that a chosen portion of it stands under the centre of the pupil; uncover the other eye and when the squinting eye returns to its deviation, it can be seen over which point the centre of the pupil stands, and the linear measure of the deviation is thus obtained. The secondary deviation of the other eye is measured of course in the same way. If, in consequence of amblyopia, the squinting eye possesses no certain fixation, the measure may be so held that the nil point of the division coincides with the lower punctum, and then in unchanged fixation the portion lying under the centre of the pupil is determined, first in the sound and then in the squinting eye.
The execution of one or other of these forms of measurement is in every case to be recommended, and if their exactness is not as perfect as can be desired, still, on the other hand it should be remembered, that for surgical treatment, an exact measurement of the deviation does not possess the importance sometimes assigned to it, as in most cases the squint angle shows considerable variations.
In a large number of cases these variations are so great, that a correct position of the eyes alternates with a more or less considerable squint, which as the case may be, appears seldom or often, sometimes only under certain conditions, and sometimes quite unexpectedly (periodic squint). In some cases stationary or permanent squint begins with the periodic form, however, one must not conclude that periodic squint is invariably the precursor of the permanent form. In by far[Pg 7] the greater number of cases periodic squint continues unchanged without ever becoming permanent.
The transition from squint to the normal condition is formed by those cases, in which the proper position of the eyes is maintained by a desire for binocular single vision, while the elastic tensions of the muscles are such, that squinting sets in as soon as binocular single vision is rendered impossible (latent squint).
The squint is generally one sided (monolateral), for the eyes in this case are usually of unequal value, and the best is always preferred for use. The eye which has the acuter vision is always made use of when something has to be carefully observed. But when the acuteness of vision is equal, and one eye is emmetropic and the other hypermetropic, or if both are hypermetropic but in varying degree, the most hypermetropic eye is always the squinting one; for with a greater power of accommodation it does not accomplish more than the emmetropic or less hypermetropic one with slighter expenditure of strength. Why should a man strain his accommodation when no advantage is thereby gained?
In most cases the squinting eye has also an available power of vision and is on that account used for fixing objects which lie in the direction of its visual axis; it can also be made to fix objects in front, this occurs as soon as the other eye is covered; it remains as the fixing eye till the next blinking of the lids, or movement to another object for fixation, or till both eyes are closed for a short time, when it returns to its former deviation.
A true alternating strabismus, i. e. alternate use of first one eye and then the other to fix objects straight ahead, only occurs when both eyes are of equal value as regards weakness and acuteness of vision, or when one is more conveniently used for near, and the other for distant vision. In these circumstances one eye is always short-sighted and is used[Pg 8] for near objects, while the other is emmetropic (or in less degree near-sighted or long-sighted) and is preferred for distant things. The reason for the alternation lies in the necessity for the act of vision itself; it begins regularly whenever distant and near objects are alternately fixed. Alternating squint is usually divergent, with short sight on one side, still convergent strabismus may occur under these conditions.
To Donders belongs the merit of having pointed out the presence of hypermetropia in about two thirds of all cases of convergent strabismus. The fact is undeniable, the theories built upon it are doubtful. Donders declares no other conclusion to be possible, than this, that the hypermetropia is the cause of the squint. "To see clearly, the hypermetrope must accommodate vigorously for each distance. In looking even at distant objects he must overcome his hypermetropia by exerting his accommodation, and in proportion as the object approaches him, he must add to it as much accommodation as the normal emmetropic eye would use. The inspection of near objects requires then a special amount of exertion. There exists, however, a certain connection between accommodation and convergence of the visual lines. The stronger one converges the more one has to put into action the accommodation. A certain tendency to convergence cannot then be absent during any effort of the faculty of accommodation."
Right as these conclusions may appear, and as they really are, as far as emmetropia is concerned, they leave out of sight the fact, that the connection between accommodation and convergence is an individual and acquired one. The weak side of the theory lies in the fact, that that relation between accommodation and convergence which is developed in emmetropia in consequence of daily practice, is given as being in itself normal and the one for all conditions of refraction. The[Pg 10] relation between accommodation and convergence depends on the state of refraction, and alters with any of its changes in the course of life. In proportion as myopia is gradually developed in originally existing emmetropia, myopes learn to converge to the neighbourhood of their far point without allowing their accommodation to come into action. With hypermetropia it is just the contrary. By far the greater number of hypermetropes learn to use their accommodation without difficulty, even with parallel lines of vision, for they see distant objects clearly, while they neutralise their hypermetropia by accommodation, without sacrificing the parallelism of the visual lines.
It is important to notice that Donders' theory makes convergent squint appear as almost a necessary consequence of hypermetropia. According to Donders, hypermetropes have to choose between the advantages of binocular vision with an effort of accommodation corresponding to the hypermetropia, and relief to the accommodation by too strong convergence with the sacrifice of binocular fixation; and the decision will tend to the latter condition, if circumstances exist which deprecate the value of binocular vision.
The demand for binocular fusion of the retinal images will be greater if both eyes are of equal value; on the contrary it will be less, if the retinal image or the visual acuteness of one eye is less perfect than that of the other. Varieties of weakness; when one eye always receives a clear retinal image, the other an indistinct one; lowering of the visual acuteness of one eye by nebulæ, astigmatism or any other cause. According to Donders all these furnish a reason why, in existing hypermetropia, binocular fixation should be abandoned and convergent strabismus developed.
It cannot be denied that the relation existing between convergent strabismus and hypermetropia may be as Donders represents it; the only question is, whether it really is so. A[Pg 11] theory may appear very acceptable, and may rest on a firm physiological basis; it will, however, be more perfect if it answers to facts. Physiological possibility is not always pathological reality, for other unusual causes besides physiological ones acquire value, and so things become pathological. If Donders' theory is right, convergent strabismus must really begin, as soon as double hypermetropia meets with causes which depreciate the value of binocular vision. The theory may be tested then by statistics, which confront the cases of hypermetropia and convergent strabismus with those cases in which hypermetropia meets with Donders' conditions and normal binocular vision still remains.
The statistics, which I have collected, relate to all the cases which have appeared in my private practice during the last ten years. The number would be much more considerable if I had included the patients of the University Clinic; however, the reliability of the single elements of which the statistics are composed was to me more important than the number. In my private practice I have myself examined every case with reference to these statistics for at least five years.
In a large clinic, where more than 5000 new patients annually come under treatment, one must frequently content oneself by satisfying the demands of the moment; thus the sources of inaccuracy in the statistics would be augmented.
Included in the statistics were not merely the cases which came under treatment for squint, but all in which squinting was present or those in which it could be objectively proved (for example, by scars left by previous operations for squint), that squint had formerly existed.
Further, in the following statistics, only those cases were included, where an exact determination of the amount of error was possible; in most cases this was also verified objectively with the ophthalmoscope. In many cases, especially in children, the objective determination of refraction alone is possible,[Pg 12] and is practicable only with the greatest difficulty and by the use of atropine.
Those cases deserve particular mention, in which it remained doubtful whether hypermetropia of slight degree or emmetropia was present. Even in full visual acuteness it is not unusual that with weak convex glasses (of less than a dioptre) binocular vision is just as clear as with the naked eyes, while in monocular investigation convex glasses cause a slight indistinctness of vision. Are we to recognise hypermetropia here or not? Opposed to the objection that in covering one eye the hypermetropia is more easily neutralised by accommodation, stands the observation that binocular is, as a rule, clearer than monocular vision, wherefore, in the usual method for testing the sight, unless special precautions are taken, full binocular visual acuteness does not prove the presence of absolutely distinct retinal images. These doubts arise much oftener in lowered visual acuteness. All conclusions which we derive from visual acuteness become very inexact as soon as it is lowered. In such cases, in determining anomalies of refraction we are accustomed to consider the strongest convex—relatively, the weakest concave glass, with which the visual acuteness individually present is reached, as the most correct expression of the hypermetropia or myopia, and with good reason if it is a case of ordering spectacles, as all sources of error in the method of examination are then avoided as far as possible; but it is quite another question if in such cases an exact measurement of the amount of error is required solely for diagnostic purposes; investigation with the ophthalmoscope is then alone decisive and furnishes proof at the same time of how unreliable the determination of the error by testing the vision is, in cases of short sight. One can realise this most readily in cases of myopia with congenital amblyopia; one gets frequently with the most exact correction possible of the objectively determined myopia no better visual[Pg 13] acuteness than with a very imperfect one. In one case, for instance, which I have repeatedly examined in the course of years, the degree of myopia determinable by means of the ophthalmoscope amounted to at least 6·5 D., while the weakest concave glass with which the full visual acuteness of 5/24 was attainable was 2·5 D. Under these circumstances, if one relies merely on the trial of vision, the degree of myopia appears too small, that of the hypermetropia, on the contrary, just as much too great.
But even the ophthalmoscopic diagnosis of refraction has its limits of error. It is a question of determining the conditions under which the image of the fundus of the eye still appears distinct. We will except those circumstances which prevent our obtaining a clear erect image of the fundus of the eye, as, for example, high degrees of astigmatism, nebulæ, &c.—even under normal circumstances the fundus of the eye does not always present such sharply-defined lines, that one could form a perfectly safe opinion from the clearness of the image.
When we call the ophthalmoscopic diagnosis of refraction objective, we only mean to say that we count the subjective opinion of the patient to be of less value, than that of the physician who examines him. The determination of the glass even, with which we believe we are able distinctly to see the fundus of the eye, is also an objective one. Whoever, for instance, is firmly convinced that convergent strabismus depends on hypermetropia, will, in doubtful cases, very easily carry his subjective conviction into the objective examination, and will still see clearly the fundus of even an emmetropic eye with a weak convex glass—the objective signs for the clearness of the image have no absolutely defined limits. But apart from this, other sources of error are possible. A person using the ophthalmoscope, for instance, who, without knowing it—and such a thing may happen—possesses a slight degree of latent hypermetropia, will find his own hypermetropia everywhere,[Pg 14] just also as a myope, who deceives himself slightly about the degree of his myopia in the calculation of the ophthalmoscopic diagnosis of refraction, lays rather too high a value on his own myopia.
Finally it must be added, that if the ophthalmoscopic estimation of refraction is to be exact, mydriasis by atropine is required, when, as is known, even emmetropic eyes may show a slight degree of hypermetropia. Enough, we must not over-rate the value of the objective determination of the error of refraction, and I would estimate the limit of error at half a dioptre at least. If the examination is rendered more difficult, as is frequently the case with children, by a restless and impatient demeanour of the patient, even the objective diagnosis may afford very doubtful results; such cases were, of course, excluded from the statistics. Moreover, ophthalmoscopic determination of the error in convergent strabismus is specially difficult, for one cannot advise the patient as to a suitable direction for the eye not under investigation. It is generally best to keep the eye not under investigation closed.
In practice it is immaterial whether emmetropia or a minimum degree of hypermetropia is present; for statistics essentially devoted to theoretical questions it seemed more suitable to unite these cases in a separate group.
Accurately taken, the statistics should give the condition of refraction at the age at which the squint begins. But, if there is a thankless task, it is that of examining the erect image in children from two to three years of age. To furnish accurate results this method requires a certain tractability on the patient's side, which is never present at this age, and not always in adults. A number of the cases surveyed in the following table also came under observation long after the squint commenced, and in some short-sighted persons in particular, the degree of myopia at the time when squinting[Pg 15] began, may have been less than it was at the time of the examination.
Further, it seemed to me desirable to keep periodic, separate from permanent squint; this, however, could not be accomplished with exactness. It may easily happen that children with periodic squint always squint just when one sees them, and in those cases which had already been operated on when they came to be examined, it was quite impossible to determine whether periodic or permanent squint had formerly been present. Therefore I have represented separately in each particular group the number of those previously operated on.
In the following table the refraction of the fixing eye and the visual acuteness of the squinting eye are given. In alternating squint the refraction of the emmetropic eye was taken, as determining it for insertion in the lower division of the statistics.
A. Convergent squint with myopia:
1. Slight myopia to M. = 1·75 D.
(a) Permanent squint 11 cases (3 previously operated on). Anisometropia in 2 cases (one with M. 1·25 D. of the fixing, M. 4 D. of the squinting eye; the other with M. 1·25 D. of the fixing, H. 4 D. and V. = 1 of the squinting eye). The examination of the visual acuteness of the squinting eye showed:
| V. more than 1/7 | 4 cases. |
| V. 1/12 - 1/18 | 1 case. |
| V. 1/24 - 1/36 | 1 case. |
| V. Less than 1/36 | 4 cases (among them one with H. 2 D. in the squinting eye.) |
| [Pg 16] | |
| V. indeterminable | 1 case. |
(b) Periodic squint 2 cases with very slight anisometropia and good vision.
2. M. 2 D. to M. 3 D. 11 cases, all permanent (6 cases previously operated on), anisometropia with good vision in both eyes in 2 cases (in both, the less myopic eye squints). V. of the squinting eye more than 1/7 in 6 cases.
| V. 1/12 - 1/18 | 1 case. | |
| V. 1/24 - 1/36 | 2 cases. | |
| V. less than 1/36 | 2 cases (one with H = 5 D). |
3. M. 3·5 D. to 6 D.
(a) Permanent 11 cases (one previously operated on). Anisometropia in 2 cases, of which one consisted of alternating squint, while the other possessed in the fixing eye M. 4 D., in the squinting one M. 7·5 D. with good vision on both sides.
| V. more than 1/7 | 7 cases. |
| V. 1/24 | 1 case. |
| V. 1/36 | 1 case (in fixation with this eye; the visual axis shows a linear deviation of 2 mm. The presence of emmetropia is detected with the ophthalmoscope). |
Two cases were excluded from the statistics of vision, one on account of congenital capsular cataract, covering almost the whole pupil area, the other on account of choroiditis of the macula lutea.
(b) Periodic squint 4 cases with good vision, anisometropia in 2 cases.
4. M. 6·5 D. and more.
(a) Permanent 11 cases, among them 9 with V. more than 1/7, 2 excluded from the statistics, one on account of complication with corneal nebulæ, cataract, [Pg 17] &c., the other possessed in the fixing eye M. 6·5 D. V. = 10/70 and slight nystagmus, in the squinting eye a smaller amount of sight not accurately noted, and strong nystagmus in fixing with this eye.
(b) Periodic squint in 4 cases with good vision.
5. Myopia with nystagmus and congenital amblyopia on both sides, 2 cases (not included in the statistics of vision). Altogether 56 cases, among them 10 with periodic squint.
B. Convergent squint in emmetropia, including simple myopic astigmatism, 98 cases.
(a) Permanent 81 cases (13 previously operated on). Visual acuteness more than 1/7 in 44 cases. V. less than 1/7 to V. = 1/12 6 cases; V. less than 1/12 to V. = 1/36 20 cases; V. less than 1/36 7. Excluded from statistics of vision 4 (3 on account of complications, 1 on account of lack of accurate information).
(b) Alternating convergent squint with emmetropia in one, myopia in the other eye, 4 cases. The degree of the myopia was 3·75 D., 5 D., 6 D., 12 D. Vision good on both sides.
(c) Periodic squint 13 cases (in 6 of them the refraction was objectively and subjectively determined in mydriasis by atropine). No anisometropia worth mentioning was present in any of these cases. Visual acuteness more than 1/7 9 cases. V. < 1/7 to V. = 1/12 2. V. < 1/12 to V. = 1/36 1; one case with choroiditis excluded.
C. Convergent squint with doubtful hypermetropia to H. = 1 D., including simple hypermetropic astigmatism, 38 cases.
(a) Permanent 30 cases (5 previously operated on). [Pg 18] Visual acuteness more than 1/7 7 cases. V < 1/7 to V. = 1/12 2. V. < 1/12 to V. = 1/36 5. V. < 1/36 2 cases. 4 excluded (3 complicated with cataract, one on account of impossibility of a trial of vision).
(b) Periodic squint 8 cases. V. more than 1/7 7. V. < 1/7 to V. = 1/12 1 case.
D. Hypermetropia 1 D. to 1·5 D. 37 cases.
(a) Permanent 23 (4 cases previously operated on). V. more than 1/7 13, V. < 1/7 to V. = 1/12 3. V. < 1/12 to V. = 1/36 3. V. < 1/36 3. One case excluded (choroiditis of the macula lutea).
(b) Periodic squint 14 cases. V. more than 1/7 12. V. < 1/12 to V. = 1/36 1 case. One excluded on account of choroiditis.
E. Hypermetropia 1·5 D. to 2 D. 61 cases.
(a) Permanent 41 (3 previously operated on). V. more than 1/7 26 cases. V. < 1/7 to V. = 1/12 3; V. < 1/12 to V. = 1/36 3; V. < 1/36 2; (7 cases excluded, 2 as complicated, 5 on account of the impossibility of testing the vision).
(b) Periodic 20 cases. V. more than 1/7 16; V. < 1/7 to V. = 1/12 2; V. < 1/12 to 1/36 1; V. < 1/36 1 case.
F. Hypermetropia 2 D. to 3 D. 88 cases.
(a) Permanent 58 cases. V. more than 1/7 26 cases; V. < 1/7 to V. = 1/12 5 cases (among them one with V. = 1/12 in both eyes); V. < 1/12 to V. = 1/36 17; V. < 1/36 4 cases. Six cases excluded as indeterminable.
(b) Periodic 30 cases. V. to 1/7 24; V < 1/7 to V. = 1/12 3; V. < 1/12 to V. = 1/36 1; V < 1/36 1. One case [Pg 19] excluded as indeterminable.
G. Hypermetropia 3 D. to 4·5 D. 54 cases.
(a) Permanent 35 cases (9 previously operated on). V. more than 1/7 18 cases; V. < 1/7 to V. = 1/12 1 case; V. < 1/12 to 1/36 9; 7 cases excluded.
(b) Periodic 19 cases. V. more than 1/7 14; V. < 1/7 to V. = 1/12 1; V. < 1/12 to V. = 1/36 3; V. < 1/36 1 case.
H. H. 5 D. and more, 16 cases.
(a) Permanent 9; V. to 1/7 3; V. < 1/7 to V. = 1/12 3; V. < 1/12 to V. = 1/36 2; V. < 1/36 1 case.
(b) Periodic 7; V. to 1/7 4; V. < 1/7 to V. = 1/12 3 cases.
| Convergent strabismus. | Permanent | V. to 1/7. | V. < 1/7 to V 1/12. | V. < 1/12 to V. 1/36. | V. < 1/36. | Excluded. | Periodic. | V. to 1/7. | V. < 1/7 to V. 1/12. | V. < 1/12. to V. 1/36. | V. < 1/36. | Excluded. |
| Myopia | 44 | 26 | 2 | 4 | 7 | 5 | 10 | 10 | — | — | — | — |
| Emmetropia | 85 | 48 | 6 | 20 | 7 | 4 | 13 | 9 | 2 | 1 | — | 1 |
| H ? to H. 1 D. | 30 | 17 | 2 | 5 | 2 | 4 | 8 | 7 | 1 | — | — | — |
| H. 1 D. to H. 1·5 D. | 23 | 13 | 3 | 3 | 3 | 1 | 14 | 12 | — | 1 | — | 1 |
| H. 1·5 D. to H. 2 D. | 41 | 26 | 3 | 3 | 2 | 7 | 20 | 16 | 2 | 1 | 1 | — |
| H. 2 D. to H. 3 D. | 58 | 26 | 5 | 17 | 4 | 6 | 30 | 24 | 3 | 1 | 1 | 1 |
| H. 3 D. to H. 4·5 D. | 35 | 18 | 1 | 9 | — | 7 | 19 | 14 | 1 | 3 | 1 | — |
| H. 5 D. and more | 9 | 3 | 3 | 2 | 1 | — | 7 | 4 | 3 | — | — | — |
| 325 | 177 | 25 | 63 | 26 | 34 | 121 | 96 | 12 | 7 | 3 | 3 |
According to this the percentage of the hypermetropia (including doubtful cases) amounts to 66 per cent. Dr. Isler in his dissertation, 'The Dependence of Strabismus on Refraction,' gives the percentage of hypermetropia in convergent squint as 88 per cent.—a great difference, which can, however, be partly accounted for. Isler found in hypermetropia of 2 to 10 dioptres squinting in 75 per cent.; in my statistics H. 1·5 D. to the highest degrees of hypermetropia are likewise represented by 75 per cent. As the difference between H. 2 D. and H. 1·5 D. amounts to only half a dioptre, the results of the statistics agree perfectly within these limits; the difference lies only in the slighter degrees of hypermetropia, for the diagnosis of which refer to pp. 12 to 14.
The influence of hypermetropia is very apparent in the percentage of periodic squint. While in myopia, emmetropia, and slight hypermetropia, the sum total of permanent as compared to periodic squint is as 100: 19·5, this number mounts in hypermetropia of 1 D. to H. = 3 D. to 52·5 and in the higher degrees to 59 per cent. Despite the small number of cases it is probably no mere accident that in the highest degrees (of H. = 5 D. and more) this percentage is calculated at 77·7.
But just this undoubted favouring of periodic squint by hypermetropia, helps to show that this condition is one of the causes of squint, but not the only one, for in periodic squint just those conditions are wanting which induce a permanent deviation.
It is further proved by the table that in convergent strabismus, myopia appears just about as frequently as the higher degrees of hypermetropia (of 3 dioptres and more). The fact that these are not so strongly represented in convergent strabismus, as one would have expected according to his theory, had also struck Donders. "This cannot be wondered at," he continues, "the power of accommodation, even with[Pg 21] increased convergence, does not here suffice to produce clear images. One gains much better ideas by practice from imperfect retinal images than by correcting, as far as possible, the retinal images by a maximum of accommodation." I can concede neither to the facts on which the theory is based nor to the theoretical structure itself.
An additional statistic which I drew up of the cases of hypermetropia which occurred during one year in my private practice, showed that the higher degrees are rare in the same proportion as cases of convergent strabismus are, with the corresponding degrees of hypermetropia. Further, however, I maintain that as a rule, at the age when squint usually begins, the accommodation really suffices to overcome even high degrees of hypermetropia. In all cases where we find full acuity of vision without correction of extreme hypermetropia—and this is frequently the case in young persons who do not squint—we may assume that the accommodation perfectly suffices to produce clear retinal images, without excessive convergence. In full acuity of vision even high degrees of hypermetropia are no trouble to children. Asthenopia, which occurs in children in connection with hypermetropia, is nearly always accompanied by defective vision. Were the increased demand on the accommodation really the cause of convergent strabismus, asthenopia would be far more common than it is among hypermetropic children who do not squint.
One can assert, with far greater right, that a sufficient ground for squint is not given by slight degrees of hypermetropia, for the latter are accommodatively overcome and binocular fixation retained by youthful persons without any difficulty, even when the additional motives enumerated by Donders are present. I have endeavoured to obtain a foundation for the depreciating influence of these circumstances favorable to squint, for I counted in my private practice, at the same time with the cases of squint, those cases also in[Pg 22] which, despite those conditions which lessen the value of binocular vision, squinting was not present. Taking notice then of those cases in which the hypermetropia of the better or less hypermetropic eye amounted to at least 1·5 D., in order to allow the influence of the hypermetropia to be more conspicuous. The patients from which the above-cited 219 cases of convergent strabismus with a hypermetropia of at least 1·5 D. are drawn, comprised also 117 cases in which, with the same degree of hypermetropia and simultaneous difference of refraction or monocular amblyopia, no convergent squint was present; of these cases 101 had acuity of vision to 1/7; less than 1/7 to V. = 1/12 7, and V. less than 1/12 to V. 1/36 9 cases. The percentage 219: 117 = 100: 53, which is yielded for the middle and higher degrees of hypermetropia, is not exactly convincing for the accommodative theory of squint; it would be placed still less favorably if we were to include the lowest degrees of hypermetropia in the statistics.
In face of these facts I do not consider it a happy question, that of seeking after "reasons for the prevention of squint." We do not want to quarrel with Donders over the question why all hypermetropes do not squint. Here, of course, I quite agree with Ulrich that squint does not occur if the necessary muscular conditions are absent. The identity of the fields of vision, on the other hand, seems to me to be of no importance for the age at which squint usually commences. This identity presupposes the habit of binocular fusion; but convergent squint arises, as a rule, before this habit is acquired. But even if binocular fusion were already learnt, it is given up with astonishing rapidity by children as soon as squint develops itself (see Case 16). The fixed habit of binocular fusion and the identity of the fields of vision dependent on it, is contracted only when squint does not occur, notwithstanding the presence of conditions favorable to it.
However, the number of cases is so considerable in which,[Pg 23] despite the presence of the causative motives suggested by Donders, no convergent strabismus is present, that the co-operation of other causes is necessary for the production of squint, and the first thing we do is to think of those causes which lead to squint even without hypermetropia.
The attempt has really been made to attribute the commencement of convergent strabismus to the accommodation even in emmetropia, and offers fresh proof how easily facts are overwhelmed by theories. Donders originally gave it as his opinion, that loss of power or paresis of the accommodation produces strabismus just as little as the decrease in the amount of accommodation which comes with increase of years; a year later, because he could not agree with Donders' theory, Javal declared the principal cause to be due to weakening of the accommodation and not the refraction, but without producing any other ground for the assertion than that of his own good pleasure. Afterwards, Donders sought to explain the occurrence of convergent strabismus in emmetropia by paresis of accommodation, which must indeed, according to his theory, produce the same result as hypermetropia.
I content myself by reminding my readers, that at the age when convergent strabismus usually arises, between the second and third year of life, a determination of the near point is utterly impossible; a foundation in fact is therefore wanting to the theory. But, further, if paresis of accommodation really had the significance assigned to it, atropine, which is so frequently used in the ophthalmic treatment of children, would be followed by convergent strabismus. This is still more the case with diphtheritic paralysis of accommodation, which is present more frequently than we are aware of, for it is only a trouble to children in the schoolroom, in younger children it passes through its natural uninterrupted course of recovery unobserved, in hypermetropia as well as in emmetropia. If the accommodation were really of great importance in the[Pg 24] occurrence of squint, convergent strabismus would frequently be an after symptom of diphtheria, which, as is known, is not the case. The few cases of squint which I have seen after diphtheria, had their origin in paresis of the external rectus, which was proved by the objective defect in movement, as well as by the disappearance of the squint, with the recovery of the paralysis of the abducens.
That the accommodation can play a part, is shown by the rarity of periodic accommodative squint, but for the great majority we must seek the chief cause of squint in emmetropia and myopia, in elastic preponderance of the internal recti and insufficiency of the externi, and it is apparent that the same causes will also be influential in hypermetropia.
In hypermetropia, if one causes fixation at about 30 cm. and then covers the eye with the hand, it frequently deviates inwards. Donders infers from this, that most hypermetropes prefer to sacrifice comfortable and clear vision in order to retain binocular vision. Now, it is easy to convince oneself that youthful hypermetropes see distinctly even without correction of their hypermetropia, and we may assume that they see comfortably if they do not complain of asthenopia; but that is by no means always the case, for the appearance of asthenopia is conditional on the relation of the degree of the hypermetropia to the amount of the accommodation, which, apart from a few other causes, depends chiefly on the age of the patient.
Just as we refer the deviation outwards of the covered eye to insufficiency of the interni or preponderance of the externi, we may conclude an inward deviation of the covered eye to be due to insufficiency of the externi or preponderance of the interni, and this all the more, as in hypermetropia the covered eye very frequently remains in fixation, and falls away exceptionally into relative divergence.
Just as in myopia even in the lesser degrees, insufficiency of[Pg 25] the interni or preponderance of the externi is not rare, so in hypermetropia insufficiency of the externi or preponderance of the interni appears to be frequent; and if this disturbance of the muscular balance be followed even in myopia or emmetropia by convergent strabismus, this will of course happen still more easily if at the same time hypermetropia, or even without hypermetropia, the remaining favouring conditions mentioned by Donders are present. Of course I do not deny the effect of the hypermetropia and of those other favouring conditions, but only wish to draw attention to the fact with reference to them, that as a rule they do not of themselves suffice to produce convergent strabismus.
Nebulæ have always been regarded as one of the causes of squint; here I quite agree with Donders that they may operate, firstly, as general causes of weak sight; secondly, through this, that the irritated condition, combined with the keratitis, may produce a spasmodic, afterwards a trophic shortening of the muscles; but this seldom happens.
Whether nebulæ are found rarely or often in squint, depends in great measure on the statistic materials which are worked out. In my statistics they do not occur in any quantity worth mentioning, because in private practice purulent ophthalmia keratitis, and in short, the whole army of external inflammations of the eye is much rarer, than in that portion of the populace which fills public clinics. Further, it is to be observed that the mere occurrence of nebulæ in squint proves nothing—even squinting eyes may develop keratitis. We must at least require to be assured that the squint began after the keratitis.
Among the causes which promote the occurrence of squint, Donders mentions also conditions which diminish convergence. We have ascribed a very important rôle to the muscles, and have only to occupy ourselves here with the relation between the visual line and the axis of the cornea, which we have already mentioned on page 2. Donders has measured the[Pg 26] angle a in ten cases of hypermetropia with convergent strabismus, and from the comparison with hypermetropic non-squinting eyes draws the conclusion, that in similar degrees of hypermetropia a higher amount of a specially disposes to strabismus. I will not repeat here the witty deduction by which Donders seeks to point out that a higher value of a must be followed by insufficiency of the externi and preponderance of the interni; the concession is enough that these circumstances exist and are the cause of the squint.
The opinion is prevalent that convergent strabismus usually begins in the form of periodic squint, and that a permanent deviation is developed in this way only. In many cases it may be so; on the other hand I have sometimes seen convergent strabismus arise suddenly, without a preliminary stage of periodic squint. This question, however, is of no special interest. It is more important to note that periodic squint frequently continues to exist unchanged, without ever becoming permanent.
Like the whole doctrine of strabismus, opinions on periodic squint have been governed by Donders' theory, regardless of facts, but as the accommodation frequently exercises a perceptible influence, it is judicious to consider first of all the cases in which this does not happen.
Convergent squint in myopia begins as a rule with periodic squint, and may continue to exist in this form: some patients who would not be operated upon have been under my observation for years; sometimes a correct position was retained for a long time, and sometimes strong convergent squint was present, proving that accommodation had nothing whatever to do with it. In myopia of higher degree the accommodation is scarcely used—unless concave glasses are worn; still periodic squint occurs under these circumstances. For example:
Case 1. Miss B—, æt. 22, possesses in both eyes myopia of 6·5 D. with full visual acuteness and without posterior staphyloma. A concave eyeglass of 4·5 D. is used off and on for[Pg 28] distance, and the eyes have never been over-exerted in looking at near objects. For a long time tendency to convergent squint, which is combined with diplopia, has existed on the left side. The eyes generally have a perfectly normal position, but occasionally convergent squint occurs, remains in existence a few hours, perhaps for a whole day even, and disappears again. The deviation here amounts to 4 or 5 mm. As the patient did not wish for an operation, I have been able to observe the condition for years without any change in it or without the squint becoming permanent. The cause of periodic squint is certainly not to be sought for here, in the accommodation.
Many cases of convergent strabismus with myopia constantly offer such a peculiar phase of the defect, that one has accepted the statements which ascribe to short-sightedness a determining influence on this form of squint, without asking for further proof. It may, therefore, be useful for our purpose to cite a few cases of periodic convergent strabismus with emmetropia. For instance:
Case 2. Louise S—, æt. 6-1/2, came under treatment for follicular conjunctivitis, convergent strabismus appearing simultaneously on the right side; the investigation showed the acuity of vision of left eye = 5/12, right V. = 5/36, the ophthalmoscope, and also mydriasis by atropine, proved the presence of emmetropia. The squint had first been observed when the child was about two years old, then it disappeared spontaneously and returned again three or four months ago.
In the course of treatment, which extended over about six months, the child came repeatedly into my consulting room, sometimes with squint, sometimes without, in the periods during which correct fixation existed, no squint occurred even when working. Examination with the stereoscope showed no normal binocular fusion even during normal position of the eyes.[Pg 29]
Case 3. Vera von K—, æt. 6; tendency to convergent strabismus, mostly on right side, has existed one and a half years. Normal position as a rule, on covering the eye immediate convergence, with a deviation of 5 mm.; with additional aid of a red glass and weak prisms deviating in a vertical direction, homonymous diplopia is very easily provoked. Visual acuteness on both sides 5/12, the left slightly better than the right; emmetropia in mydriasis by atropine. A year later a repeated examination gave the same result.
The cause of periodic squint in these cases can only be sought in the bearing of the ocular muscles; an elastic preponderance of the interni existed, which ceased, as a rule, on using the externi. A special influence of the accommodation was not traceable, which does not of course prevent this from acting differently in other cases. But in periodic squint it may frequently be observed that the deviation commences under influences which have nothing to do with the accommodation, but, on the contrary, under those which weaken the muscular energy generally, for example, fatigue, anxiety, &c.
Like convergent squint generally, the periodic form is also more frequent in hypermetropia than in emmetropia or myopia, and we admit that in hypermetropia the strain on the accommodation has more influence in producing the deviation. But as the appearance of periodic squint in emmetropia or myopia is proved without participation of the accommodation, solely on the ground of the muscular forces—so the presence of the same forces in hypermetropia ought not to be ignored.
It happens, indeed, that in considerable degrees of hypermetropia a slight convergent deviation occurs only from time to time, the cause of which, on closer investigation, can only be sought in the ocular muscles. For example:
Case 4. Paul F—, was first introduced to me in 1872 as a child of three years and two months, with a tendency to convergent[Pg 30] strabismus on the right side of two months' standing, which was sometimes greater, sometimes less, and sometimes was not present at all. In 1877 I saw him again suffering from conjunctivitis, without perceiving any squint; no examination respecting it was made. In 1880 his elder brother came under treatment for apparent myopia, which with the ophthalmoscope proved to be hypermetropia, and my attention, being again drawn to the eyes of the family, I requested the younger brother to come for examination. At first sight the position of the eyes appeared to be quite normal, on more careful inspection slight convergent squint of the right eye showed itself occasionally. On both sides apparent emmetropia or very slight hypermetropia, acuity of vision on left side 5/9, on the right 5/18, ophthalmoscopic diagnosis of refraction was impossible on account of restless fixation.
With the addition of a red glass diplopia cannot be produced, the left field of vision is observed in the stereoscope, then the right one on covering the left eye; never both together. In mydriasis by atropine hypermetropia of high degree (about 4 dioptres) is ophthalmoscopically detected on both sides, with convex 4·5 D., V. = 5/9 with slight convergent deviation of the right eye.
What has here prevented the transition to permanent squint with a deviation corresponding to the great strain on the accommodation? That the accommodation was really in action is proved simply by the apparent emmetropia and the school-work, that no retention of binocular single vision took place is shown by the proved incapacity for binocular fusion of the retinal images. Nothing then remains but to accept the fact that in the ocular muscles inducement was only given for a slight periodic squint, not for a permanent one answering to the amount of accommodation used.
As further proof that periodic squint may occur even in hypermetropia quite independently of the accommodation, I[Pg 31] should like to cite a case of intermittent convergent strabismus which a number of other oculists have seen besides myself.
Case 5. Sophie S—, æt. 7-3/4, has suffered for two years from a strong convergent squint on the left side, occurring every other day. The deviation amounts to 7 mm. (the same deviation is transferred to the left eye, when the right is put into fixation). On the intervening days the position of the eyes is quite normal, on covering one only a slight deviation takes place. The visual acuteness amounts to 5/12 on the left, 5/24 on the right, ophthalmoscopically with atropine hypermetropia of two dioptres. Quinine has been given without avail, a convex glass of 2 D. also, which has been worn for the last half year, has not affected the deviation.
Diplopia was not present—on the intervening days free from squint, with the aid of a red glass, homonymous diplopia could be detected without perceptible deviation, still it was impossible to bring about a union of the double images by prisms. In the stereoscope the left field of vision was first inspected, then both, still fusion of the fields of vision was not traceable. The statements, moreover, as indeed could not be expected otherwise in a child of such tender age, were not free from contradictions, but the existence of normal binocular vision was very doubtful. I therefore performed tenotomy of the left internal rectus, after which normal position continued to exist on the following squint days. After three quarters of a year I saw the child again; the squint was perfectly cured, even on looking down, convergence was no longer present. Whether a permanent cure was thus obtained, seems to me doubtful, owing to the rare peculiarities of this case.
Mannhardt also describes a similar case of intermittent squint; that of a girl aged eight years, in whom periodic convergent strabismus had begun four years previously, and for two years had occurred regularly every other day. On undecided[Pg 32] vision the eyes were normally placed, but as soon as a near or distant object was fixed, a considerable deviation inwards of the left eye occurred. Under the covering hand both eyes deviated inwards equally. On the non-squinting days strabismus could in no way be produced even by fixation of the nearest objects, only under the covering hand a deviation inwards ensued. The squint could not be removed by quinine, but only by correction of the hypermetropia of 3 D. In any case, then, hypermetropia was one of the causes of the squint, but not the only one, as it cannot operate on alternate days only.
Javal, who tries to make this case coincide with his theory, accepting an intermitting paresis of accommodation as the cause of squint, is manifestly in error, as Mannhardt particularly mentions that acuity of vision, refraction and accommodation remained perfectly equal on both days.
If it is thus proved, that also in periodic inward squint the deviation may occur quite independently of the accommodation, on the other hand it is apparent, that if once a tendency to squint exists, a disproportionately strong convergence may very easily unite itself with the accommodation. Particularly of course in hypermetropes, who are able to fix nothing without using their accommodation, a remarkable fluctuation of the squint angle very frequently takes place. Sometimes the deviation is exceedingly strong, sometimes so slight that it seems to be absent. It is usually impossible to determine if it is really absent, for as soon as we single out a point for fixation to make the investigation feasible, strong deviation sets in. If in such cases we perfectly atropise both eyes, restore the attainable acuity of vision by neutralisation of the hypermetropia with convex glasses, and yet, nevertheless, as is generally the case, the customary strong convergence takes place on fixation of a distant object, there can be no talk of a strain on the accommodation; at most we can say, that the[Pg 33] impulse for accommodation, habitually united with the intention to see distinctly, and the too strong convergence combined with it, also takes place, though by paralysis of the accommodation the participation of the same has become impossible. As accommodative squint those cases are chiefly indicated in which the deviation only takes place when there is a claim on the accommodation. In most cases of this kind hypermetropia is present. I have occasionally seen periodic accommodative squint with emmetropia of the fixing eye.
Case 6 may serve as an example: H. B—, æt. 15, shows a considerable and very varying periodic inward squint. Sometimes correct position is present, sometimes strong deviation, indeed the latter only occurs on looking at distant objects, while for near ones correct position of the eyes generally takes place. The examination showed for the right eye hypermetropia 1·5, for the left myopia 3·5 D.; full acuity of vision on both sides. The squint occurring in the left eye on looking at distant objects was therefore accommodative; the effort of the accommodation necessary for correcting the hypermetropia united itself to an excessively strong innervation of the interni, as the interests of binocular vision came but slightly into consideration on account of the myopia in the left eye. For near objects the myopic eye is used without accommodation and therefore also without convergent strabismus of the right. But if one caused a point about 25 cm. distant to be fixed first with the right (hypermetropic) eye while the left was covered and then caused fixation to be transferred to the left, the accommodative convergent strabismus induced was alternately transferred to the left eye and continued, although the left eye fixed without any effort of the accommodation on account of its myopia. Double tenotomy of the interni and correction of the hypermetropia effected the cure of the squint.
The clearest cases of accommodative strabismus are those in[Pg 34] which usually a correct position and sometimes even binocular fusion is present, while squint occurs only during the strain on the accommodation necessary for distinct vision.
Case 7. Miss Bertha v. Pr—, æt. 27, shows strong accommodative squint of the right eye, said to have been observed by her parents when she was fifteen months old. Correct position of the eyes is generally present with indistinct vision; the endeavours to see clearly immediately causes striking convergence of the right eye. On the left hypermetropia 3·5 D., vision normal; on the right the same degree of hypermetropia, vision not more than 1/12 of the normal, no ophthalmoscopic report. On correction of the hypermetropia and with aid of a red glass crossed diplopia immediately appears, which is corrected by a prism of 5° base inwards; prisms of 12° with the bases inwards are overcome on fixation of an object about 12 ft. distant by divergence. The elastic tension of the ocular muscles necessitates then a preponderance of the externi, and an effort of the accommodation necessary to overcome the hypermetropia, which on account of the congenital amblyopia of the right eye unites itself with excessive convergence. Had the elastic tension of the ocular muscles made a preponderance of the interni a condition, permanent convergent squint would have been the result, and one would have called the weak sight of the right eye amblyopia from want of use.
Typical accommodative squint occurs quite independently of the will on each effort of the accommodation, and is not combined with diplopia. It is otherwise in those cases of hypermetropia of high degree in which patients voluntarily call forth convergent squint, and retain it for a short time for the purpose of distinct vision. They are then perfectly conscious of the squint, and perceive also as a rule the double images which occur at the same time; I have seen such cases in adults who could only produce the accommodation necessary for distinct vision by the aid of a too strong convergence; they,[Pg 35] however, only now and then made use of this help. Although differing much from the typical form, these cases of voluntary accommodative squint were also included in the statistics.
In involuntary periodic (even if not accommodative) squint, the patient as a rule is not conscious of the occurrence of the false position; that exceptions to this occur Case 1 has given us an instance.
For the ætiology of convergent strabismus it is of interest to ascertain the age at which it is developed, and one of the first results we obtain is the exceptional position which the union of myopia with convergent strabismus takes in this category. Of the 56 cases contained in the above statistics I possess reliable information of the time of commencement in 11 cases; the squint was twice observed before the fourth year of life, once between four and ten years of age, eight times between the tenth and thirty-third years of life.
I must first state prominently with regard to the connection of myopia with convergent squint that I see no reason for holding short sight to be the cause of the squint, as v. Graefe does.
A specially severe strain of the eyes, as v. Graefe assumes, was not traceable in the cases observed by me. Excessive convergence and strain on the accommodation is often enough present in weak sight, for example, in astigmatism without the existence of squint; were short sight in general an inducement to convergent squint these cases would appear much oftener than they actually do, owing to the frequency of myopia. In my opinion the cause of their rarity lies in the fact that myopia is frequently combined with insufficiency of the interni and preponderance of the externi, but only rarely with the reverse condition of the muscles. If, however, a preponderance of the interni develops itself together with the myopia, convergent strabismus is easily produced, for[Pg 37] without correction of the myopia by spectacles, the desire for retaining binocular single vision for everything beyond the far point is lessened by the indistinctness of the retinal images. Within the range of their field of distinct vision these squinting myopes frequently retain binocular vision, while the capacity for accepting parallel rays or retaining them for long, is lost.
Strictly speaking, the periodic squint present in these cases is of a peculiar kind, for the binocular single vision present within range of the convergence excludes the notion of squint; the latter only occurs when an object lying outside the point of convergence is fixed. Moreover, according to the common use of language, I have only used the expression periodic convergent squint for the change between a parallel direction of the visual axes and pathological convergence.
As squint in myopia usually commences at an age when binocular fusion has already become a fixed habit, diplopia regularly takes place with it, but patients become more easily accustomed to this than in paralysis of the ocular muscles, because the retinal images are indistinct and the double images in the field of vision always keep at about the same distance, while in paralysis of the ocular muscles the distance is constantly changing.
The myopia, in these cases, is not the cause of the squint, but only a favouring circumstance. If the same preponderance of the interni is developed at the same age in emmetropia, squint is not so easily caused, as the distinct retinal images present in the whole field of vision render it easy to retain binocular single vision. Therefore we see the same form of squint arise less often in emmetropia (see Case 45) when childhood is past, than in myopia. As a rule preponderance of the interni in hypermetropia leads eventually to convergent squint even in childhood.
In emmetropia and hypermetropia convergent strabismus seldom arises after the tenth year (paresis of the abducens of[Pg 38] course excepted), therefore in my investigations as to the time of commencement of typical squint I have only considered those patients who came under my treatment before their tenth year. We must rely for the most part on the vague statements of the parents, which lose in exactness in proportion as the origin of the squint is of distant date; moreover, I have myself seen a great many of the children before they were four years old. In this way I have collected reliable information respecting the origin of the squint in 193 cases, and of these (a) 88 cases occurred in children one to three years old, (b) 53 in children three to four years old, (c) 35 cases in children of over four years of age. It is thus at once seen that in the great majority of cases, convergent strabismus commences in children under four years of age, who have not yet begun to read and write, and have no inducement to use their accommodation severely, and still less continuously.
Convergent squint as a result of paralysis of the abducens is not very often seen. It is first to be observed that a convergent squint, including the whole field of vision, occurs by no means in all cases; in about half the cases binocular fusion is retained towards the healthy side, diplopia then only occurs when the weak abducens is exerted beyond its strength. In those cases in which convergent squint is present in the whole field of vision paralysis of the abducens cannot be the sole cause, but some other cause than the most apparent one must co-operate. An insufficiency of the externi of previous existence, or an elastic preponderence of the interni may be considered. I have not been able to persuade myself of the fact that hypermetropia can play any part therein.
In by far the greater number of cases paralytic convergent squint recovers together with the paralysis of the abducens, the field of single vision transfers itself gradually from the healthy side to the side of the weak abducens, and at length governs the whole field of vision. In proportion as the muscle again fulfils its normal functions, the habit of binocular fixation regains its power, and it seldom happens that the elastic tension of the muscles has so changed during paralysis that the desire for binocular single vision does not suffice to overcome it. Case 48 furnishes an example of the fact that although the squint occurred as a consequence of paralysis of the abducens, it certainly remained in existence after healing of the paralysis on account of previously existing insufficiency of the externi.[Pg 40]
Congenital paralysis of the abducens seems more frequently to have convergent squint as a result. If, for example, convergent squint is observed in the first year of life, and we find a complete defect of motion on the part of one abducens when the children become old enough to be examined, we may certainly assume that the case is one of congenital paralysis of this muscle, or at least that the paralysis originated soon after birth. Doubtless, however, cases appear, of congenital paralysis of the abducens without squint, and as these cases are so rare I will describe two which I observed in adults.
Case 8. Miss H—, æt. 17, has nominally since her birth a considerable defect in the outward movement of the left eye. On looking to the left homonymous diplopia is present, on looking to the front and the right binocular single vision and no squint; on both sides emmetropia and full acuity of vision.
Case 9. Mr. V. W—, æt. 24, has likewise congenital paralysis of the left abducens. No squint, but as soon as the left eye is used for fixation in the left direction there occurs in the right one a strong secondary movement inwards.
In the hysterical form we see rather a rare variety of convergent squint, which is conditional on contraction of the interni through restriction of movement of the externi. Hysterical symptoms may at the same time appear in the eyes or elsewhere, still this does not always happen. As these cases are rare I will relate a few of those I have observed. (These cases are not included in the above statistics.)
Case 10. Anna R—, æt. 20, came under treatment in February, 1878, stating that on the previous day she perceived blindness of the right eye on waking; in the afternoon she felt particularly weary, and after she had slept about an hour woke with blindness in both eyes. No perception of light, good pupillary reaction, ophthalmoscopic report normal. Patient was treated with copious enemata and dismissed on the fifth day cured.
In February, 1880, she again came under treatment with blindness of both eyes, also perceived the previous day on waking. Convergent strabismus was present at the same time, of such a degree that the eyes converged to a point 10 to 20 cm. distant. The outward movement was suspended in both eyes. The attempt to turn the eye outwards is accompanied by short convulsive movements, and followed by an immediate rebound to the convergent position. She asserts her inability to see the movements of a hand before her eyes, is able, however, to move about in a strange room, unsteadily certainly, but with avoidance of obstacles; she sits down on a chair indicated to her, &c. The position of the eyes proves that there was no simulation[Pg 42] in all this; it would be impossible for any person to simulate a strong convergent squint continuously for four to five days. Eight days after her admission the patient was dismissed with normal movement of the eyes and good vision.
Case 11. Miss Antonie E—, æt. 15, who has been treated by her family physician for various hysterical disturbances, suffered since the middle of December, 1879, from convergent strabismus with permanent but very varying deviation, which is at times very slight, and sometimes amounted to more than 7 mm. The movement outwards is in both eyes rendered difficult, still the outer edge of the cornea is brought to the outer angle of the lids with trouble and twitching movements. Homonymous double images are present, their mutual distance is alike in the whole field of vision, but is (six or eight weeks after the commencement of the squint) signified as being slight; at the same time a difference in height is present, the image of the left eye stands lower, prism 30°, base outwards, places the images just above one another. Nystagmus occasionally occurs in monocular fixation (with exclusion of the other eye). In due course a gradual improvement set in, the deviation and the distance apart of the double images became slighter, the outward movement better, and in the middle of April, 1880, four months after the trouble began, no squint and no diplopia were present, the outward movement normal, facultative divergence = 0.
The hysterical character of the visual disturbance showed itself when the vision was tested. I will first observe that repeated investigations with atropine showed emmetropia, while in the first investigation on the left side, No. 36 at 5 m. was not recognised with the naked eye, but only with weak concave glasses (with - ·5 D. V. = 5/18). With the right eye No. 0·8 was read fluently, from 0·75 she asserted she was unable to recognise a word, with - 2 D. V. = 5/36. It would be wrong to conclude from this myopia or[Pg 43] spasm of the accommodation, for here, as in most cases of hysterical weak sight, it could be shown that whatever glass one chose to hold before the patient's eyes, was followed by an improvement in the statements. The same improvement in visual acuteness was repeatedly obtained in this case by a weak prism (3°), held before the fixing eye during monocular examination, and in the end, V. 5/12 was obtained for the right eye, as against 5/6 with a prism of 3°.
Finally, on May 1st, full visual acuteness was present on both sides. Field of vision and sense of colour normal.
Case 12. Mrs. B—, æt. 30, previously treated for various hysterical disturbances, has complained for about eight days of disordered vision, the binocular nature of which was proved as patient had herself observed that on closing one eye she could at once see clearly. Near objects to 15 cm. are seen distinctly. With all this, at the first examination it was impossible to produce diplopia, either with the aid of a red glass or prisms, &c., the images of first one eye, then the other were always seen by turns. A few days later, on repeating the examination, double images were perceived, they were homonymous with slight difference in height (image of the right eye lower), the lateral displacement is corrected by a prism of 28°. Micropsia of one image was also perceived. On both sides the outward movement is rather difficult. Full visual acuity on both sides—in the first examination slight myopia - ·75 D. is specified, afterwards emmetropia. The visual disturbance was removed by goggles with faintly ground glass on the right side—preparations of iron, bromide salts, shampooing with cold water and electricity were used. In six weeks' time binocular single vision was again restored; the facultative divergence = 0. With red glass and vertically deviating prisms homonymous diplopia corrected by prism 3°. Field of vision and sense of colour remained normal throughout.
If we want to draw a comparison between convergent and divergent squint, we must consider only absolute divergent strabismus, for convergent strabismus does not offer a parallel to relative divergent squint. In absolute divergent squint the direction of the visual axes is such that they would meet behind the patient's head; in the relative divergent squint the axes of vision are parallel or slightly convergent, but they do not cross at the point fixed by the one eye, but at a greater distance off.
If we then only compare that which admits of comparison, we first find out that divergent squint is rarer than the convergent form, and the cause contained in the ocular muscles is here brought to light still more clearly than there.
We must next distinguish between permanent and periodic squint, and we see the latter so frequently continue as such, that we must not consider the transition from this variety to the permanent one to be the rule.
In 183 cases of absolute divergent strabismus which appeared in my private practice in the same space of time as the cases of convergent squint above discussed I have been able to obtain exact determinations of the refraction and visual acuteness. The weakness of the fixing eye was the test for classing them among the statistics, and in patients who had been long under observation, the first certain determination of refraction, which was necessary, as several children are included who came[Pg 45] under treatment with divergent strabismus and emmetropia whilst myopia developed itself later.
A. Divergent squint with hypermetropia.
(a) Permanent 4 cases. Visual acuteness of the squinting eye more than 1/7 1 case, V. less than 1/36 1 case, 2 excluded, one on account of complication with detachment of retina, the other on account of impossibility of testing vision.
(b) Periodic squint 5 cases. Among them 3 with double hypermetropia, 2 with emmetropia in one, and hypermetropia in the other eye. Visual acuteness of more than 1/7 in 3 cases; V. = 1/9 1 case; V. = 1/36 1 case.
B. Divergent squint in emmetropia.
(a) Permanent 32 cases. Among them 10 with alternating strabismus and anisometropia of at least 2 D. And in 9 cases emmetropia in one, myopia in the other eye; once simple hypermetropic astigmatism in one, with myopic astigmatism in the other eye. Visual acuteness of both eyes in these 10 cases more than 1/7. In the 22 cases of monocular squint the visual acuteness of the squinting eye amounted 8 times to more than 1/7 -, 10 times 1/12 to 1/36 (in 1 case V. = 1/36 with nystagmus of the squinting eye when put into fixation). V. less than 1/36 in 3 cases; 6 cases excluded on account of complications.
(b) Periodic squint 28 cases. Among them 5 with anisometropia of at least 2 D. (emmetropia in one, myopia in the other eye). Visual acuteness of the squinting eye more than 1/7 in 27 cases, less than 1/7 to V. = 1/12 in 1 case.[Pg 46]
C. Divergent squint in myopia to M. = 2 D.
(a) Permanent 24 cases (among them 6 with anisometropia of at least 2 D.). Visual acuteness of the squinting eye more than 1/7 in 15 cases. V. less than 1/7 to V. = 1/12 2; V. less than 1/12 to V. = 1/36 3; V. less than 1/36 2 cases; 2 cases excluded on account of complications (one on account of atrophy of the optic nerve, the other on account of posterior polar cataract).
(b) Periodic squint 23 cases. Among them 10 cases with anisometropia of at least 2 D. Visual acuteness more than 1/7 in all 23 cases.
D. Divergent squint in myopia 2 D. to M. = 4 D.
(a) Permanent 17 cases. Among them 2 with anisometropia of more than 2 D. V. to 1/7 9 cases. V. < 1/7 to V. = 1/12 1 case. V. < 1/12 to V. = 1/36 2 cases. V. < 1/36 1 case. Four cases excluded (2 with choroiditis, 1 with congenital cataract, 1 with traumatic cataract).
(b) Periodic 8 cases. Among them 4 with anisometropia of at least 2 D. V. to 1/7 7 cases. V. 1/36 1 case.
E. Divergent squint in myopia 4 D. to M. 6·5 D.
(a) Permanent 10 cases. V. more than 1/7 in 5; V. less than 1/36 in 3 cases, 2 excluded (one on account of large anterior synechia, one on account of choroiditis of the macula lutea).
(b) Periodic 9 cases. Among them one with anisometropia of more than 2 D. V. more than 1/7 5 cases. V. = 1/9 1 case; 3 cases excluded on account of complications.
F. Divergent squint in myopia more than 6·5 D.[Pg 47]
(a) Permanent 8 cases. V. more than 1/7 4 cases, 4 excluded on account of choroiditis of the macula lutea.
(b) Periodic 10 cases. V. to 1/7 9 cases; V. = 1/12 in one case.
| Permanent. | V. to 1/7. | V. < 1/7 to V. = 1/12. | V. < 1/12 to V. = 1/36. | V. < 1/36. | Excluded. | Periodic. | V. to 1/7. | V. < 1/7 to V. = 1/12. | V. < 1/12 to V. = 1/36. | V. < 1/36. | Excluded. | |
| Hypermetropia | 4 | 1 | — | — | 1 | 2 | 5 | 3 | 1 | 1 | — | — |
| Emmetropia | 37 | 18 | — | 10 | 3 | 6 | 28 | 27 | 1 | — | — | — |
| Myopia to M. 2 D. | 24 | 15 | 2 | 3 | 2 | 2 | 23 | 23 | — | — | — | — |
| M. 2 D. to 4 D. | 17 | 9 | 1 | 2 | 1 | 4 | 8 | 7 | — | 1 | — | — |
| M. 4 D. to 6·5 D. | 10 | 5 | — | — | 3 | 2 | 9 | 5 | 1 | — | — | 3 |
| M. more than 6·5 D. | 8 | 4 | — | — | — | 4 | 10 | 9 | 1 | — | — | — |
| 100 | 52 | 3 | 15 | 10 | 20 | 83 | 74 | 4 | 2 | — | 3 |
It follows then from this, that periodic absolute divergent squint is just about as frequent as the permanent form and that both become more rare as the degrees of myopia increase. As, however, in spite of this, myopia is present in about 60 per cent. of all cases, the connection can be no other than this, that myopia frequently unites itself with insufficiency of the interni and preponderance of the externi; in this respect, as in every other, myopia and hypermetropia are directly opposed.
The setting up of a "hypermetropic divergent strabismus," dependent on hypermetropia, seems to me only to show how much people have been carried away by the idea that the cause of the squint must be given by the state of refraction.[Pg 48] Isler claims 17 to 29 per cent. of the cases for hypermetropic divergent strabismus; of these, however, the half possess only slight hypermetropia of 2 D. or less, which perfectly agrees with the fact that the same observer has also found in convergent squint a remarkably high percentage of the lower degrees of hypermetropia.
Whether squint originates in the permanent or periodic form depends chiefly on whether the movement of convergence is retained or lost. There are cases of considerable divergent squint, in which the near point of the convergence is scarcely removed, while on the other hand, the physiological innervation for convergence may be lost, without absolute divergence ever being brought about. In a number of emmetropic or slightly myopic cases with absolute preponderance of the externi, the physiological connection between accommodation and convergence is maintained in a relaxed way; thus, for example, it is impossible to converge voluntarily to a large object, as, for instance, a pencil held in the vertical line, while accurate convergence immediately follows on reading at the same distance; in other cases accommodation can be exerted to the near point, without inducing the slightest impulse to convergence. This circumstance is worthy of consideration for the prognosis of the operation. A mere relaxing of the tie between accommodation and convergence may be strengthened by practice, but if the impulse to innervation is completely lost, it will scarcely be possible to restore it again; as after complete laying aside of absolute divergence the relative form still continues to exist.
Those cases deserve special consideration in which emmetropia is present in one eye, in the other myopia. Slight degrees of one-sided myopia reconcile themselves with the continuance of a normal binocular act of vision. If the far point of the myopic eye lies at an inconvenient proximity even[Pg 49] for reading, then, as a rule, the emmetropic eye is used for near as well as distant objects; if, on the contrary, the degree of myopia answers to a range of vision convenient for working, and visual acuteness is normal, then the temptation to use the emmetropic eye only for distance and the myopic one only for near objects is so overpowering, and the advantages on the other hand which would be offered by clinging to binocular vision so slight, that a convenient monocular vision is generally preferred. Even for objects which lie nearer the eye than the far point of the myopic, and at the same time farther than the near point of the emmetropic eye, for which, therefore, both eyes could secure clear retinal images, binocular vision is not used. In cases in which the patient can read with proper binocular fixation, if one covers all but one line and then makes with prisms double images standing one above another, it is the myopic eye alone which almost invariably shows a clear retinal image.
The usual result of this is, first a relaxing of binocular vision, and as together with this the motive for convergence, namely, the effort of the accommodation ceases, the conditions for the commencement of divergence are produced. Still the elastic tension of the ocular muscles decides even here; if the interni preponderate, convergent squint results, when the myopic eye is used for near objects, the emmetropic for distant ones. If the externi preponderate, then permanent or periodic divergent strabismus is caused. Nevertheless, in a remarkable minority of cases the elastic tension of the ocular muscles is so regulated that, despite relaxation of binocular fusion, neither convergent squint nor absolute divergence occurs, but simple relative divergence remains with employment of the myopic eye for near objects.
The habit of binocular single vision, when it has once reached its normal development, governs the movements of our eyes to a great degree; the desire to avoid double images makes itself continually felt; and where this is not possible, an uncomfortable feeling of uncertainty arises at every movement of the body. Double images are prevented as far as possible by movements of the eyes, which we must designate as voluntary when we are conscious of their occurrence.
If we follow a moving object with the eyes, the latter make corresponding movements in order to keep the image in the centre of both retinæ. For example, if we look at a distant object which approaches in the direction of one visual axis, this eye will necessarily remain still, while the other will be put into convergence in proportion as the object advances. If this did not happen, if this eye remained also immovable, the retinal image would deviate outwards more and more from the macula lutea and diplopia would arise. In order then to avoid diplopia the macula lutea moves to where the retinal image is formed. We can, however, move the images on the retina by the aid of prisms without movement of the object. If, for example, we hold a prism before the eye so that the base lies towards the temporal side, the retinal image will be displaced towards the base of the prism, outwards then from the macula, and double images will[Pg 51] occur, which are at once removed by a distinctly perceptible inward movement of the eye. In this way, by means of a prism applied with the base inwards, outward deviation may be produced, and even in a modified way deviations in height of the visual axes by means of prisms with the base upwards or downwards. Here the force of habit is apparent, for in the daily use of our eyes we continually practise the inward movement of the visual axes; we can also easily restore the customary degree of convergence by means of prisms with the bases outwards; physiologically indeed, it is quite immaterial whether an object is in a proximity to our eyes attainable by convergence, which causes double images until it is binocularly fixed, or whether by the aid of prisms we bring the retinal images of a distant object to parts of the retinæ which do not correspond. If we look at a distant object fixed with parallel visual axes, under normal circumstances, prisms of 6° to 8° with the base inwards can be overcome, that is to say, as in weak prisms the deviation is equal to about half of the prism, an absolute divergence of the visual axes of 3° to 4° may be produced by which the double images are blended. It is immaterial whether we apply a prism of, say 8° to one eye, or prisms of 4° with the bases inwards to both. The facultative divergence thus attainable remains the same, which speaks for the fact, that this monolateral movement attainable by prisms is also combined with double innervation; and of course in the eye remaining in unmoved fixation, with impulses to innervation which are reciprocally abolished.
In the physiological use of our eyes we certainly never have occasion to practise absolute divergence, but we constantly practise the transition from the inward to the outward movement of the eyes, and experiments with prisms teach us, that the innervation of the externi therewith connected may even be carried somewhat beyond the physiological[Pg 52] limits of parallelism. Moreover, the extent of the "facultative" divergence attainable by prisms shows a considerable latitude.
The case is similar with deviation in height of the visual axes. In looking upwards or downwards the innervation of both eyes is usually precisely the same, but on looking at any point when holding the head obliquely, the difference in height of the eyes then present must be balanced by a corresponding difference in the direction of the visual axes. The same thing happens, if we hold a vertically deviating prism in front of one eye in binocular vision; prisms of 2° to 3° may then be overcome by difference in height of the eyes; rarely is a much greater difference in height of the visual axes attainable. I have seen this particularly in those cases where facultative divergence also was greater than usual.
It happens especially in myopia that prisms of considerably more than 6° to 8° are overcome by divergence, and certainly without causing any inconvenience. Among the cases presented for examination, those, of course, are most numerous where the patients have some complaint to make, even if this have quite a different cause. In any case a divergent position of the axes of vision corresponds to the balance of the muscles, and this does not generally occur, for this reason, because retaining binocular single vision necessitates a parallel or convergent position of the eyes. Frequently, however, even a slight impediment to binocular fusion, such as the application of a red glass to one eye, suffices to procure preponderance in the elastic tensions of the muscles, and to cause the fixed point to appear double. We can put a stop to binocular single vision still more surely by applying to one eye a prism with the base upwards or downwards. If the double images of a point 4 to 5 meters distant show a crossed lateral position besides the difference in height[Pg 53] caused by the prism, we may assume that an absolute divergent position of the eyes corresponds to the elastic tension of the muscles; and the measure of the deviation will be given by those prisms which, placed with the bases inwards before one or both eyes, bring the double images perpendicularly over one another. As a rule, in these cases the degree of divergence which occurs on cessation of binocular single vision, is almost as great as the facultative divergence, which may be reached in the interest of binocular single vision.
V. Graefe designates as "dynamic squint" that condition in which the position of divergence corresponding to the state of tension of the muscles does not occur because binocular vision is retained. Without clearly defined limits these conditions pass on into periodic squint, when either diplopia occurs together with the divergence, or the habit of binocular fusion becomes less frequent or is quite forgotten, while, however, according to the varying state of the muscles sometimes normal position, sometimes divergence, is present. A correct position of the eyes is quite possible even without binocular fusion, then only the regulator is wanting, which, in the varying play of the muscular forces, ensures the balance of position and movement.
The older ophthalmologists had a parallel strabismus and probably understood by that, what we now designate as relative divergence. The connection between relative divergence and myopia, pointed out by Donders, is universally admitted; on the other hand, in more modern literature we scarcely find any intimation of the fact that a parallel squint occurs, which is quite independent of myopia, and rests solely on the fact that the impulse of innervation for convergence is lost. A few examples may explain this condition.
Case 13.—Auguste T—, æt. 28. On the left emmetropia, V. 12/20. On the right the visual acuteness is variously given,[Pg 54] but certainly does not amount to more than 1/5 nor less than 1/10 of the normal. Ophthalmoscopic report normal. The left eye is naturally the fixing one, the right always remains parallel—for near objects double images are present. A convergent movement is not attained, either for near objects, or by means of prisms with bases outwards for distant ones. Prisms with the bases inwards are not overcome; with vertically deviating prisms the double images of distant objects stand perpendicularly above one another.
Case 14.—Ludwig v. K—, æt 32, has complained of diplopia repeatedly for fifteen years. Statement in August, 1877: Convergence to a pencil held before patient on the median line is only retained to about 50 cm., nearer, crossed diplopia occurs. In reading, binocular fixation is possible with an effort at a nearer point. The facultative divergence does not amount to more than 3°; even by convergence to a distance of 4 mtr. prisms of 3° only are overcome. Emmetropia and full visual acuity on both sides. In Sept., 1880, three years after, the statement remained unaltered. Patient has only used the prismatic spectacles then prescribed off and on, as the symptoms are sometimes more troublesome, sometimes less so, and he exerts his eyes but little on the whole.
A restriction of movement of the internal recti did not exist in these cases; the absence of the convergent movement is not then to be set down to the interni not possessing the proper power for acting, but only to the fact that the impulse for their simultaneous innervation was wanting. We frequently find this absence of innervation in divergent squint, and then generally consider it to be a consequence of the squint, which, however, as the above cases show, need not necessarily be the case. If preponderance of the externi is at the same time present, absolute divergence is the result, but not always permanent squint, frequently only the periodic form. The anomaly of innervation may also usually be[Pg 55] proved in such cases, in that after the removal by operation of the absolute divergence it continues to exist in the relative form; it can indeed happen that for a few days after the operation convergent squint is present for distance, together with relative divergence for near objects.
The highest phases of this anomaly, as represented in Cases 13 and 14, are seldom seen. Slighter degrees, which, like so many other things, are usually designated as "insufficiency of the interni," are more frequently met with and are combined with asthenopia. On the one hand, in looking at near objects a tendency exists to the formation of double images, which are removed by the action of the interni; on the other hand, however, the habit of binocular single vision is relinquished on account of the frequent diplopia. In all forms of squint we see that binocular fusion is forgotten; still it seems more natural to assume this to be the result, and not the cause of the squint, as Krenchel does.
Another form of relative divergence is that which is brought about in consequence of extreme myopia. The change in form of the myopic eye diminishes its mobility, associated movements of the eyes may be replaced by turning the head, but this is not possible for the movement of convergence. Further, in extreme myopia the far point is generally used for reading, &c., and sometimes even a somewhat greater distance, because on account of the close proximity of the objects the retinal images are so large that they are sufficiently clearly recognised even if they are not quite distinct. At all events accommodation certainly does not take place, hence one motive favouring convergence is removed.
Finally, however, such considerable convergence as clear vision demands in high degrees of myopia, would be difficult even for a normally movable eye. Reasons enough therefore exist for giving up binocular fixation and using only the[Pg 56] more convenient eye for reading, without effort to the accommodation and convergence. In myopia of high degree patients almost always read with relative divergence, and these myopes do just what we must advise them to do, they avoid strain of the accommodation and convergence of the visual axes and thus keep well.
Notwithstanding that this condition necessarily results from the nature of extreme myopia, it is frequently held to be pathological, which it certainly is not in itself. At most, the short-sightedness and change in form of the eye are pathological; the relative divergence on the other hand is simply a harmless result of the above conditions.
No doubts whatever exist about this relative divergence. The theory that the demands on the working eye must be very much increased is quite unfounded. If any harmful influence were to be feared for the fixing eye, one would observe the same in convergent squint, when, as a rule, one eye only is used for fixation even after operation.
In convergent strabismus, however, no one, at least no ophthalmologist, thinks of entertaining such fears for the eye used in fixation, and where is the physiological basis of this whole idea to be found? Is the visual purple more active in monocular than in binocular vision, or what physiological activity is thereby taxed in increased degree?
I have found no confirmation of Alfred Graefe's theory that in myopia the eye chiefly used in fixation is frequently affected with choroiditis of the macula lutea, &c., but have only observed that patients to whom this happens seek the advice of a physician more eagerly than when the same intra-ocular troubles befall the other usually neglected eye in connection with myopia.
Muscular asthenopia undoubtedly occurs; it is only a question whether it is as frequent as it is diagnosed. It has its foundation in that the convergence necessary for reading,[Pg 57] writing, &c., can only be sustained by an effort of the internal recti, which exceeds their strength, and finally results in painful fatigue of the muscles, just as accommodative asthenopia depends on painful fatigue of the muscles of accommodation. The similarity reaches still further. We occasionally find that despite considerable degrees of hypermetropia no asthenopia occurs even in persons who strain their eyes; while, on the other hand, asthenopic troubles appear in hypermetropia which are not removed by correction of the refraction and must consequently have some other motive. Yet still more is this the case with those disorders, of which muscular asthenopia may be supposed to be the cause. Notwithstanding the existence of a considerable preponderance of the externi, muscular asthenopia may be entirely absent. If we find, for example, that as soon as we do away with binocular single vision absolute divergence occurs even on looking at a distant fixed point, and that prisms of 12° to 30° are overcome by divergence, we may safely assume that the elastic preponderance of the externi must be overcome in reading, &c., in the interest of binocular, single vision by a stronger muscular effort of the interni, which is, however, very frequently accomplished without fatigue. Asthenopic disorders are also frequently present together with preponderance of the externi, which continue to exist despite the removal of the same by operation, and must consequently have some other cause. The diagnosis of accommodative asthenopia is as a rule confirmed ex juvantibus; this cannot be asserted for the muscular form.
For example, Case 15.—Mathilde F—, æt. 21, has suffered from asthenopic disorders for three years. The investigation at the beginning of January, 1880, shows: On the left, myopia 4 D., V. = 5/18, No. 0·3 is read at 10 cm.; on the right, myopia 6 D., V. 5/24, 0·3 is read with difficulty, cylindrical glasses cause no improvement. Patient converges to about 8 cm., on[Pg 58] exclusion absolute divergence of 3 to 4 mm. follows, with slight upward deviation of the right eye.
On correction of the myopia the facultative divergence amounts to = 26°. Here one might easily have concluded the asthenopia to be a result of fatigue of the interni, but this opinion was refuted by the effect of the treatment. The double tenotomy of the externi performed on January 2nd was first followed by convergent squint with homonymous double images, which were united by a prism of 12° with the base inwards. In the course of a few days single vision was again restored. A fortnight after the operation, on correction of the myopia, patient could see singly to 3 mtr.: towards both sides homonymous double images were still present, and in fixation to 30 cm. relative divergence on exclusion of one eye. Six months after the operation, on correction of the myopia and application of red glass to one eye, crossed double images occur close together, which become homonymous by means of a prism of 3° with the base inwards. Patient sees double images always, without being much disturbed by them, yet they cannot be united by means of prisms. The habit of binocular single vision has also gradually been lost. In reading (without correction) a movement of convergence takes place (it cannot be determined whether this answers exactly to the distance of the object). If, on the other hand, one asks the patient to fix binocularly larger objects, such as a pencil close to her, she is unable to do it, relative divergence occurs then, as well as on exclusion of one eye. The asthenopic disorders remain unchanged and are not removed even by prismatic spectacles. Despite all reasons then for the supposition the asthenopia was certainly not of a muscular nature.
The uncertainty as to diagnosis is still greater in those cases which, according to v. Graefe, were to be designated as dynamic relative divergence; cases in which with parallel[Pg 59] visual axes a disturbed balance is not present but occurs on convergence in such a way that the interni only perform their destined work with difficulty, and are nevertheless urged on in the interest of binocular single vision, till they give way in painful fatigue.
According to v. Graefe the diagnosis of this condition must be carried out in the following way. First of all the convergence must be fixed on a near object in the median line; if one eye remains behind in the movement it may be accounted for in various ways, for example, the impediment of movement caused by the change in form of the eye in myopia or the faulty innervation of the interni mentioned on p. 54. In both cases for the most part no dynamic, but manifest relative divergence is present in viewing near objects. It may also happen that the patient does not converge sufficiently, merely because accommodation is absent. This experiment does not then prove the presence of dynamic relative convergence, and v. Graefe came to the conclusion, therefore, that a normal position of the eyes obtained only by the habit of binocular single vision must be relinquished so soon as we cause binocular single vision to cease. Just as under these circumstances dynamic absolute divergence is manifested in the observance of distant objects, so must this be the case in dynamic relative divergence in the observance of near objects. One eye is first excluded while looking at an object about 25 cm. distant, to determine whether it still remains in a proper position for fixation. We have reason to believe that the position which occurs in the excluded eye answers to the given conditions of tension of the muscles. Still it is not necessary to cause binocular vision quite to cease, it is sufficient and even more advantageous, simply to make binocular single vision impossible, which we are able to do by means of prisms. If, for example, a point be fixed lying at the usual distance for work of 25 to 30 cm., or, according to v. Graefe, a large spot intersected[Pg 60] by a vertical line, and one then applies a vertically deviating prism to one eye, the influence of binocular single vision on the ocular muscles is removed, as the fusion of the double images standing above one another is impossible; and nothing prevents the assumption of a relative position of divergence instead of a proper convergent one; as a result of this the double images show a crossed lateral position as well as the difference in height produced by the prism. The extent of this lateral deviation may be measured by means of prisms, which being applied to the eyes with the bases inwards place the double images again perpendicularly above one another. Von Graefe holds it to be of importance to determine the strongest prisms which can be overcome for the given distance by means of convergence and by the outward movement of the eyes.
On the strength of this method of inquiry there is a prevalence of opinion that the asthenopic disorders common in myopia are caused by over-exertion of the ocular muscles; indeed people believe this so strongly that they assume the presence of muscular asthenopia even in individuals in whom the habit of working with relative divergence is already firmly rooted. Relative divergence may perchance cause annoyance through double images, though this really seldom happens, but it can never cause muscular asthenopia, for the internal recti muscles protect themselves by means of relative divergence from any stronger exertion.
Asthenopic disturbances are certainly frequent in myopia, but the above method of inquiry does not at all prove that their cause lies in the ocular muscles, for those appearances from which one concludes dynamic relative divergence and muscular asthenopia, are found in almost all myopes, even when the latter have no asthenopic troubles, for they owe their origin to the nature of the myopia. Myopes learn to converge to the distance of their far point, without exerting the accommodation; if we now cause a point at this distance[Pg 61] to be fixed and then exclude one eye, or make binocular fusion impossible by means of vertical prisms, what imaginable reason is there for the excluded eye to remain in proper fixation? In emmetropia the habitual relation between accommodation and convergence will be able to ensure that the excluded eye also remains covering the fixed object, convergently as well as accommodatively; in myopia, every discretionary relative divergence up to parallelism of the lines of vision is perfectly justified, because no effort of the accommodation takes place. How in the world can it be held to be pathological that a movement of convergence does not occur, when one has just artificially removed all those physiological conditions which could possibly have brought it about? If one now likes, as v. Graefe proposes, to determine the prisms, which can be overcome by means of the outward movement, there is no doubt about the fact, that with the aid of prisms the lines of vision may be made parallel or even divergent, the retinal images indeed, always retaining the same distinctness, in so far as they are not injured by the prismatic diffusion of colours. There is just as little reason why the convergence usually attainable should not also be restored by the aid of prisms with the bases outwards, the retinal images are not only impaired by the prisms, but the accommodation united with the convergence, no longer corresponds to the real distance of the fixed point.
Enough, all these incidents, which are to prove the presence of muscular asthenopia in myopia, occur when the investigation is carried out as usual in the region of the far point, entirely on a physiological basis, and must not therefore be held to be pathological without further proof.
The proof of muscular asthenopia in slight degrees of myopia, emmetropia, or hypermetropia, is somewhat more certain; a deviation from physiological laws is certainly present, if we find that the corresponding convergence does[Pg 62] not unite itself with the accommodation for a near object, we must be quite sure that an exact accommodation for the fixed point is also really present. It by no means follows because one causes a large black spot to be observed at a distance of 25 to 30 cm., that an exact accommodation takes place; one can see these things even with circles of diffusion, the retinal images are already dimmed by means of the prisms, and one can easily convince one's self that, on the renunciation of clear retinal images, normal eyes can reach every attainable convergence or relative divergence by means of prisms. Insufficient accommodation and defective convergence are, however, easily caused by all painful sensations situated near the eye, which make the accommodation uncomfortable and fatiguing. This applies to every common head- or tooth-ache, and in the same manner to disturbances arising in the conjunctiva, or which depend on the stretching of the collective tunics of the eye in myopia, or which allow any other so-called "nervous" origin to be suspected.
We must place the same claims to the diagnosis of muscular asthenopia as to that of the accommodative form. Just as the latter is only detected if convex glasses really give the expected relief, so the proof of muscular asthenopia is only furnished when relief to the interni is brought about by means of the appropriate remedies. For myopes, who do not fall back on the aid of relative divergence, notwithstanding that they possess a clear field of vision only attainable with difficulty through convergence, it is the simplest plan to remove the far point to about 25 to 30 cm. by specially adapted concave glasses. If only slight myopia or none at all is present, but the relation between accommodation and convergence is disturbed, the latter can be corrected by means of prisms with the bases inwards—to be sure, only in a slight degree, as prisms of more than 4° are scarcely suited for spectacles, partly on account of their weight and partly[Pg 63] on account of the diffusion of colours. Prisms may be ground with concave or convex surfaces, according to the requirements of refraction or accommodation.
Finally, if an elastic preponderance of the externi can be proved by means of considerable facultative divergence, the same may be lessened by tenotomy of one or both externi; still after my own experience I cannot advise the performance of this operation unless prisms of at least 16° are overcome by absolute divergence, for I have seen many patients in other practices who have acquired convergent squint and diplopia for distance as the sole result of the operation, while the asthenopic troubles for near objects continue. The proof that it is not a case of muscular asthenopia is sometimes only obtained by the operation.
The fact that those who squint do not as a rule have diplopia, while squints depending on paralysis of the ocular muscles are combined with diplopia, was difficult to explain as long as the view was adhered to of identical retinal areas founded on anatomical construction. The first explanation hit upon was that a false identity became established, an inequality of the retinæ; were this the case diplopia must of necessity occur on correction of the squint by tenotomy.
Commencing with the assumption of a congenital identity which led under all circumstances to the occurrence of diplopia as soon as the images of the same object fell in both eyes upon non-identical points of the retinæ, the hypothesis was next advanced that the image of the squinting eye was not perceived, that a constant suppression of the sensations in the squinting eye took place. Suppression of sense-impressions does take place; as soon as our attention is entirely engrossed upon anything, we are in a position to disregard the impressions upon all other organs of sense; they do not reach our consciousness. That visual sensations are easily disregarded may be proved by experiments. Hold a small plane mirror obliquely before one eye, with the brim pressed into the angle of the nose so that the objects lying at the side and behind are seen in the mirror. If the other eye is now used to read with, it is quite easy to disregard the objects seen in the mirror provided that our attention is not attracted to places by a particularly bright light. No doubt those who squint also[Pg 65] possess this physiological power, and it is therefore certain that they make use of it under certain circumstances; but the suppression theory necessitates that they should constantly and always do so, since diplopia is bound to occur directly they do not do it.
The absence of double vision is in fact the only evidence that can be adduced in favour of the exclusion theory; this negative fact, however, proves nothing, and is, moreover, capable of other explanations, as soon as one abandons the theory of congenital retinal identity. The examination of those who squint demonstrates the untenability of this theory. People who squint seldom complain of diplopia, but double images can be rendered apparent in a comparatively large proportion of cases, usually with the greatest ease, by covering the best eye with a red glass and squinting with a vertically deviating prism. Many squinters now admit the presence of double images, but their position by no means corresponds to the identity theory, their lateral displacement is far too slight, or patients find themselves unable to localise the position of the image. It sometimes happens that alternating vision with both eyes is mistaken for diplopia, the images are then invariably specified as homonymous; however, with attention it is easy to distinguish this alternating vision from the simultaneous perception of two images of one and the same object.
There can be no doubt that in most cases the position of the double images does not correspond to the principle of identity, and just as little doubt that one to whom double images are easily made apparent cannot possess the confirmed habit of always suppressing the image of the squinting eye. A certain number of cases remain in which it is impossible to produce diplopia; that these, however, do not constantly suppress the image of the squinting eye may be proved in the very simple way I have indicated. An object of fixation is[Pg 66] placed in a darkened room, on one side of and behind the squinting eye is placed a small flame, the reflection of which, by means of a plane mirror before the squinting eye is thrown upon its retina. The reflection of the flame is seen on the cornea of the squinting eye, by slight rotation of the glass it can be brought into the area of the pupil, and at the same instant the patient sees the light, the reflection of which can easily be made to coincide with the image of the fixation object seen by the other eye. The experiment has then an entirely objective basis, it always succeeds, a fact on which I lay special stress, even in eyes whose vision is very defective; therefore here also the habit of suppression of the retinal images of the squinting eye is not present.
That the squinting eye really possesses its full share of the visual field can easily be proved (especially in divergent squint) by the aid of a perimeter. The best eye is covered with a red glass, so that the objects projected from the fixation point, as well as the excentric field of vision of this eye, appear red. As soon as the test object moves towards the side of the squinting eye and enters the visual area covered by the latter, it appears in its natural white colour, and this in most cases before it has reached the centre of the retina of this eye.
Another proof that the squinting eye is really used for vision appears to me to lie in the fact that persons who squint, provided of course that the vision of the eye concerned is not very defective, do not show that uncertainty in the estimation of distance, which is apt to prove so troublesome to those who have only monocular vision.[Pg 67]
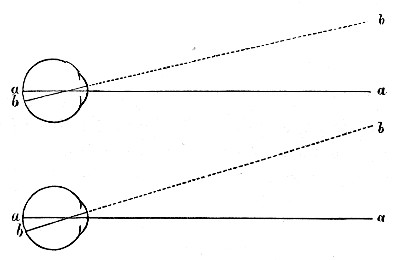 Fig. 1.
Fig. 1.
If, then, the view of the constant suppression of the retinal images of the squinting eye is untenable, how is it to be explained that squint as the result of paralysis of the ocular muscles causes diplopia, while concomitant squint does not? The answer to this question is clear as soon as we abandon the supposition of a congenital retinal identity, and look instead upon the relation of the eyes to each other as harmonious; identity, or co-ordination as something acquired. Central fixation is congenital and depends upon anatomical conditions, for as the macula lutea is anatomically the most perfect part of the retina, it is natural that the new-born child soon learns to place this part of the retina opposite objects which attract its attention, and therefore those relations of the eyes to each other are naturally developed. For instance, if both eyes (Fig. 1) are directed to the distant point a, the image of point b, situated at the same distance, will fall on the inner half of the retina of the left eye; the left eye will now learn by experience to refer inner retinal images to objects lying to the left of the fixation point; at the same time, however, with binocular fixation, the right eye learns to seek the images of the temporal half of its retina in the left field of vision, and vice versâ. From this it is easy to trace the laws of binocular diplopia. For example, let a in Fig. 2 be the fixation point, while at the same time the image of b belongs in both eyes to the temporal half of the retina. Now, as we have already seen, the right eye has learnt to refer temporal retinal images, to objects lying to the left of the fixation point,[Pg 68] while for the same reasons the left eye projects temporal images to the right. While then point a is seen binocularly singly, point b appears double, and certainly the image of the right eye is projected to the left of the fixation point, and that of the left eye to the right of it, in other words, crossed diplopia is present. But the eyes are divergent relative to point b; double images then which occur as a result of divergence (whether relative or absolute) must appear crossed, and one will easily be able to infer that for the same reasons those double images which occur in consequence of convergence, must be homonymous. All this, however, only with the presupposition, that the habit of binocular fixation is already fully developed; any disturbance of the same, in whatever way (by prisms, mechanical displacement of the eyes, paralyses of the ocular muscles, or by those forms of squint which arise after childhood is past) causes the double images to illustrate the law above explained. Certainly diplopia may be absent even then, but only in very rare instances. Now and then this happens in objectively proved ailments of the ocular muscles, where the patients complain of disturbed vision, which disappears immediately on the exclusion of one eye (see Case 12), a method of relief they usually discover for themselves; thus the indistinct vision is seen at once to be a disturbance of[Pg 69] binocular vision. Many such patients learn to see the double images which formerly escaped them, after they have been instructed how to do so during the examination. With others, all efforts are in vain, it is impossible to render them conscious of the double images, notwithstanding that the presence of the binocular disturbance of vision proves that the habit of binocular fixation exists. This apparent contradiction is explained, if one reflects that the physiological basis of vision rests on a series of conclusions. The first thing which strikes us as a result of binocular fixation is, that the images of the centres of the retinæ may be referred to one and the same region of the room, and this experience will be retained, even if the images on the centres of the retinæ represent different objects in consequence of paralysis of the ocular muscles; the images are notwithstanding referred to one and the same part of the room, all objects are thrown together promiscuously, and the consequent embarrassment is of course removed directly one eye is shut. The experience of those patients whom it is impossible to render conscious of double images, despite the habit of binocular fixation, reaches up to this point. A second conclusion belongs to diplopia, and for that it is necessary to seek out from the confusion of objects, the two retinal images belonging to one and the same object, and the majority of people, though not all, take this second step also. It is seen at the same time that the opinion held by Donders, that diplopia is absent in squint, does not suffice, for this reason, because the image in the deviating eye is too excentric. What becomes then of the image lying in the centre of the retina?
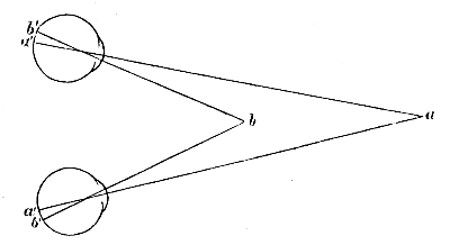 Fig. 2.
Fig. 2.
The absence of diplopia in squint may be explained quite simply by the fact that the habit of binocular fixation has not been learnt or has been forgotten; one can learn nothing that cannot be again forgotten. The normal fusion of the visual fields can only develop in consequence of binocular fixation,[Pg 70] and diplopia is only possible when some kind of binocular fusion exists. If no binocular fusion exists, then all possibility of diplopia is excluded. And why should those who squint from their earliest childhood not see well with both eyes, but yet with each separately, just as is the case with animals with laterally placed eyes? For example, in Fig. 3 there is convergent squint of the left eye, the right eye fixes the point a, whose retinal image is cast at a' in the left eye; the direction outwards in which these images are projected is discovered by drawing a straight line from a to c (the optical centre of the eye); suffice it to say that point a is seen by each eye in the direction in which it really stands.
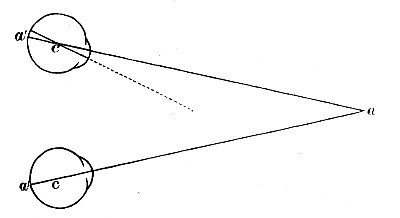 Fig. 3.
Fig. 3.
But although both eyes see at the same time, yet the close relation which in binocular fixation develops between the centres of the retinæ does not occur in squint; firstly, because the retinal area in the squinting eye which corresponds to the fixation point is too excentric, and secondly, because the angle of the squint often changes. In binocular fixation, the fixation point of one retina answers to the corresponding point of the other; in squint, on account of the varying size of the squint angle, if a like relation develops between the eyes, the fixation point of one retina must correspond to a larger area of the other. Possibly this explains a fact that is often to be observed.[Pg 71] In those cases of squint where diplopia can easily be caused by covering one eye with a red glass and the other with a vertically deviating prism, the double images disappear on rotation of the prism round the axis of vision, as soon as the angle of the prism reaches an angle of about 45°. The occurrence of double images shows that there exists for the upper and lower parts of the retinæ a community of vision by no means coinciding with the identity principle. The disappearance of the diplopia can be explained by the fact that the variations of the squint angle take place chiefly in the horizontal direction. Therefore the area in the squinting eye that corresponds to the fovea centralis of the fixing eye must be more extensive in the horizontal than in the vertical direction. Alfred Graefe has designated this phenomenon as "regional exclusion." Whilst then a sort of community of vision exists for the upper and lower parts of the retinæ, the sensations of the retinal area lying in the horizontal plane of the macula lutea of the squinting eye must be suppressed. The physiological occurrence of a suppression of the retinal images, as far as we are able to investigate it, always refers to the whole retina; however, the possibility of a "regional exclusion" should not be excluded to begin with; but in the inductive sciences it is for us to ask first, whether an incident really happens, and not whether it is possible. The fact from which Alfred Graefe draws his inference is not, as we have just seen, to be explained in any other way, and the ophthalmoscopic test described on p. 65 proves that also in these cases of "regional exclusion" both eyes are used for vision.
In many cases of periodic squint the condition of binocular vision is very interesting. Binocular fusion may be quite absent even in normal position of the eyes; on the other hand the non-occurrence of diplopia in squint does not prevent the occurrence of perfect binocular fusion with a normal position. In periodic outward squint I have sometimes seen binocular[Pg 72] fixation without the existence of binocular fusion; the excluded eye deviates outwards, but as soon as it is free it puts itself into fixation, whilst neither with prisms nor stereoscope can anything other than alternating vision be proved, i. e. neither binocular diplopia nor fusion.
If squint arises when the habit of binocular single vision has become confirmed, diplopia is always present, at least at first; even children of six to seven years old make this statement uninvited, but they soon get accustomed to the new relations, and after a short time it is impossible to make them see double images (see Case 42). Habits cling more closely in adults, therefore that form of convergent squint in particular, which usually develops quickly in myopia of average degree, causes annoying diplopia to last for a longer time. For just when these patients want to employ binocular vision in order to estimate distance correctly, diplopia occurs to hinder and confuse them.
It is otherwise with the relative divergence which is developed in consequence of myopia. At first diplopia is present here for a short time; in this case circumstances are specially favorable to a temporary suppression of the deviating eye; the fixing eye receives large distinct images to which the attention is directed. Meanwhile the relatively divergent eye is usually turned to other more distant objects that furnish indistinct retinal images, from which the attention is easily diverted. The habit of suppression may become so dominant that binocular fixation continues to exist for distant objects and the presence of binocular fusion is easily traceable, while for near objects, which are monocularly fixed with relative divergence, it is impossible to render the patient conscious of the images of the deviating eye.
Considerable squint is by no means necessary for the cessation of normal binocular single vision; slight, frequently recurring deviations are quite sufficient, as in those cases[Pg 73] where want of control renders physiological innervation for convergence more difficult. Double images are present here, although not in a troublesome way, as is usual in relative divergence, but binocular single vision does not exist even for distance. The reason for this does not lie in the impossibility of fixing the same object simultaneously with both eyes, for the objectively proved deviation may be extremely slight. A union cannot be obtained even by prisms. If crossed double images are present close together, a prism of a few degrees base inwards suffices to make them homonymous. The habit of binocular single vision is lost, in consequence of that disturbance to the innervation of the interni which is designated as insufficiency of the same.
The stereoscope, as well as the prism, is useful for testing binocular single vision, especially when it is suitably modified for the purpose. The prismatic glasses usually attached to stereoscopes are here quite superfluous. The advantage of the prismatic deviation consists solely in the fact that the centres of the images fixed for the macula lutea on each side can be removed farther from one another than the distance apart of the eyes amounts to, so that a greater extension of the visual area is rendered possible. Ordinary stereoscopic pictures are quite useless for testing binocular vision; it is a question here of employing diagrams, which contain on the one hand very prominent identical figures stimulating binocular fusion but which, on the other hand, offer for each eye special attractions not present in the visual field of the other. Further, it is desirable to regulate the stereoscope so that the glasses are not firmly inserted, but that glasses from the trial case may be applied according to the condition of refraction of the patient and the distance of the stereoscopic images.
The stereoscope is generally used with the greatest advantage in those cases where there is no conspicuous deviation, and by testing binocular vision conclusions may be drawn as[Pg 74] to whether normal binocular fusion exists or has disappeared in consequence of the squint.
It is desirable to use both methods of investigation, that with the stereoscope as well as prisms, as each test has its own value. One who at once combines the stereoscopic fields of vision certainly has binocular single vision; in other cases this is only so far lost that the stereoscopic combination does not take place at once but only after some trouble. Care must be taken, especially when one eye has defective vision, that the corresponding visual field contains objects sufficiently large and easily recognisable, as very small objects which do not correspond to the lowered visual acuity are easily overlooked. It sometimes happens that both fields are seen at the same time, but that there is no fusion; finally it happens frequently that there is complete suppression of one visual field. In testing with prisms it may appear doubtful as to whether binocular fusion or suppression of one eye exists; however, the stereoscope at once gives us certain information. It must not be forgotten that the altered relations between the eyes, which are always possible in squint, also appear at the same time; he who sees double with prisms, may yet be able completely to suppress the stereoscopic visual field of one eye. Binocular fusion, suppression of the squinting eye and simultaneous vision with both eyes without binocular fusion can alternate in the same individual. Von Kries has come to the same conclusion, and if our colleague is unable to explain all the phenomena of binocular vision that he could observe in his own case, we need not be astonished if we sometimes hear from our patients statements that appear incomprehensible and unphysiological.
At any rate it is evident that the absence of diplopia in squint can easily be understood, without adopting the arbitrary idea of a constant, habitual suppression of the image of the squinting eye.
Whether the state of refraction or the condition of the muscular equilibrium is held to be the chief cause of squint, defective vision of one eye will always have to be acknowledged as one of the most important favouring circumstances; in order to cure squint it is important to have regard to the visual acuity of both eyes, and not only to the defective condition. But this is no easy matter.
First it is to be observed, that most cases arise at an age when an objective determination of refraction is possible, but when the visual acuteness cannot be determined. Even in children who have received slight instruction, it is frequently difficult to distinguish whether imperfect knowledge of the letters or faulty visual acuteness is the cause of the non-recognition of the test-letters; when testing the vision of children it is often better to use figures than letters.
Further, in these cases it is much to be desired that the habit of determining the refraction and visual acuteness at the same time should be discontinued, particularly in reduced visual acuteness, as the test-tables only contain a few letters, which have to be recognised at a distance of 5 to 6 metres. If they have once been read with one eye it may easily happen that in testing the second eye they are repeated from memory, without being clearly recognised; even a child soon learns the few letters by heart. Therefore, when it has been a case of determining the visual acuteness I have always conducted the examination at a distance of one metre, as the choice[Pg 76] of letters or figures which can be employed at this distance is much larger than for greater distances. In every case the reading of test-letters must be used as an additional means of examination. We must never forget that the test of vision is a perfectly subjective examination, and that we are obliged first of all to accept the statements of patients as they are given without knowing what they are worth. I have met with patients in the most highly educated classes of society who, in intra-ocular troubles, for example, hæmorrhage of the retinal artery in the macula lutea, could not distinguish the largest type in the first examination, and the next day (perhaps with slight difficulty) could read small print.
Such inaccuracies may continue to exist during repeated examinations and for long periods. One of my patients, for instance, who first came under treatment in the year 1873, had extreme myopia in the left eye with good visual acuity; with the right eye, which was also myopic, and had suffered for several years from choroiditis of the macula lutea he could read only No. 20 Snellen, and a year later 7-1/2 was read with difficulty, word by word. Choroiditis of the macula lutea gradually developed in the left eye, and in the same proportion the statements as to visual acuteness of the right eye improved, so that finally at the end of 1881, 0·5 was read with difficulty with this eye, while the left still sufficed to read 0·4 (at about 5 cm.). As I tried to comfort the patient, who was very anxious about his left eye, with the fact that the right eye had considerably improved in the course of the year, he replied that he might previously have seen just as well with the right eye if he had only taken the trouble, this was certainly my own opinion.
The attention and intelligence shown by patients during examination materially influences its results, and one should never hold the first trial of vision to be conclusive. We must always remember, however, that all conclusions drawn from[Pg 77] visual acuteness become more unreliable in proportion as the latter is slight. We must attend to some peculiar difficulties in testing the vision of those who squint or we shall be liable to make great mistakes. When testing the squinting eye, particularly in children, it is not sufficient merely to cover the other or to hold the hand over it, for they know how to bring the usual eye into fixation by holding the head on one side or peeping between the fingers; we must keep it carefully closed with a bandage.
It is still more frequently the case that visual acuteness is stated to be less than it is in reality. The result of always using the better eye for fixation is, that fixation is not learnt with the weaker one. Even where there is no squint we see very frequently that in one-sided hypermetropia the accommodation is only used in that proportion which has become habitual to the emmetropic eye and does not therefore suffice to produce clear retinal images, while good visual acuteness is obtained by means of the correcting convex glasses. In the case of squinters (even without difference of refraction) it happens very frequently that the first statements as to the visual power are considerably below the truth. Patients who assert that they can only read the largest print with difficulty, frequently read smaller, and even the smallest type without more trouble, and we must be careful to ascertain this at first. Accurate reports are usually obtained more quickly by means of convex glasses or eserine. In any case insufficient accommodation is, according to this, one of the difficulties, but not the only one, which has to be overcome before the squinting eye can be put into fixation. We can understand that the innervation necessary for distinct vision can be set aside even without loss of visual acuteness, just as we see the movement of convergence disappear without the interni losing their capacity for contraction.
In order to explain the relation between squint and defective[Pg 78] vision, we must first consider the question hitherto neglected, or what is worse, answered with preconceived opinion, as to whether the same form of defective sight which is so common in squint also occurs without squint. No one doubts the existence of congenital amblyopia, nevertheless it has received but little attention in the handbooks on ophthalmology. Leber, for instance (in the well-known compilation, vol. v), does not mention it at all.
A more or less considerable reduction of visual acuteness, with good field of vision, normal sense of colour and normal ophthalmoscopic condition, are characteristic of congenital amblyopia. Colour-blindness may of course be present at the same time. I also hold as probable the very rare occurrence of congenital defects of the visual field in good central vision, but I will reserve for the present the few observations I possess on the subject.
Together with congenital defective vision we must consider the depreciation in visual acuteness usually present in nystagmus, although it might be asserted that it can neither be the cause nor the result of the nystagmus, for we find very considerable degrees of congenital defective sight in both eyes without nystagmus, as well as nystagmus with remarkably good visual acuteness. Not to complicate the question, however, I have excluded all cases of nystagmus from the following investigation. All cases of myopia of higher degree (i. e. of more than 6 D.) have also been excluded, as in such cases for various well-known reasons the full visual acuteness is never present. In the case of individual patients who remained for years under my observation I have been able to convince myself that visual acuteness decreased in accordance with the increase of myopia; on the other hand, however, it appeared to me very probable that just those cases of myopia, which from the beginning do not possess full visual acuteness, have a special tendency to increase quickly.[Pg 79]
For instance, if the examination of a hypermetropic eye, whose defect can be exactly determined by means of the ophthalmoscope, shows very faulty visual acuteness which is but slightly or not at all improved on correction of the hypermetropia, it is clear that the cause of defective sight is not to be sought in the hypermetropia. It is just the same with astigmatism. In defective vision with astigmatism proved by means of the ophthalmoscope, how frequently it is the case that not even the slightest improvement can be obtained with cylindrical glasses. This is usually attributed to the presence of an irregular astigmatism situated near the asymmetric meridian. If we illuminate the eye by means of a plane mirror, and observe one spot on the pupillary area which looks sometimes bright, sometimes dark, during slight rotations of the glass, this appearance can only be caused by the above-mentioned irregularity of the refraction of light, and it will be easy to determine whether the same takes place in the cornea or in the lens. But if this appearance is not present then irregular astigmatism cannot be proved. It is purely intentional, or a play upon words, if we refer an existing defective sight to an optic cause which cannot be proved. For instance, if haziness of the cornea exists, it is not difficult to learn to estimate by practical experience whether the amount of visual disturbance corresponds to the optic irregularities caused by the opacities and irregular refraction of the cornea. Slightly nebulous corneæ with disproportionately bad vision were therefore included in the following statistics; however, they do not influence the result as there are only ten cases in all. On the other hand, considerable opacity of the corneæ or cases which were complicated with anterior synechia, &c., were excluded from the statistics.
If then we find defective vision, the development of which has not been noticed by the patient, together with normal ophthalmoscopic condition and full visual field, and if it is[Pg 80] further seen that the condition remains unchanged for years, we have every reason for considering the defective sight to be congenital. The statements of patients must of course be received with caution. If congenital amblyopia of moderate degree exists in both eyes, patients do not usually know that it is possible for anyone to see better; if the congenital defect is one sided, it is generally only casually noticed on closing the better eye. We can scarcely doubt that it is a case of congenital amblyopia if it happens in children. Acquired defective sight without ophthalmoscopic cause seldom occurs among children. I have seen a few cases as a result of severe cerebral disease (hydrocephalus, for example); so-called anæsthesia retinæ, or amblyopia marked by contraction of the visual field is not quite so rare. It is easy to avoid confounding both these cases with congenital amblyopia.
One must be more careful about drawing conclusions with regard to adults, for on the one hand it happens that gradually developed monocular visual disturbances are only accidentally observed by patients after they have reached a high degree, and it is very difficult then to persuade these attentive observers that it is not a case of sudden blindness of one eye. (Only a few people seem to be really aware that they have two eyes, and still fewer appear to suspect the existence of a visual field.)
In all these cases opportunity is hardly given for mistakes with reference to the diagnosis of congenital amblyopia, as slowly developed monocular defect scarcely occurs without ophthalmoscopic cause. On the other hand, ophthalmoscopic symptoms (such as hæmorrhage of the retinal artery in the macula lutea) may disappear without leaving a trace, while defective vision remains. The law of habit, however, usually helps us here. In congenital monocular defect patients are generally accustomed to this condition, and only notice it when special claim is made on the visual faculty of this eye,—he,[Pg 81] on the other hand, who is accustomed to see with two equally good eyes, may not observe a gradually occurring blindness of one eye, if his talent of observation be faulty, but I have never had reason to suppose that a rapid depreciation of the central visual acuteness of one eye is also overlooked. Rapidly occurring monocular visual disturbances are noticed, whether detected with or without the ophthalmoscope.
Two peculiarities appear in isolated cases of congenital amblyopia, which may render the testing of vision difficult: rapid fatigue of the retina, and depreciation of the central visual acuteness in such a way, that an adjoining part of the retina possesses a better visual faculty than the centre.
Rapid fatigue of the retina occurs in comparatively good visual acuteness. For example:
Case 16.—Mr. W—, æt. 35, came under treatment for conjunctivitis. In testing the vision, emmetropia (or doubtful hypermetropia) was found on the left, V. = 5/6. Refraction of right eye similar to that of left, V. = 5/18 to 5/12, but with rapidly occurring fatigue of the retina. Patient had observed this fifteen years before, when shooting during his period of army service. Position and movements of the eyes are normal.
This peculiarity occurs more often in higher degrees of defective vision. For example:
Case 17.—Mrs. von G—, æt. 60, has always seen badly with the left eye. On the right H. 1·25 D., V. 5/12. On the left with + 2 D., V. 1/12 with + 5 D. words of No. 1·75 were recognised; but the visual acuteness above stated is only present at the first moment; after a few seconds everything disappears in a fog. The left eye has a slightly conical nebulous cornea, detected only on focal illumination, which does not, however, cause the slightest irregular astigmatism, and cannot, therefore, serve as explanation of the defective sight.
This rapid fatigue, which only permits the visual acuity[Pg 82] present to be estimated for a short period at a time, may easily result in the visual acuity being supposed to be worse than it is.
The other phenomenon above mentioned, which occurs in defective vision without being actually a necessary symptom, is the depreciation of the central visual acuity, which we designate as central scotoma in acquired amblyopia. It should be remembered that the visual acuteness which we determine under these conditions is something different from what we are usually accustomed to designate by this idea. When we simply talk of visual acuity we always imply the central visual acuity; however, in cases where the centre of the retina is so injured in its function, that the peripheral parts lying near are too often called into requisition, we do not determine the central visual acuity at all, but that of the nearest and at the same time best, excentric part. We cannot prevent patients from using that part of the retina which seems best to them for recognising the test objects. In such cases (just as in acquired central scotoma) continuous print is read badly, and with more trouble than one would expect from the visual acuteness which is specified in the recognition of single letters. Of course spelling and reading are two different things; the excentric visual acuity may perfectly suffice for the recognition of single letters, central and also excentric visual acuity is necessary for reading. There are patients who, despite full visual acuteness, are unable to read continuously, as soon as a defect in the right half of the visual field extends close to the fixation point. To read fluently, the excentric vision must work on in advance for the width of several letters, but if the first letter is seen excentrically, the excentric visual acuteness rapidly sinking in a physiological way, does not suffice for the following ones.
When testing the vision these circumstances should be carefully regarded. The apparent contradiction between the[Pg 83] visual acuteness specified with test-letters, and the uncertainty in reading continuous print, may be taken for simulation (I have seen some sad examples of this in acquired central scotoma), and, on the other hand, if in the form of defective vision now under discussion we content ourselves by merely employing reading tests, we take the visual acuteness to be worse than it is, or than we find it later when single test-letters are used, for even though excentric, it is yet always visual acuteness. The excentricity of that part of the retina put into fixation is usually so slight, that the oblique direction of the visual axis cannot be seen with the naked eye; if considerable and extensive defect of the centre of the retina is present, either varying fixation occurs, sometimes parts lying to the nasal and sometimes to the temporal side are put into fixation; or excentric fixation exists; an inner retinal area but sometimes also a temporal then usually has comparatively the best visual acuteness.
A third peculiarity which sometimes occurs in extreme degrees of congenital amblyopia, is monocular nystagmus of the weak eye. This trembling may be so slight that it is only observable during investigation with the ophthalmoscope; in other cases it is most marked as soon as the weak eye is put into fixation by exclusion of the sound one.
Cases of congenital amblyopia in both eyes, where no explanatory cause can be traced, and no nystagmus is present, are rare, but all the more interesting. For instance:
Case 18.—Mr. F—, æt. 56, has seen badly from childhood; the visual acuteness of each eye singly examined amounts to 1/18 to 1/12, binocular 1/12. No. 0·75 is read with difficulty at 8 cm. Ophthalmoscopic condition is normal. In mydriasis by atropine hypermetropia of 3 to 4 dioptres results. With convex 3· 5 D. on the right V. 1/18 to 1/12, on the left V. 1/12, binocular V. 1/12 to 1/9, with convex 6 D. still only 0·75 can be read, but more fluently than with the naked eyes.[Pg 84]
Normal binocular fusion may continue to exist even in extreme degrees of monocular weak sight; I have observed it up to a visual acuteness of 1/24. The stereoscope is well adapted to prove binocular fusion in these cases; only we must then take care that sufficiently large letters are present in the visual field of the defective eye, so that they may easily be recognised with the existing visual acuteness. Binocular fusion is naturally rendered still more difficult if the weak-sighted eye is at the same time hypermetropic to a high degree, as it then receives simultaneously indistinct retinal images on account of the difference of refraction; and yet in the above table there are 117 cases with hypermetropia of at least 2 D. in the better eye, and faulty visual acuteness in the other, 7 with visual acuteness of less than 1/7 to V. 1/12, and 9 with less than 1/12 to V. 1/36.
In the highest degrees of congenital defective vision, binocular fusion cannot as a rule be proved; partly because the methods of investigation by which we are able to prove binocular fusion presuppose the existence of a sufficient visual acuteness. On the other hand, it cannot be expected that normal binocular vision can be learnt with such a large amount of monocular defective vision. If the relative strength of the muscles is normal, so also are the position and movements of the eyes, if elastic preponderance on the part of the muscles is present, which in monocular defective vision of considerable degree is no longer governed by binocular fusion, and this is frequently the case, squint is developed.
Sometimes other congenital anomalies are present at the same time with congenital defective vision (for example, congenital dermoid growths on the edge of the cornea), and undoubtedly hereditary influences play a considerable rôle therein.
In order to determine the relation of congenital defective vision without squint, to defective vision with squint, I have[Pg 85] taken those cases where congenital defective vision without squint was observed, together with the cases of squint, from the diaries of my private practice for the last ten years. I have personally investigated every case, and the observations on each were carefully examined before being included in the statistics; all cases with myopia of six or more dioptres, all cases of double nystagmus, and, finally, all those cases where the previous existence of squint might be suspected, were excluded, as above stated. I must also remark that before the last ten years I had not begun to collect these cases. In order to find monocular congenital defective vision one must seek for it, as patients usually come under treatment for quite different disorders, and in the consulting-room there is not always time carefully to investigate what possesses interest for us but none for the patient. In cases of squint the opportunity for investigating the power of vision does not escape us so easily, and yet the same list, which contains among 629 patients 177 cases of squint with a visual acuteness of 1/8 to less than 1/36, furnished at the same time 98 cases with undoubted congenital defective vision of the same high degree without squint, which I place together in the following review.
Cases of congenital amblyopia with visual acuteness of 1/7 are so frequent, that I have not drawn up special statistics of them. I was not anxious to collect a large number of cases but only material for evidence. I have therefore divided the 98 cases I observed into 3 groups. (1) Cases with visual acuteness of less than 1/7 to V. 1/12; (2) V. less than 1/12 to V. 1/36; (3) visual acuteness less than 1/36. The limits between these groups are of course not very sharply defined, for what is designated as "measurement" of visual acuteness contains, even if we accept the statements of patients as trustworthy, not an inconsiderable number of sources of error; and we often find a remarkable absence of conformity in the analysed causes[Pg 86] of congenital amblyopia, according as we seek to determine the visual acuteness by means of single test-letters or by reading printed matter. In a case of visual acuteness of 1/12 No. 0·75 with convex 6 was the smallest type that could be read, and that with difficulty, larger type was usually required; and in one case where at first only single words of No. 2·25 were read with difficulty—this test was on that account repeated in myosis by eserine—No. 1·75 was finally the smallest print which could with the same difficulty be deciphered. In the division of the groups here arranged the best visual acuteness ascertained in the various examinations was always used as the basis.
A. Vision less than 1/7 to V. 1/12 38 cases. The examination of the better eye showed:
(a) Emmetropia in 18 cases. A determination of refraction, mostly ophthalmoscopic, of the weaker eye is submitted in 11 cases, which divide themselves into, 4 with emmetropia, 3 with hypermetropia (of H. 2 D. and 2·25 D.), 3 with hypermetropic astigmatism, I with myopic astigmatism.
(b) Myopia in 5 cases (3 of M. 1 D. to 1·5 D., 2 of M. 4·5 D. and 4 D.), the condition of the defective eye was determined in 3 cases, and was twice hypermetropic, once astigmatic.
(c) Hypermetropia in 8 cases, hypermetropic astigmatism in 3. In 4 cases an exact determination of refraction even of the better eye was for some reason impracticable.
There are 4 cases in this group where the visual acuteness in both eyes did not exceed the above-stated small amount, and one which was interesting from another point of view.
Case 19.—Max L—, æt. 8-1/2, recognises No. 24, and a few letters of 18 at 5 metres with the better eye with convex[Pg 87] 6 D.; at 1 metre V. 1/4 to 1/3, the left eye recognises only No. 60 at 5 m. with + 6 D. at 1 m. No. 0·75 is read with difficulty. If we exclude one eye it lapses into now less, now greater convergence, and still no squint is present, but diplopia as well as binocular fusion can be proved by the aid of prisms. The theory of Donders that squint is less frequent in hypermetropia of high degree because too strong convergence would not suffice to furnish clear retinal images, is scarcely tenable in the face of such cases. If indistinct retinal images are added to a visual acuteness of only 1/3 to 1/4 still, even with faulty accommodation, it is difficult to believe how a child could learn to read if it did not hold the book close to its eyes, which was not the case here, and indeed seldom happens. Therefore, in spite of defective vision the accommodation must have sufficed, without sacrificing binocular fusion, whilst in all probability accommodative convergence followed on exclusion of one eye.
B. 48 cases had visual acuteness from 1/12 to 1/36. The better eye was—
(a) Emmetropic in 16 cases; in 6 of them the refraction of the defective eye was determined, which showed in one case emmetropia, 3 hypermetropia, 2 astigmatism.
(b) Myopia of the better eye was present in 7 cases (in 3 myopia of 1 D., in 4 M. 3 D. to 6 D.).
(c) Hypermetropia in 18, astigmatism in 4 cases. In 3 cases the condition of the better eye was, for some reason or other, indeterminable.
In this group I should like to point out the following cases as worthy of attention:
Case 20.—Margarethe T—, æt. 16, has hypermetropia 2 D. in the right eye, V. 5/6, in the left the ophthalmoscope shows[Pg 88] with an otherwise normal condition a higher degree of hypermetropia, with + 6·5 D., V. 1/18, with + 10 D. No. 3·0 is read. No spectacles have been used until now; for the past few years school tasks have been performed with a certain effort, only during the last year the asthenopia has increased. Squint is not present, and with prisms as well as with the stereoscope (by the use of objects, whose size corresponds to the defective sight on the left side) binocular fusion can be proved.
The case is the same as regards divergent strabismus.
Case 21.—Mr. H—, æt. 28, has myopia 6 D., V. 6/9 in the right eye; the left eye has always been weak sighted, emmetropia is detected with the ophthalmoscope, with normal fundus, V. 1/18. No squint, binocular fusion can be proved with prisms.
Case 22.—Mr. B—, æt. 47, has hypermetropia 5 D., V. 5/9 in the right eye. Left eye with + 5 D., V. 1/18 (a few letters of 12 also were recognised at 1 m.). It seems, however, that the patient is not able exactly to indicate the position of the retinal images of his left eye, he does not know, as he expresses himself, "whether the letters stand here or there." Patient observed the defective sight long ago; the ophthalmoscopic condition is normal. Patient really comes on account of his son, aged 7-1/2, in whom hypermetropia of 3·5 dioptres is detected with the ophthalmoscope, right eye with + 3·5 V. 5/9. Left eye has convergent squint, V. 1/36, No. 3·0 is read with + 6·5 D.
The hereditary tendency is seen also in the following case:
Case 23.—Mrs. S—, æt. about 46, on the left H. 4 D., V. 5/18 to 5/12, has used no spectacles until now, and reads No. 0·75 without glasses at about 15 cm. R. with + 4 D., V. 1/18, with + 6·5 D. large letters of No. 5·0 are recognised.
Two sons, present at the same time, are hypermetropic. One has in either eye V. 1/4, the other a slighter degree of congenital amblyopia.[Pg 89]
Case 24.—Johanna L—, æt. 4, came under treatment for a congenital fibroma covered with hair, about the size of a cherry-stone, situated on the outer corneal margin of the left eye, which was removed. Three years later, when the child had learnt to read, emmetropia and full visual acuteness was observed in the right eye, with the left No. 4·0 only is read with difficulty. The ophthalmoscope shows a slight degree of irregular astigmatism of the cornea, which in no way explains the defective vision; the image of the fundus is perfectly clear and quite normal.
Case 25 afforded me a not altogether pleasant surprise. Martin M—, æt. 58, has matured cataract in the right eye, with perfectly satisfactory light reflex, proper projection, &c. On the left progressive cloudiness of the lens has begun. The course of operation and cure were regular in every respect, but the power of vision finally was so small that with a clear pupillary area, and otherwise normal condition, only single words of No. 3·0 were recognised with difficulty at 10 to 15 cm. with convex 20 D. For the first time the patient remembers that he noticed the defective sight in his right eye at the age of sixteen, and was for this exempt from army service. The operation performed later on the left eye procured satisfactory vision.
C. Visual acuteness of less than 1/36 12 cases.
Determination of refraction of the better eye is given in 6 cases, and showed twice emmetropia, twice slight myopia, twice hypermetropia. I only possess an exact ophthalmoscopic determination of the condition of the defective-sighted eye in one instance with H. 2·5 D.
This group is of special interest in that it represents the extreme degrees of congenital amblyopia, and, on the other hand, because it contains 5 cases of children under 10 years of age.[Pg 90]
Case 26.—Constanze von M—, æt. 9-1/2. Defective vision on the left side had been noticed long before by the child's parents. On May 1, 1879, emmetropia was observed in right eye, V. 5/12 to 5/9. No. 0·4 is read at 15 cm. On the left, only movements of the hand are seen, fingers cannot be counted even when close to the eye; the visual field is good, that is, on moving the hand in the periphery of the visual field the child sees "something" without being able to state what it is. Reaction of the pupils as rapid and equal as usual. The ophthalmoscopic condition (even with dilated pupils) is perfectly normal. All tests for simulation were of course applied.
On account of the importance of the case, I suggested another examination a year and a half later, on the 22nd December, 1880, which showed precisely the same result as the former one—optic disc, macula lutea, &c., perfectly normal, the ophthalmoscopic determination of the refraction shows H. 2·5 D.
The child's father also possesses in the left eye a slight degree of congenital defective sight, observed for many years, with normal ophthalmoscopic condition; No. 0·5 is read with + 6·5 D. at 10 cm.
Case 27.—Tina S—, æt. 6. The defective sight of the left eye had been remarked some months previously; report on July 16th, 1878: R. full visual acuteness, L. movements of the hand are scarcely visible. The child cannot count fingers. Normal ophthalmoscopic condition. Eserine and separate use were prescribed. On September 9th, 1878, fingers were counted with the left eye at 1·5 m., single words of No. 4·0 were recognised, No. 3·5 with convex 6·5 D., but always with oscillating fixation. The improvement in the child's statements may be referred to the fact that she had meanwhile learnt to form right conclusions from the very imperfect sensual impressions of her left eye.[Pg 91]
Case 28.—Frank J—, æt. 10. Left eye. V. 10/50 to 10/40, No. 1-1/2 Snellen is read at 4 inches. On the right, nystagmus on fixation, fingers are counted at 5-6 feet. The ophthalmoscopic condition is normal. A sister of the boy squints.
Case 29.—Ernest G—, æt. 8, has slight nebulæ on both corneæ. On the left V. 15/40. On the right, fingers are counted at 4 inches with visual axis deviating inwards.
Case 30.—I operated on Moritz L— for congenital cataract before he was a year old in 1869 by means of a needle operation. In June, 1877, a thin ophthalmoscopically transparent secondary cataract appeared in both eyes; on the left, with convex 12 D. V. 3/24 to 3/18, with convex 16 D. No. 0·4 is read at 10 cm. On the right, with convex 12 D., fingers are counted with difficulty at about 1 m., with inward deviation of visual axis.
Case 31 is also worthy of note. Carl H—, æt. 22, shows quite a number of congenital anomalies on the left side of the face, harelip, deformed nostril and a skin defect on the inner corner of the eyelid. There is a congenital dermoid growth of the size of half a pea situated on the inner lower corneal margin. A slight irregularity in the curve of the cornea near the dermoid is detected with the ophthalmoscope; the fundus of the eye is perfectly normal. Fingers are not counted further off than a metre with visual axis deviating inwards. The right eye is emmetropic (perhaps slightly hypermetropic), and has full visual acuteness. There is no squint.
It is customary to "explain" these cases of monocular amblyopia by previously existing squint, and one is quite satisfied if by the examination of patients it is only possible to prove that they have occasionally squinted, although the advocates of the amblyopia ex anopsia disallow the presence of the same under these conditions, that is, in periodic squint. Of course a theory which cannot exist without the assertion that occasional alternation suffices to hinder the development[Pg 92] of defective vision caused by disuse, cannot possibly hold periodic squint to be the cause of it. Certainly permanent squint may also disappear, but this much I have been able to determine, that this seldom happens before the twelfth year of life, and one may surely reckon that children in whom permanent squint is developed at the usual early period of life, still squint at the age of ten years. Cases 24 and 26 to 30 can under no circumstances be explained by previous squint, notwithstanding that they represent the extremest degrees of amblyopia, but the question is undoubtedly that of congenital defective vision; moreover I have excluded from the statistics of congenital amblyopia all cases in which the previous presence of squint could even be supposed.
A table of the cases above described with reference to the defective condition is interesting; when a determination of refraction existed for the weak eye I have given it, and when this was not the case I have stated that of the better eye, thus it is seen that among 85 cases in which the refraction was determined, hypermetropia (including hypermetropic astigmatism) was present in 39. Hypermetropia was found then in 47 per cent of all the cases. The percentage would probably be higher, if all weak-sighted eyes had been examined from the beginning as to their state of refraction, but as I only learnt to know the relation between hypermetropia and the higher degrees of congenital amblyopia from my statistics, I did not take notice of this relation when investigating individual cases.
How does congenital amblyopia now stand in relation to that disturbance of vision which we observe in squint? I see no difference; whether squint is present or not, the form of defective vision is precisely the same, and nothing happens in the combination with squint which could not also be proved without it. The relation to hypermetropia, which is proved with congenital amblyopia, also appears in squint.[Pg 93]
A collective table of cases of convergent and divergent squint included in the statistics (pp. 19 and 47) shows:
(a) In myopia, emmetropia, and doubtful hypermetropia, with convergent and divergent squint together 329 cases. Among them:
| Visual acuteness | to 1/7 | 239 | |
| " | less than | 1/7 to V. 1/12 | 19 |
| " | " | 1/12 to V. 1/36 | 46 |
| " | " | 1/36 | 25 |
Defective sight of higher degree than 1/7, 27·3 per cent.
(b) In hypermetropia 1 to 3 D., including the few cases of hypermetropia with divergent squint, 177 cases. Among them:
| Visual acuteness | to 1/7 | 121 | ||
| " | less than | 1/7 to V. 1/12 | 17 | |
| " | " | 1/12 to V. 1/36 | 27 | |
| " | " | 1/36 | 12 |
Defective sight then, 31·6 per cent.
(c) In hypermetropia 3 D. and more, 70 cases with convergent squint, with:
| Vision to 1/7 | 39 |
| V. < 1/7 to V. 1/12 | 8 |
| V. < 1/12 to V. 1/36 | 14 |
| V. < 1/36 | 9 |
Defective sight then, 44·2 per cent.
This regular increase of defective sight with the increase of the hypermetropia can be no mere accident, and speaks strongly for the identity of defective vision in squint with congenital amblyopia. Were defective vision caused by the squint the various states of refraction would show no difference in the percentage of defective vision.[Pg 94]
Further, the circumstance is worthy of remark that among 198 cases of periodic squint (convergent and divergent) which are applicable for the statistics of visual acuteness—
| 170 | possess | V. to 1/7. |
| 16 | " | V. < 1/7 to V. 1/12. |
| 9 | " | V. < 1/12 to V. 1/36. |
| 3 | " | V. < 1/36. |
| 14·2 per cent. then of defective vision of considerable degree. | ||
That defective sight on the whole plays an influential part as a cause of squint is doubted by no one, indeed we see blind eyes lapse into squint as soon as the conditions necessary to it are supplied by the muscles. Of all the prevailing causes present defective vision will be the more decisive in proportion as it is of high degree; for the motive which despite the presence of favouring circumstances can prevent the real occurrence of squint, binocular vision, becomes less efficacious as the defective vision becomes more considerable. As binocular fusion takes place frequently in periodic squint, for a time at least, that is as long as proper fixation lasts, one can understand that periodic squint exists chiefly in cases where the visual faculty of both eyes is good. Even the highest degrees of congenital amblyopia are not excluded, for periodic squint appears where the faculty of binocular fusion has been completely lost. Further, that considerable congenital defective sight is more frequent with than without squint, may be accounted for quite simply by the fact that, in extreme degrees of it, binocular fusion cannot be learnt at all, while in the lesser degrees it is more easily forgotten again.
If defective vision is undoubtedly one of the causes of squint, we must seek for the grounds upon which it has been taken to be a consequence of squint, and described as amblyopia ex anopsia. I will not inquire to whom the honour of this[Pg 95] invention belongs. I do not want to write a history of mistakes but only to examine the basis of the views now current. The most complete record of the same may be found in the well-known journal on the 'Cure of Eye Diseases,' vol. v, p. 1011. Leber, who does not seem to recognise the existence of congenital amblyopia, has shown quite a special predilection for amblyopia ex anopsia.
Amblyopia from want of use, which formerly included all possible disturbances to vision, great and small, is now only accepted in two cases, for squint and congenital cataract, if the latter is not operated on very early in the first or second year of life.
The fact is simply this, that in congenital cataract even the most successful operation is frequently deceiving as to its issue without ophthalmoscopic report; this is the more disagreeable as the most exact reflection test before the operation fails to prove the existence of this defective sight. But does it follow from this, that congenital cataract has induced defective sight from want of use? We find the same defective vision also in congenital defective development of the transparent lenses (so-called luxation of the lens). On the whole, we often find several congenital defects in the same individual. The very circumstance that the cataract is congenital makes it probable that the defective sight is so also, or are we to take congenital cataract as being a guarantee against congenital amblyopia?
Von Graefe, who first considered this defective sight to be congenital, designated it in his later lectures as originating from want of use, probably in order to advise the earliest possible performance of an operation. There is no mention of his having brought forward evidence for this assertion; that the great master himself said it was enough, and the host of believers felt themselves to be the happy possessors of a new dogma.[Pg 96]
A number of children appeared in my practice, in whom congenital cataract was needled by von Graefe in the first or second year of life with recovery of transparent media, who showed, however, the extremest degrees of defective vision when they were sufficiently intelligent to have their vision tested. Whoever is interested in this can find a number of such cases in the Royal Institution for the Blind at Steglitz, which I am accustomed to visit several times a year by request of the committee. On p. 91 I have related a case of monocular congenital defective sight in congenital cataract of both eyes.
Everywhere then the principle holds good, that whoever makes an assertion must be prepared to verify it; amblyopia from non-use is denoted as an inherited trouble, and still not a single observation exists which furnishes proof that an eye of previously ascertained good visual acuteness has become amblyopic in consequence of disuse, a fact I drew attention to ten years ago. Leber replies to this, he remembers "to have seen patients with complete amblyopia in the squinting eye, who stated that its visual faculty had been found to be good during an examination instituted years before." Is this intended as an observation? By that I mean is it a proof of facts, for the trustworthiness of which he holds himself responsible: in the handling of scientific questions I do not place the least reliance on the dim recollections of unnamed individuals. Even in personally conducted examinations we must be on our guard to avoid mistakes, and now we are confronted with mere recollections of tests of vision!
By means of the above observations the theory that "the peculiar variety of monocular amblyopia which is so frequent in monocular squint is hardly observed without squint" is sufficiently disproved.
Leber seeks to enfeeble Alfred Graefe's statement that the presence of extremely defective vision may sometimes be proved at a very early age, in children who have only squinted[Pg 97] a short time (the rapid development of amblyopia in consequence of the squint really appears incredible), by the assertion "that just at the earliest age, when the activity of the optic nerve is not yet sufficiently strengthened by use, the conditions for producing amblyopia from non-use are most favorable with complete exclusion of one eye," but complete exclusion of the squinting eye does not take place even in extremely defective sight, as can easily be seen by the mirror test (p. 66) I described fourteen years ago. Which activities of the optic nerve apparatus are strengthened then by use? Perhaps visual acuteness? The physiological conditions of this are only to be sought in the anatomical structure, and the physiological arrangements of the retina or the visual organs, which cannot be changed much by use. What we can learn from the visual act relates solely to the conclusions which we are able to draw from sensual impressions; but visual acuteness, i. e. the faculty for the recognition of distinct points, is an anatomical, physiological gift, and not a thing to be acquired.
The opposing observation, that squint, even of monolateral character dating from earliest childhood, continued to the middle and later years of life, can still exist with very good visual faculty, may easily be explained by alternation from time to time. If that is so indeed, if squint begins during the presence of good visual acuteness, and nothing further is necessary to its maintenance than alternation from time to time, why should defective vision from non-use ever be developed? With good visual faculty on both sides alternations also occur from time to time.
Still more convincing are those cases which are numerous where the visual acuteness of the squinting eye only amounts to about 1/7 to 1/12, and where, on this account, there is no alternation. Were this defective sight acquired through non-use it must of necessity be progressive; it must exist in proportion[Pg 98] to the duration of the squint. A moderate experience will suffice to show that this is not the case. And further, defective sight must continue progressive even after removal of the squint by operation, for by the operation nothing is changed in the relations of the binocular vision present in squint, which are dismissed with the one word, "suppression," by the advocates of defective vision from non-use.
Moreover, suppression may exist for years without the slightest disadvantage to the visual faculty.
Case 32.—In November, 1873, I operated on Fritz F— for a slight divergent squint of the left eye. Slight hypermetropia was present on both sides, and nearly full visual acuteness. In October, 1880, perfectly normal position of the eyes showed itself with the same visual acuity and emmetropia in both eyes; at the same time, however, the boy affirmed that when reading he could never see with his left eye but only with the right; in reality only the right visual field was perceived in the stereoscope.
The second reason brought forward is, that the variety of amblyopia from non-use is quite a peculiar one; "it consists of a functional disturbance of those parts of the retina whose images belong to the common V. F., and are suppressed in squint in order to render vision distinct—the macula and the temporal and only a part of the nasal halves of the retina." Does this hold good for all cases of amblyopia in squint, or do those cases only belong to amblyopia from non-use where excentric fixation takes place with an inward deviating visual axis? It would be difficult to draw the line. I have seen a case in which the squinting eye possessed a visual acuteness of 5/36 together with excentric fixation and nystagmus; however, I attach no value to isolated cases. We frequently find excentric fixation with a visual acuteness of 1/12 to 1/36. Further, those cases cannot possibly be regarded as results of squint, which possess unsteady oscillating fixation or rapidly trembling[Pg 99] nystagmus, which occurs as soon as the squinting eye fixes. But this conclusion is false, even for the excentric fixation with visual axis deviating inwards; if it were right the angle at which the eye deviates inwards on fixation in convergent squint would always be greater than the squint angle. Those cases are, of course, more remarkable where this is not the case; however, on close investigation those cases are more frequent where the angle of deviation is about the same size or smaller than the squint angle, and is fixed with a part of the retina which undoubtedly belongs to the common visual field.
On p. 91 I have described two cases of excentric fixation in children who had never squinted, and it is only necessary to take a little trouble to repeat the mirror test which I described, to be convinced that squinting eyes have not lost the power "of using those parts of the retina," even if they are amblyopic to an extreme degree; without the slightest doubt the reflection is perceived as soon as it falls on the retina.
Value is attached to the improvement produced by the separate use of the squinting eye. According to my experience no higher visual acuity can be attained by use of the amblyopic eye, than that which is best detected by the aid of eserine in the first examination, if it is only carried out thoroughly enough. No doubt if we proceed otherwise, and rest content with whatever statements the patient likes to make, without giving ourselves any more trouble, we may expect the most superficial diagnoses to show the most astonishing therapeutic results, as, indeed, often happens. And now, talking of strychnine injections! When two celebrated ophthalmologists occupy themselves simultaneously with the therapeutics of strychnine, one of whom obtains the most astonishing results in atrophic troubles of the optic nerves, but, on the other hand, obtains no real improvement in "amblyopia from non-use," while the other can show brilliant success in the last-named form of defective vision, and, on the[Pg 100] other hand, none in atrophy of the optic nerves, we may perhaps conclude that both are right, if even really on the negative side, and that the circumstances are the same in the tests of vision. Again, we must examine more closely some of the cases, in which strychnine injections showed a brilliant result. (Anyone interested in the original work can read up the 'Vienna Weekly Medical News' for the year 1873.)
"1. Wilhelm H—, a strong healthy boy, æt. 12, complains of defective vision. Right eye has nothing abnormal in its outward appearance, and just as little in the fundus. V. 16/100, H. 2·5 D., Snellen IV-I/II; is the smallest type he reads at 3 to 7 inches. With + 10, I-I/II is read at 4 to 6 inches. Left eye V. 16/70. H. 2·75 D. II-I smallest type legible at 3 to 12 inches. With + 4 D. I-I/II is read at 4 to 6 inches. On March 14th, 1872, first injection of strychnine with 0·002 gr. in the temples. An hour later V. of right eye 16/70, left unchanged. On March 23rd, 1872, after one injection daily, V. of each eye is 16/50."
Patient shows then in the right eye visual acuity 16/100, with manifest hypermetropia 2·5 D.; in all probability the total hypermetropia really present was higher, and was scarcely corrected by means of convex 4 D. If the patient now reads No. I-I/II Snellen with + 4 D. at 6 inches, this proves a visual acuity of 1/3 during the first investigation before the strychnine injection, and shows that the estimate of 16/100 was inaccurate. At the close of the treatment, only a visual acuity of 16/50 (almost exactly 1/3) is specified for distance. The result seems to me, then, to be this, that the patient during repeated examinations has gradually learned to make more accurate statements, indeed, with a boy twelve years old one can scarcely expect it to be otherwise.
"4. Paul A—, æt. 18, was operated on ten years ago for internal squint of the right eye, and dismissed with + 2 D. for distance, and + 6·6 D. for near use. He now complains[Pg 101] of decrease of his visual acuity. The eyes are normal externally and internally. Hyperopic formation in a high degree. Right eye V. 1/20, with and without convex glasses, without glass only VIII-I/II with difficulty, with + 6 V-I/II the smallest. Left eye appears emmetropic, but is decidedly hyperopic. V. 5/4. Glasses are rejected; I-I/II is read fluently at 6 to 12 inches. After one injection the right eye recognises III-I/II with + 6, after the second II-I/II, after the eighteenth I-I/II with difficulty. The visual acuity, however, remains at 1/20, and is not changed after six months, although latterly patient daily practised with + 3 D."
Visual acuity of 1/20 suffices to read III-I/II at 2·5 inches, II-I/II at 1·5 inches, and I-I/II at about 1 inch; clear, retinal images are then scarcely obtainable, but we know what hypermetropes can do in that case; besides this, if the patient is examined for weeks by Snellen's method, he may get so far as to realise fairly well "the strange fate of that man" of I-I/II, despite larger diffusion circles; in any case vision remained at 1/20, despite strychnine and separate use.
In extremely defective vision little importance should be paid to the fact of slight diversity in the statements, as where visual acuity amounts only to about 1/36, or where fingers are counted at a distance of 1 to 2 metres, it is quite immaterial, as far as the usefulness of the eyes is concerned, whether fingers are counted at a half or a whole metre, and we ought never to forget that all conclusions which we draw from the state of the visual acuity, are unreliable in proportion as the latter is lowered. Indeed, on repeated examination of such cases we frequently find considerable fluctuation in the statements of the patients, therefore we ought not to expect accurate statements for very inexact sensual impressions.
By separate use, even in extremely defective vision, no improvement in visual acuteness is developed, but only a more[Pg 102] complete acquirement of the power of deducing right conclusions from imperfect sensual impressions. That which has been most unscientifically designated as "suppression of diffusion circles," depends solely on this method of use. As with indistinct retinal images so with facial impressions which are insufficient, one can never learn to recognise larger objects aright.
We must never forget that vision is a conclusive act acquired by practice; whoever sees well with one eye, and is weak sighted with the other, acquires this end only for the sensual impressions of the better eye, and must first collect experience for the defective eye, before he can use it.
Leber has recently joined those cases which are described as blindness through blepharospasm, to amblyopia from disuse. First, I wish to observe that blepharospasm is not a necessary cause; I have seen the same disturbance of vision follow severe double blenorrhœa, which destroyed one eye but left the other uninjured. These children are always of an age which renders any trial of vision impossible, and we are therefore obliged to draw conclusions as to visual power from the movements of the body. If children move as though they were blind, it need not necessarily follow that they are so in the common meaning of the word. The art of vision is a difficult one, the acquisition of which begins with the earliest days of life; we do not call every person blind who does not see what is before his eyes, because he does not understand how to see it. A child who has only imperfectly learnt the conclusive act of vision, and forgotten it again during a continued disuse of both eyes, will not know how to use perfect visual acuity, and will move like a blind person till he again learns to estimate the relations between his retinal images and the things of the material world, which happens in a very short time.
After this digression let us turn again to amblyopia from disuse, and to the last trump which is played for it. "Those[Pg 103] cases are very remarkable where an immediate improvement occurs after tenotomy in amblyopia of high degree, which according to this is certainly produced and maintained by the squint." As proof a case is cited by Knapp, who describes it in the following words:—"The improvement in visual power varied very much. In many cases it was indefinable, in others very pronounced; for example, in one case, where it was very great before the operation, only No. 16 Jaeger could be read at 1 inch, while after it No. 2 was read at 8 to 9 inches."
And we are to believe wonders on the strength of this scanty communication! It is an every-day experience that a person who squints, who has just asserted his inability to read the largest type, immediately afterwards reads smaller and the smallest type, and it would at least first have to be determined that all endeavours to produce a better visual result before tenotomy were unsuccessful; but as the communication stands, the conclusion as to the effect of tenotomy is quite a superficial post hoc ergo propter hoc. Moreover, I had this case in view when I spoke on this matter in the first edition of my 'Handbook:'—"The frequently repeated assertion that a considerable improvement of vision may occur as a direct result of tenotomy, is so little in accordance with all the laws of physiology, that inquiries must be instituted ad hoc, and carried out with the most perfect exactitude. Only trials of vision which are carefully carried out and repeated several times before the operation, and which have regard to visual acuteness for distance as well as for near objects, the latter indeed by the aid of convex glasses or Calabar extract, can be recognised as proving anything in face of such a perfectly improbable assertion. In the course of examinations so instituted I have not myself found that tenotomy exercises any direct influence on visual acuity."
I would not have given so much space to this explanation had not a principle been in question. The occurrence of[Pg 104] amblyopia as a result of non-use has been deductively constructed and is not inductively proved by observation. It is just an article of faith, and in science we cannot rely on such things; we must not depart from the inductive method.
Therapeutic investigations have their safest and most instructive basis in observation of the course of a disease as it appears without complications, and with no unusual symptoms; we can only arrive at a certain decision as to the extent of our therapeutics when we know exactly what will happen without skilled assistance. When squint is once present it is seldom complicated by fresh symptoms; on the other hand, spontaneous cures unquestionably take place. We must certainly not rely simply on the statements of patients themselves. On p. 1 we have seen what mistakes occur, even when it is a question of whether squint is present or not. How little such vague statements are worth is seen by the fact, that the question as to the direction of the previous squint very seldom finds a satisfactory answer; as a rule it is impossible to determine whether periodic or permanent squint has been present.
If we undertake the task of converting the statements of patients as to previous squint into observations, in order to confirm the statements from the objective material, we must first prove whether the squint cannot by some means be still produced (by excluding the eye or by raising or lowering the eyes). Thus the condition of binocular vision offers us valuable guides. If we find that binocular fusion does not exist with available power of vision on both sides, but that the same conditions of sight appear in the eyes as we have learnt to attribute to squint, there is no reason for doubting the statements about a previously existing squint. It is otherwise[Pg 106] in those cases of extreme amblyopia where normal binocular vision is never expected, or at least cannot be proved on account of the enormous difference between the two eyes.
If we discover the existence of normal binocular fusion, squint may nevertheless have been present at a former time, for in many cases, of periodic squint particularly, the habit of binocular fusion is never quite lost.
That squint can disappear of itself is unquestionable; how often this happens it is difficult to say. The fact that in ophthalmic practice we see many more squinting children than adults is best explained by this,—that squinting children are brought to us by their parents, while adults who still squint have usually given up any desire for a cosmetic improvement, and only come under treatment accidentally or on account of other ailments; lastly, a considerable number of cases are cured by operation. If the squint has disappeared we only discover by accident that it was ever present. The fact of its previous existence may usually be determined by other signs more positive than mere statements from memory; with reference, however, to the age at which the spontaneous cure takes place we are left to depend almost entirely on the patient's statement. As far as I have been able to determine, the period from the ninth or tenth up to the sixteenth year seems to offer the most favorable conditions.
We rarely have an opportunity of watching the disappearance of squint, still I have observed two cases in which a permanent convergent squint disappeared after about a year. In both cases the squint had arisen in young people (of eight and nineteen years of age) in the course of irido-choroiditis which terminated in blindness, and disappeared with the sight. The fixing eye was emmetropic in one case, in the other the condition of error could not be determined owing to nebulæ of the cornea.
We more frequently see periodic squint disappear.[Pg 107]
Case 33.—M—, a boy æt. 10, was first examined by me in April, 1873; the right eye has hypermetropia 4·5 D., and almost full visual acuteness, the left has convergent squint, and recognises No. 6-1/2 (Snellen) with convex 10 D.; V. = 1/18 at 1 metre. (The boy's father also squints with the left eye, which is amblyopic to a high degree (V. = 1/36), right eye has emmetropia, and full visual acuteness). The prescribed spectacles (convex, 4·5 D.) were used for working, but not continually; still three years later, in 1877, the deviation was considerably less and only occurred occasionally. In March, 1880, nothing more was seen of the squint, only slight convergence still recurred on excluding the left eye. Patient now wears convex 4·5 D. constantly.
On account of the importance which the disappearance of squint possesses in hypermetropia I will describe a few more cases which belong here.
Case 34.—Mrs. B—, æt. 32, has on the left H. 1·5 D., V. 5/9; on the right H. 1·5 D., V. 5/12, binocular vision (H. =·75 D., V. = 5/6 to 5/9). Asthenopic troubles are the cause of her present complaint. She says she squinted with the right eye as a child till her eighth or ninth year; the present position of the eyes is quite normal; ordinary type is read at the usual distance with normal fixation without glasses. Particularly keen fixation is rarely followed by squint, which may be produced by excluding the right eye; the latter then deviates about 5 mm. inwards and slightly upwards; the secondary deviation of the left eye is rather less. Only the left visual field is seen in the stereoscope.
Case 35.—Mrs. W—, æt. 31, has on the right H. 3·5 D., V. 5/9, on the left V. = 1/16 with + 4 D., single words of No. 0·8 are read (mother and aunt have also congenital weak sight in this eye). Position and movement of the eyes are perfectly normal, exclusion of the left eye is followed by slight relative divergence. In answer to my question whether she had not[Pg 108] previously squinted, patient replied that she did not know, it had always been a matter of dispute in her family; as, however, only the right visual field was seen in the stereoscope, we may be sure that squint had been present and that binocular fusion had been lost in consequence.
Case 36.—Mrs. G—, æt. 49, report in March, 1876: On the right H. 3 D., V. 10/10, on the left H. 4 D., V. 10/40; a previously existing squint had disappeared of itself; the position of the eyes appears perfectly normal, but binocular fusion is not present; with red glass before one eye and a prism deviating in a vertical direction before the other, patient does not see double, but first with one eye and then with the other. The squint as well as its disappearance occurred however, at a time when it would have been regarded as an error to allow children to use convex glasses.
Case 37.—Miss H—, governess, æt. about 30, came under treatment for asthenopic disorders; on both sides hypermetropia 2·5 D., visual acuteness 5/18. She owns to have squinted as a child,—it had often been remarked when she was at school. The squint gradually disappeared, but still occurred sometimes on keen fixation. The usual position of the eyes appears perfectly normal, and gives no suspicion of squint; convergence occurs on exclusion, sometimes with downward deviation of the right eye. With the aid of a red glass changing fixation is easily produced even without prisms, but never diplopia. At first only the left visual field was seen with the stereoscope; then the right on exclusion of the left eye; never both at the same time. According to this the condition of binocular vision speaks entirely for the fact, that squint had existed long enough to prevent the development of a normal binocular visual act, and the squint had disappeared without the help of convex glasses in spite of the hypermetropia.
Case 38.—Bertha W—, æt. 18, reads with the naked eye on the right No. 0·75 at 10 cm., on the left only 1·75 at the same[Pg 109] distance; hypermetropia of 6 D. is detected with the ophthalmoscope, with + 5·5 the visual acuteness of the right eye amounts at 1 metre to 1/9 (if the test-letters had contained No. 8 or 7·5, that would probably have been recognised also), on the left with + 5·5 D., V. = 1/12, with + 6 D. No. 0·8 is read with difficulty. Patient admits to have squinted as a child; no squint is present now; binocular fusion can be detected with prisms and she only squints now and then on the left side to assist vision, with which, patient states without being questioned, diplopia is combined. Spectacles have not been used till now.
I could cite several more such cases, but they would prove no more than these. At any rate the fact is settled that squint can disappear spontaneously, and without the aid of convex glasses even in high degrees of hypermetropia.
Wecker's announcement that "this spontaneous cure goes hand in hand with the progressive decrease of the accommodation, and depends on the fact that the squinter, on the strength of this progressive decrease, renounces more and more the aid which he finds in the increased convergence during the act of accommodation," only proves to how great an extent one may be prejudiced by theories. A limitation of the accommodation must necessarily increase the claims which are made on it, and can only afford inducement for calling forth all the help possible to support the accommodation.
The fact that squint spontaneously disappears after normal binocular fusion is completely and permanently lost, and in individuals who accommodate without the occurrence of a too strong convergence, notwithstanding their hypermetropia and without the help of the controlling influence of binocular single vision, seems to me quite irreconcilable with Donders' theory. Every motive for the same, hypermetropia, difference of refraction, monocular defective vision, &c., may not only be present without the occurrence of squint, they do not even prevent the[Pg 110] spontaneous recurrence of a squint already cured. Of course I will not affirm that the causes made so prominent by Donders exercise no influence on the origin of squint, but will only emphasize the fact, that other causes exist which possess a greater influence, and which we can find only in the ocular muscles.
We have no experience as to whether this spontaneous cure occurs in myopia with divergent squint. This is not to be wondered at, as hypermetropia is present in the great majority of cases of squint, and the observations as to spontaneous cure are also rare in these. But I can vouch for one case where a slight absolute divergent squint, with crossed diplopia, which I treated shortly after its origin in a youthful myope, with prismatic spectacles, soon disappeared, and remained permanently cured.
The inclination to preponderance of the interni appears to be peculiar to youth, while later on circumstances change in favour of the externi, and that seems to me the chief ground for the spontaneous cure of convergent squint. The cure is not always complete; deviation still occurs on exclusion, or on particularly keen fixation; sometimes, however, also under conditions which can only be put down to a change in the elastic tensions of the muscles. The following is an interesting illustration of this:
Case 39.—Miss S—, æt. 20, states that she squinted frequently as a child from her fifth to her tenth year; the squint gradually disappeared, but returned again from time to time during the last half year without apparent cause. The examination showed normal position of the eyes, slight convergence only on exclusion. Visual acuteness on the right 5/6, with atropine ophthalmoscopic and functional emmetropia, the visual acuteness is lowered to 5/12 by convex 1 D.; on the left hypermetropia 7 D., visual acuteness 5/18; the same degree of hypermetropia is found with the ophthalmoscope.[Pg 111]
Crossed diplopia with a difference in height is distinguished with the aid of a red glass, the difference being corrected by a prism of 4°, with the base downwards before the right eye; a prism of 4° with the base inwards suffices to place the double images immediately above one another. Spontaneous diplopia does not take place; only the right visual field is seen in the stereoscope. As patient lived in Brandenburg and only came to consult me occasionally I never had an opportunity of seeing the squint till she decided to stay here for some time. It was then seen that a peculiar oscillating deviation of the left eye of about 4 mm. inwards often occurred. As the previous spontaneous disappearance of the squint and the crossed diplopia made one fear that tenotomy of the internus might be followed by divergence, instillations were used in order to make a more exact measurement of the deviation,—by this means the condition was so improved in the course of a few weeks, that deviation no longer occurred even on exclusion of the right eye.
The spontaneous cure of squint may, however, be quite complete; indeed I have seen one case where convergent squint became divergent.
Case 40.—A young lady, slightly over twenty years of age, showed on the right M. ·75 D., V = 10/10, on the left H. 1·5 D., V. 10/40 to 10/30, and slight divergent squint on the left side. Crossed diplopia could be produced with a red glass, tenotomy of the left abducens sufficed to correct it. I had not concealed my doubts as to her statement that she had previously squinted inwards, but they were quite dispelled by a photograph taken about twelve years before, in which decided right convergent squint could not be mistaken. There is something to be said for the fact that it may have been a periodic squint, which occurred during the taking of the picture, as the photographer would have taken pains to hide a permanent squint in some way.[Pg 112]
Conscious suppression of squint happens now and then, although very rarely.
Case 41.—Miss A. L—, æt. 27, is stated to have commenced to squint in her first year, until at the age of eighteen she took pains to cure the habit, and with perfect success as far as regards the position of the eyes; the only disagreeable symptom was that she could no longer read with the naked eye. Spectacles were therefore prescribed for her, convex 5 D., but even they did not quite remove the trouble in reading; it was now a disagreeable, painful sensation to have recourse to squint in order to see more clearly. It was easiest to read with greatly lowered field of vision and with the help of a convex eyeglass as well as the spectacles. During the examination I found on the right hypermetropia 5·5 D., visual acuteness 5/12 to 5/9, on the left with + 5·5 D., V = 1/12. With convex 6 D. No. 0·5 was read at 12 inches from the glass, but not nearer, with normal fixation on both sides. The binocular near point (if we may employ this expression in the absence of normal binocular fusion) was considerably removed without the existence of paresis of the accommodation, despite the over-correction of the hypermetropia. It was rather a question of the same disposition of the relative amplitude of accommodation as I have previously described in a similar case. By methodical practice of binocular vision, I had taught an intelligent boy to fix binocularly, not only for distance, but also for near objects, but here again the relative amplitude for accommodation was diminished, so that with correct binocular fixation he could only read with convex glasses, which greatly over-corrected the hypermetropia. Finally, the normal amplitude of accommodation was restored by tenotomy of the left internal rectus, and when I saw the patient twelve years later I was able to satisfy myself that both were perfectly preserved. In the case of Miss L—, I believed I ought to give up all thoughts of an operation; the position of the eyes could not be improved,[Pg 113] convex 5·5 D. eyeglass perfectly sufficed for distance, and convex 7 D. spectacles for reading. It seemed to me senseless to perform tenotomy merely to enable her to use the same glass for distance and for near objects, without any possibility of a cosmetic improvement. Moreover the condition of binocular vision quite confirmed the statements as to the previous squint. Diplopia could only be produced now and then with the help of prisms and red glass, at first the right visual field only was seen in the stereoscope, on closer observation also the left, but without binocular fusion.
Besides, the proved decrease of the relative power of accommodation in both these cases, marked by a voluntary suppression of the squint, does not appear in those cases where squint disappears of itself, the state of the accommodation, therefore, shows nothing unusual.
The spontaneous cure of squint teaches us two important facts, firstly, that the conditions of tension of the ocular muscles may change in the course of time, and secondly, that normal binocular fusion of the retinal images is not necessary for a correct position of the eyes; neither the spontaneous nor the operative cure of squint presupposes the presence or the restoration of a normal binocular fusion. If this were the case the operation for squint would not be of much use.
Observation of these cases further teaches, that treatment with convex glasses has prospects of success, particularly in periodic squint with hypermetropia, if squint can disappear spontaneously even without correction of the hypermetropia. At the same time, however, it appears that we need not form hasty conclusions about it. Periodic squint frequently arises during the earliest years of life, and everyone (perhaps with the exception of a few ophthalmologists) will at once reject the idea of allowing children of two to three years old to wear spectacles; constant wearing of spectacles even by older children seems to me not to be without risk as long as there[Pg 114] is any chance of their falling when running, playing, &c., in which case the eyes as well as the spectacles would be in danger. As a rule I only order children to wear convex spectacles when they are distinctly indicated, and then only during sedentary occupations, when working and eating. Of course, exceptions may be made according to the individuality of the child, and the care with which it is looked after at home.
We are more rarely able to remove permanent convergent squint by means of convex glasses than the periodic form; that it is possible, however, I should like to show by an account of a patient, who offers, besides, other interesting peculiarities.
Case 42.—Marie S—, æt. 6, came under treatment on November 28th, 1878, for recent superficial marginal keratitis of the left eye, which was treated first with atropine; a few days later slight blepharitis appeared also. On December 9th, atropine was discontinued; on the 14th, the position of the eyes was still quite normal; on the 19th, permanent convergent squint of the left eye was present. Squint had never been observed in the child before. Double images were voluntarily announced without my having inquired for them, they were homonymous and moved further apart at both sides of the visual field. On December 28th, the squint still remained the same, the double images were, however, scarcely noticed by the child, so quickly do the relations of the corresponding points of the retina change even in the sixth year. Both eyes were atropinised for the better determination of the error, when a slight degree of hypermetropia was shown by the ophthalmoscope, at most 1·5 D.; certainly a higher degree was specified when the vision was tested, namely, on the right H. 2·5 D., V. = 5/12 to 5/9, on the left H. 1·75 D., V. = 5/18, probably, however, the objective determination was more exact than the child's statements. If a child of six knows its letters and figures sufficiently well to undergo a visual test, that is as much as we can expect; in any case, however, the[Pg 115] forms of the letters and figures which we use for the visual test are not easy to children, and the more objective the way in which the child comprehends the examination, the less it perplexes itself by guesses, but only names the letters which it really distinctly recognises, the less deficient are the reports as to the visual acuteness; the proportionately larger retinal images are still recognised, even if they are no longer quite distinct, but consist of diffusion circles as a result of over-correction of the hypermetropia. That these observations were right for the case in point, is seen by the fact that eight days later, after the effects of the atropine had passed off, the child could see better with the naked eyes than with convex glasses, and that finally, when it had become accustomed to the forms of the letters and figures employed, V. = 5/9 was announced on the right, and V. = 5/12 on the left.
Mydriasis by atropine had no influence whatever on the squint, therefore, on December 31st, convex spectacles 2 D. were prescribed for permanent use. On January 4th, the linear deviation still amounted to 4 mm.; on January 15th, convergence was no longer discernible for distance, with red glass double images occurred at once; on January 21st, no squint was present, and binocular fusion was again restored; prisms immediately caused double images, the facultative divergence was = 0. I thought it prudent to order the spectacles to be worn till the middle of March, when they were discontinued; squint has not appeared since then.
In this case it is impossible to determine what really induced the squint, certainly not the slight hypermetropia, for the child had already learnt to read without squinting, and was spared any exertion at the time when the squint arose. Neither can we look for the cause in the inflammatory condition for which the child first came under treatment, this was as good as removed before the squint began and no exciting condition worth naming was present. Moreover, most cases of[Pg 116] squint arise without directly assignable causes. It seems to me unquestionable that the permanent use of convex glasses made the pathological relation between accommodation and convergence normal, before it had firmly established itself, and before the muscular relations were definitely changed, and that the squint was really thus cured. But if the child had not been under treatment I should scarcely have seen the squint so soon after its first occurrence, and most cases of squint arise at an age which forbids the permanent wearing of spectacles.
If permanent squint has already existed for a long time, nothing can be hoped for from the use of convex glasses; for the conditions of the muscles are then so much changed, that they are no longer influenced by such weak physiological powers. I have been able to convince myself in the case of several squinting persons, who conscientiously wore the spectacles prescribed for them elsewhere, that the squint was concealed by this means; that may suffice in some cases, but if it is a question of young girls we may well ask, which is to be preferred for appearance sake, squint or spectacles.
Tenotomy effects essentially a cosmetic improvement—its object is to restore the correct position of the eyes by equalising the elastic muscular tensions. The means at our disposal are, the simple separation of the tendon of the too-tense muscle from the sclerotic, the distribution of the operation between both eyes, and finally, increasing the strength of the antagonist by moving forwards its insertion.
The method of tenotomy as I carry it out is as follows: The conjunctiva is seized with fine forceps exactly over the insertion of the muscle to be divided, and the fold thus raised cut into with the smallest possible wound. Provided we operate on the right spot we enter this opening with the forceps and immediately seize the tendon close to its insertion on the sclerotic, which is drawn forwards, as was the conjunctiva, and[Pg 117] loosened with flat, curved scissors, the points of which must be rounded off. The incision must only be large enough to allow a small hook with a knob to be inserted through it and behind the insertion of the tendon, which is now lifted up and divided with fine pointed scissors close to its insertion into the sclerotic. It is important to make sure that a few threads coming off from the tendon at the ends of the insertion do not remain uncut; we can only consider the operation to be complete when the hook, carried behind the edge of the insertion made clearly visible by the foregoing proceeding, slides up to the margin of the cornea without any interruption.
The method of performing advancement is as follows: An incision is made in the conjunctiva over the tendon of the muscle to be brought forward and just at the outer bend of the latter, then loosened together with the subconjunctival tissue to the corneal margin; it is desirable to carry out this loosening close to the sclerotic, as the flap of the conjunctiva thus formed must afford sufficient support to the muscle to be brought forward. Then the capsule of Tenon is cut into at one edge of the insertion, a flat, curved, blunt hook without a knob is carried between muscle and sclerotic, and out again at the other edge of the insertion. We must be careful to get the muscle as clean as possible on the hook in the whole width of its insertion, that is without the capsule of Tenon, for the suture put in ought only to enclose the muscle, without at the same time dragging the capsule of Tenon. For the suture I always use fine catgut which is provided at both ends with curved needles; needles of slightly different form may be chosen in order that the threads may be easily distinguished from one another. A needle is carried behind the hook from each thread, one through the upper, the other through the lower edge of the muscle, between it and the sclerotic, then the thread is tied in a knot on the muscle to make sure that it does not slip back through the loop of the thread after its[Pg 118] separation from the sclerotic. Then the threads are knotted on the muscle, and the insertion is separated from the sclerotic. As the edge of the insertion is now exposed we can see how the land lies, and can carry the threads exactly in the direction of the muscle under the conjunctiva to the corneal margin, where they are passed through, and ends tied in a knot. By this means the muscle is drawn forwards precisely in its normal direction and stretched tighter. The wound in the conjunctiva is closed by a suture.
It is desirable to slightly stretch the muscle that is to be brought forward in both the above operations while the eye is rolled towards the opposite side with forceps. Further, as I always operate under chloroform, I dispense with the usual test of the immediate effect of the operation; such tests have no value before the effects of the narcotic have completely disappeared, and one must be sure in the way above described that no single fibres are left undivided. I lay special stress on the fact that the operation is so performed, that it is able to bring about the desired mechanical effect.
The immediate mechanical effects of simple tenotomy may be easily deduced; the divided muscle retracts as far as its elasticity and its relations with the surrounding tissues permit. With reference to the internal and external rectus with which strabotomy specially has to do, those relations come principally under observation which the front part of the muscle enters into with the conjunctival tissues; the greater the extent to which we loosen these relations, the farther the muscle can retract. If it is a question of obtaining a greater effect, I am accustomed to loosen the subconjunctival tissue at the front part of the muscle behind the lachrymal caruncle to a greater extent—this offers the additional advantage that the distorting sinking in of the caruncle is avoided.
By dividing one rectus its antagonist gains in proportion and rolls the eye towards it as far as its own elastic tension[Pg 119] and the powers still present on the other side permit. The improvement in position which we strive to obtain is brought about by the elastic power of the antagonist, and not by the tenotomy itself, and it is seen by this then, that the term strabotomy simply, does not quite express the circumstances of the case. Tenotomy is nothing more than the means for procuring a preponderance of the elastic power of the antagonist, therefore the effect attainable on the position of the eye does not depend solely on the division of the muscle, but to a great extent on the elasticity of the antagonist, and may be nullified at once, if the antagonist does not perform what we expect from it, and that may happen without our being able to foresee it. For example:
Case 43.—Julie B—, æt. 21, is stated to have squinted inwards since her third year, principally with the right eye, but with occasional alternation. The deviation amounts to 5 mm., the outward movement of both eyes is perfectly normal. Hypermetropia 2 D., visual acuteness 5/18 on both sides. Ophthalmoscopically with atropine the same degree of hypermetropia. Tenotomy of both interni on March 7th, 1879. On March 14th, deviation 5 mm., just as before. Then renewed division of the internal rectus and shortening of the external rectus of the right eye; but still the result was insufficient. Therefore, on March 21st, the left eye was dealt with in the same way. By this means a normal position of the eye was obtained, which was perfectly preserved when I saw the patient again a year and a half later. Everything led me to suppose beforehand that simple tenotomy of both internal recti would perfectly suffice to remove the squint, yet it was of no use, but had to be supplemented by shortening both external recti. In such cases I would not advise repeated tenotomies, but for the correction of the insufficient result as soon as possible by advancement of the antagonist.
Advancement very frequently gives us an opportunity of[Pg 120] seeing with our own eyes the insufficiency of the antagonist and its faulty anatomical development. We may suppose this to be the case if the mobility towards the side of the antagonist is faulty, however that is no proof; considerable insufficiency may co-exist with perfectly normal mobility. If limitation of movement is present, to which insufficiency of the antagonist may be assigned as the cause, or if it is desirable to obtain the greatest possible result by means of an operation on the squinting eye, we must combine tenotomy of the deviating muscle with advancement of the antagonist. The same is stretched tighter, and rolls the eye more strongly to its side, and we can regulate the degree of shortening of the muscle, by the distance behind the insertion at which we place the threads in the muscle, also by the distance from the corneal margin at which we place our anterior sutures, although the rapidly increasing ductility of the conjunctiva makes it desirable that we should not go far from the corneal margin.
The exact rules for the application of the methods of operation differ according to the nature of the case under consideration. If we contemplate first the largest group, that of the ordinary permanent convergent squint, the choice of the method is principally determined by the average degree of deviation, the condition of error, and the visual power, lastly by the mobility, particularly the outward movement of the eyes. If the visual power of both eyes is nearly the same, or if the squinting eye possesses such a visual acuteness that it can be used in fixation, it is advisable as a rule to arrange the relations of the muscles as equally as possible in both eyes—simple division of the internal recti is therefore, as a rule, to be performed in both eyes. If, on the other hand, the vision of the squinting eye is in a high degree defective, so that only the better one is used, it is generally advisable to confine the operation as far as possible to the squinting eye; in that case, tenotomy of the internal rectus and advancement of the external[Pg 121] rectus is usually indicated in the squinting eye, and frequently suffices.
Deviations which are so slight, that the careful division of both interni without loosening the conjunctiva at the front part of the muscle makes us fear an excessive result, are seldom the subject of operative treatment; if the deviation is slight but still a disfigurement, if it amounts to 3 to 4 mm., distribution between both eyes is suitable, because, when the squinting eye possesses requisite visual acuteness it is put into fixation more frequently after the operation than before. Under these circumstances, if the operation is confined to the squinting eye, and a sufficient result is thereby obtained, as soon as this eye is used for fixation a remarkable secondary deviation of the other eye occurs, which is not the case if the tensions of the muscles have been balanced by an operation on both sides.
A deviation of 5 to 6 mm. may usually be balanced by means of simple double tenotomy if the conjunctiva is considerably loosened behind the caruncle; not unfrequently, however, we must be careful to strengthen the result by means of the after-treatment. Commonly, during the first twenty-four hours, the result appears to be quite satisfactory, whilst on the second or third day troublesome convergence again sets in. By practice of the outward movement we then usually obtain at once a perceptible improvement of the position. Both eyes are repeatedly turned as far as possible to the right and left, by which means is obtained on the one hand, exercise of the external recti, on the other, increase of the effect of the tenotomy of the internal recti. I order these exercises to be begun on the day after the operation.
Besides this, however, in the relation between accommodation and convergence of the visual axes there is a very essential cause which is able to lessen the immediate effect of the operation. Persons who squint inwards, even if emmetropic, have the habit of combining accommodation for near objects with[Pg 122] excessive convergence of the visual axes, thus the immediate effect of the operation is diminished as soon as they begin to use their eyes again. This happens, not by a lessening of the effect of the tenotomy, which could, indeed, only be increased by exertion of the internal recti, but in that sufficient time is not given for the external rectus to regain its normal elastic tension. Nothing is changed at first by the operation in the customary relation between accommodation and innervation of the internal recti—it is a question, then, of avoiding every exertion of the accommodation for some time, in order that no inducement for strong convergence should be given. I am accustomed, therefore, even in the case of emmetropes, to paralyse the accommodation by means of atropine twenty-four hours after the operation, and to remove the far-point by convex glasses to about 0·70 m.; the spectacles must, of course, be worn constantly, for only by that means can we be sure that they are always used for near objects. After a few weeks the spectacles are discontinued, first for distance, then for near objects also. This after-treatment is not necessary under all circumstances; but I have repeatedly assured myself that an originally sufficient result which perceptibly diminished after a few days, could by this means be restored and permanently maintained even in emmetropes.
In the case of hypermetropes, we more often meet with the same experience; in permanent convergent squint it is by no means necessary to neutralise the hypermetropia permanently after the operation, but it happens here more often than in emmetropia, that a perfectly good immediate effect is lost within the first week after the operation, and can be restored again by permanently wearing the correcting convex glasses. In such cases also, I am accustomed after a few months to discontinue the spectacles for distance as an experiment, while they are still used for working.
Simple tenotomy of both internal recti does not, as a rule,[Pg 123] suffice for deviations of more than 7 mm.; therefore, even if both eyes possess good visual power, we must still decide on tenotomy of both internal recti together with advancement of the external rectus of the squinting eye, or anticipate repeated tenotomies of the internal recti, or seek to obtain the greatest possible effect by means of slight modification of the method of procedure.
Provided that the muscle was completely divided, and sufficiently loosened from the conjunctiva during the first operation, a repetition of the tenotomy can only aim at an increase of the effect if the elastic tension of the antagonist has improved in the meantime. I very rarely therefore carry out repeated tenotomies; it seems to me much more desirable to obtain a sufficient result at one operation whenever that is possible.
In some cases where there is a deviation of 7 to 9 mm., the effect of the tenotomy may be increased by inducing a strong divergence immediately after the tenotomy of the internal recti, which is maintained for 6 to 8 hours. For this a thread is passed through the conjunctiva at the outer edge of the cornea about 4 mm. above the horizontal meridian, and out again about 2 mm. below the horizontal meridian, then from below upwards in the same way, so that the conjunctiva is contained in a loop. The needle is then passed through the external canthus from the conjunctival surface and fastened by tying it over a roll of paper. This procedure is only to be recommended in exceptional cases; a greater effect on the internal recti is thus obtained, while with reference to the position the result depends on the elastic tension of the external rectus just as in simple tenotomy.
If the squinting eye has only an unavailable visual acuteness, a combination of tenotomy of the internal rectus with shortening of the external rectus is the best procedure. As a rule, simple tenotomy of the internal rectus of the squinting[Pg 124] eye is of very little use in such cases, as the abducens, weakened by continual extension and wanting practice, places too slight an opposing power in the balance. The chief effect of the operation then devolves on the other solely available eye, which is not a desirable circumstance, and is also frequently insufficient. On the other hand, the combination of tenotomy of the internal rectus with advancement of the external rectus enables us successfully to change the opposing muscular tensions. As a rule, the operation may be confined to the squinting, weak-sighted eye, as that suffices to obtain a correction of 5 to 6 mm.
If the result is seen to be insufficient, it may be supplemented by tenotomy of the internal rectus of the other eye; in the case of deviations of more than 7 mm. it is advisable to divide the operation between the eyes in this way.
The suture has a special use in so-called artificial strabismus; that is, in those cases where convergent is converted into divergent squint through unskilful treatment, or where tenotomy of the abducens, performed on account of "insufficiency of the internal recti," is followed by convergent strabismus. I have not found confirmation of the fear expressed by Arlt, that the method proposed by me could be scarcely practicable if it is a case of the advancement of a muscle too far forward, and I have corrected a large number of such cases in other practices. It is seldom profitable to take up things in which others have been unsuccessful, but it bring its own reward in the case of artificial squint.
Periodic convergent squint offers a less certain ground for the operation. The change between normal position and a very considerable squint gives rise to the fear that an operation which would be able to remove the convergence might finally induce divergent strabismus. This fear is certainly not groundless, but at the same time it must be remembered that, with the exception perhaps of a few cases of clearly[Pg 125] accommodative deviation, elastic preponderance of the internal recti or insufficiency of the external recti is generally the cause of periodic squint also. I have frequently, in periodic squint, performed double tenotomy of the internal recti with the slightest possible loosening of the conjunctiva. I have also attempted to confine the operation to the shortening of the external rectus without loosening the internal recti and with success, but not frequently enough to be able to deliver a certain opinion upon it.
In periodic squint, the first care must always be to determine the condition of refraction, if possible with atropine, and to neutralise or over-correct hypermetropia if present. If squint is absent during the use of convex glasses, which happens frequently under these circumstances, the operation offers no further advantages, as the constant use of convex glasses afterwards can hardly be avoided. If the periodic deviation continues to exist, the operation can be carried out according to the above rules and so as to cause a slight effect.
The final result is usually attained after two to three weeks in convergent squint; it is better to allow a slight degree of convergence to exist, as divergence, however slight, existing at this time, brings with it the fear of a gradual increase. It happens occasionally, that after years, convergence asserts itself again; I have observed it in spontaneous (see Case 39) as well as in operative cure of squint; still, this is so unusual, that I should like to give an illustration of the latter observation on account of its rarity.
Case 44.—Hedw. von L—, æt 10, came under treatment in April, 1874, for convergent squint on the left side which arose in her seventh year, with occasional alternation. Emmetropia, determined with atropine on both sides and good visual acuteness. Diplopia was present at the commencement of the squint. Patient can only be rendered conscious of double images by the help of a red glass and vertically deviating prisms.[Pg 126] Double tenotomy of the internal recti effected a normal position, and at the end of December, 1874, the continuance of the same could be proved as well as binocular fusion with prisms. At the beginning of 1880, I was informed that from time to time periodic squint had occurred with diplopia. In the middle of March, I had an opportunity of seeing the young lady. Myopia 2 D. had meanwhile developed on both sides, visual acuteness almost = 1. The position of the eyes was perfectly good, slight convergence occurred during covering, homonymous double images with a red glass which, at a distance of 5 m., were joined by a prism of 8°; stereoscopic fusion was not perfectly certain. A true squint could not be proved. On April 3rd, as patient stopped for a few hours on her journey through, a striking convergent squint of the left eye was seen. The deviation amounted to 4 to 5 mm. Single vision existed at a distance of 15 to 20 cm., then homonymous double images appeared, which did not correspond to the objective deviation; the double images were however corrected by a prism of 6° (base outwards) for an object 5 m. distant.
We cannot conclude the consideration of the operative treatment of convergent squint without once more returning to the relation between the line of vision and the position of the cornea. The angle [Greek: a] still deserves mention in a few thankful words—hic mihi angulus praeter omnes ridet—it is a very useful guide in tenotomy. In tenotomy we may count as gain the apparent divergence which it causes in hypermetropes who do not squint. We obtain a perfect cosmetic result, while a convergence, objectively determinable, but not otherwise easily visible, continues to exist. It would be folly to exceed this; and for cases where binocular fusion does not exist, and where diplopia is not present, to wish to remove this covered convergence due to the angle [Greek: a], the cosmetic result would be impaired by it.
Those cases where it is a question of uniting homonymous[Pg 127] double images are very instructive when considering tenotomy. Only when squint arises after childhood (after the fifteenth year) does it cause troublesome diplopia, this accords naturally with the laws of normal binocular fusion learnt meanwhile. (On the other hand those cases, which sometimes occur after tenotomy, with the double images in a position which does not correspond to the normal physiological laws and which cannot therefore be united by prisms, are naturally unsuitable for the operative removal of diplopia.) Cases in which convergent squint is followed by troublesome double images, appear, with the exception of the hysterical form mentioned on p. 41, chiefly in myopia, more seldom in emmetropia, and very rarely in hypermetropia; for if the conditions contained in the ocular muscles are coincident with hypermetropia, squint usually arises in the course of childhood, before normal binocular vision has become a fixed habit.
As the cases here under consideration are not very common, I will relate a few from which conclusions may be derived as to the effect of tenotomy.
Case 45.—Miss von B—, æt. 14, came under treatment on May 1st, 1875, for diplopia, which made its appearance about a year previously. Emmetropia and full visual acuteness exist on both sides. The double images are homonymous and further apart on both sides of the visual field. At first single vision existed only to about 0·75 m.; gradually, however, the area of single vision was extended by practice of the outward movement, supported by the use of prismatic spectacles, so that after a year patient could see singly to a great distance. This improvement was not maintained. At the beginning of 1879, diplopia was again present to a troublesome degree, particularly on looking downwards; on looking straight forwards the left eye showed a slight convergent deviation, amounting at most to 2 mm. During various examinations the distance of the double images was stated to be now less, now greater,[Pg 128] a prism of at least 5°, at most of 9°, was requisite for correction. Diplopia was at once removed by tenotomy of the left internal rectus, with very slight loosening of the conjunctiva, and has not appeared since.
Case 46.—Miss A—, æt. 17, suffered from diplopia for a few weeks, a year and a half ago; for the last half year the diplopia is continuous, and striking squint is stated to be sometimes present. Myopia 2 D. on both sides, visual acuteness = 5/9. On fixation of an object about 4 m. distant, the left eye deviates inwards at most 2 mm.; homonymous double images, with a red glass and on correction of the myopia, which were united by means of prism 14° at a distance of 5 m., without red glass (with retinal images alike on both sides) prism 8° sufficed to unite them. If a vertically deviating prism is held before one eye, the double images stand just above one another when looking at an object 20 cm. off, on nearer approach they are crossed. On May 3rd, 1879, tenotomy of the left internal rectus with small conjunctival wound without loosening of the conjunctiva, and union of the conjunctival wound by a suture. On May 8th, single vision, also with correction of the myopia and with red glass. Facultative divergence = 2°. On May 14th, with correction of the myopia, there was still single vision for distance; however, with red glass double images occurred again; and at the end of May the condition of the double images was just the same as before the operation. On vertical shifting of one visual field by a weak prism the double images are brought into a vertical line by means of prism 16°, with the base outwards. Therefore, on July 1st, the right internal rectus was also divided, with small conjunctival wound without loosening of the conjunctiva and without suture. The evening after the operation slight divergence on covering. On July 24th, binocular single vision is present; with red glass homonymous double images at 5 m., corrected by prism 4°. This time the result was final;[Pg 129] for in the middle of October, three months after the operation, the report was exactly like the one of July 24th above stated.
Case 47.—Mrs. A—, æt. 33, has suffered for six months from alternating convergent squint with diplopia, for a short time even a parallel position is still possible. On the right myopia 4 D., V. = 6/12. On the left myopia 4 D., V. 6/9. Single vision occurs to 22 cm., at a greater distance homonymous double images, whose mutual distance remains the same when looking to one side. On correction of the myopia a prism of at least 32° is necessary for the union of the double images for an object at 4 m. Two days after tenotomy of the internal recti on both sides, the facultative divergence amounted to 7° (at 4 m.) on correction of the myopia. Single vision was also present when looking strongly to one side, and with differentiation of one retinal image by a red glass.
Case 48.—Mr. B—, æt. 32, first observed the occurrence of diplopia at the beginning of April, 1877. Myopia 6 D. is present in both eyes, visual acuteness on the right 1/2, on the left rather more than 1/2 (5/9). The double images are homonymous and sometimes (not always) move farther apart at the limits of the visual field. Patient could only decide after two years, in July, 1879, on the operative treatment then proposed. Diplopia continued to exist; single vision was only now and then possible for a short time. On correction of the myopia (if one eye is provided with a red glass) prism 12° suffices for union of the double images. If one visual field is moved in a vertical direction by a prism of 5° during the trial of convergence, prism 38° is necessary in order to equalize the lateral deviation of the double images, and to place them perpendicularly above one another for an object 5 m. distant. On July 14th, tenotomy of the internal rectus of the left eye; single vision next day on correction of the myopia, prism 6° is overcome by divergence; if, however, double images are produced by a vertically deviating prism of 5° they immediately show[Pg 130] homonymous lateral deviation, which is corrected by prism 18° at a distance of 5 m.
Two months after the operation the diplopia was certainly better, but by no means removed; squint occurred periodically as before, so that sometimes single vision was possible at 3 to 4 m., sometimes troublesome diplopia was present.
During the test of convergence with prisms deviating in a vertical direction, a prism of 38° was necessary for the equalization of the lateral deviation just as before the operation. Therefore in the middle of October the internal rectus of the right eye was divided, and the conjunctiva loosened as far as the caruncle. Three days afterwards single vision, facultative divergence = prism 5°; in the trial of convergence, equalization by means of prism 8°. In the middle of October, two months after the operation, diplopia had not appeared again; facultative divergence = 0; homonymous double images are produced by a red glass before one eye, slight convergent deviation on covering it, which in the trial of convergence is equalized by prism 20°. The preponderance of the interni was now so far lessened for the ordinary use of the eyes, that permanent binocular single vision was possible.
Notwithstanding the small number of these cases we may conclude from them, that homonymous diplopia in typical convergent squint (not paralytic) can only be corrected occasionally by one-sided tenotomy when the deviation is slight. As a rule it is necessary to distribute the operation between the eyes. A result seems attainable by means of simple tenotomy on both sides, which is expressed by prism 20° in the trial of convergence. In future cases it would be desirable to determine during correction of the anomalies of refraction (1) the weakest prism which is able to unite the double images at about 5 m. distant (without red glass); (2) the distance at which the double images stand apart from one another during the trial of convergence with prisms deviating in a vertical[Pg 131] direction; and (3) the prism which brings the double images immediately above one another in the case of objects about 5 m. off.
Next to the cases above discussed stand those where convergent squint remains after paralysis of the abducens; at the same time slightly defective mobility and a distinct moving apart of the double images towards the affected side can usually be detected. In a few such cases I could restrict myself to tenotomy of the internal rectus of the affected eye, but in those cases which I was able to attend to more particularly, double tenotomy was necessary, and did not always suffice. Here also the advancement of the external rectus is suitably applied, which I should like to illustrate by means of a few examples.
Case 49.—Mr. B—, æt. 20, was seized by paralysis of the abducens of the right eye in November, 1877. In April, 1878, convergent squint was still present, and as it continued patient decided on an operation in February, 1879. Both eyes are emmetropic and possess full visual acuteness.
Immediately before the operation the double images were united at 4 to 5 m. in the horizontal plane by a prism of 39°; towards the right their deviation rather increased. The measurable deviation amounted to 4 mm. in the right eye, the secondary deviation of the left to 5 mm. In order to proceed carefully, I confined myself at first to tenotomy of the internal rectus of the right eye. After the space of a week single vision was present at the distance of 1 metre in the middle line and at the height of the eyes; at about 5 m. homonymous double images corrected by prism 12°, together with slight difference in height (= prism 4°, base upwards before the right eye). The area of double vision extended from the limit of the right visual field to about 20° the other side of the middle line.
This result would have sufficed perfectly for a cosmetic[Pg 132] tenotomy where binocular fusion did not exist; the annoyance caused to patient by diplopia, however, was only slightly relieved. I decided, therefore, on a second operation, not without fearing an excessive result, and performed tenotomy of the left internal rectus with a very small conjunctival wound and by closing the wound by means of a suture. The result was by no means excessive, for it was perfectly nil, apparently even negative at first, for a few days after the operation the area of single vision approached the eye to less than 0·5 m. and at 4 to 5 m. a prism of 20° was requisite for correction; however, eighteen days after the tenotomy of the left internus everything was as before. Single vision to 1 m. while prism 12° corrected for a distance of 4 to 5 m. The tenotomy then had no effect at all on the position of the eye; however, the restriction of movement dependent on it, asserted itself in that the double images were crossed on the limit of the right visual field (about 45° towards the right). On the supposition that this insufficient result might be caused by the suture of the conjunctival wound I decided to repeat the separation of the internal rectus. The agglutination of the muscle with the sclerotic is so slight for two to three weeks after the operation that the strabismus hook perfectly suffices to sever the connection; no suture was put in, but the result again was nil, and on the day after the operation single vision was only present to 0·5 m. in the middle line, just as after the previous tenotomy of the left internal rectus. It was now clear that the result with respect to the position of the eye was only unsuccessful because the antagonist did not do its duty. I shortened the abducens (without touching the internus again). The immediate effect, during the chloroform narcosis, was a terrible divergence, but on the same evening it was less, and twenty-four hours after the operation with a red glass, homonymous double images were present close together at a distance of 4 m. Ten days afterwards binocular single vision was[Pg 133] insured, facultative divergence = 3° at 4 m., crossed double images towards the limits of both visual fields, but only on moving the eyes in a lateral direction; no practical use was made of this. If one could have diagnosed beforehand the insufficiency of the externi assuredly present here, which was probably the reason for the development of squint on the healing of the paralysis of the abducens, one would have been able to combine shortening of the right abducens with tenotomy of the internus in the first operation, whereas the necessity for the advancement was only shown by the abnormally slight effect of the tenotomy on the left side. According to accounts received by letter the favorable result has continued.
We obtain a result more quickly by the immediate advancement of the abducens. For example:
Case 50.—Mr. K—, æt. 29, suffered from paresis of the right abducens in the autumn of 1877. In December, 1878, convergent squint is present, linear deviation 5 mm. (scarcely more on the left than on the right). The defect of movement towards the side of the right abducens amounts to about 2 or 3 mm. Diplopia is present in the whole visual field with increase of the deviation towards the right. Emmetropia and full visual acuteness on both sides. Tenotomy of the internal rectus and advancement of the abducens of the right eye at the end of December. Three weeks later single vision is present in the middle line; on the left limit of the visual field crossed double images, on the right side homonymous ones, beginning about 20° from the middle line. The result was by no means excessive.
In convergent squint with congenital paresis of the abducens, not much can be attained without shortening the abducens. Of course only the squint can be removed, not the paralysis, but if once a correct position is attained for the middle line, cosmetic demands are satisfied; the outward movement, which is absent, must be replaced by turning the head.[Pg 134]
The chief method for absolute divergent squint is the combination of shortening with tenotomy of the externus. If the impulse for convergence is once lost, so that an associated movement occurs in place of an accommodative one on fixation of a point situated on the middle line, a removal of the squint cannot be obtained by simple tenotomy of the externi—another proof that a change of position of the eye is by no means a necessary result of tenotomy.
Moreover, this slight aid given by tenotomy has its ground not solely in the condition of the opposing recti muscles. In other practices I have seen cases enough in which tenotomy of the externi, performed on account of relative divergence, was followed by convergent squint, just as injudicious division of the interni may induce divergent squint. It is probable, therefore, that the faulty effect of simple tenotomy in permanent absolute divergent squint depends on other causes, which, in my opinion, are to be found in the obliques. The loop formed by the obliques round the posterior circumference of the eye is most stretched, when the visual line falls in with the muscular plane of the obliques in a medial direction of the eyes. On the whole, then, it is proved that the obliques are extended on turning the eyes inwards, but shortened on turning the eyes outwards by means of their muscular action. In divergent squint, if the movement inwards occurs but seldom or not at all, the obliques consequently are not extended in a normal way—it follows then that they lose in ductility, offer greater resistance to the inward movement, and by means of their elastic tension continually draw the posterior pole of the eye inwards and the cornea outwards. As in strabotomy we cannot get at the obliques, it seems all the more desirable to offer them stronger resistance by greater tension of the internus by means of advancement. Certainly tenotomy of the external rectus of the fixing eye is as a rule also necessary. A sufficient result is usually thus obtained at[Pg 135] once; if it is much lessened in the course of one or two months there is nothing to prevent the repetition of the tenotomy of one or the other external rectus.
The innervation for the movement of convergence is not always perfectly lost; it withdraws itself from the influence of binocular fusion because this is gradually forgotten while a convergence, even if an insufficient one, unites itself with the effort of accommodation. If we ask such patients to fix a large object lying near, a pencil, for example, they cannot usually converge upon it, whilst if we ask them to read at the same distance, a distinct convergent movement occurs; large objects are sufficiently clearly recognised, even without distinct retinal images, and the supposition that an effort of accommodation is present is only justified if we employ sufficiently small objects at the examination, in order to distinguish which, clear retinal images are necessary. Of course we must have regard to the condition of refraction; myopes, who use their far point for reading, want no accommodation, therefore no convergent movement occurs, even if the impulse of innervation for it, is not yet quite lost. However, the innervation for convergence may be lost, without the internal recti losing in elastic tension. The operative importance of this relation may be illustrated by an example.
Case 51.—Bertha K—, æt. 10, has myopia 5 D. on both sides, visual acuteness 12/20, and divergent strabismus. At 4 mm. the crossed diplopia is corrected by prism 23°; a convergent movement is no longer attained, at most parallelism of the visual axes. Tenotomy of both interni on October 2nd, 1873. The immediate result was convergent squint, with a defect in movement outwards amounting to 4 to 5 mm. in both eyes. On October 9th prism 37° was still necessary to unite the homonymous double images at a distance of 4 m.; single vision existed only to about 20 cm. The area of single vision gradually extended itself; at the end of October[Pg 136] it was restored for distance also, facultative divergence nil; however, relative divergence was present for near objects. Naturally this was not the result of muscular weakness of the interni, for they had proved their capabilities by a convergent squint, fortunately only temporary, which made one anxious, but was solely the result of a faulty innervation. The further course was also interesting. After three years, in October, 1876, the myopia of the left eye amounted to 8 D., that of the right 7 D., visual acuteness 1/2 on the right, on the left 3/4 of the normal; a posterior staphyloma measuring about 1/3 of the diameter of the optic disc was present. The left eye was used for near objects with relative divergence of the right and the occasional occurrence of diplopia; there was convergence only to about 15 cm. Facultative divergence nil.
We very frequently have the opportunity of seeing, that myopia increases even after tenotomy of the externus, and if von Graefe's assertion that the progress of myopia would be brought to a standstill by means of tenotomy still finds believers, I should like to cite one example which offers proof to the contrary.
In permanent divergent squint we shall have, as a rule, to combine shortening of the internus of the squinting eye with tenotomy of both externi, even if the convergent movement is still possible to a slight degree. The result thus obtained differs somewhat; sometimes it suffices at once, sometimes a repetition of the separation of the externi is necessary later on. Two examples may illustrate this.
Case 52.—Miss Marie M—, æt. 22, has squinted on the left side since her third year, nominally after a keratitis, which left behind in the left eye a nebula of the cornea of small circumference. The deviation amounts to 8 mm. The visual power is much worse than the opacity of the cornea leads us to suppose, with visual axes deviating inwards fingers were only counted at a distance of about 1 m.[Pg 137]
On the right myopia 1 D., V. = 4/5. A slight convergent movement is still practicable. At the end of May, 1879, shortening of the left internal rectus, tenotomy of both externi. The next day slight convergence on viewing distant objects, correct position after four days. In January, 1880, correct position of the eyes, convergence possible to about 20 cm. While a correction of 8 mm. was immediately obtained here, the same operation does not always permanently suffice for slighter deviations.
Case 53.—Ernest Sp—, æt. 11-1/2; divergent squint had been observed as early as his second year. The deviation amounts to 5 or 6 mm., is sometimes alternating, generally the left eye deviates. No convergent movement on fixing a pencil about 25 cm. distant; the right eye is then used for reading, the left one makes a distinct, but not a sufficient, movement inwards. Emmetropia on both sides, visual acuteness nearly perfect on the right, on the left 2/3 of the normal. Even with red glass and prisms deviating in a vertical direction, double images not perceived. On October 2nd, 1879, shortening of the left internal rectus, tenotomy of both externi. A week later divergence was no longer present. When reading, the left eye makes a distinct, perhaps rather too great, movement of convergence, and yet six weeks after the operation, distinct divergent squint was again present, even if to a slighter degree than before; the left eye deviates 3 to 4 mm., the right 2 to 3 mm. outwards. The result obtained amounted then to not more than about 3 mm. In the middle of December the tenotomy of both externi was therefore repeated. A week after the operation convergent squint of 2 mm. is present with homonymous diplopia. A pencil made to approach on the middle line is seen double to about 20 cm., on approaching nearer, double images are not perceived in spite of distinct relative divergence. Double images at a distance of 4 m. are corrected by prism 25°; as, however,[Pg 138] normal binocular vision is not present, the value of this statement is very questionable. Three weeks after the second operation the position of the eyes was normal, and the slightest convergence was perceived only on close investigation. Double images are no longer observed, however they may still be brought to view.
In periodic divergent squint, if the deviation is considerable and frequent, if at the same time the normal near point of convergence is only attained with difficulty or not at all, we can hardly combine shortening of the internus with tenotomy of the externus; more often indeed, additional tenotomy of the externus of the other eye is necessary in order to obtain a permanent cure. In exceptional cases (when it seemed to me as if the squint depended more on insufficiency of the internus than on preponderance of the externus) I have confined myself to shortening the internus without separating the externus; I will quote just one example of this.
Case 54.—Ida K—, æt. 11. On the right, hypermetropia 3 D. with the ophthalmoscope, visual acuteness 5/24. No. 0·3 is read with difficulty. On the left, with the ophthalmoscope hypermetropia 4·5 D. with asymmetric meridian. Single letters of 3·0 m. are recognised with convex 6·5 D. Fingers are counted at about 1-1/2 m. The choroid is slightly and unequally pigmented, no ophthalmoscopically assignable reason exists for the considerable visual defect. The left eye frequently deviates outwards, convergence is attainable to 15 cm. On May 2nd, 1877, shortening of the internus (without tenotomy of the externus). Two weeks later slight convergent squint was present; in November, 1877, six months after the operation, the position of the left eye was perfectly normal.
Tenotomy of the externi suffices when the divergent deviation is inconsiderable and does not occur often, if the normal near point of convergence can still be reached, and binocular fusion is possible.[Pg 139]
If we want to increase the effect of simple tenotomy of the externi, this may be done just as well by practice of the associated movements of the eyes as by practice of the convergence, of course for a short time only after the operation. As long as the detached tendon of the external rectus is not re-attached firmly with the sclerotic, all these movements of the eyes help to strengthen the result of the tenotomy. In order to practise convergence we can bring a suitable fixed point on to a mirror and so make it possible for the patient himself to see the position of his eyes, of course only in cases where binocular fusion is no longer present. He who possesses a normal binocular vision is troubled in these exercises by diplopia; but this is not the case in the suppression of binocular fusion so frequent as a result of squint.
Periodic divergent squint is divided by no sharply defined limits from those cases in which only a preponderance of the externi exists without insufficiency of the interni. We frequently find very considerable degrees of facultative divergence as a casual symptom, without the occurrence of manifest divergence or the presence of asthenopic troubles. If this is accompanied by weakness of the interni, absolute divergence occurs on looking at near objects, sometimes for distance also and certainly if we suppress binocular fusion by covering one eye or render it difficult by colouring one visual field with a red glass.
In these cases the indications for the operation are given either by asthenopia, by troublesome double images or by the disfigurement inseparable from periodic squint; it will depend on the degree of the facultative divergence, whether we confine the tenotomy of the externus to one eye or whether we distribute it between both eyes.
Finally, it may be desirable to still say a few words as to the most favorable period for the operation. The comprehension of the defective sight often present in squint as caused by[Pg 140] "non-use" has resulted in the preposterous advice that tenotomy should be carried out as early as possible. I can vouch for the fact that even the earliest tenotomy of the ocular muscles is of no avail against congenital amblyopia. I have repeatedly seen children on whom tenotomy had been performed in their first year, usually with bad cosmetic result but with continuance of defective sight of the squinting eye.
The final result of the operation is almost always very unsatisfactory when performed on children before their fourth year. I can show a number of good results in children on whom I operated between their fifth and sixth year; however, the more I considered the subject, the more it seemed to me advisable to raise the tests which must be imposed on the patients. With children it is not so much a question of determining the limit of age, but whether their intelligence is sufficiently developed to render a reliable examination possible. A sufficient knowledge of letters and the power of reading is necessary to an accurate trial of vision; the entire bearing of the children must permit of the ophthalmoscopic diagnosis of the weak condition and should raise no scruples as to wearing spectacles which may be necessary after the operation. Under any circumstances no harm is done by deferring the operation until these conditions are fulfilled; the interval may be filled up by practising the mobility of the eyes, which does more good than the customary strabismus spectacles or even tying up the eye. If we tie up the fixing eye, the squinting one is certainly put into fixation, but the other squints instead, and of course it is just the same with the plan, as childish as it is antiquated, of tying on a pierced walnut shell before each eye.
Strabismus spectacles, i. e. those with a leather band to go round the head, provided with leaden discs which cover one eye completely and leave only a side aperture for the other, of course only induce a transfer of the squint to the covered eye,[Pg 141] together with practice of the eye in a lateral direction; but apart from their unsightly appearance they require a constant lateral direction of the eye, which is followed even after a short time by fatigue of the muscles employed and soon becomes unbearable. This is not the case if we cause the mobility to be practised alternately and towards both sides; here we must insist that the limits of the outward movement are really reached. These exercises are at least rational and tend to increase the strength of the antagonist, on which we must depend so much in the operation and to diminish an insufficiency made worse by want of practice.
Catalogue B] London, 11, New Burlington Street March, 1887
N.B.—As far as possible, this List is arranged in the order in which medical study is usually pursued.[Pg 2]
J. & A. CHURCHILL publish for the following Institutions and Public Bodies:—
ROYAL COLLEGE OF SURGEONS.
CATALOGUES OF THE MUSEUM.
Twenty-three separate Catalogues (List and Prices can be obtained of J.
& A. Churchill).
GUY'S HOSPITAL.
REPORTS BY THE MEDICAL AND SURGICAL STAFF.
Vol. XXVIII., Third Series. 7s. 6d.
FORMULÆ USED IN THE HOSPITAL IN ADDITION TO THOSE
IN THE B. P. 1s. 6d.
LONDON HOSPITAL.
PHARMACOPŒIA OF THE HOSPITAL. 3s.
CLINICAL LECTURES AND REPORTS BY THE MEDICAL AND
SURGICAL STAFF. Vols. I. to IV. 7s. 6d. each.
ST. BARTHOLOMEW'S HOSPITAL.
CATALOGUE OF THE ANATOMICAL AND PATHOLOGICAL
MUSEUM. Vol. I.—Pathology. 15s. Vol. II.—Teratology, Anatomy
and Physiology, Botany. 7s. 6d.
ST. GEORGE'S HOSPITAL.
REPORTS BY THE MEDICAL AND SURGICAL STAFF.
The last Volume (X.) was issued in 1880. Price 7s. 6d.
CATALOGUE OF THE PATHOLOGICAL MUSEUM. 15s.
SUPPLEMENTARY CATALOGUE (1882). 5s.
ST. THOMAS'S HOSPITAL.
REPORTS BY THE MEDICAL AND SURGICAL STAFF.
Annually. Vol. XV., New Series. 7s. 6d.
MIDDLESEX HOSPITAL.
CATALOGUE OF THE PATHOLOGICAL MUSEUM. 12s.
WESTMINSTER HOSPITAL.
REPORTS BY THE MEDICAL AND SURGICAL STAFF.
Annually. Vol. II. 6s.
ROYAL LONDON OPHTHALMIC HOSPITAL.
REPORTS BY THE MEDICAL AND SURGICAL STAFF.
Occasionally. Vol. XI., Part III. 5s.
OPHTHALMOLOGICAL SOCIETY OF THE UNITED KINGDOM.
TRANSACTIONS.
Vol. VI. 12s. 6d.
MEDICO-PSYCHOLOGICAL ASSOCIATION.
JOURNAL OF MENTAL SCIENCE.
Quarterly. 3s. 6d. each, or 14s. per annum.
PHARMACEUTICAL SOCIETY OF GREAT BRITAIN.
PHARMACEUTICAL JOURNAL AND TRANSACTIONS.
Every Saturday. 4d. each, or 20s. per annum, post free.
BRITISH PHARMACEUTICAL CONFERENCE.
YEAR BOOK OF PHARMACY.
In December. 10s.
BRITISH DENTAL ASSOCIATION.
JOURNAL OF THE ASSOCIATION AND MONTHLY REVIEW
OF DENTAL SURGERY.
On the 15th of each Month. 6d. each, or 7s. per annum, post free.
N.B.—J. & A. Churchill's Descriptive List of Works on Chemistry, Materia Medica, Pharmacy, Botany, Photography, Zoology, the Microscope, and other Branches of Science, can be had on application.
Practical Anatomy: A Manual of Dissections. By Christopher Heath, Surgeon to University College Hospital. Sixth Edition. Revised by Rickman J. Godlee, M.S. Lond., F.R.C.S., Demonstrator of Anatomy in University College, and Assistant Surgeon to the Hospital. Crown 8vo, with 24 Coloured Plates and 274 Engravings, 15s.
Wilson's Anatomist's Vade-Mecum. Tenth Edition. By George Buchanan, Professor of Clinical Surgery in the University of Glasgow; and Henry E. Clark, M.R.C.S., Lecturer on Anatomy at the Glasgow Royal Infirmary School of Medicine. Crown 8vo, with 450 Engravings (including 26 Coloured Plates), 18s.
Braune's Atlas of Topographical Anatomy, after Plane Sections of Frozen Bodies. Translated by Edward Bellamy, Surgeon to, and Lecturer on Anatomy, &c., at, Charing Cross Hospital. Large Imp. 8vo, with 34 Photolithographic Plates and 46 Woodcuts, 40s.
An Atlas of Human Anatomy. By Rickman J. Godlee, M.S., F.R.C.S., Assistant Surgeon and Senior Demonstrator of Anatomy, University College Hospital. With 48 Imp. 4to Plates (112 figures), and a volume of Explanatory Text. 8vo, £4 14s. 6d.
Harvey's (Wm.) Manuscript Lectures. Prelectiones Anatomiæ Universalis. Edited, with an Autotype reproduction of the Original, by a Committee of the Royal College of Physicians of London. Crown 4to, half bound in Persian, 52s. 6d.
Anatomy of the Joints of Man. By Henry Morris, Surgeon to, and Lecturer on Anatomy and Practical Surgery at, the Middlesex Hospital. 8vo, with 44 Lithographic Plates (several being coloured) and 13 Wood Engravings, 16s.
Manual of the Dissection of the Human Body. By Luther Holden, Consulting Surgeon to St. Bartholomew's Hospital. Edited by John Langton, F.R.C.S., Surgeon to, and Lecturer on Anatomy at, St. Bartholomew's Hospital. Fifth Edition. 8vo, with 208 Engravings. 20s.
By the same author.
Human Osteology. Sixth Edition, edited by the Author and James Shuter, F.R.C.S., M.A., M.B., Assistant Surgeon to St. Bartholomew's Hospital. 8vo, with 61 Lithographic Plates and 89 Engravings. 16s.
Also.
Landmarks, Medical and Surgical. Fourth Edition. 8vo. [In the Press.
The Student's Guide to Surgical Anatomy. By Edward Bellamy, F.R.C.S. and Member of the Board of Examiners. Third Edition. Fcap. 8vo, with 81 Engravings. 7s. 6d.
The Student's Guide to Human Osteology. By William Warwick Wagstaffe, late Assistant Surgeon to St. Thomas's Hospital. Fcap. 8vo, with 23 Plates and 66 Engravings. 10s. 6d.
The Anatomical Remembrancer; or, Complete Pocket Anatomist. Eighth Edition. 32mo, 3s. 6d.[Pg 4]
Diagrams of the Nerves of the Human Body, exhibiting their Origin, Divisions, and Connections, with their Distribution to the Various Regions of the Cutaneous Surface, and to all the Muscles. By W. H. Flower, F.R.S., F.R.C.S. Third Edition, with 6 Plates. Roya. 4to, 12s.
General Pathology. An Introduction to. By John Bland Sutton, F.R.C.S., Sir E. Wilson Lecturer on Pathology, R.C.S.; Assistant Surgeon to, and Lecturer on Anatomy at, Middlesex Hospital. 8vo, with 149 Engravings, 14s.
Atlas of Pathological Anatomy. By Dr. Lancereaux. Translated by W. S. Greenfield, M.D., Professor of Pathology in the University of Edinburgh. Imp. 8vo, with 70 Coloured Plates, £5 5s.
A Manual of Pathological Anatomy. By C. Handfield Jones, M.B., F.R.S., and E. H. Sieveking, M.D., F.R.C.P. Edited by J. F. Payne, M.D., F.R.C.P., Lecturer on General Pathology at St. Thomas's Hospital. Second Edition. Crown 8vo, with 195 Engravings, 16s.
Post-mortem Examinations: A Description and Explanation of the Method of Performing them, with especial reference to Medico-Legal Practice. By Prof. Virchow. Translated by Dr. T. P. Smith. Second Edition. Fcap. 8vo, with 4 Plates, 3s. 6d.
The Human Brain: Histological and Coarse Methods of Research. A Manual for Students and Asylum Medical Officers. By W. Bevan Lewis, L.R.C.P. Lond., Medical Superintendent, West Riding Lunatic Asylum. 8vo, with Wood Engravings and Photographs, 8s.
Manual of Physiology: For the use of Junior Students of Medicine. By Gerald F. Yeo, M.D., F.R.C.S., Professor of Physiology in King's College, London. Crown 8vo, with 300 Engravings, 14s.
Principles of Human Physiology. By W. B. Carpenter, C.B., M.D., F.R.S. Ninth Edition. By Henry Power, M.B., F.R.C.S. 8vo, with 3 Steel Plates and 377 Wood Engravings, 31s. 6d.
Syllabus of a Course of Lectures on Physiology. By Philip H. Pye-Smith, B.A., M.D., F.R.C.P., Physician to Guy's Hospital. Crown 8vo, with Diagrams, Notes, and Tables, 5s.
A Treatise on Human Physiology. By John C. Dalton, M.D. Seventh Edition. 8vo, with 252 Engravings, 20s.
Elementary Practical Biology: Vegetable. By Thomas W. Shore, M.D., B.Sc. Lond., Lecturer on Comparative Anatomy at St. Bartholomew's Hospital. 8vo. 6s.
Histology and Histo-Chemistry of Man. By Heinrich Frey, Professor of Medicine in Zurich. Translated by Arthur E. J. Barker, Assistant Surgeon to University College Hospital. 8vo, with 608 Engravings, 21s.
A Text-Book of Medical Physics, for Students and Practitioners. By J. C. Draper, M.D., LL.D., Professor of Physics in the University of New York. With 377 Engravings. 8vo, 18s.
The Law of Sex. By G. B. Starkweather, F.R.G.S. With 40 Illustrative Portraits. 8vo, 16s.
Influence of Sex in Disease. By W. Roger Williams, F.R.C.S., Surgical Registrar to the Middlesex Hospital. 8vo, 3s. 6d.
Medical Jurisprudence: Its Principles and Practice. By Alfred S. Taylor, M.D., F.R.C.P., F.R.S. Third Edition, by Thomas Stevenson, M.D., F.R.C.P., Lecturer on Medical Jurisprudence at Guy's Hospital. 2 vols. 8vo, with 188 Engravings, 31s. 6d.
By the same Authors.
A Manual of Medical Jurisprudence. Eleventh Edition. Crown 8vo, with 56 Engravings, 14s.
Also.
Poisons, In Relation to Medical Jurisprudence and Medicine. Third Edition. Crown 8vo, with 104 Engravings, 16s.
Lectures on Medical Jurisprudence. By Francis Ogston, M.D., late Professor in the University of Aberdeen. Edited by Francis Ogston, Jun., M.D. 8vo, with 12 Copper Plates, 18s.
The Student's Guide to Medical Jurisprudence. By John Abercrombie, M.D., F.R.C.P., Lecturer on Forensic Medicine to Charing Cross Hospital. Fcap. 8vo, 7s. 6d.
Microscopical Examination of Drinking Water and of Air. By J. D. Macdonald, M.D., F.R.S., Ex-Professor of Naval Hygiene in the Army Medical School. Second Edition. 8vo, with 25 Plates, 7s. 6d.
Pay Hospitals and Paying Wards throughout the World. By Henry C. Burdett. 8vo, 7s.
By the same Author.
Cottage Hospitals—General, Fever, and Convalescent: Their Progress, Management, and Work. Second Edition, with many Plans and Illustrations. Crown 8vo, 14s.[Pg 5]
A Manual of Practical Hygiene. By F. A. Parkes, M.D., F.R.S. Sixth Edition, by F. de Chaumont, M.D., F.R.S., Professor of Military Hygiene in the Army Medical School. 8vo, with numerous Plates and Engravings. 18s.
A Handbook of Hygiene and Sanitary Science. By Geo. Wilson, M.A., M.D., F.R.S.E., Medical Officer of Health for Mid-Warwickshire. Sixth Edition. Crown 8vo, with Engravings. 10s. 6d.
By the same Author.
Healthy Life and Healthy Dwellings: A Guide to Personal and Domestic Hygiene. Fcap. 8vo, 5s.
Sanitary Examinations Of Water, Air, and Food. A Vade-Mecum for the Medical Officer of Health. By Cornelius B. Fox, M.D., F.R.C.P. Second Edition. Crown 8vo, with 110 Engravings, 12s. 6d.
Dangers to Health: A Pictorial Guide to Domestic Sanitary Defects. By T. Pridgin Teale, M.A., Surgeon to the Leeds General Infirmary. Fourth Edition. 8vo, with 70 Lithograph Plates (mostly coloured), 10s.
Hospitals, Infirmaries, and Dispensaries: Their Construction, Interior Arrangement, and Management; with Descriptions of existing Institutions, and 74 Illustrations. By F. Oppert, M.D., M.R.C.P.L. Second Edition. Royal 8vo, 12s.
Hospital Construction and Management. By F. J. Mouat, M.D., Local Government Board Inspector, and H. Saxon Snell, Fell. Roy. Inst. Brit. Architects. In 2 Parts, 4to, 15s. each; or, the whole work bound in half calf, with large Map, 54 Lithographic Plates, and 27 Woodcuts, 35s.
Manual of Anthropometry: A Guide to the Measurement of the Human Body, containing an Anthropometrical Chart and Register, a Systematic Table of Measurements, &c. By Charles Roberts, F.R.C.S. 8vo, with numerous Illustrations and Tables, 8s. 6d.
By the same Author.
Detection of Colour-Blindness and Imperfect Eyesight. 8vo, with a Table of Coloured Wools, and Sheet of Test-types, 5s.
Illustrations of the Influence of the Mind upon the Body in Health and Disease; Designed to elucidate the Action of the Imagination. By Daniel Hack Tuke, M.D., F.R.C.P., LL.D. Second Edition. 2 vols, crown 8vo, 15s.
By the same Author.
Sleep-Walking and Hypnotism. 8vo, 5s.
A Manual of Psychological Medicine. With an Appendix of Cases. By John C. Bucknill, M.D., F.R.S., and D. Hack Tuke, M.D., F.R.C.P. Fourth Edition. 8vo, with 12 Plates (30 Figures) and Engravings, 25s.
Mental Diseases. Clinical Lectures. By T. S. Clouston, M.D., F.R.C.P. Edin., Lecturer on Mental Diseases in the University of Edinburgh. With 8 Plates (6 Coloured). Crown 8vo, 12s. 6d.
Private Treatment of the Insane as Single Patients. By Edward East, M.R.C.S., L.S.A. Crown 8vo, 2s. 6d.
Manual of Midwifery. By Alfred L. Galabin, M.A., M.D., F.R.C.P., Obstetric Physician to, and Lecturer on Midwifery, &c. at, Guy's Hospital. Crown 8vo, with 227 Engravings, 15s.
The Student's Guide to the Practice of Midwifery. By D. Lloyd Roberts, M.D., F.R.C.P., Lecturer on Clinical Midwifery and Diseases of Women at the Owens College; Obstetric Physician to the Manchester Royal Infirmary. Third Edition. Fcap. 8vo, with 2 Coloured Plates and 127 Wood Engravings, 7s. 6d.
Lectures on Obstetric Operations: Including the Treatment of Hæmorrhage, and forming a Guide to the Management of Difficult Labour. By Robert Barnes, M.D., F.R.C.P., Consulting Obstetric Physician to St. George's Hospital. Fourth Edition. 8vo, with 121 Engravings, 12s. 6d.
By the same Author.
A Clinical History of Medical and Surgical Diseases of Women. Second Edition. 8vo, with 181 Engravings, 28s.
Clinical Lectures on Diseases of Women: Delivered in St. Bartholomew's Hospital, by J. Matthews Duncan, M.D., LL.D., F.R.S. Third Edition. 8vo, 16s.
By the same Author.
Sterility in Woman. Being the Gulstonian Lectures, delivered in the Royal College of Physicians, in Feb., 1883. 8vo, 6s.
Notes on Diseases of Women: Specially designed to assist the Student in preparing for Examination. By J. J. Reynolds, L.R.C.P., M.R.C.S. Third Edition. Fcap. 8vo, 2s. 6d.
By the same Author.
Notes on Midwifery: Specially designed for Students preparing for Examination. Second Edition. Fcap. 8vo, with 15 Engravings, 4s.[Pg 6]
The Student's Guide to the Diseases of Women. By Alfred L. Galabin, M.D., F.R.C.P., Obstetric Physician to Guy's Hospital. Third Edition. Fcap. 8vo, with 78 Engravings, 7s. 6d.
West on the Diseases of Women. Fourth Edition, revised by the Author, with numerous Additions by J. Matthews Duncan, M.D., F.R.C.P., F.R.S.E., Obstetric Physician to St. Bartholomew's Hospital. 8vo, 16s.
Dysmenorrhœa, its Pathology and Treatment. By Heywood Smith, M.D. Crown 8vo, with Engravings, 4s. 6d.
Obstetric Aphorisms: For the Use of Students commencing Midwifery Practice. By Joseph G. Swayne, M.D. Eighth Edition. Fcap. 8vo, with Engravings, 3s. 6d.
A Manual of Obstetrics. By A. F. A. King, A.M., M.D., Professor of Obstetrics, &c., in the Columbian University, Washington, and the University of Vermont. Third Edition. Crown 8vo, with 102 Engravings, 8s.
Handbook of Midwifery for Midwives: By J. E. Burton, L.R.C.P. Lond., Surgeon to the Hospital for Women, Liverpool. Second Edition. With Engravings. Fcap. 8vo, 6s.
A Handbook of Uterine Therapeutics, and of Diseases of Women. By E. J. Tilt, M.D., M.R.C.P. Fourth Edition. Post 8vo, 10s.
By the same Author.
The Change of Life In Health and Disease: A Clinical Treatise on the Diseases of the Nervous System incidental to Women at the Decline of Life. Fourth Edition. 8vo, 10s. 6d.
The Principles and Practice of Gynæcology. By Thomas Addis Emmet, M.D., Surgeon to the Woman's Hospital, New York. Third Edition. Royal 8vo, with 150 Engravings, 24s.
Diseases of the Uterus, Ovaries, and Fallopian Tubes: A Practical Treatise by A. Courty, Professor of Clinical Surgery, Montpellier. Translated from Third Edition by his Pupil, Agnes McLaren, M.D., M.K.Q.C.P.I., with Preface by J. Matthews Duncan, M.D., F.R.C.P. 8vo, with 424 Engravings, 24s.
The Female Pelvic Organs: Their Surgery, Surgical Pathology, and Surgical Anatomy. In a Series of Coloured Plates taken from Nature; with Commentaries, Notes, and Cases. By Henry Savage, M.D., F.R.C.S., Consulting Officer of the Samaritan Free Hospital. Fifth Edition. Roy. 4to, with 17 Lithographic Plates(15 coloured) and 52 Woodcuts, £1 15s.
Ovarian and Uterine Tumours: Their Pathology and Surgical Treatment. By Sir T. Spencer Wells, Bart., F.R.C.S., Consulting Surgeon to the Samaritan Hospital. 8vo, with Engravings, 21s.
By the same Author.
Abdominal Tumours: Their Diagnosis and Surgical Treatment. 8vo, with Engravings, 3s. 6d.
A Practical Treatise on the Diseases of Women. By T. Gaillard Thomas, M.D., Professor of Diseases of Women in the College of Physicians and Surgeons, New York. Fifth Edition. Roy. 8vo, with 266 Engravings, 25s.
Backward Displacements of the Uterus and Prolapsus Uteri: Treatment by the New Method of Shortening the Round Ligaments. By William Alexander, M.D., M.Ch.Q.U.I., F.R.C.S., Surgeon to the Liverpool Infirmary. Crown 8vo, with Engravings, 3s. 6d.
The Student's Guide to Diseases of Children. By Jas. F. Goodhart, M.D., F.R.C.P., Physician to Guy's Hospital, and to the Evelina Hospital for Sick Children. Second Edition. Fcap. 8vo, 10s. 6d.
Diseases of Children. For Practitioners and Students. By W. H. Day, M.D., Physician to the Samaritan Hospital. Second Edition. Crown 8vo, 12s. 6d.
A Practical Treatise on Disease in Children. By Eustace Smith, M.D., Physician to the King of the Belgians, Physician to the East London Hospital for Children. 8vo, 22s.
By the same Author.
Clinical Studies of Disease in Children. Second Edition. Post 8vo, 7s. 6d.
Also.
The Wasting Diseases of Infants and Children. Fourth Edition. Post 8vo, 8s. 6d.
A Practical Manual of the Diseases of Children. With a Formulary. By Edward Ellis, M.D. Fifth Edition. Crown 8vo, 10s.
A Manual for Hospital Nurses and others engaged in Attending on the Sick. By Edward J. Domville, Surgeon to the Exeter Lying-in Charity. Fifth Edition. Crown 8vo, 2s. 6d.
A Manual of Nursing, Medical and Surgical. By Charles J. Cullingworth, M.D., Physician to St. Mary's Hospital, Manchester. Second Edition. Fcap. 8vo, with Engravings, 3s. 6d.
By the same Author.
A Short Manual for Monthly Nurses. Fcap. 8vo, 1s. 6d.[Pg 7]
Notes on Fever Nursing. By J. W. Allan, M.B., Physician, Superintendent Glasgow Fever Hospital. Crown 8vo, with Engravings, 2s. 6d.
By the same Author.
Outlines of Infectious Diseases: For the use of Clinical Students. Fcap. 8vo.
Hospital Sisters and their Duties. By Eva C. E. Lückes, Matron to the London Hospital. Crown 8vo, 2s. 6d.
Diseases and their Commencement. Lectures to Trained Nurses. By Donald W. C. Hood, M.D., M.R.C.P., Physician to the West London Hospital. Crown 8vo, 2s. 6d.
Infant Feeding and its Influence on Life; By C. H. F. Routh, M.D., Physician to the Samaritan Hospital. Fourth Edition. Fcap. 8vo. [Preparing.
Manual of Botany: Including the Structure, Classification, Properties, Uses, and Functions of Plants. By Robert Bentley, Professor of Botany in King's College and to the Pharmaceutical Society. Fifth Edition. Crown 8vo, with 1,178 Engravings, 15s.
By the same Author.
The Student's Guide to Structural, Morphological, and Physiological Botany. With 660 Engravings. Fcap. 8vo, 7s. 6d.
Also.
The Student's Guide to Systematic Botany, including the Classification of Plants and Descriptive Botany. Fcap. 8vo, with 350 Engravings, 3s. 6d.
Medicinal Plants: Being descriptions, with original figures, of the Principal Plants employed in Medicine, and an account of their Properties and Uses. By Prof. Bentley and Dr. H. Trimen. In 4 vols., large 8vo, with 306 Coloured Plates, bound in Half Morocco, Gilt Edges, £11 11s.
The National Dispensatory: Containing the Natural History, Chemistry, Pharmacy, Actions and Uses of Medicines. By Alfred Stillé, M.D., LL.D., and John M. Maisch, Ph.D. Fourth Edition. 8vo, with 311 Engravings, 36s.
Royle's Manual of Materia Medica and Therapeutics. Sixth Edition, including additions and alterations in the B. P. 1885. By John Harley, M.D., Physician to St. Thomas's Hospital. Crown 8vo, with 139 Engravings, 15s.
Materia Medica. A Manual for the use of Students. By Isambard Owen, M.D., F.R.C.P., Lecturer on Materia Medica, &c., to St. George's Hospital. Second Edition. Crown 8vo, 6s. 6d.
Materia Medica and Therapeutics: Vegetable Kingdom—Organic Compounds—Animal Kingdom. By Charles D. F. Phillips, M.D., F.R.S. Edin., late Lecturer on Materia Medica and Therapeutics at the Westminster Hospital Medical School. 8vo, 25s.
The Student's Guide to Materia Medica and Therapeutics. By John C. Thorowgood, M.D., F.R.C.P. Second Edition. Fcap. 8vo, 7s.
The Pharmacopœia of the London Hospital. Compiled under the direction of a Committee appointed by the Hospital Medical Council. Fcap. 8vo, 3s.
A Companion to the British Pharmacopœia. By Peter Squire, Revised by his Sons, P. W. and A. H. Squire. 14th Edition. 8vo, 10s. 6d.
By the same Authors.
The Pharmacopœias of the London Hospitals, arranged in Groups for Easy Reference and Comparison. Fifth Edition. 18mo, 6s.
The Prescriber's Pharmacopœia: The Medicines arranged in Classes according to their Action, with their Composition and Doses. By Nestor J. C. Tirard, M.D., F.R.C.P., Professor of Materia Medica and Therapeutics in King's College, London. Sixth Edition. 32mo, bound in leather, 3s.
Clinical Medicine: A Systematic Treatise on the Diagnosis and Treatment of Disease. By Austin Flint, M.D., Professor of Medicine in the Bellevue Hospital Medical College. 8vo, 20s.
By the same Author.
A Treatise on the Principles and Practice of Medicine. Sixth Edition. By the Author, and W. H. Welch, M.D., and Austin Flint, jun., M.D. 8vo, with Engravings, 26s.
Climate and Fevers of India, with a series of Cases (Croonian Lectures, 1882). By Sir Joseph Fayrer, K.C.S.I., M.D. 8vo, with 17 Temperature Charts, 12s.
Family Medicine for India. A Manual. By William J. Moore, M.D., C.I.E., Honorary Surgeon to the Viceroy of India. Published under the Authority of the Government of India. Fifth Edition. Post 8vo, with Engravings. [In the Press.
By the same Author.
A Manual of the Diseases of India: With a Compendium of Diseases generally. Second Edition. Post 8vo, 10s.
Also.
Health-Resorts for Tropical Invalids, in India, at Home, and Abroad. Post 8vo, 5s.[Pg 8]
Practical Therapeutics: A Manual. By Edward J. Waring, C.I.E., M.D., F.R.C.P., and Dudley W. Buxton, M.D., B.S. Lond. Fourth Edition. Crown 8vo, 14s.
By the same Author.
Bazaar Medicines of India, And Common Medical Plants: With Full Index of Diseases, indicating their Treatment by these and other Agents procurable throughout India, &c. Fourth Edition. Fcap. 8vo, 5s.
A Commentary on the Diseases of India. By Norman Chevers, C.I.E., M.D., F.R.C.S., Deputy Surgeon-General H. M. Indian Army. 8vo, 24s.
The Principles and Practice of Medicine. By C. Hilton Fagge, M.D. Edited by P. H. Pye-Smith, M.D., F.R.C.P., Physician to, and Lecturer on Medicine at, Guy's Hospital. 2 vols. 8vo, 1860 pp. Cloth, 36s.; Half Persian, 42s.
The Student's Guide to the Practice of Medicine. By Matthew Charteris, M.D., Professor of Materia Medica in the University of Glasgow. Fourth Edition. Fcap. 8vo, with Engravings on Copper and Wood. 9s.
Hooper's Physicians' Vade-Mecum. A Manual of the Principles and Practice of Physic. Tenth Edition. By W. A. Guy, F.R.C.P., F.R.S., and J. Harley, M.D., F.R.C.P. With 118 Engravings. Fcap. 8vo, 12s. 6d.
The Student's Guide to Clinical Medicine and Case-Taking. By Francis Warner, M.D., F.R.C.P., Physician to the London Hospital. Second Edition. Fcap. 8vo, 5s.
How to Examine the Chest: Being a Practical Guide for the use of Students. By Samuel West, M.D., F.R.C.P., Physician to the City of London Hospital for Diseases of the Chest; Medical Tutor and Registrar at St. Bartholomew's Hospital. With 42 Engravings. Fcap. 8vo, 5s.
The Contagiousness of Pulmonary Consumption, and its Antiseptic Treatment. By J. Burney Yeo, M.D., Physician to King's College Hospital. Crown 8vo, 3s. 6d.
The Operative Treatment of Intra-thoracic Effusion. Fothergillian Prize Essay. By Norman Porritt, L.R.C.P. Lond., M.R.C.S. With Engravings. Crown 8vo, 6s.
Diseases of the Chest: Contributions to their Clinical History, Pathology, and Treatment. By A. T. Houghton Waters, M.D., Physician to the Liverpool Royal Infirmary. Second Edition. 8vo, with Plates, 15s.
The Student's Guide to Medical Diagnosis. By Samuel Fenwick, M.D., F.R.C.P., Physician to the London Hospital, and Bedford Fenwick, M.D., M.R.C.P. Sixth Edition. Fcap. 8vo, with 114 Engravings, 7s.
By the same Author.
The Student's Outlines of Medical Treatment. Second Edition. Fcap. 8vo, 7s.
Also.
On Chronic Atrophy of the Stomach, and on the Nervous Affections of the Digestive Organs. 8vo, 8s.
The Microscope in Medicine. By Lionel S. Beale, M.B., F.R.S., Physician to King's College Hospital. Fourth Edition. 8vo, with 86 Plates, 21s.
Also.
On Slight Ailments: Their Nature and Treatment. Second Edition. 8vo, 5s.
The Spectroscope in Medicine. By Charles A. MacMunn, B.A., M.D. 8vo, with 3 Chromo-lithographic Plates of Physiological and Pathological Spectra, and 13 Engravings, 9s.
Notes on Asthma: Its Forms and Treatment. By John C. Thorowgood, M.D., Physician to the Hospital for Diseases of the Chest. Third Edition. Crown 8vo, 4s. 6d.
What is Consumption? By G. W. Hambleton, L.K.Q.C.P.I. Crown 8vo, 2s. 6d.
Winter Cough (Catarrh, Bronchitis, Emphysema, Asthma). By Horace Dobell, M.D., Consulting Physician to the Royal Hospital for Diseases of the Chest. Third Edition. 8vo, with Coloured Plates, 10s. 6d.
By the same Author.
Loss of Weight, Blood-Spitting, and Lung Disease. Second Edition. 8vo, with Chromo-lithograph, 10s. 6d.
Also.
The Mont Doré Cure, and the Proper Way to Use it. 8vo, 7s. 6d.
Pulmonary Consumption: A Practical Treatise on its Cure with Medicinal, Dietetic, and Hygienic Remedies. By James Weaver, M.D., L.R.C.P. Crown 8vo, 2s.
Croonian Lectures on Some Points in the Pathology and Treatment of Typhoid Fever. By William Cayley, M.D., F.R.C.P., Physician to the Middlesex and the London Fever Hospitals. Crown 8vo, 4s. 6d.
Treatment of Some of the Forms of Valvular Disease of the Heart. By A. E. Sansom, M.D., F.R.C.P., Physician to the London Hospital. Second Edition. Fcap. 8vo, with 26 Engravings, 4s. 6d.[Pg 9]
Diseases of the Heart and Aorta: Clinical Lectures. By G. W. Balfour, M.D., F.R.C.P., F.R.S. Edin., late Senior Physician and Lecturer on Clinical Medicine, Royal Infirmary, Edinburgh. Second Edition. 8vo, with Chromo-lithograph and Wood Engravings, 12s. 6d.
Medical Ophthalmoscopy: A Manual and Atlas. By William R. Gowers, M.D., F.R.C.P., Assistant Professor of Clinical Medicine in University College, and Senior Assistant Physician to the Hospital. Second Edition, with Coloured Autotype and Lithographic Plates and Woodcuts. 8vo, 18s.
By the same Author.
Pseudo-Hypertrophic Muscular Paralysis: A Clinical Lecture. 8vo, with Engravings and Plate, 3s. 6d.
Also.
Diagnosis of Diseases of the Spinal Cord. Third Edition. 8vo, with Engravings, 4s. 6d.
Also.
Diagnosis of Diseases of the Brain. 8vo, with Engravings, 7s. 6d.
Also.
A Manual of Diseases of the Nervous System. Vol. I. Diseases of the Spinal Cord and Nerves. Roy. 8vo, with 171 Engravings (many figures), 12s. 6d.
Diseases of the Nervous System. Lectures delivered at Guy's Hospital. By Samuel Wilks, M.D., F.R.S. Second Edition. 8vo, 18s.
Diseases of the Nervous System: Especially in Women. By S. Weir Mitchell, M.D., Physician to the Philadelphia Infirmary for Diseases of the Nervous System. Second Edition. 8vo, with 5 Plates, 8s.
Nerve Vibration and Excitation, as Agents in the Treatment of Functional Disorder and Organic Disease. By J. Mortimer Granville, M.D. 8vo, 5s.
By the same Author.
Gout in its Clinical Aspects. Crown 8vo, 6s.
Regimen to be adopted in Cases of Gout. By Wilhelm Ebstein, M.D., Professor of Clinical Medicine in Göttingen. Translated by John Scott, M.A., M.B. 8vo, 2s. 6d.
Diseases of the Nervous System. Clinical Lectures. By Thomas Buzzard, M.D., F.R.C.P., Physician to the National Hospital for the Paralysed and Epileptic. With Engravings, 8vo. 15s.
By the same Author.
Some Forms of Paralysis from Peripheral Neuritis: of Gouty, Alcoholic, Diphtheritic, and other origin. Crown 8vo, 5s.
Diseases of the Liver: With and without Jaundice. By George Harley, M.D., F.R.C.P., F.R.S. 8vo, with 2 Plates and 36 Engravings, 21s.
By the same Author.
Inflammations of the Liver, and their Sequelæ. Crown 8vo, with Engravings, 5s.
Gout, Rheumatism, And the Allied Affections; with Chapters on Longevity and Sleep. By Peter Hood, M.D. Third Edition. Crown 8vo, 7s. 6d.
Diseases of the Stomach: The Varieties of Dyspepsia, their Diagnosis and Treatment. By S. O. Habershon, M.D., F.R.C.P. Third Edition. Crown 8vo, 5s.
By the same Author.
Pathology of the Pneumogastric Nerve: Lumleian Lectures for 1876. Second Edition. Post 8vo, 4s.
Also.
Diseases of the Abdomen, Comprising those of the Stomach and other parts of the Alimentary Canal, (Esophagus, Cæcum, Intestines, and Peritoneum) Third Edition. 8vo, with 5 Plates, 21s.
Also.
Diseases of the Liver, Their Pathology and Treatment. Lettsomian Lectures. Second Edition. Post 8vo, 4s.
Acute Intestinal Strangulation, And Chronic Intestinal Obstruction (Mode of Death from). By Thomas Bryant, F.R.C.S., Senior Surgeon to Guy's Hospital. 8vo, 3s.
A Treatise on the Diseases of the Nervous System. By James Ross, M.D., F.R.C.P., Assistant Physician to the Manchester Royal Infirmary. Second Edition. 2 vols. 8vo, with Lithographs, Photographs, and 332 Woodcuts, 52s. 6d.
By the same Author.
Handbook of the Diseases of the Nervous System. Roy. 8vo, with 184 Engravings, 18s.
Also.
Aphasia: Being a Contribution to the Subject of the Dissolution of Speech from Cerebral Disease. 8vo, with Engravings, 4s. 6d.
Spasm in Chronic Nerve Disease. (Gulstonian Lectures.) By Seymour J. Sharkey, M.A., M.B., F.R.C.P., Assistant Physician to, and Joint Lecturer on Pathology at, St. Thomas's Hospital. 8vo, with Engravings, 5s.
On Megrim, Sick Headache, and some Allied Disorders: A Contribution to the Pathology of Nerve Storms. By E. Liveing, M.D., F.R.C.P. 8vo, 15s.[Pg 10]
Food and Dietetics, Physiologically and Therapeutically Considered. By F. W. Pavy, M.D., F.R.S., Physician to Guy's Hospital. Second Edition. 8vo, 15s.
By the same Author.
Croonian Lectures on Certain Points connected with Diabetes. 8vo, 4s. 6d.
Headaches: Their Nature, Causes, and Treatment. By W. H. Day, M.D., Physician to the Samaritan Hospital. Fourth Edition. Crown 8vo, with Engravings. [In the Press.
Health Resorts at Home and Abroad. By Matthew Charteris, M.D., Physician to the Glasgow Royal Infirmary. Crown 8vo, with Map, 4s. 6d.
The Principal Southern and Swiss Health-Resorts: their Climate and Medical Aspect. By William Marcet, M.D., F.R.C.P., F.R.S. With Illustrations. Crown 8vo, 7s. 6d.
Winter and Spring On the Shores of the Mediterranean. By Henry Bennet, M.D. Fifth Edition. Post 8vo, with numerous Plates, Maps, and Engravings, 12s. 6d.
By the same Author.
Treatment of Pulmonary Consumption by Hygiene, Climate, and Medicine. Third Edition. 8vo, 7s. 6d.
The Riviera: Sketches of the Health-Resorts of the Coast of France and Italy, from Hyères to Spezia: its Medical Aspect and Value, &c. By Edward I. Sparks, M.B., F.R.C.P. Crown 8vo, 8s. 6d.
Medical Guide to the Mineral Waters of France and its Wintering Stations. With a Special Map. By A. Vintras, M.D., Physician to the French Embassy, and to the French Hospital, London. Crown 8vo, 8s.
The Ocean as a Health-Resort: A Practical Handbook of the Sea, for the use of Tourists and Health-Seekers. By William S. Wilson, L.R.C.P. Second Edition, with Chart of Ocean Routes, &c. Crown 8vo, 7s. 6d.
Ambulance Handbook for Volunteers and Others. By J. Ardavon Raye, L.K. & Q.C.P.I., L.R.C.S.I., late Surgeon to H.B.M. Transport No. 14, Zulu Campaign, and Surgeon E.I.R. Rifles. 8vo, with 16 Plates (50 figures), 3s. 6d.
Ambulance Lectures: To which is added a Nursing Lecture. By John M. H. Martin, Honorary Surgeon to the Blackburn Infirmary. Crown 8vo, with 53 Engravings, 2s.
Handbook of Medical and Surgical Electricity. By Herbert Tibbits, M.D., F.R.C.P.E., Senior Physician to the West London Hospital for Paralysis and Epilepsy. Second Edition. 8vo, with 95 Engravings, 9s.
By the same Author.
How to Use a Galvanic Battery in Medicine and Surgery. Third Edition. 8vo, with Engravings, 4s.
Also.
A Map of Ziemssen's Motor Points of the Human Body: A Guide to Localised Electrisation. Mounted on Rollers, 35 × 21. With 20 Illustrations, 5s.
Also.
Electrical and Anatomical Demonstrations Delivered at the School of Massage and Electricity. Crown 8vo, with Illustrations, 5s.
Surgical Emergencies: Together with the Emergencies attendant on Parturition and the Treatment of Poisoning. By Paul Swain, F.R.C.S., Surgeon to the South Devon and East Cornwall Hospital. Third Edition. Crown 8vo, with 117 Engravings, 5s.
Operative Surgery in the Calcutta Medical College Hospital. Statistics, Cases, and Comments. By Kenneth McLeod, A.M., M.D., F.R.C.S.E., Surgeon-Major, Indian Medical Service, Professor of Surgery in Calcutta Medical College. 8vo, with Illustrations, 12s. 6d.
A Course of Operative Surgery. By Christopher Heath, Surgeon to University College Hospital. Second Edition. With 20 coloured Plates (180 figures) from Nature, by M. Léveillé, and several Woodcuts. Large 8vo, 30s.
By the same Author.
The Student's Guide to Surgical Diagnosis. Second Edition. Fcap. 8vo, 6s. 6d.
Also.
Manual of Minor Surgery and Bandaging. For the use of House-Surgeons, Dressers, and Junior Practitioners. Eighth Edition. Fcap. 8vo, with 142 Engravings, 6s.
Also.
Injuries and Diseases of the Jaws. Third Edition. 8vo, with Plate and 206 Wood Engravings, 14s.
Injuries and Diseases of the Neck and Head, the Genito-Urinary Organs, and the Rectum. Hunterian Lectures, 1885. By Edward Lund, F.R.C.S., Professor of Surgery in the Owens College, Manchester. 8vo, with Plates and Engravings, 4s. 6d.[Pg 11]
The Practice of Surgery: A Manual. By Thomas Bryant, Surgeon to Guy's Hospital. Fourth Edition. 2 vols, crown 8vo, with 750 Engravings (many being coloured), and including 6 chromo plates, 32s.
The Surgeon's Vade-Mecum: A Manual of Modern Surgery. By R. Druitt, F.R.C.S. Twelfth Edition. By Stanley Boyd, M.B., F.R.C.S. Assistant Surgeon and Pathologist to Charing Cross Hospital. Crown 8vo, with 373 Engravings 16s.
Regional Surgery: Including Surgical Diagnosis. A Manual for the use of Students. By F. A. Southam, M.A., M.B., F.R.C.S., Assistant Surgeon to the Manchester Royal Infirmary. Part I. The Head and Neck. Crown 8vo, 6s. 6d.—Part II. The Upper Extremity and Thorax. Crown 8vo, 7s. 6d. Part III. The Abdomen and Lower Extremity. Crown 8vo, 7s.
Surgical Enquiries: Including the Hastings Essay on Shock, the Treatment of Inflammations, and numerous Clinical Lectures. By Furneaux Jordan, F.R.C.S., Professor of Surgery, Queen's College, Birmingham. Second Edition, with numerous Plates. Royal 8vo, 12s. 6d.
Illustrations of Clinical Surgery. By Jonathan Hutchinson, F.R.S., Senior Surgeon to the London Hospital. In occasional fasciculi. I. to XVIII., 6s. 6d. each. Fasciculi I. to X. bound, with Appendix and Index, £3 10s.
By the same Author.
Pedigree of Disease: Being Six Lectures on Temperament, Idiosyncrasy, and Diathesis. 8vo, 5s.
Treatment of Wounds and Fractures. Clinical Lectures. By Sampson Gamgee, F.R.S.E., Surgeon to the Queen's Hospital, Birmingham. Second Edition. 8vo, with 40 Engravings, 10s.
Electricity and its Manner of Working in the Treatment of Disease. By Wm. E. Steavenson, M.D., Physician and Electrician to St. Bartholomew's Hospital. 8vo, 4s. 6d.
Lectures on Orthopædic Surgery. By Bernard E. Brodhurst, F.R.C.S., Surgeon to the Royal Orthopædic Hospital. Second Edition. 8vo, with Engravings, 12s. 6d.
By the same Author.
On Anchylosis, and the Treatment for the Removal of Deformity and the Restoration of Mobility in Various Joints. Fourth Edition. 8vo, with Engravings, 5s.
Also.
Curvatures and Diseases of the Spine. Third Edition. 8vo, with Engravings, 6s.
Diseases of Bones and Joints. By Charles Macnamara, F.R.C.S., Surgeon to, and Lecturer on Surgery at, the Westminster Hospital. 8vo, with Plates and Engravings, 12s.
Injuries of the Spine and Spinal Cord, and NERVOUS SHOCK, in their Surgical and Medico-Legal Aspects. By Herbert W. Page, M.C. Cantab., F.R.C.S., Surgeon to St. Mary's Hospital. Second Edition, post 8vo, 10s.
Face and Foot Deformities. By Frederick Churchill, C.M., Surgeon to the Victoria Hospital for Children. 8vo, with Plates and Illustrations, 10s. 6d.
Clubfoot: Its Causes, Pathology, and Treatment. By Wm. Adams, F.R.C.S., Surgeon to the Great Northern Hospital. Second Edition. 8vo, with 106 Engravings and 6 Lithographic Plates, 15s.
By the same Author.
On Contraction of the Fingers, and its Treatment by Subcutaneous Operation; and on Obliteration of Depressed Cicatrices, by the same Method. 8vo, with 30 Engravings, 4s. 6d.
Also.
Lateral and other Forms of Curvature of the Spine: Their Pathology and Treatment. Second Edition. 8vo, with 5 Lithographic Plates and 72 Wood Engravings, 10s. 6d.
Spinal Curvatures: Treatment by Extension and Jacket; with Remarks on some Affections of the Hip, Knee, and Ankle-joints. By H. Macnaughton Jones, M.D., F.R.C.S. I. and Edin. Post 8vo, with 63 Engravings, 4s. 6d.
On Diseases and Injuries of the Eye: A Course of Systematic and Clinical Lectures to Students and Medical Practitioners. By J. R. Wolfe, M.D., F.R.C.S.E., Lecturer on Ophthalmic Medicine and Surgery in Anderson's College, Glasgow. With 10 Coloured Plates and 157 Wood Engravings. 8vo, £1 1s.
Hints on Ophthalmic Out-Patient Practice. By Charles Higgens, Ophthalmic Surgeon to Guy's Hospital. Third Edition. Fcap. 8vo, 3s.
Short Sight, Long Sight, and Astigmatism. By George F. Helm, M.A., M.D., F.R.C.S., formerly Demonstrator of Anatomy in the Cambridge Medical School. Crown 8vo, with 35 Engravings, 3s. 6d.
Manual of the Diseases of the Eye. By Charles Macnamara, F.R.C.S., Surgeon to Westminster Hospital. Fourth Edition. Crown 8vo, with 4 Coloured Plates and 66 Engravings, 10s. 6d.[Pg 12]
The Student's Guide to Diseases of the Eye. By Edward Nettleship, F.R.C.S., Ophthalmic Surgeon to St. Thomas's Hospital. Fourth Edition. Fcap. 8vo, with Engravings and a Set of Coloured Papers illustrating Colour-Blindness, [Nearly Ready.
Normal and Pathological Histology of the Human Eye and Eyelids. By C. Fred. Pollock, M.D., F.R.C.S. and F.R.S.E., Surgeon for Diseases of the Eye to Anderson's College Dispensary, Glasgow. Crown 8vo, with 100 Plates (230 drawings), 15s.
Atlas of Ophthalmoscopy. Composed of 12 Chromo-lithographic Plates (59 Figures drawn from nature) and Explanatory Text. By Richard Liebreich, M.R.C.S. Translated by H. Rosborough Swanzy, M.B. Third edition, 4to, 40s.
Glaucoma: Its Causes, Symptoms, Pathology, and Treatment. By Priestley Smith, M.R.C.S., Ophthalmic Surgeon to the Queen's Hospital, Birmingham. 8vo, with Lithographic Plates, 10s. 6d.
Refraction of the Eye: A Manual for Students. By Gustavus Hartridge, F.R.C.S., Assistant Physician to the Royal Westminster Ophthalmic Hospital. Second Edition. Crown 8vo, with Lithographic Plate and 94 Woodcuts, 5s. 6d.
The Electro-Magnet, And its Employment in Ophthalmic Surgery. By Simeon Snell, Ophthalmic Surgeon to the Sheffield General Infirmary, &c. Crown 8vo, 3s. 6d.
Hare-Lip and Cleft Palate. By Francis Mason, F.R.C.S., Surgeon to St. Thomas's Hospital. 8vo, with 66 Engravings, 6s.
By the same Author.
The Surgery of the Face. 8vo, with 100 Engravings, 7s. 6d.
A Practical Treatise on Aural Surgery. By H. Macnaughton Jones, M.D., Professor of the Queen's University in Ireland, late Surgeon to the Cork Ophthalmic and Aural Hospital. Second Edition. Crown 8vo, with 63 Engravings, 8s. 6d.
By the same Author.
Atlas of Diseases of the Membrana Tympani. In Coloured Plates, containing 62 Figures, with Text. Crown 4to, 21s.
Endemic Goitre or Thyreocele: Its Etiology, Clinical Characters, Pathology, Distribution, Relations to Cretinism, Myxœdema, &c., and Treatment. By William Robinson, M.D. 8vo, 5s.
Diseases and Injuries of the Ear. By Sir William B. Dalby, Aural Surgeon to St. George's Hospital. Third Edition. Crown 8vo, with Engravings, 7s. 6d.
By the Same Author.
Short Contributions to Aural Surgery, between 1875 and 1886. 8vo, with Engravings, 3s. 6d.
Diseases of the Throat and Nose: A Manual. By Morell Mackenzie, M.D. Lond., Senior Physician to the Hospital for Diseases of the Throat.
Vol. II. Diseases of the Nose and Naso-Pharynx; with a Section on Diseases of the Œsophagus. Post 8vo, with 93 Engravings, 12s. 6d.
By the same Author.
Diphtheria: Its Nature and Treatment, Varieties, and Local Expressions. 8vo, 5s.
Lectures on Syphilis of the Larynx (Lesions of the Secondary and Intermediate Stages). By W. M. Whistler, M.D., Physician to the Hospital for Diseases of the Throat. Post 8vo, 4s.
Sore Throat: Its Nature, Varieties, and Treatment. By Prosser James, M.D., Physician to the Hospital for Diseases of the Throat. Fifth Edition. Post 8vo, with Coloured Plates and Engravings, 6s. 6d.
A Treatise on Vocal Physiology and Hygiene. By Gordon Holmes, M.D., Physician to the Municipal Throat and Ear Infirmary. Second Edition, with Engravings. Crown 8vo, 6s. 6d.
By the same Author.
A Guide to the Use of the Laryngoscope in General Practice. Crown 8vo, with Engravings, 2s. 6d.
A System of Dental Surgery. By Sir John Tomes, F.R.S., and C. S. Tomes, M.A., F.R.S. Third Edition. Fcap. 8vo, with many Engravings. [Nearly Ready.
Dental Anatomy, Human and Comparative: A Manual. By Charles S. Tomes, M.A., F.R.S. Second Edition. Crown 8vo, with 191 Engravings, 12s. 6d.
The Student's Guide to Dental Anatomy and Surgery. By Henry Sewill, M.R.C.S., L.D.S. Second Edition. Fcap. 8vo, with 78 Engravings, 5s. 6d.
Notes on Dental Practice. By Henry C. Quinby, L.D.S. R.C.S.I. 8vo, with 87 Engravings, 9s.
Mechanical Dentistry in Gold and Vulcanite. By F. H. Balkwill, L.D.S. R.C.S. 8vo, with 2 Lithographic Plates and 57 Engravings, 10s.[Pg 13]
A Practical Treatise on Mechanical Dentistry. By Joseph Richardson, M.D., D.D.S., late Emeritus Professor of Prosthetic Dentistry in the Indiana Medical College. Fourth Edition. Roy. 8vo, with 458 Engravings, 21s.
Principles and Practice of Dentistry: including Anatomy, Physiology, Pathology, Therapeutics, Dental Surgery, and Mechanism. By C. A. Harris, M.D., D.D.S. Edited by F. J. S. Gorgas, A.M., M.D., D.D.S., Professor in the Dental Department of Maryland University. Eleventh Edition. 8vo, with 750 Illustrations, 31s. 6d.
A Manual of Dental Mechanics. By Oakley Coles, L.D.S. R.C.S. Second Edition. Crown 8vo, with 140 Engravings, 7s. 6d.
Elements of Dental Materia Medica and Therapeutics, with Pharmacopœia. By James Stocken, L.D.S. R.C.S., Pereira Prizeman for Materia Medica, and Thomas Gaddes, L.D.S. Eng. and Edin. Third Edition. Fcap. 8vo, 7s. 6d.
Dental Medicine: A Manual of Dental Materia Medica and Therapeutics. By F. J. S. Gorgas, A.M., M.D., D.D.S., Editor of "Harris's Principles and Practice of Dentistry," Professor in the Dental Department of Maryland University. 8vo, 14s.
Atlas of Skin Diseases. By Tilbury Fox, M.D., F.R.C.P. With 72 Coloured Plates. Royal 4to, half morocco, £6 6s.
Diseases of the Skin: With an Analysis of 8,000 Consecutive Cases and a Formulary. By L. D. Bulkley, M.D., Physician for Skin Diseases at the New York Hospital. Crown 8vo, 6s. 6d.
By the same Author.
Acne: its Etiology, Pathology, and Treatment: Based upon a Study of 1,500 Cases. 8vo, with Engravings, 10s.
On Certain Rare Diseases of the Skin. By Jonathan Hutchinson, F.R.S., Senior Surgeon to the London Hospital, and to the Hospital for Diseases of the Skin. 8vo, 10s. 6d.
Diseases of the Skin: A Practical Treatise for the Use of Students and Practitioners. By J. N. Hyde, A.M., M.D., Professor of Skin and Venereal Diseases, Rush Medical College, Chicago. 8vo, with 66 Engravings, 17s.
Parasites: A Treatise on the Entozoa of Man and Animals, including some Account of the Ectozoa. By T. Spencer Cobbold, M.D., F.R.S. 8vo, with 85 Engravings, 15s.
Manual of Animal Vaccination, preceded by Considerations on Vaccination in general. By E. Warlomont, M.D., Founder of the State Vaccine Institute of Belgium. Translated and edited by Arthur J. Harries, M.D. Crown 8vo, 4s. 6d.
Leprosy in British Guiana. By John D. Hillis, F.R.C.S., M.R.I.A., Medical Superintendent of the Leper Asylum, British Guiana. Imp. 8vo, with 22 Lithographic Coloured Plates and Wood Engravings, £1 11s. 6d.
Cancer of the Breast. By Thomas W. Nunn, F.R.C.S., Consulting Surgeon to the Middlesex Hospital. 4to, with 21 Coloured Plates, £2 2s.
On Cancer: Its Allies, and other Tumours; their Medical and Surgical Treatment. By F. A. Purcell, M.D., M.C., Surgeon to the Cancer Hospital, Brompton. 8vo, with 21 Engravings, 10s. 6d.
Sarcoma and Carcinoma: Their Pathology, Diagnosis, and Treatment. By Henry T. Butlin, F.R.C.S., Assistant Surgeon to St. Bartholomew's Hospital. 8vo, with 4 Plates, 8s.
By the same Author.
Malignant Disease of the Larynx (Sarcoma and Carcinoma). 8vo, with 5 Engravings, 5s.
Cancerous Affections of the Skin. (Epithelioma and Rodent Ulcer.) By George Thin, M.D. Post 8vo, with 8 Engravings, 5s.
Cancer of the Mouth, Tongue, and Alimentary Tract: their Pathology, Symptoms, Diagnosis, and Treatment. By Frederic B. Jessett, F.R.C.S., Surgeon to the Cancer Hospital, Brompton. 8vo, 10s.
Clinical Notes on Cancer, Its Etiology and Treatment; with special reference to the Heredity-Fallacy, and to the Neurotic Origin of most Cases of Alveolar Carcinoma. By Herbert L. Snow, M.D. Lond., Surgeon to the Cancer Hospital, Brompton. Crown 8vo, 3s. 6d.
Lectures on the Surgical Disorders of the Urinary Organs. By Reginald Harrison, F.R.C.S., Surgeon to the Liverpool Royal Infirmary. Second Edition, with 48 Engravings. 8vo, 12s. 6d.
Hydrocele: Its several Varieties and their Treatment. By Samuel Osborn, late Surgical Registrar to St. Thomas's Hospital. Fcap. 8vo, with Engravings, 3s.
By the same Author.
Diseases of the Testis. Fcap. 8vo, with Engravings, 3s. 6d.[Pg 14]
Diseases of the Urinary Organs. Clinical Lectures. By Sir Henry Thompson, F.R.C.S., Emeritus Professor of Clinical Surgery in University College. Seventh (Students') Edition. 8vo, with 84 Engravings, 2s. 6d.
By the same Author.
Diseases of the Prostate: Their Pathology and Treatment. Sixth Edition. 8vo, with 39 Engravings, 6s.
Also.
Surgery of the Urinary Organs. Some Important Points connected therewith. Lectures delivered in the R.C.S. 8vo, with 44 Engravings. Students' Edition, 2s. 6d.
Also.
Practical Lithotomy and Lithotrity; or, An Inquiry into the Best Modes of Removing Stone from the Bladder. Third Edition. 8vo, with 87 Engravings, 10s.
Also.
The Preventive Treatment of Calculous Disease, and the Use of Solvent Remedies. Second Edition. Fcap. 8vo, 2s. 6d.
Also.
Tumours of the Bladder: Their Nature, Symptoms, and Surgical Treatment. 8vo, with numerous Illustrations, 5s.
Also.
Stricture of the Urethra, and Urinary Fistulaæ: their Pathology and Treatment. Fourth Edition. With 74 Engravings. 8vo, 6s.
Also.
The Suprapubic Operation of Opening the Bladder for the Stone and for Tumours. 8vo, with 14 Engravings, 3s. 6d.
The Surgery of the Rectum. By Henry Smith, Professor of Surgery in King's College, Surgeon to the Hospital. Fifth Edition. 8vo, 6s.
Modern Treatment of Stone in the Bladder by Litholopaxy. By P. J. Freyer, M.A., M.D., M.Ch., Bengal Medical Service. 8vo, with Engravings, 5s.
Diseases of the Testis, Spermatic Cord, and Scrotum. By Thomas B. Curling, F.R.S., Consulting Surgeon to the London Hospital. Fourth Edition. 8vo, with Engravings, 16s.
Diseases of the Rectum and Anus. By W. Harrison Cripps, F.R.C.S., Assistant Surgeon to St. Bartholomew's Hospital, &c. 8vo, with 13 Lithographic Plates and numerous Wood Engravings, 12s. 6d.
Urinary and Renal Derangements and Calculous Disorders. By Lionel S. Beale, F.R.C.P., F.R.S., Physician to King's College Hospital. 8vo, 5s.
Fistula, Hæmorrhoids, Painful Ulcer, Stricture, Prolapsus, and other Diseases of the Rectum: Their Diagnosis and Treatment. By William Allingham, Surgeon to St. Mark's Hospital for Fistula. Fourth Edition. 8vo, with Engravings, 10s. 6d.
Pathology of the Urine. Including a Complete Guide to its Analysis. By J. L. W. Thudichum, M.D., F.R.C.P. Second Edition, rewritten and enlarged. 8vo, with Engravings, 15s.
Student's Primer on the Urine. By J. Travis Whittaker, M.D., Clinical Demonstrator at the Royal Infirmary, Glasgow. With 16 Plates etched on Copper. Post 8vo, 4s. 6d.
Syphilis and Pseudo-Syphilis. By Alfred Cooper, F.R.C.S., Surgeon to the Lock Hospital, to St. Mark's and the West London Hospitals. 8vo, 10s. 6d.
Genito-Urinary Organs, including Syphilis: A Practical Treatise on their Surgical Diseases, for Students and Practitioners. By W. H. Van Buren, M.D., and E. L. Keyes, M.D. Royal 8vo, with 140 Engravings, 21s.
Lectures on Syphilis. By Henry Lee, Consulting Surgeon to St. George's Hospital. 8vo, 10s.
Diagnosis and Treatment of Syphilis. By Tom Robinson, M.D., Physician to St. John's Hospital for Diseases of the Skin. Crown 8vo, 3s. 6d.
Coulson on Diseases of the Bladder and Prostate Gland. Sixth Edition. By Walter J. Coulson, Surgeon to the Lock Hospital and to St. Peter's Hospital for Stone. 8vo, 16s.
The Medical Adviser in Life Assurance. By Sir E. H. Sieveking, M.D., F.R.C.P. Second Edition. Crown 8vo, 6s.
A Medical Vocabulary: An Explanation of all Terms and Phrases used in the various Departments of Medical Science and Practice, their Derivation, Meaning, Application, and Pronunciation. By R. G. Mayne, M.D., LL.D. Fifth Edition. Fcap. 8vo, 10s. 6d.
A Dictionary of Medical Science: Containing a concise Explanation of the various Subjects and Terms of Medicine, &c. By Robley Dunglison, M.D., LL.D. Royal 8vo, 28s.
Medical Education And Practice in all parts of the World. By H. J. Hardwicke, M.D., M.R.C.P. 8vo, 10s.
Abercrombie's Medical Jurisprudence, 4
Adams (W.) on Clubfoot, 11;
on Contraction of the Fingers, 11;
on Curvature of the Spine, 11
Alexander's Displacements of the Uterus, 6
Allan on Fever Nursing, 7;
Outlines of Infectious Diseases, 7
Allingham on Diseases of the Rectum, 14
Anatomical Remembrancer, 3
Balfour's Diseases of the Heart and Aorta, 9
Balkwill's Mechanical Dentistry, 12
Barnes (R.) on Obstetric Operations, 5;
on Diseases of Women, 5
Beale's Microscope in Medicine, 8;
Slight Ailments, 8;
Urinary and Renal Derangements, 14
Bellamy's Surgical Anatomy, 3
Bennet (J. H.) on the Mediterranean, 10;
on Pulmonary Consumption, 10
Bentley and Trimen's Medicinal Plants, 7
Bentley's Manual of Botany, 7;
Structural Botany, 7;
Systematic Botany, 7
Braune's Topographical Anatomy, 3
Brodhurst's Anchylosis, 11;
Curvatures, &c., of the Spine, 11;
Orthopædic Surgery, 11
Bryant's Acute Intestinal Strangulation, 9;
Practice of Surgery, 11
Bucknill and Tuke's Psychological Medicine, 5
Bulkley's Acne, 13;
Diseases of the Skin, 13
Burdett's Cottage Hospitals, 4;
Pay Hospitals, 4
Burton's Midwifery for Midwives, 6
Butlin's Malignant Disease of the Larynx, 13;
Sarcoma and Carcinoma, 13
Buzzard's Diseases of the Nervous System, 9;
Peripheral Neuritis, 9
Carpenter's Human Physiology, 4
Cayley's Typhoid Fever, 8
Charteris on Health Resorts, 10;
Practice of Medicine, 8
Chavers' Diseases of India, 8
Churchill's Face and Foot Deformities, 11
Clouston's Lectures on Mental Diseases, 5
Cobbold on Parasites, 13
Coles' Dental Mechanics, 13
Cooper's Syphilis and Pseudo-Syphilis, 14
Coulson on Diseases of the Bladder, 14
Courty's Diseases of the Uterus, Ovaries, &c., 6
Cripps' Diseases of the Rectum and Anus, 14
Cullingworth's Manual of Nursing, 6;
Short Manual for Monthly Nurses, 6
Curling's Diseases of the Testis, 14
Dalby's Diseases and Injuries of the Ear, 12
Dalton's Human Physiology, 4
Day on Diseases of Children, 6;
on Headaches, 10
Dobell's Lectures on Winter Cough, 8;
Loss of Weight, &c., 8;
Mont Doré Cure, 8
Domville's Manual for Nurses, 6
Draper's Text Book of Medical Physics, 4
Druitt's Surgeon's Vade-Mecum, 11
Duncan on Diseases of Women, 5;
on Sterility in Woman, 5
Dunglison's Medical Dictionary, 14
East's Private Treatment of the Insane, 5
Ebstein on Regimen in Gout, 9
Ellis's Diseases of Children, 6
Emmet's Gynæcology, 6
Fagge's Principles and Practice of Medicine, 8
Fayrer's Climate and Fevers of India, 7
Fenwick's Chronic Atrophy of the Stomach, 8;
Medical Diagnosis, 8;
Outlines of Medical Treatment, 8
Flint on Clinical Medicine, 7;
on Principles and Practice of Medicine, 7
Flower's Diagrams of the Nerves, 4
Fox's (C. B.) Examinations of Water, Air, and Food, 5
Fox's (T.) Atlas of Skin Diseases, 13
Freyer's Litholopaxy, 14
Frey's Histology and Histo-Chemistry, 4
Galabin's Diseases of Women, 6;
Manual of Midwifery, 5
Gamgee's Treatment of Wounds and Fractures, 11
Godlee's Atlas of Human Anatomy, 3
Goodhart's Diseases of Children, 6
Gorgas' Dental Medicine, 13
Gowers' Diseases of the Brain, 9;
Diseases of the Spinal Cord, 9;
Manual of Diseases of Nervous System, 9;
Medical Ophthalmoscopy, 9;
Pseudo-Hypertrophic Muscular Paralysis, 9
Granville on Gout, 9;
on Nerve Vibration and Excitation, 9
Guy's Hospital Formulæ, 2;
Reports, 2
Habershon's Diseases of the Abdomen, 9;
Liver, 9;
Stomach, 9;
Pneumogastric Nerve, 9
Hambleton's What is Consumption?, 8
Hardwicke's Medical Education, 14
Harley on Diseases of the Liver, 9;
Inflammations of the Liver, 9
Harris's Dentistry, 13
Harrison's Surgical Disorders of the Urinary Organs, 13
Hartridge's Refraction of the Eye, 12
Harvey's Manuscript Lectures, 3
Heath's Injuries and Diseases of the Jaws, 10;
Minor Surgery and Bandaging, 10;
Operative Surgery, 10;
Practical Anatomy, 3;
Surgical Diagnosis, 10
Helm on Short and Long Sight, &c., 11
Higgens' Ophthalmic Out-patient Practice, 11
Hills' Leprosy in British Guiana, 13
Holden's Dissections, 3;
Human Osteology, 3;
Landmarks, 3
Holmes' (G.) Guide to Use of Laryngoscope, 12;
Vocal Physiology and Hygiene, 12
Hood's (D. C.) Diseases and their Commencement, 7
Hood (P.) on Gout, Rheumatism, &c., 9
Hooper's Physician's Vade-Mecum, 8
Hutchinson's Clinical Surgery, 11;
Pedigree of Disease, 11;
Rare Diseases of the Skin, 13
Hyde's Diseases of the Skin, 13
James (P.) on Sore Throat, 12
Jessett's Cancer of the Mouth, &c., 13
Jones (C. H.) and Sieveking's Pathological Anatomy, 4
Jones' (H. McN.) Aural Surgery, 12;
Atlas of Diseases of Membrana Tympani, 12;
Spinal Curvatures, 11
Jordan's Surgical Enquiries, 11
Journal of British Dental Association, 2;
Mental Science, 2
King's Manual of Obstetrics, 6
Lancereaux's Atlas of Pathological Anatomy, 4
Lee (H.) on Syphilis, 14
Lewis (Bevan) on the Human Brain, 4
Liebreich's Atlas of Ophthalmoscopy, 12
Liveing's Megrim, Sick Headache, &c., 9
London Hospital Reports, 2
Lückes' Hospital Sisters and their Duties, 7
Lund's Hunterian Lectures, 10
Macdonald's (J. D.) Examination of Water and Air, 4
Mackenzie on Diphtheria, 12;
on Diseases of the Throat and Nose, 12
McLeod's Operative Surgery, 10
MacMunn's Spectroscope in Medicine, 8
Macnamara's Diseases of the Eye, 11;
Bones and Joints, 11
Marcet's Southern and Swiss Health-Resorts, 10
Martin's Ambulance Lectures, 10
Mason on Hare-Lip and Cleft Palate, 12;
on Surgery of the Face, 12
Mayne's Medical Vocabulary, 14
Middlesex Hospital Reports, 2
Mitchell's Diseases of the Nervous System, 9
Moore's Family Medicine for India, 7;
Health-Resorts for Tropical Invalids, 7;
Manual of the Diseases of India, 7
Morris' (H.) Anatomy of the Joints, 3
Mouat and Snell on Hospitals, 5
Nettleship's Diseases of the Eye, 12
Nunn's Cancer of the Breast, 13
Ogston's Medical Jurisprudence, 4
Ophthalmic (Royal London) Hospital Reports, 2
Ophthalmological Society's Transactions, 2
Oppert's Hospitals, Infirmaries, Dispensaries, &c., 5
Osborn on Diseases of the Testis, 13;
on Hydrocele, 13
Owen's Materia Medica, 7
Page's Injuries of the Spine, 11
Parkes' Practical Hygiene, 5
Pavy on Diabetes, 10
Pavy on Food and Dietetics, 10
Pharmaceutical Journal, 2
Pharmacopœia of the London Hospital, 7
Phillips' Materia Medica and Therapeutics, 7
Pollock's Histology of the Eye and Eyelids, 12
Porritt's Intra-Thoracic Effusion, 8
Purcell on Cancer, 13
Pye-Smith's Syllabus of Physiology, 4
Quinby's Notes on Dental Practice, 12
Raye's Ambulance Handbook, 10
Reynolds' (J. J.) Diseases of Women, 5;
Notes on Midwifery, 5
Richardson's Mechanical Dentistry, 13
Roberts' (C.) Manual of Anthropometry, 5;
Detection of Colour-Blindness, 5
Roberts' (D. Lloyd) Practice of Midwifery, 5
Robinson (Tom) on Syphilis, 14
Robinson (W.) on Endemic Goitre or Thyreocele, 12
Ross's Aphasia, 9;
Diseases of the Nervous System, 9;
Handbook of ditto, 9
Routh's Infant Feeding, 7
Royal College of Surgeons Museum Catalogues, 2
Royle and Harley's Materia Medica, 7
St. Bartholomew's Hospital Catalogue, 2
St. George's Hospital Reports, 2
St. Thomas's Hospital Reports, 2
Sansom's Valvular Disease of the Heart, 8
Savage on the Female Pelvic Organs, 6
Sewill's Dental Anatomy, 12
Sharkey's Spasm in Chronic Nerve Disease, 9
Shore's Elementary Practical Biology, 4
Sieveking's Life Assurance, 14
Smith's (E.) Clinical Studies, 6;
Diseases in Children, 6;
Wasting Diseases of Infants and Children, 6
Smith's (Henry) Surgery of the Rectum, 14
Smith's (Heywood) Dysmenorrhœa, 6
Smith (Priestley) on Glaucoma, 12
Snell's Electro-Magnet in Ophthalmic Surgery, 12
Snow's Clinical Notes on Cancer, 13
Southam's Regional Surgery, 11
Sparks on the Riviera, 10
Squire's Companion to the Pharmacopœia, 7;
Pharmacopœias of London Hospitals
Starkweather on the Law of Sex, 4
Steavenson's Electricity, 11
Stillé and Maisch's National Dispensatory, 7
Stocken's Dental Materia Medica and Therapeutics, 13
Sutton's General Pathology, 4
Swain's Surgical Emergencies, 10
Swayne's Obstetric Aphorisms, 6
Taylor's Medical Jurisprudence, 4
Taylor's Poisons in relation to Medical Jurisprudence, 4
Teale's Dangers to Health, 5
Thin's Cancerous Affections of the Skin, 13
Thomas's Diseases of Women, 6
Thompson's (Sir H.) Calculous Disease, 14;
Diseases of the Prostate, 14;
Diseases of the Urinary Organs, 14;
Lithotomy and Lithotrity, 14;
Stricture of the Urethra, 14;
Suprapubic Operation, 14;
Surgery of the Urinary Organs, 14;
Tumours of the Bladder, 14
Thorowgood on Asthma, 8;
on Materia Medica and Therapeutics, 7
Thudichum's Pathology of the Urine, 14
Tibbits' Medical and Surgical Electricity, 10;
Map of Motor Points, 10;
How to use a Galvanic Battery, 10;
Electrical and Anatomical Demonstrations, 10
Tilt's Change of Life, 6;
Uterine Therapeutics, 6
Tirard's Prescriber's Pharmacopœia, 7
Tomes' (C. S.) Dental Anatomy, 12
Tomes' (J. and C. S.) Dental Surgery, 12
Tuke's Influence of the Mind upon the Body, 5;
Sleep-Walking and Hypnotism, 5
Van Buren on the Genito-Urinary Organs, 14
Vintras on the Mineral Waters, &c., of France, 10
Virchow's Post-mortem Examinations, 4
Wagstaffe's Human Osteology, 3
Waring's Indian Bazaar Medicines, 8;
Practical Therapeutics, 8
Warlomont's Animal Vaccination, 13
Warner's Guide to Medical Case-Taking, 8
Waters' (A. T. H.) Diseases of the Chest, 8
Weaver's Pulmonary Consumption, 8
Wells' (Spencer) Abdominal Tumours, 6;
Ovarian and Uterine Tumours, 6
West and Duncan's Diseases of Women, 6
West's (S.) How to Examine the Chest, 8
Whistler's Syphilis of the Larynx, 12
Whittaker's Primer on the Urine, 14
Wilks' Diseases of the Nervous System, 8
Williams' (Roger) Influence of Sex, 4
Wilson's (Sir E.) Anatomists' Vade-Mecum, 3
Wilson's (G.) Handbook of Hygiene, 5;
Healthy Life and Dwellings, 5
Wilson's (W. S.) Ocean as a Health-Resort, 10
Wolfe's Diseases and Injuries of the Eye, 11
Year Book of Pharmacy, 2
Yeo's (G. F.) Manual of Physiology, 4
Yeo's (J. B.) Contagiousness of Pulmonary Consumption, 8
The following Catalogues issued by J. & A. Churchill will be forwarded post free on application:—
A. J. & A. Churchill's General List of about 650 works on Anatomy, Physiology, Hygiene, Midwifery, Materia Medica, Medicine, Surgery, Chemistry, Botany, &c., &c., with a complete Index to their Subjects, for easy reference. N.B.—This List includes B, C, & D.
B. Selection from J. & A. Churchill's General List, comprising all recent Works published by them on the Art and Science of Medicine.
C. J. & A. Churchill's Catalogue of Text Books specially arranged for Students.
D. A selected and descriptive List of J. & A. Churchill's Works on Chemistry, Materia Medica, Pharmacy, Botany, Photography, Zoology, the Microscope, and other branches of Science.
E. The Half-yearly List of New Works and New Editions published by J. & A. Churchill during the previous six months, together with particulars of the Periodicals issued from their House.
[Sent in January and July of each year to every Medical Practitioner in the United Kingdom whose name and address can be ascertained. A large number are also sent to the United States of America, Continental Europe, India, and the Colonies.]
America.—J. & A. Churchill being in constant communication with various publishing houses in Boston, New York, and Philadelphia, are able, notwithstanding the absence of international copyright, to conduct negotiations favourable to English Authors.
LONDON: 11, NEW BURLINGTON STREET.
Pardon & Sons, Printers,] [Wine Office Court, Fleet Street, E.C.
End of the Project Gutenberg EBook of Schweigger on Squint, by C. Schweigger
*** END OF THIS PROJECT GUTENBERG EBOOK SCHWEIGGER ON SQUINT ***
***** This file should be named 35639-h.htm or 35639-h.zip *****
This and all associated files of various formats will be found in:
https://www.gutenberg.org/3/5/6/3/35639/
Produced by Ian Deane, Josephine Paolucci and the Online
Distributed Proofreading Team at https://www.pgdp.net.
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License (available with this file or online at
https://gutenberg.org/license).
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS' WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTIBILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation web page at https://www.pglaf.org.
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Its 501(c)(3) letter is posted at
https://pglaf.org/fundraising. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at
809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887, email
business@pglaf.org. Email contact links and up to date contact
information can be found at the Foundation's web site and official
page at https://pglaf.org
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit https://pglaf.org
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including including checks, online payments and credit card
donations. To donate, please visit: https://pglaf.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart was the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For thirty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
https://www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.