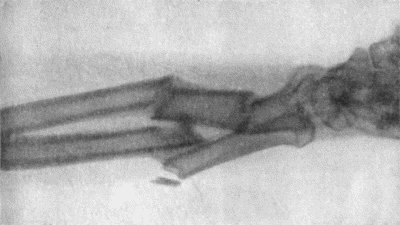
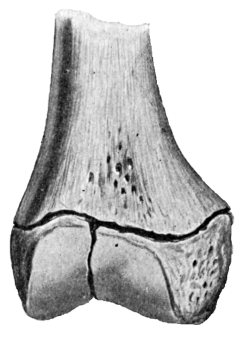
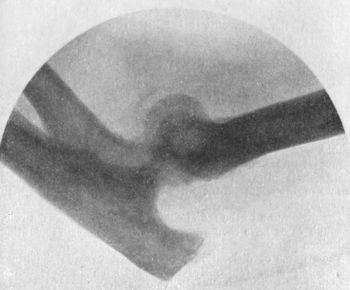
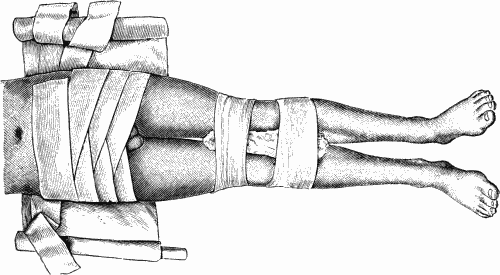
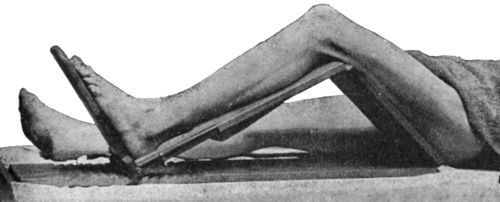
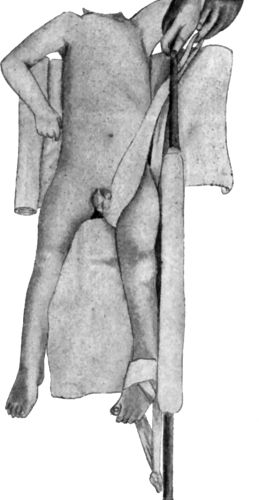
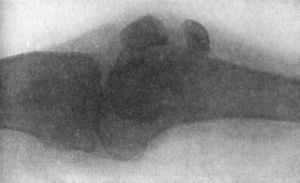
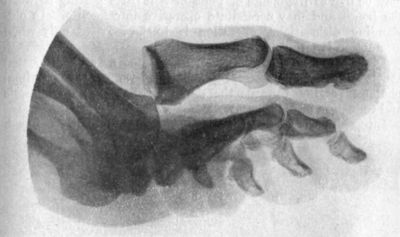
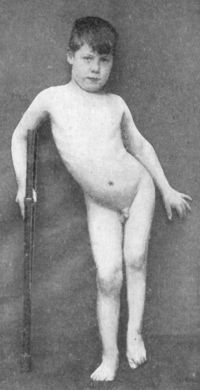
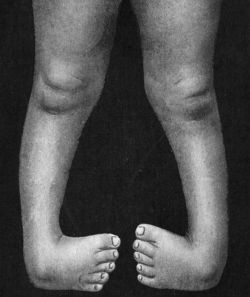
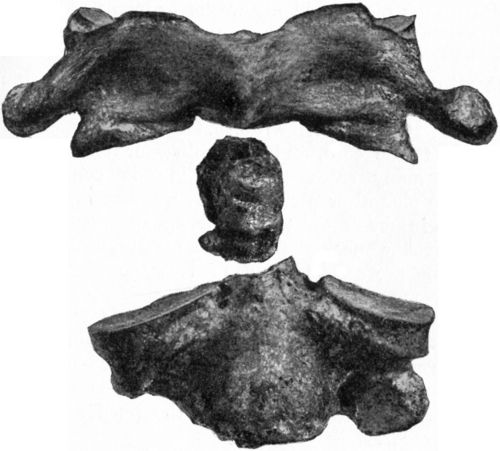
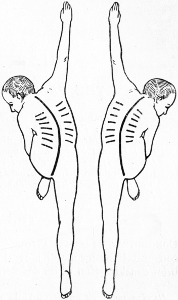
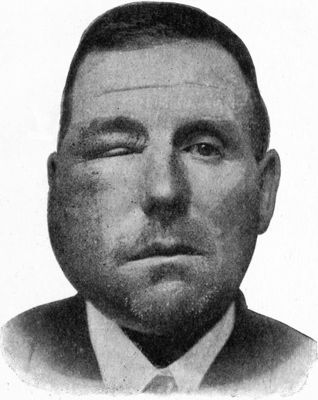
Fig. 1.—Multiple Fracture of both Bones of Leg.
Fig. 1.—Multiple Fracture of both Bones of Leg.
The Project Gutenberg EBook of Manual of Surgery Volume Second:
Extremities--Head--Neck. Sixth Edition., by Alexander Miles and Alexis Thomson
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
Title: Manual of Surgery Volume Second: Extremities--Head--Neck. Sixth Edition.
Author: Alexander Miles
Alexis Thomson
Release Date: March 29, 2009 [EBook #28428]
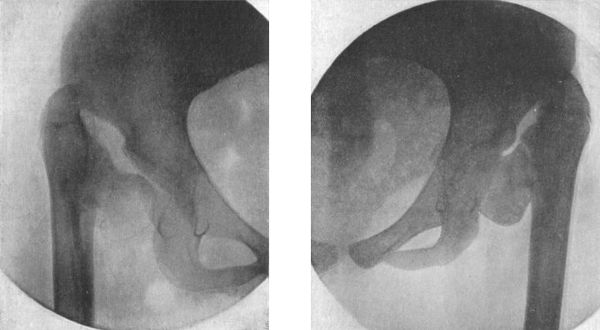
Language: English
Character set encoding: ISO-8859-1
*** START OF THIS PROJECT GUTENBERG EBOOK MANUAL OF SURGERY ***
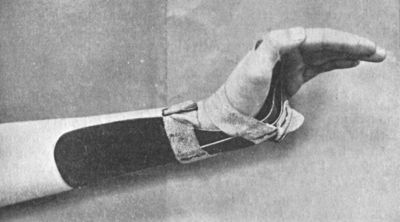
Produced by Jonathan Ingram, Chris Logan and the Online
Distributed Proofreading Team at http://www.pgdp.net
Transcriber's note: The inverted 'Y' symbol used in this book has been transcribed as [inverted Y].
VOLUME SECOND
EXTREMITIES—HEAD—NECK
SIXTH EDITION REVISED AND ENLARGED
WITH 288 ILLUSTRATIONS
LONDON
HENRY FROWDE and HODDER & STOUGHTON
THE LANCET BUILDING
1 & 2 BEDFORD STREET, STRAND, W.C. 2
| First Edition | 1904 |
| Second Edition | 1907 |
| Third Edition | 1909 |
| Fourth Edition | 1912 |
| ""Second Impression | 1913 |
| Fifth Edition | 1915 |
| ""Second Impression | 1919 |
| Sixth Edition | 1921 |
Printed in Great Britain by
Morrison and Gibb Ltd., Edinburgh
| page | |
|---|---|
| CHAPTER I | |
| Injuries of Bones | 1 |
| CHAPTER II | |
| Injuries of Joints | 32 |
| CHAPTER III | |
| Injuries in the Region of the Shoulder and Upper Arm | 44 |
| CHAPTER IV | |
| Injuries in the Region of the Elbow and Forearm | 79 |
| CHAPTER V | |
| Injuries in the Region of the Wrist and Hand | 102 |
| CHAPTER VI | |
| Injuries in the Region of the Pelvis, Hip-Joint, and Thigh | 122 |
| CHAPTER VII | |
| Injuries in the Region of the Knee and Leg | 155 |
| CHAPTER VIII | |
| Injuries in Region of Ankle and Foot | 185 |
| CHAPTER IX | |
| Diseases of Individual Joints | 201 |
| CHAPTER X | |
| Deformities of the Extremities | 241 |
| CHAPTER XI | |
| The Scalp | 319 |
| CHAPTER XII | |
| The Cranium and its Contents | 328 |
| CHAPTER XIII | |
| Injuries of the Skull | 361 |
| CHAPTER XIV | |
| Diseases of the Brain and Membranes | 373 |
| CHAPTER XV | |
| Diseases of the Cranial Bones | 406 |
| CHAPTER XVI | |
| The Vertebral Column and Spinal Cord | 411 |
| CHAPTER XVII | |
| Diseases of the Vertebral Column and Spinal Cord | 431 |
| CHAPTER XVIII | |
| Deviations of the Vertebral Column | 461 |
| CHAPTER XIX | |
| The Face, Orbit, and Lips | 474 |
| CHAPTER XX | |
| The Mouth, Fauces, and Pharynx | 496 |
| CHAPTER XXI | |
| The Jaws, including the Teeth and Gums | 507 |
| CHAPTER XXII | |
| The Tongue | 528 |
| CHAPTER XXIII | |
| The Salivary Glands | 543 |
| CHAPTER XXIV | |
| The Ear | 553 |
| CHAPTER XXV | |
| The Nose and Naso-Pharynx | 567 |
| CHAPTER XXVI | |
| The Neck | 582 |
| CHAPTER XXVII | |
| The Thyreoid Gland | 604 |
| CHAPTER XXVIII | |
| The Œsophagus | 616 |
| CHAPTER XXIX | |
| The Larynx, Trachea, and Bronchi | 634 |
| INDEX | 645 |
| fig. | page | |
|---|---|---|
| 1. | Multiple Fracture of both Bones of Leg | 4 |
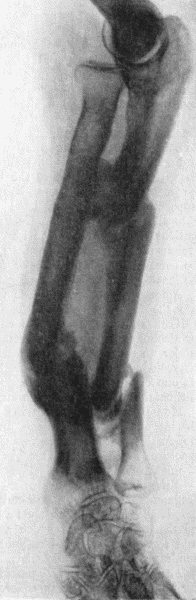
| 2. | Radiogram showing Comminuted Fracture of both Bones of Forearm | 5 |
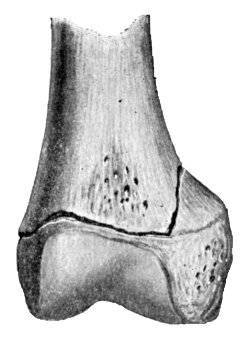
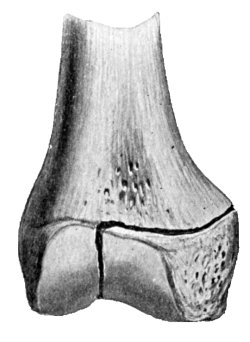
| 3. | Oblique Fracture of Tibia; with partial Separation of Epiphysis of Upper End of Fibula; and Incomplete Fracture of Fibula in Upper Third | 6 |
| 4. | Excess of Callus after Compound Fracture of Bones of Forearm | 9 |
| 5. | Multiple Fractures of both Bones of Forearm showing Mal-union | 11 |
| 6. | Radiogram of Un-united Fracture of Shaft of Ulna | 13 |
| 7. | Excessive Callus Formation after Infected Compound Fracture of both Bones of Forearm | 27 |
| 8. | Partial Separation of Epiphysis, with Fracture running into Diaphysis | 29 |
| 9. | Complete Separation of Epiphysis | 29 |
| 10. | Partial Separation with Fracture of Epiphysis | 29 |
| 11. | Complete Separation with Fracture of Epiphysis | 29 |
| 12. | Os Innominatum showing new Socket formed after Old-standing Dislocation | 41 |
| 13. | Oblique Fracture of Right Clavicle in Middle Third, united | 45 |
| 14. | Fracture of Acromial End of Clavicle | 46 |
| 15. | Adhesive Plaster applied for Fracture of Clavicle | 49 |
| 16. | Forward Dislocation of Sternal End of Right Clavicle | 51 |
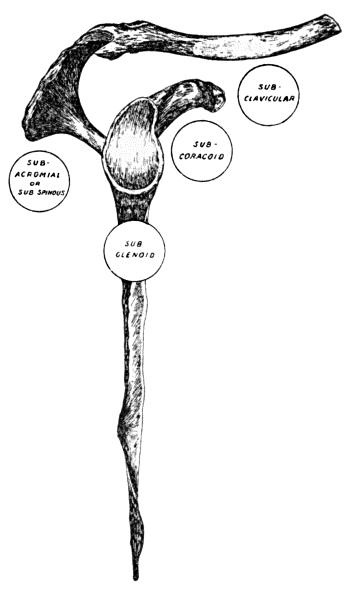
| 17. | Diagram of most common varieties of Dislocation of the Shoulder | 53 |
| 18. | Sub-coracoid Dislocation of Right Shoulder | 55 |
| 19. | Sub-coracoid Dislocation of Humerus | 56 |
| 20. | Kocher's Method of reducing Sub-coracoid Dislocation—First Movement | 57 |
| 21. | Kocher's Method—Second Movement | 58 |
| 22. | Kocher's Method—Third Movement | 59 |
| 23. | Miller's Method of reducing Sub-coracoid Dislocation—First Movement | 60 |
| 24. | Miller's Method—Second Movement | 61 |
| 25. | Dislocation of Shoulder with Fracture of Neck of Humerus | 64 |
| 26. | Transverse Fracture of Scapula | 68 |
| 27. | Fracture of Surgical Neck of Humerus, united with Angular Displacement | 70 |
| 28. | Impacted Fracture of Neck of Humerus | 71 |
| 29. | Ambulatory Abduction Splint for Fracture of Humerus | 72 |
| 30. | Radiogram of Separation of Upper Epiphysis of Humerus | 73 |
| 31. | “Cock-up” Splint | 77 |
| 32. | Gooch Splints for Fracture of Shaft of Humerus; and Rectangular Splint to secure Elbow | 77 |
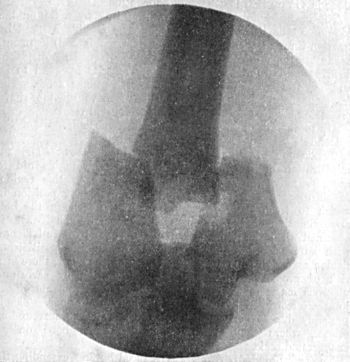
| 33. | Radiogram of Supra-condylar Fracture of Humerus in a Child | 81 |
| 34. | Radiogram of T-shaped Fracture of Lower End of Humerus | 83 |
| 35. | Radiogram of Fracture of Olecranon Process | 86 |
| 36. | Backward Dislocation of Elbow in a Boy | 89 |
| 37. | Bony Outgrowth in relation to insertion of Brachialis Muscle | 90 |
| 38. | Radiogram of Incomplete Backward Dislocation of Elbow | 91 |
| 39. | Forward Dislocation of Elbow, with Fracture of Olecranon | 93 |
| 40. | Radiogram of Forward Dislocation of Head of Radius, with Fracture of Shaft of Ulna | 95 |
| 41. | Greenstick Fracture of both Bones of the Forearm | 98 |
| 42. | Gooch Splints for Fracture of both Bones of Forearm | 99 |
| 43. | Colles' Fracture showing Radial Deviation of Hand | 103 |
| 44. | Colles' Fracture showing undue prominence of Ulnar Styloid | 103 |
| 45. | Radiogram showing the Line of Fracture and Upward Displacement of the Radial Styloid in Colles' Fracture | 104 |
| 46. | Radiogram of Chauffeur's Fracture | 107 |
| 47. | Radiogram of Smith's Fracture | 108 |
| 48. | Manus Valga following Separation of Lower Radial Epiphysis in Childhood | 109 |
| 49. | Radiogram showing Fracture of Navicular (Scaphoid) Bone | 111 |
| 50. | Dorsal Dislocation of Wrist at Radio-carpal Articulation | 113 |
| 51. | Radiogram showing Forward Dislocation of Navicular Bone | 114 |
| 52. | Extension Apparatus for Oblique Fracture of Metacarpals | 117 |
| 53. | Radiogram of Bennett's Fracture of Base of Metacarpal of Right Thumb | 118 |
| 54. | Splints for Bennett's Fracture | 119 |
| 55. | Multiple Fracture of Pelvis through Horizontal and Descending Rami of both Pubes, and Longitudinal Fracture of left side of Sacrum | 123 |
| 56. | Fracture of Left Iliac Bone; and of both Pubic Arches | 124 |
| 57. | Many-tailed Bandage and Binder for Fracture of Pelvic Girdle | 125 |
| 58. | Nélaton's Line | 128 |
| 59. | Bryant's Line | 129 |
| 60. | Section through Hip-Joint to show Epiphyses at Upper End of Femur, and their relation to the Joint | 130 |
| 61. | Fracture through Narrow Part of Neck of Femur on Section | 131 |
| 62. | Impacted Fracture through Narrow Part of Neck of Femur | 132 |
| 63. | Fracture of Neck of Right Femur, showing Shortening, Abduction, and Eversion of Limb | 133 |
| 64. | Fracture of Narrow Part of Neck of Femur | 134 |
| 65. | Coxa Vara following Fracture of Neck of Femur in a Child | 136 |
| 66. | Non-impacted Fracture through Base of Neck | 137 |
| 67. | Fracture through Base of Neck of Femur with Impaction into the Trochanters | 137 |
| 68. | Non-impacted Fracture through Base of Neck | 138 |
| 69. | Fracture of the Femur just below the small Trochanter, united, showing Flexion and Lateral Rotation of Upper Fragment | 140 |
| 70. | Adjustable Double-inclined Plane | 141 |
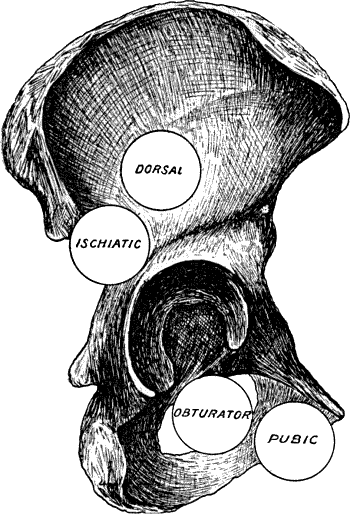
| 71. | Diagram of the most Common Dislocations of the Hip | 142 |
| 72. | Dislocation of Right Femur on to Dorsum Ilii | 143 |
| 73. | Dislocation on to Dorsum Ilii | 144 |
| 74. | Dislocation into the Vicinity of the Ischiatic Notch | 145 |
| 75. | Longitudinal Section of Femur showing Fracture of Shaft with Overriding of Fragments | 148 |
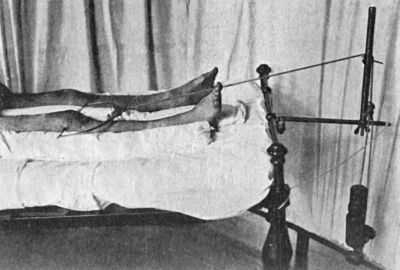
| 76. | Radiogram of Steinmann's Apparatus applied for Direct Extension to the Femur | 150 |
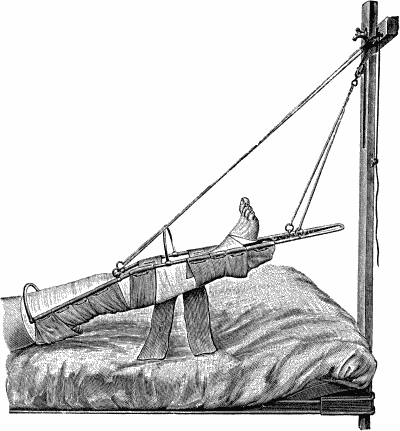
| 77. | Hodgen's Splint | 151 |
| 78. | Long Splint with Perineal Band | 152 |
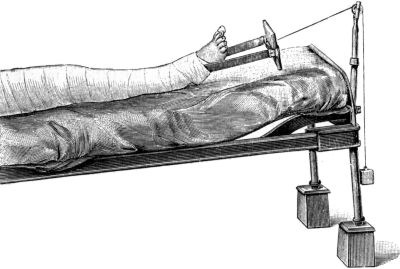
| 79. | Fracture of Thigh treated by Vertical Extension | 153 |
| 80. | Section of Knee-joint showing Extent of Synovial Cavity | 156 |
| 81. | Extension applied by means of Ice-tong Callipers for Fracture of Femur | 158 |
| 82. | Radiogram of Separation of Lower Epiphysis of Femur, with Backward Displacement of the Diaphysis | 160 |
| 83. | Separation of Lower Epiphysis of Femur, with Fracture of Lower End of Diaphysis | 161 |
| 84. | Radiogram of Fracture of Head of Tibia and upper Third of Fibula | 163 |
| 85. | Radiogram illustrating Schlatter's Disease | 164 |
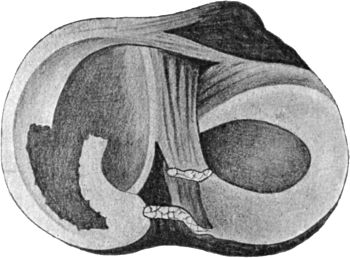
| 86. | Diagram of Longitudinal Tear of Posterior End of Right Medial Semilunar Meniscus | 171 |
| 87. | Radiogram of Fracture of Patella | 173 |
| 88. | Fracture of Patella, showing wide Separation of Fragments | 175 |
| 89. | Radiogram of Transverse Fracture of both Bones of Leg by Direct Violence | 178 |
| 90. | Radiogram of Oblique Fracture of both Bones of Leg by Indirect Violence | 178 |
| 91. | Box Splint for Fractures of Leg | 180 |
| 92. | Box Splint applied | 181 |
| 93. | Section through Ankle-joint showing relation of Epiphyses to Synovial Cavity | 186 |
| 94. | Radiogram of Pott's Fracture, with Lateral Displacement of Foot | 187 |
| 95. | Ambulant Splint of Plaster of Paris | 189 |
| 96. | Dupuytren's Splint applied to Correct Eversion of Foot | 190 |
| 97. | Syme's Horse-shoe Splint applied to Correct Backward Displacement of Foot | 191 |
| 98. | Radiogram of Fracture of Lower End of Fibula, with Separation of Lower Epiphysis of Tibia | 192 |
| 99. | Radiogram of Backward Dislocation of Ankle | 195 |
| 100. | Compound Dislocation of Talus | 197 |
| 101. | Radiogram of Fracture-Dislocation of Talus | 198 |
| 102. | Radiogram of Dislocation of Toes | 199 |
| 103. | Arthropathy of Shoulder in Syringomyelia | 203 |
| 104. | Radiogram of Specimen of Arthropathy of Shoulder in Syringomyelia | 204 |
| 105. | Radiogram showing Multiple partially Ossified Cartilaginous Loose Bodies in Shoulder-joint | 205 |
| 106. | Diffuse Tuberculous Thickening of Synovial Membrane of Elbow | 206 |
| 107. | Contracture of Elbow and Wrist following a Burn in Childhood | 207 |
| 108. | Advanced Tuberculous Disease of Acetabulum with Caries and Perforation into Pelvis | 210 |
| 109. | Early Tuberculous Disease of Right Hip-joint in a Boy | 212 |
| 110. | Disease of Left Hip; showing Moderate Flexion and Lordosis | 213 |
| 111. | Disease of Left Hip; Disappearance of Lordosis on further Flexion of the Hip | 213 |
| 112. | Disease of Left Hip; Exaggeration of Lordosis | 214 |
| 113. | Thomas' Flexion Test, showing Angle of Flexion at Diseased Hip | 214 |
| 114. | Tuberculous Disease of Left Hip: Third Stage | 215 |
| 115. | Advanced Tuberculous Disease of Left Hip-joint in a Girl | 216 |
| 116. | Extension by Adhesive Plaster and Weight and Pulley | 220 |
| 117. | Stiles' Double Long Splint to admit of Abduction of Diseased Limb | 221 |
| 118. | Thomas' Hip-splint applied for Disease of Right Hip | 222 |
| 119. | Arthritis Deformans, showing erosion of Cartilage and lipping of Articular Edge of Head of Femur | 225 |
| 120. | Upper End of Femur in advanced Arthritis Deformans of Hip | 226 |
| 121. | Femur in advanced Arthritis Deformans of Hip and Knee Joints | 227 |
| 122. | Tuberculous Synovial Membrane of Knee | 230 |
| 123. | Lower End of Femur from an Advanced Case of Tuberculous Arthritis of the Knee | 231 |
| 124. | Advanced Tuberculous Disease of Knee, with Backward Displacement of Tibia | 233 |
| 125. | Thomas' Knee-splint applied | 236 |
| 126. | Tuberculous Disease of Right Ankle | 239 |
| 127. | Female Child showing the results of Poliomyelitis affecting the Left Lower Extremity | 243 |
| 128. | Radiogram of Double Congenital Dislocation of Hip in a Girl | 249 |
| 129. | Innominate Bone and Upper End of Femur from a case of Congenital Dislocation of Hip | 250 |
| 130. | Congenital Dislocation of Left Hip in a Girl | 251 |
| 131. | Contracture Deformities of Upper and Lower Limbs resulting from Spastic Cerebral Palsy in Infancy | 255 |
| 132. | Rachitic Coxa Vara | 258 |
| 133. | Coxa Vara, showing Adduction Curvature of Neck of Femur associated with Arthritis of the Hip and Knee | 260 |
| 134. | Bilateral Coxa Vara, showing Scissors-leg Deformity | 260 |
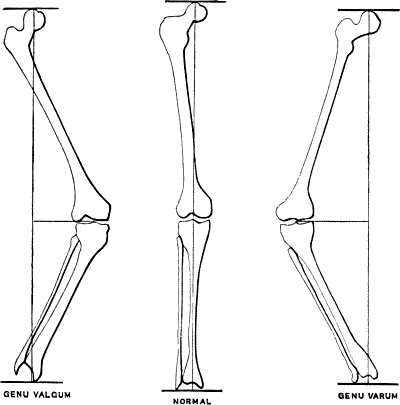
| 135. | Genu Valgum and Genu Varum | 265 |
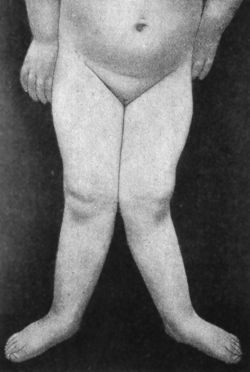
| 136. | Female Child with Right-sided Genu Valgum, the result of Rickets | 266 |
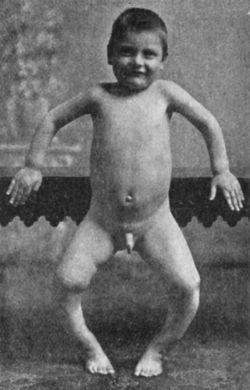
| 137. | Double Genu Valgum; and Rickety Deformities of Arms | 267 |
| 138. | Radiogram of Case of Double Genu Valgum in a Child | 268 |
| 139. | Genu Valgum in a Child. Patient standing | 269 |
| 140. | Genu Valgum. Same Patient as Fig. 139, sitting | 270 |
| 141. | Bow-knee in Rickety Child | 271 |
| 142. | Bilateral Congenital Club-foot in an Infant | 274 |
| 143. | Radiogram of Bilateral Congenital Club-foot in an Infant | 275 |
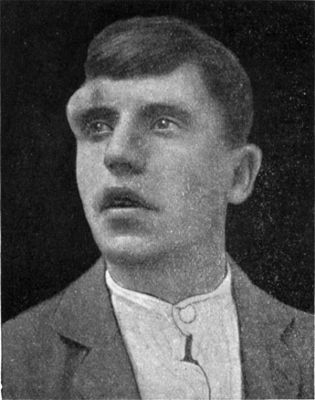
| 144. | Congenital Talipes Equino-varus in a Man | 277 |
| 145. | Bilateral Pes Equinus in a Boy | 280 |
| 146. | Extreme form of Pes Equinus in a Girl | 281 |
| 147. | Skeleton of Foot from case of Pes Equinus due to Poliomyelitis | 282 |
| 148. | Pes Calcaneo-valgus with excessive arching of Foot | 284 |
| 149. | Pes Calcaneo-valgus, the result of Poliomyelitis | 285 |
| 150. | Pes Cavus in Association with Pes Equinus, the Result of Poliomyelitis | 286 |
| 151. | Radiogram of Foot of Adult, showing Changes in the Bones in Pes Cavus | 286 |
| 152. | Adolescent Flat-Foot | 287 |
| 153. | Flat-Foot, showing Loss of Arch | 288 |
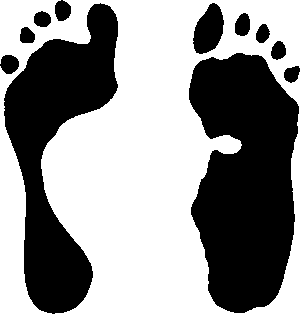
| 154. | Imprint of Normal and of Flat Foot | 290 |
| 155. | Bilateral Pes Valgus and Hallux Valgus in a Girl | 293 |
| 156. | Radiogram of Spur on Under Aspect of Calcaneus | 295 |
| 157. | Radiogram of Hallux Valgus | 296 |
| 158. | Radiogram of Hallux Varus or Pigeon-Toe | 298 |
| 159. | Hallux Rigidus and Flexus in a Boy | 299 |
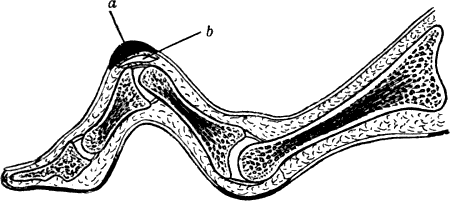
| 160. | Hammer-Toe | 300 |
| 161. | Section of Hammer-Toe | 301 |
| 162. | Congenital Hypertrophy of Left Lower Extremity in a Boy | 302 |
| 163. | Supernumerary Great Toe | 303 |
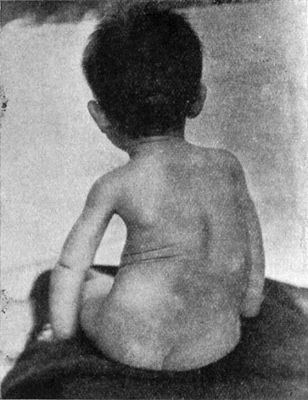
| 164. | Congenital Elevation of Left Scapula in a Girl: also shows Hairy Mole over Sacrum | 304 |
| 165. | Winged Scapula | 305 |
| 166. | Arrested Growth and Wasting of Tissues of Right Upper Extremity | 307 |
| 167. | Lower End of Humerus from case of Cubitus Varus | 309 |
| 168. | Intra-Uterine Amputation of Forearm | 310 |
| 169. | Radiogram of Arm of Patient shown in Fig. 168 | 310 |
| 170. | Congenital Absence of Left Radius and Tibia in a Child | 311 |
| 171. | Club-Hand, the Result of Imperfect Development of Radius | 312 |
| 172. | Congenital Contraction of Ring and Little Fingers | 314 |
| 173. | Dupuytren's Contraction | 315 |
| 174. | Splint used after Operation for Dupuytren's Contraction | 316 |
| 175. | Supernumerary Thumb | 317 |
| 176. | Trigger Finger | 318 |
| 177. | Multiple Wens | 324 |
| 178. | Adenoma of Scalp | 325 |
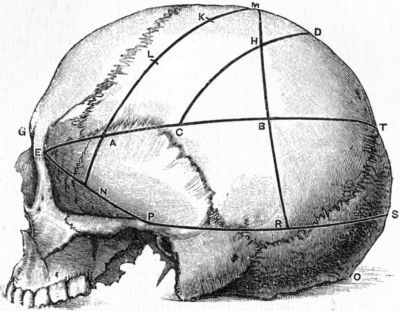
| 179. | Relations of the Motor and Sensory Areas to the Convolutions and to Chiene's Lines | 330 |
| 180. | Diagram of the Course of Motor and Sensory Nerve Fibres | 333 |
| 181. | Chiene's Method of Cerebral Localisation | 336 |
| 182. | To illustrate the Site of Various Operations on the Skull | 337 |
| 183. | Localisation of Site for Introduction of Needle in Lumbar Puncture | 338 |
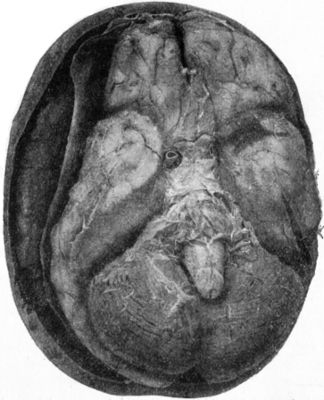
| 184. | Contusion and Laceration of Brain | 343 |
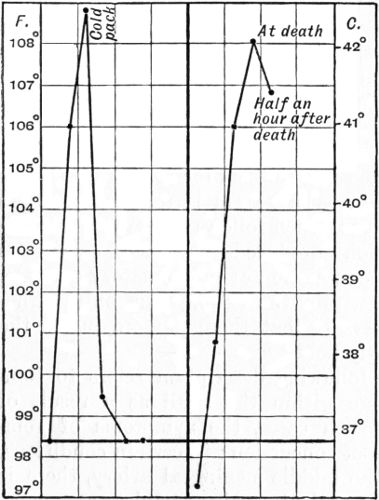
| 185. | Charts of Pyrexia in Head Injuries | 348 |
| 186. | Relations of the Middle Meningeal Artery and Lateral Sinus to the Surface as indicated by Chiene's Lines | 353 |
| 187. | Extra-Dural Clot resulting from Hæmorrhage from the Middle Meningeal Artery | 354 |
| 188. | Depressed Fracture of Frontal Bones with Fissured Fracture | 365 |
| 189. | Depressed and Comminuted Fracture of Right Parietal Bone: Pond Fracture | 365 |
| 190. | Pond Fracture of Left Frontal Bone, produced during Delivery | 366 |
| 191. | Transverse Fracture through Middle Fossa of Base of Skull | 368 |
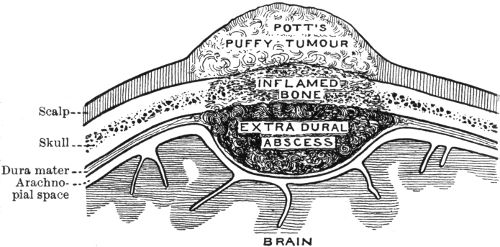
| 192. | Diagram of Extra-Dural Abscess | 374 |
| 193. | Pott's Puffy Tumour in case of Extra-Dural Abscess following Compound Fracture of Orbital Margin | 375 |
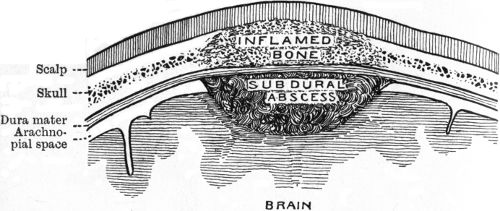
| 194. | Diagram of Sub-Dural Abscess | 376 |
| 195. | Diagram illustrating sequence of Paralysis, caused by Abscess in Temporal Lobe | 380 |
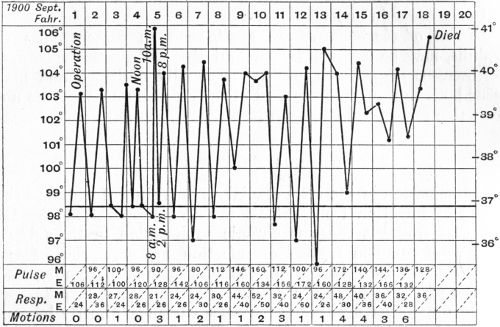
| 196. | Chart of case of Sinus Phlebitis following Middle Ear Disease | 384 |
| 197. | Occipital Meningocele | 388 |
| 198. | Frontal Hydrencephalocele | 389 |
| 199. | Nævus at Root of Nose, simulating Cephalocele | 390 |
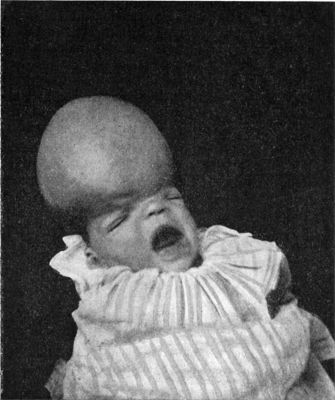
| 200. | Hydrocephalus in a Child | 391 |
| 201. | Patient suffering from Left Facial Paralysis | 402 |
| 202. | Skull of Woman illustrating the appearances of Tertiary Syphilis of Frontal Bone—Corona Veneris—in the Healed Condition | 408 |
| 203. | Sarcoma of Orbital Plate of Frontal Bone in a Child at Age of 11 months and 18 months | 409 |
| 204. | Destruction of Bones of Left Orbit, caused by Rodent Cancer | 410 |
| 205. | Distribution of the Segments of the Spinal Cord | 417 |
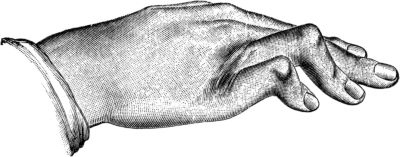
| 206. | Attitude of Upper Extremities in Traumatic Lesions of the Sixth Cervical Segment | 418 |
| 207. | Compression Fracture of Bodies of Third and Fourth Lumbar Vertebræ | 426 |
| 208. | Fracture-Dislocation of Ninth Thoracic Vertebra | 428 |
| 209. | Fracture of Odontoid Process of Axis Vertebra | 429 |
| 210. | Tuberculous Osteomyelitis affecting several Vertebræ at Thoracico-Lumbar Junction | 432 |
| 211. | Osseous Ankylosis of Bodies (a) of Dorsal Vertebræ, (b) of Lumbar Vertebræ following Pott's Disease | 434 |
| 212. | Radiogram of Museum Specimen of Pott's Disease in a Child | 435 |
| 213. | Radiogram of Child's Thorax showing Spindle-shaped Shadow at Site of Pott's Disease of Fourth, Fifth, and Sixth Thoracic Vertebræ | 437 |
| 214. | Attitude of Patient suffering from Tuberculous Disease of the Cervical Spine | 441 |
| 215. | Thomas' Double Splint for Tuberculous Disease of the Spine | 442 |
| 216. | Hunch-back Deformity following Pott's Disease of Thoracic Vertebræ | 443 |
| 217. | Attitude in Pott's Disease of Thoracico-Lumbar Region of Spine | 444 |
| 218. | Arthritis Deformans of Spine | 449 |
| 219. | Meningo-Myelocele of Thoracico-Lumbar Region | 454 |
| 220. | Meningo-Myelocele of Cervical Spine | 454 |
| 221. | Meningo-Myelocele in Thoracic Region | 456 |
| 222. | Tail-like Appendage over Spina Bifida Occulta in a Boy | 457 |
| 223. | Congenital Sacro-Coccygeal Tumour | 458 |
| 224. | Scoliosis following upon Poliomyelitis affecting Right Arm and Leg | 463 |
| 225. | Rickety Scoliosis in a Child | 464 |
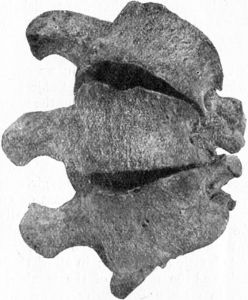
| 226. | Vertebræ from case of Scoliosis showing Alteration in Shape of Bones | 466 |
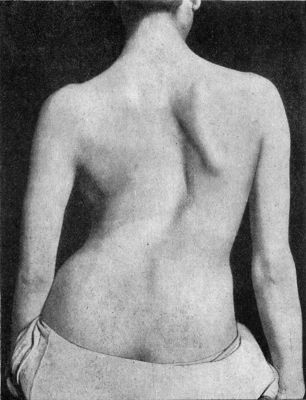
| 227. | Adolescent Scoliosis in a Girl | 467 |
| 228. | Scoliosis with Primary Curve in Thoracic Region | 468 |
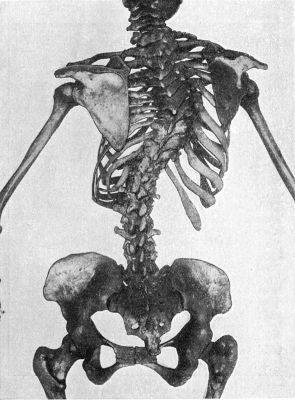
| 229. | Scoliosis showing Rotation of Bodies of Vertebræ, and widening of Intercostal Spaces on side of Convexity | 469 |
| 230. | Diagram of Attitudes in Klapp's Four-Footed Exercises for Scoliosis | 473 |
| 231. | Head of Human Embryo about 29 days old | 475 |
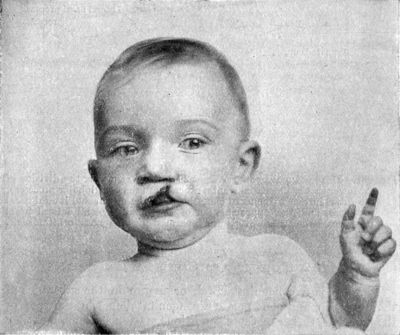
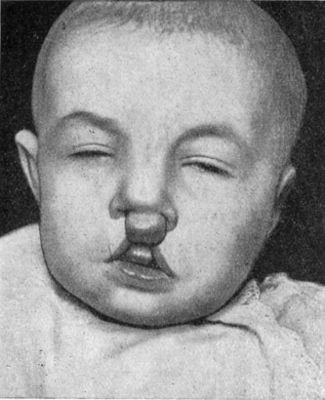
| 232. | Simple Hare-Lip | 476 |
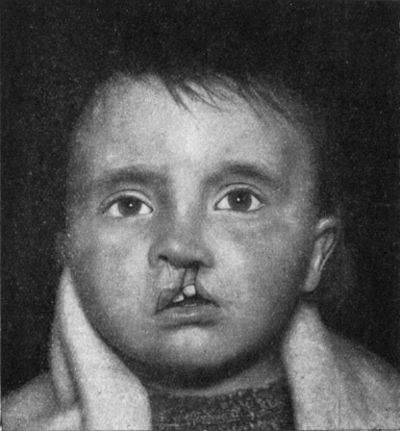
| 233. | Unilateral Hare-Lip with Cleft Alveolus | 477 |
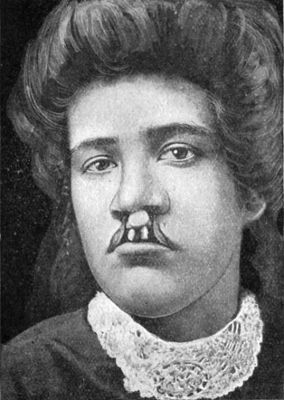
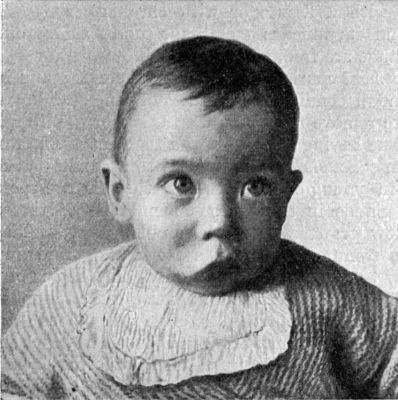
| 234. | Double Hare-Lip in a Girl | 478 |
| 235. | Double Hare-Lip with Projection of the Os Incisivum | 479 |
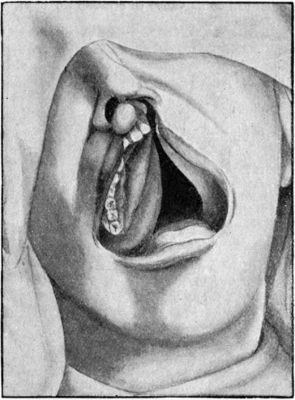
| 236. | Asymmetrical Cleft Palate extending through Alveolar Process on Left Side | 480 |
| 237. | Illustrating the Deformities caused by Lupus Vulgaris | 483 |
| 238. | Sarcoma of Orbit causing Exophthalmos and Downward Displacement of the Eye, and Projecting in Temporal Region | 488 |
| 239. | Sarcoma of Eyelid in Child | 489 |
| 240. | Dermoid Cyst at Outer Angle of Orbital Margin | 490 |
| 241. | Macrocheilia | 492 |
| 242. | Squamous Epithelioma of Lower Lip in a Man | 493 |
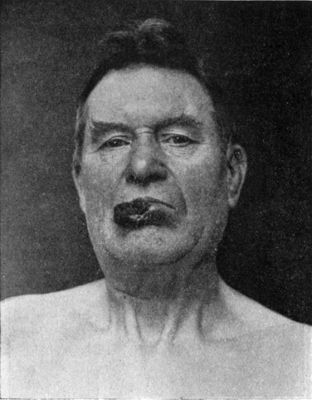
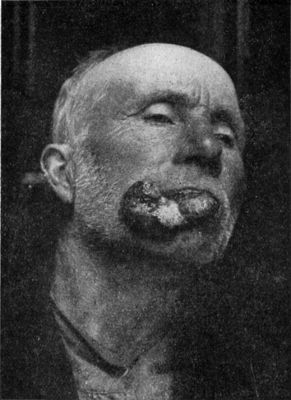
| 243. | Advanced Epithelioma of Lower Lip | 494 |
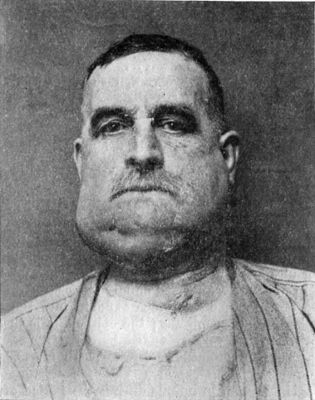
| 244. | Recurrent Epithelioma in Glands of Neck adherent to Mandible | 495 |
| 245. | Cancrum Oris | 497 |
| 246. | Perforation of Palate, the Result of Syphilis, and Gumma of Right Frontal Bone | 498 |
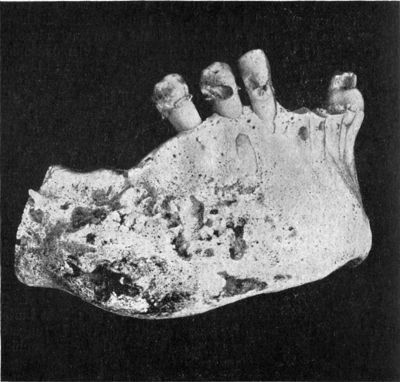
| 247. | Cario-necrosis of Mandible | 510 |
| 248. | Diffuse Syphilitic Disease of Mandible | 512 |
| 249. | Epulis of Mandible | 513 |
| 250. | Sarcoma of the Maxilla | 515 |
| 251. | Malignant Disease of Left Maxilla | 516 |
| 252. | Dentigerous Cyst of Mandible containing Rudimentary Tooth | 517 |
| 253. | Osseous Shell of Myeloma of Mandible | 518 |
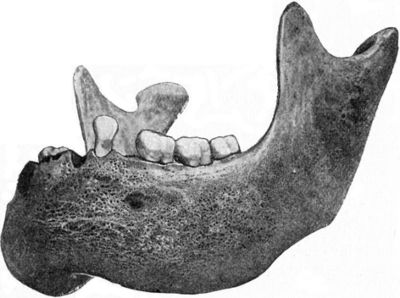
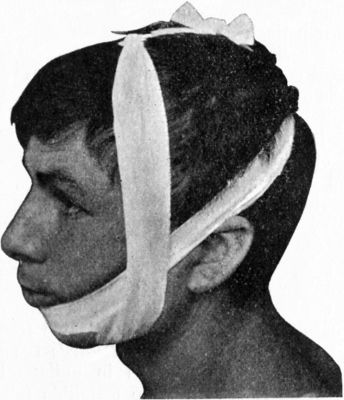
| 254. | Multiple Fracture of Mandible | 520 |
| 255. | Four-Tailed Bandage applied for Fracture of Mandible | 522 |
| 256. | Defective Development of Mandible from Fixation of Jaw due to Tuberculous Osteomyelitis in Infancy | 526 |
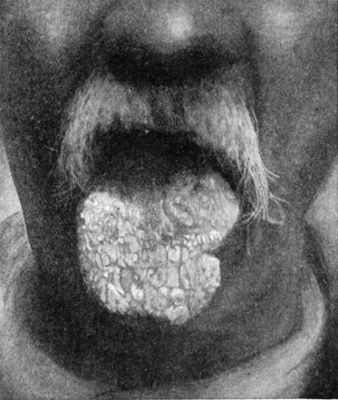
| 257. | Leucoplakia of the Tongue | 531 |
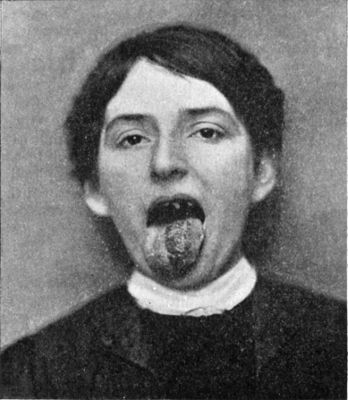
| 258. | Papillomatous Angioma of Left Side of Tongue in a Woman | 538 |
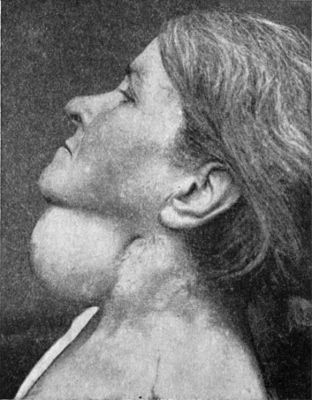
| 259. | Dermoid Cyst in Middle Line of Neck | 539 |
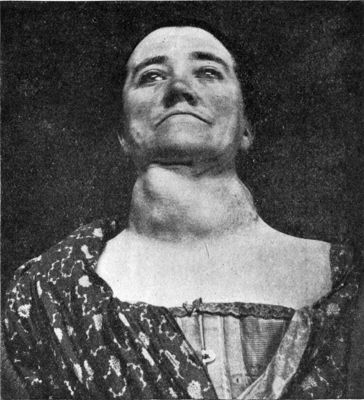
| 260. | Temporary Unilateral Paralysis of Tongue | 541 |
| 261. | Series of Salivary Calculi | 545 |
| 262. | Acute Suppurative Parotitis | 546 |
| 263. | Mixed Tumour of Parotid | 550 |
| 264. | Mixed Tumour of the Parotid of over twenty years' duration | 551 |
| 265. | Acute Mastoid Disease showing Œdema and Projection of Auricle | 565 |
| 266. | Rhinophyma or Lipoma Nasi | 569 |
| 267. | The Outer Wall of Left Nasal Chamber after removal of the Middle Turbinated Body | 571 |
| 268. | Congenital Branchial Cyst in a Woman | 584 |
| 269. | Bilateral Cervical Ribs | 586 |
| 270. | Transient Wry-Neck | 587 |
| 271. | Congenital Wry-Neck in a Boy | 589 |
| 272. | Congenital Wry-Neck seen from behind to show Scoliosis | 590 |
| 273. | Recovery from Suicidal Cut-Throat after Low Tracheotomy and Gastrostomy | 596 |
| 274. | Hygroma of Neck | 599 |
| 275. | Lympho-Sarcoma of Neck | 600 |
| 276. | Branchial Carcinoma | 601 |
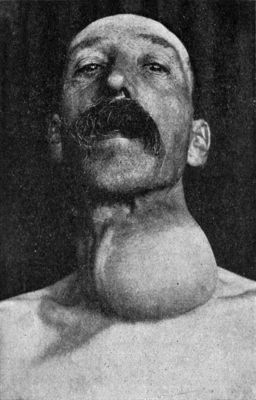
| 277. | Parenchymatous Goitre in a Girl | 606 |
| 278. | Larynx and Trachea surrounded by Goitre | 607 |
| 279. | Section of Goitre shown in Fig. 278 to illustrate Compression of Trachea | 607 |
| 280. | Multiple Adenomata of Thyreoid in a Woman | 611 |
| 281. | Cyst of Left Lobe of Thyreoid | 612 |
| 282. | Exophthalmic Goitre | 614 |
| 283. | Radiogram of Safety-Pin impacted in the Gullet and Perforating the Larynx | 620 |
| 284. | Denture Impacted in Œsophagus | 621 |
| 285. | Radiogram, after swallowing an Opaque Meal, in a Man suffering from Malignant Stricture of Lower End of Gullet | 626 |
| 286. | Diverticulum of the Œsophagus at its Junction with the Pharynx | 627 |
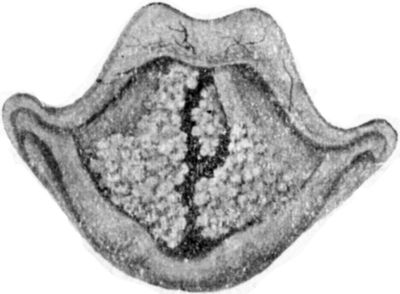
| 287. | Larynx from case of Sudden Death due to Œdema of Ary-Epiglottic Folds | 637 |
| 288. | Papilloma of Larynx | 641 |
The injuries to which a bone is liable are Contusions, Open Wounds, and Fractures.
Contusions of Bone are almost of necessity associated with a similar injury of the overlying soft parts. The mildest degree consists in a bruising of the periosteum, which is raised from the bone by an effusion of blood, constituting a hæmatoma of the periosteum. This may be absorbed, or it may give place to a persistent thickening of the bone—traumatic node.
Open Wounds of Bone of the incised and contused varieties are usually produced by sabres, axes, butcher's knives, scythes, or circular saws. Punctured wounds are caused by bayonets, arrows, or other pointed instruments. They are all equivalent to compound, incomplete fractures.
A fracture may be defined as a sudden solution in the continuity of a bone.
A pathological fracture has as its primary cause some diseased state of the bone, which permits of its giving way on the application of a force which would be insufficient to break a healthy bone. It cannot be too strongly emphasised that when a bone is found to have been broken by a slight degree of violence, the presence of some pathological condition should be suspected, and a careful examination made with the X-rays and by other means, before arriving at a conclusion as to the cause of the fracture. Many cases are on record in which such an accident has first drawn attention to the presence of a new-growth, or other serious lesion in the bone. The following conditions, which are more fully described with diseases of bone, may be mentioned as the causes of pathological fractures.
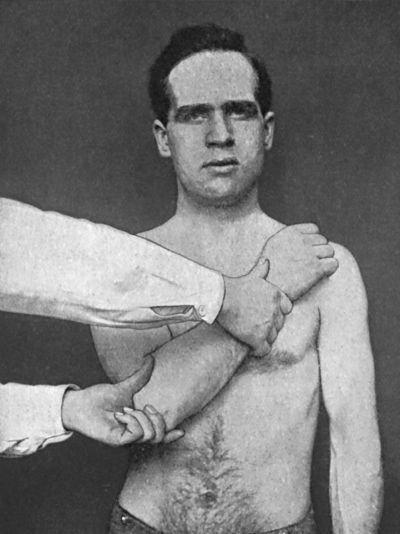
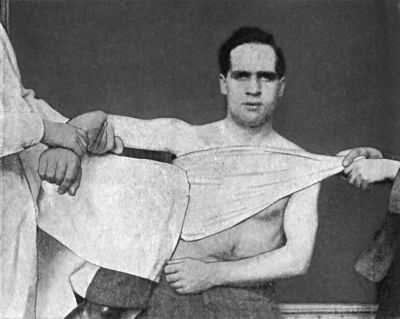
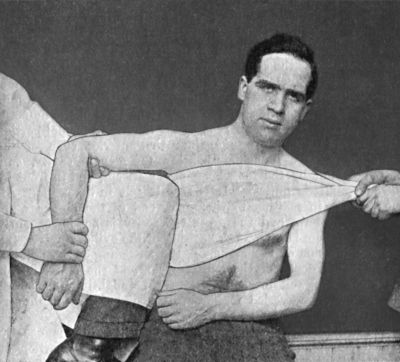
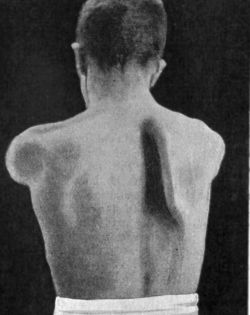
Atrophy of bone may proceed to such an extent in old people, or in those who for long periods have been bed-ridden, that slight violence suffices to determine a fracture. This most frequently occurs in the neck of the femur in old women, the mere catching of the foot in the bedclothes while the patient is turning in bed being sometimes sufficient to cause the bone to give way. Atrophy from the pressure of an aneurysm or of a simple tumour may erode the whole thickness of a bone, or may thin it out to such an extent that slight force is sufficient to break it. In general paralysis, and in the advanced stages of locomotor ataxia and other chronic diseases of the nervous system, an atrophy of all the bones sometimes takes place, and may proceed so far that multiple fractures are induced by comparatively slight causes. They occur most frequently in the ribs or long bones of the limbs, are not attended with pain, and usually unite satisfactorily, although with an excessive amount of callus. Attendants and nurses, especially in asylums, must be warned against using force in handling such patients, as otherwise they may be unfairly blamed for causing these fractures.
Among diseases which affect the skeleton as a whole and render the bones abnormally fragile, the most important are rickets, osteomalacia, and fibrous osteomyelitis. In these conditions multiple pathological fractures may occur, and they are prone to heal with considerable deformity. In osteomalacia, the bones are profoundly altered, but they are more liable to bend than to break; in rickets the liability is towards greenstick fractures.
Of the diseases affecting individual bones and predisposing them to fracture may be mentioned suppurative osteomyelitis, hydatid cysts, tuberculosis, syphilitic gummata, and various forms of new-growth, particularly sarcoma and secondary cancer. It is not unusual for the sudden breaking of the bone to be the first intimation of the presence of a new-growth. In adolescents, fibrous osteomyelitis affecting a single bone, and in adults, secondary cancer, are the commonest local causes of pathological fracture.
Intra-uterine fractures and fractures occurring during birth are usually associated with some form of violence, but in the majority of cases the fœtus is the subject of constitutional disease which renders the bones unduly fragile.
Traumatic fractures are usually the result of a severe force acting from without, although sometimes they are produced by muscular contraction.
When the bone gives way at the point of impact of the force, the violence is said to be direct, and a “fracture by compression” results, the line of fracture being as a rule transverse. The soft parts overlying the fracture are more or less damaged according to the weight and shape of the impinging body. Fracture of both bones of the leg from the passage of a wheel over the limb, fracture of the shaft of the ulna in warding off a stroke aimed at the head, and fracture of a rib from a kick, are illustrative examples of fractures by direct violence.
When the force is transmitted to the seat of fracture from a distance, the violence is said to be indirect, and the bone is broken by “torsion” or by “bending.” In such cases the bone gives way at its weakest point, and the line of fracture tends to be oblique. Thus both bones of the leg are frequently broken by a person jumping from a height and landing on the feet, the tibia breaking in its lower third, and the fibula at a higher level. Fracture of the clavicle in its middle third, or of the radius at its lower end, from a fall on the outstretched hand, are common accidents produced by indirect violence. The ribs also may be broken by indirect violence, as when the chest is crushed antero-posteriorly and the bones give way near their angles. In fractures by indirect violence the soft parts do not suffer by the violence causing the fracture, but they may be injured by displacement of the fragments.
In fractures by muscular action the bone is broken by “traction” or “tearing.” The sudden and violent contraction of a muscle may tear off an epiphysis, such as the head of the fibula, the anterior superior iliac spine, or the coronoid process of the ulna; or a bony process may be separated, as, for example, the tuberosity of the calcaneus, the coracoid process of the scapula, or the larger tubercle (great tuberosity) of the humerus. Long bones also may be broken by muscular action. The clavicle has snapped across during the act of swinging a stick, the humerus in throwing a stone, and the femur when a kick has missed its object. Fractures of ribs have occurred during fits of coughing and in the violent efforts of parturition.
Before concluding that a given fracture is the result of muscular action, it is necessary to exclude the presence of any of the diseased conditions that lead to pathological fracture.
Although the force acting upon the bone is the primary factor in the production of fractures, there are certain subsidiary factors to be considered. Thus the age of the patient is of importance. During infancy and early childhood, fractures are less common than at any other period of life, and are usually transverse, incomplete, and of the nature of bends. During adult life, especially between the ages of thirty and forty, the frequency of fractures reaches its maximum. In aged persons, although the bones become more brittle by the marrow spaces in their interior becoming larger and filled with fat, fractures are less frequent, doubtless because the old are less exposed to such violence as is likely to produce fracture.
Males, from the nature of their occupations and recreations, sustain fractures more frequently than do females; in old age, however, fractures are more common in women than in men, partly because their bones are more liable to be the seat of fatty atrophy from senility and disease, and partly because of their clothing—a long skirt—they are more exposed to unexpected or sudden falls.
Clinical Varieties of Fractures.—The most important subdivision of fractures is that into simple and compound.
In a simple or subcutaneous fracture there is no communication, directly or indirectly, between the broken ends of the bone and the surface of the skin. In a compound or open fracture, on the other hand, such a communication exists, and, by furnishing a means of entrance for bacteria, may add materially to the gravity of the injury.
A simple fracture may be complicated by the existence of a wound of the soft parts, which, however, does not communicate with the broken bone.
Fractures, whether simple or compound, fall into other clinical groups, according to (1) the degree of damage done to the bone, (2) the direction of the break, and (3) the relative position of the fragments.
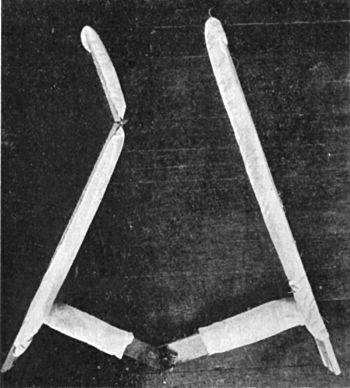
(1) According to the Degree of Damage done to the Bone.—A fracture may be incomplete, for example in greenstick fractures, which occur only in young persons—usually below the age of twelve—while the bones are still soft and flexible. They result from forcible bending of the bone, the osseous tissue on the convexity of the curve giving way, while that on the concavity is compressed. The clavicle and the bones of the forearm are those most frequently the seat of greenstick fracture (Fig. 41). Fissures occur on the flat bones of the skull, the pelvic bones, and the scapula; or in association with other fractures in long bones, when they often run into joint surfaces. Depressions or indentations are most common in the bones of the skull.
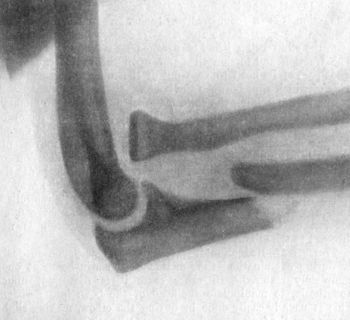
The bone at the seat of fracture may be broken into several pieces, constituting a comminuted fracture. This usually results from severe degrees of direct violence, such as are sustained in railway or machinery accidents, and in gun-shot injuries (Fig. 2).
Sub-periosteal fractures are those in which, although the bone is completely broken across, the periosteum remains intact. These are common in children, and as the thick periosteum prevents displacement, the existence of a fracture may be overlooked, even in such a large bone as the femur.
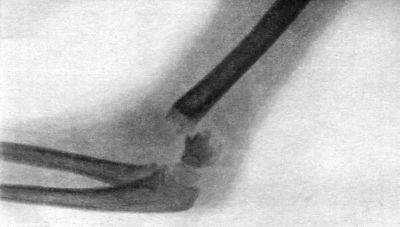
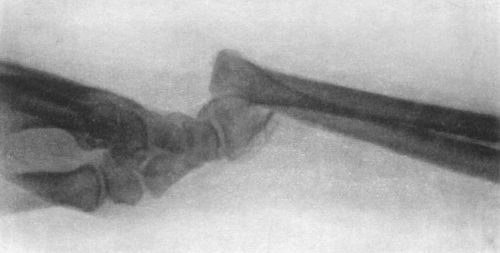
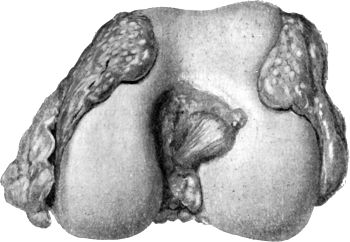
 Fig. 3.—Showing (1) Oblique fracture of Tibia; (2)
Oblique fracture with partial separation of Epiphysis of upper end of
Fibula; (3) Incomplete fracture of Fibula in upper third. Result of
railway accident. Boy æt. 16.
Fig. 3.—Showing (1) Oblique fracture of Tibia; (2)
Oblique fracture with partial separation of Epiphysis of upper end of
Fibula; (3) Incomplete fracture of Fibula in upper third. Result of
railway accident. Boy æt. 16.
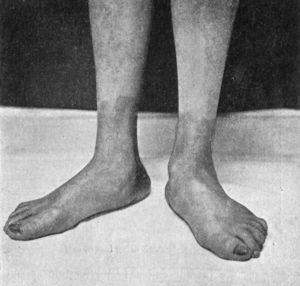
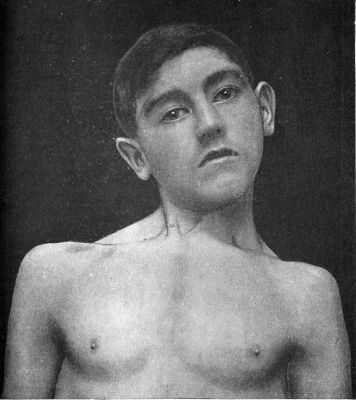
A bone may be broken at several places, constituting a multiple fracture (Fig. 1).
Separation of bony processes, such as the coracoid process, the epicondyle of the humerus, or the tuberosity of the calcaneus, may result from muscular action or from direct violence. Separation of epiphyses will be considered later.
(2) According to the Direction of the Break.—Transverse fractures are those in which the bone gives way more or less exactly at right angles to its long axis. These usually result from direct violence or from end-to-end pressure. Longitudinal fractures extending the greater part of the length of a long bone are exceedingly rare. Oblique fractures are common, and result usually from indirect violence, bending, or torsion (Fig. 3). Spiral fractures result from forcible torsion of a long bone, and are met with most frequently in the tibia, femur, and humerus.
(3) According to the Relative Position of the Fragments.—The bone may be completely broken across, yet its ends remain in apposition, in which case there is said to be no displacement. There may be an angular displacement—for example, in greenstick fracture. In transverse fractures of the patella or of the olecranon there is often distraction or pulling apart of the fragments (Fig. 35). The broken ends, especially in oblique fractures, may override one another, and so give rise to shortening of the limb (Fig. 2). Where one fragment is acted upon by powerful muscles, a rotatory displacement may take place, as in fracture of the radius above the insertion of the pronator teres, or of the femur just below the small trochanter. The fragments may be depressed, as in the flat bones of the skull or the nasal bones. At the cancellated ends of the long bones, particularly the upper end of the femur and humerus, and the lower end of the radius, it is not uncommon for one fragment to be impacted or wedged into the substance of the other (Fig. 28).
Causes of Displacement.—The factors which influence displacement are chiefly mechanical in their action. Thus the direction and nature of the fracture play an important part. Transverse fractures with roughly serrated ends are less liable to displacement than those which are oblique with smooth surfaces. The direction of the causative force also is a dominant factor in determining the direction in which one or both of the fragments will be displaced. Gravity, acting chiefly upon the distal fragment, also plays a part in determining the displacement—for example, in fractures of the thigh or of the leg, where the lower segment of the limb rolls outwards, and in fractures of the shaft of the clavicle, where the weight of the arm carries the shoulder downwards, forwards, and medially. After the break has taken place and the force has ceased to act, displacement may be produced by rough handling on the part of those who render first aid, the careless or improper application of splints or bandages, or by the weight of the bedclothes.
In certain situations the contraction of unopposed, or of unequally opposed, groups of muscles plays a part in determining displacement. For example, in fracture immediately below the lesser trochanter of the femur, the ilio-psoas tends to tilt the upper fragment forward and laterally; in supra-condylar fracture of the femur, the muscles of the calf pull the lower fragment back towards the popliteal space; and in fracture of the humerus above the deltoid insertion, the muscles inserted into the inter-tubercular (bicipital) groove adduct the upper fragment.
In a simple fracture the vessels of the periosteum and the marrow being torn at the same time as the bone is broken, blood is poured out, and clots around and between the fragments. This clot is soon permeated by newly formed blood vessels, and by leucocytes and fibroblasts, the latter being derived from proliferation of the cells of the marrow and periosteum. The granulation tissue thus formed resembles in every particular that described in the repair of other tissues, except that the fibroblasts, being the offspring of cells which normally form bone, assume the functions of osteoblasts, and proceed to the formation of bone. The new bone may be formed either by a direct conversion of the fibrous tissue into osseous tissue, the osteoblasts arranging themselves concentrically in the recesses of the capillary loops, and secreting a homogeneous matrix in which lime salts are speedily deposited; or there may be an intermediate stage of cartilage formation, especially in young subjects, and in cases where the fragments are incompletely immobilised. The newly formed bone is at first arranged in little masses or in the form of rods which unite with each other to form a network of spongy bone, the meshes of which contain marrow.
The reparative material, consisting of granulation tissue in the process of conversion into bone, is called callus, on account of its hard and unyielding character. In a fracture of a long bone, that which surrounds the fragments is called the external or ensheathing callus, and may be likened to the mass of solder which surrounds the junction of pipes in plumber-work; that which occupies the position of the medullary canal is called the internal or medullary callus; and that which intervenes between the fragments and maintains the continuity of the cortical compact tissue of the shaft is called the intermediate callus. This intermediate callus is the only permanent portion of the reparative material, the external and internal callus being only temporary, and being largely re-absorbed through the agency of giant cells.
Detached fragments or splinters of bone are usually included in the callus and ultimately become incorporated in the new bone that bridges the gap.
In time all surplus bone is removed, the medullary canal is re-formed, the young spongy bone of the intermediate callus becomes more and more compact, and thus the original architectural arrangement of the bone may be faithfully reproduced. If, however, apposition is not perfect, some of the new bone is permanently required and some of the old bone is absorbed in order to meet the altered physiological strain upon the bone resulting from the alteration in its architectural form. In overriding displacement, even the dense cortical bone intervening between the medullary canal of the two fragments is ultimately absorbed and the continuity of the medullary canal is reproduced.
The amount of callus produced in the repair of a given fracture is greater when movement is permitted between the broken ends. It is also influenced by the character of the bone involved, being less in bones entirely ossified in membrane, such as the flat bones of the skull, than in those primarily ossified in cartilage.
If the fragments are widely separated from one another, or if some tissue, such as muscle, intervenes between them, callus may not be able to bring about a bony union between the fragments, and non-union results.
Bones divided in the course of an operation, for example in osteotomy for knock-knee, or wedge-shaped resection for bow-leg, are repaired by the same process as fractures.
Excess of Callus.—In comminuted fractures, and in fractures in which there is much displacement, the amount of callus is in excess, but this is necessary to ensure stability. In fractures in the vicinity of large joints, such as the hip or elbow, the formation of callus is sometimes excessive, and the projecting masses of new bone restrict the movements of the joint. When exuberant callus forms between the bones in fractures of the forearm, pronation and supination may be interfered with (Fig. 4). Certain nerve-trunks, such as the radial (musculo-spiral) in the middle of the arm, or the ulnar at the elbow-joint, may become included in or pressed upon by callus.
Absorption of Callus.—It sometimes happens that when an acute infective disease, especially one of the exanthemata, supervenes while a fracture is undergoing repair, the callus which has formed becomes softened and is absorbed. This may occur weeks or even months after the bone has united, with the result that the fragments again become movable, and it may be a considerable time before union finally takes place.
Tumours of Callus.—Tumours, such as chondroma and sarcoma, and cysts which are probably of the same nature as those met with in osteomyelitis fibrosa, are liable to occur in callus, or at the seat of old fractures, but the evidence so far is inconclusive as to the causative relationship of the injury to the new-growth. They are treated on the same lines as tumours occurring independently of fracture.
Badly United Fracture—Mal-Union.—Union with marked displacement of the fragments is most common in fractures that have not been properly treated—as, for example, those occurring in sailors at sea; and in cases in which the comminution was so great that accurate apposition was rendered impossible. It may also result from imperfect reduction, or because the apparatus employed permitted of secondary displacement. Restlessness on the part of the patient from intractability, delirium tremens, or mania, is the cause of mal-union in some cases; sometimes it has resulted because the patient was expected to die from some other lesion and the fracture was left untreated.
Whether or not any attempt should be made to improve matters depends largely on the degree of deformity and the amount of interference with function.
When interference is called for, if the callus is not yet firmly consolidated, it may be possible, under an anæsthetic, to bend the bone into position or to re-break it, either with the hands or by means of a strong mechanical contrivance known as an osteoclast. In the majority of cases, however, an open operation yields results which are more certain and satisfactory. When the deformity is comparatively slight, the bone is divided with an osteotome and straightened; when there is marked bending or angling, a wedge is taken from the convexity, as in the operation for bow-leg. To maintain the fragments in apposition it may be necessary to employ pegs, plates, bone-grafts, or other mechanical means. Splints and extension are then applied, and the condition is treated on the same lines as a compound fracture.
Delayed Union.—At the time when union should be firm and solid, it may be found that the fragments are only united by a soft cartilaginous callus, which for a prolonged period may undergo no further change, so that the limb remains incapable of bearing weight or otherwise performing its functions. The normal period required for union may be extended from various causes. The most important of these is general debility, but the presence of rickets or tuberculosis, or an intercurrent acute infectious disease, may delay the reparative process. The influence of syphilis, except in its gummatous form, in interfering with union is doubtful. The influence of old age as a factor in delaying union has been overestimated; in the great majority of cases, fractures in old people unite as rapidly and as firmly as those occurring at other periods of life.
Treatment.—The general condition of the patient should be improved, by dieting and tonics. One of the most reliable methods of hastening union in these cases is by inducing passive hyperæmia of the limb after the method advocated by Bier, and this plan should always be tried in the first instance. An elastic bandage is applied above the seat of fracture, sufficiently tightly to congest the limb beyond, and, to concentrate the congestion in the vicinity of the fracture, an ordinary bandage should be applied from the distal extremity to within a few inches of the break. The hyperæmia should be maintained for several hours (six to twelve) daily. An apparatus should be adjusted to enable the patient to get into the open air, and in fractures of the lower extremity the patient should move about with crutches in the intervals, putting weight on the fractured bone. This method of treatment should be persevered with for three or four weeks, and the limb should be massaged daily while the constricting bandage is off.
Among the other methods which have been recommended are the injection between the fragments of oil of turpentine (Mikulicz), a quantity of the patient's own blood (Schmieden), or alcohol and iodine; the forcible rubbing of the ends together, under an anæsthetic if necessary; and the administration of thyreoid extract. If these methods fail, the case should be treated as one of un-united fracture. As a rule, satisfactory union is ultimately obtained, although much patience is required.
Non-Union.—Sometimes the fragments become united by a dense band of fibrous tissue, and the reparative process goes no further—fibrous union. This is frequently the case in fractures of the patella, the olecranon, and the narrow part of the neck of the femur.
False Joint—Pseudarthrosis.—In rare cases the ends of the fragments become rounded and are covered with a layer of cartilage. Around their ends a capsule of fibrous tissues forms, on the inner aspect of which a layer of endothelium develops and secretes a synovia-like fluid. This is met with chiefly in the humerus and in the clavicle.
Failure of Union—“Un-united Fracture.”—As the time taken for union varies widely in different bones, and ossification may ultimately ensue after being delayed for several months, a fracture cannot be said to have failed to unite until the average period has been long overpassed and still there is no evidence of fusion of the fragments. Under these conditions failure of union is a rare complication of fractures. In adults it is most frequently met with in the humerus, the radius and ulna (Fig. 6), and the femur; in children in the bones of the leg and in the forearm.
In a radiogram the bones in the vicinity of the fracture, particularly the distal fragment, cast a comparatively faint shadow, and there may even be a clear space between the fragments. When the parts are exposed by operation, the bone is found to be soft and spongy and the ends of the fragments are rarefied and atrophied; sometimes they are pointed, and occasionally absorption has taken place to such an extent that a gap exists between the fragments. The bone is easily penetrated by a bradawl, and if an attempt is made to apply plates, the screws fail to bite. These changes are most marked in the distal fragment.
The want of union is evidently due to defective activity of the bone-forming cells in the vicinity of the fracture. This may result from constitutional dyscrasia, or may be associated with a defective blood supply, as when the nutrient artery is injured. Interference with the trophic nerve supply may play a part, as cases are recorded by Bognaud in which union of fractures of the leg failed to take place after injuries of the spinal medulla causing paraplegia. The condition has been attributed to local causes, such as the interposition of muscle or other soft tissue between the fragments, or to the presence of a separated fragment of bone or of a sequestrum following suppuration. In our experience such factors are seldom present.
If the treatment recommended for delayed union fails, recourse must be had to operation, the most satisfactory procedure being to insert a bone graft in the form of an intra-medullary splint. In certain cases met with in the bones of the leg in children, the degree of atrophy of the bones is such that it has been found necessary to amputate after repeated attempts to obtain union by operative measures have failed.
In the tibia we have found that with the double electric saw a rod of bone can be rapidly and accurately cut, extending well above as well as below the site of fracture but unequally in the two directions; the rod is then reinserted into the trough from which it was taken with the ends reversed, so that a strong bridge of bone is provided at the seat of non-union.
In the first place, the history of the accident should be investigated, attention being paid to the nature of the violence—whether a blow, a twist, a wrench, or a crush, and whether the violence was directly or indirectly applied. The degree of the violence may often be judged approximately from the instrument inflicting it—whether, for example, a fist, a stick, a cart wheel, or a piece of heavy machinery. The position of the limb at the time of the injury; whether the muscles were braced to meet the blow or were lax and taken unawares; and the patient's sensations at the moment, such as his feeling something snap or tear, may all furnish information useful for purposes of diagnosis.
Signs of Fracture.—The most characteristic signs of fracture are unnatural mobility, deformity, and crepitus.
Unnatural mobility—that is, movement between two segments of a limb at a place where movement does not normally occur—may be evident when the patient makes attempts to use his limb, or may only be elicited when the fragments are seized and moved in opposite directions. Deformity, or the part being “out of drawing” in comparison with the normal side, varies with the site and direction of the break, and depends upon the degree of displacement of the fragments. Crepitus is the name applied to the peculiar grating or clicking which may be heard or felt when the fractured surfaces are brought into contact with one another.
The presence of these three signs in association is sufficient to prove the existence of a fracture, but the absence of one or more of them does not negative this diagnosis. There are certain fallacies to be guarded against. For example, a fracture may exist and yet unnatural mobility may not be present, because the bones are impacted into one another, or because the fracture is an incomplete one. Again, the extreme tension of the swollen tissues overlying the fracture may prevent the recognition of movement between the fragments. Deformity also may be absent—as, for instance, when there is no displacement of the fragments, or when only one of two parallel bones is broken, as in the leg or forearm. Similarly, crepitus may be absent when impaction exists, when the fragments completely override one another, or are separated by an interval, or when soft tissues, such as torn periosteum or muscle, are interposed between them. A sensation simulating crepitus may be felt on palpating a part into which blood has been extravasated, or which is the seat of subcutaneous emphysema. The creaking which accompanies movements in certain forms of teno-synovitis and chronic joint disease, and the rubbing of the dislocated end of a bone against the tissues amongst which it lies, may also be mistaken for the crepitus of fracture.
It is not advisable to be too diligent in eliciting these signs, because of the pain caused by the manipulations, and also because vigorous handling may do harm by undoing impaction, causing damage to soft parts or producing displacement which does not already exist, or by converting a simple into a compound fracture.
It is often necessary for purposes of diagnosis to administer a general anæsthetic, particularly in injuries of deeply placed bones and in the vicinity of joints. Before doing so, the appliances necessary for the treatment of the injury should be made ready, in order that the fracture may be reduced and set before the patient regains consciousness.
Radiography in the Diagnosis of Fractures.—While radiography is of inestimable value in the diagnosis of many fractures and other injuries, particularly in the vicinity of joints, the student is warned against relying too implicitly on the evidence it seems to afford.
A radiogram is not a photograph of the object exposed to the X-rays but merely a picture of its shadow, or rather of a series of shadows of the different structures, which vary in opacity. As the rays emanate from a single point in the vacuum tube, and as they are not, like the sun's rays, approximately parallel, the shadows they cast are necessarily distorted. Hence, in interpreting a radiogram, it is necessary to know the relative positions of the point from which the rays proceed, the object exposed, and the plate on which the shadow is registered. The least distortion takes place when the object is in contact with the plate, and the shadow of that part of the object which lies perpendicularly under the light is less distorted than that of the parts lying outside the perpendicular. The light and the plate remaining constant, the amount of distortion varies directly with the distance between the object and the plate.
To ensure accuracy in the diagnosis of fracture by the X-rays, it is necessary to take two views of the limb—one in the sagittal and the other in the coronal plane. By the use of the fluorescent screen, the best positions from which to obtain a clear impression of the fracture may be determined before the radiograms are taken. Stereoscopic radiograms may be of special value in demonstrating the details of a fracture that is otherwise doubtful.
Imperfect technique and faulty interpretation of the pictures obtained lead to certain fallacies. In young subjects, for example, epiphysial lines may be mistaken for fractures, or the ossifying centres of epiphyses for separated fragments of bone. The os trigonum tarsi has been mistaken for a fracture of the talus. In the vicinity of joints the bones may be crossed by pale bands, due to the rays traversing the cavity of the joint. In this way fracture of the olecranon or of the clavicle may be simulated. The neck of the femur may appear to be fractured if a foreshortened view is taken.
It is possible, on the other hand, to overlook a fracture—for example, if there is no displacement, or if the line of fracture is crossed by the shadow of an adjacent bone. In deeply placed bones such as those about the hip, or in bones related to dense, solid viscera—for example, ribs, sternum, or dorsal vertebræ—it is sometimes difficult to obtain conclusive evidence of fracture in a radiogram.
It is to be borne in mind also, and especially from the medico-legal point of view, that, as early callus does not cast a deep shadow in a radiogram, the appearance of fracture may persist after union has taken place. The earliest shadow of callus appears in from fourteen to twenty-one days, and can hardly be relied upon till the fourth or sixth week. The disturbed perspective produced by divergence of the rays may cause the fragments of a fracture to appear displaced, although in reality they are in good position. If the limb and the plate are not parallel, the bones may appear to be distorted, and errors in diagnosis may in this way arise. In this relation it should be mentioned that perfect apposition of the fragments and anatomically accurate restoration of the outline of the bones are not always essential to a good functional result.
As most of the remaining signs are common to all the lesions from which fractures have to be distinguished, their diagnostic value must be carefully weighed.
Interference with Function.—As a rule, a broken bone is incapable of performing its normal function as a lever or weight-bearer; but when a fracture is incomplete, when the fragments are impacted, or when only one of two parallel bones is broken, this does not necessarily follow. It is no uncommon experience to find a patient walk into hospital with an impacted fracture of the neck of the femur or a fracture of the fibula; or to be able to pronate and supinate the forearm with a greenstick fracture of the radius or a fracture of the ulna.
Pain.—Three forms of pain may be present in fractures: pain independent of movement or pressure; pain induced by movement of the limb; and pain elicited on pressure or “tenderness.” In injuries by direct violence, pain independent of movement and pressure is never diagnostic of fracture, as it may be due to bruising of soft tissues. In injuries resulting from indirect violence, however, pain localised to a spot at some distance from the point of impact is strongly suggestive of fracture—as, for example, when a patient complains of pain over the clavicle after a fall on the hand, or over the upper end of the fibula after a twist of the ankle. Pain elicited by attempts to move the damaged part, or by applying pressure over the seat of injury, is more significant of fracture. Pain elicited at a particular point on pressing the bone at a distance, “pain on distal pressure,”—for example, pain at the lower end of the fibula on pressing near its neck, or at the angle of a rib on pressing near the sternum,—is a valuable diagnostic sign of fracture. When nerve-trunks are implicated in the vicinity of a fracture, pain is often referred along the course of their distribution.
Localised swelling comes on rapidly, and is due to displacement of the fragments and to hæmorrhage from the torn vessels of the marrow and periosteum.
Discoloration accompanies the swelling, and is often widespread, especially in fracture of bones near the surface and when the tension is great. It is not uncommon to find over the ecchymosed area, especially over the shin-bone, large blebs containing blood-stained serum. In fractures of deep-seated bones, discoloration may only show on the surface after some days, and at a distance from the break.
Alterations in the relative position of bony landmarks are valuable diagnostic guides. Alteration in the length of the limb, usually in the direction of shortening, is also an important sign. Before drawing deductions, care must be taken to place both limbs in the same position and to determine accurately the fixed points for measurement, and also to ascertain if the limbs were previously normal.
Shock is seldom a prominent symptom in uncomplicated fractures, although in old and enfeebled patients it may be serious and even fatal. During the first two or three days after a fracture there is almost invariably some degree of traumatic fever, indicated by a rise of temperature to 99° or 100° F.
Complications.—Injuries to large arteries are not common in simple fractures. The popliteal artery, however, is liable to be compressed or torn across in fractures of the lower end of the femur; extravasation of blood from the ruptured artery and gangrene of the limb may result. If large veins are injured, thrombosis may occur, and be followed by pulmonary embolism.
Injuries to nerve-trunks are comparatively common, especially in fractures of the arm, where the radial (musculo-spiral) nerve is liable to suffer.
The nerve may be implicated at the time of the injury, being compressed, bruised, lacerated, or completely torn across by broken fragments, or it may be involved later by the pressure of callus. The symptoms depend upon the degree of damage sustained by the nerve, and vary from partial and temporary interference with sensation and motion to complete and permanent abrogation of function.
In rare instances fat embolism is said to occur, and fat globules are alleged to have been found in the urine. In persons addicted to excess of alcohol, delirium tremens is a not infrequent accompaniment of a fracture which confines the patient to bed.
Prognosis in Simple Fractures.—Danger to life in simple fractures depends chiefly on the occurrence of complications. In old people, a fracture of the neck of the femur usually necessitates long and continuous lying on the back, and bronchitis, hypostatic pneumonia, and bed-sores are prone to occur and endanger life. Fractures complicated with injury to internal organs, and fractures in which gangrene of the limb threatens, are, of course, of grave import.
The prognosis as regards the function of the limb should always be guarded, even in simple fractures. Incidental complications are liable to arise, delaying recovery and preventing a satisfactory result, and these not only lead to disappointment, but may even form a ground for actions for malpraxis.
The chief and most frequent cause of permanent disability after fracture is angular displacement. A comparatively small degree of angularity may lead to serious loss of function, especially in the lower limb; the joints above and below the fracture are placed at a disadvantage, arthritic changes result from the abnormal strain to which they are subjected, and rarefaction of the bone may also ensue.
Fibrous union is a common result in fractures of the neck of the femur in old people and in certain other fractures, such as fracture of the patella, of the olecranon, coronoid and coracoid processes, and although this does not necessarily involve interference with function, the patient should always be warned of the possibility.
Impairment of growth and eventual shortening of the limb may result from involvement of an epiphysial junction.
Stiffness of joints is liable to follow fractures implicating articular surfaces, or it may result from arthritic changes following upon the injury.
Osseous ankylosis is not a common sequel of simple fractures, but locking of joints from the mechanical impediment produced by the union of imperfectly reduced fragments, or from masses of callus, is not uncommon, especially in the region of the elbow.
Wasting of the muscles and œdema of the limb often delay the complete restoration of function. Delayed union, want of union, and the formation of a false joint have already been referred to.
Treatment.—The treatment of a fracture should be commenced as soon after the accident as possible, before the muscles become contracted and hold the fragments in abnormal positions, and before the blood and serum effused into the tissues undergo organisation.
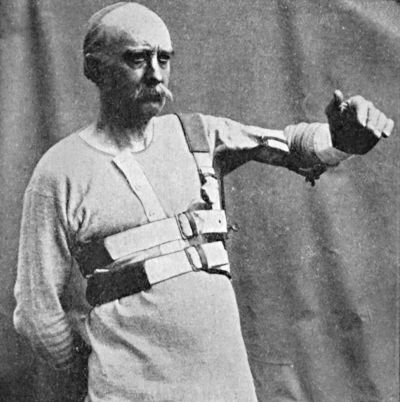
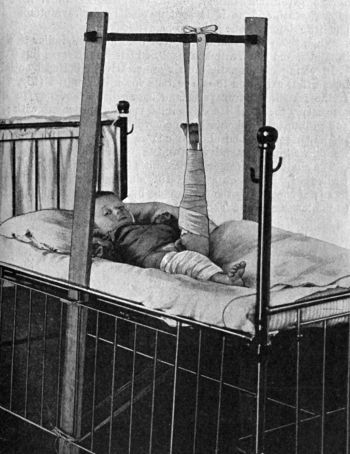
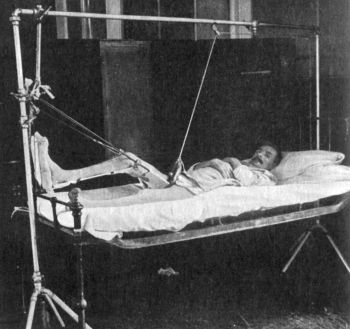
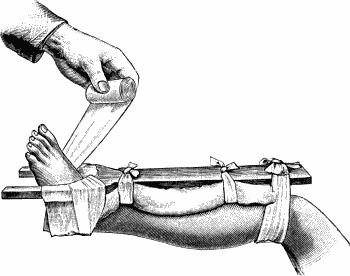
Care must be taken during the transport of the patient that no further damage is done to the injured limb. To this end the part must be secured in some form of extemporised splint, the apparatus being so designed as to control not only the broken fragments, but also the joints above and below the fracture.
When the ordinary method of removing the clothes involves any risk of unduly moving the injured part, they should be slit open along the seams.
The patient should be placed on a firm straw, horse-hair, or spring mattress, stiffened in the case of fractures of the pelvis or lower limbs by fracture-boards inserted beneath the mattress. Special mattresses constructed in four pieces, to facilitate the nursing of the patient, are sometimes used.
In many cases, particularly in muscular subjects, in restless alcoholic patients, and in those who do not bear pain well, a general anæsthetic is a valuable aid to the accurate setting of a fracture, as well as a means of rendering the diagnosis more certain.
The procedure popularly known as “setting a fracture” consists in restoring the displaced parts to their normal position as nearly as possible, and is spoken of technically as the reduction of the fracture.
The Reduction of Fractures.—In some cases the displacement may be overcome by relaxing the muscles acting upon the fragments, and this may be accomplished by the stroking movements of massage. In most cases, however, it is necessary, after relaxing the muscles, to employ extension, by making forcible but steady traction on the distal fragment, while counter-extension is exerted on the proximal one, either by an assistant pulling upon that portion of the limb, or by the weight of the patient's body. The fragments having been freed, and any shortening of the limb corrected in this way, the broken ends are moulded into position—a process termed coaptation.
The reduction of a recent greenstick fracture consists in forcibly straightening the bend in the bone, and in some cases it is necessary to render the fracture complete before this can be accomplished.
In selecting a means of retaining the fragments in position after reduction, the various factors which tend to bring about re-displacement must be taken into consideration, and appropriate measures adopted to counteract each of these.
In addition to retaining the broken ends of the bone in apposition, the after-treatment of a fracture involves the taking of steps to promote the absorption of effused blood and serum, to maintain the circulation through the injured parts, and to favour the repair of damaged muscles and other soft tissues. Means must also be taken to maintain the functional activity of the muscles of the damaged area, to prevent the formation of adhesions in joints and tendon sheaths, and generally to restore the function of the injured part.
Practical Means of Effecting Retention—By Position.—It is often found that only in one particular position can the fragments be made to meet and remain in apposition—for example, the completely supine position of the forearm in fracture of the radius just above the insertion of the pronator teres. Again, in certain cases it is only by relaxing particular groups of muscles that the displacement can be undone—as, for instance, in fracture of the bones of the leg, or of the femur immediately above the condyles, where flexion of the knee, by relaxing the calf muscles, permits of reduction.
Massage and Movement in the Treatment of Fractures.—Lucas-Championnière, in 1886, first pointed out that a certain amount of movement between the ends of a fractured bone favours their union by promoting the formation of callus, and advocated the treatment of fractures by massage and movement, discarding almost entirely the use of splints and other retentive appliances. We were early convinced by the teaching of Lucas-Championnière, and have adopted his principles in fractures.
In the majority of cases the massage and movement are commenced at once, but circumstances may necessitate their being deferred for a few days. The measures adopted vary according to the seat and nature of the fracture, but in general terms it may be stated that after the fracture has been reduced, the ends of the broken bone are retained in position, and gentle massage is applied by the surgeon or by a trained masseur. The lubricant may either be a powder composed of equal parts of talc and boracic acid, or an oily substance such as olive oil or lanolin. The rubbing should never cause pain, but, on the contrary, should relieve any pain that exists, as well as the muscular spasm which is one of the most important causes of pain and of displacement in recent fractures. The parts on the proximal side of the injured area are first gently stroked upwards to empty the veins and lymphatics, and to disperse the effused blood and serum. The process is then applied to the swollen area, and gradually extended down over the seat of the fracture and into the parts beyond. In this way the circulation through the damaged segment of the limb is improved, the veins are emptied of blood, the removal of effused fluid is stimulated, and the muscular irritability allayed. The joints of the limb are gently moved, care being taken that the broken ends of the bone are not displaced. After the rubbing has been continued for from fifteen to twenty minutes, the limb is placed in a comfortable position, and retained there by pillows, sand-bags, or, if found more convenient, by a light form of splint.
The massage is repeated once each day; the sittings last from ten to fifteen minutes. The sequence should be, first, massage; second, passive movement; and third, active movement. At first massage predominates, and more passive than active movement; gradually massage is lessened and movements are increased, active movements ultimately preponderating.
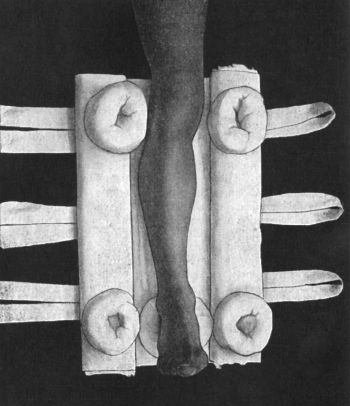
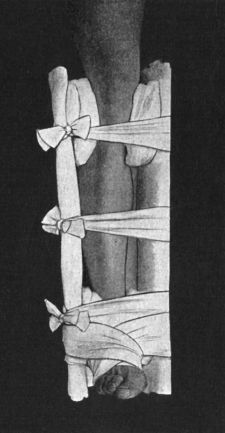
Splints and other Appliances.—The appropriate splints for individual fractures and the method of applying them will be described later; but it may here be said that the general principle is that when dealing with a part where there is a single bone, as the thigh or upper arm, the splint should be applied in the form of a ferrule to surround the break; while in situations where there are two parallel bones, as in the forearm and leg, the splint should take the form of a box.
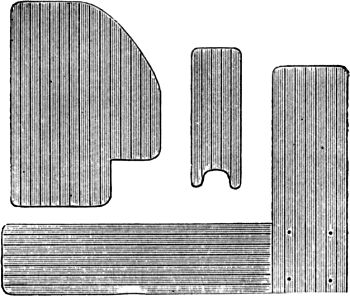
Simple wooden splints of plain deal board or yellow pine, sawn to the appropriate length and width; or Gooch's splinting, which consists of long strips of soft wood, glued to a backing of wash-leather, are the most useful materials. Gooch's splinting has the advantage that when applied with the leather side next the limb it encircles the part as a ferrule; while it remains rigid when the wooden side is turned towards the skin. Perforated sheet lead or tin, stiff wire netting, and hoop iron also form useful splints.
When it is desirable that the splint should take the shape of the part accurately, a plastic material may be employed. Perhaps the most convenient is poroplastic felt, which consists of strong felt saturated with resin. When heated before a fire or placed in boiling water, it becomes quite plastic and may be accurately moulded to any part, and on cooling it again becomes rigid. The splint should be cut from a carefully fitted paper pattern. Millboard, leather, or gutta-percha softened in hot water, and moulded to the part, may also be employed.
In conditions where treatment by massage and movement is impracticable, and where movable splints are inconvenient, splints of plaster of Paris, starch, or water-glass are sometimes used, especially in the treatment of fractures of the leg. When employed in the form of an immovable case, they are open to certain objections—for example, if applied immediately after the accident they are apt to become too tight if swelling occurs; and if applied while swelling is still present, they become slack when this subsides, so that displacement is liable to occur.
When it is desired to enclose the limb in a plaster case, coarse muslin bandages, 3 yards long, and charged with the finest quality of thoroughly dried plaster of Paris, are employed. The “acetic plaster bandages” sold in the shops set most quickly and firmly. Boracic lint or a loose stocking is applied next the skin, and the bony prominences are specially padded. The plaster bandage is then placed in cold water till air-bubbles cease to escape, by which time it is thoroughly saturated, and, after the excess of water is squeezed out, is applied in the usual way from below upward. From two to four plies of the bandage are required. In the course of half an hour the plaster should be thoroughly set. To facilitate the removal of a plaster case the limb should be immersed for a short time in tepid water.
A convenient and efficient splint is made by moulding two pieces of poroplastic felt to the sides of the limb, and fixing them in position with an elastic webbing bandage; this apparatus can be easily removed for the daily massage.
Padding is an essential adjunct to all forms of splints. The whole part enclosed in the splint must be covered with a thick layer of soft and elastic material, such as wool from which the fat has not been removed. All hollows should be filled up, and all bony projections specially protected by rings of wadding so arranged as to take the pressure off the prominent point and distribute it on the surrounding parts. Opposing skin surfaces must always be separated by a layer of wool or boracic lint. A bandage should never be applied to the limb underneath the splints and pads, as congestion or even gangrene may be induced thereby.
Operative Treatment of Simple Fractures.—Operation in simple fracture is specially called for (1) in fracture into or near a joint where a permanently displaced fragment will cause locking of the joint; (2) when fragments are drawn apart, as in fractures of the patella or olecranon; (3) when displacement, especially shortening, cannot be remedied by other means; (4) when complications are present, such as a torn nerve-trunk or a main artery; (5) when non-union is to be feared, as in certain cases of fracture of the neck of the femur in old people. Under such circumstances it is necessary to expose the fracture by operation, and to place the fragments in accurate apposition, if necessary, fixing them in position by wires, pegs, plates, or screws (Op. Surg., p. 52). Operative interference is usually delayed till about five to seven days after the injury, by which time the effect of other measures will have been estimated, accurate information obtained by means of the X-rays regarding the nature of the lesion and the position of the fragments, and the tissues recovered their normal powers of resistance. Such operations, however, are not to be undertaken lightly, as they are often difficult, and if infection takes place the results may be disastrous. Arbuthnot Lane and Lambotte advocate a more general resort to operative measures, even in simple and uncomplicated fractures, and it must be conceded that in many fractures an open operation affords the only means of securing accurate apposition and alignment of the fragments.
Both before and after operation, massage and movement are to be carried out, as in fractures treated by other methods.
The essential feature of a compound fracture is the existence of an open wound leading down to the break in the bone. The wound may vary in size from a mere puncture to an extensive tearing and bruising of all the soft parts.
A fracture may be rendered compound from without, the soft parts being damaged by the object which breaks the bone—as, for example, a cart wheel, a piece of machinery, or a bullet. Sloughing of soft parts resulting from the pressure of improperly applied splints, also, may convert a simple into a compound fracture. On the other hand, a simple fracture may be rendered compound from within—for example, a sharp fragment of bone may penetrate the skin; this is the least serious variety of compound fracture.
As a rule, it is easy to recognise that the fracture is compound, as the bone can either be seen or felt.
The prognosis depends on the success which attends the efforts to make and to keep the wound aseptic, as well as on the extent of damage to the tissues. When asepsis is secured, repair takes place as in simple fracture, only it usually takes a little longer; sometimes the reason for the delay is obvious, as when the compound fracture is the result of a more severe form of violence and where there is comminution and loss of one or more portions of bone that would have contributed to the repair. Sometimes the delay cannot be so explained; Bier suggested that it is due to the escape of blood at the wound, whereas in simple fractures the blood is retained and assists in repair.
If sepsis gains the upper hand in a compound fracture there is, firstly, the risk of infection of the marrow—osteomyelitis—which in former times was liable to result in pyæmia; in the second place, not only do loose fragments tend to die and be thrown off as sequestra, but the ends of the fragments themselves may undergo necrosis; involving as this does the dense cortical bone of the shaft, the dead bone is slow in being separated, and until it is separated and thrown off, no actual repair can take place. The sepsis stimulates the bone-forming tissues and new bone is formed in considerable amount, especially on the surface of the shaft in the vicinity of the fracture; in macerated specimens it presents a porous, crumbling texture. Sometimes the new bone—which corresponds to the involucrum of an osteomyelitis—imprisons a sequestrum and prevents its extrusion, in which case one or more sinuses may persist indefinitely. Cases are met with where such sinuses have existed for the best part of a long life and have ultimately become the seat of epithelioma.
It should be noted that all the above changes can be followed in skiagrams.
Treatment.—The leading indication is to ensure asepsis. Even in the case of a small punctured wound caused by a pointed fragment coming through the skin it is never wise to assume that the wound is not infected. It is much safer to enlarge such a wound, pare away the bruised edges, and disinfect the raw surfaces.
In cases of extensive laceration of the soft parts, all soiled, bruised, or torn portions of tissue should be clipped away with scissors, blood-clots removed, and the bleeding arrested by forci-pressure or ligature. If there is any reason to believe that the wound is infected, any fragments of bone completely separated from the periosteum should be removed. In comminuted fractures, extension applied by strips of plaster or by means of ice-tong callipers or Steinmann's apparatus (p. 150) often facilitates replacement of the fragments and their retention in position. Plates and screws are not recommended for comminuted fractures, owing to the mechanical difficulty of fixing a number of small fragments and the risks of infection. The wound should be purified with eusol, and the surrounding parts painted with iodine. On the whole, it is safer not to attempt to obtain primary union by completely closing such wounds, but rather to drain or pack them. To increase the local leucocytosis and so check the spread of infection, a Bier's constricting bandage may be applied.
In other respects the treatment is carried out on the same lines as in simple fractures, provision being made for dressing the wound without disturbance of the fracture. Massage and movement should be commenced after the wound is healed and the condition has become analogous to a simple fracture.
Question of Amputation in Compound Fractures.—Before deciding to perform primary amputation of a limb for compound fracture, the surgeon must satisfy himself (1) that the attainment of asepsis is impossible; (2) that the soft parts are so widely and so grossly damaged that their recovery is improbable; (3) that the vascular and nervous supply of the parts beyond has been rendered insufficient by destruction of the main blood vessels and nerve-trunks; (4) that the bones have been so shattered as to be beyond repair; and (5) that the limb, even if healing takes place, will be less useful than an artificial one.
In attempting to save the limb of a young subject, it is justifiable to run risks which would not be permissible in the case of an older person. To save an upper limb, also, risks may be run which would not be justifiable in the case of a lower limb, because, while a serviceable artificial leg can readily be procured, any portion of the natural hand or arm is infinitely more useful than the best substitute which the instrument-maker can contrive. The risk involved in attempting to save a limb should always be explained to the patient or his guardian, in order that he may share the responsibility in case of failure.
Whether or not the amputation should be performed at once, depends upon the general condition of the patient. If the injury is a severe one, and attended with a profound degree of shock, it is better to wait for twenty-four or forty-eight hours. Meanwhile the wound is purified, and the limb wrapped in a sterile dressing. Means are taken to counteract shock and to maintain the patient's strength, and evidence of infection or of hæmorrhage is carefully watched for. When the shock has passed off, the operation is then performed under more favourable auspices. Clinical experience has proved that by this means the mortality of primary amputations may be materially diminished, especially in injuries necessitating removal of an entire limb.
Having decided to amputate, it is important to avoid having bruised, torn, or separated tissues in the flaps, as these are liable to slough or to become the seat of infection. In this connection it should be borne in mind that the damage to soft tissues is always wider in extent than appears from external examination.
The attempt to save a limb may fail and amputation may be called for later because of spreading infective processes, osteomyelitis, or gangrene; to prevent exhaustion from prolonged suppuration and toxin absorption; or on account of secondary hæmorrhage.
Gun-shot Injuries of Bone.—Fractures resulting from the impact of bullet or fragments of shell are of necessity compound, and are usually infected from the outset by organisms carried in by the missile or by portions of clothing or other foreign material. Not infrequently the missile lodges in the bone.
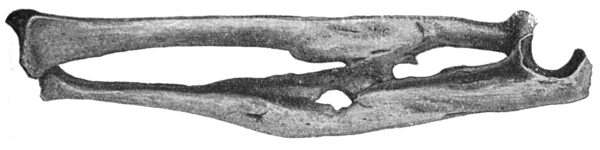 Fig. 7.—Excessive Callus Formation after infected
Compound Fracture of both Bones of Forearm—result of gun-shot wound.
Fusion of Bones across Interosseous Space.
Fig. 7.—Excessive Callus Formation after infected
Compound Fracture of both Bones of Forearm—result of gun-shot wound.
Fusion of Bones across Interosseous Space.
The extent of the injury to the bone varies infinitely, from a mere chip or gutter-shaped wound to complete pulverisation of the portion struck. The fracture is of the comminuted and fissured variety, the cracks radiating from the point of impact and extending for a considerable distance, sometimes even implicating the articular surface of the bone some inches away. In comminuted fractures of the shafts of long bones there is often a large wedge-shaped fragment completely isolated from the rest, and in the presence of infection this may form a sequestrum. Healing is often delayed by the separation of sequestra, which takes place slowly, and union is attended with excessive formation of callus. When a considerable section of the shaft has been lost, want of union, fibrous union, or the formation of a false joint may result.
The treatment is carried out on the same lines as in other forms of compound fracture, except that mention should be made of the irrigation method of Carrel, found to be the most potent means of overcoming the associated infection.
[1] We do not employ the term “diastasis,” which has been used in different senses by different writers.
In young subjects before the bones are fully developed the epiphyses may be separated from the diaphyses. The use of the X-rays has added greatly to our knowledge of these lesions.
It is useful to remember that in the upper extremity the epiphyses in the regions of the shoulder and wrist, and, in the lower extremity, those in the region of the knee, are the latest to unite; and that it is in these situations that growth in length of the bone goes on longest and most actively (twenty to twenty-one years). Injuries of these epiphyses, therefore, are most liable to interfere with the growth of the limb.
An epiphysis is nourished from the articular arteries and through the vessels of the periosteum.
Pathological Separation of Epiphyses.—There are certain pathological conditions, such as rickets, scurvy, congenital syphilis, tubercle, suppurative conditions, and tumour growths, which render separation of the epiphyses liable to occur from injuries altogether insufficient to produce such lesions under normal conditions.
Traumatic Separations.[2]—Speaking generally, it may be said that injuries which in an adult would be liable to produce dislocation, are in a young person more apt to cause separation of an epiphysis. Indirect violence, especially when exerted in such a way as to combine traction with torsion,—for example, when the foot is caught in the spokes of a carriage wheel,—is the commonest cause of epiphysial separation. Direct violence is a much less frequent cause. Muscular action occasionally produces separation of the epiphyses—for example, the anterior superior iliac spine, the small trochanter of the femur, or the upper end of the fibula.
[2] We desire here to acknowledge our indebtedness to Mr. John Poland's work on Traumatic Separation of the Epiphyses.
The majority of separations take place between the eleventh and the eighteenth years, chiefly because during this period the injuries liable to produce such lesions are most common. They do not occur after twenty-five, because by that time all the epiphyses have united. In females this form of injury is rare, and almost invariably occurs before puberty.
The following are the most common seats of separation in the order of their frequency: (1) the lower end of the femur; (2) the lower end of the radius; (3) the upper end of the humerus; (4) the lower end of the humerus; (5) the lower end of the tibia; and (6) the upper end of the tibia.
Morbid Anatomy.—In a true separation the epiphysial cartilage remains attached to the epiphysis. As a rule the epiphysis is not completely separated from the diaphysis, the common lesion being a separation along part of the epiphysial line, with a fracture running into the diaphysis (Fig. 8). It is not uncommon for more than one epiphysis to be separated by the same accident—for example, the lower end of the femur and the upper ends of the tibia and fibula. Epiphysial separations, like fractures, may be simple or compound. Incomplete separations are liable to be overlooked at the time of the accident, but there is reason to believe that they may form the starting-point of disease. Strain of the epiphysial junction—the juxta-epiphysial strain of Ollier—is a common injury in young children.
Clinical Features.—The symptoms simulate those of dislocation rather than of fracture. Thus, unnatural mobility at an epiphysial junction may closely resemble movement at the adjacent joint, especially when the epiphysis is an intra-capsular one. The relationship of the bony points, however, serves to indicate the nature of the lesion. The degree of deformity is often slight, because the transverse direction of the lesion, the breadth of the separated surfaces, and the firmness of the periosteal attachment along the epiphysial line often prevent displacement. In many cases a distinct, rounded, smooth, and regular ridge, caused by the projection of the diaphysis, can be felt. The peculiar “muffled” nature of the crepitus is one of the most characteristic signs. The older the patient, and the further ossification has progressed, the more does the crepitus resemble that of fracture.
Of the subsidiary signs, loss of power in the limb is one of the most constant; indeed, in young children it is sometimes the first, and may be the only, sign that attracts attention. Pain and tenderness along the epiphysial line are valuable signs, particularly when the lesion is due to indirect or muscular violence and there is no bruising of soft parts. Localised swelling, accompanied by ecchymosis, is often marked; and the adjacent joint may be distended with fluid.
As distinguishing this injury from a dislocation, it may be noted that in epiphysial separation there is no snap felt when the deformity is reduced, the tendency to re-displacement is greater, and the amount of relief given by reduction less than in dislocation. The use of the Röntgen rays at once establishes the diagnosis.
Prognosis and Results.—In the majority of cases union takes place satisfactorily by the formation of callus in the spongy tissue of the diaphysis and on the deep surface of the periosteum. In spite of the favourable nature of the prognosis in general, however, the friends of the patient should be warned that a completely satisfactory result cannot always be relied upon.
Deformity, with stiffness and locking at the adjacent joint, especially at the elbow, may result from imperfect reduction, or from exuberant callus. Arrest of growth of the bone in length is a rare sequel, and when it occurs, it is due, not to premature union of the epiphysis with the shaft, but to diminished action at the ossifying junction.
When the growth of one of the bones of the leg or forearm is arrested after separation of its epiphysis while the other bone continues to grow, the foot or hand is deviated towards the side of the shorter one.
Partial separations may be overlooked at the time of the accident and cause trouble later from bending of the bone, as in one variety of coxa vara. The epiphysis at the lower end of the femur may be displaced into the ham and press on the popliteal vessels.
Treatment.—The general principles which govern the treatment of fractures apply equally to epiphysial separations, the essential being the accurate replacement of the epiphysis.
In compound separations of epiphysis, the end of the diaphysis may be pushed through the skin. The entrance of sepsis may prove an obstacle to any operative measure that would otherwise be indicated.
Surgical Anatomy.—The function of a joint is to permit of the movement of one bone upon another. The articular surfaces are covered with a thin layer of hyaline cartilage, and are retained in apposition by the tension of ligaments and of the muscles surrounding the joint. The articular capsule (capsular ligament) is directly continuous with the periosteum, and is lined by a synovial layer, which at the line of attachment of the capsule is reflected on to the bone as far as the articular cartilage. The synovial layer invests intra-articular ligaments, and is projected into the interior of the joint in the form of loose folds wherever the articulating surfaces are not in immediate contact. The surface of the synovial layer is covered with minute processes or villi, which in diseased conditions may become hypertrophied. The synovia owes its lubricating property to mucin, derived from the solution of the endothelial cells on the free surface of the synovial layer. The opposing surfaces of a joint being always in accurate contact, the so-called cavity is only a potential one. If fluid is poured out into the joint, the synovial layer and the capsule are put upon the stretch, causing discomfort or actual pain, which is partly relieved by slightly flexing the joint. If the distension persists, the ligaments become elongated and the joint unstable.
The common origin of bone, cartilage, periosteum, and synovial layer from one parent tissue of the embryo, accords with the readiness with which any one of these tissues may be converted into another under traumatic or pathological influences; and how in ligaments and in synovial membrane foci of hyaline cartilage may form and, after increasing in size, undergo ossification.
Joints derive an abundant blood supply through the articular arteries. The lymphatics, which take origin in the synovial layer, pass to efferent vessels which run in the intermuscular and other connective-tissue planes of the limb. The nerve supply is derived chiefly from the nerves distributed to the muscles acting on the joint and to the skin over it.
Sources of Joint Strength.—The capacity of a joint to resist dislocation depends upon (1) the shape of its osseous elements; (2) the strength and arrangement of its ligaments; (3) the support it receives from muscles or tendons placed in relation to it; and (4) the relative stability of adjacent structures. While all these factors contribute to the strength of a given joint, one or other of them usually predominates, so that certain joints are osseously strong, others are ligamentously strong, while a few depend chiefly upon adjacent muscles for their stability.
The hip and elbows are the best examples of joints deriving their strength mainly from the architectural arrangement of the constituent bones. These joints are dislocated only by extreme degrees of violence, and not infrequently—especially in the elbow—portions of the bones are fractured before the articular surfaces are separated.
The knee, the wrist, the carpal, the tarsal, and the clavicular joints depend for their stability almost entirely on the strength of their ligaments. These joints are rarely dislocated, but as the main incidence of the violence falls on the ligaments they are frequently sprained.
The shoulder is the typical example of a joint depending for its security chiefly upon the muscles and tendons passing over it, and hence the frequency with which it is dislocated when the muscles are taken unawares. At the same time the great mobility of the scapula and clavicle materially increases the stability of the shoulder-joint. The tendons passing in relation to the knee, ankle, and wrist add to the stability of these joints.
The proximity of an easily fractured bone also contributes to prevent dislocation of certain joints—for example, fracture of the clavicle prevents an impinging force expending itself on the shoulder-joint; and the frequency of Colles' fracture of the radius, and of Pott's fracture of the fibula, doubtless accounts to some extent for the rarity of dislocation of the wrist and ankle-joints respectively. The immunity from dislocation which the joints of young subjects enjoy is partly due to the ease with which an adjacent epiphysis is separated.
The mechanical axiom that “what is gained in movement is lost in stability” applies to joints, those which have the widest range of movement being the most frequently dislocated.
The injuries to which a joint is liable are Contusions, Wounds, Sprains, and Dislocations.
Contusions of Joints.—Contusion is the mildest form of injury to a joint. Whether the violence is transmitted from a distance, as in contusion of the hip from a fall on the feet, or acts more directly, as in a fall on the great trochanter, the bones are violently driven against one another, and the force expends itself on their articular surfaces. The articular cartilages and the underlying spongy bone, as well as the synovial lining, are bruised, and there is an effusion of blood and serous fluid into the joint and surrounding tissues.
The most prominent clinical features are swelling and discoloration. The swelling, especially in superficially placed joints, is an early and marked symptom, and is mainly due to the effusion of blood into the joint (hæmarthrosis). In deeply placed joints, discoloration may not appear on the surface for some days, especially if the violence has been indirect. The joint is kept in the flexed position, and is painful only when moved. In hæmophilic subjects, considerable effusion of blood into a joint may follow the most trivial injury.
A slight degree of serous effusion into the joint (hydrarthrosis) often persists for some time, and tuberculous affections of joints not infrequently date from a contusion.
The treatment is the same as for sprains (p. 36).
Wounds of Joints.—The importance of accidental wounds of joints—such, for example, as result from a stab with a penknife or the spike of a railing—lies in the fact that they are liable to be followed by infection of the synovial cavity. The infection may involve only the synovial layer (septic synovitis), or may spread to all the elements of the joint (septic arthritis). These conditions are described with diseases of joints.
Penetration of the joint may sometimes be recognised by the escape of synovia from the wound, or the synovial layer or articular cartilage may be exposed. When doubt exists, the wound should be enlarged. The use of the probe is to be avoided, on account of the risk of carrying infective material from the track of the wound into the joint.
Penetrating wounds of joints are treated on the same lines as compound fractures. If the penetrating instrument is to be regarded as infected,—as, for example, when the spoke of a motor bicycle is driven through the upper pouch of the knee,—the injury is to be looked upon as serious and capable of endangering the function of the joint, loss of the limb, or even life itself. Reliance is chiefly laid on primary excision of the edges and track of the wound, and other measures employed in the treatment of gun-shot wounds. While the wound in the synovialis and capsule is sutured, that in the soft parts is left open. If drainage is employed, the tube extends down to the opening in the synovialis, but not into the joint itself. If sepsis supervenes, the joint is opened and irrigated by Carrel's method. Some form of splint and a Bier's bandage are valuable adjuncts. The final recourse is to amputation.
Gun-shot injuries of joints vary in severity from a mere puncture of the synovial layer by a chip of shell to complete shattering of the articular surfaces. Between these extremes are cases in which the capsular and synovial layer are extensively lacerated without involvement of the bones, and others in which the bones are implicated without serious damage being done to ligaments or synovial layer—for example, by a bullet passing through and through the cancellated part of one of the constituent bones, or by a fissure extending into the articular surface.
In all degrees the great risk is from septic infection, which may be assumed to be present in all but the last-named variety.
The treatment consists in immediately cleansing the wound by excising grossly damaged tissue and removing any foreign body that may have lodged; disinfecting the exposed part of the joint cavity with eusol, “bipp,” or other antiseptic, and closing the wound or establishing drainage, according to circumstances. The joint is then immobilised till the wound has healed, after which massage and movement are commenced. When the bones are shattered or when sepsis gets the upper hand and disorganises the joint, amputation is called for.
Sprains.—A sprain results from a stretching or twisting form of violence which causes the joint to move beyond its physiological limits, or in some direction for which it is not structurally adapted. The main incidence of the force therefore falls upon the ligaments, which are suddenly stretched or torn. The synovial layer also is torn, and the joint becomes filled with blood and synovial fluid.
Muscles and tendons passing over the joint are stretched or torn, and their sheaths filled with serous effusion. It is not uncommon for portions of bone to be torn off at the site of attachment of strong ligamentous bands or tendons, constituting a “sprain fracture”; or for intra-articular cartilages to be torn and displaced, as in the knee.
Clinical Features.—The injury is accompanied by intense sickening pain, and this may persist for a considerable time. At first it is aggravated by moving the joint, but if the movement is continued it tends to pass off. The particular ligaments involved may be recognised by the tenderness which is elicited on making pressure over them, or by putting them on the stretch. In this way a sprain may often be diagnosed from a fracture in which the maximum tenderness is over the injury to the bone.
The effusion of blood and synovia into the joint and into the tissues around gives rise to swelling and discoloration, and the fluid effused into tendon sheaths often produces a peculiar creaking sensation, which may be mistaken for the crepitus of fracture. In sprains, the bony points about the joint retain their normal relations to one another, and this usually enables these injuries to be diagnosed from dislocations. When the swelling is great, it is often necessary to have recourse to the Röntgen rays to make certain that there is no fracture or dislocation. The special features and complications of sprains of the knee are discussed with other injuries of that joint.
Repair of Sprains.—Blood and synovia are absorbed and torn structures become reunited, but in this process adhesions may form inside the joint and in the surrounding tendon sheaths and interfere with the movement of the joint.
Prognosis.—Stiffness, lasting for a longer or shorter time, follows most sprains, but may be largely prevented by proper treatment. In old and rheumatic persons, changes of the nature of arthritis deformans are liable to supervene, interfering greatly with movement. While suppuration is rare, tuberculous disease is alleged to have resulted from a sprain.
Treatment.—If seen immediately after the accident, firm pressure should be applied by means of an elastic bandage over a thick layer of cotton wool, to prevent bleeding and effusion of synovia. Later the best treatment is by massage and movement. In the ankle, for example, massage should be commenced at once, the part being gently stroked upwards. If the massage is light enough there is no pain, it is actually soothing. The rubbing is continued for from fifteen to twenty minutes, and the patient is encouraged to move the toes and ankle; a moderately firm elastic bandage is then applied. The massage is repeated once or twice a day, the sittings lasting for about fifteen minutes. The patient should be encouraged to move the joint from the first, beginning with the movements that put least strain upon the damaged ligaments, and gradually increasing the range. In the course of a few days he is encouraged to walk or cycle, or otherwise to use the joint without subjecting it to strain, or to a repetition of the movement that caused the accident. Alternate hot and cold douching, or hot-air baths, followed by massage, are also useful. Complete rest and prolonged immobilisation are to be condemned.
A dislocation or luxation is a persistent displacement of the opposing ends of the bones forming a joint. We are here concerned only with such dislocations as immediately follow upon injury. Those that are congenital or that result from disease will be studied later.
Causes.—The majority of dislocations are the result of indirect violence, the more movable bone acting as a lever, on a fulcrum furnished by the natural check to movement in the form of ligament, bone, or muscle. It is in this way that most dislocations of the shoulder, hip, and elbow are produced.
At the moment the violence is applied, the muscles are relaxed or otherwise taken at a disadvantage, so that the joint is for the time being deprived of their support. The joint is moved beyond its physiological range, and the end of one of the bones being brought to bear upon the capsule, tears it, and passes through the rent thus made. The muscles then contract reflexly, and pull the head of the bone into an unnatural position outside the capsule. The position assumed will depend upon such factors as the direction of the force, the structure of the joint, the position of the limb at the time of the accident, and the relative strength of the different groups of muscles acting upon the bone which is displaced.
Violence applied directly to the joint is a much less frequent cause of dislocation. In this way, however, the knee-joint may be dislocated, one bone being driven past the other—for example, by a kick from a horse; or the acromio-clavicular joint by a blow on the shoulder.
Muscular contraction is not often the sole cause of dislocation, although, as has been mentioned, it plays an important rôle in the production of the majority of these injuries. The shoulder, mandible, and patella are, however, not infrequently displaced by muscular action alone. Acrobats sometimes acquire the power of dislocating certain joints by voluntary contraction of their muscles.
Age and Sex.—Dislocations occur most frequently in adult males, doubtless on account of the nature of their occupations and recreations. In children the epiphyses are separated, and in old people the bones are broken by such forms of violence as cause dislocation in the middle-aged.
Muscular debility and undue laxness of ligaments resulting from disease or previous dislocation are also predisposing factors.
Clinical Varieties.—The separation between the bones may be complete or partial. When partial, portions of the articular surfaces remain in apposition, and the injury is known as a sub-luxation. Like fractures, dislocations may be simple or compound, the latter being specially dangerous on account of the risk of infection. When seen within a few days of its occurrence, a dislocation is looked upon as recent; but when several weeks or months have elapsed, it is spoken of as an old-standing dislocation. The latter will be described later.
Dislocations, like fractures, may be complicated by injuries to large blood vessels or nerve-trunks, by injuries to internal organs, or by a wound of the soft tissues which does not communicate with the joint. Further, a fracture may coexist with a dislocation—a most important complication.
Clinical Features.—The most characteristic signs of dislocation are preternatural rigidity, or want of movement where movement should naturally take place; mobility in abnormal directions; and deformity, the part being “out of drawing” as compared with the uninjured side (Fig. 18). The bony landmarks lose their normal relationship to one another; and the deformity is characteristic, and is common to all examples of the same dislocation.
Although any of the subsidiary signs may occur in lesions other than dislocations, due weight must be given to them in making a diagnosis. Loss of function is complete as a rule. Pain is much more intense than in fracture, usually because the displaced bone presses upon nerve-trunks, and from the same cause there is often numbness and partial paralysis of the limb beyond. Swelling of the soft parts due to effused blood is usually less marked in dislocation than in fracture, but is often sufficiently great to interfere with diagnostic manipulations. The displaced bone, and sometimes the empty socket, may be palpable. Discoloration is usually later of appearing than in fractures. Alteration in the length of the injured limb—usually in the direction of shortening—is a common feature; while girth measurements usually show an increase. A peculiar soft grating or creaking sensation is often felt on attempting to move the joint; this is due to cartilaginous or ligamentous structures rubbing on one another, and must not be mistaken for the crepitus of fracture. In the majority of cases, although not in all, after reduction has been effected, the bones retain their proper relations without external support, a point in which a dislocation differs from a fracture. A careful investigation of the kind of force which produced the injury, particularly as regards its intensity and direction of action, may aid in the diagnosis. The diagnosis can always be verified by the use of the Röntgen rays, and this should be had recourse to whenever possible, as a fracture may be shown that otherwise would escape recognition.
Prognosis.—After having once been dislocated, a joint is seldom as strong as it was formerly, although for all practical purposes the limb may be as useful as ever. Some degree of stiffness, of limited movement, or of muscular weakness, and occasional arthritic changes and a liability to re-dislocation, are the commonest sequelæ. Prolonged immobilisation is liable to lead to stiffness by permitting of the formation of adhesions; while too early movement tends to produce a laxity of the ligaments which favours re-displacement from slight causes.
Treatment.—Reduction should be attempted at the earliest possible moment. Every hour of delay increases the difficulty. The guiding principle is to cause the displaced bone to re-enter its socket by the same route as that by which it left it—that is, through the existing rent in the capsule. This is done by carrying out certain manipulations which depend upon the anatomical arrangement of the parts, and which vary, not only with different joints, but also with different varieties of dislocation of the same joint. In general terms it may be said that the main impediments to reduction are: the contraction of the muscles acting upon the displaced bone; the entanglement of the bone among tendons or ligamentous bands which fix it in its abnormal position; and the rent in the capsule being small or valvular, so that it forms an obstacle to the bone reentering the socket.
Muscular contraction is best overcome by the administration of a general anæsthetic, and in all but the simplest cases this should be given to ensure accurate and painless reduction. Failing this, however, the muscles may be wearied out by the surgeon making steady and prolonged traction on the limb, while an assistant makes counter-extension on the proximal segment of the joint. Advantage may also be taken of such muscular relaxation as occurs when the patient is already faint, or when his attention is diverted from the injured part, to carry out the manipulations necessary to restore the bone to its normal position.
The appropriate manœuvres for disengaging the head of the bone from tendons, ligaments, or bony processes with which it may be entangled, will be suggested by a consideration of the anatomy of the particular joint involved, and will be described with individual dislocations.
In reducing a dislocation, no amount of physical force will compensate for a want of anatomical knowledge. All tugging, twisting, or wrenching movements are to be avoided, as they are liable to cause damage to blood vessels, nerves, or other soft parts, or even—and especially in old people—to fracture one of the bones concerned.
After reduction, great benefit is gained by the systematic use of massage and movement. Before any restraining apparatus is applied the whole region should be gently stroked in a centrifugal direction for fifteen or twenty minutes; and this is to be repeated daily, each sitting lasting for about twenty minutes. From the first day onward, movement of the joint is carried out in every direction, except that which tends to bring the head of the bone against the injured part of the capsule; and the patient is encouraged to move the joint as early as possible. The appropriate apparatus and the period during which it should be worn will be considered with the individual dislocations.
Operation in Simple Dislocations.—In a limited number of cases, even with the aid of an anæsthetic, reduction by manipulation is found to be impossible. Resort must then be had to operation, which is a comparatively safe and satisfactory proceeding, although often difficult. It may happen in rare instances that the undoing of the displacement is only possible after the removal of a portion of one or other of the bones.
Compound Dislocations.—Compound dislocations are usually the result of extreme violence produced by machinery or railway accidents, or by a fall from a height. In the majority of cases they are complicated by fracture of one or more of the constituent bones of the joint, as well as by laceration of muscles, tendons, and blood vessels. In the region of the ankle, wrist, and joints of the thumb, however, compound dislocation is sometimes met with uncomplicated by other lesions. The great risk is infection, which may result in serious impairment of the usefulness of the joint or even in its complete destruction, results towards which the concomitant injuries materially contribute. In many instances where infection has occurred, ankylosis is the best result that can be hoped for.
Treatment.—As a rule, the first question that arises is whether amputation is necessary or not, and the considerations that determine this point are the same as in compound fractures (p. 26). If an attempt is to be made to save the limb, the treatment is the same as in compound fracture (p. 25).
Dislocation complicated by Fracture.—In certain dislocations the separation of small portions of bones or of epiphyses is of common occurrence—for example, fracture of the tip of the coronoid process in dislocation of the elbow backwards, and chipping off of a portion of the edge of the acetabulum in dislocation of the hip.
The most important example of a fracture complicating a dislocation is fracture of the surgical neck of the humerus coexisting with dislocation of the shoulder. Here the difficulty of diagnosis is greatly increased, and the treatment of both injuries requires to be modified. The dislocation must be reduced—by operation if necessary—before the fracture is treated, and in many cases it is advisable to secure the fragments of the broken bone by pegs, or plates, to admit of movement being commenced early, and so to prevent stiffness of the joint.
Old-standing Dislocations.—When, from want of recognition—and, curiously enough, a dislocation is much more liable to be overlooked than would have been thought possible—or from unsuccessful treatment, a dislocation is left unreduced, changes take place in and around the joint which render reduction increasingly difficult or impossible. The rent in the capsule closes upon the neck of the bone, and fibrous adhesions form between muscles, tendons, and other structures that have been torn. The articular cartilage of the head, being no longer in contact with an opposing cartilage, tends in time to be converted into fibrous tissue, and may become adherent to other fibrous structures in its vicinity. By pressing on adjacent structures it may form for itself a new socket of dense fibrous tissue which in time becomes lined with a secreting membrane. When the displaced head lies against a bone, the continuous pressure produces a new osseous socket, from the margins of which osteophytic outgrowths may spring, and as the surrounding fibrous tissue becomes condensed and forms a strong capsule, a new joint results. The occurrence of these changes in the direction of a new ball-and-socket joint is largely dependent on the behaviour of the patient: a vigorous man, anxious to recover the use of the limb, will employ it with a degree of determination and indifference to pain that could not be expected in a sensitive elderly female. The most perfect example of a new ball-and-socket joint, following upon an unreduced dislocation at the hip, that has come under our observation, was in a hunting dog, given one of us by an Australian pupil, who testified that the animal was as fleet with the new joint as it had been with the original one. Meanwhile the cartilage of the original socket is converted into fibrous tissue, which may come to fill up the cavity. Changes resembling those of arthritis deformans may occur. The large blood vessels and nerves in the vicinity may be pressed upon or stretched by the displaced bone, or may be implicated in fibrous adhesions. In course of time they become lengthened or shortened in accordance with the altered attitude of the limb.
 Fig. 12.—Os Innominatum showing new socket formed
after old-standing dislocation. The acetabulum is almost obliterated.
Fig. 12.—Os Innominatum showing new socket formed
after old-standing dislocation. The acetabulum is almost obliterated.
In many cases the new joint is remarkably mobile and useful; but in others, pain, limited movement, and atrophy of muscles render it comparatively useless, and surgical intervention is called for.
Treatment.—It is always a difficult problem to determine the date after which it is inadvisable to attempt reduction by manipulation in an old dislocation and no rules can be laid down which will cover all cases. Rather must each case be decided on its own merits, due consideration being had to the risks that attend this line of treatment. The chief of these are: rupture of a large blood vessel or nerve that has formed adhesions with the displaced bone, or has become shortened in adaptation to the altered shape or length of the limb; tearing of muscles or tendons, or even of skin; fracture of the bone, especially in old people; and separation of epiphyses in the young.
Before carrying out the manipulations appropriate to the particular dislocation, all adhesions must first be broken down; and during the proceedings no undue force is to be employed. The first attempt at reduction may fail, and yet subsequent efforts, at intervals of a few days, may ultimately prove successful; the vigorous traction and twisting of the soft parts, matted together as they are by scar-tissue, causes reactive changes in the vessels and tissues which render them more liable to yield on subsequent attempts at reduction. In old people, and where there is an absence of suffering from pressure on nerves or vessels, it may be wiser to leave the dislocation unreduced, and strive rather by massage and movement to obtain a useful variety of false joint. If the conditions are otherwise, it may be better to improve the function of the limb by an open operation. Tight ligaments and other structures are divided, and the socket is cleared out. If reduction is still impossible, a partial excision may be performed and a flap of fascia lata introduced to prevent ankylosis (arthroplasty). In the case of the hip, the dislocation may be left alone and the femur divided below the trochanter, especially if there is pronounced flexion.
Habitual or recurrent dislocation is almost exclusively met with in the shoulder, and will be described with the injuries of that joint.
Pathological Dislocations.—Joints may become dislocated in the course of certain diseases. These pathological dislocations fall into different groups: (1) those due to gradual stretching of the capsular and other ligaments weakened by inflammatory and suppurative processes, such as sometimes follow on typhoid, scarlet fever, or diphtheria, and in pyæmia; (2) those due to destructive changes in the ligaments and bones—typically seen in tuberculous arthritis, in arthritis deformans, in Charcot's disease, and in nerve lesions, e.g. dislocation of the hip in spastic conditions, such as Little's disease; (3) those associated with deformed attitudes of the limb; (4) those due to changes in the articular surfaces, e.g. the phalanges in arthritis deformans. These will be considered with the conditions which give rise to them.
Congenital Dislocations.—Congenital dislocations are believed to be the result of abnormal or arrested development in utero, and are to be distinguished from dislocations occurring during birth, which are essentially traumatic in origin. They will be described along with the Deformities of the Extremities.
The injuries met with in the region of the shoulder include fractures and dislocations of the clavicle, fractures of the scapula, dislocations and sprains of the shoulder-joint, and fractures of the upper end of the humerus.
Surgical Anatomy.—For the examination of an injury in the region of the shoulder the patient should be seated on a low stool or chair. After inspecting the parts from the front, the surgeon stands behind the patient and systematically examines by palpation the shoulder girdle and upper end of the humerus. The uninjured side should be examined along with the other for purposes of comparison.
Immediately lateral to the supra-sternal notch, the sterno-clavicular articulation may be felt, the large end of the clavicle projecting to a varying degree beyond the margins of the small and shallow articular surface on the sternum. Any dislocation of this joint is at once recognised. The clavicle being subcutaneous throughout its whole length, any irregularity in its outline can be easily detected. A small tubercle (deltoid tubercle) which frequently exists near the acromial end is liable to suggest the presence of a fracture. The lateral end forms with the acromion the acromio-clavicular joint, which, however, is not always readily identified. The fingers are now carried over the acromion, which often exhibits in the situation of its epiphysial cartilage a prominent ridge, which must not be mistaken for a fracture. The tip of the acromion is usually employed as a fixed point in measuring the length of the upper arm.
The outline of the spine of the scapula can be traced back to the vertebral border; and the body of the bone may be manipulated, and its movements tested by moving the arm.
The coracoid process can be recognised in the upper and lateral angle of the triangular depression bounded by the pectoralis major, the deltoid, and the clavicle.
The head and surgical neck of the humerus may now be felt from the axilla, if the axillary fascia is relaxed by bringing the arm to the side. The great tuberosity can be indistinctly felt on the lateral aspect of the shoulder through the fibres of the deltoid. It lies vertically above the lateral epicondyle, and may be felt to rotate with the shaft. The inter-tubercular (bicipital) groove looks forward, and lies in a line drawn vertically through the biceps muscle.
The subclavian artery, with its vein to the median side and the cords of the brachial plexus to the lateral side, passes under the middle of the clavicle, and may be compressed against the first rib immediately above this bone.
Fracture of the clavicle is one of the commonest injuries met with in practice. As about one-third of the cases occur in children, the fracture is often of the greenstick variety. The fractures are seldom compound or complicated, unless as a result of gun-shot injuries; but occasionally one of the fragments pierces the skin, or comes to press upon the subclavian vessels or the cords of the brachial plexus, arresting the pulsation in the vessels of the limb, and causing severe pain in the arm.
The most common site of fracture is in the middle third (Fig. 13), and this usually results from indirect violence, such as a fall on the outstretched hand, the elbow, or the outer aspect of the shoulder, the force being transmitted through the glenoid cavity to the scapula, and thence by the coraco-clavicular ligaments to the clavicle. The violence is therefore of a twisting character, and the bone gives way near the junction of the lateral and middle thirds, just where the two natural curves of the bone meet, and where the supporting muscular and ligamentous attachments are weakest.
The fracture so produced is usually oblique from above, downwards and inwards. The sternal fragment may be slightly drawn upwards by the clavicular fibres of the sterno-mastoid, while the acromial fragment falls by the weight of the arm, and the fragments usually overlap to the extent of about half an inch. The shoulder, having lost the buttressing support of the clavicle, falls in towards the chest wall, narrowing the axillary space, while the weight of the arm pulls it downward, and the muscles inserted in the region of the bicipital groove pull it forward.
Fracture of the middle third may result also from a direct stroke, such as the recoil of a gun, or from violent muscular contraction, the fracture as a rule being transverse, and the displacement less marked than in fracture by indirect violence.
Clinical Features.—The attitude of the patient is characteristic: the elbow is flexed and is supported by the opposite hand, while the head is inclined towards the affected shoulder to relax the muscles of the neck. Crepitus is elicited on bracing back the shoulders, or on attempting to raise the arm beyond the horizontal, and these movements cause pain. Tenderness is elicited on making pressure over the seat of fracture, and also on distal pressure. The sternal fragment almost invariably overrides the acromial, and can usually be palpated through the skin; on measurement, the clavicle is found to be shortened. When the fracture is incomplete (greenstick) or transverse, the symptoms are less marked.
 Fig. 14.—Fracture of Acromial End of Clavicle. Shows
forward rotation of lateral fragment, and line of fracture united by
bone.
Fig. 14.—Fracture of Acromial End of Clavicle. Shows
forward rotation of lateral fragment, and line of fracture united by
bone.
Fracture of the lateral or acromial third of the clavicle is a common form of accident at football matches, and usually results from direct violence, the bone being driven down against the coracoid process, and broken as one breaks a stick over the knee. The fracture may take place through the attachment of the conoid and trapezoid ligaments, in which case the only symptoms are pain and tenderness at the seat of fracture, with impaired movement of the limb. Displacement and crepitus are prevented by the splinting action of the ligaments.
When the break is lateral to the attachment of the trapezoid ligament, the fracture is usually transverse, and is almost always due to a fall on the back of the shoulder—the angle between the spine and the acromion process striking the ground. The acromial fragment rotates forward (Fig. 14), sometimes even to a right angle, causing the tip of the shoulder to pass forwards, and so to lie slightly nearer the middle line. The integrity of the coraco-clavicular ligaments prevents any marked drooping of the shoulder. It is noteworthy that the displacement is not always evident at first.
Fractures of the medial or sternal third are rare, are usually oblique, and result either from an indirect force acting in the line of the clavicle, or, less frequently, from direct violence or muscular action. As a rule, the deformity is insignificant, except when the costo-clavicular ligament is torn, in which case the medial end of the distal fragment is tilted up by the weight of the arm. The shoulder passes downwards, forwards, and medially. When close to the sternal end, this fracture may simulate a dislocation of the sterno-clavicular joint or a separation of the clavicular epiphysis. This last is a rare accident, which may occur between the seventeenth and the twenty-fifth years, and is usually the result of violent muscular action. It differs from the other injuries in this region in being more easily reduced and retained in position, the epiphysis lying entirely within the limits of the articular capsule of the sterno-clavicular joint.
Simultaneous fracture of both clavicles usually results from a severe transverse crush of the upper part of the thorax or from a fall on the outstretched hands—for example, in hunting. The middle third of the bone is implicated, and there is marked displacement and overriding. The patient is rendered helpless, and from the extrinsic muscles of respiration being thrown out of action and the weight of the powerless limbs pressing on the chest, there is considerable difficulty in breathing, and this is often increased by the fracture being complicated by injuries of the lung or pleura.
The prognosis as to union in all these injuries is good. Firm bony union usually occurs within twenty-one days. Non-union, false-joint, or fibrous union is but rarely met with. At the same time it is to be borne in mind that, in spite of all precautions, some deformity and shortening may result, without, however, interfering with the usefulness of the limb.
Treatment.—The displacement in complete fractures of the clavicle is readily reduced by supporting the elbow, bracing back the shoulders, and levering out the tip of the affected shoulder. In a few cases the interposition of some fibres of the subclavius muscle between the fragments has prevented perfect reduction.
In the greenstick variety the bone may be bent back into its normal position, but no great force should be employed, as, in spite of imperfect reduction, the clavicle usually straightens as it grows, and although some deformity may persist, the function of the limb is not interfered with.
Recumbent Position.—There is little doubt that the most perfect æsthetic results are obtained by treating the patient in the recumbent position. In girls, therefore, in whom it is desired that the shoulders should be perfectly symmetrical, the best results are obtained from placing the patient on a firm mattress, with a narrow, firm cushion between the shoulder-blades, so that the weight of the shoulder may carry the acromial fragment laterally and backwards. A pad is inserted in the axilla, the elbow raised, and the arm placed by the side on a pillow and steadied with sand-bags. Massage is applied daily. As this position must be maintained uninterruptedly for two or three weeks, it proves too irksome for most patients. When both clavicles are fractured, however, it is, short of operation, the only available method of treatment.
In ordinary cases the arm should be placed in that position which gives the best alignment of the fragments and least deformity. A thin layer of wool is placed in the axilla to separate the skin surfaces. A sling, supporting the elbow, is now applied, maintaining the arm in position, and a body bandage fixes the arm to the side. Massage and movement should be commenced at once.
A simple method, which yields satisfactory results, is that suggested by Wharton Hood. The fracture having been reduced, three strips of adhesive plaster, each an inch and a half wide, are applied from a point immediately above the nipple to a point 2 inches below the angle of the scapula (Fig. 15). The middle strap covers the seat of fracture, and is applied first: the others, slightly overlapping it, extend about half an inch on either side. The elbow is supported in a sling. This plan has the advantage that it permits of movement of the shoulder being carried out from the first, but the plaster rather interferes with massage.
The Handkerchief Method.—In cases of emergency, one of the best methods applicable to all fractures of the clavicle is to brace back the shoulders by means of two padded handkerchiefs, folded en cravate, placed well over the tips of the shoulders and tied, or interlaced, between the scapulæ. The forearm is then supported by a third handkerchief applied as a sling, the base of which is placed under the elbow, the ends passing over the sound shoulder.
Operative treatment may be called for in compound or comminuted fractures when the fragments have injured, or are likely to injure, the subclavian vessels or the cords of the brachial plexus, or when it is otherwise impossible to reduce the fracture or to retain the fragments in apposition. It is also indicated in some cases of fracture of both clavicles.
These various methods of treatment are not equally applicable to all cases. In our experience, in the circumstances indicated, the following methods have proved the most satisfactory: (1) As a temporary means of retention in emergency cases,—for example, accidents occurring on the football field,—the handkerchief method. (2) In uncomplicated fractures of average severity in any part of the bone, the method of sling and body bandage. (3) In cases where, for æsthetic reasons, the chief consideration is the avoidance of deformity and the maintenance of the symmetry of the shoulders, as in girls, the treatment by recumbency. (4) When retentive apparatus fails, or when the fragments are exerting injurious pressure, operative treatment.
In quite a number of cases, there is an excessive amount of pain, preventing sleep; where this is due to cramp-like contractions of the muscles and movements of the fragments, it is relieved by more accurate fixation, as by strips of plaster; otherwise a hypodermic injection of heroin or morphin is indicated.
Dislocation of the acromial end—sometimes, and perhaps more correctly, spoken of as dislocation of the scapula—is more frequent than that at the sternal end, and it usually results from a blow from behind, or from a fall on the tip of the shoulder, driving down the scapula, so that the clavicle projects upwards and overrides the acromion process.
Downward displacement of the acromial end of the clavicle is much rarer, and may follow a fall on the elbow or a blow over the clavicle. The end of the bone lies under the acromion process, in contact with the capsule of the shoulder-joint, and the acromion stands out prominently.
The clinical features are so well marked that the diagnosis is unmistakable. The head inclines towards the affected side, and the tip of the shoulder tends to pass slightly downward, forward, and medially. The displaced end of the bone can be seen and felt as a prominence under the skin, or the empty socket can be palpated, while the muscles attached to the displaced clavicle stand out in relief. The movements at the shoulder are restricted, particularly in the direction of abduction above the level of the shoulder. These injuries are sometimes associated with fracture of the ribs, a complication which adds materially to the difficulties of treatment.
Treatment.—Reduction is easily effected by bracing back the shoulders and replacing the bone in its socket by manipulation; but retention is invariably difficult, and in many cases impossible; even when the displacement is permanent, however, the usefulness of the arm is not necessarily impaired.
Treatment is similar to that for fracture of the clavicle by sling and body bandage. Another plan is to place a pad over the acromial end of the clavicle, and fix it in this position by a few turns of elastic bandage carried over the shoulder and under the elbow. The forearm is placed in a sling with the elbow well supported, and the arm is bound to the side by a circular bandage. When the bone cannot be kept in position and the usefulness of the limb is impaired, the joint surfaces may be rawed and the bones wired, with a view to obtaining ankylosis.
The sternal end may be dislocated forwards, backwards, or upwards.
Forward dislocation is the most common; the end of the clavicle lies on the front of the sternum, somewhat below the level of the sterno-clavicular joint, and its articular surface can be distinctly palpated (Fig. 16). The inter-articular cartilage sometimes remains attached to one bone, sometimes to the other; the rhomboid ligament is usually intact.
In the backward dislocation the end of the clavicle lies behind the manubrium sterni and the muscles attached to it; there is a marked hollow in the position of the joint, and the facet on the sternum can be felt. In a comparatively small number of cases the bone exerts pressure upon the trachea and œsophagus, producing difficulty in breathing and swallowing. It has also been known to press upon the subclavian artery and on other important structures at the root of the neck.
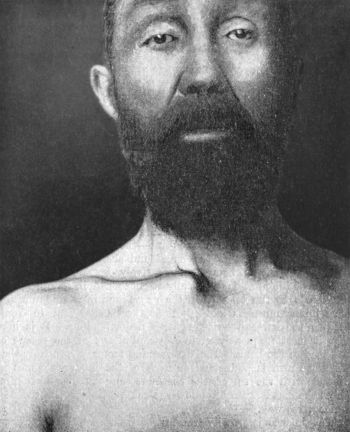 Fig. 16.—Forward Dislocation of Sternal End of Right
Clavicle. From a fall on a polished floor, in a man æt. 40.
Fig. 16.—Forward Dislocation of Sternal End of Right
Clavicle. From a fall on a polished floor, in a man æt. 40.
In rare cases the rhomboid ligament is torn, and the end of the clavicle passes upwards, and rests in the episternal notch behind the sterno-mastoid muscle.
The bone may be retained in position by keeping the shoulders braced back by a figure-of-eight bandage, or by padded handkerchiefs, and making pressure over the displaced end of the bone with a pad. The forearm is supported by a sling, and the arm fixed to the side. Massage is employed from the first, and the patient is allowed to move the arm by the end of a week. Imperfect reduction interferes so little with the functions of the limb that operative measures are seldom required except for æsthetic reasons.
Dislocation of both ends of the clavicle has occasionally occurred from a severe crush. The ultimate result has been satisfactory, as one or other end has always healed in normal position, and the function of the arm has thus been maintained.
The shoulder is more frequently dislocated than all the other joints in the body taken together. This is explained by its exposed position, the wide range of movement of which it is capable, the length of the lever afforded by the humerus, and the anatomical construction of the joint—the large, round humeral head imperfectly fitting the small and shallow glenoid cavity, and the ligaments being comparatively lax and thin. The capsule of the joint is materially strengthened in its upper and back parts by the tendons of the supra- and infra-spinatus and teres minor muscles; while it is weakest below and in front, between the subscapularis and teres major tendons. It is here that it most frequently gives way and allows of the escape of the head of the bone. The determining factor is probably that when the arm is abducted the neck of the humerus comes in contact with the tip of the acromion, and further abduction forces the head against the lower, weak portion of the capsule, which gives way.
The violence is usually transmitted from the hand or elbow, less frequently from the lateral aspect of the shoulder, the limb being usually abducted and the muscles relaxed and taken unawares. The head of the humerus, thus brought to bear on the weakest part of the capsule, ruptures it and passes out through the rent. Dislocation is readily produced in an unconscious person—as, for example, in conducting artificial respiration in a patient suffering from opium poisoning, the arms being hyper-abducted to exert traction on the chest.
Varieties.—Several varieties of dislocation are recognised, according to the position in which the head of the humerus finally rests (Fig. 17). The simplest of these is the sub-glenoid variety, in which the head rests on the long tendon of the triceps, where it arises from the axillary border of the scapula just below the glenoid cavity. In almost all dislocations of the shoulder the head of the bone is at least momentarily in this position, but the sharp edge of the scapula and the rounded head are ill adapted to one another, and the position is not long maintained. The subsequent course taken by the humerus depends upon the nature and direction of the force, the position of the limb at the moment of injury, and the relative strength and capacity for effective action of the different groups of muscles acting upon the bone.
In the great majority of cases it passes forward and medially, and comes to lie against the anterior surface of the neck of the scapula, under cover of the tendons of origin of the biceps and coraco-brachialis muscles, constituting the sub-coracoid dislocation. Much less frequently it passes under cover of the pectoralis minor and against the edge of the clavicle—the sub-clavicular variety. In rare cases the head passes backward and lies against the spine on the dorsum of the scapula, beneath the infra-spinatus muscle—the sub-spinous variety. Other varieties are so rare that they do not call for mention.
Clinical Features common to all Varieties.—Dislocation of the shoulder is commonest in adult males; in advanced life the proportion of female sufferers increases. It is usually attended with great pain, and there is often numbness of the limb due to pressure of the head of the bone upon the large nerve-trunks. There is sometimes considerable shock. The patient inclines his head towards the injured side, and, while standing, the forearm is supported by the hand of the opposite side. The acromion process stands out prominently, the roundness of the shoulder giving place to a flattening or depression immediately below it, so that a straight-edge applied to the lateral aspect of the limb touches both the acromion and the lateral epicondyle. The vertical circumference of the shoulder is markedly increased; this test is easily made with a piece of tape or bandage and is compared with a similar measurement on the normal side—we lay great stress on this simple measure, as it is a most reliable aid in diagnosis. The head of the bone can usually be felt in its new position, and the axis of the humerus is correspondingly altered, the elbow being carried from the side—forward or backward according to the position of the head. The empty glenoid may sometimes be palpated from the axilla. In most cases, although not in all, the patient is unable at one and the same time to bring his elbow to the side and to place his hand upon the opposite shoulder (Dugas' symptom). Measurements of the length of the limb from acromion to lateral epicondyle are rarely of any diagnostic value.
The sub-coracoid dislocation (Fig. 18) is that most frequently met with. It usually results from hyper-abduction of the arm while the scapula is fixed, as in a fall on the medial side of the elbow when the arm is abducted from the side. The surgical neck of the humerus is then brought to bear upon the under aspect of the acromion, which forms a fulcrum, and the head of the bone is pressed against the medial and lower part of the capsule. In some cases muscular action produces this dislocation; it may also result from force applied directly to the upper end of the humerus.
The head leaves the capsule through the rent made in its lower part, and, either from a continuation of the force or from contraction of the muscles inserted into the inter-tubercular (bicipital) groove, particularly the great pectoral, passes medially under cover of the biceps and coraco-brachialis till it comes to rest against the anterior surface of the neck of the scapula, just below the coracoid process. The anatomical neck of the humerus presses against the anterior edge of the glenoid, and there is frequently an indentation fracture of the head of the humerus where the two bones come into contact (F. M. Caird). The subscapularis is bruised or torn, the muscles inserted into the great tuberosity are greatly stretched, or the tuberosity itself may be avulsed, allowing the long tendon of the biceps to slip laterally, where it may form an impediment to reduction. The axillary (circumflex) nerve is often bruised or torn, and the head of the humerus is liable to press injuriously on the nerves and vessels in the axilla.
The clinical features common to all dislocations are prominent, although Dugas' symptom is not constant.
 Fig. 19.—Sub-coracoid Dislocation of Humerus.
Fig. 19.—Sub-coracoid Dislocation of Humerus.Treatment.—The guiding principle in the reduction of these dislocations is to make the head of the bone retrace the course it took in leaving the socket. The main obstacles to reduction being muscular contraction and the entanglement of the head with tendons, ligaments, or bony points, appropriate means must be taken to counteract each of these factors.
A general anæsthetic is an invaluable aid to reduction, and should be given unless there is some reason for withholding it. It is specially indicated in strong muscular subjects, and in nervous patients who do not bear pain well, and particularly when the dislocation has existed for a day or two. In quite recent cases, however, the surgeon may succeed in replacing the bone by taking advantage of a temporary faintness, or by engaging the patient's attention with other matters while he carries out the appropriate manipulations.
When an anæsthetic is employed, the patient should be laid on a mattress on the floor, or on a narrow, firm table; otherwise he should be seated on a chair.
Kocher's method is suitable for the great majority of cases of sub-coracoid dislocation. (1) The elbow is firmly pressed against the side, and the forearm flexed to a right angle. The surgeon grasps the wrist and elbow and firmly rotates the humerus away from the middle line (Fig. 20) till distinct resistance is felt and the deltoid becomes more prominent. In this way the rent in the lower part of the capsule is made to gape, and the head of the humerus rolls away from the middle line till it lies opposite the opening, rotation taking place about the fixed point formed by the contact of the anatomical neck of the humerus with the anterior lip of the glenoid cavity (D. Waterston). (2) The elbow is next carried forward, upward, and towards the middle line (Fig. 21); the humerus acting as the long arm of a lever on the fulcrum furnished by the muscles inserted in the region of the surgical neck, the head, which forms the short arm of the lever, is carried backward, downward, and laterally, and is thus directed towards the socket. (3) The humerus is now rotated towards the middle line by carrying the hand across the chest towards the opposite shoulder (Fig. 22). The anatomical neck of the humerus is thus disengaged from the edge of the glenoid, and the head is pulled into the socket by the tension of the surrounding muscles.
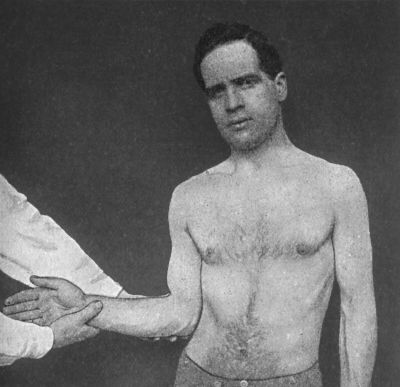 Fig. 20.—Kocher's Method of reducing Sub-coracoid
Dislocation—First Movement; Rotation of Arm away from Middle Line.
Fig. 20.—Kocher's Method of reducing Sub-coracoid
Dislocation—First Movement; Rotation of Arm away from Middle Line.
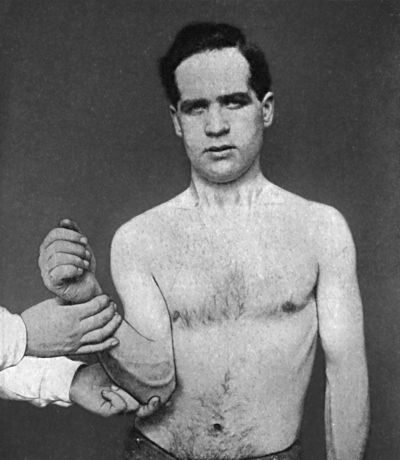 Fig. 21.—Kocher's Method—Second Movement; Elbow
carried forward, upward, and towards the Middle Line.
Fig. 21.—Kocher's Method—Second Movement; Elbow
carried forward, upward, and towards the Middle Line.
A method of reduction has been formulated by A. G. Miller, which we have found to be quite as successful as Kocher's method. The limb is grasped above the wrist and elbow, the forearm flexed to a right angle, and the upper arm abducted to the horizontal (Fig. 23). While an assistant makes counter-extension and fixes the scapula, the surgeon gradually draws the arm away from the body till the head of the humerus is felt to pass laterally. The humerus is then rotated medially by dropping the hand (Fig. 24), and the bone gradually glides into the socket.
In a certain number of cases reduction can be effected by hyper-abduction of the shoulder with traction. The patient is laid upon a firm mattress, and the surgeon, seated behind him while an assistant fixes the acromion, slowly and steadily extends the arm until it is raised well above the head. In some cases the head of the humerus spontaneously slips into its socket; in others it may be manipulated into position by pressure from the axilla. This method is restricted to recent cases, as in those of long standing the axillary vessels are liable to be stretched or torn.
The method of reduction by traction on the arm with the heel in the axilla is only to be used when other measures have failed, as it depends for its success on sheer force.
After-Treatment.—After reduction, the part is gently massaged for ten or fifteen minutes, a layer of wool is placed in the axilla, the forearm is supported by a sling, and the arm fixed to the side by a circular bandage. Massage is carried out from the first, and movement of the shoulder in every direction except that of abduction may be commenced on the first or second day. The circular bandage may be dispensed with at the end of a week, and abduction movements commenced, and by the end of a month the patient should be advised to use the arm freely.
The sub-clavicular dislocation (Fig. 17) is to be looked upon as an exaggerated degree of the sub-coracoid rather than as a separate variety. It is produced by the same mechanism, but the violence is greater, and the damage to the soft parts more severe. The head passes farther upwards and towards the middle line under cover of the pectoralis minor, resting under the clavicle against the serratus anterior and chest wall. The symptoms are usually so marked that they leave no doubt as to the diagnosis. The outline of the head of the humerus in its abnormal position is visible through the skin, and the shortening of the limb is more marked than in the sub-coracoid variety. The treatment is the same as for sub-coracoid dislocation.
Sub-glenoid dislocation (Fig. 17) is less frequently met with than the sub-coracoid variety, and almost always results from forcible abduction of the arm. The head of the humerus passes out through a small rent in the lower and medial portion of the capsule, and rests against the anterior edge of the triangular surface immediately below the glenoid cavity, supported behind by the long head of the triceps, and in front by the subscapularis muscle. It is readily felt in the axilla. All the tendons in relation to the upper end of the humerus are stretched or torn, and the great tuberosity is not infrequently avulsed. There is sometimes bruising of the axillary nerve.
The projection of the acromion, the flattening of the deltoid, the increased depth of the axillary fold, and the abduction of the elbow are well marked; the arm is slightly lengthened, rotated out, and carried forward. It is reduced by the hyper-abduction method (p. 60).
Sub-spinous Dislocation.—Backward dislocation is usually termed sub-spinous, although in a considerable proportion of cases the head of the humerus does not pass beyond the root of the acromion process (sub-acromial) (Fig. 17). This dislocation is usually produced by a fall on the elbow, the arm being at the moment adducted and rotated medially, so that the head of the humerus is pressed backwards and laterally against the capsule, which ruptures posteriorly. All the muscles attached to the upper end of the humerus are liable to be torn, and the tuberosities are frequently avulsed. The long tendon of the biceps may slip from its position between the tuberosities, and prevent reduction or favour re-dislocation, necessitating an open operation.
In the milder cases the clinical features are not always well marked, and on account of the swelling this dislocation is apt to be overlooked. In addition to the ordinary symptoms, the shoulder is broadened, there is a marked hollow in front in which the coracoid projects, and the arm is held close to the side with the elbow directed forward. The head of the bone may be seen and felt in its abnormal position below the spine of the scapula.
Reduction can usually be effected by making traction on the arm with medial rotation, and pressing the head forward into position, while counter-pressure is made upon the acromion.
Prognosis.—The ultimate prognosis in dislocations of the shoulder should always be guarded. The axillary nerve may be stretched or torn, and this may lead to atrophy of the deltoid; or other branches of the brachial plexus may be injured and the muscles they supply permanently weakened. In a certain number of cases traumatic neuritis has resulted in serious disability of the limb. The movements of the shoulder-joint may be restricted by cicatricial contraction of the torn portion of the capsule and of the damaged muscles. A marked tendency to recurrent dislocation may follow if abduction movements are permitted before repair of the capsule has had time to occur.
Dislocation of the Shoulder complicated with Fracture of the Upper End of the Humerus.—In these injuries the dislocation is almost always of the sub-coracoid variety, and the most common fractures by which it is complicated are those of the surgical neck, the anatomical neck, or the greater tuberosity. The most common cause is a fall directly on the shoulder, and it seems probable that the head of the bone is first dislocated, and, the force continuing to act, the upper end of the humerus is then broken; or the two lesions may be produced synchronously.
When seen soon after the accident, the existence of the fracture of the humerus is liable to be overlooked, the condition being mistaken for dislocation alone, or for a fracture through the neck of the scapula. On careful examination under an anæsthetic, however, it is observed that not only is the head of the humerus absent from the glenoid cavity, but that it does not move with the rest of the bone, abnormal mobility and crepitus are recognised at the seat of fracture, and the upper arm is shortened. The extravasation in the axilla is usually greater than that accompanying a simple dislocation, and the pain and shock are more severe. A fracture through the neck of the scapula alone is readily recognised by the ease with which the deformity is reduced, and the way in which it at once recurs when the support is withdrawn. In many cases it is only by the aid of a radiogram that an accurate diagnosis can be made (Fig. 25).
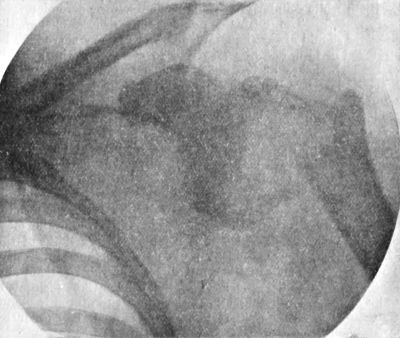 Fig. 25.—Dislocation of Shoulder with Fracture of Neck
of Humerus.
Fig. 25.—Dislocation of Shoulder with Fracture of Neck
of Humerus.Treatment.—Unless the dislocation is reduced at once, the movements of the arm are certain to be seriously restricted, and painful pressure effects from excess of callus are liable to ensue. An attempt should first be made, under anæsthesia, to replace the head in its socket, by making extension on the arm in the hyper-abducted (vertical) position, and manipulating the upper fragment from the axilla.
On no account should the lower fragment be employed as a lever in attempting reduction. When reduction by manipulation fails, recourse should be had to an open operation. The upper fragment should be exposed by an incision over its lateral aspect, and made to return to the socket by using Arbuthnot Lane's levers or M'Burney's hook, or a long steel pin may be inserted into the fragment to give the necessary leverage.
Reduction having been accomplished, the fracture is adjusted in the usual way, advantage being taken of the open wound, if necessary, to fix the fragments together by plates. The best position in which to fix the limb is that of abduction at a right angle. Massage and movement should be commenced early to prevent stiffness of the joint.
When it is found impossible to reduce the dislocation, it is usually advisable to remove the upper fragment.
The method of allowing the fracture to unite without reducing the dislocation, and then attempting reduction, usually results in re-breaking the bone, or else in failure to replace the head in the socket, and has nothing to recommend it.
Old-standing Dislocation of the Shoulder.—It is impossible to lay down definite rules as to the date after which it is inadvisable to attempt reduction by manipulation of an old-standing dislocation of the shoulder. Experience of a hundred cases in Bruns' clinic led Finckh to conclude that, provided there are no complications, reduction can generally be effected within four weeks of the accident; that within nine weeks the prospect of success is fairly good; but that beyond that time reduction is exceptional.
The patient is anæsthetised, and all adhesions broken down by free yet gentle movement of the limb. The appropriate manipulations for the particular dislocation are then carried out, care being taken that no undue force is employed, as the humerus is liable to be broken. If these are not successful, they should be repeated at intervals of two or three days, as it is frequently found that reduction is successfully effected on a second or third attempt.
Should manipulative measures fail, it may be advisable to have recourse to operation if the age of the patient and his general health warrant it, and if the condition of the limb is interfering with his occupation or involves serious disability. If operation is deemed advisable, a few days should be allowed to elapse to permit of the parts recovering from the effects of the manipulations. The joint is freely exposed, the capsule divided, the head of the bone freed and returned to the glenoid cavity. It is sometimes so difficult to replace the head of the bone that it is necessary to resect it and aim at the formation of a new joint, an operation which usually yields satisfactory results.
Habitual or Recurrent Dislocation.—Cases are occasionally met with in which the shoulder-joint shows a marked tendency to be dislocated from causes altogether insufficient to produce displacement under ordinary circumstances. This condition is usually met with in young women, and, in some cases at least, appears to be due to too early and too free movement of the joint after an ordinary dislocation, so that the capsule is stretched and remains lax. In some cases it would appear that the liability to dislocation is due to some structural defect in the joint, and under these conditions both sides are sometimes affected, and the accident is not attended with the usual pain and disability either at the time or after reduction. The facility and frequency with which dislocation recurs render the limb comparatively useless, and may seriously incapacitate the patient. We have had cases under observation in which dislocation resulted from the hyper-abduction of the arm in swimming, from throwing the arms above the head in dancing and in gymnastic exercises, and even in “doing” the hair.
The treatment consists in preventing the patient making the particular movements which tend to produce the dislocation. These are chiefly movements of hyper-abduction and overhead movements; we have found an apparatus consisting of a belt applied around the thorax, and fixed to another around the upper arm by a band which passes above the axillary fold of the dress, useful in restraining these movements. If these measures fail, it may be advisable to have recourse to operation; this may consist in tightening up the capsule, the results of which are said to be uncertain, or in detaching a portion of the deltoid or subscapularis muscle and stitching it beneath the joint to cover and strengthen the weakened portion of the capsule. It is suggestive that in performing this operation no rent in the capsule is discovered.
The condition is also met with in epileptics; and it is generally found that the head of the bone is deficient, as a result either of fracture or disease; that the muscles which naturally support the joint are atrophied or torn; and that the capsule is unduly lax.
Sprain of the shoulder-joint is comparatively rare, because of the wide range of movement of which it is capable. The region of the shoulder becomes swollen and tender to pressure, the point of maximum tenderness being over the front of the joint, just below the acromion process; pain is elicited also when the ligaments or tendons are put upon the stretch.
Contusion of the region of the shoulder, on the other hand, is exceedingly common. In most cases it is merely the deltoid muscle and the subcutaneous tissue over it that are bruised, but sometimes a hæmatoma forms either in the muscle or in the sub-deltoid bursa. There is pain on moving the limb, and the patient may be unable to abduct the arm at the shoulder-joint. Under treatment by massage and movement, the symptoms usually pass off completely in two or three weeks. The affections of the bursa are described elsewhere.
In other cases, the cords of the brachial plexus above the clavicle are stretched, or the axillary nerve is bruised, and these injuries are liable to be followed by prolonged pain, loss of abduction, and stiffness in the arm. The deltoid frequently undergoes considerable atrophy, and there is severe neuralgic pain in the axillary nerve, especially marked in the region of the insertion of the deltoid.
In addition to maintaining the limb in the abducted position, it is necessary to keep up the nutrition of the muscles by massage and electricity.
Fractures of the scapula may implicate the body, the surgical neck, the acromion, or the coracoid process. They are rarely compound.
Fracture of the Body.—Considering its exposed position, the body of the scapula is comparatively seldom fractured, doubtless because of its mobility, and the support it receives from the elastic ribs and soft muscular cushions on which it lies. Apart from gun-shot injuries, it is most frequently broken by a severe blow or crush. The scapula presents two natural arches—one longitudinal, the other transverse—and when the bone is crushed or struck, the force produces fracture by undoing its curves (E. H. Bennett). A main fissure usually runs transversely across the infra-spinous fossa, and secondary cracks radiate from it (Fig. 26). In other cases the line of the primary fracture is longitudinal, passing through the spine and involving both fossæ.
The clinical features are obscured by swelling of the overlying soft parts. Crepitus may sometimes be elicited by placing one hand firmly over the bone, and with the other moving the arm and shoulder. When the spine is implicated, the fragments may be grasped and made to move one upon another. The displacement, which usually consists in overlapping of the fragments—although sometimes they are drawn apart—is partly due to the action of the serratus anterior and teres major muscles, and partly depends on the direction of the force. Movement is restricted and painful. Osseous union usually takes place rapidly, and although displacement often persists, the function of the limb is unimpaired.
Treatment.—As these fractures are usually complicated by other injuries, especially of the thorax, and are accompanied by severe shock, it is necessary to confine the patient to bed. It is usually sufficient to fix the arm and shoulder to the chest wall by a firm binder, in the position which admits of the most complete apposition of fragments. This retentive apparatus is employed for about three weeks, after which the patient is allowed to use his arm. The bandages are removed daily to admit of massage.
Fracture of the surgical neck of the scapula, although a rare accident, is of importance, as it is liable to be mistaken for dislocation of the shoulder. The line of fracture runs through the scapular notch, downwards and laterally to the lower margin of the glenoid, so that the glenoid and the coracoid process are separated from the rest of the bone.
The coraco-acromial and coraco-clavicular ligaments are usually torn, and the detached fragment, along with the head of the humerus, sinks into the axilla, causing a flattening of the shoulder, and leaving a depression below the projecting acromion. These signs may be obscured by the general swelling of the shoulder. The arm may be lengthened about an inch. By supporting the arm the deformity is at once reduced, but recurs as soon as the support is withdrawn. Crepitus is usually detected on carrying out this manipulation; and the coracoid process is found to move with the arm and not with the scapula. By these tests, and by the X-rays, this injury is distinguished from a dislocation.
A partial fracture carrying away the lower part of the glenoid cavity simulates a sub-glenoid dislocation. This is, however, a rare injury.
The treatment consists in bracing back the shoulders and supporting the elbow, and this is most satisfactorily done by a body bandage and sling for the elbow, as for fracture of the middle third of the clavicle. Passive movements and massage are employed from the first.
Fracture of the acromion process may result from a blow or fall on the shoulder. It is often overlooked on account of the swelling resulting from bruising of the soft parts, and the absence of marked displacement. On palpation, crepitus and an irregularity at the seat of fracture may sometimes be detected. The shoulder is slightly flattened, and abduction of the arm is difficult. In rare cases the fracture passes into the acromio-clavicular joint, and is associated with dislocation of the clavicle.
In connection with this fracture, reference must be made to a condition frequently met with, in which the epiphysial portion of the acromion is found to be separate from the body of the process—separate acromion. This is by some (Symington, Hamilton) looked upon as a want of union of the epiphysis, but the weight of evidence seems to prove that it is rather of the nature of an un-united fracture at this level, even when, as sometimes happens, it is bilateral (Struthers, Arbuthnot Lane).
Between the fourteenth and twenty-second years a true separation of the epiphysis may be met with, but it is seldom possible to make a positive diagnosis of this injury. As is the case in all fractures of the acromion, bony union seldom takes place.
The treatment is the same as for fracture of the lateral end of the clavicle.
Fracture of the coracoid process is rare. It may result from direct violence, such as the recoil of a gun, but it is more often an accompaniment of dislocation of the shoulder or of the lateral end of the clavicle upward. As the coraco-clavicular ligaments usually remain intact, there is no displacement; but when these are torn the coracoid is dragged downwards and laterally by the combined action of the pectoralis minor, biceps, and coraco-brachialis muscles. Crepitus may be elicited on moving the fragment. Separation of the epiphysial portion of the coracoid may occur up to the seventeenth year.
The treatment consists in placing the arm across the front of the chest, to relax the muscles causing the displacement, and retaining it in that position by a sling and roller bandage.
It is most convenient to study fractures of the upper end of the humerus in the following order: (1) fracture of the surgical neck; (2) separation of the epiphysis; (3) fracture of head, anatomical neck, or tuberosities.
 Fig. 28.—Impacted Fracture of Neck of Humerus, in man
æt. 75.
Fig. 28.—Impacted Fracture of Neck of Humerus, in man
æt. 75.Fracture of the Surgical Neck.—The surgical neck of the humerus extends from the level of the epiphysial junction to the insertion of the pectoralis major and teres major muscles, and it is within these limits that most fractures of the upper end of bone occur. This fracture is most common in adults, and usually follows direct violence applied to the shoulder, but may result from a fall on the hand or elbow, or from violent muscular action, as, for example, in throwing a stone. It is usually transverse, and there is often little or no displacement, the fragments being retained in position by the long tendon of the biceps and the long head of the triceps. When the fracture is oblique, the fragments are often comminuted, and sometimes impacted. The displacement of the upper fragment seems to depend upon the attitude of the limb at the moment of fracture. When the upper arm is approximated to the side, the upper fragment retains its vertical position, but is slightly rotated laterally by the muscles inserted into the greater tuberosity, while the lower fragment is drawn upwards and medially towards the coracoid process by the muscles inserted into the inter-tubercular groove and the longitudinal muscles of the upper arm, and can be felt in the axilla. The elbow points laterally and backwards, and the upper arm is shortened. The shoulder retains its rotundity, but there is a slight hollow some distance below the acromion. On grasping the elbow and moving the shaft, it is found that the head and tuberosities do not move with it, and unnatural mobility and crepitus at the seat of fracture may be detected. When the upper arm is abducted at the moment of fracture, the upper fragment is retained in that position by the lateral rotator and abductor muscles inserted into it, while the lower fragment passes upwards and medially.
Although there is sometimes overlapping and broadening after union, beyond some limitation of the range of abduction the usefulness of the limb is seldom impaired.
Treatment.—Massage, by allaying spasm of the muscles, soon overcomes the moderate amount of displacement which is usually met with. Further, the skin surfaces of the axilla having been separated by a thin layer of cotton wool, a sling is applied to support the wrist, and the arm is bound to the side by a body bandage.
In comminuted fractures and those with marked displacement, a general anæsthetic may be required to ensure accurate reduction; and to maintain the fragments in apposition, and to avoid any limitation of abduction after union, the limb may be fixed in the position of abduction at a right angle by means of a Thomas' arm splint with swivel ring, and extension applied, if necessary, to maintain this attitude. After a week or ten days the patient is allowed up, wearing an abduction frame (Fig. 29), or a splint, such as Middeldorpf's, which consists of a double inclined plane, the base of which is fixed to the patient's side, while the injured arm rests on the other two sides of the triangle. Massage and movement are employed daily.
Should these measures fail, the fracture may be exposed by an incision carried along the anterior border of the deltoid, and the ends mechanically fixed, after which the limb is put up in the abducted position for three or four weeks. Massage is commenced on the second or third day. Union is usually complete in about four weeks.
Separation of Epiphysis.—The upper epiphysis of the humerus includes the head, both tuberosities, and the upper fourth of the inter-tubercular groove. On its under aspect is a cup-like depression into which the central pyramidal-shaped portion of the diaphysis fits. This epiphysis unites about the twenty-first year.
Traumatic separation is met with chiefly between the fifth and fifteenth years, and is most common in boys. It usually results from forcible traction of the arm upwards and away from the side, as in lifting a child by the upper arm, or from direct violence, but may be caused by a fall on the lateral side of the elbow.
The epiphysis, especially in young children, may be separated without being displaced, or the displacement may be incomplete.
When the epiphysis is completely separated from the shaft, the clinical features closely resemble those of fracture of the surgical neck, and the diagnosis is made by a consideration of the age of the patient, and the muffled character of the crepitus, when it can be elicited. The upper end of the diaphysis forms a projecting ridge which may be felt below and in front of the acromion. The diagnosis can usually be established by the use of the X-rays (Fig. 30). Dislocation is rare at the age when separation of the epiphysis occurs.
Reduction is often difficult on account of the periosteum and other soft tissues getting between the fragments, and on account of the small size of the upper fragment. Union almost invariably results, but the growth of the limb may be interfered with and its shape altered, especially when the injury occurs at an early age and its nature is overlooked.
Treatment.—This injury is treated on the same general lines as fracture of the surgical neck. General anæsthesia is almost always necessary to secure satisfactory reduction, and retention is most easily secured if the patient is confined to bed with the upper arm fixed in the fully abducted position. Operative treatment is called for in exceptional cases.
Fractures of the Head, Anatomical Neck, and Tuberosities of Humerus.—These fractures are met with as accompaniments of dislocation of the shoulder, and as results of gun-shot injuries, blows, or falls.
In sub-coracoid dislocation the head of the humerus may be indented by coming in contact with the anterior edge of the glenoid cavity (F. M. Caird).
The anatomical neck may be fractured in an old person by a direct blow on the shoulder. In a few cases the fracture is entirely intra-capsular, the head of the bone remaining loose in the cavity of the joint. As a rule, however, the fracture passes laterally and implicates the tuberosities. In some cases there is impaction, and in others comminution of the fragments. The use of the X-rays has shown that in many cases in which prolonged stiffness has followed a severe blow of the shoulder, there has been a fracture of the anatomical neck.
The tuberosities may be implicated in other fractures in this region and in dislocation of the shoulder; and either of them may be separated by muscular contraction or by direct violence.
Clinically all these injuries are difficult to diagnose with accuracy, and, without the use of the X-rays, it is impossible in many cases to go further than to say that a fracture exists above the level of the surgical neck. Fracture of the anatomical neck is attended with little deformity beyond slight flattening of the shoulder and sometimes slight shortening of the upper arm.
When the great tuberosity is torn off, considerable antero-posterior broadening of the shoulder may be recognised by grasping the region of the tuberosities between the fingers and thumb. Crepitus can be elicited on rotating the humerus. At the same time it will be recognised that the tuberosity does not move with the shaft. Firm union, with considerable formation of callus and some broadening of the shoulder, usually results, but the usefulness of the joint is not necessarily impaired. There may, however, be prolonged stiffness and impaired movement from adhesion; or pain and crackling in the joint may result from arthritic changes like those of arthritis deformans.
Treatment.—These fractures are treated on the same lines as fracture of the surgical neck of the humerus.
The combination of fracture of the upper end of the humerus with dislocation of the shoulder has already been referred to.
Fractures occurring in the shaft of the humerus between the surgical neck and the base of the condyles may, for convenience of description, be divided into those above, and those below, the level of the deltoid insertion—the majority being in the latter situation.
Direct violence is the most common cause of these fractures, but they may occur from a fall on the elbow or hand; and a considerable number of cases are on record where the bone has been broken by muscular action—as in throwing a cricket-ball. Twisting forms of violence may produce spiral fractures.
The fracture is usually transverse in children and in cases in which it is due to muscular action. In adults, when due to external violence, it is usually oblique, the fragments overriding one another and causing shortening of the limb. The displacement depends largely on the direction of the force and the line of fracture, but to a certain extent also on the action of muscles attached to the fragments. Thus, in fractures above the insertion of the deltoid the upper fragment is usually dragged towards the middle line by the muscles inserted into the inter-tubercular groove, while the lower is tilted laterally by the deltoid. When the break is below the deltoid insertion the displacement of the fragments is reversed. The signs of fracture—undue mobility, deformity, shortening, and crepitus—are at once evident, and the patient himself usually recognises that the bone is broken.
The nerve-trunks in the arm—the median, ulnar, and radial (musculo-spiral)—are apt to be damaged in these injuries; in fractures of the lower part of the shaft the radial nerve is specially liable to be implicated. This may occur at the time of the injury, the nerve being contused by the force causing the fracture, or pressed upon by one or other of the fragments, or its fibres may be partly or completely torn across. When there is evidence of nerve injury, the practitioner should draw the attention of the patient to it then and there, and so guard himself against actions for malpraxis should paralysis of the muscles ensue. Later, the nerve may become involved in callus, or be damaged by the pressure of ill-fitting splints. Weakness or paralysis of the extensors of the wrist and hand results, giving rise to the characteristic “wrist-drop.” The actions of the muscles should always be tested before applying splints, and each time the apparatus is removed or readjusted, to assure that no undue pressure is being exerted on the nerves.
Union takes place in from four to six weeks in adults, and in from three to four weeks in children. Delayed union, or want of union and the formation of a false joint, is more common in fractures of the middle of the shaft of the humerus than in any other long bone—a point to be borne in mind in treatment. Arrest of growth in the bone from injury to the nutrient artery is also said to have occurred.
Treatment.—To restore the alignment of the bone, extension is made on the lower fragment and the ends are manipulated into position. This may necessitate the use of a general anæsthetic, and care must be taken that no soft tissue intervenes between the fragments, as is evidenced radiographically by the persistence of a clear space between the ends even when they appear to be in apposition.
In transverse fractures the position may be maintained by a simple ferrule of poroplastic or Gooch-splinting. The elbow is flexed at a right angle, and the forearm supported in a sling midway between pronation and supination. For a few days the limb may be bound to the chest by a broad roller bandage.
The splints are removed daily to admit of massage and movement being carried out, and while the splints are off, the patient is allowed to exercise the fingers and wrist. If at the end of four or five weeks, osseous union has not occurred, the reparative process may be hastened by inducing venous congestion by Bier's method.
In oblique and spiral fractures it is often necessary to control the shoulder and elbow-joints to prevent re-displacement. This can be done by means of a plaster of Paris case enclosing the upper part of the thorax, together with the upper arm, abducted, and the elbow, at right angles.
It is sometimes necessary to apply continuous extension to the lower fragment to prevent overriding. For this purpose a Thomas' arm splint is employed, the extension tapes being attached to its lower end, but care must be taken that the traction is not sufficient to separate the fragments and leave a gap between them. The elbow should not be retained in the extended position for more than three weeks.
In rare cases it is necessary to have recourse to operative treatment.
When there is evidence that the radial nerve has been injured, and no sign of improvement appears within three or four days of the accident, operative interference is indicated. An incision is made on the lateral side of the arm, and the nerve exposed and freed from pressure, or stitched, as may be necessary; the opportunity should also be taken of dealing with the fracture. The limb is put up in a “cock-up” splint, with the hand in the attitude of marked dorsiflexion (Fig. 31).
Satisfactory results have been obtained without the use of splints, by relying upon massage to overcome the spasm of muscles, and allowing the weight of the arm to act as an extending force (J. W. Dowden and A. Pirie Watson).
In cases of un-united fracture, a vertical or semilunar incision is made over the lateral aspect of the bone, and the muscles separated from one another till the fracture is exposed, care being taken to avoid injuring the radial nerve. The fibrous tissue is removed from the ends of the bone, and the rawed surfaces fixed in apposition; the wound is then closed, and appropriate retentive apparatus applied. As soon as the wound has healed, massage and movement are employed.
The injuries met with in the region of the elbow-joint include the various fractures of the lower end of the humerus, and upper ends of the bones of the forearm, including the olecranon; and dislocations and sprains of the elbow-joint. The differential diagnosis is often exceedingly difficult on account of the swelling and tension which rapidly supervene on most of these injuries, the pain caused by manipulating the parts, and the difficulty of determining whether movement is taking place at the joint or near it.
Surgical Anatomy.—The medial epicondyle of the humerus is more readily felt through the skin than the lateral. The two epicondyles are practically on the same level, and a line joining them behind passes just above the tip of the olecranon when the arm is fully extended. On flexing the joint, the tip of the olecranon gradually passes to the distal side of this line, and when the joint is fully flexed the tip of the olecranon is found to have passed through half a circle. The head of the radius can be felt to rotate in the dimple on the back of the elbow just below the lateral epicondyle. The coronoid process may be detected on making deep pressure in the hollow in front of the joint. As the line of the radio-humeral joint is horizontal, while that of the ulno-humeral joint slopes obliquely downwards, the arm forms with the fully extended and supinated forearm an obtuse angle, opening laterally—the “carrying angle.” This angle is usually more marked in women, in harmony with the greater width of the female pelvis. The ulnar nerve lies in the hollow between the olecranon and the medial condyle, and the median nerve passes over the front of the joint, with the brachial artery and biceps tendon to its lateral side. The radial nerve divides into its superficial and deep (posterior interosseous) branches at the level of the lateral condyle.
In examining an injured elbow, the thumb and middle finger are placed respectively on the two epicondyles, while the index locates the olecranon and traces its movements on flexion and extension of the joint. The movements of the head of the radius are best detected by pressing the thumb of one hand into the depression below the lateral epicondyle, while movements of pronation and supination are carried out by the other hand. The uninjured limb should always be examined for purposes of comparison.
In injuries about the elbow much aid in diagnosis is usually obtained by the use of the X-rays; but in young children it is sometimes impossible, even with excellent pictures, to make an accurate diagnosis by means of radiograms alone. In cases of suspected fracture, a radiogram should be taken with the back of the limb resting on the plate, the forearm being extended and supinated. If a dislocation is suspected and a lateral view is desired, the arm should be placed on its medial side. In obscure cases it is useful to take radiograms of the healthy limb in the same position.
The following fractures occur at the lower end of the humerus: (1) supra-condylar fracture; (2) inter-condylar fracture; (3) separation of epiphyses; (4) fracture of either condyle alone; and (5) fracture of either epicondyle alone.
All these injuries are common in children, and result from a direct fall or blow upon the elbow, or from a fall on the outstretched hand, especially when at the same time the joints are forcibly moved beyond their physiological limits, more particularly in the direction of pronation or abduction. While it is generally easy to diagnose the existence of a fracture, it is often exceedingly difficult to determine its exact nature. Although the ulnar and median nerves are liable to be injured in almost any of these fractures, they suffer much less frequently than might be expected.
Ankylosis, or, more frequently, locking of the joint, is a common sequel to many of these injuries. This is explained by the difficulty of effecting complete reduction, and by the wide separation of periosteum which often occurs, favouring the production of an excessive amount of new bone, particularly in young subjects.
The supra-condylar fracture usually results from a fall on the outstretched hand with the forearm partly flexed, from a direct blow, or from a twisting form of violence. The line of fracture is generally transverse, or but slightly oblique from behind downwards and forwards, so that the lower fragment is forced backward together with the bones of the forearm, simulating backward dislocation of the elbow; the lower end of the upper fragment lies in front (Fig. 33).
Clinical Features.—The elbow is flexed at an angle of 120° or 130°, and the forearm, held semi-pronated, is supported by the other hand. Around the seat of fracture great swelling rapidly ensues. The olecranon projects behind, but the mutual relations of the bony points of the elbow are unaltered. The lower end of the upper fragment may be felt in front above the level of the joint, as a rough and sharp projection, and this sometimes pierces the soft parts and renders the fracture compound. Movement at the joint is possible, but unnatural mobility may be detected above the level of the joint. Crepitus and localised tenderness may be elicited. The displacement is readily reduced by manipulation, but usually returns when the support is withdrawn. The arm is shortened to the extent of about half an inch.
In rare cases the obliquity of the fracture is downward and backward, and the lower fragment is displaced forward.
The inter-condylar fracture is a combination of the supra-condylar with a vertical split running through the articular surface, and so implicating the joint. The condyles are thus separated from one another, as well as from the shaft, by a T- or Y-shaped cleft. As such fractures usually result from severe forms of direct violence, they are often comminuted and compound. In addition to the signs of supra-condylar fracture, the joint is filled with blood. The condyles may be felt to move upon one another, and coarse crepitus, which has been likened to the feeling of a bag of beans, may be elicited if the fragments are comminuted.
Separation of the lower epiphysis of the humerus is met with in children of three or four years of age, but it may occur up to the thirteenth or fourteenth year. The more common lesion, however, is a combination of separated epiphysis with fracture, and this lesion is produced by the same forms of violence as cause supra-condylar fracture. If the periosteum is not torn, there is little or no displacement, but as a rule the clinical features closely resemble those of transverse fracture above the condyles, or of dislocation of the elbow. In separation of the epiphysis there is a peculiar deformity of the posterior aspect of the joint, consisting of two projections—one the olecranon, and the other the prominent capitellum with a scale of cartilage which it carries with it from the lateral condyle (R. W. Smith and E. H. Bennett). The end of the diaphysis may be palpated through the skin in front. Muffled crepitus can usually be elicited, and there is pain on pressing the segments against one another. Sometimes the separation is compound, the diaphysis protruding through the skin.
Union takes place more rapidly than in fracture, but, owing to the excessive formation of callus from the torn periosteum in front of the joint, full flexion is often interfered with. If the displaced epiphysis is imperfectly reduced, serious interference with the movements of the elbow is liable to ensue, and may call for operative treatment.
Fracture of either Condyle alone.—The lateral condyle or trochlea is more frequently separated from the rest of the bone than is the medial or capitellum. In either, the size of the fragment varies, but the line of fracture is partly extra-capsular and partly intra-capsular, so that the joint is always involved. Pain, crepitus, and the other signs of fracture are present. As the ligaments of the joint are not as a rule torn, there is little or no immediate displacement of the fragment. Secondary displacement is liable to occur, however, during the process of union, producing alterations in the “carrying angle” of the limb—cubitus varus or cubitus valgus.
Fracture of Epicondyles.—Fracture of the lateral epicondyle alone is so rare that it need only be mentioned.
The medial epicondyle may be chipped off by a fall on the edge of a table or kerbstone, or it may be forcibly avulsed by traction through the ulnar collateral (internal lateral) ligament, as an accompaniment of dislocation. It is usually displaced downwards and forwards by the flexor muscles attached to it, and may thus come to exert pressure on the ulnar nerve. The fragment may be grasped and made to move on the shaft, producing crepitus. Fibrous union is the usual result.
Up to the age of seventeen or eighteen the epiphysis of the epicondyle may be separated.
Treatment of Fractures in Region of Elbow.—The administration of a general anæsthetic is a valuable aid to accurate reduction and fixation of fractures in this region. Much discussion has taken place as to the best position in which to treat these fractures. In our experience the best approximation of the fragments, as shown by the X-rays, is obtained when the limb is fixed in the position of full flexion with supination. American surgeons favour the position of flexion at a right angle. In the region of the elbow there is a risk of promoting too much callus formation by early and vigorous massage, with the result that the movements of the joint are restricted by locking of the bony projections. This is probably due to bone cells being forced into the surrounding tissues, where they multiply and form new bone on an exaggerated scale.
The supra-condylar fracture is reduced by first extending the elbow to free the lower fragment from the triceps, and then, while making traction through the forearm, manipulating the fragments into position, and finally flexing the elbow to an acute angle and supinating the forearm. In this way the triceps is put upon the stretch and forms a natural posterior splint. A layer of wadding is placed in the bend of the elbow to separate the apposed skin surfaces, the arm placed in a sling so arranged as to support the elbow, and fixed to the side by a body bandage. This position is maintained for three weeks, with daily massage and movement. The last movement to be attempted is that of complete extension. Operative treatment is rarely called for.
Separation of the epiphysis and fracture of the medial epicondyle are treated on the same lines as supra-condylar fracture.
T- or Y-shaped fractures and fractures of the condyles, inasmuch as they implicate the articular surfaces, present greater difficulties in treatment, but they are treated on the same lines as the supra-condylar. In young subjects whose occupation entails free movement of the elbow-joint, it is sometimes advisable to expose the fracture by operation and secure the fragments in position. The details of the operation vary in different cases, and depend upon the line of obliquity of the fracture, and the disposition of the individual fragments, points which may usually be determined by the use of the X-rays. In performing the operation, care must be taken to disturb the periosteum as little as possible, otherwise there may follow excessive formation of new bone.
Operative interference is sometimes necessary for ankylosis or locking of the joint after the fracture is united, or to relieve the ulnar nerve when it is involved in callus. Volkmann's ischæmic contracture is liable to occur after fractures in the region of the elbow from impairment of the blood supply as a result of tight bandaging.
Fracture of the olecranon is a comparatively common injury in adults. It usually follows a fall on the flexed elbow, and results from the direct impact, supplemented by the traction of the triceps muscle. In a few cases it has been produced by muscular action alone. The line of fracture may pass through the tip of the process, or through its middle, less frequently through the base. It may be transverse, oblique, T- or V-shaped, but is rarely comminuted or compound.
Clinical Features.—As the fracture almost invariably implicates the articular surface, there is considerable swelling from effusion of blood into the joint. The power of extending the forearm is impaired, and other symptoms of fracture are present. The amount of displacement depends upon the level of the fracture, and the extent to which the aponeurotic expansion of the triceps is torn. As the fracture is usually near the tip, the displacement is comparatively slight, the prolongation of the fibres of insertion of the triceps on to the sides and posterior part of the process holding the small fragment in position; and the fracture may easily escape recognition. When the line of fracture is nearer the base, however, the contraction of the triceps tends to separate the fragments widely (Fig. 35), and a distinct gap, which is increased on flexing the elbow, may often be felt between them, and if the elbow is passively extended, the fragments may be brought into apposition, and crepitus elicited.
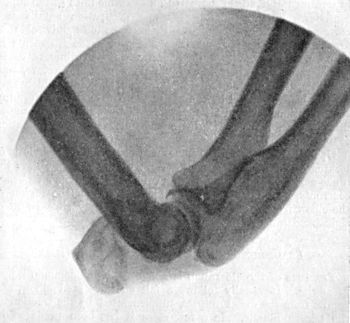 Fig. 35.—Radiogram of Fracture of Olecranon Process,
showing marked degree of displacement.
Fig. 35.—Radiogram of Fracture of Olecranon Process,
showing marked degree of displacement.When there is little displacement, bony union may result, but in many cases the fragments are united only by fibrous tissue. The upper fragment sometimes forms attachments to the shaft of the humerus, and this leads to stretching of the fibrous band between the fragments and to marked wasting of the triceps.
Separation of the olecranon epiphysis is one of the rarest forms of epiphysial detachment (Poland). When the epiphysis is displaced upwards and unites in this position, it may interfere with complete extension of the elbow.
Treatment.—It would appear that too much stress has hitherto been laid on the necessity of bringing the fragments into perfect apposition, and too little attention paid to the importance of maintaining the functions of the triceps and the movements of the elbow-joint.
Massage and movements are carried out from the first, and the forearm is supported in a sling. Full flexion is the last movement to be attempted. In carrying out the movements, the tip of the olecranon is pressed down with the thumb, so that it is obliged to follow the movements of the ulna, and is prevented from adhering to the humerus.
It was formerly the practice to have the arm almost, but not quite, fully extended, and a Gooch splint, extending from the lower border of the axilla to the finger-tips, and cut to the shape of the extended limb, applied anteriorly and fixed in position by a bandage, the region of the elbow being covered by a convergent spica.
Operative Treatment.—Operative treatment may be had recourse to, particularly in cases in which there is wide separation of the fragments. The fracture is exposed, the joint cavity opened up and cleared of clots, and silver-wire sutures passed through the fragments without encroaching upon the articular cartilage. The limb is fixed with the elbow-joint in the position of almost complete extension. Movement may be commenced at the end of a week, the angle at which the joint is fixed being changed morning and evening. During the day the flexed position should be maintained and the arm carried in a sling; during the night the limb is fixed to a pillow in the extended position. The patient is allowed to use the joint cautiously within a fortnight.
Old-standing Fracture.—When union fails to take place, the interval between the fragments tends to increase by the contraction of the triceps gradually stretching the intermediate fibrous tissue, so that a wide gap comes to separate the fragments. It is quite common that the function of the arm is all that can be desired in spite of a gap between the fragments, but, if this is not the case, the fragments may be united by operation.
Fracture of the coronoid process is rare except as a complication of backward dislocation of the elbow. It may be produced by direct violence, as well as by muscular action. As the fracture is usually within a quarter of an inch of the tip, the fibres of insertion of the brachialis prevent displacement. The ordinary evidence of fracture is often absent, and the diagnosis is seldom completed without the aid of the X-rays. The treatment consists in flexing the elbow and supporting the forearm in a sling. In some cases associated with dislocation, however, the small fragment has been so far displaced as to become attached to the back of the humerus (Annandale).
Intra-capsular fracture of the head of the radius may result from direct violence, from a fall on the pronated hand, or from forcible pronation or abduction—that is, deviation of the forearm to the radial side. It may accompany dislocation of the elbow or fracture of adjacent bones. The head may be completely separated, or may be split into two or more fragments. Up to the seventeenth year, the epiphysis, which is entirely intra-articular, may be separated.
The clinical features are localised pain, crepitus, interference with pronation and supination, while the elbow can be almost fully extended and flexed, and in some cases the fragment may be felt through the skin, although it usually continues to move with the shaft in pronation and supination.
Union generally takes place satisfactorily, but in some cases the fragments form new attachments resulting in impaired movement at the elbow, and necessitating operative interference.
Fracture of the neck of the radius between the capsule and the tubercle is rare.
Avulsion of the tubercle may occur from forcible contraction of the biceps, or, in children, from traction made on the forearm (A. L. Hall).
These injuries are treated with the elbow in the flexed position, and massage and movement are carried out as already described.
Dislocations of the elbow-joint may involve one or both bones of the forearm, and may be complete or incomplete.
Dislocation of both bones backward is the most common of all dislocations of the elbow, and is the only dislocation that is frequently met with in children. It usually results from a fall on the outstretched hand, causing hyper-extension of the joint with abduction—that is, deviation towards the radial side; but it may follow a direct blow on the back of the humerus, a fall on the elbow, or a twist of the forearm.
 Fig. 36.—Backward Dislocation of Elbow, in a boy æt.
10, caused by a fall off a wall, landing on the elbow.
Fig. 36.—Backward Dislocation of Elbow, in a boy æt.
10, caused by a fall off a wall, landing on the elbow.
Morbid Anatomy.—All the ligaments of the elbow, except the annular (orbicular), are torn or stretched. The radius and ulna pass backward, the coronoid process coming to rest opposite the olecranon fossa behind the humerus, and the head of the radius behind the lateral condyle. The condyles of the humerus bear their normal relations to one another. The olecranon and the triceps tendon form a marked prominence on the back of the elbow, the tip of the olecranon lying above and behind the condyles. The lower end of the humerus lies in the flexure of the joint with the biceps tendon tightly stretched over it. The coronoid process is often broken, or the tendon of the brachialis torn. The median and ulnar nerves may be stretched or torn. Not infrequently the bones of the forearm are displaced towards the medial side as well as backward.
Occasionally, as a sequel to the dislocation, processes of bone develop in relation to the insertion of the brachialis and interfere with the movements of the joint. These outgrowths are due to displacement of bone-forming elements, either at the time of the original injury or as a result of forcible efforts at reduction. According to D. M. Greig, they do not develop in the tendon of the brachialis, but under it, and are not of the nature of myositis ossificans. In from four to six weeks after reduction of the dislocation, the movements begin to be restricted, and a hard mass can be felt in the cubital fossa, which with the X-rays is seen to be a bony outgrowth springing from the quadrilateral space on the front of the elbow below the coronoid process (Fig. 37). This gradually increases in size and leads to fixation of the joint. In most cases the effects reach their maximum in about six months, and then reabsorption of the mass begins.
 Fig. 37.—Bony Outgrowth in relation to insertion of
Brachialis Muscle, following Backward Dislocation of Elbow.
Fig. 37.—Bony Outgrowth in relation to insertion of
Brachialis Muscle, following Backward Dislocation of Elbow.If the disability shows no sign of abatement within a year, or if the bony outgrowth is producing pressure effects on the median nerve, it should be removed by operation.
It is important not to mistake this condition for the effects of a fracture which has complicated the dislocation and been overlooked at the time of the accident.
Clinical features.—The elbow is held fixed at an angle of about 120°, pronated or midway between pronation and supination. Any attempt at movement causes great pain, and is followed by an elastic rebound to the abnormal position. The antero-posterior diameter of the joint is increased, and the forearm, as measured from the lateral epicondyle to the tip of the styloid process of the radius, is shortened to the extent of about an inch. If examined before swelling ensues, the outlines of the articular surfaces may be recognised in their abnormal positions, but swelling usually comes on rapidly, and, by obscuring the bony landmarks, renders the diagnosis difficult.
This injury has to be diagnosed from supra-condylar fracture with backward displacement of the lower fragment and from separation of the lower humeral epiphysis. A general anæsthetic is often necessary to enable an accurate diagnosis to be made. When the deformity is once reduced, there is no tendency to its reproduction unless the coronoid process is also fractured. In a considerable number of cases—according to E. H. Bennett, in the majority—this dislocation is incomplete, the coronoid process resting at the level of the trochlea, and the backward projection of the olecranon being scarcely appreciable. The head of the radius, however, is unduly prominent. In such cases the lesion is liable to be overlooked, and therefore to go untreated, leading to permanent stiffness at the elbow.
Dislocation forward is much less common than the backward variety. It is produced by severe force acting from behind on the flexed elbow, the ulna being driven forward, tearing the ligaments of the joint and the muscles attached to the condyles. The olecranon is frequently fractured at the same time (Fig. 39). When it remains intact, it may rest below the condyles (incomplete or first stage of dislocation), or may pass in front of them, especially if the triceps is ruptured (complete or second stage). The forearm is lengthened, the elbow slightly flexed, the posterior aspect of the joint flattened, and the condyles, in their abnormal relationship, can be palpated from behind.
Medial and Lateral Dislocations.—Dislocation towards the ulnar side is always incomplete, some portion of the articular surface of the bones of the forearm remaining in contact with the condyles.
The dislocation to the radial side is also incomplete as a rule, although cases have been recorded in which complete separation had taken place.
These forms of dislocation are rare, that towards the ulnar side being more frequently observed. Each form is often combined with other injuries in the vicinity.
The most common cause of these dislocations is a fall on the outstretched hand, the forearm at the moment being strongly pronated. Forced abduction favours the displacement to the ulnar side; adduction to the radial side. The limb is held flexed and pronated, and the facility with which the bony points can be palpated renders the diagnosis easy.
In a few cases diverging dislocations have been met with, the radius and ulna being separated from one another, the annular (orbicular) ligament being torn and no longer holding them together.
Treatment of Dislocations of Elbow.—The chief obstacle to reduction is the spasmodic contraction of the muscles passing over the joint, and, in the backward variety, the hitching of the coronoid process against the edge of the olecranon fossa. In recent cases, to effect reduction the patient is seated on a chair, while the surgeon grasps the humerus and wrist, and places his knee in the bend of the elbow. The limb is first fully extended, or even hyper-extended, to relax the triceps and free the coronoid process. Traction is then made in opposite directions upon the forearm and arm, the surgeon's knee meanwhile making pressure, in a backward direction, upon the lower end of the humerus. The joint is next slowly flexed, and the bones slip into position, often with a distinct snap. If the patient be anæsthetised, these manipulations must be adapted to the recumbent position.
When some days have elapsed before reduction is attempted, forcible manipulations are to be deprecated as they greatly increase the risk of ossification occurring in relation to the brachialis (D. M. Greig); and recourse should be had to open operation, and the tearing or bruising of the soft parts should be reduced to a minimum.
After reduction, the limb is flexed to rather less than a right angle and supported by a sling. Massage and movement are commenced at once.
Fracture of the coronoid process predisposes to recurrence of the dislocation; when this complication exists, therefore, the limb should be fixed at an acute angle, and movements of full extension postponed for a fortnight. Massage and limited movements, however, may be carried out from the first.
If there is a fracture of the olecranon, the treatment must be modified accordingly (p. 87).
 Fig. 39.—Forward Dislocation of Elbow, with Fracture
of Olecranon.
Fig. 39.—Forward Dislocation of Elbow, with Fracture
of Olecranon.Comminuted and compound injuries usually call for operative treatment, the fractured bones being wired after reduction of the dislocation, or the loose fragments removed.
The forward dislocation is reduced by fully flexing the elbow, and then pushing the bones of the forearm backward, while the humerus is pulled forward.
Old-standing Dislocations.—No attempt should be made to reduce by manipulation a dislocation of the elbow which has remained displaced for five or six weeks, especially when it has been complicated by a fracture. The joint surfaces become welded together by adhesions, and separated fragments often form attachments which lock the joint. Attempts to break these down are attended with considerable risk of re-fracturing the bone or of tearing the soft parts. In such cases it is best to expose the joint, and if reduction is not easily effected a sufficient amount of the lower end of the humerus should be removed to provide a movable joint.
Dislocation of the ulna alone is a rare injury, and is usually associated with fracture of one or other of its processes or of the inner condyle.
Dislocation of the radius alone, on the other hand, is comparatively common, especially as a concomitant of fracture of the upper third of the shaft of the ulna (Fig. 40).
The injury may result from a blow on the back of the upper end of the radius, a fall on the outstretched hand, or, in children, from forcible traction on the forearm while in the pronated position. The displaced head usually passes forward, and rests on the anterior edge of the capitellum, thus preventing complete flexion and supination of the limb.
The limb is held partly flexed and pronated. The displaced head of the radius can be felt to rotate with the shaft in its abnormal position, and the articular facet on the head of the radius may also be felt; there is a depression posteriorly below the lateral epicondyle where the head should be. The radial side of the forearm is slightly shortened. The superficial and deep (posterior interosseous) branches of the radial nerve are liable to be pressed upon or torn by the displaced head of the radius, especially if the ulna is fractured, leading to disturbances in the area of their distribution.
In a few cases the displacement of the head has been backwards or laterally.
Treatment.—To effect reduction, the forearm should be alternately flexed and extended, while traction is made upon it from the wrist, and the head of the radius is pressed backward with the thumb in the fold of the elbow. When reduction is prevented by the interposition of a portion of the torn ligaments between the bones, it is sometimes necessary to open the joint to ensure accurate adjustment. The joint is fixed in acute flexion to relax the biceps, to allow of union of the torn ligaments, and to prevent recurrence.
In old-standing cases, to obtain a useful joint, or to remove pressure from the branches of the radial nerve, resection of the head of the radius may be necessary.
Sub-luxation of the head of the radius, or “dislocation by elongation,” is a comparatively common injury in children between the ages of two and six. It almost invariably results from the child being lifted or dragged by the hand or forearm. The traction and torsion thus put upon the radius causes the front part of its head to pass out of the annular ligament, the edge of which slips between the bones.
The person holding the child may feel a click at the moment of displacement. The child complains of pain in the region of the elbow: the arm at once becomes useless, and is held flexed, midway between pronation and supination. All movements are painful, but especially movements in the direction of supination. The deformity is slight, but the head of the radius may be unduly prominent in front. From the way in which the injury is produced the wrist also is often swollen, and in some cases the patient is brought to the surgeon on account of the condition of the wrist, and attention is not directed to the elbow.
Treatment.—Reduction frequently takes place spontaneously or during examination, the function of the arm being at once completely restored. In other cases it is necessary, under anæsthesia, to manipulate the head of the bone into position. This is usually easily done by flexing the elbow, making slight traction on the forearm, and alternately pronating and supinating it. After reduction, a few days' massage is all that is necessary, the joint in the intervals being kept at rest in a sling.
Sprain of the elbow is comparatively common as a result of a fall on the hand or a twist of the forearm. The point of maximum tenderness is usually over the radio-humeral joint, the radial collateral and annular ligaments being those most frequently damaged. Effusion takes place into the synovial cavity, and a soft, puffy swelling fills up the natural hollows about the joint. The bony points about the elbow retain their normal relationship to one another—a feature which aids in determining the diagnosis between a sprain and a dislocation or fracture. In children it is often difficult to distinguish between a sprain and the partial separation of an epiphysis. Sprains of the elbow are treated on the same lines as similar lesions elsewhere—by massage and movement.
The condition known as tennis elbow is characterised by severe pain over the attachment of one or other of the muscles about the elbow, particularly the insertion of the pronator teres during the act of pronation, and is due to stretching or tearing of the fibres of that muscle, and of the adjacent intermuscular septa. A similar injury—sculler's sprain—occurs in rowing-men from feathering the oar. The treatment consists in massage and movement, care being taken to avoid the movement which produced the sprain.
The shafts of the bones of the forearm may be broken separately, but it is much more common to find both broken together.
Fracture of both bones may result from a direct blow, from a fall on the hand, or from their being bent over a fixed object. The line of fracture is usually transverse, both bones giving way about the same level. The common situation is near the middle of the shafts. In children, greenstick fracture of both bones is a frequent result of a fall on the hand—this indeed being one of the commonest examples of greenstick fracture met with (Fig. 41).
The displacement varies widely, depending partly upon the force causing the fracture, partly on the level at which the bones break, and on the muscles which act on the respective fragments. It is common to find an angular displacement of both bones to the radial or to the ulnar side. In other cases the four broken ends impinge upon the interosseous space, and may become united to one another, preventing the movements of pronation and supination. There may be shortening from overriding of fragments.
When the radius is broken above the insertion of the pronator teres, its upper fragment may be supinated by the biceps and supinator muscles, while the lower fragment remains in the usual semi-prone position. If union takes place in this position, the power of complete supination is permanently lost.
The usual symptoms of fracture are present, and there is seldom any difficulty in diagnosis.
The prognosis must be guarded, especially with regard to the preservation of pronation and supination. These movements are interfered with if union takes place in a bad position with angular or rotatory deformity of one or both bones, or if callus is formed in excess and causes locking of the bones. In some cases the callus fuses the two bones across the interosseous space, and pronation and supination are rendered impossible.
Persistent angular deformity of the forearm is also liable to ensue, either from failure to correct the displacement primarily, or from subsequent bending due to ill-applied splints or slings. Want of union, or the formation of a false joint in one or both bones, is sometimes met with, particularly in children, and, like the corresponding fracture of the leg, is liable to prove intractable.
A considerable number of cases of gangrene of the hand after simple fracture of the forearm are on record. This is sometimes attributable to damage inflicted upon the blood vessels by the fractured bones, or to the force that caused the fracture, but is oftener due to a roller bandage applied underneath the splints strangulating the limb, to injudiciously applied pads, or to too tight bandaging over the splints. Volkmann's ischæmic contracture occasionally develops after fractures of the forearm.
In uncomplicated cases, union takes place in from three to four weeks.
 Fig. 42.—Gooch Splints for Fracture of both Bones of
Forearm. (These are applied with the wooden side towards the skin.)
Fig. 42.—Gooch Splints for Fracture of both Bones of
Forearm. (These are applied with the wooden side towards the skin.)
Treatment.—To ensure accurate reduction and coaptation, a general anæsthetic is usually necessary. In the greenstick variety the bones must be straightened, the fracture being rendered complete, if necessary, for this purpose.
To retain the bones in position, anterior and posterior splints are then applied. These are made to overlap the forearm by about half an inch on each side, to avoid compressing the forearm from side to side, and so making the fractured ends encroach upon the interosseous space. The dorsal splint is usually made to extend from the olecranon to the knuckles, and the palmar one from the bend of the elbow to the flexure in the middle of the palm, a piece being cut out to avoid pressure on the ball of the thumb (Fig. 42). The splints are applied with the elbow flexed to a right angle, and, except when the radius is broken above the level of the insertion of the pronator teres, with the forearm midway between pronation and supination. The limb is placed in a sling, so adjusted that it supports equally the hand and elbow in order to avoid angular deformity. The use of special interosseous pads is to be avoided.
When the fracture of the radius is above the insertion of the pronator teres, the forearm should be placed in the position of complete supination, with the elbow flexed to an acute angle, and retained in this position by a moulded posterior splint, and the arm fixed to the side by a body bandage. Great care is necessary in the adjustment of the apparatus to prevent pronation.
Massage and movement should be carried out from the first. It is usually necessary to continue wearing the splints for about three weeks.
In cases of mal-union, especially when the bones are ankylosed to one another across the interosseous space, operation may be necessary, but it is neither easy in its performance nor always satisfactory in its results. The seat of fracture should be exposed by one or more incisions so placed as to enable the muscles to be separated and to give access to the callus. When the limb is straight, it is only necessary to gouge away the exuberant callus that interferes with rotatory movements; but when there is an angular deformity the bones must, in addition, be divided and re-set, and, if necessary, mechanically fixed in good position. In comparatively recent cases it is sometimes possible, without operation, to re-fracture the bones and to set them anew.
Un-united fracture of both bones of the forearm is not uncommon and is treated on the usual lines; the gap between the fragments of the radius is bridged by a portion of the fibula, that should be long enough to overlap by at least an inch at either end; it is rarely necessary to bridge the gap in the ulna, unless it alone is the seat of non-union.
Fracture of the shaft of the radius alone may be due to a direct blow; to indirect violence, such as a fall on the hand; or to forcible pronation against resistance, as in wringing clothes. It is rare in comparison with fracture of both bones. When broken above the insertion of the pronator teres, the upper fragment is flexed and supinated by the biceps and supinator, while the lower fragment remains semi-prone, and is drawn towards the ulna by the pronator quadratus.
When the fracture is below the pronator teres, the displacement depends upon the direction of the force and the obliquity of the fracture. In fractures of the lower third of the shaft, the hand may be flexed toward the radial side, and the styloid lies at a higher level, as in a Colles' fracture. From the frequency with which this fracture occurs while cranking a motor-car, it is conveniently described as Chauffeur's fracture; we have observed in doctors, who have sustained this fracture in their own persons, that they were under the impression that they had sustained a trivial sprain of the wrist.
In addition to the ordinary signs of fracture, there is partial or complete loss of pronation and supination. The head of the radius as a rule does not move with the lower part of the shaft, but may do so if the fracture is incomplete or impacted.
Fracture of the shaft of the ulna alone is also comparatively rare. It is almost always due to a direct blow sustained while protecting the head from a stroke, or to a fall on the ulnar edge of the forearm, as in going up a stair.
The upper third is most frequently broken, and this injury is often associated with dislocation of the head of the radius (Fig. 40), or some other injury implicating the elbow-joint. On account of the superficial position of the bone, this fracture is frequently compound.
The displacement depends on the direction of the force, the fragments being usually driven towards the interosseous space. There is seldom marked deformity unless the head of the radius is dislocated at the same time. The diagnosis is, as a rule, easy.
The treatment is the same as for fracture of both bones, but the splints may be discarded at the end of a fortnight.
For some unexplained reason, a fracture of the upper third of the shaft of the ulna frequently fails to unite.
These include fractures of the lower ends of the bones of the forearm and separation of their epiphyses; sprains and dislocations of the inferior radio-ulnar, and of the radio-carpal articulations; and fractures and dislocations of the carpus.
Surgical Anatomy.—The most important landmarks in the region of the wrist are the styloid processes of the radius and ulna. The tip of the radial styloid is palpable in the “anatomical snuff-box” between the tendons of the long and short extensors of the thumb, and it lies about half an inch lower than the ulnar styloid. The ulnar styloid is best recognised on making deep pressure a little below and in front of the head of the ulna, which forms the rounded subcutaneous prominence seen on the back of the wrist when the hand is pronated.
The tubercle of the navicular (scaphoid) and the greater multangular (trapezium) can be felt between the radial styloid and the ball of the thumb, a little below the radial styloid; and the pisiform and hook of the hamatum (unciform) are palpable, slightly below and in front of the ulnar styloid.
In examining an injured wrist, the different bony points should be located, and their relative positions to one another and to the adjacent joints noted; and the shape, position, and relations of any unnatural projection or depression observed, using the wrist on the other side as the normal standard for comparison. The power and range of movement—active and passive—at the various joints should also be tested.
Colles' Fracture.—This injury, which was described by Colles of Dublin in 1814, is one of the commonest fractures in the body, and is especially frequent in women beyond middle age. It is almost invariably the result of a fall on the palm of the hand, in the three-quarters pronated position, the force being received on the ball of the thumb, and transmitted through the carpus to the lower end of the radius which is broken off, the lower fragment being driven backwards.
The fracture takes place through the cancellated extremity of the bone, within a half to three-quarters of an inch of its articular surface (Fig. 45). It is usually transverse, but may be slightly oblique from above downwards and from the radial to the ulnar side. In a considerable proportion of cases it is impacted, and not infrequently the lower fragment is comminuted, the fracture extending into the radio-carpal joint.
 Fig. 43.—Colles' Fracture showing radial deviation of
hand.
Fig. 43.—Colles' Fracture showing radial deviation of
hand.
|
 Fig. 44.—Colles' Fracture showing undue prominence of
ulnar styloid.
Fig. 44.—Colles' Fracture showing undue prominence of
ulnar styloid.
|
When impaction takes place, it is usually reciprocal, the dorsal edge of the proximal fragment piercing the distal fragment, and the palmar edge of the distal fragment piercing the proximal. The periosteum is usually torn and stripped from the palmar aspect of the fragments, while it remains intact on the dorsum.
In the majority of cases the styloid process of the ulna is torn off by traction exerted through the medial ulno-carpal (internal lateral) ligament, and in a considerable proportion there is also a fracture of one of the carpal bones.
The resulting displacement is of a threefold character: (1) the distal fragment is displaced backwards; (2) its carpal surface is rotated backwards on a transverse diameter of the forearm; while (3) the whole fragment is rotated so that the radial styloid comes to lie at a higher level than normal.
 Fig. 45.—Radiogram showing the line of fracture and
upward displacement of the radial styloid in Colles' Fracture.
Fig. 45.—Radiogram showing the line of fracture and
upward displacement of the radial styloid in Colles' Fracture.
Clinical Features.—In a typical case there is a prominence on the dorsum of the wrist, caused by the displaced distal fragment, with a depression just above it (Fig. 43); and the wrist is broadened from side to side. The natural hollow on the palmar aspect of the radius is filled up by the projection of the proximal fragment. The carpus is carried to the radial side by the upward rotation of the distal fragment, and the radial styloid is as high, or even higher, than that of the ulna. The lower end of the ulna is rendered unduly prominent by the flexion of the hand to the radial side. The fingers are partly flexed and slightly deviated towards the ulnar side; and the patient supports the injured wrist in the palm of the opposite hand, and avoids movement of the part. Occasionally the median nerve is bruised or torn, causing motor and sensory disturbances in its area of distribution.
The general outline of the wrist and hand has been compared not inaptly to that of “an inverted spoon.” Pronation and stipulation are lost, the joint is swollen, and there is tenderness on pressure, especially over the line of fracture. Tenderness over the position of the ulnar styloid may indicate fracture of that process, although it is sometimes present without fracture. No attempt should be made to elicit crepitus in a suspected case of Colles' fracture as the manipulations are painful, and are liable to increase the displacement.
Treatment.—It cannot be too strongly insisted upon that success in the treatment of Colles' fracture with displacement and impaction depends chiefly upon complete and accurate reduction, and to enable this to be effected a general anæsthetic is almost essential. The surgeon grasps the patient's hand, as if shaking hands with him, and, resting the palmar surface of the wrist on his bent knee, makes traction through the hand, and counter-extension through the forearm, with lateral movements, if necessary, to undo impaction. When the fragments are freed from one another, the wrist is flexed, and the hand carried to the ulnar side, while the lower fragment is moulded into position by the thumb of the surgeon's disengaged hand. When reduction is complete, the deformity disappears, and the two styloid processes regain their normal positions relative to one another.
As there is no tendency to re-displacement and no risk of non-union, no retentive apparatus is required, but, if it adds to the patient's sense of security, a bandage or a poroplastic wristlet may be applied. In severe cases, however, anterior and posterior splints, similar to those used for fracture of both bones of the forearm, or a dorsal splint padded so as to flex the wrist to an angle of 45°, but somewhat narrower, may be employed. The hand and forearm are in any case supported in a sling.
To avoid the stiffness that is liable to follow, massage and movement of the wrist and fingers should be carried out from the first, the range of movement being gradually increased until the function of the joints is perfectly restored. If splints are used, they should be discarded in a week, and the patient is then encouraged to use the wrist freely.
The various special splints recommended for the treatment of Colles' fracture, such as Carr's, Gordon's, the “pistol splint,” and many others, are all designed to correct the deformity as well as to control the fragments. It has already been pointed out that if reduction is complete there is no deformity to correct, and if it is not complete the deformity cannot be corrected by any form of splint.
Unreduced Colles' Fracture.—When union has been allowed to take place without the displacement having been reduced, an unsightly deformity results. In young subjects whose occupation is likely to be interfered with, and in women for æsthetic reasons, the fracture is reproduced and the displacement of the lower fragment corrected. This is conveniently done by means of Jones' wrench, which grasps the distal fragment and affords sufficient leverage to break the bone.
Chauffeur's Fracture.—A fracture of the lower end of the radius frequently occurs from the recoil of the crank, “by back firing,” in starting the engine of a motor-car. The injury may be produced either by direct violence, the handle as it recoils striking the forearm, or by indirect violence, from forcible hyper-extension of the hand while grasping the handle. The fracture may pass transversely through the lower end of the radius, as in Colles' fracture, but is more often met with two or three inches above the wrist (Fig. 46). It is treated on the same lines as Colles' fracture.
A fracture of the lower end of the radius with forward displacement of the carpal fragment, was first described by R. W. Smith of Dublin (Colles' fracture reversed, or Smith's fracture) (Fig. 47). It is nearly always due to forcible flexion, as from a fall on the back of the hand. Like Colles' fracture, it may be transverse or slightly oblique, impacted, or comminuted. The deformity is characterised by an elevation on the dorsum running obliquely upwards from the ulnar to the radial side of the wrist, and caused by the head of the ulna, which remains in position, and the distal end of the proximal fragment. Below this, over the position of the distal radial fragment, is a gradual slope downwards on to the dorsum of the hand. Anteriorly there is a prominence in the flexure of the wrist, and the distal fragment may be felt under the flexor tendons. The hand deviates to the radial side, and thereby still further increases the prominence caused by the lower end of the ulna. The radial styloid is displaced forward, upward, and to the radial side, and the ulnar styloid may be torn off.
When the deformity is not well marked, this injury may be mistaken for forward dislocation of the wrist, for fracture of both bones low down, or for sprain of the joint.
The treatment is carried out on the same lines as in Colles' fracture.
Longitudinal fractures of the lower end of the radius opening into the joint usually result from the hand being crushed by a heavy weight or in machinery. They are often compound and comminuted.
Separation of the lower epiphysis of the radius, which is on the same level as that of the ulna and lies above the level of the synovial membrane of the wrist-joint, is comparatively common between the ages of seven and eighteen, especially in boys, and is caused by the same forms of violence as produce Colles' fracture.
Although clinically the appearances in these two injuries bear a general resemblance to one another, separation of the epiphysis may usually be identified by the directly transverse line of the dorsal and palmar projections, the folding of the skin observed in the palmar depression, the absence of abduction of the hand and the ease with which muffled crepitus can be elicited (E. H. Bennett). The deformity is readily reduced, and the fragments are easily retained in position.
This injury is often complicated with fracture of the shaft or styloid process of the ulna, or with dislocation of the radio-ulnar joint, and it is not infrequently compound, the lower end of the shaft being driven through the skin on the palmar aspect immediately above the wrist. Impairment of growth in the radius seldom occurs; when it does, it results in a valgus condition of the hand (Fig. 48), calling for resection of the lower end of the ulna.
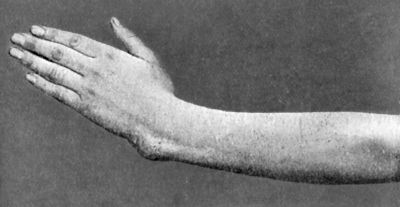 Fig. 48.—Manus Valga following separation of lower
radial epiphysis in childhood.
Fig. 48.—Manus Valga following separation of lower
radial epiphysis in childhood.The treatment is the same as for Colles' fracture.
Fracture of the Lower End of the Ulna.—The lower end of the shaft of the ulna is seldom fractured alone. The styloid process, as has already been pointed out, is frequently broken in association with Colles' and other fractures of the lower end of the radius.
Separation of the lower epiphysis of the ulna sometimes occurs, and in rare cases results in arrest of the growth of the bone, leading to a varus condition of the hand and bending of the radius. Sometimes the separated epiphysis fails to unite, and although this gives rise to no disability, it is liable to lead to errors in the interpretation of skiagrams.
The treatment is similar to that for the corresponding injuries of the radius.
Simultaneous separation of the epiphysis of both radius and ulna sometimes occurs, and, as a result of severe violence, may be compound, the lower ends of the diaphyses projecting through the skin on the palmar aspect above the wrist.
Fracture of Carpal Bones.—The use of the Röntgen rays has shown that fracture of individual carpal bones is commoner than was previously supposed, and that many cases formerly looked upon as severe sprains are examples of this injury.
The navicular (scaphoid) and lunate (semilunar) are those most commonly fractured, usually by indirect violence, by forced dorsiflexion from a fall on the extended hand. The clinical features are: localised swelling on the radial side of the wrist, increase in the antero-posterior diameter of the carpus, marked tenderness in the anatomical snuff-box when the hand is moved laterally, especially in the direction of adduction, and, rarely, crepitus. The median nerve is sometimes over-stretched or partly torn. In many cases, however, the symptoms are so obscure that an accurate diagnosis can only be made by the use of the X-rays (Fig. 49). Codman recommends taking pictures of the navicular by placing the two wrists of the patient in adduction, and of the lunate, in abduction.
The treatment of simple fractures consists in massage and movement. Codman and Chase recommend excision of the proximal half of the fractured bone, through a dorsal incision to the lateral side of the extensor digitorum communis. When the fracture is compound, the loose fragments should be removed.
Dislocation may occur at the inferior radio-ulnar, the radio-carpal, mid-carpal, inter-carpal, or carpo-metacarpal joints, but the strong ligaments of these articulations, the comparatively free movement at the various joints, and the relative weakness of the lower end of the radius whereby it is so frequently fractured, render dislocation a rare form of injury.
Dislocation of the inferior radio-ulnar articulation may complicate fracture of the lower end of the radius, or accompany sub-luxation of the head of the radius. The head of the ulna usually passes backward.
In children, the commonest cause is lifting the child by the hand, and the displacement is only partial. In adults, it may result from forcible efforts at pronation or supination, as in wringing clothes, or from direct violence, the separation being frequently complete, and sometimes compound.
The head of the ulna is unduly prominent, and there is a depression on the opposite aspect of the joint. The hand is generally pronated, the rotatory movements at the wrist are restricted and painful, while flexion and extension are comparatively free.
Reduction is effected by making pressure on the displaced bone and manipulating the joint, especially in the direction of supination. If the ligaments fail to unite, the head of the ulna tends to slip out of place in pronation and supination—recurrent dislocation.
Dislocation at the radio-carpal articulation, usually spoken of as dislocation of the wrist, is attended by tearing of the ligaments and displacement of tendons, and is frequently compound. The carpus may be displaced backward or forward, and the articular edge of the radius towards which it passes may be chipped off.
Backward dislocation is commonest, the injury resulting from a severe form of violence, such as a fall from a height on the palm while the hand is dorsiflexed and abducted. The clinical appearances closely simulate those of Colles' fracture, or of separation of the lower radial epiphysis, but the unnatural projections, both in front and behind, are lower down, and end more abruptly (Fig. 50). The hand is more flexed, and the palm is shortened. The styloid processes retain their normal relations to one another, and the carpal bones lie on a plane posterior to the styloids, the articular surfaces may be recognised on palpation. The forearm is not shortened.
Forward dislocation of the carpus may result from any form of forced flexion, such as a fall on the back of the hand, or from direct violence. The displaced carpus forms a marked projection on the palmar aspect of the wrist, and there is a corresponding depression on the dorsum. The attitude of the hand and fingers is usually one of flexion.
In both varieties reduction is readily effected by making traction on the hand and pushing the carpus into position. A moulded poroplastic splint, which keeps the hand slightly dorsiflexed, adds to the comfort of the patient, but this should be removed daily to admit of movement and massage being employed.
Dislocation of Carpal Bones.—The two rows of carpal bones may be separated from one another, or any one of the individual bones may be displaced. These injuries are rare, and result from severe forms of violence, usually from a fall on the extended hand. Pain, deformity, and loss of function are the ordinary symptoms. The treatment consists in making direct pressure over the displaced bone, while traction is made on the hand, which is alternately flexed and extended.
Of these injuries that most frequently observed is displacement of the head of the capitate bone (os magnum) from the navicular (scaphoid) and lunate (semilunar) bones. Frequently these bones are fractured, and fragments accompany the displaced os magnum. In full palmar flexion of the wrist the displaced head of the os magnum forms a prominence on the dorsum opposite the base of the third metacarpal, which temporarily disappears when the hand is dorsiflexed. There is an increase in the antero-posterior diameter of the wrist, situated on a lower level than that which accompanies fracture of the lower end of the radius; flexion and extension of the wrist are limited; and in some cases there are symptoms referable to pressure on the median nerve. By keeping the hand in the dorsiflexed position for a week or ten days, the bone may become fixed in its place and the function of the wrist be restored, but it is often necessary to excise the bone.
The lunate may be displaced forward by forcible dorsiflexion of the hand, and forms a projection beneath the flexor tendons; there is usually loss of sensibility in the distribution of the ulnar nerve in the hand. The most satisfactory treatment is removal of the bone.
In a few cases the navicular has been displaced (Fig. 51), and has had to be subsequently replaced by operation. Separation of any of the other bones is rare.
Carpo-metacarpal Dislocations.—Any or all of the metacarpal bones may be separated from the carpus by forced movements of flexion or extension. The commonest displacement is backward. The thumb seems to suffer oftener than the other digits. These injuries, however, are so rare, and the deformity is so characteristic, that a detailed description is unnecessary.
Sprain of the wrist is a common injury, and results from a fall on the hand, a twist of the wrist, or from the back-firing of a motor-crank dorsiflexing the hand. The marked swelling which rapidly ensues may render it difficult to distinguish a sprain from the other injuries that are liable to result from similar causes—Colles' fracture, separation of the lower radial epiphysis, dislocation of the wrist, and fractures and dislocations of the carpal bones.
In a sprain the normal relations of the styloid processes and other bony points about the wrist are unaltered, and there is no radial deviation of the hand, as in Colles' fracture. The most marked swelling is over the line of the articulation on the anterior and posterior aspects of the joint. There is usually some effusion into the sheaths of the tendons passing over the joint, and in some cases on moving the fingers a peculiar creaking, which may simulate crepitus, can be elicited. There is marked tenderness on making pressure over the line of the joint, as well as over one or other of the collateral ligaments, depending upon which ligament has been over-stretched or torn. Movements that tend to put the damaged ligaments on the stretch also cause pain. It has to be borne in mind, however, that in many cases of Colles' fracture there is extreme tenderness on pressing over the ulnar styloid and medial ulno-carpal ligament, as these structures are frequently injured as well as the radius, but the point of maximum pain and tenderness is over the seat of fracture of the radius. In all doubtful cases the X-rays should be employed to establish the diagnosis.
The treatment consists in the immediate employment of massage and movement, supplemented by alternate hot and cold douches, on the same lines as in sprains of other joints.
Fracture.—Fractures of the metacarpals of the fingers are comparatively common. When they result from direct violence, such as a crush between two heavy objects, they are often multiple and compound. Indirect violence, acting in the long axis of the bone and increasing its natural curve, such as a blow on the knuckle in striking with the closed fist, usually produces an oblique fracture about the middle of the shaft, the proximal end of the distal fragment projecting towards the dorsum. Apart from this there is little deformity, as the adjacent metacarpals act as natural splints and tend to retain the fragments in position. A sudden sharp pain may be elicited at the seat of fracture on making pressure in the long axis of the finger; and unnatural mobility and crepitus may usually be detected. These fractures are readily recognised by the X-rays. Firm union usually results in three weeks.
The shaft of the metacarpal of the thumb is frequently broken by a blow with the closed fist. The fracture is usually transverse, and situated near the proximal end of the shaft; frequently it is comminuted, and in some instances there is a longitudinal split.
Treatment.—When the fracture is transverse, and especially when it implicates the middle or ring fingers, the most convenient method is to make the patient grasp a firm pad, such as a roller bandage covered with a layer of wool, and to fix the closed fist by a figure-of-eight bandage. In this way the adjoining metacarpals are utilised as side splints. Active and passive movements must be carried out from the first, and the bandage may be dispensed with at the end of a week or ten days.
In oblique fractures with a tendency to overriding of the fragments, especially in the case of the index and little fingers, it is sometimes necessary to apply extension to the distal segment of the digit, by means of adhesive plaster, to which elastic tubing is attached and fixed to the end of a bow splint, reaching well beyond the finger-tips (Fig. 52). This should be worn for a week or ten days.
Bennett's Fracture of the Base of the First Metacarpal Bone.—Bennett of Dublin described an injury of the thumb which, although comparatively common, is often mistaken for a sub-luxation backward of the carpo-metacarpal joint, or a simple “stave of the thumb.” It consists in an “oblique fracture through the base of the bone, detaching the greater part of the articular facet with that piece of the bone supporting it which projects into the palm” (Fig. 53). We have frequently observed the fracture extend for a considerable distance along the palmar aspect of the shaft.
It usually results from severe force applied directly to the point of the thumb, driving the metacarpal against the greater multangular bone (trapezium), and chipping off the palmar part of the articular surface, but it may result from a blow with the closed fist. The rest of the metacarpal slips backward, forming a prominence on the dorsal aspect of the joint. The pain and swelling in the region of the fracture often prevent crepitus being elicited, and as the deformity is not at once evident, the nature of the injury is liable to be overlooked. The fracture is recognised by the use of the X-rays. Unless properly treated this injury may result in prolonged impairment of function, full abduction and fine movements requiring close apposition of the thumb being specially interfered with.
The treatment consists in reducing the fracture by extension in the attitude of full abduction and applying an accurately fitting pad over the extremity of the displaced bone, maintained in position by a light angular splint. This splint is first fixed to the extended and abducted thumb, and while extension is made by pushing it downwards the upper end is fixed to the wrist (Fig. 54 A). The apparatus is worn for three weeks, being carefully readjusted from time to time to maintain the extension and abduction. A moulded poroplastic splint added on the same principle may be employed, and is more comfortable (Fig. 54 B). Excellent results are obtained after reduction of the displacement, by massage and movement from the first, and the support merely of a figure-of-eight bandage (Pirie Watson).
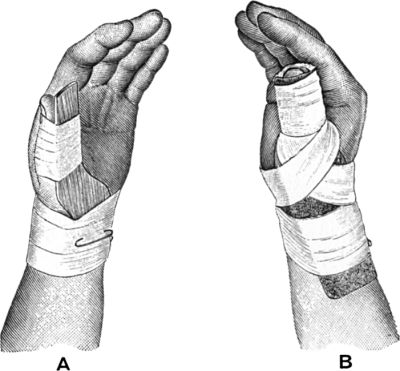 Fig. 54.—A. Splint applied as used by Bennett. B.
Poroplastic Moulded Splint for Bennett's Fracture.
Fig. 54.—A. Splint applied as used by Bennett. B.
Poroplastic Moulded Splint for Bennett's Fracture.
Fractures of phalanges usually result from direct violence, and on account of the superficial position of the bones, are often compound, and attended with much bruising of soft parts. Force applied to the distal end of the finger may also fracture a phalanx. The proximal phalanges are broken oftener than the others. The deformity is usually angular, with the apex towards the palm, and if union takes place in this position, the power of grasping is interfered with. Unnatural mobility and crepitus can usually be recognised, but, on account of the swelling and tenderness, the fracture is apt to be overlooked. Firm union takes place in two or three weeks. In oblique and comminuted fractures, union may take place with overlapping, producing a deformity which may prevent the wearing of a glove or of rings. In compound fractures, non-union sometimes occurs, and causes persistent disability. In doubtful cases radioscopy renders valuable aid, as the parts are readily seen with the screen.
Treatment.—Early movement and massage are all-important. The contiguous fingers may be utilised as side splints, and a long palmar splint projecting beyond the fingers is applied. In oblique and comminuted fractures it may be necessary to anæsthetise the patient to effect reduction. When it is particularly desirable to avoid deformity, an open operation may be advisable.
Dislocation.—Dislocation of the Metacarpo-phalangeal Joint of the Thumb.—The commonest dislocation at this joint is a backward displacement of the proximal phalanx, which may be complete or incomplete. Its special clinical importance lies in the fact that much difficulty is often experienced in effecting reduction.
This dislocation is usually produced by extreme dorsiflexion of the thumb, whereby the volar accessory (palmar) and the collateral ligaments are torn from their metacarpal attachments, the phalanx carrying with it the volar accessory ligament and sesamoid bones. The head of the metacarpal passes forward between the two heads of the short flexor of the thumb, and the tendon of the long flexor slips to the ulnar side. The phalanx passes on to the dorsum of the metacarpal, where it is held erect by the tension of the abductor and adductor muscles.
The attitude of the thumb is characteristic. The metacarpal is adducted, its head forming a marked prominence on the front of the thenar eminence, and the phalanges are displaced backwards, the proximal being dorsiflexed and the distal flexed towards the palm.
Many explanations of the difficulty so often experienced in reducing this variety of dislocation have been offered, but the consensus of opinion seems to be that it is due to the interposition of the volar accessory ligament and the sesamoid bones between the phalanx and the metacarpal, and that this is most frequently the result of ill-advised efforts at reduction. In some cases the tension of the long flexor tendon may be a factor in preventing reduction, but the “button-holing” by the short flexor is probably of no importance.
Reduction is to be effected by flexing and abducting the metacarpal while the phalanx is hyper-extended and pushed down towards the joint and levered over the head of the metacarpal.
When this manipulation fails, the volar accessory ligament should be divided longitudinally through a puncture made with a tenotomy knife on the dorsal aspect of the joint, so as to separate the sesamoid bones and permit the passage of the head between them. An open operation is seldom necessary.
Dislocation forward is rare. It results from forced flexion of the thumb with abduction, tearing the posterior and medial collateral ligaments. The deformity is characteristic: the rounded head of the metacarpal projecting behind the level of the joint, while the base of the phalanx forms a prominence among the muscles of the thenar eminence.
Reduction is easily effected by making traction on the phalanges and carrying out movements of flexion and extension. The deformity, however, is liable to be reproduced unless a retentive apparatus is securely applied.
Dislocation of the thumb to one or other side is rare.
Dislocations of the metacarpo-phalangeal joint of the fingers may be backward or forward. They are less common than those of the thumb, but present the same general characters. In the backward variety the same difficulty in reduction occurs as is met with in the corresponding dislocation of the thumb, and is to be dealt with on the same lines.
Inter-phalangeal Dislocation.—The second and the ungual phalanges may be displaced backwards, forwards, or to the side. The clinical features are characteristic, and the diagnosis, as well as reduction, is easy. These dislocations are frequently the result of machinery accidents, and being compound and difficult to render aseptic, often necessitate amputation.
Persistent flexion of the terminal phalanx of the thumb or fingers (drop or mallet finger) may result from violence applied to the end of the digit when in the extended position—as, for example, in attempting to catch a cricket-ball. The terminal phalanx is flexed towards the palm, and the patient is unable to extend it voluntarily. A palmar splint is applied securing extension of the distal joint for three or four weeks. If the deformity has been allowed to occur it can only be corrected by an open operation, suturing or tightening the extensor tendon at its insertion into the base of the terminal phalanx.
For descriptive as well as for practical purposes, it is useful to divide fractures of the pelvis into those that involve the integrity of the pelvic girdle as a whole, and those confined to individual bones.
In all, the prognosis depends upon the severity of the visceral lesions which so frequently complicate these injuries, rather than upon the fractures themselves.
Fractures implicating the pelvic girdle as a whole usually result from severe crushing forms of violence, such as the fall of a mass of coal or a pile of timber, or the passage of a heavy wheel over the pelvis. The force may act in the transverse axis of the pelvis, or in its antero-posterior axis. The pelvic viscera may be lacerated by the tearing asunder of the bones, or perforated by sharp fragments, or they may be ruptured by the same violence as that causing the fracture.
As a rule, more than one part of the pelvis is broken, the situation of the lesions varying in different cases.
Separation of the pubic symphysis may result from violence inflicted on the fork, as in coming down forcibly on the pommel of a saddle; from forcible abduction of the thighs; or it may happen during child-birth. In some cases the two pubic bones at once come into apposition again, and there is no permanent displacement, the only evidence of the injury being localised pain in the region of the symphysis elicited on making pressure over any part of the pelvis. In other cases the pubic bones overlap one another, and the membranous portion of the urethra, or the bladder wall, is liable to be torn. The displaced bones may be palpated through the skin, or by vaginal or rectal examination.
The pubic portion of the pelvic ring is the most common seat of fracture. The bone gives way at its weakest points—namely, through the superior (horizontal) ramus of the pubes just in front of the ilio-pectineal eminence, and at the lower part of the inferior (descending) ramus (Fig. 55). The intervening fragment of bone is isolated, and may be displaced. These fractures are frequently bilateral, and are often associated with separation of the sacro-iliac joint, with longitudinal fracture of the sacrum (Fig. 55), or with other fractures of the pelvic-bones.
 Fig. 55.—Multiple Fracture of Pelvis through
Horizontal and Descending Rami of both Pubes, and Longitudinal
Fracture of left side of Sacrum.
Fig. 55.—Multiple Fracture of Pelvis through
Horizontal and Descending Rami of both Pubes, and Longitudinal
Fracture of left side of Sacrum.
Injuries of the membranous urethra and bladder are frequent complications, less commonly the rectum, the vagina, or the iliac blood vessels are damaged.
Localised tenderness at the seat of fracture, pain referred to that point on pressing together or separating the iliac crests, and mobility of the fragments with crepitus, are usually present. The fragments may sometimes be felt on rectal or vaginal examination. In all cases shock is a prominent feature.
The lateral and posterior aspects of the pelvic ring may be implicated either in association with pubic fractures or independently. Thus a fracture of the iliac bone may run into the greater sciatic notch; or a vertical fracture of the sacrum or separation of the sacro-iliac joint may break the continuity of the pelvic brim. In rare cases these injuries are accompanied by damage to the intestine, the rectum, the sacral nerves, or the iliac blood vessels.
Treatment.—It is of importance that the patient be moved and handled with care lest fragments become displaced and injure the viscera. He should be put to bed on a firm mattress, which may be made in three pieces, for convenience in using the bed-pan and for the prevention of bed-sores.
Before the treatment of the fracture is commenced, the surgeon must satisfy himself, by the use of the catheter and by other means, that the urethra and bladder are intact. Should these or any other of the pelvic viscera be damaged, such injuries must first receive attention.
The treatment of the fracture itself consists in adjusting the fragments, as far as possible by manipulation, applying a firm binder or many-tailed bandage round the pelvis, and fixing the knees together by a bandage (Fig. 57).
When there is displacement of fragments extension should be applied to both legs, with the limbs abducted and steadied by sand-bags.
Compound fractures, being commonly associated with extravasation of urine, are liable to infective complications. Loose fragments should be removed, as they are prone to undergo necrosis.
The patient is confined to bed for six or eight weeks, and it may be several weeks more before he is able to resume active employment.
The acetabulum may be fractured by force transmitted through the femur, usually from a fall on the great trochanter, less frequently from a fall on the feet or other form of violence. It may merely be fissured, or the head of the femur may be forcibly driven through its floor into the pelvic cavity, either by fracturing the bone or, in young subjects, by bursting asunder the cartilaginous junction of the constituent bones. When the femoral head penetrates into the pelvis—the central dislocation of the hip of German writers—the condition simulates a fracture of the neck of the femur, but the trochanteric region is more depressed and the trochanter lies nearer the middle line. The limb is shortened, and movements of the joint are painful and restricted, especially medial rotation. In some cases there is pain along the course of the obturator nerve.
On rectal or vaginal examination there is localised tenderness over the pelvic aspect of the acetabulum, and in some cases a convex projection, or even crepitating fragments can be detected. The diagnosis is completed by an X-ray picture.
When the head of the femur penetrates the acetabulum, reduction should be attempted by traction and manipulation. The pelvis is held rigid, and the thigh is flexed and forcibly adducted, while the medial side of the thigh rests against a firm sand-bag; the femoral head is thus lifted out of the pelvis. In a recent injury the amount of force required is relatively slight. The head is kept in its corrected position by extension.
Fracture of the upper and back part of the rim of the acetabulum may accompany or simulate dorsal dislocation of the hip. Crepitus may be present in addition to the symptoms of dislocation, and after reduction the displacement is easily reproduced. The treatment is by extension with the limb adducted.
Fracture of Individual Bones of the Pelvis.—Ilium.—The expanded portion of the iliac bone is often broken by direct violence, the detached fragments varying greatly in size and position (Fig. 56).
The whole or part of the crest may be separated by similar forms of violence.
When the fracture implicates the ala of the bone, it usually starts at the triangular prominence near the middle of the crest, and runs backwards or forwards, passing for a variable distance into the iliac fossa. The displaced fragment can sometimes be palpated and made to move when the muscles attached to it are relaxed. This is done by flexing the thighs and bending the body forward and towards the affected side. Pain and crepitus may be elicited on making this examination.
These fractures are treated by applying a roller bandage or broad strips of adhesive plaster over the seat of fracture, and by placing the patient in such a position as will relax the muscles attached to the displaced fragment—in the case of the iliac spine by flexing the thigh upon the pelvis; in the case of the crest or ala by raising the shoulders. Union takes place in three or four weeks.
In young persons, the anterior superior spine has been torn off and displaced downwards by powerful contraction of the sartorius muscle; and the anterior inferior spine by strong traction on the ilio-femoral or [inverted Y]-shaped ligament. These injuries are best treated by fixing the displaced fragment in position by a peg or silver wire sutures and relaxing the muscles acting on it.
Fracture of the ischium alone is rare. It results from a fall on the buttocks, the entire bone or only the tuberosity being broken. There is little or no displacement, and the diagnosis is made by external manipulation and by examination through the rectum or vagina.
A longitudinal fracture of the sacrum may implicate the posterior part of the pelvic ring, as has already been mentioned. In rare cases the lower half of the bone is broken transversely from a fall or blow, and the lower fragment is bent forward so that it projects into the pelvis and may press upon or tear the rectum, or the sacral nerves may be damaged, and partial paralysis of the lower limbs, bladder, or rectum result. These fractures are frequently comminuted and compound, and the soft parts may be so severely bruised and lacerated that sloughing follows. On rectal examination the lower segment of the bone can be felt, and on manipulating it pain and crepitus may be elicited.
Fracture of the coccyx may be due to a direct blow, or may occur during parturition. As a result of this injury the patient may have severe pain on sitting or walking, and during defecation. The loose fragment can be palpated on rectal examination. There is considerable difficulty in keeping the fragment in position, and if it projects towards the rectum it should be removed. If the lower fragment unites at an angle so as to cause pressure on the rectum, it gives rise to the symptoms of coccydynia, which may call for excision.
These include the various fractures of the upper end of the femur; dislocation and sprain of the hip-joint; and contusion of the hip.
Surgical Anatomy.—The strength of the hip-joint depends primarily on its osseous elements—the rounded head of the femur filling the deep socket of the acetabulum, to the bottom of which it is attached through the medium of the ligamentum teres. The edge of the acetabulum is specially strong above and behind, while at its lower margin there is a gap, bridged over by the labrum glenoidale (cotyloid ligament).
In relation to fractures of the upper end of the femur, it is to be borne in mind that as the antero-posterior diameter of the neck is less than that of the shaft, and as a considerable portion of the great trochanter lies behind the junction of the neck with the shaft, the greater part of any strain put upon the upper end of the femur is borne by the neck of the bone and not by the trochanter. The head and neck of the femur are nourished chiefly by the thick, vascular periosteum, and through certain strong fibrous bands reflected from the attachment of the capsule—the retinacular or cervical ligaments of Stanley. The integrity of these ligaments plays an important part in determining union in fractures of the neck of the femur, both by keeping the fragments in position and by maintaining the blood-supply to the short fragment. Whether it be true or not that an alteration in the angle of the femoral neck takes place with advancing years, it is generally recognised that this change is of no importance in relation to fractures in this region.
The articular capsule of the hip is of exceptional strength. It is attached above to the entire circumference of the acetabulum, and below to the neck of the femur in such a way that while the whole of the anterior and inferior aspects of the neck lies within its attachment, only the inner half of the posterior and superior aspects is intra-capsular. The capsule is augmented by several accessory bands, the most important of which is the ilio-femoral or [inverted Y]-shaped ligament of Bigelow, which passes from the anterior inferior iliac spine to the anterior inter-trochanteric line, its fasciculi being specially thick towards the upper and lower ends of this ridge. The medial limb of this ligament limits extension of the thigh, while the lateral limits eversion and adduction. The weakest part of the capsular ligament lies opposite the lower and back part of the joint.
The hip-joint is surrounded by muscles which contribute to its strength, the most important from the surgical point of view being the obturator internus, which plays an important part in certain dislocations, and the ilio-psoas, which influences the attitude of the limb in various lesions in this region.
Except in thin subjects, the constituent elements of the hip-joint cannot be palpated through the skin. A line drawn vertically downwards from the middle of Poupart's ligament passes over the centre of the joint, which in adults lies on the same level as the tip of the great trochanter. In children it is somewhat higher.
For purposes of clinical diagnosis it is necessary to locate certain bony prominences, the most important being—(1) The anterior superior iliac spine, which is most readily recognised by running the fingers along Poupart's ligament towards it. (2) The ischial tuberosity, which in the extended position of the limb is overlapped by the lower margin of the gluteus maximus muscle, and is therefore not easily located with precision. By flexing the limb and making pressure from below upwards in the gluteal fold, the smooth, rounded prominence can usually be detected. (3) The quadrilateral great trochanter is readily recognised on the lateral aspect of the hip. Its highest point or tip can best be felt by pressing over the gluteal muscles from above downwards.
Clinical Tests.—If a line is drawn from the anterior superior iliac spine to the most prominent part of the ischial tuberosity, it just touches the tip of the great trochanter. This is known as Nélaton's line (Fig. 58).
Bryant's test (Fig. 59) is applied with the patient lying on his back, and consists in dropping a perpendicular AB from the anterior superior iliac spine, and drawing a line CD from the tip of the great trochanter to intersect the perpendicular at right angles. This is done on both sides of the body, and the length of the lines CD compared. Shortening on one side indicates an upward displacement of the trochanter, lengthening a downward displacement. The third side AC of the triangle indicates the distance between the anterior spine and the tip of the trochanter.
Chiene's test, which is simpler than either of these, consists in applying a strip of lead or tape across the front of the body at the level of the anterior superior iliac spines, and another touching the tips of the two trochanters. Any want of parallelism in these lines indicates a change in the position of one or other trochanter.
The fractures of the upper end of the femur that are liable to be confused with one another and with dislocations of the hip, include fractures of the head, the neck, the trochanters, and separation of the upper epiphyses, and fracture of the shaft just below the trochanters.
Fracture of the head of the femur is rare, and is usually a complication of backward dislocation of the hip. It takes the form of a split of the articular surface caused by impact against the edge of the acetabulum, and is analogous to the indentation fracture of the head of the humerus, which may accompany dislocation of the shoulder.
The epiphysis of the head, which lies entirely within the capsule of the joint (Fig. 60), is occasionally separated, and the symptoms closely simulate those of fracture of the narrow part of the neck. If the condition is overlooked or imperfectly treated, it may in course of time be followed by coxa vara.
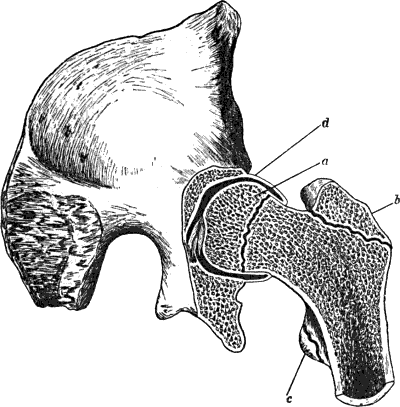 Fig. 60.—Section through Hip-Joint to show epiphyses
at upper end of femur, and their relation to the joint.
Fig. 60.—Section through Hip-Joint to show epiphyses
at upper end of femur, and their relation to the joint.It has long been customary to divide fractures of the neck of the femur into two groups—“intra-” and “extra-capsular”; but as in a considerable proportion of cases the line of fracture falls partly within and partly without the capsule, this classification is wanting in accuracy. It is more correct to divide these fractures into (1) those occurring through the narrow part of the neck, which are nearly always purely intra-capsular; and (2) those occurring through the base of the neck in which the line of fracture lies inside the capsule in front, but outside of it behind.
It is of considerable importance to distinguish between fractures in these two positions. The first group occurs almost exclusively in old persons as a result of slight forms of indirect violence, and it is liable, on account of the feeble vascular supply to the upper fragment, to be followed by absorption of the neck, which delays or may even entirely prevent union (Fig. 61). The second group usually occurs in robust adults, and results from severe forms of violence applied to the trochanter. In this group firm osseous union usually takes place.
 Fig. 61.—Fracture through Narrow Part of Neck of Femur
on section. The Neck of the bone has undergone absorption.
Fig. 61.—Fracture through Narrow Part of Neck of Femur
on section. The Neck of the bone has undergone absorption.
Fracture of the Narrow Part of the Neck or Intra-capsular Fracture.—This fracture is most frequently met with in elderly persons, especially women, and is usually produced by comparatively slight forms of indirect violence—such, for example, as result from the foot catching on the edge of a carpet, a stumble in walking, or missing a step in going downstairs.
The line of fracture, which is usually transverse but may be oblique or irregular, lies for the most part within the capsule, and the posterior part of the neck is more comminuted than the anterior. The distal fragment, which includes the base of the neck, the trochanters, and the shaft, is usually displaced upward and rotated laterally. If the periosteum and the retinacular ligaments remain intact, displacement is prevented and union favoured.
Impaction is less common than in fracture through the base of the neck; it usually results from the patient falling on the trochanter, the distal fragment being driven as a wedge into the proximal (Fig. 62).
Clinical Features.—In non-impacted cases the limb is at once rendered useless, and the patient is unable to rise. There is pain and tenderness in the region of the hip on making the slightest movement; and a specially tender spot may be localised, indicating the seat of fracture.
On placing the pelvis as square as possible, and comparing the measurements of the limbs from the anterior superior spine to the medial malleolus, shortening of the injured limb to the extent of from 1 to 3 inches may be found. On applying Nélaton's, Bryant's, or Chiene's test, the tip of the great trochanter will be found elevated. It is also farther back and less prominent than normal.
The whole limb is usually everted to a greater or less degree, and is slightly abducted. In some cases, when the impaction is of the anterior portion of the neck, the limb is inverted. On comparing the ilio-tibial band of the fascia lata on the two sides, it is found to be relaxed on the side of the injury.
The violence being as a rule indirect, there is at first little or no discoloration in the vicinity of the hip, but this may appear a few days later.
Crepitus is not a constant sign, and should not be sought for, as the necessary manipulations are liable to disengage the fragments and to increase the deformity. For the same reason rotatory movements are to be avoided.
In all cases in which the diagnosis is uncertain, the patient should be put to bed, and treated as for a fracture. In the course of a few days it is nearly always possible to make an accurate diagnosis.
In examining an old person who has sustained an injury in the region of the hip, it should be borne in mind that the limb may be shortened and everted as a result of arthritis deformans, and that the symptoms of that disease may simulate those of fracture. In arthritis deformans, however, the ilio-tibial band of the fascia lata is not relaxed as it is in fracture.
In some cases, and particularly in those in which the periosteum of the neck and the retinacular ligaments remain intact, the shortening does not become apparent till a few days after the accident. As the other symptoms are correspondingly obscure, the condition is apt to be mistaken for a bruise. In all doubtful cases the part should be examined from day to day, and, if possible, the X-rays should be used.
In impacted cases the signs of fracture are often obscure, and the patient may even be able to walk after the accident. The skin over the trochanter is generally discoloured from bruising. Eversion is usually present, but there may be little shortening. Crepitus is absent. In old people it is never advisable to undo impaction, as the interlocking of the bones favours the occurrence of osseous union.
 Fig. 64.—Fracture of Narrow Part of Neck of Femur. The
neck has become absorbed, the head has not united, and a false joint
has formed.
Fig. 64.—Fracture of Narrow Part of Neck of Femur. The
neck has become absorbed, the head has not united, and a false joint
has formed.
Prognosis.—A fracture of the neck of the femur in an old person is always attended with danger to life, a considerable proportion of the patients dying within a few weeks or months of the accident from causes associated with it. In some cases the mental and physical shock so far diminishes the vitality of the patient that death ensues within a few days. It is possible that fat embolism may account for death in some of the more rapidly fatal cases. In others, the continued dorsal position induces hypostatic congestion of the lungs, or, owing to the difficulties of nursing, bed-sores may form and death result from absorption of toxins. Frequently the prolonged confinement to bed, the continuous pain, and the natural impairment of appetite wear out the strength. In many cases the patient becomes peevish, irritable, or mentally weak.
Osseous union is the exception in intra-capsular fracture, especially when the periosteum and the retinacular ligaments have been completely torn, but in sub-periosteal and in impacted fractures it sometimes occurs. As a rule, however, the neck of the femur becomes absorbed and disappears, the head of the bone comes to lie in contact with the base of the trochanter, and a false joint forms (Fig. 64). Chronic changes of the nature of arthritis deformans may occur in and around such false joints.
When osseous union fails to take place, although the patient may eventually be able to get about, he can do so only with the aid of a stick or crutch, and as there is marked shortening, he walks with a decided limp. There is considerable antero-posterior thickening of the neck of the femur, and the femoral vessels may be pushed forward in Scarpa's triangle.
Treatment.—In treating a fracture through the narrow part of the neck, it is necessary to consider the age and general condition of the patient; whether the fracture is impacted or not; and the site of the fracture—whether in the narrow part of the neck or at its base. “The first indication is to save life, the second to get union, and the third to correct or diminish displacements” (Stimson).
In old and debilitated patients, bony or even firm fibrous union seldom takes place, and it is generally advisable to get them out of bed as speedily as possible. For the first few days the patient may be kept on his back, the limb massaged daily, and in the interval steadied by sand-bags; but on the first sign of respiratory or cardiac trouble he should be propped up in bed, and as soon as possible lifted into a chair. In all such cases care should be taken to avoid undoing impaction.
When the general condition of the patient permits of it, an attempt should be made to secure bony union.
Extension is applied by one or other of the methods described for fracture of the shaft (p. 149), so modified as to maintain the limb in the abducted position, which ensures the most accurate apposition of the fragments (Royal Whitman). This position may be maintained by a hinged long-splint, an adaptation of Thomas' hip splint. The fragments may be fixed to one another by a long steel peg introduced through the skin over the great trochanter, and passed so as to transfix them; or they may be exposed by operation and sutured together. Albe uses a bone peg.
Fracture of the Neck of the Femur in Children.—The use of the X-rays has shown that this fracture is comparatively common in children, as a result of a fall or a forcible twist of the leg. The fracture is most frequently of the greenstick variety; when complete, it is usually impacted. There is shortening to the extent of a half or three-quarters of an inch, a slight degree of eversion, the movements of the hip are restricted, and there is some pain. The patient is often able to move about after the accident, but walks with a limp. Unless the use of the X-rays reveals the fracture, the condition is liable to be overlooked.
When the lesion is diagnosed, the deformity should be completely corrected, any impaction that exists being undone; and the limb is put up in a wide abduction splint (p. 221) or in a plaster-of-Paris case in the position of extreme abduction.
If the condition is not recognised and treated, it is liable to be followed by the development of coxa vara (Royal Whitman) (Fig. 65).
Fracture through the Base of the Neck.—This fracture is usually produced by a fall on the great trochanter, although it is occasionally due to a fall on the feet or knees.
Although often spoken of as “extra-capsular,” the line of fracture is generally partly within and partly without the capsule. The fracture usually lies close to the junction of the neck with the shaft, and in the great majority of cases is accompanied by breaking of one or both trochanters. This is due to the neck being driven as a wedge into the trochanters, splitting them up. When the fragments remain interlocked, the fracture is of the impacted variety (Fig. 67).
 Fig. 66.—Non-impacted Fracture through Base of Neck.
Fig. 66.—Non-impacted Fracture through Base of Neck.
|
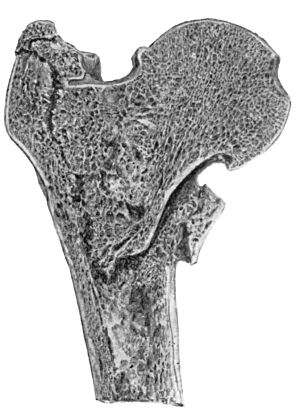 Fig. 67.—Fracture through Base of Neck of Femur with
Impaction into the Trochanters.
Fig. 67.—Fracture through Base of Neck of Femur with
Impaction into the Trochanters.
|
Clinical Features.—Although this fracture is commonly met with in strong adults, it may occur in the aged.
The lateral aspect of the hip shows marks of bruising, and there is severe pain and a considerable degree of shock. The limb lies helpless; there is generally marked eversion, with shortening, which, in non-impacted cases, may amount to 11/2 or 2 inches, and is evident immediately after the accident; it is due to the distal fragment being drawn up by the muscles inserted into the great trochanter and upper end of the shaft. In a limited number of cases the distal fragment lies in front of the proximal, and there is inversion of the limb.
 Fig. 68.—Non-impacted Fracture through Base of Neck.
Union has occurred with diminution of angle of neck—Coxa Vara.
Fig. 68.—Non-impacted Fracture through Base of Neck.
Union has occurred with diminution of angle of neck—Coxa Vara.
On applying the various tests, the great trochanter is found to be displaced upwards, there is some antero-posterior broadening of the trochanteric region, and the ilio-tibial band is relaxed. On pressing the fingers into the lateral part of Scarpa's triangle, a mass consisting of the bony fragments may be felt, and is tender on pressure. Unnatural mobility with crepitus may be elicited.
In the impacted variety, the shortening seldom exceeds one inch; the eversion is less marked; there is some power of voluntary movement; and crepitus is absent. The broadening of the trochanteric region is greater, and the great trochanter is approximated to the acetabulum.
Prognosis.—The risks to life in the aged are similar to those of intra-capsular fracture. In youths and healthy adults the chief danger is that the limb may be shortened and its function thereby impaired.
As the periosteum and retinacular ligaments which transmit the blood vessels to the proximal fragments are intact, bony union is the rule. There is always, however, considerable thickening in the region of the trochanter due to displaced fragments and callus, and in a certain number of cases, even with the greatest care in treatment, there is a varying degree of shortening and eversion of the limb. In cases in which the distal fragment lies in front of the proximal there is permanent inversion.
Treatment.—As this fracture usually occurs in robust patients, there is no danger from prolonged confinement to bed; and as union without deformity can be attained in no other way, this is always advisable. When the shortening and eversion are excessive, they should be completely corrected under anæsthesia before the retentive apparatus is applied, any impaction that exists being undone. When the deformity resulting from impaction is slight, however, it is best to leave it, as it facilitates speedy and firm union.
Extension is obtained by the same appliances as are used in fracture of the shaft, and the limb should be kept in the abducted position.
Fracture of the greater trochanter occurring apart from fracture of the neck usually results from direct violence, but may be due to muscular action. The trochanter is displaced by the gluteal muscles, causing broadening of the lateral aspect of the hip. In young persons the epiphysis of the great trochanter may be separated, but this is rare. The treatment consists in retaining the fragments in position by keeping the limb abducted between sand-bags, or by pegs driven in through the skin.
Fracture immediately below the lesser trochanter may be produced by direct or by indirect violence, and the displacement depends largely on whether the line of fracture is transverse or oblique. The proximal fragment is kept tilted forward, rotated laterally, and abducted by the ilio-psoas muscle and the lateral rotators inserted in the region of the great trochanter. The lower fragment passes upward, and is rotated laterally by the weight of the limb; the displacement is aggravated by the contraction of the flexor and adductor muscles. The tilting of the proximal fragment may be increased by the displaced distal fragment pushing it forward.
On account of the difficulty of controlling the short proximal fragment, union is liable to take place with considerable shortening and deformity (Fig. 69).
 Fig. 69.—Fracture of the Femur just below the Small
Trochanter united, showing flexion and lateral rotation of upper
fragment.
Fig. 69.—Fracture of the Femur just below the Small
Trochanter united, showing flexion and lateral rotation of upper
fragment.
Treatment.—When it is found, under an anæsthetic, that the displacement can be completely reduced, and does not tend to recur, this fracture is treated on the same lines as fracture of the shaft of the bone.
In cases in which the proximal fragment cannot be brought into line with the distal one, however, it is necessary to flex, evert, and abduct the thigh in order to get the fragments into apposition and into line. A Hodgen's splint (Fig. 77) is applied with the highest sling under the upper end of the lower fragment and with sufficient extension to correct overriding. The upper end is then strongly lifted by a counter-weight of about 15 lbs. This secures apposition of the fragments with slight forward angulation at the seat of fracture. By the end of a month sufficient callus has formed to prevent re-displacement, and if the counter-weight is gradually diminished the two fragments sag back together into a normal alignment (J. N. J. Hartley). A double-inclined plane (Fig. 70), with extension applied in the axis of the thigh, gives satisfactory results.
It is unnecessary for our present purpose to attempt a comprehensive classification of the numerous varieties of dislocation that have been met with at the hip-joint. It will suffice if we divide them into those in which the head of the femur passes backward, and comes to rest on the dorsum ilii, or in the vicinity of the great sciatic notch; and those in which it passes forward and comes to rest in the obturator foramen, or on the pubes (Fig. 71).
The backward are much more common than the forward dislocations, in contrast to what obtains at the shoulder, where the forward varieties predominate.
On account of the great strength of the hip-joint, dislocation is by no means a common injury. It occurs most frequently in strong adults after the epiphyses have ossified, and before the bones have commenced to become brittle; and it is much more common in men than in women. It is invariably the result of severe violence, the limb at the moment being in such a position that the ligaments are on the stretch and the muscles taken at a disadvantage. The head of the femur usually leaves the joint at the lower and back part, where the socket is most shallow and the ligaments weakest. The ligamentum teres is almost always torn from its femoral attachment, and one or more of the muscles inserted in the region of the trochanters may be ruptured. The [inverted Y]-shaped ligament, on the other hand, is seldom torn, and so long as it remains intact the dislocation belongs to one or other of the types above named. All atypical dislocations, such as the supra-cotyloid, infra-cotyloid, ilio-pectineal, are due to rupture of some part of the [inverted Y]-ligament, and are so rare as not to call for individual description. The central dislocation of German authors, in which the head is driven through the floor of the acetabulum, is described on page 126.
Like other dislocations, those of the hip may be complicated by laceration of muscles, blood vessels, or nerves, or by fracture of one or other of the bones in the vicinity.
Dislocation on to the Dorsum Ilii.—This, the commonest form of dislocation of the hip, is usually the result of the patient falling from a height, or receiving a heavy weight on the back while stooping forward with the thigh flexed, slightly adducted, and rotated medially. It is also said to have occurred from muscular action. The shaft of the femur acts as the long limb of a lever of which the neck is the short limb, the femoral attachment of the [inverted Y]-ligament forming the fulcrum. The head, thus brought to bear upon the lower and back part of the capsule, tears it and leaves the socket, passing upwards and coming to rest on the dorsum of the ilium, above and anterior to the tendon of the obturator internus (Fig. 73). The articular surface is directed backward, while the trochanter looks forward.
Clinical Features.—The affected limb is flexed, adducted, and inverted, so that the knee crosses the lower third of the opposite thigh, and the ball of the great toe lies on the dorsum of the sound foot. There is shortening to the extent of from 11/2 to 2 inches, the trochanter being displaced above Nélaton's line, and lying nearer to the anterior superior iliac spine than on the normal side. The patient is unable to move the limb or to bear weight upon it; abduction and lateral rotation are specially painful; and traction fails to restore the limb to its proper length. On making these attempts a characteristic elastic resistance is felt.
The head of the femur in its new position may sometimes be felt through the fibres of the gluteus maximus, but swelling of the soft parts often obscures this sign. The normal depression behind the great trochanter is lost, the gluteal fold is raised, and there is often a degree of lordosis which compensates for the flexion. The fingers can be pressed more deeply into Scarpa's triangle on the dislocated than on the normal side—a point in which this injury differs from fracture of the base of the neck of the femur.
In a certain number of cases the lateral limb of the [inverted Y]-ligament is ruptured and the limb is everted—dorsal dislocation with eversion.
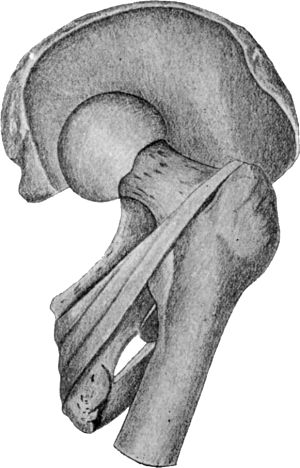 Fig. 73.—Dislocation on to Dorsum Ilii. Note relation
of neck of femur to tendons of obturator internus and gemelli
(diagrammatic).
Fig. 73.—Dislocation on to Dorsum Ilii. Note relation
of neck of femur to tendons of obturator internus and gemelli
(diagrammatic).
Dislocation into the Vicinity of the Great Sciatic Notch, or “dislocation below the tendon.”—This variety of backward dislocation is less common than that on to the dorsum, although produced in the same way. The head of the femur passes beneath the obturator internus, and this tendon, catching on its neck, checks its upward movement (Fig. 74).
The clinical features are the same as those of the dorsal variety, but, on the whole, are less marked.
Differential Diagnosis.—Backward dislocation of the hip is usually easily recognised. When dislocation below the tendon occurs in a stout person, however, it is liable to be overlooked on account of the difficulty of feeling the displaced bone, and of the comparatively slight amount of deformity present. The nature of the accident, the absence of broadening of the trochanter, and the adduction and inversion of the limb are usually sufficient to prevent a dislocation being mistaken for an impacted extra-capsular fracture.
Dislocation into the Obturator Foramen (Fig. 71).—This dislocation is produced by great force applied from behind while the thigh is flexed and abducted, as when a weight falls on the back of a man stooping forward with the legs wide apart. It may also result from violent abduction by wide separation of the thighs.
The capsule gives way at its medial and lower part, and the head of the femur comes to rest on the surface of the external obturator muscle, its articular surface looking forward, while the trochanter looks backward.
Clinical Features.—In the standing position the thigh is slightly flexed and abducted, with the foot pointing directly forward or a little outward. The body is bent forward to relax the ilio-psoas muscle and the [inverted Y]-ligament, the foot is advanced and the heel drawn up. It is not uncommon for the patient to be able to walk after the accident, and only to seek advice some time later on account of inability to adduct and extend the limb. There is apparent lengthening of the limb due to tilting of the pelvis downward on the affected side. The hip is flattened, the trochanter less prominent than usual, and the head of the bone may sometimes be felt in its abnormal position.
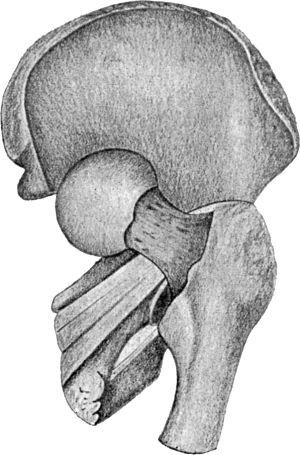 Fig. 74.—Dislocation into the vicinity of the
Ischiatic Notch. Note relation of neck of femur to tendons of
obturator and gemelli, “Dislocation below the tendon” (diagrammatic).
Fig. 74.—Dislocation into the vicinity of the
Ischiatic Notch. Note relation of neck of femur to tendons of
obturator and gemelli, “Dislocation below the tendon” (diagrammatic).
Dislocation on to the pubes is a further degree of the obturator form (Fig. 71). It is usually produced by forcible hyper-extension and lateral rotation of the hip, such as occurs when the body is bent back while the thigh remains fixed.
The capsule is torn farther forward than in the other varieties, and the head rests on the horizontal ramus of the pubes against the ilio-pectineal line.
Clinical Features.—There is marked eversion, flexion, and abduction, but the shortening is inconsiderable. The ilio-psoas and [inverted Y]-ligament are tense. The head of the femur may be felt in the groin, with the femoral vessels over, or to one or other side of it. There is sometimes pain and numbness in the distribution of the femoral (anterior crural) nerve. The prominence of the great trochanter is lost.
Treatment of Dislocation of the Hip.—For the reduction of a dislocation of the hip complete anæsthesia is necessary, and the patient should be placed on a firm mattress on the floor to give the surgeon the best possible purchase upon the limb. The surgeon grasps the ankle with one hand, while the other is placed behind the head of the tibia, the leg being held at right angles to the thigh. An assistant meantime steadies the pelvis by making firm pressure over the iliac crests.
As the chief obstacle to reduction is the tension of the ilio-femoral ligament, the first indication is to relax this structure by flexing the hip to its fullest extent.
In the backward varieties (dorsal and sciatic) the [inverted Y]-ligament is relaxed by flexing the thigh upon the pelvis in the position of adduction. The thigh is then fully abducted, to cause the head of the bone to retrace its steps forwards towards the rent in the capsule; and at the same time rotated laterally to relax the rotator muscles. This combined movement tends also to open up the rent in the capsule. Finally, the limb is quickly extended to cause the head to enter the socket. This object is often aided by making vertical traction or lifting movements on the abducted and laterally rotated limb before extending.
For the reduction of the forward varieties (obturator and pubic), the thigh is first fully flexed on the pelvis, but in the abducted position. The limb is then strongly rotated medially and abducted, and finally extended. Lifting movements may be found useful in these cases also.
All methods of reduction by forcible traction on the extended limb are to be avoided, as they fail to meet the primary indication of relaxing the [inverted Y]-ligament.
After reduction, the limb is steadied by sand-bags; massage is carried out from the first, and movement after a few days. The range of movement is gradually increased, and the patient is allowed to use the limb with caution in from two to three weeks.
When the rim of the acetabulum has been fractured, the patient must be confined to bed with extension for six to eight weeks, to avoid the risk of re-dislocation.
Changes of the nature of chronic arthritis are liable to occur in and around the joint in old and rheumatic subjects; and atrophy or paralysis of muscles may follow, if their nerves are implicated.
Old-standing Dislocation.—It is impossible to lay down any time-limit for attempting reduction in old-standing dislocations of the hip. Manipulation may succeed in cases of some months' standing, and may fail when the bone has been out only a few weeks. In certain cases, even after reduction has been effected, there is a marked tendency to re-displacement. In any case, the attempt does good by breaking down adhesions, provided no undue force is employed such as may damage the sciatic nerve or vessels, or fracture the neck of the femur, and success may attend on a second or even a third attempt at intervals of from three to five days. If manipulation fails, and if the deformity is great and the usefulness of the limb seriously impaired, an attempt may be made to effect reduction by operation; the operation, however, is one of considerable difficulty, and in the event of failure the head of the bone should be excised. If the head has formed a new socket for itself and there is a fairly useful joint, the condition should be left alone.
Congenital dislocation of the hip is described with Deformities of the Extremities.
Sprain of the hip is comparatively rare. It results from milder degrees of the same forms of violence as produce dislocation. The ligaments are stretched or partly torn, and there is effusion of fluid into the joint. Pressure over the joint elicits tenderness; and the limb assumes the position of slight flexion, abduction, and lateral rotation, but there is no alteration in length. Such injuries, unless carefully treated by massage and movement from the outset, are apt to be followed by the formation of adhesions, resulting in stiffness of the joint.
Contusion in this region, on the other hand, is not uncommon. It is produced by a fall on the trochanter, and gives rise to symptoms which simulate to some extent those of fracture of the neck. The limb lies in the position of slight flexion, but the bony points retain their normal relationship to one another, and there is no shortening. The swelling and tenderness often prevent a thorough examination being made, and when any doubt remains as to the diagnosis, the patient should be kept in bed till the doubt is cleared up by the use of the X-rays. If the bone has been broken, this will reveal itself in the course of a few days by the occurrence of shortening and other evidence of fracture.
In elderly patients, contusion of the hip may be followed by changes in the joint of the nature of arthritis deformans; and it has been stated, although proof is wanting, that absorption of the neck of the femur sometimes occurs. These injuries are treated by rest in bed, massage, and the other measures already described as applicable to sprains and contusions.
This group includes all fractures between that immediately below the lesser trochanter and the supra-condylar fracture.
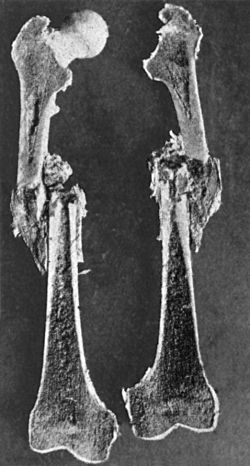 Fig. 75.—Longitudinal section of Femur showing recent
Fracture of Shaft with overriding of Fragments.
Fig. 75.—Longitudinal section of Femur showing recent
Fracture of Shaft with overriding of Fragments.
In adults, when due to direct violence, the fracture is usually transverse, and may be attended with comparatively little displacement. Indirect violence, on the other hand, usually produces an oblique fracture, which is frequently comminuted and often compound. The break is most commonly situated a little above the middle of the shaft, the obliquity being downward, forward, and medially, and of such a nature that the fragments tend to override one another (Fig. 75). The most serious forms are those associated with gun-shot wounds.
The direction and nature of the displacement depend more upon the fracturing force, the weight of the lower part of the limb, and the action of the muscles attached to the respective fragments, than upon the direction of the obliquity. As a rule, the proximal fragment passes forward and laterally, and is maintained in this position by the ilio-psoas and glutei muscles, while the distal fragment is displaced upward and medially and is rotated outward by the combined action of the weight of the limb, the longitudinal muscles, and the adductors.
Clinical Features.—The limb is at once rendered useless, and there is great swelling from effusion of blood in the region of the fracture. This, together with the muscularity of the part, often renders an accurate diagnosis as to the site and direction of the fracture exceedingly difficult. The shortening varies from 1/2 inch to 3 or 4 inches—averaging about 1 inch in adults—and eversion is always marked. Mobility may be detected and crepitus elicited without disturbing the patient, by placing the hand under the seat of fracture and gently attempting to raise the limb; or by fixing the proximal fragment by one hand placed in front of it while the distal part of the limb is carefully lifted. It will be found that the great trochanter does not rotate with the lower segment of the femur. These tests must be employed with great caution lest the deformity be increased or the fracture rendered compound.
In many fractures of the thigh, and especially in those produced by indirect violence, the knee is sprained, and there is a considerable effusion into the joint, and this may lead to stiffness unless massage is employed from the outset.
Treatment.—Fracture of the shaft of the femur is one of the most difficult fractures in the body to treat successfully. In cases of oblique fracture, the patient should be warned that shortening to the extent of from 3/4 to 1 inch is liable to result, however carefully the treatment may be carried out. This does not necessarily imply a permanent limp, as by tilting the pelvis he may be enabled to walk quite well; if this is not sufficient to equalise the length of the limbs, the sole of the boot may be raised. A general anæsthetic is necessary to ensure accurate reduction, and extension must be applied to maintain the fragments in apposition and prevent shortening. The splint which has been found most generally useful is the Thomas' knee splint, the ring of which rests against the ischial tuberosity. To admit of flexion at the knee the Thomas' splint should have a hinged attachment on which the leg is supported. This leaves the knee free and allows of movement being made to prevent stiffness. The limb is suspended by broad strips of flannel or linen, fixed to the side bars of the splint by means of safety pins or strong spring paper clips.
In simple fractures extension may be obtained by means of broad strips of adhesive plaster applied to each side of the thigh and reaching well above its middle. The plaster is secured by a bandage, and to its lower ends are attached broad tapes which are buckled to a stirrup through which traction is made by means of a cord passing over a pulley fixed to an upright at the foot of the bed.
The lower end of the splint is suspended, and the counter-extension is obtained by pressing the ring against the ischial tuberosity. To prevent the ring overriding the tuberosity and pressing on the soft tissues of the buttock, it is slung by the rope to a cross-bar above the bed, e.g. the Balkan frame (Fig. 81).
In compound fractures the presence of a wound may prevent adhesive plaster being used, and it is necessary to take the extension directly through the bone. A posterior gutter splint is applied to prevent sagging. After pulling the skin upward, a small incision is made over the upper expanded border of each condyle, and the points of an ice-tong calliper are made to grip the bone without penetrating into the cancellous tissue. A cord attached to the handles of the calliper passes over a pulley and supports the weight necessary to give the desired amount of traction (Fig. 81).
An alternative method of exerting traction directly through the bone is by means of Steinmann's apparatus (Fig. 76). In a moderately muscular adult, a weight of from 12 to 15 pounds by means of strips of plaster applied to the skin, or 10 to 25 pounds by direct traction on the bone, should be applied in the first instance. The correct weight to employ is that which maintains the length of the limb at its normal, and is therefore liable to revision from time to time.
Hodgen's splint is a comfortable and efficient means of treating these fractures, as it allows the patient a certain amount of movement, admits of the part being massaged, and facilitates nursing.
It consists of a wire frame (Fig. 77) to one side of which a series of strips of flannel about 4 inches wide are attached. Extension strapping is first applied, and then the frame, which extends from the level of Poupart's ligament to well beyond the sole, is placed over the front of the limb, and the loose ends of the flannel strips brought round behind the limb, and fixed to the other side of the frame, convert it into a sling. The tapes attached to the extension strapping are now tied to the end of the frame. By suspending the limb in this splint by means of cords passing obliquely over a pulley attached to an upright at the foot of the bed, the weight of the limb is made to act as the extending force.
The retentive apparatus should be worn for from six to eight weeks, after which the patient is allowed up with crutches, which he usually requires to use for three or four weeks longer, before he can bear his weight upon the limb. The old dictum of Nélaton, that the treatment of fracture of the thigh should last for a hundred days, is a safe working-rule. In fractures of the shaft an ordinary Thomas' knee splint, or a “walking calliper splint” which is fixed to the heel of the boot, may be worn when the patient gets up.
Union may be exceedingly slow in fracture of the femur, and may even be delayed for months. Mal-union sometimes occurs, the fracture uniting with an angular deformity outward and forward.
Re-fracture is liable to occur if the patient falls or twists the limb within a few months of the original injury. It has happened not infrequently just after the retentive apparatus has been removed from the nurse raising the limb by the foot in order to wash it.
Liston's long splint is only employed as a temporary expedient for immobilising the fragments during transport; a Thomas' splint, if available, is better for this purpose.
Operative treatment is sometimes called for when simpler measures fail to reduce the displacement, and in cases of un-united fracture or of vicious union. The incision, which must be free, is preferably placed in the line of the lateral intermuscular septum; the periosteum is interfered with as little as possible. The application of extension by the calliper method is often of great service, during the operation, in enabling the operator to get the fragments into position; sometimes no fixation is required, but, if necessary, recourse is had to plating or pegging, or an intra-medullary pin. The extension apparatus is retained for three or four weeks. The after-treatment is carried out on the same lines as for simple fracture, but the retentive apparatus must be worn for a considerably longer period.
Fracture of the Femur in Children.—In children, especially below the age of ten, this fracture is quite common. It is often of the greenstick variety, or, if complete, is transverse and sub-periosteal, and as it is accompanied by few symptoms and but little deformity, is liable to be overlooked.
When there is displacement, the deformity is similar to that in adults, and the treatment is carried out on the same lines.
In young children the nursing is greatly facilitated by applying vertical extension to one or both lower extremities (Fig. 79). If the fracture is transverse and shows little tendency to displacement, the local Gooch splints may be dispensed with; in any case, massage should be employed from the first.
The patient may be allowed out of bed in from three to four weeks, wearing a retentive apparatus.
The shaft of the femur is sometimes fractured during delivery, particularly in breech cases. The simplest and most efficient means of controlling the fracture is by extension strapping fixed to the lower end of a Thomas' knee splint.
These include the supra-condylar fracture of the femur, the T- or Y-shaped fracture opening into the joint, separation of the lower femoral epiphysis; fracture of the head of the tibia, and separation of its upper epiphysis; the various sprains and dislocations of the knee, as well as its internal derangements; and fractures and dislocations of the patella.
Surgical Anatomy.—Of the two epicondyles the medial is the more prominent and palpable. The adductor tubercle, which is situated on the upper and back part of the medial epicondyle, gives attachment to the round tendon of the adductor magnus, and marks the level of the epiphysial line and of the upper limit of the trochlear surface of the femur. Between the medial condyle of the femur and the medial condyle (tuberosity) of the tibia, when the limb is in the flexed position, the line of the joint can be recognised as a groove or cleft, and this is made use of in measuring the length of the tibia. The lateral condyle (tuberosity) of the tibia can also be palpated, and must not be mistaken for the head of the fibula, which lies farther back and at a slightly lower level, and can readily be identified by tracing to it the tendon of the biceps. The tuberosity of the tibia, into which the quadriceps extensor tendon is inserted, lies on the same level as the head of the fibula. In the extended position of the limb, the patella is loose and movable on the front of the trochlear surface of the femur, while in the flexed position it sinks between the condyles, resting chiefly on the lateral one and becoming fixed.
The popliteal artery and vein and the tibial (internal popliteal) nerve lie in close relation to the posterior aspect of the joint; and the common peroneal (external popliteal) nerve passes behind and to the medial side of the biceps tendon.
The knee is an example of a joint which depends for its strength chiefly on its ligaments. Not only are the tibial and fibular collateral (external and internal lateral) ligaments and the posterior part of the capsular ligament particularly strong, but the cruciate ligaments and the menisci (semilunar cartilages) inside the cavity of the joint further add to its stability. The powerful tendon of the quadriceps extensor muscle, in which the patella is developed as a sesamoid bone, protects and strengthens the front of the joint and functionates as the anterior ligament of the joint. In the attitude of complete extension in which the joint is locked, no demand is made on the quadriceps apparatus; with the commencement of flexion, the stability of the joint, and the weight-bearing capacity of the limb as a whole, depend largely on the controlling influence of the quadriceps muscle; this becomes evident on going down an incline and more markedly on going down stairs. Hence it is, that in recurrent sprains of the knee, including under this term the various forms of internal derangement of the joint, the wasting with loss of tone of the quadriceps is an important factor in aggravating the disability of the limb and in retarding and preventing recovery. In the treatment of recurrent sprains of the knee, therefore, special attention must be directed towards the wasting of the quadriceps by means of massage and appropriate exercises.
The synovial cavity extends from the level of the head of the tibia to an inch or more above the trochlear surface of the femur, passing slightly higher on the medial aspect of the joint than on the lateral (Fig. 80). The large bursa between the quadriceps muscle and the femur (sub-crural bursa) generally communicates with the cavity of the joint. The synovial cavity of the superior tibio-fibular articulation is usually distinct from that of the knee-joint, but may communicate with it through the popliteal bursa.
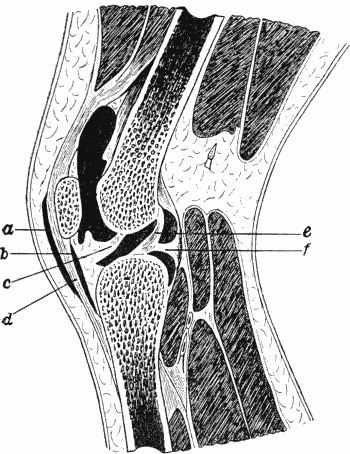 Fig. 80.—Section of Knee-joint showing extent of
Synovial Cavity.
Fig. 80.—Section of Knee-joint showing extent of
Synovial Cavity.A large bursa (pre-patellar) lies over the lower part of the patella and upper part of the ligamentum patellæ; and a smaller one separates the ligamentum patellæ from the tuberosity of the tibia. Several important bursæ are found in the popliteal space, one of which—the semi-membranosus bursa—sometimes communicates with the knee-joint.
Fractures involving the lower end of the femur, especially the supra-condylar and T-shaped fractures, are to be looked upon as serious injuries, on account of the difficulties attending their treatment, and the risk of damage to the popliteal vessels and of impairment of the usefulness of the knee-joint.
Supra-condylar fracture is usually the result of a fall on the feet or knees, or of direct violence, and is most common in adult males. The line of fracture is generally irregularly transverse, or it may be slightly oblique from above downwards and forwards, so that the proximal fragment passes forward towards the patella, while the distal is rotated backward on its transverse axis by the gastrocnemius muscle.
Clinical features.—Soon after the accident a copious effusion of blood and synovia takes place into the cavity of the knee-joint, adding to the swelling caused by the displaced bones, and rendering it difficult to recognise the precise nature of the lesion. As it is important to make an accurate diagnosis, the X-rays should be employed if possible, and a general anæsthetic should be given when necessary.
The proximal end of the distal fragment is usually palpable in the popliteal space, while the proximal fragment is unduly prominent in front. By flexing the knee the fragments may be brought into apposition and crepitus elicited. In oblique fractures, the pointed lower end of the proximal fragment may transfix the quadriceps extensor muscle and may be felt under the skin, or it may perforate the skin and thus render the fracture compound. It should be disengaged by fully flexing and making traction on the knee. The thigh is shortened to the extent of from 1/2 to 1 inch.
The popliteal vessels lie so close to the bone that they are liable to be torn by the displaced distal fragment, giving rise to the usual signs of ruptured artery. Sometimes, owing to the feeble state of the circulation from shock, the bleeding does not take place at the time of the accident, but ensues some hours later. The vessels may merely be pressed upon by the displaced bone, but the nutrition of the limb beyond is endangered and gangrene may ensue if early reduction be not effected.
Treatment.—The small size of the distal fragment, its depth from the surface, and the accompanying effusion into and around the joint, render its control difficult. In the majority of cases the two fragments can only be brought into apposition when the knee is flexed on the thigh and the thigh on the pelvis, and it is almost always necessary to carry out the reduction under anæsthesia.
In the few cases in which the fragments can be accurately approximated in the extended position of the limb, retention may be effected by means of a box splint reaching well up the thigh (p. 180).
In the majority, however, flexion is necessary, and a Thomas' knee splint with flexion attachment bent to an angle of 30° (Fig. 81) and extension by means of ice-tong callipers secures the best apposition. If this apparatus is not available the limb must be fixed on a double-inclined plane, so constructed that the angle of flexion can be adjusted to meet the requirements of the individual case (Fig. 70).
Hodgen's splint, bent nearly to a right angle, may also be employed.
A careful watch must be kept on the circulation of the limb during the first few days, lest it be interfered with by the pressure of the apparatus.
In a considerable number of cases these means of retaining the fragments in apposition prove ineffectual, and it is necessary to have recourse to operative measures for mechanical fixation. Division of the tendo calcaneus (Achillis) is not to be recommended as a means of combating the backward tilting of the distal fragment.
In all cases the retentive apparatus must be worn for about four weeks, after which the limb is flexed over a pillow; but massage and movement should be employed as soon as possible, as persistent stiffness of the knee is one of the most troublesome sequelæ of these injuries.
Compound and complicated fractures are dealt with on the general principles governing the treatment of such injuries. Amputation may become necessary should gangrene ensue from injury to the popliteal vessels, or if infective complications threaten the life of the patient.
Operative interference may be called for to rectify deformities resulting from mal-union.
The T- or Y-shaped fracture is, as a rule, produced by direct violence, the force first breaking the bone above the condyles and then causing the proximal fragment to penetrate the distal and split it up into two or more pieces. The fracture implicates the articular surface, and the main fissure is usually through the inter-condylar notch; the lower end of the bone is sometimes severely comminuted.
The knee is broadened, and pain and crepitus are readily elicited on moving the condyles upon one another or on pressing them together. On moving the patella transversely, it may be felt to hitch against the edge of one or other of the fragments. The shortening may amount to one or two inches.
The treatment is carried out on the same lines as in supra-condylar fracture, but as the joint is implicated there is greater risk of subsequent impairment of its functions.
Separation of the lower epiphysis is a comparatively common injury. It is seldom pure, a portion of the diaphysis usually being broken off and remaining attached to the epiphysis. It occurs usually in boys between the ages of thirteen and eighteen, from severe violence such as results from the limb being caught between the spokes of a revolving wheel, or from hyper-extension of the knee. It has also been produced in attempting forcibly to rectify knock-knee and other deformities in this region, and in making traction on the limb to correct deformities following recovery from tuberculous disease of the knee. As a rule, there is little displacement of the loose epiphysis, but it may pass in any direction, forward being much the most common (Fig. 82), and when displaced it is difficult to reduce and to maintain in position. The age of the patient, the mode of injury, the finding of the smooth broad end of the diaphysis in the popliteal space or on the front of the thigh, according to the displacement, usually serve to establish the diagnosis. The X-rays afford reliable information as to the position of the fragments. Pressure on the popliteal vessels is a serious aggravation of the injury, and adds greatly to the difficulties of treatment.
 Fig. 82.—Radiogram of Separation of Lower Epiphysis of
Femur, with backward displacement of the diaphysis; pressure on
popliteal vessels caused sloughing of calf.
Fig. 82.—Radiogram of Separation of Lower Epiphysis of
Femur, with backward displacement of the diaphysis; pressure on
popliteal vessels caused sloughing of calf.
The treatment is the same as for supra-condylar fracture, but, owing to the serious disability that follows on incomplete reduction, it may be necessary to have recourse to operation. After an epiphysial separation, the growth of the limb is sometimes, although not always, interfered with.
Either condyle may be broken off without the continuity of the shaft being interrupted, by a direct blow or fall on the knee, or by violent twisting of the leg. The separated condyle may not be displaced, or it may be pushed upwards or rotated on its transverse axis.
There is broadening of the knee but no shortening of the thigh, and the ecchymosis, crepitus, and pain are localised to the affected side of the joint; the knee can usually be moved towards the injured side in a way that is characteristic. If allowed to unite with the condyle displaced, the articular surface is oblique and bow- or knock-knee results.
If there is difficulty in replacing the broken condyle and maintaining it in position, it may be fixed by means of a steel nail inserted through the skin.
Fracture of the head of the tibia is a comparatively rare injury. It may result from a direct blow, such as the kick of a horse, or from indirect forms of violence, and the line of fracture may be transverse or oblique. Occasionally the distal fragment is impacted into the proximal and comminutes it. In oblique fracture a gliding displacement is liable to occur and cause bow- or knock-knee. Transverse fracture of the head of the fibula sometimes accompanies fracture of the head of the tibia, and there is always considerable effusion into the knee-joint. One or other of the condyles may be chipped off by forcible adduction or abduction at the knee.
The ordinary clinical features of fracture are well marked, and the diagnosis is easy. From some unexplained cause this fracture may take a long time, sometimes several months, to consolidate.
Separation of the upper epiphysis of the tibia, which includes the tongue-like process for the tubercle and the facet for the fibula, is also rare. It usually occurs between the ages of three and nine. The displacement of the epiphysis is almost always forward or lateral, and is accompanied by the usual signs of such lesions. The growth of the limb is sometimes arrested, and shortening and angular deformity may result.
Treatment.—After reduction under an anæsthetic these fractures are usually satisfactorily treated in a box splint (Fig. 91), carried sufficiently high to control the knee-joint. When the head of the tibia is comminuted or split obliquely, weight-extension—direct from the bone, the ice-tong callipers grasping the malleoli or the calcaneus—may be used. Massage and movement are employed from the outset.
Avulsion of the tuberosity of the tibia occasionally occurs in youths, from violent contraction of the quadriceps—as in jumping. The limb is at once rendered powerless; the osseous nodule can be felt, and on moving it crepitus is elicited.
This is best treated by pegging the tuberosity in position, and fixing the extended limb on an inclined plane to relax the quadriceps muscle.
In young, athletic subjects, the tongue-like process of the epiphysis (Fig. 85), into which the ligamentum patellæ is inserted, may be partly or completely torn away, giving rise to localised swelling, and pain which is aggravated by any muscular effort—Schlatter's disease or “rugby knee.” It has been frequently observed in cadets as a result of kneeling at drill. The treatment consists in rest and massage, but the symptoms are slow to disappear.
The condition is liable to be mistaken for some chronic inflammatory condition of the bone, such as tubercle, unless an X-ray examination is made.
The upper end of the fibula is seldom broken alone. The chief clinical interest of this fracture lies in the fact that it may implicate the common peroneal nerve, and cause drop-foot.
Dislocation of the knee is a rare injury, and occurs as a result of extreme degrees of violence, especially of a wrenching or twisting character.
Rupture of the popliteal vessels, or pressure exerted on them by the displaced bones, may lead to gangrene of the limb, and necessitate amputation. The common peroneal nerve is frequently damaged. When the lesion is compound, also, amputation may become necessary on account of infective complications.
The varieties of dislocation are named in terms of the direction in which the tibia passes: forward, backward, medial, and lateral.
Dislocation forward is the most common variety, and results from sudden hyper-extension of the knee, tearing the collateral and cruciate ligaments. The leg remains fully extended, and lies on a plane anterior to that of the thigh. The condyles of the femur are palpable posteriorly, and the skin is tightly stretched over them, or may even be torn, rendering the dislocation compound. The patella is projected forward, the quadriceps tendon is lax, and the skin over it is thrown into transverse folds. The limb is shortened by two or three inches.
Dislocation backward is usually due to a direct blow driving one of the bones past the other. The leg remains hyper-extended, the head of the tibia occupies the popliteal space, while the lower end of the femur projects forward with the patella either in front or to one side of it.
The medial and lateral dislocations are generally incomplete, and are liable to be mistaken for separation of the lower epiphysis of the femur. When the tibia passes medially, the lateral condyle of the femur forms a prominence, and there is a depression below it. The head of the tibia projects on the medial side, and the medial condyle is in a depression.
When the tibia is displaced laterally, the relative position of the prominences and depressions is reversed.
Treatment.—In dislocations of the knee no special manipulations are necessary to restore the displaced bone to its place, and reduction is not accompanied by a distinct snap.
If, while the patient is fully anæsthetised, traction is made on the leg and counter-traction on the thigh with the knee in the flexed position, the bones can usually be replaced by manipulation.
After reduction has been effected, in antero-posterior dislocations, the limb should be flexed and placed on a pillow, massage and movement being employed from the first. The patient is usually able to walk within a month.
In medial and lateral dislocations there is at first considerable tendency to re-displacement, and it is therefore necessary to secure the joint in a box splint, specially padded, for about fourteen days, massage being employed from the first, and movement commenced when the splint is removed. It is usually about six weeks before the patient can use the limb with freedom.
In compound dislocations, and in those complicated by injury to the popliteal vessels, the question of amputation may have to be considered.
Dislocation of the Superior Tibio-Fibular Articulation.—This joint may be dislocated by twisting forms of violence applied to the foot or leg, or by forcible contraction of the biceps muscle. The displacement may be forward or backward, and the head of the fibula can be felt in its new position with the prominent tendon of the biceps attached to it. The movements of the knee are quite free, but the patient is unable to walk on account of pain. Reduction and retention are, as a rule, easy, and the ultimate result satisfactory. We have frequently met with this injury accompanying compound fractures of both bones of the leg resulting from railway and similar accidents.
By applying direct pressure over the displaced bone with the knee flexed, the dislocation is easily reduced. It is kept in position by a firm bandage or a light rigid splint.
Total Dislocation of Fibula.—Very rarely the fibula is separated from the tibia at both ends and displaced upwards. Bennett of Dublin has pointed out that in some persons the upper end of the fibula does not reach the facet on the tibia—a condition which might be mistaken for a dislocation.
The semilunar menisci are two crescentic plates of white fibro-cartilage, which lie upon the upper end of the tibia, and serve to deepen the articular surface for the condyles of the femur. Each cartilage is firmly attached to the tibia by its anterior and posterior ends, and, through the medium of the coronary ligaments, is loosely attached along its peripheral, convex edge to the head of the tibia, the medial meniscus being connected also to the capsular ligament of the joint. The tendon of the popliteus muscle intervenes between the lateral meniscus and the capsule. The central, concave edges of the menisci are thin and unattached.
The cartilages enjoy a limited range of movement within the joint, passing backwards during flexion, and forwards again when the limb is extended; under normal conditions the lateral moves more freely than the medial. While the limb is partly flexed, a slight degree of rotation of the leg at the knee is possible, and during this movement the cartilages glide from side to side, and the tibia rotates below them.
Any abnormal laxity of the ligaments of the joint may render the cartilages unduly mobile, so that they are liable to be displaced from comparatively slight causes, and when so displaced it is not uncommon for one or other to be torn by being nipped between the femur and the tibia. It is convenient to consider these “internal derangements of the knee-joint” separately, according to whether the meniscus is merely abnormally mobile, or is actually torn.
Mobile Meniscus—Displacement of Medial Semilunar Cartilage (Fig. 86).—The medial meniscus exhibits undue mobility much more frequently than the lateral, and the condition is usually met with in adult males who engage in athletics, or who follow an employment which entails working in a kneeling or squatting position for long periods, with the toes turned outwards—for example, coal-miners. The tibial collateral ligament, and through it the coronary ligament, are thus gradually stretched, so that the cartilage becomes less securely anchored, and is rendered liable to be displaced towards the centre of the joint during some sudden movement which combines flexion of the knee with medial rotation of the femur upon the tibia, as, for example, in rising quickly from a squatting position, or turning rapidly and pushing off with the foot, in the course of some game such as football or tennis. It may occur also from tripping on a loose stone or slipping off the kerbstone.
What actually happens when the meniscus is displaced would appear to be, that the combined flexion and abduction of the knee opens up the medial side of the joint by separating the medial condyles of the femur and tibia, and that the medial meniscus in its movement backward during flexion slips under the femoral condyle and is caught between it and the tibia. It may even slip past the condyle and into the intercondyloid notch, and come to lie against the cruciate ligaments.
The mechanism by which this lesion is produced doubtless explains the greater frequency with which the left knee is affected, as most sudden movements are made from right to left, thus throwing the strain upon the left knee.
Clinical Features.—When seen immediately after the accident, the patient usually gives the history that while making a sudden movement he was seized with an intense sickening pain in the knee, accompanied, it may be, by a sensation of something giving way with a distinct crack, and followed by locking of the joint. He may fall to the ground and be unable to rise. On examination, the knee is found to be fixed in a slightly flexed position; and while the surgeon may be able to carry out movements of flexion to a considerable extent without increasing the pain, any attempt to extend the joint completely is extremely painful. Tenderness may be elicited on making pressure to the medial side of the ligamentum patellæ in the groove between the femur and the tibia, but the meniscus cannot be recognised by palpation. Considerable effusion rapidly takes place into the synovial cavity.
The condition is liable to be mistaken for a sprain of the joint, particularly one implicating the tibial collateral ligament, but whereas in the lesion of the meniscus the maximum tenderness is in the interval between the bones, in the sprain of the ligament the maximum tenderness is over its attachment to the bone, usually the tuberosity of the tibia.
Treatment.—To reduce the displacement, the patient is placed on a couch, and, after the knee is fully flexed, the leg is rotated laterally and abducted, to separate the medial femoral condyle from the tibia, and while the rotation and abduction are maintained the leg is quickly extended. The return of the meniscus to its place is sometimes attended with a distinct snap, but in other cases reduction is only recognised to have taken place by the fact that the joint can be completely extended without causing pain.
Alternate flexion and extension combined with rotatory movements is sometimes successful. Several attempts are often necessary, and a general anæsthetic may be called for. After reduction, the limb is fixed with sand-bags, and massage and movement are employed to get rid of effusion, care being taken that no rotatory movement at the knee is permitted. Rest and support are necessary to allow of repair of the torn ligaments, and when the patient begins to use the limb he must be careful to avoid movements which throw strain on the damaged ligaments.
In a considerable proportion of cases no recurrence takes place, and in the course of a month or two the patient is able to resume an active life with a perfectly useful joint. In other cases there is a tendency to recurrence of the displacement.
Recurrent Displacement.—In cases of recurrent displacement, each attack is accompanied by symptoms similar in kind to those above described, but less severe, and the patient usually learns to carry out some manipulation by which he is able to return the meniscus into position. He seeks advice with a view to having something done to prevent displacement occurring, and to restore the stability of the joint, which, in many cases, is impaired, preventing him following his occupation. There persists a variable amount of fluid in the joint, the ligaments are stretched and slack, and the quadriceps muscle is markedly wasted.
The symptoms closely resemble those of a “loose body,” and it is often difficult to differentiate between them. In the case of a body free in the cavity of the joint, the site of the pain varies in different attacks, and the body can sometimes be palpated. Loose bodies wholly or partly composed of bone may be identified with the X-rays.
Attempts may be made to retain the meniscus in position by pads, bandages, or other forms of apparatus, so arranged as to prevent rotation and side-to-side movement at the knee. In the majority of cases, however, the best results are obtained by opening the joint and excising the meniscus in whole or in part, as may be necessary.
The limb is flexed on a splint until the wound has healed, after which massage should be employed and movement of the joint commenced. At the end of two or three weeks the patient is allowed up, wearing an elastic bandage. In most cases the use of the joint is completely regained in from four to six weeks. As an indication of the perfect recovery of the functions of the joint after removal of the meniscus, professional football players are often able to resume their occupation.
Displacement of the lateral meniscus is comparatively rare. It is in every way comparable to displacement of the medial meniscus, and is treated on the same lines.
Torn or Lacerated Meniscus.—In a large proportion of cases of displaced meniscus in which the condition assumes the recurrent type, it is found, on opening the joint, that, in addition to being unduly mobile, the meniscus is torn or lacerated. The experience of surgeons varies regarding the nature of the laceration. In our experience the most common form is a longitudinal split, whereby a portion of the inner edge of the cartilage is separated from the rest and projects as a tag towards the centre of the joint (Fig. 86). As a rule, it is the anterior end that is torn, less frequently the posterior end. Sometimes the meniscus is split from end to end, the outer crescent remaining in position, while the inner crescent passes in between the condyles and lies curled up against the cruciate ligaments. Occasionally the anterior end is torn from its attachment to the tibia, less frequently the posterior end. In one case we found the meniscus separated at both ends and lying between the bones and the capsule.
The clinical features are similar to those of mobile meniscus with displacement, and as a rule the exact nature of the lesion is only discovered after opening the joint.
The treatment consists in excising the loose tag or the whole meniscus, according to circumstances. The recovery of function is usually complete. It is not advisable to attempt to stitch the torn portion in position.
Rupture of the Cruciate Ligaments.—A few cases have been recorded in which, as a result of severe twisting forms of violence, the cruciate ligaments have been torn from their attachments, leaving the joint loose and unstable, so that the tibia and the femur could be moved from side to side on one another. When the disability persists, the joint may be opened and the ligaments sutured in position (Mayo Robson).
Sprains of the knee are comparatively common as a result of sudden twisting or wrenching of the joint. In addition to the stretching or tearing of ligaments, there is usually a considerable effusion of fluid into the synovial cavity, and examination with the X-rays occasionally reveals that a portion of bone has been torn away with the ligament—sprain-fracture. The swelling fills up the hollows on either side of the patella, and extends for some distance in the synovial pouch underneath the quadriceps. The patella is raised from the front of the femur by the collection of fluid in the joint—“floating patella”—and, if firmly pressed upon, it may be made to rap against the trochlear surface.
A sprain is to be diagnosed from separation of one or other of the adjacent epiphyses, fracture involving the articular ends of the bones, and displacement of the semilunar menisci. On account of the swelling, which obscures the outline of the part, the differential diagnosis is often difficult, but as the swelling goes down under massage it becomes easier. Chief reliance is to be placed upon the bony points retaining their normal relationships, and upon the fact that the points of maximum tenderness are over the attachments of one or other of the collateral ligaments. As the tibial collateral ligament suffers most frequently, the most tender spot is usually over its attachment to the medial aspect of the head of the tibia—less frequently over the medial condyle of the femur.
Unless efficiently treated, a sprain of the knee is liable to result in weakness and instability of the joint from stretching of the ligaments, and this is often associated with effusion of fluid in the synovial cavity (traumatic hydrops). This is more likely to occur if the joint is repeatedly subjected to slight degrees of violence, such as are liable to occur in football or other athletic exercises—hence the name “footballer's knee” sometimes applied to the condition.
A further cause of disability, following upon sprains of the knee, is wasting of the quadriceps muscle. The stability of the joint, whenever the position of full extension has been departed from, is largely dependent upon its capacity of controlling the amount of flexion, notably in descending a stair or in walking on uneven ground, hence it is that with a wasted quadriceps there is increasing liability to a repetition of the sprain. With each repetition of the sprain, there is an addition to the fluid in the joint, stretching of ligaments, and further wasting of the quadriceps. A form of vicious circle is established in which there is at the same time increased liability to sprain and diminished capacity of recovering from it. Even after the repair of the damaged ligament or the removal of the mobile or torn meniscus, wasting of the quadriceps remains a source of weakness and disability and calls for treatment by massage and electricity.
Treatment.—In recent and severe cases the patient must be confined to bed, and firm pressure applied over the joint by means of cotton wool and a bandage. This may be removed once or twice a day to admit of the joint being douched, and at the same time it should be massaged and moved to promote absorption of the effusion and prevent the formation of adhesions.
Chronic effusion into the joint is most rapidly got rid of by rest and blistering. If the patient is unable to lie up, massage should be systematically employed, and a firm elastic bandage worn. A patient who has once had a severe sprain of the knee, or who has developed the condition of “footballer's knee,” must give up violent forms of exercise which expose him to further injuries, otherwise the condition is liable to be aggravated and to result in permanent impairment of the stability of the joint.
Fracture of the patella is a comparatively common injury in adult males. Most frequently it is due to muscular action the patella being snapped across the lower end of the femur by a sudden and forcible contraction of the quadriceps extensor muscle while the limb is partly flexed—as, for example, in the attempt to avoid falling backward. The bone is then broken as one breaks a stick by bending it across the knee, and the line of fracture, which is transverse or slightly oblique, crosses the bone a little below its middle. Fractures produced in this way are almost never compound.
The degree of displacement of the fragments depends upon the extent to which the expansion of the quadriceps tendon is lacerated. As a rule, it is but slightly torn, so that the separation of the fragments does not exceed an inch. In other cases it is widely torn, and the contraction of the quadriceps muscle is then able to separate the fragments by three or four inches, and sometimes causes tilting of the upper fragment. The blood effused into the joint tends still further to increase the separation. As the periosteum is usually torn at a level lower than the fracture, its free margin hangs as a fringe from the proximal fragment, and by getting between the broken ends may form a barrier to osseous union (Macewen).
 Fig. 88.—Fracture of Patella, showing wide separation
of fragments, which are united by a fibrous band.
Fig. 88.—Fracture of Patella, showing wide separation
of fragments, which are united by a fibrous band.Clinical Features.—Immediately the bone breaks, the patient falls, and he is unable to rise again, as the limb is at once rendered useless, and in attempting to do so we have known him to fracture the patella of the other limb. The power of extending the limb is lost, and the patient is unable to lift his foot off the ground. The knee-joint is filled with blood and synovia, which usually extend into the bursa under the quadriceps. The two fragments can be detected, separated by an interval which admits of the finger being placed between them, and which is increased on flexing the knee. On relaxing the quadriceps, the fragments may be approximated more or less completely.
Prognosis.—In cases with little displacement, if the fragments have been kept in perfect apposition, osseous union may take place, but in the great majority of cases the union is fibrous. The shortening of the quadriceps and the gradual stretching and thinning of the connecting fibrous band may allow of further separation of the fragments (Fig. 88), which to a variable extent interferes with the stability and functions of the limb. The proximal fragment sometimes becomes attached to the front of the femur, and moves with it, and the fibrous band between the two fragments gradually becomes stretched. After bony union has occurred, it is not uncommon for the patella to be fractured again by a fall within a month or two of the original accident.
Treatment.—It is probably true that the best functional results are most speedily obtained by operative measures. The laceration of the aponeurosis of the quadriceps, the tilting of the fragments, and the interposition of the torn periosteum between them, can in no other way be rectified with certainty. The operation, however, should only be undertaken by those who are familiar with wound technique, and who have the means at their disposal for carrying it out. Operative treatment is specially indicated in young subjects who lead an active life, and in labouring men, particularly those who follow dangerous employments necessitating stability of the knee.
As soon as the wound is healed,—in a week or ten days,—massage and movement of the limb are commenced, and the patient is encouraged to move his limb in bed. At the end of another week he may be allowed up with sticks or crutches.
Non-operative Treatment.—In the majority of cases occurring in patients who do not follow a laborious occupation or otherwise lead an active life, a satisfactory result can be obtained without having recourse to operation. We have reason to be satisfied with the following method: the patient is kept in bed for a few days, the injured region being supported on a pillow and massaged daily, and the patella moved from side to side as a whole to prevent adhesion to the femur. About the fourth day he is allowed to get about with crutches. As osseous union of the fragments is not essential to a good functional result, and as fibrous union does not necessarily entail any material interference with the usefulness of the limb, no attempt need be made to approximate the fragments, but every effort must be made to maintain the function of the quadriceps muscle and the mobility of the joint.
If it is desired to bring the fragments into contact and to secure osseous union, the limb should be placed upon an inclined plane to relax the quadriceps muscle, and means taken to arrest effusion and to diminish the swelling by systematic massage and a supporting bandage. When, in the course of a few days, this has been accomplished, the attempt is made to approximate the fragments, by fixing a large horseshoe-shaped piece of adhesive plaster to the front of the thigh, embracing the proximal fragment. Extension is made upon this by means of rubber tubing, which is fixed to the foot-piece of the splint. The bandage which binds the limb to the splint should make upward pressure on the distal fragment, or this may be done by a special piece of adhesive plaster with elastic tubing pulling in an upward direction.
The retentive apparatus is kept on for about three weeks, and a rigid, but easily removable, apparatus is thereafter applied, and the patient allowed up on crutches, the limb being massaged and exercised daily to improve the tone of the muscles.
When the fracture is caused by direct violence, such as a fall on the knee or the kick of a horse, it may be transverse, oblique, or vertical, but in many cases it is stellate, the bone being broken into several irregular pieces. These comminuted fractures are frequently compound. In transverse and oblique fractures, the displacement depends upon the same causes as in fracture by muscular action. In vertical and stellate fractures, unless the knee has been forcibly flexed after the bone has been broken, there is little or no displacement. The treatment is governed by the same considerations as in fractures by muscular action.
Old-standing Fracture.—As fibrous union, even with an interval of several inches between the fragments, is not incompatible with a useful limb, it is not often necessary to operate for this condition, but when the usefulness of the limb is seriously impaired, operative treatment is indicated. The operation is carried out on the same lines as for recent fracture, the ends of the bones being rawed and adhesions divided. When the proximal fragment has become attached to the femur, it should be separated and a layer of fascia interposed; it is sometimes necessary to lengthen the quadriceps muscle by making a number of V-shaped incisions through its substance; or a flap may be turned down from the rectus and stitched to the patella and the ligamentum patellæ.
When operative treatment is contra-indicated, the patient should be fitted with a firm apparatus which will limit flexion of the knee and support the fragments.
Dislocation of the patella is rare. It results from exaggerated muscular movements when the limb is in the fully extended position, or from a blow on one or other edge of the bone. Laxity of the ligaments and knock-knee are predisposing factors. It is sometimes associated with fracture of the edge of the trochlear surface, which renders retention in position difficult.
The lateral is the most common variety—the medial being rare. Either may be complete or incomplete. Sometimes the bone is rotated so that its edge rests on the front of the femur—vertical dislocation; and in a few cases it has been completely turned round, so that the articular surface is directed forwards.
Clinical Features.—The joint is fixed, usually in a position of slight flexion, and the displaced patella can readily be palpated. The deformity is a striking one, and at first sight suggests a much more serious injury. Although easily reduced, the dislocation is liable to recur.
To effect reduction, the quadriceps must be thoroughly relaxed by extending the leg upon the thigh and flexing the thigh upon the pelvis; the patella is then tilted by making firm pressure on that edge which lies farthest from the middle of the joint, and at the same time pushing towards the middle line. The limb is placed on a posterior splint, and firm elastic pressure made on the joint to prevent or diminish effusion. Massage and movement are carried out from the first.
As the displacement is liable to recur, the patient should wear a firm elastic bandage or a strong knee-cap.
Permanent and recurrent dislocation of the patella will be described later.
The bones of the leg may be broken together or separately.
Fracture of both Bones.—The features of this injury depend to a large extent upon the nature of the violence producing it. In fracture by direct violence, such as the passage of a wheel over the limb or a severe blow, the bones give way at the point of impact, and the line of fracture tends to be transverse, both bones being broken at the same level (Fig. 89). There is little or no displacement, and such as there is is angular, and is determined by the direction of the fracturing force.
 Fig. 89.—Radiogram of Transverse Fracture of both
Bones of Leg by direct violence.
Fig. 89.—Radiogram of Transverse Fracture of both
Bones of Leg by direct violence.
|
 Fig. 90.—Radiogram of Oblique Fracture of both Bones
of Leg by indirect violence.
Fig. 90.—Radiogram of Oblique Fracture of both Bones
of Leg by indirect violence.
|
When the violence is indirect, as from a fall on the feet, or a twist of the leg, the tibia usually gives way at the junction of its lower and middle thirds, and the fibula at a higher level (Fig. 90). Torsion of the tibia is probably the most important factor in the production of the fracture, the distal fragment being fixed by the pressure of the foot upon the ground, while the proximal fragment is rotated by the impetus of the body. Both fractures are usually oblique—that in the tibia running from above downward, forward, and medially, and it is generally found that the obliquity of the fibular fracture corresponds with that in the tibia.
There is usually considerable displacement, the weight of the lower portion of the limb causing it to fall backwards and to roll away from the middle line, and the traction of the calf muscles pulling up the heel and pointing the toes. The proximal fragment forms a projection on the front of the limb.
On account of the superficial position of the tibia and the pointed character of the fragments, this fracture is frequently rendered compound by the bone being forced through the skin. The projecting piece of bone is usually the distal end of the proximal fragment. This fracture is often comminuted. It has been observed that when the line of fracture forms the letter V on the subcutaneous surface of the tibia, there is invariably a fissure passing down along the back of the bone into the ankle-joint—a complication which adds to the risk of subsequent stiffness and impaired usefulness of the limb. Apart from this, the ankle is usually sprained in fractures by indirect violence, and we have frequently found the superior tibio-fibular articulation torn open in severe fractures of both bones of the leg from indirect violence.
Clinical Features.—The tibial fracture is readily recognised by detecting an irregularity on running the fingers along the crest of the shin, and at this point abnormal mobility, tenderness, and crepitus can usually be elicited. It is often difficult to detect the fibular fracture, and it is not always advisable to attempt to do so, especially if the manipulations cause pain or tend to increase the displacement. The condition of the fibula is usually to be inferred by noting the amount of displacement and the extent of mobility of the tibial fragments. Not infrequently the seat of fracture may be recognised by locating a point at which pain is elicited on making pressure over the bone at a distance—pain on distal pressure.
On account of the close connection of the skin to the periosteum on the subcutaneous aspect of the tibia, the tension caused by extravasated blood is often extreme; blisters frequently form over the area of ecchymosis, and when these become infected, sloughing of the skin may take place and the fracture thus be rendered compound.
The vessels and nerves of the leg are seldom seriously damaged.
Treatment.—If there is marked displacement, reduction is most satisfactorily accomplished under anæsthesia. Traction is made upon the foot and the fragments are manipulated into position, the pointing of the toes and the outward rotation of the foot being at the same time corrected. The normal outline of the foot in relation to the leg is restored when the ball of the great toe, the medial malleolus, and the medial edge of the patella are in the same vertical plane. As in other fractures of the lower extremity, the limb should be placed in the natural position of slight eversion: not with the toes pointing straight forward.
The retentive apparatus to be applied depends upon the tendency to re-displacement, the degree of swelling, and the extent of the damage to the skin.
In the average case, the leg is supported between sand-bags, and massage and movements are employed from the outset. When there is a tendency to re-displacement, the limb may be immediately enclosed in a rigid apparatus, such as lateral poroplastic splints retained in position by an elastic bandage, or a Cline's splint, which can readily be removed to admit of massage. When the fracture is in the lower third of the leg, the ambulatory splint gives excellent results, and is of special service in hospital practice (Fig. 95).
As an emergency appliance, for example for purposes of transport, the box splint (Fig. 91) is simple and efficient. We have not found it effectual in controlling the fragments, particularly in oblique fractures, and it requires constant supervision and readjustment. It consists of two pieces of wood extending from above the knee to an inch or two beyond the sole, and a little broader than the maximum diameter of the leg. These are rolled into the opposite ends of a folded sheet, so as to form two sides of a box, of which the sheet constitutes a third side. It is found advantageous to insert another board, fitted with a foot-piece, between the folds of the sheet forming the third side of the box, to add to the rigidity of the splint, and to aid in controlling the foot. By folding one side of the sheet somewhat obliquely, the box is made a little wider at the knee than at the ankle, and so fits the limb more accurately.
The limb is placed in this box, the sides of which have been carefully padded. Ring pads are applied to take pressure off the condyles, the head of the fibula, the malleoli, and the prominence of the heel, and a large supporting pad is placed behind the tendo calcaneus. A folded towel is laid over the front of the leg, forming a lid to the box, and the whole is bound to the limb by three slip-knots. Finally, the foot is fixed at right angles to the leg and slightly abducted by a figure-of-eight bandage or a piece of elastic webbing. Sand-bags placed alongside serve to steady the limb. In fractures of the lower third of the leg, the box splint may stop short of the knee and the limb may then be suspended in a Salter's cradle, which allows the patient to move about more freely in bed.
To prevent shortening in oblique fractures and in those near the ankle-joint, where it is often difficult to control the lower fragment, extension, applied by weight and pulley, or through a Thomas' knee splint, may be of service. The strapping may be applied only to the distal fragment, but we prefer to carry it to the upper third of the leg. If the overriding of the fragments persists, extension may be taken directly from the bone, the ice-tong callipers gripping the malleoli or the calcaneus.
When the skin is damaged, as it so frequently is on the medial aspect of the tibia, means must be taken to prevent infection.
Massage is carried out daily, and, to prevent stiffness, the ankle is moved from the first. In the course of three weeks, lateral poroplastic splints retained by an elastic bandage may be substituted, and the patient allowed up on crutches. In simple fractures without displacement, union is usually complete in from six to eight weeks, but when the fracture is oblique, comminuted, or compound, union is often delayed, and the functions of the limb may not be fully regained for three or even four months after the accident.
Operative Treatment.—When overriding cannot otherwise be corrected, it is advisable to replace the fragments by operation. A curved incision with its convexity backward is made over the medial side of the tibia, exposing the fragments, which are then levered into position and if necessary plated or otherwise fixed according to circumstances. It is seldom necessary to deal separately with the fibula. A box splint is applied till the wound has healed, after which a poroplastic splint is substituted and massage commenced.
We do not share in the dissatisfaction expressed by some surgeons, notably Arbuthnot Lane, as to the results obtained by non-operative means in the common fractures of the leg, and do not recommend a systematic resort to operative treatment.
Un-united fracture of the bones of the leg is sometimes met with. It is treated on the same lines as in other situations, but may prove extremely intractable, especially in children, in whom, indeed, it is sometimes incurable.
Mal-union, on account of the disability it entails, may call for operative treatment in the form of osteotomy of one or both bones.
Compound fractures of the leg are common, and are treated on the lines already laid down for the treatment of compound fractures in general (p. 25).
Fracture of the tibia alone, when due to direct violence, is usually transverse, there is little displacement, and as the fibula retains the fragments in position, union usually takes place rapidly and without deformity. Oblique and spiral fractures result from indirect violence.
Fracture of the fibula alone may result from direct violence, and, on account of the support given by the tibia, is usually unattended by displacement. Bennett of Dublin has pointed out that it is common to meet with an oblique fracture of the upper third of the fibula as the result of an outward twist of the ankle while the foot is extended. It is characterised by pain localised at the seat of the break, on moving the foot in such a way as to bring the talus to bear against the fibula. Local pressure also may make the fibula yield and may elicit crepitus. In some cases this fracture is associated with sprain of the ankle-joint. It is often overlooked, and from want of proper treatment may result in prolonged impairment of usefulness.
Fractures of the tibia or fibula alone are treated on the same lines as fractures of both bones, and splints are rarely necessary. The ambulant method is useful in these cases (Fig. 95).
The fractures in this region include Pott's fracture, and its converse; separation of the lower epiphysis of the tibia; fractures of the talus, calcaneus, and other tarsal bones; and fractures of the metatarsals and phalanges. Various dislocations also occur, the most important being those of the ankle joint, of the talus, and the sub-taloid dislocation.
Surgical Anatomy.—For the study of injuries in the region of the ankle-joint it is of importance to define the terms employed in describing the movements of the foot. Thus by flexion or dorsiflexion is meant that movement which approximates the dorsum of the foot to the front of the leg; while extension or plantar flexion means the drawing up of the heel so that the toes are pointed. In inversion the medial edge of the foot is drawn up so that the sole looks towards the middle line of the body, an attitude which is analogous to supination of the hand. In eversion the lateral edge of the foot is drawn up, the sole looking away from the middle line—analogous to pronation of the hand. Adduction indicates the rotation of the foot so that the toes are turned towards the middle line of the body; while in abduction the toes are turned away from the middle line.
The most prominent bony landmarks in the region of the ankle are the two malleoli, the lateral lying slightly farther back, and about half an inch lower than the medial. On the medial side of the foot from behind forward may be felt the medial process (internal tuberosity) of the calcaneus; the sustentaculum tali, which lies about 1 inch vertically below the tip of the malleolus; the tubercle of the navicular, about 1 inch in front of the malleolus, and at a slightly lower level; the first (internal) cuneiform, and the base, shaft, and head of the first metatarsal.
On the lateral side may be recognised the lateral process (external tuberosity) of the calcaneus; the trochlear process (peroneal tubercle) on the same bone; the cuboid; and the prominent base of the fifth metatarsal.
The talo-navicular joint lies immediately behind the tuberosity of the navicular, and a line drawn straight across the foot at this level passes over the calcaneo-cuboid joint.
The ankle-joint, formed by the articulation of the tibia and fibula with the talus, lies about half an inch above the tip of the medial malleolus, and is so constructed that when the foot is at a right angle with the leg it is only possible to flex and extend the joint. When the toes are pointed, however, slight side-to-side and rotatory movements are possible. The chief seat of side-to-side movement of the foot is at the talo-navicular and calcaneo-cuboid articulations—“the mid-tarsal or Chopart's joint.”
The ankle-joint owes its strength chiefly to the malleoli and the collateral ligaments, and to the inferior tibio-fibular ligaments, which bind together the lower ends of the bones of the leg. The numerous tendons passing over the joint on every side also add to its stability.
The synovial membrane of the ankle-joint passes up between the bones of the leg to line the inferior tibio-fibular joint; but it is distinct from that of the intertarsal joints, which communicate with one another in a complicated manner. The epiphysial cartilage at the lower end of the fibula lies on the level of the talo-tibial articulation, while that of the tibia is about half an inch higher (Fig. 93).
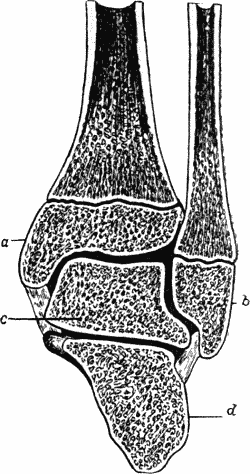 Fig. 93.—Section through Ankle-Joint showing relation
of epiphyses to synovial cavity.
Fig. 93.—Section through Ankle-Joint showing relation
of epiphyses to synovial cavity.Pott's Fracture.—It must be understood that various lesions occurring in the region of the ankle-joint are included under the clinical term “Pott's fracture.” Although of a similar nature, and produced by the same forms of violence, these vary considerably in their anatomy and clinical features. They are all the result of combined eversion and abduction of the foot—produced, for example, by slipping off the kerbstone, or by jumping from a height and landing on the medial side of the foot.
When forcible eversion is the chief movement, the tightening of the deltoid (internal lateral) ligament usually tears off the medial malleolus across its base. The talus is then brought to bear on the lateral malleolus, and the force continuing to act, the lower end of the fibula is pressed laterally, and breaks close above the malleolus. The tibio-fibular interosseous ligament may rupture, or the outer portion of the tibia, to which it is attached, may be avulsed. This form is sometimes called Dupuytren's fracture. When the bones are widely separated in Dupuytren's fracture the talus may be forced up between them.
When the movement of abduction predominates, the deltoid ligament is usually ruptured, or the anterior edge or tip of the medial malleolus torn off. The tibio-fibular interosseous ligament usually resists, and an oblique fracture of the fibula 2 or 4 inches above its lower end results.
Clinical Features.—In a considerable proportion of cases—in our experience in the majority—this fracture is not accompanied by any marked deformity of the foot, and the patient is often able to walk after the injury with only a slight limp.
In others, however, the deformity is marked and characteristic (Fig. 94). The foot is everted, its inner side resting on the ground. The medial malleolus is unduly prominent, stretching the skin, which may give way if the patient attempts to walk. The foot, having lost the support of the malleoli, is often displaced backward, and the toes are pointed by the contraction of the calf muscles. There is abnormal mobility—both from side to side and antero-posteriorly—and crepitus may be elicited. The points of tenderness are over the deltoid ligament or medial malleolus, the inferior tibio-fibular joint, and at the seat of fracture of the fibula. Distal pressure over the shaft of the fibula, or on the extreme tip of the malleolus, may elicit pain and crepitus at the seat of fracture. There is usually considerable ecchymosis and swelling in the hollows below and behind the malleoli; and the malleoli appear to be nearer the level of the sole. In Dupuytren's fracture, when the talus passes up between the tibia and fibula, there is great broadening of the ankle.
There is often considerable difficulty in distinguishing a sprain of the ankle from a fracture without displacement, as both forms of injury result from the same kinds of violence, and are rapidly followed by swelling and discoloration of the overlying soft parts. In a sprain, the point of maximum tenderness is over the ligaments and tendon sheaths that have been damaged, while in fracture the site of the break is the most tender spot. The X-rays are useful in the diagnosis of doubtful cases.
Treatment.—In those cases of fracture of the lower end of the fibula in which there is no marked displacement,—and they constitute a considerable proportion,—the limb should be massaged and laid on a pillow between sand-bags, or placed in a box splint for two or three days, until the swelling subsides. Some form of rigid apparatus, such as side poroplastic splints fixed in position with an elastic bandage, which will allow the patient to get about with crutches, is then applied. This is removed daily to permit of massage and movement being carried out—a point of great practical importance, because, if this is neglected, not only does union take place more slowly, but the stiffness of the ankle and œdema of the leg and foot which ensue, prolong the period of the patient's incapacity and endanger the usefulness of the limb.
It is in cases of this kind that the ambulatory method of treatment yields its best results. When, in the course of two or three days, the swelling has subsided, a plaster-of-Paris case (Fig. 95) is applied in such a way that when the patient walks the weight is transmitted from the condyles of the tibia through the plaster case to the ground, no weight being borne by the bones at the seat of fracture. The apparatus is applied as follows: A boracic lint bandage is applied to the limb as far as the knee, and protecting pads or rings of wool are placed over the condyles of the tibia, the head of the fibula, and the malleoli. A pad of wool about 3 inches thick is then placed under the sole and fixed in position by a plaster-of-Paris bandage, which is carried up the limb in the usual way. The case is made specially strong on the sole, around the ankle, up the sides of the leg, and at the bearing-point at the head of the tibia. After the plaster has thoroughly set, the patient is allowed to walk about with a stick, crutches being unnecessary. In the course of three weeks the plaster case may be removed and the limb massaged. It is usually found that the movements of the ankle are scarcely interfered with, and the patient is generally able to resume work within a month of the accident.
When there is marked eversion of the foot, it may be necessary to administer a general anæsthetic to reduce the deformity; and to prevent recurrence of the displacement Dupuytren's splint (Fig. 96) may be used. This splint, which is of the same shape as Liston's long splint, but on a small scale, is applied to the medial side of the leg extending from just below the knee to well beyond the sole of the foot. A large pad is placed in the hollow above the medial malleolus, and it must be thick enough to carry the splint so far from the limb that when the foot is fully inverted it does not touch the splint. The upper end of the splint having been fixed to the leg at the level of the condyles of the tibia, a bandage is applied to correct the eversion of the foot, and at the same time to support the heel, and, as far as possible, to overcome the pointing of the toes. Care must be taken to avoid carrying the turns of this bandage over the seat of fracture. The limb may then be slung in a cradle, or placed on a pillow resting on its lateral side with the knee flexed. In the course of a few days, a poroplastic splint may be substituted and massage commenced.
When backward displacement of the heel is the prominent deformity, Syme's horse-shoe or stirrup splint (Fig. 97) may be employed. It is applied to the anterior aspect of the limb, which is carefully padded to prevent undue pressure on the edge of the shin bone. After the upper end of the splint has been fixed, the heel is pulled forward by a few turns of bandage passed over the prongs at the lower end of the splint. The foot is then inverted and brought up to a right angle by a few supplementary turns of the bandage. In a few days this appliance may be replaced by a poroplastic splint.
Operative Treatment.—If the displacement is not completely corrected by the measures described, the fibular fracture is exposed by a free incision and the fragments are levered into position, and if necessary fixed by lashing with catgut or by other mechanical means.
Mal-union of Pott's fracture may necessitate re-fracture by means of a Jones' wrench, used in the same manner as for club-foot, or the parts are exposed by operation; the bone is divided by means of an osteotome, the foot forcibly inverted, and the limb put up in the same way as in a recent fracture.
The Converse of Pott's Fracture—sometimes called “Pott's Fracture with Inversion.”—This injury is fairly common, and results from forcible inversion of the foot. The lateral malleolus is broken across its base, or, in young subjects, along the epiphysial line. The medial malleolus alone may be carried away, or a portion of the broad part of the tibia may accompany it.
The foot is inverted, the heel falls back, and the toes are pointed. In other respects it corresponds to the typical Pott's fracture, and is treated on the same principles. When Dupuytren's splint is required, it is, of course, applied to the lateral side of the leg.
Separation of the lower epiphysis of the tibia is not common. It occurs most frequently between the ages of eleven and eighteen, as a result of forcible eversion or inversion of the foot. It is usually accompanied by fracture of the diaphysis of the fibula (Fig. 98), and is not infrequently compound. When the epiphysis is displaced to one side, the deformity is characteristic. In rare cases the growth of the tibia is arrested, the continued growth of the fibula causing the foot to become inverted. The treatment is the same as for Pott's fracture.
Fracture of the talus usually occurs as a result of a fall from a height, the bone being crushed between the tibia and the calcaneus. It is usually associated with other fractures, and is sometimes impacted, the foot assuming the position of equino-varus. The diagnosis is only to be made by exclusion, or by the use of the Röntgen rays. In interpreting radiograms of injuries in this region, care must be taken not to mistake the os trigonum tarsi for a fracture. In uncomplicated cases, the treatment consists in immobilising the foot and leg in a poroplastic splint and applying massage. In comminuted and in impacted fractures with persistent deformity, complete excision of the bone yields good results.
The calcaneus is most frequently broken by the patient falling from a height and landing on the sole of the foot, and the injury may occur simultaneously in both feet.
The primary fracture is usually longitudinal, passing through the facets for the talus and cuboid, and from this various secondary fissures radiate; the cancellated tissue is much crushed, so that the whole bone is flattened out. In spite of the great comminution, it is often impossible to elicit crepitus, as the fragments are held together by the investing soft parts. In other cases the foot may feel like “a bag of bones.” The lesion is often mistaken for a fracture of the lower end of the fibula, or is not diagnosed at all. The chief clinical feature is pain on movement of the foot, or on attempting to walk; the foot appears flat, and the hollows on either side of the tendo Achillis are filled up. In many cases there is a persistent tenderness which delays restoration of function for some months, but the ultimate result is usually satisfactory.
Treatment.—In simple comminuted fractures the patient should be anæsthetised, and the foot moulded into position, care being taken to restore the arch in order to avoid any tendency to flat foot. The foot is supported on a pillow, and to prevent stiffness, massage and movements of the ankle and tarsal joints should be commenced without delay.
Compound fractures confined to the calcaneus may be treated on conservative lines, but if associated with other injuries of the foot they may necessitate amputation.
The tuberosity of the calcaneus, into which the tendo Achillis is inserted, is sometimes separated by forcible contraction of the calf muscles, or from a fall on the ball of the foot. The separated fragment may be pulled up for a distance of 1 or 2 inches, and the rough surface from which it has been torn may be recognisable. The patient may be able to walk immediately after the accident, although with difficulty; or he may have pain for many months.
A good functional result is usually obtained by relaxing the calf muscles and fixing the foot in the position of extreme plantar flexion with the knee flexed, but in some cases it is advisable to peg the fragments, either through the skin or after exposing them by operation.
The other bones of the tarsus are rarely fractured separately. The tuberosity of the navicular is sometimes torn away by violent traction on the ligaments attached to it.
Fractures of the metatarsals and phalanges usually result from direct violence, such as a crush of the foot, in which the soft parts are severely damaged. The use of the Röntgen rays has shown, however, that certain painful conditions in the foot following comparatively slight injuries, such as kicking a stone, are due to a fracture of one of the metatarsals or phalanges.
When simple, these injuries are often overlooked, on account of the difficulty of eliciting the signs of fracture from the swelling which accompanies them. They are best treated in a moulded splint.
Compound fractures are more common, and are to be treated on the same principles as govern such injuries elsewhere.
A fracture of the base of the fifth metatarsal has been described by Sir Robert Jones. It is produced by the patient coming down forcibly on the lateral edge of the foot while the foot is inverted and the heel raised—as, for example, in dancing. There is a localised swelling over the base of the fifth metatarsal, and pain when the patient puts weight on the foot. There is no crepitus or deformity. The fracture is readily recognised by the Röntgen rays. Massage and movement are employed from the first.
Dislocation of the Ankle-Joint.—In describing dislocation of the talus from the tibio-fibular socket, the varieties are named according to the direction in which the foot passes—backward, forward, medially, laterally, or upward.
All of them may be complete, but they are more frequently incomplete, and are liable to be rendered compound, either from tearing of the skin at the time of the injury, or by its sloughing later. Although as a rule there is little difficulty in effecting reduction by manipulation, these injuries are liable to be followed by stiffness and impaired usefulness of the joint.
The backward dislocation is the most common, and results from extreme plantar flexion of the foot, as from a fall backwards while the foot is fixed, wedging the talus between the tibia and fibula. The collateral ligaments are torn, and one or both malleoli may be broken, or the posterior part of the articular edge of the tibia chipped off (Fig. 99).
The foot appears shortened, the heel is unduly prominent behind, and the lower ends of the tibia and fibula project in front, sometimes coming through the skin. The tendons around the joint are stretched or torn.
Forward dislocation results from extreme dorsal flexion at the ankle-joint. The foot appears lengthened, the heel is less prominent than normal, and the hollows on each side of the tendo Achillis are obliterated. The talus is felt in front of the tibia, and the malleoli appear to be displaced backwards and to lie nearer the sole.
Medial or lateral dislocation is only possible after fracture of one or both malleoli, and may be looked upon as a complication of these injuries.
In cases in which the interosseous ligament is ruptured, and in severe cases of Dupuytren's fracture, the talus may be driven upwards between the bones of the leg. There is great broadening in the region of the ankle, and the malleoli are unduly prominent under the skin, which is tightly stretched over them. They are also nearer to the sole than normally. The movements of the ankle-joint are lost.
Dislocation of the inferior tibio-fibular joint is exceedingly rare, except in association with fractures of the lower ends of the bones of the leg, particularly Dupuytren's fracture, or with dislocation of the ankle-joint proper.
Treatment of Dislocation of Ankle.—The patient having been anæsthetised, the foot is extended and the knee and hip joints flexed to relax the calf muscles as completely as possible. Traction is then made upon the foot, while counter-extension is applied to the leg, and the bones are manipulated into position. Reduction usually takes place gradually without the characteristic snap which accompanies reduction of most dislocations. It is sometimes necessary to divide the tendo Achillis, particularly in cases of forward dislocation.
When the talus passes upwards between the tibia and fibula, it is sometimes impossible to effect reduction by manipulation, and the best results are then obtained by operation.
The after-treatment consists in keeping the leg on a pillow between sand-bags, and carrying out the usual massage and movement.
In compound dislocations which have become infected, primary amputation may be indicated, but in young and healthy subjects an attempt may be made to save the foot.
Dislocation of the talus from its articulations with the bones of the leg above and the calcaneus and navicular below, is a comparatively common injury, and results from a violent wrench of the foot. It may be incomplete or complete. When the foot is plantar flexed at the moment of injury, the displacement is generally forward with a tendency outward. The talus comes to rest on the third cuneiform and cuboid bones, the foot being abducted, inverted, and displaced medially. In a large proportion of cases the dislocation is compound, more or less of the talus being forced through the skin (Fig. 100).
When the foot is dorsiflexed at the moment of injury the displacement is backward, but this is rare, as is also dislocation to one or other side, and dislocation by rotation, in which the talus is rotated in its socket. In all these injuries the body of the talus loses its normal relationship with the malleoli.
An attempt should be made to reduce the dislocation under anæsthesia, the limb being placed in the same position as for reduction of dislocation of the ankle. While traction is made upon the foot, an assistant presses directly on the displaced bone and endeavours to manipulate it into position. In incomplete dislocations this usually succeeds, but it not infrequently fails in those which are complete, and under these circumstances it may be necessary to chisel through the lateral malleolus to admit of reduction, or to excise the talus. In most cases of compound dislocation also, this bone should be removed.
Sub-taloid Dislocation.—In this dislocation, which results from the same kinds of violence as the last, the talus retains its position in the tibio-fibular socket, and the calcaneus and navicular, with the rest of the foot, are carried away from it. The body of the talus, therefore, maintains its normal relationship with the malleoli—a point of importance in the differential diagnosis between this injury and dislocation of the talus. The displacement is usually incomplete, and the foot may either pass backward and medially, or backward and laterally. When the foot passes backward and medially, the head of the talus projects on the outer part of the dorsum, resting on the cuboid. The dorsum of the foot is shortened, the heel lengthened, the toes adducted, and the medial border of the foot raised. The lateral malleolus is unduly prominent, and reaches nearly to the sole.
In the backward and lateral variety, the medial malleolus and head of the talus project unduly towards the medial side of the foot, which is abducted and everted.
In neither variety is there any mechanical obstacle to movement at the ankle-joint.
The treatment is carried out on the same lines as for dislocation of the talus, reduction being effected without difficulty in most cases. If this fails, as it occasionally does, it may be necessary to excise the talus.
Mid-tarsal or transverse tarsal dislocation—that is, at the talo-navicular and calcaneo-cuboid articulations—is extremely rare. The distal segment of the foot is usually displaced towards the sole; the foot is foreshortened, the malleoli raised from the sole, the arch of the foot is lost, and the first row of tarsal bones projects on the dorsum. The treatment consists in reducing the displacement by manipulation, after which massage and movement are employed.
Tarso-metatarsal Dislocations.—One, several, or all of the metatarsals may be separated from the distal row of tarsal bones—the usual cause being a fall from a horse, the foot being fixed in the stirrup. The bases of the metatarsal bones are displaced laterally and towards the dorsum. The base of the second metatarsal and the first cuneiform are sometimes fractured. Reduction by manipulation is generally easy in dorsal dislocations, but may be difficult when the bones are displaced laterally. This may be due to fragments of bone or soft parts getting between the bones, and may necessitate operative interference. In old-standing dislocations, operation is to be advised only when locomotion is seriously interfered with.
Dislocation of the Toes.—The great toe may be dislocated at its metatarso-phalangeal joint, the base of the proximal phalanx passing towards the dorsum (Fig. 102). Diagnosis and reduction are alike easy.
Inter-phalangeal dislocations are rare and are easily reduced.
The shoulder is seldom the seat of disease, and most affections of the joint are met with in adults. In young subjects, infective processes result chiefly from extension of disease from the upper epiphysial junction of the humerus, which is partly included within the limits of the synovial cavity. The synovial membrane, in addition to lining the capsular ligament, is prolonged down the inter-tubercular (bicipital) groove around the long tendon of the biceps, and pus may escape from the joint by this diverticulum and gravitate down the arm; we have also observed loose bodies of synovial origin in this diverticulum. There is frequently a communication between the joint and the sub-deltoid bursa. There is no attitude characteristic of disease of the shoulder-joint, but the girdle is usually elevated, the upper arm held close to the side and rotated medially, while the elbow is carried a little backwards. In the later stages, the head of the humerus may be drawn upwards and medially towards the coracoid process. Fixation of the shoulder-joint is largely compensated for by movement of the scapula on the thorax, so that when testing for rigidity the scapula should be fixed with one hand while passive movements of the arm are carried out with the other. The deltoid is usually atrophied, allowing the acromion, coracoid, and great tuberosity of the humerus to stand out prominently beneath the skin. Swelling is rarely a prominent feature, except when there is a collection of synovial fluid or of pus in the bursa beneath the deltoid.
Tuberculous Disease is usually met with in young adults, and is more common in the right shoulder. The prominent features are pain, rigidity, and wasting of the deltoid and scapular muscles. The pain is sometimes severe, shooting down the arm and interfering with sleep, and it may be associated with tenderness on pressure over the upper end of the humerus. In cases with carious destruction of the articular surfaces there are starting pains, and the arm is shortened. If a cold abscess forms in the bursa underneath the deltoid, the pus may burrow and appear at the anterior or posterior boundary of the axilla or in the axillary space. Pus formed in the joint tends to gravitate along the inter-tubercular groove. The axillary glands may be infected.
The primary lesion is either a caseating focus in one of the bones—most often in the upper end of the humerus—or it is of the nature of caries sicca. The greater part of the head may disappear, and the upper end of the shaft be drawn against the socket. In exceptional cases, portions of the glenoid or humerus are found separated as sequestra, or the disease involves parts outside the joint, such as the acromion or coracoid process. Hydrops with melon-seed bodies is rare. In young subjects, destruction of the tissues at the ossifying junction may result in considerable shortening of the arm.
The diagnosis is to be made from (1) arthritis deformans, in which the movements are less restricted, and are attended with grating and cracking; (2) paralysis involving the deltoid and scapular muscles—by the absence of pain, and the flail-like character of the movements; (3) disease in the sub-deltoid bursa—by the absence of rigidity and other evidence of implication of the articular surfaces; and (4) sarcoma of the upper end of the humerus—by the history of the case, the use of the X-rays or an exploratory incision. Injuries in the region of the upper epiphysis resulting in loss of movement, may, in the absence of a reliable history, be mistaken for tuberculous disease.
While the prognosis is favourable on the whole, recovery is usually attended with fibrous ankylosis and incapacity to raise the arm above the level of the shoulder. The disease often progresses slowly, and may last for years.
Treatment.—The limb should be immobilised in the position of abduction with the forearm and hand directed forwards; the most efficient apparatus is a plaster spica embracing the thorax and the upper limb down as far as the wrist. If the articular surfaces are affected and the disease is likely to lead to ankylosis, the arm should be abducted to a right angle. The severe pain of caries sicca may be relieved by blistering or by the application of the cautery. To inject iodoform, the needle is introduced either immediately outside the coracoid process, or just below the junction of the acromion process and spine of the scapula. When the disease does not yield to conservative measures, or the X-rays show a gross lesion in the bone, excision of the joint should be performed; a close fibrous ankylosis usually results, and the arm is quite a useful one provided the abducted position has been maintained throughout.
Pyogenic Diseases.—The shoulder-joint may be infected by extension of suppurative osteomyelitis from the upper end of the humerus, or from suppuration in the axilla, or through the blood stream by ordinary pus organisms, pneumococci, typhoid bacilli, or gonococci. Extension should be applied to the arm abducted at a right angle. When it is necessary to open the joint, the incision should be placed anteriorly in the line of the inter-tubercular groove; if a counter-opening is required it is made on the posterior aspect by cutting on the point of a dressing forceps introduced through the anterior incision.
Arthritis Deformans.—The shoulder is seldom affected alone, except when the arthritis is a sequel to injury, such as a fracture of the neck of the humerus. The common type of lesion is a dry arthritis with fibrillation and eburnation of the articular surfaces. The long tendon of the biceps is usually destroyed, the head of the bone is drawn upwards, and, after wearing through the capsule, rubs on the under surface of the acromion, which also becomes eburnated. The clinical features are pain, stiffness, and cracking on movement, and as these symptoms may also be caused by loose bodies in the joint, an X-ray picture should be taken to differentiate between them.
Neuro-arthropathies of the shoulder are met with chiefly in syringomyelia. In some cases there is a large fluctuating and painless swelling; in others marked and rapid wasting of the deltoid and scapular muscles with flail-like movements of the joint associated with disappearance of the upper end of the humerus (Fig. 104).
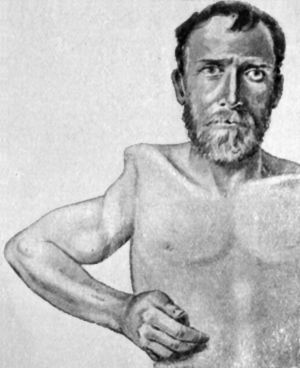 Fig. 103.—Arthropathy of Shoulder in Syringomyelia.
The upper end of the humerus has disappeared and the movements are
flail-like (cf. Fig. 104).
Fig. 103.—Arthropathy of Shoulder in Syringomyelia.
The upper end of the humerus has disappeared and the movements are
flail-like (cf. Fig. 104).
 Fig. 104.—Radiogram of specimen of Arthropathy of
Shoulder in Syringomyelia. The head of the humerus has disappeared and
masses of new bone have formed in the surrounding muscles (cf. Fig. 103).
Fig. 104.—Radiogram of specimen of Arthropathy of
Shoulder in Syringomyelia. The head of the humerus has disappeared and
masses of new bone have formed in the surrounding muscles (cf. Fig. 103).
Loose bodies are rare in the shoulder; we have met with a case in which the joint-cavity was distended with loose bodies of synovial origin, and as most of these had undergone ossification, the X-ray appearances were highly characteristic. They were removed through an anterior incision.
Ankylosis is not so disabling at the shoulder as at other joints, as the mobility of the scapula on the chest wall largely compensates for the fixation of the joint.
In disease of the elbow, the usual attitude is that of flexion with pronation of the hand. Swelling of the joint, whether from effusion of fluid or from thickening of the synovial membrane, is observed chiefly on the posterior aspect, above and on either side of the olecranon, because the synovial sac is here nearest the surface. The free communication between the elbow and the superior radio-ulnar joint should be borne in mind.
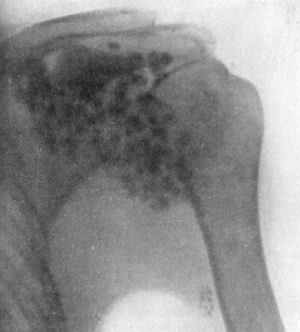 Fig. 105.—Radiogram showing Multiple partially
ossified Cartilaginous Loose Bodies in Shoulder-joint. The lowest one
is in the synovial prolongation along the tendon of the biceps.
Fig. 105.—Radiogram showing Multiple partially
ossified Cartilaginous Loose Bodies in Shoulder-joint. The lowest one
is in the synovial prolongation along the tendon of the biceps.
Tuberculous disease is the most common and important affection (Fig. 106). It usually occurs in patients under twenty, but may be met with at any age; in children the age-incidence is earlier than in the other large joints, a considerable proportion being met with in the first two years of life (Stiles). When the disease is confined to the synovial membrane, its onset is insidious, there is little or no pain, and no interference with any movement except complete extension. The chief evidence of disease is a white swelling on either side of and above the olecranon, obscuring the bony landmarks. The further progress is attended with wasting of the triceps, symptoms of involvement of the articular surfaces, and with abscess formation.
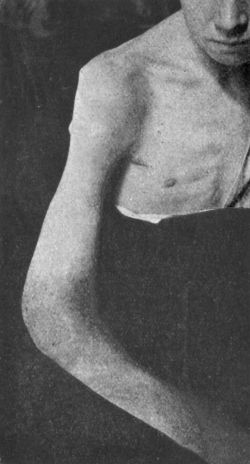 Fig. 106.—Diffuse Tuberculous Thickening of Synovial
Membrane of Elbow (white swelling) in a boy æt. 12.
Fig. 106.—Diffuse Tuberculous Thickening of Synovial
Membrane of Elbow (white swelling) in a boy æt. 12.
The occurrence of articular caries without swelling of the synovial membrane is exceptional, and is associated with a good deal of pain and considerable restriction of movement. Rigidity from muscular contraction occurs late, and is rarely complete. Tuberculous foci in the bones are met with chiefly in the lower end of the diaphysis of the humerus; in children, the epiphyses are so small that the ossifying junction is intra-articular. Foci are also met with in the upper end of the ulna. The grosser osseous lesions cause enlargement of the bone, and are readily demonstrated by skiagraphy. Abscess formation most commonly occurs beneath the triceps, and the abscess points at one or other edge of that muscle. A subcutaneous abscess may form over the upper end of the ulna or over the radio-humeral joint. Tuberculous hydrops with melon-seed bodies is rare.
 Fig. 107.—Contracture of Elbow and Wrist following a
burn in childhood. Treated by resection of both joints, and the
insertion, on the palmar aspect of each, of a flap from the abdominal
wall.
Fig. 107.—Contracture of Elbow and Wrist following a
burn in childhood. Treated by resection of both joints, and the
insertion, on the palmar aspect of each, of a flap from the abdominal
wall.
Treatment.—Conservative measures are persevered with so long as there is a prospect of securing a movable joint. The limb is placed in a light form of splint reaching from the axilla to the wrist, flexed to rather less than a right angle and with the hand semi-pronated and dorsiflexed. To inject iodoform or other anti-tuberculous agent, the needle of the syringe is easily introduced between the lateral condyle and the head of the radius. A localised focus of disease in one or other of the bones may be eradicated without opening into the synovial cavity.
If the articular surfaces are so involved that recovery is likely to be attended with ankylosis, the disease should be removed by operation, and cure with a useful and movable joint may then be reasonably anticipated within two or three months. When the patient's occupation is such that a strong stiff joint is preferable to a weaker movable one, bony ankylosis at rather less than a right angle should be aimed at.
Arthritis deformans occurs as a hydrops with hypertrophy of the synovial fringes and loose bodies, or as a dry arthritis with eburnation and lipping of the articular margins.
Neuro-arthropathies are met with chiefly in syringomyelia, and are attended with striking alterations in the shape of the bones and with abnormal mobility.
Pyogenic diseases result from staphylococcal osteomyelitis—chiefly of the humerus or ulna—and from gonorrhœa.
The remaining diseases at the elbow include syphilitic disease in young children, bleeder's joint, hysterical affections, and loose bodies, and do not call for special description.
Ankylosis of the elbow-joint, if interfering with the livelihood of the patient, may be got rid of by resecting the articular ends of the bones, or by inserting between them a flap of fascia and subcutaneous fat derived from the posterior aspect of the upper arm—arthroplasty.
The close proximity of the flexor sheaths to the carpal articulations permits of infective processes spreading readily from one to the other. The arrangement of the synovial membranes also favours the extension of disease throughout the numerous articulations in the region of the wrist.
Tuberculous disease is met with chiefly in young adults, but may occur at any age. It usually originates in the synovial membrane, but foci are frequently present in the carpal bones, and less commonly in the lower ends of the radius and ulna, or in the bases of the metacarpals. The clinical features are almost invariably those of white swelling, which is most marked on the dorsum where it obscures the bony prominences and the outlines of the extensor tendons. Wasting of the thenar and hypothenar eminences, and filling up of the hollows above and below the anterior annular ligament, render the appearance on the palmar aspect characteristic.
The attitude is one of slight flexion with drooping of the hand and fingers. The fingers become stiff as a result of adhesions in the tendon sheaths, and the power of opposing the thumb and fingers may be lost. Pain is usually absent until the articular surfaces become carious. Softening of the ligaments may permit of lateral mobility, and sometimes partial dislocation occurs. Abscess may be followed by sinuses and infection of the tendon sheaths, especially those in the palm.
The localisation of disease in individual bones or joints can be determined by the use of the X-rays.
Treatment.—Conservative measures may be persevered with over a longer period than in most other joints. The forearm, wrist, and metacarpus are immobilised in the attitude of dorsal flexion, while the fingers and thumb are left free to allow of passive movements. It may be necessary to give an anæsthetic to obtain the necessary degree of dorsiflexion. To inject iodoform, the needle is inserted immediately below the radial or the ulnar styloid process. Sometimes the carpal bones are so soft that the needle can be made to penetrate them in different directions. Operative treatment is indicated in cases which resist conservative measures, or when the general health calls for speedy removal of the disease.
Other diseases of the wrist are comparatively rare. They include pyogenic affections, such as those resulting from infective conditions in the palm of the hand, different types of gonorrhœal, rheumatic, and gouty affections, and arthritis deformans. An interesting feature, sometimes met with in arthritis deformans, consists in eburnation of the articular surfaces of the carpal bones, although the range of movement is almost nil.
Owing to the depth of this joint from the surface, it is not possible to detect the presence of effusion or of synovial thickening as readily as in other joints, hence in the recognition of hip disease we have to rely largely upon indirect evidence, such as a limp in walking, an alteration in the attitude of the limb, or restriction of its movements.
The whole of the anterior and fully one-half of the posterior aspect of the neck of the femur is covered by synovial membrane, so that lesions not only of the epiphysis and epiphysial junction, but also of the neck of the bone, are capable of spreading directly to the synovial membrane and to the cavity of the joint. Conversely, disease in the synovial membrane may spread to the bone in relation to it. Infective material may escape from the joint into the surrounding tissues through any weak point in the capsule, particularly through the bursa which intervenes between the capsule and the ilio-psoas, and which in one out of every ten subjects communicates with the joint.
Tuberculous disease of the hip, morbus coxæ, or “hip-joint disease,” is especially common in the poorer classes. It is a frequent cause of prolonged invalidism, and of permanent deformity, and is attended with a considerable mortality. It is essentially a disease of early life, rarely commencing after puberty, and almost never after maturity.
Pathological Anatomy.—Bone lesions bulk more largely in hip disease than they do in disease of other joints—five cases originating in bone to one in synovial membrane being the usual estimate. The upper end of the femur and the acetabulum are affected with about equal frequency.
In addition to primary tuberculous lesions, secondary changes result from the inflamed and softened bones pressing against one another subsequent to the destruction of their articular cartilages. The head of the femur undergoes absorption from above downwards, becoming flattened and truncated, or disappearing altogether. In the acetabulum the absorption takes place in an upward and backward direction, whereby the socket becomes enlarged and elongated towards the dorsum ilii. To this progressive enlargement of the socket Volkmann gave the suggestive name of “wandering acetabulum” (Fig. 108). The displacement of the femur resulting from these secondary changes is one of the causes of real shortening of the limb.
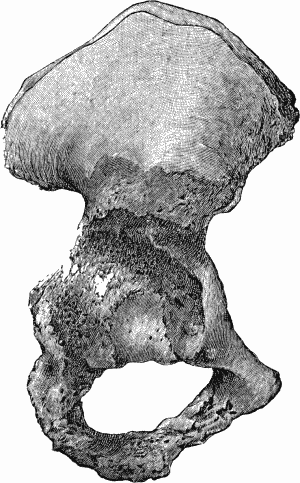 Fig. 108.—Advanced Tuberculous Disease of Acetabulum
with caries and perforation into pelvis.
Fig. 108.—Advanced Tuberculous Disease of Acetabulum
with caries and perforation into pelvis.Clinical Features.—It is customary to describe three stages in the progress of hip disease, but this is arbitrary and only adopted for convenience of description.
Initial Stage.—At this stage the disease is confined to a focus in the bone which has not yet opened into the joint or to the synovial membrane. The onset is insidious, and if injury is alleged as an exciting cause, some weeks have usually elapsed between the receipt of the injury and the onset of symptoms. The child is brought for advice because he has begun to limp and to complain of pain. There is a history that he has become pale and has ceased to take food well, that his sleep has been disturbed, and that the pain and the limp, after coming and going for a time, have become more pronounced. On walking, the affected limb is dragged in such a way as to avoid movement at the hip, and to substitute for it movement at the lumbo-sacral junction. The child throws the weight of the trunk as little as possible on to the affected limb, and inclines to rest on the balls of the toes rather than on the sole. There is usually some wasting of the muscles of the thigh and flattening of the buttock. Diminution or loss of the gluteal fold indicates flexion at the hip which might otherwise escape notice. Pain is complained of in the hip, or is referred to the medial side of the knee, in the distribution of the obturator nerve. Sometimes the pain is confined to the knee, and if the examination is restricted to that joint the disease at the hip may be overlooked. At this stage the attitude of the limb is not constant; at one time it may be natural, and at another slightly flexed and abducted. Tenderness of the joint may be elicited by pressing either in front or behind the head of the bone, but is of little diagnostic importance. Pain elicited on driving the head against the acetabulum may occasionally assist in the recognition of hip disease, but the diagnostic value of this sign has been overrated and, in our opinion, this test should be omitted.
Most information is gained by testing the functions of the joint, and if this is done gently and without jerking, it does not cause pain. The child should lie on his back, either on his nurse's knee or on a table; and to reassure him the movements should be first practised on the sound limb. On slowly flexing the thigh of the affected limb, it will be found that the range of flexion at the hip is soon exhausted, and that any further movement in this direction takes place at the lumbo-sacral junction. The child is next made to lie on his face with the knees flexed in order that the movements of rotation may be tested. The thigh is rotated in both directions, and on comparing the two sides it will be found that rotation is restricted or abolished on the side affected, any apparent rotation taking place at the lumbo-sacral junction. These tests reveal the presence of rigidity resulting from the involuntary contraction of muscles, which is the most reliable sign of hip disease during the initial stage, and they possess the advantage of being universally applicable, even in the case of young children.
Second Stage.—This probably corresponds with commencing disease of the articular surfaces, and progressive involvement of all the structures of the joint. The child complains more, and usually exhibits the attitude of abduction, eversion, and flexion (Fig. 109).
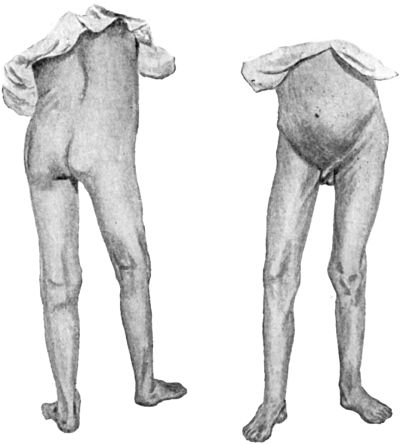 Fig. 109.—Early Tuberculous Disease of Right Hip-joint
in a boy æt. 14, showing flexion, abduction, and apparent lengthening
of the limb.
Fig. 109.—Early Tuberculous Disease of Right Hip-joint
in a boy æt. 14, showing flexion, abduction, and apparent lengthening
of the limb.
At first the attitude is maintained entirely by the action of muscles; but when it is prolonged, the muscles, fasciæ, and ligaments undergo shortening, so that it becomes fixed.
On looking at the patient, the abnormal attitude may not be at once evident, as he usually restores the parallelism of the limbs by lowering the pelvis on the affected side and adducting the sound limb. This obliquity or tilting of the pelvis causes apparent lengthening of the diseased limb, and is best demonstrated by drawing one straight line between the anterior iliac spines, and another to meet it from the xiphoid cartilage through the umbilicus; if the pelvis is in its normal position, the two lines intersect at right angles; if it is tilted, the angles at the point of intersection are unequal. The flexion may be largely compensated for by increasing the forward curve of the lumbar spine (lordosis), and by flexing the leg at the knee. There may also be an attempt to compensate for the eversion of the limb by rotating the pelvis forwards on the affected side.
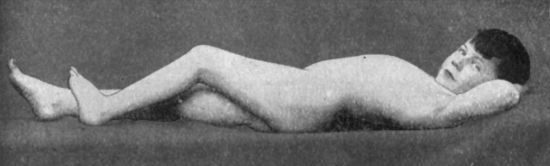 Fig. 110.—Disease of Left Hip: position of ease
assumed by patient, showing moderate flexion and lordosis.
Fig. 110.—Disease of Left Hip: position of ease
assumed by patient, showing moderate flexion and lordosis.
To demonstrate the lordosis, the patient should be laid on a flat table; in the resting position the lordosis is moderate, when the hip is flexed it disappears, when it is extended the lordosis is exaggerated, and the hand or closed fist may be inserted between the spine and the table (Fig. 112).
When the functions of the joint are tested, it will be found that there is rigidity, and that both active and passive movements take place at the lumbo-sacral junction instead of at the hip. While rigidity is usually absolute as regards rotation, it may sometimes be possible with care and gentleness to obtain some increase of flexion. For diagnostic purposes most stress should therefore be laid on the presence or absence of rotation.
If the sound limb is flexed at the hip and knee until the lumbar spine is in contact with the table, the real flexion of the diseased hip becomes manifest, and may be roughly measured by observing the angle between the thigh and the table (Fig. 113). This is known as “Thomas' flexion test,” and is founded upon the inability to extend the diseased hip without producing lordosis.
Swelling is seen on the anterior aspect of the joint; it may fill up the fold of the groin and push forward the femoral vessels. It is doughy and elastic, but may at any time liquefy and form a cold abscess. Swelling about the trochanter and neck of the bone may be estimated by measuring the antero-posterior diameter with callipers, and comparing with the sound side. Swelling on the pelvic aspect of the acetabulum can sometimes be discovered on rectal examination.
Third Stage.—This probably corresponds with caries of the articular surfaces, since pain is now a prominent feature, and there are usually startings at night. The attitude is one of adduction, inversion, flexion, and apparent or real shortening of the limb (Fig. 114). The flexion is usually so pronounced that it can no longer be concealed by lordosis, so that when the patient is recumbent, although the spine is arched forwards, the limb is still flexed both at the hip and at the knee; with the spine flat on the table, the flexion of the thigh may amount to as much as a right angle. The adduction varies greatly in degree; when it is slight, as is most often the case, the toes of the affected limb rest on the dorsum of the sound foot. When moderate, it is compensated for by raising the pelvis on the affected side, with apparent shortening of the limb, this being the result of an effort on the part of the patient to restore the normal parallelism of the limbs, the sound limb being abducted to the same extent as the affected limb is adducted. It is important to recognise the cause of this shortening, as it can be corrected by treatment. As a result of the obliquity of the pelvis, the patient, when erect, exhibits a lateral curvature of the spine with the dorso-lumbar convexity to the sound side.
 Fig. 115.—Advanced Tuberculous Disease of Left
Hip-joint in a girl æt. 14, showing flexion, adduction, shortening,
and iliac abscess.
Fig. 115.—Advanced Tuberculous Disease of Left
Hip-joint in a girl æt. 14, showing flexion, adduction, shortening,
and iliac abscess.
When adduction is pronounced, the patient is unable to restore the normal parallelism of the limbs, and the knee on the affected side may cross the sound limb. There is a deep groove at the junction of the perineum and thigh, great prominence of the trochanter, and the pelvis may be tilted to such an extent that the iliac crest comes into contact with the lower ribs.
As a result of the pressure of the carious articular surfaces against one another, the acetabulum is enlarged and the upper end of the femur is drawn gradually upwards and backwards within the socket. Examination will then reveal the existence of a variable amount of actual shortening; it will also be found that the trochanter is displaced above Nélaton's line, while above and behind the trochanter there is a prominent hard swelling corresponding to the enlarged acetabulum.
There may, therefore, be a combination of real and apparent shortening together amounting to several inches (Fig. 115).
In cases of long standing, beginning in childhood, the shortening is still further added to by deficient growth in length of the femur, and it may be of all the bones of the limb; even the foot is smaller on the affected side.
The most reasonable explanation of the attitudes assumed in hip disease is that given by König. If the patient walks without crutches, as he is usually able to do at an early stage of the disease, the attitude of abduction, eversion, and slight flexion enables him to save the limb to the utmost extent; on the other hand, if he uses a crutch, as he is obliged to do at a more advanced stage, he no longer uses the limb for support, and therefore draws it upwards and medially into the position of adduction, inversion, and greater flexion. Similarly, if he is confined to bed, he lies on the sound side, and the affected limb sinks by gravity so as to lie over the normal one in the position of adduction, inversion, and flexion. König's explanation accords with the fact that in the exceptional cases which begin with adduction and inversion we have usually to deal with a severe type of the disease, associated with grave osseous lesions—precisely those cases in which the patient is compelled from the outset to lie up or to adopt the use of crutches. Further, the transition from the abducted to the adducted position usually follows upon such an aggravation of the symptoms that the patient is no longer able to walk without the assistance of a crutch.
During the third stage the other signs and symptoms become more pronounced; the patient looks ill and thin, he is usually unable to leave his bed, his sleep is disturbed by startings of the limb, and the rigidity of the joint and the wasting of the muscles are well marked. The temperature may rise slightly after examination of the limb, or after a railway journey.
Abscess Formation in Hip Disease.—The formation of abscess is not related to any stage of the disease; it may occur before there is deformity, and it may be deferred until the disease is apparently cured. Its importance lies in the fact that if a mixed infection with pyogenic organisms occurs, the gravity of the condition is greatly increased.
An abscess may appear in the thigh in front or behind the joint. The anterior abscess emerges on one or other side of the psoas muscle; from the resistance offered by the fascia lata, the pus may gravitate down the thigh before perforating the fascia. It has occasionally happened that when such an abscess has been opened and become infected with pyogenic organisms, the femoral vessels have been eroded, and serious or even fatal hæmorrhage has resulted. The posterior abscess appears in the buttock and may make its way to the surface through the gluteus maximus; more often it points at the lower border of this muscle in the region of the great trochanter, or it may gravitate down the thigh.
Abscesses which form within the pelvis originate either in connection with the acetabulum or in relation to the psoas muscle where it passes in front of the joint. Those that are directly connected with disease of the acetabulum may remain localised to the lateral wall of the pelvis, or may spread backwards towards the hollow of the sacrum. They may open into the bladder or rectum, or may ascend into the iliac fossa and point above Poupart's ligament (Fig. 115), or descend towards the ischio-rectal fossa. The abscess which develops in relation to the psoas muscle may be shaped like an hour-glass, one sac occupying the iliac fossa, the other filling up Scarpa's triangle, the two sacs communicating with each other through a narrow neck beneath Poupart's ligament.
So long as the skin is intact, the abscess is unattended with symptoms, and may escape notice. If it bursts externally, pyogenic infection is almost inevitable, and the patient gradually passes into the condition of hectic fever or chronic toxæmia; he loses ground from day to day, may become the subject of waxy disease in the viscera, or may die of exhaustion, tuberculous meningitis, or general tuberculosis.
Dislocation is a rare complication of hip disease, and is most likely to occur during the stage of adduction with inversion. It has been known to take place during sleep, apparently from spasmodic contraction of muscles. In the dorsal dislocation, which is the most common form, adduction and inversion are exaggerated, the trochanter projects above and behind Nélaton's line, and the head of the bone may be felt on the dorsum ilii. It is a striking fact that after dislocation has occurred there is less complaint of pain or of startings than before, and passive movements may be carried out which were previously impossible.
Diagnosis of Hip Disease.—The diagnosis is to be made not only from other affections of the joint, but also from morbid conditions in the vicinity of the hip, as in any of these the patient may seek advice on account of pain and a limp in walking. The patient should be stripped, and if able to walk, his gait should be observed. He is then examined lying on his back, and attention is directed to the comparative length of the limbs, to the attitude of the limbs and pelvis, and to the movements at the hip-joint, especially those of rotation. When there is any doubt as to the diagnosis, the examination should be repeated at intervals of a few days. In children, there are three non-febrile conditions attended with a limp and with shortening of the limb, which may be mistaken for hip disease,—congenital dislocation, coxa vara, and paralysis following poliomyelitis—but in all of these the movements are not nearly so restricted as they are in disease of the joint.
In tuberculous disease of the sacro-iliac joint, while the pelvis may be tilted, and the limb apparently lengthened, the movements at the hip are retained. In tuberculous disease of the great trochanter, or of either of the bursæ over it, while there may be abduction, eversion, impairment of mobility, and swelling in the region of the trochanter followed by abscess formation, the movements are less restricted than in disease of the joint.
In psoas abscess associated with spinal disease, or in disease of the bursa underneath the psoas, the limb is flexed and everted, there may be lordosis, and the patient may limp in walking, but the movements at the hip are restricted only in the directions of extension and inversion, while in hip disease they are restricted in all directions.
New-growths in the vicinity of the hip—especially central sarcoma of the upper end of the femur—are difficult to differentiate from hip disease without the help of the X-rays.
Among other conditions which by interfering with the free mobility of the hip may simulate hip disease, are appendicitis, inflammation of the glands in the groin, staphylococcal disease of the upper end of the femur, and sciatica.
The diagnosis from other diseases of the hip-joint is made by careful consideration of the history, symptoms, and X-ray appearances.
Prognosis.—The prognosis in hip disease is more serious than in tuberculosis of other joints, excepting only those of the spine, and it is most unfavourable when there are gross lesions of the bones and infected sinuses.
Whatever the stage of the disease, recovery is a slow process, and even in early and mild cases it seldom takes place in less than one or two years, and is liable to be attended with some impairment of function. During the process of cure, complications are liable to occur, and after apparent recovery relapses are not uncommon. When arrested during the initial stage, recovery may be complete; but when there has been destruction of the articular surfaces, there is apt to be ankylosis of the joint and shortening of the limb.
In cases which terminate fatally, death usually results from meningeal, pulmonary, or general tuberculosis, or from pyogenic complications and waxy degeneration.
Treatment.—A large proportion of cases recover under conservative treatment, and the functional results are so much better than those following operative interference that unless there are special indications to the contrary, conservative measures should always be adopted in the first instance.
Conservative Treatment.—The first essential is to take the weight off the limb and secure its fixation in the attitude of almost complete extension and moderate abduction. When the symptoms are well marked, the child is kept in bed and the limb is extended with a weight and pulley.
Extension by Weight and Pulley (Fig. 116).—The weight employed varies from one to four pounds in children, to ten or more pounds in adolescents and adults, and must be adjusted to meet the requirements of each case. If pain returns after having been relieved, it is due to stretching of the ligaments, and the weight should be diminished or removed for a time. If there is deformity, the line of traction should be in the axis of the displaced limb until the deformity is got rid of. The extension should be continued until pain, tenderness, and muscular contraction have disappeared, and the limb has been brought into the desired attitude.
In restless children, in addition to the extension, a long splint is applied on the sound side and a sand-bag on the affected one; or, better still, a double long splint and cross-bar, the long splint on the affected side being furnished with a hinge opposite the hip to permit of varying the degree of abduction (Fig. 117).
When the deformed attitude does not yield rapidly to extension, it should be corrected under an anæsthetic, and if the adductor tendons and fasciæ are so contracted that this is difficult, they should be forcibly stretched or divided.
The immediate correction of deformed attitudes under anæsthesia has largely replaced the more gradual method by extension with weight and pulley; and in hospital practice it is usually followed by the application of a plaster case. The plaster bandages are applied over a pair of knitted drawers; the pelvis and both thighs, the diseased one in the abducted position, are included. The case may be strengthened by strips of aluminium, and should be renewed every six weeks or two months.
Ambulant Treatment.—When the patient is able to use crutches, the affected limb is prevented from touching the ground by fixing a patten on the sole of the boot on the sound side. This may suffice, or, in addition, the hip-joint is kept rigid by a Thomas' (Fig. 118) or a Taylor's splint. The Thomas' splint must be fitted to the patient under the supervision of the surgeon, who must make himself familiar with the construction of the splint, and its alteration by means of wrenches.
 Fig. 118.—Thomas' Hip Splint applied for disease of
Right Hip. Note patten under sound foot. The foot on the affected side
is too near the ground.
Fig. 118.—Thomas' Hip Splint applied for disease of
Right Hip. Note patten under sound foot. The foot on the affected side
is too near the ground.
In children who are unable to use crutches, a double Thomas' splint is employed; the child thereby is converted into a rigid object, capable of being carried from one room to another and into the open air. Personally we have obtained satisfaction from the double Thomas' splint employed for spinal disease, which extends from the occiput to the soles of the feet.
The fixation of the hip-joint and the taking of the weight off the limb by one or other of the above methods, should, as a general rule, be continued for at least a year.
Should an abscess develop, it is treated on the usual lines.
Operative Interference.—Widely diverse opinions are held on the question as to whether or not recourse should be had to operative interference.
Some surgeons are opposed to operative interference, on the grounds that however advanced the disease may be it will yield to conservative measures if judiciously and perseveringly carried out. Other surgeons advocate operative treatment in all cases which do not speedily show improvement under conservative treatment. An intermediate attitude may be adopted which recommends operation in cases in which the disease progresses in spite of conservative treatment, and in which periodic examination with the X-rays shows that there are progressive lesions in the upper end of the femur or in the acetabulum.
It is claimed by those who advocate operation under these conditions that pain and suffering are at once got rid of, sleep is restored, appetite returns, and there is a marked improvement in the general health, and that this result is obtained in months instead of years, and that the cure is more likely to be permanent. It is certainly unwise to delay operation until sinuses have formed, as such a course is largely responsible for the bad results which formerly followed excision of the joint.
Amputation for tuberculous disease of the hip has become one of the rarest of operations, but is still required in cases which have continued to progress after excision, and when there is disease of the pelvis or of the shaft of the femur, with sinuses, albuminuria, and hectic fever.
The Correction of Deformity resulting from Antecedent Disease of the Hip.—From neglect or from improper treatment, deformity may have been allowed to persist, while the disease has undergone cure. It is associated with ankylosis of the joint, or contracture of the soft parts or both. The contracture of the soft parts involves specially the tendons, fasciæ, and ligaments on the anterior and medial aspects of the joint, and is usually present to such a degree that, even if the joint were rendered mobile, these shortened structures would prevent correction of the deformity. The usual deformity is a combination of shortening, flexion, and adduction.
Bilateral Hip Disease.—Both hip-joints may become affected with tuberculous disease, either simultaneously or successively, and abscesses may form on both sides. The patient is necessarily confined to bed, and if the disease is recovered from, his capacity for walking may be seriously impaired, especially if the joints become fixed in an undesirable attitude. The most striking deformity occurs when both limbs are adducted so that they cross each other—one variety of the “scissor-leg” or “crossed-leg” deformity—in which the patient, if able to walk at all, does so by forward movements from the knees. An attempt should be made by arthroplasty to secure a movable joint at least on one side.
Pyogenic Diseases are met with in childhood and youth as a result of infection with the common pyogenic organisms, gonococci, pneumococci, or typhoid bacilli. While the organisms usually gain access to the tissues of the joint through the blood stream, a direct infection is occasionally observed from suppuration in the femoral lymph glands or in the bursa under the ilio-psoas.
The clinical features are sometimes remarkably latent and are much less striking than might be expected, especially when the hip affection occurs as a complication of an acute illness such as scarlet fever. It may even be entirely overlooked during the active stage, and only noticed when the head of the femur is found dislocated, or the joint ankylosed. In the acute arthritis of infants also, the clinical features may be comparatively mild, but as a rule they assume a type in which the suppurative element predominates. The limb usually becomes flexed and adducted, and a swelling forms in front of the joint at the upper part of Scarpa's triangle; the upper femoral epiphysis may be separated and furnish a sequestrum.
The flexion and adduction of the limb favour the occurrence of dislocation. A child who has recovered with dislocation on to the dorsum ilii is usually able to walk and run about, but with a limp or waddle which becomes more pronounced as he grows up. The condition closely resembles a congenital dislocation, but the history, and the presence of gross alterations in the upper end of the femur as seen with the X-rays, should usually suffice to differentiate them.
Treatment.—In the acute stage the limb is extended by means of the weight and pulley, and kept at rest with the single or double long splint, or by sand-bags. If there is suppuration, the joint should be aspirated or opened by an anterior incision, and Murphy's plan of filling the joint with formalin-glycerine may be adopted. In children, it is remarkable how completely the joint may recover.
If there is dislocation, the head of the femur should be reduced by manipulation with or without preliminary extension; it has been successful in about one-half of the cases in which it has been attempted. Preliminary tenotomy of the shortened tendons is required in some cases. When reduction by manipulation is impossible, the joint structures should be exposed by operation and the head of the bone replaced in the acetabulum. When the upper end of the femur has disappeared, the neck should be implanted in the acetabulum, and the limb placed in the abducted position.
Arthritis Deformans.—This disease is comparatively common at the hip, either as a mon-articular affection or simultaneously with other joints.
 Fig. 119.—Arthritis Deformans, showing erosion of
cartilage and lipping of articular edge of head of femur.
Fig. 119.—Arthritis Deformans, showing erosion of
cartilage and lipping of articular edge of head of femur.
The changes in the joint are characteristic of the dry form of the disease, and affect chiefly the cartilage and bone. The atrophy and wearing away of the articular surfaces are accompanied by new formation of cartilage and bone around their margins. The head of the femur may acquire the shape of a helmet, a mushroom, or a limpet shell, and from absorption of the neck the head may come to be sessile at the base of the neck, and to occupy a level considerably below that of the great trochanter (Fig. 120). These changes sometimes extend to the upper part of the shaft, and result in curving of the shaft and neck, suggesting a resemblance to a point of interrogation (Fig. 121). The acetabulum may “wander” backwards and upwards, as in tuberculous disease. It is usually deepened, and its floor projects on the pelvic aspect; its margins may form a projecting collar which overhangs the neck of the femur, or grasps it, so that even in the macerated condition the head is imprisoned in the socket and the joint locked. There is eburnation of the articular surfaces in those areas most exposed to friction and pressure.
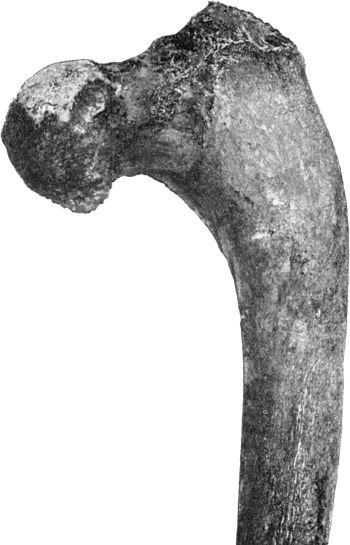 Fig. 120.—Upper End of Femur in advanced Arthritis
Deformans of Hip. The shaft is curved and the head of the bone is at a
lower level than the great trochanter.
Fig. 120.—Upper End of Femur in advanced Arthritis
Deformans of Hip. The shaft is curved and the head of the bone is at a
lower level than the great trochanter.
 Fig. 121.—Femur in advanced Arthritis Deformans of Hip
and Knee Joints. The upper end of the bone shows the condition of coxa
vara; the lower end shows enlargement of the medial condyle and
alteration in the axis of the articular surface.
Fig. 121.—Femur in advanced Arthritis Deformans of Hip
and Knee Joints. The upper end of the bone shows the condition of coxa
vara; the lower end shows enlargement of the medial condyle and
alteration in the axis of the articular surface.
These changes are necessarily associated with restriction of movement, and in advanced cases with striking deformity, which consists in shortening of the limb, usually with eversion and displacement of the trochanter upwards and backwards in relation to Nélaton's line.
The clinical features are usually so characteristic that there is little difficulty in diagnosis. Restriction of the movements of abduction and adduction, the presence of cracking and of grating of the articular surfaces, and the aggravation of the pain and stiffness after resting the limb, are characteristic of arthritis deformans. The prominence of sciatic pain may lead to the disease being regarded as sciatica.
The greatest difficulty is met with in cases in which the disease occurs as mon-articular affection in adolescents, for the resemblance to tuberculous disease of the hip and to coxa vara may be close. Skiagrams do not always enable one to differentiate between them.
Treatment is conducted on the same lines as in other joints. The normal movements are maintained by suitable exercises, and an effort is made to diminish the pressure on the articular surfaces in walking by the use of sticks or crutches.
Shortening of the limb may be compensated by raising the sole of the boot. When the X-rays show that the disability is mainly due to new bone locking the head of the femur, such new bone may be removed by operation, cheilotomy (Sampson Handley). Excision of the joint has in some cases yielded satisfactory results; it is indicated in young patients who are otherwise healthy, and who are unable to walk on account of pain and deformity.
Osteo-chondritis Deformans Juvenilis.—Under this term Perthes describes an affection of the hip in children which differs in many respects from the juvenile form of arthritis deformans. Islands of cartilage appear in the epiphysis of the head of the femur, and the epiphysis itself becomes flattened without involvement of the articular surface or of the acetabulum.
The disease is met with in children between five and ten; there is a limp in walking without pain or sensitiveness, so that the child continues to take part in games. Abduction is markedly restricted and the trochanter is elevated and prominent. There is no crepitation on movement or other signs of involvement of the articular surfaces. The X-rays show the deformity of the head and clear areas in the interior of the upper epiphysis corresponding to the islands of cartilage; these clear areas resemble those due to caseous foci in tuberculous coxitis.
The disease runs a chronic course, and in the course of a year or two the limp and the restriction of abduction disappear, so that no active treatment is called for.
Neuro-Arthropathies.—Charcot's disease is usually met with in men over thirty who suffer from tabes dorsalis. One or both hip-joints may be affected. Sometimes the first manifestation is a hydrops and a fluctuating swelling in the upper part of Scarpa's triangle. In many of the recorded cases, however, attention has first been directed to the disease by the deformity and limp associated with disappearance of the head of the femur, or by the occurrence of pathological dislocation. The absence of pain and tenderness is characteristic. When dislocation has occurred, the limb is short, and the upper end of the femur is freely movable on the dorsum ilii. When both hips are dislocated, the attitude and gait are similar to those observed in bilateral congenital dislocation. The rotation arc of the great trochanter may be much reduced as a result of the disappearance of the head of the femur. There may be considerable formation of new bone, giving rise to large tumour-like masses in relation to the capsular ligament and the muscles surrounding the joint.
The treatment consists in protecting and supporting the joint. When the affection is unilateral, advantage may be derived from a Thomas' or other form of splint, along with a patten and crutches; in bilateral cases, from the use of crutches alone.
Loose bodies in the hip are mostly the result of hypertrophy of synovial fringes in arthritis deformans and in Charcot's disease, and do not figure in the clinical features of these affections; Caird has observed a case in which the cavity of the joint and the bursa beneath the psoas were filled with loose bodies, many of which had undergone ossification and gave a characteristic picture with the X-rays.
Hysterical affections of the hip resemble those in other joints.
The knee is more often the seat of disease than any other joint in the body.
The synovial membrane extends beneath the quadriceps extensor as a cul-de-sac, which either communicates with the sub-crural bursa, or forms with it one continuous cavity. When the joint is distended with fluid, this upper pouch bulges above and on either side of the patella, and this bone is “floated” off the condyles of the femur. When there is only a small amount of fluid, it is most easily recognised while the patient stands with his feet together and the trunk bent forwards at the hip-joints, and the quadriceps completely relaxed; the fluid then bulges above and on each side of the patella, and its presence is readily detected, especially on comparison with the joint of the other side.
On account of the great extent of the synovial membrane, a large quantity of serous effusion may accumulate in the joint in a comparatively short time, as a result either of injury or disease. The villous processes and fringes may take on an exaggerated growth, and give rise to pedunculated and other forms of loose body.
The bursæ in the popliteal space, especially that between the semi-membranosus and the medial head of the gastrocnemius, as well as the sub-crural bursa, frequently communicate with the synovial cavity of the knee and may share in its diseases.
As the epiphyses at the knee are mainly responsible for the growth in length of the lower extremity, and are late in uniting with their respective shafts—twenty-one to twenty-five years—serious shortening of the limb may result if their functions are interfered with, whether by disease or injury. The epiphysial cartilages lie beyond the limits of the synovial cavity, so that infective lesions at the ossifying junctions are less likely to spread to the joint than is the case at the hip or shoulder, where the upper epiphysis lies partly or wholly within the joint; disease in the lower end of the femur is more likely to implicate the knee-joint than disease in the upper end of the tibia.
One of the commonest causes of prolonged disability and feeling of insecurity in the knee, is to be found in the wasting and loss of tone in the quadriceps extensor muscle; the feeling of insecurity is most marked in coming down stairs. The instability of the joint is often added to by stretching of the ligaments and lateral mobility. As a result of both of these factors the joint is liable to repeated slight strains or jars which irritate the synovial membrane and tend to keep up the effusion and excite the overgrowth of its tissue elements.
While tuberculous disease of the knee is specially common in childhood and youth, it may occur at any period of life, and is not uncommon in patients over fifty. The disease originates in the synovial membrane and in the bones respectively with about equal frequency.
When the synovial membrane is diseased, it tends to grow inwards over the articular surfaces (Fig. 122), shutting off the supra-patellar pouch and fixing the knee-cap to the femur, and diminishing the area of the articular surfaces. The ingrowth of synovial membrane may fill up the cavity of the joint, or may divide it up into compartments. Ulceration of the cartilage and caries of the articular surfaces are common accompaniments.
 Fig. 123.—Lower End of Femur from an advanced case of
Tuberculous Arthritis of the Knee. Towards the posterior aspect of the
medial condyle there is a wedge-shaped sequestrum, of which the
surface exposed to the joint is polished like porcelain.
Fig. 123.—Lower End of Femur from an advanced case of
Tuberculous Arthritis of the Knee. Towards the posterior aspect of the
medial condyle there is a wedge-shaped sequestrum, of which the
surface exposed to the joint is polished like porcelain.The femur and tibia are affected with about equal frequency, and the nature and seat of the bone lesions are subject to wide variations. Multiple small foci may be found beneath the articular cartilage of the tibia, or along the margins of the femoral condyles—especially the medial. Caseating foci are comparatively rare, but they sometimes attain a considerable size—especially in the head of the tibia, where they may take the form of a caseous abscess. Sclerosed foci, which form sequestra, are comparatively common (Fig. 123).
Clinical Types.—(1) Hydrops usually arises from a purely synovial lesion, but the joint may suddenly become distended with fluid when an osseous focus ruptures into the synovial cavity.
It is met with chiefly in young adults. As the fluid accumulates it gradually stretches the capsule, and pushes the patella forwards, so that it floats. There is little pain or interference with function; the patient is usually able to walk, but is easily tired. The amount of fluid diminishes under rest, and increases after use of the limb. In a certain number of cases it may be possible to recognise localised thickening of the synovial membrane, or the presence of floating masses of fibrin or melon-seed bodies. This is best appreciated if the knee is alternately flexed and extended by the patient while the surgeon grasps and compresses it with both hands. If the joint is opened, fibrinous material, often in the form of melon-seed bodies, may be found lining the synovial membrane.
Tuberculous hydrops is to be diagnosed from the effusion that results from repeated sprain, from the hydrops of loose body, gonorrhœa, arthritis deformans, Charcot's disease, and Brodie's abscess in the adjacent bone, and from the hæmarthrosis met with in bleeders.
(2) Papillary or Nodular Tubercle of the Synovial Membrane.—This is a condition in which there is a fringy, papillary, or polypoidal growth from the synovial membrane. It is most often met with in adult males. The onset and progress are gradual, and the chief complaint is of stiffness and swelling which are worse after exertion. Sometimes there are symptoms of loose body, such as occasional locking of the joint, with pain and inability to extend the limb; but the locking is easily disengaged, and the movements are at once free again. The patient may give a history of several years' partial and intermittent disability, with lameness and occasional locking, although he may have been able to go about or even to continue his occupation.
There is a moderate degree of effusion into the joint, and when this has subsided under rest it may be possible to feel ill-defined cords, or tufts, or nodular masses, and to grasp between the fingers those in the supra-patellar pouch. There is little wasting of muscles, and it is exceptional to have signs of disease of the articular surfaces or of cold abscess.
On opening the joint, there may escape fluid and loose bodies similar to those described under hydrops, and if the finger is introduced into the cavity, the upper pouch is felt to be occupied by fringes or polypoidal processes derived from the synovial membrane.
The diagnosis is to be made from arthritis deformans, and in some cases from loose body of other than tuberculous origin.
(3) Cold abscess or empyema of the knee is a rare condition, in which the joint becomes filled with pus. It usually results from a primary tuberculosis of the synovial membrane occurring in children reduced in health and the subject of tuberculosis elsewhere.
(4) Diffuse Thickening of the Synovial Membrane—White Swelling.—So long as this form of the disease remains confined to the synovial membrane, the chief feature is that of an indolent elastic swelling in the area of the joint. The swelling tapers off above and below, so that it acquires a fusiform shape, and from the wasting of the muscles it appears greater than it really is. The range of movement is moderately restricted.
At first the patient limps, keeps the knee slightly flexed, and complains of tiredness and stiffness after exertion. As the articular surfaces become affected, there is pain, which is readily excited by jarring of the limb, or by any attempt at movement; the joint is held rigid, and there may be startings at night. If untreated, flexion becomes more pronounced—it may be to a right angle—the leg and foot are everted, and, in children, the tibia may be displaced backwards (Fig. 124). The wasting of muscles continues, the part becomes hot to the touch, the swelling increases, and may show areas of softening or fluctuation from abscess formation.
White swelling is to be differentiated from peri-synovial gummata, from myeloma and sarcoma of the lower end of the femur, and from bleeder's knee. In the first of these the swelling is nodular and less uniform, and there may be tertiary ulcers or depressed scars in the neighbourhood of the patella. In tumours the swelling is more marked on one side of the joint, it is uneven or nodular, it does not correspond to the shape of the synovial membrane, and may extend beyond the limits of the joint, and it involves the bone to a greater extent than is usual in disease of the joint. Skiagrams show expansion of the bone in central tumours, or abundant new bone in ossifying sarcoma. The diagnosis of bleeder's knee is to be made from the history.
(5) Primary Tuberculous Disease in the Bones of the Knee.—So long as the foci are confined to the interior of the bone, it is impossible to recognise their existence, unless they are of sufficient size to cause enlargement of the bone or to be discernible in a skiagram.
The formation of peri-articular abscess takes place in rather more than fifty per cent. of cases. When left to themselves, such abscesses tend to spread up the thigh, or down the back of the leg between the superficial and deep layers of calf muscles, and numerous sinuses may result from their rupture through the skin.
Attitudes of the Limb in Knee-Joint Disease.—The attitude most often assumed is that of flexion, with or without eversion of the leg and foot. The flexion is explained by its being the resting attitude of the joint, and that which affords most ease and comfort to the patient. Once the joint is flexed, the involuntary contraction of the flexor muscles maintains the attitude, and if the patient is able to use the limb in walking, the weight of the body is a powerful factor in increasing it. The eversion of the leg is probably associated with contraction of the biceps muscle. Backward displacement of the tibia is met with chiefly in neglected cases of chronic disease of the knee when the child has walked on the limb after it has become flexed.
In certain cases, genu valgum or abduction of the leg is present along with a slight degree of flexion. The valgus attitude is associated with slight lateral displacement of the patella, with prominence and apparent enlargement of the medial condyle, with depression of the pelvis on the diseased side and apparent lengthening of the limb.
Treatment of Tuberculous Disease of the Knee.—Conservative measures are always indicated in the first instance, and are persevered with so long as there is a prospect of obtaining a movable joint.
Conservative Treatment.—If the joint is sensitive and tends to be flexed, the patient is confined to bed, the limb is secured to a posterior splint, and extension with weight and pulley persevered with until these symptoms have disappeared; during this time, from three to six weeks, methods of inducing hyperæmia and other anti-tuberculous procedures are employed. If it is proposed to inject iodoform or other drug, the needle is inserted into the interval between the bones on the medial side of the ligamentum patellæ or into the upper pouch when this is distended with fluid.
If there is no pain or tendency to flexion, or when these have been overcome, the limb is put up in a Thomas' splint (Fig. 125) and the patient allowed to go about. The splint is worn for a period varying from six to twelve months; before being discarded it may be left off at night; it is ultimately replaced by a bandage.
 Fig. 125.—Thomas' Knee Splint applied. Note extension
strapping applied to affected leg, and patten under sound foot.
Fig. 125.—Thomas' Knee Splint applied. Note extension
strapping applied to affected leg, and patten under sound foot.
The indications for operative treatment are: (1) marked symptoms of destruction of the articular cartilages; (2) a deformed attitude incapable of being rectified without operation; (3) a condition of the general health which requires that the disease should be got rid of as speedily as possible; (4) progress or persistence of the disease in spite of conservative treatment. When there is no prospect of recovery with a movable joint it is a waste of time and a possible source of danger to persevere with conservative measures. Operation permits of the disease being eradicated and the restoration of a useful limb within a reasonable time, averaging from three to six months.
In adults, the operation consists in excising the joint; in children the aim is to remove the diseased tissues without damaging the epiphysial cartilages.
Amputation is performed when the disease has relapsed after excision and there is persistent suppuration, and when life is threatened by the occurrence of tuberculosis in the lungs or elsewhere.
Treatment of Deformities resulting from Antecedent Diseases of the Knee.—Flexion is the commonest of these; when due to contracture of the soft parts, these are either stretched by degrees, the limb being encased in plaster after each sitting, or they are divided by open dissection in the popliteal space. If there is fibrous or osseous ankylosis, the choice lies between arthroplasty, the removal of a wedge of bone which includes the joint, or, in patients who are still growing, of a wedge from the femur above the level of the epiphysial cartilage. Backward displacement of the tibia, genu recurvatum, and genu valgum also require operative treatment.
Pyogenic diseases result from infection through the blood stream, from one of the adjacent bones, or from a penetrating wound of the joint. The commoner types include the synovitis associated with disease in the adjacent bone, acute arthritis of infants, joint suppuration in pyæmia, pyogenic arthritis following upon penetrating wounds, and the affections which result from gonorrhœal or pneumococcal infection.
Treatment.—The limb is immobilised on a posterior splint so padded as to allow slight flexion at the knee, and extension applied with sufficient weight to relieve the pain; it is also of benefit to induce hyperæmia by one or other of the methods devised by Bier. To tap the joint, the needle is introduced obliquely into the supra-patellar pouch, and if it is necessary to open the joint, the incision is made on one or on both sides of the patella, and Murphy's plan of inserting formalin-glycerine may be employed. If the infection progresses and threatens the life of the patient, it may be necessary to lay the joint freely open from side to side, sawing across the patella, and, the limb being flexed, the whole wound is left open and packed with gauze. As the infection subsides, the limb is gradually straightened. If these methods fail, amputation through the thigh may be the only means of saving life.
Arthritis deformans affects the knee more frequently than any of the other large joints. The changes related to the synovial membrane here attain their maximum development, and may assume the form of hydrops with or without fibrinous bodies, or of overgrowth of the synovial fringes and the formation of pedunculated loose bodies. It is suggested that these synovial changes follow upon repeated sprains or upon a previous pyogenic infection of the joint. The effusion and stretching of the ligaments that follow upon a sprain are incompletely recovered from; the synovial membrane becomes puckered, the quadriceps atrophies and no longer puts the ligamentum mucosum on the stretch; and the infra-patellar pad of fat, not undergoing the normal compression during extension, is readily nipped between the femur and tibia. Each nipping implies a fresh sprain, with return of the effusion, and so a vicious circle is set up which terminates in what has been called a villous arthritis, with fringes and loose bodies; in time, the articular cartilage at the line of the synovial reflection undergoes fibrillation and conversion into connective tissue, and the process spreading to the articular surfaces, the picture of a rheumatoid arthritis is complete. Fibrillation of the cartilage imparts a feeling of roughness when the joint is grasped during flexion and extension, and lipping of the margins of the trochlear surface of the femur may be felt when the joint is flexed; it is also readily seen in skiagrams. When a portion of the “lipping” is broken off, it may give rise to a loose body. In advanced cases with destruction of the cartilages, there may be movement from side to side, with grating of the articular surfaces.
In the early stages, treatment consists in limiting the movements of extension by means of a splint provided with a hinge that locks at thirty degrees from full extension and vigorous massage of the quadriceps. In the dry, creaking forms of arthritis, the symptoms are relieved by introducing liquid vaseline into the joint. When the symptoms are due to the presence of fringes and loose bodies, these may be removed by operation. When the disease is of a severe type, and is confined to one knee, the question of excising the joint may be considered.
Bleeder's knee, Charcot's disease, hysterical knee, and loose bodies in the joint have already been described.
There is a common synovial cavity for the ankle and the inferior tibio-fibular joints. The epiphysial cartilage of the tibia lies above the level of this synovial cavity, but that of the fibula is included within its limits (Fig. 93). The talus is related to three articulations—the ankle above, the talo-navicular joint in front, and the calcaneo-taloid joint below. The tendon sheaths, especially those of the peronei and of the tibialis posterior, are liable to be infected by the spread of infective disease from the joint.
Tuberculous Disease.—Tuberculous disease at the ankle is met with at all ages. In the majority of cases the disease affects both bone and synovial membrane. Gross lesions in the bones are comparatively rare, and are chiefly met with in the head or neck of the talus.
Primary synovial disease usually exhibits the features of white swelling, projecting beneath the extensor tendons on the dorsum, and, posteriorly, filling up the hollows on either side of the tendo Achillis and below the malleoli (Fig. 126). The foot may retain its normal attitude, or the toes may be pointed and adducted. The calf muscles are wasted, there is little complaint of pain, and the movements of the joint may be so little interfered with that the patient can walk without a limp. When the disease involves the articular surfaces, there is pain and sensitiveness, the movements are restricted or abolished, and the patient is unable to put the foot on the ground.
A primary focus in the bone causes localised pain and tenderness, and a limp in walking, but the first sign may be the formation of abscess or the rapid development of articular symptoms. In such cases skiagrams afford valuable information.
Abscess formation is an early and prominent feature, whether the disease is of osseous or synovial origin, and sinuses are liable to form around the joint. Outlying abscesses and sinuses are usually the result of infection of the tendon sheaths in the neighbourhood.
Diagnosis.—When teno-synovitis occurs independently of disease of the ankle, the swelling is confined to one aspect of the joint. In sarcoma of the lower end of the tibia, the swelling lacks the uniform distribution of that met with in joint disease. In Brodie's abscess of the lower end of the tibia there may be swelling of the ankle, but there is an area of special tenderness on percussion over the bone.
Treatment.—The foot is immobilised at a right angle to the leg by splints or plaster of Paris; if articular symptoms are absent or have subsided, a Thomas' knee splint should be applied to enable the patient to move about without bearing his weight on the affected foot (Fig. 125). To inject iodoform, the point of the needle is inserted below either malleolus, and is then pushed upwards alongside of the talus. If localised disease in one of the bones is recognised before the joint is infected, it should be eradicated by operation.
When the disease is diffuse and resists conservative treatment, excision should be performed, the articular surfaces of the constituent bones being removed, and if necessary the whole of the talus.
Amputation is only called for in adults with rapidly progressing disease and diffuse suppuration, and in cases which have relapsed after excision.
The other diseases of the ankle include pyogenic, gonorrhœal, rheumatic, gouty, and hysterical affections, arthritis deformans, and Charcot's disease. The last-named is generally associated with a rapid and painless disintegration of the bones of the ankle and tarsus, resulting in great deformity and loss of the arch of the foot—sometimes associated with perforating ulcer of the sole.
Tuberculous disease in the tarsus, metatarsus, and phalanges has been considered in the chapter on Diseases of Bone.
The surgery of the extremities is so largely concerned with the correction of deformities that it is necessary at the outset to refer briefly to some points relating to the time and mode of origin of these.
1. Congenital deformities—that is, those which originate in utero and are present at birth—are comparatively common and may be due to a variety of causes. Some result from errors of development—for example, supernumerary fingers or toes, and deficiencies in the bones of the leg or forearm. A larger number are to be attributed to a persistent abnormal attitude of the fœtus, usually associated with want of room in the uterus—for example, the common form of club-foot and congenital dislocation of the hip. Less frequently amniotic bands so constrict the digits or the limbs as to produce distortion, or even to sever the distal part—intra-uterine amputation. Lastly, certain diseases of the fœtus, and particularly such as affect the skeleton—for example, achondroplasia—cause congenital deformities.
2. Deformities originating during birth are all traceable to the effects of injuries sustained in the course of a difficult labour. Examples of these are: wry-neck resulting from rupture of the sterno-mastoid; lesions of the shoulder-joint and brachial plexus due to hyper-extension of the arm; a spastic condition of the lower limbs—Little's disease—resulting from tearing of blood vessels on the surface of the brain with hæmorrhage and interference with the function of the cortical motor area.
3. Deformities acquired after birth arise from widely different causes, of which diseases of bone, including rickets, diseases of joints, and affections of the nervous system attended with paralysis, are amongst the commonest. Other deformities are produced by unsuitable clothing, such as a tight corset, or ill-fitting shoes distorting the toes, prolonged standing in growing subjects overstraining the mechanism of the foot and giving rise to the common form of flat-foot.
The part played by the palsies of children in the surgical affections of the extremities necessitates a short description of their more important features.
Anterior poliomyelitis is the lesion underlying what was formerly known as infantile paralysis—a name to be avoided, because the condition is not confined to infants and it is not the only form of paralysis met with in young children. Anterior poliomyelitis is characterised by an illness attended with fever, in which the child is found to have lost the power of one, less frequently of both lower extremities; or, it may be, of one or both arms. After a period, varying from six weeks to three months, the paralysis tends to diminish both in extent and degree, and in the majority of cases it ultimately persists only in certain muscles or groups of muscles. At the onset of the paralysis the affected limb is helpless and relaxed, the reflexes are lost, the muscles waste, and those that are paralysed exhibit the reaction of degeneration. In severe cases, and especially if proper treatment is neglected, the nutrition of the limb is profoundly affected; its temperature is subnormal, the skin is bluish in cold weather and readily becomes the seat of pressure sores. In course of time the limb lags behind its fellow in growth, and tends to assume a deformed attitude, which at first can easily be corrected, but later becomes permanent.
 Fig. 127.—Female child showing the results of
Poliomyelitis affecting the left lower extremity; the limb is short
and poorly developed, the pelvis is tilted and the spine is curved.
Fig. 127.—Female child showing the results of
Poliomyelitis affecting the left lower extremity; the limb is short
and poorly developed, the pelvis is tilted and the spine is curved.
When the acute stage of the illness is past, the chief question is to what extent recovery of function can be looked for in the paralysed muscles.
It would appear to be established that if a muscle reacts to faradism it will recover, but the contrary proposition does not follow. It was formerly accepted that a muscle which exhibits the reaction of degeneration is incapable of recovery, but observation has shown that this is not the case. Complete destruction of the motor cells in the anterior horn of grey matter as a result of poliomyelitis is now known to be exceptional; as a matter of fact, damage to the nerve cells is usually capable of being repaired. The muscles governed by these cells may appear to be completely paralysed, but with appropriate treatment their functional activity can be restored. As functional disability is frequently due to the affected muscle being over-stretched, it is of the first importance, when the acute symptoms are on the wane, that every care should be taken to prevent the weak muscular groups being put upon the stretch, and the greatest attention should be paid to the posture of the limb during convalescence. For example, if the child is allowed to lie with the wrist flexed, the flexor muscles undergo shortening, and the extensors are over-stretched and are therefore placed at a mechanical disadvantage. As the inflammatory changes in the anterior horn of the cord subside, the flexor tendons, from their position of advantage, are in a condition to respond to the first stimuli that come from their recovering motor cells, while the extensors are not in a position to do so. If, on the other hand, the wrist and fingers are maintained in the attitude of extreme dorsiflexion, the extensors become shortened, and, relieved of strain, they soon begin to respond to the stimuli sent them from the recovering nerve cells. Similarly in the lower extremity, when, for example, the muscles innervated through the peroneal (external popliteal) nerve are paralysed, if the foot is allowed to remain in the attitude of inversion with the heel drawn up—paralytic equino-varus—an attitude which is rendered more pronounced by the pressure of the bedclothes, the chance of the muscles recovering their function is seriously diminished. Another potent factor in preventing recovery, especially in the lower limbs, is erroneous deflection of the body weight. If, for example, there is weakness in the tibial group of muscles, and the child is allowed to walk, the eversion of the foot will steadily increase, the tibial muscles will be more and more stretched, the opposing peroneal muscles will shorten, and, in time, the bones of the tarsus will undergo structural alterations which will perpetuate the deformity. If, on the other hand, by some alteration of the boot, the foot is maintained in the attitude of inversion, the weakened or paralysed tibial muscles are placed in a much more favourable condition for recovery.
It must be emphasised that no operation should be performed in these cases until the question whether it be possible or not to restore the apparently paralysed muscle is settled. The clinical test of the recoverability of a muscle is to keep it for a long period—six or even twelve months—in a condition of relaxation. This test should be made, no matter how many months or years the muscle may have been paralysed.
The first stage in the treatment, therefore, is the correction of existing deformity, after which the limb should be kept immovable until the ligaments, muscles, and even the bones have regained their normal length and shape. The slightest stretching of a muscle which is in process of recovery disables it again.
The age of the patient influences the method of treatment. In young children in whom the structures are soft and yielding, gradual correction of the deformity is to be preferred to the more rapid methods employed in older children. The proper sequence consists in correcting the deformity, providing the simplest apparatus to keep the limb in good position, preventing erroneous deflection of body weight during walking, and then allowing the child to grow and develop until he has reached the age of five before considering such an operation as transplanting tendons, and the age of ten before deciding to ankylose a flail-like joint.
Reposition, Manipulations, Supports.—An attempt is made to correct the deformity by manipulation, and the proper attitude is maintained by a mechanical support. If the foot has become rotated so that the sole looks laterally, the medial side of the boot must be raised, and an iron worn which extends from the knee down the lateral side of the leg, to end, without a joint, in the heel of the boot. In pes equinus, the iron is let into the back of the heel and extends forwards into the waist of the boot, to keep the foot at right angles to the leg and to relax the weak extensor muscles.
Division of Contractions.—Bands of fascia and contracted tendons which prevent correction of deformity may have to be divided or lengthened. This is best done by the open method.
Removal of Skin.—To assist in maintaining the desired attitude, Jones recommends the plan of excising an area of the redundant skin on the weaker aspect of the limb; in equinus, the skin is taken from the dorsum; in equino-varus, from the front and lateral aspect of the foot. When the edges of the gap have united, the foot is maintained in the desired attitude for some months, even if parents carelessly remove the iron support to let the child run about.
Tendon transplantation, a procedure introduced by Nicoladoni, is to be considered in children of five and upwards. It may be employed for different purposes: (1) To reinforce a weak muscle by a healthy one—for example, by transplanting a hamstring tendon into the patella to reinforce a weak quadriceps, or reinforcing the weak invertors of the foot by a transplanted extensor hallucis longus. (2) Transplantation may also be performed to replace a muscle which is quite inactive and does not show any sign of recovery—for example, the tibiales being paralysed, the peroneus longus may be implanted into the navicular or first metatarsal to act as an invertor of the foot.
Wherever possible a tendon should be transplanted directly into bone, as, if it is attached to soft parts it rarely holds firmly enough. The bone should if possible be tunnelled, and the tendon passed through the tunnel and securely fixed. When bringing a tendon to its new point of attachment, it should pass in as straight a line as possible, avoiding any bend or angle which might impair its action. Fat is the best medium for the transplanted tendon to traverse, as it acts as a sheath and prevents the formation of adhesions which would interfere with the function of the new tendon. All deformity must be corrected before transferring the tendon; if the tendon is too short to admit of this, it can be lengthened by means of silk threads (Lange).
According to Jones, the most successful transplantations are the following, in order: (1) The tibialis anterior into the lateral tarsus in paralysis of the peronei; (2) the peroneus longus into the navicular in paralysis of the tibial group; (3) the extensor hallucis longus into any part of the foot where it may be wanted; (4) the hamstrings into the patella, to reinforce the quadriceps, provided the strictest after-treatment can be secured; (5) deflection of part of the tendo Achillis to one or other side of the foot.
Arthrodesis.—This operation, first performed by Albert in 1877, consists in removing the cartilage covering the articular surfaces of bones with the object of producing a firm ankylosis. The procedure is most successful in the ankle and mid-tarsal joints, and as a result of it there is obtained a secure and firm base of support in walking. Before performing arthrodesis, the surgeon must decide whether the patient will be better off with a stiff joint or with a weak and movable ankle supported by apparatus. This is often a matter of social position; in the poor, an ankylosed joint is more useful and less expensive. An arthrodesis should seldom be performed at the ankle until the child has passed his eighth year, or at the knee until he has reached his twentieth year. There is plenty to be done during the period of waiting, and if this is done well, it is possible that the operation may not be required. The existing deformities, for example, will have to be corrected, areas of skin removed to relieve functionless muscles of strain, the body weight appropriately deflected, and the child must be taught to walk with the aid of a support, swinging his limb about, and using it effectively in a correct position. Such exercise is a powerful agent in promoting physiological and functional development.
Nerve anastomosis, which seeks to provide a new channel for the transmission of motor impulses to the paralysed muscles, has as yet a restricted field of application—for example, the tibial and peroneal nerves may be anastomosed when the muscles supplied by one of them are paralysed. Stoffel of Heidelberg lays stress on regard being paid to the anatomical arrangement of the nerve bundles within the nerve-trunk so that motor fibres may be joined to motor ones and not to sensory. It is necessary also to cut across some of the fibres of the healthy nerve in order that they may grow into the nerve which is degenerated.
In extreme cases in which the limb is hopelessly paralysed and useless, it may be amputated to admit of an artificial limb being worn; it must be borne in mind, however, that such limbs furnish poor stumps, usually quite unable to bear pressure.
Cerebral Palsies of Childhood—Spastic Paralysis.—These may be due to arrest of development of the brain, to injuries of the head at birth, to meningeal hæmorrhage, or to other lesions of the brain, with secondary degenerative changes in the spinal cord. The commonest cause is hæmorrhage occurring during child-birth from the veins which ascend from the middle part of the convexity of the hemisphere to open into the superior sagittal (superior longitudinal) sinus. The blood is poured out beneath the dura on one or on both sides of the falx cerebri, and as it accumulates near the vertex, the damage to the motor centres for the legs is usually more extensive than that to the centres for the arms. The paralysis may affect one side of the body—hemiplegia, or both sides—diplegia; less commonly one extremity alone is involved—monoplegia. In diplegia, in which both arms and both legs are affected in the first instance, the arms may recover while the lower extremities remain in a spastic state, a condition known as Little's disease. The mental functions may be normal but more frequently they are imperfectly developed, the impairment in some cases amounting to idiocy. The affected limbs exhibit muscular rigidity or spasm, which is aggravated on movement but disappears under an anæsthetic; the reflexes are exaggerated, and sometimes there are perverted involuntary movements (athetosis). The growth of the limb is impaired, and contracture deformities may supervene (Fig. 131). The amount of power in the limb is often astonishing, in marked contrast to what is observed to follow upon anterior poliomyelitis. The degree of natural improvement is by no means great, and normal function is almost never regained.
The treatment is concerned in the first place with improving the condition of the muscles by methodical exercises and massage. When reflex irritability of the muscles with consequent spasm is a prominent feature, the reflex arc may be interrupted by resection of the posterior nerve roots corresponding to the part affected. This operation, first suggested by Spiller but chiefly popularised by Foerster, has yielded the best results in cases of Little's disease, in which there still remains a considerable amount of voluntary movement, and yet there is inability to walk on account of involuntary spasm. In the case of the lower extremities, three or more of the lumbar and one or more of the sacral nerve roots are resected within the vertebral canal. Sensation is diminished but not abolished in the area of skin involved. Massage and exercises and, it may be, splints or apparatus are essential factors in promoting the recovery of function. It has not yet been decided whether the results of the resection of nerve roots justify the risk.
Apart from Foerster's operation, or when it has failed, the spasm of any individual muscle or group of muscles may be got rid of by diminishing the nerve supply to the muscle or by lengthening the tendon. Diminishing the nerve supply was suggested by Stoffel; it consists in exposing the motor nerve as it enters the muscle and resecting one-third or one-half of the fibres so as to reduce the innervation to the required degree. The method is still on its trial.
Lengthening the Tendons.—In spastic paraplegia, for example, Jones resects the origins of the adductors longus and brevis, lengthens the tendo Achillis, divides the popliteal fascia and hamstrings, and transplants the biceps into the quadriceps; after which the limbs are put up in the attitude of wide abduction for six weeks. It is important that the patient should begin to walk with the legs wide apart and learn to balance himself without any feeling of insecurity; he should be taught to look at an object straight in front of him rather than on the ground.
This is the commonest of all congenital dislocations. Its frequency varies in different countries, being greater on the continent of Europe than in this country. It is more often unilateral than bilateral (about 4 to 1), and is about three times more common in girls than in boys.
The dislocation takes place in the early months of intra-uterine life, and may be associated with deficiency of the liquor amnii.
Pathological Anatomy.—In the infant, the anatomical changes in the joint are less marked than they are after the child has borne its weight on the limb. The acetabulum, never having been occupied by the head of the femur, is imperfectly developed; it remains flat and shallow, is partly filled with fibro-fatty tissue derived from the synovial membrane, and is always too small for the head of the femur. The cotyloid ligament being broader and thicker than usual, makes the osseous portion of the socket appear deeper than it really is. In unilateral cases the affected half of the pelvis is contracted, so that the pelvic basin is narrowed and oblique. The head of the femur is small, flattened, and, in some cases, conical; and the angle formed by the neck with the shaft is altered, sometimes diminished, it may be to a right angle—coxa vara (Fig. 129); sometimes increased—coxa valga. There is also a variable degree of torsion of the neck, ante-torsion being of practical importance as it increases the difficulty of retaining the head in the socket. The capsule is lax and admits of the head passing upwards for a variable distance on to the dorsum ilii. In unilateral cases the ligamentum teres is elongated and thickened; in bilateral cases it is frequently absent.
In children who have walked, the head of the femur is pushed farther upwards on the dorsum ilii; the capsule becomes lengthened by supporting the weight of the body. That part of the capsule which arises from the lower margin of the acetabulum stretches across the socket and partly shuts it off from the rest of the joint cavity. In course of time the capsule becomes greatly thickened, and may present an hour-glass constriction about its middle, which may prove a serious obstacle to reduction. The socket becomes small and triangular, and there is almost no ledge against which the head of the femur can rest. A superficial depression may form on the ilium where it is pressed upon by the head of the femur, covered by the capsule; and in the course of years, as the head changes its position, several secondary sockets may be formed. No proper new bony socket forms like that in traumatic dislocations that remain unreduced because in the congenital variety the thickened capsule intervenes between the head of the bone and the dorsum ilii. The displacement of the head is most frequently backwards (dorsal luxation), and as the point of support thus falls behind the acetabulum the pelvis tilts forwards, and the lumbar spine becomes unduly concave (lordosis). The muscles of the hip and thigh alter in consequence of the changed relations; the gemelli, obturators, and piriformis are lengthened, the adductors, hamstrings, and ilio-psoas are shortened, while the glutei and quadriceps are but little altered. In rare cases the head is displaced upwards and lies immediately above the acetabulum.
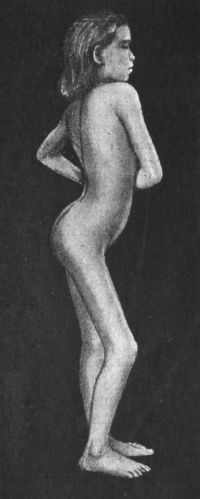 Fig. 130.—Congenital Dislocation of Left Hip in a girl
æt. 8. The patient is putting the whole weight on the dislocated
limb.
Fig. 130.—Congenital Dislocation of Left Hip in a girl
æt. 8. The patient is putting the whole weight on the dislocated
limb.
Clinical Features.—The condition rarely attracts attention until the child begins to walk, but sometimes the unusual breadth of the pelvis, the presence of a lump in the buttock, snapping about the hip, or a peculiar way of holding the limb, leads the parents to seek advice early. In unilateral cases, when the child has learned to walk at the late age of two, three, or it may even be four years, it is noticed that the back is hollow and the buttocks unduly prominent, and that there is a peculiar and characteristic limp; each time the weight of the body is put upon the affected limb, the trunk makes a sudden dip towards that side. There is no pain on walking. The affected limb is shortened, as is shown by the projection of the great trochanter above Nélaton's line; the shortening gradually increases, and in time may amount to several inches. It is partly compensated for by resting the affected limb on the balls of the toes and flexing the knee on the sound side. The gluteal fold is shorter, deeper, and higher than on the healthy side, and on account of the obliquity of the pelvis the spine shows a lateral curvature, with its concavity to the affected side. The movements at the hip-joint are free in all directions except abduction; on practising external rotation it is often found to be abnormally free; lastly, in young children, if the pelvis is fixed, the head of the bone may be made to glide up and down on the ilium.
In bilateral cases the trunk appears well grown in contrast to the short lower limbs, the hollow of the back is exaggerated, the abdomen protrudes, the perineum is broadened, and the buttocks are unduly prominent. The gait is waddling like that of a duck, the trunk lurching from one side to the other with each step. In untreated cases the deformity and disability become more pronounced as the capsular and round ligaments are further stretched, the shortening and limp become more marked, the patient is easily fatigued by walking or standing, and is usually unfitted for earning a living. We have had under observation, however, an adult male with bilateral dislocation and extroversion of the bladder, who efficiently performed the duties of a carrier for many years.
Except in fat infants, the diagnosis is not difficult; the absence of pain and tenderness, the freedom of motion and the absence of the head of the femur from its normal position, differentiate the condition from tuberculous disease of the joint, and from coxa vara and other deformities in the region of the hip. Trendelenburg's test consists in noting the relative level of the buttocks when the patient stands on the affected leg. Normally the buttocks remain on the same level when the patient stands on one leg; in congenital dislocation the buttock of the limb raised from the ground drops to a lower level; in coxa vara it rises higher.
In paralytic conditions at the hip there may be considerable resemblance to dislocation, but the muscles are slack and wasted, and the normal attitude can easily be restored by pulling on the limb. The most certain means of diagnosis is by the X-rays, which show the position of the head of the bone in relation to the acetabulum, and any torsion of the neck of the femur that may be present. This last point is determined by taking a series of skiagrams in different positions of the limb; these are also useful in correcting erroneous impressions as to the angle of the neck of the femur.
Treatment.—We are indebted to Paci, Schede, Calot, Lorenz, and Hoffa for the rational treatment which seeks to reduce the dislocation by manipulation.
Reduction by Manipulation (Method of Lorenz).—The child is anæsthetised and placed on its back with the legs over the end of the table. While an assistant steadies the pelvis, the surgeon pulls on the limb so as to bring the trochanter down to Nélaton's line; this is followed by forced rotation outwards and inwards and forcible abduction to a right angle, and by kneading the adductors till they are stretched and torn. The next step is to stretch the hamstrings, and this is done by raising the foot, without bending the knee, until the front of the thigh meets the abdomen, and the toes the face. To stretch the anterior muscles, the patient is turned on the side or face, and the hip is hyper-extended both in the straight and in the abducted position. The stage is now reached at which attempts at reduction may be made; the child is again laid on its back, the surgeon grasps the knee, flexes the thigh to a right angle, rotates laterally, and slowly flexes and abducts, while the thumb pushes from behind on the trochanter, trying to guide and lift it over the rim of the socket as the hip reaches the over-abducted position. Lorenz uses a wedge of wood padded with leather about 3 inches high to rest the trochanter upon while attempting to lift it forward. When reduction takes place, there is generally a sound and a sudden jump, as in reducing a traumatic dislocation.
To keep the head in the socket, the limb must be maintained in the position of right-angled abduction and external rotation (90°) by a plaster case, which includes the lower part of the trunk and both limbs down to the knee. Under the plaster, stockinette drawers are worn, and the bony prominences are padded with cotton wool. The plaster should overlap the costal margin. The first case is worn for two months or more, and is then renewed at shorter intervals, the degree of abduction being diminished at each renewal until the limbs are nearly parallel. The child is only kept in bed for a week or two, and is then allowed up, being provided with a boot and high sole on the affected side, but should not use crutches. At the end of six months, by which time the capsule has become tightened up round the head of the femur, the plaster is given up and massage and exercises are employed.
In bilateral cases both dislocations are reduced at one sitting if possible, and a plaster case applied with both thighs abducted and flexed to a right angle, the so-called “frog position.”
In the event of failure to reduce a dislocation at the first attempt, the limb should be fixed in plaster in the abducted attitude for ten days or a fortnight, and then another attempt made. The greatest number of successes in bilateral cases is met with under five years of age, and in unilateral cases under seven. Reduction may sometimes be accomplished, however, in older children.
If it is found impossible to restore the head of the femur to the acetabulum, an attempt should be made by similar manipulations to wedge it under the long head of the rectus femoris, or, failing this, below the anterior iliac spine under the sartorius and tensor fasciæ femoris. By thus converting a posterior into an anterior dislocation, the tilting of the pelvis and the lordosis are greatly diminished. This procedure, named by Lorenz anterior transposition of the head of the femur, is specially applicable to cases in which relapse has taken place after reduction, and to those above the age when reduction should be attempted.
Reduction by open operation may be had recourse to in cases in which, after several attempts, reduction has failed, or in which re-dislocation has occurred; it is, however, a serious operation. Attempts have also been made by means of pegs and other contrivances to fix the head of the bone and prevent it sliding upwards on the ilium. When reduction is impossible by any means, a stiff leather jacket with prolongations around the thighs may diminish the deformity and improve the walking.
Snapping Hip (Hanche à ressort).—This is a rare affection, met with in children and young adults, and characterised by the occurrence of a sudden, snapping sound, sometimes attended with pain in the region of the great trochanter. This usually occurs when the limb is slightly flexed or adducted, and rotated either inwards or outwards. On palpation a cord-like structure may be felt, which slips forwards and backwards over the trochanter when the position of the limb is altered.
The condition was formerly described as a voluntary dislocation of the hip; it is now believed to be due to a cord-like band of tissue slipping backwards and forwards over the trochanter. The band is usually derived from the fascia lata, sometimes reinforced by the anterior fibres of the gluteus maximus, sometimes by the tensor fasciæ femoris. The condition seldom gives rise to any appreciable disability and surgical treatment is rarely called for. In a number of cases the muscle has been fixed by sutures with satisfactory results. In a recent case, an extensive open dissection proved negative, but the stitching of the gluteus to the trochanter was followed by the disappearance of the snapping.
Paralytic Deformities of the Hip.—In anterior poliomyelitis the paralysis of muscles may be so widespread that the limb is unable to support the weight of the body, or certain groups of muscles only are paralysed and the child may be able to walk with the help of apparatus. Even if the ilio-psoas is paralysed, flexion is still possible by the anterior fibres of the gluteus medius, the anterior adductors, and when the leg is rotated out by the tensor fasciæ and sartorius, the dislocation differs from the traumatic variety in that the head, although it leaves the socket, remains within the capsule. Dislocation tends to occur from the disturbance of muscular balance, anterior dislocation being commoner than posterior in about the proportion of two to one; the nature of the dislocation is best demonstrated by means of the X-rays. Reduction is rarely possible without an open operation. Tendon and nerve-transplantation are scarcely possible, and arthrodesis is rarely to be recommended; contracture deformities, however, are often benefited by tenotomy in young children, and in older children by osteotomy through the trochanter, and putting the limb up in the abducted position.
In spastic paralysis of cerebral origin, the tendency is towards contracture, usually in the attitude of flexion, with adduction and inversion. This may result in dislocation backwards on to the dorsum ilii, and may occur in patients confined to bed (Fig. 131).
 Fig. 131.—Contracture Deformities of Upper and Lower
Limbs resulting from Spastic Cerebral Palsy in infancy.
Fig. 131.—Contracture Deformities of Upper and Lower
Limbs resulting from Spastic Cerebral Palsy in infancy.Contractures and Ankyloses of the Hip.—Various forms of contracture are met with as a result of cicatricial contraction, or from shortening of the fasciæ, muscles, and ligaments when the hip has been maintained in the flexed position for long periods—for example, in psoas abscess, chronic rheumatism, or hysteria. The majority, however, result from tuberculous disease of the hip-joint. In osseous ankylosis, an attempt may be made to restore movement by the operation of Murphy, which consists in chiselling through the osseous junction between the bones, deepening the acetabulum if necessary, and then interposing between the bony surfaces a portion of fat-bearing fascia derived from the fascia lata over the great trochanter. The operation of Jones consists in detaching the great trochanter (the insertions of the glutei into it being left intact), dividing the neck of the femur, and then securing the separated portion of the trochanter to the proximal end of the neck to prevent union of the fragments.
These deformities depend on abnormalities of the angle of the neck of the femur; the average or normal elevation is 125° for the adult and 135° for the child; variations between 120° and 140° are considered normal. If the angle is less than 120° the condition is one of coxa vara; if greater than 140°, coxa valga. The angle of inclination of the neck of the femur is dependent upon the adjustment of certain forces, namely, the weight of the body, the action of muscles, and the resistance of the bone. The most obvious cause of deviation of the neck from the normal angle is some condition which causes softening of the bone so that it yields under weight-pressure, the most common being partial fractures, rickets, and other diseases of the bone.
Coxa Vara—Incurvation of the Neck of the Femur.—There may be a simple adduction bend of the neck, the head sinking to, or even below, the level of the great trochanter (Fig. 132); or this may be combined with a curve of the neck, of which the convexity is upwards and forwards, so that the lower border of the neck is greatly shortened and the head approximated to the lesser trochanter. At the same time the shaft of the femur is adducted and rotated outwards.
Adolescent Coxa Vara.—This, the most common clinical type, is met with in boys between the ages of twelve and eighteen. The unilateral form is nearly always the result of injury to the neck of the femur or to the epiphysial junction, although the deformity may not show itself for months or a year or two after the injury. The deformity may be the first indication, or it is preceded by pain and stiffness; the patient complains of being easily tired, of difficulty in kneeling and sitting, difficulty in riding, and of an increasing limp in walking. On examination, the limb is found to be shortened, the great trochanter is displaced upwards and backwards and is unduly prominent, and the muscles of the buttock and thigh are a little smaller and softer than on the normal side. The limb is adducted, its normal range of abduction, and sometimes also of flexion, is restricted, and there is, as a rule, some degree of lateral rotation, so that the toes point outwards. It should be noted that the same picture—shortening with eversion and stiffness at the hip—results from the common fracture of the neck of the bone in old people. The adduction element of the deformity is partly compensated for by upward tilting of the pelvis on the affected side and curvature of the spine with its concavity towards the affected limb.
When the condition is bilateral it is usually the result of disease in the bone, rickets most frequently in this country. The attitude and gait are highly characteristic, as the adducted and everted legs tend to cross each other at the knee, the deformity being of the scissors-like type (Fig. 134), and in extreme cases the patient is only able to walk with the aid of crutches.
Diagnosis.—Pain in the hip and a limp in walking suggest hip-joint disease, but while in coxa vara the movements are chiefly restricted in the direction of abduction, in hip disease they are restricted or absent in all directions. From congenital dislocation of the hip the diagnosis can usually be made by the history, the examination of the joint and of its movements; and by the Trendelenburg test (p. 252). In sacro-iliac disease, the pain and tenderness are over the sacro-iliac joint and the movements at the hip are free in all directions. Valuable evidence is obtained from skiagrams.
Treatment.—In the early stages, especially if there is pain and tenderness, the patient must lie up and extension is applied in the abducted position of the limb; after a fortnight or so recourse is had to massage and exercises and the patient is allowed up for a little each day, attention being paid to flat-foot, which is a common accompaniment. When deformity is the prominent feature and interferes with locomotion it must be corrected. The bloodless method is to be preferred; under general anæsthesia, the shortened adductors are stretched or divided, and forcible movements are carried out in all directions, until the limb can be brought into an attitude of marked abduction and internal rotation. A plaster-case is then applied, from the pelvis to the middle of the calf, the knee being slightly flexed for greater comfort; in a week or so the patient is able to go about, and in a couple of months a second plaster-case is applied, this time leaving the knee free. After another six weeks or so a moulded splint is used, which can be removed at bedtime. The traumatic forms can nearly always be corrected by this bloodless method. In advanced cases the deformity can only be corrected by open operation, which consists in dividing the femur obliquely downwards and medially through the great trochanter, and, the adductor muscles having been ruptured or divided, the limb is put up in the abducted position along with, if required, powerful weight extension.
 Fig. 133.—Coxa Vara, showing adduction curvature of
neck of femur associated with arthritis of the hip and knee.
Fig. 133.—Coxa Vara, showing adduction curvature of
neck of femur associated with arthritis of the hip and knee.
|
 Fig. 134.—Bilateral Coxa Vara, showing scissors-leg
deformity.
Fig. 134.—Bilateral Coxa Vara, showing scissors-leg
deformity.
|
In cases of traumatic origin—epiphysial separation—Sprengel has obtained good results by forcibly abducting and internally rotating the limb under an anæsthetic, and then applying a plaster-case which extends down to the knee.
Other Forms of Coxa Vara.—In rickety children, coxa vara is most often associated with pronounced eversion of both lower extremities, without the capacity for abduction being necessarily restricted, and with but little impairment of function. The child should be treated for rickets, and put up in a double long splint with the limbs abducted and inverted.
In arthritis deformans of the hip, it is not uncommon to have considerable depression of the head of the bone and diminution in the angle of its neck, with consequent restriction of abduction. Sometimes the upper end of the shaft is also curved.
In osteomyelitis fibrosa, involving the upper end of the femur, a gross form of coxa vara may be observed, of which a marked example is shown in figures on pp. 476, 478, Volume I.
The congenital variety of coxa vara is due to various intra-uterine conditions, of which the chief is defective development of the upper end of the femur; as it does not manifest itself until the child begins to walk, the resemblance to congenital dislocation of the hip is very close.
Coxa Valga.—Coxa valga is the reverse of coxa vara, the angle at the neck of the femur being over 140°. It is not nearly so important in practice as coxa vara. It may result from incomplete fractures or epiphysial separations, rickets, or various forms of osteomyelitis, but it is also a frequent accompaniment of other deformities, such as congenital dislocation of the hip and paralysis following anterior poliomyelitis. It is commoner in boys than in girls, and is more often single than bilateral. The limb is lengthened, abducted, and rotated outwards; there is flattening of the buttock, and the trochanter is depressed so that it lies below Nélaton's line. The patient is unable to adduct the limb, and shows a peculiar gait, which has frequently caused the condition to be mistaken for unilateral congenital dislocation at the hip.
In recent cases it may be possible under anæsthesia forcibly to adduct the limb and rotate it inwards, and to retain it in this position with a plaster bandage. In advanced cases the length of the limbs may be equalised by a high sole on the sound side, or by performing an osteotomy through the great trochanter.
Congenital dislocation at the knee-joint is rare; it is usually incomplete, and the patella is sometimes absent. The dislocation may be permanent, or may only occur from accidental movements of the limb. In some cases it can be produced at will by the patient or the surgeon. We have observed one such case in a professional cyclist in whom this capacity of partially dislocating the knee entailed no disability. When the child begins to walk, an apparatus which will prevent hyper-extension and lateral motion should be fitted to the limb.
Congenital absence of the patella usually complicates other abnormalities of the knee-joint. The tubercle of the tibia is prominent and the extensor tendon unusually thick. In flexion the tendon rises on to the lateral condyle of the femur.
Congenital Dislocation of the Patella Laterally.—This may be persistent or intermittent. In the persistent form the dislocation is present from birth; the patella rests on the trochlear surface of the lateral condyle, and when the knee is flexed may pass farther outwards and become completely dislocated, lying against the lateral aspect of the condyle.
In the intermittent or recurrent form the patella lies in its normal place, but is liable to be displaced outwards when the joint is flexed; the displacement occurs suddenly and unexpectedly in walking, and the patient may fall to the ground, suffering intense pain. The knee-cap is readily replaced on extending the joint, but the sprain of the joint is followed by effusion, and the patient is usually disabled for a day or two. It is met with chiefly in girls, and there may be a history that the child was late in walking and learned with difficulty. On examination, the patella is found to have an abnormal range of movement outwards, although it cannot be completely dislocated without considerable pain. If the child is brought for advice when there is fluid in the joint, the condition is liable to be mistaken for tuberculous synovitis. The observation that the undue mobility of the knee-cap is present in both knees is of assistance in arriving at a diagnosis, and also the history that the girl has repeatedly hurt her knee in falling.
The cause of the abnormal mobility of the patella varies in different cases; in some there is congenital laxity of the ligaments, in others a faulty formation of the lower end of the femur. Bade has observed families in which several children were affected, and although there was nothing abnormal in the shape of the bones, the knee was slender and delicately formed.
The use of a strong knee-cap may prevent falling, but as a rule an operation is required, and there is quite a number to choose from, the principle of them all being to prevent displacement of the bone without unduly restricting flexion of the joint. That devised by Goldthwait consists in exposing, by means of a vertical incision, the whole length of the patellar ligament, splitting it longitudinally, separating the lateral half from the tibia, passing it under the medial portion and suturing it to the periosteum; this gives the quadriceps a straight line of pull. We have achieved the same result by dividing the lax capsule and synovial membrane on the medial side of the patella, and overlapping the edges with a double line of catgut sutures.
Lateral dislocation of the patella is met with in extreme forms of knock-knee, and after correction of this deformity by osteotomy, and its possible occurrence should be guarded against at the time of the operation.
Genu Recurvatum.—In this deformity the knee is hyper-extended, the thigh and leg forming an angle which is open forwards; the attitude may be permanent or may only appear on walking. It is an extremely disabling and unsightly deformity.
There are several varieties. In the congenital form, which is apparently due to a faulty attitude of the lower extremities in utero, the patella may be imperfectly developed or absent; the knee is convex backwards, and attempts to flex the joint cause pain. Other deformities frequently coexist. The treatment consists in flexing the joint to a right angle under an anæsthetic, and maintaining this attitude by means of plaster-of-Paris or splints until the growth of parts overcomes any tendency to relapse.
Acquired Forms.—The most common acquired form is the result of anterior poliomyelitis, and is described in the next section.
The deformity may also be due to rickets which has caused a backward bend of the tibia immediately below its upper epiphysis—sometimes combined with an exaggerated forward curve of the femur. If there is no prospect of spontaneous rectification, the upper end of the tibia should be divided with the osteotome, and the limb straightened.
It may result also from fracture or from separation of one of the epiphyses in the region of the knee, or from cicatricial contraction of the quadriceps. As a result of bone and joint disease, it is met with chiefly in neuro-arthropathies when the knee has become disorganised and flail-like.
Deformities of the Knee resulting from Anterior Poliomyelitis and from Spastic Paralysis.—When there is paralysis of all the muscles acting on the knee, the joint may be so flail-like that the patient is unable to stand without the aid of a crutch, or when weight is put on the limb, it assumes the attitude of genu recurvatum. The usefulness of the limb may be improved by the application of a rigid apparatus with a lock at the joint so that it can be used in the extended position for walking or in the flexed position for sitting. The rigid knee produced by arthrodesis affords good support but is inconvenient in sitting.
When the quadriceps alone is paralysed, the patient is obliged to maintain the joint in the position of extreme extension, because the least degree of flexion results in the limb giving way under him. In course of time the posterior ligament is stretched, and the joint becomes hyper-extended, acquiring the attitude of genu recurvatum. When it is bilateral the gait is seriously impaired. The treatment consists in applying an apparatus which prevents hyper-extension, in improving the condition of the thigh muscles, and in wearing a splint at night which secures the flexed position. Recourse may be had to operative measures, such as transplanting one of the hamstrings into the patella, so as to compensate for the loss of power in the quadriceps, arthrodesis, or supra-condylar osteotomy of the femur.
When the quadriceps is overcome by a contraction of the hamstrings, as in spastic paraplegia, the knee is fixed in the flexed position and the child is unable to walk. The flexion may be corrected by lengthening the hamstring tendons, bringing the divided biceps tendon through an opening in the vastus lateralis, and attaching it to the rectus and to the patella. If there is a combination of flexion and genu valgum, the knee-joint should be resected and ankylosed in the straight position.
Contracture and Ankylosis at the Knee.—In addition to the different paralytic forms above described, contracture may result from ulceration and suppuration in the popliteal space, and from disease (osteomyelitis) in one of the adjacent bones. The greater number of contractures and ankyloses are the result of disease in the joint, and have already been described.
In the normal limb, a line drawn from the centre of the head of the femur to a point midway between the malleoli passes through the centre of the knee-joint. If the line passes outside the centre of the knee-joint, the condition is one of genu valgum; if inside, it is one of genu varum (Fig. 135).
Genu Valgum—Knock-knee.—In this deformity the leg joins the thigh at an angle which is open outwards, and when the affection is bilateral, the projecting knees tend to knock against each other in walking; the term X-legs is sometimes applied to it.
Etiology.—The observations of Macewen and of Mikulicz, and information afforded by the Röntgen rays, have shown that the primary cause of the deformity is an inequality of growth at the ossifying junction of the femur or tibia or of both. This inequality of growth is nearly always due to rickets, and its direction is determined by a faulty attitude of the limbs in standing and walking. The legs being abducted, the weight of the body falls unequally on the medial and lateral parts of the ossifying junctions, and inequality of growth results.
Pathological Anatomy.—Examination of the femur usually shows that the lower third of the diaphysis is lengthened on its medial side and shortened on its lateral side, and that the epiphysis, itself unaltered, is fitted on to the diaphysis obliquely, so that the medial condyle appears to be increased in length and to occupy a level distinctly below that of the lateral condyle. In many cases the tibia shows corresponding alterations. On section of the bones, the epiphysial cartilage and the zone of ossification are found to be unduly broad and irregular.
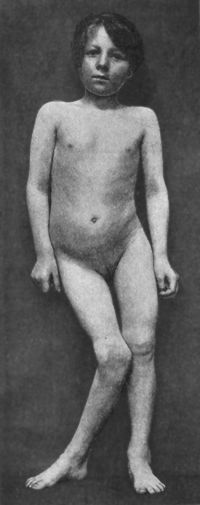 Fig. 136.—Female child with right-sided Genu Valgum,
the result of Rickets. The pelvis is tilted, and the spine is curved.
Fig. 136.—Female child with right-sided Genu Valgum,
the result of Rickets. The pelvis is tilted, and the spine is curved.
The neck of the femur is shortened and its angle diminished. The bones of the leg are sometimes bent inwards in their lower thirds, and this compensates partly for the valgus deformity at the knee. The articular cartilage of the lateral condyle and the lateral meniscus are usually thickened. In pronounced cases the quadriceps tendon and the patella are displaced laterally, and this may be so pronounced that on flexion of the joint the patella is dislocated on to the lateral condyle of the femur. The biceps tendon and ilio-tibial band are shortened and more prominent as a result of the approximation of their attachments, and they are also displaced laterally. The sartorius and gracilis are displaced backwards, so that they descend behind instead of on the medial side of the knee. The popliteal artery lies on the back of the lateral condyle instead of in the hollow between the condyles, and the tibial (internal popliteal) nerve is displaced even farther outwards. The capsular and other ligaments are slack, so that the joint is unstable and easily hyper-extended. There is often some effusion into the joint.
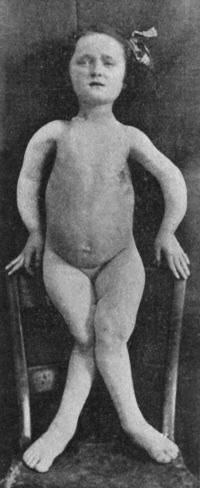 Fig. 137.—Female child with Rickety deformities of
upper and lower extremities.
Fig. 137.—Female child with Rickety deformities of
upper and lower extremities.Radiograms reveal the changes in the bones (Fig. 138); the shaft of the femur or tibia, or both, which may also be curved, is set obliquely on its epiphysis; and the clear zone, corresponding to the epiphysial cartilage, is uneven and broader than normal. There are also less obvious changes in the density of the shadow and in the arrangement of the trabecular structure of the bones.
Clinical Features.—In the infantile form (Fig. 139) the knock-knee is commonly associated with rickets in other parts of the skeleton, and especially with bending of the tibia and femur, and in extreme cases the child may be unable to walk.
The deformity is about as frequently bilateral as unilateral. There may be knock-knee on the one side and bow-knee on the other. If, as is usually the case, the deformity is due to obliquity of the femur, it disappears on flexing the joint (Fig. 140), because in flexion the tibia glides behind the projecting median condyle; if the deformity affects the tibia only, the influence of flexion in disguising it is not so marked. It is usually possible to hyper-extend the joint, and, in the extended position, to rotate the leg outwards to a greater extent than is normal. In unilateral knock-knee, the affected limb is a little shorter than its fellow, but the patient compensates for this by depressing the pelvis on the affected side.
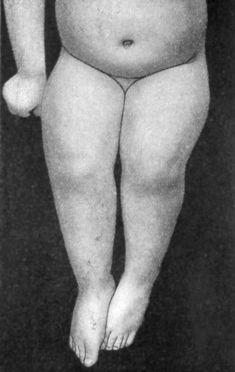 Fig. 140.—Genu Valgum. Same patient as Fig. 139.
Sitting, to show disappearance of deformity on flexion of knee.
Fig. 140.—Genu Valgum. Same patient as Fig. 139.
Sitting, to show disappearance of deformity on flexion of knee.
Prognosis.—In children below the age of six, the bones naturally tend to straighten if the child is kept off its feet. After this age, there is no such prospect.
The treatment of knock-knee in children is directed towards curing the rickets and preventing the child from putting its feet to the ground. If it cannot have the services of a nurse and the use of a perambulator, a light padded splint is applied on the lateral side of the limb, extending from the iliac crest to 3 inches beyond the foot. The splint is fixed above and below by bandages, and the projecting knee is drawn towards it by a few turns of elastic webbing. A method specially applicable to hospital out-patients, is to straighten the limbs as far as possible under anæsthesia, and apply a plaster bandage; the bandage is renewed at intervals of three weeks until the deformity is corrected. Whatever plan is adopted, it must be persevered with for at least six months, until the rickety changes in the bones have been entirely recovered from.
If the child is approaching the age of five or six before it comes under treatment, or if the deformity does not yield to treatment by splints, it is better to straighten the limb by osteotomy.
In adolescent knock-knee the patient seeks advice because of the deformity or of pain after exertion, especially at the medial side of the epiphysial junctions, of being easily tired, and of incapacity for any occupation involving standing. The bones are coarse and badly formed, and there is frequently a spinous process projecting downwards from the medial side of the tibia about three finger-breadths below the joint.
When the deformity is bilateral, the patient abducts the thigh and rotates the limb outwards at the hip to disguise the deformity, and to allow the projecting knees to pass each other. He usually supinates or inverts the foot, with the object of bringing the whole length of the lateral border of the sole into contact with the ground. Flat-foot is exceptional. The boots are usually more worn along the lateral than along the medial border of the sole and heel.
No apparatus that allows of the patient walking is of any value. If the deformity is marked, there should be no hesitation in having recourse to operation by one or other of the various methods of osteotomy.
In severe cases it may be found that when the deformity is corrected by osteotomy, the patella shows a tendency to be dislocated laterally on flexion of the knee. This may be prevented by putting up the limb in the attitude of slight genu varum.
The most difficult cases to treat are those in which, owing to curving of the lower part of the shaft of the femur with the convexity forwards, the knee is permanently flexed and cannot be completely extended.
Other forms of genu valgum are relatively rare. There is a congenital form arising from faulty position of the limbs in utero; a traumatic form following fracture or epiphysial separation in the region of the knee; and a paralytic form, usually combined with flexion, in cases of spastic paralysis. Finally, genu valgum may be a result of various forms of osteomyelitis of the lower end of the femur, or of disease in the knee-joint, such as tuberculosis, arthritis deformans, or Charcot's disease.
Genu Varum—Bow-knee.—In this deformity, which is the converse of genu valgum, the leg joins the thigh at an angle which is open medially. It is almost invariably bilateral, is of rachitic origin, and is frequently associated with bow-legs (Fig. 141). The tibia takes a greater share in its production than the femur. Although an ungainly deformity, it is much less frequently the source of complaint than knock-knee, because it scarcely interferes with locomotion—as a matter of fact, the subjects of bow-knee, although short in stature, are unusually sturdy on their legs. An extreme example of the deformity is shown in Fig. 141.
Treatment is carried out on the same lines as in genu valgum.
Rickety Deformities of the Bones of the Leg—Bow-leg.—These deformities are common in children; are nearly always bilateral and symmetrical, and may be associated with knock-knee or bow-knee. They may occur before the child is able to walk, the bones bending in the attitude in which the limbs are habitually placed—over the nurse's knee, for example, or as they are crossed underneath the child in sitting. In children who are able to walk, the curve is due to the weight of the body acting on the softened bones. In either case, the bending may be increased by the traction of muscles, and sometimes by the occurrence of greenstick fracture. The most common deformity is a uniform curvature of the bones laterally and forwards, or a more acute bend in the lower thirds of their shafts. In some cases the chief curvature is forwards. The ungainliness in walking may be added to by flat-foot. Backward curving of the upper end of the tibia has been already described as one of the causes of genu recurvatum. The most extreme deformities are met with in rickety dwarfs.
Treatment.—Under the age of six, and particularly in children, who are actively growing, the bones will probably straighten if the child is treated for rickets and kept off his feet; well-padded lateral splints are applied as recommended for knock-knee, and these should be taken off at intervals for massage and douching. Above the age of six, the choice lies between osteoclasis and osteotomy. In performing osteotomy the bone is either simply divided or a segment is resected. The fibula can usually be forcibly straightened, but may require to be divided through a separate incision. In aggravated cases it may also be necessary to lengthen the tendo Achillis.
The deformities of the bones of the leg in inherited syphilis, ostitis deformans, and osteomalacia have already been described.
Congenital Deficiencies of the Bones of the Leg.—The tibia may be absent completely or in part, more often on one side than on both sides. In either case the leg is short and stunted, the knee is flexed, the foot occupies the position of extreme equino-varus, and the limb is useless. The extent of the defects is demonstrated by the Röntgen rays. Among other defects with which it may be associated, absence or deficient development of the patella is the most frequent. When the upper end of the tibia is absent, the fibula articulates with the lateral condyle of the femur. The operative treatment aims at correcting the flexion at the knee, the equino-varus deformity of the foot, and at substituting the fibula for the absent tibia. The deficiency of the upper end may be compensated for by implanting the head of the fibula between the condyles of the femur, and that at the lower end by splitting the fibula so as to form a socket for the talus. Amputation should be avoided, as even a dwarfed leg and foot improves the service of an artificial limb. A modification of the O'Connor extension boot may be employed.
The fibula may be absent completely or in part. The clinical appearances depend upon the condition of the tibia. When the tibia is normal, the most notable feature is the absence of the lateral malleolus, and the extreme valgus attitude of the foot. More commonly the tibia makes a sharp forward bend just below its middle, and the overlying skin presents a dimple or scar-like depression. This has usually been regarded as an evidence of intra-uterine fracture, but the observations of Hoffa suggest that both the bend of the bone and the depression on the skin are due to pressure exercised upon the leg from without by an amniotic band or adhesion. The leg fails to grow, the deformity becomes more pronounced, and the toes become pointed. If the tibia is markedly bent, it may be straightened by osteotomy; and the tendons, Achillis and peronei, may require to be lengthened. If the ankle is unstable as a result of the absence of the lateral malleolus, it may be artificially ankylosed, or the lower end of the tibia may be split vertically so as to make a socket for the talus. In either case, the foot is placed in the equinus attitude to compensate for the shortening of the leg. Deficiency of the tibia is frequently associated with imperfect development of the great toe; deficiency of the fibula with absence of the lateral toes and their metatarsal bones.
Volkmann's Supra-malleolar Deformity.—This condition, which is closely allied to that just described, consists in a congenital deficiency in the development of the bones of the leg, and especially of the fibula, as a result of which the articular surface is oblique and the foot deviates to one or other side. The foot usually occupies a valgus position, the sole looking laterally, and only its medial border coming into contact with the ground. It is treated by supra-malleolar osteotomy.
Various deformities are met with in the region of the ankle and tarsus. The term “talipes” is commonly used to include all these, but here it will be restricted to that form in which the heel is more or less elevated, and the foot supinated so that it rests on its lateral border—talipes equino-varus. In pes equinus the foot is in the position of plantar-flexion, and the patient walks on the toes. In pes calcaneus the foot is dorsiflexed so that the tip of the heel comes in contact with the ground; this deformity may be combined with eversion of the foot, pes calcaneo-valgus, or with inversion, pes calcaneo-varus. When the instep is unduly arched, the terms pes cavus, pes arcuatus or hollow claw-foot are employed; while loss of the arch constitutes flat-foot, and eversion of the sole, pes valgus.
Talipes Equino-varus.—This deformity may be congenital or acquired.
Congenital talipes equino-varus (Fig. 142) is a common malformation which is sometimes associated with other deformities, such as hare-lip or spina bifida, and may be met with in several members of one family. It is nearly twice as common in boys as in girls, and is slightly more frequently bilateral than unilateral. Its etiology is obscure, and various hypotheses have been put forward to account for it, but no one is convincing. It may be pointed out, however, that the fœtal foot is very easily moulded into abnormal attitudes by external pressure such as might be exercised by the wall of the uterus when the liquor amnii is deficient. In a number of cases there are indications of such pressure over the bony prominences of the foot, in the shape of circumscribed scar-like areas in which the skin is atrophied; and in the infant, the intra-uterine position can be reproduced, thus demonstrating its method of origin. The occurrence of club-foot in several generations is alleged to support the Mendelian law.
Pathological Anatomy.—In well-marked cases the foot presents a concavity towards the medial side, the maximum point of the curve being opposite the mid-tarsal joint. When the patient attempts to stand, only the lateral border of the foot touches the ground, and the weight is borne on the fifth metatarsal, the cuboid, and the greater process of the calcaneus.
The individual tarsal bones, especially the talus and calcaneus, are altered in shape as well as in their relations to one another and to the tibio-fibular socket. The navicular and cuboid are rotated medially around the anterior ends of the talus and calcaneus respectively, and the tubercle of the navicular comes to lie close to the medial malleolus. The lower third of the tibia is twisted medially on its vertical axis.
The changes in the soft parts follow the general law that tissues which are relaxed become shortened, while those that are put on the stretch are lengthened. All the tissues on the medial, concave side of the foot are shortened, the structures most affected being the medial and the posterior ligaments of the ankle, and the inferior calcaneo-navicular ligament. There is also shortening of the muscles inserted into the tendo Achillis, and to a less extent of the tibiales anterior and posterior. The extensor tendons on the dorsum are displaced medially.
Clinical Features.—In children who have not walked, the degree of deformity varies, sometimes being very slight; in pronounced cases, the foot is turned medially, and in that position forms a right angle with the leg; the sole looks backwards and the medial border upwards. The foot appears shortened because it is curved on itself, the heel is narrower and more vertical than normal, the medial malleolus is obscured by the approximation of the navicular, and the lateral malleolus is unduly prominent.
In extreme cases, the supinated foot forms an acute angle with the leg, and there is frequently a deep transverse depression across the sole, the result of contraction of the plantar fascia—a feature which is distinctive of the congenital form of club-foot.
In children who have walked, the deformity becomes aggravated. The dorsum of the foot is markedly uneven, partly because of the prominence of the individual tarsal bones, and especially of the head of the talus and greater process of the calcaneus, and partly because of a depression over the neck of the talus. Instead of resting on its lateral border, the foot may finally rest on the dorsum, the sole looking upwards and backwards. While the skin over the heel remains comparatively thin and delicate, that covering the lateral border and dorsum of the foot becomes the seat of callosities, beneath which adventitious bursæ are formed. These bursæ are liable to become inflamed, and are then a source of great suffering, and if they suppurate may cause persistent sinuses. The muscles of the leg and foot, although not paralysed, undergo atrophy from disuse. In walking, the patient lifts one foot over the other in an ungainly and laborious manner, without any spring, as if walking on stilts.
In adults, these features are further aggravated, and there are permanent changes in the bones (Fig. 144).
Treatment.—This should be commenced as soon as the viability of the infant is beyond question, as the younger the patient the more easily and completely is the deformity rectified. Manipulations to correct the deformity should be carried out twice or thrice daily, and the limbs are also massaged and douched. At the end of two or three months, assistance may be derived from the use of a simple lateral poroplastic or aluminium splint with a foot-piece, or more simply by a strip of rubber plaster. The foot is held in the over-corrected attitude and the plaster is applied so as to maintain this attitude. If this regime is systematically persevered with from within a few days after birth, by the time the child begins to walk the sole can be brought into contact with the ground, and the weight of the body will aid in correcting the deformity. If the equinus element resists correction, the tendo Achillis should be lengthened.
The turning in of the toes may be overcome by strapping the feet at night to a wooden board with the whole lower limb rotated laterally so that the toes of each foot point directly outwards. On account of the tendency towards relapse, the manipulations and massage must be persevered with for at least a year.
Tenotomy and Forcible Correction under Anæsthesia.—In more severe cases we have to deal not only with the contracted soft parts, but with changes in the bones resulting from their having grown in adaptation to the deformed attitude. The majority of surgeons defer operative measures until the child is about a year old.
The soft parts to be divided are the tendo Achillis, the medial and posterior ligaments of the ankle, the plantar fascia, the calcaneo-navicular ligaments, and the tibialis posterior tendon. The varus deformity may then be corrected by laying the foot on its lateral side on a padded triangular wooden block, and pressing forcibly on the anterior and posterior ends of the foot so as to undo the curve on its medial side and allow of abduction of the foot; this is usually attended with cracking as the shortened ligaments give way. The equinus element is next dealt with by forcibly dorsiflexing the foot until the deformity is over-corrected. If it is preferred to correct the deformity in stages instead of at one sitting, the equinus element is left to the last. In older children, the strength of the hands is usually insufficient to stretch the tissues, and mechanical wrenches may be employed, such as those devised by Thomas, Bradford, or Lorenz.
Resection of a wedge from the tarsus (Davies Colley, 1876) is reserved for the most severe cases in which the shape and rigidity of the bones prevent correction of the deformity by any other means. The base of the wedge is on the lateral aspect, and the bone removed includes parts of the calcaneus, cuboid, talus, and navicular.
Removal of the talus is an alternative operation to resection of the tarsus, and may yield equally good results.
In children, before the tarsal bones have become completely ossified, Ogston's method yields good results; instead of removing a wedge from the tarsus, the osseous nucleus of each bone is gouged out, leaving the cartilaginous shell. In this way the intertarsal joints are not interfered with, and the cartilaginous tarsus can be moulded so that when ossification is completed the bones differ but little from the normal.
After any of these operative procedures, manipulations, massage, exercises, electrical stimulation of the muscles, and the wearing of some apparatus must be persevered with for at least twelve months. Failures are due to not sufficiently over-correcting the deformity in the first instance, and to neglect of after-treatment; in hospital practice it is difficult to ensure continuous supervision over long periods.
Finally, amputation may be called for when other methods have failed, and the patient is unable to put the foot to the ground because of suppurating bursæ and ulceration of the skin.
Acquired Talipes Equino-varus.—In the great majority of cases this condition results from anterior poliomyelitis. It especially affects the peronei and the extensors of the toes, and is unilateral. The patient is unable to dorsiflex and abduct the foot, which hangs with the toes pointed and the sole turned medially.
At first the joints are flaccid, and the attitude can easily be corrected by manipulation. In course of time, however, the opposing muscles—those inserted into the tendo Achillis, the tibialis posterior, and the long flexors of the toes—become shortened, and there is secondary contraction of the plantar fascia and of the ligaments on the medial side of the foot, and the deformity is thus rendered permanent. The bones also are altered in their shape and mutual relations, the talus being rotated forwards so that a large portion of its trochlear surface protrudes from the tibio-fibular socket. The skin is cold and livid, and readily suffers from pressure sores. The whole limb is ill-developed, and may be shorter than its fellow, and the paralysed muscles are wasted and exhibit for a time the reaction of degeneration.
A similar deformity may result from section of the peroneal (external popliteal) nerve, from the peroneal form of progressive muscular atrophy, and from peripheral neuritis.
The treatment of paralytic equino-varus, short of operation, has been referred to under anterior poliomyelitis (p. 242). If tendon transplantation is indicated, the tendon of the tibialis anterior is attached to the cuboid, and a strip of the tendo Achillis to the dorsal aspect of the tarsus. Jones displaces the tibialis anterior into the base of the fifth metatarsal.
If the paralysis is widely distributed, and the joints are flail-like, it is better to ankylose the ankle and mid-tarsal joints. It may be necessary to divide in several places the plantar fascia and other structures that have undergone secondary shortening.
As using the limb hastens the restoration of function, the child should be got on to his feet as soon as possible.
The spastic form of talipes equino-varus is comparatively rare. The plantar flexors and invertors distort the foot into the equino-varus attitude. The heel is drawn up, the anterior part of the foot is adducted and inverted at the mid-tarsal joint. The muscles are tense and rigid, and the reflexes exaggerated. The condition is frequently bilateral, and is often associated with other deformities of the lower limb and with a characteristic spastic gait. Considerable improvement may be brought about by lengthening the tendons of the shortened muscles. In severe cases it may be necessary to resect a portion of the tarsus.
The occurrence of varus without equinus is so exceptional as not to call for separate description.
Pes Equinus.—This deformity, in which the foot is in the position of plantar-flexion with the heel drawn up and the toes pointed, is nearly always acquired as a result either of poliomyelitis or of spastic paralysis. In typical cases the patient walks on the balls of the toes (Fig. 145). It is seldom met with as a congenital condition. Occasionally it is due to nerve lesions such as peripheral neuritis, or to injuries and diseases in the region of the ankle, when the foot has been allowed to remain for long periods in the attitude of plantar-flexion. In a limited number of cases the equinus attitude is assumed to compensate for shortening of the limb.
In poliomyelitis the deformity is most often unilateral (Fig. 146), while in spastic paralysis it is frequently bilateral (Fig. 145), and is usually accompanied by excessive arching of the foot—pes cavus—as a result of plantar-flexion at the mid-tarsal joint, and hyper-extension of the first phalanges and plantar-flexion of the second and third phalanges of the toes—“clawing of the toes.”
Clinical Features.—In the mildest cases the patient is able to bring the foot to a right angle. In average cases the heel is raised off the ground, and the foot rests on the balls of the toes. In extreme cases, and especially when the extensors are completely paralysed, the toes may be flexed towards the sole, and the weight is borne on the dorsum of the foot (Fig. 146). The patient suffers from painful corns and callosities, and from inflammation of bursæ which form over the points of pressure. When unilateral, the patient compensates for the lengthening of the limb by flexing the knee and throwing the limb outwards in walking. In severe cases, especially when both limbs are affected, the patient may be dependent on crutches.
The talus projects on the dorsum, the anterior part of its trochlear surface escapes from the tibio-fibular socket, and the calcaneus is drawn up so that it comes into contact with the bones of the leg (Fig. 147).
Shortening of the soft parts affects chiefly the muscles inserted into the tendo Achillis, the posterior ligament, and posterior parts of the lateral ligaments of the ankle. The fasciæ, ligaments, and muscles of the sole of the foot are also shortened. The flexors of the toes, the tibialis posterior, and the peroneus longus are shortened to a less degree.
Treatment.—Of all the deformities of the foot, pes equinus is that most easily rectified. In recent cases a great deal may be done by regular manipulations, and by the wearing of some corrective splint or apparatus between times.
In well-marked cases it is necessary to lengthen the shortened structures, and especially the tendo Achillis. When the equinus is corrected, the excessive arching of the foot (pes cavus) and the clawing of the toes usually disappear, but it may be necessary to lengthen the flexor tendons, especially that of the great toe, and also the plantar fascia.
Jones divides the tendo Achillis and the flexors of the toes subcutaneously, and maintains the dorsiflexion by excising an oval flap of skin from the front of the ankle.
In aggravated cases, the bones must be attacked, for example by excising the talus. Arthrodesis of the ankle alone or along with the mid-tarsal joint may be indicated when these joints are flail-like. Amputation is reserved for cases which are otherwise hopeless, such as that shown in Fig. 147.
When the deformity is compensatory to shortening of the limb, it is usually said to be a mistake to correct the equinus. Experience shows, however, that in young patients growth is stimulated by walking on the limb after the deformity has been corrected; the sole of the boot is then raised to the necessary extent.
Pes Calcaneus.—In this deformity the foot is dorsiflexed at the ankle-joint. It is sometimes combined with eversion of the foot—pes calcaneo-valgus, or with inversion—pes calcaneo-varus.
Pes calcaneus may be congenital or acquired. In the congenital form the deformity is frequently bilateral. There is dorsiflexion at the ankle-joint, and if an attempt is made to flex the foot towards the sole, the extensor tendons stand out prominently. In marked cases the long axis of the calcaneus is vertical, the tendo Achillis lies in close contact with the tibia, and the hollows on either side of the tendon are absent. The peronei are displaced from their grooves, and may lie in front of the lateral malleolus.
Corrective manipulations are commenced within a few days after birth, and a malleable splint is worn between times. When the child begins to walk there is a natural tendency towards recovery. In severe cases it may be necessary to lengthen the contracted tendons—the extensor digitorum, the extensor hallucis, and, it may be also, the peroneus tertius and tibialis anterior; the tendo Achillis may require to be shortened.
In the acquired form, the appearances are different, because the anterior part of the foot is usually flexed towards the sole, thus disguising to a certain extent the dorsiflexion at the ankle. This form is nearly always due to poliomyelitis, but it may also result from accidental division of the tendo Achillis. The anterior part of the foot is flexed towards the sole by the contraction of the plantar fascia and short muscles of the sole, the balls of the toes are approximated to the heel, and a deep transverse groove is formed in the sole opposite the mid-tarsal joint. The deformity presents a combination of the hollow foot—pes cavus—with pes calcaneus, and resembles that of a Chinese lady's foot. The foot rests on the heel and on the balls of the great and little toes, the sole of the foot being so deeply hollowed that even the lateral border does not touch the ground.
In paralysis of the calf muscles alone, the tendons of the peronei or flexor digitorum longus may be divided and stitched to the calcaneus, to take the place of the tendo Achillis. If the calf muscles are not completely paralysed and the tendo Achillis is merely stretched, this tendon may be shortened by splitting it longitudinally and making the ends overlap, or its insertion may be displaced downwards. When the ankle is flail-like, it may be necessary to perform arthrodesis.
Jones gets rid of the cavus deformity by resecting a wedge with its base towards the dorsum from the middle of the tarsus; the foot is then placed in a position of extreme calcaneus, the dorsum coming into contact with the front of the leg. Four weeks later a wedge is taken from the posterior part of the talus large enough to bring the foot down to a right angle with the leg; the articular surfaces of the tibia and fibula being denuded of cartilage, ankylosis takes place in a good position.
Pes Calcaneo-valgus.—This deformity, which consists in a combination of dorsiflexion at the ankle and eversion of the foot, is as common as pure calcaneus (Figs. 148 and 149); the heel is depressed, the sole looks laterally, and its medial border is convex. Although it may be congenital, it is usually acquired as a result of poliomyelitis. The calf muscles are paralysed while the peronei retain their power, and, along with the tibialis anterior and the extensors of the toes, become secondarily contracted. Treatment is conducted on the same lines as in pes calcaneus, and the valgus may be controlled by implanting the peroneus brevis into the navicular.
Pes Calcaneo-varus.—In this rare deformity the heel is depressed and the sole of the foot looks inwards.
Pes Cavus.—In this deformity, which is known also as hollow claw-foot, pes arcuatus, or pes excavatus, the longitudinal arch of the foot is exaggerated as a result of the approximation of the balls of the toes to the heel (Fig. 150). It is most frequently met with as an addition to pes equinus or pes calcaneus of paralytic origin, and has already been described. There is a mild form which is congenital, and which is quite independent of paralysis; another variety occurs in diseases of the spinal cord, such as Friedreich's ataxia.
The name hollow claw-foot appropriately indicates the clinical appearances. The arch is exaggerated and the instep abnormally high; there is hyper-extension of the toes at the metatarso-phalangeal joints, and plantar-flexion at the inter-phalangeal joints; the plantar fascia and muscles are shortened. The footprint shows that neither border of the foot touches the ground. The patient complains of pain in the instep, of painful corns over the heads of the metatarsal bones, and of difficulty in getting properly fitting boots.
Treatment should first be directed towards the equinus or calcaneus element of the deformity, for if these are corrected the cavus condition tends to disappear. Exercises and massage should be persevered with, and boots without heels should be worn. The contracted structures in the sole may require to be divided, either subcutaneously or by the open method, as a preliminary to forcible correction, and the hallucis tendon may be brought through the head of the first metatarsal. In aggravated cases the talus and the heads of the metatarsal bones may be excised.
Flat-foot or splay-foot is that deformity in which there is loss of the arch, and the foot tends to be pronated and abducted. The term pes planus is applicable when there is merely loss of the arch; pes valgus when the foot is pronated and the sole looks laterally. Of all deformities of the foot, flat-foot is the one for which advice is most frequently sought; it is also a common complication of other disabilities of the foot and of the lower extremity. It is usually bilateral, and is about twice as common in the male as in the female. Various types are met with; they are known according to their cause, as static, congenital, traumatic, paralytic, rachitic, rheumatic, arthritic, gonorrhœal, and tabetic.
Static or Adolescent Flat-foot.—This, by far the most common and important variety (Fig. 152), generally develops between the ages of fourteen and twenty. It is called static because the essential factor in its production is a disproportion between the weight of the body and the supporting power of the arch of the foot.
It is met with in rapidly growing children or adolescents of feeble muscular development and with long narrow feet, and those especially who, after leaving school, begin some occupation which entails much standing—such as that of a factory hand, message boy, or domestic servant. To enable him to stand with the least effort for long periods, the patient adopts an attitude which makes little demand on the muscles, and throws nearly all the strain of the body weight on the ligaments and bones of the feet. This, which has been called “the attitude of rest,” consists in standing with the limbs apart, the knees slightly flexed, the legs slightly rotated laterally at the knee, and the feet pronated, with the toes pointing laterally. The most important local factors predisposing to flat-foot are weakness of those muscles which normally support the ankle and the tarsal arches, especially the tibiales; weakness of the ligaments of the foot; and softness of the tarsal bones. When these conditions are present and a faulty method of standing and walking is adopted, the undue strain to which the tendons and ligaments are exposed results in their being stretched; the bones are altered in position, and flat-foot results. The head of the talus is displaced medially, and is protruded between the calcaneus and navicular, tending to separate them from one another, stretching the inferior calcaneo-navicular ligament and causing the anterior part of the foot to be abducted. The plantar ligaments—especially the inferior calcaneo-navicular—are stretched and lengthened. In something like 80 per cent. there is the combined deformity—pes plano-valgus—in those who apply for treatment.
Clinical Features.—The patient complains of being easily tired, and of pain in the foot after walking or standing. There is generally more pain before the appearance of the deformity than when it has developed, and at this stage it is not so easily recognised, and is apt to be called “rheumatism.” The most common seat of pain is at the medial border of the foot behind the tubercle of the navicular, and this is due to stretching of the inferior calcaneo-navicular ligament. Pain is also complained of in the middle of the dorsum across the instep, from stretching of the interosseous ligaments. Later, there is pain over the greater process of the calcaneus in front of the lateral malleolus, from these bones coming into contact. There may be nocturnal cramp in the muscles of the leg and foot.
The faulty attitude of the foot in standing and walking is usually evident. The foot appears longer and broader than normal, and when the body weight is put on it, it spreads out with the toes extended until the entire sole is in contact with the ground. In advanced cases, the medial border of the foot may be actually convex. Below and in front of the prominent medial malleolus, the head of the talus forms a rounded eminence, and a little farther forwards and lower still is the projection of the tubercle of the navicular. The eversion of the foot as a whole is best seen from behind; if the central axis of the leg is prolonged downwards, it approaches the medial border of the heel instead of passing through its centre; or, stated differently, instead of the axis of the calcaneus being a continuation of that of the leg, it deviates laterally and the medial malleolus is abnormally prominent. When the eversion is more pronounced, the sole looks laterally and the tendons of the peronei stand out in relief. The anterior part of the foot is displaced laterally. Flat-foot is frequently associated with stiff great toe; the patient having lost the power of dorsiflexing the toe, the first phalanx and first metatarsal are in a straight line, instead of forming an angle open towards the dorsum.
The muscles of the leg are flabby and poorly developed. When the patient is seated and asked to move the foot in different directions, there is a characteristic stiffness, ungainliness, and restriction in the range of movement. The feet are usually cold and sweat excessively. The gait is slouching, and there is a want of spring and elasticity. The lengthening of the foot results in the tendons, especially the flexors, being too short, hence hammer-like contraction of the toes may be brought about. The boots, after being worn, show a bulging of the instep towards the sole, greater wearing away of the sole along the medial border, and, when there is stiff great toe, an absence of the transverse crease on the dorsum opposite the balls of the toes. Footprints may be obtained by wetting the soles of the feet. The print of a normal foot shows only the heel, the lateral border of the foot, and the balls and tips of the toes. In flat-foot the medial border appears in the print to a greater or less extent (Fig. 154). If a record is wanted to estimate the progress of treatment, the sole of the foot is painted with a 5 per cent. solution of ferro-cyanide of potassium, and the patient stands on paper painted with the liquor of the perchloride of iron diluted one-half; the print appears dark blue on a yellow ground.
Skiagrams are useful for showing displacement of bones and differences between sitting and standing, and for recording the results of treatment.
Prophylaxis of Flat-foot.—Stress is to be laid on a supervised training of the whole muscular system, and especially of that of the legs. In walking and standing, the feet should be kept parallel and not pointed outwards, as was formally taught in schools of gymnastics and insisted upon by drill instructors. Children should be taught to walk properly, rising on the balls of the toes with each foot in succession. Attention should also be directed to the boots, which should be so fashioned that the medial side of the boot is kept straight and the end of the boot is opposite the big toe.
Treatment.—This is directed towards restoring and maintaining the arch of the foot. As the measures adopted necessarily vary with the extent to which the condition has progressed, it is convenient for purposes of treatment to recognise the following four degrees. A first degree, in which the arch reappears when the weight is taken off the foot or the patient rises on the balls of the toes; a second, in which the normal attitude can be restored by manipulation; a third, in which this is only possible under anæsthesia; a fourth, in which the bones are so displaced and altered in shape that correction is impossible without operation.
Cases of the First Degree.—If there is marked pain and tenderness, the patient must lie up. The general health is improved by a nourishing diet and by cod-liver oil and tonics; and the legs and feet are douched and massaged thrice daily. When pain and tenderness have disappeared, the patient is instructed how to walk and exercise the feet. In walking, the medial edges of the feet should be parallel with one another, first the heel should touch the ground and then the balls of the toes. He should neither stand nor walk long enough to cause fatigue, and in standing he should alter the attitude of the feet from time to time, and occasionally rise on the balls of the toes. The following exercises, devised by Ellis of Gloucester, should be practised: (1) Rising on the balls of the toes, the toes being directed straight forwards; (2) rising on the balls of the toes, with the points of the great toes touching each other, and the heels directed out, so that the medial borders of the feet meet in front at a right angle; (3) in the same attitude, after rising on to the balls of the toes, the knees are flexed and then extended before the heels descend again; (4) while seated in a chair, one leg crossed over the other, circumduction movements of the foot are carried out; (5) while standing, the medial border of the foot is raised off the ground several times, then the patient walks to and fro on the lateral border of the foot, and in the same attitude lifts one foot over the other. These exercises should be carried out slowly and deliberately, with the feet bare, and they should be carefully supervised until the patient thoroughly understands what is aimed at. The movements should be performed a definite number of times at regular intervals, but should not be pushed so as to cause pain or fatigue. The patient should be fitted with well-made lacing boots, with the heel and sole raised about half an inch on the medial side so that the foot rests mainly on its lateral border. The additional leather, which can be applied by any bootmaker, is in the form of a wedge, with its base to the medial side, one on the sole and one on the heel. The wedge fades away towards the lateral border, and also forwards towards the tip. In time, the limbs are further strengthened by sea-bathing, cycling, skipping, and other exercises.
In cases of the second degree, the patient should be provided with a metal plate inside the boot. That known as Whitman's spring is the most popular. A plaster cast is taken of the sole while the foot is held in its proper position, and on this a metal plate, preferably of aluminium bronze, is modelled. This is covered with leather and inserted into the boot. We have found the supports devised by Scholl simple and efficient. The treatment described for cases of the first degree is carried out in addition.
In cases of the third degree, the deformity is corrected under an anæsthetic. The foot is forcibly moved in all directions so as to stretch the shortened ligaments and to break down adhesions, it is then rotated into an extreme varus position, and fixed in plaster-of-Paris or to a Dupuytren's splint. It may be necessary to have recourse to the Thomas' wrench, employed in the correction of club-foot. When the reaction consequent upon this procedure has subsided, the question of shortening or of reinforcing the tendons concerned in the support of the arch of the foot may be considered; one of the peronei, for example, may be attached to the tubercle of the navicular. We have not found it necessary to employ this procedure.
In cases of the fourth degree, in which the displacement and alterations in shape of the bones constitute an insuperable bar to correction, operative treatment may be considered, either resection of a wedge including the talo-navicular joint or forward displacement of the tuberosity of the calcaneus.
Spasmodic Flat-foot.—There are cases of flat-foot in which pain and spasm of the peronei muscles are the predominant features. If the spasm is not allayed by rest in bed and hot fomentations, the foot should be inverted under an anæsthetic; and in this position it is encased in plaster-of-Paris. Jones resects an inch of each of the peroneal tendons about 21/2 inches above the tip of the lateral malleolus; Armour and Dunn claim to have obtained better results from crushing the peroneal nerve in the substance of the peroneus longus.
Paralytic Flat-foot (Fig. 155).—In typical cases this results from poliomyelitis affecting the tibial muscles. When other groups of muscles are affected at the same time, compound deformities, such as pes calcaneo-valgus, are more likely to result.
 Fig. 155.—Bilateral Pes Valgus and Hallux Valgus in a
girl æt. 15, the result of Anterior Poliomyelitis.
Fig. 155.—Bilateral Pes Valgus and Hallux Valgus in a
girl æt. 15, the result of Anterior Poliomyelitis.
In paralytic valgus the medial border of the foot is depressed and convex towards the sole, and although the foot can readily be restored to the normal position by manipulation, it at once resumes the valgus attitude. The leg is wasted, the skin is cold and livid, and the ankle is flail-like. The treatment consists in reinforcing the paralysed tibial muscles by attaching the peronei, or a strip of the tendo Achillis, to the scaphoid, or in bringing about an ankylosis of the joints above and in front of the talus.
Traumatic flat-foot is that form which results directly from injury. It is most often due to a fall from a height on to the feet; the ligaments supporting the arch are ruptured, and the bones are displaced, either at the time of the injury or later when the patient gets out of bed. The arch can only be restored by a wedge-resection of the tarsus. Loss of the arch may follow as a result of walking on the everted foot after injuries about the ankle, especially a badly united Pott's fracture; the foot may be displaced laterally and pronated, the sole looking laterally. This variety is very unsightly and disabling; it is treated by supra-malleolar osteotomy of the tibia and fibula.
Other Forms of Flat-foot.—Flat-foot is sometimes met with in rickety children, in association with knock-knee or curvature of the bones of the leg, and is treated on the same lines as other rickety deformities. It may follow upon an attack of acute rheumatism or upon diseases in the region of the ankle and tarsus, such as gonorrhœa, arthritis deformans, tuberculosis, and Charcot's disease; the gonorrhœal flat-foot is extremely resistant to treatment. There is a congenital form in which the sole is convex and the dorsum concave, the result of the persistence of an abnormal attitude of the fœtus in utero. Lastly, there is a racial variety, chiefly met with in the negro and in Jews, which is inherited and developmental, and which, although unsightly, is rarely a cause of disability.
Pes Transverso-planus.—Lange describes under this head a sinking or flattening of the anterior arch formed by the heads of the metatarsal bones, of which normally only the heads of the first and fifth rest on the ground. In this condition all may be on the same level or the arch is actually convex towards the sole. It may coexist along with the common form of flat-foot, or it may be associated with the neuralgic pain known as metatarsalgia.
Painful Affections of the Heel.—These include inflammation of the bursa between the posterior aspect of the calcaneus and the lower end of the tendo Achillis, inflammation of the tendon itself and its sheath of cellular tissue, and the presence of a spur of bone projecting from the plantar aspect of the tuberosity of the calcaneus. The spur of bone is the source of considerable pain on standing and walking, and tenderness is elicited on making pressure on the plantar aspect of the heel; it is well demonstrated by the X-rays (Fig. 156). The condition is usually bilateral. Complete relief is obtained by removing the spur by operation.
Sever of Boston calls attention to a painful condition of the heel met with in children, and associated with changes in the epiphysial junction, allied to those met with in the epiphysis of the tubercle of the tibia in Schlatter's disease. The changes in the epiphysial junction can be demonstrated in skiagrams. Treatment is conducted on the same lines as in teno-synovitis of the tendo Achillis.
Metatarsalgia.—This affection, which was first described by Morton of Philadelphia (1876), is a neuralgia on the area of the anterior metatarsal arch, specially located in the region of the heads of the third and fourth metatarsal bones. It is most often met with in adults between thirty and forty, is commoner in women than in men, and is often combined with flat-foot. The patient complains of a dull aching or of intense cramp-like pain in the anterior part of the foot. The pain is usually relieved by rest and by taking off the boot. It may be excited by pressing the heads of the metatarsals together or by grasping the fourth metatarso-phalangeal joint between the finger and thumb. In advanced cases the pain may be so severe as to cripple the patient, so that she is obliged to use a crutch. On examination, the sole may be found to be broadened across the balls of the toes, and there may be corns over the heads of the third and fourth metatarsals. Skiagrams may show a downward displacement of the head of one or other of these bones, and prints of the foot may show an increased area of contact in the region of the balls of the toes. The affection is of insidious development, and is usually ascribed to sinking of the transverse arch of the foot—pes transverso-planus—the result of weakness or of wearing badly fitting boots. The intense pain is believed to be due to stretching of, or pressure upon, the interdigital nerves or the communicating branch between the medial and lateral plantar nerves; Whitman believes it is due to abnormal side pressure on the depressed articulations.
Treatment.—Great improvement usually results from treating coexisting flat-foot, and pain is relieved by rest, massage, and douching. A tight bandage or strip of plaster applied round the instep before putting on the stocking may relieve pain. Boots should be made from a plaster cast of the foot, high and narrow at the instep so as to compress the bases of the metatarsals, and with the medial edge of the sole and heel slightly raised; a support may be worn in the sole, like that used for flat-foot, with both the longitudinal and transverse arches exaggerated. Scholl has devised a support for the anterior arch which we have used with benefit. When the head of one of the metatarsals is displaced, it may be removed through a dorsal incision running parallel with the tendon of the long extensor.
Hallux Valgus and Bunion.—Hallux valgus is that deformity in which the great toe deviates towards the middle line of the foot and comes to lie on the top of, or beneath, the second toe (Figs. 155, 157). The head of the first metatarsal projects on the medial border of the foot, and, as a result of the pressure of the boot, an adventitious bursa is formed, which, when thickened by chronic inflammation, constitutes a prominent swelling or bunion. It is a common affection in civilised and especially in urban communities, and reaches its acme of development in adult women. It may occur on one or on both sides, and is sometimes associated with flat-foot.
 Fig. 157.—Radiogram of Hallux Valgus. The sesamoid
bone is seen displaced towards middle line of the foot.
Fig. 157.—Radiogram of Hallux Valgus. The sesamoid
bone is seen displaced towards middle line of the foot.
The deformity develops slowly, and is usually attributed to the wearing of stockings which are unduly tight at the toes, and of improperly made boots. The boot that favours the occurrence of hallux valgus is one which is too short and has pointed toes, with the apex in the middle line of the foot instead of being in line with the great toe. The pressure of the boot displaces the great toe into the valgus position, especially if a high heel is worn, as the toes are then driven forward into the apex of the boot. Once the great toe is abducted by the pressure of the boot, the deformity is increased by bearing unduly on the medial side of the ball of the great toe, and by pointing the foot outwards in walking.
Arthritis deformans is rarely the cause of hallux valgus, but the changes characteristic of that affection are commonly present in the joint of the great toe. In pronounced cases, the base of the first phalanx is displaced on to the lateral aspect of the head of the first metatarsal, the exposed head of which frequently shows fibrillation and wearing away of the cartilage, and is often surrounded by new bone, sometimes amounting to an exostosis. There are also fringes from the synovial membrane that may be caught between the articular surfaces. The distal end of the first metatarsal is displaced medially, broadening the tread of the foot, and in severe cases its shaft is rotated on its long axis, so that its dorsal surface looks medially; the great toe is then similarly rotated (Fig. 157). The flexor and extensor tendons and the sesamoid bones are displaced laterally. The ligaments and other soft parts on the medial side are elongated, while those on the lateral side are contracted.
In women, the chief complaint may be of the disfigurement of the boot; in others, of pain and disability resulting from the sensitiveness of the joint and of the enlarged bursa over the head of the first metatarsal. The inflamed bursa, which sometimes communicates with the joint, may suppurate, and the infection may spread to the joint.
The treatment varies with the severity of the deformity. In mild cases, a great deal can be done by wearing properly made boots and stockings with a separate compartment for the great toe, or a pad of cotton wool or tent of rubber between the great and second toes. The patient should practise manipulations and exercises of the toes and feet, and putting the foot to the ground properly in walking. In pronounced cases, the pain and tenderness must first be got rid of by rest and soothing applications. At night, the attitude of the toe may be corrected by a moulded splint fixed to the medial aspect of the foot by strips of plaster; the toe is then bandaged to the distal end of the splint. Scholl has devised a prop, made of rubber, to be worn between the great and second toes. If there is flat-foot, this must receive appropriate treatment.
In aggravated cases, the deformity can only be corrected by an operation which consists in resecting the head of the metatarsal bone, and the tendon of the long extensor may be detached from its insertion and secured to the medial side of the first phalanx. A bar may be placed across the sole just behind the balls of the toes, and the boot should also comply with the anatomical shape of the foot.
Hallux Varus or Pigeon-toe (Fig. 158).—In this deformity, which is extremely rare, the great toe deviates from the middle line of the foot; it occurs chiefly in children in conjunction with other deformities, and interferes with the wearing of boots. Treatment consists in straightening the toe and retaining it in position by a splint or plaster of Paris. The medial collateral ligament and the tendon of the abductor hallucis may require to be divided.
Hallux Rigidus and Hallux Flexus (Fig. 159).—These terms indicate two stages of an affection of the metatarso-phalangeal joint of the great toe, first described by Davies Colley. In the earlier stage—hallux rigidus—the toe is stiff and incapable of being dorsiflexed, although plantar-flexion is, as a rule, but little restricted. When the joint, in addition to being stiff, is painful, sensitive, and swollen, the term hallux dolorosus is applied.
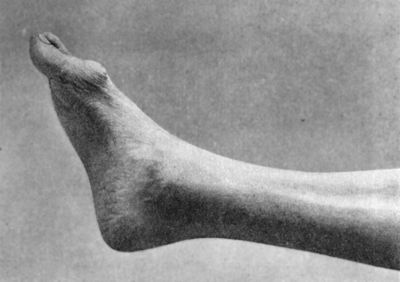 Fig. 159.—Hallux Rigidus and Flexus in a boy æt. 17.
There is a suppurating corn over the head of the first metatarsal
bone.
Fig. 159.—Hallux Rigidus and Flexus in a boy æt. 17.
There is a suppurating corn over the head of the first metatarsal
bone.
As the disease progresses, the toe is drawn towards the sole and becomes permanently flexed—hallux flexus—and any attempt at dorsiflexion is attended with pain.
The condition is met with chiefly in adolescent males, is nearly always associated with flat-foot, and is then usually bilateral. The patient's gait, in addition to having the characteristic features associated with flat-foot, is peculiarly wooden and inelastic, as instead of rising on the balls of the toes with each step, he puts down and lifts the sole as if it were a rigid plate. The pain is increased by walking. The boot tends to become worn away at the point of the toes and at the posterior edge of the heel, and the usual crease across the dorsum is absent.
On dissection it is found, especially in hallux flexus, that the inferior portions of the collateral ligaments are contracted, and that the cartilage of that part of the head of the metatarsal which is exposed on the dorsum is converted into fibrous tissue; there may also be other changes characteristic of arthritis deformans. Bony ankylosis has not been observed.
Treatment.—In early cases, great benefit results from measures directed towards the cure of the accompanying flat-foot, and especially the wearing of the support of the anterior arch devised by Scholl. If the joint of the big toe is painful and sensitive, absolute rest should be enforced until these symptoms have disappeared. The patient must wear a properly shaped boot with a pliable sole, and be instructed how to manipulate and exercise the toe. Later, when the toe is already rigid or flexed towards the sole, the above treatment is not feasible. It is then best to correct the deformity either by wrenching the toe into the dorsiflexed position, under anæsthesia, and fixing it with a plaster-of-Paris bandage; or, when this is impossible, by excising the articular end of the metatarsal bone and interposing a layer of fatty or bursal tissue between the distal end of the metatarsal and the base of the first phalanx. When these measures are impracticable, the suffering may be relieved by inserting in the boot a rigid metal plate which will prevent any attempt at dorsiflexion in walking.
Hammer-toe.—This is a flexion-contracture which generally involves the second, but sometimes also other toes. It may be congenital and inherited, but usually develops about puberty, and is then, as a rule, bilateral, and often associated with flat-foot.
The first phalanx is dorsiflexed, and the second is plantar-flexed, while the third varies in its attitude, sometimes being in line with the second (Fig. 160), sometimes even more plantar-flexed, and sometimes dorsiflexed. When the second toe alone is affected, as is commonly the case, it is partly buried by those on either side of it, only the knuckle of the first inter-phalangeal joint projecting above the level of the other toes (Fig. 160). The skin over the head of the first phalanx being pressed upon by the boot usually presents a corn, under which a bursa forms (Fig. 161). Both the corn and the bursa are subject to attacks of inflammation, which cause suffering and disability in walking. The soft parts at the distal extremity of the toe are flattened out by contact with the sole of the boot—hence the supposed resemblance to the head of a hammer.
On dissection, it is found that the contracture is maintained by shortening of the plantar portions of the collateral ligaments of the first inter-phalangeal joint and of the glenoid ligament upon which the head of the first phalanx rests.
Hammer-toe is usually ascribed to the use of tight socks and of ill-fitting boots, especially those which are median-pointed and are too short for the feet, but in some persons there appears to be an inherited predisposition to the deformity.
While corrective manipulations, strapping, and the use of splints may be of service in slight cases, it is usually necessary to perform an operation in order to extend the toe permanently. Before operating, any infective condition, such as a suppurating corn or bursa, must be corrected. The collateral and glenoid ligaments are divided subcutaneously—Spitzy also divides the flexor tendons and capsule—and if the toe can then be straightened, the foot is secured to a metal splint moulded to the sole and provided with longitudinal slots opposite the intervals on either side of the toe affected. The toe is drawn down to the splint by passing a loop of cotton or elastic bandage round the toe and through the slots. In many cases the contraction of all the tissues on the plantar aspect, including the skin, prevents the toe being straightened even after division of the ligaments, and it is then necessary to remove the head and neck of the first phalanx through a lateral incision. This is more satisfactory than amputation of the affected toe at the metatarso-phalangeal joint, as after this the adjacent toes tend to fall together and favour hallux valgus. If amputation is performed, a pad of cotton wool or rubber prop should be worn to fill up the vacant space.
The term Gampsodactyly has been applied to a deformity in which all the toes assume the position of hammer-toe, usually from a spastic condition of the muscles controlling the toes.
Hypertrophy of the Toes.—One or more of the toes may be the seat of hypertrophy or local giantism. This is usually present at birth or appears in early childhood, and may form part of an overgrowth involving the entire lower extremity (Fig. 162). The overgrowth may involve all the tissues equally, or the subcutaneous fat may be specially affected. The medial toes are those most commonly hypertrophied. In addition to being enlarged, the toe may be displaced from its normal axis. The hypertrophy may affect two or more toes which are fused together or webbed (Fig. 162). The treatment consists in amputating as much of the toe as will allow of an ordinary boot being worn.
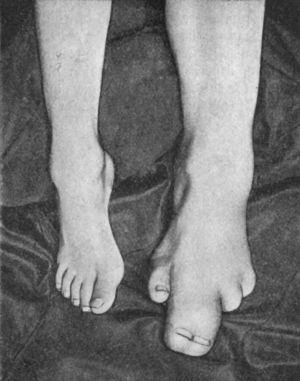 Fig. 162.—Congenital Hypertrophy of Left Lower
Extremity in a boy æt. 5. The second and third toes are fused.
Fig. 162.—Congenital Hypertrophy of Left Lower
Extremity in a boy æt. 5. The second and third toes are fused.
Supernumerary Toes (Polydactylism).—These vary from mere appendages of skin to fully developed toes (Fig. 163); if they interfere with the wearing of boots they should be removed.
Webbing of the Toes (Syndactylism).—This may affect two or more toes, which may be united merely by a web of skin, or so completely fused that the individual digits are only indicated by the nails; the degree of fusion is shown by means of skiagrams. Unless associated with congenital hypertrophy, no treatment is called for.
Congenital Absence of the Clavicle.—Both clavicles may be absent, and it is possible for the patient voluntarily to bring his shoulders into contact with one another in front of the chest; there is little or no impairment of function.
Displacements of the Scapula.—Congenital Elevation of the Scapula (Sprengel's shoulder, 1891).—This abnormality is rare, and is not usually recognised till several years after birth. In one variety there is a bridge of bone or fibrous tissue connecting the superior angle of the scapula with the spinous process of one of the cervical vertebræ, and there may be a false joint at one end of the bridge permitting a certain amount of movement of the scapula. Associated abnormalities in the vertebræ and in the ribs are shown in skiagrams. In the more common type, the scapula seems to be held in its elevated position by shortening of the muscles attached to its body, and it is often rotated so that its lower angle is close to the spine and its axillary border nearly horizontal, or the axillary border may lie in close to the ribs, and the vertebral border project from the chest wall. The shoulder is generally higher and farther forward on the affected side, and there is a moderate degree of scoliosis. There is a want of purchase in the movements of the shoulder and upper arm.
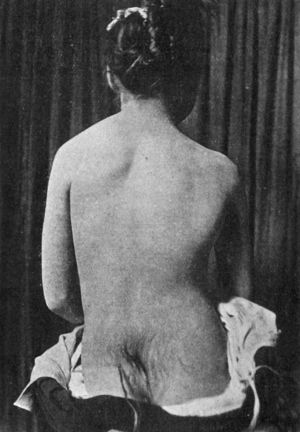 Fig. 164.—Congenital elevation of Left Scapula in a
girl: also shows hairy mole over Sacrum.
Fig. 164.—Congenital elevation of Left Scapula in a
girl: also shows hairy mole over Sacrum.When the deformity is bilateral, which is rare, the neck is short and thick, the chin lies close to the sternum, and the arms can scarcely be raised to the horizontal.
Gymnastic exercises and the wearing of a brace to hold the shoulders back and down may be followed by some improvement, but, as a rule, it is necessary to mobilise the scapula by operation. An X-ray photograph should first be taken, because, when the scapula is connected with the spine by a bridge of bone, this must be resected. The muscles attached to the vertebral border and spine of the scapula are divided, the bone is drawn down to its proper position, and the parts are fixed by plaster bandages.
Winged Scapula.—This condition consists in a marked displacement backwards of the lower angle and vertebral border of the scapula, when the patient attempts to raise the arm from the side (Fig. 165). Under normal conditions, in making this movement the serratus and rhomboid muscles pull forward the vertebral border and inferior angle of the scapula, and so fix the bone firmly against the chest wall. When these muscles are paralysed, as a result of anterior poliomyelitis, neuritis, or injury of the long thoracic nerve of Bell, or of the fifth and sixth cervical nerve-roots through which they receive their supply, the patient is unable to abduct the arm, and the deltoid having lost its point d'appui, its contraction merely results in tilting the angle of the scapula backward (Fig. 165).
Treatment.—In the majority of recent cases the condition yields to the administration of strychnin and other muscle and nerve tonics, and the use of massage and the faradic current. The application of a carefully adjusted padded belt is sometimes useful. The method of treatment by stitching the latissimus dorsi over the lower angle of the scapula is based on the erroneous assumption that the displacement is due to the slipping of that muscle off the bone; at the same time, it must be admitted that the operation sometimes diminishes the deformity and adds to the patient's comfort.
A more efficient method consists in detaching the clavicular portion of the pectoralis major from its insertion, and stitching it to the serratus anterior so as to make it take on the function of this muscle, or stitching it to the axillary border of the scapula. Success has also followed suture of the vertebral border of the scapula to the subjacent ribs (Eiselsberg).
Displacement of the scapula upwards and laterally has been observed as a result of partial paralysis of the trapezius when the nerves supplying it have been divided in removing tuberculous glands from the neck. In these acquired displacements, treatment is directed towards the nerve lesion and towards the improvement of the muscles by electricity, massage, and exercises; when the paralysis of the trapezius is permanent, the disability is gradually overcome by the compensatory hypertrophy of the levator muscle.
Congenital Dislocation of the Shoulder.—This rare condition is usually bilateral, and is associated with other congenital defects. The glenoid cavity is deformed or absent, and the dislocation may be sub-coracoid, sub-acromial, or sub-spinous. The movements of the arm are restricted, and the development of the extremity as a whole is imperfect. It is sometimes possible to reduce the dislocation by manipulation, or, if this fails, by operation. Unilateral dislocation is sometimes mistaken for dislocation that has occurred during delivery and vice versa.
Habitual Dislocation is described on p. 65.
Paralytic Deformities—Paralytic Dislocation of the Shoulder.—The muscles in the region of the shoulder may have their innervation interfered with as a result of various conditions, of which poliomyelitis and injuries of the brachial plexus at birth are the most important. The capsular ligament of the shoulder-joint, being no longer kept tense by the scapular muscles—especially the deltoid and lateral rotators—becomes relaxed, and is gradually stretched by the weight of the arm. The appearances are characteristic; the muscles of the shoulder are wasted, the acromion is prominent, and between it and the upper end of the humerus there is a marked hollow into which one or more fingers may be inserted. The arm hangs flaccid by the side, rotated medially and pronated, and moves in a flail-like fashion in all directions, the patient having little control over it. The best results are obtained by the transplantation of muscles, the trapezius being detached from the clavicle and stitched to the surface of the deltoid, and the upper arm fixed in the position of horizontal abduction with the arm rotated laterally and supinated. Bradford inserts a portion of the trapezius into the humeral insertion of the deltoid. When these methods are impracticable, the upper arm may be fixed to the trunk by some form of apparatus, or arthrodesis is performed so that the movements of the scapula are communicated to the upper arm; the best attitude for ankylosis is one of abduction with medial rotation, so that the hand can be brought to the mouth.
In cases of poliomyelitis, when all the muscles governing the elbow are paralysed while the muscles of the hand have escaped, it may be of great service to fix this joint permanently at rather less than a right angle. This may be effected by arthrodesis, or by removing an extensive diamond-shaped portion of skin from the flexor aspect of the joint and bringing the raw surfaces together, commencing the stitching at the lateral apices of the gap.
 Fig. 166.—Arrested Growth and Wasting of Tissues of
Right Upper Extremity, the result of Anterior Poliomyelitis in
childhood.
Fig. 166.—Arrested Growth and Wasting of Tissues of
Right Upper Extremity, the result of Anterior Poliomyelitis in
childhood.
Congenital Dislocations at the Elbow.—The head of the radius may be dislocated forwards, backwards, or laterally—usually in association with imperfect development of the radius and of the lateral condyle of the humerus. When the displaced head of the bone interferes with supination, or with extension, it should be removed. Congenital dislocation of both bones of the forearm is extremely rare.
Cubitus Valgus and Cubitus Varus.—When the normal arm hangs by the side with the palm of the hand directed forward, the forearm and upper arm form an angle which is open outwards—known as the “carrying angle”; it is usually more marked in women in association with the greater breadth of the pelvis and the relative narrowness of the shoulders. When this angle is increased, the attitude is described as one of cubitus valgus. This deformity may be acquired as a result of rickets, but more commonly it is due to fracture of the lateral condyle of the humerus, in which the separated fragment has been displaced upwards.
Cubitus varus is the reverse of cubitus valgus. It is more common, is always pathological, and is nearly always a result of fracture of the lower end of the humerus or separation of the lower humeral epiphysis and subsequent interference with growth. These deformities may be corrected by supra-condylar osteotomy of the humerus.
Synostosis of the superior radio-ulnar joint is a rare congenital condition, in which the hinge movements at the elbow are free, but supination is impossible; an attempt may be made by operation to form a new joint.
Volkmann's ischæmic contracture of the muscles of the forearm, resulting in the production of claw-hand, is described in Volume I., p. 415.
Deformities of the Forearm and Hand.—The radius may be absent completely or in part, frequently in combination with other malformations. The most evident result is a deviation of the hand to the radial side—one variety of club-hand. The forearm is shortened, the ulna thickened and often bent, and the thumb and its metacarpal bone are often absent, so that the usefulness of the hand and arm is greatly impaired (Fig. 171). For this condition Bardenheuer devised an operation which consists in splitting the lower end of the ulna longitudinally and inserting the proximal bones of the carpus into the cleft.
Congenital deficiency of the ulna is extremely rare.
Intra-uterine amputation by constriction of amniotic bands sometimes occurs (Figs. 168, 169).
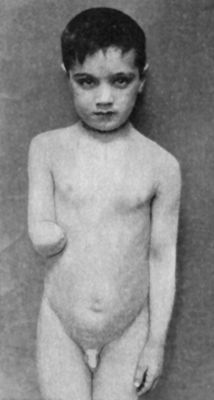 Fig. 168.—Intra-uterine Amputation of Forearm.
Fig. 168.—Intra-uterine Amputation of Forearm.
|
 Fig. 169.—Radiogram of Arm of patient shown in Fig. 168.
Fig. 169.—Radiogram of Arm of patient shown in Fig. 168.
|
Drop Wrist from Anterior Poliomyelitis.—In this condition the capacity of extending the fingers is deficient or absent. Recovery can be confidently predicted if, on still further flexing the fingers, they can be voluntarily extended towards the point from which they are flexed (Tubby and Jones). Considerable improvement may result from fixing the hand by means of a splint in the attitude of dorsal flexion. The splint is removed at frequent intervals to allow of massage and other treatment being carried out, and it has usually to be worn for a period of one to two years. In some cases recourse should be had to arthrodesis.
In spastic paralysis the most pronounced deformity is flexion of the forearm and pronation and flexion of the hand (Fig. 166). Gradual extension at the wrist may be brought about by the use of a malleable splint, in which the angle is gradually increased, over a period of at least twelve months. Failing success by this method, operation may be had recourse to, and this consists in lengthening of tendons, and tendon transplantation. Tubby has devised an operation for converting the pronator radii teres into a supinator, and Robert Jones another in which the flexors of the carpus are made to take the place of the extensors. “These operations, combined if necessary with elongation of the flexors of the fingers, pave the way for diminution of the angle of flexion at the elbow, lessening of the pronator spasm, increase of the supinating power, reduction of the carpal flexion, and addition to the extensor power at the wrist” (Tubby and Jones).
Congenital Club-hand.—This rare deformity corresponds to congenital club-foot, and probably arises in the same way. The hand and fingers are rigidly flexed to the ulnar or radial side, so that the patient is incapable of moving them. Treatment is carried out on the same lines as for club-foot.
A deformity resembling this, acquired club-hand, is brought about when the growth of either of the bones of the forearm has been arrested as a result of disease or of traumatic separation of its lower epiphysis. The hand deviates to the side on which the growth has been arrested—manus valga or vara. The treatment consists in resecting a portion of the longer bone.
 Fig. 171.—Club-hand, the result of imperfect
development of radius. The thumb is absent.
Fig. 171.—Club-hand, the result of imperfect
development of radius. The thumb is absent.Madelung's Deformity of the Wrist.—In 1878, Madelung called attention to a deformity also called sub-luxation of the hand, in which the lower articular surface of the radius is rotated so that it looks towards the palm; there is palmar displacement of the carpus, and the lower end of the ulna projects on the dorsum. The cause of the condition is obscure, but it is met with chiefly in young women with slack ligaments, whose laborious occupation or athletic pursuits subject the hand and wrist to long-continued or repeated strain. It is as frequently unilateral as bilateral and may recur in successive generations. There is a good deal of pain, the grasping power of the hand is impaired, and dorsiflexion is considerably restricted. The deformity disappears on forcible traction, but at once reappears when the traction is removed. A wristlet of poroplastic or leather extending from the mid-forearm to the knuckles is moulded to the limb in the corrected position, and is taken off at intervals for massage and exercises.
When operative treatment is called for, it takes the form of osteotomy of the radius and ulna about an inch or more above their articular surfaces.
Congenital dislocation of the wrist is rare.
Deformities of the Fingers.—Various forms of congenital dislocation of the fingers are met with, but they are of little clinical importance, as they interfere but slightly with the usefulness of the digit affected.
Congenital lateral deviation of the phalanges is more unsightly than disabling; it is met with chiefly in the thumb, in which the terminal phalanx deviates to the radial or to the ulnar side in extension; the deviation disappears on flexion.
Congenital contraction of the fingers is comparatively common. It is an inherited deformity, and is often met with in several members of the same family. It most frequently affects the little or the ring and little fingers (Fig. 172), and is usually bilateral. The second and third phalanges are flexed towards the palm; the first phalanx is dorsiflexed, this being the reverse of what is observed in Dupuytren's contraction. Duncan Fitzwilliams suggests that it should be called “hook-finger,” and that it is probably due to imperfect development of the anterior ligament of the first inter-phalangeal joint. He has observed it in association with laxity of the ligaments of the other joints of the body.
The affection is usually disregarded in infancy and childhood as being of no importance. In young children, the deformity is corrected by wearing a light splint fixed with strips of plaster, or a piece of whalebone or steel inside the finger of a glove. In older children, the finger may be straightened by subcutaneous division of the ligament over the palmar aspect of the base of the middle phalanx, or failing this by lengthening the flexor tendons and resecting a wedge from the dorsal aspect of the first phalanx close to the inter-phalangeal joint.
Dupuytren's Contraction.—This is an acquired deformity resulting from contraction of the palmar fascia and its digital prolongations (Fig. 173). It is rare in childhood and youth, but is common after middle life, especially in men. It is often hereditary, and is said to occur in those who are liable to gout and to arthritis deformans. While it is met with in the working-classes and attributed to the pressure of some hard object on the palm of the hand—such as a hammer or shovel or whip—its greater frequency in those who do no manual work, and the fact that it is very often bilateral, indicate that the constitutional factor is the more important in its causation.
 Fig. 173.—Dupuytren's Contraction.
Fig. 173.—Dupuytren's Contraction.
In the initial stage there is a localised induration in the palm opposite the metacarpo-phalangeal joint, and the skin over it is puckered and closely adherent to the underlying fascia. After a variable interval, the finger is gradually and progressively flexed at the metacarpo-phalangeal joint. The ring finger is usually the first to be affected, less often the fifth, although both are commonly involved. It is rarest of all in the index. The flexion may be confined to the metacarpo-phalangeal joint, or the middle and distal phalanges may also be flexed; and as the deformity becomes more pronounced, the nail of the affected finger may come into contact with the skin of the palm. Dissections show that the flexion of the finger is the result of a chronic interstitial overgrowth or fibrositis and subsequent contraction of the palmar fascia and of its prolongations on to the sides of the fingers. The digital processes of the fascia are thickened and shortened, and come to stand out like the string of a bow. The adipose tissue in the skin of the palm disappears, and the skin and fascia thus brought into contact become fused. The tendons and their sheaths are not implicated; they are found lying deeply in the concavity of the curve of the flexed digit. There is no pain, but the grasp of the hand is interfered with, the patient is unable to wear an ordinary glove, and he may be incapacitated from following his occupation.
The condition is easily diagnosed from congenital contraction by the fact that in the latter the proximal phalanx is dorsiflexed.
Treatment.—When seen in the initial stage, contraction may be prevented by passive movements of the finger and by massage of the indurated fascia; we have observed cases in which these measures have held the malady in check for many years, but when flexion has already occurred, they are useless, and according to the social position, habits, or occupation of the patient, the condition is left alone or the deformity is corrected by operation.
Adam's operation consists in multiple subcutaneous division of the contracted fascia in the palm and of its prolongations on to the finger; in addition to dividing the fascia, the tenotomy knife should be used also to separate the skin from the fascia. The finger is then forcibly extended, and a well-padded splint secured to the hand and forearm. The skin on the palmar aspect opposite the first inter-phalangeal joint may give way when the finger is extended; should this occur, the resulting gap may be covered by a skin graft.
After healing has occurred, massage and movements must be persevered with, and a splint (Fig. 174) worn at night, as there is an inveterate tendency to recurrence of the contraction. In view of this tendency there is much to be said in favour of the radical operation which consists in removal of the fascia by open dissection. Owing to the long time required for healing and the sensitiveness of the scar, the results of excision of the fascia are sometimes disappointing. Greig has obtained good results by resecting the head of the metacarpal bone. When the little finger is completely flexed towards the palm it may be amputated, as it is always in the way.
Supernumerary Fingers (Polydactylism).—These may coexist with supernumerary toes, and the condition is often met with in several members of the same family. Sometimes the extra finger is represented by a mere skin appendage, the nature of which may only be indicated by the presence of a rudimentary nail; sometimes it contains bone representing one or more phalanges, or it may be fully formed (Fig. 175). In the majority of cases the superfluous finger should be removed.
Congenital Deficiencies in the Number of Fingers.—One or more fingers may be absent, such deficiency being often associated with imperfect development of the radius or ulna; or they may be represented by short rounded stumps, which are ascribed to the strangulation of the digits by amniotic bands in utero—the so-called intra-uterine amputation.
Webbing of Fingers (Syndactylism).—Congenital webbing or fusion of the fingers may be associated with polydactylism or with congenital hypertrophy, and, like other digital deformities, may affect several members of the same family. The degree of fusion ranges from a web of skin joining the fingers to a fusion of the bones, the latter being well seen in skiagrams. If an operation is decided upon, it should not be performed until the age of five or six years. In the simplest cases it is only necessary to divide the web and to unite the cut edges of skin along each finger by sutures, a skin graft being inserted into the angle between the fingers. An operation in which the skin is dissected up in the form of flaps may be required, but it should not be lightly entered upon, as in young children it has been known to be followed by gangrene of one or more of the digits.
Congenital Hypertrophy of the Fingers.—This is a form of local giantism affecting one or more digits, and involving all the tissues. The finger is usually of abnormal size at birth, and continues to grow more rapidly than the others, and it may also come to deviate from its normal axis. Such a finger should be trimmed down or removed, to permit of the use of the other digits.
Trigger Finger (Fig. 176).—This is an acquired condition in which movement of a finger or thumb, either in flexion or extension, is arrested, and is only completed with the assistance of the other hand. The obstacle to movement is usually overcome with a jerk or snap suggesting a resemblance to the trigger of a gun or the blade of a clasp-knife. The commonest cause is a disproportion between the size of the tendon and its sheath, such as may result from a localised thickening of the tendon. Recovery usually takes place under massage and passive movements. Failing this, the thickened portion of the tendon is pared down to its normal size; if it is the sheath of the tendon that is narrow, it is laid freely open.
Drop or mallet finger is described on p. 121.
Surgical Anatomy.—The skin of the scalp is intimately united to the epicranial aponeurosis by a network of firm fibrous tissue containing some granular fat, and representing the subcutaneous connective tissue. These three layers constitute the scalp proper, and they are so closely connected as to form a single structure which can be moved to a certain extent by the action of the epicranius muscle. The epicranius (occipito-frontalis) muscle with its aponeurosis extends from the superciliary ridge in front to the superior nuchal (curved) line of the occipital bone behind, and laterally to the level of the zygoma where it blends with the temporal fascia. Between the scalp proper and the pericranium is a quantity of loose areolar tissue, in the meshes of which extravasated blood or inflammatory products can rapidly spread over a wide area. Blood extravasated under the pericranium is limited by the attachments of this membrane at the sutures.
The blood supply of the frontal region is derived from the internal carotid arteries through their supra-orbital branches; the remainder of the scalp is supplied from the external carotids through their temporal, posterior auricular and occipital branches. The vessels, which run in the subcutaneous tissue, superficial to the epicranial aponeurosis, anastomose freely with one another and across the middle line. The main branches run towards the vertex, and incisions should, as far as possible, be directed parallel with them.
The venous return is through the frontal, temporal, and occipital veins. These have free communications, through the emissary veins, with the intra-cranial sinuses, and by these routes infective conditions of the scalp may readily be transmitted to the interior of the skull. The most important of the emissary veins are: the mastoid, condyloid, and occipital, passing to the transverse (lateral) sinus; the parietal, which enters the superior sagittal (longitudinal) sinus; and a branch from the nose which traverses the foramen cæcum and enters the anterior end of the superior sagittal sinus.
The supra-trochlear, supra-orbital and auriculo-temporal branches of the trigeminal nerve, together with the greater and lesser occipital nerves, supply the scalp with sensation, while the muscles are supplied from the facial nerve.
The lymph vessels pass to the parotid, occipital, mastoid, and submaxillary groups of glands, the different areas of drainage being ill-defined.
Subcutaneous Injuries.—In simple contusion of the superficial layers, owing to the density of the tissues, the blood effused is small in quantity and remains confined to the area directly injured, which is firm and tender to the touch, swollen and discoloured. The disappearance of the swelling may be hastened by elastic pressure and massage.
Hæmatoma of the scalp results when lacerated vessels bleed into the sub-aponeurotic space. Owing to the laxity of the connective tissue in this area, the effused blood tends to diffuse itself widely, and, according to the position assumed by the patient, gravitates to the region of the eyebrow, the occiput, or the zygoma. When a large artery is torn the swelling may pulsate. A hæmatoma of the scalp may readily be mistaken for a depressed fracture of the skull, owing to the fact that the margins of the effusion are often raised and of a firm resistant character. A differential diagnosis can usually be made by observing that the swelling is on a higher level than the rest of the skull; that the raised margin can to a large extent be dispersed by making firm, steady pressure over it with the finger; and that, on doing so, the smooth and intact surface of the skull can be recognised. When a fracture exists, the finger sinks into the depression and the irregular edge of the bone can be felt. In doubtful cases, if cerebral symptoms are present, an exploratory incision should be made.
Even a large hæmatoma is usually completely absorbed, but the dispersion of the clot may be hastened by massage and elastic pressure. Any excoriation or wound of the skin must be disinfected.
Sometimes a blood-cyst, consisting of a connective-tissue capsule filled with a yellowish-red fluid, remains, and may require to be emptied with a hollow needle.
These effusions are to be distinguished from the cephal-hæmatoma, in which the blood collects between the pericranium and the bone. This is oftenest seen in newly born children as a result of pressure on the head during delivery, and is characterised by its limitation to one particular bone—usually the parietal—the further spread of the blood being checked by the attachment of the pericranium at the sutures. Occasionally a permanent thickening of the edges of the bone remains after the absorption of the extravasated blood. This condition is to be diagnosed from traumatic cephal-hydrocele (p. 390).
Wounds of the Scalp.—So long as a scalp wound, however extensive, is kept free from infection, it involves comparatively little risk, but the introduction of organisms to even the most trivial wound is fraught with danger, on account of the ease and rapidity with which the infection may spread along the emissary veins to the meninges and intra-cranial sinuses.
The deeper the wound, the greater is the risk. If the epicranial aponeurosis is divided, the “dangerous area” between it and the pericranium is opened, and if infection occurs, it may lead to widespread suppuration. Should the wound extend through the pericranium, infection is more liable to spread to the bone and to the cranial contents.
The usual varieties of wounds—incised, punctured, contused, and lacerated—are met with in the scalp, and they vary in degree from a simple superficial cut to complete avulsion. For medico-legal purposes it is important to bear in mind that a scalp wound produced by the stroke of a blunt weapon, such as a stick or baton, may closely simulate a wound made with a cutting instrument.
On account of the density of the integument and its close connection with the aponeurosis, scalp wounds do not gape unless the epicranial aponeurosis is widely divided. This facilitates union in incised wounds, but interferes with drainage in the long narrow tracts which result from punctures, and which are so liable to be infected and to implicate the sub-aponeurotic space, the pericranium, or even the bone. It also favours the inclusion in the wound of a foreign body, such as the broken point of a knife, or a piece of glass. The bleeding from scalp wounds is often profuse and difficult to control, because the vessels, fixed as they are in the dense subcutaneous tissue, cannot retract and contract so as to bring about the natural arrest of hæmorrhage, and it is difficult to apply forceps or ligatures to their cut ends, suture ligatures are more efficient. On account of the free arterial anastomosis in the deeper layers of the integument, large flaps of scalp will survive when replaced, even if badly bruised and torn, and it is never advisable to cut away any un-infected portion of the scalp, however badly it may be lacerated or however narrow may be the pedicle which unites it to the head.
Gun-shot wounds of the scalp are usually associated with damage to the skull and brain. A spent shot, however, may pierce the scalp, and then, glancing off the bone, lodge in the soft parts.
Complete Avulsion.—In women, the scalp is sometimes torn from the cranium as a result of the hair being caught in revolving machinery. The portion removed, as a rule, consists of integument and aponeurosis with portions of muscle attached. In a few cases the pericranium also has been torn away. So long as any attachment to the intact scalp remains, the parts should be replaced, and, if asepsis is maintained, a satisfactory result may be hoped for. When the scalp is entirely separated, recourse must be had to skin-grafting.
Treatment of recent Scalp Wounds.—To ensure asepsis, the hair should be shaved from the area around the wound, and the part then purified. Gross dirt ground into the edges of lacerated wounds is best removed by paring with scissors. Undermined flaps must be further opened up and drained—by counter-openings if necessary. When there is reason to suspect their presence, foreign bodies should be sought for. Bleeding is arrested by forci-pressure or by ligature; when, as is often the case, these measures fail, the hæmorrhage may be controlled by passing a needle threaded with catgut through the scalp so as to include the bleeding vessel. The wound is stitched with horse-hair or silk, and, except in very small and superficial wounds, it is best to allow for drainage. With the use of iodine as a disinfectant, it is often advantageous to dispense with dressings altogether.
Complications of Scalp Wounds.—The most common complications are those due to infection, which not only aggravates the local condition, but is apt to lead to spreading cellulitis, osteomyelitis, meningitis, or inflammation of the intra-cranial sinuses. These dangerous sequelæ are liable to follow infection of any scalp wound, but more especially such as implicate the sub-aponeurotic area, or the pericranium. In the integument, a small localised abscess, attended with pain and œdema of surrounding parts, may form. Pus forming under the aponeurosis is liable to spread widely, pointing above the eyebrow, in the occipital region, or in the line of the zygoma. Suppuration under the pericranium tends to be limited by the inter-sutural attachments of the membrane. Necrosis of the outer table, or even of the whole thickness of the skull, may follow, although it is by no means uncommon for large denuded areas of bone to retain their vitality.
The onset of infection is indicated by restlessness, throbbing pain and heat in the wound, a feeling of chilliness or the occurrence of a rigor, and tension of the stitches from œdema of the surrounding tissues. The œdema often extends to the eyelids and face; a puffiness of the eyelids, indeed, is not infrequently the first evidence of the occurrence of infection in the wound.
Treatment.—When suppuration ensues, the stitches should be removed, the wound opened up and purified with eusol, and packed. A dressing of ichthyol and glycerine should be employed for a few days.
Erysipelas of the scalp may originate even in wounds so trivial as to be almost invisible, or from suppurative processes in the region of the frontal sinuses or nasal fossæ. It tends to be limited by the attachments of deep fasciæ, and seldom spreads to the cheek or neck. Symptoms of cerebral complications, in the form of delirium or coma, and of meningitis may supervene. Cellulitis beneath the aponeurosis from mixed infection is a dangerous complication.
Infective Conditions.—It is not uncommon for localised abscesses to occur in the subcutaneous cellular tissue in delicate children, and such collections are not infrequently associated with pediculi, impetigo, or chronic dermatitis. They develop slowly and painlessly, and are only covered by a thin, bluish pellicle of skin. It is not improbable that they result from a mixed infection by pyogenic and tuberculous organisms. As a rule they heal quickly after incision and drainage, but when they are allowed to burst, tedious superficial ulcers may form. Localised abscesses may also form in connection with disease of the cranial bones. Suppuration following upon injuries has already been referred to.
Boils and carbuncles are not common on the hairy part of the scalp. Lupus rarely originates on the scalp, although it may spread thither from the face. Syphilitic lesions are common and present the same characters as elsewhere. Gummata may develop in the soft parts, but more commonly they take origin in the pericranium or bone. Eczema capitis is of surgical importance only in so far as it often forms the starting-point of infection of lymph glands by pyogenic and other organisms.
Cystic and Solid Tumours.—A great variety of swellings is met with in the scalp.
Sebaceous cysts or wens are of frequent occurrence, and have been described in Volume I.
A dermoid cyst is most commonly situated over the position of the anterior fontanelle, in the region of the occipital protuberance, or at the lateral angle of the orbit. As it frequently lies in a gap in the skull, it may be connected by a pedicle with the dura mater, and is liable to be mistaken for a meningocele.
Serous cysts are occasionally found in the occipital region, and are believed to be meningoceles that have become shut off from the interior of the skull before birth.
Adenomas originating in the sebaceous or sweat glands are sometimes multiple, of a purplish colour, and the skin covering them is thin and glistening. They show a tendency to ulcerate and fungate, giving rise to a fœtid discharge, and may be mistaken for epithelioma; they are also liable to become the seat of epithelioma. They are treated by excision.
Large, flat papillomas or warts may be single or multiple; they are of slow growth, and as they may also become the starting-point of epithelioma, they should be removed.
The plexiform neuroma forms a loose soft tumour situated in the course of one or more branches of the trigeminal nerve, especially the supra-orbital branch. In its most aggravated form the tumour hangs over the face or neck in large pendulous masses, and is described as a pachydermatocele (V. Mott).
A sarcoma usually has its origin in the bones of the skull, and only implicates the scalp secondarily.
Epithelioma of the scalp may originate in relation to a wart, an ulcerated wen or sebaceous adenoma, or the cicatrix of a burn. It may affect comparatively young persons, may spread over a wide area, or pass deeply and involve the bone. Free and early removal is indicated.
Rodent cancer may originate on the scalp, but usually spreads thither from the face.
In operating for extensive tumours of the scalp the hæmorrhage is sometimes formidable. It may be controlled by an elastic tourniquet applied horizontally round the head, or if, on account of the position of the tumour or from other causes, this is not practicable, by ligation or temporary clamping of the external carotid on one or on both sides.
Air-containing Swellings—Pneumatocele Capitis.—Cases have been recorded in which, as a result of pathological or traumatic perforations of the mastoid, and less frequently of the frontal cells, air has passed under the pericranium and given rise to a tense rounded tumour, resonant on percussion, and capable of being emptied by firm pressure. Such swellings exhibit neither pulsation nor fluctuation; and as they are painless, and give rise to almost no inconvenience, they do not call for treatment.
Emphysema of the scalp may follow fractures implicating any of the air sinuses of the skull, the air infiltrating the loose cellular tissue between the pericranium and the aponeurosis, and on palpation yielding a characteristic crepitation. It usually disappears in a few days.
Vascular Tumours.—Nævi on the scalp present the same features as elsewhere. If placed over one of the fontanelles, a nævus may derive pulsation from the brain, and so simulate a meningocele.
Cirsoid aneurysm is usually met with in the course of the temporal artery, and may involve the greater part of the scalp. Large, distended, tortuous, bluish vessels pulsating synchronously with the heart are seen and felt. They can be emptied by pressure, but fill up again at once on removal of the pressure. The patient complains of dizziness, headache, and a persistent rushing sound in the head. Ulceration of the skin over the dilated vessels, leading to fatal hæmorrhage, may take place.
They may be treated by excision, after division and ligation of the larger vessels entering the swelling; or the dilated vessels may be cut across at several points and both ends ligated. Krogius recommends the introduction of a series of subcutaneous ligatures so as to surround the whole periphery of the pulsating tumour, and interrupt the blood flow. Ligation of the main afferent vessels, or of the external or common carotid, has been followed by recurrence, owing to the free anastomatic circulation in the scalp. In some cases electrolysis has yielded good results.
Traumatic aneurysm of the temporal artery was comparatively common in the days when the practice of bleeding from this vessel was in vogue, but it is seldom met with now.
Arterio-venous aneurysm may also occur in the course of the temporal artery, as a result of injury, and is best treated by complete extirpation of the segments of the vessels implicated.
Anatomy and Physiology.—The Cranium is irregularly ovoid in shape, and its floor is broken up by various projections to form three separate fossæ—anterior, middle, and posterior—in which rest respectively the frontal, the temporal, and the occipital lobes of the brain; the cerebellum, pons, and medulla oblongata also occupy the posterior fossa.
The outer table is the most elastic layer of the calvarium, and it varies greatly in thickness in different skulls and in different parts of the same skull. It is nourished chiefly from the pericranium which is firmly bound down along the lines of the sutures. The inner or vibreous table is thin and fragile, and its smooth internal surface is grooved by the middle meningeal and other arteries of the dura mater, and by the large venous sinuses. The intermediate layer—the diploë—is highly vascular, branches of the meningeal vessels anastomosing freely in its open porous substance with branches derived from the pericranial vessels. Some of its veins open into the external veins, and others into the intra-cranial sinuses, and they communicate with the emissary veins as these pass through the bone, which explains the spread of infective processes from the structures outside the skull to those within. The possibility of withdrawing blood from the interior of the skull by leeching, bleeding, or cupping depends on the existence of the emissary veins.
The Membranes of the Brain.—The dura mater is a fibro-serous membrane, the outer, fibrous layer constituting the endosteum of the skull, the inner, serous layer forming one of the coverings of the brain. Between the fibrous layer and the bone the meningeal vessels ramify; and along certain lines the two layers split to form channels in which run the cranial venous sinuses. Inside the dura, and separated from it by a narrow space—the sub-dural space—lies the arachno-pial membrane, consisting of an outer (arachnoid) layer which envelops the brain but does not pass into the sulci, and a highly vascular inner layer—the pia mater—which closely invests the brain and lines its entire surface.
The space between these layers—the sub-arachnoid space—is traversed by a network of fine fibrous strands, in the meshes of which the cerebro-spinal fluid circulates. Each nerve-trunk as it leaves the skull or spinal canal carries with it a prolongation of each of these membranes and their intervening spaces. The membranes gradually become lost in the fibrous sheaths of the nerves, and the sub-dural and sub-arachnoid spaces become continuous with the lymph spaces of the nerves.
The cerebro-spinal fluid is secreted by the choroid plexuses and fills the cerebral ventricles, the central canal of the cord, the sub-dural and sub-arachnoid spaces, and the sheaths of the intra-cerebral blood vessels. At the base of the brain, particularly in the posterior fossa, the sub-arachnoid space is wider than elsewhere, forming “cisterns” filled with cerebro-spinal fluid which supports the cerebral structures. Through the foramen of Magendie in the roof of the fourth ventricle the sub-arachnoid fluid of the cranial cavity communicates with that of the vertebral canal.
Although it differs in its chemical constitution from true lymph, the cerebro-spinal fluid seems to functionate as lymph, in addition to acting as a lubricating agent, and playing a part in regulating the vascular supply of the brain. In cases of cerebral hæmorrhage, abscess, tumour, or depressed fracture, room is made up to a certain point for the extraneous matter by displacement of cerebro-spinal fluid.
Vascular supply.—The free anastomosis between the vessels entering into the formation of the circulus arteriosus (circle of Willis) ensures an abundant supply of blood to the brain. The larger arteries run in the sub-arachnoid space and give off branches which ramify in the pia mater before entering the cerebral substance. Within the brain, each artery being more or less terminal, there is no free anastomosis between adjacent vessels, with the result that if any individual artery is obstructed the vitality of the area supplied by it is seriously impaired. The venous arrangements are also peculiar in that the veins are thin-walled and valveless, and open into the rigid, incompressible sinuses which run between the layers of the dura mater. Most of the blood passes to the internal jugular vein, and any increase in the pressure of this vessel is immediately transmitted back to the cerebral veins. As the blood vessels project into a rigid case filled with incompressible material, and as the total volume of blood in the brain is constant (Munro and Kelly), any alteration in the supply of blood to the cerebral tissue must be due to an increased velocity of flow, and this in turn depends upon changes in the aortic and vena cava pressure. Thus, if the aortic pressure rises, more blood will enter the cerebral vessels and will move along more rapidly; while if the pressure in the vena cava rises there is obstruction to the passage of blood in the arteries and diminished velocity of flow. The ebb and flow of cerebro-spinal fluid in and out of the spinal canal may also help to control the pressure.
Nerve Elements.—The nervous system is composed of a multitude of units, called neurones, each neurone consisting of a nucleated cell, with branching protoplasmic processes or dendrites and one axis-cylinder or axon. The nutrition of an axis cylinder depends on its continuity with a living cell. If the cell dies, the axis cylinder degenerates. If the axis cylinder is severed at any point, it degenerates beyond that point, and the nucleus of the nerve-cell disintegrates—chromatolysis.
The axis cylinder of one cell ends in a number of fine filaments which arborise around another nerve-cell, thus bringing it into physiological, if not anatomical, relationship with the first cell. The termination is called a cell-station or synapsis. In this way the various sections of the nervous system are kept in association with one another and with the rest of the body.
Motor Functions and Mechanism.—The nerve centres, which together make up the motor area, and govern the voluntary muscular movements of the body, are situated in the grey matter of the præcentral or ascending frontal gyrus, and of the frontal aspect of the central sulcus (fissure of Rolando). The upper limit of the motor area reaches on to the mesial aspect of the paracentral lobule, and the lower limit stops short of the lateral cerebral fissure (fissure of Sylvius) (Fig. 179).
 Fig. 179.—Relations of the Motor and Sensory Areas to
the Convolutions and to Chiene's Lines.
Fig. 179.—Relations of the Motor and Sensory Areas to
the Convolutions and to Chiene's Lines.Each group of muscles has its own regulating centre, the size of the area representing any group depending upon the character and complexity of the movements performed by the muscles, rather than upon the amount of muscular tissue that is governed by the centre—for example, the centre for the mouth, tongue, and vocal cords is larger than that for the muscles of the trunk.
The motor centres have been localised on the surface of the brain with approximate accuracy. For example, above the superior genu of the præcentral gyrus, the centres governing the hip, knee, and toes are grouped; opposite the genu are the centres for the movements of the trunk; between the superior and middle genua lie the centres for the upper extremity; opposite the middle genu, those for the neck, and below it, those for the face, jaws, and tongue, pharynx and larynx.
The Motor Tracts.—It is now generally accepted that there are two paths by which motor impulses pass from the brain: one—the rubro-spinal tract—which controls the more elemental movements of the body, such as standing, walking, breathing, etc.; the other—the pyramidal tract—developed later in the evolution of the nervous system, and concerned with the finer and more skilled movements.
The pyramidal tract is the more important clinically. From the pyramidal cells in the cortex of the Rolandic area, the axis cylinders pass through the centrum ovale towards the base of the brain. They converge at the internal capsule, and pass through the anterior two-thirds of its posterior limb (Figs. 180 and 195). The fibres for the eyes, face, and tongue lie farthest forward, and next in order from before backward, those for the arm and the leg.
From the internal capsule, the motor fibres pass as the pyramidal tract through the crusta of each crus cerebri, the pons and the medulla oblongata. Throughout this part of its course, numerous axons leave the tract, and enter the mid-brain, pons, and medulla in which lie the nuclei of the motor cranial nerves.
At the decussation of the pyramids in the lower third of the medulla, the main mass of the motor fibres crosses the middle line, and enters the lateral column of the spinal cord as the crossed pyramidal tract. The remaining fibres pass down as the direct pyramidal tract, and decussate in the cord near their termination.
The fibres forming the second path pass through the red nucleus in the cerebral peduncle (crus cerebri) and thence by way of the rubro-spinal tract in the lateral column of the cord.
The existence of this double motor path explains how after a hemiplegic stroke in which the pyramidal tract is destroyed while the rubro-spinal tract escapes, the patient is able to perform such primitive movements as are involved in walking or standing, while he is unable to carry out finer movements that require higher education.
The pyramidal and rubro-spinal tracts, in addition to conveying motor impulses, convey impulses that influence muscle tonus and the deep reflexes. The pyramidal tract conveys impulses that inhibit muscle tonus, while the rubro-spinal tract is the path by which excitatory impulses travel. When the inhibitory influences are cut off, as in a lesion of the internal capsule, the paralysed muscles become spastic, and the deep reflexes are exaggerated. When the excitatory impulses are also lost, as in a total transverse lesion of the cord, the paralysed muscles are flaccid and the deep reflexes disappear. In destructive lesions of the lower neurones, the muscles are always flaccid.
The axons passing from the cerebral cortex terminate at different levels in the cord by breaking up into dendrites which arborise around the cells on the grey matter of the posterior horns—this system of cells, axons, and dendritic processes forming an upper neurone. From this synapsis the lower neurone proceeds, its axons travelling to the anterior horn and arborising around the motor cells. The axis cylinders pass out in the anterior nerve roots to the spinal nerves and are continued in them to their distribution in voluntary muscles.
If the continuity of any group of these lower neurones is interrupted, not only do the nerve fibres degenerate, but the nutrition of the muscles supplied by them is interfered with and they rapidly degenerate and waste, and after an interval show the reaction of degeneration. In addition, the reflex arc is disturbed, and reflexes are lost. As these changes do not occur in lesions of the upper neurones, an appreciation of the differences enables us to distinguish between lesions implicating the upper and the lower neurones.
Sensory Functions and Mechanism.—Three kinds of sensory impulses pass from the periphery to the brain; (1) deep, or muscular sensibility, (2) protopathic sensibility, and (3) epicritic sensibility.
Deep sensibility includes the recognition of (a) deep pressure, say by the blunt end of a pencil; (b) the position of a joint on passive movement (joint sense); (c) active muscular contraction (kinesthetic sense). The fibres that convey these impulses to the spinal cord pass in the afferent nerves from the muscles, tendons, and bones, and so long as these nerves are intact these sensations are retained, even if the surface of the skin is quite anæsthetic.
Protopathic sensibility is of a lower order than epicritic. It consists in the recognition of painful cutaneous stimuli and of extreme degrees of heat and cold. The fibres concerned are non-medullated and regenerate comparatively quickly after injury, so that protopathic sensibility is regained before epicritic.
Epicritic sensibility is the most highly specialised and permits of the recognition of light touch, e.g., with a wisp of cotton wool, of fine differences of temperature, and of discriminating as separate the points of a pair of compasses 2 cm. apart. These sensations are carried by medullated nerve fibres, and are slow to return after injury to the nerves.
The sensory nerve fibres conveying these different impulses pass to the ganglionic cells of the posterior nerve roots. From each of these cells a process passes into the cord and bifurcates into an ascending and a descending branch. In the cord the fibres rearrange themselves and pass to the brain by a double path. Those that convey sensations of pain and of temperature pass by the spino-thalamic route by way of the tract of Gowers and the fillet to the optic thalamus; those that are concerned with the muscular sense, the joint sense, and tactile discrimination pass up the posterior columns in the tracts of Goll and Burdach to the nuclei gracilis and cuneatus in the medulla, whence they pass to the optic thalamus.
From the cell station in the optic thalamus the fibres proceed to the cortical sensory centres, that for tactile sensation being situated in the post-central (ascending parietal) gyrus; that for muscular and stereognostic sense lying probably in the adjacent portions of the parietal lobe.
In a unilateral lesion of the cord, pain and the temperature sense may be disturbed in one limb, and motor power and tactile sensibility in the other, as the fibres that convey impressions of pain, and those that subserve the discrimination of temperature, pass up and decussate in the cord a few segments above their point of entrance.
Effects of Lesions of the Motor and Sensory Mechanisms.—Lesions of the motor mechanism differ in their fundamental characters according as they affect the upper or the lower neurones. The signs also vary according as the affected area is destroyed or merely irritated, say by the pressure of a tumour. Irritative lesions in general produce muscular spasms or convulsions, while destructive lesions cause paralysis. The essential differences in the effects of destructive lesions of upper and lower neurones may be indicated thus:—
| Upper Neurone Lesion. | Lower Neurone Lesion. |
|---|---|
| Spastic paralysis of voluntary muscles. | Flaccid paralysis of voluntary muscles. |
| No marked wasting of paralysed muscles. | Marked wasting of paralysed muscles. |
| No reaction of degeneration. | Reaction of degeneration. |
| Exaggeration of reflexes. | Loss of reflexes. |
Irritative lesions of the sensory mechanism cause numbness and tingling (paræsthesia); more extensive paralytic lesions produce anæsthesia, astereognosis, loss of muscle sense, loss of pain, or inability to distinguish temperature, according to the tracts that are affected.
Lesions of the Upper Motor Neurone may occur in any part of its course. Localised lesions of the motor cortex of an irritative kind, for example, a patch of meningitis, a tumour, meningeal hæmorrhage, or a spicule of bone, produce spasms in those groups of muscles on the opposite side of the body that are supplied by the centres implicated—Jacksonian epilepsy. The cortical discharge may overflow into neighbouring centres and cause more widespread convulsive movements, or, if strong and long-continued, may even lead to general convulsions. Consciousness is usually lost before the whole of one side becomes implicated in the spasms; always before they spread to the opposite side. Contracture may occur in the muscles affected after the spasms cease.
If an area of the cortex is destroyed by the lesion, paralysis is produced of the corresponding muscles on the opposite side of the body. At first the paralysed muscles are flaccid, but spasticity soon develops. In some cortical lesions, for reasons not yet understood, the paralysis remains of the flaccid type. The seat and extent of the paralysis depend upon the area of the cortex destroyed. In rare cases the whole motor area is destroyed—cortical hemiplegia; more generally the lesion affects one or more groups of muscles, and occasionally all the muscles of one limb are paralysed—cortical monoplegia. Lesions are often both irritative and destructive, and lead to paralysis of one or more groups of muscles associated with spasms and convulsions of the muscles governed by neighbouring areas of the cortex. Irritation or destruction of the sensory centres may also exist, giving rise to areas of paræsthesia and anæsthesia.
Lesions in the centrum ovale, which destroy the fibres proceeding from the overlying cortex, produce a corresponding spastic paralysis on the opposite side of the body. No irritative phenomena are associated with such a sub-cortical lesion.
Lesions in the region of the internal capsule often produce complete spastic hemiplegia of the opposite side of the body. When the posterior part of the capsule is involved, there are, in addition, hemianæsthesia and hemianopia, and sometimes disturbances of hearing, smell, and taste.
A lesion of the crus may in like manner produce spastic hemiplegia and hemianæsthesia of the opposite side, often associated with a lower neurone paralysis of the third and fourth nerves of the same side (crossed paralysis). The optic tract, which crosses the crus, may also be affected, and hemianopia result.
Lesions of the corpora quadrigemina cause interference with the reaction of the pupil, disturbance of the functions of the oculo-motor nerve and of mastication, ataxia, and inco-ordination of the movements of the limbs.
The symptoms produced by lesions of the pons and medulla vary according to the position of the lesion. If it is unilateral, there may be spastic hemiplegia and hemianæsthesia of the opposite side; if it is situated in the lower part of the pons or in the medulla, there is often also a lower neurone paralysis of one or more of the cranial nerves on the same side as the lesion (crossed paralysis). Paralysis of the external rectus of one eye and of the internal rectus of the other (conjugate paralysis) is frequently found in pontine, and in cortical and internal capsule lesions.
Cerebellar lesions are associated with special symptoms. In ataxia, there is inco-ordination of muscular movements, especially of the coarse movements, such as walking. The gait becomes irregular and staggering, with a tendency to fall, sometimes to the side on which the lesion is situated, sometimes to the opposite side. In patients who cannot walk, ataxia may be tested by ordering repeated pronation and supination of the forearm. Paresis or asthenia may be found in the trunk muscles, or evidenced by weakness of the grip, or drooping of the head to one side. Changes in muscle tone may arise and lead to exaggerated or decreased reflexes, often varying from day to day. Vertigo and nystagmus may also be present, in addition to occipital headache and tenderness on percussion. When one lateral lobe is implicated, the symptoms are referred to the same side; when the median lobe is involved, they are bilateral, and there may be retraction of the neck with extension of the legs, probably as the result of the associated internal hydrocephalus.
A unilateral lesion of the spinal cord causes a lower neurone paralysis of the muscles supplied from the cord at the level of the lesion, with spastic paralysis of the muscles of the same side of the body supplied from a lower level of the cord. The sensory symptoms are variable. Typically there is some anæsthesia in the structures supplied from the damaged section of the cord—incomplete owing to the overlapping by other sensory nerves. Just above the lesion there is irritation of spinal nerves, and hyperæsthesia and pain referred to their distribution. On the same side below the lesion, there is a loss of epicritic, stereognostic and deep sensibility, and on the opposite side below the lesion, loss of the sense of pain and the discrimination between heat and cold. Ordinary tactile sensibility, which is governed by a double path, may or may not be lost on either side below the lesion.
Other Special Centres.—The cortical centres for vision lie on the median surfaces of the occipital lobes in the neighbourhood of the calcarine fissure. Each half-vision centre—for there is one in each occipital lobe—receives the fibres from the same side of both retinæ. Destruction of one half-vision centre produces the condition known as homonymous hemianopia, in which the medial (nasal) half of one visual field and the lateral (temporal) half of the other is affected, so that there is an inability to see objects situated on the side opposite to the lesion.
Auditory impulses are received in the posterior part of the superior temporal convolution.
Aphasia.—The use of language, spoken or written, as a means of expression depends upon the co-ordination of four different centres: the visual, the auditory, the graphic, and the articulatory. These are situated in different parts of the brain and are connected by sub-cortical association tracts, the main pathway of which lies in the vicinity of the upper end of the fissure of Sylvius. Marie has proved that aphasia results from lesions in this area.
The olfactory and gustatory centres are situated in the uncus close to the pituitary fossa.
Lesions of the frontal cortex anterior to the motor centres, even if extensive, may produce few or no symptoms, and in consequence this region has been called a “silent” area. Occasionally there results a change in temperament or intelligence, and the region is on this account supposed to be concerned with the higher psychical functions. There is evidence that the pre-frontal cortex has a centre for the conscious initiation of movements, and that lesions produce “apraxia,” i.e., inability to perform, or clumsiness in voluntarily performing fine movements such as touching the nose with the finger, though such movements may be perfectly carried out unintentionally. This centre is probably situated in the superior and middle left frontal convolutions in right-handed people. The fibres from the centre to the right motor area cross in the anterior part of the corpus callosum.
Cerebral Localisation.—The various parts of the brain can be localised in relation to the surface by various methods. That devised by Professor Chiene has been found reliable.
Relation of Cerebral Centres to the Surface.—Numerous attempts have been made to formulate rules for locating the different parts of the brain in relation to the surface of the head. The method devised by Chiene is free from many of the difficulties and fallacies common to most other methods, inasmuch as the results obtained do not depend upon making definite measurements in inches, or determining particular angles. Certain fixed and easily recognised bony landmarks—the glabella, the external occipital protuberance, the lateral angular process, and the root of the zygoma—are taken, and connected by lines, which are further subdivided—always being bisected. Figs. 179 and 181 explain the method. The head being shaved, a line (GO) is drawn along the vertex from the glabella (G) to the external occipital protuberance (O). This line is bisected in M, which constitutes the “mid-point.” The posterior half of the line MO is bisected in T, constituting the “three-quarters point,” and the posterior half TO is bisected in S—“the seven-eighths point.” The lateral angular process (E) is next connected to the root of the zygoma (P) by a line EP, and the root of the zygoma with the seven-eighths point by PS; the line EPS thus forms the base line. The lateral angular process is now joined to the three-quarters point by ET. The two segments of the base line EP and PS are bisected in N and R respectively, and these points connected with the mid-point (M) by lines NM and RM. These lines cut off a part of ET—AB, which is now bisected in C, and from C the line CD is drawn parallel to AM.
In this way practically all the points of the brain which are wanted for operative purposes may be mapped out. Thus the quadrilateral space MDCA contains the Rolandic area. MA represents the præcentral sulcus, and if it be trisected in K and L, these points will correspond to the origins of the superior and inferior frontal sulci. The pentagon ABRPN corresponds to the temporal lobe. The apex of the temporal lobe extends a little in front of N. The supra-marginal convolution lies in the triangle HBC. The angular gyrus is at B. A is over the anterior branch of the middle meningeal artery, and the bifurcation of the lateral or Sylvian fissure; AC follows the horizontal limb of the lateral fissure. The transverse or lateral sinus at its highest point touches the line PS at R (Fig. 181).
The fissure of Rolando or central sulcus may be marked out by taking a point half an inch behind the mid-point (M) (Fig. 181), and drawing a line downwards and forwards for a distance of about three and a half inches, at an angle of 67.5° with the line GO. The angle of 67.5° can be readily determined by folding a square piece of paper on itself so as to make a triangle. The angle at the fold equals 45°. By folding the paper again upon itself in the same direction, the right angle of the paper is divided into four angles of 22.5° each. Three of these angles taken together make up the 67.5°. If the straight edge of the paper be placed along the sagittal suture with the angle of folding over the upper end of the fissure of Rolando, the folded edge falls over the line of the fissure (Chiene).
Quincke, in 1891, first suggested the withdrawal of cerebro-spinal fluid from the theca in the lumbar region, as a means of relieving excessive intra-cranial tension in tuberculous meningitis, and to obtain specimens of the fluid for diagnostic purposes. The scope of the procedure, both as a therapeutic and as a diagnostic measure, has since been widely extended.
Technique.—The puncture may be made with the patient either lying on his left side, the spine being fully flexed by approximating the knees and shoulders; or sitting on the table with the knees drawn up and the body bent forward. The upper edge of the fourth lumbar spine is identified by drawing a horizontal line across the back at the level of the highest part of the iliac crests (Fig. 183). The space between the fourth and fifth lumbar vertebræ being the widest, is that usually selected. The skin having been purified, an exploring needle, about three inches long, is introduced about half an inch below the fourth lumbar spine in the middle line, and passed for about two inches in a direction forwards and slightly upwards. The needle usually encounters some resistance as it pierces the interspinous ligament, and then enters the sub-arachnoid space. If bone is struck, the needle should be withdrawn and introduced at a different level. If the cerebro-spinal fluid does not escape at once, a stylet should be passed through the needle to clear it of blood-clot or shreds of tissue. When the intra-thecal tension is normal, the fluid trickles away drop by drop, but if it is increased, as, for example, in meningitis, intra-cranial tumour, hydrocephalus, or uræmia, it may escape in a jet.
The normal cerebro-spinal fluid is clear and colourless, has a specific gravity of 1004–1008, and contains a trace of serum globulin and albumose, some chlorides, and a substance which reduces Fehling's solution. Microscopically, it may contain some large endothelial cells and a few lymphocytes, or may be entirely devoid of cells. It does not contain the antitoxins and opsonins which are normally found in the plasma and lymph, hence the liability to infective meningitis after injuries and operations on the central nervous system. With a view to diminishing these risks, hexamine, which is excreted into the cerebro-spinal fluid, is administered for its antiseptic properties in cases of head injury and before intra-cranial operations.
Diagnostic Puncture.—Examination of the fluid withdrawn has proved useful in diagnosis in cases of intra-cranial and intra-spinal hæmorrhage, in various forms of meningitis, in cerebral abscess, and in some cases of cerebral tumour.
The first few drops should be discarded, as they may be stained with blood from the puncture, and about 5 c.c. collected in each of two sterile tubes. To determine whether blood in the fluid is due to the puncture or to a pre-existing intra-cranial or intra-thecal hæmorrhage, the fluid should be centrifugalised; in the former case the supernatant fluid is clear and limpid, in the latter it retains a yellow tinge. In extra-dural hæmorrhage there is no blood in the cerebro-spinal fluid.
In acute meningitis the fluid is turbid, and contains an excess of albumin. Organisms also are present, such as the diplococcus intracellularis in acute cerebro-spinal meningitis; staphylococci, streptococci, and pneumococci, particularly in the intra-cranial complications of middle ear disease. In all cases of acute microbic infection, and especially in the suppurative forms, polynuclear leucocytes are found in the fluid; while in chronic affections, such as tubercle and syphilis, there is an excess of lymphocytes (Purves Stewart). The detection of the tubercle bacillus is confirmatory of a diagnosis of tuberculous meningitis, but, as it is often difficult to find, its absence does not negative this diagnosis. In tuberculous meningitis the clot which forms floats in the centre of the fluid, and is translucent, grey, and flaky; in the pyogenic forms it is yellow, and sticks to the side of the vessel.
In a few cases of malignant tumour of the spinal cord and its membranes, characteristic cells have been found in the fluid after centrifugalising.
In uræmia there is a diminution of chlorides, and an increase of phosphates and sulphates.
The Wasserman test is sometimes positive in the cerebro-spinal fluid, when it is negative in the blood.
Therapeutic Puncture.—In certain cases of cerebral tumour, and of tuberculous meningitis associated with an excessive quantity of fluid in the arachno-pial space, temporary relief of such symptoms of increased intra-cranial tension as headache, vertigo, blindness, or coma, has followed the withdrawal of from 30 to 40 c.cm. of the fluid. Terrier and others have found this measure useful in relieving pain in the head, delirium, and even coma, in cases of basal fracture. Carrière has found it beneficial in some cases of uræmia. The quantity withdrawn must not exceed 40 c.cm., lest the ventricles be emptied and pressure be exerted directly on the basal ganglia (Tuffier). In a number of cases sudden death has followed the withdrawal of cerebro-spinal fluid.
This route is sometimes selected for the induction of spinal anæsthesia, and for the injection of antitoxin in cases of tetanus.
The brain is protected from injury by moderate degrees of violence applied to the head, by the dense and mobile scalp, the dome-like shape of the skull, the elasticity of its outer table and the buffer-like sutural membrane between the numerous bones of which it is composed, and the various internal osseous projections with the membranes attached to them, all of which tend to diminish vibrations and to disperse forces so that they expend themselves before they reach the brain. Further protection is provided by the water-bed of cerebro-spinal fluid, and by the external buttresses formed by the zygomatic arch and the thick muscular pads related to it, as well as by the mobility of the skull upon the spine.
In all cases of head injury, the questions that dominate the whole clinical outlook are, whether the brain is directly damaged or not, and whether it is likely to become the seat of infection.
It is impossible to consider separately in their clinical aspects injuries of the cranium and injuries of the brain. It seldom happens that one is seriously damaged without the other suffering to a greater or less extent. Sometimes the skull suffers comparatively little, while the brain is severely damaged, but it is rare for a serious injury to the bone to be unaccompanied by definite brain lesions. In any case it is the damage to the brain, however slight, that gives to the injury its clinical importance. It is an old and a true saying that “no injury of the head is so trivial as to be despised or so serious as to be despaired of.” Injuries at first sight apparently slight may prove fatal from hæmorrhage or infection; on the other hand, recovery has followed injuries of great severity—for example, the famous “American crowbar case,” in which a bar of iron three and a half feet long and one and a half inches thick passed through the head, and yet the patient recovered.
It is convenient to consider the injuries of the brain before those of the skull.
It is probable that in all cases of injury to the head in which a patient loses consciousness, there is some definite damage to the cerebral tissue. This takes the form of a greater or less degree of contusion or laceration, and the lesions are usually most severe and dangerous when the skull is fractured and fragments are driven in upon the brain, but they may exist—indeed they may be very extensive—in the absence of fracture.
Several degrees are recognised.
(1) Numerous minute petechial hæmorrhages may be found widely scattered throughout the brain substance, as a result of a diffused blow on the head, which has shaken up the brain and caused symptoms of cerebral shock or “concussion.” We have found, on microscopic examination in such cases, in addition to these small extravasations, collections of colloid bodies, patches of miliary sclerosis, and chromatolysis and vacuolation of nerve-cells.[3]
[3] Miles, Laboratory Reports, Royal College of Physicians, Edinburgh, vol. iv.
(2) In more severe cases there are often several visible areas of extravasation, most commonly in the grey matter of the cortex (Fig. 184). These foci vary in size from a split-pea to a hazel-nut, and consist of a dark central zone of extravasated blood, surrounded by an area of “red softening” of the brain matter, beyond which are numerous minute capillary hæmorrhages. These intra-cerebral lesions may be accompanied by an effusion of blood into the meshes of the arachno-pial membrane, and they may occur either at the part of the head struck, or at the opposite pole of the axis of percussion—the so-called point of contre-coup. The symptoms vary with the size and site of the extravasations. It is probable that the phenomena of “cerebral irritation” are to be explained by the occurrence of such hæmorrhages widely scattered through the cerebral cortex. Effusions into the cortical motor areas give rise to irritation or paralysis of the muscles governed by the affected centres. Different forms of aphasia and interference with vision or with hearing follow implication of the centres governing these functions. In the pre-frontal and in the lower temporal convolutions no special symptoms seem to follow. When the hæmorrhages are extensive and numerous, symptoms of compression may ensue, and these are aggravated when œdema of the brain is superadded.
Localised hæmorrhages also occur, although less frequently, in the crura cerebri, the pons, the floor of the fourth ventricle, and the cerebellum. In these situations they usually prove fatal by causing rapidly advancing coma and interference with the respiratory and cardiac centres. The temperature immediately rises to 106° or even 108° F., and a modified form of Cheyne-Stokes respiration is present.
(3) Still more gross lesions, in the form of distinct lacerations, are comparatively common at the tips of the frontal, temporal, and occipital lobes, on the surface of the cerebellum, and at the base of the brain. These are usually associated with symptoms of compression in its most typical form, and as a rule prove fatal. The grey matter is torn, and extensive effusion of blood takes place into the brain substance, and on the surface, filling up the sulci, and distending the arachno-pial space (Fig. 184). In a compound fracture, brain matter may be extruded through the opening in the skull.
(4) The extravasated blood may burst into the lateral ventricles, in which case the pulse becomes small and rapid—130, 160, or even 170. The respiration also is rapid—45 to 60—and greatly embarrassed, and the temperature suddenly rises to 103° or 104° F., and continues to rise till death ensues.
(5) Traumatic Œdema.—It is not uncommon for a diffuse œdematous infiltration of the brain substance or of the arachno-pial membrane to take place in the vicinity of the injured portion of brain. This serous exude, on account of the natural adhesions of the arachno-pia, usually remains limited to the damaged area, but it may become generalised.
Mechanism.—The explanation of these widespread hæmorrhages is to be found, according to Duret, in the disturbance of the cerebro-spinal fluid which accompanies a severe blow on the head. This fluid not only surrounds the brain, but it also fills the ventricles, and permeates its substance in every direction in the peri-vascular and perilymphatic spaces. As the brain tissue is incompressible, if an area of the skull is momentarily depressed by a localised blow, space is provided for it by displacement of a quantity of cerebro-spinal fluid, which sets up a fluid wave, and this by hydrostatic pressure increases the tension of the fluid throughout the entire brain. Vessels may be lacerated at any point, either by the flow of this wave or during the ebb which follows the recoil. Hence it is that the lesion is not always at the seat of impact, but may be at the opposite side of the skull or at other remote points.
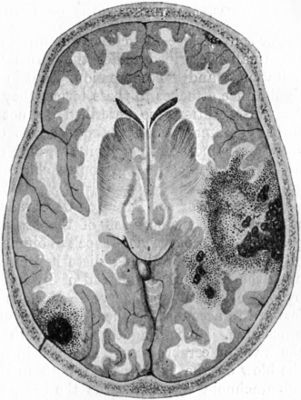 Fig. 184.—Contusion and Laceration of Brain. Note
limited lesion at point of impact on left side, and more extensive
damage at point of contre-coup on right.
Fig. 184.—Contusion and Laceration of Brain. Note
limited lesion at point of impact on left side, and more extensive
damage at point of contre-coup on right.Repair.—As the disintegrated brain matter is replaced by cicatricial tissue, neither the nerve cells nor the fibres being regenerated, the loss of function of the parts destroyed is usually permanent. A localised extravasation of blood may become encapsulated, and constitute a “hæmorrhagic cyst.” We have experimentally confirmed Duret's observations and agree with his conclusions.
For convenience, the clinical manifestations of cerebral injury are usually described under the terms “concussion,” “cerebral irritation,” and “compression,” but no precise pathological significance attaches to these terms, they are essentially clinical. As the conditions so described do not occur as independent entities and may overlap or merge into one another their differentiation is more or less arbitrary, and cases are frequently met with that do not run the course characteristic of any of these groups.
Concussion of the Brain or Cerebral Shock.—The symptoms associated with concussion of the brain are to all intents and purposes those of surgical shock (Volume I., p. 250), the activity of the vital centres being disturbed by violence acting directly upon the brain tissue instead of by impulses transmitted to it by way of the afferent nerves. Various theories have been put forward to account for the depression of the vital functions in concussion. According to Duret, with whose views we agree, the wave of cerebro-spinal fluid set in motion by the impact of the blow on the skull, passes, both in the ventricles and in the sub-arachnoid space, towards the base, where it impinges upon the pons and medulla, stimulating the restiform bodies and so inducing a fall in the blood pressure and a profound anæmia of the brain. The disturbance of the cerebro-spinal fluid may at the same time produce the microscopic lesions in the brain tissues described on p. 341.
The symptoms of shock may be the only evidence of injury, or they may be superadded to those of fracture of the skull, or laceration of the brain.
The clinical features vary according to the severity of the violence. In the slightest cases the patient does not lose consciousness, but merely feels giddy, faint, and dazed for a few seconds. His mind is confused, but he rapidly recovers, and, perhaps after vomiting, feels quite well again, save for a slight shakiness in his limbs.
In more severe cases, immediately on receiving the blow the patient falls to the ground unconscious. Sometimes he suffers from a general tetanic seizure associated with arrest of respiration, which is usually of short duration and is frequently overlooked, but may prove fatal. The pulse is slow, small, and feeble, and is sometimes irregular in force and frequency. The respirations are short, shallow, slow, and frequently sighing in character. The temperature falls to 97° F., or even lower. The skin is cold and pallid and covered with clammy sweat, and the features are pinched and pale.
In uncomplicated cases the pupils are usually equal, moderately dilated, and react sluggishly to light. The patient can be partially roused by shouting or by other forms of external stimulation, but he soon subsides again into a lethargic condition. Although voluntary movement and the deep reflexes are abolished, there is no true muscular paralysis.
After a period, varying from a few minutes to several hours, he rallies, the first evidence often being vomiting, which is usually repeated. Sometimes reaction is ushered in by a mild epileptiform seizure. He then turns on his side, the face becomes flushed, and gradually the symptoms pass off and consciousness returns. The temperature rises to 99° or 100° F., and in some cases remains elevated for a few days. In most cases it falls again to 97° or 97.5°, and remains persistently subnormal for one or two weeks. During reaction the pulse becomes quick and bounding, but after a few hours it again becomes slow, and usually remains abnormally slow (40 to 60) for ten or fourteen days. There is sometimes a tendency to constipation, and for the bladder to become distended, although he has no difficulty in passing water. Very commonly the patient complains of pain in the head for some days after the return of consciousness. Children often sleep a great deal during the first few days, but sometimes they are very fretful.
In cases complicated by gross brain lesions the symptoms of concussion may imperceptibly merge into those of compression or there may be a “lucid interval” of some hours duration.
After-Effects of Concussion.—The majority of patients recover completely. A number complain for a time of headache, languor, muscular weakness, and incapacity for sustained effort—traumatic neurasthenia. Sometimes there is a condition of mental instability, the patient is easily excited, and is unduly affected by alcohol or other stimulants. Occasionally there is permanent mental impairment. It is not uncommon to find that the patient has entirely forgotten the circumstances of the injury and of the events which immediately preceded it. In some instances the memory is permanently impaired. On the other hand, it has occurred that a patient, after concussion, has recovered his memory of a foreign language long since forgotten.
As it is never possible to determine the precise extent of the damage to the brain, the immediate prognosis, even in the mildest cases of concussion, should always be guarded. If the patient has been actually unconscious, the condition should be looked upon as a serious one, and treated accordingly.
Treatment.—The immediate treatment is the same as that of shock. Absolute rest and quietness are called for. When the symptoms begin to pass off, the head should be raised on pillows to prevent congestion and to diminish the risk of bleeding from damaged blood vessels in the brain. The value of applying an ice-bag or Leiter's tubes with a view to arresting hæmorrhage inside the skull, is more than doubtful. Lumbar puncture, venesection, or the application of leeches over the temple or behind the ear may be employed with benefit. The use of small doses of atropin and ergotin was recommended by von Bergmann. The bowels should be thoroughly opened by calomel, croton oil, or Henry's solution, and a light milk diet given. The patient is kept in a shaded room, and should be confined to bed for from fourteen to twenty-one days. It is often difficult to convince the patient of the necessity for such prolonged confinement, but the responsibility for curtailing it must rest upon him or his friends. Reading, conversation, and argument must be avoided to ensure absolute rest to the brain.
Cerebral Irritation.—In some cases of injury to the head—particularly of the anterior part and the parietal region—as the symptoms of concussion are passing off, the patient begins to exhibit a peculiar train of symptoms, which was graphically described by Erichsen under the name of cerebral irritation. “The attitude of the patient is peculiar, and most characteristic: he lies on one side and is curled up in a state of general flexion. The body is bent forwards and the knees are drawn up on the abdomen, the legs bent, the arms flexed, and the hands drawn in. He does not lie motionless, but is restless, and often, when irritated, tosses himself about. But, however restless he may be, he never stretches himself out nor assumes the supine position, but invariably maintains an attitude of flexion. The eyelids are firmly closed, and he resists violently every effort made to open them; if this be effected, the pupils will be found to be contracted. The surface is pale and cool, or even cold. The pulse is small, feeble, and slow, seldom above 70. The sphincters are not usually affected, and the patient will pass urine when the bladder requires to be emptied; there may, however, though rarely, be retention.
“The mental state is equally peculiar. Irritability of mind is the prevailing characteristic. The patient is unconscious, takes no heed of what passes, unless called to in a loud tone of voice, when he shows signs of irritability of temper or frowns, turns away hastily, mutters indistinctly, and grinds his teeth. It appears as if the temper, as much as or more than the intellect, were affected in this condition. He sleeps without stertor.
“After a period varying from one to three weeks, the pulse improves in tone, the temperature of the body increases, the tendency to flexion subsides, and the patient lies stretched out. Irritability gives place to fatuity; there is less manifestation of temper, but more weakness of mind. Recovery is slow, but though delayed, may at length be perfect....”
The treatment consists in keeping the patient quiet, in a darkened room, on much the same lines as for concussion.
Compression of the Brain.—This term is used clinically to denote the train of symptoms which follows a marked increase of the intra-cranial tension produced by such causes as hæmorrhage, œdema, the accumulation of inflammatory exudate, or the growth of tumours within the skull. The only pathological idea the term conveys is that there is more inside the skull than it can conveniently hold.
Clinical Features.—The following description refers to compression due to hæmorrhage within the skull as a result of injury. In a majority of such cases, the symptoms of compression supervene on those of concussion; in certain conditions, notably hæmorrhage from the middle meningeal artery, there is an interval, during which the patient regains complete consciousness, in others the symptoms of concussion gradually and imperceptibly merge into those of compression. The rapidity of onset of the symptoms and their course and duration vary widely according to the nature and extent of the brain lesion. Death may occur in a few hours, or recovery may take place after the patient has been unconscious for several weeks.
The first symptoms are of an irritative character—dull pain in the head, restlessness, and hyper-sensitiveness to external stimuli. The face is suffused, and the pupils at first are usually contracted. The temperature falls to 97°, or even to 95° F. Vomiting is not infrequent.
As the pressure increases, paralytic symptoms ensue. The patient gradually loses consciousness, and passes into a condition of coma. The face is cyanosed, and the distension of the veins of the eyelids furnishes an index of the severity of the intra-cranial venous stasis (Cushing). The pulse becomes slow, full, and bounding. The respiration is slow and deep, and eventually stertorous or snoring in character from paralysis of the soft palate, and the lips and cheeks are puffed out from paralysis of the muscles of these parts. The temperature, which at first falls to 97° or even 95° F., in the course of three or four hours usually rises (100.5° or 102.5° F.). If the temperature reaches 104° F., or higher, the condition usually proves fatal. Sometimes it rises as high as 106° or 108° F.—cerebral hyperpyrexia (Fig. 185). Retention of urine from paralysis of the bladder, and involuntary defecation from paralysis of the sphincter ani, are common.
During the progress of the symptoms there is frequently evidence of direct pressure upon definite cortical centres or cranial nerves, giving rise to focal symptoms. Particular groups of muscles on the side opposite to the lesion may first show spasmodic jerkings or spasms (unilateral monospasm), and later the same groups become paralysed (monoplegia). The paralysis frequently affects the whole of one side of the body (hemiplegia) and the oculo-motor nerve is often paralysed at the same time.
The pupils vary so widely in different cases that their condition does not form a reliable diagnostic sign. Perhaps it is most common for the pupil on the same side as the lesion to be contracted at first and later to become fully dilated, while that on the opposite side remains moderately dilated. As a rule, they are irresponsive to light. Ophthalmoscopic examination shows swelling of the disc, and the vessels of the papilla are distended and tortuous.
In cases which go on to a fatal termination, the coma deepens and the muscular and sensory paralyses become general and complete. The vital centres in the medulla oblongata gradually become involved, and death results from paralysis of the respiratory centre. The fatal issue is often hastened by the onset of hypostatic pneumonia. Not infrequently a modified type of Cheyne-Stokes respiration is observed for some time before death ensues.
A similar train of symptoms may ensue in cases of head injury as a result of pyogenic infection having given rise to meningitis or abscess with accumulation of inflammatory exudate.
Pathology.—When any addition is made to the bulk of matter inside the cranial cavity, room is gained in the first instance by the displacement into the vertebral canal of a certain amount of cerebro-spinal fluid. The capacity of the spinal sheath, however, is limited, and as soon as the tension oversteps a certain point, the pressure comes to bear injuriously on the cerebral capillaries, disturbing the circulation, and so interfering with the nutrition of the brain tissue. As the intra-cranial tension still further increases, the pressure gradually comes to affect the cerebral tissue itself, and so the extreme symptoms of compression are produced. The vagus and vaso-motor centres are irritated, and this causes slowing of the pulse, contraction of the small arteries, and increase of the arterial tension which tends to maintain an adequate circulation in the vital centres in the medulla. The Cheyne-Stokes respiration is due to rhythmical variations in the arterial tension: during the period of fall the centres become anæmic and the respiration fails; during the rise the medulla is again supplied with blood, and breathing is resumed (Eyster).
The parts of the brain directly pressed upon become anæmic, while the other parts become congested, and the nutrition of the whole brain is thus seriously interfered with. Different parts of the brain and cord show varying powers of resistance to this circulatory disturbance. The cortex is the least resistant part, and next in order follow the corona radiata, the grey matter of the spinal cord, the pons, and, last, the medulla oblongata. Hence it is that the respiratory and cardiac centres hold out longest.
Depressed Bone as a Cause of Compression.—It is more than doubtful whether a depressed portion of bone is of itself capable of inducing symptoms of compression of the brain. When such symptoms accompany depressed fracture, they are to be attributed either to associated hæmorrhage, or to interference with the circulation and consequent œdema which the displaced bone produces. Fragments of bone may, however, aggravate the symptoms by irritating the cerebral tissue on which they impinge.
Foreign Bodies.—The rôle of foreign bodies, such as bullets, in the production of compression symptoms is similar to that of depressed bone. That foreign bodies of themselves are not a cause of compression seems evident from the fact that it is not uncommon for them to become permanently embedded in the brain substance without inducing any symptoms. Not only have bullets, the points of sharp instruments, and other substances remained embedded in the brain for years without doing harm, but in many cases the patients have continued to occupy important and responsible positions in life.
Differential Diagnosis.—It not infrequently happens that a patient is found in an insensible condition under circumstances which give no clue to the cause of his unconsciousness. He is usually removed to the nearest hospital, and the house-surgeon under whose charge he comes must exercise the greatest care and discretion in dealing with him. In attempting to arrive at the cause of the condition, numerous possibilities have to be borne in mind, but it is often impossible to make a definite diagnosis. The chief of these causes are trauma, apoplexy or cerebral embolism, epileptic coma, alcohol and opium poisoning, uræmic and diabetic coma, sunstroke, and exposure to cold. The commonest error is to mistake a case of cerebral compression for one of drunkenness. It is scarcely necessary to say that a man who smells of alcohol is not necessarily intoxicated; the drink may have been given with the object of reviving him. It may be that one or other of the above-named conditions has caused the patient to fall, and in his fall he has incidentally sustained an injury to the head, which, however, is in no way responsible for his unconsciousness. Whenever there is the least doubt, therefore, the patient should be admitted to hospital.
In the first instance, careful search should be made for any sign of injury, especially on the head. The discovery of a severe scalp wound or of a fracture of the skull, in association with the symptoms of concussion or compression, will in most cases raise the presumption that the unconsciousness is due to some traumatic intra-cranial lesion. Examination of the fluid withdrawn by lumbar puncture may furnish useful information (p. 338).
In the absence of evidence of a head injury, the stomach should be washed out and its contents examined to see if any narcotic poison is present. The urine also should be drawn off and examined for albumin and sugar.
In hæmorrhage due to the rupture of diseased cerebral arteries (apoplexy), or to embolism, the symptoms are essentially those of compression, and, in the absence of a definite history of injury to the head, it is seldom possible to arrive at an accurate diagnosis as to the cause of the condition. The history that the patient has previously had “an apoplectic shock,” and the fact that he is up in years and shows signs of arterial degeneration and of cardiac hypertrophy which would favour such hæmorrhage, are presumptive evidence that the lesion is not traumatic.
If a history is forthcoming that the patient is an epileptic, there is a strong presumption that the symptoms are those of epileptic coma.
In alcoholic poisoning the examination of the stomach contents will furnish evidence. The patient is not completely unconscious, nor is he paralysed; the pupils are usually contracted, but react; and the temperature is often markedly subnormal. Improvement soon takes place after the stomach has been emptied.
In opium poisoning the general condition of the patient is much the same as in poisoning by alcohol. The pupils, however, are markedly contracted, and do not react to light. When the poison has been taken in the form of laudanum, this may be recognised by its odour.
In the coma of uræmia or of diabetes there is no true paralysis, nor is there stertor. The urine contains albumin or sugar, and there may be œdema of the feet and legs.
Prognosis.—The prognosis depends so much on the nature and extent of the injury to the brain that it is impossible to formulate any general statements with regard to it. It may be said, however, that the symptoms which indicate a bad prognosis are immediate rise of temperature, particularly if it goes above 104° F., the early onset of muscular rigidity, extreme and persistent contraction of the pupils, with loss of the reflex to light, conjugate deviation of the eyes, and the early appearance of bed-sores.
In the majority of cases compression ends fatally in from two to seven days. On the other hand, recovery may ensue after the stuporous condition has lasted for several weeks.
The treatment of compression is considered with the different lesions which cause it; the principle in all cases being to remove, if possible, the cause of the increased pressure within the skull.
Traumatic Œdema.—In practice, cases are frequently met with, particularly in children, that do not conform to the classical description of either concussion, cerebral irritation, or compression. The injury may be followed by a varying degree of concussion which soon passes off but leaves the patient in a listless, drowsy state that may persist for days or even for weeks. The cerebration is disturbed, so that while the patient is not unconscious, he is apathetic and has lost his bearings and fails to recognise where or with whom he is. He complains of headache, there is tenderness on percussion over the skull, the knee jerks are diminished or absent, but there is no motor paralysis. In some cases there are localised jerkings, in others generalised convulsive attacks during which the patient becomes deeply cyanosed. The condition differs from compression due to middle meningeal hæmorrhage in that it is less severe and is not steadily progressive.
When the symptoms are localised, the condition is probably due to œdematous infiltration of the injured portion of brain; when generalised, to increased intra-cranial tension from serous effusion into the arachno-pial space.
The treatment consists in diminishing the intra-cranial tension by purgation, leeches, bleeding, or lumbar puncture, or if life is threatened, by opening the skull over the seat of injury, or failing evidence of this, by a decompression operation in the temporal region.
Apart from the hæmorrhage that accompanies laceration of brain tissue, bleeding may occur inside the skull, either from arteries or from veins. The effused blood may collect either between the dura mater and the bone (extra-dural hæmorrhage), or inside the dura (intra-dural hæmorrhage).
Middle Meningeal Hæmorrhage.—The commonest cause of extra-dural hæmorrhage is laceration of the middle meningeal artery. This artery—a branch of the internal maxillary—after entering the skull through the foramen spinosum, crosses the anterior inferior angle of the parietal bone, and divides into an anterior and a posterior branch which supply the meninges and calvaria (Fig. 186). Either branch may be injured in association with fractures, or from incised, punctured, or gun-shot wounds. The vessel may be ruptured without the skull being fractured, and sometimes it is the artery on the side opposite to the seat of the blow that is torn. The most common situations for rupture are at the anterior inferior angle of the parietal bone, in which case the anterior branch is torn (90 to 95 per cent.); and on the inner aspect of the temporal bone, where the posterior branch is torn (5 to 10 per cent.).
 Fig. 186.—Relations of the Middle Meningeal Artery and
Lateral Sinus to the surface as indicated by Chiene's Lines.
Fig. 186.—Relations of the Middle Meningeal Artery and
Lateral Sinus to the surface as indicated by Chiene's Lines.It is probable that the size of the hæmorrhage depends on the nature, extent, and severity of the injury to the head. The recoil of the skull after the blow separates the dura from the bone, and if the meningeal artery is lacerated or punctured, blood is effused into the space thus formed (Fig. 187). A localised blow therefore results in a small area of separation and a correspondingly small clot; while a diffuse blow is followed by more extensive lesions. It is believed that, once the dura is partly separated, the force of the blood poured out from the lacerated artery is—on the principle of the hydraulic press—sufficient to continue the separation.
Clinical Features.—The typical characteristics of middle meningeal hæmorrhage are met with only when the bleeding takes place between the dura and the bone. Under these conditions the symptoms of concussion are usually most prominent at first, and those of compression only ensue after a varying interval, during which the patient as a rule regains consciousness. In some cases, indeed, he is able to continue his work, or to walk home or to hospital, before any evidence of intra-cranial mischief manifests itself. This “lucid interval” helps to distinguish the symptoms due to middle meningeal hæmorrhage from those of laceration of the brain substance, as in the latter the symptoms of concussion merge directly into those of compression. Lumbar puncture may aid in the differential diagnosis between extra-and intra-dural hæmorrhage, as blood is present in the fluid withdrawn in the latter, but not in the former.
A few hours after the accident the patient experiences severe pain in the head, and he usually vomits repeatedly. For a time he is restless and noisy, but gradually becomes drowsy, and the stupor increases more or less rapidly until coma supervenes. The pulse usually becomes slow and full. The respiration is rapid (30 to 50), and becomes greatly embarrassed and stertorous. The temperature progressively rises, and before death may reach 106° F., or even higher. Monoplegia, usually beginning in the face or arm on the side opposite to the lesion, gradually comes on, and is followed by hemiplegia, from pressure on the motor areas, underlying the clot. The condition of the pupils is so variable as to have no diagnostic value; but if both are widely dilated and irresponsive to light, the prognosis is grave. Death usually ensues in from twenty-four to forty-eight hours, unless the pressure within the skull is relieved by operation; even after removal of the clot death may ensue if the brain has been lacerated, or if there is hæmorrhage at the base.
When the hæmorrhage takes place from the anterior branch, the clot tends to spread towards the base, and may press upon the cavernous sinus, causing congestion and protrusion of the eye, with paralysis of the oculo-motor nerve and wide dilatation of the pupil.
In some cases of middle meningeal hæmorrhage there is no gross injury to the brain; the area underlying the clot is merely compressed and emptied of blood, and, on being exposed, the brain is found flattened, or even deeply indented by the blood-clot, and it does not pulsate. If the clot is removed, the brain may regain its normal contour and its pulsation return. The mortality is over 50 per cent.
If the fracture is compound, the blood can escape, and therefore the pressure symptoms are less evident or may be entirely absent.
It is a fact of some medico-legal importance that hæmorrhage from the middle meningeal may not take place till some days, or even weeks, after an injury, which at the time was only attended with symptoms of concussion. This condition is known as traumatic apoplexy.
Treatment.—Immediate operation is imperatively called for, not only to arrest the hæmorrhage and remove the clot, but also to ward off the œdema of the brain, which is often responsible for the fatal issue. When there is no external wound, the point at which the skull is to be opened is determined by the symptoms; for example, paralysis of the arm and face on one side indicates trephining over the centres governing these parts on the side opposite to the paralysis.
If the bleeding cannot otherwise be arrested it may be necessary to ligate the external carotid artery. It has been suggested by J. B. Murphy that, when the patient is seen while the symptoms of compression are coming on, instead of trephining, the hæmorrhage from the meningeal vessels should be arrested by applying a ligature to the external carotid, under local anæsthesia.
Injury to the internal carotid artery within the skull may result from penetrating wounds, or may be associated with a fracture of the base. It is almost invariably fatal. In some cases a communication is established between the artery and the cavernous sinus, and an arterio-venous aneurysm is thus produced. Ligation of the internal carotid in the neck or of the common carotid is the only feasible treatment.
Injuries of the venous sinuses may occur apart from gross lesions of the skull, but as a rule they accompany fractures and penetrating wounds. The transverse (lateral), superior sagittal (longitudinal), and cavernous sinuses are those most frequently damaged. On account of the low pressure in the sinuses, spontaneous arrest of extra-dural hæmorrhage usually takes place, and recovery ensues. In some cases, however, the amount of blood extravasated is sufficient to cause compression. If the dura mater is torn, and the blood passes into the sub-arachnoid space, it may spread over the whole surface of the brain. Sometimes the bleeding only commences after a depressed fracture has been elevated.
In the presence of an open wound, the venous source of the bleeding is recognised by the dark colour of the blood and the continuous character of the stream. It may be arrested by pressure with gauze pads or by packing a strand of catgut into the sinus (Lister), or, if this fails, by grasping the sinus with forceps and leaving these in position for twenty-four or forty-eight hours. A small puncture in the outer wall of the sinus may be closed with sutures. Signs of increasing compression call for trephining and opening of the dura if this is necessary to admit of the clot being removed.
Intra-cranial Hæmorrhage in the Newly-Born.—An extravasation of blood into the arachno-pial space frequently occurs during birth. The observations of Cushing seem to show that this is usually due to tearing of the delicate cerebral veins which pass from the cortex to the superior sagittal sinus, from the strain put upon them by the overlapping of the parietal bones, in the moulding of the head. It may sometimes be due to an excessive degree of asphyxia during birth. The extravasation is usually most marked over the central area of the cortex near the middle line, and it is often bilateral.
This condition is most frequently met with in a first-born child—and more often in boys than in girls—the labour having been prolonged and difficult, and the presentation abnormal. There is usually a history that the infant was deeply cyanosed when born, and that there was difficulty in getting it to breathe. As a rule, there is no external evidence of trauma. The anterior fontanelle is tense and does not pulsate, the pulse is slow, and for several days the child appears to have difficulty in sucking and swallowing, and is abnormally still. In the course of a few days definite symptoms of localised pressure appear. It is noticed that one leg or arm, or one side of the body is not moved, or both sides may be affected; when the paralysis is bilateral, the absence of movement is more liable to be overlooked. The infant may suffer from convulsions; there may be paralysis of certain of the ocular muscles, and inequality of the pupils; sometimes there is blindness. Persistent rigidity of the limbs, with turning of the thumbs towards the palm, is present in some cases. Lumbar puncture may reveal the presence of blood corpuscles in the cerebro-spinal fluid, and increase in the tension of the fluid.
If untreated, the condition is usually followed by the development of spastic paralysis of one or more limbs, on one or on both sides of the body (Little's disease), by blindness, deafness, and varying degrees of mental deficiency, or by Jacksonian epilepsy.
Treatment.—To obviate these after-effects the clot may be removed by raising an osteo-plastic flap, including nearly the whole of the parietal bone. The operation should be undertaken within the first week or two, and great care must be taken to keep up the body-warmth, and to prevent undue loss of blood. It may be necessary to operate on both sides, an interval being allowed to elapse between the two operations.
For the immediate relief of increased intra-cranial tension, the daily withdrawal of 10–12 c.c. of cerebro-spinal fluid by lumbar punctures may be employed, or a sub-temporal decompression operation may be performed.
Wounds of the Brain.—Incised wounds of the brain usually result from sabre-cuts, hatchet blows, or circular saws. A portion of the scalp and cranium may be raised along with a slice of brain matter, and in some cases the whole flap is severed. The extent of the injury, the conditions under which it is received, and the liability to infection, render such wounds extremely dangerous.
Punctured wounds may be inflicted on the vault by stabs with a knife or dagger, or by other sharp objects, such as the spike of a railing. More frequently a pointed instrument, such as a fencing foil, the end of an umbrella, or a knitting needle, is thrust through the orbit into the base of the brain. Occasionally the base of the skull has been perforated through the roof of the pharynx, for example, by the stem of a tobacco-pipe. All such wounds are of necessity compound, and the risk of infection is considerable, particularly if the penetrating object is broken and a portion remains embedded within the skull. The infective complications of such injuries are described later.
Bullet wounds have many features in common with punctured wounds. There is more contusion of the brain substance, disintegrated brain matter is usually found in the wound of entrance, and the bullet often carries in with it pieces of bone, cloth, or wad, thus adding to the risk of infection.
Aseptic foreign bodies, especially bullets, may remain embedded in the brain without producing symptoms.
The treatment of punctured wounds consists in enlarging the wounds in the soft parts, trephining the skull, and removing any foreign body that may be in it, purifying the track, and establishing drainage.
Various after-effects may follow injuries of the head. Thus, for example, chronic interstitial changes (sclerosis) may spread from an area of cicatrisation in the brain; or softening may ensue, either in the form of pale areas of necrosis (white softening) or of hæmorrhagic patches (red softening). The symptoms vary with the area implicated. Adhesions between the brain and its membranes may produce severe headache and attacks of vertigo, especially on the patient making sudden exertion.
After a head injury, the patient's whole mental attitude is sometimes changed, so that he becomes irritable, unstable, and incapacitated for brain-work—traumatic neurasthenia. In some cases self-control is lost, and alcoholic and drug habits are developed.
Traumatic epilepsy may ensue as a result of some circumscribed cortical lesion, such as a spicule of bone projecting into the cortex, the presence of adhesions between the membranes and the brain, a cicatrix in the brain tissue leading to sclerosis or a hæmorrhagic cyst in the membranes or cerebral tissue.
The convulsive attacks are of the Jacksonian type, beginning in one particular group of muscles and spreading to neighbouring groups till all the muscles of the body may be affected. The convulsions may begin soon after the injury, for example, when the cause is a fragment of bone irritating the cortex; in other cases it may be several years before they make their appearance. The onset is usually sudden, and the “signal symptom”—for example, jerking of the thumb, conjugate deviation of the eyes, or motor aphasia—indicates the seat of the lesion. At first the attacks only recur at intervals of, it may be weeks or months, but as time goes on they become more and more frequent, until there may be as many as forty or fifty in a day. Sometimes the patient loses consciousness during the fit; sometimes he remains partly conscious. In course of time the same degenerative changes as occur in other forms of epilepsy ensue: certain groups of muscles may become paralysed; the patient may pass into a state of idiocy, or into what is known as the “status epilepticus,” in which the fits succeed one another without remission, the breathing becomes stertorous, the temperature rising, the pulse becoming very rapid; finally coma supervenes, and the patient dies.
Treatment.—The administration of bromides is only palliative. Operation is indicated only when the “signal symptom” indicates a limited and accessible portion of the brain as the seat of the lesion, or when there is a depression of the skull or other definite evidence of cranial injury. The more recent the injury the better is the prospect, as secondary changes are less likely to have taken place, and the peculiarly irritable state of the brain—sometimes referred to as the “epileptic habit”—has not developed. The operation consists in opening the skull freely, and removing any discoverable cause of irritation—depressed bone, thickened and adherent membranes, a cyst, or sclerosed patch of cortex; it may be necessary to interpose a layer of tissue, a flap of fascia lata, for example, between the bone and the cortex of the brain. The point at which the skull is opened is determined by the seat of the injury and the focal brain symptoms.
The return of fits within a few days of the operation does not necessarily mean failure, as they often pass off again. Complete and permanent cure is not common, but the number and severity of the attacks are usually so far diminished that life is rendered bearable.
Traumatic insanity may follow injury to any part of the brain, and it may come on either immediately or after an interval. It may or may not be associated with epilepsy. Any form of insanity may occur, either as a direct result of the trauma, or from the resistance of the brain being lowered by the injury in a patient predisposed to insanity. When insanity follows as a direct consequence of injury, the organic lesion is usually a superficial one, and the disturbance of brain function is generally due to reflex irritation of the dura mater (Duret). These facts possibly explain the immediate improvement which occasionally follows the opening of the skull at the point of injury and removal of the exciting cause. Cases occurring within a few days of the injury usually recover within a month or two. The later the condition is in developing the less obvious is the relationship between the trauma and the insanity, and therefore the worse is the prognosis.
Meningitis, sinus thrombosis, and cerebral abscess may follow upon any form of head injury attended with infection. The clinical features—save for the history of a trauma—correspond so closely with those of the same conditions occurring apart from injury, that they are most conveniently considered together (p. 374).
The bones of the skull may be contused or fractured. These injuries are not in themselves serious: their clinical importance is derived from the injury to the intra-cranial contents with which they are liable to be associated.
Contusion of the skull may result from a fall, a blow, or a gun-shot injury. In the majority of cases the damage to soft parts—scalp, meningeal vessels, or brain—overshadows the osseous lesion, which of itself is comparatively unimportant.
While it is convenient to consider separately fractures of the vault and fractures of the base of the skull, it is to be borne in mind that it is not uncommon for a fracture to involve both the vault and the base. Fractures in either situation may be simple or compound.
Mechanism.—When the skull is broken by direct violence, the fracture takes place at the seat of impact, and its extent varies with the nature of the impinging object and the degree of violence exerted. If, for example, a pointed instrument, such as a bayonet, a foil, or a spike, is forcibly driven against the skull, the weapon simply crashes through the bone, disintegrating it at the point of entrance, and cracking or splintering it for a variable, but limited, distance beyond. On the other hand, when the head is struck by a “blunt” object—for example, a batten falling from a height—the force is applied over a wider area and the elastic skull bends before it. If the limits of its elasticity are not exceeded, the bone recoils into its normal position when the force ceases to act; but if the bone is bent beyond the point from which it can recoil, a fracture takes place—“fracture by bending.” The bone gives way over a wide area, the affected portion may be comminuted, and one or more of the fragments may remain depressed below the level of the rest of the skull. Cracks and fissures spread widely in different directions—often (70 to 75 per cent.) extending into the base. In almost all fractures of the vault the inner table splinters over a wider area than the outer, partly because it is more brittle and is not supported from within, but also because the diffusion of the force as it passes inwards affects a wider area. If a bullet traverses the cranial cavity the inner table is more widely shattered at the aperture of entrance, and the outer table at the aperture of exit. Von Bergmann reported thirty cases in which the inner table alone was fractured by a blow on the head.
Fractures by indirect violence—that is, fractures in which the bone breaks at a point other than the seat of impact—are almost always due to violence inflicted with a blunt object, and acting over a wide area—such, for example, as when the head strikes the pavement. Much discussion has taken place as to the method of their production. It has been shown that when the skull is depressed at one point by a force impinging on it, it bulges at another, so that its whole contour is altered. But the elasticity of the bone varies at different parts of the skull, owing to differences in thickness and in structure. If, therefore, the part which is depressed—that is, the part directly struck—happens to be less elastic than the part which bulges, it gives way, and a fracture by “bending” results; but if the bulging part is the less elastic, it bursts outwards—fracture by “bursting.” The term “fracture by contre-coup” has been incorrectly applied to such fractures when the area of bulging happens to be opposite to the seat of impact. Contre-coup, properly so-called, is only possible in a perfectly spherical body, which, of course, the skull is not.
When a high-velocity bullet penetrates the head, it exerts on the incompressible, semi-fluid brain an explosive (hydro-dynamic) force, which is transmitted to all points on the inner surface of the skull and leads to shattering of the bone.
Repair.—The repair of fractures of the skull is usually attended with an exceedingly small amount of callus. Except in the presence of infection, separated fragments live and become reunited, but they may unite in such a manner as to project towards the brain and, by irritating the cortical centres, cause traumatic epilepsy. In comminuted fractures, the lines of fracture remain permanently visible on the bone, but fissured fractures may leave no trace. Gaps left in the skull by injury or operation are, after a time, filled in by a fibrous membrane, which may undergo ossification from the periphery towards the centre, but unless the aperture is a small one it is seldom completely closed by bone. The new bone which forms is derived from the old bone at the margins of the opening. Permanent defects in the skull are chiefly injurious if they are accompanied by lesions of the underlying dura, such as adhesions to the brain; large gaps may cause giddiness on stooping, or on forcible expiration, as in blowing the nose or playing a wind instrument.
Varieties.—For descriptive purposes, fractures of the vault are divided into the fissured, the punctured, the depressed, and the comminuted varieties. Clinically, however, these varieties are often combined. The practical importance of a given fracture depends upon whether it is simple or compound, rather than upon the exact nature of the damage done to the bone. Compound fractures which open the dura mater are the most serious. Simple fractures result, as a rule, from diffuse forms of violence, and are liable to spread far beyond the seat of impact. Compound fractures result from severe and localised violence—for example, the kick of a horse or the blow of a hammer—and tend to be limited more or less to the seat of impact. In gun-shot injuries, however, there are usually numerous fissures radiating from the point at which the missile enters the skull.
Fissured fractures generally result from blows by blunt objects or from falls, and they usually extend far beyond the area struck, in most cases passing into the base. The fissure may pass through the bone vertically or obliquely, and it may implicate one or both tables. So long as the fracture is simple, it can scarcely be diagnosed except by inference from the associated symptoms of meningeal or cerebral injury. When compound, the crack in the bone can be seen and felt. It is recognised by the eye as a split in the bone, filled with red blood, which, as often as it is sponged away, oozes again into the gap. In fractures by bursting a tuft of hair may be caught between the edges of the fracture, and this adds to the difficulty of purifying the wound.
Diagnosis.—A normal suture may be mistaken for a fissured fracture. A suture, however, may generally be recognised by its position, the irregularity of its margins, and the absence of blood between its edges. At the same time, it is not uncommon, especially in children, for a suture to be sprung by violence applied to the head, or for a fissured fracture to enter a suture and, after running in it for some distance, to leave it again. The edges of a clean cut in the periosteum may be mistaken for a fissure in the bone, especially if reliance is placed on the probe for diagnosis. This error can be avoided by raising the edge of the periosteum from the bone, with the gloved finger. On combined auscultation and percussion a peculiar “hollow-cask” sound may be detected in some cases of fissured fracture of the vault.
Fissured fractures as such call for no treatment. When compound, the wound must be disinfected; and intra-cranial complications, such as meningeal hæmorrhage, laceration of the brain, or infection, are to be treated on the lines already described.
Punctured fractures are of necessity compound, and on account of the risks of infection are to be looked upon as serious injuries. They result from the localised impact of a sharp, and usually infected object the point of which is not infrequently left either in the bone or inside the skull. Fragments of bone are often driven into the brain, and short fissures frequently pass in various directions from the central aperture.
Diagnosis.—When the instrument impinges on the head obliquely, after piercing the scalp it may pass for some distance under it before perforating the skull, so that on its withdrawal a valvular wound is left, and at first sight it appears that only the scalp is involved. Sometimes a foreign body left in the gap so fills it up that it is difficult to detect the fracture with a probe or even with the finger. In all doubtful cases the scalp wound should be sufficiently enlarged to exclude such errors. We have known of a case of a man who died of meningitis resulting from a punctured fracture of the vault caused by the spoke of an umbrella, the fracture having escaped recognition until the meningeal symptoms developed.
Treatment.—The scalp wound must be purified, being opened up as far as necessary for this purpose. The infected portion of bone should be removed to render possible the purification of the membranes and brain, and to permit of drainage.
Depressed and Comminuted Fractures.—As these varieties almost always occur in combination, they are best considered together. The terms “indentation fracture,” “gutter fracture,” “pond fracture,” have been applied to different forms of depressed fracture, according to the degree of damage to the bone and the disposition of the fragments (Figs. 188, 189, 190). These fractures may be simple or compound.
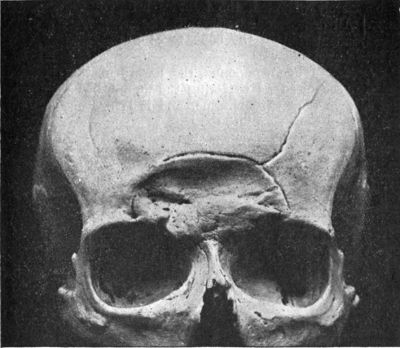 Fig. 188.—Depressed Fracture of Frontal
Bones—involving the air sinus on both sides—with a fissured fracture
radiating from it.
Fig. 188.—Depressed Fracture of Frontal
Bones—involving the air sinus on both sides—with a fissured fracture
radiating from it.
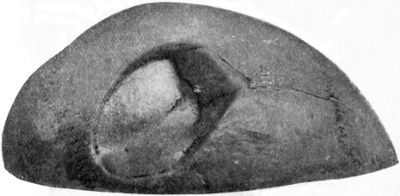 Fig. 189.—Depressed and Comminuted Fracture of Right
Parietal Bone: Pond Fracture. The patient sustained the injury twenty
years before death.
Fig. 189.—Depressed and Comminuted Fracture of Right
Parietal Bone: Pond Fracture. The patient sustained the injury twenty
years before death.
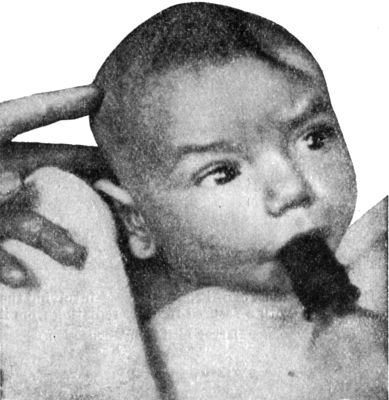 Fig. 190.—Pond Fracture of Left Frontal Bone, produced
during delivery.
Fig. 190.—Pond Fracture of Left Frontal Bone, produced
during delivery.As a rule the whole thickness of the skull is broken, and, as usual, the inner table suffers most. In infants the bones may be merely indented, the fracture being of the greenstick variety. All degrees of severity are met with, from a simple, localised indentation of the bone, to complete smashing of the skull into fragments.
Diagnosis.—When compound, the nature of these fractures is readily recognised on exploring the wound, but their extent is not always easy to determine, and it is not uncommon for extensive fissures to pass into the base.
A hæmatoma of the scalp may readily be mistaken for a depressed fracture. The condensation of the tissues round the seat of impact and the soft coagulum in the centre, closely simulate a depression in the bone; but if firm pressure is made with the finger, the irregular edge of the bone can be recognised, and the depressed portion is felt to be on a lower level. On the other hand, a depression in the bone is sometimes obscured by an overlying hæmatoma, and unless great care is taken the fracture may be overlooked.
Treatment.—All are agreed that compound depressed and comminuted fractures—whether associated with cerebral symptoms or not—should be operated on to enable the wound to be purified, and the normal outline of the skull to be restored by elevating or removing depressed or separated fragments. Except in young children, in whom considerable degrees of depression are frequently righted by nature, most surgeons recommend operative interference even in simple fractures with the object of elevating the depressed bone, and to anticipate subsequent complications such as persistent headache, attacks of giddiness, traumatic epilepsy, or insanity. Others, including von Bergmann and Tilmanns, consider that the risk of such sequelæ ensuing is not sufficient to justify a prophylactic operation of such severity as trephining.
The operation is described in Operative Surgery, p. 93.
The base of the skull may be fractured by a pointed object, such as a fencing foil, a knitting pin, or the end of an umbrella, being forced through the orbit, the nasal cavities, or the pharynx. These injuries will be referred to in describing fractures of the anterior fossa.
The majority of basal fractures result from such accidents as a fall from a height, the patient landing on the vertex or on the side of the head, or from a heavy object falling on the head. The violence is therefore indirect in so far as the bone breaks at a point other than the seat of impact.
In other cases the base is broken by the patient falling from a height and landing on his feet or buttocks, the force being transmitted through the spine to the occiput, and the bone giving way around the foramen magnum. Sometimes the condyle of the lower jaw is driven through the base of the skull by a blow or fall on the chin, and fissures radiate into the base from the glenoid cavity. It is usual to describe these also as fractures by indirect violence, but as the skull gives way at the point where it is struck, these are really fractures by direct violence. Von Bergmann, Bruns, and Messerer have done much to elucidate the mechanism of basal fractures.
In the consideration of the mode of production of basal fractures by indirect violence, the irregular shape of the cavity, the varying strength and thickness of its different parts, and the existence of the foramina through the bone are to be borne in mind. The force acting on the skull tends to increase one diameter of the cavity, and to diminish the opposite diameter. The resulting fracture, therefore, is due to bursting of the skull, and tends to take place at the part which has least elasticity—that is, at the base. It has been found that the site and direction of basal fractures bear a fairly constant relation to the direction of the force by which they are produced. When, for example, the skull is compressed from side to side, the line of fracture through the base is usually transverse, and it may implicate one or both sides (Fig. 191). On the other hand, when the pressure is antero-posterior, the fracture tends to be longitudinal; and when oblique, it tends to be diagonal.
Fractures of the base usually take the form of a single fissure, or a series of fissures, which, as a rule, run through the foramina in their track. Small portions of bone are sometimes completely separated. It is common for a fissure through the base to be continued for a considerable distance on to the vault.
The fracture may involve only one fossa, but as a rule fissures radiate into two or all of them. Fractures of the anterior and middle fossæ are usually rendered compound by tearing of the mucous membrane of the nose, the pharynx, or the ear.
Basal fractures are frequently associated with contusion and laceration of the brain, and also with injuries of one or more of the cranial nerves.
Fracture of the anterior fossa may result from a blow on the forehead, nose, or face; or from a punctured wound of the orbit or of the nasal cavity. Often the injury is at first considered trivial, and it is only when infective complications, in the form of meningitis or cerebral abscess, develop, that its true nature is suspected. This fossa may also be implicated in fractures of the vault, fissures extending from the vertex to the orbital plate of the frontal bone, or to the lesser wing of the sphenoid.
Clinical Features.—Unless the fracture is compound through opening into the nose or pharynx, there are few symptoms by which it can be recognised. When compound, there may be bleeding from the pharynx or nose from tearing of the periosteum and mucous membrane related to the basi-sphenoid and ethmoid respectively. When the hæmorrhage is profuse, it is probable that the meningeal vessels or even the venous sinuses have been torn. Cerebro-spinal fluid may escape along with the blood, but it is seldom possible to recognise it. If the flow is long continued, the patient may be conscious of a persistent salt taste in the mouth, due to the large proportion of sodium chloride which the fluid contains. In very severe injuries, brain matter may escape through the nose or mouth.
Fracture of the anterior fossa is often accompanied by extravasation of blood into the orbit, pushing forward the eyeball and infiltrating the conjunctiva (sub-conjunctival ecchymosis). This occurs especially when the orbital plate of the frontal bone is implicated. The blood which infiltrates the conjunctiva passes from behind forwards, appearing first at the outer angle of the eye and spreading like a fan towards the cornea. Later it spreads into the upper eyelid. When the orbital ridge is chipped off, without the cavity of the skull being opened into, the hæmorrhage shows at once both under the conjunctiva and in the upper lid. If the frontal sinus is opened, air may infiltrate the scalp.
The olfactory, optic, oculo-motor, pathetic, ophthalmic division of the trigeminal, and the abducens nerves are all liable to be implicated.
Diagnosis.—It is scarcely necessary to state that bleeding from the nose or mouth may occur after a blow on the face without the occurrence of a fracture of the skull. It is only when it is long continued and profuse that the bleeding suggests a fracture. Similarly effusion of blood in the region of the orbit may be due to a simple contusion of the soft parts ("black eye"), or to gravitation of blood from the forehead or temple. Sub-conjunctival ecchymosis also may occur independently of a fracture implicating the anterior fossa—for example, in association with an ordinary black eye, or with fracture of the orbital ridge or of the zygomatic (malar) bone.
Finally, paralysis of the cranial nerves may result from pressure of blood-clot, or from the nerves being torn without the skull being fractured.
Fracture of the middle fossa is usually the result of severe violence applied to the vault, as, for example, when a man falls from a height, or is thrown from a horse and lands on his head.
Clinical features.—The most conclusive sign of fracture of the middle fossa is the escape of dark-coloured blood in a steady stream from the ear, followed by oozing of cerebro-spinal fluid. The bleeding from the ear may go on for days, the blood gradually becoming lighter in colour from admixture with cerebro-spinal fluid. Finally the blood ceases, but the clear fluid continues to drain away, sometimes for weeks, and in such quantity as to soak the dressings and the pillow. In our experience, the escape of cerebro-spinal fluid is much less common than is generally supposed. In most cases, on examining the ear with a speculum, the tympanic membrane is found to be ruptured; when it is intact, the blood and cerebro-spinal fluid may pass down the Eustachian tube into the pharynx. The escape of brain matter from the ear is exceedingly rare. Emphysema of the scalp sometimes results when the fracture passes through the mastoid cells. The facial and acoustic nerves and the maxillary and mandibular divisions of the trigeminal are frequently implicated. Deafness is a serious and not uncommon accompaniment of fracture of the middle fossa, as the fracture involves the labyrinth and is attended with hæmorrhage and the formation of new bone.
Diagnosis.—Care must be taken not to mistake blood which has passed into the ear from a scalp wound, or which has its origin in a fracture of the wall of the external auditory meatus or a laceration of the tympanic membrane, for blood escaping from a fracture of the base. Under these conditions the blood is usually bright red, is not accompanied by cerebro-spinal fluid, and the flow soon stops. It is on record[4] that blood and cerebro-spinal fluid may escape along the sheath of the acoustic nerve without the bone being broken.
[4] Miles, Edinburgh Medical Journal, 1895.
Fracture of the posterior fossa is produced by the same forms of violence as cause fracture of the middle fossa; it is specially liable to result if the patient falls on the feet or buttocks.
Clinical Features.—Sometimes a comparatively limited fracture of the occipital bone results, and in the course of a few days blood infiltrates the scalp in the region of the occiput and mastoid, or may pass down in the deeper planes of the neck. As a rule, however, there is no immediate external evidence of fracture. The patient is generally unconscious, and shows signs of injury to the pons and medulla, causing interference with respiration, which soon proves fatal. The rapidly fatal issue of these cases usually prevents the manifestation of any injury to the posterior cranial nerves.
Diagnosis of Basal Fractures.—In the diagnosis of fractures of the base, reliance is to be placed chiefly upon: (1) the nature of the injury; (2) the diffuse character of the cerebral symptoms; (3) the evidence of injury to individual cranial nerves; (4) the occurrence of persistent bleeding from the nose, mouth, or ear; (5) the extravasation of blood under the conjunctiva or behind the mastoid process; and (6) the presence of blood in the cerebro-spinal fluid withdrawn by lumbar puncture. In rare cases the diagnosis is made certain by the escape of cerebro-fluid or of brain matter from the nose, mouth, or ear.
It must be admitted, however, that in a large proportion of cases which end in recovery, the diagnosis of fracture of the base is little more than a conjecture. The external evidence of damage to the bone is so slight and so liable to be misleading, that little reliance can be placed upon it. The associated cerebral and nervous symptoms also are only presumptive evidence of fracture of the bone. In all cases, however, in which there is reason to suspect that the base is fractured, the patient should be treated on this assumption. It is often found that, when there are no cerebral symptoms present, it is difficult to convince the patient of the necessity for undergoing treatment, and of the risk involved in his leaving his bed and resuming work.
Prognosis in Basal Fractures.—The prognosis depends upon the severity of the cerebral lesions, and on the occurrence of traumatic œdema or infective intra-cranial complications. Many cases prove fatal within a few hours from the associated injury to the brain, the patient dying from cerebral compression due to hæmorrhage. If the patient survives two days, the prognosis is more hopeful (Wagner). It is possible that the free escape of blood from the nose or ear may in some cases prevent compression, and to a certain extent render the prognosis more favourable. Punctured fractures are frequently fatal from infective complications—meningitis, sinus thrombosis, and cerebral abscess. These complications are also liable to occur in fractures rendered compound by opening into the nose, pharynx, or ear, but they are less common than might be expected.
Treatment.—The general treatment includes that for all head injuries. In a number of cases attended with symptoms of compression, benefit has followed the relief of intra-cranial tension by a decompression operation. The withdrawal of 30 or 40 c.c. of cerebro-spinal fluid by lumbar puncture has also proved beneficial in the same way; Quenú strongly recommends repeated puncture in serious cases. In a few cases this procedure has been followed by sudden death.
Steps must be taken to prevent infection from the mucous surfaces implicated. This is exceedingly difficult in fractures opening into the pharynx and nose. Owing to the general condition of the patient, it is usually impossible to employ nasal douching or mouth washes, but spraying the cavities with peroxide of hydrogen or other antiseptics may be employed with benefit. In fractures of the middle fossa, the ear should be gently sponged out and the meatus plugged with gauze, retained in position by adhesive plaster or a bandage. When there is a persistent escape of blood or cerebro-spinal fluid, the dressing requires to be changed frequently.
In compound fractures of the anterior fossa due to perforation through the orbit, the frontal bone should be trephined to admit of the removal of loose fragments or of any foreign body that may have entered the skull and to provide for drainage.
The most important intra-cranial conditions that result from infection with pyogenic bacteria are: meningitis, abscess of the brain, and phlebitis of the venous sinuses.
The organisms most frequently associated with these conditions are the staphylococcus aureus and the streptococcus, but it is not uncommon to meet with mixed infections in which other bacteria are present—particularly the pneumococcus, the bacillus fœtidus, the bacillus coli, the bacillus pyocyaneus, and the diplococcus intracellularis.
By far the most common source of intra-cranial infection is chronic suppuration of the middle ear and mastoid antrum, the organisms passing from these cavities to the interior of the skull directly through a perforation of the tegmen tympani or of the wall of the sigmoid groove, or being carried in the blood stream by the emissary veins. In some cases the infection travels along the sheaths of the facial and acoustic nerves.
Less frequently infective conditions of the nasal cavity and its accessory air sinuses, and compound fractures of the skull, particularly punctured fractures, are followed by intra-cranial complications; or infection is conveyed to the inside of the skull, by way of the emissary veins, from wounds of the scalp, or from such conditions as erysipelas of the face and scalp, malignant pustule, carbuncles, or boils.
At the bedside there is often difficulty in discriminating between the various pyogenic intra-cranial complications, because many of the symptoms are common to all the members of this group, and because more than one condition is frequently present. Thus a localised meningitis spreading to the brain may set up a cerebral abscess; a sinus phlebitis may give rise to a purulent lepto-meningitis; or a cerebral abscess bursting into the sub-arachnoid space may produce meningitis.
Pachymeningitis.—This term is applied when the infection involves the dura mater—a condition which is usually due to the spread of infection from a localised osseous lesion, such as erosion of the tegmen tympani in chronic suppuration of the middle ear, of the wall of the sigmoid groove in mastoid disease, or of the posterior wall of the frontal sinus in suppuration of that cavity. It also occurs in relation to septic lesions of the cranial bones such as a broken-down gumma, after operations on the cranial bones, and in cases of compound fracture attended with a mild degree of infection and with imperfect drainage. In contusion of the skull without an external wound, the infection may take place through the blood stream.
The layer of the dura in contact with the affected portion of bone is inflamed, thickened, and covered with a layer of granulations—external pachymeningitis—and between it and the bone there is an effusion of fluid. Up to this point the process is largely protective in its effects, and gives rise to no symptoms, beyond perhaps some pain in the head.
In the majority of cases, however, suppuration occurs between the dura and the bone—suppurative pachymeningitis—and leads to the formation of an extra-dural abscess (Fig. 192). When this happens in association with disease in the middle ear or frontal sinus, it is attended with severe headache referred to the seat of the abscess, a sudden rise of temperature preceded by shivering, and other evidence of the absorption of toxins. Over the situation of the abscess, the scalp becomes swollen and œdematous—a condition which Percival Pott, in 1760, first observed to be characteristic of extra-dural suppuration, hence the name, Pott's puffy tumour, applied to it (Fig. 193). Under these circumstances the abscess is seldom of sufficient size to cause a marked increase in the intra-cranial tension, or to give rise to localised cerebral symptoms by pressing on the brain.
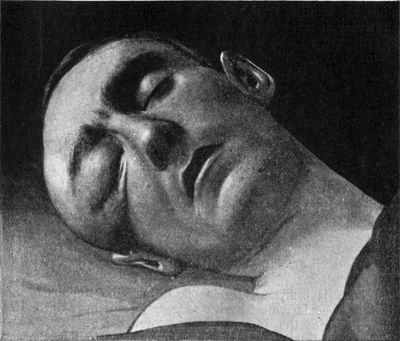 Fig. 193.—Pott's Puffy Tumour in case of extra-dural
abscess following compound fracture of orbital margin; infected with
road-dust; operation; recovery. At the time of the photograph the man
was unconscious.
Fig. 193.—Pott's Puffy Tumour in case of extra-dural
abscess following compound fracture of orbital margin; infected with
road-dust; operation; recovery. At the time of the photograph the man
was unconscious.
When associated with a punctured wound implicating the skull, an extra-dural abscess may develop within a few days of the injury, or not till after the lapse of several weeks, and it may spread over a wide area and come to encroach on the cranial cavity sufficiently to raise the intra-cranial tension and cause symptoms of compression, or even to press upon cortical centres and produce localised paralyses. As discharge can escape from the wound in the scalp, the puffy tumour does not necessarily form.
Treatment.—When the abscess is secondary to middle ear disease, the mastoid must be opened, the eroded bone exposed, and sufficient of it removed with rongeur forceps to admit of free drainage. When the infection has spread from the frontal sinus, the skull is trephined in the frontal region, the precise site being indicated by the œdematous area in the scalp, and the diseased bone is removed. In cases of compound fracture, drainage is established by enlarging the scalp wound, and removing loose, depressed, or inflamed portions of bone; if the bone is comparatively intact, it must be trephined, and further bone is removed with rongeur forceps over the entire area in which the dura has been separated.
Lepto-meningitis.—If the infection spreads to the adjacent arachno-pia (localised lepto-meningitis), adhesions usually form, and shut off the infected area from the general arachno-pial space.
Pus may form among these adhesions, constituting a sub-dural abscess, and may infiltrate the superficial layers of the cortex (purulent encephalitis, or meningo-encephalitis) (Fig. 194). The symptoms are similar to those of extra-dural abscess, but may be more severe; and it is seldom possible to distinguish between them before exposing the parts by operation. The treatment is carried out on the same lines.
Acute General Lepto-Meningitis.—In bone lesions, particularly compound fractures, infection of the arachno-pia may take place before protective adhesions form, and a diffuse lepto-meningitis results. The open structure of the arachno-pial membrane favours the rapid spread of the infection, which may extend over the surface of the hemispheres, or downwards towards the base (basal meningitis), or in both directions. The process is at first attended with a copious effusion of cerebro-spinal fluid into the arachno-pial space and into the ventricles (serous lepto-meningitis), but this fluid tends to become purulent, the pus forming in a thin layer over the surface of the brain, and in the sulci between the convolutions (purulent lepto-meningitis). The membranes are congested and thickened, the veins of the arachno-pia engorged, and the superficial layers of the cortical grey matter may share in the process (encephalitis).
Clinical features.—The earliest and most prominent symptom is violent pain in the head, often referred to the frontal region, or, in cases starting from middle ear disease, to the temporal region. This is accompanied by a sudden rise of temperature, usually without an antecedent rigor; the temperature remains persistently elevated (102° to 105° F.), and the pulse is small, rapid, and irregular both in rate and force. The patient, especially if a child, is extremely irritable, all his sensations are hyper-acute, and he periodically utters a peculiarly sharp, piercing cry.
Vomiting of the cerebral type—that is, unattended with nausea and not related to the taking of food or to gastric disturbance—is common, and persists through the illness. The bowels are usually constipated. There is an increase in the number of leucocytes in the cerebro-spinal fluid, and organisms also are found in the fluid. As this does not occur in cerebral abscess, examination of the cerebro-spinal fluid may be useful in differential diagnosis. There is a higher leucocytosis in the blood in meningitis than in cerebral abscess.
When the inflammation is most marked over the cerebral hemisphere, there may be paralysis of the side of the body opposite to the seat of the original lesion; sometimes there is erratic rigidity of the limbs, sometimes clonic spasms of groups of muscles. The superficial reflexes disappear early on both sides; the abdominal reflexes being lost sooner than the knee-jerks. In basal meningitis, temporary squinting due to irritation of the ocular muscles, retraction of the head, and an excessively high temperature are usually prominent features. The pupils at first are equally contracted; later they become dilated and fixed. Both optic discs are œdematous and swollen.
Gradually the patient becomes unconscious, shows signs of increasing intra-cranial tension, slowing of the pulse, and laboured respiration, and the condition almost always proves fatal within three or four days.
Treatment.—The treatment consists in removing the source of infection when this is possible, but as a rule little can be done to arrest the spread of the meningitis or to ward off its effects. In cases resulting from a sub-dural abscess in relation to a compound fracture, a sinus phlebitis, or an erosion of the tegmen tympani, an attempt should be made, after exposing this, to purify and drain the meningeal spaces. Temporary relief of symptoms sometimes follows the withdrawal of cerebro-spinal fluid by repeated lumbar puncture, bleeding by leeches or cupping, or the use of an ice-bag or Leiter's tubes. The bowels should be freely moved by purgatives or enemata.
Cerebro-spinal Meningitis.—This form of meningitis, which is due to the diplococcus intracellularis, may occur sporadically, but is more frequently met with in an epidemic form. It is attended with the formation of a profuse sero-purulent exudate, which covers the brain, the cord, the nerves, and the membranes.
The clinical features are similar to those of acute general lepto-meningitis, and in sporadic cases the diagnosis is only completed by discovering the diplococcus intracellularis in the fluid withdrawn by lumbar puncture. Although recovery sometimes takes place, the disease is attended with a high mortality. In the early stages, before the exudate has become too thick, repeated lumbar puncture followed by the injection of Flexner's serum has proved beneficial. Recovery may be attended with paralysis of one or other of the cranial nerves.
Abscess due to Middle Ear Disease.—The most common cause of abscess in the brain is chronic middle ear disease, and the majority of cerebral abscesses are therefore situated in the temporal lobe. Some are due to direct spread from a collection of pus in relation to an erosion of the tegmen tympani, either inside or outside the dura, others to infection carried by the veins, and in this way the infective material reaches the white matter; less frequently infection from the middle ear takes place along the peri-vascular lymph spaces. Macewen has pointed out that cerebral abscess never occurs from pyogenic organisms passing from the middle ear by way of the internal auditory meatus, although lepto-meningitis may do so. Cerebral abscess is much more frequently met with in the white matter of the centrum ovale than in the cortex, and in the majority of cases the abscess is single.
The pus is often of a greenish-yellow colour, or it may be dark brown from admixture with broken-down blood-clot; in some cases it is thin and serous and contains sloughs of brain matter, and it frequently has a fœtid odour. In quantity it varies from a few drops to several ounces.
The arachno-pia over an abscess usually has a turbid and milky appearance.
In an acute abscess the surrounding brain tissue is engorged and infiltrated with pus; in a chronic abscess it is condensed, and the pus may be encapsulated by the formation of a zone of young fibrous tissue round its periphery. In this condition the abscess may remain “latent,” giving rise to no symptoms for many weeks or even months.
Clinical features.—The initial formation of pus in the cerebral tissue is associated with the sudden onset of severe pain in the head, shivering and well-marked cutis anserina, and vomiting of the cerebral type. The discharge from the ear usually diminishes or may even cease.
As a localised abscess develops the patient gradually passes, into a stuporous condition; he does not lose consciousness, but, his cerebration is slow, he seems unable to sustain his attention, for any length of time, and he answers questions “slowly, briefly, but, as a rule, correctly” (Macewen). The pain in the region of the ear becomes less intense, but the mastoid and temporal areas on the affected side are tender on percussion. The temperature falls, and, as a rule, remains subnormal. Rigors are unusual: their occurrence usually indicating the development of some complication such as sinus phlebitis. The pulse is full, regular, and slow (40 to 60). Vomiting frequently occurs, and the bowels are often obstinately constipated.
There is no actual paresis, but there is a “gradual diminution of the ability to apply his strength.” The superficial reflexes are late of disappearing and the disturbance is unilateral. The optic discs are moderately swollen. “The face is expressionless, passive, and cloudy. It may assume a meaningless smile, with which the features are not lit; it is too mechanical” (Macewen).
Differential Diagnosis.—In the early stages it is often difficult to distinguish between meningitis and cerebral abscess. The chief points on which reliance is to be placed are that in meningitis the pulse shows an irregularity, both in rate and force, which is wanting in cases of uncomplicated abscess. In meningitis the temperature is raised, while in abscess it is persistently subnormal. The superficial reflexes, particularly the abdominal reflexes, disappear early in meningitis and the disturbance is bilateral; in abscess they are slower to disappear, and one side only is affected. Retraction of the neck, when present, is a characteristic sign of meningitis. In meningitis the optic discs are highly œdematous and are more swollen than in abscess, and the condition is equally marked on the two sides.
Localisation of Cerebral Abscess—Temporal Abscess.—The existence of middle ear disease is always presumptive evidence that the abscess is in the temporal lobe on the same side. A small abscess in this lobe may produce no localising symptoms; one of large size may press indirectly on the motor cortex, on the fibres passing through the internal capsule, or on individual cranial nerves.
It is important to observe the order in which paralysis of the opposite side of the body comes on. When it begins in the face and passes successively to the arm and leg, the pressure is on the cortical centres. When the paralysis progresses in the opposite direction—leg, arm, face—the pressure is on the nerve fibres passing through the internal capsule (Fig. 195). The paralysis may be spastic in lesions of the cortex or internal capsule; if it is flaccid the lesion is almost certainly cortical.
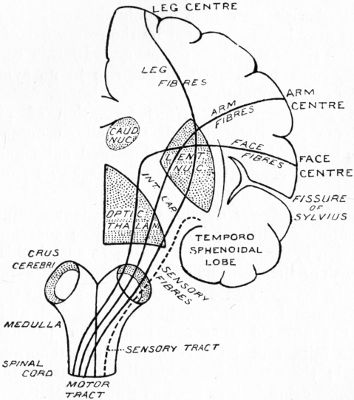 Fig. 195.—Diagram illustrating Sequence of Paralysis,
caused by abscess in temporal lobe. (After Macewen.)
Fig. 195.—Diagram illustrating Sequence of Paralysis,
caused by abscess in temporal lobe. (After Macewen.)
Motor aphasia may result from pressure on the left inferior frontal convolution; auditory aphasia from abscess in the posterior part of the superior temporal convolution. Ptosis and lateral squint, with a fixed and dilated pupil, indicates pressure on the oculo-motor nerve of the same side.
Abscess in the parietal lobe gives rise to paralysis of the face and limbs on the opposite side of the body. Abscess in the occipital lobe produces interference with the visual functions. An abscess in the frontal lobe may give rise to no localising symptoms, but if it is on the left side, the power of making co-ordinated movements may be lost—apraxia—or the motor speech centre may be implicated.
Terminal Stage.—If left to itself, a cerebral abscess usually ends fatally by causing gradually increasing stupor and coma, or by bursting, either into the ventricles or into the sub-arachnoid space, and setting up a diffuse purulent lepto-meningitis.
When the abscess bursts into the ventricles, the patient suddenly becomes much worse and dies within a few hours. “The pupils become widely dilated, the face livid, the respiration greatly hurried, and either shallow or stertorous. The temperature rises within a few hours with a bound from subnormal to 104° to 105° F.; the pulse from 40 or 50 per minute quickly reaches 120 and over. There are muscular twitchings all over the body, possibly associated with convulsions and tetanic seizures, and these are followed by coma and speedy death” (Macewen).
Spontaneous evacuation of a temporal abscess may take place through the middle ear.
Cerebellar Abscess.—Next to the temporal lobe, the cerebellum is the most common seat of abscess. Cerebellar abscess is usually due to spread of infection from a thrombosed sigmoid sinus, either directly from a sub-dural abscess formed in relation to the walls of the sinus, or by extension of the thrombotic process along the cerebellar veins. While the abscess is small, it may give rise to few symptoms, and the patient may be able to go about, but as it increases in size serious symptoms develop. There may be nystagmus, and the patient suffers from vertigo, and is unable to co-ordinate his movements. If he attempts to walk, he reels from side to side; even when sitting up in bed, he may feel giddy and tend to fall, usually towards the side opposite to that on which the abscess is situated. The head and neck are retracted, the pulse is slow and weak, and the temperature subnormal. There is frequent yawning, and the speech is slow, syllabic, and jerky. There may be optic neuritis and blindness. There is sometimes unilateral or even bilateral spastic paralysis of the limbs from pressure on the medulla oblongata. The respiration may assume the Cheyne-Stokes character, occasionally being interrupted for a few minutes, while the heart continues to beat vigorously. This arrest of respiration is especially liable to occur during anæsthesia.
Treatment.—The abscess having been localised, the skull must be opened and the pus removed.
Abscess from causes other than Middle Ear Disease.—From the nasal passages, infection may spread to the interior of the skull directly through the walls of the frontal, ethmoidal, or sphenoidal air sinuses, or indirectly by way of the veins, and give rise to a cerebral abscess, usually in the frontal lobe. The symptoms are similar to those of abscess following middle ear disease, but focal symptoms are seldom present. When the abscess is on the left side, apraxia and motor aphasia may be present. Spontaneous evacuation may take place by the abscess bursting into the nose through the cribriform plate.
The treatment consists in trephining through the frontal bone or through the temporal fossa, according to the site of the abscess and its seat of origin. The primary focus of infection must also be dealt with.
In infected compound fractures, an abscess may form in the cortical grey matter within a few days of the injury from direct spread of infection from the bone and membranes. This is usually associated with a spreading lepto-meningitis, the symptoms of which predominate. The condition usually proves fatal, but by opening up the original wound, removing depressed fragments of bone, and establishing drainage, the patient's life may be saved.
There is evidence that an abscess may form in the brain after a simple contusion without fracture or other external injury (Ehrenvooth).
An abscess may develop in the white matter of the centrum ovale some weeks, or even months, after an injury, particularly if a fragment of bone or a foreign body has been driven into the brain. If the infection has spread along the track of the missile, the abscess is usually near to the seat of the brain injury, but if it is due to spread of a thrombo-phlebitis it may be a considerable distance from it, even on the opposite side of the head. These chronic abscesses are usually in the parietal or frontal lobes, and as the pus is encapsulated they may remain latent for long periods, during which they may cause some degree of headache, neuralgic pains in the distribution of the trigeminal nerve, and occasional rises of temperature. When the abscess becomes active, general symptoms similar to those of other forms of abscess develop, and there may be localised paralysis of the opposite side of the body, the distribution of which depends upon whether the cortical centres or the motor fibres are implicated.
The treatment consists in opening up the original wound, removing any depressed bone or foreign body that may be present, and establishing drainage.
Bronchiectasis and other infective diseases of the lungs are less common causes of cerebral abscess, which is usually single, and may occur in any part of the brain.
Disease of the bones of the skull, such as osteomyelitis or syphilis, may be followed by cerebral abscess.
Abscesses of pyæmic origin are usually multiple, and may occur both in the cerebrum and in the cerebellum; they are not amenable to surgical treatment.
Inflammation of the intra-cranial venous sinuses is due to the spread of infection from a local focus of suppuration; by far the most frequent cause is chronic suppuration in the middle ear. Less common sources of infection are erysipelas of the face or scalp, infective conditions of the mouth or nose, and diseases of the bones of the skull.
The organisms may reach the affected sinus directly by continuity of tissue, as, for instance, when the transverse (lateral) sinus becomes infected from a focus of suppuration in the mastoid process spreading through the bone to the sigmoid groove and involving the walls of the vessel; or they may reach it by extension of thrombosis in a tributary vein—for example, when the superior sagittal (longitudinal) sinus is infected from an anthrax pustule of the lip, which has caused thrombosis of the emissary vein that passes through the foramen cæcum.
The pathological changes are the same as occur in the suppurative form of thrombo-phlebitis in the peripheral veins (Volume I., p. 285). The soft clot that forms adheres to the inflamed wall of the sinus, and, being infected with pyogenic bacteria, it soon undergoes purulent disintegration.
The infective process may spread backward along tributary vessels, and so give rise to cerebral or cerebellar abscess, or to purulent meningitis; or it may spread into the internal jugular vein and lead to the development of a diffuse purulent cellulitis along its course.
General pyæmic infection may take place from pus or bacteria getting into the circulation, either directly or by reversed flow through tributary veins. Infective emboli are liable to lodge in the lung or pleura, and set up pulmonary abscess, gangrene of the lung, or empyema.
Clinical Features.—In all cases, pain in the head, referred to the region of the affected sinus, and so severe as to prevent sleep, is an early and prominent feature. The patient is usually excited, hypersensitive, and irritable in the early stages, and becomes dull and even comatose towards the end. Rigors, followed by profuse perspiration, occur early and increase in frequency as the disease progresses. The temperature is markedly remittent, varying from 103° to 106° F. (Fig. 196). The pulse is rapid, small, and thready. Loss of appetite, vomiting, and diarrhœa are almost constant symptoms.
Phlebitis of Individual Sinuses.—The transverse (lateral or sigmoid sinus), from its proximity to the middle ear and mastoid air cells, is that most commonly affected, especially in young adults. With the onset of the phlebitis the discharge from the ear stops; there is severe pain in the ear and violent headache. The temperature rises, but shows marked remissions, and rigors are common. Vomiting is frequently present. Turgescence of the scalp veins draining into this sinus, and œdema over the mastoid, are occasionally observed; but as these signs may accompany various other conditions, they are of little diagnostic value. Not infrequently phlebitis spreads to the internal jugular vein, which may then be felt as a firm, tender cord running down the neck, and the head is held rigid, sometimes in the position characteristic of wry-neck.
Three clinical types of sinus phlebitis are recognised—pulmonary, abdominal, and meningeal—but it is often impossible to relegate a particular case to one or other of these groups. Many cases present symptoms characteristic of more than one of the types.
In the pulmonary type evidence of infection of the lungs appears towards the end of the second week, in the form of dyspnœa, cough, and pain in the side, coarse moist râles, and dark fœtid sputum. Death usually takes place from gangrene of the lung. The brain functions may remain active to the end.
In the abdominal type the symptoms closely resemble those of typhoid fever, for which the condition may be mistaken. The absence of a rash and the coexistence of middle ear disease are important factors in diagnosis.
When the disease is of the meningeal type, symptoms of general purulent lepto-meningitis assert themselves, and soon come to dominate the clinical picture. Evidence of the presence of meningitis may be obtained by lumbar puncture. The mind at first is clear, but the patient is irritable; later he becomes comatose.
The prognosis is always grave, on account of the risk of general infection.
Treatment.—The primary focus of infection must first be removed, and this usually involves clearing out the middle ear and mastoid process. The sigmoid sinus is then exposed, and after any granulation tissue or pus that may be in the groove has been cleared away, the sinus is opened and the thrombus removed. With the object of preventing the dissemination of infective material, a ligature should be applied to the internal jugular vein in the neck before the sinus is opened, as was first recommended by Victor Horsley. If the phlebitis is accompanied by other intra-cranial infections, these are, of course, treated at the same time.
The superior sagittal or longitudinal sinus is liable to be infected from pyogenic lesions of the scalp. There are no symptoms that are pathognomonic, but œdema of the scalp with turgescence of its veins, epistaxis, and convulsions followed by paralysis, are those most likely to be met with.
The cavernous sinus is usually implicated by spread of the process from other sinuses—for instance, from the petrosal or transverse (lateral) sinuses—or from the ophthalmic veins in cases of orbital cellulitis. Although at first unilateral, the thrombosis usually spreads across the middle line to the sinus of the opposite side. The special symptoms—exophthalmos, œdema of the eyelids, and paralysis of the ocular nerves—are due to pressure on the structures entering the orbit.
Operative interference is seldom feasible in phlebitis of the superior sagittal (longitudinal) or cavernous sinuses.
Intra-cranial Tuberculosis.—Tuberculous meningitis is most frequently met with in patients below the age of twenty, and the infection takes place by the blood stream from some focus elsewhere in the body or from the spinal membranes. In cases of tuberculous disease of the middle ear infection may spread to the membranes by way of the internal auditory meatus (Macewen). The arachno-pia, especially at the base, is studded over with miliary tubercles, and an excess of fluid collects in the arachno-pial space and in the ventricles (acute hydrocephalus).
At first the symptoms of irritation of the brain predominate: severe headache, photophobia, inequality of the pupils, stiffness of the neck, cutaneous hyperæsthesia, vomiting and convulsions. Kernig's sign—pain on flexing the hip while the knee is extended, and inability to extend the knee while in the sitting posture—is present. There is usually obstinate constipation, and the abdomen is retracted. Later, signs of increased intra-cranial tension develop: unconsciousness deepening into coma, paralysis of ocular muscles, rapid pulse, Cheyne-Stokes respiration, and sometimes hyperpyrexia. An excess of mono-nuclear lymphocytes and, sometimes, tubercle bacilli may be discovered in the cerebro-spinal fluid withdrawn by lumbar puncture. The absence of the diplococcus intracellularis helps to differentiate the disease from cerebro-spinal meningitis, which it may closely simulate.
The only surgical measure that is justifiable is lumbar puncture, which often affords marked relief of symptoms, although the benefit is only temporary.
Localised tuberculous nodules sometimes develop in the brain and form definite tumours. They vary in size from a pea to a hen's egg, are rounded and encapsulated. Sometimes the centre is caseous, sometimes fibrinous or calcified. In children they are usually multiple; in adults they may be single—the so-called “solitary tubercle.” They are most common in the pons, basal ganglia, and cerebellum, but occur also in the cerebral cortex and sometimes in the centrum ovale. They usually originate in the pia and invade the brain substance, but do not as a rule involve the dura. The membranes in the vicinity of the growth are often the seat of tuberculous disease.
As these nodules give rise to the same symptoms as other forms of cerebral tumour, and as their nature can be diagnosed only in exceptional cases, their clinical features and treatment are described with tumours of the brain.
Intra-cranial Syphilis.—Syphilitic meningitis is usually secondary to cario-necrosis of the bones of the vault or to a localised gumma of the brain. When primary, it usually affects the inter-peduncular region of the base, and takes the form of a diffuse gummatous infiltration of the membranes which gives rise to symptoms referable to the parts pressed upon, and especially paralysis of one or other of the cranial nerves. As in other intra-cranial syphilitic lesions, the symptoms show a variability in intensity which is characteristic. The diagnosis is made by the history, and the treatment is carried out on the same lines as in other syphilitic lesions.
Localised gummata are described with tumours of the brain.
The term “cephalocele” is applied to a protrusion of a portion of the cranial contents through a congenital deficiency in the bones of the skull. This malformation is believed to be due to an irregularity in development, whereby a portion of the primary cerebral vesicle remains outside the mesoblastic layer of the embryo. It is usually associated with adhesion of the membranes in the region of the fourth ventricle, and with internal hydrocephalus. Cephaloceles are covered by the scalp, and are most commonly met with in the occipital region and at the root of the nose; less frequently at the anterior inferior angle of the parietal bone, and in the line of the sagittal suture. Very rarely they occur at the base of the skull and project into the pharynx, the mouth, or the nose, where they are liable to be mistaken for polypi. Cephaloceles vary greatly in size, some being so small as almost to escape detection, while others are larger than a child's head. In many cases the condition is incompatible with life.
Several varieties are recognised. They are known as (1) meningocele, which consists of a protrusion of a cul-de-sac of the arachno-pial membrane, containing cerebro-spinal fluid; (2) encephalocele, in which a portion of the brain is protruded in addition to the membranes; and (3) hydrencephalocele, in which the protruded portion of brain includes a part of one of the ventricles.
Clinical Features.—The meningocele is commonest in the occipital region, where it escapes through a cleft in the bone between the foramen magnum and the occipital protuberance (Fig. 197). It forms a tense, smooth, translucent globular swelling, which may be sessile or pedunculated, and is usually covered by thin, smooth skin in which the vessels are dilated and nævoid. The tumour does not pulsate, but increases in size and tension when the child cries or coughs. It may be diminished in size or even made to disappear by pressure, and so permit of the opening in the bone being felt. This manipulation, however, may be followed by slowing of the pulse, vomiting, loss of consciousness, or convulsions.
Small meningoceles may remain stationary for a long time, or may even undergo spontaneous cure. Those of larger size usually progress till they eventually burst, and death results from the escape of the cerebro-spinal fluid or from meningitis. Infection may also occur from eczema or from excoriation of the overlying skin.
Encephaloceles are much commoner than meningoceles, and usually occur in the frontal region, where they form broad-based, elastic, and pulsatile tumours, which vary greatly in size.
The hydrencephalocele is usually met with in the occipital region, and is generally so large and associated with such great cerebral deformity as to be inconsistent with life. It does not as a rule pulsate (Fig. 198).
Cephaloceles have to be diagnosed from dermoid cysts, nævi (Fig. 199), cephal-hydrocele, and cephal-hæmatoma. Their recognition is seldom attended with difficulty. If the margins of the gap in the skull can be distinctly felt, or the gap in the bone can be shown by the X-rays, the diagnosis is greatly simplified.
 Fig. 199.—Nævus at Root of Nose, simulating
Cephalocele.
Fig. 199.—Nævus at Root of Nose, simulating
Cephalocele.Treatment.—Only small cephaloceles are amenable to surgical treatment; those that are large and contain brain substance are best left alone, being merely protected from irritation and infection.
While the immediate effects of operation are, on the whole, satisfactory, the ultimate results are disappointing, as the essential cause of the intra-cranial pressure persists, and the child develops hydrocephalus. The method of tapping the sac and injecting iodine has nothing to recommend it.
Traumatic Cephal-hydrocele.—Certain rare cases of simple fracture of the vault occurring in early childhood have been followed by the development beneath the scalp of a localised fluid swelling, which varies in size from time to time and is partly reducible by pressure. The swelling results from laceration of the membranes, and sometimes of the brain substance, so that the cerebro-spinal fluid of the sub-arachnoid space, or even of the lateral ventricle, escapes through the opening in the skull and bulges beneath the scalp. In a majority the swelling pulsates synchronously with the heart, and becomes tense on exertion. A distinct opening in the skull may sometimes be felt. When associated, as it frequently is, with mental deficiency or the occurrence of fits, the cyst may be tapped or its neck ligated (Hogarth Pringle). Otherwise it should be left alone.
An excess of cerebro-spinal fluid may collect in the arachno-pial space surrounding the brain, or in the interior of the ventricles, constituting in the former case an external, and in the latter an internal hydrocephalus. Hydrocephalus may be acute or chronic.
Acute hydrocephalus is practically synonymous with tuberculous meningitis, although it may result from other forms of meningeal infection. The excess of fluid is found both in the arachno-pial space and in the ventricles. This condition only calls for mention here as attempts have been made to treat it by surgical measures, such as lumbar puncture, or drainage through the occipital fossa. The results, however, have not been encouraging.
Chronic Hydrocephalus.—Chronic external hydrocephalus is rare, and usually results from some definite intra-cranial lesion, such as meningitis, tumour, or cerebral atrophy. It is not amenable to surgical treatment.
Chronic internal hydrocephalus, on the other hand, is a comparatively common condition. It may be of congenital origin, or may develop in young rickety children, usually as a result of some chronic inflammatory process in the membranes at the base, the choroid plexuses, or the ependyma of the ventricles, causing obstruction to the outflow of blood through the internal cerebral veins of Galen. In the acquired form the communication between the ventricles and the sub-arachnoid space, by way of the foramen of Magendie, is obstructed, so that the cerebro-spinal fluid is pent up in the ventricles and gradually distends them. The pressure causes the head to enlarge, the fontanelles to bulge, and the bones to be separated from one another, the interval between the bones being occupied by a thin translucent membrane.
The cerebral tissue is greatly thinned out, but the cerebellum and cranial nerves usually remain unaffected.
The appearance of the patient is characteristic (Fig. 200). The enormous dome of the skull surmounts a puny and preternaturally old face; the eyes are pushed downwards and forwards by the pressure on the orbital plates, and the eyebrows are displaced upwards. The head rolls helplessly from side to side; the child moans and cries a great deal; and vomiting is often a prominent symptom. In most cases the intelligence is defective, and epileptic seizures and other functional disturbances of the brain may be present.
In mild cases, especially when associated with rickets or syphilis, recovery sometimes takes place, but in the majority the condition progresses, and death results either from convulsions or from some intercurrent disease. Few hydrocephalic subjects reach adult life.
Treatment.—Hydrocephalus being a symptom rather than a disease, no method of treatment which does not remove the primary cause can be permanently curative. Anti-syphilitic treatment should be tried in the hydrocephalus of infants and young children. The rachitic element, when present, must also be treated.
In congenital hydrocephalus, as there is no blocking of the passages at the fourth ventricle, the foramina being as a rule much larger than normal, no form of drainage is beneficial. Ligation of the common carotids, one some weeks after the other, has been successful in restoring the balance which normally exists between the secretion and absorption of the cerebro-spinal fluid (H. J. Stiles). In acquired hydrocephalus, puncture of the ventricles is sometimes followed by a remarkable improvement in the symptoms, and may even result in apparent cure. An exploring needle is introduced at the lateral angle of the anterior fontanelle, to avoid the superior sagittal (longitudinal) sinus, and from a half to one ounce of cerebro-spinal fluid withdrawn. This is repeated once a week for several weeks. Continuous drainage of the fourth ventricle through an opening made in the occipital region (Parkin), and the establishment of a communication between the ventricle and sub-arachnoid space (Watson-Cheyne), or between the sub-arachnoid space of the spinal cord and the peritoneal cavity, or the retro-peritoneal space (Cushing), have been tried, with little more than temporary benefit in the majority of cases. Operative treatment, if it is to do good, must be undertaken early, before permanent changes in the brain have taken place.
Micrencephaly.—This condition is due to defective development of the brain, and not to premature closure of the cranial sutures and fontanelles, and as the subjects of it are mentally deficient, and often blind, deaf and dumb, the removal of segments of the skull with a view to enable the brain to develop have proved futile.
As a comparatively small proportion of tumours of the brain—using the term “tumour” in its widest sense—are amenable to surgical treatment, it is only necessary here to refer to those aspects of this subject that have a distinctively surgical bearing.
Various forms of growth occur in the brain, the most common being tuberculous nodules, syphilitic gumma, endothelioma, glioma, and sarcoma. Less frequently fibroma, osteoma, and parasitic, hæmorrhagic, and other cysts are met with. The growth may originate in the brain tissue primarily, or may spread thence from the membranes, or from the skull. In relation to operative treatment, it is an unfortunate fact that those forms that are well defined and do not tend to infiltrate the brain tissue, usually occur at the base, where they are difficult to reach; while those that develop in more accessible regions are for the most part infiltrating growths of a gliomatous or sarcomatous nature, and are therefore irremovable.
Clinical Features.—The presence of a tumour in the brain inevitably results sooner or later in an increase in the intra-cranial tension, and to this the symptoms are chiefly due.
The earliest and most prominent of the general symptoms are severe paroxysmal headache, optic neuritis, with choked disc and limitation of the field for blue, amounting sometimes to blue-blindness (Cushing). The relative degree of neuritis in the two eyes is a reliable guide to the side on which the tumour is situated (Horsley). The symptoms are seldom absent, and are common to all forms of tumour, wherever situated. Vomiting, which is without relation to the taking of food and is usually unattended by nausea, is a characteristic symptom when present, but it is wanting in two-thirds of the cases (Cushing). Vertigo, general convulsions, and signs of mental deterioration are also present in a considerable proportion of cases.
In addition, certain localising symptoms may be present. When, for example, the tumour is situated in the cortex of the Rolandic area, attacks of Jacksonian epilepsy, preceded by an aura, which is usually referable to the centre primarily implicated, are common. The group of muscles first involved, and the order in which other groups become affected, are important localising factors. As the tumour increases in size, these irritative phenomena are replaced by localised paralyses. The tactile and muscular sensations are also disturbed, and motor and sensory aphasia may be present. In some cases localised tenderness on percussing the skull may be of assistance in indicating the site of the tumour.
When the tumour is sub-cortical, that is, in the centrum ovale, there are no Jacksonian spasms, the motor paralysis is more widespread, and sensation also is lost on the opposite side of the body. There is no special tenderness on percussion. It is not always possible, however, to distinguish between cortical and sub-cortical tumours, and in many cases both areas are invaded.
Tumours situated in the region of the internal capsule, and in the deeper parts of the brain, are not attended with Jacksonian spasms, paralysis develops more rapidly than in cortical and sub-cortical tumours, and there is complete loss of sensation on the opposite side of the body. The cranial nerve-trunks also are liable to be pressed upon.
Tumours and cysts in the cerebellum give rise to symptoms similar to those of cerebellar abscess (p. 381).
Tumours in the cerebello-pontine angle, in addition to the special symptoms associated with cerebellar lesions, give rise to symptoms of interference with nerve-roots of the same side. The facial and acoustic nerves are most frequently affected, resulting in facial weakness, tinnitus, loss of perception for high-pitched notes, as tested by Galton's whistle, or absolute unilateral deafness. Any of the other cranial nerves from the fifth to the twelfth may be either irritated or paralysed. Pressure on the pons may produce hemiplegia of the opposite side, with spasticity and exaggeration of reflexes. Sudden death may occur from crowding of the cerebellum into the foramen magnum.
With the growth of the tumour the symptoms become aggravated, the optic neuritis is followed by optic atrophy and blindness, the patient gradually becomes stuporous, and finally dies in a state of coma. The severity of the symptoms depends to a large extent on the rapidity of growth of the tumour; thus an osteoma growing slowly from the inner table of the skull and implicating the brain may reach a considerable size without producing cerebral symptoms, while a comparatively small sarcoma or syphilitic gumma of rapid growth may endanger life. A sudden and serious aggravation of symptoms may result from hæmorrhage into a soft tumour, such as glioma.
The diagnosis of the pathological nature of a cerebral tumour is generally “hardly more than a guess” (Gowers). At the same time it may be borne in mind that syphilitic gummata occur in adults, from forty to sixty years of age, who have suffered from acquired syphilis, and who may present other evidence of the disease. They tend to increase somewhat rapidly. A negative Wassermann reaction does not necessarily exclude a diagnosis of brain syphilis. Severe nocturnal pain which interferes with sleep is often a prominent symptom. Gummata are generally situated on the surface of the brain; they often originate in the dura mater, and when exposed are easily enucleated. Improvement in the symptoms may follow the administration of iodides and mercury, or organic arsenical salts of the salvarsan group, but in many cases the growth is very resistant to anti-syphilitic treatment.
Tuberculous masses occur most frequently in children and adolescents, and other signs of tuberculosis are usually present. The cerebellum is a common seat of these tumours, and they are often multiple. Their growth may be rapid at first, and then become arrested for a time. Spasmodic growth of a tumour strongly suggests its tuberculous nature, and superadded signs of basal meningitis confirm the diagnosis.
Endothelioma grows from the dura mater, and in so far as it is a well-defined and non-infiltrating growth it lends itself to removal by operation. Unfortunately, however, it is usually located at the base of the brain and is not readily accessible.
Glioma is usually met with in the young; it tends to grow slowly at first, but may take on a rapid growth at any time, and hæmorrhage is liable to occur into the substance of the tumour, causing a sudden aggravation of the symptoms.
Sarcoma occurs between puberty and middle life; it grows slowly, and compresses rather than destroys the brain tissue. It is sharply defined from the surrounding cerebral tissue, and is therefore more favourable for operation than glioma.
The prognosis is grave in all forms of brain tumour. Even in syphilitic growths, although the more urgent symptoms may be ameliorated by the use of drugs, recurrence is liable to occur, and the structural changes induced in the cerebral tissue, and the contraction of the cicatrix which results, may permanently interfere with the functions of the brain, or may induce Jacksonian epilepsy. Tuberculous tumours also may become arrested, and may cease for a time to cause symptoms, but permanent cure is extremely rare. We have known a sarcoma to recur as late as five years after removal. Death sometimes occurs suddenly from hæmorrhage, from acute œdema, or from implication of vital centres.
Treatment.—It is to be borne in mind that gummatous growths in the brain are seldom influenced to any extent by anti-syphilitic remedies, and time should not be wasted in trying this form of treatment.
The question of removal by operation arises in cases in which there is reason to believe that the tumour is situated near the surface of the brain and that it is circumscribed and of moderate size. Unfortunately it is only in a small proportion of cases that these conditions are present and can be recognised before opening the skull.
In many cases in which there is no hope of being able to remove the tumour, it is advisable to relieve symptoms due to excessive intra-cranial tension, such as blindness, severe headache, and persistent vomiting, by performing a “decompression operation” (Operative Surgery, p. 108). The relief that follows such operations is often remarkable.
Lumbar puncture, frequently repeated, has also been practised for the relief of tension in inoperable cases, but it is not free of danger and is not to be looked upon as a substitute for a decompression operation.
When surgical treatment is contra-indicated, all that can be done is to palliate the symptoms by bromides, opium, phenacetin, caffein, and other drugs.
Tumours of the Pituitary Body or Hypophysis Cerebri.—The tumours most frequently met with in the pituitary body are of the nature of adenoma with hyperplasia and cystic degeneration; carcinoma and sarcoma also occur. They develop slowly and give rise to comparatively slight increase in the intra-cranial tension. When the anterior lobe is implicated and there is a pathological increase in the functional activity of the gland (hyperpituitarism), signs of acromegaly may ensue. Diminution of function (hypopituitarism) is attended with infantilism, a rapid deposition of fat in the subcutaneous tissue, and a decrease or loss of the genital functions. In women, amenorrhœa is an early and constant symptom. Intense drowsiness is a marked feature in some cases.
From their position close to the back of the optic chiasma these growths affect the fibres passing to the nasal half of each retina, and so give rise to bilateral temporal hemianopsia, and although there is no choked disc, the optic nerves undergo primary atrophy from pressure, and there is failure of sight.
Marked temporary benefit has followed the administration of thyreoid extract. Operative treatment has been successful in a number of cases, but as the anterior lobe is essential to life, the operation is merely directed towards the relief of pressure on the optic chiasma with a view to preventing loss of vision. We have seen marked relief follow a temporal decompression operation.
Epilepsy.—The surgical aspects of Jacksonian epilepsy following head injuries have already been considered (p. 358). For the cure of those forms of epilepsy in which there is no gross lesion of the brain, numerous surgical procedures have been suggested, but from none of these have the results been encouraging.
Hernia Cerebri.—This term is applied to a protrusion of brain substance through an acquired opening in the skull and dura mater, such as may result from a compound fracture or a gun-shot wound. The protrusion is due to increased intra-cranial tension, and is almost invariably associated with infection of the brain and its membranes, and with the presence of a foreign body or fragments of bone. Other things being equal, a hernia is more likely to occur through a small than through a large opening in the skull.
So long as the extruded portion of brain matter is small, it pulsates, but as it increases in size and is pressed upon by the edges of the opening through which it escapes, the pulsation ceases, and the herniated portion may become strangulated and undergo necrosis.
In cases of compound fracture, and in other conditions associated with necrosis of bone, masses of redundant granulation tissue growing from the soft parts outside the skull may simulate a hernia cerebri.
The treatment consists in counteracting the septic infection by purifying the protruding mass, and if necessary by enlarging the opening in the skull with rongeur forceps to admit of the removal of foreign bodies or bone fragments and to relieve the inter-cranial tension. Steps must also be taken to prevent meningitis, which, if it occurs, is usually fatal. Pressure over the hernia, with the object of returning it to the skull, is to be avoided, and the herniated portion should not be cut away unless it is sloughing, or has become pedunculated. It may be got rid of by painting it with 40 per cent. formalin, which causes a dry, horny crust to form on the surface; this is picked off, and the formalin re-applied.
After the hernia has disappeared and the wound is aseptic, steps should be taken to close the gap in the skull. This may be done by an osteo-plastic operation in which a flap, comprising a segment of the outer table, is raised from an adjacent part of the skull and placed in the gap; or by transplanting a portion of periosteum-covered bone from the scapula, tibia, or other suitable source. An alternative method is to implant a plate of celluloid, silver or other metal, or a portion of the fascia lata, in the gap. When a permanent hole is left in the bone, the patient should wear over it a leather or metal shield to protect the brain.
The protrusion of brain resulting after a decompression operation deliberately performed for the relief of intra-cranial tension, unless it becomes infected, has nothing in common with a hernia cerebri.
Irritation, or paralysis, of one or more of the cranial nerves may result from lesions implicating their centres or trunks.
When the trunk of the nerve is affected, the paralysis is on the same side as the lesion, and is of the lower neurone type; when the cortical centre or the upper axons are involved, it is on the opposite side, and is of the upper neurone type (p. 334). The lesions of the cerebral centres with which nerve symptoms are most frequently associated are: laceration of the brain, hæmorrhage, meningitis, tumour, and syphilitic gumma.
The nerve-trunks may be contused or torn across, especially in basal fractures which traverse their foramina of exit; blood may be effused into their sheaths as a result of injuries not attended with fracture; or they may be pressed upon by an inflammatory effusion, a tumour, a gumma, or an aneurysm invading the base of the skull. When the nerve is merely contused, or pressed upon by blood-clot, the paralysis tends to pass off in the course of a few days. When it is torn across, or compressed by a new growth, the paralysis is permanent. In some traumatic cases paralysis does not come on until a few days after the injury, and is then due either to gradually increasing pressure from blood-clot, or more probably to the onset of meningitis or of ascending neuritis.
I. The branches of the Olfactory Nerve may be ruptured as they pass through the cribriform plate in fractures implicating the anterior fossa of the skull, and there results complete and permanent loss of smell (anosmia). Hæmorrhage into the nerve sheath or contusion of the nerve may cause a transitory loss of smell. The trunk of the nerve may be implicated also in tumours and meningitis in the anterior fossa. In all cases in which anosmia results there is also interference with the power of recognising different flavours, thus greatly impairing the sense of taste.
II. Optic Nerve.—Temporary paralysis of one or both optic nerves is a comparatively common result of traumatic effusion of blood into their sheaths; the resulting blindness may pass off in a few days, or may last for some weeks. When a large effusion takes place, the prolonged pressure on the nerve may result in optic atrophy and permanent blindness. Complete severance of the nerve by a bullet, the point of a sharp instrument, or a fragment of bone, results in loss of sight in the eye on the same side. In cellulitis of the orbit, intra-orbital tumour, gumma and aneurysm in the region of the cavernous sinus, also, the optic nerve may be implicated.
Lesions implicating the cortical centre for sight in the occipital lobe give rise to hemianopia—that is, loss of sight in the lateral halves of the fields of vision of both eyes—colour-blindness, subjective sensations of light and colour, and other eye symptoms.
Double optic neuritis, followed by optic atrophy, is one of the most constant effects of the growth of a tumour within the skull, and is not uncommon in cases of cerebral abscess and meningitis. Pressure on the optic chiasma, for example by a tumour of the pituitary body, is associated with bilateral temporal hemianopsia.
III. Oculo-Motor Nerve.—One or more of the branches of this nerve may be compressed by extravasated blood, or be contused and lacerated in fractures implicating the region of the sphenoidal fissure. Fixed dilatation of one pupil may result from pressure by blood-clot, without other functional disturbance of the nerve. A tumour or an aneurysm growing in this region also may press upon the nerve. Sometimes both nerves are involved—for example, in fracture implicating both sides of the anterior fossa, and in tumours, particularly gumma, growing in the region of the floor of the third ventricle. In lesions of the cerebral hemispheres the third nerve is frequently paralysed. Its cortical centre lies in close proximity to the centre for the face (Fig. 179).
The most prominent symptoms of complete paralysis are ptosis or drooping of the upper eyelid, lateral strabismus, and slight downward rotation of the eye with diplopia. There are also dilatation of the pupil from paralysis of the circular fibres of the iris, and loss of accommodation and reaction to light from paralysis of the ciliary muscle.
Paralysis of the muscle supplied by the third nerve is frequently associated with paralysis of other ocular muscles. When all the muscles of the eye are paralysed, the condition is known as “opthalmoplegia externa”; it is usually due to syphilitic disease in the floor of the third ventricle.
IV. The Trochlear or Patheticus Nerve, which supplies the superior oblique muscle, may suffer in the same way as the oculo-motor nerve. When it is paralysed, there is defective movement of the eye downward and medially, and the patient may complain of diplopia when he looks downward.
V. Trigeminal Nerve.—The most important surgical affection of this nerve is “trigeminal neuralgia,” which has already been described (Volume I., p. 373). One or other of the divisions of the nerve may be torn in fractures of the base of the skull, and there results anæsthesia in the area supplied by it. In fractures crossing the apex of the petrous portion of the temporal bone, the great and small superficial petrosal nerves may be ruptured, and the soft palate and uvula are paralysed and there is difficulty in swallowing; there are also painful sensations in the ear. When the ophthalmic division is implicated, the conjunctiva is rendered insensitive, and conjunctivitis, which may be followed by ulceration of the cornea, results from exposure to dust and other foreign bodies, which, on account of the anæsthetic condition of the eye, are allowed to remain and cause irritation.
VI. Abducens Nerve.—This nerve, which supplies the lateral rectus muscle, has the longest course within the skull of any of the cranial nerves. In spite of this fact, it is comparatively seldom torn in basal fractures; but it is prone to be pressed upon by tumours, gummas, or aneurysms in the region of the base of the brain. When it is paralysed, medial strabismus results.
VII. Facial Nerve.—Paralysis of the facial muscles, more or less complete, is the most characteristic symptom of lesions of this nerve.
Paralysis of the Cerebral Type.—When the fibres of the nerve are implicated in any part of their course between the cortical centre and the nucleus in the lower part of the pons, the paralysis is of the upper neurone (cerebral) type. It affects the side of the face opposite to that of the lesion, and the defective movement is more marked in the lower than in the upper half of the face.
This form of facial paralysis may be due to the pressure of an intra-cranial tumour, abscess, or hæmorrhage, or to degenerative processes in the cerebral tissue, and as a rule other cranial nerves are also affected. Its recognition is chiefly of diagnostic and localising importance.
Paralysis of the Peripheral Type.—When the trunk of the nerve is implicated between the pontine nucleus and its peripheral distribution, the paralysis is of the lower neurone (peripheral) type, the muscles on the same side as the lesion being flaccid and atrophied.
The majority of cases are of the so-called “rheumatic” variety, and are attributed to exposure to cold. Others result from fractures implicating the middle fossa of the skull, or are associated with chronic suppuration in the middle ear.
In fractures passing across the petrous temporal, the nerve may be torn at the time of the injury, or may become pressed upon by a traumatic effusion or by callus later, but considering the frequency of these fractures it is comparatively seldom damaged.
Suppurative disease of the middle ear is a more common cause of facial paralysis. The nerve, as it traverses the facial canal (aqueductus Fallopii), may be pressed upon by inflammatory effusions or granulations, or may be destroyed by the suppurative process, particularly in young children, as in them the osseous wall of the aqueduct is very thin. It may also be involved in tuberculous and in malignant disease of the middle ear.
The nerve may be injured also in the course of operations on the mastoid or middle ear, or in the removal of tumours or glands in the parotid region. As the nerve breaks up into numerous branches soon after it leaves the stylo-mastoid foramen, the paralysis may be confined to one or more of its branches.
Temporary paralysis may result from inflammatory conditions such as parotitis, or from blows or pressure over the nerve, for example by the forceps in delivery.
Symptoms.—In complete unilateral facial paralysis (Bell's paralysis) the affected side of the face is expressionless and devoid of voluntary or emotional movement. The muscles are flaccid, the cheek is flattened and smooth, all its folds and wrinkles being obliterated. When the patient speaks or smiles, the face is drawn to the sound side (Fig. 201). The eye on the affected side cannot be closed, and on making the attempt the eyeball rolls upwards and outwards. The lower lid droops, the patient cannot wink, and the conjunctiva therefore becomes dry, and is irritated by exposure to cold and dust. The tears run over the cheek. From paralysis of the buccinator muscle there is inability to whistle or to puff out the cheeks and food collects between the cheek and the gums. The orbicularis oris being also paralysed, the patient is unable to show his upper teeth, and the labial consonants are pronounced indistinctly. The sense of taste is often impaired from involvement of the chorda tympani nerve.
 Fig. 201.—Patient suffering from left facial
Paralysis. Note smoothness of left side of face, imperfect closure of
left eye, and deviation of face to right side.
Fig. 201.—Patient suffering from left facial
Paralysis. Note smoothness of left side of face, imperfect closure of
left eye, and deviation of face to right side.When the paralysis is bilateral, the symmetrical appearance of the face renders the condition liable to be overlooked.
Treatment.—In addition to removing the cause, when this is possible, recovery of function may be promoted by the administration of drugs, such as potassium iodide, strychnin, or iron, by the application of blisters, or by massage and electricity. These measures are most useful in cases due to blows or exposure to cold. When the nerve is accidentally divided in the course of an operation on the face, it should immediately be sutured. So long as the electrical reactions of the affected muscles indicate an incomplete lesion, recovery may be confidently expected (Sherren). When the reaction of degeneration is present and the paralysis has lasted for more than six months, there is little hope of recovery, and recourse should be had to operation, to restore the function of the nerve by grafting its distal end on to the trunk of the hypoglossal nerve. To prevent paralysis of the tongue the lingual nerve may be divided, and its proximal end anastomosed with the distal end of the hypoglossal.
The facial may be grafted on the accessory nerve, but the associated movements of the face which then accompany movements of the shoulder often prove inconvenient.
Facial Spasm.—Clonic contraction of the facial muscles (histrionic spasm) occasionally results from irritative lesions in the cortex or pons. Sometimes all the muscles are involved, sometimes only one, for example the orbicularis oculi (palpebrarum)—blepharospasm. This condition may be induced reflexly from irrigation of the trigeminal nerve, notably of branches that supply the nasal cavities and the teeth.
The treatment consists in removing any source of peripheral irritation that may be present, in employing massage, and in administering nerve tonics, bromides, and other drugs. In severe cases, the facial nerve may be stretched with benefit, either at its exit from the stylo-mastoid foramen or on the face.
VIII. Acoustic or Auditory Nerve.—The acoustic nerve is liable to be damaged along with the facial in tumours of the cerebello-pontine angle, and in fractures which traverse the internal auditory meatus. Both nerves also may be torn across just before they enter the meatus in severe brain injuries apart from fracture. Complete and permanent deafness results. Effusion of blood into the nerve sheath, or into the internal or middle ear, causes transitory deafness, and the patient suffers from noises in the ear, giddiness, and interference with equilibration.
IX. The Glosso-pharyngeal Nerve is comparatively seldom injured. When it is compressed by a tumour in the region of the medulla, there is interference with speech and deglutition, ulcers form on the tongue, and œdema of the glottis may supervene.
X. The Vagus or Pneumogastric Nerve is seldom injured within the cranial cavity.
In the neck, it is liable to be divided or ligated in the course of operations for the removal of malignant or tuberculous glands, for goitre, or for ligation of the common carotid. Division of the nerve on one side, or even removal of a portion of it, is not as a rule followed by any change in the pulse or respiration. If it is irritated, however, for example by being grasped with an artery forceps, there is inhibition of the heart, and if it is accidentally ligated, there may be persistent vomiting.
Division of the main trunk, or of its recurrent branch on one side, results in paralysis of the corresponding posterior crico-arytænoid muscle—the muscle that opens the glottis. This condition is known as unilateral abductor paralysis, and is accompanied by interference with inspiration and phonation. If both nerves are divided, bilateral abductor paralysis results: the vocal cords flap together, producing a crowing sound on inspiration and embarrassment of breathing, and tracheotomy may be necessary to prevent asphyxia.
The vagus and recurrent nerves have been successfully sutured after having been divided accidentally.
XI. Accessory or Spinal Accessory Nerve.—This nerve is seldom damaged within the skull. It supplies the sterno-mastoid and trapezius; but as these muscles usually have an additional nerve supply from the cervical plexus, the accessory may be divided, or a considerable portion of it resected, as, for example, in the treatment of spasmodic torticollis, without any serious disablement resulting. It is liable to be accidentally divided in excising malignant or tuberculous glands in the neck. When, however, the accessory is the only source of supply to these muscles, its division is followed by considerable disablement, which appears to depend almost entirely on the paralysis of the trapezius. The head is inclined slightly forward, the shoulder is depressed, the arm hangs heavily by the side and is slightly rotated forward, the scapula is drawn away from the spine and rotated on its horizontal axis, and there is slight cervical scoliosis with the concavity towards the affected side. The trapezius is markedly wasted, and is, therefore, less prominent in the neck than normally, and the functions of the arm and shoulder are impaired, especially in making overhead movements. In time other muscles compensate in part for the loss of the trapezius.
When divided accidentally, the nerve should be immediately sutured. Even when the paralysis has lasted for some time, secondary suture should be attempted; if this is impossible, the peripheral end should be anastomosed with the anterior primary divisions of the third and fourth cervical nerves (Tubby). Massage, electricity, and the administration of tonics are also indicated.
XII. Hypoglossal Nerve.—This nerve has been ruptured in fractures passing through the canalis hypoglossi (anterior condylar foramen). It is also liable to be divided in wounds of the submaxillary region—for example, in cut throat, or during the operation for ligation of the lingual artery, or the removal of diseased lymph glands.
The paralysed half of the tongue undergoes atrophy. When the tongue is protruded, it deviates towards the paralysed side, being pushed over by the active muscles of the opposite side. Speech and mastication are interfered with, the tongue feeling too large for the mouth; in time this disability is to a large extent overcome.
The Cervical Sympathetic.—The cervical sympathetic cord and its ganglia may be injured in the neck by stabs or gun-shot wounds, or in the course of deep dissections in the neck; and in injuries of the lower part of the cervical enlargement of the spinal cord (p. 417) or of the first dorsal nerve root.
Paralysis of the cervical sympathetic is characterised by diminution in the size of the pupil on the affected side. The pupil does not dilate when shaded, nor when the skin of the neck is pinched—“loss of the cilio-spinal reflex.” The palpebral fissure is smaller than its fellow, and the eyeball sinks into the orbit. There is anidrosis or loss of sweating on the side of the face, neck, and upper part of the thorax, and on the whole upper extremity of the affected side.
Suppurative Periostitis and Osteomyelitis.—These conditions may be the result of infection through the blood stream, but as a rule they follow upon a breach of the surface caused by a wound, a severe burn as in epileptics, a tertiary syphilitic ulcer, or a compound fracture that has become infected. Sometimes they follow suppuration in the middle ear and mastoid or in the frontal sinus, and epithelioma and rodent cancer that has ulcerated and become infected after spreading from the face towards the vertex. They are occasionally associated with acute cellulitis of the scalp. When the infection is blood-borne suppuration occurs on both aspects of the bone—a point of importance in treatment.
The illness is usually ushered in by a rigor, and this is soon followed by other signs of suppuration—high temperature, pain and tenderness, and the formation of a fluctuating swelling in relation to the bone. When pus forms between the bone and the dura, there is a characteristic œdema of the overlying area of the scalp—spoken of as Pott's puffy tumour—which is of value as indicating the extent of the disease in the bone, and of the collection of pus between it and the dura. When suppuration occurs under the pericranium, an incision gives exit to a quantity of pus, and exposes an area of bare bone. If the incision is made early, this bone may soon be covered by granulations and recover its vitality; but if operation is delayed, it usually undergoes necrosis. The sequestrum that forms includes, as a rule, only the outer table, but in some cases the whole thickness of the bone undergoes necrosis. In either case the separation of the sequestrum is an exceedingly slow process, and is not accompanied by the formation of new bone. When the whole thickness of the skull is lost, there may be a protrusion of the contents of the skull—hernia cerebri; should the patient survive, the gap becomes filled in by a dense fibrous membrane which is fused with the dura mater.
Serious complications, in the form of meningitis, cerebral abscess, sinus phlebitis, and general pyæmia, are liable to develop at any time during the progress of the infection, and we have seen pyæmia develop after the suppuration in the skull had been recovered from.
Treatment.—Early, free, and, if necessary, multiple incisions are indicated to admit of disinfection of the affected area, and of the establishment of drainage. If the symptoms point to suppuration having occurred between the bone and the dura, the skull should be trephined and further bone removed with the rongeur forceps as may be required.
Time may be saved by separating the sequestrum with the aid of an elevator or sharp spoon, or by chiselling away the dead part till healthy vascular bone is reached.
Tuberculosis of the cranial vault is usually met with in children. The disease commences in the diploë, and results in the formation of a central sequestrum, around and beneath which the tuberculous process spreads. Granulations form between the skull and the dura, and on the outer aspect lifting up the pericranium. The sequestrum is slowly thrown off, and when separated is circular like a coin and presents worm-eaten edges.
A circumscribed, tender swelling forms, at first yielding an obscure sensation of fluctuation, but later, when the pus is no longer confined under the pericranium, assuming the characters of a cold abscess, which gradually becomes superficial, and eventually bursts through the scalp, forming one or more sinuses.
The abscess should be laid open, all tuberculous granulations scraped away, and the sequestrum removed, with the aid of the chisel if it has not already become loose. On inserting the finger through the opening, it appears to penetrate to an alarming extent; this is due to the accumulation of tuberculous material between the skull and the dura mater, depressing the latter. After healing is completed, a depression or gap in the bone remains.
Syphilis.—Syphilitic affections occur during the tertiary period of the disease, and usually implicate the frontal and parietal bones (Fig. 202). They are described in Volume I., p. 462.
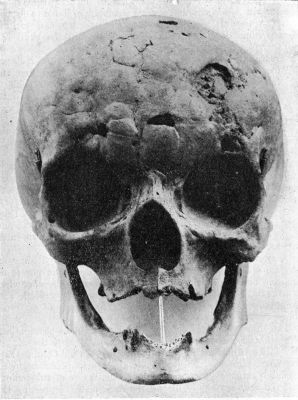 Fig. 202.—Skull of woman illustrating the appearances
of Tertiary Syphilis of Frontal Bone—Corona Veneris—in the healed
condition.
Fig. 202.—Skull of woman illustrating the appearances
of Tertiary Syphilis of Frontal Bone—Corona Veneris—in the healed
condition.
Tumours.—Osteoma of the skull has been described with diseases of bone (Volume I., p. 481).
Sarcoma.—All forms of sarcoma are met with, implicating the bones of the skull. They may originate in the pericranium, in the diploë, or in the dura mater, and usually involve the bones of the vault. They sometimes occur in children (Fig. 203).
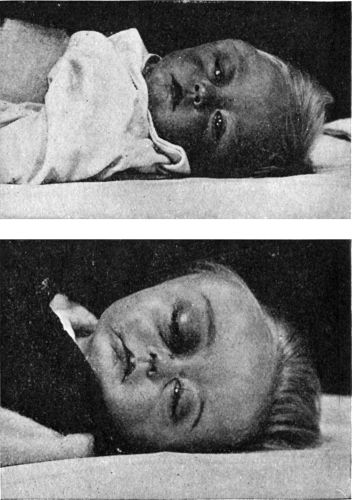 Fig. 203.—Sarcoma of Orbital Plate of Frontal Bone in
a child at age of 11 months, and 18 months.
Fig. 203.—Sarcoma of Orbital Plate of Frontal Bone in
a child at age of 11 months, and 18 months.The tumour grows chiefly towards the surface, but it also tends to invade the cranial cavity, and may thus assume the shape of a dumb-bell. Its growth is usually rapid, and results in the formation of a diffuse soft swelling, which sometimes pulsates, and sooner or later fungates through the skin. On account of its rapid growth the tumour is liable to be mistaken for an abscess, and in some cases the nature of the disease is only discovered after making an exploratory incision, and finding that the finger passes through a softened area in the bone.
When the cranial cavity is encroached upon, signs of compression ensue. After the tumour has fungated, infective complications within the skull are liable to develop. In all cases the prognosis is extremely unfavourable.
If diagnosed sufficiently early, an attempt may be made to remove the tumour, but often the operation has to be abandoned, either on account of the hæmorrhage which attends it, or because of the extent of the disease.
The bones of the skull may become the seat of secondary growths by the direct spread of cancer from the soft parts, e.g. rodent cancer (Fig. 204), or by metastasis of cancer or sarcoma from distant parts of the body, or of thyreoid tumours. Metastatic cancer would appear to be conveyed by the blood stream; it may occur in a diffuse form—cancerous osteomalacia—softening the calvaria so that at the post-mortem examination it may be removed with the knife instead of the saw; or it occurs in a discrete or scattered form, and then the macerated skull presents a number of circular and oval perforations.
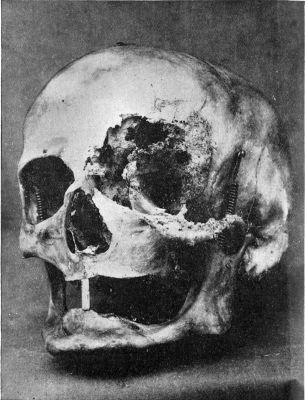 Fig. 204.—Destruction of Bones of Left Orbit, caused
by Rodent Cancer. The patient died of septic meningitis.
Fig. 204.—Destruction of Bones of Left Orbit, caused
by Rodent Cancer. The patient died of septic meningitis.Surgical Anatomy.—The veretebral column is the central axis of the skeleton, and affords a protecting casement for the spinal cord.
The spine is movable in all directions—flexion, extension, lateral flexion, and rotation around the long axis of the column. Flexion is accompanied by compression of the intervertebral discs, and by a slight forward movement of each vertebra on the one below it. This forward movement is checked by the tension of the ligamenta flava which stretch between the laminæ.
In the infant, the spine is either straight or presents one long antero-posterior curve with its convexity backwards. With the assumption of the erect posture the normal S-shaped curve is developed, the cervical and lumbar segments arching forward, while the thoracic and sacral segments arch backward.
Through the skin it is often difficult to identify with certainty the individual spinous processes. The spine of the seventh cervical vertebra,—vertebra prominens—and that of the first thoracic, are those most readily felt. While the arm hangs by the side, the root of the spine of the scapula is opposite the third thoracic spine, and the lower angle of the scapula is on the same level as the seventh. The twelfth thoracic vertebra may be recognised by tracing back to it the last rib. A line joining the highest points of the iliac crests crosses the fourth lumbar spine; and the second sacral spine is on the same level as the posterior superior iliac spine. The bodies of the upper cervical vertebræ may be felt through the posterior wall of the pharynx. The cricoid cartilage corresponds in level to that of the lower border of the sixth cervical vertebræ and its transverse process.
It is important for surgical purposes to bear in mind that most of the spinous processes do not lie on the same level as their corresponding bodies. The tips of the spines of the cervical and first two or three thoracic vertebræ lie, roughly speaking, opposite the lower edge of their respective bodies; those of the remaining thoracic vertebræ lie opposite the body of the vertebræ below; while the spines of the lumbar vertebræ lie opposite the middle of their corresponding bodies.
The vertebral canal contains the spinal cord so suspended within its membranes that it does not touch the bones, and is not disturbed by the movements of the vertebral column.
The membranes of the cord are continuous with those of the brain. The arachno-pia invests the cord and furnishes a sheath to each of the spinal nerves as it passes out through the intervertebral foramen. The arachno-pial space is filled with cerebro-spinal fluid, which forms a water-bed for the cord, continuous with that at the base of the brain. The dura mater constitutes the enveloping sheath of the cord. It hangs from the edge of the foramen magnum as a tubular sac, and is connected to the bones only opposite the intervertebral foramina, where it is prolonged on to each spinal nerve as part of its sheath. Between the dura and the bony wall of the canal is a space filled with loose areolar tissue and traversed by large venous sinuses. The dura extends as far as the upper edge of the sacrum.
The spinal cord extends from the foramen magnum to the level of the disc between the first and second lumbar vertebræ. The cervical enlargement, which includes the lower four cervical and the upper two thoracic segments, ends opposite the seventh cervical spine. The lumbar enlargement lies opposite the last three thoracic spines.
One pair of spinal nerves leaves each “segment” of the cord. On leaving the cord the nerves incline slightly downwards towards the foramina by which they make their exit from the canal. The obliquity of the nerves gradually increases, till in the lower part of the canal—from the second lumbar vertebra onward—they run parallel with the filum terminale and together constitute the cauda equina.
It is to be borne in mind that owing to the fact that the cord is relatively shorter than the canal, the tips of the spinous processes lie a considerable distance lower than the segments of the cord with which they correspond numerically. To estimate the level of the segment of the cord which is injured: in the cervical region add one to the number of the vertebra counted by the spines; in the upper thoracic region add two, in the lower thoracic region add three, and this will give the corresponding segment. The lower part of the eleventh thoracic spinous process and the space below it are opposite the lower three lumbar segments. The twelfth thoracic spinous process and the space below it are opposite the sacral segments (Chipault).
Functions.—The essential function of the spinal cord is to transmit motor and sensory impulses between the brain and the rest of the body. The general course of the fibres by which these impulses travel has already been described (p. 331).
In the grey matter there are groups of nerve-cells—“centres”—which govern certain reflex movements. The most important of these—the centres for the rectal, the vesical, and the patellar reflexes—are situated in the lumbar enlargement.
In the great majority of cases of spinal disease or injury coming under the notice of the surgeon the symptoms are bilateral, that is, are of the nature of paraplegia, and the whole of the body below the level of the segment affected is involved in the paralysis. Lesions affecting only one-half of the cord are rare and give rise to symptoms which are exceedingly complicated. When the lesion implicates the nerve-roots only, the symptoms are confined to the area supplied by the affected nerves.
As the clinical importance of a spinal injury depends almost entirely on the degree of damage done to the cord, we shall consider injuries of the cord before those of the vertebral column. They will be described under the headings: Concussion of the Cord; Traumatic Spinal Hæmorrhage; Total Transverse Lesions; Partial Lesions of the Cord and Nerve Roots; and “Railway Spine.”
Concussion of the Spinal Cord.—Concussion of the cord is now regarded as a definite entity closely resembling concussion of the brain. In some cases, the underlying lesion is of a temporary character, usually in the form of a vascular disturbance such as œdema or vascular engorgement, and possibly an arterial anæmia; in other cases there is definite evidence of injury, of the nature of contusion, minute hæmorrhages and blood-staining of the cerebro-spinal fluid. It must be clearly stated, that concussion of the cord may be attended with an immediate arrest of all its functions closely resembling the condition following upon complete crushing of the cord—total transverse lesion,—and it may be impossible to differentiate between the two conditions until two or more days have elapsed after the accident; it is usual, however, in concussion, as contrasted with crushing of the cord, that although motor conduction may be completely abolished, sensation is only impaired and evidence of sensory conduction can usually be elicited. If the lesion is merely a concussion, the functions of the cord will be restored within a day or two, first to full sensation and then to full motor power.
A classical instance is that of a late Governor-General of India, who on being thrown in the hunting-field was found to be paralysed in all four extremities; Paget diagnosed a total transverse lesion of the cervical cord with the necessary inference that it would inevitably have a fatal termination. The fact that the patient recovered completely, and was later able to fill two Viceroyalties, proved that the lesion must have been of the nature of a concussion of the cord.
The treatment consists in adopting the same measures as in crushing of the cord, while careful watch is observed for the signs of recovery of conduction. The usual order of recovery is first the reflexes, then sensation, and lastly, the motor functions.
Traumatic Spinal Hæmorrhage.—Hæmorrhage into the vertebral canal is a common accompaniment of all forms of injury to the spine, but the lower cervical region is the common seat of the severe type of hæmorrhage resulting from acute flexion of the spine such as occurs especially in a fall on the head from a horse or a vehicle in motion. The blood may be effused around the cord—between it and the dura—(extra-medullary), or into its substance (intra-medullary).
Extra-medullary Hæmorrhage—Hæmatorrachis.—The symptoms associated with extra-medullary hæmorrhage are at first of an irritative kind—muscular cramps and jerkings, radiating pains along the course of the nerves pressed upon, and hyperæsthesia. It is only when the blood accumulates in sufficient quantity to exert definite pressure on the cord that symptoms of paralysis ensue, and it is characteristic of extra-medullary hæmorrhage that the paralysis comes on gradually. When the effusion is in the cervical region—the commonest situation—the arms are more affected than the legs. The paralysis of the arms is of the lower neurone type, and the muscles are flaccid and undergo atrophy; the legs may exhibit a more complete degree of paralysis of the upper neurone type, with exaggeration of the knee-jerks. Blood may trickle down the canal and collect at a level lower than that of the lesion which causes the bleeding, and produce paralysis which slowly spreads from below upwards—gravitation paraplegia (Thorburn). There is blood in the cerebro-spinal fluid.
The treatment is on the same lines as in total transverse lesions. When there is evidence of progressive pressure on the cord, the blood is removed by spinal puncture if possible, or by laminectomy performed at the level suggested by the symptoms; operation is, however, rarely called for.
Intra-medullary Hæmorrhage—Hæmatomyelia.—Traumatic hæmorrhage into the substance of the cord occurs almost invariably in the lower cervical region, and results from forcible stretching of the cord by acute flexion of the neck. The blood is usually effused into the anterior cornua of the grey matter and into the central canal, and there is a varying degree of laceration of the nerve tissue, in addition to pressure exerted by the extravasated blood.
The severity of the clinical features depends upon the extent of the lesion. In contrast with what results in extra-medullary hæmorrhage, the symptoms are paralytic from the outset.
When the hæmorrhage is only sufficient to cause pressure on the cord, the paralysis is usually most marked in the lower extremities because the conducting fibres are pressed upon. This is associated with evanescent anæsthesia for temperature and pain, while tactile sensibility is preserved. There is retention of urine and fæces, and in young men, priapism. As the fibres which supply the dilator pupillæ are involved, the pupils are contracted. The symptoms gradually subside as the extravasated blood is re-absorbed, sensation being restored before motion, and recovery may be comparatively rapid.
When the blood extravasated in the cord causes disintegration of its substance, there is complete paralysis with atrophy, and anæsthesia in the area supplied by the segments of the cord directly implicated. The paralysis in the parts below the lesion assumes the spastic form. As the lesion is usually in the upper part of the cord, it is the arms that are most frequently affected. In less severe degrees of damage the paralysis of the most distant parts, e.g. the feet, may be transitory. Even in cases in which the loss of function below the level of the lesion has been complete, recovery may take place, but it is apt to be marred by a spastic condition of the muscles concerned, due to sclerotic changes in the cord.
Except that operative treatment is contra-indicated, the treatment is the same as for extra-medullary hæmorrhage, and at a later period measures may be employed to relieve the spastic condition of the muscles.
Total Transverse Lesions.—Total transverse lesions, that is, those in which the cord is completely crushed or torn across, are much more common than partial lesions, being an almost invariable accompaniment of a complete dislocation or of a fracture-dislocation of the spine. Even when the displacement of the vertebræ is only partial and temporary, the cord may be completely torn across. Similar lesions may result from stabs or bullet-wounds.
From the records of cases in which the vertebræ were injured by modern rifle bullets, even although the bony walls of the spinal canal had not been fractured and no hæmorrhage had occurred within the spinal canal, the cord in the vicinity was degenerated into a “custard-like material” incapable of any conducting power (Makins). According to Stevenson, “this must have been due to the vibratory concussion communicated to it by the passage of the bullet at a high rate of velocity.” The importance of this observation lies in the fact that in such cases no benefit can follow operative interference.
The clinical features vary with the level at which the cord is injured, and the diagnosis as to the nature and site of the lesion is to be made by a careful analysis of the symptoms. By gently passing the fingers under the patient's back as he lies recumbent, any irregularity in the spinous processes or laminæ may be detected, but movement of the patient to admit of a more direct examination of the spine is attended with considerable risk, and should be avoided. Skiagrams are indispensable, as they show the exact site and nature of the lesion.
Immediate Symptoms.—At whatever level the cord is damaged there is immediate and complete paralysis of motion and sensation (paraplegia) below the seat of injury, and the paralysed limbs at once become flaccid. On careful examination, a narrow zone of hyperæsthesia may be mapped out above the anæsthetic area, and the patient may complain of radiating pain in the lines of the nerves derived from the segments of the cord directly implicated. In complete transverse lesions the paralytic symptoms are symmetrical; any marked difference on the two sides indicates an incomplete lesion.
Retention of urine and retention or incontinence of fæces are constant symptoms. In young men priapism is common—the corpus cavernosum penis is filled with blood without actual erection. There is other evidence of vaso-motor paralysis in the form of dilatation of the subcutaneous vessels, and local elevation of temperature in the paralysed parts. The deep reflexes, including the tendon reflexes, are permanently lost.
Unless regularly emptied by the catheter, the bladder becomes distended, and there is dribbling of urine—the overflow from the full bladder. As the bladder is unable to empty itself, and its trophic nerve supply is interfered with, the use of the catheter involves considerable risk of infection, unless the most rigid precautions are adopted. Hypostatic pneumonia is liable to develop. Great care in nursing is necessary to prevent trophic sores occurring over parts subjected to pressure, such as the sacrum, the scapulæ, the heels, and the elbows.
Later symptoms are the result of descending degeneration taking place in the antero-lateral columns of the cord. There are often violent and painful jerkings of the muscles of the limbs; the muscles become rigid and the limbs flexed.
Treatment.—When the cord is completely divided, no benefit can follow operative interference, and treatment is directed towards the prevention of infective complications from cystitis and bed-sores.
Injuries of the Cord at Different Levels.—Cervical Region.—Complete lesions of the first four cervical segments—that is, above the level of the disc between the third and fourth cervical vertebræ—are always rapidly, if not instantaneously, fatal, as respiration is at once arrested by the destruction of the fibres which go to form the phrenic nerve. It is from this cause that death results in judicial hanging.
In lesions between the fifth cervical and first thoracic segments inclusive, all four limbs are paralysed. Sensation is lost below the second intercostal space. The parts above this level retain sensation, as they are supplied by the supra-clavicular nerves which are derived from the fourth cervical segment (Fig. 205). Recession of the eyeballs, narrowing of the palpebral fissures, and contraction of the pupils result from paralysis of the cervical sympathetic. Respiration is almost exclusively carried on by the diaphragm, and hiccup is often persistent. There is at first retention of urine, followed by dribbling from overflow, and sugar is sometimes found in the urine. Priapism is common. The pulse is slow (40 to 50) and full; and the temperature often rises very high—a symptom which is always of grave omen.
When the lesion is confined to the sixth cervical segment, the arms assume a characteristic attitude as a result of the contraction of the muscles supplied from the higher segments. The upper arm is abducted and rotated out, the elbow is sharply flexed, and the hand supinated and flexed (Fig. 206). Sensation is retained along the radial side of the limb.
 Fig. 206.—Attitude of Upper Extremities in Traumatic
Lesions of the Sixth Cervical Segment. The prominence of the abdomen
is due to gaseous distension of the bowel.
Fig. 206.—Attitude of Upper Extremities in Traumatic
Lesions of the Sixth Cervical Segment. The prominence of the abdomen
is due to gaseous distension of the bowel.
Total lesions of the lower cervical segments are usually fatal in from two to three days to as many weeks, from embarrassment of respiration and hypostatic pneumonia.
When the lesion is confined to the first thoracic segment, the attitude of the arms is usually that of slight abduction at the shoulder and flexion at the elbow, the forearms lie semi-pronated on the chest or belly, and there is slight flexion of the fingers. There is complete anæsthesia as high as the level of the second interspace, and along the distribution of the ulnar nerve (Fig. 205); the respiration is entirely diaphragmatic; and the ocular changes depending on paralysis of the cervical sympathetic are present.
Thoracic Region.—In injuries of the thoracic region—second to eleventh thoracic segments inclusive—the anæsthesia below the level of the lesion is complete and its upper limit runs horizontally round the body, and not parallel with the intercostal nerves. Above the anæsthetic area there is a zone of hyperæsthesia, and the patient complains of a sensation as if a band were tightly tied round the body—“girdle-pain.”
The motor paralysis and the anæsthesia are co-extensive. The intercostal muscles below the seat of the lesion and the abdominal muscles are paralysed. The respiratory movements are thus impeded, and, as the patient is unable to cough, mucus gathers in the air-passages and there is a tendency to broncho-pneumonia. As the patient is unable to aid defecation or to expel flatus by straining, the bowel is liable to become distended with fæces and gas, and the meteorism which results adds to the embarrassment of respiration by pressing on the diaphragm. There is retention of urine followed by dribbling from overflow. As the reflex arc is intact there may be involuntary and unconscious micturition whenever the bladder fills.
If infection of the bladder and the formation of bed-sores are prevented, the patient may live for months or even for years. At any time, however, infection of the bladder may occur and spread to the kidneys, setting up a pyelo-nephritis; or the patient may develop an ascending myelitis, and these conditions are the most common causes of death.
Lumbo-sacral Region.—All the spinal segments representing the lumbar, sacral, and coccygeal nerves lie between the level of the eleventh thoracic and first lumbar vertebræ. Injuries of the lower thoracic and upper lumbar vertebræ, therefore, may produce complete paralysis within the area of distribution of the lumbar and sacral plexuses. The anæsthesia reaches to about the level of the umbilicus. There is incontinence of urine and fæces from the first. Priapism is absent. Bed-sores and other trophic changes are common, and there is the usual risk of complications in relation to the urinary tract.
Conus Medullaris.—A lesion confined to the conus medullaris may result from a fall in the sitting position. It is attended with slight weakness of the legs, anæsthesia involving a saddle-shaped area over the buttocks and back of the thighs, the perineum, scrotum, and penis. The urethra and anal canal are insensitive, and there is paralysis of the levatores ani, the rectal and the vesical sphincters. The testes retain their sensation.
Cauda Equina.—As the cord terminates opposite the lower border of the first lumbar vertebra, injuries below this level implicate the cauda equina. The extent of the motor and sensory paralysis varies with the level of the lesion and with the particular nerves injured. Sometimes it is complete, sometimes, selective. As a rule all the muscles of the lower extremity are paralysed, except those supplied by the femoral (anterior crural), obturator, and superior gluteal nerves. The perineal and penile muscles are also implicated. There is anæsthesia of the penis, scrotum, perineum, lower half of the buttock, and the entire lower extremity, except the front and lateral aspects of the thigh, which are supplied by the lateral cutaneous nerve and the cutaneous branches of the femoral (anterior crural). There is incontinence of urine and fæces. The prognosis is more favourable than in lesions affecting the cord itself, and the only risk to life is the occurrence of infective complications.
Partial Lesions of the Cord and Nerve Roots.—Partial lesions, such as bruises, lacerations, or incomplete ruptures, are always attended with hæmorrhage into the substance of the cord, and usually result from distortions or incomplete fractures and dislocations of the spine, or from bullet wounds. They are comparatively rare.
When the nerve roots alone are injured, sensory phenomena predominate. Formication, radiating pains, and neuralgia are present in the area of distribution of the nerves implicated. There is motor paresis or paralysis, which may disappear either suddenly or gradually, or may persist and be followed by atrophy of the muscles concerned. In contrast to what is observed from pressure by tumours and inflammatory products, twitchings and cramps are rare.
In partial lesions of the cord the motor phenomena predominate. Paresis extends to the whole of the motor area below the seat of the lesion, but the weakness is more marked on one side of the body. The distal parts—feet and legs—suffer more than the proximal—arms and hands, and the extensors more than the flexors. The paresis develops slowly, varies in extent and degree, and may soon improve. Vaso-motor disturbances accompany the motor symptoms. Irritative phenomena, such as twitchings or contractures, may come on later.
The deep reflexes, particularly the knee-jerks, may be absent at first, but they soon return, and are usually exaggerated; a well-marked Babinski response may appear later. Abolition of the reflexes, therefore, does not necessarily indicate complete destruction of the cord, but their return is conclusive evidence that the lesion is a partial one. It is necessary, therefore, to defer judgment until it is determined whether the abolition of the reflexes is temporary or permanent.
Sensory disturbances may be entirely absent. When present, they are incomplete, and are chiefly irritative in character. They may not reach the same level as the motor phenomena, and the different sensory functions are unequally disturbed in the areas corresponding to the several nerve roots. There is sometimes a combination of hyperæsthesia on one side and anæsthesia on the other.
Retention of urine is not always present even in those cases in which the limbs are completely paralysed, as the fibres of one side of the cord are sufficient to maintain the functions of the bladder. The patient may be aware that the bladder is full, although he is unable to empty it. Similarly, sensation in the rectum and anus may be retained although the control of the sphincters is lost. Priapism may be present, but tends to disappear.
In partial lesions, the difficulties of diagnosis are sometimes increased by the occurrence of hæmorrhage into the substance of the cord, so that symptoms of generalised pressure are superadded to those of the partial lesion. In time the symptoms due to the intra-medullary hæmorrhage pass off, but those due to the tearing of the cord persist.
The prognosis is generally favourable, but must be guarded, as permanent organic changes in the cord may take place, causing a spastic condition of the muscles. When recovery is taking place the first signs are the return of the knee-jerks, and a gradual change in the limbs from the flaccid to the spastic condition. Sensibility returns in the order—touch, pain, temperature, and the parts supplied by the lowest sacral segments usually become sentient first. Voluntary power returns earlier in the flexors than in the extensors, and flexion of the toes is almost invariably the earliest voluntary movement possible. Infection from bed-sores or from the urinary tract is the most common cause of death in cases that terminate fatally.
The treatment is carried out on the same lines as for total lesions. Laminectomy, however, is indicated when there is reason to believe that the pressure is due to some cause, such as a blood-clot or a displaced fragment of bone, which is capable of being removed.
In practice when a person has lost the power of the lower extremities as the result of an accident, there are three conditions requiring ultimate differentiation—a concussion of the cord alone, a total transverse lesion and a partial lesion of the cord together with concussion. It must again be emphasised that it may not be possible to differentiate between these immediately after the accident. Two or three days may elapse before it is possible to give a definite opinion.
“Railway Spine.”—This term is employed to indicate a disturbance of the nervous system which may develop in persons who have been in railway accidents, but a similar group of symptoms is met with in men engaged in laborious occupations such as coal-miners, who, after an injury to the back, develop symptoms referable to the nervous system on account of which they claim compensation not infrequently in the law-courts. It is a remarkable fact that it seldom occurs in railway employees, or in passengers who sustain gross injuries, such as fractures or lacerated wounds.
Clinical Features.—The patient usually gives a history of having been forcibly thrown backwards and forwards across the carriage at the time of the accident. He is dazed for a moment and suffers from shock or, it may be, is little the worse at the time, and is able to continue his journey. On reaching his destination, however, he feels weak and nervous, and complains of pain in his back and limbs. There is rarely any sign of local injury. For a few days he may be able to attend to business, but eventually feels unfit, and has to give it up.
The symptoms that subsequently develop are for the most part subjective, and it is difficult therefore either to corroborate or to refute them; it will be observed that while some of them are referable to the cord the greater number are referable to the brain. They usually include a feeling of general weakness, nervousness, and inability to concentrate the attention on work or on business matters. The patient is sleepless, or his sleep is disturbed by terrifying dreams. His memory is defective, or rather selective, as he can usually recall the circumstances of the accident with clearness and accuracy. He becomes irritable and emotional, complains of sensations of weight or fullness in the head, of temporary giddiness, is hypersensitive to sounds, and sometimes complains of noises in the ears. There are weakness of vision and photophobia, but there are no ophthalmoscopic changes. He has pain in the back on making any movement, and there is a diffuse tenderness or hyperæsthesia along the spine. There is weakness of the limbs, sometimes attended with numbness, and he is easily fatigued by walking. There may be loss of sexual power and irritability of the bladder, but there is seldom any difficulty in passing urine. The patient tends to lose weight, and may acquire an anxious, careworn expression, and appear prematurely aged. Special attention should be directed to the condition of the deep reflexes and to the state of the muscles, as any alteration in the reflexes or atrophy of the muscles indicates that some definite organic lesion is present.
As the symptoms are so entirely subjective, it is often extremely difficult to exclude the possibility of malingering; it is essential that the patient should be examined with scrupulous accuracy at regular intervals and careful notes made for purposes of comparison, and also that the doctor should retain an impartial attitude and not develop a bias either in favour of or against the patient's claim for compensation.
So long as litigation is pending the patient derives little benefit from treatment, but after his mind is relieved by the settlement of his claim—whether favourable to him or not—his health is usually restored by the general tonic treatment employed for neurasthenia.
Partial lesions include twists or sprains, isolated dislocations of articular processes, isolated fractures of the arches and spinous processes, and isolated fractures of the vertebral bodies. The most important complete lesions are total dislocations and fracture-dislocations.
In partial lesions, the continuity of the column as a whole is not broken, and the cord sustains little damage, or may entirely escape; in complete lesions, on the other hand, the column is broken and the cord is always severely, and often irreparably, damaged.
Twists and dislocations are most common in the cervical region, that is, in the part of the spine where the forward range of movement—flexion—is greatest. Fractures are most common in the lumbar region, where flexion is most restricted. Fracture-dislocations usually occur where the range of flexion is intermediate, that is, in the thoracic region.
In all lesions accompanied by displacement, the upper segment of the spine is displaced forwards.
Twists or sprains are produced by movements that suddenly put the ligamentous and muscular structures of the spine on the stretch—in other words, by lesser degrees of the same forms of violence as produce dislocation. When the interspinous and muscular attachments alone are torn, the effects are confined to the site of these structures, but when the ligamenta flava are involved, blood may be extravasated and infiltrate the space between the dura and the bone and give rise to symptoms of pressure on the cord. The nerve roots emerging in relation to the affected vertebræ may be stretched or lacerated, and as a result radiating pains may be felt in the area of their distribution.
In the cervical region, distortion usually results either from forcible extension of the neck—for example from a violent blow or fall on the forehead forcing the head backwards—or from forcible flexion of the neck. The patient complains of severe pain in the neck, and inability to move the head, which is often rigidly held in the position of wry-neck. There is marked tenderness on attempting to carry out passive movements, and on making pressure over the affected vertebræ or on the top of the head. The maximum point of tenderness indicates the vertebra most implicated. In diagnosis, fracture and dislocation are excluded by the absence of any alteration in the relative positions of the bony points, and by the fact that passive movements, although painful, are possible in all directions.
In the lumbar region sprains are usually due to over-exertion in lifting heavy weights, or to the patient having been suddenly thrown backwards and forwards in a railway collision. The attachments of the muscles of the loins are probably the parts most affected. The back is kept rigid, and there is pain on movement, particularly on rising from the stooping posture.
Treatment.—Unless carefully treated, a sprain of the spine is liable to cause prolonged disablement. The patient should be kept at rest in bed, and, when the injury is in the cervical region, extension should be applied to the head with the nape of the neck supported on a roller-pillow. Early recourse should be had to massage, but active movements are forbidden till all acute symptoms have disappeared. In patients predisposed to tuberculosis, the period of complete rest should be materially prolonged.
Isolated Dislocation of Articular Processes.—This injury, which is most frequently met with in the cervical region and is nearly always unilateral, is commonly produced by the patient falling from a vehicle which suddenly starts, and landing on the head or shoulders in such a way that the neck is forcibly flexed and twisted. The articular process of the upper vertebra passes forward, so that it comes to lie in front of the one below.
The pain and tenderness are much less marked than in a simple twist, as the ligaments are completely torn and are therefore not in a state of tension. The patient often thinks lightly of the condition at the time of the accident, and may only apply for advice some time after on account of the deformity. The head is flexed and the face turned towards the side opposite the dislocation, the attitude closely resembling that of ordinary wry-neck, only it is the opposite sterno-mastoid that is tight. The bony displacement is best recognised by palpating the transverse process of the dislocated vertebra. In the case of the upper vertebræ this is done from the pharynx, in the lower between the sterno-mastoid and the trachea. There is pain on attempting movement, and tenderness on pressure, particularly on the side that is not displaced, as the ligaments there are on the stretch. There are often radiating pains along the line of the nerves emerging between the affected vertebræ. As the bodies are not separated, damage to the cord is exceptional. The lesion can usually be recognised in a radiogram.
Treatment.—Reduction should be attempted at once, before the vertebræ become fixed in their abnormal position. Under anæsthesia gentle extension is made on the head by an assistant, and the abnormal attitude is first slightly exaggerated to relax the ligaments and to restore mobility to the locked articular processes. The head is then forcibly flexed towards the opposite side, after which it can be rotated into its normal attitude (Kocher). Haphazard movements to effect reduction are attended with risk of damaging the cord. After reduction has been effected, the treatment is the same as that of a sprain.
Isolated Fractures of the Arches, Spinous and Transverse Processes.—Fractures of the arches and spinous processes usually result from direct violence, such as a blow or a bullet wound, and are accompanied by bruising of the overlying soft parts, irregularity in the line of the spines, and by the ordinary signs of fracture. Skiagrams are useful in showing the exact nature of the lesion. These fractures are most common in the lower cervical and in the thoracic regions, where the spines are most prominent and therefore most exposed to injury.
 Fig. 207.—Compression Fracture of Bodies of Third and
Fourth Lumbar Vertebræ. Woman, æt. 28, who fell three storeys and
landed on the buttocks.
Fig. 207.—Compression Fracture of Bodies of Third and
Fourth Lumbar Vertebræ. Woman, æt. 28, who fell three storeys and
landed on the buttocks.
In many cases there are no symptoms of damage to the cord or spinal nerves, but when both laminæ give way the posterior part of the arch may be driven in and cause direct pressure on the cord, or blood may be effused between the bone and the dura. In such cases immediate operation is indicated. When there are no cord symptoms, the treatment consists in securing rest, with the aid of extension, if necessary, for several weeks until the bones are reunited.
The use of the X-rays has shown that one or more of the transverse processes of the lumbar vertebræ may be chipped off by direct violence. The symptoms are pain and tenderness in the region of the fracture, and marked restriction of movement, especially in the direction of flexion. This lesion may explain some of the cases of persistent pain in the back following injuries in workmen. It is important to remember, however, that in a radiogram an un-united epiphysis may simulate a fracture.
Isolated Fracture of the Bodies—“Compression Fracture.”—The “compression fracture” consists in a crushing from above downwards of the bodies—and the bodies only—of one or more vertebræ. It is due to the patient falling from a height and landing on the head, buttocks, or feet in such a way that the force is transmitted along the bodies of the vertebræ while the spine is flexed.
If the patient lands on his head, the compression fracture usually involves the lower cervical or upper thoracic vertebræ. When he lands on his buttocks or feet it is usually the lumbar or the lower thoracic vertebræ that are fractured (Fig. 207).
As a rule, there are no external signs of injury over the spine. The sternum, however, is often fractured, and irregularity and discoloration may be detected on examining the front of the chest. The recognition of a fracture of the sternum should always raise the suspicion of a fracture of the spine. On examination of the back a more or less marked projection of the spinous processes of the damaged vertebræ may be recognised. In the cervical and lumbar regions this projection may merely obliterate the normal concavity. The spinous process which forms the apex of the projection belongs to the vertebra above the one that is crushed. The cord usually escapes, but the nerves emerging in relation to the damaged vertebræ may be bruised, and this gives rise to girdle-pain.
Local tenderness is elicited on pressing over the affected vertebræ. As might be expected from the nature of the accident producing this lesion, it is often associated with serious injuries to the head, limbs, or internal organs which gravely affect the prognosis.
The treatment consists in taking the pressure off the injured vertebræ in order that the reparative material may be laid down in such a way as to restore the integrity of the column. In the cervical region, extension is applied to the head, and a roller-pillow placed beneath the neck. In the lumbar region, the extension is applied through the lower limbs, and the pillow placed under the loins. The patient is confined to bed for six or eight weeks, and before he gets up a poroplastic or plaster-of-Paris jacket is applied. This is worn for a month or six weeks.
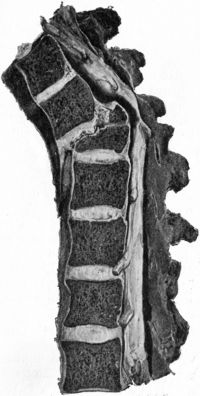 Fig. 208.—Fracture—Dislocation of Ninth Thoracic
Vertebra, showing downward and forward displacement of upper segment,
and compression of cord by upper edge of lower segment.
Fig. 208.—Fracture—Dislocation of Ninth Thoracic
Vertebra, showing downward and forward displacement of upper segment,
and compression of cord by upper edge of lower segment.Traumatic Spondylitis.—This condition is liable to develop in patients who have sustained a severe injury to the back. It is believed to originate in a compression fracture which has not been recognised, and is probably due to the callus thrown out for the repair of the fracture being subjected to strain and pressure too early, or to a progressive softening of the injured vertebra and of the bodies of those adjacent to it. This leads to an alteration in the shape of the affected bones, which can be demonstrated by means of the X-rays. The usual history is that some considerable time after the patient has resumed work he suffers from pain in the back, and radiating pains round the body and down the legs. He becomes more and more unfit for work, and a marked projection appears in the back and may come to involve several vertebræ. While the condition is progressive, the prominent vertebræ are painful and tender. In course of time the softening process is arrested, and the affected bones become fused, so that the area of the spine involved becomes rigid and permanent deformity results. So long as the condition is progressive the patient should be kept in the recumbent and hyper-extended position over a roller-pillow and, when he gets up, the spine should be supported by a jacket.
Dislocation and Fracture-Dislocation.—It is seldom possible at the bedside to distinguish between a complete dislocation of the spine and a fracture-dislocation. Fracture-dislocation is by far the more common lesion of the two, and is the injury popularly known as a “broken back.” It may occur in any part of the column, but is most frequently met with in the thoracic and thoracico-lumbar regions. It usually results from forcible flexion of the spine, as, for example, when a miner at work in the stooping posture is struck on the shoulders by a heavy fall of coal. The spine is acutely bent, and breaks at the angle of flexion and not at the point struck. The lesion consists in a complete bilateral dislocation of the articular processes, together with a fracture through one or more of the bodies. This fracture is usually oblique, running downwards and forwards. The upper fragment with the segment of the spine above it is displaced downwards and forwards, and the cord is crushed between the posterior edge of the broken body and the arch of the vertebra above it (Fig. 208). In almost every case the cord is damaged beyond repair.
Total dislocation, in which the articular processes on both sides are displaced and the contiguous intervertebral disc separated, is rare, and is met with chiefly in the lower cervical region.
Clinical Features.—The outstanding symptoms of total lesions are referable to the damage inflicted on the cord. The diagnosis should always be made by a consideration of the mechanism of the injury and the condition of the nerve functions below the lesion. On no account should the patient be moved to enable the back to be examined, as this is attended with risk of increasing the displacement and causing further damage to the cord. On passing the fingers under the back as the patient lies recumbent, it is usually found that there is some backward projection of the spinous processes, the most prominent being that of the broken vertebra. The spinous process immediately above it is depressed as the upper segment has slipped forward. Pain, tenderness, swelling and discoloration may be present over the injured vertebræ. It is usually possible to have skiagrams taken without risk of further damage to the spine. There is complete loss of motion and sensation below the seat of the lesion. The symptoms of total transverse lesions of the cord at different levels have already been described (p. 416).
Treatment.—An attempt may be made to reduce the displacement under anæsthesia, gentle traction being made in the long axis of the spine by assistants, while the surgeon attempts to mould the bones into position. No special manipulations are necessary, as the ligaments are extensively torn, and the bones are, as a rule, readily replaced. A roller-pillow is placed under the seat of fracture to allow the weight of the body above and below to exert gentle traction, and so to relieve pressure on the cord. Operative treatment is almost never of any avail, as the cord is not merely pressed upon, but is severely crushed, or even completely torn across. Even when the cord is only partially torn, operative treatment is not likely to yield better results than are obtained by reduction and extension. The usual precautions must be taken to prevent cystitis and bed-sores.
Total fracture-dislocation between the atlas and epistropheus (axis), if attended with displacement, is instantaneously fatal (Fig. 209). This is the osseous lesion that occurs in judicial hanging. Fracture of the odontoid process may occur, however, without displacement, the transverse ligament retaining the fragment in position and protecting the cord from injury. The patient complains of stiff neck and pain, and the lesion may be recognised in a radiogram. A number of cases are recorded in which death took place suddenly weeks or months after such an injury, from softening of the transverse ligament and displacement of the bones.
Penetrating Wounds.—These result from stabs or gun-shot accidents, and are practically equivalent to compound fractures of the spine; their severity depends on the extent of the damage done to the cord, and on whether or not the wound is infected. In many cases the condition is complicated by injuries of the pleural or peritoneal cavities and their contained viscera, or by injury of the trachea, œsophagus, or large vessels and nerves of the neck. When the membranes of the cord are opened, the profuse and continued escape of cerebro-spinal fluid may prove a serious complication.
Treatment.—The wound of the soft parts is treated on the usual lines. When the spinous processes and laminæ are driven in upon the cord, they must be elevated at once by operation. In injuries involving the lumbo-sacral region it is sometimes advisable to perform laminectomy for the purpose of suturing divided nerve cords.
When there is evidence that the spinal cord is completely divided, operation is contra-indicated. Attempts have been made to unite the two ends of the divided cord by sutures, but there is as yet no authentic record of restoration of function following the operation.
Percival Pott, in 1779, first described a disease of the vertebral column which is characterised by erosion and destruction of the bodies of the vertebræ. It is liable to produce an angular deformity of the spine, and to be associated with abscess formation and with nervous symptoms referable to pressure on the cord. This disease is now known to be tuberculous. It may occur at any period of life, but in at least 50 per cent. of cases it attacks children below the age of ten and rarely commences after middle life.
Morbid Anatomy.—The tuberculous process may affect any portion of the spine, and as a rule is limited to one region; several vertebræ are usually simultaneously involved. The disease may begin either in the interior of the bodies of the vertebræ—tuberculous osteomyelitis—or in the deeper layer of the periosteum on the anterior surface of the bones—tuberculous periostitis.
Osteomyelitis is the form most frequently met with in children. The disease commences as a tuberculous infiltration of the marrow, which results in softening of the bodies of the affected vertebræ, particularly in their anterior parts, and, as the disease progresses, caseation and suppuration ensue, and the destructive process spreads to the adjacent intervertebral discs. In some cases a sequestrum is formed, either on the surface or in the interior of a vertebra. The pus usually works its way towards the front and sides of the bones, and burrows under the anterior longitudinal (common) ligament. Less frequently it spreads towards the vertebral canal and accumulates around the dura, causing pressure on the cord.
The compression of the diseased vertebræ by the weight of the head and trunk above the seat of the lesion, and by the traction of the muscles passing over it, produces angling of the vertebral column. The anterior portions of the bodies being more extensively destroyed, sink in, while the less damaged posterior portions and the intact articular processes prevent complete dislocation. In this way the integrity of the canal is maintained, and the cord usually escapes being pressed upon. The spinous processes of the affected vertebræ project and form a prominence in the middle line of the back. When, as is usually the case, only two or three vertebræ are implicated, this prominence takes the form of a sharp angular projection, while if a series of vertebræ are involved, the deformity is of the nature of a gentle backward curve (Fig. 210).
The periosteal form of vertebral tuberculosis is that most frequently met with in adults. The disease begins in the deeper layer of the periosteum on the anterior aspect of the vertebræ, and extends along the surface of the bones, causing widespread superficial caries. It may attack the discs at their margins, and spread inwards between the discs and the contiguous vertebræ. Owing to the comparatively wide area of the spine implicated, this form of the disease is not attended with angular deformity, but rather with a wide backward curvature which corresponds in extent to the number of vertebræ affected. The accumulation of tuberculous pus under the periosteum and anterior longitudinal ligament is the first stage in the formation of the large abscesses with which this form of spinal tuberculosis is so commonly associated.
Effects on the Spinal Cord and Nerve Roots.—In some cases the cord and nerve roots are pressed upon by an œdematous swelling of the membranes; in others, the tuberculous process attacks the dura mater and gives rise to the formation of granulation tissue on its outer aspect—tuberculous pachymeningitis. Less frequently a collection of pus forms between the bone and the dura, and presses the cord back against the laminæ. The cord is rarely subjected to pressure as a result of curving of the spine alone, but occasionally, especially in the cervical region, a sequestrum becomes displaced backward and exerts pressure on it, and it sometimes happens, also in the cervical region, that the cord is nipped by sudden displacement of diseased vertebræ—a condition comparable to a fracture-dislocation of the spine.
The severity of the symptoms is aggravated by the occurrence of inflammation of the cord—myelitis—which is not due to tuberculous disease, but to interference with its blood-supply from the associated meningitis.
Repair.—When the progress of the disease is arrested, the natural cure of the condition is brought about by the bodies of the affected vertebræ becoming fused by osseous ankylosis (Fig. 211). While this reparative process is progressing, the cicatricial contraction renders the angular deformity more acute, and it may go on increasing until the bones are completely ankylosed; this reparative process can be followed in successive skiagrams. An increase in the projection in the back, therefore, is not necessarily an unfavourable symptom, although, of course, it is undesirable.
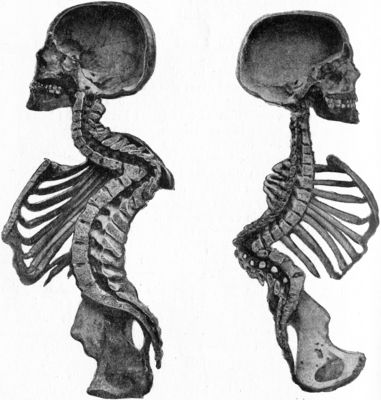 Fig. 211.—Osseous Ankylosis of Bodies (a) of Dorsal
Vertebræ, (b) of Lumbar Vertebræ following Pott's disease. There is
marked kyphosis at the seat of the disease and compensatory lordosis
above and below.
Fig. 211.—Osseous Ankylosis of Bodies (a) of Dorsal
Vertebræ, (b) of Lumbar Vertebræ following Pott's disease. There is
marked kyphosis at the seat of the disease and compensatory lordosis
above and below.
 Fig. 212.—Radiogram of Museum Specimen of Pott's
disease in a Child; the disease is located at the thoracico-lumbar
junction.
Fig. 212.—Radiogram of Museum Specimen of Pott's
disease in a Child; the disease is located at the thoracico-lumbar
junction.In rare cases the disease affects only the articular or the spinous processes, producing superficial caries and a localised abscess.
Clinical Features.—The clinical features of Pott's disease vary so widely in different regions of the spine, that it is necessary to consider each region separately. To avoid repetition, however, certain general features may be first described.
Pain.—In the earliest stages, the patient complains of a feeling of tiredness, which prevents him walking far or standing for any length of time. Later, there is a constant, dull, gnawing pain in the back, increased by any form of movement, particularly such as involves jarring or bending of the spine. If the patient is a child, it is noticed that he ceases to play with his companions, and inclines to sit or lie about, usually assuming some attitude which tends to take the weight off the affected segment of the spine (Figs. 214, 217). If he is going about, the pain increases as the day goes on, but may pass off during the night. It is often referred along the course of the nerves emerging between the diseased vertebræ, and takes the form of headache, neuralgic pains in the arms or side, girdle-pain, or belly-ache, according to the seat of the lesion. Tenderness may be elicited on pressing over the spinous or transverse processes of the diseased vertebræ, or on making pressure in the long axis of the spine. These tests, however, are not of great diagnostic value, and they should be omitted, as they cause unnecessary suffering. It is to be borne in mind that in some cases the disease is not attended with any pain.
Rigidity.—The pain produced by movement of the diseased portion of the spine causes reflex contraction of the muscles passing over it, and the affected segment of the column is thus rendered rigid. If the palm of the hand is placed over the painful area while the patient attempts to make movements of stooping, nodding, or turning to the side, it is found that the vertebræ implicated move en bloc instead of gliding on one another. This rigidity of the diseased portion of the column with “boarding” of the muscles of the back is one of the earliest and most valuable diagnostic signs of Pott's disease.
Deformity.—The most common and characteristic deformity is an abnormal antero-posterior curvature, with its convexity backwards. The situation, extent, and acuteness of the bend vary with the region of the spine affected, the situation of the disease in the bone, and the number of vertebræ implicated. When the disease has destroyed the bodies of one or two vertebræ, a short, sharp, angular deformity results; when it affects the surface of several bones, a long, wide curvature.
Lateral deviation is occasionally met with in the early stages of the disease as a result of unequal muscular contraction, and in the later stages from excessive destruction of one side of a vertebra, or from partial luxation between two diseased vertebræ.
Abscess Formation.—Spinal abscesses occur with greater frequency and at an earlier stage in adults than in children, because in adults the disease usually begins on the surface of the vertebræ. Pyogenic infection of such abscesses after they have burst externally constitutes one of the chief risks to life in Pott's disease.
X-Ray Appearances.—These, when considered along with the clinical signs, usually afford valuable information as to the exact seat and nature of the lesion and the number of vertebræ involved. It is recommended to compare the skiagram with that of the normal spine from the same region and from a patient of approximately similar age. The outlines of the bodies are woolly or blurred; in the early stage there may be clear areas corresponding to cheesy foci. In progressive cases the bodies may be altered in shape and in size, and from destruction and collapse of the bones there is altered spacing, both of the bodies and of the ribs. In the interpretation of skiagrams, help is often obtained from an alteration in the axis of bodies, an angular deviation often drawing attention to the lesion which is located at the “angle.” In children (Fig. 213) there is often a spindle-shaped shadow, outlined against the vertebral column, which is due to a cold abscess, and which extends above and below the bodies actually involved in the tuberculous process. The fusion of the bodies by new bone, which accompanies repair, can be followed in skiagrams taken at intervals.
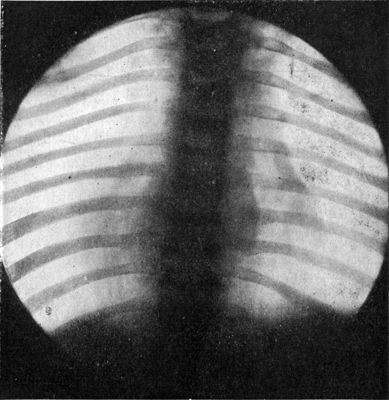 Fig. 213.—Radiogram of Child's Thorax, showing
spindle-shaped shadow at site of Pott's disease of fourth, fifth, and
sixth thoracic vertebræ.
Fig. 213.—Radiogram of Child's Thorax, showing
spindle-shaped shadow at site of Pott's disease of fourth, fifth, and
sixth thoracic vertebræ.
Cord and Nerve Symptoms.—When the spinal cord is pressed upon, the motor fibres are first affected as they lie superficially on the antero-lateral aspects of the cord, and are more sensitive to pressure. There is at first weakness or paresis of the muscles supplied from the part of the cord below the seat of pressure. The knee-jerks and plantar reflexes are exaggerated, and there is marked ankle clonus. Later, there is paralysis of the spastic type, varying in extent and sometimes amounting to complete paraplegia, and this may come on gradually or quite suddenly. There is wasting of muscles from disuse, and later a tendency to contracture and the development of deformities, as a result of sclerosis or descending degeneration of the cord.
The sensory fibres usually escape, although in some cases there is partial anæsthesia and perversion of sensation. When there is also myelitis, loss of sensibility to pain (analgesia) below the level of the lesion is one of the most characteristic symptoms. In severe cases there is incontinence of urine and of fæces, as the patient loses control of the sphincters. Acute bed-sores are not uncommon.
The symptoms referable to pressure on the nerve roots at their points of emergence are pain and hyperæsthesia along the course of the nerves that are pressed upon, and occasionally weakness and wasting of the muscles supplied by them; girdle-pain is often a prominent symptom in adults.
In the diagnosis of Pott's disease in young children, chief stress is laid on the demonstration of rigidity of the affected portion of spine; the child is laid prone and is lifted by the legs and feet so as to hyper-extend the spine; in Pott's disease the spine is held rigid, while in the rickety and other conditions that resemble it, the movements are normal.
Treatment of Pott's Disease.—In addition to the general treatment of tuberculosis, the essential factor consists in immobilising the spine in the recumbent posture and in the attitude of hyper-extension; this must be persisted in until the diseased vertebræ become fused together or ankylosed by new bone, a result which is estimated partly by the disappearance of all symptoms and more accurately by observing the formation of the new bone in successive skiagrams.
Under conservative measures it is estimated that this reparative process entails an immobilisation of the spine of from one to three years; the operative procedures introduced by Albe and Hibbs bring about a bony ankylosis of the vertebræ in as many months, and may be accepted as reducing the period of spinal immobilisation in the recumbent posture to one year at the most.
The immobilisation of the recumbent spine in the attitude of hyper-extension is most efficiently carried out by an apparatus on the lines of the Bradford frame; this is made of gas-piping covered by canvas, and is easily bent as may be required in the progress of the case towards convalescence. The frame does not interfere with such extension as may be necessary, to the head, for example, in recent cervical caries, or to the lower extremities where flexion at the hip from spasmodic contraction of the psoas muscle may be efficiently relieved by weight-extension.
Gauvain's “wheel-barrow” splint and the double Thomas' splint (Fig. 215) are efficient substitutes, but Phelps' box has been discarded because it fails to secure immobilisation of the spine.
When the stage of convalescence is arrived at, and recumbency is no longer essential, the child is allowed to sit up, stand, and go about, with the restraint, however, of some apparatus that will prevent movement of the spine, except to a limited extent. The plaster-of-Paris jacket, applied over a woollen jersey, as introduced by Sayre of New York, is probably the best; the jacket is accurately moulded to the trunk while the child is partly suspended by means of a tripod and the necessary strings under the chin, occiput, and armpits. Poroplastic felt, celluloid, papier mâché, and other materials, reinforced by strips of metal, may be substituted for the plaster of Paris. Various forms of jury-masts and collars have been employed to diminish the weight of the head in children with cervical caries, but have been very properly discarded as failing to perform the function expected of them.
Correction of the Angular Projection.—In cases in which the angular projection or gibbus, as it is called by continental authors, is of recent origin, it may be corrected by the method so successfully employed by Calot of Berck-sur-Mer—a plaster jacket is accurately moulded to the trunk, and a diamond-shaped window is cut in the jacket opposite the gibbus; a series of layers of cotton-wool are then applied, one on top of the other, so as to exert firm pressure on the gibbus, a plaster or elastic webbing bandage being employed to retain them and reinforce the pressure. The padding is renewed at intervals of three weeks or a month; in successful cases the projection may ultimately be replaced by a hollow.
Treatment of Abscess.—If a spinal abscess is causing symptoms or is approaching the surface, and there appears to be a risk of mixed infection, the abscess should be asperated and injected with iodoform emulsion.
Treatment of Cord-Complications.—Extension is applied, in the first instance, to the head or to the lower limbs, or to both, while some form of pillow is inserted at the seat of the disease; if the condition is merely one of œdema, the symptoms usually yield with remarkable rapidity; if they persist, in spite of extension, for three to six weeks, recourse should be had to laminectomy; it is usual to find evidence of mechanical pressure by granulation tissue, pus, or displaced bone, the relieving of which is followed by disappearance of the nerve symptoms. Some authors are lukewarm in their advocacy of this operation, but we can cite a number of cases in which, after laminectomy, an apparently hopeless paraplegia has been entirely got rid of.
Prognosis.—As regards the survival of persons who have suffered from Pott's disease, and as having an important bearing on prognosis, it may be noted that surgical museums contain many specimens illustrating the “cured” stage of the disease, in which the bodies of the vertebræ, formerly the seat of tuberculous destruction or caries, are represented by a ridge-shaped mass of new bone, forming a solid union between the segments above and below (Fig. 211), or the remains of the original bodies may still be identifiable, although they are surrounded and fused together by new bone. The latter condition is the more liable to a recrudescence of the tuberculous infection. Further, it may be inferred from the number of “cured” cases of Pott's disease met with in everyday life, that the malady is one from which recovery may be expected.
The cervical cases are recognised by the “telescoping” of the neck, the head and thorax being unduly approximated; the dorsal cases by the well-known hump or hunch-back, in which the spinous processes of the collapsed vertebræ constitute the apex of the hump; the thorax is telescoped from above downwards, the ribs are crowded together, the lower ones, it may be, inside the iliac crests, and the sternum projected forwards. The hunch-back from Pott's disease is often a remarkably capable person, both physically and intellectually.
Upper Cervical Region, including Atlo-axoid Disease.—When the disease affects the first and second cervical vertebræ, the atlo-axoid articulation becomes involved, and as a result of the destruction of its component bones and ligaments, the atlas tends to be dislocated forward. When this occurs suddenly, the odontoid process may impinge on the medulla and upper part of the cord and cause sudden death. When the displacement occurs gradually, the atlas and axis may be separated to a considerable extent without the cord being pressed upon, and recovery with ankylosis may ensue. When the third, fourth, and fifth vertebræ are affected, the tendency to dislocation and compression of the cord is not so great, but a portion of bone may be displaced backwards and exert pressure on the cord.
The patient complains of a fixed pain in the back of the neck, and of radiating pains along the course of the sub-occipital and other cervical nerves. The neck is held rigid, and to look to the side the patient turns his whole body round. As the disease advances the head may be bent to one side as in wry-neck, or it may be retracted and the chin protruded. To take the weight of the head off the diseased vertebræ the patient often supports the chin on the hands (Fig. 214).
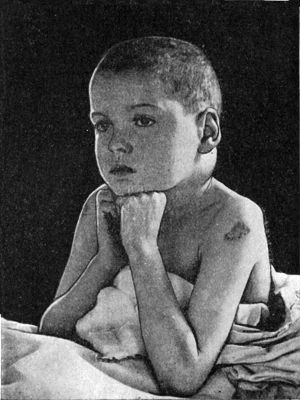 Fig. 214.—Attitude of patient suffering from
Tuberculous disease of the Cervical Spine. The swelling on the left
side of the neck is due to a retro-pharyngeal abscess.
Fig. 214.—Attitude of patient suffering from
Tuberculous disease of the Cervical Spine. The swelling on the left
side of the neck is due to a retro-pharyngeal abscess.
An abscess may form between the vertebræ and the wall of the pharynx—retro-pharyngeal abscess—the pus accumulating between the diseased bones and the prevertebral layer of the cervical fascia. The abscess may project towards the pharynx as a soft fluctuating swelling, and may cause difficulty in swallowing and breathing, and snoring during sleep; if it bursts internally it may cause suffocation. The abscess may bulge towards one or both sides of the neck, and come to the surface behind the posterior border of the sterno-mastoid muscle (Fig. 214). In some cases it comes to the surface in the sub-occipital region.
If the cord is pressed upon by inflammatory products, there is muscular weakness, beginning in the arms and extending to the legs, and sometimes followed by complete paralysis. In the early stages there is retention of urine and constipation; later the bladder and rectum are paralysed, and there is incontinence.
Sudden death may result when dislocation of the atlo-axoid joint takes place.
Cervical caries has to be diagnosed from rheumatic torticollis, and from the effects of injuries, such as a sprain or twist of the spine. When a retro-pharyngeal abscess points behind the sterno-mastoid, it is apt to be mistaken for a cold abscess originating in tuberculous cervical glands. Retro-pharyngeal abscess due to other causes is described with diseases of the pharynx.
Treatment.—Extension is applied to the head, preferably by means of an elastic band fixed to the top of the bed, and the head of the bed is raised on blocks so that the weight of the body may furnish the necessary counter-extension. Lateral movements of the head are prevented by means of sand-bags. After the acute symptoms have subsided, the spine should be fixed by some rigid apparatus, such as a double Thomas' splint prolonged so as to support the occiput (Fig. 215).
When it is considered advisable to open a retro-pharyngeal abscess, this should be done from the side of the neck by an incision along the posterior border of the sterno-mastoid, as first recommended by John Chiene. The abscess is evacuated, and the cavity filled with iodoform emulsion, and closed without drainage. An opening made through the mouth is attended with the risks of pus being inhaled into the air-passages and of pyogenic infection.
When the patient is allowed to get up, a poroplastic collar and jacket of the Minerva type which supports the head and controls the movement of the cervical and thoracic vertebræ must be worn until the cure is complete.
 Fig. 216.—Hunch-back Deformity following Pott's
disease of Thoracic Vertebræ.
Fig. 216.—Hunch-back Deformity following Pott's
disease of Thoracic Vertebræ.Cervico-thoracic Region.—When the lower cervical and upper thoracic vertebræ are affected, in addition to the fixed pain in the diseased bones, the patient complains of pain radiating along the distribution of the superficial cervical nerves and down the arms. There is often marked angular deformity. If an abscess forms, it may come to the surface in the lower part of the posterior triangle, or may spread into the posterior mediastinum or into the axilla. Sometimes the pus burrows behind the œsophagus and trachea, and it may find its way into the pleural cavity. The cord is not often pressed upon; when it is, the cervical sympathetic is implicated.
Thoracic or Dorsal Region.—When the disease is confined to the thoracic region, stiffness of the back and boarding of the vertebral muscles are prominent features. On being asked to pick up an object from the floor, the patient reaches it by bending his knees and hips, while he keeps his back rigid. He refuses to make any movement that involves jolting of the spine, such, for example, as jumping from a chair to the ground. Children often attempt to take the weight off the diseased vertebræ by placing the palms of the hands on the edge of a chair so that the weight is borne by the arms.
Angular deformity is often well marked, and may implicate several vertebræ. In order to maintain the head erect, the spine above and below the seat of disease becomes unduly arched forward—compensatory lordosis. In advanced cases the ribs become approximated, and the lower end of the sternum is projected forward. The antero-posterior diameter of the thorax is thus increased, while its vertical diameter is diminished. These changes, together with the telescoping of the vertebral bodies, lead to the deformity characteristic of the tuberculous hunch-back (Fig 216). The alterations in the shape of the chest may lead to functional disturbances of the heart and lungs.
Dorsal Abscess.—As already mentioned, the earliest stage of abscess is well seen in skiagrams (Fig. 213), especially in children. When there is an extension of the suppurative process, the pus may pass directly backwards along the posterior branches of the intercostal vessels and nerves, and come to the surface behind the transverse processes, or it may travel forward between the pleura and the ribs, and, passing along the course of the lateral cutaneous branches of the intercostals, come to the surface opposite the middle of the rib. In the latter case, the abscess is liable to be mistaken for one associated with tuberculous disease of the rib, particularly as the rib is usually found to be bare. In rare cases the pus opens into the pleura, giving rise to empyema. When the disease is on the anterior surface of the bodies of the lower thoracic vertebræ, the pus may spread down through the pillars of the diaphragm and reach the sheath of the psoas muscle.
Treatment is on the usual lines.
Thoracico-lumbar Region.—The symptoms are similar to those of disease in the thoracic region. Children while standing often assume a characteristic attitude—the hips and knees are slightly flexed, and the hands grasp the thighs just above the knees (Fig. 217). In this way the weight is partly taken off the affected vertebræ and borne by the arms. If the child is laid on its back and lifted by the heels, the spine remains rigid. By this test a projection due to tuberculous disease may be differentiated from one due to rickets, as in the latter case the projection disappears.
The patient often complains of pain in the abdomen—which in children may be mistaken for a simple “belly-ache”—and of pain shooting down the buttocks and into the legs. If the cord is pressed upon at the level of the lumbar enlargement the anal and vesical sphincters are paralysed, and the reflexes are exaggerated.
Psoas Abscess.—When an abscess forms, it usually occupies the sheath of the psoas muscle, in which it spreads down towards the iliac fossa, and into the thigh, passing beneath Poupart's ligament, posterior and lateral to the femoral vessels. The communication between the pelvis and the thigh is often very narrow, so that the abscess cavity has to some extent the shape of an hour-glass. The pus may reach the surface in the region of the saphenous opening, or may spread farther down the thigh under cover of the deep fascia. In some cases it is liable to be mistaken for a femoral hernia, as the swelling becomes smaller when the patient lies down, and has an impulse on coughing.
Lumbar Abscess.—Sometimes the pus travels along the posterior branches of the lumbar vessels and nerves to the lateral border of the sacro-spinalis (erector spinæ) and comes to the surface in the space between the edges of the latissimus dorsi and external oblique muscles—the triangle of Petit.
In rare cases it passes through the sacro-sciatic foramen and forms a swelling in the buttock (sub-gluteal abscess); or it may pass through the obturator foramen and reach the adductor region of the thigh or even the perineum.
Lumbo-sacral Region.—Pott's disease in the lumbo-sacral region usually affects adults, and, on account of the breadth of the vertebral bodies and the limited range of movement in this segment of the spine, is seldom accompanied by marked symptoms or deformity. The diagnosis, therefore, is often difficult, unless good skiagrams are available. The disease may be associated with pain in the distribution of the sciatic nerve, which is liable to be mistaken for sciatica. Single or double iliac abscess frequently forms without the patient showing any characteristic signs of spinal disease. When the disease begins in childhood it may induce a permanent deformity of the pelvis, the conjugate diameter at the brim being increased, while the transverse diameter at the outlet is diminished—kyphotic pelvis, and, in females, this may lead to complications in parturition.
Tuberculous Disease of the Sacro-iliac Joint.—This condition may occur as a primary affection, but is much more frequently secondary to disease in the ilium, sacrum, or lower lumbar vertebræ, and is most common in adolescents and young adults of the male sex. It is attended with pain in the lumbar region, and sometimes in the buttock and along the course of the sciatic nerve. The pain is aggravated by movements, especially such as involve sudden and violent contraction of the lumbar and abdominal muscles, for example, coughing, sneezing, or straining during defecation. Tenderness is elicited on making pressure over the joint, on pressing together the iliac bones, or on attempting to abduct the limb while the pelvis is fixed. The muscles of the buttock and thigh are wasted. As any attempt to bear weight on the affected limb causes pain, the patient walks with a limp, and to save the joint he assumes an attitude which is characteristic: he throws his weight on the sound limb, leans forward, using a stick for support, tilts the affected side of the pelvis downwards, and flexes the hip and knee-joints of the diseased limb. The anterior superior spine is unduly prominent on the affected side, and the limb appears to be lengthened. Sooner or later, in most cases, an abscess forms, and the pus may reach the surface over the posterior aspect of the joint. When the pus forms in front of the joint, it may spread laterally in the iliac fossa as an iliac abscess or may gravitate downwards in the hollow of the sacrum and emerge on the buttock through the sacro-sciatic foramen—sub-gluteal abscess. Sometimes it passes into the ischio-rectal fossa or into the perineum. The presence of an abscess in the pelvis may sometimes be recognised on rectal examination. The appearance of an abscess is sometimes the first thing to draw attention to the condition.
As pain across the small of the back and along the course of the sciatic nerve may be among the early symptoms of sacro-iliac disease, the condition is liable to be mistaken for lumbago or for sciatica. From hip disease it is recognisable by noting that the movements of the hip-joint are not restricted. It is not always possible without the aid of skiagrams to differentiate sacro-iliac disease from disease of the lumbar spine, and the two conditions sometimes coexist.
The prognosis is unfavourable, particularly in cases complicated by extensive disease of the ilium with abscess formation and mixed infection.
Treatment.—In early cases the patient should use crutches and wear a patten on the foot of the sound side; in more advanced cases he must be confined to bed, and have absolute rest to the joint secured by means of extension applied to both legs, or by other apparatus. In children a double Thomas' splint or Stiles' abduction frame is a convenient appliance. Counter-irritation by blisters or the actual cautery may be had recourse to in dry cases in which pain is a prominent feature. If operative treatment becomes necessary, as it may, for removal of a sequestrum, access to the seat of disease is obtained by removing the posterior portion of the iliac bone. Cold abscess is treated on the usual lines.
Syphilitic Disease of the Vertebræ.—All the clinical features of Pott's disease may be simulated by gummatous disease of the vertebræ. This is usually met with in adults who have suffered from acquired syphilis; it is most common in the upper cervical vertebræ, and begins on the anterior surface of the bodies. The onset is more sudden than that of tuberculous caries, and the progress more rapid. The bone is early and extensively destroyed, but abscess formation is rare. Severe nocturnal pains are complained of, and some degree of angular deformity may develop. In almost all cases other evidence of tertiary syphilis is present, and this, together with the history and the effects of anti-syphilitic treatment, aids in diagnosis. The local treatment is carried out on the same lines as for tuberculous disease.
Malignant Disease of the Vertebræ.—Sarcoma is the most important of the primary tumours met with in the vertebral column. It gives rise to symptoms which are liable to be mistaken for those of Pott's disease or of arthritis deformans. The pain, however, is more intense, and the disease progresses more continuously, and is uninfluenced by treatment. The changes in the vertebræ, as seen in skiagrams, are helpful in diagnosis. The growth may encroach upon the vertebral canal and cause pressure on the cord (p. 451). In the sacrum—the most common site—the tumour implicates the sacral nerves, and causes symptoms of intractable sciatica; and the real nature of the disease is often only detected on making a rectal examination.
Secondary cancer is a common disease, particularly in cases of advanced scirrhus of the breast. It leads to extensive softening of the bodies of the vertebræ, so that they yield under the weight of the body, as in Pott's disease. Clinically it is associated with severe pain in the region of the vertebræ affected, and along the course of the nerves emerging in the neighbourhood. If paralysis occurs from the cancerous bodies pressing upon the cord (paraplegia dolorosa), it is of rapid development, often becoming complete in a few hours. When the cervical cord is compressed all four limbs are paralysed, and from interference with respiration, the condition is fatal within a few days.
Actinomycosis, Blastomycosis, and Hydatid Cysts also occur in the vertebræ, and are difficult to diagnose from tuberculous disease.
Typhoid Spine.—An acute infective condition of the vertebræ, intervertebral discs, and spinal ligaments occasionally occurs during convalescence from typhoid fever. The lumbar region is most frequently affected, and the X-rays reveal inflammatory changes in the bones, disappearance of the discs, and, in the later stages, deposits of new bone leading to synostosis of adjacent vertebræ. The onset, which may be gradual or sudden, is attended with intense pain, and tenderness over the affected vertebræ. The temperature is raised, and other signs of an acute infective process are present. In a few cases there are symptoms of involvement of the membranes and cord. With prolonged rest and immobilisation of the spine the inflammation usually subsides, but sometimes it goes on to suppuration.
Hysterical Spine.—This term is applied to a functional affection of the spine occasionally met with in neurotic females between the ages of seventeen and thirty, and liable to be mistaken for Pott's disease. The patient complains of pain in some part of the spine—usually the cervico-thoracic or thoracico-lumbar region—and there is marked hyperæsthesia on making even gentle pressure over the spinous processes. As the patients are usually thin, the pressure of the corset is apt to redden the skin over the more prominent vertebræ, and give rise to an appearance which at first sight may be mistaken for a projection. The general condition of the patient, the freedom of movement of the vertebral column, and the entire absence of rigidity, are sufficient to exclude tuberculosis. The condition is treated on the same lines as other hysterical affections.
 Fig. 218.—Arthritis Deformans of Spine. The vertebræ
are fixed to one another by outgrowths of bone which bridge across the
intervertebral spaces, and there is a slight lateral deviation to the
left in the mid-dorsal region.
Fig. 218.—Arthritis Deformans of Spine. The vertebræ
are fixed to one another by outgrowths of bone which bridge across the
intervertebral spaces, and there is a slight lateral deviation to the
left in the mid-dorsal region.Acute osteomyelitis of the vertebræ is a rare affection, and is met with in young subjects. It attacks the more mobile portions of the spine—cervical and lumbar—and may begin either in the bodies or in the arches. It is attended with extreme sensitiveness on movement, severe localised pain in the region of the vertebræ attacked, and a marked degree of fever. Pus usually forms rapidly, but, being deeply placed, is not easily recognised unless it points towards the surface. The infection is liable to spread to the meninges of the cord and give rise to meningitis, particularly when the disease begins in the arches. A milder form occurs, in which the main incidence is on the periosteum; the symptoms are less severe, it does not tend to suppurate, and is usually recovered from. The treatment consists in applying extension to the spine and in opening any abscess that may be detected. The suppurative form usually proves fatal, and, indeed, is often only diagnosed on post-mortem examination.
Arthritis Deformans.—This disease usually begins between the ages of thirty-five and forty, and attacks men who follow some laborious occupation which involves exposure to cold and wet. It is met with, however, in women who lead a sedentary life. There is sometimes a recent history of gonorrhœa, rheumatism, or other toxic disease, and occasionally the condition follows upon injury. The discs disappear, osteophytic outgrowths develop at the margins of the bodies and in connection with the transverse processes, and bridge across the space between neighbouring vertebræ (Fig. 218). The articulations between the ribs and the vertebræ show similar changes, and the ligaments of the several joints tend to undergo ossification, so that the bones are fused together.
In the early stage the patient complains of pain and stiffness in the back; later the spine becomes rigid, and gradually develops a kyphotic curve, sometimes accompanied by lateral deviation. In some cases, the curvature of the spine assumes an extreme type, the shoulders are rounded, and the head depressed, the face approximating the sternum, so that to see an object such as a picture on a wall, the patient must turn his back to it. The chest is flattened and restricted in its movements, with the result that respiration is embarrassed and becomes almost entirely abdominal. The muscles of the back, shoulders, and hips undergo atrophy, and may exhibit tremors, and the deep reflexes become exaggerated. The nerves are liable to be pressed upon as they pass through the intervertebral foramina, and this gives rise to pain and other disturbances of sensation in their area of distribution. These pains may simulate those associated with renal or gastro-intestinal affections.
The disease may simulate tuberculous caries or malignant disease. The changes in the bones are demonstrated by the use of the X-rays.
The treatment is carried out on general principles (Volume I., p. 530), but it is seldom possible to do more than arrest the progress of the disease.
Coccydynia is the name applied to a condition in which the patient experiences severe pain in the region of the coccyx on sitting or walking, and during defecation. The pathology is uncertain. In some cases there is a definite history of injury, such as a kick or blow, causing fracture of the coccyx, or dislocation of the sacro-coccygeal joint. These lesions have also been produced during labour. In other cases the pain appears to be neuralgic in character, and is referable to the fifth sacral and the coccygeal nerves, or to the terminal branches of the sacral plexus distributed in this region. The affection is almost entirely confined to females, and the patients are usually of a neurotic type. On rectal examination the coccyx is exceedingly tender, and it is sometimes found to be less movable than normal, and unduly arched forward. When medicinal treatment fails to give relief, the coccyx may be excised.
Tumours of the Spinal Cord and Membranes.—Tumours may develop in the substance of the cord (intra-medullary), in the membranes (meningeal), or in the tissues between the dura and the bone (extra-dural); or the cord may be pressed upon by a tumour originating in the vertebræ. It is seldom possible to diagnose the nature of a tumour before operation, and it is often difficult to determine in which of the above situations it has originated.
Tumours growing in the substance of the cord are nearly as common as extra-medullary growths, and as the growth is usually sarcoma, glioma, tuberculoma, or gumma, and infiltrates the cord, it is seldom capable of being removed by operation.
The great majority of meningeal tumours are primary sarcomas, and in about 25 per cent. of cases they are multiple. Hydatid cysts and fibromas are also met with in this situation, and they too may be multiple.
Extra-dural growths are comparatively rare. The forms usually met with are sarcoma and lipoma.
These extra-medullary tumours seldom infiltrate the cord; they simply compress it, and should be subjected to operative treatment before secondary changes are produced in the cord.
The symptoms vary according as the tumour presses on the nerve roots, on one half, or on both halves of the cord. Pressure on nerve roots is a characteristic sign in extra-medullary growths. It gives rise to pain, which, according to the level of the tumour, passes round the trunk (girdle-pain), or shoots along the nerve-trunks of the upper or lower limbs.
When the cord is pressed upon, intense neuralgic pain related to the segment first involved is one of the earliest symptoms, particularly in extra-medullary tumours. The pain is at first unilateral, but later becomes bilateral—a point of importance in diagnosis. The painful areas are anæsthetic, but the anæsthesia does not always reach to the level of the lesion. There may be a zone of hyperæsthesia at the upper limit of the anæsthesia, or in the area corresponding to the roots on which the tumour is situated, but there is never diffuse hyperæsthesia (V. Horsley). In intra-medullary tumours the pain is less severe, it is rarely an initial symptom, and is seldom referable to individual nerve roots.
The next symptom to appear is motor paresis, followed by complete paralysis, and later by contracture of the paralysed muscles—spastic paraplegia. In intra-medullary tumours the paraplegia is usually less complete than in those that are extra-medullary. When only one lateral half of the cord is pressed upon, the motor paralysis and loss of ordinary sensation are on the same side as the tumour, and the loss of the sense of pain and of the temperature sense is on the opposite side. Retention of urine accompanies the onset of paralysis, and later gives place to incontinence. The rectum becomes paralysed, and cystitis and pressure sores develop.
Anti-syphilitic treatment should be employed in the first instance to exclude the possibility of the lesion being of the nature of a gumma. Radical operative treatment is contra-indicated in intra-medullary and in metastatic growths, but decompressive measures may be employed for the relief of pain. In meningeal and extra-dural tumours, however, in view of the hopeless prognosis if the condition is allowed to take its course, an attempt may be made to remove the tumour by operation. It is to be borne in mind that the lesion may be two or three segments higher than the complete anæsthesia would appear to indicate; the vertebral canal, therefore, should be opened about four inches above the level of the anæsthesia.
When the tumour is not removable, the patient's suffering may sometimes be alleviated by resecting the posterior roots of the nerves emerging in the vicinity of the lesion.
Chronic Spinal Meningitis.—Victor Horsley (1909) described by this name a condition which gives rise to symptoms closely simulating those of a tumour of the cord. He believes it to consist in a pachymeningitis combined with a certain degree of sclero-gliosis of the periphery of the cord. The theca is greatly distended over a variable extent of the cord; the cerebro-spinal fluid is increased in quantity and is under considerable tension; and the cord itself presents a shrunken appearance. Sometimes there is thickening of the arachno-pia and matting of the nerve roots. The condition appears to begin in the lower part of the cord, and to spread up, usually as far as the mid-thoracic region. There is frequently a history of syphilis, sometimes of recent gonorrhœa, but in some cases no cause can be assigned for the lesion.
Clinical Features.—This affection is almost always met with in adults, and the earliest symptoms are pain and weakness in the legs, and sometimes a slight kyphotic projection of the spinous processes. The loss of power, which is sometimes attended with spasticity, usually manifests itself in one leg first, and later affects the other; it is progressive, and ultimately ends in complete paraplegia. The pain is not confined to the region supplied by any one nerve root, but affects a diffuse area, and the patient complains also of a sensation of tightness in the limbs. There is never absolute anæsthesia, but there is relative anæsthesia for all forms of sensation, which extends as a rule as far as the sixth or eighth thoracic root.
There are no vaso-motor phenomena, and no tendency to the formation of pressure sores. Sometimes the patient complains of pain in the spine, but this is not aggravated by movement.
Treatment.—The treatment recommended by Horsley consists in performing laminectomy, opening the theca, and washing it out with 1 in 1000 mercurial lotion. After the wound has healed, mercurial inunction over the spine is employed to hasten the absorption of inflammatory products. The administration of anti-syphilitic drugs has not proved beneficial.
Acute Spinal Meningitis.—The spinal membranes may become implicated by direct spread in cases of acute intra-cranial lepto-meningitis, or they may be infected from without—for example, in gun-shot injuries or in cases of spina bifida.
When the infection spreads from the cranial cavity, the cerebral symptoms dominate the clinical picture, but evidence of involvement of the membranes of the cord may be present in the form of rigidity of the cervical muscles with retraction of the neck; deep-seated pain in the back, shooting round the body (girdle-pain) and down the limbs; painful cramp-like spasms in the muscles of the back and limbs, with increased reflex excitability, sometimes so marked as to simulate the spasms of tetanus.
When the theca of the cord is directly infected the spinal symptoms predominate at first, but as the condition progresses it involves the cerebral membranes, and symptoms of acute general lepto-meningitis ensue.
Once the condition has started little can be done to arrest its progress, but the symptoms may be relieved by repeated lumbar puncture.
Spinal Myelitis.—The term “myelitis” is applied to certain changes which occur in the spinal cord as a result, for example, of hæmorrhage into its substance (hæmorrhagic myelitis); or of pressure exerted on it by fragments of bone, blood-clot, tuberculous material, or new growths (compression myelitis).
In another group of cases myelitis is a result of the action of organisms or their toxins. Syphilis is a common cause, but the condition may follow on infections with ordinary pyogenic cocci, pneumococci, the influenza bacillus or the bacillus coli.
In addition to the use of anti-syphilitic remedies, or of sera directed to neutralise the toxins of the causative organism, attention must be directed to the bladder, and steps taken to prevent cystitis and the formation of bed-sores.
Spina Bifida.—Spina bifida is a congenital defect in certain of the vertebral arches, which permits of a protrusion of the contents of the vertebral canal. It is due to an arrest of development, whereby the closure of the primary medullary groove and the ingrowth of the mesoblast to form the spines and laminæ fail to take place. The cleft may implicate only the spinous processes, but as a rule the laminæ also are deficient. The defect usually extends over several vertebræ (Fig. 219). While the protrusion varies much in size, there is no constant ratio between the dimensions of the swelling and the extent of the defect in the neural arches.
 Fig. 219.—Meningo-myelocele of Thoracico-lumbar
Region.
Fig. 219.—Meningo-myelocele of Thoracico-lumbar
Region.
|
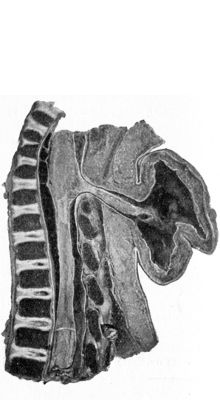 Fig. 220.—Meningo-myelocele of Cervical Spine.
Fig. 220.—Meningo-myelocele of Cervical Spine.
|
The condition is comparatively common, being met with in about one out of every thousand births. It is most frequent in the lumbar and sacral regions (Fig. 219), but occurs also in the cervical (Fig. 220) and thoracic regions. It is not uncommon to find spina bifida associated with other congenital deformities such as hydrocephalus, club-foot, and extroversion of the bladder.
Varieties.—Four varieties are usually described according to the character of the protrusion. They are analogous, to a certain extent, to the varieties of cephalocele (p. 387). (1) Spinal meningocele, in which only the membranes, filled with cerebro-spinal fluid, are protruded. (2) Meningo-myelocele, the form most commonly met with clinically, in which the cord and some of the spinal nerves are protruded, and spread out over the inner aspect of the sac (Figs. 219, 220). (3) Syringo-myelocele, in which there is a dilatation of the central canal in the protruded part of the cord. In these three forms the protrusion may be covered by healthy skin, or by a thin, smooth, translucent membrane through which the contents are visible. Frequently this thin covering sloughs or ulcerates, and permits the cerebro-spinal fluid to drain away. (4) In the myelocele, this skin, as well as the vertebral arches and membranes, is absent, and the cord lies exposed on the surface. This form is comparatively common, but as the infants are either dead born or die within a few days of birth, it seldom comes under the notice of the surgeon.
Clinical Features.—The presence of a swelling in the middle line of the back, which has existed since birth, and which contains fluid and increases in size and tenseness when the child cries, renders the diagnosis of spina bifida easy. The defect in the bone may be seen in skiagrams. The swelling is usually sessile, but may be pedunculated; it is usually possible to palpate the edges of the gap in the bones. It may be reduced in size by making gentle pressure over it, and in young children this may cause a bulging of the fontanelles. This test, however, must be employed with caution, as it is liable to induce convulsions. A meningocele, as it contains no nerve elements, may be translucent. In a meningo-myelocele the shadows of the cord and nerves stretched out in the sac may be recognised. The presence of the cord is sometimes indicated by a median furrow, and after withdrawal of some of the fluid the cord can sometimes be palpated. It is, however, often difficult to distinguish between a meningocele and meningo-myelocele.
Sometimes there are no nervous disturbances, and this is especially the case when the defect is in the lower lumbar and sacral regions below the termination of the cord. In most cases, however, there are paralytic symptoms referable to the lower extremities, the bladder, and the rectum, and there may also be trophic disturbances in the parts below. Paralytic symptoms may be absent during infancy, and develop during childhood or adolescence.
Prognosis.—Comparatively few children born with spina bifida survive longer than four or five years. The great majority die within a few weeks of birth, death being due to the escape of cerebro-spinal fluid, or to spinal meningitis following on infection. The condition in some cases remains stationary for years, but spontaneous disappearance is rare.
Treatment.—The more severe forms of spina bifida only call for palliative treatment, which consists in protecting the protrusion against infection and applying a sterilised dressing and a supporting bandage. A meningocele may be tapped with a fine needle passed through healthy skin, and the empty sac compressed by a pad of wool and an elastic bandage.
Operative treatment is seldom to be recommended in a young child unless it is otherwise viable and the swelling is increasing rapidly and threatening to burst, and there is reason to believe that the paralysis is due to pressure. The immediate results of operation are usually satisfactory, but in a large proportion of cases the child subsequently develops hydrocephalus, from which it ultimately succumbs. The hope of improvement in the motor symptoms after operation depends on the site of the spina bifida; above the twelfth thoracic vertebra there is no prospect of improvement; below this level, inasmuch as it is the tip of the conus or the cauda equina that is involved, there may be regeneration of nerve fibres and return of power in the lower extremities, and control of the sphincters may be regained. Murphy has practised resection of cicatricial or atrophied portions of the cauda, with end-to-end suture.
The term spina bifida occulta is applied to a condition in which there is no protrusion of the contents of the vertebral canal, although the vertebral arches are deficient. The skin over the gap is often puckered and adherent, and is frequently covered with a growth of coarse hair.
A mass of fat may project towards the surface, and when situated in the lumbo-sacral region may suggest a caudal appendage or tail (Fig. 222).
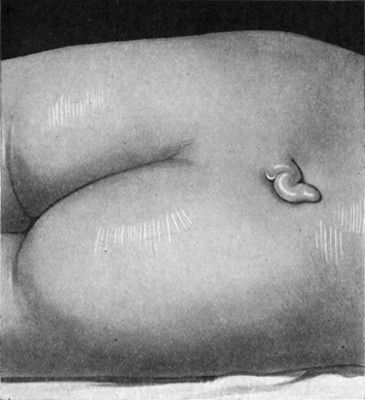 Fig. 222.—Tail-like Appendage over Spina Bifida
Occulta in a boy æt. 5, and associated with incontinence of urine.
Operation was followed by temporary retention.
Fig. 222.—Tail-like Appendage over Spina Bifida
Occulta in a boy æt. 5, and associated with incontinence of urine.
Operation was followed by temporary retention.
The clinical importance of spina bifida occulta lies in the fact that it is sometimes associated with congenital club-foot, and with nerve symptoms, in the form of sensory, motor, and trophic disturbances referable to the lower limbs, such as perforating ulcer, and to the sphincters. These nerve symptoms usually result from the presence of a tough cord composed of connective tissue, fat, and muscle, stretching from the skin through the vertebral canal to the lower end of the spinal cord. As this strand of tissue does not grow in proportion with the body, in the course of years it drags the cord against the lower border of the membrana reuniens, which closes in the vertebral canal posteriorly. These symptoms may be relieved by the removal of this strand of tissue from the gap in the vertebral arches, or by incising the membrana reuniens.
Congenital Sacro-coccygeal Tumours—Teratoma.—Many varieties of congenital tumours are met with in the region of the sacrum and coccyx. The majority are developed in relation to the communication which exists in the embryo between the neural canal and the alimentary tract—the post-anal gut or neurenteric canal. Some are evidently of bigerminal origin, and contain parts of organs, such as limbs, partly or wholly formed, nerves, parts of eyes, mammary, renal, and other tissues.
Among other tumours met with in this region may be mentioned: the congenital lipoma—a small, rounded, fatty tumour which often suggests a caudal appendage (Fig. 222); the sacral hygroma, which forms a sessile cystic tumour growing over the back of the sacrum, and is believed to be a meningocele which has become cut off in utero by the continued growth of the vertebral arch; dermoids, sarcoma, and lymphangioma.
The treatment consists in removing the tumour, as from its situation it is exposed to injury, and this is liable to be followed by infection. From the position of the wound, and the fact that many of these tumours extend into the hollow of the sacrum and therefore necessitate an extensive dissection, there is considerable risk from infection, especially in young children. The risk is increased when the tumour communicates with the vertebral canal.
Congenital Sacro-coccygeal Sinuses and Fistulæ.—The post-anal dimple, a shallow depression frequently observed over the tip of the coccyx, may be due to traction exerted on the skin at this spot by the remains of the neurenteric canal, or by the caudal ligament of Luschka. Sometimes the integument is retracted to such an extent that one or more sinuses are formed, lined with skin which is furnished with hairs, sweat, and sebaceous glands. The bursting of a dermoid, or its being incised in mistake for an abscess, may result in the formation of such a sinus, which fails to heal and may persist for years.
In some cases the depression communicates with the vertebral canal, constituting a complete sacro-coccygeal fistula, which may be lined with cylindrical or ciliated epithelium.
From the accumulation of secretions and subsequent infection, these conditions may be associated with a persistent offensive discharge, and they are liable to be mistaken for ano-rectal fistulæ. They are best dealt with by complete excision, and as primary union cannot be expected, the wound should be treated by the open method.
Three main deviations of the vertebral column are described: Lordosis, in which it is unduly arched forwards; Kyphosis, in which it is unduly arched backwards; and Scoliosis or lateral deviations, in which the spine deviates to one side of the middle line.
Lordosis or anterior curvature of the spine with the convexity forwards, is chiefly met with in the lumbar region as an exaggeration of the natural curvature. A minor degree of lordosis sometimes occurs as a peculiarity in the conformation of the individual and may be present in several members of the same family; also in street-hawkers and others who carry weights suspended in front of them; in very obese persons; in those who suffer from large abdominal tumours, such as fibroids; and in pregnant women. In its more marked and typical forms it is met with as a compensatory deviation when the pelvis is tilted forwards in association with flexion of one or of both hip-joints. Illustrations of this association are found in congenital dislocation of the hip, particularly when this is bilateral, in tuberculous disease of the hip when recovery has occurred with ankylosis in the flexed position, and in Charcot's disease of the hip. The resuming of the erect position with tilting of the pelvis from flexion at the hip is necessarily attended by an exaggeration of the forward curvature of the lumbar spine. Its relationship to the erect posture is readily demonstrated by noting its partial or complete disappearance when the patient is sitting and the tilting of the pelvis is thus eliminated.
Lordosis elsewhere than in the lumbar segment is met with as a compensatory deviation to kyphotic or backward curvature of the spine: in Fig. 211, for example, a kyphotic projection in the mid-thoracic region has led to a lordosis in the cervico-thoracic segment above, and in the thoracico-lumbar segment below, the forward curve being again a necessary outcome of the resuming of the erect posture. The absence of a compensatory lordosis in such a condition would warrant the inference that the patient had been bed-ridden.
Kyphosis or posterior curvature of the spine with the convexity backwards, is met with at all periods of life, and results from a wide range of conditions.
In infancy it is a common result of general debility. The child need not appear to be badly nourished, it may even be fat and look well, but there is a want of muscular vigour such as should enable it to hold itself erect in the sitting posture. It is to be noted that a considerable degree of kyphosis may exist without interference with the normal outlook in the erect posture, and, therefore, the question of compensatory curvature does not arise. In the adolescent a degree of kyphosis in the cervico-thoracic region is common, and is spoken of as “round shoulders”; it is largely a matter of habit that requires correction by the governess or nurse. Among agricultural labourers and gardeners after middle life, and in the aged, this type of curvature is of common occurrence and is evidently associated with their occupation. An exaggerated form of the same cervico-thoracic kyphosis is met with in patients suffering from progressive muscular atrophy, poliomyelitis, osteitis deformans of Paget, acromegaly, and many allied conditions in which either the muscular or the mental vigour is deficient, and the patient adopts the cervico-thoracic kyphosis as the attitude of rest.
Another type of diffuse kyphosis without compensatory curvature is met with in arthritis deformans, in which the kyphosis is associated with the disappearance of the intervertebral discs and ankylosis of the vertebral bodies by bridges of new bone in the position of the anterior common ligament.
Partial or localised kyphosis, on the other hand, is the result of organic changes in the bodies of the vertebræ of the segment of spine affected. It is most often met with in Pott's disease in which the extent of the curve depends on the number of bodies affected, and its degree on the amount of destruction that the bodies have undergone. With the resumption of the erect posture, and in order that the eyes should look directly forwards, a compensatory lordosis is acquired above and below the segment that is the seat of kyphosis (Fig. 211). A similar but less marked type of kyphosis may follow upon compression fracture of the spine—in the condition known as traumatic spondylitis; and as a result of other lesions, such as osteomalacia, or malignant disease, in which the bodies undergo softening and yield, so that the spinous processes project posteriorly.
Scoliosis or lateral curvature is by far the commonest and most important deviation of the spine. The student will obtain a clearer conception of the nature of this deformity if we consider in the first place those types for which an obvious explanation is available.
Static scoliosis, for example, when one leg is shorter than the other, the pelvis is tilted down on the short side, the thoracico-lumbar spine deviates laterally to the normal side, and to restore the equilibrium of the trunk the cervico-thoracic spine deviates again in the opposite direction. The causes of one leg being shorter than the other are numerous and varied; they include such conditions as unilateral congenital dislocation of the hip, fractures united with overriding of the fragments, diseases of the joints, e.g., hip disease, or of the bones, especially such as interfere with the function of ossifying junctions; and acquired deformities such as unilateral flat-foot, knock-knee, or bow-leg. Clinically, this type of scoliosis is identified by observing that when the patient sits down the deviation of the spine disappears; it is relieved or got rid of by raising the sole and the heel of the boot on the short side, and, if required, by inserting an “elevator” inside the boot.
When there is shortening of the muscles on one side of the trunk there develops a lateral curvature of the spine with its convexity to the normal side; a good example of this is afforded in cases of infantile hemiplegia (Fig. 224) in which the deviation affects the entire column: a localised form is seen in congenital wry-neck, in which the convexity of the cervico-dorsal curve is on the side of the normal sterno-mastoid with a compensatory deviation to the opposite side in the spine below (Fig. 272). Unilateral paralysis of muscles acting on the trunk may also cause a lateral deviation of the spine, as is well seen in paralysis of the trapezius, which results in a cervical scoliosis with the convexity to the non-paralysed side.
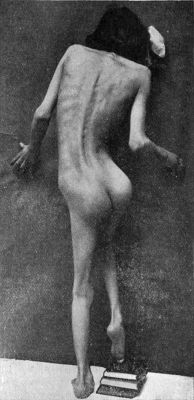 Fig. 224.—Scoliosis following upon Poliomyelitis
affecting right arm and leg.
Fig. 224.—Scoliosis following upon Poliomyelitis
affecting right arm and leg.Asymmetry of the thorax, such as may follow on empyema with defective expansion of the lung, causes a lateral deviation of the dorsal spine with the convexity towards the normal side.
Attitudes adopted to relieve pain, such as that caused by sciatica, sacro-iliac or hip disease, in which the weight of the body is transferred to the normal side, cause a scoliosis similar to that due to irregularity in the length of the lower extremities, and is similarly made to disappear when the patient sits upon a flat surface.
Malformation or disease of the vertebræ themselves is a well recognised cause of scoliosis; the best known, as it may be also the most severe and the most intractable, is that due to rickets, under which heading it has already been described (Fig. 225). In a few cases a rudimentary wedge-shaped vertebra has been revealed by the X-rays.
In all of these forms or types of scoliosis the primary cause must be searched for and when found is made the first object of treatment; the treatment of the scoliosis as such is on the same lines as in the postural variety that now falls to be described.
Habitual or Postural Scoliosis.—These names have been given to the type of scoliosis that develops in young girls and for which there is no mechanical explanation.
It is most frequently met with in rapidly growing girls of poor physique who are overworked at school or lessons, or on commencing an apprenticeship for which they are physically unfit. In some cases there is nasal obstruction from adenoids, in others the development and free play of the chest are interfered with by tight and ill-fitting garments; in all of them the muscular system is weak and the muscles of the trunk do not take their proper share in maintaining the erect posture. The most important determining factor would appear to be the habitual or repeated assumption of faulty attitudes, partly from carelessness, largely from fatigue, in order to relieve the feeling of tiredness in the back. So far as is known, the condition does not occur in communities living under aboriginal conditions. In some cases there is a hereditary tendency to scoliosis; we have seen it, for example, in a father and his daughters.
The excessive use of one arm in the carrying of weights, the habit of resting on one leg more than the other, or the assumption of a faulty attitude in writing or in playing the piano or violin, doubtless, determine the seat and direction of the curvature, and, when it has once commenced, tend to aggravate and to perpetuate it.
It is probable that the greater frequency of the primary curvature towards the right is associated with the more general use of the right hand and arm, although primary curvatures towards the left are not confined to left-handed persons.
Morbid Anatomy.—The original deviation or “primary curve” is usually in the thoracic region, and has its convexity directed towards the right side. To re-establish the equilibrium of the column, “secondary” or “compensatory” curves, with their convexities to the left, develop in the regions above and below the primary curve. It has been proved experimentally that lateral deviation of the spine is inevitably accompanied by rotation of the vertebræ around a vertical axis, in such a way that their bodies look towards the convexity of the curve, while their spines, laminæ, and articular processes are directed towards the concavity (Fig. 226).
As the deformity increases, the individual vertebræ are distorted, the bodies becoming wedge-shaped from side to side, the base of the wedge looking towards the convexity of the curve, while the narrow end looks towards the concavity (Fig. 228). As the spine, laminæ, and articular processes also undergo alterations in shape, a line uniting the tips of the spinous processes does not furnish an accurate index of the degree of lateral deviation but minimises it considerably. The muscles and ligaments are altered in length in accordance with the changes in the shape and position of the bones.
In the thoracic region, the ribs necessarily accompany the transverse processes, so that on the side of the convexity they form an undue prominence behind—the “rib-hump” (Fig. 227), while on the side of the concavity the chest is flattened and the ribs crowded together so that the intercostal spaces are diminished or even obliterated. The converse—flattening on the side of the concavity—is seen on the front of the chest.
The general shape of the thorax is altered: on the side of the convexity it is longer and narrower than normal and its capacity diminished, while on the side of the concavity it is shorter and broader and its capacity is increased.
The viscera are distorted and displaced in accordance with the altered shape of the thoracic and abdominal cavities. The twisting of the spine causes the patient to lose in stature, and the limbs appear to be disproportionately long. In advanced cases the pelvis becomes obliquely contracted—a deformity known as the scoliotic pelvis.
In spite of the marked deformity the spinal cord is never compressed.
Clinical features.—The development of scoliosis is always slow and insidious. As a rule, attention is first attracted to the deformity about the age of puberty, but in most cases it has existed for a considerable time before it is observed. The patient—usually a girl, although it also occurs in boys—is easily fatigued, has difficulty in keeping herself erect, and often complains of pain in the back and shoulders and along the intercostal spaces on the side of the convexity. To relieve the muscles of the back she is inclined to lounge in easy and ungainly attitudes.
The most common form of scoliosis met with in adolescents is a primary thoracic curvature with its convexity to the right (Fig. 227), and with more or less marked compensatory curves towards the left in the lumbar and cervical regions. The thoracic spines lie towards the right of the middle line. On account of the prominence of the ribs, the right scapula is projected backwards, and its inferior angle is on a higher level and farther from the middle line than that of the left scapula. The right shoulder seems higher than the left, and is popularly said to be “growing out”—a point which is often first observed by the dressmaker. The right side of the back is unduly prominent, while the left side is flattened. A deep sulcus forms in the left flank below the costal margin, and the space between the arm and the chest wall—the “brachio-thoracic triangle”—on the left side is much more marked than on the right; and the left iliac crest usually projects upwards and backwards. As seen from the front, the right side of the chest is flattened, while the left side is abnormally prominent, the breasts are asymmetrical, and the right nipple is on a higher level than the left.
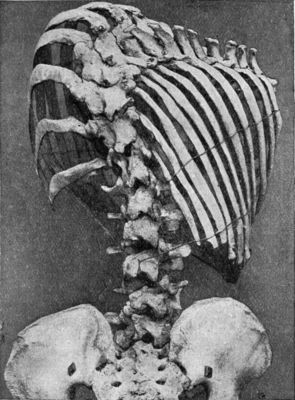 Fig. 229.—Scoliosis showing rotation of bodies of
vertebræ, and widening of intercostal spaces on side of convexity.
Fig. 229.—Scoliosis showing rotation of bodies of
vertebræ, and widening of intercostal spaces on side of convexity.
In aggravated cases, the patient may suffer from shortness of breath on exertion, and the respiratory difficulty may react on the heart, causing dilatation of the right side, palpitation, and precordial pain.
Sometimes, and particularly in males, the primary curvature is in the lumbar region, and the convexity is to the left. The deviation of the lumbar vertebræ produces a prominence in the left flank which masks the outline of the iliac crest on that side, while the right flank shows a deep furrow and the right half of the pelvis is unduly prominent. There is a slight compensatory curve to the right in the thoracic region, and the right side of the chest projects backwards. The brachio-thoracic triangle is much more marked on the right than on the left side.
Diagnosis of Adolescent Scoliosis.—In many cases the patient is brought to the surgeon on account of pain and weakness in the back before any distinct deviation has developed, and, unless a careful examination is made, the real cause of the symptoms is liable to be overlooked.
The patient should be stripped and examined in a good light in various attitudes; for example, standing in an easy position, standing as straight as she can, and sitting on a flat stool. She should also be asked to read from a book and to write, in order to exhibit her usual attitudes. In early cases, an inequality in the level of the angles of the scapulæ is often the only physical sign to be detected. It should also be observed whether the line of the spines is altered when the patient hangs from a horizontal bar or trapeze. Any backward projection of the ribs on one side is rendered more obvious if the patient folds the arms across the chest and bends well forward, while the surgeon looks along the back from behind.
Pott's disease may be excluded by the absence of rigidity. Any mechanical cause of deviation of the spine, such, for example, as inequality in the length of the limbs or contraction of the chest after empyema, must be sought for. Scoliosis that depends upon inequality in the length of the limbs or tilting of the pelvis, disappears on sitting.
Treatment.—The treatment of postural scoliosis implies a comprehensive programme, including attention to the general health, habits, and exercises out of doors and in the gymnasium, clothing, etc., all requiring supervision over a period of months, or even of years. The object of the treatment is to correct the deformity before the position has become fixed by rotation of the vertebræ and alteration in their shape. The child must not be allowed to assume awkward attitudes while reading, writing, or playing the piano; she must sit on a low chair, the seat of which slopes slightly downwards and backwards, and the back rest of which reaches as high as the shoulders, and is at an angle of 100°–110° with the seat. The feet should rest on a sloping stool, and when the child is reading or writing, a desk sloping at an angle of 45° should be used. In weakly girls approaching the period of puberty, special care should be taken to avoid compression of the trunk by tight corsets. Adenoids or other sources of respiratory obstruction must be removed; and if the patient is myopic she should be provided with suitable glasses. Standing should be avoided, as there is a great tendency to throw the weight on to one leg; but walking, running, and other exercises which bring both sides of the body into action equally are permitted under supervision. Horse-riding is a suitable form of exercise, but girls must ride astride; cycling is not to be recommended.
In mild cases—that is, those in which the curvature is obliterated when the patient is suspended—the prophylactic measures above mentioned must be rigidly enforced, and gymnastic exercises should be prescribed. The exercises should not be commenced, however, until, after a period of rest in bed, all pain and feeling of tiredness in the back have disappeared.
In cases in which the curvature is not affected by suspension, the deformity is usually permanent, but by suitable exercises it may be prevented from becoming worse, and the patient may be educated to disguise it to a considerable extent. Training is also directed towards regaining the muscular sense; with the eyes shut before a mirror, the child should endeavour to assume the correct posture; on opening the eyes, the faulty attitude is seen and corrected. Forcible correction by means of successive plaster jackets, applied in the flexed position, somewhat on the lines employed by Calot in Pott's disease, has yielded results which may be described as encouraging. Only in very advanced cases should the patient be allowed to wear a supporting jacket; such appliances have no curative effect, and can only be expected to relieve symptoms.
Exercises for Lateral Curvature.—The particular exercises given must be carefully selected to meet the indications present in each case, the movements prescribed being designed to strengthen the weak muscles and ligaments, to increase the mobility of the spine as a whole, and to correct the deviation that exists. The exercises should be taken twice daily, preferably in the morning and afternoon, and after each spell the patient should rest for an hour, lying flat on the back. During the exercises the breathing should be carefully regulated, and at the end of each movement one or two deep breaths should be taken. Each movement should be carried out slowly, the number of times it is repeated varying from four to twelve or more, according to the nature of the exercise and the strength of the patient. The exercises should be stopped if the patient feels fatigued. Hot-air baths and massage are useful adjuvants to all forms of exercise.
Special Exercises for Thoracic Curvature with convexity to right.—1. Stand with arms by side; palms directed forward; shoulders braced back. This is referred to as the “best standing position” or original position. 2. Slowly raise arms from sides until level with shoulders, with palms directed forward; carry left arm straight upward—“the keynote position.” Then slowly lower left arm to level of shoulder; lower both arms into original position. 3. Assume keynote position: slowly bend body forwards at hips until stooping position is reached, with legs kept quite straight, head bent slightly backwards, and eyes directed forward. Gradually return to keynote and original positions. 4. Keynote position: slowly bend whole spine to right; resume keynote and original positions. 5. Keynote position: turn body forward sideways. 6. Keynote position: rise on to balls of toes. 7. Keynote position: rise on to balls of toes; bend knees; back to original position in reverse order. 8. Patient suspended from bar or rings, the left end of the bar or left ring being three inches higher than the right. (a) Draw right knee upwards and forwards against resistance. (b) Draw legs apart against resistance. (c) Draw legs together against resistance. 9. Patient lying on back. (a) Bend right knee- and hip-joints against resistance. (b) Extend right knee and hip against resistance. (c) Rotate right hip against resistance. 10. Patient lying on face with pillow under chest; slowly raise arms to keynote position. While limbs are firmly held by a nurse, raise the body backwards and to the right. 11. Same position: make swimming movements. 12. Patient astride a narrow table or chair, without a back. (a) Repeat exercises 3, 4, 5, and 11. (b) Bend body forwards, backwards; and rotate to right and left against slight resistance made by nurse grasping patient's shoulders.
Klapp's “four-footed” Exercises.—Rudolf Klapp has devised a series of exercises designed to strengthen the muscles and ligaments of the spine, and to increase the mobility of the column. To take the weight of the body off the spine, and to render both ends of the column mobile, these exercises are carried out in the “all-fours” attitude, the patient crawling in imitation of a quadruped, that is, in such a way that the hand and knee of one side are approximated, while those of the other side are separated; in other words, the hand and knee of one side should not move forward simultaneously (Fig. 230). With each step the spine is curved laterally, the concavity of the curve being towards the side on which the hand and knee are approximated. The exercises, for a case of dorsal curvature with the convexity to the right, for example, are graduated as follows: (1) The child crawls in a straight line till he has acquired the “quadruped gait”; (2) with each step forward the head is inclined towards the side on which the hand and knee are approximated; (3) at each step the hand and knee which are wide apart are brought over and cross the limbs on the other side; (4) to open out the concave left side, he crawls in a circle towards the right. The exercises are practised morning and afternoon for from fifteen to sixty minutes at a time. If there is a marked double curve, it is best neutralised by imitating the “pacing” action of a quadruped, i.e., the limbs of the same side moving forward together. The hands, knees, and toes should be protected by suitable gloves and leather pads. Hot-air baths and massage are useful adjuvants to the exercises.
Abbott has introduced a method of treatment applicable to cases in which the deformity has become permanent. Under general anæsthesia, the patient being slung in a bracket-frame with the spine flexed, the curvature is over-corrected and a plaster-case is then applied to maintain the attitude; the plaster-case is renewed at intervals of two or three months.
Congenital Malformations.—The description of the various congenital malformations of the face will be simplified by a brief consideration of its development.
Development.—About the middle of the first month of intra-uterine life the prosencephalon bends acutely forward over the end of the notochord and sends out from its base a series of processes, which ultimately blend to form the face (Fig. 231). These processes surround a stellate depression, the primitive buccal cavity or stomatodæum, from which the mouth and nasal cavities are developed. The buccal cavity is bounded above by the fronto-nasal process, which is divided by a fissure—the nasal cleft or olfactory pit—into a lateral nasal process, and a mesial nasal process, at the outer angle of which a spheroidal elevation appears—the globular process.
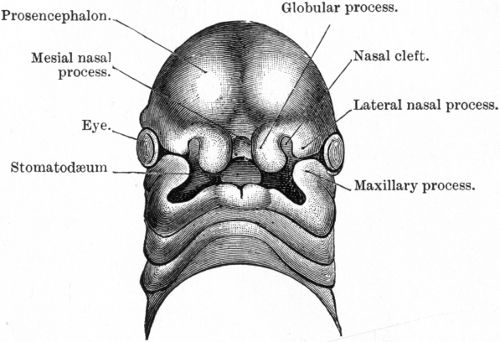 Fig. 231.—Head of human embryo about 29 days old,
showing the division of the lower part of the mesial frontal process
into the two globular processes, the intervention of the nasal clefts
between the mesial and lateral nasal processes, and the approximation
of the maxillary and lateral nasal processes, which, however, are
separated by the nasal-orbital cleft. (After His.)
Fig. 231.—Head of human embryo about 29 days old,
showing the division of the lower part of the mesial frontal process
into the two globular processes, the intervention of the nasal clefts
between the mesial and lateral nasal processes, and the approximation
of the maxillary and lateral nasal processes, which, however, are
separated by the nasal-orbital cleft. (After His.)
From the mesial nasal and globular processes the septum of the nose, the mesial segment of the premaxillary bone, and the middle portion of the upper lip are developed; while the lateral nasal process forms the roof of the nasal cavity, the ala nasi and adjacent portion of the cheek, and the lateral segment of the os incisivum or premaxillary bone. Each segment of the os incisivum carries one of the incisor teeth, and each of the mesial segments may contain in addition an accessory tooth. The nasal cleft ultimately becomes the anterior nares.
The primitive buccal cavity is bounded below by the mandibular arch, which contains Meckel's cartilage, and from which are developed the mandible, the lower lip, and the floor of the mouth.
From the lateral and back part of the mandibular arch springs the maxillary process, which grows upwards and blends with the lateral nasal process across the naso-orbital cleft—the deeper portion of which persists as the nasal duct. From the maxillary process are developed the cheeks, certain of the facial bones, the lateral portions of the upper lip, the soft and hard palate (with the exception of the os incisivum). The development of the face is completed about the end of the second month of intra-uterine life.
Hare-lip is a congenital notch or fissure in the substance of the upper lip, and cleft palate a congenital defect in the roof of the mouth. Either of these conditions may exist alone, but they occur so frequently in combination that it is convenient to consider them together.
In hare-lip the cleft may be median or lateral, and it may or may not be associated with a cleft in the palate. The resemblance to the Y-shaped cleft in the upper lip of the hare, suggested by the name, is in most cases only superficial.
Median hare-lip is extremely rare. It occurs in two forms: one in which there is a simple cleft in the middle of the lip, the result of non-union of the two globular processes; another in which there is a wide gap due to entire absence of the parts developed from the mesial nasal process—the central portion of the lip, the mesial segment of the os incisivum, and the septum of the nose. The second form is usually associated with cleft palate.
Lateral hare-lip is much more common. It is due to imperfect fusion of the globular process with the labial plates of the maxillary process. There may be a cleft only on one side of the lip, or the condition may be bilateral. In some cases the cleft merely extends into the soft parts of the lip—simple hare-lip (Fig. 232) forming a notch with rounded margins on which the red edge of the lip shows almost to the apex. In other cases the cleft passes into the alveolus of the jaw—alveolar hare-lip—partly or completely separating the mesial and lateral segments of the premaxillary bone (Fig. 233). These cases are usually combined with cleft palate (Fig. 236).
When the hare-lip is bilateral, the two clefts may be unequal, one forming a simple notch in the lip, the other passing into the nostril. In most cases, however, both clefts are complete, and the mesial portion of the lip is entirely separated from the lateral portions. The central portion or prolabium is usually smaller than normal, and is closely adherent to the os incisivum. This bone may retain its normal position in line with the alveolar processes of the maxilla (Fig. 234), or it may be tilted forward so that the incisor teeth, when present, project beyond the level of the prolabium (Fig. 235). In aggravated cases, the os incisivum and prolabium are adherent to the end of the nose. In these cases there is a Y-shaped cleft in the palate.
Cleft Palate.—It has already been mentioned that the palate is formed by the blending of the two palatal plates of the maxillary processes with the four segments of the os incisivum, derived from the nasal processes. The foramen incisivum (anterior palatine foramen) marks the point at which these elements of the palate unite. The process of fusion begins in front and spreads backwards, the two halves of the uvula being the last part to unite.
As development may be arrested at any point, several varieties of cleft palate are met with. The uvula, for example, may be bifid, or the cleft may extend throughout the soft palate. In more severe cases, it extends into the hard palate as far forward as the foramen incisivum. In these varieties the whole cleft is mesial. In still more aggravated cases, the cleft passes farther forward, deviating to one or to both sides in the fissures between the mesial and lateral segments of the os incisivum or between the lateral segments and the maxillæ. These cases are combined with double hare-lip.
The cleft varies considerably in width. It may be so wide that the imperfectly developed nasal septum is seen between its edges, and gives to the cleft the appearance of being double, or the septum is adherent to one edge of the palate—usually the right—and the cleft appears to be to the left of the middle line. In most cases the roof of the mouth is unduly arched, and is narrower than normal (Fig. 236).
Clinical Features.—Single hare-lip is about twice as common on the left as on the right side, and it occurs more frequently in boys than in girls. In a considerable proportion of cases there is a well-marked hereditary tendency to these deformities, and they frequently occur in several members of a family.
The nose is characteristically broad and flattened, the ala being bound down to the alveolar margin of the maxilla by fibrous tissue. The margins of the cleft in the lip are also attached to the alveolus by firm reflections of the mucous membrane. The orbicularis oris and other muscles of expression about the mouth being defective, the deformity is exaggerated when the child cries or laughs. In simple hare-lip the child may have difficulty in sucking, but this can usually be overcome by some mechanical contrivance to occlude the cleft.
When the hare-lip is double and combined with cleft palate, the child is unable to suck, and food introduced into the mouth tends to regurgitate through the nose. The nutrition can only be maintained by having recourse to spoon-feeding, and in feeding the child it is necessary to throw the head well back and to introduce the food directly into the back of the pharynx. Many of these infants are of such low vitality, however, that in spite of the most careful feeding they emaciate and die.
In those who survive, the voice has a peculiar nasal twang, as in phonation the air is expelled through the nose instead of through the mouth, and the articulation, especially of certain consonants, is very indistinct. Taste and smell are deficient. The constant exposure of the nasal and pharyngeal mucous membrane renders it liable to catarrhal inflammation and granular pharyngitis.
Treatment.—The only means of correcting these deformities is by operation, and, speaking generally, it may be said that the earlier the operation is performed the better, provided the general condition of the child is equal to the strain. In simple hare-lip the best time is between the sixth and the twelfth weeks. When cleft palate coexists with hare-lip, the lip should be operated on first, as the closure of the lip often exerts a beneficial influence on the cleft in the palate, causing it to become narrower.
Considerable difference of opinion exists as to when the cleft in the palate should be dealt with. Some surgeons, notably Arbuthnot Lane, recommend that it should be done in early infancy, as soon as the viability of the child is assured. We agree with R. W. Murray, James Berry, and others in preferring to wait until the child is between two and a half and three years old. It should not be delayed longer, because, even if the cleft in the palate is repaired, the nasal character of the voice persists, as the patient cannot overcome the habit of expelling the air through the nose.
Before the operation is undertaken, the child must be got into the best possible condition; and arrangements must be made for its constant supervision by a competent nurse. Success depends largely on the avoidance of infective complications, and on absence of tension between the rawed surfaces that are brought into apposition. More than one operation is sometimes required to effect complete closure of the cleft.
Voice Training.—The treatment of cleft palate does not cease with a successful operation; the importance of voice training must be explained to the parents. The child must be taught, in speaking, to send the stream of air through the mouth, instead of through the nose. If the soft palate is not sufficiently large and mobile to shut off the mouth from the nasal cavity, little improvement in speaking can be looked for.
In adolescents and adults, if the cleft is wide and the soft tissues of the palate are thin and atrophied, better physiological results may be obtained by the use of an artificial obturator or velum. With the aid of the dentist a plate of vulcanite or gold is fitted to the teeth and kept in position by suction.
Other Congenital Deformities of the Face.—Macrostoma is an abnormal enlargement of the mouth in its transverse diameter, due to imperfect fusion of the maxillary and mandibular processes.
Microstoma is due to excessive fusion of the maxillary and mandibular processes. In some cases the buccal orifice is so small as only to admit a probe.
Facial cleft is due to non-closure of the fissure between the nasal and maxillary processes. It passes upwards through the lip and cheek to the lateral angular process of the frontal bone.
Mandibular cleft occurs in the middle line of the lower lip, and may extend to, or even beyond, the chin; it is due to non-union of the two lateral halves of the mandibular arch.
These various deformities are treated by plastic operations carried out on the same principles as for hare-lip.
Fistulæ of the Lower Lip.—Two small openings, about the size of a pin's head, are occasionally met with on the free border of the lower lip, near the middle line. On passing a probe, each is found to lead into a narrow cul-de-sac, which runs for about an inch laterally and backwards under the mucous membrane. Watery, saliva-like fluid exudes through the openings. These fistulæ frequently occur in several members of the same family, and are usually associated with hare-lip. The treatment consists in dissecting them out.
Injuries of the Soft Parts of the Face.—Owing to its free blood supply, the skin of the face has great vitality, and even when severely lacerated it not only survives, but shows such resistance to bacterial infection that primary union frequently takes place. In plastic operations, also, even extensive flaps seldom become infected, and they heal so rapidly that the sutures can be removed in two or three days.
In incised wounds the bleeding is usually free at first, but unless one of the larger arteries, such as the external maxillary (facial) or temporal, is injured, it soon ceases. Paralysis of the muscles of expression may follow if the facial nerve is injured; and loss of sensation may result from injury to the supra-orbital or infra-orbital nerves. If the parotid gland is implicated, saliva may escape from the wound, but it usually ceases in a few days; if the duct is involved, a persistent salivary fistula may form.
Punctured wounds may perforate the orbit, the cranial cavity, or the maxillary sinus, and be followed by infective complications, particularly if the point of the instrument breaks off and is left in the wound.
Contused and lacerated wounds result from explosions and injuries by firearms, and foreign bodies, such as particles of stone or coal, or grains of gunpowder and small shot, may lodge in the tissues. Every effort should be made to remove such foreign bodies, as if left embedded they cause unsightly pigmentation of the skin. Ligatures are seldom necessary for the arrest of hæmorrhage unless the larger branches are injured, as the bleeding from smaller twigs is arrested by the sutures. The edges of the wound are approximated by means of Michel's clips, or by a series of interrupted horse-hair stitches, and for this purpose a fine Hagedorn needle is to be preferred, as it leaves less mark than the ordinary bayonet-shaped needle. If the mucous membrane of the mouth or of the eyelid is implicated, its edges should be approximated by a separate row of catgut stitches.
Cicatricial contraction after severe burns may lead to marked deformities of the eyelids (ectropion), mouth, and nose. When the burn has implicated the neck, the chin may be drawn towards the chest, and the movements of the lower jaw and head seriously impeded.
Bacterial Disease.—Boils, carbuncles, and anthrax pustules frequently occur on the face, and when situated near the middle line, and particularly on the upper lip, are liable to give rise to general infection and to intra-cranial complications which may prove fatal. The primary infection of glanders and of actinomycosis may also occur on the face.
The various forms of tuberculous lupus are met with more frequently on the face than in any other situation (Fig. 237). Tuberculous disease of the facial bones, particularly of the lateral half of the orbital margin at the junction of the zygomatic (malar) bone with the maxilla, is not uncommon in children.
 Fig. 237.—Illustrating the deformities caused by Lupus
Vulgaris, which dated from adolescence.
Fig. 237.—Illustrating the deformities caused by Lupus
Vulgaris, which dated from adolescence.The primary lesion of syphilis, and the various forms of secondary and tertiary syphilides, may simulate tuberculous lupus, cancer, and other ulcerative conditions.
Tumours.—The simple tumours met with on the face include sebaceous and dermoid cysts, nævus, plexiform neuroma and adenoma; the malignant forms include the squamous epithelioma, and rodent, paraffin, and melanotic cancers.
Epithelioma occurs most frequently in men beyond the age of forty. The affection usually begins at the margin of the lip, the edge of the nostril, or the angle of the eye. There is generally a history of prolonged or repeated irritation, or the condition may develop in connection with a scar, a wart, a cutaneous horn, or an ulcerating sebaceous cyst. It may begin as a hard nodule, or as a papillary growth which breaks down on the surface, leaving a deep ulcer with a characteristically indurated base—the crateriform ulcer. The neighbouring lymph glands are infected early, but metastases to other organs are not common. The treatment consists in excising the growth and the associated lymph glands as early and as freely as possible. When excision is impracticable, benefit may be derived from the use of radium or of the X-rays.
The face is the commonest seat of rodent cancer (Volume I., p. 395).
Injuries.—Wounds of the eyelids are liable to be complicated by damage to the lachrymal apparatus, leading to stenosis of the canaliculus and persistent watering of the eye. If the wall of the lachrymal sac or nasal duct is torn, the patient should be warned not to blow his nose for some days lest air be forced into the tissues and produce emphysema. In suturing wounds of the lids care must be taken to secure accurate apposition at the free margins, and to avoid constricting the canaliculi.
Contusion of the eyelids and circum-orbital region—the ordinary “black eye”—is associated with extravasation of blood into the loose cellular tissue of these parts, and is followed within a few hours of the injury by marked ecchymosis. The lids may swell to such an extent that the eye is completely closed. In some cases the impinging object lacerates the vessels of the conjunctiva and produces a sub-conjunctival ecchymosis, which may be situated under the palpebral conjunctiva of the lower lid, or close to the corneal margin on the front of the globe. The blood effused under the conjunctiva remains bright red as it is aerated from the atmospheric air. The characteristic play of colours which attends the disappearance of effused blood is observed within a week or ten days of the injury.
Firm pressure applied by means of a pad of cotton wadding and an elastic bandage, if employed early, may limit the effusion of blood; and massage is useful in hastening its absorption.
A black eye is to be distinguished from the effusion which sometimes follows such injuries as fracture of the anterior fossa of the skull, fracture of the orbital ridges, or a bruise of the frontal region of the scalp, chiefly by the facts that in the former the discoloration comes on within a very short time of the injury, the swelling appears simultaneously in both lids, and the sub-conjunctival ecchymosis, when present, is coeval with the ecchymosis of the lids. In fractures of the orbital plate and bruises of the forehead, on the other hand, the ecchymosis does not appear in the eyelids for several days, and that under the conjunctiva is usually disposed on the globe as a triangular patch towards the lateral canthus.
Wounds of the orbit result from the introduction of pointed objects, such as knitting pins, pencils, or fencing foils, or from chips of stone or metal, or small shot. They are attended with considerable extravasation of blood, which may be diffused throughout the cellular tissue of the orbit, or may form a defined hæmatoma. In either case the eyeball is protruded, and the cornea is exposed to irritation and may become inflamed and ulcerated. The optic nerve may be lacerated, and complete and permanent loss of vision result. Sometimes the ocular muscles and nerves are damaged, and deviation of the eye or loss of motion in one or other direction results. The globe itself may be injured. Foreign bodies lodged in the orbit, so long as they are aseptic, may give rise to little or no disturbance, and are liable to be overlooked. The Röntgen rays are useful in determining the presence and position of a foreign body.
Infective complications are liable to follow injuries by bullets or fragments of shell, and they not only endanger the eyeball, but are liable to be associated with suppurative conditions in the adjacent air sinuses—frontal, maxillary, and ethmoidal—or in the cranial cavity. In purifying wounds of the orbit, and in extracting foreign bodies, great care is necessary to avoid injury of the eyeball or of its muscles or nerves.
Fracture of the margin of the orbit results from a direct blow, and is followed by circum-orbital and sub-conjunctival ecchymosis, and sometimes is associated with paralysis of the optic nerve, or of the other ocular nerves. Implication of the frontal sinus may be followed by emphysema of the orbit and lids, and if there is infection by suppurative complications.
The roof of the orbit is implicated in many fractures of the anterior fossa of the skull produced by indirect violence. It is also liable to be fractured by pointed instruments thrust through the orbit, in which case intra-cranial complications are prone to ensue, and these in a large proportion of cases prove fatal. When the medial wall is fractured and the nasal fossa opened into, epistaxis and emphysema of the orbit are constant symptoms. Sub-conjunctival ecchymosis, and some degree of exophthalmos, are almost always present. Treatment is directed towards the complications. When the nasal fossæ or the air sinuses are opened into, the patient should be warned against blowing his nose, as this is liable to induce or increase emphysema of the orbit or lids.
Injuries of the Eyeball.—These injuries may be divided into two groups—(1) those in which the globe is contused without its outer coat being ruptured, and (2) those in which the outer coat is ruptured.
In cases belonging to the first group, while the sclerotic coat and cornea remain intact, the iris may be partly torn from its ciliary origin, and the blood effused collects in the lower portion of the anterior chamber; or the pupillary margin of the iris may be ruptured at several points, causing apparent dilatation of the pupil. The lens may be partly or completely dislocated, and in the latter case it may pass forward into the anterior chamber or backward into the vitreous. Among other injuries resulting from contusion of the eye may be mentioned hæmorrhage into the vitreous, rupture of the choroid, and detachment of the retina.
Injuries in which the outer coat of the eyeball is ruptured may be further subdivided into two groups according to whether or not a foreign body is lodged in the globe.
Rupture of the outer coat, especially when it results from a punctured wound, adds greatly to the risk of the injury, by opening up a path through which infective material may enter the globe, and this risk is materially increased when a foreign body is retained in the cavity of the eyeball.
When the globe is burst by a blow with a blunt object, the sclerotic usually gives way, and as the rupture takes place from within outward, there is less risk of infection than in punctured wounds. The lens may be extruded through the wound, and the iris prolapsed. If the rupture is large, the conjunctiva torn, and the globe collapsed from loss of vitreous, the eye should be removed without delay. If sight is not entirely lost and there is no marked collapse of the globe, an attempt should be made to save the eye.
Wounds produced by stabs or punctures are liable to be followed by infective complications ending in panophthalmitis. When this is threatened, removal of the eye is indicated, not only because the affected eye is destroyed beyond hope of recovery, but to avoid the risk of “sympathetic ophthalmia” affecting the other eye.
Orbital Cellulitis.—Infection of the cellular tissue of the orbit by pyogenic bacteria is specially liable to follow punctured wounds and compound fractures, if a foreign body has lodged in the orbital cavity. It may also result from the spread of a suppurative process from the globe of the eye, the conjunctiva, or the nasal fossæ or their accessory air sinuses. Both orbits may be affected simultaneously.
Clinical Features.—The disease is ushered in by rigors, high temperature, and severe pain, which radiates all over the affected side of the head. There is exophthalmos and fixation of the globe, with redness, swelling and tenderness of the eyelids, and congestion and ecchymosis of the conjunctiva. The pupil is usually dilated, the cornea becomes opaque and may ulcerate, and there is photophobia and sometimes diplopia. Suppuration usually ensues, and the pus burrows in every direction, and may ultimately point through the eyelids or conjunctiva. Sometimes the infection spreads to the meninges, and to the ophthalmic vein, and the phlebitis may then extend to the cavernous sinus. The eyeball may be infected and destructive panophthalmitis result. The prognosis therefore is always grave.
The treatment consists in making one or more incisions into the cellular tissue for the purpose of removing the pus and establishing drainage. A narrow bistoury is passed in parallel to the wall of the orbit, care being taken to avoid injuring the globe. When possible, the incision should be made through the reflection of the conjunctiva, but in some cases efficient drainage can only be established by incising through the lid. When the eye is destroyed by panophthalmitis, the propriety of eviscerating or enucleating it will have to be considered.
Tumours of the Orbit.—Tumours may originate in the orbit or may invade it by spreading from adjacent cavities. Those which originate in the orbit may be solid or cystic. Of the solid tumours the glioma and the sarcoma are the most common, and when they originate in the pigmented structures of the globe they present the characters of melanotic growths. Primary carcinoma begins in the lachrymal gland. Osteoma—usually the ivory variety—may originate in the wall of the orbit, or may spread from the adjacent sinuses.
Clinical Features.—In children, the tumour is usually a glioma, and it is frequently bilateral. It generally occurs before the age of four, is associated with increased intra-ocular tension, protrusion of the eyeball, and dilatation of the pupil, and soon produces blindness. The tumour fungates and bleeds, and rapidly invades adjacent structures and spreads along the optic nerve to the brain. It is highly malignant, and recurrence usually takes place, even when the tumour is removed early.
In adults melanotic sarcoma is most common. It occurs between the ages of forty and sixty, and is almost always unilateral; and while it shows little tendency to invade the brain, the adjacent lymph glands are early infected, and death usually results from dissemination.
In all varieties of intra-orbital tumour exophthalmos is a prominent feature (Figs. 238, 239), and when the protrusion of the eyeball is marked the lids become swollen, œdematous, and dusky. The eye is seldom pushed directly forward except when the tumour is growing in the optic nerve or its sheath. When the tumour is solid, the eye cannot be pressed back into the orbit, but in cystic tumours it may to some extent. The movements of the eyeball are restricted in a varying degree, and ptosis often results from paralysis of the levator palpebræ superioris. In almost all cases there is also more or less visual disturbance. The cornea being unduly exposed is liable to become inflamed, or even ulcerated. Pain is a variable symptom; when present, it usually radiates along the branches of the first and second divisions of the trigeminal nerve. Tenderness on pressure is not always present. It is comparatively uncommon for a tumour of the orbit to invade the globe directly.
 Fig. 238.—Sarcoma of Orbit, causing exophthalmos and
downward displacement of the eye, and projecting in temporal region.
Fig. 238.—Sarcoma of Orbit, causing exophthalmos and
downward displacement of the eye, and projecting in temporal region.
Treatment.—When practicable, removal of the tumour is the only method of treatment, and in malignant tumours it is often necessary to sacrifice the eye to ensure complete removal. When the tumour has invaded the orbit secondarily, its removal may be impossible, but it may be necessary to remove the eye for the relief of pain.
The orbital dermoid usually occurs at the lateral end of the supra-orbital ridge (Fig. 240). A less common situation is the anterior part of the orbit, near the nasal wall, and this variety, from its position and from the fact that it is usually met with in children, is liable to be confused with orbital meningocele or encephalocele. Treatment consists in its removal by careful dissection, and this can usually be done under local anæsthesia.
Orbital aneurysms have already been described, Volume I., p. 317.
Herpes of the lips, due to a mild staphylococcal infection, is common in delicate children and in the early stages of pneumonia. A crop of vesicles forms and, after bursting, these leave dry scabs.
A more severe staphylococcal infection may give rise to a carbuncular swelling with great œdema, and lead to infective phlebitis of the facial vein and general septicæmia. Excision of the focus is indicated.
The lip is sometimes the seat of the malignant pustule of anthrax.
Painful cracks and fissures are frequently met with in the middle line of the lip and at the angle of the mouth in young subjects. They usually develop during frosty weather, and as they are constantly being torn open by the movements of the mouth, they are difficult to heal. If local applications fail, it may be necessary to cocainise the fissure and scrape it with a sharp spoon.
Chronic Induration of the Lips (Strumous Lip).—A chronic œdematous infiltration, probably of the nature of a lymphangitis, sometimes affects the submucous tissue of the lips of delicate children. It is most common on the upper lip, and may be associated with a fissure or with chronic coryza. The lip is everted, and its mucous membrane unduly prominent. The cervical glands are frequently enlarged.
The treatment consists in removing the cause and in improving the general condition. In cases of long standing it may be necessary to remove from the inner aspect of the lip a horizontal strip of tissue having the shape of a segment of an orange.
The term “double lip” is applied to a condition occasionally met with in young men, in which there is a hypertrophy of the labial glands in the mucous membrane of the upper lip. It is of slow growth, and forms an elongated swelling on each side of the frenum, covering the teeth, and projecting the lip. It is shotty to the feel, and the only complaint is of disfigurement. The treatment consists in excising the redundant fold of mucous membrane, including the enlarged mucous glands.
Tuberculous disease may occur in the form of lupus or of ulcers. The ulcers generally occur in patients suffering from advanced pulmonary or laryngeal phthisis. They are usually superficial, may be single or multiple, and are exceedingly painful.
Syphilitic Lesions.—The upper lip is the most frequent seat of extra-genital chancre. The chancre of the lip begins on the mucous surface as a small crack or blister, which becomes the seat of a rounded, indurated swelling, about a quarter of an inch in diameter. The surface is smooth, of a greyish colour, and exudes a small quantity of sero-purulent fluid. The lip is swollen and everted, and there is a considerable area of induration around. The submental and submaxillary lymph glands on one or on both sides soon become enlarged, and may reach the size of a pigeon's egg. At first they are firm, but they may subsequently soften and become painful. In some cases the sore is much less characteristic, resembling an ordinary crack or fissure, and its true nature is only revealed when the secondary manifestations of syphilis appear.
Mucous patches and superficial ulcers are frequently met with on the mucous surface of the lips and at the angles of the mouth during the secondary stage of syphilis. In the inherited form of the disease deep cracks and fissures form, and often leave characteristic scars which radiate from the angles of the mouth.
Gummatous lesions occur on the lips, and are liable to be mistaken for epithelioma.
Tumours.—Nævi are not uncommon on the lips. When confined to the mucous surface they may be dissected out, but when they invade the skin they are best treated by electrolysis.
Lymphangioma.—The term macrocheilia is applied to a congenital hypertrophy of the lip (Fig. 241), which is probably of the nature of a lymphangioma (Middeldorpf). One or both lips may be affected. The lip is protruded, the mucous membrane everted, and, when the lower lip is implicated, it becomes pendulous and is liable to ulcerate. The substance of the lip is uniformly firm and rigid, so that it moves in one piece, and sucking, mastication, and phonation are interfered with.
The treatment consists in removing a wedge-shaped portion of the swelling on the same lines as for “strumous lip,” or in employing electrolysis.
Mucous cysts occur as small rounded tumours, projecting from the inner surface of the lip. They are of a bluish colour, and contain a glairy fluid. They are treated by removal of the cyst wall, together with the overlying portion of mucous membrane.
Epithelioma of the lip is of the squamous-celled variety, and is met with either as a fungating wart-like projection, or as an indurated ulcer. It almost exclusively occurs on the lower lip of men over forty years of age. The growth begins about midway between the middle line and the angle of the mouth, either as a horny epidermal thickening, or as a warty excrescence, which bleeds readily and soon ulcerates. The affection is said to be especially common in those who smoke short clay pipes, and it is a suggestive fact that, while epithelioma of the lip is rare in women, the majority of those who do suffer are smokers.
The ulceration spreads along the lip, chiefly towards the angle of the mouth, and downwards towards the chin, and the substance of the lip becomes swollen and indurated (Figs. 242, 243). The edges are characteristically raised and hard, and the raw surface is extremely painful, especially when irritated by hot food or fluids. The growth is liable to spread to the mucous membrane and gum, and to invade the mandible. The disease spreads early to the submental and submaxillary glands, which are best felt with one finger inside the mouth, under the tongue, and another outside, behind the mandible. The infected glands tend to become fixed to the bone, and while at first extremely hard, so much so that they simulate a bony tumour of the jaw, they later soften, liquefy, and fungate (Fig. 244). Metastasis to internal organs is rare. Unless removed by operation, the disease usually proves fatal in from three to three and a half years.
The treatment consists in early and free removal of the affected portion of lip and of all the lymphatic connections in the submaxillary region and neck. Recurrence in the scar is rare; it is nearly always located in the glands.
The operation of cleaning out the glands below the mandible on both sides in men who are advanced in years is not free from risk to life, especially from respiratory complications which may or may not be traceable to the anæsthetic.
In inoperable cases benefit may follow the use of the X-rays, or of radium.
Epithelioma of the upper lip is less common. It occurs with equal frequency in the two sexes, progresses more slowly, and is, on the whole, less malignant. It sometimes appears to be due to contact infection from the lower lip. It is treated on the same lines as cancer of the lower lip.
Stomatitis.—The term stomatitis is applied to any inflammation of the buccal mucous membrane. The catarrhal form is often associated with the presence of carious teeth or an infected wound; the mucous membrane is hyperæmic and swollen, and exudes an excessive amount of viscid mucous secretion, and the epithelium desquamates in patches, leaving small superficial erosions or ulcers, which are very sensitive. The aphthous form, met with in unhealthy, underfed children, is characterised by the occurrence of patches of fibrinous exudate into the superficial layers of the mucous membrane; the epithelium is shed, leaving a series of whitish spots surrounded by a red hyperæmic zone, which may become confluent and form small ulcers. The condition known as thrush, which closely resembles aphthous stomatitis, is met with in infants during the period of teething, and is due to the oïdium albicans, a fungus met with in sour milk. The spots, which are most numerous on the lips, tongue, and throat, have the appearance of curdled milk.
The treatment of these forms consists in improving the general condition of the patient, and in employing a mouth-wash, such as peroxide of hydrogen, Condy's fluid, chlorate of potash, or boro-glyceride. The superficial ulcers may be touched with silver nitrate or with a 1 per cent. solution of chromic acid.
Ulcerative stomatitis is frequently met with in debilitated subjects with decayed teeth, and is specially liable to occur during the course of acute febrile diseases in which sordes accumulate about the teeth and gums. It also occurs in syphilitic subjects while under treatment by mercury—mercurial stomatitis. Some patients show a special susceptibility to mercury, and one of the first signs of intolerance of the drug is some degree of stomatitis, which may ensue after a comparatively small quantity has been administered. It begins in the gums, which become swollen and spongy, growing on to the teeth and into the interstices. The gums assume a bluish-red colour and bleed readily, and the teeth may become loose and fall out. The tongue may share in the swelling—mercurial glossitis. There is also profuse salivation, and the breath has a characteristically offensive odour. In severe cases the alveolar margin of the jaw undergoes necrosis. A similar condition occurs in lead and in phosphorus poisoning, and in patients suffering from scurvy.
The treatment consists in removing the cause, and in employing antiseptic and astringent mouth-washes. The internal administration of chlorate of potash is also indicated, as this drug is excreted in the saliva. Loose teeth should not be removed as they become fixed again when the stomatitis subsides.
Gangrenous stomatitis, or cancrum oris (Fig. 245), has already been described (Volume I., p. 102).
Roof of the Mouth.—Suppuration in the muco-periosteum of the palate is usually secondary to suppuration at the root of a carious tooth. It may also arise in excoriations caused by an ill-fitting tooth-plate, or from the impaction of a foreign body, such as a fish or game bone, in the mucous membrane. The inflammation begins close to the alveolus, and may spread back along the palate. The muco-periosteum becomes swollen, red, and exceedingly tender, and, as pus forms, is raised from the bone, forming a prominent, firm, elongated swelling, which on bursting or being incised gives exit to foul-smelling pus.
The syphilitic gumma, which begins as a rounded indolent swelling, is usually situated in the middle line near the posterior edge of the hard palate. The swelling gradually softens and ulcerates, and a sequestrum may separate and leave a perforation in the palate (Fig. 246). The treatment consists in employing the usual remedies for tertiary syphilis. If the perforation persists and causes trouble by allowing food to pass into the nose, or by giving a nasal tone to the voice, it may be closed by an operation on the same principle as that performed for cleft palate, or an obturator may be fitted to occlude the opening.
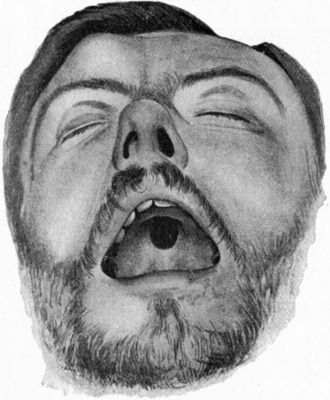 Fig. 246.—Perforation of Palate, the result of
Syphilis, and Gumma of Right Frontal Bone.
Fig. 246.—Perforation of Palate, the result of
Syphilis, and Gumma of Right Frontal Bone.Tuberculous disease is chiefly met with in the form of lupus which has spread from the nose or lips, and it may lead to widespread destruction of the soft tissues, or even to perforation of the bony palate.
Mucous cysts, dermoids, adenomas, lipomas, and fibromas are occasionally met with. Papillomatous thickening of the mucous membrane sometimes occurs in association with leucoplakia. It resists anti-syphilitic treatment, but yields to scraping with the sharp spoon. Endotheliomas, or mixed tumours, similar to those met with in the parotid gland, also occur in young subjects, and grow in the submucous tissue of the soft palate, usually to one side of the middle line. In their early stages they are of slow growth, and give rise to no inconvenience save from their size, are easily removed, and show no tendency to recur. Later, they grow more rapidly, tend to infiltrate their surroundings and to assume malignant characters, so that complete removal becomes difficult or impossible.
Epithelioma may originate in the hard palate as a result of local irritation, or may spread from adjacent parts. When it is confined to the palate it is treated by removal of the palatal and alveolar portions of the maxilla.
Elongation of the uvula is usually due to a chronic inflammatory engorgement combined with glandular hypertrophy of the mucous membrane. It often occurs in children, and is associated with a constant hacking cough, which is usually worst when the patient is lying down. By tickling the back of the tongue and pharynx it may induce vomiting after meals. The treatment consists in snipping off the redundant portion with scissors.
Epithelioma of the floor of the mouth frequently originates in the mucous membrane between the frenum of the tongue and the inner aspect of the gum. It develops insidiously, grows slowly, and gradually spreads to the mandible and to the substance of the tongue, tacking it down so that it cannot be protruded. The glands are early involved, and their enlargement not infrequently first draws attention to the condition. It is to be regarded as a particularly unfavourable site, as local recurrence is frequent. For the complete removal of the disease it is necessary to excise the tissues in the floor of the mouth, and a variable portion of the tongue and mandible, and to clear out the glands and fat from the submaxillary and submental regions.
Infective Conditions.—The majority of the infective conditions included under the popular term “sore throat” originate in the tonsils, and are due to the action of bacteria which under normal conditions are present in the crypts of the tonsils and of the mucous membrane of the naso-pharynx. The most important of these organisms are streptococci, various forms of staphylococci and of pneumo-bacteria, and diphtheritic and pseudo-diphtheritic bacilli. So long as the health is good these organisms are harmless, but when there is any lowering of the vitality they become virulent and give rise to various forms of infection.
Catarrhal tonsillitis—usually attributed by the laity to “catching cold”—is characterised by hyperæmia and congestion of the tonsils and mucous membrane of the pharynx, soft palate, and uvula. It is often met with in those who are much exposed to air contaminated with organisms—for example, patients who have been long in hospital, or the resident staff of hospitals (septic or hospital throat), and particularly in persons of a “rheumatic” tendency. There is slight pain on swallowing, and a tickling sensation passes along the Eustachian tube to the ear; the throat feels dry, and the patient has a constant desire to clear it, and there is usually a rise of temperature to 101°–102° F. As a rule the symptoms pass off in three or four days, but the condition may spread along the Eustachian tube to the ear, and interfere with hearing, or it may set up chronic suppuration of the middle ear.
A similar condition of the pharynx is frequently one of the initial symptoms in acute febrile diseases, such as scarlet fever, measles, influenza, or acute rheumatism.
The treatment of the throat affection consists in employing antiseptic and soothing gargles, inhalations of chloride of ammonium, or a spray of peroxide of hydrogen, menthol, or eucalyptol. Lozenges or pastilles containing chloride of ammonium, chlorate of potash, and cubebs may be employed. In rheumatic cases, salicin, aspirin, and salicylate of soda are indicated.
In follicular tonsillitis, the infection first implicates the lymphoid follicles. The crypts are distended with yellowish-white plugs, composed of inflammatory exudate, leucocytes, and desquamated epithelium, and these may project from the openings, giving the tonsil a spotted appearance. Sometimes the exudate accumulates on the surface of the tonsils and pharynx, forming a thin, greyish-white film, which is liable to be mistaken for the false membrane of diphtheria. It can, however, usually be wiped off, and when examined microscopically does not contain the typical Löffler's bacillus.
The tonsils are enlarged, and project so that they obstruct the isthmus of the fauces, sometimes even meeting in the middle line. There is pain on swallowing, and the respiration is impeded and noisy during sleep. There is usually some degree of fever, and the glands behind the angle of the jaw are enlarged and tender and may suppurate and set up cellulitis. The acute symptoms usually subside in four or five days, but if the deeper crypts are filled with plugs of exudate the condition may prove obstinate. The patient is liable to periodic attacks, particularly if the tonsils are chronically enlarged.
The treatment is carried out on the same lines as for the catarrhal form. In recurrent cases the tonsils should be removed.
Acute Suppurative Tonsillitis and Peri-tonsillitis—Quinsy.—This is an acute suppurative inflammation of the tonsils and peritonsillar tissue, due to infection with pyogenic bacteria. It affects the whole substance of the tonsils, and the cellular tissue of the pillars of the fauces, the soft palate, and the pharynx.
Clinical Features.—The onset is usually sudden, and the affection is ushered in by a rigor, high fever, and a feeling of malaise. There is persistent thirst and dryness of the throat, and the patient has the sensation of a foreign body being in the pharynx, with a constant desire to swallow. Swallowing is extremely painful, the pain shooting up to the ears, and the patient has difficulty in taking nourishment. The saliva accumulates in the mouth; the voice is thick and nasal; and the respiration impeded and noisy. If the patient can open the mouth sufficiently to afford a view of the back of the throat (which, however, is seldom the case), the inflamed parts are seen to be of a dull reddish-violet colour. One tonsil is often more swollen than the other, and the corresponding anterior pillar of the fauces more prominent. The uvula is swollen and œdematous, and is deviated towards the side on which there is least swelling. Suppuration occurs in from three to seven days; in adults it is usually in the peritonsillar tissue of the anterior pillar of the fauces, and extends into the soft palate. In children the pus sometimes forms in the substance of the tonsil. If left to burst, the abscess discharges itself into the mouth, and the patient experiences instant relief. The pus is always offensive, and if the abscess bursts during sleep, it may enter the air-passages and cause septic pneumonia. The lymph glands in the neck are usually enlarged and tender, and sometimes they suppurate and give rise to a diffuse cellulitis. General infection of the blood may follow, leading to metastatic invasion of different tissues and organs, particularly one or other of the large joints.
Treatment.—In the early stages soothing antiseptic gargles are indicated. Later, when the patient is unable to gargle, the inhalation of steam impregnated with the vapour of carbolic acid or friar's balsam, and the application of hot fomentations or a large linseed poultice to the neck may afford relief. When an abscess is formed, it should be opened by means of a fine-pointed pair of sinus forceps, thrust through the soft palate at a point opposite the base of the uvula, and in the line of the anterior pillar of the fauces. As those who suffer from quinsy are liable to have attacks coming on periodically, if the tonsils remain permanently enlarged they should be removed between attacks.
Hypertrophy of the tonsils is most commonly met with in children between five and ten years of age, and is often associated with adenoid vegetations in the naso-pharynx and chronic thickening of the pharyngeal mucous membrane.
The whole tonsil is enlarged, the mucous membrane thickened, and the connective tissue more or less sclerosed. The crypts appear on the surface as deep clefts or fissures, and the lymph follicles are enlarged and prominent. Secretion accumulates in the crypts, and a calculus may form from the deposit of lime salts. Sometimes food particles lodge in the crypts, and they may collect and form accumulations of considerable size, requiring the use of a scoop to dislodge them.
Clinical Features.—The hypertrophy is bilateral, but not always symmetrical. Sometimes the tonsils project to such an extent as almost to meet in the middle line; sometimes they scarcely pass beyond the level of the pillars of the fauces. They are usually sessile, but sometimes the base is so narrow as almost to form a pedicle. During childhood they are usually soft and spongy, but when they persist into adolescence or adult life they become firm and indurated. This sclerotic change is due to the repeated attacks of catarrhal or suppurative tonsillitis to which the patient is subject. The lymph glands behind the angle of the jaw are frequently enlarged. Swallowing is sometimes interfered with, and the patient is liable to attacks of nausea and vomiting. Respiration is always more or less impeded; the patient breathes through the open mouth, and snores loudly during sleep; and the hindrance to respiration interferes with the development of the chest. In some cases alarming suffocative attacks occasionally supervene during sleep, but the difficulty in breathing disappears as soon as the child is wakened. The voice is characteristically thick and nasal, especially when adenoids are present, and in many cases the patient has a vacant and stupid expression. Hearing is often impaired from obstruction of the Eustachian tube.
Treatment.—In early and mild cases, the tonsils should be painted with glycerine of tannic acid, or some other astringent, and an antiseptic mouth-wash, or spray of hydrogen peroxide, should be used several times a day. When the condition is interfering with the general health or with the development of the chest, or when there is deafness or disturbance of sleep, the tonsils should be removed.
Calculi composed of phosphate or carbonate of lime are sometimes formed in the crypts of enlarged tonsils; as a rule they are about the size of a pea, but they may be much larger. They cause a sharp stabbing pain on swallowing, and sometimes a persistent hacking cough. They are easily shelled out through a small incision into the tonsil.
Syphilis.—The fauces and tonsils are occasionally the seat of a hard chancre, and the condition may simulate malignant disease. The submaxillary glands, however, become enlarged sooner and increase more rapidly than in cancer, and they are tender. The secondary manifestations of the disease usually appear before the chancre has healed.
Early in secondary syphilis, mucous patches and superficial ulcers are frequently met with. Later, severe phagedænic ulceration sometimes occurs, especially in alcoholic subjects, and may rapidly eat through the soft palate, leading to marked deformity from contraction when cicatrisation takes place.
In the tertiary stage, a diffuse gummatous infiltration occurs, and is liable to be followed by ulceration, which spreads to the pharyngeal wall and soft palate, and, by causing cicatricial contraction and adhesions, may lead to narrowing or even complete occlusion of the communication between the pharynx and the naso-pharynx.
Tuberculous lesions of the fauces and tonsils are almost invariably secondary to tubercle of the larynx or lungs, or to lupus of the face or naso-pharynx. They are attended with more pain than syphilitic lesions; are less prone to spread to the palate and cause perforation; but, when cicatrisation takes place, they are equally liable to produce contraction and deformity.
Tumours.—Innocent tumours—fibroma, lipoma, myoma—are comparatively rare. When sessile they cause inconvenience only by their bulk; when pedunculated they may hang down into the pharynx and interfere with swallowing and breathing. They may be shelled out, or ligated at the base and cut off, according to circumstances.
Malignant Disease.—The tonsil is frequently the primary seat of lympho-sarcoma, a very malignant form of round-celled sarcoma. The tumour is at first confined to the tonsil, which differs in appearance from simple hypertrophy only in being paler and more nodular. The growth rapidly infiltrates the peritonsillar connective tissue and adjacent palatal mucous membrane, which becomes pale and œdematous, and the condition at this stage may simulate a suppurative tonsillitis. As it increases, the tumour encroaches upon the cavity of the pharynx, causing interference with swallowing and breathing; the mucous membrane soon gives way, and widespread ulceration and sloughing of the tumour substance occurs, sometimes leading to serious and even fatal hæmorrhage. The patient emaciates rapidly. The adjacent lymph glands are early infected.
Removal by operation is seldom practicable, but the introduction of a tube containing radium for several days has in some cases proved beneficial.
Carcinoma is more common than sarcoma. It may take the form of squamous epithelioma or of medullary cancer, and may originate in the tonsil, in the groove between the tonsil and the tongue, or in the soft palate. By the time the patient seeks advice it has usually implicated the fauces, soft palate, and pharyngeal wall as well as the tonsil.
Males suffer more frequently than females. The disease may exist for a considerable time before giving rise to marked symptoms, and attention may first be drawn to it by pain and difficulty in swallowing, or by pain shooting towards the ear. In some cases enlargement of the glands behind the angle of the jaw is the first thing to attract the patient's attention. The other symptoms are very like those of cancer of the tongue—pain during eating or drinking, salivation and fœtid breath. Sometimes fluids regurgitate through the nose, and the voice may become nasal and indistinct. As the patient is usually unable to open the mouth widely, it is seldom possible to learn much by inspection, but a digital examination may reveal an irregular, hard, and ulcerated growth. The swelling is sometimes palpable from the outside, filling up the hollow behind the angle of the jaw, and in this situation also the enlarged lymph glands may be felt. These are often enlarged out of all proportion to the size of the primary growth. The disease tends to spread locally, causing increasing difficulty in swallowing and breathing. The patient gradually loses strength, and may die from exhaustion induced by pain and insomnia, from hæmorrhage, or from septic pneumonia.
In early cases an attempt may be made to remove the disease by operation. In our experience radium has proved less efficacious in cancer than in sarcoma.
In advanced cases, it is only possible to relieve the patient's suffering by palliative measures. Antiseptic mouth-washes are used to diminish the fœtor of the breath and the risk of pneumonia, and heroin or morphin to relieve pain. The use of the nasal tube, or even a gastrostomy, may be necessary to enable the patient to take sufficient food, and tracheotomy may be called for to relieve dyspnœa.
Retro-pharyngeal Abscess.—The chronic retro-pharyngeal abscess associated with tuberculous disease of the cervical vertebræ, in which the pus accumulates behind the prevertebral fascia, has already been described (p. 441).
The acute abscess occurs in the space between the prevertebral fascia and the wall of the pharynx. The infection usually begins in one of the lymph glands that occupy this space, and rapidly ends in suppuration, which spreads to the surrounding cellular tissue. It is most common in children during the first and second years, and the patient may be convalescent after one of the eruptive fevers attended with inflammation of the bucco-pharyngeal mucous membrane—such as scarlet fever, measles, or chicken-pox—or may suffer from nasal excoriations or coryza. In some cases the irritation of dentition is the only discoverable cause.
In infants, the condition is usually very acute, and is attended with fever, rigors, vomiting, and often with convulsions. The head is held rigid, and usually twisted to one side, and there is pain on attempting to move it. The child has great pain on swallowing, there is regurgitation of food, and the saliva dribbles from the mouth. There is marked dyspnœa and a short, dry cough. The back of the throat is red and swollen, and a localised projection, which is soft and fluctuating, and is usually asymmetrical, may be recognised by digital examination. Sometimes the voice is lost, and the patient has severe attacks of choking—symptoms which have led to the disease being mistaken for membranous laryngitis. In some cases a soft swelling is palpable on one or on both sides of the neck. Unless the abscess is promptly opened the condition usually proves fatal. The mouth is opened by means of a gag, the head allowed to hang over the end of the table, and the abscess incised, with a guarded bistoury, through the wall of the pharynx. The dangers associated with opening the abscess from the mouth appear to have been exaggerated.
A less acute form of retro-pharyngeal abscess sometimes develops in the course of chronic middle ear disease, the inflammatory process spreading along the Eustachian tube, in the wall of which an abscess forms and burrows into the retro-pharyngeal space.
Dental caries is a process of disintegration which begins in the enamel of a tooth—usually in the region of its neck—and gradually extends through the dentine till the pulp cavity is reached.
Infection of the exposed pulp cavity may set up an acute purulent pulpitis. This is associated with severe pain, which is not confined to the diseased tooth, but may spread to adjacent teeth, and sometimes to all the branches of the trigeminal nerve on the same side of the face.
The infection may spread from the tooth to the alveolo-dental periosteum, and set up a periodontitis. In the affected tooth there is at first a feeling of uneasiness, which is relieved by the patient biting against it. Later there is severe lancinating or throbbing pain. The affected tooth usually projects beyond its neighbours, and is excessively tender when the opposing tooth comes in contact with it in mastication. The gum becomes red and swollen, and the cheek is œdematous.
Periodontitis is usually followed by the formation of an alveolar abscess. The pus, which forms at the root of the tooth, in most cases works its way through the bone and into the gum, constituting a “gum-boil.” The pus may then burst through the gum, or may spread underneath the external periosteum of the jaw and lead to necrosis.
In some cases the cheek becomes adherent to the gum and to the jaw before the abscess bursts, and the pus escapes through the skin, leaving a sinus which leads down to the defaulting tooth, and which is slow to heal, usually because there is a small sequestrum at the bottom of it. The opening of the sinus is most commonly situated at the under margin of the mandible a little in front of the masseter muscle. An alveolar abscess deeply seated in the maxilla may open into the maxillary antrum and set up suppuration in that cavity. To avoid a scar on the face, the abscess should be opened from the mouth. A periodontal abscess of one of the upper central incisors spreads backwards between the muco-periosteum and the bony palate, causing an elongated swelling in the roof of the mouth.
In all cases the extraction of the carious tooth is necessary before the abscess will cease discharging and the sinus heal. If a sequestrum is present it must be removed, and the bone scraped with a sharp spoon. Among the other effects of dental caries may be mentioned localised necrosis of the alveolar margin, cellulitis of the neck, and enlargement of the cervical lymph glands.
A cyst is frequently found attached to the root of a decayed tooth. It is lined with epithelium, and is probably derived from a belated portion of the enamel organ which has been stimulated to active growth by infective processes in the pulp cavity. It is seldom larger than a pea, and contains a pultaceous mass like inspissated pus. It gives rise to no symptoms, and is only recognised after extraction of the root.
Odontomas have already been described (Volume I., p. 192).
A localised swelling of the mandible, associated with pain referred to the ear and neck, and in some cases with spasmodic contraction of the muscles of mastication, may be due to impaction of the wisdom tooth (lower third molar). If the tooth is merely embedded in the gum, incision may allow of its eruption; if the X-rays show that it is wedged under the second molar it must be extracted, and this may prove a difficult dental operation.
Affections of the Gums.—Inflammation of the gums—gingivitis—usually occurs in association with a general stomatitis. The gums are swollen and spongy, and may show superficial ulceration, associated with bleeding and extreme fœtor of the breath. The teeth become loose, project from the alveoli, and sometimes fall out. These symptoms are prominent in cases of scurvy, and of chronic mercurial poisoning. In chronic lead-poisoning a characteristic blue line is seen on the gums near the dental margin. The treatment consists in removing the cause, improving the hygienic and dietetic conditions of the patient, and administering lime-juice, iodide of potash, quinine, or cod-liver oil, according to the cause. Antiseptic mouth-washes and dentifrices are also indicated. Chlorate of potash, being excreted in the saliva, is particularly useful.
Pyorrhœa alveolaris is a chronic form of gingivitis, met with after middle life, which begins in relation to the necks of the teeth and the alveolo-dental periosteum. It is due to bacterial infection, and is associated with an accumulation of tartar between the gums and the teeth. A muco-purulent discharge escapes from within the free edge of the gum and alveolus. The alveolar borders and the gum subsequently undergo atrophy, so that the roots are exposed, and the teeth are liable to become loose and eventually to fall out. The condition may only affect a few teeth, or it may spread to them all, in which case the patient may in the course of some years become edentulous. Gastro-intestinal disturbances, chronic joint affections of the nature of arthritis deformans, a form of pernicious anæmia, and other general conditions have been attributed to the absorption of toxic products. The treatment consists in removing the tartar from the teeth, applying strong antiseptics to the groove between the teeth and the gums, and employing mouth-washes and dentifrices. Massage of the gums night and morning, and rubbing in a paste of chlorate of potash and menthol, is often of great value. Good results have followed the use of vaccines and improvement of the general health.
Hypertrophy of the gums is occasionally met with in children and young adults who are mentally defective, and the teeth appear early and are abnormally large. The gum almost buries the teeth, and large polypoid masses form which tend to fungate. The treatment consists in removing not only the hypertrophied gums, but also the affected alveolus (Heath).
A localised hypertrophy—polypus of the gum—sometimes results from the irritation of a carious tooth, or from the pressure of an artificial denture, and may simulate an epulis (p. 513). The swelling is usually pedunculated, and if cut away close to the alveolar margin does not tend to recur.
Epithelioma sometimes originates in the gum in relation to a carious tooth or to an artificial tooth-plate. The growth tends to invade the bone and to spread to the cheek or buccal mucous membrane, or to the maxillary antrum, and its malignant nature is suggested by its persisting after the removal of the irritation. The only treatment is early and complete removal of the growth and the adjacent segment of bone.
Other tumours of the gums, such as angioma and papilloma, are rare.
Pyogenic Infections.—The jaws may be infected in fractures communicating with the mouth or as a result of the unskilful extraction of teeth, but the majority of pyogenic infections originate in relation to carious teeth, beginning as a periodontitis which is followed by diffuse periostitis that may lead to necrosis of considerable portions of bone. In workers exposed to the fumes of yellow phosphorus, the bone may be so devitalised that it readily becomes infected with pyogenic organisms and undergoes a process of cario-necrosis—the phosphorus necrosis of the older writers.
Acute osteomyelitis occasionally attacks the mandible, less frequently the maxilla. Pus rapidly forms under the periosteum, and a considerable area of bone may undergo necrosis.
In cancrum oris, also, the bones are frequently attacked and may undergo necrosis.
The treatment is to let out the pus, and, whenever possible, this should be done from the mouth to avoid a cicatrix on the face. When the angle or the ascending ramus of the mandible or the facial portion of the maxilla is involved, it is not possible to avoid making an external opening. Drainage is secured, and the mouth kept sweet by the frequent use of antiseptic washes. When the condition is due to a carious stump or to an unerupted tooth, this should be extracted at the same time as the abscess is opened.
The separation of a sequestrum is usually slow, taking from two to four months according to the acuteness of the infection and the extent of the necrosis. In the mandible the sequestrum becomes surrounded by a sheath of new periosteal bone, so that, even if the greater part of the jaw undergoes necrosis, the arch is reproduced, and after removal of the sequestrum little or no deformity results. The sequestrum can usually be removed after dividing the mucous membrane and gouging away a portion of the outer aspect of the new sheath. The cavity is packed with iodoform or bismuth gauze. When the ascending ramus is involved, precautions must be taken to prevent fixation of the jaw taking place during the healing process. In the maxilla no new case is formed, and deformity results from sinking in of the cheek, unless this is prevented by wearing a plate made by the dentist.
Tuberculous disease is comparatively rare. It is occasionally met with on the orbital margin of the maxilla and in the region of the zygomatic (malar) bone. In the mandible it usually occurs near the angle. Stockman isolated the tubercle bacillus from a series of cases of “phosphorus necrosis” investigated by him. The sinuses that form when a cold abscess bursts on the surface are peculiarly intractable and only heal after the diseased bone has been removed, leaving a characteristically depressed scar, which is adherent to the bone.
Syphilitic affections are also rare. A localised gumma may develop in the neighbourhood of the angle of the mandible, or the whole of the body of that bone may be the seat of a diffuse gummatous infiltration (Fig. 248). In either case the clinical importance of the condition lies in the fact that it is liable to be mistaken for a new growth, such as an osteo-sarcoma, or for actinomycosis.
Actinomycosis.—This condition is met with in the jaws more frequently than in any other part, and the mandible is attacked oftener than the maxilla. The actinomyces gain access to the bone through a carious tooth or through the gum.
At the outset the patient complains of pain and tenderness referred to one or more carious teeth. Within a few weeks a swelling forms—in the mandible near the angle as a rule, and in the maxilla in some part of the cheek. The swelling, which varies in consistence, implicates the bone and cannot be moved apart from it. The skin over it becomes red, suppuration occurs, and sinuses form and give exit to a sero-purulent fluid in which the characteristic yellow “sulphur grains” may be detected. The surrounding soft tissues are infiltrated, and the part becomes riddled with sinuses, which lead down to bare bone. The disease usually runs a chronic course, lasting for one or two years, and, unless pyogenic infection is superadded, is not attended with fever.
In the absence of the characteristic yellow granules, actinomycosis may readily be mistaken for tuberculous or syphilitic disease, or for sarcoma.
The treatment consists in removing the diseased tissue with the knife or sharp spoon, and in the administration of large doses of potassium iodide. The insertion of tubes of radium has a beneficial effect.
Tumours of the Alveolar Process.—Epulis.—The tumours that grow from the alveolar processes of the jaws appear at first sight to spring from the gums, hence the term epulis, generally applied to them. They really originate in the periosteum of the alveolus or in the periodontal membrane, and are essentially of the nature of fibro-sarcoma. In some, the fibrous element predominates, but the frequency with which they recur after removal, unless the segment of bone from which they spring is also excised, indicates their malignant tendency. In most cases the tumour is of the myeloid type—myeloma; in others new bone is formed in its substance—osteo-sarcoma.
An epulis usually begins in the gap between two teeth, and grows slowly, either towards the cavity of the mouth, or more frequently towards the lip or cheek, where it appears as a bright red, smooth, firm, rounded swelling, which is adherent to the jaw, and may be sessile or pedunculated (Fig. 249). It causes little pain, but is liable to interfere with mastication. As it increases in size it spreads over the alveoli of several teeth, becomes softer, and assumes a dark violet colour, and if subjected to pressure or irritation may ulcerate and bleed.
The true alveolar tumour is to be diagnosed from a mass of redundant granulations such as may form in relation to a carious tooth, from a polypus or an epithelioma of the gum, a tumour of the body of the jaw, or an angioma.
The treatment consists in removing the tumour together with a wedge-shaped or quadrilateral portion of the alveolar process from which it grows. A dental plate should be fitted to fill up the gap in the alveolus. After such free removal these tumours show little tendency to recur and metastases are rare.
Malignant Tumours of the Maxilla.—All varieties of sarcoma and carcinoma are met with; of the former, the round and spindle-celled are the most common. Carcinoma occurs chiefly in two forms, less commonly a columnar epithelioma arising from glandular epithelium, much more commonly a squamous epithelioma either originating within the antrum and causing its expansion, or spreading to the maxilla from the mucous membrane of the nose or mouth. Clinically it is practically impossible to differentiate sarcoma from carcinoma; in the later stages the infection of the glands below the mandible is more marked in carcinoma. An important point to determine is whether the growth arises within the maxilla or has spread to it from adjacent parts, such as the base of the skull, the nose, or the palate. In this the X-rays are helpful. Their malignancy is evidenced by the rapidity of their growth, the manner in which they infiltrate adjacent parts, and the frequency with which they recur after removal. They occur at all ages, and have been met with even in children.
The clinical features vary according to whether the tumour originates on the anterior aspect of the bone, in the maxillary antrum, or on the posterior aspect.
When the tumour originates in the periosteum covering the front of the bone, it forms a swelling under the cheek, usually in the vicinity of the zygomatic (malar) bone, and grows towards the mouth as well as towards the surface. The cheek is gradually invaded, and in some cases the growth extends into the maxillary sinus.
The typical malignant tumour of the upper jaw originates in the lining membrane of the antrum; it first fills the cavity and then bulges its walls in every direction, so that, on pressure being made over the swelling, the osseous shell of the sinus dimples and crackles under the finger. The sinus is dark on trans-illumination. The tumour may obstruct the nostril on the same side, and, by pressing on the tear duct, may cause the tears to flow over the cheek. It may be seen through the anterior nares, and may be attended with a sanious discharge from the nose. The eyeball is liable to be displaced upward, and if the ethmoid cells are invaded, it is also pushed outward; the palate may be depressed and the cheek projected (Figs. 250, 251).
When the tumour grows from the periosteum of the posterior aspect of the bone, and extends into the spheno-maxillary or pterygo-maxillary fossa, the eyeball is usually protruded by the invasion of the orbit from behind, and a swelling appears in the temporal region. If the sinus is invaded, the tumour spreads in the various directions already indicated. Not infrequently a tumour, which appears to have its seat in the maxilla, is really a downward prolongation of a growth originating in the base of the skull, a point on which the X-rays may yield valuable information.
In all cases the tumour tends to infiltrate the surrounding tissues indiscriminately. There is severe pain referred to the distribution of the maxillary division of the trigeminal nerve. Hæmorrhage is liable to occur when exposed portions of the tumour ulcerate—for example in the nasal fossæ. Sarcoma is to be distinguished from the solid and cystic forms of odontoma, which also may distend the bone, bulging the hard palate and projecting on the face.
Treatment of Malignant Disease.—Without the help of radiation the results of operative treatment of malignant disease of the maxilla are far from encouraging. Probably the best line to follow is to embed several tubes of radium in different parts of the tumour for several days, and when the resulting shrinkage of the growth appears to have attained its limits, the maxilla should be excised. If on microscopic examination it is found to be a carcinoma, the glands on the same side of the neck should be removed at a second operation on lines similar to those in Butlin's operation in cancer of the tongue. The aid of the dentist is required to fit a denture which will at least restore the hard palate and alveolar margin. The operation of excising the upper jaw is not a dangerous one, especially if the risk of broncho-pneumonia is minimised by the intra-tracheal administration of ether. The final illness in cases of malignant disease of the upper jaw left to nature, or when it has recurred after operation, is a terrible one; the growth displaces and destroys the globe, blocks the nose and fungating on the face, causes hideous disfigurement.
Simple tumours are rare. Fibroma may originate in the periosteum or in the lining membrane of the maxillary sinus. It usually tends to assume the characters of sarcoma. Chondroma usually begins either on the nasal surface of the bone or in the maxillary sinus. Osteoma occurs in two forms: the exostosis, which may be composed of cancellated or of compact tissue, and the diffuse osteoma or leontiasis ossea (Volume I., p. 485). All intermediate forms are met with, and when confined to the maxilla, the resulting disfigurement may be improved or remedied by operation; the cheek is raised or reflected and the bone shaved away with a strong knife or osteotome.
Tumours of the Mandible.—The same varieties are met with as in the maxilla. The non-malignant forms—osteoma, chondroma, and fibroma—are rare.
A dentigerous cyst appears as a smooth, rounded, and painless swelling, usually in the region of the molar teeth. The bone gradually becomes expanded and crackles on pressure. The cyst is filled with a glairy mucoid fluid, and may contain one or more unerupted teeth (Fig. 252). The X-ray appearances are characteristic. The treatment consists in removing the anterior wall of the cyst, scraping the interior, and packing the cavity with iodoform or bismuth gauze.
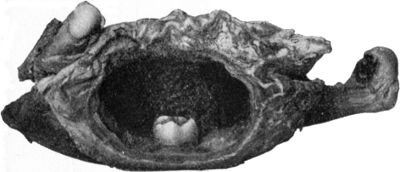 Fig. 252.—Dentigerous Cyst of Mandible containing
rudimentary tooth.
Fig. 252.—Dentigerous Cyst of Mandible containing
rudimentary tooth.The myeloid tumour or myeloma is comparatively common. It develops in the interior of the bone and expands the affected segment (Fig. 253). It grows slowly, is more or less encapsulated, and therefore does not infiltrate the surrounding tissues. Sometimes it so weakens the bone that pathological fracture occurs. There is no glandular involvement, and the tumour shows little evidence of malignancy.
The periosteal sarcoma is the most malignant form. It grows rapidly, and infiltrates the surrounding tissues. The submaxillary salivary glands and the cervical lymph glands are usually implicated, and the disease tends to spread by metastasis to distant parts.
Epithelioma is the commonest new growth affecting the mandible; it usually involves the central portion of the bone, being a direct spread from the lower lip, tongue, or floor of the mouth. When it originates in the pillars of the fauces it implicates the ascending ramus. In all cases the infection of the cervical lymph glands is a serious factor both in prognosis and treatment.
Treatment.—Partial removal of the mandible may be undertaken for myeloma, and in cases of sarcoma and epithelioma in which the tumour is limited to a small area of the bone—for example, to the alveolar process, the angle, the horizontal ramus, or the symphysis; in other cases, the whole bone must be removed.
Fracture of the Maxilla.—Fractures of the maxilla are nearly always due to direct violence, such as a blow on the face, a stab, or a gun-shot wound. They are often rendered compound by opening into the mouth, into the maxillary sinus, or on to the skin of the cheek. The alveolar process, in whole or in part, may be separated from the body of the bone by a severe blow, such as the kick of a horse, and when the whole alveolus is detached, it may carry with it the hard palate. Limited portions of the alveolus are frequently broken in the extraction of teeth. The main trouble after severe alveolar fractures is that the upper teeth do not accurately oppose the lower ones, and mastication is thereby interfered with.
When the frontal (nasal) portion of the maxilla is broken, the lachrymal sac and nasal duct may be damaged and the flow of the tears obstructed. In such cases emphysema is also liable to develop. Fractures of the facial portion are frequently complicated by hæmorrhage from the infra-orbital vessels, and anæsthesia of the area supplied by the infra-orbital nerve. Suppuration may occur in the maxillary sinus. In some cases the maxilla is driven in as a whole, and in others the fracture radiates to the base of the skull and cerebral symptoms develop.
The treatment consists in reducing any deformity that may be present, ensuring efficient drainage, and keeping the mouth as aseptic as possible. Union takes place rapidly, and owing to the vascularity of the parts necrosis is rare, even when suppuration ensues. When the alveolar portion is comminuted, the fragments may be kept in position by fixing the mandible against the maxilla by means of a four-tailed bandage (Fig. 255), or by adjusting a moulded lead or gutta-percha splint to the alveolus and palate.
The zygomatic (malar) bone is sometimes fractured by direct violence, along with the adjacent portion of the maxilla. It may be possible to manipulate the displaced fragments into position with the fingers introduced between the cheek and the gum; if this fails, a small incision should be made in the mucous membrane anterior to the masseter, and the bone levered into position with an elevator.
The zygomatic arch is occasionally fractured by a direct blow. As the depressed fragments are liable to interfere with the movement of the mandible, they should be elevated either by manipulation or through an incision.
Fractures of the Mandible.—The most common situation for fracture of the mandible is through the body of the bone in the vicinity of the canine tooth (Fig. 254). The depth of the socket of this tooth, and the comparative narrowness of the jaw at this level, render it the weakest part of the arch. The fracture is usually due to direct violence, such as a blow with the fist, the kick of a horse, or a fall from a height. It is sometimes bilateral, the bone giving way at the canine fossa on one side and just in front of the masseter on the other; or both fractures may be at the canine fossæ. The fracture is usually oblique from above downwards and outwards, and is nearly always rendered compound by tearing of the mucous membrane of the mouth.
When only one side is broken, the smaller fragment is usually displaced outwards and forwards by the masseter and temporal muscles, so that it overlaps the larger fragment. In bilateral fractures the central loose segment is driven downwards and backwards towards the hyoid bone by the force causing the fracture, and is held in this position by the muscles attached to the chin, while both lateral fragments are tilted outwards and forwards by the masseters and temporals. The amount of displacement is best recognised by observing the degree of irregularity in the line of the teeth. Abnormal mobility and crepitus are readily elicited, and there is severe pain, particularly if the inferior dental nerve is stretched or crushed. The patient's attitude is characteristic; he supports the broken jaw with his hands, and keeps it as steady as possible when he attempts to speak or swallow. Saliva dribbles from the open mouth, and the speech is indistinct.
In adults, the bone may be broken at the symphysis as a result of lateral compression of the jaw—for example, pressing together of the angles. The general characters of the fracture are the same as those of fracture of the body, but the displacement is inconsiderable.
Fractures of the angle and through the ramus are less common, and are not attended with deformity, as the fragments are retained in position by the masseter and internal pterygoid muscles. Fracture of the coronoid process is rare.
The condyle is usually fractured just below the insertion of the external pterygoid muscle (Fig. 254) by a fall on the chin or by a severe blow on the side of the face. When the fracture is unilateral, the broken condyle is tilted inwards and forwards by the external pterygoid, and can be palpated from the mouth, while the rest of the jaw is displaced towards the affected side, and not away from it, as happens in unilateral dislocation. When the fracture is bilateral, the mandible falls backwards, so that the lower teeth lie behind those of the maxilla.
In a few cases the condyle has been driven through the floor of the glenoid cavity, causing fracture of the base of the skull. The diagnosis may be established by means of the X-rays.
Complications.—As the majority of these fractures are compound, suppuration is comparatively common during the process of repair, but if means are taken to keep the mouth clean it can usually be kept in check, and seldom leads to necrosis. The teeth adjacent to the fracture are liable to be loosened or displaced. If merely loosened they should be left in place, as they usually become firmly fixed in the course of a few days. Care must be taken that a displaced tooth does not pass between the fragments, as this has been the cause of difficulty in reducing a fracture and of its failure to unite. Irregular union, by destroying the alignment of the teeth, leads to interference with mastication. The bone usually unites in from four to six weeks. Want of union is a rare event.
Treatment.—In the majority of cases of unilateral fracture after reduction, the fragments can be kept in apposition by closing the mouth and keeping the lower jaw fixed against the upper by means of a four-tailed bandage (Fig. 255). Care must be taken that the posterior tails of the bandage do not pull the mandible backward. Additional security may be given by a light poroplastic or gutta-percha splint fitted to the chin, the vertical portion passing well up the ramus of the jaw. After a few days the apparatus is removed, the patient is encouraged to move the jaw, and massage is employed. The mouth must be regularly cleansed by an antiseptic mouth-wash, or by a spray of hydrogen peroxide.
In certain fractures implicating the body of the jaw, and particularly when bilateral, the co-operation of the dentist is necessary to obtain the best results. After the fragments have been coapted, a plaster impression is taken of the jaw and teeth, and from this a silver frame is cast which surrounds but does not envelop the teeth. This frame is then applied to the fractured jaw, and restrains movement of the fragments without interfering with the action of the jaw (W. Guy). The use of an intra-oral frame obviates the necessity of wiring the fragments.
Even in badly united fractures the original contour of the bone is eventually restored by the movements of the tongue moulding it into shape.
Dislocation of the Mandible.—Dislocation of the lower jaw may be unilateral or bilateral. The bilateral form is the more common, and is met with most frequently in middle life, and in females. The liability to dislocation is greatest when the mouth is widely open—for example, in yawning, laughing, or vomiting—as under these conditions the condyle, accompanied by the meniscus, passes forwards out of the glenoid cavity and rests on the summit of the articular eminence. If, while the bone is in this position, the external pterygoid muscle is thrown into contraction, it pulls the condyle forward over the eminence into the hollow beneath the root of the zygoma, and the contraction of the masseter and temporal muscles retains it there. Muscular contraction is therefore an important factor in its production.
Dislocation may be produced also by a downward blow on the chin, by the unskilful introduction of a mouth gag, particularly while the patient is anæsthetised, or even in the attempt to take a big bite—say, of an apple. The dislocation that results from such causes is usually unilateral.
In some persons the ligaments of the joint are unnaturally lax, and dislocation is liable to occur repeatedly from comparatively slight causes—recurrent dislocation.
Clinical Features.—The appearance of a patient suffering from bilateral dislocation is characteristic. The mouth is open, the jaw fixed, and the chin protruded so that the lower teeth project beyond the upper. The patient has difficulty in swallowing, and the saliva dribbles from the mouth. As the lips cannot be approximated, the speech is indistinct and guttural. Just in front of the auditory meatus a deep hollow can be felt, and in front of this the condyle forms an undue projection. The coronoid process is displaced below and behind the zygomatic (malar) bone, and may be felt through the mouth. The contracted temporal muscle forms a prominence above the zygoma.
In unilateral dislocation the deformity is the same in character, but is less marked, and in mild cases its cause is liable to be overlooked. In most cases the chin deviates towards the sound side.
Treatment.—In recent cases, reduction is usually easily effected. The patient should be seated on a low chair or stool, an assistant supporting the head from behind. The surgeon, standing in front, places his thumbs, well protected by a roll of lint, far back on the molar teeth, and with his other fingers grasps the body of the jaw. Pressure is now made downwards and backwards to free the condyles from the articular eminence, and to overcome the tension of the temporal and masseter muscles, and as this is effected the tip of the chin is carried upward, while the whole jaw is pushed directly backward. The condyle slips into position, sometimes with a distinct snap. When difficulty is experienced in levering the condyle from its abnormal position, a cork may be placed between the molar teeth on each side to act as a fulcrum. After reduction the jaw is fixed by means of a four-tailed bandage for a few days. The patient is warned to avoid for some weeks opening the mouth widely.
Old-standing Dislocation.—It sometimes happens that, from having been overlooked or neglected, the dislocation remains unreduced. In such cases the movement of the jaw is in time partly restored, and the patient acquires sufficient control of the lips to be able to articulate intelligibly and to prevent dribbling of saliva. The power of masticating the food, however, remains impaired. The hollow behind the condyle and the projection of the chin persist. Reduction by manipulation is seldom possible after the dislocation has existed for more than three months, but it has been effected as long as ten months after the accident. Several attempts at reduction should be made at intervals of two or three days, and if these fail recourse may be had to operation. As the masseter and internal pterygoid muscles have assumed a vertical position and become shortened, they form an obstacle to reduction, and to overcome their action it is necessary to separate them from their insertion to the ascending ramus of the bone through an incision carried round the angle. If the adhesions about the dislocated condyle are then separated, reduction can be effected (Samter). In some cases it is necessary to excise the condyle to restore movement.
Internal Derangements of the Temporo-mandibular Joint.—The intra-articular cartilage is liable to be displaced by excessive traction exerted on it by the external pterygoid muscle during some sudden movement of the joint, particularly in closing the mouth. There is acute pain in the region of the joint, the teeth on the affected side cannot be brought into apposition, so that mastication is interfered with, and the patient is conscious of something locking inside the joint. The joint is tender to the touch, but there is no external swelling. Replacement is effected by keeping up firm pressure at the back of the condyle with the mouth open, and slowly closing the jaw. If recurrence takes place repeatedly, the disc may be sutured to the periosteum (Annandale), or excised (Hogarth Pringle).
Arthritis of the temporo-mandibular joint occurs in two forms, non-suppurative and suppurative.
The non-suppurative form is usually due to gonorrhœal infection, and as a rule is bilateral. The patient complains of neuralgic pains shooting towards the ears and temples, and of pain in the joint on movement. The jaw is therefore kept fixed, usually with the mouth slightly open and the chin protruded. Mastication is impossible, and the speech is indistinct. There is effusion into the joint, and a swelling may be detected in front of the ear. The inflammation may subside and movement restored, or fibrous ankylosis may ensue.
The suppurative form may be due either to direct spread of infection from adjacent parts, as, for example, in middle ear disease, suppurative parotitis, or pyogenic affections of the mandible, or it may be part of a general pyæmic infection, as sometimes occurs after exanthematous fevers and in gonorrhœa. The clinical features are similar to those of the non-suppurative form, but the signs referable to the joint are often masked by those of the primary lesion. When the pus originates in the joint, it may point either towards the skin or into the external auditory meatus through the petro-tympanic (Glaserian) fissure. The joint is usually completely disorganised and ankylosis results.
Tuberculous arthritis is rare, and is usually secondary to disease of the mandible, the temporal bone, or the middle ear. It leads to destruction of the joint and ankylosis. It is treated by incision and scraping, or by excision of the condyle.
Arthritis deformans is a comparatively common affection, and is generally bilateral. In the earlier stages the condyle is usually hypertrophied and distorted, and the glenoid cavity is correspondingly broadened and flattened, and in time may be filled up by new bone. Osteophytic outgrowths form around the joint and lead to fixation or locking. The enlarged condyle may be felt in front of the ear, and there is pain and cracking on movement; the pain is worst at night and in wet weather. The jaw is usually depressed and the chin protruded. The disease runs a chronic course, with occasional acute exacerbations. Excision of the condyle may be advisable when non-operative measures have failed to give relief. In the later stages, the condyle, together with the meniscus, may be worn away and completely disappear.
Closure or Fixation of the Mandible.—Temporary fixation is due to spasmodic contraction of the muscles of mastication, particularly the masseter. This may be symptomatic of some inflammatory condition in the vicinity, such as a pyogenic affection of the lower jaw—for example, that associated with a carious root or an unerupted wisdom tooth, or with parotitis or tonsillitis. In such cases the spasm passes off on the removal of the cause. It is occasionally a manifestation of hysteria. The administration of a general anæsthetic and the introduction of a wedge or separator is usually necessary to confirm the diagnosis and, it may be, to permit of operative measures, such as the extraction of a wisdom tooth.
Muscular fixation may be due to rheumatic or syphilitic myositis, and this is sometimes followed by fibroid degeneration of the muscles, rendering the fixation permanent.
Permanent fixation may be due to a variety of causes. Fibroid degeneration of muscles following myositis has already been mentioned. Much more frequently it results from cicatricial contraction of the soft parts of the face or mouth following such conditions as cancrum oris, ulceration, or burns. Fixation following upon prolonged immobilisation after fracture or dislocation, or any of the forms of arthritis or suppurative or tuberculous disease of the adjacent portions of the mandible, is also met with. The ankylosis may be fibrous or osseous, and may be intra- or extra-articular.
The clinical features vary with the degree of separation of the jaws. There is always some deformity, and more or less interference with mastication and speech. The patient usually feeds himself by pushing small portions of bread or meat with the fingers through some gap between the badly opposed and badly formed and preserved teeth. As the patient is unable to keep the mouth clean, particles of food lodge and decompose there, causing irritation of the mucous membrane, caries of the teeth, and fœtor of the saliva and breath. When osseous ankylosis occurs in childhood, it leads to arrest of development of the mandible, which is small and markedly receding, so that the teeth do not oppose those of the maxilla (Fig. 256).
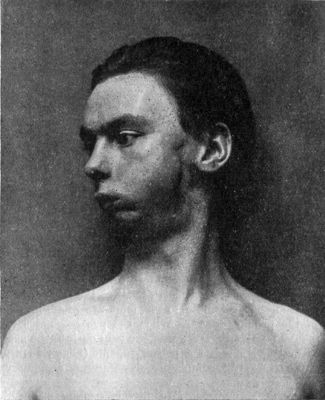 Fig. 256.—Defective development of Mandible from
fixation of jaw due to tuberculous osteomyelitis in infancy.
Fig. 256.—Defective development of Mandible from
fixation of jaw due to tuberculous osteomyelitis in infancy.
Treatment.—When the cause of the fixation is in the joint itself, the best treatment is to resect one or both condyles.
When the fixation is due to cicatricial contraction of the soft parts, mobility is best restored by forming an artificial joint well in front of the cicatricial tissue, as suggested by Esmarch.
Surgical Anatomy.—The tongue is composed of interlaced, striped muscle fibres, partly consisting of the terminations of the extrinsic muscles, and partly of the intrinsic muscles. A median fibrous septum divides it into two lateral halves so completely that but little communication takes place between the blood vessels and lymphatics of the two sides. It is covered by stratified squamous epithelium. For practical purposes it is described as consisting of an anterior or oral part, and a posterior or pharyngeal part.
The oral part, which includes the anterior two-thirds of the organ, is mobile, and the epithelium on its dorsal aspect is modified so as to form several varieties of papillæ. A slight median depression is recognisable on the dorsum as far back as the vallate (circumvallate) papillæ, which mark the boundary between the oral and pharyngeal parts. A double fold of mucous membrane—the frenum—connects the under aspect of the tip with the floor of the mouth and the mandible. On each side of the frenum, under the mucous membrane of the tip, are mucous glands—apical glands—in which cysts sometimes form. On the lateral border of the tongue, just in front of the anterior palatine arch, are several vertical folds of mucous membrane—the folia linguæ, or foliate papillæ.
The pharyngeal part, or base of the tongue, forms the anterior wall of the pharynx, and is attached to the hyoid bone. Its mucous membrane is devoid of papillæ, but contains numerous lymphoid follicles—the lingual tonsil. The foramen cæcum lies just behind the apex of the vallate papillæ in the middle line.
The chief artery, the lingual, a branch of the external carotid, passes forward beneath the hyoglossus muscle, and is continued to the apex as the ranine, lying nearer the under than the upper aspect of the tongue. The pharyngeal part is supplied by the dorsalis linguæ branch. The blood is returned to the internal jugular by the ranine vein, which can be seen under the mucous membrane on the inferior aspect near the frenum, and by the venæ comites of the lingual artery and its branches.
The hypoglossal is the motor nerve of the tongue. The lingual branch of the mandibular (inferior maxillary) supplies the anterior two-thirds with common sensation. It is accompanied by the chorda tympani branch of the facial, which probably carries the taste fibres. The glosso-pharyngeal supplies the posterior third of the tongue with both common and gustatory sensation.
The lymph vessels of the anterior two-thirds of the tongue drain into the submental and submaxillary glands, and these in turn into the deep cervical group which accompany the internal jugular vein. The vessels of the base converge into several large trunks which pass out behind the tonsils and drain directly into the deep cervical glands. One of these, which lies in the angle between the internal jugular and common facial veins, is frequently infected in cancer of the tongue.
Wounds are commonly produced by the teeth, as, for instance, when a child falls on the chin with the tongue protruded, or when an epileptic bites his tongue during a fit. Less frequently a foreign body, such as a pipe-stem, a bullet, or a displaced tooth, is driven into the tongue. The immediate risk is hæmorrhage, particularly when the posterior part of the tongue is implicated and the wound penetrates deeply. Of the later complications, infections and secondary hæmorrhage are the most serious, and they are most liable to occur when a foreign body is embedded in the tongue.
Treatment.—In superficial wounds near the tip the oozing is efficiently arrested by sutures, but in deeper wounds a ligature must be applied to the bleeding vessel. Secondary hæmorrhage is much more difficult to arrest on account of the friable state of the tissues, and it may be necessary to ligate the lingual or even the external carotid in the neck.
To prevent infective complications any foreign body must be removed and an antiseptic mouth-wash regularly employed.
Cases have been recorded in which such a foreign body as a bullet, a needle, or a piece of a pipe-stem, has remained embedded in the substance of the tongue for a long period, and caused a firm, indolent swelling liable to be mistaken for a new growth.
Dental Ulcer.—The continuous friction of a jagged tooth, or of an ill-fitting dental plate, is liable to cause swelling and excoriation of the side of the tongue. A painful superficial ulcer forms, and if the irritation continues and infection occurs, the surrounding parts become indurated, the ulcer assumes a crater-like appearance, not unlike that of a commencing epithelioma. If such an ulcer does not promptly heal on the removal of the irritant, a portion of the margin should be removed and submitted to microscopic examination to make sure that it is not cancerous.
Inflammatory Affections.—Acute Parenchymatous Glossitis is usually due to the action of streptococci. Although it affects mainly the mucous membrane and submucous tissue, it causes a diffuse œdematous swelling of the whole organ, and this may extend to the ary-epiglottic folds and give rise to œdema of the glottis. As a rule it does not go on to suppuration.
The onset is sudden, and is marked by pain and stiffness of the tongue, particularly when the patient attempts to masticate or to speak. The tongue rapidly swells, and in the course of twenty-four or forty-eight hours may fill the mouth and protrude beyond the teeth. There is profuse salivation, and in addition to difficulty in swallowing and speaking there may be considerable interference with respiration. The salivary and lymph glands in the submaxillary space are enlarged and tender. The symptoms begin to subside in three or four days, unless suppuration occurs.
The treatment consists in administering a sharp purge and employing a mouth-wash; leeches may be applied to the submaxillary region with benefit. When the swelling is excessive, it may be necessary to make longitudinal incisions into the substance of the tongue, and dyspnœa may call for laryngotomy. If an abscess forms it must be opened.
A similar condition has been met with in patients who have contracted the “foot and mouth disease” of cattle. Vesicles form on the mucous membrane, and after bursting, ulcerate, and a mixed infection with streptococci occurs, leading to diffuse œdema. Portions of the tongue may become gangrenous, and the infection may spread to the tissues of the neck and set up one form of angina Ludovici. The condition is usually fatal.
Acute Hemi-glossitis.—An acute transitory swelling, confined to one half of the tongue, in the distribution of the lingual nerve, is occasionally met with. It is attended with great pain and high temperature, and is believed to be analogous to herpes zoster (Güterbock).
Mercurial Glossitis may accompany mercurial stomatitis (p. 496).
Chronic Superficial Glossitis.—Several forms of chronic superficial glossitis are met with. The most important, as it is frequently followed by the development of epithelioma, is that known as leucoplakia or leucokeratosis.
The tongue is studded over with white patches, which result from overgrowth and cornification of the surface epithelium, whereby it becomes thickened and raised above the surface, and at the same time there is small-celled infiltration of the submucous tissue. The patches are irregularly lozenge-shaped, and when crowded together they present the appearance of a mosaic (Fig. 257). Similar patches are often present on the mucous membrane lining the cheek.
The disease is met with almost invariably in men between the ages of forty and fifty. Syphilis appears to be a predisposing factor, and any form of irritation—for example, the chewing or smoking of tobacco, the drinking of raw spirits, friction by a rough tooth or tooth-plate—plays an important part in inducing or in aggravating the condition.
The milder forms give rise to no discomfort, but when the condition is advanced the patient complains of dryness and hardness of the tongue, with impairment of the sense of taste and persistent thirst. When cracks, fissures, or warts develop, there is pain on chewing or speaking, or on taking hot or irritating food. The glands below the jaw may be enlarged.
The disease is most intractable and persistent, and even after disappearing for a time is liable to recur. After a variable number of years epithelioma is prone to develop, usually in one or other of the fissures which accompany the condition.
The treatment consists in removing all sources of irritation, particularly smoking, and in employing mouth-washes. Butlin recommends antiseptic ointments applied before going to bed. In some cases painting the patches with chromic acid (10 grains to the ounce) or lactic acid (20 per cent.) is useful in removing the excess of epithelium, but stronger caustics are to be avoided. Constitutional treatment is of little use even when the patient has suffered from syphilis. The best results have been attained by the use of radium.
The “smoker's patch” consists of a small oval area on the front of the tongue from which the papillæ have disappeared. It is slightly raised, smooth and red, and may be covered with a yellowish-brown or yellowish-white crust. It causes no discomfort unless the crust is removed, when a raw, sensitive surface is exposed. The condition is liable to spread over the tongue if the patient persists in smoking. It may eventually assume the characters of leucoplakia. The treatment consists in stopping the use of tobacco, and painting the patches with chromic acid, tannic acid, or alum, and employing a chlorate of potash mouth-wash.
Tuberculous Disease.—The tongue is rarely the primary seat of tuberculosis. The majority of cases occur in adult males, who suffer from advanced pulmonary or laryngeal phthisis, the tongue being infected by bacilli from the sputum or through the blood stream. In other cases the infection is due to direct spread of lupus from the face or nose.
The condition may begin as a firm, painless lump, seldom larger than a hazel-nut, on one side of the tongue, or near its tip. At first the swelling is covered by epithelium; in time caseation takes place, the epithelium gives way, and an open sore is formed.
The tuberculous ulcer is the form most frequently met with. The surface of the ulcer is uneven, pale and flabby, and is covered with a yellowish-grey discharge, with here and there feeble granulations showing through. The edges are shreddy, sinuous in outline, and there is little or no induration. The surrounding parts are slightly swollen, and may be studded with small tuberculous foci. The ulcer may be quite superficial, or it may extend into the muscular substance, and the tip of the tongue may be completely eaten away so that it looks as if it had been cut off with a knife. As the disease advances there is severe pain and usually profuse salivation. The submaxillary glands may be, but are not always, enlarged. The ulcer may heal, but tends to break down again.
Unless there is advanced pulmonary disease or other contraindication to operation, the ulcer should be excised under local anæsthesia. Care must be taken to avoid reinfecting the raw surface. When excision is impracticable, it is only possible to palliate the symptoms by dusting with orthoform, or applying local anæsthetics, and by attending to the hygiene of the mouth and removing all sources of irritation.
Syphilitic Affections.—A primary lesion on the tongue is accompanied by marked enlargement and tenderness of the submaxillary lymph glands on one or on both sides. It is most common in men, infection usually taking place through the medium of tobacco pipes, or implements such as the blow-pipes of glass-blowers.
During the secondary stage—particularly in the later periods—mucous patches and ulcers are common, and they may assume a condylomatous or warty appearance.
The tertiary manifestations in the tongue are sclerosing glossitis, gummas, and gummatous ulcers.
Sclerosing glossitis is the term applied by Fournier to a condition in which there is an abundant new formation of granulation tissue in the substance of the tongue, leading to the appearance of tuberous masses on the dorsum. These tend to be oval in outline, are elevated above the normal mucous membrane, and present a dull red mammilated or lobulated surface, comparable to the surface of a cirrhotic liver. They are firm, elastic, and insensitive.
A gumma is usually situated on the dorsum and more often towards the centre than at the edges. As it seldom implicates the floor of the mouth or the base of the tongue, the tongue can usually be protruded freely. It forms an indolent swelling, which tends to break down slowly and to ulcerate. So long as it remains unbroken it does not cause pain, and there is no enlargement of the adjacent lymph glands. Two forms are met with—the superficial, and the deep or parenchymatous.
A superficial gumma appears as a small hard nodule under the mucous membrane, varying in size from a pin's head to a pea. The mucous membrane over it is redder than normal, and in the early stages retains its papillæ but later becomes smooth. It tends to break down early, forming a superficial ulcer. Superficial gummas are often multiple.
The deep or parenchymatous form varies in size from a hazel-nut to a walnut, and feels like a hard body in the substance of the tongue. The mucous membrane over the swelling is of normal colour, but is usually devoid of papillæ. The gumma may remain for months unchanged, or may approach the surface, soften, and break down, leaving a deep, ragged ulcer.
Syphilitic ulcers and fissures are nearly always due to the softening and breaking down of gummas. The ulcers have seldom the typically rounded or serpiginous outline of gummatous ulcers on other parts of the body. The base is ragged and unhealthy, and on it a yellowish-grey slough resembling wash-leather may be seen. The edges are steep, ragged, and often undermined, and the surrounding parts thickened and indurated. The neighbouring glands are not usually enlarged. The ulcer is extremely painful when irritated by food, hot fluids, or spirits. If untreated, the sore may remain indolent and for months show no sign either of spreading or healing, but at any time it may become the seat of cancer.
Syphilitic fissures are met with as long, narrow, deep clefts, or as stellate or sinous cracks in the substance of the tongue. After the healing of these ulcers and fissures permanent furrows and depressed scars remain.
Treatment.—The tertiary manifestations of syphilis in the tongue are treated on the same lines as other tertiary lesions. Locally, the use of mouth-washes, such as chlorate of potash or black wash diluted with lime-water, the insufflation of powdered iodoform and borax with a small quantity of morphin, or the application of mercurial ointment is useful. The sore must be thoroughly cleansed before these remedies are applied.
Carcinoma is by far the most common form of new growth met with in the tongue, and it is almost invariably a squamous epithelioma.
Epithelioma generally occurs between the ages of forty and sixty, and attacks males oftener than females, in the proportion of about six to one. Its development is favoured by any long-continued irritation, such as the rubbing of the tongue against a carious tooth, an ill-fitting tooth-plate, or the rough end of a short clay pipe, particularly when such irritation leads to the formation of an ulcer. Chronic superficial glossitis associated with leucoplakia, and syphilitic fissures, ulcers, or scars, also act as predisposing factors. The repeated application of strong caustics to chronic inflammatory conditions is, according to Butlin, a determining cause of cancer. The degree of malignancy appears to vary in different cases, and is probably lowest when the disease originates in a patch of leucoplakia or other pre-cancerous lesion.
The disease is usually situated in the anterior half of the tongue, and more commonly on the edge than on the dorsum. It may begin as an excoriation, ulcer, or fissure, or as a warty growth, particularly in association with a patch of leucoplakia. In all cases ulceration begins early, and the base of the ulcer and the surrounding parts become indurated. The lymph glands are, as a rule, early infected.
Clinical Features.—The clinical appearances vary widely. Sometimes the surface presents a warty growth; sometimes it is excavated, forming a deep ulcer with raised nodular edges; in other cases the ulcer is smooth, and its edges even and rounded. Extreme hardness of the edges and base of the ulcer is always a characteristic feature. The tongue tends to become fixed, especially when the disease spreads to the floor of the mouth, so that it cannot be protruded, and the restriction of its movement produces a characteristic interference with articulation, certain words being slurred, and when the fixation is extreme it may interfere with mastication and swallowing. The patient complains of a constant gnawing pain in the tongue, and of severe pain shooting along the branches of the trigeminal nerve, and especially towards the ear. In the advanced stages there is salivation and fœtor of the breath.
When the disease is situated on the edge of the tongue it tends to spread to the floor of the mouth and the muco-periosteum of the mandible. If situated far back on the dorsum, it spreads on to the epiglottis, the pillars of the fauces, and the tonsil.
The neighbouring lymph glands—particularly those under the jaw and along the line of the carotid vessels—soon become infected and are palpable. The submaxillary and sublingual salivary glands are also liable to be affected. The enlarged cervical glands later undergo softening, or suppurate and burst on the skin surface, forming fungating ulcers. Metastasis to the liver, lungs, and other viscera is exceptional. If the disease is allowed to run its course, the patient usually dies in from twelve to eighteen months from repeated small hæmorrhages, toxin absorption, or septic broncho-pneumonia.
Differential Diagnosis.—Cancer of the tongue has to be diagnosed from syphilitic and tuberculous affections, from papilloma, and from simple ulcer and fissure. It is to be borne in mind that any of these conditions may take on malignant characters and develop into epithelioma. The microscopic examination of a portion of the growth removed under local anæsthesia from the base of the ulcer at some distance from its epithelial core is often the only certain means of establishing the diagnosis, and should be had recourse to as early as possible. When there is still doubt as to the nature of the growth, it should be treated as if it were cancerous.
An unbroken gumma is liable to be confused only with the uncommon form of epithelioma which begins as a nodule under the mucous membrane. Gumma, however, are often multiple, and the tongue shows old scars or other evidence of syphilis.
Gummatous ulcers are usually situated on the dorsum, are frequently multiple, and have sloughy, undermined edges; the surrounding parts, although indurated, are not so densely hard as in cancer; there is not necessarily any involvement of lymph glands. The cancerous ulcer is usually single and situated on the margin of the tongue; its edges are hard, raised, and nodular; and the glands are usually enlarged and hard. Little reliance is to be placed on the therapeutic effects of anti-syphilitic drugs in the differential diagnosis, as they are often inconclusive, and their use results in loss of time.
Tuberculous ulcers usually occur in association with other and unmistakable evidences of tuberculosis. A papilloma, when sessile, may simulate cancer; these tumours show a marked tendency to become malignant. Simple ulcers and fissures are usually recognised by the history of the condition, the absence of induration and of glandular involvement, and by the fact that they heal quickly on removal of the cause.
Treatment.—The only treatment that offers any hope of cure is free removal of the disease, and experience has proved that unless this is done early the prospect of the cure being a radical one is remote. Not only must the segment of the tongue on which the growth is situated be widely excised, but all the lymphatic connections must also be removed whether the glands are palpably enlarged or not.
The chief risk after operation is pneumonia resulting from the inhaling of blood and products of infection: hence the importance of rendering the mouth as dry and as sweet as possible before operation, special attention being paid to the teeth, and precautions being taken at the operation to prevent the passage of blood down the trachea. The patient is usually able to be out of bed on the second or third day, and is well in a fortnight or three weeks. The operation, even when followed by recurrence, usually prolongs life by six or eight months, and renders the patient more comfortable by removing the foul ulcer from the mouth. The speech, although impaired by the removal of one-half or even more of the tongue, is distinct enough for ordinary purposes. When recurrence takes place it is usually in the glands, and may be attended with great suffering.
Treatment of Inoperable Cases.—The mouth must be kept as sweet as possible. The pain may be relieved to some extent by cocain or orthoform, but as a rule the free administration of morphin is called for. Pain shooting up to the ear may be relieved by resection of the lingual nerve, or the injection of alcohol into its substance. If hæmorrhage takes place from the ulcerated surface and cannot be controlled by adrenalin, or other local styptics, it may be necessary to ligate the lingual, or even the external carotid artery. Interference with respiration may necessitate tracheotomy. When the patient has difficulty in taking food, recourse should be had to the use of the stomach-tube or to gastrostomy. The use of radium or of the X-rays appears to have a restraining influence on the disease in the glands, but has not proved curative.
Sarcoma of the tongue is rare, and is sometimes met with in children. The round-cell type is the most common; it grows rapidly, and tends to ulcerate and fungate, pain becoming severe when the growth has broken down. The diagnosis is always difficult, and is seldom made until a portion of the growth has been removed and examined microscopically. The more slowly growing forms, if removed before ulceration has taken place, show little tendency to recur, but those which grow rapidly and break down, not only recur locally, but are liable to give rise to metastases. The treatment is the same as for cancer; the use of radium is more likely to be beneficial than in epithelioma.
Innocent Tumour and Cysts.—Lipoma, fibroma, and various forms of angioma (Fig. 258) are occasionally met with. They are all of slow growth, and give rise to inconvenience chiefly by their bulk, and should be removed.
Papilloma may occur on any part of the tongue, and at any age. It may be single or multiple, pedunculated or sessile, and is liable to become malignant, especially when associated with leucoplakia. It should be freely removed by excising a wedge-shaped portion of the tongue.
Dermoid cyst is met with beneath the tongue, lying in the middle line, between the genio-glossi (genio-hyoglossi), and on the upper surface of the mylo-hyoid muscles. It may be noticed soon after birth, or may only attract attention during adult life. The cyst usually projects under the chin, forming a soft swelling of putty-like consistence, which varies in size from a pigeon's to a turkey's egg (Fig. 259). When it bulges towards the mouth it is liable to be mistaken for a retention cyst of one of the salivary glands. It is distinguished by its medial position, its yellow colour, and its opacity, the retention cyst being to one side of the middle line, purplish in colour, translucent and fluctuating. The cyst should be dissected out, either from the mouth or from under the chin, according to circumstances.
A sebaceous cyst may reach such dimensions as to simulate a dermoid or thyreo-glossal cyst.
Hydatid and cysticercus cysts have also been met with in the tongue.
Thyreo-glossal Tumours and Cysts.—Tumours may develop in the embryonic tract which passes from the isthmus of the thyreoid gland to the foramen cæcum at the base of the tongue—the thyreo-glossal tract of His. They have the same structure as the thyreoid gland, and occupy the dorsum of the tongue, extending from the foramen cæcum backwards towards the epiglottis, in some cases attaining considerable size. They are of a bluish-brown or dark red colour, and are liable to repeated attacks of hæmorrhage. These tumours sometimes become cystic, the cysts being lined with ciliated epithelium and containing colloid material. Bleeding may take place into a cyst, causing it to become suddenly enlarged, or the cyst may burst and the blood escape into the mouth. These variations in size and repeated attacks of bleeding help to distinguish thyreo-glossal cysts from other swellings of the tongue. Treatment is only called for when the swelling causes interference with speech or swallowing; it consists in removing the tumour by dissection.
When the lower end of the tract becomes cystic it forms a swelling in the neck (p. 583).
Malformations.—Complete or partial absence of the tongue is exceedingly rare.
Occasionally the fore part of the tongue is bifid. The function of the organ is not interfered with, and the operation of paring and suturing the two halves is only called for on account of the disfigurement.
Congenital tongue-tie is a condition in which the tip of the tongue is bound down to the floor of the mouth by an abnormally short and narrow frenum, or by folds of mucous membrane on each side of the frenum, so that the tongue cannot be protruded. Although this deformity is rare, it is common for parents to blame an imaginary tongue-tie when a child is slow in learning to speak, or when he speaks indistinctly or stammers, and the doctor is frequently requested to divide the frenum under such circumstances. In the vast majority of cases nothing is found to be wrong with the frenum. In the rare cases of true tongue-tie the edges of the shortened bands should be snipped with scissors close behind the incisor teeth, and then torn with the finger-nail.
Excessive length of the frenum is occasionally met with, and in children may allow of the tongue falling back into the throat and causing sudden suffocative attacks, one of which may prove fatal. In some cases the patient is able voluntarily to fold the tongue back behind the soft palate.
Macroglossia is the term applied to a variety of conditions in which the tongue becomes unduly large, so that it tends to be protruded from the mouth, and to become scored by the teeth. The typical form—lymphangiomatous macroglossia—is due to a dilatation of the lymph spaces of the tongue. It is often congenital, and may affect the whole or only a part of the tongue. The enlargement may be progressive from the first, or may remain stationary for years, and then begin to develop somewhat suddenly, sometimes after an injury or as a result of some infective condition. The treatment consists in removing a wedge-shaped portion of the tongue.
In certain cases of macroglossia in children, the lesion has been found to be a fibromatosis of the nerves of the tongue, analogous to the plexiform neuroma.
Atrophy of the tongue is rare as a congenital condition. Hemi-atrophy occurs in various diseases of the central nervous system, as well as after injuries and diseases implicating the hypoglossal nerve.
Nervous Affections of the Tongue.—Neuralgia confined to the distribution of the lingual nerve is comparatively rare. It usually yields to medical treatment, but in inveterate cases it is sometimes necessary to resect the nerve.
It is more common to meet with a condition in which the patient complains of severe burning or aching pain in the region of the foliate papilla, which is situated on the edge of the tongue just in front of the anterior pillar of the fauces. The patient is usually a middle-aged, neurotic woman, and often with a gouty or rheumatic tendency. The pain, for which it is seldom possible to discover any cause, is usually worst at night, and may last for months, or even years. The practical importance of the condition is that, as the foliate papilla is prominent and red, it is liable to be mistaken on superficial examination for a commencing epithelioma. An inspection of the opposite side of the tongue, however, will reveal an exactly similar condition, which is not painful. The first and most important step in treatment is to assure the patient that the condition is not cancerous. Caustics and other irritating applications are to be avoided.
Spasm of the tongue sometimes occurs after injuries of the head implicating either the centre or the trunk of the hypoglossal nerve. It may also appear as a reflex condition in infective affections of the teeth and gums, or as a manifestation of some general disease of the central nervous system.
Paralysis of the tongue—unilateral or bilateral—may be due to injury or disease of the nerve centres of the hypoglossal nerve, more frequently to injury of or pressure on the nerve-trunk. The nerve may be bruised or divided in operations for the removal of tuberculous glands or other tumours in the neck. When the tongue is protruded it deviates towards the paralysed side, being pushed over by the active muscles of the opposite side (Fig. 260), and speech and mastication may be interfered with. The paralysed half of the tongue subsequently undergoes atrophy, but the functional disability largely disappears.
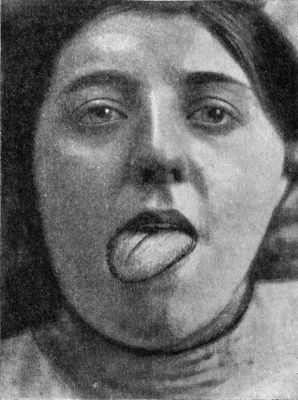 Fig. 260.—Temporary Unilateral Paralysis of Tongue,
from bruising of hypoglossal nerve during operation for tuberculous
cervical glands.
Fig. 260.—Temporary Unilateral Paralysis of Tongue,
from bruising of hypoglossal nerve during operation for tuberculous
cervical glands.
Surgical Anatomy.—The parotid gland lies on the side of the face below and in front of the ear, and extends deeply behind the mandible reaching almost to the side wall of the pharynx. Its deeper part lies in close relation with the internal carotid artery, the internal jugular vein, and the vagus, glosso-pharyngeal, accessory, and hypoglossal nerves. The external carotid artery passes through the substance of the parotid, and bifurcates opposite the neck of the condyle into the temporal and internal maxillary arteries. It is accompanied by the venous trunk formed by the junction of the temporal and internal maxillary veins. The facial nerve and its branches traverse the lower third of the gland from behind forwards. The facial portion of the gland lies on the surface of the masseter muscle, and the parotid duct (Stenson's duct) emerges from its anterior border. After crossing the masseter, the duct pierces the buccinator muscle and the mucous membrane obliquely, and opens into the mouth opposite the second upper molar tooth. Its course is indicated by a line passing from the upper part of the lobule of the ear to a point midway between the ala of the nose and the margin of the upper lip—that is, at a higher level than the facial nerve. Several lymph glands—pre-auricular—lie inside the capsule of the parotid just in front of the ear.
The submaxillary gland lies under the integument and fascia in the triangle formed by the lower jaw and the two bellies of the digastric muscle. Its anterior part is crossed by the facial vessels, and several lymph glands lie inside its capsule. The submaxillary duct (Wharton's duct) opens into the mouth by the side of the frenum of the tongue.
The sublingual gland lies in the floor of the mouth just beneath the mucous membrane. It has numerous ducts, some of which open directly into the mouth, others into the submaxillary duct.
Injuries.—The parotid is frequently injured by accidental wounds and in the course of operations. If the blood vessels traversing the gland are divided, such wounds are liable to bleed freely, and if the facial and auriculo-temporal nerves are damaged, motor and sensory paralysis of the parts supplied by them ensues. Wounds of the parotid heal rapidly and without complications so long as infection is prevented, but if suppuration takes place they are liable to be followed by the escape of saliva, which may go on for weeks; in some cases a salivary fistula is thus established.
The parotid duct may be divided and a salivary fistula result. If the external wound heals rapidly, a salivary cyst may develop in the substance of the cheek, forming a swelling, which fills up at meals, and may be emptied by external pressure, the saliva escaping into the mouth.
In a wound implicating the whole thickness of the cheek the skin should be accurately sutured, care being taken that the stitches do not include the duct, but in order that the saliva may readily reach the mouth, the mucous membrane should not be stitched.
Salivary Fistulæ.—A salivary fistula may occur in relation to the glandular substance of the parotid or in relation to the duct. Fistula in connection with the glandular substance—parotid fistula—seldom results from a wound, made, for example, in the removal of a tumour or in an operation on the ramus of the jaw, so long as it is aseptic; but as a sequel of suppuration in the gland, and particularly of an abscess developing around a concretion, it is not uncommon. The fistulous opening is usually small, and may occur at any point over the gland. The fistula may be dry between meals, or the saliva may escape in small transparent drops, but the quantity is always greatly increased when food is taken. A parotid fistula, although it may continue to discharge for weeks, or even for months, usually closes spontaneously.
In persistent cases, the edges of the fistula may be pared and brought together with sutures, or the actual cautery may be applied to induce cicatricial contraction.
Fistula of the parotid duct is more serious. It is usually due to a wound, less frequently to abscess or impacted calculus. From the minute opening, which is most frequently situated over the buccinator muscle, there is an almost continuous flow of clear limpid saliva, which is greatly increased in quantity while the patient is eating. These fistulæ show little tendency to close spontaneously. Attempts to close the opening by the external application of collodion, by cauterising the edges, or even by paring the edges and introducing sutures, usually fail. It is necessary to establish an opening into the mouth, either by opening up the original duct or by making an internal fistula in place of the external one.
Salivary Calculi.—Salivary calculi are most commonly met with in the submaxillary gland or its duct. They consist of phosphate and carbonate of lime with a small proportion of organic matter, and result from the chemical action of bacteria on the saliva. In rare cases a foreign body, such as a piece of straw, a fruit-seed, or a fish-bone, forms the nucleus of the concretion. They vary in size from a pea to a walnut, and are hard, of a whitish or grey colour, and rough on the surface. Those that form in the gland itself are usually irregular, while those met with in the duct are rounded or spindle-shaped (Fig. 261).
A calculus in the duct gives rise to sharp lancinating pain, which is aggravated when the patient takes food. The duct is seldom completely obstructed, but the flow of saliva is usually so much impeded that the gland becomes greatly swollen during meals. The swelling gradually subsides between meals, or can be made to disappear by external pressure. The calculus can usually be felt by means of a probe passed along the duct, or by puncturing the swelling with a needle; or, with one finger inside the mouth and another under the jaw, a hard lump can be detected under the mucous membrane of the floor of the mouth. It may be revealed by the X-rays. When the obstruction is complete, a retention cyst forms in which suppuration is liable to occur, causing marked aggravation of the symptoms. In some cases the wall of the duct and the surrounding tissues become thickened and indurated, forming a swelling which is liable to be mistaken for a malignant growth. The treatment consists in making an incision through the mucous membrane over the calculus and extracting it with a scoop or forceps.
Infective Conditions.—Parotitis.—Inflammation of the parotid gland may be non-suppurative or suppurative.
Of the non-suppurative varieties the most common is the epidemic form known as mumps. This is an acute infective condition, which usually attacks young children, and implicates both glands, either simultaneously or consecutively. It runs a definite course, which lasts for from one to two weeks, and almost invariably ends in resolution. The parotid gland is swollen and tender, there is pain on attempting to open the mouth, difficulty in swallowing, and dribbling of saliva. The surgical interest of this disease lies in the fact that it is frequently complicated by pain and swelling of the testis, œdema of the scrotum, and occasionally by a urethral discharge, and atrophy of the testis has been observed after such an attack. In females there is sometimes pain in the ovary, tenderness and swelling of the mamma, and a vaginal discharge.
The parotid on one or both sides may suddenly become swollen and tender in patients who are taking large doses of mercury, in gouty subjects, or in patients suffering from infective conditions of the genito-urinary organs, such as orchitis, ovaritis, urethritis, or cystitis. The condition is usually transient and leads to no complications.
Recurrent enlargement of the parotid and submaxillary glands, as well as of the lachrymal glands, is occasionally met with in adults, and was first described by Mikulicz. It may be associated with salivary lithiasis, xerostomia, or organic narrowing of the ducts, but in the majority of cases no such cause can be discovered (D. M. Greig). When the parotid is affected the condition tends to be bilateral and there is some constitutional disturbance. The submaxillary form is usually unilateral and the symptoms are entirely local. The affected gland rapidly becomes swollen, painful and tender to the touch, and the swelling increases markedly while the patient is eating. Each attack lasts for a few hours to one or two weeks, and then subsides spontaneously. The intervals between attacks vary from a few weeks to a year or more. In the course of a few years there is considerable deformity, and sometimes deficiency in the glandular secretion, but the disease is not attended by other inconvenience. Benefit has followed the administration of arsenic and iodides, and the use of radium and X-rays.
The treatment of these non-suppurative forms of parotitis consists in relieving the symptoms.
Suppurative parotitis may be due to direct spread of infection from the mouth along the parotid duct, or to extension of suppurative processes from the temporo-mandibular joint, the jaw, or a lymph gland. It is liable to occur also in the course of any disease in which there is an infection of the blood with pyogenic bacteria, and has been met with in diphtheria, typhoid fever, scarlet fever, measles, and other eruptive fevers.
The post-operative form of parotitis is most frequently met with after laparotomy for such conditions as suppurative appendicitis, perforated gastric ulcer, ovarian cyst, and pyosalpinx.
These secondary forms are probably due to infection from the mouth under conditions in which the secretion of saliva is arrested or its escape from the gland interfered with.
The early symptoms are apt to be overshadowed by those of the general disease from which the patient suffers. At first the gland is swollen, hard, and tender, and the seat of constant, dull, boring pain; later there is redness, œdema, and fluctuation. The movements of the jaw are restricted and painful, the patient is unable to open the mouth, and has difficulty in swallowing. The inflammation reaches its height on the third or fourth day, and usually ends in suppuration. The pus is scattered in numerous foci throughout the gland, and sometimes large sloughs form. The dense capsule of the gland prevents the pus reaching the surface and causes it to burrow among the tissues of the neck, giving rise to dyspnœa and dysphagia. It may find its way downwards towards the mediastinum, inwards towards the pharynx—where it constitutes one form of retro-pharyngeal abscess—or upwards towards the base of the skull. Not infrequently it burrows into the temporo-mandibular joint, or escapes by bursting into the external auditory meatus. Serious hæmorrhage may result from erosion of the vessels traversing the gland or of the internal jugular vein, or venous thrombosis may ensue. Persistent paralysis may follow destruction of the facial nerve; and salivary fistulæ may form. Death may take place from toxæmia even before pus forms.
Treatment.—During the first two or three days hyperæmia is induced by means of poultices, hot fomentations, or Klapp's suction bells, and the mouth is frequently washed out with an antiseptic. As soon as there is reason to believe that pus has formed an incision is made behind the angle of the jaw, parallel to the branches of the facial nerve, the abscess opened by Hilton's method, a finger passed into the gland, and all septa broken down and drainage secured.
Acute infection of the submaxillary gland is met with under the same conditions as that of the parotid. Both glands are occasionally attacked at the same time.
The acute phlegmonous peri-adenitis of the submaxillary gland, known as angina Ludovici, is referred to at p. 597.
The treatment consists in making incisions through the deep fascia in order to relieve the tension, or to let out pus if it has formed.
Acute suppurative inflammation of the sublingual gland may occur under the same conditions as in the parotid, and is associated with the formation of an exceedingly painful and tender swelling under the tongue. The tongue is gradually pushed against the roof of the mouth, so that swallowing is difficult and respiration may be seriously impeded. There is marked constitutional disturbance. An incision into the swelling is immediately followed by relief of the symptoms.
Tuberculous disease of the salivary glands is rare. It usually begins in the lymph glands within the capsule of the parotid or submaxillary, and spreads thence to the salivary gland tissue.
Tumours.—Cystic Tumours—Ranula.—The term ranula is applied to any cystic tumour formed in connection with the glands in the floor of the mouth. Formerly these tumours were believed to be retention cysts due to blocking of the salivary ducts. They are now known to be the result of a cystic degeneration of one or other of the secreting glands in the floor of the mouth. They contain a thick glairy fluid, which differs from saliva in containing a considerable quantity of mucin and albumin, while it is free from any amylolytic ferment or sulpho-cyanide of potassium. Numerous degenerated epithelial cells are found in the fluid.
The sublingual ranula is the most common variety. It appears as a painless, smooth, tense, globular swelling of a bluish colour. It usually lies on one side of the frenum, and over it the mucous membrane moves freely. As it increases in size it gradually pushes the tongue towards the roof of the mouth, and so causes interference with speech, mastication, and swallowing. It is to be differentiated from a retention cyst of the submaxillary gland by the fact that a probe can usually be passed down the submaxillary duct alongside of the swelling, and from sublingual dermoid (p. 539).
The treatment consists in making an incision through the mucous membrane over the swelling, dissecting away the whole of the cyst wall if possible, and, if any portion cannot be removed, swabbing it with a solution of chloride of zinc (40 grains to the ounce), after which the cavity is stuffed with bismuth gauze and allowed to close by granulation. It is sometimes found more satisfactory to dissect out the cyst through an incision below the jaw, and in the event of recurrence this should be undertaken.
Cystic tumours, similar to the sublingual ranula, form in the other glands in the floor of the mouth—for example, the incisive gland, which lies just behind the symphysis menti, as well as in the apical gland on the under aspect of the tip of the tongue. The latter is distinguished by the fact that it moves with the tongue. In rare cases children are born with a cystic swelling in the floor of the mouth—the so-called congenital ranula. It is usually due to an imperfect development of the duct of the submaxillary or sublingual gland.
Solid Tumours—Mixed Tumours of the Parotid.—The most important of the solid tumours met with in the salivary glands is the so-called “mixed tumour of the parotid.” This was formerly believed to be an endothelioma derived from a proliferation of the endothelial cells lining the lymph spaces and blood vessels of the gland. A more probable view is that it develops from rests derived from the first branchial arch an not from the parotid. The matrix of the tumour is made up of cartilaginous, myxomatous, sarcomatous, or angiomatous tissue, the proportion of these different elements varying in individual specimens, and it may include some portions that are adenomatous. A gelatinous substance forms in the intercellular spaces of the tumour, and may accumulate in sufficient quantity to give rise to cysts of various sizes. There is reason to believe that the tumours of the parotid previously described as adenoma, chondroma, angioma, myxoma, and many of the cases of sarcoma, were really mixed tumours in which one or other of these tissues predominated.
The tumour usually develops in the vicinity of the parotid, and presses on the salivary tissue, thinning it out and causing it to undergo atrophy.
Clinical Features.—The mixed tumour is usually first observed between the ages of twenty and thirty. It is of slow growth and painless, and forms a rounded, nodular swelling, the consistence of which varies with its structure. The skin over the swelling is normal in appearance and is not attached to the tumour (Figs. 263, 264). Only in rare cases does paralysis result from pressure on the facial nerve.
Although usually benign, these tumours may, after lasting for years, take on malignant characters, growing rapidly, implicating adjacent lymph glands, and showing a marked tendency to recur after removal.
The treatment consists in shelling out the tumour, care being taken to avoid injuring the facial nerve or the parotid duct by making the incision and the subsequent cuts in the dissection run parallel to them. If the tumour is removed early and completely, recurrence is the exception.
Sarcoma and carcinoma are rare. They are very malignant, grow rapidly, infiltrate surrounding parts, including the skin, and infect the adjacent lymph glands. There is severe neuralgic pain, and paralysis from involvement of the facial nerve is an early symptom.
The treatment consists in excising the whole of the parotid gland with the tumour, no attempt being made to conserve the facial nerve or other structures traversing it. Recourse should be had to the use of radium both before and after operation, otherwise recurrence is all but inevitable.
The submaxillary and sublingual glands may be the seat of the same varieties of tumour as the parotid. These glands are particularly liable to become invaded along with the adjacent lymph glands in epithelioma of the tongue and floor of the mouth.
[5] We desire here to acknowledge our indebtedness to Dr. Logan Turner for again revising this chapter.
Surgical Anatomy.—The anatomical subdivision of the ear into three parts—the external, middle, and internal ear—forms a satisfactory basis for the study of ear lesions. The outer ear consists of the auricle and external auditory meatus, the latter being made up of an outer cartilaginous portion half an inch in length, and a deeper osseous portion three-quarters of an inch long. The canal forms a curved tube, which can be straightened to a considerable extent for purposes of examination by pulling the auricle upwards and backwards. It is closed internally by the tympanic membrane, which separates it from the tympanic cavity or middle ear. The middle ear includes the tympanum proper, which is crossed by the chain of ossicles—malleus, incus, and stapes—the Eustachian tube, which communicates with the naso-pharynx, and the tympanic antrum and mastoid cells. As these cavities lie in close relation to the middle and posterior cranial fossæ, infective conditions in the tympanum and mastoid cells are liable to spread to the interior of the skull. The internal ear or labyrinth lies in the petrous part of the temporal bone, its outer boundary being the inner wall of the middle ear.
Physiologically the different parts of the auditory mechanism may be divided into (1) the sound-conducting apparatus, which includes the outer and middle ears; and (2) the sound-perceiving apparatus—the internal ear and central nerve tracts. Impairment of hearing may be due to causes existing in one or other or both of these subdivisions. The condition of the sound-conducting apparatus can be investigated by direct inspection through the speculum, and by inflation of the Eustachian tube and tympanum, while that of the sound-perceiving apparatus is ascertained partly by testing the hearing, and partly by excluding affections of the outer and middle ear. When the sound-conducting apparatus is at fault, the resulting deafness is spoken of as “obstructive”; when the sound-perceiving apparatus is affected, the term “nerve deafness” is used. The semicircular canals, which are peripheral organs concerned in the maintenance of equilibration, form part of the inner ear apparatus.
Cardinal Symptoms of Ear Disease.—The most important symptom of ear disease is impairment of hearing, which varies in degree, and may be due to lesions either in the sound-conducting or in the sound-perceiving apparatus. The sudden onset of deafness may be due to impaction of wax in the external meatus or to hæmorrhage or effusion into the labyrinth. A gradual onset is more common. In children there is a great tendency for acute inflammatory conditions of the middle ear to arise in connection with the exanthemata and in association with adenoids. In adult life chronic catarrhal processes are more common causes of gradually increasing deafness, while in advanced age there is a tendency to acoustic nerve impairment. Certain anomalous conditions of hearing are occasionally met with, such as the “paracusis of Willis”—a condition in which the patient hears better in a noise; “diplacusis,” or double hearing; and “hyperæsthesia acustica,” or painful impressions of sound.
Tinnitus aurium, or subjective noises in the ear, may constitute a very annoying and persistent symptom. These sounds vary in their character, and may be described by the patient as ringing, hissing, or singing, or may be compared to the sound of running water or of a train. They are usually compared to some sound which, from his occupation or otherwise, the patient is accustomed to hear. They may be purely aural in origin, being due, for example, to increased pressure on the acoustic nerve endings from causes in the labyrinth itself or in the middle or external ear; or they may be due to certain reflex causes, such as naso-pharyngeal catarrh or gastric irritation. Vascular changes such as occur in anæmia, Bright's disease, and heart disease may also be concerned in their production.
Pain, or earache, varies in degree from a mere sense of discomfort to acute agony. The pain associated with a boil in the external meatus is usually aggravated by movements of the jaw, by pulling the auricle, and by pressure upon the tragus. The pain of acute middle-ear inflammation is deep-seated, intermittent in character, and worse at night, and is aggravated by blowing the nose, coughing, and sneezing—acts which increase middle-ear tension by forcing air along the Eustachian tube. Mastoid pain and tenderness are indicative of inflammation in the antrum or cells, and when these symptoms supervene in the course of a chronic middle-ear suppuration, they should always be regarded as of grave import. Severe neuralgia of the ear may simulate the pain of acute mastoiditis, and it must not be forgotten that earache may be traced to a diseased tooth. A careful examination, not only of the ear, but also of the throat and teeth, should therefore be made in all cases of earache.
Vertigo, or giddiness, may be produced by causes which alter the tension of the labyrinthine fluid, such, for example, as the pressure of wax upon the tympanic membrane, or exudation into the middle ear or into the labyrinth. Giddiness occurring in the course of chronic middle-ear suppuration may be significant of labyrinthine or of intra-cranial mischief, but is not necessarily so. Giddiness preceded by nausea suggests a gastric origin; if followed by nausea it points to an aural origin. In cases of suspected aural vertigo, the patient's “static sense” should be carefully tested. He should be asked (1) to stand with both feet together with the eyes closed, (2) to stand on one or other foot with eyes closed, (3) to walk in a straight line, (4) to hop backwards and forwards off both feet. His incapacity for performing such movements should be noted. As nystagmus may be associated with disturbance of equilibrium due to ear disease, the movements of the eyeballs must be carefully tested.
Labyrinthine nystagmus is of a rhythmic character, and consists of a slow and a rapid movement. Physiological nystagmus can be induced by stimulating the movement of the endolymph in the semicircular canals, by syringing the ear with hot and cold water (caloric test), by rotating the individual (rotation test), and by the galvanic current. Any departure from the normal reactions which these tests may produce, should raise the suspicion of a pathological condition of the semicircular canals.
Discharge from the ear, or otorrhœa, is occasionally due to an eczematous condition of the skin lining the external meatus. It is then usually of a thin, watery character, and contains epithelial flakes and débris. An aural discharge is, however, most commonly of middle-ear origin. It may be muco-purulent and stringy, or purulent and of thicker consistence. A peculiar, offensive odour is characteristic of chronic middle-ear suppuration. The surgeon should smell the speculum in suspicious cases. He should never accept the patient's statement as regards the absence of discharge, but should satisfy himself by inspection and by the introduction of a cotton-wool wick.
The Hearing Tests.—In testing the hearing, a definite routine method should be adopted, the watch, whisper, voice, and tuning-fork tests being systematically employed. Although the patient only complains of one ear, both must be examined. Each ear should be tested separately, and the patient should be so placed that he cannot see the lips of the examiner. While one ear is being tested, the other should be closed with the finger, and each test should be commenced outside the probable normal range of hearing. All the results should be written down at once, and the date of the test recorded, as this is essential for following the progress of the case.
Tuning-fork Tests.—To differentiate between deafness due to a lesion in the sound-conducting apparatus and that due to labyrinthine causes, it is necessary to enter into a little more detail. The tone produced by a vibrating tuning-fork is conducted to the nerve terminations in the labyrinth both through the air column in the external meatus (air-conduction), and through the cranial bones (bone-conduction). When, in a deaf ear, the vibrations of a tuning-fork placed in contact with the mastoid process are heard better than when the fork is held opposite the meatus, the lesion is in the sound-conducting apparatus. When, on the other hand, the vibrations are heard better by air-conduction, the lesion is in the sound-perceiving apparatus. In addition to these facts, we find also that in obstructive deafness low tones tend to be lost first, while in nerve deafness the higher notes are the first to go. This may be investigated by tuning-forks of different pitch or with the aid of a Galton's whistle. Again, in middle-ear deafness, hearing may be better in a noisy place, and be improved by inflation of the tympanum; while in labyrinthine deafness, hearing may be better in a quiet room, and be rendered worse by inflation.
Inspection of the Ear.—This should be carried out by the aid of reflected light, the ear to be examined being turned away from the window, lamp, or other source of light that may be employed. A small ear reflector, either held in the hand or attached to a forehead band, and a set of aural specula are required. Before introducing the speculum, the outer ear and adjacent parts should be examined, and the presence of redness, swelling, sinuses or cicatrices over the mastoid, displacement of the auricle, or any inflammatory condition of the outer ear observed. To inspect the tympanic membrane, a medium-sized speculum held between the thumb and index finger is insinuated into the cartilaginous meatus, the auricle being at the same time pulled upwards and backwards by the middle and ring fingers, so as to straighten the canal. The tympanic membrane is then sought for and its appearance noted.
The normal membrane is concave as a whole on its meatal aspect; it occupies a doubly oblique plane, being so placed that its superior and posterior parts are nearer the eye of the examiner than the anterior and inferior parts. While varying to some extent in colour, polish, and transparency, it presents a bluish-grey appearance. The handle of the malleus traverses the membrane as a whitish-yellow ridge, which appears to pass from its upper and anterior parts downwards and backwards to a point a little below the centre. At the lower end of the handle of the malleus a bright triangular cone of light passes downwards and forwards to the periphery of the membrane. At the upper end of the handle is a white knob-like projection, the short process of the malleus. Passing forwards and backwards from this are the anterior and posterior folds. The portion of the membrane situated above the short process is known as the membrana flaccida or Shrapnell's membrane. Behind the malleus the long process of the incus may be visible through the membrane. The mobility of the membrana tympani should be tested by inflating the tympanum or by means of Siegle's pneumatic speculum.
Various departures from the normal may be observed. Atrophy of the membrane is characterised by extreme transparency of the whole disc. Circumscribed atrophic patches appear as dark transparent areas, which show considerable mobility and bulge prominently on inflation. A cicatrix in the membrane is evidence of a healed perforation, and is also transparent, but differs from an atrophic patch in being more sharply defined from the surrounding membrane. A thickened membrane presents an opaque white appearance. Calcareous or chalky patches are markedly white, and when probed are hard to the touch; they are often evidence of past suppuration. An indrawn or retracted membrane, resulting from Eustachian obstruction, is characterised by increased concavity, undue prominence of the lateral short process of the malleus and of the anterior and posterior folds, and by the handle of the malleus assuming a more horizontal position. An inflamed membrane, showing congestion of the vessels about the malleus or a general diffuse redness, is evidence of middle-ear inflammation. A yellow appearance of the lower part of the membrane, limited above by a dark line stretching across the drum-head, is indicative of sero-purulent exudation into the tympanum. The membrane may be bulged outwards into the meatus by the fluid, and thus lie nearer the observer's eye than normally. A perforation is usually single, and varies in size from a small pinhead to complete destruction of the membrane. The labyrinthine (inner) wall of the tympanum may be visible through the perforation, and is recognised by being on a deeper plane than the membrane, and by its hard bony consistence when touched with the probe. The diagnosis of a perforation associated with middle-ear discharge may be further assisted by inspection during inflation, when bubbles of air and secretion are visible. When the perforation is invisible, its existence may be inferred if a small pulsating spot of light can be recognised through the speculum. Granulations in the tympanum appear as red fleshy masses of different sizes. When large they constitute aural polypi, which are recognised by their proximity to the outer end of the meatus, their soft consistence and mobility, and the fact that the probe may be passed round them. Granulations and polypi usually indicate the presence of middle-ear suppuration.
Inflation of the Middle Ear.—Before proceeding to inflate the middle ear, the examiner should inspect the nose, naso-pharynx, and pharynx. This should be made a routine part of the examination in all cases of ear disease. As inflation is not only an aid in diagnosis, but is also of great assistance in prognosis, it is necessary that the hearing should be tested and noted before the ear is inflated. There are three methods of inflating the tympanum: Valsalva's method, Politzer's method, and by means of the Eustachian catheter.
In Valsalva's inflation the patient himself forces air into his Eustachian tubes, by holding his nose, closing his mouth, and forcibly expiring. This method of inflation has only a limited application and is of little therapeutic value.
Politzer's Method.—For this a Politzer's air-bag and an auscultating tube, one end of which is inserted into the patient's ear and the other into the ear of the examiner, are required. The nasal end of the bag should be protected with a piece of rubber tubing or be provided with a nozzle. The patient retains a small quantity of water in his mouth until directed to swallow. The nozzle of the bag is inserted into one nostril, and the other is occluded by the fingers of the surgeon. The signal to swallow is then given, and, simultaneously with the movement of the larynx during this act, the bag is sharply and forcibly compressed. Holt's modification of this method consists in directing the patient to puff out his cheeks while the lips are kept firmly closed.
Inflation through the Eustachian Catheter.—For this method, in addition to the Politzer's bag and the auscultating tube, a silver or vulcanite Eustachian catheter is required. The silver instrument has the advantage that it can be sterilised by boiling. The patient is seated facing the light, while the surgeon stands in front of him, and, having placed the auscultating tube in position, with his left thumb he tilts up the tip of the patient's nose. The beak of the catheter is now inserted into the inferior meatus, point downwards, and carried horizontally backwards along the floor of the nose until the convexity of the curve touches the posterior wall of the naso-pharynx. When the posterior pharyngeal wall is felt, the point of the instrument is rotated inwards through a quarter of a circle; the position of the point is indicated by the metal ring upon the outer end of the catheter. The finger and thumb of the left hand should now grasp the stem of the catheter just beyond the tip of the nose so as to steady it. It is now gently withdrawn until the concavity of the beak is brought against the posterior edge of the septum nasi. With the right hand the point of the instrument is then rotated downwards and outwards through a little more than half a circle, so that the point slips into the Eustachian orifice and the metal ring looks outwards and upwards towards the external canthus of the eye of the same side. While the instrument is maintained in this position by the left hand, the nozzle of the Politzer's bag is inserted into the funnel-shaped outer extremity of the catheter, and inflation is gently carried out with the least possible jerking. Before withdrawing the catheter its point must be disengaged from the Eustachian opening by turning it slightly downwards. Difficulties in introducing the catheter may arise from the presence of spines and ridges upon, and deviations of, the septum, and it may be necessary to pass the instrument under the guidance of the mirror and speculum.
More accurate information is gained from the use of the catheter than from Politzer's inflation, and it is the safer method to employ when a cicatrix or atrophied patch exists in the tympanic membrane, as by the latter method rupture of these areas might occur. Further, the catheter has the advantage of only inflating one ear, and thus preventing any undue strain being put upon the other. In children the catheter can seldom be employed, on account of the difficulty in passing it.
Considerable information may be derived from inflation. If the Eustachian tube is patent, a full clear sound is heard close to the examiner's ear through the auscultating tube. If the Eustachian tube is obstructed, the sound is fainter and more distant. If there is fluid in the tympanum, a fine moist sound may be detected, which must not be confounded with the coarser and more distant gurgling sound associated with moisture at the pharyngeal opening of the tube. If a small dry perforation exists in the tympanic membrane, the air may be heard whistling through it, while if the perforation is large, a sensation which is almost painful may be produced in the examiner's ear. If there is fluid associated with the perforation, these sounds may be accompanied by a bubbling noise. The effect of inflation upon the hearing must be carefully tested and recorded.
Deformities.—The auricle, together with the external auditory meatus, may be congenitally absent on one or on both sides. The condition is not amenable to surgical treatment. Double auricles are occasionally met with; more frequently rudimentary auricular appendages about the size of a pea, consisting of skin, subcutaneous connective tissue and nodules of cartilage occur in front of the tragus, on the lobule or in the neck. These appendages should be snipped off with scissors. These congenital deformities are due to errors in development of the mandibular arch, and are frequently associated with macrostoma, facial clefts, and other malformations of the face.
Outstanding ears may be treated by excising a triangular or elliptical portion of skin and cartilage from the posterior surface of the pinna and uniting the cut edges with sutures. Abnormally large ears may be diminished in size by the removal of a V-shaped portion from the upper part of the auricle.
The term hæmatoma auris is applied to a sub-perichondrial effusion of blood, which may occur either as the result of injury to the auricle, for example in football players, or as a result of trophic changes in the cartilage and perichondrium. The latter form is not uncommon among the insane. A more or less tense fluctuating swelling forms on the anterior surface of the auricle, presenting in some cases a distinctly bluish coloration. Inflammation may ensue, and in some cases suppuration and even necrosis of cartilage may follow.
The treatment in a recent case consists in applying cold or elastic compression with cotton-wool and a bandage, or in withdrawing the effused blood by means of a hollow needle. In the event of suppuration supervening, incision and drainage must be carried out.
Epithelioma may attack the auricle and extend along the external auditory meatus. It begins as a small abrasion which refuses to heal, and is attended with a constant fœtid discharge and intense pain. The disease may spread to the middle ear and invade the temporal bone, and facial paralysis then ensues. The adjacent lymph glands are early infected. The treatment consists in removing the growth freely, and excising the associated lymph glands at an early stage of the disease. In inoperable cases radium or the X-rays may be employed.
Rodent cancer also may attack the outer ear.
Impaction of Wax or Cerumen.—Hyper-secretion may result from unknown causes, or it may accompany or be induced by the discharge from a chronic middle-ear suppuration. The association of these two conditions should be borne in mind. An accumulation of wax may be caused by the too zealous attempts of the patient to keep the ear clean, the wax being forced into the narrow deeper part of the meatus.
The chief symptom of impacted wax is deafness, which is often of sudden onset. Impaction of wax causes deafness only when the lumen of the auditory canal becomes completely occluded by the plug. Tinnitus aurium and vertigo are sometimes present, and may be troublesome if the wax rests upon the tympanic membrane. Pain is occasionally complained of, and is usually due to the pressure of the plug upon an inflamed area of skin. Certain reflex symptoms, such as coughing and sneezing, have been met with.
It is only by an objective examination of the ear that the diagnosis can be made. The plug varies in colour and consistence, and may be yellow, brown, or black in appearance. Sometimes from the admixture of a quantity of epithelium it is almost white in colour.
Treatment.—The ear should be syringed with a warm antiseptic or sterilised solution. The lotion is at a suitable temperature if the finger can be comfortably held in it. The ear should be turned to the light, a towel placed over the patient's dress, and a kidney basin held under the auricle and close to the cheek. A syringe provided with metal rings for the fingers and armed with a fine ear nozzle should be held with the point inserted just within the aperture of the external meatus and in contact with the roof of the canal. Care must be taken that all the air is first removed from the syringe. To straighten the canal, the pinna should be pulled upwards and backwards by the left hand. It may be necessary to exert some considerable degree of force before the plug becomes dislodged, but this must be done with caution. The ear should then be dried out with cotton-wool, and a small plug of wool inserted for a few hours. If pain is complained of, or if the wax is hard and cannot be readily removed, the syringing should be stopped, and means taken to soften it by the instillation of a few drops of a solution of bicarbonate of soda (10 grains to the ounce of water or glycerine), or of peroxide of hydrogen, several times daily.
Eczema of the external meatus is often associated with eczema of the auricle and of the surrounding parts. Not infrequently there also exists a chronic middle-ear suppuration, which may be the cause of the eczema. Intense itchiness is the most characteristic symptom, and a watery discharge may also be complained of. Deafness and tinnitus are dependent upon the accumulation of epithelium and débris. After the ear is syringed the skin may present a dry, scaly appearance, while sometimes fissures and an indurated condition of the outer end of the meatus may be noted. Rarely is the outer surface of the tympanic membrane itself involved.
Treatment consists in keeping the ear clean by syringing and careful drying. Probably the best local application is nitrate of silver (10 grains to the ounce of spiritus ætheris nitrosi). This is applied by means of a grooved probe dressed with a small piece of cotton-wool. Care should be taken that none of the fluid is allowed to escape upon the cheek, otherwise staining of the skin occurs. A plug of cotton-wool is inserted, and the solution is re-applied at the end of a week. Sometimes the condition is very intractable.
Occasionally the vegetable parasite aspergillus is present in the external meatus, and produces a condition that is liable to be mistaken for eczema. Strong antiseptic lotions are required to kill the fungus.
Furunculosis or Boils.—Boils in the ear may arise singly or in crops, and may be associated with eczema of the meatus or with chronic suppuration of the middle ear. Pain is the chief symptom complained of, and it may be very acute. Deafness ensues when the meatus becomes completely blocked by the swelling. The boil occurs in the cartilaginous meatus, and it is to be borne in mind that the skin may present a normal appearance even when suppuration has occurred. Palpation of the affected area with the probe causes intense pain. Sometimes œdema over the mastoid with displacement forwards of the pinna supervenes, and simulates acute inflammation of the mastoid.
Treatment.—If seen in the earliest stages, an attempt may be made to relieve the pain by the application of a 20 per cent. menthol and parolein solution, or by the use of carbolic acid and cocain, 5 grains of each to a dram of glycerine. When suppuration has occurred, the best treatment is by early incision, transfixing the base of the swelling with a narrow knife and cutting into the meatus. If the tendency to boils persists, a staphylococcal vaccine will be found of value.
Foreign Bodies.—It is unnecessary to enumerate all the varieties of foreign bodies that may be met with in the ear. They may be conveniently classified into the animate—for example maggots, larvæ, and insects; and the inanimate—for example beads, buttons, and peas. Pain, deafness, tinnitus, and giddiness may be produced, and such reflex symptoms as coughing and vomiting have resulted.
The main practical point consists in identifying the body by inspection. The mere history of its introduction should not be taken as proof of its presence. In children it is advisable to give a general anæsthetic so that a thorough examination may be made with the aid of good illumination. If previous attempts to remove the body have caused œdema of the meatal walls, and if the symptoms are not urgent, no further attempt should be made until the swelling has been allayed by syringing with warm boracic lotion, and by applying one or more leeches to the tragus. An attempt should always be made in the first instance to remove the body by syringing. It is rare to find this method fail. Should it do so, a small hook should be used, sharp or blunt according to the consistence of the body. Maggots, larvæ, and insects should first be killed by instillations of alcohol and then syringed out.
Traumatic Rupture of the Tympanic Membrane.—Perforating wounds may result from direct violence caused by the patient—for example, in attempts to remove wax or foreign bodies, or by clumsiness on the part of the surgeon. It is also a comparatively common complication of fracture of the middle fossa of the base of the skull. More commonly, perhaps, the membrane is ruptured from indirect violence due to great condensation of the air in the external auditory meatus, following blows upon the ear, heavy artillery reports, or diving from a height. The injury is followed by pain in the ear, often by considerable deafness and tinnitus, and bleeding is frequently observed. If early examination of the ear is made, coagulated blood may be found in the meatus or upon the membrane, or ecchymosis may be visible on the latter. A rupture in the membrane following indirect violence is usually lozenge-shaped. During inflation by Valsalva's method the air may be heard to whistle through the perforation. In all such injuries the hearing should be carefully tested, and the possibility of an injury to the labyrinth investigated by means of the tuning-fork test. Prognosis as regards hearing should be guarded at first. As a rule the rupture heals rapidly, and no treatment is necessary save the introduction of a piece of cotton-wool into the meatus. Syringing should be avoided unless suppuration has already occurred, in which case treatment for this condition must be adopted. As these injuries frequently have a medico-legal bearing, careful notes should be made.
Acute Infection of the Middle Ear.—This usually arises in connection with infective conditions of the throat and naso-pharynx. It varies considerably in its severity, and may run a mild or a severe course. It is characterised by pain in the ear, deafness, and a certain degree of fever. In children the symptoms may simulate those of meningitis. When the tympanic membrane is examined in the mild forms of the affection or in the early stages of the more severe type, the vessels about the handle of the malleus and periphery of the membrane are injected, and possibly a number of injected vessels may be seen coursing across the surface of the membrane. In the later stages the whole membrane presents a red surface, the anatomical landmarks being indistinguishable, the membrane bulges outwards into the meatus, and, if an abscess is pointing, a yellowish area may be visible upon it. The sudden cessation of pain and the appearance of a discharge from the meatus indicate perforation of the membrana tympani.
The treatment of acute otitis media varies with the severity of the attack. The patient should be confined to the house or to bed, alcohol and tobacco should be forbidden, and the bowels must be freely opened. Pain may be allayed by repeated instillations of cocain and carbolic acid (5 grains of each to a dram of glycerine). A few drops of laudanum, hot boracic instillations, or the application of a dry hot sponge, may prove soothing. Two or three leeches may be applied over the mastoid, but should the pain persist or should rupture of the membrane appear imminent, paracentesis must be carried out. After spontaneous perforation or puncture, the meatus must be kept clean. It is probably safer not to inflate through the Eustachian tube in the acute stage. Attention must be paid to any affection of the nose or throat that may be present.
Chronic Suppuration in the Middle Ear.—Acute suppuration may pass into the chronic variety, which is characterised by a perforation of the tympanic membrane, a persistent purulent or muco-purulent discharge from the middle ear, and a certain amount of deafness.
Various complications may arise in the course of chronic middle-ear disease, and so long as a person is the subject of a chronic otorrhœa, he is liable to one or more of these. The complications may be extra-cranial or intra-cranial. Those affecting the middle ear itself include granulations, polypi, cholesteatoma, caries and necrosis of the temporal bone, destruction and loss of one or more of the ossicles, facial paralysis, hæmorrhage from the carotid artery or jugular vein, and malignant disease. As mastoid complications may be mentioned: suppurative mastoiditis, leading to destruction of the bone, mastoid fistula, and sub-periosteal mastoid abscess. The intra-cranial complications that may arise are: extra-dural abscess, sub-dural abscess, meningitis, cerebral and cerebellar abscess, and lateral sinus phlebitis with general septicæmia and pyæmia.
The treatment of chronic middle-ear suppuration consists in keeping the parts clean by syringing with antiseptic lotions. The installation of hydrogen peroxide, followed by syringing with boiled water or boracic lotion, and inflation through the Eustachian tube once, twice, or thrice daily, according to the requirements of the case, constitute a routine method. Packing the meatus with antiseptic gauze after washing out may be practised.
Suppuration in the Tympanic Antrum and Mastoid Cells, or Acute Suppurative Mastoiditis.—Acute suppuration may occur in the mastoid cells in the course of an attack of acute otitis media, or as a result of interference with drainage in chronic suppuration of the antrum and middle ear. As the outer wall of the mastoid is liable to be perforated by cario-necrosis, the pus may find its way externally and form an abscess over the mastoid process behind the ear. In some cases the pus escapes into the external auditory meatus by perforating its posterior wall; in others a sinus forms on the inner side of the apex of the mastoid, and the pus burrows in the digastric fossa under the sterno-mastoid—Bezold's mastoiditis. If the posterior wall or roof of the antrum is destroyed, intra-cranial complications are liable to ensue.
The clinical features are pain behind the ear, tenderness on pressure or percussion over the mastoid, redness and œdematous swelling of the skin, and, when pus forms under the periosteum, the œdema may be so great as to displace the auricle downwards and forwards (Fig. 265). The deeper part of the posterior osseous wall of the meatus may be swollen so that it conceals the upper and back part of the membrane.
Treatment.—When arising in connection with acute otitis, the application of several leeches behind the ear, free incision of the membrane, and syringing with hot boracic lotion may be sufficient. As a rule, however, it is necessary to expose the interior of the antrum by opening through the mastoid cells—Schwartze's operation. When mastoid suppuration is associated with chronic middle-ear disease, it is usually necessary to perform the complete radical operation—Stacke-Schwartze operation. The operations are described in Operative Surgery, p. 98.
[6] Revised by Dr. Logan Turner.
Fracture of the Nasal Bones and Displacement of the Cartilages.—These injuries are always the result of direct violence, such as a blow or a fall against a projecting object, and in spite of the fact that the fracture is usually compound through tearing of the mucous membrane, infective complications are rare. The fracture usually runs transversely across both nasal bones near their lower edge, but sometimes it is comminuted and involves also the frontal processes of the maxillæ. In nearly all cases the cartilage of the septum is bent or displaced so that it bulges into one or other nostril, and not infrequently a hæmatoma forms in the septum (p. 573). Sometimes the perpendicular plate of the ethmoid is implicated, and the fracture in this way comes to involve the base of the skull. The nasal ducts may be injured, obstructing the flow of the tears, and a lachrymal abscess and fistula may eventually form.
The clinical features are pain, bleeding from the nose, discoloration, and swelling. Crepitus can usually be elicited on pressing over the nasal bones. The deformity sometimes consists in a lateral deviation of the nose, but more frequently in flattening of the bridge—traumatic saddle nose. Within a few hours of the injury the swelling is often so great as to obscure the nature of the deformity and to render the diagnosis difficult. Subcutaneous emphysema is not a common symptom; when it occurs, it is usually due to the patient forcing air into the connective tissue while blowing his nose. The lateral cartilages may be separated from the nasal bones and give rise to clinical appearances which simulate those of fracture. Sometimes the septum is displaced laterally without the bone being broken, and this causes symptoms of nasal obstruction.
Treatment.—As the bones unite rapidly, it is of great importance that any displacement should be reduced without delay, and to facilitate this a general anæsthetic should be administered, or the nasal cavity sprayed with cocain. The bones can usually be levered into position with the aid of a pair of dressing forceps passed into the nostrils, the blades being protected with rubber tubing. After the fragments have been replaced and moulded into position, it is seldom necessary to employ any retaining apparatus, but the patient must be warned against blowing or otherwise handling the nose. When the septum is damaged and the bridge of the nose tends to fall in, rubber tubes may be placed in the nostrils to give support, or, if this is not sufficient, a soft lead or gutta-percha splint should be moulded over the nose, and the splint and the fragments transfixed with one or more hare-lip pins. These may be removed on the fourth or fifth day. Rigid appliances introduced into the nostrils are to be avoided if possible, as they are uncomfortable and interfere with proper cleansing and drainage of the nose. The inside of the nose should be smeared with vaseline to prevent crusting of blood, and the nasal cavities should be frequently irrigated.
Deformities of the Nose.—The most common deformity is that known as the sunken-bridge or saddle nose (Volume I., p. 174). It is most frequently a result of inherited syphilis, the nasal bones being imperfectly developed, and the cartilages sinking in so that the tip of the nose is turned up and the nostrils look directly forward. The bridge of the nose may sink in also as a result of necrosis of the nasal bones, particularly in tertiary syphilis, and less frequently from tuberculous disease. A similar, but as a rule less marked deformity may result from fracture of the nasal bones or from displacement of the cartilages.
When the condition is due to mal-union of a fracture, the contour of the nose may be restored by operation. A narrow knife is passed in at the nostril and the skin freely separated from the bone; the bone is then broken into several pieces with necrosis forceps, and the fragments moulded into shape. A rubber drainage tube introduced into each nostril maintains the contour of the nose till union has taken place.
When it results from disease, it is much less amenable to treatment. The present-day tendency is to discard the use of subcutaneous paraffin injection and to employ grafts of cartilage or bone. An artificial bridge has been made by turning down from the forehead a flap, including the periosteum and a shaving of the outer table of the skull, or by implanting portions of bone or plates of gold, aluminium, or celluloid.
Portions of the alæ nasi may be lost from injury, or from lupus, syphilis, or rodent cancer. After the destructive process has been arrested, the gap may be filled in by a flap taken from the cheek or adjacent part of the nose. When the tip of the nose is lost, it may be replaced by Syme's operation, which consists in raising flaps from the cheeks and bringing them together in the middle line.
The whole of the nose, including the cartilages and bones, may be destroyed by syphilitic ulceration or by lupus. In parts of India the nose is sometimes cut off maliciously or as a punishment for certain crimes.
In reconstructing the nose it is necessary to provide skin, a supporting structure in the form of cartilage or bone, and an epithelial lining. In the “Indian operation” a racket-shaped flap, including skin and periosteum, is turned down from the forehead and fixed in position, the edges of the flap being inturned to provide a lining for the passage. An implant of free cartilage may be necessary to support the skin flaps and to prevent subsequent contraction. Flaps of skin may be formed by Gillies' tube-pedicle method from the cheek, the forehead, or the neck, and utilised to form the covering of the nose. When the deformity cannot be corrected by operation, the appearance may be greatly improved by wearing an artificial nose held in position by spectacles.
The term Rhinophyma has been applied by Hebra to a condition in which the skin of the tip and alæ of the nose becomes thick and coarse, and presents large, irregular, tuberous masses on which the orifices of the sebaceous follicles are unduly evident—potato or hammer nose (Fig. 266). The capillaries of the skin are dilated and tortuous, and the nose assumes a bluish-red colour, and its surface is soft and greasy. The condition is met with in elderly men, and the masses appear to be chiefly composed of sebaceous adenomas. The term lipoma nasi, formerly employed, is therefore misleading.
The treatment consists in paring away the protuberant masses until the normal size and contour of the nose are restored, care being taken not to encroach on the cartilages or on the orifices of the nostrils. There is comparatively little bleeding, and the raw surface rapidly becomes covered with epidermis.
Examination of the Nasal Cavities.—For the examination of the interior of the nose the following appliances are necessary: A reflector, such as is used in laryngoscopy, attached to a forehead band or spectacle frame; one of the various forms of nasal speculum; a long, pliable probe; a tongue depressor; and a small-sized mirror. As additional aids, a 10 per cent. solution of cocain, a grooved probe as a cotton-wool holder, and a palate retractor should be in readiness. Good illumination is important, and may be obtained from an electric light, or from a Welsbach or Argand burner. The light should be placed close to, and on a level with, the patient's left ear. Both the anterior and posterior nares should be examined.
Anterior Rhinoscopy.—Before the introduction of the speculum the tip of the nose should be tilted up and the interior of the vestibule and the anterior part of the septum examined. In this way the existence of eczema or small furuncules, the presence of dilated or bleeding vessels upon, or a perforation of, the anterior part of the septum may be noted, and the general appearances observed. After inserting the speculum into the vestibule and dilating it, the following parts should be sought for and examined:—Close to the floor, and attached to the outer wall of the nasal cavity, is the anterior end of the inferior concha or turbinated body (Fig. 267), which overhangs the inferior meatus. It presents a pink appearance, and its size varies in different persons. At a higher level and on a posterior plane is the anterior end of the middle concha or turbinated body, which is of a paler colour than the inferior, and is only visible when the head is tilted backwards. Between it and the inferior turbinated body is the middle meatus, with which communicate the openings of the maxillary sinus, the frontal sinus, and the anterior ethmoidal cells. A considerable area of the anterior part of the nasal septum is also visible by anterior rhinoscopy, and between it and the middle turbinal is a narrow chink—the olfactory sulcus.
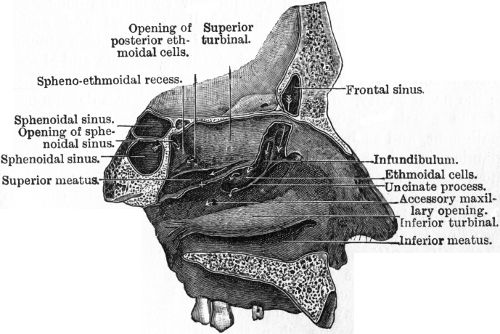 Fig. 267.—The outer wall of Left Nasal Chamber, after
removal of the middle turbinated body. (After Logan Turner.)
Fig. 267.—The outer wall of Left Nasal Chamber, after
removal of the middle turbinated body. (After Logan Turner.)
Posterior Rhinoscopy.—Examination of the posterior nares and naso-pharynx is frequently attended with difficulty. The patient is directed to breathe through the nose, the tongue is depressed with a spatula, and a small-sized laryngeal mirror, comfortably warmed and with its reflecting surface turned upwards, is introduced behind the soft palate. When a good examination of the naso-pharynx is obtained, the following parts may be seen reflected in the mirror: the posterior surface of the uvula and soft palate, and above them, in the mesial plane, the posterior free edge of the septum nasi; on each side of the septum the apertures of the posterior nares, in which may be seen the upper part of the posterior end of the inferior turbinal, the middle meatus, the posterior end of the middle turbinal, the superior meatus, and occasionally a portion of the superior turbinal. On the lateral wall of the naso-pharynx the Eustachian opening and cushion can be seen, while by tilting the mirror backwards the vault of the naso-pharynx can be inspected.
Digital examination of the naso-pharynx may be required, especially in children. The examiner passes his left arm and hand round the back of the child's head, and with one of his fingers presses the cheek inwards, between the jaws. His right forefinger is carried along the dorsum of the tongue, passed up behind the soft palate and a rapid examination made of the post-nasal space.
Cardinal Symptoms of Nasal Affections.—The chief symptoms of nasal disease are: nasal obstruction, nasal discharge, anomalies of smell and taste, and certain reflex phenomena.
Nasal Obstruction.—This may be partial or complete, intermittent or constant, and may be the cause of such symptoms as alteration in the tone of the voice, catarrh of the respiratory passages, snoring, cough, headache, inability to concentrate the attention, alteration in the physiognomy, or deformity of the chest. The half-open mouth, drooping jaw, lengthened appearance of the face, narrow nostrils, and vacant expression are characteristic signs of nasal obstruction.
Nasal obstruction may be due to intra-nasal or to post-nasal (naso-pharyngeal) causes. Amongst the former may be noted as the more common, erectile swelling and hypertrophy of the mucous membrane covering the inferior turbinated bones, and nasal polypi growing from the middle turbinal and middle meatal region. Causes originating in the septum include deviations, spines, and ridges, and septal hæmatoma and abscess. Obstruction may also be due to the presence of a foreign body in the nasal cavity, to a rhinolith, and to imperfect development of the nasal chambers. Further, tumours, both simple and malignant, and such conditions as tubercle, lupus, syphilis, and glanders may interfere more or less with nasal respiration. The most common cause of post-nasal obstruction is the presence of adenoids; more rarely fibro-mucous polypi, fibrous tumours, malignant disease, and cicatricial contractions and adhesions resulting from syphilis are met with.
Erectile swelling of the inferior turbinated bodies is due to engorgement of the venous spaces contained in the mucous membrane. Obstruction from this cause is usually intermittent in character, and may be unilateral or bilateral. It is influenced by posture, being worse when the patient is in the horizontal position, and also by changes in atmospheric conditions and temperature. It is characterised objectively by a swelling of the mucous membrane, which is pink or red in appearance and of a soft consistence, pitting when touched with the probe, and shrinking on the application of a 5 per cent. solution of cocain. Its soft consistence and the fact that it becomes smaller when painted with cocain differentiate it from true hypertrophy of the mucous membrane. Its situation and immobility, its pink colour, and the shrinkage under cocain, distinguish it from the mucous polypus of the nose. The turgescence may involve the whole extent of the mucosa of the inferior turbinated bodies, including their posterior ends. After anæsthetising with cocain, the electric cautery, or fused chromic acid applied on a probe, may be employed for the relief of the condition. If a true hypertrophy exists, it is better to remove it with a nasal snare.
Nasal polypi spring from the mucous membrane covering the middle turbinated bone and from the adjacent parts of the middle meatus, but rarely from the septum. They consist of œdematous masses of mucous membrane, and are as a rule multiple. They are usually pedunculated, and as they increase in size they become pendulous in the nasal cavity. They are smooth, rounded in outline, of a translucent bluish-grey colour, soft in consistence, and freely movable. These characters, and the fact that the probe can be passed round the greater part of the polypus, serve to differentiate this affection from the erectile swelling. It must not be forgotten that nasal polypi may be associated with suppuration in one or more of the accessory sinuses. They are frequently present also in malignant disease, and in these cases they bleed readily. They are best removed by means of the cold snare, with the aid of the speculum and a good light. Several sittings are usually necessary.
Carcinoma and sarcoma sometimes grow from the muco-periosteum in the region of the ethmoid. They tend to invade adjacent parts, giving rise to hæmorrhage and symptoms of nasal obstruction, and as they increase in size they may cause considerable deformity of the face. If diagnosed early, an attempt should be made to remove the growth.
Deviations, spines, and ridges of the septum may produce partial or complete occlusion of the anterior nares. In deviation of the septum, the obstructed nostril is more or less occluded by a smooth rounded swelling of cartilaginous or bony hardness, which is covered with normal mucous membrane, while the opposite nostril shows a corresponding concavity or hollowing of the septum. Sometimes the convex side is thickened in the form of a ridge. A simple spine of the septum is usually situated anteriorly, and presents an acuminate appearance, often pressing against the inferior turbinated body; it is hard to the touch. Ridges and spines may be cut or sawn off, or removed with the chisel. Many methods of dealing with a deviated septum have been suggested, such as forcible fracture or excision of a portion of the cartilage. A submucous resection of the deflected portion is to be preferred.
Hæmatoma of the septum is usually traumatic in origin. As the result of a blow, an extravasation of blood takes place beneath the perichondrium on each side of the septum, and a bilateral, symmetrical swelling, smooth in outline and covered with mucous membrane, is visible immediately within the anterior nares. The blood is usually absorbed and should not be interfered with. If suppuration occurs, however, the swelling becomes soft, fluctuation can be detected, and the patient's discomfort increases. The abscess must then be incised and the cavity drained. It is sometimes found that a portion of the cartilage undergoes necrosis, leading to perforation of the septum.
Nasal discharge may be mucous, muco-purulent, or purulent in character. When it is of a clear, watery nature, it is usually associated with erectile swelling of the inferior turbinated bodies. A purulent discharge may be complained of from one or both nostrils. If unilateral, it should suggest, in the case of children, the presence of a foreign body; in adults, the possibility of suppuration in one or more of the accessory sinuses. In infants, a purulent discharge from both nostrils may be due to gonorrhœal infection or to inherited syphilis. Nasal discharge may be constant or intermittent. It is sometimes influenced by changes in posture; for example, it may be chiefly complained of at the back of the nose and in the throat when the patient occupies the horizontal position, or it may flow from the nostril when he bends his head forward or to one side. The discharge may be intra-nasal in origin, or due altogether to naso-pharyngeal catarrh. It varies somewhat in colour and consistence, and may be associated with such intra-nasal conditions as purulent rhinitis following scarlet fever and other exanthemata or ulceration accompanying malignant disease, syphilis, or tuberculosis. Sometimes it contains shreds of false membrane, for example in nasal diphtheria; or white cheesy masses as in coryza cascosa. The formation of crusts is significant of fœtid atrophic rhinitis (ozæna) and syphilis, and in these conditions the discharge is associated with a most objectionable and distinctive fœtor. Pus from the maxillary sinus is often fœtid, and the odour is noticed by the patient; while the odour of ozæna is not recognised by the patient, although very obvious to others.
Foreign bodies of various descriptions have been met with in the nasal cavities, particularly of children. They set up suppuration and give rise to a unilateral discharge, which is often offensive in character. The surgeon must not be satisfied with the history given by the parents, but, with the aid of good illumination, and, in young children, under general anæsthesia, the nose should be carefully inspected and probed. If there is much swelling, the introduction of a 5 per cent. solution of cocain will facilitate the examination by diminishing the congestion of the mucous membrane. No attempt should be made to remove a foreign body from the nose by syringing. If fluid is injected into the obstructed nostril, it is liable to force the body farther back, while, if injected into the free nostril, it is apt to accumulate in the naso-pharnyx and to pass into the Eustachian tubes. A fine hook should be passed behind the body and traction made upon it, or sinus forceps or a snare may be employed. Care must be taken that the body is not pushed still deeper into the cavity. Fungi and parasites should first be killed with injections of chloroform water, or by making the patient inhale chloroform vapour.
Rhinoliths.—Concretions having a plug of inspissated mucus or a small foreign body as a nucleus sometimes form in the nose. They are composed of phosphate and carbonate of lime, and have a covering of thickened nasal secretion. They are rough on the surface, dark in colour, and usually lie in the inferior meatus. They give rise to the same symptoms as a foreign body, and are treated in the same way. The stone, which is usually single, may be so large and so hard that it is necessary to crush it before it can be removed.
Ozæna, or fœtid atrophic rhinitis, is characterised by atrophy of the nasal mucous membrane, and sometimes even of the turbinated bones, and is accompanied by a muco-purulent discharge and the formation of crusts having a characteristic offensive odour, which is not recognised by the patient. It is usually bilateral, and the nasal chambers, owing to the atrophy, are very roomy. It may be differentiated from a tertiary syphilitic condition by the absence of ulceration and necrosis of bone, by the odour, and by the fact that it is not influenced by anti-syphilitic treatment.
Various methods of treatment are in vogue, but thorough cleanliness is the most essential factor, and this is best secured by regular syringing. Plugging of the nostrils with cotton-wool for half an hour before washing out the nose greatly facilitates the detachment of the crusts. A pint of lukewarm solution containing a teaspoonful of bicarbonate of soda or of common salt, is then used with a Higginson's syringe, the patient leaning over a basin and breathing in and out quickly through the open mouth. The patient should then forcibly blow down each nostril in turn, the other being occluded with the finger, so that the infective material may thus be blown out without risk of it entering the Eustachian tubes, as may happen when the handkerchief is used in the ordinary way. Antiseptic sprays, such as peroxide of hydrogen, and ointments may be applied to the mucous membrane after cleansing.
Epistaxis.—Bleeding from the nose may be due either to local or to general causes. Among the former may be cited injuries such as result from the introduction of foreign bodies, blows on the face, and fractures of the anterior fossa of the skull, and the ulceration of syphilitic, tuberculous, or malignant disease. Amongst the general conditions in which nasal hæmorrhage may occur are typhoid fever, anæmia, and purpura cardiac and renal disease, cirrhosis of the liver, and whooping-cough. Prolonged oozing of blood may be an evidence of hæmophilia. Nasal hæmorrhage usually takes place from one or more dilated capillaries situated at the anterior inferior part of the septum close to the vestibule, and in such cases the bleeding point is readily detected. Occasionally bleeding occurs from one of the anterior ethmoidal veins, and under these circumstances the blood flows downwards between the middle turbinal and the septum. Before steps are taken to arrest the bleeding, the interior of the nose should, if possible, be inspected and the bleeding point sought for. As a preliminary to the use of local applications, the nose should be washed out with boracic lotion or salt solution to remove all clots from the cavity. In many cases this is all that is necessary to stop the bleeding. If the bleeding is not very copious, it may be stopped by grasping the alæ nasi between the finger and thumb, or by spraying the nasal cavity with adrenalin. If the blood is evidently flowing from the olfactory sulcus, a strip of gauze soaked in adrenalin, turpentine, or other styptic should be packed between the septum and middle turbinated body. If recurrent hæmorrhage takes place from the anterior and lower part of the septum, the application of the electric cautery at a dull red heat, or of the chromic acid bead fused on a probe, is the best method of treatment. Plugging of the posterior nares is rarely necessary, as, in the majority of cases, an anterior plug suffices. In bleeders, the administration of sheep serum by the mouth has proved efficacious.
Suppuration in the Accessory Nasal Sinuses.—As already stated, the presence of pus in the nose should always direct attention to its possible origin in one or more of the accessory sinuses, especially if the discharge is unilateral. The condition is usually a chronic one, and may be present for months, or even years, without the patient suffering much inconvenience save from the presence of the discharge.
If on examination by anterior rhinoscopy, pus is seen in the middle meatus, suspicion should be aroused of its origin in the maxillary sinus, frontal sinus, or anterior ethmoidal cells, as all these cavities communicate with that channel. If, on the other hand, the pus is detected in the olfactory sulcus, attention must be directed to the posterior ethmoidal cells and sphenoidal sinus (Fig. 267). Further evidence of its source in the last-named cavities may be gained by finding pus in the superior meatus above the middle turbinal on examination by posterior rhinoscopy.
As the anterior group of sinuses is most frequently affected, and of these most commonly the maxillary sinus, attention should first be turned to this cavity. Pain, tenderness on pressing over the canine fossa or on tapping the teeth of the upper jaw, and swelling of the cheek are rarely met with save in acute inflammation. The complaint of a bad odour or taste, the reappearance of pus in the middle meatus after mopping it away and directing the patient to bend his head well forwards, and opacity on trans-illumination of the suspected cavity, are signs which strongly suggest an affection of the maxillary sinus. The withdrawal of pus by a puncture through the thin outer wall of the inferior meatus of the nose with a fine trocar and cannula will establish the diagnosis.
The treatment consists in opening and draining the sinus. If the infection is due to a carious tooth, this should be extracted, the socket opened up and drainage established through it in recent cases. If the teeth are sound, and the case is of long duration, the sinus is opened through the canine fossa and its walls curetted. To avoid the risk of reinfecting the cavity from the mouth, an opening may be made into the nose by removing a portion of the nasal wall of the sinus and part of the inferior turbinated bone, after which the incision in the buccal mucous membrane is closed with sutures.
Suppuration in the frontal sinus is attended with frontal headache, vertigo, especially on stooping, and tenderness on pressure, particularly over the internal orbital angle, or on percussion over the frontal region. Pus escapes into the middle meatus of the nose, and if wiped away will reappear if the head is kept erect for a few minutes. After removal of the anterior end of the middle turbinated bone, it may be possible to catheterise the sinus and wash out pus from its interior. The diseased sinus may present a darker shadow than the healthy one on trans-illumination, or in an X-ray photograph.
The treatment consists in exposing the anterior wall of the sinus, chiselling away sufficient bone to admit of free removal of all infected tissue, and establishing efficient drainage through the infundibulum (Fig. 267) into the nose.
The anterior ethmoidal cells (Fig. 267) are frequently affected in conjunction with the frontal, and sometimes with the maxillary sinus. The presence of polypi and granulations, with pus oozing out from between them, and increasing after withdrawal of the probe, and the detection of carious bone are significant of ethmoidal suppuration.
The treatment consists in extending the operation for the frontal or maxillary sinus so as to ensure drainage of the ethmoidal cells.
Suppuration in the sphenoidal sinus (Fig. 267) is characterised in many cases by the presence of eye symptoms. Pus in the olfactory sulcus, on the upper surface of the middle turbinal posteriorly, and on the vault of the naso-pharynx, is suggestive of sphenoidal suppuration. The removal of the middle turbinated bone permits of inspection of the ostium sphenoidale by anterior rhinoscopy, and pus may be seen escaping from the orifice. A probe is then passed into the ostium, and the anterior wall of the sinus is removed with a curette or rongeur forceps.
The posterior ethmoidal cells (Fig. 267) are frequently affected along with the sphenoidal sinus. The nasal appearances just noted are present, and if the sphenoidal sinus can be washed out and its ostium temporarily plugged, and pus rapidly reappears, its origin from these cells is probable. The operation for draining the sphenoidal sinus is extended by removing the inner wall of the posterior ethmoidal cells.
Anomalies of Smell and Taste.—Anosmia or loss of smell and impairment or loss of the sense of recognising flavours may follow fracture of the anterior fossa attended with injury of the olfactory nerves, and is a common sequel of influenza. Any lesion that prevents the passage of the odoriferous particles to the olfactory region of the nose interferes with the sense of smell. In ozæna also the sense of smell is lost. Parosmia, or the sensation of a bad odour, may be of functional origin; it sometimes occurs after influenza. It may also be associated with maxillary suppuration.
Reflex Symptoms of Nasal Origin.—It is only necessary here to draw attention to the relation that exists between affections of the nose and asthma. When present in asthmatic subjects, nasal polypi, erectile swelling of the inferior turbinated bodies, spines of the septum in contact with the inferior turbinal, or areas on the mucous membrane which, when probed, produce coughing, call for treatment with the object of modifying the asthma.
Post-nasal Obstruction—Adenoid Vegetations.—The most common cause of post-nasal obstruction is hypertrophy of the normal lymphoid tissue which constitutes the naso-pharyngeal or Luschka's tonsil. Adenoids form a soft, velvety mass, which projects from the vault of the naso-pharynx and extends down its posterior and lateral walls, in some cases filling up the fossæ of Rosenmüller behind the Eustachian cushions. They do not grow from the margins of the posterior nares. Adenoids are frequently associated with hypertrophy of the faucial tonsils, and the patient often suffers from granular pharyngitis and chronic nasal catarrh.
These growths are sometimes met with in infants, but are most common between the ages of five and fifteen, after which they tend to undergo atrophy. They may, however, persist into adult life.
Clinical Features.—The most prominent symptom in most cases is interference with nasal respiration, so that the patient is compelled to breathe through the mouth. The facies of adenoids is characteristic: the mouth is kept partly open, the face appears lengthened, the nose is flattened by the falling in of the alæ nasi, the inner angles of the eyes are drawn down, and the eyelids droop, while the whole facial expression is dull and stupid. As the respiratory difficulty is increased during sleep, the patient snores loudly, and his sleep is frequently broken by sudden night terrors. Owing to the disturbed sleep, to imperfect oxygenation of the blood, and to frequent attacks of nasal and bronchial catarrh, the child's nutrition is interfered with, and he becomes languid and backward at his lessons.
When the adenoids encroach upon the Eustachian cushions, the patient suffers from deafness, frequent attacks of earache, and sometimes from suppurative otitis media with a discharge from the ear.
Among the rarer conditions attributed to adenoids are asthma, inspiratory laryngeal stridor, persistent cough, chorea, and nocturnal enuresis.
A diagnosis should never be made from the symptoms alone; an attempt must be made to examine the naso-pharynx by posterior rhinoscopy and by digital examination. The interior of the nose must always be examined and any further cause of obstruction excluded.
Treatment.—Thorough removal is the only satisfactory line of treatment, and this should be done under general anæsthesia. The following instruments are necessary: two Gottstein's adenoid curettes, one provided with a cradle and hooks, the other without, a Hartmann's lateral ring knife, and one pair of adenoid forceps—Kuhn's or Lœwenberg's—a tongue depressor, a gag, and one or two throat sponges on holders. The patient having been anæsthetised, his head should be drawn over the end of the table. An assistant standing on the left side inserts the gag and maintains it in position. The operator, being on the patient's right, depresses the tongue and insinuates the curette provided with the hooks behind the soft palate, carrying it to the roof of the naso-pharynx between the growth and the posterior free edge of the nasal septum. Firm pressure is then made against the vault of the naso-pharynx, and the curette is carried backwards and downwards in the mesial plane and withdrawn with the main mass of the adenoids caught in the hooks. The unguarded curette is then introduced and several strokes are made with it, the instrument being carried on either side of the mesial plane. With Hartmann's lateral ring knife the posterior naso-pharyngeal wall and fossæ of Rosenmüller are curetted. The curette should not be used on the lateral pharyngeal wall in case the Eustachian orifices and cushions are damaged. Bleeding soon ceases when the head is again elevated, and the patient should be at once laid well over upon his side so that the blood may escape from the mouth.
No local after-treatment is required, and spraying or syringing may prove harmful. The patient should remain in the house for five or six days. If nasal obstruction has been the outstanding symptom, respiratory exercises through the nose should be carried out for some considerable time; on the other hand, if Eustachian obstruction and deafness have been the main features of the case, a course of Politzer inflation should be conducted after the wound has healed.
Tumours of the Naso-Pharynx.—Tumours are occasionally met with growing from the muco-periosteum of the basi-sphenoid and basi-occipital, and projecting from the vault of the naso-pharynx—naso-pharyngeal tumour or retro-pharyngeal polypus. This usually occurs between the ages of fifteen and twenty, and while it may originally be a fibroma, it tends to assume the characters of a fibro-sarcoma and to exhibit malignant tendencies. At first the tumour is firm, rounded, and of slow growth, but later it becomes softer, more vascular, and grows more rapidly, spreading forwards towards the nasal cavity and downwards towards the pharynx.
Clinical Features.—In its growth the tumour blocks the nostrils, and so interferes with nasal respiration and causes the patient to snore loudly, especially during sleep. It may also bulge the soft palate towards the mouth and interfere with deglutition. In some cases the face becomes flattened and expanded and the eyes are pushed outwards, giving rise to the deformity known as frog-face. Deafness may result from obstruction of the Eustachian tube. The patient suffers from intense frontal headache, and there is a persistent and offensive mucous discharge from the nose. Profuse recurrent bleeding from the nose is a common symptom, and the patient becomes profoundly anæmic. The tumour can usually be seen on examination with the nasal speculum or by posterior rhinoscopy, and its size and limits may be recognised by digital examination.
Unless removed by operation these tumours prove fatal from hæmorrhage, interference with respiration, or by perforating the base of the skull and giving rise to intra-cranial complications.
Treatment.—These growths are seldom recognised before they have attained considerable dimensions, and owing to the fact that they are permeated by numerous large, thin-walled venous sinuses, their removal is attended with formidable hæmorrhage. Attempts to remove them by the galvanic snare are seldom satisfactory, because the base of the tumour is left behind and recurrence is liable to take place. The operative treatment is described in Operative Surgery, p. 153.
Surgical Anatomy.—In the middle line the following structures may be recognised on palpation: (1) the hyoid bone, lying below and behind the body of the lower jaw, on a level with the fourth cervical vertebra; (2) the hyo-thyreoid membrane, behind which lies the base of the epiglottis and the upper opening of the larynx; (3) the thyreoid cartilage, to the angle of which the vocal cords are attached about its middle; (4) the crico-thyreoid membrane, across which run transversely the crico-thyreoid branches of the superior thyreoid arteries; (5) the cricoid cartilage, one of the most important landmarks in the neck. It lies opposite the disc between the fifth and sixth cervical vertebræ, and at this level the common carotid artery may be compressed against the carotid tubercle on the transverse process of the sixth cervical vertebra. The cricoid also marks the junction of the larynx with the trachea, and of the pharynx with the œsophagus; at this point there is a constriction in the food passage, and foreign bodies are frequently impacted here. At the level of the cricoid cartilage the omo-hyoid crosses the carotid artery—a point of importance in connection with ligation of that vessel. The middle cervical ganglion of the sympathetic lies opposite the level of the cricoid. (6) Seven or eight rings of the trachea lie above the level of the sternum, but they cannot be palpated individually. The isthmus of the thyreoid gland covers the second, third, and fourth tracheal rings. As the trachea passes down the neck, it gradually recedes from the surface, till at the level of the sternum it lies about an inch and a half from the skin. The thyreoidea ima artery—an inconstant branch of the anonyma (innominate) or of the aorta—runs in front of the trachea as far up as the thyreoid isthmus. The inferior thyreoid plexus of veins also lies in front of the trachea. In the superficial fascia, cross branches between the anterior jugular veins cross the middle line.
In children under two years of age the thymus gland may extend for some distance into the neck in front of the trachea and carotid vessels, under cover of the depressors of the hyoid bone.
Cervical Fascia.—This fascia completely envelops the neck, and from its deep aspect two strong processes—the prevertebral and pretracheal layers—pass transversely across the neck, dividing it into three main compartments. The posterior or vertebral compartment contains the muscles of the back of the neck, the vertebral column and its contents, and the prevertebral muscles. This compartment is limited above by the base of the skull, and below is continued into the posterior mediastinum. The middle or visceral compartment contains the pharynx and œsophagus, the larynx and trachea with the thyreoid gland, and the carotid sheath and its contents. These different structures derive their special fascial coverings from the processes that bound this compartment. The middle compartment extends to the base of the skull and passes into the anterior mediastinum as far as the pericardium. The connective tissue space around the subclavian vessels is continued into the axilla. The anterior or muscular compartment contains the sterno-mastoid muscle and the depressor muscles of the hyoid bone. It extends upwards as far as the hyoid bone and base of the mandible, and downwards as far as the sternum and clavicle. The arrangement and limits of the different layers of the cervical fascia explain the course taken by inflammatory products and by new growths in the neck.
Malformations of the Neck.—Various congenital deformities result from interference with the developmental processes which take place in and around the fore-gut. These malformations are associated chiefly with imperfect development of the visceral or branchial arches and clefts, or of the hypoblastic diverticula from which the thyreoid and thymus glands are formed.
The term cervical auricles is applied to small outgrowths, composed of skin, connective tissue, and yellow elastic cartilage, found usually along the anterior border of the sterno-mastoid. These appendages are usually unilateral, and are derived from the second visceral arch. Sometimes they are situated near the orifice of a lateral fistula. When, on account of their size, or their situation on an exposed part of the neck, they give rise to disfigurement, they should be removed.
Thyreo-glossal Cysts and Fistulæ.—The thyreo-glossal cyst is developed in relation to the thyreo-glossal tract of His, which in early embryonic life extends from the foramen cæcum at the base of the tongue to the isthmus of the thyreoid. Those that form in the upper part of the tract, in relation to the base of the tongue, have already been described (p. 538). Those arising from the lower part form a swelling in the middle line of the neck, usually above, but sometimes below the hyoid bone. They have to be diagnosed from other forms of cyst occurring in the middle line of the neck—sebaceous and dermoid cysts—and when giving rise to disfigurement they should be excised.
Such a cyst may rupture on the surface, usually as a result of superadded infection, and give rise to a thyreo-glossal or median fistula of the neck. As a rule the external opening of the fistula is above the hyoid bone, only the upper part of the duct having remained pervious. When the whole length of the duct has persisted, the fistula extends from the skin to the foramen cæcum, passing usually in front of, but sometimes through the substance of, the hyoid bone. Occasionally the fistula only extends as high as the hyoid.
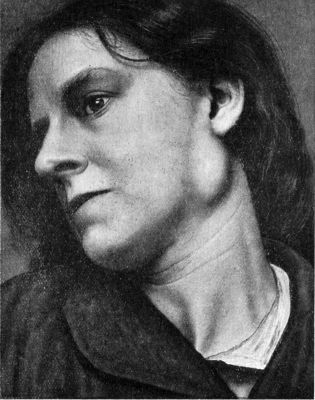 Fig. 268.—Congenital Branchial Cyst in a woman æt. 33.
Fig. 268.—Congenital Branchial Cyst in a woman æt. 33.The part of the tract near the tongue is lined by squamous epithelium; the lower part by columnar epithelium, which, below the level of the hyoid, is usually ciliated. Lymphoid tissue and mucous glands are found in its wall.
The treatment consists in excising the duct and the connections, and it is usually necessary to resect the central portion of the hyoid bone to ensure complete removal.
The lateral fistula of the neck—formerly described as a branchial fistula—according to Weglowski, usually takes origin from the remains of the hypoblastic diverticulum, which arises from the pharyngeal part of the third visceral cleft and extends downwards to form the thymus gland. The internal opening is situated in the lateral wall of the pharynx in the region of the posterior palatine arch close to the tonsil, and the fistula passes out above the hypoglossal nerve, and runs downwards and laterally between the carotids and along the medial border of the sterno-mastoid muscle. When the fistula is complete, the external opening is situated a short distance above the sterno-clavicular joint. As the lower part of the thymus canal most often persists, an incomplete external fistula is the form most frequently met with. It is lined with ciliated columnar epithelium.
The fistula may be present at birth, or may result from the rupture of a cystic swelling, which has become infected. Clear viscous fluid exudes from it, and, when the fistula is complete and the lumen sufficiently wide, particles of food may escape. As the track is tortuous, it is seldom possible to pass a probe along it, but its extent and course may be recognised by injecting an emulsion of bismuth and taking an X-ray photograph.
The treatment consists in excising the fistula in its whole length, but, owing to its long and tortuous course, and its relations to important structures, the operation is a tedious and difficult one. Less radical measures, such as scraping with the sharp spoon, cauterising, or packing, are seldom successful.
Cervical Ribs.—Supernumerary ribs are not infrequently met with in connection with the seventh cervical vertebra, and in the majority of cases the condition is bilateral. The extra rib may be thin and pointed, and project straight out from the transverse process terminating in a free end, in which case, as it passes above the subclavian artery and the brachial plexus, it gives rise to no trouble. In other cases it arches downwards and forwards, and is attached by dense fibrous tissue to the first thoracic rib about the level of the scalene tubercle, or to the sternum by cartilage like an ordinary rib. When it encroaches upon the posterior triangle the scalene muscles are attached to it, and the subclavian artery and the lower trunk and medial cord of the brachial plexus pass over it in a groove behind the scalenus anterior. The pleura may reach as high as the medial border of the rib.
Clinical Features.—The condition, which is more common in women than in men, is seldom recognised before the age of twenty, and is often discovered accidentally, for example after some emaciating illness, or by a tight collar causing pain. The diagnosis is established by the X-rays.
When symptoms arise, they may be referable either to pressure on the artery or on the nerve roots. When the subclavian artery is displaced upwards it may be recognisable as a prominent pulsatile swelling, and as the part of the vessel distal to the rib is sometimes dilated and yields a systolic bruit, it may simulate an aneurysm (Sir William Turner). The pulse beyond is weakened while the arm hangs by the side, but may be restored by raising the hand above the head. Gangrene of the tips of the fingers has been observed in rare instances, but it is probably nervous rather than vascular in origin.
Symptoms referable to pressure on the nerve roots usually affect the right arm, and may be either neuralgic or paralytic in character (Wm. Thorburn). In the neuralgic group there is tingling pain, a feeling of numbness, and sensations of cold in the limb, most marked along the ulnar border of the forearm; the arm is weak, and susceptible to cold. This condition may be mistaken for brachial neuritis; it is relieved, however, by holding the arm above the head, for example, during sleep.
In the paralytic group, the pressure symptoms are referred to the first dorsal, or first dorsal and eighth cervical roots. The paralysis is most marked in the muscles of the thumb, and becomes less towards the ulnar side; the affected muscles atrophy, especially those forming the thenar eminence, and the finer movements of the thumb and fingers are impaired.
When pressure symptoms are present, the extra rib should be removed through an incision which exposes the posterior triangle sufficiently to admit of the bone and its periosteum being excised, without damage being inflicted on the brachial plexus, the subclavian artery, or the pleura.
Similar clinical features to those of cervical rib may be caused by a prominent transverse process of the first thoracic vertebra and similarly got rid of by its removal.
Branchial cysts and branchial tumours are described with tumours of the neck (p. 598).
Wry-Neck or Torticollis.—The term wry-neck or torticollis is applied to a condition in which the head assumes an abnormal attitude, which is usually one of combined lateral flexion and rotation.
The most important form is due to faulty action of the cervical muscles, and three varieties of muscular wry-neck are recognised—(1) the acute or transient; (2) the chronic or permanent; and (3) the spasmodic.
Acute or transient wry-neck—so-called “rheumatic torticollis”—comes on suddenly, usually after the patient has been exposed to a draught of cold air or to damp. The condition is popularly known as “stiff neck,” and is probably associated with fibrositis of the affected muscles. The sterno-mastoid, and often the trapezius, are contracted, and pull the head to one side, twisting the face slightly towards the opposite side (Fig. 270). There is tenderness on pressing over the affected muscles, and sometimes over the vertebral spines, and in the lines of the cervical nerves, and severe pain on attempting to move the head. Usually in the course of a few days the condition passes off as suddenly as it came on, but in some cases a certain amount of wasting of the affected muscles ensues.
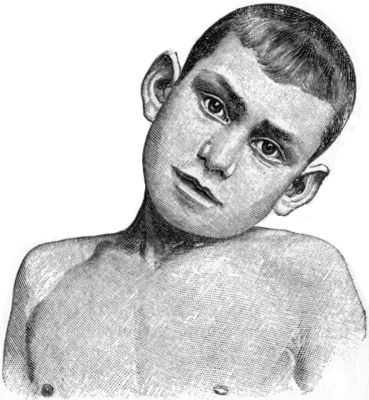 Fig. 270.—Transient Wry-neck, which came on suddenly
after sitting in a draught, and passed off completely in a few days.
Fig. 270.—Transient Wry-neck, which came on suddenly
after sitting in a draught, and passed off completely in a few days.
In the diagnosis of this form of wry-neck it is necessary to exclude such conditions as cellulitis, inflammation of the cervical glands, and disease of the cervical spine, in which the head may assume an abnormal attitude, the position being that which gives the patient greatest comfort.
The treatment consists in ensuring free action of the bowels and kidneys, in inducing hyperæmia by means of heat, and applying gentle massage. Salicylates and similar drugs are useful in relieving the pain.
Permanent or true wry-neck is due to an organic shortening of the sterno-mastoid muscle. The trapezius, the splenius, the scaleni, and the levator scapulæ muscle may also undergo shortening, along with their investing sheaths derived from the cervical fascia.
The sternal head of the sterno-mastoid is always markedly shortened, and stands out as a tight cord; sometimes the clavicular head is also prominent.
There is evidence that in the majority of cases the deformity results from some interference with the development of the muscles during intra-uterine life. This is probably the effect of undue pressure on the fœtus diminishing the arterial supply to the central part of the muscle, with the result that the muscle fibres undergo degeneration with subsequent sclerosis and contraction. It may result also from cicatricial contraction of the muscle following rupture of its fibres during delivery. In such cases there is a history that the birth was a difficult one, the presentation having been abnormal; and that a swelling was observed in the sterno-mastoid shortly after birth. This swelling—a hæmatoma of the sterno-mastoid—is at first soft, later becomes smaller, and eventually disappears. In course of time, sometimes months, sometimes years after the disappearance of the swelling, shortening of the muscle takes place, and the deformity is established.
Clinical Features.—Although the condition is usually described as “congenital,” it is the common experience in practice that the child has reached the age of from seven to ten years before advice is sought. The appearance of the patient is characteristic (Fig. 271). The shortening of the sterno-mastoid pulls the head towards the affected side, usually the right, so that the ear is approximated to the shoulder. At the same time the head is rotated towards the opposite side and slightly tilted backwards, with the result that the chin is directed towards the opposite side, and is somewhat raised. The shortened sterno-mastoid stands out prominently, and, on any attempt to straighten the head, can be felt as a firm, fibrous band. The skin of the affected side of the neck may be thrown into transverse folds. The patient is unable to correct the deformity, but it is usually possible to diminish it by manipulation.
If the condition is not corrected, all the structures on the affected side of the neck undergo organic shortening, with the result that the deformity becomes accentuated. In advanced cases a lateral curvature, with the convexity towards the normal side, occurs in the cervical region, the vertebræ becoming wedge-shaped from side to side, and a compensatory curve may develop in the thoracic region (Fig. 272).
There is also asymmetry of the head and face, the affected side being the smaller. The eye on this side lies on a lower level, and is more oblique than its neighbour, the cheek is flattened, and the mouth asymmetrical. Instead of the eyebrows and the lips forming parallel lines, their axes converge towards the side of the contracted muscles and fasciæ.
Treatment.—While it may be possible when the condition is recognised during infancy to counteract the tendency to contraction and deformity by manipulations, massage, and exercises alone, it is usually necessary to divide the shortened structures as a preliminary to orthopædic measures.
Subcutaneous tenotomy—at one time the favourite method of treatment—has been entirely replaced by the open operation, which admits of all the structures at fault, including the cervical fascia, being thoroughly divided, without risk of injuring other structures in the neck. The result of division of the shortened tissues is seen at once in a marked increase in the interval between the sterno-clavicular joint and the mastoid process. As in other deformities, the operation is only a preliminary, although an essential one, to the treatment by massage, movement, and exercises which must be persevered with for months, and it may be for years. When the torticollis attitude has been corrected in childhood, the asymmetry of the skull disappears.
Spasmodic wry-neck is the term applied to a condition in which clonic contractions of certain muscles produce jerkings of the head. The muscles most frequently at fault are the sterno-mastoid and trapezius of one side, and the posterior rotators of the opposite side. By these muscles the head is pulled into the wry-neck position, and is at the same time retracted, and there is more or less constant nodding or jerking of the head.
The condition is usually met with in adults of a neurotic disposition who are in a depressed state of health, and is due to some lesion, as yet undiscovered, in the nerve mechanism of the affected muscles—most probably in their cortical centres. It would appear that in some cases the spasmodic jerkings are originated by certain movements habitually made by the patient in the course of his work. In others, as a result of astigmatism and other errors of refraction, the patient has acquired the habit of repeatedly tilting his head to enable him to see clearly, and these movements have become continuous and uncontrollable.
The affection tends to become progressively worse until the patient is incapacitated for work or enjoyment. Sleep even may be interfered with.
Treatment.—In well-marked cases the use of drugs, electricity, or restraining apparatus is never curative, but these measures combined with massage have been temporarily beneficial in milder cases.
Of the operative procedures, resection of portions of the accessory nerve on one side, and of the posterior primary divisions of the first five cervical nerves on the opposite side, seems to offer the best prospect of recovery. Simple division of these nerves or resection of the accessory alone has not proved permanently curative. Open division of the offending muscles without interfering with the nerves has given good results, and is a much simpler operation (Kocher).
Spasmodic wry-neck must be distinguished from the hysterical variety, which after lasting for weeks, or even months, may pass off completely, but, like other hysterical affections, is liable to recur.
Deviations of the neck simulating torticollis may occur in cervical caries, and in unilateral dislocation of the spine.
The cicatricial contraction of the integument of the neck that results from extensive burns, abscesses, or ulcers, may cause unsightly deformity and fixation of the head in an abnormal attitude, and call for surgical treatment. The contraction which follows the disappearance of a gumma of the sterno-mastoid may also produce a deformity resembling wry-neck.
Contusion of the neck may result from a blow or crush, as, for example, the passage of a wheel over the neck, or from throttling, strangling, or hanging. In medico-legal cases the distribution of the discoloration should be carefully noted. When due to throttling, the marks of the fingers may be recognisable, and nail-prints may be present. In cases of strangling, the mark of the cord passes straight round the neck, while in suicidal hanging it is more or less oblique and is higher behind than in front. When due to a direct blow, for example by a fist, the discoloration is limited, while it is usually diffused over the neck when due to the passage of a wheel over the part.
The clinical importance of these injuries depends on the complications that may ensue; for example, extravasation of blood under the cervical fascia may press upon the air-passage and œsophagus to such an extent as to cause interference with breathing and swallowing; the larynx or the trachea may be so grossly damaged that death results immediately from suffocation, or later from gradually increasing œdema causing obstruction of the glottis. If the mucous membrane of the air-passage or the apex of the lung and its investing pleura is torn, emphysema of the connective tissue may develop and spread widely over the body. In contusions of the lower part of the neck the cords of the brachial plexus may be injured.
Fractures of the Hyoid, Larynx, and Trachea.—The hyoid bone, on account of its mobility and the protection it receives from the body of the mandible, is seldom fractured, except in old people in whom the great cornu has become ossified to the body of the bone. It is usually broken either by a direct blow, or by transverse pressure as in garrotting. The fracture is almost always at the junction of the great cornu with the body, and there is marked displacement of the fragments, which may injure the pharyngeal mucous membrane.
The thyreoid and cricoid cartilages are also liable to be fractured in run-over accidents, particularly in old people after calcification or ossification has taken place.
The trachea may be lacerated, or even completely torn from the larynx, by the same forms of injury as produce fracture of the laryngeal cartilages.
The clinical features common to all these injuries are swelling and discoloration; and if the mucous membrane is torn, air may escape into the tissues and produce emphysema. There is always more or less difficulty in breathing, which may amount to actual suffocation, and this may come on immediately, or in the course of a few hours from œdema of the glottis. Blood may pass into the lungs and be coughed up. Swallowing is usually difficult and painful, especially in fracture of the hyoid bone. There is also pain on speaking, the voice is husky and indistinct, and spasmodic coughing is common. When blood has entered the air-passages there is considerable risk of septic pneumonia.
Treatment.—As the immediate risk to life is from suffocation, it is usually necessary to perform tracheotomy at once. In fracture of the hyoid the fragments may be replaced by manipulation through the mouth, after which the head and neck are immobilised by a poroplastic collar.
Wounds—Cut-throat.—The most important variety of wound of the neck met with in civil practice is that known as “cut-throat”—an injury usually inflicted with suicidal, less frequently with homicidal intent.
Suicidal wounds are usually directed from left to right (if the patient is right-handed), and they run more or less obliquely from below upwards across the neck; the wound being deepest towards its left end, that is where the weapon enters, and gradually tailing off towards the right. In most cases the would-be suicide throws his head so far back at the moment of inflicting the wound, that the main vessels are carried backward under cover of the tense sterno-mastoid muscles, and so escape injury. The knife may even reach the vertebral column without damaging the contents of the carotid sheath.
Homicidal wounds are usually more directly transverse, and are of equal depth throughout. The main vessels are generally divided, the œsophagus and trachea opened into, and in some cases the vertebral canal is opened and the cord and its membranes injured.
Clinical Features.—The clinical features vary with the level of the wound and with its depth. In all cases the contraction of the platysma causes the wound to gape widely, and its edges tend to be turned in.
In a large proportion of suicidal attempts the patient only succeeds in inflicting one or more comparatively superficial wounds across the front of the neck. In many cases the hæmorrhage from these is trifling, but if the external jugular and other large superficial veins are divided, it may be fairly profuse, although it is seldom immediately fatal, unless the blood is sucked in to the wounded air-passage.
Occasionally, but rarely, the wound is made above the hyoid bone, and opens directly into the mouth. There may then be sharp hæmorrhage from the base of the tongue or from the lingual and external maxillary (facial) arteries or their branches in the submaxillary region, and asphyxia may result from the base of the tongue and the epiglottis falling back and obstructing the larynx.
The hyo-thyreoid membrane is frequently divided, and the pharynx thus opened. As the depressor muscles of the hyoid are divided, there is interference with deglutition and phonation, but respiration is not affected. In such cases the upper portion of the epiglottis is often cut off, and the base of the tongue, the tonsil or the soft palate may be injured. The lingual, external maxillary and superior thyreoid arteries, and the hypoglossal nerve are also liable to be divided at this level, but the main vessels of the neck usually escape. There is pain and difficulty in swallowing, and food and saliva tend to escape through the wound. Particles of food may pass into the air-passages and cause violent fits of coughing.
In more severe cases the knife enters the larynx or the trachea. Sometimes the thyreoid cartilage is divided—as a rule only partly—and the vocal cords are injured; in other cases the trachea is opened, or it may be completely cut across. The bleeding is serious, as the superior thyreoid arteries are usually damaged. If the common carotid and the internal jugular vein also are wounded, the hæmorrhage usually proves fatal. The fatal issue may be contributed to by blood entering the air-passages and causing asphyxia, or by air being sucked into the open veins and causing air embolism. The laryngeal branches of the vagus may be divided and paralysis of the larynx ensue.
In all cases there is more or less dyspnœa and persistent coughing. The voice is husky, and the patient can only express himself in a hoarse whisper. There is difficulty in swallowing, and the food may enter the trachea. When the external wound is small, there may be a considerable degree of emphysema of the cellular tissue.
The prognosis depends largely on the general condition of the patient. The majority of those who attempt to take their own lives are in a low state of health from alcoholic excess, mental worry, privation or other causes, and many succumb even when the wound in the neck is comparatively slight. Shock, loss of blood, asphyxia from blood entering the air-passages, and œdema of the glottis are the most frequent causes of death soon after the injury. Cellulitis, inhalation, pneumonia, and delirium tremens are later complications that may prove fatal.
Treatment.—The first indication is to arrest hæmorrhage, and this may be done by applying digital compression over the bleeding points. The bleeding vessels are then sought for and ligated, the wound being enlarged if necessary.
If the food and air-passages are intact, any muscles that have been divided should be sutured.
When the epiglottis is cut across in wounds opening into the pharynx, it should be united, preferably with fine silk sutures, as catgut is absorbed before healing has time to take place. The wall of the pharynx and the muscles should then be sutured layer by layer.
When the air-passage is opened, it is usually advisable to introduce a tracheotomy tube (Fig. 273), and pack gauze round it to avoid the risk of œdema of the glottis and to prevent blood entering the lungs. The soft tissues may then be brought together layer by layer.
 Fig. 273.—Recovery from Suicidal Cut-throat after low
tracheotomy and gastrostomy.
Fig. 273.—Recovery from Suicidal Cut-throat after low
tracheotomy and gastrostomy.In all cases the superficial part of the wound should be drained, and in applying the bandage the head should be flexed on the chest to take all tension off the stitches. The patient must be kept under constant supervision lest he should interfere with the dressings, or make a further attempt on his life. In some cases it is necessary to feed him through a tube passed into the stomach either through the mouth or through the nose; when this is not feasible, nourishment must be given by the rectum, or by a gastrostomy tube (Fig. 273).
Wounds of the thoracic duct have been described with affections of the lymphatics (Volume I., p. 324), and wounds of the brachial plexus with injuries of individual nerves (Volume I., p. 360).
Cellulitis may occur in any of the cellular planes in the neck, the most important form being that which occurs under the cervical fascia, for example in the course of acute infective diseases, such as scarlet fever, measles, or pyæmia. The pus tends to spread widely throughout the neck, infiltrating the connective-tissue spaces around the blood vessels, the air-passages, and the œsophagus. The density and tension of the cervical fascia cause the pus to burrow downwards towards the mediastinal spaces of the thorax, where it may give rise to such complications as empyema, infective pericarditis, or gangrene of the lung. The pus may also reach the axilla by spread of the infection along the subclavian vessels.
An acute phlegmonous peri-adenitis sometimes occurs in the loose cellular tissue around the submaxillary gland, and spreads with great rapidity through the cellular planes of the neck. The condition—which goes by the name of angina Ludovici—is usually met with in adults, and appears to originate in some infective focus in the mouth.
Clinical Features.—In all forms the process spreads rapidly, and the neck becomes swollen, brawny, and of a dusky red colour. The head is flexed towards the affected side, and there is pain on movement and on palpating the swelling. Pus forms early, but, as it is under great tension, fluctuation can seldom be detected. Respiration may be interfered with by pressure on the air-passages, or by the onset of œdema of the glottis, and tracheotomy may be urgently called for. Swallowing may also be affected by pressure on the pharynx and œsophagus. Pressure on the important nerves traversing the neck may give rise to irritative or paralytic symptoms. The main vessels may become thrombosed or eroded—particularly when the cellulitis is associated with scarlet fever—and in the latter case copious hæmorrhage may follow incision of the abscess.
There is always marked constitutional disturbance, as evidenced by rigors, high temperature, a small, rapid pulse, and delirium; and death may result within a few days from toxæmia.
Treatment.—In the earliest stages hot fomentations or ichthyol and glycerine should be applied, but if the process does not begin to abate within twenty-four hours, and if the swelling becomes brawny in character, one or more incisions should be made through the deep fascia where the signs of inflammation are most intense, and the deeper planes of the neck opened up by dissection. Drainage is secured by tubes or strips of rubber tissue. If profuse hæmorrhage occurs it may be necessary to ligate the main artery lower in the neck.
Actinomycosis manifests itself in the neck as a diffuse, painless swelling, which slowly infiltrates the superficial structures, becoming brawny at some places, and at others breaking down and forming sinuses from which the ray fungus escapes in the discharge.
Boils and carbuncles frequently occur on the back of the neck, where the skin is thick and coarse and is rubbed by the collar.
The affections of the cervical lymph glands have already been described (Volume I., p. 330).
Cystic Tumours.—A great variety of cystic tumours is met with in the neck.
Branchial cysts are formed by the distension of an isolated and unobliterated portion of one of the branchial clefts. They usually form in connection with the third cleft, and are met with in the region of the great cornu of the hyoid bone, to which the wall of the cyst is almost always attached. Less frequently they take origin in the second cleft, and lie below the mastoid process, in which case the cyst is adherent either to the mastoid or to the styloid process. In some cases these cysts project towards the floor of the mouth. When near the skin they are of the nature of dermoid cysts, being lined with squamous epithelium and filled with sebaceous material. When deeply placed, they are lined by cylindrical or ciliated epithelium and contain a glairy mucoid fluid.
Although of congenital origin, these cysts do not usually attract attention till about the age of puberty, when they are noticed as small, soft, fluctuating tumours over which the skin moves freely. They grow slowly, but may attain great dimensions. The only treatment that yields satisfactory results is complete excision.
The cystic lymphangioma, hygroma, or hydrocele of the neck (Fig. 274), has been described with affections of lymphatics (Volume I., p. 327); and thyreo-glossal cysts in the neck at p. 583.
Blood Cysts.—These may originate in a diverticulum of a vein that has become isolated, or in a cavernous angioma; or they may be due to hæmorrhage taking place into a branchial or thyreo-glossal cyst. The diagnosis is often only possible by exploratory puncture; and the treatment consists in complete excision.
Cystic Bursæ.—Cystic degeneration may occur in the supra-hyoid and thyreo-hyoid bursæ, and give rise to a rounded swelling which moves with the thyreoid on swallowing, and is only troublesome from the disfigurement it causes. It is treated by excision.
Solid Tumours, apart from the common enlargements of lymph glands, and the various forms of goitre, are not often met with in the neck.
The circumscribed lipoma usually occurs over the nape of the neck or in the supra-clavicular region. It may attain considerable size, and from its weight become pedunculated and hang down over the back or shoulder.
Diffuse lipomatosis usually begins over the nape and spreads more or less symmetrically till it completely surrounds the neck. As the new-formed fat is not encapsulated, extirpation of the mass is difficult and is seldom called for.
Fibroma originating in the ligamentum nuchæ, or the periosteum of the vertebral processes, is of slow growth, but it may attain considerable size, and on account of its deep attachments the operation for its removal may be difficult.
Mixed tumours like that described as occurring in the vicinity of the parotid, and taking origin from branchial rests, are sometimes met with in the upper part of the anterior triangle.
Osseous and cartilaginous tumours occasionally grow in connection with the transverse processes of the lower cervical vertebræ.
Sarcoma and fibro-sarcoma of the slowly growing type may develop from any of the fascial structures in the neck, or from the connective tissue surrounding the blood vessels. In those taking origin beneath the sterno-mastoid, there is difficulty in removing them completely on account of their deep attachments, and when they are found to infiltrate the surrounding tissues the attempt should be abandoned. This rule may be relaxed in view of the aid that may be afforded by the insertion of a tube of radium, which is capable of rendering inert such portions of the growth as are not capable of being removed. Sacrifice of the common carotid artery is attended with the risk of hemiplegia and cerebral softening, especially in persons over fifty; resection of a portion of the vagus is less dangerous to life than stimulation by irritation of its fibres; resection of the internal jugular vein and of the cervical sympathetic cord are factors which add to the shock of the operation but do not carry with them any special risk.
Carcinoma.—The commonest form of primary cancer is the branchial carcinoma, a squamous epithelioma which originates in connection with the second visceral cleft (Fig. 276). It appears as a rule under the sterno-mastoid at the level of the hyoid bone, and extends towards the submaxillary region, infiltrating the muscles and the sheath of the vessels.
It is more common in men than in women, and there is often a history of a small swelling having been present for many years, or even since birth. About middle life more active growth begins, the swelling becomes more fixed and is painful, and once it begins to grow, it increases rapidly and within a month or two may reach the size of a child's head. In spite of its size, however, it seldom causes interference with breathing or swallowing, and it has comparatively little effect on the general health. Clinically, the induration and fixation of the tumour suggest its epitheliomatous character, but the absence of a primary growth in the mouth or pharynx excludes its being a metastasis in the lymph glands.
Unless completely removed at an early stage, recurrence inevitably takes place.
Primary carcinoma may also occur in a supernumerary thyreoid, and in the para-thyreoid glands.
We have met with a case of paraffin epithelioma on the neck, and a similar type of epithelioma may be met with in a lupus or a burn of long standing.
The Thymus Gland.—The thymus gland begins to diminish in size towards the end of the second year, and by the time puberty is reached it has entirely disappeared. In some cases, however, the process of involution fails to take place, and the gland may even undergo hyperplasia and exert pressure on the trachea, the great blood vessels, or the left vagus nerve and its recurrent branch. The enlargement of the thymus may be part of a general lymphatic hyperplasia—known as the status lymphaticus.
The pressure effects may be entirely referable to the trachea—thymus stenosis of the trachea—giving rise to progressive dyspnœa accompanied by stridor, with paroxysmal exacerbations during which the child becomes asphyxiated. It is only expiration that is interfered with, as with each inspiratory effort the gland is sucked in towards the mediastinum and so frees the air-passages, while with expiration it rises again, and, becoming jammed in the upper opening of the thorax, exerts pressure on the trachea, and during expiration a soft swelling is sometimes recognisable in the episternal notch. The paroxysms occur at irregular intervals, and any one of them may prove fatal. In some cases the symptoms seem to be associated with pressure on the blood vessels and nerves rather than on the air-passages, and in these there is distension of the veins and a tendency to syncopal attacks.
The only way to afford relief is to expose the gland and withdraw it from behind the sternum by making traction on its capsule. If the breathing is not thereby improved, the capsule should be opened and the gland shelled out.
The term thymic asthma has been applied to another form of disturbed respiration due to a large thymus, which comes on suddenly in infants otherwise apparently healthy. Without warning, the child seems to choke, has great difficulty in breathing, with inspiratory stridor and indrawing of the epigastrium; he rapidly becomes cyanosed, and in the majority of cases dies in a few minutes—thymus death. No satisfactory explanation of the sudden onset of the symptoms is forthcoming, but it appears to be associated with something which suddenly narrows the mediastinal space, such as backward bending of the head, or venous engorgement of the thymus gland. Cases are recorded in which an attack has come on during the administration of a general anæsthetic; in some instances the patient has suffered from the generalised status lymphaticus.
Tumours of the Carotid Gland or Glomus Carotica (Potato-like tumour of the neck).—The carotid gland under normal conditions is about the size of a grain of corn, and lies to the posterior aspect of the bifurcation of the carotid. It is sometimes the seat of endothelioma. The tumour has a definite capsule, is moderately firm and elastic, increases in size slowly and gradually for a time, and then may grow more rapidly. Its relation to the vessels is characteristic: as it grows it envelops the common carotid and its branches, and becomes adherent to the internal jugular vein; and it may come to implicate the nerves in the neck, particularly the vagus and its recurrent branch, and the cervical sympathetic.
It gives rise to few symptoms, and in the majority of cases the surgeon is consulted on account of the disfigurement resulting from the presence of the swelling in the neck. This swelling is ovoid, smooth or slightly lobulated; it lies at the level of the bifurcation of the carotid, and tends to grow upwards rather than downwards; it is movable from side to side, but not up and down; it lies under the sterno-mastoid, and the skin is not implicated. There is transmitted pulsation in the tumour, but no expansion.
The diagnosis has to be made from lymphoma, adenoma, tuberculous glands, sarcoma, and carcinoma.
In a large proportion of the cases operated upon it has been necessary to ligate the carotids and to excise portions of the internal jugular vein, and as severe cerebral symptoms are liable to ensue the mortality has hitherto been high. Operation is therefore only to be recommended when the growth is rapid, or the symptoms have become urgent.
Surgical Anatomy.—The thyreoid gland consists of two lateral lobes connected by an isthmus. The lateral lobes lie in contact with the side of the larynx up to the middle of the thyreoid cartilage, and with the sides of the first five or six rings of the trachea. The isthmus lies in front of the second, third and fourth rings of the trachea, and from it a process of gland tissue—the pyramidal lobe—passes up in the middle line towards the hyoid bone.
The gland lies under cover of the superficial muscles of the neck, and is surrounded by a process of the cervical fascia—the external thyreoid capsule of Kocher—which connects it with the larynx, trachea, and œsophagus, so that it moves with these structures on swallowing. In this capsule are numerous veins; and in the groove between the œsophagus and trachea the recurrent (laryngeal) nerve runs. Enclosing the gland substance is the capsule proper, which sends in processes to form its fibrous stroma. The arteries of supply—the superior and inferior thyreoids—are very large for the size of the gland, and enter it at its four corners. The thyreoidea ima, when present, goes to the isthmus. Isolated nodules of thyreoid tissue—accessory thyreoids—are sometimes met with in different parts of the neck; they are liable to the same diseases as the main gland.
The secretion of the gland is absorbed into the general circulation through the veins; it consists of a complex colloid substance which contains an iodine-albumin—iodothyrin—and plays an important part in maintaining the normal metabolism of the body, particularly of the central nervous and cutaneous tissues in adults, and of the bones in children. Disturbance of the function of the thyreoid gland plays a part in producing the symptoms characteristic of myxœdema, cretinism, and goitre.
The para-thyreoid glands—usually two on each side—lie in the external capsule along the posterior edge of the lobes of the thyreoid. They are flattened, elliptical bodies, averaging a quarter of an inch in length and an eighth of an inch in width, of a light brown colour, smooth and glistening on the surface, and of a soft, flabby consistence (W. G. MacCallum). When tetany follows operations for goitre it is due to the removal of these glands.
Physiological Hyperæmia.—The thyreoid varies greatly in size even within normal limits, and may become engorged and swollen from physiological causes, particularly in the female. Before the onset of menstruation at puberty, for example, the thyreoid frequently becomes engorged, and the enlargement may recur with each period for months or even years. During pregnancy also the gland may become swollen.
Acute Thyreoiditis may occur in a healthy thyreoid or in one that is the seat of goitre, and may end within a few days in resolution, or go on to suppuration. It is due to infection with pyogenic bacteria, which usually gain access to the gland by the blood stream, as, for example, in typhoid fever, pyæmia, influenza, and other acute infective diseases. Direct infection sometimes occurs from an abscess, a cellulitis, or an infected wound in the neck; it has also occurred from a foreign body impacted in the œsophagus ulcerating through and perforating the gland.
One lobe is usually more involved than the other, but the condition may be diffused. When pus forms it may infiltrate the stroma of the gland, or may be collected into several small foci.
Clinical Features.—The usual signs of inflammation are present; there is severe headache of a congestive nature, and sometimes vertigo. The swelling takes the shape of the thyreoid, and although the skin may not be red, the subcutaneous veins are dilated. In severe cases there is pain and difficulty in swallowing and dyspnœa.
When suppuration ensues, all the symptoms are aggravated, and repeated rigors occur. The pus may burst into the cellular tissue of the neck, or into the air-passage or the œsophagus.
Treatment.—In the non-suppurative stage the ordinary treatment of acute inflammatory conditions is employed; if pus forms, the abscess should be opened and drained.
Tuberculous and syphilitic affections of the thyreoid are very rare.
The term goitre is applied clinically to any non-inflammatory enlargement of the thyreoid gland.
Etiology.—Parenchymatous goitre, sometimes called also simple, or non-toxic goitre, is endemic in certain hilly districts in England—particularly Derbyshire and Gloucestershire—and in various parts of Scotland. It is exceedingly common in certain valleys in Switzerland. It is met with less frequently in men than in women, and it occurs chiefly during the child-bearing period of life. The toxic agent that causes goitre has been traced to certain mountain springs in goitrous districts; it has been observed that a patient with goitre may, through fæcal contamination apparently, infect the water supply, and that conscripts in order to avoid military service have drunk from goitrous springs with success. Children born in a goitrous district are liable to be cretins, while if goitrous parents move to a healthy district, the children are born healthy. If the water supply of a goitrous valley be changed to a healthy spring, goitre and cretinism disappear. Thorough boiling of the water rids it of its toxic properties.
Morbid Anatomy.—Both the secreting and the fibrous elements share in the hyperplasia, and the gland as a whole becomes enlarged and forms a horseshoe-shaped swelling of moderate size in the neck. This swelling is soft and smooth on the surface, and is seldom quite symmetrical. In some cases the hypertrophy involves chiefly the isthmus. In others an outlying accessory lobule of thyreoid tissue constitutes the bulk of the swelling, and this may extend a considerable distance from the position of the normal thyreoid, reaching even behind the sternum into the thorax—infra-thoracic or retro-sternal goitre.
When the secreting elements increase out of proportion to the stroma, numerous rounded or irregular spaces filled with a thick yellow colloid material are formed in the substance of the goitre—colloid goitre. The majority of these spaces are not larger than a pea, but one or more may enlarge and form cysts of considerable size—cystic goitre. These varieties, especially the cystic form, attain greater dimensions than any other form of goitre.
When the fibrous stroma is greatly in excess—fibrous goitre—the swelling is smaller, firmer, and shows a greater tendency to contract and compress the trachea. If the sclerosis is extreme and the secretory tissue undergoes atrophy, myxœdema may result.
In some cases the hyperplasia affects chiefly the blood vessels of the thyreoid—vascular goitre. The capillaries, veins, and arteries are increased in size and number; the swelling pulsates and increases in size when the patient makes any muscular effort. Hæmorrhagic cysts may also develop in the substance of these goitres.
Effects on the Trachea.—The trachea may be displaced laterally when the enlargement of the gland affects one lobe more than the other; or it may be compressed and narrowed from side to side—the scabbard trachea—when both lobes are about equally affected and the enlargement extends posteriorly so as almost to surround the air-passage (Figs. 278, 279). The third effect is that of softening of the cartilaginous rings of the trachea so that the air-tube, instead of having a considerable degree of elastic resiliency, is soft and flaccid and readily yields to pressure. Under these conditions an alteration in the attitude of the patient, from the erect or sitting to the recumbent position, would appear to be sufficient to permit of a compression of the trachea.
Further changes in the trachea consist in catarrh and engorgement of the blood vessels of its mucous membrane, attended with an abundant secretion of mucus, which, if it accumulates behind a narrowed segment of the trachea, may still further encroach on the lumen.
Pressure on other Structures.—The recurrent nerve may be pressed upon intermittently causing spasms and choking, or continuously causing abductor paralysis and hoarseness.
The gullet is rarely compressed; if marked difficulty in swallowing develops, some additional factor should be suspected, notably carcinoma at the junction of the pharynx with the œsophagus. The carotid arteries are displaced laterally beneath the sterno-mastoids without detriment; the superficial veins—anterior and external jugular—are greatly distended in those cases in which the goitre grows downwards behind the sternum.
Clinical Features.—The symptoms vary widely in different cases, and their severity is not proportionate to the size of the goitre. The disfigurement produced by the swelling is often the only cause of complaint. In some cases the symptoms are due to the pressure of the enlarged thyreoid on surrounding structures. In others toxic effects, in the form of cardiac, nervous, muscular, and general metabolic disturbances, predominate, and are due to absorption of excessive or abnormal thyreoid secretion. This thyreoid toxæmia varies in degree; in the milder cases it merely amounts to a nervousness or excitability that may unfit the patient for occupation; it reaches its maximum in the condition of hyperthyreoidism characteristic of exophthalmic goitre or Graves' disease (p. 614).
The skin over the goitre is freely movable, and the tumour itself can be moved transversely, carrying the larynx and trachea with it, but it cannot be moved vertically. It moves up and down with the larynx on swallowing—a point of great diagnostic value. Of the mechanical symptoms dyspnœa is the most constant. It may only amount to shortness of breath on exertion, or the patient may suffer from sudden and severe dyspnœic attacks, especially when lying on the back during sleep, and such an attack may prove fatal. This may be due to the weight of the tumour pressing on the trachea, which has been softened and distorted by the goitre, or to temporary congestion and engorgement of the mucous membrane of the air-passages. In these cases there is marked stridor both on inspiration and expiration, but no aphonia. In rare cases the goitre presses upon the recurrent nerve, causing spasmodic dyspnœa, hoarseness, and aphonia from impaired movement of the vocal cords, and these symptoms, especially if accompanied by pain, raise the suspicion of malignancy. Disturbance of the heart's action may cause palpitation and sudden attacks of syncope; and pressure on the blood vessels may give rise to a feeling of fullness in the head, and giddiness.
The occurrence of hæmorrhage into the substance of the goitre or into a cyst, produces a sudden aggravation of the symptoms.
In intra-thoracic or retro-sternal goitre the tumour displaces and compresses the trachea and causes dyspnœa, and there are occasional paroxysmal attacks of breathlessness, which may be mistaken for asthma, particularly as the patient is usually the subject also of bronchitis and emphysema. In some cases the patient can, by a violent expiratory effort, such as coughing, project the goitre upwards into the neck. When the goitre is fixed in the thorax, the clinical features are those of a mediastinal tumour with lateral displacement of the trachea, and engorgement of the veins of the neck.
Treatment.—The patient should change his residence to a non-goitrous district. The evidence regarding the benefit derived from the internal administration of thyreoid extract, or of preparations of phosphorus or of iodine, is conflicting.
Operative treatment is indicated when there are symptoms referable to pressure on the air-passage, and in goitres which are steadily increasing in size. Kocher considers it advisable to operate if the patient becomes breathless on making pressure on the goitre from side to side. The suspicion of a goitre becoming malignant is also a reason for removing it by operation.
The operation—thyreoidectomy—consists in excising that portion of the thyreoid which is causing pressure symptoms, and this usually involves removal of one-half of the gland. The chief danger in operations for goitre is cardiac insufficiency, as evidenced by disturbed rhythm of the heart-beats, lowering of the blood pressure, or dilatation of the cavities of the heart (Kocher).
It is sometimes advisable to perform the operation under local anæsthesia. A general anæsthetic is, however, preferred in this country. The injection of 1/6th grain of morphin and 1/120th grain of atropin half an hour before the operation, and the administration of ether by the open method, or by intra-tracheal insufflation, is safe and satisfactory.
There is reason to believe that the absorption of thyreoid secretion squeezed from the divided surfaces gives rise to a condition known as acute thyreodism during the first few hours after operation; its symptoms are elevation of temperature, increase in the pulse-rate (150–200), rapid respiration with dyspnœa, flushing of the face, muscular twitchings, and mental excitement. The gentle handling of the tumour and the employment of a drainage tube for the first forty-eight hours diminishes this risk.
Tetany, as evidenced by the occurrence of cramp-like contractions of the thumb and fingers, may supervene within a few days of the operation if one or more of the para-thyreoids have been inadvertently removed. It may be controlled by large doses of calcium lactate. On no account may the whole of the thyreoid gland be removed, as this is followed by the development of symptoms closely resembling those of myxœdema—operative myxœdema or cachexia strumipriva.
Treatment of Sudden Dyspnœa.—When dyspnœa suddenly supervenes and threatens life, it is sometimes possible to relieve the pressure on the trachea by open division of the skin, superficial fascia, platysma and deep fascia in the middle line of the neck, so as to relax the tension on the goitre. If this is insufficient, the isthmus may be divided. Should relief not follow, tracheotomy must be performed, and a long tube or a large-sized gum-elastic catheter with a terminal aperture be passed along the trachea beyond the seat of obstruction.
Adenoma of the Thyreoid.—In this condition the swelling of the thyreoid is due to the growth within its substance of one or more adenomas of variable size and surrounded by a capsule. The rest of the gland may be normal, or may show some degree of hyperplasia. Some are solid, others undergo cystic degeneration, the glandular tissue being replaced by a quantity of clear or yellowish fluid, sometimes mixed with blood. The cysts thus formed may be unilocular or multilocular, and intra-cystic papillary vegetations frequently grow from their walls. The walls of the cysts may be thin, soft, and flaccid, or thick and firm, or they may even be calcified.
The thyreoid is enlarged, but instead of the uniform enlargement which characterises the parenchymatous goitre, it tends to be uneven, with hillocky projections corresponding to the individual cysts (Fig. 280), and in these fluctuation may be detected. It is to be noted that there are no toxic symptoms in cystic adenoma.
The treatment is necessarily operative; cystic tumours may be tapped and injected with iodine, but the more satisfactory procedure, both with the solid and cystic forms, is to incise freely the overlying thyreoid tissue and enucleate the tumour.
Malignant Disease of the Thyreoid.—This, whether in the form of carcinoma or sarcoma, usually develops in a gland that has been the seat of goitre for several years, although it may begin in a previously healthy gland.
Clinical Features.—Both sexes, above the age of fifty, are affected in about equal proportion. The characteristic features are that the tumour undergoes a progressive increase in size, that it becomes fixed to its surroundings, that its surface tends to be uneven and nodular, and its consistence densely hard. The voice often becomes hoarse from abductor paralysis due to infiltration by the growth, usually of the left recurrent nerve. The effects upon the trachea are more decided and more progressive than in parenchymatous goitre; it displaces and compresses the trachea and frequently overlaps it, so as to bury the air-passage completely. If the tumour tissue has actually penetrated the trachea, the expectoration is tinged with blood. Dysphagia is rarely a prominent symptom. The lymph glands become enlarged after the tumour bursts through the capsule; and metastases to the lungs and bones, particularly the skull, sternum, and mandible, are common. When the goitre extends behind the sternum—the malignant form of retro-sternal goitre—the pressure symptoms are due to the encroachment upon the limited accommodation of the upper opening of the thorax; the trachea especially suffers, and the pressure on the veins causes distension of the anterior and external jugulars and their tributaries. The patient is unable to lie down; there are violent paroxysms of coughing, and an abundant frothy expectoration. Death may take place suddenly from asphyxia, from heart failure, or from displacement of a thrombus from one of the veins in the neck.
Treatment.—It is only in the earliest stages that a malignant goitre can be successfully removed. In the later stages complete extirpation is not to be attempted, as it usually involves the removal of a portion of the trachea or œsophagus, and the operation is attended with grave risk to life.
Operative interference is often called for, however, for the relief of respiratory embarrassment. Tracheotomy may prove a difficult and dangerous procedure, owing to the trachea being buried under the goitre and displaced or narrowed by it, so that it is not easy to reach it or to introduce an efficient tube beyond the point of obstruction. A more certain method consists in exposing the goitre by an incision as for thyreoidectomy, rapidly removing sufficient of the growth to expose the trachea and admit of a tube being introduced. If there is a retro-sternal prolongation compressing the trachea within the thorax, a long flexible tube may have to be passed beyond the site of the compression before the dyspnœa is relieved. The benefit is immediate and decided; the accumulated secretion is coughed up, and after a few deep breaths the patient is able to lie down, and usually falls asleep. The stridor disappears. Unfortunately the relief is only temporary, and the patient soon succumbs to a broncho-pneumonia, or to secondary hæmorrhage from the trachea.
Toxic Goitre—Exophthalmic Goitre—Graves' or Basedow's Disease.—These terms are applied to a variety of goitre in which the symptoms due to absorption of thyreoid secretion—thyreotoxicosis—predominate. The name “exophthalmic goitre” is misleading, as in some cases the enlargement of the thyreoid, and in others the eye symptoms, are scarcely appreciable, while the general symptoms are well marked. The term toxic goitre or hyperthyreoidism, suggested by C. H. Mayo, is preferable, as the manifestations of the disease depend upon excessive or abnormal action of the thyreoid tissue.
The condition is chiefly met with in young adult women, and may develop suddenly after a shock to the nervous system. The intoxication affects the higher cerebral functions and causes nervousness, irritability, and tremor; the cardiac and vaso-motor centres, causing tachycardia and pallor of the skin; the sympathetic fibres to the eye, causing protrusion of the eyeballs, staring of the eyes without winking, narrowing of the palpebral fissure, dilatation of the pupil, and lagging behind of the upper lid, and sometimes also of the lower lid—von Graefe's symptom. There may be diarrhœa and vomiting, loss of weight, and in the worst cases there is delirium at night. In course of time there develops cardiac insufficiency with fibroid degeneration of the myocardium. Coagulation of the blood is retarded, and there is a marked diminution in the number of leucocytes, especially the neutrophils, and an increase in the lymphocytes (Kocher).
In the early stages the thyreoid is enlarged and pulsatile, and bruits may be heard over it; later, these vascular symptoms disappear, and only a firm, diffuse, uniform swelling implicating all parts of the gland remains.
Prognosis.—The tenure of life is uncertain as the patient offers little resistance to intercurrent affections such as influenza and pneumonia. If the average course of the disease is represented by a curve, the greatest height is reached during the second half of the first year and then descends. For the next two to four years it fluctuates with occasional exacerbations of symptoms due to fright or worry.
Treatment.—Medical measures, along with the external application of radium, the strict observance of rest in bed with the exclusion of all forms of excitement and worry, the administration of bromides, heroin or other sedatives, and of digitalis or other cardiac tonics, are to be prescribed in the first instance, and in any case, as a desirable preparation for operation.
Operative measures consist in the ligation of the vessels and nerves at one or other pole of the gland—usually the superior on one side—followed by, if necessary, a partial thyreoidectomy.
Crile of Cleveland has organised his clinic in the direction of arranging that the operation shall be performed without the patient knowing that it is to take place—what he calls “stealing the goitre”—the thorough preparation of the patient for the operation, the minimising the risk from the anæsthetic by the combination of novocain locally and of nitrous oxide and oxygen; and of diminishing the risk of absorption of thyreoid secretion by packing the (open) wound with gauze wrung out of a solution of flavin.
Operations on the cervical sympathetic cord have been abandoned.
The presence of toxic goitre may influence the question of operation in the treatment of other surgical conditions, and may determine the selection of one or other form of anæsthesia.
Surgical Anatomy.—The œsophagus extends from the level of the cricoid cartilage to about the level of the lower end of the sternum. The distance from the upper incisor teeth to the commencement of the œsophagus is about 5 or 6 inches, and the œsophagus measures from 9 to 10 inches. The whole distance, therefore, from the teeth to the stomach is from 14 to 16 inches.
The cervical portion of the œsophagus, extending from the cricoid cartilage to the upper edge of the sternum, measures about 2 inches. It lies behind and to the left of the trachea, and in the groove between them on each side runs the recurrent nerve. The thoracic portion is about 7 inches long, and traverses the posterior mediastinum lying slightly to the left of the middle line. It is crossed by the left bronchus, and below this level has the pericardium immediately in front of it. The left pleura is closely related to the anterior surface of the œsophagus throughout, while the right pleura passes behind it in its lower part. This accounts for the frequency with which growths in the œsophagus invade the pleura. The œsophagus passes through the diaphragm about an inch above the cardiac opening of the stomach.
There are three points at which the œsophagus shows narrowing of the lumen: (1) at the lower border of the cricoid—the “mouth of the œsophagus”; (2) where it is crossed by the left bronchus; and (3) where it passes through the diaphragm. It is at these points that foreign bodies tend to become impacted. The mucous membrane of the œsophagus is insensitive to tactile and painful stimuli, but is sensitive to heat and cold and to exaggerated peristaltic contractions.
Methods of Examination.—It is sometimes possible to detect an impacted foreign body, a distended diverticulum, or a new growth in the cervical portion of the œsophagus by palpation.
Auscultation while the patient is drinking sometimes aids in the diagnosis of stricture; the stethoscope is placed at various points along the left side of the dorsal spine, and abnormal sounds may be heard as the fluid impinges against the stricture or trickles through it.
Introduction of Bougies.—Œsophageal bougies or probangs are used for diagnostic purposes in cases of suspected stricture, and to aid in the detection of foreign bodies. Various forms are employed, of which the most generally useful are the round-pointed gum-elastic or silk-web bougie, and the olive-headed metal bougie, consisting of a flexible whalebone stem, to which one of a graduated series of aluminium or steel bulbs is screwed. For some purposes, such as pushing onward an impacted bolus of food, the sponge probang—which consists of a small round sponge fixed on a whalebone stem—is to be preferred.
Before passing bougies, it is necessary to make certain that the symptoms are not due to the pressure of an aneurysm on the œsophagus, as cases have been recorded in which a thin-walled aneurysm has been perforated by a bougie. The existence of ulceration or of an abscess pressing on the gullet also contra-indicates the use of bougies.
For the passage of a bougie the patient should be seated on a chair with the head thrown back and supported from behind by an assistant, and he is directed to take full deep breaths rapidly. The bougie, lubricated with butter or glycerine, and held like a pen, is guided with the left forefinger. As soon as the instrument engages in the opening of the œsophagus, the chin is brought down towards the chest, and if the patient is now directed to swallow, the instrument may be carried down the œsophagus, or can be passed on by gentle pressure. Great gentleness must be exercised, and no attempt should be made to force the instrument past any obstruction. The instrument may catch against the hyoid bone, and this may be mistaken for an obstruction.
It is to be borne in mind that in some cases the passage of a bougie may be attended with a considerable degree of shock, and cases are on record in which this has proved fatal without any gross lesion being found after death.
Intubation, or the passage of a cannula through a stricture, is referred to later.
Œsophagoscopy.—The œsophagoscope—a form of speculum which enables the œsophagus to be illuminated by an electric lamp—is employed for the detection and removal of foreign bodies, for the examination of ulcers, diverticula, and strictures of the tube, and with its aid it is possible to remove a portion of a growth for microscopic examination. The mouth, pharynx, and entrance to the œsophagus having been cleansed and cocainised, the patient is placed in the recumbent or sitting posture, and the tube introduced. For prolonged examinations a general anæsthetic is preferred.
The mouth of the œsophagus is closed by the sphincter-like action of the lower fibres of the inferior constrictor muscle, and the cervical part of the tube appears as a transverse slit, due to the backward pressure of the trachea. The thoracic portion is more open and may contain air, so that it is possible to see down to the lower end, the closed cardiac orifice appearing as an oblique cleft surrounded by a rosette-like cushion of mucous membrane. The pulsation of the aorta can be seen just above the prominence formed by the left bronchus.
Radiography.—Opaque foreign bodies can be detected by the screen or in a radiogram; and the position of a stricture by making the patient swallow capsules containing bismuth and examining with the screen. To determine the position and size of a diverticulum, a radiogram is taken after the patient has swallowed some food, such as porridge mixed with bismuth.
Wounds of the œsophagus inflicted from without, for example stabs, cut-throat or gun-shot injuries, are rare, and are almost invariably accompanied by lesions of other important structures in the neck, which may rapidly prove fatal. It is more common to meet with wounds inflicted from within, for example by the swallowing of rough and irregularly shaped foreign bodies, or by unskilful attempts to remove such bodies or to pass bougies along the œsophagus. The severity of the lesion varies from a scratch of the mucous membrane to a perforation of the tube. The less severe injuries are attended with pain on swallowing and a sensation as if something had lodged in the œsophagus. In more severe cases there is bleeding, followed by attacks of coughing and expectoration of blood-stained mucus. When the œsophagus is perforated, diffuse cellulitis of the neck or of the posterior mediastinum may ensue. In the treatment of these injuries the chief point is to give the œsophagus rest by feeding the patient entirely by the rectum or through an opening made in the stomach—gastrostomy.
Rupture of the œsophagus has occurred during violent vomiting, and during lavage. The tear is longitudinal and is usually near the cardiac orifice. It is probably due to increased pressure within the gullet. The accident has usually been met with in alcoholics, and has proved fatal by setting up left-sided empyema or cellulitis.
Swallowing of Corrosive Substances.—The œsophagus is damaged by the swallowing of strong chemicals, such as sulphuric acid, nitric acid, carbolic acid, or caustic potash. These substances produce their worst effects at the two ends of the œsophagus, but in some cases the whole length of the tube suffers. The mucous membrane alone may be destroyed, or the muscular and even the fibrous coats may also be implicated. The damaged tissue undergoes necrosis, and when the sloughs separate, raw surfaces are left, and are very slow to heal.
If not rapidly fatal from shock and œdema of the glottis, these injuries are usually attended with intense pain, severe thirst, and vomiting, the vomit containing shreds of mucous membrane and blood. Complications, such as cellulitis, perforation of the œsophagus, or peri-œsophageal abscess, may follow. Later, cicatricial contraction takes place at the injured portions, producing the most intractable form of fibrous stricture.
The treatment consists in administering solutions of carbonate of potash, of soda, or of magnesia when an acid has been swallowed, or vinegar diluted with water in the case of an alkali. When carbolic acid has been swallowed, a large quantity of olive oil should be administered. The stomach should be washed out with water, the tube being passed with the greatest gentleness to avoid perforating the softened œsophageal wall. Subsequently the patient should be fed by the rectum, but, in the majority of cases, gastrostomy is called for to enable the patient to take nourishment and put the gullet at rest.
As soon as the œsophagus has healed, say in three or four weeks, bougies should be passed every three or four days to prevent cicatricial contraction. As the calibre of the tube is restored, the instruments may be passed less frequently, but for some years—it may be for the rest of the patient's life—a full-sized bougie should be passed at least once a month.
Impaction of Foreign Bodies in the Pharynx and Œsophagus.—It is an interesting fact that foreign bodies, even as large as a dinner fork, when intentionally swallowed, can pass through the pharynx and œsophagus and enter the stomach without apparent difficulty. When the body is accidentally swallowed impaction is more liable to take place, probably on account of the spasm induced by fright and by inco-ordinated attempts to eject it. For obvious reasons the accident is most liable to occur in children, in epileptics, and in those who are under the influence of alcohol. It happens also during anæsthesia for the extraction of teeth or if the patient vomits solid substances. The clinical aspects vary according as the object is impacted in the pharynx or in the œsophagus.
In the Pharynx.—If a large bolus of unmasticated food becomes impacted in the pharynx, it blocks the openings of both the œsophagus and the larynx, and the patient may, without manifesting the usual signs of suffocation, suddenly fall back dead, and if he happens to be alone at the time of the accident, the cause of death is liable to be overlooked unless the pharynx is examined at the post-mortem examination. Most surgical museums contain specimens illustrating the impaction of a bolus of meat in the pharynx; this fatal accident has occurred especially in men in a condition of alcoholic intoxication.
An object of irregular shape, for example a large denture, also, is most likely to lodge in the pharynx, obstructing the openings of both the œsophagus and the larynx, and causing suffocation. The face immediately becomes blue and engorged, the patient is speechless, and violent efforts are made to eject the object by retching and coughing. It may be seen from the mouth and touched with the finger.
In the case of small sharp bodies, such as fish, game, and mutton bones, there is not the same urgency, and a methodical search for the foreign body is carried out. Even after the foreign body has been got rid of, the patient may have the sensation that it is still present. This may be due to a scratch of the mucous membrane, or to spasm, in which case the swallowing of a few drops of cocain solution will cause the sensation to disappear.
Treatment.—In the presence of impending suffocation, the mouth must be forced open by an extemporised gag, the finger passed into the back of the throat, and the body hooked out. If this is impossible, and if suitable forceps are not at hand, it may be necessary at once to perform laryngotomy, followed by artificial respiration, because, although the patient may appear lifeless, the heart continues to beat after breathing has ceased. The foreign body should then be removed with forceps. Sub-hyoid pharyngotomy, which consists in opening the pharynx by a mesial vertical incision carried through the hyo-thyreoid membrane, may be called for, as in the case of a denture, the hooks of which have penetrated the wall of the pharynx.
In the Œsophagus.—Smaller bodies, such as coins, bones, or pins, usually enter the œsophagus, and the great majority become impacted above the level of the manubrium sterni. Those that pass farther down are liable to stick where the tube is narrowed at the crossing of the bronchus, or at the opening through the diaphragm. In children, coins predominate and are nearly always arrested at the level of the upper end of the sternum; in adults, dentures are the commonest foreign bodies, and may be impacted anywhere.
At the moment of impaction there is pain, which assumes the character of cramp due to spasm of the muscular coat, and which is increased on attempting to swallow, and violent retching and coughing are set up; in many cases, as when bodies are impacted in the pharynx, respiratory distress is again the predominant feature. If the passage is completely obstructed, food and saliva—sometimes blood-stained—are regurgitated with retching soon after being swallowed. When the obstruction is incomplete, fluids may pass into the stomach while solids are regurgitated.
If the mucous membrane is injured, there is severe stabbing pain and choking attacks, both due to spasm, sometimes even after the body has passed on, and the pain is not always referred to the seat of the injury.
The diagnosis is made by the history, and by the use of the fluorescent screen, or X-ray photographs (Figs. 283, 284). The œsophagoscope is also of great value, both for diagnostic purposes and as an aid in the removal of the impacted body. Bougies are to be employed with great care, as there is a danger of pushing the foreign body farther down, or of wedging it more firmly in the œsophagus, and the information obtained is often misleading.
 Fig. 283.—Radiogram of Safety-pin impacted in the
Gullet and perforating the Larynx.
Fig. 283.—Radiogram of Safety-pin impacted in the
Gullet and perforating the Larynx.
It should be borne in mind that drunkards may suffer from a form of spasm of the œsophagus, which simulates the impaction of a foreign body; hospital records also show that the patient may only have dreamt that he has swallowed a foreign body, usually a denture. These possibilities should be always excluded before further procedures are undertaken.
Treatment.—There being no urgency, a careful examination is carried out, not only to confirm the impaction of a foreign body, but its site and its relation to the wall of the gullet. In skilled hands, the safest and most certain means of removing impacted foreign bodies is with the aid of the œsophagoscope. If this apparatus is not available, other measures must be adopted varying with the nature of the body, its site, and the manner of its impaction.
A bolus of food, for example, or a small smooth object that is likely to pass safely along the alimentary canal, if it cannot be extracted with forceps, may be pushed on into the stomach by the aid of a bulbous-headed or sponge probang. This must be done gently, especially if the body has been impacted for any time, as the inflammatory softening of the œsophageal wall may predispose to rupture.
Small, sharp, or irregular objects, such as fish bones, tacks, or pins, may be dislodged by the “umbrella probang”—an instrument which, after being passed beyond the foreign body, is expanded into the form of a circular brush which, on withdrawal, carries the foreign body out among its bristles.
Coins usually lodge edgewise in the œsophagus, and are best removed by means of an instrument known as a “coin-catcher”, which is passed beyond the coin, and on being withdrawn catches it in a hinged flange. In emergencies a loop of stout silver wire bent so as to form a hook makes an excellent substitute for a coin-catcher.
In difficult cases the removal of solid objects is facilitated by carrying out the manipulations in the dark room with the aid of the X-rays and the fluorescent screen.
Irregular bodies with projecting edges or hooks, such as tooth-plates, tend to catch in the mucous membrane, and attempts to withdraw them by forceps or other instruments are liable to cause laceration of the wall. When situated in the cervical part of the œsophagus, these should be removed by the operation of œsophagostomy (Operative Surgery, p. 195).
If the foreign body is lodged near the lower end of the gullet, it may be necessary to perform gastrostomy (Operative Surgery, p. 291), making an opening in the anterior wall of the stomach large enough to admit suitable forceps, or, if necessary, the whole hand, in order that the body may be extracted by this route; experience shows that an impacted body is more easily extracted from below, that is, from the stomach, than from above.
When the surgeon fails to remove the body by either of these routes, gastrostomy must be performed both to feed the patient and to place the gullet at rest. Smooth bodies may lie latent for long periods, but those with points or hooks damage the mucous membrane, cause ulceration and perforation with the risk of erosion of vessels and secondary hæmorrhage or of cellulitis of the neck or mediastinum and empyema.
Other complications include septic broncho-pneumonia from damage to the air-passage, and suppurative thyreoiditis.
Infective conditions due to pyogenic infection (œsophagitis and peri-œsophagitis) are rare.
A chronic form of œsophagitis is occasionally met with in alcoholic subjects, giving rise to symptoms that simulate those of impacted foreign body, or of stricture.
In tuberculous lesions the symptoms are pain, dysphagia, and regurgitation of food mixed with blood, and the condition is liable to be mistaken for gastric ulcer or for cancer of the œsophagus.
Syphilitic affections of the œsophagus are rare.
Varix at the lower end of the œsophagus may give rise to hæmatemesis, and be mistaken for gastric ulcer. Bleeding from the dilated veins may follow the use of bougies or of the œsophagoscope.
Difficulty in swallowing may arise from a wide variety of causes which it is convenient to consider together.
Impaction of Foreign Bodies has already been discussed, and attention has been drawn to the importance of the history given by the patient and to the various sources of fallacy or deception—in children it may be artful reticence or misrepresentation, in adults, the possibility of nightmare and of dreams.
Compression of the Gullet from without.—Any one of the numerous structures in relation to the gullet may, when enlarged as a result of disease, give rise to narrowing of its lumen, for example a lymph-sarcoma at the root of the lung, or any enlargement of the thyreoid or of the mediastinal lymph glands. The possibility of aneurysm must always be kept in mind because of the risk attending the passage of instruments for diagnostic purposes.
Spasm of the Muscular Coat.—As in other tubular structures containing circular muscular fibres, sudden contraction or spasm may occur in the œsophagus and cause narrowing of the lumen, attended with difficulty in swallowing. This spasmodic dysphagia includes such widely varying conditions as the “globus hystericus” of neurasthenic women, the spasm of chronic alcoholics, and the affection known as cardiospasm or “hiatal œsophagismus.”
In contrast with other affections causing difficulty in swallowing, spasmodic dysphagia usually has a sudden and unexplained onset, the progress of symptoms is irregular and erratic, while the remission of symptoms common to all affections of the œsophagus, and the influence of mental impressions, such as excitement, hurry in the presence of strangers, are exaggerated.
In testing the calibre of the gullet it is found that on one occasion a full-sized bougie may pass easily and be completely arrested at another.
Apart from the treatment of the neurosis underlying the dysphagia, reliance is placed upon dilatation of the portion of gullet affected.
Cardiospasm is the name given to “a recurrent interference with deglutition by spasmodic contraction of the lower end of the œsophagus.” As there is no muscular or nervous mechanism at the cardiac end of the œsophagus forming a true sphincter, the term “œsophagospasm” would be more accurate (D. M. Greig).
According to H. S. Plummer, who has had an experience of 130 cases, there are three stages in the development of this condition. In the initial stage, the first attack occurs suddenly and unexpectedly; a choking sensation is felt at some point in the gullet, usually at its lower end. Attacks of choking with difficulty in swallowing occur chiefly at meals, but they have also been known to occur apart from the taking of food. In this stage the peristalsis of the gullet is sufficient to force the food through the cardia.
In the second stage, the peristalsis of the gullet above being no longer able to overcome the contraction, there is regurgitation of food, which at first is returned to the mouth immediately after being swallowed, but, as the gullet becomes dilated, is retained for longer periods.
In the third stage, the gullet becomes more and more dilated, and the food collects in it and is regurgitated at irregular intervals. The patient complains of a sensation of weight and discomfort in the lower part of the chest, and sometimes of regurgitation of food into the nasal passages during sleep.
Cardiospasm should be suspected as the cause of difficulty in swallowing if a rubber tube cannot be passed into the stomach while a solid one can. When it is impossible to pass a solid instrument in the ordinary way it can always be passed on a silk thread as a guide. The patient is directed to swallow 6 yards of silk thread, half in the afternoon and the remainder on the following morning. The first portion forms a snarl in the gullet or stomach which passes out into the intestine during the night; the proximal end is fixed to the cheek by a strip of plaster. The olive heads of the bougies are drilled for threading from the tip to one side of the base.
The treatment consists in dilating the contracted segments by a bougie. The results are immediate and are most striking, the patients being almost invariably able to take any kind of food at the following meal, and the gain in weight and strength is rapid. In a small proportion of cases, dilatation fails to give relief, and recourse has been had to anastomosing the lower end of the dilated and pouched œsophagus with the stomach.
Paralysis of the Gullet.—As the passage of the food along the gullet is entirely dependent upon muscular peristalsis, when the muscular coat is paralysed, as it may be after diphtheria, for example, the patient is unable to swallow and the food materials are regurgitated, with consequent loss of flesh and strength. The difficulty may be tided over for a time by feeding through a rubber tube, but it is to be remembered that, in children, struggling in resisting the passage of the tube may seriously strain a heart that is already threatened by the toxins of diphtheria.
Diverticula or Pouches of the Gullet.—A diverticulum consists in the protrusion of the mucous and submucous coats through a defect or weak part in the muscular tunic; it is therefore of the nature of a hernia and not a localised dilatation of the tube as a whole. Anatomically, there is such a weak spot in the posterior wall opposite the cricoid cartilage, known as the pharyngeal dimple, between the circular and oblique fibres of the crico-pharyngeus muscle. As the pouch increases in size by pressure from within, it usually extends downwards and to the left. This pouch is described as a pressure or pulsion diverticulum because the hernial protrusion is ascribed to increased pressure within the pharynx, not only the normal increase caused by the act of swallowing, but an abnormal pressure from the too rapid swallowing or bolting of imperfectly masticated food materials.
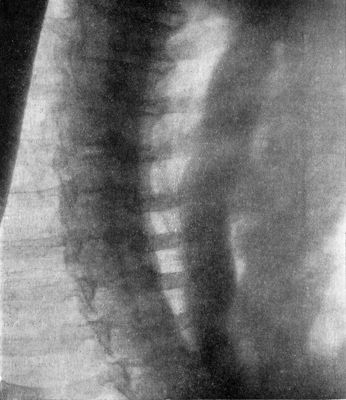 Fig. 285.—Radiogram, after swallowing an opaque meal,
in a man suffering from malignant stricture of lower end of Gullet.
Fig. 285.—Radiogram, after swallowing an opaque meal,
in a man suffering from malignant stricture of lower end of Gullet.
The clinical features are not so characteristic of difficulty in swallowing as might be expected. The patient, usually a man over forty years of age, complains of dryness in the throat and of a sensation as of a foreign body; later there is regurgitation of saliva and of food with occasional choking. In about one-third of the cases, there is a fullness, or a palpable tumour in the neck, about three times more often on the left than on the right side, which may increase in size after a meal, and pressure on which may cause a gurgling sound and, it may be, regurgitation of food.
It is suggestive of a pouch, if the patient regurgitates food materials which can be identified as having been swallowed several days before, currants perhaps being those most easily recognised and remembered.
Diverticula are also met with at a lower level, springing from the gullet at or below the upper opening of the thorax; the distension of the pouch with food materials presses upon the gullet with more serious effect, even to the extent of complete obstruction and consequent rapid emaciation. In men over fifty, the resemblance to carcinoma may be very close.
In this, as in all cases of difficulty in swallowing, chief stress should be laid on the X-ray appearances after the administration of an opaque meal; a pouch shows as a uniform, spherical shadow of from one to two inches in circumference.
Treatment is influenced by the manner in which the patient may have learned to overcome the difficulty of getting food into his stomach—Lord Jeffrey, who was the possessor of the pharyngeal pouch shown in Fig. 286, was in the habit of emptying it, after a meal, by means of a long silver spoon. Some patients learn to feed themselves through a soft rubber tube.
 Fig. 286.—Diverticulum of the Œsophagus at its
junction with the Pharynx.
Fig. 286.—Diverticulum of the Œsophagus at its
junction with the Pharynx.If an operation is decided upon, and for this it is essential that the pouch should be accessible from the neck, the general condition is improved by feeding through a stomach tube and by rectal and subcutaneous salines. The operation consists in exposing and isolating the pouch by a dissection on the left side of the neck, and either excising it as if it were a tumour or cyst, or if the risk of infection of the deeper planes of cellular tissue is regarded with apprehension, the pouch may be infolded into the lumen of the gullet, or the excision be carried out in two stages. At the first stage, the pouch is isolated and rotated on its pedicle, in which condition it is fixed by sutures; after an interval of from ten to fourteen days it is excised.
Should the diverticulum be inaccessible from the neck, and the difficulty of swallowing be attended with progressive emaciation, gastrostomy may be required to avert death by starvation.
Traction diverticula are due to the contraction of scar tissue outside the gullet, as for example that resulting from tuberculous glands in the posterior mediastinum; they are rarely attended with symptoms, and are rather of pathological than surgical interest.
Innocent Stricture or Cicatricial Stenosis of the Gullet.—The innocent or fibrous stricture follows upon the swallowing of corrosive substances, usually by inadvertence, sometimes with suicidal intent. Having recovered from the initial effects of the corrosive agent, the patient suffers from gradually increasing difficulty in swallowing, first with solids and later with fluids. There is the usual variation or intermittence of symptoms that attend upon all conditions causing difficulty of swallowing, the exacerbations being due to superadded spasm of the muscular coat and congestion of all the coats. As the gullet dilates above the stricture, there is an increasing accumulation of what has been swallowed, and this the patient regurgitates at intervals; this is usually described as “vomiting,” but the material ejected shows no signs of gastric digestion. There is pain referred to the epigastrium or between the shoulder-blades, the patient suffers from hunger and thirst, and may present an extreme degree of emaciation.
The diagnosis is suggested by the history, and is confirmed by the œsophagoscope or by the X-rays after an opaque meal. The use of bougies has taken a secondary place since the introduction of these methods of examination, but, when other means are not available, the passage of bougies having a whalebone shaft and a series of metal heads shaped like an olive, may give useful information regarding the site, number, and size of the strictures that require to be dealt with.
Treatment.—If the patient is in a critical state from starvation, gastrostomy must be performed to enable him to be fed; otherwise he is prepared for treatment of the stricture by rest in bed, sedatives, and suitable liquid or some solid foods to improve his general condition and eliminate the muscular spasm and congestion already referred to. If the passage of bougies with the object of dilating the stricture is difficult or impossible, it may be made easier or possible by getting a silk thread through the stricture. The patient swallows several yards of a reliable silk thread a day or two before the proposed dilatation is carried out; the thread is expected to pass through the stricture of the stomach, and to enter for some distance into the small intestine; the metal head of the bougie, which is canalised in its long axis, is “threaded” on the silk, and the latter acting as a guide, the bougie is passed safely and confidently through the stricture. Larger olive-shaped heads are passed at intervals until the normal calibre of the gullet is exceeded, after which it is usually easy to pass an ordinary full-sized instrument at intervals of a month or so.
In the event of failure, recourse must be had to gastrostomy, and through the stomach it may be possible to dilate the stricture by the “retrograde” route. In aggravated cases, the gastrostomy opening must be retained in order to prevent death from starvation.
Malignant Stricture—Carcinoma of the Gullet.—This is met with in two forms which present widely different pathological and clinical features.
Cancer of the cervical portion affects the gullet at its junction with the pharynx, and for some unexplained reason is much more common in women, and at the comparatively early age of between thirty and fifty. Cancer of the thoracic portion affects the extreme lower end of the gullet, and is met with almost exclusively in men over fifty.
Cancer of the Cervical Portion.—Difficulty of swallowing may arise suddenly; more often it is slow and progressive over a period of months and, in some cases, even of years. Pain on swallowing is not a constant or prominent feature; it may be referred to the site of the lesion or to one or both ears. In a considerable number of cases, the complaints of the patient are referred to the larynx; coughing, with abundant mucous expectoration disturbing the night's rest, hoarseness, or even loss of voice, which symptoms are due either to direct invasion of the larynx or to implication of one or other recurrent nerve; for the same cause, difficulty of breathing may supervene, sometimes of such a nature as to render tracheotomy imperative. A gurgling noise on swallowing, and regurgitation of food are occasionally observed.
Palpation of the neck, and particularly of the larynx and trachea, should be carried out in all cases presenting the symptoms described; and as bearing on the question of operation, enlargement of the cervical lymph glands and of the thyreoid should be looked for; cancer of the thyreoid is sometimes secondary to disease at the pharyngo-œsophageal junction.
Direct and indirect laryngoscopic examination is then made; if the laryngeal mirror fails to reveal anything abnormal, suspension laryngoscopy, which gives a more extensive view of that part of the pharynx lying behind the larynx, may be employed, or the œsophagoscope may be preferred. A portion of the growth may be removed for microscopical examination.
The use of the œsophageal bougie as a diagnostic agent must be deprecated; it gives no satisfactory explanation of the cause of the obstruction, and its employment when malignant ulceration is present, is not free from serious risk to the patient (Logan Turner).
Treatment.—The surgeon is dependent on the help of the laryngologist not only for the diagnosis of the disease at the earliest stage possible, but also for information as to its extent, especially with regard to involvement of the larynx.
Œsophagectomy, or resection of the cancerous segment of the gullet, in suitable cases, even if it does not yield a permanent cure, not only prolongs life but relieves the patient of her most distressing symptoms. It is rarely possible to secure an end-to-end anastomosis, but the feeding by means of a tube introduced into the open end of the gullet is more satisfactory and the laryngeal symptoms are more efficiently relieved, than by either of the purely palliative operations. In the majority of cases, however, only the palliative measures of œsophagostomy or gastrostomy can be adopted. Œsophagostomy presents the advantage, that by exposing the cervical portion of the gullet, the operator is enabled to investigate the extent of the disease and to revise his opinion on the feasability of its removal if necessary. In advanced cases, when the disease has spread widely in the neck and involved, it may be, the thyreoid and the larynx, it may only be possible to relieve the urgent distress of the patient by gastrostomy. Tracheotomy may also become necessary because of the spread of the cancer to the interior of the larynx.
Cancer of the Lower End of the Gullet.—The remarkable preference of this location of œsophageal cancer for the male sex has already been referred to; it affects the same type of male patients as are subject to squamous epithelioma in other parts of the body. So far as we have observed, its association with chronic irritation of the mucous membrane in which it takes origin, or with any pre-cancerous condition, has not been demonstrated.
The clinical features resemble those of cicatricial stricture; the difficulty of swallowing is usually of gradual onset, it concerns solids in the first instance, then semi-solids like porridge or bread and milk, and finally fluids. As in other forms of œsophageal obstruction, the difficulty of swallowing varies quite remarkably from time to time, presumably from variations in the degree of congestion of the mucous membrane and of spasm of the muscular coat, but also from mere nervousness, the patient having greater difficulty when in a hurry, as in a railway refreshment room, or embarrassed by the presence of strangers.
As the lumen of the gullet becomes narrower, the food materials accumulate above the obstruction, and the consequent dilatation of the gullet above the stricture accounts for the large amount that may be regurgitated and for the patient describing it as vomiting. Along with food materials there is abundant saliva, and, if the cancer has ulcerated, of pus and blood. Contrary to what might be expected, there is little or no complaint of hunger, in spite of the progressive starvation and emaciation which inevitably supervene.
Death takes place within a year or so of the onset of symptoms, usually from starvation, but the fatal issue may be precipitated by ulceration and perforation of the gullet into a large blood vessel or into the left pleural sac; in the latter event, there follows a basal empyema which may contain gas and food materials.
Diagnosis.—In the majority of cases the history is so characteristic that there is little doubt regarding the diagnosis; the most reliable corroboration, with least risk and distress to the patient, is obtained by radiographic examination after an opaque meal; the appearance of the dilated gullet is that of an elongated sausage, parallel with the vertebral column, and terminating abruptly at the site of stricture (Fig. 285). A filiform, tortuous shadow of the bismuth may be continued downwards and show up the lumen of the stricture. The use of the œsophagoscope and of bougies is to be deprecated as not free from risk.
Treatment.—The lower end of the gullet is one of the most inaccessible portions of the body, and although it has been removed by operation the prospects of success are so small that it is not at present regarded as justifiable.
Among palliative measures, may be mentioned intubation of the stricture with a view to increasing the amount of food that can be swallowed; a funnel-shaped tube like that of Symonds or of Hill is introduced into the lumen of the stricture by means of a bougie or with the help of the œsophagoscope. The tube is anchored to a denture, or by means of a silk thread to the cheek by sticking-plaster. Our experience of intubation is that it merely serves to tide the patient over a critical period of starvation, so that he may regain some strength for any other procedure that may be indicated.
The value of making a fistula in the stomach—gastrostomy—in order to feed the patient, is a question about which widely different opinions are held both by patients and by surgeons. Many patients allege that they would prefer to die rather than prolong a precarious existence by being fed through a tube; some surgeons look upon the operation with disfavour because they doubt whether it even prolongs life, and it is often followed by a pneumonia which rapidly proves fatal. Variation in the results of gastrostomy observed by different surgeons is partly due to differences in the stage of the disease at which the operation is performed, and probably to a greater extent to the confusion between cases of slowly growing squamous epithelioma of the lower end of the gullet and cases of glandular carcinoma of the cardiac end of the stomach, these being grouped together under the clinical heading of “malignant stricture of the lower end of the gullet.” In our experience cases of epithelioma of the gullet (in the strict sense of the term) benefit greatly if subjected to gastrostomy as soon as the condition is recognised. In a case operated upon by Thomas Annandale the patient survived the operation for three years and some months.
Radiation.—The introduction of a tube of radium into the stricture and its retention there, the silk thread attached to the tube being secured to the cheek by a strip of plaster, is described by Hill and Finzi as the most valuable palliative measure that has so far been employed in cancer of the gullet; the capacity of swallowing may be regained to a considerable extent. The employment of radium is rendered easier and more efficient if it is preceded by gastrostomy.
The Roux-operation.—This consists in making a new gullet to replace that which is obstructed; the abdomen is opened and a loop of jejunum is isolated; its lower end is anastomosed—end to side—to the stomach; the intestine is brought upwards through a tunnel made for it between the skin and the sternum, and the upper end is brought out and fixed to the skin, in the supra-sternal notch. It has scarcely passed beyond the experimental stage.
[7] Revised by Dr. Logan Turner.
Examination of the Larynx.—For this purpose the examiner requires a laryngeal reflector with forehead attachment, one or two sizes of laryngeal mirror, a tongue cloth, and the means of obtaining good illumination. The source of light should be by preference placed opposite to and on the same horizontal plane as the patient's left ear. The forehead reflector is placed over the observer's right eye so that he may look through the central aperture, while at the same time he throws a good circle of light into the patient's mouth. The patient should be seated with the head thrown slightly back; the tongue is protruded and covered with the cloth, and held lightly but firmly between the finger and thumb of the left hand. A full-sized mirror, warmed so as to prevent the condensation of the breath upon it, is inserted with the reflecting surface turned downwards, and pressed gently against the soft palate so as to push that structure upwards. The handle of the instrument is carried towards the left angle of the mouth, and by slightly altering the plane of the reflecting surface of the mirror the different parts of the larynx are in turn brought into view. The movements of the vocal cords should be observed during both respiration and phonation, and for the latter purpose the patient should be directed to phonate the vowel sound “eh.”
In the upper part of the mirror the epiglottis usually comes first into view: it is of a pinkish yellow colour, and presents a thin, sharply defined free margin. In front of the epiglottis are the median and lateral glosso-epiglottic folds passing forwards to the base of the tongue, and enclosing the two valleculæ. Extending backwards and downwards from the lateral margins of the epiglottis are the two ary-epiglottic folds which reach the arytenoid cartilages posteriorly. Between the two layers of mucous membrane of which the ary-epiglottic folds are composed are the cartilages of Wrisberg and Santorini. In the interval between the two arytenoid cartilages is the inter-arytenoid fold of mucous membrane, which forms the upper margin of the posterior wall of the larynx. The upper aperture of the larynx is bounded by the epiglottis in front, the ary-epiglottic folds laterally, and the inter-arytenoid fold behind. In the interior of the larynx the vocal folds (true vocal cords) form the most prominent features, being conspicuous as two flat white bands, which form the boundary of the rima glottidis or glottic chink. Above each true cord, and parallel with it, the ventricular fold or false cord is evident as a pink fold of mucous membrane. Between the ventricular fold and the vocal fold on each side is a linear interval, which indicates the entrance to the ventricle of the larynx.
Direct Laryngoscopy.—The larynx may also be examined by the direct method by means of Jackson's or Killian's spatulæ. After cocainisation of the base of the tongue, the soft palate, and the posterior surface of the epiglottis, the patient is seated upon a low stool and his head supported by an assistant. The light is obtained from a small lamp in the handle of the instrument or reflected from a forehead mirror. The spatula is warmed and introduced under the guidance of the eye, its end being passed over the epiglottis, and pressure exerted so as to draw the latter structure forward. In children a general anæsthetic is required, and the examination is made with the head hanging over the end of the table. Killian's “suspension laryngoscopy” affords the best method of examining the larynx in young children.
Tracheoscopy and Bronchoscopy.—Direct examination of the trachea and larger bronchi may be carried out in a similar way, by passing through the mouth and larynx metal tubes, after the method devised by Killian. This procedure is described as direct upper tracheoscopy and bronchoscopy. The examination may also be made through a tracheotomy wound—direct lower tracheoscopy. These procedures have proved of great service in the recognition of foreign bodies in the lower air-passages, and in their extraction; in the diagnosis of stenosis of the trachea, and of aneurysm pressing on the trachea.
The cardinal symptoms of laryngeal affections are interference with the voice and with respiration, and pain on swallowing. Laryngeal cough of a croupy or barking character may be present, and is usually associated with a lesion of the posterior wall or inter-arytenoid fold. Hæmoptysis is seldom of laryngeal origin, and unless the bleeding spot is visible in the mirror, the source of the bleeding is much more likely to be in the bronchi or lungs.
Interference with the Voice.—Hoarseness results from some affection of the vocal cords: it may be simple laryngitis, some specific cause such as tuberculosis or syphilis, or some condition which prevents the proper approximation of the cords, as in tumours and certain forms of paralysis. Huskiness of voice occurring in a middle-aged person, lasting for a considerable period, and unattended by any other local or constitutional symptom, should always arouse suspicion of malignant disease, and calls for an examination of the larynx. Should this reveal a congested condition of one vocal cord, associated with some infiltration, and should the mobility of the cord be impaired, suspicion of the malignant character of the affection is still further increased. The hoarseness in these cases is sometimes greater than the local appearances would seem to account for.
Aphonia, or loss of voice, sudden in origin, and sometimes transient, occurs more often in women, and is usually functional or hysterical in nature. Although the patient is unable to speak, she is quite able to cough. In these cases there is a bilateral paralysis of the adductor muscles, so that the cords do not approximate on attempted phonation; or the internal tensors may be paretic, leaving an elliptical space between the cords on attempted phonation. If the arytenoideus muscle alone is paralysed, a triangular interval is left between the cords posteriorly. There is no inflammation or other evidence of local disease.
The treatment of functional aphonia should be general and local; tonics such as strychnin, iron, and arsenic should be administered; the intra-laryngeal application of electricity usually effects a sudden cure. In obstinate cases the use of the shower-bath and cold douching, the administration of chloroform, and even hypnotism may be tried.
An examination of the lungs should be made in all cases of adductor paralysis, as this functional condition may be met with in early pulmonary tuberculosis.
Dysphagia.—Pain on swallowing, due to causes originating in the larynx, is usually associated with ulceration of the mucous membrane covering the epiglottis, ary-epiglottic folds, or arytenoid cartilages, that is, in connection with those parts with which the food is brought into direct contact.
The most frequent causes of such ulceration are tuberculosis, syphilis, and malignant disease. The differential diagnosis is often difficult from local inspection alone. The Wasserman test, the previous history, the state of the lungs and sputum, and the results of anti-syphilitic treatment may clear it up.
The treatment of dysphagia, apart from that of the disease associated with it, resolves itself into the use of local sedative applications, such as a weak cocain or eucain spray before meals, insufflations of acetate of morphin and boracic acid, and the use of a menthol spray. One of the best anæsthetic applications is orthoform powder, introduced by means of the ordinary laryngeal insufflator. Its action is more prolonged than that of any of the others, often lasting for from twenty-four to forty-eight hours.
Injection of the superior laryngeal nerve with a 60 per cent. solution of alcohol has been found satisfactory where other means have failed.
Interference with Respiration.—It is only necessary here to refer to such causes of interference with respiration as may call for surgical treatment.
The chief forms of laryngitis to be considered in connection with the production of dyspnœa, are membranous or diphtheritic laryngitis and acute inflammatory œdema.
Diphtheria of the larynx is described on p. 110, Volume I.
Acute Œdema of the Larynx.—Œdema of the larynx may be inflammatory or non-inflammatory in origin. The former is the more common, and may arise in connection with disease of the larynx, such as tuberculosis or syphilis, or it may be secondary to acute infective conditions at the base of the tongue, or in the fauces or pharynx; more rarely it results from infective conditions of the cellular tissue or glands of the neck. The non-inflammatory form may be a local dropsy in renal or cardiac disease, may be induced by pressure on the large cervical veins, and in some cases it appears to follow the administration of potassium iodide in the treatment of laryngeal affections.
The œdema consists of an exudation into the loose submucous areolar tissue, which may be of a simple serous character or may become sero-purulent. The situations mainly involved are the glosso-epiglottic fossæ between the base of the tongue and the epiglottis, the ary-epiglottic folds (Fig. 287), and the false cords. If the infective process commences in front of the epiglottis this structure becomes swollen and rigid, and often livid in colour—points which are readily discerned on examination with the mirror, or even without its aid in some cases. The patient complains of great pain on swallowing, and has the sensation of a foreign body in the throat. Should the œdema spread to the ary-epiglottic folds, either from the interior of the larynx or from the fauces and pharynx, dyspnœa becomes a prominent and grave symptom. The patient may rapidly become cyanosed, the inspirations assume a noisy, stridulous character, and great distress and imminent suffocation supervene. If laryngoscopic examination is possible, the ary-epiglottic folds may be found greatly swollen and the upper aperture of the larynx partly occluded. Digital examination may reveal the swollen condition of the parts. The urine should be examined for albumin and tube casts.
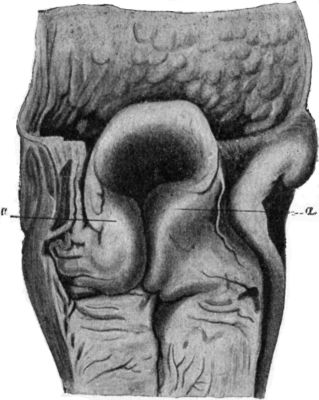 Fig. 287.—Larynx from case of sudden death, due to
œdema of ary-epiglottic folds, a, a.
Fig. 287.—Larynx from case of sudden death, due to
œdema of ary-epiglottic folds, a, a.Treatment.—In the milder forms, the sucking of ice, the inhalation of medicated steam, or spraying with a solution of adrenalin, and the application of poultices to the neck, may suffice to relieve the condition. Scarification of the epiglottis and ary-epiglottic folds with a knife, followed by free bleeding, may give complete relief. Diaphoretic and purgative treatment should not be neglected. If suffocation is imminent, tracheotomy or intubation is called for.
In performing tracheotomy, a roller pillow is placed beneath the neck to put the parts on the stretch, and an incision is carried from the lower margin of the cricoid cartilage downwards for about 2 inches. The sterno-hyoids and sterno-thyreoids are separated; the cross branch between the anterior jugular veins, and any other veins met with, secured with forceps before being divided; and the trachea exposed by dividing transversely the layer of deep fascia which passes from the cricoid to the isthmus of the thyreoid. If the isthmus cannot be pulled downwards sufficiently, it may be divided in the middle line. All active bleeding having been arrested, the larynx is steadied by inserting a sharp hook into the lower edge of the cricoid cartilage, and the trachea is opened by thrusting a short, broad-bladed knife through the exposed rings. The back of the knife should be directed downwards, and the opening in the trachea enlarged upwards sufficiently to admit the tracheotomy tube. In children it is sometimes found necessary to divide the cricoid for this purpose (laryngo-tracheotomy). The slit in the trachea is then opened up with a tracheal dilator, and the outer tube inserted and fixed in position with tapes. The inner tube is not fixed, so that it may be coughed out if it becomes blocked, and that it may be frequently removed and cleaned by the nurse. The tube should be discarded as soon as the patient is able to breathe by the natural channel.
Intubation of the Larynx.—This procedure is employed as a substitute for tracheotomy, especially in children suffering from membranous and œdematous forms of laryngitis. As experience is required to carry out the manipulations successfully, and as its use is attended with certain risks which necessitate that the surgeon should be constantly within call, the operation is more adapted to hospital than to private practice. O'Dwyer's apparatus is that most generally employed. The operation consists in introducing through the glottis, by means of a specially constructed guide, a small metal or vulcanite tube furnished with a shoulder which rests against the false vocal cords. The part of the tube which passes beyond the true vocal cords is bulged to prevent it being coughed out.
In an emergency a gum-elastic catheter with a terminal aperture may be passed, as recommended by Macewen and Annandale.
Bilateral Abductor Paralysis.—Both recurrent nerves may be interfered with by such conditions as enlargement of the thyreoid, tumour of the œsophagus, or intra-thoracic tumour, or by injury in the course of operations for goitre. A gradually increasing inspiratory dyspnœa is developed, which at first is only noticed on exertion, when the desire for air is increased; later it becomes permanent, and even during sleep the stridor may be marked. Suffocation may become imminent. When the larynx is examined with the mirror, the vocal cords are seen to lie near each other, and on inspiration their approximation is still greater.
The treatment is directed to removing the cause of pressure on the nerves. In the majority of cases tracheotomy is called for and the tube must be worn permanently.
Syphilitic Affections of the Larynx.—Secondary syphilitic manifestations in the form of congestion of the mucous membrane, mucous patches, or condylomata, are occasionally met with, and give rise to a huskiness of the voice. These conditions usually disappear rapidly under anti-syphilitic treatment.
In tertiary syphilis, whether inherited or acquired, the most common lesion is a diffuse gummatous infiltration, which tends to go on to ulceration and to lead to widespread destruction of tissue. It usually attacks the epiglottis, the arytenoids, and the ary-epiglottic folds, but may spread and implicate all the structures of the larynx. Syphilitic ulcers are usually single, deep, and crateriform; the base is covered with a dirty white secretion, and the surrounding mucosa presents an angry red appearance. When the perichondrium becomes invaded, necrosis of cartilage is liable to occur.
Hoarseness, dyspnœa, and, when the epiglottis is involved, dysphagia, are the most prominent symptoms.
Cicatricial contraction leading to stenosis may ensue, and cause persistent dyspnœa.
The usual treatment for tertiary syphilis is employed, but on account of the tendency of potassium iodide to increase the œdema of the larynx, this drug must at first be used with caution. Intubation or tracheotomy may be called for on account of sudden urgent dyspnœa or of increasing stenosis. The stenosis is afterwards treated by gradual dilatation with bougies, which, if a tracheotomy has been performed, may conveniently be passed from below upwards. An annular stricture causing occlusion may be excised, and the ends of the trachea sutured.
Tuberculosis.—The larynx is seldom the primary seat of tubercle. In the majority of cases the patient suffers from pulmonary phthisis, and the laryngeal mucous membrane is infected from the sputum. The disease may take the form of isolated nodules in the vicinity of the arytenoid cartilages, of superficial ulceration of the vocal cords and adjacent parts, or of a diffuse tuberculous infiltration of all the structures bounding the upper aperture of the larynx. The mucous membrane becomes œdematous and semi-translucent. The nodules coalesce and break down, leading to the formation of multiple superficial ulcers. The parts adjacent to the ulcers are pale in colour. Perichondritis may occur and be followed by necrosis of cartilage and the formation of abscesses in the submucous tissue of the larynx or in the cellular tissue of the neck.
The voice becomes hoarse or may be lost, there is persistent and intractable cough, and in some cases dyspnœa supervenes. When the epiglottis is involved there is pain and difficulty in swallowing.
In the presence of advanced pulmonary phthisis the treatment is chiefly palliative, but if the disease in the lungs is amenable to treatment, and the laryngeal lesion limited, the electric cautery may be used. Tracheotomy may be called for on account of urgent dyspnœa.
Tumours.—The commonest form of simple tumour met with in the larynx is the papilloma. It may occur at any age, and is comparatively common in children. It most frequently springs from the vocal cords and adjacent parts, forming a soft, pedunculated, cauliflower-like mass of a pink or red colour, which may form a fringe hanging from the edge of the cord (Fig. 288), or may spread until it nearly fills the larynx. In children, the growths are frequently multiple and show a marked tendency to recur after removal. They sometimes disappear spontaneously about puberty.
The most prominent symptoms are hoarseness, aphonia, and dyspnœa, which in children may be paroxysmal.
The treatment consists in removing the growth by means of laryngeal forceps or the snare, under cocain and adrenalin anæsthesia. For the removal of multiple papillomata, the removal of the growths through Killian's tubes or by suspension laryngoscopy has now taken the place of the external operation in children. In a certain number of cases it has been found that the tumour disappears after the larynx has been put at rest by the operation of tracheotomy.
Cancer.—Epithelioma of the larynx is almost always primary, and usually occurs in males between the ages of forty and seventy. It is important to distinguish between those cases in which the growth first appears in the interior of the larynx—on the vocal cords, the ventricular bands, or in the sub-glottic cavity (intrinsic cancer)—and those in which it attacks the epiglottis, the ary-epiglottic folds, or the posterior surface of the cricoid cartilage (extrinsic cancer).
Clinical Features.—In the great majority of cases of intrinsic cancer the first and for many months the only symptom is huskiness of the voice, which may go on to complete aphonia before any other symptoms manifest themselves. When the larynx is examined in an early stage, the presence of a small warty growth on the posterior part of one vocal cord, or a papillary fringe extended along the free edge of the cord, should raise the suspicion of malignancy, especially if the affected cord is congested and moves less freely than its fellow. Early diagnosis is essential in intrinsic cancer, and the absence of enlargement of lymph glands, or of fœtor and cachexia, must in no way influence the surgeon against making a diagnosis of malignancy. The impaired mobility of the affected cord is an important point in determining the malignant nature of the growth.
Intrinsic cancer may spread over the upper boundaries of the larynx and become extrinsic, or the disease may be extrinsic from the outset.
In cases of extrinsic cancer the early symptoms are much more marked, pain and difficulty in swallowing, and the secretion of frothy, blood-stained mucus being among the earliest manifestations. The cervical glands are infected early, sometimes even before there are any symptoms of laryngeal disease. Difficulty of breathing is also an early symptom on account of the growth obstructing the entrance of air. Tracheotomy may therefore be called for. In other respects the course and terminations are similar to those of intrinsic cancer.
When the growth spreads into the tissues of the neck the patient's sufferings are greatly increased. The œsophagus may be invaded with resulting dysphagia; the nerve-trunks may be pressed upon, causing intense neuralgic pains; the lymph glands become infected and break down, and the growth fungates through the skin. The general health deteriorates and death results, usually from septic pneumonia set up by the passage of food particles into the air-passages, from absorption of toxins, or from hæmorrhage. The duration of this form of the disease varies from one to three years.
The treatment consists in removing the growth. In early and limited forms of intrinsic cancer laryngo-fissure (thyreotomy) gives good results; in more advanced cases the entire larynx must be removed—complete laryngectomy—and at the same time, or after an interval, the associated lymph glands are removed from the anterior triangle of the neck on both sides.
In cases in which excision is impracticable, the sufferings of the patient may be alleviated by performing low tracheotomy, and by feeding with the stomach tube or by nutrient enemata. In some cases the difficulty of feeding the patient may make it necessary to perform gastrostomy.
Sarcoma of the larynx gives rise to the same symptoms as cancer, and can seldom be diagnosed from it before operation.
Foreign Bodies in the Air-Passages.—Foreign bodies impacted in the pharynx usually consist of unmasticated pieces of meat or large tooth-plates, and they occlude both the food and the air-passages, frequently causing sudden death. They are considered with affections of the pharynx.
The bodies most frequently impacted in the larynx are small tooth-plates in the case of adults, and buttons, beads, sweets, coins, and portions of toys in children. These are drawn from the mouth into the air-passage during a sudden inspiratory effort, for example while laughing or sneezing. If the glottis is completely blocked, rapidly fatal asphyxia ensues. If the obstruction is incomplete, the patient experiences severe pain, difficulty of breathing, and a terrifying sensation of being choked. The irritation of the foreign body causes spasmodic coughing and retching, and may induce spasm of the glottis, with threatening suffocation.
Small round bodies may lodge in the upper aperture or in one of the ventricles, and give rise to hoarseness and repeated attacks of dyspnœa and spasmodic cough. Wherever the body is situated, the symptoms may suddenly become urgent from its displacement into the glottis, or from the onset of œdema. The position of the body may often be ascertained by the use of the X-rays.
Treatment.—If the symptoms are urgent, laryngotomy, which consists in opening the larynx below the glottis by dividing the crico-thyreoid membrane, or tracheotomy must be performed at once, and an attempt made to remove the foreign body thereafter. In less severe cases in adults, the throat should be sprayed with cocain, and the larynx examined with the mirror; in children, the direct method must be employed. In both instances an attempt should be made to extract the body by the direct method. As these manipulations are liable to induce sudden spasm of the glottis, the means of performing tracheotomy must be at hand. If it is found impossible to remove the body through the mouth, laryngotomy or tracheotomy should be performed, and the body extracted through the wound, or pushed up into the pharynx and removed by this route. In the case of small bodies, a strand of gauze pushed up from the tracheotomy wound, through the larynx and out of the mouth, catches the foreign body and carries it out (Walker Downie).
The foreign bodies that are most likely to become impacted in the trachea are tooth-plates with projecting hooks, and small coins. The position of the foreign body may be ascertained by the use of Killian's tracheoscope, or by means of the X-rays. If the body remains movable in the trachea, it is apt to be displaced when the patient moves or coughs, and it may be driven up and become impacted in the glottis, setting up violent attacks of coughing and spasmodic dyspnœa.
Tracheotomy should be performed at once, and the edges of the tracheal wound held widely open with retractors, the patient being inverted, or coughing induced by tickling the mucous membrane with a feather. The foreign body is usually expelled, but it may be inhaled into one of the bronchi. One of Killian's tracheal tubes may be introduced through the tracheotomy wound and the body extracted by means of suitable forceps.
Foreign Bodies in the Bronchi.—Rounded objects, which pass through the larynx, usually drop into one or other of the bronchi, usually the right, which is the more vertical and slightly the larger. The body may act as a ball-valve, permitting the escape of air with expiration, but preventing its entrance on inspiration, with the result that the portion of lung supplied by the bronchus becomes collapsed. The physical signs of collapse of a portion or of the whole lung may be recognised on examination of the chest. In some cases the body is dislodged and driven up into the larynx, causing severe dyspnœic attacks and spasms of coughing. The irritation caused by the foreign body in the bronchus may set up bronchitis or pneumonia, and abscess of the lung may supervene. This has frequently followed the entrance of an extracted tooth into the air-passage, and it may be a considerable time before pulmonary symptoms arise. Sometimes the tooth is ultimately coughed up and the symptoms disappear. In some cases the physical signs closely simulate those of pulmonary phthisis.
The treatment consists in removing the body by the aid of Killian's or Jackson's tube passed through the mouth. If this is not successful, low tracheotomy is performed and the tube is passed through the tracheotomy opening.
| A | B | C | D | E | F | G | H | I | J | K | L | M |
| N | O | P | Q | R | S | T | U | V | W | X | Y | Z |
End of the Project Gutenberg EBook of Manual of Surgery Volume Second:
Extremities--Head--Neck. Sixth Edition., by Alexander Miles and Alexis Thomson
*** END OF THIS PROJECT GUTENBERG EBOOK MANUAL OF SURGERY ***
***** This file should be named 28428-h.htm or 28428-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/2/8/4/2/28428/
Produced by Jonathan Ingram, Chris Logan and the Online
Distributed Proofreading Team at http://www.pgdp.net
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License (available with this file or online at
http://gutenberg.org/license).
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH F3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS' WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTIBILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need, are critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation web page at http://www.pglaf.org.
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Its 501(c)(3) letter is posted at
http://pglaf.org/fundraising. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at
809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887, email
business@pglaf.org. Email contact links and up to date contact
information can be found at the Foundation's web site and official
page at http://pglaf.org
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit http://pglaf.org
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations.
To donate, please visit: http://pglaf.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart is the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For thirty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
http://www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.