
The Project Gutenberg EBook of Cases of Organic Diseases of the Heart, by John Collins Warren This eBook is for the use of anyone anywhere at no cost and with almost no restrictions whatsoever. You may copy it, give it away or re-use it under the terms of the Project Gutenberg License included with this eBook or online at www.gutenberg.org Title: Cases of Organic Diseases of the Heart Author: John Collins Warren Release Date: October 7, 2008 [EBook #26836] Language: English Character set encoding: ISO-8859-1 *** START OF THIS PROJECT GUTENBERG EBOOK HEART DISEASE *** Produced by Bryan Ness, Irma Spehar and the Online Distributed Proofreading Team at http://www.pgdp.net (This book was produced from scanned images of public domain material from the Google Print project.)
WITH DISSECTIONS AND SOME REMARKS INTENDED TO POINT OUT THE
DISTINCTIVE SYMPTOMS OF THESE DISEASES.
READ BEFORE THE COUNSELLORS OF THE MASSACHUSETTS
MEDICAL SOCIETY.
BOSTON:
PRINTED BY THOMAS R. WAIT AND COMPANY.
COURT-STREET.
1809.
PLATE I.
Appearance of the valves of the aorta in Case 3d, Article 10.
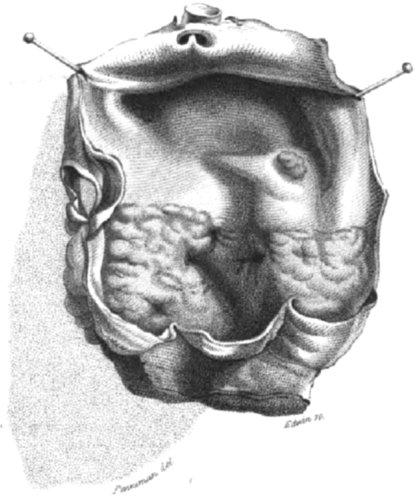
PLATE II.
Is a representation of the fleshlike thickening of the aorta in case 7th. The valves are smaller than usual, and their form is in some degree changed. A round spot, thickened, is seen at a little distance from the seat of the principal disease.
Morbid changes in the organization of the heart are so frequent, as to have attracted the observation of those, who have devoted any attention to the study of morbid anatomy. Derangements of the primary organ of the circulation cannot exist without producing so great disorder of the functions of that and of other parts, as to be sufficiently conspicuous by external signs; but, as these somewhat resemble the symptoms of different complaints, especially of asthma, phthisis pulmonalis, and water in the thorax, it has happened, that each of these has been sometimes confounded with the former[1]. The [2]object of the following statement of cases is to shew, that, whatever resemblance there may be in the symptoms of the first, when taken separately, to those of the latter diseases, the mode of connection and degree of those symptoms at least is quite dissimilar; and that there are also symptoms, peculiar to organic diseases of the heart, sufficiently characteristic to distinguish them from other complaints.
The symptoms of organic disease of the heart are marked with extraordinary clearness in the following case. The opportunity for observing them was very favourable; and there was every incitement to close observation, which could arise from the important and interesting character of the patient. These advantages will justify an uncommon minuteness in the detail of the case; especially, as the most accurate [3]knowledge of a complaint is obtained from a successive view of its stages.
The late Governour of this commonwealth was endowed with most vigorous powers of mind and body. At the age of sixteen he was attacked with fits of epilepsy, which first arose from a sudden fright, received on awaking from sleep in a field, and beholding a large snake erecting its head over him. As he advanced in life they became more frequent, and were excited by derangement of the functions of the stomach, often by affections of the mind, by dreams, and even by the sight of the reptile which first produced the convulsions.
At the commencement of the American revolution he became deeply engaged in public affairs; and from that time devoted himself to intense application to business, with which the preservation of his health was never allowed to interfere. In the expedition against Rhode Island, an attack of inflammation of the lungs had nearly proved fatal to him.
In the beginning of the year 1807, he suffered severely from the epidemic catarrh; and a remarkable irregularity of the pulse was then perceived to be permanent, though there is some reason to believe, that this irregularity had previously existed, during the fits of epilepsy, and for a few days after them. In the summer, while he was apparently in good health, the circulation in the right arm was suddenly and totally suspended; yet, without loss of motion or sensation. This affection lasted from noon till midnight, when it as suddenly ceased, and[4] the circulation was restored. In the autumn he was again seized with the influenza, which continued about three weeks, leaving a troublesome cough of two or three months’ duration, and a slight occasional difficulty of breathing, which at that time was not thought worth attention. Soon after, in November, he had one or two singular attacks of catarrhal affection of the mucous membrane of the lungs, which commenced with a sense of suffocation, succeeded by cough and an expectoration of cream coloured mucus, to the quantity of a quart in an hour, with coldness of the extremities, lividity of the countenance, and a deathlike moisture over the whole body. These attacks lasted six or eight hours, were relieved by emetics, and disappeared, without leaving a trace behind.
At this time he began to complain of palpitations of the heart; yet, it is probable, that he had been affected with these before, since he was unaccustomed to mention any complaint, which was not sufficiently distressing to require relief. He experienced a difficulty of respiring, as he ascended the stairs, and became remarkably susceptible of colds, from slight changes of clothing, moisture of the feet, or a current of cold air. His sleep was unquiet in the night, and attended with very profuse perspiration; and, in the latter part of the day, a troublesome heaviness occurred. The sanguiferous vessels underwent an extraordinary increase, or, at least, became remarkably evident. The pulsation of the carotid arteries was uncommonly strong; the radial[5] arteries seemed ready to burst from their sheaths; the veins, especially the jugulars, in which there was often a pulsatory motion, were every where turgid with blood. The countenance was high coloured, and commonly exhibited the appearance of great health; but, when he was indisposed from catarrh, this florid red changed to a livid colour; which also, after an attack of epilepsy, was observable for two or three days on the face and hands. This livid hue was often attended, under the latter circumstances, with something like ecchymosis over the face, at first formidable in its aspect, and gradually subsiding, till it had the general appearance of an eruption, which also soon vanished.
These symptoms increased, almost imperceptibly, during the five first months of the year 1808. Much of this time was passed in close application to official duties; and it seemed that a constant and regular occupation of the mind had the effect of obviating the occurrence of any paroxysm of disease, as well of epilepsy, as of difficult respiration; and that a very sudden and disagreeable impression generally produced either one or the other. There were, indeed, independently of such circumstances, some occasional aggravations of those symptoms. Some nights, for example, were passed in sitting up in bed, under a fit of asthma, as it was called; sometimes the mind became uncommonly impatient and irritable; the body gradually emaciated; yet the appetite and digestive functions remained principally unimpaired; and persons around were not sensible[6] of any material alteration in the condition of the patient.
On the approach of warm weather, in June, the violence of the symptoms increased. Paroxysms of dyspnœa occurred more frequently, and were more distressing. They commenced with symptoms of slight febrile affection, such as hot skin, hard, frequent, and more irregular pulse, disordered tongue, loss of appetite, and derangement of the digestive functions. This kind of paroxysm lasted two or three days. Evacuations of blood from the nose and hæmorrhoidal vessels, which before rarely occurred, became frequent; a fulness at the upper and right side of the abdomen was sometimes perceptible, formed apparently by temporary enlargement of the liver; the difficulty in ascending an eminence increased sensibly. In the intervals of these attacks, which were variable, but generally continuing ten or twelve days, the strength was frequently good, and accompanied by a great flow of spirits, and an aptitude, or rather ardour, for business.
Such was the course of this complaint until the latter part of August, when a very severe paroxysm occurred. It commenced, like the former, with febrile symptoms, but those more violent than before. The countenance became high coloured; the dyspnœa excessive, and rendered almost suffocating by a slight movement, or attempt to speak; the pulse hard, very irregular, intermittent, and vibrating; and the digestive functions were suspended. These symptoms soon increased to the highest[7] degree. The respiration was so distressing, as to produce a wish for speedy death; the eyes became wild and staring. No sleep could be obtained; for, after dosing a short time, he started up in violent agitation, with the idea of having suffered a convulsion. During the few moments of forgetfulness, the respiration was sometimes quick and irregular, sometimes slow, and frequently suspended for the space of twenty five, and even so long as fifty seconds. At the end of three days the febrile heat was less permanent; the red colour of the face changed to a death like purple; the hands and face were cold, and covered with an adhesive moisture; the hardness of the pulse diminished, and a degree of insensibility took place. I seized this opportunity to examine the region of the heart, which had not been done before, from fear of alarming the active and irritable mind of the patient. The heart was perceived palpitating, obscurely, about the 7th and 8th ribs; its movements were very irregular, and consisted in one full stroke, followed by two or three indistinct strokes, and sometimes by an intermission, corresponding with the pulse at each wrist. The pulsation was felt more distinctly in the epigastric region. During this paroxysm a recumbent posture was very uneasy, and the patient uniformly preferred sitting in a chair. When the recumbent posture was assumed, the head was much raised, inclined to the right side, and supported by the hand; the knees were drawn up as much as possible. He could not bear an horizontal posture; nor[8] did he ever lie on the left side, except a short time after the application of a blister. At the end of the fifth day his sufferings abated, but the sudden affusion of a small portion of a cold liquid on the head produced a severe fit of epilepsy. This was followed by a return of the symptoms equally distressing, and more durable, than in the first attack[2].
This violent agitation gradually subsided, and was followed by a pleasant calm. The natural functions resumed their ordinary course; his appetite returned; his enjoyment of social intercourse was unusually great; and he amused and instructed his friends by the immense treasures of information, which his talents and observations had afforded him, and which, he seemed to feel, would soon be lost. At the end of September the feet began to swell, and after some time the enlargement extended up to the legs and thighs, and increased to an extraordinary degree; the abdomen next swelled, and, after it, the face. Toward the end of October there were some indications of water in the chest; there was a constant shortness and difficulty of breathing; the cough, till now rare, became more frequent and troublesome; the contraction of the thoracic cavity rendered the action of the heart more painful, to that [9]beside an uniform stricture across the breast, he sometimes described a dreadful sensation like twisting of the organs in the thorax. He suspected the existence of water there, and was inclined to consider it as his primary disease, but was easily convinced of the contrary. At one time he had a suspicion of a complaint of the heart, and, although he had never heard of a disease of that organ, slightly intimated it to one of his friends, and mentioned a sensation he had experienced in the chest, which he compared to a fluid driven through an orifice too narrow for it to pass freely. In this month, beside the dropsical affections and increase of cough, he had occasional painful enlargements of the liver, frequent starting up from sleep, a slight degree of dizziness, a great disposition for reveries, and sometimes extraordinary illusions, one of which was, that he was two individuals, each of whom was dying of a different disease. This idea often occurred, and gave him much uneasiness. He was also afflicted with long continued frightful dreams, and sometimes a slight delirium.
After the use of much medicine, on the 6th of November, the effused fluids began to be absorbed, and passed out through the urinary organs with such rapidity, that on the 12th the dropsical enlargements had nearly disappeared. The pulse was much reduced, in hardness and frequency, by the medicine, and, as it fell, he became more easy. On the 10th the state legislature convened, and the call of business roused, like magic, the vigor of his mind; and the[10] symptoms of his disease almost disappeared. During this session he made little complaint, dictated many important communications, and attended to all the duties of his office, without neglecting the most minute. As soon as the legislature adjourned, he declared, that his work was finished, and that he had no desire to remain longer in this world. He entreated that no farther means should be used to prolong his existence, and immediately yielded himself to the grasp of disease, which appeared waiting with impatience to inflict its agonies.
From this moment the distressing difficulty of breathing had very slight remissions. The consequent disposition to incline the superior part of the body forward, for the purpose of facilitating respiration, increased so much, that he frequently slept with his head reposed on his knees. The cough became occasionally very violent, and was always attended with an expectoration of a brown coloured mucus, sometimes tinged with blood. The abdominal viscera lost their activity. The face was sometimes turgid and high coloured, at other times pallid and contracted. A gradual abolition of the powers of the mind ensued, with a low delirium, and two short fits of phrenzy. The state of the circulation was very variable; the pulse at the wrists principally hard and vibrating, rarely soft and compressible; the less pulsations becoming more indistinct, and at length scarcely perceptible. No perfectly distinct beat of the heart was felt, but a quick undulating motion, not corresponding with the pulse at the[11] wrist. Three days before death the arteries assumed this undulatory motion, corresponded with the motion of the heart, and, for forty-eight hours, lost the irregularity of pulsation[3].
Once or twice the expiring faculties brightened. On the 30th of November he awoke, as if from death, conversed very pleasantly for two or three hours, and humorously described scenes, which he had witnessed in his youth.
On the 4th of December came on the second attack of furious delirium. Insensibility, and great prostration of strength, ensued. The respiration became very slow, and obstructed by the accumulation of mucus in the lungs; the pulse very intermittent, then regular, and finally fluctuating. A hiccough commenced; coldness of the extremities and lividity of the face followed, and continued three days before death. On the 9th the incurvated posture was relinquished, and the head sunk back upon the pillow; the respirations then diminished in frequency, till they became only two in a minute; and [12]at the end of twenty-four hours they very gradually ceased.[4]
The whole body was much emaciated; the face pale and contracted. The hands were slightly œdematous. Discolourations, answering to the ribs, were observed on the thorax; many small purple spots, hard and prominent, on the back; excoriations on the nates; and purple spots, resembling incipient mortification, on the heel and toe.
The integuments of the thorax were free from fat: the cartilages of the ribs ossified in various degrees, some perfectly, others slightly. Upon laying open the cavity of the thorax, it was found to contain about three pints of water, the proportion being greatest on the left side.
The lungs were contracted into a smaller compass than usual, and were very firm to the touch. Their colour anteriorly was whitish, with small distinct purple spots; posteriorly, of a deep red, with similar spots. The right lobe adhered closely to the pericardium; it also adhered to the pleura costalis, by a great number of strong cords, which seemed to be elongations of the original adhesions. Some of them were nearly as hard as ligament, and many an inch in length. Internally the lungs presented a very [13]compact structure. Their cells were crowded with mucus, and their vessels filled with black blood, partly fluid, and partly coagulated. Some portions were firmer and more condensed than others, but no tubercles were discovered.
The pericardium, viewed externally, appeared very large, and occupied almost the whole space behind the opening formed by removing the sternum and cartilages of the ribs. It was situated principally on the left side, and contained about double the usual quantity of water; but was principally filled by the enlarged heart, to which it adhered anteriorly about two inches, near its base. Its parietes were, in every part, very much thickened and hardened.
The heart presented nearly its usual colour and form, excepting on its anterior surface, which was somewhat discoloured by coagulated lymph. It was enlarged in bulk to, at least, one half more than the healthy size. The auricles and ventricles contained coagulated blood. The tricuspid valves were in a sound state. The left auricle was double the usual size. The left ventricle was enlarged, about three times thicker and much firmer than usual. The mitral valves were very much thickened, and near the insertion of their columnæ, which were sound, cartilaginous, so that they were quite rigid, and the opening made by them, from the auricle to the ventricle, was scarcely large enough to admit the passage of a finger. The semilunar valves of the aorta were ossified at their bases and apices, and the portion[14] intermediate, between the base and apex, partly ossified, and partly cartilaginous, so as to render the valves very rigid. The aorta was at least one half larger than usual, especially at its arch. The arteria innominata, the carotid, and subclavian arteries, were uncommonly large and thick. The coronary arteries were considerably ossified.
The omentum was destitute of fat. The stomach distended with flatus on the pyloric side; its cardiac extremity, lying under the liver, was pressed down and contracted. The liver was shrunk; its tunic corrugated, as if it had been distended, and bearing marks of inflammation; its substance harder than usual; its vessels, when divided, pouring out liquid black blood. The gall bladder was filled with bile. The kidneys were thicker, and more irregular in form, than is common. The abdominal cavity contained some water.
The bones of the cranium were unusually thick. The dura mater, which was thickened, and in many places bore marks of former inflammation, adhered to the bone at the vertex. On its internal surface, near the longitudinal sinus, there was a small ossified portion, half an inch long and the eighth of an inch thick. The convolutions of the brain were narrow, and very strongly marked. The pia mater bore marks of pretty extensive inflammation, and adhered to the dura mater at the vertex. The cortical[15] substance ran deep into the medullary part of the brain. The ventricles contained about double the usual quantity of water; their parts were all remarkably well defined. The vessels of the pia mater, over the corpora striata, were unusually injected with blood. The velum interpositum was very firm; the plexus choroides uncommonly thick, but pale; the opening from the right to the left ventricle large. The vessels of the brain were generally not much filled with blood.
The blood appeared every where fluid, except in some portions of the lungs, and in the cavities of the heart. It was very dark coloured, perhaps more than ordinarily thin, and oozed from every part, which was cut.
The cellular membrane, in all dependent parts, effused, when cut, a serous fluid.
Mr. John Jackson, fifty-two years of age, had been affected for more than two years with palpitations of the heart, and paroxysms of dyspnœa. These symptoms increased in October, 1808, and were followed by strong cough, uneasiness in lying down, sudden startings in sleep, and an inclination to bend the body forward and to the left side. His cough, during the last part of his life, was attended with copious bloody expectoration. His countenance was florid; his pulse very irregular, though not quite intermittent. The occasional variations in the[16] state of the disease were remarkable. Some periods were marked with uncommon mental irritability. Pain in the region of the liver, œdema of the inferior extremities, paucity and turbidness of the urine, yellowness of the skin, and great emaciation attended the latter stages of the disease. A degree of stupor occurred. The termination on the 30th of January, 1809, was tolerably quiet. Two days before death he sank into the recumbent posture, and his pulse became more regular[5].
On opening the thorax, its right cavity was found to contain a large quantity of water; the left, a smaller quantity.
The lungs were of a firm, condensed texture, especially at the lower part, where their solidity was nearly equal to that of a healthy liver. They contained black blood.
The heart was much enlarged, and proportionally thickened. Its tunic was in some places covered with coagulated lymph, especially over the coronary arteries. Its cavities were filled with black coagulum, which in the right auricle and ventricle had a slight appearance of polypus. The semilunar valves of the pulmonary artery and aorta were unusually small, and their bases cartilaginous. Those of the aorta had lost their form, and were slightly ossified. [17]The remaining valves were partially thickened. The arch of the aorta was very much dilated, its internal coat covered with a bony crust, which extended through the remaining thoracic portion, gradually diminishing. This portion was also considerably dilated.
The liver was indurated; its peritonæal coat exhibited a flaccid or wrinkled appearance, and bore marks of slight inflammation. The gall bladder was filled with bile, and the pancreas indurated.
Captain Job Jackson, forty-five years of age, a man of vigorous constitution, after an indisposition of some years continuance, was seized with palpitations of the heart and dyspnœa, occurring by variable paroxysms, especially on ascending an eminence, and attended by hardness, irregularity, and intermission of the pulse. To these symptoms were superadded dizziness and severe head-ache, a disposition to bend the body forward, sudden starting from sleep, with dread of suffocation, violent cough with copious expectoration, which for fifteen days before death consisted of black blood, distressing pain across the chest, especially on the left side, great œdema of the lower extremities, and paucity of urine.
He died painfully in January, 1809, after violent struggles for breath. The day before death the pulse became regular. He rested his head upon an[18] attendant, and made no attempts to lie down for some days previous[6].
The skin was of a yellow colour. The inferior extremities, quite to the groins, were œdematous.
The left cavity of the thorax was filled with water; the right contained only a small quantity. The pleura costalis, on the left side opposite to the heart, was thickened and covered with a very thick flocculent coat of coagulated lymph, and the pericardium opposite to it had the same marks of inflammation. The lungs on that side were pushed up into a narrow space. They were dense and dark coloured.
The pericardium contained little more than the usual quantity of water. The heart, which exhibited marks of some inflammation on its surface, was astonishingly large, and firm in proportion. Its cavities were principally filled with coagulum. The semilunar valves of the pulmonary artery had their bases slightly ossified, and the remaining part thickened. There were only two valves of the aorta, and these were disorganized by the deposition of ossific matter about their bases, and a fleshlike thickening of the other part[7]. The parietes of the heart, especially of the left ventricle, were greatly thickened, and somewhat ossified near the origin of the aorta.
The liver had the same appearance as in case second.
Thomas Appleton, thirty-eight years of age, of a robust constitution, was affected with excessive difficulty of breathing, occurring at intervals of different duration. It commenced three years before his death, and gradually increased. He was subject to palpitations of the heart for at least two years before his death, and was distressed with violent cough, attended with copious expectoration, which finally became very bloody. The palpitation and dyspnœa were greatly augmented by ascending stairs. His countenance was very florid.
Sometimes he was seized with violent head-ache and dizziness, which, as well as the other symptoms, were greatly relieved by venesection. About two months before death œdema of the legs appeared, which was soon followed by frequent and alarming syncope. His pulse was irregular, intermittent, hard, and vibrating. When lying down he frequently awoke, and started up in great terror. His usual posture was that of sitting, with his trunk and head bent forward, and inclining to the left side. For some time before death a recumbent posture threatened immediate suffocation; yet, three days previous to the occurrence of that event, he sank back upon the pillow. He was, at intervals, so much better as to think himself free from disease. Slight delirium preceded his death, which occurred in January, 1809[8].
The countenance continued florid. The inferior extremities were much distended with water, and the cellular membrane abounded in fat.
The right cavity of the pleura contained a moderate quantity of water; the left, scarcely any. The lungs were firm, condensed, and dark coloured, from venous blood. The pleura, on the left side opposite to the pericardium, appeared to have been inflamed, as there was an effusion of coagulated lymph on its surface.
The pericardium was much distended with water. The heart, on the anterior surface of which were some appearances of inflammation, was very much enlarged. Its parietes were thickened; its cavities unnaturally large, and filled with black coagulum. Each of the valves had lost, in some degree, its usual smoothness, and those of the aorta were, in some points, thickened, and partly cartilaginous.
The liver was small, and, when cut, poured out dark blood. Its tunic was whitish, opaque, and corrugated.
A. B. a negro, about thirty-five years of age, had paroxysms of dyspnœa and violent cough, attended with œdema of the extremities and ascites, violent head-ache, dizziness, brightness of the eyes, palpitations[21] of the heart, irregular, intermittent, slow, and soft pulse. These symptoms slowly increased, during three or four years, in which time the dropsical collections were repeatedly dispersed. He gradually and quietly died in the alms-house, in January, 1809.
On dissection, the cavities of the pleura were found to contain a considerable quantity of water. The pericardium was filled with water; the heart considerably enlarged; its parietes very thin, and its cavities, especially the right auricle and ventricle, morbidly large[9].
Mrs. M‘Clench, a washer-woman, forty-eight years of age, of good constitution and regular habits, was attacked, in the summer of 1808, with palpitations of the heart and dyspnœa on going up stairs, severe head-ache, and discharges of blood from the anus. These symptoms did not excite much attention. In the winter of 1808-9, all of them increased, except the palpitations. The inferior extremities and abdomen became distended with water; the region of the liver painful; the skin quite yellow; the pulse was hard, regular, and vibrating; the countenance very florid. Violent cough followed, and blood was profusely discharged from the lungs. [22]This discharge being suppressed, evacuations of blood from the anus ensued, under which she died, in March, 1809.
The right cavity of the thorax was filled with water; the left contained none. The lungs were sound, but very dense, full of dark coloured blood, and, on the right side, pressed into the upper part of the thorax. The heart was one half larger than natural; its substance firm, and its anterior part, especially near the apex, covered with coagulated lymph. The right auricle and ventricle were large, and their parietes thin. The parietes of the left auricle and ventricle, particularly of the latter, were much thickened, and their cavities were filled with black coagulum.
The liver was contracted; its coat wrinkled, and marked with appearances of recent inflammation.
MY DEAR SIR,
Your important communication to our society, which is about to be published, will lay before the American public much more knowledge respecting the diseases of the heart, and large vessels, than has hitherto been presented to them. A case has lately fallen under my observation, having so much similarity to those of organic diseases of the heart, which[23] have occurred to you, as to mark its affinity, yet with some differences, which characterize it as a variety. If the statement of it will add any value to your collection of cases, you are at liberty to publish it.
A. S. twenty-eight years of age, and of middle stature, was attacked, after a debauch, with pain in the region of the heart, which subsided, but returned a year after on a similar occasion. He then became affected with palpitations of the heart for six months, great difficulty of breathing, which was augmented by ascending an eminence, severe cough, dizziness, and violent head-ache, attended by a disposition to bend the body forward, and sudden startings from sleep. His pulse was always regular, and never remarkably hard. His countenance, till within a few weeks of death, presented the appearance of blooming health. His feet and legs did not swell at any period of the disease. He suffered exceedingly from flatulence, to which he was disposed to attribute all his complaints. This symptom might have been aggravated by his habits of free living, and occasional intoxication, which he acknowledged, and to which he traced the origin of his disease.
After death, water was discovered in the thorax; but the lungs had not that appearance of accumulation of blood, in particular spots, which is commonly observed in cases of organic disease of the heart. The only very remarkable morbid appearance about the heart was in the aorta, and its valves. The valves had lost their transparency, and were considerably[24] thickened in various spots. The inner surface of the aorta, for about an inch from its commencement, was elevated and thickened, and the external surface singularly roughened and verrucated. This appearance was so peculiar, that no words will give a competent idea of it, and perhaps it would be sufficient for me to call it a chronic inflammation[10].
I am, my dear sir,
Your friend and obedient servant,
JAMES JACKSON.
Col. William Scollay, aged fifty-two, of a plethoric habit of body, was attacked, in the year 1805, with dyspnœa and palpitation of the heart, attended with irregularity of the pulse, and œdema of the lower extremities. By the aid of medicine, the dropsical collections were absorbed, and he recovered his health, so far as to follow his usual occupations, nearly a year; but was then compelled to relinquish them. The symptoms afterwards underwent various aggravations and remissions, till the beginning of the winter of 1808-9, when the attacks became so violent, as to confine him to the house. His face was then high coloured. The faculties of his mind were much impaired. The dyspnœa became more constant, and was occasionally attended by cough; the palpitations rather lessened in violence; the pulse was more irregular, and exceedingly intermittent. The abdomen and inferior extremities [25]were sometimes enormously distended with water, and afterwards subsided nearly to their usual size. One of the earliest, most frequent, and distressing symptoms, was an intense pain in the head. About two months before death, a hemiplegia took place, but after a few days disappeared. This so much impaired the operations of the mind, that the patient afterwards found great difficulty in recollecting words sufficient to form an intelligible sentence. During the existence of the last symptom the pulse was regular.
He gradually expired, on the 15th of March, 1809.
The countenance was somewhat livid and pale; the lips were very livid. The chest resounded, when struck, except over the heart. The abdomen was tumid, and marked by cicatrices like those of women, who have borne children. The superior extremities were emaciated, and marked like the abdomen. The lower extremities were œdematous.
The cartilages of the ribs were ossified. The left cavity of the pleura contained about twelve ounces of water; the right, about three ounces. The lungs, externally, were dark coloured, especially the posterior lobes; internally, they were very firm, and, in some places, as dense as the substance of the liver. A frothy mucus was effused from them in great[26] quantities. They were coloured by very dark blood, especially in the middle portion of the left superior lobe. One or two calcareous concretions were observed in them. The pericardium was a little firmer than usual, and contained about five ounces of water. The heart was enlarged, and covered with tough fat. In the right auricle, and ventricle, was some coagulated blood. The tricuspid valves had lost their smoothness and transparency; the semilunar valves of the pulmonary artery were cartilaginous at their bases. The left auricle and ventricle, particularly the first, contained coagulum. The mitral valves were roughened by many bony spots. Considerable ossification had taken place in the semilunar valves of the aorta, so that one of them had quite lost its form; and the aorta was ossified for the space of a square inch, at a small distance from the valves. The coronary arteries were also ossified.
The coat of the liver was somewhat wrinkled, as if shrunk. Its substance was hard, and discharged, when cut, great quantities of blood. The veins of the omentum, mesentery, and intestines, were full of blood. The abdomen contained a considerable quantity of water.
Water was found between the dura and pia mater, and between the pia mater and arachnoides. The vertical portion of the pia mater bore marks of[27] former inflammation. The convolutions of the brain were very distinct; their external surface was pale. The veins were empty[11]. No bloody points were observed in the medullary portion of the brain, when cut. The ventricles contained between one and two ounces of water; the communication between them was very large. The plexus choroides was pale.
A lady, about forty-five years of age, the mother of many children, has been troubled during the course of the past year with violent palpitations of the heart, and great difficulty of respiration, especially on going up stairs. These complaints have lately increased, so that she has kept in her chamber about two months. Her countenance is florid; her eyes are clear and bright. She has dizziness, especially on moving, without pain in her head. She had for some time, a severe cough, which is now relieved. The dyspnœa is not yet very distressing, except on using motion; it often occurs in the night, and obliges her to rise and sit up in bed. The palpitations are very hard, and so strong, that they may be perceived through her clothes; the tumult in the thorax is indescribable. The functions of the abdominal viscera are unimpaired. The pulse is hard, vibrating, irregular, intermittent, very variable, corresponding [28]with the motions of the heart, and similar in each arm. There is not yet the slightest reason to suspect any dropsical collection. The alternations of ease and distress are very remarkable, but on the whole, the violence of the symptoms increases rapidly.
There is no difficulty in discovering in this case an organic disease of the heart, which probably consists in an enlargement and thickening of the heart, and an ossification of the semilunar valves of the aorta.
Levi Brown, a cabinet-maker, forty-eight years of age, complained in February, 1809, of great difficulty of breathing, and an indescribable sensation in the chest, which he said was sometimes very distressing, and at other times quitted him entirely. Being a man of an active mind, he had read some medical books, whence he got an idea, that he was hypochondriac.
On examining his pulse, it was found to be occasionally intermittent, contracted, and vibrating. He had some years previously been attacked with copious hæmorrhages from the stomach or lungs, which have occasionally recurred, though they have lately been less frequent. Eight years since he suffered from an inflammation of the lungs; and about two or three years ago he first experienced a beating in the chest, and pain in the region of the heart, which[29] increased till within six or eight months, since which the beating has been stationary, and the pain has much increased. In the course of the last summer, dyspnœa, on using exercise, and especially ascending any eminence, commenced. This has greatly increased, so as to render it almost impossible for him to go up stairs. His countenance is turgid, and uniformly suffused with blood; his eyes are bright and animated; his lips livid. The pulsation of the heart cannot be felt on the left side, and is barely perceptible on the right side of the sternum, and in the epigastric region. When he is distressed with fits of dyspnœa, he feels something as if rising to the upper part of the thorax, and the heart then seems to him to be beating through the ribs. I have not witnessed any of these paroxysms. The inferior extremities and abdomen have been swelled about three weeks. When in bed, he has his head and shoulders elevated, and, upon the attack of his paroxysms, sits up and inclines his head forward; but he keeps from the bed as much as possible. In his sleep he is apt to start up, suddenly, in distress, especially when he first slumbers. His dreams are often frightful, and, when awake, he is affected with reveries, during which, though conscious of being awake, strange illusions present themselves. At intervals he seems slightly delirious. He has a violent cough, with very copious expectoration of thick mucus. He often suffers from severe head-ache, and the least exercise produces dizziness.[30]
This man has a very robust frame of body, and has been accustomed to a free use of ardent spirits, and of opium, of which he now takes about twelve grains in a day. His appearance is such, that, on a slight survey, one would not suppose him diseased, but, on observing him with a little attention, a shortness and labour of respiration are perceived, with some interruption in speaking, and a frequent catching of the breath, or sighing.
April. Since writing the above account, the dropsical collections were absorbed, and the palpitations and other symptoms moderated, so that he considered himself nearly well, and attended to his usual business. Within a few days, however, the symptoms have returned with more violence. The dyspnœa is at times very distressing; the pulse more irregular and intermittent; the palpitations are more constant. His sufferings from lying in bed are so increased, that in the most comfortable nights he passes, he sits up once in an hour or two. The appetite is keen. The legs begin to swell again.
Some organic disease of the heart exists in this case. The indistinctness of the palpitations, the want of hardness in the pulse, and the slow progress of the disease, indicate a loss of power in the heart, the effect of the distention and thinness of its parietes. The irregularity of the pulse affords some reason to suspect disorder of the aortal valves, which is not yet very considerable.[31]
ENUMERATION of the principal morbid changes, observed in the organization of the heart, in the preceding cases.
| Enlargement of the volume of the heart, or aneurism.[12] | |
| Increase of the capacity, or aneurism of the right auricle, of the right ventricle, of the left auricle of the left ventricle, of the aorta, with thickening of its coats. |
with thickened, or thin, parietes. |
| Fleshlike[13] thickening of the mitral valves. of the aortal valves. of the aorta. | |
| Cartilaginous thickening of the internal membrane of the heart, and generally of its valves. | |
| Ossification of the parietes of the heart. mitral valves. aortal valves. aorta. coronary arteries. |
ENUMERATION of the principal morbid appearances, observed in these cases of disease of the heart, which may be considered secondary.
The symptoms, which are most observable, in some or all of the preceding cases, are the following:
The first notice of disorder is commonly from an irregular and tumultuous movement of the heart, which occurs some time before any perceptible derangement of the other functions. This irregularity slowly increases, and arrives at its height before the strength of the patient is much impaired, at least in the cases which I have noticed; and as the vigour of the patient lessens, the force of the palpitations diminishes. These palpitations are often so strong, as to be perceptible to the eye at a considerable distance. They are seldom most distinct in the place where the pulsation of the heart is usually felt. Sometimes they are perceived a little below; often in the epigastric region; and not unfrequently beneath, and on the right side, of the sternum.
After the palpitations have lasted some time, a little difficulty of breathing, accompanied with sighing, is perceived, especially on any great exertion, ascending an eminence, or taking cold, of which there is an uncommon susceptibility. This dyspnœa becomes, as it increases, a most distressing symptom. It is induced by the slightest cause; as by an irregularity in diet, emotions of the mind, and especially movement of the body; so that on ascending stairs quickly, the patient is threatened with immediate suffocation. It occurs at no stated periods, but is never long absent, nor abates much[33] in violence during the course of the disease. It is attended with a sensation of universal distress, which perhaps may arise from the circulation of unoxygenated blood, or the accumulation of carbon in the system; for the countenance becomes livid, and the skin, especially that of the extremities, receives a permanent dark colour. This dyspnœa soon causes distress in lying in an horizontal posture. The patient raises his head in bed, gradually adding one pillow after another, till he can rarely, in some cases never, lie down without danger of suffocation; he inclines his head and breast forward, and supports himself upon an attendant, or a bench placed before him. A few hours before death the muscular power is no longer capable of maintaining him in that posture, and he sinks backward. The dyspnœa is attended with cough, sometimes through the whole of the disease, sometimes only at intervals. The cough varies in frequency. It is always strong, and commonly attended with copious expectoration of thick mucus, which, as the disease advances, becomes brown coloured, and often tinged with blood; a short time before death it frequently consists entirely of black blood.
The changes in the phœnomena of the circulation are very remarkable. The sanguiferous system is increased in capacity; the veins, especially, are swelled with blood; the countenance is high coloured, except in fits of dyspnœa, when it becomes livid; and it is very frequently puffed, or turgid. The brightness of the eyes, dizziness, which is a[34] common, and head-ache, which is a frequent symptom, and in some cases very distressing, are probably connected with these changes. The motions of the heart, as has already been stated, are inordinate, irregular, and tumultuous. The pulse presents many peculiarities. In some cases, probably where there is no obstruction in the orifices of the heart, it remains tolerably regular, and is either hard, full, quick, vibrating and variable, or soft, slow, compressible and variable. Most commonly, perhaps always, when the orifices of the heart are obstructed, it is vibrating, very irregular, very intermittent, sometimes contracted and almost imperceptible, very variable, often disagreeing with the pulsations of the heart, and sometimes differing in one of the wrists from the other.
The functions of the brain suffer much disturbance. Melancholy, and a disposition for reverie, attend the early stages of the complaint; and there is sometimes an uncommon irritability of mind. The dreams become frightful, and are interrupted by sudden starting up in terror. Strange illusions present themselves. The mental faculties are impaired. The termination of the disease is attended with slight delirium; sometimes with phrenzy, and with hemiplegia.
The abdominal viscera are locally, as well as generally, affected. Although the digestive functions are occasionally deranged, the appetite is at some periods remarkably keen. The action of the intestines is sometimes regular, but a state of costiveness[35] is common. The liver is often enlarged, probably from accumulation of blood. This distention is attended with pain, varies much, and, in all the cases I have seen, has subsided before death, leaving the coats of the liver wrinkled, flaccid, and marked with appearances of inflammation, caused by the distention and pressure against the surrounding parts. An effect of the accumulation of blood in the liver, and consequently in the mesenteric veins, is the frequent discharge of blood from the hæmorrhoidal vessels. This occurs both in the early and late stages of the disease, and may become a formidable symptom. Evacuations of blood from the nose are not uncommon.
Dropsical swellings in various parts of the body succeed the symptoms already enumerated. They commence in the cellular membrane of the feet, and gradually extend up the legs and thighs; thence to the abdominal cavity, to the thorax, sometimes to the pericardium, to the face and superior extremities; and, lastly, to the ventricles and meninges of the brain. These collections of water may be reabsorbed by the aid of medicine; but they always return and attend, in some degree, the patient’s death.
There is no circumstance more remarkable in the course of this complaint, than the alternations of ease and distress. At one time the patient suffers the severest agonies, assumes the most ghastly appearance, and is apparently on the verge of death; in a day or a week after, his pain leaves him, his[36] appetite and cheerfulness return, a degree of vigour is restored, and his friends forget that he has been ill. The paroxysms occasionally recur, and become more frequent, as the disease progresses. Afterwards the intermissions are shorter, and a close succession of paroxysms begins. If the progress of the complaint has been slow, and regular, the patient sinks into a state of torpor, and dies without suffering great distress. If, on the contrary, its progress has been rapid, the dyspnœa becomes excessive; the pain and stricture about the præcordia are insupportable; a furious delirium sometimes succeeds; and the patient expires in terrible agony.
Such are the symptoms, which a limited experience has enabled me to witness. Others, equally characteristic of the disease, may probably exist.
From this description of the symptoms it would appear, that there could be no great difficulty in distinguishing this from other diseases; yet probably it has sometimes been confounded with asthma, and very frequently with hydrothorax. Some may think, that there is no essential difference in the symptoms of these diseases. The resemblance between them, however, is merely nominal.
The cough in hydrothorax, unlike that which attends organic diseases of the heart, is short and dry; the dyspnœa constant, and not subject to violent aggravations. An uneasiness in a horizontal posture attends it, but no disposition to incurvate the body forward. These are some of the points, in which these two diseases slightly resemble each[37] other. Those, in which they totally differ, are still more numerous; but as most of them have been already mentioned, it is unnecessary to indicate them here.
It is probable, that the two diseases commonly arise in patients of opposite physical constitutions; the hydrothorax in subjects of a weak relaxed fibre; the organic diseases of the heart in a rigid and robust habit. The subjects of the latter affection, in the cases which have fallen under my observation, were, with the exception of one or two instances, persons of ample frame, and vigorous muscularity, and who had previously enjoyed good health. In nearly all these cases the collection of water was principally on one side, yet the patients could lie as easily on the side where there was least fluid, as on the other; which, in the opinion of most authors, is not the case in primary hydrothorax. It should also be observed, that, in many of the cases, there was only a small quantity of water in the chest, and that in neither of them was there probably sufficient to produce death. May not primary hydrothorax be much less frequent, than has commonly been imagined?
Idiopathic dropsy of the pericardium may, perhaps, produce some symptoms similar to those of organic disease of the heart; but it appears to be an uncommon disorder, and I have had no opportunity of observing it. In the fourth case, a remarkable disposition to syncope, on movement, distinguished the latter periods of the disease, and might[38] have arisen from the great collection of water in the pericardial sac.
The causes of this disease may, probably, be whatever violently increases the actions of the heart. Such causes are very numerous; and it is therefore not surprising, that organic diseases of the heart should be quite frequent. Violent and long continued exercise, great anxiety and agitation of mind[14], excessive debauch, and the habitual use of highly stimulating liquors, are among them.
The treatment of this complaint is a proper object for investigation. Some of its species, it is to be feared, must forever remain beyond the reach of art; for it is difficult to conceive of any natural agent sufficiently powerful to produce absorption of the thickened parietes of the heart, and at the same time diminish its cavities; but we may indulge better hopes of the possibility of absorbing the osseous matter and fleshy substance deposited in the valves of the heart and coats of the aorta. A careful attention to the symptoms will enable us to distinguish the disease, in its early stages, in which we may undoubtedly combat it with frequent success.
Although it may not admit of cure, the painful symptoms attending it may be very much palliated; and, as they are so severely distressing, we ought to resort to every probable means of [39]alleviating them. Remedies, which lessen the action of the heart, seem to be most commonly indicated. Blood-letting affords more speedy and compleat relief, than any other remedy. Its effect is quite temporary, but there can be no objection to repeating it. The digitalis purpurea seems to be a medicine well adapted to the alleviation of the symptoms, not only by diminishing the impetus of the heart, but by lessening the quantity of circulating fluids. Its use is important in removing the dropsical collections; and for this purpose it may often be conjoined with quicksilver. Expectoration is probably promoted by the scilla maritima, which, in a few cases, seemed also to alleviate the cough and dyspnœa. Blisters often diminish the severe pain in the region of the heart, and the uneasiness about the liver. It has been seen, that the excessive action of the heart sometimes produces inflammation of the pleura and pericardium, and that the distention of the coat of the liver has the same effect upon that membrane in a slighter degree. Vesication may probably lessen those inflammations. When the stomach and bowels are overloaded, a singular alleviation of the symptoms may be produced by cathartics, and even when that is not the case, the frequent use of moderate purgative medicines is advantageous. Full doses of opium are, at times, necessary through the course of the complaint. The antiphlogistic regimen should be carefully observed. The food should be simple, and taken in small quantities, stimulating liquors[40] cautiously avoided, and the repose of body and mind preserved, as much as possible.
The causes of some of the phœnomena of this disease are easily discovered; those of the others are involved in obscurity, and form a very curious subject for investigation. I shall not at present trouble you with the ideas relating to them, which have occurred to me, but hope to be able to present some additional remarks on the subject, at a future period. In the mean time, I beg leave to invite the attention of the society to the observation of the symptoms of this interesting disorder, and of the morbid appearances in the dead bodies of those, who have become its victims.
At the time the preceding pages were going to the press, the subjects of the ninth and tenth cases died, on the same day, and an opportunity was given of ascertaining whether their complaints had been rightly distinguished.
It is a proof of an enlightened age and country, that no objections were made in any instance to the examinations, which have afforded us so much useful information.
The lady, who was the subject of this case, died on the 10th of May, but she was not seen by me after the 29th of March; so that it is not in my[41] power to relate exactly the symptoms which attended the latter stages of her complaint. I was informed, however, that they increased in violence, especially the difficulty of breathing, and inability to lie down; that her cough returned, and her expectoration was sometimes bloody; and that, for sometime before death she suffered inexpressible distress.
We found the body somewhat emaciated, and the lower extremities and left arm œdematous. Might not this swelling of the left arm have depended on her constant posture of inclining to her left side?
The face, especially at the lips, was livid, though not so much as in many other cases of this disease. On the left shoulder were small, hard, and prominent livid spots.
The cellular membrane, both on the outside and inside of the thorax, was quite bloody, which is not usually the case in dead bodies. The cartilages of the ribs were slightly ossified, and, upon their removal, it appeared that the pericardium and its contents occupied an extraordinary space, for the lungs were quite concealed by them. These organs being drawn forward, appeared sound and free from adhesions; their colour, anteriorly, was rather dark; posteriorly, still darker; their consistence firm. Their vessels were so crowded with blood, as to cause an uniform dark colour in the substance of the lungs, especially in some particular spots, where the blood appeared to be accumulated; but whether[42] this accumulation was confined to the blood vessels, or extended to the bronchial vesicles, could not be satisfactorily determined. No one can doubt that blood may be frequently forced through the thin membrane of the air vesicles, who considers, that in these cases the heart often acts with uncommon violence, that, when it is enlarged, it attempts to send toward the lungs more blood than their vessels can contain, and that there is commonly some obstruction to the return of blood from the lungs into the heart, from derangement either in the mitral or aortal valves, or in the aorta. The consequent accumulation of blood in the lungs seems to me to be the probable cause of the dyspnœa, which so much distresses those affected with diseases of the heart; for if there be an inordinate quantity of blood, there must be a deficiency of air.
This accumulation of blood in the lungs has, by some writers, been considered as an appearance belonging to idiopathic hydrothorax. Whether it ever exists in that complaint seems to me uncertain. The pressure of water upon the lungs, may possibly interrupt the free circulation of blood through their vessels, yet probably the same pressure would prevent the entrance of blood into the vessels, unless there be some other cause to overcome it, such as increased action of the heart, which attends only the first stage of hydrothorax. It has beside been proved by the experiments of Bichat, that the collapsion of the lungs does not obstruct the circulation of blood through the pulmonary vessels. It seems[43] probable, therefore, that those who have thought this collection of blood an appearance belonging to idiopathic hydrothorax, have mistaken for it the secondary hydrothorax produced by diseases of the heart.
On pursuing the examination, we found, behind the lungs, about five or six ounces of yellowish serum in each cavity of the pleura, and about one ounce in the cavity of the pericardium. The heart was then seen enlarged to more than double its natural size. Its surface, especially along the course of the branches of the coronary arteries, was whitened by coagulated lymph. In the cavities of the heart, which were all enlarged and thickened, particularly the left, were found portions of coagulum mixed with fluid blood. Near its apex, over the left ventricle, was a small soft spot which, to the finger, seemed like the point of an abscess ready to burst. The tricuspid valves, and the valves of the pulmonary artery, had lost somewhat of their transparency, and were a little thickened, though not materially. It is worthy of remark, that these valves have not exhibited any great appearance of disease in any of these cases, while those of the left side of the heart have scarcely ever been found healthy. So it appeared in this case. The mitral valves were uniformly thickened, and partly cartilaginous; the left portion adhered to the side of the heart. The valves of the aorta had lost their usual form, were entirely cartilaginous, and almost equal in firmness to the aorta, which was cartilaginous under the valves, sound in[44] other parts, and rather small, compared to the size of the heart.
It may be thought that the symptoms, on which reliance was placed to distinguish disorder of the valves of the aorta, are fallacious, because it was supposed that these valves would be found ossified, when they were in reality only cartilaginous. The difference, however, would be small in the effects produced on the circulation by such a state of the valves as existed in this case, and a very considerable ossification; for, if the valves were rigid and unyielding, it is of little importance whether they were rendered so by bone, or cartilage. Whether the irregularity of the pulse in these diseases generally depends on the disorganized state of the aortal, or other valves, we have not at present observations sufficient to decide. In the sixth case no irregularity of the pulse could be observed, although the other symptoms were unequivocal, and no disease was found in the valves; while, on the other hand, we find that the valves in the fourth case were not importantly deranged, and yet there was an irregularity and intermission of the pulse, which however might be attributed to the dropsy of the pericardium. In the seventh case, where the pulse was not irregular, the valves of the aorta were “considerably thickened in various spots;” in the fifth, the pulse was irregular, and the valves were not materially altered, but there was water in the pericardium. In all the other cases, the pulse was irregular, and the valves were much disordered:[45] On a review of these cases, therefore, we find some reason to believe, that the irregularity of the pulse depends much on disease of the valves, especially those of the aorta.
The cavity of the abdomen being opened, no water was discovered in it, nor any other uncommon appearance, except about the liver, the coat of which had been rendered opaque by coagulated lymph, and was studded over with soft, dark coloured tubercles. The substance of the liver was tender, and full of bile and venous blood.
The symptoms of disease in this patient did not alter much, except in degree, from the middle of April to the 10th of May. He became weaker, had more straitness and pain about the heart on moving, an increase of swelling in the legs and abdomen, return of the cough, and a pain from the left shoulder to the middle of the arm. After his relapse in April, he had been directed to employ blisters, the submuriate of quicksilver, and the tincture of the digitalis purpurea. The dose of the tincture he gradually increased, till he took two hundred drops, two or three times in a day. Notwithstanding a profuse flow of urine, the legs became so hard and painful, that I made punctures to discharge the water from them. He would have had the water in the abdomen drawn off, but believing it would not afford him great relief, I dissuaded him from it. On[46] the 10th of May, after having passed an unusually comfortable night, he rose and left his chamber for five or six hours, then retiring to it again, said he would be tapped that day, and, after lying down, was quitted by his attendant, who went in an hour after and found him dead. This was rather unexpected, for he had the appearance of sufficient vigour to struggle with disease three or four weeks longer.
A number of medical gentlemen being assembled, as has been usual on these occasions, we first remarked, that the face was swollen, and extraordinarily livid; for, although a considerable degree of lividity, and sometimes of redness, after death, is peculiar to these cases, we had seen none which resembled this. Hard and prominent purple spots were observed upon the shoulders, side, and back. The surface of the body was moderately covered with fat; the legs and abdomen were much swollen with water, the arms more slightly. The integuments of the thorax being cut through, the cellular membrane discharged a serous fluid from every part; these being turned aside, to lay bare the cartilages of the ribs, we found them completely ossified; and having divided them, with a saw, the cavity of the thorax was opened. The cellular membrane, inside the thorax, about the mediastinum, had not so bloody an appearance as we witnessed in the preceding cases, nor were the lungs, either externally or internally, so dark coloured as usual, though they were much darker, firmer, and more filled with[47] blood, than is common in subjects of other diseases. The lungs of the left side adhered closely to the pleura costalis, and those of the right were tied by loose and membranous adhesions; beside which there was no appearance of disease about them. The cavity of the pleura did not contain any water; that of the pericardium held about six ounces.
The anterior surface of the heart exhibited a considerable whiteness of its coat over the coronary arteries. This appearance differed from that of other cases, in being contained in the substance of the membrane, instead of lying on its surface; and, either from this circumstance, or from the length of time since it had existed, its aspect was so peculiar that it might be supposed to be the first stage of an ossification. A deposition of lymph on the heart has been observed in every one of these cases of organic disease, and it has existed principally over the branches of the coronary arteries, or else near the apex of the heart, which is to be attributed to the irritation of the membrane by the combined impulse of the heart and coronary arteries, and to the stroke of the apex upon the ribs. This is an appearance that, as it belongs to this complaint, might be useful in a case otherwise dubious, if any such should occur, to aid in deciding whether the action of the heart had been inordinate.
The heart was enlarged to double its usual size, as we judged with confidence, for pains had been taken to examine hearts in a healthy state, for the purpose of forming a comparison. Its firmness was[48] not proportioned to its bulk, but it was considerably flaccid. Near the apex, over the left ventricle, was a soft spot, similar to that found in the preceding case. The venæ cavæ were then divided, and a torrent of black blood issued from each of the orifices, in spite of our efforts to restrain it. All the cavities of the heart were filled, as we afterwards saw, with similar blood; in which circumstance this resembles the other cases; though in this case the blood was entirely fluid, and thinner than in cases of different disease: whereas, in every other instance, was partly or wholly coagulated. This therefore must be considered as another appearance peculiar to this complaint, because it is well known, that blood is not usually found in the left cavities of the hearts of those who die of other disorders. The cause of it is doubtless an obstruction, which opposes the free discharge of blood from the heart, whether that obstruction be in the aortal valves, in the aorta itself, or in the disproportion between the heart, or more precisely the left ventricle, and the parts it supplies with blood.
Why was the blood entirely fluid in this case? If we compare the appearance of the cellular membrane, and of the lungs, in both of which there was a deficiency of blood, with the aspect of the face, where there was an accumulation of blood, and consider at the same time the mode of termination of this case, we shall find reason to believe, that death was produced by a violent pressure of the brain from a congestion of blood in its vessels, in consequence[49] of the obstruction to the return of that fluid to the heart. An additional proof of this opinion is derived from the great quantity of blood, which poured from the vena cava superior, during the whole time of the examination, and afterward; so that it was found impossible to preserve the subject from the blood flowing between the ligatures, notwithstanding the thorax was entirely emptied, before it was closed. In cases of sudden death from apoplexy, related by Morgagni, the blood was frequently fluid, and this may be supposed to be the cause of that appearance in the present case. The extraordinary thinness or watery state of the blood is a distinct circumstance, which will be presently noticed.
An examination of the brain, to ascertain the truth of the supposition above mentioned, was relinquished with regret, but this was impracticable; for the want of time on these occasions frequently obliged us to content ourselves with investigating the state of the most important parts. This must serve as our apology for not oftener relating the appearance of all the principal organs; yet it should be observed, that such methods have been employed to ascertain with accuracy the most interesting morbid phœnomena, as would satisfy the most scrupulous anatomist.
The tricuspid valves and the semilunar valves of the pulmonary artery had lost their healthy transparency, but were not otherwise diseased. In all the above cases these valves had been found without[50] important derangement of their structure; a circumstance not less remarkable, than difficult to be satisfactorily explained. The basis of the mitral valves was marked by a bony projection, which nearly surrounded the orifice of the ventricle; the valves themselves were thickened, and one of them was smaller than the other. The semilunar valves of the aorta were lessened in size, and somewhat thickened. One of them was ossified sufficiently to annihilate its valvular function; the others were slightly. The aorta under the valves was semicartilaginous, ossified in one small spot, roughened by fleshlike prominences in others, entirely deprived of the smoothness of its internal coat, and in size proportioned to the heart.
The parietes of the heart were thicker than those of a healthy heart, but thin when compared with its whole volume; whence it follows, that the cavities were enlarged. That of the left ventricle was disproportionately larger than the others, but no difference of size could be ascertained between the auricles. When a cavity of the heart is situated in the course of the circulation immediately behind a contracted orifice, it seems probable that the contraction may have an important influence in originating the enlargement or aneurism of that cavity; but, where there is no contraction of an orifice, what is the obstruction which impedes the free discharge of blood from the heart, and causes the first yielding of its parietes? Perhaps a violent simultaneous action of many muscles, from great exertion, may, during[51] the systole of the heart, impede the passage of the blood through the arteries, drive it back upon the valves of the aorta, and resist the heart at the moment of its contraction. If the parietes of the heart yield, in one part, it is easy to conceive a consequent distension of the remainder to any degree; for, during the systole of the heart, the columnæ approximate, till their sides are in contact, to protect the parietes of the heart; but, if these be distended, the columnæ can no longer come in contact with each other, and the blood passing between them will be propelled against the parieties, and increase their distention. The left ventricle being thus dilated, the mitral valves will not be able to completely cover its orifice, and part of the blood will escape from the ventricle, when it contracts, into the auricle when dilated with the blood from the lungs; and this undue quantity of blood will gradually enlarge the auricle. A resistance will arise, from the same cause, to the passage of the blood from the lungs, thence to that from the right ventricle and auricle, and thus these cavities may become enlarged in their turns. When an ossification of the aorta, or of its valves, exists, there will be a resistance to the passage of the blood from the left ventricle, either by a loss of dilatability in the artery, or a contraction of the orifice by the ossified parts. In either case, the blood will reflow upon the heart, and dilate the left ventricle, as in case the first, and others; and, if the mitral valves be thickened and rigid, the left auricle will[52] be more dilated than in a case of simple aneurism of the left ventricle, as appeared also in the first case.
The coronary arteries, at their origin from the aorta, and a considerable distance beyond, were ossified. How far does the existence of this ossification in this and other cases related by different authors, without symptoms of angina pectoris, disprove the opinion that it is the cause of that disease?
The abdomen being opened, the organs generally appeared sound, except the liver, which had its tunic inflamed, its substance indurated and filled with blood. The vestiges of inflammation in the coat of the liver were traced in every instance already related, while at the same time the liver, in all, appeared shrunken. The diminution of size in the liver, after death, cannot at present be well explained; for it is very certain that such a diminution is not an attendant of this disorder, during most of its stages, but that on the contrary a state exists precisely opposed to it. The indications of distention of the liver, clearly perceived in some cases, have been pain, tenderness, and sense of distention, in the right hypochondrium, and, what is less equivocal than these, very considerable swelling and prominence of the liver. The inflammation of its tunic is an effect of this distention and of the consequent pressure against the adjacent parts.
The cause of this phœnomenon can easily be explained. If an obstruction exist in either side of the heart, or in the lungs, the blood to be poured[53] into the right auricle, from the vena cava inferior, must be obstructed, its flow into that vessel from the liver will be equally checked, the thin coats of the hepatic veins and of the branches of the vena porta will yield and distend the soft substance of the liver. Hence are caused the discharges of blood from the hæmorrhoidal veins, which form one of the characteristic symptoms of the disease; for as these vessels empty their blood into the meseraic veins, which open into the vena porta, if the meseraic veins be obstructed, the hæmorrhoidals must consequently be also affected, and they easily burst open from too great distention. The hæmoptoe, which also is so frequent, is as easily explained on the same principle.
The cause of the serous collections is not so readily discovered. In this case, as in most of the others, we found a considerable quantity of water in the abdominal cavity. Dropsy is commonly considered as a disease of debility, but in these cases it often appeared, while the strength was unimpaired, and the heart acted with very extraordinary force. If the blood was driven with rapidity through the arteries, while an obstruction existed at the termination of the venous system in the heart, the consequences must have been accumulation in the venous system, difficult transmission of the blood from the extreme arteries to the veins, overcharge of the arterial capillary system, consequent excitement of the exhalant system to carry off the serous part of the blood, for which it is adapted, and thence a serous discharge[54] into the cavities, and also on the surface of the body; for great disposition to sweating is a common symptom. In addition to these, there is another cause of the universality of these effusions. The blood, in all the cases which I have examined, is both before and after death, more thin and watery than healthy blood. How this happens, our knowledge of the theory of sanguification does not enable us to determine. Perhaps, as the imperfect respiration must cause a deficiency of air, and consequently of oxygen, in the lungs; and as the absorption of oxygen is a cause of solidity in many bodies, this tenuity of the blood may proceed from a deficient absorption of oxygen. However this may be, it is certain that the blood is very much attenuated, though with considerable variations in degree, as it is sometimes found thin on opening a vein, and at a subsequent period is thicker; varying perhaps according to the continuance of ease or difficulty in respiration. It is certain, that this attenuation of the blood must tend to an increase of the serous exhalations.
That these secondary dropsies are not the effect of debility appears pretty evident from considering, that they often exist while the strength of the patient is yet undiminished, while all the other secretions, except that of the urine, are carried on with vigour, and while the appetite and digestive functions are not only unimpaired, but improved.
The examinations of the ninth and tenth cases are particularly valuable, because they confirm what had been observed in other subjects; they exhibit[55] two well marked instances of aneurism of the heart, and present us a view of organic disease unattended by dropsy of the pleura. This must be sufficient to remove the suspicion, that the symptoms we have attributed to the former disease might arise from the existence of the latter. No one probably will be willing to impute a chronic disease, terminated by a sudden death, to five or six ounces of water in the pericardium; for such a quantity, though it might produce inconvenience, could not prove fatal, unless it were suddenly effused; and, if this were true, it of course could not have been the cause of the long train of symptoms observed in case tenth.
Dr. William Hamilton, the author of a valuable treatise on the digitalis purpurea, thinks the hydrothorax a more frequent disease than has commonly been imagined, because he conceives that it has often been mistaken for organic disease of the heart. He names, with some precision, many symptoms of the latter complaint; but how remote he is from an accurate knowledge of it may be discovered by his opinion, that, in diseases of the heart, “the patient can lie down with ease, and seldom experiences much difficulty of breathing.” The limits of this paper do not admit a discussion of this and other points, respecting which he seems to be mistaken. We must therefore submit them to be decided by the evidence adduced in Dr. Hamilton’s “observations,” and by that which may be drawn from these cases, and future investigations of the subject. It will perhaps hereafter appear surprising,[56] that derangements in the structure of so important an organ as the heart should have been lightly estimated by very respectable authors.
While concluding these observations, a case of this disease presented itself, which comprehends so many of the symptoms, that I cannot neglect an opportunity of recording it, especially as it exhibits the complaint in an earlier stage than the others, with appearances equally unequivocal. I may here be allowed to remark, that no cases have been introduced which occurred before my attention was directed to a close observation of this disorder, and that there are many others, under the care of practitioners of eminence belonging to this society, with symptoms perfectly well marked, which it has not been thought necessary to adduce. In proof of this, reference may be had to Dr. Warren, sen. who has a number of cases, and also to Dr. Dexter, Dr. Jackson, and Dr. J. C. Howard.
A lady from the country, of a robust habit, whose age is about thirty-four years, complains of uneasiness in the right side below the edge of the ribs, sometimes attended with swelling, external soreness, and a throbbing pain, which often reaches to the shoulder, and produces a numbness of the right arm. She is rather uncertain at what time her complaints commenced. About two years since she lost her husband, and was left with but small means to support a number of children. She became[57] in consequence, much dejected. While nursing a child, about a year since, she first was sensible of palpitations of the heart, which, in about three months, were followed by dyspnœa very much augmented by ascending an eminence; and profuse discharges of blood from the mouth, first raised, she believes, by vomiting, and afterwards by coughing. Evacuations of blood from the hæmorrhoidal vessels appeared about the same time, and occasionally since, till within six weeks, during which time there have been no sanguineous discharges, and this suppression has aggravated her other complaints.
The pulsation of the heart is felt most distinctly quite on the left side of the thorax, where there is a painful spot; it is perceptible also in the epigastric region. It is irregular and variable, at one moment hard, strong, distinct, and vibrating; at another, feeble and confused. There is also sometimes perceived a pulsation above the left clavicle, within the insertion of the mastoid muscle, commonly attended with a visible fulness of the superior part of the breast. The thorax feels, to the patient, as if it were girt across, and there is a distinct pain in the heart. Both these sensations are aggravated by a very hard, frequent, and dry cough, which however begins to be less violent from the use of the scilla maritima. The countenance is animated, and rather flushed, but not so much overcharged with blood as happens in many instances; perhaps it little exceeds a blush, so moderate that it might be considered as an indication of perfect health; yet the head is greatly disturbed[58] with dizziness, and frequent and intense pain, and is seen to be shaken by the palpitations.
The functions of the abdominal viscera are not much deranged. The appetite varies, though it is commonly good; the intestinal evacuations, and the menstrual discharges, are regular; the urine is turbid, and so small in quantity as sometimes to produce strangury. The abdomen and inferior extremities are swelled, and the distention produces an uneasiness in the former, and pain and a livid colour about the gastroenemii muscles in the latter. The pulse is hard, without strength or fulness, slightly intermittent, variable, and irregular; yet it has not so much irregularity as in most of the cases recorded above.
This patient is uneasy in bed, though she raises her head almost upright; her sleep is disturbed by unpleasant dreams, and by startings, sometimes quite to an upright posture, without any cause discoverable to herself. She can incline a little to the left side, but never to the right, because it brings on a singular oppression, and a sense of weight drawing on the left side. When most distressed by dyspnœa she bends her head and trunk forward, and remains thus seated a considerable portion of the night, often sighing quickly and convulsively. She is subject to profuse sweatings, and very liable to take cold, and is then more uneasy.
This lady is still corpulent. She has taken much medicine, under the direction of eminent physicians, sometimes with temporary relief, but most commonly[59] without any. The exercise of walking slowly, in pleasant weather, although it increases the palpitations at the moment, is followed with relief from the distressing feelings, which are increased when she sits still for a long time. She has no suspicion of her hopeless situation, and confidently expects relief from medicine, yet labours under a melancholy which is unnatural to her.
The following case of hydrothorax will shew, that water may exist in the chest without the symptoms, which we have attributed to organic diseases of the heart.
Mrs. T——, aged 56 years, of an excessively corpulent habit, had been affected for a great number of years with a scirrhus of the right breast. Finding her health decline, she at last disclosed it, and in coincidence with the opinion of Dr. Warren, sen. I amputated it on the 30th of May, of the present year. We however informed her friends, that the probability of eradicating the disease was extremely small. The skin was in many places hardened and drawn in, and in others discoloured, and ulcerated at the nipple, so that it was found necessary to remove, not only what covered the breast, but some portion of that which surrounded it. A long[60] chain of diseased glands, extending quite to the axillary vessels, was also extirpated. She bore the operation well, lost no great quantity of blood, and recovered her appetite and strength surprisingly in a few days, while the wound healed rapidly. At the end of twenty days a difficulty of breathing commenced, and soon became so oppressive, that she could no longer lie in bed; partly, no doubt, on account of her extraordinary obesity. The pulse was small, quick, and commonly feeble, but sometimes a little hard, when any degree of fever was present. The countenance became pale, the lips of a leaden hue, the eyes dim. We were surprised at the change, and conjectured that the cancerous action had suddenly extended to the lungs. Yet she had not the slightest cough; and it was remarked by Dr. Warren, sen. that he had never observed that diseased action to increase, while the wound remained open. At last the lower extremities swelled, which might be attributed to the upright posture, and the pressure on the absorbent vessels in that posture. The appetite failed; she complained of a constant sense of depression at the stomach, and, without any remission of the difficulty of breathing, died on the 1st of July.
On the next morning the body was examined. The pleura in both cavities of the thorax was studded with small, white, and apparently homogeneous tubercles; the lungs contained a great number of similar bodies. The right cavity of the pleura was entirely filled with water, of which we removed at[61] least three quarts. The heart was of the usual size, very flaccid and tender; but not otherwise disordered. The liver was enlarged, of its usual colour, much hardened, and had on its surface, and in its substance, many tubercles like those in the thorax. It had also a great number of encysted cavities, each about the size of a hazle nut, which contained a thin yellow fluid. The gall bladder was wanting, and in its place there was a small, but very remarkable depression, without a vestige of any former gall bladder, for the coat of the liver was as smooth and perfect there as in any other part[15]. The pancreas was in a scirrhous state. The abdomen did not contain any water.
It seems, then, that water may exist in the cavity of the thorax, without any remarkable symptoms, except dyspnœa and difficulty in assuming the horizontal posture. But in organic diseases of the heart, there is a long train of frightful symptoms, distinguishable by the most superficial observers. We infer that these disorders have been unnecessarily confounded.
[1] A careful examination of the works of some of the most eminent English practical writers does not afford evidence of any clear distinction of these diseases of the heart. Dr. Cullen, whose authority is of the highest estimation, evidently enumerates symptoms of them in his definition and description of the hydrothorax. In § 1702 Th. and Pr. he places much confidence on a particular sign of water in the chest, and remarks, that the same sign is not produced by the presence of pus. Now, there is no sufficient reason, why this symptom should not arise from the presence of pus, as well as from that of water; but it probably can depend on neither of those alone. See Morgagni de causis et sedibus morborum, Epist. 16. art. 11. The experienced Heberden says in the chapter “De palpitatione cordis,” “Hic affectus manifesta cognitione conjunctus est cum istis morbis, qui existimantur nervorum proprii esse, quique sanguinis missione augentur; hoc igitur remedium plerumque omittendum est.”—“Ubi remediis locus est, ex sunt adhibenda, quæ conveniunt affectibus hypochondriacis.”
Dr. Baillie’s knowledge of morbid anatomy has enabled him to make nearer approaches to truth; yet it will probably be found, when this subject shall be fully understood, that his descriptions of the symptoms of diseases of the heart and of hydrothorax are not quite accurate, and, that with respect to the former, they are very imperfect.
Some of the French physicians have devoted much attention to this subject; especially M. Corvisart, professor in the hospital of La Charite, at Paris, from whose clinical lectures is derived the most important information.
[2] During this time it was thought adviseable to acquaint his friends, that an organic disease of the heart existed, which doubtless consisted in an ossification of the semilunar valves of the aorta, attended, perhaps, by enlargement of the heart; that the disease was beyond the reach of art, and would prove fatal within three months, possibly very soon; that if it lasted so long, it would be attended by frequent recurrences of those distressing symptoms, general dropsical affections, and an impaired state of the mental faculties.
[3] The celebrated Morgagni has recorded some cases of organic disease of the heart discovered by dissection, the symptoms of which do not exactly accord with those observed in this and the succeeding cases. It should be remembered, however, that many of the subjects of those cases were not examined by him, while living, and others but a very short time before death. But it appears, that, in the last stage of this disorder, some of the most important symptoms may be materially changed, especially the state of the pulse, dyspnœa and palpitations. Thus in the case related above, and in some others, the pulse became regular, the palpitations subsided, and the dyspnœa was less observable. The cases of that accurate anatomist, therefore, are not so contradictory of those related here, as might at first be imagined.
[4] Governour Sullivan was born December 4th, 1744, and died December 10th, 1809.
[5] The symptoms of this patient were related by Dr. Rand, sen. to whose politeness and love of medical improvement I am indebted for the opportunity of examining this and the following case.
[6] The symptoms of this case were related to me by Dr. Rand, sen.
[7] See plate first.
[8] The symptoms in this case were related to me by Dr. Warren, sen.
[9] This dissection was performed by Dr. Gorham.
[10] See plate second.
[11] In this case, and in case first, the vena cava ascendens had been divided, before the brain was examined.
[12] Morgagni uses this term, which he borrows from Ambrose Pare, to express dilatation of the cavities of the heart. It seems to be as applicable to the dilatation of the heart, as to that of an artery. I have therefore adopted it in this enumeration.
[13] The term fleshlike is employed to express that roughness of the valves, which somewhat resembles flesh in its appearance, but which is very different from the thickening of the parietes of the heart.
[14] It has been remarked by the French physicians, and particularly by M. Corvisart, physician to the emperor of France, that these organic diseases were very prevalent after the revolution, and that the origin of many cases was distinctly traced to the distressing events of that period.
[15] See Soemmerring de corporis humani fabrica, vol. 6, pag. 188 and Baillie’s morbid anatomy, pag. 248.
End of the Project Gutenberg EBook of Cases of Organic Diseases of the Heart, by
John Collins Warren
*** END OF THIS PROJECT GUTENBERG EBOOK HEART DISEASE ***
***** This file should be named 26836-h.htm or 26836-h.zip *****
This and all associated files of various formats will be found in:
http://www.gutenberg.org/2/6/8/3/26836/
Produced by Bryan Ness, Irma Spehar and the Online
Distributed Proofreading Team at http://www.pgdp.net (This
book was produced from scanned images of public domain
material from the Google Print project.)
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License (available with this file or online at
http://gutenberg.org/license).
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH F3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS' WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTIBILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need, is critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation web page at http://www.pglaf.org.
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Its 501(c)(3) letter is posted at
http://pglaf.org/fundraising. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at
809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887, email
business@pglaf.org. Email contact links and up to date contact
information can be found at the Foundation's web site and official
page at http://pglaf.org
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit http://pglaf.org
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including checks, online payments and credit card donations.
To donate, please visit: http://pglaf.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart is the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For thirty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
http://www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.