 FRONTISPIECE.
FRONTISPIECE.Photo, H. Kisch Ladysmith. Engraved and Printed by Bale and Danielsson, Ltd.
The Project Gutenberg EBook of Surgical Experiences in South Africa,
1899-1900, by George Henry Makins
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
Title: Surgical Experiences in South Africa, 1899-1900
Being Mainly a Clinical Study of the Nature and Effects
of Injuries Produced by Bullets of Small Calibre
Author: George Henry Makins
Release Date: May 3, 2007 [EBook #21280]
Language: English
Character set encoding: ISO-8859-1
*** START OF THIS PROJECT GUTENBERG EBOOK SURGICAL EXPERIENCES ***
Produced by Jonathan Ingram, Josephine Paolucci and the
Online Distributed Proofreading Team at https://www.pgdp.net
FRONTISPIECE.
SURGEON TO ST. THOMAS'S HOSPITAL, LONDON
JOINT LECTURER ON SURGERY IN THE MEDICAL SCHOOL OF ST. THOMAS'S HOSPITAL
MEMBER OF THE COURT OF EXAMINERS OF THE ROYAL COLLEGE OF
SURGEONS OF ENGLAND, AND LATE ONE OF THE CONSULTING SURGEONS
TO THE SOUTH AFRICAN FIELD FORCE
LONDON
SMITH, ELDER, & CO., 15 WATERLOO PLACE
1901
TO
SURGEON-GENERAL W. D. WILSON
PRINCIPAL MEDICAL OFFICER TO THE SOUTH AFRICAN FIELD FORCE
THE MEMBERS OF THE ROYAL ARMY MEDICAL CORPS
EMPLOYED IN SOUTH AFRICA
AND TO THE
CIVIL SURGEONS TEMPORARILY ATTACHED TO THAT CORPS
These Experiences are Dedicated
AS AN EXPRESSION OF APPRECIATION
OF THE INVARIABLE KINDNESS AND SYMPATHY EXTENDED
TO THE AUTHOR
WITHOUT WHICH THE BOOK COULD NOT
HAVE BEEN WRITTEN
A word of explanation is perhaps necessary as to the form in which these experiences have been put together. The matter was originally collected with the object of sending a series of articles to the British Medical Journal. Various circumstances, however, of which the chief was the feeling that extending experience altered in many cases the views adopted at first sight, prevented the original intention from being carried into execution, and the articles, considerably expanded, are now published together.
As to the illustrative cases introduced in support of various statements made in the text, only those have been chosen from my notes which were under my own observation for a considerable time, and many of these have been brought up to date since my return to England. I have, as a rule, avoided the inclusion of cases seen cursorily, and few simple ones have been quoted since their character is sufficiently indicated in the text. These remarks seem necessary since the mode of selection has resulted in the inclusion of a number of cases of exceptional severity, and any attempt to draw statistical conclusions from them would be most misleading.
The first two chapters have been added with a view to affording some information, first, as to the conditions under which a great part of the surgical work was done, and, secondly, as to the mechanism and causation of the injuries, which would not readily be at hand in the case of the general surgical reader. For much of the information contained in Chapter II. I must express my indebtedness to the work of MM. Nimier and Laval, so frequently quoted.[Pg viii]
The only other object of this Preface is to express my thanks to the many who have aided me in the task of amplifying the observations on which the articles are founded, and I think no writer ever received more sympathetic and kindly help in such particulars than the author.
My first thanks, those due to the Members of the Royal Army Medical Corps, I endeavour to express by the dedication of this volume. Any attempt to make individual acknowledgment to either the Members of the Service, or to the Civil Surgeons temporarily attached, would be impossible. I have, however, tried to associate the names of many of those in charge of cases in the recital of histories and treatment throughout.
My thanks are not less due to the Military Heads of Departments at the War Office, who have helped me in the collection of details as to the subsequent course of many of the cases described, and in the acquisition of information regarding the weapons and ammunition treated of. I should particularly express my gratitude to Colonel Robb, of the Adjutant-General's Department, and Colonel Montgomery, of the Ordnance Department.
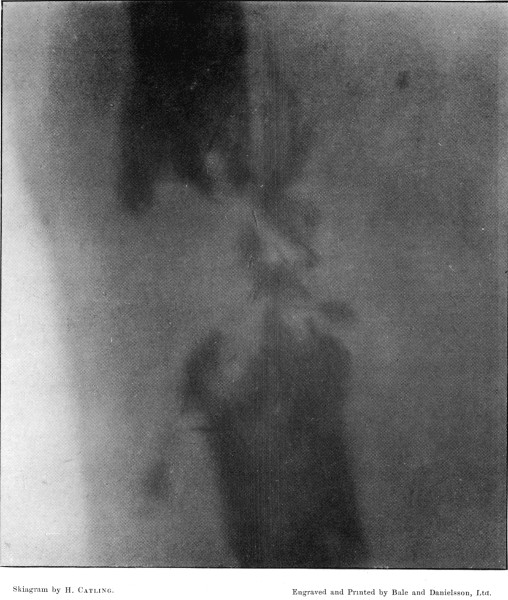
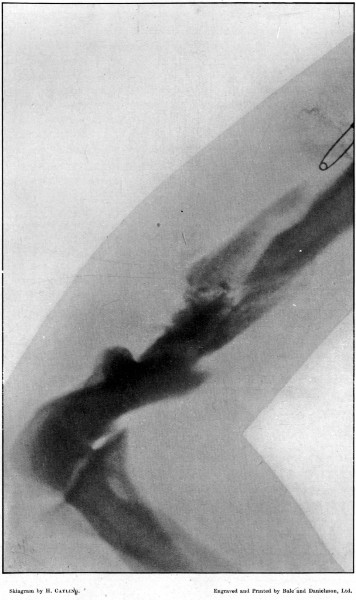
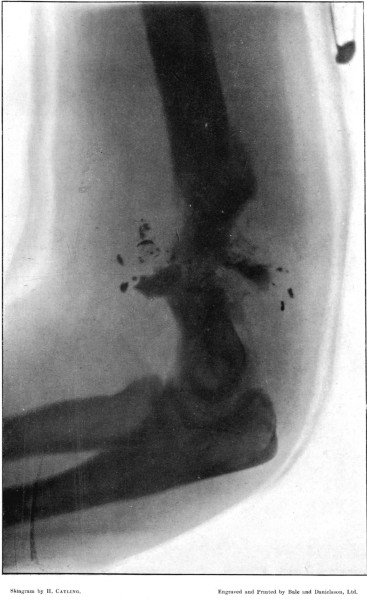
I am greatly indebted to my former colleague Mr. Cheatle for two of the illustrations of wounds, and for permission to quote some of his other experience, and to Mr. Henry Catling, to whose skill I owe the majority of the skiagrams of the fractures under my observation at Wynberg and elsewhere.
I must also express my thanks to Mr. Danielsson and his artist, Mr. Ford, for the trouble they have taken in converting my rough sketches into the illustrations contained in the volume.
Lastly, my warmest gratitude is due to my friends, Mr. Cuthbert Wallace, who has read some of my chapters, and to Mr. F. C. Abbott, who has read the whole book for the press and suggested many improvements and modifications.
47 Charles Street, Berkeley Square, W.
February 1901.
PAGE
CHAPTER I
INTRODUCTORY
ItineraryLinen Holdall with surgical instrumentsSurgical outfit—Personal transport—General health of the
troops—Climate—Consideration of the number of men killed and
wounded—Transport of the wounded—Vehicles—Trains—Ships—Hospitals 1
CHAPTER II
MODERN MILITARY RIFLES AND THEIR ACTION
General type—Calibre, length, and weight of
bullet—Velocity—Trajectory—Revolution—Varieties of rifle in common
use by the Boers—Penetration—Comparison of bullets—Use of
wax—Comparative efficiency of different types 40
CHAPTER III
GENERAL CHARACTERS OF WOUNDS INFLICTED BY BULLETS OF SMALL CALIBRE
Type wounds—Nature of external apertures—Direct course of wound
track—Multiple wounds—Small bore and sharp localisation of
tracks—Clinical course—Mode of healing—Suppuration—Wounds of
irregular type—Ricochet—Mauser bullet—Lee-Metford bullet—Expanding
bullets—Altered bullets—Large sporting bullets—Symptoms—Psychical
disturbance and shock—Local
[Pg x]shock—Pain—Hæmorrhage—Diagnosis—Prognosis—Treatment
55
CHAPTER IV
INJURIES TO THE BLOOD VESSELS
Nature of lesions; contusion, laceration, perforation—Results of
injuries—Primary hæmorrhage—Recurrent hæmorrhage—Secondary
hæmorrhage—Treatment of hæmorrhage—Traumatic aneurisms—Arterial
hæmatoma—True traumatic aneurism—Aneurismal varix and varicose
aneurism—Conditions affecting development—Effects of aneurismal varix
or varicose aneurism on the general circulation—Prognosis and treatment
of aneurismal varix—Prognosis and treatment of varicose
aneurism—Gangrene after ligation of arteries 112
CHAPTER V
INJURIES TO THE BONES OF THE LIMBS
Nature of wounds—Explosive wounds—Types of fracture of shafts of long
bones—Stellate, wedge, notch, oblique, transverse,
perforating—Fractures by old types of bullet—Lesions of the short and
flat bones—Special character of the symptoms in gunshot fracture, and
of the course of healing—Prognosis—Treatment—Special fractures—Upper
extremity—Pelvis—Lower extremity154
CHAPTER VI
INJURIES TO THE JOINTS
General character—Vibration synovitis—Wounds of
joints—Classification—Course and symptoms—General treatment—Special
joints225
CHAPTER VII
INJURIES TO THE HEAD AND NECK
Anatomical lesions—Scalp wounds—Fracture of the skull without evidence
of gross lesion of the brain—Fractures with concurrent brain
injury—Classification—General injuries—Effect of ricochet—Vertical
or coronal wounds in frontal region—Glancing or oblique wounds of any
region—Gutter fractures—Superficial perforating fractures—Fractures
of the base—Symptoms of fracture of the skull, with concurrent injury
to the brain—Concussion—Compression—Irritation—Frontal
injuries—Fronto-parietal and parietal injuries—Occipital
injuries—Forms of hemianopsia—Abscess of the brain—General
[Pg xi]diagnosis—General prognosis—Traumatic epilepsy—General
treatment—Wounds of the head not involving the brain—Mastoid
process—Orbit—Globe of the eye—Nose—Malar bone—Upper
jaw—Mandible—Wounds of the neck—Wounds of the pharynx, larynx, and
trachea 241
CHAPTER VIII
INJURIES TO THE VERTEBRAL COLUMN AND SPINAL CORD
Fractures in their relation to nerve injury—Transverse
processes—Spinous processes—Centra—Signs of fracture of the
vertebra—Injuries to the spinal cord—Effects of high
velocity—Concussion, slight, severe—Contusion—Hæmorrhage,
extra-medullary, hæmatomyelia—Symptoms of injury to the spinal
cord—Concussion—Hæmorrhage—Total transverse lesion—Diagnosis of form
of lesion—Prognosis—Treatment314
CHAPTER IX
INJURIES TO THE PERIPHERAL NERVES
Anatomical lesions—Concussion—Contusion—Division or
laceration—Secondary implication of the nerve—Symptoms of nerve
injury—Traumatic neuritis—Scar implication—Ascending
neuritis—Traumatic neurosis—Injuries to special nerves—Cranial
nerves—Cervical, brachial, lumbar, and sacral plexuses—Cases of nerve
injury—General prognosis and treatment 341
CHAPTER X
INJURIES TO THE CHEST
Non-penetrating wounds of the chest wall—Penetrating wounds, special
characters of entrance and exit apertures—Fracture of the ribs,
symptoms, treatment—Wounds of the diaphragm—Wounds of the
heart—Wounds of the lung, symptoms—Pneumothorax—Hæmothorax—
Empyema—Diagnosis, prognosis, and treatment of hæmothorax—Cases
of hæmothorax374
CHAPTER XI
INJURIES TO THE ABDOMEN
Introductory remarks—Wounds of the abdominal wall—Penetration of
the intestinal area without definite evidence of visceral injury—Wounds
of explosive character—Anatomical characters of intestinal wounds—Wounds
of the mesentery—-Wounds of the omentum—Results of intestinal
[Pg xii]wounds, fæcal extravasation, peritoneal infection, septicæmia—Reasons
for the escape of severe injury in wounds traversing the
abdomen—Wounds of the stomach—Wounds of the small intestine—Wounds
of the large intestine—Prognosis in intestinal injuries—Treatment
of intestinal injuries—Wounds of the urinary bladder—Wounds
of the kidney—Wounds of the liver—Wounds of the spleen—General
remarks on the prognosis in abdominal injuries—Wounds of
the external genital organs—Wounds of the urethra 407
CHAPTER XII
ON SHELL WOUNDS
Varieties of shells employed—Large shells—Wounds produced by different
varieties—Pom-Pom shells—Wounds produced by fragments and fuses—Shrapnel—
Boer segment shells—Leaden shrapnel bullets—Treatment of shell wounds474
Index of Contents487
PLATES
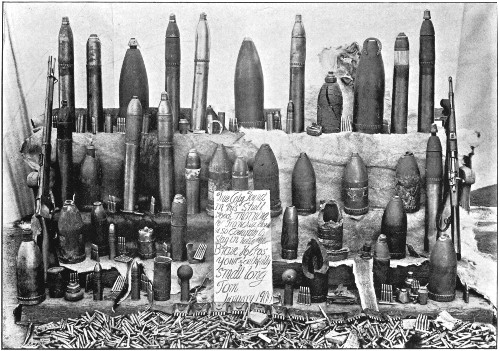
Varieties of Ammunition collected at LadysmithFrontispiece
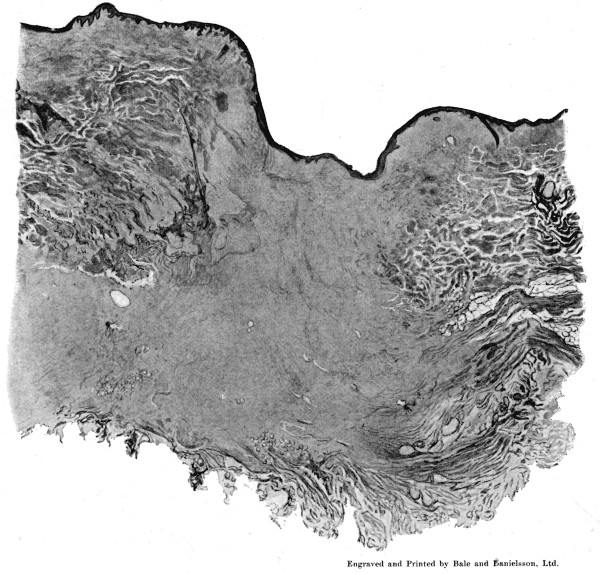
1. Section of Mauser Aperture of Entry To face p. 73
2. Section of Mauser Aperture of Exit 76
3. Punctured Fracture of Clavicle162
4. Comminuted Fracture of Shaft of Humerus180
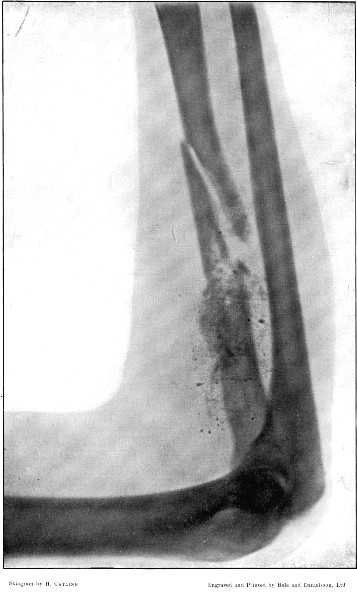
5. Comminuted Fracture of Humerus accompanied by an Explosive Exit182
6. Comminuted Fracture of Humerus due to Oblique Impact184
7. Same Fracture healed186
8. Low Velocity Fracture of Humerus With Retained Bullet188
9. Localised Fracture of Humerus Showing Fragmentation of the Bullet190
10. Wedge-shaped Fracture of the Radius192
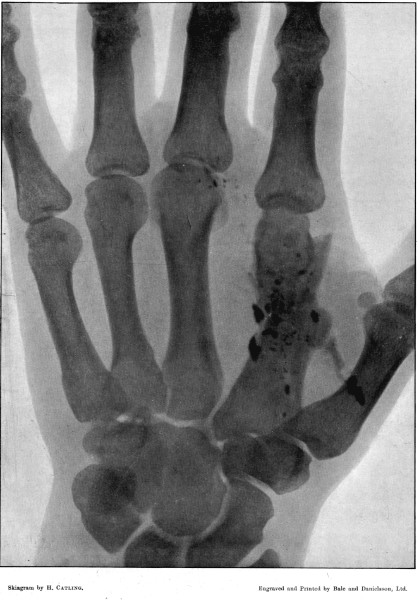
11. Fracture of the Metacarpus, showing Fragmentation of the Bullet194
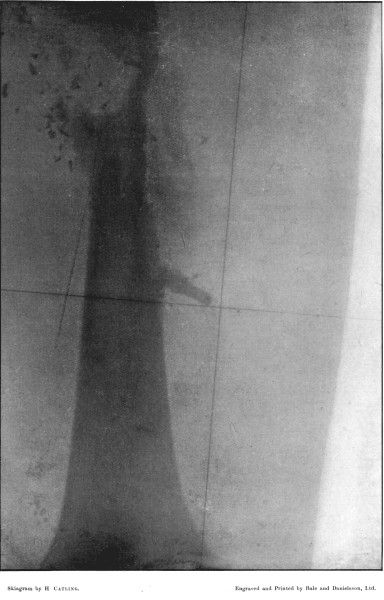
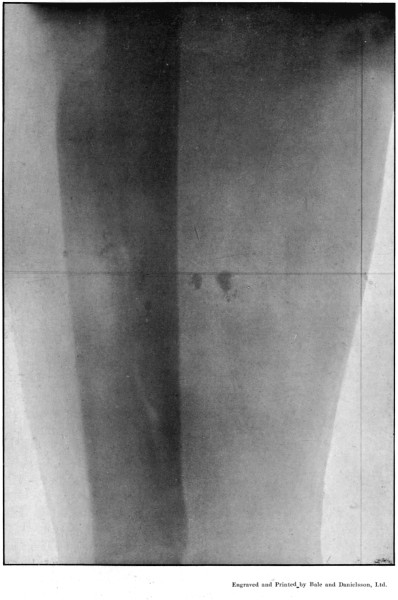
12. Finely Comminuted Fracture of the Femur196
13. The same Fracture Healed198
14. Stellate 'Butterfly' Fracture of the Femur200
15. Lateral Impact of Bullet, with Comminution of the Femur202
16. Rectangular Impact of Bullet, with highly Oblique Line of Fracture of the Femur204
17. Punctured Fracture of the Femur with Exit Bone-flap206
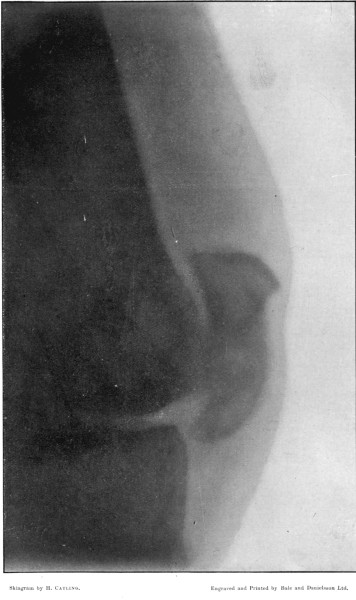
18. Fractured Patella208
19. Oblique Comminuted Fracture of the Tibia210
20. Transverse Fracture of the Tibia212
21. Puncture of the Tibia, with an Oblique Fissure214
22. Notched Fracture of the Tibia216
23. Punctured Fracture of the Fibula218
24. The same Fracture, Lateral View 220
25. Vickers-Maxim Fracture of the Humerus 482
FIG. PAGE
1. Linen Hold-all with Instruments4
2. Instrument Hold-all Rolled for Packing5
3. Tin Water-bottle for Emergency Operations6
4. Buggy on the Veldt7
5. McCormack-Brook Wheeled Stretcher Carriage19
6. Indian Tonga20
7. Service Ambulance Wagon21
8. Buck-wagon Loaded with Wounded Men22
9. Interior of a Wagon of No. 2 Hospital Train24
10. P. & O. Hospital Ship 'Simla'25
11. Type of General Hospital 32
12. Type of Tortoise Tent Hospital 33
13. Single Tortoise Hospital Tent 35
14. Five Types of Cartridge in Common Use During the War47
15. Sections of Four Bullets To Show Relative Thickness of Mantles51
16. Entry and Exit Mauser Wounds56
17. Gutter Wound of Shoulder56
18. Oblique Gutter Exit Wound 57
19. Oval Entry, Starred Exit Wounds58
20. Circular Entry, Slit Exit Wounds59
21. Circular Entry, Starred Exit Wounds59
22. Entry and Exit Wounds in Six Successive Spots made by same Bullet61
23. Four Successive Entry and Exit Wounds of same Bullet62
24. Superficial Abdomino-thoracic Track64
25. Superficial Linear Ecchymosis of Thigh65
25a. Sections of Mauser Entry and Exit Wounds74
25b. Prolapsed Omentum77
26. Sections of Four Bullets82
27. Normal Mauser Bullet83
28. Four Mauser Ricochets 84
29. Mauser Ricochet, Disc Form 85
30. Fissured Mauser Mantle 86
31. Mausers Deformed by Impact on Femur 86
32. Apical Mauser Ricochet 87
33. Spiral Ricochet88
[Pg xv]
34. Normal Lee-Metford Bullet89
35. Apical Lee-Metford Ricochets90
36. " " " 91
37. Four Types of Soft-nosed Bullets92
38. 'Set-up' Soft-nosed Lee-Metford Bullets92
39. Flattened, Solid-based Mantle From Ricochet93
40. Mauser Bullet, Jeffreys-Tweedie Modification94
41. Section of Mark IV. and Soft-nosed Mauser94
42. Tampered Bullets95
43. Large Leaden Sporting Bullets98
44. Explosive Wound of Back100
45. Dead Men on Field of Battle102
46. Flattened Leaden Cores from Mantled Bullets105
47. Explosive Exit Wound over Fractured Ulna156
48. Explosive Exit Wound over Fractured Humerus158
49. Explosive Exit and Entry Wounds of Legs159
50. Types of Gunshot Fracture161
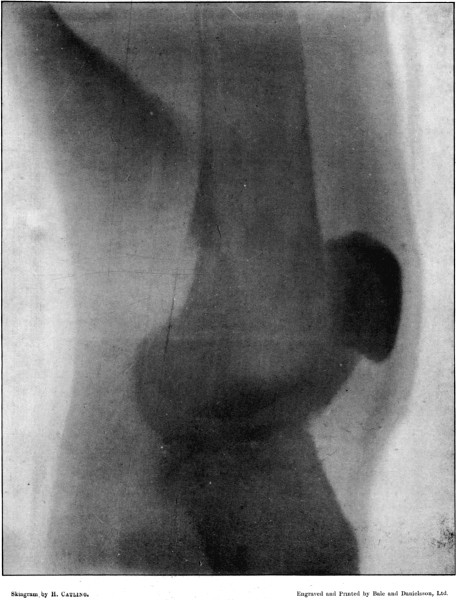
51. Lower End of Fractured Femur164
52. Oblique Perforation of Femur, Separation of Fragment at Exit Aperture in Bone169
53. Gutter Fracture of Head of Humerus178
53a. Diagram of 'Butterfly' Type180
54. Wire Gauze Splint 187
55. Gutter Fracture of Pelvis 191
55a. Diagram of 'Butterfly' Type 200
56. Cane Field Splint for Lower Extremity 209
57. Tunnel Fracture at Surface of Tibia 219
58. Cane Field Splint for Leg 222
59. Skiagram of Injury to Interphalangeal Joint 237
60. Skiagram of Bullet in Nasal Fossa 244
61. Diagram of Aperture of Entry into Cranium 245
62. Aperture of Entry into Frontal Bone 252
63. Fragment of Inner Table Displaced from Opening seen in Fig. 62 253
64. Gutter Fracture of First Degree in Parietal Bone 255
65. Diagram of Gutter Fractures 256
66. Gutter Fracture of Second Degree in Parietal Bone 257
67. Diagrams of Gutter Fractures 258
68. Superficial Perforating Fracture of Parietal Region 259
69. Diagram of Superficial Perforating Fracture 260
70. Fragment Forming Floor of Temporal Gutter Fracture 260
[Pg xvi]
71. Scale of External Table in Low Velocity Injury of Frontal Bone 261
72. Frontal Perforation, Aperture of Exit 261
73. Visual Field in Occipital Injury 279
74. " " " 279
75. " " " 281
76. " " " 281
77. " " " 283
78. " " " 283
79. Contused Spinal Cord 333
80. Divided Spinal Cord 334
81. Superficial Track in Anterior Body-wall 377
82. Spirally Grooved Bullet 381
83. Ecchymosis in Fractured Ribs with Hæmothorax392
84. Subcutaneous Division of Abdominal Muscles409
85. Lateral Incomplete Wound of Small Intestine. Slit Form416
86. Lateral Perforation of Small Intestine. Gutter Form417
87. Entry and Exit Wounds in a Transverse Perforation of Intestine418
88. Inner Aspect of Piece of Intestine Shown in Fig. 87419
89. Impaction of Omentum in Exit Wound of Abdominal Wall421
90. Fragments of Large Shells 475
91. Fragments of Percussion and Time Fuses 477
92. Complete 1-lb. Pom-pom Shell 479
93. Fragments of Exploded Pom-pom Shells 480
94. Percussion Fuse From 1-lb. Pom-pom Shell481
95. Fragments of Boer Segment Shells 483
96. Normal and Deformed Leaden Shrapnel Bullets 485
1. Case of Axillary Hæmatoma, Blood Temperature 119
2. Case of Hæmothorax with Recurrent Hæmorrhages 395
3. Primary and Secondary Rises of Temperature in Hæmothorax, Recovering Spontaneously 402
4. Secondary Rise of Temperature in Hæmothorax 403
5. Falls of Temperature in Hæmothorax following Paracentesis 404
6. Secondary Hæmothorax, Spontaneous Fall of Temperature 405
The following pages are intended to give an account of personal experience of the gunshot wounds observed during the South African campaign in 1899 and 1900. For this reason few cases are quoted beyond those coming under my own immediate observation, and in the few instances where others are made use of the source of quotation is indicated. It will be noted that my experience was almost entirely confined to bullet wounds, and in this respect it no doubt differs from that of surgeons employed in Natal, where shell injuries were more numerous. This is, however, of the less moment for my purpose as there is probably little to add regarding shell injuries to what is already known, while, on the other hand, the opportunity of observing large numbers of injuries from rifle bullets of small calibre has not previously been afforded to British surgeons.
I think the general trend of the observations goes to show that the employment of bullets of small calibre is all to the advantage of the men wounded, except in so far as the increased possibilities of the range of fire may augment the number of individuals hit; also that such variations as exist between wounds inflicted by bullets of the Martini-Henry and Mauser types respectively, depend rather on the form and bulk of the projectile than on any inherent difference in the nature of the injuries. Thus in the chapter devoted to the general characters of the wounds, it will be seen that most of the older types[Pg 2] of entry and exit aperture are produced in miniature by the small modern bullet, and that the main peculiarity of the deeper injuries is the frequent strict localisation of the direct damage to an area of no greater width than that crossed by narrow structures of importance such as arteries or nerves.
It is to be regretted that I am unable to furnish any important statistical details, but incomplete numbers, such as are at my disposal, would be of little value. In view, however, of the considerable interval which must elapse before the Royal Army Medical Corps is able to arrange and publish the large material which will have accumulated, it has seemed unwise to defer publication until the completion of a report which will deal with such matters thoroughly.
It may be of interest to premise the opportunities which I enjoyed of gaining experience during the campaign. I arrived in South Africa on November 19, 1899; two days later I proceeded to Orange River with Surgeon-General Wilson, and on the day three weeks after leaving home performed some operations in the field hospitals on patients from the battle of Belmont. I remained at Orange River during the three next engagements, Graspan, Enslin, and Modder River, and on the day of Magersfontein I went forward to the Field hospitals at Modder River, arriving during the bringing in of the patients from the field of battle. I returned to Orange River with the patients and remained there a further period of three weeks, during which time the patients were gradually transferred to the Base hospitals at Wynberg. At Christmas I followed the patients down to the base, and thus was able to observe the course of the cases from their commencement to convalescence. I remained at Wynberg six weeks, during which time a number of cases from the neighbourhood of Rensburg and some from Natal were received. On February 7, I left Wynberg, following Lord Roberts up to my old quarters at Modder River, where I saw a few wounded men brought in from the engagements at Koodoosberg Drift. On Lord Roberts's departure for Bloemfontein he requested me to return to Wynberg to await the wounded who might be sent down from the fighting which might occur during his advance. I therefore had the disappointment of seeing the start of the[Pg 3] army, and then returning to Wynberg, where I remained for another six weeks in attendance at Nos. 1 and 2 General Hospitals.
During this period a very large number of the wounded from Paardeberg Drift and other battles were sent down and treated, after which surgical work began to flag.
On April 14, I was recalled to the front and journeyed to Bloemfontein, where I stayed three weeks, making one journey out to the Bearer Company of the IX. Division at the Waterworks.
On May 4, I left Bloemfontein with Lord Roberts's army, and shortly after joined the IX. Division, with which I journeyed until the commencement of June, seeing a good deal of scattered work in the field and Field hospitals, and in the small temporary improvised hospitals in the towns of Winberg, Lindley, and Heilbron. Early in June I left Heilbron with Lord Methuen's division, and spent the next four weeks with this division in the field. Thence I journeyed to Pretoria and Johannesburg, seeing a small number of wounded in each town, and on July 10, with Lord Roberts's consent, I started for home, visiting a number of the hospitals in the Orange River Colony and Natal on my way down to Cape Town. During the movements briefly recorded above, which absorbed a period of nine months, my time was fairly evenly divided between Field, Stationary, and Base hospitals; hence I had opportunities of observing the patients in every stage of their illnesses, and in all some thousands of men came under my notice.[Pg 4]
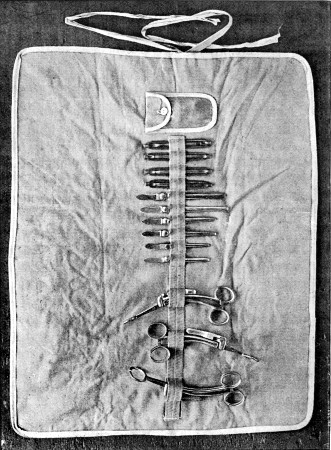 Fig. 1.—Linen Holdall with surgical instruments
Fig. 1.—Linen Holdall with surgical instruments
My departure for the seat of war was rather hurried, hence my surgical equipment was not of an extensive nature. It may be of interest, however, to shortly recount what it consisted in, since it proved an ample one, and yet was carried in a small satchel. The plan of selection adopted consisted in carefully going through the equipment of the British Field Hospital, and then adding such other instruments as seemed to me likely to be useful. With few exceptions, therefore, designed to meet emergencies, my set of instruments formed a supplement to the actual necessities carried by the Service hospitals, and was as follows:—4 trephines, Horsley's elevator, brain knife and seeker. 2 pairs of Hoffman's and 1 pair of Lane's fulcrum gouge forceps, 3 bone gouges, 1 pair straight 1 curved necrosis forceps, 1 pair bone forceps. 1 Wood's 1 Horsley's skull saws, 18 Gigli's saws with an extra handle, and two Podrez' directors for the same. 1 set Lane's bone drills, broaches, screw-drivers, and counter-sink with eight ounces of screws: silver patella wire, and 1 pair Peter's bone forceps. 2 aneurism needles, 1 bullet probe, 1 pair Egyptian Army pattern bullet forceps. 4 Lane's and 3 pairs Makins's bowel[Pg 5] clamps, Nos. 3 4 and 5 Laplace's bowel forceps, 6 Murphy's buttons, 1 pair Morris's retractors, 6 dozen intestine needles, 2 Macphail's needle-holders, Nos. 4 5 6 Thomas's slot-eyed needles, 1 mouth gag, 1 Durham's double raspatory, 3 strong plated raspatories, 1 pair tongue forceps, 1 tracheal dilator, 1 pair hernia needles, 1 hernia and 1 ordinary steel director, 1 transfusion set with metal funnel, and a stock of Messrs. Burroughes and Wellcome's compound saline infusion soloids. 1 antitoxin syringe. 6 scalpels, 2 blunt-pointed curved bistouries, 6 forcipressure forceps, 1 pair Jordan Lloyd's retractors, 1 pair ordinary retractors, 2 pairs of forceps, 3 pairs of Scissors, 1 skin-grafting razor and roll of perforated tin foil, 1 metal pocket case, and 1 hypodermic syringe with tabloids. A stock of silkworm gut, horsehair and silk ligatures, the latter prepared and sterilised for me by Miss Taylor, the Theatre Sister at St. Thomas's Hospital. Some pairs of McBurney's india-rubber, and cotton-thread operating gloves.
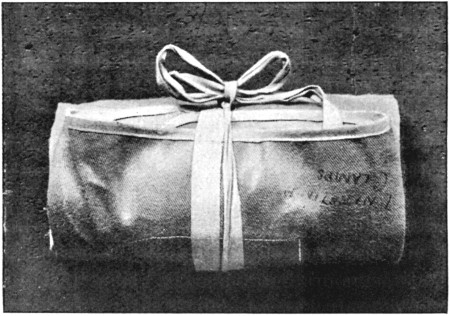 Fig. 2.—Instrument Holdall rolled
Fig. 2.—Instrument Holdall rolled
The instruments were packed in sets in small linen holdalls suggested and made by Messrs. Down Bros., who also devised my satchel. In the light of the experience gained I should have preferred a tin case to the satchel, as it never needed to be carried on horseback.
For dressings I trusted entirely to the Royal Army Medical Corps, and at my request Colonel Gubbins, R.A.M.C., sent out[Pg 6] to the Cape a quantity of sterilised sponges and pads made by Messrs. Robinson & Co. Ltd. of Chesterfield, which fully met all requirements in this direction.
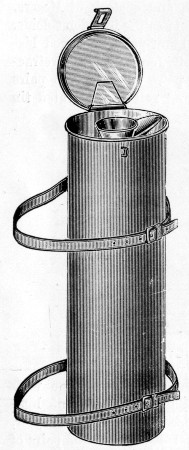 Fig. 3.—Tin Water-bottle for the march (Military Equipment Company)
Fig. 3.—Tin Water-bottle for the march (Military Equipment Company)
This equipment was superfluous at the Base hospitals, but when in the field with the troops proved very useful. In the early part of the campaign I was able to do all my travelling by train, but later I travelled by road only. I received the greatest kindness and help in this particular. General Sir William Nicholson, Chief Director of Transport, provided me with a buggy, a pair of horses, and a driver, and Prince Francis of Teck, the Chief Remount Officer, selected a pony suitable to my equestrian powers. The buggy proved a very great success; the box seat carried my instruments and dressings, the front a 4-gallon tin water-bottle for emergency operations, and the rear shelf my personal belongings. The water-bottle was lent to me by the Portland Hospital. (Fig. 3.)
The cart was able to cross any drifts or dongas, and when an engagement was in progress was able to accompany the Ambulance wagons, so that I had all my necessaries on the spot, even at the first dressing station. In point of fact when with the Highland Brigade, on some occasions, we did all necessary operations on the spot during the progress of fighting; a most useful performance, since fighting on several days did not cease till dark, and the evenings were much too cold to allow of operations being done with safety to the patients. The great advantage of the buggy was its lightness and smallness.[Pg 7] On one occasion it accompanied me between 500 and 600 miles without a single accident, beyond the fact that one night I was relieved of both my horses by some troopers whose own were worn out.
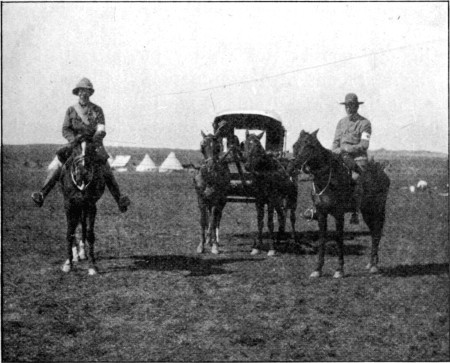 Fig. 4.—My Buggy on the veldt at Bloemfontein. (Photo by Mr. Bowlby)
Fig. 4.—My Buggy on the veldt at Bloemfontein. (Photo by Mr. Bowlby)
With regard to the general health of the troops as subjects of surgical wounds, I suppose a better class of patient could scarcely be found. The men were young, sound, well set and nourished, and hard and fit from exercise in the open air. Beyond this, in spite of the scarcity of vegetables, a certain amount of fruit, rations of jam, and lime juice made any sign of scurvy a rare occurrence—I never saw a case during the whole of my wanderings. The meat was good, especially in the early part of the campaign, when it was for the most part brought from Australia and New Zealand, and we enjoyed the two collateral advantages of getting plenty of the ice which had been used for the preservation of the meat, in the camps, and the still greater one of having no butchers' offal to need destruction or prove a source of danger. When bread was to be got it was fairly good, and the biscuit was at all times excellent. Except on the advance from Modder River to Bloemfontein,[Pg 8] as far as I could judge, no large bodies of the men ever really suffered from shortness of food, and then only for a few days. Drink was a more serious problem: in the early days beer was to be got at the canteens, but with the increase of numbers and difficulties of transport this ceased to be the case, and water was the sole fluid available. This was often muddy, and the soldiers would take very little care what they drank unless under constant supervision; hence a great quantity of very undesirable water was drunk. None the less I think the water was more often the cause of sand diarrhœa than of enteric fever. A large quantity of fluid was by no means a necessity if the men would only have exercised some self-control. During the first week I spent at Orange River, I drank lime juice and water all day, but after that time, by a very slight amount of determination, I thoroughly broke myself of the habit, and drank at meal-times only. Most of the men however emptied their water-bottles during the first hour of the march, and the rest of the day endured agony, seizing the first opportunity of drinking any filthy water they met with. When, for instance, we camped near a vlei, and the General took the greatest care that the mules and horses should be watered at one spot only, in order to preserve the cleanliness of the rest of the pool, the men would often go and fill their water-bottles amongst the animals' feet rather than take the trouble to walk the few necessary yards round. In such particulars they needed constant supervision.
The climate on the western side was a great element no doubt both in the general healthiness of the men and in the general good results seen in the healing of wounds. The days were often hot; thus even in November at Orange River the thermometer registered 115°F. in the single bell tents, but on the other hand the nights were cool and refreshing. The air was very pure and exceedingly dry, while the constant sunshine not only kept up the spirits, but also proved the most efficient disinfector of any ground fouled to less than a serious extent. Dust was our principal bugbear; and when a camp had been settled for a few days, flies; both of these evils increasing rapidly as the stay on any one spot was prolonged. My personal experience of rain was small, but I was twice in[Pg 9] camp, once at Orange River and once at Bloemfontein, when very heavy rain fell, and this was sufficient to make the camps terribly uncomfortable for a few days.
Under these conditions, as might be expected, until the outbreak of enteric fever the health of the men was remarkably good, minor ailments alone prevailing. One of the most troublesome of these was diarrhœa, which gained the appellation of 'the Modders,' already a classical name as far as South Africa is concerned. This most frequently, I think, depended on errors of diet, combined with the swallowing of a large amount of sand with the food as dust, and in the water drunk. Cases of severe dysentery, however, were also not very uncommon. Rheumatic pains were a common ailment, which, considering the dryness of the atmosphere, would hardly have been expected. Continued fever of a somewhat special type was not uncommon, and was sometimes spoken of under the name of the district, sometimes as veldt fever—of this I will say nothing, as others better fitted to point out its peculiarities will no doubt deal with it. Enteric fever, our chief scourge, I will pass over for the same reason. I might, however, remark from the point of view of one not very experienced in this disease, that in a large number of the fatal cases I happened to see, the actual cause of death seemed to me to be septicæmia from absorption from the mouth. The mouths were unusually bad, even allowing for the often insufficient cleansing that was able to be carried out, and I was inclined to attribute these in some degree to the dryness of the atmosphere, which very quickly and effectively dried up the mucous membrane of the mouth in patients not breathing through the nose, and encouraged the formation of large cracks. Pneumonia was rare, and this was rendered the more striking from the comparatively large number of men who contracted the disease on board ship on the voyage out from England.
As will be gathered from the above, medical disease seldom called for the aid of the surgeon. Abdominal section was occasionally considered in cases of perforation in enteric fever, and was, I believe, a few times performed, but as far as I know without success. It was also proposed to treat some[Pg 10] of the severe dysentery cases by colotomy, but I never saw the method tried. As far as I was concerned I never met with a case of either disease I thought suitable for the treatment. I saw one case in which an abscess of the liver had followed an attack of enteric, which had been successfully treated by incision, and a few cases of tropical abscess which probably came into the country were also subjected to operation. Some cases of appendicitis, as would be expected, also needed surgical treatment. In a few instances empyema followed influenza, and a few cases of mastoid suppuration had to be dealt with.
Of surgical diseases the one most special to the campaign, although not of great importance, was the veldt sore. This was a small localised suppuration most common on the hands and neck, but sometimes invading the whole trunk, more particularly the lower extremities however, when the covered parts of the body were attacked. The sores were no doubt the result of local infections; they reminded me most of the sores seen on the hands of plasterers, and I think there is no doubt the dust was responsible for them. I think piles were somewhat more prevalent than they should have been among the men, but this was probably dependent on the strain involved in defæcation in the squatting position, since the soldiers were for the most part regularly attentive to the calls of nature.
I saw a good many cases of lightning stroke, and some were fatal. Sunstroke was not common, and, considering the heat, it was very remarkable how little the men suffered from this condition. This was no doubt in part attributable to the absence of the possibility of getting alcoholic drinks, but it is not common for any one in South Africa to suffer in this way, probably as a result of the continuous nature of the sunshine.
In spite of the labours of hospital surgeons at home, it was rather instructive to see the number of men who suffered with hernia, varicocele, and varicose veins to a sufficient degree to necessitate going to the base. The experience quite sufficed to explain the trouble which is taken to prevent men with these complaints entering the service.[Pg 11]
I will now pass to the question of the proportionate frequency with which the men were killed or wounded during the present campaign. I propose to take only one series of battles, with which I was personally acquainted throughout, to illustrate this point. This seems the more satisfactory course to follow, since the number of casualties is still undergoing continuous gradual increase, and besides this the warfare has assumed a peculiar and irregular form, statistics from which scarcely possess general application.
The battles included, those of the first Kimberley Relief Force, were fought under fair average conditions as to the nature of the ground. In the first two the defending enemy occupied heights, in the two following the ground advanced over by our men was comparatively even; thus at Modder River there was only a gradual slope upwards, and at Magersfontein the advanced trenches of the Boers were only slightly above the level of the ground over which the advance was made. At the same time, at the latter battle a great number of the Boers engaged were on the sides of the hill well above the advanced trenches. In no case were the Boers in such a position as to have to fire upwards, to them a considerable advantage. It must also be noted that throughout the Boers were able to rest their rifles; hence the fire should have been at any rate of an average degree of accuracy. In the advances of our own men, anthills and stones were practically the only cover to be obtained, and little or no help was given by variations in the general surface. All these points seem to favour a large proportional number of hits on the part of the riflemen. I very much regret that I am unable to say what was the proportional number of shell wounds among the men hit, but I can say with some confidence that among the wounded it was not as great as ten per cent. I should be inclined to place it as low as five per cent. Again, I cannot fix the proportionate occurrence of wounds from bullets of large calibre such as the Martini-Henry, but this was certainly not large. I think if ten per cent. is deducted to represent the[Pg 12] number of hits from either of these forms of projectile, that we may fairly assume the remaining 90 per cent. of the wounds to have been produced by bullets of small calibre. The numbers of the opposing forces were probably fairly even.
Taking all these circumstances together, and bearing in mind that our army was always in the position of having to make frontal attacks on men well protected in strong positions, I think it must be allowed that a fair idea should be possible of the effectiveness of the modern weapons. Only one circumstance, one inseparable from any fighting with the Boers, seems to affect the numbers in an important manner. This consists in the fact that the Boer rarely fights to the bitter end, hence the greater proportion of his hits are obtained at long distances.
| Number of troops engaged | Killed | Wounded | Missing | Total | Percentage of killed and wounded to number of men engaged | |
| Belmont: | ||||||
| Officers | 297 | 3 | 23 | 0 | 26 | 8.75 |
| Non.-com. officers and men | 8,396 | 55 | 206 | 4 | 265 | 3.15 |
| Total | 8,693 | 58 | 229 | 4 | 291 | 3.34 |
| Graspan: | ||||||
| Officers | 326 | 3 | 7 | 0 | 10 | 3.06 |
| Non.-com. officers and men | 8,213 | 18 | 163 | 7 | 188 | 2.29 |
| Total | 8,539 | 21 | 170 | 7 | 198 | 2.31 |
| Modder River: | ||||||
| Officers | 335 | 3 | 19 | 0 | 22 | 6.56 |
| Non.-com. officers and men | 9,856 | 67 | 377 | 18 | 462 | 4.68 |
| Total | 10,191 | 70 | 396 | 18 | 484 | 4.74 |
| Magersfontein: | ||||||
| Officers | 379 | 18 | 48 | 2 | 68 | 17.94 |
| Non.-com. officers and men | 11,068 | 148 | 669 | 101 | 918 | 8.29 |
| Total[1] | 11,447 | 166 | 717 | 103 | 986 | 8.43 |
Table I. gives the number of men engaged, and also that of the killed and wounded at each of four battles. Table III. shows for comparison the relative number of killed and wounded in some former campaigns while older forms of weapon were in use.
With regard to the numbers in Tables I. and II. it should be at once said that they are only to be regarded as approximate, since they do not exactly tally with those officially reported in the 'Times' at a later date. Sources of error may, however, have crept into both, and as there is little difference in the gross numbers, I have preferred to retain the series compiled by Major Burtchaell, R.A.M.C., as Table II. contains interesting information as to the proportionate number of men who died during the first 48 hours, after being wounded.
| Percentage mortality | |||||||
| Number of troops engaged | Total number of men hit | Killed | Died within forty-eight hours | Total | To men hit | To force employed | |
| Belmont: | |||||||
| Officers | 297 | 26 | 3 | 3 | 6 | 23 | 2.02 |
| Non.-com. officers and men | 8,396 | 265 | 55 | 8 | 63 | 23.77 | 0.75 |
| Total | 8,693 | 291 | 58 | 11 | 69 | 23.71 | 0.79 |
| Graspan: | |||||||
| Officers | 326 | 10 | 3 | 1 | 4 | 40[2] | 1.22 |
| Non.-com. officers and men | 8,213 | 188 | 18 | 3 | 21 | 11.17 | 0.25 |
| Total | 8,539 | 198 | 21 | 4 | 25 | 12.62 | 0.29 |
| Modder River: | |||||||
| Officers | 335 | 22 | 3 | 1 | 4 | 18.18 | 1.19 |
| Non.-com. officers and men | 9,856 | 462 | 67 | 9 | 76 | 16.45 | 0.77 |
| Total | 10,191 | 484 | 70 | 10 | 80 | 16.53 | 0.78 |
| Magersfontein: | |||||||
| Officers | 379 | 68 | 18 | 4 | 22 | 32.35 | 5.80 |
| Non.-com. officers and men | 11,068 | 918 | 148 | 20 | 168 | 18.30 | 1.51 |
| Total | 11,447 | 986 | 166 | 24 | 190 | 19.26 | 1.66 |
The high death rate among the officers will at once arrest attention, but this has been noticed in other campaigns, particularly in the Franco-German war. It is mainly attributable to the circumstance that the officers, as leading, are always in the front and most exposed position. I much doubt whether at the end of the campaign the entire abandonment of distinctive badges will be found to have had any very important result in decreasing the relative number of casualties as between officers and men. At close quarters distinctive uniform is no doubt a danger, but at the common ranges of 1,000 yards and upwards the enemy's fire is rather directed to cover a zone than to pick out individuals.
The especially high mortality among the officers at the battle of Graspan was attributable to the casualties among the naval officers, and the men of the brigade suffered most severely also.
It will be noted that the most expensive battles were those of Belmont and Magersfontein.
If the numbers of the men actually taking part in the fighting in these battles as given in Table I. are massed, we get an approximate total of 12,420.[3]
Of this number, 1,959 or 15.06 per cent. were reported as killed, wounded, or missing. Thus: killed, 315 or 2.53 per cent.; wounded, 1,512 or 12.17 per cent.; missing, 132 or 1.06 per cent. Reference to Table III. shows that these percentages almost exactly correspond with those obtaining in the entire Crimean campaign, and are greater than those observed in the German army during the entire Franco-German campaign.
The mortality statistics given in Table II. are of great[Pg 15] interest, since to those dying on the field are added all men dying within the first 48 hours in the Field hospitals. From the surgical point of view these men all received mortal injury, and are therefore properly included among the fatalities. Their inclusion, moreover, makes an appreciable difference in the percentage proportion of mortal injuries to wounds. Thus, if the numbers are massed (omitting the 'missing'), we find that in the four battles 1,827 men were hit, of whom 315, or 17.24 per cent., were killed. Among the wounded carried off the field, however, 49 received mortal injuries, and if these are added to the 315, we find that the proportion of mortal injuries reaches 19.92 per cent.
| 1815. | 1854. | 1871. | 1877. | 1899. | |
| Waterloo | Crimean War | Franco-German War | Russo-Turkish War | Kimberley Relief Force | |
| (English troops) | (English troops) | (German troops) | (Russian troops) | (English troops) | |
| Number of troops engaged | 36,240 | 97,864 | 887,876 | 300,000 | 15,748 |
| Number of killed | 1,759 | 2,775 | 17,570 | 32,780 | 315 |
| Percentage | 4.85 | 2.81 | 1.97 | 10.92 | 2 |
| Number of wounded | 5,892 | 12,094 | 96,189 | 71,268 | 1,512 |
| Percentage | 16.25 | 12.35 | 10.83 | 23.75 | 9.60 |
| Number of missing | 807 | — | 4,009 | — | 132 |
| Percentage | 2.19 | — | 0.45 | — | .83 |
| -Total killed, wounded, and missing | 8,458 | 14,849 | 117,768 | 104,050 | 1,959 |
| Percentage | 23.31 | 15.17 | 13.26 | 34.68 | 12.43 |
The proportion of men killed to those wounded was as follows: killed 315, wounded 1,512, or 1 to 4.8. If we add to the men killed on the field of battle the 49 dying in the next 48 hours, the proportion of fatalities is increased to 1 to 4.15. The higher of these proportions is certainly the surgically correct one.
With regard to the general accuracy of the numbers given above, a comparison of those published for the campaign up to September 15, 1900, is of value, as the two series substantially tally. Thus, up to that date, 17,072 men were[Pg 16] hit, and of these 2,998 were killed. The proportion killed to wounded was therefore 1 to 4.69.
If it be borne in mind that of the wounded men included in Table I., 1.5 per cent. died later in the Base hospitals, the percentages are almost identical.
Table III. is inserted with a view to instituting a comparison between the number of casualties in the present and earlier campaigns.
For the purposes of this table it is necessary to take the approximate number of men at Lord Methuen's disposal, irrespective of their active participation in the fighting.
The result of this addition to the total is to show that the percentage of men killed and wounded was slightly lower than in the Crimean war, and nearly corresponded with that observed in the Franco-German campaign.
As it has been shown that our numbers correspond in general with those of the whole war up to September 15, 1900, there can be little doubt that the same ratios will be maintained to the close of the campaign.
On the face of the numbers, therefore, there is little ground for assuming that the change in the nature of the weapons has materially influenced the deadliness of warfare at all. This is capable of explanation on the ground that in the Crimea the battles were fought at much closer quarters, and hence the weapons of the time were as effective, or more so, than the present ones. That this increased distance between the combatants will always counterbalance the increased deadliness of the weapons in the future is more than probable, since the range of effectiveness has been increased both in rifle and in artillery fire. In the present campaign the effect of the latter was very noticeable, since the Boers were, as a rule, quickly displaced by shell fire, unless they were in especially favourable positions, and this although no great number of men was hit by the projectiles. Under these circumstances, except on some occasions, neither side derived all the advantage from the increased shooting powers of their rifles which might have been expected. To a lesser degree this will probably always be the case in the future.
In connection with these remarks, however, I would point[Pg 17] to column 4 of Table III., as showing how difficult it is to draw definite deductions from any particular set of numbers alone. This column shows that in the Russo-Turkish War of 1877 all the percentages were practically doubled or more, and in the case of the number of men killed on the field of battle, the number was nearly five times as great as either in the Crimea or the present campaign. The explanation here depends on the race of men and their tenacity in resistance alone. In the case of either nation death in battle is little feared, and slight inclination to avoid it exists. When the theory of war held by the Boer—i.e. going out to shoot an enemy without incurring risk of being yourself shot—is borne in mind, the special circumstances attending the present campaign are sufficiently obvious to need little further remark. A future campaign in which the combatants are as equally well armed, but each side stands to the last, will probably give very different results.
It is unfortunate that no details can be given as to the influence of range in altering the relative numbers of killed to wounded. It may be stated, however, that in no instance did the percentage of killed to wounded reach 25 per cent. At the battle of Magersfontein it amounted to 19.26 per cent., at Colenso to 17.97 per cent., and at both these engagements there is little doubt that a considerable number of the men were hit within a distance of 1,000 yards. When the distances were very short the injuries were frequently multiple; and this character was a more common source of danger than increase of severity in the individual wounds received at a short range.
A short consideration of the circumstances especially influencing the ultimate mortality amongst the wounded subsequent to the reception of the injury is here necessary, although I shall be obliged to make my remarks as short as possible. The subject is best treated of under the two headings of Transport and Hospital Accommodation.
Transport.—The importance of transport is felt from the moment of the injury till the time of arrival of the patient in the mother country. To the surgeon it is of the same vital importance as the carrying of food for the troops is to the combatant general.[Pg 18]
(a) Removal of the wounded from the field of battle. My experience was opposed to hurried action in this matter, although it is necessary to gather up the wounded before nightfall if possible. As a rule wounded men should not be removed from the field of battle under fire, at any rate when the troops are in open order at a range of 1,000 yards or more. I saw several instances in which mortal wounds were incurred by previously wounded men or their bearers during the process of removal, while it was astonishing how many scattered wounded men could lie out under a heavy fire and escape by the doctrine of chances. The erect position and small group necessary to bear off a wounded man at once draws a concentrated fire, if fighting is still proceeding.
As to the best and quickest method of removing the patients to the first dressing station, there were few occasions when this was not more satisfactorily done by bearers with stretchers than by wagons. The movement was more easy to the wounded men, and, as a rule, time was saved. Over rough ground the wagons travel slowly, and patients with only provisional splints were shaken undesirably. A stretcher party in my experience easily outstripped the wagon unless a road or very smooth veldt existed. A larger number of men is of course required, but I take it that on the occasion of a great war men are both more easily obtained and fed than are transport animals. From what I have been able to learn, both the Indian dhoolie-bearers and the hastily recruited Colonial bearer companies were most successful in the removal of the large number of wounded men from the field of Colenso. I had several opportunities of comparing the two methods on a smaller scale during the fighting in Orange River Colony, and felt very strongly in favour of the stretcher parties.
For removal of patients from one part of a hospital to another, or sometimes in loading trains, &c., great economy of men, and increased comfort to the patients, may be attained by the use of some form of ambulance trolly.
I append an illustration of what seemed to me the simplest and best I came across among several in use in South Africa. The description beneath is by Major McCormack, R.A.M.C., its inventor (fig. 5).[Pg 19]
When wagons were necessary or preferable, the Indian Tongas (fig. 6), presented by Mr. Dhanjibhoy, were most useful; they carried two men lying down, the same number as the big service wagon, and were drawn by two ponies only. Although somewhat highly springed, the vehicle is so well arranged and padded, that the occupants are seldom hurt by striking against the sides with rough jolting, unless quite helpless. I occasionally made long journeys in this vehicle with much comfort.
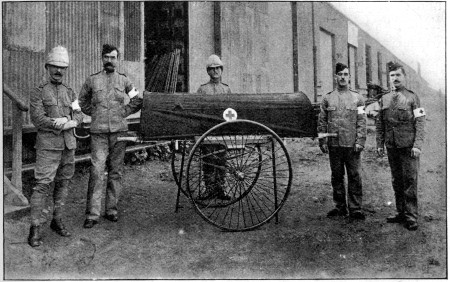 Fig. 5.—The McCormack-Brook Wheeled Stretcher Carriage.
Fig. 5.—The McCormack-Brook Wheeled Stretcher Carriage.
It consists of an under-carriage built up of two light wheels with steel spokes and rims with rubber tyres and ball bearings; on the axle are two light elliptic springs, to which is attached a transverse seat for the stretcher-carrier proper. This is securely bolted on to the seat, and consists of two pieces of hard wood, suitably worked, and forming an angle frame. On the bottom side the stretcher poles rest, and the sides of the L formed by the carrier proper prevent most effectually any jerking or turning of the stretcher when once it has been laid in the carrier. The carrier is about thirty inches long, but can be increased to any length desired. It has been found that this length is admirably suited for all purposes. To prevent the stretcher from any lateral or upward movement, two buttons with tightening screws are attached to the top of the carrier on each side. When the stretcher is laid on the carrier the screws are tightened and the stretcher is held rigid.
Two iron supports are provided, one at each end and on opposite sides of the carrier. These are lowered when it is desired either to place the stretcher on the carriage or remove it therefrom, which can be effected in a second. The carriage meanwhile remains perfectly still. When the carriage is in motion the iron supports are turned up, and lie along the respective sides of the carrier, where each rests in a small clip. The great object of this stretcher carriage has been to obtain mobility, strength, and lightness combined with efficiency and a ready and easy means of transport for sick and wounded, no matter where a patient has to be transported from. The loaded stretcher and wheeled carriage can be readily handled by one man on good roads, and by two men in rough country. The springs prevent any jar being felt by the patient on the stretcher.
(b) For the longer journeys to the Field or Stationary[Pg 20] hospitals, the service wagon and other transport vehicles came into use, particularly the South African ox-wagon.
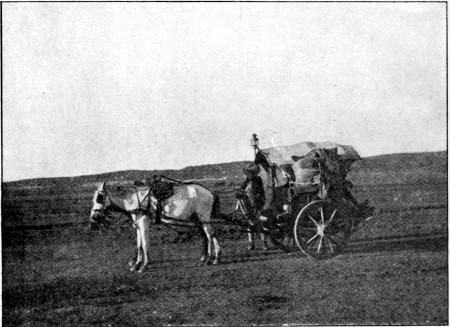 Fig. 6—Indian Tonga on the march. (Photo by Mr. Bowlby)
Fig. 6—Indian Tonga on the march. (Photo by Mr. Bowlby)
The service wagon (fig. 7) is a heavy four-wheeled vehicle, drawn by ten mules. The good construction of the wagon was amply proved by the manner in which it stood the hard wear and tear of the present campaign. It is, however, very heavy, and in comparison with its size affords very small accommodation. Two lying-down patients and six sitting is its entire capacity. Some modified patterns were in use, notably those with the Irish and Imperial Yeomanry Field Hospitals, capable of carrying four lying-down cases, the men being arranged in two tiers. Major Hale, R.A.M.C., made a very successful trek from Rhenoster to Kroonstadt with some of these, carrying twice the regulation number of lying-down cases in his wagons. Some modification in the mode of fixation is, however, necessary to increase the security of the stretchers of the upper series.
A really satisfactory wagon, combining both strength and comfort, still remains to be devised.[Pg 21]
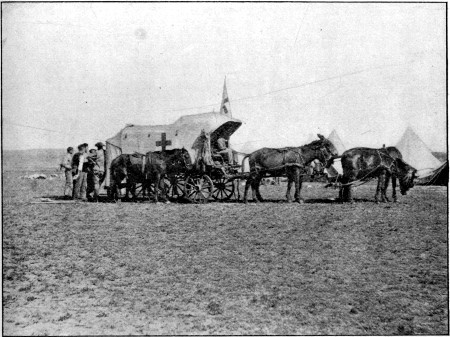 Fig. 7.—Service Ambulance Wagon, the six front mulesremoved.
Fig. 7.—Service Ambulance Wagon, the six front mulesremoved.During the later stages of the campaign, a very large number of patients were transported by the South African ox- or mule- (buck) wagons. Although not of prepossessing appearance, and unprovided with any sort of springs, these vehicles were far from unsatisfactory. The ox-wagon consists of a long simple platform, 19 ft. 2 in. in length, 4 ft. 6 in. in width, from the sides of which a slanting board rises over the wheels for the posterior two-thirds. These bulwarks increase the actual width to 6 ft. 6 in., which corresponds with the gross width occupied by the wheels. One third is covered by a small hood 5 ft. 6 in. in height erected on wooden stave hoops. The latter was often absent in transport wagons. The two hind wheels are large, the fore somewhat smaller. They are attached to very heavy wooden cross-beams bearing the axles, and the two beams are connected by a longitudinal bar, continuous with the düssel boom or pole. This latter bar is in two sections, the connection of which allows considerable play in the long axis and serves to break the jolts occurring when either pair of wheels passes over uneven spots on the[Pg 22] ground. When some sacks of oats or hay were spread over the floor the wounded men travelled comparatively comfortably in these wagons, the great distance between the fore and hind wheels tending to minimise the jolting. The principal objection to them was the slow pace of the oxen, and the fact that to obtain the greatest amount of work from these animals a major part of the journey must be performed during the night. The ox-wagon carries, with comfort, four lying-down cases on stretchers, or six without stretchers; or twenty sitting-up cases.
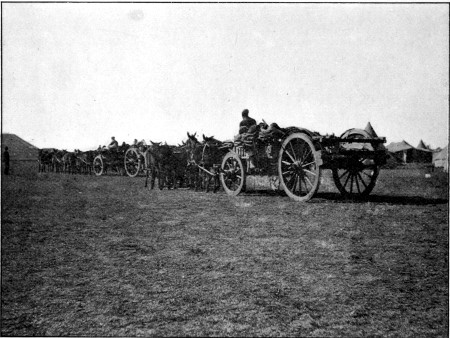 Fig. 8.—South African Wagon, loaded with patients, and
mule transport. (Photo by Mr. C. S. Wallace)
Fig. 8.—South African Wagon, loaded with patients, and
mule transport. (Photo by Mr. C. S. Wallace)
The mule- or buck-wagon, which is of the same class but smaller, can only accommodate two stretchers, four lying-down men without stretchers, or 12-14 sitting-up cases. As a rule, the wagons were loaded with recumbent cases in the centre, while more slightly wounded men sat around, and were able to give help to those lying down when needed. The wagons can be covered with canvas throughout.[Pg 23]
The steady even pace of the oxen is a great advantage, and I was often surprised to see how well men bore transport in these wagons, who seemed utterly unfit to be moved had it not been an absolute necessity. A very large number of the wounded from Paardeberg Drift were transported to Modder River in them.
One other advantage of these wagons, the possibility of converting them into an excellent laager, is not to be underrated. Any one who saw the comfortable encampment which a naval contingent on the march made by massing the wagons with intervals covered by macintosh sheets, could at once appreciate their capabilities for a long trek.
Traction engines were, as far as I know, never employed as a means of transporting the sick. The tendency of these heavy machines to stick in the mud and to break down bridges is so well known that it hardly needs mention. Putting these disadvantages on one side, with a supply of fuel ensured, and such roads as are afforded by a civilised country, a great future is probably before this means of transport for the wounded. A large number of patients might be carried at an even pace, and the camps would be saved all the trouble and worry of the transport animals.
Trains.—In many cases in Natal, and in a few instances on the western side, the wounded men were able to be transferred from the first dressing station directly into the trains. Space will not allow me to describe any of those in use, but the accompanying illustration shows the general arrangement of the beds in Nos. 2 and 3 trains (fig. 9). The carriages were converted from ordinary bogie wagons of the Cape Government Railway stock under the supervision of Colonel Supple, R.A.M.C., P.M.O. of the Base at Cape Town. Each train was provided with accommodation for two medical officers, two nursing Sisters, orderlies, a kitchen, and a dispensary, and each carried some 120 patients. The trains were under the charge of Major Russell, R.A.M.C., and Dr. Boswell (and later other civilian medical officers) and of Captain Fleming, R.A.M.C., D.S.O., and Mr. Waters, and carried many thousand patients from all parts of the country to the Base and Station hospitals. They were most admirably worked, and seemed[Pg 24] to offer little scope for improvement except in minor details. To them much of the success in the treatment of the wounded who had to traverse the immense distances incident to South Africa must be attributed. I made many pleasant journeys in each of them. Later, two additional trains, Nos. 4 and 5, of a similar nature, were added. Two trains, No. 1, and the Princess Christian train, which I was not fortunate enough to see, performed similar duties for Natal.
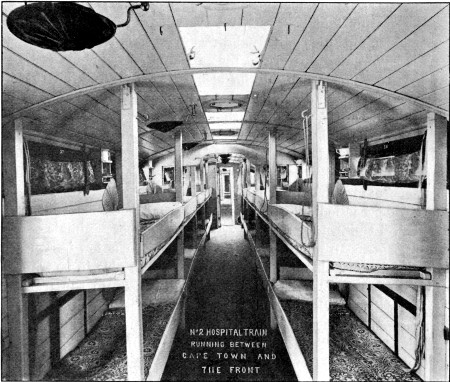 Fig. 9.—Interior of one of the Wagons of No. 2 Hospital
Train
Fig. 9.—Interior of one of the Wagons of No. 2 Hospital
Train
Hospital Ships.—These were numerous and some especially well arranged. Fig. 10 is of the 'Simla,' a P. & O. vessel which was admirably adapted to the requirements of a hospital ship. On her main deck some 250 patients were accommodated in a series of wards all on the same level, which much lightened the difficulties of service usually experienced. During the present campaign the abundance of[Pg 25] transport vessels rendered the transhipment of patients to England a matter of comparative ease, and good vessels were always available. Considering the constant transhipment of invalids from India and our other colonial possessions, it would seem advisable that, in place of having to hurriedly improvise hospital ships, the Government should possess two or three hospital ships of the 'Simla' type. It is true this would deprive our naval transport officers of a duty which in this war was performed with extraordinary celerity and success; thus the 'Simla' was fitted in seven days, and sailed with a cargo of invalids ten days after her arrival at Durban; but on the other hand it would ensure that really suitable vessels were always provided.
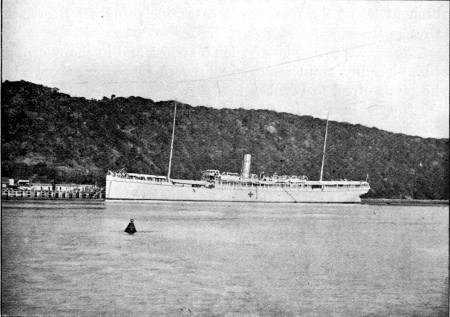 Fig. 10.—P. & O. Hospital Ship 'Simla' in Durban
Harbour
Fig. 10.—P. & O. Hospital Ship 'Simla' in Durban
Harbour
To give some idea of the amount of work contingent on the transport of wounded men from an army of some 15,000, fighting its way against continued opposition, I will quote the approximate number of men moved during Lord Methuen's advance from Orange River to Magersfontein. (The number[Pg 26] of men actually present at each battle is shown in Table I., p. 12.)
Belmont, the first battle, was fought on November 23.
November 24.—No. 2 hospital train removed 152 cases to the Stationary Field hospitals at Orange River, then returned and loaded up with 130 more. Some of the most severe cases in the latter were detrained at Orange River, and the remainder were taken direct to Wynberg (591½ miles).
The division marched, and the battle of Graspan was fought during the day.
November 26.—A train of specially constructed trucks brought 90 of the less severe cases, including 20 Boers, to Orange River.
November 27.—The division marched, and in the morning No. 3 hospital train removed 80 severe cases from the Field hospitals direct to Wynberg.
November 28.—Battle of Modder River.
November 29.—339 patients, including a few sick, and some wounded Boers, were sent down to Orange River in open trucks with impromptu shelters made with rifles and blankets.
Later, 97 severe cases were sent down in ordinary carriages, of which some had doors sawn out to admit lying-down patients.
December 10.—The division marched, and on the next day the battle of Magersfontein was fought.
December 11.—Nos. 2 and 3 trains were loaded up during the night and early morning of the 12th, in part from the Field hospitals, in part directly from the Ambulance wagons. During the day of the 12th, No. 3 train made three journeys to Orange River, and No. 2 was sent direct to Wynberg.
In all some 800 patients needed transport; they were picked up by 10 ambulance wagons and 5 buck wagons for slighter cases and the two bearer companies sent out from Modder River. On the 12th Lord Methuen sent out a number of bearers with stretchers, and at 12 noon all the wounded were collected, but many had lain out through the night. The bearers had to retire under a shell fire kept up by the Boers as long as our army was within range of their position.[Pg 27]
Four Field hospitals were present, but only that of the IX. Brigade at Modder River was so situated as to be of general use. This hospital, under the command of Major Harris, R.A.M.C., did an immense amount of work most expeditiously and with great success.
The nature of the advance on Kimberley necessitated the evacuation of the Field hospitals with extreme promptitude, as the troops were in constant action, and the arrangements for this were carried out with great success by Colonel Townsend, the P.M.O. of the First Division.
The amount of fighting far exceeded anything that had been expected, and the Stationary hospitals on the lines of communication at Orange River and De Aar were unable to cope with the number of severe cases thrown on their hands, with the constant possibility of new arrivals. Hence a number of severe cases had to be sent direct to Wynberg.
This experience strongly illustrated the necessity of possessing Stationary hospitals of greater mobility and a higher degree of equipment than the service at present possesses. In these a large number of severe cases could have been retained, and only the slighter ones exposed to the fatigue and general disadvantage of transport. In South Africa very special difficulties existed in the length of the line of communication, the single line of rails, and the absence of any source of supply within 500 to 600 miles; but in any other country mobile Stationary hospitals, although more easily equipped, would be equally valuable.
The difficulties of transport experienced in the advance of the Kimberley Relief Force were many times multiplied in that upon Bloemfontein, since the whole of the severely wounded men had to be sent back thirty to forty miles to the railway. The ambulance accommodation on the occasion of this march, although, if untouched, proportionately smaller than that possessed by Lord Methuen, was reduced to one-fifth to meet the exigencies of warfare. Beyond this the equipment transport of the Field hospitals was reduced from four ox-wagons to two, and the Scotch cart was cut off, only two ox-wagons and the two water-carts being allowed. This greatly hampered the Field hospitals on the march, and when they arrived at[Pg 28] Bloemfontein and had to undertake the work of Stationary hospitals, their efficiency was seriously impaired. Again, on the advance from Bloemfontein to Kroonstadt many of the Field hospitals were unable to accompany their respective divisions, not alone on account of the number of patients remaining in them, but also because the mule transport had been otherwise employed for military purposes.
The transport of the ambulances and hospitals stands in a very special position. As far as my experience went, neither ambulances nor hospitals were ever taken or retained by the Boers, and consequently the transport animals originally devoted to this purpose should have been held sacred to it.
Hospitals.—Accommodation for the wounded was provided under canvas in the Field hospitals, also in the large General hospitals. Beyond this iron huts were erected in many of the Base and Station hospitals. At Capetown, Maritzburg, and Ladysmith barrack huts were modified and equipped as hospitals, and in towns such as Bloemfontein, Kimberley, and Johannesburg large civil hospitals were at our disposal. Beyond these sources of accommodation, churches, schools, public institutions, and private houses were made use of in the smaller towns.
As to the broad question of canvas v. buildings, experience amply showed that in a climate such as is possessed by South Africa, canvas affords the greater advantages. The hospitals are more mobile, more readily extended, and the more healthy. Except under unusual conditions of rain and dust, the patients did excellently in the tents.
Rain and dust were occasionally most troublesome, especially when combined with wind. I once saw a whole hospital, fortunately unoccupied, levelled to the ground in the course of some twenty minutes. Under such circumstances iron huts present advantages, and were on many occasions utilised with much success. They are readily erected, and it would have been a considerable improvement if a number of them had been ready for use at the earliest part of the campaign. Except in the matter of weight, they possess in a considerable degree the advantage of mobility possessed by canvas, and in addition they offer much more[Pg 29] protection from the weather. On the other hand, they are more liable to become unhealthy from prolonged use.
Churches and public institutions were mainly troublesome from the necessity of having to improvise sanitary arrangements, and sometimes the disadvantage of the collection of a large number of men in one chamber could not be avoided. None the less I cannot look back without admiration on the temporary hospitals established in the Raadzaal at Bloemfontein, and the Irish hospital in the Palace of Justice in Pretoria.
The State schools in the smaller towns of the Orange River Colony also afforded excellent accommodation as small temporary hospitals.
Private houses, possessing the disadvantages of ill-adapted construction and the necessity of a considerably increased staff to work them, were on the whole little used as hospitals. The scattered farmhouses occasionally afforded shelter to very severely wounded men. In most of the country I traversed, however, the farms were so wide apart as to be of little use in this respect; and again, under the special circumstances, patients left in them might have to be abandoned to the enemy.
The chief interest during the campaign centred in the working of the Field and General hospitals.
Two types of Field hospital were employed, one the Home, the other the Indian. The latter differs from the Home in that in it the bearer company is attached and consists of Indian natives, and that the hospital is separable into four sections in place of two only.
The amalgamation of the Field hospital and bearer company into one unit is much to be desired in the Home service, both for economy of working and the more equal distribution of duties to the medical officers engaged. Again the divisibility of the hospital into four sections is also an advantage. It allows of the advance or the leaving of sections, in the case of either small expeditions or the presence of a number of severely wounded men unfit to travel. As far as I could judge, it necessitates very small addition to the present equipment, and is in every way desirable.
As to the working of the Field hospitals in the present[Pg 30] campaign, it was universally acknowledged to possess a very high degree of excellence. The equipment, with small exceptions, proved equal to the demands made upon it. The mobility of the camps was proved again and again, and the rules governing their administration evidenced by their effectiveness the care and experience which have been bestowed on the organisation of the hospitals.
It is difficult for any one who has not had an opportunity of observing the actual amount of work performed in the Field hospitals either to appreciate the storm and stress following an important engagement when the wounded men are first brought in, or the demands that are made on the powers of the medical officers in charge. To a civilian the first feeling is one of impotence, followed by an attempt to see no further than the case under immediate observation, and to nurture the conviction that the work is to be got through if it is only stuck to. I gathered that this first impression was absent in the minds of the officers in charge of the Field hospitals, as work commenced at once, and was carried on without intermission during the persistence of daylight, in the winter often by the aid of lanterns, and eventually the huge task was accomplished. In early days at Orange River work commenced at 4 a.m., and was steadily continued until 6 p.m. or later, and this state of things persisted sometimes for many days together.
The officers of the Field hospitals, the bearer companies, and those doing regimental duty carried out their duties with a calmness and efficiency which not only impressed observers like myself, but also excited the admiration of our German colleagues sent by their government to observe the working of the British system.
I saw on several occasions the German and Dutch ambulances, and was much struck by the excellence of their equipment. In some details there was much to be learned from them, especially in the matter of appliances, dressings, and instruments. The Dutch ambulance I saw at Brandfort had a complete installation of acetylene gas, which was carried, gasometer and all, in one Scotch cart. They were, however, really designed to fill the combined position of our[Pg 31] Field, Stationary, and General hospitals, and when it became necessary for them to move about frequently, the inferior mobility they possessed in comparison with our own Field hospitals was at once demonstrated.
The large General hospitals of 500 beds were a great feature in the campaign. Although designed and organised some time since, the present was the first occasion on which they have come into general use, and they may be said to have actually been on trial. The organisation of these hospitals proved itself excellent, and in the case of the best of them left little to be desired.
In some cases the accommodation was temporarily strained enormously, and the number of patients was extended beyond more than three times the regulation limit. The additional patients were then accommodated in marquees and bell tents, according to the nature of their diseases. Under these circumstances the working of the hospitals was difficult, and the officers both of the R.A.M.C. and the civilian surgeons were placed at a great disadvantage.
My space does not allow me to give any description of the general arrangement of these hospitals, but I would suggest that a certain number of them should be so modified as to increase their mobility and allow of their being more readily utilised as Stationary hospitals.
During the whole campaign it seemed to me that the Stationary hospitals (that is to say, the hospitals necessary to receive patients when the Field hospitals were rapidly evacuated), were those in which some increased uniformity of organisation was most needed.
It scarcely needs to be pointed out that this is the most difficult link of the whole hospital chain to be uniformly well organised and equipped. It is needed at short notice, and often for a short period, and it is difficult to maintain a regular staff of officers ready for any emergency without keeping a certain number of men idle.
The conversion of Field hospitals to Stationary purposes is undesirable, as the troops move with only a regulation number of the former, which under ordinary circumstances is the minimum that may be necessary.[Pg 32]
Stationary hospitals as individual units are undesirable for the reasons above given.
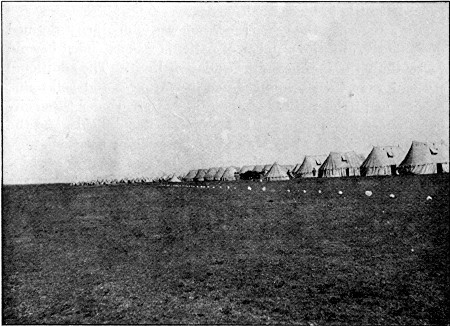 Fig. 11.—Type of a General Hospital (No. VIII.
Bloemfontein) extended by use of bell tents in the distance. (Photo by
Mr. C. S. Wallace)
Fig. 11.—Type of a General Hospital (No. VIII.
Bloemfontein) extended by use of bell tents in the distance. (Photo by
Mr. C. S. Wallace)
The difficulty might be met by increasing the mobility of a certain number of the General hospitals, by making them divisible into five sections, each of which should be able to move independently, and to the last of which should be attached the heavy part of the equipment, such as the iron huts for operating and X-ray rooms, kitchens, store sheds, &c. The tents might also be lightened by the substitution of the tortoise tent for the service marquee. The tortoise tent is lighter (360 as against 500 lbs.), easily pitched and moved, and holds at least two more patients with ease. The capabilities of this tent were amply proven during its use by the Portland, Irish, and other civil hospitals attached to the army. It withstood wind and weather, the former better than the service marquee. Figs. 11 and 12 show the appearance of camps composed of the two varieties. I must admit a warm preference for the appearance of the service pattern,[Pg 33] but I think it is indubitable that the other is the more useful.
Given the possibility of division of a General hospital in this manner, single sections could readily be sent up the lines of communication to serve as Stationary hospitals at various points behind the advance of the troops, and on the cessation of active need, the sections could be reunited at any point to form an advanced Base hospital. The sections could be kept in touch throughout by visits from the officer of the lines of communication. This would appear a ready means of providing well-organised Stationary hospitals at short notice, and would save the disadvantage of a definitely separate series.
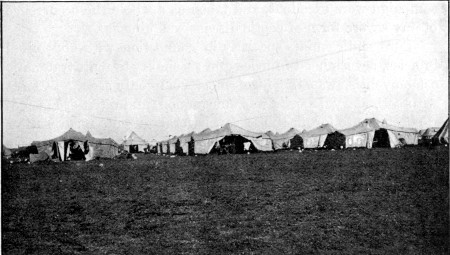 Fig. 12.—Type of Tortoise Tent Hospital. Portland
Hospital, Bloemfontein. (Photo by Mr. C. S. Wallace)
Fig. 12.—Type of Tortoise Tent Hospital. Portland
Hospital, Bloemfontein. (Photo by Mr. C. S. Wallace)
Such hospitals might have been used on many occasions when the transport of an entire General hospital was an impossibility. The service, moreover, has some experience in this direction, since at one time No. 3 General Hospital was divided into two definite sections.
Bearing in mind the extreme readiness and promptitude with which the officers during the present campaign extended the accommodation of either Field or General hospitals, one of[Pg 34] such sections as are proposed might readily be made far more capacious than its regulation number would suggest.
My duties being entirely in connection with the service hospitals, I did not become intimately acquainted with any of the volunteer hospitals which did such excellent service, except the Portland, to the staff of which I was indebted for much hospitality and kindness. This hospital was practically of about the capacity proposed for the above-mentioned sections, and the report of its work will no doubt furnish many points of detail as to equipment, &c., which may be useful.
The general results of the surgical work done during the campaign were excellent, and taken as a whole the occurrence of any severe form of septic disease was unusual.
Pure septicæmia, especially in connection with abdominal injuries, severe head injuries and secondary to acute traumatic osteo-myelitis, was the form most commonly seen. Pyæmia with secondary deposits was uncommon, and often of a somewhat subacute form; thus I saw several patients recover after secondary abscesses had been opened, or the primary focus of infection removed. The only really acute case of joint pyæmia I heard of, developed in connection with a blistered toe followed by cellulitis of the foot.
Cutaneous erysipelas I never happened to see, and really acute phlegmonous inflammation was rare.
I may mention the occurrence of acute traumatic gangrene in two cases. This developed in each instance with gunshot fracture of the femur; in one amputation was performed, and the process extended upwards on to the abdomen. The cases occurred with the army in the field in the neighbourhood of Thaba-nchu and not in a stationary hospital.
Acute traumatic tetanus occurred only in one instance to my knowledge. In this case the primary injury was a shell wound of the thigh, and the patient developed the disease and died within ten days.
To the civil surgeon the performance of operations, and the dressing of severe wounds at the front, proved on occasions a somewhat trying ordeal.
When operations were necessary in the field, during the daytime, it was often possible to perform them in the open[Pg 35] air, provided tolerable protection could be obtained from the sun. A number of cases were so operated upon during the march of the Highland Brigade from Wynberg to Heilbron, and gave excellent results, the patients deriving considerable benefit from the early cleansing and closure of the wounds.
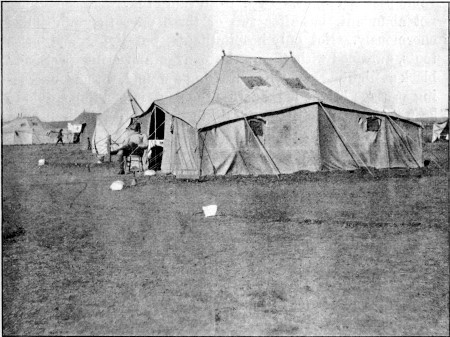 Fig. 13.—Tortoise Hospital Tent. Portland Hospital.
(Photo by Mr. C. S. Wallace)
Fig. 13.—Tortoise Hospital Tent. Portland Hospital.
(Photo by Mr. C. S. Wallace)
In camp, in the Field, or Stationary hospitals, the difficulties were often much greater. The operations were necessarily performed under shelter for reasons of privacy. In the tents the draught carrying the dust from the camp was one of the commonest troubles. The exclusion of dust was impossible, and it not only found its way into open wounds, but permeated bandages with ease. Often when a bandage was removed, an even layer of dust moistened by perspiration covered the whole area included with a coating of mud. Again, in dust storms a similar layer of mud sometimes covered the whole of the exposed parts of the bodies of patients lying on the ground in the tents.[Pg 36]
It is of some interest to remark with regard to this dust, that Dr. L. L. Jenner lately kindly examined a specimen collected at Modder River after the camp had been more than two months established, and discovered no pathogenic organisms in it. As a period of seven months had elapsed since this dust was collected, the fact is of no practical import, beyond showing that, if such organisms had existed, at any rate they were not of a resistent nature.
Insects, particularly common house-flies, were an intolerable pest at times. In a fresh camp they were sometimes not abundant, but after two or three days they multiplied enormously. Not only hospital tents, but living and mess tents, swarmed with them, the canvas appearing positively black at night. Even when dressing a wound, without unceasing passage of the hand across the part, it was impossible to keep them from settling, and during operations the nuisance was much greater.
Storms of rain were occasionally as troublesome as, though perhaps less harmful than, those of dust. On one occasion a whole Field hospital was flooded only a few hours after a number of important operations had been performed, and the patients were practically washed out of the tents. It was somewhat remarkable that none of the men suffered any serious ill as a result.
At times the temperature was sufficiently high to make either dressing or operating a most exhausting process to the surgeon. The heat of the day was not on the whole so disadvantageous from the point of view of the operator, as the cold of the nights during the winter in Orange River Colony. On one or two occasions serious operations had to be left undone, as it was only possible to consider them in camp, where, as we arrived at night only, the temperature was too low to justify the necessary exposure.
Water for use at operations was often a great difficulty. Even at Orange River, where, though muddy, the water was wholesome, it was impossible to get water suitable for operations unless it had previously gone through the complicated processes of precipitation by alum, boiling, and filtration. At Orange River a small room in the house of one of the railway[Pg 37] servants was obtained and fitted as a rough operating room by the Royal Engineers. The necessary utensils were provided by Colonel Young, Commissioner of the Red Cross Societies. Here a stock of prepared water was kept for emergencies.
The remaining difficulties mainly consisted in those we are familiar with in civil practice, such as the securing of suitable assistance in the handling of instruments and dressing, when the rush of work was very great.
At the Base hospitals accommodation for operating in properly equipped rooms obviated many of the difficulties above referred to.
In concluding this introduction I should sum up in a few words my experience of the general working of the hospital system during my stay in South Africa.
The excellence of the Field hospitals for their purpose has been already alluded to, and, as far as I could ascertain, won the confidence and approval of patients, military commanders, and civilians such as myself.
The Stationary hospitals (by which I intend to indicate those receiving the patients directly from the Field hospitals before the establishment of advanced Base hospitals), as already indicated, were not in my opinion so perfectly conceived or organised. The requirements of these are, however, far greater than those of the Field hospitals, and they of all others are dependent on the possession of facilities for rapid transport. In South Africa the difficulties of supplying them were enormous, and no doubt the conditions of the campaign in this, as so many other particulars, were novel and unusual. None the less the experience gained will no doubt be utilised in the future. With regard to the extravagant criticisms levelled at the Field hospitals serving as Stationary hospitals at the time of the early period of the occupation of Bloemfontein, it may be pointed out that the only proper ground for comparison was not between the patients at Bloemfontein and those in hospital at the base, but between the men in hospital and those in the field at that time, since the conditions were equally adverse to both. Besides, it must not be forgotten that a large proportion of the patients, at that time, were really comfortably housed in[Pg 38] the Raadzaal and other buildings, the preparation of which entailed a very great amount of both labour and resource.
The difficulties experienced at that time will, it is hoped, go far towards securing greater facilities and rights of transport to the Royal Army Medical Corps in the future. As a civilian, one cannot but recognise that the conditions of modern warfare are much altered from those of the past. Prisoners are well cared for and kindly treated, the sick and wounded are respected by both sides, and except in the actual horrors of fighting the condition of the soldier is a happier one. Under these circumstances the limitation of the transport facilities of a department so closely concerned with the well-being of all, and which has been organised on a most moderate scale, must soon become a tradition of the past in civilised armies.
As to the efficiency of the organisation of the General hospitals, either at the advanced or actual base, I have already testified. Naturally the working of these hospitals varied with the personal equation of the officer in charge of them, but as a whole the service has every reason to be proud of their success. As far as surgical results are concerned, and with these I had special acquaintance, the success of the hospitals was amply demonstrated.
Adverse criticism was not however wanting, and often expressed in the strongest terms by persons totally unacquainted with hospital methods, and apparently unconscious that such excellence as is exhibited in a London hospital is the result of continuous work and development for some centuries, and that such institutions are worked by committees and staffs of permanent constitution.
The proportion of female nurses employed in these hospitals underwent steady increase from the commencement of the campaign, and the immense value of the nursing reserve was fully proved. There is no doubt that in Base hospitals the actual nursing should always be entrusted to women.
The demands of the campaign necessitated the employment of a large number of civil surgeons in the various hospitals. These gentlemen accommodated themselves with[Pg 39] true British aptitude to the conditions under which they were placed, and in all positions their sterling work contributed in no small degree to the success that was attained.
One class of hospital still remains for mention. I refer to the improvised hospitals prepared in the Boer towns prior to the British occupation. They were met with in all the smaller towns, and also in the larger ones such as Johannesburg and Pretoria.
The Burke hospital in Pretoria, started by a private citizen and his daughter, and the Victoria hospital in Johannesburg, presided over by Dr. and Mrs. Murray, were two of the largest, but each and all deserve due recognition.
I am sure that many of our wounded officers and men who were cared for in these hospitals while prisoners in the hands of the Boers, will never lose their sense of gratitude to those inhabitants who spared no effort to render their position as happy as possible under the circumstances; and the existence of these hospitals was no small boon to the service when called upon to take charge of the sick and wounded therein contained.
I cannot close this chapter without recognition of the immensity of the task which has fallen on the Royal Army Medical Corps in the treatment of the sick and wounded during the course of the campaign and full appreciation of the manner in which that task has been met. The strain thrown upon this department of the service, originally organised for the needs of an army less than half the magnitude of that eventually taking the field, was incalculably great, and the medical profession may well be proud of the efforts made by its military representatives to do the best possible work under the circumstances.
[1] 3,328 men of the IX. Brigade present are not included, as they never came into action.
[2] The high mortality was due to deaths amongst the officers of the Naval Brigade.
[3] To obtain this total the numbers of killed, wounded, and missing, after the three earlier battles, have been massed, and added to the total number of men known to have taken part in the battle of Magersfontein. The inaccuracy dependent on the fact that some of the men reported as wounded or missing in the earlier battles had already returned to their regiments, and are included in the total of 11,447, must be disregarded.
[4] Numbers quoted from Fischer, Handbuch der Kriegschirurgie, vol. i. p. 22, 1882.
Before proceeding to the actual description of the wounds inflicted by modern military rifles, it is necessary to prefix a few remarks on the mechanism and mode of production of these injuries.
Recent tendency in the construction of military rifles has been in the direction of reduction of bore, and a corresponding one in the calibre of the bullet, the resulting loss of weight in the latter as an element in striking power being compensated for by the attainment of an augmentation of velocity in the flight of the projectile, and a comparatively flat trajectory.
Changes in this direction have endowed the weapons with increase both in range and accuracy of fire; while the greater rapidity with which magazine rifles can be discharged and, in consequence of reduction in weight, the greater number of cartridges which can be carried by each man, also form important factors in the possible deadliness of warfare at the present day. None the less the experience of the present campaign has scarcely justified the early prognostications expressed as to a great increase in the number and severity of wounds amongst the combatants.[5] This comparative immunity is to be explained mainly on two grounds. The increased distance which for the most part separated the two bodies of men, a feature no doubt accentuated by the mode of warfare adopted by the Boer, and his strong sense of the folly of close combat on equal terms, tended to efface one of the chief characters, velocity of flight, on the part of the projectile. The want of[Pg 41] effectiveness of the small-calibre bullet as an instrument of serious mischief also kept down the mortality.
Since the year 1889 the calibre of the bullet in our own army has been reduced from that of the Martini-Henry (.450 in.) to one of .309 in. in the Lee-Metford, and a consequent reduction in weight from 480 to 215 grains. To allow of the satisfactory assumption of the more complicated rifling by the more rapidly projected bullet, the lead core has been ensheathed in a mantle of denser metal. The bullet itself is of an original calibre (.309 in.) somewhat exceeding the bore of the rifle barrel (.303 in.), in which way a species of 'choke' is obtained and deep rifling of the surface ensured. Beyond this the comparative transverse and longitudinal measurements and shape have been altered in order to maintain weight, preserve a proper balance during flight, and increase the power of penetration. These alterations with slight differences in detail embody the general principles that underlie the construction of each of the weapons adopted by European nations. It will be well here to consider the influence of each alteration from the point of view of the surgeon.
Calibre.—The effect of the diminution of calibre is (a) to reduce the area of impact of the bullet on the part impinged upon, and hence to lower the degree of resistance offered by the tissues; this to a certain extent tends to neutralise the augmented striking force resulting from the increased velocity of flight. (b) To limit considerably the destructive powers of the bullet, as a smaller area of tissue is exposed to its action. (c) To allow of the production of very 'neat' injuries and the frequent escape of important structures, also the production of remarkably prolonged subcutaneous tracks in positions where such would be regarded as scarcely possible, and in point of fact were impossible with the older and larger projectiles.
Length.—The comparative increase in length of the bullet is, from the surgical point of view, only of material importance in increasing the weight and therefore the striking power, and in so far as it is a mechanical necessity for the flight of the projectile on an axis parallel to its long diameter,[Pg 42] and so tends to ensure impact on the body by the tip of the bullet. This latter is, however, surgically favourable as ensuring a smaller wound.
Weight.—The decrease in weight must be regarded on the whole as altogether to the advantage of the wounded individual, since it cannot be considered to be entirely compensated for by the resulting increased velocity of flight, unless the range of fire is moderately close.
Shape.—The ogival tip and general wedge-like outline, while decreasing the aerial resistance to and increasing the power of penetration possessed by the bullet, at the same time allow the escape of some structures by displacement, while others are saved from complete destruction by undergoing perforation. Beyond this the sharper the tip, the smaller is the area of the body primarily impinged upon, the less the resistance offered to perforation, and to some degree the less the destruction of surrounding tissues.
Increased velocity of flight.—This multiplies the striking force, and compensates in part for decrease in volume and weight of the bullet. It is customary to speak of the velocity as 'initial' and 'remaining.' Initial velocity is the term employed to express the velocity at the time of the escape of the bullet from the barrel; this is also designated as 'muzzle velocity.' 'Remaining velocity' expresses that obtaining during any subsequent portion of the flight of the projectile.
The greatest initial velocity is obtained with the use of bullets of the smallest calibre, but this is not of the practical importance which might be assumed, since the remaining velocity of flight of such projectiles falls more rapidly than that of those of slightly greater mass. Thus, although there may be a difference of a hundred metres per second in initial velocity between two rifles of calibres varying from 6.5 to 8 millimetres (.303-.314 in.), at the end of 1,000 metres the discrepancy is greatly reduced, while at 2,000 metres it hardly exists. Under such circumstances the projectile of greater weight and volume, as possessing the greater striking force, is considerably the more formidable of the two. This is the more important if it be allowed, as I believe to be the case, that velocity per se is of no practical import in the[Pg 43] case of wounds of the soft parts of the body, which after all form the preponderating number of all gunshot injuries. The effect of the higher degrees of velocity differs, however, with the amount of resistance met with on the part of the body; hence its serious import is well exemplified when parts of the osseous skeleton are implicated, although even here considerable variations exist, dependent upon the structure of that part of the bone actually involved. The most obvious ill effect of injuries from bullets travelling at high rates is seen in the case of the various parts of the nervous system, and here it is undeniable. High velocity and striking force are also responsible for the prolonged course sometimes taken by bullets through the body.
The actual degree of velocity, as judged by the range of fire at which an injury is received and the resulting injury, is very hard to estimate on account of the many and varying factors which enter into its determination. The mere recital of some of these will suffice to make this evident.
1. Quality of the individual cartridge employed, as to loading, the materials employed, and their condition.
2. The condition of the rifle as to cleanliness, heating, and the state of the grooves of the barrel.
3. The angle of impact of the bullet with the part injured.
4. Resistance dependent on the weight of the whole body of the man struck, or of an isolated limb.
5. Special peculiarities of build in the individual struck, such as thickness and density of the integument and fasciæ, strength and thickness of the bones, &c.
6. State of tension of the muscles, fasciæ, and ligaments at the moment of impact, and fixity or otherwise of the part of the body struck.
7. The degree of wind, temperature, and hygroscopic conditions of the atmosphere.
These form some of the more important points which have to be taken into consideration, in addition to a mere calculation of the actual distance from which a wound has been received from a particular rifle, and taken with the unsatisfactory nature of the evidence as to the latter, which is usually alone obtainable, it is clear that definite assumptions are scarcely[Pg 44] possible. In a great number of cases I came to the conclusion that the only indisputable evidence of low velocity was the lodgment of an undeformed bullet. There is little doubt, moreover, that the general tendency of wounded men was to minimise the range of fire at which they were struck, and again that in the majority of cases in this campaign it was quite impossible to determine whence any particular bullet had come, since the enemy was seldom arranged in one line, but rather in several. Again, smokeless powder was generally employed. Beyond this, in some cases where there was no doubt of the short distance from which the bullet was fired, the wounds were due to 'ricochet' of portions of broken-up bullets. The following instance well illustrates this. A sentry fired five times at two men within a distance of six paces, knocking both down. One man received a severe direct fracture of the ilium, the bullet entering between the anterior superior and inferior iliac spines and emerging at the upper part of the buttock. The entry and exit apertures were large but hardly 'explosive,' as a subcutaneous track four to five inches long separated them. Besides this both men had other lesser injuries; thus in the second two perforating wounds of the arm existed. The latter were not unlike type Lee-Metford wounds, and were regarded as such until a few days afterwards when a hard body was felt in the distal portion of one track and removed. This proved to be a part of the leaden core only, and the similar wound had no doubt been produced by a like fragment, the bullet having broken up on striking the stony ground.
Trajectory.—The comparative flatness of this depends on the construction of the rifle and the propulsive force employed, and varies as does velocity with the nature, excellence, and amount of the explosive, the correctness of the principles upon which the bullet is devised, and the mechanical perfection of its manufacture. Its importance naturally consists in the manner in which it affects the possibility of covering objects on a wide area of ground and thus creating a broad 'dangerous zone.' A bullet fired on level ground from any one of three of the rifles referred to later (Lee-Metford, Mauser, Krag-Jörgensen), sighted to 500[Pg 45] yards and fired from the shoulder in the standing position, will cover some part of an erect man of average height during the whole extent of its flight. A body of men within that distance is therefore in a position of extreme peril in the face of a good shooting enemy.
The importance of a flat trajectory is progressively lost, however, with any rifle, as the weapon is gradually sighted to greater distances. Thus when sighted to 2,000 yards the bullet from the Lee-Metford rifle rises 174 feet, and a whole army might comfortably be situated over a considerable area within that distance. The importance of flatness of trajectory is also influenced by the nature of the ground occupied by the combatants. Thus when the area to be covered consists in ground first rising then falling from the rifleman, the trajectory will become more or less parallel to the surface crossed, and the 'dangerous zone' will be correspondingly increased in extent. On the other hand, when the ground slopes away from the rifleman the rise of the projectile is exaggerated, and reaches its most limited capacity of covering an intervening space when the flight crosses a hollow.
Revolution of the bullet.—It only remains in this place to say a few words concerning the revolution imparted to the bullet by the rifling of the barrel. This ensures the flight of the projectile on a line parallel to its long axis, and notably increases its power of penetration.
Both these properties of the flight are to the advantage of the wounded, since, as already mentioned, the more exactly the impact corresponds to a right angle with the skin, the more limited will be the area of contusion, even if it be of the most severe character, while to the twist of the bullet must be ascribed a not inconsiderable part in the explanation of the ready and neat perforations of narrow structures which are frequently produced.
It has been pointed out that the Lee-Metford bullet turns on its own axis once in a distance of ten inches, while the Mauser revolves once in a distance of eight and eleven-sixteenths inches; hence not more than at most two revolutions are made in tracks crossing the trunk, and not more than half a full revolution in the perforation of a limb. None the[Pg 46] less, no one can deny the influence of the one half turn of supination in entering a perforating tool of any description, both as preventing splintering, and in preserving the surrounding parts from damage.
Beyond this, the spiral turn of the bullet, by diverting a part of the transmitted vibrations into a second direction, must, in the case of wounds of the body, help to throw off contiguous structures, and while those that are in actual contact are more severely contused, the surrounding ones suffer somewhat less direct injury. It must be borne in mind, also, that rapidity of revolution does not fall pari passu with that of velocity of flight, but that the former undergoes a comparatively slighter diminution until the bullet is actually spent. Hence, the influence of revolution is felt, however low the velocity may be, provided sufficient striking force is retained to enter the body. A word must be added here as to the surface of a discharged bullet; this, in taking the rifling of the barrel, becomes permanently grooved. The depth of the groove differs with the variety of rifle. In the Lee-Metford the grooves are deep (.009), in the Mauser slightly less so (.007), but the surface of both bullets is comparatively roughened when revolving in the body, and this circumstance, since the projectile exactly fits its track, may influence the degree of the surface destruction of tissue, and somewhat aid in the clean perforation of bone, since a little bone dust is always found at the entrance aperture of a canal in cancellous bone.
During the campaign many varieties of rifle projecting bullets of widely differing calibre were employed by the Boers, many of whom as sportsmen preferred the rifle to which they were accustomed to a regulation weapon, and an illustration of a large variety of bullets from cartridges which I collected from arsenals and camps is given below (p. 96). The great majority of the men, however, were armed with small-calibre weapons of some sort, and as the wounds produced by these are of chief interest at the present day, I shall say little of any others, beyond an occasional reference to Martini-Henry rifle wounds which may be considered to represent approximately those made by large leaden sporting bullets.[Pg 47]
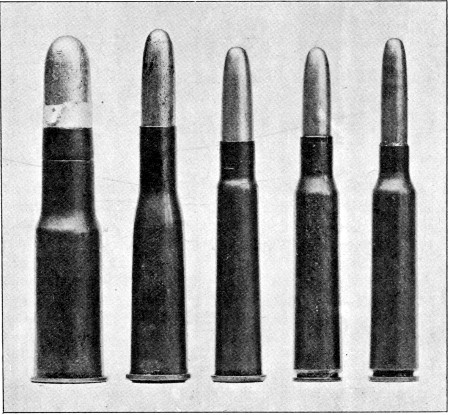 Fig. 14.—Type Cartridges in common use during the war.
Fig. 14.—Type Cartridges in common use during the war.
From left to right: Martini-Henry, Guedes, Lee-Metford, (Spanish) Mauser, Krag-Jörgensen
The most important, as the most frequently employed, rifles projecting small-calibre bullets were the Krag-Jörgensen, Mauser, Lee-Metford, and Guedes, given in the order of increase of calibre (from 6.5 to 8 millimetres, or .254-.314 in.) in the bullets. As to the seriousness of wounds produced by these there is little to choose, differences in character being only those of degree. Such differences depended on the area of tissue implicated, corresponding with the calibre of the particular bullet, the comparative weight of the bullet, and the degree of velocity of flight maintained at the moment of impact. When, however, any of these bullets have been exposed in their flight to influences capable of causing deformity of their outline and symmetry, peculiarities of construction and in the composition of the metals employed in their manufacture may materially alter the character of the wounds produced and revolutionise a classification founded purely on the relative weight, calibre, and degree of velocity with which each is endowed.[Pg 48]
| Martini-Henry | Guedes | Lee-Metford | Lee-Enfield | Mauser | Krag-Jörgensen | |
| Calibre of rifle | .45 in. | .314 in. | .303 in. | .303 in. | .276 in. | .254 in. |
| Number of grooves | 7 | 4 | 7 | 5 | 4 | 4 |
| One twist in | 22 in. to right | 9.85 in. to right | 10 in. to left | 10 in. to left | 8-11/16 in. to right | 8 in. to left |
| Muzzle velocity | 1,300 f.s. | 1,988 f.s. | 2,000 f.s. | 2,000 f.s. | 2,262 f.s. | 2,309 f.s. |
| Sighted to | 1,450 yds. | 2,600 paces | 2,800 yds. | 2,800 yds. | 2,187 yds. | 2,406 yds. |
| Weight of cartridge | 758 grains | 464.05 grains[6] | 416½ grains | 416½ grains | 384.5 grains | 372.1 grains |
| Weight of bullet | 480 grains | 244 grains | 215 grains | 215 grains | 173.3 grains | 156.4 grains |
| Length of bullet | 1.250 in. | 1.250 in. | 1.250 in. | 1.250 in. | 1 in. | 1.250 in. |
| Calibre of bullet | .450 in. | .315 in. | .309 in. | .309 in. | .280 in. | .260 in. |
| Charge of powder | 85 grains (black powder) | 20-23 (grains nitro-smokeless) | 31½ grains (cordite) | 31½ grains (cordite) | 38.0 grains (smokeless) | 36 grains (nitro-smokeless) |
| Nature of alloy used for mantle of bullet | — | Mantle: Mild steel, greased | Cupro-nickel | Cupro-nickel | Mantle: Steel with alloy of copper on surface | Mantle: Mild steel coated with copper nickel, the composition of the latter being that of the cupro-nickel of the Lee-Enfield bullet |
| Thickness of mantle | — | — | Mark II. bullet | Mark II. bullet | — | — |
| Tip | — | .031 | .036 | .036 | .031 | .022 |
| Sides .984 from tip | — | .011 | .015 | .015 | .015 | .015 |
Some particulars of the four rifles and their projectiles are collated in Table I., to which is added the corresponding information regarding the Martini-Henry for the purposes of comparison.
The penetration of the Martini-Henry and the Lee-Metford or Lee-Enfield rifle with Mark II. bullet is as follows:
| Martini-Henry | 15½ in. of 1 in. deal boards 1 in. apart | 19 in. of sand containing 15 per cent. of moisture |
| Lee-Metford {Mark II. } | 42 in. of 1 in. deal boards 1 in. apart | 60 in. of sand containing 15 per cent. of moisture |
| Lee-Enfield {bullet } |
The penetration of bullets of .314 calibre differs little from that possessed by the Lee-Metford or Lee-Enfield, of which the muzzle velocities are very little lower, with Mark II. bullet. The Belgian Mauser perforates 55 inches of fir-wood at 12 metres distance. With regard to the penetration of bullets of smaller calibre that of the Roumanian Mannlicher (.256) may be taken as typical. When fired into a sand butt at 25 yards the bullet enters 9 inches and then breaks up.
The comparative size of the different cartridges is shown in fig. 14.
The general remarks already made as to the effect of weight, calibre, and velocity sufficiently explain the importance of the particulars given in this table, but it will be noted that the Lee-Metford rifle is inferior to both the Krag-Jörgensen and Mauser rifles in the initial velocity transmitted to its bullet. The tendency to equalisation, in this particular, when the remaining velocity is considered, has been mentioned; but it may be of interest if I quote from Nimier and Laval[7] the scale on which the decrease in velocity takes place in the case of the three weapons.
| Lee-Metford | Mauser | Krag-Jörgensen | |
| Initial velocity | 630 | 718 | 720 |
| Remaining velocity: | |||
| At 100 metres | 574 | 699 | 718 |
| At 1,000 metres | 249 | 264 | 269 |
| At 2,000 metres | 159 | 165 | 165.9 |
Giving full importance to the effects of velocity as a factor in the severity of the injuries produced, when the large proportion of wounds received at distances above 1,000 yards is borne in mind, we see how rapidly the superiority of the smaller projectiles is lost. This loss, even in the early stages, is probably more than made up for in the case of the Lee-Metford, when the superiority in weight, calibre, and bluntness of extremity as contributing to striking force is taken into consideration.
The striking force (kinetic energy) of a bullet is indicated by the following formula: f = 1/2 mv.2; that is to say, the striking force is equal to half the weight of the bullet multiplied by the square of the velocity.
In point of fact, with unaltered regulation bullets I was never able to determine any very material difference between the wounds produced, further than that the wounds of entry and exit in the soft parts tended to correspond with the calibre of the particular bullet concerned. Although the immense majority of the wounds which came under my notice were caused by the Mauser bullet, yet I saw some hundreds of wounded Boers and a good many of our own men wounded by Lee-Metford bullets, in the latter case no doubt by some of the sporting varieties. The only cases that I can call to mind or have noted as exhibiting a superior wounding power in the Lee-Metford bullet are some injuries to bone. Thus I saw a considerable number of clean perforations of the patella produced by Mauser bullets, while the only two Boers whom I saw with injured patellæ had suffered transverse fractures. Again, I have a lively recollection of an old Boer who had suffered a fracture of the middle third of the femur, in the thigh of whom, with small apertures of entry[Pg 51] and exit, a cavity of destroyed tissue, five inches across, was found beneath the fascia lata at the distal side of the fracture. I cannot however say that I did not observe many equally severe injuries to the femur produced by Mauser bullets in our own men, and as far as fractures of the skull went, a somewhat crucial test, among the men brought off the battlefield alive, I never saw any difference in severity whatever.
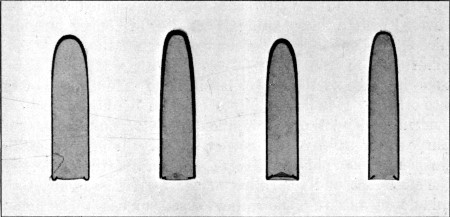 Fig. 15.—Sections of four Bullets to show relative shape
and thickness of mantles.
Fig. 15.—Sections of four Bullets to show relative shape
and thickness of mantles.
From left to right: 1. Guedes; regular dome-shaped tip; mild steel mantle; thickness at tip 0.8 mm.; at sides of body 0.3 mm. 2. Lee-Metford; ogival tip; cupro-nickel mantle; thickness at tip 0.8 mm.; gradual decrease at sides to 0.4 mm. 3. Mauser; pointed dome tip, steel mantle plated with copper alloy; thickness at tip 0.8 mm.; gradual decrease at sides to 0.4 mm. 4. Krag-Jörgensen; ogival tip as in Lee-Metford; steel mantle plated with cupro-nickel; thickness at tip 0.6 mm.; gradual decrease at sides to 0.4 mm. The measurements of the sides are taken 2.5 cm. from the tip. Note the more gradual thinning in the Lee-Metford mantle.
These points of comparison having been made, it only remains to consider one other point, that of the relative stability of the bullets. This is a matter of the greatest importance as regards the regularity or otherwise of the wounding power of the projectile, and, as far as my experience went, I believe the Mauser to far exceed the Lee-Metford in instability of structure.
The core of all four bullets is composed of lead hardened by a certain admixture of tin or antimony, but the mantle differs in composition, thickness both general and in different parts of the bullet, mode of fixation, and consequently in its power of resistance to violence.[Pg 52]
Fig. 15 gives an exact representation of the relative thickness of the mantles, and shows the general tendency to a thickening of the mantle at its upper extremity, designed to increase both the stability and striking power of the projectile. It will be noted that in general stoutness the Lee-Metford stands first, as the case increases gradually in thickness from base to apex.
Beyond this it must be noted that the Lee-Metford is the only one of the four that is ensheathed with a mantle composed of a definite alloy, this consisting of 80 parts of nickel and 20 of copper. Two of the remaining bullets, the Mauser and Krag-Jörgensen, are ensheathed with steel covered with a thin coating of an alloy of copper or cupro-nickel, to take the rifling of the barrel, while the third has a plain steel mantle which is covered with a layer of wax to take the place of the nickel used in the manufacture of the two others. It is interesting to mention here that the Boers evidently found the copper alloy coating insufficient for its purpose, or at any rate not satisfactory in preserving the weapon from the ill-effects consequent on the friction between the steel case and the rifling of the barrel, as at about the middle of the campaign they began to use their bullets waxed, as in the case of the Austrian Mannlicher; hence the legend of the poisoned bullets which caused such a sensation for a short period amongst the uninitiated. It is possible also that the additional layer of wax was necessitated by the wearing of the barrel.
The wax employed for the Mauser bullets was not originally green. Mr. Leslie B. Taylor informs me that it is probably paraffin wax, the green colour depending on the formation of verdigris from the copper alloy with which the steel envelopes are plated. This completely corresponds with my own experience, since on the bullets in my possession the green colour, originally pale, has steadily increased in depth. Many old leaden bullets I found in the Boer arsenals were also waxed, but in this case no alteration in colour had taken place. The Guedes bullets, which are cased in mild steel, become somewhat brown with exposure from a similar oxidation or rusting of the surface.[Pg 53]
As far as my experience went, however, the steel casing has an important surgical bearing beyond the mere question of wear and tear on the rifle barrel. That it possesses elasticity and capability of bending is obvious, and in a later chapter, devoted to irregular wounds, several illustrations of such deformities are given; but when it strikes stone I believe it splits and tears with very much greater freedom than the cupro-nickel mantle of the Lee-Metford. At any rate, I never came across Lee-Metford bullets deformed to the same degree as Mauser bullets, either when removed from the body, or as ricochet projectiles on the field of battle. For this reason, therefore, provided the fighting takes place on stony ground, I believe the Mauser bullet and others ensheathed in steel to be much more dangerous surgically than those encased in cupro-nickel. I fancy this would be equally the case even if the mantles were of exactly the same thickness.
The layer of copper alloy on the steel mantles is also a physical characteristic worthy of mention. This very readily chips off in a manner similar to that we are accustomed to see with nickel-plated instruments. This may be due to the compression into the grooving of the rifle, or as the result of passing impact of the bullet with an obstacle previous to entering the body or contact with a bone within it. Small scales of metal set free in one of these ways are seen in a very large proportion of Mauser wounds, and although they are so small as usually to be of little importance, the presence of such in, for instance, the substance of one of the peripheral nerves which has been perforated cannot be considered a desirable complication.
To recapitulate, it would appear that at mean ranges, both in striking force and as regards the area of the tissues affected, the Lee-Metford is a superior projectile to the Mauser, in spite of the greater initial velocity possessed by the latter. On the other hand the comparative ease with which the Mauser bullet undergoes deformation either without or within the body, so ensuring more extensive injury and laceration, renders it the less desirable bullet to receive a wound from when not in its normal shape and condition.[Pg 54]
I can say little about the remaining two rifles. The Krag-Jörgensen was little used, and beyond pointing out its capacity to inflict very neat individual injuries, in which it must surpass even the Mauser, I can only add that I had no opportunity of forming an opinion as to the danger dependent on the great initial velocity imparted to the bullet. The Guedes rifle has been included in the table because it approximates in bore to the other three. Its bullet is of the same calibre as the Austrian Mannlicher, one of the most powerful military rifles in use, and it was used to a considerable extent during the war by the Boers.[8] As to its capabilities, it appeared an inferior weapon, since want of velocity and striking power of the bullets was indicated by the number of these which were retained in the body, and by the fact that I never saw one extracted that had undergone any more serious deformation than some flattening on one side of the tip. On the other hand wounds of the soft parts occasioned by it were only to be distinguished from Mauser wounds by their slightly greater size, and at a short range of fire the weight and volume of the bullet made it a dangerous projectile.
The question of deformed bullets will be again referred to at length in the section on wounds of irregular type, and a number of type specimens are there figured and described (p. 76). In the same chapter will be found illustrations of a number of sporting bullets of small calibre, as well as of large calibres in lead, found in the Boer arsenals and camps. I have placed them in that position as mainly of interest in connection with the occurrence of large and irregular wounds (see figs. 42 and 43, pp. 95 and 98).
The small sporting bullets were mostly of the Mauser (.276), Lee-Metford (.303), or Mannlicher (.315) calibre.
[5] See tables, pp. 12, 13, 15, Chapter I.
[6] The weights are from cartridges brought home. The charge of powder was small and variable.
[7] H. Nimier and E. Laval, Les Projectiles des Armes de Guerre, p. 20. F. Alcan. 1899.
[8] Mr. Leslie B. Taylor informs me that this rifle is a discarded Portuguese regulation pattern, with which a copper-ensheathed soft-nosed bullet was originally employed. For the purposes of the present campaign a modified cartridge was constructed. Examination of some specimens in my possession showed the charge of powder to be very small. (Table I. p. 48.)
The effects of injuries inflicted by bullets of small calibre may be divided into two classes:
1. Direct or immediate destruction of tissue.
2. Remote changes induced by the transmission of vibratory force from the passing projectile to neighbouring tissues or organs.
Those of the first class will be mainly considered in this chapter; the remote effects will be dealt with under the headings devoted to special regions.
In dealing with the wounds as a whole I shall first describe those of uncomplicated character as type injuries, and deal with those possessing special or irregular characters separately.
1. Nature of the external apertures.—The apertures of entry and exit in uncomplicated cases are very insignificant, but the size naturally varies slightly with that of the special form of bullet concerned. As will be shown moreover, the difference in size is the only real distinguishing characteristic in many cases between wounds produced by the modern bullet of small calibre and those resulting from the use of the older and larger projectiles of conical form. I have been very much struck on looking over my diagrams of entry, and especially exit, wounds to find that they reproduce in miniature most of those figured in the History of the War of the Rebellion; some of these diagrams are reproduced in this chapter.
Aperture of entry.—The typical wound of entry with a normal undeformed bullet varies in appearance according to whether the projectile has impinged at a right angle or[Pg 56] at increasing degrees of obliquity, or again, to whether the skin is supported by soft tissues alone, or on those of a more resistent nature such as bone or cartilage.
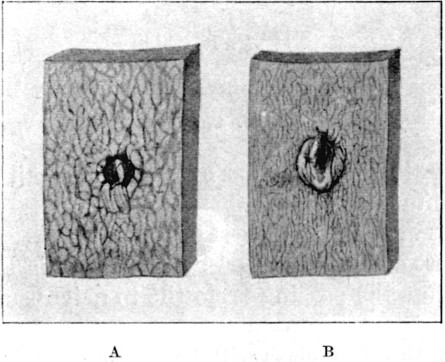 Fig. 16.—Mauser Entry and Exit Wounds.
Fig. 16.—Mauser Entry and Exit Wounds.
A, entry in buttock; circular opening filled with clot and crossed by a tag of tissue. B, exit in epigastrium near mid-line; irregular slit form, with well-marked prominence. Specimens hardened in formalin immediately after death; the resulting contraction has slightly exaggerated the irregularity of outline of the entry wound
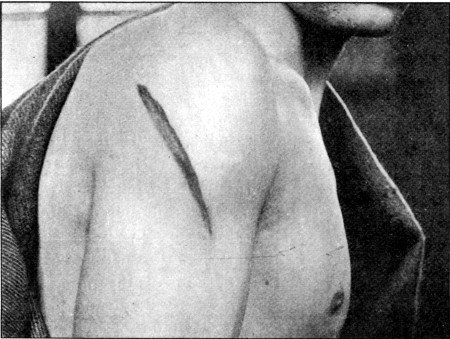 Fig. 17.
Fig. 17.
Gutter Wound of outer aspect of shoulder, caused by a normal Mauser, which subsequently perforated a man's leg. At the central part the gutter was 3/4 in. deep a few days after the injury
When the bullet impinges at a right angle the wound is circular, with more or less depressed margins, and of a[Pg 57] diameter, corresponding to the size of the bullet occasioning it, from a quarter to a third of an inch. The description 'punched out' has been sometimes applied to it, but it would be more correct to reverse the term to 'punched in,' since the appearance is really most nearly simulated by a hole resulting from the driving of a solid punch into a soft structure enveloped in a denser covering. The loss of substance, moreover, in the primary stage is not actually so great as appears to be the case, fragments of contused tissue from the margin being turned into the opening of the wound track. The true margin therefore is not sharp cut, and the nature of the line differs somewhat according to the structure of the skin in the locality impinged upon. Thus the granular scalp and the comparatively homogeneous skin of the anterior abdominal wall will furnish good examples of the nature of the slight difference in appearance. From the first the margin is also often somewhat discoloured by a metallic stain, similar to that seen when a bullet is fired through a paper book. This ring is, however, narrow, and not likely to be noticeable when the bullet has passed through the clothing. In any case it is subsequently obscured by the development of a narrow ring of discoloration due to the contusion. This latter varies in width, and still later a halo of ecchymosis half an inch or more in diameter surrounds the original wound.
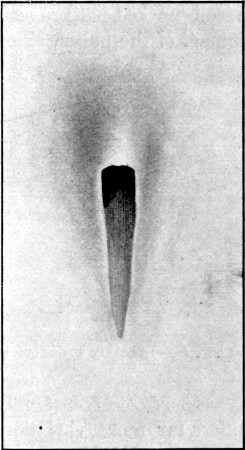 Fig. 18.—Oblique Exit Gutter.
Fig. 18.—Oblique Exit Gutter.
Diagram enlarged to actual size from case shown in fig. 24, p. 64.
With increasing degrees of obliquity of impact more and more pronounced oval openings of entry result, culminating in an actual gutter such as is seen in fig. 17.
In all oval openings the loss of substance is more pronounced[Pg 58] at the proximal margin, while the wound is liable to undergo secondary enlargement at the distal margin, since in the former the epidermis is mainly affected, while in the latter the epidermis is spared as an ill-nourished bridge, the deeper layers of the skin suffering the more severely. When the wound occurs in regions, such as the chest-wall or over the sacrum, where the skin is firmly supported, the oval openings are often very considerable in size, reaching a diameter at least double that of the circular ones. In the case of the oval openings the depression of the margins is not such a well-marked feature as in wounds resulting from rectangular impact of the bullet, since the distal margin is really lifted.
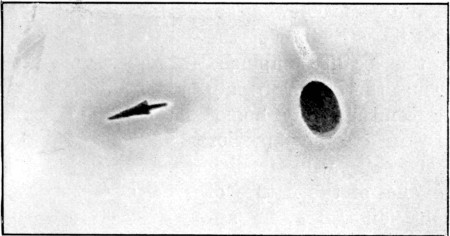 Fig. 19.
Fig. 19.
Oval Entry Wound over third sacral vertebra. Exit wound, anterior abdominal wall. Slightly starred variety. Diagram made on second day
Aperture of exit.—The wound of exit in normal cases offers far more variation in appearance than that of entry, this variation depending on several circumstances: first, the want of support to the skin from without, and such other factors as the degree of velocity retained by the travelling bullet, the locality of the opening, and the density, tension, and resistance offered by the particular area of skin implicated.
When the range has been short and the velocity high, it is often difficult to discriminate between the two apertures. Both may be circular and of approximately the same size, and the only distinguishing characteristic, the slight depression of the margin of the wound of entrance, may be absent if any time has elapsed between the infliction of the injury and examination by the surgeon. One very strong characteristic if present is[Pg 59] the general tendency of the margins, and even the area surrounding the exit wound itself, to be somewhat prominent. Fig. 16 shows this point, although the wound from which it was drawn had been produced thirty-six hours before death. The specimen was then hardened in formalin and still preserves its original aspect. This character is, however, more frequently displayed in wounds received at mean, or longer, ranges. In wounds produced by bullets travelling at the highest degrees of velocity it is often absent.
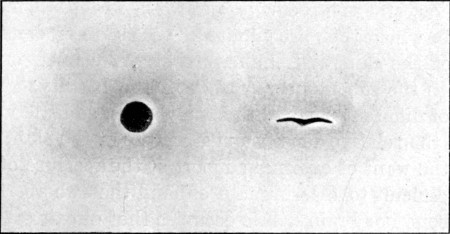 Fig. 20.
Fig. 20.
Circular Entry back of arm; exit (bird-like) in anterior elbow crease
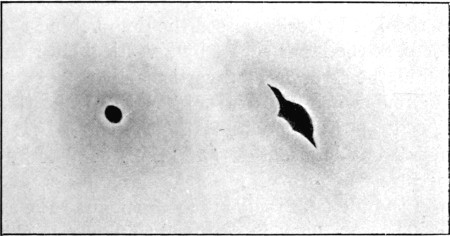 Fig. 21.
Fig. 21.
Circular Entry over patella. Starred exit of elongated form in popliteal crease
When the range of fire has been greater and the velocity retained by the bullet lower, slit wounds are common, or some of the slighter degrees of starring. Actual starring I never saw, but reference to figs. 20 and 21 will show a tendency in this direction, also a close resemblance to the starred wounds[Pg 60] resulting from perforations by large leaden bullets. Such wounds, I believe, are usually the result of a somewhat low degree of velocity.
Slit exit wounds may be vertical or transverse (fig. 20) in direction, and the production of these is dependent on the locality in which they are situated, the thickness, density, and tension of the skin, and the nature of the connection of the latter with the subcutaneous fascia in the locality. Thus in wounds of different parts of the hairy scalp, so little variation exists in the relative density and structure of the skin, that, in spite of the want of external support at the aperture of exit, it is often difficult to discriminate offhand the two apertures, if neither bone nor brain débris occupies that of exit.
If, however, a wound crosses from side to side a region such as the thigh where well-marked differences exist in the subjacent support, thickness, and elasticity of the skin implicated in the apertures, the wound of entry, if in the thick skin of the outer aspect, was usually circular, while the exit in the thin elastic skin of the inner aspect was either slit-like or starred. The difficulty in laying down any general rule as to the occurrence of circular or slit apertures of exit in any definite region is, however, great, as may be seen by reference to the accompanying diagrams taken from two patients wounded at Paardeberg (figs. 22 and 23).
In fig. 22 the bullet entered the outer and posterior aspect of the left buttock, crossed the limb behind the femur, and emerged at the inner aspect by a vertical slit: the bullet then entered the scrotum by a vertical slit, and emerged by a typical circular aperture; re-entered the right thigh by a transverse slit aperture, and, striking the femur in its further course, underwent deformation, and finally escaped by an irregular aperture 3/4 of an inch in diameter. The occurrence of exit slits in the adductor region is common, and to be explained by the tendency of the comparatively thin elastic skin to be carried before the bullet; the slit entry in this position must, I suppose, be explained by the comparatively slight support afforded by the underlying structures, which are often in a condition of hollow tension. The scrotal wounds are perhaps more difficult to account for, but in this case the fact of the distal aperture being directly supported by the right thigh is a ready explanation of the circular exit, while the skin corresponding to the slit entry was no doubt carried before the bullet, and finally gave way in the line of a normal crease.[Pg 61]
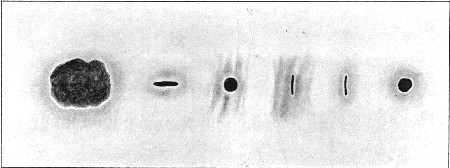 Fig. 22.
Fig. 22.
Entry and Exit Wounds in both thighs and
scrotum.
From right to left: 1. Circular entry in left buttock behind
trochanter. 2. Vertical slit exit in adductor region. 3. Slit entry in
scrotum (probably inverted before bullet broke the surface, and then a
slit occurred in a normal crease). 4. Circular exit in scrotum (here
supported by surface of right thigh). 5. Transverse slit entry in right
adductor region. 6. Irregular 'explosive' exit, the bullet having set up
on contact with the front surface of the femur, but without having
caused solution of continuity of the bone
In fig. 23 all the wounds are circular except the final exit, which was irregular as a result of the bullet in this case also having struck the femur in the second thigh. Considerable variation also exists in the size of the circular apertures; this illustrates the secondary enlargement often occurring in such wounds, and most marked at the apertures of entry, as the more contused. Both diagrams were made from patients eight days after the reception of the wounds.
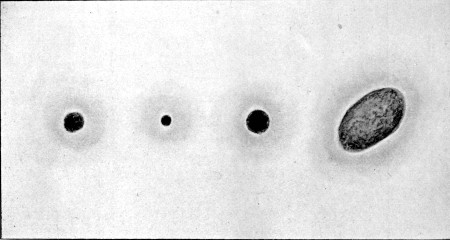 Fig. 23.
Fig. 23.
Wound of both Thighs. First and second entry typical circular wounds. First exit a small circular wound; the bullet 'set up' on contact with the femur without causing solution of continuity of the bone, and second exit is irregular and large.
This diagram is of considerable interest when compared with fig. 22. I believe the comparative regularity in the wounds to have been due to a higher degree of velocity of flight on the part of the bullet
Lastly, vertical or transverse slits may be looked for with considerable confidence in situations in which transverse oblique or vertical folds or creases normally exist in the skin, and depend on the lines of tension maintained by the connection of the skin in these situations to the underlying fascia. Thus I saw well-marked transverse and vertical slits in the forehead corresponding with the creases normally found there, and in this situation I noted some slit entries. Transverse slits[Pg 63] were common in the folds of the neck, the flexures of the joints (fig. 20), and the anterior abdominal wall either in the mid line or in creases like those stretching across from the anterior superior iliac spines. Again they were seen in the palms and soles, but here more readily tended to assume the stellate forms. Vertical slits are less common; they occurred with the greatest frequency in the posterior axillary folds.
Oval apertures of exit are far less common than those of entry, since the most common factor for the production of an oval opening, bony support, is never present. In long subcutaneous tracks, or very superficial wounds, they are however sometimes met with and may terminate in a pointed gutter (see figs. 18 and 24).
The greatest modifications in the appearance and nature of the apertures of entry are dependent on previous deformation of the bullet, when all special characteristics are lost, and it becomes impossible to form any opinion as to the type of bullet concerned. These modifications are naturally far more common in the aperture of exit, since the bullet so often acquires deformity in the body as the result of impact with the bones. Further remarks on this subject will be found with the description and comparison of the various bullets on p. 81.
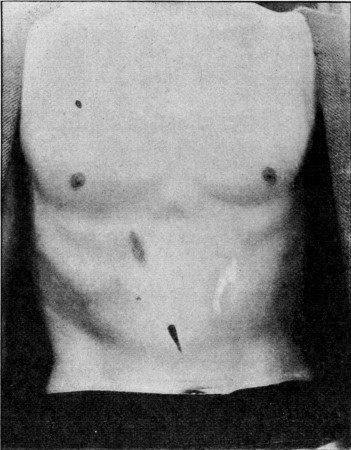 Fig. 24.—Superficial Thoracico-abdominal Track.
Fig. 24.—Superficial Thoracico-abdominal Track.
Small entry: discoloration of surface over costal margin from deep injury to skin; well-marked 'flame' gutter exit (see fig. 18)
2. Direct course taken by the wound track.—This character primarily depends on the velocity with which bullets of small calibre are made to travel, and on the small area of the tissues upon which they operate. In this relation the degree of velocity retained by the bullet is often of minor importance, provided it be sufficient to penetrate the body. Fired within a distance of 2,500 yards there is little doubt that a bullet of the Lee-Metford, Mauser, or Krag-Jörgensen types, passes straight between the apertures of entry and exit when these are of the type outline, even when the bones are implicated. By reason of the small size of the projectiles, their shape, and the spin and velocity transmitted to them, there is no reason why at a sufficiently short range they should not traverse the body from the crown of the head to the sole of the foot. The necessary conditions of position and distance for such an injury are obviously not[Pg 64] often obtained, but it may be pointed out that the Belgian Mauser rifle at a distance of five yards is capable of driving a bullet 55 inches or nearly five feet into a log of pine-wood. Many examples of long tracks will be referred to later, but the following instances may be of interest in this relation. A bullet entering at the occipital protuberance traversed the muscles of the neck, passed through the thoracic cavity, fractured the bodies of the third and fourth and grooved the seventh and eighth dorsal vertebræ, grooved the seventh and eighth and fractured the ninth and tenth ribs, traversed the muscles of the back and finally lodged against the ilium; the whole length of this track measured some 25 inches. Again, at the battle of Belmont a Mauser bullet entered the pelvis of a horse just below the anus, and traversed the entire trunk before emerging from the front of the chest: it may be of interest to[Pg 65] mention that this animal was alive and moving about the next day, but I am sorry I can give no further information regarding his fate.
 Fig. 25.—Superficial Track on external surface of Thigh.
Fig. 25.—Superficial Track on external surface of Thigh.The possibility of contour tracks travelling around the walls of the chest or abdomen has therefore rarely to be considered, except in occasional instances where the bullet fired from a long range has impinged against a bone and is retained in the body. The small volume of the bullets, however, allows the production of very prolonged direct subcutaneous tracks in the body wall, in positions where they would be manifestly impossible with projectiles of larger calibre.[Pg 66]
Figs. 24 and 25 illustrate wounds of this nature. In the case figured in fig. 24 the bullet entered over the third rib in a vertical line above the right nipple; it then coursed obliquely down, crossing the seventh costal cartilage, and finally emerged 3 inches above the umbilicus. Where the track crossed the prominence of the thoracic margin the skin was so thinned as to undergo subsequent discoloration, while a distinct groove was evident there on palpation. In some similar cases I have seen the central part of the track secondarily laid open as a result of the thinning of the skin and consequent sloughing due to the interference with its vitality.
Short of sloughing, the skin may show signs of alteration of vitality for a long period after the injury; thus fig. 25 depicts the condition seen in a superficial wound of the thigh five weeks after the injury. The line of passage of the bullet between the two openings was still clearly visible as a dark red coloured streak. Grooves in such cases are generally readily palpable in the early stages, while later the want of resistance is replaced by the readily felt firm cord representing the cicatrix. These points are of much importance in discriminating between perforating and non-perforating wounds of the abdomen, and are again referred to in that connection.
The direction of the tracks obviously depends on the attitude assumed by the patient at the moment of impact of the bullet and the direction whence the firing has proceeded. The frequent assumption of the prone position during the campaign led to the occurrence of a large proportion of longitudinal tracks in the trunk, or trunk and head, which will be referred to later. Certain battles were in fact strongly characterised by the nature of the wounds sustained by the men. Thus at Belmont and Graspan, where some rapid advances were made in the erect attitude, fractured thighs were proportionately numerous, while at Modder River, where many of the men lay for a great part of the day in the prone position, glancing wounds of the uplifted head, of the occipital region, or longitudinal tracks in the trunk and limbs were particularly frequent. I very much regret that the material at my disposal does not allow me to add some remarks[Pg 67] as to variation in the nature of the wounds according to whether they were received from an enemy firing from a height or from below, but it is possible that some information on this subject may be forthcoming when the returns of the Service are made up, since it is naturally of great importance as to the effect of trajectory in the proportionate occurrence of hits.
3. Multiple character of the wounds.—The same conditions responsible for the length and directness of the tracks, account for the frequently multiple character of the wounds implicating either the limbs or viscera—thus, lung, stomach, liver; neck, thorax, abdomen; abdomen, pelvis, thigh. Also for the frequent infliction of two or more separate tracks by the same bullet—thus, arm and forearm with the elbow in the flexed position; both lower extremities; both lower extremities, penis or scrotum; leg, thigh, and abdomen, with a flexed knee; upper extremity and trunk, and more rarely one upper and one lower extremity. Again, it was remarkable how often the same bullet would inflict injuries on two or more separate men, not unfrequently dealing lightly with the first and inflicting a fatal injury on the second, or vice versâ. The small calibre of the bullet, moreover, allows of the neatest and most exact multiple injuries. Thus in a patient who was crawling up a kopje on all fours, the flexed middle digit of the hand was struck. The bullet entered at the base of the nail, first emerged at the distal interphalangeal flexor fold, re-entered the metacarpo-phalangeal fold, and finally emerged from the back of the hand between the third and fourth metacarpal bones.
4. Small 'bore' of the tracks, and tendency of the injury to be localised to individual structures of importance.—Here we meet with the most striking characteristic of the injuries, and evidence that reduction of calibre affects more strongly the nature of the lesion than does any other element in the structure of the modern rifle. The diameter of the track slightly exceeds that of the external apertures, probably as a result of the more ready separability of the elements of the structures perforated than exists in the skin. The calibre, moreover, tends to be fairly even throughout[Pg 68] when soft structures only are implicated, though local enlargements result wherever increased resistance is met with. Thus a strong fascia may offer such resistance as to increase locally the bore of the track, and in this particular the state of tension of the fascia when struck will affect the degree of the enlargement. The most striking instances of local enlargement of the track are of course seen when a bone lies in the course of the bullet, but we must here bear in mind the introduction of a new element—the propulsion of comminuted fragments together with the bullet itself. In cases of fracture the distal portion of the track is in consequence many times larger than the proximal. The most striking examples of small even tracks are seen, on the other hand, in punctures of the elastic and practically homogeneous lung tissue, where the wounds are extremely small.
On transverse section of the track the gross amount of actual tissue destruction occupies a lesser area than that corresponding to the diameter of the bullet. The destructive action of the projectile is in fact exerted mainly on the tissues directly lying in its course, the track being opened up during the rush of the passage of the bullet, partly as a result of its wedge-like shape and partly as a result of the throwing off of the tissues forming the walls of the track by a diversion of a portion of the force in the form of spiral vibrations dependent on the revolution of the bullet. Again, the opening out of the tissues may be aided by the direction taken by the first and strongest as well as the simplest series of vibrations transmitted, which would assume the shape of a cone of which the point of impact forms the apex.
The escape from actual destruction by structures lying in the immediate neighbourhood of the track is indeed often surprising, but not perhaps so astonishing as the perforation of long narrow structures such as the peripheral nerves and vessels, without irreparable damage to the parts remaining, and this although the structures themselves may be of a diameter not exceeding that of the bullet itself. The capacity of these projectiles to split such structures as tendons was already well known before our experience in this campaign, but the injuries to the nerves and vessels of the same character came as[Pg 69] a surprise to most of us. The lateral displacement of tissues seems to bear a strong resemblance to what is seen on the passage of an express train, when solid bodies of considerable weight are displaced by the draught created without ever coming into contact with the train itself. The tendency to lateral displacement is still more strongly exhibited when dense hard structures such as bone are implicated. Here the fragments at the actual points of impact on the proximal and distal surfaces of a shaft are driven forwards, while the lateral walls of the track in the bone are simply comminuted and pushed on one side without loss of continuity with their covering periosteum.
The extension of this form of displacement to a degree amounting to a so-called explosive character in the case of the soft tissues, even when the bullet passed at the highest degrees of velocity, was, however, never witnessed by me, and I very much doubt the existence of a so-called 'explosive zone' so far as wounds of the soft parts are concerned. On the contrary, I am inclined to believe that the highest degrees of velocity are favourable to clean-cut neat injuries of the soft tissues. I saw a large number of type wounds of entry and exit inflicted at a range of under fifty yards.
5. Clinical course of the wounds.—The tendency of simple wounds such as are above described to run an aseptic course was very marked, and, given satisfactory conditions, deep suppuration and cellulitis were distinctly rare. It may also be confidently affirmed that when suppuration did occur, with apertures of entry and exit of the normal small type, this was always the result of infection from the skin, or infection subsequent to the actual infliction of the wound. The infrequency of suppuration depended on the aseptic nature of the injury, the smallness of the openings, the small tendency of the track to weep and furnish serous discharge in any abundance, the comparative rarity of the inclusion of fragments of clothing or other foreign bodies, and possibly in some degree on the purity and dryness of the atmosphere, which favoured a firm dry clotting of the blood in the apertures of entry and exit, and consequent safe 'sealing of the wound.'[Pg 70]
As to the aseptic nature of the injury, it will be well to first consider the question of the sterility of the bullet. Putting laboratory experiments on one side, the large experience of this campaign seems to prove to absolute demonstration that, bearing in mind the very large proportion of instances of primary union in simple tracks, the surgeon has nothing to fear on the part of the bullet itself. This is the more striking when we remember that these bullets shortly before their employment were carried in a dirty bandolier, and freely handled by men whose opportunities of rendering either their hands or implements aseptic were as bad as it is possible to conceive.
Several explanations are to hand, but none of them conclusive. Two must, however, be shortly considered. First, the surface of the bullet, except its tip and base, is practically renewed by passage through the barrel. Secondly, there is the question of the heat to which it is subjected. As far as cauterisation of the tissues is concerned, this question has been practically settled in the negative, since actual determinations of the heat immediately after the moment of impact have been made, and again it has been shown that butter is not melted, and that neither gunpowder nor dynamite is exploded, by firing bullets through small quantities of those materials. Again, the absence of any sign of scorching of the clothes of the wounded is strong evidence against the possibility of any considerable heat being applied to the tissues of the body; while another observation, although of less importance as affecting spent bullets only, that bullets, which have perforated the body but lie between the skin and the clothing, leave no sign of cauterising action on either, may be mentioned. None the less, the sources of heating while the bullet is passing from the barrel are many and obvious. Thus there is the heat consequent on explosion of the powder, the warm state of the barrel itself when the rifle has been fired a few times consecutively, and the heat resulting from the force and friction essential to the propulsion of the bullet through the barrel. Again, bullets covered with wax before their introduction into the barrel retain no trace of this when they have been fired, although at any rate[Pg 71] the portion covering the tip is not exposed to friction on the part of the rifle, and lastly the base of the bullet has no other explicable reason for its innocuousness than subjection to a certain degree of heat. While not claiming any cauterising action on the tissues by the bullet, I should therefore still be inclined to allow the probability of the heat to which the surface of the bullet is exposed exerting a cleansing action on the projectile. In regard to this point it is interesting to bear in mind that shots from an ordinary gun seldom or never give rise to infection.
Foreign bodies were rarely carried into the wounds with the bullet. I saw several instances in which portions of the metal of cigarette cases and of cartridge cases when the bullet had perforated cartridges in the wounded man's bandolier, and in one instance small pieces of glass from a pocket mirror, must have been carried in without any obvious ill effect. Fragments of clothing, on the other hand, in every case caused suppuration: clothing was not often carried in, the khaki linen was perforated with a clean aperture, most commonly a slit; but the thick woollen kilts of the Highlanders, and thick flannel shirts, occasionally furnished fragments. The introduction of large pieces of clothing is a sure proof of irregularity of impact on the part of the bullet. The frequency with which portions of cloth were introduced from the kilt was one of the strongest surgical objections to its retention as a part of the uniform on active service.
Retained bullets themselves remained as foreign bodies in a certain number of cases. I cannot say that suppuration never followed the retention of a bullet, since in two of the instances where I saw such removed they lay in a small cavity containing at any rate a 'purulent fluid.' In one of these the bullet was a Martini-Henry, and in both the bullet had been imbedded for some weeks, and had certainly not occasioned a primary suppuration of the wound.
The favourable influence of the pure and dry nature of the atmosphere in this campaign must certainly not be underrated, and in support of this influence I think I may say, from the experience of cases that I saw coming from Natal where the climate and surroundings were not so favourable as[Pg 72] on the western side, that suppuration was more common and more severe in the moister atmosphere.
Putting aside all the above remarks, however, I am inclined to think that a general tendency to primary union and the absence of suppuration will always be a feature of wounds from bullets of small calibre, and that this favourable tendency is attributable to certain inherent characters of the injuries. Of these the nature and small size of the openings, the dry character of the lining of the track due to superficial destruction and condensation of the tissue forming its wall, the small disposition to prolonged primary hæmorrhage, and the absence of any great amount of serous exudation during the early stages of healing are the most important.
A mechanical factor of great importance also exists in the spontaneous collapse and automatic apposition of the walls of the track. This closure is rendered additionally effective in many cases by the interruption of the continuous line in the wounded tissues consequent on alteration in the position of the parts traversed when an attitude of rest is assumed by the injured part. The indisposition to suppuration and the apparent unsuitability of the tissue lining the track for the development and spread of infecting organisms are well illustrated by several observations. Thus, even if the bullet be thoroughly aseptic, the fragments of destroyed skin driven into the track by the bullet can scarcely be free from organisms; yet these seldom give rise to trouble. Again, if for any reason a deep portion of a track becomes infected and suppurates, there is no tendency for the spread of infection along the line of wounded tissue, but rather for the development of a local abscess, pointing in the ordinary direction of least resistance, irrespective of the course originally taken by the bullet.[Pg 73]
Mauser Wound of Entrance, a little more than 48 hours after infliction. About 12/1.
G. L. Cheatle.
Section of the entry segment of an aseptic Mauser wound removed a little over forty-eight hours after its infliction. Magnified twelve diameters.
The margins of the opening are still sloping and depressed, indicating the originally 'punched-in' nature of the aperture. A thin stratified layer of epidermis completely closes it. No scab remains.
The wound track is occluded by an effusion of lymph, commencing organisation of which is shown under a higher magnifying power by the presence of leucocytes near the margin of the bounding tissue, and some giant cells. The effusion of lymph occupies a slightly wider area immediately beneath the papillary layer of the skin, then narrows, and broadens again as the subcutaneous fascia is reached, indicating the effect of resistance in widening the area of damage.
The subcutaneous connective tissue bounding the track shows little sign of alteration beyond a general slight tendency of the lines of structure to deviate in the direction of the passage of the bullet.
No hæmorrhage is apparent beyond a small collection of blood situated immediately beneath the new layer of epidermis at the left-hand corner of the opening.
Range probably within 800 yards. Seat of wound, abdominal wall a highest point of iliac crest.[Pg 74]
Fig. 25 (a), a (plate I.) represents a section carried across an aseptic aperture of entry. The specimen was removed by Mr. Cheatle from a patient who died forty-eight hours after reception of the injury. It shows well the small amount of gross destruction suffered by the subcutaneous tissue, and the rapid repair which follows, since macroscopically the track is scarcely discernible. Reference to plate I. shows the remarkable fact that even at this early date considerable progress towards definite healing has occurred, and a thin layer of stratified epidermis covers the original opening. The question may be raised whether the origin of this epidermal layer is not in part a floating up of the margins of the main aperture.
During the course of healing some variation takes place in the appearance of the apertures, especially that of entry. This, at first contracted, later becomes somewhat relaxed, while in many cases a small halo of ecchymosis develops around it. The blood-clot occupying its centre now contracts, the margins rapidly become approximated centripetally, and a small circular dark spot only remains, which is later replaced by a small red cicatrix. The dark central spot under these circumstances consists of the contused margin of the wound in the skin, and a small proportion of blood-clot which finally comes away as a small dry scab. When slight local infection occurs in place of simple contraction and dry scabbing, the process is prolonged, the contused margin separates by granulation, the clot in the opening breaks down, and a small ulcer of somewhat larger proportions than the original wound remains and takes some days to heal.
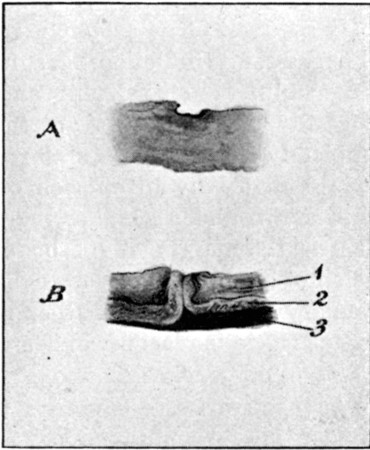 Fig. 25 (a).
Fig. 25 (a).
A. Wound of entry 48 hours after reception. B. Wound of exit, 7½ days after reception. 1. Skin. 2. Subcutaneous fat carried into the lips of the wound by the bullet. 3. Infected blood extravasation in subcutaneous tissue. Exact size. (See plates I. and II.)
The aperture of exit in simple wounds of the soft parts sometimes heals even more rapidly than that of entry, and[Pg 75] if of the slit form may be almost invisible at the end of ten days or a fortnight, actual primary union having taken place as after a simple small incision. Larger or irregular exit apertures, however, take a longer period to close than entry wounds, and this is most often observed when the bullet has undergone deformation within the body, or bone fragments have been driven out with the bullet.
Fig. 25 (a), b (plate II.) represents a section of an infected exit aperture from a patient who died seven and a half days after its infliction. Two main points of interest are at once apparent: 1. The carrying forwards of the subcutaneous fat into the lips of the skin wound by the bullet. This illustrates the manner in which lightly supported structures are carried forward by the bullet, and throws some light on the mode by which vessels and nerves may escape by a process of displacement. This figure may be compared with fig. 25 (b) which shows a tag of omentum similarly carried forward by a bullet crossing the abdominal cavity and plugging the exit wound. 2. The second feature of interest is the amount of hæmorrhage into the subcutaneous tissue. In this respect the contrast between the exit and entry apertures is marked, since in the latter hæmorrhage is scarcely apparent. The presence of such hæmorrhages is explained by the same dragging action as the extrusion of the fat, and is of course dependent on consequent rupture of small vessels. It is of importance as predisposing the exit wound to more easy infection, and it accounts for the persisting subcutaneous induration more often detected beneath healed exit than entry apertures. Again, it suggests that the presence of blood in the deeper parts of the tracks may be the determining cause of the indurated cords often replacing them.[Pg 76]
G. L. Cheatle.
Mauser Wound of Exit, 7½ days after infliction. Healing delayed by Infection. About 12/1.
Section of the exit segment of a Mauser wound, removed seven and a half days after infliction. Magnified twelve diameters.
The healing process has been delayed by infection.
There is no attempt at closure by a layer of epidermis, and the margins are not depressed.
The wound track is narrower than that seen in the entry wound plate I., and completely occluded by a plug of the subcutaneous fat which has been carried forward by the bullet in its passage. A small wedge-shaped plug of lymph indicates the position of the actual track at its termination.
Dragging on the surrounding tissue consequent on the extrusion of the plug of fat has ruptured some capillaries, and given rise to considerable extravasation of blood, which is seen as a darker layer in the deepest portion of the wound.
Comparison of this plate with the exit wound depicted in fig. 16, p. 56, explains the nature of the tags of tissue there seen to protrude from the convex opening.
Range 800 yards. Seat of wound, abdominal wall below 9th costal cartilage.
Pari passu with the closure of the external openings, healing of the track takes place, but this is not always so rapid a process as is apparently the case. In many instances the closure, and even definite healing, of the external wounds is complete long before the track has actually healed, even though it be contracted up to complete closure as far as any cavity is concerned. This is well seen in many cases in which the exit opening is large as a result of deformation of the bullet, or the passage of bone splinters in conjunction with it; here, in spite of absence of all suppuration, the track may remain patent for many weeks. This may point to infection, but the tardiness in actual consolidation corresponds with what we are well acquainted with in the case of all aseptic wounds when a slough has to separate or become absorbed, and it is therefore only what might be reasonably expected when we remember that every such bullet track is lined by a thin layer of damaged tissue.
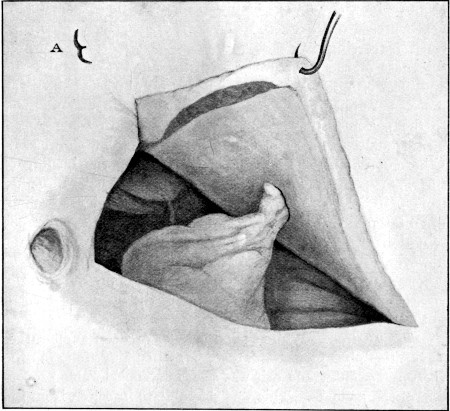 Fig. 25 (b).
Fig. 25 (b).
Great Omentum carried by the bullet into an exit track leading from the abdominal cavity. A. Outline of opening in the peritoneum
When fully healed, the points of entry and exit are so insignificant as to be less obvious than ordinary acne scars, and later are often hardly visible, but for a considerable period they are often more palpable than apparent. This depends upon the induration of the line of cicatrix corresponding[Pg 78] to the course of the original track which is adherent to the two points. The induration is indeed so marked as to occasionally give rise to the suspicion that a foreign body such as a fragment of lead or of the mantle of the bullet has been enclosed during the healing of the wound.
In the deeper portions of the tracks the extreme density of the cicatrix is a factor of great prognostic importance, since if it implicates muscles, tendons, vessels, or nerves, impairment of movement, circulatory disturbance, or signs of neuritis or nerve pressure are often witnessed. Thus, for instance, a track traversing the calf, will more or less tie the whole thickness of the structures perforated at one spot, and the apertures of entry and exit may be visibly retracted when the muscles are put in action with consequent pain and stiffness to the patient. Such pain and stiffness form some of the most troublesome after-consequences of many simple wounds. It is remarkable for how long a period after the healing of the wound and resumption of active duty the patients suffer from pain in and radiating from the locality of the wound, when fatigued or suffering from stiffness from the prolonged retention of one attitude or exposure to cold. The cords, however, eventually completely disappear, and the cicatrices become moveable. The effects of secondary pressure on the vessels and nerves are considered under the headings devoted to those structures.
Suppuration.—While the occurrence of deep suppuration or septic phlegmon was rare, local suppuration of the apertures of entry and exit was seen in a considerable proportion of the wounds. This was referable to infection from the skin itself, or to infection from without subsequent to the infliction of the injury. Infection from the skin, difficult to obviate at all times, is especially likely to occur in wounds the first dressing of which is often delayed, and which happen to men sweating freely into clothes the condition of which is at least undesirable for contact with a recent wound. Beyond this, the first dressing materials, removed from a soiled tunic by possibly a comrade or a stretcher-bearer, are scarcely above reproach of the probability of containing septic organisms themselves. Again, once applied, the exigencies of the[Pg 79] situation often necessitate an amount of movement fatal to the retention of the dressing over the wound, and a second opportunity of infection arises before the patient comes into the hands of the surgeon in the Field hospital.
The general tendency of such suppurations when they occurred in uncomplicated flesh wounds was to remain superficial, either involving the contused margin of the cutaneous opening and the plug of blood-clot occupying it, and resulting in a slight enlargement of the wound only, or at most involving the subcutaneous tissue and not extending into the deep planes of the trunk or limbs. In either case a slight delay in healing was the most serious result, while constitutional signs of infection were either absent or of the slightest nature. The same indisposition to spread by the track was equally noted when a deep portion became infected from, for instance, the intestine in a belly wound.
Wounds of irregular type, however, such as those caused by ricochet bullets, or accompanying severe fractures, or those caused by fragments of larger projectiles, often suppurated freely in spite of exposure to no more unsatisfactory surrounding conditions than the wounds of small bore. This appears to show conclusively that the first element in the general slight consequences of small-bore wounds is their calibre, and, secondly, that increase of velocity on the part of the bullet, while it in some measure compensates for the loss of volume in the projectile, on the other hand reacts in favour of the wounded in so far as the injuries it effects on the soft tissues are ill suited to the development of septic organisms in the parts.
Retained bullets.—These were met with more frequently than might have been expected, but I can give no idea as to their proportional occurrence, since so many of the slighter injuries never came under my observation. Experience, however, showed that the bullets of large calibre and low velocity employed during the campaign were far more commonly lodged in proportion to the frequency of their use. Thus I saw a considerable number of Martini-Henry, Snider, large leaden sporting bullets, and shrapnel retained. Again, among the bullets of smaller calibre, the Guedes 8-mm.[Pg 80] bullet, which travels at a comparatively low rate of velocity and with moderate spin, was far more frequently lodged than the Lee-Metford or Mauser in comparison with the number of Guedes rifles in use.
Bullets of small calibre were, however, also retained with some degree of frequency, either as the result of striking at a long range, or in such a direction as to need to traverse a large segment of the body before escaping, or as striking large or several bones, or making some irregular form of impact: the last was a not infrequent explanation of lodgment, especially when a bone lay in the course of the track. Ricochet bullets naturally were especially likely to be retained, both on account of the low velocity with which they often travel and the irregularity of their surface with consequent loss of penetrating power.
Many of the wounds met with deviated so greatly in appearance and general characters from what has been described above as to afford little or no evidence of having been inflicted by small-calibre bullets, and before describing these it is necessary to give a short account of the circumstances which are responsible for such departures from the common type. In the case of the wound of entry, the simplest explanations are lateral impact on the part of the cylindro-conoidal projectile, due to the position of the part struck or the direction in which the bullet has been fired, wobbling on the part of the bullet due simply to loss of velocity and force in flight, or to turning of the bullet by impact with an obstacle to its course (ricochet) which may amount to actual reversal of the striking end. As a rule, in such cases the size of the aperture of entry exceeds that of exit, and in a large proportion the bullet is retained within the body.
Of these explanations that of the 'wobble' needs some passing notice. In its simplest form it depends merely on loss of velocity of flight on the part of the bullet, the centre of gravity of which lies behind its middle; hence a tendency to turn over and over is acquired. As a result of this, either the side of the tip, the side of the bullet, the side of the base,[Pg 81] or the base itself may form the portion of the projectile which comes into contact with the body. The tendency to wobble is naturally greatly increased in ricochet bullets, since the contact, if lateral, serves to check the spin on which the bullet depends for its flight on an axis parallel to its long diameter. The first effect of wobbling is to increase the size and interfere with the regularity of outline of the wound of entry; but it also acts in a more serious manner, since the increase of the area of impact augments the resistance offered by the body; therefore the degree of damage to the tissues is accentuated and becomes greater than it would be from a bullet travelling at the same rate on its normal axis. Hence the wounds are both large and severe, or if the velocity is very low, the projectile is especially likely to be retained.
Actual reversal of the bullet usually only slightly enlarges the aperture of entry, but injuries to cancellous bone are apt to be more severe when the bullet enters in this manner, or again it is often retained. I saw several such cases during the campaign.
Another form of wobble is suggested by Nimier and Laval,[9] of which I can offer no experience. They suggest that, as rotation slows, the bullet may on impact wobble like a top before it ceases to spin. Probably the power of penetration possessed by a bullet wobbling in this manner would not be very great, but its effect would mainly be altered in the direction of an abnormal increase in the size of the aperture of entry, or possibly in the degree of comminution in fractures.
It is probable that some of the more serious wounds observed were merely the result of unusual forms of impact with normal flight on the part of the bullet. The majority, however, depended, in the case of the wound of exit, on deformation of the bullet within the body, or the propulsion of bone fragments with it, and, when both apertures were affected, to previous ricochet on the part of the projectile.
It is here necessary to give a short account of the more common deformities met with, and to refer to the special characters possessed by different types of bullet of small[Pg 82] calibre which may affect the ease with which deformity is produced, and the degree to which it is commonly carried. The effect of ricochet is to lower the velocity of flight, and at the same time to effect certain alterations of form in the bullet. These with rectangular impact in the case of bullets travelling at a low degree of velocity consist in a bending and deformation of the tip; in the higher degrees, of bending, shortening, extensive destruction, or complete fragmentation. If the bullet makes lateral impact, only widening and flattening result, often with the escape of the lead core from the mantle. That a ricochet bullet may travel a considerable distance is shown by the following observations quoted from Nimier and Laval.[10]
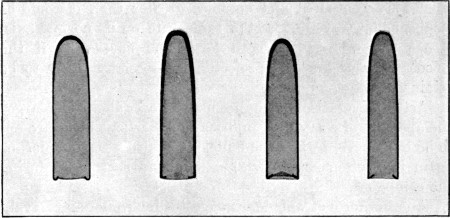 Fig. 26.—Sections of four Bullets to show relative shape
and thickness of mantles.
Fig. 26.—Sections of four Bullets to show relative shape
and thickness of mantles.
From left to right: 1. Guedes; regular dome-shaped tip; mild steel mantle; thickness at tip 0.8 mm.; at sides of body 0.3 mm. 2. Lee-Metford; ogival tip; cupro-nickel mantle; thickness at tip 0.8 mm.; gradual decrease at sides to 0.4 mm. 3. Mauser; pointed dome tip, steel mantle plated with copper alloy; thickness at tip 0.8 mm.; gradual decrease at sides to 0.4 mm. 4. Krag-Jörgensen; ogival tip as in Lee-Metford; steel mantle plated with cupro-nickel; thickness at tip 0.6 mm.; gradual decrease at sides to 0.4 mm. The measurements of the sides are taken 2.5 cm. from the tip. Note the more gradual thinning in the Lee-Metford mantle.
Up to a distance of 1,700 to 1,800 metres the bullet may make several ricochet bounds. When the bullet strikes first at short distances (as 600 metres), it may make several bounds of from 300 to 400 metres: at moderate distances (as from 600 to 1,200 metres), bounds of 200 to 300 metres; and at distances above 1,200 metres, bounds of 100 to 200[Pg 83] metres. The length of the ricochet bounds depends on the angle of impact of the bullet with the ground, the nature of the slope of the latter, and the velocity of the bullet.
Putting aside the question of calibre and volume of the bullets we are concerned with, I believe the most important variations as serious effects of ricochet depend on the relative thickness and the composition of the mantles. Fig. 26 illustrates the relative thickness of the mantles in the Krag-Jörgensen, Mauser, Lee-Metford, and Guedes bullets. Given an equal degree of force and velocity on the part of the bullet at the moment of impact, the assumption is justifiable that the thinner mantles would tear or burst more readily in direct ratio to their relative thinness. I believe this assumption to be borne out by my own experience of the common deformities that occurred; but the great relative frequency with which Mauser bullets came under my observation, and the difficulty of forming any estimate of the velocity and force retained by any particular bullet at the moment of impact, make it impossible for me to express myself with the confidence which I should wish.
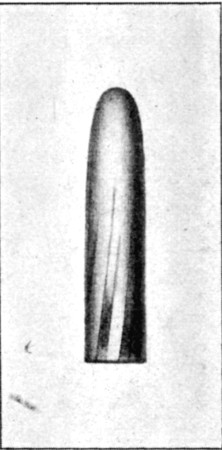 Fig. 27.—Normal Mauser Bullet
Fig. 27.—Normal Mauser Bullet
The second condition which influences the nature and degree of the deformities depends on the relative tenacity or brittleness peculiar to the metal employed in the manufacture of the mantles. In the case of the Lee-Metford this consists of an alloy of 80 parts of nickel with 20 of copper. The Krag-Jörgensen and Mauser are ensheathed in steel plated with cupro-nickel, and the Guedes has a plain steel envelope coated with wax.
Both as a result of experience in the field gained from ricochet bullets, and in the hospitals from bullets which had undergone deformation within the body, I am under the firm impression that the thin nickel-plated steel envelope of the Mauser bullet splits more readily than the thicker and more tenacious cupro-nickel envelope of the Lee-Metford, that the[Pg 84] direction of the ruptures is more purely longitudinal, and the fissuring itself more extensive and complete.
I append below a series of deformities observed in Mauser bullets, some of which were collected on the field of battle, but all of which were familiar to me in bullets removed from the bodies of patients, except the complete disc shape shown in fig. 29. They correspond with specimens of which I made sketches at the time of removal from the body, but which I had not the heart to retain in view of the natural wish of the patients to keep them as mementoes of their wounds.
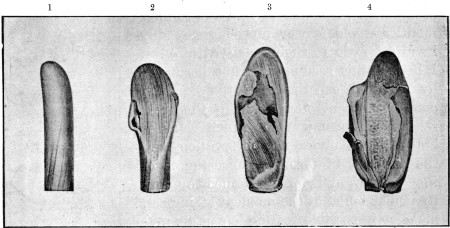 Fig. 28.—Four common types of lateral Mauser Ricochet
Bullets.
Fig. 28.—Four common types of lateral Mauser Ricochet
Bullets.
From left to right: 1. Slipper form; slight broadening and turning of tip. 2. More pronounced degree of form 1, with laceration of the mantle opposite the shoulder of the bullet. This is the weakest spot, for two reasons: the alteration in curve at this position, and the junction of the thickened point of the mantle with the thinner sides. 3. Lateral ricochet involving nearly whole length of bullet. Rupture of mantle from broadening of core opposite shoulder. 4. Similar lateral ricochet with extensive longitudinal rupture of mantle, the latter being turned out and forming a cutting 'flange.'
Slight indentations and deviations from strict symmetry of form of such degree as not seriously to influence the outline and nature of the apertures were very common. Beyond these one of the most frequent primary deformities was that we familiarly spoke of as the 'slipper form' (No. 1, fig. 28). This results from light glancing contact of the tip with a hard body: in it the mantle of the bullet is rarely fractured, and the deformity itself is of slight importance, except in so far as it may influence the direction of the wound track, which acquires a tendency to be curved. The tip of the bullet is slightly flattened and turned up, down, or to one side,[Pg 85] according to the point struck. I saw this deformity frequently, both with Lee-Metford and Mauser bullets. Nos. 2, 3, and 4 are more pronounced degrees of the same type of deformity, accompanied by more or less extensive fissuring of the mantle. No. 4 illustrates the turning out of the longitudinally fissured mantle in such a way as to make a cutting flange. I have seen such bullets removed, and the variety is of some importance as materially increasing the cutting capabilities of the bullet, and augmenting its area of destructive action. No. 5, fig. 29, is the only form I have not seen removed, but such a bullet would account for some of the long irregular gutter wounds observed, if it retained sufficient velocity to strike with any force.
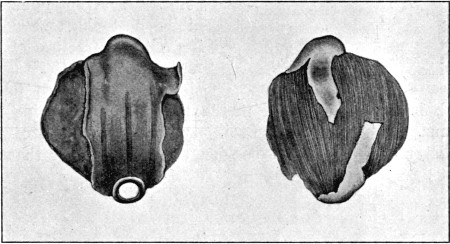 Fig. 29.—'Disc'-shaped Lateral Ricochet.
Fig. 29.—'Disc'-shaped Lateral Ricochet.
This form is of little practical importance, as the velocity retained by the bullet is low, and no perforating power would be retained. It is inserted separately in order to complete the series, shown in fig. 28.
Fig. 30 illustrates complete longitudinal fissuring of the mantle. Such mantles are common, and still more so are the opened-out sheets such as is shown still attached in fig. 29. Free mantles are often very numerous on stony ground, but are of little importance, since I never saw fragments of them removed or impacted. They probably travel a very short distance after their formation, and if they did strike would possess little power of penetration. The freed leaden cores do, however, sometimes enter the body, and some of the specimens removed have been referred to the[Pg 86] use of expanding bullets. In all the Mauser specimens the longitudinal direction of the fissuring of the mantle is striking.
 Fig. 30.—Ruptured Mauser Mantle, to illustrate the
tendency to complete longitudinal fissuring
Fig. 30.—Ruptured Mauser Mantle, to illustrate the
tendency to complete longitudinal fissuring
Fig. 31 represents bullets removed from the body and illustrates types of deformity due to impact with the bones. The deformity resembles in some degree that of the mushroomed lead cores, and also indicates that the shoulder of the cased bullet is its weakest point. Each specimen exhibits shortening and widening without fracture of the mantle, the latter being simply thrown into folds; both bullets were lodged in the thigh after fracturing the femur. The localisation of injury to the fore part of the bullet, and the fact of expansion, allow us to infer that the degree of velocity retained on impact with the bone was comparatively low, and that neither bullet had been exposed to very severe strain.
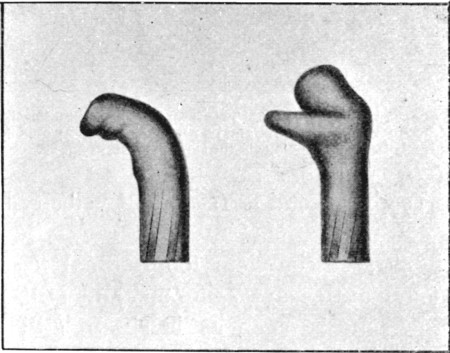 Fig. 31.
Fig. 31.
Two retained Mauser Bullets which had produced comminuted fractures of the femur of moderate severity. Each has given way at the shoulder, but the mantle has developed creases without rupture, and the bullets are correspondingly bent. Both bullets were travelling at a moderate if not low degree of velocity
Fig. 32 is also of a retained bullet in which the fore part of the mantle is very extensively fissured and the core set free. In this the mantle has suffered severely and the leaden core to a less extent. As an apical ricochet it corresponds with the Lee-Metford shown in fig. 36.
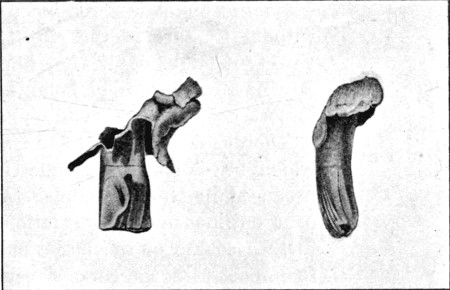 Fig. 32.
Fig. 32.
Apical Ricochet Mauser Bullet (see text). The 'mushrooming' of the core is moderate, but the destruction of the anterior part of the mantle very considerable
The deformity found in fig. 32 I met with both in retained bullets and also in those which had been fired into sand or anthills. The particular specimen figured was removed from the thigh of a patient wounded at the battle of Belmont. An irregular entry wound was situated over the internal tuberosity of the tibia, while a large fluctuating hæmatoma existed in the lower third of the thigh, at the upper part of which a hard elongated body was palpable. As was so often the case with internal hæmorrhages, the patient's temperature rose high, and on the third day the hæmatoma was incised by Major Coutts, R.A.M.C. The core of the bullet was then found in the blood cavity near the surface, but on introduction of the finger a second body was discovered entangled in the quadriceps muscle, and this proved to be the tattered mantle. I saw similar deformity produced within the body by a bullet, which, entering by a small type aperture in the left ala of the nose, struck the margin of the right malar bone, and lodged beneath the latter. The similarity of this bullet to that seen in the ricochet in fig. 32 was exact. The form[Pg 88] is of great importance both on account of the degree of laceration it effects in the track, the presence of two foreign bodies in the wound, and from the fact that it can be produced by making the bullet travel through sand or antheaps, since both the former in the shape of sandbags and the latter in their natural state so often formed the cover to men during the campaign. Bullets of 6.5 mm., such as the Krag-Jörgensen, with steel envelopes apparently break up with great ease in sand.
Fig. 33 shows a form not uncommon when the bullet comes into contact with the ribs. It is produced in bullets travelling at a low rate of velocity and striking by their side. I several times met with it when the bullet was retained, and also without fracture of the rib. In some variety it might occur after impact with any narrow margin of bone, and some importance attaches to the form, since it affords evidence as to the ease with which alterations in symmetry can be produced in Mauser bullets. Again its bent outline favours deviation in the further course of the bullet subsequent to impact with the bone, a result which I observed on more than one occasion.
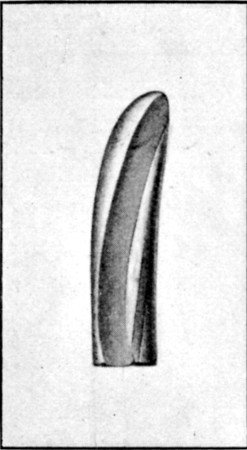 Fig. 33.
Fig. 33.
Grooved Mauser removed from anterior abdominal wall after crossing the ribs. I saw several such removed from the thoracic wall, and am inclined to attribute the grooving to impact with the margin of the ribs
Lastly, the question of actual spluttering or breaking up of the bullets must be considered. It is extraordinary into how many fragments either a Lee-Metford or a Mauser bullet may break up if it strike a hard body while travelling at a high rate of velocity. Fragmentation is exhibited in the skiagram forming the subject of plate XI. p. 194. It is somewhat remarkable how often this occurred when the short hard bones of the metacarpus were struck. With regard to the casing, the separation of small scales of the nickel plating has already been referred to; reference to the skiagrams, plates IX. and XVI., shows how readily the whole thickness of the mantle breaks up into small fragments, even when the bullet is travelling at moderately[Pg 89] low degrees of velocity, and this I believe to be a special characteristic of the thin cupro-nickel-plated steel mantles.
Any variety of cased bullet, however, when it strikes against a stone, hard ground, or a bone, may be broken into innumerable fragments. The leaden fragments occasionally show a simple fractured surface, such as is illustrated on a larger scale by the broken shrapnel bullets shown in fig. 96, p. 485. More commonly, however, the fragments, if of any size, appear torn, and if small, are mere spicules. These if of lancet shape often bury themselves in the skin only, while larger ones may penetrate deeply or even perforate. Thus, of a group of three officers standing near a stone on which a bullet struck, all were spattered about the face; most of the fragments lodged in the skin, but one perforated the concha of the ear and bruised the mastoid area, while others caused small jagged cuts. In another instance, both thighs of the patient were spattered after perforation of the clothes, and a large fragment lodged beneath the skin of the penis. A case in which larger fragments perforated and simulated type wounds has already been referred to on p. 44.
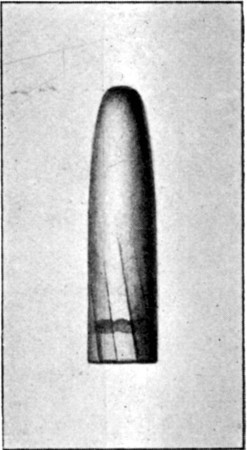 Fig. 34.—Normal Lee-Metford Bullet
Fig. 34.—Normal Lee-Metford Bullet
The above remarks apply, for the most part, to Mauser bullets only, because my experience of that projectile was far wider than of the Lee-Metford. The only deformed Lee-Metford bullets that I saw removed from the body were of the 'slipper' variety, exactly corresponding to the similarly altered Mausers, and with no fissuring of the mantle. I saw none so freely deformed as the Mausers depicted in figs. 28, 29, 31, and 32.
In spite of diligent search on several battlefields, I was unable to collect many forms of Lee-Metford ricochet, although I found many undeformed bullets. I insert here, therefore, some illustrations I obtained through the kindness of Colonel Hopton, Director of the School of Musketry at Hythe, which are of interest, and in some degree substantiate the impression[Pg 90] I formed in South Africa as to the greater stability of the Mark II. Lee-Metford bullet (fig. 34). I am aware that, as meeting a smooth target at right angles, some of these are not strictly comparable to the Mauser bullets forming the subjects of the preceding illustrations, which struck stones, and these mainly by their sides (if we except figs. 31 and 32), but they sufficiently exhibit the characters on which I wish to insist. That they support my opinion is the more probable as, with the exception of the type included above, I am under the impression that the large majority, if not all, of the Mauser bullets which struck stones fairly with their tips were broken to pieces, otherwise I must have met with some among the immense number which I saw. On the top of Tabanyama, for instance, the whole ground was littered at the time of my visit with shattered mantles and leaden cores, deformed almost past recognition.
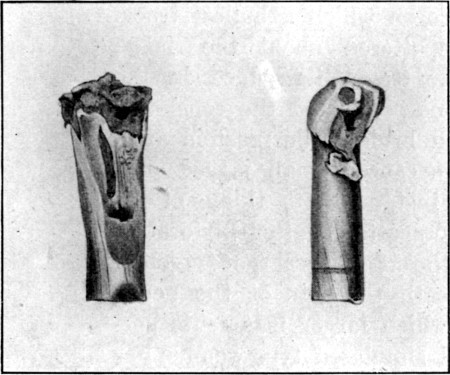 Fig. 35.—Apical Lee-Metford Ricochets.
Fig. 35.—Apical Lee-Metford Ricochets.
From Hythe targets. Tendency of cupro-nickel envelope to tear in transverse direction
The specimens depicted in figs. 35 and 36 indicate—(1) a greater malleability on the part of the mantle; thus in fig. 35 the cupro-nickel is obviously hammered and flattened out, while the fissures are neither numerous nor extensive. (2) Both bullets exhibit transverse tearing of the mantle, a common feature in Lee-Metford ricochets, of which I could offer other examples, but which I less often observed in Mauser[Pg 91] bullets. (3) Tear is the term best expressing the nature of the fissures, while fracture more nearly expresses the nature of the fissures in the Mauser mantles. (4) Fig. 36 shows a mushroomed core and split mantle, which may be compared with the similarly deformed Mauser depicted in fig. 31. I think the variation in appearance is characteristic, the fissuring of the mantle being much less extreme, while the leaden core is normal at its base in consequence of the support afforded by the more tenacious cupro-nickel mantle. With regard to complete splitting of the mantles, however, I must add that free Lee-Metford mantles are often found from bullets fired at the target or elsewhere, and Nimier and Laval figure numerous forms.[11]
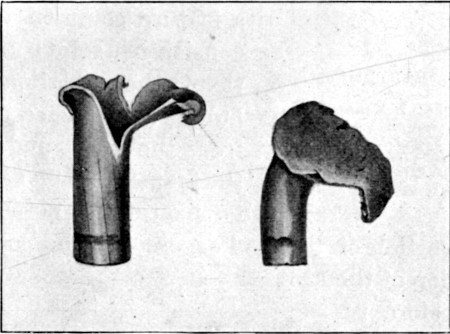 Fig. 36.—Apical Lee-Metford Target Ricochet.
Fig. 36.—Apical Lee-Metford Target Ricochet.
Well-marked 'mushrooming' of core. 'Torn' nature of the fissures in the mantle and limited extent. Compare with fig. 32
Expanding bullets.—The wounds resulting from perforation with deformed regulation bullets, such as are described above, differ for the most part by deviation from the type appearances, and a tendency to take a less favourable course on account of their increased size and of the greater degree of laceration of the tissues accompanying them. I must now pass on to the consideration of the forms of bullet especially likely to occasion those wounds spoken of as 'explosive' in character, and my remarks on these must be prefaced by a short description of the varieties which were in use during the campaign.[Pg 92]
 Fig. 37.—
Fig. 37.—
From left to right: 1. Mauser (.275); small amount of core exposed. 2. Lee-Metford (.303). 3. Lee-Metford, with larger amount of exposed core, also cupped apex. This is probably the most effective of these forms. 4. Mannlicher (.315)
These consisted in soft-nosed bullets of the Mauser and Lee-Metford patterns, Tweedie and Jeffreys modifications of the Lee-Metford and Mauser, several soft-nosed bullets of a slightly larger calibre, mostly old Mauser or Mannlicher types, and a large variety of sporting leaden bullets of larger calibre and volume. Figs. 37 and 43.
With regard to the various soft-nosed bullets of small calibre, I will first advert to a feature common to all, which consists in a solid base to the mantle. In the regulation whole-cased bullets the leaden core is inserted from the base, and the edge of the mantle is then so turned over for fixation purposes as to leave the central portion of the lead exposed. The position of the exposed portion of the core is therefore reversed in the two varieties. The small experience I had the opportunity of obtaining was all to the effect that the solid base considerably increases the stability of the mantle, and I never saw the latter seriously torn in any specimen either collected on the field or removed from the body.
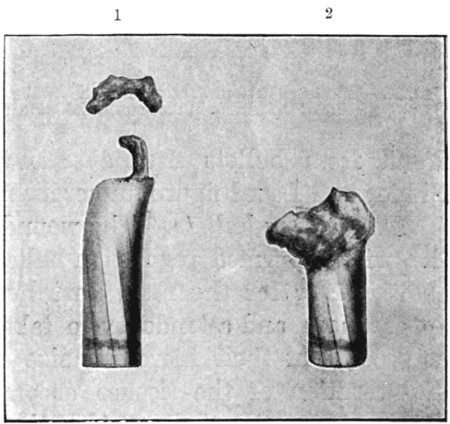 Fig. 38.
Fig. 38.
Two Soft-nosed Lee-Metford Bullets (see text). 1. Removed from forearm. 2. Removed from beneath skin of back after it had perforated the scapula. In both the velocity retained was no doubt low, and neither encountered great resistance
Fig. 38, 1, represents a soft-nosed Lee-Metford removed from just below the lesser sigmoid cavity of the ulna, after it had perforated the[Pg 93] elbow-joint. The soft nose appears to have been torn, and separated by impact with the bone, but the mantle is little altered. There can be little doubt, however, that the bullet was travelling at a comparatively low rate of velocity, since it was retained in the forearm, whence its various parts were removed by Major Lougheed, R.A.M.C. I picked up a number of similarly deformed bullets on the field. No. 2 represents a soft-nosed Lee-Metford which perforated the scapula from the front; the bullet was retained, hence again velocity cannot have been very high, and the comminution was slight. If it had passed out, a large exit wound would, however, have resulted.
 Fig. 39.—Soft-nosed Lee-Metford Mantle.
Fig. 39.—Soft-nosed Lee-Metford Mantle.
Lateral ricochet. Illustrating effect of solid base in maintaining the stability of the mantle
Fig. 39 represents a type of ricochet sometimes found on the field. In spite of a considerable amount of violence which has caused the escape of the core, the fissuring of the mantle is comparatively slight. In point of fact, the casing is, as a rule, preserved from the severe violence it suffers when complete, by the flattening and turning over of the soft nose. I am sorry I cannot append an illustration of a damaged soft-nosed Mauser, but I am of opinion that those used during the campaign were not of a very dangerous nature on account of the small amount of lead exposed. To gain the full advantage of the soft nose at least a third of the core should be exposed. No. 3, fig. 37, of a Lee-Metford, probably represents the most effective form of such bullets. I am inclined to think these bullets as a class, however, are not more dangerous to the wounded man than the regulation Mauser fired at short range, if the latter either comes into contact with bone or suffers ricochet.
The Tweedie and Jeffreys bullets come under a somewhat different category. In the Tweedie the top of the bullet is sawn off in such a manner as to flatten the tip and widen the surface of direct impact, and to expose the[Pg 94] leaden core over a small area. The general principle of the flat tip resembles that of the French Lebel bullet. In the Jeffreys modification the mantle is sawn down for about half the length of the whole mantle, the slits neither reaching tip nor base. I seldom saw these bullets removed, but they were used to a considerable extent. Fig. 40 illustrates one of Mauser calibre in the possession of Mr. Cuthbert S. Wallace. It perforated the abdomen, producing fatal injuries, but the only alteration in outline consists in slight bulging and shortening. This specimen, however, manifestly suffered but slight resistance. A somewhat general impression existed that a number of severe injuries had been produced by the Jeffreys bullets, but it was a matter of conjecture, as few of them were removed. A weekly illustration appears in the advertisement sheet of the 'Field,' showing the deformity of some of them shot into animals, which bear a strong resemblance to the Mauser figured earlier (fig. 31), and which we have seen can be produced in the human body by contact of a regulation fully cased bullet with a bone like the malar. A tendency on the part of the longitudinal slits to become caught in the rifling of the barrel militates against the use of this bullet.
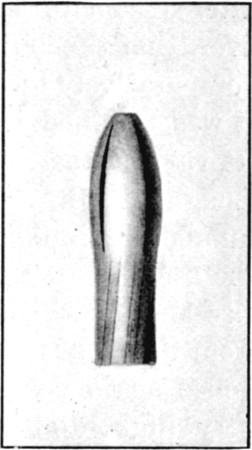 Fig. 40.—Jeffreys modification of Mauser.
Fig. 40.—Jeffreys modification of Mauser.
The bullet is in the possession of Mr. C. S. Wallace. It perforated the abdomen and caused death. The bullet is only slightly shortened by bulging at the shoulder
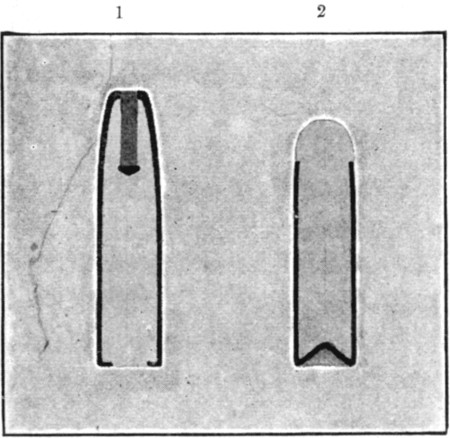 Fig. 41.
Fig. 41.
1. Section of Mark IV. Lee-Metford. Note thickness of mantle and exposed core at base. 2. Soft-nosed Mauser. Note solid base. Short pattern
Fig. 41 represents sections of the soft-nosed Mauser, and the British Mark IV. bullet, and shows the different method of[Pg 95] closure of the base. If the former remarks on the influence of the closed base in maintaining the stability of the bullet be correct, Mark IV. should be a very destructive bullet. I have no experience of its use, but I am inclined to think that here, as elsewhere, the thickness and resistance of the cupro-nickel mantle would endow it with considerable stability, unless it met with very great resistance.
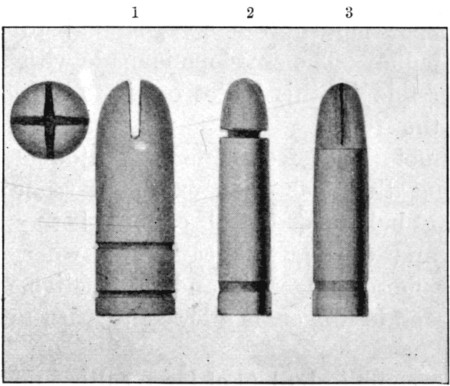 Fig. 42.
Fig. 42.
Types of Bullets tampered with by the Boers in the trenches. 1 and 3. Cross-cut tips, Martini-Henry and Lee-Metford. 2. Groove cut at base of exposed tip of Lee-Metford. Another modification of the Martini-Henry consisted in boring it longitudinally and inserting a wooden plug
In connection with the subject of soft-nosed bullets, I should mention that the Boers occasionally extemporised various modifications of them, such as are shown in fig. 42, with intent to increase the wounding power of the projectiles. I am unable, however, to give any information as to the effects produced by these, and I do not think they were often employed. The illustrations are from cartridges found in trenches which had been occupied for some time by the Boers, who had no doubt used their spare time in exercising their ingenuity on the bullets.
'Explosive' bullets of small calibre were also said to have been employed; with regard to these I can only say that I never met with any example of a hollow bullet containing explosive material.
One officer in a Colonial corps who spoke freely about them, told me he had 'sawn' them in half and found the[Pg 96] cavities, but the method of investigation he had employed seemed against the presence of any fulminant in the body of the bullets. Others based their statements on the fact that they had frequently heard the bullets burst in the air; but this is probably to be explained by the breaking up of regulation bullets on impact with stones, which makes a smart crack like a small explosion.
A clip of soft-nosed Mauser cartridges, in which a copper centre to the bullet suggested a percussion-cap, was sent home to the War Office. Colonel Montgomery has kindly furnished me with the following report on the bullet:
'The bullet contains no explosive matter, it is fitted with a hollow copper tube in the nose, similar to the ordinary "Express" bullet. The envelope is made with a solid base, which is possible in this bullet owing to the core being inserted from the front.'
One cannot help feeling some astonishment at the strong feeling that has been exhibited regarding the use of expanding bullets of small calibre, both at the Hague Conference and during this campaign, when the Martini-Henry, a far more dangerous and destructive missile in its effects at moderate ranges, is allowed to pass muster without notice.
Lastly, we come to bullets of large calibre unprovided with a mantle. The Martini-Henry is practically representative of all these, but I append a photograph of some twenty out of thirty varieties which came into my possession during searches amongst captured ammunition. Some of these were provided with a copper core to facilitate 'setting up,' others were cupped at the top, and others flattened, to increase the resistance on impact. I can say little about them except that I believe some of the forms were responsible for a considerable proportion of the most severe injuries we met with, in some of which a large and regular entry made their use certain, while a considerable proportion of them were retained. In the case of the viscera their power of doing serious damage was very striking compared with that of the bullets of small calibre. As with the small sporting bullets I think their use was often due to the fact that the sporting[Pg 97] Boer preferred to use the weapon he was accustomed to rather than his military weapon.
A considerable number of the Boers were armed with Martini-Henry rifles, and this was particularly the case with small bodies of men, rather than with the larger commandos fighting regular engagements. The Transvaal Government, moreover, had Martini-Henry rifles made as late as 1898. The Martini-Henry bullet was responsible for some of the worst fractures that came under my notice, but it is of interest to remark that its capability to do damage did not satisfy some of the Boers, who cut them as is shown in fig. 43. I cannot say what the effect of this manœuvre was, although it may have accounted for some of the wounds of the calf such as are mentioned below.
Some odd missiles were met with during the campaign; thus, at Ladysmith, I was told ball bicycle bearings were at one time in use amongst the Boers.
Anatomical characters of wounds of irregular type.—It will be seen from the above that in dealing with wounds of irregular type we have to consider those due to irregular impact of normal regulation bullets, to bullets deformed by contact with bone, to ricochet bullets, and lastly to bullets of the expanding type.
No further mention of those due to irregular impact is needful beyond what has already been said under the heading of wobbling, except to point out that, given a fair degree of velocity, these injuries may assume an actual explosive character, especially in the case of skull fractures. The description of extensive wounds accompanying comminuted fractures finds its most appropriate place under the heading of injuries to the bones, and will be there considered (Chapter V. p. 155).
'Explosive' exit apertures are, however, described as occasionally occurring in injuries involving the soft parts only. I saw no cases substantiating this belief, but several were described to me as having been met with in abdominal injuries, which terminated fatally at an early date.[Pg 98]
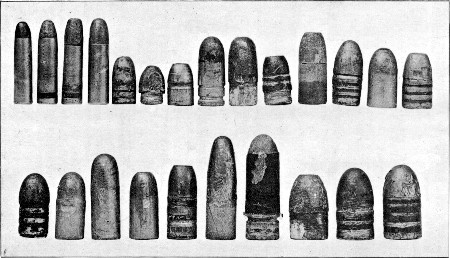 Fig. 43.
Fig. 43.
Four Soft-nosed Bullets of small calibre shown in fig. 37. Twenty large-calibre leaden carbine and rifle bullets from cartridges found in Boer arsenals. These were not very extensively used, but specimens of most varieties were at times removed from our wounded men. It will be noted that some are of great weight, and a large proportion either cupped or flattened at the apex to increase area of impact and consequent resistance. The 'express' bullet with a copper core is included in this series. It is worth remarking that all the bullets of this nature in the Pretoria Arsenal were waxed, and that the wax retained its white colour on the lead.
I still, however, incline to the opinion that the bullet in these cases had come into contact with some bone, or was one of the larger varieties of projectile. A few cases of wound of the calf did, however, come under my observation which presented fairly typical 'explosive' characters without evidence of solution of continuity of the bones. I will shortly recount two of them. In the first the exit opening was very large and on the outer aspect of the limb in the upper third. The bullet had apparently passed between the bones. Secondary hæmorrhage from the anterior tibial artery necessitated exploration of the wound and ligature of the vessel (Mr. Carré). When the wound was thus laid open no injury to the bones could be detected, but I do not consider that it could be actually excluded. In the second case a wound traversed the calf transversely, just above the centre; the exit aperture was large and ragged. Deep suppuration occurred, and the wound had to be laid open, when a fracture of the tibia without solution of continuity was discovered. I also saw one or two wounds of the buttock in which very large exit apertures were present with small entry openings; in these again it was impossible to exclude passing contact of the bullet with a part of the pelvic wall. Unfortunately in all these cases it is impossible to obtain the bullet responsible for the injury. In this relation I append a diagrammatic illustration of a peculiar wound shown to me by Mr. Hanwell. In this case a typical small entry wound was situated at the outer margin of the left erector spinæ muscle in the loin. The bullet had taken a subcutaneous course of not more than three-quarters of an inch, while the exit opening was a long shallow wound measuring 4½ in. in length by 1½ in. width. (Fig. 44.)
The wound was stated to have been received at a distance of from fifty to a hundred yards. I think we can scarcely assume that impact with the margin of the erector spinæ could have resulted in 'setting up' of the bullet, while an irregular tongue of skin at the point where the wound crossed the spines of the lumbar vertebræ did suggest possible bony contact. That the latter must have been of the slightest nature is evident, as no signs of concussion of the spinal cord were noted. I should rather be inclined to compare this case to one of gutter wound quoted on p. 56, and to assume that[Pg 100] the bullet passed so closely beneath the surface as either to entirely sever the skin, or at any rate to allow it to give way on flexion of the back on movement.
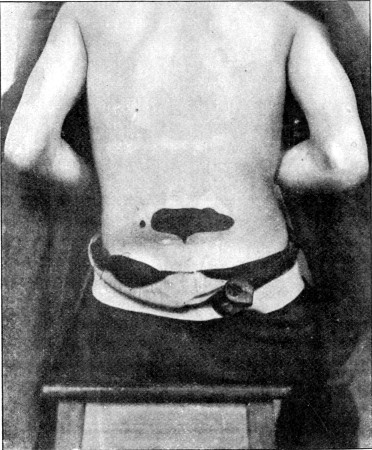 Fig. 44.
Fig. 44.
Small Circular Entry, large 'explosive' skin wound of back. Track only an inch or less in length (see text)
On the ground of the observations made in the foregoing pages it will be gathered that the opinion I formed was against either the very free use or the great wounding power of so-called expanding bullets of small calibre. I believe that a great number of the injuries which were attributed to the employment of these missiles were produced either by ricochet regulation bullets of small calibre, or by large leaden bullets of the Martini-Henry type.
Symptoms.—I very much doubt whether the general symptoms observed as the result of wounds from bullets of[Pg 101] small calibre differ in more than slight degree from those described when larger bullets were regularly employed. Great variation was met with, but I do not think a diminution in serious results in this direction corresponding to the comparatively limited nature of the direct injury to the organs or tissues can be affirmed. It is true that the immediate symptoms in many patients were amazingly slight, but after all, this has always been a feature of gunshot injuries on the field of battle and cannot be assigned a position of distinctive importance.
1. Psychical disturbance and shock.—Some remarkable instances of psychical disturbance were observed, and although perhaps in no way influenced by the calibre of the projectile, they seem worthy of note in this place. Thus a patient wounded over the cervical spine and who suffered later with a slight degree of spinal concussion emitted an involuntary shriek like that of a wounded hare on being struck; another (Martini wound), after receiving a wound of the chest, lost all sense of his surroundings for a considerable period, and occupied himself in attempts to write on a white stone lying near him on the veldt; then suddenly realising his position he was greatly bewildered in trying to account for his own action. A similar instance of preoccupation is probably offered by the dead man in the accompanying photograph (fig. 45), whose arms, forearms, and hands had evidently been in play until the actual moment of death. Again the influence of the psychical state on the actual occurrence of shock was often illustrated by the mental condition of the wounded after a battle; thus after the battles of Belmont and Graspan the patients came into hospital in excellent spirits, and minimised their injuries in the wish of rapidly regaining the front; while after the battle of Magersfontein the men were depressed and miserable, shock was more pronounced, and their sufferings were undoubtedly greater.
On the whole, however, shock was by no means a prominent symptom in the small-bore injuries of soft parts, and was possibly less than when larger bullets were the rule, and again it was often remarkably slight after the infliction of serious visceral injury. Still shock was observed in a[Pg 102] considerable proportion of the patients, and its occurrence appeared to vary under very much the same conditions as obtain in civil practice. Grades of severity depended on individual idiosyncrasy, on the degree of excitement or preoccupation at the moment of injury, and to a certain degree on the range of fire at which the injury was received.
 Fig. 45.—Note position of head, neck, and forearms in
upper figure
Fig. 45.—Note position of head, neck, and forearms in
upper figure
The last is the only special factor, and as far as my observation went it was one of considerable importance. When the soft parts only were affected, even high velocity did not produce much effect; but when to a flesh wound a severe bone fracture or injury to any part of the nervous system was added, shock might be severe or profound. The question of shock dependent on visceral injury will be considered in succeeding chapters, but it may be well to state here that the most severe shock appeared to follow injuries to the central nervous system especially to the spinal cord, fracture of the larger bones, and wounds of the abdominal and thoracic[Pg 103] viscera, the latter especially when the cardiac neighbourhood was encroached upon: hence the severity depended almost solely on the importance of the part injured and the degree of damage inflicted. I never observed instances of entire absence of shock in visceral injuries, unless the range of fire had been an especially long one.
To these remarks on constitutional shock I should add a few on the 'local shock' exhibited by the actual part of the body struck. The phenomena were of a severity I was quite unacquainted with in civil practice, and apparently were attributable to the local vibration transmitted to the whole structure of a limb or part of the trunk. In many fractures, and in some wounds of the soft parts alone, without the direct implication of any large nerve trunk, the loss of functional capacity of the limb was complete, and this condition persisted for hours or even days.
2. Pain.—As an initial symptom the occurrence of pain varied greatly with the idiosyncrasy of the patient, and according to the circumstances under which the wound was received. Some individuals are remarkably insensitive, and in these the fact of a wound being a gunshot injury in no way altered their habitual insensibility, but in persons of what may be termed the normal type in this particular great differences were observed.
When a wound was received in the full excitement of battle during a rapid advance, pain was often slight, or so trifling in degree that it was almost unnoticed; many patients did not realise that they had been struck until a second wound, possibly implicating a bone or some specially sensitive structure, was superadded. In such instances the pain was often described as 'burning' in character, or even likened to a 'sting from an insect.' Occasionally the pain was referred to a distant part; thus a man struck in the head first felt pain in the great toe, and another struck in the abdomen also felt pain in his foot only. Again in some multiple injuries, pain was only felt in the more sensitive of the regions implicated; thus a patient in whom a bullet (Martini) traversed the arm and chest emerging in the neck to again enter the chin and comminute the mandible, only felt pain[Pg 104] in the chin and first realised that he had been wounded elsewhere when he undressed. A striking instance of the entire absence of initial pain was afforded by a man shot through the buttock, the bullet then traversing the abdomen: this patient remained unaware that he had been hit until on undressing he found blood in his trousers and exclaimed: 'Why I have got this bloody dysentery!' None the less his internal injuries were sufficiently severe to lead to death during the next thirty-six hours.
Although initial pain might be slight or absent, practically all the patients complained of some of varying severity at the end of an hour after reception of the wound.
In a large proportion of the wounded, however, pain was more or less severe from the first, and this was especially the case when the men had been exposed to fire for some hours behind inadequate 'cover.' The most common descriptions under these circumstances were that they felt as if they had been struck by 'a brick,' 'a ton of lead,' or 'a sledge-hammer.'
3. Hæmorrhage.—This question is fully treated under the heading of injuries to the blood-vessels. It will suffice here to say that hæmorrhage was rarely of a dangerous nature so far as life was concerned, unless the large visceral vessels or those in the walls of serous cavities were concerned, when death was often rapid. From limb wounds, even when the largest trunks were implicated, the general tendency was to spontaneous cessation of the hæmorrhage. Consequently, except these patients were seen on the field, one seldom had to deal with serious bleeding. None the less, the condition of the patients' clothes bore testimony to a free rush immediately after the injury, and pools of blood were occasionally found where patients had lain. In nearly all cases the rush of the bullet determined the initial flow of the blood from the exit wound, and this aperture usually furnished any hæmorrhage of importance.
Diagnosis.—The only diagnostic point which it is necessary to consider in this chapter is the determination of the nature of the bullet which has caused the particular injury under observation, and this is more a matter of interest than importance.[Pg 105]
The primary indication lies in the size of the aperture of entry, which naturally varies with the calibre of the bullet employed, and the difference, except in the case of large projectiles, is not always easily determined, unless we can be sure that the impact of the bullet was at right angles. In the latter case it is possible to distinguish even between, for instance, a Lee-Metford and a Mauser wound, if the resistance likely to be offered by the part struck is kept in mind. A ricochet bullet, on the other hand, may upset all our calculations, if size alone be taken as an indication; but here the irregularity of the wound often serves to exclude one of the larger varieties as the cause. The appearances of the exit wound are less useful in determining the nature of the bullet employed, as irregularities of outline are so much more common whatever projectile may have emerged; but examination of this wound often gives us useful information as to the existence of an injury to the bones not involving loss of continuity.
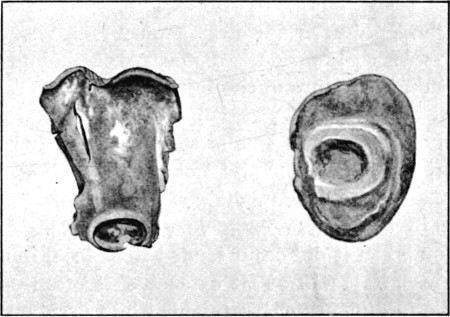 Fig. 46.
Fig. 46.
Two flattened Leaden Cores to illustrate means of determination of nature of bullet. Note ring at base. The right-hand bullet is probably a 'man-stopping' revolver bullet; it flattened against bone
Other information beyond that furnished by the external wounds may be gleaned from the presence of fragments of lead in the wound; these, if unaccompanied by portions of casing, afford some presumptive evidence of the use of an unsheathen bullet, especially if found on the fractured surface of the[Pg 106] bones; but it must be borne in mind that in the case of ricochet bullets the leaden core often perforates when entirely freed from its mantle. Pieces of the mantle again may give useful information both from examination of their thickness and composition. Lastly a naked core nearly always retains the marking on its base corresponding to the turning over of the mantle, this not being likely to suffer impact calculated to efface the groove. When this groove existed the employment of any of the soft-nosed bullets used in this campaign might be safely excluded (fig. 46).
Prognosis.—The question of general mortality amongst the wounded has already been considered (Chapter I. p. 11), and it has been shown, putting aside those dying at once on the field, or during the first twenty-four hours, that the mortality was a low one. Some other points specially dependent on the nature of the injury are, however, worthy of mention in this place. First, it has been shown, with a slight reservation as to when a wound can be considered definitely sound, that if suppuration did not occur, healing was rapid, and that many men with slight wounds were back with their regiments in the course of a very few days. Again, that suppuration when it did occur tended to be local in character; none the less, if it was at all extensive, it often proved very prolonged and difficult of treatment, while residual abscesses after apparent healing were not uncommon. In connection with this subject I may quote from Colonel Stevenson[12] an observation that limbs the subject of marked local shock are especially liable to furnish septic discharges. Parts the subject of local shock when infected show a lesser degree of vitality and power of resistance to the spread of infection than do normal ones, and if infected do badly. I think I convinced myself of this on many occasions, and also of the fact that cases of fracture in which this condition was marked were slow in consolidating. Again I am inclined to think that the bad results which sometimes followed the tying of the limb arteries were also consequent on lowered vitality, and possibly vaso-motor disturbance due to the effects of the exquisite vibratory force to which the nerves had been subjected. On[Pg 107] this account I was never anxious to hurry operations in such cases, unless obviously necessary at the moment.
The larger question of general nervous breakdown as the result of injuries from bullets of small calibre is at present hardly capable of an answer, and is so complicated by the co-existence of concurrent mental anxiety, exposure, &c., that a definite answer will always be difficult. I think there is already sufficient evidence, however, to suggest that the remote effects of many of these injuries may be far more serious than we expected at the moment, especially in the direction of sclerotic changes in the nervous system.
Treatment.—In view of the remarks on the treatment of special injuries contained in succeeding chapters, I shall confine myself here to the question of the treatment of wounds of the soft parts alone.
This consisted during the campaign in the primary application of the regulation first field dressing by one of the wounded man's comrades, an orderly, or less commonly an officer or a medical man. This dressing is composed of a piece of gauze, a pad of flax charpie between layers of gauze, a gauze bandage 4½ yards long, a piece of mackintosh water-proof, and two safety pins, enclosed in an air-tight cover. Mr. Cheatle,[13] in insisting on the importance of an immediate antiseptic dressing in the field, recommends the following. A paste contained in a collapsible tube, made up in the following proportions: Mercury and zinc cyanide grs. 400, tragacanth in powder gr. 1, carbolic acid grs. 40, sterilised water grs. 800; sufficient bicyanide gauze and wool for the dressing of two wounds, a bandage, and four safety pins; the whole enclosed in a mackintosh bag. The paste possesses the advantage over any liquid or powder, that it can be applied in any position of the body to severe wounds, and its application in the open air is not interfered with by draughts of wind. Mr. Cheatle used a similar preparation with success during the campaign.
On arrival at the Field hospital, or in some cases at the station of the bearer company, the wounds were then commonly dressed as follows: The parts around the wound[Pg 108] were cleansed with an antiseptic lotion, either solution of perchloride of mercury 1 in 1,000, or 2½ per cent. solution of carbolic acid. The wound itself was then cleansed, and a dressing of double cyanide of mercury and zinc applied. This was covered with a pad of wool and secured with a bandage. The gauze was usually wrung out in the lotion before application as a precaution against previous contamination, and the moistening was also useful as helping to ensure the dressing from subsequent displacement. It was early recognised that the drier the dressing the better, and hence anything like a mackintosh layer was carefully avoided. In some instances, antiseptic powders were employed, but they did not find much favour, and because they tended to favour slipping of the dressing, and to prevent the adhesion of the gauze dressing to the wound, they were certainly not desirable when there was any necessity for the patient to travel. In the absence of reliable water the use of antiseptic lotions was obligatory, and such is likely to be the case in most campaigns; in the present one, filtration of the thick muddy water was impossible, without a considerable expenditure of time, which could only be obtained when the hospitals were fairly stationary. I very much preferred carbolic acid lotions.
The wound having been once cleansed, or rather the surroundings of the wound, the drier the surface was kept the better; hence a too heavy or impervious dressing was not satisfactory; in point of fact, I think some of the slighter wounds in which all the dressings slipped off, and in which there was less consequent chance of the dressing being moistened with the sweat of the patient, did as well as any.
I do not think the bicyanide gauze, absorbent wool, and common open-wove bandages, together with a good supply of nail brushes, soap, and carbolic acid for the primary disinfection of the skin and the external wound, are to be greatly bettered at the present day as materials for the first permanent dressing of cases in the field. The wound itself should be carefully shielded during the preliminary cleansing of the skin by a firmly applied antiseptic pad, and then the dressing applied as above described. The one desirable improvement is some mode of ensuring the dressing being kept in good[Pg 109] position, and for this some form of adhesive covering for the gauze and wool should be devised. When the atmosphere is such as to allow of rapid drying, thin moistened book-muslin bandages would be preferable to the plain open-wove ones. The one period of danger is that of transport, and when that is over, the dressing in Stationary or Base hospitals should give no trouble.
As a rule the wounds themselves need no interference, but in some instances either the exit or entrance wounds may be in undesirable positions for purposes of asepsis, when a large opening may seem safer closed and actually sealed. I saw this method tried in a few cases, but without much success. It is one which might be of much use in Base hospitals if the patients were brought directly into them, but in the Field hospitals, in face of the rush with which the first dressings have to be done, I think it is seldom applicable, and consider the interference with the wound as rather likely to increase the danger of infection than to decrease it.
Dressings should not be too frequent; two should suffice for simple wounds with type forms of entry and exit; there is little discharge and usually no bleeding: hence the more the dry scab form of healing can be simulated the better. When a dressing needs changing from fouling of its outer parts, it is preferable to cut round the adherent part of the deep layers and apply some fresh gauze over the central scab rather than to remove it. One point should be kept in mind: the first dressing in the Field hospital seals the fate of the wound as to the chances of primary union, and hence too much care is impossible with it.
Operations in the Field hospitals were proportionately not numerous, and they should be kept down in number, as far as possible. At the same time such operations as are necessary are mostly of capital importance, such as the treatment of fractures of the skull, abdominal section, the ligature of arteries, and amputations. Of these only the first and last classes occur with any degree of frequency. In order to be prepared for these a stock of filtered water which has been boiled, and some special sterilised sponges, should be at hand if possible, also some small towels which can be[Pg 110] wrung out in antiseptic lotion. If sterilised sponges are not to be had, wool pads wrung out in carbolic lotion must be substituted.
Primary amputations bore transport badly. I saw few sent down from the front within a few days of their performance in which the flaps did not slough, or worse consequences ensue. On the other hand, if the first fortnight could be tided over at the front, they did well enough. The head cases on the other hand bore movement fairly well, provided only that asepsis was ensured.
Retained bullets are rarely suitable for removal in the rush of the first work of a Field hospital after an engagement. A short delay is of no importance, and ensures their being removed safely if necessary. With regard to the broad question of the advisability of removing them at all, it may be laid down that they should not be interfered with unless some obvious reason exists. Those most commonly calling for removal are as follows: 1. Bullets lying immediately beneath the skin or quite superficially in any region, or those which, although they have produced an exit opening, yet lie within the body. 2. Those which lie at the bottom of an infected track, or cause secondary suppuration. 3. Those causing pressure on important structures, particularly nerves. 4. Those which interfere with the movements of joints when lodged in the bones or soft tissues in close proximity, or those which lie within the articular cavity itself. Bullets sunk in the great body cavities or in positions difficult of access should never be interfered with. Retained bullets sometimes give rise to unexpected surprises; thus in a man with a retained bullet in the pelvis no steps for its removal were taken. During the man's voyage home on a transport he had an attack of retention of urine. As a catheter would not pass, he was placed in a warm bath, and shortly after passed a Mauser bullet per urethram, and thus saved himself a cystotomy.
One word may be added as to the treatment of shock when severe. Quiet in the supine position, and the administration of a small amount of stimulant, was usually all that was required. Hypodermic injections of strychnine sulph. grs. 1/30 to 1/10 were useful, and in some severe cases, especially where[Pg 111] operations were needed, saline infusions with a small amount of stimulant were made into the veins, either at the elbow, or in amputation cases into one of the large veins exposed.
The treatment of hæmorrhage is dealt with in Chapter IV.
The after treatment of simple wounds needs little comment, but bearing in mind what has been said as to the definite healing of the internal portion of the tracks, it will be obvious that in parts such as the thigh or calf, care was needed as to not commencing active work at too early a date. On the other hand, a too long period of absolute rest is also to be deprecated. The best results were obtained by careful movement and massage, commenced after the first week or ten days, according to the appearance presented by the external wound, followed by a gradual resumption of active movement. It was a striking fact that some of the patients suffering from such wounds took longer to become apparently well than many of those who had suffered visceral injuries.
[9] Loc. cit. p. 31.
[10] Loc. cit. p. 100.
[11] Loc. cit. pp. 54, 55.
[12] Wounds in War, p. 83. Longmans & Co. 1897.
[13] A First Field Dressing, Brit. Med. Jour. 1900, vol. ii. p. 668.
The small calibre of the modern bullet, and its tendency to take a direct course, naturally favour the occurrence of more or less uncomplicated wounds of the large vascular trunks, and both the nature of these wounds and the results which follow them are in some respects most characteristic.
1. Contusion or laceration without perforation.—(a)The vessel may be struck laterally, the injured portion then forming a part of the bounding wall of the wound track, or (b) one or more layers of the vessel wall may be destroyed over a limited area. Given primary union, these conditions are only of importance in so far as subsequent contraction of the lumen of the vessel may result from implication in the neighbouring cicatrix. One of the most striking features of the wounds as a whole was seen in the hair-breadth escapes of the large limb vessels with no subsequent ill effects, and such injuries were seen in every situation.
In a certain proportion of wounds in close proximity to large vessels, however, a diminution of the normal calibre of the arteries was observed, either shortly after the injury or later in the advanced stages of cicatrisation. As an example of early obstruction, the following may be related. A Mauser bullet passed from the inner side of the thigh across the neck and great trochanter of the femur beneath the femoral vessels, and probably struck and grooved the bone, since the aperture of exit was large and irregular, some 3/4 of an inch in diameter. One week later no pulse was palpable in either anterior or posterior tibial arteries at the ankle, and[Pg 113] pulsation which was strong in the common femoral artery was very weak in the superficial femoral. Slight fulness existed in the hollow of Scarpa's triangle, but not sufficient to make any serious difference in the contour of the two limbs. No thrill or abnormal murmur was discoverable. There was no œdema of the limb, which was also normal in temperature. The patient was kept at rest in the supine position for three weeks, during which time the tibial pulses gradually returned. Three weeks later he was invalided home, the pulses, however, still remaining considerably smaller than normal.
In the advanced stages of cicatrisation narrowing of the lumen of the trunk vessels was far from uncommon, especially in cases of wounds of the arm crossing the course of the brachial artery; in many of these the radial pulse was diminished almost to imperceptibility. How far this condition may prove permanent there has been little opportunity of judging; nor as to the possible ultimate weakening of the vessel wall and the development of a secondary aneurism has time allowed the acquisition of experience. In the light of the observation of so many cases in which large vessels were wounded without the occurrence of severe hæmorrhage, either primary or secondary, it is impossible to be certain whether some of the cases of arterial obstruction were not secondary to perforating lesions of the vessels.
Pressure on, or minor lesion of the vessel was sometimes evidenced by the development of a murmur, as in the following case. A Mauser bullet entered immediately within and below the left coracoid process, and emerged at the back of the arm at its inner margin, 2½ inches above the junction of the right posterior axillary fold. During the first week dysphagia and some pain and soreness in the episternal notch, with pain and difficulty of respiration, were noticed. Eight weeks later no trouble with the pharynx or œsophagus remained, but a short sharp systolic murmur was audible over the first part of the left axillary artery, which could be extinguished by pressure on the subclavian; the radial pulse was normal.[14]
When primary union failed or was prevented by infection[Pg 114] and suppuration, lesions, although incomplete, of the vessel coat naturally frequently gave rise to secondary hæmorrhage.
2. Perforation of the vessels.—(a) This may be oblique or transverse to the long axis of a trunk; when the vessel is impinged upon laterally, an oval or circular notch, as the case may be, is produced; or (b) the bullet may strike more or less in the centre of the vessel, perforating both in front and behind, while lateral continuity is maintained; (c) beyond these degrees a vessel may, of course, be completely divided. Cases of notching of the vessel will be referred to under the heading of traumatic aneurism; those of perforation under that of aneurismal varix and varicose aneurism, the perforations in these cases affecting a parallel artery and vein.
1. Hæmorrhage.—The fact that hæmorrhage was not a prominent feature in the wounds received during this campaign can scarcely be regarded as an experience confined to injuries caused by bullets of small calibre. The same observation was often made in the case of larger bullets in old days, and the absence of severe hæmorrhage has previously been regarded as a special characteristic of gunshot wounds. None the less, as high a proportion as 50 per cent. of deaths occurring on the field in earlier days has been ascribed to this cause.
Unfortunately no new facts can be furnished on this point, although a few cases of rapid death from primary hæmorrhage will be found recounted under the heading of visceral injuries. Beyond these the general evidence offered by observations on men brought in from the field with vascular injuries, was opposed to the frequent occurrence of death from hæmorrhage, at any rate of an external nature. This subject will be dealt with under the classical three headings of primary, recurrent, and secondary hæmorrhage.
Primary hæmorrhage.—A marked distinction needs to be drawn between external and internal hæmorrhage. External hæmorrhage from the great vessels of the limbs, or even of the neck, proved responsible for a remarkably small proportion of the deaths on the battlefield. This statement[Pg 115] may be made with confidence, since it is not only my own experience, but coincides with what I was able to glean from many medical officers with the Field bearer companies. It is, moreover, supported by the facts that cases in which primary ligature had been resorted to were extremely rare at the Base hospitals, while, on the other hand, traumatic aneurisms and aneurismal varices of any one of the great trunks of the neck and limbs were comparatively common. Again, primary amputation for small-calibre bullet wounds, except when complicated by severe injury to the bones, was so rare as to render more than doubtful the frequent occurrence of severe primary hæmorrhage on the field. Only one case of rapid death due to bleeding from a limb artery was recounted to me. In this a wound of the first part of the axillary artery proved fatal in the twenty minutes occupied by the removal of the patient to the dressing station. The amount of hæmorrhage in many instances was no doubt checked by the application of pressure at the time of the first field dressing; but it can scarcely be argued that such dressings as were applied were of sufficient firmness to control bleeding from such trunks as the brachial, femoral, or carotid arteries.
The spontaneous cessation of hæmorrhage is rather to be ascribed to the special method of production and the consequent nature of the wound. The lesions were the result of immense force strictly localised in its application, which might well induce very complete and rapid contraction of the vessel wall; while the track in the soft parts was not only narrow, but also lined by a thin layer of tissue possibly so devitalised superficially as to specially favour rapid coagulation of the blood. Beyond this the tracks were often sinuous when the position of the limb at the time of reception of the injury was replaced by one of rest. The influence of mere narrowness of the track is illustrated by classical experience in the development of aneurismal varices after stabs by knives or bayonets; and in the injuries under consideration the frequent development of large interstitial hæmorrhages into the tissues of the limbs indicated that blood does not readily travel along the wound track. It was noteworthy that when hæmorrhage did occur it was most free from, or often limited[Pg 116] to, the wound of exit. This is due to the direction of the active current set up by the rush of the bullet through the tissues. The mechanical factor is, no doubt, the most important.
Control of primary hæmorrhage from a wounded vessel by the impaction of a foreign body was of much less frequent occurrence than appears to have been the case with the older bullets. I saw a case in which, on removal of a fragment of shell (Mr. S. W. F. Richardson), very free hæmorrhage occurred from a wound of one of the circumflex arteries of the thigh, but not a single one in which a similar result followed the extraction of a bullet of small calibre. The comparative infrequency of retention of modern bullets is probably one of the main elements in this relation. A very curious instance of provisional plugging of a wound in the upper part of the brachial artery by an inserted loop of the musculo-spiral nerve was related to me by Mr. Clinton Dent. This instance must, I think, be regarded as an accident definitely dependent on the size and outline of the bullet and on the nature of the force transmitted by it to neighbouring structures.
While, however, deaths from external primary hæmorrhage were rare, a considerable number resulted from primary internal hæmorrhage. In some of these, injury to the largest trunks in the thorax or abdomen led to an immediately fatal issue; in others wounds of the large visceral arteries, as of the lungs, liver, or mesentery, were scarcely less rapid in their results. In such cases the potential space offered by the peritoneal or pleural cavities favours the ready escape of blood from the wounded vessel, while the tendency of the blood effused into serous cavities to rapid coagulation is notably slight. Beyond this the comparative deficiency in direct support afforded by surrounding structures to vessels running in the large body cavities is also an important element in their behaviour when wounded.
These remarks receive support from the observation that few, if any, patients survived an injury to the external iliac vessels within the abdomen, while the remarkable instances of escape from fatal hæmorrhage from large vessels recorded below (cases 1-19) indicate that the mere size of a wounded vessel is not to be regarded as the sole factor in prognosis.[Pg 117]
Recurrent hæmorrhage was occasionally met with both in the case of the limb and trunk vessels. In the limbs it often necessitated ligature of the artery. I saw several cases in the lower extremity where recurrent hæmorrhage on the second or third day was treated by ligature of the femoral or popliteal artery, and it also occurred during the course of development of one of the carotid aneurisms recounted below. On two occasions I saw rapid death follow recurrent abdominal hæmorrhage; in one I was standing in a tent when a man who had been wounded the day before suddenly exclaimed: 'Why, I am going to die after all.' The appearance of the man was ghastly, and on examining the abdomen it was found greatly distended, and with dulness in the flanks; the patient expired a few minutes later. Another example of recurrent abdominal hæmorrhage is related in case 169, p. 432.
Secondary hæmorrhage.—In simple wounds of the soft parts by small-calibre bullets this was decidedly rare. In wounds complicated by fractures of the bones, especially when they exhibited the so-called 'explosive' character, secondary hæmorrhage was not uncommon, and this not necessarily in conjunction with infection and suppuration.
In the chapter on fracture some remarks will be found on the prolongation of healing often observed in the exit portion of the wound track, which is explained by the well-known fact that, given an aseptic condition of the wound, sloughs of tissue separate very slowly. Secondary hæmorrhage in these cases is due to lesions of the vessel short of perforation, but severe enough to so lower the vitality that local gangrene of the wall occurs. In such instances hæmorrhage most usually occurred on the tenth to the fourteenth day, but occasionally still later. In one instance of ligature of the anterior tibial artery for such hæmorrhage three-quarters of the whole lumen of the vessel had been devitalised. The resemblance of some cases of secondary hæmorrhage of this class to those occasionally observed after amputation, and due to accidental non-perforative injury of the artery at the time of operation above the point of ligature, was very striking.
In other cases secondary hæmorrhage was the result of perforation of the vessel by a sharp spicule of bone, but in[Pg 118] the large majority sepsis and suppuration were the cause. Naturally therefore the accident was commoner in the more severe kinds of wound, and in those caused by large bullets or fragments of shell. The symptoms in nearly all cases were the classical ones of repeated small hæmorrhages followed by a sudden copious gush.
The forms of secondary hæmorrhage, however, which afforded most interest were the interstitial and the internal, mainly on account of the scope they allowed for diagnosis.
Characteristic examples of internal secondary hæmorrhage are furnished by cases of chest injury accompanied by hæmothorax and fully dealt with under that heading (Chapter X.). Cases of interstitial secondary hæmorrhage are also described under the heading of traumatic aneurism and abdominal injuries (No. 194, p. 445). It therefore suffices here merely to remark on the diagnostic difficulties the condition gave rise to. These mainly depended upon the elevation of general bodily temperature by which the hæmorrhage was often accompanied. Further evidence of the condition was furnished by the development of local swellings, or physical signs indicative of the collection of fluid in a serous cavity. These signs developed rapidly, and the rise of temperature was sudden and decided enough to suggest commencing suppuration. In several cases incisions were made under the supposition that this had already occurred.
The fever accompanying blood effusions was generally a somewhat special feature in the wounds of the campaign. At first bearing in mind that in every case a track, even if closed, led from the surface to the effused blood, one was disposed to suspect an infection of the clot of a somewhat innocuous nature. The absence of subsequent suppuration, however, was definitely opposed to this view, and suggested that the fever resulted from absorption of some element of the blood, possibly the fibrin ferment, or some form of albumose. A pronounced illustration was in fact afforded of the evanescent rise of temperature usually the accompaniment of simple fractures in the case of the limbs, and of the more marked rise not uncommon in cases of traumatic blood effusion into the peritoneal cavity, or when the pleuræ or joints[Pg 119] were the seats of the mischief. In the case of interstitial hæmorrhages I only remember to have seen fever of such marked continued type in the subjects of hæmophilia with recent effusions, although one is of course acquainted with it in a less pronounced form as a result of hæmorrhage into operation wounds.
In primary interstitial hæmorrhages a similar continued rise of temperature was also common, and I cannot perhaps better illustrate its character than by the brief relation of two instances.
In a patient wounded at Kamelfontein the bullet entered four inches below the acromion, pierced the deltoid, splintered the humerus, and crossed the axilla. A large blood extravasation developed in the axilla, accompanied by cutaneous ecchymosis extending halfway down the arm. There was no perceptible pulsation in either the brachial or radial artery, but the limb was warm. There was partial paralysis of the parts supplied by the ulnar and musculo-spiral nerves and complete loss of power and sensation in the area of distribution of the median nerve. Six months later the radial pulse was still absent in this patient, but there was no sign of the development of an aneurism.
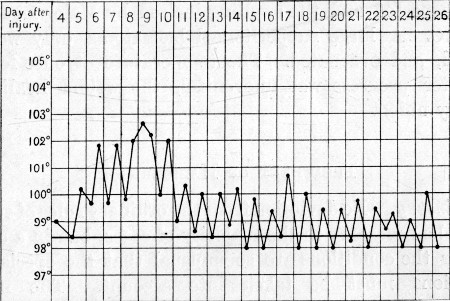 Temperature Chart 1.
Temperature Chart 1.
Axillary Hæmatoma. Shows range of temperature during process of absorption and consolidation without suppuration
The accompanying temperature chart is characteristic.[Pg 120] The blood effusion gradually gained in consistency and underwent steady diminution in size. No suppuration occurred.
The median paralysis was found to be accompanied by the inclusion of the nerve in a sort of foramen of callus, when the patient was explored at a later date by Mr. Ballance.
In a patient wounded at Paardeberg, a Mauser bullet entered by the left buttock, pierced the venter ilii, traversed the pelvis, and emerging at the brim of the latter, crossed the back, fractured the spine of the fourth lumbar vertebra, and escaped below the twelfth right rib. The track suppurated where it crossed the back, but the man did well until the twentieth day, when a swelling developed in the left iliac fossa and the general temperature rose to 102°. An abscess was at once suspected and the swelling incised by Major Lougheed, R.A.M.C. A large subperitoneal hæmatoma only was discovered, and evacuated. The temperature at once fell and the after progress was uneventful, the wound healing by primary union.
Primary.—No deviation from the ordinary rules of surgery should be necessary in the majority of cases, but in a certain number the conditions are so unusual that the special considerations must be taken into account. The natural tendency to spontaneous cessation of primary hæmorrhage in small-calibre wounds is the first of these. Experience has shown that often mere dressing, or at any rate slight pressure, suffices to efficiently stanch immediate bleeding. Although, however, immediate control is to be obtained by such means, the cases of traumatic aneurism of every variety related in the next section show that the ultimate result is in many such cases by no means satisfactory.
Under these circumstances it may be said that the classical rule of ligation at the point of injury should never be disregarded. Against this, however, certain objections may be at once raised; thus in many cases both artery and vein need ligature, a consideration of much importance in the case of such vessels as the carotid and femoral arteries. Again in[Pg 121] many of the injuries to the popliteal artery the wound directly communicated with the knee joint, a complication which, while it may be disregarded in civil practice, must take a much more important place in the circumstances under which many operations in military surgery are performed.
On the whole, it seems clear that the military surgeon must be guided by circumstances, since it may be far better to risk the chances of recurrent hæmorrhage, or the development of an aneurism or varix, all of which are amenable to successful treatment later, than those of gangrene of a limb or softening of the brain. As a general rule, therefore, on the field or in a Field hospital, primary ligature of the great vessels is best reserved for those cases only in which hæmorrhage persists, while in those in which spontaneous cessation has occurred, or in which bleeding is readily controlled by pressure, rest and an expectant attitude are to be preferred.
A word must be added as to the objections to distant proximal ligature for primary or recurrent hæmorrhage. In some situations this may be unavoidable, and it is sometimes successful, but none the less it is opposed to all rules of good surgery and a most uncertain procedure. It leaves the patient exposed to all the risks attendant on the employment of simple pressure. In one case which I saw, the third part of the subclavian artery had been ligatured for axillary bleeding; secondary hæmorrhage, as might have been expected, occurred, and that as late as five weeks after the operation. In another case ligature of the femoral artery for popliteal hæmorrhage was followed by the development of a traumatic aneurism in the ham.
Secondary.—In secondary hæmorrhage the treatment to be adopted depends upon the nature of the case. When the wound is aseptic, and bleeding the result of the separation of sloughs, local ligature is the proper treatment, and this was often successfully adopted, especially in the case of such arteries as the tibials. In septic cases, on the other hand, it is usually far better if possible to amputate, unless the general state of the patient and the local conditions are especially favourable.
When neither amputation nor direct local ligature is[Pg 122] practicable, proximal ligature may be of use. Sometimes this may be obligatory in consequence of the difficulties attendant on direct local treatment. I saw a few cases successfully treated in this manner: in one the common carotid was tied (Mr. Jameson) for hæmorrhage from an arterial hæmatoma in connection with the internal maxillary artery. Although ligature of the external carotid would perhaps have been preferable, the result was excellent. When even this expedient is impracticable, local pressure is the only resort.
Lastly, as to the treatment of secondary interstitial blood effusions, I believe the best initial treatment is the expectant. If interference is needed, it is much more likely to be satisfactory the more chronic the condition has become, since the source of the bleeding may be impossible to discover. I never saw a patient's life endangered by the amount of such hæmorrhage, but if this should seem to be likely, local treatment is of course unavoidable. In several cases quoted below, incision and evacuation were followed by excellent results; in any such operation too much care to ensure asepsis is impossible.
The experience of the campaign fully bears out that of the past as to the steady increase of the number of aneurisms from gunshot wounds in direct ratio to diminution in the size of the projectiles employed. Every variety of traumatic aneurism was met with, and most frequently of all, perhaps, aneurismal varices and varicose aneurisms. While so experienced a military surgeon as Pirogoff could say, in 1864, that he had never seen a case of aneurismal varix, every young surgeon lately in South Africa has met with a series. Again, although the condition is a well-known one, it has been rather in connection with civil life; for the great majority of recorded cases were the result of stabs or punctured wounds such as are liable to be received in street brawls, or as a result of accidents with the tools of mechanics. Thus of ninety cases collected by K. Bardeleben in 1871, only 12 or 13.33 per cent. were the result of gunshot wound.[Pg 123]
False traumatic aneurism or arterial hæmatoma.—This condition was met with comparatively frequently, and bears a very close relation to that already described under the heading of interstitial hæmorrhages. The latter might almost have been included here, since the difference between the two conditions depended merely on the size of the vessels implicated. The exact correspondence in the period of development of some of the arterial hæmatomata, and of the occurrence of the aseptic form of secondary hæmorrhage, also explains the pathology of the two conditions as identical; except that in the former the effused blood is retained in the tissues, while in the latter it escapes externally. The history of these cases was uniform and characteristic. A wound of the soft parts, or sometimes a fracture, was accompanied by a certain degree of primary interstitial hæmorrhage, which might or might not have been associated with external bleeding. A hæmatoma resulted in connection with the wounded vessel, the general tendency in the effusion being to coagulation at the margins and subsequent contraction. Meanwhile the opening in the artery became more or less securely closed by the development of thrombus, and possibly by retraction of the inner and middle coats of the vessel. With the return of full circulatory force as shock passed off, or with the resumption of activity and consequent freer movement of the limb, the temporary thrombus became washed away. The newly formed wall of soft clot bounding the effusion proved insufficient to withstand the full force of the blood pressure, and extension of the cavity resulted. In the more rapidly developing hæmatomata, temporary pressure by the effused blood on the bleeding vessels was also, no doubt, a common explanation of temporary cessation of increase in size.
A diffuse soft fluctuating swelling, sometimes accompanied by pulsation, but oftener without, developed, and not uncommonly diffusion was accompanied by some discoloration of the surface and elevation of the general temperature. Such arterial hæmatomata commonly developed from ten days to three weeks after the original wound. A few examples will suffice.
(1) A patient wounded at Elandslaagte was sent down to Wynberg. The antero-posterior wound in the upper third of the[Pg 124] arm was healed, but a month after the injury a large fluctuating arterial hæmatoma developed in the axilla and upper third of the arm. This was incised (Colonel Stevenson) and a wound of the axillary artery in its third part discovered, and the vessel ligatured. The patient made an excellent recovery.
(2) A patient received a wound at Doornkop which traversed the calf in an obliquely antero-posterior longitudinal direction. Three weeks later a soft fluctuating swelling developed at the inner margin of the tendo Achillis occupying the lower third of the leg. Neither pulsation nor murmur was detected. There was anæsthesia in the area of distribution of the posterior tibial nerve. No tendency to further increase was observed, and operation was postponed. The temperature was normal.
(3) An Imperial Yeoman was struck at Zwartskopfontein at a range of one hundred yards. The man rode four miles on his horse after being hit, but the horse then fell and rolled over him twice. The man was treated successively in the Van Alen, Boshof, and Kimberley Hospitals, and from the last he was sent to Wynberg which place he reached on the twenty-third day. When admitted into No. 2 General Hospital the wounds of type form and size (entry, in posterior fold of axilla; exit, 1½ inch below junction of anterior fold with arm) were healed. The whole upper arm was swollen and discoloured, while an indurated mass extended along the line of the vessels into the axilla. This was considered a blood effusion; it was not obviously distensile, and pulsation was very slight. The brachial radial and ulnar pulses were absent. A fluctuating swelling was present along the anterior border of the deltoid. There were some signs of nerve contusion, but no paralysis, beyond tactile anæsthesia in the area of distribution of the median nerve.
Four days later little alteration had been noticed beyond a tendency to variation in firmness of the different parts of the swelling. On the thirty-first day considerable enlargement was observed. This enlargement, together with continued rise of temperature, aroused the suspicion of suppuration, and an exploratory puncture with a von Graefe's knife was made by Major Lougheed, R.A.M.C., after consultation with Professor Chiene. Blood clot first escaped, followed by free arterial hæmorrhage. The incision was enlarged while compression of the third part of the subclavian was maintained; a large quantity of clot was turned out, and an obliquely oval wound half an inch in long diameter was found in the axillary artery. Ligatures were applied above and below the opening between the converging heads[Pg 125] of the median nerve. The veins were not damaged. The wound healed by first intention. On the twelfth day a feeble radial pulse was perceptible, and shortly afterwards the man left for England, diminished median tactile sensation being the only remnant of the original symptoms.
(4) A private of the 2nd Rifle Brigade was struck while doubling at Geluk, at a range of one hundred yards. The Mauser bullet entered four inches above the upper border of the left patella, internal to the mid line of the limb, and escaped in the centre of the popliteal space. The man lay in a farmhouse during the night and bled considerably from both wounds. He did not fall when struck, but could not walk. He was sent to No. 2 General Hospital in Pretoria. On arrival there the external wounds were scabbed over, and a large tumour existed beneath the entrance wound. There was much discoloration from ecchymosis, but no pulsation could be detected. The posterior tibial pulse was good. At the end of ten days pulsation became marked both in the front of the limb and in the popliteal space. There were no symptoms of nerve injury. On the thirteenth day an Esmarch's bandage was applied and Major Lougheed laid the tumour open opposite the opening in the adductor magnus. Much clot was removed, and both artery and vein, which were found divided in the adductor canal, were ligatured.
The foot remained very cold for the first twenty-four hours, but otherwise progress was satisfactory, the wound healing by first intention. No pulsation was palpable in the tibials at the end of a month.
For the last two cases I am very much indebted to Major Lougheed. I am glad to include them, as they illustrate one or two points of special importance. No. 3 shows the tendency to variation in the tension and firmness of the tumours, the tendency to primary contraction of the sac, followed by diffusion, and the rise of temperature often accompanying the latter occurrence. This is of great interest in relation to the similar rise of temperature seen with the increase of hæmorrhage in cases of hæmothorax. For purposes of comparison, the progress may well be considered alongside of that in the case related on p. 119, in which the wounded vessel was probably also the main trunk itself.
No. 4 differs from any of the others in depending on a complete division of a large artery and vein. The development[Pg 126] of the hæmatoma was consequently more rapid and continuous. Another point of interest was the maintenance of pulsation in the tibial vessels, in spite of complete solution of continuity in the parent trunk. That this was independent of the collateral circulation seems evident from its complete disappearance and slowness of return after ligation of the wounded vessels.
Prognosis and treatment.—The treatment in these cases is sufficiently obvious, and consists in direct incision and ligature of the wounded vessels. The cases related show the success with which this procedure was attended, since uniformly good results were obtained. When possible, an Esmarch's tourniquet should be applied in the case of the lower limb. In the upper, compression of the subclavian is necessary during interference with axillary hæmatomata, combined with direct pressure on the bleeding spot after the clot has been removed. In the case of the arm, digital compression is always to be preferred, in view of the well-known danger of damage to the brachial nerves from the tourniquet.
Proximal ligature is always to be avoided. It is inadequate, and proved more dangerous as far as the vitality of the limb was concerned, the latter point probably depending on the interference with the collateral circulation by pressure from the extravasated blood, which is unrelieved by the operation. I know of at least two cases of gangrene which occurred consecutively to proximal ligature of the femoral artery for this condition.
True traumatic aneurisms.—The cases met with differed so little from those seen in ordinary civil practice, that but slight notice of them is necessary. They differed from the last variety mainly in the more localised nature of the tumour, the greater firmness of its walls, and the more pronounced expansile pulsation. The development of this form of aneurism was probably influenced by several circumstances, such as the more complete rest secured for the patient, the locality in the limb as affecting movement of the spot in the vessel actually wounded, the size of the opening in the vessel, and the degree of support afforded by surrounding structures. (Examples are furnished by cases 6-9.)[Pg 127]
Under the influence of rest, all that I saw tended to contract and become firmer, and they so far resembled spontaneous aneurisms as to be readily cured by proximal ligature of the artery. The ideal treatment no doubt consists in local incision and ligature on either side of the wounded spot, with or without ablation of the sac. The choice of direct or proximal ligature in any case depends on the position of the aneurism, and the ease with which the former operation can be carried out. In all these cases a very great advantage in the localisation and diminution of the tumours was gained by postponing interference until they became stationary. I need scarcely add that any evidence of diffusion indicated immediate operation. The preference of direct or proximal ligation will probably, to a certain extent, always depend on the personal predilection of the surgeon, but while proximal ligature has often given good immediate results during this campaign, it cannot be with certainty decided whether the patients are definitely protected from the dangers of recurrence.
Reference to cases 7 and 9 as illustrating the possible spontaneous cure of traumatic aneurisms is of great interest.
I saw a number of cases successfully treated by proximal ligature; also a number where continuous improvement followed rest, and which were sent home for further treatment. None of these demand any special mention.
One case of a very special nature, which terminated fatally, is of great interest:—
(5) In a man wounded at Belmont the bullet entered the second left intercostal space and was retained in the thorax. He was sent directly to the Base and came under the care of Mr. Thornton at No. 1 General Hospital, Wynberg. Signs of wound of the lung developed in the form of hæmoptysis and left hæmothorax. The left radial pulse was almost imperceptible.
The entry wound did not close by primary union, and three weeks later an incision was made into the chest in consequence of the presence of fever, progressive emaciation, and weakness. Breaking down blood clot was evacuated: general improvement followed, and the radial pulse increased considerably in volume.
A fortnight later sudden severe hæmorrhage occurred from the external wound, and the man rapidly collapsed and died. At the post-mortem a traumatic aneurism the size of an orange was[Pg 128] found in connection with an oval wound in the first portion of the left subclavian artery which admitted the tip of the forefinger.
This case is noteworthy as an illustration of the magnitude of an artery which can be wounded without leading to rapid death from primary hæmorrhage, even when in communication with a serous sac, and still more as emphasising the importance of weakening of the radial pulse as a sign in connection with a wound of the upper part of the chest on the left side. It is somewhat surprising that this sign was not marked in two cases (Nos. 13 and 14, p. 140) recorded below, in which the innominate and right carotid arteries respectively were probably perforated.
(6) Traumatic popliteal aneurism.—Wounded at Modder River. Entry (Mauser), over centre of tibia 1 inch above the tubercle. Exit, about centre of popliteal space. No hæmorrhage of any importance occurred from the wound, but there was a typical hæmarthrosis, which subsided slowly. Twelve days after the injury a pulsating swelling the size of a hen's egg, to which attention was drawn on account of pain, was noted in popliteal space. The pulsation extended upwards in the line of the artery some 3 inches. The limb was placed on a splint and treated by rest, and a month later the aneurism had decreased to one half its former size, the wall having greatly increased in firmness. Pulsation was easily controlled by pressure above the tumour; there was no thrill present, but a high-pitched bellows murmur. The patient was sent home on February 1.
When admitted at Netley the patient came under the care of Major Dick, R.A.M.C., who ligatured the popliteal artery on the proximal side by an incision in the line of the tendon of the adductor magnus. The aneurism then consolidated.
(7) Traumatic popliteal aneurism.—Wounded at Magersfontein. Entry (Mauser), centre of patella. Exit, centre of popliteal space; the knee was bent at the time it was struck. There was considerable primary external hæmorrhage, and so much blood collected in the knee-joint that it was aspirated. On the eighth day secondary hæmorrhage occurred from the exit wound and the femoral artery was tied in Hunter's canal. No further hæmorrhage occurred, but at the end of three weeks feeble pulsation was[Pg 129] palpable in the popliteal space, suggesting an aneurism; the latter decreased and the patient was sent home apparently well.
(8) Traumatic axillary aneurism.—Wounded at Karree. The bullet entered 2½ inches below the acromial end of the right clavicle and emerged over the 9th rib in the posterior axillary line. The Mauser bullet was found in the patient's haversack. Both apertures were of the slit form, and healed per primam. Three weeks later at Wynberg a large arterial hæmatoma which pulsated was noted in the axilla. Signs of injury to the musculo-spiral nerve were also observed. The tumour altered little, but a fortnight later Major Burton, R.A.M.C., cut down upon it through the pectorals. The aneurism was of the third part of the axillary artery, and a ligature was applied at the lower margin of the pectoralis minor. The wound healed by primary union and the aneurism rapidly shrank. The patient left for England a month later; the musculo-spiral paralysis was improving. I am indebted to Major Burton for the notes of this case.
(9) Traumatic popliteal aneurism.—Wounded in Natal. Entry (Mauser), immediately above head of fibula. Exit, immediately inside semi-tendinosus tendon at level of central popliteal crease. Fulness but no pulsation was noted at end of three weeks; seven days later pulsation was evident, and an aneurism the size of a pigeon's egg, with firm walls, became localised and palpable. It gave rise to no symptoms, and patient refused operation during the three weeks he remained in hospital. The aneurism continued to contract, and the patient was sent home. The aneurism has since spontaneously consolidated.
Aneurismal varix and varicose (arterio-venous) aneurism.—Uncomplicated cases of aneurismal varix, as might be expected, were less common than those in which the arterio-venous communication was accompanied by the formation of a traumatic sac. The initial lesion accountable for each condition was, however, probably identical, and dependent on the passage of a bullet of small calibre across the line of large parallel arteries and veins. Thus, obliquely coursing antero-posterior wounds of the neck produced carotid and jugular varices; vertically coursing tracks laid the subclavian vessels in communication; antero-posterior tracks the brachial, popliteal, and lower part of the femoral; and transverse tracks, the vessels of the calf and forearm. Given an arterial wound, the mode of development of the aneurismal sac in no way[Pg 130] differs from that of the ordinary traumatic variety; the main point of interest, therefore, is to seek an explanation of the causes which may restrict the ultimate result to the formation of a pure aneurismal varix. The explanation is possibly to be found in some of the following circumstances.
Size, position, and symmetry of the vascular wound.—It seems scarcely necessary to insist on the calibre of the projectile, since this alone determined the frequency of these conditions, but it must be borne in mind that in the diameter of the bullets, classed as of small calibre during this war, a range of from 6.5-8 mm. existed. In the case of both the Krag-Jörgensen and Mauser, the shape of the bullet also was better adapted to pure perforation of the vessels. I saw no case of arterio-venous communication in which a larger bullet than one of the four types chosen had been responsible for the primary injury, but a difference of 1½ mm. in calibre in the small projectile might well determine the division, the pure and symmetrical perforation of the two vessels, or the giving way of one side, so that they were deeply notched instead of perforated.
Such positive evidence as was afforded by operation as to the exact condition of the vessels in two cases of femoral arterio-venous aneurism was, that in either case a clean perforation existed.
It is improbable that notching of the two vessels can primarily produce a pure varix, although it may result in the formation of an arterio-venous aneurism, especially if the bullet should have passed between the two vessels in such a way as to notch the contiguous sides. It is impossible to say, in any given case, what the result of secondary contraction of a sac produced in this manner may be in the determination of the ultimate relation of the vessels. In many of the cases clinically designated pure varix, the remains of such a sac may still actually persist. In the case also of pure perforation of the vessels, it is difficult to believe that a localised blood cavity has not originally existed. Given complete division of the vessels, as far as my experience went, arterial hæmatoma was the uniform result.
Under these circumstances I am inclined to believe that a[Pg 131] symmetrical perforation of both vessels is the most common precursor of either condition; that the pure varix is the rarer and less likely result, and that its formation is dependent mainly on certain anatomical conditions. The most important of these conditions are the proximity and degree of cohesion of the two vessels, the comparative spaciousness or the opposite of the vascular cleft, and the degree of support afforded by surrounding structures.
Thus, the close proximity of the popliteal artery and vein, together with the particularly firm adhesion which exists between the vessels, probably favours the formation of a varix; again, a varix more readily forms if the femoral artery and vein are wounded in Hunter's canal than if the injury is situated high in Scarpa's triangle, where the vessels lie in a large areolar space. The passage of a bullet between an artery and vein may perhaps produce either condition, but wide separation of the two vessels, as for instance of the subclavian artery and vein, renders an aneurismal sac almost a certainty. These suggestions seem borne out by the cases recounted below, since the pure varices are one femoral, one popliteal, and one axillary. I cannot include the calf and forearm cases, as the existence of a small sac could not be disproved.
To these anatomical factors certain others must be added. In most cases a false sac exists at first, which tends to undergo contraction and spontaneous cure, as is observed in some of the ordinary traumatic sacs. This history of development is moreover supported by the observation that proximal ligature of the artery usually converts an arterio-venous aneurism into an aneurismal varix. The process is no doubt favoured by cleanness and small size of the perforation, moderation in the amount of primary hæmorrhage, the tone and resistance of the surrounding tissues, special points in the circulatory force and condition of the blood, and the possibility of maintaining the part at rest after the injury.
Aneurismal varix, when pure, was evidenced by the presence of purring thrill and machinery murmur alone. In none of the cases I saw was pain or swelling of the limb present. In one popliteal varix, slight varicosity of the superficial veins of[Pg 132] the leg was present, but it was not certain that the development of this was not antecedent to the injury, as the patient did not notice it until his attention was drawn to its existence. In none of the cases under observation in South Africa had enough time elapsed for sufficient dilatation of the artery above the point of communication to give rise to any confusion from this cause as to the presence of a sac.
When an arterio-venous sac has once formed, clinical observation shows that the general tendency is towards extension in the direction of least resistance. This direction of course varies with the situation of the aneurism, and also with the nature of the wound track.
Speaking generally the direction of least resistance in a typically pure perforation is towards the vein. Initial flow of blood from the wounded artery is naturally favoured towards the potential space afforded by a canal occupied by blood flowing at a lower degree of pressure. The partial collapse of the vein dependent on the wound in its wall also probably helps in determining the initial flow in its direction. Examples are afforded by the carotid aneurisms (cases 10, 11, and 14), and here it must be borne in mind that the outer limits of the cervical vascular cleft are those least likely to offer resistance to extension of the sac. In each the aneurisms mainly occupied the exit segment of the track; this is the general rule, as in the case of external hæmorrhage, and is determined by the same cause.
The latter rule however finds exceptions when the entry segment is so situated as to cross a region of lesser resistance, and case 12 illustrates this point with regard to the cervical vascular cleft. Examples of the tendency to spread in the anatomical direction of least resistance are also offered by the cases of aneurism at the root of the neck, where extension was into the posterior triangle.
The further clinical history and signs are as follows. A local swelling is found, usually at first diffuse, often commencing to develop with cessation of the external hæmorrhage. It increases, for the first few days maintaining its diffuse character. If near the surface, it may be superficially ecchymosed. At the end of this time a tendency to localisation,[Pg 133] as evidenced by increasing firmness and more definite margination, takes place, and this is followed by general contraction and rounding off of the tumour. The latter process may be continuous, and eventually the sac may become small and stationary or ultimately disappear and a pure varix be the result. The latter is only likely to be the case under the most satisfactory of the conditions enumerated above. Occasionally an opposite course may be followed, and fresh extension take place, as evidenced by enlargement of the tumour, disappearance of sharp definition, softening, and pain. The natural termination of such cases in the absence of interference would no doubt be rupture, and possibly death in some positions, loss of the limb in others. The former I never saw.
Purring thrill.—This, the pathognomonic sign of either condition, was always present in the fully developed stage, and is probably present from the first unless a temporary thrombosis obstructs the vascular openings. It was noted as early as the third day in case 13. In many of the other patients it was palpable only with the subsidence of the primary swelling attendant on the injury. In some of the forearm and calf aneurisms, and in some of the popliteal, it was only discovered by accident some weeks even after the injury, but this often because no serious vascular lesion had been suspected. The thrill was widely conducted, often apparently superficial on palpation, and much more pronounced with light than with forcible digital pressure.
In case 10 the visible vibration in consonance with the thrill when the vein was exposed during the operation of ligature of the carotid was a novel experience to me.
Murmur.—The typical 'bee in the bag,' or 'machinery' murmur was present in every case, and was often very widely distributed, especially over the thorax. (Cases 13, 14, and 20.)
In all three carotid cases the murmur was troublesome, being audible to the patient at night when the head was rested on the side corresponding to the aneurism.
Expansile pulsation.—Pulsation in combination with the existence of a tumour is the main feature in the diagnosis between the conditions of pure varix and varicose aneurism.[Pg 134] It was not always existent or prominent in the earliest stages, probably from temporary blocking of the artery, or from the diffuse and irregular nature of the cavity offering conditions unsuitable to the satisfactory transmission of the wave. When localisation had occurred it was always present.
(a) General.—The most striking feature in these injuries is the remarkable effect of the disturbance to the even flow of the circulation on the heart. This first struck me in two of the cases of carotid arterio-venous aneurism recorded below (Nos. 10 and 11). In these I was inclined at first to attribute the rapid and irritable character of the pulse solely to injury to the vagus, as in each laryngeal paralysis pointed to concussion or contusion of the nerve. The pulse reached a rate of 120-140 to the minute. This disturbance was not of a transitory nature, for in the two cases referred to the rapid pulse persists, in spite of entire recovery of the laryngeal muscles, and the fact that in one case the aneurismal sac has been absolutely cured, and in the second only a small sac remains, in each as a result of proximal ligature of the carotid artery. In the former a varix still exists, and at the end of seven months the pulse is still over 100. In the latter, in which a sac is still present, the pulse rate varies from 110 to 130. In each case the condition has now existed twelve months. My attention once directed to this point, I noted a similar acceleration of the pulse in the case of these aneurisms elsewhere; thus in a femoral aneurism the rate was 120, and in an axillary varix of twenty years' standing which came under my observation the pulse rate varied from 110 to 120, according to the position of the patient. Unfortunately I had not directed my attention to this point in the early series of cases which came under observation.
It will be remarked in cases 13 and 14 that at the expiration of a year the pulse rate was still high, but these again are cervical aneurisms each in contact with or near the vagus.[Pg 135]
In a case of aneurismal varix of the femoral artery of three years' standing, which was under the charge of Mr. Mackellar, the pulse rate was normal. In this instance great dilatation of the vessels had occurred.
These observations raise the interesting question whether the irritable circulation which has been classically considered one of the predisposing causes of spontaneous aneurism should not rather be regarded as a result of the condition.
(b) Local.—In none of the cases of varix was the period of observation long enough to allow me to determine the development of dilatation of the arterial trunk above the point of obstruction. This, however, is the common sequence, and no doubt will occur in those patients who resume active occupation without operation.
The effects of either condition on the distal circulation were remarkably slight. The distal pulses were little, if at all, modified in strength or volume, and signs of venous obstruction, if present at first, disappeared with much rapidity. In one case (No. 15) of a large arterio-venous popliteal aneurism there was considerable swelling of the leg, but in this case the sac was large and situated at the apex of the space, and no doubt exercised external pressure on the vein.
In the case of the carotid aneurisms, especially that probably on the internal carotid, transient faintness was a symptom in the early stages of the case. All three of the cases recorded here, however, had been the subjects of very free hæmorrhage, either primary or recurrent.
(10) Carotid arterio-venous aneurism.—Wounded at Paardeberg. Entry (Mauser) to the right side of the Pomum Adami, exit at anterior margin of left trapezius, two inches below the angle of the jaw. There was some hæmorrhage at the time from the exit wound, but no hæmoptysis; about four hours later, however, in the Field hospital bleeding was so free that an incision was made with the object of tying the common carotid. During the preliminary stages of the operation bleeding ceased and the wound was closed without exposing the vessel. The patient remained a week in the Field hospital, and then made a three day and night's journey in a bullock waggon to Modder River (40 miles), and fourteen days later he was transferred to the Base hospital at[Pg 136] Wynberg, when the condition was as follows. Operation and bullet wounds healed. Considerable extravasation of blood in the posterior triangle. Beneath the sterno-mastoid in the course of the bullet track, swelling, thrill and pulsation over an area 1½ inch wide in diameter. Loud machinery murmur audible to the patient when the left side of the head is placed on the pillow, and widely distributed on auscultation. The left eye appears prominent, but the pupils are normal and equal in size. Voice weak and husky, and there is cough. Laryngoscopic examination showed the cords to be untouched, but some swelling still persisted. No headache, but giddiness is troublesome at times. Pulse 100, regular but somewhat irritable.
The patient was kept quiet in the supine position for a month, and during this time the condition in many ways improved. The voice improved in strength, the pulse steadied, falling to 80, the prominence of the left eye disappeared, and all the blood effusion in the posterior triangle became absorbed. Meanwhile the aneurism contracted at first, until it became oval in outline, with a long axis of 2 inches by 1½ broad extending in the line of the wound track, but mainly situated in the exit half. During the last fortnight, however, it remained quite stationary in size, and as it showed no further signs of diminution in spite of the favourable conditions under which the patient had been placed, it was considered best to try to ensure its consolidation by a proximal ligature. Thrill had become slightly less pronounced, and was less evident to the patient himself, but was otherwise unchanged. The probabilities in this case seemed rather in favour of wound of the internal carotid artery, and it was decided to bare the upper part of the common carotid, follow up the main trunk, and if possible apply the ligature to the internal branch. On April 12, 61 days after the injury, the classical incision for securing the common carotid was made, and the sterno-mastoid slightly retracted. It was found that the sac of the aneurism extended over the bifurcation of the artery, reaching to the wall of the larynx. The omo-hyoid muscle was therefore divided, and the artery ligatured beneath, in order to ensure against any interference with the sac. Some difficulty was met with, for on opening the vascular cleft the vein was exposed and found to completely overlie the artery: although it was on the left side of the neck, the position of the vein was so completely superficial that there seemed no doubt that it had been displaced by the development of the aneurismal sac. A striking appearance was noted on[Pg 137] exposure of the vein, the coats of which vibrated visibly, quivering in exact consonance with the palpable thrill. On tightening the silk ligature all pulsation ceased in the aneurism, and the vibratory thrill in the vein became much lessened.
The patient made a good recovery, only disturbed by a slight attack of vomiting, and at the end of a week the wound had healed, and pulsation in the aneurism had completely ceased. The thrill persisted as before.
Six months later, a small sac still exists beneath the sterno-mastoid. The pulse still reaches 110-120 in pace. The purring thrill is very slight. The condition gives rise to little or no trouble. Pulsation is strong in the external carotid artery, there is little in the common carotid. The voice is strong and good. This aneurism is either at the bifurcation of the common carotid, or on the immediate commencement of the internal carotid. Ligature of the external carotid will probably cure it.
(11) Arterio-venous aneurism, probably affecting both carotids. Wounded at Paardeberg. Entry (Mauser), at dimple of chin immediately below mandibular symphysis. Exit, at margin of right trapezius, the track crossing the carotids about the level of normal bifurcation. The patient was lying on his back with the head down when struck. Some hæmorrhage from the exit wound occurred at the time, and later on the way to Jacobsdal this was so profuse as to be nearly fatal. A considerable hæmorrhage also occurred on the tenth day. The patient made the journey to Modder River safely, and was then under the charge of Mr. Cheatle. A large diffuse pulsating swelling developed on the right side of the neck, with well-marked thrill and machinery murmur. During the next three weeks the swelling steadily contracted, and the patient was sent down to the Base one month after receiving the wound, when the condition was as follows. There is no evidence of any fracture of the jaw. On the right side of the neck a large aneurism fills the carotid triangle, extending from the mid-line backwards to the margin of the trapezius, and from the level of the top of the larynx upwards to the margin of the mandible. The wall is fairly firm, pulsation is both visible and palpable, and a well-marked thrill and machinery murmur are present. The latter annoys him by its buzzing when the head rests on the right side. The pupils are equal. Pulse somewhat irritable, about 100. The voice is weak and husky, and there is difficulty in swallowing solids. The[Pg 138] actual swelling is somewhat remarkable in outline, on the one hand following up the course of the external carotid and facial arteries, and on the other extending backwards in the line of the wound track towards the exit. The patient was kept on his back with sandbags around the head during the next fortnight. For the first eight days such change as occurred was in the direction of localisation and contraction, but during the last six, evident extension occurred both backwards and downwards; this extension was accompanied by severe pain in the cutaneous cervical nerve area of the neck. The larynx became pushed over 3/4 of an inch to the left of the median line, and the extension beneath the sterno-mastoid downwards raised a doubt as to whether the common carotid could be exposed without encroaching on the walls of the sac. Owing to indisposition I had not been able to see the patient for some days, but now, after consultation with Major Simpson and Mr. Watson, it was decided that the best plan would be to expose and tie the common carotid as high as could be safely done. The operation was performed six weeks after the injury, and somewhat to our surprise offered little difficulty. The carotid was exposed at the upper border of the omo-hyoid, only a small amount of infiltration having occurred in the vascular cleft. No dilatation of the jugular was noticeable, and when a silk ligature was applied to the artery all pulsation was controlled, and the thrill in the vein disappeared completely. The after progress was satisfactory, but four days later the wound was dressed, as the patient's temperature had risen above 100°. The tumour was consolidated: no pulsation could be felt, but there was little apparent diminution in its size. A loud blowing murmur was audible, especially at the posterior part of the swelling.
On the morning of the fifth day the patient mentioned that he again heard the whirr during the night. There had been no sign of any cerebral disturbance and the pupils had remained equal throughout.
A week after the operation the stitches were removed, there was evidence of some blood clot in the lower part of the wound, and this later liquefied and was let out on the eleventh day. At that time a slight bubbling thrill could be felt at the upper part of the tumour, also slight pulsation in the line of the external carotid and at the most posterior part of the sac. The latter was much contracted, diminished in size and apparently solid, so that it was hoped that such pulsation as existed was communicated.[Pg 139] Ten months later, no trace of the aneurismal sac exists. Neck normal, except for purring thrill. Voice strong and good. Pulse 100. Following his usual work.
(12) Carotid arterio-venous aneurism.—Wounded at Paardeberg. Aperture of entry (Mauser), at the posterior border of the left sterno-mastoid, 1 inch above the clavicle; exit, near the posterior border of the right sterno-mastoid, 2 inches from the sterno-clavicular joint. The injury was followed by very free hæmorrhage, mainly from the wound of entry, some 'quarts' of blood escaping; at any rate his clothes were saturated. The voice was hoarse and weak, and there was much difficulty in swallowing; for the first twenty-four hours he could swallow nothing, but gradual improvement took place. The patient was carried two miles to the Field hospital, and three days later travelled 36-40 miles in a bullock waggon to Modder River. Thence he travelled to Orange River 55 miles by train on the next day. A swelling was first noted when the wound was dressed some seven days after the injury. No evidence was ever existent of gross damage to either trachea or œsophagus beyond the initial dysphagia. The hoarseness of voice due to left laryngeal paralysis slowly improved, and was probably the effect of concussion or contusion of the left recurrent laryngeal nerve. During the patient's stay at Orange River a large pulsating swelling with a strong thrill developed. This was at first diffuse, but under the influence of rest it steadily contracted and localised. During this period the patient was seen several times by Mr. Cheatle, who noted considerable temporary enlargement of the thyroid gland.
At the end of eight weeks he had been allowed up some days, and travelled 570 miles to Wynberg. The aneurism was about 1½ inch in diameter, smooth and rounded, extending just beneath the left clavicle and nearly the whole width of the sterno-mastoid, but well defined in all directions. There was well-marked expansile pulsation, purring thrill along the jugular vein and over the tumour, and loud machinery murmur widely diffused along the whole neck and into the thorax. The voice was still weak and husky, but there was no dysphagia or dyspnœa. The left pupil was larger than the right.
The patient acquired enteric fever at Wynberg and when convalescent was sent to Netley, whence he returned home. The aneurism caused little discomfort. It may possibly have been of the inferior thyroid artery.
(13) Innominate arterio-venous varix.—Wounded at Modder[Pg 140] River. Entry (Mauser) posterior margin of left sterno-mastoid, close above the clavicle. Exit in anterior axillary line one inch below the right anterior axillary fold. Soon after the injury a considerable amount of blood was coughed up, and occasional hæmoptysis persisted for the next four days. The patient was moved from the Field hospital by train to Orange River, a journey of 55 miles and some four hours' duration, on the fourth day. When examined there was slight fulness over an area roughly circular and about 2½ inches in extent, of which the sterno-clavicular joint lay just within the centre. Over this area there was faint pulsation with a strongly marked thrill and loud systolic bruit. The radial pulses were even, the right pupil larger than the left. No pain, and no dyspnœa. The right eye was partially closed, but could be opened by the levator palpebræ superioris. The patient was shortly afterwards sent to the Base, and when seen there twenty-five days after the injury, there was little change in the condition except that the fulness had disappeared, the thrill was more marked, and a typical machinery murmur transmitted along both carotid and subclavian arteries had developed. There was no headache and the man himself did not notice the bruit. Evidence of mediastinal hæmorrhage existed in the presence of subcutaneous discoloration of the abdominal wall, below the ensiform cartilage and extending slightly over the costal margin of the thorax. In the absence of an aneurismal swelling, or of the development of any further symptoms, the patient was sent home to Netley in January.
I saw this patient in Glasgow a year later. He was employed as a lamplighter, and was able to do his work well, only complaining of attacks of shortness of breath on exertion. He said these were apt to come on each evening about 6 p.m. The pulse was 100 when the erect position was maintained, and 84 to 88 in the sitting posture. The right pupil was still dilated, reacting for accommodation but little to light. The palpebral fissure was normal in size and there was little, if any, diminution in strength of the right radial pulse.
On inspection no pulsation was visible; in fact, the pulsation of the normal left subclavian was more apparent in the posterior triangle of that side. The sterno-mastoid was prominent, also the sternal third of the clavicle. On firm[Pg 141] pressure some pulsation was palpable beneath the sterno-mastoid, but no definite evidence of the presence of a sac could be detected. Purring thrill and machinery murmur were still present, but the former was slight, and palpable only with the lightest pressure. The machinery murmur had ceased to be audible to himself, and was by no means loud or very widely distributed.
The condition had, in fact, steadily improved, and become far less obvious. The prominence of the sterno-mastoid and clavicle still present was difficult of explanation, except on the theory of an injury to the bone, or that an aneurismal sac had consolidated spontaneously.
(14) Arterio-venous aneurism, root of right carotid.—Wounded at Magersfontein. Entry (Mauser), centre of right infra-spinous fossa. Exit, 3/4 of an inch above clavicle, through point of junction of the heads of the right sterno-mastoid muscle. Range 200-300 yards. When wounded the man ran two hundred yards to seek cover. There was no serious external hæmorrhage, but the injury was followed by some difficulty in swallowing, and hæmoptysis, which lasted for the first two days. The right radial pulse was noted to be smaller than the left, and weakness in flexion of the fingers, with hyperæsthesia in the ulnar nerve distribution, was observed. The right pupil was also noted to be larger than the left.
The patient was sent down to the Base, and on the twenty-fourth day the condition was as follows. A pulsating swelling existed extending 1¼ inch upwards beneath the right sterno-mastoid, from the mid line of the neck backwards to the centre of the posterior triangle, and downwards over 2 inches of the first intercostal space, which latter was dull on percussion. There was some evidence of a bounding wall, but it was thin and the tumour was soft and yielding. A loud machinery murmur was audible over the tumour, over nearly the whole extent of the thorax, and in the distal vessels as far as the temporal upwards, and the brachial as far down as the bend of the elbow. The murmur was audible to the patient with his ears closed. Over the swelling a strong thrill was palpable; this extended some little distance into the distal vessels and felt remarkably superficial. It was particularly evident in the line and course of the anterior jugular vein, and appeared to be extinguished by local pressure. Although readily felt in the posterior triangle, it was impalpable[Pg 142] on deep pressure in the suprasternal notch, a fact which seemed in favour of localising the aneurismal varix to the subclavian artery and vein. The right pulse was good, although smaller than the left, and was said to have improved in volume. The right pupil was slightly larger than the left, but reacted normally. There was no pain or difficulty in swallowing. Weakness in power of flexion of the fingers persisted, and there was some impairment of sensation in the area of distribution of the ulnar nerve.
Three weeks later no material change had occurred, except that the swelling was perhaps softer and the thrill more superficial, and at the end of two months the patient was sent to England.
I saw this patient a year later in Glasgow, when the condition was as follows. He was living at home, and out of employment. He complained of shortness of breath on exertion, and said that when he mounted stairs he felt 'as if his heart were going to leave him.' The heart's apex beat in the sixth interspace in the nipple line, and the precordial dulness was somewhat increased. The pulse numbered 80 to 84. The muscles supplied by the ulnar nerve were very weak, but not much wasted, and ulnar sensation was imperfect.
The aneurism had considerably altered in form and outline; its walls were dense and firm; it extended 2½ inches upwards in the line of the carotid artery, beneath the sterno-mastoid, but projected beyond the posterior border of that muscle. The larynx was displaced 1/2 an inch to the left of the median line; the voice was still husky, although much stronger than it was; the anterior jugular vein was dilated. The purring thrill was very superficial, and chiefly palpable over the subclavian vessels. The machinery murmur was still loud, but much less widely distributed than before; it was still audible to the patient when he lay on his right side.
This case was of much interest from the diagnostic point of view. When I first saw the patient I considered the injury to have implicated the innominate vessels. Later, from the facts that the thrill was imperceptible in the episternal notch, and that the main part of the tumour was situated in the posterior triangle, that the wound was of the root of the right subclavian vessels.[Pg 143]
It now appears that, at any rate, the root of the right carotid is the artery implicated.
In spite of the continued existence of a large aneurism, the localisation of the sac, which had taken place, was very striking, considering that the man had been walking about freely, and living an ordinary life, except that he had undertaken no work.
(15) Popliteal arterio-venous aneurism.—Wounded at Paardeberg. Entry (Mauser), at lower margin of patella. Exit, at centre of back of thigh. Perforation of lower end of femur. The patient was lying down with crossed knees when the injury was received. Much œdema of the foot and leg followed the injury, and on the third day a thrill was discovered. Three weeks later there was still some swelling of the calf, the posterior tibial pulse was imperceptible, the anterior very small. An aneurism was palpable at the inner part of the top of the popliteal space, about the size of a pigeon's egg; a strong thrill was to be felt, especially when the knee was flexed, and with this expansile pulsation and a loud machinery murmur. The entry wound was firmly healed; the exit still furnished blood-stained serous discharge. The synovial cavity of the knee was distended and doughy on palpation. During the next three weeks the aneurism contracted considerably and the patient was sent home.
When admitted to the Herbert Hospital the patient complained chiefly of pains in the foot and leg. The aneurism was cured by ligation of the vein above and below the communication and proximal ligature of the popliteal artery.[15]
(16) 'Femoral arterio-venous aneurism.—A private of the West Yorkshire Regiment was hit on February 11, 1900, at Monte Christo by a bullet which passed through the inner border of his right thigh above its middle. On arrival at Woolwich the patient was found to have a varicose aneurism at the upper end of Hunter's canal. On May 31 the femoral artery was ligatured just above its communication with the vein, and as this stopped all pulsation in the vein, it was decided to postpone ligature of the latter to a subsequent occasion, if it should ever be necessary; such a procedure would, it was thought, interfere less with the circulation of the limb, and would therefore be less likely to be followed by gangrene, which is so frequent a result of high ligature of the femoral. But a few days after the operation the foot became[Pg 144] cold and mummified, and there was no alternative but to amputate the limb through the condyles of the femur. From this operation the patient made a good recovery, and when discharged there was no sign of an aneurism of the vein.'
Case 16 is quoted from a paper in the Lancet by Lieut.-Colonel Lewtas, I.M.S. It illustrates a result with which I became acquainted in three other instances not under my own observation.
(17) Axillary.—Wounded at Modder River. Entry (Mauser), at inner margin of front of left arm, just below level of junction of axillary fold. Exit, at about centre of hollow of axilla. A month later when the wound was healed a typical thrill and machinery murmur were noticed. The latter was audible down to the elbow and upwards into the neck. The radial pulse appeared normal. No swelling or pulsation existed. At the end of three months the condition was unaltered; the patient said he noticed nothing abnormal in his arm, except that it was sometimes 'sort of numb' at night.
(18) Popliteal.—Wounded at Magersfontein. Entry (Mauser), in centre of popliteal space. Exit, about centre of patella, which latter was cleanly perforated. Three weeks later the typical thickening of the knee-joint following hæmarthrosis was present, also a well-marked thrill and machinery murmur in the popliteal vessels with no evidence of a tumour. The leg was normal except for slight enlargement of the internal saphenous vein and its branches, probably independent of the arterial lesion.
(19) Femoral.—Wounded at Magersfontein. Entry (Mauser), 7 inches below left anterior superior iliac spine. Exit, at inner aspect of thigh. One month later slight fulness without pulsation was discovered on the inner side of the femoral vessels just above the level of the wound track. Some blood-staining still remained in the fold between the scrotum and thigh. Machinery murmur and a well-marked thrill, most palpable to the inner side of the superficial femoral artery, were noted. No further symptoms developed and the patient was sent home.
Prognosis and treatment.—No one can help being struck with the disinclination shown by the older surgeons to[Pg 145] interference in cases of either aneurismal varix or varicose aneurism, even after the time that ligation of the vessels had become a favourite and successful operation. The objections lay in the technical difficulties of local treatment, and the danger of gangrene after proximal ligature. Modern surgery has lightened the difficulties under which our predecessors approached these operations, but none the less the experience in this campaign fully supports the objections to indiscriminate and ill-timed surgical interference, as accidents have followed both direct local and proximal ligature.
In pure varix no doubt can exist as to the advisability of non-interference in the early stage, in the absence of symptoms. This is the more evident when we bear in mind that a stage in which an aneurismal sac exists can seldom be absent. In many cases an expectant attitude may lead to the conviction that no interference is necessary, especially in certain situations where the danger of gangrene has been fully demonstrated. In connection with this subject I cannot help recalling the first case of femoral varix that ever came under my own observation. I discovered the condition accidentally in a man admitted into the hospital for other reasons. The patient remarked: 'For heaven's sake, sir, do not say anything about that. I have had it many years, and it has never given any trouble. If it is known, I shall be worried to death by people examining it.'
None the less it must be borne in mind that beyond enlargement of the vein dilatation of the artery above the seat of obstruction does occur, and gives trouble in some situations. Again the disturbance of the general circulation already adverted to shows that the existence of this condition is sometimes of importance in its influence on the cardiac action.
Under these circumstances the treatment varies with regard to the vessels affected, and the degree of disturbance the condition gives rise to.
With regard to locality, experience appears to have shown clearly that communications between the carotid arteries and jugular veins usually give rise to so little serious trouble that, in view of the grave nature of the operation and its possible after consequences on the brain, interference is as a rule better[Pg 146] avoided. I should, however, be inclined to draw a distinction between operations on the common and internal carotid arteries in this particular, and should regard varix of the latter vessel and the internal jugular vein as especially undesirable for interference.
The vessels at the root of the neck are probably to be regarded from the same point of view, as to surgical interference.
The arteries of the upper extremity are the most suitable for operation, and the axillary may perhaps be the vessel in which interference is most likely to be useful. In this relation it may be of interest to include here a case of a man who took part in the campaign when already the subject of an aneurismal varix of the axillary artery.
(20) Twenty years previously the patient suffered a punctured wound of the left axilla from a pencil. A varix developed, but was only discovered by accident ten years later. The patient was seen by several surgeons, and treatment was discussed; the balance of opinion was, however, in favour of non-interference, and nothing was done beyond giving injunctions as to care in the use of the limb. Up to the time of discovery of the varix no inconvenience had been felt, although the patient was of athletic habits. Subsequently, the patient himself was positive that a swelling existed, but he pursued his usual work. In 1899-1900 he took part in the operations in South Africa as a combatant, and during this time was subjected to very hard manual work. During this he was seized with sudden pain in the left side of the head and neck, and in consequence invalided. No restriction in the movements of the upper extremity, and no subcutaneous ecchymosis developed, but the patient was positive as to the tumour having greatly enlarged.
Four months later the condition was little altered. A pulsating swelling 1½ inch broad existed along the line of the upper two-thirds of the axillary artery, and along the subclavian in the neck, rising some 1½ inch into the posterior triangle. Pulsation was visible; the murmur was audible when sitting beside the patient, and widely distributed over the whole chest, the neck, and upper extremity on auscultation. The pulse rate varied with the mental condition of the patient, which was excitable, between 96 and 120. There was neuralgic pain in the neck and scalp, and down the distribution of the brachial plexus. The pupils[Pg 147] were equal, but flushing of the face and profuse sweating followed any exertion. I concluded the tumour in this case to be mainly due to dilatation of the trunk above the point of obstruction on account of its outline, the absence of any restriction of movement in the upper extremity, and the non-occurrence of subcutaneous ecchymosis at the time of the attack of severe pain. Difficulties arose as to undertaking any active form of treatment for this patient, which, to be satisfactory, needed an antecedent period of absolute rest, and he passed from my observation. I think, however, operation by ligature above and below the communication would have been possible. The case affords a good example of the course the condition may sometimes take if precaution is neglected.
The vessels of the arm or forearm may in almost all cases be interfered with, but in many instances an absence of any serious symptom renders operation unnecessary.
With regard to the femoral varices, I would refer to the remarks below, and those on the treatment of varicose aneurism as indicating that a certain amount of caution should be exercised in interfering with them.
The same remarks in a lesser degree apply to the popliteal vessels. In the leg the tibials may readily and safely be attacked, but it may be mentioned that the widespread and diffused nature of the thrill may in some cases give rise to considerable difficulty in sharp localisation of the varix to either of the vessels, or to any particular spot in their course. In one case in my experience the posterior tibial was cut down upon, when the varix was probably peroneal in situation.
The operation most in favour consists in ligation of the artery above and below the varix, the vein remaining untouched. Even this operation, however, in two cases of femoral varix failed to effect more than a temporary cessation of the symptoms, although the ligatures were placed but a short distance from the communication. Failure is due to the presence of collateral branches, which are not easy of detection. Even when the vessels lie exposed, the even distribution of the thrill renders determination of the exact point of communication difficult, and the difficulty is augmented by the temporary arrest of the thrill following the[Pg 148] application of a proximal ligature to the artery. A successful case is reported by Deputy Inspector-General H. T. Cox, R.N., in which the ligatures were placed 1/2 an inch from the point of communication.[16] Single ligation, or proximal ligature, is useless.
If the vein cannot be spared, excision of a limited part of both vessels may be preferable, particularly in those of the upper extremity.
Proximal ligation of the artery combined with double ligature of the vein, as adopted in case 15 by Colonel Lewtas for a varicose aneurism, might offer advantages in some situations.
Given suitable surroundings and certain diagnosis, the ideal treatment of this condition, as of the next, is preventive—i.e. primary ligation of the wounded artery. Many difficulties, however, lie in the way of this beyond mere unsatisfactory surroundings. It suffices to mention the two chief: uncertainty as to the vessel wounded, and the necessity of always ligaturing the vein as well as the artery in a limb often more or less dissected up by extravasated blood, to show that this will never be resorted to as routine treatment.
Arterio-venous aneurism.—Many of the remarks in the last section find equal application here, but in the presence of an aneurismal sac non-intervention is rarely possible or advisable. In the early stages the proper treatment in any case consists in placing the patient in as complete a condition of rest as possible, and affording local support to the limb by a splint, preferably a removable plaster-of-Paris case. Should no further extension, or, what is more likely, should contraction and diminution occur, it will be well to continue this treatment for some weeks at least.
When the aneurism has reached a quiescent stage the question of further treatment arises, and whether this should consist in local interference or proximal ligature. The answer to this mainly depends on the size and situation of the vessels concerned. To take of the cases above described the five instances in which the cervical vessels were the seat of the aneurism. In No. 13 the symptoms appeared fairly conclusive of[Pg 149] the injury being to the innominate artery and vein, or possibly innominate artery and jugular vein. Fortunately the aneurismal sac in this case was small and showed a tendency to decrease, but in any case no interference would have been justifiable. I think a similar opinion was unavoidable in No. 14, probably affecting the root of the right carotid. Here under any circumstances interference would have been most hazardous. The position of large aneurism made the route of approach to the wounded spot necessarily through the sac, exposing the patient to the double danger of immediate hæmorrhage and of entrance of air into the great veins. Nos. 10, 11, and 12 fall into the same category, except that in No. 11 the immediate indication for interference was extension. In each, ligature of the artery above and below the point of communication would have necessitated so near an approach to the sac which must remain in communication with the vein as to have entailed injury to the latter, when both artery and vein must have been ligatured, probably risking serious cerebral trouble. In No. 11 I believe both the external and internal carotids were implicated; in No. 10 I believe the internal alone, close to its origin. The operation of proximal ligature ensured primary consolidation of the sac in both cases 10 and 11, but left the thrill unaltered, except in so far as it was temporarily weakened. It, in fact, converted these cases from arterio-venous aneurisms into pure aneurismal varices. In No. 10 a sac subsequently redeveloped. No. 12 stood on a different basis. No operation was done for him in South Africa, but the first portion of the carotid might have been ligatured in the episternal notch, or by aid of removal of a part of the sternum, and a second ligature placed above the sac. Here a ligature above and below the communication would have been comparatively easy.
As a general rule proximal ligature is to be reserved for those cases alone in which double ligature is either impracticable or inadvisable, and it can only be expected to convert a varicose aneurism into the less dangerous condition of aneurismal varix.
In the case of arterio-venous aneurisms in the limbs the possibilities of treatment are enlarged, and here the alternatives[Pg 150] of (a) local interference with the sac and direct ligature of the wounded point, (b) simple ligature above and below the sac, (c) proximal ligature (Hunterian operation), come into consideration.
Direct incision of the sac is suitable, and the best method of treatment for aneurisms in the calf, forearm, and probably arm. Several cases in the two former situations were successfully treated by this method. On the other hand, the only case I saw in which a proximal ligature had been applied for an arterio-venous aneurism of the leg resulted most unsatisfactorily. The sac in the calf suppurated at a later date, and for many weeks the escape of small quantities of blood from the remaining sinus kept up the fear of a severe attack of secondary hæmorrhage until the sinus closed.
In the case of femoral and popliteal aneurisms the method of Antyllus is often unsuitable. A case of arterio-venous aneurism of the femoral artery quoted in the Lancet[17] will illustrate the difficulty which may be met with in determining the actual bleeding point in the irregular cavity laid open. In any case the necessary ligature of both artery and vein is a serious objection to the direct method either in the thigh or ham, and more particularly if adopted before the damage dependent on the dissection of the limb by extravasated blood has been repaired.
Proximal ligature (Hunterian) even, offers dangers under these circumstances. In one case with which I became acquainted, it was followed by gangrene, necessitating amputation. The lesion in this instance was a perforating one of the femoral artery and vein.
For either femoral or popliteal arterio-venous aneurisms ligature of the artery above and below the aneurism is the best and safest treatment. In view of the healthy state of the vascular wall in most of these cases, the advantage of placing the ligatures as near to the wounded spot as can be managed without interference with the sac is afforded. A number of popliteal cases treated in this way did perfectly. In the femoral cases a considerable period of rest to allow of[Pg 151] consolidation of the sac, and readjustment of the circulation, should always be allowed to elapse.
In the case of popliteal arterio-venous aneurisms a number were successfully treated by proximal (Hunterian) ligature, and by single ligature immediately above the sac. In a considerable proportion of the latter both artery and vein were tied. This was apparently the result of the difficulty of isolating the vessels in the tangled mass of clot and cicatricial tissue surrounding them, and is a strong argument against too early interference. The late Sir William Stokes expressed himself as in favour of ligature of the artery in Hunter's canal, combined with that of the great anastomotic branch, and quoted some successful cases to me. I have grave doubts, however, whether the varix can often be permanently cured by this operation.
I can give no useful statistics on this subject, but with regard to the popliteal aneurisms I may state that in three instances gangrene of the leg followed early operative interference in the popliteal space.
My own opinion on this subject is strong, and to the effect that none of these operations should be undertaken before a period of from two to three months after the injury, unless there is evidence of progressive enlargement. In every case which came under my own observation progressive contraction and consolidation took place up to a certain point under the influence of rest. When this process has become stationary, and the surrounding tissues have regained to a great extent their normal condition, the operations are far easier, and beyond this more likely to be followed by success.
It appears to me that one argument only can be raised against the above opinion, viz. the possibility of healing of the recent wound in the vessels when the force of the circulation is lowered by proximal ligature. Such experience as that quoted from Sir W. Stokes and two of Mr. Ker's cases, mentioned below, support this possibility, but in all the reported results were recent. Against them I can only advance my knowledge of several mishaps following early operation.[Pg 152]
In concluding these observations on injuries to the arteries and aneurisms, a few general remarks as to the occurrence of gangrene after operation must be added. This was not uncommon, and in the main was no doubt attributable—(1) to the lowering of the vitality of the surrounding tissues by creeping blood extravasation, and sometimes to actual pressure by the extravasation on the vessels necessary for the establishment of the collateral circulation. (2) To the frequency with which both artery and vein required to be ligatured.
Beyond these common causes, however, others must be advanced, dependent on the general and local condition of the nervous system in these cases. In general mental state many of the patients were much shaken, and in others the condition spoken of as local shock in a former chapter had been marked. In a third series obvious individual nerve lesions were co-existent with those to the vessels. Beyond this a fourth nervous element of unknown quantity, the effect of the form of injury on the vaso-motor nerves accompanying the great vessels, must be taken into consideration.
I believe all these factors were of importance, since it appeared to me that gangrene occurred more often than I should have expected. In one case which I have heard of, gangrene followed a very slight injury to the foot in a patient who had apparently made an excellent recovery after ligature of the femoral artery.
The nervous factor seems another element in favour of reasonable delay in active interference with traumatic aneurisms of the above varieties in the absence of threatening symptoms.
It is worthy of remark that no case of gangrene due to aneurism came under my notice, except subsequently to operation.
Since the above chapter was written, my friend, Mr. J. E. Ker, has sent me his experience in the treatment of four aneurisms, which is of such interest that I insert it as an addendum.
Arterial hæmatomata.—(1) Popliteal, treated by local incision. Both artery and vein completely divided. Ligature[Pg 153] of the four ends. Cure. (2) Traumatic aneurism of upper third of forearm. Treated by rest and pressure by bandage. On the eighth day pulsation and bruit ceased spontaneously, and the remains of the sac steadily consolidated until the man's discharge on the twenty-sixth day.
Arterio-venous aneurisms.—(1) At junction of brachial and axillary arteries. Proximal ligature. Cure. (2) Arterio-venous aneurism at the bend of the elbow. Ligature of the brachial at the junction of the middle and lower thirds of the arm. Cure.
[14] The murmur is still present at the expiration of one year, but no other change.
[15] Lieut.-Colonel Lewtas, I.M.S. See Lancet, 1900, vol. ii. p. 1073.
[16] Lancet, 1900, vol. ii. p. 1074.
[17] Sir W. MacCormac, Lancet, vol. i. 1900, p. 876.
Injuries to the bones of the limbs formed a very large proportion of the accidents we were called upon to treat, and afforded as much interest as any class, since they possessed many special features. I shall hope to show, however, as in some of the other injuries, that these features differed only in degree from those exhibited by injuries from the old leaden bullets of larger calibre, although with few exceptions they were of a distinctly more favourable character.
It is of considerable interest to note that, taking the fractures as a whole, there was a somewhat striking change in their nature during the earlier and later portions of the campaign. In the earlier stages I think there is no doubt that punctured fractures were proportionately more common than in the later, when comminuted fractures were much more often seen. There was, I believe, a source of error in this opinion, as far as I myself was concerned, in that the first cases I saw were at Capetown and had come from Natal. There is no doubt that the punctured fractures were earlier fit to travel, and hence a larger number of them found their way to the Base hospitals at a period when the comminuted fractures were still in the Field or Stationary hospitals. I do not, however, rely on the cases seen at Capetown alone for my opinion, as while at the front I saw the same large proportion of clean punctures in the early engagements of the Kimberley relief force.
I am inclined to attribute the change to two reasons: first, I believe that the use of regulation weapons was more universal in the earlier part of the war, while later, as more men were engaged, the Martini-Henry came more into evidence,[Pg 155] and the Boers took more freely to the use of sporting rifles and ammunition. Another element also in the less clean punctures of the short and cancellous bones was probably the less accurate and hard shooting of the Mauser rifles as they became worn; the bullets seemed to evidence this by the comparative shallowness of their rifle grooves, which, I take it, would mean less velocity and accuracy in flight. This would be of importance, since the clean puncture of cancellous bone was no doubt favoured by a high rate of velocity.
The special features of the fractures caused by the small-calibre bullets were: (1) The nature of the exit wound, which in a certain proportion of the cases exhibited the so-called 'explosive' character. (2) The presence, in a marked degree in the severe cases, of the condition spoken of in Chapter III. as 'local shock.' (3) The striking contrast of clean perforation and extreme comminution in different cases. (4) The occasional occurrence of fractures of a very high degree of longitudinal obliquity. (5) The rarity of any that could be termed transverse fractures. (6) The general tendency of longitudinal fissuring when it occurred to stop short of the articular extremities of the bones.
It will perhaps be most convenient to consider first the explanation of the development of the so-called explosive apertures, and then to pass on to a general consideration of the types of fracture commonly met with, before proceeding to the description of the injuries to the separate bones.
Explosive wounds in connection with fractures.—The aperture of entry in these injuries presented little or no deviation from the normal, unless it was due to the passage of ricochet bullets, when it might be very irregular, but usually not of great size.[Pg 156]
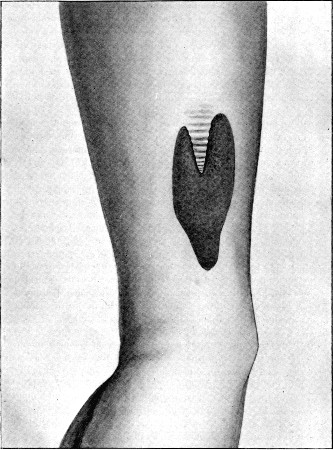 Fig. 47
Fig. 47
(21) 'Explosive' Exit Wound of Forearm over margin of ulna. Note creased tongue of skin originally covering whole wound. The entry wound was a small typical circular one
The aperture of exit offered special features beyond simple increase in size. First of all, as in the small type wounds, the actual extent of destruction of the skin was small, this having been projected outwards by the passing bullet and then either burst or torn by the bullet and accompanying bony fragments. Fig. 47 well illustrates this feature. A triangular tongue of skin was lifted by the passing bullet and probably by the lower end of the upper fragment of the fractured ulna; through the resulting opening a mass of soft tissues and bone fragments, bound together by an infiltration of coagulated blood, was extruded, separating the lateral lips of the aperture, while the original tongue has shortened and retracted up to the top of the wound.
The small extent of skin actually destroyed is an important element in the rapid contraction often seen in these wounds when they progress favourably. Thus the large wound portrayed in fig. 48 contracted to one-fourth its original size ten days after the diagram and measurements were made. The large mass of protruded tissue was often most striking when a muscle such as the biceps in fig. 48 had been divided; but the herniæ were more persistent when the mass projected in regions where tendons formed a large integral constituent, as at the wrist or lower third of the forearm. The protruding tissues naturally consisted of many varieties, according to what lay in the track of any particular wound.
It should be added that for 'explosive' features to reach their strongest development, it is necessary that the bone affected should lie near the surface of the body; hence the most characteristic explosive wounds were met with in the forearm or leg, over the metacarpus or metatarsus, or in the arm. In the thigh, on the other hand, where the femur in a great part of its course not only lies deeply, but is also protected by particularly strong and resistent skin and fascia, another type of wound was met with. The explosive exit aperture, although large, was still only moderate in extent, sometimes, as in the front of the lower third, exposing a somewhat angular large track walled by the divided quadriceps extensor cruris. In other cases, on introducing the finger through a moderate exit opening on the inner aspect of the thigh, a large cavity, sometimes 4 or 5 inches in diameter, was discovered, full of clot and shreds of destroyed tissue and lined by a layer of similar material. In either of these latter cases the fractured bone ends were situated too deeply to take part in the actual laceration of the skin, while the force transmitted to the bone fragments, although sufficient to cause them to widely destroy the first soft tissues met with, did not suffice to cause them to burst or lacerate the skin widely.[Pg 158]
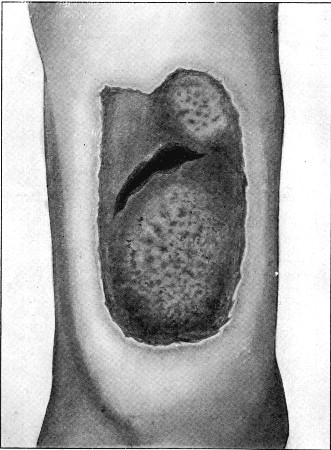 Fig. 48.
Fig. 48.
(22) 'Explosive' Exit Wound of front of Arm. Wound actual size eight days after its infliction. The prominences in the upper and lower parts correspond with the lacerated biceps. The dark crater led down to the fracture. In another week the wound had contracted to half the size. The entry aperture was a normal circular one. The arm a year later was used in the patient's employment as a hammer-man
With regard to the theories of the production of these phenomena, that of the transmission of a part of the force of the bullet to the comminuted fragments, which thus themselves acquire the characters of secondary projectiles, seems quite adequate.[18] Examination of any of the skiagrams in which considerable comminution has taken place, shows that the fragments are carried forward and perforate the tissues distal to the fracture.
 Fig. 49.
Fig. 49.
'Explosive' Wounds of Legs. Large irregular entry (1 ×3/4 in.). First exit (2 in.) roughly circular. Second entry wound, produced by bone fragments driven out of left leg, very large and irregular (5 ×3½ in.). The measurements were taken eight days after infliction of the wounds. The right limb was amputated later for secondary hæmorrhage
Fig. 49, although a poor delineation of the actual condition, shows well the possible action of projected fragments, even after they have been driven from the wound. In this case either a large or a ricochet bullet entered on the outer aspect of the upper third of the left tibia; it produced a severe comminuted fracture, the fragments from which,[Pg 160] together with the deformed bullet, then struck and perforated the upper third of the right tibia. A large irregular entry wound 5 inches in transverse diameter was produced in the second limb together with a comminuted fracture of the bone. The right limb had eventually to be amputated for secondary hæmorrhage, but I am unacquainted with the later history of the patient.
The mode of displacement of the lateral fragments when a wide shaft such as that of the femur is struck, throws some light on that of the displacement of soft tissues such as the component parts of a perforated nerve or artery. The bullet, passing through, expends the chief part of its energy in driving before it the fragments produced in its direct course, while a minor part of the energy is expended on displacing the lateral fragments, which are pushed to either side without becoming separated from their periosteal attachment. The appearance, in fact, somewhat suggests what might be expected were a small charge of dynamite introduced into the centre of a small tunnel made across the shaft of the bone. Examination of some of the skiagrams also illustrates another point of interest, viz. that a certain degree of recoil on the part of the bone results from the blow, since in many of them portions of the mantle of the bullet and bone fragments are seen in that portion of the track proximal to the fractured bone.
The importance of 'setting up' of the bullet is at once evident in relation to the production of wounds of an explosive type in connection with fractures of the bones. There can be no doubt that a considerable number of the most severe injuries we saw were produced by the various soft-nosed or expanding forms of bullet, also that others of an equally serious nature were produced by Martini-Henry or large leaden sporting bullets. Allowing for this, however, I think a considerable proportion were the result of deformation from bony impact, or ricochet deformities external to the body acquired by regulation Mauser bullets, and I think these bullets can be quite as formidable as any of the sporting varieties met with. The soft-nose varieties of small calibre may not set up enough to cause severe injury, while the large leaden bullets often flatten out so completely as to lose all penetrating power. As[Pg 161] far as my impressions went, the small soft-nosed bullets needed to be travelling at a very considerable rate of velocity to be dangerous. In the form of soft-nose Mauser employed, the soft-nose was too short to allow of as successful a mushrooming of the bullet as often occurred with the regulation projectile, because, as already explained, the mantle acquires increased stability from its closed base.
Types of fracture.—The common types of fracture of shafts of the long bones are illustrated diagrammatically in fig. 50. Of the whole series comminuted fractures were by far the most frequently met with, while the various wedge-shaped forms were the most strongly characteristic of the special form of injury in which we are interested.
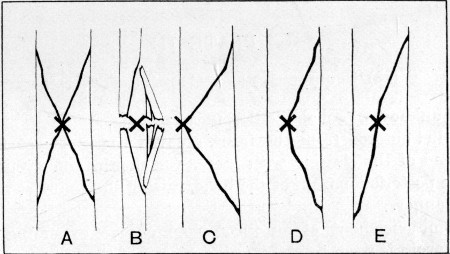 Fig. 50.
Fig. 50.
Five Types of Fracture: A. Primary lines of stellate fracture; wedges driven out laterally and pointed extremities left to main fragments. B. Development of same lines by a bullet travelling at a low degree of velocity; suppression of two left-hand limbs and substitution of a transverse line of fracture; a spurious form of perforation. See plate XXIII. C. Typical complete wedge. See plate VII. D. Incomplete wedge; impact of bullet, lateral or oblique, and two left-hand lines seen in A are suppressed. E. Oblique single line, one right and one left hand line seen in A, suppressed. The influence of leverage from weight of the body probably acts here. Compare plates XVI. and XXI.
(23) Spurious Perforation of Clavicle
Range unknown, probably either mean or long.
The bullet entered from the front, grooved the under surface of the acromial end of the clavicle with increasing depth, and eventually perforated the posterior margin of the bone, raising the compact tissue in an angular manner.
The commencement of an incomplete groove extending from the anterior margin is seen, resembling the groove of the humerus, fig. 58.[Pg 163]
1. Stellate comminuted fractures.—a shows the primary nature of the lesion in all comminuted fractures of compact bone, consisting in the production of a number of radiating fissures, which assume a stellate form of which the point of impact corresponds to the centre. b shows an incomplete development of this form, the fragments being simply displaced laterally with slight loss of substance, so as to simulate a real punctured fracture. An illustration of this fracture produced by a bullet travelling at a low degree of velocity is seen in plate XXIII., which also shows the unaltered bullet lying in close proximity to the injured fibula.
The degree of comminution in these fractures depends first on the range of fire and consequent striking force retained by the bullet, a high degree of velocity producing extreme comminution of compact bone. The severity of the latter again may be influenced by the measure of resistance dependent on the density and brittleness of any individual bone, or on the possession of the same characters as a special property by the tissues of the man struck. Thus plate IV. shows a fracture of the humerus produced by a bullet shot from a short range, and the fragments are comparatively large and of even dimensions, while plate XIV. shows extreme comminution of the portion of the femur exposed to direct impact, with elongated large fragments at the sides of the track. Plate XIX. shows less extreme comminution and less separation of the fragments, and was probably produced by a bullet from a longer range of fire.
The separation of elongated lateral fragments is a special feature, and best marked when the portion of bone struck is considerably wider than the bullet, as in the case of the shaft of the femur. These fragments correspond in the method of their production to those seen in the wedge fractures described below, while their separation leaves a pointed extremity to either segment of the shaft. This fracture in its purest type is, I believe, spoken of as the 'butterfly fracture.'
With regard to the spread of the fissures in the long axis of the bone into neighbouring articulations I think fractures produced by bullets of small calibre differ considerably from those produced by larger projectiles, in that their general tendency is not to extend beyond the commencement of the cancellous bone forming the joint end. This is perhaps capable of explanation on several grounds: first, the smaller area of impact results in the assumption of a strongly marked stellate figure, the radiating fissures of which rapidly reach the lateral limits of the shaft, producing a solution of continuity in the bone which interrupts the continuance of the action of the wedge represented by the bullet. Secondly, the small size[Pg 164] of the wedge itself is opposed to the wide separation of the parts directly implicated, which is necessary for the continued progress of the process of fissuring, and again the rapidity of passage minimises the period during which the force is exerted. It is in these points that I believe the chief differences between the modern and old gunshot fractures find their explanation, since with the larger bullets fractures extending from some distance into the joints were a somewhat special feature. In addition it is probable that the alteration in structure at the junction of the shafts with the cancellous ends also tends to check the regular extension of the fissures, as a similar limitation is illustrated even in some fractures by Snider bullets. Fig. 51 of the lower end of the femur illustrates a not uncommon lower limit to a comminuted injury in this region.
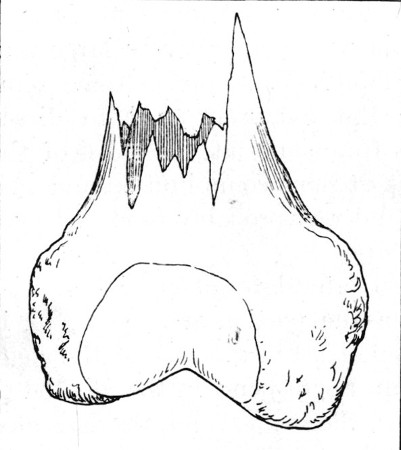 Fig. 51.—Lower end of Femur.
Fig. 51.—Lower end of Femur.
From Case needing amputation. It shows the usual tendency of the fissures to stop short of the articular ends of the long bones
The degree and nature of the comminution also vary with the directness of impact on the part of the bullet. The more nearly this approaches at a right angle, the more severe is the local comminution, but probably a lesser area of the shaft is implicated. Plate V. shows an example of this: all trace of continuity is lost, a wide gap separates the bone ends, while the fragments themselves have been for the most part driven altogether out of the wound. Oblique impact, on the other hand, may widen the comminuted area at the point of impact, while, if the bullet retains sufficient force and regularity of outline, it may then travel 'cutting its way' through the remainder of the bone in an oblique direction. It will be of course recognised that the exact impact of the bullet depends not alone on the direction of the projectile, but also[Pg 165] on the nature of the slope offered by the surface of bone struck.
2. Wedge fractures.—This form (c and d, fig. 50) is equally characteristic of gunshot injury with pure perforation; it is met with in two varieties. c illustrates the more strongly marked type; in it the bullet makes passing lateral impact with the shaft, and from the point struck radiating fissures extend to the opposite margin, so that a wedge-shaped piece of bone often secondarily comminuted is separated from the remainder of the shaft; see plate X. of the radius.
The second variety, d, is an incomplete development of the stellate fracture in which the fissures pass to one margin of the bone only. The explanation of this variation is probably to be sought in the direction of impact on the part of the bullet, since the main fissure is often accompanied by secondary lines which run a somewhat parallel course to the main one, and suggest the dispersion of the force in the form of concentric waves. Such fractures were most strongly marked in the tibia, the breadth of the surfaces of this bone presenting especially favourable conditions for their production.
3. Notched fractures.—These may be a slight degree of the form of wedge fracture last described; such a one is depicted in plate XXII. where a portion of the spine of the tibia has been carried away by a passing bullet. Other notched fractures approximate themselves more nearly to perforations, the notch being a groove secondary to the opening up of such a track as is shown in the illustration of a perforation of the lower third of the shaft of the tibia (fig. 57 on p. 219). Notching or grooving is naturally much more common in the cancellous portions of bones.
4. Oblique fractures.—These also occur in two varieties: the first has been already alluded to; in it the bullet actually cuts an oblique track in the bone; the main line of fracture is often considerably comminuted, usually at the proximal end of the track (see plates XV. and XIX.).
The second variety (e, fig. 50) is less common; in it two of the main limbs of the simple stellate figure are suppressed, while the remaining two form a continuous line from one margin of the shaft to the other, the point of impact lying[Pg 166] approximately in the centre of the line of fracture. Such a fracture is illustrated by the skiagram of a femur in plate XVI. in which the bullet traversed the soft parts transversely at the level of the centre of the fracture, which was 9 inches in length. In another case the line of fracture occupied the lower third of the femur, passing from the inner border of the shaft, the lower end of the upper fragment was formed by the compact tissue forming the outer wall of the external condyle. This latter perforated the vastus externus and lay beneath the skin; as it could not be disentangled, an incision was made over it, and the fragments when reduced were screwed together by Mr. S. W. F. Richardson. In neither fracture was there any comminution. Such fractures most nearly resemble the oblique or spiral ones met with in civil practice as the results of falls. In all the instances I observed the patients were supported on the lower extremities at the time of the accident, and one can only assume that a twist of the trunk consequent on the fall of the body diverts the most forcible vibrations resulting from the impact of the bullet into one line, and thus produces a solution of continuity of a simple oblique nature. In both the cases mentioned above the bullet was probably travelling at a low degree of velocity; in the first it was a ricochet and was retained. I never saw one of these fractures in the upper extremity.
Plate XXI. affords an excellent example of this mechanism. The patient was standing when struck, and then fell backwards. An incomplete fissure 7 inches in length is seen to extend from an otherwise pure perforation of the shaft of the tibia.
5. Transverse fractures.—Throughout these were of very rare occurrence. Plate XX. illustrates a pure transverse fracture produced by passing contact of a bullet probably fired at a distance not exceeding 400 yards, and which subsequently struck the fibula plumb and produced considerable comminution. No fissure extended into the ankle-joint. Comminutions such as that illustrated by plate V. more or less simulated transverse fractures, but I saw no examples of transverse tracks comparable to the oblique ones described above 'cut through' the shaft of a bone.
6. Perforations.—Although these were common in cancellous bone, they were comparatively rare in the compact[Pg 167] shafts. I saw, however, complete pure perforations of the shafts of the tibia, femur, clavicle, and other bones. These perforations were, I believe, always the result of low degrees of velocity, and they took the place of simple transverse fractures of the 'cut' variety. The apertures of entry and exit in the bones resembled in character those seen in the soft parts, or in the bones of the skull in low-velocity injuries (see figs. 71 and 72, p. 261). The entry was more or less cleanly cut, while at the exit a plate of bone was raised, and either separated or turned back on a hinge by the bullet (fig. 52), (plate XVII.) Such a projecting hinged fragment was sometimes a source of some trouble; thus in a case of postero-anterior perforation of the lower third of the shaft of the femur, the long exit fragment projected into the substance of the quadriceps extensor muscle, and interfered with flexion of the knee-joint. Fig. 57 of a superficial tunnel of the lower third of the tibia is especially interesting as bringing such injuries of the long bones into line with fractures of the flat bones of the skull, such as are illustrated in fig. 68, p. 259.
Plate XXI. affords an excellent example of perforation of the shaft of the tibia, although complicated by the secondary fissure.
Plates XXIII., VIII., and III., of the fibula, humerus, and clavicle, exhibit examples of what may be called spurious perforations of the shafts of bones, since comminution or loss of continuity accompanies all three.
Subsequently to writing the above paragraphs, I took the opportunity of re-examining the magnificent series of gunshot fractures collected during the Franco-German campaign by Sir William MacCormac, and afterwards presented by him to the museum of St. Thomas's Hospital.
The close approximation in type between the main features in these and those in the fractures produced by the modern bullet is very striking. In the case of the shafts of the long bones, the same stellate, oblique, wedge-shaped, and even perforating injuries are illustrated on a coarser scale. In a specimen of a patella, a perforation of the lower half, implicating also the tendon of the quadriceps muscle is, though large, almost as pure as a Mauser perforation.[Pg 168]
The difference in the nature of the lesions of the bones is seen to be, firstly, one of pure magnitude, corresponding to the size of the large Snider bullet by which they were produced. Thus the fragments generally are larger, and occupy a wider area of the shafts, the first character depending on the lesser degree of velocity of the bullet, the latter on its volume and weight. Fine comminution, however, the most striking feature of the modern injury, is throughout absent.
The effect of the larger size of the wedge provided by the bullet in increasing the length of secondary longitudinal fissures is well marked, and for the same reason the perforations are usually accompanied by fissures of considerable extent. It is interesting to note, however, that even in the case of the large bullets, and the special tendency shown by them to cause the extension of fissures into the joints, one or two specimens still show that these fissures incline to stop short when the point of junction between the portion of the shaft occupied by the medullary canal and that built on a foundation of cancellous tissue is reached.
The above types of fracture are those common to the shafts of the long bones, but the difference in structure of the articular ends and the short and flat bones endows lesions of these with somewhat different characters, the nature of which varies between grooving, perforation, and great comminution.
The most typical injury consists in the production of a clean perforation of the cancellous bone; this was common both in the articular ends and in the short bones. The tunnel differed little in character from those already described, a tendency always existing to the lifting of a lid of compact tissue at the exit end of the track.
For the production of the cleanest forms of injury I believe high rates of velocity were distinctly favourable, although I am unable to maintain this statement by proof in the case of injuries received at the shortest ranges of fire. When the velocity was lower, yet with force still sufficient to[Pg 169] produce a perforating injury, the separation of an extensive scale of bone at the exit aperture was a marked feature not seen in perforations produced by higher degrees of velocity. Fig. 52, of a perforation of the lower end of the femur, well exhibits this feature; but it must be borne in mind in this case that the illustration is not a pure one, both shaft and epiphysis taking part in the walls of the track, and the exit opening is in the former, where a thicker layer of compact bone exists than would cover any epiphysis, and hence the fragment is larger. I use the example, however, because it so forcibly illustrates the effect of increased resistance on the part of the bone struck in widening the area of the lesion. When the track was entirely limited to the articular ends the small amount of damage at either aperture was shown by clinical evidence in the rarity of subsequent limitation of joint movements due to bony deformity.
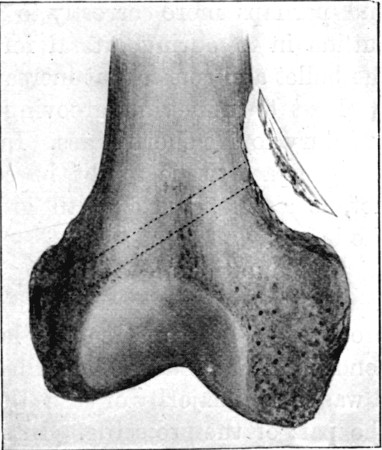 Fig. 52.
Fig. 52.
Oblique perforation, implicating both epiphysis and diaphysis. Large fragment detached at exit aperture. Caused by a bullet travelling at a low rate of velocity. Compare with figs. 71 and 72 of a skull fracture. The dotted lines indicate the course of the track
Again, it was rare for fissuring to extend from these tunnels to the articular surfaces; thus many instances could be given of perforation of the head of the humerus, the olecranon, or the femoral condyles, in which no evidence of joint fissure was discoverable. The slight amount of resistance offered by the cancellous ends was also clinically illustrated by the absence of severe synovial effusions when they were struck. When the joint cavity was not crossed, slight effusion only resulted, while in the case of fractures of the femoral shaft great effusion into the knee-joint, resulting from the forcible vibration transmitted to the limb, was a common feature, even when the point fractured was situated[Pg 170] above the centre of the bone. Again, when the joint cavity was crossed a moderate degree only of hæmarthrosis was the most common result.
With regard to the implication of joints, either primary or secondary, in connection with fractures of the articular ends, I am inclined to place the lesions of the upper end of the tibia in a more important position than those of any other bone. Evidence of this implication was in my experience more frequent here than in any other situation. This may in part be attributable to the complexity of structure of this epiphysis, and perhaps more correctly to the influence of its irregular outline in favouring lateral forms of impact on the part of the bullet and consequent increase in the area of damage.
Next to tunnelling, grooving was the most common form of injury to the short bones. In the case of superficial tracks the compact tissue might be considerably comminuted, but not, as a rule, over a width greatly exceeding the calibre of the bullet.
Comminution and crushing of a single or several bones were rare in proportion to the occurrence of similar injuries produced by Martini-Henry or large leaden bullets. When the condition was produced by bullets of small calibre, I believe it was in the majority of cases the result of irregular impact on the part of the projectile. In support of this view it may be added that such injuries were most common in the bones of the tarsus, bones especially liable to be struck by ricochet bullets.
It was generally believed that bullets travelling at a very high degree of velocity were liable to cause severe comminution of the short bones, but I never saw any cases supporting this opinion; in point of fact, all the short-range lesions of this nature that I saw were of the clean perforating variety. I believe that this is capable of satisfactory explanation on the ground of the thin character of the layer of compact tissue which for the most part ensheaths the short bones; this decreases the resistance offered to the bullet and so tends to localise the lesion. This statement may be supported by two observations with regard to the long and flat bones. First, if the shaft of a long bone be hit above the junction of diaphysis and epiphysis, the cancellous tissue in and extending from the medullary[Pg 171] cavity is pulverised, and examination of fragments from such fractures gives the impression of the inner aspect having been scraped clean. Secondly, I saw one fracture of the ilium produced by a bullet taking a course between its compact layers for 3 inches from the notch between the anterior superior and anterior inferior spines; the bone to the extent of 2½ square inches was pulverised, the cancellous tissue blown away as dust, and the compact tissue only represented by scales still adhering by their periosteum to the muscles attached to the two surfaces of the bone. This injury was produced from a rifle fired at five yards distance, and was an extreme example; but, on the other hand, it illustrates only what we are thoroughly well acquainted with in the case of flat bones, such as those of the cranium, where the compact element is abundant in comparison with the cancellous, and the resistance offered to the bullet is consequently great.
Some remarks on transverse fractures of the patella will be found under the heading devoted to that bone.
Lesions of the flat bones are considered at some length in Chapter VII., which deals with injuries to the head, and their special features are there described; some further remarks on these injuries will be found under the headings of the individual bones.
Special characters of the symptoms observed, and of the course of healing of the fractures.—Peculiarities in the initial signs may be rapidly passed over. The first depended on the large number of lesions of the bone which were unaccompanied by loss of continuity. In the case of perforations attention to the course of the track, external palpation, and possibly the detection of bone dust in the aperture of exit, were usually sufficient to indicate injury to the bones. When these did not suffice the introduction of a probe would usually set the question at rest; but this is always to be avoided if possible, as adding a fresh item of risk to the wound. The X rays were not always to hand, and are not always capable of giving reliable information in the matter of perforations, although very useful in detecting grooves or notching. The latter injuries are those in which information[Pg 172] as to the condition of the bones is often of most interest in view of the characters of the external wounds.
Fractures with solution of continuity were, as a rule, easy of detection, but the relative prominence of the classical signs varied somewhat from what we are accustomed to see in civil practice.
The first striking peculiarity noted in comminuted fractures of the long bones was the degree of local shock; the limbs were often quite powerless, the muscles flaccid, and common sensation lowered. This was of importance in two ways; firstly, shortening of the limb was often absent as a sign, and, secondly, pain was sometimes not at all pronounced even when the patient was moved. The primary absence of shortening, even persisting for the first two or three days, was a phenomenon always important to bear in mind, as it affected the degree of extension needed in the treatment of the fracture, which, if sufficient at the moment, often proved quite inadequate with the return of tone in the muscles. Secondly, abnormal mobility was usually strongly marked, and this sometimes without very definite crepitus, as a result of the fine nature of the comminution and the displacement of the small fragments.
During the course of healing some other peculiarities are worthy of mention. First of all, union was tardy and often not strong. On the other hand, an abundance of provisional callus was common, which formed large swellings apt to implicate neighbouring nerves, and sometimes to interfere with the movements of joints. The slowness of healing was particularly noticeable in those cases where the degree of local shock had been marked, and was probably to some extent dependent on disturbance of the general nutrition of the tissues of the affected limb. Beyond this, however, it was in many cases a direct result of the degree of comminution and displacement of the fragments, which necessitated the formation of a large amount of provisional callus, and time for the proper consolidation and contraction of the same. In many cases a large ball-like mass of callus surrounding the fragments was developed, into which the actual ends of the broken bone only dipped, and hence union was weak and insecure. As to[Pg 173] those cases in which the wounds closed by primary union, we must bear in mind in this relation the tardy union often observed in civil practice, when the irritation of suppuration and consequent inflammation are absent.
Another peculiarity of a similar nature was the occasional late necrosis of fragments; the wounds apparently healed well, only to break down weeks or months later for the discharge of a sequestrum. Such cases were quite distinct from those in which primary suppuration had occurred. I saw one or two instances in fractures of the humerus, the trouble arising with commencing use of the limb, and I suppose that fragments which suffered death at the time of the injury had been enclosed, and only caused irritation as foreign bodies when the muscles again came into action. In the absence both of evident necrosis and suppuration, however, in some cases the exit portion of the track in the soft parts was extremely slow in healing. Although no discharge beyond a small quantity of blood-tinged serum escaped, the wounds remained open for many weeks, even when the fracture consolidated well. I ascribed this to slow separation of aseptic sloughs, a point which has already been mentioned under the heading of wounds in general.
Superabundance of callus, as far as I had an opportunity of judging, comparatively seldom gave rise to permanent mechanical trouble. This was no doubt due to the infrequency of extension of the comminuted fractures beyond the junction of diaphysis and epiphysis.
Lastly, with regard to suppuration, only a small proportion of the fractures, accompanied by the presence of large wounds, escaped infection. When infection did occur, the results offered some special features dependent on the small relative amount of damage to the soft tissues, compared with that suffered by the bone. In an ordinary compound fracture, such as we meet with in civil practice, whether the result of direct or indirect violence, a considerable amount of contusion or laceration, as the case may be, accompanies the injury to the bone. The result of this is a widespread effusion of blood into the limb, which tears and strips up the various layers of soft parts, and opens up the way to the spread of infection, often into the[Pg 174] whole length of the segment of the limb affected. In fractures produced by bullets of small calibre, even when the exit portion of the track is large, the injury to the soft parts is far more localised, except in extreme cases, while the bone itself is the tissue which has suffered the most severe violence and contusion. When infection occurred, its spread corresponded with this anatomical feature of the lesion, and the bone itself and its immediate neighbourhood suffered the most severely.
At the present day one is naturally not very familiar with a large series of suppurating compound fractures, but during my whole experience I have never seen so many cases of what might be regarded as fairly pure instances of acute osteo-myelitis. The symptoms corresponded with the main seat of the suppuration; only moderate swelling of the limbs occurred, this mainly consisting in soft superficial œdema; often there was no redness, and fluctuation was difficult to determine. At the same time symptoms of constitutional infection, such as continued fever, rapid pulse, restlessness, loss of strength, progressive anæmia, and emaciation, were marked. Pyæmia, as evidenced by secondary deposits, was, however, rare; I only saw two cases, both in fractures of the femur; in both recovery followed secondary amputation.
Prognosis.—This depended almost entirely on the nature of the injury to the soft parts; given moderate injury to these, and the preservation of the wound from infection, scarcely any degree of injury of the bones precluded recovery, even if this were slow and prolonged. The existence of perforations scarcely increased to an important extent the gravity of a wound of the soft parts alone; in fact, this injury could not be regarded as more severe than an ordinary surgical osteotomy, putting the risks of infection of the wound under the special circumstances on one side.
With regard to the functional results, these depended on the degree of comminution; when this was extreme, union was slow and for a time weak, and shortening was often considerable, but a fair result was as a rule obtained.
Suppuration and osteo-myelitis were the dangerous features when they occurred; still, even in the presence of these, I never saw a fatal result in an upper extremity fracture, although[Pg 175] in the lower extremity a considerable mortality followed fractures both of the leg and thigh, the deaths being most commonly from septicæmia, or from a combination of this with secondary hæmorrhage.
Treatment.—The general treatment was of a simple character. The perforations may be at once dismissed, since nothing more was needed than what has been already described under the heading of wounds of the soft parts. Again, with regard to the co-existence of vascular injury, or injury to the soft parts generally, the ordinary rules guiding us in civil practice were followed.
The first point of importance, and needing consideration in the treatment of severely comminuted fractures, was as to whether in these it was better simply to try to obtain union of the wound with as little disturbance as possible, or to anæsthetise the patient and explore the wound, removing such fragments as were free or widely displaced. I think the answer to this question depends entirely on the nature of the external wounds. If these be of the small type forms, or if the exit aperture is, at any rate, of only moderate size, a strictly conservative attitude is the better when the risk of making an exploration under the circumstances is borne in mind, the more so as an exploration, to be safe and useful, ought to be done at once. If the exit wound is of the large or explosive type, on the other hand, there is no doubt that the best results are to be obtained by early exploration and the removal of all loose fragments. I saw several excellent results obtained in this way, even when the patients had to undergo the risk of transport shortly, in some cases the very next day, after the operation. The loose fragments are an immediate source of danger, and later may interfere with the healing of the fracture, even if suppuration does not occur. In all the cases that I saw the exit wound was dressed, but left freely open, and I do not think any attempt to close it should ever be made.
The question of operative fixation rarely needs consideration; it occasionally happens, however, that oblique fractures, such as one mentioned on p. 166, are met with, in which screwing or wiring of the bone ends is advisable. What[Pg 176] has been said above as to fractures, accompanied by loss of continuity, applies equally to cases of severe wedge-fracture, where many loose fragments exist.
As to the disinfection of the limb, primary cleansing, mainly by soap and water, of course precedes the exploration, and when the latter has been carried out a second cleansing and disinfection, preferably with spirit and carbolic acid lotion, are imperative.
Immobilisation is a more difficult problem. In practised hands plaster-of-Paris splints answer most requirements except in the case of the thigh; but the splints take time to apply and also to set firmly, and, as sometimes needing frequent removal, are not altogether suitable for Field hospital work. Of all the splints I saw in use, I think the best were wire splints, and the Dutch cane folding splints for the thigh and leg (figs. 56, 58); wire-gauze splints with steel at the margins (fig. 54), or strips of ordinary cardboard applied with some variety of adhesive bandage for the arm and forearm; and plain wooden of various lengths for any situation.
A question of constant difficulty was that of frequency of dressing; in a Stationary or Base hospital this is not difficult, as the same surgeon has the patient continuously under his charge, and can readily decide as to the proper moment for the renewal of the dressing. When the patient is, however, being moved from the Field to the Stationary hospital, and thence to the Base, a constant succession of surgeons has the case in hand for short periods, the movements during transport disturb the fixity of the dressing, and, in consequence, dressings are apt to be far more frequent than is advisable. This question raises the larger one of the advisability of any transport beyond what may be an actual necessity. There is only one answer to this. No fractures of the thigh or leg, and few of the arm, can be transported for any distance without material disadvantage. The risks attendant on disturbance of the fracture and tissue injury, septic infection as a result of slipping of the dressing and the impracticability of efficiently renewing it, far more than counterbalance any advantage to be gained from the superior comforts available at a Base hospital. For these reasons, if possible,[Pg 177] all fractures of the arm, thigh, or leg should be kept at a Stationary hospital for a period of three or more weeks, and, as far as splints and appliances are concerned, these should be as numerous and complete as at a Base hospital. I have had a useful set made of aluminium. A word will be added later as to the splints suitable for different regions of the body.
The necessity for primary amputation chiefly depends on the nature of the injury to the soft parts, less commonly on the extent of the injury to the bones, and should be decided on exactly the same lines as in civil practice. So-called intermediate amputations are always to be avoided if possible; the results were consistently bad, and the operation should only be undertaken in cases of severe sepsis where little can be hoped from it, or for secondary hæmorrhage. When the operation could be tided over until the septic process had settled down and localised itself, secondary amputation gave very fair results. In either intermediate or secondary amputation for suppurating fractures, it was necessary to bear in mind the special likelihood of the existence of extensive osteo-myelitis. If this condition affected the upper fragment, an amputation was of little use unless the whole bone was removed, as septic infection continued and brought about a fatal issue, or a fresh amputation was required in order to obtain a stump that would heal.
Upper Extremity.—Fractures of the scapula were not uncommon, but were mostly of the perforative variety; thus perforations both of the spine in longitudinal wounds of the back, and of the ala in perforating wounds of the thorax, were tolerably frequent. They possessed little practical interest; as a rule, the openings were not large, and the most unexpected feature was the small interference with the movements of the bone on the chest wall that resulted. It might be assumed that comminuted fragments would project into the muscles and cause both pain and interference with movement; but neither was the case. I saw grooving of the crest of the[Pg 178] spine, but never happened to meet with a fracture of the acromion process. Many axillary tracks passed in the closest proximity to the coracoid, but this again I never saw separated. One practical point of importance with regard to the scapula was the frequency with which bullets lodged in the venter, or the firmly bound-down muscles of the supra- and infra-spinous fossæ. These retained bullets often gave rise to remarkably little trouble in this situation; thus I have a skiagram of a shrapnel bullet lying in the deepest part of the subscapular fossa, which did not inconvenience its possessor.
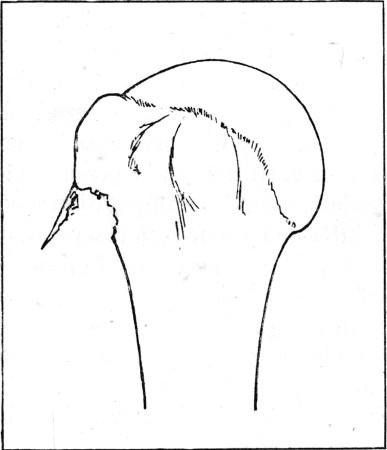 Fig. 53.
Fig. 53.
Head of Humerus, showing broken perforation. The roof forms a hinged covering to a groove
Every variety of fracture of the clavicle was met with, even perforation of the most compact portion of the shaft; comminuted, wedge, or notched fractures were, however, the more common, and were accompanied by the development of very large masses of provisional callus during the process of healing. An interesting skiagram is reproduced in plate III., which shows a compound form of injury to the clavicle. The bullet has passed obliquely beneath the acromial end, rising to perforate the posterior compact margin, and producing one of the diamond-shaped openings sometimes occurring in compact bone with the passage of bullets at a low rate of velocity. No case of perforation of the subclavian vein by comminuted fragments of the clavicle came under my notice.
Fractures of the humerus of every variety were common, and I think when the statistics of the campaign are published, it will be shown that the humerus was the most frequently injured individual bone in the whole body. I remember to[Pg 179] have seen thirteen fractures of the shaft of the humerus in one pavilion alone at Wynberg after the battle of Paardeberg.
Perforations of the upper articular extremity were common, and as a rule gave rise to wonderfully little trouble in the shoulder-joint. The outer aspect of the head of the humerus is a common situation for the production of a special form of broken canal or groove (fig. 53). The slope from the greater tuberosity to the shaft naturally favours the production of the injury in this position.
I saw only one case in which a vertical fissure extended from a fracture of the shaft into the shoulder-joint; in this case the transverse solution of continuity was at the upper part of the middle third of the bone. Skiagram, plate IV., illustrates a well-marked stellate comminution of the shaft with large fragments. Plate V. shows extreme comminution with fragments blown out of the wound. Two plates, Nos. VI. and VIII., illustrate well the difference resulting from the oblique passage of a bullet at high and low rates of velocity respectively. In both cases good results were obtained; in the more severe the resultant mass of ensheathing callus was very large, temporarily interfered with flexion of the elbow-joint, and consolidation was very slow (see plate VII.). The patient was wounded at Belmont in November 1899, but he was able to row at the end of the summer of 1900, although very prolonged suppuration occurred, and the elbow movements became practically normal. Plate IX. illustrates a transverse track, the bullet having undergone considerable injury during its passage through the bone, as evidenced by the presence of fragments both of mantle and lead in the limb. This might be called an example of transverse fracture, and illustrates the nearest approach to one seen when the bone is struck fairly plumb.[Pg 180]
(24) Comminuted Fracture of the Humerus
Range about '300 yards.'
The wound track took a directly antero-posterior course. Impact rectangular. The musculo-spiral nerve was completely divided.
The plate affords a good example of the so-called 'butterfly' fracture. Two long doubly wedge-shaped lateral fragments, and pointed extremities to both main fragments, are shown.
The fracture healed well, with the deposition of a large mass of provisional callus. The musculo-spiral nerve was united by suture some three months later.
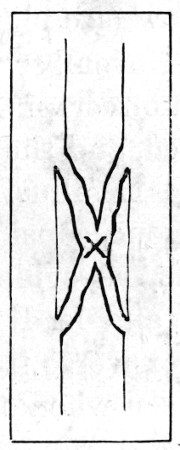 Fig. 53 a.—Diagram of "butterfly' type
Fig. 53 a.—Diagram of "butterfly' type
Plate VIII. exhibits an oblique fracture of the lower part of the shaft produced by a bullet passing at a low rate of velocity. It does not widely differ from a perforation, and the illustration possesses some further interest as showing the deviation of a bullet likely to occur when a bone lies in its course. Although the velocity with which this bullet was travelling must have been very low, when the bone had been traversed the deviation in its course was slight. A few bony fragments from the compact tissue of the posterior surface of the humerus have been carried into the distal portion of the track.
Fractures of the various prominences of the lower articular extremity were not uncommon, but deviated little from the types with which we are familiar in civil practice; the after results were good, both as to union and movement of the elbow.
Explosive wounds of the soft parts were not infrequent in the arm, and fig. 48, p. 158, exhibits an extreme example. The humerus in respect of depth of covering, however, comes between the femur and the bones of the leg and forearm; hence such injuries were not so easily produced as in the latter segments of the limbs.
In connection with the subject of fractures of this bone, one word must be added as to the occurrence of the most characteristic of its complications, musculo-spiral paralysis. This was frequent in every position of the fracture, and came on either immediately, or, at a subsequent period, as a result of callus irritation or pressure. Its frequency is only what would be expected when the nature of the fracture is considered, but the chief interest of the condition lay in the difficulty of certainly detecting it in the initial stages of the cases; this depended on the fact that in many of them the local shock to the limb was so severe that the function of the whole of the muscles was lowered, or in some cases, although the musculo-spiral was the nerve chiefly affected, the other large trunks had also suffered concussion or contusion. In consequence of this difficulty the actual localised paralysis often only became evident at the end of a week, or even more, when there was difficulty in deciding as to whether the paralysis was primary or due to secondary trouble. In the fracture illustrated by skiagram, plate IV., the nerve suffered complete division, and was united some three months later, improvement in the symptoms being very slow. The latter was a common experience, and although not unusual in civil practice, I think it is more marked in these injuries as a result of the more widespread character of the nerve lesion.[Pg 182]
(25) Comminuted Fracture of the Humerus
Range '50 yards.' Velocity extreme.
Impact somewhat oblique. The bullet entered anteriorly about 3 inches above the elbow crease. The wound of exit was on the inner aspect of the arm and explosive in character; it still measured 4 inches by 2 inches three weeks after the injury was received.
The wounds suppurated locally, but at the end of six weeks fair union of the bone had taken place and the wound of exit had contracted to a sinus. The musculo-spiral nerve was concussed, but not divided.
The skiagram was taken three weeks after the reception of the injury.
Comparison with plate IV. demonstrates the effect of high velocity in free comminution of the bone, the sharper radiation of the stellate lines of fracture, and the propulsion of bone fragments.[Pg 183]
The bones of the forearm were also often fractured. The principal peculiarity of these fractures was the common localisation of the injury to one bone, which is readily seen to be probable.
Each bone offered some special features dependent on its structural character and anatomical position. In the case of the ulna, pure perforation of the olecranon process, without obvious evidence of implication of the elbow, was seen on several occasions. The other important feature with regard to this bone depends on its subcutaneous position, which accounted for the frequency with which highly developed explosive exit wounds were met with. One is figured in the general section (fig. 47, p. 156). This, however, is a very slight instance compared with what was often seen in the upper and middle thirds of the bone, where the lateral soft parts often protruded as a much larger tumour, the particular illustration being mainly designed to show the nature of the injury to the skin. The radius, as more deeply placed in the upper part of its course, was less often the seat of such well-marked explosive injuries; but when the lower end was struck this character was sometimes very striking: thus in a track passing antero-posteriorly through this bone, the whole lower end appeared shattered, all the tendons at the back of the wrist being implicated in the protruding mass, while the bone itself seemed shortened, so that the hand took up the position common in Colles's fracture. It was found impossible to place the bone in good position; nevertheless the patient retained his hand, which is still of use in writing.
Plate X. is a good example of a high-velocity injury in which lateral contact with the radius has produced local comminution, some slight injury to the casing of the bullet, and the separation of a large wedge. The case from which this was taken also illustrated well one of the chief troubles of such fractures of the forearm; the degree of splintering resulted in the formation of a large mass of callus, which for a time rendered any degree of pronation and supination impossible.[Pg 184]
(26) Comminuted Fracture of the Humerus
Range '250 yards.'
Impact oblique. Wound of entry 1 inch below the insertion of the deltoid; exit, on inner aspect of arm at a slightly lower level. The bullet probably struck the bone laterally, and drove out the central fragment.
Prolonged suppuration resulted, but the humerus healed well, and good movement of the elbow was preserved.
The effect of oblique impact together with high velocity is well illustrated. Had the resistance been greater, as in the case of the femur, a nearer resemblance to the effect seen in plate XV. would have been the result.[Pg 185]
Of fractures of the hand I have little to say. In the case of the carpus, the slight degree of resistance offered by the bones rendered injuries of an explosive character rare. I never saw one. Fractures of the metacarpus, on the other hand, presented exactly the opposite features. The density of these small bones was well illustrated by the frequency with which the bullet suffered injury, even amounting to fragmentation, and the great comminution they themselves suffered. The breaking up of the bullet in these fractures was a curious feature, which may perhaps be explained by the tendency of the distal part of the limb to be driven in the course of the bullet, with the result of somewhat lengthening the period of contact of the projectile, or more probably by somewhat frequently occurring irregular impact. Plate XI. is a good example of an injury of this nature of moderate severity. The soft parts suffered much in these injuries, the tendons were torn and lacerated at the moment, and were very apt to acquire more or less permanent adhesion. This latter condition was sometimes to be improved by the removal of bone fragments, and I have freed tendons from actual clefts in the bones where they had been carried in by the bullet. In some cases very great deformity of the digits, due to shortening, developed, even when no fragments were removed beyond those blown away by the bullet.
One form of injury of some interest was multiple fracture of the phalanges produced by a bullet travelling in a course parallel to the length of the rifle when pointed by the patient. Occasionally several digits were lost.
Treatment of fractures of the upper extremity.—The general lines of this have already been foreshadowed in the general section, the remarks as to transport being applicable to all serious fractures of the shaft of the humerus, and this is the only one of the bones of the upper extremity on which anything special need be said, as the treatment of all the other fractures exactly coincides with that of ordinary civil practice.[Pg 186]
(26a) Condition of the same Fracture shown in Plate VI., a year after its production
The ensheathing callus is still very abundant, but less so than at an earlier date. No trouble with the musculo-spiral nerve was noted, but residual abscesses occurred from time to time in connection with the fracture.[Pg 187]
 Fig. 54.—German Wire Gauze Splint on steel wire
foundation.
Fig. 54.—German Wire Gauze Splint on steel wire
foundation.
(German Ambulance, Heilbron)
The treatment of wounds should be on the lines already laid down: thorough cleansing, and then an attempt to seal. In severely comminuted fractures, however, the exit wound may be of very large size, and then frequent dressings are necessary. Loose fragments, by which those freed from their periosteal connections are meant, need removal. The question which most interested me was the best method of fixation. This needs to be sufficient to effect immobility, but on the other hand in many cases the weight of the arm as a means of extension is very valuable. Some of the most successfully treated cases that I saw were fixed by means of simple strips of pasteboard, applied moist, and fixed with an adhesive bandage. Ordinary book-muslin bandages are as good as anything for this purpose, as they can be reinforced by a stronger form outside them. Where necessary, an angular piece of cardboard can be applied on the inner aspect, or a wooden angular splint may be substituted, if it is at hand; but in this case most of the advantage of the weight of the arm as a means of extension is lost. The cardboard cases possess the great advantage of being readily cut off and reapplied much as is done with plaster of Paris. During the period in which dressing may be necessary I believe this form of splint is as good as can be got for use in Field hospitals, the only point needing care being to ensure that the bandaging is not too tight. It is much more reliable than are ordinary splints if transport is unavoidable, and is much lighter and less irksome to the patient. With such strips of cardboard, a few of the gauze splints (fig. 54), and a few angular and wooden splints, I believe a Field hospital is fully equipped for the treatment of any fractures of the upper extremity.[Pg 188]
(27) Oblique Fracture of the Humerus of the nature of a Perforation
Range more than '1,000 yards.'
The distance was probably much greater, as the bullet was retained and undeformed, and the comminution of the bone was very slight. The wound of entry was just below the elbow.
The bullet has cut its way through the inner half of the humerus, producing little comminution and mere solution of continuity of the bone without displacement[Pg 189]
Fractures of the pelvis.—These, as a rule, were of so slight a nature as to form a very insignificant part of the entire injury with which they were associated, or when uncomplicated they were of little more importance than simple wounds of the soft parts. The very great majority were of the simple perforating type. I had the opportunity of examining three at the brim of the pelvis, these all passing in a downward direction. The openings were of about the same calibre as the bullet, and at their entrance was a small amount of bone dust such as would be found at the entry hole of a gimlet. It was these that made me consider the possibility of the rifle grooves having some part in the ease with which certain perforations are made. Of a large number of cases in which bullets traversed the ilium, the openings in the bone, as a rule, were with difficulty palpated. I must say that I was astonished that I never met with an instance of an extensive stellate fracture in the case of the ilium. Such may have occurred in some of the cases fatal on the field or shortly afterwards, but I never came across one in the hospital. It says much for the combined density and toughness of the human pelvis.
Comminuted fractures were, however, occasionally met with when the bullet passed in a track parallel to the plane of the bone. One such of an unusual character has already been mentioned on p. 171. A still more interesting form, and one highly characteristic of flat bone injuries, is shown in fig. 55. The patient, a man wounded at Modder River, was struck at a range of 300 to 400 yards. The bullet entered over about the centre of the ilium and emerged in the anterior abdominal wall about 2 inches above the anterior-superior spine. As there was some doubt as to penetration of the abdomen, and as the exit wound was of considerable size, the wound was explored, an anæsthetic having been given. A clean-cut track in the bone was discovered which allowed the middle finger to be placed in it. There was little splintering of either inner or outer table of the bone beyond the width of the track, but plates of each table adhered on the one side to the origin of the gluteus medius, and on the other to the iliacus, the latter muscle being somewhat widely separated from the venter ilii by effused blood. There was no perforation of the abdominal cavity.[Pg 190]
(28) Localised Comminuted Fracture of the Humerus
Range '100 yards.'
The entry and exit wounds were on the front and back aspects of the arm, about 3 inches above the elbow.
Fragmentation of the mantle of the bullet has occurred. It will be noted that the fragments are lodged in both the proximal and distal segments of the track. This may indicate that the bullet was damaged prior to entry, or the recoil of fragments. I incline to the latter view. The skiagram was taken a fortnight after the injury.
The large median fragment carried forwards, and the small degree of comminution, suggest the decrease of resistance and prolongation of impact by carriage back of the arm when struck.
The fracture is one of the nearest approaches to a transverse cleft that I met with.
The plate may well be compared with No. XII., where the effect of increased resistance in augmenting the degree of comminution is seen.[Pg 191]
Lesser degrees of the same kind of injury amounting to grooving of the surface or notching of the crest of the ilium were not uncommon, and the occasional large character of exit openings in buttock wounds pointed to contact of travelling bullets with other parts of the external pelvic wall.
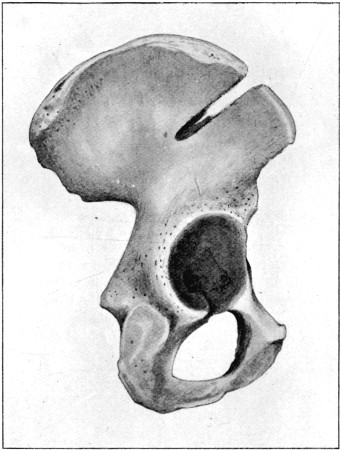 Fig. 55.
Fig. 55.
Clean Gutter Fracture of the Ilium (range placed by patient at 300 yards. Highland Brigade, Magersfontein). The gutter was clean cut, and admitted the forefinger. The inner and outer tables of the bone were in part blown out of a large irregularly circular exit opening about 1½ in. above the crest of the ilium. The cancellous tissue was probably entirely blown out. Plates of the outer and inner tables still remained connected by their periosteum to the deep aspects of the iliacus and gluteus medius muscles. The peritoneal cavity was not opened. The patient did well. Compare with the gutter fractures of the skull shown in figs. 64, 66
Certain portions of the pelvis were subject to more severe comminution; thus in one case in which the bladder was wounded, a very much comminuted fracture of the horizontal ramus of the pubes was produced by a bullet which subsequently lodged in the thigh behind the femoral vessels. In this case the track was so oblique as to have necessitated almost pure lateral impact on the part of the bullet; hence the form of injury was nearly allied to the comminutions of the ilium already described.[Pg 192]
(29) Wedge-shaped Fracture of the Radius
Range 'a few yards.'
The officer shot the man, his assailant, with a revolver. The entry wound was on the posterior aspect of the forearm at the junction of the middle and lower thirds. The exit wound was on the anterior aspect of the forearm, 1 inch below the elbow crease, and of moderate size.
Some fine fragmentation of the mantle of the bullet is indicated, and very fine comminution of the bone. The fracture healed well, but the resulting mass of callus at the end of three months prevented any movements of pronation or supination.[Pg 193]
I never observed a fracture of the floor of the acetabulum by a bullet which had entered from the back of the pelvis, although tracks entering by the great sciatic notch were not infrequent. I saw one case in which a bullet which traversed the upper part of the shoulder and emerged at the axilla entered a second time an inch behind and above the anterior superior spine, and split off a layer of the outer table of the ilium of the extent of two square inches, which involved the upper portion of the rim of the acetabulum. No displacement upwards of the femur resulted; but external rotation was accompanied by crepitus. The wound suppurated, and some general infection resulted, but six weeks later there was no evidence of fluid in the hip-joint, the limb was adducted and slightly rotated outwards, and some movement in each direction could be made without causing any great amount of pain. I can say nothing of the further course of this case, as I neglected to take the patient's name.
I saw one or two instances of perforation of the sacrum. One is mentioned in the chapter on injuries to the abdomen, in which a central puncture at the level of the fourth vertebra was accompanied by temporary incontinence of fæces.
Fractures of the femur were fairly numerous and formed one of the most serious classes of case we had to treat, as well as one of the most fertile sources of mortality in the Base hospitals. In spite of the last observation, however, it is probable that the results in this campaign will be far better than in any previous war, both as to the smaller proportion in which amputation was needed and as to recovery.[Pg 194]
(30) Comminuted Fracture of the Second Metacarpal Bone
Large fragments of the mantle of the bullet.
Fragmentation of the bullet was comparatively common when the metacarpal bones were struck, also free comminution of a somewhat coarser variety than that seen when bones offering greater resistance were struck.
This may be a result of the more frequent lateral impact of the bullet on these small bones.[Pg 195]
In spite of a considerable experience, I never saw a case of perforation of either the head or neck of the thigh bone. I saw numerous tracks emerging at the side of the femoral vessels and entering at the buttock or vice versa, but never one accompanied either by effusion into the hip-joint or impairment of movement. Considering the regularity with which hæmarthrosis occurred when the other joints were crossed, and also the nature of the compact tissue of the neck of the femur, which must have ensured some splintering, I do not think I can have overlooked an injury of this nature. No doubt also the escape of the neck of the bone was explained in some of the cases by the fact that the injuries were received while the hip-joint was in a position of flexion, the bullet passing over the neck of the femur. In two cases of extensive comminution of the upper third of the femur that I saw, the fissures stopped short at the inter-trochanteric line anteriorly, but in one of them a large angular fragment was torn out of the posterior surface of the neck.
Excepting transverse fracture every form was met with in the shaft, although I saw only two instances of perforation. One has been already alluded to and was situated in the broadening portion of the lower third, the bullet taking an antero-posterior course. The second is seen in plate XVII.
Plate XII. shows an instance of extreme comminution of the upper third accompanied by the presence of two typical elongated fragments. The course taken by the bullet was almost directly antero-posterior, and the wounds were of moderate size even in the case of the exit one. This seems to preclude the possibility of the injury having been produced by a ricochet bullet, while the fact of perforation and escape of the bullet in spite of the serious damage suffered by the mantle points to the injury having been produced at a short range of fire. The patient himself owns to being quite unable to give any estimate of the distance. Although no suppuration occurred, this fracture was very slow in consolidating, and the free comminution with consequent inaccurate apposition led to the development of four inches shortening of the limb. The skiagram was taken about six weeks after the occurrence of the injury, a few days after I first saw the patient; I have, however, had the opportunity of seeing a second skiagram taken some four months later. This is of considerable interest, as throwing light on the mode of union of such fractures. The two elongated fragments in the later skiagram are widened to three times their original breadth, and form buttresses on either side of the point of union, while the irregular ends of the shaft are rounded off, and the mass of fine fragments behind is consolidated. Beyond this the second skiagram shows that the upper fragment, apparently intact in the first, was really split longitudinally, and therefore was far less useful as a point of support than might have been assumed from the earlier skiagram, plate XIII. The case illustrates well the chief difficulty in the treatment of such fractures: that of maintaining the fragments in line, since absolutely no help is received from the apposition of the two ends, and artificial traction alone must be relied upon.[Pg 196]
(31) Highly Comminuted Fracture of the Upper Third of the Shaft of the Femur
Range 'short.'
Impact fairly direct. The wounds were of moderate size and at nearly the same level. The exit wound near the buttock fold was of moderate size, and presented no special features.
Considerable fragmentation of the bullet occurred. The comminution of the bone is very fine, suggesting high velocity, and great resistance by the bone. The skiagram was taken five weeks after the injury was received, and at that time no union had occurred.
Reference to plate XIII. will explain more fully the difficulty experienced in maintaining this fracture in position. The upper fragment is seen to be split into fragments, beyond the separation of the long splinter on the inner side; hence no aid was to be obtained from the apposition of the ends. About 2 inches of the shaft were actually pulverised; the fine fragments seen in a mass to the inner side of the bone in the exit portion of the back, eventually formed a large mass of callus, and the fracture united, with considerable shortening.[Pg 197]
Plate XIV. offers a good contrast; the fracture here presents a typical stellate form, and a good result without shortening was readily obtained. I assume that the difference in character of these two fractures depended mainly on the rate of velocity with which the bullet was travelling, since it passed fairly directly across the limb in each. I think it is clear, however, that the bullet struck the femur rather nearer the centre of the width of the shaft and therefore more directly, in the more severe injury.
This brings me to the question of explosive exit wounds in the thigh. In spite of the great tendency to comminution of the shaft, these were rare in a severe form. This depended simply on the depth and thickness of the coverings of the bone, and, as already mentioned, although the skin openings were often comparatively small, a large cavity or area of destroyed soft tissues may be contained within the limb. I do not think I ever saw an exit wound in the thigh exceeding 1½ inch in diameter.
The oblique fracture illustrated by plate XVI. has been already referred to, and the influence of the weight and movement of the trunk on its production has been considered.
Plate XV. illustrates an obliquely comminuted fracture of another character. The bullet has here been stripped of its mantle, which has undergone fragmentation, but the leaden core is little altered in shape. This is of much interest, since it shows that the bullet struck the bone by its side. The effect of such lateral impact on the part of the projectile is well shown: there is great bone comminution of a less regular character than usual, and the bullet is retained. Retention in this case was probably not a result of low velocity of flight, but of the increased resistance offered by the broad area of bone struck, and the check exerted on the axial rotation of the bullet by the lateral contact.[Pg 198]
(31a) The Fracture Shown in Plate XII., six months after reception of the injury
The amount of callus furnished around the loose fragments is very striking.
The upper end of the bone is shown to have been divided into at least two fragments, hence one of the difficulties of maintaining the ends in apposition. The stoppage of the fissuring short of the epiphysis is characteristic.[Pg 199]
Slighter injuries to the femur in which the shaft was chipped or grooved without loss of continuity were not uncommon, and showed well the capacity of the bone to withstand the lateral shock transmitted by small bullets. Two figures inserted in the chapter on wounds in general (figs. 22, 23, pp. 61, 62) are of cases in which, from the appearance of the wound of exit, the bullet probably underwent deformation, or was so deflected as to escape on a considerably altered axis. Beyond the nature of the exit wound in the case depicted in fig. 22, some thickening beneath the femoral vessels denoted bone injury, but unfortunately no skiagram was taken.
I saw no case in which a transverse fracture of the shaft accompanied such injuries, but am under the impression that, if they had been produced by bullets of greater volume and weight, transverse solution of continuity would have been more common. In point of fact, no case of pure transverse fracture of the femur ever came under my notice.
The diagram depicted in fig. 51, p. 164, is from a sketch made of the lower end of a femur in which a severely comminuted fracture followed by suppuration necessitated an amputation of the thigh, performed by Major Lougheed, R.A.M.C. It is inserted as an illustration of the tendency of the fissures to stop short above the actual articular extremities of the bones. In this case the comminution was extreme and accompanied by the usual long lateral fragments, one of which measured five inches in length and might well have extended into the knee-joint had that been an ordinary occurrence.
Perforations of the lower extremity of the bone were very common. These were sometimes transverse and limited to the articular extremity itself, or the same limitation occurred to the antero-posterior tracks. These were the slightest forms of injury, putting on one side incomplete tunnels and grooves on the surface of the bone. With regard to the latter, however, when they invaded the joint cavity the injury was liable to be more severe than a complete perforation, in consequence of the projection of comminuted fragments into the joint cavity near the line of reflection of the synovial capsule and ulterior interference with freedom of movement.[Pg 200]
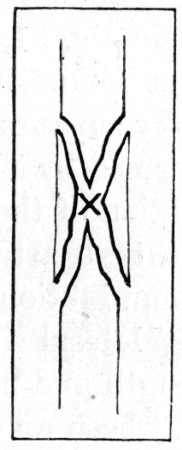 Fig. 55a.—Diagram of 'Butterfly' type.
Fig. 55a.—Diagram of 'Butterfly' type.
(32) Typical Stellate (Butterfly) Comminuted Fracture of the Femur
Range 'short.'
Wounds small, impact direct, very little fine comminution. The bone united without shortening of the limb.[Pg 201]
Other tracks took a direction of longitudinal obliquity, and then implicated both epiphysis and diaphysis. Fig. 52, p. 169, shows an example, and also the peculiarity likely to be assumed by the exit aperture in the bone, especially if the bullet was travelling at a low rate of velocity, a considerable plate of the compact bone being driven out. In some cases these oblique tracks involved both femur and tibia. They will be referred to again under the heading of injuries to the joints, and some remarks will also be found there regarding the synovial effusion so often occurring into the knee-joint in cases of fracture of the shaft of the bone.
It may be of interest to insert here a few remarks as to the clinical characteristics of fractures of the femur. First with regard to the primary signs and symptoms. A very considerable degree of general or constitutional shock usually accompanied them, and this was perhaps more constant than in the case of any other injury in the body. This was, moreover, no doubt increased by the unfavourable conditions in which patients on the field of battle are situated in regard to transport. When the patients were brought into hospital some delay in the primary treatment was often necessary until reaction took place. Local shock to the part was also a prominent feature. Abnormal mobility was very free in the badly comminuted cases. Crepitus was often loose, and of 'the bag of bone' variety. The result of local shock and consequent flaccidity of the muscles was to reduce the development of primary shortening; in some cases of severe comminution this was practically nil during the first day or two, when, with return of tone in the muscles, it sometimes became very considerable. Swelling of the limb was often very great, and vascular injury definitely far more common than in the fractures of civil practice, in consequence, no doubt, not only of the number and sharpness of the fragments, but also of the force with which they were driven into the surrounding tissues. The exit segment of the track was out of all proportion in size to the entry, as a result of the propulsion of bone fragments through it. This often made the closure of the exit wound a very protracted event, the track continuing to discharge a small quantity of bloody serum and fragments of necrosed tissue for many weeks.[Pg 202]
(33) Comminuted Fracture of the Femur
Range 'short.'
Normal entry wound of slightly oval form.
Oblique lateral impact on the part of the bullet, the mantle of which burst into numerous fragments. The bullet is seen to the inner side of the shaft, almost devoid of its mantle, and little deformed at the tip. The comminution of the upper portion of the fracture is very fine; the bullet has merely cut its way down the lower portion, and one or two long fragments are separated. The skiagram shows well the result of lateral impact by the side of the bullet.
Compare this plate with No. VI. as illustrating lesser resistance, and No. VIII. as illustrating the effect of lower velocity.
In a large proportion of the cases which were transported for any distance suppuration occurred; this must have been the case in at least 60 per cent. of the fractures. Suppuration was of the character already described in the general section, affecting particularly the bone itself, and accompanied by very marked signs of general infection.
Prognosis in fractures of the femur.—As regards mortality fractures in the upper third of the bone proved one of the most formidable injuries which came under treatment. Suppuration was common, at least 60 per cent. of the wounds becoming infected. This depended on several reasons, often inseparable from the injuries, or from their treatment in Field hospitals: such as (1) the exit wound being situated in the dangerous region of the thigh; (2) ineffective dressing and fixation; (3) the impossibility of ensuring primary cleansing and removal of detached fragments of bone; (4) the necessity of the early transport of patients to the Stationary or Base hospitals, often for great distances; (5) the comparatively long period that often had to elapse before the opportunity of doing the first efficient dressing arrived.
Fractures in the middle and lower thirds of the bone were more easy to treat successfully, but these also added to the list both of amputations and fatalities.
Punctured fractures of the lower articular extremity were usually of little importance, as they progressed without exception, as far as my experience went, favourably.
I can give no idea of the general results obtained during the whole campaign, but I am able to state the results of the fractures of the shaft treated at No. 1 General Hospital during my stay in South Africa. Thirty-two cases of fracture of the shaft of the bone came under treatment, and of these 6 or 18.7 per cent. needed amputation, and of the whole number 5 or 15.6 per cent. died. To emphasise the satisfactory nature of these figures I need only quote the results attained in the American War of the Rebellion; mortality in upper third, 46 per cent.; middle third, 40.6 per cent.; lower third, 38.2 per cent.[Pg 204]
(34) Oblique Fracture of the Shaft of the Femur
Range '300 to 400 yards.'
Aperture of entry just above the centre of the outer aspect of the thigh. Exit, about 2 inches lower, at the junction of the inner and posterior aspects. The bullet was retained just within the wound, and when removed the mantle fell off in two parts. The leaden core was mushroomed. The bullet had passed through another soldier previous to entering the patient's thigh. Only two small fragments of the mantle were retained, as seen in the skiagram. These were in the substance of the great sciatic nerve, and were subsequently removed by Sir Thomas Smith.
It is difficult to determine how the bone was struck; reference to plate XXI. would suggest that the shaft may have been perforated, but no evidence of this remains in the skiagram taken, which was five months later.
The patient was standing at the moment of reception of the injury, and the obliquity of the fracture no doubt depended on his fall and the resulting influence of the weight of the body. The length of the fracture cleft was 9 inches.
I need hardly dwell upon the difference between the nature of the injuries received in the American War of the Rebellion and in the present campaign, as in the former the old large bullets were employed, and shell injuries are possibly included; but I ought to add in this relation, that the numbers quoted from No. 1 General Hospital included, to my knowledge, at least three severe Martini-Henry wounds.
The first element for a favourable prognosis is a small wound, and opportunity for an efficient primary treatment of the same; the second the absence of necessity for transport of the patient. With regard to the second of these requirements, we were unfortunately situated in South Africa, and the majority of the cases which did badly were moved during the first few days and for a distance of between five and six hundred miles. On the other hand, as a rule, the external wounds were small.
As to functional result, the fractures did well. I think an average of an inch and a half would well cover the shortening, and in many the length was little altered. Considering the serious nature of many of these fractures, this was good.
Treatment.—In all punctured fractures of the lower extremity, dressing of the wounds like uncomplicated ones and a short period of immobilisation were all that was necessary. In oblique fractures, and those with slight comminution, closure of the wound by dressings, after it had been carefully cleansed, was all that was necessary prior to applying the splints for immobilisation.[Pg 206]
(35) Perforation of the Shaft of the Femur. Flap of bone raised at the aperture of exit in the popliteal surface of the shaft.
Range 'over 1,000 yards.'
Compare with fig. 52, p. 169.
In the highly comminuted fractures a more radical treatment was indicated, especially if the exit wound was large. In these, after careful preliminary cleansing of the limb, the wounds, especially the exit aperture, needed exploration and, if necessary, enlargement, and all free splinters needed removal. If interference with the entry wound could be avoided, this was always preferable, as it was rare for this not to heal by primary union unless free suppuration occurred. Under Field hospital conditions I think the exit wound should never be sutured, whatever its situation; and in the present campaign, where carbolic acid lotion was freely used, this step was manifestly inadvisable, in view of the abundant serous discharge always to be expected when this disinfectant has been employed. Except in cases manifestly infected at the time of exploration, the use of drainage tubes or plugs is not to be recommended. I would point out also that in the majority of cases it is quite hopeless to attempt to make the entry wound the safety-valve for drainage, as its natural tendency, even if enlarged, is to heal, while the condition of the tissues in the exit segment of the track usually renders primary union an impossibility.
The wound having been dealt with, the next indications were for the reduction of deformity, immobilisation of the limb, and the provision of a proper degree of extension. As to the reduction of the fracture, this was always a matter of ease, needing only slight axis traction. The provision of efficient means of extension and immobilisation was a very different matter. These questions had to be considered under two sets of conditions: (1) when it was possible to keep the patient at rest in the hospital he was first deposited in; (2) when it was necessary for him to be transported for a considerable distance, probably not less than 500 miles.
When transport is a necessity, the best method of immobilisation is the application of breeches of plaster of Paris, and a long outside splint. The latter we often had excellently made on emergency by the Ordnance Department or the Royal Engineers. A perineal band is the only form of extension possible under these circumstances. The Dutch ambulances were provided with a very excellent emergency splint for cases of fractured thigh, which is illustrated in fig. 56. I think something of this kind should be carried in one of the ambulances going on to every field of battle, as being far more suitable than a long outside splint for hasty and inaccurate application. This splint, fixed with some kind of firm bandage, is an excellent temporary one for use during transport.[Pg 208]
(36) Obliquely Transverse Fracture of the Patella
Range 'short.'
The entry and exit wounds were small, and a distinct grooving from loss of substance of the bone was palpable superficial to the actual cleft of the fracture.
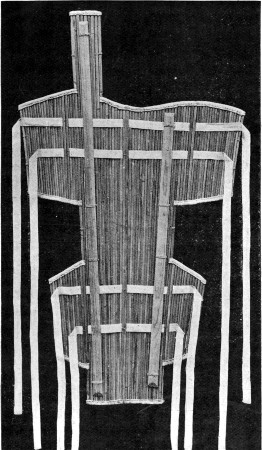 Fig. 56.—Dutch Cane Field Emergency Splint for Thigh or
Lower Extremity. (Dutch Ambulance, Winberg)
Fig. 56.—Dutch Cane Field Emergency Splint for Thigh or
Lower Extremity. (Dutch Ambulance, Winberg)
In cases which can be treated at a Stationary hospital near at hand, a long outside splint supplemented by plaster breeches, and a well-applied American extension, is a very good method of treatment, the only point to bear in mind being frequent examination of the position of the limb to ensure the extension being efficient. As already mentioned, the shortening in the primary stages is often slight and easily combated, but in many of these cases if examined in a few days the limbs are found to have shortened considerably, principally as a result of recovery of tone by the muscles, and the absence of any help from the resting of the two fragments end to end. The weight, therefore, has often to be progressively increased and the fracture readjusted if necessary. Although this method of treatment is satisfactory in cases with a small wound, it is very troublesome to carry out, even when a bracket is inserted opposite the wound, when frequent dressing is necessary, as is generally at first the case when the wounds are large. For this purpose a much more satisfactory method is the use of Hodgen's splint. This allows of automatic adjustment of the degree of extension, and the dressing of the wound without interference with the position of the fracture. A continuous many-tailed bag is preferable to the strips usually employed for the suspension of the limb, as more easily adjustable and as offering a more even support to the limb.[Pg 210]
(37) Oblique Comminuted Fracture of the Tibia
Range '600 yards.'
The entrance wound was large and the exit also. The fracture may have been caused by a Mannlicher (8 mm.) soft-nosed bullet, or possibly a ricochet. The fragmentation is somewhat coarse at the periphery, but very fine in the track of the bullet. Several fragments of the mantle are visible.
The fracture affords a good example of obliquity due to cutting by the bullet, and contrasts well with those due to rectangular impact such as are shown in plates IV. and XIV.[Pg 211]
While at Orange River, in conjunction with Major Knaggs, R.A.M.C., and Mr. Langmore, we treated several cases of fracture of the shaft of the femur by this method. The splints were made for us by the Ordnance Department, while the Royal Engineers erected a kind of gallows for us down the centre of a commissariat marquee in order to avoid the risk of using the tent poles for suspension. The patients were then ranged on each side of the tent in two rows so that the pull of the two sets of limbs opposed each other on the gallows from which they were suspended. Although these patients had to lie on the ground, they were really comfortable compared with those treated with long outside splints, and the results obtained were very good: in three cases which I had the opportunity of measuring later the bones were in good position and the shortening was less than one inch.
I have no doubt whatever that Hodgen's splint is by far the best method of treating all cases of fractured thigh in the Stationary field hospitals; and, more than this, I believe it is the only practicable and efficient one. It can be applied without the use of an anæsthetic without causing undue suffering to the patient, it allows of ready change of the dressing, it is comfortable and permits considerable range of movement on the part of the patient, it is as efficient with patients lying on the ground as in a bed, it keeps the limb in good position and allows of constant inspection on this point, and it is the only method which provides satisfactory extension without constant readjustment.[Pg 212]
(38) Transverse Fracture of the Tibia, Comminuted Fracture of the Fibula
Range '300 yards.'
Wound of soft parts nearly transverse, entry on tibial aspect. The bullet crossed and grooved the posterior aspect of the tibia, but struck the fibula full. This is the only instance of a transverse cleft which came under my notice.
The wound suppurated, and a number of fragments of the fibula needed removal; hence the amount of callus present.[Pg 213]
Cases in which operative fixation is indicated are rare, but a few oblique fractures may be treated with advantage in this manner if the conditions surrounding the patient admit of it. Screwing is generally preferable to wiring.
Lastly, we come to the cases in which primary amputation is necessary. I may say at once that I saw no case of wound from a bullet of small calibre in which this was indicated, and only one shell injury in which it was performed. I believe with small bullets that injury to the main blood-vessels is almost the only indication which is likely to be met with, and this by no means always indicates an amputation. First of all the question arises as to whether the wound in the vessel is caused by a bone fragment or by the bullet itself; reference to the chapter on blood-vessels would seem to prove that a bullet wound is by no means a necessary indication for amputation. Given favourable conditions, it might be treated locally by ligature at the time, while if hæmorrhage is not proceeding, developments should be awaited before proceeding to amputation. In the case of bone fragment punctures, secondary hæmorrhage is a more likely indication for amputation than primary.
Broadly, it may be laid down that very extensive injury to the soft parts is the only indication for primary amputation beyond primary hæmorrhage, and it may be added that the condition is rare with wounds from small-calibre bullets. If a primary amputation is necessary the observations as to the transport of fractured thighs are equally applicable. I never saw a primary amputation do well that was moved during the first week; sloughing of flaps or hæmorrhage followed as a rule, and often death.
Intermediate amputations were indicated in cases of septic infection and those of hæmorrhage; they seldom did well, and should be avoided if possible. Secondary amputations for sepsis or hæmorrhage were attended by fair results, but I can give no statistics. Unless extensive osteo-myelitis is evident, or very widespread cellulitis of the limb exists, I am strongly of opinion that the amputations when the fractures are above the middle of the thigh should be through the fracture, and not at the hip-joint, even if a subsequent secondary operation is risked.[Pg 214]
(39) Perforation of the Shaft of the Tibia, and Incomplete Oblique Fissure extending from the lower part of The opening to the crest of the bone.
Range medium. Entry and exit wounds at same level.
The patient was standing when struck, and fell backwards, his rifle falling at the same time and striking the shin. The fibula is intact.
The perforation indicated by the well-marked translucent spot is small.
The forking of the lower extremity of the cleft suggests the starting of the fissure from above. The fissure comes to the surface at the seat of election, but its position may possibly have been determined by the blow from the falling rifle.
The backward fall of the patient clearly explains the mechanism of production of the fissure, and throws light on the production of an oblique fracture such as shown in plate XVI.[Pg 215]
Fractures of the patella.—Punctured fractures of the patella were common with direct impact of the bullet; these were often difficult to palpate, and were only to be certainly diagnosed by attention to the direction of the track, and the development of hæmarthrosis. I saw at least three or four in which the bullet, in addition to traversing the knee-joint, injured the popliteal vessels. I have notes of one case in which a bullet traversed the soft parts from above downwards and scored a vertical groove on the surface of the patella; this was readily palpable, but produced no solution of continuity. In several cases the margin of the patella was notched by a passing bullet.
I never saw a case of stellate fracture, and by this my experience in the case of the ilium was confirmed.
On two occasions I saw pure transverse fractures of the bone; in each the wound was produced by a Lee-Metford bullet. This is of some interest as denoting that the greater volume and weight, in conjunction with the blunter tip, of the Lee-Metford may produce more severe injury to the bones than the Mauser. I believe this to be the case, given an equal degree of velocity on the part of the bullet at the moment of impact; but it is probable that the position of the patella with regard to the condyles of the femur when struck is of far greater importance in relation to the production of transverse fractures. The skiagram represented in plate XVIII. shows an obliquely transverse fracture, which in this instance resulted from a crossing bullet, which grooved the surface of the bone.
With regard to the two cases of transverse fracture above referred to, I may add that one occurred in a youth under twenty, and a good result was obtained by treatment with splints, and later by massage. In the second the patient was a man over fifty, who had received other injuries. The wound over the patella healed and some union had occurred, when the patient fell and burst both the bone union and the skin cicatrix. Secondary suppuration of the knee-joint, necessitating an amputation of the thigh, followed, but the patient made a good recovery. The third case also did well.[Pg 216]
(40) Notch Fracture of the Crest of the Tibia
Range 'short.'
The raising of the margins of the notch suggests a perforation. Compare with figs. 51 and 57 in the text.[Pg 217]
The treatment of these injuries differed in no way from that adopted in civil practice, given satisfactory surroundings. Suture might be indicated in some cases of transverse fracture, but this would only be necessary if the fragments were widely separated. The punctured fractures needed treatment as for simple wounds, combined with a short period of rest and pressure for the condition of hæmarthrosis. It was important not to prolong the period of rest beyond a week or ten days if the effusion was slight, in view of possible ulterior interference with range of movement in the knee-joint.
Fractures of the tibia.—Some remarks have already been made regarding fractures of the head of the tibia, and the importance of the overhanging prominent margins in the production of somewhat irregular injuries (p. 170). Putting these peculiarities on one side, the cancellous ends are subject to the type forms of injury; thus perforations either of the head of the bone or the malleolus were common injuries. The fractures of the shaft also deviated from the type in so far as the broad flat surfaces in the upper two thirds of the bone rendered it especially liable to the results of lateral impact, and to the production of the extreme wedge-shaped types of fracture. Plate XXII. illustrates the different result of a bullet striking the dense and strong spine at a low rate of velocity, a notch only resulting. If, on the other hand, the lateral surfaces were struck, a wedge with the base corresponding to the posterior surface was the most common injury, the spine in many cases remaining intact and maintaining the continuity of the bone. Wedge-shaped fractures of this bone were apt to show multiple secondary wave fissures concentric with the main line, and consequently free comminution. I saw several examples, the loose fragments being remarkably numerous. Plate XIX. is an example of an oblique fracture produced by a bullet which has ploughed across the bone, displacing large fragments anteriorly, but finely comminuting the bone in its course, and leaving small fragments of the mantle on its way. Plate XX. is an example of the rare condition of transverse fracture.[Pg 218]
(41) Spurious Perforation of the Fibula
Moderate range, 'about 1,000 yards.'
The injury was caused by an 8 mm. bullet, which entered base foremost and lodged in the calf. The fracture is really an incomplete stellate form, two well-marked transverse fissures extending from the point struck. The position of the bullet suggests its entry into the limb base foremost, and as it is retained low velocity may be assumed.[Pg 219]
This fracture was produced by a bullet travelling at a high rate of velocity, which struck the posterior surface of the tibia, and caused a grooving, accompanied by a horizontal fissure through the whole thickness of the bone; later it struck the fibula more directly, and produced an ordinary comminuted fracture two inches above the malleolus. Perforations of the shaft were far more common than in the case of the femur, and I saw them in every part of the length of the bone (plate XXI.). Fig. 57 illustrates a form of peculiar interest as showing the gradual transition of the tunnel to the groove, and also as bringing fractures of the long bones into line with such fractures of the flat bones of the skull as are depicted in fig. 68.
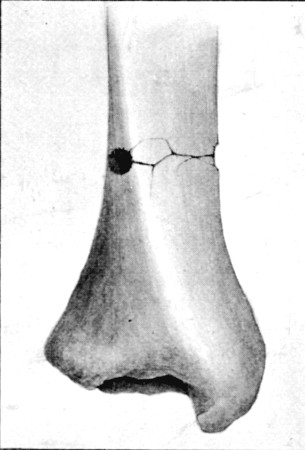 Fig. 57.
Fig. 57.
(42) Perforation of lower third of Tibia, showing lifting and fissuring of the compact roof of the tunnel. Compare with fig. 68, p. 259, of a fracture of the cranial vault.
Fractures of the fibula offered no special features of importance. Any form might occur. The plate No. XXIII. is of interest as showing a spurious form of perforation, and also the primary form of displacement of the fragments in stellate fractures. It was produced by a reversed ricochet, but undeformed, bullet, still seen in position in the skiagram; the bullet only possessed sufficient force to perforate the bone, and then appears to have turned on its transverse axis. The following plate, No. XXIV., is inserted to show the depth at which the bullet lay, and its distance from the surface of the tibia, which appears in the first plate to be nil. It is also of interest as showing the ease with which a false impression may be obtained from a single picture, as, beyond a spot of transparency, no obvious injury to the fibula, and certainly no displacement, is discernible.[Pg 220]
(41a) This skiagram is inserted to show the depth at which the bullet lay from the surface. It is also interesting to note the insignificance of the fracture of the fibula from this aspect. Without the second skiagram the injury might have passed for a simple perforation or a transverse fracture.[Pg 221]
Fractures of the bones of the leg possessed an unenviable degree of importance. First, on account of the very severe injuries to the soft parts that often accompanied them, without an apparently correspondingly serious damage to the bone. Secondly, on account of the frequency with which the vessels were implicated in these injuries to the soft parts, either by the bullet or bone fragments. Beyond this, fracture of either articular end of the tibia was certainly more frequently followed by troublesome joint complications than occurred in the case of any other bone.
In the matter of 'explosive' injuries, I think more were seen in the calf of the leg than in any other part of the body, and this often without solution of continuity of the bones, and sometimes without evidence even of contact of the bullet with either tibia or fibula. Some remarks on this subject have already been made in the chapter on wounds in general, and some sources of fallacy exposed. I believe that in practically all these so-called explosive injuries the wound was either caused by a ricochet, or a bullet which deformed with great ease on bony contact during its progress through the limb. A considerable number of the wounds which were referred by the men to the use of expanding bullets were probably the result of the use of Martini-Henry or large leaden sporting bullets, and evidence of this was often forthcoming on examination of the entry wounds. In other cases the irregularity of the opening plainly pointed to ricochet of a small bullet as the explanation of the character of the injury. The greater frequency of ricochet injuries in the leg and foot when the men were standing is readily understood.
Concurrent injury to the vessels of the leg was common, but primary hæmorrhage, as was the case generally, usually ceased spontaneously. The importance of injury to the vessels was rather in view of secondary hæmorrhage, which occurred with some frequency, and I think more commonly from the anterior than the posterior tibial vessels, usually occurring at the end of a week or ten days, and naturally most frequently in cases which suppurated.
Prognosis and treatment in fractures of the leg.—In fractures of the leg, except those of extreme severity, almost any form of splint sufficed to maintain the bones in position, but for field purposes the Dutch cane splint (fig. 58, p. 222) was certainly very convenient. For later use in cases that needed frequent[Pg 222] dressing, a wooden back splint, with a foot-piece, or, if obtainable, a Neville's splint with a suspension cradle, was the best. Where the wounds were small and frequent dressing was not required, nothing was so good as plaster of Paris, especially when transport was a necessity.
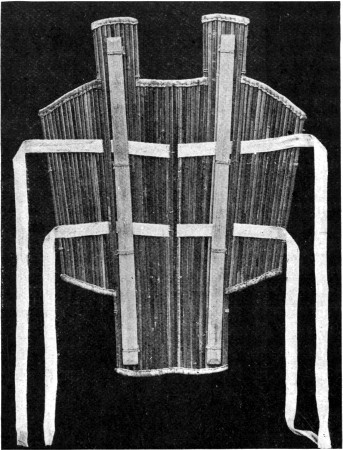 Fig. 58.—Dutch Cane Field Emergency Splint for Leg
Fig. 58.—Dutch Cane Field Emergency Splint for Leg
In cases with large wounds suppuration was very frequent, and in connection with this secondary hæmorrhage, or in the case of fractures near the articular ends, especially the upper, joint suppuration. The treatment of these cases varied: in many an amputation was the best or only treatment advisable; but I several times saw good results follow ligation of the anterior tibial artery for secondary hæmorrhage, even when suppuration existed, and occasional good results[Pg 223] after incision and drainage of joints if the infection was not of the most acute form.
Primary amputation was rarely needed for any case of injury from a bullet of small calibre, since it was only necessary either in the case of injury to both main arteries, and this was rare, or in cases of very extensive injury to the soft parts. I saw many of the latter make fair results when treated conservatively, even though the condition seemed almost hopeless at first sight. All the primary amputations that I saw were either for shell or large bullet injuries. A word may be inserted here as to the weight that ought to attach to nerve injuries in this relation. From the experience gained elsewhere it is clear that we should attach little importance to these unless the divided nerves are actually in sight, as far as deciding on amputation is concerned. On the other hand, there is little doubt that the presence of concurrent nerve injury, be it only concussion or contusion, exerts an important ulterior influence on the healing of the wound, whether the part be amputated or not. Amputation flaps in such cases possess a very considerably lowered degree of vitality.
Secondary amputations were often needed for sepsis, and on the whole did very well; both for the same cause and for hæmorrhage intermediate amputations had occasionally to be performed; the results of these, as elsewhere, were bad.
Fractures of the tarsus.—Wounds of these short bones were as a rule of slight importance, given fairly direct impact on the part of the bullet. They then consisted of either simple perforations or surface grooving. A single bone might be implicated or several might be tunnelled; in the latter case the implication of the joints very considerably influenced the prognosis, since the addition of the joint injury caused much more prolonged weakening of the foot.
Wounds of the foot were common from the fact that when the men lay out in the prone position, the foot was often the part least protected by the cover chosen, and particularly the heel. In these circumstances the os calcis was the bone most frequently implicated, and that by tracks taking an oblique course downwards from the leg to the sole. Again the foot was often struck by ricochet bullets, as a result of its position[Pg 224] when the erect attitude was assumed. The latter fact was of much importance with regard to the nature of the injury sustained by the bones, as under these circumstances the mode of impact was irregular, and consequently comminution was often produced.
The behaviour of the different bones of the tarsus varied somewhat. On the whole the prognosis in cases of injury to the os calcis was the best, since the injury was more often individual and did not implicate any joint, and also because of the comparatively regular architecture of the bone. In the smaller bones concurrent injury to a joint was more frequent. In the astragalus the central hard core extending upwards from the interosseous groove, as increasing resistance, I think accounted for the fact that comminution was more marked in this bone than in any other. The effect of wound of bones of the tarsus in producing a certain degree of laxity in the mediotarsal joint resulting in a slightly flexed position of the fore part of the foot and some projection of the head of the astragalus did not seem to me easy of explanation, but it occurred with some regularity.
The injuries to the metatarsus corresponded so nearly to those already spoken of in the case of the metacarpus that they need no further mention. They were less common, however, and I am under the impression that fragmentation of the bullet was not such a marked feature, probably on account of the lower degree of density of the bones, and their greater fixity of position.
[18] Col. W. F. Stevenson. Loc. cit. p. 69.
Until recent times gunshot injuries of the joints formed a class entailing the gravest anxiety to the surgeon, both in regard to the selection of primary measures of treatment and in the conduct of the after progress of the cases. The external wounds were severe, comminution of the bones was great, and retention of the bullet within the articulation was not uncommon. Operative surgery therefore found a large field in the extraction of bullets, removal of bone fragments, excision of the joints, or even amputation of the limbs.
The introduction of bullets of small calibre has robbed these injuries of much of the importance they possessed in earlier days and during the present campaign direct clean wounds of the joints were little more to be dreaded than uncomplicated wounds of the soft parts alone. No more striking evidence of the aseptic nature of the wounds, and the harmless character of the projectile as a possible infecting agent, than that offered by the general course of these injuries in this campaign, is to be found in the whole range of military surgery.
The aseptic nature of the wounds, and the slight and localised character of the bone lesions, have in fact justified the opinion previously expressed by Von Coler, that these injuries in the future would be less feared than fractures of the diaphyses of the bones.
Not less important than the localised character of the bone lesion itself is the fact that the accompanying wounds of the soft parts retain the small or type forms. Thus I occasionally observed more troublesome results from minor shell wounds in the neighbourhood of joints, but not implicating the synovial[Pg 226] cavity, than in actual perforating injuries produced by bullets of small calibre.
Vibration synovitis.—Before proceeding to the consideration of wounds of the joints, a short account is necessary of a condition of some importance which is, I believe, more or less special to injuries from bullets of small calibre travelling at high rates of velocity. This condition, if not novel, at any rate excited little comment in the descriptions of the older forms of injury, although this may have depended on the more serious nature of the primary local lesions accompanying wounds from the larger bullets, among which it formed a comparatively unimportant element.
The condition referred to was the occurrence of considerable synovial effusion into the joints of limbs in which the articulation itself was primarily untouched. These effusions sometimes occurred even when the soft parts alone were perforated, especially when the wounds were situated above or below the knee-joint. They were apparently the direct result of vibratory concussion of the entire limb dependent on the blow received from the bullet.
The effusions were most strongly marked in cases of fractures of the diaphyses, although this was more noticeable in some situations than others. Thus with fractures of the shaft of the femur anywhere below the junction of the upper and middle thirds of the bone, and in some cases even higher, effusion into the knee-joint was very common, and sometimes extreme. On the other hand, similar effusions into the hip-joint were less marked, since I failed to determine their existence in the majority of cases. I am inclined to ascribe this to the different anatomical arrangement of the two joints, particularly to the fact that the head of the femur is included in a bony cup, into the hollow of which it is accurately fixed by the resilient cotyloid fibro-cartilage. The latter by its firm grasp of the head allows of little play in the joint; hence vibrations are conveyed directly to the acetabulum in continuous waves, and rocking of the articular surfaces is prevented. Beyond this no doubt the difficulty of detecting small effusions in this joint is an element which must be taken into consideration.
I do not think that wrenches of the knee-joint in the act[Pg 227] of falling can be suggested as an explanation of the frequency of effusions into that articulation, since the fractures of the femur were not always received while the erect position was maintained, and effusion was most marked when the diaphysis was the part affected, the latter point illustrating the greater resistance offered by compact bone. Again, when fracture had taken place, the solution of continuity rendered the directly injured point the most mobile, and tended to prevent lateral strain from falling on the joints.
Effusion into the knee or ankle, or sometimes both joints, was common in fractures of the shaft of the tibia.
In the articulations of the upper extremity the condition was also common, but somewhat less marked than in the lower limb. Effusions into the shoulder or elbow occurred. In the former these were less striking; again, perhaps, as a result of the difficulty of detecting small effusions in this situation. The elbow was to a certain extent protected by the possession of a degree of fixity somewhat resembling that already mentioned in the case of the hip-joint, although here depending on the conformation of the bones alone. I think this explained the absence of free effusion in many cases of fracture of the humeral shaft, but when the latter affected the lower third effusion into the elbow was usually abundant.
The lighter weight and greater mobility of the upper extremity as a whole, as decreasing the resistance to the bullet, were also probably an element in the fact that these effusions were less severe than those in the joints of the lower limb.
The nature of the effusions was apparently simple, since they were rapidly reabsorbed, and little thickening of the synovial membrane remained to suggest either a marked degree of inflammation, or the deposition of blood-clot on the inner aspect of the same.
The only treatment indicated was a short period of rest, accompanied in the early stages by pressure and slight fixation, followed later by massage and movement if necessary.
Before dismissing this subject, I should like to particularly emphasise the fact, that in the cases described there was no reason to suspect the extension of fissures from the point of[Pg 228] fracture in the shafts into the articular ends of the bones. This was as far as possible excluded by clinical examination, and in the cases where wounds of the soft parts only were present, the rapid return of the patients to active duty, with absence of remaining joint trouble, negatived the possibility of such fractures.
I only saw one case in which a longitudinal fracture actually extended for any considerable distance into a neighbouring joint. In this a comminuted fracture occurred just above the centre of the shaft of the humerus. At the time of examination and putting up of the fracture there was considerable swelling of the whole arm, and nothing special was noticed about the shoulder-joint. Three weeks later, however, when the fracture was consolidating, difficulty in abduction of the shoulder was noted, and the arm could not be placed closely in contact with the trunk. There was no evident displacement of the head of the humerus forwards. A skiagram, which I much regret I have not been able to insert, showed that a longitudinal fissure extended from the seat of fracture upwards in such a manner as to divide the upper fragment into two parts, of which the outer bore the greater tuberosity, the inner the articular surface of the head. The latter fragment had become somewhat displaced downwards, and had united in such a manner that the head rested on the lower part of the glenoid cavity. Abduction of the limb therefore brought the greater tuberosity into contact with the acromion process, and movement was checked. This case passed out of my observation shortly afterwards, and I have no knowledge of the final result as to movement.
Fractures of the bony processes surrounding the elbow-joint, and of the malleoli of the tibia and fibula, were not infrequent, but offered no special features.
One other form of injury indirectly affecting the joints is perhaps worthy of mention, but I observed it only once, and that in the case of the shoulder, the only joint where it is likely to be marked. I refer to the displacement of the head of the humerus by the force of gravity, when the circumflex nerve is injured. In the instance I refer to, a fracture of the surgical neck of the humerus was accompanied by complete[Pg 229] motor paralysis of the deltoid and very rapid wasting of the muscle. Circumflex sensation was impaired, but not absent at the time the condition of the muscle was noted—a favourable prognostic sign of much importance. At the end of five weeks, when the fracture of the bone was consolidated, the head of the humerus had dropped vertically at least an inch, but could be replaced with ease. Shortly afterwards an improvement in the condition of the muscle commenced, and with this the head of the humerus was gradually raised. This patient later recovered his power in great part, but not completely.
In a few cases bullets lodged in the neighbourhood of joints in such positions as to limit movement by mechanical impact with the bones. Thus I saw one case in which a bullet lay between the radius and ulna just below the lesser sigmoid cavity; in another the bullet lay in front of the ankle-joint, and limited the possibility of flexion; and in a case related to me by Mr. Bowlby, a bullet was removed by him from the wall of the acetabulum where it was tightly fixed in the substance of the bone. In two other cases I saw bullets lying deeply on the anterior surface of the hip capsule and so limiting flexion. In all such cases the indication for removal of the bullet was sufficiently strongly marked.
These may be divided into several classes, varying much in comparative severity, and in prognostic importance.
1. The comparatively rare instances in which a wound implicated a joint cavity, without accompanying lesion of any bone.
2. Perforating wounds in which the bullet was retained within the articular cavity. These were also rare.
3. Wounds of the joints accompanied by grooving of the articular extremities of the bones.
4. Complete perforating tracks through the articular ends of the bones, crossing the joint cavity in various directions.
5. Comminuted fractures of the terminal parts of the diaphyses extending into joints.[Pg 230]
Of these several classes, the first was of the least prognostic importance. In the absence of bone injury the wounds usually healed without any obvious ill effect beyond the transient effusion into the joints of a mixture of blood and synovial fluid. When suppuration of the wound in the soft parts occurred, however, the remarks made as to the injuries classed under the third heading also apply here in a lesser degree.
With regard to the retention of the bullet, in the case of bullets of small calibre this was a distinctly rare occurrence. I never happened to see an instance of retention of either a Mauser or Lee-Metford bullet in an articulation. It is only possible with bullets practically spent, or travelling at a very low rate of velocity and making irregular impact.
The influence of both volume and velocity of flight was well illustrated by my own small experience of retained bullets. In one case a Martini-Henry was found impacted between the femoral condyles, having slipped in beneath the margin of the patella. It caused a semiflexed position to be assumed by the joint, and was removed by Mr. Brown in No. 1 General Hospital at Wynberg. The second instance I saw in the Portland Hospital at Bloemfontein in a patient of Mr. Bowlby's. The bullet was a Guedes, a form which has been already described as possessing low velocity and deficient power of penetration; beyond this, in the particular instance irregular impact was evidenced by the presence of a large irregular contused wound of entry over the tuberosity of the tibia.
The presence of the bullet in the knee-joint was later determined by the X-rays, and Mr. Bowlby removed it successfully. Seven months later the range of movement was nearly normal.
I may add that I saw several instances of large leaden bullets lodging in the popliteal space, and a comparatively insignificant number of bullets of small calibre in the same situation. This was very striking, in view of the immense relative frequency of use of the latter forms. There is no doubt, moreover, that small bullets rarely lodge even in the neighbourhood of joints, unless at the distal end of a long track. To take the extreme example of large bullets,[Pg 231] those employed as shrapnel, in comparison with the frequency with which wounds were produced by them, bullets lying at the bottom of short tracks in the neighbourhood of joints were not uncommon. Thus I saw one lying over the hip-joint, and another in close proximity to the shoulder capsule.
Wounds of the third class, where the bones had been superficially grooved, were in some respects the most serious. This was especially so in the knee and ankle joints, and some cases will be quoted later under the heading of the special joints to illustrate this point. Danger only arose in the event of suppuration; and here the presence of the long oblique superficial track in a neighbourhood liable to comparatively free movement was the important element. Such tracks usually opened the synovial sac more extensively than direct perforating wounds, and if suppuration occurred in any portion of the track, the pus was very liable to be sucked into the joint on any free movement. The presence of fine splinters of the bone displaced in the production of the groove was also a special character of wounds of this class. Another point worthy of mention is that in these cases it was not always easy to be quite certain whether the joint cavity had been implicated or not, since cases often occurred in which, although the bones had been grooved, the joint cavity escaped. The indication, however, was to consider any wound in the immediate proximity of a joint as perforating until it was healed. This course was the more easy to take, since a large proportion of such wounds were accompanied by some degree of synovial effusion, even when the neighbouring joint had escaped puncture.
Wounds of the fourth class, although the most highly characteristic of the form of accident, were in many instances the most favourable in regard to their course. The tracks might course directly across the joint in any direction, or they might course obliquely, traversing either one or both the component bones. In the latter case the exit might be in the diaphysis, and be accompanied by the separation of an exit fragment such as is illustrated in fig. 52, p. 169. The particularly favourable character of the direct transverse and antero-posterior wounds depended on the slight amount of splintering of the bones, the limited nature of the opening into the joint,[Pg 232] and the shortness of the tracks in the soft parts, which ensured that, even if infection did occur, the resulting pus was near the surface, and generally spread in that direction and escaped.
Wounds of the fifth class were the most dangerous, but the danger was entirely a secondary one, dependent on the occurrence of infection. These injuries were liable to be accompanied by the presence of extensive irregular wounds of the soft parts, in which suppuration was frequent, and the suppuration of the joint frequently meant subsequent amputation, if not a worse result.
Course and symptoms of wounds of the joints.—The immediate result of any perforation of a joint was the development of intra-articular effusion. This consisted of synovial fluid admixed with a varying proportion of blood. The degree of synovitis was apt to vary with the amount of force expended in the production of the injury; for this reason both high velocity and irregular impact were of importance in this relation.
The constant feature, however, depended on the effusion of blood; this was not rapid, or, as a rule, very abundant, but tended to increase during the first twenty-four hours. It resulted in a swelling of the joint, which possessed some peculiar features. At first elastic and resilient, it slowly decreased in volume with the assumption of a soft doughy character on palpation. In the case of the knee, where readily palpated, it very much resembled a tubercular synovial membrane, except for its extreme regularity of surface; still more closely the condition noted in a hæmophilic knee of some duration. Absorption took place with some rapidity, and except for slight thickening, the joints might appear almost normal, in a period of from two to four weeks. With the development of the effusion there was local rise in temperature of the surface, and in a considerable number of the cases a general rise of temperature.
This latter was sometimes very marked, as in the case of all the other traumatic blood effusions, but not quite so regular in occurrence. It was important, as I have seen it give rise to the suspicion of suppuration, when tapping resulted in[Pg 233] nothing more than the evacuation of turbid synovia mixed with blood. Pain was rarely a prominent symptom in consequence of the generally moderate degree of distension.
As a rule, these injuries were characterised by the small tendency to the development of adhesions; but this in great part depended on the care expended on their treatment. If kept too long quiet, either from necessity when the effusion was followed by much thickening, or when the external wound was large and so situated as to be harmfully influenced by movement, or in the ordinary course of treatment, troublesome stiffness, even amounting to firm anchylosis, sometimes followed. I saw several such cases, some of the most confirmed being wounds of the knee-joint complicated by injury to the popliteal vessels or nerves. The latter complication I saw altogether six times, but only once with a thoroughly bad knee, and in this case the injury had affected both the vessels and the internal popliteal nerve. The joint in that case was straightened out by continuous extension by Major Lougheed, when it came under his charge some six weeks after the primary injury, but I hear has again relapsed, and the popliteal paralysis is not much improved.
The small tendency to formation of adhesions in uncomplicated cases probably depended on the coagulation of a layer of blood over the whole internal lining of the joint. This kept the synovial surfaces apart at the lines of reflection of the membrane, and, given sufficiently active treatment, mobility was restored before any firm union could take place.
The primary escape of synovial fluid was rarely observed, as the wounds of the soft parts were too small and valvular to permit of it. Synovia in some abundance, mixed with pus, sometimes escaped in considerable quantity when infection had opened up the tracks.
Primary suppuration in any joint as a result of small and direct wounds was very rare. I observed it only on one occasion. On the other hand, a considerable number of cases in which secondary suppuration occurred came under my notice. In some of these the suppuration was secondary to comminuted fractures of the shaft of the tibia, in which the articular extremity was implicated. These offered no special[Pg 234] peculiarity. In others infection of the joint was secondary to infection and suppuration in the deep part of long oblique wound tracks, and these were of sufficient interest to warrant the insertion of two illustrative cases.
(43) In a man wounded at Paardeberg the bullet entered the leg to the inner side of the crest of the tibia, about 3 inches below the tubercle; thence it coursed upwards to emerge about 2 inches above the cleft of the knee-joint on the outer side. Regulation dressings were applied, and a week later the man arrived at the Base, with little apparent mischief in the knee-joint. He was placed in bed and warned against movement; on the second day, however, he got up and walked to the latrine. When bending his knee to sit down he was seized with agonising pain in the joint, and had to call out for help; he was then carried back to bed in a more or less collapsed condition. The knee commenced to swell; there was rise of temperature and great pain, together with extreme restlessness. I was asked to see him two days later, and after a consultation, Major Burton, R.A.M.C., freely incised the knee-joint bi-laterally. One opening was closed, the second plugged for drainage, as there was a large quantity of pus. No improvement followed, and a week later Major Burton amputated through the thigh. An attack of secondary hæmorrhage a few days later, combined with the degree of septic infection, ended the man's life. On examination of the joint, a groove forming three-fourths of a tunnel was found in the external tuberosity of the tibia, leading into the knee-joint beneath the external semilunar cartilage. The bullet had then passed upwards over the outer border of the cartilage, bruised the margin of the external condyle of the femur in such a manner as to depress the outer compact layer, and finally escaped from the joint near the upper reflection of the synovial membrane. The synovial membrane was granular in appearance and reddened, but there was no suppuration outside the confines of the joint, except in a cavity corresponding to 2 inches of the track before it actually perforated the tibia. A localised abscess had evidently formed here and been diffused into the joint by the movement of flexion already described.
(44) A man wounded during General Hamilton's advance on Heilbron was struck on the outer aspect of the heel. An oval opening of some size led down to a track in the os calcis; the bullet was retained. The foot was dressed, and put up later in a plaster-of-Paris splint. On the tenth day the splint was removed to see to the wound, which looked satisfactory and was re-dressed.[Pg 235]
A few hours later the man was seized with very severe pain in the ankle, and a day later I was asked to see him by Mr. Alexander. The man was anæsthetised, and I examined the wound with care, and also removed the retained bullet from the inner margin of the leg. The bullet was reversed, having no doubt suffered ricochet, hence the large aperture of entry, but it was in no way deformed. I could not certainly determine the presence of any fluid in the ankle-joint, and as the pain was apparently localised to the distribution of the musculo-cutaneous nerve, I decided not to freely open the joint. In this, however, I erred, and two days later, after consultation, the joint was freely incised by Mr. Alexander. It was then found that the bullet in its passage had just touched the posterior aspect of the tibia and wounded the ankle-joint. A localised collection of pus which had formed in the deep part of the wound had been diffused into the joint by the movements made when the splint was removed, in a similar manner to that described in the last case. This joint also did badly, and an amputation of the leg had to be performed by Mr. Alexander to save the man's life.
These two cases are particularly instructive as showing, first, how quietly a small amount of deep suppuration may sometimes take place; and, secondly, the importance of keeping the joints quiet on a splint when there is any reason to suspect their implication by wounds of this character.
The general treatment of the wounded joints was simple. The old difficulties of deciding on partial as against full excision, or amputation, were never met with by us. We had merely to do our first dressings with care, fix the joint for a short period, and be careful to commence passive movement as soon as the wounds were properly healed, to obtain in the great majority of cases perfect results. Careful light massage, if available, was used to promote absorption of blood.
If suppuration occurred, the choice between incision and amputation had to be considered. In the early stages this choice depended entirely on the nature of the injury to the bones. If this were slight, incision was the best plan to adopt. I saw several cases so treated which did well, although convalescence was often prolonged, and only a small amount of movement was regained. Amputation was sometimes indicated in cases of severe bone-splintering, when the shafts were implicated,[Pg 236] but was as a rule only performed after an ineffectual trial to cut short general infection of the septicæmic type by incision.
I have dwelt at such length on the subject of suppuration on account of its importance, but I should add that, on the whole, suppuration of the joints was uncommon, except in the case of injuries far exceeding the average in primary severity.
Special joints.—Such deviations from the general type of injury as above described depended entirely on peculiarities of anatomical arrangement, and peculiarities in the situation of the joint clefts in the different parts of the body. A few words as to these are perhaps necessary.
Shoulder-joint.—Wounds of this articulation were by no means common. This depended, I think, on two points in the architecture of the joint: first, a bullet to enter the front of the cavity and traverse the joint needed to come with great exactitude from the immediate front; secondly, wounds received from a purely lateral direction calculated to pierce the head of the humerus and the glenoid cavity were naturally of very rare occurrence. Wounds of the prominent tip of the shoulder received while the men were in the prone position were not uncommon, but it was remarkable how rarely the shoulder-joint was implicated in these. The question of the narrow nature of the cleft exposed also comes up in this position. As far as my experience went, injuries to the lower portion of the capsule accompanying wounds of the axilla were those most often met with. The ease and neatness with which pure perforations of the head of the humerus can be produced was also an important element in the frequent escape of this joint. No case of fracture of the glenoid cavity happened to come under my notice.
I saw few instances in which the joint needed incision, and cannot recall or find in my notes any case in which serious trouble arose.
Elbow-joint.—Injuries to this joint came second in frequency in my experience to those of the knee. They were, in fact, comparatively common, especially in conjunction with fractures of the various bony prominences surrounding the articulation. Fractures of the lower end of the humerus[Pg 237] were of worse prognostic significance than those of the ulna, on account of the greater tendency to splintering of the bone. I saw several cases of pure perforation of the olecranon without any signs of implication of the elbow-joint. In a case which has been utilised for the illustration of some of the types of aperture (fig. 20, p. 59), at the end of a week there was no sign of any joint lesion, although the bullet had obviously perforated the articulation.
Several cases of suppuration which came under my notice did well. I saw one of them a few days ago, six months after the injury, with perfect movement. In another of which I took notes, the bullet entered over the outer aspect of the head of the radius, to emerge just above the internal condyle anteriorly. A considerable amount of comminution of the olecranon resulted, and when the man came into hospital some ten days later the joint was suppurating. The joint was opened up from behind, and some fragments of bone removed by Mr. Hanwell. On the 26th day this joint was doing well, and considerable flexion and extension were possible without pain. There was a somewhat abundant discharge of bloody synovia during the first few days after the operation.
 Fig. 59.
Fig. 59.
Illustrates the very neat and limited injury to the Phalanges over the dorsal aspect of the first inter-phalangeal joint of the Middle Finger, accompanying a gutter wound received by the patient while holding a rifle
I never saw any troublesome results from perforations of the carpus. The joints of the fingers also offered little[Pg 238] special interest, except in so far as they afforded astonishing examples of the extreme neatness of the injuries which a small-calibre bullet can produce. Fig. 59 is a good example of such an injury.
Hip-joint.—I can only repeat with regard to this joint what I have already said as to the injuries to the head of the femur. I had practically no experience of small-calibre bullet injuries to the femoral constituent, and beyond the single case of injury to the acetabular margin mentioned on p. 193 I saw no obvious wounds of the joint at all.
The knee, as usual, proved itself par excellence the joint most commonly injured, no doubt as a result of its size, the extent of its capsule anteriorly, and its exposed position. In spite, however, of the frequency with which it suffered injury, and the opportunities it afforded for observation of the progress of the effusions towards absorption, the injuries to the joint gave less anxiety and attained a more favourable prognostic character than is the case in civil practice. This depended on the very favourable course observed in the frequent pure perforations following a direct line. These occurred in every direction, the accompanying hæmarthrosis usually disappearing completely in an average period of little over a month. The extremes can be fairly placed at a fortnight and six weeks. Limitation of movement was slight or non-existent in many cases; in others it was of a very moderate character, and I only remember to have seen one case in which a really serious anchylosis developed. In this the man was struck from a distance of 300 yards, and a considerable amount of bone dust from the femur was found in the lips of the exit aperture. The wounds healed per primam, but when I saw the man two months later anchylosis in the straight position was apparently complete.
The comparatively frequent association of popliteal aneurisms with wounds of the knee-joint has already been spoken of in relation to anchylosis. Wounds of the popliteal space from larger bullets sometimes caused more troublesome after-stiffness than wounds of the articulation itself. Again I remember a small pom-pom wound at the inner margin of the ligamentum patellæ without obvious wound of the joint,[Pg 239] which was accompanied by synovitis from contusion, and was followed by very considerable limitation of movement. This had only been partially improved when the patient returned home, in spite of prolonged massage and passive movement.
The general remarks on the joints cover all that need be said as to suppuration of the knee-joint.
The ankle-joint maintained the undesirable character which it has always held as a subject for gunshot injuries. This is entirely a question of sepsis, and in great measure depends on the fact that the foot, as enclosed in a boot, is invested with skin particularly difficult to thoroughly cleanse; while the socks are an additional source of infection to the wounds before the patients come under proper treatment.
Of seven cases of suppurating ankle-joint, of which I have notes, only two retained the foot, and one of these after a very dangerous illness. This case was one of special interest as exemplifying the results dependent on variations in velocity on the part of the bullet. The patient was struck at a distance of twenty yards. The bullet entered the front of the right ankle-joint and emerged through the internal malleolus, just behind its centre, causing no comminution of the latter. It then entered the left foot by a type wound one inch behind and below the tip of the internal malleolus, traversed and comminuted the astragalus, and emerged one inch below the tip of the external malleolus. The first joint healed per primam. The second produced by the bullet when passing at a lower rate of velocity was accompanied by considerable comminution of the bone. It suppurated, and gave rise to great anxiety both for the fate of the foot and the life of the patient. It is probable that the more abundant hæmorrhage which took place from the second wound was in part responsible for the occurrence of infection.
The second of the two cases is of some interest in relation to the doctrine of chances as to the position in which a wound may be received. The man was wounded in one of the earlier engagements, a bullet passing transversely through his leg immediately behind the bones and about half an inch above the level of the ankle-joint. He recovered, and rejoined his regiment,[Pg 240] only to receive at Paardeberg a second wound, about an inch lower, which traversed the ankle-joint. On his return to Wynberg he happened to be sent to the same pavilion, and occupied the same bed he had left on returning to the front.
The subject of the result of wounds of the joints of the foot has received sufficient consideration under the heading of wounds of the tarsus.
The repetition of the fact that, among the whole series of cases on which this chapter is founded, not a single instance of primary or secondary excision of a joint, either partial or complete, is recorded, forms an apt conclusion to my remarks on this subject.
Injuries to the head formed one of the most fruitful sources of death, both upon the battlefield and in the Field hospitals. It has been suggested that the mere fact of wounds of the head being readily visible ensured all such being at once distinguished and correctly reported, while wounds hidden by the clothing often escaped detection. When the external insignificance of many of the fatal wounds of the trunk is taken into consideration this is possible; but, on the other hand, it must be borne in mind that the head is in any attitude the most advanced, and often the most exposed, part of the body, and even when the soldier had taken 'cover,' it was frequently raised for purposes of observation. For the latter reasons I believe injury to the head fully deserved the comparative importance as a fatal accident with which it was credited.
A number of somewhat sensational immediate recoveries from serious wounds of the head have been placed upon record. Observation, however, shows that these, with but few exceptions, belonged either to certain groups of cases the relatively favourable prognosis in which is familiar to us in civil practice, or that the wounds were received from a very long range of fire, and hence the injuries were strictly localised in character.
Wounds of the scalp.—Nothing very special is to be recorded with regard to these; they either formed the terminals of perforating wounds, or were the result of superficial glancing shots. The glancing wounds were of the nature of[Pg 242] furrows, varying in depth from mere grazes to wounds laying bare the bone. Their peculiarity was centred in the fact that a definite loss of substance accompanied them, the skin being actually carried away by the bullet; hence gaping was the rule. Every gradation in depth was met with, but the only situations in which wounds of considerable length could occur were the frontal region in tranverse shots, or, when the bullet passed sagitally, the sides of the head, or the flat area of the vertex.
The danger of overlooking injuries to the bone was of special importance in the short subcutaneous tracks occasionally met with at the points at which the surface of the skull makes sharp bends. In all such wounds it was a safe rule to assume a fracture of the skull until this was excluded by direct examination. In some of the gutter wounds and subcutaneous tracks crossing the forehead and sides of the head, signs of intracranial disturbance were occasionally observed in the absence of external fracture, such as transient muscular weakness, unsteadiness in movements, giddiness, diplopia, or loss of memory and intellectual clearness. In connection with such symptoms the classical injury of splintering of the internal table of the skull, the external remaining intact, had to be borne in mind, but I observed no proven instance of this accident. I am of opinion, moreover, that its occurrence with small bullets travelling at a high degree of velocity must be very rare, since little deflection is probable unless the contact has been sufficiently decided to fracture the external table; while in the cases of spent bullets the injury is unlikely, as requiring a considerable degree of force.
Injuries to the cranial bones, without evidence of gross lesion to the brain.—It may be premised that these were of the rarest occurrence, and they may be most readily described by shortly recounting the conditions observed in a few cases I noted at the time. The injuries resulted from blows with spent bullets, from bullets barely striking the skull directly, or those striking over the region of the frontal sinuses. Wounds of the mastoid process will not be considered in this connection as being of a special nature (see p. 299).[Pg 243]
I saw only one case of escape of the internal, with depressed fracture of the external, table of the skull.
(45) In marching on Heilbron a man in the advance guard was struck by a bullet at right angles just within the margin of the hairy scalp. The regiment was at the time to all intents and purposes outside the range of rifle fire, and the patient was the only individual struck among its number. When brought into the Highland Brigade Field Hospital, a single typical entry wound was discovered; examination with the probe gave evidence of a slight depression in the external table of the frontal bone just above the temporal ridge. Although no perforation was detectible by the probe, and this was positively excluded on the raising of a flap (Major Murray, R.A.M.C.), it was considered advisable to remove a 1/4-inch trephine crown, the pin of the instrument being applied to the margin of the depression. No depression or splintering of the internal table was discovered, nor any injury to the dura, nor blood upon the surface of that membrane. The man made an uninterrupted recovery.
(46) A case of frontal injury was shown to me at Wynberg, in which a distinct furrow could be traced across the upper part of the frontal sinuses. There had been no symptoms beyond temporary diplopia, and the wound was healed; no surgical interference had been deemed necessary.
(47) In a man wounded at Poplar Grove, a single typical wound of entry was found 3/4 of an inch above the right eyebrow and the same distance from the median line. No primary symptoms were observed, but on the evening of the second day the temperature rose above 100° F., and the man seemed somewhat heavy and dull. The patient was examined by Major Fiaschi and Mr. Watson Cheyne, and it was decided to explore the wound. Mr. Cheyne removed fragments both of external and internal tables, one of the latter having made a punctiform opening, not admitting the finest probe, in the dura-mater. The bullet was traced into the nasal fossæ, where it was subsequently localised with the aid of the Roentgen rays when the patient came under my observation at Wynberg some days later (fig. 60).
Gunshot fracture of the skull with concurrent brain injury.—This was the commonest form of head injury, and possessed two main peculiarities; firstly, the large amount of brain destruction compared with the extent of the bone lesion; secondly, the fact that any region of the skull was[Pg 244] equally open to damage. In consequence of the second peculiarity, the position and direction of secondary fissures are not so dependent on anatomical structure as in the corresponding injuries of civil practice. Thus, fractures of the base, for instance, were less constant in their course and position. The cases as a whole are best divided into four classes.
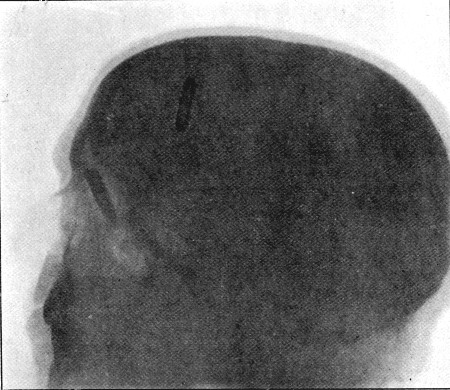 Fig. 60.—Mauser Bullet in Nasal Fossa. (Skiagram by H.
Catling.) Case No. 47
Fig. 60.—Mauser Bullet in Nasal Fossa. (Skiagram by H.
Catling.) Case No. 47
1. Extensive sagittal tracks passing deeply through the brain, and vertical wounds passing from base to vertex or vice versa, in the posterior two thirds of the skull. These will be referred to as general injuries.
2. Vertical or coronal wounds in the frontal region.
3. Glancing or obliquely perforating wounds of varying depth in any part of the head.
4. Fractures of the base.
Of these classes the first was nearly uniformly fatal; the[Pg 245] second relatively favourable, and with low degrees of velocity often accompanied by surprisingly slight immediate effects; while the third had perhaps the best prognosis of all, but this varied as to the defects that might be left, and with the region of the head affected.
1. General injuries.—Fractures of this class may be treated of almost apart. For their production the retention of a considerable degree of velocity on the part of the bullet was always necessary, and the results were consequently both extensive and severe.
The aperture of entry was comparatively small, since to take so direct and lengthy a course through the skull the impact of the bullet needed to be at nearly an exact right angle to the surface of the bone. Any disposition to assume the oval form, therefore, depended mainly upon the degree of slope of the actual area of the skull implicated. In size the aperture of entry did not greatly exceed the calibre of the bullet; in outline it was seldom exactly circular, but rather roughly four-sided, with rounded angles, slightly oval, or pear-shaped. The margin of the opening consisted of outer table alone, the inner being always considerably comminuted. Fragments of the latter, together with the majority of those corresponding to the loss of substance of the outer table, were driven through the dura mater and embedded in the brain. These bony fragments were more or less widely distributed over an area of a square inch or more, and not confined to a narrow track.
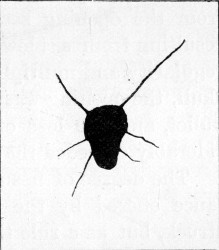 Fig. 61.
Fig. 61.
Diagram of Aperture of Entry in Occipital Bone, showing radiating fissures exact length. The exit in the frontal region was of typical explosive character. Range '100 yards'
The amount of fissuring at the aperture of entry was often not so extensive as I had been led to expect. Fig. 61 is a diagram illustrating a fairly typical instance; in some cases no fissuring existed. As a rule the nearer to the base, the greater was the amount of fissuring observed. The fissures were sometimes very extensive in this position, probably as a[Pg 246] result of the lesser degree of elasticity in this region of the skull. Again, when the aperture of entry was near the parts of the vertex where sudden bends take place, considerable fissuring of the same nature as that seen in the superficial tracks (fig. 68) was produced in the flat portion of the skull above the point of entrance.
Radial fissuring around the aperture of entry in the skull scarcely corresponds in degree with that seen when the shafts of the long bones are struck, and is far less marked and regular than when one of these small bullets strikes a thick sheet of glass set in a frame. I saw several apertures in the thick glass of the windows of the waterworks building at Bloemfontein produced by Mauser bullets. They differed little from the opening seen in an ordinary plate-glass window resulting from a blow from a stone, except perhaps in the regularity and multiplicity of the radial fissures. As in the skull, the opening was a little larger than the calibre of the bullet, and the loss of substance on the inner aspect considerably exceeded that on the outer.
The degree of fissuring is probably affected by the resistance offered by the particular skull, or the special region struck, but as a rule the elasticity and capacity for alteration in shape possessed by the bony capsule, is opposed to the production of the extreme radial starring observed in the long bones or a fixed sheet of glass. Corroborative evidence of the influence of elasticity in the prevention of starring is seen in the limited nature of the comminution of the ribs in cases of perforating wounds of the thorax.
In the most severe cases we can only speak of the 'aperture' of exit in a limited sense in so far as the opening in the scalp is concerned; this was often comparatively small, not exceeding 3/4 of an inch in diameter. Beneath this limited opening in the soft parts, the bone of the skull was smashed in a most extensive manner. The portion exactly corresponding to the point of exit of the bullet was carried altogether away, but around this point a number of large irregularly shaped fragments of bone, from 3/4 to 1 inch in diameter, were found loose, and often so displaced as to expose a considerable area of the dura-mater. Beyond the[Pg 247] area of these loose fragments, fissures extended into the base and vertex, in the latter case often being limited in their extent by the nearest suture.
Over extensive fractures of this nature general œdema and infiltration of the scalp, due to extravasation of blood, were present. When the exit was situated in the frontal region ecchymosis often extended to the eyelids and down the face, while in the occipital region similar ecchymosis was often seen at the back of the neck.
The opening in the dura mater at the aperture of entry was either slitlike, or more often irregular from laceration by the fragments of bone driven in by the bullet. At the point of exit a similar limited opening corresponded with the spot at which the bullet had passed, while separate rents of larger size were often seen at some little distance. The latter were the result of laceration of the outer surface of the membrane by the margins of the large loose fragments of bone above described.
Injury to the brain more than corresponded in extent to the fractures of the bone. Pulping of its tissue existed over a wide area both at the points of entrance and of exit. In the former position the amount of damage was the less, the gross changes roughly corresponding with the tissue directly implicated by the bullet itself, and the fragments of bone carried forward by it. The degree of splintering of the skull therefore in great part determined the severity of the lesion. At the exit aperture much more widespread destruction existed, while masses of brain tissue, small shreds of the membranes, fragments of bone, and débris from the scalp were found occasionally bound together by coagulated blood and protruding from an exit opening of some size. The largest masses of such débris were most often seen in instances in which the bullet had entered by the base to escape at the vertex of the skull.
The brain in the line of injury suffered comparatively slightly, but small parenchymatous hæmorrhages into its tissue indicated in lesser degree the same type of injury undergone by the mass of brain pulp and small blood-clots found at the external limits of the wound. Beyond this extensive hæmorrhages at the base of the skull were common.[Pg 248]
With regard to the extensive character of the brain destruction in the region of the aperture of exit, it must be borne in mind that this lesion corresponds in position with one which would exist even if the injury were of a non-penetrating degree. A large proportion of the contusion and destruction is therefore explained by violent impact of the projected brain with the skull prior to the passage of the bullet, and not to the direct action of the bullet on the tissues.
These cases of 'general injury' afford a marked example of the lesions to which the term 'explosive' has been applied, and as such have an important bearing on the theories held as to the mode of production of explosive effect. The increased area of tissue damage at the aperture of exit favours the theory of direct transmission of a part of the force with which the bullet is endowed, to the molecules of tissue bounding the track made by the projectile. Thus the area of destruction corresponds with the cone-like figure which one would expect to be built up by the vibrations spreading from the primary point of impact. The exit region of the skull is subjected not alone to the force of the travelling bullet, but also to that exerted over a much wider area by the tissue to which secondary vibrations have been communicated. The brain itself is, in fact, dashed with such violence against the bone as to cause a great part of the injury.
No doubt the brain in its reaction to the bullet forms as near an approach to a fluid as any solid tissue in the human body, and experimental observation has shown how greatly its presence or absence in the skull affects the degree of comminution on the exit side; hence the fondness for the so-called hydraulic theory that has been always exhibited in the case of these injuries. The localisation of the injury in its highest degree to the neighbourhood of the exit aperture, however, shows that in any case the main wave takes a definite direction in a course corresponding to that of the bullet.
The real importance of the presence of the brain within the skull in increasing the amount of damage at the exit end of the track, is as a medium for the ready transmission of[Pg 249] forcible vibrations. That the latter are to some extent conveyed as by a fluid is evidenced by the occasional presence of brain matter and fragments of bone in the aperture of entry, which suggests recoil or splash such as would be expected from a fluid wave.
Experience of the character of the lesions observed after severe concussion by the ordinarily somewhat coarser forms of violence common to civil life, fully explains the severity of the damage to the brain tissue met with in injuries due to bullets of small calibre. Viewing the elaborate arrangements which exist for the preservation of the central nervous system from the moderate vibration incidental to ordinary existence, it is easy to appreciate the harmfulness of such exquisite vibratory force as that transmitted by a bullet of small calibre travelling at a high rate of velocity.
Effect of ricochet in the production of severe forms of injury.—In connection with the lesions above described mention must be made of cases in which the aperture of entry reaches a large size, or a portion of the skull is actually blown away.
Examples of the former class were not uncommon; I will briefly relate one.
(48) A Highlander while lying in the prone position at Rooipoort, was struck by a bullet probably at a distance of about 1,000 yards. A large entry wound in the scalp was produced, while the defect in the skull was coarsely comminuted and was capable of admitting three fingers into a mass of pulped brain. Both brain matter and fragments of bone were found in the external wound, which was situated just anterior to the right parietal eminence. The bullet passed onwards through the base of the skull, crossing the external auditory meatus, fracturing the zygoma and probably the condyle of the mandible, and eventually lodged beneath the masseter muscle. Blood and brain matter escaped from the external auditory meatus.
The patient was brought off the field in a semi-conscious condition, the pupils moderately contracted but equal, the pulse 66, very small and irregular in beat, the respiration quiet and easy, and with paralysis of the left side of the body. The fæces had been passed involuntarily.
The wound was cleansed and bone fragments removed. The patient had to travel in a wagon for the next three days until the column halted. The progress of the case was unsatisfactory, as the wound became infected, and the man eventually died on the 14th day of general septicæmia, but with little evidence of local extension of septic inflammation.
In this instance the head was no doubt struck by a bullet which had previously made ricochet contact with the ground. I saw several such cases.
Closely connected with such injuries are those in which large portions of the skull and scalp were actually blown away. I never witnessed one of these myself, but I recall two instances described to me by officers who lay near the wounded men on the field. In one the frontal region was carried away so extensively that, to repeat the familiar description given by the officer, 'he could see down into the man's stomach through his head.' In a second case the greater part of the occipital region was blown away in a similar manner, and this was of especial interest as the wounded man was seen to sit up on the buttocks and turn rapidly round three or four times before falling apparently dead. The observation offers interesting evidence of the result of an extensive gross lesion of the cerebellum.
In the absence of exact information, it may well be that such injuries as the two latter were produced by some special form of bullet, but as both were produced while the patients were lying on the ground, and therefore especially liable to blows from ricochet bullets, I am inclined to attribute both to this cause.
In considering injuries of the above nature, one cannot help speculating on the possible influence of a head-over-heels ricochet turn on the part of the bullet while traversing the long sagittal axis of the skull. It is not uncommon for apical target ricochets to present evidence of damage to the apex and base of the mantle alone. This must depend on a rapid turn on impact, which might well be imitated in the case of the skull, and would then go far to explain the production of some of the most severe forms of explosive exit wounds met with. See cases 48, 54, 68.
Short of ricochet, the influence of simple wobbling must[Pg 251] also be considered in shots from a long range. The entry wound may be large as a result of this condition, but as the velocity possessed by the bullet is low, the injuries would probably not be of a very severe nature.
In connection with the subject of wobbling, reference should be made to the form suggested by Nimier and Laval, in which the wobble, as the result of resistance to the apex of the revolving bullet, assumes the form of movement seen when the spin of a top is failing. This would explain a peculiarity in some wounds of entry over the skull first pointed out to me by Mr. J. J. Day. When such wounds were explored, as well as the presence of brain in the entry aperture, a number of fragments of the external table of the skull were found everted and fixed in the tissues of the scalp. As already suggested, this may be mere evidence of splash, but it may be equally well explained by a process of wobble around the axis of revolution of the bullet. This might, no doubt, also be invoked to explain the displacement of some of the fragments in fractures of the long bones, where considerable resistance to the passage of the bullet is offered.
II. Vertical or coronal wounds in the frontal region.—These injuries were common, and offered some of the most interesting illustrations of the variations in symptoms and effects following apparently exactly identical lesions, judging from the condition of the external soft parts alone; since the latter sometimes gave little indication of the force (dependent on the rate of velocity) which had been applied.
With the lower degrees of velocity simple punctured fractures of the skull resulted, without extensive lesion of the frontal lobes as evidenced by immediate symptoms. The nature of the fractures differed in no way from the punctured fractures we are familiar with in civil practice. The openings of entry in the bone were irregularly rounded, corresponding in size to the particular calibre of the bullet concerned. The margin consisted of outer table alone, while the inner table was either considerably comminuted, or a large piece was depressed, wounding the dura-mater and projecting into the brain substance (see fig. 63). The aperture of exit presented exactly the opposite characters, the splintering comminution[Pg 252] or separation of a large fragment affecting the outer table, while the inner presented a simple perforation. The latter condition is represented in figs. 71 and 72, and I will here give short notes of four illustrative cases, as being the shortest and most satisfactory method of conveying a correct idea of the nature of such injuries.
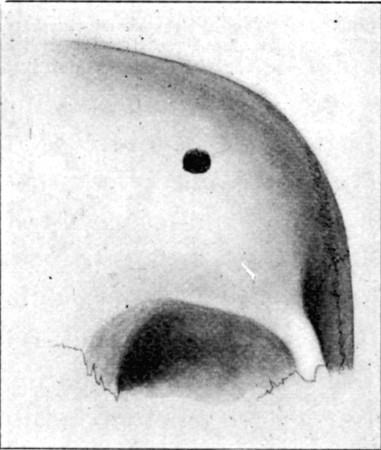 Fig. 62—Aperture of Entry in Frontal Bone. Case No. 50.
1/2
Fig. 62—Aperture of Entry in Frontal Bone. Case No. 50.
1/2
(49) Vertical perforation of frontal bone.—Wounded at Belmont, while in the prone position. Aperture of entry (Mauser), at the anterior margin of the hairy scalp on the left side; course, through the anterior part of the left frontal lobe, roof of the left orbit, cutting the optic nerve and injuring the back of the eyeball, floor of the orbit, the antrum, the hard palate, and tongue. Exit, in mid line of the submaxillary region. No cerebral symptoms were noted, and on the fifth day the man was sent to the Base hospital without operation; the pulse was then 70 and the temperature normal. The movements of the eyeball were perfect, but blindness was absolute. At the Base hospital the eye suppurated and was removed. The patient was then sent home apparently well. He has since been discharged from the service, and is now employed as a painter in Portsmouth Dockyard.
(50) Vertical perforation of frontal bone.—Wounded at Paardeberg while in the prone position. Range, 600-700 yards. Aperture of entry (Mauser), at the fore margin of the hairy scalp above the centre of the right eyebrow; course, through the anterior third of the right frontal lobe, roof of orbit, front of eyeball, margin of floor of orbit making a distinct palpable notch, and cheek; exit through the red margin of the upper lip, 1/2 an inch from the right angle of mouth. The bullet slightly grooved the lower lip.
The patient rose almost immediately after being struck, and walked about a mile, although feeling dizzy and tired. The wounds, which both bled considerably, were then dressed. After three days' stay in a Field hospital, the patient was sent in a bullock wagon three days and nights' journey to Modder River and thence to the Base.[Pg 253]
There was anæsthesia over the area supplied by the outer branch of the supra-orbital nerve, extending from the supra-orbital notch backwards into the parietal region, but none over the area supplied by the second division of the fifth nerve.
On the tenth day there were no signs of cerebral disturbance except a pulse of 48. The eyeball was suppurating, and the temperature rose to 99° at night. The lids were still swollen and closed.
A few days later the eyeball was removed and at the same time a flap was raised and the fracture explored (Major Burton, R.A.M.C.). An opening somewhat angular, 1/3 of an inch in diameter, was found with a thin margin in the outer table of the skull (fig. 62); when this was enlarged with a Hoffman's forceps, an opening in the dura was discovered, and cerebro-spinal fluid escaped. A piece of the inner table of the skull (fig. 63), 3/4 by 1/3 an inch in size, was discovered projecting downwards vertically into the brain. This latter was removed and the wound closed. Healing by primary union followed, and no further symptoms were observed.
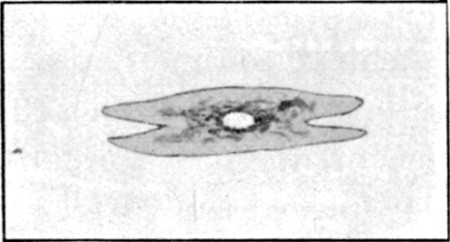 Fig. 63.
Fig. 63.
Fragment of Inner Table depending vertically from lower margin of puncture shown in fig. 62. The centre was perforated. Exact size
(51) Transverse frontal wound.—Wounded at Paardeberg. The man was sitting down at the time he was struck, in the belief that he was out of the range of fire. The entry and exit wounds were almost symmetrical, placed on the two sides of the forehead at the margin of the hairy scalp, 2¼ inches above the level of the external angular processes of the frontal bone. The patient lost consciousness for about half an hour, then rose and walked half a mile to the Field hospital. The wounds were dressed, and after a stay of three days in hospital, the man was sent the three days' journey to Modder River; during the journey he got in and out of the wagon when he wished. After two days' stay at Modder, a journey was again made by rail to De Aar (122½ miles). The wounds were healed. The man stayed at De Aar nearly a month, and then, rejoining his regiment, made a two days' march of some 22 miles on hot days. He had to fall out twice on the way by reason of headache, feeling dizzy, and 'things looking black.' He did not own to any loss of memory or intellectual trouble, but was invalided to England. This patient returned to South Africa [Pg 254]later, and is now on active service.
(52) Transverse frontal wound.—Within a few days an almost identical symmetrical wound in the frontal region occurred in the same district, from a near range. The patient became immediately unconscious, and remained so until his death some four days later, his symptoms being in no way alleviated by operation and the removal of a quantity of bone fragments and cerebral débris. At the post-mortem examination, extensive destruction of both hemispheres of the brain was revealed, and large fissures extended into the base of the skull.
III. Glancing or oblique perforating wounds of varying depth in any portion of the cranium.—These injuries were the most common, the most highly characteristic of small-calibre bullet wounds, the most interesting from the point of view of diagnosis, prognosis, and treatment, and beyond this they formed the variety most unlike any that we meet with in civil practice.
They were met with in every region of the cranium, and in every degree of depth and severity. The lesser are best designated as gutter fractures, the deeper are perforating and gradually approximate themselves to the type of injury described as class 1.
When the bullet struck a prominent or angular spot on the skull a considerable oval-shaped fragment was occasionally carried away, leaving an exposed surface of the diploë (case 60, p. 274). Under these circumstances the apparent lesion on raising a flap was slight, but exploration often showed extensive intra-cranial mischief. Thus in the case referred to both dura and brain were wounded, and continuing hæmorrhage led to the development of progressive paralysis, relieved only by operation.
From the more deeply passing bullets a more or less oval opening resulted, in which both tables were freely comminuted and displaced. These cases differed from the typical gutter fracture only in length and outline, and the nature of the accompanying intra-cranial lesion was identical, while in the latter particular they differed much from fractures in which the impact of the bullet was direct, in spite of a near resemblance in the appearances in the osseous defect.
I saw one instance in which a circular fissure about 1½ inch from the actual opening of entry surrounded the latter, the area of bone within the circle being somewhat depressed, though radial fissures were absent.
In several of these cases fragments of lead were either found on the fractured surface of the bone or within the cranial cavity, showing that the bullets had undergone fissuring of the mantle, or had actually broken up on impact.
Gutter fractures.—The nature of the injury to the bones in these is best illustrated by a series of diagrams of sections such as are shown below.
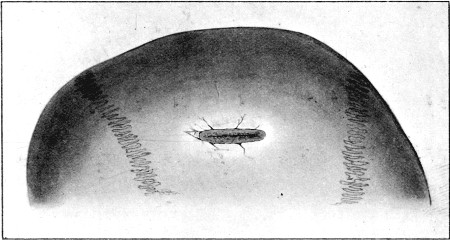 Fig. 64.
Fig. 64.
Gutter Fracture of first degree. The drawing does not show well the small fragments of bone usually carried from the margins of the depression by the bullet
In the most superficial injuries the outer table was grooved and depressed, usually with loss of substance from small fragments directly shot away: these latter had either been driven through the wound in the soft parts, or remained embedded on the deep aspect of the enveloping scalp (fig. 64). In the less common variety the scalp was slit to a length corresponding with the injury to the bone, but more often oval openings in the skin existed at either end of the track. The inner table was practically never intact, but the amount of comminution naturally varied with the depth to which the outer table was implicated (fig. 65 A, and B).
The following is an illustrative example of this degree,[Pg 256] and also emphasises the consequences which may follow primary non-interference.
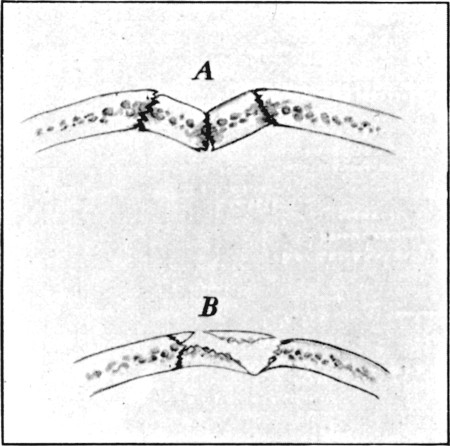 Fig. 65.
Fig. 65.
Diagrammatic transverse sections of varying condition of bones in Gutter Fractures of the first degree. A. With no loss of substance. B. With comminution
(53) Superficial gutter fracture in parietal region. Convulsive twitchings. Secondary paralysis.—Wounded at Modder River. Range, 400 yards. A scalp wound 3 inches in length ran vertically downwards, commencing 1 inch from the median line, and situated immediately over the upper third of the right fissure of Rolando. The patient was unconscious for several hours after the injury, and later suffered with severe headache, and twitchings in the left shoulder and arm.
The wound healed, but a well-marked groove was palpable in the bone beneath, and the twitchings persisted. The latter came on about every twenty minutes, and loss of power in the left upper extremity, and to a less degree in the lower, developed. The memory was defective, and the patient suffered at times with headache. The pupils were equal but sluggish in action. No changes were discovered in the fundus beyond a well-developed myopic crescent at the lower and outer part of the left disc (Mr. Hanwell).
The twitchings became more frequent and latterly were accompanied by somewhat severe muscular contractions in the upper extremity, while the loss of power in the lower extremity became more marked. Headache was also more troublesome.
The patient throughout refused any operation, saying he would rather go home first, and at the end of a month he left for England.
In the deeper injuries more and more of the outer table was cut away, and the inner became gradually more depressed, fractured, or comminuted (fig 66).
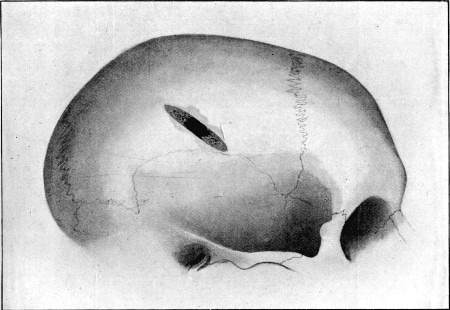 Fig. 66.
Fig. 66.
Gutter Fracture of the second degree. Perforating the skull in the centre of its course. External table alone carried away at either end
Bevelling at the expense of the outer table at both entry and exit ends of the course existed, but in either case a portion of the inner table was also detached and depressed. Sometimes the depressed portion of the inner table was mainly composed of one elongated fragment; this was either when the bullet had not implicated a great thickness of the outer table, or had passed with great obliquity through especially dense bone (see fig. 70). When the bullet had passed more deeply the inner table was comminuted into numberless fragments. I have frequently seen 50 or 60 removed. Where such tracks[Pg 258] crossed convex surfaces of the skull, the two conditions were often combined; thus at one portion of the track, usually the centre, the comminution was extreme, while at either end a considerable elongated fragment of inner table was often found, the latter perhaps more commonly at the distal or exit extremity (fig. 67).
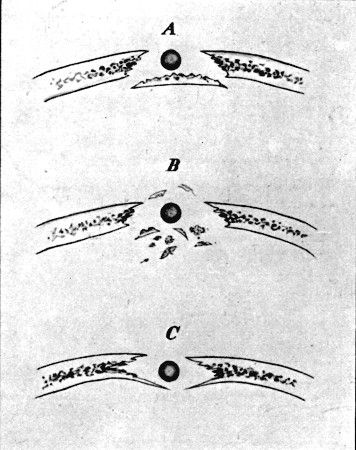 Fig. 67.
Fig. 67.
Diagrammatic transverse sections of complete Gutter Fracture. A. External table destroyed, large fragment of internal table depressed. (Low velocity or dense bone.) B. Comminution and pulverisation of both tables centre of track. C. Depression of inner table (low velocity)
The nature of the injury to the bone when the flight of the bullet actually involved the whole thickness of the calvarium was comparable to that seen in the case of the long bones when struck by a bullet travelling at a moderate rate (see plate XIX. of the tibia, or what is illustrated in the case of the pelvis in fig. 55). In point of fact, a clean longitudinal track appeared to have been cut out. The length of these tracks naturally depended upon the region of the skull struck. When a point corresponding to a sharp convexity, or a sudden bend in the[Pg 259] surface, was implicated, an oval opening of varying length in its long axis was the result; when a flat area, as exists in the frontal or lateral portions of the skull, was the seat of injury, a long track was cut.
Superficial perforating fractures.—These formed the next degree; the chief peculiarity in them was the lifting of nearly the whole thickness of the skull at the distal margin of the entry, and the proximal edge of the exit, openings; the flatter the area of skull under which the bullet travelled the more extensive was the comminution. In some cases nearly the whole length of the bone superficial to the track would be raised; in fact, the bullet having once entered, the force is applied from within in exactly the same way that it operates on the inner table in the gutter fractures. A corresponding injury is met with in the case of the bones of the extremities (see fig. 57 of the tibia), and again the resemblance between these injuries of the skull and such perforations of the long bones as are illustrated by skiagrams Nos. III. and XXIII. of the clavicle and fibula is a close one.
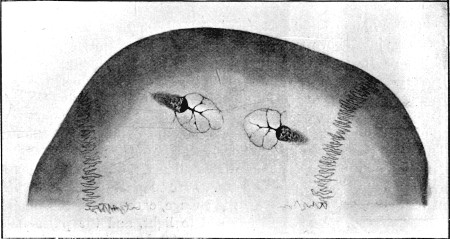 Fig. 68.
Fig. 68.
Superficial Perforating Fracture. Illustrating lifting of roof at both entry and exit openings
I will add here a case of coexistent gutter fracture and perforating wound of the skull, the conditions of the bone in[Pg 260] which will illustrate the behaviour of the outer and inner tables respectively, when struck with moderate force.
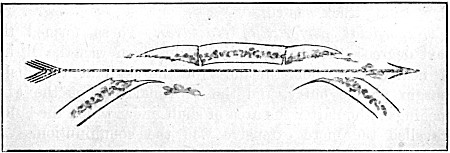 Fig. 69.
Fig. 69.
Diagrammatic longitudinal section of Fracture shown in fig. 68
 Fig. 70.
Fig. 70.
Fragment forming the main part of the floor of Gutter Fracture in the squamous portion of the temporal bone. (Low velocity, hard bone)
(54) Wounded at Thaba-nchu. Guedes bullet. Entry behind left ear, just above posterior root of zygoma; gutter fracture; bullet retained within skull. Above and corresponding to right frontal eminence there was a hæmatoma, beneath which a loose fragment of bone was readily palpable. When brought into the Field hospital, twenty-four hours after the injury, the man appeared to understand when spoken to, but made no answers to questions. The urine was passed unconsciously, the bowels were confined.
He was drowsy, the pupils widely dilated, the pulse 68, of good strength, and the temperature 104°. He slept well the following night and midday there was little change, except that the pupils acted to light, and the pulse had risen to 88, becoming dicrotic and small. The temperature was 103°, the tongue furred and dry, but he was lying with the mouth wide open.
At 2 p.m. the wound was explored. The entry led down to a typical gutter fracture in the squamous portion of the temporal bone, at the point of junction of the vertical with the horizontal part; the floor of the gutter had been displaced inwards as a single fragment (fig. 70). A flap was raised in the frontal region, where a scale of outer table (fig. 71), clothed with diploic tissue, was found loose. Beneath this a puncture on the frontal bone, about corresponding in size to the bullet, was[Pg 261] discovered. This opening was enlarged, and a bullet detected and removed. The bullet was a Guedes, with no marks of rifling, and was in no way deformed. At least a square inch of the right frontal lobe was pulped, so that the bullet lay in a cavity.
The patient improved somewhat during the next two days, and on the third took a 16 hours' journey to Bloemfontein, where Mr. Bowlby (who was present at the operation) kindly took him into the Portland Hospital. The pulse gradually rose to 112, the temperature remained on an average from 102° to 103°, the respiration rose to 36, the face became somewhat livid, and on the sixth day death occurred rather suddenly, apparently from respiratory failure. For two days before his death the patient sometimes asked for food, &c.; there was occasional twitching of the left angle of the mouth, and, when the posterior wound was manipulated, some twitching of the fingers of the left hand. When the wound was dressed on the fourth day, there were breaking-down blood-clot and signs of incipient suppuration.
Mr. Bowlby made a post-mortem examination, and found considerable pulping of the tip of the right frontal and left temporo-sphenoidal lobes, and a thick layer of hæmorrhage extending over the whole base of the brain.
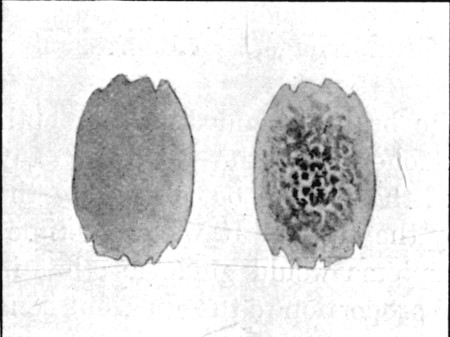 Fig. 71.
Fig. 71.
Scale of outer table of Frontal Bone and Diploë. Exact size, from fracture shown in fig. 72
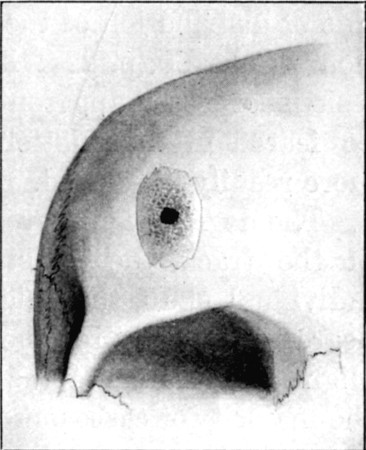 Fig. 72.—Perforating Fracture of Frontal Bone from
within Separation of plate outer table. (Low velocity.) 1/2
Fig. 72.—Perforating Fracture of Frontal Bone from
within Separation of plate outer table. (Low velocity.) 1/2
The injury to the cranial contents varied with the degree of bone injury. Hæmorrhage on the surface of the dura may in rare instances have been the sole gross lesion; I never met with such a condition, however. In all the cases in which comminution had occurred, some laceration of the dura, even if[Pg 262] not more than surface damage or a punctiform opening, had resulted. In the more serious gutter fractures an elongated rent of some extent usually existed. In the perforating fractures two more or less irregular openings were the rule. The amount of hæmorrhage, even if the venous sinuses were implicated, was on the whole surprisingly small, when the cases were such as to survive the injury long enough to be brought to the Field hospital. I never saw a typical case of middle meningeal hæmorrhage, although many fractures crossing the line of distribution of the large branches came under observation. Case 60, p. 274, illustrated the fact that the osseous lesions of lesser apparent degree are sometimes the more to be feared in the matter of hæmorrhage, as compression is more readily developed.
The degree of injury to the brain depended on the depth of the track, the resistance offered by the bones of any individual skull, the weight of the patient, but chiefly on the degree of velocity retained by the bullet. It was sometimes slight and local as far as symptoms would guide us; but in the majority of cases out of all proportion to the apparent bone lesion, if the range was at all a short one. Cases illustrative of these injuries are included under the heading of symptoms.
It will be, of course, appreciated that the coarse brain lesions under the third heading differed in localisation and in extent alone, and in no wise in nature, from those observed in the two preceding classes. The damage consisted in direct superficial laceration and contusion, and beyond the limits of the area of actual destruction, abundant parenchymatous hæmorrhages more or less broke up the structure of the brain, such hæmorrhages decreasing both in size and number as macroscopically uninjured tissue was reached. No opportunity was ever afforded of examining a simple wound track in a case in which no obvious cerebral symptoms had been present.
IV. Fractures of the base.—In addition to the above classes, a few words ought to be added regarding the gunshot fractures of the base of the skull. These possessed some striking peculiarities; first in the fact that they might occur in any position, and hence differed from the typically coursing[Pg 263] 'bursting' fractures we are accustomed to in civil life as the consequence of blows and falls, and consequently were often present without any of the classical symptoms by which we are accustomed to locate such fissures. Secondly, the peculiar form was not uncommon in which extensive mischief was produced from within by direct contact of a passing bullet.
As far as could be judged from clinical symptoms, indirect fractures of the base such as we are accustomed to meet in civil practice in connection with fractures of the vault were decidedly rare, and, as has already been mentioned, ocular evidence of extensive fissures extending from perforating wounds of the vertex was wanting, except in the extreme cases classed under heading I. For these reasons I am inclined to regard them as uncommon.
Direct fractures of the base, on the other hand, were of common occurrence, especially in the anterior fossa of the skull. These might be produced either from within, the most characteristic form of gunshot injury, or from without. The fractures from within were often simple punctures of the roof of the orbit or nose.
Punctured fractures of the roof of the orbit caused little trouble as far as the cranium was concerned, but the orbital structures often suffered severely. I saw one or two very severe comminutions of the roof of the orbit caused by bullets which had crossed the interior of the skull; in one case the whole roof was in small fragments, while the damage in others was not greater than chipping off some portion of the lesser wing of the sphenoid. The roof of the orbit again was sometimes very severely damaged by bullets which first traversed that cavity itself; thus in one case which recovered, the bullet passed transversely, smashing both globes, and fracturing the roof of both orbits and the cribriform plate so severely as to lacerate both dura-mater and brain, portions of the latter being found in the orbit on removal of the damaged eyes.
Fractures of the middle and posterior fossæ were met with far less frequently, partly I think because vertical wounds passing from the vertex to the base in these regions were with few exceptions rapidly fatal, and partly from the[Pg 264] fact that the occipital region, being ordinarily sheltered from the line of fire, was rarely exposed to the danger of direct fracture from without. As an odd coincidence I may mention that in my whole experience during the war I only once saw bleeding from the ear as a sign of fracture of the base, apart from direct injuries to the tympanum or external auditory meatus.
Symptoms of fracture of the skull, with concurrent injury to the brain.—These consisted in various combinations of the groups of signs indicative of the conditions of concussion, compression, cerebral irritation, or destruction. Although the symptoms possessed no inherent peculiarities, yet certain characteristics exhibited served to illustrate the fact that, as a result of the special mechanism of causation of the injuries, the type deviated in many ways from that accompanying the corresponding injuries of civil practice.
The characters of the external wounds will be first considered, followed by some remarks concerning the symptoms attendant on the different degrees and types of lesion, the symptoms special to injuries to different regions of the head, and on the subsequent complications observed.
In the simplest injuries the type forms of entry and exit wound were found, and it has already been observed that in these, if symmetrical, considerable difficulty existed in discriminating between the two apertures. This is to be explained by the fact that the arrangement and structure of the scalp are identical in corresponding regions; hence the only difference in the conditions of production of the entry and exit wounds exists in the absence of support to the skin in the latter. The granular structure of the hairy scalp is opposed to the occurrence of the slit forms of exit, hence the openings were usually irregularly rounded. Any increase of size in the exit wound in the soft parts due to the passage of bone fragments with the bullet, was equalised in that of entry by the fact that the latter, as supported by a hard substratum, was usually larger than those met with in situations where the skin covers soft parts alone.
In some cases of gutter fracture the wounds of entry were large and irregular, as a result of upward splintering of the[Pg 265] bone at the distal margin of the aperture of entry in the skull, and consequent laceration of the scalp. Again, on the forehead very pure types of slit exit wound were often met with in the position of the vertical or horizontal creases. With higher degrees of velocity on the part of the bullet and consequent comminution at the aperture of exit in the bone, the scalp was more extensively lacerated, and large irregular openings in the soft parts, often occupied by fragments of bone and brain pulp, were met with. It is well to repeat here, however, that the presence of brain pulp in a wound by no means necessarily indicated the aperture of exit, for it was sometimes found in the entry opening also.
In the most severe cases, such as are included in class I., the exit wound often possessed in the highest degree the so-called 'explosive' character. From an opening in the skin with everted margins two or more inches in diameter a mass of brain débris, bone fragments and particles of dura-mater, skin, and hair, bound together by coagulated blood, protruded as a primary hernia cerebri if the patient survived the first few hours after the injury. In other cases of the same class the actual opening was smaller, but the whole scalp was swollen and œdematous, sometimes crackling when touched from the presence of extravasated blood in the cellular tissue, while firm palpation often gave the impression that the head consisted of a bag of bones over a considerable area.
Gutter fractures of the scalp were sometimes situated beneath an open furrow, gaping from loss of substance, or beneath a bridge of skin; in the latter case they were usually palpable. Simple punctures were also usually palpable, but the smallness of the openings sometimes rendered their detection more difficult than might be assumed.
I never saw a case in which the skull escaped injury when the bullet struck the scalp at right angles, but the frequency with which Mauser bullets were found within the helmets of men would suggest that this must have sometimes occurred. A case of injury to the external table alone has been described (p. 243). An illustration of the next degree of injury is afforded by the following:—A bullet lodged in the centre of the forehead, the point lying within the cranial cavity, while[Pg 266] the base projected from the surface: this patient suffered but slight immediate trouble, so little, indeed, that he merely asked his officer to remove the bullet for him, as it was inconvenient. The bullet was subsequently removed in the Field hospital.
In a few cases the bullet entered the skull and was retained, when only a single wound was found. Such cases are described in Nos. 54 and 68, where the position of the bullet was determined by palpable fractures beneath the skin. With regard to the retention of bullets, however, in small-calibre wounds, it was always necessary to examine the other parts of the body with great care, and to ascertain, if possible, the direction from which the wound was received, as an exit was often found some distance down the neck or trunk. Again the possibility of the opening having been produced by glancing contact had to be considered.
In cases which survived the injury on the field, free hæmorrhage, as in wounds of other regions, was rare, and although general evidence of loss of blood was often noted in patients brought in, progressive bleeding was seldom observed. Again, when the wounds were explored, the amount of blood, although considerable, was usually not more than sufficed to fill up the space consequent on the loss of brain tissue. This was especially striking when large venous sinuses, as the superior longitudinal, were involved in the injury. None the less, hæmorrhage at the base of the brain was, I believe, responsible for early death in many of the severe cases, especially when the wounds were near the lower regions of the skull.
Escape of cerebro-spinal fluid was not so prominent a feature as might have been expected, considering how freely the arachnoid space was opened up in many cases. I think this was usually checked by early coagulation of the blood, and later by adhesions. It must be remembered also that extensive wounds were most common on the vertex, or at any rate over the convex surface of the brain, while fractures of the middle fossa were usually rapidly fatal.
Concussion.—Cases exhibiting symptoms of pure uncomplicated concussion were distinctly rare, as would be expected[Pg 267] from the mechanism of the injuries. On the other hand, symptoms of concussion formed the dominant feature of all severe cases.
The symptoms in many instances consisted in great part in transitory signs of the so-called 'radiation' type, such as are seen in destructive lesions where the signs of nervous damage rapidly tend to diminish and localise themselves.
As to the causation of the 'radiation' symptoms, it is difficult to discriminate the effects of neighbouring parenchymatous hæmorrhages from those of local vibratory concussion of the nervous tissue. The local character of the signs seems, however, to point to causation by molecular disturbance, resulting from the conduction of forcible mechanical vibration to the brain tissue rather than to upset in the intra-cranial pressure. Again the limited nature of the paralysis observed, sharply defines it from the general loss of power accompanying ordinary cases of concussion of the brain. The similarity of the phenomena to those described in other parts of the body under the heading of 'local shock' is sufficiently obvious.
The following instance well exemplifies the condition in question:
(55) Wounded at Spion Kop. A scalp wound 3 inches in length crossed the left parietal bone nearly transversely, starting 1½ and ending 2 inches from the median line: the centre of the wound corresponded with the position of the fissure of Rolando. The patient was struck at a distance of fifty yards while kneeling; he fell and remained unconscious an hour and a half. Right hemiplegia without aphasia followed. The wound was cleansed and sutured, and in three days both arm and leg could be moved, after which time the man improved rapidly. Three weeks later when I saw him at Wynberg there was still comparative weakness of the right side, but beyond some neuralgia of the scalp, the man considered himself well. No groove could be detected on the bone on palpation. (This case offers a good example of the ease with which bone injury may be overlooked. The man came over to England 'well;' but while on furlough, two pieces of bone came away spontaneously. He is now again on active service.)
Compression.—Equally rare was it for pure symptoms of compression to be exhibited. This depended on two circumstances:[Pg 268] first, the rarity of injuries giving rise to meningeal hæmorrhage; secondly, the fact that in nearly every case a more or less extensive destructive lesion was present, at the margins of which less completely destroyed tissue remained, capable of giving rise to symptoms of irritation. Again, as we have seen, free hæmorrhage into, or from the walls of, the cavities produced in the brain was not a marked feature, and beyond this the large defect in the cranial parietes was calculated to render a high degree of compression impossible.
As the most serious head injuries presented a remarkable similarity in their symptoms, I will shortly summarise their common features.
Every degree of mental stupor up to complete unconsciousness was met with, but in some instances where the pulse, respiration, and general bodily condition pointed to speedy dissolution, the patients answered rationally often between moans or cries indicative of pain.
Widespread paralysis often existed, but this was seldom completely general; more commonly it was combined with extreme restlessness of the unparalysed parts, or sometimes, even when the whole of one hemisphere was tunnelled, and in all probability widely destroyed, restlessness was the only symptom. In some cases twitching of the features or the limbs or severe convulsions were superadded.
The pupils were rarely unequal, and at the stage in which these patients were first seen were usually moderately contracted. Wide dilatation was uncommon throughout.
The pulse was with very few exceptions slow, sometimes irregular. In some instances, when the wounds had been thought suitable for exploration, the slow pulse was altered after operation to a rapid one, and death usually quickly supervened.
Respiration was irregular, sometimes sighing; in the late stage often of the Cheyne-Stokes type; actual stertor was exceptional, but the respiration was often noisy.
The temperature was often raised from an early stage to 99° or 100°, and if the patient survived a day or two, it often rose to 103° or 104°. How far the secondary rise[Pg 269] depended on sepsis it was not always easy to determine. The urine was usually retained.
Cases presenting the above characters were usually those suffering from lesions such as are described in class I., and mostly died in twenty-four to forty-eight hours. The correspondence of the train of symptoms with those due to combined brain destruction and severe concussion is at once apparent.
To illustrate the nature of the symptoms in patients suffering from the less extensive forms of injury, such as those included in classes II. and III. under the heading of anatomical lesion, the relation of a short series of histories will be advisable. I may first premise, however, that the special characteristics of these were in some instances the almost entire absence of primary symptoms of gravity; in others general symptoms of a severity out of apparent proportion to the external lesion; while in all destructive lesions, very widely distributed radiation symptoms developed, often disappearing with great rapidity.
The symptoms consisted in those of concussion, irritation, local pressure, and actual destruction.
The symptoms of concussion were either general, and then usually transient, or local paralysis of the radiation variety, which also rapidly improved.
Signs of irritation consisted in irritability of temper, drowsiness, closure of the eyes and objection to light, contracted pupils sometimes unequal, a tendency to the assumption of the flexed position at all the joints, twitchings, and sometimes convulsions. Sometimes these appeared early as a direct result of mechanical irritation from bone fragments or blood-clot; sometimes only in the course of a few days, as a result of irritation of parts recovering from the radiation effects which had prevented earlier nervous reaction. Possibly in some cases the symptoms of irritation depended upon an increase in the amount of hæmorrhage, and in others upon the development of local inflammatory changes.
Local pressure, or actual destruction of brain tissue, was evidenced by temporary paralysis in the former, permanent loss of function in the latter, condition.[Pg 270]
Fractures of the anterior fossa of the skull were attended by very marked evidence of orbital hæmorrhage, as subconjunctival ecchymosis (rarely pure), increased tension, and proptosis.
Injuries to the cranial nerves at the base, with the single exception of lesion of the optic nerves, which was not rare, were in my experience uncommon in the hospitals—a fact pointing to the very fatal nature of direct basal injuries, except in the anterior fossa of the skull. Signs indicative of injury to the olfactory lobe were occasionally observed.
I should, perhaps, again insist here on the rarity with which acute diffuse septic infection occurred in cases of these degrees of severity, also on the fact that interference with the wounds in the way of secondary exploration, even when they were manifestly the seat of local infection, was followed almost without exception by good immediate results; and, lastly, that when suppuration did occur, it was usually strictly local in character. The influence of the climate of South Africa and our surroundings has already been discussed, but whether climate, condition of the patients, or peculiarity in the nature of causation of the wounds was responsible, in no series of cases was the absence of acute inflammatory troubles more striking than in this one of brain injuries.
Frontal injuries were those most frequently unaccompanied by primary symptoms of severity; slowing of the pulse—this often fell to 40—and occasional irregularity, were almost the only constant signs of cerebral damage. Some patients temporarily lost consciousness, others rose at once and walked to the dressing station, and in few cases was any psychical disturbance noted in the early stages.
I think, however, it may be affirmed that frontal injuries, accompanied by trivial signs, resulted without exception from the passage of bullets travelling at a low rate of velocity. Thus in several of the instances here related the patients at the time of reception of the wound were under the impression that they were entirely beyond the range of fire, and in one, in which well-marked signs of concussion followed, the bullet, which had traversed the head, retained only sufficient force to perforate the skin of the neck and bury itself[Pg 271] in the posterior triangle without even fracturing the clavicle, against which it impinged. In men struck at a shorter range, signs of concussion, often followed by transient radiation signs of injury to the parietal lobe, were common. These signs were, I think, not as a rule due to surface hæmorrhage, since they were of a purely paralytic nature and not irritative. Several cases with partial or complete hemiplegia, hemiplegia and aphasia, or facial paralysis are recorded below.
(56) Frontal injury.—Wounded at Magersfontein. In prone position when struck, distance 700 to 800 yards. Entry (Mauser), at the margin of the hairy scalp above and to the left of the frontal eminence; course, through anterior third of left frontal lobe, roof of orbit, obliquely across line of optic nerve, inner wall of orbit, nose, right superior maxilla piercing alveolar process, and passing superficial to inferior maxilla: exit, one inch anterior to angle of jaw. The bullet again entered the posterior triangle of the neck, struck the right clavicle, and turned a somersault, so that its base lay deepest in the wound.
The patient was unconscious for a short time, suffered with general headache and giddiness, and was somewhat irritable. On the third day the pulse was 70, temperature normal, and he was sent to the Base. There was considerable proptosis, œdema and discoloration of the eyelid, and subconjunctival ecchymosis, but the movements of the eyeball could be made and light could be distinguished. The sense of smell was apparently absent. A week later the headache was gone, the pulse numbered 80 to 90, the temperature was normal, he slept well, sat up in bed and smoked, took his food well, and exhibited no cerebral symptoms. He could detect the smell of tobacco, but not as a definite odour.
No further symptoms were noted, the sense of smell returned, the swelling of the eyelid and proptosis decreased, but the upper lid could not be raised. When the lid was drawn up, there appeared to be vision at the margins of the field with a large central blind spot. The patient left for England at the end of a month apparently well.
(57) Gutter fracture of frontal bone.—Wounded at Paardeberg. Entry (Mauser), 3/4 of an inch within the margin of hairy scalp above outer extremity of right eyebrow; gutter fracture; exit, 2 inches nearer middle line, at the same distance from the margin of the hairy scalp. The patient was knocked head over heels, his main feeling being a sense of dulness in the right great toe. He sat up[Pg 272] and got a first field dressing applied, then lay down, but as he was still under fire, he retired 1,000 yards to the collecting station; here he dressed some patients, and later mounted an ambulance wagon and was driven to the Field hospital. The next day he helped with the work of the hospital, amongst other things controlling the artery during an amputation of the arm. He then took a three days' and nights' journey to Modder River in a bullock wagon, during which journey he had a fit, which was general, the thumbs being turned in and a wedge being necessary between the teeth to prevent him biting his tongue.
On the sixth day the wound was examined, and between this and the tenth day he had several fits of the same nature as the first, accompanied by stertorous breathing and profuse sweating. On the tenth day Mr. Cheatle opened up the wound and removed numerous fragments of bone, leaving a clean gutter 2 inches by 3/4 of an inch. After the operation no further fits occurred, and eight days later he was conscious, but was excitable and talked at random. On the twentieth day he arrived at the Base after 30 hours' railway journey (623 miles). He was then quite rational, but unable to make any demands on his memory and very sensitive to noise; at times he wandered in the evenings and his temperature rose as high as 100°. The wound was open and granulating, the floor pulsating freely.
Three weeks later the wound was still open, and the skin dipped in at the lower margin. The mental condition was much improved, although attempts at giving a history of his case were obviously tiresome.
The wounds in the leather headband of this patient's helmet were interesting, the round aperture of entry in the exterior of the helmet being followed by a starred exit aperture in the leather band, the second entry opening in the leather band being again circular, and the external opening in the puggaree a transverse slit.
(58) Transverse superficial perforating frontal injury.—Wounded at Graspan. Aperture of entry (Lee-Metford), at upper and outer part of left frontal eminence; exit, at margin of hairy scalp over outer third of right eyebrow. On the second day the patient complained of giddiness and headache; the pulse was 60. He was then walking about. The wounds were explored and typical entry and exit apertures discovered in the frontal bone from which cerebral matter was protruding. Both openings were enlarged (Mr. S. W. F. Richardson) with Hoffman's forceps, and a considerable number of splinters of the inner table were removed from the aperture of entry.[Pg 273]
The headache gradually passed off, but there was throbbing about the scar, and pulsation was visible for some three weeks, after which no further symptoms were observed.
(59) Oblique frontal gutter fracture.—Wounded at Magersfontein. Entry (Mauser), 1/2 an inch to right of median line of forehead, 3/4 of an inch from the margin of the hairy scalp; exit, about 3/4 of an inch anterior to the lower extremity of the right fissure of Rolando. Weakness of left facial muscles, especially of angle of mouth. No further motor symptoms. Wounds explored (Mr. Stewart); numerous fragments of bone and some pulped cerebral matter were removed. Patient developed no further signs; the paralysis, although improved, did not completely disappear. The man a year later was still on active duty, the paralysis almost well, and no further ill effects of the injury remained.
In the fronto-parietal or parietal regions, signs of damage to the cortical motor area were seldom absent, sometimes evanescent, at others prolonged. In some cases the signs were permanent and followed by evidence of local sclerosis.
The motor area on both sides of the brain was sometimes implicated; thus in a child shot at Kimberley the bullet entered in the right frontal region, and emerged to the left of the line connecting bregma and inion a little behind its centre. Paralysis of both lower extremities resulted, power rapidly returning in the right, while incomplete paralysis persisted in the left.
In only one instance (see case 73, p. 292) was any permanent sensory defect observed, and the mental condition of this patient would have certainly suggested a functional explanation for its presence, had it not been for the accompanying inequality in the axillary surface temperatures.
In a second case (No. 67) blunting of sensation followed a definite lesion of the inferior parietal lobule. In this instance an occipital lesion was associated with the parietal.
(60) Parietal gutter fracture.—Wounded at Magersfontein. A scalp wound 3 inches in length ran transversely across the right parietal bone at the level of the lower third of the fissure of Rolando. A second wound of entry was found crossing the third dorsal spine; the bullet was retained and was palpable over the right scapula. There was left facial paralysis, weakness and numbness[Pg 274] of both upper extremities, especially of the left, and some difficulty in swallowing. The man was sent to the Base, where he arrived on the fourth day. The symptoms had then become much more marked, consciousness was incomplete, and articulation slow and imperfect. There was complete left hemiplegia, and deviation of the tongue to the right. The pulse was 40. An exploration (Mr. J. J. Day) showed that an oval plate of the outer table of the parietal bone had been struck off. A trephine was applied to the exposed diploë and a crown of bone removed; considerable comminution of the inner table had occurred, several large fragments having perforated the dura-mater. The latter did not pulsate; it was therefore freely incised, and many more fragments of bone and a large quantity of blood-clot removed.
The first effect of the operation was slight, but ten days later rapid improvement commenced, the first sign being acceleration of the pulse, which rose to 70. On the eighteenth day the original symptoms still remained to a diminished extent, but a fortnight later there remained traces of the facial weakness only, and there was little difference in the grip of the two hands. The patient was shortly afterwards sent home. Ten months later he returned to South Africa on active service.
(61) Fronto-parietal gutter fracture.—Wounded at Graspan. Entry (Mauser), 1 inch within the margin of the hairy scalp, 1/2 an inch to the left of the median line; exit, 3½ inches posterior in same line. Complete right-sided hemiplegia. The wounds were explored on the fourth day (Major Moffatt, R.A.M.C.) and a gutter fracture involving the frontal and parietal bones exposed. The dura-mater was lacerated and brain matter from the frontal lobe escaped freely. A large number of bone fragments were removed. On the fourth day after the operation, the patient became unconscious with right-sided twitchings, but rapidly improved, and at the end of three weeks, except for slight headache, he was well, the power of the right side being good. Ten months later he rejoined his regiment in South Africa, no apparent ill effects remaining.
(62) Fronto-parietal perforating fracture.—Wounded at Magersfontein. Entry, within the margin of the hairy scalp; exit, behind and below the left parietal eminence, the track crossing about the centre of the fissure of Rolando. Right hemiplegia, the lower half of the face only being involved. The wounds were explored and a large number of fragments of bone and a quantity of pulped cerebral matter removed. Six days later the hemiplegia persisted, speech was slow, headache was troublesome and the pulse not above 45. After this, gradual improvement took place,[Pg 275] and a month later the lower extremity and face had regained good power. The upper extremity remained flaccid and paralysed, except for some slight power of movement of the shoulder.
(63) Fronto-parietal perforating fracture.—Wounded at Magersfontein. Entry (Mauser), 2½ inches from the median line, 3½ inches from the occipital protuberance; exit, 3/4 of an inch from the median line, 4½ inches from the glabella; sanious fluid escaped from both ears. There was left facial paralysis, complete paralysis of the left upper extremity, and partial paralysis of the left lower extremity. The patient was deaf, drowsy, and the pulse 45.
Exploration showed the entry wound to be in the parietal, the exit to involve both parietal and frontal bones. The openings were enlarged, and a number of fragments of bone, together with pulped cerebral matter and blood-clot, were removed. The wound healed, except at the front part, where a small prominence suggested a hernia cerebri.
The patient improved slowly; fourteen days after the operation he could hear well, and the flow from the ears had ceased. The facial weakness was slight, the upper extremity was still powerless, but he could move the lower and draw it up in bed. At the end of six weeks the wound had healed, and he was got up and dressed.
At the end of two months he was well enough to be sent home; there was only a trace of facial weakness; the right upper extremity, however, was powerless and slightly rigid, occasional twitchings occurring in it. Considerable power had been regained in the lower extremity, so that the patient could walk with help, but foot-drop persisted; the gait was spastic in character, the reflexes were much exaggerated, and there was marked clonus. The patient was sensible, but his manner suggested some mental weakness. Both the openings in the skull were closed by very firm material, apparently bony.
This patient became a Commissionaire some ten months later. His mental condition is normal, and loss of memory seems confined to the events immediately following the injury. The lower extremity has improved, but the upper is useless.
(64) Parietal injury: retained bullet.—Wounded at Paardeberg. Aperture of entry (Mauser), 1 inch diagonally below and anterior to left parietal eminence. No exit. The patient was trephined by the surgeons of the German ambulance at Jacobsdal.
Sixteen days later he arrived at the Base. A circular pulsating trephine opening was then to be felt beneath the flap, but no information was forthcoming as to the bullet. The patient could[Pg 276] speak, but lost words and the gist of sentences; he could remember nothing as to himself since the day of the injury. There was right facial weakness; he could not close the right eye or whistle, but there was little apparent want of symmetry; there was weakness in the grip of both hands, more marked on the right side; both lower extremities could be moved. The reflexes were normal, although the left limb was slightly rigid. The pupils were equal, reflex normal; slight nystagmus. Pulse 72, small and regular. Temperature normal. Rapid improvement followed.
During the fourth week the temperature rose to 103°, and remained elevated for six days, but no local or general signs appeared; at the end of five weeks there was little evidence of the paralysis remaining. The patient was discharged from the service on his return home.
In the upper part of the occipital region glancing or superficial injuries were comparatively favourable; those near the base, especially if perforating, were very dangerous. Two such cases are referred to elsewhere. Case 69 is included as the only example of cerebellar injury I happened to see who lived any appreciable time after the accident.
The main interest in these cases centres in the defects produced in the area of the visual field. I am extremely indebted to my colleague, Mr. J. H. Fisher, who has kindly determined this for me in three of the following cases. It will be noted that in two instances the injury was to the left occipital lobe. In these the resulting hemianopsia was of the pure lateral homonymous character, and in both the visual symptoms were accompanied by a certain degree of amnesic aphasia (65 and 68).
In 65 the injury was definitely unilateral, and at the time of the operation I decided that at least an inch and a half of the posterior extremity of the left occipital lobe was totally destroyed.
In 68 the lesion was probably confined to the left lobe, but it is impossible to exclude slight injury to the right lobe also. In this instance amnesic aphasia was a far more marked symptom than in 65, and the position of the lesion suggested damage both to the visual and auditory word centres.[Pg 277]
Cases 66 and 67 are instances of damage to both occipital lobes. In 66, although the wound was a glancing one, and did not perforate, it was so near the median line, and accompanied by such severe damage to the bone, that a symmetrical lesion of the cuneate and precuneate lobules of both right and left sides is to be inferred. In 67 the great longitudinal fissure was traversed by the bullet obliquely. It is of great interest to observe that in each of these cases the lesion of the visual field was a horizontal one and affected the lower half in place of assuming a lateral distribution.
In all four cases the primary effect of the occipital injury was the same—viz. absolute blindness—while the return of vision in each was of the nature of the dawning of light. I regret that I am unable to furnish any detail as to increase of the field of vision in the progress of the cases, but circumstances rendered continuous observation of the patients impossible.
In each case deafness was apparently the direct result of concussion of the ear on the side corresponding to the wound. Deafness of the opposite ear was never noted.
In case 67 some general blunting of sensation was noted in the paralysed upper extremity, and in this patient, no doubt, injury to the inferior parietal lobule accompanied the occipital lesion.
(65) Injury to left occipital lobe.—Wounded at Belmont. A single transverse wound, 2 inches in length, extended across the occipital bone, 2 inches above the level of the external protuberance. When seen on the third day the wound was gaping and pulped cerebral matter was found in it. The patient was very drowsy, lying with closed eyes, and complaining of great coronal and frontal headache. He could distinguish light and darkness, but not persons. Total blindness immediately followed the injury, persisting some three days, and the patient spoke of return of sight as of the appearance of dawn. The pupils were equal, moderately dilated and acted to light, which was unpleasant to him. He was somewhat irritable and silent, but apparently rational. Temperature 99°. Pulse 56 full. Tongue clean. No sickness, no difficulty in micturition.
Fifty-six hours after the injury the wound was opened up and cleaned, and an oval fractured opening about 3/4 by 1/2 inch was[Pg 278] exposed 3/4 inch to the left, and 2 inches above the occipital protuberance. The margins of the opening showed several small fragments of lead attached to the bone. A 3/4-inch trephine was applied at the left extremity of the opening, and it was found that about a square inch of the internal table was comminuted and driven into the brain, together with several small fragments of lead. On introducing the finger, about 1½ square inches of the occipital lobe were found to be pulped, and the finger could be swept across the tentorium. There was no sinus hæmorrhage (nor did the history suggest that hæmorrhage had ever been severe). The cavity was carefully sponged out, and the wound closed with a drainage aperture. Little change followed in the patient's condition, and on the sixth day he was sent to the Base hospital.
Three weeks later the wound was firmly healed. The patient still complained of frontal headache, and wore a shade, as the light hurt his eyes and made them water freely. The pupils acted, but were wide; objects could be distinguished, and also persons. Otherwise, the man's condition was good: he began to get up, and at the end of six weeks returned to England.
A year later the man was earning his living as a Commissionaire porter. He complains of giddiness when he stoops, or when he looks upwards, and at times he suffers much with headache both in the region of the injury and across the temples.
There is a bony defect and slight pulsation at the site of the injury, but no prominence. When attempts are made to read the lines run together, and a dark shadow comes before his eyes. He speaks of the latter as still terribly weak. Speech is slow and somewhat simple, but he makes no mistakes as to words. Memory is bad for recent events.
Mr. Fisher makes the following report as to the eyes: Pupils and movement of eyes normal in every respect. No changes in fundi.
| Vision, | R. | 5/12 | with—0.5 | 5/6 |
| L. | 5/9 | with—0.5 | 5/5 |
There is therefore practically full direct vision. Though the man chooses a concave glass he is not really myopic. There is typical right homonymous hemianopsia; the answers, when tested with the perimeter, are quite certain, and the fields absolutely reliable.
The man's statements confirm the condition; he is aware of his inability to see objects to his right-hand side, and is apt to collide with persons or objects on that side.
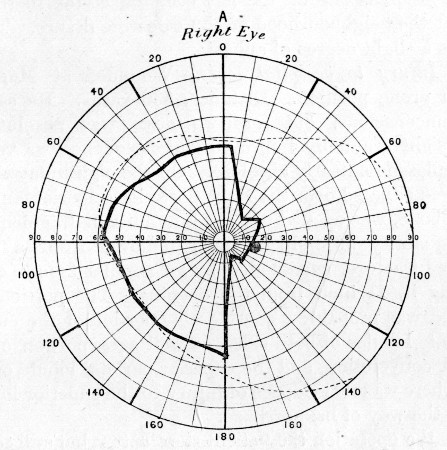 Fig. 73.
Fig. 73.
Right Visual Field, in case 65. Injury to left occipital lobe. Field for white. Test spot 10 mm. Good daylight. Right homonymous hemianopsia
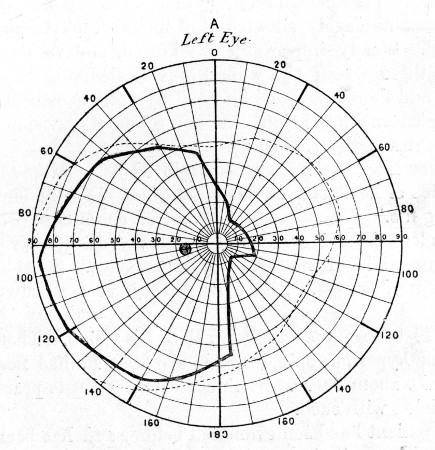 Fig. 74.—Left Visual Field, case 65
Fig. 74.—Left Visual Field, case 65
The lesion is one of the left occipital cortex in the cuneate lobe and the neighbourhood of the calcarine fissure. The speech suggests a slight degree of aphasia.
(66) Injury to occipital lobes.—Wounded at Magersfontein while in prone position. Distance, 500 yards. He says he was never unconscious, but for two days was absolutely blind. His eyesight gradually improved, but headache was very severe, and sleeplessness nearly absolute. On the eighth day the wound, which was situated over the right posterior superior angle of the parietal bone, was opened up, and a number of fragments of bone and a quantity of pulped brain removed from a depressed punctured fracture, surrounded by an annular fissure, completely encircling it, 1½ inch from the opening. The portion of brain destroyed was probably a considerable portion of the cuneate and precuneate lobules of both sides, as well as a portion of the first occipital convolution, and the superior parietal lobule of the right side. There was no evidence of injury to the superior longitudinal sinus in the way of hæmorrhage.
After the operation the patient slept better, but still complained of headache, and when he arrived at the Base, the flap became œdematous, and the stitch holes and also the central part of the wound suppurated. The temperature rose to 101°. The wound was therefore re-opened, and a number of additional fragments of bone, some as deeply situated as 2 inches from the surface, were removed. Steady improvement followed, and at the end of a further three weeks the wound was healed, the headache had ceased, and there were no abnormal symptoms, except that light was unpleasant to the right eye, and the field of vision was manifestly contracted (Mr. Pooley).
A year later the man was employed as a letter-carrier. He complains of headache at times, and on six occasions has had 'fainting fits.' He says that the latter commence with tremor, that his legs then give way and he falls. In a quarter of an hour he gets up, and feels no further inconvenience. Speech is perfect, there is no deafness. The bone defect is very nearly completely closed.
Mr. Fisher reports as follows as to the vision. There is a high degree of hypermetropia in each eye, the R. has nearly 6.0 D and the L. about 5.0 D. With correction he gets practically full direct vision with each.
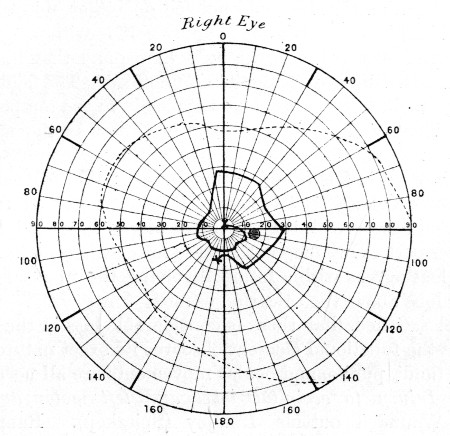 Fig. 75.
Fig. 75.
Right Visual Field, in case 66. Injury to both occipital lobes. Field for white. Test spot 10 mm. Good artificial light. Defect in field complicated by functional symptoms
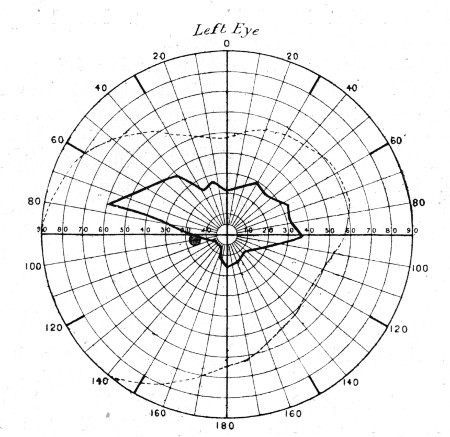 Fig. 76.—Left Visual Field, in case 66. Defect in lower
half of field
Fig. 76.—Left Visual Field, in case 66. Defect in lower
half of field
The patient has been examined before, and has been informed that his vision quite incapacitates him from further service. He began by stating that he could not see on either side of him, but only straight in front; that he is apt to collide with people in walking, was nearly knocked down by a horse, and that his acquaintances accuse him of passing them unnoticed. The fields of vision are very small, but the loss is not typically in the temporal half of either. That of the right eye which we know as the spiral field, becoming more and more contracted as the perimeter test is continued, is what is found in functional cases; that of the left, however, shows a characteristic loss of the lower part of the field of vision, and agrees with the statement of the man that he can see the upper part of my face but not the lower when he looks at me. Such a loss agrees with a lesion involving the upper part of the cuneate lobe above the calcarine fissure.
I feel satisfied that there is considerable loss in the right field also, but the functional element obscures its exact nature.
The fundi, pupils, and ocular movements are all normal.
(67) Injury to occipital lobes and left motor and sensory areas.—Wounded outside Lindley (Spitzkop). Range within 1,000 yards. Entry, one inch within the right lateral angle of the occipital bone, external wound more than 1/2 an inch in diameter; exit, 2 inches from the median line, over the upper half of the left fissure of Rolando. Behind the wound of exit comminution of the parietal bone, extending back to the lambdoid suture, existed. I attributed this to oblique lateral impact by the bullet on the inner surface of the skull.
The patient could afterwards remember being struck, but became rapidly unconscious. When brought into the Field hospital some five hours later the condition was as follows: Semi-conscious, can speak, apparently blind, pupils equal, of moderate size, do not react to light. Right hemiplegia. No sickness. Moans with pain in head. Passes water normally.
Considerable hæmorrhage had occurred from each wound, the scalp was puffy, and the bones yielded on pressure over the left parietal bone, indicating considerable comminution.
The night was so cold that no operation could be considered, so the head was partly shaved, the wounds cleansed, and a dressing applied. The next morning the Division marched at 5 a.m., and it was considered wise to leave the man at Lindley in the local hospital.
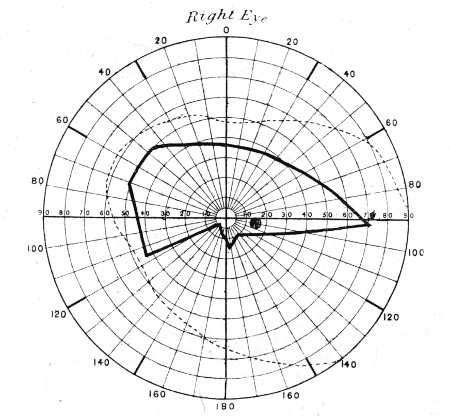 Fig. 77.—Right Visual Field, in case 67.
Fig. 77.—Right Visual Field, in case 67.
Injury to both occipital lobes. Field for white. Test spot 10 mm. Good artificial light. Defect in lower half of field
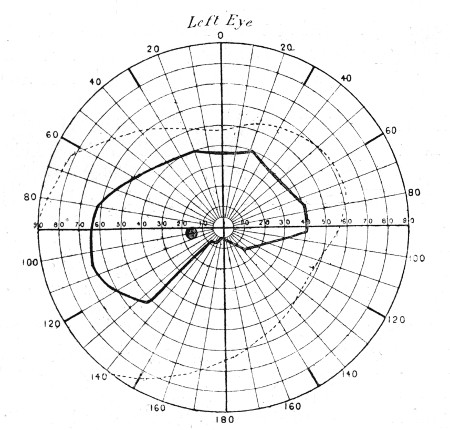 Fig. 78.—Left Visual Field, in case 67
Fig. 78.—Left Visual Field, in case 67
No operation was performed there, but I heard later that the man recovered full consciousness at the end of five days, and at the end of a fortnight he commenced to see again.
Six weeks later he travelled to Kroonstadt, thence to Bloemfontein, and thence to Cape Town and home to Netley. The paralytic symptoms meanwhile steadily improved.
Seven months later his condition is as follows: Scarcely a trace of facial paralysis. Slight power of movement of arm, forearm, and fingers, but grip is very weak. Little power of abduction of the shoulder or of straightening the elbow. The latter movement is made with effort and in jerks. Sensation over the back of the arm is somewhat lowered, and is 'furry' at the finger tips. There is very little wasting of the muscles noticeable.
Walks well, but with some foot-drop. Slight increase of patellar reflex. He says that he does not walk in the street with confidence, as he often feels as if omnibuses &c. were coming too near him.
He is absolutely deaf in the right ear.
The openings in the skull are closed, the occipital lies about halfway between the external auditory meatus and the external occipital protuberance, while the parietal still affords evidence of the earlier comminution, one fissure passing backwards as far as the lambda, and the whole surface is lumpy and uneven.
The track through the brain no doubt involved a considerable extent of the outer aspect of the right occipital lobe and the cuneate lobule. It must also have crossed the great longitudinal fissure, and penetrated the left Rolandic region, just above its centre, probably involving the precuneate lobule, and a portion of the internal capsular fibres as well as the cortex on the left side. The deafness was probably due to concussion of the internal ear.
Mr. Fisher has kindly furnished the following note regarding the vision. The pupils, movements, and fundi are quite healthy. There is good direct vision R. or L. 5/5 fairly, and together 5/5. The man complains he has lost his side sight, also the lower; he demonstrates the latter quite obviously with his hand, and says he has to repeatedly look down when walking. He thinks no improvement has taken place during the last month. The accompanying fields of vision show the loss quite characteristically.
(68) Injury to left occipital lobe.—Wounded at Paardeberg. Entry (Mauser), through the lambdoid suture on the right side of the mid line. Bullet retained, but a palpable prominence behind the left ear suggested its localisation.
The patient became at once unconscious and remained so for several days. He was completely blind; vision returned later, but[Pg 285] only to a limited degree. There was complete loss of memory as to the events of the day.
When admitted at Rondebosch into No. 3 General Hospital the condition was as follows: The field of vision is limited, and examination shows right homonymous hemianopsia. When any one comes into the tent the patient sees a shadow only until his bed is reached.
When spoken to the patient 'thinks and thinks,' and then apologises for not answering, saying he will remember at some future time. He is absolutely unable to remember times, names, or localities, but places his hand to his head and appears to think deeply in the effort to recall them. Occasionally when you go into his tent he suddenly remembers something he has been trying to think of for some days, and will tell you.
A fortnight later after an attack of influenza the patient was not so well, and vision was apparently becoming more impaired.
An incision was made (Mr. J. E. Ker) so as to raise a flap the centre of the convexity of which was 2½ inches behind the left external auditory meatus. A slight prominence and a fissure was discovered in the temporal bone, and over this a trephine was applied. On removal of the crown of bone the bullet was discovered with the point turned backwards (having evidently undergone a partial ricochet turn) on the upper surface of the petrous bone, just above the lateral sinus. The dura-mater was healed but thickened, and some clot upon its surface was removed.
The wound healed per primam, and a rapid recovery was made. Ten days later a running water-tap was able to be detected 120 yards from the tent door. The hemianopsia however persisted.
The following letter, dictated by the patient to his wife, and sent to me, gives a clear account of his condition ten months later:—
I am pleased to say my memory is better than it was some time ago, though at times I am entirely lost and really forget all that I was speaking about. I also find that I often call things and places by their wrong names. I sometimes try to read a paper or book which I have to read letter by letter, sometimes calling out the wrong letter, such as B for D &c., and by the time I have read almost halfway through, I have forgotten the commencement.
My sight is about the same. There is no improvement in the right eye, and the doctor at Stoke said that the left eye was not as it ought to be and might get worse.[Pg 286]
I ofttimes go to take up a thing, but find I am not near to it, though it appears to me so.
I have no pain to speak of in the head, though at times a shooting pain.
I have a continual noise in the left ear as if of a locomotive blowing off steam, and a deafness in the left ear which I had not before being wounded.
I am extremely indebted to my friend Mr. J. Errington Ker for the notes of the above case, so successfully treated by him.
(69) Injury to occipital lobe.—Wounded at Modder River. Scalp wound in occipital region. Two days later on arrival at the Base the patient was extremely restless and in a condition of noisy delirium. The wound was explored (Mr. J. J. Day) and a vertical gutter fracture discovered 1/2 an inch above and to the left of the occipital protuberance. The gutter was 1½ inch in length and finely comminuted, the dura wounded, and the left occipital lobe pulped. A number of fragments of bone (one lodged in the wall of, but not penetrating, the lateral sinus) and pulped brain were removed. No improvement took place in the general condition, but the patient lived twenty-two days, during which time he coughed up a large quantity of gangrenous lung tissue and foul pus.
At the post-mortem examination a wound track was found extending to the crest of the left ilium, where the bullet was lodged. The patient was no doubt lying with his head dipped into a hole scooped out in the sand (a common custom) when struck; the bullet then traversed the muscles of the neck, entered the upper opening of the thorax, where it struck the bodies of the second and third dorsal vertebræ, one third of the bodies of each of which were driven into an extensive laceration of the lung; it then grooved the inner surfaces of the eighth and ninth ribs, fractured the tenth and eleventh, and passing the twelfth traversed the deep muscles of the back to the pelvis. Beyond the injury to the occipital lobe, the cerebellum was found to be lacerated and extensively bruised and ecchymosed.
Complications.—Hernia cerebri as a primary feature has already been mentioned as one of the peculiarities of some explosive wounds. In the later stages of the cases in which primary union did not take place the development of granulation tumours was often seen, sometimes in connection with[Pg 287] slight local suppuration, sometimes over a cerebral abscess. In some cases a wound which had once closed reopened and a hernia developed. This sequence was chiefly of prognostic significance as an indication of intra-cranial inflammation, usually of a chronic character, and affecting rather the lowly organised granulation tissue formed in the cavity than the brain itself. When primary union of the skin flap and wound failed, the process of definitive closure of the subjacent cavity was always a very prolonged one, and it was in such cases that a great proportion of the so-called herniæ developed.
Abscess of the brain.—Local abscesses formed in a considerable proportion of the cases where serious damage to the brain had occurred, in whatever region this happened to be. I never saw one develop in cases where primary union had taken place, even when bone fragments had not been removed; neither did I ever see an abscess situated at a distance from the original injury. I take it that the latter is to be explained by the early date of the suppuration, and the fact that in the great majority of small-calibre wounds the exit opening exists in the situation of the contre-coup damages of civil practice.
The main feature in the symptoms when abscesses developed was the insidious mode of their appearance, usually at the end of fourteen to twenty-one days, and their comparative mildness.
Very slight evidences of compression were observed; thus, varying degrees of headache, drowsiness, irritability of temper or depression, twitchings, or in some cases Jacksonian seizures, combined with slow pulse and slight rises of temperature. I never happened to see complete unconsciousness. The slight evidence of compression was perhaps explained in most cases by the large bony defect in the skull, which acted as a kind of safety-valve. Again the firm nature of the cicatricial tissue which formed at the periphery of the injury and extended up to the skull and there formed a more or less firm attachment, also preserved the actual brain tissue to some degree from either pressure or direct irritation. After evacuation of the pus, the usual difficulty was experienced in ensuring free drainage, and definitive healing and closure of the cavities was very slow. The following two cases will[Pg 288] illustrate the character of the cases of cerebral abscess we met with:—
(70) Fronto-parietal abscess.—Wounded at Magersfontein (Mauser). Entry, 1¾ inch above the line from the lower margin of the orbit to the external auditory meatus, and 1¾ inch behind the external angular process; exit, a little posterior to the left parietal eminence. There was right hemiplegia. The wounds were explored, and a large number of fragments of bone and pulped brain were removed, especially from the anterior wound. No great improvement followed, and the patient was sent to the Base. At this time there was a large hernia cerebri at the anterior wound which was suppurating.
A further operation was here performed (Mr. J. J. Day). The hernia cerebri was removed, also several fragments of bone which were found deeply imbedded in the brain. The patient then improved, but a month later his temperature rose, and on exploration an abscess was discovered in the frontal lobe and drained.
Subsequently the patient suffered with Jacksonian seizures, sometimes starting spontaneously, sometimes following interference with the wound. The convulsions commenced in the muscles of the face, and the twitchings then became general. Meanwhile the right upper extremity remained weak, although the fist could be clenched, and all movements of the limb made in some degree.
Some difficulty was experienced in maintaining a free exit for the pus, which was however overcome by the use of a silver tube. All twitchings ceased about a month after the opening of the abscess, the man improved steadily, and he left for England fifteen weeks after the reception of the injury, walking well, with a firm hand-grip, and the wounds soundly healed.
(71) Frontal injury. Secondary abscess.—Wounded at Modder River. Aperture of entry (Mauser), just external to the centre of the right eyebrow; exit, above the centre of the right zygoma. The wound did not render the man immediately unconscious, but he lost all recollection of what had happened to him for the next three or four days. The wounds were explored on the second day, at which time the patient was in a semi-conscious drowsy state, the pupils contracted and the pulse slow. A number of fragments of bone and pulped brain matter were removed.
Subsequently to the operation the patient showed more signs of cerebral irritation than usual, lying in a semi-conscious state and more or less curled up. He answered questions on being bothered. He improved somewhat, and was sent to the Base,[Pg 289] where the improvement continued, but he suffered much from headache.
Later the headache became much more severe, and eleven weeks after the injury the man complained of great pain both locally and over the whole right hemisphere; he lay moaning, with the temperature subnormal, and the pulse very slow. At times there was nocturnal delirium.
The wound had remained closed and apparently normal, but now a small fluctuating pulsating nipple-like swelling developed in the situation of the aperture of entry. This was incised, and two ounces of sweet pus evacuated (Professor Dunlop). A tube was introduced, and removed later on the cessation of discharge.
Removal of the tube was followed by a recurrence of the same symptoms, and this occurred on no fewer than six occasions whenever the wound closed.
At the end of twenty weeks the patient appeared quite well, the wound had been closed six weeks, the previously irritable mental state was replaced by placidity, and he was sent home.
Diagnosis.—The importance of proper exploration of scalp wounds to determine the condition of the bone has already been insisted upon. The localisation of the position and extent of the injury to the cranial contents depended simply on attention to the symptoms, and needs no further mention here.
Prognosis.—This subject can only be very imperfectly considered at the present time, since only the more or less immediate results of the injuries are known to us, while the more important after consequences remain to be followed up.
As to life the immediate prognosis has been already foreshadowed in the section on the anatomical lesions. It is there shown that the first point of general importance is the range of fire at which the injury has been received. At short ranges, as evidenced by the history, the characters of the wounds, and the severity of the symptoms, the immediate prognosis was uniformly bad, a very great majority of the patients dying, and that at the end of a few hours or days.
The rapidity with which death followed depended in part on the actual severity of the wound, and still more on the region it affected; the nearer the base and the longer the track the more rapidly the patients died, and this always with[Pg 290] signs of failure of the functions of the heart and lungs due to general concussion, pressure from basal hæmorrhage, or rapid intracranial œdema. In my experience no patients survived direct fracture of the base in any region but the frontal, although many, no doubt, got well in whom fissures merely spread into the middle or posterior fossa. Patients with very extensive injuries at a higher level, on the other hand, often survived days, or even a week, then usually dying of sepsis.
The actual relative mortality of these injuries I can give little idea of, but it was a high one both on the field and in the Field hospitals; thus of 10 cases treated in one Field hospital, after the battle at Paardeberg Drift, no less than 8 died; while of 61 cases from various battles who survived to be sent down to the Base during a period of some months, only 4 or 6.55 per cent. died. Many of the latter, as is seen from the cases here recorded which were among the number, were none the less of a very serious nature. The early causes of death in patients dying during the first forty-eight hours have been already mentioned; the later one was almost always sepsis.
As in civil practice the best immediate results were seen in injuries to the frontal lobes, and after these in injuries to the occipital region. In the latter permanent lesions of vision were, however, common. The above injuries apart, the prognosis depended on the severity and depth of the lesion. The frequency and extent of radiation symptoms often made it possible to give a more hopeful prognosis than the immediate conditions seemed to warrant, if the exact situation of the lesion, and the probable velocity at which the bullet was travelling, were taken into account; since the actual destructive lesion, when the velocity had been insufficient to cause damage of a general nature, was often very strictly localised.
Another very important point in the immediate prognosis was the primary union of the scalp wound; if this could only be ensured, few cases went wrong afterwards. Such remote effects as I witnessed were mainly the results of the actual destructive lesion, such as paralyses and contraction. I know of only one case in which early maniacal symptoms[Pg 291] closely followed on a frontal injury, and here the symptoms accompanied the development of an abscess. Some patients were depressed and irritable, and some were blind or deaf, probably from gross lesion; in one patient the mental faculties generally were lowered.
In spite of the surprising immediate recoveries which occurred, and the small amount of experience I am able to record as to remote ill effects of these injuries, I feel certain that a long roll of secondary troubles from the contraction of cicatricial tissue, irritation from distant remaining bone fragments, as well as mental troubles from actual brain destruction, await record in the near future.
Since my return to England I have heard of four cases of injury to the head, which died on their return, as the result of the formation of secondary residual abscesses; and of one who died suddenly, soon after his return to active service in South Africa apparently well. These occurrences are sufficiently suggestive.
It may be of interest to add here two cases of secondary traumatic epilepsy of differing degree:—
(72) Gutter fracture over left temporo-sphenoidal lobe. Traumatic epilepsy.—A trooper in Brabant's Horse was wounded at Aliwal North, in March, in several places. A Mauser bullet entered the head 1½ inch above the junction of the anterior border of the left pinna with the side of the head. The exit wound was situated just below and behind the left parietal eminence. The patient stated that the shot was fired by a man he recognised in a laager 150 yards distant from him.
The man remained unconscious eleven days, and when he came round paralysis of the right upper extremity, and weakness of both lower extremities, were noted. There was also ataxic aphasia.
The wounds healed, but two months later the man began to suffer from fits every few days. He spoke of them as fainting fits, but they were accompanied by general twitchings.
The patient was shown to me in July by Major Woodhouse, R.A.M.C. The strength of the right upper extremity was then good, and he walked well. Speech was slow, but correct. The pupils were equal, and acted normally.
The mental condition was weak, and the temper irritable. The man had hallucinations, and was very obstinate: there was[Pg 292] complete deafness of the left ear. He refused surgical treatment, but was really hardly a responsible individual.
(73) Gutter fracture in right frontal region. Traumatic epilepsy.—Wounded at Pieter's Hill. Gutter fracture crossing the outer aspect of the frontal lobe, immediately above the level of the right Sylvian fissure. The wound was perforating at the central part, but only reached as far back as the lower end of the ascending frontal convolution. The patient was rendered unconscious and was removed to Mooi River. He was there seen by Sir William MacCormac, who removed a number of fragments of bone. The patient rapidly recovered consciousness after the operation, but was completely hemiplegic. After a month he suddenly found he was able to move his lower extremity, and later the paralysis became steadily less.
On his return home the man obtained employment as a Commissionaire, but nine months after the injury, while his wife was helping him on with his coat one morning, he was suddenly seized with a fit; the paralysed arm was jerked up, and convulsions became general, a wedge needing to be inserted to prevent the tongue suffering injury.
When admitted into the hospital, the cicatrix of the wound was considerably depressed, and the central part was evidently continuously attached to the surface of the brain. Pulsation was both visible and palpable, there was little or no tenderness on examination, and the patient did not complain of pain.
Little trace of the left facial paralysis remained. The man walked well, but with foot-drop. The left upper extremity was rigid, but chiefly from the elbow downwards. The fingers were flexed, but a slight increase of grip could be effected. No other active movements of hand. The elbow was held flexed, but could be straightened to about 3/4 range on effort. The shoulder could be slightly abducted, but wide movements were made by the scapular muscles.
Sensation was dull over the left side of the face, also over the left side of the neck. There was complete loss of cutaneous sensibility over the lower half of the forearm and hand, and a similar patch in the left axilla. Over the rest of the extremity the sensation was better on the flexor than on the extensor aspects. There was little alteration in the common sensation elsewhere, except that the contrast between that of the dorsum and sole of the foot was somewhat more marked than usual. The temperature of the insensitive axilla was one degree higher than that of the right.[Pg 293]
The left knee jerk was somewhat exaggerated.
On December 15 an incision was made through the old cicatrix directly over the defect in the skull. On separating the skin it was found directly adherent to the cicatrised dura, and when this was incised a large vicarious arachnoid space was opened up. The space was crossed by a number of strands of connective tissue, and the cavity had no epithelial lining. The fluid ran out freely, and the space was evidently in free communication with the general arachnoid cavity. A trephine crown was taken out at the posterior end of the gutter, and the surface of the brain explored, but no fragments of bone were found. I therefore replaced the crown, and closed the bony defect in the floor of the gutter with a plate of platinum fitted into a groove made in the bony margin. The wound was then sutured. Primary union took place, and there was no constitutional disturbance beyond one temperature of 100° on the evening of the second day; otherwise the temperature remained normal, and the pulse did not rise above 75.
On the second evening a fit occurred, coming on while the patient was apparently asleep. It lasted about a quarter of an hour and was general, the patient becoming for a short time unconscious, and passing water involuntarily.
On the third morning two similar fits occurred, the first a severe one, during which the patient passed a motion involuntarily. The commencement of all three fits was observed by the nurse only, but in each the convulsions apparently commenced in the face and then became general.
Three months later no further fits had occurred, and the patient, who throughout had said he felt remarkably well, complained of nothing. The upper extremity was apparently slightly less rigid than before the exploration, and the patient said he walked somewhat better than before. The closure of the skull was perfect.
Treatment.—The treatment of fractures of the skull possesses a degree of surgical interest that attaches to no other class of gunshot injury, since operative interference is necessary in every case in which recovery is judged possible. The injuries are, without exception, of the nature of punctured wounds of the skull, and the ordinary rule of surgery should under no circumstances be deviated from. An expectant attitude, although it often appears immediately satisfactory, exposes the patient to future risks which are incalculable,[Pg 294] but none the less serious. Happily the operations needed may be included amongst the most simple as well as the most successful, and expose the patient with ordinary precautions to no increase of risk beyond that dependent on the original injury.
Cases of a general character, or in which the base has been directly fractured other than in the frontal region, are seldom suitable for operation, since surgical skill is in these of no avail; but in all others an exploration is indicated. I use the word 'exploration' advisedly, since what may be called the formal operation of trephining is seldom necessary except in the case of the small openings due to wounds received from a very long range of fire; in all others there is no difficulty, but very great advantage, in making such enlargement of the bone opening as is necessary with Hoffman's forceps.
The scalp should be first shaved and cleansed; if for any reason an operation is impossible, this procedure at least should be carried out, with a view to ensuring, as far as possible, future asepsis, infection in head injuries being almost the only danger to be feared. The shaving may need to be complete, but local clearance of the hair suffices in many cases. The hair having been removed, the scalp is cleansed with all care, a flap is raised of which the bullet opening forms the central point, and the wound explored. In slight cases the entry opening is the one of chief importance, and the exit may be simply cleansed and dressed. In some instances, as in direct fracture of the roof of the orbit from above, the exit should not be touched.
The flap having been raised, if the wound be a small perforation, a 1/2-inch trephine crown may be taken from one side; but it is rare for the opening to be so small that the tip of a pair of Hoffman's forceps cannot be inserted. The trephine is more often useful in cases of non-penetrating gutter fractures where space is needed for exploration, and the elevation or removal of fragments of the inner-table. Loose fragments may need to be removed from beneath the scalp, but the important ones are those within the cranium. These may either be of some size, or fine comminuted splinters of either table, often at as great a distance as[Pg 295] 2 inches or more from the surface. The cavity must be thoroughly explored and all splinters removed. I have seen more than fifty extracted in one case of open gutter fracture. The brain pulp and clot should then be gently removed or washed away, and the wound closed without drainage. Fragments of bone, as a rule, are better not replaced, but complete suture of the skin flap is always advisable in view of the great importance of primary union, and the fact that a drainage opening exists at the original wound of entry, and that the wound is readily re-opened to its whole extent, should such a step be advisable.
The detection of fragments is easiest and most satisfactorily done with the finger, and in all but simple punctures the opening should be large enough to allow thoroughly effective digital exploration; the remarks already made as to the factors determining the size of fragments are of interest in this connection. The determination of the amount of brain pulp which should be removed is somewhat more difficult; one can only say that all that washes readily away should be removed, and its place is usually taken up by blood.
Few fractures of the base are suitable for treatment; the only ones I saw were those of direct fracture of the roof of the orbit or nose, produced by bullets passing across the orbits; here the advisability of interference with the injured eye led to opening of the orbit, and sometimes exposed the fracture. Some patients recovered, even when the damage had been sufficient to cause escape of pulped brain into the orbit.
The after treatment simply consisted in keeping the patients as quiet as circumstances would permit, and the administration of a fluid diet. In some cases recurring symptoms pointed to the continued presence of bone fragments; these were usually indicated by signs of irritation, or often of local inflammation, in the latter case infection taking the greater share in the causation. Such cases needed secondary exploration, and the wonderful success of this operation, even when the wound was evidently infected, was perhaps one of the most striking experiences of the surgery in general.[Pg 296]
I should add a word here as to the most satisfactory time for the performance of these operations; as in all cases the earlier they could be undertaken the better, but in the head injuries the advantages of early interference were more evident than in any other region. This depended on the fact that, as in civil practice, the scalp is one of the most dangerous regions as far as auto-infection of the wound is concerned, and one of the most difficult to cleanse, except by thorough shaving. Beyond this the extreme simplicity of the operative procedure needed, called for few precautions beyond those for asepsis, and very little armament in the way of instruments, &c.
When on the march from Winberg to Heilbron with the Highland Brigade we had some five days' continuous fighting, and on this occasion several perforating fractures of the skull were brought in. The coldness of the nights at that time made evening operations an impossibility; hence the operations on these men were performed at the first dressing station, in the open air, at the side of the ambulance wagons, often during the progress of fighting around. Of several cases so operated on, all healed by primary union without a bad symptom of any kind, except one (see p. 249), in whom a very large entrance opening over the right cortical motor area led down to an extensive destruction of the brain, complicated by a fracture of the base in the middle fossa. This wound, from the first considered hopeless, became septic during the four days' travelling in an ambulance wagon that was necessary, and the man died at the end of fourteen days. As the whole cortical motor area was destroyed, death was, perhaps, the end most to be desired; but the fight that this man made for recovery, and the fact that his death, after all, was due to general infection and not to any local extension of the injury, very strongly impressed me with the possibility of recovery, even in such extensive cases, if only an aseptic condition can be maintained. I saw many other cases of the same nature, particularly in men who, as a result of unfortunate circumstances, were necessarily left out on the field for more than twenty-four hours. In some of these maggots were found[Pg 297] in the wounds only thirty-six hours after the infliction of the injury.
I have said nothing as to the treatment of the large primary herniæ cerebri in wounds of an explosive nature, since these were rarely subjects suitable for operation; but in the instances of minor severity they were treated as the other cases where the pulped brain lay mostly within the skull.
In cases where the wounds were in the frontal or fronto-parietal regions, and hemiplegia existed, the rapid improvement in the paralytic symptoms, after operation, was very marked, showing that the signs were mainly, or entirely, due to 'radiation' injury. I am inclined to think that temporary injury of this kind from vibratory disturbance and small parenchymatous hæmorrhages, were far more often the cause of the paralysis than surface hæmorrhage, since the latter was rarely found in large quantity. Large clots, however, no doubt growing in both size and firmness, occasionally occupied the area of destroyed brain, and these sometimes manifestly exercised pressure that was at once relieved by their evacuation.
In cases where inflammatory hernia cerebri developed, a secondary exploration was often indicated for the removal of fragments of bone or the evacuation of pus, otherwise the condition was best treated by dry dressings and gentle support.
Abscess of the brain was treated by simple evacuation and drainage by metal or rubber tubes: the operations were always of extreme simplicity, since the abscess in every case I saw was in the direct line of the wound track, and was readily opened by the insertion of a director or blunt knife. The only trouble in the after treatment was that already referred to, of preventing premature closure of the drainage opening.
I have made no special reference to the method of dressing, since it was of the ordinary routine kind. The most important factor in success was the efficient primary disinfection of the scalp; a piece of antiseptic gauze and some absorbent wool, efficiently secured, was all that was needed later.
As usual the consideration of the treatment of cases in which the bullet was retained may be considered last. Such accidents were distinctly rare. I operated in only one (No. 54,[Pg 298] p. 260) in whom the indications both for localisation and interference were obvious, since the bullet had palpably fractured the bone, although it had not retained sufficient force to enable it to leave the skull. In two other cases that I saw, in one the bullet was lodged in the zygomatic fossa, in the second just below the mastoid process. The former patient died; the latter exhibited symptoms indicative of injury to the occipital lobe (No. 68), and was successfully treated by Mr. J. E. Ker. I never happened to see a case in which a retained bullet in the skull was localised by the X rays, but such might have been possible in case No. 64, p. 275. In no case is primary interference indicated, unless a fracture exists where the bullet has tried to escape, or secondary symptoms develop pointing to irritation.
Under ordinary circumstances, moreover, the indications for removal of a bullet are not likely to be sufficiently imperative to necessitate the operation being undertaken until the patient can be placed under the best conditions that can be secured. This is the more advisable since such operations need the infliction of an additional wound, require great delicacy, and may be very prolonged in performance. The experience of civil practice has already sufficiently proved the small amount of inconvenience likely to follow the retention of a bullet in the skull.
I may again mention the fact that in explorations for the removal of bone fragments, fragments of lead, from breaking or setting up of the bullet, are sometimes found.
Taken as a whole, the operations on the head were extremely satisfactory from a technical point of view; the large depressed pulsating cicatrix so often left was the chief defect observed. The circumstances under which many of the operations had to be performed militated strongly, however, against the successful replacement of separated bone fragments, which might have rendered the defects less serious.
Secondary operations for traumatic epilepsy scarcely come within the scope of these experiences. In case 73, p. 292, it is of interest to note the manner in which the cavity due to loss of brain substance was filled up. No doubt a similar[Pg 299] vicarious arachnoid space develops in all cases in which a soft pulsating swelling fills an aperture in the bones of the skull.
Mastoid process.—The most important wound of the cranium not already mentioned was that involving the mastoid process and the bony capsule of the ear. Wounds of the mastoid process obtained their chief interest in connection with paralysis of the seventh nerve. This nerve rarely or never escaped, and, as far as my experience went, the facial paralysis was permanent (see cases 111-114, p. 355). I think the same prognosis holds good with regard to the deafness resulting from these injuries, and it is difficult to believe, with our experience of the effect of vibration on other nerve centres and organs, that the internal ear could ever escape permanent damage.
In a number of cases the tympanum itself, or the external auditory meatus, was directly implicated in tracks; in these, also, loss of hearing was the rule.
Wounds of the pinna when produced by undeformed bullets were usually of the same slitlike nature remarked in perforations of the cartilages of the nose, and healed with equal rapidity.
Wounds of the orbit.—Injuries to the orbit were very numerous and serious in their results, both to the globe of the eye and the surrounding structures.
Anatomical lesions.—The wound tracks, with regard to the injuries produced, may be well classified according to the direction they took; thus—vertical, transverse, and oblique.
Vertical wound tracks were on the whole the least serious, but this mainly from the fact of limitation of the injury to one orbital cavity. They were usually produced by bullets passing from above downwards through the frontal region of the cranium, and were received by the patients while in the prone position.
Transverse and oblique wounds owed their greater importance to the fact that both eyes were more likely to be implicated.[Pg 300]
Besides these tracks, which actually crossed the cavities, a number involved the bony boundaries, producing almost as severe lesions in the globe of the eye, many of the patients being rendered permanently blind. The only difference in nature of such cases was the escape of orbital structures, and this was of minor importance in the presence of the graver lesion to vision. The following is an illustrative case:—
(74) Wounded at Colenso. Entry (Mauser), 1 inch below the centre of the margin of the right orbit; exit, behind the right angle of the mandible. Fracture of lower jaw, and development of a diffuse traumatic aneurism of the external carotid artery. The common carotid artery was tied for secondary hæmorrhage (Mr. Jameson) some three weeks later.
Vision was affected at the time of the accident; the fingers could be seen, but not counted. After ligation of the carotid the condition was possibly worse, and this needs mention as transitory loss of power in the left upper extremity also followed the operation.
Fractures of the bony wall were of every degree. The most severe that I saw were two in which lateral impact by a bullet crossing the cranial cavity caused general comminution of the whole orbital roof. Fissures of the roof were common in connection with 'explosive' exit apertures in the frontal region of the skull. Pure perforations usually accompanied the vertical or transverse wounds of the cavity, fragments at the aperture of entry then being projected into the orbit, sometimes penetrating the muscles.
Occasionally the margin of the cavity was merely notched.
The ocular muscles were often divided more or less completely, and occasionally some difficulty arose in determining whether loss of movement of the globe in any definite direction depended on injury to the muscle itself, or to the nerve supplying the muscle. The following case illustrates this point:—
(75) Entry (Mauser), 2 inches behind the right external canthus; the bullet pierced the external wall and traversed the floor of the right orbit beneath the globe, crossed the nasal cavity, and a part of the left orbit; exit, at the lower margin of the left orbit, beneath the centre of the globe of the eye.[Pg 301]
Complete loss of sight followed the injury, and persisted for one week. Modified vision then returned.
Three weeks later there was diplopia; loss of function of the right external and inferior recti, although the ball could be turned downward to some extent by the superior oblique when the internal rectus was in action. Movements of the left globe were not seriously affected.
The pupils were immobile and moderately dilated, but atropine had been employed two days previously.
A year later the condition was as follows: There is some weakness of the right seventh nerve, as evidenced by want of symmetry in all the folds of the face, and in narrowing of the palpebral fissure.
When at rest the right eye is somewhat raised and turned outwards. Active movements outwards or downwards are restricted. There is diplopia, and the vision of the right eye is much impaired; the man can see persons, but cannot count fingers with certainty, although he sees the hand. Putting on one side the loss of free movement, there is no obvious external appearance of injury to the eye.
Mr. J. H. Fisher reported as follows:
Ophthalmoscopic examination shows the left eye and fundus to be normal. The right disc is not atrophied, but the whole of the lower half of the fundus is coated with masses of black retinal pigment. There is atrophy in spots of the capillary layer of the choroid, and the larger vessels of the deeper layer are exposed between the interstices of the pigment masses. There is no definite choroidal rupture. The lesion encroaches upon and implicates the macular region.
The injury is a concussion one, not necessarily resulting from contact, and certainly not due to a perforation. The loss of movement and faulty position are the result of injury to the muscles, and not to nerve implication.
The man complained that when he blew his nose the left eye filled with water and air came out. The left nasal duct was however shown to be intact, as water injected by the canaliculus passed freely into the nose.
Intra-orbital bleeding, subconjunctival hæmorrhage with proptosis and ecchymosis of the lids were usually well marked. The latter was sometimes extreme.
Injury to the nerves was naturally of a very mixed character. In many instances the branches of the first two[Pg 302] divisions of the fifth nerve were obviously implicated and regional anæsthesia was common. This was often transitory when the result of vibratory concussion, contusion, or pressure from hæmorrhage. In other cases it was more prolonged as a result of actual division of the nerve. As is usually the case, when a small area of distribution only was affected, sensation was rapidly regained from vicarious sources, even when section had been complete.
As individual injuries, those to the optic nerve were the most frequently diagnosed. I am sorry to be unable to attempt a discrimination of injuries to the nerve alone from those in which both nerve and globe suffered, but the globe can rarely have escaped injury, either direct or indirect, when the bullet actually traversed the orbital cavity. (A few further remarks concerning injuries to the optic nerve will be found in Chapter IX.)
Injuries to the globe of the eye, either direct or indirect, accompanied most of the orbital wounds.
In some the lesion was of the nature of concussion. In such the bone injury was usually at the periphery of the orbit, or to the bones of the face in the neighbourhood. The loss of vision might then be temporary, persisting from two to ten days, then returning, often with some deficiencies.
In other similar external injuries, the lesion of the globe was more severe, and permanent blindness followed.
In variability of degree of completeness, these lesions of the globe corresponded exactly with those produced in other parts of the nervous system by bullets striking the bones in their vicinity, and they were no doubt the result of a similar transmission of vibratory force.
In a third series of cases the globe suffered direct contusion, and in a fourth was perforated and destroyed.
In cases in which permanent blindness was produced without solution of continuity of the sclerotic coat, the nature of the lesion was probably in most cases vibratory concussion and the development of multiple hæmorrhages from choroidal ruptures of a similar nature to those seen in the brain and spinal cord. The actual hæmorrhagic areæ varied in size; but, as far as my experience went, gross hæmorrhages into[Pg 303] the anterior chamber did not occur without severe direct contact of the bullet.
In the vast majority of the cases blindness, whether transitory or permanent, developed immediately on the reception of the injury, and was possibly in its initial stage the result of primary concussion.
Cases were, however, seen occasionally in which the symptoms were less sudden, of which the following is an example. I did not think that the mode of progress seen here could be referred to simple orbital hæmorrhage, although this existed, but rather to intravaginal hæmorrhage into the sheath of the optic nerve. On external inspection the globes appeared normal.
(76) Wounded at Paardeberg. Entry (Mauser), over the centre of the right zygoma; the bullet traversed the right orbit, nose, and left orbit. Exit, immediately above the outer extremity of the left eyebrow.
The patient stated that he could 'see' for thirty minutes with the right eye and for an hour with the left, immediately after the injury. He then became totally blind, and has since remained so. During the next three weeks there were occasional 'flashes of light' experienced, but these then ceased.
At the end of three weeks the condition was as follows: Ocular movements good in every direction except that of elevation of the globe. The levator palpebræ superioris acted very slightly; the right, however, better than the left.
There were marked right proptosis, less left proptosis, and slight patchy subconjunctival hæmorrhage of both eyes. The pupils were dilated, motionless, and not concentric.
The patient was invalided as totally blind (November, 1900).
Mr. Lang, who saw this patient on his return to England, kindly furnishes me with the following note as to the condition. There was extensive damage to both eyes, hæmorrhage, and probably retinal detachment as well as choroidal changes.
The quotation of a few illustrative examples typical of the ordinary orbital injuries may be of interest:—
(77) Vertical wound.—Entry, into left orbit in roof posterior to globe, and internal to optic nerve; exit, from orbit through junction of inner wall and floor into nose.[Pg 304]
Complete blindness followed the injury, but upon the second day light was perceived on lifting the upper lid. There was marked proptosis, subconjunctival ecchymosis, swelling and ecchymosis of the upper lid, and ptosis. Anæsthesia in the whole area of distribution of the frontal nerve.
At the end of three weeks, fingers could be recognised, but a large blind spot existed in the centre of the field of vision. The general movements of the globe were fair, but the upper lid could not be raised. The proptosis and subconjunctival hæmorrhage cleared up.
Little further improvement occurred; six months later the patient could only count the fingers excentrically. A very extensive scotoma was present. The optic disc was much atrophied, the calibre of the arteries diminished and the veins full (Mr. Critchett). The ptosis persisted. It was doubtful in this case whether the ptosis depended on injury to the nerve of supply, or on laceration and fixation of the levator palpebræ superioris. The latter seemed the more probable, as the superior rectus acted. The absence of any sign of gross bleeding into the anterior chamber is opposed to the existence of a perforating lesion of the globe in this case.
(78) Entry (Mauser), from cranial cavity, just within the centre of the roof of the right orbit; exit, from the orbit by a notch in the lower orbital margin internal to the infra-orbital foramen; track thence beneath the soft parts of the face to emerge from the margin of the upper lip near the left angle of the mouth. Collapse of globe, proptosis, subconjunctival hæmorrhage, œdema and ecchymosis of lids.
Shrunken ball removed on twenty-fourth day (Major Burton, R.A.M.C.).
(79) Entry (Mauser), at the posterior border of the left mastoid process, 3/4 inch above the tip; exit, in the inner third of the left upper eyelid. Globe excised at end of seven days. Facial paralysis and deafness.
(80) Entry (Mauser), from cranial cavity through centre of roof of orbit; exit, through maxillary antrum. Total blindness. Movements of ball good, no loss of tension. Proptosis, subconjunctival hæmorrhage, ecchymosis of eyelids. No improvement in sight followed. One month later the globe suppurated and was removed. The bullet had divided the optic nerve and contused the ball.
Prognosis and treatment of wounds of the orbit.—Except in those cases in which return of vision was rapid, the[Pg 305] prognosis was consistently bad in the injuries to the globe. When the globe was ruptured it, as a rule, rapidly shrank. The case (80) quoted above is the only one in which I saw secondary suppuration.
With regard to active treatment, the majority of the cases were complicated by fracture of the roof of the orbit, and in many instances concurrent brain injury was present. In all of these, as a general rule, it was advisable to await the closure of the wound in the orbital roof prior to removal of the injured eye, if that was considered necessary. The only exception to this rule was offered by instances in which the bullet passed from the orbit into the cranium; in these primary removal of fragments projecting into the frontal lobe was preferable. As already indicated, such wounds were comparatively rare except in the case of bullets coursing transversely or obliquely.
The wounds were, as a rule, followed by considerable matting of the orbital structures.
Wounds of the nose.—I will pass by the external parts, with the remark that perforating wounds of the cartilages were remarkable for their sharp limitation and simple nature. I remember one case shown to me in the Irish Hospital in Bloemfontein by Sir W. Thomson, in which at the end of the third day small symmetrical vertical slits in each ala already healed were scarcely visible. This case very strongly impressed one with the doctrine of chances, since on the same morning I was asked to see a patient in whom a similar transverse shot had crossed both orbits, destroying both globes and injuring the brain.
A retained bullet in the upper portion of the nasal cavity has already been referred to (fig. 60). This accident was naturally a rare one; in that instance the bullet had only retained sufficient force to insert itself neatly between the bones.
Wounds crossing the nasal fossæ were comparatively common. The interference with the sense of smell often resulting is discussed in Chapter IX.
Wounds of the malar bone were not infrequent. The small amount of splintering was somewhat remarkable considering the density of structure of the bone. In this[Pg 306] particular the behaviour of the malar corresponded with what was observed in the flat bones in general. A case quoted in Chapter III. p. 87, illustrates the capacity of the hard edge of the bone to check the course of a bullet, and cause considerable deformity and fissuring of the mantle.
Wounds of the jaws. Upper jaw.—A large number of tracks crossing the antrum transversely, obliquely, or vertically were observed. In the first case the nasal cavity, in the others the orbital or buccal cavity, were generally concurrently involved. It was somewhat striking that I never observed any trouble, immediate or remote, from these perforations of the antrum. If hæmorrhage into the cavity occurred, it gave rise to no ultimate trouble. I never saw an instance of secondary suppuration even in cases where the bullet entered or escaped through the alveolar process with considerable local comminution. The branches of the second division of the fifth nerve were sometimes implicated. In one instance a bullet traversed and cut away a longitudinal groove in the bones, extending from the posterior margin of the hard palate, and terminating by a wide notch in the alveolar process.
A good example of a troublesome transverse wound of the bones of the face is afforded by the following instance:—
(81) Entry (Mauser), through the left malar eminence, 1 inch below and external to the external canthus; exit, a slightly curved tranverse slit in the lobe of the right ear.
The injury was followed by no signs of orbital concussion, and no loss of consciousness. There was free bleeding from both external wounds and from the nose. The sense of smell was unaffected, but taste was impaired, and there was loss of tactile sensation in the teeth on the left side also on the hard palate. There was no evidence of fracture of the neck of the mandible, nor of the external auditory meatus, but there was considerable difficulty in opening the mouth widely or protruding the teeth. The latter difficulty persisted for some time, and was still present when I last saw the patient.
Mandible.—Fractures of the lower jaw were frequent and offered some peculiarities, the chief of which were the liability of any part of the bone to be damaged, and the absence of the obliquity between the cleft in the outer and inner tables so common in the fractures seen in civil practice.[Pg 307]
The neck of the condyle I three times saw fractured; in each instance permanent stiffness and inability to open the mouth resulted. This stiffness was of a degree sufficient to raise the question whether the best course in such cases would not be to cut down primarily and remove a considerable number of loose fragments, and thus diminish the amount of callus likely to be thrown out.
Fractures of the ascending ramus and body were more frequent. They were accompanied by considerable comminution, but all that I observed healed remarkably well, and in good position, in spite of the fact that many of the patients objected to wear any form of splint.
The most special feature was the occurrence of notched fractures, corresponding to the type wedges described in Chapter V. When these fractures were at the lower margin of the bone, the buccal cavity occasionally escaped in spite of considerable comminution, the latter confining itself to the basal portion of the bone.
When the base of the teeth, or the alveolus, was struck, a wedge was often broken away, and from the apex of the resulting gap a fracture extended to the lower margin of the bone.
When fractures of the latter nature resulted from vertically coursing bullets, much trouble often ensued. I will quote two cases in illustration:—
(82) Wounded at Rooipoort. Entry (Mauser), through the lower lip; the bullet struck the base of the right lateral incisor and canine teeth, knocked out a wedge, and becoming slightly deflected, cut a vertical groove to the base of the mandible; exit, in left submaxillary triangle. The bullet subsequently re-entered the chest wall just below the clavicle, and escaped at the anterior axillary fold. The appearance of these second wounds suggested only slight setting up of the bullet; the original impact was no doubt of an oblique or lateral character.
The injury was followed by free hæmorrhage and remarkably abundant salivation (I was inclined to think that the latter symptom was particularly well marked in gunshot fractures of the body of the mandible), and very great swelling of the floor of the mouth.[Pg 308]
The patient could not bear any form of apparatus, but was assiduous in washing out his mouth, and made a good recovery, the fragments being in good apposition.
(83) Entry (Mauser), over the right malar eminence; the bullet carried away all the right upper and lower molars, fractured the mandible, and was retained in the neck.
A fortnight later an abscess formed in the lower part of the neck, which was opened (Mr. Pooley), and portions of the mantle and leaden core, together with numerous fragments of the teeth, were removed. The bullet had undergone fragmentation on impact, probably on the last one (teeth of mandible), and still retained sufficient force to enter the neck.
This case affords an interesting example of transmission of force from the bullet to the teeth, and bears on the theory of explosive action.
In the treatment of fractures of the upper jaw, interference was rarely needed. In the case of the mandible, a remark has already been made as to the advisability of removing fragments when the neck of the condyle has suffered comminution. The removal of loose fragments is necessary in all cases in which the buccal cavity is involved. Experience in fracture of the limbs has shown a tendency to quiet necrosis when comminution was severe, in spite of primary union. This is no doubt dependent on the very free separation of fragments on the entry and exit aspects from their enveloping periosteum. In the case of the mandible, considerable necrosis is inevitable, and much time is saved by the primary removal of all actually loose fragments.
A splint of the ordinary chin-cap type with a four-tailed bandage meets all further requirements, but the patients often object to them. Cases in which the fragments could be fixed by wiring the teeth were not common, as the latter had so frequently been carried away. The usual precautions as to maintaining oral asepsis were especially necessary.
The results of fractures of the mandible were, in so far as my experience went, remarkably good, as deformity was seldom considerable. The absence of obliquity and the effect of primary local shock were no doubt favourable elements, little primary displacement from muscular action occurring.[Pg 309]
Wounds of the cheek healed readily, and the same was noticeable of the lips. Wounds of the tongue healed with remarkable rapidity when of the simple perforating type, often with little or no swelling or evidence of contusion. At the end of a few days it was often difficult to localise them.
In connection with this subject a remarkable case which occurred at the fighting at Koodoosberg Drift is worthy of mention, although the projectile was a shell fragment and not a bullet of small calibre.
(84) A Highlander was the unfortunate possessor of an entire set of upper teeth set in a gold plate. A small fragment of a shell perforated the upper lip by an irregular aperture, and struck the teeth in such a manner as to turn the posterior edge of the plate towards the tongue, which latter was cut into two halves transversely through to the base.
The patient asserted that the plate had been driven down his throat, but nothing was palpable either in the fauces or on external examination of the neck. He spoke distinctly, but there was dysphagia as far as solids were concerned.
On the second day swelling of the neck due to early cellulitis developed, especially on the left side, and signs of laryngeal obstruction became prominent. Chloroform was administered, but on the introduction of the finger into the fauces, respiration failed and a hasty tracheotomy had to be performed. No foreign body was palpable with the finger in the pharynx.
Tracheitis and septic pneumonia developed, and the man died of acute septicæmia thirty-six hours later. Death occurred just as the Division received marching orders, and no post-mortem examination was made. As a result of palpation at the time of the tracheotomy, the probabilities seemed against the presence of the tooth plate in the pharynx, but the absence of positive evidence scarcely allows the case to be certainly classed as one of cellulitis and septicæmia secondary to wound of the tongue.
Wounds of the neck were not unfrequent and were of the gravest importance; there can be little doubt that they accounted for a considerable proportion of the deaths on the field. On the other hand, the neck as a region offered[Pg 310] some of the most striking examples of hairbreadth escape of important structures. Consideration of a number of the vascular lesions (see cervical aneurisms, p. 135) also shows conclusively that in no region did the small size of the bullet more materially influence the result, since no doubt can exist that all these wounds would have proved immediately fatal if produced by projectiles of larger calibre.
In this place only a few general considerations will be entered into, as most of the important cases are dealt with under the general headings of vessels, nerves, and spine; but it is convenient to include here the few remarks that have to be made concerning the cervical viscera.
The wounds of the soft parts might course in any direction, but vertical tracks from above downwards were rare. In point of fact, these occurred only in connection with perforations of the head, and as vertical wounds of the latter were received in the prone position, usually when the head was raised, the necessary conditions for longitudinal tracks were seldom offered. One case of a complete vertical track in the muscles of the back of the neck has been already quoted (No. 69, p. 286).
Tracks coursing upwards from the trunk were somewhat more frequent in occurrence; thus a considerable number traversing the thorax were seen. In such instances the aperture of exit was generally situated in the posterior triangle, and some of the brachial nerves often suffered.
The commonest forms of wound were the transverse or the oblique. A large number of cases with such tracks will be found among the cases of injury to the cervical vessels and nerves. In some instances the course was restricted to the neck alone, in others the trunk or upper extremity was also implicated.
The favourable influence of the arrangement of the structures of the neck, which allows of the ordinary displacement excursions necessary for deglutition, respiration, and their cognate movements, was very strongly marked. Thus in several cases the bullet traversed the neck behind the pharynx and œsophagus without injuring either viscus, and the escape of the main vessels and nerves was equally[Pg 311] striking. In such wounds the wedge-like bullet without doubt separated and displaced all these structures, causing mere superficial contusion.
In connection with the latter statement, the rarity of direct sagittal wounds in the hospitals should be mentioned. This is probably to be explained by the facts that wounds in the mid-line of the neck implicated the cervical spinal cord, and that sagittal wounds implicating the vessels were apt to lead more directly to the surface, and thus external hæmorrhage was favoured. A few examples of cervical tracks will suffice to illustrate these remarks:—
(85) Entry (Lee-Metford), below angle of scapula; exit, centre of posterior triangle. Injury to the lung, and hæmothorax. No damage to neck structures.
(86) Entry (Mauser), over Pomum Adami; exit, below right scapular spine. Median and musculo-spiral paralysis.
(87) Entry, a large oval aperture through ninth right rib, 1/2 an inch external to scapular angle; exit, anterior border of sterno-mastoid opposite Pomum Adami. Second entry, opposite angle of mandible; exit, in centre of cheek.
Wound of lung. Musculo-spiral paralysis still persisting at the end of nine months.
(88) Entry (Mauser), 2 inches above left clavicle at margin of trapezius; exit, 1 inch from sternum in left first intercostal space. Contusion of brachial plexus, with mixed signs, which disappeared in two months. No signs of vascular injury.
See also cases of cervical aneurism, &c.
Wounds of the pharynx.—I saw only three cases of wound of the pharynx; in each the injury was in the nasal or buccal segment of the cavity, and in each the soft palate was injured, in two instances the wound being a small perforation.
All three cases belong to the somewhat miraculous class. The first (89) was the only one in which the wound gave rise to subsequent trouble. The second was under the charge of Mr. Bowlby, and will no doubt be more fully recounted by him, as interesting signs of injury to the cervical cord were present. In the third the occipital neuralgia was the only troublesome symptom.[Pg 312]
In both cases 90 and 91 the high position of the wound in the fixed portion of the pharynx no doubt accounted for the absence of any infective trouble.
(89) Wounds of the pharynx.—Entry (Lee-Metford), immediately below the tip of right mastoid process; the bullet traversed the neck, entering the pharynx close to the right tonsil, crossed the cavity of the pharynx and the mouth, emerging through the left cheek. Great swelling of the fauces and dysphagia persisted for some days after the injury, and there was considerable hæmorrhage.
Infection of the posterior portion of the track from the pharynx resulted, and suppuration continued for some weeks: a small sequestrum eventually needed to be removed from the tip of the transverse process of the atlas.
(90) Entry (Mauser), through mouth; the bullet pierced the soft palate and the posterior wall of the pharynx, and passed out between the transverse process of atlas and the occiput. No serious pharyngeal symptoms.
(91) Entry (Mauser), through the mouth, knocking out the left upper canine and bicuspid teeth. Perforation of the soft palate just to the right of the base of the uvula and the posterior wall of the pharynx; exit, 1½ inch internal to and 1/2 an inch below the tip of the right mastoid process. Hæmorrhage persisted for half an hour, and the patient could not swallow solids for a week. Great occipital neuralgia followed the wound.
Wounds of the larynx.—I saw only one wound of the larynx (see No. 10, p. 135). In this instance the thyroid cartilage was wounded on either side at the level of the Pomum Adami. Transitory hæmorrhage and signs of œdema were the only signs referable to the wound, but in addition the bullet contused the left vagus and gave rise to temporary laryngeal paralysis. The same course was observed in a second case of perforation of the larynx of which I was told.
Wounds of the trachea.—The two cases recounted below are the only tracheal injuries I met with; in one the œsophagus was also implicated. This patient died from mediastinal emphysema. In the second case the wide development of emphysema was prevented by the early introduction of a tracheotomy tube.[Pg 313]
(92) Entry (Mauser), on the outer side of the right arm, 3½ inches below the acromion; exit, 3 inches below the tip of the left mastoid process, through the sterno-mastoid. Thirty six hours later there was very free hæmorrhage into the right posterior triangle, emphysema at the episternal notch, dysphagia, and complete obliteration of the cardiac area of dulness. Respiration was rapid (40) and extremely noisy. Pulse 130, small and weak.
A tracheotomy was performed (Mr. Stewart), but the patient died an hour later. When the operation was performed a considerable amount of mucus from the œsophagus was discovered in the wound. The bullet had passed obliquely between trachea and œsophagus, wounding both tubes.
(93) Entry, at the centre of the margin of the left trapezius; exit, in mid line of the neck over the trachea. Dyspnœa was noted the next morning, which increased during a journey in a wagon. On the third day the dyspnœa was more troublesome and emphysema began to develop in the neck. A tracheotomy was performed (Mr. Hunter), and the tube was kept in for four days. No further trouble was experienced, and the wound shortly closed, and the patient, a surgeon, returned to his duties. Temporary signs of median nerve concussion and contusion were noted.
Every degree of local injury to the constituent vertebræ and the contents of the spinal canal was met with considerable frequency. Pure uncomplicated fractures of the bones were of minor importance, except in so far as they exemplified the general tendency to localised injury in small-calibre bullet wounds. Injuries implicating the spinal medulla, on the other hand, were proportionately the most fatal of any in the whole body to the wounded who left the field of battle or Field hospital alive, and these cases formed one of the most painful and distressing features of the surgery of the campaign.
The prognostic gravity of any spinal injury depended upon two factors: first, the obvious one of relative contiguity or direct implication of the cord or nerves in the wound track; secondly, the degree of velocity retained by the bullet at the moment of impact with the spine. Observation of the serious ill effects produced by bullets passing in the immediate proximity of large strongly ensheathed peripheral nerves surrounded by soft tissue, such as those of the arm or thigh, would lead one to expect that a comparatively thin-clad bundle of delicate nerve tissue like the spinal cord, enclosed in a bony canal so well disposed for the conveyance of vibrations, would suffer severely, and such proved to be the case.
Fractures in their relation to nerve injury will be first dealt with, and secondly injuries to the cord itself.
Isolated fractures of the processes were not uncommon, the determination of the injury to anyone being naturally dependent on the position and direction taken by the wound track.
For implication of the transverse processes sagittal wounds[Pg 315] coursing in varying degrees of obliquity were mainly responsible. Such injuries might be unaccompanied by any nerve lesion. Thus a Boer received a Lee-Metford wound at Belmont which passed from just below the tip of the right mastoid process across the pharynx and through the opposite cheek. No bone damage was at first suspected; suppuration in the neck, however, followed infection from the pharynx, and when a sinus which persisted was opened up later, a number of small comminuted fragments were found detached from the transverse process of the axis. In other cases more or less severe symptoms of nerve lesion were observed, varying from transient hyperæsthesia, due to implication of the issuing nerves, to symptoms of spinal hæmorrhage, such as are portrayed in the following:—
(94) A private in the Black Watch was wounded at Magersfontein from within a distance of 1,000 yards. Among other wounds, one track entered 1 inch to the right of the second lumbar spinous process, and emerged 1 inch internal to the right anterior superior iliac spine. There were signs of wound of the kidney, and in addition, retention of urine, incontinence of fæces, complete motor and sensory paralysis of the right lower extremity, and total absence of all reflexes. Anæsthesia existed over the whole area of skin supplied by the nerves of the sacral plexus, hyperæsthesia over that supplied by the lumbar nerves.
On the tenth day subsequent to the injury, the hyperæsthesia in the area of lumbar supply was replaced by normal sensation, motor power began to be slowly regained in the muscles supplied by the anterior crural and obturator nerves, and the patellar reflex returned. At this time lowered sensation returned in the area supplied by the sacral plexus, but no improvement in motor power took place, and no control was regained over the bladder and rectum.
During the succeeding week some sciatic hyperæsthesia developed, but on the twenty-eighth day the patient developed secondary peritonitis from other causes and died on the thirty-first. A fracture of the transverse process existed, but unfortunately the spinal canal was not opened for examination and no details can be given as to the condition of the cord. (See case 201, p. 463.)
Fractures of the spinous processes, or those involving both the process and laminæ, were not uncommon. Isolated[Pg 316] separation of the spinous process was usually the result of wounds crossing the back obliquely or transversely. Examples of this injury were numerous, especially in the dorsal region, as being the most prominent, particularly when the patients assumed the prone position when advancing on the enemy.
Cervical injuries, owing to the comparatively sheltered position of the more deeply sunk spines, and from the fact that the head was usually under cover of a stone or ant-heap, were less common; in one instance hyperæsthesia was noted in one upper extremity as the result of a crossing bullet having struck the fourth cervical spine. In a man wounded at Paardeberg Drift the bullet entered at the centre of the buttock, traversed the bones of the pelvis, and, leaving that cavity above the crest of the ilium, crossed the spine to emerge in the opposite loin. Suppuration occurred, and when the wound was laid open the third and fourth lumbar spinous processes were found to be loosened, but still connected to the surrounding soft parts. There were no nerve symptoms in this case; these would not have been expected, since by the time that the bullet had traversed the bones of the pelvis its velocity must have been considerably lessened, even if high at the moment of primary impact. In another case a dorsal spine, together with its lamina, was separated and moveable; the only nerve symptoms were slight pain and a crop of herpes on the line of distribution of the corresponding intercostal nerve, the bullet having probably struck the nerve in passing across the intercostal space. In one instance of a retained bullet lying beneath the skin of the back, its passage between two contiguous dorsal spines without fracture of either was determined during an extraction operation.
When the prone position was assumed by the men, more or less longitudinal wounds in the course of the spine were naturally liable to occur. These tracks assumed somewhat greater importance than the transverse ones, because the injury to bone was more often multiple, and the laminæ were frequently implicated. The relative importance of such injuries was dependent on the velocity of the bullet and the[Pg 317] depth at which it travelled. As an instance of a more serious character the following may be given:—
(95) In a Highlander wounded at Magersfontein, probably at a range within 1,000 yards, the bullet entered at the right side of the sixth cervical vertebra; tracking downwards, it loosened the laminæ of the fifth and sixth dorsal vertebræ from the pedicles, and separated the tip of the seventh spine. The bullet was extracted from beneath the skin at the latter spot, its force having been no doubt exhausted by the resistance of the firm neural arches supported by the weight of the man's body. Symptoms of total transverse lesion of the cord followed, and the patient died at the end of fifty-four days. The bone had not apparently been sufficiently depressed to exert continuous pressure, but the cord was diffluent and actually destroyed over an area corresponding with the fourth, fifth, sixth, and seventh dorsal segments.
I saw no instance of wound of the neural arch from a direct shot in the back in any of our men, neither was I ever able to detect an injury to the articular processes as a localised lesion.
Injuries to the centra were very frequent, but differed extraordinarily in their importance. Perforation by bullets travelling at a relatively low grade of velocity, but still one sufficient to allow them to pass through the body, produced in many instances no symptoms whatever when the track did not lie in immediate contiguity to the spinal canal or perforate it.
In all the wounds which I had the opportunity of examining post mortem, the fracture was of the nature of a pure perforation of the cancellous tissue of the centrum, with no comminution beyond slight splintering of the compact tissue at the aperture of exit. In one instance the bullet passed in a coronal direction so close to the back of the centrum as to leave a septum of only the thickness of stout paper between the track and the spinal canal. In this case signs of total transverse lesion were present. I never happened to meet with a case in which the canal was encroached upon from the front by displaced bone. In some cases at the end of six weeks there was difficulty in determining the position of the openings, and section of the bone was necessary in order to assure oneself as to the direction of the track.[Pg 318]
In some instances the centra were pierced in the coronal direction with varying degrees of obliquity; in others the direction was more sagittal; in two of the latter the bullet was retained in the spinal canal. The tracks were sometimes confined to one vertebra, but often implicated two. In others the bullet passed longitudinally through the thorax, grooving or perforating one or more centra.
The accompanying evidences of nerve injury varied from nil to those of pressure or irritation of the nerve roots, transient signs of spinal concussion, signs of contusion and hæmorrhage, or to evidence of total transverse lesion. Instances of all these conditions will be quoted under the heading of injuries to the cord or nerves.
Signs of injury to the vertebræ.—Separation of the spinous processes was often indicated by slight deformity, either evident or palpable, local pain, tenderness, mobility, and crepitus. In some cases these local signs were reinforced by evidence of cord injury. Fractures involving the laminæ differed merely in the degree to which the above signs were developed. Fractures of the transverse processes were generally only to be assumed from the position and direction of the wounds, the assumption being sometimes strengthened in probability by evidence of injury to the cord and nerves.
Fractures of the centra were also frequently only to be assumed from the direction of the wound tracks, and possibly from evidence of nerve injury. When no paralysis supervened, interference with the movements of the back, or pain, was so slight as to be inappreciable, especially in the presence of concurrent injury to other parts, which was seldom absent. I only once saw any angular deformity from this injury, and that slight, and not apparent before the end of three weeks. In this particular a very striking difference exists between injuries from small-calibre bullets and larger ones such as the Martini-Henry. In the only instance of Martini-Henry fracture of the spine that came under my notice, the centrum was severely comminuted and deformity was obvious. Still, as in so many particulars, the difference was only one of degree, since comminution of the centra in gunshot wounds has always been observed to be slight in nature[Pg 319] compared with what is met with in the compression fractures of civil life.
A few words will suffice to dismiss the questions of diagnosis, prognosis, and treatment of the above injuries. The diagnosis depended on attention to the signs above indicated, the prognosis almost entirely on the concurrent injury to the nervous system, which will be considered later, and the treatment consisted in enforcing rest alone.
Anatomical lesions.—In introducing the subject of the nature of the lesions of the spinal cord and membranes, I should again enforce the statement that their character and degree, in comparison with the slight accompanying bone damage, are pathognomonic of gunshot wounds, and that these characters find their completest exemplification in injuries produced by bullets of small calibre, endowed with a high grade of velocity. Again, that the varying degrees of damage depend comparatively slightly on the position of the bone lesion, apart from actual encroachment on the canal, while the degree of velocity retained by the bullet at the moment of impact is all-important. In no other way are the divergent results to be explained which follow an apparently identical injury, in so far as extent, position, and external evidence of damage to the spinal column are concerned.
Injuries to the nerve roots of the nature of concussion and contusion, are dealt with in Chapter IX.
Pure concussion of the spinal cord may, I believe, be studied from a better standpoint in the case of small-calibre bullet injuries than in any others, since in many instances it is, I think, possible to exclude any complications such as wrenches and strains of the vertebral column, and ascribe the symptoms to the pure effect of extreme vibratory force communicated to the cord by its enveloping bony canal. The condition must be considered under the two headings of slight and severe.
In slight concussion the usually transient effects of the[Pg 320] injury, and its happy tendency not to destroy life, place us in a state of uncertainty as to the occurrence of anatomical changes, since no opportunity of post-mortem examination occurred. The clinical condition included under this term corresponds with that implied in 'spinal concussion' in civil practice. One point of extreme interest, whether the subjects of small-calibre bullet spinal concussion will in the future suffer from the remote effects common to similar sufferers in civil life from other causes such as railway collisions, still remains for future determination. An ample field for such observations has at any rate been created by the present war.
In severe concussion a far more highly destructive action is exerted. This condition may be followed by complete disorganisation of the cord, accompanied or not by multiple parenchymatous hæmorrhages into its substance. Either or both of these pathological conditions are produced by the impact of the bullet with the spine, given a sufficiently high degree of velocity, and it is difficult to separate clinically the resulting symptoms. This is a matter perhaps of less importance, since it stands to reason that a vibratory force, capable of rupturing the spinal capillaries, would at the same time damage the nervous tissue.
In speaking of concussion of this degree, it should be clearly recognised that a general condition, such as is indicated by the use of the term 'concussion of the brain,' is in no wise implied. The condition is really far more nearly allied to one of contusion, a strictly localised portion of the spinal cord undergoing the destructive process which affects the segments below only in so far as it interrupts the normal channels of communication with the higher centres.
Case 102 is an instance of such a lesion, the post-mortem examination showing clearly that the spinal canal was not encroached upon by the bullet. The cord in this instance appeared little changed macroscopically, and this fact was observed in other instances, both during operations and post mortem.
Contusion.—This condition is very closely allied to the last. In cases 101 and 103 the spinal canal was as little encroached upon as in 102, but the bullet struck the somewhat[Pg 321] elastic neural arch in each case, and post mortem an adhesion between the cord and the enveloping dura opposite the point at which impact of the bullet was closest suggests that, in spite of the escape of the bone from fracture, it may have been momentarily depressed to a sufficient degree to contuse the cord, or the latter may have suffered a contre-coup injury. For these reasons the inclusion of the cases as instances of pure concussion is not warranted. In both Nos. 99 and 100 the neural arch had actually suffered fracture, and although the bone was not depressed or exercising pressure at the time of the autopsies, it was no doubt driven in temporarily at the moment of impact of the bullet.
At the post-mortem examinations of injuries of this nature it was common to find one to four segments of the spinal cord completely disorganised. At the end of some five weeks, the common duration of life, the structure of the cord was represented by a semi-diffluent yellowish material, the consistence of which was so deficient in firmness as to allow the partial collapse of the membranes covering the affected portion, so as to exhibit a definite narrowing when the whole was held up (see fig. 79). In such cases traces of extra- or intra-dural hæmorrhage sometimes still persisted.
Hæmorrhage.—This occurred as surface extravasation and in the form of parenchymatous hæmorrhages. I saw the former both in the extra-dural and peri-pial forms, but never in sufficient quantity to exert a degree of pressure calculated to produce symptoms of total transverse lesion. Here again, however, it is difficult to speak with confidence since the conditions which regulate the tension within the normal spinal canal are so complicated and liable to variation, that it is very difficult to estimate the effect of any given hæmorrhage discovered.
My friend Mr. R. H. Mills-Roberts described to me one fatal case under his care in the Welsh Hospital in which extra-dural hæmorrhage was so abundant as, in his opinion, to have taken a prominent part in the production of the paralytic symptoms.
Examples of both extra- and intra-dural (peri-pial) hæmorrhage are afforded by cases 99, 102, and 103; in none was it large in amount or widely distributed. The condition was[Pg 322] probably also frequently associated in varying degree with that to be immediately described below.
Intra-medullary hæmorrhage (hæmato-myelia).—The importance of this condition is lessened in small-calibre bullet injuries by the fact already alluded to, that it is almost invariably accompanied by concussion changes. In one instance in which death took place at the end of eight days, partly as the result of concurrent injury, in a man in whom signs of total transverse lesion of the cord were present, the substance of the cord was found to be closely scattered over with hæmorrhages of various sizes and extending for a longitudinal area of some three inches.
As to the frequency with which hæmorrhage into the substance of the cord occurred, I regret to be unable to give an opinion. In the late post-mortem examinations I witnessed, a yellow discoloration of the softened cord was the only macroscopic evidence of hæmorrhage.
Hæmorrhages of this nature may, however, account for the grave paralytic symptoms in some cases of partial or total transverse lesion not due to direct compression or laceration.
The conditions of concussion, contusion, or hæmatomyelia were, I believe, responsible for at least nine-tenths of the cases in which a total transverse lesion was indicated by the symptoms. The extreme importance of realising this fact and the rarity of the production of symptoms by continuing compression both from the prognostic and the therapeutic point of view is obvious.
The analogous injuries termed generally in Chapter IX. nerve contusion, although frequently accompanied by tissue destruction, may be followed by reparative change, and are capable of complete or almost complete spontaneous recovery; while the lesions in the spinal cord are permanent, and complete recovery is only witnessed in the parts affected by the remote pressure or irritation from blood extravasation, or in those influenced by concussion.
I include below short abstracts of all the cases of lesion of the spinal cord which terminated fatally, in which I had the opportunity of witnessing the post-mortem conditions. In a considerable proportion of the cases at the end of six weeks[Pg 323] the spinal cord was softened over an area of from two to four segments in such degree as to have practically lost all continuity. Although the autopsies were made on patients who had died slowly and in summer weather, often twelve to sixteen hours after death, I think it can be but fair to assume, when the consistency of the remaining portion of the spinal cord is considered, that the softening was only in slight degree if at all exaggerated by post-mortem change. Again symptoms of secondary myelitis and meningitis had been observed in some of the fatal cases prior to death.
I had but one opportunity of observing a case in which a retained bullet exercised compression, and none in which this was due to displaced bone fragments. I also only once came across a case of complete section, but no doubt both bone pressure and section may have occurred with greater frequency amongst patients dying on the field or shortly after. The case of section is illustrated in fig. 80. It will be noted that, although the section is complete, the bullet lies to one side of the canal, and hence the bullet, as fixed in its course by the bone of the centrum, directly struck but half of the whole width of the cord.
It was striking how little secondary change in the cord had occurred in the neighbourhood of the spot of division. This well illustrates the comparatively slight vibratory effect of a bullet travelling with a degree of velocity insufficient to completely perforate the vertebral column.
Symptoms of injury to the spinal cord.—In slight spinal concussion these exactly resembled those of the more severe lesions, except in their transitory nature. They consisted in loss of cutaneous sensibility, motor paralysis, and vesical and rectal incompetence. The phenomena persisted from periods of a few hours to two or three days, return of function being first noticeable in the sensory nerves, and often with modification in the way of lowered acuteness, or minor signs of irritation, such as formication, slight hyperæsthesia or pain, pointing to a combination with the least extensive degrees of hæmorrhage; later, motor power was rapidly regained. The subjects of such symptoms often suffered from weakness and unsteadiness in movement for some days or weeks; a[Pg 324] sharp line of discrimination between such cases and those described in the next paragraphs is manifestly impossible.
Spinal hæmorrhage.—The symptoms of this condition developed differently according to whether concurrent concussion existed. Occasionally very typical instances of pure hæmorrhage were observed with transient symptoms:—
(96) A private in the Yorkshire Light Infantry was wounded at Modder River; the bullet entered between the eleventh and twelfth ribs, just posterior to the left mid-axillary line, emerging in the posterior axillary fold, at its junction with the right side of the trunk. On the second day after the injury the lower extremities became drawn up, the knees and hips assuming a flexed position, and this was followed shortly by the advent of complete motor and sensory paraplegia, accompanied by retention of urine. Two days later, the patient again passed water normally, and gradual and rapid return of both sensation and motor power took place. At the end of fourteen days no trace of the condition remained, and the patient was shortly after sent home.
The symptoms, however, were rarely so simple as in this example; it was very much more common to meet with an admixture of signs of primary concussion, or at any rate symptoms of radiation. The following is an extreme but excellent example of more complicated and prolonged effects:
(97) A lance-corporal of the Black Watch was wounded at Magersfontein at a range of from 400 to 500 yards. The bullet entered over the left malar bone 2½ inches from the outer canthus, while the aperture of exit was 2¼ inches above the inferior angle of the right scapula, 3/4 of an inch anterior to its axillary margin.
Very shortly after the injury complete motor and sensory paralysis developed in both upper extremities, followed by the development of a similar condition in the left lower limb, and retention of urine and fæces, but the latter unaccompanied by the marked abdominal intestinal distension so characteristic in cases of total transverse lesion. The right side of the chest continued to work well, but the intercostals of the left side were paralysed. No disturbance of the normal action or condition of the pupils was noted. After the first few days the condition began to improve.
Three weeks later, the chest was moving symmetrically and well, sensation and motor power had returned in considerable[Pg 325] degree in the left lower extremity, with marked increase in both the plantar and patellar reflexes; sensation had returned in both upper extremities, a slight amount of motor power was regained in the right, but the left remained entirely flaccid and incapable of movement.
At the end of a month power was regained over both bladder and rectum, some slight movement of the left thumb was possible, and a certain degree of hyperæsthesia developed over the back of the forearm.
At the end of six weeks there was little further alteration, but that in the direction of improvement. There was some wasting of the muscles of the left upper extremity, and this was most marked in the muscles supplied by the ulnar nerve.
At the end of ten weeks the patient had been up some days; he could stand and walk, but was unable to rise from the sitting posture without help. The plantar and patellar reflexes were much exaggerated, and there was ankle clonus, most marked in the left limb. The right upper extremity was normal, but weak; there was wrist-drop on the left side and the deltoid was wasted and powerless; on the other hand the fingers could be flexed, and although the elbow could not be, there were signs of returning power in the biceps, and some movements of the shoulder could be performed by the capsular muscles. It was remarkable that common sensation was more acute in the left than the right lower extremity, but I attributed this to the remains of hyperæsthesia on the left side. The patient left for home shortly after the last note.
In both these cases the absence of marked hyperæsthesia or pain points to medullary hæmorrhage (hæmato-myelia) as the pathological condition produced by the injury. In this particular they contrast well with case 94 quoted on page 315, where the degree of both hyperæsthesia and pain indicated a combination of pressure and irritation of the nerve roots by surface hæmorrhage on the affected side. In case 97 the persistence for four weeks of paralysis of the bladder and rectum suggested medullary hæmorrhage in addition, while the return of patellar reflex in the paralysed limb negatived the occurrence of an extensive destructive lesion.
In view of the extreme interest of these cases I will shortly detail one other in which the cauda equina alone was affected.
I must confess my inability to place the case definitely in[Pg 326] the category either of concussion or medullary hæmorrhage. As so often happened, both conditions probably took part in the lesion. The immediate development of the primary symptoms is no doubt to be referred to concussion, while the patchy nature of the prolonged lesion and gradual recession of the symptoms point to the presence of hæmorrhages. We find here the link most nearly connecting the spinal cord and the peripheral systemic nerves. Such a case goes far to show that the condition which I have in the next chapter often referred to as nerve contusion may in fact be produced by an injury far short of actual contact.
(98) A trooper in the Imperial Yeomanry, while advancing in the crouching attitude, was struck by a bullet from his left front, at an estimated distance of 300 yards. The bullet traversed the right arm anteriorly to the humerus, entered the trunk in the line of the posterior axillary fold, 1½ inch below the level of the nipple, crossed the thoracic and abdominal cavities, deeply striking the lumbar spine, and finally lodged beneath the skin over the venter of the left ilium. The skin was broken, but the force of the bullet was not sufficient to cause it to pass through, and it was later expressed from the wound by the surgeon. The bullet was a Mauser, and not in any way deformed, although it must at any rate have struck the spine and perforated the ilium.
Immediate paraplegia resulted, both sensation and motor power were completely abolished, but there was no trouble either with the bladder or rectum. No symptoms of injury to either thoracic or abdominal viscera were noted.
Three days after the injury sensation and some return of motor power were observed in the left extremity, and some power of movement in the toes of the right foot.
During the next eight weeks steady but slow improvement took place; during the last three weeks of this period he made the voyage to England. Ever since the injury some elevation of temperature was noted, a rise at night to 100° or at times to 102°; for this no definite cause was discovered. In the tenth week the condition was as follows: The temperature has become normal. The patient has lost flesh to a considerable extent since the reception of the injury. The lower extremities are much wasted, especially the peroneal muscles. Patellar reflexes can be obtained, but the knee jerks are uncertain. Unevenly distributed paralysis exists in both lower extremities. Left—Sensation fairly[Pg 327] good throughout. Quadriceps very weak; does not react to electrical stimulation. Calf muscles act fairly. Anterior tibial and musculo-cutaneous groups are paralysed. Right—Quadriceps acts better than on left, muscles below the knee paralysed, and in the same area there is complete absence of sensation. The patient complains of shooting pains in both legs, and there is some deep muscular tenderness.
Three weeks later an abundant crop of vesicles appeared over the front of the right thigh and leg, above and below the knee. Sensation in the limb at the same time returned to a considerable degree, anæsthesia persisting on the outer aspect of the thigh only.
At the end of four months very considerable improvement had taken place, but there was no return of motor power in the right leg, or the muscles supplied by the peroneal nerve in the left leg. There was some general œdema of the legs, especially of the right, possibly in connection with the herpetic eruption which was now disappearing. Muscular tenderness had disappeared. There was also definite improvement in the size and tone of the peroneal muscles, although no motor power was regained.
At the end of five months, slight gradual improvement was still taking place, but the loss of power was nearly as extensive as when the last note was taken. The skin of the right leg was glossy, that of the left apparently normal. At times some hyperæsthesia of the soles was noted, and the plantar reflex was very brisk.
The right anterior tibial and musculo-cutaneous groups of muscles reacted to the strongest faradic current, not to any galvanic current below 20-25 m.a., contraction very sluggish. The same muscles in the left leg also reacted to the strongest faradic current, but only locally, with no sort of effect on the tendons. Similar contractions could be induced in the right quadriceps, but none in the left (Dr. Turney).
Appreciation of heat and cold applied to the skin was fair, but, in the case of heat, distinctly slow in the right leg and foot.
At the end of seven months improvement was still taking place; the patient could now stand, walk a little with crutches, and even ascend and descend a staircase.
Severe concussion, contusion, or medullary hæmorrhage producing signs of total transverse lesion, and complete transverse section.—The symptoms of these conditions will be taken together, because, with very slight variations, they may be[Pg 328] considered as lesions of equal degree as to severity, bad prognosis, and unsuitability for active interference.
All were characterised by the exhibition of the same essential phenomena, symmetrical abolition of sensation and motor power on either side of the body, absence of any signs of irritation in the paralysed area, and loss of patellar reflex. In a small number of the cases of medullary hæmorrhage some return of sensation was observed prior to death; in a still smaller, traces of motor power, and in one or two irritability of the muscles or feeble reflexes pointed to the fact that destruction of the cord was not absolute. As abstracts of a series of cases are appended on page 330, it is only necessary to add a few remarks as to any slight peculiarities which seemed directly dependent on the mode of causation.
It may be first stated that these severe injuries were accompanied by signs of a very high degree of shock. In fact, the shock observed in them was more severe than in any other small-calibre bullet injuries that I witnessed. The patients lay still with the eyes closed, great pallor of surface, sometimes moaning with pain, the sensorium much benumbed, or occasionally early delirium was noted. The pulse was small, often slow and irregular, and the respiration shallow. The originally quiet state was often changed to one of great restlessness of the unparalysed part of the body, with the appearance of reaction.
The degree of primary pain varied greatly, but as a rule it was considerable; in some cases it was excruciating in the parts above the level of the totally destructive lesion, and commonly of the zonal variety. A hyperæsthetic zone at the lower limit of sensation usually existed.
In the majority of the cases pain must have depended on meningeal hæmorrhage. In one of the cases related, positive evidence was offered as to this particular by the autopsy, although this was made as long as six weeks after the original injury, since no other source of pressure or irritation was discovered. When I first saw this patient some twenty-four hours after the injury he was moaning with pain, although a strong and plucky man; I hastened to give him an injection of morphia, and assured him that it would relieve[Pg 329] his suffering: as I left I heard him say to his neighbour: 'That is no use; they gave me three last night, and I was no better,' and his remark proved true.
In high dorsal and cervical injuries the temperature rose high, in one case to 108° F.; I had no opportunity, however, of observing the temperature in any case immediately before and after death. During the hot weather the profuse sweating of the upper part of the body contrasted very strongly with the dry skin of the paralysed part.
The heart's action was often particularly irregular in the dorsal injuries, and the respiration slow and irregular; as these cases, however, were often complicated by severe concurrent injuries to internal organs, the irregularities could hardly be ascribed to the spinal-cord lesion alone. In cases of pure diaphragmatic respiration, the rate did not as a rule exceed the normal of 16 or 20 to the minute, and it was quite regular; this was noted soon after the injury and persisted throughout the course of the cases. As is usually the case, both respiration and the heart's action were most embarrassed in the cases in which abdominal distension was a prominent feature. In some of the neck cases the Cheyne-Stokes type of respiration was very strongly marked.
In cases of low dorsal injury intestinal distension was extreme, and I think more troublesome than the same condition as seen in civil practice. The distension was accompanied by most persistent vomiting, continuing for days, and in the cases that lived for some time severe gastric crises of the same type occurred in some instances.
Priapism was a common symptom; but, as is seen from the cases quoted, was rarely due to any gross direct laceration of the cord.
Trophic sores were both early to develop, and extensive; primary decubitus occurred in all the cases I saw, and steady extension followed. In one case a remarkable symmetrical serpiginous ulceration developed in the area of distribution of the cutaneous branches of the external popliteal nerve on the outer side of the leg.
The paralysis in nearly every case was of the utterly flaccid type, and wasting of the muscles was early and[Pg 330] extreme. This was occasionally accentuated by the supervention of myelitis.
Opportunities for making observations on the quantity of urine secreted were not great, and I can offer no remark as to the occurrence of polyuria. In one rapidly fatal case, however, suppression of urine occurred.
(99) Lumbar region. Transverse lesion.—Range under 1,000 yards. Wound of entry (Mauser), over the seventh rib 1 inch from the left posterior axillary fold; exit, over the centre of the right iliac crest. Complete symmetrical motor and sensory paralysis of lower extremities, entire abolition of reflexes, retention of urine.
On the ninth day there was some return of sensation in the lower extremities, and a cremasteric reflex was to be obtained. A large bedsore had developed over the sacrum. No further change occurred in the lower extremities. The patient became progressively emaciated and exhausted, cystitis persisted, the bedsore deepened. The man eventually developed signs of a large basal abscess in the left lung, and died on the forty-second day.
At the post-mortem a fracture of the first lumbar lamina was discovered, with some splintering of the bone; the lumbar spinous process was attached and in its normal position. Opposite the centre of the cauda equina were the remains of a considerable hæmorrhage, both extra- and intra-dural, the nerves appearing somewhat compressed, but of normal consistency. The muscles of the back were infiltrated with putrid pus on both sides. A pulmonary abscess cavity the size of a hen's egg occupied the upper part of the lower lobe of the left lung. The kidneys were congested, and the bladder thickened and chronically inflamed.
(100) Cervico-dorsal region. Total transverse lesion.—Wound of entry (Mauser), to the right of the sixth cervical vertebra: the bullet was removed on the field from the left of the seventh dorsal spinous process, which was somewhat prominent. Complete motor and sensory paralysis extended upwards to the third intercostal space; the breathing was almost entirely diaphragmatic. Retention of urine. Entire abolition of reflexes in lower limbs and trunk. Hyperæsthesia was present in both upper extremities, with a zone of hyperæsthesia around the chest. The patient suffered greatly for some weeks from pain in the hyperæsthetic area, he developed severe cystitis and later incontinence of urine. A large trophic sacral bed-sore steadily increased in depth and size.
About ten days before death, which occurred on the fifty-third[Pg 331] day from exhaustion and septicæmia, the patient complained of pains in his legs; but there was no return of sensation, motion, or reflexes.
At the post-mortem, the seventh dorsal spinous process was found to be loose and the laminæ of the fifth, sixth, and seventh vertebræ were separated from the pedicles, and somewhat depressed on the left side. These laminæ were adherent to the dura, as were also a few small separated bony spiculæ. There was no sign of old hæmorrhage. The spinal cord was practically gone between the levels of the fourth and seventh dorsal vertebræ, and diffluent from myelitis up to the third cervical.
(101) Dorsal region; total transverse lesion.—Wound of entry (Mauser), in the left supra-spinous fossa of the scapula; exit, between the eleventh and twelfth ribs of the right side. Complete motor and sensory paralysis, with absence of reflexes from mid-dorsal region downwards. Upper intercostals working. Retention of urine, penis turgid. Sensation perfect to lower extremity of sternum. Early trophic sacral bed-sores developed and steadily increased in depth and extent, slighter ones developed on the heels. The paralysis was flaccid throughout. The patient gradually emaciated with fever, and died on the seventy-eighth day.
At the post-mortem the wound proved not to have penetrated the thorax, and both the vertebral spines and laminæ were intact, no trace of bony injury being discoverable. Opposite the sixth dorsal vertebra, for a distance of 1½ inch, the cord and dura were adherent, and over the same area the cord was represented by soft custard-like material. There was no sign of old hæmorrhage.
(102) Dorsal region; total transverse lesion; slight extra-dural hæmorrhage.—Wound of entry (Mauser), at the posterior aspect of the right shoulder; exit, 2 inches to the left of the spine below the ninth rib.
Complete motor and sensory paralysis below the site of the lesion, with absence of superficial and deep reflexes. Retention of urine. Great abdominal distension, pain, and vomiting. Bed-sores over the sacrum developed on the third day; meanwhile the vomiting continued on and off for a week, and very severe girdle pain persisted.
One month later when seen at the Base hospital considerable improvement had occurred. Sensation had returned in both lower limbs; but flaccid paralysis persisted and both were wasted, especially the left. There was no return of reflexes in the lower[Pg 332] limbs, the urine was passed in gushes, and the patient was cognisant when these occurred. The sacral bed-sores were, however, very extensive and becoming larger and deeper.
At the end of the fifth week slight power was regained in the flexors and abductors of the right thigh, and the same muscles of the left limb could be made to contract feebly. Meanwhile the patient suffered with severe fever, accompanied by frequent rigors and profuse sweats; the bed-sore continued to extend, and the urine was foul and contained pus.
The patient continued in a similar condition, progressive emaciation and exhaustion taking place, and at the end of six weeks he died.
At the post-mortem the bullet was found to have tracked beneath the right scapula, entering the chest by the fifth intercostal space and lacerating the right lung; thence it entered the eighth dorsal centrum and tunnelled both this and the ninth diagonally, to escape beneath the ninth rib. On opening the spinal canal the tunnel was found to be separated only by the compact tissue of the centrum from the cavity, while a thin extra-dural hæmorrhage separated the dura from the bones anteriorly. The spinal cord exhibited no sign of pressure and was firm and continuous, but up to the lower limit of the dorsal region there was septic myelitis and meningitis, the result of pus having tracked up the canal from the sacral bedsore. Suppurative cystitis and pyelitis were present. The patient was the subject of an old urethral stricture which had given rise to trouble during treatment.
(103) Dorsal region; total transverse lesion; slight intra-dural hæmorrhage.—Wound of entry (Mauser), below spine of scapula, close to right axilla; exit, 2½ inches to left of tenth dorsal spinous process.
Complete motor and sensory paralysis below ensiform cartilage, with well-marked hyperæsthetic zone around trunk. All reflexes absent. Retention of urine. Incontinence of fæces. Bed-sores in sacral region developed during the first two days, and seventeen days later well-developed serpiginous trophic sores developed on the outer side of each leg and continued to increase slowly until death. The paralysis remained of the absolutely flaccid variety. Great emaciation occurred, accompanied by hectic fever, the temperature ranging from normal to 102.5°. During the third week double pleurisy developed.
At the post-mortem no bone injury could be detected. The cord and dura-mater were adherent over an area corresponding to the[Pg 333] fifth to the eighth dorsal vertebræ, and opposite the seventh the cord was soft and of the consistence of butter. A small intra-dural hæmorrhage was still evident below the main lesion, not extensive enough to give rise to serious compression. General adhesions in each pleura. Cystitis.
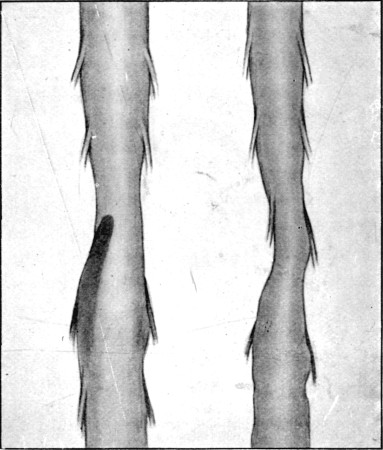 Fig. 79.
Fig. 79.
Appearance of Spinal Cord enclosed in membranes in case 103 after removal from the canal. When the membranes were opened a white custard-like substance took the place of the cord. Slight evidence of extra-dural hæmorrhage existed
(104) Dorsal region; section of cord; retained bullet.—Wound of entry (Mauser), in seventh right intercostal space, 4½ inches from the dorsal spinous processes, oval in outline; bullet retained.
Complete motor and sensory paralysis, with absence of reflexes below umbilicus. Retention of urine, incontinence of fæces. Large sacral bed-sore developed rapidly. Right hæmothorax.
The patient emaciated rapidly, and for the last fourteen days the temperature ranged to 104°, the bed-sore steadily increasing in size. Death occurred on the forty-second day.
At the post-mortem a Mauser bullet was found embedded in the centrum of the twelfth dorsal vertebra. The bullet was slightly curved; its anterior extremity had passed across the spinal canal, and wounding the dura posteriorly rested against the left lamina. The plating of the mantle of the bullet was stripped from half the area of the tip. The dura was not adherent,[Pg 334] and the cord was softened for half an inch above the point of section; above this it was normal, the vessels coursing normally to the softened spot. Below the point of section the cord was blanched, but offered no other macroscopic evidence of disease. No evidence of either intra- or extra-dural hæmorrhage was detectible.
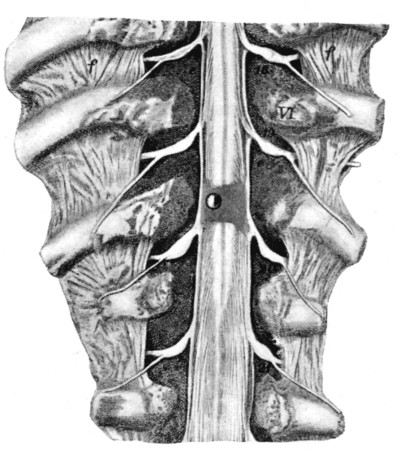 Fig. 80.
Fig. 80.
Complete division of Spinal Cord. The bullet is retained, and from its position can be seen to have struck the right half of the cord only. The nickel plating of half of the tip of the bullet is stripped off. Case No. 104
The right pleura contained a large quantity of dark cocoa-like fluid. Extensive adhesions were present in both pleural cavities. The spleen was much enlarged. At the base of the bladder a large submucous hæmorrhage had occurred, the blood-clot had assumed a dark orange colour, and on first opening the viscus the appearance was that of a mass of fæces. The mucous lining elsewhere was slaty grey, with small hæmorrhages. The kidneys were large, but no abscesses or pyelitis were present.
(105) Cervico-dorsal region; total transverse lesion.—Wound of entry (Mauser), opposite right sixth cervical transverse process; exit, on left side of third dorsal spinous process. Slight grasping power was present in the hands, and the patient could hold his arms across his chest. Complete motor and sensory paralysis, with absence of all reflexes below. The pupils were moderately contracted. Retention of urine. On the second day blebs appeared on each buttock, and the patient complained of very severe pain in the neck: the temperature rose to 103°, and on the third day he died suddenly. No post-mortem examination was made.
I observed two similar cases in the Field Hospital at Orange River, the patients dying on the third day; pain and high temperature were prominent symptoms in both. In one patient early delirium was present.
(106) Dorsal region; Martini-Henry wound.—Wound of entry, oval, 1 inch ×3¼ inches; long axis obliquely crossing infra-spinous fossa of right scapula; bullet retained (Martini-Henry). Spine of third dorsal vertebra loose, and a distinct thickening to its right side. Complete symmetrical paralysis extending up to upper extremities. No sensation on surface of trunk below cervical area. Respiration entirely diaphragmatic. Retention of urine, penis turgid. Total absence of reflexes, superficial and deep. Reddening of buttocks, but no bullæ.
General hyperæsthesia of upper extremities, with severe spasmodic attacks of pain.
On the third day an exploration was decided upon, in view of the local deformity, and the severe pain in the upper extremities. The third dorsal spine was found to be loose, as a result of bilateral fracture of the neural arch; the bullet had crossed the right limit of the spinal canal, and destroyed the body of the vertebra, and passing onwards had entered the left pleural cavity, into which air entered freely from the operation wound.
The patient was relieved from his pain by the exploration, and lived four days. On the second day after operation, however, the temperature rose to 107°, while on the last two days the temperature was normal in the mornings, rising to 105° in the evenings. No alteration resulted in the trunk symptoms.
Diagnosis.—The pure question of the fact of injury of the spinal cord needs no discussion; but it is necessary to make some remarks on the discrimination between concussion, contusion and hæmorrhage, meningeal and medullary hæmorrhage, the latter condition and compression, and on partial and complete severance of the cord.
The sharp discrimination of cases of concussion from those of slight medullary hæmorrhage was necessarily impossible. I think the only points of any importance in diagnosing pure concussion were the transitory nature of the symptoms, and the uniformity of recovery, without persistence of any signs of minor destructive lesion. In medullary hæmorrhage the tendency for a certain period was[Pg 336] towards increase in gravity in the signs. It goes almost without saying that the latter point was seldom accurately determined in patients struck on the field of battle; these perhaps lay out for hours before they were brought in, and when they were placed in the Field hospital the rush of work did not usually allow the careful observation necessary to clear up this difference in the development of the symptoms. Nevertheless it is preferable to consider the cases in which transitory symptoms persist for a period of hours, or even a couple of days, as instances of pure concussion, unless the existence of this condition can be disproved by actual observation.
Extra-medullary hæmorrhage, accompanied by only slight encroachment on the spinal canal, certainly results with some frequency from small-calibre wounds. Some of the quoted cases show this decisively by post-mortem evidence, others by such clinical signs of irritation as pain and hyperæsthesia. I think its presence may also be assumed in cases of total transverse lesion due to medullary hæmorrhage or severe concussion, accompanied by well-marked pain and hyperæsthesia above the level of paralysis. As affecting treatment, however, determination of its presence is of small importance.
The important conditions for discriminative diagnosis are those of local compression, actual destructive lesion, whether from concussion changes, contusion, or medullary hæmorrhage, and partial and total section of the cord.
First, with regard to compression of the cord, the possible sources are three; (i) extra-dural hæmorrhage, which may, I think, be dismissed with mention as rarely capable of producing severe symptoms. (ii) The displacement of bone fragments. This is of less importance than in civil practice, because an injury by a bullet of small calibre, capable of seriously displacing fragments, has probably at the same time produced grave changes in the cord. In the presence of severe immediate symptoms we may tentatively assume that a simultaneous destructive lesion has been produced. In such injuries pain, combined with a tendency to improvement in the paralytic symptoms and return of reflexes, is the only point in favour of bone pressure, unless considerable deformity[Pg 337] of the spinal column can be detected by palpation or examination with the X-rays.
(iii) Pressure from the bullet. This is the most important form of compression, because the mere fact of retention of the bullet is evidence of a low degree of velocity, and therefore opposed to the existence of the most severe form of intramedullary lesion. In a case of apparent transverse lesion with retained bullet, shown to me at No. 3 General Hospital by Mr. J. E. Ker, the pain was very severe, and so greatly aggravated by movement that an anæsthetic had to be administered prior to the renewal of some necessary dressings. The general condition of this patient precluded a projected operation, and after death the bullet was found to be pressing laterally upon a cord not materially altered on macroscopic inspection. In the case of retained bullet recorded (No. 104), the slight degree to which the severed ends of the cord appeared altered has been already remarked upon.
Beyond this we are helped by the position of the aperture of entry, and its shape, as evidence of the direction in which the bullet passed, the presence of pain, and positive proof may be obtained by examination with the X-rays.
Lastly, we come to the discrimination of total or partial section, destruction by vibratory concussion or contusion, and severe intramedullary hæmorrhage. Except in the case of partial section with localised symptoms, which must be rare, I believe this to be impossible from the primary symptoms, although some indication of possible encroachment on the canal may be obtained from careful consideration of the course of the wound, as evidenced by the position and shape of the openings, the position of the patient's body at the time of reception of the injury being taken into consideration. Later we may get some aid from the possible improvement in the symptoms in the case of hæmorrhage. In cases with signs of total transverse lesion, however, the discrimination of the conditions is of little practical importance, since either is equally unfavourable and unsuitable for surgical treatment.
In closing these remarks reference must be made to the occasional occurrence of paraplegic symptoms of an apparently purely functional nature. I saw these on one or two occasions,[Pg 338] of which the following is a fair example. A man was wounded in the lower extremity and fell. When brought into the hospital he complained of loss of power in the legs and inability to straighten his back. No very definite evidence was present of serious impairment either of motor or sensory nerves, and the man was got up and walked with crutches. While moving about the hospital camp, another man pushed him down, and the patient then became completely paraplegic. He was placed in bed, and the next day moved his limbs without any difficulty, and gave rise to no further anxiety.
Prognosis.—In slight concussion the importance of prognosis is as to remote effects, and upon this no opinion can be given at the present time. The same may be said concerning cases in which transient symptoms followed the slighter degrees of surface and medullary hæmorrhage. In the case of the latter, however, I think it would be rash to give a too confident opinion as to the future non-occurrence of secondary changes.
Severe concussion is probably irrecoverable.
Meningeal hæmorrhage of either form is one of the slighter lesions, and less dangerous, both as an immediate condition and as to the probabilities of after trouble. None the less the possibilities of secondary chronic meningitis, or chronic trouble from adhesions, must be kept in mind.
Cases of medullary hæmorrhage with incomplete signs are favourable in prognosis, as far as life is concerned; as to complete recovery, however, this is hardly possible; in many cases serious functional deficiency at any rate will remain, while in others the healing of the lacerated tissue and subsequent contraction can scarcely fail to influence unfavourably an already imperfect recovery.
I think it must be a rare occurrence for pressure from bone fragments to be able to be regarded as a favourable prognostic condition, since in the very large majority of cases the velocity of the bullet causing the injury will have been such as to inflict irreparable damage on the cord. Still, cases may occasionally be met with where the velocity has been sufficiently low, or contact with the bone slight enough, to allow of the comparative escape of the cord. In this relation[Pg 339] cases in which the bullet is retained, especially if the symptoms of transverse lesion are incomplete, may be regarded as relatively favourable.
Cervical and high dorsal injuries, as in civil practice, offered the worst prognosis. In cases in which symptoms of total transverse lesion were present, as far as my experience went, it was, however, only a matter of importance as to the prolongation of a miserable existence. All the patients eventually died; those with higher lesions at the end of a few days; the lower ones, at the completion on an average of six weeks of suffering.
The actual causes of death resembled exactly those met with in civil practice, except in so far as it was more often influenced or determined by concurrent injuries, a complication so characteristic of modern gunshot wounds. Thus exhaustion, septicæmia from absorption from suppurating bed-sores or from severe cystitis, secondary myelitis, and pulmonary complications, carried off most of the patients.
Treatment.—The general treatment of the cases demanded nothing special to military surgery, except in so far as it was modified by the disadvantage to the patient of necessarily having to be transported, often for some distance. The ill effects of this, particularly in cases of hæmorrhage, are obvious, but in so far as fracture was concerned the question of transport did not acquire the importance that it does in civil practice, since the nature of the fractures and their strict localisation did not render movement either painful or particularly hurtful. It was indeed striking how little pain movement, made for the purposes of examination, caused these patients. The treatment of bed-sores, cystitis, or other secondary complications possessed no special features.
The importance of insuring rest in the early stages of the cases of hæmorrhage is self-evident; hence, if the possibility exists of not moving the patient, its advantage cannot be too strongly insisted upon. Again, if transport is inevitable, the shorter distance that can be arranged for the better. It should be borne in mind, also, that from the peculiar nature of causation of the injuries, stretcher or wagon transport for short distances is preferable to the vibratory movements of[Pg 340] a long railway journey. Beyond this the administration of opium, and in some cases the assumption of the prone position, are both useful in the recent or possibly progressive stage of hæmorrhage.
Lastly, as to active surgical treatment by operation. In no form of spinal injury is this less often indicated, or less likely to be useful. It is useless in the cases of severe concussion, contusion, or medullary hæmorrhage which form such a very large proportion of those exhibiting total tranverse lesion, and equally unsuited to cases of partial lesion of the same character. Extra-medullary hæmorrhage can rarely be extensive enough to produce signs calling for the mechanical relief of pressure; the section of the cord cannot be remedied. In one case with signs of total transverse lesion, in which a laminectomy was performed, no apparent lesion was discovered, and this would frequently be the case, since the damage is parenchymatous. The experience was indeed exactly comparable to that which followed early exposure of the peripheral nerves.
Only three indications for operation exist. 1. Excessive pain in the area of the body above the paralysed segment; operation is here of doubtful practical use, except in so far as it relieves the immediate sufferings of the patient.
2. An incomplete or recovering lesion, when such is accompanied by evidence furnished by the position of the wounds, pain, and signs of irritation of pressure from without, or possibly palpable displacement of parts of the vertebra, that the spinal canal is encroached upon by fragments of bone.
3. Retention of the bullet, accompanied by similar signs to those detailed under 2.
In both the latter cases the aid of the X-rays should be invoked before resorting to exploration.
Operation, if decided upon, in either of the two latter circumstances, may be performed at any date up to six weeks; but if pressure be the actual source of trouble, it is obvious that the more promptly operation is undertaken the better for early relief and ulterior prognostic chances.
In only one case of the whole series I observed did it seem possible to regret the omission of an exploration.
The occurrence of these injuries has undoubtedly increased in frequency with the employment of bullets of small calibre, and no other class of case more strikingly illustrates the localised nature of the lesions produced by small projectiles of high velocity. Again, no other series of injuries affords such obvious indications of the firm and resistent nature of the cicatricial tissue formed in the process of repair of small-calibre wounds, and in none is the advantage of a conservative and expectant attitude so forcibly impressed upon the surgeon. Implication of the nerves may be primary, or secondary to an injury which left them originally unscathed.
Nature of the anatomical lesions.—In degree these vary in mathematical progression, but the extent of the lesion is not always readily differentiated by the early clinical manifestations, and again the actual damage is not to be estimated by the gross apparent anatomical lesion alone; but, in addition, consists in part in changes of a less easily demonstrable nature, varying with the velocity with which the bullet was travelling and the consequent comparative degree of vibratory force to which the nerve has been subjected. In these injuries, as in those of every part of the nervous system, the degree of velocity appears to gain especial importance both in regard to the general symptoms and the local effect on the functional capacity of the nerve.
This is perhaps a fitting place for the introduction of a few further remarks as to the significance of the term 'concussion' in connection with the injuries produced by bullets of small calibre, since the most striking exemplification of the results following the transmission of the vibratory force of the projectile[Pg 342] is afforded by the behaviour of the comparatively densely ensheathed and supported peripheral nerves.
As already pointed out in Chapters VII. and VIII. the chief concussion effects on the nervous tissue of the brain and spinal cord are of a destructive nature, far exceeding those accompanying the injuries designated by the same term seen in the ordinary accidents met with in civil practice, and this damage is comparatively localised in extent.
In the case of the peripheral nerves I have still employed the terms 'concussion' and 'contusion' to designate certain groups of symptoms and clinical phenomena, but any sharp distinction between the two conditions on a morbid anatomical basis is impossible. The results of severe vibratory concussion may, in fact, be more generally destructive than those of contusion, and the subsequent effects more prolonged. A certain length of the affected nerve is apparently completely destroyed as a conductor of impulses, the connective-tissue element alone remaining intact. Under these circumstances a nerve, the subject of the most serious degree of vibratory concussion, which, if cut down upon, may exhibit no macroscopic change, may take a longer period to recover than one in which the presence of considerable local thickening points to direct contact with the bullet, with resulting hæmorrhage into the nerve sheath and perhaps partial gross rupture of nerve fibres.
The therapeutic and prognostic importance of the above remarks, if correct, is obvious. The course of the nerve is preserved by its intact connective-tissue framework, and ultimate recovery by a regeneration of the nerve fibres is more likely to be complete, and will be just as rapid, if nature be relied on and the nerve be left untouched by the hand of the surgeon.
It is, I think, undeniable that nerve trunks may escape severe or irrecoverable injury by lateral displacement. The mere fact that the trunk itself may be perforated by a slit in its long axis would suggest the possibility of displacement of the whole structure, and this no doubt occurred with some frequency. Displacement would naturally be most frequent in the case of nerves, such as those of the arm, which run long courses in comparatively loose tissue. In a remarkable[Pg 343] case already narrated, an exploratory operation showed the musculo-spiral nerve in the upper part of the arm to have been driven into a loop which projected into, and provisionally closed, an opening in the brachial artery.
I. Simple concussion.—Anatomically, or histologically, no information exists as to the changes which give rise to the often transitory symptoms dependent on this condition. We are reduced to the same theories of molecular disturbance and change which have been invoked to account for similar affections of the central nervous system. The causation of concussion is, however, materially influenced in its degree by the velocity of flight of the bullet and consequent severity of the vibratory force exerted. Hence actual contact of the bullet with the nerves is not necessary for its production, as is seen in the temporary complete loss of functional capacity in the limbs in many cases of fracture, where the vibrations are rendered still more far-reaching and effective as the result of their wider distribution from the larger solid resistance afforded by the bone. The relative density and resistance offered by the different parts of the bone acquire great significance in this relation, since local shock due to nerve concussion is far more profound when the shafts are struck than when the cancellous ends furnish the point of impact.
The form of concussion which most nearly interests us in this chapter is that affecting single nerve trunks in wounds of the soft parts alone, and here the passage of the bullet is, as a rule, so contiguous to the nerve that there is difficulty in drawing a strict line of demarcation between such cases and those dealt with in the next paragraph.
II. Contusion.—Clinically this was the form of nerve injury both of greatest comparative frequency and of interest from the points of view both of diagnosis and prognosis.
The seriousness of a contusion depends on two factors: first, the relative degree of violence exerted upon the nerve, which is dependent on the force still retained by the travelling bullet; and, secondly, on the extent of tissue actually implicated. The range of fire at which the injury was received determines the importance of the first factor; the second varies[Pg 344] with the degree of exactness with which the nerve is struck, and on the direction taken by the bullet. Naturally transverse wounds affect a small area; while an oblique or longitudinal direction of the track may indefinitely increase the extent of injury to the nerve trunk, and hence acquire prognostic significance in direct ratio to the amount of tissue which needs to be regenerated.
As to the actual anatomical lesion resulting in the cases which we designated clinically as contusion I can give no information. On many occasions when the symptoms were considered of such a nature as to render an exploration advisable, no macroscopic evidence of gross injury was obtained. It was therefore impossible to draw a definite line of demarcation between such cases and those which we considered merely concussion. It could only be assumed that the vibration transmitted to the nerve had occasioned such changes as to destroy its capacity as a conductor of impressions.
In some cases the presence of a certain amount of interstitial blood extravasation was suggested clinically by early hyperæsthesia and signs of irritation; in others the paralysis was of such a degree as to lead to the inference that a complete regeneration of the existing nerve would be necessary prior to the restitution of functional capacity.
In a certain proportion of the injuries the development of a distinct fusiform swelling in the course of the nerve pointed to the existence of considerable tissue damage, while in others this was evidenced clinically by early signs of neuritis.
III. Division or laceration.—The varying mechanical conditions affecting the last class of injury play a similar rôle here. Thus the degree of laceration depends on the direction of the wound track, and as all lacerations are accompanied by contusion, the relative velocity retained by the travelling bullet assumes the same importance.
I saw every degree of injury to the trunks, from notching to complete solution of continuity, and in some cases destruction and disappearance of pieces from one to two or more inches in length. Such lesions as the latter were most common in the forearm. In this segment of the limbs tracks of varying degrees of longitudinal obliquity are readily produced,[Pg 345] whether the patient be in the upright or prone position, since the upper extremities are commonly in forward action whichever position is assumed.
The most peculiar form of injury consisted in perforation of the trunk without gross destruction of its fibres, and without in many cases prolonged or permanent loss of functional capacity. I cannot speak with any confidence as to the comparative frequency of occurrence of this form of injury, but judging by the analogous perforations of the vessels, it is probably not uncommon in trunks large enough to allow of its production. The trunk nerves of the arm, and the great sciatic nerve, were probably the most frequent seats of such wounds. As, however, a very short experience of the futility of early interference in the case of nerve lesions warned me against exploration before a date at which observations of this nature were unsatisfactory, I gained less experience on this point than I could have wished.
In the case of completely divided nerves the development of a bulbous enlargement on the proximal end was constant, and very marked in degree. I saw few cases in which primary effects could be certainly referred to pressure or laceration by bone spicules, excepting in some fractures of the humerus, and perhaps some injuries of the seventh nerve accompanying perforating wounds of the mastoid process.
IV. Secondary implication of the nerves.—This was a striking characteristic in many at first apparently simple wounds of the soft parts. In such cases it was due to implication of the contiguous trunk in the process of cicatrisation, and its importance varied with the size of the nerve in question. In the smaller sensory trunks it was often evidenced by the occurrence of neuralgic pain, especially liable to be influenced by climatic changes; in the larger, by signs of more or less severe motor, sensory, and trophic disturbance. Musculo-spiral paralysis from implication in, or pressure from, callus in cases of fracture of the humerus was very frequent. This would naturally be expected from the extreme degree the comminution of the bone often reached, and the consequently large amount of callus developed.
The effect of cicatrisation of the tissues surrounding the[Pg 346] nerves varied somewhat according to the degree of fixation of the individual nerve implicated. Thus if a nerve lay in a fixed bed some form of circular constriction resulted; if, on the other hand, the nerve was readily displaceable, the cicatrix often drew it considerably out of its course; in either case symptoms corresponding with those of pressure resulted.
Symptoms of nerve lesion.—These differed little in character from those common to such injuries in civil practice, except in the relative frequency with which they assumed a serious aspect. After all in civil practice nerve concussion is most familiar to us in the degree common after knocking the elbow against a hard object, and the same may be said in regard to the allied injury of contusion. It is in small-calibre bullet wounds alone that the occurrence of such severe and sharply localised injury to deep parts as was observed is possible.
Concussion.—Temporary loss of function was often observed in the limbs, corresponding to the distribution of one or more nerve trunks when wound tracks had passed in their vicinity. Interference with function sometimes amounted to loss of sensation alone: in others to loss of both sensation and motor power. Such symptoms were of a transitory character, lasting for a few days or a week; if both sensation and motion were impaired, sensation was usually the first to be regained. In these cases secondary trouble was not uncommon, since the near proximity of the track to the originally affected nerve offered every chance for implication of the latter in the resulting cicatrix. This sequence was often observed, and its symptoms are described under the heading of secondary implication below. Equally striking were the instances of concussion in the case of the nerves of special sense and their end organs, temporary loss of smell, vision, or hearing being not uncommon, often passing off in the course of a few days with no apparent ulterior ill-effect.
One of the most interesting illustrations of the occurrence of concussion was furnished by cases in which complete paralysis of a limb rapidly cleared up with the exception of that corresponding to a single individual nerve of the complex apparently originally implicated. Instances of severe contusion[Pg 347] or division of one nerve of the arm, for instance, accompanied by transient signs of concussion of varying degrees of severity in all the others, were by no means uncommon.
Contusion.—The symptoms of contusion were somewhat less simple, since, in addition to lowering or loss of function, signs of irritation were often observed. In the slighter cases irritation was often a marked feature, as was evidenced by hyperæsthesia and pain combined with loss of power. In cases in which pain and hyperæsthesia were primary symptoms, these were often transitory. I will quote an illustrative case which, though affecting the nerve roots, is characteristic of the effects of slight contusion in the case of the nerve trunks in any part of their course:—
(107) Contusion of cervical nerve roots.—Range probably about 1,000 yards. Wounded at Belmont. Aperture of entry (Lee-Metford), immediately posterior to the right fifth cervical transverse process; exit, immediately anterior to the space between the third and fourth left cervical transverse processes. The movements of the neck were perfect, there was neither pain nor difficulty in swallowing. Extreme hyperæsthesia was present in both palms and down the front of the forearms. The grip in either hand was weak, this being possibly explained in part by the hyperæsthesia of the palms, as all movements of the upper extremities could be made, although not with full power. On the fourth day the condition was much improved on the left side, and at the end of a week the left upper extremity was normal; the right (side of entry, and therefore exposed to greater force from the bullet) improved more slowly, becoming normal only at the end of three weeks.
I observed an identical case of injury to the cervical roots, and many similar instances in injuries of the nerve trunks of the limbs in which the course was exactly parallel. In the more severe, pain was often added to hyperæsthesia.
In the most severe cases the signs corresponded in all particulars, except in the early entire loss of reaction of the muscles to electricity, with those of complete section. Loss of sensation and motion was immediate, complete, and prolonged, the limbs being lowered in temperature, flaccid, and powerless. General systemic shock was also severe. In the[Pg 348] case either of plexus or multiple contusions, or where the injury was more local, correspondingly complete signs were present in the area supplied by the affected nerves.
In the cases in which the contusion was not of extreme degree, hyperæsthesia often developed as a later sign, and was probably due to the irritation of hæmorrhage, when the sensory portion of the nerve began to regain functional capacity. The date of appearance of the hyperæsthesia varied from a few days to a week or later. It might then persist for weeks or many months.
In a few instances large blebs rose on the back of the hand, or patches of vesicles appeared over the terminal distribution of the nerve, pointing to early trophic changes.
The period of recovery varied greatly; in some instances of very complete paralysis, function was regained and became apparently normal at the end of three or four weeks; in others, even after severe wasting of muscles for weeks, rapid improvement occurred often suddenly, while in some there was no apparent recovery at the end of months. In cases of long-deferred improvement, wasting of the muscles became a very prominent feature; but this without complete loss of reaction of the muscles to electrical stimulation.
Recovery of sensation usually preceded by some time that of motion, the former often reappearing in some degree at an early date, and, even if very modified in character, it formed a most useful and valuable aid both in diagnosis and prognosis.
When in a position allowing of direct examination, the contused portion of the nerve sometimes developed a palpable fusiform thickening, manipulation of which might give rise to formication in the area of distribution—a favourable prognostic sign.
Many of the cases bore a very marked resemblance in character to those in which paralysis results from tight constriction of the limb, as in the arm after the application of an Esmarch's tourniquet.
Laceration.—If incomplete, the signs corresponded very nearly to those of severe contusion, since partial section is impossible without the occurrence of the latter. The[Pg 349] condition indeed was only to be distinguished by the partial nature of the recovery, and even this latter might be only more prolonged.
The same remarks hold good with regard to perforation of the nerve trunks; but, as regards function, these injuries are not so serious in prognosis as very much more limited transverse divisions or mere notching, and in some cases the disturbance of function was by no means profound or prolonged.
Absolute loss of reaction to electrical stimulus from above was the only pathognomonic sign of actual section, unless the position of the nerve was such as to allow of palpation, when the presence of a bulbous end at once settled the difficulty. In many cases of superficial tracks with division of such nerves as the long or short saphenous, the early development of bulbs in the course of the trunks gave positive information, and these were often observed.
Traumatic neuritis.—This was a common sequence of contusion of the nerve itself, or of its subsequent inclusion in a cicatrix or callus. It was evidenced by hyperæsthesia both superficial and deep, pain, contracture, wasting of the muscles, local sweating, and the development of glossy skin.
Examples of this condition were seen in the case of nearly every nerve in the body. In frequency of occurrence, degree of severity, and in its selection of individual nerves considerable variation was met with. With regard to the two former points, personal idiosyncrasy, and degree of or peculiarity in the nature of the injury, are the only explanations I can suggest. Perhaps in some instances exposure to wet or cold in the early stages of the injury was of some import. Thus, I saw several severe cases of musculo-spiral neuritis in men who were wounded during the trying and wet march on Bloemfontein. I did not observe that suppuration or wound complications seemed important explanatory moments, as most of the cases occurred in wounds that healed rapidly.
With regard to the question of selection; the same nerves that appear particularly liable to suffer from idiopathic inflammations, toxic influences, or to be the seat of ascending[Pg 350] changes (e.g. ulnar, musculo-spiral, and external popliteal), were those most often affected by secondary neuritis. Many of the most severe cases I saw were in the musculo-spiral nerve.
Scar implication.—The signs of this most commonly commenced with neuralgia, or painful sensations when such movements were made as to put the cicatrix on the stretch. Although such neuralgia might not be constant, it was often observed to be troublesome when the patients were exposed to cold in sleeping out at night, or to extra fatigue, as in long marches. The results in many cases stopped at this point, but the size and wide distribution of certain nerves rendered even such slight symptoms of importance; while in others well-marked signs of neuritis declared themselves, such as glossy skin, pain, muscular wasting, and paralysis.
Ascending neuritis.—In a few cases I observed very remarkable instances of ascending neuritis, after comparatively slight wounds. I will quote three of these as illustrations and make no further remarks as to the symptoms. It will be observed that one is a case of ulnar, both the others of external popliteal, neuritis:—
(108) Ulnar nerve: secondary ascending neuritis.—Boer wounded at Elandslaagte. Wound of hand, implicating anterior two-thirds of third metacarpal bone. This bone, together with the middle finger, was removed, and healing took place by granulation slowly.
The resulting gap allowed considerable overlapping of the fingers, and shortening of the corresponding digit; the index finger also became flexed as a result of destruction of the extensor tendons. Three months later the man was still in hospital in consequence of the tardiness with which the wound had healed: at this time pain was noted, which became very severe in the whole course of the ulnar nerve; superficial hyperæsthesia and deep muscular tenderness developed, but no wasting. Several crops of herpetic vesicles also developed over the distribution of the radial nerve in the hand. This pain was followed by spastic contracture, first of the ulnar fingers and later of the wrist and elbow, which could only be straightened by the application of considerable force. The limb was, therefore, kept straight by the application of a splint; and warm baths, and a blister applied over the course of the ulnar nerve, were resorted to: under this[Pg 351] treatment the condition improved until the patient was well enough to be transferred as a prisoner, and I saw him no more.
(109) Peroneal nerve branches.—Wounded at Colenso. Entry, at the anterior margin of the fibula 5 inches above the external malleolus; the track crossed the anterior aspect of the leg obliquely, to its exit 1 inch above the centre of the ankle joint. Incomplete paralysis of the peronei muscles followed, combined with progressive wasting of the whole limb, which at the end of a month was marked, and then commenced to improve.
(110) In a second case the wound took a similar course in the centre of the leg, crossing the line of the branches of the musculo-cutaneous nerve. Motor paralysis of the peronei followed, together with general lowering of tactile sensation in the musculo-cutaneous area.
Traumatic neurosis.—In connection with the cases just quoted, mention must be made of the fact that the functional element was often somewhat prominent. The influence of this factor was not to be neglected in case 108; again, its presence was a feature in cases 132 and 134, of injury to the sciatic nerve and of peripheral injury to the seventh nerve (p. 355). A remark has been made as to the occurrence of functional paraplegia on p. 337. Again, in the case of the organs of special sense. Case 66, of injury to the occipital lobes, showed that a mixture of organic and functional phenomena might be a source of error, even in the determination of the visual field in the subject of an undoubted destructive lesion. On more than one occasion an injury was accompanied by loss of the power of speech; thus a patient who received a slight wound of the neck did not speak again until the application of a battery by my colleague, Mr. H. B. Robinson. A patient was also for a short time an inmate of No. 1 General Hospital, Wynberg, who had become deaf and dumb as a result of the explosion of a shrapnel shell over his head. This patient also did not recover his powers until he returned to the mother-country.
In many other cases of nerve concussion or contusion, the recovery of power and sensation, or the disappearance of neuralgia or contractures, was so sudden and rapid after prolonged continuance of the symptoms, as to suggest a very[Pg 352] strong functional element in their origin. The influence of the general shock to the nervous system received by the patients had an important bearing on these phenomena, and their interest from a prognostic point of view was very great.
Cranial nerves.—It will be convenient first to make a few remarks concerning the nerves of special sense.
Olfactory.—I observed temporary loss of smell on three occasions. In two instances this accompanied transverse wounds of the bones of the face in which the upper third of the nasal cavities was crossed; in the third a track passing obliquely downwards from the frontal region passed through the inner wall of the orbit, and crossed the nose at a lower level. In view of the small area of the olfactory distribution which was directly implicated, I was at first inclined to regard the loss of smell as dependent on the presence of dried blood on the surface of the mucous membrane, or on obstruction of the cavities from the same cause. Further observation, however, appeared to show that it was due to concussion of the branches of the olfactory nerve, since the loss of function persisted when the cavities were manifestly clear.
In all these cases we were confronted with the same difficulty which was experienced both in lesions of sight and hearing, the determination as to whether the concussion was of the branches or of the olfactory bulb. When the symptom was the accompaniment of a fracture of the roof of the orbit, the possibility of concussion of the olfactory lobe was manifest. In all, again, it was difficult to say what part the accompanying concussion of the branches of the fifth nerve took in the production of the symptom. In all three cases mentioned the return of function was gradual, but apparently fairly complete at the end of three weeks. In one it was noted that at first the patient was conscious of an odour before he was able to discriminate its actual nature; later he could determine the latter readily.
Optic.—Some remarks concerning lesions of the optic nerve have already been made under the heading of wounds of the orbit. Concussion and contusion of the nerve both[Pg 353] occurred, but I was unable to differentiate between the effects of these on the nerve itself, apart from the effects on the globe of the eye, which usually accompanied wounds of the orbit.
In some cases the nerve was directly divided in orbital wounds, and either pressure on or division of the nerve in the intra-cranial portion of its course, or as it traversed the optic foramen, was not uncommon.
Auditory.—Loss of hearing was also not infrequent; thus it accompanied all three wounds of the mastoid process quoted under the heading of the seventh nerve, also two cases of fracture of the occipital bone near the ear quoted on p. 278. In all these instances it was impossible to attribute the deafness to lesion of the nerve alone, as the causative injury equally affected the internal ear, and in at least two the bullet implicated the tympanum as well in its course. The deafness was absolute in each case, and in none had any improvement occurred at the end of nine months. Deafness was a symptom in a certain number of the more severe cerebral injuries in which the course of the bullet was not so near to the internal ear: probably some of these were central in origin.
I only once observed any interference with the sense of taste.
Remaining cranial nerves.—I have little to say regarding the third, fourth, and sixth nerves. In the case of the third nerve, ptosis was occasionally seen in wounds of the skull involving the roof of the orbit, but the relative parts taken by injury to nerve and laceration or fixation of muscle respectively, were usually hard to determine. Again, the fourth and sixth nerves may have been damaged in some of the more extensive orbital wounds, especially those in which the globe suffered injury, but the signs under such circumstances were difficult to discriminate, and the injury was of slight practical importance, in view of the major injury to the globe itself.
Fifth nerve.—Concussion, contusion, or laceration of the different branches of the three divisions of the fifth nerve were common in wounds of the head, but most frequent in fractures of the upper or lower jaws. Localised anæsthesia[Pg 354] was common from one or other of these causes, but for the most part transitory in the cases of contusion or concussion. I saw no case of entire loss of function in any one division, symptoms being mostly confined to certain branches, as the supra-orbital, the temporo-malar, the dental branches of the second division, the auriculo-temporal nerve, and the lingual, dental, and mental branches of the third division. I did not observe any cases in which modification of the special senses accompanied these injuries beyond those mentioned in the remarks already made on the subject of anosmia, and one case in which some modification of the sense of taste accompanied an injury to the floor of the mouth. It was a matter of surprise, considering the frequency with which subsequent neuritis was met with in the nerves generally, that trifacial neuralgia in some form was not more often met with. I never observed any serious case. Perhaps this is one of the fields in which a longer after-period may increase our knowledge. Lastly, I never observed motor paralysis in the case of the third division, although sensory symptoms in some of the branches were common, evident proof that injuries to the trunk were rare.
Seventh nerve.—Facial paralysis was most commonly observed in cases of wound of the mastoid process, apart from central cortical facial paralyses, of which several are quoted in the chapter on injuries of the head. All the wounds of the mastoid process were, in addition, accompanied by absolute deafness. I am sorry to be unable to give any details as to the electrical condition of the muscles in these cases, but I believe that in the great majority the paralysis was mainly the result of nerve concussion, since the perforations were clean in character and not obviously accompanied by comminution. Pressure from hæmorrhage into the Fallopian canal may, of course, have been present, and in some instances, particularly those in which the bullet traversed the tympanic cavity, spicules of bone may have caused laceration. In every case, however, all the branches were equally affected; the paralysis was absolute, and in none did any improvement occur while the cases were under my observation.[Pg 355]
The following are a few illustrative examples:—
(111) Boer wounded at Belmont. Entry, immediately above zygoma; the bullet passed through the temporal fossa, fractured the neck of the mandible, traversed the mastoid process, and emerged at the lower margin of the hairy scalp, 1 inch from the median line. Facial paralysis was complete, and there was no improvement at the end of ten weeks.
(112) Wounded at Magersfontein. Entry, at the posterior border of the left mastoid process, 1/2 an inch above the tip; exit, through the right upper lip at the junction of the middle and outer thirds. There was considerable hæmorrhage from the left ear. The injury was followed by complete deafness, and facial paralysis, which showed no sign of improvement.
There was complete anæsthesia over the area of distribution of the third division of the fifth nerve; this improved rapidly, and at the end of five weeks was hardly to be detected; neither at that time could any impairment of power on the part of the muscles of mastication be detected. No impairment of the sense of taste was noted.
(113) Entry, above the anterior extremity of the zygoma, bullet retained. Primary hæmorrhage from ear. Complete facial paralysis and deafness. Anæsthesia over distribution of temporal branch of temporo-malar nerve, part of supra-orbital area, auriculo-temporal nerve, and small occipital cervical nerve. The muscles of mastication acted well. Ecchymosis below the right mastoid process.
(114) Wounded at Paardeberg. 300 yards. Entry, at the posterior border of the right mastoid process, 3/4 of an inch above the tip; exit, the inner third of the left upper eyelid. (Eye destroyed.) Complete right facial paralysis; deaf, on right side cannot hear tick of watch either held close or in contact. Purulent otitis media.
In this place I might mention two other cases of lesion of the seventh nerve secondary to wound of peripheral branches. In one a patient was struck by several fragments of lead from a bullet which broke up against a neighbouring stone. These for the most part lodged in the skin over the left orbicularis muscle, but one also lodged in the conjunctiva and was removed. Some ten days later the patient complained that he could not lift the upper lid. The levator palpebræ was normal, but spasm of the orbicularis held the[Pg 356] eye firmly closed. The condition did not improve, and the patient was invalided home. He recovered later.
In another patient a bullet entered above the right zygoma and traversed the orbits, without wounding the globes. At the time no want of power of the muscles of the face was noted, but a year later there was evident weakness of the whole of the muscles of the right side of the face, with loss of symmetry.
In the former case the functional element was strong, but in both an ascending neuritis was probably present.
Tenth nerve.—The pneumogastric was implicated in many wounds of the neck. I never observed an uncomplicated case, but laryngeal paralysis was temporarily present in two of the cases of cervical aneurism in which the wound crossed above the level of origin of the recurrent laryngeal branch, while in two others the recurrent branch itself was in close contact with the wall of the aneurism (p. 135). In all such cases signs of concussion or contusion of the nerve would be expected, judging from the similar results observed in the brachial nerves when the neighbouring artery was implicated. The only obvious symptoms occurring, however, were laryngeal paralysis and acceleration of the pulse. As the latter symptom was often observed in the cases of arterio-venous communication, wherever situated, and as the sympathetic nerve also lay in close contiguity to the wound track, it was difficult to ascribe it with certainty solely to the vagus lesion. In the two cases of high vagus injury the laryngeal paralysis steadily improved, and at the end of six months was apparently well; in the two others it persisted at the end of three months and a year respectively.
The nerve must have been very frequently damaged in wounds of the neck; it is possible that this injury may have been an important factor in the death of some of the patients with cervical wounds upon the field.
Eleventh nerve.—I append the only case of localised spinal accessory paralysis I observed. This was one of my earliest experiences, and when I examined the neck, in the Field hospital, I assumed from the completeness of the sterno-mastoid and trapezius paralysis that the nerve was severed.[Pg 357] The patient, however, made such a rapid recovery that it became evident that the nerve had been contused only, and that the recovery of function was not due, as is so often the case, to vicarious compensation by the cervical supply to the muscles.
(115) Entry, immediately to the right of the fourth cervical spinous process; exit, at the anterior border of the left sterno-mastoid opposite the angle of the mandible. The left shoulder was depressed, the head inclined to the injured side. There was evident spinal accessory paralysis, and marked hyperæsthesia of the whole left upper extremity, most severe in the circumflex area. The hyperæsthesia gradually disappeared in a few days, and was clearly due to concussion and possibly slight contusion of the cervical nerve roots. The spinal accessory paralysis improved, so that the patient returned to the front at the end of a month: when I saw him some four months later the shoulders were held quite symmetrically.
The twelfth nerve was occasionally damaged in wounds of the floor of the mouth. I saw no case of permanent paralysis.
Injury to the systemic nerves. Cervical plexus.—Evidence of injury to the superficial branches of the cervical plexus was not rare; thus I saw cases of small occipital anæsthesia, and great occipital neuralgia, but none of motor paralysis from injury to the deeper muscular branches. I take it that the smallness of the branches, and the multiple supply possessed by many of the muscles of the neck, would both take part in rendering certain evidence of the injury of an individual motor nerve rare.
Brachial plexus.—Injury to this plexus in the neck was common; the main peculiarity observed was the partial nature of the damage inflicted.
Thus injury to a single nerve, or to a complex of two or more, was far more common than one implicating the whole plexus. Again, while complete paralysis might affect one set of nerves, another might simply exhibit signs of irritation in the form of hyperæsthesia or pain.
The wounds producing these injuries varied much in[Pg 358] direction; thus some crossed the neck transversely, some were obliquely transverse, while others took a more or less vertical course.
These same remarks hold good in the case of the nerves of the arm. In the upper half, especially, complex injury was not rare, while in the lower third affection of individual nerves was more common. Another important difference must be mentioned in regard to the upper and lower segments of the course of the brachial nerves; they are not only more widely distributed below, but also more fixed in position, a fact antagonistic to the escape of the nerve by displacement and liable to expose it to more severe contusion.
The latter point holds good in the forearm also; here, individual injuries often occurred.
While at work in the Field hospital alone I gained the impression that the musculo-spiral nerve would not retain the unenviable character of being the most vulnerable nerve of the upper extremity, since the chances of each individual nerve seemed about equal, putting the question of the long course of the musculo-spiral nerve against the humerus out of question. This expectation was, however, not confirmed, since the musculo-spiral itself, if not primarily affected, was so often the seat of secondary mischief in fractures of the humerus. The posterior interosseous branch seemed to exhibit a similar vulnerability to slight injuries, to be referred to later under the external popliteal of the lower extremity. Again, in complex injuries of the brachial plexus, or nerve trunks, the musculo-spiral branch rarely escaped being a member, if not individually singled out.
Of the thoracic nerves I have little to say. They must have been often injured in the thoracic wounds, yet, as far as my experience went, intercostal neuralgia was uncommon, or at any rate not a special feature. One observation of interest, however, does exist; in the cases in which the ribs were fractured by bullets travelling across them within the thorax, pain was distinctly a prominent feature. This was no doubt referable to the facts that in such instances the intercostal nerves were especially liable to direct injury, and that this was often multiple. On one occasion a crop of herpetic[Pg 359] vesicles developed along the course of a dorsal nerve in an injury implicating a single intercostal space posteriorly.
Lumbar plexus.—Although not quite so well arranged to escape bullet wounds as the thoracic nerves, the lumbar, by reason of their deep position and the comparatively wide area they cover, together with the rarity of wounds taking a sufficiently longitudinal direction to cross the course of more than one or two branches, were also comparatively rarely damaged. I never saw an uncomplicated case of anterior crural paralysis, and rarely cruralgia. I think this is to be explained in two ways: first, that the trunk course of the nerve is short; secondly, that it lies in the inguinal fossa. The second fact is of importance, since wounds in this region were in my experience responsible for a considerable percentage of the deaths on the field or shortly afterwards. Such deaths probably occurred from internal hæmorrhage from the iliac arteries, and it was in such cases that the anterior crural nerve stood in greatest danger of injury. I also never saw a case of localised obturator paralysis. On the other hand, anæsthesia or hyperæsthesia in the area of distribution of the lumbar nerves in the groin, the external cutaneous and the long saphenous in the thigh, were not uncommon. Hyperæsthesia developed in more than one case in which injury to the psoas had led to hæmorrhage into the muscle sheath.
Sacral plexus.—The sacral plexus is far more liable to extensive direct injury than either of the two preceding. Its cords are larger, gathered up into a much smaller space, and more liable to injury, from the fact that the slope in which they lie is more readily followed by a bullet track. Again, the cords rest for a considerable portion of their course on a bony bed, a particularly dangerous position in gunshot wounds, since the nerves are not only exposed to the danger of direct wound, or pressure from bony spicules, but also readily receive transmitted vibrations secondary to impact of the bullet with the bone.
None the less I had few occasions to observe extensive injuries of the plexus. In one instance damage particularly affecting the lumbo-sacral cord occurred, but this was complicated by signs of irritation of the anterior crural[Pg 360] and obturator nerves, as the result of retro-peritoneal hæmorrhage and injury to the psoas muscle. Two cases in which the sacro-coccygeal plexus suffered isolated injury on account of their characteristic nature as gunshot injuries will be shortly quoted:
(116) Sacro-coccygeal plexus.—Entry, at the junction of the middle and posterior thirds of the left iliac crest; the bullet passed obliquely downwards through the pelvis to lodge 3 inches below the right trochanter major. Incontinence of soft fæces persisted for five weeks, and retention of urine during three weeks.
This patient subsequently died on the homeward voyage, but I am unable to say from what cause.
(117) Entry, over third sacral vertebra; exit, 2 inches from the median line, and 1½ inch above Poupart's ligament on the anterior abdominal wall. Incontinence, with involuntary passage of fæces, persisted during the first twenty-four hours, and for two days the urine had to be withdrawn with a catheter. No further signs of nerve injury were noted.
The same explanation of the comparative rarity of injuries to the sacral plexus that has been already given in the case of the anterior crural nerve holds good—viz. that in a great many of the pelvic wounds involving the plexus early death followed from the severity of the concurrent injuries.
Injuries to the great sciatic nerve outside the pelvis, or to one of its constituent elements, on the other hand, formed one of the most familiar of the nerve lesions. The wounds giving rise to these were of the most diverse character; some crossed the buttock in a vertical, transverse, or oblique direction; others travelled through the thigh in corresponding directions, while a third series involved both buttock and thigh.
The size of the great sciatic nerve renders complete laceration by a bullet of small calibre a matter almost of impossibility; hence complete division may almost be left out of consideration in the case of this nerve. On the other hand, partial division, perforation, and severe contusion are each and all favoured by the same factor.
With an extended thigh the nerve is in a state of comparatively slight tension, and this may be still lessened if the[Pg 361] knee be flexed. This factor, together with the density of the sheath of the nerve, favours the possibility of displacement, and this occurrence is more likely in the lower segment than in the upper, which is comparatively fixed in position.
Clinical experience appeared to illustrate the importance of these anatomical factors, as the worst cases of sciatic injury that I saw were in connection with wounds of the buttock or the junction of that segment of the trunk with the thigh.
The most striking observation with regard to the injuries of the great sciatic nerve was the comparatively frequent escape of the popliteal element and the severe lesion of the peroneal. This was so pronounced as to amount to as high a proportion of peroneal symptoms as 90 per cent., and often when the whole nerve was implicated the popliteal signs were of the irritative, the peroneal of the paralytic type. When bullets crossed the popliteal space, given wounds of equal severity in corresponding degrees of contiguity to the respective nerves, the peroneal element always suffered in greater degree. Again, the peroneal nerve symptoms were more obstinate and prolonged, and instances of ascending neuritis were more common than in the case of any other nerve of the lower extremity, and the trophic wasting of muscles was more marked.
The peroneal nerve, therefore, acquires the same unenviable degree of importance in the lower extremity enjoyed by the musculo-spiral in the upper. Here, again, we are confronted with the fact that the peroneal element of the great sciatic nerve is the more prone to idiopathic inflammations or toxic influences, and hence we can only assume it to possess a special vulnerability. The peroneal element is of course somewhat the more exposed, as lying posterior; but it seems unreasonable to assume that so large a proportion of the injuries can implicate the posterior segment of the nerve as to make the startling difference in the incidence of degeneration explicable. In this relation we may bear in mind that the muscles supplied by this nerve suffer most in the degeneration subsequent to anterior polio-myelitis, and again that in cerebral hemiplegia or spinal-cord injuries they are the last to recover. Unfortunately no explanation of these[Pg 362] remarkable facts, so forcibly impressed by the large series of cases with peroneal symptoms seen in a short time, is forthcoming.
I may dismiss the other branches of the sacral plexus in a few words. The small sciatic was occasionally injured in its course in the buttock, and the small saphenous in the leg. When either element of the latter was injured, it was surprising how sharply the imperfections in the anæsthesia corresponded with the composite character of the nerve.
The following cases are added mainly to give some idea of the comparative frequency with which the individual nerves were injured, and also to exemplify the more common forms of complex injury met with. Circumstances, unfortunately, did not always allow of extended observation at the time, and I have not been very fortunate in my attempts to obtain subsequent information on this series since my return. A certain amount of prognostic information is, however, furnished by some of the records, and I am very much indebted to my colleague, Dr. Turney, for help in this matter.
(118) Brachial plexus.—Entry, 2 inches above the clavicle at the anterior margin of the trapezius; exit, first intercostal space, 1 inch from the sternal margin. Heavy dull pain developed at once, extending down the upper extremity. A fortnight later this pain still persisted; there was lowered sensation in the ulnar area with formication, also lowered sensation in the internal cutaneous area of distribution; sensation in the lesser internal cutaneous area was normal. The patient went home with the nerve symptoms well at the end of a month.
(119) Brachial plexus injury.—Wounded at Magersfontein. Entry, at the anterior border of the sterno-mastoid opposite the pomum Adami; exit, through the ninth rib below and 1/2 an inch external to the scapular angle. Emphysema and considerable blood extravasation developed in the posterior triangle of the neck, also loss of power in the musculo-spiral distribution, but no anæsthesia. At the end of the first fortnight there was evident wasting of the muscles, but some power was returning in the triceps. At the end of a month the man left for England, with[Pg 363] fair power in the triceps, but well-marked wrist-drop. A year later the wrist-drop still persisted.
(120) Plexus injury.—Wound of entry, over pomum Adami; exit, below scapular spine, about centre. Complete median and musculo-spiral paralysis.
(121) Median, musculo-cutaneous, and musculo-spiral nerves.—The wound traversed the axilla from just beneath the anterior fold; three weeks later a firm mass in the axilla corresponded to the wound track. Hyperæsthesia developed in the area of median distribution, with deep pain in the muscles. There was rigidity of the biceps cubiti and slight wasting in the radial extensors. The patient improved slowly, and eventually was discharged and passed out of sight.
(122) Brachial nerves.—Wounded at Paardeberg. Range 500 yards. Entry, at the front of the arm, 2 inches below the junction of the anterior axillary fold; exit, a little lower, at the back of the arm, in the line of junction of the posterior axillary fold.
Considerable shock attended the primary injury; when reaction had taken place, complete motor and sensory paralysis was noted of the whole upper extremity, with the exception of some power of movement of the posterior interosseous group of muscles. Three weeks later the patient could extend the wrist, but sensation was imperfect in the arm, and completely absent in the forearm and hand. The track was now hard and palpable, but there was no hyperæsthesia in any area; when the track was manipulated slight formication in the hand was experienced. The biceps and triceps were equally paralysed. There was no wasting in any of the muscles.
(123) Brachial nerves.—Wounded at Modder River. Entry, through the anterior axillary fold at its junction with the arm; exit, on the posterior wall of the thorax, 1/2 an inch from the median line at a level with the angle of the scapula. Complete musculo-spiral paralysis; hæmothorax. Three weeks later, radial sensation returned; but the triceps was very weak, and wrist-drop was complete. There was some wasting of the muscles supplied by the median and ulnar nerves, and complete obliteration of the radial pulse. A year later the musculo-spiral paralysis still persisted.
(124) Musculo-spiral and median.—Wounded at Magersfontein. Entry, 3 inches below the anterior axillary fold, on the inner aspect of the arm; track passed obliquely downwards behind the humerus to a point on the outer aspect of the arm 1½ inch[Pg 364] below the level of the entry. The humerus escaped injury. Musculo-spiral paralysis was complete; hyperæsthesia in the distribution of the median followed some days later. One month subsequently radial sensation had returned, and a feeling of numbness had taken the place of the median hyperæsthesia. The triceps and marginal muscles were much wasted, and only interosseous extension was possible in the fingers.
(125) Brachial nerves.—Wounded at Magersfontein. Entry and exit, in the upper third of the arm internal to the humerus. Complete median paralysis, anæsthesia in the ulnar area, and in the radial supply to the dorsum of the middle and ring fingers. Could flex, extend, and adduct and abduct the wrist; some power of flexion in index finger, in others none. The flexion of the wrist was dependent on the ulnar supply to the muscles of the forearm. No wasting of the interossei, skin normal except for a large trophic blister on the dorsum of the hand. Little improvement had taken place in this patient at the end of a year.
(126) Brachial nerves.—Wounded at Magersfontein. The wound traversed the lower part of the upper third of the arm, fracturing the humerus. Immediate complete loss of power in the arm was experienced, together with loss of all sensation. Three weeks later the humerus was united; the fracture was evidently the result of passing contact, and not of direct impact. The paralysis was still complete in the distribution of the median, ulnar, and musculo-spiral nerves. There was considerable wasting of the hand and forearm, and a good deal of thickening in the lower third of the arm.
Four months after the original injury, the nerves were explored by Mr. Eve, who kindly gives me the following information. All the nerves and vessels of the arm were united into one firm bundle by cicatricial tissue. When dissected clear, the median nerve was found to be thickened and enlarged for about 1½ inch of its length; the ulnar was not completely freed, but was found to be continuous and indurated; the musculo-spiral was also intact, but at its entrance into the humeral groove a mass of callus was felt. A sclerosed and thickened portion of the median nerve 3½ inches in length was resected, also 1 inch of sclerosed ulnar nerve, and both were sutured. The musculo-spiral nerve was left for future exploration. A small traumatic aneurism was found on the brachial artery, and the vessel was ligatured above it.
Ten months later no improvement in the median or ulnar nerves. Electrical reaction present in musculo-spiral group of muscles.[Pg 365]
(127) Musculo-spiral.—Transverse wound through arm posterior to humerus. Slight suppuration. Triceps weakened only, complete paralysis of radial extensors and posterior interosseous group. Radial sensation lowered only.
(128) Musculo-spiral.—Entry, 2 inches above and 1/2 an inch behind the external humeral condyle; exit, at the inner edge of the biceps, 1/2 an inch lower in the arm than the entry. It is doubtful whether the paralysis was noted at first, but a few days later complete posterior interosseous paralysis and lowered radial sensation were remarked. No change except a deepening of the anæsthesia, and the development of formication on manipulation of the wound occurred, and at the end of three weeks the nerve was exposed (Mr. Watson), and it was found that a notch had been cut in its outer border, which had opened out into a V shape. The margins of this notch were refreshed and the gap closed. Ten days later radial sensation was fairly good, but the motor symptoms remained unchanged. Nine months later steady but very slow improvement was reported.
(129) Ulnar and musculo-cutaneous nerves.—Entry, back of forearm; the bullet passed between the bones and was retained at the posterior aspect of the arm. Three weeks later the hand was glossy and stiff, the fingers extended and adducted, the thumb was held stiffly in the palm with no power of extension. The forearm was held semiprone, and the elbow flexed by a rigid biceps. Six months later the same position was maintained, but the contracture disappeared under an anæsthetic.
(130) Median and posterior interosseous.—Entry, over the external margin of the radius at the centre of the forearm; exit, at the inner margin of the olecranon 1½ inch below the tip. Lowered cutaneous sensation in median distribution, and loss of median flexion of wrist and fingers. Complete wrist-drop. The triceps supinator longus and extensor carpi radialis longior were perfect. Twelve days later the wrist could be raised into a direct line with forearm, but there was no change in the median symptoms. A week after this the anæsthetic median area became hyperæsthetic both as to skin and on deep pressure over the muscles.
(131) Sacral plexus. Great sciatic nerve.—Wounded at Modder River. Entry, in left loin; exit, at lower margin of buttock. The wound was followed immediately by complete peroneal paralysis, both motor and sensory. Fourteen days later hyperæsthesia developed in the area of distribution of the internal popliteal nerve, the superficial pain being greatest in the sole; the muscles of the[Pg 366] calf were also very tender on manipulation. The pain increased, and at the end of twenty-four days the patient's sufferings were so great that Mr. Thornton cut down upon and exposed the nerve. It was found embedded in firm cicatricial tissue close to the sciatic notch; this compressed the nerve to such a degree that a waist was apparent upon it.
The nerve was freed and resumed its normal outline. For a few days the patient was much relieved, but the neuralgia then returned in greater intensity than ever. Morphia was injected hypodermically, and other hypnotics employed, but with little effect, the patient developing the hysterical condition so common in the subjects of severe sciatica. Some five weeks later a sudden improvement took place, the morphia was decreased, and the patient became sufficiently well to return to England, but there was still deep tenderness in the calf, and well-marked hyperæsthesia of the sole.
A year later the patient had been discharged from the Service, but was earning his living in a shop. He walked fairly well, but still with foot-drop, and complained of tenderness in the sole. I am indebted to Dr. Turney for the following report on the condition of the muscles.
Calf muscles practically normal. In the anterior tibial and peroneal groups the faradic irritability is much diminished, that in the peroneus longus being the lowest of all. Contraction can be induced in the extensor longus hallucis, extensor longus digitorum, and peroneus brevis; but reaction is doubtful in the case of the tibialis anticus and peroneus longus.
With the galvanic current contraction is sluggish, and the irritability diminished. No serious changes are present except in the peroneus longus. ACC > KCC at 10 m. a.
(132) Great sciatic.—Entry, at outer aspect of the thigh, just above the centre; exit, at the junction of the inner and posterior aspects of thigh, about 2 inches lower. The wound was produced by a ricochet bullet, and beyond the perforation of the sciatic nerve the femur was fractured obliquely (see plate XVI.). Hyperæsthesia of the sole was noted early, and when I saw the patient three months later, there was wasting of the muscles of the leg, and foot-drop, although he walked with a stick.
These symptoms persisted, and on his return to England an exploration was made by Sir Thomas Smith, and the two fragments of mantle seen in the skiagram were removed from the substance of the sciatic nerve. Eight months after the injury, the[Pg 367] patient still walked with foot-drop; there was modified sensation in the musculo-cutaneous area, and a feeling as if the bones of the foot were uncovered when he walked. The circumference of the affected leg was more than 1 inch less than that of the sound one. Steady but slow improvement was taking place.
(133) Great sciatic.—In a third patient with a buttock track, the symptoms were identical with those observed in case 131. In this an exploration showed that the nerve had been perforated. Although the symptoms were never so severe as in No. 131, yet recovery was very much slower and less complete, the muscular weakness remained more marked, and the skin exhibited more evidence of trophic lesion. Some contracture of the knee and rigid foot-drop took place, and at the end of twelve months the patient walked poorly with a stick. Improvement is, however, continuing.
(134) Great sciatic.—Wounded at Ladysmith. Entry, immediately below left buttock fold; exit, at anterior aspect of thigh, 3½ inches below Poupart's ligament. The left leg was paralysed, and patient was sent down to the Base, where he remained two months. The wound closed by primary union, the paralysis improved, and the man rejoined his regiment. After he had been in camp four days, his leg gave way, and he returned to hospital, where he contracted enteric fever. Later, he was sent home, and eight months after the reception of the injury his condition was as follows:
Left lower limb somewhat wasted, a diminution of 1 inch in the circumference of the leg and 1/2 an inch in the thigh being found. The patient walks with foot-drop, and the flexor muscles of the knee are weak. On examination the peroneal muscles reacted but sluggishly to faradic irritation. There is complete anæsthesia of the foot to above the ankle, and up to the knee tactile sensation and appreciation of pain were dulled. The left plantar reflex was absent, the right slight, the left patellar reflex was abnormally brisk. There was neither ankle nor patellar clonus, and the other reflexes were present and normal. The gait was spastic, and the patient was more troubled by a contraction of the calf muscles, which prevented his putting the heel to the ground, than by the foot-drop.
Beyond these local phenomena there was marked tremor of the upper extremities on any exertion, and slight lateral nystagmus. The patient was not sure that this had not been present ever since he recovered from the enteric fever, but it was sufficiently marked to give rise to the suspicion of the development of disseminated sclerosis.[Pg 368]
The patient was a hard-headed, sensible man. He remained in the hospital under the care of Dr. Turney, to whom I am indebted for notes of the case, forty-six days. During this period he was treated by faradic electricity, and, with some checks, notably the development of passive effusion into the left knee-joint, and a fugitive attack of redness over the dorsum of the foot, both suggesting trophic changes, steadily improved. The anæsthesia became limited to the outer half of the leg, at the end of one month was limited to the dorsum of the foot only, and at the end of six weeks entirely disappeared. Meanwhile the tendency to drawing up of the heel by the calf muscles became less, and the gait improved. The man left the hospital at the end of two months, very satisfied with his condition, although the tremor of the hands was still present in a lessened degree.
(135) External popliteal.—Wounded at Magersfontein, 250-300 yards. Entry, at the outer side of the thigh, 5 inches above the lower extremity of the external condyle; exit, at the inner margin of the adductors, at a level 4 inches higher in the thigh. The track crossed behind the femur. Complete peroneal motor paralysis and anæsthesia, except in the hinder part of the region supplied by the mixed external saphenous. Slight hyperæsthesia of the sole. Improving at the end of three weeks, but paralysis still nearly complete.
(136) External popliteal.—Wounded at Magersfontein. Entry, 5 inches below the highest part of the right iliac crest, on outer aspect of hip; exit, at the posterior margin of the gracilis, 2 inches from the perineum. Complete peroneal paralysis followed, which rapidly improved, and on the twenty-second day was nearly well.
(137) Internal popliteal. Secondary anæsthesia.—Shell wounds of the right popliteal space. Wounded at Belmont. Anæsthesia of the outer side of the calf, the leg and sole of foot. No motor paralysis. As cicatrisation progressed, the anæsthesia became more marked and was complete over the whole of the external saphenous area.
(138) Internal popliteal.—Wounded at Paardeberg. 400-500 yards. Entry, about the centre of the outer half of the patella; exit, at the centre of the calf, about 2 inches from the popliteal crease. Five days after the injury severe burning pain developed in the sole. A fortnight later the pain was much less severe, but varied in degree with the heat of the weather, being worse when cool. At this date, however, rubbing became comforting.[Pg 369]
(139) External popliteal.—-Wounded at Magersfontein. Entry, 1 inch above the upper end of the internal margin of the patella; exit, at the margin of leg, just below the outer tuberosity of the tibia. Complete peroneal paralysis followed the injury. A month later the nerve was bared and found slightly thickened. An improvement in cutaneous sensation followed quickly, and a much slower improvement in the motor power commenced.
(140) External popliteal nerve.—Wounded at Beacon Hill. A bayonet entered over upper quarter of fibula, and passed between the bones of leg into the calf. An aneurismal varix of the calf vessels developed, also incomplete peroneal paralysis. The scar was raised from the nerve (Major Simpson, R.A.M.C.) six weeks later, and at the end of a fortnight the power and sensation were both much improved and the patient returned to England.
(141) External popliteal.—Wounded at Modder River. Entry, 1/2 an inch above the internal border of the patella; exit, 1½ inch from the head of the fibula and over that bone. The wound was followed by peroneal paralysis. Six weeks later sensation was still diminished in the anterior tibial and musculo-cutaneous nerve areas, and marked foot-drop, little improved, persisted. The patient came to England, and at the end of twelve months is reported as very little improved.
(142) Anterior tibial.—Entry, 1 inch in front and below the external malleolus; exit, at the centre of the sole, just anterior to the bases of the metatarsal bones. Wasting and paralysis of extensor brevis digitorum.
(143) Small sciatic and small saphenous.—Wounded at Magersfontein. 200 yards. Two wounds: (i) Entry, below the centre of the twelfth rib on the left side; exit, immediately to the left of the buttock furrow at upper part, (ii) Entry, in the right loin, midway between the last rib and iliac crest; exit, just within the centre of the left buttock; the two wounds crossed diagonally. Hyperæsthesia in area of distribution of small saphenous and small sciatic nerves, which rapidly improved.
(144) Lumbar plexus.—Boer, wounded at Magersfontein. Entry, eleventh interspace, posterior axillary line; exit, tenth interspace, right mid-axillary line. Impaired sensation in area of distribution of external cutaneous and crural branch of genito-crural nerves. At the end of a fortnight anæsthesia was less apparent, but a feeling of numbness persisted, which soon disappeared.
Prognosis and treatment.—In considering the prognosis in cases of nerve injury, several of the points already raised as[Pg 370] to the nature of the lesion are of importance. Short of actual section, it may be broadly stated that no lesion is too serious to render ultimate recovery impossible.
In cases in which the injury has been produced by a bullet fired at a short range, or in which contact with the nerve has been close, the return of functional activity is very slow. In such instances the condition probably resembles that in which a divided nerve has been sutured, with the additional disadvantage that a considerable portion of the nerve, both above and below the point actually struck, has been destroyed as far as the conduction of nervous impulses is concerned. This may reasonably be concluded in the light of the evidence offered by the injuries of the spinal cord, in which several segments usually suffered if the velocity of the bullet was great, and also if the fact is remembered that, when thickening takes place, a considerable length of the nerve is usually implicated.
Recovery is notably slow in the case of certain nerves, e.g. musculo-spiral and peroneal, even when the injury has not been of extreme severity. Again, these same nerves are apparently more seriously affected by moderate degrees of damage than are others.
As favourable prognostic elements we may bear in mind: low velocity on the part of the travelling bullet, and with this a lesser degree of contiguity of the track to the nerve. The early return of sensation is a favourable sign, and in this relation the development of hyperæsthesia, whether preceded by anæsthesia or no, points to the maintenance of continuity of, and a moderate degree of damage to, the nerve. The early return of sensation, even if modified in acuteness, was always a very hopeful sign; also the production of formication in the area of distribution of the nerve on manipulation of the injured spot. As in the case of nerve injuries of every nature, the disposition and temperament of the patient exerted considerable influence on the course of the cases.
Complete section of the nerves in these bullet wounds only obtained special importance in two ways: first, in that a considerable portion of the trunk might be shot away in oblique tracks, and, secondly, in that very severe contusion[Pg 371] might affect the nerve for a considerable distance beyond the point actually implicated. In point of fact, complete section when treated by suture was often more rapidly recovered from than an injury in which only a portion of the width of a trunk was divided. This was no doubt to be explained on the theory that the contiguous portion of the nerve suffered less when tension and resistance were lessened by complete severance of the cord.
The treatment of slight nerve contusion was simple; rest alone was necessary, and in the course of hours or days paralysis was recovered from. The symptoms were most troublesome in patients of a neurotic temperament, or those who had suffered from severe systemic shock.
In severe concussions and contusions the first care had to be devoted to the discrimination of the lesion from that of division. A period of rest then needed to be followed by one of massage and movement, to maintain the nutrition of the muscles. In a considerable portion of the cases a stage of neuritis had to be expected. In all cases, either of severe concussion, contusion, or complete section, accompanied by the fracture of a bone, especial care was necessary that the bandaging and fixation of the limb were not sufficiently tight to add the dangers of muscular ischæmia to those of the nerve injury already present.
Neuritis, whether dependent on local injury, implication in the scar, pressure from callus, or of the ascending variety, needed the same treatment: rest, preservation of the limb from cold or damp, and the local application of anodynes, as belladonna, or hot laudanum fomentations. In some cases a general anodyne, as morphia, was preferable; then always to be used with caution, as the patients soon craved inordinately for it, and were unwilling to give it up. Later, local blisters in the line of the nerve trunk, careful massage and exercise when muscular and cutaneous tenderness had subsided, the application of the continuous current to the nerves, and perhaps faradisation of the muscles, were all useful.
Splints were often temporarily required to resist contracture, or the assumption of false positions; in either case[Pg 372] they needed to be frequently removed, and movement &c. made, in order to avoid any chance of troublesome stiffness.
Operative treatment.—Early interference was only warranted by positive knowledge that some source of irritation or pressure could be removed; thus a bone spicule, or a bullet, or part of one, particularly portions of mantles.
In case of contusion the expiration of three months is the earliest date at which any operation should be taken into consideration, and interference is only then advisable if there is good prospect of freeing the nerve from compressing adhesions. The two strongest indications for operation are (1) signs pointing to the secondary implication of the nerve in a cicatrix, especially when these are of such a nature as to indicate local tension, fixation, or pressure; (2) the possibility of the irritation being the result of the presence of some foreign body, such as a bone spicule, or portions of a bullet mantle; in such cases the X rays will often give useful help.
With regard to the early exploration of cases of traumatic neuralgia, it may be pointed out that when this was undertaken the results were as a rule very temporary. In many cases in which the measure was resorted to, either no macroscopic evidence of injury to the nerve was discovered, or a bulbous thickening was met with of such extent as to make excision inadvisable, even if it were considered otherwise the most suitable treatment.
Even when complete section of the nerve was assured by the absence of any power of reaction to stimulation by electricity from above on the part of the muscles, operation was better not undertaken until cicatrisation had reached a certain stage. If done earlier than at the end of three weeks, the sutured spot became implicated in a hard cicatrix, and any advantage to be obtained by early interference was lost. When partial division of a trunk was determined, the same date was the most favourable one for exploration, the gap in the nerve being freshened and closed by suture. There is little doubt, however, that in some cases such injuries were recovered from spontaneously.
In view of the uniformly bad results observed in the case of the seventh nerve, I am inclined to think that the above[Pg 373] rules might be tentatively relaxed, and the nerve primarily explored by an operation resembling that for mastoid suppuration. It is of course doubtful whether the trouble does not generally result from the vibratory concussion alone; but as this is not certain, and the operation would only have to be performed on patients already permanently deaf, it might be worth while at any rate opening the Fallopian canal with the object of relieving tension. It is not probable that in any of the cases quoted much splintering of the bone had occurred, as the wounds appeared to be of the nature of pure perforations.
In regard to Prognosis wounds of the chest furnished the most hopeful class of the whole series of trunk or visceral injuries. Cases of wound of the heart and great vessels afforded the only exceptions to an almost universally favourable course, both as regards life and the non-occurrence of serious after-effects.
This was mainly explicable on two grounds: first, the sharply localised character of the lesion produced by the bullet of small calibre; and, secondly, the fact that the lung, the most frequently injured organ, is not materially affected by the grade of velocity with which the bullet strikes. In point of fact, wounds of this organ probably afford an instance in which high grades of velocity are distinctly favourable to the nature of the injury, and this is possibly true in the case of wounds of the chest-wall also.
The significance of the calibre of the bullet in wounds of the chest is evident. The late Mr. Archibald Forbes, in one of his letters from the seat of the Franco-German war, remarked that in crossing a battlefield it was easy to recognise the patients who had suffered a wound of the lung from the fact that the whistle of the air entering and leaving the chest was plainly audible. This was, indeed, not uncommonly the case in wounds produced by the older bullets of large calibre, but with the employment of the smaller projectile it has become an experience of the past. Some evidence as to the comparative severity of wounds produced by the larger forms of bullet was, moreover, afforded by the present campaign, since Martini-Henry wounds were occasionally met with. Of some instances observed by myself, in one, external hæmorrhage was a prominent symptom; in another, a piece of lung[Pg 375] was prolapsed from a wound in the back, and twice I observed pneumothorax, an uncommon sequela to wounds from bullets of small calibre.
It may be remarked, however, that all these more serious injuries were recovered from, also that when we consider that the patients were comparatively young and healthy subjects, the favourable prognosis was what might have reasonably been expected. When, as occasionally happened, a patient of more mature years, with enlarged facial capillaries, received a wound of the lung, the course was in no way so favourable as that witnessed in the case of the younger men.
In support of this opinion I may add that wounds from shrapnel and fragments of shell also did remarkably well, although they sometimes gave rise to more troublesome symptoms than did wounds produced by bullets of the Mauser type. Again, these injuries as a whole were of nothing like so serious a nature as the lacerations of the lung produced by fractured ribs, which we commonly have to treat in civil practice, and are not accustomed to regard as especially dangerous.
It is also a striking fact that the most common and troublesome complication of wounds of the chest, hæmothorax, was usually the result of the wound of the chest-wall and not of the lung. I preface these remarks to the detailed account of the thoracic injuries, because I think the favourable course usually taken by patients with wounds of the lung has been accorded somewhat greater prominence than the circumstances warranted.
Non-penetrating wounds of the chest-wall.—Surface wounds were not very common, and were chiefly of interest in so far as they illustrated the very superficial course that may be occasionally taken by a bullet without breach of the integument, and as sometimes affording opportunity for the exercise of diagnostic skill when the track traversed the axilla.
The most common situation for tracks taking a long course on the surface of the thoracic skeleton was the back. Such wounds were usually received while the patients were prone on the ground; thus I might instance a case in[Pg 376] which the bullet entered the posterior aspect of the shoulder 3 inches above the spine of the scapula, passed downwards, pierced that process, and emerged 2 inches below the inferior angle of the bone. Wounds of a similar nature coursing in transverse and oblique directions, and not implicating bone, were also seen. Those implicating the vertebræ have been already dealt with. The scapular region was also a favourite one for the lodgment of retained bullets, some resting in the supra- and infra-spinatus muscles, others lying beneath the bone itself.
On the anterior aspect of the chest, bullets coming from the front sometimes traversed and fractured the clavicle, and then took a short course downwards, emerging over the ribs or sternum. Figure 81 represents a particularly long track in this region. In other cases the precordial region was crossed, but I never witnessed any serious effect on the heart's action in any such injury at the time the patients came under my notice.
Wounds received with the arm outstretched and traversing the axilla sometimes gave considerable trouble in excluding with certainty a perforation of the thoracic cavity. Thus a bullet entered below the centre of the right clavicle and emerged 2½ inches below, above the angle of the scapula, at its axillary margin. The arm was outstretched at the moment of the reception of the injury; but when the wound was viewed with the limb placed alongside the trunk, it seemed almost impossible that the chest cavity could have escaped. In some cases of this kind the difficulty was at once cleared up by noting evidence of injury to the axillary nerves.
A word will suffice as to the treatment of these wounds. The only special indication was to keep the scapula at rest for a sufficient period. I have dealt with the anatomy of them at such length only because in their extreme form they are so highly characteristic of the nature of the injuries which may be produced by bullets of small calibre.
Penetrating wounds of the chest.—Tracks crossing the thoracic cavity in every direction were common. When the erect attitude was maintained, frontal and sagittal wounds,[Pg 377] pure or oblique, were received; when the prone position was assumed, longitudinal tracks, either purely or obliquely vertical, were the rule. Experience of wounds of the latter class was extensive in the present campaign, from the fact that so many of the advances were made in prone or crawling attitudes. The vertical and transverse tracks each possessed the special characteristic of frequently implicating both the thoracic and abdominal cavities, but the vertical were often prolonged into the neck, or even downwards through the pelvis. The vertical wounds in addition sometimes exhibited one very important feature, the fracture of several ribs from within, often at a very considerable distance from the aperture of either entry or exit.
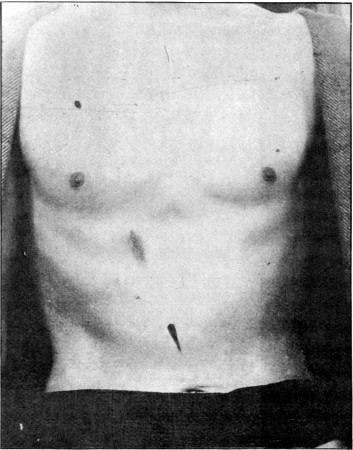 Fig. 81.—Superficial Track in anterior Wall of Trunk
Fig. 81.—Superficial Track in anterior Wall of Trunk
Characters of the apertures of entry and exit.—As has already been mentioned, the chest-wall was one of the situations in which the aperture of entry was often large, and the oval form due to obliquity of impact on the part[Pg 378] of the bullet was particularly well marked. The exit wounds were often smaller than those of entry, especially if the bullet emerged by an intercostal space; even when the ribs were comminuted, the fragments were, as a rule, too small to occasion more than a slightly enlarged and irregular aperture. Taken as a class, however, and putting aside explosive exit wounds, wounds of the chest afforded more numerous examples of irregular outline and variation in size than were met with in any other region of the body.
When the tracks penetrated the broad upper intercostal spaces, an interesting feature, due to the tense and rigid nature of the muscles closing the intervals, and their large admixture of fibrous tissue, was sometimes noticed. The bullet, especially if passing obliquely, was apt to cut a slit in the muscles far exceeding in size the opening in the overlying integument, with the result of leaving a palpable subcutaneous defect. Under these circumstances the yielding spot was often noticed to rise and fall with the movements of respiration, external palpation met with an absence of normal resistance, and there was impulse on coughing.
Fractures of the ribs.—These injuries were produced in either transverse or longitudinal coursing tracks, their special feature being a sharp localisation of the lesion of the bone.
In tracks crossing the chest transversely the injury to the ribs might consist in notching, perforation, or complete solution of continuity, sometimes with fine comminution. In the incomplete injuries some importance attached to the localisation of the lesion to the upper or lower border of the rib, in so far as the intercostal artery was concerned. Comminution at the wound of entry was, as a rule, not so extensive as at the aperture of exit, and in any case was less apparent, since the fragments were driven inward. The wider comminution at the exit aperture depends on the lesser degree of support afforded by the thoracic coverings to the convex outer surface of the rib, and on the fact that the velocity of the bullet has been lowered by its passage through the opposite rib and the chest cavity.
The splinters of comminuted ribs are small, and wide-reaching[Pg 379] fissures rare. These characters depend on the elastic nature of the resistance offered by the curved rib to the passage of the bullet, which is calculated to preserve the bone from the full force of impact, except at the point actually impinged upon.
Fractures of the ribs, produced from within by bullets taking a longitudinal course through the thorax, were still more special in character. They were also more important, as giving rise to troublesome symptoms.
In these, again, the degree of injury to the bones varied considerably. In some cases the bones were merely grooved internally, without any external deformity; in other cases a sort of green-stick fracture was produced, accompanied by the projection of a tender salient angle externally; in others complete solution of continuity was effected.
Another feature of importance was the occasional implication of several ribs. In this case the symptoms accompanying the injury were very much more like those observed in the corresponding injuries resulting from indirect violence seen in civil practice.
Injuries to the costal cartilages closely resembled those to the ribs. Perforation, bending from injury to the inner aspect, and comminution were observed. The latter condition differed from the similar one seen in the case of the ribs only in so far as the tougher consistence of the cartilage did not lend itself to such free comminution, and the splinters remained in great part attached. The nature of the fractures, in fact, somewhat resembled that seen on breaking a piece of cane.
I saw no fracture of the sternum except of the nature of a pure perforation; these were not uncommon in the hospitals, either in the upper or the extreme lower portions of the bone. Fractures in other portions were no doubt usually associated with fatal injuries to the heart. The openings were usually so small as to be difficult of palpation, and I never had the opportunity of examining one post mortem.
Perforations of the body of the scapula were common, but they were of little importance in symptoms or prognosis.
Symptoms of fracture of the ribs.—Fractures accompanying transverse wounds of the chest were characterised by the[Pg 380] insignificance of the symptoms produced. Every common sign of fracture of the rib was in fact absent. Neither pain, stitch on inspiration, nor crepitus, either audible or palpable, was, as a rule, present. This absence of signs was accounted for by the nature of the lesion: thus in perforations or notchings there was no loss of continuity, while in the freely comminuted fractures the loss of continuity was so absolute as to allow no possibility of the main fragments rubbing together. Again, part of the symptoms attending these injuries, as seen in civil practice, depends upon contusion and laceration of the surrounding structures—a condition precluded by the localised nature of the application of the violence by a bullet of small calibre. In order to establish a diagnosis, therefore, we were in many cases reduced to palpation, and occasionally to direct examination of the wound.
Fractures accompanying longitudinal tracks formed a class rather apart in the matter of symptoms. In these mere groovings might also be accompanied by no signs, or at the most by slight local pain and tenderness. When, however, the grooving was sufficiently deep to be accompanied by deformity, or a complete solution of continuity was effected, the signs were often severe. The tender salient angle, or, in the absence of this, a highly tender localised spot, often pointed to the less severe injuries, and when the fractures were complete or multiple, pain was a very prominent symptom, both constant and in the form of inspiratory stitch. The severity of the pain was probably to be in part ascribed to implication of the intercostal nerves, which in these injuries was direct and often multiple. Again, severe contusion or actual laceration of the nerves, with resulting anæsthesia, was less common than when the bullet directly implicated the nerves in transverse wounds. Free comminution and absolute solution of continuity were also less common than in the fractures accompanying transverse wounds; hence pain from rubbing of the fragments on inspiratory movement or palpation was more common, and crepitus, either on auscultation or palpation, was more often met with. Patients with this class of fracture often suffered greatly from painful dyspnœa, and were unable to assume the supine position.[Pg 381]
External hæmorrhage of severity was rare from these thoracic wounds; in many cases it did not amount to more than local staining of the shirt; altogether I saw only one or two cases where any serious bleeding occurred. Internal hæmorrhage into the pleura, in consequence of the position of the intercostal arteries, was common, and often abundant; this will be treated of under the heading of hæmothorax.
Treatment of fractured ribs.—Transverse wounds of the thorax, with no symptoms of fractured ribs, needed to be dealt with as wounds of the soft parts alone.
In multiple fractures accompanying longitudinal tracks, bandaging or strapping for the purpose of fixation was necessary to relieve pain. A few fragments of bone sometimes needed primary removal, and occasionally small sequestra were removed at a later date; but necrosis was rare, unless some complication led to the development of a fistula.
Retained bullets were occasionally met with in the chest wall. In such cases the last remaining energy of the bullet often seemed to have been spent in diving under the margin of a rib and turning longitudinally up or down. Removal was sometimes necessary, either from the prominence produced, the presence of pain, or the continuance of suppuration. Some of the specimens removed offered interesting evidence of the capacity of the ribs to withstand considerable violence from a bullet. These were slightly bent, and marked by a half-spiral groove. I saw such bullets removed from the thoracic and the abdominal wall, and the evidence seemed rather against the groove having been produced prior to their entrance into the body.
 Fig. 82.—Spirally grooved Mauser Bullet
Fig. 82.—Spirally grooved Mauser Bullet
Wounds of the diaphragm.—Perforations of the diaphragm were very frequent, and as a rule of small significance. When, however, the course taken by the bullet was parallel with that of the slope of the diaphragm, a more or less extensive slit was the result. I saw such a wound still[Pg 382] gaping, and 2 inches in length, in the body of a patient who died three weeks after the infliction of a fatal abdominal injury.
In several other obliquely transverse thoracic wounds there was reason to assume the existence of similar slits. Certain signs were more or less constant under these circumstances. These consisted in shallow respiration, often accompanied by a groan or the slightest degree of hiccough on inspiration, and considerable increase in respiratory frequency. In one patient the respirations were at first 48, only dropping to 36 some seventy hours after the reception of the injury. In some of the cases in which the abdominal cavity was implicated, wound to the diaphragm seemed a more likely explanation of early, frequent, and painful vomiting than did visceral injury. The possibility of the later development of diaphragmatic herniæ in some of these patients will have to be borne in mind in the future.
Visceral injuries.—The frequent escape of the thoracic viscera from injury, putting aside the lungs which fill so great a part of the cavity, was very remarkable. I never saw a case in which I could assume injury to any of the posterior mediastinal viscera, although such may have occurred on the field of battle. An injury to the œsophagus, for instance, would almost of necessity be accompanied by wound of either one of the large vessels, even the thoracic aorta, or the spinal column. I was somewhat surprised, however, to learn on enquiry from surgeons who had seen a large number of the dead and dying on the field, that thoracic wounds, putting aside those that directly implicated the heart, were responsible for but a small proportion of the fatalities.
The escape of the posterior mediastinal viscera, the great vessels, and the heart, is, I believe, to be explained by the fact that all are supported and held in position by the loose meshed mediastinal tissue, which allows for their displacement after the manner observed in the case of the vessels and nerves lying in the loose tissue of the great vascular clefts.
Wounds of the heart.—Perforating wounds of the heart were probably fatal in all instances, in spite of the fact that, in some patients who survived, the position of wound apertures[Pg 383] on the surface of the body made it difficult to believe that the heart had not been penetrated. (See cases below.)
In the case of this organ, we must bear in mind its constant variations in bulk, its elastic compressibility, and its variations in position in systole and diastole. The variations in bulk and position would be capable of explaining the escape of the organ from injury at some particular moment, when a second shot apparently through the same wound track might implicate it. Beyond this, reasoning from the case of analogous hollow viscera, as the arteries or the intestine, a bullet might readily score the surface of the heart without perforating its cavity.
Such accidents were observed. Thus, in a case examined by Mr. Cheatle, the patient died of suppurative pericarditis, secondary to a wound of which the external apertures had closed. In this patient both auricle and ventricle were scored externally by the passage of the bullet.
I am, however, disinclined to allow that many patients survived direct blows on the heart, since I believe that in the majority if not in all cardiac wounds the actual cause of death was not hæmorrhage, but sudden stoppage of the heart's action. This is to be inferred from the fact that severe external hæmorrhage did not occur; in some cases the shirt was hardly stained, and in all death occurred in the course of a very few minutes. Again, in none of the patients whom I saw who had received possible wounds of the heart-wall were there evident signs of hæmo-pericardium. In view of the difficulty of detecting this condition from physical signs, this argument is naturally not of great weight, but must be allowed.
One or two death scenes from cardiac wound were described to me. In one the patient muttered 'They have got me this time,' and died quietly; in a second the patient's face became ghastly pale, he lay on his back with the knees flexed, clutching the ground, gasping for breath, and died only after some minutes of evident great agony. The absence of any post-mortem details as to the condition of the heart in these injuries is much to be regretted.
(145) Entry, in the seventh left intercostal space, in the posterior axillary line; exit, immediately below the ninth costal cartilage, close to the position of the gall bladder.[Pg 384]
This track in all probability involved the diaphragm twice, both lungs and pleuræ, and passed immediately beneath the heart. The liver was also perforated, but the spleen and stomach probably escaped as far as could be judged from the symptoms. The patient afterwards developed a pneumo-hæmo-thorax on the right side. The immediate symptoms were great distress in breathing and rapid irregular pulse. The difficulty in respiration was probably in part accounted for by the injuries to the lung and diaphragm. The pulse remained from 112 to 120 for three days, at first soft and hardly perceptible, later very irregular, and dropping one every fifth or sixth beat; and it seemed fair to attribute this to the shock to the nervous mechanism of the heart. The patient recovered from the chest injury.
In some other patients in whom the track passed close below the heart a disturbance of the pulse rate was noted, but this was in some cases a slowing, not below 48, in others quickening to 100, with irregularity both in force and beat.
(146) Entry, in the fourth right interspace, 3 inches from the middle line; exit, in the seventh left interspace, in the mid-axillary line. This wound was received at a distance of 500-600 yards, but the bullet penetrated both sides of a stout silver cigarette case and some cigarettes before entering the body. There were minor signs of pulmonary injury, 'coughing day and night,' and slight discoloration of the sputum on three or four occasions. The respirations were quickened to 32, and as much as ten days after the injury the pulse only beat 48 to the minute; it then rose to 56, but beat in a very deliberate manner.
In other cases the signs were almost nil.
(147) Entry, in the fourth right intercostal space 3/4 of an inch from the sternum; exit, in the sixth left interspace in the posterior axillary line. This patient had no symptoms, beyond quickening of the pulse to 100, and a 'feeling of tightness at the heart.' He shortly returned to active duty.
(148) Entry, situated in the third right interspace 3 inches from the sternal margin; exit, in the fourth left space 2¾ inches from the sternal margin. In this case the bullet without doubt passed through the anterior mediastinum, and slight injury to the lung was evidenced by transient hæmoptysis.
Some remarks regarding wounds of the thoracic vessels have already been made in Chapter IV., where instances of[Pg 385] injury to the innominate and left subclavian arteries are recounted. The escape of the large trunks was generally quite as astonishing as in other parts of the body, especially in the superior mediastinum.
(149) Entry, over the first right intercostal space beneath the centre of the clavicle; exit, at left anterior axillary fold. The great vessels must have been crossed here in immediate contact, and considerable hæmorrhage from the wound of entry caused great anxiety; this ceased spontaneously, however, and, beyond transient hæmoptysis and a right pneumo-thorax, no further trouble occurred.
(150) Entry, in the ninth interspace, just anterior to the anterior axillary line; exit, through the right half of the sternum, 1/2 an inch below the upper border. No primary hæmorrhage of importance followed, but I believe this patient subsequently died. The wound was received at a range of within fifty yards.
Wounds of the lungs.—Numerically, pulmonary wounds formed the most important series of visceral injuries met with in the thorax, the frequency of incidence corresponding with the proportionate sectional area occupied by the organs. Although these injuries did well, and needed little interference on the part of the surgeon, many points of interest were raised by them.
Thus the comparative importance of the wound in the chest-wall to that in the lung itself, was scarcely what, without actual experience, would have been expected, the former proving so very much the more important element of the two.
The question of velocity on the part of the bullet took a very secondary position in these injuries. I saw a number of cases in which the patients estimated the range at which they received their wounds as from 30 to 50 yards, and although some of the wounds were of a severe type, the increased gravity depended rather on the injury to the chest-wall than to that of the lung. If the bullet passed by the intercostal space, avoiding the rib, I very much doubt if the relative velocity was of any importance, further than from the fact that a sufficiently low degree to allow of lodgment of the bullet was distinctly unfavourable.
In view of the general lack of significance in these injuries it was interesting to note how very definite was the ill effect of[Pg 386] early transport on the after course. This depended on the frequent development of parietal hæmothorax in patients who were not kept absolutely at rest.
The tracks produced in the lungs by the bullets were very minute, and in the few cases in which opportunity arose for their examination post mortem some little time after the infliction of the wound, there was great difficulty in localising them. The slight damage incurred by the pulmonary tissue is due to its elasticity and non-resistent character.
Pulmonary hæmothorax was distinctly rare. Reasoning from the analogous wounds of the liver, tracks scoring the surface of these organs might be much more to be feared than clean perforations. The elasticity of the lung tissue, however, must make such lesions rare. In point of fact, there is no reason why a perforation by a bullet of small calibre should be much more feared than a puncture from an exploring trocar, and the danger of the two wounds is probably very nearly the same.
The only points of importance as to the particular region of the lung traversed were the distance from the periphery as affecting the probable size of the vessels injured, and perhaps the implication of the base or apex of the organ respectively. I am under the impression that wounds in the apical region were somewhat more liable to be followed by the development of pneumothorax, and possibly hæmothorax, while wounds at the base gained their chief importance from the frequency of concurrent injury to the abdominal viscera. I had no experience of the immediate results of wound of the great vessels at the root of the lung, but assume that they led to speedy death.
Symptoms of wound of the lung.—I shall describe the whole complex usually observed, although it is obvious that the wound of the chest-wall is responsible for a large proportion of the signs.
The majority of these injuries were accompanied by a certain degree of systemic shock, and this was more marked in wounds received at a short range. The shock was, however, rather to be attributed to the injury to the chest-wall and thoracic concussion than to that to the lung itself. I think it[Pg 387] may also be stated that few patients were inclined to walk or remain in the erect position after receiving these wounds; this feature was also noted in horses in whom a bullet passed through the lungs.
The remarks made as to the pain accompanying fractures of the ribs apply equally here. Pain was not a prominent symptom, except in so far as the actual impact caused temporary suffering. It was striking how often patients who received wounds through the arm prior to the same bullet traversing the chest appreciated the chest wound only, yet the chest might pass unnoticed when a still more sensitive part was struck later, as has been already mentioned in the section on wounds in general.
Dyspnœa was not a prominent primary symptom. The patients sometimes had 'all the wind knocked out of them' at the moment of impact, but when seen at the Field hospitals a short time later, the respirations were shallow, but easy and regular, and only moderately quickened; thus 24 was a not uncommon rate. Naturally if accumulation of blood in the pleura began early and continued, these remarks do not hold good; and again in some older men of full-blooded type and the subjects of recurrent attacks of bronchitis, a considerable degree of pain, dyspnœa, and even cyanosis was sometimes present soon after the injury. The complication of wound of the diaphragm has already been referred to in this relation.
Local respiratory immobility of the thoracic parietes and consequent asymmetry of movement were constant. This was especially a marked feature when the upper part of the chest was implicated on one side only. It rather corresponded, however, to the local shock observed in wounds of the limbs than to the instinctive immobility accompanying fractures of the ribs; since, as already explained, small-calibre bullet wounds of the ribs are not necessarily painful on movement, and the sign existed even when the bullet had passed by an intercostal space. This sign was naturally a transitory one.
Hæmoptysis was a fairly constant sign, but sometimes quite absent when no doubt could exist as to the perforation of the lung. As a rule, a considerable quantity of blood might be coughed up shortly after the injury; but I never knew this to be[Pg 388] sufficient in amount to give rise to any misgivings as to danger from the hæmorrhage. After the first evacuation of blood from the wounded lung, the sign varied much; in the majority of instances the patients continued to expectorate small quantities of blood mixed with mucus, for some three or four days, the blood gradually assuming a coagulated condition. Sometimes only the primary hæmoptysis was noted, and still more rarely the expectoration of clots was continued for a week, or even longer. This probably depended partly on personal idiosyncrasy, partly on the size of the vessels which had been implicated in the track.
Cough was not commonly the troublesome symptom noted in the contused wounds of the lung seen in civil practice accompanying fracture of the ribs. Moist sounds were usually audible on auscultation, but in many cases over a very limited area and only on the first few days.
Cellular emphysema was distinctly rare, and usually limited in extent: thus I saw it in the posterior triangle of the neck alone in an apical wound; over about a third of the upper part of the thorax in another wound through the second intercostal space, and in this case oddly enough the emphysema was the only sign of injury to the lung; and very occasionally widely distributed—in the latter case there were also usually multiple fractures of the ribs. Neither issue of air from the external wound nor frothy blood was ever seen with small-calibre wounds, but I saw one instance in a case of Martini-Henry wound.
Pneumothorax was also rare. I saw pneumothorax three times out of about half a dozen Martini-Henry wounds, but I do not think it occurred as often in 100 small-calibre wounds. The Martini-Henry wounds all recovered; but convalescence was very prolonged, and the same remark to a less degree holds good in the small-calibre cases.
That the slow recovery in cases of pneumothorax in the Martini-Henry wounds was due mainly to the size of the opening in the thoracic parietes was, I think, proved by the fact that in the small-calibre bullet wounds, followed by the development of pneumothorax, the external wounds were usually large and irregular in type; also, that in the only[Pg 389] pneumothorax which I saw produced during an extraction operation, the air was very rapidly absorbed. In the latter case, however, there was little reason to conclude that wound of the lung had occurred primarily, and certainly no opening existed at the time the thorax was incised.
Hæmothorax.—This was the most frequent and also the most interesting of the complications of wound of the chest. In 90 per cent. or more of the cases, the hæmorrhage was of parietal source, and due either to direct injury to the intercostal vessels by the bullet or to laceration by spicules of comminuted ribs. For this reason, the passage of the bullet whether by an intercostal space, or through a rib, provided the wound was not at the posterior part of the space where the artery crosses, was a point of considerable prognostic importance. Exclusion of the lung as the source of hæmorrhage was, I think, amply justified by the absence of continuous recurrent or progressive hæmoptysis in the majority of the cases, and by the very small trace of injury found in the lungs of patients who died some weeks after the injury. In such it was difficult to discriminate the tracks at all. I only happened to see one case where free hæmoptysis, during the course of development of a hæmothorax, pointed to the lung as the source of the blood.
Hæmorrhage into the pleural cavity occurred in some degree in a very large proportion of the chest wounds, but it was especially interesting to note how greatly its extent was influenced by the amount of transport to which the patients were subjected in the early stages after the injury. During the early part of the campaign, on the western side, I saw a large number of chest wounds, and had I been asked my opinion as to the relative frequency of occurrence of hæmothorax I should have placed it at about 30 per cent. The patients in these early battles needed little wagon transport, and when sent down to the Base travelled in comfortable ambulance trains. After the commencement of the march from Modder River to Bloemfontein, however, these conditions were changed, and all the chest as other cases were exposed to the necessity of three days and nights' journey to the Stationary hospitals and afterwards to the long journey to[Pg 390] Cape Town. Of these patients, at least 90 per cent. suffered with hæmothorax of varying degrees of severity.
In some cases, the least common, signs of considerable intra-pleural hæmorrhage immediately followed the wound; in others, the accumulation of blood was gradual, and only manifest in any degree at the end of three or four days, when it became stationary if the patient was kept at rest. In a second series the hæmorrhage was of the recurrent variety; these cases differing little in character from those of slight continuous hæmorrhage. In a third, the bleeding was definitely of a secondary character, corresponding with one of the classes of secondary hæmorrhage described in Chapter IV., and occurring on the eighth or tenth day from giving way of an imperfectly closed wounded vessel. In either of the two latter classes the development of the hæmothorax often corresponded with a journey, or with allowing the patient to get up.
The general course of these effusions was towards spontaneous absorption and recovery. Coagulation of the blood took place early, the fluid serum separated, and tended to undergo absorption with some rapidity, leaving a small amount of coagulum at the base, which evidenced its presence for many weeks by a persistence of a certain degree of dulness on percussion. Early coagulation, I think, accounted for the usual absence of gravitation ecchymosis as a sign.
The course to recovery was sometimes broken by signs of slight pleuritic inflammation, which, as affecting the amount of effusion, will be spoken of under the heading of symptoms. In some cases the amount of blood was so great as to necessitate means being taken for its removal; in these a reaccumulation often took place. Occasionally an empyema followed in cases thus treated.
The nature of the blood evacuated on tapping varied much. In very early aspirations unchanged blood was often met with, but clot sometimes made evacuation difficult and necessitated a second puncture. In the tappings done at the end of a week or more a dark porter-like fluid was common, while when suppuration was imminent a brick-red-coloured grumous fluid replaced normal blood. In the cases where early incision was resorted to, blood both fluid and in clots[Pg 391] was often mixed with a certain proportion of lymph flakes, perhaps indicating the part taken by inflammatory reaction to the irritation of the clot in producing the rise of temperature.
Symptoms of hæmothorax.—In the more severe cases of primary bleeding the symptoms did not, as a rule, reach their full height until the third or fourth day after the injury. The patients then often suffered severely. The pulse and temperature rose, and to general symptoms of loss of blood were added: occasional lividity of countenance; severe dyspnœa, accompanied by inability to lie on the sound side or to assume the supine position; absence of respiratory movement on the injured side; pain, restlessness, cough, and sometimes continuance of hæmoptysis, small clots usually being expectorated.
Accompanying these symptoms were the usual physical signs of fluid in the pleura in differing degrees and combination. Dulness of varying extent up to complete absence of resonance on one side, often accompanied in the incomplete cases by well-marked skodaic resonance anteriorly. Loss of vocal resonance, and fremitus; œgophony, tubular respiration over the root of the lung or at the upper limit of the dulness, and more or less extensive displacement of the heart. Obvious increase in girth, fulness of the intercostal spaces, or gravitation ecchymosis was rare. The latter was most common in instances in which multiple fracture of the ribs existed (see fig. 83). I think the rarity of the last sign must have been due to the early coagulation of the blood, and its retention by the pleura, as I saw well-marked gravitation ecchymosis in one or two cases of mediastinal hæmorrhage.
The above complex of symptoms was common to all the cases, but in the slighter ones they gave rise to little trouble, and cleared up with great rapidity.[Pg 392]
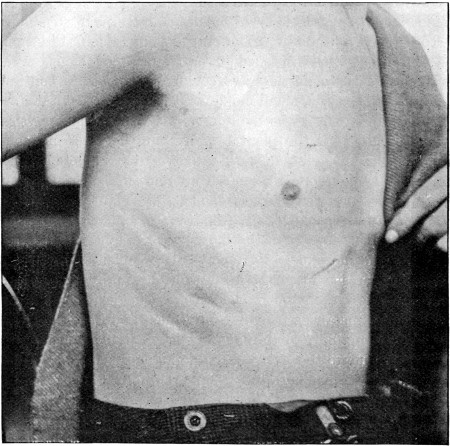 Fig. 83.
Fig. 83.
Gravitation Ecchymosis in a case of Hæmothorax, accompanying fracture of three ribs from within. The influence of the fractures on the development of the ecchymosis is shown by the linear arrangement of the discoloration
The most interesting feature was offered by the temperature, as this was very liable to lead one astray. A primary rise always occurred with the collection of blood in the pleura, this reaching its height on the third or fourth day, usually about 102° F. in well-marked cases; it then fell, and in favourable instances remained normal. In a large number of cases, however, where the amount of blood was considerable, this was not the case, the primary fall not reaching the normal, and a second rise occurred which reached the same height as before or higher. The second rise was accompanied by sweating, quickened pulse, and the probability of the development of an empyema had always to be considered. I believe in most cases this secondary rise was an indication of a further increase in the hæmorrhage, for the dulness usually increased in extent, and such rises were often seen when the patient had been moved or taken a journey. Again, the temperature often fell to normal after paracentesis and removal of the blood, to rise again with a fresh accumulation, which was not uncommon. I have already mentioned the large proportional incidence of hæmothorax observed in the patients who had to[Pg 393] travel down from Paardeberg, and I might instance another case related to me by Dr. Flockemann of the German ambulance, which was very striking. A Boer, wounded at Colesberg, developed a hæmothorax which quieted down, and he was removed to Bloemfontein; on arrival at the latter place the temperature rose, and other signs of fever suggested the development of an empyema; an exploring needle, however, only brought blood to light. After a short stay at Bloemfontein the symptoms entirely subsided, and the man was sent to Kroonstadt, when an exactly similar attack resulted, again quieting down with rest.
Similar recurrent attacks of hæmorrhage and fever occurred, however, in patients confined to their beds without moving after the first journey. Some temperature charts, in illustration of this point, are added to the cases quoted later. The explanation of the recurrent hæmorrhages is, I think, to be found in the reduction of the intra-thoracic pressure with coagulation and shrinkage of the clot in the pleura in the patients kept quiet in bed, while in the patients who had to travel it was probably the result of direct mechanical disturbance.
In many of these cases a pleural rub was audible at the upper margin of the dulness with the development of the fresh symptoms. Whether this was due to actual pleurisy or to the rubbing of surfaces rough from the breaking down of slight recent adhesions which had formed a barrier to the effusion, I am unable to say, but the signs were fairly constant. In some instances the increase in the amount of fluid was, no doubt, due to pleural effusion resulting from irritation from the presence of blood-clot, or perhaps the shifting of the latter; in these the secondary rise of temperature may well be ascribed to the development of pleurisy.
I am inclined to believe, however, that the primary rise of temperature was similar to that seen when blood accumulates in the peritoneal cavity as the result of trauma, and the secondary rises in most cases to those which we saw so frequently accompanying the interstitial secondary hæmorrhages spoken of in Chapter IV., and are to be explained on the theory of absorption of a blood ferment. The secondary rises[Pg 394] always occurred with a fresh effusion, often of blood, occasioning an extension, which broke down probable light adhesions and exposed a fresh area of normal pleural membrane to act as a surface for absorption.
It is, of course, manifest that the fever might also be ascribed to the infection of the clot or serum from without, and in the first cases I saw I was inclined to take this view, since we had in every case the primary wounds of chest-wall, and possibly of lung, and in some the addition of a puncture by an exploring needle between the first and second rise. After a wider experience, however, I abandoned the infection theory, as it seemed opposed by the very infrequent sequence of suppuration. The effect of simple removal of the blood or serum was also often so striking as to strongly suggest that it alone was responsible for the fever. Exactly the same result, moreover, followed evacuation of the interstitial blood effusions already mentioned elsewhere.
The common course of all the cases of hæmothorax was to spontaneous recovery, the rapidity of the subsidence of the signs depending mainly on the quantity of the primary hæmorrhage, and the occurrence of further increases. The blood serum tended to collect at the upper limit of the original blood effusion (as was often proved on tapping), and this was first absorbed; the clot deposited on the pleural surface and at the basal part of the cavity was, however, not absorbed with the same rapidity. In the majority of the patients when they left the hospitals, at the end of six weeks on an average, some dulness and deficiency of vesicular murmur always remained, and the clot and the surrounding surface, irritated by its presence, will, no doubt, be responsible for permanent adhesions in many cases. That such adhesions do form in the majority of cases I feel certain, as, although these patients when they left the hospital were to all intents and purposes apparently well, few of them could undertake sustained exertion without getting short of breath, and sometimes suffering from transitory pain, and for this reason it became customary to invalid them home.
In a small proportion of the cases empyema followed; but I never saw this in any case that had neither been tapped nor[Pg 395] opened, and I saw only one patient die from a chest wound uncomplicated by other injuries. This case was an interesting one of recurrent hæmorrhage followed by inflammatory troubles:—
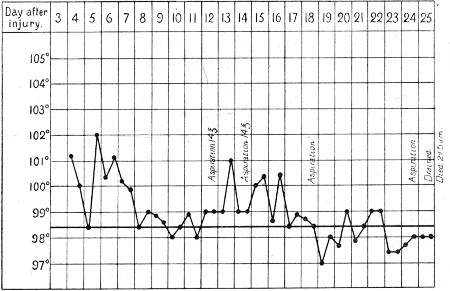 Temperature Chart 2.—Secondary Hæmorrhages in a case of Hæmothorax. Case No. 151
Temperature Chart 2.—Secondary Hæmorrhages in a case of Hæmothorax. Case No. 151
(151) The wound was received at short range, probably at from 100 to 200 yards. Entry, 1 inch from the left axillary margin in the first intercostal space; exit, at the back of the right arm 1½ inch below the acromial angle; both pleuræ were therefore crossed. The patient expectorated at first fluid, then clotted, blood in considerable quantity. When brought into the advanced Base hospital on the third day, there were signs of blood in the left pleura, cellular emphysema over the right side of the chest, and signs of collapse of the right lung. The temperature chart gives shortly the course of the case: the right pneumo-thorax cleared up spontaneously, also the emphysema; but the left pleura needed tapping to relieve symptoms of pressure on four occasions, the 13th, 15th, 19th, and 25th days respectively. On the first two occasions blood was removed, on the third blood serum only, and on the last pus. The patient was relieved after each aspiration; after the third, the temperature fell to normal, the general condition also improved, and he promised to do well. None the less, reaccumulation took place, the evacuated fluid assumed an inflammatory character, and an incision to evacuate pus was eventually followed by death on the twenty-seventh day. The amount of hæmoptysis throughout was considerable, and the case was possibly one of pulmonary hæmothorax, as after death no source of hæmorrhage[Pg 396] could be localised in the intercostal space. The track in the lung was almost healed, and although a part of it allowed the introduction of a probe for about an inch, it could be traced no further even on section of the organ, and no special vessel could be located as the original bleeding spot.
Empyema.—I may here add the little that I have to say on this subject. During the whole campaign the single case of primary empyema that I saw was the one recorded below, which deserves special mention as illustrating the disadvantage of extracting bullets on the field. Under the conditions which necessarily accompanied this operation the ensurance of asepsis was impossible, and the additional wound no doubt proved the source of infection.
(152) Entry, at the posterior margin of the sterno-mastoid muscle, 2 inches above the clavicle; the bullet came to the surface beneath the skin over the fifth rib, in the nipple line of the right side. There was never any hæmoptysis, but the patient suffered with some dyspnœa throughout. After a three days' stay in the Field hospital, where the subcutaneous bullet was removed, the patient was transported by wagon and train to the Base, a journey of about 600 miles.
On the fifth day pus escaped from the extraction wound, and when the case was examined at the Base, the temperature was 101°, the pulse over 100, the respirations 30, and the whole side of the chest was dull, with the exception of a patch of boxy resonance over the apex anteriorly. On the following day the chest was drained, and a considerable amount of pus evacuated, which was mixed with breaking-down blood-clot. A fortnight later a second operation had to be performed to improve the drainage, and the patient made a tedious recovery.
The following case well illustrates the symptoms in a severe case of hæmothorax, and empyema following aspiration:—
(153) The patient was wounded at Paardeberg at a range of from 500 to 700 yards. Entry, just to the left of the episternal notch; exit, in the fifth left interspace posteriorly, midway between the spine and vertebral margin of the scapula. A quantity of bright blood was brought up at once, and later blood was coughed up in clots.
There was no great pain at the moment of the injury; the[Pg 397] man again got up to the firing line, and later walked two miles to the Field hospital without aid. He remained here a week, when he was sent down to the Base, and during the first three days' journey in the wagon he began to get worse. On the fourth day cough began to be very troublesome.
When he arrived at the Base, fifteen days after the original injury, there was much dyspnœa; the temperature was 102°, and the pulse 110. The left side of the chest was dull throughout; an aspirating needle was introduced, and a pint of very dark liquid blood drawn off. The whole of the blood was not removed on account of the very severe cough and pain which the evacuation occasioned. The man appeared to steadily improve until three weeks later, when the temperature, which throughout had been uneven, became consistently high, and signs of fluid at the base increased. An aspirating needle was introduced, and 16 ounces of pus were drawn off. Two days later a piece of rib was resected (Mr. Pegg) and another pint of pus evacuated. After this, rapid improvement took place, and in ten days the man was able to be up and dressed, although a small amount of discharge still persisted. He eventually made an excellent recovery.
Secondary empyemata not uncommonly followed incision of the chest, or excision of a rib for draining a hæmothorax. These operations in the early part of the campaign were more freely undertaken on the supposition that rise of temperature and other symptoms of fever pointed to incipient breaking down of the clot. Subsequent experience showed this not to be the case, and early operations for drainage ceased to be undertaken. In these operations a primary difficulty was met with in effectively clearing out the clot, a drain had to be left, and suppuration occurred later in a considerable proportion. The suppurations were most troublesome; local adhesions formed, and the pus collected in small pockets, which were difficult to find and to drain, and even when the collections seemed to have been successfully dealt with at the time, residual abscesses often followed at a very late date. Thus, I saw a case with a contracted chest and a fresh abscess the day before I left Cape Town, in whom I had advised and witnessed an operation for the evacuation of clot in the presence of signs of fever a week after my arrival in the country, nine months previously. I saw another case where general infection[Pg 398] followed incision of a hæmothorax, but the patient fortunately recovered.
The question of pleurisy has already been mentioned in connection with hæmothorax; it no doubt accounted for secondary effusion in some cases, and beyond this I have nothing to add to what has been there said.
Pneumonia was rare; there were occasionally signs of consolidation, but, I think, quite as often in the opposite lung as in the one injured. I never saw a fatal case, and I am inclined to think that when it occurred it was as often the result of cold and exposure as of the injury to the lung. Abscess of the lung I only saw once, and that in a case in which the injury to the chest was complicated by paraplegia from spinal injury and septicæmia, and it was possibly pyæmic.
Diagnosis.—No difficulties special to small-calibre wounds were experienced, except such as have been already dealt with. The only class of case which frequently gave rise to difficulty was hæmothorax. Here two points especially needed consideration. (1) The source of the hæmorrhage as parietal or visceral. As has been already foreshadowed, this was mainly to be decided by the amount and persistence of the hæmoptysis, but naturally free hæmoptysis did not negative concurrent parietal bleeding. Then the actual source of the bleeding other than from the lung had to be considered; in the great majority of cases the intercostal vessels were responsible, and attention to the course of the tracks often allowed this to be definitely decided upon.
A case included in the chapter on Injuries to the Blood Vessels (No. 5, p. 127) is of great interest in this particular; in that instance feebleness of the radial pulse, together with the position of the wound, was a valuable indication of injury to the subclavian artery, but weakened somewhat by the fact of retention of the bullet, and hence uncertainty as to the exact course that it had taken, and as to whether the bullet itself was not responsible for pressure on the vessel. Such indications, however, should make one very chary of interference with a hæmothorax, even with extremely urgent symptoms, in the light of our present knowledge of the nature of the lesions to the great vessels[Pg 399] produced by small-calibre bullets, and their tendency to be incomplete.
(2) The imminence of suppuration or its actual occurrence.—In most cases it sufficed to preserve an expectant attitude, and in the persistence or increase of symptoms, to have recourse to an exploratory puncture as the best means of solution of the difficulty.
Prognosis.—The prognosis both as to life and as to subsequent ill-effects was remarkably good; in many cases of uncomplicated injury to the lung the patients rejoined their regiments at the end of a month or six weeks. In the more serious cases complicated by the collection of blood in the pleura, convalescence was more prolonged, and an average time of six to eight weeks often elapsed before the patients could be safely discharged from hospital. In the more serious a certain amount of dulness always persisted at this time over the base of the lung, and the chest was usually somewhat contracted on the injured side, with evidence in the way of decreased vesicular murmur that the lung was still not free from compression. With regard to the persistence of dulness on percussion, it is well to bear in mind that a thin layer of blood apparently produces as serious impairment of resonance as a much larger quantity of serum. The signs appeared to favour the view that the space necessary for the location of the hæmorrhage had been obtained at the expense of the lung rather than by distension of the thoracic parietes, and also, I think, denoted the presence of adhesions. Possibly they will entirely disappear with the return of full excursion movements of respiration, the latter being often still somewhat restricted when the patients left hospital. All the patients with such signs were liable to attacks of pain and shortness of breath on actual bodily exertion. I happened to meet with an officer, the subject of a Lee-Metford wound of the thorax, sustained five years previously, and he told me that he was nine months before he could take active exercise without feeling short of breath.
As to the cases of hæmothorax and empyema which needed drainage, all did well; but expansion of the lung was much less satisfactory than would have been expected,[Pg 400] probably on account of especially firm adhesions. The importance of concurrent injury I need hardly dwell on; but I might add that perforation of one or both arms, the most common one, did not materially affect the general statements above made.
Treatment.—In the early stages of the pulmonary wounds rest was the all-important indication, and when this was assured few serious cases of hæmothorax occurred. Beyond simple rest, the administration of opium with a view to checking internal hæmorrhage was used with good effect. The wounds needed simple dressing only.
The treatment of hæmothorax at a later date, however, was of much interest and difficulty. I think the following lines may be laid down for guidance in such cases:—
(i) Hæmothorax, even of considerable severity, will undergo spontaneous cure. An early rise of temperature may be disregarded.
(ii) Tapping the chest is indicated when pressure signs on the lung are sufficiently severe to cause serious symptoms, and the removal of the blood undoubtedly shortens the period of recovery, as well as relieves symptoms.
In such cases the collection of blood has usually been rapid and continuous; hence a fresh hæmorrhage is always probable when the local pressure has been removed. Tapping therefore should not necessarily mean complete evacuation, and should be followed by careful firm binding up of the chest, the administration of opium, and the most stringent precautions for rest.
(iii) Tapping may be needed as a diagnostic aid, and in such circumstances as much fluid as can be removed should be evacuated with the same precautions as mentioned in the last paragraph.
(iv) Tapping may be indicated for the evacuation of serum expressed from the blood-clot, or due to pleural effusion, on the same lines as in any other collection of fluid in the pleural cavity.
(v) Early free incision is, as a rule, to be steadfastly avoided. Some cases already quoted fully illustrate its disadvantages.[Pg 401]
(vi) Cases in which an incision and the ligature of a parietal artery are indicated are very rare. I never saw such a one myself.
(vii) If a hæmothorax suppurates, it must be treated on the ordinary lines of an empyema. In view of the constant formation of adhesions and difficulty in drainage, a portion of a rib should always be resected in order to ensure sufficient space for after-treatment. The cavities, as a rule, are better irrigated, the usual precautions being taken where there is any reason to fear that the lung is still in communication with the cavity.
Care in carrying out asepsis in tapping, which should be performed with an aspirator, need hardly be more than mentioned. It will be noted that in some of the cases quoted suppuration followed tapping, but it must be remembered that in these the two primary wounds already existed as possible channels of infection.
Retained bullets of small calibre in the thoracic cavity were not common, unless the lodgment had occurred in the bodies of the vertebræ. I saw very few. Shrapnel bullets and fragments of shells, however, were, in proportion to the frequency of wounds from such projectiles, more commonly retained. The rules to be followed in such cases do not materially deviate from those to be observed in the body generally.
When the bullet is causing no trouble, and is lodged in either the bone of the spine or the lung substance, no interference is advisable. When, on the other hand, the bullet as viewed by the X-rays is seen to be in the pleural cavity, and any symptoms of its presence exist, it may be justifiable to remove it. I saw this done in one case for the removal of a shrapnel bullet from the lower reflexion of the pleura on account of fixed pain and tenderness complained of by the patient. The bullet, a shrapnel, had perforated the arm, which the patient was sure was by his side at the moment of injury, and the X-rays showed it to lie at the bottom of the pleural cavity, where we assumed it had fallen. When, however, the bullet was removed by Mr. Watson, he found that the fixed pain and tenderness had been the result of a fracture of a rib from the inner side, not involving loss of continuity; hence the actual[Pg 402] indication for the operation had been a delusive one, since the bullet had not fallen, but expended its last force in injuring the rib. The patient made an excellent recovery, and rejoined his regiment at the end of six weeks. I saw several cases in which the bullet was lodged in either the lung or bones of the spine do well with no interference. The great disadvantage of primary removal in inducing an artificial pneumo-thorax and in laying open a hæmothorax is obvious.
In case of lodgment of the bullet in the lung, bearing in mind the infrequency of untoward symptoms, the latter should be watched for prior to interference.
The following cases illustrate some typical instances of wound of chest accompanied by the development of hæmothorax:—
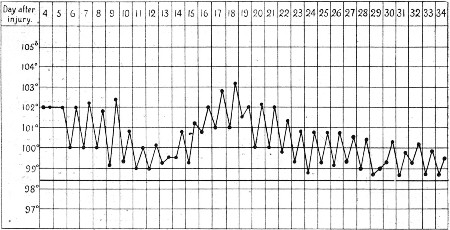 Temperature Chart 3.—Primary Hæmothorax, with rise of
temperature. Secondary rise, with fresh effusion and pneumonia.
Spontaneous recovery. Case No. 154
Temperature Chart 3.—Primary Hæmothorax, with rise of
temperature. Secondary rise, with fresh effusion and pneumonia.
Spontaneous recovery. Case No. 154
(154) Severe hæmothorax. Spontaneous recovery.—Wounded at Modder River at a distance of 30 yards. Entry, at the junction of the left anterior axillary fold with the chest-wall; exit, immediately to the left of the seventh dorsal spinous process. The patient arrived at the Base with signs of an extensive hæmothorax, accompanied by a temperature which reached 102° on the fourth day, and on the evening of the tenth 103°. The man was very ill, and an exploring needle was inserted, by which about an ounce of blood was evacuated. The signs of fluid in the left pleura were accompanied by those of consolidation over the lower[Pg 403] fourth of the right lung, and the sputa were rusty. Evidence of perforation of the left axillary artery existed in feebleness of the radial pulse; and there was musculo-spiral paralysis.
After the preliminary puncture, the man refused any further operative treatment, although a second rise of temperature commenced on the fifteenth day, culminating in a temperature of 103.2° on the eighteenth. The further treatment of the patient consisted in the ensurance of rest and the alleviation of pain. A steady fall in the temperature extended over another three weeks, together with diminution in the signs of fluid in the pleura. At the end of seventy-four days the man was sent home, some slight dulness at the left base, and contraction of the chest sufficient to influence the spine in the way of lateral curvature, being the only remaining signs.
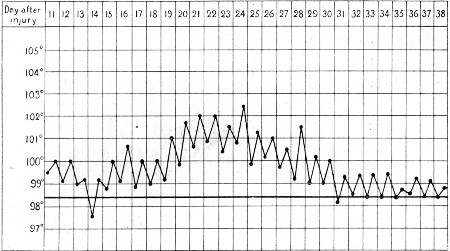 Temperature Chart 4.—Primary Hæmothorax. Secondary rise
of temperature, with increase in the effusion. Spontaneous recovery.
Case No. 155
Temperature Chart 4.—Primary Hæmothorax. Secondary rise
of temperature, with increase in the effusion. Spontaneous recovery.
Case No. 155
(155) Severe hæmothorax. Secondary effusion. Spontaneous recovery.—Wounded at Koodoosberg Drift, at a distance of 200 yards. Entry, at angle of the right scapula; exit, at the junction of the left anterior axillary fold with the chest-wall. No signs of spinal cord injury. The patient was brought in from the field twelve miles by an ambulance wagon on the second day, and in crossing the Modder River he was accidentally upset into the stream. For the first four days there was no hæmoptysis, but for the succeeding nine days small brightish red clots were expectorated. There was some tenderness over the ribs from the fifth to the ninth in the axillary line, and on the ninth day some gravitation ecchymosis appeared over the same region. Cough[Pg 404] was an early troublesome symptom in this case, and when admitted to the Base hospital, about the seventh day, there was evidence of fluid extending about a third of the way up the back.
On the tenth day after admission a pleural rub was detected at the upper margin of the dulness, and the latter shortly extended upwards over a little more than half the back. Meanwhile, there was no further hæmoptysis, respiration was fairly easy, 24 per minute, but accompanied by slight dilatation of the alæ nasi, and the temperature, which had been ranging from 99° to 100°, began to rise steadily, on the fifteenth day reaching 102.5°. The patient refused even an exploratory puncture, and was treated on the expectant plan. The temperature slowly subsided, with a steady improvement in the physical signs, and at the end of about ten weeks he left for home with only slight dulness and incapacity for active exertion remaining. (Now again on active service.)
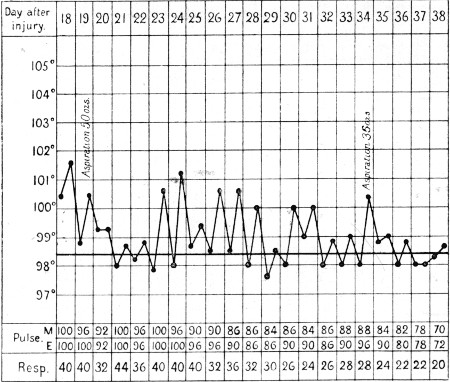 Temperature Chart 5.—Hæmothorax, primary and secondary
rises of temperature, on each occasion falling on the evacuation of the
blood. Case No. 156
Temperature Chart 5.—Hæmothorax, primary and secondary
rises of temperature, on each occasion falling on the evacuation of the
blood. Case No. 156
(156) Severe hæmothorax. Recurrent secondary effusion. Tapping on two occasions. Cure.—The patient was wounded at Paardeberg, and arrived at the Base on the eighteenth day. Entry, below the first rib, just external to its junction with the costal cartilage; exit, through the ninth rib, just within the posterior axillary line. The whole right side of the chest was dull, with signs of the presence of fluid, the heart being displaced to the left. There was considerable distress; the respirations averaged 40, the[Pg 405] pulse 100, and the temperature reached 101.5° the first evening after arrival.
On the nineteenth day the thorax was aspirated (Mr. Hanwell) and 50 ounces of dirty red-coloured fluid, half clot, half serum, were evacuated. Considerable relief was afforded; the respirations became slightly less frequent; the heart returned to a normal position, and distant tubular respiration was audible. The temperature dropped to normal the third day after evacuation of the fluid, but on the sixth day it again commenced to rise, and meanwhile fluid again began to collect.
On the twenty-sixth day a second aspiration resulted in the evacuation of 35 ounces of bloody fluid in which flakes of lymph were found. Three days later the temperature became normal. The respirations fell to 22, and the patient made an uninterrupted recovery.
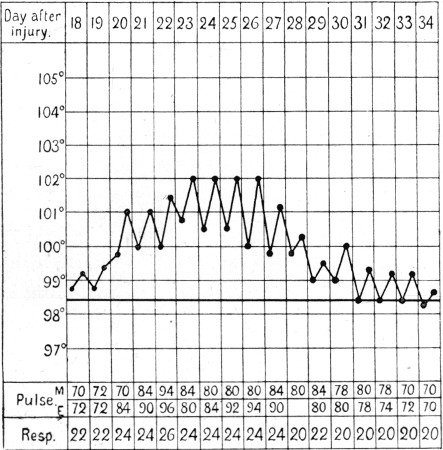 Temperature Chart 6.—Wound of Lung. Secondary
development of Hæmothorax, with rise of temperature. Spontaneous
recovery. Case No 157
Temperature Chart 6.—Wound of Lung. Secondary
development of Hæmothorax, with rise of temperature. Spontaneous
recovery. Case No 157
(157) Moderate hæmothorax. Secondary effusion at the end of twenty days. Spontaneous recovery.—Wounded at Paardeberg; range from 700 to 1,000 yards. Entry, in the centre of the second right intercostal space, anteriorly; exit, at the level of the sixth rib posteriorly, through the scapula, close to its vertebral margin.
The patient arrived at the Base on the sixth day; he said he expectorated some blood at the end of about ten minutes after being shot, and experienced a 'half-choking sensation.' A small quantity of phlegm and occasional clots had been expectorated[Pg 406] since. He had walked about a good deal; movement occasioned cough, and he became 'blown' very rapidly.
On admission there were signs of fluid in the lower third of the pleural cavity, but no general symptoms beyond an evening rise of temperature to an average of 99°. About the twentieth day the temperature commenced to rise, and on the twenty-third and four following evenings reached 102°. The fever was accompanied by some distress, and a well-marked increase in the physical signs of the presence of fluid in the chest. The pulse rose to 96, and the respirations considerably above the average of 24, which was at first noted. A strictly expectant attitude was maintained, and the temperature steadily fell in a curve corresponding to the rise, gradually reaching the normal at the end of a week. The physical signs at the base steadily cleared up, and at the end of six weeks the patient returned to England convalescent.
Perhaps no chapter of military surgery was looked forward to with more eager interest than that dealing with wounds of the abdomen. In none was greater expectation indulged in with regard to probable advance in active surgical treatment, and in none did greater disappointment lie in store for us.
Wounds of the solid viscera, it is true, proved to be of minor importance when produced by bullets of small calibre; but wounds of the intestinal tract, although they showed themselves capable of spontaneous recovery in a certain proportion of the cases observed, afforded but slight opportunity for surgical skill, and results generally deviated but slightly from those of past experience. Such success as was met with depended rather on the mechanical genesis and nature of the wounds than upon the efforts of the surgeon, and operative surgery scored but few successes.
It is true that to the Civil Surgeon accustomed to surroundings replete with every modern appliance and convenience, and the possibility of exercising the most stringent precautions against the introduction of sepsis from without, abdominal operations presented difficulties only faintly appreciated in advance; but this alone scarcely accounted for the want of success attending the active treatment of wounds of the intestine when occasion demanded. Failure was rather to be referred to the severity of the local injury to be dealt with, or to the operations being necessarily undertaken at too late a date. Many fatalities, again, were due to the association of other injuries, a large proportion of the wound tracks involving other organs or parts beyond the boundaries of the abdominal cavity.[Pg 408]
The frequent association of wounds of the thoracic cavity with those of the abdomen afforded many of the most striking examples of immunity from serious consequences as a result of wound of the pleura. It must be conceded that in a large number of such injuries only the extreme limits of the pleural sac were encroached upon, yet in some the tracks passed through the lungs, although without serious consequences. Under the heading of injury to the large intestine a somewhat special form of pleural septicæmia will be referred to.
It may at once be stated that such favourable results as occurred in abdominal injuries were practically limited to wounds caused by bullets of small calibre, and that, although in the short chapter dealing with shell injuries a few recoveries from visceral wounds will be mentioned, I never met with a penetrating visceral injury from a Martini-Henry or large sporting bullet which did not prove fatal.
Wounds of the abdominal wall.—It is somewhat paradoxical to say that these injuries possessed special interest from their comparative rarity of occurrence, since they were not of intrinsic importance. Their infrequency depended on the difficulty of striking the body in such a plane as to implicate the belly wall alone, and their interest in the diagnostic difficulty which they gave rise to.
In many cases the position of the openings and the strongly oval or gutter character possessed by them were sufficient proof of the superficial passage of the bullet; in others we had to bear in mind that the position of the patient when struck was rarely that of rest in the supine position, in which the surgical examination was made, and considerable difficulty arose. Some superficial tracks crossing the belly wall have already been referred to in the chapter on wounds in general and in that dealing with injuries to the chest, in which the above characters sufficed to indicate that penetration of the abdominal cavity had not occurred. In other instances a definite subcutaneous gutter could be traced, and often in these a well-marked cord in the abdominal wall corresponding to the track could be felt at a later date. Again, limitation to the abdominal wall was sometimes proved by the position of the retained bullet, or sometimes by the presence in the[Pg 409] track of foreign bodies carried in with the projectile. See case 160.
Fig. 84 illustrates an example where the limitation to the abdominal wall was evident on inspection. Here the division of the thick muscles of the abdominal wall had led to the formation of a swelling exactly similar to that seen after the subcutaneous rupture of a muscle, and two soft fluctuating tumours bounded by contracted muscle existed in the substance of the oblique and rectus muscles.
 Fig. 84.
Fig. 84.
Wound of Abdominal Wall (Lee-Metford). Division of fibres of external oblique and rectus abdominis muscles. Case 159
The cases which presented the most serious diagnostic difficulty in this relation were those in which the wound was situated in the thicker muscular portions of the lower part of the abdominal and pelvic walls. Such a case is illustrated in the chapter on fractures (see fig. 55, p. 191). I saw one or two such instances, in which only the exploration necessary for treatment of the fracture decided the point. In many of the wounds affecting the lateral portion of the abdominal wall the question of penetration could never be definitely cleared up, as wounds of the colon sometimes gave rise to absolutely no symptoms.
In a certain proportion of the injuries the peritoneal cavity[Pg 410] was no doubt perforated without the infliction of any further visceral injury, and in these also the doubt as to the occurrence of penetration was never solved.
(158) Wound of belly wall.—Wounded at Modder River. Entry (Mauser), 2 inches below the centre of the left iliac crest; exit, 1½ inch above and internal to the left anterior superior iliac spine. The patient was on horseback at the time of the injury and did not fall; he got down, however, and lay on the field an hour, whence he was removed to hospital. Probably the track pierced the ilium, and remained confined to the abdominal wall. There were no signs of visceral injury.
(159) Cape Boy. Wounded at Modder River. Entry (Lee-Metford), immediately above and outside right anterior superior spine; exit, 1½ inch below and to right of umbilicus. A well-marked swelling corresponded with division of the fibres of the oblique muscles and of the rectus, and on palpation a hollow corresponding with the track was felt. The abdominal muscles were exceptionally well developed (fig. 84).
(160) Wounded at Magersfontein while lying prone. Entry, irregular, oblique, and somewhat contused, over the eighth left rib, in the anterior axillary line; exit, a slit wound immediately above and to the left of the umbilicus. The bullet struck a small circular metal looking-glass before entering, hence the irregularity of the wound. The patient developed a hæmothorax, but no abdominal signs; the former was probably parietal in origin, secondary to the fractured rib, and the whole wound non-penetrating as far as the abdominal cavity was concerned.
(161) Wounded at Magersfontein. Entry (Mauser), 1½ inch external to and 1/2 inch below the left posterior superior iliac spine; exit, 1 inch internal horizontally to the left anterior superior spine.
No signs of intra-peritoneal injury were noted, but free suppuration occurred in left loin; the ilium was tunnelled.
The same patient was wounded by a Jeffrey bullet in the hand; the third metacarpal was pulverised, although the bullet, which was longitudinally flanged, was retained.
(162) Wounded outside Heilbron. Entry, below the eighth right costal cartilage; exit, below the eighth cartilage of the left side. The wound of entry was slightly oval; that of exit continued out as a 'flame'-like groove for 2 inches. A week later the wound track could be palpated as an evident hard continuous cord.
Penetration of the intestinal area without definite evidence of visceral injury.—This accident occurred with a sufficient degree of frequency to obtain the greatest importance, both from the point of view of diagnosis and prognosis, and as affecting the question of operative interference. Amongst the cases reported below a number occurred in which it was impossible to settle the question whether injury to the bowel had occurred or not, and I will here shortly give what explanation I can for the apparent escape of the intestine from serious injury.
We may first recall the general question of the escape of structures lying to one or other side of the track of the bullet. I believe that there can be no doubt as to the accuracy of the remarks already made as to the escape of such structures as the nerves by means of displacement, and that the occurrence of such escapes is manifestly dependent on the degree of fixity of the nerve or the special segment of it implicated. The general tendency of the tissues around the tracks to escape extensive destruction from actual contusion has also been referred to, and is, I think, indisputable.
If these observations be accepted, I think there can be no difficulty in allowing that the small intestine is exceptionally well arranged to escape injury. First of all, it is very moveable; secondly, it is so arranged that in certain directions a bullet may pass almost parallel to the long axis of the coils; thirdly, it is elastic, capable of compression, and light, and hence offers but a small degree of resistance to the passage of the bullet across the abdominal cavity.
Certain evidence both clinical and pathological supports the contention that the small intestine may escape injury from the passing bullet.
First of all, the fact may be broadly stated that injuries to the small intestine were fatal in the great majority of certainly diagnosed cases, while, on the other hand, many tracks crossed the area occupied by the small intestine without serious symptoms of any kind resulting. Secondly, experience showed that when the bullet crossed the line of the fixed portions of the large intestine the gut rarely escaped, and that, although a considerable proportion of these cases recovered spontaneously,[Pg 412] in a large number of them immediate symptoms, or secondary complications, clearly substantiated the nature of the original injury. As far as my experience went, however, I never saw any instance in which an undoubted injury of the small intestine was followed by the development of a local peritoneal suppuration and recovery, a sequence by no means uncommon in the case of wounds of the large intestine. Although, therefore, I am not prepared to deny the possibility of spontaneous recovery from an injury to the small intestine, under certain conditions which will be stated later, I believe that in the immense majority of cases in which a bullet crossed the small intestine area without the supervention of serious symptoms, the small intestine escaped perforating injury.
Beyond the clinical evidence offered above, certain pathological observations support the view that the intestine escapes perforation by displacement. Most of my knowledge on this subject was derived from the limited number of abdominal sections I performed on cases of injury to the small intestine, and may be summed up as follows.
The small intestine may present evidence of lateral contusion in the shape of elongated ecchymoses, either parallel, oblique, or transverse to its long axis. These ecchymoses resemble in extent and outline those which ordinarily surround a wound of the intestinal wall produced by a bullet (see fig. 87, p. 418).
The wall of the small intestine may be wounded to an extent short of perforation, either the peritoneal coat alone being split, or the wound implicating the muscular coat and producing an appearance similar to that seen when the intestine is dragged upon during an operation, but without so much gaping of the edges (see fig. 85, p. 416).
I met with these conditions in association with co-existing complete perforations of the small intestine, and in one case of intra-peritoneal hæmorrhage in which no complete perforation was discoverable (No. 169, p. 432).
The implication and perforation of the small intestine are to some extent influenced by the direction of the wound. A striking case is included below, No. 201, in which a bullet passed from the loin to the iliac fossa on each side of the body, approximately[Pg 413] parallel to the course of the inner margin of the colon, and I also saw some other wounds in this direction in which no evidence of injury to the small intestine was detected, and which got well. Again wounds from flank to flank were, as a rule, very fatal; but I saw more than one instance where these wounds were situated immediately below the crest of the ilium, in which the intestine escaped injury (see case 171). A very striking observation was made by Mr. Cheatle in such a wound. The patient died as a result of a double perforation of both cæcum and sigmoid flexure; none the less the bullet had crossed the small intestine area without inflicting any injury.
The sum of my experience, in fact, was to encourage the belief that, unless the intestine was struck in such a direction as to render lateral displacement an impossibility, the gut often escaped perforation.
As a rule, the wounds of the abdomen which from their position proved the most dangerous to the intestine were—
1. Wounds passing from one flank to the other were very dangerous, as crossing complicated coils of the small intestine, and two fixed portions of the colon. This danger was most marked when the wounds were situated between the eighth rib in the mid axillary line and the crest of the ilium; above this level the liver, or possibly liver and stomach, were sometimes alone implicated, and the cases did well. Again, when the wounds crossed the false pelvis the patients sometimes escaped all injury to viscera.
2. Antero-posterior wounds in the small intestine area were very fatal if the course was direct; in such the small intestine seldom escaped injury.
3. Wounds with a certain degree of obliquity from anterior wall to flank, or from flank to loin, were on the other hand comparatively favourable, as the small intestine often escaped, and if any gut was wounded, it was often the colon.
4. Vertical wounds implicating the chest and abdomen, or the abdomen and pelvis, were on the whole not very unfavourable. For instance, when the bullet entered by the buttock and emerged below the umbilicus, a number of patients escaped fatal injury; this depended on the comparatively good prognosis in wounds of the rectum and bladder. A good many patients[Pg 414] in whom the bullet entered by the upper part of the loin, and escaped 1½ inch within the anterior superior spine of the ilium, also did well. The same holds good when the wounds either entered or emerged under the anterior costal margin of the thorax, either prior to or after traversing the thorax.
Wounds passing directly backward from the iliac regions were in my experience very unfavourable; but I believe mainly as a result of hæmorrhage from the iliac arteries.
The occurrence of wounds of the abdomen of an 'explosive' character.—The vast majority of the abdominal wounds observed in the Stationary or Base hospitals were of the type dimensions. A certain number of the abdominal injuries which proved fatal on the field or shortly afterwards were described as explosive in character, and were referred by the observers to the employment of expanding bullets.
A few words on this subject seem necessary, because it seems doubtful whether such injuries could be produced by any of the forms of expanding bullet of small calibre in use, unless the track crossed one of the bones in the abdominal or pelvic wall. That this was sometimes the case there is no doubt: thus I saw two cases in which the splenic flexure of the colon was wounded, in which the external opening was large, and a comminuted fracture of the ribs of the left side existed. One can well believe that bullets passing through the pelvic bones might 'set up' to a considerable extent, and although I never happened to see such a case, an explanation of some of the wounds described by others might be found in this occurrence.
In instances in which the soft parts alone were perforated, I am disinclined to believe that bullets of small calibre, either regulation or soft-nosed, were responsible for the injuries. I had the opportunity of examining two Mauser bullets of the Jeffreys variety which crossed the abdomen and caused death. In the first (figured on page 94, fig. 40) very little alteration beyond slight shortening had occurred. In the second the deformity was almost the same, except that the side of the bullet was indented, probably from impact with some object prior to its entry into the body. In each case the bullet was of course travelling at a low rate of velocity;[Pg 415] hence no very strong inference can be drawn from either. In the case of the second specimen, which was removed by Mr. Cheatle, a remarkable observation was made, which tends to throw some light on one possible mode of production of large exit apertures. This bullet crossed the cæcum, making two small type openings; but later, when it crossed the sigmoid flexure, it tore two large irregular openings in the gut. This might be explained on the ground that the velocity was so small as only just to allow of perforation, which therefore took the nature of a tear. I am inclined to suggest, as a more likely explanation, that the spent bullet turned head over heels in its course across the abdomen, and made lateral or irregular impact with the last piece of bowel it touched. A slightly greater degree of force would have allowed a similar large and irregular opening to be made in the abdominal wall also.
In this relation the question will naturally be raised as to how far the explosive appearances may have been due to high velocity alone on the part of the bullet. I am disinclined from my general experience to believe that explosive injuries of the soft parts were to be thus explained. On the other hand, I believe that the possession of a low degree of velocity very greatly increased the danger in abdominal wounds. I believe that the bowel was, under these circumstances, less likely to escape by displacement, and was more widely torn when wounded; again, that inexact impact led to increase of size in the external apertures, and the bullet was of course more often retained.
Mr. Watson Cheyne[19] published a very remarkable instance of one of the dangers of an injury from a spent bullet, in which, in spite of non-penetration of the abdominal cavity, the small intestine was ruptured in two places.
I believe the majority of the wounds designated as explosive were the result of the passage of large leaden bullets, either of the Martini-Henry or Express type. The small opportunity of observing such injuries in the hospitals of course depended on the fact that the majority were rapidly fatal.
Nature of the anatomical lesion in wounds of the intestine.—The openings in the parietal peritoneum tended to[Pg 416] assume the slit or star forms, probably on account of the elasticity of the membrane. A diagram of one of these forms is appended to fig. 89. In this instance the opening in the peritoneum was made from the abdominal aspect, prior to the escape of the bullet from the cavity, and on the impact of the tip, the long axis of the bullet was oblique to the surface of the abdominal wall.
In the intestinal wall the openings varied in character according to the mode of impact.
In some cases the gut was merely contused by lateral contact of the passing bullet. The result of this was evidenced later by the presence of localised oval patches of ecchymosis. These were identical in appearance with the patches shown surrounding the wounds in fig. 87.
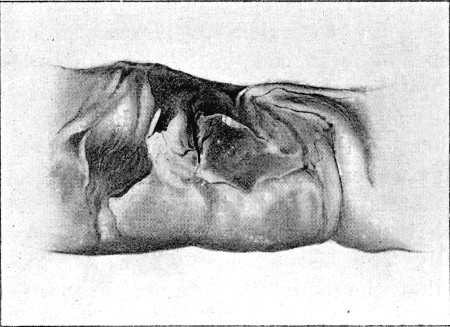 Fig. 85.
Fig. 85.
Lateral Slit in Small Intestine produced by passage of bullet. Slit somewhat obscured by deposition of inflammatory lymph. (St. Thomas's Hospital Museum)
More forcible lateral impact produced a split of the peritoneum, or of this together with the muscular coat. Such a lateral slit is shown in fig. 85, although the clearness of outline is somewhat impaired by the presence of a considerable amount of inflammatory lymph.
Fig. 86 exhibits a lateral injury of a more pronounced form. The bullet here struck the most prominent portion of the under surface of the bowel, and produced a circular perforation not very unlike one produced by rectangular impact, except in[Pg 417] the lesser degree of eversion of the mucous membrane. Here again the appearance is somewhat altered by the presence of a considerable amount of lymph, but this is of less importance in this figure because the lymph is localised to the portion of the bowel in the immediate neighbourhood of the opening which had suffered contusion and erasion.
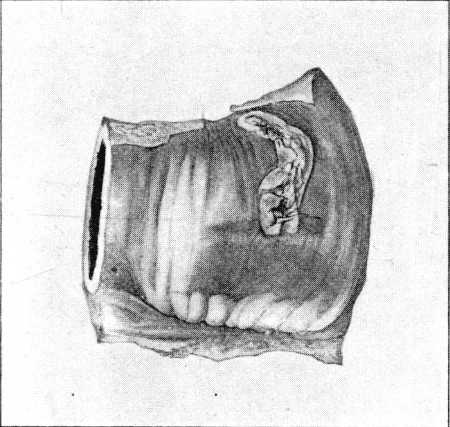 Fig. 86.
Fig. 86.
Gutter Wound of Small Intestine caused by lateral impact. Position of shallow portion of gutter indicated by deposition of inflammatory lymph. Circular perforation. (St. Thomas's Hospital Museum)
Fig. 87, a b, illustrates a symmetrical perforation of the small intestine; the aperture of entry (a) is roughly circular, and a ring of mucous membrane protrudes and partially closes the opening. The aperture of exit is a curved slit, again partially occluded by the mucous membrane. The same amount of difference between the two apertures did not always exist; in many cases both were circular, and apparently symmetrical. Beyond this I have seen three apertures in close proximity, two lying on the same aspect of the bowel, and the first of these was no doubt an opening due to lateral impact similar to that seen in fig. 86. In the recent condition little difference existed between the three apertures.
The localised ecchymosis surrounding the apertures is quite characteristic of this form of injury, and is a valuable aid to finding the openings during an operation.[Pg 418]
Fig. 88 shows the interior of the same segment of bowel, as fig. 87. It shows the localised ecchymosis as seen from the inner surface, here rather more extensive from the fact that the blood spreads more readily in the submucous tissue.
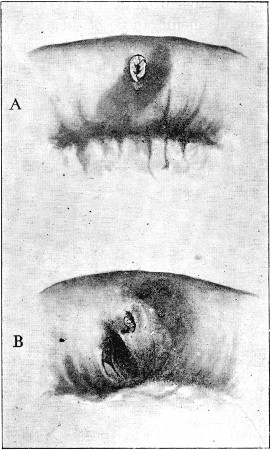 Fig. 87.—Perforating Wounds of Small Intestine.
Fig. 87.—Perforating Wounds of Small Intestine.
A. Entry; note circular outline and eversion of mucous membrane. B. Wound of exit; curved slit-like character, eversion of mucous membrane. Note the localised ecchymosis, more abundant round exit aperture. (St. Thomas's Hospital Museum)
It will be noted that the main feature of the form of injury is the regular outline and the small size of the wounds. Another feature not illustrated by the figures should also be mentioned. In the ruptures of intestine with which we are acquainted in civil practice the wound in the gut is almost without exception situated at the free border of the bowel, but in these injuries it was just as frequently at the mesenteric margin. The importance of this factor is considerable, since wounds near[Pg 419] the mesenteric edge are much more likely to be accompanied by hæmorrhage, and thus the opportunity for diffusion of infection is considerably multiplied, to say nothing of the danger from loss of blood.
Beyond these more or less pure perforations, long slits or gutters were occasionally cut. I saw instances of these in the case of the ascending colon, and in the small curvature of the stomach. The comparative fixity of the portion of bowel struck is a matter of great importance in the production of this form of injury.
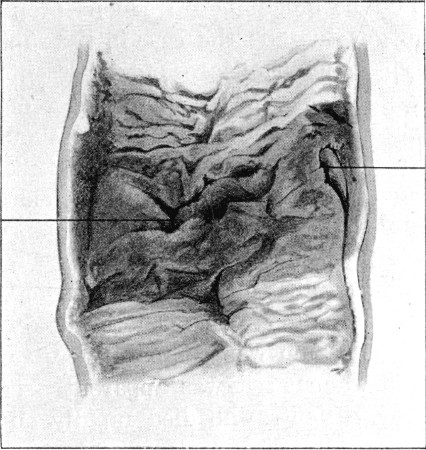 Fig. 88.
Fig. 88.
The same piece of Intestine as that shown in fig. 87, laid open to show the ecchymosis on the inner aspect of the Bowel. The two indicating lines lead to the openings, which appear slit-like, and are sunk at the bottom of folds. (St. Thomas's Hospital Museum)
It may be well to add that, although the figures inserted are all taken from small-intestine wounds, the nature of the wounds of the peritoneum-clad part of the large intestine in no way differed from them, except in so far as fixity of the bowel exposed it to a more extensive wound when the bullet took a parallel course to its long axis.
A more important point in the injuries to the large intestine was the possibility of an extra-peritoneal wound. I saw several such lesions of the colon, every one of which ended fatally. I became still more fully convinced of the greater seriousness of[Pg 420] extra- to intra-peritoneal rupture of this portion of the gut than I was when I expressed a similar opinion in a former paper.[20] It will be seen later that the results of intra- and extra-peritoneal wounds of the bladder fully confirm this view, as all extra-peritoneal injuries died, while many intra-peritoneal perforations recovered spontaneously.
Wounds of the mesentery.—I had little experience of this injury; in fact, case 169, on which I operated, was my sole observation. It stands to reason, however, that injuries to the mesentery would be much more frequent proportionately to wounds of the gut than is the case in the ruptures seen in civil practice, since the whole area of the mesentery is equally open to injury. Viewing the extreme danger of hæmorrhage into the peritoneal cavity in these injuries, I should be inclined to expect that a considerable proportion of those deaths from abdominal wounds which took place on the field of battle were due to this source.
Wounds of the omentum.—Here, again, I am unable to express any opinion, although the supposition that hæmorrhage from this source took place is natural.
Prolapse of omentum was comparatively rare, except in cases with large wounds; it was apparently seen with some frequency among patients who died rapidly on the field of battle. I only saw it twice, and on each occasion in shell wounds. The wounds from small-calibre bullets were as a rule too small to allow of external prolapse.
Fig. 89, however, illustrates a very interesting observation. A patient in the German Ambulance in Heilbron, under Dr. Flockemann, died as a result of suppuration and hæmorrhage secondary to an injury to the colon. At the autopsy a portion of the omentum was found adherent in the wound of exit, but it had not reached the external surface. The chief interest of the observation lies in the light it throws on the mechanism of these injuries. It is impossible to conceive that a small-calibre bullet coming into direct contact with the omentum could do anything but perforate it. It, therefore, appears clear that in a displacement like that figured, only lateral impact[Pg 421] occurred with the omentum, which was carried along by the spin and rush of the bullet into the canal of exit, where it lodged.
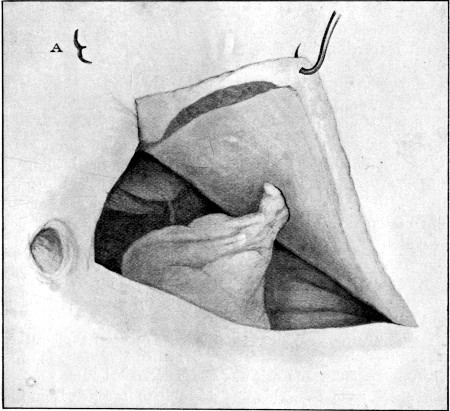 Fig. 89.
Fig. 89.
Great Omentum carried by the bullet into an exit track leading from the abdominal cavity. A. Outline of opening in the peritoneum
Results of injury to the intestine. 1. Escape of contents and infection of the peritoneal cavity.—I think there is little special to be said on this subject. The escape of contents into the peritoneal cavity was by no means free, unless the injury was multiple. Thus in one case of injury to the small intestine, No. 166, on which I operated, there was absolutely no gross escape until the bowel was removed from the abdominal cavity, when the contents spurted out freely. In one case of very oblique injury to the colon there was a considerable quantity of fæcal matter in a localised space, but as a rule the ordinary condition best described as 'peritoneal[Pg 422] infection' from the wound was found. The bad effect of anything like free escape was well shown in multiple perforations; in these suppurative peritonitis rapidly developed and the patients died at the end of thirty-six hours or less. A typical case is quoted in No. 168.
2. Peritoneal infection, and general septicæmia.—As is evident from the results quoted among the cases, the degree which this reached varied greatly. It may of course be assumed that in some measure it occurred in every case in which the bowel was perforated, but it was sometimes so slight as to be scarcely noticeable. This may be said to have been most common in injuries to the large intestine. Wounds of the cæcum, ascending and descending colon, the sigmoid flexure, or the rectum, were sometimes followed by no serious symptoms, either local or general. Again in these portions of the bowel the development of local signs, and the later formation of an abscess, were by no means uncommon.
In the case of the small intestine I never observed this sequence, and the same may be said of the transverse colon, which in its anatomical arrangement and position so nearly approximates to the small bowel. In suspected wounds of these portions of the bowel either the symptoms were so slight as to render it doubtful whether a perforation had occurred, or marked signs of general peritoneal septicæmia developed, and death resulted.
The condition of the peritoneum in fatal cases varied much. In some a dry peritonitis, or one in which a considerable quantity of slightly turbid fluid was effused, was found. In others a rapid suppurative process, accompanied by the effusion of large quantities of plastic lymph, was met with. My experience suggested that the latter condition was the result of free infection from multiple wounds of the gut, the former the accompaniment of single wounds. Hence I should ascribe the difference mainly to the extent of the primary infection.
This is perhaps a suitable place to further discuss the explanation of the escape of a considerable number of the patients who received wounds of the abdomen, possibly implicating the bowel. Although this was not, I think, so common an[Pg 423] occurrence as has been sometimes assumed, yet many examples were met with. Several reasons have been advanced.
(1) Great importance has been given to the fact that many of the men were wounded while in a state of hunger, no food having been taken for twelve or more hours before the reception of the injury. In view of the well-proved fact in these, as in other intestinal injuries, that free intestinal escape does not occur, and that it is usually a mere question of infection, this explanation, in my opinion, is of small importance. It might with far more justice be pointed out that many of these wounded men were for them in the happy position of not having friends freely dosing them with brandy and water after the reception of the injury, and this was possibly an element of some importance.
Some of the men did, however, drink freely, and in one case which terminated fatally a comrade gave a man wounded through the belly an immediate dose of Beecham's pills.
(2) Mr. Treves has suggested that the effect of the severe trauma on the muscular coat of the bowel is to cause a cessation of peristaltic movement. This, as in the case of 'local shock' elsewhere, may no doubt be of importance, and to it should be added the simultaneous cessation of abdominal respiratory movements in the segment of the belly wall covering the injured part. The occurrence of general cessation of peristaltic movement is, however, to some extent opposed by the fact that in a certain number of the cases early passage of motions was seen just as happens in the intestinal ruptures seen in civil practice.
I should be inclined to ascribe the escape from serious infection in these injuries to the same cause which accounts for their comparative insignificance in other regions—namely, the small calibre of the bullet and consequent small size of the lesion: in point of fact to the minimal nature of the primary infection. I very much doubt if any patient who had more than one complete perforation of the small intestine got well during the whole campaign. This opinion is, moreover, supported by the fact that the prognosis was so far better in cases of injury to the large than to the small intestine, in which former segment of the bowel we have the advantages of a[Pg 424] position beyond the region in which intestinal movement is most free, the unlikelihood of multiple injury, and a drier and more solid type of fæcal contents.
In the instances in which recovery followed perforating injuries without any bad signs we can only assume a minimal infection, and sufficient irritation and reaction on the part of the bowel to produce rapid adhesion between contiguous coils, and thus provisional closure.
The other mode of spontaneous recovery which I saw several times take place in the injuries to the large bowel consisted in the limitation of the spread of infection by early adhesions and the development of a local abscess. The non-observance of this process in any case of injury to the small intestine raises very great doubts in my mind as to the frequent recovery of patients in whom the small intestine was perforated.
1. Wounds of the stomach.—A considerable number of wounds in such a situation as to have possibly implicated the stomach were observed, and of these a certain number recovered spontaneously. The only two instances that came under my own observation are recorded below. It will be noted that in each the special symptoms were the classic ones of vomiting and hæmatemesis. In the first case blood was also passed per anum, and in the second the diagnosis was reinforced by the escape of stomach contents from the external wound.
The second case was a surgical disappointment. No doubt the fatal issue was mainly dependent on the fact that the external wound had to be kept open to allow of the escape of the abundant discharge from the wounded liver. In the absence of the hepatic wound, however, I believe it would have been possible for this patient to have got well spontaneously, in view of the firm adhesions which had formed around the opening in the stomach, and the consequent localisation which had been effected. Another unfortunate element in this case was the comminuted fracture of the seventh costal cartilage, which maintained the patency of the aperture of[Pg 425] exit. The latter point, however, was of doubtful importance from this aspect, as the vent provided for the gastric and biliary secretions may have been the safety-valve that had allowed localisation to develop.
I believe that the secondary hæmorrhage was the main element in robbing us of a success in this case, and that this depended on the digestion of the wound by the gastric secretion. The early troubles which arose in the treatment of this patient well illustrate the difficulties by which the military surgeon is at times met; but the patient was admirably attended to and nursed by my friend Mr. Pershouse, and an orderly who was specially put on duty for the purpose.
(163) Wounded at Rensburg. Entry (Mauser), in ninth left intercostal space in posterior axillary line; exit, a transverse slit 1/2 an inch in length to left of xiphoid appendage. Patient was retiring when struck; he did not fall, but ran for about 1,000 yards, whence he was conveyed to hospital. He vomited half an hour after the injury (last meal bread and 'bully beef,' taken two hours previously), and during the evening three times again, the vomit consisting mainly 'of dark thick blood.' He was put on milk diet, and not completely starved; on the third day a large quantity of dark clotted blood was passed per rectum with the stool, and this continued for two days.
Ten days after the injury the temperature was still rising to 100°, and did not become normal till the fourteenth day. The pulse averaged 80. The abdomen, meanwhile, moved fairly well, respirations 18 to 20. Some tenderness was present in the epigastrium and towards the spleen. Resonance throughout. Ordinary diet was now resumed, and beyond slight epigastric pain on deep inspiration, no further symptoms were observed, and the patient left for England at the end of the month. The spleen may have been traversed in this patient, as well as the lower margin of the right lung.
(164*) Wounded at Enslin. Entry (Mauser), 3/4 of an inch from the spine, opposite the eighth intercostal space; exit, through the seventh left costal cartilage, 1 inch from the median line. The patient was lying in the prone position when shot: he vomited blood freely, and the bowels acted three times before he was seen forty hours after the accident, each motion containing dark blood.
On the commencement of the third day the patient's expression was extremely anxious, and he was suffering great pain.[Pg 426] Pulse 96, temperature 100°. Tongue moist, occasional vomiting, bowels open yesterday. Has taken fluid nourishment since injury. The abdomen moved with respiration, but was moderately distended, especially in the line of the transverse colon; it was tympanitic on percussion, there was no dulness in the flanks, and only moderate rigidity of the wall on palpation. Frothy fluid stained with bile and fæcal in odour was escaping from the wound of exit, and the everted margins of the latter were bile-stained.
A vertical incision was carried downwards from the wound for 4 inches. A rugged furrow was found on the under surface of the left lobe of the liver; the stomach was contracted and firmly adherent by recent lymph to the under surface of the liver and the diaphragm. The transverse colon was much distended. On separating the stomach a slit wound was found at the lesser curvature, immediately to the right of the œsophagus. This wound was closed with some difficulty with two tiers of sutures; the cavity was mopped out, and then irrigated with boiled water; a plug was introduced along the line of the furrow in the liver, and the lower part of the abdominal incision closed.
The patient stood the operation well, and was removed to his tent; during the day, however, two thunder showers occurred during each of which water, several inches if not a foot deep, rushed through the camp. After the second flood he was removed to the operating room, the only house we had, and slept there. The pulse rose to 120, and respiration to 26, and there was pain, which was subdued by 1/3 grain of morphia, administered subcutaneously. A fair amount of urine was passed, and the bowels acted once, the motion containing blood.
On the second day after operation there was some improvement; the pulse still numbered 116, and the temperature was raised to 100°, but the belly moved fairly, and pain was moderate. Abundant foul-smelling, bile-stained discharge came from the wound when the plug was removed. Rectal feeding was supplemented by small quantities of milk and soda by the mouth.
The condition did not materially change, but on the fourth day it was evident that the suturing of the stomach wound had given way, and liquid food escaped readily when taken. The discharge remained bile-stained and very foul. No extension of inflammation to the general peritoneal cavity occurred, but it was evident that the patient was suffering from constitutional infection from the foul wound, the lower part of which opened up somewhat[Pg 427] after the removal of the stitches on the seventh day. The wound was irrigated three times daily with 1-300 creolin lotion, but remained very foul. The man slowly lost strength, although escape from the stomach considerably decreased. On the tenth day a sudden severe hæmorrhage occurred, presumably from a large branch of the cœliac axis. The bleeding was readily controlled by a plug, and did not recur; but the patient rapidly sank, and died on the twelfth day after the operation, and fourteen days after reception of the injury. No post-mortem examination was made.
2. Wounds of the small intestine.—These were comparatively common, but offered little that was special either in their symptoms or the results attending them. Wounds were met with in every part of the small gut; but I saw no case in which an injury to the duodenum could be specially diagnosed.
As to the symptoms which attended these injuries, it is somewhat difficult to speak with precision, and it must be left to my readers to form an opinion as to how many of the cases recounted below were really instances of perforating wounds. My own view is that in the majority of the cases that got well spontaneously, the injury was not of a perforating nature, and that for reasons which have been already set forth. It will, however, be at once noted that in all the five cases in which the injury was certainly diagnosed in hospital death occurred.
The cases of injury to the small intestine are perhaps best arranged in three classes.
1. Those who died upon the field, or shortly after removal from it. In these the external wounds were often large, the omentum was not rarely prolapsed, and escape of fæces sometimes occurred early. Shock from the severity of the lesion, and hæmorrhage, were no doubt important factors in the early lethal issue in this class. Many of the injuries were no doubt produced by bullets striking irregularly, by ricochets, by bullets of the expanding forms, or by bullets of large calibre. As being beyond the bounds of surgical aid, this class possessed the least interest.
2. Cases brought into the Field, or even the Stationary hospitals, with symptoms of moderate severity, or even of an[Pg 428] insignificant character, in which evidence of septic peritonitis suddenly developed and death ensued.
3. Cases in which the position of the wounds raised the possibility of injury to the intestine, but in which the symptoms were slight or of moderate severity, and which recovered spontaneously.
The whole crux in diagnosis lay in the attempt to separate the two latter classes, and, personally, I must own to having been no nearer a position of being able to form an opinion on this point, in the late than in the early stage of my stay in South Africa. The advent of peritoneal septicæmia was in many instances the only determining moment. On this matter I can only add that, in civil practice, an exploratory abdominal section is often the only means of determination of a rupture of the bowel wall.
With regard to the cases of suspected injury to the bowel which recovered spontaneously, the symptoms were somewhat special in their comparative slightness, and in the limited nature of the local signs. Thus the pulse seldom rose to as much as 100 in rate, 80 was a common average. Respiration was never greatly quickened, 24 was a common rate. The temperature rarely exceeded 100°. Vomiting was occasionally severe, but usually not persistent, ceasing on the second day. A good quantity of urine was passed. As to the local signs, these again were of a limited nature; distension did not occur, or was slight; movement of the abdominal wall was only restricted in the neighbourhood of the wound, the affected area amounted to a quarter, or at most half, the abdominal wall, and rigidity was localised to a similar segment. Local tenderness usually existed; but, as a rule, there was little or no dulness to point to the occurrence either of fluid effusion or a considerable deposition of lymph.
Again many of the patients suffered with very slight symptoms of constitutional shock, although there was considerable variation in this particular.
(165*) Wounded at Graspan, sustaining a compound fracture of the fibula. While being carried off the field, a second bullet (Lee-Metford) entered immediately outside the left posterior superior[Pg 429] iliac spine, perforated the pelvis, and emerged 1½ inch within the left anterior superior spine. The patient was then put down and left on the field ten hours; later he was carried to shelter for the night, and arrived at Orange River on the second day. He suffered with some pain in the abdomen, especially during the journey in the train, but was not sick; the bowels were confined.
When seen on the third day at 6 p.m., some pain was complained of in the abdomen, which moved freely in the upper part, but was motionless below the umbilicus. No distension. Tenderness around wound of exit and some rigidity. The bowels had acted four times during the day; motions loose, dark brown, and containing no blood. Face not anxious, eyes bright, temperature 102°. Pulse 96, regular, and of good strength. Tongue moist and little furred.
The abdomen was opened at 5 a.m. on the fourth day, as the local signs had become more pronounced, and the patient had passed a restless night in great abdominal pain. A local incision was chosen, as the wound was presumably in the sigmoid flexure. The sigmoid flexure was adherent to the abdominal wall opposite the wound of exit, and a dark ecchymosed patch was found, but no perforation could be detected. Foul pus and gas escaped freely from the pelvis, but no wound of the large bowel could be discovered here. On enlarging the incision upwards three openings were found in a coil of jejunum, probably that about five feet from the duodenal junction usually provided with the longest mesentery. No fourth opening could be found. The openings were circular, about 1/3 inch in diameter, clean cut, with a ring of everted mucous membrane, and the wall of the bowel in the neighbourhood was thickened. All three openings were included within a length of 2½ inches. There was no surrounding ecchymosis of the bowel wall. Very little escaped intestinal contents were found in the situation of the bowel. The latter had apparently been retracted upwards, and lay to the left of the lumbar spine. The wounds were readily closed by five Lembert's sutures, three crossing the openings, and one at each end. The belly was then washed out with boiled water and closed. The delay in finding the wounds due to the mistaken impression that they would be found in the pelvis materially prolonged the operation, which lasted an hour and a half. The patient never rallied, and died seventeen hours later. It is possible that a wound in the sigmoid flexure was present which had already closed at the time of operation.
(166*) Wounded at Magersfontein. Entry (Mauser), opposite[Pg 430] central point of left ilium; exit, 1½ inch above the centre of the right Poupart's ligament. Vomiting commenced soon after the injury, and this was continuous until the patient's arrival in the Stationary hospital on the fourth day, when the condition was as follows:—
Face extremely anxious in expression. Temperature 101°, sweating freely. Pulse 110, fair strength. Tongue moist. Abdomen much distended, rigid, motionless, tympanitic throughout. Bowels confined. No urine had been passed for twenty-four hours, ℥ij in bladder on catheterisation, clear, and containing no blood.
Abdominal section. Median incision. A considerable quantity of bloody effusion was evacuated. Intestine generally congested and distended. No lymph. Two wounds were found in the ileum on the opposite sides of one coil; the openings were circular, with the mucous membrane everted. No escape of fæcal matter was visible until the intestine was delivered, when intestinal contents spurted freely across the room. The openings were sutured with five Lembert's stitches. The bowel was punctured in two places to relieve distension, and then returned into the belly, after washing with boiled water.
Four pints of saline solution were infused into the median basilic vein, and 1/30 grain strychnine sulph. was injected hypodermically.
The patient did not rally, and died twelve hours after the operation.
(167*) Wounded at Graspan. Entry (Lee-Metford), midway between the umbilicus and pubes; exit, 1 inch to the left of the fifth lumbar spine. The patient was seen on the third day in the following condition: in great pain, expression extremely anxious, vomiting constantly. Pulse 150 running, respirations 48. Temperature 100°, sweating freely. Great distension, rigidity, and general tenderness of immobile abdomen. No improvement followed the administration of brandy and hypodermic injection of strychnine 1/30 grain, and operation was deemed hopeless.
In the evening the patient was apparently dying. Face blue and sunken and covered with sweat, eyes dull, speechless, pulse imperceptible, restlessness extreme, bowels acting involuntarily, no urine in bladder.
The man was placed in a tent by himself, and to my surprise was alive and better the next morning; the expression was still anxious, but the face brighter and not sweating; the pulse only[Pg 431] numbered 100, but was very weak, and the hands and feet were cold. The condition of the abdomen was unaltered, but the thoracic respiration had decreased in rapidity from 48 to 28.
His condition still seemed to preclude any chance of successful intervention, but none the less life was retained until the morning of the seventh day, the state alternating between a moribund one and one of slight improvement. He was lucid at times, although for the most part wandering, and was so restless that no covering could be kept upon him. Vomiting was continuous, so that no nourishment could be retained; the bowels acted frequently involuntarily, and little or no urine was passed. Meanwhile, the abdomen became flat, then sunken, an area of induration and tenderness about 6 inches in diameter developing around the wound of entry. Slight variations in the pulse, and from normal to subnormal in the temperature, were noted, and death eventually occurred from septicæmia and inanition.
(168*) Wounded at Driefontein. Entry (Mauser), above the posterior third of the left iliac crest, at the margin of the last lumbar transverse process (probably through ilio-lumbar ligament); exit, 1 inch below and to the left of the umbilicus.
The patient was wounded at 3 p.m., but not brought into the Field hospital until 9 p.m., when the temperature of the tents was below 28°F. He was considerably collapsed, suffering much pain, and vomited freely. The abdomen was flat, but very tender. Bowels confined. The column had to move at 5 a.m. the next morning, when the temperature was still near freezing, and during the day continuous fighting prevented any chance of operation. The man steadily sank during the day, and died thirty-six hours after the reception of the injury.
Post-mortem condition.—Belly not distended, dull anteriorly in patches, and right flank dull throughout. When the belly was opened, extensive adhesion of omentum and intestine enclosing numerous collections of pus were disclosed, and on disturbing the adhesions a large collection of turbid blood-stained fluid was set free from the right loin. The great omentum was much thickened and matted, with deposition of thick patches of lymph; very firm recent adhesions also united numerous coils of small intestine. The pus was fœtid, but no appreciable quantity of intestinal contents was detected in it. The lower half or more of the small intestine was injected, reddened, and thickened. The wounds which were situated in the lower part of the jejunum and ileum were multiple, and seven perforations were detected;[Pg 432] besides these the intestine was marked by bruises, and some gutter slits affecting the serous and muscular coats only. Considerable ecchymosis surrounded these latter. The clean perforations were circular, less than 1/4 inch in diameter, and for the most part closed by eversion of the mucous membrane. Intestinal contents were not apparent, but escaped freely on manipulation of the bowel.
(169*) Wounded at Magersfontein. Entry (Mauser), over the eighth rib in the anterior axillary line; exit, 1 inch to the left of second lumbar spinous process, just below the last rib. Vomiting commenced almost immediately after reception of the injury, and the bowels acted frequently. This condition persisted until the fourth day, when the patient was brought down to Orange River, and the signs were as follows. Considerable pain in left half of abdomen, pulse 110, fair strength, temperature 101°. Some general distension of abdomen with complete disappearance of hepatic dulness. Some movement of right half of abdomen, left half immobile, dulness extending from the flank as far forwards as linea semilunaris. An incision was made in left linea semilunaris, and Oj blood evacuated from the left loin. There was no lymph on the intestines nor sign of inflammation. No perforation was discovered in either stomach or intestine, but on two coils of jejunum there were deep slits 3/4 inch long, extending through both peritoneal and muscular coats. Beyond these wounds, on other coils oval patches of ecchymosis, due to direct bruising, were present. The peritoneal cavity was sponged free of all blood and irrigated with boiled water; no bleeding point was discovered, and the abdomen was closed.
The next morning the patient was comfortable; temperature 100.2°, pulse 100. Tongue clean and moist; he vomited once during the night.
Some bloody discharge had collected in the dressing, and at the lower angle of wound there was a local swelling, apparently in the abdominal wall. The flank was resonant.
During the afternoon the patient became faint, and when seen at 6 p.m. was in a state of collapse, in which he shortly died.
Death was apparently due to renewal of the previous hæmorrhage. No post-mortem examination was made.
(170*) Wounded at Magersfontein. Entry (Mauser), 1/2 inch to the left of the second sacral spine; exit, immediately below the left anterior superior iliac spine; the patient was kneeling at the time, and the same bullet traversed his left thigh in the lower[Pg 433] third. When seen on the third day, the lower part of the abdomen was motionless, tumid, and tender. The bowels had been confined for three days; there had been no sickness, and the tongue was moist and clean. Temperature 100°, pulse 90, fair strength, respirations 38. The patient had once had an attack of acute appendicitis, and he himself said he was sure he now had 'peritonitis,' as he had pain exactly similar in the belly to that he had suffered in his previous illness.
No further signs, however, developed under an expectant treatment, and he remained some two months in hospital, while the wound in the thigh and a third injury to the elbow-joint were healing.
(171) Entry (Mauser), at the highest point of the left crista ilii; exit, through the right ilium, 2 inches horizontally anterior to the posterior superior spine. Absolutely no abdominal symptoms followed. The bowels were confined five days, and then opened by enema. The patient complained of some stiffness in the lumbo-sacral region, but the right synchondrosis was no doubt implicated in the track.
(172) Wounded at Paardeberg (range 800 yards). Entry (Mauser), 2 inches diagonally below and to the right of the umbilicus; exit, not discoverable. For the first two days the patient had to lie out with the regiment; on the fourth he was removed to the Field hospital. During the first three days the patient vomited (green matter) frequently, and the belly was hard and painful; as biscuit was the only available food, no nourishment was taken. The bowels acted on the second night. At the end of a week the patient was sent by bullock wagon (three days and nights) to Modder River, and then down to Capetown, where he walked into the hospital on the thirteenth day, apparently well.
Two days later the temperature rose to 104°, and enteric fever was diagnosed, no local signs pointing to the injury existing. The patient made a good recovery.
(173) Wounded at Colenso. Entry (Mauser), at junction of outer 2/5 with inner 3/5 of line from right anterior superior iliac spine to umbilicus; exit, at upper part of right great sacro-sciatic foramen, in line of posterior superior iliac spine. Advancing on foot when struck; he then fell and crept fifty yards to behind a rock, where he remained seven and a half hours. For two days subsequently he vomited freely; the bowels acted nine hours after the injury, and then became constipated. No further symptoms[Pg 434] were noted, and at the end of three weeks the abdomen was absolutely normal. The man is now again on active service.
(174*) Wounded at Modder River while retiring on foot. Entry (Mauser), at highest point of right iliac crest; exit, 2½ inches to right of and 1/2 inch above level of umbilicus. The injury was not followed by sickness, and the bowels remained confined. During the first two days 'pain struck across the abdomen' when micturition was performed.
When the patient came under observation on the third day the condition was as follows:—Complains of little pain, temperature normal, pulse 72, respirations 24, tongue moist, bowels confined. Rigidity of abdominal wall and deficient mobility of nearly whole right half of belly, the whole lower half of which moves little with respiration. No track palpable in abdominal parietes. No dulness, no distension. The temperature rose to 99.5° at night. On the fourth day the bowels acted freely, the pulse fell to 60, the respirations were 24, and the temperature normal.
Tenderness and rigidity persisted in the right flank to the end of a week, after which time no further signs persisted.
(175*) Wounded at Modder River while lying on right side. Range 500 yards. Walked 400 yards after injury. Entry (Mauser), at the junction of the posterior and middle thirds of the right iliac crest; exit, 3 inches to right of and 1/2 inch below the level of the umbilicus. The injury was followed by no signs of intra-abdominal lesion; on the third day the temperature was normal, pulse 80, and the tongue clean and moist. Some soreness at times and tenderness on pressure were complained of, but the man was discharged well at the end of one month.
(176*) Wounded while doubling in retirement at Modder River. Entry (Mauser), immediately above the junction of the posterior and middle thirds of the left iliac crest; exit, 1 inch below costal margin (eighth rib), 3 inches to the right of the median line. The bullet was lying in the anterior wound, whence it was removed by the orderly who applied the first dressing on the field. The patient remained on the field seven and a half hours, and when brought into hospital at once commenced to vomit. The ejected matter, at first green in colour, during the next forty-eight hours changed to a dirty brown. Meanwhile, the abdomen was somewhat painful. When seen on the third day he had ceased to vomit for three hours. The face was slightly anxious, and the[Pg 435] patient lay on the ground with the lower extremities extended. Temperature 99°, pulse 72, fair strength. Respirations 32, shallow. Tongue moist, lightly furred, bowels not open for four days. He slept fairly last night. Abdomen soft, moving well with respiration, no distension, slight tenderness below and to the right of the umbilicus, and local dulness in right flank.
The next day the pulse fell to 60 and the bowels acted, but there was no change in the local condition. The man looked somewhat ill until the end of a week, but was then sent to the Base, and at the expiration of a month was sent home well.
(177*) Wounded at Modder River. Two apertures of entry (Mauser); (a) below cartilage of eighth rib in left nipple line; (b) 2 inches below and 4½ inches to the left of the median line. No exit wound discovered, and no track could be palpated between the two openings, which were both circular and depressed. When seen on fourth day there was tenderness in the lower half of the abdomen, and the left thigh was held in a flexed position. Respirations 20, respiratory movement confined to upper half of abdominal wall. Pulse 70, temperature 99°. Tongue moist, covered with white fur; bowels confined since the accident; no sickness. The patient remained under observation thirteen days, during which time pain and difficulty in movement of the left thigh persisted, also slight tenderness in the lower part of the abdomen; but at the end of a month he was sent to England well, but unfit to take further part in the campaign. I thought the bullet might be in the left psoas, but it was not localised.
(178*) Wounded at Modder River. Entry (Mauser), 3½ inches above and 1½ inch within the left anterior superior iliac spine; exit, 1½ inch to the right of the tenth dorsal spinous process. The same bullet had perforated the forearm just above the wrist prior to entering the abdomen. No local or constitutional signs indicated either bowel injury or perforation of liver. The man, however, was suffering from a slight attack of dysentery, passing blood and mucus per rectum with great tenesmus. He was sent to the Base at the end of a week, and returned to England well three weeks later. He attributed his dysentery to the wound, as the symptoms did not exist prior to its reception; but as the disease coincided exactly with what was very prevalent amongst the troops at the time, I do not think there was any connection between it and the injury.
(179) Wounded near Thaba-nchu. Entry, over the centre of the sacrum at the upper border of fourth segment; exit, 1½ inch[Pg 436] above left Poupart's ligament, 2 inches from the median line. Aperture of entry oval, with long vertical axis. Exit wound a transverse slit, with slight tendency to starring (see fig. 19, p. 58). One hour after being shot the patient vomited once. There was some evidence of shock and considerable pain. The bowels acted involuntarily simultaneously with the vomiting, and incontinence of fæces and retention of urine persisted for four days. The vomit was bilious in appearance; no blood was seen either in it or the motions.
Forty-six hours after the injury the condition was as follows: Face slightly anxious and pale; skin moist, temperature 100.4°; pulse 116, regular and of fair strength; respirations 24; abdomen slightly tumid; tenderness over lower half, especially on left side; the lower half moves little with respiration.
Twenty-four hours later the patient had improved. He was comfortable and hopeful; slept well with morphia 1/3 grain hypodermically. Tongue moist, covered with white fur; has been taking milk only, ℥ij every half-hour. No sickness. Temperature
99°. Pulse 104. Respirations 24. Abdomen flatter; general respiratory movement; tenderness now mainly localised to an area 2½ inches in diameter, to the left of the umbilicus, above exit wound.
The patient continued to improve, and on the fifth day travelled six hours in a bullock wagon to Bloemfontein. Soon after arrival his temperature was normal: pulse 80, respirations 16, with good abdominal movement. Local tenderness persisted in the same area, but was less in degree. Tongue rather dry, bowels confined. Micturition normal. Two drachms of castor oil and an enema were given.
On the ninth day patient was practically well, except for slight deep tenderness. He remained in bed on ordinary light diet, but at the end of the third week he was seized by a sudden attack of pain, the temperature rising to 103° and the pulse to 140, the abdomen becoming swollen and tender. He was then under the charge of Mr. Bowlby, who ordered some opium, and the symptoms rapidly subsided. Although this wound crossed the small intestine area, it is probable that the symptoms may have been due to an injury of the rectum or sigmoid flexure.
3. Wounds of the large intestine.—Injuries to every part of the large bowel were observed, and spontaneous recoveries were seen in all parts except the transverse colon, which,[Pg 437] as already remarked, is near akin to the small intestine with regard to its position and anatomical arrangement.
The only case of perforation of the vermiform appendix that I heard of, one under the care of Mr. Stonham, died of peritoneal septicæmia. Several cases of recovery from wounds of the cæcum and ascending colon are recounted below. The only points of importance in the nature of the signs of these injuries were their primary insignificance, and the comparative frequency with which local peritoneal suppuration followed them. The absence of a similar sequence in some of the cases in which wounds of the small intestine were assumed, was, in my opinion, one of the strongest reasons for doubting the correctness of the diagnosis. It is also a significant fact that injuries of the ascending colon—that is to say, of the portion of the large bowel which perhaps lies most free from the area occupied by the small intestine—were those which most frequently recovered.
The following cases afford examples of the course followed in a number of injuries to the large intestine, and illustrate both the uncomplicated and the complicated modes of spontaneous recovery.
No. 180 affords a good example of an extra-peritoneal injury, and of the especially fatal character of such lesions. This case was also one of my surgical disappointments.
Nos. 182, 183 are of great interest in several particulars. First, the aperture of exit was large and allowed the escape of fæces, not a very common feature in wounds not proving immediately fatal. Secondly, in neither were any peritoneal signs observed. Thirdly, in each the exit wound communicated with the pleura, and the patients died from septicæmia mainly due to absorption from the surface of that membrane (Pleural septicæmia).
No. 190 is a most striking instance of spontaneous cure, since no doubt can exist that both rectum and bladder were perforated.
(180*) Injury to the cæcum and ascending colon.—Boer, wounded at Graspan while sheltering behind a rock, lying on his back.
Entry (Lee-Metford), in right thigh, 3 inches below and 1 inch[Pg 438] within anterior superior spine of ilium; exit, in back, on a level with the fourth lumbar spinous process and 3 inches from that point.
Half an hour after the wound the patient commenced to suffer severe stabbing pain; he lay on the field one hour; later he was taken to a Field hospital, and on the second day was sent by train a distance of twenty-five miles.
When seen at the end of fifty hours the condition was as follows. Face anxious, complexion dusky. Great abdominal pain, especially about the umbilicus. Vomiting frequent and distressing; bowels confined since the accident; tongue dry and furred. Urine scanty. Pulse full and strong, 125; respirations, entirely thoracic, 30.
Abdomen generally distended and tympanitic, wall rigid and motionless. Dulness in right flank, together with superficial œdema and emphysema.
Abdominal section fifty-three and a half hours after accident. Incision in right linea semilunaris. Great omentum adherent to ascending colon, which was covered with plastic lymph. Gas and intestinal contents escaped from an opening at the line of reflexion of the peritoneum from the ascending colon; retro-peritoneal extravasation and emphysema extended the whole length of the ascending colon and around duodenum, the wall of the colon itself exhibiting subperitoneal emphysema. The colon was freed and the rent sewn up with interrupted sutures. About ℥iv of foul fæcal fluid were evacuated from loin, and a free counter-opening made. The opening in the ilium by which the bullet had entered the abdomen was found at the brim of the pelvis; the loin and peritoneal cavity were sponged dry and flushed with boiled water; no lymph was seen on the small intestine. A large gauze plug was inserted into the posterior wound, one end of the plug being brought out of the operation incision.
During the succeeding six days progress was not unsatisfactory: the abdomen became soft, moved with respiration, there was no sickness, and the bowels acted. The pulse fell to 90, respirations to 20, and the temperature did not exceed 102° F. The wound suppurated freely, however, and although there were no further signs of peritoneal septicæmia, it was evident that general infection had taken place, and on the sixth day a parotid bubo developed on the right side, which was opened.
On the seventh day the patient suddenly commenced to fail rapidly; vomiting was almost continuous—at first curdled milk, later frothy watery fluid—and on the eighth day he died. The[Pg 439] abdomen remained soft, sunken, and flaccid, and death no doubt resulted from general septicæmia rather than from peritoneal infection, absorption taking place from the large foul cavity behind the colon. As the cavity in part surrounded the descending duodenum, this possibly accounted for the attack of vomiting which preceded death.
(181*) Ascending colon.—Wounded at Graspan while lying in prone position. Entry (Mauser), over ninth rib in line of right linea semilunaris; exit, in right buttock, just below and behind the top of the great trochanter.
The injury was followed by little abdominal pain, but a strange sensation of local gurgling was noted. The bowels acted as soon as the patient reached camp, some hours after being wounded. There was no sickness and nothing abnormal was noted in the motions, except that they were loose and light-coloured.
On the evening of the third day the patient came under observation in the ambulance train for Capetown. He looked somewhat anxious and ill, but he complained of little pain; the temperature was 102°, pulse 88, fair strength, soft and regular. There was local dulness, tenderness, and deficiency of movement in the right iliac region. As it was night, he was removed from the train and an operation was performed the next morning.
Prior to operation the condition was as follows: Pulse 84, temperature 100°; respiration easy, 20. Tongue moist, but thickly coated in centre. Abdomen moves fairly, and is resonant, except in right lower quadrant. No distension. Dulness, tenderness, and rigidity in right iliac region, marked to outer side of cæcum. Entry wound nearly and exit quite healed. Cannot flex right thigh. The following operation was performed. Appendix incision, about ℥j of fæcal fluid and fæces in a localised cavity on outer and anterior aspect of cæcum evacuated; adhesions very firm. Cavity sloughy throughout and cæcum covered with dull grey lymph. The opening in the bowel was not localised, and it was considered wiser to treat the case like one of perforation from appendicitis than to run the risk of breaking down adhesions. A small awl-like opening was found in the ilium with powdered bone at its entrance leading to the wound of exit.
The after-treatment of the case gave rise to no anxiety, but healing of the resulting sinus was slow; fæcal-smelling pus escaped for some days, and a number of small sloughs came away. On the twelfth day the patient was sent down to Wynberg, where he remained twelve weeks. A counter-incision was needed in the[Pg 440] loin to drain the suppurating cavity three weeks after the primary operation, and five weeks after the operation an escape of gas and fæces took place from the anterior wound, while the bowels were acting, as a result of a dose of castor oil. No further escape of fæces occurred, and he left for England with a small sinus only. No extension of inflammation into the original wound track ever occurred, both openings and the canal healing by primary union.
The sinus remained open, and occasionally discharged for a further period of six months, and then healed firmly; since when the patient has been in perfect health.
(182*) Splenic flexure, descending colon.—Wounded at Magersfontein. Entry (Mauser), in sixth left intercostal space in mid-axillary line; exit, in left loin, below last rib, at outer margin of erector spinæ. The patient remained in the Field hospital three days, during which time he exhibited no serious abdominal symptoms, but during the journey to Orange River (53½ miles) he was sick. He remained at Orange River two days, and while there an enema was administered, producing a normal motion. The abdomen was slightly distended; it moved fairly, there was slight rigidity, but little tenderness. Temperature 100.8°, pulse 120. No appearance of fæces in wound.
When seen on the sixth day the condition was as follows:—Patient cheerful and not in great pain. Temperature 99.2°; pulse 120; respirations 48, very shallow. Abdomen soft, moving freely, no distension or general tenderness. Fluid fæces escaping in abundance from the wound in loin. Redness of skin and swelling below level of wound, and cellular emphysema above. Fæcal-smelling fluid was also escaping from the thoracic wound.
The wound was enlarged, but the patient rapidly sank, and died of septicæmia on the seventh day.
(183*) An exactly similar case came under observation from the battle of Modder River, except that the opening in the loin was somewhat larger, and earlier and freer escape of fæces took place from it. In this also fæcal matter passed freely into the left pleural cavity, and fæcal matter was expectorated, while there was an almost complete absence of abdominal symptoms. Death occurred on the fourth day.
No post-mortem examination was made in either case, but I believe in both the extra-peritoneal aspect of the colon was implicated and that the septicæmia was in great part due to absorption from the pleural rather than the peritoneal cavity, since in neither case were the abdominal symptoms a prominent feature.[Pg 441]
(184) Possible wound of cæcum.—Wounded at Spion Kop. Bullet (Mauser) perforated the right forearm, then entered belly. Entry, 3 inches from the right anterior superior iliac spine, in the line of the supra-pubic fold of the belly wall (a transverse slit); exit, in right buttock, on a level with the tip of the great trochanter and 2 inches within it. The wound was received immediately after breakfast had been eaten. There was retention of urine and constipation for three days, but no sickness. Local pain and tenderness were severe, and at the end of three weeks there was still local tenderness, slight induration, and dragging pain on defæcation. The patient returned to England at the end of a month well, except for slight local tenderness.
(185) Possible wound of colon.—Wounded at Paardeberg; range 200 yards. Walking at time. The bullet (Mauser) perforated the left forearm, just below the elbow-joint. Entry, into belly 1 inch anterior to the tip of the left eleventh costal cartilage; no exit.
The injury was followed by pain in the left half of the abdomen and vomiting, which continued for two days. The bowels acted on the third day; no nourishment was taken for two days, but a small quantity of water was allowed. No further symptoms were noted, and at the end of a fortnight the patient was well, except for slight local tenderness. The bullet could not be detected with the X-rays.
(186) Wound of cæcum.—Wounded at Paardeberg. Entry (Mauser), 2 inches diagonally above and within right anterior superior iliac spine; exit, immediately to the right of the fifth lumbar spinous process; the patient was lying on his left side when struck. A burning pain down the right thigh immediately followed the accident, and lasted some days. There was no sickness, the bowels were confined three days, and there was pain across the back and down the thigh.
On the tenth day he arrived at the Base, when he was lying on his back suffering considerable pain. The temperature ranged to 101°. There was diarrhœa and cystitis, with a considerable amount of pus in the urine, which was very offensive. A small fluctuating spot existed on the back, just to the right of the original exit wound which was firmly healed. The abdomen moved fairly with respiration in its upper part, but was motionless below, especially in the right iliac fossa; some induration was to be felt here. The right thigh was kept flexed.
During the next few days the pus disappeared from the urine,[Pg 442] and with this change the induration in the right iliac fossa increased. An incision (Mr. Gairdner) was made into the fluctuating spot behind, and pus evacuated. The patient recovered.
(187) Possible wound of cæcum.—Wounded outside Heilbron. Entry (Mauser), in the right loin, 2½ inches above the iliac crest, at the margin of the erector spinæ; exit, 1½ inch above and within the right anterior superior spine of the ilium. There was little shock. The patient was brought six miles in a wagon into camp, and slept comfortably with a small morphia injection. Prior to the accident the patient was suffering from diarrhœa, but afterwards the bowels were confined. The next morning there had been no sickness and little pain. The tongue was moist and clean, the pulse 80, the respirations 24, the belly moved generally, although inspiration was shallow; the temperature was 99°. Slight tenderness in the belly to the inner side of the exit wound, but no dulness.
The patient was starved for the first thirty-six hours, a little warm water then being allowed. No symptoms developed, and a perfect recovery followed.
(188) Colon, liver.—Wounded outside Heilbron. Entry (Mauser), midway between the last right rib and the crista ilii; exit, below the eighth costal cartilage in nipple line. There were no serious primary symptoms, but ten days after the accident the temperature rose, swelling and pain developed in the right loin, and on the fourteenth day a large tympanitic abscess was opened (Dr. Flockemann, German Ambulance.) Fæcal-smelling gas and pus were evacuated. There was no extension of the abscess forwards. A week later the patient had much improved, although there were evident signs of general absorption, and the discharge from the abscess cavity was abundant and very foul. On the thirteenth day a serious hæmorrhage occurred from the loin wound, which was opened up, but no evident source was discovered; hæmorrhage was repeated the next day, and the man died.
At the post-mortem examination a large quantity of chocolate-coloured fluid was found free in the abdomen and pelvis. A chain of small local abscesses was found surrounding the ascending colon, and a larger one over the front of the cæcum. The wall of the ascending colon was generally thickened, and from this, in three places, openings with rounded margins connected the abscess cavities with the lumen of the bowel. One of the openings, larger than the others, was possibly the[Pg 443] aperture of entry of the bullet; the others were apparently spontaneous.
At the anterior border of the right lobe of the liver an abscess cavity existed in connection with the wound of the liver, and this was continuous with the aperture of exit, although not discharging. The aperture of exit was plugged by a tag of omentum (see fig. 89). No obvious source of the hæmorrhage was forthcoming, but it probably originated in one of the large branches of the vena cava. The bullet had struck the transverse process of the lumbar vertebra, but had not given rise to any signs of spinal concussion.
(189*) Ascending colon.—Wounded at Modder River. Entry (Mauser), midway between the tip of the tenth right rib and the iliac crest. Bullet retained. A second wound existed over the centre of the left sterno-mastoid, and the bullet here was also retained and never localised. The patient stated that he brought up blood at short intervals for half an hour immediately after he was wounded. This might have been explained by the wound in the neck, but no difficulty in swallowing was noted. The bowels acted the day after he was shot, and, except for some local tenderness and immobility, no abdominal signs were noted. Three weeks later a swelling was obvious to the right side of the umbilicus, and a tympanitic abscess developed; this was opened, and a deformed Mauser bullet extracted. Foul pus, but no fæcal matter, was evacuated, and after discharging for a fortnight the wound closed, and the man was sent home as 'well.' In this case I assumed a wound of the ascending colon had occurred.
(190*) Rectum and bladder.—Wounded at Graspan, while retiring at the double. Entry (Mauser), 1 inch to the right of the coccyx; exit, 1 inch above the junction of the middle and outer thirds of left Poupart's ligament. The man suffered with some pain in the abdomen, and for first two days with retention of urine. The urine was drawn off with the catheter, and contained blood. During the next five days micturition was hourly or more frequent; gas was passed per urethram, and the urine was very foul, containing evident fæcal matter. Micturition continued frequent, with purulent cystitis for one month. Local tenderness, pain, and immobility developed over the lower quarter of the abdomen, extending to the right iliac fossa. A local abscess pointed a little to the right of the mid line, and 2 inches above the symphysis, and from this foul-smelling pus, but no fæces, was discharged for three months, during which period the surrounding dulness and[Pg 444] induration gradually decreased and the sinus healed. When the patient left for England there was still occasional slight discharge from the original wound of entry, and there was slight discomfort on micturition, but he was otherwise well.
A year later the man had resumed active duty, and, except for occasional pain on stooping, considered himself well.
The following cases are appended as of some general interest. The first two (191, 192) illustrate extra-peritoneal injuries to the rectum. In neither did positive evidence exist of wound of the bowel, but the symptoms in each rendered this accident probable. Case 193 is an illustration of apparent escape of the anal canal in a wound in which from the position of the external apertures this escape would have appeared impossible.
Wounds of the extra-peritoneal portion of the rectum, as a rule, appeared to have a somewhat better prognosis than would have been expected; in any case, the prognosis was far better than that obtaining in wounds of the base of the urinary bladder. My experience on the subject of these wounds was, however, limited to the two cases quoted.
Case 194 is inserted as an example of the complicated nature of the abdominal injuries not so very unfrequently met with. It illustrates well the difficulty which may arise at any stage in the course of treatment of an injury, in the certain determination or exclusion of wound of a part of the alimentary canal.
(191) Wounded at Magersfontein. Entry (Mauser), in the right loin, immediately below the ribs in the mid-axillary line; exit, about the centre of the left buttock, on a level with the tip of the great trochanter. A second lacerated shell wound of back was present. All the wounds suppurated. For the first sixteen days following the injury all control was lost over the anal sphincter, and bloody fæces, and later slime, constantly escaped, but no fæcal matter ever escaped from the wound in the buttock. There was no history of previous dysentery, and rectal examination afforded no information. The buttock wound had to be opened up, disclosing a tunnel in the ilium.
The wounds granulated slowly with continuous suppuration, but were healed, and the patient returned home at the end of fourteen weeks, the bowels acting normally.[Pg 445]
(192) Wounded at Paardeberg. Entry (Mauser), at the junction of the middle and posterior thirds of the left iliac crest; the bullet was retained, and removed (Mr. Pegg) from the back of the right thigh, 3 inches below the back of the great trochanter. After the injury retention of urine followed, with incapacity to control loose motions, though solid ones could be retained. The retention was treated by catheterisation, which was followed by cystitis. The power of micturition was slowly recovered, and three weeks later he could pass water, at times in a dribbling stream only; the cystitis had improved. The man returned to England very much improved, but not quite well, at the end of five weeks.
(193) Wounded at Modder River. Entry, in the right buttock, near the outer border at the upper part; exit, at the lower part of outer border of left buttock. The line of the wound exactly crossed the position of the anus, but no sign of injury to the rectum could be discovered.
(194) Wounded at Magersfontein. Entry (Mauser), 1/2 inch below the margin of the iliac crest, at the junction of its middle and posterior thirds, and on a level with the fifth lumbar spinous process; exit, below the cartilage of the eighth rib, just within the left nipple line. Struck while retiring; fell at once, and remained thirty hours on the field. Patient stated that he vomited 'blood like coffee grounds' six times while lying on the field, and twice after being brought in. His bowels were confined for three days. His right lower extremity was paralysed.
On the fifth day there was considerable induration around the wound of exit, and the upper half of the abdomen was immobile and tender. The temperature rose to 100°, and the pulse was 96. Shortly afterwards a similar condition was noted in the lower half of the abdomen; the temperature continued to be raised and the pulse quickened, when on the thirteenth day a considerable quantity of pus was passed per rectum, and diarrhœa set in; this continued for three days, with marked improvement in the general symptoms. Micturition, which had been painful, became normal; the pulse and temperature fell, and the expression became less anxious. The patient continued to sleep badly, however, and complained of pain.
At the end of the third week he still looked ill, but was easier. Temperature normal in the morning, 100° in evening, pulse 80. Tongue thickly furred, but moist. Still on milk diet; appetite bad; bowels irregular.[Pg 446]
The abdomen moved little in the lower half, induration persisted in the left iliac fossa, the left thigh continued flexed, and resonance was impaired to the left of the umbilicus.
At the end of six weeks a distinct hard swelling in two parts, separated by a resonant area, was noted to the left of the umbilicus and in the left iliac fossa. The abdomen moved fairly, and there was little tenderness over the swelling. During the next week the swelling appeared to increase and to fluctuate; at the same time the temperature again began to rise to 100° and 101° at eve. The swelling was taken to be a localised peritoneal suppuration, and an incision was made over it; but this led down to a free peritoneal cavity, with a tumour pressing up from the posterior abdominal wall. The wound was therefore closed, and a fresh extra-peritoneal incision made, immediately above Poupart's ligament, when the swelling proved to be a large retro-peritoneal hæmatoma. As the cavity extended into the pelvis and up to the level of the costal margin, it was deemed wise only to evacuate a part of the blood-clot. The origin of the bleeding was not determined, and the wound was closed and healed by first intention. The man continued to improve, and left for home five weeks later.
This patient has continued to improve since his return, but the left thigh is still somewhat flexed.
Prognosis in intestinal injuries.—This was of a most discouraging character compared with the prognosis in abdominal injuries as a whole. The cases were of two classes, however: those that died within twenty-four hours, and those that died at the end of from three days to a week.
Cases falling into the first category are obviously of little importance from the point of view of surgical treatment. Many of them died from the widespread nature of the injury, and the shock produced by it; others from hæmorrhage from the large abdominal vessels. It is unlikely that any could have been saved, even under the most satisfactory conditions.
In the following small table, therefore, I have included only the cases which have been already quoted, which survived long enough to be amenable to surgical treatment, and which were for some days under my own observation. Some of them, in fact almost all, I watched until they were either convalescent, or died, and in six I performed operations.[Pg 447]
I am aware, and have short details of the histories of eight patients wounded in the same battles who died prior to the termination of the first thirty-six hours; but these are not included, for the reason stated above, and also because I am uncertain whether all the injuries were produced by bullets of small calibre.
| Viscous wounded | Number of cases | Localised Secondary suppuration occurred | Recovered | Died |
| Stomach certain | 2 | — | 1 | 1 |
| Stomach possible | 1 | — | 1 | — |
| Small intestine certain | 5 | 0 | — | 5 |
| Small intestine possible | 10 | 0 | 10 | — |
| Large intestine certain | 8 | 4[21] | 4 | 4 |
| Large intestine possible | 4 | — | 4 | — |
| Bladder certain | 3 | 3 | 1 | 2 |
| Bladder possible | 1 | — | 1 | — |
| Liver | 6 | — | 6 | — |
| Kidneys | 6 | — | 4 | 2 |
| Spleen | 3 | — | 2 | 1 |
| Total | 49[22] | — | 34 | 15 |
Included in the above table are thirty instances of intestinal injury, and these are divided up according to the segment of the intestinal canal implicated, and also as to whether the perforation was certain, or only assumed from the position of the external apertures and the presence of abdominal symptoms of a noticeable grade.
From this analysis it appears clear—
1. That wounds of the stomach have a comparatively good prognosis, and that they may recover spontaneously. It is true that only two examples are included in my table; but I was at various times shown patients with similar injuries and histories, and a number of cases which have been published appear to substantiate the opinion. From our experience of the occasional spontaneous recovery of gastric perforations from disease, I think we might be prepared to expect that the stomach would offer a comparatively favourable[Pg 448] seat for these wounds. It may be pointed out, however, that hæmatemesis, the main feature in the symptoms pointing to wound, is by no means direct proof of more than contusion.
2. That perforating wounds of the small intestine are very fatal injuries; every patient in whom the condition was certainly diagnosed died.
3. That in the cases in which a perforation was inferred from the position of the external apertures and the symptoms, not one patient suffered from the secondary complications—e.g. local peritonitis and suppuration, which were common in the case of the large intestine, and which we are accustomed to see after perforation from disease. This renders the occurrence of actual perforation in the majority of the cases a matter of very grave doubt.
If spontaneous recovery does take place after this injury, it is only in cases in which the wounds are single, and slight in character.
4. That in eight cases in which perforation of the large intestine was certain, four recoveries took place; but in each instance suppuration occurred. I am, however, quite prepared to believe that perforation may have occurred in some or all of the other four cases included as 'possible,' provided the wounds were intra-peritoneal.
Wounds of the cæcum and ascending colon are those which have the best prognosis, and after these of the rectum. The comparatively good prognosis in these parts is what would be expected, on account of their greater fixity, and lesser tendency to be covered by the small intestine.
An extra-peritoneal wound of any of these portions of the bowel is more dangerous than an intra-peritoneal, and more likely to give rise to septicæmia.
Of the cases included in my table eighteen of the possible intestinal injuries were observed among the wounded of the four battles of the Kimberley relief force. These cases I saw early and followed to their termination, and I believe the list contains the great majority of all the patients who received intestinal wounds in those battles. On inquiry I could not learn of others from the officers of the Field hospitals; but no doubt[Pg 449] some patients died before their reception into hospital, and some may have been overlooked; again, I know of two cases in which death took place within the first week, but which went direct to the Base and did not come under my observation. These exceptions being made, we have a fairly complete series, from which some deductions may be drawn. The cases included are marked with an asterisk.
Of the eighteen cases, eight or 44.4 per cent. died. These were made up as follows:—Stomach, one case; this patient died at the end of fourteen days, as a result of secondary hæmorrhage and septicæmia. It was complicated by a severe wound of the liver and also one of the lung.
Small intestine, four certain cases; all died, two after operation in the stage of septicæmia, and one after operation from recurrent hæmorrhage, possibly from the mesentery. Of the other six cases one can only say that the position of the wounds was such as to render wound of the intestine possible, and that all suffered with abdominal symptoms of some severity.
Large intestine. Of six cases in which wound was certain, three died, one after operation. One recovered after operation, two recovered with local peritoneal suppuration. In one case the injury could only be returned as possible.
In connection with this subject I have received permission from Mr. Watson Cheyne to quote the statistics published by him[23] concerning the abdominal wounds observed after the fighting at Karree Siding, on March 29, which are as follows:—
'The number of the wounded was 154, and in fifteen it was considered that the abdominal cavity had been penetrated. Of these patients, five had already died within twenty-four to twenty-eight hours after the injury, and I saw ten who were still alive. Of these nine were left alone, and four died within the next twenty-four or thirty-six hours; five were still alive when I left Karee on Sunday afternoon, April 1. On one I operated, but he died on April 2.
The Karee statistics are really the only complete ones which I have as yet been able to obtain. The following are the notes of the cases above alluded to.[Pg 450]
Besides the five cases of abdominal wounds which had already died, and of which I could get no complete details, the following ten are cases which I saw from twenty-four to thirty hours after they were shot:—
Case I.—The point of entrance was 2 inches to the right of the umbilicus, and the bullet was found lying under the skin far back in the left loin. The patient was pulseless, and there was much rigidity of the abdomen, tenderness, and vomiting. He died a few hours later.
Case II.—The bullet, coming from the side, had entered the abdomen 4 inches below and behind the right nipple. There was no exit wound. The patient had been vomiting a good deal, but not any blood; the abdomen was very rigid and tender. He was obviously very ill, and died the next morning. The bullet had probably perforated the liver and stomach.
Case III.—There was a large wound above the right anterior iliac spine (probably the point of exit), and a small opening behind and near the spine on the same side. There was great tenderness and rigidity of the abdomen. He died a few hours later.
Case IV.—In this case there was a transverse wound of the abdomen, the bullet having entered on the right side in the middle of the lumbar region and passed out on the left side, rather higher up and further back. All the symptoms of acute peritonitis were present. The patient died the next morning.
Case V.—The bullet had entered the anterior end of the sixth intercostal space on the left side, and was found lying under the skin over the seventh intercostal space on the right side and about 2 inches further back. He had vomited blood on the previous day. The bullet may have perforated the stomach. The epigastrium was somewhat tender, but there were no marked symptoms. On April 1 he was going on well.
Case VI.—The place of entrance of the bullet was 1 inch in front of the right anterior superior spine, and of exit behind the left sacro-iliac synchondrosis. There was much hæmorrhage at the time. His condition when I saw him was fair, and there was no marked abdominal tenderness. On April 1 his morning temperature was 101°. There were no signs of general peritonitis, and his condition was good.
Case VII.—The bullet had entered from behind, about the tip of the twelfth rib on the left side, and had left about the middle of the epigastrium, and rather to the left of the middle line.[Pg 451]
Vomiting was still going on, but not of blood. There was much tenderness and rigidity of the abdomen, and he was almost pulseless. On April 1 his general condition was better, but the abdomen was very rigid and tender. (Subsequently died.)
Case VIII.—The point of entrance of the bullet was about 2 inches from the anterior end of the seventh left intercostal space, and of exit rather lower down and further back on the right side. The patient said that he had vomited brown fluid after the injury. There was much abdominal pain, but his general condition was fair. On April 1 there was still much pain, but his general condition was good.
Case IX.—The bullet had entered about 1½ inch in front of the anterior inferior spine on the right side, had gone directly backwards, and had come out in the buttock. The patient, however, suffered very little. On March 31 there was slight tympanites and tenderness in the right iliac fossa. The bowels acted well, and no blood was passed. On April 1 he was very well, and it was considered very doubtful if any viscus was wounded.
Case X.—The point of entrance was in the middle of the right buttock, a little above the level of the trochanter; the exit was through the anterior abdominal wall in the right semilunar line at the level of the umbilicus. The patient was decidedly ill; the abdomen was a good deal distended, and pressure on it caused an escape of gas through the anterior opening. There was a good deal of abdominal tenderness and rigidity. I opened the abdomen outside the right linea semilunaris, and found a perforation in the anterior wall of the ascending colon, without any adhesions around, which was easily stitched up. The posterior opening was found about 2 inches lower down, with a piece of omentum firmly adherent to it and completely closing it. As the patient was in a bad state, I thought it better, instead of excising the piece of intestine beyond the holes or tearing off the omentum, to leave the wounds alone, merely cleaning out the peritoneal cavity as well as I could and arranging for free drainage. He rallied from the operation very well, and for twenty-four hours it looked as if he might get better; but he gradually got worse and died on April 2.'
The above statistics are particularly valuable, as they give the incidence of abdominal injuries compared with those in general in one definite battle. This amounted to the high number of 15 in 154 or 9.74 per cent. wounded. I am inclined to think that this is a higher proportion than the[Pg 452] average of the campaign, and that more of the men must have been exposed in the erect position than was ordinarily the case during the fighting.
The statistics also show that 33.33 per cent. of the patients with abdominal injuries died within from twenty-four to twenty-eight hours, and that the percentage of deaths had risen to 73.33 per cent. at the end of the third day. These numbers again seem high, but in this relation it may be noted that, as a small force only was present, and as all the patients were together, Mr. Cheyne had unusually good opportunities for seeing all the cases.
One other point is doubtful from the report, and that is what percentage of the wounds were caused by bullets of small calibre. In one case it is definitely stated that the wound was large, and in the second that gas escaped from the wound; both of these may have been instances in which a large bullet, or some expanding form, had been employed, and there is no doubt that the use of such projectiles was more common at this stage of the campaign than it was earlier.
Treatment of injuries to the intestine.—Some general rules for the immediate treatment of all cases may be laid down. First, the patients must be removed with as little disturbance as possible, and absolute starvation must be insisted upon. If the patients be suffering from severe shock, hypodermic injections of strychnine should be administered, or possibly some stimulant by the rectum.
After a battle, when these cases may be brought in in considerable number, they should be collected and placed in the same tent. The objection to congregating a number of severely wounded patients together must be disregarded in the face of the manifest advantage of being able to treat all alike in the matter of feeding. After the battles of the Kimberley relief force, Surgeon-General Wilson, at my request, had all the abdominal cases placed in a large marquee, where we were able to carefully watch the whole of the patients from hour to hour, and little chance existed for any indiscretion on the part of the patients in the way of eating or drinking.[Pg 453]
If possible, the patients should be kept absolutely quiet until they are evidently out of danger. A week's stay at Orange River sufficed for this object in the cases referred to. The avoidance of transport is manifestly of extreme prognostic importance.
When feeding is commenced at the end of twenty-four or thirty-six hours, it must be in the form at first of warm water, then milk administered in tea-spoonfuls only.
In doubtful cases the use of morphia must be avoided.
Operative treatment is required in a certain number of the cases, but in the majority of instances we are met with the extreme difficulty that in a very large proportion of the occasions upon which these wounds are received an exploratory abdominal section is not warranted in consequence of the conditions under which it has to be performed.
A word must be added as to these difficulties; they are in part purely of an administrative nature, partly surgical. After a great battle the wounded are numerous, and amongst them a very considerable proportion of the wounds and injuries are of such a nature as to do extremely well if promptly dealt with, and each of these makes small demands on the time of the staff. Abdominal operations, on the other hand, are unsatisfactory from a prognostic point of view, and their performance requires much time and the assistance of a considerable number of the men, who are obliged to neglect the treatment of the more promising cases for those of doubtful issue. This difficulty, although not surgical in its nature, is nevertheless a practical one of great importance and appeals strongly to the Principal Medical Officers in charge of the arrangements. It is only to be avoided by an increase of the staff, which is not likely to be made except on very special occasions.
Other difficulties are purely surgical. First, the difficulty of diagnosing with certainty a perforating lesion. In the presence of the fact that many incomplete lesions follow wounds crossing the intestinal area, and that these give rise to modified symptoms, I believe this determination to be impossible without the aid of an exploratory incision. Here we are met with the remaining surgical difficulties—disadvantages such as the absence of sufficient aid to the operating[Pg 454] surgeon, difficulties connected with the temperature, wind, and dust, and as to the subsequent treatment of the patient. Again difficulty in obtaining the most important adjunct, suitable water, or indeed any water in a sufficient quantity.
It is of course obvious that conditions may exist in which all these troubles may be avoided. Again, the practical difficulty adverted to above does not come in the way when a single man happens to sustain an abdominal wound on the march. Under such circumstances an exploration may be not only justifiable, but obligatory, and the general rules of surgery must be followed rather than such incomplete indications as are suggested below.
My own experience led me to the following conclusions:
1. A wound in the intestinal area should be watched with care. In the face of the numerous recoveries in such cases, habitual abdominal exploration is not justified, under the conditions usually prevailing in the field.
2. The very large class of patients excluded by this rule from operation leads us to a smaller and less satisfactory number to be divided into two categories:
Patients who die during the first twelve hours. The whole of these are naturally unfit for operation, and their general condition when seen often precludes any thought of it.
Patients with very severe injuries, as evidenced by the escape of fæces, or with wounds from flank to flank or taking an antero-posterior course in the small intestinal area. These patients die, and the majority of them will always die whether operated upon or not. The undertaking of operations upon them is unpleasant to the surgeon, as being unlikely to be attended with any great degree of success, whence the impression may gain ground that patients are killed by the operations. None the less, I think these operations ought to be undertaken when the attendant conditions allow, and it is from this class of case that the real successes will be drawn in the future. The history of such injuries, after all, corresponds exactly with what we were long familiar with in traumatic ruptures in civil practice, and now know may be avoided by a sufficiently early interference. The whole question here is one of time, and this will always be the trouble in military work.[Pg 455]
3. The expectant attitude which is obligatory under the above rules in doubtful cases, brings us face to face with a large proportion of patients in the early or late stage of peritoneal septicæmia. These cases run on exactly the same lines as those in which the same condition is secondary to spontaneous perforation of the bowel, in which we consider it our duty to operate, and in which a definite percentage of recoveries is obtained. Hence another unpleasant duty is here imposed upon the surgeon. Two such cases on which I operated are recounted above, and although I cannot say they give much encouragement, I should add that in the only one I left untouched, I regretted my want of courage for the five days during which the patient continued to carry on a miserable existence.
4. The treatment of the cases in which an expectant attitude is followed by the advent of localised suppuration presents no difficulty; simple incision alone is needed, and healing follows.
As a rule this is a late condition. In one case of injury to the ascending colon recounted above, however, considerable local escape of fæces had occurred, and a successful result was obtained by a local incision on the third day without suture of the bowel. In this case I believe the wound in the bowel to have been of the nature of a long slit, but the surrounding adhesions were so firm as to render any interference with them a great risk, and a successful result was obtained at the cost of a somewhat prolonged recovery. I am convinced that the best course was followed here. (No. 131.)
When the suppuration was of a less acute character, it was generally advisable to allow the pus to make its way towards the surface before interference.
5. Cases of injury to the colon in which the posterior aspect is involved should be treated by free opening up of the wound, and either by suture of the bowel or else its fixation to the surface. I operated on one such case, and although the patient eventually died on the eighth day, from septicæmia, he certainly had a chance. Two cases where the opening looked so free that one almost thought the wound could be regarded as a lumbar colotomy did badly; in both infection of the pleura[Pg 456] took place, besides extension of suppuration into the retro-peritoneal areolar tissue. In the future I should always feel inclined to enlarge such wounds and bring the bowel to the surface.
As regards actual technique the majority of the wounds are particularly well suited to suture; three stitches across the opening and one at either end of the resulting crease sufficed to close the opening effectively. The openings in the small intestine were not as a rule difficult to find, on account of the ecchymosis which surrounded them. From what I have seen stated in the reports given by other surgeons, there seems to have been more difficulty in discovering wounds in the large gut. Under ordinary circumstances the only instruments specially needed are a needle and some silk. At my first two operations, as my instruments had gone astray, the wounds were readily closed by a needle and cotton borrowed from the wife of a railway porter.
If aseptic sponges or pads are not available, boiled squares of ordinary lint may be employed for the belly, and towels wrung out of 1 to 20 carbolic acid solution used to surround the field of operation. Whenever there is any likelihood of the necessity for operations, water boiled and filtered should be kept ready in special bottles.
When septic peritonitis was already present, the ordinary procedure of dry mopping, followed by irrigation, was necessary, before closing the belly.
The after-treatment should be on the usual lines as to feeding, &c.
I am unaware to what degree success followed intestinal operations generally during the campaign. I saw only one case in which the small intestine had been treated by excision and the insertion of a Murphy's button in which a cure followed: this case was in the Scottish Royal Red Cross hospital under the care of Mr. Luke. I heard of two cases in which the large intestine was successfully sutured, and of one other in which recovery followed the removal of a considerable length of the small bowel for multiple wounds.
In concluding these most unsatisfactory remarks, I should add that the impressions are those that were gained as the[Pg 457] result of the conditions by which we were bound in South Africa, and which might recur even in a more civilised region. Under really satisfactory conditions nothing I saw in my South African experience would lead me to recommend any deviation from the ordinary rules of modern surgery, except in so far as I should be more readily inclined to believe that wounds in certain positions already indicated might occur without perforation of the bowel when produced by bullets of small calibre; and further in cases where I believed the fixed portion of the large bowel was the segment of the alimentary canal that had been exposed to risk, I should not be inclined to operate hastily.
A careful consideration of the whole of the cases that I saw leaves me with the firm impression that perforating wounds of the small intestine differ in no way in their results and consequences when produced by small-calibre bullets, from those of every-day experience, although when there is reason merely to suspect their presence an exploration is not indicated under circumstances that may add a fresh danger to the patient.
Wounds of the urinary bladder.—Perforating wounds of the bladder are the injuries nearest akin to those we have just considered, but a great gulf separates them, in so far as the escape of a few drops or even a considerable quantity of normal urine does not necessarily mean peritoneal infection. The difference in this particular was very forcibly demonstrated in my experience, since an uncomplicated perforation of the bladder in the intra-peritoneal portion of the viscus proved to be an injury that not infrequently recovered spontaneously, I believe in a considerable proportion of the cases.
I include only one such case in my list because it was the only example which happened to be under my personal observation during its whole course, but from time to time I was shown several others in which the position of the external apertures and the transient presence of hæmaturia left little doubt as to the nature of the injury. The case recounted above, No. 190, is of especial interest, since the patient recovered from an injury which involved both the bladder and a fixed portion of the large intestine in contact with its posterior surface.[Pg 458]
In another, No. 194, a transient inflammatory thickening pointed to a local inflammation of a non-infective character, since no suppuration ensued, and this may have been a case of extra-peritoneal wound; on the other hand, the bladder may have entirely escaped injury. In wounds of the portions of the viscus not clad in peritoneum, as a rule, a very different prognosis obtains. Two typical cases are related, which I believe fairly represent the general results which follow when the bladder is either wounded behind the symphysis or at the base. The first case, No. 195, exemplifies a very characteristic form of wound when small-calibred bullets are concerned. The bullet, taking a course more or less parallel to that of the wall of the viscus, cut a long slit in its anterior wall. This bullet in its onward passage comminuted the horizontal ramus of the pubes, and lodged in the thigh. Into the latter region the greater part of the extravasated urine escaped. I think the history of this case fully shows that I made a blunder in not performing a proper exploration, instead of contenting myself with an incision in the thigh. My only excuse was that the patient at the time I saw him was in a very collapsed state, and a severe grade of abdominal distension suggested that septic peritonitis was already in an advanced stage. In point of fact, the patient at once improved, sufficiently so to be able to undergo a second exploration at a later date by Mr. Hanwell at the Base, only dying of septicæmia at the end of twenty-one days. Even a free supra-pubic vent might, I believe, have given him a chance of life.
When the perforation was at the base of the bladder, however, the prognosis was very bad, and, as far as I know, not a single patient escaped death. The increase of risk in an extra-peritoneal wound of this viscus is indeed very great, while an intra-peritoneal perforation may be considered an injury of lesser severity, provided the urine be of normal character.
(194a) Possible wound of the bladder.—Wounded at Magersfontein. Entry (Mauser), immediately above the symphysis pubis; exit, in the buttock, behind the tip of the left great trochanter. The man was struck while advancing, and fell, thinking at the time 'that he was struck in the foot.' He lay twelve hours on[Pg 459] the field, and passed water for the first time when the bearer removed him. During the next two days he passed urine only twice, and no blood was noticed. The bowels acted on the evening of the third day. When seen on the fourth day he complained of aching pain in the lower part of the belly, and a concentric patch of tender induration extended for about 1½ inch around the wound. The abdominal wall was moving well. The tongue was clean and moist. There was no blood in the urine, and micturition was not frequent. Temperature 99.4°. Pulse 80, good strength. The patient was then sent to the Base. At the end of seventeen days there was still a little tenderness in the left iliac fossa; but the man was otherwise well, and at the end of a month he was sent home.
(195) Extra-peritoneal wound of the bladder.—Wounded at Magersfontein. Entry (Mauser), at the fore part of the right buttock. No exit. The patient was seen on the third day. He had an expression of extreme anxiety, and complained of very great pain in the abdomen and thigh. The abdomen was greatly distended and tympanitic, and the left thigh and groin were very much swollen and œdematous, with some redness of surface. Temperature 100°, pulse 120. No sickness, tongue moist, bowels confined. Retention of urine. The condition of the patient was very grave; but he was anæsthetised, clear urine was withdrawn from the bladder by catheter, and an incision was made into the thigh just below the inner third of Poupart's ligament, where fluctuation was evident. Two pints of bloody urine were evacuated, and when a finger was introduced it passed over a fracture of the pubes into the pelvis, but not into the peritoneal cavity. In view of the patient's condition it was not thought wise to proceed further, and he somewhat improved later, and was sent to the Base. Loss of power in the right lower extremity pointed to injury to the anterior crural nerve.
On the patient's arrival at Wynberg there were signs of local peritonitis in the lower half of the abdomen, and all his urine was passed from the wound in the left thigh. Some days later this wound was enlarged to allow of the freer exit of pus, and a fragment of bone was removed. The wound granulated healthily, but the man steadily emaciated and lost ground, with signs of chronic septicæmia, and he died on the twenty-first day. At the post-mortem examination a transverse wound of the anterior wall of the bladder behind the pubes, below the peritoneal reflexion, was found gaping somewhat widely, and 2 inches in[Pg 460] length. There was little sign of previous peritonitis. The retained bullet was discovered beneath the femoral vessels in the left thigh.
(196) Extra-peritoneal perforation of the bladder.—Wounded at Paardeberg. Entry (Mauser), 3 inches above the left tuber ischii; exit, above the symphysis, immediately over the right margin of the penis. The patient was retiring to fetch ammunition when shot. Urine was noted to escape from both apertures the day after, and this continued until he was sent down to the Base on the fourteenth day. The patient was then considerably emaciated, complained of great pain, especially down the left thigh (sciatic nerve), the temperature averaged 100°, the pulse 80, tongue clean and moist, bowels acted regularly, no sign of injury to the rectum. He was taking food fairly, but was very sleepless. Urine was passed per urethram, and also escaped by both wounds. The abdomen was flaccid and sunken, respiratory movements being confined to the upper half.
As there was evidence of considerable infiltration in the buttock, the original entry wound was enlarged, and a catheter was tied into the bladder. Little change occurred in the symptoms and the local condition, urine and pus continued to escape freely from the posterior wound, and the patient gradually sank, dying on the thirty-eighth day. At the post-mortem examination the peritoneum was found intact and unaltered, but there was extensive pelvic cellulitis around the bladder, a large slough and some pus lying in the cavum Retzii. An aperture of entry still open existed in the centre of the anterior wall of the bladder, and a patent exit opening at the base of the trigone. The bullet had passed out of the pelvis by the great sciatic notch.
The above remarks and cases sufficiently set forth the prognosis in these injuries. For the intra-peritoneal lesions an expectant plan of treatment may be followed by uncomplicated recovery. Mention has already been made of a case in which a Mauser bullet was retained in the bladder and was subsequently passed per urethram. In such a case a cystotomy would be indicated were the bullet discovered in the viscus.
As to extra-peritoneal injuries it is difficult to lay down guiding lines. I believe the ideal treatment would be a supra-pubic cystotomy and drainage of the bladder by a Sprengel's pump apparatus, such as we employ at home. Under these circumstances, with the possibility of keeping the bladder actually[Pg 461] empty, I believe good results might be obtained. Certainly drainage of the bladder by a catheter tied in proved worse than useless, and I very much doubt whether a simple supra-pubic opening would give any better results under the circumstances under which a patient has to be treated in a Field hospital.
Cases might, however, occur in which oblique passage of the bullet cuts a groove and makes a large opening in the peritoneum-clad portion of the viscus. Under satisfactory conditions a laparotomy would be here indicated. I take it that this condition would most probably be accompanied by retention of bloody urine, which fact would arouse suspicion.
Wounds of the kidney.—Tracks implicating the kidneys were of comparatively common occurrence. As uncomplicated injuries they healed rapidly, and without producing any serious symptoms beyond transient hæmaturia.
The nature of the lesion appeared to vary with the direction of the wound. In many cases a simple puncture no doubt alone existed, an injury no more to be feared than the exploratory punctures often made for surgical purposes. In other cases the wounds may have been of the nature of notches and grooves.
Two of the cases recounted below were of a more severe variety; in one (No. 201) both kidneys were implicated by symmetrical wounds of the loin, and in the case of the right organ a transverse rupture was produced, which was followed by the development of a hydro-nephrosis, and later by suppuration. This injury was probably the result of a wound from a short range, as the patient was one of those wounded in the early part of the day at the battle of Magersfontein. It was complicated by a wound of the spleen and an injury to the spinal cord producing incomplete paraplegia accompanied by retention of urine. The last complication was responsible for the death of the patient, since ascending infection from the bladder led to the development of pyo-nephrosis and death from secondary peritonitis.[Pg 462]
Case 202 is an instance of a transverse wound of the upper part of the abdominal cavity; it is impossible to say what further complications were present. The early development of a tympanitic abscess suggested an injury to the colon, but this was not by any means certain. The condition of the kidney was very likely similar to that in the last case, but the ultimate recovery of the patient left this a matter of doubt. The case was also one dependent on a short-range wound, since the patient, one of the Scandinavian contingent, was wounded at Magersfontein during close fighting.
The common history of the symptoms after a wound of the kidney was moderate hæmorrhage from the organ, persisting for two to four days. In one of the cases recounted below the hæmaturia was accompanied by the passage of ureteral clots, but this was not a common occurrence.
For the sake of comparison I have included one case of wound of the kidney from a large bullet, in which death was due to internal hæmorrhage. In this instance the injury was a complex one, the lung certainly, and the back of the liver probably, being concurrently injured. None the less if the same track had been produced by a bullet of small calibre I believe the injury would not have proved a fatal one. I never saw such free renal hæmorrhage in any of the Mauser or Lee-Metford wounds.
(197) Wound of right kidney.—Wounded at Modder River while lying in the prone position; retired 100 yards at the double with his company, and walked a further 1½ mile. There was very slight bleeding. Entry (Mauser), in the tenth right intercostal space in the mid-axillary line; exit, in eleventh interspace, 2 inches from the spinous processes. Cylindrical blood-clots, 3 inches in length, were passed on the first two occasions of micturition after the accident, and the urine contained blood. For four days he could only lie on the wounded side. When seen on the third day the urine was normal, and there were no signs of injury to either thoracic or abdominal viscera. He returned to England well at the end of a month.
(198) Wound of right kidney.—Wounded at Modder River while kneeling to dress another man's wound. Entry (Mauser), in the seventh right intercostal space in the nipple line; exit,[Pg 463] 1 inch to the right of the twelfth dorsal spine. The man was carried off the field, and during the first day vomited frequently. For two days there was blood in his urine, and he passed water four to five times daily. He returned to duty at the end of three weeks.
(199) Wound of the left kidney.—Wounded at Magersfontein. Entry (Mauser), 2 inches to the left and 1 inch below the left nipple. No exit. Lying in prone position when struck. Bloody urine was passed at normal intervals for four days, when the hæmaturia ceased. No thoracic signs, and no other sign of abdominal injury. There was tenderness in the left loin below the twelfth rib for some days, possibly over the position of the bullet, but the latter was neither localised nor removed.
(200) Wound of the right kidney.—Wounded at Magersfontein while retiring on his feet. Entry (Mauser), immediately to the right of the second lumbar spinous process; bullet retained and lay beneath margin of ninth right costal cartilage. The man passed urine containing blood twelve times during the first day, and hæmaturia continued until the evening of the third day. On the third day the belly was tumid and did not move well; there was no dulness in the right flank. Pulse 120, fair strength. Temperature 99°. Respirations 20. Tongue moist, bowels confined for four days. The fifth day the pulse fell to 76, and the bowels were moved by an enema. Great tenderness over bullet. The tenderness persisted over the bullet and also in the right flank until the tenth day, when the bullet was removed. At the end of a month the patient returned to England well but during the third week there was occasionally blood in the urine.
(201) Wound of both kidneys (rupture of right) and spleen.—Wounded at Magersfontein. Entry (Mauser), (a) 1 inch to right of second lumbar spinous process; (b) above angle of left ninth rib: exits, (a) 1 inch internal to right anterior superior iliac spine; (b) in seventh intercostal space in mid-axillary line. The wound on the right side gave rise to a lesion of the lumbar bulb (see p. 315), and the patient suffered throughout with retention. There was complete paralysis of the right lower extremity, both motor and sensory. For ten days there was hæmaturia, and very severe cystitis developed, while the patient suffered with severe abdominal pain. The cystitis persisted, also retention, which gradually gave way to dribbling, while irregular rise of temperature and tenderness in the loins pointed to ascending inflammation[Pg 464] in the ureters. The patient gradually lost ground, and a month later suddenly developed signs of peritonitis, severe vomiting, distension, and dulness in the right flank; and in two days he died.
At the post-mortem examination the following condition was found:—On the right side general pleural adhesions, recent lymph over ascending colon and cæcum, ࡍvj of bloody fluid in a localised cavity between colon, kidney, stomach, and liver. Lower quarter of right kidney in half its width separated from main part of organ, yellow in colour, and enveloped in disintegrating clot. Blood-staining of psoas sheath; no injury to vertebral column or to bowel detected.
On the left side recent pleural adhesions and consolidation of base of lung, rent of diaphragm; spleen soft and disorganised and presenting a yellow cicatrix at its upper end, and at antero-external aspect of left kidney was a soft yellow puckered spot about the size of a florin, dipping 3/4 of an inch into the organ, which was otherwise healthy, beyond congestion. The capsules of both kidneys were adherent, but there was no sign of suppuration.
(202) Wound of right kidney. Traumatic hydronephrosis.—Wounded at Magersfontein. Entry (Lee-Metford), in the eleventh intercostal space in the posterior axillary line; exit, in the tenth right interspace, in mid axillary line. The patient was in the prone position when struck, and lay on the field from 5 a.m. until 6 p.m. There was no sickness, and the bowels did not act. When seen on the fourth day he was cheerful, but in some pain. The abdominal wall moved well, but was rigid; there was some general distension, and very marked local distension of the gastric area extending across to the right, so that a depressed band extended between the upper and lower parts of the belly. There was marked local dulness in the right flank, which did not shift on movement; the abdomen was elsewhere tympanitic. Tongue furred, bowels confined; there has been no sickness, and no hæmatemesis. Urine normal, and in good quantity. Temperature 100°. Pulse 84, good strength. There was impairment of sensation in the area of distribution of the external cutaneous and crural branch of the genito-crural nerves.
On the sixth day the bowels acted, after the administration of ℥j of sulphate of magnesia, and the distension was much lessened, although the belly retained its unusual appearance. The dulness in the flank was unaltered. Temperature 100.8°, pulse 92.[Pg 465]
A week later the man was much improved, suffering no pain. Temperature ranged from 99 to 100°, and the pulse about 80. The abdomen was normal in appearance, except for general prominence of the right thorax in the hepatic area.
During the third week a large tympanitic abscess developed at the aperture of exit, and this was opened (Mr. S. W. F. Richardson) through the chest, and a large collection of foul-smelling pus, but no fæcal matter, evacuated. The patient again improved, but a fortnight later a swelling and apparent signs of local peritonitis developed in the right inguinal and lower umbilical and lumbar regions. An incision made over this, however, disclosed a normal peritoneal cavity and was closed.
At the end of ten weeks the patient was sent to the Base hospital; a large firm swelling was then evident, extending from the liver to the inguinal region, and nearly to the median line. This gradually increased until it filled half the belly; it was at first thought to be a retro-peritoneal hæmatoma (similar to that described in case 194), but it became quite soft and fluctuating, and was then tapped, and ℥50 of blood-stained fluid, which proved to be urine, were removed. The urine rapidly reaccumulated, and the cavity was then laid freely open. Urine continued to discharge in large quantity for two months, the man meanwhile remaining well, and passing a somewhat variable daily quantity of urine (℥xxiv-℥lx).
At the end of six months the wound had healed, and the man was serving as an orderly in the hospital.
(203) Wound of right kidney and lung.—Wounded near Paardekraal, while crawling on hands and knees. Entry (Martini-Henry, or small bullet making lateral impact), just above the right nipple, opening ragged and large, bullet retained. There was very severe shock, accompanied by vomiting, but no hæmatemesis. Later there was some hæmoptysis. Pulse 120, respirations 48.
Twenty-four hours later the vomiting had ceased; the patient had passed a restless night, in spite of an injection of morphia. He lay on his right side, pale and collapsed, but answered questions and was quite collected. Pulse imperceptible, respirations 56; the abdomen moved freely. The urine had been passed twice, and was chiefly blood. The patient died shortly afterwards, apparently mainly from internal hæmorrhage, although restlessness was not a prominent feature. As the Column was on the march no autopsy was possible.
The treatment of uncomplicated wounds of the kidney consisted in the ensurance of rest, either alone, or with the administration of opium if the hæmaturia was severe. The after-treatment in the event of the development of hydronephrosis is on ordinary lines. Tapping, or incision followed by extirpation of the injured viscus, if the less severe procedures failed. I never saw a case where renal hæmorrhage suggested the removal of the kidney as a primary step, and much doubt whether such a case is likely to be met with, as the result of a wound from a bullet of small calibre.
Wounds of the liver.—Wounds of the liver were, I believe, responsible for more cases of death from primary hæmorrhage than those of the kidney. I heard of a few cases in which this occurred, although I never saw one. Case 204 is of considerable interest as illustrating the result of an injury to one of the large bile ducts. Putting the deaths from primary hæmorrhage on one side, the prognosis in hepatic wounds was as good as in those of the kidneys. A few fairly uncomplicated cases are quoted below, but wounds of the liver occurred in connection with a large number of other injuries both of the chest and abdomen, and except in the case of wound of the stomach, recorded on page 425, No. 164, and in case 188, I never saw any troublesome consequences ensue.
Nature of the lesions.—I never saw any case of so-called explosive lesion of the liver, such as have been described from experimental results; this may have been due to the fact that such patients rapidly expired, but such were never admitted into the hospitals.
The most favourable cases were those in which a simple perforation was effected; such were usually attended by a practical absence of symptoms, unless a large bile duct had been implicated, when a temporary biliary fistula resulted.
Biliary fistulæ were, however, much more common when the bullet scored the surface of the organ. One such case is recounted under the heading of injuries to the stomach, No. 164. Here a deep gaping cleft with coarsely granular margins extended the whole antero-posterior length of the under surface of the left lobe, and the escape of bile was[Pg 467] free. This was the nearest approach to one of the so-called explosive injuries I met with.
Case 207 is an example of a superficial injury from a bullet possibly of small calibre in which a superficial groove was followed by temporary escape of bile, and it is of interest to note a very similar condition in a shell injury (No. 210) recorded on p. 477.
Although both these cases recovered, I think notching and superficial grooving must be considered much more serious injuries than pure perforation. (See case 188, p. 442.)
The symptoms observed in these injuries have been already indicated in the above description of the nature of the lesions. They consisted in the pure perforations of practically nothing, in the grooves or the perforations implicating a large duct in the escape of bile. In two of the cases in which a biliary fistula was present transient jaundice was noticed.
In many cases the accompanying wound of the diaphragm gave rise to much discomfort; again, in the transverse wounds the action of the heart was often affected by the local cardiac shock accompanying the injury. In one case in which the colon was at the same time wounded (No. 188), an abscess formed at the site of the hepatic wound, as might have been expected.
As uncomplicated injuries, these wounds were little to be feared. Except as a source of hæmorrhage in rapidly dying patients, I never heard of a fatality. As a complication of other injuries, however, the wound of the liver, as has been shown, was sometimes of importance. It was remarkable in case 204 how little trouble the biliary fistula gave rise to, although the bile was discharged across the pleural cavity.
The treatment consisted in rest, and morphia in the cases of suspected progressive hæmorrhage, or in the presence of great pain. In cases where bile was escaping, it was important to ensure a free vent for the secretion.
(204) Wound of liver. Biliary fistula.—Wounded at Magersfontein. Entry (Lee-Metford), below the seventh rib, in the left nipple line; exit, through the eighth rib, in the mid axillary line on the right side. The patient lay for seventeen hours on the[Pg 468] field, during which time the bowels acted once, but there was no sickness. The bowels then remained confined. When seen on the third day the abdomen was normal and the chest resonant throughout on both sides; bile to the amount of some ounces escaped from the wound on the right side. Suffering no pain; temperature 99°, pulse 100. The bowels acted freely the following day.
During the next fortnight there was little change; ℥ii-iij of bile escaped daily, and there was occasional diarrhœa. At the end of that time, however, the temperature rose; there was local redness and evidence of retention of pus. The wound was therefore enlarged, some fragments of rib removed, and a drainage tube inserted. After this the temperature fell, and for the next two months the patient suffered little except from the discharge from the sinus; this persisted for three months, becoming less in amount and less bile-stained, the fistula eventually closing in the fourteenth week, when the patient was sent home on parole.
(205) Wound of liver.—Entry (Mauser), 1 inch below and to the left of the ensiform cartilage; exit, in the sixth right intercostal space, just behind the posterior axillary line. The trooper was sitting bolt upright on his horse at the time; both were shot and fell together. 'Stitch' on coughing or laughing was the only sign noted after the accident; this rapidly subsided.
(206) Wound of the liver.—Wounded at Magersfontein. Entry (Mauser), through the seventh left costal cartilage, 1 inch from the base of the ensiform cartilage; exit, below the twelfth rib 2 inches to the right of the lumbar spines. The patient lay on the field some hours and was brought in at night very cold, and suffering with much shock. No signs of abdominal injury developed, but the pulse remained as slow as 66 for some days, and there was some pain and stiffness about back and sides, or on taking a deep breath. These signs persisted some days, but no others developed, and in six weeks the patient returned to duty.
Some three months later this patient suffered from a short severe attack suggesting local peritonitis, but he again returned to duty.
(207) Wound of the liver.—Wounded at Tweefontein. Entry, in eighth intercostal space in right mid axillary line; exit, 1½ inch below the point of the ensiform cartilage, 1/2 an inch to the right of the mid line. The wounds were large, and although the impact had been oblique, they were possibly produced by a Martini-Henry or Guedes bullet.[Pg 469]
On the second day bile began to escape from the exit aperture, and this together with a little pus continued to be discharged for a week, when the wound rapidly healed up. The only symptom which occasioned any trouble was a stitch on inspiration, probably attributable to the wound of the diaphragm. There was no fracture of the rib.
(208) Wound of the liver.—Wounded outside Heilbron at a range of fifty yards. Entry (Mauser), in the tenth right interspace 2 inches to the right of the dorsal spines; exit, through the gladiolus, immediately to the right of the median line, and just above the junction with the ensiform cartilage. There was considerable shock on reception of the injury, and a great feeling of dizziness. Continuous vomiting set in and persisted for the first two days, then became occasional, and ceased only at the end of a week. There was also occasional hiccough, and stitch on drawing a long breath. The respiration was shallow and rapid. The bowels acted twice shortly after the injury.
The pulse was rapid and small, and a week after the injury was still above 100. The abdomen was then normal and moving symmetrically, and the respiration fairly easy. There were no signs of chest trouble, but some mucous expectoration. A slight icteric tinge existed. The patient made a good recovery.
Wounds of the spleen.—Uncomplicated wounds of the spleen were necessarily rare, and beyond this the strict localisation of a track to the spleen is not a matter of great ease. None the less the spleen must have been implicated in a considerable number of the wounds crossing the chest and abdomen. I know of only one case in which a wound which crossed the splenic area caused death from hæmorrhage, and of this I can give no details, as I never saw the patient. In this instance, however, a wound of the spleen was diagnosed after death from the position of the wounds. The patient continued to perform his duty as an officer in the fighting line for at least an hour after being struck, and then died rapidly apparently from an internal hæmorrhage.
In case No. 201, included amongst the renal injuries, a wound of the spleen existed, but had given rise to no symptoms, and at the time of death, some three weeks later, was cicatrised. The only other assertion of importance that I can make is,[Pg 470] that, as far as I could judge, wounds of the spleen from bullets of small calibre were not, as a rule, accompanied by hæmorrhage, since I never saw a case in which dulness in the left flank suggested the presence of extravasated blood, and in no case that I saw was there any history of general symptoms pointing to the loss of blood.
This is only to be explained by our similar experience with regard to wounds of the liver unaccompanied by puncture of main vessels, and perhaps hæmorrhage is still less to be expected in the case of the spleen, in consequence of the contractile muscular tunic with which the organ is provided.
I can quote no case of certain injury to the spleen, except that already referred to discovered at a post-mortem examination, but many wounds were observed in positions of which the following may be taken as a type. Entry, through the seventh left costal cartilage, 3/4 of an inch from the sternal margin; exit, 2½ inches from the left lumbar spines at the level of the last rib.
As an instance of the doctrine of chances I might quote the position of the wound in the patient who lay in the next bed. Both patients were wounded while fighting at Almonds Nek. Entry, through right seventh costal cartilage, 3/4 of an inch from the sternal margin; exit, 1½ inch from the lumbar spines, at the level of the last right rib.
In neither of these cases did anything except the position of the external apertures point to the infliction of visceral injury.
General remarks as to the prognosis in abdominal injuries. The prognosis in each form of individual visceral injury has been already considered, but a few points affecting these injuries as a class should perhaps be further considered.
First, as to the influence of range on the severity of the injuries inflicted; I am not able to confirm the greater danger of short range, except in so far as there is no doubt that more shock attends such injuries, and possibly some of the most severely wounded were killed outright as a direct consequence of the greater striking force of the bullet.
Among the cases in which but slight effects were noted, however, many were said to have been hit within a range[Pg 471] of 200 yards, as for instance the two injuries quoted under the heading of wounds of the spleen.
I personally saw no cases in which explosive injuries of the solid viscera were to be ascribed to this cause.
Secondly, as to the immediate prognosis in all abdominal injuries, the ensurance of rest and limitation as far as possible of transport were of the highest importance, either in the case of wound of the alimentary canal, or in wounds of the solid viscera in which hæmorrhage was a possible result.
Thirdly, as to the later prognosis in these injuries; very few men are fit to resume active service without a prolonged period of rest. In spite of the insignificance of the primary symptoms, or of the favourable course taken by the injuries, active exertion was almost always followed for some months by the appearance of vague pains and occasionally by indications of recurrent peritoneal symptoms, pointing to the disturbance of quiescent hæmorrhages, or of adhesions. Wounds of the kidney are apparently those least liable to be followed by trouble.
Lastly, the prognosis was influenced in the case of many of the viscera by coexisting injury to other organs or parts.
For instance, at least thirty per cent. of the abdominal wounds were complicated by wound of the thorax; and in the lower segment of the abdomen injury to the extra-peritoneal portions of the pelvic organs was common.
Both the immediate and ultimate prognosis were influenced greatly by this fact.
As to the individual injuries:
1. Wounds in the intestinal area, except in certain directions, often traverse the abdomen without inflicting a perforating injury on the bowel.
2. If the alimentary canal is perforated, injuries in certain segments, even if perforating, may be followed by spontaneous recovery. I should say the prognosis from this point of view is best in the ascending colon, then in the rectum; after these most favourable segments, I should place the others in the following order: stomach, sigmoid flexure, descending colon. As to perforating wounds of the transverse[Pg 472] colon and small intestine, I believe spontaneous recovery to be very rare.
3. Wounds of the solid viscera generally, usually heal spontaneously, and give no trouble unless one of the great vessels has been injured. I include in this category all organs except the pancreas, of wounds of which I had no experience.
4. Wounds of the bladder, if of the nature of pure perforations in the intra-peritoneal segment, often heal spontaneously.
5. As a rule, injuries to the organs in their intra-peritoneal course have a far better prognosis than those which implicate the organs in their uncovered portions.
6. The small calibre of the bullet is alone responsible for the favourable results observed.
7. The danger or otherwise of an intestinal injury depends mainly on mechanical conditions; for instance, the fixity of the ascending colon, and its comparative freedom from a covering of small intestine capable by movement of diffusing any infective material, account chiefly for such favourable results as are seen when that segment of the bowel is implicated.
Wounds of the scrotum were not uncommon, especially in connection with perforations of the upper part of the thigh. They offered no special feature, beyond the common tendency of every-day experience to the development of extensive ecchymosis.
Wounds of the testicles I saw on several occasions. I remember only one out of some half-dozen in which castration became necessary. I was told of one case, for the accuracy of which I cannot vouch, in which destruction of one testicle was followed by an attack of melancholia, culminating in the suicide of the patient.
Wounds of the penis also occurred, but as a rule were unimportant. I append a case, however; in which the penile urethra was wounded, which is of some interest.
(209) Wounded at Heilbron. Range 1,500 yards. Entry, 2½ inches below the right anterior superior iliac spine; the bullet traversed the groin superficially in the line of Poupart's ligament,[Pg 473] emerged, and crossed both penis and scrotum. The trooper was in the saddle when struck, and the penis probably somewhat coiled up. Three wounds were found, one at the junction of the penis and scrotum which opened the urethra, a second one about 3/4 of an inch along the under surface of the penis, and a third on the left side of the base of the prepuce. A considerable amount of œdema and ecchymosis of the scrotum developed, but no extravasation of urine. A catheter was kept in the urethra for some days, and the opening eventually closed by granulation.
I only once saw a patient with an injury to the deep urethra; in this case concurrent injury to other pelvic organs led to death on the third day. As a good many of the patients with pelvic wounds died rapidly, the accident may have been more common than my experience would suggest.
[19] British Med. Journal, May 12, 1900, i. 1195.
[20] 'On Traumatic Rupture of the Colon.' Annals of Surgery, vol. xxx. 1899, p. 137.
[21] Two of these died.
[22] The cases of injury to the solid viscera are those only which happen to be quoted in the text, and give no idea of relative mortality.
[23] British Medical Journal, May 12, 1900, vol. i. p. 1194.
The title of this work hardly allows of its conclusion without a brief mention of the shell wounds observed during the campaign.
As already pointed out, these formed but a very small proportion of the injuries treated in the hospitals, and beyond this they possessed comparatively small surgical interest, since, as a rule, the features presented were those of mere lacerated wounds, while the more severe of the cases which survived only offered scope for operations of the mutilating class so uncongenial to modern surgical instincts.
The fatal wounds consisted in extensive lacerations resulting in the destruction of the head or limbs, the laying open of the abdominal or thoracic cavities, or the production of visceral injuries beyond the possibility of repair. Of such injuries no further mention will be made.
A very great variety of shells was employed during the campaign, especially on the part of the Boers, and the frontispiece gives some idea of these. The photograph was taken by Mr. Kisch after the relief of Ladysmith. For the want of more extended knowledge I shall confine myself to the description of a few injuries caused by two classes of large shell, those of the Vickers-Maxim or 'Pom-pom,' and two varieties of shrapnel.
The large shells employed may be divided into classes according to the metal used in their construction, and the nature of the explosive with which they were filled. These details are of some surgical import, because they affect the nature of the fragments into which the shells are broken up.[Pg 475]
Fragments of shells constructed with cast iron and burst with powder, and also of forged steel exploded with lyddite, are depicted in fig. 90.
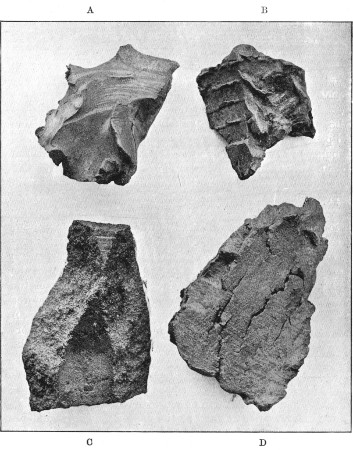 Fig. 90.
Fig. 90.
A, B, D. Fragments of 200 lb. forged Steel Howitzer Shell exploded by lyddite. C. Fragment of Cast-iron Shell exploded by powder. B exhibits transverse markings which might be mistaken for the lines seen in the Boer segment shells, but which really correspond to the area of fixation of the copper driving band
Examination of fragment C of a cast-iron shell exploded by powder shows the characteristic granular fracture, and[Pg 476] edges, although sharp, yet of a comparatively rounded nature. The fragment is also heavier for its surface measurement, as the metal is thicker than that seen in the remaining fragments, although the cast-iron shell was of a much smaller calibre than the steel one. The lesser degree of penetrative power, and increased capacity to contuse, possessed by such fragments are obvious.
a b and d are fragments of a large forged steel howitzer shell exploded by lyddite, such as were cast by our guns. The photograph well shows the more tenacious structure of the metal in the incomplete longitudinal fissuring exhibited, while the margins are of a sharp knifelike character, well calculated to penetrate or, in the case of superficial injuries, to produce wounds of a more sharply incised character than the cast-iron shell. Fragments a and b also show an appearance suggestive of partial fusion, characteristic of high explosive action, in the turning of the prominent margins.
The larger fragments of such shells were responsible for the most serious mutilating injuries, while small fragments sometimes caused comparatively simple perforating wounds. I remember a fragment of the fused character not larger than a small nut which had perforated the front of the thigh of a Boer, and lodged near the inner surface of the femur. Removal of the fragment was followed by a free gush of hæmorrhage. When the wound was opened up an opening was found in the external circumflex artery, hæmorrhage from which had been controlled by the impaction of the piece of shell. As an example of the cutting power of sharp fragments of shell I might instance the case of another Boer in whom light passing contact had been made by the missile. A gaping incised wound extended from above the angle of the scapula down to the outer surface of the buttock. The wound involved the latissimus dorsi, and the external and internal oblique muscles of the abdomen. The separate muscular layers were sharply defined in the lateral parts of the floor of the wound, and remained so for some time during the gradual contraction of the large granulating surface produced. The degree of contusion was in fact slight, while the incised character was strongly marked.[Pg 477]
In some cases the fragments merely struck the soldiers on the flat without producing any wound. In one such case a blow upon the epigastrium was, according to the patient, followed by the vomiting of a considerable amount of blood. A fluid diet was ordered, and no further ill effects were noted. The following case illustrates an oblique blow of a perforating character, which was nevertheless recovered from.
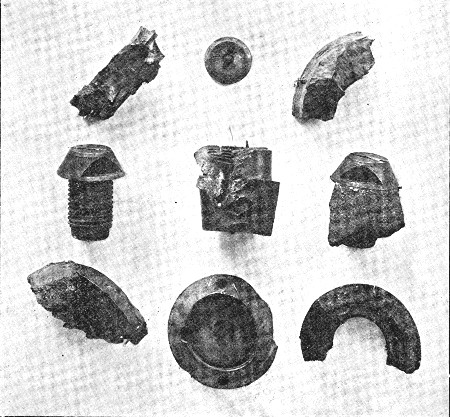 Fig. 91.—Various portions of Brass Percussion and Time
Fuses
Fig. 91.—Various portions of Brass Percussion and Time
Fuses
(210) Shell-wound of abdomen. Injury to liver.—Wounded at Paardeberg by a fragment of shell. Aperture of entry, a ragged opening in the median line. The fragment of shell was retained over the ninth costal cartilage in the nipple line. The wound bled freely, but the man was taken into camp, and then four miles on to the hospital, where he was anæsthetised and the fragment[Pg 478] extracted. The wound of entry was at the same time enlarged, cleansed, and partly sutured. The patient vomited once after the anæsthetic, and the bowels remained confined for three or four days after the injury. The extraction wound healed readily, but a considerable amount of slimy, bile-stained discharge was still escaping from the ragged entrance wound on the man's arrival at the Base on the fourteenth day. The abdomen was then normal in appearance, and as to physical signs, except for a tympanitic note over the hepatic area to the right of the wound. The temperature was normal, the pulse 90, the tongue clean, and the bowels were acting. At the end of four weeks pleurisy, with effusion, developed on the right side; the chest was aspirated and ℥xx of clear serum drawn off. The man then rapidly improved; the bile-stained discharge ceased at the end of five weeks, and a small granulating wound eventually closed at the end of two months, when the man returned to England.
Fig. 91 is inserted to illustrate the multifarious nature of the fragments into which the component parts of shells may break up. The pieces are for the most part of brass, and formed parts of either time or percussion fuses.
Fig. 92 represents the one-pound Vickers-Maxim shell in its actual size. The wounds produced by this shell are of some interest, since the Vickers-Maxim may be said to have been on trial during this campaign. The general opinion seems to have been to the effect that the moral influence produced by the continuous rapid firing of the gun and the attendant unpleasant noise were its chief virtues. A considerable number of wounds must, however, have been produced by it, which, if not of great magnitude and severity, were, at any rate, calculated to put the recipients out of action, and these wounds, moreover, were slower in healing than many of the rifle-bullet injuries.
The shell is so small that it was said to occasionally strike the body as a whole, and perforate. I was shown a case in which a wounded officer was confident that an entire shell had perforated his arm. The entry wound was at the outer part of the front of the forearm, the exit at the inner aspect of the arm, just above the elbow. Two ragged contused wounds existed, which healed slowly, but no serious nervous or[Pg 479] vascular injury had been produced. Although it is probable that only a fragment perforated in this case, it is of interest in connection with the following.
In a case shown to me by Sir William Thomson in the Irish Hospital at Bloemfontein, an entire shell had passed between the left arm and body of a trooper, perforating the haversack, as also a non-commissioned officer's notebook contained within it, without exploding. The only injury sustained by the trooper was a contusion on the inner aspect of the elbow-joint, with slight signs of contusion of the ulnar nerve. The case is of some importance, as showing that a comparatively resistent body can be perforated without necessary explosion on the part of the shell; hence the possibility of a similar perforation of the soft parts of the body.
 Fig. 92.—Unexploded 1-lb. Vickers-Maxim Shell. (Actual
size)
Fig. 92.—Unexploded 1-lb. Vickers-Maxim Shell. (Actual
size)
Fig. 93 is of a number of fragments of Vickers-Maxim shells, and it was by such that the great majority of the wounds were produced.
Wounds from fragments of these shells were, indeed, not at all rare. They were met with on any position; but, as far as my experience went, they were more common on the lower extremities than in other parts of the body, if the sufferers were in the erect position when wounded. I saw a good many wounds in the neighbourhood of the knee, some of which implicated the joint. When the injuries were received by patients in the lying or crouching positions, any part of the body was equally likely to be affected, or, again, the presence of large stones or rocks in the vicinity might determine the scattering of the[Pg 480] flying fragments at a more dangerous height than when the shells burst from contact with the actual ground.
The relation of one or two examples of wounds from pom-pom fragments may not be without interest, the more so as they illustrate the favourable influence of a low degree of velocity on the part of a projectile. I saw three wounds produced by the percussion fuses of these shells, an experience which shows that they were not very uncommon.
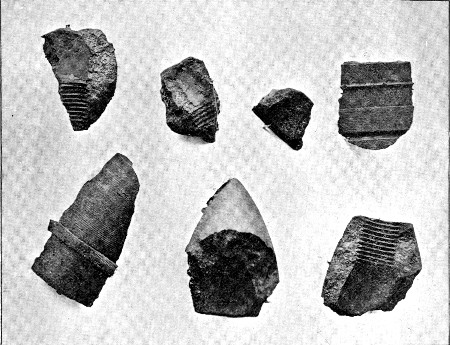 Fig. 93.
Fig. 93.
Fragments of Vickers-Maxim 1-lb. Shells. The centre fragment of the lower row is the point of a steel armour-piercing shell; although unsuitable for the purpose, they were occasionally employed in the field by the Boers
(211) Perforating shell-wound of abdomen.—Wounded at Magersfontein by the fuse screw of a small shell (Vickers-Maxim). Aperture of entry ragged, roughly circular, and 2 inches in diameter, with much-contused margins situated in the median line, nearly midway between the ensiform cartilage and umbilicus. The screw was lodged in the abdominal wall at the margin of the thorax, just outside the left nipple line. The aperture of entry was cleansed by Major Harris, R.A.M.C., who determined the fact that penetration of the peritoneal cavity had occurred, and removed[Pg 481] the fuse (see fig. 94) by a separate incision. The patient made an uneventful and uninterrupted recovery, the wound healing by granulation and leaving little weakness of the abdominal wall. He returned to England at the end of five weeks.
In a second case the fuse, together with a fragment of the iron case, entered the buttock by a ragged opening. The fragment of iron escaped by an exit aperture of about the same size. When the patient arrived at the Base some days after the injury, a hard body was felt in the wound, and on exploration the fuse was found and removed.
In a third case the fuse struck the side of the foot below the outer malleolus and comminuted the astragalus, and then passing forwards lodged beneath the extensor tendons of the toes. The wound was explored at the time of the injury and some fragments of bone removed; considerable cellulitis supervened, and the fuse was only discovered some days later when the patient came under the care of Sir W. Thomson in the Irish Hospital in Pretoria. It was there removed, together with some more fragments of bone, and the wound slowly granulated. The patient then returned to England, when the wound rapidly healed after the removal of some further necrosed fragments of cancellous tissue. The astragalus had been reduced to a mere shell of compact tissue, and the convexity of the articular surface was altogether lost. The deformity, together with the formation of adhesions in the ankle-joint, led to the development of a firm anchylosis.
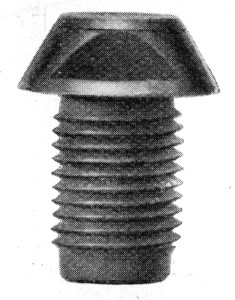 Fig. 94.—Pom-pom Percussion Fuse, exact size
Fig. 94.—Pom-pom Percussion Fuse, exact size
My friend Mr. Abbott removed a similar fuse from the substance of the lung after the lapse of nine months, the patient having developed an empyema, and a chronic fistula, which rapidly closed after the removal of the foreign body.[Pg 482]
Oblique Fracture of the Humerus caused by a Fragment of a Vickers-Maxim or Pom-pom Shell
The entire absence of comminution is very striking[Pg 483]
I will add one further case, that illustrated by plate XXV. In this a fragment of a pom-pom shell entered the outer aspect of the right shoulder to escape on the inner aspect of the arm, just below the confines of the axilla. An oblique, non-comminuted fracture of the humerus resulted, which in spite of moderate suppuration united well in the course of six weeks. The case is of particular interest as illustrating the nature of the fracture to be expected when the velocity retained by the missile is low.
The above instances show that such peculiarities as belong to wounds produced by pom-pom shells depend on the comparatively small size and weight of the fragments, and on the small degree of impetus with which they are propelled.
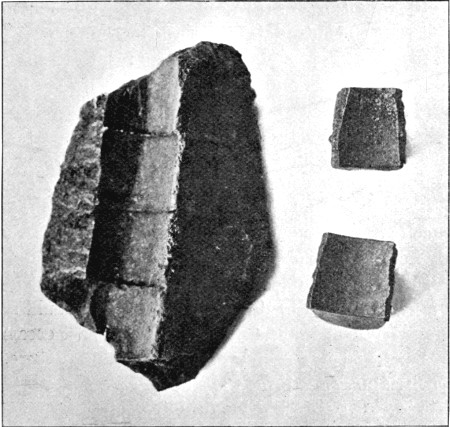 Fig. 95.—Boer Segment Shell, or Shrapnel.
Fig. 95.—Boer Segment Shell, or Shrapnel.
The large fragment is a piece of the case, the smaller are two of the pieces of iron packed within
Fig. 95 illustrates a form of shrapnel employed by the Boers, the case of which is of cast metal arranged in definite segments, while the interior is filled with small fragments of iron so shaped as to pack in concentric layers. As to the wounds produced by the contained fragments I have no experience, since I never saw one of the pieces of iron removed. This no doubt depended in part on the very unsatisfactory practice made by the Boers with shrapnel generally. Even when they fired English shrapnel, the shells were, as a rule, exploded far[Pg 484] too high to cause any serious danger to the men beneath. I saw on one occasion a large number of shrapnel shells exploded over a body of Imperial Yeomanry, but as a result of the great height at which all the shells were exploded, not a single casualty resulted.
The segment casing of the shell, however, I several times saw removed from the body. The fragment shown in fig. 95 was removed from the buttock of a man after one of Lord Methuen's early battles. It may be remarked that the buttock is rather a common, and also a favourable, seat for shell wounds with retention of the fragment. This no doubt depends on the fact that the buttock is one of the few superficial regions in which sufficient depth of tissue exists for the retention or the passage of so large an object as a fragment of shell.
Fig. 96 is of a number of leaden shrapnel bullets from our own shells. A normal undeformed bullet, such as was the usual cause of wounds, is shown at the left-hand upper corner. The remainder show common forms of deformity caused by striking on the ground or against rocks. I attribute small importance to the deformed bullets, as I never saw one removed, and it is probable that a ricochet shrapnel bullet would rarely retain sufficient force to penetrate. The lower fragments are inserted to illustrate a fact that would scarcely have been assumed, that these bullets on impact occasionally suffer a fracture of a somewhat crystalline nature. The occurrence of this gross form of fracture is of some interest in relation to the extreme fragmentation sometimes undergone by the hardened leaden cores of the small-calibre bullets.
A considerable number of wounds from leaden shrapnel bullets were met with among our own men, as well as among the Boers. The wounds possessed little special interest, except from the fact that the bullets were often retained. I saw bullets in the chest on several occasions, also in the abdomen, pelvis, the neighbourhood of joints, and in the limbs.
I saw one patient who had suffered no less than six perforating wounds as the result of the bursting of one shrapnel shell.
I will here quote one case of interest as completing the[Pg 485] various forms of perforating wound of the abdomen met with during the campaign.
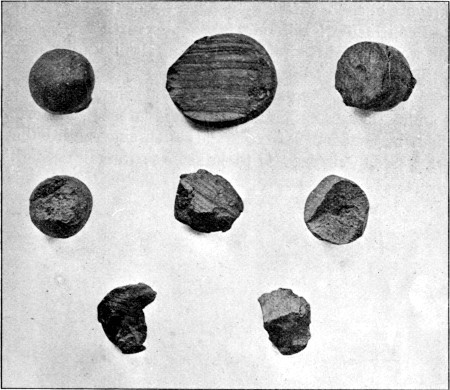 Fig. 96.—Normal, Deformed, and Fractured Leaden Shrapnel
Bullets
Fig. 96.—Normal, Deformed, and Fractured Leaden Shrapnel
Bullets
(212) Perforating shrapnel-wound of abdomen.—Boer wounded at Graspan. Aperture of entry (shrapnel), opposite eighth left costal cartilage, 1 inch external to nipple line. The opening was circular, and surrounded by an area of ecchymosis 4 inches in diameter; exit, 4½ inches above and to the right of the umbilicus. Patient was at first in a Boer ambulance, and only seen by me on the ninth day. At that date he was dressed and walking with a gauze pad and bandage over the wounds. From the exit wound, which was 1 inch in diameter, protruded a piece of sloughing omentum, the margin of the wound being everted and raised over a circular indurated area.
It was thought best to allow the sloughing omentum, which was very foul, to separate spontaneously, and then to return the stump. At the end of three weeks, however, the slough had not only separated, but the stump had retracted, and only a small granulating surface was left, which healed spontaneously.
I have little to say regarding the treatment of shell wounds. The mutilating injuries, if not of a fatal character, necessitated treatment of a corresponding nature to the damage. In all such cases the general rules of surgery indicate the lines to be followed.
In the case of shrapnel wounds the bullets were often better removed; but when in dangerous positions, as sunk deeply in the chest, abdomen, or pelvis, they were best left, unless some very special indication for removal existed. Large fragments of shell always demanded removal.
In conclusion I will only make the further remark, that shell wounds, with the exception of clean leaden shrapnel tracks, always suppurated.
I make this closing statement with the view of emphasising the influence exerted on the aseptic course of modern rifle wounds by the small calibre of the bullet, since both bullet and shell wounds were exposed to the same surrounding conditions.
Abdomen, injuries to, 407
General prognosis in, 470
Abdominal wounds:
Explosive, 414
Non-perforating, 409
Perforating, 411
Abscess of the brain, 287
Acetabulum, fracture of, 193
Acetylene light, 30
Ambulance:
Foreign, 30
Trolly (McCormack-Brook), 18
Wagons, 19
Amputations:
Effect of transport on, 110
for fracture, 177
Aneurisms:
Effect of rest on, 127
Gangrene after, 152
Traumatic, 122
False, 123
True, 126
Treatment of, 127
Aneurismal varix:
Arm and forearm, 147
Effect on circulation, 134
Carotid, 146
Femoral, 147
Mode of development, 130
Popliteal, 147
Prognosis in, 144
Signs of, 131
Treatment of, 144
Anosmia, 348
Antrum, wounds of, 306
Aphasia:
Amnesic, 276
Ataxic, 273
Functional, 351
Arterial hæmatoma, 123
Prognosis in, 126
Treatment of, 126
Arteries:
Compression by cicatrices, 113
Contusion of, 112
Division of, 114
Perforation of, 114
Arterio-venous aneurism:
Arm and forearm, 150
Cervical, 149
Femoral, 150
Leg, 150
Popliteal, 151
Treatment of, 148
Biliary fistula, 467
Bladder:
Wounds of, 443, 457
Extra-peritoneal, 458
Intra-peritoneal, 457
Retained bullet in, 110, 460
Bones. See Fractures
Bowlby, Mr.:
Retained bullets in joints, 229, 230
Wound of pharynx, 311
Brain:
Abscess of, 287
Cerebral irritation, 269
Compression of, 267
Concussion of, 266
Effect of ricochet on, 249
Explosive injury of, 247, 248
Frontal injuries, 247, 249, 266
Fronto-parietal injuries, 273
Occipital injuries, 276
Parietal injuries, 273
Prognosis in cerebral injuries, 289
Treatment, 289
Bread, 7
Buck wagon, 21
Bullets:
Characters directly affecting wounds:
Aseptic nature, 70
Calibre, 41
Composition of, 51
Deformities of, 81
Fragmentation, 88
Length, 41
Mantles of, 52, 82, 83
Penetration, 49
Revolution, 45
Ricochet, 82
Shape, 42
Stability, 51
Striking force, 50
Velocity of flight, 42
Weight, 42
Effect of resistance of bones on, 86, 87, 88, 93
Retention of, 71, 79
Indications for removal of, 110
in bladder, 110, 460
in chest, 381, 401
in nasal fossa, 244
in or near joints, 229, 230
in skull, 244, 249, 260, 266, 284, 298
in spinal canal, 337
Reversal of, 81
Varieties of:
Determination of, 105
Expanding, 91
Explosive, 95
Guedes, 48, 51
Krag-Jörgensen, 48, 51
Jeffreys, 94
Large leaden, 95
Lee-Metford, 52, 89
Mark IV., 94
Mauser, 52, 83
Soft-nosed, 93
Tampered, 95
Tweedie, 94
Waxed, 52
Cauda equina, injury to, 325, 330
Cellulitis, 34
Cervical nerve roots, injury to, 107
Plexus, 357
Cheatle, Mr. G. L.:
Entry and exit wounds, 72
First field dressing, 107
Wound of heart, 383
" " intestine, 413
Cheek, wounds of, 309
Chest, injuries to, 374
Character of wounds, 377
Influence of small calibre of bullet on, 374
Martini wounds, 374, 388
Non-penetrating wounds, 375
Penetrating wounds, 376
Cheyne, Mr. W. W., F.R.S.:
Abdominal wounds, 449
Spent bullets, 243, 449
Civil surgeons, 38
Climate, 8, 36, 71
Comparison of South African with other campaigns, 14
Compression of brain, 267
Spinal cord, 319
Concussion of brain, 266
Eye, 300
Joints, 226
Nerves, 341, 343
Spinal cord, 315
Contour wounds, 65
Contusion:
Nerves, 343
Spinal cord, 316
Costal cartilages, fractures of, 379
Cox, Dep. Insp.-Gen.:
Case of varix, 148
Day, Mr. J. J.:
Fractures of the skull, 251
Deadliness of modern weapons, 16
Diaphragm, wounds of, 381
Displacement of structures by the bullet, 68
Abdomen, 411
Nerves, 342
Vessels, 382, 384
Viscera, 310, 382, 411
Drink, 8
Dust, 8, 35
Bacteriology of, 36
Empyema, 394, 396
Enteric fever, 9
Epilepsy, traumatic, 291
Equipment of foreign ambulances, 31
Surgical, 4
Erysipelas, 34
Expanding bullets, 91
Explosive bullets, 95
Explosive wounds:
of abdomen, 414
of fractures, 155
of head, 245
of leg, 221
of soft parts, 97
of thigh, 197
Eye, injuries to, 299
Facial paralysis:
Cortical, 273-277
Peripheral, 355
First field dressings, 107
Flies, 36
Flockemann, Dr.:
Hæmothorax, 393
Injury to abdomen, 420
Fractures:
Course of healing of, 172
Explosive wounds in, 155
into joints, 163, 228
Limb bones, 154
Local shock in, 172
Long bones, types of, 161
Longitudinal, 163
Notch, 165
Oblique, 165
Perforating, 166
Stellate, 161
Transverse, 166
Wedge, 165
Osteomyelitis in, 174
Pom-pom fractures, 483
Prognosis, general, in, 174
Special features of, 155
Special bones:
Acetabulum, 193
Carpus, 183
Clavicle, 178
Femur, 193
Fibula, 219
Humerus, 178
Jaws, 306
Malar, 305
Mastoid process, 299
Metacarpus, 185
Metatarsus, 224
Orbital walls, 300
Patella, 215
Pelvis, 189
Radius, 183
Ribs, 377
Scapula, 177, 379
Skull:
Base, 262
Glancing, 254
Gutter, 255
Perforating, deep, 245
Superficial, 259
Treatment of, 293
Spine, 314
Sternum, 379
Tarsus, 223
Tibia, 217
Short and flat bones, 168
Suppuration of soft parts in, 173
Symptoms of, 171
Treatment of:
General, 175
Femur, 205
Leg, 221
Upper Extremity, 135
Variation in character during the campaign, 154
Fractures in Franco-German war (Sir W. MacCormac), 167
Fragmentation of bullets, 88
Fuses of shells, wounds by, 481
Gangrene:
Acute traumatic, 34
After ligature of main vessels, 152
Genital organs, wounds of, 472
Guedes rifle, 65
Gutter wounds:
of bladder, 458
of bones, 231
of intestine, 417
of joints, 231
of liver, 466
of pelvis, 189
of scalp, 242
of skull, 255
of soft parts, 157
Hæmarthrosis, 232
Hæmorrhage, 104, 114
Control by bullets, 116
by loop of nerve, 116
Deaths from, 116
Fever dependent upon, 118
Internal, 116
Interstitial, 118
Primary, 114
Recurrent, 117
Secondary, 117
Treatment of, 120
Hæmorrhoids, 10
Hæmothorax, 386, 389
Behaviour of blood in, 390
Course of, 390, 394
Diagnosis of, 398
Effect of transport on, 389
Empyema after, 394
Pleuritic effusion in, 390
Prognosis in, 399
Recurrent bleeding in, 393
Parietal, 389, 398
Pulmonary, 386, 389
Symptoms of, 391
Temperature in, 391, 393
Treatment of, 400
Head, injuries to, 241
Health of the troops, 7
Heart, wounds of, 382
in neighbourhood of, 384
Hemianopsia, 276
Altitudinal, 277
Lateral, 276
Hospitals:
Field, 29, 37
Foreign, 30
General, 31, 38
Improvised, 28, 39
Indian Field, 29
Stationary, 27, 31, 33, 37
Varieties of, 28
Hospital ships, 24
Tents, 32
Trains, 23
Hydronephrosis, 464
Impact, irregular, 80, 82
Instruments, 4
Intestine, injuries to:
Diagnosis of, 428
Difficulties of operation, 453
Indications for operation, 454
Lateral contusion, 416
Prognosis, 446
Treatment, 452
Wounds of, 415
Extra-peritoneal, 419
Large intestine, 436, 444
Results of, 421
Small intestine, 427
Irregular wounds, 97
Itinerary, 2
Jam, 7
Jaws, fractures of:
Lower, 306
Upper, 306
Treatment of, 308
Jenner, L. L., bacteriology of dust, 36
Joints, injuries to, 225
Arterial wounds in, 121, 233
Classification of, 229
Course after, 232
Fractures into, 228
Signs and symptoms, 232
Suppuration of, 233
Treatment, general, 235
Joints, retained bullets in or near, 229, 230
Joints, special:
Ankle, 239
Elbow, 236
Hand, 237
Hip, 238
Knee, 238
Shoulders, 236
Tarsus, 240
Ker, J. E., cases of aneurism, 152
Kidney, wounds of, 461
Krag-Jörgensen rifle, 65
Laminectomy, 335, 340
Larynx, wounds of, 312
Leaden bullets, 95
Lee-Metford rifle, 53, 64
Lewtas, Col. I. M. S., cases of aneurism, 144
Lightning stroke, 10
Liver, wounds of, 466
Local shock, 103
in fractures, 172
Lower jaw, fractures of, 306
Lungs, wounds of, 385
Diagnosis, 398
Effect of velocity on, 385
Prognosis, 399
Retained bullets in, 401
Symptoms of, 386
Treatment of, 400
Lyddite shells, 475
MacCormac, Sir W.:
Aneurism, 150
Fractures, 167
Malar bone, fractures, 305
Mandible, fractures, 306
Mantles, stability of, 51, 83
Martini-Henry rifle, 48
Wounds by, 96
Mastoid process, 299
Mauser rifle, 64
Meat, 7
Mediastinal wounds, 382, 384
Mesentery, wounds of, 420
Mills-Roberts, Mr. H. R.:
Spinal hæmorrhage, 321
'Modders, the,' 9
Mortality, general, 11
amongst officers, 14
in battles of Kimberley Relief Force, 12
Nasal fossæ, bullet in, 244
Neck, wounds of, 309
Nerves, injuries to, 341
Concussion, 341, 343, 346
Contusion, 343, 347
Displacement of, 342
Laceration, 344, 348
Perforation, 345
Prognosis in, 370
Scar, implication of, 345, 350
Section, 344
Symptoms of, 346
Treatment of, 371
Velocity in relation to, 341
Nerves, special:
Cranial:
Fifth, 353
Fourth, 353
Eighth, 353, 354
Eleventh, 356
Olfactory, 352
Optic, 352
Seventh, 354, 372
Sixth, 353
Tenth, 356
Third, 353
Twelfth, 357
Spinal:
Brachial, 357
Cervical, 347, 357
Lumbar, 359
Sacral, 359
Sacro-coccygeal, 360
Thoracic, 358
Neuritis:
Ascending, 350
Peripheral, 355
Traumatic, 349
Neurosis, traumatic 351
Nose, wounds of, 305, 348
Nurses, 38
Officers, mortality among, 14
Olecranon, fracture of, 183, 237
Omentum, wounds of, 420
Prolapse of, 420
Operations:
Difficulties of, 35
in field, 296
in Field hospitals, 109
Orbit, wounds of, 299
Prognosis and treatment of, 304
Osteomyelitis in fractures, 174
Outfit, surgical, 3
Pain in wounds, 103
Paraplegia, functional, 337
Penetration of bullets, 49
Penis, wounds of, 472
Peritoneal infection, 412
Pharynx, wounds of, 311
Pleural septicæmia, 437
Pleurisy, 390, 398
Pneumonia, 9, 398
Pneumo-thorax, 388
Pom-pom shells, 478
Portland Hospital, 34
Psychical disturbance, 101
Rain, 9, 36
Range of fire:
Difficulty of judging influence on mortality, 17
Rectum, wounds of, 443, 444
Removal of wounded from the field, 18
Respiration in spinal injuries, 329
Retained bullets. See Bullets
Reversed bullets, 81
Revolution of bullet, 45, 46
Ribs, fractures of, 377
Signs of, 379
Ricochet, 82
Effect on wound type, 249
Lee-Metford, 89
Mauser, 84
Within body,
Abdomen, 415
Skull, 249
Rifles:
Bore, 41
Guedes, 47, 54
Krag-Jörgensen, 47, 54
Lee-Metford, 47, 64
Martini-Henry, 47, 97
Mauser, 47, 64
Modern principles of, 40
Trajectory, 44
Varieties employed, 47, 48
Scalp wounds, 242, 264
Scapula, fractures of, 177, 379
Scrotum, wounds of, 472
Septic disease, 34
Septicæmia:
General, 34
in enteric fever, 9
Peritoneal, 421
Pleural, 437
Shells, 474
Varieties of, 475
Vickers-Maxim, 478
Lyddite, 476
Shrapnel, 483
Shell wounds:
of abdomen, 480, 485
Proportionate occurrence of, 11
Shell fuse wounds, 481
Ships, hospital, 24
Shock:
General, 101
Local, 103
Treatment of, 110
Shrapnel, 483
Simla, 25
Skull. See Fractures
Fractures independent of gross brain lesion, 242
with brain lesion, 248
Spinal column:
Injuries to, 314
Fractures of centra, 317
Spinous processes, 315
Transverse processes, 314
Spinal cord, injuries to, 315
Compression by bullets, 319
Concussion, 319
Contusion, 320
Diagnosis, 335
Hæmato-myelia, 322
Section of, 323
Shock accompanying, 328
Signs of, 323
Transport of, 339
Treatment of, 339
Spinal hæmorrhage:
Epidural, 321
Hæmato-myelia, 322
Peri-pial, 321
Spleen, wounds of, 469
Splints:
Aluminium, 177
Field cane, 209, 221
Hodgen's, 211
Wire gauze, 187
Sternum, fractures of, 379
Stevenson, Col. W. F.:
Local shock, 106
Explosive wounds, 159
Stokes, Sir W.:
Treatment of aneurism, 151
Stomach, wounds of, 424
Stonham, Mr. C.:
Wound of vermiform appendix, 437
Sunstroke, 10
Suppuration of wounds, 78
in fracture, 173
Synovitis, vibration, 226
Temperature of air, 8, 36
in blood effusions, 118, 391, 393
Tents, 32
Testicle, wounds of, 472
Tetanus, 34
Thirst, 8
Thomson, Sir W.:
Pom-pom wounds, 479
Wound of nose, 305
Thoracic vessels, wounds of, 384
Tonga, the, 19
Tongue, wounds of, 309
Trachea, wounds of, 312
Traction engines, 23
Trains, hospital, 23
Trajectory, 44
Transport:
after battles, 26
of wounded men from field, 18
of wounded of the Kimberley Relief Force, 25
of chest injuries, 386
of fractures, 176
of spinal injuries, 339
Traumatic aneurism. See Aneurism
Traumatic epilepsy, 291
Traumatic gangrene, 34
Traumatic neurosis, 107, 351
Treves, Mr. F.: on cessation of intestinal peristalsis, 423
Trolly (McCormack-Brook), 19
Upper jaws, 306
Urethra, wounds of, 472
Urinary Bladder. See Bladder
Varix. See Aneurismal varix
Vegetables, 7
Veldt sores, 10
Velocity of bullet:
Circumstances influencing, 43
Initial, 42, 49
Remaining of various rifles, 49
Velocity, influence of:
on fractures of long bones, 163
on fractures of short and flat bones, 168
on wounds of abdomen, 414
of chest, 385
of joints, 226, 230
of lungs, 385
of nerves, 341
of skull, 251
of spine, 319
Vermiform appendix, wounds of, 437
Vibration synovitis, 226
Vickers-Maxim shell, 478
Vomiting in spinal injuries, 329
Wagons:
Ambulance, 20
Buck, 22
Ox, 20
Warfare, deadliness of, 40
Water in South Africa:
Character of, 8, 36
Transport of, 5
Waxed bullets, 52
Wobble, 80, 81, 251
Wounded men, removal from the field, 18
Wounds, general:
Aperture of entry, 55, 72
Aperture of exit, 58, 74
Climate, influence on, 71
Clinical, course of, 69
Contour tracks, 65
Direct nature of tracks, 63
Directions of tracks, 66
Displacement of structures, 68
Explosive exit wounds, 97
Foreign bodies in, 71
First field dressing, 107
Hæmorrhage, 104
Irregular types of, 80, 97
Mode of healing, 72
Multiple character, 67
Nature of tracts, 68
Pain, 103
Prognosis, 106
Psychical disturbance, 101
Shock, 101
Small bore, 67
Superficial tracts, 65
Suppuration, 69, 78
Symptoms, 100
Tracks, nature of, 68
Treatment, 107
PRINTED BY
SPOTTISWOODE AND CO. LTD., NEW-STREET SQUARE
LONDON
End of the Project Gutenberg EBook of Surgical Experiences in South Africa,
1899-1900, by George Henry Makins
*** END OF THIS PROJECT GUTENBERG EBOOK SURGICAL EXPERIENCES ***
***** This file should be named 21280-h.htm or 21280-h.zip *****
This and all associated files of various formats will be found in:
https://www.gutenberg.org/2/1/2/8/21280/
Produced by Jonathan Ingram, Josephine Paolucci and the
Online Distributed Proofreading Team at https://www.pgdp.net
Updated editions will replace the previous one--the old editions
will be renamed.
Creating the works from public domain print editions means that no
one owns a United States copyright in these works, so the Foundation
(and you!) can copy and distribute it in the United States without
permission and without paying copyright royalties. Special rules,
set forth in the General Terms of Use part of this license, apply to
copying and distributing Project Gutenberg-tm electronic works to
protect the PROJECT GUTENBERG-tm concept and trademark. Project
Gutenberg is a registered trademark, and may not be used if you
charge for the eBooks, unless you receive specific permission. If you
do not charge anything for copies of this eBook, complying with the
rules is very easy. You may use this eBook for nearly any purpose
such as creation of derivative works, reports, performances and
research. They may be modified and printed and given away--you may do
practically ANYTHING with public domain eBooks. Redistribution is
subject to the trademark license, especially commercial
redistribution.
*** START: FULL LICENSE ***
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg-tm mission of promoting the free
distribution of electronic works, by using or distributing this work
(or any other work associated in any way with the phrase "Project
Gutenberg"), you agree to comply with all the terms of the Full Project
Gutenberg-tm License (available with this file or online at
https://gutenberg.org/license).
Section 1. General Terms of Use and Redistributing Project Gutenberg-tm
electronic works
1.A. By reading or using any part of this Project Gutenberg-tm
electronic work, you indicate that you have read, understand, agree to
and accept all the terms of this license and intellectual property
(trademark/copyright) agreement. If you do not agree to abide by all
the terms of this agreement, you must cease using and return or destroy
all copies of Project Gutenberg-tm electronic works in your possession.
If you paid a fee for obtaining a copy of or access to a Project
Gutenberg-tm electronic work and you do not agree to be bound by the
terms of this agreement, you may obtain a refund from the person or
entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. "Project Gutenberg" is a registered trademark. It may only be
used on or associated in any way with an electronic work by people who
agree to be bound by the terms of this agreement. There are a few
things that you can do with most Project Gutenberg-tm electronic works
even without complying with the full terms of this agreement. See
paragraph 1.C below. There are a lot of things you can do with Project
Gutenberg-tm electronic works if you follow the terms of this agreement
and help preserve free future access to Project Gutenberg-tm electronic
works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation ("the Foundation"
or PGLAF), owns a compilation copyright in the collection of Project
Gutenberg-tm electronic works. Nearly all the individual works in the
collection are in the public domain in the United States. If an
individual work is in the public domain in the United States and you are
located in the United States, we do not claim a right to prevent you from
copying, distributing, performing, displaying or creating derivative
works based on the work as long as all references to Project Gutenberg
are removed. Of course, we hope that you will support the Project
Gutenberg-tm mission of promoting free access to electronic works by
freely sharing Project Gutenberg-tm works in compliance with the terms of
this agreement for keeping the Project Gutenberg-tm name associated with
the work. You can easily comply with the terms of this agreement by
keeping this work in the same format with its attached full Project
Gutenberg-tm License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern
what you can do with this work. Copyright laws in most countries are in
a constant state of change. If you are outside the United States, check
the laws of your country in addition to the terms of this agreement
before downloading, copying, displaying, performing, distributing or
creating derivative works based on this work or any other Project
Gutenberg-tm work. The Foundation makes no representations concerning
the copyright status of any work in any country outside the United
States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate
access to, the full Project Gutenberg-tm License must appear prominently
whenever any copy of a Project Gutenberg-tm work (any work on which the
phrase "Project Gutenberg" appears, or with which the phrase "Project
Gutenberg" is associated) is accessed, displayed, performed, viewed,
copied or distributed:
This eBook is for the use of anyone anywhere at no cost and with
almost no restrictions whatsoever. You may copy it, give it away or
re-use it under the terms of the Project Gutenberg License included
with this eBook or online at www.gutenberg.org
1.E.2. If an individual Project Gutenberg-tm electronic work is derived
from the public domain (does not contain a notice indicating that it is
posted with permission of the copyright holder), the work can be copied
and distributed to anyone in the United States without paying any fees
or charges. If you are redistributing or providing access to a work
with the phrase "Project Gutenberg" associated with or appearing on the
work, you must comply either with the requirements of paragraphs 1.E.1
through 1.E.7 or obtain permission for the use of the work and the
Project Gutenberg-tm trademark as set forth in paragraphs 1.E.8 or
1.E.9.
1.E.3. If an individual Project Gutenberg-tm electronic work is posted
with the permission of the copyright holder, your use and distribution
must comply with both paragraphs 1.E.1 through 1.E.7 and any additional
terms imposed by the copyright holder. Additional terms will be linked
to the Project Gutenberg-tm License for all works posted with the
permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg-tm
License terms from this work, or any files containing a part of this
work or any other work associated with Project Gutenberg-tm.
1.E.5. Do not copy, display, perform, distribute or redistribute this
electronic work, or any part of this electronic work, without
prominently displaying the sentence set forth in paragraph 1.E.1 with
active links or immediate access to the full terms of the Project
Gutenberg-tm License.
1.E.6. You may convert to and distribute this work in any binary,
compressed, marked up, nonproprietary or proprietary form, including any
word processing or hypertext form. However, if you provide access to or
distribute copies of a Project Gutenberg-tm work in a format other than
"Plain Vanilla ASCII" or other format used in the official version
posted on the official Project Gutenberg-tm web site (www.gutenberg.org),
you must, at no additional cost, fee or expense to the user, provide a
copy, a means of exporting a copy, or a means of obtaining a copy upon
request, of the work in its original "Plain Vanilla ASCII" or other
form. Any alternate format must include the full Project Gutenberg-tm
License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying,
performing, copying or distributing any Project Gutenberg-tm works
unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing
access to or distributing Project Gutenberg-tm electronic works provided
that
- You pay a royalty fee of 20% of the gross profits you derive from
the use of Project Gutenberg-tm works calculated using the method
you already use to calculate your applicable taxes. The fee is
owed to the owner of the Project Gutenberg-tm trademark, but he
has agreed to donate royalties under this paragraph to the
Project Gutenberg Literary Archive Foundation. Royalty payments
must be paid within 60 days following each date on which you
prepare (or are legally required to prepare) your periodic tax
returns. Royalty payments should be clearly marked as such and
sent to the Project Gutenberg Literary Archive Foundation at the
address specified in Section 4, "Information about donations to
the Project Gutenberg Literary Archive Foundation."
- You provide a full refund of any money paid by a user who notifies
you in writing (or by e-mail) within 30 days of receipt that s/he
does not agree to the terms of the full Project Gutenberg-tm
License. You must require such a user to return or
destroy all copies of the works possessed in a physical medium
and discontinue all use of and all access to other copies of
Project Gutenberg-tm works.
- You provide, in accordance with paragraph 1.F.3, a full refund of any
money paid for a work or a replacement copy, if a defect in the
electronic work is discovered and reported to you within 90 days
of receipt of the work.
- You comply with all other terms of this agreement for free
distribution of Project Gutenberg-tm works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg-tm
electronic work or group of works on different terms than are set
forth in this agreement, you must obtain permission in writing from
both the Project Gutenberg Literary Archive Foundation and Michael
Hart, the owner of the Project Gutenberg-tm trademark. Contact the
Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable
effort to identify, do copyright research on, transcribe and proofread
public domain works in creating the Project Gutenberg-tm
collection. Despite these efforts, Project Gutenberg-tm electronic
works, and the medium on which they may be stored, may contain
"Defects," such as, but not limited to, incomplete, inaccurate or
corrupt data, transcription errors, a copyright or other intellectual
property infringement, a defective or damaged disk or other medium, a
computer virus, or computer codes that damage or cannot be read by
your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the "Right
of Replacement or Refund" described in paragraph 1.F.3, the Project
Gutenberg Literary Archive Foundation, the owner of the Project
Gutenberg-tm trademark, and any other party distributing a Project
Gutenberg-tm electronic work under this agreement, disclaim all
liability to you for damages, costs and expenses, including legal
fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT
LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE
PROVIDED IN PARAGRAPH F3. YOU AGREE THAT THE FOUNDATION, THE
TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE
LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR
INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH
DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a
defect in this electronic work within 90 days of receiving it, you can
receive a refund of the money (if any) you paid for it by sending a
written explanation to the person you received the work from. If you
received the work on a physical medium, you must return the medium with
your written explanation. The person or entity that provided you with
the defective work may elect to provide a replacement copy in lieu of a
refund. If you received the work electronically, the person or entity
providing it to you may choose to give you a second opportunity to
receive the work electronically in lieu of a refund. If the second copy
is also defective, you may demand a refund in writing without further
opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth
in paragraph 1.F.3, this work is provided to you 'AS-IS' WITH NO OTHER
WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO
WARRANTIES OF MERCHANTIBILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied
warranties or the exclusion or limitation of certain types of damages.
If any disclaimer or limitation set forth in this agreement violates the
law of the state applicable to this agreement, the agreement shall be
interpreted to make the maximum disclaimer or limitation permitted by
the applicable state law. The invalidity or unenforceability of any
provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the
trademark owner, any agent or employee of the Foundation, anyone
providing copies of Project Gutenberg-tm electronic works in accordance
with this agreement, and any volunteers associated with the production,
promotion and distribution of Project Gutenberg-tm electronic works,
harmless from all liability, costs and expenses, including legal fees,
that arise directly or indirectly from any of the following which you do
or cause to occur: (a) distribution of this or any Project Gutenberg-tm
work, (b) alteration, modification, or additions or deletions to any
Project Gutenberg-tm work, and (c) any Defect you cause.
Section 2. Information about the Mission of Project Gutenberg-tm
Project Gutenberg-tm is synonymous with the free distribution of
electronic works in formats readable by the widest variety of computers
including obsolete, old, middle-aged and new computers. It exists
because of the efforts of hundreds of volunteers and donations from
people in all walks of life.
Volunteers and financial support to provide volunteers with the
assistance they need, is critical to reaching Project Gutenberg-tm's
goals and ensuring that the Project Gutenberg-tm collection will
remain freely available for generations to come. In 2001, the Project
Gutenberg Literary Archive Foundation was created to provide a secure
and permanent future for Project Gutenberg-tm and future generations.
To learn more about the Project Gutenberg Literary Archive Foundation
and how your efforts and donations can help, see Sections 3 and 4
and the Foundation web page at https://www.pglaf.org.
Section 3. Information about the Project Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a non profit
501(c)(3) educational corporation organized under the laws of the
state of Mississippi and granted tax exempt status by the Internal
Revenue Service. The Foundation's EIN or federal tax identification
number is 64-6221541. Its 501(c)(3) letter is posted at
https://pglaf.org/fundraising. Contributions to the Project Gutenberg
Literary Archive Foundation are tax deductible to the full extent
permitted by U.S. federal laws and your state's laws.
The Foundation's principal office is located at 4557 Melan Dr. S.
Fairbanks, AK, 99712., but its volunteers and employees are scattered
throughout numerous locations. Its business office is located at
809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887, email
business@pglaf.org. Email contact links and up to date contact
information can be found at the Foundation's web site and official
page at https://pglaf.org
For additional contact information:
Dr. Gregory B. Newby
Chief Executive and Director
gbnewby@pglaf.org
Section 4. Information about Donations to the Project Gutenberg
Literary Archive Foundation
Project Gutenberg-tm depends upon and cannot survive without wide
spread public support and donations to carry out its mission of
increasing the number of public domain and licensed works that can be
freely distributed in machine readable form accessible by the widest
array of equipment including outdated equipment. Many small donations
($1 to $5,000) are particularly important to maintaining tax exempt
status with the IRS.
The Foundation is committed to complying with the laws regulating
charities and charitable donations in all 50 states of the United
States. Compliance requirements are not uniform and it takes a
considerable effort, much paperwork and many fees to meet and keep up
with these requirements. We do not solicit donations in locations
where we have not received written confirmation of compliance. To
SEND DONATIONS or determine the status of compliance for any
particular state visit https://pglaf.org
While we cannot and do not solicit contributions from states where we
have not met the solicitation requirements, we know of no prohibition
against accepting unsolicited donations from donors in such states who
approach us with offers to donate.
International donations are gratefully accepted, but we cannot make
any statements concerning tax treatment of donations received from
outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg Web pages for current donation
methods and addresses. Donations are accepted in a number of other
ways including including checks, online payments and credit card
donations. To donate, please visit: https://pglaf.org/donate
Section 5. General Information About Project Gutenberg-tm electronic
works.
Professor Michael S. Hart was the originator of the Project Gutenberg-tm
concept of a library of electronic works that could be freely shared
with anyone. For thirty years, he produced and distributed Project
Gutenberg-tm eBooks with only a loose network of volunteer support.
Project Gutenberg-tm eBooks are often created from several printed
editions, all of which are confirmed as Public Domain in the U.S.
unless a copyright notice is included. Thus, we do not necessarily
keep eBooks in compliance with any particular paper edition.
Most people start at our Web site which has the main PG search facility:
https://www.gutenberg.org
This Web site includes information about Project Gutenberg-tm,
including how to make donations to the Project Gutenberg Literary
Archive Foundation, how to help produce our new eBooks, and how to
subscribe to our email newsletter to hear about new eBooks.